User login
The Hair-Cut Sign for Scalp Biopsy Site Identification
Practice Gap
Accurate biopsy site identification prior to Mohs micrographic surgery (MMS) can be challenging, particularly on the scalp, where excellent healing, field cancerization, prior procedures, large surface area, and hair density may complicate localization. Accurate site identification is further hindered when patients are unable to recall the biopsy location, when the biopsy and MMS are performed by different clinicians, or when photographic documentation is absent. Scalp lesions pose an additional challenge because even high-quality photographs may fail to capture subtle landmarks that are obscured by hair.
Wrong-site surgery was the most common serious error reported in a survey of 150 dermatologists, accounting for 19.0% of these errors.1 Research has shown that dermatologists may misidentify biopsy sites in up to 17.6% of cases, and patients (eg, if a patient goes to a dermatologic surgeon and is asked to identify the biopsy site for the surgeon) in up to 25.5% (N=278).2 Additionally, a survey of Mohs surgeons revealed that 14.0% of 42 malpractice cases were due to wrong-site surgery.3 A Delphi consensus study assessing possible preventive interventions found that the best way to document the site is with a photograph in association with landmarks and diagrams.4
The Technique
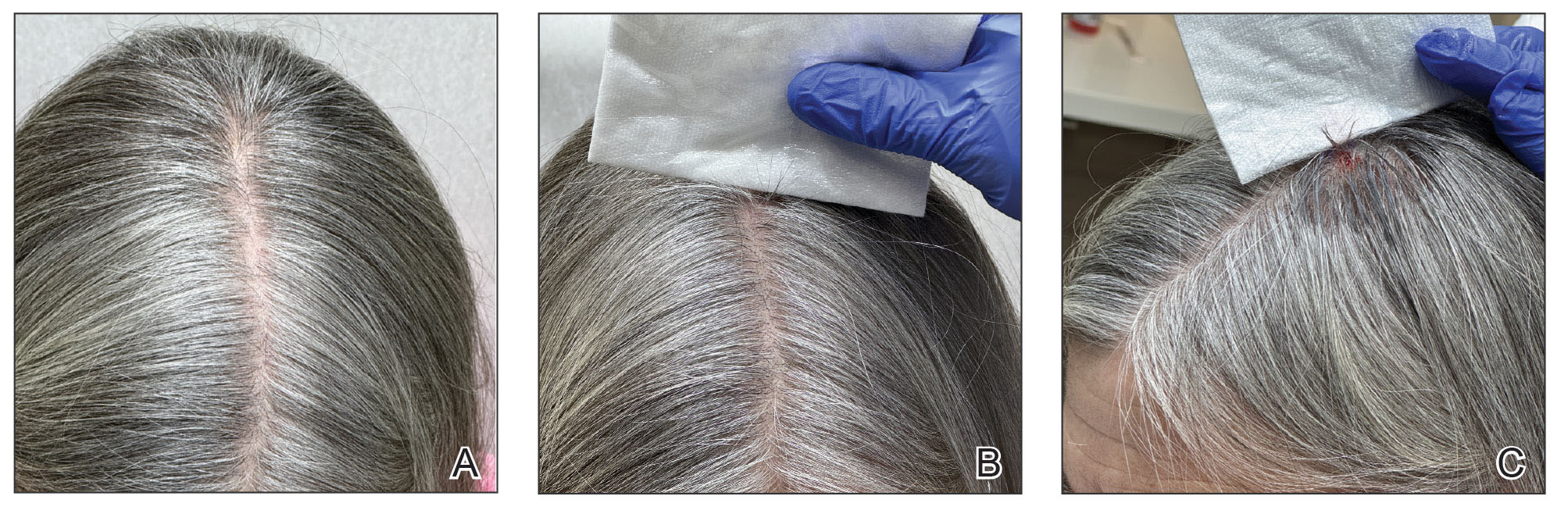
The hair-cut sign is a simple and effective technique for identifying biopsy sites on the scalp. Hair at the biopsy site typically is cut during biopsy; as the surrounding hair grows, the resulting short tuft serves as an anatomic marker that can persist for weeks to months to facilitate accurate site localization by the Mohs surgeon (Figure). This noninvasive, equipment-free method may be particularly useful when documentation or photography is limited. To maximize its effectiveness, clinical staff should avoid trimming the area before physician verification of the site. The technique is most effective in patients with longer hair and when the interval between biopsy and surgery is less than 3 months, as hair regrowth may reduce contrast with the surrounding scalp.
Practice Implications
Accurate biopsy site identification is a critical component of patient safety in dermatologic surgery, particularly on the scalp, where traditional localization strategies may be unreliable. The hair-cut sign is a simple, reliable, no-cost, and reproducible adjunct to photography, anatomic documentation, and patient verification that may improve site localization and help reduce the risk for wrong-site surgery in select patients to complement standard practices. Incorporating the hair-cut sign into routine scalp surgery workflow represents a low-burden intervention that may improve accuracy when other documentation is limited.
- Watson AJ, Redbord K, Taylor JS, et al. Medical error in dermatology practice: development of a classification system to drive priority setting in patient safety efforts. J Am Acad Dermatol. 2013;68:729-737. doi:10.1016/j.jaad.2012.10.058
- Nijhawan RI, Lee EH , Nehal KS. Biopsy site selfies—a quality improvement pilot study to assist with correct surgical site identification. Dermatol Surg. 2015;41:499-504. doi:10.1097/DSS.0000000000000305
- Perlis CS, Campbell RM, Perlis RH, et al. Incidence of and risk factors for medical malpractice lawsuits among Mohs surgeons. Dermatol Surg. 2006;32:79-83. doi:10.1111/1524-4725.2006.32009
- Alam M, Lee A, Ibrahimi OA, et al. A multistep approach to improving biopsy site identification in dermatology: physician, staff, and patient roles based on a Delphi consensus. JAMA Dermatol. 2014;150:550-558. doi:10.1001/jamadermatol.2013.9804
Practice Gap
Accurate biopsy site identification prior to Mohs micrographic surgery (MMS) can be challenging, particularly on the scalp, where excellent healing, field cancerization, prior procedures, large surface area, and hair density may complicate localization. Accurate site identification is further hindered when patients are unable to recall the biopsy location, when the biopsy and MMS are performed by different clinicians, or when photographic documentation is absent. Scalp lesions pose an additional challenge because even high-quality photographs may fail to capture subtle landmarks that are obscured by hair.
Wrong-site surgery was the most common serious error reported in a survey of 150 dermatologists, accounting for 19.0% of these errors.1 Research has shown that dermatologists may misidentify biopsy sites in up to 17.6% of cases, and patients (eg, if a patient goes to a dermatologic surgeon and is asked to identify the biopsy site for the surgeon) in up to 25.5% (N=278).2 Additionally, a survey of Mohs surgeons revealed that 14.0% of 42 malpractice cases were due to wrong-site surgery.3 A Delphi consensus study assessing possible preventive interventions found that the best way to document the site is with a photograph in association with landmarks and diagrams.4
The Technique
The hair-cut sign is a simple and effective technique for identifying biopsy sites on the scalp. Hair at the biopsy site typically is cut during biopsy; as the surrounding hair grows, the resulting short tuft serves as an anatomic marker that can persist for weeks to months to facilitate accurate site localization by the Mohs surgeon (Figure). This noninvasive, equipment-free method may be particularly useful when documentation or photography is limited. To maximize its effectiveness, clinical staff should avoid trimming the area before physician verification of the site. The technique is most effective in patients with longer hair and when the interval between biopsy and surgery is less than 3 months, as hair regrowth may reduce contrast with the surrounding scalp.
Practice Implications
Accurate biopsy site identification is a critical component of patient safety in dermatologic surgery, particularly on the scalp, where traditional localization strategies may be unreliable. The hair-cut sign is a simple, reliable, no-cost, and reproducible adjunct to photography, anatomic documentation, and patient verification that may improve site localization and help reduce the risk for wrong-site surgery in select patients to complement standard practices. Incorporating the hair-cut sign into routine scalp surgery workflow represents a low-burden intervention that may improve accuracy when other documentation is limited.
Practice Gap
Accurate biopsy site identification prior to Mohs micrographic surgery (MMS) can be challenging, particularly on the scalp, where excellent healing, field cancerization, prior procedures, large surface area, and hair density may complicate localization. Accurate site identification is further hindered when patients are unable to recall the biopsy location, when the biopsy and MMS are performed by different clinicians, or when photographic documentation is absent. Scalp lesions pose an additional challenge because even high-quality photographs may fail to capture subtle landmarks that are obscured by hair.
Wrong-site surgery was the most common serious error reported in a survey of 150 dermatologists, accounting for 19.0% of these errors.1 Research has shown that dermatologists may misidentify biopsy sites in up to 17.6% of cases, and patients (eg, if a patient goes to a dermatologic surgeon and is asked to identify the biopsy site for the surgeon) in up to 25.5% (N=278).2 Additionally, a survey of Mohs surgeons revealed that 14.0% of 42 malpractice cases were due to wrong-site surgery.3 A Delphi consensus study assessing possible preventive interventions found that the best way to document the site is with a photograph in association with landmarks and diagrams.4
The Technique
The hair-cut sign is a simple and effective technique for identifying biopsy sites on the scalp. Hair at the biopsy site typically is cut during biopsy; as the surrounding hair grows, the resulting short tuft serves as an anatomic marker that can persist for weeks to months to facilitate accurate site localization by the Mohs surgeon (Figure). This noninvasive, equipment-free method may be particularly useful when documentation or photography is limited. To maximize its effectiveness, clinical staff should avoid trimming the area before physician verification of the site. The technique is most effective in patients with longer hair and when the interval between biopsy and surgery is less than 3 months, as hair regrowth may reduce contrast with the surrounding scalp.
Practice Implications
Accurate biopsy site identification is a critical component of patient safety in dermatologic surgery, particularly on the scalp, where traditional localization strategies may be unreliable. The hair-cut sign is a simple, reliable, no-cost, and reproducible adjunct to photography, anatomic documentation, and patient verification that may improve site localization and help reduce the risk for wrong-site surgery in select patients to complement standard practices. Incorporating the hair-cut sign into routine scalp surgery workflow represents a low-burden intervention that may improve accuracy when other documentation is limited.
- Watson AJ, Redbord K, Taylor JS, et al. Medical error in dermatology practice: development of a classification system to drive priority setting in patient safety efforts. J Am Acad Dermatol. 2013;68:729-737. doi:10.1016/j.jaad.2012.10.058
- Nijhawan RI, Lee EH , Nehal KS. Biopsy site selfies—a quality improvement pilot study to assist with correct surgical site identification. Dermatol Surg. 2015;41:499-504. doi:10.1097/DSS.0000000000000305
- Perlis CS, Campbell RM, Perlis RH, et al. Incidence of and risk factors for medical malpractice lawsuits among Mohs surgeons. Dermatol Surg. 2006;32:79-83. doi:10.1111/1524-4725.2006.32009
- Alam M, Lee A, Ibrahimi OA, et al. A multistep approach to improving biopsy site identification in dermatology: physician, staff, and patient roles based on a Delphi consensus. JAMA Dermatol. 2014;150:550-558. doi:10.1001/jamadermatol.2013.9804
- Watson AJ, Redbord K, Taylor JS, et al. Medical error in dermatology practice: development of a classification system to drive priority setting in patient safety efforts. J Am Acad Dermatol. 2013;68:729-737. doi:10.1016/j.jaad.2012.10.058
- Nijhawan RI, Lee EH , Nehal KS. Biopsy site selfies—a quality improvement pilot study to assist with correct surgical site identification. Dermatol Surg. 2015;41:499-504. doi:10.1097/DSS.0000000000000305
- Perlis CS, Campbell RM, Perlis RH, et al. Incidence of and risk factors for medical malpractice lawsuits among Mohs surgeons. Dermatol Surg. 2006;32:79-83. doi:10.1111/1524-4725.2006.32009
- Alam M, Lee A, Ibrahimi OA, et al. A multistep approach to improving biopsy site identification in dermatology: physician, staff, and patient roles based on a Delphi consensus. JAMA Dermatol. 2014;150:550-558. doi:10.1001/jamadermatol.2013.9804
The Hair-Cut Sign for Scalp Biopsy Site Identification
The Hair-Cut Sign for Scalp Biopsy Site Identification
