User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Suicide factors: UNSAFE or SAFER?
The basic function of a suicide assessment is to identify fixed and modifiable risk factors for suicide and existing or amendable protective factors.1 Epidemiologic studies have defined a range of suicide risk and protective factors for the general population.2 Other research has delineated suicide risk and protective factors for individuals with specific psychiatric disorders.3 The presence of disorder-specific risk and protective factors for suicide must be identified during suicide risk assessment.
Risk factors
Lack of support from family, peers, or the community is a critical concern. Noncompliance with treatment may be associated with onset of suicidality. Help-seeking is impeded by stigma associated with suicide and shame for past attempts. History of physical, sexual, or psychological abuse is tied to subsequent suicidal behavior. Alcohol abuse plays a role in suicide. Many patients who attempt suicide have backgrounds involving suicide loss or attempts by family members. Recurring psychiatric symptoms—particularly depression, anxiety, and panic—can trigger suicidality. Symptom relapse may lead to hospitalization, which is followed by a high-risk period after discharge.
These suicide risk factors can be summarized by the mnemonic UNSAFE:
Unconnected—no support; sense of not belonging or being a burden
Nonadherence—unmanaged mental illness or co-occurring disorders
Stigma/shame related to past attempts or suicidal behavior
Abuse history and/or alcohol misuse; prior attempt
Family history of suicide or suicide attempts
Exacerbations—worsened mental illness, hospitalizations
Protective factors
The presence of a personal crisis or safety self-help plan shows patient insight. Maintaining prescribed treatment indicates a patient’s likelihood of complying with clinical and self-care measures to avert future suicidality. Accessible support from family, peers, and the community demonstrates social integration. The recovery concept promotes these factors as well as wellness and resilience. Awareness of the warning signs of suicide and personal risk factors and precipitants is essential for self-help and help-seeking.
Protective factors for suicide can be summarized by the mnemonic SAFER:
Self-help skills, personal crisis/suicide prevention plan
Adherence to treatment plan
Family and community support
Education about risk factors, warning signs, and triggers for suicide
Recovery and resilience
In our emergency psychiatric facility the UNSAFE and SAFE mnemonics are posted next to the desk of the on-duty psychiatrist. Crisis center staff use these mnemonics to screen patients during psychiatric evaluations. Allied therapists use them during in-patient psychoeducation about suicidality. Peer specialists use them to help patients prepare personal safety plans.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufactures of competing products.
These mnemonics were developed by Tony Salvatore in consultation with Rocio Nell, MD, CPE.
1. Simon R, Shuman DW. The standard of care in suicide risk assessment: an elusive concept. CNS Spectr. 2006;11(6):442-445.
2. Goldsmith SK, Pellmar TC, Kleinman AM, et al. eds. Reducing suicide: a national imperative. Washington, DC: The National Academies Press; 2002.
3. Harris EC, Barraclough B. Suicide as an outcome for mental disorders. A meta-analysis. Br J Psychiatry. 1997;170(3):205-228.
The basic function of a suicide assessment is to identify fixed and modifiable risk factors for suicide and existing or amendable protective factors.1 Epidemiologic studies have defined a range of suicide risk and protective factors for the general population.2 Other research has delineated suicide risk and protective factors for individuals with specific psychiatric disorders.3 The presence of disorder-specific risk and protective factors for suicide must be identified during suicide risk assessment.
Risk factors
Lack of support from family, peers, or the community is a critical concern. Noncompliance with treatment may be associated with onset of suicidality. Help-seeking is impeded by stigma associated with suicide and shame for past attempts. History of physical, sexual, or psychological abuse is tied to subsequent suicidal behavior. Alcohol abuse plays a role in suicide. Many patients who attempt suicide have backgrounds involving suicide loss or attempts by family members. Recurring psychiatric symptoms—particularly depression, anxiety, and panic—can trigger suicidality. Symptom relapse may lead to hospitalization, which is followed by a high-risk period after discharge.
These suicide risk factors can be summarized by the mnemonic UNSAFE:
Unconnected—no support; sense of not belonging or being a burden
Nonadherence—unmanaged mental illness or co-occurring disorders
Stigma/shame related to past attempts or suicidal behavior
Abuse history and/or alcohol misuse; prior attempt
Family history of suicide or suicide attempts
Exacerbations—worsened mental illness, hospitalizations
Protective factors
The presence of a personal crisis or safety self-help plan shows patient insight. Maintaining prescribed treatment indicates a patient’s likelihood of complying with clinical and self-care measures to avert future suicidality. Accessible support from family, peers, and the community demonstrates social integration. The recovery concept promotes these factors as well as wellness and resilience. Awareness of the warning signs of suicide and personal risk factors and precipitants is essential for self-help and help-seeking.
Protective factors for suicide can be summarized by the mnemonic SAFER:
Self-help skills, personal crisis/suicide prevention plan
Adherence to treatment plan
Family and community support
Education about risk factors, warning signs, and triggers for suicide
Recovery and resilience
In our emergency psychiatric facility the UNSAFE and SAFE mnemonics are posted next to the desk of the on-duty psychiatrist. Crisis center staff use these mnemonics to screen patients during psychiatric evaluations. Allied therapists use them during in-patient psychoeducation about suicidality. Peer specialists use them to help patients prepare personal safety plans.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufactures of competing products.
These mnemonics were developed by Tony Salvatore in consultation with Rocio Nell, MD, CPE.
The basic function of a suicide assessment is to identify fixed and modifiable risk factors for suicide and existing or amendable protective factors.1 Epidemiologic studies have defined a range of suicide risk and protective factors for the general population.2 Other research has delineated suicide risk and protective factors for individuals with specific psychiatric disorders.3 The presence of disorder-specific risk and protective factors for suicide must be identified during suicide risk assessment.
Risk factors
Lack of support from family, peers, or the community is a critical concern. Noncompliance with treatment may be associated with onset of suicidality. Help-seeking is impeded by stigma associated with suicide and shame for past attempts. History of physical, sexual, or psychological abuse is tied to subsequent suicidal behavior. Alcohol abuse plays a role in suicide. Many patients who attempt suicide have backgrounds involving suicide loss or attempts by family members. Recurring psychiatric symptoms—particularly depression, anxiety, and panic—can trigger suicidality. Symptom relapse may lead to hospitalization, which is followed by a high-risk period after discharge.
These suicide risk factors can be summarized by the mnemonic UNSAFE:
Unconnected—no support; sense of not belonging or being a burden
Nonadherence—unmanaged mental illness or co-occurring disorders
Stigma/shame related to past attempts or suicidal behavior
Abuse history and/or alcohol misuse; prior attempt
Family history of suicide or suicide attempts
Exacerbations—worsened mental illness, hospitalizations
Protective factors
The presence of a personal crisis or safety self-help plan shows patient insight. Maintaining prescribed treatment indicates a patient’s likelihood of complying with clinical and self-care measures to avert future suicidality. Accessible support from family, peers, and the community demonstrates social integration. The recovery concept promotes these factors as well as wellness and resilience. Awareness of the warning signs of suicide and personal risk factors and precipitants is essential for self-help and help-seeking.
Protective factors for suicide can be summarized by the mnemonic SAFER:
Self-help skills, personal crisis/suicide prevention plan
Adherence to treatment plan
Family and community support
Education about risk factors, warning signs, and triggers for suicide
Recovery and resilience
In our emergency psychiatric facility the UNSAFE and SAFE mnemonics are posted next to the desk of the on-duty psychiatrist. Crisis center staff use these mnemonics to screen patients during psychiatric evaluations. Allied therapists use them during in-patient psychoeducation about suicidality. Peer specialists use them to help patients prepare personal safety plans.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufactures of competing products.
These mnemonics were developed by Tony Salvatore in consultation with Rocio Nell, MD, CPE.
1. Simon R, Shuman DW. The standard of care in suicide risk assessment: an elusive concept. CNS Spectr. 2006;11(6):442-445.
2. Goldsmith SK, Pellmar TC, Kleinman AM, et al. eds. Reducing suicide: a national imperative. Washington, DC: The National Academies Press; 2002.
3. Harris EC, Barraclough B. Suicide as an outcome for mental disorders. A meta-analysis. Br J Psychiatry. 1997;170(3):205-228.
1. Simon R, Shuman DW. The standard of care in suicide risk assessment: an elusive concept. CNS Spectr. 2006;11(6):442-445.
2. Goldsmith SK, Pellmar TC, Kleinman AM, et al. eds. Reducing suicide: a national imperative. Washington, DC: The National Academies Press; 2002.
3. Harris EC, Barraclough B. Suicide as an outcome for mental disorders. A meta-analysis. Br J Psychiatry. 1997;170(3):205-228.
Therapeutic alliances: Conveying our sacred calling
Before modern medications and managed care, we tended to focus more on our relationships with patients. The goal was to establish a therapeutic alliance. Perhaps the idea of this kind of physician-patient relationship was what philosopher Martin Buber described as the “I-Thou” interaction. Instead of the “I-It” relationship where we mainly look at reducing symptoms, “I-Thou” recognizes the authenticity of the other and recommends reciprocity and respect.1
After Buber, research found that a positive and hopeful relationship is a common ingredient of successful psychotherapy of any theoretical persuasion and technique.2 Because the therapeutic alliance is crucial even during a brief medication check—and likely will enhance compliance—maybe we need to bring Buber back into prominence. Here’s how:
The nature of our work. Shortened time and reliance on medication can make us feel as if we are doing factory work. Think of psychiatry as much as a calling as a career.
The greeting. One of the most rewarding clinical experiences I’ve had occurred when a new patient came into my office. Before I could ask how she was feeling about seeing a new psychiatrist, she quickly said how pleased she was that I was her physician. Thinking that she might have looked up some of my writings on the Internet, I asked her why. She said that she had noticed that I smiled when I greeted my patients in the waiting room, as if I was happy to see them.
Look at your patient, not your computer. When my practice was transferring from paper to electronic records, I tried to talk to patients as I typed. One patient joked, “Hey, Doc, who are you talking to on that computer?” I got the message. I used to be able to scribble notes as we talked. Now, I maintain eye contact when I begin the session, and leave the computer until the end.
Know who your patients are. Find out what is most important to each patient, and refer to it often. What gives meaning to patients’ lives despite their psychiatric disorder will give meaning to your relationship.
You’re in this together. Make clear the limitations you are working under. Indicate that despite these obstacles, you will do whatever you can as a partnership. You may even want to apologize at times for what you can’t do, but would like to.
Saying goodbye. Always leave time for questions. Given the trend for less frequent appointments, which can make patients feel rejected, ask them if coming back at a later date seems acceptable. Let your patients know you look forward to seeing them again. Be sure to close with a handshake or other culturally appropriate gesture.
Disclosure
Dr. Moffic reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Before modern medications and managed care, we tended to focus more on our relationships with patients. The goal was to establish a therapeutic alliance. Perhaps the idea of this kind of physician-patient relationship was what philosopher Martin Buber described as the “I-Thou” interaction. Instead of the “I-It” relationship where we mainly look at reducing symptoms, “I-Thou” recognizes the authenticity of the other and recommends reciprocity and respect.1
After Buber, research found that a positive and hopeful relationship is a common ingredient of successful psychotherapy of any theoretical persuasion and technique.2 Because the therapeutic alliance is crucial even during a brief medication check—and likely will enhance compliance—maybe we need to bring Buber back into prominence. Here’s how:
The nature of our work. Shortened time and reliance on medication can make us feel as if we are doing factory work. Think of psychiatry as much as a calling as a career.
The greeting. One of the most rewarding clinical experiences I’ve had occurred when a new patient came into my office. Before I could ask how she was feeling about seeing a new psychiatrist, she quickly said how pleased she was that I was her physician. Thinking that she might have looked up some of my writings on the Internet, I asked her why. She said that she had noticed that I smiled when I greeted my patients in the waiting room, as if I was happy to see them.
Look at your patient, not your computer. When my practice was transferring from paper to electronic records, I tried to talk to patients as I typed. One patient joked, “Hey, Doc, who are you talking to on that computer?” I got the message. I used to be able to scribble notes as we talked. Now, I maintain eye contact when I begin the session, and leave the computer until the end.
Know who your patients are. Find out what is most important to each patient, and refer to it often. What gives meaning to patients’ lives despite their psychiatric disorder will give meaning to your relationship.
You’re in this together. Make clear the limitations you are working under. Indicate that despite these obstacles, you will do whatever you can as a partnership. You may even want to apologize at times for what you can’t do, but would like to.
Saying goodbye. Always leave time for questions. Given the trend for less frequent appointments, which can make patients feel rejected, ask them if coming back at a later date seems acceptable. Let your patients know you look forward to seeing them again. Be sure to close with a handshake or other culturally appropriate gesture.
Disclosure
Dr. Moffic reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Before modern medications and managed care, we tended to focus more on our relationships with patients. The goal was to establish a therapeutic alliance. Perhaps the idea of this kind of physician-patient relationship was what philosopher Martin Buber described as the “I-Thou” interaction. Instead of the “I-It” relationship where we mainly look at reducing symptoms, “I-Thou” recognizes the authenticity of the other and recommends reciprocity and respect.1
After Buber, research found that a positive and hopeful relationship is a common ingredient of successful psychotherapy of any theoretical persuasion and technique.2 Because the therapeutic alliance is crucial even during a brief medication check—and likely will enhance compliance—maybe we need to bring Buber back into prominence. Here’s how:
The nature of our work. Shortened time and reliance on medication can make us feel as if we are doing factory work. Think of psychiatry as much as a calling as a career.
The greeting. One of the most rewarding clinical experiences I’ve had occurred when a new patient came into my office. Before I could ask how she was feeling about seeing a new psychiatrist, she quickly said how pleased she was that I was her physician. Thinking that she might have looked up some of my writings on the Internet, I asked her why. She said that she had noticed that I smiled when I greeted my patients in the waiting room, as if I was happy to see them.
Look at your patient, not your computer. When my practice was transferring from paper to electronic records, I tried to talk to patients as I typed. One patient joked, “Hey, Doc, who are you talking to on that computer?” I got the message. I used to be able to scribble notes as we talked. Now, I maintain eye contact when I begin the session, and leave the computer until the end.
Know who your patients are. Find out what is most important to each patient, and refer to it often. What gives meaning to patients’ lives despite their psychiatric disorder will give meaning to your relationship.
You’re in this together. Make clear the limitations you are working under. Indicate that despite these obstacles, you will do whatever you can as a partnership. You may even want to apologize at times for what you can’t do, but would like to.
Saying goodbye. Always leave time for questions. Given the trend for less frequent appointments, which can make patients feel rejected, ask them if coming back at a later date seems acceptable. Let your patients know you look forward to seeing them again. Be sure to close with a handshake or other culturally appropriate gesture.
Disclosure
Dr. Moffic reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Shattering dogmas
Like all other medical specialties, psychiatry has its share of dogmas that are perpetuated via the clinical apprenticeship model from one generation of physicians to the next, despite the lack of hard evidence. They become “articles of faith” that go unchallenged by trainees who acquire them from their supervisors. A dogma masquerades as a truism and eventually becomes a sacred feature of the “clinical lore.”
Sooner or later, however, the bright light of scientific evidence will reveal the ersatz nature of a dogma and it will come crashing down. Similar to a revolution to depose a dictator, the demise of a dogma will have a salutary effect on medical practice and a liberating effect on practitioners.
Here are examples of psychiatric dogmas that were part of my training but have been/or are in the process of being taken to the slaughterhouse of obsolete tenets:
Psychiatrists should not touch their patients. Really! How can we be practicing physicians if we don’t? This dogma arbitrarily sexualized the physical exam, including drawing blood, measuring blood pressure or waist circumference, assessing neuroleptic-induced cogwheeling, or checking the body for a drug-induced rash. This dogma is the antithesis of good medical care for psychiatric patients, who frequently suffer from serious physical ailments and often do not have a primary care provider. It was created during the primordial phase of psychiatry (aka psychoanalysis) and is irrelevant in modern-era psychiatry.
Push the dose of neuroleptics higher and higher until the patient becomes parkinsonian, which is the sign that psychosis will improve. This dogma dominated the pharmacotherapy of schizophrenia for 40 years because of the erroneous linkage of extrapyramidal symptoms (EPS) with therapeutic response to antipsychotics. We did not realize the neurologic harm of this dogma until the computer revolution and related scientific advances enabled researchers to measure the dopamine receptor occupancy in patients’ brains.1 Positron emission tomography (PET) scan studies revealed that only 60% to 65% of dopamine D2 receptors need to be blocked to suppress psychotic symptoms, whereas EPS will occur at ≥78% occupancy. Millions of patients needlessly suffered intolerable rigidity, dyskinesia, restlessness, and tremors and routinely received large doses of anticholinergic drugs that destroyed their quality of life due to memory loss, dry mouth, constipation, and blurry vision.
Medications must be administered daily. The same landmark receptor imaging studies described above may soon debunk this ubiquitously entrenched clinical dogma. Recent data showed that administering the same antipsychotic dose every other day instead of every day was equally efficacious.2 Dopamine receptors do not require 24/7 blockade to treat psychosis as was formerly believed; apparently, intermittent occupancy is sufficient. Shattering this dogma can save 50% of the cost of the (expensive) antipsychotic medications, which chronic schizophrenia patients have to take for many years.
Patients with schizophrenia will ingest their oral medications as prescribed. This dogma continues to dominate clinical practice despite numerous studies that show up to 80% of schizophrenia patients relapse due to poor adherence to oral antipsychotics. Yet many psychiatrists continue to prescribe oral medications even though they know core symptoms of schizophrenia—lack of insight, amotivation, impaired memory, suspiciousness, and substance use—contribute heavily to nonadherence. The dogma of oral meds has been “attenuated” in Europe, where 30% of patients are treated with long-acting injectable depot medications, compared with about 7% in the United States.3
Academic psychiatrists must not collaborate with the pharmaceutical industry. This dogma was hatched recently and ignores the huge unmet needs of psychiatric patients. More than 80% of DSM-IV disorders do not have any FDA-approved drug.4 Whether we like it or not, the pharmaceutical industry is the only source of new medication. Instead of avoiding an academic-industry collaboration, Europe has boldly moved ahead of the United States by formalizing a unique initiative called Novel Methods leading to New Medications in Depression and Schizophrenia (NEWMEDS).
This large collaboration intends to accelerate new drug discovery via a partnership between several prestigious European academic psychiatry institutes and global drug companies. By discarding the strident, dogmatic attitudes of shirking collaboration, NEWMEDS promises to expedite and accelerate the discovery and development of urgently needed therapeutic agents with innovative mechanisms. Dr. S. Kapur, the PET imaging pioneer, serves as the academic leader of NEWMEDS.
Psychiatrists are experts at detecting erroneous thinking in individuals or groups. We should vigorously rid our specialty of unproven tenets and detrimental dogmas. The best and only way to accomplish that worthy goal is to seek scientific basis for everything we do or teach.
1. Kapur S, Seeman P. Does fast dissociation from the dopamine d(2) receptor explain the action of atypical antipsychotics?: a new hypothesis. Am J Psychiatry. 2001;158:360-369.
2. Remington G, Kapur S. Antipsychotic dosing: how much but also how often? Schizophr Bull. 2010;36(5):900-903.
3. Adams CE, Fenton MK, Quraishi S, et al. Systematic meta-review of depot antipsychotic drugs for people with schizophrenia. Br J Psychiatry. 2001;179:290-299.
4. Devulapalli K, Nasrallah HA. An analysis of the high psychotropic off-label use in psychiatric disorders: the majority of psychiatric diagnoses have no approved drug. Asian J Psychiatr. 2009;2:29-36.

Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://CurrentPsychiatry.blogspot.com or https://www.currentpsychiatry.com/forms/reader_feedback.asp
Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://CurrentPsychiatry.blogspot.com or https://www.currentpsychiatry.com/forms/reader_feedback.asp
Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://CurrentPsychiatry.blogspot.com or https://www.currentpsychiatry.com/forms/reader_feedback.asp
Like all other medical specialties, psychiatry has its share of dogmas that are perpetuated via the clinical apprenticeship model from one generation of physicians to the next, despite the lack of hard evidence. They become “articles of faith” that go unchallenged by trainees who acquire them from their supervisors. A dogma masquerades as a truism and eventually becomes a sacred feature of the “clinical lore.”
Sooner or later, however, the bright light of scientific evidence will reveal the ersatz nature of a dogma and it will come crashing down. Similar to a revolution to depose a dictator, the demise of a dogma will have a salutary effect on medical practice and a liberating effect on practitioners.
Here are examples of psychiatric dogmas that were part of my training but have been/or are in the process of being taken to the slaughterhouse of obsolete tenets:
Psychiatrists should not touch their patients. Really! How can we be practicing physicians if we don’t? This dogma arbitrarily sexualized the physical exam, including drawing blood, measuring blood pressure or waist circumference, assessing neuroleptic-induced cogwheeling, or checking the body for a drug-induced rash. This dogma is the antithesis of good medical care for psychiatric patients, who frequently suffer from serious physical ailments and often do not have a primary care provider. It was created during the primordial phase of psychiatry (aka psychoanalysis) and is irrelevant in modern-era psychiatry.
Push the dose of neuroleptics higher and higher until the patient becomes parkinsonian, which is the sign that psychosis will improve. This dogma dominated the pharmacotherapy of schizophrenia for 40 years because of the erroneous linkage of extrapyramidal symptoms (EPS) with therapeutic response to antipsychotics. We did not realize the neurologic harm of this dogma until the computer revolution and related scientific advances enabled researchers to measure the dopamine receptor occupancy in patients’ brains.1 Positron emission tomography (PET) scan studies revealed that only 60% to 65% of dopamine D2 receptors need to be blocked to suppress psychotic symptoms, whereas EPS will occur at ≥78% occupancy. Millions of patients needlessly suffered intolerable rigidity, dyskinesia, restlessness, and tremors and routinely received large doses of anticholinergic drugs that destroyed their quality of life due to memory loss, dry mouth, constipation, and blurry vision.
Medications must be administered daily. The same landmark receptor imaging studies described above may soon debunk this ubiquitously entrenched clinical dogma. Recent data showed that administering the same antipsychotic dose every other day instead of every day was equally efficacious.2 Dopamine receptors do not require 24/7 blockade to treat psychosis as was formerly believed; apparently, intermittent occupancy is sufficient. Shattering this dogma can save 50% of the cost of the (expensive) antipsychotic medications, which chronic schizophrenia patients have to take for many years.
Patients with schizophrenia will ingest their oral medications as prescribed. This dogma continues to dominate clinical practice despite numerous studies that show up to 80% of schizophrenia patients relapse due to poor adherence to oral antipsychotics. Yet many psychiatrists continue to prescribe oral medications even though they know core symptoms of schizophrenia—lack of insight, amotivation, impaired memory, suspiciousness, and substance use—contribute heavily to nonadherence. The dogma of oral meds has been “attenuated” in Europe, where 30% of patients are treated with long-acting injectable depot medications, compared with about 7% in the United States.3
Academic psychiatrists must not collaborate with the pharmaceutical industry. This dogma was hatched recently and ignores the huge unmet needs of psychiatric patients. More than 80% of DSM-IV disorders do not have any FDA-approved drug.4 Whether we like it or not, the pharmaceutical industry is the only source of new medication. Instead of avoiding an academic-industry collaboration, Europe has boldly moved ahead of the United States by formalizing a unique initiative called Novel Methods leading to New Medications in Depression and Schizophrenia (NEWMEDS).
This large collaboration intends to accelerate new drug discovery via a partnership between several prestigious European academic psychiatry institutes and global drug companies. By discarding the strident, dogmatic attitudes of shirking collaboration, NEWMEDS promises to expedite and accelerate the discovery and development of urgently needed therapeutic agents with innovative mechanisms. Dr. S. Kapur, the PET imaging pioneer, serves as the academic leader of NEWMEDS.
Psychiatrists are experts at detecting erroneous thinking in individuals or groups. We should vigorously rid our specialty of unproven tenets and detrimental dogmas. The best and only way to accomplish that worthy goal is to seek scientific basis for everything we do or teach.
Like all other medical specialties, psychiatry has its share of dogmas that are perpetuated via the clinical apprenticeship model from one generation of physicians to the next, despite the lack of hard evidence. They become “articles of faith” that go unchallenged by trainees who acquire them from their supervisors. A dogma masquerades as a truism and eventually becomes a sacred feature of the “clinical lore.”
Sooner or later, however, the bright light of scientific evidence will reveal the ersatz nature of a dogma and it will come crashing down. Similar to a revolution to depose a dictator, the demise of a dogma will have a salutary effect on medical practice and a liberating effect on practitioners.
Here are examples of psychiatric dogmas that were part of my training but have been/or are in the process of being taken to the slaughterhouse of obsolete tenets:
Psychiatrists should not touch their patients. Really! How can we be practicing physicians if we don’t? This dogma arbitrarily sexualized the physical exam, including drawing blood, measuring blood pressure or waist circumference, assessing neuroleptic-induced cogwheeling, or checking the body for a drug-induced rash. This dogma is the antithesis of good medical care for psychiatric patients, who frequently suffer from serious physical ailments and often do not have a primary care provider. It was created during the primordial phase of psychiatry (aka psychoanalysis) and is irrelevant in modern-era psychiatry.
Push the dose of neuroleptics higher and higher until the patient becomes parkinsonian, which is the sign that psychosis will improve. This dogma dominated the pharmacotherapy of schizophrenia for 40 years because of the erroneous linkage of extrapyramidal symptoms (EPS) with therapeutic response to antipsychotics. We did not realize the neurologic harm of this dogma until the computer revolution and related scientific advances enabled researchers to measure the dopamine receptor occupancy in patients’ brains.1 Positron emission tomography (PET) scan studies revealed that only 60% to 65% of dopamine D2 receptors need to be blocked to suppress psychotic symptoms, whereas EPS will occur at ≥78% occupancy. Millions of patients needlessly suffered intolerable rigidity, dyskinesia, restlessness, and tremors and routinely received large doses of anticholinergic drugs that destroyed their quality of life due to memory loss, dry mouth, constipation, and blurry vision.
Medications must be administered daily. The same landmark receptor imaging studies described above may soon debunk this ubiquitously entrenched clinical dogma. Recent data showed that administering the same antipsychotic dose every other day instead of every day was equally efficacious.2 Dopamine receptors do not require 24/7 blockade to treat psychosis as was formerly believed; apparently, intermittent occupancy is sufficient. Shattering this dogma can save 50% of the cost of the (expensive) antipsychotic medications, which chronic schizophrenia patients have to take for many years.
Patients with schizophrenia will ingest their oral medications as prescribed. This dogma continues to dominate clinical practice despite numerous studies that show up to 80% of schizophrenia patients relapse due to poor adherence to oral antipsychotics. Yet many psychiatrists continue to prescribe oral medications even though they know core symptoms of schizophrenia—lack of insight, amotivation, impaired memory, suspiciousness, and substance use—contribute heavily to nonadherence. The dogma of oral meds has been “attenuated” in Europe, where 30% of patients are treated with long-acting injectable depot medications, compared with about 7% in the United States.3
Academic psychiatrists must not collaborate with the pharmaceutical industry. This dogma was hatched recently and ignores the huge unmet needs of psychiatric patients. More than 80% of DSM-IV disorders do not have any FDA-approved drug.4 Whether we like it or not, the pharmaceutical industry is the only source of new medication. Instead of avoiding an academic-industry collaboration, Europe has boldly moved ahead of the United States by formalizing a unique initiative called Novel Methods leading to New Medications in Depression and Schizophrenia (NEWMEDS).
This large collaboration intends to accelerate new drug discovery via a partnership between several prestigious European academic psychiatry institutes and global drug companies. By discarding the strident, dogmatic attitudes of shirking collaboration, NEWMEDS promises to expedite and accelerate the discovery and development of urgently needed therapeutic agents with innovative mechanisms. Dr. S. Kapur, the PET imaging pioneer, serves as the academic leader of NEWMEDS.
Psychiatrists are experts at detecting erroneous thinking in individuals or groups. We should vigorously rid our specialty of unproven tenets and detrimental dogmas. The best and only way to accomplish that worthy goal is to seek scientific basis for everything we do or teach.
1. Kapur S, Seeman P. Does fast dissociation from the dopamine d(2) receptor explain the action of atypical antipsychotics?: a new hypothesis. Am J Psychiatry. 2001;158:360-369.
2. Remington G, Kapur S. Antipsychotic dosing: how much but also how often? Schizophr Bull. 2010;36(5):900-903.
3. Adams CE, Fenton MK, Quraishi S, et al. Systematic meta-review of depot antipsychotic drugs for people with schizophrenia. Br J Psychiatry. 2001;179:290-299.
4. Devulapalli K, Nasrallah HA. An analysis of the high psychotropic off-label use in psychiatric disorders: the majority of psychiatric diagnoses have no approved drug. Asian J Psychiatr. 2009;2:29-36.
1. Kapur S, Seeman P. Does fast dissociation from the dopamine d(2) receptor explain the action of atypical antipsychotics?: a new hypothesis. Am J Psychiatry. 2001;158:360-369.
2. Remington G, Kapur S. Antipsychotic dosing: how much but also how often? Schizophr Bull. 2010;36(5):900-903.
3. Adams CE, Fenton MK, Quraishi S, et al. Systematic meta-review of depot antipsychotic drugs for people with schizophrenia. Br J Psychiatry. 2001;179:290-299.
4. Devulapalli K, Nasrallah HA. An analysis of the high psychotropic off-label use in psychiatric disorders: the majority of psychiatric diagnoses have no approved drug. Asian J Psychiatr. 2009;2:29-36.
Atypical antipsychotics for delirium: A reasonable alternative to haloperidol?
Discuss this article at http://currentpsychiatry.blogspot.com/2011/01/atypical-antipsychotics-for-delirium.html#comments
Ms. B, age 48, is admitted to our hospital after overdosing on unknown amounts of amitriptyline, diphenhydramine, and laxatives. Three days after admission, the psychiatry service is consulted to assess her for “bipolar disorder.” Although Ms. B does not have a psychiatric history, her internist believes her pressured speech and psychomotor agitation warrant investigation.
During the initial psychiatric interview, Ms. B is disoriented, with fluctuating alertness and cognition. The Confusion Assessment Method for the Intensive Care Unit (CAM-ICU)1 is positive for delirium. We perform a delirium workup while we start Ms. B on olanzapine, 5 mg/d orally and 5 mg intramuscular (IM) every 8 hours as needed.
Ms. B’s laboratory results (complete blood count, complete metabolic profile, urinalysis, chest roentgenogram, vitamin B12 level, blood alcohol level, urine drug screen, arterial blood gas, and head CT) are unremarkable except for her amitriptyline/nortriptyline level, which is in the toxic range. On physical examination, Ms. B’s heart rate and temperature are elevated, her pupils are dilated and sluggish, and her skin is hot and dry. Based on these findings, we determine that Ms. B’s delirium most likely is an anticholinergic syndrome from amitriptyline/diphenhydramine toxicity.2 We discontinue olanzapine after only 2 doses because of its potential anticholinergic effects.3
In hospitalized patients, delirium is one of the most frequently encountered mental disorders, but because of its variable presentation the condition often is underrecognized and undertreated, which leads to longer hospitalizations and increased mortality.4,5 Ms. B’s case illustrates the classical delirium presentation (Table 1),6 highlighting 2 hallmark features of the disorder: inattention and an acute fluctuating course.4 Unfortunately, delirium is a diverse disorder that may present with numerous nonclassical symptoms—including lethargy, emotionality, sleep irregularities, and neurologic abnormalities—in lieu of more commonly recognized symptoms.4,5
In addition to recommending identifying and addressing the underlying acute illness, American Psychiatric Association guidelines suggest prescribing psychotropic medications to treat delirium symptoms.5,7 Antipsychotics are considered first-line pharmacotherapy because they have been shown to lower hospital mortality rates8 and improve delirium symptoms even before underlying medical etiologies are treated.5 Haloperidol is the mainstay of delirium treatment.8 Compared with atypical antipsychotics in delirium treatment, haloperidol doses <3.5 mg/d have not been associated with an increase in extrapyramidal symptoms (EPS).9
Although not devoid of side effects, atypical antipsychotics are an alternative to haloperidol.8,10 This article briefly summarizes the current evidence on the use of atypicals for treating delirium.
Table 1
Delirium: Diagnostic criteria
| Delirium describes a group of related disorders with variable clinical presentations and differing causation. Regardless of the etiology, all types of delirium share a set of common symptoms that include: |
| Disturbances of consciousness and attention |
| Changes in cognition such as memory deficit, language disturbance, or disorientation |
| Perceptual disturbances not better accounted for by dementia |
| Abrupt onset (usually hours to days) |
| Fluctuating symptoms throughout the course of the day |
| Source: Adapted from reference 6 |
CASE CONTINUED: IM ziprasidone
After reassessing our treatment options, we prescribe ziprasidone, 10 mg IM twice a day, and an additional 10 mg IM every 12 hours as needed. Ziprasidone’s minimal anticholinergic and sedative effects3 seem favorable for Ms. B’s delirium; however, this medication has several drawbacks, including IM administration, greater expense compared with intravenous haloperidol, and risk of adverse cardiac affects, specifically prolonged corrected QT (QTc) interval.11 Bioavailability of oral ziprasidone is markedly less than the IM preparation (~60% vs 100%, respectively), and oral bioavailability decreases to approximately 30% when taken without food.12 Given Ms. B’s her current mental state, we feel that IM ziprasidone is a more reliable means to achieve therapeutic efficacy.13
With respect to cardiac concerns, we evaluate Ms. B’s predisposing and precipitating risk factors.11 Family members confirm that she had no cardiac history. We obtain baseline ECGs and continually monitor her QTc interval, which remained at <500 msec during ziprasidone treatment.
Ms. B tolerates ziprasidone and we note modest improvement in her mental status after 2 days of treatment; her vigilant-A portion of the CAM-ICU improves, but she still screens positive for delirium. During the next week Ms. B develops several medical comorbidities, including ileus, urinary tract infection, and methicillin-resistant Staphylococcus aureus infection. Despite these complications her mental status continues to improve. Within 6 days, Ms. B’s attention and cognition improve dramatically. She is oriented and able to engage in medical decision-making, and she screens negative for delirium on the CAM-ICU. We begin to assess her for psychiatric disorders that may have contributed to her hospitalization.
Evidence for antipsychotics
Haloperidol has been the antipsychotic of choice for treating delirium symptoms. It is recommended by the Society of Critical Care Medicine7 and is regarded as safe, cost-effective, and efficacious for delirium5 despite a risk of dose-related EPS and potential cardiac conduction alterations.5,14
Risperidone is not indicated for treating delirium but is one of the most extensively studied atypical antipsychotic alternatives to haloperidol. Evidence consisting primarily of case reports has illustrated the potential efficacy of risperidone in treating delirium (Table 2).10,15-19
In 2004, Parellada et al17 observed significant mean improvements in all measures (Delirium Rating Scale [DRS], Mini-Mental State Exam [MMSE], positive subscale of the Positive and Negative Syndrome Scale [PANSS-P], and Clinical Global Impressions scale [CGI]) in 64 delirium patients treated with risperidone. In a 2004 double-blind trial of 28 delirium patients randomly assigned to risperidone or haloperidol, risperidone was effective but not significantly more efficacious than low-dose haloperidol for acute delirium treatment.18
Advantages of using risperidone include its lack of anticholinergic effects. Potential side effects include dose-related EPS and weight gain, which were observed in patients with schizophrenia and other psychotic disorders and dementia-related behavioral disorders.20,21
Olanzapine. Much like risperidone, olanzapine’s use in delirium is relatively well described in the literature (Table 3).22-24 In a randomized, placebo-controlled study comparing olanzapine with haloperidol, 175 patients were treated for 7 days with olanzapine, haloperidol, or placebo. Olanzapine and haloperidol showed significantly greater DRS score improvement than placebo.24 There was no difference between olanzapine and haloperidol outcomes; however, olanzapine showed significant improvement by days 2 and 3 compared with haloperidol. Haloperidol was associated with a significantly higher rate of dystonia compared with olanzapine.
Olanzapine carries a risk of anticholinergic effects. This can be a drawback, especially in patients such as Ms. B whose delirium has an anticholinergic component. Olanzapine is available in an IM formulation, which can be an advantage when addressing agitation and medical comorbidities of delirium.
Quetiapine. Case reports have suggested quetiapine is effective for delirium (Table 4).10,25-27 In a prospective, open-label trial, Sasaki et al26 treated 12 delirium patients with a single bedtime dose of quetiapine. All patients achieved remission within several days of beginning quetiapine, and the drug was well tolerated with no detected EPS or excessive sedation.
In 2010 Devlin et al27 reported on the efficacy and safety of quetiapine in a prospective double-blind, placebo-controlled study of 36 adult ICU patients. Compared with those receiving placebo, patients taking quetiapine had a statistically significant shorter time to first resolution of delirium, reduced duration of delirium, and less agitation as measured by the Sedation-Agitation Scale. Mortality, ICU length of stay, and incidence of QTc prolongation did not differ, but patients treated with quetiapine were more likely to be discharged home or to rehabilitation and to have more somnolence. Quetiapine’s side effect profile includes a low occurrence of EPS, sedation, and dose-related anticholinergic effects.25
Ziprasidone. The literature on ziprasidone for delirium so far is limited to a few anecdotal case reports (Table 5).28-31 In 2002, Leso and Schwartz28 successfully used ziprasidone to treat delirium in a patient with human immunodeficiency virus and cryptococcal meningitis. Ziprasidone was chosen for its lack of sedating effects and low EPS risk. The patient experienced significant clearing of his delirium and lowering of his DRS score. Ziprasidone eventually was discontinued because a fluctuating QTc interval associated with comorbid electrolyte imbalances—a potential drawback to ziprasidone.
In the case of Ms. B, ziprasidone appeared to be efficacious; however, improvement in her medical condition, rather than ziprasidone treatment, is the most likely explanation for the resolution of her delirium symptoms.
Aripiprazole. Alao et al30 reported on 2 delirium patients treated with 30 mg and 15 mg aripiprazole; improvement was monitored using the MMSE and DRS (Table 5).28-31 In both cases, confusion, disorientation, and agitation improved within 7 days of treatment. In the first case, the patient’s MMSE score improved from 5 to 28 and his DRS score decreased from 28 to 6. The second patient’s MMSE score improved from 7 to 27 and her DRS score went from 18 to 6.
Straker et al31 reported on 14 delirium patients treated with aripiprazole. Twelve patients had a ≥50% reduction in DRS, Revised-98 scores, and 13 showed improvement on CGI scores. The rate of adverse side effects was low. Three patients had prolonged QTc interval, but no patients developed arrhythmia or discontinued aripiprazole.
Table 2
Risperidone for delirium: What the evidence says
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Sipahimalani et al, 199715 | N=2 (age 14 and 60). Initial dose: 1 mg/d; maintenance dose: 2 mg/d | 10 to 14 days | MMSE score increased. AEs: extrapyramidal symptoms (dystonia and cogwheeling) |
| Schwartz et al, 200210 | N=11 (age range 14 to 74). Mean dose: 1.59 ± 0.8 mg/d | 5.1 ± 4.3 days | CGI score decreased. No reported AEs |
| Horikawa et al, 200316 | N=10 (mean age: 56.8; range: 22 to 81). Mean dose: 1.7 mg/d | 7.1 days | DRS score decreased significantly in 80% of patients (P=.03) AEs: sleepiness (30%), mild drug-induced parkinsonism (10%) |
| Parellada et al, 200417 | N=64 (mean age: 67.3 ± 11.4 years). Mean dose: 2.6 ± 1.7 mg/d | 3 to 7 days | Effective in 90.6% of patients with significant decreases in DRS, PANSS-P, and CGI and increase in MMSE (P < .001). AEs: drowsiness (3.1%), nausea (1.6%) |
| Hans et al, 200418 | N=12 (mean age: 65.6). Mean dose: 1.02 mg/d | 4 to 7 days | MDAS scores decreased significantly (P < .05). No reported AEs |
| Bourgeois et al, 200519 | N=1 (age 57). Initial dose: 8 mg/d; maintenance dose: 2 mg/d | 9 days | MMSE score increased. No reported AEs |
| CGI: Clinical Global Impressions scale; DRS: Delirium Rating Scale; MDAS: Memorial Delirium Assessment Scale; MMSE: Mini-Mental State Exam; PANSS-P: positive subscale of the Positive and Negative Syndrome Scale | |||
Table 3
Olanzapine may have a role in treating delirium symptoms
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Sipahimalani et al, 199822 | N=11 (mean age: 63.5 ± 23.2 years). Mean dose: 8.2 ± 3.4 mg/d | 6.8 ± 3.5 days | Marked decrease (>50%) in DRS score for 5 patients. No reported AEs |
| Breitbart et al, 200223 | N=79 (mean age: 60.6 ± 17.3 years; range: 19 to 89). Initial dose: 3 ± 0.14 mg/d; mean dose: 4.6 to 6.3 mg/d | 2 to 7 days | MDAS decreased significantly (P < .001), with 76% of patients’ delirium reaching resolution (MDAS ≤10). AEs: sedation (30%) |
| Hu et al, 200424 | N=74 (mean age: 74). Mean dose: 1.25 to 2 mg/d | 2.78 ± 1.85 days | DRS score decreased significantly (P < .01) in 72.2% of patients. AEs: drowsiness (18.9%), dystonia (2.7%), dry mouth (2.7%) |
| DRS: Delirium Rating Scale; MDAS: Memorial Delirium Assessment Scale | |||
Table 4
Evidence suggests quetiapine could reduce delirium symptoms
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Schwartz et al, 200210 | N=11 (age range: 19 to 91). Mean dose: 211.4 mg/d | 6.5 days | Decrease in DRS score (>50% reduction in global delirium symptoms) for 10 patients. AEs: sedation |
| Al-Samarrai et al, 200325 | N=2 (age 50 and 52). Mean dose: 200 to 400 mg/d | 2 to 4 days | No specific rating scale used but clinical reduction in agitation and improvement in cognition were reported. AEs: drowsiness |
| Sasaki et al, 200326 | N=12 (mean age: 67.3 ± 14.8 years). Mean dose: 44.9 ± 31.0 mg/d | 4.8 ± 3.5 days | Decrease in DRS score and remission of delirium for all patients. Significant increase in MMSE (P=.0256). No reported AEs |
| Devlin et al, 201027 | N=18 (adult ICU patients). Initial dose: 100 mg/d | 36 to 87 hours | Significantly shorter time to first resolution of delirium and duration of delirium compared with placebo. AEs: somnolence |
| DRS: Delirium Rating Scale; ICU: intensive care unit; MMSE: Mini-Mental State Exam | |||
Table 5
Limited data support ziprasidone and aripiprazole for treating delirium
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Ziprasidone | |||
| Leso et al, 200228 | N=1 (age 34). Initial dose: 40 mg/d; maintenance dose: 100 mg/d | 21 days | DRS score decreased from 26 to 14. AEs: 8.4% increase in QTc interval |
| Young et al, 200429 | N=1 (age 47). Initial dose: 20 mg IV bolus, followed by an oral taper over 7 days. | 7 days | No specific rating scale was used but dramatic improvement in patient’s restlessness was reported. No AEs reported |
| Aripiprazole | |||
| Alao et al, 200630 | N=2 (age 62 and 37). Mean dose: 15 and 30 mg/d | 2 to 7 days | Patient 1: DRS score decreased from 28 to 6 and MMSE score increased from 5 to 28. Patient 2: DRS score decreased from 18 to 6 and MMSE score increased from 7 to 27. No AEs reported |
| Straker et al, 200631 | N=14 (age range: 18 to 85). Mean dose: 8.9 mg/d | 2 to 14 days | 12 of 14 patients had a ≥50% decrease in DRS-R-98. AEs: 3 patients had prolonged QTc interval |
| DRS: Delirium Rating Scale; DRS-R-98: Delirium Rating Scale–Revised-98; MMSE: Mini-Mental State Exam | |||
Anticholinergic activity
Decreased acetylcholine activity (AA) is suspected in delirium pathogenesis.32 By extension of this theory, medications that block muscarinic receptors could worsen delirium. Haloperidol, risperidone, and ziprasidone have negligible or no AA, as reported in atropine equivalents. Quetiapine and olanzapine have mild (0.5 to 5 pmol/ mL) and moderate (5 to 15 pmol/mL) dose-related AA, respectively. For example, olanzapine, 5 mg/d, has roughly the same AA as quetiapine, 300 mg/d, whereas olanzapine, 10 mg/d, has about the same AA as quetiapine, 600 mg/d.32,33
Although we used this evidence, in part, to select an atypical antipsychotic for Ms. B, this model should be used only to estimate the possible anticholinergic burden associated with a specific medication or combination. The risk of anticholinergic burden needs to be considered along with a medication’s potential nonanticholinergic adverse effects and the patient’s overall clinical history (eg, past sensitivity to anticholinergic agents, memory complaints, effectiveness of an agent, concomitant medications, disease state, adherence concerns). For example, an atypical antipsychotic that is potently anti-histaminergic and therefore sedating could be beneficial when treating an agitated delirium patient. Establishing the presence of a risk of anticholinergic burden cannot be equated with the presence of anticholinergic toxicity, because the exact relationship between AA and cognitive performance is still unknown.32,33
Cardiovascular safety
The most common cardiovascular effects of atypical antipsychotics are tachycardia, hypotension (usually mild), and prolongation of QTc interval.34 For example, haloperidol, 15 mg/d, was found to increase mean QTc by 7 msec, with a reported odds ratio ranging from 2.2 to 6.1 for ventricular dysrhythmia and sudden cardiac death,35 although risk may be more strongly associated with high-dose, IV haloperidol.36
QTc interval prolongation warrants concern because it suggests that patients may be predisposed to torsades de pointes (TdP). Conventional antipsychotics— especially phenothiazines—have the highest risk of inducing TdP. One review concluded that compared with other antipsychotics, chlorpromazine, pimozide, thioridazine, and the atypical clozapine have a higher risk of cardiac arrhythmias and sudden cardiac death.11 Another review found cases of TdP with haloperidol, ziprasidone, olanzapine, and thioridazine.37 When prescribing an antipsychotic, consider both pharmacologic and nonpharmacologic risks factors, including preexisting cardiovascular disease, female sex, hepatic insufficiency, electrolyte abnormalities, stimulant drug abuse,36 and genetic predisposition (Table 6).11,35-37
Table 6
Risk factors for antipsychotic-induced QT interval prolongation and torsades de pointes*
| Pharmacologic |
|---|
| Antipsychotic selection |
| Drug interaction (QT-prolonging agents) |
| Drug interaction (slow metabolism by cytochrome P450 inhibitors of 2D6, 3A4, 1A2) |
| Nonpharmacologic |
| Advanced age (>65) |
| Bradycardia |
| Hypokalemia |
| Hypomagnesemia |
| Hepatic/renal dysfunction |
| Genetic predisposition |
| Female sex |
| Screening (major risk factors) |
| Structural cardiac disease |
| Congenital long QT syndrome |
| Family history of sudden cardiac death |
| Previous episodes of drug-induced QT prolongation or torsades de pointes |
| * Serial electrocardiograms are recommended for patients with a major risk factor or multiple pharmacologic/ nonpharmacologic risk factors Source: References 11,35-37 |
Related Resource
- Stern TA, Celano CM, Gross AF, et al. The assessment and management of agitation and delirium in the general hospital. Prim Care Companion J Clin Psychiatry 2010;12(1):e1–e11. www.psychiatrist.com/private/pccpdf/article_wrapper.asp?art=2010/09r00938yel/09r00938yel.htm.
Drug Brand Names
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Atropine • Sal-Tropine
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Diphenhydramine • Benadryl
- Haloperidol • Haldol
- Nortriptyline • Aventyl
- Olanzapine • Zyprexa
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thioridazine • Mellaril
- Ziprasidone • Geodon
Disclosures
Dr. Spiegel is a speaker for AstraZeneca, Pfizer, Inc., and Janssen Pharmaceuticals.
Drs. Ahlers, Yoder, and Qureshi report no financial relationship with any company whose products are mention in this article or with manufacturers of competing products.
1. Ely EW, Inouye SK, Bernard GR, et al. Delirium in the mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286:2703-2710.
2. Rudolph JL, Salow MJ, Angelini MC, et al. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med. 2008;168(5):508-513.
3. Albers LJ, Hahn RK, Reist C. Handbook of psychiatric drugs 2008. Blue Jay, CA: Current Clinical Strategies Publishing; 2007.
4. Inouye SK. Delirium in older persons. N Engl J Med. 2006;354(11):1157-1165.
5. American Psychiatric Association. Practice guideline for the treatment of patients with delirium. Am J Psychiatry. 1999;156(suppl 5):1-20.
6. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
7. Seitz DP, Gill SS, van Zyl LT. Antipsychotics in the treatment of delirium: a systematic review. J Clin Psychiatry. 2007;68(1):11-21.
8. Lacasse H, Perreault MM, Williamson DR. Systematic review of antipsychotics for the treatment of hospital-associated delirium in medically or surgically ill patients. Ann Pharmacother. 2006;40(11):1966-1973.
9. Lonergan E, Britton AM, Luxenberg J, et al. Antipsychotics for delirium. Cochrane Database Syst Rev. 2007;(2):CD005594.-
10. Schwartz TL, Masand PS. The role of atypical antipsychotics in the treatment of delirium. Psychosomatics. 2002;43(3):171-174.
11. Sicouri S, Antzelevitch C. Sudden cardiac death secondary to antidepressant and antipsychotic drugs. Expert Opin Drug Saf. 2008;7(2):181-194.
12. Citrome L. Using oral ziprasidone effectively: the food effect and dose-response. Adv Ther. 2009;26(8):739-748.
13. Preskorn SH. Pharmacokinetics and therapeutics of acute intramuscular ziprasidone. Clin Pharmacokinet. 2005;44(11):1117-1133.
14. Girard TD, Pandharipande PP, Carson SS, et al. Feasibility, efficacy, and safety of antipsychotics for intensive care unit delirium: the MIND randomized, placebo-controlled trial. Crit Care Med. 2010;38(2):428-437.
15. Sipahimalani A, Masand PS. Use of risperidone in delirium: case reports. Ann Clin Psychiatry. 1997;9(2):105-107.
16. Horikawa N, Yamazaki T, Miyamoto K, et al. Treatment for delirium with risperidone: results of a prospective open trial with 10 patients. Gen Hosp Psychiatry. 2003;25(4):289-292.
17. Parellada E, Baeza I, de Pablo J, et al. Risperidone in the treatment of patients with delirium. J Clin Psychiatry. 2004;65(3):348-353.
18. Hans CS, Kim YK. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics. 2004;45(4):297-301.
19. Bourgeois JA, Hilty DM. Prolonged delirium managed with risperidone. Psychosomatics. 2005;46(1):90-91.
20. Naber D, Lambert M. The CATIE and CUtLASS studies in schizophrenia: results and implications for clinicians. CNS Drugs. 2009;23(8):649-659.
21. Zheng L, Mack WJ, Dagerman KS, et al. Metabolic changes associated with second-generation antipsychotic use in Alzheimer’s disease patients: the CATIE-AD study. Am J Psychiatry. 2009;166(5):583-590.
22. Sipahimalani A, Masand PS. Olanzapine in the treatment of delirium. Psychosomatics. 1998;39(5):422-430.
23. Breitbart W, Tremblay A, Gibson C. An open trial of olanzapine for the treatment of delirium in hospitalized cancer patients. Psychosomatics. 2002;43(3):175-182.
24. Hu H, Deng W, Yang H. A prospective random control study comparison of olanzapine and haloperidol in senile dementia. Chongqing Medical Journal. 2004;8:1234-1237.
25. Al-Samarrai S, Dunn J, Newmark T, et al. Quetiapine for treatment-resistant delirium. Psychosomatics. 2003;44(4):350-351.
26. Sasaki Y, Matsuyama T, Inoue S, et al. A prospective, open-label, flexible-dose study of quetiapine in the treatment of delirium. J Clin Psychiatry. 2003;64(11):1316-1321.
27. Devlin JW, Roberts RJ, Fong JJ, et al. Efficacy and safety of quetiapine in critically ill patients with delirium: a prospective, multicenter, randomized, double-blind, placebo-controlled pilot study. Crit Care Med. 2010;38(2):419-427.
28. Leso L, Schwartz TL. Ziprasidone treatment of delirium. Psychosomatics. 2002;43(1):61-62.
29. Young CC, Lujan E. Intravenous ziprasidone for treatment of delirium in the intensive care unit. Anesthesiology. 2004;101(3):794-795.
30. Alao AO, Moskowitz L. Aripiprazole and delirium. Ann Clin Psychiatry. 2006;18(4):267-269.
31. Straker DA, Shapiro PA, Muskin PR. Aripiprazole in the treatment of delirium. Psychosomatics. 2006;47(5):385-391.
32. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc. 2008;56(7):1333-1341.
33. Chew ML, Mulsant BH, Pollock BG, et al. A model of anticholinergic activity of atypical antipsychotic medications. Schizophr Res. 2006;88(1-3):63-72.
34. Buckley NA, Sanders P. Cardiovascular adverse effects of antipsychotic drugs. Drug Saf. 2000;23:215-228.
35. Stöllberger C, Huber JO, Finsterer J. Antipsychotic drugs and QT prolongation. Int Clin Psychopharmacol. 2005;20(5):243-251.
36. Zemrak WR, Kenna GA. Association of antipsychotic and antidepressant drugs with Q-T interval prolongation. Am J Health Syst Pharm. 2008;65(11):1029-1038.
37. Alvarez PA, Pahissa J. QT alterations in psychopharmacology: proven candidates and suspects. Curr Drug Saf. 2010;5(1):97-104.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/01/atypical-antipsychotics-for-delirium.html#comments
Ms. B, age 48, is admitted to our hospital after overdosing on unknown amounts of amitriptyline, diphenhydramine, and laxatives. Three days after admission, the psychiatry service is consulted to assess her for “bipolar disorder.” Although Ms. B does not have a psychiatric history, her internist believes her pressured speech and psychomotor agitation warrant investigation.
During the initial psychiatric interview, Ms. B is disoriented, with fluctuating alertness and cognition. The Confusion Assessment Method for the Intensive Care Unit (CAM-ICU)1 is positive for delirium. We perform a delirium workup while we start Ms. B on olanzapine, 5 mg/d orally and 5 mg intramuscular (IM) every 8 hours as needed.
Ms. B’s laboratory results (complete blood count, complete metabolic profile, urinalysis, chest roentgenogram, vitamin B12 level, blood alcohol level, urine drug screen, arterial blood gas, and head CT) are unremarkable except for her amitriptyline/nortriptyline level, which is in the toxic range. On physical examination, Ms. B’s heart rate and temperature are elevated, her pupils are dilated and sluggish, and her skin is hot and dry. Based on these findings, we determine that Ms. B’s delirium most likely is an anticholinergic syndrome from amitriptyline/diphenhydramine toxicity.2 We discontinue olanzapine after only 2 doses because of its potential anticholinergic effects.3
In hospitalized patients, delirium is one of the most frequently encountered mental disorders, but because of its variable presentation the condition often is underrecognized and undertreated, which leads to longer hospitalizations and increased mortality.4,5 Ms. B’s case illustrates the classical delirium presentation (Table 1),6 highlighting 2 hallmark features of the disorder: inattention and an acute fluctuating course.4 Unfortunately, delirium is a diverse disorder that may present with numerous nonclassical symptoms—including lethargy, emotionality, sleep irregularities, and neurologic abnormalities—in lieu of more commonly recognized symptoms.4,5
In addition to recommending identifying and addressing the underlying acute illness, American Psychiatric Association guidelines suggest prescribing psychotropic medications to treat delirium symptoms.5,7 Antipsychotics are considered first-line pharmacotherapy because they have been shown to lower hospital mortality rates8 and improve delirium symptoms even before underlying medical etiologies are treated.5 Haloperidol is the mainstay of delirium treatment.8 Compared with atypical antipsychotics in delirium treatment, haloperidol doses <3.5 mg/d have not been associated with an increase in extrapyramidal symptoms (EPS).9
Although not devoid of side effects, atypical antipsychotics are an alternative to haloperidol.8,10 This article briefly summarizes the current evidence on the use of atypicals for treating delirium.
Table 1
Delirium: Diagnostic criteria
| Delirium describes a group of related disorders with variable clinical presentations and differing causation. Regardless of the etiology, all types of delirium share a set of common symptoms that include: |
| Disturbances of consciousness and attention |
| Changes in cognition such as memory deficit, language disturbance, or disorientation |
| Perceptual disturbances not better accounted for by dementia |
| Abrupt onset (usually hours to days) |
| Fluctuating symptoms throughout the course of the day |
| Source: Adapted from reference 6 |
CASE CONTINUED: IM ziprasidone
After reassessing our treatment options, we prescribe ziprasidone, 10 mg IM twice a day, and an additional 10 mg IM every 12 hours as needed. Ziprasidone’s minimal anticholinergic and sedative effects3 seem favorable for Ms. B’s delirium; however, this medication has several drawbacks, including IM administration, greater expense compared with intravenous haloperidol, and risk of adverse cardiac affects, specifically prolonged corrected QT (QTc) interval.11 Bioavailability of oral ziprasidone is markedly less than the IM preparation (~60% vs 100%, respectively), and oral bioavailability decreases to approximately 30% when taken without food.12 Given Ms. B’s her current mental state, we feel that IM ziprasidone is a more reliable means to achieve therapeutic efficacy.13
With respect to cardiac concerns, we evaluate Ms. B’s predisposing and precipitating risk factors.11 Family members confirm that she had no cardiac history. We obtain baseline ECGs and continually monitor her QTc interval, which remained at <500 msec during ziprasidone treatment.
Ms. B tolerates ziprasidone and we note modest improvement in her mental status after 2 days of treatment; her vigilant-A portion of the CAM-ICU improves, but she still screens positive for delirium. During the next week Ms. B develops several medical comorbidities, including ileus, urinary tract infection, and methicillin-resistant Staphylococcus aureus infection. Despite these complications her mental status continues to improve. Within 6 days, Ms. B’s attention and cognition improve dramatically. She is oriented and able to engage in medical decision-making, and she screens negative for delirium on the CAM-ICU. We begin to assess her for psychiatric disorders that may have contributed to her hospitalization.
Evidence for antipsychotics
Haloperidol has been the antipsychotic of choice for treating delirium symptoms. It is recommended by the Society of Critical Care Medicine7 and is regarded as safe, cost-effective, and efficacious for delirium5 despite a risk of dose-related EPS and potential cardiac conduction alterations.5,14
Risperidone is not indicated for treating delirium but is one of the most extensively studied atypical antipsychotic alternatives to haloperidol. Evidence consisting primarily of case reports has illustrated the potential efficacy of risperidone in treating delirium (Table 2).10,15-19
In 2004, Parellada et al17 observed significant mean improvements in all measures (Delirium Rating Scale [DRS], Mini-Mental State Exam [MMSE], positive subscale of the Positive and Negative Syndrome Scale [PANSS-P], and Clinical Global Impressions scale [CGI]) in 64 delirium patients treated with risperidone. In a 2004 double-blind trial of 28 delirium patients randomly assigned to risperidone or haloperidol, risperidone was effective but not significantly more efficacious than low-dose haloperidol for acute delirium treatment.18
Advantages of using risperidone include its lack of anticholinergic effects. Potential side effects include dose-related EPS and weight gain, which were observed in patients with schizophrenia and other psychotic disorders and dementia-related behavioral disorders.20,21
Olanzapine. Much like risperidone, olanzapine’s use in delirium is relatively well described in the literature (Table 3).22-24 In a randomized, placebo-controlled study comparing olanzapine with haloperidol, 175 patients were treated for 7 days with olanzapine, haloperidol, or placebo. Olanzapine and haloperidol showed significantly greater DRS score improvement than placebo.24 There was no difference between olanzapine and haloperidol outcomes; however, olanzapine showed significant improvement by days 2 and 3 compared with haloperidol. Haloperidol was associated with a significantly higher rate of dystonia compared with olanzapine.
Olanzapine carries a risk of anticholinergic effects. This can be a drawback, especially in patients such as Ms. B whose delirium has an anticholinergic component. Olanzapine is available in an IM formulation, which can be an advantage when addressing agitation and medical comorbidities of delirium.
Quetiapine. Case reports have suggested quetiapine is effective for delirium (Table 4).10,25-27 In a prospective, open-label trial, Sasaki et al26 treated 12 delirium patients with a single bedtime dose of quetiapine. All patients achieved remission within several days of beginning quetiapine, and the drug was well tolerated with no detected EPS or excessive sedation.
In 2010 Devlin et al27 reported on the efficacy and safety of quetiapine in a prospective double-blind, placebo-controlled study of 36 adult ICU patients. Compared with those receiving placebo, patients taking quetiapine had a statistically significant shorter time to first resolution of delirium, reduced duration of delirium, and less agitation as measured by the Sedation-Agitation Scale. Mortality, ICU length of stay, and incidence of QTc prolongation did not differ, but patients treated with quetiapine were more likely to be discharged home or to rehabilitation and to have more somnolence. Quetiapine’s side effect profile includes a low occurrence of EPS, sedation, and dose-related anticholinergic effects.25
Ziprasidone. The literature on ziprasidone for delirium so far is limited to a few anecdotal case reports (Table 5).28-31 In 2002, Leso and Schwartz28 successfully used ziprasidone to treat delirium in a patient with human immunodeficiency virus and cryptococcal meningitis. Ziprasidone was chosen for its lack of sedating effects and low EPS risk. The patient experienced significant clearing of his delirium and lowering of his DRS score. Ziprasidone eventually was discontinued because a fluctuating QTc interval associated with comorbid electrolyte imbalances—a potential drawback to ziprasidone.
In the case of Ms. B, ziprasidone appeared to be efficacious; however, improvement in her medical condition, rather than ziprasidone treatment, is the most likely explanation for the resolution of her delirium symptoms.
Aripiprazole. Alao et al30 reported on 2 delirium patients treated with 30 mg and 15 mg aripiprazole; improvement was monitored using the MMSE and DRS (Table 5).28-31 In both cases, confusion, disorientation, and agitation improved within 7 days of treatment. In the first case, the patient’s MMSE score improved from 5 to 28 and his DRS score decreased from 28 to 6. The second patient’s MMSE score improved from 7 to 27 and her DRS score went from 18 to 6.
Straker et al31 reported on 14 delirium patients treated with aripiprazole. Twelve patients had a ≥50% reduction in DRS, Revised-98 scores, and 13 showed improvement on CGI scores. The rate of adverse side effects was low. Three patients had prolonged QTc interval, but no patients developed arrhythmia or discontinued aripiprazole.
Table 2
Risperidone for delirium: What the evidence says
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Sipahimalani et al, 199715 | N=2 (age 14 and 60). Initial dose: 1 mg/d; maintenance dose: 2 mg/d | 10 to 14 days | MMSE score increased. AEs: extrapyramidal symptoms (dystonia and cogwheeling) |
| Schwartz et al, 200210 | N=11 (age range 14 to 74). Mean dose: 1.59 ± 0.8 mg/d | 5.1 ± 4.3 days | CGI score decreased. No reported AEs |
| Horikawa et al, 200316 | N=10 (mean age: 56.8; range: 22 to 81). Mean dose: 1.7 mg/d | 7.1 days | DRS score decreased significantly in 80% of patients (P=.03) AEs: sleepiness (30%), mild drug-induced parkinsonism (10%) |
| Parellada et al, 200417 | N=64 (mean age: 67.3 ± 11.4 years). Mean dose: 2.6 ± 1.7 mg/d | 3 to 7 days | Effective in 90.6% of patients with significant decreases in DRS, PANSS-P, and CGI and increase in MMSE (P < .001). AEs: drowsiness (3.1%), nausea (1.6%) |
| Hans et al, 200418 | N=12 (mean age: 65.6). Mean dose: 1.02 mg/d | 4 to 7 days | MDAS scores decreased significantly (P < .05). No reported AEs |
| Bourgeois et al, 200519 | N=1 (age 57). Initial dose: 8 mg/d; maintenance dose: 2 mg/d | 9 days | MMSE score increased. No reported AEs |
| CGI: Clinical Global Impressions scale; DRS: Delirium Rating Scale; MDAS: Memorial Delirium Assessment Scale; MMSE: Mini-Mental State Exam; PANSS-P: positive subscale of the Positive and Negative Syndrome Scale | |||
Table 3
Olanzapine may have a role in treating delirium symptoms
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Sipahimalani et al, 199822 | N=11 (mean age: 63.5 ± 23.2 years). Mean dose: 8.2 ± 3.4 mg/d | 6.8 ± 3.5 days | Marked decrease (>50%) in DRS score for 5 patients. No reported AEs |
| Breitbart et al, 200223 | N=79 (mean age: 60.6 ± 17.3 years; range: 19 to 89). Initial dose: 3 ± 0.14 mg/d; mean dose: 4.6 to 6.3 mg/d | 2 to 7 days | MDAS decreased significantly (P < .001), with 76% of patients’ delirium reaching resolution (MDAS ≤10). AEs: sedation (30%) |
| Hu et al, 200424 | N=74 (mean age: 74). Mean dose: 1.25 to 2 mg/d | 2.78 ± 1.85 days | DRS score decreased significantly (P < .01) in 72.2% of patients. AEs: drowsiness (18.9%), dystonia (2.7%), dry mouth (2.7%) |
| DRS: Delirium Rating Scale; MDAS: Memorial Delirium Assessment Scale | |||
Table 4
Evidence suggests quetiapine could reduce delirium symptoms
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Schwartz et al, 200210 | N=11 (age range: 19 to 91). Mean dose: 211.4 mg/d | 6.5 days | Decrease in DRS score (>50% reduction in global delirium symptoms) for 10 patients. AEs: sedation |
| Al-Samarrai et al, 200325 | N=2 (age 50 and 52). Mean dose: 200 to 400 mg/d | 2 to 4 days | No specific rating scale used but clinical reduction in agitation and improvement in cognition were reported. AEs: drowsiness |
| Sasaki et al, 200326 | N=12 (mean age: 67.3 ± 14.8 years). Mean dose: 44.9 ± 31.0 mg/d | 4.8 ± 3.5 days | Decrease in DRS score and remission of delirium for all patients. Significant increase in MMSE (P=.0256). No reported AEs |
| Devlin et al, 201027 | N=18 (adult ICU patients). Initial dose: 100 mg/d | 36 to 87 hours | Significantly shorter time to first resolution of delirium and duration of delirium compared with placebo. AEs: somnolence |
| DRS: Delirium Rating Scale; ICU: intensive care unit; MMSE: Mini-Mental State Exam | |||
Table 5
Limited data support ziprasidone and aripiprazole for treating delirium
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Ziprasidone | |||
| Leso et al, 200228 | N=1 (age 34). Initial dose: 40 mg/d; maintenance dose: 100 mg/d | 21 days | DRS score decreased from 26 to 14. AEs: 8.4% increase in QTc interval |
| Young et al, 200429 | N=1 (age 47). Initial dose: 20 mg IV bolus, followed by an oral taper over 7 days. | 7 days | No specific rating scale was used but dramatic improvement in patient’s restlessness was reported. No AEs reported |
| Aripiprazole | |||
| Alao et al, 200630 | N=2 (age 62 and 37). Mean dose: 15 and 30 mg/d | 2 to 7 days | Patient 1: DRS score decreased from 28 to 6 and MMSE score increased from 5 to 28. Patient 2: DRS score decreased from 18 to 6 and MMSE score increased from 7 to 27. No AEs reported |
| Straker et al, 200631 | N=14 (age range: 18 to 85). Mean dose: 8.9 mg/d | 2 to 14 days | 12 of 14 patients had a ≥50% decrease in DRS-R-98. AEs: 3 patients had prolonged QTc interval |
| DRS: Delirium Rating Scale; DRS-R-98: Delirium Rating Scale–Revised-98; MMSE: Mini-Mental State Exam | |||
Anticholinergic activity
Decreased acetylcholine activity (AA) is suspected in delirium pathogenesis.32 By extension of this theory, medications that block muscarinic receptors could worsen delirium. Haloperidol, risperidone, and ziprasidone have negligible or no AA, as reported in atropine equivalents. Quetiapine and olanzapine have mild (0.5 to 5 pmol/ mL) and moderate (5 to 15 pmol/mL) dose-related AA, respectively. For example, olanzapine, 5 mg/d, has roughly the same AA as quetiapine, 300 mg/d, whereas olanzapine, 10 mg/d, has about the same AA as quetiapine, 600 mg/d.32,33
Although we used this evidence, in part, to select an atypical antipsychotic for Ms. B, this model should be used only to estimate the possible anticholinergic burden associated with a specific medication or combination. The risk of anticholinergic burden needs to be considered along with a medication’s potential nonanticholinergic adverse effects and the patient’s overall clinical history (eg, past sensitivity to anticholinergic agents, memory complaints, effectiveness of an agent, concomitant medications, disease state, adherence concerns). For example, an atypical antipsychotic that is potently anti-histaminergic and therefore sedating could be beneficial when treating an agitated delirium patient. Establishing the presence of a risk of anticholinergic burden cannot be equated with the presence of anticholinergic toxicity, because the exact relationship between AA and cognitive performance is still unknown.32,33
Cardiovascular safety
The most common cardiovascular effects of atypical antipsychotics are tachycardia, hypotension (usually mild), and prolongation of QTc interval.34 For example, haloperidol, 15 mg/d, was found to increase mean QTc by 7 msec, with a reported odds ratio ranging from 2.2 to 6.1 for ventricular dysrhythmia and sudden cardiac death,35 although risk may be more strongly associated with high-dose, IV haloperidol.36
QTc interval prolongation warrants concern because it suggests that patients may be predisposed to torsades de pointes (TdP). Conventional antipsychotics— especially phenothiazines—have the highest risk of inducing TdP. One review concluded that compared with other antipsychotics, chlorpromazine, pimozide, thioridazine, and the atypical clozapine have a higher risk of cardiac arrhythmias and sudden cardiac death.11 Another review found cases of TdP with haloperidol, ziprasidone, olanzapine, and thioridazine.37 When prescribing an antipsychotic, consider both pharmacologic and nonpharmacologic risks factors, including preexisting cardiovascular disease, female sex, hepatic insufficiency, electrolyte abnormalities, stimulant drug abuse,36 and genetic predisposition (Table 6).11,35-37
Table 6
Risk factors for antipsychotic-induced QT interval prolongation and torsades de pointes*
| Pharmacologic |
|---|
| Antipsychotic selection |
| Drug interaction (QT-prolonging agents) |
| Drug interaction (slow metabolism by cytochrome P450 inhibitors of 2D6, 3A4, 1A2) |
| Nonpharmacologic |
| Advanced age (>65) |
| Bradycardia |
| Hypokalemia |
| Hypomagnesemia |
| Hepatic/renal dysfunction |
| Genetic predisposition |
| Female sex |
| Screening (major risk factors) |
| Structural cardiac disease |
| Congenital long QT syndrome |
| Family history of sudden cardiac death |
| Previous episodes of drug-induced QT prolongation or torsades de pointes |
| * Serial electrocardiograms are recommended for patients with a major risk factor or multiple pharmacologic/ nonpharmacologic risk factors Source: References 11,35-37 |
Related Resource
- Stern TA, Celano CM, Gross AF, et al. The assessment and management of agitation and delirium in the general hospital. Prim Care Companion J Clin Psychiatry 2010;12(1):e1–e11. www.psychiatrist.com/private/pccpdf/article_wrapper.asp?art=2010/09r00938yel/09r00938yel.htm.
Drug Brand Names
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Atropine • Sal-Tropine
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Diphenhydramine • Benadryl
- Haloperidol • Haldol
- Nortriptyline • Aventyl
- Olanzapine • Zyprexa
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thioridazine • Mellaril
- Ziprasidone • Geodon
Disclosures
Dr. Spiegel is a speaker for AstraZeneca, Pfizer, Inc., and Janssen Pharmaceuticals.
Drs. Ahlers, Yoder, and Qureshi report no financial relationship with any company whose products are mention in this article or with manufacturers of competing products.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/01/atypical-antipsychotics-for-delirium.html#comments
Ms. B, age 48, is admitted to our hospital after overdosing on unknown amounts of amitriptyline, diphenhydramine, and laxatives. Three days after admission, the psychiatry service is consulted to assess her for “bipolar disorder.” Although Ms. B does not have a psychiatric history, her internist believes her pressured speech and psychomotor agitation warrant investigation.
During the initial psychiatric interview, Ms. B is disoriented, with fluctuating alertness and cognition. The Confusion Assessment Method for the Intensive Care Unit (CAM-ICU)1 is positive for delirium. We perform a delirium workup while we start Ms. B on olanzapine, 5 mg/d orally and 5 mg intramuscular (IM) every 8 hours as needed.
Ms. B’s laboratory results (complete blood count, complete metabolic profile, urinalysis, chest roentgenogram, vitamin B12 level, blood alcohol level, urine drug screen, arterial blood gas, and head CT) are unremarkable except for her amitriptyline/nortriptyline level, which is in the toxic range. On physical examination, Ms. B’s heart rate and temperature are elevated, her pupils are dilated and sluggish, and her skin is hot and dry. Based on these findings, we determine that Ms. B’s delirium most likely is an anticholinergic syndrome from amitriptyline/diphenhydramine toxicity.2 We discontinue olanzapine after only 2 doses because of its potential anticholinergic effects.3
In hospitalized patients, delirium is one of the most frequently encountered mental disorders, but because of its variable presentation the condition often is underrecognized and undertreated, which leads to longer hospitalizations and increased mortality.4,5 Ms. B’s case illustrates the classical delirium presentation (Table 1),6 highlighting 2 hallmark features of the disorder: inattention and an acute fluctuating course.4 Unfortunately, delirium is a diverse disorder that may present with numerous nonclassical symptoms—including lethargy, emotionality, sleep irregularities, and neurologic abnormalities—in lieu of more commonly recognized symptoms.4,5
In addition to recommending identifying and addressing the underlying acute illness, American Psychiatric Association guidelines suggest prescribing psychotropic medications to treat delirium symptoms.5,7 Antipsychotics are considered first-line pharmacotherapy because they have been shown to lower hospital mortality rates8 and improve delirium symptoms even before underlying medical etiologies are treated.5 Haloperidol is the mainstay of delirium treatment.8 Compared with atypical antipsychotics in delirium treatment, haloperidol doses <3.5 mg/d have not been associated with an increase in extrapyramidal symptoms (EPS).9
Although not devoid of side effects, atypical antipsychotics are an alternative to haloperidol.8,10 This article briefly summarizes the current evidence on the use of atypicals for treating delirium.
Table 1
Delirium: Diagnostic criteria
| Delirium describes a group of related disorders with variable clinical presentations and differing causation. Regardless of the etiology, all types of delirium share a set of common symptoms that include: |
| Disturbances of consciousness and attention |
| Changes in cognition such as memory deficit, language disturbance, or disorientation |
| Perceptual disturbances not better accounted for by dementia |
| Abrupt onset (usually hours to days) |
| Fluctuating symptoms throughout the course of the day |
| Source: Adapted from reference 6 |
CASE CONTINUED: IM ziprasidone
After reassessing our treatment options, we prescribe ziprasidone, 10 mg IM twice a day, and an additional 10 mg IM every 12 hours as needed. Ziprasidone’s minimal anticholinergic and sedative effects3 seem favorable for Ms. B’s delirium; however, this medication has several drawbacks, including IM administration, greater expense compared with intravenous haloperidol, and risk of adverse cardiac affects, specifically prolonged corrected QT (QTc) interval.11 Bioavailability of oral ziprasidone is markedly less than the IM preparation (~60% vs 100%, respectively), and oral bioavailability decreases to approximately 30% when taken without food.12 Given Ms. B’s her current mental state, we feel that IM ziprasidone is a more reliable means to achieve therapeutic efficacy.13
With respect to cardiac concerns, we evaluate Ms. B’s predisposing and precipitating risk factors.11 Family members confirm that she had no cardiac history. We obtain baseline ECGs and continually monitor her QTc interval, which remained at <500 msec during ziprasidone treatment.
Ms. B tolerates ziprasidone and we note modest improvement in her mental status after 2 days of treatment; her vigilant-A portion of the CAM-ICU improves, but she still screens positive for delirium. During the next week Ms. B develops several medical comorbidities, including ileus, urinary tract infection, and methicillin-resistant Staphylococcus aureus infection. Despite these complications her mental status continues to improve. Within 6 days, Ms. B’s attention and cognition improve dramatically. She is oriented and able to engage in medical decision-making, and she screens negative for delirium on the CAM-ICU. We begin to assess her for psychiatric disorders that may have contributed to her hospitalization.
Evidence for antipsychotics
Haloperidol has been the antipsychotic of choice for treating delirium symptoms. It is recommended by the Society of Critical Care Medicine7 and is regarded as safe, cost-effective, and efficacious for delirium5 despite a risk of dose-related EPS and potential cardiac conduction alterations.5,14
Risperidone is not indicated for treating delirium but is one of the most extensively studied atypical antipsychotic alternatives to haloperidol. Evidence consisting primarily of case reports has illustrated the potential efficacy of risperidone in treating delirium (Table 2).10,15-19
In 2004, Parellada et al17 observed significant mean improvements in all measures (Delirium Rating Scale [DRS], Mini-Mental State Exam [MMSE], positive subscale of the Positive and Negative Syndrome Scale [PANSS-P], and Clinical Global Impressions scale [CGI]) in 64 delirium patients treated with risperidone. In a 2004 double-blind trial of 28 delirium patients randomly assigned to risperidone or haloperidol, risperidone was effective but not significantly more efficacious than low-dose haloperidol for acute delirium treatment.18
Advantages of using risperidone include its lack of anticholinergic effects. Potential side effects include dose-related EPS and weight gain, which were observed in patients with schizophrenia and other psychotic disorders and dementia-related behavioral disorders.20,21
Olanzapine. Much like risperidone, olanzapine’s use in delirium is relatively well described in the literature (Table 3).22-24 In a randomized, placebo-controlled study comparing olanzapine with haloperidol, 175 patients were treated for 7 days with olanzapine, haloperidol, or placebo. Olanzapine and haloperidol showed significantly greater DRS score improvement than placebo.24 There was no difference between olanzapine and haloperidol outcomes; however, olanzapine showed significant improvement by days 2 and 3 compared with haloperidol. Haloperidol was associated with a significantly higher rate of dystonia compared with olanzapine.
Olanzapine carries a risk of anticholinergic effects. This can be a drawback, especially in patients such as Ms. B whose delirium has an anticholinergic component. Olanzapine is available in an IM formulation, which can be an advantage when addressing agitation and medical comorbidities of delirium.
Quetiapine. Case reports have suggested quetiapine is effective for delirium (Table 4).10,25-27 In a prospective, open-label trial, Sasaki et al26 treated 12 delirium patients with a single bedtime dose of quetiapine. All patients achieved remission within several days of beginning quetiapine, and the drug was well tolerated with no detected EPS or excessive sedation.
In 2010 Devlin et al27 reported on the efficacy and safety of quetiapine in a prospective double-blind, placebo-controlled study of 36 adult ICU patients. Compared with those receiving placebo, patients taking quetiapine had a statistically significant shorter time to first resolution of delirium, reduced duration of delirium, and less agitation as measured by the Sedation-Agitation Scale. Mortality, ICU length of stay, and incidence of QTc prolongation did not differ, but patients treated with quetiapine were more likely to be discharged home or to rehabilitation and to have more somnolence. Quetiapine’s side effect profile includes a low occurrence of EPS, sedation, and dose-related anticholinergic effects.25
Ziprasidone. The literature on ziprasidone for delirium so far is limited to a few anecdotal case reports (Table 5).28-31 In 2002, Leso and Schwartz28 successfully used ziprasidone to treat delirium in a patient with human immunodeficiency virus and cryptococcal meningitis. Ziprasidone was chosen for its lack of sedating effects and low EPS risk. The patient experienced significant clearing of his delirium and lowering of his DRS score. Ziprasidone eventually was discontinued because a fluctuating QTc interval associated with comorbid electrolyte imbalances—a potential drawback to ziprasidone.
In the case of Ms. B, ziprasidone appeared to be efficacious; however, improvement in her medical condition, rather than ziprasidone treatment, is the most likely explanation for the resolution of her delirium symptoms.
Aripiprazole. Alao et al30 reported on 2 delirium patients treated with 30 mg and 15 mg aripiprazole; improvement was monitored using the MMSE and DRS (Table 5).28-31 In both cases, confusion, disorientation, and agitation improved within 7 days of treatment. In the first case, the patient’s MMSE score improved from 5 to 28 and his DRS score decreased from 28 to 6. The second patient’s MMSE score improved from 7 to 27 and her DRS score went from 18 to 6.
Straker et al31 reported on 14 delirium patients treated with aripiprazole. Twelve patients had a ≥50% reduction in DRS, Revised-98 scores, and 13 showed improvement on CGI scores. The rate of adverse side effects was low. Three patients had prolonged QTc interval, but no patients developed arrhythmia or discontinued aripiprazole.
Table 2
Risperidone for delirium: What the evidence says
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Sipahimalani et al, 199715 | N=2 (age 14 and 60). Initial dose: 1 mg/d; maintenance dose: 2 mg/d | 10 to 14 days | MMSE score increased. AEs: extrapyramidal symptoms (dystonia and cogwheeling) |
| Schwartz et al, 200210 | N=11 (age range 14 to 74). Mean dose: 1.59 ± 0.8 mg/d | 5.1 ± 4.3 days | CGI score decreased. No reported AEs |
| Horikawa et al, 200316 | N=10 (mean age: 56.8; range: 22 to 81). Mean dose: 1.7 mg/d | 7.1 days | DRS score decreased significantly in 80% of patients (P=.03) AEs: sleepiness (30%), mild drug-induced parkinsonism (10%) |
| Parellada et al, 200417 | N=64 (mean age: 67.3 ± 11.4 years). Mean dose: 2.6 ± 1.7 mg/d | 3 to 7 days | Effective in 90.6% of patients with significant decreases in DRS, PANSS-P, and CGI and increase in MMSE (P < .001). AEs: drowsiness (3.1%), nausea (1.6%) |
| Hans et al, 200418 | N=12 (mean age: 65.6). Mean dose: 1.02 mg/d | 4 to 7 days | MDAS scores decreased significantly (P < .05). No reported AEs |
| Bourgeois et al, 200519 | N=1 (age 57). Initial dose: 8 mg/d; maintenance dose: 2 mg/d | 9 days | MMSE score increased. No reported AEs |
| CGI: Clinical Global Impressions scale; DRS: Delirium Rating Scale; MDAS: Memorial Delirium Assessment Scale; MMSE: Mini-Mental State Exam; PANSS-P: positive subscale of the Positive and Negative Syndrome Scale | |||
Table 3
Olanzapine may have a role in treating delirium symptoms
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Sipahimalani et al, 199822 | N=11 (mean age: 63.5 ± 23.2 years). Mean dose: 8.2 ± 3.4 mg/d | 6.8 ± 3.5 days | Marked decrease (>50%) in DRS score for 5 patients. No reported AEs |
| Breitbart et al, 200223 | N=79 (mean age: 60.6 ± 17.3 years; range: 19 to 89). Initial dose: 3 ± 0.14 mg/d; mean dose: 4.6 to 6.3 mg/d | 2 to 7 days | MDAS decreased significantly (P < .001), with 76% of patients’ delirium reaching resolution (MDAS ≤10). AEs: sedation (30%) |
| Hu et al, 200424 | N=74 (mean age: 74). Mean dose: 1.25 to 2 mg/d | 2.78 ± 1.85 days | DRS score decreased significantly (P < .01) in 72.2% of patients. AEs: drowsiness (18.9%), dystonia (2.7%), dry mouth (2.7%) |
| DRS: Delirium Rating Scale; MDAS: Memorial Delirium Assessment Scale | |||
Table 4
Evidence suggests quetiapine could reduce delirium symptoms
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Schwartz et al, 200210 | N=11 (age range: 19 to 91). Mean dose: 211.4 mg/d | 6.5 days | Decrease in DRS score (>50% reduction in global delirium symptoms) for 10 patients. AEs: sedation |
| Al-Samarrai et al, 200325 | N=2 (age 50 and 52). Mean dose: 200 to 400 mg/d | 2 to 4 days | No specific rating scale used but clinical reduction in agitation and improvement in cognition were reported. AEs: drowsiness |
| Sasaki et al, 200326 | N=12 (mean age: 67.3 ± 14.8 years). Mean dose: 44.9 ± 31.0 mg/d | 4.8 ± 3.5 days | Decrease in DRS score and remission of delirium for all patients. Significant increase in MMSE (P=.0256). No reported AEs |
| Devlin et al, 201027 | N=18 (adult ICU patients). Initial dose: 100 mg/d | 36 to 87 hours | Significantly shorter time to first resolution of delirium and duration of delirium compared with placebo. AEs: somnolence |
| DRS: Delirium Rating Scale; ICU: intensive care unit; MMSE: Mini-Mental State Exam | |||
Table 5
Limited data support ziprasidone and aripiprazole for treating delirium
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Ziprasidone | |||
| Leso et al, 200228 | N=1 (age 34). Initial dose: 40 mg/d; maintenance dose: 100 mg/d | 21 days | DRS score decreased from 26 to 14. AEs: 8.4% increase in QTc interval |
| Young et al, 200429 | N=1 (age 47). Initial dose: 20 mg IV bolus, followed by an oral taper over 7 days. | 7 days | No specific rating scale was used but dramatic improvement in patient’s restlessness was reported. No AEs reported |
| Aripiprazole | |||
| Alao et al, 200630 | N=2 (age 62 and 37). Mean dose: 15 and 30 mg/d | 2 to 7 days | Patient 1: DRS score decreased from 28 to 6 and MMSE score increased from 5 to 28. Patient 2: DRS score decreased from 18 to 6 and MMSE score increased from 7 to 27. No AEs reported |
| Straker et al, 200631 | N=14 (age range: 18 to 85). Mean dose: 8.9 mg/d | 2 to 14 days | 12 of 14 patients had a ≥50% decrease in DRS-R-98. AEs: 3 patients had prolonged QTc interval |
| DRS: Delirium Rating Scale; DRS-R-98: Delirium Rating Scale–Revised-98; MMSE: Mini-Mental State Exam | |||
Anticholinergic activity
Decreased acetylcholine activity (AA) is suspected in delirium pathogenesis.32 By extension of this theory, medications that block muscarinic receptors could worsen delirium. Haloperidol, risperidone, and ziprasidone have negligible or no AA, as reported in atropine equivalents. Quetiapine and olanzapine have mild (0.5 to 5 pmol/ mL) and moderate (5 to 15 pmol/mL) dose-related AA, respectively. For example, olanzapine, 5 mg/d, has roughly the same AA as quetiapine, 300 mg/d, whereas olanzapine, 10 mg/d, has about the same AA as quetiapine, 600 mg/d.32,33
Although we used this evidence, in part, to select an atypical antipsychotic for Ms. B, this model should be used only to estimate the possible anticholinergic burden associated with a specific medication or combination. The risk of anticholinergic burden needs to be considered along with a medication’s potential nonanticholinergic adverse effects and the patient’s overall clinical history (eg, past sensitivity to anticholinergic agents, memory complaints, effectiveness of an agent, concomitant medications, disease state, adherence concerns). For example, an atypical antipsychotic that is potently anti-histaminergic and therefore sedating could be beneficial when treating an agitated delirium patient. Establishing the presence of a risk of anticholinergic burden cannot be equated with the presence of anticholinergic toxicity, because the exact relationship between AA and cognitive performance is still unknown.32,33
Cardiovascular safety
The most common cardiovascular effects of atypical antipsychotics are tachycardia, hypotension (usually mild), and prolongation of QTc interval.34 For example, haloperidol, 15 mg/d, was found to increase mean QTc by 7 msec, with a reported odds ratio ranging from 2.2 to 6.1 for ventricular dysrhythmia and sudden cardiac death,35 although risk may be more strongly associated with high-dose, IV haloperidol.36
QTc interval prolongation warrants concern because it suggests that patients may be predisposed to torsades de pointes (TdP). Conventional antipsychotics— especially phenothiazines—have the highest risk of inducing TdP. One review concluded that compared with other antipsychotics, chlorpromazine, pimozide, thioridazine, and the atypical clozapine have a higher risk of cardiac arrhythmias and sudden cardiac death.11 Another review found cases of TdP with haloperidol, ziprasidone, olanzapine, and thioridazine.37 When prescribing an antipsychotic, consider both pharmacologic and nonpharmacologic risks factors, including preexisting cardiovascular disease, female sex, hepatic insufficiency, electrolyte abnormalities, stimulant drug abuse,36 and genetic predisposition (Table 6).11,35-37
Table 6
Risk factors for antipsychotic-induced QT interval prolongation and torsades de pointes*
| Pharmacologic |
|---|
| Antipsychotic selection |
| Drug interaction (QT-prolonging agents) |
| Drug interaction (slow metabolism by cytochrome P450 inhibitors of 2D6, 3A4, 1A2) |
| Nonpharmacologic |
| Advanced age (>65) |
| Bradycardia |
| Hypokalemia |
| Hypomagnesemia |
| Hepatic/renal dysfunction |
| Genetic predisposition |
| Female sex |
| Screening (major risk factors) |
| Structural cardiac disease |
| Congenital long QT syndrome |
| Family history of sudden cardiac death |
| Previous episodes of drug-induced QT prolongation or torsades de pointes |
| * Serial electrocardiograms are recommended for patients with a major risk factor or multiple pharmacologic/ nonpharmacologic risk factors Source: References 11,35-37 |
Related Resource
- Stern TA, Celano CM, Gross AF, et al. The assessment and management of agitation and delirium in the general hospital. Prim Care Companion J Clin Psychiatry 2010;12(1):e1–e11. www.psychiatrist.com/private/pccpdf/article_wrapper.asp?art=2010/09r00938yel/09r00938yel.htm.
Drug Brand Names
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Atropine • Sal-Tropine
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Diphenhydramine • Benadryl
- Haloperidol • Haldol
- Nortriptyline • Aventyl
- Olanzapine • Zyprexa
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thioridazine • Mellaril
- Ziprasidone • Geodon
Disclosures
Dr. Spiegel is a speaker for AstraZeneca, Pfizer, Inc., and Janssen Pharmaceuticals.
Drs. Ahlers, Yoder, and Qureshi report no financial relationship with any company whose products are mention in this article or with manufacturers of competing products.
1. Ely EW, Inouye SK, Bernard GR, et al. Delirium in the mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286:2703-2710.
2. Rudolph JL, Salow MJ, Angelini MC, et al. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med. 2008;168(5):508-513.
3. Albers LJ, Hahn RK, Reist C. Handbook of psychiatric drugs 2008. Blue Jay, CA: Current Clinical Strategies Publishing; 2007.
4. Inouye SK. Delirium in older persons. N Engl J Med. 2006;354(11):1157-1165.
5. American Psychiatric Association. Practice guideline for the treatment of patients with delirium. Am J Psychiatry. 1999;156(suppl 5):1-20.
6. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
7. Seitz DP, Gill SS, van Zyl LT. Antipsychotics in the treatment of delirium: a systematic review. J Clin Psychiatry. 2007;68(1):11-21.
8. Lacasse H, Perreault MM, Williamson DR. Systematic review of antipsychotics for the treatment of hospital-associated delirium in medically or surgically ill patients. Ann Pharmacother. 2006;40(11):1966-1973.
9. Lonergan E, Britton AM, Luxenberg J, et al. Antipsychotics for delirium. Cochrane Database Syst Rev. 2007;(2):CD005594.-
10. Schwartz TL, Masand PS. The role of atypical antipsychotics in the treatment of delirium. Psychosomatics. 2002;43(3):171-174.
11. Sicouri S, Antzelevitch C. Sudden cardiac death secondary to antidepressant and antipsychotic drugs. Expert Opin Drug Saf. 2008;7(2):181-194.
12. Citrome L. Using oral ziprasidone effectively: the food effect and dose-response. Adv Ther. 2009;26(8):739-748.
13. Preskorn SH. Pharmacokinetics and therapeutics of acute intramuscular ziprasidone. Clin Pharmacokinet. 2005;44(11):1117-1133.
14. Girard TD, Pandharipande PP, Carson SS, et al. Feasibility, efficacy, and safety of antipsychotics for intensive care unit delirium: the MIND randomized, placebo-controlled trial. Crit Care Med. 2010;38(2):428-437.
15. Sipahimalani A, Masand PS. Use of risperidone in delirium: case reports. Ann Clin Psychiatry. 1997;9(2):105-107.
16. Horikawa N, Yamazaki T, Miyamoto K, et al. Treatment for delirium with risperidone: results of a prospective open trial with 10 patients. Gen Hosp Psychiatry. 2003;25(4):289-292.
17. Parellada E, Baeza I, de Pablo J, et al. Risperidone in the treatment of patients with delirium. J Clin Psychiatry. 2004;65(3):348-353.
18. Hans CS, Kim YK. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics. 2004;45(4):297-301.
19. Bourgeois JA, Hilty DM. Prolonged delirium managed with risperidone. Psychosomatics. 2005;46(1):90-91.
20. Naber D, Lambert M. The CATIE and CUtLASS studies in schizophrenia: results and implications for clinicians. CNS Drugs. 2009;23(8):649-659.
21. Zheng L, Mack WJ, Dagerman KS, et al. Metabolic changes associated with second-generation antipsychotic use in Alzheimer’s disease patients: the CATIE-AD study. Am J Psychiatry. 2009;166(5):583-590.
22. Sipahimalani A, Masand PS. Olanzapine in the treatment of delirium. Psychosomatics. 1998;39(5):422-430.
23. Breitbart W, Tremblay A, Gibson C. An open trial of olanzapine for the treatment of delirium in hospitalized cancer patients. Psychosomatics. 2002;43(3):175-182.
24. Hu H, Deng W, Yang H. A prospective random control study comparison of olanzapine and haloperidol in senile dementia. Chongqing Medical Journal. 2004;8:1234-1237.
25. Al-Samarrai S, Dunn J, Newmark T, et al. Quetiapine for treatment-resistant delirium. Psychosomatics. 2003;44(4):350-351.
26. Sasaki Y, Matsuyama T, Inoue S, et al. A prospective, open-label, flexible-dose study of quetiapine in the treatment of delirium. J Clin Psychiatry. 2003;64(11):1316-1321.
27. Devlin JW, Roberts RJ, Fong JJ, et al. Efficacy and safety of quetiapine in critically ill patients with delirium: a prospective, multicenter, randomized, double-blind, placebo-controlled pilot study. Crit Care Med. 2010;38(2):419-427.
28. Leso L, Schwartz TL. Ziprasidone treatment of delirium. Psychosomatics. 2002;43(1):61-62.
29. Young CC, Lujan E. Intravenous ziprasidone for treatment of delirium in the intensive care unit. Anesthesiology. 2004;101(3):794-795.
30. Alao AO, Moskowitz L. Aripiprazole and delirium. Ann Clin Psychiatry. 2006;18(4):267-269.
31. Straker DA, Shapiro PA, Muskin PR. Aripiprazole in the treatment of delirium. Psychosomatics. 2006;47(5):385-391.
32. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc. 2008;56(7):1333-1341.
33. Chew ML, Mulsant BH, Pollock BG, et al. A model of anticholinergic activity of atypical antipsychotic medications. Schizophr Res. 2006;88(1-3):63-72.
34. Buckley NA, Sanders P. Cardiovascular adverse effects of antipsychotic drugs. Drug Saf. 2000;23:215-228.
35. Stöllberger C, Huber JO, Finsterer J. Antipsychotic drugs and QT prolongation. Int Clin Psychopharmacol. 2005;20(5):243-251.
36. Zemrak WR, Kenna GA. Association of antipsychotic and antidepressant drugs with Q-T interval prolongation. Am J Health Syst Pharm. 2008;65(11):1029-1038.
37. Alvarez PA, Pahissa J. QT alterations in psychopharmacology: proven candidates and suspects. Curr Drug Saf. 2010;5(1):97-104.
1. Ely EW, Inouye SK, Bernard GR, et al. Delirium in the mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286:2703-2710.
2. Rudolph JL, Salow MJ, Angelini MC, et al. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med. 2008;168(5):508-513.
3. Albers LJ, Hahn RK, Reist C. Handbook of psychiatric drugs 2008. Blue Jay, CA: Current Clinical Strategies Publishing; 2007.
4. Inouye SK. Delirium in older persons. N Engl J Med. 2006;354(11):1157-1165.
5. American Psychiatric Association. Practice guideline for the treatment of patients with delirium. Am J Psychiatry. 1999;156(suppl 5):1-20.
6. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
7. Seitz DP, Gill SS, van Zyl LT. Antipsychotics in the treatment of delirium: a systematic review. J Clin Psychiatry. 2007;68(1):11-21.
8. Lacasse H, Perreault MM, Williamson DR. Systematic review of antipsychotics for the treatment of hospital-associated delirium in medically or surgically ill patients. Ann Pharmacother. 2006;40(11):1966-1973.
9. Lonergan E, Britton AM, Luxenberg J, et al. Antipsychotics for delirium. Cochrane Database Syst Rev. 2007;(2):CD005594.-
10. Schwartz TL, Masand PS. The role of atypical antipsychotics in the treatment of delirium. Psychosomatics. 2002;43(3):171-174.
11. Sicouri S, Antzelevitch C. Sudden cardiac death secondary to antidepressant and antipsychotic drugs. Expert Opin Drug Saf. 2008;7(2):181-194.
12. Citrome L. Using oral ziprasidone effectively: the food effect and dose-response. Adv Ther. 2009;26(8):739-748.
13. Preskorn SH. Pharmacokinetics and therapeutics of acute intramuscular ziprasidone. Clin Pharmacokinet. 2005;44(11):1117-1133.
14. Girard TD, Pandharipande PP, Carson SS, et al. Feasibility, efficacy, and safety of antipsychotics for intensive care unit delirium: the MIND randomized, placebo-controlled trial. Crit Care Med. 2010;38(2):428-437.
15. Sipahimalani A, Masand PS. Use of risperidone in delirium: case reports. Ann Clin Psychiatry. 1997;9(2):105-107.
16. Horikawa N, Yamazaki T, Miyamoto K, et al. Treatment for delirium with risperidone: results of a prospective open trial with 10 patients. Gen Hosp Psychiatry. 2003;25(4):289-292.
17. Parellada E, Baeza I, de Pablo J, et al. Risperidone in the treatment of patients with delirium. J Clin Psychiatry. 2004;65(3):348-353.
18. Hans CS, Kim YK. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics. 2004;45(4):297-301.
19. Bourgeois JA, Hilty DM. Prolonged delirium managed with risperidone. Psychosomatics. 2005;46(1):90-91.
20. Naber D, Lambert M. The CATIE and CUtLASS studies in schizophrenia: results and implications for clinicians. CNS Drugs. 2009;23(8):649-659.
21. Zheng L, Mack WJ, Dagerman KS, et al. Metabolic changes associated with second-generation antipsychotic use in Alzheimer’s disease patients: the CATIE-AD study. Am J Psychiatry. 2009;166(5):583-590.
22. Sipahimalani A, Masand PS. Olanzapine in the treatment of delirium. Psychosomatics. 1998;39(5):422-430.
23. Breitbart W, Tremblay A, Gibson C. An open trial of olanzapine for the treatment of delirium in hospitalized cancer patients. Psychosomatics. 2002;43(3):175-182.
24. Hu H, Deng W, Yang H. A prospective random control study comparison of olanzapine and haloperidol in senile dementia. Chongqing Medical Journal. 2004;8:1234-1237.
25. Al-Samarrai S, Dunn J, Newmark T, et al. Quetiapine for treatment-resistant delirium. Psychosomatics. 2003;44(4):350-351.
26. Sasaki Y, Matsuyama T, Inoue S, et al. A prospective, open-label, flexible-dose study of quetiapine in the treatment of delirium. J Clin Psychiatry. 2003;64(11):1316-1321.
27. Devlin JW, Roberts RJ, Fong JJ, et al. Efficacy and safety of quetiapine in critically ill patients with delirium: a prospective, multicenter, randomized, double-blind, placebo-controlled pilot study. Crit Care Med. 2010;38(2):419-427.
28. Leso L, Schwartz TL. Ziprasidone treatment of delirium. Psychosomatics. 2002;43(1):61-62.
29. Young CC, Lujan E. Intravenous ziprasidone for treatment of delirium in the intensive care unit. Anesthesiology. 2004;101(3):794-795.
30. Alao AO, Moskowitz L. Aripiprazole and delirium. Ann Clin Psychiatry. 2006;18(4):267-269.
31. Straker DA, Shapiro PA, Muskin PR. Aripiprazole in the treatment of delirium. Psychosomatics. 2006;47(5):385-391.
32. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc. 2008;56(7):1333-1341.
33. Chew ML, Mulsant BH, Pollock BG, et al. A model of anticholinergic activity of atypical antipsychotic medications. Schizophr Res. 2006;88(1-3):63-72.
34. Buckley NA, Sanders P. Cardiovascular adverse effects of antipsychotic drugs. Drug Saf. 2000;23:215-228.
35. Stöllberger C, Huber JO, Finsterer J. Antipsychotic drugs and QT prolongation. Int Clin Psychopharmacol. 2005;20(5):243-251.
36. Zemrak WR, Kenna GA. Association of antipsychotic and antidepressant drugs with Q-T interval prolongation. Am J Health Syst Pharm. 2008;65(11):1029-1038.
37. Alvarez PA, Pahissa J. QT alterations in psychopharmacology: proven candidates and suspects. Curr Drug Saf. 2010;5(1):97-104.
Bariatric procedures: Managing patients after surgery
Discuss this article at http://currentpsychiatry.blogspot.com/2011/01/bariatric-procedures-managing-patients.html#comments

Bariatric surgery is the most effective treatment for obesity (defined as a body mass index [BMI] >30 kg/m2) and is recommended for extremely obese individuals (BMI >40 kg/m2) age >18.1,2 Most patients experience significant weight loss accompanied by improvements in mood, physical comorbidities, and quality of life (Box).3-8 Despite these favorable outcomes, several aspects of postoperative care—such as management of mental health issues—remain unclear. Bariatric surgery candidates show high rates of preoperative psychopathology, particularly depression and dysphoria. Little is known about how bariatric surgery affects absorption of psychiatric medications, leaving prescribing clinicians with minimal guidance when a postoperative patient reports changes in mood symptoms.
This article discusses the psychosocial status of bariatric surgery candidates and presents a rationale for increased medication monitoring after surgery.
Weight loss after bariatric surgery is associated with significant improvements in obesity-related comorbidities, including diabetes and cardiovascular disease, and decreased mortality.3,4
Many patients are able to reduce or discontinue many of their nonpsychiatric preoperative medications as their comorbid conditions improve.5 Symptoms of depression and anxiety, health-related quality of life, self-esteem, and body image often improve dramatically in the first year after surgery and endure for several years.6,7
Psychosocial improvements, however, may not translate into changes in psychotropic use. In a sample of 114 bariatric surgery patients, 43% were taking a selective serotonin reuptake inhibitor before surgery, 40% at 12 months postsurgery, and 31% at 24 months.8 These percentages do not account for patients who were taking other types of antidepressants.
Surgical treatment of obesity
The most common surgical procedures for weight loss are adjustable gastric banding (AGB) and Roux-en-Y gastric bypass (RYGB); each can be performed laparoscopically. With both procedures, food intake is restricted by creating a gastric pouch at the base of the esophagus. RYGB (Figure)9,10 also is thought to induce weight loss through selective malabsorption and favorable effects on gut peptides11,12 and currently is the procedure of choice in the United States.13
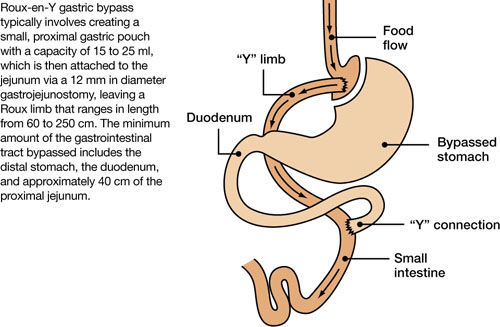
Figure Roux-en-Y: Bariatric procedure of choice
Source: References 9,10Bariatric surgery patients typically lose 25% to 35% of their initial body weight within 12 to 18 months of surgery.3,4 However, 20% to 30% of patients fail to achieve typical postoperative weight loss or regain large amounts of weight within a few years.14-16 Suboptimal results have been attributed to multiple factors, including problematic dietary intake, disordered eating, low levels of physical activity, preoperative psychopathology, and poor follow-up.6,17,18
Preop psychopathology
Twenty percent to 60% of extremely obese persons who pursue bariatric surgery have a psychiatric illness.6,7 In a study of 288 bariatric surgery candidates assessed with the Structured Clinical Interview for DSMIV, 38% received a current axis I diagnosis and 66% were given a lifetime diagnosis.19 In a separate study of 174 individuals seeking bariatric surgery, 24% met criteria for a current axis I or axis II disorder and 37% were found to have ≥1 lifetime diagnoses.20 The most common lifetime diagnoses were affective disorders (22%), anxiety disorders (16%), and eating disorders (14%).20
Psychopathology could negatively impact postoperative outcome. In an observational study, patients with a lifetime diagnosis of any axis I disorder—particularly mood and anxiety disorders—experienced less weight loss 6 months after RYGB compared with those who never received an axis I diagnosis.21 Bariatric surgery patients with ≥2 psychiatric diagnoses were more likely to stop losing weight or regain weight after 1 year compared with those with 1 or no diagnosis.22 Psychiatric illness also appears to impact longer term weight loss.23
Most bariatric surgery programs in the United States require a mental health evaluation as part of the patient selection process.24 These assessments may include evaluating a patient’s behavior patterns, motivation, expectations, and cognitive and emotional functioning, and performing psychological testing (see Related Resources). Psychiatric problems such as substance abuse, active psychosis, bulimia nervosa, and severe, uncontrolled depression1,9,25 are widely considered contraindications to bariatric surgery.24,26
Postsurgery considerations
At the time of bariatric surgery 16% to 40% of patients are receiving mental health treatment, which often includes antidepressants.27-29 Unfortunately, little is known about how medications interact with these surgical procedures. Dramatic changes in medication absorption may occur because of reduced gastrointestinal (GI) surface area. Rapid reduction in body weight and fat mass and postoperative complications also may impact the efficacy and tolerability of antidepressants.
Pharmacokinetics. Anatomic and physiologic changes with bariatric surgery may lead to changes in the pharmacokinetic (PK) parameters of certain medications, particularly after RYGB. PK studies typically are conducted by collecting a series of plasma samples at predetermined intervals after a patient takes a medication. The blood levels of the medication and its active metabolites are used to compute multiple PK parameters that illustrate drug absorption, distribution, and metabolism. Theoretically, a bariatric surgery patient may experience changes in the rate and/or extent of:
- medication absorption from the GI tract into systemic circulation
- distribution throughout the body as fat mass and total body water change after surgery
- drug metabolism.
The effects of bariatric surgery on medication PK appears to be drug-specific.30-33
The bypassed portion of the GI tract is the primary absorption site for most medications; therefore, the length of the Roux limb may affect the extent of drug absorption impairment. However, the duodenum wall is one of many locations of the cytochrome P450 (CYP) isoenzymes CYP3A4 and CYP3A5,34 which are the primary metabolic enzymes for drugs such as atorvastatin. Eliminating this portion of the bowel could increase rather than decrease bioavailability.35 Alterations in drug absorption also may result from changes in gastric emptying rate, reduced exposure to absorptive mucosal surfaces, and alterations in gastric pH that can impair drug dissolution and solubility.30 These changes could reduce medication bioavailability.33 The impact of such changes may differ according to the characteristics of the specific drug. It has been theorized that drugs that are intrinsically poorly absorbed, are highly lipophilic, and undergo enterohepatic circulation carry the highest risk of malabsorption.30 Antidepressants vary in the extent to which they demonstrate these characteristics. Progressive changes in the volume of distribution as weight is lost also could affect the blood levels of some antidepressants.
A series of small studies and case reports of PK changes in medications such as digoxin, oral contraceptives, cyclosporine, sulfisoxazole, and tacrolimus after jejunoileal bypass—an older, obsolete bariatric procedure—reveal variability in the surgery’s effect on PK parameters, although most reported reduced absorption. Data specific to RYGB consist of small studies and case series that show reduced absorption after surgery with significant variability among agents (see our bibliography of studies describing PK changes in nonpsychiatric medications after bariatric surgery). In a systematic literature review, Padwal et al found evidence for a decreased magnitude of absorption in 15 of 22 studies of jejunoileal bypass patients, 1 of 3 studies of gastric bypass/gastroplasty, and no studies examining biliopancreatic diversion.30
It is unclear if antidepressant absorption is impaired after RYGB because currently only 1 case report presents in-vivo data. Hamad et al describe an obese patient (BMI 46 kg/m2) taking sertraline, 100 mg/d, for depression.36 Researchers measured sertraline levels before and 1 month after RYGB, at which time the patient’s depression worsened. After surgery, sertraline maximum concentration was lower (14.4 ng/ml vs 41.6 ng/ml), trough concentration was lower (11.1 ng/ml vs 17.5 ng/ml), and time to maximum concentration was shorter (240 vs 300 minutes). This suggests that a shift in sertraline absorption after surgery may have contributed to the patient’s worsened mood symptoms.
An in-vitro study that simulated preand post-RYGB GI environments found that 12 of 22 psychotropic drugs tested dissolved differently between the models.37 Whereas the dissolved fractions of amitriptyline, fluoxetine, paroxetine, and sertraline were significantly less in the post-RYGB environment, bupropion dissolved to a greater extent in the pre-RYGB environment, and venlafaxine and citalopram were not different between the 2 conditions (Table).37 Although several limitations prevent translating these data into clinical recommendations, this study suggests that there may be significant variability among medications with regard to the implications of an altered GI environment.
Blouin RA, Bauer LA, Miller DD, et al. Vancomycin pharmacokinetics in normal and morbidly obese subjects. Antimicrob Agents Chemother. 1982;21(4):575-580.
Blouin RA, Brouwer KL, Record KE, et al. Amikacin pharmacokinetics in morbidly obese patients undergoing gastric-bypass surgery. Clin Pharm. 1985;4:70-72.
Chenhsu RY, Wu Y, Katz D, et al. Dose-adjusted cyclosporine c2 in a patient with jejunoileal bypass as compared to seven other liver transplant recipients. Ther Drug Monit. 2003;25(6):665-670.
Fuller AK, Tingle D, DeVane CL, et al. Haloperidol pharmacokinetics following gastric bypass surgery. J Clin Psychopharmacol. 1986;6:376-378.
Garrett ER, Süverkrup RS, Eberst K, et al. Surgically affected sulfisoxazole pharmacokinetics in the morbidly obese. Biopharm Drug Dispos. 1981;2:329-365.
Gerson CD, Lowe EH, Lindenbaum J. Bioavailability of digoxin tablets in patients with gastrointestinal dysfunction. Am J Med. 1980;69:43-49.
Hamad GG, Kozak GM, Wisner KL, et al. The effect of gastric bypass on SSRI pharmacokinetics and pharmacodynamics. Abstract presented at: American Society for Metabolic and Bariatric Surgery 25th Annual Meeting; June 15-20, 2008; Washington, DC.
Kelley M, Jain A, Kashyap R, et al. Change in oral absorption of tacrolimus in a liver transplant recipient after reversal of jejunoileal bypass: case report. Transplant Proc. 2005; 37:3165-3167.
Knight GC, Macris MP, Peric M, et al. Cyclosporine A pharmacokinetics in a cardiac allograft recipient with a jejunoileal bypass. Transplant Proc. 1988;20:351-355.
Marcus FI, Quinn EJ, Horton H, et al. The effect of jejunoileal bypass on the pharmacokinetics of digoxin in man. Circulation. 1977;55:537-541.
Magee SR, Shih G, Hume A. Malabsorption of oral antibiotics in pregnancy after gastric bypass surgery. J Am Board Fam Med. 2007;20:310-313.
Marterre WF, Hariharan S, First MR, et al. Gastric bypass in morbidly obese kidney transplant recipients. Clin Transplant. 1996;10:414-419.
Prince RA, Pincheira JC, Mason EE, et al. Influence of bariatric surgery on erythromycin absorption. J Clin Pharmacol. 1984;24:523-527.
Rogers CC, Alloway RR, Alexander JW, et al. Pharmacokinetics of mycophenolic acid, tacrolimus and sirolimus after gastric bypass surgery in end-stage renal disease and transplant patients: a pilot study. Clin Transplant. 2008;22:281-291.
Shepherd MF, Rosborough TK, Schwartz ML. Heparin thrombophylaxis in gastric bypass surgery. Obes Surg. 2003;13(2):249-253.
Skottheim IB, Stormark K, Christensen H, et al. Significantly altered systemic exposure to atorvastatin acid following gastric bypass surgery in morbidly obese patients. Clin Pharmacol Ther. 2009;86(3):311-318.
Victor A, Odlind V, Kral JG. Oral contraceptive absorption and sex hormone binding globulins in obese women: effects of jejunoileal bypass. Gastroenterol Clin North Am. 1987;16(3):483-491.
PK: pharmacokinetic
Table
Weights of dissolved portions of antidepressants before and after simulated RYGB
| Simulated pre-RYGB environment | Simulated post-RYGB environment | ||||
|---|---|---|---|---|---|
| Drug | Median weight of dissolved portion (mg) | Percentage* | Median weight of dissolved portion (mg) | Percentage* | P† |
| Amitriptyline, 75 mg/d | 80 | 28% | 60 | 21% | <.04 |
| Fluoxetine, 20 mg/d | 110 | 30% | 40 | 11% | <.04 |
| Paroxetine, 20 mg/d | 30 | 9% | 10 | 3% | <.04 |
| Sertraline, 100 mg/d | 50 | 16% | 30 | 10% | <.04 |
| Bupropion, 100 mg/d | 320 | 52% | 450 | 73% | <.05 |
| Venlafaxine, 75 mg/d | 180 | 59% | 180 | 59% | Not significant |
| Citalopram, 20 mg/d | 70 | 27% | 80 | 31% | Not significant |
| *Relative to original pill weight †Mann-Whitney U test RYGB: Roux-en-Y gastric bypass Source: Adapted from reference 37 | |||||
Altering antidepressant doses
Current PK data are insufficient to make clinical recommendations regarding appropriate postsurgical adjustment of dose or alternate dosage formulations (liquid, extended-release, etc.). However, based on theoretical considerations, Miller and Smith suggest that patients avoid extended-release preparations whenever possible after bariatric surgery, citing the rationale that decreased intestinal length and surface area leads to reduced absorption.33 No data are available to advise clinicians regarding the appropriateness of switching patients from extended-release products to immediate-release or liquid preparations following surgery.
Presently, increased medication monitoring may be the most appropriate clinical approach. If appropriate doses have little or no effect, consider the possibility of decreased medication absorption.33 Monitoring plasma levels of medications that have therapeutic ranges also is advisable.
Areas for future research
Before specific clinical recommendations for managing antidepressants following RYGB can be proposed, the extent to which the absorption, volume of distribution, drug metabolism, and other measures change after surgery need to be quantified. It is also unclear whether changes in medication absorption are subject to inter-patient variability, whether predictive characteristics can be identified, and whether any observed changes remain stable over time. Similarly, the extent to which variability in surgical procedures (eg, surgeon preference regarding remnant intestinal length) affects medication absorption is unknown. Data regarding medication absorption following AGB and other bariatric procedures also will be needed.
- American Society for Metabolic and Bariatric Surgery. Fact sheet: Metabolic and bariatric surgery. www.asbs.org/Newsite07/media/asmbs_fs_surgery.pdf.
- American Society for Metabolic and Bariatric Surgery. Suggestions for the pre-surgical psychological assessment of bariatric surgery candidates. www.asmbs.org/html/pdf/PsychPreSurgicalAssessment.pdf.
Drug Brand Names
- Amitriptyline • Elavil
- Atorvastatin • Lipitor
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Cyclosporine • Sandimmune
- Digoxin • Lanoxin
- Fluoxetine • Prozac
- Paroxetine • Paxil
- Sertraline • Zoloft
- Sulfisoxazole • Truxazole
- Tacrolimus • Prograf
- Venlafaxine • Effexor
Disclosures
Dr. Sarwer receives grant/research support from the National Institutes of Health, the American Society for Metabolic and Bariatric Surgery, and Ethicon Endo-Surgery, Inc., is consultant to Allergan, BAROnova, Inc., EnteroMedics, and Ethocon Endo-Surgery, Inc., and is on the board of directors of Surgical Review Corporation.
Dr. Roerig receives grant/research support from Eli Lilly and Company.
Drs. Faulconbridge, Steffen, and Mitchell report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Mechanick JI, Kushner RF, Sugerman HJ, et al. American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic and Bariatric Surgery Medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Endocr Pract. 2008;14:318-336.
2. NIH conference. Gastrointestinal surgery for severe obesity. Consensus Development Conference Panel. Ann Intern Med. 1991;115:956-961.
3. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724-1737.
4. Maggard MA, Shugarman LR, Suttorp M, et al. Meta-analysis: surgical treatment of obesity. Ann Intern Med. 2005;142:547-559.
5. Hodo DM, Waller JL, Martindale RG, et al. Medication use after bariatric surgery in a managed care cohort. Surg Obes Rel Dis. 2008;4:601-607.
6. Sarwer DB, Wadden TA, Fabricatore AN. Psychosocial and behavioral aspects of bariatric surgery. Obes Res. 2005;13:639-648.
7. Mitchell JE, de Zwaan M. Bariatric surgery: a guide for mental health professionals. New York, NY: Routledge; 2005.
8. Malone M, Alger-Mayer SA. Medication use patterns after gastric bypass surgery for weight management. Ann Pharmacopher. 2005;39:637-642.
9. Buchwald H. and the Consensus Conference Panel. Consensus conference statement: bariatric surgery for morbid obesity: health implications for patients, health professionals, and third-party payers. Surg Obes Rel Dis. 2005;1:371-381.
10. Needleman BJ, Happel LC. Bariatric surgery: choosing the optimal procedure. Surg Clin North Am. 2008;88:991-1007.
11. Albrecht RJ, Pories WJ. Surgical intervention for the severely obese. Baillieres Best Pract Res Clin Endocrinol Metab. 1999;13:149-172.
12. Brolin RE. Bariatric surgery and long-term control of morbid obesity. JAMA. 2002;288:2793-2796.
13. Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric surgical procedures. JAMA. 2005;294:1909-1917.
14. Brolin RE, Kenler HA, Gorman RC, et al. The dilemma of outcome assessment after operations for morbid obesity. Surgery. 1989;105:337-346.
15. Sjöström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683-2693.
16. Sjöström L, Narbro K, Sjöström CD, et al. and the Swedish Obese Subjects Study. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357:741-752.
17. Bocchieri LE, Meana M, Fisher BL. A review of psychosocial outcomes of surgery for morbid obesity. J Psychosom Res. 2002;52:155-165.
18. Herpertz S, Kielmann R, Wolf AM, et al. Do psychosocial variables predict weight loss or mental health after obesity surgery? A systematic review. Obes Res. 2004;12:1554-1569.
19. Kalarchian MA, Marcus MD, Levine MD, et al. Psychiatric disorders among bariatric surgery candidates: relationship to obesity and functional health status. Am J Psychiatry. 2007;164:328-334.
20. Rosenberger PH, Henderson KE, Grilo CM. Psychiatric disorder comorbidity and association with eating disorders in bariatric surgery patients: a cross-sectional study using structured interview based diagnosis. J Clin Psychiatry. 2006;67:1080-1085.
21. Kalarchian MA, Marcus MD, Levine MD, et al. Relationship of psychiatric disorders to 6-month outcomes after gastric bypass. Surg Obes Relat Dis. 2008;4:544-549.
22. Rutledge T, Groesz LM, Savu M. Psychiatric factors and weight loss patterns following gastric bypass surgery in a veteran population. Obes Surg. 2009;[Epub ahead of print].
23. Kinzl JF, Schrattenecker M, Traweger C, et al. Psychosocial predictors of weight loss after bariatric surgery. Obes Surg. 2006;16:1609-1614.
24. Bauchowitz AU, Gonder-Frederick LA, Olbrisch ME, et al. Psychosocial evaluation of bariatric surgery candidates: a survey of present practices. Psychosom Med. 2005;67(5):825-832.
25. Wadden TA, Sarwer DB, Womble LG, et al. Psychosocial aspects of obesity and obesity surgery. Surg Clin North Am. 2001;81:1001-1024.
26. Fabricatore AN, Crerand CE, Wadden TA, et al. How do mental health professionals evaluate candidates for bariatric surgery? Survey results. Obes Surg. 2006;16:567-573.
27. Sarwer DB, Cohn NI, Gibbons LM, et al. Psychiatric diagnoses and psychiatric treatment among bariatric surgery candidates. Obes Surg. 2004;14(9):1148-1156.
28. Larsen JK, Greenen R, van Ramshorst B, et al. Psychosocial functioning before and after laparoscopic adjustable gastric banding: a cross-sectional study. Obes Surg. 2003;13(4):629-636.
29. Clark MM, Balsiger BM, Sletten CD, et al. Psychosocial factors and 2-year outcome following bariatric surgery for weight loss. Obes Surg. 2003;13(5):739-745.
30. Padwal R, Brocks D, Sharma AM. A systematic review of drug absorption following bariatric surgery and its theoretical implications. Obes Rev. 2010;11(1):41-50.
31. Macgreggor AMC, Boggs L. Drug distribution in obesity and following bariatric surgery: a literature review. Obes Surg. 1996;6:17-27.
32. Malone M. Altered drug disposition in obesity and after bariatric surgery. Nutr Clin Pract. 2003;18:131-135.
33. Miller AD, Smith KM. Medication and nutrient administration considerations after bariatric surgery. Am J Health Syst Pharm. 2006;63:1852-1857.
34. Paine MF, Khalighi M, Fisher JM, et al. Characterization of interintestinal and intraintestinal variations in human CYP3A-dependent metabolism. J Pharmacol Exp Ther. 1997;283:1552-1562.
35. Skottheim IB, Stormark K, Christensen H, et al. Significantly altered systemic exposure to atorvastatin acid following gastric bypass surgery in morbidly obese patients. Clin Pharmacol Ther. 2009;86(3):311-318.
36. Hamad GG, Kozak GM, Wisner KL, et al. The effect of gastric bypass on SSRI pharmacokinetics and pharmacodynamics. Abstract presented at: American Society for Metabolic and Bariatric Surgery 25 Annual Meeting; June 15-20, 2008; Washington, DC.
37. Seaman JS, Bowers SP, Dixon P, et al. Dissolution of common psychiatric medications in a Roux-en-Y gastric bypass model. Psychosomatics. 2005;46:250-253.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/01/bariatric-procedures-managing-patients.html#comments
Bariatric surgery is the most effective treatment for obesity (defined as a body mass index [BMI] >30 kg/m2) and is recommended for extremely obese individuals (BMI >40 kg/m2) age >18.1,2 Most patients experience significant weight loss accompanied by improvements in mood, physical comorbidities, and quality of life (Box).3-8 Despite these favorable outcomes, several aspects of postoperative care—such as management of mental health issues—remain unclear. Bariatric surgery candidates show high rates of preoperative psychopathology, particularly depression and dysphoria. Little is known about how bariatric surgery affects absorption of psychiatric medications, leaving prescribing clinicians with minimal guidance when a postoperative patient reports changes in mood symptoms.
This article discusses the psychosocial status of bariatric surgery candidates and presents a rationale for increased medication monitoring after surgery.
Weight loss after bariatric surgery is associated with significant improvements in obesity-related comorbidities, including diabetes and cardiovascular disease, and decreased mortality.3,4
Many patients are able to reduce or discontinue many of their nonpsychiatric preoperative medications as their comorbid conditions improve.5 Symptoms of depression and anxiety, health-related quality of life, self-esteem, and body image often improve dramatically in the first year after surgery and endure for several years.6,7
Psychosocial improvements, however, may not translate into changes in psychotropic use. In a sample of 114 bariatric surgery patients, 43% were taking a selective serotonin reuptake inhibitor before surgery, 40% at 12 months postsurgery, and 31% at 24 months.8 These percentages do not account for patients who were taking other types of antidepressants.
Surgical treatment of obesity
The most common surgical procedures for weight loss are adjustable gastric banding (AGB) and Roux-en-Y gastric bypass (RYGB); each can be performed laparoscopically. With both procedures, food intake is restricted by creating a gastric pouch at the base of the esophagus. RYGB (Figure)9,10 also is thought to induce weight loss through selective malabsorption and favorable effects on gut peptides11,12 and currently is the procedure of choice in the United States.13
Figure Roux-en-Y: Bariatric procedure of choice
Source: References 9,10Bariatric surgery patients typically lose 25% to 35% of their initial body weight within 12 to 18 months of surgery.3,4 However, 20% to 30% of patients fail to achieve typical postoperative weight loss or regain large amounts of weight within a few years.14-16 Suboptimal results have been attributed to multiple factors, including problematic dietary intake, disordered eating, low levels of physical activity, preoperative psychopathology, and poor follow-up.6,17,18
Preop psychopathology
Twenty percent to 60% of extremely obese persons who pursue bariatric surgery have a psychiatric illness.6,7 In a study of 288 bariatric surgery candidates assessed with the Structured Clinical Interview for DSMIV, 38% received a current axis I diagnosis and 66% were given a lifetime diagnosis.19 In a separate study of 174 individuals seeking bariatric surgery, 24% met criteria for a current axis I or axis II disorder and 37% were found to have ≥1 lifetime diagnoses.20 The most common lifetime diagnoses were affective disorders (22%), anxiety disorders (16%), and eating disorders (14%).20
Psychopathology could negatively impact postoperative outcome. In an observational study, patients with a lifetime diagnosis of any axis I disorder—particularly mood and anxiety disorders—experienced less weight loss 6 months after RYGB compared with those who never received an axis I diagnosis.21 Bariatric surgery patients with ≥2 psychiatric diagnoses were more likely to stop losing weight or regain weight after 1 year compared with those with 1 or no diagnosis.22 Psychiatric illness also appears to impact longer term weight loss.23
Most bariatric surgery programs in the United States require a mental health evaluation as part of the patient selection process.24 These assessments may include evaluating a patient’s behavior patterns, motivation, expectations, and cognitive and emotional functioning, and performing psychological testing (see Related Resources). Psychiatric problems such as substance abuse, active psychosis, bulimia nervosa, and severe, uncontrolled depression1,9,25 are widely considered contraindications to bariatric surgery.24,26
Postsurgery considerations
At the time of bariatric surgery 16% to 40% of patients are receiving mental health treatment, which often includes antidepressants.27-29 Unfortunately, little is known about how medications interact with these surgical procedures. Dramatic changes in medication absorption may occur because of reduced gastrointestinal (GI) surface area. Rapid reduction in body weight and fat mass and postoperative complications also may impact the efficacy and tolerability of antidepressants.
Pharmacokinetics. Anatomic and physiologic changes with bariatric surgery may lead to changes in the pharmacokinetic (PK) parameters of certain medications, particularly after RYGB. PK studies typically are conducted by collecting a series of plasma samples at predetermined intervals after a patient takes a medication. The blood levels of the medication and its active metabolites are used to compute multiple PK parameters that illustrate drug absorption, distribution, and metabolism. Theoretically, a bariatric surgery patient may experience changes in the rate and/or extent of:
- medication absorption from the GI tract into systemic circulation
- distribution throughout the body as fat mass and total body water change after surgery
- drug metabolism.
The effects of bariatric surgery on medication PK appears to be drug-specific.30-33
The bypassed portion of the GI tract is the primary absorption site for most medications; therefore, the length of the Roux limb may affect the extent of drug absorption impairment. However, the duodenum wall is one of many locations of the cytochrome P450 (CYP) isoenzymes CYP3A4 and CYP3A5,34 which are the primary metabolic enzymes for drugs such as atorvastatin. Eliminating this portion of the bowel could increase rather than decrease bioavailability.35 Alterations in drug absorption also may result from changes in gastric emptying rate, reduced exposure to absorptive mucosal surfaces, and alterations in gastric pH that can impair drug dissolution and solubility.30 These changes could reduce medication bioavailability.33 The impact of such changes may differ according to the characteristics of the specific drug. It has been theorized that drugs that are intrinsically poorly absorbed, are highly lipophilic, and undergo enterohepatic circulation carry the highest risk of malabsorption.30 Antidepressants vary in the extent to which they demonstrate these characteristics. Progressive changes in the volume of distribution as weight is lost also could affect the blood levels of some antidepressants.
A series of small studies and case reports of PK changes in medications such as digoxin, oral contraceptives, cyclosporine, sulfisoxazole, and tacrolimus after jejunoileal bypass—an older, obsolete bariatric procedure—reveal variability in the surgery’s effect on PK parameters, although most reported reduced absorption. Data specific to RYGB consist of small studies and case series that show reduced absorption after surgery with significant variability among agents (see our bibliography of studies describing PK changes in nonpsychiatric medications after bariatric surgery). In a systematic literature review, Padwal et al found evidence for a decreased magnitude of absorption in 15 of 22 studies of jejunoileal bypass patients, 1 of 3 studies of gastric bypass/gastroplasty, and no studies examining biliopancreatic diversion.30
It is unclear if antidepressant absorption is impaired after RYGB because currently only 1 case report presents in-vivo data. Hamad et al describe an obese patient (BMI 46 kg/m2) taking sertraline, 100 mg/d, for depression.36 Researchers measured sertraline levels before and 1 month after RYGB, at which time the patient’s depression worsened. After surgery, sertraline maximum concentration was lower (14.4 ng/ml vs 41.6 ng/ml), trough concentration was lower (11.1 ng/ml vs 17.5 ng/ml), and time to maximum concentration was shorter (240 vs 300 minutes). This suggests that a shift in sertraline absorption after surgery may have contributed to the patient’s worsened mood symptoms.
An in-vitro study that simulated preand post-RYGB GI environments found that 12 of 22 psychotropic drugs tested dissolved differently between the models.37 Whereas the dissolved fractions of amitriptyline, fluoxetine, paroxetine, and sertraline were significantly less in the post-RYGB environment, bupropion dissolved to a greater extent in the pre-RYGB environment, and venlafaxine and citalopram were not different between the 2 conditions (Table).37 Although several limitations prevent translating these data into clinical recommendations, this study suggests that there may be significant variability among medications with regard to the implications of an altered GI environment.
Blouin RA, Bauer LA, Miller DD, et al. Vancomycin pharmacokinetics in normal and morbidly obese subjects. Antimicrob Agents Chemother. 1982;21(4):575-580.
Blouin RA, Brouwer KL, Record KE, et al. Amikacin pharmacokinetics in morbidly obese patients undergoing gastric-bypass surgery. Clin Pharm. 1985;4:70-72.
Chenhsu RY, Wu Y, Katz D, et al. Dose-adjusted cyclosporine c2 in a patient with jejunoileal bypass as compared to seven other liver transplant recipients. Ther Drug Monit. 2003;25(6):665-670.
Fuller AK, Tingle D, DeVane CL, et al. Haloperidol pharmacokinetics following gastric bypass surgery. J Clin Psychopharmacol. 1986;6:376-378.
Garrett ER, Süverkrup RS, Eberst K, et al. Surgically affected sulfisoxazole pharmacokinetics in the morbidly obese. Biopharm Drug Dispos. 1981;2:329-365.
Gerson CD, Lowe EH, Lindenbaum J. Bioavailability of digoxin tablets in patients with gastrointestinal dysfunction. Am J Med. 1980;69:43-49.
Hamad GG, Kozak GM, Wisner KL, et al. The effect of gastric bypass on SSRI pharmacokinetics and pharmacodynamics. Abstract presented at: American Society for Metabolic and Bariatric Surgery 25th Annual Meeting; June 15-20, 2008; Washington, DC.
Kelley M, Jain A, Kashyap R, et al. Change in oral absorption of tacrolimus in a liver transplant recipient after reversal of jejunoileal bypass: case report. Transplant Proc. 2005; 37:3165-3167.
Knight GC, Macris MP, Peric M, et al. Cyclosporine A pharmacokinetics in a cardiac allograft recipient with a jejunoileal bypass. Transplant Proc. 1988;20:351-355.
Marcus FI, Quinn EJ, Horton H, et al. The effect of jejunoileal bypass on the pharmacokinetics of digoxin in man. Circulation. 1977;55:537-541.
Magee SR, Shih G, Hume A. Malabsorption of oral antibiotics in pregnancy after gastric bypass surgery. J Am Board Fam Med. 2007;20:310-313.
Marterre WF, Hariharan S, First MR, et al. Gastric bypass in morbidly obese kidney transplant recipients. Clin Transplant. 1996;10:414-419.
Prince RA, Pincheira JC, Mason EE, et al. Influence of bariatric surgery on erythromycin absorption. J Clin Pharmacol. 1984;24:523-527.
Rogers CC, Alloway RR, Alexander JW, et al. Pharmacokinetics of mycophenolic acid, tacrolimus and sirolimus after gastric bypass surgery in end-stage renal disease and transplant patients: a pilot study. Clin Transplant. 2008;22:281-291.
Shepherd MF, Rosborough TK, Schwartz ML. Heparin thrombophylaxis in gastric bypass surgery. Obes Surg. 2003;13(2):249-253.
Skottheim IB, Stormark K, Christensen H, et al. Significantly altered systemic exposure to atorvastatin acid following gastric bypass surgery in morbidly obese patients. Clin Pharmacol Ther. 2009;86(3):311-318.
Victor A, Odlind V, Kral JG. Oral contraceptive absorption and sex hormone binding globulins in obese women: effects of jejunoileal bypass. Gastroenterol Clin North Am. 1987;16(3):483-491.
PK: pharmacokinetic
Table
Weights of dissolved portions of antidepressants before and after simulated RYGB
| Simulated pre-RYGB environment | Simulated post-RYGB environment | ||||
|---|---|---|---|---|---|
| Drug | Median weight of dissolved portion (mg) | Percentage* | Median weight of dissolved portion (mg) | Percentage* | P† |
| Amitriptyline, 75 mg/d | 80 | 28% | 60 | 21% | <.04 |
| Fluoxetine, 20 mg/d | 110 | 30% | 40 | 11% | <.04 |
| Paroxetine, 20 mg/d | 30 | 9% | 10 | 3% | <.04 |
| Sertraline, 100 mg/d | 50 | 16% | 30 | 10% | <.04 |
| Bupropion, 100 mg/d | 320 | 52% | 450 | 73% | <.05 |
| Venlafaxine, 75 mg/d | 180 | 59% | 180 | 59% | Not significant |
| Citalopram, 20 mg/d | 70 | 27% | 80 | 31% | Not significant |
| *Relative to original pill weight †Mann-Whitney U test RYGB: Roux-en-Y gastric bypass Source: Adapted from reference 37 | |||||
Altering antidepressant doses
Current PK data are insufficient to make clinical recommendations regarding appropriate postsurgical adjustment of dose or alternate dosage formulations (liquid, extended-release, etc.). However, based on theoretical considerations, Miller and Smith suggest that patients avoid extended-release preparations whenever possible after bariatric surgery, citing the rationale that decreased intestinal length and surface area leads to reduced absorption.33 No data are available to advise clinicians regarding the appropriateness of switching patients from extended-release products to immediate-release or liquid preparations following surgery.
Presently, increased medication monitoring may be the most appropriate clinical approach. If appropriate doses have little or no effect, consider the possibility of decreased medication absorption.33 Monitoring plasma levels of medications that have therapeutic ranges also is advisable.
Areas for future research
Before specific clinical recommendations for managing antidepressants following RYGB can be proposed, the extent to which the absorption, volume of distribution, drug metabolism, and other measures change after surgery need to be quantified. It is also unclear whether changes in medication absorption are subject to inter-patient variability, whether predictive characteristics can be identified, and whether any observed changes remain stable over time. Similarly, the extent to which variability in surgical procedures (eg, surgeon preference regarding remnant intestinal length) affects medication absorption is unknown. Data regarding medication absorption following AGB and other bariatric procedures also will be needed.
- American Society for Metabolic and Bariatric Surgery. Fact sheet: Metabolic and bariatric surgery. www.asbs.org/Newsite07/media/asmbs_fs_surgery.pdf.
- American Society for Metabolic and Bariatric Surgery. Suggestions for the pre-surgical psychological assessment of bariatric surgery candidates. www.asmbs.org/html/pdf/PsychPreSurgicalAssessment.pdf.
Drug Brand Names
- Amitriptyline • Elavil
- Atorvastatin • Lipitor
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Cyclosporine • Sandimmune
- Digoxin • Lanoxin
- Fluoxetine • Prozac
- Paroxetine • Paxil
- Sertraline • Zoloft
- Sulfisoxazole • Truxazole
- Tacrolimus • Prograf
- Venlafaxine • Effexor
Disclosures
Dr. Sarwer receives grant/research support from the National Institutes of Health, the American Society for Metabolic and Bariatric Surgery, and Ethicon Endo-Surgery, Inc., is consultant to Allergan, BAROnova, Inc., EnteroMedics, and Ethocon Endo-Surgery, Inc., and is on the board of directors of Surgical Review Corporation.
Dr. Roerig receives grant/research support from Eli Lilly and Company.
Drs. Faulconbridge, Steffen, and Mitchell report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/01/bariatric-procedures-managing-patients.html#comments
Bariatric surgery is the most effective treatment for obesity (defined as a body mass index [BMI] >30 kg/m2) and is recommended for extremely obese individuals (BMI >40 kg/m2) age >18.1,2 Most patients experience significant weight loss accompanied by improvements in mood, physical comorbidities, and quality of life (Box).3-8 Despite these favorable outcomes, several aspects of postoperative care—such as management of mental health issues—remain unclear. Bariatric surgery candidates show high rates of preoperative psychopathology, particularly depression and dysphoria. Little is known about how bariatric surgery affects absorption of psychiatric medications, leaving prescribing clinicians with minimal guidance when a postoperative patient reports changes in mood symptoms.
This article discusses the psychosocial status of bariatric surgery candidates and presents a rationale for increased medication monitoring after surgery.
Weight loss after bariatric surgery is associated with significant improvements in obesity-related comorbidities, including diabetes and cardiovascular disease, and decreased mortality.3,4
Many patients are able to reduce or discontinue many of their nonpsychiatric preoperative medications as their comorbid conditions improve.5 Symptoms of depression and anxiety, health-related quality of life, self-esteem, and body image often improve dramatically in the first year after surgery and endure for several years.6,7
Psychosocial improvements, however, may not translate into changes in psychotropic use. In a sample of 114 bariatric surgery patients, 43% were taking a selective serotonin reuptake inhibitor before surgery, 40% at 12 months postsurgery, and 31% at 24 months.8 These percentages do not account for patients who were taking other types of antidepressants.
Surgical treatment of obesity
The most common surgical procedures for weight loss are adjustable gastric banding (AGB) and Roux-en-Y gastric bypass (RYGB); each can be performed laparoscopically. With both procedures, food intake is restricted by creating a gastric pouch at the base of the esophagus. RYGB (Figure)9,10 also is thought to induce weight loss through selective malabsorption and favorable effects on gut peptides11,12 and currently is the procedure of choice in the United States.13
Figure Roux-en-Y: Bariatric procedure of choice
Source: References 9,10Bariatric surgery patients typically lose 25% to 35% of their initial body weight within 12 to 18 months of surgery.3,4 However, 20% to 30% of patients fail to achieve typical postoperative weight loss or regain large amounts of weight within a few years.14-16 Suboptimal results have been attributed to multiple factors, including problematic dietary intake, disordered eating, low levels of physical activity, preoperative psychopathology, and poor follow-up.6,17,18
Preop psychopathology
Twenty percent to 60% of extremely obese persons who pursue bariatric surgery have a psychiatric illness.6,7 In a study of 288 bariatric surgery candidates assessed with the Structured Clinical Interview for DSMIV, 38% received a current axis I diagnosis and 66% were given a lifetime diagnosis.19 In a separate study of 174 individuals seeking bariatric surgery, 24% met criteria for a current axis I or axis II disorder and 37% were found to have ≥1 lifetime diagnoses.20 The most common lifetime diagnoses were affective disorders (22%), anxiety disorders (16%), and eating disorders (14%).20
Psychopathology could negatively impact postoperative outcome. In an observational study, patients with a lifetime diagnosis of any axis I disorder—particularly mood and anxiety disorders—experienced less weight loss 6 months after RYGB compared with those who never received an axis I diagnosis.21 Bariatric surgery patients with ≥2 psychiatric diagnoses were more likely to stop losing weight or regain weight after 1 year compared with those with 1 or no diagnosis.22 Psychiatric illness also appears to impact longer term weight loss.23
Most bariatric surgery programs in the United States require a mental health evaluation as part of the patient selection process.24 These assessments may include evaluating a patient’s behavior patterns, motivation, expectations, and cognitive and emotional functioning, and performing psychological testing (see Related Resources). Psychiatric problems such as substance abuse, active psychosis, bulimia nervosa, and severe, uncontrolled depression1,9,25 are widely considered contraindications to bariatric surgery.24,26
Postsurgery considerations
At the time of bariatric surgery 16% to 40% of patients are receiving mental health treatment, which often includes antidepressants.27-29 Unfortunately, little is known about how medications interact with these surgical procedures. Dramatic changes in medication absorption may occur because of reduced gastrointestinal (GI) surface area. Rapid reduction in body weight and fat mass and postoperative complications also may impact the efficacy and tolerability of antidepressants.
Pharmacokinetics. Anatomic and physiologic changes with bariatric surgery may lead to changes in the pharmacokinetic (PK) parameters of certain medications, particularly after RYGB. PK studies typically are conducted by collecting a series of plasma samples at predetermined intervals after a patient takes a medication. The blood levels of the medication and its active metabolites are used to compute multiple PK parameters that illustrate drug absorption, distribution, and metabolism. Theoretically, a bariatric surgery patient may experience changes in the rate and/or extent of:
- medication absorption from the GI tract into systemic circulation
- distribution throughout the body as fat mass and total body water change after surgery
- drug metabolism.
The effects of bariatric surgery on medication PK appears to be drug-specific.30-33
The bypassed portion of the GI tract is the primary absorption site for most medications; therefore, the length of the Roux limb may affect the extent of drug absorption impairment. However, the duodenum wall is one of many locations of the cytochrome P450 (CYP) isoenzymes CYP3A4 and CYP3A5,34 which are the primary metabolic enzymes for drugs such as atorvastatin. Eliminating this portion of the bowel could increase rather than decrease bioavailability.35 Alterations in drug absorption also may result from changes in gastric emptying rate, reduced exposure to absorptive mucosal surfaces, and alterations in gastric pH that can impair drug dissolution and solubility.30 These changes could reduce medication bioavailability.33 The impact of such changes may differ according to the characteristics of the specific drug. It has been theorized that drugs that are intrinsically poorly absorbed, are highly lipophilic, and undergo enterohepatic circulation carry the highest risk of malabsorption.30 Antidepressants vary in the extent to which they demonstrate these characteristics. Progressive changes in the volume of distribution as weight is lost also could affect the blood levels of some antidepressants.
A series of small studies and case reports of PK changes in medications such as digoxin, oral contraceptives, cyclosporine, sulfisoxazole, and tacrolimus after jejunoileal bypass—an older, obsolete bariatric procedure—reveal variability in the surgery’s effect on PK parameters, although most reported reduced absorption. Data specific to RYGB consist of small studies and case series that show reduced absorption after surgery with significant variability among agents (see our bibliography of studies describing PK changes in nonpsychiatric medications after bariatric surgery). In a systematic literature review, Padwal et al found evidence for a decreased magnitude of absorption in 15 of 22 studies of jejunoileal bypass patients, 1 of 3 studies of gastric bypass/gastroplasty, and no studies examining biliopancreatic diversion.30
It is unclear if antidepressant absorption is impaired after RYGB because currently only 1 case report presents in-vivo data. Hamad et al describe an obese patient (BMI 46 kg/m2) taking sertraline, 100 mg/d, for depression.36 Researchers measured sertraline levels before and 1 month after RYGB, at which time the patient’s depression worsened. After surgery, sertraline maximum concentration was lower (14.4 ng/ml vs 41.6 ng/ml), trough concentration was lower (11.1 ng/ml vs 17.5 ng/ml), and time to maximum concentration was shorter (240 vs 300 minutes). This suggests that a shift in sertraline absorption after surgery may have contributed to the patient’s worsened mood symptoms.
An in-vitro study that simulated preand post-RYGB GI environments found that 12 of 22 psychotropic drugs tested dissolved differently between the models.37 Whereas the dissolved fractions of amitriptyline, fluoxetine, paroxetine, and sertraline were significantly less in the post-RYGB environment, bupropion dissolved to a greater extent in the pre-RYGB environment, and venlafaxine and citalopram were not different between the 2 conditions (Table).37 Although several limitations prevent translating these data into clinical recommendations, this study suggests that there may be significant variability among medications with regard to the implications of an altered GI environment.
Blouin RA, Bauer LA, Miller DD, et al. Vancomycin pharmacokinetics in normal and morbidly obese subjects. Antimicrob Agents Chemother. 1982;21(4):575-580.
Blouin RA, Brouwer KL, Record KE, et al. Amikacin pharmacokinetics in morbidly obese patients undergoing gastric-bypass surgery. Clin Pharm. 1985;4:70-72.
Chenhsu RY, Wu Y, Katz D, et al. Dose-adjusted cyclosporine c2 in a patient with jejunoileal bypass as compared to seven other liver transplant recipients. Ther Drug Monit. 2003;25(6):665-670.
Fuller AK, Tingle D, DeVane CL, et al. Haloperidol pharmacokinetics following gastric bypass surgery. J Clin Psychopharmacol. 1986;6:376-378.
Garrett ER, Süverkrup RS, Eberst K, et al. Surgically affected sulfisoxazole pharmacokinetics in the morbidly obese. Biopharm Drug Dispos. 1981;2:329-365.
Gerson CD, Lowe EH, Lindenbaum J. Bioavailability of digoxin tablets in patients with gastrointestinal dysfunction. Am J Med. 1980;69:43-49.
Hamad GG, Kozak GM, Wisner KL, et al. The effect of gastric bypass on SSRI pharmacokinetics and pharmacodynamics. Abstract presented at: American Society for Metabolic and Bariatric Surgery 25th Annual Meeting; June 15-20, 2008; Washington, DC.
Kelley M, Jain A, Kashyap R, et al. Change in oral absorption of tacrolimus in a liver transplant recipient after reversal of jejunoileal bypass: case report. Transplant Proc. 2005; 37:3165-3167.
Knight GC, Macris MP, Peric M, et al. Cyclosporine A pharmacokinetics in a cardiac allograft recipient with a jejunoileal bypass. Transplant Proc. 1988;20:351-355.
Marcus FI, Quinn EJ, Horton H, et al. The effect of jejunoileal bypass on the pharmacokinetics of digoxin in man. Circulation. 1977;55:537-541.
Magee SR, Shih G, Hume A. Malabsorption of oral antibiotics in pregnancy after gastric bypass surgery. J Am Board Fam Med. 2007;20:310-313.
Marterre WF, Hariharan S, First MR, et al. Gastric bypass in morbidly obese kidney transplant recipients. Clin Transplant. 1996;10:414-419.
Prince RA, Pincheira JC, Mason EE, et al. Influence of bariatric surgery on erythromycin absorption. J Clin Pharmacol. 1984;24:523-527.
Rogers CC, Alloway RR, Alexander JW, et al. Pharmacokinetics of mycophenolic acid, tacrolimus and sirolimus after gastric bypass surgery in end-stage renal disease and transplant patients: a pilot study. Clin Transplant. 2008;22:281-291.
Shepherd MF, Rosborough TK, Schwartz ML. Heparin thrombophylaxis in gastric bypass surgery. Obes Surg. 2003;13(2):249-253.
Skottheim IB, Stormark K, Christensen H, et al. Significantly altered systemic exposure to atorvastatin acid following gastric bypass surgery in morbidly obese patients. Clin Pharmacol Ther. 2009;86(3):311-318.
Victor A, Odlind V, Kral JG. Oral contraceptive absorption and sex hormone binding globulins in obese women: effects of jejunoileal bypass. Gastroenterol Clin North Am. 1987;16(3):483-491.
PK: pharmacokinetic
Table
Weights of dissolved portions of antidepressants before and after simulated RYGB
| Simulated pre-RYGB environment | Simulated post-RYGB environment | ||||
|---|---|---|---|---|---|
| Drug | Median weight of dissolved portion (mg) | Percentage* | Median weight of dissolved portion (mg) | Percentage* | P† |
| Amitriptyline, 75 mg/d | 80 | 28% | 60 | 21% | <.04 |
| Fluoxetine, 20 mg/d | 110 | 30% | 40 | 11% | <.04 |
| Paroxetine, 20 mg/d | 30 | 9% | 10 | 3% | <.04 |
| Sertraline, 100 mg/d | 50 | 16% | 30 | 10% | <.04 |
| Bupropion, 100 mg/d | 320 | 52% | 450 | 73% | <.05 |
| Venlafaxine, 75 mg/d | 180 | 59% | 180 | 59% | Not significant |
| Citalopram, 20 mg/d | 70 | 27% | 80 | 31% | Not significant |
| *Relative to original pill weight †Mann-Whitney U test RYGB: Roux-en-Y gastric bypass Source: Adapted from reference 37 | |||||
Altering antidepressant doses
Current PK data are insufficient to make clinical recommendations regarding appropriate postsurgical adjustment of dose or alternate dosage formulations (liquid, extended-release, etc.). However, based on theoretical considerations, Miller and Smith suggest that patients avoid extended-release preparations whenever possible after bariatric surgery, citing the rationale that decreased intestinal length and surface area leads to reduced absorption.33 No data are available to advise clinicians regarding the appropriateness of switching patients from extended-release products to immediate-release or liquid preparations following surgery.
Presently, increased medication monitoring may be the most appropriate clinical approach. If appropriate doses have little or no effect, consider the possibility of decreased medication absorption.33 Monitoring plasma levels of medications that have therapeutic ranges also is advisable.
Areas for future research
Before specific clinical recommendations for managing antidepressants following RYGB can be proposed, the extent to which the absorption, volume of distribution, drug metabolism, and other measures change after surgery need to be quantified. It is also unclear whether changes in medication absorption are subject to inter-patient variability, whether predictive characteristics can be identified, and whether any observed changes remain stable over time. Similarly, the extent to which variability in surgical procedures (eg, surgeon preference regarding remnant intestinal length) affects medication absorption is unknown. Data regarding medication absorption following AGB and other bariatric procedures also will be needed.
- American Society for Metabolic and Bariatric Surgery. Fact sheet: Metabolic and bariatric surgery. www.asbs.org/Newsite07/media/asmbs_fs_surgery.pdf.
- American Society for Metabolic and Bariatric Surgery. Suggestions for the pre-surgical psychological assessment of bariatric surgery candidates. www.asmbs.org/html/pdf/PsychPreSurgicalAssessment.pdf.
Drug Brand Names
- Amitriptyline • Elavil
- Atorvastatin • Lipitor
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Cyclosporine • Sandimmune
- Digoxin • Lanoxin
- Fluoxetine • Prozac
- Paroxetine • Paxil
- Sertraline • Zoloft
- Sulfisoxazole • Truxazole
- Tacrolimus • Prograf
- Venlafaxine • Effexor
Disclosures
Dr. Sarwer receives grant/research support from the National Institutes of Health, the American Society for Metabolic and Bariatric Surgery, and Ethicon Endo-Surgery, Inc., is consultant to Allergan, BAROnova, Inc., EnteroMedics, and Ethocon Endo-Surgery, Inc., and is on the board of directors of Surgical Review Corporation.
Dr. Roerig receives grant/research support from Eli Lilly and Company.
Drs. Faulconbridge, Steffen, and Mitchell report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Mechanick JI, Kushner RF, Sugerman HJ, et al. American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic and Bariatric Surgery Medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Endocr Pract. 2008;14:318-336.
2. NIH conference. Gastrointestinal surgery for severe obesity. Consensus Development Conference Panel. Ann Intern Med. 1991;115:956-961.
3. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724-1737.
4. Maggard MA, Shugarman LR, Suttorp M, et al. Meta-analysis: surgical treatment of obesity. Ann Intern Med. 2005;142:547-559.
5. Hodo DM, Waller JL, Martindale RG, et al. Medication use after bariatric surgery in a managed care cohort. Surg Obes Rel Dis. 2008;4:601-607.
6. Sarwer DB, Wadden TA, Fabricatore AN. Psychosocial and behavioral aspects of bariatric surgery. Obes Res. 2005;13:639-648.
7. Mitchell JE, de Zwaan M. Bariatric surgery: a guide for mental health professionals. New York, NY: Routledge; 2005.
8. Malone M, Alger-Mayer SA. Medication use patterns after gastric bypass surgery for weight management. Ann Pharmacopher. 2005;39:637-642.
9. Buchwald H. and the Consensus Conference Panel. Consensus conference statement: bariatric surgery for morbid obesity: health implications for patients, health professionals, and third-party payers. Surg Obes Rel Dis. 2005;1:371-381.
10. Needleman BJ, Happel LC. Bariatric surgery: choosing the optimal procedure. Surg Clin North Am. 2008;88:991-1007.
11. Albrecht RJ, Pories WJ. Surgical intervention for the severely obese. Baillieres Best Pract Res Clin Endocrinol Metab. 1999;13:149-172.
12. Brolin RE. Bariatric surgery and long-term control of morbid obesity. JAMA. 2002;288:2793-2796.
13. Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric surgical procedures. JAMA. 2005;294:1909-1917.
14. Brolin RE, Kenler HA, Gorman RC, et al. The dilemma of outcome assessment after operations for morbid obesity. Surgery. 1989;105:337-346.
15. Sjöström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683-2693.
16. Sjöström L, Narbro K, Sjöström CD, et al. and the Swedish Obese Subjects Study. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357:741-752.
17. Bocchieri LE, Meana M, Fisher BL. A review of psychosocial outcomes of surgery for morbid obesity. J Psychosom Res. 2002;52:155-165.
18. Herpertz S, Kielmann R, Wolf AM, et al. Do psychosocial variables predict weight loss or mental health after obesity surgery? A systematic review. Obes Res. 2004;12:1554-1569.
19. Kalarchian MA, Marcus MD, Levine MD, et al. Psychiatric disorders among bariatric surgery candidates: relationship to obesity and functional health status. Am J Psychiatry. 2007;164:328-334.
20. Rosenberger PH, Henderson KE, Grilo CM. Psychiatric disorder comorbidity and association with eating disorders in bariatric surgery patients: a cross-sectional study using structured interview based diagnosis. J Clin Psychiatry. 2006;67:1080-1085.
21. Kalarchian MA, Marcus MD, Levine MD, et al. Relationship of psychiatric disorders to 6-month outcomes after gastric bypass. Surg Obes Relat Dis. 2008;4:544-549.
22. Rutledge T, Groesz LM, Savu M. Psychiatric factors and weight loss patterns following gastric bypass surgery in a veteran population. Obes Surg. 2009;[Epub ahead of print].
23. Kinzl JF, Schrattenecker M, Traweger C, et al. Psychosocial predictors of weight loss after bariatric surgery. Obes Surg. 2006;16:1609-1614.
24. Bauchowitz AU, Gonder-Frederick LA, Olbrisch ME, et al. Psychosocial evaluation of bariatric surgery candidates: a survey of present practices. Psychosom Med. 2005;67(5):825-832.
25. Wadden TA, Sarwer DB, Womble LG, et al. Psychosocial aspects of obesity and obesity surgery. Surg Clin North Am. 2001;81:1001-1024.
26. Fabricatore AN, Crerand CE, Wadden TA, et al. How do mental health professionals evaluate candidates for bariatric surgery? Survey results. Obes Surg. 2006;16:567-573.
27. Sarwer DB, Cohn NI, Gibbons LM, et al. Psychiatric diagnoses and psychiatric treatment among bariatric surgery candidates. Obes Surg. 2004;14(9):1148-1156.
28. Larsen JK, Greenen R, van Ramshorst B, et al. Psychosocial functioning before and after laparoscopic adjustable gastric banding: a cross-sectional study. Obes Surg. 2003;13(4):629-636.
29. Clark MM, Balsiger BM, Sletten CD, et al. Psychosocial factors and 2-year outcome following bariatric surgery for weight loss. Obes Surg. 2003;13(5):739-745.
30. Padwal R, Brocks D, Sharma AM. A systematic review of drug absorption following bariatric surgery and its theoretical implications. Obes Rev. 2010;11(1):41-50.
31. Macgreggor AMC, Boggs L. Drug distribution in obesity and following bariatric surgery: a literature review. Obes Surg. 1996;6:17-27.
32. Malone M. Altered drug disposition in obesity and after bariatric surgery. Nutr Clin Pract. 2003;18:131-135.
33. Miller AD, Smith KM. Medication and nutrient administration considerations after bariatric surgery. Am J Health Syst Pharm. 2006;63:1852-1857.
34. Paine MF, Khalighi M, Fisher JM, et al. Characterization of interintestinal and intraintestinal variations in human CYP3A-dependent metabolism. J Pharmacol Exp Ther. 1997;283:1552-1562.
35. Skottheim IB, Stormark K, Christensen H, et al. Significantly altered systemic exposure to atorvastatin acid following gastric bypass surgery in morbidly obese patients. Clin Pharmacol Ther. 2009;86(3):311-318.
36. Hamad GG, Kozak GM, Wisner KL, et al. The effect of gastric bypass on SSRI pharmacokinetics and pharmacodynamics. Abstract presented at: American Society for Metabolic and Bariatric Surgery 25 Annual Meeting; June 15-20, 2008; Washington, DC.
37. Seaman JS, Bowers SP, Dixon P, et al. Dissolution of common psychiatric medications in a Roux-en-Y gastric bypass model. Psychosomatics. 2005;46:250-253.
1. Mechanick JI, Kushner RF, Sugerman HJ, et al. American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic and Bariatric Surgery Medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Endocr Pract. 2008;14:318-336.
2. NIH conference. Gastrointestinal surgery for severe obesity. Consensus Development Conference Panel. Ann Intern Med. 1991;115:956-961.
3. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724-1737.
4. Maggard MA, Shugarman LR, Suttorp M, et al. Meta-analysis: surgical treatment of obesity. Ann Intern Med. 2005;142:547-559.
5. Hodo DM, Waller JL, Martindale RG, et al. Medication use after bariatric surgery in a managed care cohort. Surg Obes Rel Dis. 2008;4:601-607.
6. Sarwer DB, Wadden TA, Fabricatore AN. Psychosocial and behavioral aspects of bariatric surgery. Obes Res. 2005;13:639-648.
7. Mitchell JE, de Zwaan M. Bariatric surgery: a guide for mental health professionals. New York, NY: Routledge; 2005.
8. Malone M, Alger-Mayer SA. Medication use patterns after gastric bypass surgery for weight management. Ann Pharmacopher. 2005;39:637-642.
9. Buchwald H. and the Consensus Conference Panel. Consensus conference statement: bariatric surgery for morbid obesity: health implications for patients, health professionals, and third-party payers. Surg Obes Rel Dis. 2005;1:371-381.
10. Needleman BJ, Happel LC. Bariatric surgery: choosing the optimal procedure. Surg Clin North Am. 2008;88:991-1007.
11. Albrecht RJ, Pories WJ. Surgical intervention for the severely obese. Baillieres Best Pract Res Clin Endocrinol Metab. 1999;13:149-172.
12. Brolin RE. Bariatric surgery and long-term control of morbid obesity. JAMA. 2002;288:2793-2796.
13. Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric surgical procedures. JAMA. 2005;294:1909-1917.
14. Brolin RE, Kenler HA, Gorman RC, et al. The dilemma of outcome assessment after operations for morbid obesity. Surgery. 1989;105:337-346.
15. Sjöström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683-2693.
16. Sjöström L, Narbro K, Sjöström CD, et al. and the Swedish Obese Subjects Study. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357:741-752.
17. Bocchieri LE, Meana M, Fisher BL. A review of psychosocial outcomes of surgery for morbid obesity. J Psychosom Res. 2002;52:155-165.
18. Herpertz S, Kielmann R, Wolf AM, et al. Do psychosocial variables predict weight loss or mental health after obesity surgery? A systematic review. Obes Res. 2004;12:1554-1569.
19. Kalarchian MA, Marcus MD, Levine MD, et al. Psychiatric disorders among bariatric surgery candidates: relationship to obesity and functional health status. Am J Psychiatry. 2007;164:328-334.
20. Rosenberger PH, Henderson KE, Grilo CM. Psychiatric disorder comorbidity and association with eating disorders in bariatric surgery patients: a cross-sectional study using structured interview based diagnosis. J Clin Psychiatry. 2006;67:1080-1085.
21. Kalarchian MA, Marcus MD, Levine MD, et al. Relationship of psychiatric disorders to 6-month outcomes after gastric bypass. Surg Obes Relat Dis. 2008;4:544-549.
22. Rutledge T, Groesz LM, Savu M. Psychiatric factors and weight loss patterns following gastric bypass surgery in a veteran population. Obes Surg. 2009;[Epub ahead of print].
23. Kinzl JF, Schrattenecker M, Traweger C, et al. Psychosocial predictors of weight loss after bariatric surgery. Obes Surg. 2006;16:1609-1614.
24. Bauchowitz AU, Gonder-Frederick LA, Olbrisch ME, et al. Psychosocial evaluation of bariatric surgery candidates: a survey of present practices. Psychosom Med. 2005;67(5):825-832.
25. Wadden TA, Sarwer DB, Womble LG, et al. Psychosocial aspects of obesity and obesity surgery. Surg Clin North Am. 2001;81:1001-1024.
26. Fabricatore AN, Crerand CE, Wadden TA, et al. How do mental health professionals evaluate candidates for bariatric surgery? Survey results. Obes Surg. 2006;16:567-573.
27. Sarwer DB, Cohn NI, Gibbons LM, et al. Psychiatric diagnoses and psychiatric treatment among bariatric surgery candidates. Obes Surg. 2004;14(9):1148-1156.
28. Larsen JK, Greenen R, van Ramshorst B, et al. Psychosocial functioning before and after laparoscopic adjustable gastric banding: a cross-sectional study. Obes Surg. 2003;13(4):629-636.
29. Clark MM, Balsiger BM, Sletten CD, et al. Psychosocial factors and 2-year outcome following bariatric surgery for weight loss. Obes Surg. 2003;13(5):739-745.
30. Padwal R, Brocks D, Sharma AM. A systematic review of drug absorption following bariatric surgery and its theoretical implications. Obes Rev. 2010;11(1):41-50.
31. Macgreggor AMC, Boggs L. Drug distribution in obesity and following bariatric surgery: a literature review. Obes Surg. 1996;6:17-27.
32. Malone M. Altered drug disposition in obesity and after bariatric surgery. Nutr Clin Pract. 2003;18:131-135.
33. Miller AD, Smith KM. Medication and nutrient administration considerations after bariatric surgery. Am J Health Syst Pharm. 2006;63:1852-1857.
34. Paine MF, Khalighi M, Fisher JM, et al. Characterization of interintestinal and intraintestinal variations in human CYP3A-dependent metabolism. J Pharmacol Exp Ther. 1997;283:1552-1562.
35. Skottheim IB, Stormark K, Christensen H, et al. Significantly altered systemic exposure to atorvastatin acid following gastric bypass surgery in morbidly obese patients. Clin Pharmacol Ther. 2009;86(3):311-318.
36. Hamad GG, Kozak GM, Wisner KL, et al. The effect of gastric bypass on SSRI pharmacokinetics and pharmacodynamics. Abstract presented at: American Society for Metabolic and Bariatric Surgery 25 Annual Meeting; June 15-20, 2008; Washington, DC.
37. Seaman JS, Bowers SP, Dixon P, et al. Dissolution of common psychiatric medications in a Roux-en-Y gastric bypass model. Psychosomatics. 2005;46:250-253.
How to discuss the palliative care approach with families
Immobile, mute, and at risk
CASE: Nude and mute
Mr. M, age 45, is found naked outside his apartment. He has a history of schizophrenia, paranoid type, hypertension, and diet-controlled type 2 diabetes mellitus. His schizophrenia has been treated with ziprasidone, 160 mg/d, but 2 months ago he stopped taking his medication and seeing his psychiatrist. He does not respond to questions from police and is taken to a local emergency department for medical workup of altered mental status.
Mr. M is noted to have bilateral conjunctival discharge and a white blood cell (WBC) count of 15,000/mm3. Vital signs, physical examination, laboratory studies, and head CT are otherwise within normal limits. Mr. M is medically cleared for his 15th admission to our inpatient psychiatric facility in the last 7 years. He is divorced, has 2 adult sons, and receives Social Security disability benefits.
Mr. M is alert but guarded and mute and appears to be internally preoccupied. His mood is euthymic and his facial expressions do not vary much and are similar to a blank stare. His grooming and hygiene are poor, but there is no evidence of delusions or suicidal or homicidal ideation. He paces around the unit or sits in his bed staring straight ahead, occasionally mouthing inaudible words but remaining nonverbal.
Mr. M is restarted on his previous dose of ziprasidone and referred to the primary care physician in our inpatient psychiatric facility for further evaluation. His admission vitals and laboratory values show a platelet count of 124,000/mm3, glucose of 113 mg/dL, triglycerides of 160 mg/dL, high-density lipoprotein of 37 mg/dL, and hemoglobin A1c of 6%. Mr. M needs help drinking fluids but resists solid foods as well as medications, including lorazepam, 3 mg/d, and most scheduled doses of ziprasidone. On day 3, Mr. M’s extremities are rigid and he has poor oral intake. We diagnose Mr. M with catatonia based on his immobility, negativity, and mutism.
The authors’ observations
The literature describes >40 signs of catatonia.1-11 According to DSM-IV-TR, catatonia may occur in the context of schizophrenia, a mood disorder, or a general medical condition. DSM-IV-TR criteria for catatonia include:
- motor immobility as evidenced by catalepsy or stupor
- excessive motor activity
- extreme negativism or mutism
- peculiarities of voluntary movements as evidenced by posturing, stereotypic movements, or grimacing
- echolalia or echopraxia.12
Only 2 signs are necessary to meet the diagnostic criteria for catatonia.11,12 Several catatonia rating scales—including the Bush-Francis Catatonia Rating Scale (BFCRS)—have been found to be highly reliable for screening for and rating the severity of catatonia. Such tools also can be used serially to monitor treatment efficacy. The BFCRS takes 5 minutes to administer; the screen is considered positive if ≥2 of the first 14 items on the scale are present.13 Mr. M exhibits immobility and mutism, which are the most common signs of catatonia.
In patients with catatonia, poor oral intake may result in malnutrition that often requires parenteral nutrition or intravenous fluids1,10 and dehydration that may lead to dental caries, gum disease, constipation, and ileus.1 Pneumonia may occur secondary to atelectasis or buildup of respiratory secretions and possibly aspiration.7 Vaginal infections may develop secondary to poor hygiene.1 Immobility and malnutrition may lead to infection and decubitus ulcers.1 Finally, immobility also may cause urinary incontinence,2,10 nerve palsies, flexion contractions, and rhabdomyolysis.1
EVALUATION: Venous complications
On day 3, Mr. M is referred to a local emergency department, where he is assessed for delirium and dehydration because of increased WBC count and diaphoresis. The medical staff finds bilateral pulmonary embolisms and a deep vein thrombosis (DVT) of his left lower leg.
The authors’ observations
Catatonia is associated with an increased risk of venous thromboembolism because of the increased risk of venous stasis and hypercoagulability, both elements of Virchow’s triad for thrombogenesis.1-10,14,15 The third element of Virchow’s triad, vascular injury, does not appear to directly increase the risk for thromboembolic events in catatonic states.
Catatonia-specific causes for venous stasis include immobility, prolonged use of physical restraints, and sedation as a side effect of antipsychotic use.16
Causes for hypercoagulability during catatonic states include:
- increased catecholamine levels during excited states3
- hyperhomocysteinemia secondary to poor diet, smoking, and/or high caffeine consumption16
- increased anticardiolipin and/or anti-phospholipid antibody levels secondary to use of specific antipsychotics, such as chlorpromazine and clozapine16
- increased platelet aggregation secondary to hyperprolactinemia caused by low-potency conventional antipsychotics, such as chlorpromazine16,17
- increased platelet activation caused by altered levels of platelet serotonin in depressed patients.18
Patients taking low-potency conventional antipsychotics may have a 7-fold greater risk for thromboembolic events compared with those who do not use these medications.16
Reducing thromboembolic risk
Diagnose catatonia early. Treating symptoms of catatonia early with benzodiazepines (and, in refractory cases, with electroconvulsive therapy) prevents immobility, thereby decreasing the risk of thromboembolic events.3,11 It may be useful to minimize antipsychotic use.
Monitor activity levels. Fatal thromboembolic events may appear early in the course of catatonia before risk factors associated with thromboembolic events are evident.4 However, these events may be more common when the patient resumes movement.3 Monitor patients’ activity status and encourage ambulation throughout treatment.
Monitor vital signs for signs of pulmonary embolism, including hypoxia, tachycardia, tachypnea, and fever. Take serial pulse oximetry and, if indicated, arterial blood gas measurements to monitor hemoglobin oxygen saturation. Be vigilant for other signs and symptoms of pulmonary embolism and DVT (Table).
Consider prophylactic treatment. Some studies recommend prophylaxis against thromboembolic events in catatonic patients.3-6,10,15 These measures include:
- intravenous fluids
- nasogastric tube feeding
- physical examinations to assess for signs of DVT
- support stockings
- sequential/pneumatic compression devices
- physical therapy or range-of-motion exercises
- complete anticoagulation during immobility, although there are no data that support using anticoagulation medications in catatonic patients who have not yet experienced a thromboembolic event.
Consider prophylactic antithrombotic treatment in catatonic patients and other immobile inpatients who have risk factors for thromboembolic events.9,16 Although it has not been rigorously tested, the Algorithm suggested by Malý et al15 can serve as a guideline for determining the need for prophylaxis against venous thromboembolism in psychiatric inpatient settings.
Table
Signs and symptoms of deep vein thrombosis and pulmonary embolism
| Deep vein thrombosis |
| Swelling of the leg or along a vein in the leg |
| Pain or tenderness in the leg, which may be felt only when standing or walking |
| Increased warmth in the area of the leg that is swollen or in pain |
| Red or discolored skin on the leg |
| Pulmonary embolism |
| Unexplained shortness of breath or pain with deep breathing |
| Chest pain |
| Coughing or coughing up blood |
| Arrhythmia |
| Source: National Heart, Lung, and Blood Institute. What are the signs and symptoms of deep vein thrombosis? Available at: www.nhlbi.nih.gov/health/dci/Diseases/Dvt/DVT_ SignsAndSymptoms.html. Accessed November 8, 2010 |
Algorithm
Does my patient need venous thromboembolism prophylaxis?
| Step 1. Assess risk factors for venous thromboembolism and determine risk level score | |
|---|---|
| Risk factor | Score |
| Consensus-based | |
| Immobilization | 1 |
| Hormone therapy | 1 |
| Obesity (BMI ≥30 kg/m2) | 1 |
| Age 60 to 74 | 1 |
| Varicose veins/venous insufficiency | 1 |
| Dehydration | 1 |
| Thrombophilia | 1 |
| Expert opinion | |
| Treatment with antipsychotics | 1 |
| Evidence-based | |
| History of deep vein thrombosis or pulmonary embolism | 2 |
| Cancer (active/treated) | 2 |
| Age ≥75 | 2 |
| Acute infection/respiratory disease | 2 |
| TOTAL | |
| BMI: body mass index | |
| Step 2. Determine recommended prophylaxis based on risk level score | |
| Risk level score | Recommended prophylaxis |
| All risk levels | Regular physical exercise of lower extremities, sufficient hydration, graduated compression stockings |
| Medium risk (4 to 7 points) and/or physical restraint ≥8 hours | Heparin, 5,000 units every 12 hours, or low molecular weight heparin equivalent until patient is fully mobilized |
| High risk (≥8 points) | Heparin, 5,000 units every 8 hours, or low molecular weight heparin equivalent until patient is fully mobilized |
| Source: Adapted from reference 15 | |
OUTCOME: Stable and speaking
In the hospital, Mr. M remains immobile and mute for several days. The hospital’s psychiatric consult team recommends lorazepam, 3 mg/d, to address his catatonia. Mr. M improves and begins speaking and eating after starting lorazepam, but becomes agitated, banging his head against walls and threatening to jump out the window. Because this puts him at risk for trauma, Mr. M is not a good candidate for warfarin therapy, and an inferior vena cava filter is placed on an emergency basis. Later, a Dobhoff tube is placed for feeding and administering oral medications.
Mr. M’s catatonic state gradually improves and he begins to respond to the staff with short phrases, eats all of his food, and accepts oral medications. He is transferred back to our inpatient psychiatric facility with haloperidol, 10 mg/d, lorazepam, 3 mg/d, and benztro-pine, 2 mg/d, in addition to sulfacetamide eye drops for bilateral conjunctivitis. At our facility, we start him on warfarin, 5 mg/d, and closely monitor his international normalized ratio levels, with a plan to remove the inferior vena cava filter after 6 months of anticoagulation therapy. Mr. M remains at our facility for 3 weeks to stabilize his medications and is discharged to his apartment.
Six months after being discharged from our facility, Mr. M is stable at an intensive outpatient mental health program.
Related Resources
- Fink M, Taylor MA. Catatonia: a clinician’s guide to diagnosis and treatment. Cambridge, United Kingdom: Cambridge University Press; 2003.
- Snow V, Qaseem A, Barry P, et al, and American College of Physicians; American Academy of Family Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Management of venous thromboembolism: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med. 2007;146(3):204-210.
Drug Brand Names
- Benztropine • Cogentin
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Haloperidol • Haldol
- Lorazepam • Ativan
- Sulfacetamide • Sulamyd
- Warfarin • Coumadin
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Caroff SN, Mann SC, Francis A, et al. eds. Catatonia: from psychopathology to neurobiology. Arlington, VA: American Psychiatric Publishing, Inc.; 2004.
2. Gangadhar BN, Keshavan MS, Goswami U, et al. Cortical venous thrombosis presenting as catatonia: a clinicopathologic report. J Clin Psychiatry. 1983;44:109-110.
3. McCall WV, Mann SC, Shelp FE, et al. Fatal pulmonary embolism in the catatonic syndrome: two case reports and a literature review. J Clin Psychiatry. 1995;51:21-25.
4. Morioka H, Nagatomo I, Yamada K, et al. Deep venous thrombosis of the leg due to psychiatric stupor. Psychiatry Clin Neurosci. 1997;51:323-326.
5. Lachner C, Sandson NB. Medical complications of catatonia: a case of catatonia-induced deep venous thrombosis. Psychosomatics. 2003;44:512-514.
6. Woo BK. Basal ganglia calcification and pulmonary embolism in catatonia. J Neuropsychiatry Clin Neurosci. 2007;19:472-473.
7. Regestein QR, Alpert JS, Reich P. Sudden catatonic stupor with disastrous outcome. JAMA. 1977;238:618-620.
8. Suzuki K, Takamatsu K, Takano T, et al. Safety of electroconvulsive therapy in psychiatric patients shortly after the occurrence of pulmonary embolism. J ECT. 2008;24:286-288.
9. Tsao C, Nusbaum A. Successful ECT course for catatonia after large pulmonary embolism and placement of inferior vena cava filter. Gen Hosp Psychiatry. 2007;29:374.-
10. Barbuto J. Preventing sudden death during a catatonic episode. Hosp Community Psychiatry. 1983;34:72-73.
11. Taylor MA, Fink M. Catatonia in psychiatric classification: a home of its own. Am J Psychiatry. 2003;160:1233-1241.
12. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
13. Bush G, Fink M, Petrides G, et al. Catatonia I. Rating scale and standardized examination. Acta Psychiatr Scand. 1996;93(2):129-136.
14. Lal S, Bleiman M, Brown GN. Pulmonary embolism in psychiatric patients. J Am Geriatr Soc. 1966;14:1138-1143.
15. Malý R, Masopust J, Hosák L, et al. Assessment of risk of venous thromboembolism and its possible prevention in psychiatric patients. Psychiatry Clin Neurosci. 2008;62:3-8.
16. Higg S, Jönsson AK, Spigset O. Risk of venous thromboembolism due to antipsychotic drug therapy. Expert Opin Drug Saf. 2009;8:537-547.
17. Wallaschofski H, Eigenthaler M, Kiefer M, et al. Hyperprolactinemia in patients on antipsychotic drugs causes ADP-stimulated platelet activation that might explain the increased risk for venous thromboembolism: pilot study. J Clin Psychopharmacol. 2003;23(5):479-483.
18. Arnone D, Hansen L, Davies G. Pulmonary embolism and severe depression. Am J Psychiatry. 2009;159:873-874.
CASE: Nude and mute
Mr. M, age 45, is found naked outside his apartment. He has a history of schizophrenia, paranoid type, hypertension, and diet-controlled type 2 diabetes mellitus. His schizophrenia has been treated with ziprasidone, 160 mg/d, but 2 months ago he stopped taking his medication and seeing his psychiatrist. He does not respond to questions from police and is taken to a local emergency department for medical workup of altered mental status.
Mr. M is noted to have bilateral conjunctival discharge and a white blood cell (WBC) count of 15,000/mm3. Vital signs, physical examination, laboratory studies, and head CT are otherwise within normal limits. Mr. M is medically cleared for his 15th admission to our inpatient psychiatric facility in the last 7 years. He is divorced, has 2 adult sons, and receives Social Security disability benefits.
Mr. M is alert but guarded and mute and appears to be internally preoccupied. His mood is euthymic and his facial expressions do not vary much and are similar to a blank stare. His grooming and hygiene are poor, but there is no evidence of delusions or suicidal or homicidal ideation. He paces around the unit or sits in his bed staring straight ahead, occasionally mouthing inaudible words but remaining nonverbal.
Mr. M is restarted on his previous dose of ziprasidone and referred to the primary care physician in our inpatient psychiatric facility for further evaluation. His admission vitals and laboratory values show a platelet count of 124,000/mm3, glucose of 113 mg/dL, triglycerides of 160 mg/dL, high-density lipoprotein of 37 mg/dL, and hemoglobin A1c of 6%. Mr. M needs help drinking fluids but resists solid foods as well as medications, including lorazepam, 3 mg/d, and most scheduled doses of ziprasidone. On day 3, Mr. M’s extremities are rigid and he has poor oral intake. We diagnose Mr. M with catatonia based on his immobility, negativity, and mutism.
The authors’ observations
The literature describes >40 signs of catatonia.1-11 According to DSM-IV-TR, catatonia may occur in the context of schizophrenia, a mood disorder, or a general medical condition. DSM-IV-TR criteria for catatonia include:
- motor immobility as evidenced by catalepsy or stupor
- excessive motor activity
- extreme negativism or mutism
- peculiarities of voluntary movements as evidenced by posturing, stereotypic movements, or grimacing
- echolalia or echopraxia.12
Only 2 signs are necessary to meet the diagnostic criteria for catatonia.11,12 Several catatonia rating scales—including the Bush-Francis Catatonia Rating Scale (BFCRS)—have been found to be highly reliable for screening for and rating the severity of catatonia. Such tools also can be used serially to monitor treatment efficacy. The BFCRS takes 5 minutes to administer; the screen is considered positive if ≥2 of the first 14 items on the scale are present.13 Mr. M exhibits immobility and mutism, which are the most common signs of catatonia.
In patients with catatonia, poor oral intake may result in malnutrition that often requires parenteral nutrition or intravenous fluids1,10 and dehydration that may lead to dental caries, gum disease, constipation, and ileus.1 Pneumonia may occur secondary to atelectasis or buildup of respiratory secretions and possibly aspiration.7 Vaginal infections may develop secondary to poor hygiene.1 Immobility and malnutrition may lead to infection and decubitus ulcers.1 Finally, immobility also may cause urinary incontinence,2,10 nerve palsies, flexion contractions, and rhabdomyolysis.1
EVALUATION: Venous complications
On day 3, Mr. M is referred to a local emergency department, where he is assessed for delirium and dehydration because of increased WBC count and diaphoresis. The medical staff finds bilateral pulmonary embolisms and a deep vein thrombosis (DVT) of his left lower leg.
The authors’ observations
Catatonia is associated with an increased risk of venous thromboembolism because of the increased risk of venous stasis and hypercoagulability, both elements of Virchow’s triad for thrombogenesis.1-10,14,15 The third element of Virchow’s triad, vascular injury, does not appear to directly increase the risk for thromboembolic events in catatonic states.
Catatonia-specific causes for venous stasis include immobility, prolonged use of physical restraints, and sedation as a side effect of antipsychotic use.16
Causes for hypercoagulability during catatonic states include:
- increased catecholamine levels during excited states3
- hyperhomocysteinemia secondary to poor diet, smoking, and/or high caffeine consumption16
- increased anticardiolipin and/or anti-phospholipid antibody levels secondary to use of specific antipsychotics, such as chlorpromazine and clozapine16
- increased platelet aggregation secondary to hyperprolactinemia caused by low-potency conventional antipsychotics, such as chlorpromazine16,17
- increased platelet activation caused by altered levels of platelet serotonin in depressed patients.18
Patients taking low-potency conventional antipsychotics may have a 7-fold greater risk for thromboembolic events compared with those who do not use these medications.16
Reducing thromboembolic risk
Diagnose catatonia early. Treating symptoms of catatonia early with benzodiazepines (and, in refractory cases, with electroconvulsive therapy) prevents immobility, thereby decreasing the risk of thromboembolic events.3,11 It may be useful to minimize antipsychotic use.
Monitor activity levels. Fatal thromboembolic events may appear early in the course of catatonia before risk factors associated with thromboembolic events are evident.4 However, these events may be more common when the patient resumes movement.3 Monitor patients’ activity status and encourage ambulation throughout treatment.
Monitor vital signs for signs of pulmonary embolism, including hypoxia, tachycardia, tachypnea, and fever. Take serial pulse oximetry and, if indicated, arterial blood gas measurements to monitor hemoglobin oxygen saturation. Be vigilant for other signs and symptoms of pulmonary embolism and DVT (Table).
Consider prophylactic treatment. Some studies recommend prophylaxis against thromboembolic events in catatonic patients.3-6,10,15 These measures include:
- intravenous fluids
- nasogastric tube feeding
- physical examinations to assess for signs of DVT
- support stockings
- sequential/pneumatic compression devices
- physical therapy or range-of-motion exercises
- complete anticoagulation during immobility, although there are no data that support using anticoagulation medications in catatonic patients who have not yet experienced a thromboembolic event.
Consider prophylactic antithrombotic treatment in catatonic patients and other immobile inpatients who have risk factors for thromboembolic events.9,16 Although it has not been rigorously tested, the Algorithm suggested by Malý et al15 can serve as a guideline for determining the need for prophylaxis against venous thromboembolism in psychiatric inpatient settings.
Table
Signs and symptoms of deep vein thrombosis and pulmonary embolism
| Deep vein thrombosis |
| Swelling of the leg or along a vein in the leg |
| Pain or tenderness in the leg, which may be felt only when standing or walking |
| Increased warmth in the area of the leg that is swollen or in pain |
| Red or discolored skin on the leg |
| Pulmonary embolism |
| Unexplained shortness of breath or pain with deep breathing |
| Chest pain |
| Coughing or coughing up blood |
| Arrhythmia |
| Source: National Heart, Lung, and Blood Institute. What are the signs and symptoms of deep vein thrombosis? Available at: www.nhlbi.nih.gov/health/dci/Diseases/Dvt/DVT_ SignsAndSymptoms.html. Accessed November 8, 2010 |
Algorithm
Does my patient need venous thromboembolism prophylaxis?
| Step 1. Assess risk factors for venous thromboembolism and determine risk level score | |
|---|---|
| Risk factor | Score |
| Consensus-based | |
| Immobilization | 1 |
| Hormone therapy | 1 |
| Obesity (BMI ≥30 kg/m2) | 1 |
| Age 60 to 74 | 1 |
| Varicose veins/venous insufficiency | 1 |
| Dehydration | 1 |
| Thrombophilia | 1 |
| Expert opinion | |
| Treatment with antipsychotics | 1 |
| Evidence-based | |
| History of deep vein thrombosis or pulmonary embolism | 2 |
| Cancer (active/treated) | 2 |
| Age ≥75 | 2 |
| Acute infection/respiratory disease | 2 |
| TOTAL | |
| BMI: body mass index | |
| Step 2. Determine recommended prophylaxis based on risk level score | |
| Risk level score | Recommended prophylaxis |
| All risk levels | Regular physical exercise of lower extremities, sufficient hydration, graduated compression stockings |
| Medium risk (4 to 7 points) and/or physical restraint ≥8 hours | Heparin, 5,000 units every 12 hours, or low molecular weight heparin equivalent until patient is fully mobilized |
| High risk (≥8 points) | Heparin, 5,000 units every 8 hours, or low molecular weight heparin equivalent until patient is fully mobilized |
| Source: Adapted from reference 15 | |
OUTCOME: Stable and speaking
In the hospital, Mr. M remains immobile and mute for several days. The hospital’s psychiatric consult team recommends lorazepam, 3 mg/d, to address his catatonia. Mr. M improves and begins speaking and eating after starting lorazepam, but becomes agitated, banging his head against walls and threatening to jump out the window. Because this puts him at risk for trauma, Mr. M is not a good candidate for warfarin therapy, and an inferior vena cava filter is placed on an emergency basis. Later, a Dobhoff tube is placed for feeding and administering oral medications.
Mr. M’s catatonic state gradually improves and he begins to respond to the staff with short phrases, eats all of his food, and accepts oral medications. He is transferred back to our inpatient psychiatric facility with haloperidol, 10 mg/d, lorazepam, 3 mg/d, and benztro-pine, 2 mg/d, in addition to sulfacetamide eye drops for bilateral conjunctivitis. At our facility, we start him on warfarin, 5 mg/d, and closely monitor his international normalized ratio levels, with a plan to remove the inferior vena cava filter after 6 months of anticoagulation therapy. Mr. M remains at our facility for 3 weeks to stabilize his medications and is discharged to his apartment.
Six months after being discharged from our facility, Mr. M is stable at an intensive outpatient mental health program.
Related Resources
- Fink M, Taylor MA. Catatonia: a clinician’s guide to diagnosis and treatment. Cambridge, United Kingdom: Cambridge University Press; 2003.
- Snow V, Qaseem A, Barry P, et al, and American College of Physicians; American Academy of Family Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Management of venous thromboembolism: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med. 2007;146(3):204-210.
Drug Brand Names
- Benztropine • Cogentin
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Haloperidol • Haldol
- Lorazepam • Ativan
- Sulfacetamide • Sulamyd
- Warfarin • Coumadin
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Nude and mute
Mr. M, age 45, is found naked outside his apartment. He has a history of schizophrenia, paranoid type, hypertension, and diet-controlled type 2 diabetes mellitus. His schizophrenia has been treated with ziprasidone, 160 mg/d, but 2 months ago he stopped taking his medication and seeing his psychiatrist. He does not respond to questions from police and is taken to a local emergency department for medical workup of altered mental status.
Mr. M is noted to have bilateral conjunctival discharge and a white blood cell (WBC) count of 15,000/mm3. Vital signs, physical examination, laboratory studies, and head CT are otherwise within normal limits. Mr. M is medically cleared for his 15th admission to our inpatient psychiatric facility in the last 7 years. He is divorced, has 2 adult sons, and receives Social Security disability benefits.
Mr. M is alert but guarded and mute and appears to be internally preoccupied. His mood is euthymic and his facial expressions do not vary much and are similar to a blank stare. His grooming and hygiene are poor, but there is no evidence of delusions or suicidal or homicidal ideation. He paces around the unit or sits in his bed staring straight ahead, occasionally mouthing inaudible words but remaining nonverbal.
Mr. M is restarted on his previous dose of ziprasidone and referred to the primary care physician in our inpatient psychiatric facility for further evaluation. His admission vitals and laboratory values show a platelet count of 124,000/mm3, glucose of 113 mg/dL, triglycerides of 160 mg/dL, high-density lipoprotein of 37 mg/dL, and hemoglobin A1c of 6%. Mr. M needs help drinking fluids but resists solid foods as well as medications, including lorazepam, 3 mg/d, and most scheduled doses of ziprasidone. On day 3, Mr. M’s extremities are rigid and he has poor oral intake. We diagnose Mr. M with catatonia based on his immobility, negativity, and mutism.
The authors’ observations
The literature describes >40 signs of catatonia.1-11 According to DSM-IV-TR, catatonia may occur in the context of schizophrenia, a mood disorder, or a general medical condition. DSM-IV-TR criteria for catatonia include:
- motor immobility as evidenced by catalepsy or stupor
- excessive motor activity
- extreme negativism or mutism
- peculiarities of voluntary movements as evidenced by posturing, stereotypic movements, or grimacing
- echolalia or echopraxia.12
Only 2 signs are necessary to meet the diagnostic criteria for catatonia.11,12 Several catatonia rating scales—including the Bush-Francis Catatonia Rating Scale (BFCRS)—have been found to be highly reliable for screening for and rating the severity of catatonia. Such tools also can be used serially to monitor treatment efficacy. The BFCRS takes 5 minutes to administer; the screen is considered positive if ≥2 of the first 14 items on the scale are present.13 Mr. M exhibits immobility and mutism, which are the most common signs of catatonia.
In patients with catatonia, poor oral intake may result in malnutrition that often requires parenteral nutrition or intravenous fluids1,10 and dehydration that may lead to dental caries, gum disease, constipation, and ileus.1 Pneumonia may occur secondary to atelectasis or buildup of respiratory secretions and possibly aspiration.7 Vaginal infections may develop secondary to poor hygiene.1 Immobility and malnutrition may lead to infection and decubitus ulcers.1 Finally, immobility also may cause urinary incontinence,2,10 nerve palsies, flexion contractions, and rhabdomyolysis.1
EVALUATION: Venous complications
On day 3, Mr. M is referred to a local emergency department, where he is assessed for delirium and dehydration because of increased WBC count and diaphoresis. The medical staff finds bilateral pulmonary embolisms and a deep vein thrombosis (DVT) of his left lower leg.
The authors’ observations
Catatonia is associated with an increased risk of venous thromboembolism because of the increased risk of venous stasis and hypercoagulability, both elements of Virchow’s triad for thrombogenesis.1-10,14,15 The third element of Virchow’s triad, vascular injury, does not appear to directly increase the risk for thromboembolic events in catatonic states.
Catatonia-specific causes for venous stasis include immobility, prolonged use of physical restraints, and sedation as a side effect of antipsychotic use.16
Causes for hypercoagulability during catatonic states include:
- increased catecholamine levels during excited states3
- hyperhomocysteinemia secondary to poor diet, smoking, and/or high caffeine consumption16
- increased anticardiolipin and/or anti-phospholipid antibody levels secondary to use of specific antipsychotics, such as chlorpromazine and clozapine16
- increased platelet aggregation secondary to hyperprolactinemia caused by low-potency conventional antipsychotics, such as chlorpromazine16,17
- increased platelet activation caused by altered levels of platelet serotonin in depressed patients.18
Patients taking low-potency conventional antipsychotics may have a 7-fold greater risk for thromboembolic events compared with those who do not use these medications.16
Reducing thromboembolic risk
Diagnose catatonia early. Treating symptoms of catatonia early with benzodiazepines (and, in refractory cases, with electroconvulsive therapy) prevents immobility, thereby decreasing the risk of thromboembolic events.3,11 It may be useful to minimize antipsychotic use.
Monitor activity levels. Fatal thromboembolic events may appear early in the course of catatonia before risk factors associated with thromboembolic events are evident.4 However, these events may be more common when the patient resumes movement.3 Monitor patients’ activity status and encourage ambulation throughout treatment.
Monitor vital signs for signs of pulmonary embolism, including hypoxia, tachycardia, tachypnea, and fever. Take serial pulse oximetry and, if indicated, arterial blood gas measurements to monitor hemoglobin oxygen saturation. Be vigilant for other signs and symptoms of pulmonary embolism and DVT (Table).
Consider prophylactic treatment. Some studies recommend prophylaxis against thromboembolic events in catatonic patients.3-6,10,15 These measures include:
- intravenous fluids
- nasogastric tube feeding
- physical examinations to assess for signs of DVT
- support stockings
- sequential/pneumatic compression devices
- physical therapy or range-of-motion exercises
- complete anticoagulation during immobility, although there are no data that support using anticoagulation medications in catatonic patients who have not yet experienced a thromboembolic event.
Consider prophylactic antithrombotic treatment in catatonic patients and other immobile inpatients who have risk factors for thromboembolic events.9,16 Although it has not been rigorously tested, the Algorithm suggested by Malý et al15 can serve as a guideline for determining the need for prophylaxis against venous thromboembolism in psychiatric inpatient settings.
Table
Signs and symptoms of deep vein thrombosis and pulmonary embolism
| Deep vein thrombosis |
| Swelling of the leg or along a vein in the leg |
| Pain or tenderness in the leg, which may be felt only when standing or walking |
| Increased warmth in the area of the leg that is swollen or in pain |
| Red or discolored skin on the leg |
| Pulmonary embolism |
| Unexplained shortness of breath or pain with deep breathing |
| Chest pain |
| Coughing or coughing up blood |
| Arrhythmia |
| Source: National Heart, Lung, and Blood Institute. What are the signs and symptoms of deep vein thrombosis? Available at: www.nhlbi.nih.gov/health/dci/Diseases/Dvt/DVT_ SignsAndSymptoms.html. Accessed November 8, 2010 |
Algorithm
Does my patient need venous thromboembolism prophylaxis?
| Step 1. Assess risk factors for venous thromboembolism and determine risk level score | |
|---|---|
| Risk factor | Score |
| Consensus-based | |
| Immobilization | 1 |
| Hormone therapy | 1 |
| Obesity (BMI ≥30 kg/m2) | 1 |
| Age 60 to 74 | 1 |
| Varicose veins/venous insufficiency | 1 |
| Dehydration | 1 |
| Thrombophilia | 1 |
| Expert opinion | |
| Treatment with antipsychotics | 1 |
| Evidence-based | |
| History of deep vein thrombosis or pulmonary embolism | 2 |
| Cancer (active/treated) | 2 |
| Age ≥75 | 2 |
| Acute infection/respiratory disease | 2 |
| TOTAL | |
| BMI: body mass index | |
| Step 2. Determine recommended prophylaxis based on risk level score | |
| Risk level score | Recommended prophylaxis |
| All risk levels | Regular physical exercise of lower extremities, sufficient hydration, graduated compression stockings |
| Medium risk (4 to 7 points) and/or physical restraint ≥8 hours | Heparin, 5,000 units every 12 hours, or low molecular weight heparin equivalent until patient is fully mobilized |
| High risk (≥8 points) | Heparin, 5,000 units every 8 hours, or low molecular weight heparin equivalent until patient is fully mobilized |
| Source: Adapted from reference 15 | |
OUTCOME: Stable and speaking
In the hospital, Mr. M remains immobile and mute for several days. The hospital’s psychiatric consult team recommends lorazepam, 3 mg/d, to address his catatonia. Mr. M improves and begins speaking and eating after starting lorazepam, but becomes agitated, banging his head against walls and threatening to jump out the window. Because this puts him at risk for trauma, Mr. M is not a good candidate for warfarin therapy, and an inferior vena cava filter is placed on an emergency basis. Later, a Dobhoff tube is placed for feeding and administering oral medications.
Mr. M’s catatonic state gradually improves and he begins to respond to the staff with short phrases, eats all of his food, and accepts oral medications. He is transferred back to our inpatient psychiatric facility with haloperidol, 10 mg/d, lorazepam, 3 mg/d, and benztro-pine, 2 mg/d, in addition to sulfacetamide eye drops for bilateral conjunctivitis. At our facility, we start him on warfarin, 5 mg/d, and closely monitor his international normalized ratio levels, with a plan to remove the inferior vena cava filter after 6 months of anticoagulation therapy. Mr. M remains at our facility for 3 weeks to stabilize his medications and is discharged to his apartment.
Six months after being discharged from our facility, Mr. M is stable at an intensive outpatient mental health program.
Related Resources
- Fink M, Taylor MA. Catatonia: a clinician’s guide to diagnosis and treatment. Cambridge, United Kingdom: Cambridge University Press; 2003.
- Snow V, Qaseem A, Barry P, et al, and American College of Physicians; American Academy of Family Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Management of venous thromboembolism: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med. 2007;146(3):204-210.
Drug Brand Names
- Benztropine • Cogentin
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Haloperidol • Haldol
- Lorazepam • Ativan
- Sulfacetamide • Sulamyd
- Warfarin • Coumadin
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Caroff SN, Mann SC, Francis A, et al. eds. Catatonia: from psychopathology to neurobiology. Arlington, VA: American Psychiatric Publishing, Inc.; 2004.
2. Gangadhar BN, Keshavan MS, Goswami U, et al. Cortical venous thrombosis presenting as catatonia: a clinicopathologic report. J Clin Psychiatry. 1983;44:109-110.
3. McCall WV, Mann SC, Shelp FE, et al. Fatal pulmonary embolism in the catatonic syndrome: two case reports and a literature review. J Clin Psychiatry. 1995;51:21-25.
4. Morioka H, Nagatomo I, Yamada K, et al. Deep venous thrombosis of the leg due to psychiatric stupor. Psychiatry Clin Neurosci. 1997;51:323-326.
5. Lachner C, Sandson NB. Medical complications of catatonia: a case of catatonia-induced deep venous thrombosis. Psychosomatics. 2003;44:512-514.
6. Woo BK. Basal ganglia calcification and pulmonary embolism in catatonia. J Neuropsychiatry Clin Neurosci. 2007;19:472-473.
7. Regestein QR, Alpert JS, Reich P. Sudden catatonic stupor with disastrous outcome. JAMA. 1977;238:618-620.
8. Suzuki K, Takamatsu K, Takano T, et al. Safety of electroconvulsive therapy in psychiatric patients shortly after the occurrence of pulmonary embolism. J ECT. 2008;24:286-288.
9. Tsao C, Nusbaum A. Successful ECT course for catatonia after large pulmonary embolism and placement of inferior vena cava filter. Gen Hosp Psychiatry. 2007;29:374.-
10. Barbuto J. Preventing sudden death during a catatonic episode. Hosp Community Psychiatry. 1983;34:72-73.
11. Taylor MA, Fink M. Catatonia in psychiatric classification: a home of its own. Am J Psychiatry. 2003;160:1233-1241.
12. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
13. Bush G, Fink M, Petrides G, et al. Catatonia I. Rating scale and standardized examination. Acta Psychiatr Scand. 1996;93(2):129-136.
14. Lal S, Bleiman M, Brown GN. Pulmonary embolism in psychiatric patients. J Am Geriatr Soc. 1966;14:1138-1143.
15. Malý R, Masopust J, Hosák L, et al. Assessment of risk of venous thromboembolism and its possible prevention in psychiatric patients. Psychiatry Clin Neurosci. 2008;62:3-8.
16. Higg S, Jönsson AK, Spigset O. Risk of venous thromboembolism due to antipsychotic drug therapy. Expert Opin Drug Saf. 2009;8:537-547.
17. Wallaschofski H, Eigenthaler M, Kiefer M, et al. Hyperprolactinemia in patients on antipsychotic drugs causes ADP-stimulated platelet activation that might explain the increased risk for venous thromboembolism: pilot study. J Clin Psychopharmacol. 2003;23(5):479-483.
18. Arnone D, Hansen L, Davies G. Pulmonary embolism and severe depression. Am J Psychiatry. 2009;159:873-874.
1. Caroff SN, Mann SC, Francis A, et al. eds. Catatonia: from psychopathology to neurobiology. Arlington, VA: American Psychiatric Publishing, Inc.; 2004.
2. Gangadhar BN, Keshavan MS, Goswami U, et al. Cortical venous thrombosis presenting as catatonia: a clinicopathologic report. J Clin Psychiatry. 1983;44:109-110.
3. McCall WV, Mann SC, Shelp FE, et al. Fatal pulmonary embolism in the catatonic syndrome: two case reports and a literature review. J Clin Psychiatry. 1995;51:21-25.
4. Morioka H, Nagatomo I, Yamada K, et al. Deep venous thrombosis of the leg due to psychiatric stupor. Psychiatry Clin Neurosci. 1997;51:323-326.
5. Lachner C, Sandson NB. Medical complications of catatonia: a case of catatonia-induced deep venous thrombosis. Psychosomatics. 2003;44:512-514.
6. Woo BK. Basal ganglia calcification and pulmonary embolism in catatonia. J Neuropsychiatry Clin Neurosci. 2007;19:472-473.
7. Regestein QR, Alpert JS, Reich P. Sudden catatonic stupor with disastrous outcome. JAMA. 1977;238:618-620.
8. Suzuki K, Takamatsu K, Takano T, et al. Safety of electroconvulsive therapy in psychiatric patients shortly after the occurrence of pulmonary embolism. J ECT. 2008;24:286-288.
9. Tsao C, Nusbaum A. Successful ECT course for catatonia after large pulmonary embolism and placement of inferior vena cava filter. Gen Hosp Psychiatry. 2007;29:374.-
10. Barbuto J. Preventing sudden death during a catatonic episode. Hosp Community Psychiatry. 1983;34:72-73.
11. Taylor MA, Fink M. Catatonia in psychiatric classification: a home of its own. Am J Psychiatry. 2003;160:1233-1241.
12. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
13. Bush G, Fink M, Petrides G, et al. Catatonia I. Rating scale and standardized examination. Acta Psychiatr Scand. 1996;93(2):129-136.
14. Lal S, Bleiman M, Brown GN. Pulmonary embolism in psychiatric patients. J Am Geriatr Soc. 1966;14:1138-1143.
15. Malý R, Masopust J, Hosák L, et al. Assessment of risk of venous thromboembolism and its possible prevention in psychiatric patients. Psychiatry Clin Neurosci. 2008;62:3-8.
16. Higg S, Jönsson AK, Spigset O. Risk of venous thromboembolism due to antipsychotic drug therapy. Expert Opin Drug Saf. 2009;8:537-547.
17. Wallaschofski H, Eigenthaler M, Kiefer M, et al. Hyperprolactinemia in patients on antipsychotic drugs causes ADP-stimulated platelet activation that might explain the increased risk for venous thromboembolism: pilot study. J Clin Psychopharmacol. 2003;23(5):479-483.
18. Arnone D, Hansen L, Davies G. Pulmonary embolism and severe depression. Am J Psychiatry. 2009;159:873-874.
Reconsidering delusions
I appreciate Dr. Henry A. Nasrallah’s refreshing, mind-bending thoughts about delusions in, “Are some nonpsychotic psychiatric disorders actually psychotic?” (From the Editor, Current Psychiatry, November 2010, p. 16-19). I am moved to contemplate delusions in a new way and to try an antipsychotic in select cases. If delusional thinking were like a closed circuit with its associated neurotransmitter pathway and no access to cortical modification, it would make sense to use a “circuit breaker” (such as dopamine inhibitors and anxiolytics) to open up a pathway to cortical modification. Cognitive-behavioral therapy would help with the transition to cortical control.
Justine Forbes, MD
Private Practice
Los Gatos, CA
I appreciate Dr. Henry A. Nasrallah’s refreshing, mind-bending thoughts about delusions in, “Are some nonpsychotic psychiatric disorders actually psychotic?” (From the Editor, Current Psychiatry, November 2010, p. 16-19). I am moved to contemplate delusions in a new way and to try an antipsychotic in select cases. If delusional thinking were like a closed circuit with its associated neurotransmitter pathway and no access to cortical modification, it would make sense to use a “circuit breaker” (such as dopamine inhibitors and anxiolytics) to open up a pathway to cortical modification. Cognitive-behavioral therapy would help with the transition to cortical control.
Justine Forbes, MD
Private Practice
Los Gatos, CA
I appreciate Dr. Henry A. Nasrallah’s refreshing, mind-bending thoughts about delusions in, “Are some nonpsychotic psychiatric disorders actually psychotic?” (From the Editor, Current Psychiatry, November 2010, p. 16-19). I am moved to contemplate delusions in a new way and to try an antipsychotic in select cases. If delusional thinking were like a closed circuit with its associated neurotransmitter pathway and no access to cortical modification, it would make sense to use a “circuit breaker” (such as dopamine inhibitors and anxiolytics) to open up a pathway to cortical modification. Cognitive-behavioral therapy would help with the transition to cortical control.
Justine Forbes, MD
Private Practice
Los Gatos, CA
Bupropion controversy
I am writing to question publication of “Bupropion: Off-label treatment for cocaine and methamphetamine addiction” (Pearls, Current Psychiatry, July 2010, p. 52). The author recommends use of bupropion during in-patient detoxification and continuing after discharge. The only support given for this recommendation is the unreferenced statement that “some clinicians have found it helpful during the initial treatment.” No actual supporting data are given, either directly or by citing published literature. I believe that this article does a serious disservice to readers by giving a clinical recommendation based solely on the author’s unsubstantiated opinion. No evidence is provided at any level of scientific rigor, whether anecdotal case series or controlled clinical trial. Readers are left unable to judge for themselves the validity of the recommendation.
David A. Gorelick, MD, PhD
National Institute on Drug Abuse
Baltimore, MD
Dr. Gorelick is supported by the Intramural
Research Program, National Institutes of
Health, National Institute on Drug Abuse
I am writing to question publication of “Bupropion: Off-label treatment for cocaine and methamphetamine addiction” (Pearls, Current Psychiatry, July 2010, p. 52). The author recommends use of bupropion during in-patient detoxification and continuing after discharge. The only support given for this recommendation is the unreferenced statement that “some clinicians have found it helpful during the initial treatment.” No actual supporting data are given, either directly or by citing published literature. I believe that this article does a serious disservice to readers by giving a clinical recommendation based solely on the author’s unsubstantiated opinion. No evidence is provided at any level of scientific rigor, whether anecdotal case series or controlled clinical trial. Readers are left unable to judge for themselves the validity of the recommendation.
David A. Gorelick, MD, PhD
National Institute on Drug Abuse
Baltimore, MD
Dr. Gorelick is supported by the Intramural
Research Program, National Institutes of
Health, National Institute on Drug Abuse
I am writing to question publication of “Bupropion: Off-label treatment for cocaine and methamphetamine addiction” (Pearls, Current Psychiatry, July 2010, p. 52). The author recommends use of bupropion during in-patient detoxification and continuing after discharge. The only support given for this recommendation is the unreferenced statement that “some clinicians have found it helpful during the initial treatment.” No actual supporting data are given, either directly or by citing published literature. I believe that this article does a serious disservice to readers by giving a clinical recommendation based solely on the author’s unsubstantiated opinion. No evidence is provided at any level of scientific rigor, whether anecdotal case series or controlled clinical trial. Readers are left unable to judge for themselves the validity of the recommendation.
David A. Gorelick, MD, PhD
National Institute on Drug Abuse
Baltimore, MD
Dr. Gorelick is supported by the Intramural
Research Program, National Institutes of
Health, National Institute on Drug Abuse
Bupropion for cocaine users
The article by Heidi Magyar, MS, ARNP, “Bupropion: Off-label treatment for cocaine and methamphetamine addiction” (Pearls, Current Psychiatry, July 2010, p. 52) was quite interesting. Over the last 2 decades studies assessing the efficacy of bupropion for cocaine and methamphetamine addiction treatment have had conflicting results, with more negative than positive findings. There have been at least 4 studies since 2006, some of which have found statistically significant results when comparing bupropion with placebo in specific subgroups.
A double-blind, randomized, placebo-controlled trial by Shoptaw et al1 that used bupropion or placebo combined with cognitive-behavioral therapy showed no statistically significant difference. A study of 106 methadone-maintained patients carried out by Poling et al2 evaluated 4 treatment conditions: contingency management and placebo, contingency management and bupropion, 300 mg/d, voucher control and placebo, and voucher control and bupropion. The contingency management and bupropion group was the only one that showed a significant decrease in cocaine use. Su et al3 found that in mice prenatal bupropion exposure could enhance cocaine sensitivity.
In the case of methamphetamine treatment, a double-blind placebo-controlled study by Elkashef et al4 randomized patients to either placebo or bupropion, 300 mg/d. Initial generalized results showed no statistically significant difference, but a mixed model regression analysis that adjusted for sex, baseline level of methamphetamine use, and severity of depression showed significantly increased abstinence, mainly in male patients and those with low-to-moderate methamphetamine use at baseline.
Adegboyega Oyemade, MD
Addiction Psychiatrist
Southern Illinois Healthcare Foundation
Belleville, IL
1. Shoptaw S, Heinzerling KG, Rotheram-Fuller E, et al. Bupropion hydrochloride versus placebo, in combination with cognitive behavioral therapy, for the treatment of cocaine abuse/dependence. J Addict Dis. 2008;27(1):13-23.
2. Poling J, Oliveto A, Petry N, et al. Six-month trial of bupropion with contingency management for cocaine dependence in a methadone-maintained population. Arch Gen Psychiatry. 2006;63(2):219-228.
3. Su SW, Cherng CF, Lin YC, et al. Prenatal exposure of bupropion may enhance agitation, anxiety responses, and sensitivity to cocaine effects in adult mice. Chin J Physiol. 2007;50(1):1-8.
4. Elkashef AM, Rawson RA, Anderson AL, et al. Bupropion for treatment of methamphetamine dependence. Neuropsychopharmacology. 2008;33(5):1162-1170.
The article by Heidi Magyar, MS, ARNP, “Bupropion: Off-label treatment for cocaine and methamphetamine addiction” (Pearls, Current Psychiatry, July 2010, p. 52) was quite interesting. Over the last 2 decades studies assessing the efficacy of bupropion for cocaine and methamphetamine addiction treatment have had conflicting results, with more negative than positive findings. There have been at least 4 studies since 2006, some of which have found statistically significant results when comparing bupropion with placebo in specific subgroups.
A double-blind, randomized, placebo-controlled trial by Shoptaw et al1 that used bupropion or placebo combined with cognitive-behavioral therapy showed no statistically significant difference. A study of 106 methadone-maintained patients carried out by Poling et al2 evaluated 4 treatment conditions: contingency management and placebo, contingency management and bupropion, 300 mg/d, voucher control and placebo, and voucher control and bupropion. The contingency management and bupropion group was the only one that showed a significant decrease in cocaine use. Su et al3 found that in mice prenatal bupropion exposure could enhance cocaine sensitivity.
In the case of methamphetamine treatment, a double-blind placebo-controlled study by Elkashef et al4 randomized patients to either placebo or bupropion, 300 mg/d. Initial generalized results showed no statistically significant difference, but a mixed model regression analysis that adjusted for sex, baseline level of methamphetamine use, and severity of depression showed significantly increased abstinence, mainly in male patients and those with low-to-moderate methamphetamine use at baseline.
Adegboyega Oyemade, MD
Addiction Psychiatrist
Southern Illinois Healthcare Foundation
Belleville, IL
The article by Heidi Magyar, MS, ARNP, “Bupropion: Off-label treatment for cocaine and methamphetamine addiction” (Pearls, Current Psychiatry, July 2010, p. 52) was quite interesting. Over the last 2 decades studies assessing the efficacy of bupropion for cocaine and methamphetamine addiction treatment have had conflicting results, with more negative than positive findings. There have been at least 4 studies since 2006, some of which have found statistically significant results when comparing bupropion with placebo in specific subgroups.
A double-blind, randomized, placebo-controlled trial by Shoptaw et al1 that used bupropion or placebo combined with cognitive-behavioral therapy showed no statistically significant difference. A study of 106 methadone-maintained patients carried out by Poling et al2 evaluated 4 treatment conditions: contingency management and placebo, contingency management and bupropion, 300 mg/d, voucher control and placebo, and voucher control and bupropion. The contingency management and bupropion group was the only one that showed a significant decrease in cocaine use. Su et al3 found that in mice prenatal bupropion exposure could enhance cocaine sensitivity.
In the case of methamphetamine treatment, a double-blind placebo-controlled study by Elkashef et al4 randomized patients to either placebo or bupropion, 300 mg/d. Initial generalized results showed no statistically significant difference, but a mixed model regression analysis that adjusted for sex, baseline level of methamphetamine use, and severity of depression showed significantly increased abstinence, mainly in male patients and those with low-to-moderate methamphetamine use at baseline.
Adegboyega Oyemade, MD
Addiction Psychiatrist
Southern Illinois Healthcare Foundation
Belleville, IL
1. Shoptaw S, Heinzerling KG, Rotheram-Fuller E, et al. Bupropion hydrochloride versus placebo, in combination with cognitive behavioral therapy, for the treatment of cocaine abuse/dependence. J Addict Dis. 2008;27(1):13-23.
2. Poling J, Oliveto A, Petry N, et al. Six-month trial of bupropion with contingency management for cocaine dependence in a methadone-maintained population. Arch Gen Psychiatry. 2006;63(2):219-228.
3. Su SW, Cherng CF, Lin YC, et al. Prenatal exposure of bupropion may enhance agitation, anxiety responses, and sensitivity to cocaine effects in adult mice. Chin J Physiol. 2007;50(1):1-8.
4. Elkashef AM, Rawson RA, Anderson AL, et al. Bupropion for treatment of methamphetamine dependence. Neuropsychopharmacology. 2008;33(5):1162-1170.
1. Shoptaw S, Heinzerling KG, Rotheram-Fuller E, et al. Bupropion hydrochloride versus placebo, in combination with cognitive behavioral therapy, for the treatment of cocaine abuse/dependence. J Addict Dis. 2008;27(1):13-23.
2. Poling J, Oliveto A, Petry N, et al. Six-month trial of bupropion with contingency management for cocaine dependence in a methadone-maintained population. Arch Gen Psychiatry. 2006;63(2):219-228.
3. Su SW, Cherng CF, Lin YC, et al. Prenatal exposure of bupropion may enhance agitation, anxiety responses, and sensitivity to cocaine effects in adult mice. Chin J Physiol. 2007;50(1):1-8.
4. Elkashef AM, Rawson RA, Anderson AL, et al. Bupropion for treatment of methamphetamine dependence. Neuropsychopharmacology. 2008;33(5):1162-1170.