For patients with carotid artery stenosis, percutaneous intervention with stenting is as good as surgery (carotid endarterectomy). This was the major finding of the recently completed Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)1—with some qualifications.
CREST is the latest in a series of clinical trials of treatment of carotid stenosis that have generated reams of numbers and much debate. The topic of surgery vs percutaneous intervention is a moving target, as techniques evolve and improve. We believe the CREST results are valuable and should help inform decisions about treatment in the “real world.”
In this article, we offer a critical review of CREST, with a careful evaluation of its methods, results, and conclusions.
AN EVOLVING FIELD
Despite improvements in diagnosis and management, stroke remains one of the leading causes of morbidity and death in the United States, with an annual incidence of 780,000 cases and 270,000 deaths.2,3
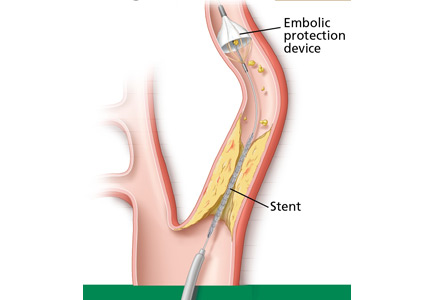
Figure 1. Carotid endarterectomy has long been an established treatment in selected patients with symptomatic carotid artery stenosis of 50% or greater or asymptomatic stenosis of 60% or greater. However, percutaneous carotid artery angioplasty with stenting and placement of an embolic protection device is gaining ground as a reasonable, safe, less invasive alternative.
From 10% to 30% of ischemic strokes are due to emboli from the carotid arteries.4–6 Carotid endarterectomy is an established treatment in selected patients with symptomatic carotid stenosis of 50% or greater or asymptomatic stenosis of 60% or greater.7,8 However, percutaneous techniques such as carotid artery angioplasty with stenting have improved, making them a viable, less invasive option (Figure 1).
Randomized trials of stenting have had mixed results, leading the Centers for Medicare and Medicaid Services (CMS) to adopt strict reimbursement policies. Currently, CMS reimburses for stenting only in symptomatic cases with at least 50% carotid artery stenosis. It also reimburses for stenting in asymptomatic cases in patients at high risk with 80% or greater stenosis, but only if the patients are enrolled in ongoing clinical trials or registries.
CREST compared stenting with endarterectomy and provided important insights into each approach.1
BEFORE CREST
Endarterectomy is superior to medical therapy for symptomatic stenosis
First described in 1953, carotid endarterectomy became the most widely used invasive treatment for significant carotid stenosis.9 Several studies have described patient subsets that benefit from this procedure.
NASCET (the North American Symptomatic Carotid Endarterectomy Trial)10 assigned 2,226 patients with symptomatic stenosis (transient ischemic attack or stroke within the past 180 days) to medical management or endarterectomy.
Surgery was associated with a 65% lower rate of ipsilateral cerebral events in patients with 70% or greater stenosis.10 Surgery was also found to be superior in patients with moderate disease (50% to 69% stenosis), but the difference only approached statistical significance. In patients with stenosis of less than 50%, the outcomes were similar with endarterectomy and medical management.11
ECST (the European Carotid Surgery Trial)12 included a similar population of 3,024 patients. Those with high-grade disease (stenosis ≥ 80%) had significantly better outcomes with endarterectomy, but in those with stenosis less than 70%, surgery was no better than drug therapy.
Comment. NASCET and ECST taught us that endarterectomy is clearly superior to medical therapy in patients with severe symptomatic carotid disease. However, both trials excluded patients at high surgical risk, eg, those with severe coronary artery disease, kidney disease, or heart failure. Additionally, medical management was not aggressive by today’s standards in terms of control of blood pressure and hyperlipidemia, and this could have skewed the results in favor of carotid endarterectomy.
The case for carotid endarterectomy for asymptomatic stenosis
Endarterectomy has also been compared with drug therapy for asymp tomatic carotid artery stenosis in several trials.13–15
ACAS (the Asymptomatic Carotid Atherosclerosis Study)15 assigned 1,662 patients who had no symptoms and had at least 60% carotid artery stenosis to endarterectomy or to medical management, and found a relative risk reduction of 53% in favor of surgery.15
The Veterans Affairs Cooperative Study Group14 corroborated these results in 444 patients with asymptomatic stenosis of greater than 50%. Endarterectomy was associated with a 61% lower risk of transient ischemic attack, transient monocular blindness, or stroke compared with medical therapy. However, there was no statistically significant difference in rates of stroke or death at 30 days.14
ACST (the Asymptomatic Carotid Surgery Trial),13 the largest study to compare carotid endarterectomy with drug therapy for asymptomatic stenosis, randomized 3,120 patients to surgery or drug therapy. The net 5-year risk of stroke was 6.4% with endarterectomy vs 11.8% with drug therapy (P < .0001). The rate of fatal stroke was also lower with endarterectomy: 2.1% vs 4.2% (P = .006).13
Comment. The results of these and other studies of endarterectomy vs medical therapy may not be applicable to current practice, since medical therapy has evolved and the risks with current drug therapy are likely much lower than seen in these trials, some of which began 2 decades ago. Another problem with interpreting these trials is that they excluded surgically “high-risk” patients, which limits the generalizability of the findings to this particular patient population.
The American Heart Association and the American Stroke Association have, on the basis of these trials, recommended carotid endarterectomy in patients with7,8,16:
Ipsilateral, symptomatic carotid artery stenosis of 70% to 99% (class I, level of evidence A)
Symptomatic stenosis of 50% to 69%, depending on patient-specific factors such as age, sex, and comorbidities
High-grade asymptomatic carotid stenosis, if the patients are carefully selected and the surgery is performed by surgeons with procedural morbidity and mortality rates of less than 3% (class I, level of evidence A).
In all cases, treatment should be individualized according to the patient’s comorbid conditions and preferences, with a thorough discussion of risks and benefits (Table 1).7,8,16
The case for percutaneous intervention
While carotid endarterectomy is proven to be more efficacious than medical management in certain patient subsets, studies favoring surgery over medical therapy have been criticized because they excluded patients with significant comorbidities. In addition, surgery has been associated with significant cardiovascular events, wound complications, and cranial nerve damage, and it requires general anesthesia in most cases.12,17–19 These and other factors spurred the development of less invasive, percutaneous approaches for patients with substantial comorbidities.
So far, several trials have investigated carotid angioplasty with or without stents and with or without devices to capture distal emboli. This interest set the stage for CREST.20,21
Initial attempts at angioplasty without distal protection were not very successful. A meta-analysis of nonrandomized trials that included 714 patients from the initial 13 studies of angioplasty (with or without stenting) and 6,970 patients from 20 studies of carotid endarterectomy found angioplasty to be possibly associated with higher rates of stroke within 30 days of the procedure.20
With improvements in technology, routine use of embolic protection devices, more experience, and better selection of patients, the outcome of carotid stenting has improved. In fact, a meta-analysis comparing stenting without an embolic protection device (26 trials with 2,357 patients) vs stenting with an embolic protection device (11 trials with 839 patients) showed that embolic protection led to significantly better outcomes with fewer strokes—outcomes arguably similar to those of carotid endarterectomy.21
SAPPHIRE (the Stenting and Angioplasty With Protection in Patients at High Risk for Endarterectomy trial)22 was the only completed US trial until CREST that compared carotid artery stenting with distal protection against surgery. It included 334 high-risk patients with either symptomatic stenosis of 50% or greater or asymptomatic stenosis of 80% or greater.
The results suggested that the outcomes with stenting with embolic protection were in fact similar to those of endarterectomy, with possibly fewer complications.23 The benefit persisted up to 2 years.22
The US Food and Drug Administration (FDA), on the basis of these data, approved the use of stenting with distal protection for high-risk patients, and the CMS reimburses for symptomatic stenosis of 50% or greater and for asymptomatic stenosis of 80% or greater as long as the patient is enrolled in a registry.
SPACE (the Stent-Protected Angioplasty Versus Carotid Endarterectomy in Symptomatic Patients trial),24 conducted in Germany, included 1,214 patients with symptomatic stenosis of at least 50%. Results were similar in terms of the combined primary end point of stroke or death at 30 days. However, the results were not similar enough to prove that stenting is not inferior to surgery, according to preset study criteria.
EVA-3S (the Endarterectomy Versus Stenting in Patients With Symptomatic Severe Carotid Stenosis trial),25 in France, evaluated 527 patients with symptomatic carotid disease (stenosis ≥ 60%), but was terminated early due to significantly higher rates of death or stroke at 30 days in the stenting group.
Comment. SPACE and EVA-3S have been widely criticized for not mandating the use of an embolic protection device (used in 27% of cases in SPACE and in 91.9% of cases in EVA-3S). Questions were also raised about the experience level of the operators who performed the carotid stenting: up to 39% of the primary operators involved in stent placement were trainees.26 Also, myocardial infarction (MI), an important complication of carotid endarterectomy, was not included in the primary end point.
ICSS (the International Carotid Stenting Study)27 compared stenting with endarterectomy in 1,713 patients with symptomatic carotid stenosis of greater than 50%. The primary end point was the rate of fatal or disabling stroke at 3 years.
An interim safety analysis at 120 days of follow-up showed the primary end point had occurred in 4.0% of stenting cases vs 3.2% of endarterectomy cases, a difference that was not statistically significant (hazard ratio [HR] 1.28, 95% confidence interval [CI] 0.77–2.11). However, the risk of any stroke was higher with stenting, with a rate of 7.7% vs 4.1% in the surgical group—a statistically significant difference (HR 1.92, 95% CI 1.27–2.89).
In a substudy of ICSS,28 the investigators corroborated these findings, using magnetic resonance imaging to evaluate for new ischemic brain lesions periprocedurally. They found more new ischemic brain lesions in patients who underwent stenting than in patients who underwent surgery—a statistically significant finding.
Comment. ICSS had limitations: eg, it included only patients with symptoms, and the training for the stenting procedure was not standardized. Furthermore, the use of embolic protection devices was not mandated in stenting procedures.
Because of the controversial and incongruous findings of the above trials, there has been much anticipation for further large, appropriately conducted, randomized controlled trials such as CREST.
CREST STUDY DESIGN
CREST was a prospective, multicenter randomized controlled trial with blinded end point adjudication. Assignment to stenting or surgery occurred in a one-to-one fashion, and patients were stratified by medical center and symptomatic status.
Conducted at 108 sites in the United States and nine sites in Canada, CREST was supported by a grant from the National Institutes of Health and by the manufacturer of the catheter and stent delivery and embolic protection systems. The manufacturer’s representative held a nonvoting position on the executive committee and reviewed the manuscript of the results before submission.
CREST included patients with or without symptoms
CREST was initially designed to compare carotid artery stenting vs carotid endarterectomy in patients with symptoms, but enrollment was later extended to patients without symptoms.
Patients with symptoms were included if they had stenosis of at least 50% on angiography, at least 70% on ultrasonography, or at least 70% on computed tomographic angiography or magnetic resonance angiography if stenosis on ultrasonography was 50% to 69%. Carotid artery stenosis was considered symptomatic if the patient had a transient ischemic attack, amaurosis fugax, or minor disabling stroke in the hemisphere supplied by the target vessel within 180 days of randomization.
Patients without symptoms were eligible if they had at least 60% stenosis on angiography, at least 70% stenosis on ultrasonography, or at least 80% stenosis on computed tomographic angiography or magnetic resonance angiography if the stenosis was 50% to 69% on ultrasonography.
Other eligibility criteria included favorable anatomy and clinical stability for both stenting and surgical procedures.
Exclusion criteria were evolving stroke, history of major stroke, chronic or paroxysmal atrial fibrillation on anticoagulation therapy, MI within the previous 30 days, and unstable angina.
Patients received antiplatelet agents
Patients undergoing stenting received aspirin and clopidogrel (Plavix) before and up to 30 days after the procedure. Continuation of antiplatelet therapy was recommended beyond 1 month.
Patients undergoing endarterectomy received aspirin before surgery and continued to receive aspirin for at least 1 year.
Alternatives to aspirin in both groups were ticlopidine (Ticlid), clopidogrel, or aspirin with extended-release dipyridamole (Aggrenox).
End points: Stroke, MI, death
The primary end point was a composite of periprocedural clinical stroke (any type), MI, or death, and of ipsilateral stroke up to 4 years after the procedure. Secondary analyses were also planned for evaluation of treatment modification by age, symptom status, and sex.
Stroke was defined as any acute neurologic ischemic event lasting at least 24 hours with focal signs and symptoms.
Two separate definitions were applied to distinguish major stroke from nonmajor stroke. Major stroke was defined as a National Institutes of Health Stroke Scale (NIHSS) score greater than 9 or records suggesting that the event was a disabling stroke if admitted to another facility. Nonmajor stroke included an event that did not fit these criteria. The stroke review process was initiated with a significant neurologic event, a positive transient ischemia attack or stroke questionnaire, or a two-point or greater increase in the NIHSS score.
MI was defined as a combination of an elevation of cardiac enzymes to at least twice the laboratory upper limit of normal, as well as clinical signs suggesting MI or electrocardiographic evidence of ischemia.29
Stroke was adjudicated by two independent neurologists, and MI was adjudicated by two independent cardiologists blinded to treatment group assignment.
The Rankin scale, the transient ischemic attack and stroke questionnaire, and the Medical Outcomes Survey were also used to assess for disability and quality of life in long-term follow-up.
Intention-to-treat analysis
Intention-to-treat survival analysis was used along with time-to-event statistical modeling with adjustment for major baseline covariates. Differences in outcomes were assessed, and a noninferiority analysis was performed. Kaplan-Meier estimates were constructed of the proportion of patients remaining free of the composite end point at 30 days, 6 months, 1 year, and annually thereafter, and of the associated confidence intervals. The hazard ratios between groups were estimated after adjustment for important covariates.
Most patients enrolled were available for analysis
From December 2000 to July 2008, 2,522 patients were enrolled; 1,271 were assigned to stenting, and 1,251 were assigned to surgery. After randomization, 2.8% of the patients assigned to stenting withdrew consent, 5.7% underwent surgery, and 2.6% were lost to follow-up. Of those assigned to surgery, 5.1% withdrew consent, 1.0% underwent stenting, and 3.8% were lost to follow-up.
A ‘conventional-risk’ patient population
The trial sought to include a “conventional-risk” patient population to make the study more applicable to real-world practice. The mean age was 69 years in both groups. Of the 2,522 patients enrolled:
35% were women
47% had asymptomatic carotid disease
86% had carotid stenosis of 70% or greater
86% had hypertension
30% had diabetes mellitus
83% had hyperlipidemia
26% were current smokers
42% had a history of cardiovascular disease
21% had undergone coronary artery bypass grafting surgery.
The only statistically significant difference in measured baseline variables between the two treatment groups was a slightly higher rate of dyslipidemia in the group undergoing surgery.
The interventionalists and surgeons were highly experienced
Operators performing stenting underwent a lead-in phase of training, with close supervision and scrutiny before eligibility. Of patients undergoing stenting, 96.1% also received an embolic protection device. Antiplatelet therapy was continued in 99% of the patients.
The surgeons performing endarterectomy were experienced and had documented low complication rates. General anesthesia was used in 90% of surgical patients. Shunts were used during surgery in 57%, and patches were used in 62%. After endarterectomy, 91% of the patients received antiplatelet therapy.
CREST STUDY RESULTS: STENTING WAS AS GOOD AS SURGERY
Periprocedural outcomes
Stroke, MI, or death: 5.2% with stenting vs 4.5% with surgery, HR 1.18, 95% CI 0.82–1.68, P = .38
Stroke: 4.1% vs 2.3%, HR 1.79, 95% CI 1.14–2.82, P = .01
Major ipsilateral stroke: 0.9% vs 0.3%, HR 2.67, 95% CI 0.85–8.40, P = .09.
MI: 1.1% vs 2.3%, HR 0.50, 95% CI 0.26–0.94, P = .03
Cranial nerve palsy: 0.3% vs 4.8%, HR 0.07, 95% CI 0.02–0.18, P < .0001 (Table 2).
Outcomes at 4 years
Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.
Figure 2. Kaplan-Meier analysis of the primary outcome (stroke, myocardial infarction, or death during the periprocedural period or any ipsilateral stroke within 4 years after randomization) for patients undergoing carotid artery stenting or carotid endarterectomy.
The primary end point (periprocedural stroke, MI, or death, or ipsilateral stroke within 4 years after the procedure): 7.2% with stenting vs 6.8% with surgery, HR 1.11, 95% CI 0.81–1.51, P = .51. A Kaplan-Meier analysis showed similar findings with statistically similar outcomes (Figure 2).
Ipsilateral stroke: 2.0% vs 2.4%, HR 0.94, 95% CI 0.50–1.76, P = .85.
The primary outcome was analyzed for interactions of baseline variables, and no effect was detected for symptomatic status or sex. There was a suggestion of an interaction with age, with older patients (over age 70) benefiting more from endarterectomy.
Quality-of-life indices showed that both major and minor strokes were likely to produce long-term physical limitations, with minor stroke associated with worse mental and physical health at 1 year. The effect of periprocedural MI on long-term physical and mental health was less certain. The increased incidence of cranial nerve palsy noted with endarterectomy has been found before and has had no effect on quality of life.
WHAT DO THE CREST FINDINGS MEAN?
CREST is the largest trial to date to compare stenting and surgery. It is an important addition to the literature, not only because of its size, but also because it focused on a real-world patient population. For this reason, its results are more applicable to patients seen in primary care clinics, ie, with peripheral vascular disease, coronary artery disease, diabetes mellitus, hypertension, and smoking.
As noted, previous studies of endarterectomy had strict inclusion and exclusion criteria, which selected against patients at high surgical risk. Therefore, the CREST findings are of greater relevance when comparing stenting and endarterectomy.
Periprocedural and long-term neurologic outcomes
CREST showed similar findings for the composite end point of periprocedural stroke, death, or MI (ie, within 30 days of the procedure) and long-term stroke, establishing similar outcomes in patients undergoing stenting and surgery.
However, an analysis of the individual components of the composite end point showed significant differences between the two treatments. The risk of ipsilateral periprocedural stroke was higher with stenting; these events were defined as nonmajor by NIHSS criteria. The risk of contralateral stroke was similar and low with each treatment.
While the increased risk of periprocedural ipsilateral stroke was not synonymous with an increased risk of major stroke, post hoc analysis showed that any stroke was associated with decreased physical and mental health at 1 year. Therefore, patients who had even a minor stroke did worse from a physical and mental standpoint, a finding that argues for the superiority of surgery in selected patients at risk of periprocedural stroke.
If periprocedural stroke is excluded, the risk of long-term ipsilateral stroke was similar for each treatment, and extremely low (2% for stenting, 2.4% for surgery). Despite this, given the importance of periprocedural minor and major stroke, better predictive models are needed to identify patients at risk of procedural neurologic events. These prediction models will allow better patient selection.
The CREST data and medical therapy
The rates of stroke in this trial were similar to those observed with current medical treatment (approximately 1% per year), especially for patients with asymptomatic disease. Such findings introduce fresh controversy in the necessity of performing either procedure for this patient subset and may lead to further studies evaluating current medical therapy vs intervention.
Periprocedural myocardial infarction
Vascular surgery has long been associated with high cardiovascular risk, especially an increased risk of periprocedural MI.30 Findings from CREST provide further evidence of the risk of MI with endarterectomy in a real-world patient population. Given the evidence of a strong correlation between periprocedural cardiac enzyme elevations and adverse outcomes, the increased incidence of periprocedural MI is worrisome.31 As with risk assessment for periprocedural stroke, better predictive models are needed for patients at risk of cardiovascular events during endarterectomy.
Procedural complications
Carotid endarterectomy entails incisions in the neck with disruption of tissue planes, as opposed to catheter entry site wounds with stenting. The more invasive nature of endarterectomy thus carries a higher risk of wound complications. In fact, in the NASCET trial, the risk of wound complications was 9.3%.10,19 In CREST, surgery carried a higher risk of wound complications compared with stenting (42 vs 0 cases), although stenting involved more periprocedural transfusions, presumably due to retroperitoneal bleeding in four patients.
Use of general anesthesia is also associated with adverse outcomes.17,18 In CREST, 90% of endarterectomy procedures required general anesthesia, whereas none of the stenting procedures required this.
Cranial nerve palsy is an often overlooked but real complication after these procedures. Cranial nerve palsies can lead to vocal, swallowing, and sensory problems that can have a transient or permanent impact on quality of life. In CREST, as in EVA-3S, SAPPHIRE, and ICSS, this risk was substantially higher with surgery,23,25,27 although the long-term consequences of these palsies were not found to affect quality of life at 1 year of follow-up.
HOW CREST FINDINGS COMPARE WITH PREVIOUS STUDIES
Patients in CREST enjoyed overall better outcomes than in previous studies. In earlier trials of surgery vs medical therapy, the rates of adverse outcomes were higher than in CREST. In NASCET, the risk of ipsilateral stroke was 9% with surgery, with 2.5% being fatal or disabling strokes.10 In the ECST, rates of major stroke or death with endarterectomy were 7.0% within 30 days of surgery and 37.0% at a mean follow-up of 6.1 years.12
In earlier studies of surgery vs stenting, outcomes at 30 days were also substantially worse than those in CREST. In the EVA-3S trial, the 30-day incidence of stroke or death was 3.9% after surgery and 9.6% after stenting. These findings were similar at 6 months in EVA-3S, with a 6.1% rate of adverse events after surgery and 11.7% after stenting.25 In the SAPPHIRE trial, the cumulative incidence of stroke and death at 1 year was 21.4% for surgery and 13.6% for stenting.23
Overall, the CREST results show better outcomes than in previous trials. This may be due to improvements in technical aspects of the interventions and to more aggressive drug therapy. Also, because of the high number of patients enrolled in CREST, surgeons and interventionalists were required to meet eligibility criteria, which could have contributed to the improved outcomes.32
CREST was also unique in that stenting was done with an embolic protection device whenever possible, and this also likely had an impact on outcomes.
The CREST data suggest that interventions for carotid artery stenosis should only be performed by rigorously trained, experienced personnel at high-volume centers, as this provided lower event rates compared with previous studies. Additional data should also help identify those at risk of periprocedural stroke and MI, thereby helping to match the patient to the most appropriate procedure. The pros and cons of surgery and stenting are shown in Table 3.1,10,23,25,27
CREST vs ICSS
CREST and ICSS, published within a few months of each other, seem to have arrived at entirely different conclusions. As both studies are well-designed randomized controlled trials, these distinct results have yielded much controversy. However, closer scrutiny sheds light as to why the results may be different.
While ICSS focused only on patients with symptoms, CREST also included those without symptoms. The difference in patient populations is itself enough to account for the different outcomes.
Also, the interim analysis of ICSS was at 120 days, which makes periprocedural events a more dominant factor in outcomes, whereas these events likely do not last into the long term, as was the case in CREST. Analysis of the ICSS data at a later follow-up date may show results more similar to those of CREST.
The design of ICSS was also different than CREST. In ICSS, the use of an embolic protection device in stenting was not mandated, and the study lacked a lead-in phase of intensive training for those performing stenting. Furthermore, MI was adjudicated only when clinically recognized, which is different than the more rigorous method used in CREST.
Yet despite these differences, CREST and ICSS shed light on a controversial area of carotid stenosis management, and both studies boasted low rates of periprocedural complications. Clinicians should keep in mind the inclusion criteria and the technical specificities of these trials in order to explain to patients the risks and benefits of stenting and surgery, and to arrive at a decision together.
Limitations
The results of CREST should also be reviewed carefully due to a number of limitations. The study began in 2000 with symptomatic patients only, and began enrolling asymptomatic patients in 2005, so that the methodology of the study was changed midway. However, the investigators performed a subgroup analysis to distinguish between outcomes of the symptomatic and the asymptomatic groups and found no statistical interaction for the primary end point based on symptom status.
Despite careful patient selection, many of the predictors of adverse outcomes with stenting, such as lesion length, level of calcification, and lesion location, were not accounted for in the earlier days of enrollment. This may have had an impact on the incidence of stroke in patients enrolled in the early years of the trial. We await the analysis of predictors of perioperative stroke from CREST.
TAKE-HOME POINTS AND FUTURE DIRECTIONS
The CREST findings show that outcomes with stenting are similar to those with surgery in both the short term and the long term, and that the choice of management should be individualized. Each patient’s risk of MI and stroke should be considered based on a variety of factors, including the severity of coronary artery disease, the length of the carotid lesion, the level of calcification, the location of the lesion, and aortic atheroma. The treatment should be selected after also taking into account the patient’s preference and the available expertise, and only after a comprehensive discussion with the patient.
References
Brott TG, Hobson RW, Howard G, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med2010; 363:11–23.
Thom T, Haase N, Rosamond W, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation2006; 113:e85–e151.
Rosamond WD, Folsom AR, Chambless LE, et al. Stroke incidence and survival among middle-aged adults: 9-year follow-up of the Atherosclerosis Risk in Communities (ARIC) cohort. Stroke1999; 30:736–743.
Chaturvedi S, Bruno A, Feasby T, et al; Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Carotid endarterectomy—an evidence-based review: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology2005; 65:794–801.
Howell GM, Makaroun MS, Chaer RA. Current management of extracranial carotid occlusive disease. J Am Coll Surg2009; 208:442–453.
Barnett HJ, Gunton RW, Eliasziw M, et al. Causes and severity of ischemic stroke in patients with internal carotid artery stenosis. JAMA2000; 283:1429–1436.
Biller J, Feinberg WM, Castaldo JE, et al. Guidelines for carotid endarterectomy: a statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation1998; 97:501–509.
Goldstein LB, Adams R, Alberts MJ, et al; American Heart Association; American Stroke Association Stroke Council. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council: cosponsored by the Atherosclerotic Peripheral Vascular Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation2006; 113:e873–e923.
Strully KJ, Hurwitt ES, Blankenberg HW. Thrombo-endarterectomy for thrombosis of the internal carotid artery in the neck. J Neurosurg1953; 10:474–482.
Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1991; 325:445–453.
Barnett HJ, Taylor DW, Eliasziw M, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1998; 339:1415–1425.
Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet1998; 351:1379–1387.
Halliday A, Mansfield A, Marro J, et al; MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet2004; 363:1491–1502.
Hobson RW, Weiss DG, Fields WS, et al. Efficacy of carotid endarterectomy for asymptomatic carotid stenosis. The Veterans Affairs Cooperative Study Group. N Engl J Med1993; 328:221–227.
Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA1995; 273:1421–1428.
Sacco RL, Adams R, Albers G, et al; American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention: the American Academy of Neurology affirms the value of this guideline. Circulation2006; 113:e409–e449.
Watts K, Lin PH, Bush RL, et al. The impact of anesthetic modality on the outcome of carotid endarterectomy. Am J Surg2004; 188:741–747.
Weber CF, Friedl H, Hueppe M, et al. Impact of general versus local anesthesia on early postoperative cognitive dysfunction following carotid endarterectomy: GALA Study Subgroup Analysis. World J Surg2009; 33:1526–1532.
Ferguson GG, Eliasziw M, Barr HW, et al. The North American Symptomatic Carotid Endarterectomy Trial: surgical results in 1415 patients. Stroke1999; 30:1751–1758.
Golledge J, Mitchell A, Greenhalgh RM, Davies AH. Systematic comparison of the early outcome of angioplasty and endarterectomy for symptomatic carotid artery disease. Stroke2000; 31:1439–1443.
Kastrup A, Gröschel K, Krapf H, Brehm BR, Dichgans J, Schulz JB. Early outcome of carotid angioplasty and stenting with and without cerebral protection devices: a systematic review of the literature. Stroke2003; 34:813–819.
Gurm HS, Yadav JS, Fayad P, et al; SAPPHIRE Investigators. Long-term results of carotid stenting versus endarterectomy in high-risk patients. N Engl J Med2008; 358:1572–1579.
Yadav JS, Wholey MH, Kuntz RE, et al; Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy Investigators. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med2004; 351:1493–1501.
Eckstein HH, Ringleb P, Allenberg JR, et al. Results of the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: a multinational, prospective, randomised trial. Lancet Neurol2008; 7:893–902.
Mas JL, Chatellier G, Beyssen B, et al; EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med2006; 355:1660–1771.
Roffi M, Sievert H, Gray WA, et al. Carotid artery stenting versus surgery: adequate comparisons?Lancet Neurol2010; 9:339–341.
International Carotid Stenting Study Investigators; Ederle J, Dobson J, Featherstone RL, et al. Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International Carotid Stenting Study): an interim analysis of a randomised controlled trial. Lancet2010; 375:985–997.
Bonati LH, Jongen LM, Haller S, et al; ICSS-MRI study group. New ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid stenosis: a sub-study of the International Carotid Stenting Study (ICSS). Lancet Neurol2010; 9:353–362.
Sheffet AJ, Roubin G, Howard G, et al. Design of the Carotid Revascularization Endarterectomy vs. Stenting Trial (CREST). Int J Stroke2010; 5:40–46.
Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery) developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. J Am Coll Cardiol2007; 50:e159–e241.
Bhatt DL, Topol EJ. Does creatinine kinase-MB elevation after percutaneous coronary intervention predict outcomes in 2005? Periprocedural cardiac enzyme elevation predicts adverse outcomes. Circulation2005; 112:906–915.
Hobson RW, Howard VJ, Roubin GS, et al; CREST. Credentialing of surgeons as interventionalists for carotid artery stenting: experience from the lead-in phase of CREST. J Vasc Surg2004; 40:952–957.
Olcay Aksoy, MD Department of Cardiovascular Medicine, Cleveland Clinic
Samir R. Kapadia, MD Department of Cardiovascular Medicine, Cleveland Clinic
Christopher Bajzer, MD Department of Cardiovascular Medicine, Cleveland Clinic
Wayne M. Clark, MD Department of Neurology, Oregon Health & Science University, Portland; Investigator, Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)
Mehdi H. Shishehbor, DO, MPH, PhD Department of Cardiovascular Medicine, Cleveland Clinic
Address: Mehdi H. Shishehbor, DO, MPH, Heart & Vascular Institute, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail [email protected]
Dr. Shishehbor has disclosed teaching and speaking for Abbott Vascular.
Olcay Aksoy, MD Department of Cardiovascular Medicine, Cleveland Clinic
Samir R. Kapadia, MD Department of Cardiovascular Medicine, Cleveland Clinic
Christopher Bajzer, MD Department of Cardiovascular Medicine, Cleveland Clinic
Wayne M. Clark, MD Department of Neurology, Oregon Health & Science University, Portland; Investigator, Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)
Mehdi H. Shishehbor, DO, MPH, PhD Department of Cardiovascular Medicine, Cleveland Clinic
Address: Mehdi H. Shishehbor, DO, MPH, Heart & Vascular Institute, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail [email protected]
Dr. Shishehbor has disclosed teaching and speaking for Abbott Vascular.
Author and Disclosure Information
Olcay Aksoy, MD Department of Cardiovascular Medicine, Cleveland Clinic
Samir R. Kapadia, MD Department of Cardiovascular Medicine, Cleveland Clinic
Christopher Bajzer, MD Department of Cardiovascular Medicine, Cleveland Clinic
Wayne M. Clark, MD Department of Neurology, Oregon Health & Science University, Portland; Investigator, Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)
Mehdi H. Shishehbor, DO, MPH, PhD Department of Cardiovascular Medicine, Cleveland Clinic
Address: Mehdi H. Shishehbor, DO, MPH, Heart & Vascular Institute, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail [email protected]
Dr. Shishehbor has disclosed teaching and speaking for Abbott Vascular.
For patients with carotid artery stenosis, percutaneous intervention with stenting is as good as surgery (carotid endarterectomy). This was the major finding of the recently completed Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)1—with some qualifications.
CREST is the latest in a series of clinical trials of treatment of carotid stenosis that have generated reams of numbers and much debate. The topic of surgery vs percutaneous intervention is a moving target, as techniques evolve and improve. We believe the CREST results are valuable and should help inform decisions about treatment in the “real world.”
In this article, we offer a critical review of CREST, with a careful evaluation of its methods, results, and conclusions.
AN EVOLVING FIELD
Despite improvements in diagnosis and management, stroke remains one of the leading causes of morbidity and death in the United States, with an annual incidence of 780,000 cases and 270,000 deaths.2,3
Figure 1. Carotid endarterectomy has long been an established treatment in selected patients with symptomatic carotid artery stenosis of 50% or greater or asymptomatic stenosis of 60% or greater. However, percutaneous carotid artery angioplasty with stenting and placement of an embolic protection device is gaining ground as a reasonable, safe, less invasive alternative.
From 10% to 30% of ischemic strokes are due to emboli from the carotid arteries.4–6 Carotid endarterectomy is an established treatment in selected patients with symptomatic carotid stenosis of 50% or greater or asymptomatic stenosis of 60% or greater.7,8 However, percutaneous techniques such as carotid artery angioplasty with stenting have improved, making them a viable, less invasive option (Figure 1).
Randomized trials of stenting have had mixed results, leading the Centers for Medicare and Medicaid Services (CMS) to adopt strict reimbursement policies. Currently, CMS reimburses for stenting only in symptomatic cases with at least 50% carotid artery stenosis. It also reimburses for stenting in asymptomatic cases in patients at high risk with 80% or greater stenosis, but only if the patients are enrolled in ongoing clinical trials or registries.
CREST compared stenting with endarterectomy and provided important insights into each approach.1
BEFORE CREST
Endarterectomy is superior to medical therapy for symptomatic stenosis
First described in 1953, carotid endarterectomy became the most widely used invasive treatment for significant carotid stenosis.9 Several studies have described patient subsets that benefit from this procedure.
NASCET (the North American Symptomatic Carotid Endarterectomy Trial)10 assigned 2,226 patients with symptomatic stenosis (transient ischemic attack or stroke within the past 180 days) to medical management or endarterectomy.
Surgery was associated with a 65% lower rate of ipsilateral cerebral events in patients with 70% or greater stenosis.10 Surgery was also found to be superior in patients with moderate disease (50% to 69% stenosis), but the difference only approached statistical significance. In patients with stenosis of less than 50%, the outcomes were similar with endarterectomy and medical management.11
ECST (the European Carotid Surgery Trial)12 included a similar population of 3,024 patients. Those with high-grade disease (stenosis ≥ 80%) had significantly better outcomes with endarterectomy, but in those with stenosis less than 70%, surgery was no better than drug therapy.
Comment. NASCET and ECST taught us that endarterectomy is clearly superior to medical therapy in patients with severe symptomatic carotid disease. However, both trials excluded patients at high surgical risk, eg, those with severe coronary artery disease, kidney disease, or heart failure. Additionally, medical management was not aggressive by today’s standards in terms of control of blood pressure and hyperlipidemia, and this could have skewed the results in favor of carotid endarterectomy.
The case for carotid endarterectomy for asymptomatic stenosis
Endarterectomy has also been compared with drug therapy for asymp tomatic carotid artery stenosis in several trials.13–15
ACAS (the Asymptomatic Carotid Atherosclerosis Study)15 assigned 1,662 patients who had no symptoms and had at least 60% carotid artery stenosis to endarterectomy or to medical management, and found a relative risk reduction of 53% in favor of surgery.15
The Veterans Affairs Cooperative Study Group14 corroborated these results in 444 patients with asymptomatic stenosis of greater than 50%. Endarterectomy was associated with a 61% lower risk of transient ischemic attack, transient monocular blindness, or stroke compared with medical therapy. However, there was no statistically significant difference in rates of stroke or death at 30 days.14
ACST (the Asymptomatic Carotid Surgery Trial),13 the largest study to compare carotid endarterectomy with drug therapy for asymptomatic stenosis, randomized 3,120 patients to surgery or drug therapy. The net 5-year risk of stroke was 6.4% with endarterectomy vs 11.8% with drug therapy (P < .0001). The rate of fatal stroke was also lower with endarterectomy: 2.1% vs 4.2% (P = .006).13
Comment. The results of these and other studies of endarterectomy vs medical therapy may not be applicable to current practice, since medical therapy has evolved and the risks with current drug therapy are likely much lower than seen in these trials, some of which began 2 decades ago. Another problem with interpreting these trials is that they excluded surgically “high-risk” patients, which limits the generalizability of the findings to this particular patient population.
The American Heart Association and the American Stroke Association have, on the basis of these trials, recommended carotid endarterectomy in patients with7,8,16:
Ipsilateral, symptomatic carotid artery stenosis of 70% to 99% (class I, level of evidence A)
Symptomatic stenosis of 50% to 69%, depending on patient-specific factors such as age, sex, and comorbidities
High-grade asymptomatic carotid stenosis, if the patients are carefully selected and the surgery is performed by surgeons with procedural morbidity and mortality rates of less than 3% (class I, level of evidence A).
In all cases, treatment should be individualized according to the patient’s comorbid conditions and preferences, with a thorough discussion of risks and benefits (Table 1).7,8,16
The case for percutaneous intervention
While carotid endarterectomy is proven to be more efficacious than medical management in certain patient subsets, studies favoring surgery over medical therapy have been criticized because they excluded patients with significant comorbidities. In addition, surgery has been associated with significant cardiovascular events, wound complications, and cranial nerve damage, and it requires general anesthesia in most cases.12,17–19 These and other factors spurred the development of less invasive, percutaneous approaches for patients with substantial comorbidities.
So far, several trials have investigated carotid angioplasty with or without stents and with or without devices to capture distal emboli. This interest set the stage for CREST.20,21
Initial attempts at angioplasty without distal protection were not very successful. A meta-analysis of nonrandomized trials that included 714 patients from the initial 13 studies of angioplasty (with or without stenting) and 6,970 patients from 20 studies of carotid endarterectomy found angioplasty to be possibly associated with higher rates of stroke within 30 days of the procedure.20
With improvements in technology, routine use of embolic protection devices, more experience, and better selection of patients, the outcome of carotid stenting has improved. In fact, a meta-analysis comparing stenting without an embolic protection device (26 trials with 2,357 patients) vs stenting with an embolic protection device (11 trials with 839 patients) showed that embolic protection led to significantly better outcomes with fewer strokes—outcomes arguably similar to those of carotid endarterectomy.21
SAPPHIRE (the Stenting and Angioplasty With Protection in Patients at High Risk for Endarterectomy trial)22 was the only completed US trial until CREST that compared carotid artery stenting with distal protection against surgery. It included 334 high-risk patients with either symptomatic stenosis of 50% or greater or asymptomatic stenosis of 80% or greater.
The results suggested that the outcomes with stenting with embolic protection were in fact similar to those of endarterectomy, with possibly fewer complications.23 The benefit persisted up to 2 years.22
The US Food and Drug Administration (FDA), on the basis of these data, approved the use of stenting with distal protection for high-risk patients, and the CMS reimburses for symptomatic stenosis of 50% or greater and for asymptomatic stenosis of 80% or greater as long as the patient is enrolled in a registry.
SPACE (the Stent-Protected Angioplasty Versus Carotid Endarterectomy in Symptomatic Patients trial),24 conducted in Germany, included 1,214 patients with symptomatic stenosis of at least 50%. Results were similar in terms of the combined primary end point of stroke or death at 30 days. However, the results were not similar enough to prove that stenting is not inferior to surgery, according to preset study criteria.
EVA-3S (the Endarterectomy Versus Stenting in Patients With Symptomatic Severe Carotid Stenosis trial),25 in France, evaluated 527 patients with symptomatic carotid disease (stenosis ≥ 60%), but was terminated early due to significantly higher rates of death or stroke at 30 days in the stenting group.
Comment. SPACE and EVA-3S have been widely criticized for not mandating the use of an embolic protection device (used in 27% of cases in SPACE and in 91.9% of cases in EVA-3S). Questions were also raised about the experience level of the operators who performed the carotid stenting: up to 39% of the primary operators involved in stent placement were trainees.26 Also, myocardial infarction (MI), an important complication of carotid endarterectomy, was not included in the primary end point.
ICSS (the International Carotid Stenting Study)27 compared stenting with endarterectomy in 1,713 patients with symptomatic carotid stenosis of greater than 50%. The primary end point was the rate of fatal or disabling stroke at 3 years.
An interim safety analysis at 120 days of follow-up showed the primary end point had occurred in 4.0% of stenting cases vs 3.2% of endarterectomy cases, a difference that was not statistically significant (hazard ratio [HR] 1.28, 95% confidence interval [CI] 0.77–2.11). However, the risk of any stroke was higher with stenting, with a rate of 7.7% vs 4.1% in the surgical group—a statistically significant difference (HR 1.92, 95% CI 1.27–2.89).
In a substudy of ICSS,28 the investigators corroborated these findings, using magnetic resonance imaging to evaluate for new ischemic brain lesions periprocedurally. They found more new ischemic brain lesions in patients who underwent stenting than in patients who underwent surgery—a statistically significant finding.
Comment. ICSS had limitations: eg, it included only patients with symptoms, and the training for the stenting procedure was not standardized. Furthermore, the use of embolic protection devices was not mandated in stenting procedures.
Because of the controversial and incongruous findings of the above trials, there has been much anticipation for further large, appropriately conducted, randomized controlled trials such as CREST.
CREST STUDY DESIGN
CREST was a prospective, multicenter randomized controlled trial with blinded end point adjudication. Assignment to stenting or surgery occurred in a one-to-one fashion, and patients were stratified by medical center and symptomatic status.
Conducted at 108 sites in the United States and nine sites in Canada, CREST was supported by a grant from the National Institutes of Health and by the manufacturer of the catheter and stent delivery and embolic protection systems. The manufacturer’s representative held a nonvoting position on the executive committee and reviewed the manuscript of the results before submission.
CREST included patients with or without symptoms
CREST was initially designed to compare carotid artery stenting vs carotid endarterectomy in patients with symptoms, but enrollment was later extended to patients without symptoms.
Patients with symptoms were included if they had stenosis of at least 50% on angiography, at least 70% on ultrasonography, or at least 70% on computed tomographic angiography or magnetic resonance angiography if stenosis on ultrasonography was 50% to 69%. Carotid artery stenosis was considered symptomatic if the patient had a transient ischemic attack, amaurosis fugax, or minor disabling stroke in the hemisphere supplied by the target vessel within 180 days of randomization.
Patients without symptoms were eligible if they had at least 60% stenosis on angiography, at least 70% stenosis on ultrasonography, or at least 80% stenosis on computed tomographic angiography or magnetic resonance angiography if the stenosis was 50% to 69% on ultrasonography.
Other eligibility criteria included favorable anatomy and clinical stability for both stenting and surgical procedures.
Exclusion criteria were evolving stroke, history of major stroke, chronic or paroxysmal atrial fibrillation on anticoagulation therapy, MI within the previous 30 days, and unstable angina.
Patients received antiplatelet agents
Patients undergoing stenting received aspirin and clopidogrel (Plavix) before and up to 30 days after the procedure. Continuation of antiplatelet therapy was recommended beyond 1 month.
Patients undergoing endarterectomy received aspirin before surgery and continued to receive aspirin for at least 1 year.
Alternatives to aspirin in both groups were ticlopidine (Ticlid), clopidogrel, or aspirin with extended-release dipyridamole (Aggrenox).
End points: Stroke, MI, death
The primary end point was a composite of periprocedural clinical stroke (any type), MI, or death, and of ipsilateral stroke up to 4 years after the procedure. Secondary analyses were also planned for evaluation of treatment modification by age, symptom status, and sex.
Stroke was defined as any acute neurologic ischemic event lasting at least 24 hours with focal signs and symptoms.
Two separate definitions were applied to distinguish major stroke from nonmajor stroke. Major stroke was defined as a National Institutes of Health Stroke Scale (NIHSS) score greater than 9 or records suggesting that the event was a disabling stroke if admitted to another facility. Nonmajor stroke included an event that did not fit these criteria. The stroke review process was initiated with a significant neurologic event, a positive transient ischemia attack or stroke questionnaire, or a two-point or greater increase in the NIHSS score.
MI was defined as a combination of an elevation of cardiac enzymes to at least twice the laboratory upper limit of normal, as well as clinical signs suggesting MI or electrocardiographic evidence of ischemia.29
Stroke was adjudicated by two independent neurologists, and MI was adjudicated by two independent cardiologists blinded to treatment group assignment.
The Rankin scale, the transient ischemic attack and stroke questionnaire, and the Medical Outcomes Survey were also used to assess for disability and quality of life in long-term follow-up.
Intention-to-treat analysis
Intention-to-treat survival analysis was used along with time-to-event statistical modeling with adjustment for major baseline covariates. Differences in outcomes were assessed, and a noninferiority analysis was performed. Kaplan-Meier estimates were constructed of the proportion of patients remaining free of the composite end point at 30 days, 6 months, 1 year, and annually thereafter, and of the associated confidence intervals. The hazard ratios between groups were estimated after adjustment for important covariates.
Most patients enrolled were available for analysis
From December 2000 to July 2008, 2,522 patients were enrolled; 1,271 were assigned to stenting, and 1,251 were assigned to surgery. After randomization, 2.8% of the patients assigned to stenting withdrew consent, 5.7% underwent surgery, and 2.6% were lost to follow-up. Of those assigned to surgery, 5.1% withdrew consent, 1.0% underwent stenting, and 3.8% were lost to follow-up.
A ‘conventional-risk’ patient population
The trial sought to include a “conventional-risk” patient population to make the study more applicable to real-world practice. The mean age was 69 years in both groups. Of the 2,522 patients enrolled:
35% were women
47% had asymptomatic carotid disease
86% had carotid stenosis of 70% or greater
86% had hypertension
30% had diabetes mellitus
83% had hyperlipidemia
26% were current smokers
42% had a history of cardiovascular disease
21% had undergone coronary artery bypass grafting surgery.
The only statistically significant difference in measured baseline variables between the two treatment groups was a slightly higher rate of dyslipidemia in the group undergoing surgery.
The interventionalists and surgeons were highly experienced
Operators performing stenting underwent a lead-in phase of training, with close supervision and scrutiny before eligibility. Of patients undergoing stenting, 96.1% also received an embolic protection device. Antiplatelet therapy was continued in 99% of the patients.
The surgeons performing endarterectomy were experienced and had documented low complication rates. General anesthesia was used in 90% of surgical patients. Shunts were used during surgery in 57%, and patches were used in 62%. After endarterectomy, 91% of the patients received antiplatelet therapy.
CREST STUDY RESULTS: STENTING WAS AS GOOD AS SURGERY
Periprocedural outcomes
Stroke, MI, or death: 5.2% with stenting vs 4.5% with surgery, HR 1.18, 95% CI 0.82–1.68, P = .38
Stroke: 4.1% vs 2.3%, HR 1.79, 95% CI 1.14–2.82, P = .01
Major ipsilateral stroke: 0.9% vs 0.3%, HR 2.67, 95% CI 0.85–8.40, P = .09.
MI: 1.1% vs 2.3%, HR 0.50, 95% CI 0.26–0.94, P = .03
Cranial nerve palsy: 0.3% vs 4.8%, HR 0.07, 95% CI 0.02–0.18, P < .0001 (Table 2).
Outcomes at 4 years
Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.
Figure 2. Kaplan-Meier analysis of the primary outcome (stroke, myocardial infarction, or death during the periprocedural period or any ipsilateral stroke within 4 years after randomization) for patients undergoing carotid artery stenting or carotid endarterectomy.
The primary end point (periprocedural stroke, MI, or death, or ipsilateral stroke within 4 years after the procedure): 7.2% with stenting vs 6.8% with surgery, HR 1.11, 95% CI 0.81–1.51, P = .51. A Kaplan-Meier analysis showed similar findings with statistically similar outcomes (Figure 2).
Ipsilateral stroke: 2.0% vs 2.4%, HR 0.94, 95% CI 0.50–1.76, P = .85.
The primary outcome was analyzed for interactions of baseline variables, and no effect was detected for symptomatic status or sex. There was a suggestion of an interaction with age, with older patients (over age 70) benefiting more from endarterectomy.
Quality-of-life indices showed that both major and minor strokes were likely to produce long-term physical limitations, with minor stroke associated with worse mental and physical health at 1 year. The effect of periprocedural MI on long-term physical and mental health was less certain. The increased incidence of cranial nerve palsy noted with endarterectomy has been found before and has had no effect on quality of life.
WHAT DO THE CREST FINDINGS MEAN?
CREST is the largest trial to date to compare stenting and surgery. It is an important addition to the literature, not only because of its size, but also because it focused on a real-world patient population. For this reason, its results are more applicable to patients seen in primary care clinics, ie, with peripheral vascular disease, coronary artery disease, diabetes mellitus, hypertension, and smoking.
As noted, previous studies of endarterectomy had strict inclusion and exclusion criteria, which selected against patients at high surgical risk. Therefore, the CREST findings are of greater relevance when comparing stenting and endarterectomy.
Periprocedural and long-term neurologic outcomes
CREST showed similar findings for the composite end point of periprocedural stroke, death, or MI (ie, within 30 days of the procedure) and long-term stroke, establishing similar outcomes in patients undergoing stenting and surgery.
However, an analysis of the individual components of the composite end point showed significant differences between the two treatments. The risk of ipsilateral periprocedural stroke was higher with stenting; these events were defined as nonmajor by NIHSS criteria. The risk of contralateral stroke was similar and low with each treatment.
While the increased risk of periprocedural ipsilateral stroke was not synonymous with an increased risk of major stroke, post hoc analysis showed that any stroke was associated with decreased physical and mental health at 1 year. Therefore, patients who had even a minor stroke did worse from a physical and mental standpoint, a finding that argues for the superiority of surgery in selected patients at risk of periprocedural stroke.
If periprocedural stroke is excluded, the risk of long-term ipsilateral stroke was similar for each treatment, and extremely low (2% for stenting, 2.4% for surgery). Despite this, given the importance of periprocedural minor and major stroke, better predictive models are needed to identify patients at risk of procedural neurologic events. These prediction models will allow better patient selection.
The CREST data and medical therapy
The rates of stroke in this trial were similar to those observed with current medical treatment (approximately 1% per year), especially for patients with asymptomatic disease. Such findings introduce fresh controversy in the necessity of performing either procedure for this patient subset and may lead to further studies evaluating current medical therapy vs intervention.
Periprocedural myocardial infarction
Vascular surgery has long been associated with high cardiovascular risk, especially an increased risk of periprocedural MI.30 Findings from CREST provide further evidence of the risk of MI with endarterectomy in a real-world patient population. Given the evidence of a strong correlation between periprocedural cardiac enzyme elevations and adverse outcomes, the increased incidence of periprocedural MI is worrisome.31 As with risk assessment for periprocedural stroke, better predictive models are needed for patients at risk of cardiovascular events during endarterectomy.
Procedural complications
Carotid endarterectomy entails incisions in the neck with disruption of tissue planes, as opposed to catheter entry site wounds with stenting. The more invasive nature of endarterectomy thus carries a higher risk of wound complications. In fact, in the NASCET trial, the risk of wound complications was 9.3%.10,19 In CREST, surgery carried a higher risk of wound complications compared with stenting (42 vs 0 cases), although stenting involved more periprocedural transfusions, presumably due to retroperitoneal bleeding in four patients.
Use of general anesthesia is also associated with adverse outcomes.17,18 In CREST, 90% of endarterectomy procedures required general anesthesia, whereas none of the stenting procedures required this.
Cranial nerve palsy is an often overlooked but real complication after these procedures. Cranial nerve palsies can lead to vocal, swallowing, and sensory problems that can have a transient or permanent impact on quality of life. In CREST, as in EVA-3S, SAPPHIRE, and ICSS, this risk was substantially higher with surgery,23,25,27 although the long-term consequences of these palsies were not found to affect quality of life at 1 year of follow-up.
HOW CREST FINDINGS COMPARE WITH PREVIOUS STUDIES
Patients in CREST enjoyed overall better outcomes than in previous studies. In earlier trials of surgery vs medical therapy, the rates of adverse outcomes were higher than in CREST. In NASCET, the risk of ipsilateral stroke was 9% with surgery, with 2.5% being fatal or disabling strokes.10 In the ECST, rates of major stroke or death with endarterectomy were 7.0% within 30 days of surgery and 37.0% at a mean follow-up of 6.1 years.12
In earlier studies of surgery vs stenting, outcomes at 30 days were also substantially worse than those in CREST. In the EVA-3S trial, the 30-day incidence of stroke or death was 3.9% after surgery and 9.6% after stenting. These findings were similar at 6 months in EVA-3S, with a 6.1% rate of adverse events after surgery and 11.7% after stenting.25 In the SAPPHIRE trial, the cumulative incidence of stroke and death at 1 year was 21.4% for surgery and 13.6% for stenting.23
Overall, the CREST results show better outcomes than in previous trials. This may be due to improvements in technical aspects of the interventions and to more aggressive drug therapy. Also, because of the high number of patients enrolled in CREST, surgeons and interventionalists were required to meet eligibility criteria, which could have contributed to the improved outcomes.32
CREST was also unique in that stenting was done with an embolic protection device whenever possible, and this also likely had an impact on outcomes.
The CREST data suggest that interventions for carotid artery stenosis should only be performed by rigorously trained, experienced personnel at high-volume centers, as this provided lower event rates compared with previous studies. Additional data should also help identify those at risk of periprocedural stroke and MI, thereby helping to match the patient to the most appropriate procedure. The pros and cons of surgery and stenting are shown in Table 3.1,10,23,25,27
CREST vs ICSS
CREST and ICSS, published within a few months of each other, seem to have arrived at entirely different conclusions. As both studies are well-designed randomized controlled trials, these distinct results have yielded much controversy. However, closer scrutiny sheds light as to why the results may be different.
While ICSS focused only on patients with symptoms, CREST also included those without symptoms. The difference in patient populations is itself enough to account for the different outcomes.
Also, the interim analysis of ICSS was at 120 days, which makes periprocedural events a more dominant factor in outcomes, whereas these events likely do not last into the long term, as was the case in CREST. Analysis of the ICSS data at a later follow-up date may show results more similar to those of CREST.
The design of ICSS was also different than CREST. In ICSS, the use of an embolic protection device in stenting was not mandated, and the study lacked a lead-in phase of intensive training for those performing stenting. Furthermore, MI was adjudicated only when clinically recognized, which is different than the more rigorous method used in CREST.
Yet despite these differences, CREST and ICSS shed light on a controversial area of carotid stenosis management, and both studies boasted low rates of periprocedural complications. Clinicians should keep in mind the inclusion criteria and the technical specificities of these trials in order to explain to patients the risks and benefits of stenting and surgery, and to arrive at a decision together.
Limitations
The results of CREST should also be reviewed carefully due to a number of limitations. The study began in 2000 with symptomatic patients only, and began enrolling asymptomatic patients in 2005, so that the methodology of the study was changed midway. However, the investigators performed a subgroup analysis to distinguish between outcomes of the symptomatic and the asymptomatic groups and found no statistical interaction for the primary end point based on symptom status.
Despite careful patient selection, many of the predictors of adverse outcomes with stenting, such as lesion length, level of calcification, and lesion location, were not accounted for in the earlier days of enrollment. This may have had an impact on the incidence of stroke in patients enrolled in the early years of the trial. We await the analysis of predictors of perioperative stroke from CREST.
TAKE-HOME POINTS AND FUTURE DIRECTIONS
The CREST findings show that outcomes with stenting are similar to those with surgery in both the short term and the long term, and that the choice of management should be individualized. Each patient’s risk of MI and stroke should be considered based on a variety of factors, including the severity of coronary artery disease, the length of the carotid lesion, the level of calcification, the location of the lesion, and aortic atheroma. The treatment should be selected after also taking into account the patient’s preference and the available expertise, and only after a comprehensive discussion with the patient.
For patients with carotid artery stenosis, percutaneous intervention with stenting is as good as surgery (carotid endarterectomy). This was the major finding of the recently completed Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)1—with some qualifications.
CREST is the latest in a series of clinical trials of treatment of carotid stenosis that have generated reams of numbers and much debate. The topic of surgery vs percutaneous intervention is a moving target, as techniques evolve and improve. We believe the CREST results are valuable and should help inform decisions about treatment in the “real world.”
In this article, we offer a critical review of CREST, with a careful evaluation of its methods, results, and conclusions.
AN EVOLVING FIELD
Despite improvements in diagnosis and management, stroke remains one of the leading causes of morbidity and death in the United States, with an annual incidence of 780,000 cases and 270,000 deaths.2,3
Figure 1. Carotid endarterectomy has long been an established treatment in selected patients with symptomatic carotid artery stenosis of 50% or greater or asymptomatic stenosis of 60% or greater. However, percutaneous carotid artery angioplasty with stenting and placement of an embolic protection device is gaining ground as a reasonable, safe, less invasive alternative.
From 10% to 30% of ischemic strokes are due to emboli from the carotid arteries.4–6 Carotid endarterectomy is an established treatment in selected patients with symptomatic carotid stenosis of 50% or greater or asymptomatic stenosis of 60% or greater.7,8 However, percutaneous techniques such as carotid artery angioplasty with stenting have improved, making them a viable, less invasive option (Figure 1).
Randomized trials of stenting have had mixed results, leading the Centers for Medicare and Medicaid Services (CMS) to adopt strict reimbursement policies. Currently, CMS reimburses for stenting only in symptomatic cases with at least 50% carotid artery stenosis. It also reimburses for stenting in asymptomatic cases in patients at high risk with 80% or greater stenosis, but only if the patients are enrolled in ongoing clinical trials or registries.
CREST compared stenting with endarterectomy and provided important insights into each approach.1
BEFORE CREST
Endarterectomy is superior to medical therapy for symptomatic stenosis
First described in 1953, carotid endarterectomy became the most widely used invasive treatment for significant carotid stenosis.9 Several studies have described patient subsets that benefit from this procedure.
NASCET (the North American Symptomatic Carotid Endarterectomy Trial)10 assigned 2,226 patients with symptomatic stenosis (transient ischemic attack or stroke within the past 180 days) to medical management or endarterectomy.
Surgery was associated with a 65% lower rate of ipsilateral cerebral events in patients with 70% or greater stenosis.10 Surgery was also found to be superior in patients with moderate disease (50% to 69% stenosis), but the difference only approached statistical significance. In patients with stenosis of less than 50%, the outcomes were similar with endarterectomy and medical management.11
ECST (the European Carotid Surgery Trial)12 included a similar population of 3,024 patients. Those with high-grade disease (stenosis ≥ 80%) had significantly better outcomes with endarterectomy, but in those with stenosis less than 70%, surgery was no better than drug therapy.
Comment. NASCET and ECST taught us that endarterectomy is clearly superior to medical therapy in patients with severe symptomatic carotid disease. However, both trials excluded patients at high surgical risk, eg, those with severe coronary artery disease, kidney disease, or heart failure. Additionally, medical management was not aggressive by today’s standards in terms of control of blood pressure and hyperlipidemia, and this could have skewed the results in favor of carotid endarterectomy.
The case for carotid endarterectomy for asymptomatic stenosis
Endarterectomy has also been compared with drug therapy for asymp tomatic carotid artery stenosis in several trials.13–15
ACAS (the Asymptomatic Carotid Atherosclerosis Study)15 assigned 1,662 patients who had no symptoms and had at least 60% carotid artery stenosis to endarterectomy or to medical management, and found a relative risk reduction of 53% in favor of surgery.15
The Veterans Affairs Cooperative Study Group14 corroborated these results in 444 patients with asymptomatic stenosis of greater than 50%. Endarterectomy was associated with a 61% lower risk of transient ischemic attack, transient monocular blindness, or stroke compared with medical therapy. However, there was no statistically significant difference in rates of stroke or death at 30 days.14
ACST (the Asymptomatic Carotid Surgery Trial),13 the largest study to compare carotid endarterectomy with drug therapy for asymptomatic stenosis, randomized 3,120 patients to surgery or drug therapy. The net 5-year risk of stroke was 6.4% with endarterectomy vs 11.8% with drug therapy (P < .0001). The rate of fatal stroke was also lower with endarterectomy: 2.1% vs 4.2% (P = .006).13
Comment. The results of these and other studies of endarterectomy vs medical therapy may not be applicable to current practice, since medical therapy has evolved and the risks with current drug therapy are likely much lower than seen in these trials, some of which began 2 decades ago. Another problem with interpreting these trials is that they excluded surgically “high-risk” patients, which limits the generalizability of the findings to this particular patient population.
The American Heart Association and the American Stroke Association have, on the basis of these trials, recommended carotid endarterectomy in patients with7,8,16:
Ipsilateral, symptomatic carotid artery stenosis of 70% to 99% (class I, level of evidence A)
Symptomatic stenosis of 50% to 69%, depending on patient-specific factors such as age, sex, and comorbidities
High-grade asymptomatic carotid stenosis, if the patients are carefully selected and the surgery is performed by surgeons with procedural morbidity and mortality rates of less than 3% (class I, level of evidence A).
In all cases, treatment should be individualized according to the patient’s comorbid conditions and preferences, with a thorough discussion of risks and benefits (Table 1).7,8,16
The case for percutaneous intervention
While carotid endarterectomy is proven to be more efficacious than medical management in certain patient subsets, studies favoring surgery over medical therapy have been criticized because they excluded patients with significant comorbidities. In addition, surgery has been associated with significant cardiovascular events, wound complications, and cranial nerve damage, and it requires general anesthesia in most cases.12,17–19 These and other factors spurred the development of less invasive, percutaneous approaches for patients with substantial comorbidities.
So far, several trials have investigated carotid angioplasty with or without stents and with or without devices to capture distal emboli. This interest set the stage for CREST.20,21
Initial attempts at angioplasty without distal protection were not very successful. A meta-analysis of nonrandomized trials that included 714 patients from the initial 13 studies of angioplasty (with or without stenting) and 6,970 patients from 20 studies of carotid endarterectomy found angioplasty to be possibly associated with higher rates of stroke within 30 days of the procedure.20
With improvements in technology, routine use of embolic protection devices, more experience, and better selection of patients, the outcome of carotid stenting has improved. In fact, a meta-analysis comparing stenting without an embolic protection device (26 trials with 2,357 patients) vs stenting with an embolic protection device (11 trials with 839 patients) showed that embolic protection led to significantly better outcomes with fewer strokes—outcomes arguably similar to those of carotid endarterectomy.21
SAPPHIRE (the Stenting and Angioplasty With Protection in Patients at High Risk for Endarterectomy trial)22 was the only completed US trial until CREST that compared carotid artery stenting with distal protection against surgery. It included 334 high-risk patients with either symptomatic stenosis of 50% or greater or asymptomatic stenosis of 80% or greater.
The results suggested that the outcomes with stenting with embolic protection were in fact similar to those of endarterectomy, with possibly fewer complications.23 The benefit persisted up to 2 years.22
The US Food and Drug Administration (FDA), on the basis of these data, approved the use of stenting with distal protection for high-risk patients, and the CMS reimburses for symptomatic stenosis of 50% or greater and for asymptomatic stenosis of 80% or greater as long as the patient is enrolled in a registry.
SPACE (the Stent-Protected Angioplasty Versus Carotid Endarterectomy in Symptomatic Patients trial),24 conducted in Germany, included 1,214 patients with symptomatic stenosis of at least 50%. Results were similar in terms of the combined primary end point of stroke or death at 30 days. However, the results were not similar enough to prove that stenting is not inferior to surgery, according to preset study criteria.
EVA-3S (the Endarterectomy Versus Stenting in Patients With Symptomatic Severe Carotid Stenosis trial),25 in France, evaluated 527 patients with symptomatic carotid disease (stenosis ≥ 60%), but was terminated early due to significantly higher rates of death or stroke at 30 days in the stenting group.
Comment. SPACE and EVA-3S have been widely criticized for not mandating the use of an embolic protection device (used in 27% of cases in SPACE and in 91.9% of cases in EVA-3S). Questions were also raised about the experience level of the operators who performed the carotid stenting: up to 39% of the primary operators involved in stent placement were trainees.26 Also, myocardial infarction (MI), an important complication of carotid endarterectomy, was not included in the primary end point.
ICSS (the International Carotid Stenting Study)27 compared stenting with endarterectomy in 1,713 patients with symptomatic carotid stenosis of greater than 50%. The primary end point was the rate of fatal or disabling stroke at 3 years.
An interim safety analysis at 120 days of follow-up showed the primary end point had occurred in 4.0% of stenting cases vs 3.2% of endarterectomy cases, a difference that was not statistically significant (hazard ratio [HR] 1.28, 95% confidence interval [CI] 0.77–2.11). However, the risk of any stroke was higher with stenting, with a rate of 7.7% vs 4.1% in the surgical group—a statistically significant difference (HR 1.92, 95% CI 1.27–2.89).
In a substudy of ICSS,28 the investigators corroborated these findings, using magnetic resonance imaging to evaluate for new ischemic brain lesions periprocedurally. They found more new ischemic brain lesions in patients who underwent stenting than in patients who underwent surgery—a statistically significant finding.
Comment. ICSS had limitations: eg, it included only patients with symptoms, and the training for the stenting procedure was not standardized. Furthermore, the use of embolic protection devices was not mandated in stenting procedures.
Because of the controversial and incongruous findings of the above trials, there has been much anticipation for further large, appropriately conducted, randomized controlled trials such as CREST.
CREST STUDY DESIGN
CREST was a prospective, multicenter randomized controlled trial with blinded end point adjudication. Assignment to stenting or surgery occurred in a one-to-one fashion, and patients were stratified by medical center and symptomatic status.
Conducted at 108 sites in the United States and nine sites in Canada, CREST was supported by a grant from the National Institutes of Health and by the manufacturer of the catheter and stent delivery and embolic protection systems. The manufacturer’s representative held a nonvoting position on the executive committee and reviewed the manuscript of the results before submission.
CREST included patients with or without symptoms
CREST was initially designed to compare carotid artery stenting vs carotid endarterectomy in patients with symptoms, but enrollment was later extended to patients without symptoms.
Patients with symptoms were included if they had stenosis of at least 50% on angiography, at least 70% on ultrasonography, or at least 70% on computed tomographic angiography or magnetic resonance angiography if stenosis on ultrasonography was 50% to 69%. Carotid artery stenosis was considered symptomatic if the patient had a transient ischemic attack, amaurosis fugax, or minor disabling stroke in the hemisphere supplied by the target vessel within 180 days of randomization.
Patients without symptoms were eligible if they had at least 60% stenosis on angiography, at least 70% stenosis on ultrasonography, or at least 80% stenosis on computed tomographic angiography or magnetic resonance angiography if the stenosis was 50% to 69% on ultrasonography.
Other eligibility criteria included favorable anatomy and clinical stability for both stenting and surgical procedures.
Exclusion criteria were evolving stroke, history of major stroke, chronic or paroxysmal atrial fibrillation on anticoagulation therapy, MI within the previous 30 days, and unstable angina.
Patients received antiplatelet agents
Patients undergoing stenting received aspirin and clopidogrel (Plavix) before and up to 30 days after the procedure. Continuation of antiplatelet therapy was recommended beyond 1 month.
Patients undergoing endarterectomy received aspirin before surgery and continued to receive aspirin for at least 1 year.
Alternatives to aspirin in both groups were ticlopidine (Ticlid), clopidogrel, or aspirin with extended-release dipyridamole (Aggrenox).
End points: Stroke, MI, death
The primary end point was a composite of periprocedural clinical stroke (any type), MI, or death, and of ipsilateral stroke up to 4 years after the procedure. Secondary analyses were also planned for evaluation of treatment modification by age, symptom status, and sex.
Stroke was defined as any acute neurologic ischemic event lasting at least 24 hours with focal signs and symptoms.
Two separate definitions were applied to distinguish major stroke from nonmajor stroke. Major stroke was defined as a National Institutes of Health Stroke Scale (NIHSS) score greater than 9 or records suggesting that the event was a disabling stroke if admitted to another facility. Nonmajor stroke included an event that did not fit these criteria. The stroke review process was initiated with a significant neurologic event, a positive transient ischemia attack or stroke questionnaire, or a two-point or greater increase in the NIHSS score.
MI was defined as a combination of an elevation of cardiac enzymes to at least twice the laboratory upper limit of normal, as well as clinical signs suggesting MI or electrocardiographic evidence of ischemia.29
Stroke was adjudicated by two independent neurologists, and MI was adjudicated by two independent cardiologists blinded to treatment group assignment.
The Rankin scale, the transient ischemic attack and stroke questionnaire, and the Medical Outcomes Survey were also used to assess for disability and quality of life in long-term follow-up.
Intention-to-treat analysis
Intention-to-treat survival analysis was used along with time-to-event statistical modeling with adjustment for major baseline covariates. Differences in outcomes were assessed, and a noninferiority analysis was performed. Kaplan-Meier estimates were constructed of the proportion of patients remaining free of the composite end point at 30 days, 6 months, 1 year, and annually thereafter, and of the associated confidence intervals. The hazard ratios between groups were estimated after adjustment for important covariates.
Most patients enrolled were available for analysis
From December 2000 to July 2008, 2,522 patients were enrolled; 1,271 were assigned to stenting, and 1,251 were assigned to surgery. After randomization, 2.8% of the patients assigned to stenting withdrew consent, 5.7% underwent surgery, and 2.6% were lost to follow-up. Of those assigned to surgery, 5.1% withdrew consent, 1.0% underwent stenting, and 3.8% were lost to follow-up.
A ‘conventional-risk’ patient population
The trial sought to include a “conventional-risk” patient population to make the study more applicable to real-world practice. The mean age was 69 years in both groups. Of the 2,522 patients enrolled:
35% were women
47% had asymptomatic carotid disease
86% had carotid stenosis of 70% or greater
86% had hypertension
30% had diabetes mellitus
83% had hyperlipidemia
26% were current smokers
42% had a history of cardiovascular disease
21% had undergone coronary artery bypass grafting surgery.
The only statistically significant difference in measured baseline variables between the two treatment groups was a slightly higher rate of dyslipidemia in the group undergoing surgery.
The interventionalists and surgeons were highly experienced
Operators performing stenting underwent a lead-in phase of training, with close supervision and scrutiny before eligibility. Of patients undergoing stenting, 96.1% also received an embolic protection device. Antiplatelet therapy was continued in 99% of the patients.
The surgeons performing endarterectomy were experienced and had documented low complication rates. General anesthesia was used in 90% of surgical patients. Shunts were used during surgery in 57%, and patches were used in 62%. After endarterectomy, 91% of the patients received antiplatelet therapy.
CREST STUDY RESULTS: STENTING WAS AS GOOD AS SURGERY
Periprocedural outcomes
Stroke, MI, or death: 5.2% with stenting vs 4.5% with surgery, HR 1.18, 95% CI 0.82–1.68, P = .38
Stroke: 4.1% vs 2.3%, HR 1.79, 95% CI 1.14–2.82, P = .01
Major ipsilateral stroke: 0.9% vs 0.3%, HR 2.67, 95% CI 0.85–8.40, P = .09.
MI: 1.1% vs 2.3%, HR 0.50, 95% CI 0.26–0.94, P = .03
Cranial nerve palsy: 0.3% vs 4.8%, HR 0.07, 95% CI 0.02–0.18, P < .0001 (Table 2).
Outcomes at 4 years
Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.
Figure 2. Kaplan-Meier analysis of the primary outcome (stroke, myocardial infarction, or death during the periprocedural period or any ipsilateral stroke within 4 years after randomization) for patients undergoing carotid artery stenting or carotid endarterectomy.
The primary end point (periprocedural stroke, MI, or death, or ipsilateral stroke within 4 years after the procedure): 7.2% with stenting vs 6.8% with surgery, HR 1.11, 95% CI 0.81–1.51, P = .51. A Kaplan-Meier analysis showed similar findings with statistically similar outcomes (Figure 2).
Ipsilateral stroke: 2.0% vs 2.4%, HR 0.94, 95% CI 0.50–1.76, P = .85.
The primary outcome was analyzed for interactions of baseline variables, and no effect was detected for symptomatic status or sex. There was a suggestion of an interaction with age, with older patients (over age 70) benefiting more from endarterectomy.
Quality-of-life indices showed that both major and minor strokes were likely to produce long-term physical limitations, with minor stroke associated with worse mental and physical health at 1 year. The effect of periprocedural MI on long-term physical and mental health was less certain. The increased incidence of cranial nerve palsy noted with endarterectomy has been found before and has had no effect on quality of life.
WHAT DO THE CREST FINDINGS MEAN?
CREST is the largest trial to date to compare stenting and surgery. It is an important addition to the literature, not only because of its size, but also because it focused on a real-world patient population. For this reason, its results are more applicable to patients seen in primary care clinics, ie, with peripheral vascular disease, coronary artery disease, diabetes mellitus, hypertension, and smoking.
As noted, previous studies of endarterectomy had strict inclusion and exclusion criteria, which selected against patients at high surgical risk. Therefore, the CREST findings are of greater relevance when comparing stenting and endarterectomy.
Periprocedural and long-term neurologic outcomes
CREST showed similar findings for the composite end point of periprocedural stroke, death, or MI (ie, within 30 days of the procedure) and long-term stroke, establishing similar outcomes in patients undergoing stenting and surgery.
However, an analysis of the individual components of the composite end point showed significant differences between the two treatments. The risk of ipsilateral periprocedural stroke was higher with stenting; these events were defined as nonmajor by NIHSS criteria. The risk of contralateral stroke was similar and low with each treatment.
While the increased risk of periprocedural ipsilateral stroke was not synonymous with an increased risk of major stroke, post hoc analysis showed that any stroke was associated with decreased physical and mental health at 1 year. Therefore, patients who had even a minor stroke did worse from a physical and mental standpoint, a finding that argues for the superiority of surgery in selected patients at risk of periprocedural stroke.
If periprocedural stroke is excluded, the risk of long-term ipsilateral stroke was similar for each treatment, and extremely low (2% for stenting, 2.4% for surgery). Despite this, given the importance of periprocedural minor and major stroke, better predictive models are needed to identify patients at risk of procedural neurologic events. These prediction models will allow better patient selection.
The CREST data and medical therapy
The rates of stroke in this trial were similar to those observed with current medical treatment (approximately 1% per year), especially for patients with asymptomatic disease. Such findings introduce fresh controversy in the necessity of performing either procedure for this patient subset and may lead to further studies evaluating current medical therapy vs intervention.
Periprocedural myocardial infarction
Vascular surgery has long been associated with high cardiovascular risk, especially an increased risk of periprocedural MI.30 Findings from CREST provide further evidence of the risk of MI with endarterectomy in a real-world patient population. Given the evidence of a strong correlation between periprocedural cardiac enzyme elevations and adverse outcomes, the increased incidence of periprocedural MI is worrisome.31 As with risk assessment for periprocedural stroke, better predictive models are needed for patients at risk of cardiovascular events during endarterectomy.
Procedural complications
Carotid endarterectomy entails incisions in the neck with disruption of tissue planes, as opposed to catheter entry site wounds with stenting. The more invasive nature of endarterectomy thus carries a higher risk of wound complications. In fact, in the NASCET trial, the risk of wound complications was 9.3%.10,19 In CREST, surgery carried a higher risk of wound complications compared with stenting (42 vs 0 cases), although stenting involved more periprocedural transfusions, presumably due to retroperitoneal bleeding in four patients.
Use of general anesthesia is also associated with adverse outcomes.17,18 In CREST, 90% of endarterectomy procedures required general anesthesia, whereas none of the stenting procedures required this.
Cranial nerve palsy is an often overlooked but real complication after these procedures. Cranial nerve palsies can lead to vocal, swallowing, and sensory problems that can have a transient or permanent impact on quality of life. In CREST, as in EVA-3S, SAPPHIRE, and ICSS, this risk was substantially higher with surgery,23,25,27 although the long-term consequences of these palsies were not found to affect quality of life at 1 year of follow-up.
HOW CREST FINDINGS COMPARE WITH PREVIOUS STUDIES
Patients in CREST enjoyed overall better outcomes than in previous studies. In earlier trials of surgery vs medical therapy, the rates of adverse outcomes were higher than in CREST. In NASCET, the risk of ipsilateral stroke was 9% with surgery, with 2.5% being fatal or disabling strokes.10 In the ECST, rates of major stroke or death with endarterectomy were 7.0% within 30 days of surgery and 37.0% at a mean follow-up of 6.1 years.12
In earlier studies of surgery vs stenting, outcomes at 30 days were also substantially worse than those in CREST. In the EVA-3S trial, the 30-day incidence of stroke or death was 3.9% after surgery and 9.6% after stenting. These findings were similar at 6 months in EVA-3S, with a 6.1% rate of adverse events after surgery and 11.7% after stenting.25 In the SAPPHIRE trial, the cumulative incidence of stroke and death at 1 year was 21.4% for surgery and 13.6% for stenting.23
Overall, the CREST results show better outcomes than in previous trials. This may be due to improvements in technical aspects of the interventions and to more aggressive drug therapy. Also, because of the high number of patients enrolled in CREST, surgeons and interventionalists were required to meet eligibility criteria, which could have contributed to the improved outcomes.32
CREST was also unique in that stenting was done with an embolic protection device whenever possible, and this also likely had an impact on outcomes.
The CREST data suggest that interventions for carotid artery stenosis should only be performed by rigorously trained, experienced personnel at high-volume centers, as this provided lower event rates compared with previous studies. Additional data should also help identify those at risk of periprocedural stroke and MI, thereby helping to match the patient to the most appropriate procedure. The pros and cons of surgery and stenting are shown in Table 3.1,10,23,25,27
CREST vs ICSS
CREST and ICSS, published within a few months of each other, seem to have arrived at entirely different conclusions. As both studies are well-designed randomized controlled trials, these distinct results have yielded much controversy. However, closer scrutiny sheds light as to why the results may be different.
While ICSS focused only on patients with symptoms, CREST also included those without symptoms. The difference in patient populations is itself enough to account for the different outcomes.
Also, the interim analysis of ICSS was at 120 days, which makes periprocedural events a more dominant factor in outcomes, whereas these events likely do not last into the long term, as was the case in CREST. Analysis of the ICSS data at a later follow-up date may show results more similar to those of CREST.
The design of ICSS was also different than CREST. In ICSS, the use of an embolic protection device in stenting was not mandated, and the study lacked a lead-in phase of intensive training for those performing stenting. Furthermore, MI was adjudicated only when clinically recognized, which is different than the more rigorous method used in CREST.
Yet despite these differences, CREST and ICSS shed light on a controversial area of carotid stenosis management, and both studies boasted low rates of periprocedural complications. Clinicians should keep in mind the inclusion criteria and the technical specificities of these trials in order to explain to patients the risks and benefits of stenting and surgery, and to arrive at a decision together.
Limitations
The results of CREST should also be reviewed carefully due to a number of limitations. The study began in 2000 with symptomatic patients only, and began enrolling asymptomatic patients in 2005, so that the methodology of the study was changed midway. However, the investigators performed a subgroup analysis to distinguish between outcomes of the symptomatic and the asymptomatic groups and found no statistical interaction for the primary end point based on symptom status.
Despite careful patient selection, many of the predictors of adverse outcomes with stenting, such as lesion length, level of calcification, and lesion location, were not accounted for in the earlier days of enrollment. This may have had an impact on the incidence of stroke in patients enrolled in the early years of the trial. We await the analysis of predictors of perioperative stroke from CREST.
TAKE-HOME POINTS AND FUTURE DIRECTIONS
The CREST findings show that outcomes with stenting are similar to those with surgery in both the short term and the long term, and that the choice of management should be individualized. Each patient’s risk of MI and stroke should be considered based on a variety of factors, including the severity of coronary artery disease, the length of the carotid lesion, the level of calcification, the location of the lesion, and aortic atheroma. The treatment should be selected after also taking into account the patient’s preference and the available expertise, and only after a comprehensive discussion with the patient.
References
Brott TG, Hobson RW, Howard G, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med2010; 363:11–23.
Thom T, Haase N, Rosamond W, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation2006; 113:e85–e151.
Rosamond WD, Folsom AR, Chambless LE, et al. Stroke incidence and survival among middle-aged adults: 9-year follow-up of the Atherosclerosis Risk in Communities (ARIC) cohort. Stroke1999; 30:736–743.
Chaturvedi S, Bruno A, Feasby T, et al; Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Carotid endarterectomy—an evidence-based review: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology2005; 65:794–801.
Howell GM, Makaroun MS, Chaer RA. Current management of extracranial carotid occlusive disease. J Am Coll Surg2009; 208:442–453.
Barnett HJ, Gunton RW, Eliasziw M, et al. Causes and severity of ischemic stroke in patients with internal carotid artery stenosis. JAMA2000; 283:1429–1436.
Biller J, Feinberg WM, Castaldo JE, et al. Guidelines for carotid endarterectomy: a statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation1998; 97:501–509.
Goldstein LB, Adams R, Alberts MJ, et al; American Heart Association; American Stroke Association Stroke Council. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council: cosponsored by the Atherosclerotic Peripheral Vascular Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation2006; 113:e873–e923.
Strully KJ, Hurwitt ES, Blankenberg HW. Thrombo-endarterectomy for thrombosis of the internal carotid artery in the neck. J Neurosurg1953; 10:474–482.
Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1991; 325:445–453.
Barnett HJ, Taylor DW, Eliasziw M, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1998; 339:1415–1425.
Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet1998; 351:1379–1387.
Halliday A, Mansfield A, Marro J, et al; MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet2004; 363:1491–1502.
Hobson RW, Weiss DG, Fields WS, et al. Efficacy of carotid endarterectomy for asymptomatic carotid stenosis. The Veterans Affairs Cooperative Study Group. N Engl J Med1993; 328:221–227.
Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA1995; 273:1421–1428.
Sacco RL, Adams R, Albers G, et al; American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention: the American Academy of Neurology affirms the value of this guideline. Circulation2006; 113:e409–e449.
Watts K, Lin PH, Bush RL, et al. The impact of anesthetic modality on the outcome of carotid endarterectomy. Am J Surg2004; 188:741–747.
Weber CF, Friedl H, Hueppe M, et al. Impact of general versus local anesthesia on early postoperative cognitive dysfunction following carotid endarterectomy: GALA Study Subgroup Analysis. World J Surg2009; 33:1526–1532.
Ferguson GG, Eliasziw M, Barr HW, et al. The North American Symptomatic Carotid Endarterectomy Trial: surgical results in 1415 patients. Stroke1999; 30:1751–1758.
Golledge J, Mitchell A, Greenhalgh RM, Davies AH. Systematic comparison of the early outcome of angioplasty and endarterectomy for symptomatic carotid artery disease. Stroke2000; 31:1439–1443.
Kastrup A, Gröschel K, Krapf H, Brehm BR, Dichgans J, Schulz JB. Early outcome of carotid angioplasty and stenting with and without cerebral protection devices: a systematic review of the literature. Stroke2003; 34:813–819.
Gurm HS, Yadav JS, Fayad P, et al; SAPPHIRE Investigators. Long-term results of carotid stenting versus endarterectomy in high-risk patients. N Engl J Med2008; 358:1572–1579.
Yadav JS, Wholey MH, Kuntz RE, et al; Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy Investigators. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med2004; 351:1493–1501.
Eckstein HH, Ringleb P, Allenberg JR, et al. Results of the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: a multinational, prospective, randomised trial. Lancet Neurol2008; 7:893–902.
Mas JL, Chatellier G, Beyssen B, et al; EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med2006; 355:1660–1771.
Roffi M, Sievert H, Gray WA, et al. Carotid artery stenting versus surgery: adequate comparisons?Lancet Neurol2010; 9:339–341.
International Carotid Stenting Study Investigators; Ederle J, Dobson J, Featherstone RL, et al. Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International Carotid Stenting Study): an interim analysis of a randomised controlled trial. Lancet2010; 375:985–997.
Bonati LH, Jongen LM, Haller S, et al; ICSS-MRI study group. New ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid stenosis: a sub-study of the International Carotid Stenting Study (ICSS). Lancet Neurol2010; 9:353–362.
Sheffet AJ, Roubin G, Howard G, et al. Design of the Carotid Revascularization Endarterectomy vs. Stenting Trial (CREST). Int J Stroke2010; 5:40–46.
Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery) developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. J Am Coll Cardiol2007; 50:e159–e241.
Bhatt DL, Topol EJ. Does creatinine kinase-MB elevation after percutaneous coronary intervention predict outcomes in 2005? Periprocedural cardiac enzyme elevation predicts adverse outcomes. Circulation2005; 112:906–915.
Hobson RW, Howard VJ, Roubin GS, et al; CREST. Credentialing of surgeons as interventionalists for carotid artery stenting: experience from the lead-in phase of CREST. J Vasc Surg2004; 40:952–957.
References
Brott TG, Hobson RW, Howard G, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med2010; 363:11–23.
Thom T, Haase N, Rosamond W, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation2006; 113:e85–e151.
Rosamond WD, Folsom AR, Chambless LE, et al. Stroke incidence and survival among middle-aged adults: 9-year follow-up of the Atherosclerosis Risk in Communities (ARIC) cohort. Stroke1999; 30:736–743.
Chaturvedi S, Bruno A, Feasby T, et al; Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Carotid endarterectomy—an evidence-based review: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology2005; 65:794–801.
Howell GM, Makaroun MS, Chaer RA. Current management of extracranial carotid occlusive disease. J Am Coll Surg2009; 208:442–453.
Barnett HJ, Gunton RW, Eliasziw M, et al. Causes and severity of ischemic stroke in patients with internal carotid artery stenosis. JAMA2000; 283:1429–1436.
Biller J, Feinberg WM, Castaldo JE, et al. Guidelines for carotid endarterectomy: a statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation1998; 97:501–509.
Goldstein LB, Adams R, Alberts MJ, et al; American Heart Association; American Stroke Association Stroke Council. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council: cosponsored by the Atherosclerotic Peripheral Vascular Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation2006; 113:e873–e923.
Strully KJ, Hurwitt ES, Blankenberg HW. Thrombo-endarterectomy for thrombosis of the internal carotid artery in the neck. J Neurosurg1953; 10:474–482.
Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1991; 325:445–453.
Barnett HJ, Taylor DW, Eliasziw M, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1998; 339:1415–1425.
Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet1998; 351:1379–1387.
Halliday A, Mansfield A, Marro J, et al; MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet2004; 363:1491–1502.
Hobson RW, Weiss DG, Fields WS, et al. Efficacy of carotid endarterectomy for asymptomatic carotid stenosis. The Veterans Affairs Cooperative Study Group. N Engl J Med1993; 328:221–227.
Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA1995; 273:1421–1428.
Sacco RL, Adams R, Albers G, et al; American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention: the American Academy of Neurology affirms the value of this guideline. Circulation2006; 113:e409–e449.
Watts K, Lin PH, Bush RL, et al. The impact of anesthetic modality on the outcome of carotid endarterectomy. Am J Surg2004; 188:741–747.
Weber CF, Friedl H, Hueppe M, et al. Impact of general versus local anesthesia on early postoperative cognitive dysfunction following carotid endarterectomy: GALA Study Subgroup Analysis. World J Surg2009; 33:1526–1532.
Ferguson GG, Eliasziw M, Barr HW, et al. The North American Symptomatic Carotid Endarterectomy Trial: surgical results in 1415 patients. Stroke1999; 30:1751–1758.
Golledge J, Mitchell A, Greenhalgh RM, Davies AH. Systematic comparison of the early outcome of angioplasty and endarterectomy for symptomatic carotid artery disease. Stroke2000; 31:1439–1443.
Kastrup A, Gröschel K, Krapf H, Brehm BR, Dichgans J, Schulz JB. Early outcome of carotid angioplasty and stenting with and without cerebral protection devices: a systematic review of the literature. Stroke2003; 34:813–819.
Gurm HS, Yadav JS, Fayad P, et al; SAPPHIRE Investigators. Long-term results of carotid stenting versus endarterectomy in high-risk patients. N Engl J Med2008; 358:1572–1579.
Yadav JS, Wholey MH, Kuntz RE, et al; Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy Investigators. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med2004; 351:1493–1501.
Eckstein HH, Ringleb P, Allenberg JR, et al. Results of the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: a multinational, prospective, randomised trial. Lancet Neurol2008; 7:893–902.
Mas JL, Chatellier G, Beyssen B, et al; EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med2006; 355:1660–1771.
Roffi M, Sievert H, Gray WA, et al. Carotid artery stenting versus surgery: adequate comparisons?Lancet Neurol2010; 9:339–341.
International Carotid Stenting Study Investigators; Ederle J, Dobson J, Featherstone RL, et al. Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International Carotid Stenting Study): an interim analysis of a randomised controlled trial. Lancet2010; 375:985–997.
Bonati LH, Jongen LM, Haller S, et al; ICSS-MRI study group. New ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid stenosis: a sub-study of the International Carotid Stenting Study (ICSS). Lancet Neurol2010; 9:353–362.
Sheffet AJ, Roubin G, Howard G, et al. Design of the Carotid Revascularization Endarterectomy vs. Stenting Trial (CREST). Int J Stroke2010; 5:40–46.
Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery) developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. J Am Coll Cardiol2007; 50:e159–e241.
Bhatt DL, Topol EJ. Does creatinine kinase-MB elevation after percutaneous coronary intervention predict outcomes in 2005? Periprocedural cardiac enzyme elevation predicts adverse outcomes. Circulation2005; 112:906–915.
Hobson RW, Howard VJ, Roubin GS, et al; CREST. Credentialing of surgeons as interventionalists for carotid artery stenting: experience from the lead-in phase of CREST. J Vasc Surg2004; 40:952–957.
In CREST, stenting and surgery had similar combined rates of stroke, MI, and death when performed by highly qualified interventionalists and surgeons in carefully selected patients.
The risk of periprocedural stroke was higher with stenting; most of those strokes were nonmajor. Both major and nonmajor strokes were associated with decreased quality of life in long-term follow-up.
Endarterectomy was associated with higher rates of periprocedural MI than stenting.
Endarterectomy carried a significantly higher rate of cranial nerve damage than stenting.
 Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.
Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.