User login
Hip Fracture Rates Rose as Use of HT Waned
Major Finding: The Women's Health Initiative reported in May 2002 that risks of coronary heart disease and cancer were associated with HT. Between July 2002 and December 2008, HT use in this population decreased from 85% to 18%. After adjustment for age and race, women who did not use HT in the previous year had a 55% increased risk of hip fracture.
Data Source: A study of 80,995 patients in the Kaiser Permanente Southern California database.
Disclosures: Dr. Karim said she had no financial conflicts of interest. The study was supported by the University of Southern California.
CHICAGO – Prescriptions for hormone therapy for elderly postmenopausal women declined significantly after the results of the Women's Health Initiative were reported in May 2002, and it now appears that there has been a correspondingly steep rise in hip fracture rates, said Roksana Karim, Ph.D., of the University of Southern California, Los Angeles, at the meeting.
“The rise in hip fracture rates in elderly postmenopausal women may be partially attributed to the continued decline in hormone therapy use,” she said.
This was the conclusion of a longitudinal observational study of 80,995 postmenopausal women aged 60 years or older using data from 11 Kaiser Permanente medical centers in southern California. The study was designed to assess the risk of hip fracture for women who stopped taking hormone therapy (HT), compared with those who continued the therapy. It was also designed to evaluate the risk of hip fracture over time after stopping HT, and to measure bone mineral density (BMD) over time after stopping HT.
Data were collected on hip fracture, HT use, and the use of antiosteoporotic medication from June 2002 through December 2008. All hip fractures were verified by chart review by an orthopedic surgeon who was blinded to patients' HT status. Exclusion criteria included fractures secondary to tumors or high-energy trauma, and periprosthetic fractures. Patients were considered to be HT users if they had filled at least two prescriptions in a given year, as each prescription provides a 3-month supply of medication. HT was defined as estrogen alone or estrogen plus progesterone.
BMD data of the hip and lumbar regions were available for 54,209 women (67%). The 80,955 women had a mean age of 68.8 years and a mean body mass index of 26.9 kg/m
Between July 2002 and December 2008, HT use in this population decreased from 85% to 18%. After adjustments for age and race, women who did not use HT in the previous year had a 55% increased risk of hip fracture (hazard ratio, 1.55), said Dr. Karim. She also said that hip fracture risk significantly increased with 2 or more years of HT cessation. Mean BMD was significantly and inversely associated with cumulative years of HT nonuse, she said.
Dr. Karim acknowledged that the study was limited by lack of body mass index data in 47% of the population, or information on history of past HT use or on previous fractures.
“Women at risk of hip fracture should consider carefully before making a decision of stopping using hormone therapy,” she said.
{kind=link}
Women at risk of hip fracture should consider carefully before they stop using hormone therapy.
Source DR. KARIM
Major Finding: The Women's Health Initiative reported in May 2002 that risks of coronary heart disease and cancer were associated with HT. Between July 2002 and December 2008, HT use in this population decreased from 85% to 18%. After adjustment for age and race, women who did not use HT in the previous year had a 55% increased risk of hip fracture.
Data Source: A study of 80,995 patients in the Kaiser Permanente Southern California database.
Disclosures: Dr. Karim said she had no financial conflicts of interest. The study was supported by the University of Southern California.
CHICAGO – Prescriptions for hormone therapy for elderly postmenopausal women declined significantly after the results of the Women's Health Initiative were reported in May 2002, and it now appears that there has been a correspondingly steep rise in hip fracture rates, said Roksana Karim, Ph.D., of the University of Southern California, Los Angeles, at the meeting.
“The rise in hip fracture rates in elderly postmenopausal women may be partially attributed to the continued decline in hormone therapy use,” she said.
This was the conclusion of a longitudinal observational study of 80,995 postmenopausal women aged 60 years or older using data from 11 Kaiser Permanente medical centers in southern California. The study was designed to assess the risk of hip fracture for women who stopped taking hormone therapy (HT), compared with those who continued the therapy. It was also designed to evaluate the risk of hip fracture over time after stopping HT, and to measure bone mineral density (BMD) over time after stopping HT.
Data were collected on hip fracture, HT use, and the use of antiosteoporotic medication from June 2002 through December 2008. All hip fractures were verified by chart review by an orthopedic surgeon who was blinded to patients' HT status. Exclusion criteria included fractures secondary to tumors or high-energy trauma, and periprosthetic fractures. Patients were considered to be HT users if they had filled at least two prescriptions in a given year, as each prescription provides a 3-month supply of medication. HT was defined as estrogen alone or estrogen plus progesterone.
BMD data of the hip and lumbar regions were available for 54,209 women (67%). The 80,955 women had a mean age of 68.8 years and a mean body mass index of 26.9 kg/m
Between July 2002 and December 2008, HT use in this population decreased from 85% to 18%. After adjustments for age and race, women who did not use HT in the previous year had a 55% increased risk of hip fracture (hazard ratio, 1.55), said Dr. Karim. She also said that hip fracture risk significantly increased with 2 or more years of HT cessation. Mean BMD was significantly and inversely associated with cumulative years of HT nonuse, she said.
Dr. Karim acknowledged that the study was limited by lack of body mass index data in 47% of the population, or information on history of past HT use or on previous fractures.
“Women at risk of hip fracture should consider carefully before making a decision of stopping using hormone therapy,” she said.
Women at risk of hip fracture should consider carefully before they stop using hormone therapy.
Source DR. KARIM
Major Finding: The Women's Health Initiative reported in May 2002 that risks of coronary heart disease and cancer were associated with HT. Between July 2002 and December 2008, HT use in this population decreased from 85% to 18%. After adjustment for age and race, women who did not use HT in the previous year had a 55% increased risk of hip fracture.
Data Source: A study of 80,995 patients in the Kaiser Permanente Southern California database.
Disclosures: Dr. Karim said she had no financial conflicts of interest. The study was supported by the University of Southern California.
CHICAGO – Prescriptions for hormone therapy for elderly postmenopausal women declined significantly after the results of the Women's Health Initiative were reported in May 2002, and it now appears that there has been a correspondingly steep rise in hip fracture rates, said Roksana Karim, Ph.D., of the University of Southern California, Los Angeles, at the meeting.
“The rise in hip fracture rates in elderly postmenopausal women may be partially attributed to the continued decline in hormone therapy use,” she said.
This was the conclusion of a longitudinal observational study of 80,995 postmenopausal women aged 60 years or older using data from 11 Kaiser Permanente medical centers in southern California. The study was designed to assess the risk of hip fracture for women who stopped taking hormone therapy (HT), compared with those who continued the therapy. It was also designed to evaluate the risk of hip fracture over time after stopping HT, and to measure bone mineral density (BMD) over time after stopping HT.
Data were collected on hip fracture, HT use, and the use of antiosteoporotic medication from June 2002 through December 2008. All hip fractures were verified by chart review by an orthopedic surgeon who was blinded to patients' HT status. Exclusion criteria included fractures secondary to tumors or high-energy trauma, and periprosthetic fractures. Patients were considered to be HT users if they had filled at least two prescriptions in a given year, as each prescription provides a 3-month supply of medication. HT was defined as estrogen alone or estrogen plus progesterone.
BMD data of the hip and lumbar regions were available for 54,209 women (67%). The 80,955 women had a mean age of 68.8 years and a mean body mass index of 26.9 kg/m
Between July 2002 and December 2008, HT use in this population decreased from 85% to 18%. After adjustments for age and race, women who did not use HT in the previous year had a 55% increased risk of hip fracture (hazard ratio, 1.55), said Dr. Karim. She also said that hip fracture risk significantly increased with 2 or more years of HT cessation. Mean BMD was significantly and inversely associated with cumulative years of HT nonuse, she said.
Dr. Karim acknowledged that the study was limited by lack of body mass index data in 47% of the population, or information on history of past HT use or on previous fractures.
“Women at risk of hip fracture should consider carefully before making a decision of stopping using hormone therapy,” she said.
Women at risk of hip fracture should consider carefully before they stop using hormone therapy.
Source DR. KARIM
From the Annual Meeting of the North American Menopause Society
Choosing CT or Ultrasound for Acute Abdominal Pain
CHICAGO – The choice of computed tomography versus ultrasound for diagnosis of right lower quadrant pain is not only about radiation, but also about the operator’s level of training, the patient’s age and sex, and several other factors, according to Dr. Stephanie R. Wilson and Dr. Ajay Singh.
"I would choose ultrasound for everyone," Dr. Wilson said at the annual meeting of the Radiological Society of North America. But Dr. Singh praised CT "because of its high sensitivity, high specificity, accuracy, availability, lack of operator dependence, and finally the wide range of disease processes it can diagnose."
Acute abdominal pain accounts for 8 million* emergency department visits in the United States each year, and CT is the diagnostic modality of choice, said Dr. Singh of the radiology department at Harvard Medical School, Boston. Exceptions are suspected appendicitis in children and in pregnancy, right upper quadrant pain, and pelvic pain in young women. "CT is considered the most appropriate modality for adults with right lower quadrant pain. Ultrasound is the most appropriate imaging modality for assessing right lower quadrant pain in children and in pregnant patients," he said.
However, ultrasound is quite effective for diagnosing the scope and extent of disease in the GI tract, with excellent spatial and temporal resolution, said Dr. Wilson of the department of radiology at the University of Calgary (Alta.). The modality is inexpensive, portable, and safe, and has no requirement for radiation or for functioning kidneys, she said. Choosing ultrasound is especially important for patients with a chronic condition like inflammatory bowel disease because of the high likelihood of excess radiation when CT is used for multiple imaging studies. Its only negatives are operator dependency and a small number of technically inadequate examinations, she added.
For confirmation of appendicitis, the American College of Radiology (ACR) appropriateness rating for CT of the abdomen (intravenous contrast) for acute right lower quadrant pain is 8, compared with 6 for ultrasound (graded compression), Dr. Singh pointed out.
A properly trained physician can confirm suspected appendicitis with ultrasound, Dr. Wilson countered. The main reason that reports of accuracy vary in the literature is that ultrasound is an operator-dependent modality, she said. Ultrasound has a sensitivity of 76%-89% and a specificity of 85%-92% for diagnosis of appendicitis. For a differential diagnosis of acute appendicitis, the physician should image the area that hurts, she said, calling this "the sonographic McBurney’s sign."
Compared with ultrasound, CT for appendicitis has a higher sensitivity (90%-100%) and specificity (95%-97%) (Radiology 2000;215:337-48). CT is widely available and does not depend on operator experience, Dr. Singh said; its drawbacks are ionizing radiation and high cost.
The risks of radiation in inflammatory bowel disease should not be disregarded, Dr. Wilson emphasized. The onset of Crohn’s disease is generally in youth or young adulthood, and the lifelong chronic disease has frequent exacerbations with corresponding demands for imaging. Diagnosis, surveillance, monitoring disease response to therapy, and evaluation at the time of exacerbation are better managed with ultrasound, she said, especially as a patient with the disease may require as many as 50 scans over a period of a lifetime.
Ileoscopy is the standard for Crohn’s disease, Dr. Singh said. Fluoroscopic barium studies have traditionally been the mainstay of small intestine imaging, he said, and the advantages of CT are the ease of evaluating superimposed small intestine loops and extraintestinal disease. The ACR appropriateness rating for CT enterography at initial presentation is 9, compared with 5 for ultrasound of the abdomen and pelvis, he noted. "For initial assessment of Crohn’s disease in adult patients, one should perform CT enterography. For assessment of Crohn’s disease in pediatric patients, one can perform CT enterography or MR enterography," Dr. Singh said.
Ultrasound "shows bowel wall layers and perienteric tissues with really exquisite detail," Dr. Wilson said. It also shows peristalsis, and the extent and scope of disease, he added. "Operator dependency – this is definitely true. But everyone with effort can be proficient at it. The deterioration of the practice of ultrasound in North America is related to lack of attention of this modality, rather than to a failure of the technique," Dr. Wilson said.
Dr. Singh conceded that "in the United States, ultrasounds are done by residents, fellows, ultrasound technologists. Not everybody is able to achieve the sensitivities that are achieved in some of the European papers."
Dr. Singh reported no relevant financial disclosures. Dr. Wilson disclosed receiving a research grant from Lantheus Medical Imaging and being on the advisory board of Koninklijke Philips Electronics.
*CORRECTION, 1/20/2011: The original version of this article stated an incorrect figure for the number of ED visits for abdominal pain in the U.S. each year. The correct figure is 8 million.
CHICAGO – The choice of computed tomography versus ultrasound for diagnosis of right lower quadrant pain is not only about radiation, but also about the operator’s level of training, the patient’s age and sex, and several other factors, according to Dr. Stephanie R. Wilson and Dr. Ajay Singh.
"I would choose ultrasound for everyone," Dr. Wilson said at the annual meeting of the Radiological Society of North America. But Dr. Singh praised CT "because of its high sensitivity, high specificity, accuracy, availability, lack of operator dependence, and finally the wide range of disease processes it can diagnose."
Acute abdominal pain accounts for 8 million* emergency department visits in the United States each year, and CT is the diagnostic modality of choice, said Dr. Singh of the radiology department at Harvard Medical School, Boston. Exceptions are suspected appendicitis in children and in pregnancy, right upper quadrant pain, and pelvic pain in young women. "CT is considered the most appropriate modality for adults with right lower quadrant pain. Ultrasound is the most appropriate imaging modality for assessing right lower quadrant pain in children and in pregnant patients," he said.
However, ultrasound is quite effective for diagnosing the scope and extent of disease in the GI tract, with excellent spatial and temporal resolution, said Dr. Wilson of the department of radiology at the University of Calgary (Alta.). The modality is inexpensive, portable, and safe, and has no requirement for radiation or for functioning kidneys, she said. Choosing ultrasound is especially important for patients with a chronic condition like inflammatory bowel disease because of the high likelihood of excess radiation when CT is used for multiple imaging studies. Its only negatives are operator dependency and a small number of technically inadequate examinations, she added.
For confirmation of appendicitis, the American College of Radiology (ACR) appropriateness rating for CT of the abdomen (intravenous contrast) for acute right lower quadrant pain is 8, compared with 6 for ultrasound (graded compression), Dr. Singh pointed out.
A properly trained physician can confirm suspected appendicitis with ultrasound, Dr. Wilson countered. The main reason that reports of accuracy vary in the literature is that ultrasound is an operator-dependent modality, she said. Ultrasound has a sensitivity of 76%-89% and a specificity of 85%-92% for diagnosis of appendicitis. For a differential diagnosis of acute appendicitis, the physician should image the area that hurts, she said, calling this "the sonographic McBurney’s sign."
Compared with ultrasound, CT for appendicitis has a higher sensitivity (90%-100%) and specificity (95%-97%) (Radiology 2000;215:337-48). CT is widely available and does not depend on operator experience, Dr. Singh said; its drawbacks are ionizing radiation and high cost.
The risks of radiation in inflammatory bowel disease should not be disregarded, Dr. Wilson emphasized. The onset of Crohn’s disease is generally in youth or young adulthood, and the lifelong chronic disease has frequent exacerbations with corresponding demands for imaging. Diagnosis, surveillance, monitoring disease response to therapy, and evaluation at the time of exacerbation are better managed with ultrasound, she said, especially as a patient with the disease may require as many as 50 scans over a period of a lifetime.
Ileoscopy is the standard for Crohn’s disease, Dr. Singh said. Fluoroscopic barium studies have traditionally been the mainstay of small intestine imaging, he said, and the advantages of CT are the ease of evaluating superimposed small intestine loops and extraintestinal disease. The ACR appropriateness rating for CT enterography at initial presentation is 9, compared with 5 for ultrasound of the abdomen and pelvis, he noted. "For initial assessment of Crohn’s disease in adult patients, one should perform CT enterography. For assessment of Crohn’s disease in pediatric patients, one can perform CT enterography or MR enterography," Dr. Singh said.
Ultrasound "shows bowel wall layers and perienteric tissues with really exquisite detail," Dr. Wilson said. It also shows peristalsis, and the extent and scope of disease, he added. "Operator dependency – this is definitely true. But everyone with effort can be proficient at it. The deterioration of the practice of ultrasound in North America is related to lack of attention of this modality, rather than to a failure of the technique," Dr. Wilson said.
Dr. Singh conceded that "in the United States, ultrasounds are done by residents, fellows, ultrasound technologists. Not everybody is able to achieve the sensitivities that are achieved in some of the European papers."
Dr. Singh reported no relevant financial disclosures. Dr. Wilson disclosed receiving a research grant from Lantheus Medical Imaging and being on the advisory board of Koninklijke Philips Electronics.
*CORRECTION, 1/20/2011: The original version of this article stated an incorrect figure for the number of ED visits for abdominal pain in the U.S. each year. The correct figure is 8 million.
CHICAGO – The choice of computed tomography versus ultrasound for diagnosis of right lower quadrant pain is not only about radiation, but also about the operator’s level of training, the patient’s age and sex, and several other factors, according to Dr. Stephanie R. Wilson and Dr. Ajay Singh.
"I would choose ultrasound for everyone," Dr. Wilson said at the annual meeting of the Radiological Society of North America. But Dr. Singh praised CT "because of its high sensitivity, high specificity, accuracy, availability, lack of operator dependence, and finally the wide range of disease processes it can diagnose."
Acute abdominal pain accounts for 8 million* emergency department visits in the United States each year, and CT is the diagnostic modality of choice, said Dr. Singh of the radiology department at Harvard Medical School, Boston. Exceptions are suspected appendicitis in children and in pregnancy, right upper quadrant pain, and pelvic pain in young women. "CT is considered the most appropriate modality for adults with right lower quadrant pain. Ultrasound is the most appropriate imaging modality for assessing right lower quadrant pain in children and in pregnant patients," he said.
However, ultrasound is quite effective for diagnosing the scope and extent of disease in the GI tract, with excellent spatial and temporal resolution, said Dr. Wilson of the department of radiology at the University of Calgary (Alta.). The modality is inexpensive, portable, and safe, and has no requirement for radiation or for functioning kidneys, she said. Choosing ultrasound is especially important for patients with a chronic condition like inflammatory bowel disease because of the high likelihood of excess radiation when CT is used for multiple imaging studies. Its only negatives are operator dependency and a small number of technically inadequate examinations, she added.
For confirmation of appendicitis, the American College of Radiology (ACR) appropriateness rating for CT of the abdomen (intravenous contrast) for acute right lower quadrant pain is 8, compared with 6 for ultrasound (graded compression), Dr. Singh pointed out.
A properly trained physician can confirm suspected appendicitis with ultrasound, Dr. Wilson countered. The main reason that reports of accuracy vary in the literature is that ultrasound is an operator-dependent modality, she said. Ultrasound has a sensitivity of 76%-89% and a specificity of 85%-92% for diagnosis of appendicitis. For a differential diagnosis of acute appendicitis, the physician should image the area that hurts, she said, calling this "the sonographic McBurney’s sign."
Compared with ultrasound, CT for appendicitis has a higher sensitivity (90%-100%) and specificity (95%-97%) (Radiology 2000;215:337-48). CT is widely available and does not depend on operator experience, Dr. Singh said; its drawbacks are ionizing radiation and high cost.
The risks of radiation in inflammatory bowel disease should not be disregarded, Dr. Wilson emphasized. The onset of Crohn’s disease is generally in youth or young adulthood, and the lifelong chronic disease has frequent exacerbations with corresponding demands for imaging. Diagnosis, surveillance, monitoring disease response to therapy, and evaluation at the time of exacerbation are better managed with ultrasound, she said, especially as a patient with the disease may require as many as 50 scans over a period of a lifetime.
Ileoscopy is the standard for Crohn’s disease, Dr. Singh said. Fluoroscopic barium studies have traditionally been the mainstay of small intestine imaging, he said, and the advantages of CT are the ease of evaluating superimposed small intestine loops and extraintestinal disease. The ACR appropriateness rating for CT enterography at initial presentation is 9, compared with 5 for ultrasound of the abdomen and pelvis, he noted. "For initial assessment of Crohn’s disease in adult patients, one should perform CT enterography. For assessment of Crohn’s disease in pediatric patients, one can perform CT enterography or MR enterography," Dr. Singh said.
Ultrasound "shows bowel wall layers and perienteric tissues with really exquisite detail," Dr. Wilson said. It also shows peristalsis, and the extent and scope of disease, he added. "Operator dependency – this is definitely true. But everyone with effort can be proficient at it. The deterioration of the practice of ultrasound in North America is related to lack of attention of this modality, rather than to a failure of the technique," Dr. Wilson said.
Dr. Singh conceded that "in the United States, ultrasounds are done by residents, fellows, ultrasound technologists. Not everybody is able to achieve the sensitivities that are achieved in some of the European papers."
Dr. Singh reported no relevant financial disclosures. Dr. Wilson disclosed receiving a research grant from Lantheus Medical Imaging and being on the advisory board of Koninklijke Philips Electronics.
*CORRECTION, 1/20/2011: The original version of this article stated an incorrect figure for the number of ED visits for abdominal pain in the U.S. each year. The correct figure is 8 million.
FROM THE ANNUAL MEETING OF THE RADIOLOGICAL SOCIETY OF NORTH AMERICA
Choosing CT or Ultrasound for Acute Abdominal Pain
CHICAGO – The choice of computed tomography versus ultrasound for diagnosis of right lower quadrant pain is not only about radiation, but also about the operator’s level of training, the patient’s age and sex, and several other factors, according to Dr. Stephanie R. Wilson and Dr. Ajay Singh.
"I would choose ultrasound for everyone," Dr. Wilson said at the annual meeting of the Radiological Society of North America. But Dr. Singh praised CT "because of its high sensitivity, high specificity, accuracy, availability, lack of operator dependence, and finally the wide range of disease processes it can diagnose."
[Check out our coverage of the Radiological Society of North America's annual meeting.]
Acute abdominal pain accounts for 8 million* emergency department visits in the United States each year, and CT is the diagnostic modality of choice, said Dr. Singh of the radiology department at Harvard Medical School, Boston. Exceptions are suspected appendicitis in children and in pregnancy, right upper quadrant pain, and pelvic pain in young women. "CT is considered the most appropriate modality for adults with right lower quadrant pain. Ultrasound is the most appropriate imaging modality for assessing right lower quadrant pain in children and in pregnant patients," he said.
[30-Day Outcomes Suggest Surgery for Acute Appendicitis May Be Delayed]
However, ultrasound is quite effective for diagnosing the scope and extent of disease in the GI tract, with excellent spatial and temporal resolution, said Dr. Wilson of the department of radiology at the University of Calgary (Alta.). The modality is inexpensive, portable, and safe, and has no requirement for radiation or for functioning kidneys, she said. Choosing ultrasound is especially important for patients with a chronic condition like inflammatory bowel disease because of the high likelihood of excess radiation when CT is used for multiple imaging studies. Its only negatives are operator dependency and a small number of technically inadequate examinations, she added.
For confirmation of appendicitis, the American College of Radiology (ACR) appropriateness rating for CT of the abdomen (intravenous contrast) for acute right lower quadrant pain is 8, compared with 6 for ultrasound (graded compression), Dr. Singh pointed out.
A properly trained physician can confirm suspected appendicitis with ultrasound, Dr. Wilson countered. The main reason that reports of accuracy vary in the literature is that ultrasound is an operator-dependent modality, she said. Ultrasound has a sensitivity of 76%-89% and a specificity of 85%-92% for diagnosis of appendicitis. For a differential diagnosis of acute appendicitis, the physician should image the area that hurts, she said, calling this "the sonographic McBurney’s sign."
Compared with ultrasound, CT for appendicitis has a higher sensitivity (90%-100%) and specificity (95%-97%) (Radiology 2000;215:337-48). CT is widely available and does not depend on operator experience, Dr. Singh said; its drawbacks are ionizing radiation and high cost.
[Restricted CT Scans Did Not Harm Sensitivity]
The risks of radiation in inflammatory bowel disease should not be disregarded, Dr. Wilson emphasized. The onset of Crohn’s disease is generally in youth or young adulthood, and the lifelong chronic disease has frequent exacerbations with corresponding demands for imaging. Diagnosis, surveillance, monitoring disease response to therapy, and evaluation at the time of exacerbation are better managed with ultrasound, she said, especially as a patient with the disease may require as many as 50 scans over a period of a lifetime.
Ileoscopy is the standard for Crohn’s disease, Dr. Singh said. Fluoroscopic barium studies have traditionally been the mainstay of small intestine imaging, he said, and the advantages of CT are the ease of evaluating superimposed small intestine loops and extraintestinal disease. The ACR appropriateness rating for CT enterography at initial presentation is 9, compared with 5 for ultrasound of the abdomen and pelvis, he noted. "For initial assessment of Crohn’s disease in adult patients, one should perform CT enterography. For assessment of Crohn’s disease in pediatric patients, one can perform CT enterography or MR enterography," Dr. Singh said.
Ultrasound "shows bowel wall layers and perienteric tissues with really exquisite detail," Dr. Wilson said. It also shows peristalsis, and the extent and scope of disease, he added. "Operator dependency – this is definitely true. But everyone with effort can be proficient at it. The deterioration of the practice of ultrasound in North America is related to lack of attention of this modality, rather than to a failure of the technique," Dr. Wilson said.
Dr. Singh conceded that "in the United States, ultrasounds are done by residents, fellows, ultrasound technologists. Not everybody is able to achieve the sensitivities that are achieved in some of the European papers."
Dr. Singh reported no relevant financial disclosures. Dr. Wilson disclosed receiving a research grant from Lantheus Medical Imaging and being on the advisory board of Koninklijke Philips Electronics.
*CORRECTION, 1/20/2011: The original version of this article stated an incorrect figure for the number of ED visits for abdominal pain in the U.S. each year. The correct figure is 8 million.
CHICAGO – The choice of computed tomography versus ultrasound for diagnosis of right lower quadrant pain is not only about radiation, but also about the operator’s level of training, the patient’s age and sex, and several other factors, according to Dr. Stephanie R. Wilson and Dr. Ajay Singh.
"I would choose ultrasound for everyone," Dr. Wilson said at the annual meeting of the Radiological Society of North America. But Dr. Singh praised CT "because of its high sensitivity, high specificity, accuracy, availability, lack of operator dependence, and finally the wide range of disease processes it can diagnose."
[Check out our coverage of the Radiological Society of North America's annual meeting.]
Acute abdominal pain accounts for 8 million* emergency department visits in the United States each year, and CT is the diagnostic modality of choice, said Dr. Singh of the radiology department at Harvard Medical School, Boston. Exceptions are suspected appendicitis in children and in pregnancy, right upper quadrant pain, and pelvic pain in young women. "CT is considered the most appropriate modality for adults with right lower quadrant pain. Ultrasound is the most appropriate imaging modality for assessing right lower quadrant pain in children and in pregnant patients," he said.
[30-Day Outcomes Suggest Surgery for Acute Appendicitis May Be Delayed]
However, ultrasound is quite effective for diagnosing the scope and extent of disease in the GI tract, with excellent spatial and temporal resolution, said Dr. Wilson of the department of radiology at the University of Calgary (Alta.). The modality is inexpensive, portable, and safe, and has no requirement for radiation or for functioning kidneys, she said. Choosing ultrasound is especially important for patients with a chronic condition like inflammatory bowel disease because of the high likelihood of excess radiation when CT is used for multiple imaging studies. Its only negatives are operator dependency and a small number of technically inadequate examinations, she added.
For confirmation of appendicitis, the American College of Radiology (ACR) appropriateness rating for CT of the abdomen (intravenous contrast) for acute right lower quadrant pain is 8, compared with 6 for ultrasound (graded compression), Dr. Singh pointed out.
A properly trained physician can confirm suspected appendicitis with ultrasound, Dr. Wilson countered. The main reason that reports of accuracy vary in the literature is that ultrasound is an operator-dependent modality, she said. Ultrasound has a sensitivity of 76%-89% and a specificity of 85%-92% for diagnosis of appendicitis. For a differential diagnosis of acute appendicitis, the physician should image the area that hurts, she said, calling this "the sonographic McBurney’s sign."
Compared with ultrasound, CT for appendicitis has a higher sensitivity (90%-100%) and specificity (95%-97%) (Radiology 2000;215:337-48). CT is widely available and does not depend on operator experience, Dr. Singh said; its drawbacks are ionizing radiation and high cost.
[Restricted CT Scans Did Not Harm Sensitivity]
The risks of radiation in inflammatory bowel disease should not be disregarded, Dr. Wilson emphasized. The onset of Crohn’s disease is generally in youth or young adulthood, and the lifelong chronic disease has frequent exacerbations with corresponding demands for imaging. Diagnosis, surveillance, monitoring disease response to therapy, and evaluation at the time of exacerbation are better managed with ultrasound, she said, especially as a patient with the disease may require as many as 50 scans over a period of a lifetime.
Ileoscopy is the standard for Crohn’s disease, Dr. Singh said. Fluoroscopic barium studies have traditionally been the mainstay of small intestine imaging, he said, and the advantages of CT are the ease of evaluating superimposed small intestine loops and extraintestinal disease. The ACR appropriateness rating for CT enterography at initial presentation is 9, compared with 5 for ultrasound of the abdomen and pelvis, he noted. "For initial assessment of Crohn’s disease in adult patients, one should perform CT enterography. For assessment of Crohn’s disease in pediatric patients, one can perform CT enterography or MR enterography," Dr. Singh said.
Ultrasound "shows bowel wall layers and perienteric tissues with really exquisite detail," Dr. Wilson said. It also shows peristalsis, and the extent and scope of disease, he added. "Operator dependency – this is definitely true. But everyone with effort can be proficient at it. The deterioration of the practice of ultrasound in North America is related to lack of attention of this modality, rather than to a failure of the technique," Dr. Wilson said.
Dr. Singh conceded that "in the United States, ultrasounds are done by residents, fellows, ultrasound technologists. Not everybody is able to achieve the sensitivities that are achieved in some of the European papers."
Dr. Singh reported no relevant financial disclosures. Dr. Wilson disclosed receiving a research grant from Lantheus Medical Imaging and being on the advisory board of Koninklijke Philips Electronics.
*CORRECTION, 1/20/2011: The original version of this article stated an incorrect figure for the number of ED visits for abdominal pain in the U.S. each year. The correct figure is 8 million.
CHICAGO – The choice of computed tomography versus ultrasound for diagnosis of right lower quadrant pain is not only about radiation, but also about the operator’s level of training, the patient’s age and sex, and several other factors, according to Dr. Stephanie R. Wilson and Dr. Ajay Singh.
"I would choose ultrasound for everyone," Dr. Wilson said at the annual meeting of the Radiological Society of North America. But Dr. Singh praised CT "because of its high sensitivity, high specificity, accuracy, availability, lack of operator dependence, and finally the wide range of disease processes it can diagnose."
[Check out our coverage of the Radiological Society of North America's annual meeting.]
Acute abdominal pain accounts for 8 million* emergency department visits in the United States each year, and CT is the diagnostic modality of choice, said Dr. Singh of the radiology department at Harvard Medical School, Boston. Exceptions are suspected appendicitis in children and in pregnancy, right upper quadrant pain, and pelvic pain in young women. "CT is considered the most appropriate modality for adults with right lower quadrant pain. Ultrasound is the most appropriate imaging modality for assessing right lower quadrant pain in children and in pregnant patients," he said.
[30-Day Outcomes Suggest Surgery for Acute Appendicitis May Be Delayed]
However, ultrasound is quite effective for diagnosing the scope and extent of disease in the GI tract, with excellent spatial and temporal resolution, said Dr. Wilson of the department of radiology at the University of Calgary (Alta.). The modality is inexpensive, portable, and safe, and has no requirement for radiation or for functioning kidneys, she said. Choosing ultrasound is especially important for patients with a chronic condition like inflammatory bowel disease because of the high likelihood of excess radiation when CT is used for multiple imaging studies. Its only negatives are operator dependency and a small number of technically inadequate examinations, she added.
For confirmation of appendicitis, the American College of Radiology (ACR) appropriateness rating for CT of the abdomen (intravenous contrast) for acute right lower quadrant pain is 8, compared with 6 for ultrasound (graded compression), Dr. Singh pointed out.
A properly trained physician can confirm suspected appendicitis with ultrasound, Dr. Wilson countered. The main reason that reports of accuracy vary in the literature is that ultrasound is an operator-dependent modality, she said. Ultrasound has a sensitivity of 76%-89% and a specificity of 85%-92% for diagnosis of appendicitis. For a differential diagnosis of acute appendicitis, the physician should image the area that hurts, she said, calling this "the sonographic McBurney’s sign."
Compared with ultrasound, CT for appendicitis has a higher sensitivity (90%-100%) and specificity (95%-97%) (Radiology 2000;215:337-48). CT is widely available and does not depend on operator experience, Dr. Singh said; its drawbacks are ionizing radiation and high cost.
[Restricted CT Scans Did Not Harm Sensitivity]
The risks of radiation in inflammatory bowel disease should not be disregarded, Dr. Wilson emphasized. The onset of Crohn’s disease is generally in youth or young adulthood, and the lifelong chronic disease has frequent exacerbations with corresponding demands for imaging. Diagnosis, surveillance, monitoring disease response to therapy, and evaluation at the time of exacerbation are better managed with ultrasound, she said, especially as a patient with the disease may require as many as 50 scans over a period of a lifetime.
Ileoscopy is the standard for Crohn’s disease, Dr. Singh said. Fluoroscopic barium studies have traditionally been the mainstay of small intestine imaging, he said, and the advantages of CT are the ease of evaluating superimposed small intestine loops and extraintestinal disease. The ACR appropriateness rating for CT enterography at initial presentation is 9, compared with 5 for ultrasound of the abdomen and pelvis, he noted. "For initial assessment of Crohn’s disease in adult patients, one should perform CT enterography. For assessment of Crohn’s disease in pediatric patients, one can perform CT enterography or MR enterography," Dr. Singh said.
Ultrasound "shows bowel wall layers and perienteric tissues with really exquisite detail," Dr. Wilson said. It also shows peristalsis, and the extent and scope of disease, he added. "Operator dependency – this is definitely true. But everyone with effort can be proficient at it. The deterioration of the practice of ultrasound in North America is related to lack of attention of this modality, rather than to a failure of the technique," Dr. Wilson said.
Dr. Singh conceded that "in the United States, ultrasounds are done by residents, fellows, ultrasound technologists. Not everybody is able to achieve the sensitivities that are achieved in some of the European papers."
Dr. Singh reported no relevant financial disclosures. Dr. Wilson disclosed receiving a research grant from Lantheus Medical Imaging and being on the advisory board of Koninklijke Philips Electronics.
*CORRECTION, 1/20/2011: The original version of this article stated an incorrect figure for the number of ED visits for abdominal pain in the U.S. each year. The correct figure is 8 million.
FROM THE ANNUAL MEETING OF THE RADIOLOGICAL SOCIETY OF NORTH AMERICA
Estriol Gel Reduces Vaginal Atrophy Symptoms
Major Finding: In the active treatment group, 97 of 112 (87%) rated the treatment excellent, good, or acceptable, vs. 37 of 53 (70%) in the placebo group, a significant difference.
Data Source: A study of 167 women randomized 2:1 to estriol 0.005% or to placebo.
Disclosures: Dr. Nieto is the medical director of Italfarmaco SA, maker of ITFE-2026, estriol 0.005% gel. The study was sponsored by Italfarmaco, the Spanish affiliate of Grupo Italfarmaco, a pharmaceutical company operating in Europe and South America. No other member of the investigational team disclosed a financially relevant relationship.
CHICAGO – Estrogen may safely and effectively be administered vaginally in a very low-dose 0.005% estriol gel to treat vaginal atrophy, said Dr. Concepcion Nieto of Italfarmaco S.A. of Madrid.
“The new estriol vaginal gel formulation, providing a very low amount of estriol per application [50 g], is highly efficacious in the improvement of the symptoms related to postmenopausal vaginal atrophy,” she said at the meeting.
Dr. Nieto reported the results of a randomized, double-blind, placebo-controlled multicenter study of 167 women randomized 2:1 to the investigational estriol gel or placebo. She said that the gel provides 10 times less hormone per application than the European reference product, Ovestinon 0.1%, and that it is not approved by the Food and Drug Administration for use in the United States.
The 0.005% estriol vaginal gel was approved in Europe in July 2010 and will be proximately marketed in Europe under the brand names of Blissel and Gelistrol, Dr. Nieto said in a later interview. Estriol is a metabolite of estradiol and estrone, but has lower estrogenic potency than estradiol. It also has a greater relative affinity for beta than for alpha estrogen receptors. The study's primary objective was to evaluate the efficacy of 0.005% estriol vaginal gel after 12 weeks of treatment. Safety was a secondary objective. Postmenopausal amenorrheic women with signs and symptoms of vaginal atrophy made up the study population. Symptoms of vaginal atrophy included dryness, dyspareunia, pruritus, burning, and dysuria, and signs included dry vaginal mucosa, pallor, fragility, flattening of vaginal folds, and petechiae. Medication was administered daily in weeks 1-3 and twice weekly in weeks 4-12.
The primary efficacy variable was change in maturation value of vaginal epithelium from baseline to week 12. Symptoms were evaluated by change in global symptom score at baseline and at week 12. The women in the study population (114 active, 53 placebo) averaged 56.7 years, had a mean body mass index of 26.0 kg/m
“The 0.005% estriol vaginal gel has proved to be significantly more efficacious than the placebo gel over the local symptomatology,” said Dr. Nieto. “This effect is clinically relevant, as shown by the evaluation of the patients greatly in favor of estriol regarding the general efficacy of the treatment on finishing the study.”
An audience member said, “The FDA requires now an improvement in [the] most bothersome symptom, which you recorded. Was there a statistically significant reduction in [the] most bothersome symptom?”
“Yes,” said Dr. Nieto. “We analyzed the most bothersome symptom, and we observed in vaginal dryness that at week 12, 88% of women had improved or were cured from the vaginal dryness, and 66% of women that received the placebo improved or were cured.”
Major Finding: In the active treatment group, 97 of 112 (87%) rated the treatment excellent, good, or acceptable, vs. 37 of 53 (70%) in the placebo group, a significant difference.
Data Source: A study of 167 women randomized 2:1 to estriol 0.005% or to placebo.
Disclosures: Dr. Nieto is the medical director of Italfarmaco SA, maker of ITFE-2026, estriol 0.005% gel. The study was sponsored by Italfarmaco, the Spanish affiliate of Grupo Italfarmaco, a pharmaceutical company operating in Europe and South America. No other member of the investigational team disclosed a financially relevant relationship.
CHICAGO – Estrogen may safely and effectively be administered vaginally in a very low-dose 0.005% estriol gel to treat vaginal atrophy, said Dr. Concepcion Nieto of Italfarmaco S.A. of Madrid.
“The new estriol vaginal gel formulation, providing a very low amount of estriol per application [50 g], is highly efficacious in the improvement of the symptoms related to postmenopausal vaginal atrophy,” she said at the meeting.
Dr. Nieto reported the results of a randomized, double-blind, placebo-controlled multicenter study of 167 women randomized 2:1 to the investigational estriol gel or placebo. She said that the gel provides 10 times less hormone per application than the European reference product, Ovestinon 0.1%, and that it is not approved by the Food and Drug Administration for use in the United States.
The 0.005% estriol vaginal gel was approved in Europe in July 2010 and will be proximately marketed in Europe under the brand names of Blissel and Gelistrol, Dr. Nieto said in a later interview. Estriol is a metabolite of estradiol and estrone, but has lower estrogenic potency than estradiol. It also has a greater relative affinity for beta than for alpha estrogen receptors. The study's primary objective was to evaluate the efficacy of 0.005% estriol vaginal gel after 12 weeks of treatment. Safety was a secondary objective. Postmenopausal amenorrheic women with signs and symptoms of vaginal atrophy made up the study population. Symptoms of vaginal atrophy included dryness, dyspareunia, pruritus, burning, and dysuria, and signs included dry vaginal mucosa, pallor, fragility, flattening of vaginal folds, and petechiae. Medication was administered daily in weeks 1-3 and twice weekly in weeks 4-12.
The primary efficacy variable was change in maturation value of vaginal epithelium from baseline to week 12. Symptoms were evaluated by change in global symptom score at baseline and at week 12. The women in the study population (114 active, 53 placebo) averaged 56.7 years, had a mean body mass index of 26.0 kg/m
“The 0.005% estriol vaginal gel has proved to be significantly more efficacious than the placebo gel over the local symptomatology,” said Dr. Nieto. “This effect is clinically relevant, as shown by the evaluation of the patients greatly in favor of estriol regarding the general efficacy of the treatment on finishing the study.”
An audience member said, “The FDA requires now an improvement in [the] most bothersome symptom, which you recorded. Was there a statistically significant reduction in [the] most bothersome symptom?”
“Yes,” said Dr. Nieto. “We analyzed the most bothersome symptom, and we observed in vaginal dryness that at week 12, 88% of women had improved or were cured from the vaginal dryness, and 66% of women that received the placebo improved or were cured.”
Major Finding: In the active treatment group, 97 of 112 (87%) rated the treatment excellent, good, or acceptable, vs. 37 of 53 (70%) in the placebo group, a significant difference.
Data Source: A study of 167 women randomized 2:1 to estriol 0.005% or to placebo.
Disclosures: Dr. Nieto is the medical director of Italfarmaco SA, maker of ITFE-2026, estriol 0.005% gel. The study was sponsored by Italfarmaco, the Spanish affiliate of Grupo Italfarmaco, a pharmaceutical company operating in Europe and South America. No other member of the investigational team disclosed a financially relevant relationship.
CHICAGO – Estrogen may safely and effectively be administered vaginally in a very low-dose 0.005% estriol gel to treat vaginal atrophy, said Dr. Concepcion Nieto of Italfarmaco S.A. of Madrid.
“The new estriol vaginal gel formulation, providing a very low amount of estriol per application [50 g], is highly efficacious in the improvement of the symptoms related to postmenopausal vaginal atrophy,” she said at the meeting.
Dr. Nieto reported the results of a randomized, double-blind, placebo-controlled multicenter study of 167 women randomized 2:1 to the investigational estriol gel or placebo. She said that the gel provides 10 times less hormone per application than the European reference product, Ovestinon 0.1%, and that it is not approved by the Food and Drug Administration for use in the United States.
The 0.005% estriol vaginal gel was approved in Europe in July 2010 and will be proximately marketed in Europe under the brand names of Blissel and Gelistrol, Dr. Nieto said in a later interview. Estriol is a metabolite of estradiol and estrone, but has lower estrogenic potency than estradiol. It also has a greater relative affinity for beta than for alpha estrogen receptors. The study's primary objective was to evaluate the efficacy of 0.005% estriol vaginal gel after 12 weeks of treatment. Safety was a secondary objective. Postmenopausal amenorrheic women with signs and symptoms of vaginal atrophy made up the study population. Symptoms of vaginal atrophy included dryness, dyspareunia, pruritus, burning, and dysuria, and signs included dry vaginal mucosa, pallor, fragility, flattening of vaginal folds, and petechiae. Medication was administered daily in weeks 1-3 and twice weekly in weeks 4-12.
The primary efficacy variable was change in maturation value of vaginal epithelium from baseline to week 12. Symptoms were evaluated by change in global symptom score at baseline and at week 12. The women in the study population (114 active, 53 placebo) averaged 56.7 years, had a mean body mass index of 26.0 kg/m
“The 0.005% estriol vaginal gel has proved to be significantly more efficacious than the placebo gel over the local symptomatology,” said Dr. Nieto. “This effect is clinically relevant, as shown by the evaluation of the patients greatly in favor of estriol regarding the general efficacy of the treatment on finishing the study.”
An audience member said, “The FDA requires now an improvement in [the] most bothersome symptom, which you recorded. Was there a statistically significant reduction in [the] most bothersome symptom?”
“Yes,” said Dr. Nieto. “We analyzed the most bothersome symptom, and we observed in vaginal dryness that at week 12, 88% of women had improved or were cured from the vaginal dryness, and 66% of women that received the placebo improved or were cured.”
From the Annual Meeting of the North American Menopause Society
BREEZE 2: Gabapentin-ER Tames Hot Flashes
Major Finding: Gabapentin-ER 1,800 mg/day may be effective and well tolerated for the treatment of moderate to severe hot flashes in postmenopausal women.
Data Source: BREEZE 2 trial database of 565 postmenopausal women with moderate to severe hot flashes who were randomized to gabapentin-ER in two active arms (1,800 mg or 1,200 mg) or placebo for 13 weeks in this phase III, double-blind, placebo-controlled, randomized trial.
Disclosures: The trial was sponsored by Depomed Inc., maker of gabapentin-ER. Dr. Utian is a consultant to Depomed. Some of the study investigators are Depomed employees.
CHICAGO – An extended-release formulation of gabapentin for hot flashes showed the potential both to minimize peak adverse events and to allow for less frequent dosing in a randomized, controlled trial of 565 women, said Dr. Wulf Utian.
“The results of the BREEZE 2 study suggest that gabapentin–extended release 1,800 mg/day may be effective and well tolerated for the treatment of moderate to severe hot flashes in postmenopausal women,” he noted at the meeting.
Gabapentin-ER releases over 8 hours, potentially minimizing peak adverse events and allowing once daily or twice daily dosing, said Dr. Utian, the Arthur H. Bill Professor Emeritus of Reproductive Biology and Obstetrics and Gynecology at Case Western Reserve University in Cleveland. Gabapentin is an anticonvulsant that is also used to relieve nerve-related pain.
BREEZE 2 is a prospective, multicenter, randomized, double-blind, placebo-controlled study in postmenopausal women aged 18-70 years at 45 sites across the United States. The study had two active arms: gabapentin-ER 1,200 mg given once daily, and 1,800 mg given as 600 mg in the morning and 1,200 in the evening. Efficacy was assessed at 4 and 12 weeks, and the treatment duration was 3 months. The primary efficacy end points were reductions in the mean frequency of moderate to severe hot flashes and the average severity of hot flashes.
The trial's secondary end points were the proportion of patients who were categorized as “much improved” or “very much improved” at 12 weeks in the self-reported Patient Global Impression of Change scale. Investigators also recorded their impression of the results of the therapy using the Clinician Global Impression of Change scale.
Postmenopausal women who had been experiencing seven or more moderate to severe hot flashes per day (or at least 50 per week), accompanied by sweating during at least the previous 30 days, were the trial population.
Baseline characteristics were similar across the three groups. In the 1,800-mg group, for example, the average age was 54 years, the women were 71% white, and the average body mass index was less than 30 kg/m
Data were subjected to both parametric and nonparametric analysis, said Dr. Utian, because parametric analyses can be influenced by outliers.
At 4 weeks and 12 weeks, changes in the mean severity of moderate and severe hot flashes were −0.6 and −0.8 for the 1,800-mg group, compared with the placebo group; both were significant differences.
More than 60% of patients in both active treatment groups and more than 40% in the placebo group self-reported and were clinician reported as “very much improved” at 12 weeks. “This was a particularly high placebo response,” said Dr. Utian.
Nonparametric analysis revealed a statistically significant change in median frequency of moderate to severe hot flashes at 4 weeks and 12 weeks in both active groups, compared with the placebo group.
Dizziness was the most commonly reported adverse event in both the 1,800-mg and 1,200-mg groups, whereas headache was most commonly reported in the placebo group. Somnolence was the second most common complaint in the active treatment groups. A total of 48 patients across both active treatment groups discontinued because of adverse events.
“Essentially, this long-release product was well tolerated, adverse events were mild, the difference was a slight difference in dizziness and somnolence during the titration, and [there was] no real difference in the adverse events” between the 1,800-mg and the 1,200-mg dosing regimens, said Dr. Utian. “The incidence of the adverse events declined markedly after 2-4 weeks of study therapy.”
Major Finding: Gabapentin-ER 1,800 mg/day may be effective and well tolerated for the treatment of moderate to severe hot flashes in postmenopausal women.
Data Source: BREEZE 2 trial database of 565 postmenopausal women with moderate to severe hot flashes who were randomized to gabapentin-ER in two active arms (1,800 mg or 1,200 mg) or placebo for 13 weeks in this phase III, double-blind, placebo-controlled, randomized trial.
Disclosures: The trial was sponsored by Depomed Inc., maker of gabapentin-ER. Dr. Utian is a consultant to Depomed. Some of the study investigators are Depomed employees.
CHICAGO – An extended-release formulation of gabapentin for hot flashes showed the potential both to minimize peak adverse events and to allow for less frequent dosing in a randomized, controlled trial of 565 women, said Dr. Wulf Utian.
“The results of the BREEZE 2 study suggest that gabapentin–extended release 1,800 mg/day may be effective and well tolerated for the treatment of moderate to severe hot flashes in postmenopausal women,” he noted at the meeting.
Gabapentin-ER releases over 8 hours, potentially minimizing peak adverse events and allowing once daily or twice daily dosing, said Dr. Utian, the Arthur H. Bill Professor Emeritus of Reproductive Biology and Obstetrics and Gynecology at Case Western Reserve University in Cleveland. Gabapentin is an anticonvulsant that is also used to relieve nerve-related pain.
BREEZE 2 is a prospective, multicenter, randomized, double-blind, placebo-controlled study in postmenopausal women aged 18-70 years at 45 sites across the United States. The study had two active arms: gabapentin-ER 1,200 mg given once daily, and 1,800 mg given as 600 mg in the morning and 1,200 in the evening. Efficacy was assessed at 4 and 12 weeks, and the treatment duration was 3 months. The primary efficacy end points were reductions in the mean frequency of moderate to severe hot flashes and the average severity of hot flashes.
The trial's secondary end points were the proportion of patients who were categorized as “much improved” or “very much improved” at 12 weeks in the self-reported Patient Global Impression of Change scale. Investigators also recorded their impression of the results of the therapy using the Clinician Global Impression of Change scale.
Postmenopausal women who had been experiencing seven or more moderate to severe hot flashes per day (or at least 50 per week), accompanied by sweating during at least the previous 30 days, were the trial population.
Baseline characteristics were similar across the three groups. In the 1,800-mg group, for example, the average age was 54 years, the women were 71% white, and the average body mass index was less than 30 kg/m
Data were subjected to both parametric and nonparametric analysis, said Dr. Utian, because parametric analyses can be influenced by outliers.
At 4 weeks and 12 weeks, changes in the mean severity of moderate and severe hot flashes were −0.6 and −0.8 for the 1,800-mg group, compared with the placebo group; both were significant differences.
More than 60% of patients in both active treatment groups and more than 40% in the placebo group self-reported and were clinician reported as “very much improved” at 12 weeks. “This was a particularly high placebo response,” said Dr. Utian.
Nonparametric analysis revealed a statistically significant change in median frequency of moderate to severe hot flashes at 4 weeks and 12 weeks in both active groups, compared with the placebo group.
Dizziness was the most commonly reported adverse event in both the 1,800-mg and 1,200-mg groups, whereas headache was most commonly reported in the placebo group. Somnolence was the second most common complaint in the active treatment groups. A total of 48 patients across both active treatment groups discontinued because of adverse events.
“Essentially, this long-release product was well tolerated, adverse events were mild, the difference was a slight difference in dizziness and somnolence during the titration, and [there was] no real difference in the adverse events” between the 1,800-mg and the 1,200-mg dosing regimens, said Dr. Utian. “The incidence of the adverse events declined markedly after 2-4 weeks of study therapy.”
Major Finding: Gabapentin-ER 1,800 mg/day may be effective and well tolerated for the treatment of moderate to severe hot flashes in postmenopausal women.
Data Source: BREEZE 2 trial database of 565 postmenopausal women with moderate to severe hot flashes who were randomized to gabapentin-ER in two active arms (1,800 mg or 1,200 mg) or placebo for 13 weeks in this phase III, double-blind, placebo-controlled, randomized trial.
Disclosures: The trial was sponsored by Depomed Inc., maker of gabapentin-ER. Dr. Utian is a consultant to Depomed. Some of the study investigators are Depomed employees.
CHICAGO – An extended-release formulation of gabapentin for hot flashes showed the potential both to minimize peak adverse events and to allow for less frequent dosing in a randomized, controlled trial of 565 women, said Dr. Wulf Utian.
“The results of the BREEZE 2 study suggest that gabapentin–extended release 1,800 mg/day may be effective and well tolerated for the treatment of moderate to severe hot flashes in postmenopausal women,” he noted at the meeting.
Gabapentin-ER releases over 8 hours, potentially minimizing peak adverse events and allowing once daily or twice daily dosing, said Dr. Utian, the Arthur H. Bill Professor Emeritus of Reproductive Biology and Obstetrics and Gynecology at Case Western Reserve University in Cleveland. Gabapentin is an anticonvulsant that is also used to relieve nerve-related pain.
BREEZE 2 is a prospective, multicenter, randomized, double-blind, placebo-controlled study in postmenopausal women aged 18-70 years at 45 sites across the United States. The study had two active arms: gabapentin-ER 1,200 mg given once daily, and 1,800 mg given as 600 mg in the morning and 1,200 in the evening. Efficacy was assessed at 4 and 12 weeks, and the treatment duration was 3 months. The primary efficacy end points were reductions in the mean frequency of moderate to severe hot flashes and the average severity of hot flashes.
The trial's secondary end points were the proportion of patients who were categorized as “much improved” or “very much improved” at 12 weeks in the self-reported Patient Global Impression of Change scale. Investigators also recorded their impression of the results of the therapy using the Clinician Global Impression of Change scale.
Postmenopausal women who had been experiencing seven or more moderate to severe hot flashes per day (or at least 50 per week), accompanied by sweating during at least the previous 30 days, were the trial population.
Baseline characteristics were similar across the three groups. In the 1,800-mg group, for example, the average age was 54 years, the women were 71% white, and the average body mass index was less than 30 kg/m
Data were subjected to both parametric and nonparametric analysis, said Dr. Utian, because parametric analyses can be influenced by outliers.
At 4 weeks and 12 weeks, changes in the mean severity of moderate and severe hot flashes were −0.6 and −0.8 for the 1,800-mg group, compared with the placebo group; both were significant differences.
More than 60% of patients in both active treatment groups and more than 40% in the placebo group self-reported and were clinician reported as “very much improved” at 12 weeks. “This was a particularly high placebo response,” said Dr. Utian.
Nonparametric analysis revealed a statistically significant change in median frequency of moderate to severe hot flashes at 4 weeks and 12 weeks in both active groups, compared with the placebo group.
Dizziness was the most commonly reported adverse event in both the 1,800-mg and 1,200-mg groups, whereas headache was most commonly reported in the placebo group. Somnolence was the second most common complaint in the active treatment groups. A total of 48 patients across both active treatment groups discontinued because of adverse events.
“Essentially, this long-release product was well tolerated, adverse events were mild, the difference was a slight difference in dizziness and somnolence during the titration, and [there was] no real difference in the adverse events” between the 1,800-mg and the 1,200-mg dosing regimens, said Dr. Utian. “The incidence of the adverse events declined markedly after 2-4 weeks of study therapy.”
From the Annual Meeting of the North American Menopause Society
Annual MRI a Plus in Women With Past Cancer
Major Finding: Women with a personal history of breast cancer should consider an annual screening MRI, despite American Cancer Society guidelines to the contrary.
Data Source: Retrospective review of 1,026 women who received a first screening breast MRI, of whom 973 were screened for genetic and family history of breast cancer. A total of 327 had genetic or family history of breast cancer and 646 had a personal history of breast cancer.
Disclosures: None. According to Dr. DeMartini, the study had no sponsor.
CHICAGO – Women with a personal history of breast cancer should be advised to consider an annual screening breast MRI as an adjunct to mammography, despite the American Cancer Society's current position that there is insufficient evidence to recommend for or against it, according to a retrospective study from the University of Washington Medical Center, Seattle.
“We found that the diagnostic performance of screening breast MRI was similar or higher overall in women with a personal history [of breast cancer] alone, compared to those with a genetic or family history, the latter being the group currently recommended for screening by the American Cancer Society,” said lead author Dr. Wendy B. DeMartiniat the meeting.
American Cancer Society guidelines recommend an annual screening with breast MRI as an adjunct to mammography for women with a genetic or family history of breast cancer, but not for those with a personal history of the disease. MRI is highly sensitive and allows early detection of otherwise occult breast carcinoma, and mammography is an imperfect tool for detection, Dr. DeMartini said. This is critical in women with a personal history of treated breast cancer because they are at elevated risk for a second cancer, and finding second cancers early increases their chance of survival. “Annual screening with MRI may be important in this group,” she said.
Disadvantages of MRI include the use of intravenous contrast material, the potential for false positives, and increased cost.
The American Cancer Society's most recent guidelines issued in 2007 recommend annual screening MRI in addition to mammography for women in two high-risk groups: those with genetic mutation such as the BRCA gene or first-degree relatives with the gene, and those with at least a 20%-25% lifetime risk, based on family history. The guidelines concluded that there was insufficient evidence to recommend for or against breast MRI in patients with only a personal history of the disease but no genetic or family risk.
“And thus it's been quite challenging, as you can imagine, for women and their physicians to know whether these breast cancer survivors should be having breast MRI once a year with their mammograms,” she said.
This study was designed to compare the diagnostic performance of screening breast MRI in women with a personal history of treated breast cancer alone, to that in women with a genetic or family history of breast cancer.
A review of the University of Washington's electronic medical database identified all women who underwent a first screening breast MRI for a clinical indication and had either a personal history or genetic or family history of breast cancer during the period January 2004 – June 2009. Each patient contributed ter first screening breast MRI to the study. For each examination, the highest-level final breast imaging-reporting and data system (BI-RADS) assessment was used.
Cancer status was followed for 365 days following index breast MRI and was considered positive if there was a diagnosis of invasive carcinoma or ductal carcinoma in situ.
Measures of diagnostic performance that were calculated included the recall rate, or number of women recalled for additional testing; the positive predictive value for malignancy at biopsy; the cancer yield, or percent found to be malignant among those screened; and the sensitivity and specificity.
Of the 1,026 women who underwent a first screening breast MRI in the study interval, 973 were screened for personal history and/or genetic or family history. These made up the study population. Of these, 646 (66%) were screened for personal history alone, and the remaining 327 (34%) were screened for genetic or family history. Women who fell into both categories were classified as genetic or family history.
In the 973 women, 27 malignancies were found, said Dr. DeMartini. “Twenty-five of them were found with breast MRI,” she said. The other two were not found with breast MRI and were false negatives; both occurred in the personal history group. Of the 25 malignancies, MRI detected 20 in the personal history group and 5 in the genetic family group, she said.
In diagnostic performance, the recall rate – the percentage recalled for additional testing – was 9.3% (60 of 646) in the personal history group, significantly lower than the 15.0% (49 of 327) in the genetic or family history group.
The positive predictive value of biopsy – the percentage found to be malignant – in the personal history group was 35.7% (20 of 56), significantly higher than in the genetic and family history group (12.2%, or 5 of 41).
The cancer yield – the fraction of all women screened who were found to have a malignancy – was 3.1% (20 of 646) in the personal history group, or more than twice the 1.5% (5 of 327) found in the genetic and family history group (P = .14). The sensitivity was 90.9% (20 of 22) in the personal history group (which had two false negatives not found with breast MRI) vs. 100% (5 of 5) in the genetic and family history group. Specificity was 93.6% (584 of 624) in the personal history group, higher than the genetic and family history group's 86.3% (278 of 322).
The date of original cancer was available for 18 of the 20 malignancies detected by MRI, and 11 of the 18 were detected greater than 5 years after the original cancer.
“Women with a personal history of breast cancer had a lower recall rate, higher positive predictive value, higher cancer yield (although not statistically significant), and higher specificity.,” said Dr. DeMartini.
Screening breast MRI may therefore be an important adjunct to mammography in women with a personal history of breast cancer, she said.
{kind=link}
Mammography images of the left breast (top) show no abnormality in a woman with a history of right-breast invasive cancer treated with mastectomy. MRI from the same patient shows a 15-mm mass, which biopsy revealed to be invasive cancer.
Source Courtesy Radiological Society of North America
Major Finding: Women with a personal history of breast cancer should consider an annual screening MRI, despite American Cancer Society guidelines to the contrary.
Data Source: Retrospective review of 1,026 women who received a first screening breast MRI, of whom 973 were screened for genetic and family history of breast cancer. A total of 327 had genetic or family history of breast cancer and 646 had a personal history of breast cancer.
Disclosures: None. According to Dr. DeMartini, the study had no sponsor.
CHICAGO – Women with a personal history of breast cancer should be advised to consider an annual screening breast MRI as an adjunct to mammography, despite the American Cancer Society's current position that there is insufficient evidence to recommend for or against it, according to a retrospective study from the University of Washington Medical Center, Seattle.
“We found that the diagnostic performance of screening breast MRI was similar or higher overall in women with a personal history [of breast cancer] alone, compared to those with a genetic or family history, the latter being the group currently recommended for screening by the American Cancer Society,” said lead author Dr. Wendy B. DeMartiniat the meeting.
American Cancer Society guidelines recommend an annual screening with breast MRI as an adjunct to mammography for women with a genetic or family history of breast cancer, but not for those with a personal history of the disease. MRI is highly sensitive and allows early detection of otherwise occult breast carcinoma, and mammography is an imperfect tool for detection, Dr. DeMartini said. This is critical in women with a personal history of treated breast cancer because they are at elevated risk for a second cancer, and finding second cancers early increases their chance of survival. “Annual screening with MRI may be important in this group,” she said.
Disadvantages of MRI include the use of intravenous contrast material, the potential for false positives, and increased cost.
The American Cancer Society's most recent guidelines issued in 2007 recommend annual screening MRI in addition to mammography for women in two high-risk groups: those with genetic mutation such as the BRCA gene or first-degree relatives with the gene, and those with at least a 20%-25% lifetime risk, based on family history. The guidelines concluded that there was insufficient evidence to recommend for or against breast MRI in patients with only a personal history of the disease but no genetic or family risk.
“And thus it's been quite challenging, as you can imagine, for women and their physicians to know whether these breast cancer survivors should be having breast MRI once a year with their mammograms,” she said.
This study was designed to compare the diagnostic performance of screening breast MRI in women with a personal history of treated breast cancer alone, to that in women with a genetic or family history of breast cancer.
A review of the University of Washington's electronic medical database identified all women who underwent a first screening breast MRI for a clinical indication and had either a personal history or genetic or family history of breast cancer during the period January 2004 – June 2009. Each patient contributed ter first screening breast MRI to the study. For each examination, the highest-level final breast imaging-reporting and data system (BI-RADS) assessment was used.
Cancer status was followed for 365 days following index breast MRI and was considered positive if there was a diagnosis of invasive carcinoma or ductal carcinoma in situ.
Measures of diagnostic performance that were calculated included the recall rate, or number of women recalled for additional testing; the positive predictive value for malignancy at biopsy; the cancer yield, or percent found to be malignant among those screened; and the sensitivity and specificity.
Of the 1,026 women who underwent a first screening breast MRI in the study interval, 973 were screened for personal history and/or genetic or family history. These made up the study population. Of these, 646 (66%) were screened for personal history alone, and the remaining 327 (34%) were screened for genetic or family history. Women who fell into both categories were classified as genetic or family history.
In the 973 women, 27 malignancies were found, said Dr. DeMartini. “Twenty-five of them were found with breast MRI,” she said. The other two were not found with breast MRI and were false negatives; both occurred in the personal history group. Of the 25 malignancies, MRI detected 20 in the personal history group and 5 in the genetic family group, she said.
In diagnostic performance, the recall rate – the percentage recalled for additional testing – was 9.3% (60 of 646) in the personal history group, significantly lower than the 15.0% (49 of 327) in the genetic or family history group.
The positive predictive value of biopsy – the percentage found to be malignant – in the personal history group was 35.7% (20 of 56), significantly higher than in the genetic and family history group (12.2%, or 5 of 41).
The cancer yield – the fraction of all women screened who were found to have a malignancy – was 3.1% (20 of 646) in the personal history group, or more than twice the 1.5% (5 of 327) found in the genetic and family history group (P = .14). The sensitivity was 90.9% (20 of 22) in the personal history group (which had two false negatives not found with breast MRI) vs. 100% (5 of 5) in the genetic and family history group. Specificity was 93.6% (584 of 624) in the personal history group, higher than the genetic and family history group's 86.3% (278 of 322).
The date of original cancer was available for 18 of the 20 malignancies detected by MRI, and 11 of the 18 were detected greater than 5 years after the original cancer.
“Women with a personal history of breast cancer had a lower recall rate, higher positive predictive value, higher cancer yield (although not statistically significant), and higher specificity.,” said Dr. DeMartini.
Screening breast MRI may therefore be an important adjunct to mammography in women with a personal history of breast cancer, she said.
Mammography images of the left breast (top) show no abnormality in a woman with a history of right-breast invasive cancer treated with mastectomy. MRI from the same patient shows a 15-mm mass, which biopsy revealed to be invasive cancer.
Source Courtesy Radiological Society of North America
Major Finding: Women with a personal history of breast cancer should consider an annual screening MRI, despite American Cancer Society guidelines to the contrary.
Data Source: Retrospective review of 1,026 women who received a first screening breast MRI, of whom 973 were screened for genetic and family history of breast cancer. A total of 327 had genetic or family history of breast cancer and 646 had a personal history of breast cancer.
Disclosures: None. According to Dr. DeMartini, the study had no sponsor.
CHICAGO – Women with a personal history of breast cancer should be advised to consider an annual screening breast MRI as an adjunct to mammography, despite the American Cancer Society's current position that there is insufficient evidence to recommend for or against it, according to a retrospective study from the University of Washington Medical Center, Seattle.
“We found that the diagnostic performance of screening breast MRI was similar or higher overall in women with a personal history [of breast cancer] alone, compared to those with a genetic or family history, the latter being the group currently recommended for screening by the American Cancer Society,” said lead author Dr. Wendy B. DeMartiniat the meeting.
American Cancer Society guidelines recommend an annual screening with breast MRI as an adjunct to mammography for women with a genetic or family history of breast cancer, but not for those with a personal history of the disease. MRI is highly sensitive and allows early detection of otherwise occult breast carcinoma, and mammography is an imperfect tool for detection, Dr. DeMartini said. This is critical in women with a personal history of treated breast cancer because they are at elevated risk for a second cancer, and finding second cancers early increases their chance of survival. “Annual screening with MRI may be important in this group,” she said.
Disadvantages of MRI include the use of intravenous contrast material, the potential for false positives, and increased cost.
The American Cancer Society's most recent guidelines issued in 2007 recommend annual screening MRI in addition to mammography for women in two high-risk groups: those with genetic mutation such as the BRCA gene or first-degree relatives with the gene, and those with at least a 20%-25% lifetime risk, based on family history. The guidelines concluded that there was insufficient evidence to recommend for or against breast MRI in patients with only a personal history of the disease but no genetic or family risk.
“And thus it's been quite challenging, as you can imagine, for women and their physicians to know whether these breast cancer survivors should be having breast MRI once a year with their mammograms,” she said.
This study was designed to compare the diagnostic performance of screening breast MRI in women with a personal history of treated breast cancer alone, to that in women with a genetic or family history of breast cancer.
A review of the University of Washington's electronic medical database identified all women who underwent a first screening breast MRI for a clinical indication and had either a personal history or genetic or family history of breast cancer during the period January 2004 – June 2009. Each patient contributed ter first screening breast MRI to the study. For each examination, the highest-level final breast imaging-reporting and data system (BI-RADS) assessment was used.
Cancer status was followed for 365 days following index breast MRI and was considered positive if there was a diagnosis of invasive carcinoma or ductal carcinoma in situ.
Measures of diagnostic performance that were calculated included the recall rate, or number of women recalled for additional testing; the positive predictive value for malignancy at biopsy; the cancer yield, or percent found to be malignant among those screened; and the sensitivity and specificity.
Of the 1,026 women who underwent a first screening breast MRI in the study interval, 973 were screened for personal history and/or genetic or family history. These made up the study population. Of these, 646 (66%) were screened for personal history alone, and the remaining 327 (34%) were screened for genetic or family history. Women who fell into both categories were classified as genetic or family history.
In the 973 women, 27 malignancies were found, said Dr. DeMartini. “Twenty-five of them were found with breast MRI,” she said. The other two were not found with breast MRI and were false negatives; both occurred in the personal history group. Of the 25 malignancies, MRI detected 20 in the personal history group and 5 in the genetic family group, she said.
In diagnostic performance, the recall rate – the percentage recalled for additional testing – was 9.3% (60 of 646) in the personal history group, significantly lower than the 15.0% (49 of 327) in the genetic or family history group.
The positive predictive value of biopsy – the percentage found to be malignant – in the personal history group was 35.7% (20 of 56), significantly higher than in the genetic and family history group (12.2%, or 5 of 41).
The cancer yield – the fraction of all women screened who were found to have a malignancy – was 3.1% (20 of 646) in the personal history group, or more than twice the 1.5% (5 of 327) found in the genetic and family history group (P = .14). The sensitivity was 90.9% (20 of 22) in the personal history group (which had two false negatives not found with breast MRI) vs. 100% (5 of 5) in the genetic and family history group. Specificity was 93.6% (584 of 624) in the personal history group, higher than the genetic and family history group's 86.3% (278 of 322).
The date of original cancer was available for 18 of the 20 malignancies detected by MRI, and 11 of the 18 were detected greater than 5 years after the original cancer.
“Women with a personal history of breast cancer had a lower recall rate, higher positive predictive value, higher cancer yield (although not statistically significant), and higher specificity.,” said Dr. DeMartini.
Screening breast MRI may therefore be an important adjunct to mammography in women with a personal history of breast cancer, she said.
Mammography images of the left breast (top) show no abnormality in a woman with a history of right-breast invasive cancer treated with mastectomy. MRI from the same patient shows a 15-mm mass, which biopsy revealed to be invasive cancer.
Source Courtesy Radiological Society of North America
Coronary CT Angiography Reveals Vessel Involvement in Obstructive Sleep Apnea
CHICAGO – Patients with obstructive sleep apnea have more active atherosclerotic disease with a greater degree of vessel involvement and more vulnerable plaque than do patients without the disease, according to a retrospective matched cohort study presented at the annual meeting of the Radiological Society of North America.

"We found that those folks who have obstructive sleep apnea have the more dangerous form of plaque," said Dr. U. Joseph Schoepf of the Medical University of South Carolina, Charleston, at a news conference.
"This is the first time that a noninvasive test, namely coronary CT angiography, has been applied to this, to actually demonstrate it. The clinical relevance is that we have a noninvasive tool at hand that allows us potentially to care better for our patients who have that disease."
Patients with obstructive sleep apnea (OSA) repeatedly stop breathing during sleep due to airway collapse. It is a disease of obesity, and 30% of Americans are obese, said Dr. Schoepf. Diminishing the oxygen supply exposes the cardiovascular system to oxidative stress, and may render vessel linings more vulnerable to the formation of atherosclerosis. OSA has been linked to coronary artery disease, he noted.
Computed tomography is the only noninvasive test that can directly evaluate cardiac vessel patency and analyze the composition of atherosclerotic lesions on vessel walls, said Dr. Schoepf. Therefore, it was used to study the association between OSA and coronary artery disease.
Investigators performed a retrospective search for patients who had undergone CT of the heart and polysomnogram assessment for suspected OSA. One observer measured coronary artery calcium, known informally as hard plaque. Two observers in consensus analyzed heart CT data for the presence and degree of coronary artery narrowing or blockages. The presence and extent of noncalcified or soft plaque, also known as vulnerable plaque, were also evaluated. Noncalcified plaque frequently causes acute cardiac events such as heart attack and unstable angina.
The retrospective search revealed 97 patients who had undergone both heart CT for atypical chest pain or prior equivocal test, as well as a polysomnogram. Two patients were excluded because their polysomnogram was performed more than 36 months before or after the date of their cardiac CT.
Of the 95 remaining patients, 49 (23 women, mean age 61 plus or minus 11 years, average body mass index 33 plus or minus 8 kg/m 2 ) had documented obstructive sleep apnea by polysomnogram. The other 46 patients (24 women, mean age 60 plus or minus 12 years, average BMI 30 plus or minus 6 kg/m 2 ) were found not to have obstructive sleep apnea by polysomnogram. The investigators found no significant difference in age, gender, BMI, or cardiovascular risk factors between the two groups.
Agatson calcium scores (hard plaque) were not significantly different between the two groups (mean score 272 plus or minus 422 for the group with obstructive sleep apnea versus 241 plus or minus 415 without, P = .5). The presence of any type of narrowing in the heart vessels was found to correlate with the presence of obstructive sleep apnea (P less than .0001). The total number of vessels with any narrowing was also found to correlate with the presence of obstructive sleep apnea (P = .0008). In addition, the degree of narrowing in the highest grade of lesion correlated with obstructive sleep apnea (P = .0013).
In conclusion, Dr. Schoepf said that any instance where noncalcified plaque (‘soft’ or ‘vulnerable’ plaque) was measured showed a significant correlation with obstructive sleep apnea.
If the study’s findings are sustained by larger prospective trials, cardiac CT could emerge as a useful noninvasive tool for investigating the relationship between OSA and coronary artery disease.
The study was not funded, and Dr. Schoepf made no disclosures relevant to the study. His general disclosures are that he has served on the speakers bureau of, and/or received research grants from, the Bracco Group, General Electric, and Bayer AG. He also has served on the Siemens AG Medical Advisory Board.
CHICAGO – Patients with obstructive sleep apnea have more active atherosclerotic disease with a greater degree of vessel involvement and more vulnerable plaque than do patients without the disease, according to a retrospective matched cohort study presented at the annual meeting of the Radiological Society of North America.
"We found that those folks who have obstructive sleep apnea have the more dangerous form of plaque," said Dr. U. Joseph Schoepf of the Medical University of South Carolina, Charleston, at a news conference.
"This is the first time that a noninvasive test, namely coronary CT angiography, has been applied to this, to actually demonstrate it. The clinical relevance is that we have a noninvasive tool at hand that allows us potentially to care better for our patients who have that disease."
Patients with obstructive sleep apnea (OSA) repeatedly stop breathing during sleep due to airway collapse. It is a disease of obesity, and 30% of Americans are obese, said Dr. Schoepf. Diminishing the oxygen supply exposes the cardiovascular system to oxidative stress, and may render vessel linings more vulnerable to the formation of atherosclerosis. OSA has been linked to coronary artery disease, he noted.
Computed tomography is the only noninvasive test that can directly evaluate cardiac vessel patency and analyze the composition of atherosclerotic lesions on vessel walls, said Dr. Schoepf. Therefore, it was used to study the association between OSA and coronary artery disease.
Investigators performed a retrospective search for patients who had undergone CT of the heart and polysomnogram assessment for suspected OSA. One observer measured coronary artery calcium, known informally as hard plaque. Two observers in consensus analyzed heart CT data for the presence and degree of coronary artery narrowing or blockages. The presence and extent of noncalcified or soft plaque, also known as vulnerable plaque, were also evaluated. Noncalcified plaque frequently causes acute cardiac events such as heart attack and unstable angina.
The retrospective search revealed 97 patients who had undergone both heart CT for atypical chest pain or prior equivocal test, as well as a polysomnogram. Two patients were excluded because their polysomnogram was performed more than 36 months before or after the date of their cardiac CT.
Of the 95 remaining patients, 49 (23 women, mean age 61 plus or minus 11 years, average body mass index 33 plus or minus 8 kg/m 2 ) had documented obstructive sleep apnea by polysomnogram. The other 46 patients (24 women, mean age 60 plus or minus 12 years, average BMI 30 plus or minus 6 kg/m 2 ) were found not to have obstructive sleep apnea by polysomnogram. The investigators found no significant difference in age, gender, BMI, or cardiovascular risk factors between the two groups.
Agatson calcium scores (hard plaque) were not significantly different between the two groups (mean score 272 plus or minus 422 for the group with obstructive sleep apnea versus 241 plus or minus 415 without, P = .5). The presence of any type of narrowing in the heart vessels was found to correlate with the presence of obstructive sleep apnea (P less than .0001). The total number of vessels with any narrowing was also found to correlate with the presence of obstructive sleep apnea (P = .0008). In addition, the degree of narrowing in the highest grade of lesion correlated with obstructive sleep apnea (P = .0013).
In conclusion, Dr. Schoepf said that any instance where noncalcified plaque (‘soft’ or ‘vulnerable’ plaque) was measured showed a significant correlation with obstructive sleep apnea.
If the study’s findings are sustained by larger prospective trials, cardiac CT could emerge as a useful noninvasive tool for investigating the relationship between OSA and coronary artery disease.
The study was not funded, and Dr. Schoepf made no disclosures relevant to the study. His general disclosures are that he has served on the speakers bureau of, and/or received research grants from, the Bracco Group, General Electric, and Bayer AG. He also has served on the Siemens AG Medical Advisory Board.
CHICAGO – Patients with obstructive sleep apnea have more active atherosclerotic disease with a greater degree of vessel involvement and more vulnerable plaque than do patients without the disease, according to a retrospective matched cohort study presented at the annual meeting of the Radiological Society of North America.
"We found that those folks who have obstructive sleep apnea have the more dangerous form of plaque," said Dr. U. Joseph Schoepf of the Medical University of South Carolina, Charleston, at a news conference.
"This is the first time that a noninvasive test, namely coronary CT angiography, has been applied to this, to actually demonstrate it. The clinical relevance is that we have a noninvasive tool at hand that allows us potentially to care better for our patients who have that disease."
Patients with obstructive sleep apnea (OSA) repeatedly stop breathing during sleep due to airway collapse. It is a disease of obesity, and 30% of Americans are obese, said Dr. Schoepf. Diminishing the oxygen supply exposes the cardiovascular system to oxidative stress, and may render vessel linings more vulnerable to the formation of atherosclerosis. OSA has been linked to coronary artery disease, he noted.
Computed tomography is the only noninvasive test that can directly evaluate cardiac vessel patency and analyze the composition of atherosclerotic lesions on vessel walls, said Dr. Schoepf. Therefore, it was used to study the association between OSA and coronary artery disease.
Investigators performed a retrospective search for patients who had undergone CT of the heart and polysomnogram assessment for suspected OSA. One observer measured coronary artery calcium, known informally as hard plaque. Two observers in consensus analyzed heart CT data for the presence and degree of coronary artery narrowing or blockages. The presence and extent of noncalcified or soft plaque, also known as vulnerable plaque, were also evaluated. Noncalcified plaque frequently causes acute cardiac events such as heart attack and unstable angina.
The retrospective search revealed 97 patients who had undergone both heart CT for atypical chest pain or prior equivocal test, as well as a polysomnogram. Two patients were excluded because their polysomnogram was performed more than 36 months before or after the date of their cardiac CT.
Of the 95 remaining patients, 49 (23 women, mean age 61 plus or minus 11 years, average body mass index 33 plus or minus 8 kg/m 2 ) had documented obstructive sleep apnea by polysomnogram. The other 46 patients (24 women, mean age 60 plus or minus 12 years, average BMI 30 plus or minus 6 kg/m 2 ) were found not to have obstructive sleep apnea by polysomnogram. The investigators found no significant difference in age, gender, BMI, or cardiovascular risk factors between the two groups.
Agatson calcium scores (hard plaque) were not significantly different between the two groups (mean score 272 plus or minus 422 for the group with obstructive sleep apnea versus 241 plus or minus 415 without, P = .5). The presence of any type of narrowing in the heart vessels was found to correlate with the presence of obstructive sleep apnea (P less than .0001). The total number of vessels with any narrowing was also found to correlate with the presence of obstructive sleep apnea (P = .0008). In addition, the degree of narrowing in the highest grade of lesion correlated with obstructive sleep apnea (P = .0013).
In conclusion, Dr. Schoepf said that any instance where noncalcified plaque (‘soft’ or ‘vulnerable’ plaque) was measured showed a significant correlation with obstructive sleep apnea.
If the study’s findings are sustained by larger prospective trials, cardiac CT could emerge as a useful noninvasive tool for investigating the relationship between OSA and coronary artery disease.
The study was not funded, and Dr. Schoepf made no disclosures relevant to the study. His general disclosures are that he has served on the speakers bureau of, and/or received research grants from, the Bracco Group, General Electric, and Bayer AG. He also has served on the Siemens AG Medical Advisory Board.
FROM THE ANNUAL MEETING OF THE RADIOLOGICAL SOCIETY OF NORTH AMERICA
Major Finding: Coronary CT angiography reveals a higher prevalence of stenotic coronary artery disease and more extensive vessel involvement in patients with obstructive sleep apnea than in those without it.
Data Source: A retrospective study of 95 obese patients, 49 with obstructive sleep apnea and 46 without.
Disclosures: The study was not funded, and Dr. Schoepf made no disclosures relevant to the study. His general disclosures are that he has served on the speakers bureau of, and/or received research grants from, the Bracco Group, General Electric, and Bayer AG. He also has served on the Siemens AG Medical Advisory Board.
Personal Breast Cancer History: Screening MRI, Annual Mammography Recommended
CHICAGO – Women with a personal history of breast cancer should be advised to consider an annual screening breast MRI as an adjunct to mammography, despite the American Cancer Society’s current position that there is insufficient evidence to recommend for or against it, according to a retrospective review from the University of Washington Medical Center, Seattle.
“We found that the diagnostic performance of screening breast MRI was similar to or higher overall in women with a personal history [of breast cancer] alone, compared to those with a genetic or family history, the latter being the group currently recommended for screening by the American Cancer Society,” said lead author Dr. Wendy B. DeMartini of the University of Washington. Dr.
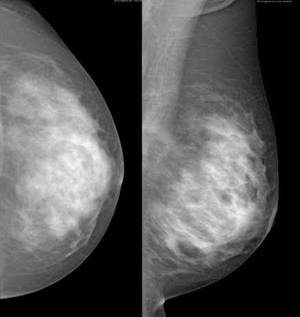
DeMartini presented her results Nov. 28 at the annual meeting of the Radiological Society of North America.
American Cancer Society guidelines recommend an annual screening with breast MRI as an adjunct to mammography for women with a genetic or family history of breast cancer, but not for those with a personal history of the disease. MRI is highly sensitive and allows early detection of otherwise occult breast carcinoma, and mammography is an imperfect tool for detection, Dr. DeMartini said. This is critical in women with a personal history of treated breast cancer because they are at elevated risk for a second cancer, and finding second cancers early increases their chance of survival. “Annual screening with MRI may be important in this group,” she said.
Disadvantages of MRI include the use of intravenous contrast material, the potential for false positives, and increased cost.

The American Cancer Society’s most recent guidelines issued in 2007 recommend annual screening MRI in addition to mammography for women in two high-risk groups: those with genetic mutation such as the BRCA gene or first-degree relatives with the gene and those with greater than or equal to 20%-25% lifetime risk, based on family history. The guidelines concluded that there was insufficient evidence to recommend for or against breast MRI in patients with only a personal history of the disease but no genetic or family risk.
“And thus it’s been quite challenging as you can imagine for women and their physicians to know whether these breast cancer survivors should be having breast MRI once a year with their mammograms,” she said.
This study was designed to compare the diagnostic performance of screening breast MRI in women with a personal history of treated breast cancer alone, to that in women with a genetic or family history of breast cancer.
A retrospective review of the University of Washington’s electronic medical database identified all women who underwent a first screening breast MRI for a clinical indication and had either a personal history or genetic or family history of breast cancer during the period January 2004 – June 2009. Each patient contributed their first screening breast MRI to the study. For each examination, the highest level final breast imaging-reporting and data system (BI-RADS) assessment was used. Cancer status was followed for 365 days following index breast MRI and was considered positive if there was a diagnosis of invasive carcinoma or ductal carcinoma in situ.
Measures of diagnostic performance that were calculated included the recall rate, or number of women recalled for additional testing; the positive predictive value for malignancy at biopsy; the cancer yield, or percent found to be malignant among those screened; and the sensitivity and specificity.
Of the 1,026 women who underwent a first screening breast MRI in the study interval, 973 were screened for personal history and/or genetic or family history. These made up the study population. Of these, 646 (66%) were screened for personal history alone, and the remaining 327 (34%) were screened for genetic or family history. Women who fell into both categories were classified as genetic or family history.
In the 973 women, 27 malignancies were found, said Dr. DeMartini. “Twenty-five of them were found with breast MRI,” she said. The other two were not found with breast MRI and were false negatives; both occurred in the personal history group. Of the 25 malignancies, MRI detected 20 in the personal history group and 5 in the genetic family group, she said.
In diagnostic performance, the recall rate – the percentage recalled for additional testing – was 9.3% (60 of 646) in the personal history group, significantly lower than the 15.0% (49 of 327) in the genetic or family history group.
The positive predictive value of biopsy – the percentage found to be malignant – in the personal history group was 35.7% (20 of 56), significantly higher than in the genetic and family history group (12.2%, or 5 of 41). The cancer yield – the fraction of all women screened who were found to have a malignancy – was 3.1% (20 of 646) in the personal history group, or more than twice the 1.5% (5 of 327) found in the genetic and family history group (P =.14). The sensitivity was 90.9% (20 of 22) in the personal history group (which had two false negatives not found with breast MRI) vs. 100% (5 of 5) in the genetic and family history group. Specificity was 93.6% (584 of 624) in the personal history group, higher than the genetic and family history group’s 86.3% (278 of 322).
The date of original cancer was available for 18 of the 20 malignancies detected by MRI, and 11 of the 18 were detected greater than 5 years after the original cancer.
“The diagnostic performance of screening breast MRI was similar to or higher overall in women with personal history alone compared to those with a genetic or family history,” said Dr. DeMartini. “Women with a personal history of breast cancer had a lower recall rate, higher positive predictive value, higher cancer yield (although not statistically significant) and higher specificity.”
Screening breast MRI may therefore be an important adjunct to mammography in women with a personal history of breast cancer, she said, and should be a step in the direction of evidence-based, personalized surveillance of women who are breast cancer survivors.
Asked later at a news conference whether other prospective studies were underway, Dr. DeMartini said that to her knowledge there were not. However she now recommends to her own patients, “that they strongly consider breast MRI and discuss it with their provider.” Dr. DeMartini said that the typical cost of breast MRI is between $1,000 and $2,000.
CHICAGO – Women with a personal history of breast cancer should be advised to consider an annual screening breast MRI as an adjunct to mammography, despite the American Cancer Society’s current position that there is insufficient evidence to recommend for or against it, according to a retrospective review from the University of Washington Medical Center, Seattle.
“We found that the diagnostic performance of screening breast MRI was similar to or higher overall in women with a personal history [of breast cancer] alone, compared to those with a genetic or family history, the latter being the group currently recommended for screening by the American Cancer Society,” said lead author Dr. Wendy B. DeMartini of the University of Washington. Dr.
DeMartini presented her results Nov. 28 at the annual meeting of the Radiological Society of North America.
American Cancer Society guidelines recommend an annual screening with breast MRI as an adjunct to mammography for women with a genetic or family history of breast cancer, but not for those with a personal history of the disease. MRI is highly sensitive and allows early detection of otherwise occult breast carcinoma, and mammography is an imperfect tool for detection, Dr. DeMartini said. This is critical in women with a personal history of treated breast cancer because they are at elevated risk for a second cancer, and finding second cancers early increases their chance of survival. “Annual screening with MRI may be important in this group,” she said.
Disadvantages of MRI include the use of intravenous contrast material, the potential for false positives, and increased cost.
The American Cancer Society’s most recent guidelines issued in 2007 recommend annual screening MRI in addition to mammography for women in two high-risk groups: those with genetic mutation such as the BRCA gene or first-degree relatives with the gene and those with greater than or equal to 20%-25% lifetime risk, based on family history. The guidelines concluded that there was insufficient evidence to recommend for or against breast MRI in patients with only a personal history of the disease but no genetic or family risk.
“And thus it’s been quite challenging as you can imagine for women and their physicians to know whether these breast cancer survivors should be having breast MRI once a year with their mammograms,” she said.
This study was designed to compare the diagnostic performance of screening breast MRI in women with a personal history of treated breast cancer alone, to that in women with a genetic or family history of breast cancer.
A retrospective review of the University of Washington’s electronic medical database identified all women who underwent a first screening breast MRI for a clinical indication and had either a personal history or genetic or family history of breast cancer during the period January 2004 – June 2009. Each patient contributed their first screening breast MRI to the study. For each examination, the highest level final breast imaging-reporting and data system (BI-RADS) assessment was used. Cancer status was followed for 365 days following index breast MRI and was considered positive if there was a diagnosis of invasive carcinoma or ductal carcinoma in situ.
Measures of diagnostic performance that were calculated included the recall rate, or number of women recalled for additional testing; the positive predictive value for malignancy at biopsy; the cancer yield, or percent found to be malignant among those screened; and the sensitivity and specificity.
Of the 1,026 women who underwent a first screening breast MRI in the study interval, 973 were screened for personal history and/or genetic or family history. These made up the study population. Of these, 646 (66%) were screened for personal history alone, and the remaining 327 (34%) were screened for genetic or family history. Women who fell into both categories were classified as genetic or family history.
In the 973 women, 27 malignancies were found, said Dr. DeMartini. “Twenty-five of them were found with breast MRI,” she said. The other two were not found with breast MRI and were false negatives; both occurred in the personal history group. Of the 25 malignancies, MRI detected 20 in the personal history group and 5 in the genetic family group, she said.
In diagnostic performance, the recall rate – the percentage recalled for additional testing – was 9.3% (60 of 646) in the personal history group, significantly lower than the 15.0% (49 of 327) in the genetic or family history group.
The positive predictive value of biopsy – the percentage found to be malignant – in the personal history group was 35.7% (20 of 56), significantly higher than in the genetic and family history group (12.2%, or 5 of 41). The cancer yield – the fraction of all women screened who were found to have a malignancy – was 3.1% (20 of 646) in the personal history group, or more than twice the 1.5% (5 of 327) found in the genetic and family history group (P =.14). The sensitivity was 90.9% (20 of 22) in the personal history group (which had two false negatives not found with breast MRI) vs. 100% (5 of 5) in the genetic and family history group. Specificity was 93.6% (584 of 624) in the personal history group, higher than the genetic and family history group’s 86.3% (278 of 322).
The date of original cancer was available for 18 of the 20 malignancies detected by MRI, and 11 of the 18 were detected greater than 5 years after the original cancer.
“The diagnostic performance of screening breast MRI was similar to or higher overall in women with personal history alone compared to those with a genetic or family history,” said Dr. DeMartini. “Women with a personal history of breast cancer had a lower recall rate, higher positive predictive value, higher cancer yield (although not statistically significant) and higher specificity.”
Screening breast MRI may therefore be an important adjunct to mammography in women with a personal history of breast cancer, she said, and should be a step in the direction of evidence-based, personalized surveillance of women who are breast cancer survivors.
Asked later at a news conference whether other prospective studies were underway, Dr. DeMartini said that to her knowledge there were not. However she now recommends to her own patients, “that they strongly consider breast MRI and discuss it with their provider.” Dr. DeMartini said that the typical cost of breast MRI is between $1,000 and $2,000.
CHICAGO – Women with a personal history of breast cancer should be advised to consider an annual screening breast MRI as an adjunct to mammography, despite the American Cancer Society’s current position that there is insufficient evidence to recommend for or against it, according to a retrospective review from the University of Washington Medical Center, Seattle.
“We found that the diagnostic performance of screening breast MRI was similar to or higher overall in women with a personal history [of breast cancer] alone, compared to those with a genetic or family history, the latter being the group currently recommended for screening by the American Cancer Society,” said lead author Dr. Wendy B. DeMartini of the University of Washington. Dr.
DeMartini presented her results Nov. 28 at the annual meeting of the Radiological Society of North America.
American Cancer Society guidelines recommend an annual screening with breast MRI as an adjunct to mammography for women with a genetic or family history of breast cancer, but not for those with a personal history of the disease. MRI is highly sensitive and allows early detection of otherwise occult breast carcinoma, and mammography is an imperfect tool for detection, Dr. DeMartini said. This is critical in women with a personal history of treated breast cancer because they are at elevated risk for a second cancer, and finding second cancers early increases their chance of survival. “Annual screening with MRI may be important in this group,” she said.
Disadvantages of MRI include the use of intravenous contrast material, the potential for false positives, and increased cost.
The American Cancer Society’s most recent guidelines issued in 2007 recommend annual screening MRI in addition to mammography for women in two high-risk groups: those with genetic mutation such as the BRCA gene or first-degree relatives with the gene and those with greater than or equal to 20%-25% lifetime risk, based on family history. The guidelines concluded that there was insufficient evidence to recommend for or against breast MRI in patients with only a personal history of the disease but no genetic or family risk.
“And thus it’s been quite challenging as you can imagine for women and their physicians to know whether these breast cancer survivors should be having breast MRI once a year with their mammograms,” she said.
This study was designed to compare the diagnostic performance of screening breast MRI in women with a personal history of treated breast cancer alone, to that in women with a genetic or family history of breast cancer.
A retrospective review of the University of Washington’s electronic medical database identified all women who underwent a first screening breast MRI for a clinical indication and had either a personal history or genetic or family history of breast cancer during the period January 2004 – June 2009. Each patient contributed their first screening breast MRI to the study. For each examination, the highest level final breast imaging-reporting and data system (BI-RADS) assessment was used. Cancer status was followed for 365 days following index breast MRI and was considered positive if there was a diagnosis of invasive carcinoma or ductal carcinoma in situ.
Measures of diagnostic performance that were calculated included the recall rate, or number of women recalled for additional testing; the positive predictive value for malignancy at biopsy; the cancer yield, or percent found to be malignant among those screened; and the sensitivity and specificity.
Of the 1,026 women who underwent a first screening breast MRI in the study interval, 973 were screened for personal history and/or genetic or family history. These made up the study population. Of these, 646 (66%) were screened for personal history alone, and the remaining 327 (34%) were screened for genetic or family history. Women who fell into both categories were classified as genetic or family history.
In the 973 women, 27 malignancies were found, said Dr. DeMartini. “Twenty-five of them were found with breast MRI,” she said. The other two were not found with breast MRI and were false negatives; both occurred in the personal history group. Of the 25 malignancies, MRI detected 20 in the personal history group and 5 in the genetic family group, she said.
In diagnostic performance, the recall rate – the percentage recalled for additional testing – was 9.3% (60 of 646) in the personal history group, significantly lower than the 15.0% (49 of 327) in the genetic or family history group.
The positive predictive value of biopsy – the percentage found to be malignant – in the personal history group was 35.7% (20 of 56), significantly higher than in the genetic and family history group (12.2%, or 5 of 41). The cancer yield – the fraction of all women screened who were found to have a malignancy – was 3.1% (20 of 646) in the personal history group, or more than twice the 1.5% (5 of 327) found in the genetic and family history group (P =.14). The sensitivity was 90.9% (20 of 22) in the personal history group (which had two false negatives not found with breast MRI) vs. 100% (5 of 5) in the genetic and family history group. Specificity was 93.6% (584 of 624) in the personal history group, higher than the genetic and family history group’s 86.3% (278 of 322).
The date of original cancer was available for 18 of the 20 malignancies detected by MRI, and 11 of the 18 were detected greater than 5 years after the original cancer.
“The diagnostic performance of screening breast MRI was similar to or higher overall in women with personal history alone compared to those with a genetic or family history,” said Dr. DeMartini. “Women with a personal history of breast cancer had a lower recall rate, higher positive predictive value, higher cancer yield (although not statistically significant) and higher specificity.”
Screening breast MRI may therefore be an important adjunct to mammography in women with a personal history of breast cancer, she said, and should be a step in the direction of evidence-based, personalized surveillance of women who are breast cancer survivors.
Asked later at a news conference whether other prospective studies were underway, Dr. DeMartini said that to her knowledge there were not. However she now recommends to her own patients, “that they strongly consider breast MRI and discuss it with their provider.” Dr. DeMartini said that the typical cost of breast MRI is between $1,000 and $2,000.
From the annual meeting of the Radiological Society of North America
Major Finding:
Women with a personal history of breast cancer should consider an annual
screening MRI, despite American Cancer Society guidelines to the contrary.
Data Source:
Retrospective review of 1,026 women who received a first screening breast MRI, of
whom 973 were screened for genetic and family history of breast cancer. A total
of 327 had genetic or family history of breast cancer and 646 had a personal
history of breast cancer
Disclosures: None.
According to Dr. DeMartini, the study had no sponsor
Metabolic Syndrome Plus HT Ups Coronary Risk
CHICAGO – The results of the Women's Health Initiative randomized clinical trial suggest that postmenopausal women who begin hormone therapy may be at risk for coronary heart disease, but a new study from the University of Oklahoma Health Sciences Center suggests that the presence or absence of the metabolic syndrome at baseline is a key determining factor.
“If the metabolic syndrome was present, indeed there was a greater risk, greater odds of event, and this was statistically significant,” said principal investigator Dr. Robert Wild, professor of ob.gyn. and adjunct professor of medicine–cardiology at the center.
The nested case-control study examined the Women's Health Initiative cohort for an effect modification between elevated baseline risk and hormone therapy (HT). It found 359 incident cases of coronary heart disease (CHD), and matched these to 817 controls without CHD. Controls were matched with a variety of criteria, including prevalent cardiovascular disease at baseline. Trials of estrogen plus progesterone and estrogen alone were studied separately and in a pooled analysis. Metabolic syndrome was defined by ATP III criteria, at least three of the following: elevated waist circumference, triglycerides, HDL cholesterol, blood pressure, and fasting glucose.
In the pooled trial analysis of estrogen plus progesterone and estrogen alone, the metabolic syndrome was found to be an effect modifier. The odds ratio for treatment effect was 0.98 for women without the metabolic syndrome and 1.72 for those with the metabolic syndrome.
The individual trials had limited power, said Dr. Wild, but the findings were similar.
“Women without metabolic syndrome had no increase in risk of coronary heart disease vs. placebo, whereas women with metabolic syndrome had elevated risk,” said Dr. Wild. The reasons for this heightened risk might be more advanced stages of atherosclerosis and a heightened thrombogenic state among women with the metabolic syndrome, he said.
“Baseline CHD risk assessment may be helpful to identify women at increased risk for CHD when taking hormone therapy,” said Dr. Wild.
He disclosed no relevant financial relationships. This study was sponsored by the University of Oklahoma Health Sciences Center, Oklahoma City.
CHICAGO – The results of the Women's Health Initiative randomized clinical trial suggest that postmenopausal women who begin hormone therapy may be at risk for coronary heart disease, but a new study from the University of Oklahoma Health Sciences Center suggests that the presence or absence of the metabolic syndrome at baseline is a key determining factor.
“If the metabolic syndrome was present, indeed there was a greater risk, greater odds of event, and this was statistically significant,” said principal investigator Dr. Robert Wild, professor of ob.gyn. and adjunct professor of medicine–cardiology at the center.
The nested case-control study examined the Women's Health Initiative cohort for an effect modification between elevated baseline risk and hormone therapy (HT). It found 359 incident cases of coronary heart disease (CHD), and matched these to 817 controls without CHD. Controls were matched with a variety of criteria, including prevalent cardiovascular disease at baseline. Trials of estrogen plus progesterone and estrogen alone were studied separately and in a pooled analysis. Metabolic syndrome was defined by ATP III criteria, at least three of the following: elevated waist circumference, triglycerides, HDL cholesterol, blood pressure, and fasting glucose.
In the pooled trial analysis of estrogen plus progesterone and estrogen alone, the metabolic syndrome was found to be an effect modifier. The odds ratio for treatment effect was 0.98 for women without the metabolic syndrome and 1.72 for those with the metabolic syndrome.
The individual trials had limited power, said Dr. Wild, but the findings were similar.
“Women without metabolic syndrome had no increase in risk of coronary heart disease vs. placebo, whereas women with metabolic syndrome had elevated risk,” said Dr. Wild. The reasons for this heightened risk might be more advanced stages of atherosclerosis and a heightened thrombogenic state among women with the metabolic syndrome, he said.
“Baseline CHD risk assessment may be helpful to identify women at increased risk for CHD when taking hormone therapy,” said Dr. Wild.
He disclosed no relevant financial relationships. This study was sponsored by the University of Oklahoma Health Sciences Center, Oklahoma City.
CHICAGO – The results of the Women's Health Initiative randomized clinical trial suggest that postmenopausal women who begin hormone therapy may be at risk for coronary heart disease, but a new study from the University of Oklahoma Health Sciences Center suggests that the presence or absence of the metabolic syndrome at baseline is a key determining factor.
“If the metabolic syndrome was present, indeed there was a greater risk, greater odds of event, and this was statistically significant,” said principal investigator Dr. Robert Wild, professor of ob.gyn. and adjunct professor of medicine–cardiology at the center.
The nested case-control study examined the Women's Health Initiative cohort for an effect modification between elevated baseline risk and hormone therapy (HT). It found 359 incident cases of coronary heart disease (CHD), and matched these to 817 controls without CHD. Controls were matched with a variety of criteria, including prevalent cardiovascular disease at baseline. Trials of estrogen plus progesterone and estrogen alone were studied separately and in a pooled analysis. Metabolic syndrome was defined by ATP III criteria, at least three of the following: elevated waist circumference, triglycerides, HDL cholesterol, blood pressure, and fasting glucose.
In the pooled trial analysis of estrogen plus progesterone and estrogen alone, the metabolic syndrome was found to be an effect modifier. The odds ratio for treatment effect was 0.98 for women without the metabolic syndrome and 1.72 for those with the metabolic syndrome.
The individual trials had limited power, said Dr. Wild, but the findings were similar.
“Women without metabolic syndrome had no increase in risk of coronary heart disease vs. placebo, whereas women with metabolic syndrome had elevated risk,” said Dr. Wild. The reasons for this heightened risk might be more advanced stages of atherosclerosis and a heightened thrombogenic state among women with the metabolic syndrome, he said.
“Baseline CHD risk assessment may be helpful to identify women at increased risk for CHD when taking hormone therapy,” said Dr. Wild.
He disclosed no relevant financial relationships. This study was sponsored by the University of Oklahoma Health Sciences Center, Oklahoma City.
Hip Fractures Rose as the Use of HT Declined
Major Finding: The Women's Health Initiative reported in May 2002 that risks of coronary heart disease and cancer were associated with HT. Between July 2002 and December 2008, HT use in this population decreased from 85% to 18%. After adjustment for age and race, women who did not use HT in the previous year had a 55% increased risk of hip fracture.
Data Source: A study of 80,995 patients in the Kaiser Permanente Southern California database.
Disclosures: Dr. Karim said she had no financial conflicts of interest. The study was supported by the University of Southern California.
CHICAGO – Prescriptions for hormone therapy for elderly postmenopausal women declined significantly after the results of the Women's Health Initiative were reported in May 2002, and it now appears that there has been a correspondingly steep rise in hip fracture rates, said Roksana Karim, Ph.D., of the University of Southern California, Los Angeles.
“The rise in hip fracture rates in elderly postmenopausal women may be partially attributed to the continued decline in hormone therapy use,” she said at the meeting. “Hormone therapy–related benefits on hip fracture do not carry over after cessation.”
This was the conclusion of a longitudinal observational study of 80,995 postmenopausal women aged 60 years or older using data from 11 Kaiser Permanente medical centers in southern California. The study was designed to assess the risk of hip fracture for women who stopped taking hormone therapy (HT), compared with those who continued the therapy. It was also designed to evaluate the risk of hip fracture over time after stopping HT, and to measure bone mineral density (BMD) over time after stopping HT.
Data was collected on hip fracture, HT use, and the use of antiosteoporotic medication from June 2002 through December 2008. All hip fractures were verified by chart review by an orthopedic surgeon who was blinded to patients' HT status. Exclusion criteria included fractures secondary to tumors or high-energy trauma, and periprosthetic fractures. Patients were considered to be HT users if they had filled at least two prescriptions in a given year, as each prescription provides a 3-month supply of medication. HT was defined as estrogen alone or estrogen plus progesterone.
BMD data of the hip and lumbar regions were available for 54,209 women (67%). The 80,955 women had a mean age of 68.8 years and a mean body mass index of 26.9 kg/m
Between July 2002 and December 2008, HT use in this population decreased from 85% to 18%. After adjustments for age and race, women who did not use HT in the previous year had a 55% increased risk of hip fracture (hazard ratio, 1.55), said Dr. Karim. She also said that hip fracture risk significantly increased with 2 or more years of HT cessation. Mean BMD was significantly and inversely associated with cumulative years of HT nonuse, she said.
Dr. Karim acknowledged that the study was limited by lack of body mass index data in 47% of the population, or information on history of past HT use or on previous fractures.
The estimated annual cost for osteoporotic fractures in the United States is $18 billion, and hip fractures result in a greater cost and disability than do all other osteoporotic fractures combined, said Dr. Karim.
“Women at risk of hip fracture should consider carefully before making a decision of stopping using hormone therapy,” she said.
During a question-and-answer session, Andrea LaCroix, Ph.D., professor of epidemiology at the University of Washington, Seattle, said, “It certainly comes as no surprise that women discontinue hormone therapy. There's some loss of bone density and an increase in hip fracture rates. I agree with the conclusion that women coming off hormone therapy should be counseled about their potential for losing bone and having an increased fracture risk, but they've never enjoyed more alternatives for the prevention of hip fracture than they do today, including many agents besides hormone therapy.”
Major Finding: The Women's Health Initiative reported in May 2002 that risks of coronary heart disease and cancer were associated with HT. Between July 2002 and December 2008, HT use in this population decreased from 85% to 18%. After adjustment for age and race, women who did not use HT in the previous year had a 55% increased risk of hip fracture.
Data Source: A study of 80,995 patients in the Kaiser Permanente Southern California database.
Disclosures: Dr. Karim said she had no financial conflicts of interest. The study was supported by the University of Southern California.
CHICAGO – Prescriptions for hormone therapy for elderly postmenopausal women declined significantly after the results of the Women's Health Initiative were reported in May 2002, and it now appears that there has been a correspondingly steep rise in hip fracture rates, said Roksana Karim, Ph.D., of the University of Southern California, Los Angeles.
“The rise in hip fracture rates in elderly postmenopausal women may be partially attributed to the continued decline in hormone therapy use,” she said at the meeting. “Hormone therapy–related benefits on hip fracture do not carry over after cessation.”
This was the conclusion of a longitudinal observational study of 80,995 postmenopausal women aged 60 years or older using data from 11 Kaiser Permanente medical centers in southern California. The study was designed to assess the risk of hip fracture for women who stopped taking hormone therapy (HT), compared with those who continued the therapy. It was also designed to evaluate the risk of hip fracture over time after stopping HT, and to measure bone mineral density (BMD) over time after stopping HT.
Data was collected on hip fracture, HT use, and the use of antiosteoporotic medication from June 2002 through December 2008. All hip fractures were verified by chart review by an orthopedic surgeon who was blinded to patients' HT status. Exclusion criteria included fractures secondary to tumors or high-energy trauma, and periprosthetic fractures. Patients were considered to be HT users if they had filled at least two prescriptions in a given year, as each prescription provides a 3-month supply of medication. HT was defined as estrogen alone or estrogen plus progesterone.
BMD data of the hip and lumbar regions were available for 54,209 women (67%). The 80,955 women had a mean age of 68.8 years and a mean body mass index of 26.9 kg/m
Between July 2002 and December 2008, HT use in this population decreased from 85% to 18%. After adjustments for age and race, women who did not use HT in the previous year had a 55% increased risk of hip fracture (hazard ratio, 1.55), said Dr. Karim. She also said that hip fracture risk significantly increased with 2 or more years of HT cessation. Mean BMD was significantly and inversely associated with cumulative years of HT nonuse, she said.
Dr. Karim acknowledged that the study was limited by lack of body mass index data in 47% of the population, or information on history of past HT use or on previous fractures.
The estimated annual cost for osteoporotic fractures in the United States is $18 billion, and hip fractures result in a greater cost and disability than do all other osteoporotic fractures combined, said Dr. Karim.
“Women at risk of hip fracture should consider carefully before making a decision of stopping using hormone therapy,” she said.
During a question-and-answer session, Andrea LaCroix, Ph.D., professor of epidemiology at the University of Washington, Seattle, said, “It certainly comes as no surprise that women discontinue hormone therapy. There's some loss of bone density and an increase in hip fracture rates. I agree with the conclusion that women coming off hormone therapy should be counseled about their potential for losing bone and having an increased fracture risk, but they've never enjoyed more alternatives for the prevention of hip fracture than they do today, including many agents besides hormone therapy.”
Major Finding: The Women's Health Initiative reported in May 2002 that risks of coronary heart disease and cancer were associated with HT. Between July 2002 and December 2008, HT use in this population decreased from 85% to 18%. After adjustment for age and race, women who did not use HT in the previous year had a 55% increased risk of hip fracture.
Data Source: A study of 80,995 patients in the Kaiser Permanente Southern California database.
Disclosures: Dr. Karim said she had no financial conflicts of interest. The study was supported by the University of Southern California.
CHICAGO – Prescriptions for hormone therapy for elderly postmenopausal women declined significantly after the results of the Women's Health Initiative were reported in May 2002, and it now appears that there has been a correspondingly steep rise in hip fracture rates, said Roksana Karim, Ph.D., of the University of Southern California, Los Angeles.
“The rise in hip fracture rates in elderly postmenopausal women may be partially attributed to the continued decline in hormone therapy use,” she said at the meeting. “Hormone therapy–related benefits on hip fracture do not carry over after cessation.”
This was the conclusion of a longitudinal observational study of 80,995 postmenopausal women aged 60 years or older using data from 11 Kaiser Permanente medical centers in southern California. The study was designed to assess the risk of hip fracture for women who stopped taking hormone therapy (HT), compared with those who continued the therapy. It was also designed to evaluate the risk of hip fracture over time after stopping HT, and to measure bone mineral density (BMD) over time after stopping HT.
Data was collected on hip fracture, HT use, and the use of antiosteoporotic medication from June 2002 through December 2008. All hip fractures were verified by chart review by an orthopedic surgeon who was blinded to patients' HT status. Exclusion criteria included fractures secondary to tumors or high-energy trauma, and periprosthetic fractures. Patients were considered to be HT users if they had filled at least two prescriptions in a given year, as each prescription provides a 3-month supply of medication. HT was defined as estrogen alone or estrogen plus progesterone.
BMD data of the hip and lumbar regions were available for 54,209 women (67%). The 80,955 women had a mean age of 68.8 years and a mean body mass index of 26.9 kg/m
Between July 2002 and December 2008, HT use in this population decreased from 85% to 18%. After adjustments for age and race, women who did not use HT in the previous year had a 55% increased risk of hip fracture (hazard ratio, 1.55), said Dr. Karim. She also said that hip fracture risk significantly increased with 2 or more years of HT cessation. Mean BMD was significantly and inversely associated with cumulative years of HT nonuse, she said.
Dr. Karim acknowledged that the study was limited by lack of body mass index data in 47% of the population, or information on history of past HT use or on previous fractures.
The estimated annual cost for osteoporotic fractures in the United States is $18 billion, and hip fractures result in a greater cost and disability than do all other osteoporotic fractures combined, said Dr. Karim.
“Women at risk of hip fracture should consider carefully before making a decision of stopping using hormone therapy,” she said.
During a question-and-answer session, Andrea LaCroix, Ph.D., professor of epidemiology at the University of Washington, Seattle, said, “It certainly comes as no surprise that women discontinue hormone therapy. There's some loss of bone density and an increase in hip fracture rates. I agree with the conclusion that women coming off hormone therapy should be counseled about their potential for losing bone and having an increased fracture risk, but they've never enjoyed more alternatives for the prevention of hip fracture than they do today, including many agents besides hormone therapy.”