User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Don’t ‘teach to the test’
I was disappointed to read Dr. Henry Nasrallah’s editorial calling for the use of clinician measurement tools in the management of psychiatric illness (“Long overdue: Measurement-based psychiatric practice,” From the Editor, Current Psychiatry, April 2009). I agree that general and vague comments such as “doing better” are of limited value. I would further argue that such documentation is the psychiatric equivalent of “WNL”—which stands for “we never looked”—in a medical review of systems. But I do not believe the answer is to further dumb down the practice of psychiatry by generating quantifiable, 1-dimensional scores that purport to measure how well our patient is doing.
In the past, when these psychometric tools were developed (approximately from 1960 to 1987), 2 primary concerns were voiced.
First, there was limited data to support their validity and reliability, although that concern is somewhat less now, at least with some of the tests Dr. Nasrallah recommended. These tests still lack criterion-related validity. For example, IQ as measured by an IQ test predicts performance on an IQ test, so it’s reliable. But to use that number to predict fitness for a job or even academic success ends up discriminating against some individuals or groups who are more than just a number.
Second, there was the concern that, similar to schoolteachers who end up teaching to a normative test, we could end up treating a patient’s test score rather than the discomfort with his or her life. I believe this also remains true. Unlike diabetes mellitus, which is defined by increased blood sugars, psychiatric diagnoses are purely syndromal and require “clinically significant distress or impairment” or they are not a disease according to DSM-IV-TR. It’s the distress and the impairment that we treat.
Today, I see 2 positive trends in our field: to find increasingly efficient methods to appropriately tailor and effectively deliver care and to be recovery-focused. It seems to me that routine and indiscriminate use of psychometrics obstructs both of these. Each test takes 30 to 40 minutes to administer and requires skilled and trained clinicians, if not psychiatrists themselves. That at least doubles the length of the visit with no evidence-based benefit. A recovery focus requires that we—as does the DSM—focus on our patients’ perceived impairments, not their test scores.
Lyle B. Forehand, Jr, MD
Modesto, CA
Dr. Nasrallah responds
I thank Dr. Forehand for his comments. I agree that psychiatric diagnoses at this time are purely syndromal and require “clinically significant distress or impairment.” What I am calling for is to quantify the various signs and symptoms of the distress and impairment before and after treatment with a standard scale widely used by all researchers and some clinicians.
The definition of remission, which is the phase that precedes recovery, actually is based on standard rating scales’ severity score for a given psychiatric illness. Therefore, clinicians must rate their patients on the scale corresponding to that illness to recognize when their patients have met the official criteria for remission.
Practitioners do not have to use a scale to rate the patient’s symptoms separate from the standard interviewing process. Rather, once clinicians become familiar with these scales, they could conduct their usual interview and then take a moment when writing their note in the chart to circle the score of each symptom they assessed during their clinical interaction, and cite the total score in the admission or progress note. A copy of the scale can be included as a supplement to the progress note and will ensure that all signs and symptoms related to an illness are assessed, rather than just some of them.
To summarize, until scientific research leads to actual lab tests for psychiatric disorders—and I believe that day will come—psychiatrists should quantify their patients’ clinical distress and impairment with the same objective measures used in evidence-based FDA trials, even if the scales’ reliability and validity are not perfect.
Henry A. Nasrallah, MD
Editor-In-Chief
I was disappointed to read Dr. Henry Nasrallah’s editorial calling for the use of clinician measurement tools in the management of psychiatric illness (“Long overdue: Measurement-based psychiatric practice,” From the Editor, Current Psychiatry, April 2009). I agree that general and vague comments such as “doing better” are of limited value. I would further argue that such documentation is the psychiatric equivalent of “WNL”—which stands for “we never looked”—in a medical review of systems. But I do not believe the answer is to further dumb down the practice of psychiatry by generating quantifiable, 1-dimensional scores that purport to measure how well our patient is doing.
In the past, when these psychometric tools were developed (approximately from 1960 to 1987), 2 primary concerns were voiced.
First, there was limited data to support their validity and reliability, although that concern is somewhat less now, at least with some of the tests Dr. Nasrallah recommended. These tests still lack criterion-related validity. For example, IQ as measured by an IQ test predicts performance on an IQ test, so it’s reliable. But to use that number to predict fitness for a job or even academic success ends up discriminating against some individuals or groups who are more than just a number.
Second, there was the concern that, similar to schoolteachers who end up teaching to a normative test, we could end up treating a patient’s test score rather than the discomfort with his or her life. I believe this also remains true. Unlike diabetes mellitus, which is defined by increased blood sugars, psychiatric diagnoses are purely syndromal and require “clinically significant distress or impairment” or they are not a disease according to DSM-IV-TR. It’s the distress and the impairment that we treat.
Today, I see 2 positive trends in our field: to find increasingly efficient methods to appropriately tailor and effectively deliver care and to be recovery-focused. It seems to me that routine and indiscriminate use of psychometrics obstructs both of these. Each test takes 30 to 40 minutes to administer and requires skilled and trained clinicians, if not psychiatrists themselves. That at least doubles the length of the visit with no evidence-based benefit. A recovery focus requires that we—as does the DSM—focus on our patients’ perceived impairments, not their test scores.
Lyle B. Forehand, Jr, MD
Modesto, CA
Dr. Nasrallah responds
I thank Dr. Forehand for his comments. I agree that psychiatric diagnoses at this time are purely syndromal and require “clinically significant distress or impairment.” What I am calling for is to quantify the various signs and symptoms of the distress and impairment before and after treatment with a standard scale widely used by all researchers and some clinicians.
The definition of remission, which is the phase that precedes recovery, actually is based on standard rating scales’ severity score for a given psychiatric illness. Therefore, clinicians must rate their patients on the scale corresponding to that illness to recognize when their patients have met the official criteria for remission.
Practitioners do not have to use a scale to rate the patient’s symptoms separate from the standard interviewing process. Rather, once clinicians become familiar with these scales, they could conduct their usual interview and then take a moment when writing their note in the chart to circle the score of each symptom they assessed during their clinical interaction, and cite the total score in the admission or progress note. A copy of the scale can be included as a supplement to the progress note and will ensure that all signs and symptoms related to an illness are assessed, rather than just some of them.
To summarize, until scientific research leads to actual lab tests for psychiatric disorders—and I believe that day will come—psychiatrists should quantify their patients’ clinical distress and impairment with the same objective measures used in evidence-based FDA trials, even if the scales’ reliability and validity are not perfect.
Henry A. Nasrallah, MD
Editor-In-Chief
I was disappointed to read Dr. Henry Nasrallah’s editorial calling for the use of clinician measurement tools in the management of psychiatric illness (“Long overdue: Measurement-based psychiatric practice,” From the Editor, Current Psychiatry, April 2009). I agree that general and vague comments such as “doing better” are of limited value. I would further argue that such documentation is the psychiatric equivalent of “WNL”—which stands for “we never looked”—in a medical review of systems. But I do not believe the answer is to further dumb down the practice of psychiatry by generating quantifiable, 1-dimensional scores that purport to measure how well our patient is doing.
In the past, when these psychometric tools were developed (approximately from 1960 to 1987), 2 primary concerns were voiced.
First, there was limited data to support their validity and reliability, although that concern is somewhat less now, at least with some of the tests Dr. Nasrallah recommended. These tests still lack criterion-related validity. For example, IQ as measured by an IQ test predicts performance on an IQ test, so it’s reliable. But to use that number to predict fitness for a job or even academic success ends up discriminating against some individuals or groups who are more than just a number.
Second, there was the concern that, similar to schoolteachers who end up teaching to a normative test, we could end up treating a patient’s test score rather than the discomfort with his or her life. I believe this also remains true. Unlike diabetes mellitus, which is defined by increased blood sugars, psychiatric diagnoses are purely syndromal and require “clinically significant distress or impairment” or they are not a disease according to DSM-IV-TR. It’s the distress and the impairment that we treat.
Today, I see 2 positive trends in our field: to find increasingly efficient methods to appropriately tailor and effectively deliver care and to be recovery-focused. It seems to me that routine and indiscriminate use of psychometrics obstructs both of these. Each test takes 30 to 40 minutes to administer and requires skilled and trained clinicians, if not psychiatrists themselves. That at least doubles the length of the visit with no evidence-based benefit. A recovery focus requires that we—as does the DSM—focus on our patients’ perceived impairments, not their test scores.
Lyle B. Forehand, Jr, MD
Modesto, CA
Dr. Nasrallah responds
I thank Dr. Forehand for his comments. I agree that psychiatric diagnoses at this time are purely syndromal and require “clinically significant distress or impairment.” What I am calling for is to quantify the various signs and symptoms of the distress and impairment before and after treatment with a standard scale widely used by all researchers and some clinicians.
The definition of remission, which is the phase that precedes recovery, actually is based on standard rating scales’ severity score for a given psychiatric illness. Therefore, clinicians must rate their patients on the scale corresponding to that illness to recognize when their patients have met the official criteria for remission.
Practitioners do not have to use a scale to rate the patient’s symptoms separate from the standard interviewing process. Rather, once clinicians become familiar with these scales, they could conduct their usual interview and then take a moment when writing their note in the chart to circle the score of each symptom they assessed during their clinical interaction, and cite the total score in the admission or progress note. A copy of the scale can be included as a supplement to the progress note and will ensure that all signs and symptoms related to an illness are assessed, rather than just some of them.
To summarize, until scientific research leads to actual lab tests for psychiatric disorders—and I believe that day will come—psychiatrists should quantify their patients’ clinical distress and impairment with the same objective measures used in evidence-based FDA trials, even if the scales’ reliability and validity are not perfect.
Henry A. Nasrallah, MD
Editor-In-Chief
Workplace mobbing is real
I found Dr. James Randolph Hillard’s article on workplace mobbing timely and extremely interesting (“Workplace mobbing: Are they really out to get your patient?” Current Psychiatry, April 2009). As clinical director of a consultation service for corporations, I am asked to assess employees suspected to be at risk for workplace violence and for fitness for duty. Mobbing seems to be more prevalent and the consequences more dire for a victim who is feeling pressured to leave his or her job when there is little hope of getting another one or is taking on responsibilities previously held by others who have been laid off.
This brings to the forefront a very important consideration for individuals who confront such assessment challenges. Gathering collateral information is critical for diagnostic accuracy and well-articulated interventions that may be recommended. Evaluators who do such assessments at the behest of corporate clients should insist that they have access to employee files investigative reports, and—if appropriate—permission to interview supervisors, employee assistance program representatives, and human resources personnel familiar with the case. Mobbing is real and deserves much greater attention by researchers and clinicians in the United States.
Scott Bresler, PhD
Clinical director
Center for Threat Assessment
Institute for Psychiatry and Law
University of Cincinnati
Cincinnati, OH
I found Dr. James Randolph Hillard’s article on workplace mobbing timely and extremely interesting (“Workplace mobbing: Are they really out to get your patient?” Current Psychiatry, April 2009). As clinical director of a consultation service for corporations, I am asked to assess employees suspected to be at risk for workplace violence and for fitness for duty. Mobbing seems to be more prevalent and the consequences more dire for a victim who is feeling pressured to leave his or her job when there is little hope of getting another one or is taking on responsibilities previously held by others who have been laid off.
This brings to the forefront a very important consideration for individuals who confront such assessment challenges. Gathering collateral information is critical for diagnostic accuracy and well-articulated interventions that may be recommended. Evaluators who do such assessments at the behest of corporate clients should insist that they have access to employee files investigative reports, and—if appropriate—permission to interview supervisors, employee assistance program representatives, and human resources personnel familiar with the case. Mobbing is real and deserves much greater attention by researchers and clinicians in the United States.
Scott Bresler, PhD
Clinical director
Center for Threat Assessment
Institute for Psychiatry and Law
University of Cincinnati
Cincinnati, OH
I found Dr. James Randolph Hillard’s article on workplace mobbing timely and extremely interesting (“Workplace mobbing: Are they really out to get your patient?” Current Psychiatry, April 2009). As clinical director of a consultation service for corporations, I am asked to assess employees suspected to be at risk for workplace violence and for fitness for duty. Mobbing seems to be more prevalent and the consequences more dire for a victim who is feeling pressured to leave his or her job when there is little hope of getting another one or is taking on responsibilities previously held by others who have been laid off.
This brings to the forefront a very important consideration for individuals who confront such assessment challenges. Gathering collateral information is critical for diagnostic accuracy and well-articulated interventions that may be recommended. Evaluators who do such assessments at the behest of corporate clients should insist that they have access to employee files investigative reports, and—if appropriate—permission to interview supervisors, employee assistance program representatives, and human resources personnel familiar with the case. Mobbing is real and deserves much greater attention by researchers and clinicians in the United States.
Scott Bresler, PhD
Clinical director
Center for Threat Assessment
Institute for Psychiatry and Law
University of Cincinnati
Cincinnati, OH
‘What do the voices tell you?’
I would like to thank Dr. Nasrallah for his wonderful editorial about assessing auditory hallucinations (“The hallucination portrait of psychosis: Probing the voices within,” From the Editor, Current Psychiatry, May 2009). He has eloquently addressed many of the concerns I have had regarding how psychiatrists respond when a patient says “I am hearing voices.” In my experience many psychiatrists simply leave it at that and don’t even attempt the briefest characterization of these hallucinations, let alone the rigorous elucidation that Dr. Nasrallah suggests.
We are doing a disservice to our patients by not performing a thorough evaluation of what a patient means when he says “I am hearing voices.” How can we really understand what our patient is experiencing if we don’t attempt to grasp the specifics of something as remarkable as a hallucination?
Unfortunately, there are patients who use statements such as “I am hearing voices telling me to kill myself and others” in order to be admitted to hospitals or for secondary gain. Getting or attempting to get details about these “voices” and documenting what we are told can be an invaluable part of a patient’s records. Inconsistencies arise that can be taken into consideration during subsequent encounters.
Bennett Cohen, MD
New York, NY
I would like to thank Dr. Nasrallah for his wonderful editorial about assessing auditory hallucinations (“The hallucination portrait of psychosis: Probing the voices within,” From the Editor, Current Psychiatry, May 2009). He has eloquently addressed many of the concerns I have had regarding how psychiatrists respond when a patient says “I am hearing voices.” In my experience many psychiatrists simply leave it at that and don’t even attempt the briefest characterization of these hallucinations, let alone the rigorous elucidation that Dr. Nasrallah suggests.
We are doing a disservice to our patients by not performing a thorough evaluation of what a patient means when he says “I am hearing voices.” How can we really understand what our patient is experiencing if we don’t attempt to grasp the specifics of something as remarkable as a hallucination?
Unfortunately, there are patients who use statements such as “I am hearing voices telling me to kill myself and others” in order to be admitted to hospitals or for secondary gain. Getting or attempting to get details about these “voices” and documenting what we are told can be an invaluable part of a patient’s records. Inconsistencies arise that can be taken into consideration during subsequent encounters.
Bennett Cohen, MD
New York, NY
I would like to thank Dr. Nasrallah for his wonderful editorial about assessing auditory hallucinations (“The hallucination portrait of psychosis: Probing the voices within,” From the Editor, Current Psychiatry, May 2009). He has eloquently addressed many of the concerns I have had regarding how psychiatrists respond when a patient says “I am hearing voices.” In my experience many psychiatrists simply leave it at that and don’t even attempt the briefest characterization of these hallucinations, let alone the rigorous elucidation that Dr. Nasrallah suggests.
We are doing a disservice to our patients by not performing a thorough evaluation of what a patient means when he says “I am hearing voices.” How can we really understand what our patient is experiencing if we don’t attempt to grasp the specifics of something as remarkable as a hallucination?
Unfortunately, there are patients who use statements such as “I am hearing voices telling me to kill myself and others” in order to be admitted to hospitals or for secondary gain. Getting or attempting to get details about these “voices” and documenting what we are told can be an invaluable part of a patient’s records. Inconsistencies arise that can be taken into consideration during subsequent encounters.
Bennett Cohen, MD
New York, NY
Ask more questions
The list of interview questions Dr. Henry Nasrallah suggested in “The hallucination portrait of psychosis: Probing the voices within” (From the Editor, Current Psychiatry, May 2009) is a much-needed reminder of the clinical importance of patients’ verbal auditory hallucinations. In 15 years of practice—much of that inpatient psychiatry—I have cared for many patients with hallucinations, and until recently I confess my interview was not as thorough as Dr. Nasrallah advises. Then after attending a workshop in January 2009, I modified my usual clinical interview when a patient reported religious, paranoid, persecutory, and/or command verbal auditory hallucinations. The results have been startling.
Anne M. Stoline, MD
Perryville, MD
The list of interview questions Dr. Henry Nasrallah suggested in “The hallucination portrait of psychosis: Probing the voices within” (From the Editor, Current Psychiatry, May 2009) is a much-needed reminder of the clinical importance of patients’ verbal auditory hallucinations. In 15 years of practice—much of that inpatient psychiatry—I have cared for many patients with hallucinations, and until recently I confess my interview was not as thorough as Dr. Nasrallah advises. Then after attending a workshop in January 2009, I modified my usual clinical interview when a patient reported religious, paranoid, persecutory, and/or command verbal auditory hallucinations. The results have been startling.
Anne M. Stoline, MD
Perryville, MD
The list of interview questions Dr. Henry Nasrallah suggested in “The hallucination portrait of psychosis: Probing the voices within” (From the Editor, Current Psychiatry, May 2009) is a much-needed reminder of the clinical importance of patients’ verbal auditory hallucinations. In 15 years of practice—much of that inpatient psychiatry—I have cared for many patients with hallucinations, and until recently I confess my interview was not as thorough as Dr. Nasrallah advises. Then after attending a workshop in January 2009, I modified my usual clinical interview when a patient reported religious, paranoid, persecutory, and/or command verbal auditory hallucinations. The results have been startling.
Anne M. Stoline, MD
Perryville, MD
The $1.2 billion CME crisis: Can eleemosynary replace industry support?
Change is coming for continuing medical education (CME). A cloud of conflict of interest has shrouded any person or activity that receives pharmaceutical funding, including the venerable institution of CME. This is a big deal because all health practitioners rely on CME programs to meet requirements for license renewal and to keep up with medical advances.
Attitudes about commercial support of CME have changed, with some organizations calling for elimination of all industry funding (Table). Pressure to strip commercial support from CME is equivalent to draining blood from a living organism; it can have dire consequences if done precipitously.
CME has grown rapidly into a big business. Its commercial support quadrupled from $300 million to $1.2 billion between 1998 and 2006, according to the Accreditation Council for Continuing Medical Education. Another $1.2 billion came from other sources. Here is who received the $2.4 billion in CME funds in 2006: 34% went to publishing and medical education companies, 33% to physician organizations, 18% to medical schools, and 15% to other CME providers (such as hospitals).
The urgent question about sustaining CME has become: where will $1.2 billion come from if not from industry? Eleemosynary is likely to provide only a fraction of support. Shifting the cost to attendees could make CME fees prohibitively high (>$1,000 for a 1-day symposium).
It’s no wonder that CME providers feel anxious about the perception of undue influence on their programs, while at the same time pharmaceutical companies are pulling back from sponsoring CME. But how do psychiatric practitioners feel about this issue?
Table
Industry support of CME: Evolution of standards
| Year | Development |
|---|---|
| 1992 | ACCME issues first standards for commercial support |
| 1994 | ACCME updates standards to ensure that CME programs are free of bias and beyond the control of persons or organizations with an economic interest in influencing the content |
| 2007 | AAMC proposes principles to guide medical schools and teaching hospitals in developing policies to manage industry gifting practices and financial support for medical education |
| 2007 | U.S. Senate finance committee expresses concern that “commercial sponsorship of CME is designed to increase sales of the sponsor’s drugs through improper influence” |
| 2008 | Josiah Macy, Jr. Foundation calls for end to industry support of CME |
| 2009 | IOM recommends eventual cessation of commercial support of CME |
| AAMC: Association of American Medical Colleges; ACCME: Accreditation Council for Continuing Medical Education; CME: continuing medical education; IOM: Institute of Medicine | |
Practitioners’ attitudes about CME funding
To find out, I polled 200 mental health professionals at a CME symposium in October 2008. The results are interesting and contrary to what one might assume to be prevailing perceptions. Most respondents (69%) said industry support biases CME content at least sometimes. Most agreed CME programs with multiple sponsors are less likely to be biased than single-sponsored programs (29% “strongly agree,” 53% “agree”). Nearly all (90%) said CME programs generally meet their educational needs.
If CME funding must come from nonindustry sources, only 17% of respondents favored higher registration fees. Other sources they endorsed were private foundations (39%), online CME (30%), and grand rounds (5%). View complete survey results.
Based on these responses, here are my predictions:
- CME will survive, but its funding sources will change.
- Industry sponsorship of CME will not disappear, but it will decline substantially (a trend that has already begun). Funds from multiple pharmaceutical companies might be pooled and allocated to applicants by a third party.
- Eleemosynary will probably increase, but charity will remain a small fraction of CME support.
- The number of CME programs will decline (the American Psychiatric Association has cut sponsored CME symposia at their annual meeting by about 70%).
- Online CME will grow.
- Health professionals will increasingly participate in online learning through educational Web sites, including those of medical journals.

Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://CurrentPsychiatry.blogspot.com or click here.
Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://CurrentPsychiatry.blogspot.com or click here.
Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://CurrentPsychiatry.blogspot.com or click here.
Change is coming for continuing medical education (CME). A cloud of conflict of interest has shrouded any person or activity that receives pharmaceutical funding, including the venerable institution of CME. This is a big deal because all health practitioners rely on CME programs to meet requirements for license renewal and to keep up with medical advances.
Attitudes about commercial support of CME have changed, with some organizations calling for elimination of all industry funding (Table). Pressure to strip commercial support from CME is equivalent to draining blood from a living organism; it can have dire consequences if done precipitously.
CME has grown rapidly into a big business. Its commercial support quadrupled from $300 million to $1.2 billion between 1998 and 2006, according to the Accreditation Council for Continuing Medical Education. Another $1.2 billion came from other sources. Here is who received the $2.4 billion in CME funds in 2006: 34% went to publishing and medical education companies, 33% to physician organizations, 18% to medical schools, and 15% to other CME providers (such as hospitals).
The urgent question about sustaining CME has become: where will $1.2 billion come from if not from industry? Eleemosynary is likely to provide only a fraction of support. Shifting the cost to attendees could make CME fees prohibitively high (>$1,000 for a 1-day symposium).
It’s no wonder that CME providers feel anxious about the perception of undue influence on their programs, while at the same time pharmaceutical companies are pulling back from sponsoring CME. But how do psychiatric practitioners feel about this issue?
Table
Industry support of CME: Evolution of standards
| Year | Development |
|---|---|
| 1992 | ACCME issues first standards for commercial support |
| 1994 | ACCME updates standards to ensure that CME programs are free of bias and beyond the control of persons or organizations with an economic interest in influencing the content |
| 2007 | AAMC proposes principles to guide medical schools and teaching hospitals in developing policies to manage industry gifting practices and financial support for medical education |
| 2007 | U.S. Senate finance committee expresses concern that “commercial sponsorship of CME is designed to increase sales of the sponsor’s drugs through improper influence” |
| 2008 | Josiah Macy, Jr. Foundation calls for end to industry support of CME |
| 2009 | IOM recommends eventual cessation of commercial support of CME |
| AAMC: Association of American Medical Colleges; ACCME: Accreditation Council for Continuing Medical Education; CME: continuing medical education; IOM: Institute of Medicine | |
Practitioners’ attitudes about CME funding
To find out, I polled 200 mental health professionals at a CME symposium in October 2008. The results are interesting and contrary to what one might assume to be prevailing perceptions. Most respondents (69%) said industry support biases CME content at least sometimes. Most agreed CME programs with multiple sponsors are less likely to be biased than single-sponsored programs (29% “strongly agree,” 53% “agree”). Nearly all (90%) said CME programs generally meet their educational needs.
If CME funding must come from nonindustry sources, only 17% of respondents favored higher registration fees. Other sources they endorsed were private foundations (39%), online CME (30%), and grand rounds (5%). View complete survey results.
Based on these responses, here are my predictions:
- CME will survive, but its funding sources will change.
- Industry sponsorship of CME will not disappear, but it will decline substantially (a trend that has already begun). Funds from multiple pharmaceutical companies might be pooled and allocated to applicants by a third party.
- Eleemosynary will probably increase, but charity will remain a small fraction of CME support.
- The number of CME programs will decline (the American Psychiatric Association has cut sponsored CME symposia at their annual meeting by about 70%).
- Online CME will grow.
- Health professionals will increasingly participate in online learning through educational Web sites, including those of medical journals.
Change is coming for continuing medical education (CME). A cloud of conflict of interest has shrouded any person or activity that receives pharmaceutical funding, including the venerable institution of CME. This is a big deal because all health practitioners rely on CME programs to meet requirements for license renewal and to keep up with medical advances.
Attitudes about commercial support of CME have changed, with some organizations calling for elimination of all industry funding (Table). Pressure to strip commercial support from CME is equivalent to draining blood from a living organism; it can have dire consequences if done precipitously.
CME has grown rapidly into a big business. Its commercial support quadrupled from $300 million to $1.2 billion between 1998 and 2006, according to the Accreditation Council for Continuing Medical Education. Another $1.2 billion came from other sources. Here is who received the $2.4 billion in CME funds in 2006: 34% went to publishing and medical education companies, 33% to physician organizations, 18% to medical schools, and 15% to other CME providers (such as hospitals).
The urgent question about sustaining CME has become: where will $1.2 billion come from if not from industry? Eleemosynary is likely to provide only a fraction of support. Shifting the cost to attendees could make CME fees prohibitively high (>$1,000 for a 1-day symposium).
It’s no wonder that CME providers feel anxious about the perception of undue influence on their programs, while at the same time pharmaceutical companies are pulling back from sponsoring CME. But how do psychiatric practitioners feel about this issue?
Table
Industry support of CME: Evolution of standards
| Year | Development |
|---|---|
| 1992 | ACCME issues first standards for commercial support |
| 1994 | ACCME updates standards to ensure that CME programs are free of bias and beyond the control of persons or organizations with an economic interest in influencing the content |
| 2007 | AAMC proposes principles to guide medical schools and teaching hospitals in developing policies to manage industry gifting practices and financial support for medical education |
| 2007 | U.S. Senate finance committee expresses concern that “commercial sponsorship of CME is designed to increase sales of the sponsor’s drugs through improper influence” |
| 2008 | Josiah Macy, Jr. Foundation calls for end to industry support of CME |
| 2009 | IOM recommends eventual cessation of commercial support of CME |
| AAMC: Association of American Medical Colleges; ACCME: Accreditation Council for Continuing Medical Education; CME: continuing medical education; IOM: Institute of Medicine | |
Practitioners’ attitudes about CME funding
To find out, I polled 200 mental health professionals at a CME symposium in October 2008. The results are interesting and contrary to what one might assume to be prevailing perceptions. Most respondents (69%) said industry support biases CME content at least sometimes. Most agreed CME programs with multiple sponsors are less likely to be biased than single-sponsored programs (29% “strongly agree,” 53% “agree”). Nearly all (90%) said CME programs generally meet their educational needs.
If CME funding must come from nonindustry sources, only 17% of respondents favored higher registration fees. Other sources they endorsed were private foundations (39%), online CME (30%), and grand rounds (5%). View complete survey results.
Based on these responses, here are my predictions:
- CME will survive, but its funding sources will change.
- Industry sponsorship of CME will not disappear, but it will decline substantially (a trend that has already begun). Funds from multiple pharmaceutical companies might be pooled and allocated to applicants by a third party.
- Eleemosynary will probably increase, but charity will remain a small fraction of CME support.
- The number of CME programs will decline (the American Psychiatric Association has cut sponsored CME symposia at their annual meeting by about 70%).
- Online CME will grow.
- Health professionals will increasingly participate in online learning through educational Web sites, including those of medical journals.
The nurse who worked the system
CASE: A ‘high utilizer’
Ms. Y, a 49-year-old intensive care registered nurse, is admitted to the psychiatric hospital for suicidal ideation for the eighth time in 1 year. Ms. Y has chronic suicidal ideation with multiple attempts and has been on disability for 3 years for treatment of severe depression. She has been hospitalized for depression with suicide ideation 49 times since her divorce 6 years ago. She is prescribed fluoxetine, 60 mg/d, quetiapine, 400 mg/d, and clonazepam, 2 mg/d.
The authors’ observations
Ms. Y possesses 7 of the 11 characteristics of a high utilizer of psychiatric services (Table 1),1,2 defined as a patient who is:
- 2 standard deviations above the mean number of visits to an urban psychiatric emergency service in 6 months or
- has 4 inpatient admissions in a quarter or 6 inpatient admissions in 1 year.
Table 1
Common characteristics of high utilizers* of psychiatric services
| Homelessness |
| Developmental delays |
| Enrolled in a mental health plan |
| History of voluntary and involuntary hospitalization |
| Personality disorders |
| Likely to be uncooperative |
| Substance abuse or dependence (or history) |
| History of incarceration |
| Unreliable social support |
| Young Caucasian women |
| * Defined as having either 2 standard deviations above the mean number of visits to an urban psychiatric emergency service in 6 months or 4 inpatient admissions in a quarter or 6 inpatient admissions in 1 year |
| Source: References 1,2 |
The author’s observations
Because previous hospitalizations and courses of ECT have provided Ms. Y with only minimal, short-lived improvement, the treatment team decides to reconsider her diagnosis and treatment plan. Ms. Y’s first psychiatrist diagnosed her with major depressive disorder. After thoroughly interviewing Ms. Y and reviewing her history, the hospital psychiatrist determines that she meets criteria for borderline personality disorder (BPD) in addition to major depression. The psychiatrist explains this diagnosis to Ms. Y, provides her with education and support, and recommends dialectical behavioral therapy (DBT) and case management. She rejects the new diagnosis and treatment plan and pleads for help establishing treatment with a new psychiatrist.
The team at the psychiatric hospital feels Ms. Y needs to receive ongoing treatment from a psychiatrist. In the hope that she will be able to establish a therapeutic alliance with a new psychiatrist and therapist, they decide to continue working with Ms. Y if she accepts the BPD diagnosis and agrees to undergo DBT.
EVALUATION: A troubling pattern
Before Ms. Y’s husband divorced her, she had not received psychiatric care and had no psychiatric diagnosis. During the contentious divorce, she experienced depressive symptoms that later intensified, and she was unable to return to her previous high level of functioning.
Ms. Y became suicidal and was hospitalized for the first time shortly after the divorce was finalized and her ex-husband remarried. She began treatment with a psychiatrist, whom she idealized and saw for 5 years.
When this psychiatrist—who had been one of the few stable relationships in Ms. Y’s life—moved to another state, Ms. Y experienced a rapid recurrence of depression. She began treatment with 3 other psychiatrists but fired them because they “never understand me” like her first psychiatrist did, and she never felt she received the consistent, supportive care she deserved. She become suicidal and again required psychiatric hospitalization. This pattern continued up to her current admission.
The authors’ observations
Ms. Y briefly returns to work between hospitalizations but is not able to tolerate the stress. At one point she was admitted to an out-of-state facility; after this 2-month stay, she remained out of the local psychiatric hospital for 6 months but then became unable to function and was readmitted to the local psychiatric hospital.
When interviewed, Ms. Y describes feeling hopeless, empty, and alone each time 2 of her 3 children return to college after summer break. Her youngest child lives at home but is involved in extracurricular high school activities, and doesn’t seem to need her. Ms. Y is estranged from both parents. Her social support is unreliable because she tends to push others away and isolate herself.
The authors’ observations
Because she has no history of mania, Ms. Y does not meet criteria for bipolar affective disorder. Her multidisciplinary treatment team feels she is too fragile to transfer care to new providers or to foster care, so we schedule a care conference and carefully compose a 6-month contract to formally articulate limits and boundaries within which we will continue to treat her.
The contract specifies that Ms. Y will participate in DBT, take her medications exactly as prescribed, and not receive any early refills of her prescriptions. We arrange with Ms. Y’s health plan to have a home healthcare agency provide her medications weekly. This benefit was not available to other health plan members. Ms. Y signs the contract.
TREATMENT: Contract violation
Ms. Y complies with the contract for 2 months, then abruptly fires her long-term therapist, whom she claims violated confidentiality by giving false information to another provider. At her next session, Ms. Y will not provide details about the alleged incident, and the issue never is resolved. She admits she did not start DBT and is not taking her medications as prescribed.
Ms. Y expresses her disagreement with the terms of the contract. She becomes very upset and asks for her care to be transferred to another psychiatrist. She demands to be followed at the current clinic because “I was born here.” She denies being actively suicidal and terminates the session early. That afternoon, she calls 1 of the inpatient psychiatrists and asks if he would treat her. She also calls the first psychiatrist she had seen to enlist help in obtaining care.
The authors’ observations
In Groves’ description of 4 types of “hateful patients,” Ms. Y represents a combination of an entitled demander and a manipulative help-rejecter. The behaviors and personality disorders associated with these types of patients—and effective management strategies—are listed in (Table 2).3 (Table 3) offers tips for successfully dealing with high utilizers of psychiatric services. High utilizers of medical services other than psychiatry are more likely than patients who are not high utilizers to have a psychiatric disorder (Box).4-9
Patients who are high utilizers of medical services other than psychiatry have up to 50% higher rates of psychiatric disorders—particularly depression—compared with less-frequent utilizers.4-6 Screening medical patients for depression helps ensure that these patients are correctly diagnosed and treated.
Depression is a risk factor for nonadherence with medical treatment, and treating depression leads to decreased utilization of medical services.7,8 Patients with successfully treated depression may have reduced functional disability as well.9
Some members of our treatment team began to experience countertransference, which also interfered with Ms. Y’s treatment. They viewed her behavior as entitled, demanding, and manipulative and dreaded caring for her. Failing to recognize such defenses can lead to consequences such as malignant alienation—a progressive deterioration in the patient’s relationship with others that includes loss of sympathy and support from staff members—which can put a patient at high risk for suicide.10
After a lengthy discussion among several psychiatrists, therapists, nurses, and attorneys, the treatment team decided to terminate outpatient care for Ms. Y at our facility because of her chronic nonadherence to treatment recommendations. Ms. Y had manipulated numerous providers in our department, called multiple doctors in our facility to ask them to care for her, and asked her ex-husband to contact the department administration on her behalf. Her behavior bordered on harassment. In addition, the interventions we provided were making her worse, not better. Factors that influenced our decision included:
- fear of Ms. Y committing suicide
- fear of setting limits
- fear of being reported to the Medical Board
- fear of a lawsuit.
Table 2
Strategies for helping 4 types of ‘hateful patients’
| Dependent clinger | |
| Behaviors | Shows extreme gratitude with flattery |
| Associated personality traits/disorders | Codependent |
| Management strategies | As early and as tactfully as possible, set firm limits on the patient’s expectations for an intense doctor-patient relationship. Tell the patient that you have limits not only on knowledge and skill but also on time and stamina |
| Entitled demander | |
| Behaviors | Intimidates, devalues, induces guilt, may try to control with threats; terrified of abandonment |
| Associated personality traits/disorders | Narcissistic, borderline personality disorder |
| Management strategies | Try to rechannel your patient’s feelings of entitlement into a partnership that acknowledges his or her entitlement not to unrealistic demands but to good medical care. Help your patient stop directing anger at the healthcare team |
| Manipulative help-rejecter | |
| Behaviors | Resists treatment; may seem happy with treatment failures |
| Associated personality traits/disorders | Psychopathy, paranoia, borderline personality disorder, negativistic, passive/aggressive |
| Management strategies | Diminish your patient’s notion that losing the symptom or illness implies losing the doctor by ‘sharing’ your patient’s pessimism. Tell your patient that treatment may not cure the illness. Schedule regular follow-up visits |
| Self-destructive denier | |
| Behaviors | Denial helps them survive |
| Associated personality traits/disorders | Borderline personality disorder, histrionic, schizoid, schizotypal |
| Management strategies | Recognize that this type of patient can make clinicians wish the patient would die and that the chance of helping a self-destructive denier is minimal. Lower unrealistic expectations of delivering perfect care. Evaluate the patient for a treatable mental illness, such as depression, anxiety, etc. |
| Source: Reference 3 | |
Table 3
Tips for managing high utilizers
Establish a collaborative treatment plan with firm limits and expectations
|
Acknowledge your feelings and countertransference
|
Explore your patient’s expectations and commitment to treatment by asking:
|
Practice safely and proactively
|
OUTCOME: The pattern continues
Ms. Y continues to receive treatment with a different outpatient psychiatrist and therapist in the area. She has not been hospitalized for almost 2 years but her financial state has deteriorated and she has had a recurrence of depression. Ms. Y’s psychiatrist recently called the hospital to ask for direct admission on the patient’s behalf, stating that Ms. Y did not want to wait hours to be seen in the ER. Hospital staff explained that she needs to first come to the ER for evaluation. Ms. Y refused to come to the ER and was not admitted. About 1 month later, Ms. Y’s psychiatrist called again, and she was directly admitted to the psychiatric hospital.
Related resource
- National Suicide Prevention Lifeline. 1-800-273-TALK (8255). www.suicidepreventionlifeline.org.
- Clonazepam • Klonopin
- Fluoxetine • Prozac
- Quetiapine • Seroquel
The authors report no financial relationship with any company whose products are mentioned in this article or manufacturers of competing products.
1. Pasic J, Russo J, Roy-Byrne P. High utilizers of psychiatric emergency services. Psychiatr Serv. 2005;56(6):678-684.
2. Geller J, Fisher W, McDermeit M, et al. The effects of public managed care on patterns of intensive use of inpatient psychiatric services. Psychiatr Serv. 1998;49:327-332.
3. Groves JE. Taking care of the hateful patient. N Engl J Med. 1978;298(16):883-887.
4. Karlsson H, Lehtinen V, Joukamaa M. Are frequent attenders of primary health care distressed? Scan J Health Care. 1995;13:32-38.
5. Karlsson H, Lehtinen V, Joukamaa M. Psychiatric morbidity among frequent attenders in primary care. Gen Hosp Psychiatry. 1995;17:19-25.
6. Lefevre F, Refiler D, Lee P, et al. Screening for undetected mental disorders in high utilizers of primary care services. J Gen Int Med. 1999;14:425-431.
7. Pearson S, Katzelnick D, Simon G, et al. Depression among high utilizers of medical care. J Gen Intern Med. 1999;14:461-468.
8. DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on medical adherence. Arch Intern Med. 2000;160:2101-2107.
9. Von Korff M, Ormel J, Katon W, et al. Disability and depression among high utilizers of health care. A longitudinal analysis. Arch Gen Psychiatry. 1992;49(2):91-100.
10. Watts D, Morgan G. Malignant alienation dangers for patients who are hard to like. Br J Psychiatry. 1994;164:11-15.
CASE: A ‘high utilizer’
Ms. Y, a 49-year-old intensive care registered nurse, is admitted to the psychiatric hospital for suicidal ideation for the eighth time in 1 year. Ms. Y has chronic suicidal ideation with multiple attempts and has been on disability for 3 years for treatment of severe depression. She has been hospitalized for depression with suicide ideation 49 times since her divorce 6 years ago. She is prescribed fluoxetine, 60 mg/d, quetiapine, 400 mg/d, and clonazepam, 2 mg/d.
The authors’ observations
Ms. Y possesses 7 of the 11 characteristics of a high utilizer of psychiatric services (Table 1),1,2 defined as a patient who is:
- 2 standard deviations above the mean number of visits to an urban psychiatric emergency service in 6 months or
- has 4 inpatient admissions in a quarter or 6 inpatient admissions in 1 year.
Table 1
Common characteristics of high utilizers* of psychiatric services
| Homelessness |
| Developmental delays |
| Enrolled in a mental health plan |
| History of voluntary and involuntary hospitalization |
| Personality disorders |
| Likely to be uncooperative |
| Substance abuse or dependence (or history) |
| History of incarceration |
| Unreliable social support |
| Young Caucasian women |
| * Defined as having either 2 standard deviations above the mean number of visits to an urban psychiatric emergency service in 6 months or 4 inpatient admissions in a quarter or 6 inpatient admissions in 1 year |
| Source: References 1,2 |
The author’s observations
Because previous hospitalizations and courses of ECT have provided Ms. Y with only minimal, short-lived improvement, the treatment team decides to reconsider her diagnosis and treatment plan. Ms. Y’s first psychiatrist diagnosed her with major depressive disorder. After thoroughly interviewing Ms. Y and reviewing her history, the hospital psychiatrist determines that she meets criteria for borderline personality disorder (BPD) in addition to major depression. The psychiatrist explains this diagnosis to Ms. Y, provides her with education and support, and recommends dialectical behavioral therapy (DBT) and case management. She rejects the new diagnosis and treatment plan and pleads for help establishing treatment with a new psychiatrist.
The team at the psychiatric hospital feels Ms. Y needs to receive ongoing treatment from a psychiatrist. In the hope that she will be able to establish a therapeutic alliance with a new psychiatrist and therapist, they decide to continue working with Ms. Y if she accepts the BPD diagnosis and agrees to undergo DBT.
EVALUATION: A troubling pattern
Before Ms. Y’s husband divorced her, she had not received psychiatric care and had no psychiatric diagnosis. During the contentious divorce, she experienced depressive symptoms that later intensified, and she was unable to return to her previous high level of functioning.
Ms. Y became suicidal and was hospitalized for the first time shortly after the divorce was finalized and her ex-husband remarried. She began treatment with a psychiatrist, whom she idealized and saw for 5 years.
When this psychiatrist—who had been one of the few stable relationships in Ms. Y’s life—moved to another state, Ms. Y experienced a rapid recurrence of depression. She began treatment with 3 other psychiatrists but fired them because they “never understand me” like her first psychiatrist did, and she never felt she received the consistent, supportive care she deserved. She become suicidal and again required psychiatric hospitalization. This pattern continued up to her current admission.
The authors’ observations
Ms. Y briefly returns to work between hospitalizations but is not able to tolerate the stress. At one point she was admitted to an out-of-state facility; after this 2-month stay, she remained out of the local psychiatric hospital for 6 months but then became unable to function and was readmitted to the local psychiatric hospital.
When interviewed, Ms. Y describes feeling hopeless, empty, and alone each time 2 of her 3 children return to college after summer break. Her youngest child lives at home but is involved in extracurricular high school activities, and doesn’t seem to need her. Ms. Y is estranged from both parents. Her social support is unreliable because she tends to push others away and isolate herself.
The authors’ observations
Because she has no history of mania, Ms. Y does not meet criteria for bipolar affective disorder. Her multidisciplinary treatment team feels she is too fragile to transfer care to new providers or to foster care, so we schedule a care conference and carefully compose a 6-month contract to formally articulate limits and boundaries within which we will continue to treat her.
The contract specifies that Ms. Y will participate in DBT, take her medications exactly as prescribed, and not receive any early refills of her prescriptions. We arrange with Ms. Y’s health plan to have a home healthcare agency provide her medications weekly. This benefit was not available to other health plan members. Ms. Y signs the contract.
TREATMENT: Contract violation
Ms. Y complies with the contract for 2 months, then abruptly fires her long-term therapist, whom she claims violated confidentiality by giving false information to another provider. At her next session, Ms. Y will not provide details about the alleged incident, and the issue never is resolved. She admits she did not start DBT and is not taking her medications as prescribed.
Ms. Y expresses her disagreement with the terms of the contract. She becomes very upset and asks for her care to be transferred to another psychiatrist. She demands to be followed at the current clinic because “I was born here.” She denies being actively suicidal and terminates the session early. That afternoon, she calls 1 of the inpatient psychiatrists and asks if he would treat her. She also calls the first psychiatrist she had seen to enlist help in obtaining care.
The authors’ observations
In Groves’ description of 4 types of “hateful patients,” Ms. Y represents a combination of an entitled demander and a manipulative help-rejecter. The behaviors and personality disorders associated with these types of patients—and effective management strategies—are listed in (Table 2).3 (Table 3) offers tips for successfully dealing with high utilizers of psychiatric services. High utilizers of medical services other than psychiatry are more likely than patients who are not high utilizers to have a psychiatric disorder (Box).4-9
Patients who are high utilizers of medical services other than psychiatry have up to 50% higher rates of psychiatric disorders—particularly depression—compared with less-frequent utilizers.4-6 Screening medical patients for depression helps ensure that these patients are correctly diagnosed and treated.
Depression is a risk factor for nonadherence with medical treatment, and treating depression leads to decreased utilization of medical services.7,8 Patients with successfully treated depression may have reduced functional disability as well.9
Some members of our treatment team began to experience countertransference, which also interfered with Ms. Y’s treatment. They viewed her behavior as entitled, demanding, and manipulative and dreaded caring for her. Failing to recognize such defenses can lead to consequences such as malignant alienation—a progressive deterioration in the patient’s relationship with others that includes loss of sympathy and support from staff members—which can put a patient at high risk for suicide.10
After a lengthy discussion among several psychiatrists, therapists, nurses, and attorneys, the treatment team decided to terminate outpatient care for Ms. Y at our facility because of her chronic nonadherence to treatment recommendations. Ms. Y had manipulated numerous providers in our department, called multiple doctors in our facility to ask them to care for her, and asked her ex-husband to contact the department administration on her behalf. Her behavior bordered on harassment. In addition, the interventions we provided were making her worse, not better. Factors that influenced our decision included:
- fear of Ms. Y committing suicide
- fear of setting limits
- fear of being reported to the Medical Board
- fear of a lawsuit.
Table 2
Strategies for helping 4 types of ‘hateful patients’
| Dependent clinger | |
| Behaviors | Shows extreme gratitude with flattery |
| Associated personality traits/disorders | Codependent |
| Management strategies | As early and as tactfully as possible, set firm limits on the patient’s expectations for an intense doctor-patient relationship. Tell the patient that you have limits not only on knowledge and skill but also on time and stamina |
| Entitled demander | |
| Behaviors | Intimidates, devalues, induces guilt, may try to control with threats; terrified of abandonment |
| Associated personality traits/disorders | Narcissistic, borderline personality disorder |
| Management strategies | Try to rechannel your patient’s feelings of entitlement into a partnership that acknowledges his or her entitlement not to unrealistic demands but to good medical care. Help your patient stop directing anger at the healthcare team |
| Manipulative help-rejecter | |
| Behaviors | Resists treatment; may seem happy with treatment failures |
| Associated personality traits/disorders | Psychopathy, paranoia, borderline personality disorder, negativistic, passive/aggressive |
| Management strategies | Diminish your patient’s notion that losing the symptom or illness implies losing the doctor by ‘sharing’ your patient’s pessimism. Tell your patient that treatment may not cure the illness. Schedule regular follow-up visits |
| Self-destructive denier | |
| Behaviors | Denial helps them survive |
| Associated personality traits/disorders | Borderline personality disorder, histrionic, schizoid, schizotypal |
| Management strategies | Recognize that this type of patient can make clinicians wish the patient would die and that the chance of helping a self-destructive denier is minimal. Lower unrealistic expectations of delivering perfect care. Evaluate the patient for a treatable mental illness, such as depression, anxiety, etc. |
| Source: Reference 3 | |
Table 3
Tips for managing high utilizers
Establish a collaborative treatment plan with firm limits and expectations
|
Acknowledge your feelings and countertransference
|
Explore your patient’s expectations and commitment to treatment by asking:
|
Practice safely and proactively
|
OUTCOME: The pattern continues
Ms. Y continues to receive treatment with a different outpatient psychiatrist and therapist in the area. She has not been hospitalized for almost 2 years but her financial state has deteriorated and she has had a recurrence of depression. Ms. Y’s psychiatrist recently called the hospital to ask for direct admission on the patient’s behalf, stating that Ms. Y did not want to wait hours to be seen in the ER. Hospital staff explained that she needs to first come to the ER for evaluation. Ms. Y refused to come to the ER and was not admitted. About 1 month later, Ms. Y’s psychiatrist called again, and she was directly admitted to the psychiatric hospital.
Related resource
- National Suicide Prevention Lifeline. 1-800-273-TALK (8255). www.suicidepreventionlifeline.org.
- Clonazepam • Klonopin
- Fluoxetine • Prozac
- Quetiapine • Seroquel
The authors report no financial relationship with any company whose products are mentioned in this article or manufacturers of competing products.
CASE: A ‘high utilizer’
Ms. Y, a 49-year-old intensive care registered nurse, is admitted to the psychiatric hospital for suicidal ideation for the eighth time in 1 year. Ms. Y has chronic suicidal ideation with multiple attempts and has been on disability for 3 years for treatment of severe depression. She has been hospitalized for depression with suicide ideation 49 times since her divorce 6 years ago. She is prescribed fluoxetine, 60 mg/d, quetiapine, 400 mg/d, and clonazepam, 2 mg/d.
The authors’ observations
Ms. Y possesses 7 of the 11 characteristics of a high utilizer of psychiatric services (Table 1),1,2 defined as a patient who is:
- 2 standard deviations above the mean number of visits to an urban psychiatric emergency service in 6 months or
- has 4 inpatient admissions in a quarter or 6 inpatient admissions in 1 year.
Table 1
Common characteristics of high utilizers* of psychiatric services
| Homelessness |
| Developmental delays |
| Enrolled in a mental health plan |
| History of voluntary and involuntary hospitalization |
| Personality disorders |
| Likely to be uncooperative |
| Substance abuse or dependence (or history) |
| History of incarceration |
| Unreliable social support |
| Young Caucasian women |
| * Defined as having either 2 standard deviations above the mean number of visits to an urban psychiatric emergency service in 6 months or 4 inpatient admissions in a quarter or 6 inpatient admissions in 1 year |
| Source: References 1,2 |
The author’s observations
Because previous hospitalizations and courses of ECT have provided Ms. Y with only minimal, short-lived improvement, the treatment team decides to reconsider her diagnosis and treatment plan. Ms. Y’s first psychiatrist diagnosed her with major depressive disorder. After thoroughly interviewing Ms. Y and reviewing her history, the hospital psychiatrist determines that she meets criteria for borderline personality disorder (BPD) in addition to major depression. The psychiatrist explains this diagnosis to Ms. Y, provides her with education and support, and recommends dialectical behavioral therapy (DBT) and case management. She rejects the new diagnosis and treatment plan and pleads for help establishing treatment with a new psychiatrist.
The team at the psychiatric hospital feels Ms. Y needs to receive ongoing treatment from a psychiatrist. In the hope that she will be able to establish a therapeutic alliance with a new psychiatrist and therapist, they decide to continue working with Ms. Y if she accepts the BPD diagnosis and agrees to undergo DBT.
EVALUATION: A troubling pattern
Before Ms. Y’s husband divorced her, she had not received psychiatric care and had no psychiatric diagnosis. During the contentious divorce, she experienced depressive symptoms that later intensified, and she was unable to return to her previous high level of functioning.
Ms. Y became suicidal and was hospitalized for the first time shortly after the divorce was finalized and her ex-husband remarried. She began treatment with a psychiatrist, whom she idealized and saw for 5 years.
When this psychiatrist—who had been one of the few stable relationships in Ms. Y’s life—moved to another state, Ms. Y experienced a rapid recurrence of depression. She began treatment with 3 other psychiatrists but fired them because they “never understand me” like her first psychiatrist did, and she never felt she received the consistent, supportive care she deserved. She become suicidal and again required psychiatric hospitalization. This pattern continued up to her current admission.
The authors’ observations
Ms. Y briefly returns to work between hospitalizations but is not able to tolerate the stress. At one point she was admitted to an out-of-state facility; after this 2-month stay, she remained out of the local psychiatric hospital for 6 months but then became unable to function and was readmitted to the local psychiatric hospital.
When interviewed, Ms. Y describes feeling hopeless, empty, and alone each time 2 of her 3 children return to college after summer break. Her youngest child lives at home but is involved in extracurricular high school activities, and doesn’t seem to need her. Ms. Y is estranged from both parents. Her social support is unreliable because she tends to push others away and isolate herself.
The authors’ observations
Because she has no history of mania, Ms. Y does not meet criteria for bipolar affective disorder. Her multidisciplinary treatment team feels she is too fragile to transfer care to new providers or to foster care, so we schedule a care conference and carefully compose a 6-month contract to formally articulate limits and boundaries within which we will continue to treat her.
The contract specifies that Ms. Y will participate in DBT, take her medications exactly as prescribed, and not receive any early refills of her prescriptions. We arrange with Ms. Y’s health plan to have a home healthcare agency provide her medications weekly. This benefit was not available to other health plan members. Ms. Y signs the contract.
TREATMENT: Contract violation
Ms. Y complies with the contract for 2 months, then abruptly fires her long-term therapist, whom she claims violated confidentiality by giving false information to another provider. At her next session, Ms. Y will not provide details about the alleged incident, and the issue never is resolved. She admits she did not start DBT and is not taking her medications as prescribed.
Ms. Y expresses her disagreement with the terms of the contract. She becomes very upset and asks for her care to be transferred to another psychiatrist. She demands to be followed at the current clinic because “I was born here.” She denies being actively suicidal and terminates the session early. That afternoon, she calls 1 of the inpatient psychiatrists and asks if he would treat her. She also calls the first psychiatrist she had seen to enlist help in obtaining care.
The authors’ observations
In Groves’ description of 4 types of “hateful patients,” Ms. Y represents a combination of an entitled demander and a manipulative help-rejecter. The behaviors and personality disorders associated with these types of patients—and effective management strategies—are listed in (Table 2).3 (Table 3) offers tips for successfully dealing with high utilizers of psychiatric services. High utilizers of medical services other than psychiatry are more likely than patients who are not high utilizers to have a psychiatric disorder (Box).4-9
Patients who are high utilizers of medical services other than psychiatry have up to 50% higher rates of psychiatric disorders—particularly depression—compared with less-frequent utilizers.4-6 Screening medical patients for depression helps ensure that these patients are correctly diagnosed and treated.
Depression is a risk factor for nonadherence with medical treatment, and treating depression leads to decreased utilization of medical services.7,8 Patients with successfully treated depression may have reduced functional disability as well.9
Some members of our treatment team began to experience countertransference, which also interfered with Ms. Y’s treatment. They viewed her behavior as entitled, demanding, and manipulative and dreaded caring for her. Failing to recognize such defenses can lead to consequences such as malignant alienation—a progressive deterioration in the patient’s relationship with others that includes loss of sympathy and support from staff members—which can put a patient at high risk for suicide.10
After a lengthy discussion among several psychiatrists, therapists, nurses, and attorneys, the treatment team decided to terminate outpatient care for Ms. Y at our facility because of her chronic nonadherence to treatment recommendations. Ms. Y had manipulated numerous providers in our department, called multiple doctors in our facility to ask them to care for her, and asked her ex-husband to contact the department administration on her behalf. Her behavior bordered on harassment. In addition, the interventions we provided were making her worse, not better. Factors that influenced our decision included:
- fear of Ms. Y committing suicide
- fear of setting limits
- fear of being reported to the Medical Board
- fear of a lawsuit.
Table 2
Strategies for helping 4 types of ‘hateful patients’
| Dependent clinger | |
| Behaviors | Shows extreme gratitude with flattery |
| Associated personality traits/disorders | Codependent |
| Management strategies | As early and as tactfully as possible, set firm limits on the patient’s expectations for an intense doctor-patient relationship. Tell the patient that you have limits not only on knowledge and skill but also on time and stamina |
| Entitled demander | |
| Behaviors | Intimidates, devalues, induces guilt, may try to control with threats; terrified of abandonment |
| Associated personality traits/disorders | Narcissistic, borderline personality disorder |
| Management strategies | Try to rechannel your patient’s feelings of entitlement into a partnership that acknowledges his or her entitlement not to unrealistic demands but to good medical care. Help your patient stop directing anger at the healthcare team |
| Manipulative help-rejecter | |
| Behaviors | Resists treatment; may seem happy with treatment failures |
| Associated personality traits/disorders | Psychopathy, paranoia, borderline personality disorder, negativistic, passive/aggressive |
| Management strategies | Diminish your patient’s notion that losing the symptom or illness implies losing the doctor by ‘sharing’ your patient’s pessimism. Tell your patient that treatment may not cure the illness. Schedule regular follow-up visits |
| Self-destructive denier | |
| Behaviors | Denial helps them survive |
| Associated personality traits/disorders | Borderline personality disorder, histrionic, schizoid, schizotypal |
| Management strategies | Recognize that this type of patient can make clinicians wish the patient would die and that the chance of helping a self-destructive denier is minimal. Lower unrealistic expectations of delivering perfect care. Evaluate the patient for a treatable mental illness, such as depression, anxiety, etc. |
| Source: Reference 3 | |
Table 3
Tips for managing high utilizers
Establish a collaborative treatment plan with firm limits and expectations
|
Acknowledge your feelings and countertransference
|
Explore your patient’s expectations and commitment to treatment by asking:
|
Practice safely and proactively
|
OUTCOME: The pattern continues
Ms. Y continues to receive treatment with a different outpatient psychiatrist and therapist in the area. She has not been hospitalized for almost 2 years but her financial state has deteriorated and she has had a recurrence of depression. Ms. Y’s psychiatrist recently called the hospital to ask for direct admission on the patient’s behalf, stating that Ms. Y did not want to wait hours to be seen in the ER. Hospital staff explained that she needs to first come to the ER for evaluation. Ms. Y refused to come to the ER and was not admitted. About 1 month later, Ms. Y’s psychiatrist called again, and she was directly admitted to the psychiatric hospital.
Related resource
- National Suicide Prevention Lifeline. 1-800-273-TALK (8255). www.suicidepreventionlifeline.org.
- Clonazepam • Klonopin
- Fluoxetine • Prozac
- Quetiapine • Seroquel
The authors report no financial relationship with any company whose products are mentioned in this article or manufacturers of competing products.
1. Pasic J, Russo J, Roy-Byrne P. High utilizers of psychiatric emergency services. Psychiatr Serv. 2005;56(6):678-684.
2. Geller J, Fisher W, McDermeit M, et al. The effects of public managed care on patterns of intensive use of inpatient psychiatric services. Psychiatr Serv. 1998;49:327-332.
3. Groves JE. Taking care of the hateful patient. N Engl J Med. 1978;298(16):883-887.
4. Karlsson H, Lehtinen V, Joukamaa M. Are frequent attenders of primary health care distressed? Scan J Health Care. 1995;13:32-38.
5. Karlsson H, Lehtinen V, Joukamaa M. Psychiatric morbidity among frequent attenders in primary care. Gen Hosp Psychiatry. 1995;17:19-25.
6. Lefevre F, Refiler D, Lee P, et al. Screening for undetected mental disorders in high utilizers of primary care services. J Gen Int Med. 1999;14:425-431.
7. Pearson S, Katzelnick D, Simon G, et al. Depression among high utilizers of medical care. J Gen Intern Med. 1999;14:461-468.
8. DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on medical adherence. Arch Intern Med. 2000;160:2101-2107.
9. Von Korff M, Ormel J, Katon W, et al. Disability and depression among high utilizers of health care. A longitudinal analysis. Arch Gen Psychiatry. 1992;49(2):91-100.
10. Watts D, Morgan G. Malignant alienation dangers for patients who are hard to like. Br J Psychiatry. 1994;164:11-15.
1. Pasic J, Russo J, Roy-Byrne P. High utilizers of psychiatric emergency services. Psychiatr Serv. 2005;56(6):678-684.
2. Geller J, Fisher W, McDermeit M, et al. The effects of public managed care on patterns of intensive use of inpatient psychiatric services. Psychiatr Serv. 1998;49:327-332.
3. Groves JE. Taking care of the hateful patient. N Engl J Med. 1978;298(16):883-887.
4. Karlsson H, Lehtinen V, Joukamaa M. Are frequent attenders of primary health care distressed? Scan J Health Care. 1995;13:32-38.
5. Karlsson H, Lehtinen V, Joukamaa M. Psychiatric morbidity among frequent attenders in primary care. Gen Hosp Psychiatry. 1995;17:19-25.
6. Lefevre F, Refiler D, Lee P, et al. Screening for undetected mental disorders in high utilizers of primary care services. J Gen Int Med. 1999;14:425-431.
7. Pearson S, Katzelnick D, Simon G, et al. Depression among high utilizers of medical care. J Gen Intern Med. 1999;14:461-468.
8. DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on medical adherence. Arch Intern Med. 2000;160:2101-2107.
9. Von Korff M, Ormel J, Katon W, et al. Disability and depression among high utilizers of health care. A longitudinal analysis. Arch Gen Psychiatry. 1992;49(2):91-100.
10. Watts D, Morgan G. Malignant alienation dangers for patients who are hard to like. Br J Psychiatry. 1994;164:11-15.
Choosing antipsychotics for children with schizophrenia: Evidence plus experience
“A patient I’ve seen for a number of years had been diagnosed in the pervasive developmental disorder spectrum, but she was quite atypical. Her perseverative thinking focused on a fantasy world, and she was so preoccupied that it was very difficult to pull her out of it. Now at age 12, she has a full-blown psychotic disorder, and the fantasy world is enveloping her. She hears people talking to her all day long.”
Jean A. Frazier, MD, who treats this patient and other children with psychotic disorders, was 1 of 4 principal investigators in the Treatment of Early-Onset Schizophrenia Spectrum Disorders (TEOSS) study, a randomized, double-blind, multisite trial funded by the National Institute of Mental Health. The study, published in November 2008,1 compared the efficacy and tolerability of 3 antipsychotics—olanzapine, risperidone, and molindone—in pediatric patients with schizophrenia or schizoaffective disorder (Box 1).
Dr. Frazier discusses the unexpected findings of the TEOSS trial with Current Psychiatry Section Editor Robert A. Kowatch, MD, PhD. Based on the trial findings and her experience, she tells how she makes decisions when prescribing antipsychotics for children and adolescents with schizophrenia and related disorders.
DR. KOWATCH: The TEOSS trial found no significant differences in efficacy between molindone and the atypical antipsychotics (olanzapine and risperidone) included in the study. You’ve prescribed both typical and atypical antipsychotics in research and in your clinical practice. Do you believe there’s any difference between the 2 classes?
DR. FRAZIER: There are some differences. For example, treatment-refractory patients, especially young children, sometimes need more D2 blockade than some atypical antipsychotics provide. I’ve seen more extra pyramidal side effects with the typical antipsychotics than the atypicals, although it’s not uncommon to see some akathisia with aripiprazole or some dystonia and dyskinesia with risperidone.
DR. KOWATCH: What are the benefits and risks of using antipsychotics in young children?
DR. FRAZIER: The benefit is that antipsychotics can decrease children’s suffering and get them more centered in reality so they can enjoy their friends and progress in school. And when that happens, it’s wonderful. What are the risks? With the atypicals my greatest concern is weight gain, and with the typical agents it’s tardive dyskinesia.
DR. KOWATCH: Have you changed the way you prescribe antipsychotics as a result of the TEOSS study?
DR. FRAZIER: Actually, I have. Clinicians have to be very careful about selecting psychotropic agents that can worsen pediatric-onset obesity. Olanzapine is an effective agent for targeting psychosis and mood symptoms, but the weight gain associated with it is a concern. I do not prescribe olanzapine as much as I have in the past, although I keep it in my armamentarium and tend to reserve it for third- or fourth-line therapy.
I have found molindone to be quite effective in children with schizophrenia or schizoaffective disorder, especially in those who have gained a lot of weight on atypical antipsychotics. They usually lose weight on molindone.
DR. KOWATCH: Do you think the TEOSS study had adequate power to demonstrate differences among molindone, olanzapine, and risperidone?
DR. FRAZIER: We enrolled 119 patients—which is large for a study such as this—but we did not reach our target of 168 patients, which might have increased our power to detect differences. Among the children we did enroll, the 3 antipsychotics showed no difference in efficacy, but the meaningful finding of this study to me was the side effect profile of these agents.
DR. KOWATCH: You mean weight gain with olanzapine and extrapyramidal symptoms with molindone?
DR. FRAZIER: Yes.
Managing side effects
DR. KOWATCH: How do you manage antipsychotic side effects?
DR. FRAZIER: For any of the antipsychotics’ side effects, you have to decide whether to continue the agent or switch to another anti psychotic. For example, I’ve had a number of children—many with significant weight problems—whose psychotic symptoms have responded only to risperidone. So we put them back on risperidone, and the decision then becomes what can we do to help with the weight gain while continuing that agent.
For weight gain, I think the best intervention is diet, exercise, and drinking a lot of water, but that can be effective only if you engage the patient’s entire family in the intervention as well. Short of that, a number of pharmacologic interventions have been studied, although not specifically in children.
In an open-label trial our group conducted with 11 children age 10 to 18 years who had gained weight while taking atypical antipsychotics, metformin decreased lipid levels and body mass index but not significantly. I’ve followed these children in my practice, however, and all those who continued taking metformin over a period of months lost weight.
TEOSS study adds to debate about efficacy and tolerability
The 5-year National Institute of Mental Health-funded Treatment of Early-Onset Schizophrenia Spectrum Disorders (TEOSS) trial began with an ambitious goal: to compare the efficacy and safety of 1 typical and 2 atypical antipsychotics in children age 8 to 19 with schizophrenia. The primary hypothesis was that atypical agents would show greater efficacy and tolerability when given for 8 weeks. Instead, the atypical agents showed no greater efficacy, and adverse effects occurred with all 3 antipsychotics. Because the trial was designed for 168 subjects but enrolled 119, it may not have been adequately powered to detect differences among the 3 agents.
Medications: Most of the 116 children who received medications were severely ill with psychotic symptoms when randomly assigned to 1 of the 3 antipsychotics for 8 weeks of double-blind treatment. Administration began at the lowest dose in a set range and usually was increased to midrange within 10 to 14 days. Dosing remained flexible within these ranges:
- molindone, 10 to 140 mg/d (mean endpoint dose 59.9 mg/d)
- olanzapine, 2.5 to 20 mg/d (mean endpoint dose 11.4 mg/d)
- risperidone, 0.5 to 6 mg/d (mean endpoint dose 2.8 mg/d).
Benztropine, ≥1 mg/d, was given to all patients treated with molindone, 14% of those treated with olanzapine, and 34% of those treated with risperidone to prevent or manage akathisia.
Efficacy: Two criteria defined treatment response: a Clinical Global Impression improvement score of 1 or 2 and a ≥20% reduction in baseline Positive and Negative Syndrome Scale (PANSS) score. Tolerability outcomes included neurologic side effects, weight changes, laboratory analyses, vital signs, ECG, serious adverse events, and treatment discontinuation. Extrapyramidal symptoms were monitored with involuntary movement and akathisia scales.
Observed PANSS total score by week of treatment
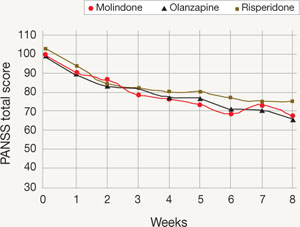
Mean Positive and Negative Symptom Scale (PANSS) total scores of observed cases during each week of the TEOSS trial. Minimum possible PANSS score is 30; scores >60 typically are viewed as problematic.
Among the 70 patients who completed treatment (25 of 40 with molindone, 17 of 35 olanzapine, and 28 of 41 with risperidone), more than one-half failed to achieve an adequate response. Response rates were 50% with molindone, 34% with olanzapine, and 46% with risperidone. The atypical antipsychotics did not show greater efficacy than molindone, and mean reductions in psychotic symptoms were modest (20% to 34% on the PANSS). Mean medication doses were midrange and considered moderate.
Tolerability: Sedation, irritability, and anxiety were frequent adverse events. Patients receiving molindone reported significantly higher rates of akathisia (P < .0008). Those receiving olanzapine reported significantly higher rates of weight gain (P < .0001) and were the only group with increased lipid and insulin serum levels and liver function tests. Patients in the risperidone group reported significantly higher rates of constipation (P < .021) and were the only group that experienced elevated serum prolactin.
Source: Sikich L, Frazier JA, McClellan J, et al. Double-blind comparison of first- and second-generation antipsychotics in early-onset schizophrenia and schizoaffective disorder: findings from the Treatment of Early-Onset Schizophrenia Spectrum disorders (TEOSS) study. Am J Psychiatry. 2008;165:1420-1431
Choosing antipsychotics
DR. KOWATCH: Let’s say you’re seeing psychosis in a 12-year-old whom you think is schizophrenic, and he or she has not yet received an antipsychotic. What are your top 3 treatment choices?
DR. FRAZIER: The first agent I usually select is risperidone. We have the most data on the use of this atypical antipsychotic in children and adolescents, and most psychotic children I see do better with a bit more D2 blockade than some of the other atypicals provide. That said, I remain concerned about risperidone’s side effects—such as weight gain and increased serum prolactin—so my usual second-line agent is aripiprazole.
I became interested in the complicated overlap between pervasive developmental disorders spectrum and psychotic disorders early in my training. More is known about prodromal symptoms in adolescents and adults than in children.
A group in the Netherlands5 compared 32 adolescents with severe early deficits in affect regulation, anxiety, disturbed social relationships, and thought disorder (characterized as “multiple complex developmental disorder” [MCDD]) with 80 adolescents with prodromal psychotic symptoms who met criteria for “at-risk mental state” (ARMS). Three-quarters of the children with MCDD (78%) were found to meet criteria for ARMS, and the 2 groups showed similar schizotypal traits, disorganization, and prodromal symptoms.
Signs of progression to psychosis and schizophrenia in children typically include:
- change in personality
- decrease in functioning or decline in ability to perform at school
- unusual thoughts or behaviors
- crippling anxiety
- supersensitivity to stress.
With experience, the clinician can more clearly differentiate the prodromal signs of psychosis from normal childhood behaviors. Children who are psychotic often don’t make good eye contact. When you try to engage them in discussion about hearing voices, they’re inattentive and internally preoccupied.
Normal vs psychotic children. You want a child in the latency age to have a rich fantasy life. If they do not, that raises concerns. Both normal and psychotic children sometimes say an imaginary friend told them something. Normal children eventually will admit this friend is imaginary. When children are psychotic, especially at an early age, you can’t pull them out of thinking about the imaginary friend, and they can’t distinguish fantasy from reality. Psychotic children also hear imaginary friends talking to them much more often.
Normal children usually are not afraid of their imaginary friends, whereas psychotic children—particularly adolescents—often are afraid of the voices they hear. However, if a psychotic child has heard voices from a young age, the voices aren’t always ego-dystonic. The girl I mentioned at the beginning of this article likes having the voices around. In fact, she gets uncomfortable when the voices are quiet.—Jean A. Frazier, MD
DR. KOWATCH: Why do you like aripiprazole for this patient population?
DR. FRAZIER: Aripiprazole doesn’t tend to be associated with as much weight gain as olanzapine or risperidone, although I’ve had children—especially in the autism spectrum—who have gained quite a bit of weight on aripiprazole. Clinically, I’ve noticed that aripiprazole seems to brighten up children’s affect. It also seems to help many children in my practice with attentional symptoms, although that’s anecdotal.
Although we don’t have a lot of data to inform this discussion about aripiprazole, a placebo-controlled study of 302 adolescents diagnosed with schizophrenia showed that aripiprazole, 10 mg/d, targeted negative symptoms fairly well, based on changes from baseline in PANSS (Positive and Negative Syndrome Scale) total scores. This was a 6-week multicenter, double-blind, randomized, trial.2
Ultimately, cognition in patients with schizophrenia is the strongest predictor of success in the workplace and in school. We need data on what happens to neurocognitive functioning with aripiprazole—and all the other atypical agents.
DR. KOWATCH: What would be your third-line agent?
DR. FRAZIER: Well, that varies for me. I’m trying to match the medication I use with the individual patient, and at this point I prescribe based on the side-effect profile more than anything else. I also consider if the child has a family member who has suffered from a similar condition and what agents the family member responded to.
Let’s say I have a child who has tried 1 or 2 atypical antipsychotics and has not had a good response. Many times I decide to try yet another atypical, and often I will try quetiapine. But after a patient has not responded to 2 atypicals, I might start thinking about a typical agent or clozapine. I use clozapine quite a bit. I find it is the most efficacious agent available, and the data speak to this as well.3,4 It has been truly remarkable for some children in my practice.
Less than 50% chance of efficacy?
DR. KOWATCH: The TEOSS study found 50% or lower response rates across 8 weeks of antipsychotic treatment. Clinically, what kind of response rates do you see with antipsychotics in children and adolescents?
DR. FRAZIER: I probably see about a 50% response rate in my practice as well. It’s variable, and the earlier the onset of the illness, the harder it is to treat.
DR. KOWATCH: Do you ever combine a typical antipsychotic with an atypical?
DR. FRAZIER: I try not to, but a number of children in the schizophrenia spectrum have enduring positive symptoms after 2 or 3 trials of atypical antipsychotics. Sometimes adding a touch of a typical agent can improve the situation. The typicals I usually try are perphenazine (around 8 to 16 mg/d) or molin done (around 20 to 60 mg/d). Sometimes I use a very low dose of haloperidol (such as 0.5 to 2 mg/d) with an atypical agent, and it can be quite effective.
DR. KOWATCH: That has been our experience as well; sometimes combining typical and atypical agents improves response. Besides medications, what do you consider an optimal treatment plan for a child or adolescent with psychosis?
DR. FRAZIER: These children need a multi-modal approach. Pharmacotherapy is the cornerstone because you want to decrease positive symptoms of psychosis, but often these children require therapeutic school placements or residential programs. If they’re old enough, cognitive-behavioral therapy can help by teaching them skills to manage ongoing psychotic symptoms. Older teens often have comorbid substance abuse and may require substance abuse intervention.
Are antipsychotics overused?
DR. KOWATCH: Do you think antipsychotics are overused in pediatric patients with psychosis?
DR. FRAZIER: In pediatric patients with psychosis? No.
DR. KOWATCH: What about in pediatric patients with behavioral disorders?
DR. FRAZIER: We need more studies to inform our practice and to be mindful of the evidence. Most children with schizophrenia have substantial developmental challenges (Box 2).5 In the autism spectrum, often an atypical antipsychotic is the only agent that can help a patient who is aggressive, self-injurious, or agitated.
In terms of bipolar disorder in children and adolescents, it would be ideal if we had more head-to-head comparator studies to inform our prescriptive practice. For example, we need more studies comparing traditional mood stabilizers such as lithium with the atypical agents.
Of course it would be ideal if we could use monotherapy in children who suffer from bipolar disorder and schizophrenia. But early-onset bipolar disorder—like early-onset schizophrenia—can be very difficult to treat and often requires more than 1 agent.
In a recent study of a pharmacotherapy algorithm for treating pediatric bipolar disorder,3 the children who did the best were on a combination of a mood stabilizer and an atypical antipsychotic. That has been my experience, too. I do my best to manage children on a mood stabilizer alone, but I rarely have been able to do that.
In terms of attention-deficit/hyperactivity disorder (ADHD), it depends on what’s going on with the child. Certain children with an ADHD diagnosis have complicated behavioral issues. First I would wonder if they have a different diagnosis, particularly if it gets to the point that an atypical agent is being considered. But sometimes it becomes a question of treating pronounced aggression. We need more studies to inform what we do. Some studies indicate that stimulants can be quite helpful for the aggressive child with ADHD.7
DR. KOWATCH: I don’t see any child and adolescent psychiatrist in the United States using antipsychotics to treat uncomplicated ADHD. The kids we see [at specialty clinics] have comorbid problems such as conduct disorder, oppositional-defiant disorder, mood instability—whatever you want to call it. And we’re seeing these patients because they haven’t done well on other medications, such as stimulants. Usually the parents are desperate because these children are moody and aggressive. I don’t think anybody wants to treat children with antipsychotics or mood stabilizers, but it’s what keeps these children well.
DR. FRAZIER: Yes, I agree.
Related resources
- Longitudinal assessment and monitoring of clinical status and brain function in adolescents and adults. Boston Center for Intervention Development and Applied Research (CIDAR) study. www.bostoncidar.org.
- Frazier JA, Hodge S, Breeze JL, et al. Diagnostic and sex effects on limbic volumes in early-onset bipolar disorder and schizophrenia. Schizophr Bull. 2008;34(1):37-46.
- Frazier JA, McClellan J, Findling RL, et al. Treatment of Early-Onset Schizophrenia Spectrum disorders (TEOSS): demographic and clinical characteristics. J Am Acad Child Adolesc Psychiatry. 2007;46:979-988.
Drug brand names
- Aripiprazole • Abilify
- Benztropine • Cogentin
- Clozapine • Clozaril
- Haloperidol • Haldol
- Metformin • Glucophage
- Molindone • Moban
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosures
Dr. Kowatch receives grant/research support from the Stanley Foundation, National Institute of Mental Health, National Institute of Child Health and Human Development, and the National Alliance for Research on Schizophrenia and Depression. He is a consultant to AstraZeneca and Forest Pharmaceuticals and a speaker for AstraZeneca.
Dr. Frazier receives grant/research support from Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, Johnson & Johnson, Neuropharm, Otsuka America Pharmaceuticals, and Pfizer Inc.
1. Sikich L, Frazier JA, McClellan J, et al. Double-blind comparison of first- and second-generation antipsychotics in early-onset schizophrenia and schizoaffective disorder: findings from the Treatment of Early-Onset Schizophrenia Spectrum Disorders (TEOSS) study. Am J Psychiatry. 2008;165:1420-1431.
2. Findling RL, Robb A, Nyilas M, et al. A multiple-center, randomized, double-blind, placebo-controlled study of oral aripiprazole for treatment of adolescents with schizophrenia. Am J Psychiatry. 2008;165(11):1432-1441.
3. Findling RL, Frazier JA, Gerbino-Rosen G, et al. Is there a role for clozapine in the treatment of children and adolescents? J Am Acad Child Adolesc Psychiatry. 2007;46(3):423-428.
4. Kim Y, Kim BN, Cho SC, et al. Long-term sustained benefits of clozapine treatment in refractory early onset schizophrenia: a retrospective study in Korean children and adolescents. Hum Psychopharmacol. 2008;23(8):715-722.
5. Sprong M, Becker HE, Schothorst PF, et al. Pathways to psychosis: a comparison of the pervasive developmental disorder subtype multiple complex developmental disorder and the “at risk mental state.” Schizophr Res. 2008;99:38-47.
6. Pavuluri MN, Henry DB, Devineni B, et al. A pharmacotherapy algorithm for stabilization and maintenance of pediatric bipolar disorder. J Am Acad Child Adolesc Psychiatry. 2004;43(7):859-867.
7. Sinzig J, Döpfner M, Lehmkuhl G, et al. Long-acting methylphenidate has an effect on aggressive behavior in children with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. 2007;17(4):421-432.
“A patient I’ve seen for a number of years had been diagnosed in the pervasive developmental disorder spectrum, but she was quite atypical. Her perseverative thinking focused on a fantasy world, and she was so preoccupied that it was very difficult to pull her out of it. Now at age 12, she has a full-blown psychotic disorder, and the fantasy world is enveloping her. She hears people talking to her all day long.”
Jean A. Frazier, MD, who treats this patient and other children with psychotic disorders, was 1 of 4 principal investigators in the Treatment of Early-Onset Schizophrenia Spectrum Disorders (TEOSS) study, a randomized, double-blind, multisite trial funded by the National Institute of Mental Health. The study, published in November 2008,1 compared the efficacy and tolerability of 3 antipsychotics—olanzapine, risperidone, and molindone—in pediatric patients with schizophrenia or schizoaffective disorder (Box 1).
Dr. Frazier discusses the unexpected findings of the TEOSS trial with Current Psychiatry Section Editor Robert A. Kowatch, MD, PhD. Based on the trial findings and her experience, she tells how she makes decisions when prescribing antipsychotics for children and adolescents with schizophrenia and related disorders.
DR. KOWATCH: The TEOSS trial found no significant differences in efficacy between molindone and the atypical antipsychotics (olanzapine and risperidone) included in the study. You’ve prescribed both typical and atypical antipsychotics in research and in your clinical practice. Do you believe there’s any difference between the 2 classes?
DR. FRAZIER: There are some differences. For example, treatment-refractory patients, especially young children, sometimes need more D2 blockade than some atypical antipsychotics provide. I’ve seen more extra pyramidal side effects with the typical antipsychotics than the atypicals, although it’s not uncommon to see some akathisia with aripiprazole or some dystonia and dyskinesia with risperidone.
DR. KOWATCH: What are the benefits and risks of using antipsychotics in young children?
DR. FRAZIER: The benefit is that antipsychotics can decrease children’s suffering and get them more centered in reality so they can enjoy their friends and progress in school. And when that happens, it’s wonderful. What are the risks? With the atypicals my greatest concern is weight gain, and with the typical agents it’s tardive dyskinesia.
DR. KOWATCH: Have you changed the way you prescribe antipsychotics as a result of the TEOSS study?
DR. FRAZIER: Actually, I have. Clinicians have to be very careful about selecting psychotropic agents that can worsen pediatric-onset obesity. Olanzapine is an effective agent for targeting psychosis and mood symptoms, but the weight gain associated with it is a concern. I do not prescribe olanzapine as much as I have in the past, although I keep it in my armamentarium and tend to reserve it for third- or fourth-line therapy.
I have found molindone to be quite effective in children with schizophrenia or schizoaffective disorder, especially in those who have gained a lot of weight on atypical antipsychotics. They usually lose weight on molindone.
DR. KOWATCH: Do you think the TEOSS study had adequate power to demonstrate differences among molindone, olanzapine, and risperidone?
DR. FRAZIER: We enrolled 119 patients—which is large for a study such as this—but we did not reach our target of 168 patients, which might have increased our power to detect differences. Among the children we did enroll, the 3 antipsychotics showed no difference in efficacy, but the meaningful finding of this study to me was the side effect profile of these agents.
DR. KOWATCH: You mean weight gain with olanzapine and extrapyramidal symptoms with molindone?
DR. FRAZIER: Yes.
Managing side effects
DR. KOWATCH: How do you manage antipsychotic side effects?
DR. FRAZIER: For any of the antipsychotics’ side effects, you have to decide whether to continue the agent or switch to another anti psychotic. For example, I’ve had a number of children—many with significant weight problems—whose psychotic symptoms have responded only to risperidone. So we put them back on risperidone, and the decision then becomes what can we do to help with the weight gain while continuing that agent.
For weight gain, I think the best intervention is diet, exercise, and drinking a lot of water, but that can be effective only if you engage the patient’s entire family in the intervention as well. Short of that, a number of pharmacologic interventions have been studied, although not specifically in children.
In an open-label trial our group conducted with 11 children age 10 to 18 years who had gained weight while taking atypical antipsychotics, metformin decreased lipid levels and body mass index but not significantly. I’ve followed these children in my practice, however, and all those who continued taking metformin over a period of months lost weight.
TEOSS study adds to debate about efficacy and tolerability
The 5-year National Institute of Mental Health-funded Treatment of Early-Onset Schizophrenia Spectrum Disorders (TEOSS) trial began with an ambitious goal: to compare the efficacy and safety of 1 typical and 2 atypical antipsychotics in children age 8 to 19 with schizophrenia. The primary hypothesis was that atypical agents would show greater efficacy and tolerability when given for 8 weeks. Instead, the atypical agents showed no greater efficacy, and adverse effects occurred with all 3 antipsychotics. Because the trial was designed for 168 subjects but enrolled 119, it may not have been adequately powered to detect differences among the 3 agents.
Medications: Most of the 116 children who received medications were severely ill with psychotic symptoms when randomly assigned to 1 of the 3 antipsychotics for 8 weeks of double-blind treatment. Administration began at the lowest dose in a set range and usually was increased to midrange within 10 to 14 days. Dosing remained flexible within these ranges:
- molindone, 10 to 140 mg/d (mean endpoint dose 59.9 mg/d)
- olanzapine, 2.5 to 20 mg/d (mean endpoint dose 11.4 mg/d)
- risperidone, 0.5 to 6 mg/d (mean endpoint dose 2.8 mg/d).
Benztropine, ≥1 mg/d, was given to all patients treated with molindone, 14% of those treated with olanzapine, and 34% of those treated with risperidone to prevent or manage akathisia.
Efficacy: Two criteria defined treatment response: a Clinical Global Impression improvement score of 1 or 2 and a ≥20% reduction in baseline Positive and Negative Syndrome Scale (PANSS) score. Tolerability outcomes included neurologic side effects, weight changes, laboratory analyses, vital signs, ECG, serious adverse events, and treatment discontinuation. Extrapyramidal symptoms were monitored with involuntary movement and akathisia scales.
Observed PANSS total score by week of treatment
Mean Positive and Negative Symptom Scale (PANSS) total scores of observed cases during each week of the TEOSS trial. Minimum possible PANSS score is 30; scores >60 typically are viewed as problematic.
Among the 70 patients who completed treatment (25 of 40 with molindone, 17 of 35 olanzapine, and 28 of 41 with risperidone), more than one-half failed to achieve an adequate response. Response rates were 50% with molindone, 34% with olanzapine, and 46% with risperidone. The atypical antipsychotics did not show greater efficacy than molindone, and mean reductions in psychotic symptoms were modest (20% to 34% on the PANSS). Mean medication doses were midrange and considered moderate.
Tolerability: Sedation, irritability, and anxiety were frequent adverse events. Patients receiving molindone reported significantly higher rates of akathisia (P < .0008). Those receiving olanzapine reported significantly higher rates of weight gain (P < .0001) and were the only group with increased lipid and insulin serum levels and liver function tests. Patients in the risperidone group reported significantly higher rates of constipation (P < .021) and were the only group that experienced elevated serum prolactin.
Source: Sikich L, Frazier JA, McClellan J, et al. Double-blind comparison of first- and second-generation antipsychotics in early-onset schizophrenia and schizoaffective disorder: findings from the Treatment of Early-Onset Schizophrenia Spectrum disorders (TEOSS) study. Am J Psychiatry. 2008;165:1420-1431
Choosing antipsychotics
DR. KOWATCH: Let’s say you’re seeing psychosis in a 12-year-old whom you think is schizophrenic, and he or she has not yet received an antipsychotic. What are your top 3 treatment choices?
DR. FRAZIER: The first agent I usually select is risperidone. We have the most data on the use of this atypical antipsychotic in children and adolescents, and most psychotic children I see do better with a bit more D2 blockade than some of the other atypicals provide. That said, I remain concerned about risperidone’s side effects—such as weight gain and increased serum prolactin—so my usual second-line agent is aripiprazole.
I became interested in the complicated overlap between pervasive developmental disorders spectrum and psychotic disorders early in my training. More is known about prodromal symptoms in adolescents and adults than in children.
A group in the Netherlands5 compared 32 adolescents with severe early deficits in affect regulation, anxiety, disturbed social relationships, and thought disorder (characterized as “multiple complex developmental disorder” [MCDD]) with 80 adolescents with prodromal psychotic symptoms who met criteria for “at-risk mental state” (ARMS). Three-quarters of the children with MCDD (78%) were found to meet criteria for ARMS, and the 2 groups showed similar schizotypal traits, disorganization, and prodromal symptoms.
Signs of progression to psychosis and schizophrenia in children typically include:
- change in personality
- decrease in functioning or decline in ability to perform at school
- unusual thoughts or behaviors
- crippling anxiety
- supersensitivity to stress.
With experience, the clinician can more clearly differentiate the prodromal signs of psychosis from normal childhood behaviors. Children who are psychotic often don’t make good eye contact. When you try to engage them in discussion about hearing voices, they’re inattentive and internally preoccupied.
Normal vs psychotic children. You want a child in the latency age to have a rich fantasy life. If they do not, that raises concerns. Both normal and psychotic children sometimes say an imaginary friend told them something. Normal children eventually will admit this friend is imaginary. When children are psychotic, especially at an early age, you can’t pull them out of thinking about the imaginary friend, and they can’t distinguish fantasy from reality. Psychotic children also hear imaginary friends talking to them much more often.
Normal children usually are not afraid of their imaginary friends, whereas psychotic children—particularly adolescents—often are afraid of the voices they hear. However, if a psychotic child has heard voices from a young age, the voices aren’t always ego-dystonic. The girl I mentioned at the beginning of this article likes having the voices around. In fact, she gets uncomfortable when the voices are quiet.—Jean A. Frazier, MD
DR. KOWATCH: Why do you like aripiprazole for this patient population?
DR. FRAZIER: Aripiprazole doesn’t tend to be associated with as much weight gain as olanzapine or risperidone, although I’ve had children—especially in the autism spectrum—who have gained quite a bit of weight on aripiprazole. Clinically, I’ve noticed that aripiprazole seems to brighten up children’s affect. It also seems to help many children in my practice with attentional symptoms, although that’s anecdotal.
Although we don’t have a lot of data to inform this discussion about aripiprazole, a placebo-controlled study of 302 adolescents diagnosed with schizophrenia showed that aripiprazole, 10 mg/d, targeted negative symptoms fairly well, based on changes from baseline in PANSS (Positive and Negative Syndrome Scale) total scores. This was a 6-week multicenter, double-blind, randomized, trial.2
Ultimately, cognition in patients with schizophrenia is the strongest predictor of success in the workplace and in school. We need data on what happens to neurocognitive functioning with aripiprazole—and all the other atypical agents.
DR. KOWATCH: What would be your third-line agent?
DR. FRAZIER: Well, that varies for me. I’m trying to match the medication I use with the individual patient, and at this point I prescribe based on the side-effect profile more than anything else. I also consider if the child has a family member who has suffered from a similar condition and what agents the family member responded to.
Let’s say I have a child who has tried 1 or 2 atypical antipsychotics and has not had a good response. Many times I decide to try yet another atypical, and often I will try quetiapine. But after a patient has not responded to 2 atypicals, I might start thinking about a typical agent or clozapine. I use clozapine quite a bit. I find it is the most efficacious agent available, and the data speak to this as well.3,4 It has been truly remarkable for some children in my practice.
Less than 50% chance of efficacy?
DR. KOWATCH: The TEOSS study found 50% or lower response rates across 8 weeks of antipsychotic treatment. Clinically, what kind of response rates do you see with antipsychotics in children and adolescents?
DR. FRAZIER: I probably see about a 50% response rate in my practice as well. It’s variable, and the earlier the onset of the illness, the harder it is to treat.
DR. KOWATCH: Do you ever combine a typical antipsychotic with an atypical?
DR. FRAZIER: I try not to, but a number of children in the schizophrenia spectrum have enduring positive symptoms after 2 or 3 trials of atypical antipsychotics. Sometimes adding a touch of a typical agent can improve the situation. The typicals I usually try are perphenazine (around 8 to 16 mg/d) or molin done (around 20 to 60 mg/d). Sometimes I use a very low dose of haloperidol (such as 0.5 to 2 mg/d) with an atypical agent, and it can be quite effective.
DR. KOWATCH: That has been our experience as well; sometimes combining typical and atypical agents improves response. Besides medications, what do you consider an optimal treatment plan for a child or adolescent with psychosis?
DR. FRAZIER: These children need a multi-modal approach. Pharmacotherapy is the cornerstone because you want to decrease positive symptoms of psychosis, but often these children require therapeutic school placements or residential programs. If they’re old enough, cognitive-behavioral therapy can help by teaching them skills to manage ongoing psychotic symptoms. Older teens often have comorbid substance abuse and may require substance abuse intervention.
Are antipsychotics overused?
DR. KOWATCH: Do you think antipsychotics are overused in pediatric patients with psychosis?
DR. FRAZIER: In pediatric patients with psychosis? No.
DR. KOWATCH: What about in pediatric patients with behavioral disorders?
DR. FRAZIER: We need more studies to inform our practice and to be mindful of the evidence. Most children with schizophrenia have substantial developmental challenges (Box 2).5 In the autism spectrum, often an atypical antipsychotic is the only agent that can help a patient who is aggressive, self-injurious, or agitated.
In terms of bipolar disorder in children and adolescents, it would be ideal if we had more head-to-head comparator studies to inform our prescriptive practice. For example, we need more studies comparing traditional mood stabilizers such as lithium with the atypical agents.
Of course it would be ideal if we could use monotherapy in children who suffer from bipolar disorder and schizophrenia. But early-onset bipolar disorder—like early-onset schizophrenia—can be very difficult to treat and often requires more than 1 agent.
In a recent study of a pharmacotherapy algorithm for treating pediatric bipolar disorder,3 the children who did the best were on a combination of a mood stabilizer and an atypical antipsychotic. That has been my experience, too. I do my best to manage children on a mood stabilizer alone, but I rarely have been able to do that.
In terms of attention-deficit/hyperactivity disorder (ADHD), it depends on what’s going on with the child. Certain children with an ADHD diagnosis have complicated behavioral issues. First I would wonder if they have a different diagnosis, particularly if it gets to the point that an atypical agent is being considered. But sometimes it becomes a question of treating pronounced aggression. We need more studies to inform what we do. Some studies indicate that stimulants can be quite helpful for the aggressive child with ADHD.7
DR. KOWATCH: I don’t see any child and adolescent psychiatrist in the United States using antipsychotics to treat uncomplicated ADHD. The kids we see [at specialty clinics] have comorbid problems such as conduct disorder, oppositional-defiant disorder, mood instability—whatever you want to call it. And we’re seeing these patients because they haven’t done well on other medications, such as stimulants. Usually the parents are desperate because these children are moody and aggressive. I don’t think anybody wants to treat children with antipsychotics or mood stabilizers, but it’s what keeps these children well.
DR. FRAZIER: Yes, I agree.
Related resources
- Longitudinal assessment and monitoring of clinical status and brain function in adolescents and adults. Boston Center for Intervention Development and Applied Research (CIDAR) study. www.bostoncidar.org.
- Frazier JA, Hodge S, Breeze JL, et al. Diagnostic and sex effects on limbic volumes in early-onset bipolar disorder and schizophrenia. Schizophr Bull. 2008;34(1):37-46.
- Frazier JA, McClellan J, Findling RL, et al. Treatment of Early-Onset Schizophrenia Spectrum disorders (TEOSS): demographic and clinical characteristics. J Am Acad Child Adolesc Psychiatry. 2007;46:979-988.
Drug brand names
- Aripiprazole • Abilify
- Benztropine • Cogentin
- Clozapine • Clozaril
- Haloperidol • Haldol
- Metformin • Glucophage
- Molindone • Moban
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosures
Dr. Kowatch receives grant/research support from the Stanley Foundation, National Institute of Mental Health, National Institute of Child Health and Human Development, and the National Alliance for Research on Schizophrenia and Depression. He is a consultant to AstraZeneca and Forest Pharmaceuticals and a speaker for AstraZeneca.
Dr. Frazier receives grant/research support from Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, Johnson & Johnson, Neuropharm, Otsuka America Pharmaceuticals, and Pfizer Inc.
“A patient I’ve seen for a number of years had been diagnosed in the pervasive developmental disorder spectrum, but she was quite atypical. Her perseverative thinking focused on a fantasy world, and she was so preoccupied that it was very difficult to pull her out of it. Now at age 12, she has a full-blown psychotic disorder, and the fantasy world is enveloping her. She hears people talking to her all day long.”
Jean A. Frazier, MD, who treats this patient and other children with psychotic disorders, was 1 of 4 principal investigators in the Treatment of Early-Onset Schizophrenia Spectrum Disorders (TEOSS) study, a randomized, double-blind, multisite trial funded by the National Institute of Mental Health. The study, published in November 2008,1 compared the efficacy and tolerability of 3 antipsychotics—olanzapine, risperidone, and molindone—in pediatric patients with schizophrenia or schizoaffective disorder (Box 1).
Dr. Frazier discusses the unexpected findings of the TEOSS trial with Current Psychiatry Section Editor Robert A. Kowatch, MD, PhD. Based on the trial findings and her experience, she tells how she makes decisions when prescribing antipsychotics for children and adolescents with schizophrenia and related disorders.
DR. KOWATCH: The TEOSS trial found no significant differences in efficacy between molindone and the atypical antipsychotics (olanzapine and risperidone) included in the study. You’ve prescribed both typical and atypical antipsychotics in research and in your clinical practice. Do you believe there’s any difference between the 2 classes?
DR. FRAZIER: There are some differences. For example, treatment-refractory patients, especially young children, sometimes need more D2 blockade than some atypical antipsychotics provide. I’ve seen more extra pyramidal side effects with the typical antipsychotics than the atypicals, although it’s not uncommon to see some akathisia with aripiprazole or some dystonia and dyskinesia with risperidone.
DR. KOWATCH: What are the benefits and risks of using antipsychotics in young children?
DR. FRAZIER: The benefit is that antipsychotics can decrease children’s suffering and get them more centered in reality so they can enjoy their friends and progress in school. And when that happens, it’s wonderful. What are the risks? With the atypicals my greatest concern is weight gain, and with the typical agents it’s tardive dyskinesia.
DR. KOWATCH: Have you changed the way you prescribe antipsychotics as a result of the TEOSS study?
DR. FRAZIER: Actually, I have. Clinicians have to be very careful about selecting psychotropic agents that can worsen pediatric-onset obesity. Olanzapine is an effective agent for targeting psychosis and mood symptoms, but the weight gain associated with it is a concern. I do not prescribe olanzapine as much as I have in the past, although I keep it in my armamentarium and tend to reserve it for third- or fourth-line therapy.
I have found molindone to be quite effective in children with schizophrenia or schizoaffective disorder, especially in those who have gained a lot of weight on atypical antipsychotics. They usually lose weight on molindone.
DR. KOWATCH: Do you think the TEOSS study had adequate power to demonstrate differences among molindone, olanzapine, and risperidone?
DR. FRAZIER: We enrolled 119 patients—which is large for a study such as this—but we did not reach our target of 168 patients, which might have increased our power to detect differences. Among the children we did enroll, the 3 antipsychotics showed no difference in efficacy, but the meaningful finding of this study to me was the side effect profile of these agents.
DR. KOWATCH: You mean weight gain with olanzapine and extrapyramidal symptoms with molindone?
DR. FRAZIER: Yes.
Managing side effects
DR. KOWATCH: How do you manage antipsychotic side effects?
DR. FRAZIER: For any of the antipsychotics’ side effects, you have to decide whether to continue the agent or switch to another anti psychotic. For example, I’ve had a number of children—many with significant weight problems—whose psychotic symptoms have responded only to risperidone. So we put them back on risperidone, and the decision then becomes what can we do to help with the weight gain while continuing that agent.
For weight gain, I think the best intervention is diet, exercise, and drinking a lot of water, but that can be effective only if you engage the patient’s entire family in the intervention as well. Short of that, a number of pharmacologic interventions have been studied, although not specifically in children.
In an open-label trial our group conducted with 11 children age 10 to 18 years who had gained weight while taking atypical antipsychotics, metformin decreased lipid levels and body mass index but not significantly. I’ve followed these children in my practice, however, and all those who continued taking metformin over a period of months lost weight.
TEOSS study adds to debate about efficacy and tolerability
The 5-year National Institute of Mental Health-funded Treatment of Early-Onset Schizophrenia Spectrum Disorders (TEOSS) trial began with an ambitious goal: to compare the efficacy and safety of 1 typical and 2 atypical antipsychotics in children age 8 to 19 with schizophrenia. The primary hypothesis was that atypical agents would show greater efficacy and tolerability when given for 8 weeks. Instead, the atypical agents showed no greater efficacy, and adverse effects occurred with all 3 antipsychotics. Because the trial was designed for 168 subjects but enrolled 119, it may not have been adequately powered to detect differences among the 3 agents.
Medications: Most of the 116 children who received medications were severely ill with psychotic symptoms when randomly assigned to 1 of the 3 antipsychotics for 8 weeks of double-blind treatment. Administration began at the lowest dose in a set range and usually was increased to midrange within 10 to 14 days. Dosing remained flexible within these ranges:
- molindone, 10 to 140 mg/d (mean endpoint dose 59.9 mg/d)
- olanzapine, 2.5 to 20 mg/d (mean endpoint dose 11.4 mg/d)
- risperidone, 0.5 to 6 mg/d (mean endpoint dose 2.8 mg/d).
Benztropine, ≥1 mg/d, was given to all patients treated with molindone, 14% of those treated with olanzapine, and 34% of those treated with risperidone to prevent or manage akathisia.
Efficacy: Two criteria defined treatment response: a Clinical Global Impression improvement score of 1 or 2 and a ≥20% reduction in baseline Positive and Negative Syndrome Scale (PANSS) score. Tolerability outcomes included neurologic side effects, weight changes, laboratory analyses, vital signs, ECG, serious adverse events, and treatment discontinuation. Extrapyramidal symptoms were monitored with involuntary movement and akathisia scales.
Observed PANSS total score by week of treatment
Mean Positive and Negative Symptom Scale (PANSS) total scores of observed cases during each week of the TEOSS trial. Minimum possible PANSS score is 30; scores >60 typically are viewed as problematic.
Among the 70 patients who completed treatment (25 of 40 with molindone, 17 of 35 olanzapine, and 28 of 41 with risperidone), more than one-half failed to achieve an adequate response. Response rates were 50% with molindone, 34% with olanzapine, and 46% with risperidone. The atypical antipsychotics did not show greater efficacy than molindone, and mean reductions in psychotic symptoms were modest (20% to 34% on the PANSS). Mean medication doses were midrange and considered moderate.
Tolerability: Sedation, irritability, and anxiety were frequent adverse events. Patients receiving molindone reported significantly higher rates of akathisia (P < .0008). Those receiving olanzapine reported significantly higher rates of weight gain (P < .0001) and were the only group with increased lipid and insulin serum levels and liver function tests. Patients in the risperidone group reported significantly higher rates of constipation (P < .021) and were the only group that experienced elevated serum prolactin.
Source: Sikich L, Frazier JA, McClellan J, et al. Double-blind comparison of first- and second-generation antipsychotics in early-onset schizophrenia and schizoaffective disorder: findings from the Treatment of Early-Onset Schizophrenia Spectrum disorders (TEOSS) study. Am J Psychiatry. 2008;165:1420-1431
Choosing antipsychotics
DR. KOWATCH: Let’s say you’re seeing psychosis in a 12-year-old whom you think is schizophrenic, and he or she has not yet received an antipsychotic. What are your top 3 treatment choices?
DR. FRAZIER: The first agent I usually select is risperidone. We have the most data on the use of this atypical antipsychotic in children and adolescents, and most psychotic children I see do better with a bit more D2 blockade than some of the other atypicals provide. That said, I remain concerned about risperidone’s side effects—such as weight gain and increased serum prolactin—so my usual second-line agent is aripiprazole.
I became interested in the complicated overlap between pervasive developmental disorders spectrum and psychotic disorders early in my training. More is known about prodromal symptoms in adolescents and adults than in children.
A group in the Netherlands5 compared 32 adolescents with severe early deficits in affect regulation, anxiety, disturbed social relationships, and thought disorder (characterized as “multiple complex developmental disorder” [MCDD]) with 80 adolescents with prodromal psychotic symptoms who met criteria for “at-risk mental state” (ARMS). Three-quarters of the children with MCDD (78%) were found to meet criteria for ARMS, and the 2 groups showed similar schizotypal traits, disorganization, and prodromal symptoms.
Signs of progression to psychosis and schizophrenia in children typically include:
- change in personality
- decrease in functioning or decline in ability to perform at school
- unusual thoughts or behaviors
- crippling anxiety
- supersensitivity to stress.
With experience, the clinician can more clearly differentiate the prodromal signs of psychosis from normal childhood behaviors. Children who are psychotic often don’t make good eye contact. When you try to engage them in discussion about hearing voices, they’re inattentive and internally preoccupied.
Normal vs psychotic children. You want a child in the latency age to have a rich fantasy life. If they do not, that raises concerns. Both normal and psychotic children sometimes say an imaginary friend told them something. Normal children eventually will admit this friend is imaginary. When children are psychotic, especially at an early age, you can’t pull them out of thinking about the imaginary friend, and they can’t distinguish fantasy from reality. Psychotic children also hear imaginary friends talking to them much more often.
Normal children usually are not afraid of their imaginary friends, whereas psychotic children—particularly adolescents—often are afraid of the voices they hear. However, if a psychotic child has heard voices from a young age, the voices aren’t always ego-dystonic. The girl I mentioned at the beginning of this article likes having the voices around. In fact, she gets uncomfortable when the voices are quiet.—Jean A. Frazier, MD
DR. KOWATCH: Why do you like aripiprazole for this patient population?
DR. FRAZIER: Aripiprazole doesn’t tend to be associated with as much weight gain as olanzapine or risperidone, although I’ve had children—especially in the autism spectrum—who have gained quite a bit of weight on aripiprazole. Clinically, I’ve noticed that aripiprazole seems to brighten up children’s affect. It also seems to help many children in my practice with attentional symptoms, although that’s anecdotal.
Although we don’t have a lot of data to inform this discussion about aripiprazole, a placebo-controlled study of 302 adolescents diagnosed with schizophrenia showed that aripiprazole, 10 mg/d, targeted negative symptoms fairly well, based on changes from baseline in PANSS (Positive and Negative Syndrome Scale) total scores. This was a 6-week multicenter, double-blind, randomized, trial.2
Ultimately, cognition in patients with schizophrenia is the strongest predictor of success in the workplace and in school. We need data on what happens to neurocognitive functioning with aripiprazole—and all the other atypical agents.
DR. KOWATCH: What would be your third-line agent?
DR. FRAZIER: Well, that varies for me. I’m trying to match the medication I use with the individual patient, and at this point I prescribe based on the side-effect profile more than anything else. I also consider if the child has a family member who has suffered from a similar condition and what agents the family member responded to.
Let’s say I have a child who has tried 1 or 2 atypical antipsychotics and has not had a good response. Many times I decide to try yet another atypical, and often I will try quetiapine. But after a patient has not responded to 2 atypicals, I might start thinking about a typical agent or clozapine. I use clozapine quite a bit. I find it is the most efficacious agent available, and the data speak to this as well.3,4 It has been truly remarkable for some children in my practice.
Less than 50% chance of efficacy?
DR. KOWATCH: The TEOSS study found 50% or lower response rates across 8 weeks of antipsychotic treatment. Clinically, what kind of response rates do you see with antipsychotics in children and adolescents?
DR. FRAZIER: I probably see about a 50% response rate in my practice as well. It’s variable, and the earlier the onset of the illness, the harder it is to treat.
DR. KOWATCH: Do you ever combine a typical antipsychotic with an atypical?
DR. FRAZIER: I try not to, but a number of children in the schizophrenia spectrum have enduring positive symptoms after 2 or 3 trials of atypical antipsychotics. Sometimes adding a touch of a typical agent can improve the situation. The typicals I usually try are perphenazine (around 8 to 16 mg/d) or molin done (around 20 to 60 mg/d). Sometimes I use a very low dose of haloperidol (such as 0.5 to 2 mg/d) with an atypical agent, and it can be quite effective.
DR. KOWATCH: That has been our experience as well; sometimes combining typical and atypical agents improves response. Besides medications, what do you consider an optimal treatment plan for a child or adolescent with psychosis?
DR. FRAZIER: These children need a multi-modal approach. Pharmacotherapy is the cornerstone because you want to decrease positive symptoms of psychosis, but often these children require therapeutic school placements or residential programs. If they’re old enough, cognitive-behavioral therapy can help by teaching them skills to manage ongoing psychotic symptoms. Older teens often have comorbid substance abuse and may require substance abuse intervention.
Are antipsychotics overused?
DR. KOWATCH: Do you think antipsychotics are overused in pediatric patients with psychosis?
DR. FRAZIER: In pediatric patients with psychosis? No.
DR. KOWATCH: What about in pediatric patients with behavioral disorders?
DR. FRAZIER: We need more studies to inform our practice and to be mindful of the evidence. Most children with schizophrenia have substantial developmental challenges (Box 2).5 In the autism spectrum, often an atypical antipsychotic is the only agent that can help a patient who is aggressive, self-injurious, or agitated.
In terms of bipolar disorder in children and adolescents, it would be ideal if we had more head-to-head comparator studies to inform our prescriptive practice. For example, we need more studies comparing traditional mood stabilizers such as lithium with the atypical agents.
Of course it would be ideal if we could use monotherapy in children who suffer from bipolar disorder and schizophrenia. But early-onset bipolar disorder—like early-onset schizophrenia—can be very difficult to treat and often requires more than 1 agent.
In a recent study of a pharmacotherapy algorithm for treating pediatric bipolar disorder,3 the children who did the best were on a combination of a mood stabilizer and an atypical antipsychotic. That has been my experience, too. I do my best to manage children on a mood stabilizer alone, but I rarely have been able to do that.
In terms of attention-deficit/hyperactivity disorder (ADHD), it depends on what’s going on with the child. Certain children with an ADHD diagnosis have complicated behavioral issues. First I would wonder if they have a different diagnosis, particularly if it gets to the point that an atypical agent is being considered. But sometimes it becomes a question of treating pronounced aggression. We need more studies to inform what we do. Some studies indicate that stimulants can be quite helpful for the aggressive child with ADHD.7
DR. KOWATCH: I don’t see any child and adolescent psychiatrist in the United States using antipsychotics to treat uncomplicated ADHD. The kids we see [at specialty clinics] have comorbid problems such as conduct disorder, oppositional-defiant disorder, mood instability—whatever you want to call it. And we’re seeing these patients because they haven’t done well on other medications, such as stimulants. Usually the parents are desperate because these children are moody and aggressive. I don’t think anybody wants to treat children with antipsychotics or mood stabilizers, but it’s what keeps these children well.
DR. FRAZIER: Yes, I agree.
Related resources
- Longitudinal assessment and monitoring of clinical status and brain function in adolescents and adults. Boston Center for Intervention Development and Applied Research (CIDAR) study. www.bostoncidar.org.
- Frazier JA, Hodge S, Breeze JL, et al. Diagnostic and sex effects on limbic volumes in early-onset bipolar disorder and schizophrenia. Schizophr Bull. 2008;34(1):37-46.
- Frazier JA, McClellan J, Findling RL, et al. Treatment of Early-Onset Schizophrenia Spectrum disorders (TEOSS): demographic and clinical characteristics. J Am Acad Child Adolesc Psychiatry. 2007;46:979-988.
Drug brand names
- Aripiprazole • Abilify
- Benztropine • Cogentin
- Clozapine • Clozaril
- Haloperidol • Haldol
- Metformin • Glucophage
- Molindone • Moban
- Olanzapine • Zyprexa
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosures
Dr. Kowatch receives grant/research support from the Stanley Foundation, National Institute of Mental Health, National Institute of Child Health and Human Development, and the National Alliance for Research on Schizophrenia and Depression. He is a consultant to AstraZeneca and Forest Pharmaceuticals and a speaker for AstraZeneca.
Dr. Frazier receives grant/research support from Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, Johnson & Johnson, Neuropharm, Otsuka America Pharmaceuticals, and Pfizer Inc.
1. Sikich L, Frazier JA, McClellan J, et al. Double-blind comparison of first- and second-generation antipsychotics in early-onset schizophrenia and schizoaffective disorder: findings from the Treatment of Early-Onset Schizophrenia Spectrum Disorders (TEOSS) study. Am J Psychiatry. 2008;165:1420-1431.
2. Findling RL, Robb A, Nyilas M, et al. A multiple-center, randomized, double-blind, placebo-controlled study of oral aripiprazole for treatment of adolescents with schizophrenia. Am J Psychiatry. 2008;165(11):1432-1441.
3. Findling RL, Frazier JA, Gerbino-Rosen G, et al. Is there a role for clozapine in the treatment of children and adolescents? J Am Acad Child Adolesc Psychiatry. 2007;46(3):423-428.
4. Kim Y, Kim BN, Cho SC, et al. Long-term sustained benefits of clozapine treatment in refractory early onset schizophrenia: a retrospective study in Korean children and adolescents. Hum Psychopharmacol. 2008;23(8):715-722.
5. Sprong M, Becker HE, Schothorst PF, et al. Pathways to psychosis: a comparison of the pervasive developmental disorder subtype multiple complex developmental disorder and the “at risk mental state.” Schizophr Res. 2008;99:38-47.
6. Pavuluri MN, Henry DB, Devineni B, et al. A pharmacotherapy algorithm for stabilization and maintenance of pediatric bipolar disorder. J Am Acad Child Adolesc Psychiatry. 2004;43(7):859-867.
7. Sinzig J, Döpfner M, Lehmkuhl G, et al. Long-acting methylphenidate has an effect on aggressive behavior in children with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. 2007;17(4):421-432.
1. Sikich L, Frazier JA, McClellan J, et al. Double-blind comparison of first- and second-generation antipsychotics in early-onset schizophrenia and schizoaffective disorder: findings from the Treatment of Early-Onset Schizophrenia Spectrum Disorders (TEOSS) study. Am J Psychiatry. 2008;165:1420-1431.
2. Findling RL, Robb A, Nyilas M, et al. A multiple-center, randomized, double-blind, placebo-controlled study of oral aripiprazole for treatment of adolescents with schizophrenia. Am J Psychiatry. 2008;165(11):1432-1441.
3. Findling RL, Frazier JA, Gerbino-Rosen G, et al. Is there a role for clozapine in the treatment of children and adolescents? J Am Acad Child Adolesc Psychiatry. 2007;46(3):423-428.
4. Kim Y, Kim BN, Cho SC, et al. Long-term sustained benefits of clozapine treatment in refractory early onset schizophrenia: a retrospective study in Korean children and adolescents. Hum Psychopharmacol. 2008;23(8):715-722.
5. Sprong M, Becker HE, Schothorst PF, et al. Pathways to psychosis: a comparison of the pervasive developmental disorder subtype multiple complex developmental disorder and the “at risk mental state.” Schizophr Res. 2008;99:38-47.
6. Pavuluri MN, Henry DB, Devineni B, et al. A pharmacotherapy algorithm for stabilization and maintenance of pediatric bipolar disorder. J Am Acad Child Adolesc Psychiatry. 2004;43(7):859-867.
7. Sinzig J, Döpfner M, Lehmkuhl G, et al. Long-acting methylphenidate has an effect on aggressive behavior in children with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. 2007;17(4):421-432.
Soft bipolarity: How to recognize and treat bipolar II disorder
WEB AUDIO
At least 25% and possibly up to 50% of patients with recurrent major depressive disorder (MDD) have features of mild hypomania (the “soft end” of the bipolar spectrum1) and might be better conceptualized as suffering from a broadly defined bipolar (BP) II disorder.2 The challenge is to differentiate MDD from BP II so that we make treatment decisions—such as antidepressants vs mood stabilizers—shown to improve the long-term course of patients’ depressive symptoms.
Diagnosis of BP II often is not straightforward and unfortunately may be delayed several years after patients first present for evaluation. To help clinicians make correct diagnostic decisions, this article:
- describes diagnostic criteria outside of DSM-IV-TR that can assist in identifying BP II disorder
- identifies subgroups of recurrently depressed patients whose primary disorder is more likely to be bipolar than unipolar
- provides a screening tool validated for identifying “soft” bipolarity
- offers a pragmatic clinical perspective on the treatment of BP II disorder.
How common is BP II disorder?
As with all psychiatric diagnoses, the prevalence of BP II disorder is a function of the diagnostic criteria used to define it.3 BP II—1 or more depressive episodes with at least 1 hypomanic episode—affects 1% to 2% of the population, based on DSM-IV-TR criteria for hypomania (Box 1). However, the DSM definition of BP II might be too restrictive. Regarding the diagnosis of hypomania, in particular:
- the symptom of “overactivity” should be given as much weight as the stem criteria of “euphoria” and “irritability”
- the 4-day threshold for a hypomanic episode probably is too long.
These deficiencies in DSM-IV-TR exclude many patients who experience brief but clinically significant periods of hypomania. A more realistic definition of hypomania within BP II disorder would:
- include overactivity as an additional stem criterion
- specify a threshold duration for hypomanic symptoms of at least 1 day rather than 4 days
- stipulate the experience of negative consequences of the episode as necessary for the diagnosis (Table 1).
- A distinct period of persistently elevated, expansive, or irritable mood, lasting at least 4 days, that is clearly different from the usual nondepressed mood
- During the period of mood disturbance, 3 or more of the following symptoms have persisted (4 if the mood is only irritable) and have been present to a significant degree:
- The episode is associated with an unequivocal change in functioning that is uncharacteristic of the person when not symptomatic
- The disturbance in mood and the change in functioning are observable by others
- The episode is not severe enough to cause marked impairment in social or occupational functioning, or to necessitate hospitalization, and there are no psychotic features
- The symptoms are not due to the direct physiological effects of a substance (a drug of abuse, a medication, or other treatment) or a general medical condition (such as hyperthyroidism)
Note: Hypomanic-like episodes that are clearly caused by somatic antidepressant treatment (such as medication, electroconvulsive therapy, or light therapy) should not count toward a diagnosis of bipolar II disorder
Proposed hypomania criteria in broadly defined BP II
| A. Euphoria, irritability, or overactivity |
| B. At least 3 of the 7 DSM-IV-TR symptoms of hypomania |
| C. Hypomanic symptoms of at least 1 day’s duration |
| D. Experience of negative consequences of hypomanic periods |
| BP II: bipolar II disorder |
| Source: Reference 4 |
Depression’s subgroups
Recurrent MDD is an extremely heterogeneous diagnosis. It includes many clinical presentations of depressive illness that may share little in terms of etiology, pathophysiology, and response to treatment. When carefully assessed, 2 subgroups of recurrently depressed patients in particular appear to be more likely to have a primary bipolar disorder:
- young patients with early-onset severe depression
- older adults with difficult-to-treat or treatment-resistant depression.
6 Other reports have indicated that at least 40% of young adults with recurrent MDD satisfy broad diagnostic criteria for bipolar disorder.7
Higher rates of unrecognized bipolar disorder have been identified in patients with treatment-resistant depression. In a prospective study of 61 consecutive MDD patients referred to a mood disorders clinic, 59% satisfied DSM-IV-TR criteria for bipolar disorder.8
Consequences. Undiagnosed BP II disorder is an important clinical issue because bipolar features in patients presumed to have recurrent MDD can adversely affect long-term outcomes. Many of these patients will be treated exclusively with antidepressants despite evidence that antidepressant monotherapy for bipolar depression—at least for some patients—can cause more frequent mood episodes, mood destabilization, and possibly an increase in suicidal behaviors.9,10
This point is highlighted in the United Kingdom’s National Institute of Health and Clinical Excellence (NICE) guidelines for bipolar disorder, which recommended that antidepressants be prescribed for bipolar depression only in combination with mood stabilizer treatment and withdrawn within 2 to 3 months of recovery.11
The American Psychiatric Association’s (APA) practice guideline for treating bipolar disorder, published in 2002, advises against antidepressants as monotherapy for bipolar depression, recommending instead that lithium or lamotrigine be used first-line. A revised APA guideline is scheduled for publication this year.12
Why is BP II underdiagnosed?
Notwithstanding the limitations of DSMIV-TR criteria for hypomania, additional factors contribute to under-recognition of BP II in clinical practice.
Dominant depressive symptoms. The clinical course of bipolar disorders is dominated by low-grade depressive symptoms and recurrent depressive episodes rather than mania or hypomania. This is especially true for BP II disorder, where the ratio of time spent with depressive symptoms relative to time with hypomanic symptoms is approximately 30:1.13 The fact that BP II patients in general seek help only during depressive periods means that consultations inevitably focus on the diagnosis and treatment of depression, rather than long-term prophylaxis of both depressive and hypomanic episodes.
Indistinguishable symptoms? Bipolar depressions are generally thought to be clinically indistinguishable from unipolar depressions, but this might not be clear-cut. Although differentiating symptoms of unipolar and bipolar depression can be difficult in clinical practice, evidence suggests that certain symptoms may be more common in bipolar than unipolar depression:
- atypical depressive features such as mood reactivity, overeating, oversleeping, and excessive fatigue14
- depressive psychotic symptoms, especially in younger patients15
- “mixed” depressive episodes (depressive episodes with concurrent manic symptoms).16
How to recognize BP II disorder
To detect and diagnose BP II disorder, systematically assess hypomanic features in all patients who present with recurrent MDD, especially those who have an early age of onset or don’t seem to be responding well to antidepressant monotherapy. As noted, a corroborative history from a close relative is essential. Within a full clinical assessment, use the features listed in Table 2 to help differentiate bipolar depression from unipolar depression.
Screening instruments for hypomania are no substitute for a careful psychiatric history but can be very helpful in everyday clinical practice. The most well-known is the Mood Disorder Questionnaire (MDQ);17 other options include the Hypomania Checklist (HCL-32)18 and the Bipolar Spectrum Diagnostic Scale (BSDS).19 In general, the MDQ performs better at detecting BP I in psychiatric practice settings, whereas the HCL-32 and BSDS may be more useful in primary care and general population settings.20
The BSDS has a particular focus on the softer end of the bipolar spectrum,19 and in my experience patients like its narrative structure. It can help prompt discussions about previous hypomania symptoms and mood instability. In this sense, the BSDS is a useful adjunct to the routine clinical assessment of patients with recurrent depressive disorders. Click here to view the BSDS.
Table 2
Possible indicators of bipolarity in apparently unipolar depression
| Atypical features |
| First-degree relative with bipolar disorder |
| Antidepressant-induced mania or hypomania |
| Multiple family members with major depression |
| Early onset of depression (age |
| Lack of response to ≥3 antidepressant trials |
| Psychotic features (before age 35) |
| Mixed depressive episodes |
| Brief but frequent episodes of depression |
| Complex comorbidity (anxiety disorders, drug and alcohol misuse, previous diagnosis of borderline personality disorder) |
| Source: References 2,13,14 |
Treatment strategies for BP II
As with all psychiatric disorders, treatment needs to multimodal and tailored to the individual. For a detailed assessment of pharmacologic and psychological options, see Goodwin and Jamison’s authoritative text, chapters 17 to 20.21
Pharmacologic options. Because few clinical trials have focused exclusively on BP II patients, much psychiatric practice has been extrapolated from trials involving BP I patients. Obviously, trials with BP II samples are needed, but these may be limited by the restrictive DSM-IV-TR definition of hypomania.
Lithium has the most supporting evidence, showing efficacy for all 3 phases of BP II—treatment of hypomania, treatment of bipolar depression, and prophylaxis against hypomanic and depressive relapses.22 Different medications used in bipolar disorder appear to have different efficacy profiles, however. For example, a systematic review of 14 randomized controlled trials with 2,526 patients found that although lithium, lamotrigine, olanzapine, and valproate were more effective than placebo at preventing relapse due to any mood episode:
- only lithium and olanzapine significantly reduced manic relapses
- only lamotrigine and valproate significantly reduced depressive relapses.23
The Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) trial did not find any therapeutic benefit or increased risk of switching to mania for anti depressants plus mood stabilizer vs mood stabilizer alone.26 Many trials of bipolar depression have recruited such heterogeneous groups of patients (including BP I, BP II, and BP NOS; schizoaffective disorder, bipolar type; and even recurrent MDD) that it is difficult to make firm recommendations about pharmacologic options for the depressive phase of BP II disorder.
In my experience, approximately one-third of BP II patients have a history of poor response to antidepressants or adverse effects from antidepressants (extreme irritability, activation, and antidepressant-induced hypomania). In the long term, these patients often do much better on mood stabilizer monotherapy or a combination of mood stabilizers such as lithium plus lamotrigine. The key is to be flexible with treatment options within recommended guidelines and to tailor treatment choices to the individual’s pattern of illness and treatment preferences.
Psychological interventions. Some evidence supports cognitive-behavioral therapy (CBT) and interpersonal and social rhythm therapy (IPSRT) in long-term treatment of bipolar disorders, although—as with medication trials—we need to be careful about extrapolating these findings to BP II disorder.29 For example, a recent large-scale randomized controlled trial of CBT for bipolar disorder was largely negative.30 Psychoeducation given in families and groups can be effective long-term options when used as adjuncts to medications.31
Table 3
Recommendations for treating patients with BP II disorder
| Most BP II patients require a multimodal team approach |
| Look for and treat psychiatric comorbidities, such as alcohol abuse |
| Lithium remains a gold standard treatment for BP II disorder |
| Quetiapine or lamotrigine may be helpful for acute bipolar II depression |
| Avoid antidepressant monotherapy for bipolar depression; some patients should avoid antidepressants altogether |
| CBT and IPSRT are useful psychological interventions |
| Family-focused and group psychoeducation are helpful in the long term |
| Always tailor treatments to the individual |
| BP II: bipolar II disorder; CBT: cognitive-behavioral therapy; IPSRT: interpersonal and social rhythm therapy |
Related Resources
- Goodwin GM and the Consensus Group of the British Association for Psychopharmacology. Evidence-based guidelines for treating bipolar disorder: revised second edition—recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2009;23(4):346-388. www.bap.org.uk/pdfs/Bipolar_guidelines.pdf.
- Goodwin FK, Jamison KR. Manic-depressive illness: bipolar disorders and recurrent depression. 2nd ed. New York, NY: Oxford University Press; 2007.
- Phelps J. Bipolar psychoeducation. www.psycheducation.org.
- Mood Disorders Treatment Team, Cardiff University. Interactive online psychoeducational treatment for bipolar disorder. www.BeatingBipolar.org.
- Goodwin GM, Geddes JR. What is the heartland of psychiatry? Br J Psychiatry. 2007;191(3):189-191.
- Lamotrigine • Lamictal
- Lithium • Various
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Valproate • Depakon
Dr. Smith receives research funding from the National Institute of Health Research UK, the MRC/Welsh Assembly Government, NARSAD, and the American Psychiatric Institute for Research and Education. He is a speaker for Eli Lilly and Company, AstraZeneca, and Bristol-Myers Squibb and is a consultant to Shire Pharmaceuticals.
1. Pies R. The “softer” end of the bipolar spectrum. J Psychiatr Pract. 2002;8(4):189-195.
2. Angst J. The bipolar spectrum. Br J Psychiatry. 2007;190(3):189-191.
3. Smith DJ, Ghaemi SN, Craddock N. The broad clinical spectrum of bipolar disorder: implications for research and practice. J Psychopharmacol. 2008;22(4):397-400.
4. Angst J, Gamma A, Bennazzi F, et al. Toward a re-definition of subthreshold bipolarity: epidemiology and proposed criteria for bipolar-II, minor bipolar disorders and hypomania. J Affect Disord. 2003;73:133-146.
5. Judd LJ, Akiskal HS. The prevalence and disability of bipolar spectrum disorders in the US population: re-analysis of the ECA database taking into account subthreshold cases. J Affect Disord. 2003;73:123-131.
6. Goldberg JF, Harrow M, Whiteside JE. Risk for bipolar illness in patients initially hospitalized for unipolar depression. Am J Psychiatry. 2001;58:1265-1270.
7. Smith DJ, Harrison N, Muir W, et al. The high prevalence of bipolar spectrum disorders in young adults with recurrent depression: toward an innovative diagnostic framework. J Affect Disord. 2005;84(2-3):167-178.
8. Sharma V, Khan M, Smith A. A closer look at treatment resistant depression: is it due to a bipolar diathesis? J Affect Disord. 2005;84(2-3):251-257.
9. Akiskal HS, Benazzi F, Perugi G. Agitated “unipolar” depression re-conceptualized as a depressive mixed state: implications for the antidepressant-suicide controversy. J Affect Disord. 2005;85(3):245-258.
10. Ghaemi SN, Wingo AP, Filkowski MA, et al. Long-term antidepressant treatment in bipolar disorder: meta-analyses of benefits and risks. Acta Psychiatr Scand. 2008;118(5):347-356.
11. National Institute of Health and Clinical Excellence. Bipolar disorder: the management of bipolar disorder in adults, children and adolescents, in primary and secondary care. Issued July 2006. Available at: http://www.nice.org.uk/CG038. Accessed June 3, 2009.
12. American Psychiatric Association practice guidelines. Treatment of patients with bipolar disorder, 2nd ed. Issued April 2002. Available at: http://www.psychiatryonline.com/pracGuide/pracGuideTopic_8.aspx. Accessed June 3, 2009.
13. Judd LL, Akiskal HS, Schletter PJ, et al. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry. 2003;60:261-269.
14. Forty L, Smith D, Jones L, et al. Clinical differences between bipolar and unipolar depression. Br J Psychiatry. 2008;192(5):388-389.
15. Mitchell PB, Wilhelm K, Parker G, et al. The clinical features of bipolar depression: a comparison with matched major depressive disorder patients. J Clin Psychiatry. 2001;62:212-216.
16. Akiskal HS, Benazzi F. Family history validation of the bipolar nature of depressive mixed states. J Affect Disord. 2003;73(1-2):113-122.
17. Hirschfeld RMA, Williams JB, Spitzer RL, et al. Development and validation of a screening instrument for bipolar spectrum disorder: The Mood Disorder Questionnaire. Am J Psychiatry. 2000;157:1873-1875.
18. Angst J, Adolfsson R, Benazzi F, et al. The HCL-32: towards a self-assessment tool for hypomanic symptoms in outpatients. J Affect Disord. 2005;88(2):217-233.
19. Ghaemi SN, Millar C, Berv DA, et al. Sensitivity and specificity of a new bipolar spectrum diagnostic scale. J Affect Disord. 2005;84:273-277.
20. Allen R, Smith DJ. Screening for bipolar disorder: strengths and limitations of currently available instruments. Primary Care and Community Psychiatry. 2008;13(2):47-51.
21. Goodwin FK, Jamison KR. Manic-depressive illness: bipolar disorders and recurrent depression. 2nd ed. New York, NY: Oxford University Press; 2007.
22. Young AH, Hammond JM. Lithium in mood disorders: increasing evidence base, declining use? Br J Psychiatry. 2007;191(6):474-476.
23. Smith LA, Cornelius V, Warnock A, et al. Effectiveness of mood stabilizers and antipsychotics in the maintenance phase of bipolar disorder: a systematic review of randomized controlled trials. Bipolar Disord. 2007;9(4):394-412.
24. Licht RW, Gijsman H, Nolen WA, et al. Are antidepressants safe in the treatment of bipolar depression? A critical evaluation of their potential risk to induce switch into mania or cycle acceleration. Acta Psychiatr Scand. 2008;118(5):337-346.
25. Smith DJ, Forty L, Russell E, et al. Sub-threshold manic symptoms in recurrent major depressive disorder are a marker for poor outcome. Acta Psychiatr Scand. 2009;119(4):325-329.Epub 2008 Dec 16.
26. Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N Engl J Med. 2007;356(17):1711-1722.
27. Thase ME, Madfadden W, Weisler RH, et al. Efficacy of quetiapine monotherapy in bipolar I and II depression: a double-blind, placebo-controlled study (the BOLDER II study). J Clin Psychopharmacology. 2006;26(6):600-609.
28. Geddes JR, Calabrese JR, Goodwin GM. Lamotrigine for treatment of bipolar depression: independent meta-analysis and meta-regression of individual patient data from five randomised trials. Br J Psychiatry. 2009;194:4-9.
29. Beynon S, Soares-Weiser K, Woolacott N, et al. Psychosocial interventions for the prevention of relapse in bipolar disorder: systematic review of controlled trials. Br J Psychiatry. 2008;192(1):5-11.
30. Scott J, Paykel E, Morriss R, et al. Cognitive-behavioural therapy for severe and recurrent bipolar disorders: randomised controlled trial. Br J Psychiatry. 2006;188(4):313-320.
31. Miklowitz DJ. Adjunctive psychotherapy for bipolar disorder: state of the evidence. Am J Psychiatry. 2008;165(11):1408-1419.Epub 2008 Sep 15.
WEB AUDIO
At least 25% and possibly up to 50% of patients with recurrent major depressive disorder (MDD) have features of mild hypomania (the “soft end” of the bipolar spectrum1) and might be better conceptualized as suffering from a broadly defined bipolar (BP) II disorder.2 The challenge is to differentiate MDD from BP II so that we make treatment decisions—such as antidepressants vs mood stabilizers—shown to improve the long-term course of patients’ depressive symptoms.
Diagnosis of BP II often is not straightforward and unfortunately may be delayed several years after patients first present for evaluation. To help clinicians make correct diagnostic decisions, this article:
- describes diagnostic criteria outside of DSM-IV-TR that can assist in identifying BP II disorder
- identifies subgroups of recurrently depressed patients whose primary disorder is more likely to be bipolar than unipolar
- provides a screening tool validated for identifying “soft” bipolarity
- offers a pragmatic clinical perspective on the treatment of BP II disorder.
How common is BP II disorder?
As with all psychiatric diagnoses, the prevalence of BP II disorder is a function of the diagnostic criteria used to define it.3 BP II—1 or more depressive episodes with at least 1 hypomanic episode—affects 1% to 2% of the population, based on DSM-IV-TR criteria for hypomania (Box 1). However, the DSM definition of BP II might be too restrictive. Regarding the diagnosis of hypomania, in particular:
- the symptom of “overactivity” should be given as much weight as the stem criteria of “euphoria” and “irritability”
- the 4-day threshold for a hypomanic episode probably is too long.
These deficiencies in DSM-IV-TR exclude many patients who experience brief but clinically significant periods of hypomania. A more realistic definition of hypomania within BP II disorder would:
- include overactivity as an additional stem criterion
- specify a threshold duration for hypomanic symptoms of at least 1 day rather than 4 days
- stipulate the experience of negative consequences of the episode as necessary for the diagnosis (Table 1).
- A distinct period of persistently elevated, expansive, or irritable mood, lasting at least 4 days, that is clearly different from the usual nondepressed mood
- During the period of mood disturbance, 3 or more of the following symptoms have persisted (4 if the mood is only irritable) and have been present to a significant degree:
- The episode is associated with an unequivocal change in functioning that is uncharacteristic of the person when not symptomatic
- The disturbance in mood and the change in functioning are observable by others
- The episode is not severe enough to cause marked impairment in social or occupational functioning, or to necessitate hospitalization, and there are no psychotic features
- The symptoms are not due to the direct physiological effects of a substance (a drug of abuse, a medication, or other treatment) or a general medical condition (such as hyperthyroidism)
Note: Hypomanic-like episodes that are clearly caused by somatic antidepressant treatment (such as medication, electroconvulsive therapy, or light therapy) should not count toward a diagnosis of bipolar II disorder
Proposed hypomania criteria in broadly defined BP II
| A. Euphoria, irritability, or overactivity |
| B. At least 3 of the 7 DSM-IV-TR symptoms of hypomania |
| C. Hypomanic symptoms of at least 1 day’s duration |
| D. Experience of negative consequences of hypomanic periods |
| BP II: bipolar II disorder |
| Source: Reference 4 |
Depression’s subgroups
Recurrent MDD is an extremely heterogeneous diagnosis. It includes many clinical presentations of depressive illness that may share little in terms of etiology, pathophysiology, and response to treatment. When carefully assessed, 2 subgroups of recurrently depressed patients in particular appear to be more likely to have a primary bipolar disorder:
- young patients with early-onset severe depression
- older adults with difficult-to-treat or treatment-resistant depression.
6 Other reports have indicated that at least 40% of young adults with recurrent MDD satisfy broad diagnostic criteria for bipolar disorder.7
Higher rates of unrecognized bipolar disorder have been identified in patients with treatment-resistant depression. In a prospective study of 61 consecutive MDD patients referred to a mood disorders clinic, 59% satisfied DSM-IV-TR criteria for bipolar disorder.8
Consequences. Undiagnosed BP II disorder is an important clinical issue because bipolar features in patients presumed to have recurrent MDD can adversely affect long-term outcomes. Many of these patients will be treated exclusively with antidepressants despite evidence that antidepressant monotherapy for bipolar depression—at least for some patients—can cause more frequent mood episodes, mood destabilization, and possibly an increase in suicidal behaviors.9,10
This point is highlighted in the United Kingdom’s National Institute of Health and Clinical Excellence (NICE) guidelines for bipolar disorder, which recommended that antidepressants be prescribed for bipolar depression only in combination with mood stabilizer treatment and withdrawn within 2 to 3 months of recovery.11
The American Psychiatric Association’s (APA) practice guideline for treating bipolar disorder, published in 2002, advises against antidepressants as monotherapy for bipolar depression, recommending instead that lithium or lamotrigine be used first-line. A revised APA guideline is scheduled for publication this year.12
Why is BP II underdiagnosed?
Notwithstanding the limitations of DSMIV-TR criteria for hypomania, additional factors contribute to under-recognition of BP II in clinical practice.
Dominant depressive symptoms. The clinical course of bipolar disorders is dominated by low-grade depressive symptoms and recurrent depressive episodes rather than mania or hypomania. This is especially true for BP II disorder, where the ratio of time spent with depressive symptoms relative to time with hypomanic symptoms is approximately 30:1.13 The fact that BP II patients in general seek help only during depressive periods means that consultations inevitably focus on the diagnosis and treatment of depression, rather than long-term prophylaxis of both depressive and hypomanic episodes.
Indistinguishable symptoms? Bipolar depressions are generally thought to be clinically indistinguishable from unipolar depressions, but this might not be clear-cut. Although differentiating symptoms of unipolar and bipolar depression can be difficult in clinical practice, evidence suggests that certain symptoms may be more common in bipolar than unipolar depression:
- atypical depressive features such as mood reactivity, overeating, oversleeping, and excessive fatigue14
- depressive psychotic symptoms, especially in younger patients15
- “mixed” depressive episodes (depressive episodes with concurrent manic symptoms).16
How to recognize BP II disorder
To detect and diagnose BP II disorder, systematically assess hypomanic features in all patients who present with recurrent MDD, especially those who have an early age of onset or don’t seem to be responding well to antidepressant monotherapy. As noted, a corroborative history from a close relative is essential. Within a full clinical assessment, use the features listed in Table 2 to help differentiate bipolar depression from unipolar depression.
Screening instruments for hypomania are no substitute for a careful psychiatric history but can be very helpful in everyday clinical practice. The most well-known is the Mood Disorder Questionnaire (MDQ);17 other options include the Hypomania Checklist (HCL-32)18 and the Bipolar Spectrum Diagnostic Scale (BSDS).19 In general, the MDQ performs better at detecting BP I in psychiatric practice settings, whereas the HCL-32 and BSDS may be more useful in primary care and general population settings.20
The BSDS has a particular focus on the softer end of the bipolar spectrum,19 and in my experience patients like its narrative structure. It can help prompt discussions about previous hypomania symptoms and mood instability. In this sense, the BSDS is a useful adjunct to the routine clinical assessment of patients with recurrent depressive disorders. Click here to view the BSDS.
Table 2
Possible indicators of bipolarity in apparently unipolar depression
| Atypical features |
| First-degree relative with bipolar disorder |
| Antidepressant-induced mania or hypomania |
| Multiple family members with major depression |
| Early onset of depression (age |
| Lack of response to ≥3 antidepressant trials |
| Psychotic features (before age 35) |
| Mixed depressive episodes |
| Brief but frequent episodes of depression |
| Complex comorbidity (anxiety disorders, drug and alcohol misuse, previous diagnosis of borderline personality disorder) |
| Source: References 2,13,14 |
Treatment strategies for BP II
As with all psychiatric disorders, treatment needs to multimodal and tailored to the individual. For a detailed assessment of pharmacologic and psychological options, see Goodwin and Jamison’s authoritative text, chapters 17 to 20.21
Pharmacologic options. Because few clinical trials have focused exclusively on BP II patients, much psychiatric practice has been extrapolated from trials involving BP I patients. Obviously, trials with BP II samples are needed, but these may be limited by the restrictive DSM-IV-TR definition of hypomania.
Lithium has the most supporting evidence, showing efficacy for all 3 phases of BP II—treatment of hypomania, treatment of bipolar depression, and prophylaxis against hypomanic and depressive relapses.22 Different medications used in bipolar disorder appear to have different efficacy profiles, however. For example, a systematic review of 14 randomized controlled trials with 2,526 patients found that although lithium, lamotrigine, olanzapine, and valproate were more effective than placebo at preventing relapse due to any mood episode:
- only lithium and olanzapine significantly reduced manic relapses
- only lamotrigine and valproate significantly reduced depressive relapses.23
The Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) trial did not find any therapeutic benefit or increased risk of switching to mania for anti depressants plus mood stabilizer vs mood stabilizer alone.26 Many trials of bipolar depression have recruited such heterogeneous groups of patients (including BP I, BP II, and BP NOS; schizoaffective disorder, bipolar type; and even recurrent MDD) that it is difficult to make firm recommendations about pharmacologic options for the depressive phase of BP II disorder.
In my experience, approximately one-third of BP II patients have a history of poor response to antidepressants or adverse effects from antidepressants (extreme irritability, activation, and antidepressant-induced hypomania). In the long term, these patients often do much better on mood stabilizer monotherapy or a combination of mood stabilizers such as lithium plus lamotrigine. The key is to be flexible with treatment options within recommended guidelines and to tailor treatment choices to the individual’s pattern of illness and treatment preferences.
Psychological interventions. Some evidence supports cognitive-behavioral therapy (CBT) and interpersonal and social rhythm therapy (IPSRT) in long-term treatment of bipolar disorders, although—as with medication trials—we need to be careful about extrapolating these findings to BP II disorder.29 For example, a recent large-scale randomized controlled trial of CBT for bipolar disorder was largely negative.30 Psychoeducation given in families and groups can be effective long-term options when used as adjuncts to medications.31
Table 3
Recommendations for treating patients with BP II disorder
| Most BP II patients require a multimodal team approach |
| Look for and treat psychiatric comorbidities, such as alcohol abuse |
| Lithium remains a gold standard treatment for BP II disorder |
| Quetiapine or lamotrigine may be helpful for acute bipolar II depression |
| Avoid antidepressant monotherapy for bipolar depression; some patients should avoid antidepressants altogether |
| CBT and IPSRT are useful psychological interventions |
| Family-focused and group psychoeducation are helpful in the long term |
| Always tailor treatments to the individual |
| BP II: bipolar II disorder; CBT: cognitive-behavioral therapy; IPSRT: interpersonal and social rhythm therapy |
Related Resources
- Goodwin GM and the Consensus Group of the British Association for Psychopharmacology. Evidence-based guidelines for treating bipolar disorder: revised second edition—recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2009;23(4):346-388. www.bap.org.uk/pdfs/Bipolar_guidelines.pdf.
- Goodwin FK, Jamison KR. Manic-depressive illness: bipolar disorders and recurrent depression. 2nd ed. New York, NY: Oxford University Press; 2007.
- Phelps J. Bipolar psychoeducation. www.psycheducation.org.
- Mood Disorders Treatment Team, Cardiff University. Interactive online psychoeducational treatment for bipolar disorder. www.BeatingBipolar.org.
- Goodwin GM, Geddes JR. What is the heartland of psychiatry? Br J Psychiatry. 2007;191(3):189-191.
- Lamotrigine • Lamictal
- Lithium • Various
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Valproate • Depakon
Dr. Smith receives research funding from the National Institute of Health Research UK, the MRC/Welsh Assembly Government, NARSAD, and the American Psychiatric Institute for Research and Education. He is a speaker for Eli Lilly and Company, AstraZeneca, and Bristol-Myers Squibb and is a consultant to Shire Pharmaceuticals.
WEB AUDIO
At least 25% and possibly up to 50% of patients with recurrent major depressive disorder (MDD) have features of mild hypomania (the “soft end” of the bipolar spectrum1) and might be better conceptualized as suffering from a broadly defined bipolar (BP) II disorder.2 The challenge is to differentiate MDD from BP II so that we make treatment decisions—such as antidepressants vs mood stabilizers—shown to improve the long-term course of patients’ depressive symptoms.
Diagnosis of BP II often is not straightforward and unfortunately may be delayed several years after patients first present for evaluation. To help clinicians make correct diagnostic decisions, this article:
- describes diagnostic criteria outside of DSM-IV-TR that can assist in identifying BP II disorder
- identifies subgroups of recurrently depressed patients whose primary disorder is more likely to be bipolar than unipolar
- provides a screening tool validated for identifying “soft” bipolarity
- offers a pragmatic clinical perspective on the treatment of BP II disorder.
How common is BP II disorder?
As with all psychiatric diagnoses, the prevalence of BP II disorder is a function of the diagnostic criteria used to define it.3 BP II—1 or more depressive episodes with at least 1 hypomanic episode—affects 1% to 2% of the population, based on DSM-IV-TR criteria for hypomania (Box 1). However, the DSM definition of BP II might be too restrictive. Regarding the diagnosis of hypomania, in particular:
- the symptom of “overactivity” should be given as much weight as the stem criteria of “euphoria” and “irritability”
- the 4-day threshold for a hypomanic episode probably is too long.
These deficiencies in DSM-IV-TR exclude many patients who experience brief but clinically significant periods of hypomania. A more realistic definition of hypomania within BP II disorder would:
- include overactivity as an additional stem criterion
- specify a threshold duration for hypomanic symptoms of at least 1 day rather than 4 days
- stipulate the experience of negative consequences of the episode as necessary for the diagnosis (Table 1).
- A distinct period of persistently elevated, expansive, or irritable mood, lasting at least 4 days, that is clearly different from the usual nondepressed mood
- During the period of mood disturbance, 3 or more of the following symptoms have persisted (4 if the mood is only irritable) and have been present to a significant degree:
- The episode is associated with an unequivocal change in functioning that is uncharacteristic of the person when not symptomatic
- The disturbance in mood and the change in functioning are observable by others
- The episode is not severe enough to cause marked impairment in social or occupational functioning, or to necessitate hospitalization, and there are no psychotic features
- The symptoms are not due to the direct physiological effects of a substance (a drug of abuse, a medication, or other treatment) or a general medical condition (such as hyperthyroidism)
Note: Hypomanic-like episodes that are clearly caused by somatic antidepressant treatment (such as medication, electroconvulsive therapy, or light therapy) should not count toward a diagnosis of bipolar II disorder
Proposed hypomania criteria in broadly defined BP II
| A. Euphoria, irritability, or overactivity |
| B. At least 3 of the 7 DSM-IV-TR symptoms of hypomania |
| C. Hypomanic symptoms of at least 1 day’s duration |
| D. Experience of negative consequences of hypomanic periods |
| BP II: bipolar II disorder |
| Source: Reference 4 |
Depression’s subgroups
Recurrent MDD is an extremely heterogeneous diagnosis. It includes many clinical presentations of depressive illness that may share little in terms of etiology, pathophysiology, and response to treatment. When carefully assessed, 2 subgroups of recurrently depressed patients in particular appear to be more likely to have a primary bipolar disorder:
- young patients with early-onset severe depression
- older adults with difficult-to-treat or treatment-resistant depression.
6 Other reports have indicated that at least 40% of young adults with recurrent MDD satisfy broad diagnostic criteria for bipolar disorder.7
Higher rates of unrecognized bipolar disorder have been identified in patients with treatment-resistant depression. In a prospective study of 61 consecutive MDD patients referred to a mood disorders clinic, 59% satisfied DSM-IV-TR criteria for bipolar disorder.8
Consequences. Undiagnosed BP II disorder is an important clinical issue because bipolar features in patients presumed to have recurrent MDD can adversely affect long-term outcomes. Many of these patients will be treated exclusively with antidepressants despite evidence that antidepressant monotherapy for bipolar depression—at least for some patients—can cause more frequent mood episodes, mood destabilization, and possibly an increase in suicidal behaviors.9,10
This point is highlighted in the United Kingdom’s National Institute of Health and Clinical Excellence (NICE) guidelines for bipolar disorder, which recommended that antidepressants be prescribed for bipolar depression only in combination with mood stabilizer treatment and withdrawn within 2 to 3 months of recovery.11
The American Psychiatric Association’s (APA) practice guideline for treating bipolar disorder, published in 2002, advises against antidepressants as monotherapy for bipolar depression, recommending instead that lithium or lamotrigine be used first-line. A revised APA guideline is scheduled for publication this year.12
Why is BP II underdiagnosed?
Notwithstanding the limitations of DSMIV-TR criteria for hypomania, additional factors contribute to under-recognition of BP II in clinical practice.
Dominant depressive symptoms. The clinical course of bipolar disorders is dominated by low-grade depressive symptoms and recurrent depressive episodes rather than mania or hypomania. This is especially true for BP II disorder, where the ratio of time spent with depressive symptoms relative to time with hypomanic symptoms is approximately 30:1.13 The fact that BP II patients in general seek help only during depressive periods means that consultations inevitably focus on the diagnosis and treatment of depression, rather than long-term prophylaxis of both depressive and hypomanic episodes.
Indistinguishable symptoms? Bipolar depressions are generally thought to be clinically indistinguishable from unipolar depressions, but this might not be clear-cut. Although differentiating symptoms of unipolar and bipolar depression can be difficult in clinical practice, evidence suggests that certain symptoms may be more common in bipolar than unipolar depression:
- atypical depressive features such as mood reactivity, overeating, oversleeping, and excessive fatigue14
- depressive psychotic symptoms, especially in younger patients15
- “mixed” depressive episodes (depressive episodes with concurrent manic symptoms).16
How to recognize BP II disorder
To detect and diagnose BP II disorder, systematically assess hypomanic features in all patients who present with recurrent MDD, especially those who have an early age of onset or don’t seem to be responding well to antidepressant monotherapy. As noted, a corroborative history from a close relative is essential. Within a full clinical assessment, use the features listed in Table 2 to help differentiate bipolar depression from unipolar depression.
Screening instruments for hypomania are no substitute for a careful psychiatric history but can be very helpful in everyday clinical practice. The most well-known is the Mood Disorder Questionnaire (MDQ);17 other options include the Hypomania Checklist (HCL-32)18 and the Bipolar Spectrum Diagnostic Scale (BSDS).19 In general, the MDQ performs better at detecting BP I in psychiatric practice settings, whereas the HCL-32 and BSDS may be more useful in primary care and general population settings.20
The BSDS has a particular focus on the softer end of the bipolar spectrum,19 and in my experience patients like its narrative structure. It can help prompt discussions about previous hypomania symptoms and mood instability. In this sense, the BSDS is a useful adjunct to the routine clinical assessment of patients with recurrent depressive disorders. Click here to view the BSDS.
Table 2
Possible indicators of bipolarity in apparently unipolar depression
| Atypical features |
| First-degree relative with bipolar disorder |
| Antidepressant-induced mania or hypomania |
| Multiple family members with major depression |
| Early onset of depression (age |
| Lack of response to ≥3 antidepressant trials |
| Psychotic features (before age 35) |
| Mixed depressive episodes |
| Brief but frequent episodes of depression |
| Complex comorbidity (anxiety disorders, drug and alcohol misuse, previous diagnosis of borderline personality disorder) |
| Source: References 2,13,14 |
Treatment strategies for BP II
As with all psychiatric disorders, treatment needs to multimodal and tailored to the individual. For a detailed assessment of pharmacologic and psychological options, see Goodwin and Jamison’s authoritative text, chapters 17 to 20.21
Pharmacologic options. Because few clinical trials have focused exclusively on BP II patients, much psychiatric practice has been extrapolated from trials involving BP I patients. Obviously, trials with BP II samples are needed, but these may be limited by the restrictive DSM-IV-TR definition of hypomania.
Lithium has the most supporting evidence, showing efficacy for all 3 phases of BP II—treatment of hypomania, treatment of bipolar depression, and prophylaxis against hypomanic and depressive relapses.22 Different medications used in bipolar disorder appear to have different efficacy profiles, however. For example, a systematic review of 14 randomized controlled trials with 2,526 patients found that although lithium, lamotrigine, olanzapine, and valproate were more effective than placebo at preventing relapse due to any mood episode:
- only lithium and olanzapine significantly reduced manic relapses
- only lamotrigine and valproate significantly reduced depressive relapses.23
The Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) trial did not find any therapeutic benefit or increased risk of switching to mania for anti depressants plus mood stabilizer vs mood stabilizer alone.26 Many trials of bipolar depression have recruited such heterogeneous groups of patients (including BP I, BP II, and BP NOS; schizoaffective disorder, bipolar type; and even recurrent MDD) that it is difficult to make firm recommendations about pharmacologic options for the depressive phase of BP II disorder.
In my experience, approximately one-third of BP II patients have a history of poor response to antidepressants or adverse effects from antidepressants (extreme irritability, activation, and antidepressant-induced hypomania). In the long term, these patients often do much better on mood stabilizer monotherapy or a combination of mood stabilizers such as lithium plus lamotrigine. The key is to be flexible with treatment options within recommended guidelines and to tailor treatment choices to the individual’s pattern of illness and treatment preferences.
Psychological interventions. Some evidence supports cognitive-behavioral therapy (CBT) and interpersonal and social rhythm therapy (IPSRT) in long-term treatment of bipolar disorders, although—as with medication trials—we need to be careful about extrapolating these findings to BP II disorder.29 For example, a recent large-scale randomized controlled trial of CBT for bipolar disorder was largely negative.30 Psychoeducation given in families and groups can be effective long-term options when used as adjuncts to medications.31
Table 3
Recommendations for treating patients with BP II disorder
| Most BP II patients require a multimodal team approach |
| Look for and treat psychiatric comorbidities, such as alcohol abuse |
| Lithium remains a gold standard treatment for BP II disorder |
| Quetiapine or lamotrigine may be helpful for acute bipolar II depression |
| Avoid antidepressant monotherapy for bipolar depression; some patients should avoid antidepressants altogether |
| CBT and IPSRT are useful psychological interventions |
| Family-focused and group psychoeducation are helpful in the long term |
| Always tailor treatments to the individual |
| BP II: bipolar II disorder; CBT: cognitive-behavioral therapy; IPSRT: interpersonal and social rhythm therapy |
Related Resources
- Goodwin GM and the Consensus Group of the British Association for Psychopharmacology. Evidence-based guidelines for treating bipolar disorder: revised second edition—recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2009;23(4):346-388. www.bap.org.uk/pdfs/Bipolar_guidelines.pdf.
- Goodwin FK, Jamison KR. Manic-depressive illness: bipolar disorders and recurrent depression. 2nd ed. New York, NY: Oxford University Press; 2007.
- Phelps J. Bipolar psychoeducation. www.psycheducation.org.
- Mood Disorders Treatment Team, Cardiff University. Interactive online psychoeducational treatment for bipolar disorder. www.BeatingBipolar.org.
- Goodwin GM, Geddes JR. What is the heartland of psychiatry? Br J Psychiatry. 2007;191(3):189-191.
- Lamotrigine • Lamictal
- Lithium • Various
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Valproate • Depakon
Dr. Smith receives research funding from the National Institute of Health Research UK, the MRC/Welsh Assembly Government, NARSAD, and the American Psychiatric Institute for Research and Education. He is a speaker for Eli Lilly and Company, AstraZeneca, and Bristol-Myers Squibb and is a consultant to Shire Pharmaceuticals.
1. Pies R. The “softer” end of the bipolar spectrum. J Psychiatr Pract. 2002;8(4):189-195.
2. Angst J. The bipolar spectrum. Br J Psychiatry. 2007;190(3):189-191.
3. Smith DJ, Ghaemi SN, Craddock N. The broad clinical spectrum of bipolar disorder: implications for research and practice. J Psychopharmacol. 2008;22(4):397-400.
4. Angst J, Gamma A, Bennazzi F, et al. Toward a re-definition of subthreshold bipolarity: epidemiology and proposed criteria for bipolar-II, minor bipolar disorders and hypomania. J Affect Disord. 2003;73:133-146.
5. Judd LJ, Akiskal HS. The prevalence and disability of bipolar spectrum disorders in the US population: re-analysis of the ECA database taking into account subthreshold cases. J Affect Disord. 2003;73:123-131.
6. Goldberg JF, Harrow M, Whiteside JE. Risk for bipolar illness in patients initially hospitalized for unipolar depression. Am J Psychiatry. 2001;58:1265-1270.
7. Smith DJ, Harrison N, Muir W, et al. The high prevalence of bipolar spectrum disorders in young adults with recurrent depression: toward an innovative diagnostic framework. J Affect Disord. 2005;84(2-3):167-178.
8. Sharma V, Khan M, Smith A. A closer look at treatment resistant depression: is it due to a bipolar diathesis? J Affect Disord. 2005;84(2-3):251-257.
9. Akiskal HS, Benazzi F, Perugi G. Agitated “unipolar” depression re-conceptualized as a depressive mixed state: implications for the antidepressant-suicide controversy. J Affect Disord. 2005;85(3):245-258.
10. Ghaemi SN, Wingo AP, Filkowski MA, et al. Long-term antidepressant treatment in bipolar disorder: meta-analyses of benefits and risks. Acta Psychiatr Scand. 2008;118(5):347-356.
11. National Institute of Health and Clinical Excellence. Bipolar disorder: the management of bipolar disorder in adults, children and adolescents, in primary and secondary care. Issued July 2006. Available at: http://www.nice.org.uk/CG038. Accessed June 3, 2009.
12. American Psychiatric Association practice guidelines. Treatment of patients with bipolar disorder, 2nd ed. Issued April 2002. Available at: http://www.psychiatryonline.com/pracGuide/pracGuideTopic_8.aspx. Accessed June 3, 2009.
13. Judd LL, Akiskal HS, Schletter PJ, et al. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry. 2003;60:261-269.
14. Forty L, Smith D, Jones L, et al. Clinical differences between bipolar and unipolar depression. Br J Psychiatry. 2008;192(5):388-389.
15. Mitchell PB, Wilhelm K, Parker G, et al. The clinical features of bipolar depression: a comparison with matched major depressive disorder patients. J Clin Psychiatry. 2001;62:212-216.
16. Akiskal HS, Benazzi F. Family history validation of the bipolar nature of depressive mixed states. J Affect Disord. 2003;73(1-2):113-122.
17. Hirschfeld RMA, Williams JB, Spitzer RL, et al. Development and validation of a screening instrument for bipolar spectrum disorder: The Mood Disorder Questionnaire. Am J Psychiatry. 2000;157:1873-1875.
18. Angst J, Adolfsson R, Benazzi F, et al. The HCL-32: towards a self-assessment tool for hypomanic symptoms in outpatients. J Affect Disord. 2005;88(2):217-233.
19. Ghaemi SN, Millar C, Berv DA, et al. Sensitivity and specificity of a new bipolar spectrum diagnostic scale. J Affect Disord. 2005;84:273-277.
20. Allen R, Smith DJ. Screening for bipolar disorder: strengths and limitations of currently available instruments. Primary Care and Community Psychiatry. 2008;13(2):47-51.
21. Goodwin FK, Jamison KR. Manic-depressive illness: bipolar disorders and recurrent depression. 2nd ed. New York, NY: Oxford University Press; 2007.
22. Young AH, Hammond JM. Lithium in mood disorders: increasing evidence base, declining use? Br J Psychiatry. 2007;191(6):474-476.
23. Smith LA, Cornelius V, Warnock A, et al. Effectiveness of mood stabilizers and antipsychotics in the maintenance phase of bipolar disorder: a systematic review of randomized controlled trials. Bipolar Disord. 2007;9(4):394-412.
24. Licht RW, Gijsman H, Nolen WA, et al. Are antidepressants safe in the treatment of bipolar depression? A critical evaluation of their potential risk to induce switch into mania or cycle acceleration. Acta Psychiatr Scand. 2008;118(5):337-346.
25. Smith DJ, Forty L, Russell E, et al. Sub-threshold manic symptoms in recurrent major depressive disorder are a marker for poor outcome. Acta Psychiatr Scand. 2009;119(4):325-329.Epub 2008 Dec 16.
26. Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N Engl J Med. 2007;356(17):1711-1722.
27. Thase ME, Madfadden W, Weisler RH, et al. Efficacy of quetiapine monotherapy in bipolar I and II depression: a double-blind, placebo-controlled study (the BOLDER II study). J Clin Psychopharmacology. 2006;26(6):600-609.
28. Geddes JR, Calabrese JR, Goodwin GM. Lamotrigine for treatment of bipolar depression: independent meta-analysis and meta-regression of individual patient data from five randomised trials. Br J Psychiatry. 2009;194:4-9.
29. Beynon S, Soares-Weiser K, Woolacott N, et al. Psychosocial interventions for the prevention of relapse in bipolar disorder: systematic review of controlled trials. Br J Psychiatry. 2008;192(1):5-11.
30. Scott J, Paykel E, Morriss R, et al. Cognitive-behavioural therapy for severe and recurrent bipolar disorders: randomised controlled trial. Br J Psychiatry. 2006;188(4):313-320.
31. Miklowitz DJ. Adjunctive psychotherapy for bipolar disorder: state of the evidence. Am J Psychiatry. 2008;165(11):1408-1419.Epub 2008 Sep 15.
1. Pies R. The “softer” end of the bipolar spectrum. J Psychiatr Pract. 2002;8(4):189-195.
2. Angst J. The bipolar spectrum. Br J Psychiatry. 2007;190(3):189-191.
3. Smith DJ, Ghaemi SN, Craddock N. The broad clinical spectrum of bipolar disorder: implications for research and practice. J Psychopharmacol. 2008;22(4):397-400.
4. Angst J, Gamma A, Bennazzi F, et al. Toward a re-definition of subthreshold bipolarity: epidemiology and proposed criteria for bipolar-II, minor bipolar disorders and hypomania. J Affect Disord. 2003;73:133-146.
5. Judd LJ, Akiskal HS. The prevalence and disability of bipolar spectrum disorders in the US population: re-analysis of the ECA database taking into account subthreshold cases. J Affect Disord. 2003;73:123-131.
6. Goldberg JF, Harrow M, Whiteside JE. Risk for bipolar illness in patients initially hospitalized for unipolar depression. Am J Psychiatry. 2001;58:1265-1270.
7. Smith DJ, Harrison N, Muir W, et al. The high prevalence of bipolar spectrum disorders in young adults with recurrent depression: toward an innovative diagnostic framework. J Affect Disord. 2005;84(2-3):167-178.
8. Sharma V, Khan M, Smith A. A closer look at treatment resistant depression: is it due to a bipolar diathesis? J Affect Disord. 2005;84(2-3):251-257.
9. Akiskal HS, Benazzi F, Perugi G. Agitated “unipolar” depression re-conceptualized as a depressive mixed state: implications for the antidepressant-suicide controversy. J Affect Disord. 2005;85(3):245-258.
10. Ghaemi SN, Wingo AP, Filkowski MA, et al. Long-term antidepressant treatment in bipolar disorder: meta-analyses of benefits and risks. Acta Psychiatr Scand. 2008;118(5):347-356.
11. National Institute of Health and Clinical Excellence. Bipolar disorder: the management of bipolar disorder in adults, children and adolescents, in primary and secondary care. Issued July 2006. Available at: http://www.nice.org.uk/CG038. Accessed June 3, 2009.
12. American Psychiatric Association practice guidelines. Treatment of patients with bipolar disorder, 2nd ed. Issued April 2002. Available at: http://www.psychiatryonline.com/pracGuide/pracGuideTopic_8.aspx. Accessed June 3, 2009.
13. Judd LL, Akiskal HS, Schletter PJ, et al. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry. 2003;60:261-269.
14. Forty L, Smith D, Jones L, et al. Clinical differences between bipolar and unipolar depression. Br J Psychiatry. 2008;192(5):388-389.
15. Mitchell PB, Wilhelm K, Parker G, et al. The clinical features of bipolar depression: a comparison with matched major depressive disorder patients. J Clin Psychiatry. 2001;62:212-216.
16. Akiskal HS, Benazzi F. Family history validation of the bipolar nature of depressive mixed states. J Affect Disord. 2003;73(1-2):113-122.
17. Hirschfeld RMA, Williams JB, Spitzer RL, et al. Development and validation of a screening instrument for bipolar spectrum disorder: The Mood Disorder Questionnaire. Am J Psychiatry. 2000;157:1873-1875.
18. Angst J, Adolfsson R, Benazzi F, et al. The HCL-32: towards a self-assessment tool for hypomanic symptoms in outpatients. J Affect Disord. 2005;88(2):217-233.
19. Ghaemi SN, Millar C, Berv DA, et al. Sensitivity and specificity of a new bipolar spectrum diagnostic scale. J Affect Disord. 2005;84:273-277.
20. Allen R, Smith DJ. Screening for bipolar disorder: strengths and limitations of currently available instruments. Primary Care and Community Psychiatry. 2008;13(2):47-51.
21. Goodwin FK, Jamison KR. Manic-depressive illness: bipolar disorders and recurrent depression. 2nd ed. New York, NY: Oxford University Press; 2007.
22. Young AH, Hammond JM. Lithium in mood disorders: increasing evidence base, declining use? Br J Psychiatry. 2007;191(6):474-476.
23. Smith LA, Cornelius V, Warnock A, et al. Effectiveness of mood stabilizers and antipsychotics in the maintenance phase of bipolar disorder: a systematic review of randomized controlled trials. Bipolar Disord. 2007;9(4):394-412.
24. Licht RW, Gijsman H, Nolen WA, et al. Are antidepressants safe in the treatment of bipolar depression? A critical evaluation of their potential risk to induce switch into mania or cycle acceleration. Acta Psychiatr Scand. 2008;118(5):337-346.
25. Smith DJ, Forty L, Russell E, et al. Sub-threshold manic symptoms in recurrent major depressive disorder are a marker for poor outcome. Acta Psychiatr Scand. 2009;119(4):325-329.Epub 2008 Dec 16.
26. Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N Engl J Med. 2007;356(17):1711-1722.
27. Thase ME, Madfadden W, Weisler RH, et al. Efficacy of quetiapine monotherapy in bipolar I and II depression: a double-blind, placebo-controlled study (the BOLDER II study). J Clin Psychopharmacology. 2006;26(6):600-609.
28. Geddes JR, Calabrese JR, Goodwin GM. Lamotrigine for treatment of bipolar depression: independent meta-analysis and meta-regression of individual patient data from five randomised trials. Br J Psychiatry. 2009;194:4-9.
29. Beynon S, Soares-Weiser K, Woolacott N, et al. Psychosocial interventions for the prevention of relapse in bipolar disorder: systematic review of controlled trials. Br J Psychiatry. 2008;192(1):5-11.
30. Scott J, Paykel E, Morriss R, et al. Cognitive-behavioural therapy for severe and recurrent bipolar disorders: randomised controlled trial. Br J Psychiatry. 2006;188(4):313-320.
31. Miklowitz DJ. Adjunctive psychotherapy for bipolar disorder: state of the evidence. Am J Psychiatry. 2008;165(11):1408-1419.Epub 2008 Sep 15.
Assessing potential for harm: Would your patient injure himself or others?
Police take Ms. L, age 23, to the emergency room (ER) after her fiancé called them. He told the police that after a “night of drinking” they argued about a girl he had flirted with. Ms. L took out a loaded gun and threatened to shoot herself. She eventually handed the gun over to the police.
In the ER, Ms. L’s blood alcohol level is 0.20%. She tells the admitting emergency room nurse, “I would never hurt myself. I drank too much and was acting stupid. I just want to go home and sleep it off. I promise not to harm myself.” Emergency room staff observe Ms. L smile and giggle while waiting for a psychiatric evaluation.
What would you do? Hospitalize Ms. L for safety, or accept her promise not to hurt herself and send her home? What criteria would you use?
Knowing how to assess patients such as Ms. L is an essential psychiatric skill, whether or not you trained in forensic psychiatry. This article includes case reports that illustrate techniques for evaluating patients who may harbor suicidal or homicidal thoughts.
Evaluating danger to self
Your role is to weigh an individual’s risk factors for suicide against potential protective factors and to make a judgment call. Potential risk factors for suicide include (but are not limited to):
- current suicidal thoughts
- prior suicide attempts
- presence of a comorbid psychiatric disorder (particularly depression)
- intoxication or ongoing substance use
- feelings of hopelessness
- marked anxiety
- recent stressors
- family history of suicide
- lack of psychosocial support.1
Also review information that is reasonably available. In the ER, records from other facilities or private psychiatric treatment notes may not be accessed easily. However, in addition to conducting a suicide risk assessment and mental status examination, consider reviewing the collateral information outlined in Table 2.
Furthermore, do not rely on “no-suicide” contracts. They do not guarantee that a person won’t attempt suicide, and they will not provide legal protection if the patient commits suicide after being released from your care.2
What to document. After completing your evaluation, specifically document:
- that a suicide risk assessment was conducted
- what risk factors were present
- interventions to address those risk factors
- the level of risk determined (minimal, moderate, or high)
- factors that may protect the patient against suicide.
Table 1
Evaluating suicidality: Sample questions to ask
| Do you wish you were dead? |
| Do you have thoughts about harming yourself? |
| Do you have an actual plan as to how you would harm yourself? If yes: Have you taken any steps to enact that plan? If so, what were they? |
| Have you ever attempted suicide before? If yes: What stopped you from enacting this plan? What do you think would keep you from acting on this plan in the future? |
| Has anyone in your family or close to you committed suicide? |
| How close have you come to killing yourself? |
Table 2
Sources of information to assess suicidality in the ER
| Police reports on circumstances that led the patient to come to the ER |
| ER nursing/physician notes |
| Family members’/friends’ statements regarding reasons for the patient’s visit |
| Observations by anyone assigned to monitor the patient while awaiting your consult |
| Laboratory and physical exam findings, particularly related to substance use and/or self-injurious behavior |
| Psychiatric records at that facility |
| Concerns expressed by anyone responsible for the patient if he/she is released from the hospital |
| ER: emergency room |
CASE REPORT: Paranoid and armed
Mr. J, age 21, is brought involuntarily to the psychiatric ER by police. His mother reports he was locked in his room with a gun, claiming “the FBI is going to kill me.”
Mr. J’s mother tells the ER psychiatrist that her son has schizophrenia, paranoid type, and stopped taking risperidone, 3 mg/d, 4 weeks ago. She explains that Mr. J sometimes “hears voices” whispering to him that his medications are poison and to not trust his family. She states that Mr. J also abuses alcohol and methamphetamine and has 2 prior arrests for assault with a deadly weapon.
She adds that Mr. J now believes his family is working with the FBI to have him placed in a “secret detention camp.” Mr. J’s mother found a loaded pistol in his room and is “scared of what might happen.” During your psychiatric interview, Mr. J appears frightened and paranoid and provides only minimal answers to your questions. He clenches his teeth while staring intently at you.
Evaluating danger to others
There is good reason to be concerned that Mr. J might behave violently, and you likely have sufficient information to hospitalize him. When creating a long-term violence risk prevention plan, divide the concept of dangerousness into 5 components:
- magnitude of potential harm
- likelihood that harm will occur
- imminence of harm
- frequency of dangerous behavior
- situational variables that promote or protect against aggressive behavior.
A person who has used weapons against others may pose a serious risk of future violence. Ask patients whether they own or have ever owned a weapon. In our experience, the recent movement of a weapon—such as transferring a gun from a closet to a nightstand—is particularly ominous in a paranoid person. The greater the psychotic fear, the more likely a paranoid person is to kill someone he misperceives as a persecutor.
Drugs and alcohol are strongly associated with violent behavior.5 Most persons involved in violent crimes are under the influence of alcohol or drugs at the time of their aggression.6 Stimulants such as cocaine, crack, amphetamines, and phencyclidine are of special concern. These drugs often are associated with feelings of disinhibition, a sense of power, and paranoia. The violence linked with cocaine use differs by gender: men are more likely to perpetrate violent crimes, whereas women are more likely to be the victims of violence.7
Table 3
10 questions to ask patients about a history of violence
| What is the most violent thing you have ever done? |
| What types of violent behavior have you engaged in? |
| What is your understanding of why this violence occurred? |
| Who was involved in prior violent incidents? |
| Have you ever been arrested for any type of violent act? |
| Have you ever been intoxicated at the time you were violent? |
| Were you experiencing mental health symptoms when violent? |
| What is the greatest degree of injury you inflicted on someone else? |
| What weapons have you used when violent? |
| Have you ever been a victim of violence? |
Mental illness and violence
Studies examining whether individuals with mental illness are more violent than the non-mentally ill have yielded mixed results.8,9 In a study of civilly committed psychiatric patients released into the community, most mentally ill individuals were not violent.10 Although researchers noted a weak relationship between mental illness and violence, violent conduct was greater only when the person was experiencing acute psychiatric symptoms. Subsequent research suggests that individuals with schizophrenia may have increased rates of violence even when not experiencing active signs of their illness.11
Psychosis. In paranoid psychotic patients, violence often is well planned and in line with their false beliefs.12 These patients usually direct the violence at a specific person they perceive as a persecutor. Paranoid individuals often target relatives or friends. In addition, community-dwelling paranoid persons are more likely to be dangerous because they have greater access to weapons than institutionalized patients.12
Carefully inquire about hallucinations—particularly auditory ones—to determine whether their presence increases the person’s risk to commit a violent act. Patients with schizophrenia are more likely to be violent if their auditory hallucinations generate negative emotions (anger, anxiety, or sadness) and if the patients have not developed successful coping strategies.13 Although most patients ignore violent command hallucinations to harm others, the presence of command hallucinations may increase the likelihood of behaving violently,14 particularly if:
- the voice is familiar to the person,15 and
- the person has delusional beliefs associated with the hallucinations.16
18
Antisocial personality disorder (APD). Violence by those with APD often is motivated by revenge or occurs during a period of heavy drinking. Violent behavior by these persons frequently is cold, calculated, and lacks emotionality.19
In addition to DSM-IV-TR personality disorders, be familiar with the psychological construct known as psychopathy. Cleckley20 used the term psychopath to describe a person who is superficially charming, lacks close relationships, is impulsive, and is primarily concerned with self-gratification. Hare et al21 developed the Psychopathy Checklist-Revised as a validated measure of psychopathy in adults. Psychopathy is a strong predictor of criminal behavior and violence among adults.22
Affect. Individuals who are angry and lack empathy for others are at increased risk for violent behavior.23 Also observe the patient for physical signs and symptoms of changes indicating incipient violence. Berg et al24 noted that signs of imminent violence can include:
- chanting
- clenched jaw
- flared nostrils
- flushed face
- darting eyes
- close proximity to the clinician
- clenched or gripping hands.
Static vs dynamic factors. When organizing strategies to decrease risk factors for violence, distinguish static from dynamic factors. Static factors include demographic information and history of violence. Dynamic factors, which are subject to change with intervention, include access to weapons, psychotic symptoms, active substance use, and a person’s living situation.
Table 4
Sample violence risk management chart for Mr. J
| Risk factor | Intervention | Status |
|---|---|---|
| Paranoia | Antipsychotic medication | Admitted to inpatient psychiatric facility; antipsychotic medications ordered with continued assessments of mental status |
| Antipsychotic medication nonadherence | Depot form of antipsychotic | Mr. J agreed to depot medication |
| Gun at home | Remove guns | His mother removed all guns from home |
| Alcohol and methamphetamine abuse | Evaluate for potential alcohol detox; urine drug screen on admission | Mr. J refused group substance treatment in the hospital; substance use treatment in the community to be arranged prior to discharge |
Related resource
- Simon RI, Hales RE, eds. The American Psychiatric Publishing textbook of suicide assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2006.
- Simon RI, Tardiff K, eds. Textbook of violence assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
- Risperidone • Risperdal
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. El-Mallakh RS, Roberts RJ, El-Mallakh RL. Mood disorders. In: Simon RI, Tardiff K, eds. Textbook of violence assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2008:86–92.
2. Resnick PJ. Recognizing that the suicidal patient views you as an “adversary.” Current Psychiatry. 2002;1:8.-
3. American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. 2nd ed. In: Practice guidelines for the treatment of psychiatric disorders compendium. Arlington, VA: American Psychiatric Publishing, Inc; 2004:835–1027.
4. Klassen D, O’Connor WA. A prospective study of predictors of violence in adult male mental health admissions. Law Hum Behav. 1988;12(3):143-158.
5. Tardiff K. Violence. In: Hales R, Yudofsky S, Talbott A, eds. American Psychiatric Press textbook of psychiatry. Arlington, VA: American Psychiatric Publishing, Inc; 1999:1405–1428.
6. Murdoch D, Phil RO, Ross D. Alcohol and crimes of violence: present issues. Int J Addict. 1990;25:1065-1081.
7. Goldstein PJ, Bellucci PA, Spunt BJ, et al. Frequency of cocaine use and violence: a comparison between men and women. In: Scholber S, Schade C, eds. The epidemiology of cocaine use and abuse. Research monograph 110. Rockville, MD: National Institute on Drug Abuse; 1991:113–138.
8. Link BG, Stueve A. Evidence bearing on mental illness as a possible cause of violent behavior. Epidemiol Rev. 1995;17:172-181.
9. Torrey EF. Violent behavior by individuals with serious mental illness. Hosp Community Psychiatry. 1994;45:653-662.
10. Monahan J. Actuarial support for the clinical assessment of violence risk. Int Rev Psychiatry. 1997;9:167-170.
11. Wallace C, Mullen PE, Burgess P. Criminal offending in schizophrenia over a 25-year period marked by deinstitutionalization and increasing prevalence of comorbid substance use disorders. Am J Psychiatry. 2004;161:716-727.
12. Krakowski M, Volavka J, Brizer D. Psychopathology and violence: a review of literature. Compr Psychiatry. 1986;27:131-148.
13. Cheung P, Schweitzer I, Crowley K, et al. Violence in schizophrenia: role of hallucinations and delusions. Schizophr Res. 1997;26:181-190.
14. McNiel DE, Eisner JP, Binder RL. The relationship between command hallucinations and violence. Psychiatr Serv. 2000;51:1288-1292.
15. Rudnick A. Relation between command hallucinations and dangerous behavior. J Am Acad Psychiatry Law. 1999;27:253-257.
16. Junginger J. Predicting compliance with command hallucinations. Am J Psychiatry. 1990;147:245-247.
17. Marjuk PM, Tardiff K, Hirsh CS. The epidemiology of murder-suicide. JAMA. 1992;267:3179-3183.
18. Tardiff K, Sweillam A. Assaultive behavior among inpatients. Am J Psychiatry. 1982;139:212-215.
19. Williamson S, Hare R, Wong S. Violence: criminal psychopaths and their victims. Canadian Journal of Behavioral Sciences. 1987;19:454-462.
20. Cleckley HM. The mask of sanity. St. Louis, MO: Mosby; 1976.
21. Hare RD. The Hare Psychopathy Checklist-Revised. Toronto, ON, Canada: Multi-Health Systems; 1991.
22. Salekin RT, Rogers R, Sewell KW. A review of meta-analysis of the Psychopathy Checklist and Psychopathy Checklist-Revised: predictive validity of dangerousness. Clinical Psychology Science and Practice. 1996;3:203-213.
23. Menzies RJ, Webster CD, Sepejak DS. The dimensions of dangerousness: evaluating the accuracy of psychometric predictions of violence among forensic patients. Law Hum Behav. 1985;9:49-70.
24. Berg AZ, Bell CC, Tupin J. Clinician safety: assessing and managing the violent patient. New Dir Ment Health Serv. 2000;(86):9-29.
Police take Ms. L, age 23, to the emergency room (ER) after her fiancé called them. He told the police that after a “night of drinking” they argued about a girl he had flirted with. Ms. L took out a loaded gun and threatened to shoot herself. She eventually handed the gun over to the police.
In the ER, Ms. L’s blood alcohol level is 0.20%. She tells the admitting emergency room nurse, “I would never hurt myself. I drank too much and was acting stupid. I just want to go home and sleep it off. I promise not to harm myself.” Emergency room staff observe Ms. L smile and giggle while waiting for a psychiatric evaluation.
What would you do? Hospitalize Ms. L for safety, or accept her promise not to hurt herself and send her home? What criteria would you use?
Knowing how to assess patients such as Ms. L is an essential psychiatric skill, whether or not you trained in forensic psychiatry. This article includes case reports that illustrate techniques for evaluating patients who may harbor suicidal or homicidal thoughts.
Evaluating danger to self
Your role is to weigh an individual’s risk factors for suicide against potential protective factors and to make a judgment call. Potential risk factors for suicide include (but are not limited to):
- current suicidal thoughts
- prior suicide attempts
- presence of a comorbid psychiatric disorder (particularly depression)
- intoxication or ongoing substance use
- feelings of hopelessness
- marked anxiety
- recent stressors
- family history of suicide
- lack of psychosocial support.1
Also review information that is reasonably available. In the ER, records from other facilities or private psychiatric treatment notes may not be accessed easily. However, in addition to conducting a suicide risk assessment and mental status examination, consider reviewing the collateral information outlined in Table 2.
Furthermore, do not rely on “no-suicide” contracts. They do not guarantee that a person won’t attempt suicide, and they will not provide legal protection if the patient commits suicide after being released from your care.2
What to document. After completing your evaluation, specifically document:
- that a suicide risk assessment was conducted
- what risk factors were present
- interventions to address those risk factors
- the level of risk determined (minimal, moderate, or high)
- factors that may protect the patient against suicide.
Table 1
Evaluating suicidality: Sample questions to ask
| Do you wish you were dead? |
| Do you have thoughts about harming yourself? |
| Do you have an actual plan as to how you would harm yourself? If yes: Have you taken any steps to enact that plan? If so, what were they? |
| Have you ever attempted suicide before? If yes: What stopped you from enacting this plan? What do you think would keep you from acting on this plan in the future? |
| Has anyone in your family or close to you committed suicide? |
| How close have you come to killing yourself? |
Table 2
Sources of information to assess suicidality in the ER
| Police reports on circumstances that led the patient to come to the ER |
| ER nursing/physician notes |
| Family members’/friends’ statements regarding reasons for the patient’s visit |
| Observations by anyone assigned to monitor the patient while awaiting your consult |
| Laboratory and physical exam findings, particularly related to substance use and/or self-injurious behavior |
| Psychiatric records at that facility |
| Concerns expressed by anyone responsible for the patient if he/she is released from the hospital |
| ER: emergency room |
CASE REPORT: Paranoid and armed
Mr. J, age 21, is brought involuntarily to the psychiatric ER by police. His mother reports he was locked in his room with a gun, claiming “the FBI is going to kill me.”
Mr. J’s mother tells the ER psychiatrist that her son has schizophrenia, paranoid type, and stopped taking risperidone, 3 mg/d, 4 weeks ago. She explains that Mr. J sometimes “hears voices” whispering to him that his medications are poison and to not trust his family. She states that Mr. J also abuses alcohol and methamphetamine and has 2 prior arrests for assault with a deadly weapon.
She adds that Mr. J now believes his family is working with the FBI to have him placed in a “secret detention camp.” Mr. J’s mother found a loaded pistol in his room and is “scared of what might happen.” During your psychiatric interview, Mr. J appears frightened and paranoid and provides only minimal answers to your questions. He clenches his teeth while staring intently at you.
Evaluating danger to others
There is good reason to be concerned that Mr. J might behave violently, and you likely have sufficient information to hospitalize him. When creating a long-term violence risk prevention plan, divide the concept of dangerousness into 5 components:
- magnitude of potential harm
- likelihood that harm will occur
- imminence of harm
- frequency of dangerous behavior
- situational variables that promote or protect against aggressive behavior.
A person who has used weapons against others may pose a serious risk of future violence. Ask patients whether they own or have ever owned a weapon. In our experience, the recent movement of a weapon—such as transferring a gun from a closet to a nightstand—is particularly ominous in a paranoid person. The greater the psychotic fear, the more likely a paranoid person is to kill someone he misperceives as a persecutor.
Drugs and alcohol are strongly associated with violent behavior.5 Most persons involved in violent crimes are under the influence of alcohol or drugs at the time of their aggression.6 Stimulants such as cocaine, crack, amphetamines, and phencyclidine are of special concern. These drugs often are associated with feelings of disinhibition, a sense of power, and paranoia. The violence linked with cocaine use differs by gender: men are more likely to perpetrate violent crimes, whereas women are more likely to be the victims of violence.7
Table 3
10 questions to ask patients about a history of violence
| What is the most violent thing you have ever done? |
| What types of violent behavior have you engaged in? |
| What is your understanding of why this violence occurred? |
| Who was involved in prior violent incidents? |
| Have you ever been arrested for any type of violent act? |
| Have you ever been intoxicated at the time you were violent? |
| Were you experiencing mental health symptoms when violent? |
| What is the greatest degree of injury you inflicted on someone else? |
| What weapons have you used when violent? |
| Have you ever been a victim of violence? |
Mental illness and violence
Studies examining whether individuals with mental illness are more violent than the non-mentally ill have yielded mixed results.8,9 In a study of civilly committed psychiatric patients released into the community, most mentally ill individuals were not violent.10 Although researchers noted a weak relationship between mental illness and violence, violent conduct was greater only when the person was experiencing acute psychiatric symptoms. Subsequent research suggests that individuals with schizophrenia may have increased rates of violence even when not experiencing active signs of their illness.11
Psychosis. In paranoid psychotic patients, violence often is well planned and in line with their false beliefs.12 These patients usually direct the violence at a specific person they perceive as a persecutor. Paranoid individuals often target relatives or friends. In addition, community-dwelling paranoid persons are more likely to be dangerous because they have greater access to weapons than institutionalized patients.12
Carefully inquire about hallucinations—particularly auditory ones—to determine whether their presence increases the person’s risk to commit a violent act. Patients with schizophrenia are more likely to be violent if their auditory hallucinations generate negative emotions (anger, anxiety, or sadness) and if the patients have not developed successful coping strategies.13 Although most patients ignore violent command hallucinations to harm others, the presence of command hallucinations may increase the likelihood of behaving violently,14 particularly if:
- the voice is familiar to the person,15 and
- the person has delusional beliefs associated with the hallucinations.16
18
Antisocial personality disorder (APD). Violence by those with APD often is motivated by revenge or occurs during a period of heavy drinking. Violent behavior by these persons frequently is cold, calculated, and lacks emotionality.19
In addition to DSM-IV-TR personality disorders, be familiar with the psychological construct known as psychopathy. Cleckley20 used the term psychopath to describe a person who is superficially charming, lacks close relationships, is impulsive, and is primarily concerned with self-gratification. Hare et al21 developed the Psychopathy Checklist-Revised as a validated measure of psychopathy in adults. Psychopathy is a strong predictor of criminal behavior and violence among adults.22
Affect. Individuals who are angry and lack empathy for others are at increased risk for violent behavior.23 Also observe the patient for physical signs and symptoms of changes indicating incipient violence. Berg et al24 noted that signs of imminent violence can include:
- chanting
- clenched jaw
- flared nostrils
- flushed face
- darting eyes
- close proximity to the clinician
- clenched or gripping hands.
Static vs dynamic factors. When organizing strategies to decrease risk factors for violence, distinguish static from dynamic factors. Static factors include demographic information and history of violence. Dynamic factors, which are subject to change with intervention, include access to weapons, psychotic symptoms, active substance use, and a person’s living situation.
Table 4
Sample violence risk management chart for Mr. J
| Risk factor | Intervention | Status |
|---|---|---|
| Paranoia | Antipsychotic medication | Admitted to inpatient psychiatric facility; antipsychotic medications ordered with continued assessments of mental status |
| Antipsychotic medication nonadherence | Depot form of antipsychotic | Mr. J agreed to depot medication |
| Gun at home | Remove guns | His mother removed all guns from home |
| Alcohol and methamphetamine abuse | Evaluate for potential alcohol detox; urine drug screen on admission | Mr. J refused group substance treatment in the hospital; substance use treatment in the community to be arranged prior to discharge |
Related resource
- Simon RI, Hales RE, eds. The American Psychiatric Publishing textbook of suicide assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2006.
- Simon RI, Tardiff K, eds. Textbook of violence assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
- Risperidone • Risperdal
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Police take Ms. L, age 23, to the emergency room (ER) after her fiancé called them. He told the police that after a “night of drinking” they argued about a girl he had flirted with. Ms. L took out a loaded gun and threatened to shoot herself. She eventually handed the gun over to the police.
In the ER, Ms. L’s blood alcohol level is 0.20%. She tells the admitting emergency room nurse, “I would never hurt myself. I drank too much and was acting stupid. I just want to go home and sleep it off. I promise not to harm myself.” Emergency room staff observe Ms. L smile and giggle while waiting for a psychiatric evaluation.
What would you do? Hospitalize Ms. L for safety, or accept her promise not to hurt herself and send her home? What criteria would you use?
Knowing how to assess patients such as Ms. L is an essential psychiatric skill, whether or not you trained in forensic psychiatry. This article includes case reports that illustrate techniques for evaluating patients who may harbor suicidal or homicidal thoughts.
Evaluating danger to self
Your role is to weigh an individual’s risk factors for suicide against potential protective factors and to make a judgment call. Potential risk factors for suicide include (but are not limited to):
- current suicidal thoughts
- prior suicide attempts
- presence of a comorbid psychiatric disorder (particularly depression)
- intoxication or ongoing substance use
- feelings of hopelessness
- marked anxiety
- recent stressors
- family history of suicide
- lack of psychosocial support.1
Also review information that is reasonably available. In the ER, records from other facilities or private psychiatric treatment notes may not be accessed easily. However, in addition to conducting a suicide risk assessment and mental status examination, consider reviewing the collateral information outlined in Table 2.
Furthermore, do not rely on “no-suicide” contracts. They do not guarantee that a person won’t attempt suicide, and they will not provide legal protection if the patient commits suicide after being released from your care.2
What to document. After completing your evaluation, specifically document:
- that a suicide risk assessment was conducted
- what risk factors were present
- interventions to address those risk factors
- the level of risk determined (minimal, moderate, or high)
- factors that may protect the patient against suicide.
Table 1
Evaluating suicidality: Sample questions to ask
| Do you wish you were dead? |
| Do you have thoughts about harming yourself? |
| Do you have an actual plan as to how you would harm yourself? If yes: Have you taken any steps to enact that plan? If so, what were they? |
| Have you ever attempted suicide before? If yes: What stopped you from enacting this plan? What do you think would keep you from acting on this plan in the future? |
| Has anyone in your family or close to you committed suicide? |
| How close have you come to killing yourself? |
Table 2
Sources of information to assess suicidality in the ER
| Police reports on circumstances that led the patient to come to the ER |
| ER nursing/physician notes |
| Family members’/friends’ statements regarding reasons for the patient’s visit |
| Observations by anyone assigned to monitor the patient while awaiting your consult |
| Laboratory and physical exam findings, particularly related to substance use and/or self-injurious behavior |
| Psychiatric records at that facility |
| Concerns expressed by anyone responsible for the patient if he/she is released from the hospital |
| ER: emergency room |
CASE REPORT: Paranoid and armed
Mr. J, age 21, is brought involuntarily to the psychiatric ER by police. His mother reports he was locked in his room with a gun, claiming “the FBI is going to kill me.”
Mr. J’s mother tells the ER psychiatrist that her son has schizophrenia, paranoid type, and stopped taking risperidone, 3 mg/d, 4 weeks ago. She explains that Mr. J sometimes “hears voices” whispering to him that his medications are poison and to not trust his family. She states that Mr. J also abuses alcohol and methamphetamine and has 2 prior arrests for assault with a deadly weapon.
She adds that Mr. J now believes his family is working with the FBI to have him placed in a “secret detention camp.” Mr. J’s mother found a loaded pistol in his room and is “scared of what might happen.” During your psychiatric interview, Mr. J appears frightened and paranoid and provides only minimal answers to your questions. He clenches his teeth while staring intently at you.
Evaluating danger to others
There is good reason to be concerned that Mr. J might behave violently, and you likely have sufficient information to hospitalize him. When creating a long-term violence risk prevention plan, divide the concept of dangerousness into 5 components:
- magnitude of potential harm
- likelihood that harm will occur
- imminence of harm
- frequency of dangerous behavior
- situational variables that promote or protect against aggressive behavior.
A person who has used weapons against others may pose a serious risk of future violence. Ask patients whether they own or have ever owned a weapon. In our experience, the recent movement of a weapon—such as transferring a gun from a closet to a nightstand—is particularly ominous in a paranoid person. The greater the psychotic fear, the more likely a paranoid person is to kill someone he misperceives as a persecutor.
Drugs and alcohol are strongly associated with violent behavior.5 Most persons involved in violent crimes are under the influence of alcohol or drugs at the time of their aggression.6 Stimulants such as cocaine, crack, amphetamines, and phencyclidine are of special concern. These drugs often are associated with feelings of disinhibition, a sense of power, and paranoia. The violence linked with cocaine use differs by gender: men are more likely to perpetrate violent crimes, whereas women are more likely to be the victims of violence.7
Table 3
10 questions to ask patients about a history of violence
| What is the most violent thing you have ever done? |
| What types of violent behavior have you engaged in? |
| What is your understanding of why this violence occurred? |
| Who was involved in prior violent incidents? |
| Have you ever been arrested for any type of violent act? |
| Have you ever been intoxicated at the time you were violent? |
| Were you experiencing mental health symptoms when violent? |
| What is the greatest degree of injury you inflicted on someone else? |
| What weapons have you used when violent? |
| Have you ever been a victim of violence? |
Mental illness and violence
Studies examining whether individuals with mental illness are more violent than the non-mentally ill have yielded mixed results.8,9 In a study of civilly committed psychiatric patients released into the community, most mentally ill individuals were not violent.10 Although researchers noted a weak relationship between mental illness and violence, violent conduct was greater only when the person was experiencing acute psychiatric symptoms. Subsequent research suggests that individuals with schizophrenia may have increased rates of violence even when not experiencing active signs of their illness.11
Psychosis. In paranoid psychotic patients, violence often is well planned and in line with their false beliefs.12 These patients usually direct the violence at a specific person they perceive as a persecutor. Paranoid individuals often target relatives or friends. In addition, community-dwelling paranoid persons are more likely to be dangerous because they have greater access to weapons than institutionalized patients.12
Carefully inquire about hallucinations—particularly auditory ones—to determine whether their presence increases the person’s risk to commit a violent act. Patients with schizophrenia are more likely to be violent if their auditory hallucinations generate negative emotions (anger, anxiety, or sadness) and if the patients have not developed successful coping strategies.13 Although most patients ignore violent command hallucinations to harm others, the presence of command hallucinations may increase the likelihood of behaving violently,14 particularly if:
- the voice is familiar to the person,15 and
- the person has delusional beliefs associated with the hallucinations.16
18
Antisocial personality disorder (APD). Violence by those with APD often is motivated by revenge or occurs during a period of heavy drinking. Violent behavior by these persons frequently is cold, calculated, and lacks emotionality.19
In addition to DSM-IV-TR personality disorders, be familiar with the psychological construct known as psychopathy. Cleckley20 used the term psychopath to describe a person who is superficially charming, lacks close relationships, is impulsive, and is primarily concerned with self-gratification. Hare et al21 developed the Psychopathy Checklist-Revised as a validated measure of psychopathy in adults. Psychopathy is a strong predictor of criminal behavior and violence among adults.22
Affect. Individuals who are angry and lack empathy for others are at increased risk for violent behavior.23 Also observe the patient for physical signs and symptoms of changes indicating incipient violence. Berg et al24 noted that signs of imminent violence can include:
- chanting
- clenched jaw
- flared nostrils
- flushed face
- darting eyes
- close proximity to the clinician
- clenched or gripping hands.
Static vs dynamic factors. When organizing strategies to decrease risk factors for violence, distinguish static from dynamic factors. Static factors include demographic information and history of violence. Dynamic factors, which are subject to change with intervention, include access to weapons, psychotic symptoms, active substance use, and a person’s living situation.
Table 4
Sample violence risk management chart for Mr. J
| Risk factor | Intervention | Status |
|---|---|---|
| Paranoia | Antipsychotic medication | Admitted to inpatient psychiatric facility; antipsychotic medications ordered with continued assessments of mental status |
| Antipsychotic medication nonadherence | Depot form of antipsychotic | Mr. J agreed to depot medication |
| Gun at home | Remove guns | His mother removed all guns from home |
| Alcohol and methamphetamine abuse | Evaluate for potential alcohol detox; urine drug screen on admission | Mr. J refused group substance treatment in the hospital; substance use treatment in the community to be arranged prior to discharge |
Related resource
- Simon RI, Hales RE, eds. The American Psychiatric Publishing textbook of suicide assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2006.
- Simon RI, Tardiff K, eds. Textbook of violence assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
- Risperidone • Risperdal
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. El-Mallakh RS, Roberts RJ, El-Mallakh RL. Mood disorders. In: Simon RI, Tardiff K, eds. Textbook of violence assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2008:86–92.
2. Resnick PJ. Recognizing that the suicidal patient views you as an “adversary.” Current Psychiatry. 2002;1:8.-
3. American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. 2nd ed. In: Practice guidelines for the treatment of psychiatric disorders compendium. Arlington, VA: American Psychiatric Publishing, Inc; 2004:835–1027.
4. Klassen D, O’Connor WA. A prospective study of predictors of violence in adult male mental health admissions. Law Hum Behav. 1988;12(3):143-158.
5. Tardiff K. Violence. In: Hales R, Yudofsky S, Talbott A, eds. American Psychiatric Press textbook of psychiatry. Arlington, VA: American Psychiatric Publishing, Inc; 1999:1405–1428.
6. Murdoch D, Phil RO, Ross D. Alcohol and crimes of violence: present issues. Int J Addict. 1990;25:1065-1081.
7. Goldstein PJ, Bellucci PA, Spunt BJ, et al. Frequency of cocaine use and violence: a comparison between men and women. In: Scholber S, Schade C, eds. The epidemiology of cocaine use and abuse. Research monograph 110. Rockville, MD: National Institute on Drug Abuse; 1991:113–138.
8. Link BG, Stueve A. Evidence bearing on mental illness as a possible cause of violent behavior. Epidemiol Rev. 1995;17:172-181.
9. Torrey EF. Violent behavior by individuals with serious mental illness. Hosp Community Psychiatry. 1994;45:653-662.
10. Monahan J. Actuarial support for the clinical assessment of violence risk. Int Rev Psychiatry. 1997;9:167-170.
11. Wallace C, Mullen PE, Burgess P. Criminal offending in schizophrenia over a 25-year period marked by deinstitutionalization and increasing prevalence of comorbid substance use disorders. Am J Psychiatry. 2004;161:716-727.
12. Krakowski M, Volavka J, Brizer D. Psychopathology and violence: a review of literature. Compr Psychiatry. 1986;27:131-148.
13. Cheung P, Schweitzer I, Crowley K, et al. Violence in schizophrenia: role of hallucinations and delusions. Schizophr Res. 1997;26:181-190.
14. McNiel DE, Eisner JP, Binder RL. The relationship between command hallucinations and violence. Psychiatr Serv. 2000;51:1288-1292.
15. Rudnick A. Relation between command hallucinations and dangerous behavior. J Am Acad Psychiatry Law. 1999;27:253-257.
16. Junginger J. Predicting compliance with command hallucinations. Am J Psychiatry. 1990;147:245-247.
17. Marjuk PM, Tardiff K, Hirsh CS. The epidemiology of murder-suicide. JAMA. 1992;267:3179-3183.
18. Tardiff K, Sweillam A. Assaultive behavior among inpatients. Am J Psychiatry. 1982;139:212-215.
19. Williamson S, Hare R, Wong S. Violence: criminal psychopaths and their victims. Canadian Journal of Behavioral Sciences. 1987;19:454-462.
20. Cleckley HM. The mask of sanity. St. Louis, MO: Mosby; 1976.
21. Hare RD. The Hare Psychopathy Checklist-Revised. Toronto, ON, Canada: Multi-Health Systems; 1991.
22. Salekin RT, Rogers R, Sewell KW. A review of meta-analysis of the Psychopathy Checklist and Psychopathy Checklist-Revised: predictive validity of dangerousness. Clinical Psychology Science and Practice. 1996;3:203-213.
23. Menzies RJ, Webster CD, Sepejak DS. The dimensions of dangerousness: evaluating the accuracy of psychometric predictions of violence among forensic patients. Law Hum Behav. 1985;9:49-70.
24. Berg AZ, Bell CC, Tupin J. Clinician safety: assessing and managing the violent patient. New Dir Ment Health Serv. 2000;(86):9-29.
1. El-Mallakh RS, Roberts RJ, El-Mallakh RL. Mood disorders. In: Simon RI, Tardiff K, eds. Textbook of violence assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2008:86–92.
2. Resnick PJ. Recognizing that the suicidal patient views you as an “adversary.” Current Psychiatry. 2002;1:8.-
3. American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. 2nd ed. In: Practice guidelines for the treatment of psychiatric disorders compendium. Arlington, VA: American Psychiatric Publishing, Inc; 2004:835–1027.
4. Klassen D, O’Connor WA. A prospective study of predictors of violence in adult male mental health admissions. Law Hum Behav. 1988;12(3):143-158.
5. Tardiff K. Violence. In: Hales R, Yudofsky S, Talbott A, eds. American Psychiatric Press textbook of psychiatry. Arlington, VA: American Psychiatric Publishing, Inc; 1999:1405–1428.
6. Murdoch D, Phil RO, Ross D. Alcohol and crimes of violence: present issues. Int J Addict. 1990;25:1065-1081.
7. Goldstein PJ, Bellucci PA, Spunt BJ, et al. Frequency of cocaine use and violence: a comparison between men and women. In: Scholber S, Schade C, eds. The epidemiology of cocaine use and abuse. Research monograph 110. Rockville, MD: National Institute on Drug Abuse; 1991:113–138.
8. Link BG, Stueve A. Evidence bearing on mental illness as a possible cause of violent behavior. Epidemiol Rev. 1995;17:172-181.
9. Torrey EF. Violent behavior by individuals with serious mental illness. Hosp Community Psychiatry. 1994;45:653-662.
10. Monahan J. Actuarial support for the clinical assessment of violence risk. Int Rev Psychiatry. 1997;9:167-170.
11. Wallace C, Mullen PE, Burgess P. Criminal offending in schizophrenia over a 25-year period marked by deinstitutionalization and increasing prevalence of comorbid substance use disorders. Am J Psychiatry. 2004;161:716-727.
12. Krakowski M, Volavka J, Brizer D. Psychopathology and violence: a review of literature. Compr Psychiatry. 1986;27:131-148.
13. Cheung P, Schweitzer I, Crowley K, et al. Violence in schizophrenia: role of hallucinations and delusions. Schizophr Res. 1997;26:181-190.
14. McNiel DE, Eisner JP, Binder RL. The relationship between command hallucinations and violence. Psychiatr Serv. 2000;51:1288-1292.
15. Rudnick A. Relation between command hallucinations and dangerous behavior. J Am Acad Psychiatry Law. 1999;27:253-257.
16. Junginger J. Predicting compliance with command hallucinations. Am J Psychiatry. 1990;147:245-247.
17. Marjuk PM, Tardiff K, Hirsh CS. The epidemiology of murder-suicide. JAMA. 1992;267:3179-3183.
18. Tardiff K, Sweillam A. Assaultive behavior among inpatients. Am J Psychiatry. 1982;139:212-215.
19. Williamson S, Hare R, Wong S. Violence: criminal psychopaths and their victims. Canadian Journal of Behavioral Sciences. 1987;19:454-462.
20. Cleckley HM. The mask of sanity. St. Louis, MO: Mosby; 1976.
21. Hare RD. The Hare Psychopathy Checklist-Revised. Toronto, ON, Canada: Multi-Health Systems; 1991.
22. Salekin RT, Rogers R, Sewell KW. A review of meta-analysis of the Psychopathy Checklist and Psychopathy Checklist-Revised: predictive validity of dangerousness. Clinical Psychology Science and Practice. 1996;3:203-213.
23. Menzies RJ, Webster CD, Sepejak DS. The dimensions of dangerousness: evaluating the accuracy of psychometric predictions of violence among forensic patients. Law Hum Behav. 1985;9:49-70.
24. Berg AZ, Bell CC, Tupin J. Clinician safety: assessing and managing the violent patient. New Dir Ment Health Serv. 2000;(86):9-29.