User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Teaching the STEPs of clinical psychopharmacology
Teaching medical students and psychiatry residents the principles of safe, effective clinical psychopharmacology can be challenging. Psychotropic agents from the same category often possess different mechanisms of action, cause various side effects, and have distinct safety profiles. Moreover, similar agents can be differentiated by the amount of evidence supporting their efficacy in treating particular disorders.
To help, I encourage prescribers to add a “STEP”—Safety, Tolerability, Efficacy, and Practicality—to their clinical decision-making. This is an invaluable “pearl” I learned nearly a decade ago and present here in a slightly modified form.1
Safety. Know the psychotropic’s safety profile, especially regarding comorbid medical illness and potential drug-drug interactions. Bupropion, for instance, may be an excellent choice for a depressed patient who recently had a myocardial infarction, but research shows the drug is risky for a person with a comorbid seizure disorder.
Tolerability. Evaluate the short- and long-term effects of each medication. Haloperidol, for example, is a reasonable choice for acute treatment of psychotic agitation in the emergency department, but a young woman struggling to manage her schizophrenia may not tolerate the drug as a maintenance therapy.
Efficacy. Familiarize yourself with the clinical evidence supporting a drug’s use for a particular disorder. Evidence strongly supports lithium carbonate for treating bipolar affective disorder, but current evidence-based clinical guidelines do not endorse gabapentin as a first choice for mood stabilization.
Practicality. Consider cost, adherence, and monitoring issues. A medication will certainly fail if the patient never fills the prescription because of cost or cannot adhere to a multiple daily dosing regimen or routine serum chemistries. This aspect may be the most essential to dispensing psychotropics because the student or resident must have a thoughtful grasp of the patient’s life circumstances, deficits, strengths, and motivation. Such understanding can be achieved only through careful, empathic listening and active involvement in the patient’s care and well-being.
Reference
1. Preskorn SH. Selection of an antidepressant: mirtazapine. J Clin Psychiatry 1997;58(suppl 6):3-8.
Dr. Christensen is associate professor of psychiatry, University of Florida College of Medicine, Jacksonville, and director of the university’s community psychiatry program.
Teaching medical students and psychiatry residents the principles of safe, effective clinical psychopharmacology can be challenging. Psychotropic agents from the same category often possess different mechanisms of action, cause various side effects, and have distinct safety profiles. Moreover, similar agents can be differentiated by the amount of evidence supporting their efficacy in treating particular disorders.
To help, I encourage prescribers to add a “STEP”—Safety, Tolerability, Efficacy, and Practicality—to their clinical decision-making. This is an invaluable “pearl” I learned nearly a decade ago and present here in a slightly modified form.1
Safety. Know the psychotropic’s safety profile, especially regarding comorbid medical illness and potential drug-drug interactions. Bupropion, for instance, may be an excellent choice for a depressed patient who recently had a myocardial infarction, but research shows the drug is risky for a person with a comorbid seizure disorder.
Tolerability. Evaluate the short- and long-term effects of each medication. Haloperidol, for example, is a reasonable choice for acute treatment of psychotic agitation in the emergency department, but a young woman struggling to manage her schizophrenia may not tolerate the drug as a maintenance therapy.
Efficacy. Familiarize yourself with the clinical evidence supporting a drug’s use for a particular disorder. Evidence strongly supports lithium carbonate for treating bipolar affective disorder, but current evidence-based clinical guidelines do not endorse gabapentin as a first choice for mood stabilization.
Practicality. Consider cost, adherence, and monitoring issues. A medication will certainly fail if the patient never fills the prescription because of cost or cannot adhere to a multiple daily dosing regimen or routine serum chemistries. This aspect may be the most essential to dispensing psychotropics because the student or resident must have a thoughtful grasp of the patient’s life circumstances, deficits, strengths, and motivation. Such understanding can be achieved only through careful, empathic listening and active involvement in the patient’s care and well-being.
Teaching medical students and psychiatry residents the principles of safe, effective clinical psychopharmacology can be challenging. Psychotropic agents from the same category often possess different mechanisms of action, cause various side effects, and have distinct safety profiles. Moreover, similar agents can be differentiated by the amount of evidence supporting their efficacy in treating particular disorders.
To help, I encourage prescribers to add a “STEP”—Safety, Tolerability, Efficacy, and Practicality—to their clinical decision-making. This is an invaluable “pearl” I learned nearly a decade ago and present here in a slightly modified form.1
Safety. Know the psychotropic’s safety profile, especially regarding comorbid medical illness and potential drug-drug interactions. Bupropion, for instance, may be an excellent choice for a depressed patient who recently had a myocardial infarction, but research shows the drug is risky for a person with a comorbid seizure disorder.
Tolerability. Evaluate the short- and long-term effects of each medication. Haloperidol, for example, is a reasonable choice for acute treatment of psychotic agitation in the emergency department, but a young woman struggling to manage her schizophrenia may not tolerate the drug as a maintenance therapy.
Efficacy. Familiarize yourself with the clinical evidence supporting a drug’s use for a particular disorder. Evidence strongly supports lithium carbonate for treating bipolar affective disorder, but current evidence-based clinical guidelines do not endorse gabapentin as a first choice for mood stabilization.
Practicality. Consider cost, adherence, and monitoring issues. A medication will certainly fail if the patient never fills the prescription because of cost or cannot adhere to a multiple daily dosing regimen or routine serum chemistries. This aspect may be the most essential to dispensing psychotropics because the student or resident must have a thoughtful grasp of the patient’s life circumstances, deficits, strengths, and motivation. Such understanding can be achieved only through careful, empathic listening and active involvement in the patient’s care and well-being.
Reference
1. Preskorn SH. Selection of an antidepressant: mirtazapine. J Clin Psychiatry 1997;58(suppl 6):3-8.
Dr. Christensen is associate professor of psychiatry, University of Florida College of Medicine, Jacksonville, and director of the university’s community psychiatry program.
Reference
1. Preskorn SH. Selection of an antidepressant: mirtazapine. J Clin Psychiatry 1997;58(suppl 6):3-8.
Dr. Christensen is associate professor of psychiatry, University of Florida College of Medicine, Jacksonville, and director of the university’s community psychiatry program.
Pros and cons of pill splitting
Clinicians and patients look to pill splitting to reduce psychotropics’ costs and fine-tune pharmacotherapy, but pill splitting has not been rigorously studied for safety or efficacy. It is important to understand the risks and benefits of pill splitting before you recommend the practice to patients.
Pros of pill splitting
Lower costs for patients. Many psychotropics come in multiple strengths, and one larger pill often costs less than 2 smaller pills of equivalent dosage.1 Writing a prescription for a higher dose and instructing the patient to cut the pill in half can lower costs.
Fine-tune titration. Pill splitting allows you to prescribe a lower strength to gradually titrate dosages up or taper them down. This practice can prevent side effects and improve adherence because a lower dose may have a more favorable pharmacokinetic profile.
Improve tolerability. Patients might better tolerate half a pill taken twice daily rather than an entire pill once daily. A smaller dose may prevent a spike in serum level, which could aid tolerability.
- Will there be a cost saving for the patient?
- Can the patient understand and follow your recommendations?
- Can the patient tolerate minor dosage variability that can occur with pill splitting?
- Is the medication’s integrity maintained when the pill is split?
If the answer is yes to all 4 questions, then pill splitting is an option.
Cons of pill splitting
Unequal dosing. In most instances, pill splitting leads to slightly unequal dosing.2 This could be a problem if:
- the medication such as lithium has a narrow therapeutic index
- the patient’s condition is unstable
- the patient’s condition is stable but minor dose variations might cause problems, such as a patient who relapses with small dosing changes.
Table
Appropriate and inappropriate medications for pill splitting
| OK to split | Do not split |
| Adderall tablets | Adderall XR capsules* |
| Effexor tablets† | Effexor-XR capsule* |
| Paxil or paroxetine tablets | Paxil CR |
| Prozac 10 mg tablet or fluoxetine tablets | Prozac 20 mg capsule |
| Risperdal tablet | Risperdal M-TAB |
| Tegretol | Tegretol XR |
| Wellbutrin and bupropion tablets | Wellbutrin XL |
| Zyprexa tablets | Zyprexa Zydis |
| Abilify tablets | Concerta capsules |
| Celexa or citalopram tablets | Cymbalta capsules |
| Lamictal tablets† | Depakote ER |
| Lexapro tablets | Equetro* |
| Luvox tablets | Eskalith CR, Lithobid tablets |
| Remeron or mirtazapine tablets | Geodon capsules |
| Seroquel tablets | Ritalin LA* |
| Zoloft tablets | Strattera capsules |
| * Capsule can be opened and contents sprinkled on food | |
| † Tablets may have uneven shapes, making even cuts difficult | |
Scoring. Cutting unscored tablets can be difficult, especially if the pills are not round or oval. Because patients can get injured using a knife, recommend pill cutters, which are available at most pharmacies.
Capsule splitting. Some psychotropics are sold only in capsules. Some capsules can be opened and sprinkled on food, but splitting the contents into approximately equal dosages can be difficult.
1. Cohen CI, Cohen SI. Potential cost savings from pill splitting of newer psychotropic medications. Psychiatr Serv 2000;51(4):527-9.
2. Teng J, Song CK, Williams RL, Polli J. Lack of medication dose uniformity in commonly split tablets. J Am Pharm Assoc 2002;42:195-9.
Dr. Rakesh Jain is director of psychopharmacology research, R/D Clinical Research, Inc., Lake Jackson, Texas.
Dr. Shailesh Jain is assistant professor, University of Texas Medical School at San Antonio.
Clinicians and patients look to pill splitting to reduce psychotropics’ costs and fine-tune pharmacotherapy, but pill splitting has not been rigorously studied for safety or efficacy. It is important to understand the risks and benefits of pill splitting before you recommend the practice to patients.
Pros of pill splitting
Lower costs for patients. Many psychotropics come in multiple strengths, and one larger pill often costs less than 2 smaller pills of equivalent dosage.1 Writing a prescription for a higher dose and instructing the patient to cut the pill in half can lower costs.
Fine-tune titration. Pill splitting allows you to prescribe a lower strength to gradually titrate dosages up or taper them down. This practice can prevent side effects and improve adherence because a lower dose may have a more favorable pharmacokinetic profile.
Improve tolerability. Patients might better tolerate half a pill taken twice daily rather than an entire pill once daily. A smaller dose may prevent a spike in serum level, which could aid tolerability.
- Will there be a cost saving for the patient?
- Can the patient understand and follow your recommendations?
- Can the patient tolerate minor dosage variability that can occur with pill splitting?
- Is the medication’s integrity maintained when the pill is split?
If the answer is yes to all 4 questions, then pill splitting is an option.
Cons of pill splitting
Unequal dosing. In most instances, pill splitting leads to slightly unequal dosing.2 This could be a problem if:
- the medication such as lithium has a narrow therapeutic index
- the patient’s condition is unstable
- the patient’s condition is stable but minor dose variations might cause problems, such as a patient who relapses with small dosing changes.
Table
Appropriate and inappropriate medications for pill splitting
| OK to split | Do not split |
| Adderall tablets | Adderall XR capsules* |
| Effexor tablets† | Effexor-XR capsule* |
| Paxil or paroxetine tablets | Paxil CR |
| Prozac 10 mg tablet or fluoxetine tablets | Prozac 20 mg capsule |
| Risperdal tablet | Risperdal M-TAB |
| Tegretol | Tegretol XR |
| Wellbutrin and bupropion tablets | Wellbutrin XL |
| Zyprexa tablets | Zyprexa Zydis |
| Abilify tablets | Concerta capsules |
| Celexa or citalopram tablets | Cymbalta capsules |
| Lamictal tablets† | Depakote ER |
| Lexapro tablets | Equetro* |
| Luvox tablets | Eskalith CR, Lithobid tablets |
| Remeron or mirtazapine tablets | Geodon capsules |
| Seroquel tablets | Ritalin LA* |
| Zoloft tablets | Strattera capsules |
| * Capsule can be opened and contents sprinkled on food | |
| † Tablets may have uneven shapes, making even cuts difficult | |
Scoring. Cutting unscored tablets can be difficult, especially if the pills are not round or oval. Because patients can get injured using a knife, recommend pill cutters, which are available at most pharmacies.
Capsule splitting. Some psychotropics are sold only in capsules. Some capsules can be opened and sprinkled on food, but splitting the contents into approximately equal dosages can be difficult.
Clinicians and patients look to pill splitting to reduce psychotropics’ costs and fine-tune pharmacotherapy, but pill splitting has not been rigorously studied for safety or efficacy. It is important to understand the risks and benefits of pill splitting before you recommend the practice to patients.
Pros of pill splitting
Lower costs for patients. Many psychotropics come in multiple strengths, and one larger pill often costs less than 2 smaller pills of equivalent dosage.1 Writing a prescription for a higher dose and instructing the patient to cut the pill in half can lower costs.
Fine-tune titration. Pill splitting allows you to prescribe a lower strength to gradually titrate dosages up or taper them down. This practice can prevent side effects and improve adherence because a lower dose may have a more favorable pharmacokinetic profile.
Improve tolerability. Patients might better tolerate half a pill taken twice daily rather than an entire pill once daily. A smaller dose may prevent a spike in serum level, which could aid tolerability.
- Will there be a cost saving for the patient?
- Can the patient understand and follow your recommendations?
- Can the patient tolerate minor dosage variability that can occur with pill splitting?
- Is the medication’s integrity maintained when the pill is split?
If the answer is yes to all 4 questions, then pill splitting is an option.
Cons of pill splitting
Unequal dosing. In most instances, pill splitting leads to slightly unequal dosing.2 This could be a problem if:
- the medication such as lithium has a narrow therapeutic index
- the patient’s condition is unstable
- the patient’s condition is stable but minor dose variations might cause problems, such as a patient who relapses with small dosing changes.
Table
Appropriate and inappropriate medications for pill splitting
| OK to split | Do not split |
| Adderall tablets | Adderall XR capsules* |
| Effexor tablets† | Effexor-XR capsule* |
| Paxil or paroxetine tablets | Paxil CR |
| Prozac 10 mg tablet or fluoxetine tablets | Prozac 20 mg capsule |
| Risperdal tablet | Risperdal M-TAB |
| Tegretol | Tegretol XR |
| Wellbutrin and bupropion tablets | Wellbutrin XL |
| Zyprexa tablets | Zyprexa Zydis |
| Abilify tablets | Concerta capsules |
| Celexa or citalopram tablets | Cymbalta capsules |
| Lamictal tablets† | Depakote ER |
| Lexapro tablets | Equetro* |
| Luvox tablets | Eskalith CR, Lithobid tablets |
| Remeron or mirtazapine tablets | Geodon capsules |
| Seroquel tablets | Ritalin LA* |
| Zoloft tablets | Strattera capsules |
| * Capsule can be opened and contents sprinkled on food | |
| † Tablets may have uneven shapes, making even cuts difficult | |
Scoring. Cutting unscored tablets can be difficult, especially if the pills are not round or oval. Because patients can get injured using a knife, recommend pill cutters, which are available at most pharmacies.
Capsule splitting. Some psychotropics are sold only in capsules. Some capsules can be opened and sprinkled on food, but splitting the contents into approximately equal dosages can be difficult.
1. Cohen CI, Cohen SI. Potential cost savings from pill splitting of newer psychotropic medications. Psychiatr Serv 2000;51(4):527-9.
2. Teng J, Song CK, Williams RL, Polli J. Lack of medication dose uniformity in commonly split tablets. J Am Pharm Assoc 2002;42:195-9.
Dr. Rakesh Jain is director of psychopharmacology research, R/D Clinical Research, Inc., Lake Jackson, Texas.
Dr. Shailesh Jain is assistant professor, University of Texas Medical School at San Antonio.
1. Cohen CI, Cohen SI. Potential cost savings from pill splitting of newer psychotropic medications. Psychiatr Serv 2000;51(4):527-9.
2. Teng J, Song CK, Williams RL, Polli J. Lack of medication dose uniformity in commonly split tablets. J Am Pharm Assoc 2002;42:195-9.
Dr. Rakesh Jain is director of psychopharmacology research, R/D Clinical Research, Inc., Lake Jackson, Texas.
Dr. Shailesh Jain is assistant professor, University of Texas Medical School at San Antonio.
How to diagnose pathologic gambling in older patients
Pathologic gambling among older patients causes more than financial losses; it also can lead to comorbid alcohol dependence, depression, anxiety disorders, and medical treatment nonadherence.1
Retirement, death of a spouse, “empty nest” syndrome, and other emotional, social, and financial stresses are common in later life. Some try to fill the gap with gambling, which can become pathologic. Early intervention and treatments addressing an older patient’s psychological and social needs can improve outcomes, however.
Screening for pathologic gambling
Late life pathologic gambling often goes undiagnosed but is thought to be on the rise. In a random sample of 843 older adults at scheduled primary-care appointments, 70% had gambled at least once in the past year and 11% were identified as at-risk gamblers.1
Diagnosing pathologic gambling requires a high degree of suspicion and inquiry. You must actively incorporate screening questions in the clinical interview to identify at-risk and pathologic gamblers in older patients.
Based on clinical experience and several DSM-IV-TR criteria,2 we developed a screening tool called PACE RULeS to identify pathologic gambling in this population (Box 1). A positive response to 5 or more of the 8 questions indicates a likely diagnosis of pathologic gambling. Lower scores may point to at-risk behavior and would require follow-up.
Diagnose maladaptive or pathologic gambling if your patient answers yes to 5 or more of these “PACE RULeS” questions:
- P—Are you often Preoccupied with thoughts of gambling?
- A—Would you often gamble with increasing Amounts of money to achieve the same excitement?
- C—Have you made repeated efforts to Control, cut back, or stop gambling?
- E—Do you gamble to Escape daily problems and stresses?
- R—After losing money, do you often Return another day to get even?
- U—Have you ever committed Unlawful acts to finance gambling?
- L—Have you Lost a significant relationship or job because of gambling?
- S—Do you use your Savings to gamble?
Psychosocial intervention
After you make a diagnosis, manage your patient’s pathologic gambling with a comprehensive plan that includes family and community resources.3 Box 2 shows interventions studied in the adult population that are appropriate for older patients.
- Screen for active gambling
- Intervene immediately if the patient is suicidal
- Refer the patient to Gamblers Anonymous
- Enlist family and friends to support treatment adherence and effectiveness. Be aware of confidentiality and ethical issues, however, especially during discussions with family members
- Refer the patient to counseling
- Actively participate in the treatment plan by assessing for relapses.
Medication
No psychotropics are FDA-approved for pathologic gambling, but adding medication to psychosocial interventions may help. Most medications studied in the general population are similarly efficacious in older adults. Slowly increase dosages, however, because of the greater risk of side effects in older patients.
Selective serotonin reuptake inhibitors help reduce gambling behavior, improve social and occupational functioning, and treat comorbid depression when used in relatively higher dosages. In anecdotal reports, the following medications have been found to be beneficial:
Although some medications treat pathologic gambling, others can cause it. Dopamine agonists such as pramipexole could cause reversible pathologic gambling in some older individuals who take it for Parkinson’s disease or restless legs syndrome.10
Drug brand names
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clomipramine • Anafranil
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Lithium • Eskalith, Lithobid
- Naltrexone • ReVia
- Paroxetine • Paxil
- Pramipexole • Mirapex
- Valproate • Depakene, Depakote
1. Levens S, Dyer AM, Zubritsky C, et al. Gambling among older, primary-care patients: an important public health concern. Am J Geriatr Psychiatry 2005;13(1):69-76.
2. Diagnostic and statistical manual of mental disorders, 4th ed. text rev. Washington, DC: American Psychiatric Association; 2000.
3. Unwin B, Davis M, DeLeeuw J. Pathological gambling. Am Fam Physician 2000;61:741-9.
4. De la Gandara JJ. Fluoxetine: open-trial in pathological gambling. Paper presented at: Annual Meeting of the American Psychiatric Association; May 16-21, 1999; Washington, DC.
5. Kim SW, Grant JE, Adson DE, et al. A double-blind placebo-controlled study of the efficacy and safety of paroxetine in the treatment of pathological gambling. J Clin Psychiatry 2002;63(6):501-7.
6. Hollander E, DeCaria CM, Mari E, et al. Short-term single-blind fluvoxamine treatment of pathological gambling. Am J Psychiatry 1998;155(12):1781-3.
7. Hollander E, DeCaria CM, Finkell JN, et al. A randomized double-blind fluvoxamine/placebo crossover trial in pathological gambling. Biol Psychiatry 2000;47(9):813-7.
8. Zimmerman M, Breen RB, Posternak MA. An open-label study of citalopram in the treatment of pathological gambling. J Clin Psychiatry 2002;63(1):44-8.
9. Kim SW, Grant JE. An open naltrexone treatment study of pathological gambling disorder. Int Clin Psychopharmacol 2001;16(5):285-9.
10. Dodd ML, Klos KJ, Bower JH, et al. Pathological gambling caused by drugs used to treat Parkinson disease. Arch Neurol 2005;62(9):1377-81.
Dr. Madaan is a fellow in child and adolescent psychiatry, Creighton University, Omaha, NE.
Dr. Padala is assistant professor, department of psychiatry, University of Nebraska Medical Center, Omaha, NE.
Dr. Sattar is assistant professor, department of psychiatry, Creighton University Medical Center, Omaha, NE.
Pathologic gambling among older patients causes more than financial losses; it also can lead to comorbid alcohol dependence, depression, anxiety disorders, and medical treatment nonadherence.1
Retirement, death of a spouse, “empty nest” syndrome, and other emotional, social, and financial stresses are common in later life. Some try to fill the gap with gambling, which can become pathologic. Early intervention and treatments addressing an older patient’s psychological and social needs can improve outcomes, however.
Screening for pathologic gambling
Late life pathologic gambling often goes undiagnosed but is thought to be on the rise. In a random sample of 843 older adults at scheduled primary-care appointments, 70% had gambled at least once in the past year and 11% were identified as at-risk gamblers.1
Diagnosing pathologic gambling requires a high degree of suspicion and inquiry. You must actively incorporate screening questions in the clinical interview to identify at-risk and pathologic gamblers in older patients.
Based on clinical experience and several DSM-IV-TR criteria,2 we developed a screening tool called PACE RULeS to identify pathologic gambling in this population (Box 1). A positive response to 5 or more of the 8 questions indicates a likely diagnosis of pathologic gambling. Lower scores may point to at-risk behavior and would require follow-up.
Diagnose maladaptive or pathologic gambling if your patient answers yes to 5 or more of these “PACE RULeS” questions:
- P—Are you often Preoccupied with thoughts of gambling?
- A—Would you often gamble with increasing Amounts of money to achieve the same excitement?
- C—Have you made repeated efforts to Control, cut back, or stop gambling?
- E—Do you gamble to Escape daily problems and stresses?
- R—After losing money, do you often Return another day to get even?
- U—Have you ever committed Unlawful acts to finance gambling?
- L—Have you Lost a significant relationship or job because of gambling?
- S—Do you use your Savings to gamble?
Psychosocial intervention
After you make a diagnosis, manage your patient’s pathologic gambling with a comprehensive plan that includes family and community resources.3 Box 2 shows interventions studied in the adult population that are appropriate for older patients.
- Screen for active gambling
- Intervene immediately if the patient is suicidal
- Refer the patient to Gamblers Anonymous
- Enlist family and friends to support treatment adherence and effectiveness. Be aware of confidentiality and ethical issues, however, especially during discussions with family members
- Refer the patient to counseling
- Actively participate in the treatment plan by assessing for relapses.
Medication
No psychotropics are FDA-approved for pathologic gambling, but adding medication to psychosocial interventions may help. Most medications studied in the general population are similarly efficacious in older adults. Slowly increase dosages, however, because of the greater risk of side effects in older patients.
Selective serotonin reuptake inhibitors help reduce gambling behavior, improve social and occupational functioning, and treat comorbid depression when used in relatively higher dosages. In anecdotal reports, the following medications have been found to be beneficial:
Although some medications treat pathologic gambling, others can cause it. Dopamine agonists such as pramipexole could cause reversible pathologic gambling in some older individuals who take it for Parkinson’s disease or restless legs syndrome.10
Drug brand names
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clomipramine • Anafranil
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Lithium • Eskalith, Lithobid
- Naltrexone • ReVia
- Paroxetine • Paxil
- Pramipexole • Mirapex
- Valproate • Depakene, Depakote
Pathologic gambling among older patients causes more than financial losses; it also can lead to comorbid alcohol dependence, depression, anxiety disorders, and medical treatment nonadherence.1
Retirement, death of a spouse, “empty nest” syndrome, and other emotional, social, and financial stresses are common in later life. Some try to fill the gap with gambling, which can become pathologic. Early intervention and treatments addressing an older patient’s psychological and social needs can improve outcomes, however.
Screening for pathologic gambling
Late life pathologic gambling often goes undiagnosed but is thought to be on the rise. In a random sample of 843 older adults at scheduled primary-care appointments, 70% had gambled at least once in the past year and 11% were identified as at-risk gamblers.1
Diagnosing pathologic gambling requires a high degree of suspicion and inquiry. You must actively incorporate screening questions in the clinical interview to identify at-risk and pathologic gamblers in older patients.
Based on clinical experience and several DSM-IV-TR criteria,2 we developed a screening tool called PACE RULeS to identify pathologic gambling in this population (Box 1). A positive response to 5 or more of the 8 questions indicates a likely diagnosis of pathologic gambling. Lower scores may point to at-risk behavior and would require follow-up.
Diagnose maladaptive or pathologic gambling if your patient answers yes to 5 or more of these “PACE RULeS” questions:
- P—Are you often Preoccupied with thoughts of gambling?
- A—Would you often gamble with increasing Amounts of money to achieve the same excitement?
- C—Have you made repeated efforts to Control, cut back, or stop gambling?
- E—Do you gamble to Escape daily problems and stresses?
- R—After losing money, do you often Return another day to get even?
- U—Have you ever committed Unlawful acts to finance gambling?
- L—Have you Lost a significant relationship or job because of gambling?
- S—Do you use your Savings to gamble?
Psychosocial intervention
After you make a diagnosis, manage your patient’s pathologic gambling with a comprehensive plan that includes family and community resources.3 Box 2 shows interventions studied in the adult population that are appropriate for older patients.
- Screen for active gambling
- Intervene immediately if the patient is suicidal
- Refer the patient to Gamblers Anonymous
- Enlist family and friends to support treatment adherence and effectiveness. Be aware of confidentiality and ethical issues, however, especially during discussions with family members
- Refer the patient to counseling
- Actively participate in the treatment plan by assessing for relapses.
Medication
No psychotropics are FDA-approved for pathologic gambling, but adding medication to psychosocial interventions may help. Most medications studied in the general population are similarly efficacious in older adults. Slowly increase dosages, however, because of the greater risk of side effects in older patients.
Selective serotonin reuptake inhibitors help reduce gambling behavior, improve social and occupational functioning, and treat comorbid depression when used in relatively higher dosages. In anecdotal reports, the following medications have been found to be beneficial:
Although some medications treat pathologic gambling, others can cause it. Dopamine agonists such as pramipexole could cause reversible pathologic gambling in some older individuals who take it for Parkinson’s disease or restless legs syndrome.10
Drug brand names
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Clomipramine • Anafranil
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Lithium • Eskalith, Lithobid
- Naltrexone • ReVia
- Paroxetine • Paxil
- Pramipexole • Mirapex
- Valproate • Depakene, Depakote
1. Levens S, Dyer AM, Zubritsky C, et al. Gambling among older, primary-care patients: an important public health concern. Am J Geriatr Psychiatry 2005;13(1):69-76.
2. Diagnostic and statistical manual of mental disorders, 4th ed. text rev. Washington, DC: American Psychiatric Association; 2000.
3. Unwin B, Davis M, DeLeeuw J. Pathological gambling. Am Fam Physician 2000;61:741-9.
4. De la Gandara JJ. Fluoxetine: open-trial in pathological gambling. Paper presented at: Annual Meeting of the American Psychiatric Association; May 16-21, 1999; Washington, DC.
5. Kim SW, Grant JE, Adson DE, et al. A double-blind placebo-controlled study of the efficacy and safety of paroxetine in the treatment of pathological gambling. J Clin Psychiatry 2002;63(6):501-7.
6. Hollander E, DeCaria CM, Mari E, et al. Short-term single-blind fluvoxamine treatment of pathological gambling. Am J Psychiatry 1998;155(12):1781-3.
7. Hollander E, DeCaria CM, Finkell JN, et al. A randomized double-blind fluvoxamine/placebo crossover trial in pathological gambling. Biol Psychiatry 2000;47(9):813-7.
8. Zimmerman M, Breen RB, Posternak MA. An open-label study of citalopram in the treatment of pathological gambling. J Clin Psychiatry 2002;63(1):44-8.
9. Kim SW, Grant JE. An open naltrexone treatment study of pathological gambling disorder. Int Clin Psychopharmacol 2001;16(5):285-9.
10. Dodd ML, Klos KJ, Bower JH, et al. Pathological gambling caused by drugs used to treat Parkinson disease. Arch Neurol 2005;62(9):1377-81.
Dr. Madaan is a fellow in child and adolescent psychiatry, Creighton University, Omaha, NE.
Dr. Padala is assistant professor, department of psychiatry, University of Nebraska Medical Center, Omaha, NE.
Dr. Sattar is assistant professor, department of psychiatry, Creighton University Medical Center, Omaha, NE.
1. Levens S, Dyer AM, Zubritsky C, et al. Gambling among older, primary-care patients: an important public health concern. Am J Geriatr Psychiatry 2005;13(1):69-76.
2. Diagnostic and statistical manual of mental disorders, 4th ed. text rev. Washington, DC: American Psychiatric Association; 2000.
3. Unwin B, Davis M, DeLeeuw J. Pathological gambling. Am Fam Physician 2000;61:741-9.
4. De la Gandara JJ. Fluoxetine: open-trial in pathological gambling. Paper presented at: Annual Meeting of the American Psychiatric Association; May 16-21, 1999; Washington, DC.
5. Kim SW, Grant JE, Adson DE, et al. A double-blind placebo-controlled study of the efficacy and safety of paroxetine in the treatment of pathological gambling. J Clin Psychiatry 2002;63(6):501-7.
6. Hollander E, DeCaria CM, Mari E, et al. Short-term single-blind fluvoxamine treatment of pathological gambling. Am J Psychiatry 1998;155(12):1781-3.
7. Hollander E, DeCaria CM, Finkell JN, et al. A randomized double-blind fluvoxamine/placebo crossover trial in pathological gambling. Biol Psychiatry 2000;47(9):813-7.
8. Zimmerman M, Breen RB, Posternak MA. An open-label study of citalopram in the treatment of pathological gambling. J Clin Psychiatry 2002;63(1):44-8.
9. Kim SW, Grant JE. An open naltrexone treatment study of pathological gambling disorder. Int Clin Psychopharmacol 2001;16(5):285-9.
10. Dodd ML, Klos KJ, Bower JH, et al. Pathological gambling caused by drugs used to treat Parkinson disease. Arch Neurol 2005;62(9):1377-81.
Dr. Madaan is a fellow in child and adolescent psychiatry, Creighton University, Omaha, NE.
Dr. Padala is assistant professor, department of psychiatry, University of Nebraska Medical Center, Omaha, NE.
Dr. Sattar is assistant professor, department of psychiatry, Creighton University Medical Center, Omaha, NE.
To protect and serve: Psychiatrists’ duty to patients
Patient discharged from group therapy kills psychiatrist, patient, and himself
Oakland County (MI) Circuit Court
The plaintiff, age 57, attended regular group therapy with a psychiatrist. Another patient, Mr. B, was dismissed from group therapy by the psychiatrist, but returned to the office with a gun during one of the regular sessions. Mr. B shot and killed the psychiatrist then entered the group meeting room and discharged his gun, fatally injuring another patient and wounding the plaintiff. Mr. B then turned the gun on himself and committed suicide. The plaintiff suffered gunshot wounds to the lower leg, foot, and hand and was away from work for 6 weeks.
The plaintiff alleged that the psychiatrist, his associates, and his daughter—who is also a psychiatrist at the office—knew Mr. B was dangerous and should not have been included in group therapy. The plaintiff claimed that Mr. B had a history of questionable psychotic behavior and other patients should not have been exposed to him. The psychiatrist’s associates contended that they had no way to anticipate this event and had used due care and caution in their practice.
- A $2 million verdict was returned
Dr. Grant’s observations
Warn and protect
In this case, several unavailable facts may have supported the successful negligence claim. For example, why was Mr. B dismissed from the group? Did he threaten someone in the group? Did he tell the group or the group leader about thoughts of violence or homicide? If so, perhaps a violent event was foreseeable.
Was Mr. B dismissed because of delusional or paranoid thoughts? What was done to help him, and were appropriate referrals in place? Instituting the right interventions requires clinicians to walk a fine line between preserving doctor-patient confidentiality and protecting other patients and the general public.
Doctor-patient confidentiality is deeply rooted in medical ethics and protected by law—in various forms—in all jurisdictions. Directives requiring a physician to reveal information without a patient’s consent are either legislated—and tend to be clear—or are based on court precedent, which is more open to interpretation. These mandated exceptions are purpose-specific and intended to preserve overall doctor-patient confidentiality.“Is this patient dangerous?” by John Battaglia, MD, and “Protect yourself from patient assault”, an interview between Dr. Battaglia and Lois E. Krahn, MD.
1. Kleinman I. Confidentiality and the duty to warn. Can Med Assoc J 1993;149:1783-5.
2. Chaimowitx G, Glancy G. The duty to protect. Can J Psychiatry 2002;47:1-4.
3. Tarasoff v. Regents of the University of California, 118 Cal. Rptr. 129 (Cal. 1974) (Tarasoff I), modified by Tarasoff v. Regents of the Univ. of Cal., 551 P.2d 334 (Cal. 1976) (Tarasoff II).
4. Naidu v. Laird, 539 A.2d 1064 (Del. 1988).
5. Davis v. Lhim, 335 N.W.2d 481 (Mich. App. 1983).
6. Beck J, Baxter P. The violent patient. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:153-65.
7. Buckner F, Firestone M. Where the public peril begins: 25 years after Tarasoff. J Legal Med 2000;21:187-222.
8. Corey G, Williams GT, Moline ME. Ethical and legal issues in group counseling. Ethics & Behavior 1995;5:161-83.
9. American Counseling Association code of ethics and standards of practice 2005. Available at: http://www.counseling.org/Resources/CodeOfEthics/TP/Home/CT2.aspx. Accessed October 23, 2006.
Patient discharged from group therapy kills psychiatrist, patient, and himself
Oakland County (MI) Circuit Court
The plaintiff, age 57, attended regular group therapy with a psychiatrist. Another patient, Mr. B, was dismissed from group therapy by the psychiatrist, but returned to the office with a gun during one of the regular sessions. Mr. B shot and killed the psychiatrist then entered the group meeting room and discharged his gun, fatally injuring another patient and wounding the plaintiff. Mr. B then turned the gun on himself and committed suicide. The plaintiff suffered gunshot wounds to the lower leg, foot, and hand and was away from work for 6 weeks.
The plaintiff alleged that the psychiatrist, his associates, and his daughter—who is also a psychiatrist at the office—knew Mr. B was dangerous and should not have been included in group therapy. The plaintiff claimed that Mr. B had a history of questionable psychotic behavior and other patients should not have been exposed to him. The psychiatrist’s associates contended that they had no way to anticipate this event and had used due care and caution in their practice.
- A $2 million verdict was returned
Dr. Grant’s observations
Warn and protect
In this case, several unavailable facts may have supported the successful negligence claim. For example, why was Mr. B dismissed from the group? Did he threaten someone in the group? Did he tell the group or the group leader about thoughts of violence or homicide? If so, perhaps a violent event was foreseeable.
Was Mr. B dismissed because of delusional or paranoid thoughts? What was done to help him, and were appropriate referrals in place? Instituting the right interventions requires clinicians to walk a fine line between preserving doctor-patient confidentiality and protecting other patients and the general public.
Doctor-patient confidentiality is deeply rooted in medical ethics and protected by law—in various forms—in all jurisdictions. Directives requiring a physician to reveal information without a patient’s consent are either legislated—and tend to be clear—or are based on court precedent, which is more open to interpretation. These mandated exceptions are purpose-specific and intended to preserve overall doctor-patient confidentiality.“Is this patient dangerous?” by John Battaglia, MD, and “Protect yourself from patient assault”, an interview between Dr. Battaglia and Lois E. Krahn, MD.
Patient discharged from group therapy kills psychiatrist, patient, and himself
Oakland County (MI) Circuit Court
The plaintiff, age 57, attended regular group therapy with a psychiatrist. Another patient, Mr. B, was dismissed from group therapy by the psychiatrist, but returned to the office with a gun during one of the regular sessions. Mr. B shot and killed the psychiatrist then entered the group meeting room and discharged his gun, fatally injuring another patient and wounding the plaintiff. Mr. B then turned the gun on himself and committed suicide. The plaintiff suffered gunshot wounds to the lower leg, foot, and hand and was away from work for 6 weeks.
The plaintiff alleged that the psychiatrist, his associates, and his daughter—who is also a psychiatrist at the office—knew Mr. B was dangerous and should not have been included in group therapy. The plaintiff claimed that Mr. B had a history of questionable psychotic behavior and other patients should not have been exposed to him. The psychiatrist’s associates contended that they had no way to anticipate this event and had used due care and caution in their practice.
- A $2 million verdict was returned
Dr. Grant’s observations
Warn and protect
In this case, several unavailable facts may have supported the successful negligence claim. For example, why was Mr. B dismissed from the group? Did he threaten someone in the group? Did he tell the group or the group leader about thoughts of violence or homicide? If so, perhaps a violent event was foreseeable.
Was Mr. B dismissed because of delusional or paranoid thoughts? What was done to help him, and were appropriate referrals in place? Instituting the right interventions requires clinicians to walk a fine line between preserving doctor-patient confidentiality and protecting other patients and the general public.
Doctor-patient confidentiality is deeply rooted in medical ethics and protected by law—in various forms—in all jurisdictions. Directives requiring a physician to reveal information without a patient’s consent are either legislated—and tend to be clear—or are based on court precedent, which is more open to interpretation. These mandated exceptions are purpose-specific and intended to preserve overall doctor-patient confidentiality.“Is this patient dangerous?” by John Battaglia, MD, and “Protect yourself from patient assault”, an interview between Dr. Battaglia and Lois E. Krahn, MD.
1. Kleinman I. Confidentiality and the duty to warn. Can Med Assoc J 1993;149:1783-5.
2. Chaimowitx G, Glancy G. The duty to protect. Can J Psychiatry 2002;47:1-4.
3. Tarasoff v. Regents of the University of California, 118 Cal. Rptr. 129 (Cal. 1974) (Tarasoff I), modified by Tarasoff v. Regents of the Univ. of Cal., 551 P.2d 334 (Cal. 1976) (Tarasoff II).
4. Naidu v. Laird, 539 A.2d 1064 (Del. 1988).
5. Davis v. Lhim, 335 N.W.2d 481 (Mich. App. 1983).
6. Beck J, Baxter P. The violent patient. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:153-65.
7. Buckner F, Firestone M. Where the public peril begins: 25 years after Tarasoff. J Legal Med 2000;21:187-222.
8. Corey G, Williams GT, Moline ME. Ethical and legal issues in group counseling. Ethics & Behavior 1995;5:161-83.
9. American Counseling Association code of ethics and standards of practice 2005. Available at: http://www.counseling.org/Resources/CodeOfEthics/TP/Home/CT2.aspx. Accessed October 23, 2006.
1. Kleinman I. Confidentiality and the duty to warn. Can Med Assoc J 1993;149:1783-5.
2. Chaimowitx G, Glancy G. The duty to protect. Can J Psychiatry 2002;47:1-4.
3. Tarasoff v. Regents of the University of California, 118 Cal. Rptr. 129 (Cal. 1974) (Tarasoff I), modified by Tarasoff v. Regents of the Univ. of Cal., 551 P.2d 334 (Cal. 1976) (Tarasoff II).
4. Naidu v. Laird, 539 A.2d 1064 (Del. 1988).
5. Davis v. Lhim, 335 N.W.2d 481 (Mich. App. 1983).
6. Beck J, Baxter P. The violent patient. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:153-65.
7. Buckner F, Firestone M. Where the public peril begins: 25 years after Tarasoff. J Legal Med 2000;21:187-222.
8. Corey G, Williams GT, Moline ME. Ethical and legal issues in group counseling. Ethics & Behavior 1995;5:161-83.
9. American Counseling Association code of ethics and standards of practice 2005. Available at: http://www.counseling.org/Resources/CodeOfEthics/TP/Home/CT2.aspx. Accessed October 23, 2006.
SGAs for resistant depression
Thanks to readers who commented on the October Instant Poll concerning my article on use of second-generation antipsychotics (SGAs) in treatment-resistant unipolar depression (Current Psychiatry, October 2006). Let me respond to several comments:
“Using SGAs in resistant depression is an unusual strategy, though they can be used as mood stabilizers.”
This reader raises an important point I would like to clarify on using SGAs for mood disorders. SGAs have acute antimanic effects and are effective for treating mixed bipolar states, rapid cycling, and psychotic features. Long-term data support use of some SGAs as mood stabilizers.October), weight gain and attendant metabolic syndrome as well as tardive dyskinesia and hyperprolactinemia temper enthusiasm for SGA use. Of note, at least two SGAs—aripiprazole3,4 and ziprasidone5—have not shown problematic metabolic effects, although evidence supporting the use of these drugs for resistant unipolar depression is limited. Taken together, these risks warrant reserving SGAs for unipolar depression that has not responded to antidepressants.
“After two failed SSRIs trials, I would try a serotonin-norepinephrine reuptake inhibitor (SNRI) and/or bupropion. Then it would depend on symptoms and risk factors.”
Compared with SNRI monotherapy or combination SSRI/bupropion therapy, a higher level of evidence supports SGAs’ benefits in resistant depression. Given the risks associated with SGAs, however, try an SNRI and SSRI/bupropion therapy before adding an SGA for most patients.
“I would not use an SGA in resistant depression without evidence of psychosis.”
SGAs’ benefit in nonpsychotic, unipolar major depression resistant to two classes of antidepressants is reasonably well-established. Psychotic depression, however, is one of the few diagnostic groups for which an SGA added to an antidepressant should be considered first line.
Richard C. Shelton, MD
James G. Blakemore Research Professor
Vanderbilt University
Nashville, TN
1. Berk M, Dodd S. Efficacy of atypical antipsychotics in bipolar disorder. Drugs 2005;65:257-69.
2. Shelton RC, Tollefson GD, Tohen M, et al. A novel augmentation strategy for treating resistant major depression. Am J Psychiatry 2001;158:131-4.
3. Papakostas GI, Petersen TJ, Kinrys G, et al. Aripiprazole augmentation of selective serotonin reuptake inhibitors for treatment-resistant major depressive disorder. J Clin Psychiatry 2005;66:1326-30.
4. Worthington JJ, III, Kinrys G, Wygant LE, Pollack MH. Aripiprazole as an augmentor of selective serotonin reuptake inhibitors in depression and anxiety disorder patients. Int Clin Psychopharmacol 2005;20:9-11.
5. Papakostas GI, Petersen TJ, Nierenberg AA, et al. Ziprasidone augmentation of selective serotonin reuptake inhibitors (SSRIs) for SSRI-resistant major depressive disorder. J Clin Psychiatry 2004;65:217-21.
Thanks to readers who commented on the October Instant Poll concerning my article on use of second-generation antipsychotics (SGAs) in treatment-resistant unipolar depression (Current Psychiatry, October 2006). Let me respond to several comments:
“Using SGAs in resistant depression is an unusual strategy, though they can be used as mood stabilizers.”
This reader raises an important point I would like to clarify on using SGAs for mood disorders. SGAs have acute antimanic effects and are effective for treating mixed bipolar states, rapid cycling, and psychotic features. Long-term data support use of some SGAs as mood stabilizers.October), weight gain and attendant metabolic syndrome as well as tardive dyskinesia and hyperprolactinemia temper enthusiasm for SGA use. Of note, at least two SGAs—aripiprazole3,4 and ziprasidone5—have not shown problematic metabolic effects, although evidence supporting the use of these drugs for resistant unipolar depression is limited. Taken together, these risks warrant reserving SGAs for unipolar depression that has not responded to antidepressants.
“After two failed SSRIs trials, I would try a serotonin-norepinephrine reuptake inhibitor (SNRI) and/or bupropion. Then it would depend on symptoms and risk factors.”
Compared with SNRI monotherapy or combination SSRI/bupropion therapy, a higher level of evidence supports SGAs’ benefits in resistant depression. Given the risks associated with SGAs, however, try an SNRI and SSRI/bupropion therapy before adding an SGA for most patients.
“I would not use an SGA in resistant depression without evidence of psychosis.”
SGAs’ benefit in nonpsychotic, unipolar major depression resistant to two classes of antidepressants is reasonably well-established. Psychotic depression, however, is one of the few diagnostic groups for which an SGA added to an antidepressant should be considered first line.
Richard C. Shelton, MD
James G. Blakemore Research Professor
Vanderbilt University
Nashville, TN
Thanks to readers who commented on the October Instant Poll concerning my article on use of second-generation antipsychotics (SGAs) in treatment-resistant unipolar depression (Current Psychiatry, October 2006). Let me respond to several comments:
“Using SGAs in resistant depression is an unusual strategy, though they can be used as mood stabilizers.”
This reader raises an important point I would like to clarify on using SGAs for mood disorders. SGAs have acute antimanic effects and are effective for treating mixed bipolar states, rapid cycling, and psychotic features. Long-term data support use of some SGAs as mood stabilizers.October), weight gain and attendant metabolic syndrome as well as tardive dyskinesia and hyperprolactinemia temper enthusiasm for SGA use. Of note, at least two SGAs—aripiprazole3,4 and ziprasidone5—have not shown problematic metabolic effects, although evidence supporting the use of these drugs for resistant unipolar depression is limited. Taken together, these risks warrant reserving SGAs for unipolar depression that has not responded to antidepressants.
“After two failed SSRIs trials, I would try a serotonin-norepinephrine reuptake inhibitor (SNRI) and/or bupropion. Then it would depend on symptoms and risk factors.”
Compared with SNRI monotherapy or combination SSRI/bupropion therapy, a higher level of evidence supports SGAs’ benefits in resistant depression. Given the risks associated with SGAs, however, try an SNRI and SSRI/bupropion therapy before adding an SGA for most patients.
“I would not use an SGA in resistant depression without evidence of psychosis.”
SGAs’ benefit in nonpsychotic, unipolar major depression resistant to two classes of antidepressants is reasonably well-established. Psychotic depression, however, is one of the few diagnostic groups for which an SGA added to an antidepressant should be considered first line.
Richard C. Shelton, MD
James G. Blakemore Research Professor
Vanderbilt University
Nashville, TN
1. Berk M, Dodd S. Efficacy of atypical antipsychotics in bipolar disorder. Drugs 2005;65:257-69.
2. Shelton RC, Tollefson GD, Tohen M, et al. A novel augmentation strategy for treating resistant major depression. Am J Psychiatry 2001;158:131-4.
3. Papakostas GI, Petersen TJ, Kinrys G, et al. Aripiprazole augmentation of selective serotonin reuptake inhibitors for treatment-resistant major depressive disorder. J Clin Psychiatry 2005;66:1326-30.
4. Worthington JJ, III, Kinrys G, Wygant LE, Pollack MH. Aripiprazole as an augmentor of selective serotonin reuptake inhibitors in depression and anxiety disorder patients. Int Clin Psychopharmacol 2005;20:9-11.
5. Papakostas GI, Petersen TJ, Nierenberg AA, et al. Ziprasidone augmentation of selective serotonin reuptake inhibitors (SSRIs) for SSRI-resistant major depressive disorder. J Clin Psychiatry 2004;65:217-21.
1. Berk M, Dodd S. Efficacy of atypical antipsychotics in bipolar disorder. Drugs 2005;65:257-69.
2. Shelton RC, Tollefson GD, Tohen M, et al. A novel augmentation strategy for treating resistant major depression. Am J Psychiatry 2001;158:131-4.
3. Papakostas GI, Petersen TJ, Kinrys G, et al. Aripiprazole augmentation of selective serotonin reuptake inhibitors for treatment-resistant major depressive disorder. J Clin Psychiatry 2005;66:1326-30.
4. Worthington JJ, III, Kinrys G, Wygant LE, Pollack MH. Aripiprazole as an augmentor of selective serotonin reuptake inhibitors in depression and anxiety disorder patients. Int Clin Psychopharmacol 2005;20:9-11.
5. Papakostas GI, Petersen TJ, Nierenberg AA, et al. Ziprasidone augmentation of selective serotonin reuptake inhibitors (SSRIs) for SSRI-resistant major depressive disorder. J Clin Psychiatry 2004;65:217-21.
Mythbusting
In “10 delirium myths debunked,” (Pearls, Current Psychiatry, October 2006) Dr. Mitchell Levy promulgates a dangerous myth about psychiatric illness. He states that a patient—a postoperative middle-aged attorney with psychotic symptoms—“is not mentally ill, but has delirium.”
Delirium, like schizophrenia, is a mental disorder. The idea that a mental syndrome with an identifiable physical cause is not a psychiatric disorder is antiquated and obviously incorrect but is not understood by many medical personnel. We need to educate our colleagues about this misconception.
This myth dehumanizes mentally ill individuals. By distinguishing the middle-aged attorney from what might be considered a typical schizophrenia patient, Dr. Levy propagates the idea that mentally ill persons come from a class beneath successful professionals. This mistaken idea contributes to misdiagnosis and inadequate treatment and disproportionately low financial allocation for treating mentally ill patients.
Ira Handler, MD
Butler Memorial Hospital
Butler, PA
Dr. Levy responds
As a psychiatrist in a large university hospital, I advocate for the mentally ill daily and would never denigrate their condition.
A differential diagnosis via DSM-IV-TR, however, requires determining that “symptoms are not due to the direct physiological effects of a substance or general medical condition.” The best way to advocate for our patients is to render proper treatment, and the standard of care for treating delirium addresses causative medical issues.
Delirium is a mental disorder just as depression is a physical disorder caused by disrupted neurobiological mechanisms. However, as most psychiatrists—but not all internists—are aware, a high-functioning person rarely suffers a first schizophrenic break in middle age. Conversely, bypass patients are at risk for cognitive and perceptual changes—which mimic schizophrenia—caused by delirium.
My article described a situation I encounter frequently in consultation-liaison psychiatry when non-psychiatrists attempt to admit their delirious patients to the psych unit instead of treating the underlying medical cause. I hope that we can advocate for our patients across multiple venues and not at the expense of any group or population.
Mitchell Levy, MD
Assistant professor in psychiatry
University of Washington, Seattle
In “10 delirium myths debunked,” (Pearls, Current Psychiatry, October 2006) Dr. Mitchell Levy promulgates a dangerous myth about psychiatric illness. He states that a patient—a postoperative middle-aged attorney with psychotic symptoms—“is not mentally ill, but has delirium.”
Delirium, like schizophrenia, is a mental disorder. The idea that a mental syndrome with an identifiable physical cause is not a psychiatric disorder is antiquated and obviously incorrect but is not understood by many medical personnel. We need to educate our colleagues about this misconception.
This myth dehumanizes mentally ill individuals. By distinguishing the middle-aged attorney from what might be considered a typical schizophrenia patient, Dr. Levy propagates the idea that mentally ill persons come from a class beneath successful professionals. This mistaken idea contributes to misdiagnosis and inadequate treatment and disproportionately low financial allocation for treating mentally ill patients.
Ira Handler, MD
Butler Memorial Hospital
Butler, PA
Dr. Levy responds
As a psychiatrist in a large university hospital, I advocate for the mentally ill daily and would never denigrate their condition.
A differential diagnosis via DSM-IV-TR, however, requires determining that “symptoms are not due to the direct physiological effects of a substance or general medical condition.” The best way to advocate for our patients is to render proper treatment, and the standard of care for treating delirium addresses causative medical issues.
Delirium is a mental disorder just as depression is a physical disorder caused by disrupted neurobiological mechanisms. However, as most psychiatrists—but not all internists—are aware, a high-functioning person rarely suffers a first schizophrenic break in middle age. Conversely, bypass patients are at risk for cognitive and perceptual changes—which mimic schizophrenia—caused by delirium.
My article described a situation I encounter frequently in consultation-liaison psychiatry when non-psychiatrists attempt to admit their delirious patients to the psych unit instead of treating the underlying medical cause. I hope that we can advocate for our patients across multiple venues and not at the expense of any group or population.
Mitchell Levy, MD
Assistant professor in psychiatry
University of Washington, Seattle
In “10 delirium myths debunked,” (Pearls, Current Psychiatry, October 2006) Dr. Mitchell Levy promulgates a dangerous myth about psychiatric illness. He states that a patient—a postoperative middle-aged attorney with psychotic symptoms—“is not mentally ill, but has delirium.”
Delirium, like schizophrenia, is a mental disorder. The idea that a mental syndrome with an identifiable physical cause is not a psychiatric disorder is antiquated and obviously incorrect but is not understood by many medical personnel. We need to educate our colleagues about this misconception.
This myth dehumanizes mentally ill individuals. By distinguishing the middle-aged attorney from what might be considered a typical schizophrenia patient, Dr. Levy propagates the idea that mentally ill persons come from a class beneath successful professionals. This mistaken idea contributes to misdiagnosis and inadequate treatment and disproportionately low financial allocation for treating mentally ill patients.
Ira Handler, MD
Butler Memorial Hospital
Butler, PA
Dr. Levy responds
As a psychiatrist in a large university hospital, I advocate for the mentally ill daily and would never denigrate their condition.
A differential diagnosis via DSM-IV-TR, however, requires determining that “symptoms are not due to the direct physiological effects of a substance or general medical condition.” The best way to advocate for our patients is to render proper treatment, and the standard of care for treating delirium addresses causative medical issues.
Delirium is a mental disorder just as depression is a physical disorder caused by disrupted neurobiological mechanisms. However, as most psychiatrists—but not all internists—are aware, a high-functioning person rarely suffers a first schizophrenic break in middle age. Conversely, bypass patients are at risk for cognitive and perceptual changes—which mimic schizophrenia—caused by delirium.
My article described a situation I encounter frequently in consultation-liaison psychiatry when non-psychiatrists attempt to admit their delirious patients to the psych unit instead of treating the underlying medical cause. I hope that we can advocate for our patients across multiple venues and not at the expense of any group or population.
Mitchell Levy, MD
Assistant professor in psychiatry
University of Washington, Seattle
Will CATIE-AD change dementia treatment?
New findings questioning the value of second-generation antipsychotics (SGAs) for treating acute behaviors in patients with Alzheimer’s disease have raised more questions on when and how to use these agents in the elderly.
The National Institute of Mental Health-sponsored Clinical Antipsychotic Trial of Intervention Effectiveness-Alzheimer’s disease (CATIE-AD) concluded that SGAs offer no overall advantage over placebo. Although SGAs helped some trial patients, the medications were discontinued for approximately 8 in 10 patients because of intolerable side effects or ineffectiveness.
CATIE-AD’s principal investigator says the findings—published in the October 12 New England Journal of Medicine1—will guide clinicians in adjusting SGA dosages and durations for older patients with dementia.
But other psychiatrists argue that the study—led by prominent researchers and published in a prestigious medical journal—will deter clinicians from trying SGAs for older patients with dementia-related psychosis, aggression, or agitation.
Barbara Kamholz, MD
Clinical associate professor, department of psychiatry, University of Michigan Medical School; staff psychiatrist, VA Medical Center, Ann Arbor
Lon Schneider, MD
Professor of psychiatry, neurology, and gerontology, University of Southern California, Los Angeles
Sumer Verma, MD
Director, geriatric psychiatry education program, McLean Hospital, Belmont, MA
“These drugs are not FDA-approved for dementia. They may cause diabetes. They cause weight gain. They carry boxed warnings that they could increase risk of stroke and—in patients over age 85—can increase risk of dying,” says Sumer Verma, MD, director of the geriatric psychiatry education program at McLean Hospital (Belmont, MA). “Doctors already were reluctant to use SGAs, and now these researchers publish this study in one of the country’s most respected journals and make an unqualified statement to the effect that [SGAs] are no better than placebo. How many clinicians will be comfortable prescribing them?”
Participants
421 outpatients with psychosis, agitation, or aggression, or who met DSM-IV-TR criteria for Alzheimer’s-type dementia or probable Alzheimer’s disease based on history, physical examination, structural brain imaging results, and Mini-Mental State Examination scores between 5 and 26, indicating some degree of cognitive deficit. These patients:
- were ambulatory
- lived at home or in an assisted-living facility
- had delusions, hallucinations, aggression, or agitation that developed after dementia onset, disrupted functioning, and justified treatment with an antipsychotic
- showed signs and symptoms of psychosis, aggression, or agitation almost daily during the previous week or intermittently for 4 weeks.
Trial duration
Up to 36 weeks
Study drugs/mean dosages at endpoint
- olanzapine (5.5 mg/d)
- quetiapine (56.5 mg/d)
- risperidone (1 mg/d)
Physicians could increase dosages or prescribe a benzodiazepine or haloperidol if problem behaviors emerged.
Key findings
- Time to discontinuing treatment for any reason did not differ significantly among the treatment and placebo groups.
- Median time to discontinuation because of lack of efficacy was significantly longer with olanzapine (22.1 weeks) or risperidone (26.7 weeks) than with quetiapine (9.1 weeks) or placebo (9.0 weeks).
- Rates of discontinuation because of intolerance, adverse effects, or death were 24% with olanzapine, 16% with quetiapine, 18% with risperidone, and 5% with placebo.
- Overall rates of discontinuation for any reason were 63% after 12 weeks and 82% after 36 weeks.
- Parkinsonism or extrapyramidal symptoms were more prevalent among the olanzapine and risperidone groups (12% in each) than among the quetiapine and placebo groups (2% and 1%, respectively).
- Sedation was more common with the three SGAs (15% to 24% of patients) than with placebo (5%).
- Confusion or mental status changes were more common with olanzapine (18%) and risperidone (11%) than with placebo (5%). Cognitive disturbances and psychotic symptoms were more common with olanzapine (5% and 7%, respectively) than with the other SGAs or placebo (0 to 2%).
- Body weight increased 0.4 to 1 lb/month among the SGA groups and decreased 0.9 lb/month in the placebo group.
- Rates of improvement—as measured with the Clinical Global Impression of Change scale—did not differ significantly among the treatment and placebo groups.
‘Discouraging’ discontinuation
CATIE-AD—a double-blind, multicenter, randomized trial (Box)—followed 421 ambulatory outpatients with Alzheimer’s disease and psychosis, aggression, or agitation. Patients received the SGAs olanzapine (mean dosage, 5.5 mg/d), quetiapine (mean 56.5 mg/d), risperidone (mean 1 mg/d), or placebo. Dosages were adjusted as needed.
After 36 weeks, times to discontinuation because of lack of efficacy were longest for olanza-pine and risperidone, but these drugs also had the highest rates of discontinuation because of intolerability (24% and 18%, respectively). Quetiapine’s rate of discontinuation because of intolerability was 16%.
SGAs were stopped because of lack of efficacy or intolerable side effects—such as parkinsonism, extrapyramidal symptoms, sedation, or weight gain—in:
- 63% of treatment and placebo group patients within 12 weeks
- 82% of all patients within 36 weeks.
Lon Schneider, MD, principal investigator for CATIE-AD, acknowledged that the findings could discourage psychiatrists from prescribing SGAs for acute dementia-related behaviors, specifically in patients with Alzheimer’s disease.
But although discontinuation because of intolerability was most prevalent among patients taking risperidone or olanzapine, both SGAs were more effective than placebo for treating problem behaviors in some participants, Dr. Schneider notes. He adds that the patient population and most SGA dosages in CATIE-AD reflected typical geriatric psychiatric practice in the community.
An editorial in the October 12 New England Journal of Medicine2 praised CATIE-AD for allowing physicians to titrate and stop SGA regimens as needed while maintaining the double-blind design. Results of fixed-dose trials with prespecified time points are more difficult to apply to clinical practice because the course of Alzheimer’s disease and patients’ ability to tolerate specific drugs change over time.2
“This study can inform clinicians that they should not be prescribing medication and then not following up or maintaining it indefinitely,” says Dr. Schneider, who is professor of psychiatry, neurology and gerontology, University of Southern California, Los Angeles.
‘Black box’ fears?
Dr. Verma, however, reports that many clinicians have been hesitant to prescribe SGAs to older patients since last year—when the FDA ordered that SGAs carry “black box” warnings of a possible increased mortality risk in that population.
“CATIE-AD will intensify clinicians’ fears of litigation by implying that the risks of using SGAs outweigh their benefits, especially when SGAs are reported to be no better than placebo,” Dr. Verma predicts. “A lawyer could say to a clinician, ‘You used an SGA on Mr. Smith despite the risks, and he developed XYZ complication?’ Try to work yourself out of that one.
“A paper like this will be snapped up by pharmacy and therapeutics committees around the country, as well as Medicare, Medicaid, and other insurers,” Dr. Verma adds. “They’ll say, ‘These expensive drugs are no better than placebo. Why bother covering them?’”
Echoing Dr. Verma’s fears, the American Association for Geriatric Psychiatry (AAGP) responded to CATIE-AD by urging regulatory agencies not to overreact to the findings or “prevent physicians from exercising clinical judgment.”3 AAGP also is calling for more research “based on clinical and evidence-based protocols designed to help physicians know when and how to start, continue, and discontinue psychotropics” for older patients.3
Another problem with generalizing the CATIE-AD findings, Dr. Verma says, is that many Alzheimer’s patients are more severely impaired than those who participated in CATIE-AD.
“These are people who cannot be managed,” adds Barbara Kamholz, MD, clinical associate professor, University of Michigan, and staff psychiatrist, VA Medical Center, Ann Arbor. “They can’t get through the day. They can’t eat or use the bathroom properly. You can’t treat their medical problems if you can’t manage grossly abusive or violent behaviors.”
Dr. Schneider, however, notes that the outpatients in CATIE-AD were nearly as symptomatic as patients in nursing homes—as suggested by CATIE-AD patients’ mean Brief Psychiatric Rating Scale and Neuropsychiatric Inventory scores (28 and 37, respectively).
Also, Dr. Schneider says, most trials of SGAs conducted among nursing home patients have not yielded statistically significant results.4
‘Informing’ practice
Dr. Schneider warns against drastic interpretation of CATIE-AD, saying the trial should guide clinical practice, not radically alter it. He says he will keep prescribing SGAs for short-term acute treatment of older patients whose behavioral problems do not respond to psychosocial interventions, distraction, redirection, environmental manipulation, or other treatments.
“I’m not sure this study has changed my use of [SGAs],” Dr. Schneider says. “What it has done is better inform my considerations in prescribing. But I use [SGAs] in patients with significant behavioral problems—and especially with delusions, paranoia and aggression—who can’t be otherwise treated.”
Studies show that despite their risks, SGAs:
- are associated with one-tenth the risk of tardive dyskinesia compared with first-generation antipsychotics (FGAs) such as haloperidol5
- are less likely to cause extrapyramidal symptoms than FGAs.6
Dr. Verma notes that the cardiac, cerebrovascular, and cardiopulmonary side effects described in the “black box” warnings on SGAs are prevalent conditions in the elderly, independent of medication.
“Despite the side effects, 20% to 30% of patients [in CATIE-AD] continued to take [SGAs] for the entire study,”
Dr. Verma adds. “[SGAs] are not perfect drugs, but they’re the best we’ve got right now and better than what we had.”
Dr. Schneider acknowledges that no evidence supports use of other drug classes to treat problem behaviors in the elderly. “Antidepressants have their own adverse effects, and you wouldn’t expect them to work for delusions or aggression. And benzodiazepines are strongly associated with falling and oversedation.”
Dr. Kamholz fears that some psychiatrists might eschew SGAs in older patients and prescribe another type of medication that carries a greater side-effect risk.
“If they’re not using [SGAs], they might be using something more dangerous,” Dr. Kamholz says. “For example, haloperidol is an old standby, but very few studies address its global effects. So we’re groping around in the dark. I’ve also seen some bad deliriums caused by benzodiazepines.”
When to prescribe SGAs
At what point does the need to manage psychosis, aggression, or agitation in Alzheimer’s disease outweigh SGAs’ risks?
“Frankly, I’d rather not use medications unless I have to—and then only enough to preserve function while treating the behavioral disturbance,” Dr. Verma says. “I don’t want to anesthetize these patients. I just want to maintain their function, dignity, and quality of life.”
Seeking other causes of acute behaviors is essential before prescribing an SGA, Drs. Verma and Schneider say. Psychotic disorientation, for example, can occur with underlying psychiatric problems (such as delirium), hearing and sight deficits, disrupted schedules, poor sleep and appetite, incontinence, pain, unrelated medical complications, or environmental stressors.
For many older patients with problem behaviors, SGAs are worth the risk after other interventions have failed, Dr. Kamholz says. Weighing behavioral against pharmacologic risks is key, Dr. Schneider adds.
“What are the consequences of the behavior or paranoid ideation?” Dr. Schneider asks. “What about when the patient is refusing food? Or when caregivers cannot approach the patient, or the behavior creates a rift between family members so that the patient’s basic needs cannot be met? If psychosocial and environmental interventions haven’t worked, [SGAs] are worth a try.”
Because acute behavior hastens caregiver burnout—a major cause of nursing home admission6—appropriate SGA use also can help older patients remain at home, Drs. Schneider, Kamholz, and Verma say.
Practical applications
Drs. Schneider, Verma, and Kamholz agree that SGAs are a short-term intervention for problem behaviors in dementia. Because Alzheimer’s symptoms wax and wane as the disease progresses, patients need to be monitored continually, and medication regimens should be modified as needed and discontinued if possible.
Dr. Verma advises starting risperidone, olanza-pine, or quetiapine at low dosages, titrating slowly, and monitoring the patient carefully (Table).
Dr. Schneider suggests discontinuing the SGA after 12 to 20 weeks in patients who have responded. If behavior worsens after an SGA is discontinued, restart the medication, he says.
“If patients have adverse events with SGAs, do not try to tough it out,” Dr. Schneider adds. “Either adjust medications to eliminate adverse events or change the medication. If patients have been tolerating the medication for, say, 12 weeks, that doesn’t mean adverse reactions cannot develop later, so be ready to make adjustments.”
To guard against medicolegal risk when prescribing SGAs to older patients, Dr. Verma suggests that you clearly document:
- the reason you are prescribing the SGA
- your understanding of the risk/benefit ratio in using SGAs and that, in your clinical judgment, using an SGA in this patient is warranted because the benefits outweigh the risks
- that you considered other medications and the reasons those medications are inappropriate (for example, “I opted against a benzodiazepine because it could be too sedating and could increase the risk of falls and consequent injury”).
Also, get updates from the patient’s primary care physician on the patient’s cardiopulmonary and cerebrovascular health. Finally, provide extensive information about SGAs’ risks to family members, and keep signed documentation that you provided these warnings.
Table
Recommended second-generation antipsychotic dosing for older patients
| Drug | Starting dosage | Titration | Most-common side effects |
|---|---|---|---|
| Olanzapine | 2.5 to 5 mg/d, depending on the patient’s body mass and frailty | 2.5 mg every 2 to 3 days to 15 to 20 mg/d or therapeutic effect | Weight gain, orthostasis, sedation |
| Quetiapine* | 25 mg/d | 25 mg every 2 to 3 days to 350 mg/d or therapeutic effect | Sedation, weight gain |
| Risperidone | 0.25 mg bid | 0.25 mg every 2 to 3 days to 2 to 3 mg bid or therapeutic effect | Extrapyramidal symptoms, orthostasis |
| * Recommended for patients with Lewy body dementia or parkinsonian movement problems. | |||
| Source: Sumer Verma, MD | |||
Related resources
- American Association for Geriatric Psychiatry. AAGP position statement: Principles of care for patients with dementia resulting from Alzheimer disease.www.aagponline.org/prof/position_caredmnalz.asp.
Drug brand names
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
Acknowledgment
Peter A. Kelly is senior editor, Current Psychiatry.
Lynn Waltz, a medical writer and editor in Norfolk, VA, helped prepare this article from transcripts of interviews with Drs. Kamholz, Schneider, and Verma.
1. Schneider LS, Tariot PN, Dagerman KS, et al. Effectiveness of atypical antipsychotic drugs in patients with Alzheimer’s disease. N Engl J Med 2006;355:1525-38.
2. Karlawish J. Alzheimer’s disease: clinical trials and the logic of clinical purpose. N Engl J Med 2006;355:1604-6.
3. American Association for Geriatric Psychiatry. New NIH study underscores complexity of Alzheimer’s disease, according to AAGP. Available at: http://www.aagponline.org/news/pressreleases.asp?viewfull=110. Accessed November 9, 2006.
4. Schneider LS, Dagerman K, Insel PS. Efficacy and adverse effects of atypical antipsychotics for dementia: meta-analysis of randomized, placebo-controlled trials. Am J Geriatr Psychiatry 2006;14:191-210.
5. Kasckow JW, Mulchahey JJ, Mohamed S. Using antipsychotics in patients with dementia. Current Psychiatry 2004;3(2):55-64.
6. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47:716-19.
New findings questioning the value of second-generation antipsychotics (SGAs) for treating acute behaviors in patients with Alzheimer’s disease have raised more questions on when and how to use these agents in the elderly.
The National Institute of Mental Health-sponsored Clinical Antipsychotic Trial of Intervention Effectiveness-Alzheimer’s disease (CATIE-AD) concluded that SGAs offer no overall advantage over placebo. Although SGAs helped some trial patients, the medications were discontinued for approximately 8 in 10 patients because of intolerable side effects or ineffectiveness.
CATIE-AD’s principal investigator says the findings—published in the October 12 New England Journal of Medicine1—will guide clinicians in adjusting SGA dosages and durations for older patients with dementia.
But other psychiatrists argue that the study—led by prominent researchers and published in a prestigious medical journal—will deter clinicians from trying SGAs for older patients with dementia-related psychosis, aggression, or agitation.
Barbara Kamholz, MD
Clinical associate professor, department of psychiatry, University of Michigan Medical School; staff psychiatrist, VA Medical Center, Ann Arbor
Lon Schneider, MD
Professor of psychiatry, neurology, and gerontology, University of Southern California, Los Angeles
Sumer Verma, MD
Director, geriatric psychiatry education program, McLean Hospital, Belmont, MA
“These drugs are not FDA-approved for dementia. They may cause diabetes. They cause weight gain. They carry boxed warnings that they could increase risk of stroke and—in patients over age 85—can increase risk of dying,” says Sumer Verma, MD, director of the geriatric psychiatry education program at McLean Hospital (Belmont, MA). “Doctors already were reluctant to use SGAs, and now these researchers publish this study in one of the country’s most respected journals and make an unqualified statement to the effect that [SGAs] are no better than placebo. How many clinicians will be comfortable prescribing them?”
Participants
421 outpatients with psychosis, agitation, or aggression, or who met DSM-IV-TR criteria for Alzheimer’s-type dementia or probable Alzheimer’s disease based on history, physical examination, structural brain imaging results, and Mini-Mental State Examination scores between 5 and 26, indicating some degree of cognitive deficit. These patients:
- were ambulatory
- lived at home or in an assisted-living facility
- had delusions, hallucinations, aggression, or agitation that developed after dementia onset, disrupted functioning, and justified treatment with an antipsychotic
- showed signs and symptoms of psychosis, aggression, or agitation almost daily during the previous week or intermittently for 4 weeks.
Trial duration
Up to 36 weeks
Study drugs/mean dosages at endpoint
- olanzapine (5.5 mg/d)
- quetiapine (56.5 mg/d)
- risperidone (1 mg/d)
Physicians could increase dosages or prescribe a benzodiazepine or haloperidol if problem behaviors emerged.
Key findings
- Time to discontinuing treatment for any reason did not differ significantly among the treatment and placebo groups.
- Median time to discontinuation because of lack of efficacy was significantly longer with olanzapine (22.1 weeks) or risperidone (26.7 weeks) than with quetiapine (9.1 weeks) or placebo (9.0 weeks).
- Rates of discontinuation because of intolerance, adverse effects, or death were 24% with olanzapine, 16% with quetiapine, 18% with risperidone, and 5% with placebo.
- Overall rates of discontinuation for any reason were 63% after 12 weeks and 82% after 36 weeks.
- Parkinsonism or extrapyramidal symptoms were more prevalent among the olanzapine and risperidone groups (12% in each) than among the quetiapine and placebo groups (2% and 1%, respectively).
- Sedation was more common with the three SGAs (15% to 24% of patients) than with placebo (5%).
- Confusion or mental status changes were more common with olanzapine (18%) and risperidone (11%) than with placebo (5%). Cognitive disturbances and psychotic symptoms were more common with olanzapine (5% and 7%, respectively) than with the other SGAs or placebo (0 to 2%).
- Body weight increased 0.4 to 1 lb/month among the SGA groups and decreased 0.9 lb/month in the placebo group.
- Rates of improvement—as measured with the Clinical Global Impression of Change scale—did not differ significantly among the treatment and placebo groups.
‘Discouraging’ discontinuation
CATIE-AD—a double-blind, multicenter, randomized trial (Box)—followed 421 ambulatory outpatients with Alzheimer’s disease and psychosis, aggression, or agitation. Patients received the SGAs olanzapine (mean dosage, 5.5 mg/d), quetiapine (mean 56.5 mg/d), risperidone (mean 1 mg/d), or placebo. Dosages were adjusted as needed.
After 36 weeks, times to discontinuation because of lack of efficacy were longest for olanza-pine and risperidone, but these drugs also had the highest rates of discontinuation because of intolerability (24% and 18%, respectively). Quetiapine’s rate of discontinuation because of intolerability was 16%.
SGAs were stopped because of lack of efficacy or intolerable side effects—such as parkinsonism, extrapyramidal symptoms, sedation, or weight gain—in:
- 63% of treatment and placebo group patients within 12 weeks
- 82% of all patients within 36 weeks.
Lon Schneider, MD, principal investigator for CATIE-AD, acknowledged that the findings could discourage psychiatrists from prescribing SGAs for acute dementia-related behaviors, specifically in patients with Alzheimer’s disease.
But although discontinuation because of intolerability was most prevalent among patients taking risperidone or olanzapine, both SGAs were more effective than placebo for treating problem behaviors in some participants, Dr. Schneider notes. He adds that the patient population and most SGA dosages in CATIE-AD reflected typical geriatric psychiatric practice in the community.
An editorial in the October 12 New England Journal of Medicine2 praised CATIE-AD for allowing physicians to titrate and stop SGA regimens as needed while maintaining the double-blind design. Results of fixed-dose trials with prespecified time points are more difficult to apply to clinical practice because the course of Alzheimer’s disease and patients’ ability to tolerate specific drugs change over time.2
“This study can inform clinicians that they should not be prescribing medication and then not following up or maintaining it indefinitely,” says Dr. Schneider, who is professor of psychiatry, neurology and gerontology, University of Southern California, Los Angeles.
‘Black box’ fears?
Dr. Verma, however, reports that many clinicians have been hesitant to prescribe SGAs to older patients since last year—when the FDA ordered that SGAs carry “black box” warnings of a possible increased mortality risk in that population.
“CATIE-AD will intensify clinicians’ fears of litigation by implying that the risks of using SGAs outweigh their benefits, especially when SGAs are reported to be no better than placebo,” Dr. Verma predicts. “A lawyer could say to a clinician, ‘You used an SGA on Mr. Smith despite the risks, and he developed XYZ complication?’ Try to work yourself out of that one.
“A paper like this will be snapped up by pharmacy and therapeutics committees around the country, as well as Medicare, Medicaid, and other insurers,” Dr. Verma adds. “They’ll say, ‘These expensive drugs are no better than placebo. Why bother covering them?’”
Echoing Dr. Verma’s fears, the American Association for Geriatric Psychiatry (AAGP) responded to CATIE-AD by urging regulatory agencies not to overreact to the findings or “prevent physicians from exercising clinical judgment.”3 AAGP also is calling for more research “based on clinical and evidence-based protocols designed to help physicians know when and how to start, continue, and discontinue psychotropics” for older patients.3
Another problem with generalizing the CATIE-AD findings, Dr. Verma says, is that many Alzheimer’s patients are more severely impaired than those who participated in CATIE-AD.
“These are people who cannot be managed,” adds Barbara Kamholz, MD, clinical associate professor, University of Michigan, and staff psychiatrist, VA Medical Center, Ann Arbor. “They can’t get through the day. They can’t eat or use the bathroom properly. You can’t treat their medical problems if you can’t manage grossly abusive or violent behaviors.”
Dr. Schneider, however, notes that the outpatients in CATIE-AD were nearly as symptomatic as patients in nursing homes—as suggested by CATIE-AD patients’ mean Brief Psychiatric Rating Scale and Neuropsychiatric Inventory scores (28 and 37, respectively).
Also, Dr. Schneider says, most trials of SGAs conducted among nursing home patients have not yielded statistically significant results.4
‘Informing’ practice
Dr. Schneider warns against drastic interpretation of CATIE-AD, saying the trial should guide clinical practice, not radically alter it. He says he will keep prescribing SGAs for short-term acute treatment of older patients whose behavioral problems do not respond to psychosocial interventions, distraction, redirection, environmental manipulation, or other treatments.
“I’m not sure this study has changed my use of [SGAs],” Dr. Schneider says. “What it has done is better inform my considerations in prescribing. But I use [SGAs] in patients with significant behavioral problems—and especially with delusions, paranoia and aggression—who can’t be otherwise treated.”
Studies show that despite their risks, SGAs:
- are associated with one-tenth the risk of tardive dyskinesia compared with first-generation antipsychotics (FGAs) such as haloperidol5
- are less likely to cause extrapyramidal symptoms than FGAs.6
Dr. Verma notes that the cardiac, cerebrovascular, and cardiopulmonary side effects described in the “black box” warnings on SGAs are prevalent conditions in the elderly, independent of medication.
“Despite the side effects, 20% to 30% of patients [in CATIE-AD] continued to take [SGAs] for the entire study,”
Dr. Verma adds. “[SGAs] are not perfect drugs, but they’re the best we’ve got right now and better than what we had.”
Dr. Schneider acknowledges that no evidence supports use of other drug classes to treat problem behaviors in the elderly. “Antidepressants have their own adverse effects, and you wouldn’t expect them to work for delusions or aggression. And benzodiazepines are strongly associated with falling and oversedation.”
Dr. Kamholz fears that some psychiatrists might eschew SGAs in older patients and prescribe another type of medication that carries a greater side-effect risk.
“If they’re not using [SGAs], they might be using something more dangerous,” Dr. Kamholz says. “For example, haloperidol is an old standby, but very few studies address its global effects. So we’re groping around in the dark. I’ve also seen some bad deliriums caused by benzodiazepines.”
When to prescribe SGAs
At what point does the need to manage psychosis, aggression, or agitation in Alzheimer’s disease outweigh SGAs’ risks?
“Frankly, I’d rather not use medications unless I have to—and then only enough to preserve function while treating the behavioral disturbance,” Dr. Verma says. “I don’t want to anesthetize these patients. I just want to maintain their function, dignity, and quality of life.”
Seeking other causes of acute behaviors is essential before prescribing an SGA, Drs. Verma and Schneider say. Psychotic disorientation, for example, can occur with underlying psychiatric problems (such as delirium), hearing and sight deficits, disrupted schedules, poor sleep and appetite, incontinence, pain, unrelated medical complications, or environmental stressors.
For many older patients with problem behaviors, SGAs are worth the risk after other interventions have failed, Dr. Kamholz says. Weighing behavioral against pharmacologic risks is key, Dr. Schneider adds.
“What are the consequences of the behavior or paranoid ideation?” Dr. Schneider asks. “What about when the patient is refusing food? Or when caregivers cannot approach the patient, or the behavior creates a rift between family members so that the patient’s basic needs cannot be met? If psychosocial and environmental interventions haven’t worked, [SGAs] are worth a try.”
Because acute behavior hastens caregiver burnout—a major cause of nursing home admission6—appropriate SGA use also can help older patients remain at home, Drs. Schneider, Kamholz, and Verma say.
Practical applications
Drs. Schneider, Verma, and Kamholz agree that SGAs are a short-term intervention for problem behaviors in dementia. Because Alzheimer’s symptoms wax and wane as the disease progresses, patients need to be monitored continually, and medication regimens should be modified as needed and discontinued if possible.
Dr. Verma advises starting risperidone, olanza-pine, or quetiapine at low dosages, titrating slowly, and monitoring the patient carefully (Table).
Dr. Schneider suggests discontinuing the SGA after 12 to 20 weeks in patients who have responded. If behavior worsens after an SGA is discontinued, restart the medication, he says.
“If patients have adverse events with SGAs, do not try to tough it out,” Dr. Schneider adds. “Either adjust medications to eliminate adverse events or change the medication. If patients have been tolerating the medication for, say, 12 weeks, that doesn’t mean adverse reactions cannot develop later, so be ready to make adjustments.”
To guard against medicolegal risk when prescribing SGAs to older patients, Dr. Verma suggests that you clearly document:
- the reason you are prescribing the SGA
- your understanding of the risk/benefit ratio in using SGAs and that, in your clinical judgment, using an SGA in this patient is warranted because the benefits outweigh the risks
- that you considered other medications and the reasons those medications are inappropriate (for example, “I opted against a benzodiazepine because it could be too sedating and could increase the risk of falls and consequent injury”).
Also, get updates from the patient’s primary care physician on the patient’s cardiopulmonary and cerebrovascular health. Finally, provide extensive information about SGAs’ risks to family members, and keep signed documentation that you provided these warnings.
Table
Recommended second-generation antipsychotic dosing for older patients
| Drug | Starting dosage | Titration | Most-common side effects |
|---|---|---|---|
| Olanzapine | 2.5 to 5 mg/d, depending on the patient’s body mass and frailty | 2.5 mg every 2 to 3 days to 15 to 20 mg/d or therapeutic effect | Weight gain, orthostasis, sedation |
| Quetiapine* | 25 mg/d | 25 mg every 2 to 3 days to 350 mg/d or therapeutic effect | Sedation, weight gain |
| Risperidone | 0.25 mg bid | 0.25 mg every 2 to 3 days to 2 to 3 mg bid or therapeutic effect | Extrapyramidal symptoms, orthostasis |
| * Recommended for patients with Lewy body dementia or parkinsonian movement problems. | |||
| Source: Sumer Verma, MD | |||
Related resources
- American Association for Geriatric Psychiatry. AAGP position statement: Principles of care for patients with dementia resulting from Alzheimer disease.www.aagponline.org/prof/position_caredmnalz.asp.
Drug brand names
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
Acknowledgment
Peter A. Kelly is senior editor, Current Psychiatry.
Lynn Waltz, a medical writer and editor in Norfolk, VA, helped prepare this article from transcripts of interviews with Drs. Kamholz, Schneider, and Verma.
New findings questioning the value of second-generation antipsychotics (SGAs) for treating acute behaviors in patients with Alzheimer’s disease have raised more questions on when and how to use these agents in the elderly.
The National Institute of Mental Health-sponsored Clinical Antipsychotic Trial of Intervention Effectiveness-Alzheimer’s disease (CATIE-AD) concluded that SGAs offer no overall advantage over placebo. Although SGAs helped some trial patients, the medications were discontinued for approximately 8 in 10 patients because of intolerable side effects or ineffectiveness.
CATIE-AD’s principal investigator says the findings—published in the October 12 New England Journal of Medicine1—will guide clinicians in adjusting SGA dosages and durations for older patients with dementia.
But other psychiatrists argue that the study—led by prominent researchers and published in a prestigious medical journal—will deter clinicians from trying SGAs for older patients with dementia-related psychosis, aggression, or agitation.
Barbara Kamholz, MD
Clinical associate professor, department of psychiatry, University of Michigan Medical School; staff psychiatrist, VA Medical Center, Ann Arbor
Lon Schneider, MD
Professor of psychiatry, neurology, and gerontology, University of Southern California, Los Angeles
Sumer Verma, MD
Director, geriatric psychiatry education program, McLean Hospital, Belmont, MA
“These drugs are not FDA-approved for dementia. They may cause diabetes. They cause weight gain. They carry boxed warnings that they could increase risk of stroke and—in patients over age 85—can increase risk of dying,” says Sumer Verma, MD, director of the geriatric psychiatry education program at McLean Hospital (Belmont, MA). “Doctors already were reluctant to use SGAs, and now these researchers publish this study in one of the country’s most respected journals and make an unqualified statement to the effect that [SGAs] are no better than placebo. How many clinicians will be comfortable prescribing them?”
Participants
421 outpatients with psychosis, agitation, or aggression, or who met DSM-IV-TR criteria for Alzheimer’s-type dementia or probable Alzheimer’s disease based on history, physical examination, structural brain imaging results, and Mini-Mental State Examination scores between 5 and 26, indicating some degree of cognitive deficit. These patients:
- were ambulatory
- lived at home or in an assisted-living facility
- had delusions, hallucinations, aggression, or agitation that developed after dementia onset, disrupted functioning, and justified treatment with an antipsychotic
- showed signs and symptoms of psychosis, aggression, or agitation almost daily during the previous week or intermittently for 4 weeks.
Trial duration
Up to 36 weeks
Study drugs/mean dosages at endpoint
- olanzapine (5.5 mg/d)
- quetiapine (56.5 mg/d)
- risperidone (1 mg/d)
Physicians could increase dosages or prescribe a benzodiazepine or haloperidol if problem behaviors emerged.
Key findings
- Time to discontinuing treatment for any reason did not differ significantly among the treatment and placebo groups.
- Median time to discontinuation because of lack of efficacy was significantly longer with olanzapine (22.1 weeks) or risperidone (26.7 weeks) than with quetiapine (9.1 weeks) or placebo (9.0 weeks).
- Rates of discontinuation because of intolerance, adverse effects, or death were 24% with olanzapine, 16% with quetiapine, 18% with risperidone, and 5% with placebo.
- Overall rates of discontinuation for any reason were 63% after 12 weeks and 82% after 36 weeks.
- Parkinsonism or extrapyramidal symptoms were more prevalent among the olanzapine and risperidone groups (12% in each) than among the quetiapine and placebo groups (2% and 1%, respectively).
- Sedation was more common with the three SGAs (15% to 24% of patients) than with placebo (5%).
- Confusion or mental status changes were more common with olanzapine (18%) and risperidone (11%) than with placebo (5%). Cognitive disturbances and psychotic symptoms were more common with olanzapine (5% and 7%, respectively) than with the other SGAs or placebo (0 to 2%).
- Body weight increased 0.4 to 1 lb/month among the SGA groups and decreased 0.9 lb/month in the placebo group.
- Rates of improvement—as measured with the Clinical Global Impression of Change scale—did not differ significantly among the treatment and placebo groups.
‘Discouraging’ discontinuation
CATIE-AD—a double-blind, multicenter, randomized trial (Box)—followed 421 ambulatory outpatients with Alzheimer’s disease and psychosis, aggression, or agitation. Patients received the SGAs olanzapine (mean dosage, 5.5 mg/d), quetiapine (mean 56.5 mg/d), risperidone (mean 1 mg/d), or placebo. Dosages were adjusted as needed.
After 36 weeks, times to discontinuation because of lack of efficacy were longest for olanza-pine and risperidone, but these drugs also had the highest rates of discontinuation because of intolerability (24% and 18%, respectively). Quetiapine’s rate of discontinuation because of intolerability was 16%.
SGAs were stopped because of lack of efficacy or intolerable side effects—such as parkinsonism, extrapyramidal symptoms, sedation, or weight gain—in:
- 63% of treatment and placebo group patients within 12 weeks
- 82% of all patients within 36 weeks.
Lon Schneider, MD, principal investigator for CATIE-AD, acknowledged that the findings could discourage psychiatrists from prescribing SGAs for acute dementia-related behaviors, specifically in patients with Alzheimer’s disease.
But although discontinuation because of intolerability was most prevalent among patients taking risperidone or olanzapine, both SGAs were more effective than placebo for treating problem behaviors in some participants, Dr. Schneider notes. He adds that the patient population and most SGA dosages in CATIE-AD reflected typical geriatric psychiatric practice in the community.
An editorial in the October 12 New England Journal of Medicine2 praised CATIE-AD for allowing physicians to titrate and stop SGA regimens as needed while maintaining the double-blind design. Results of fixed-dose trials with prespecified time points are more difficult to apply to clinical practice because the course of Alzheimer’s disease and patients’ ability to tolerate specific drugs change over time.2
“This study can inform clinicians that they should not be prescribing medication and then not following up or maintaining it indefinitely,” says Dr. Schneider, who is professor of psychiatry, neurology and gerontology, University of Southern California, Los Angeles.
‘Black box’ fears?
Dr. Verma, however, reports that many clinicians have been hesitant to prescribe SGAs to older patients since last year—when the FDA ordered that SGAs carry “black box” warnings of a possible increased mortality risk in that population.
“CATIE-AD will intensify clinicians’ fears of litigation by implying that the risks of using SGAs outweigh their benefits, especially when SGAs are reported to be no better than placebo,” Dr. Verma predicts. “A lawyer could say to a clinician, ‘You used an SGA on Mr. Smith despite the risks, and he developed XYZ complication?’ Try to work yourself out of that one.
“A paper like this will be snapped up by pharmacy and therapeutics committees around the country, as well as Medicare, Medicaid, and other insurers,” Dr. Verma adds. “They’ll say, ‘These expensive drugs are no better than placebo. Why bother covering them?’”
Echoing Dr. Verma’s fears, the American Association for Geriatric Psychiatry (AAGP) responded to CATIE-AD by urging regulatory agencies not to overreact to the findings or “prevent physicians from exercising clinical judgment.”3 AAGP also is calling for more research “based on clinical and evidence-based protocols designed to help physicians know when and how to start, continue, and discontinue psychotropics” for older patients.3
Another problem with generalizing the CATIE-AD findings, Dr. Verma says, is that many Alzheimer’s patients are more severely impaired than those who participated in CATIE-AD.
“These are people who cannot be managed,” adds Barbara Kamholz, MD, clinical associate professor, University of Michigan, and staff psychiatrist, VA Medical Center, Ann Arbor. “They can’t get through the day. They can’t eat or use the bathroom properly. You can’t treat their medical problems if you can’t manage grossly abusive or violent behaviors.”
Dr. Schneider, however, notes that the outpatients in CATIE-AD were nearly as symptomatic as patients in nursing homes—as suggested by CATIE-AD patients’ mean Brief Psychiatric Rating Scale and Neuropsychiatric Inventory scores (28 and 37, respectively).
Also, Dr. Schneider says, most trials of SGAs conducted among nursing home patients have not yielded statistically significant results.4
‘Informing’ practice
Dr. Schneider warns against drastic interpretation of CATIE-AD, saying the trial should guide clinical practice, not radically alter it. He says he will keep prescribing SGAs for short-term acute treatment of older patients whose behavioral problems do not respond to psychosocial interventions, distraction, redirection, environmental manipulation, or other treatments.
“I’m not sure this study has changed my use of [SGAs],” Dr. Schneider says. “What it has done is better inform my considerations in prescribing. But I use [SGAs] in patients with significant behavioral problems—and especially with delusions, paranoia and aggression—who can’t be otherwise treated.”
Studies show that despite their risks, SGAs:
- are associated with one-tenth the risk of tardive dyskinesia compared with first-generation antipsychotics (FGAs) such as haloperidol5
- are less likely to cause extrapyramidal symptoms than FGAs.6
Dr. Verma notes that the cardiac, cerebrovascular, and cardiopulmonary side effects described in the “black box” warnings on SGAs are prevalent conditions in the elderly, independent of medication.
“Despite the side effects, 20% to 30% of patients [in CATIE-AD] continued to take [SGAs] for the entire study,”
Dr. Verma adds. “[SGAs] are not perfect drugs, but they’re the best we’ve got right now and better than what we had.”
Dr. Schneider acknowledges that no evidence supports use of other drug classes to treat problem behaviors in the elderly. “Antidepressants have their own adverse effects, and you wouldn’t expect them to work for delusions or aggression. And benzodiazepines are strongly associated with falling and oversedation.”
Dr. Kamholz fears that some psychiatrists might eschew SGAs in older patients and prescribe another type of medication that carries a greater side-effect risk.
“If they’re not using [SGAs], they might be using something more dangerous,” Dr. Kamholz says. “For example, haloperidol is an old standby, but very few studies address its global effects. So we’re groping around in the dark. I’ve also seen some bad deliriums caused by benzodiazepines.”
When to prescribe SGAs
At what point does the need to manage psychosis, aggression, or agitation in Alzheimer’s disease outweigh SGAs’ risks?
“Frankly, I’d rather not use medications unless I have to—and then only enough to preserve function while treating the behavioral disturbance,” Dr. Verma says. “I don’t want to anesthetize these patients. I just want to maintain their function, dignity, and quality of life.”
Seeking other causes of acute behaviors is essential before prescribing an SGA, Drs. Verma and Schneider say. Psychotic disorientation, for example, can occur with underlying psychiatric problems (such as delirium), hearing and sight deficits, disrupted schedules, poor sleep and appetite, incontinence, pain, unrelated medical complications, or environmental stressors.
For many older patients with problem behaviors, SGAs are worth the risk after other interventions have failed, Dr. Kamholz says. Weighing behavioral against pharmacologic risks is key, Dr. Schneider adds.
“What are the consequences of the behavior or paranoid ideation?” Dr. Schneider asks. “What about when the patient is refusing food? Or when caregivers cannot approach the patient, or the behavior creates a rift between family members so that the patient’s basic needs cannot be met? If psychosocial and environmental interventions haven’t worked, [SGAs] are worth a try.”
Because acute behavior hastens caregiver burnout—a major cause of nursing home admission6—appropriate SGA use also can help older patients remain at home, Drs. Schneider, Kamholz, and Verma say.
Practical applications
Drs. Schneider, Verma, and Kamholz agree that SGAs are a short-term intervention for problem behaviors in dementia. Because Alzheimer’s symptoms wax and wane as the disease progresses, patients need to be monitored continually, and medication regimens should be modified as needed and discontinued if possible.
Dr. Verma advises starting risperidone, olanza-pine, or quetiapine at low dosages, titrating slowly, and monitoring the patient carefully (Table).
Dr. Schneider suggests discontinuing the SGA after 12 to 20 weeks in patients who have responded. If behavior worsens after an SGA is discontinued, restart the medication, he says.
“If patients have adverse events with SGAs, do not try to tough it out,” Dr. Schneider adds. “Either adjust medications to eliminate adverse events or change the medication. If patients have been tolerating the medication for, say, 12 weeks, that doesn’t mean adverse reactions cannot develop later, so be ready to make adjustments.”
To guard against medicolegal risk when prescribing SGAs to older patients, Dr. Verma suggests that you clearly document:
- the reason you are prescribing the SGA
- your understanding of the risk/benefit ratio in using SGAs and that, in your clinical judgment, using an SGA in this patient is warranted because the benefits outweigh the risks
- that you considered other medications and the reasons those medications are inappropriate (for example, “I opted against a benzodiazepine because it could be too sedating and could increase the risk of falls and consequent injury”).
Also, get updates from the patient’s primary care physician on the patient’s cardiopulmonary and cerebrovascular health. Finally, provide extensive information about SGAs’ risks to family members, and keep signed documentation that you provided these warnings.
Table
Recommended second-generation antipsychotic dosing for older patients
| Drug | Starting dosage | Titration | Most-common side effects |
|---|---|---|---|
| Olanzapine | 2.5 to 5 mg/d, depending on the patient’s body mass and frailty | 2.5 mg every 2 to 3 days to 15 to 20 mg/d or therapeutic effect | Weight gain, orthostasis, sedation |
| Quetiapine* | 25 mg/d | 25 mg every 2 to 3 days to 350 mg/d or therapeutic effect | Sedation, weight gain |
| Risperidone | 0.25 mg bid | 0.25 mg every 2 to 3 days to 2 to 3 mg bid or therapeutic effect | Extrapyramidal symptoms, orthostasis |
| * Recommended for patients with Lewy body dementia or parkinsonian movement problems. | |||
| Source: Sumer Verma, MD | |||
Related resources
- American Association for Geriatric Psychiatry. AAGP position statement: Principles of care for patients with dementia resulting from Alzheimer disease.www.aagponline.org/prof/position_caredmnalz.asp.
Drug brand names
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
Acknowledgment
Peter A. Kelly is senior editor, Current Psychiatry.
Lynn Waltz, a medical writer and editor in Norfolk, VA, helped prepare this article from transcripts of interviews with Drs. Kamholz, Schneider, and Verma.
1. Schneider LS, Tariot PN, Dagerman KS, et al. Effectiveness of atypical antipsychotic drugs in patients with Alzheimer’s disease. N Engl J Med 2006;355:1525-38.
2. Karlawish J. Alzheimer’s disease: clinical trials and the logic of clinical purpose. N Engl J Med 2006;355:1604-6.
3. American Association for Geriatric Psychiatry. New NIH study underscores complexity of Alzheimer’s disease, according to AAGP. Available at: http://www.aagponline.org/news/pressreleases.asp?viewfull=110. Accessed November 9, 2006.
4. Schneider LS, Dagerman K, Insel PS. Efficacy and adverse effects of atypical antipsychotics for dementia: meta-analysis of randomized, placebo-controlled trials. Am J Geriatr Psychiatry 2006;14:191-210.
5. Kasckow JW, Mulchahey JJ, Mohamed S. Using antipsychotics in patients with dementia. Current Psychiatry 2004;3(2):55-64.
6. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47:716-19.
1. Schneider LS, Tariot PN, Dagerman KS, et al. Effectiveness of atypical antipsychotic drugs in patients with Alzheimer’s disease. N Engl J Med 2006;355:1525-38.
2. Karlawish J. Alzheimer’s disease: clinical trials and the logic of clinical purpose. N Engl J Med 2006;355:1604-6.
3. American Association for Geriatric Psychiatry. New NIH study underscores complexity of Alzheimer’s disease, according to AAGP. Available at: http://www.aagponline.org/news/pressreleases.asp?viewfull=110. Accessed November 9, 2006.
4. Schneider LS, Dagerman K, Insel PS. Efficacy and adverse effects of atypical antipsychotics for dementia: meta-analysis of randomized, placebo-controlled trials. Am J Geriatr Psychiatry 2006;14:191-210.
5. Kasckow JW, Mulchahey JJ, Mohamed S. Using antipsychotics in patients with dementia. Current Psychiatry 2004;3(2):55-64.
6. Jeste DV, Lacro JP, Bailey A, et al. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc 1999;47:716-19.
Bipolar disorder: Clinical questions beg for answers
A distinguished speaker at a recent national conference was describing his classification of bipolar disorder, and his slides listed subtypes I, II, II½, III, IV, and IV½. During the question-and-answer session, a perplexed attendee announced—with tongue in cheek—that he had 4½ questions and 2½ comments about the bipolar presentation….
Let’s face it, bipolar disorder is a fascinating neuropsychiatric condition that tests every clinician’s diagnostic acumen and treatment skills. Many questions about its diagnosis and treatment remain unanswered.
Diagnosis. Bipolar disorder can present with many different symptoms and with phases that cycle spontaneously or in response to treatment. And with its many mood states and multiple comorbidities, bipolar disorder is replete with red herrings. Many of its sufferers are misdiagnosed with alcoholism, anxiety, borderline personality disorder, attention-deficit/hyperactivity disorder (child or adult), or—the most frequent misdiagnosis—major depression.
Treatment. Despite a rich literature, astonishingly few large controlled clinical trials have been conducted to guide bipolar disorder pharmacotherapy. Long-term follow-up studies indicate that depression dominates in >75% of bipolar patients’ symptomatic days. Even so, (inexplicably) 8 drugs are approved in monotherapy for bipolar mania and only 1 for bipolar depression. (Quetiapine monotherapy was FDA-approved in October, joining the combination of olanzapine/fluoxetine with this labeling.)
No antidepressants are indicated for bipolar depression, yet they have been widely used despite their inherent risk of inducing switches to mania, hypomania, mixed states, and rapid cycling.
Winging it. Most clinicians improvise when treating rapid cycling, hypomania, cyclothymia, or bipolar II. No medications have been approved for these bipolar states, which commonly are seen in outpatient settings.
Three mood stabilizers and five atypical antipsychotics are approved for mania in bipolar I disorder, but hardly a shred of controlled evidence exists to help you decide which drug to try first. Without controlled head-to-head trials, clinicians must choose treatment based on available data:
- Some may use quetiapine as first-line therapy because of evidence showing efficacy in both bipolar mania and bipolar depression.
- Others may select ziprasidone or valproate ER, the only agents approved for all three types of mania (euphoric, mixed, and psychotic).
- Still others—cognizant of high nonadherence and the relapse-inducing risk of substance abuse in bipolar patients—may choose parenteral long-acting risperidone for long-term maintenance.
Combination therapy. Most bipolar disorder patients eventually receive two or more medications, but the evidence is anemic (at best) for combination therapy as well.
What is the optimal combination for mania with severe anxiety or for bipolar II disorder with mixed features or irritable depression? Dozens of iterations are possible, with nothing for prescribers to rely on except “expert consensus” guidelines based on opinion or clinical experience. No controlled clinical trials have compared various combinations, and little is known about:
- optimal dosing of agents in combinations
- which combinations are safest in patients with coexisting medical conditions.
Much remains to be learned about diagnosis and treatment of bipolar disorder’s subtypes. Our talented and productive patients with bipolar disorder look to us to provide the safest, most effective treatments that improve functioning without compromising quality of life. For this, we need a National Institute of Mental Health-sponsored study of bipolar disorder, similar to the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) studies of schizophrenia and Alzheimer’s disease (see Will CATIE-AD change dementia treatment?).
In the meantime, good luck managing the next bipolar II½ patient you see!

A distinguished speaker at a recent national conference was describing his classification of bipolar disorder, and his slides listed subtypes I, II, II½, III, IV, and IV½. During the question-and-answer session, a perplexed attendee announced—with tongue in cheek—that he had 4½ questions and 2½ comments about the bipolar presentation….
Let’s face it, bipolar disorder is a fascinating neuropsychiatric condition that tests every clinician’s diagnostic acumen and treatment skills. Many questions about its diagnosis and treatment remain unanswered.
Diagnosis. Bipolar disorder can present with many different symptoms and with phases that cycle spontaneously or in response to treatment. And with its many mood states and multiple comorbidities, bipolar disorder is replete with red herrings. Many of its sufferers are misdiagnosed with alcoholism, anxiety, borderline personality disorder, attention-deficit/hyperactivity disorder (child or adult), or—the most frequent misdiagnosis—major depression.
Treatment. Despite a rich literature, astonishingly few large controlled clinical trials have been conducted to guide bipolar disorder pharmacotherapy. Long-term follow-up studies indicate that depression dominates in >75% of bipolar patients’ symptomatic days. Even so, (inexplicably) 8 drugs are approved in monotherapy for bipolar mania and only 1 for bipolar depression. (Quetiapine monotherapy was FDA-approved in October, joining the combination of olanzapine/fluoxetine with this labeling.)
No antidepressants are indicated for bipolar depression, yet they have been widely used despite their inherent risk of inducing switches to mania, hypomania, mixed states, and rapid cycling.
Winging it. Most clinicians improvise when treating rapid cycling, hypomania, cyclothymia, or bipolar II. No medications have been approved for these bipolar states, which commonly are seen in outpatient settings.
Three mood stabilizers and five atypical antipsychotics are approved for mania in bipolar I disorder, but hardly a shred of controlled evidence exists to help you decide which drug to try first. Without controlled head-to-head trials, clinicians must choose treatment based on available data:
- Some may use quetiapine as first-line therapy because of evidence showing efficacy in both bipolar mania and bipolar depression.
- Others may select ziprasidone or valproate ER, the only agents approved for all three types of mania (euphoric, mixed, and psychotic).
- Still others—cognizant of high nonadherence and the relapse-inducing risk of substance abuse in bipolar patients—may choose parenteral long-acting risperidone for long-term maintenance.
Combination therapy. Most bipolar disorder patients eventually receive two or more medications, but the evidence is anemic (at best) for combination therapy as well.
What is the optimal combination for mania with severe anxiety or for bipolar II disorder with mixed features or irritable depression? Dozens of iterations are possible, with nothing for prescribers to rely on except “expert consensus” guidelines based on opinion or clinical experience. No controlled clinical trials have compared various combinations, and little is known about:
- optimal dosing of agents in combinations
- which combinations are safest in patients with coexisting medical conditions.
Much remains to be learned about diagnosis and treatment of bipolar disorder’s subtypes. Our talented and productive patients with bipolar disorder look to us to provide the safest, most effective treatments that improve functioning without compromising quality of life. For this, we need a National Institute of Mental Health-sponsored study of bipolar disorder, similar to the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) studies of schizophrenia and Alzheimer’s disease (see Will CATIE-AD change dementia treatment?).
In the meantime, good luck managing the next bipolar II½ patient you see!
A distinguished speaker at a recent national conference was describing his classification of bipolar disorder, and his slides listed subtypes I, II, II½, III, IV, and IV½. During the question-and-answer session, a perplexed attendee announced—with tongue in cheek—that he had 4½ questions and 2½ comments about the bipolar presentation….
Let’s face it, bipolar disorder is a fascinating neuropsychiatric condition that tests every clinician’s diagnostic acumen and treatment skills. Many questions about its diagnosis and treatment remain unanswered.
Diagnosis. Bipolar disorder can present with many different symptoms and with phases that cycle spontaneously or in response to treatment. And with its many mood states and multiple comorbidities, bipolar disorder is replete with red herrings. Many of its sufferers are misdiagnosed with alcoholism, anxiety, borderline personality disorder, attention-deficit/hyperactivity disorder (child or adult), or—the most frequent misdiagnosis—major depression.
Treatment. Despite a rich literature, astonishingly few large controlled clinical trials have been conducted to guide bipolar disorder pharmacotherapy. Long-term follow-up studies indicate that depression dominates in >75% of bipolar patients’ symptomatic days. Even so, (inexplicably) 8 drugs are approved in monotherapy for bipolar mania and only 1 for bipolar depression. (Quetiapine monotherapy was FDA-approved in October, joining the combination of olanzapine/fluoxetine with this labeling.)
No antidepressants are indicated for bipolar depression, yet they have been widely used despite their inherent risk of inducing switches to mania, hypomania, mixed states, and rapid cycling.
Winging it. Most clinicians improvise when treating rapid cycling, hypomania, cyclothymia, or bipolar II. No medications have been approved for these bipolar states, which commonly are seen in outpatient settings.
Three mood stabilizers and five atypical antipsychotics are approved for mania in bipolar I disorder, but hardly a shred of controlled evidence exists to help you decide which drug to try first. Without controlled head-to-head trials, clinicians must choose treatment based on available data:
- Some may use quetiapine as first-line therapy because of evidence showing efficacy in both bipolar mania and bipolar depression.
- Others may select ziprasidone or valproate ER, the only agents approved for all three types of mania (euphoric, mixed, and psychotic).
- Still others—cognizant of high nonadherence and the relapse-inducing risk of substance abuse in bipolar patients—may choose parenteral long-acting risperidone for long-term maintenance.
Combination therapy. Most bipolar disorder patients eventually receive two or more medications, but the evidence is anemic (at best) for combination therapy as well.
What is the optimal combination for mania with severe anxiety or for bipolar II disorder with mixed features or irritable depression? Dozens of iterations are possible, with nothing for prescribers to rely on except “expert consensus” guidelines based on opinion or clinical experience. No controlled clinical trials have compared various combinations, and little is known about:
- optimal dosing of agents in combinations
- which combinations are safest in patients with coexisting medical conditions.
Much remains to be learned about diagnosis and treatment of bipolar disorder’s subtypes. Our talented and productive patients with bipolar disorder look to us to provide the safest, most effective treatments that improve functioning without compromising quality of life. For this, we need a National Institute of Mental Health-sponsored study of bipolar disorder, similar to the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) studies of schizophrenia and Alzheimer’s disease (see Will CATIE-AD change dementia treatment?).
In the meantime, good luck managing the next bipolar II½ patient you see!
Gender dysphoria: ‘I’m a man, but…’
History: normal on paper
Mr. C, age 65, presents to an endocrinologist complaining of hot flashes and low libido. Initial testing shows low male testosterone, but a repeat test shows normal levels. No medical cause is found for his symptoms.
“My testosterone might be normal on paper,” Mr. C tells the endocrinologist, “but I’m not. I think I’m a woman.”
Mr. C requests referral to a female psychiatrist because he feels more comfortable discussing sexual issues with a woman. The endocrinologist refers him to me for evaluation.
Over 7 years, Mr. C’s other psychiatrist—a man—has been treating him for obsessive-compulsive disorder (OCD), anxiety disorder, and bipolar disorder type II. Mr. C takes paroxetine, 60 mg/d, for depressive symptoms and was taking divalproex, 1,500 mg/d, to stabilize his mood. He recently stopped divalproex because it was causing nausea and sedation.
During our initial visit, Mr. C says he’s “through pretending to be a man.” He says he first questioned his sexual identity in early childhood, when he sometimes dressed in his mother’s clothes for play. As an adult, he mostly cross-dresses in lingerie; he wears a woman’s tank top in public once or twice weekly underneath his polo dress shirt. Fifteen years ago, he suffered anorexia and bulimia while trying to look as svelte as a woman.
At 6 feet, 2 inches with good muscle tone and short, wavy black hair, Mr. C looks strikingly masculine. Now retired, he served in the Air Force and later worked as a commercial pilot and in construction. In private, however, he prefers gardening and cooking over sports and cars.
Mr. C is married but seldom has sexual intercourse with women. He gains sexual fulfillment by visualizing himself as a woman having sex with other women or with himself as a man. He denies interest in male-male sex.
The patient has been masturbating since age 5, mostly by rubbing his scrotum against a swing set pole he still keeps in his utility shed. He often tucks his penis to mimic female genitalia and makes believe his rectum is a vagina.
- Transsexualism
- Pure transvestism (having a firm gender identity but becoming sexually aroused by cross-dressing)
- Dual-role transvestism (cross-dressing solely to experience temporary membership in the opposite sex)
- Stress-related cross-dressing
- Men who desire penectomy or castration but no other gender-reassignment interventions
- Congenital intersex conditions, such as hermaphrodism
Mr. C’s Mini-Mental State Examination score of 30 indicates no underlying dementia. He shows stable affect with no evidence of derailment, paranoia, thought blocking, or auditory hallucinations.
Medical examination results are normal. Negative urine toxicology screen rules out substance abuse, and negative rapid plasma reagin rules out syphilis. Testosterone is not rechecked because levels were normal 2 days before.
The author’s observations
I suspect gender dysphoria, which describes a heterogeneous group of persons who express varying degrees of distress with their anatomic sex and sometimes desire secondary opposite-gender sexual characteristics (Box).
Sexual identity in gender dysphoria is often fluid. Symptoms might suggest transvestism, then evolve to transsexualism. Recognizing this heterogeneity and fluidity is crucial to diagnosis and treatment.
Primary transsexualism. The term “transsexualism” describes persons who want to live and be accepted within the opposite sex.1 The transsexual identity persists for ≥ 2 years and is not caused by another mental disorder or intersexed condition. Fetishism is classically absent and cross-dressing is not sexually gratifying. Most transsexuals want surgical and hormone treatment to make their bodies as congruent as possible with the preferred sex.
In 1994, DSM-IV recognized that some late-onset transsexuals showed features of comorbid transvestism and were sexually aroused by female dress and behaviors. Gender identity disorder (GID) replaced the term “transsexualism” and includes these individuals. A secondary diagnosis of transvestism is applied.
Secondary transsexualism. Case reports2 describe psychosis-induced transsexual desires in patients with schizophrenia. Gender dysphoria improved as their schizophrenia symptoms lessened.
The relationship between transsexualism and schizophrenia has been debated. Hyde and Kenna3 view transsexualism as a schizophrenia spectrum disorder, whereas sexologists consider transsexualism and schizophrenia distinct syndromes that can occur simultaneously.
Affective disorders might also alter contentment with gender role, but the relationship is unclear. Case reports of patients with bipolar disorder suggest that gender dysphoria intensity fluctuates with affective excursions.4 O’Gorman,5 however, described a bipolar patient whose gender dysphoria was mitigated during manic episodes.
Paraphilias are sexual disorders with recurrent intense urges and fantasies that do not follow normative arousal patterns and can diminish capacity for sexual intimacy.6 Manifestations include exhibitionism, fetishism, frotteurism, pedophilia, masochism/sadism, voyeurism, and transvestic fetishism.
Dividing transsexualism and pure transvestism paraphilia into discrete categories is simplistic, as transvestites can develop secondary components of transsexualism. Hoenig and Kenna7 assert that transsexualism—though not an anomalous erotic preference—is almost always preceded by transvestism or accompanied by cross-gender fetishism.
Nonparaphilic sexual addiction—included in DSM-IV-TR as sexual disorder not otherwise specified—describes culturally acceptable sexual interests and behaviors that are frequent or intense enough to reduce capacity for sexual intimacy. Such behaviors include compulsive masturbation, repetitive promiscuity, and dependence on anonymous sexual encounters.
An addiction model conceptualizes paraphilia as a form of pleasure seeking that has become habitual and self-destructive. Treatment involves directing patients to 12-step groups patterned after Alcoholics Anonymous.
Other models place paraphilias and related disorders within the OCD spectrum.8-13 Persons with OCD often are obsessed with sexual content and might grapple with religious and moral concerns about sexual issues. They typically consider their symptoms intrusive or senseless. Selective serotonin reuptake inhibitors—the standard medication for OCD—might alleviate paraphilia, but results are mixed.14
Mr. C’s symptoms. Mr. C shows features of GID and transvestism. His strong, persistent cross-gender identification and sense of inappropriateness with being a man indicate GID. His recurrent sexual urges and fantasies and impaired capacity for sexual intimacy suggest a paraphilia or transvestism.
The significance of Mr. C’s comorbid bipolar disorder and OCD is unclear. Both appeared controlled, but the potential for mania-induced hypersexuality cannot be ignored.
Diagnosing gender dysphoria
A thorough medical, psychiatric, and sexual history can reveal sexual identity symptoms’ source.
Consider a medical cause. Your medical workup may include a genital exam to check for irregularities such as hermaphrodism that can compound questions of sexual identity, and karyotyping to probe chromosomal anomalies, such as mosaicism or chimerism.
Consider schizophrenia or bipolar disorder, as mania or psychosis can cause aberrant sexual behavior. In gender-dysphoric patients with either disorder, treating the psychiatric comorbidity might alleviate the dysphoria. Watch for fluctuations in gender dysphoria intensity when you treat other psychopathologies.
Take a thorough sexual history. Being matter-of-fact while discussing unusual sexual acts will help the patient “open up” about his sexual problems. Ask him if he:
- showed gender-atypical behavior as a child, which can predict transsexualism or homosexuality has engaged in heterosexual, homosexual, or abnormal sexual acts; ask about frequency and preference
- is married or has a girlfriend. If so, are they getting along? How often do they have sex?
- cross-dresses. Does his partner cross-dress as well and, if so, do they cross-dress for sexual gratification or to identify with the opposite gender? Has this response changed over time? Where and how often do they cross-dress?
- is achieving sexual gratification. If so, how?
- has sexual fantasies involving breast-feeding, giving birth, or forced feminization through gender-changing surgeries or other means
- “tucks” his penis, urinates sitting down, or mimics other stereotypical feminine behavior.
The answers will uncover a motivation behind these behaviors, which is key to diagnosis. Sexual gratification as a motive suggests paraphilia, whereas a desire to live as a woman points to transsexualism. Because of the myriad presentations, multiple patient visits are necessary for a specific diagnosis.
Diagnosis: ‘i enjoy womanhood, but…’
I diagnose gender dysphoria, but because Mr. C’s mood is euthymic, I cannot discern how his mood instability might affect his dysphoria. His sexual fantasies are mood-congruent and evoke no shame.
Mr. C then states that he adamantly opposes living outwardly as a woman, and fears that an overt sex change would destroy his marriage and other relationships. Even so, he desires hormone therapy and surgical breast implants so he can more closely mimic physical womanhood and make masturbation more pleasurable. He says he would flatten his breasts with gauze while in public so he can continue to look like a man.
Though comfortable with his sexual fantasies, Mr. C laments that presenting himself as an “alpha male” drains his psychic energy.
The author’s observations
Mr. C meets criteria for GID and transvestism. Some transvestites also meet criteria for autogynephilia and report erotic arousal upon seeing oneself as a woman. Character pathology, specifically sexual fantasies associated with schizoid personality, might also contribute to unusual gender presentation. Sexologists also propose fluidity in gender identification across populations and over a person’s life span.
Autogynephilia—by which a man becomes sexually aroused by imagining or seeing himself as a woman15—usually is associated with transvestism. Autogynephiles often have sexual fantasies of possessing female anatomical structures, engaging in feminine behaviors, or performing female bodily functions such as lactation, menstruation, or childbirth.
Autogynephilia may be a misdirected heterosexuality and is more prevalent among male-to-female transsexuals who are attracted to women, both sexes, or neither sex than among those attracted only to men.16
Gender identity fluidity. Clinicians have recorded fluidity in gender identity (sense of masculinity or femininity) and sexual orientation (the sex to which one is attracted). Sexologists have tried to create scales that gauge these changes.
The Kinsey Heterosexual-Homosexual Rating Scale17 is based on Kinsey’s theory that men are not strictly heterosexual or homosexual. Scores between 0 and 6 indicate some degree of both (Table).
The Benjamin Gender Disorientation Scale, which measures gender identity variations, recognizes variability of gender dysphoria expression and underscores the difficulty of classifying patients who—like Mr. C—present with varied symptoms. The scale is available at www.wpath.org.
I did not administer the Kinsey or Benjamin scales to Mr. C. Although his case shows how innate sense of masculinity or femininity can vary among patients with gender dysphoria, his presentation has been stable, albeit unusual.
Mr. C’s symptoms. Mr. C shows autogynephilic features. He lacks the schizoid’s emotional inertness and his gender presentation is static, though dramatic. He appears to meet criteria for GID and transvestism, autogynephilic variant.
Schizoid and other personality disorders are associated with unusual sexual fantasies. Mr. C lacks primary schizoid features, such as flattened affectivity and indifference to close relationships.
Table
Kinsey Heterosexual-Homosexual Rating Scale
| Score | Indicates… |
|---|---|
| 0 | Exclusively heterosexual |
| 1 | Predominantly heterosexual, incidentally homosexual |
| 2 | Predominantly heterosexual, more than incidentally homosexual |
| 3 | Equally heterosexual and homosexual |
| 4 | Predominantly homosexual, more than incidentally heterosexual |
| 5 | Predominantly homosexual, incidentally heterosexual |
| 6 | Exclusively homosexual |
| Source: Reference 17. Reprinted by permission of The Kinsey Institute for Research in Sex, Gender, and Reproduction, Inc., Indiana University, Bloomington. | |
The author’s observations
Mr. C is a poor candidate for hormone therapy or gender reassignment surgery because of his circumscribed desire to live as a woman at home. Also, sexual gratification is his primary motivation for wanting to develop breasts.
Treating gender dysphoria
Serotonergic agents such as fluoxetine have shown effectiveness for treating paraphilias and nonparaphilic sexual addiction in case reports.18,19
Behavioral techniques, however, might have a more definite impact on gender dysphoria. Marks19 reported a 4-year remission of transsexualism in a patient after comorbid OCD improved with self-exposure therapy.
Psychotherapy will not resolve gender identity disorder but can promote a stable lifestyle and improve the patient’s chances for success in relationships, education, work, and gender identity expression.20 Psychotherapy can also help determine patients’ readiness for sexual reassignment surgery.
Treatment: learning to accept
I refer Mr. C back to his primary psychiatrist, who adds aripiprazole, 5 mg/d, to address grandiosity and hypomania that emerged months after my initial evaluation.
I also refer Mr. C to a gender disorder specialist for psychotherapy directed at examining his history, understanding his dilemmas, and identifying unrealistic ideas and maladaptive behaviors. The therapist has been teaching Mr. C coping skills and educating him on gender disorders and normal gender variations in activities and interests. He has been attending weekly sessions for 4 months.
To address his resentment over trying to look manly, I assure him that he doesn’t need to assume additional “masculine” behaviors and attitudes, and that his height and features make him appear masculine.
- World Professional Association for Transgender Health, formerly the Harry Benjamin International Gender Dysphoria Association (offers links to transgender resources, gender programs, and sexologists). www.hbigda.org.
- Divalproex sodium • Depakote
- Fluoxetine • Prozac
- Paroxetine • Paxil
Dr. Martin reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Mental and behavioral disorders, diagnostic criteria for research. In: The ICD-10 classification of mental and behavioural disorders: diagnostic criteria for research. Geneva: World Health Organization; 1993.
2. Caldwell C, Keshavan MS. Schizophrenia with secondary transsexualism. Can J Psychiatry 1991;36:300-1.
3. Hyde C, Kenna JC. A male MZ twin pair, concordant for transsexualism, discordant for schizophrenia. Acta Psychiatr Scand 1977;56:265-75.
4. Habermeyer E, Kamps I, Kawohl W. A case of bipolar psychosis and transsexualism. Psychopathology 2003;36:168-70.
5. O’Gorman EC. The effect of psychosis on gender identity. Br J Psychiatry 1980;136:314-5.
6. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000:566-76.
7. Hoenig J, Kenna JC. The nosolgical position of transsexualism. Arch Sex Behav 1974;3:273-87.
8. Jenike MA. Obsessive-compulsive and related disorders: a hidden epidemic. N Engl J Med 1989;24;321:539-41.
9. Stein DJ, Hollander E. The spectrum of obsessive-compulsive related disorders. In: Hollander E, ed. The obsessive-compulsive related disorders. Washington, DC: American Psychiatric Publishing. In press.
10. Hollander E. Serotonergic drugs and the treatment of disorders related to obsessive-compulsive disorder. In: Pato MT, Zohar J, eds. Current treatments of obsessive-compulsive disorder. Washington, DC: American Psychiatric Publishing; 1991:173-92.
11. Quadland MC. Compulsive sexual behavior: definition of a problem and an approach to treatment. J Sex Marital Ther 1985;11:121-32.
12. Coleman E. Sexual compulsivity: definition, etiology, and treatment considerations. In: Coleman E, ed. Chemical dependency and intimacy dysfunction. New York: Haworth Press; 1988.
13. Anthony DT, Hollander E. Sexual compulsions. In: Hollander E, ed. The obsessive-compulsive related disorders. Washington, DC: American Psychiatric Publishing. In press.
14. Perilstein RD, Lipper S, Friedman LJ. Three cases of paraphilias responsive to fluoxetine treatment. J Clin Psychiatry 1991;52:169-70.
15. Blanchard R. Nonmonotonic relation of autogynephilia and heterosexual attraction. J Abnorm Psychol 1992;101:271-6.
16. Hirschfeld M. Sexual anomalies. New York: Emerson Books; 1948.
17. Kinsey AC, Pomeroy WB, Martin CE. Sexual behavior in the human male. Philadelphia: WB Saunders; 1948;636-59.
18. Kafka MP. Successful antidepressant treatment of nonparaphilic sexual addictions and paraphilias in men. J Clin Psychiatry 1991;52:60-5.
19. Marks IM, Mataix-Cols D. Four-year remission of transsexualism after comorbid obsessive-compulsive disorder improved with self-exposure therapy. Case report. Br J Psychiatry 1997;171:389-90.
20. Harry Benjamin International Gender Dysphoria Association’s Standards of Care for Gender Identity Disorders. Int J Transgenderism 2001; 5(1). Available at: http://www.symposion.com/ijt/index.htm. Accessed November 3, 2006.
History: normal on paper
Mr. C, age 65, presents to an endocrinologist complaining of hot flashes and low libido. Initial testing shows low male testosterone, but a repeat test shows normal levels. No medical cause is found for his symptoms.
“My testosterone might be normal on paper,” Mr. C tells the endocrinologist, “but I’m not. I think I’m a woman.”
Mr. C requests referral to a female psychiatrist because he feels more comfortable discussing sexual issues with a woman. The endocrinologist refers him to me for evaluation.
Over 7 years, Mr. C’s other psychiatrist—a man—has been treating him for obsessive-compulsive disorder (OCD), anxiety disorder, and bipolar disorder type II. Mr. C takes paroxetine, 60 mg/d, for depressive symptoms and was taking divalproex, 1,500 mg/d, to stabilize his mood. He recently stopped divalproex because it was causing nausea and sedation.
During our initial visit, Mr. C says he’s “through pretending to be a man.” He says he first questioned his sexual identity in early childhood, when he sometimes dressed in his mother’s clothes for play. As an adult, he mostly cross-dresses in lingerie; he wears a woman’s tank top in public once or twice weekly underneath his polo dress shirt. Fifteen years ago, he suffered anorexia and bulimia while trying to look as svelte as a woman.
At 6 feet, 2 inches with good muscle tone and short, wavy black hair, Mr. C looks strikingly masculine. Now retired, he served in the Air Force and later worked as a commercial pilot and in construction. In private, however, he prefers gardening and cooking over sports and cars.
Mr. C is married but seldom has sexual intercourse with women. He gains sexual fulfillment by visualizing himself as a woman having sex with other women or with himself as a man. He denies interest in male-male sex.
The patient has been masturbating since age 5, mostly by rubbing his scrotum against a swing set pole he still keeps in his utility shed. He often tucks his penis to mimic female genitalia and makes believe his rectum is a vagina.
- Transsexualism
- Pure transvestism (having a firm gender identity but becoming sexually aroused by cross-dressing)
- Dual-role transvestism (cross-dressing solely to experience temporary membership in the opposite sex)
- Stress-related cross-dressing
- Men who desire penectomy or castration but no other gender-reassignment interventions
- Congenital intersex conditions, such as hermaphrodism
Mr. C’s Mini-Mental State Examination score of 30 indicates no underlying dementia. He shows stable affect with no evidence of derailment, paranoia, thought blocking, or auditory hallucinations.
Medical examination results are normal. Negative urine toxicology screen rules out substance abuse, and negative rapid plasma reagin rules out syphilis. Testosterone is not rechecked because levels were normal 2 days before.
The author’s observations
I suspect gender dysphoria, which describes a heterogeneous group of persons who express varying degrees of distress with their anatomic sex and sometimes desire secondary opposite-gender sexual characteristics (Box).
Sexual identity in gender dysphoria is often fluid. Symptoms might suggest transvestism, then evolve to transsexualism. Recognizing this heterogeneity and fluidity is crucial to diagnosis and treatment.
Primary transsexualism. The term “transsexualism” describes persons who want to live and be accepted within the opposite sex.1 The transsexual identity persists for ≥ 2 years and is not caused by another mental disorder or intersexed condition. Fetishism is classically absent and cross-dressing is not sexually gratifying. Most transsexuals want surgical and hormone treatment to make their bodies as congruent as possible with the preferred sex.
In 1994, DSM-IV recognized that some late-onset transsexuals showed features of comorbid transvestism and were sexually aroused by female dress and behaviors. Gender identity disorder (GID) replaced the term “transsexualism” and includes these individuals. A secondary diagnosis of transvestism is applied.
Secondary transsexualism. Case reports2 describe psychosis-induced transsexual desires in patients with schizophrenia. Gender dysphoria improved as their schizophrenia symptoms lessened.
The relationship between transsexualism and schizophrenia has been debated. Hyde and Kenna3 view transsexualism as a schizophrenia spectrum disorder, whereas sexologists consider transsexualism and schizophrenia distinct syndromes that can occur simultaneously.
Affective disorders might also alter contentment with gender role, but the relationship is unclear. Case reports of patients with bipolar disorder suggest that gender dysphoria intensity fluctuates with affective excursions.4 O’Gorman,5 however, described a bipolar patient whose gender dysphoria was mitigated during manic episodes.
Paraphilias are sexual disorders with recurrent intense urges and fantasies that do not follow normative arousal patterns and can diminish capacity for sexual intimacy.6 Manifestations include exhibitionism, fetishism, frotteurism, pedophilia, masochism/sadism, voyeurism, and transvestic fetishism.
Dividing transsexualism and pure transvestism paraphilia into discrete categories is simplistic, as transvestites can develop secondary components of transsexualism. Hoenig and Kenna7 assert that transsexualism—though not an anomalous erotic preference—is almost always preceded by transvestism or accompanied by cross-gender fetishism.
Nonparaphilic sexual addiction—included in DSM-IV-TR as sexual disorder not otherwise specified—describes culturally acceptable sexual interests and behaviors that are frequent or intense enough to reduce capacity for sexual intimacy. Such behaviors include compulsive masturbation, repetitive promiscuity, and dependence on anonymous sexual encounters.
An addiction model conceptualizes paraphilia as a form of pleasure seeking that has become habitual and self-destructive. Treatment involves directing patients to 12-step groups patterned after Alcoholics Anonymous.
Other models place paraphilias and related disorders within the OCD spectrum.8-13 Persons with OCD often are obsessed with sexual content and might grapple with religious and moral concerns about sexual issues. They typically consider their symptoms intrusive or senseless. Selective serotonin reuptake inhibitors—the standard medication for OCD—might alleviate paraphilia, but results are mixed.14
Mr. C’s symptoms. Mr. C shows features of GID and transvestism. His strong, persistent cross-gender identification and sense of inappropriateness with being a man indicate GID. His recurrent sexual urges and fantasies and impaired capacity for sexual intimacy suggest a paraphilia or transvestism.
The significance of Mr. C’s comorbid bipolar disorder and OCD is unclear. Both appeared controlled, but the potential for mania-induced hypersexuality cannot be ignored.
Diagnosing gender dysphoria
A thorough medical, psychiatric, and sexual history can reveal sexual identity symptoms’ source.
Consider a medical cause. Your medical workup may include a genital exam to check for irregularities such as hermaphrodism that can compound questions of sexual identity, and karyotyping to probe chromosomal anomalies, such as mosaicism or chimerism.
Consider schizophrenia or bipolar disorder, as mania or psychosis can cause aberrant sexual behavior. In gender-dysphoric patients with either disorder, treating the psychiatric comorbidity might alleviate the dysphoria. Watch for fluctuations in gender dysphoria intensity when you treat other psychopathologies.
Take a thorough sexual history. Being matter-of-fact while discussing unusual sexual acts will help the patient “open up” about his sexual problems. Ask him if he:
- showed gender-atypical behavior as a child, which can predict transsexualism or homosexuality has engaged in heterosexual, homosexual, or abnormal sexual acts; ask about frequency and preference
- is married or has a girlfriend. If so, are they getting along? How often do they have sex?
- cross-dresses. Does his partner cross-dress as well and, if so, do they cross-dress for sexual gratification or to identify with the opposite gender? Has this response changed over time? Where and how often do they cross-dress?
- is achieving sexual gratification. If so, how?
- has sexual fantasies involving breast-feeding, giving birth, or forced feminization through gender-changing surgeries or other means
- “tucks” his penis, urinates sitting down, or mimics other stereotypical feminine behavior.
The answers will uncover a motivation behind these behaviors, which is key to diagnosis. Sexual gratification as a motive suggests paraphilia, whereas a desire to live as a woman points to transsexualism. Because of the myriad presentations, multiple patient visits are necessary for a specific diagnosis.
Diagnosis: ‘i enjoy womanhood, but…’
I diagnose gender dysphoria, but because Mr. C’s mood is euthymic, I cannot discern how his mood instability might affect his dysphoria. His sexual fantasies are mood-congruent and evoke no shame.
Mr. C then states that he adamantly opposes living outwardly as a woman, and fears that an overt sex change would destroy his marriage and other relationships. Even so, he desires hormone therapy and surgical breast implants so he can more closely mimic physical womanhood and make masturbation more pleasurable. He says he would flatten his breasts with gauze while in public so he can continue to look like a man.
Though comfortable with his sexual fantasies, Mr. C laments that presenting himself as an “alpha male” drains his psychic energy.
The author’s observations
Mr. C meets criteria for GID and transvestism. Some transvestites also meet criteria for autogynephilia and report erotic arousal upon seeing oneself as a woman. Character pathology, specifically sexual fantasies associated with schizoid personality, might also contribute to unusual gender presentation. Sexologists also propose fluidity in gender identification across populations and over a person’s life span.
Autogynephilia—by which a man becomes sexually aroused by imagining or seeing himself as a woman15—usually is associated with transvestism. Autogynephiles often have sexual fantasies of possessing female anatomical structures, engaging in feminine behaviors, or performing female bodily functions such as lactation, menstruation, or childbirth.
Autogynephilia may be a misdirected heterosexuality and is more prevalent among male-to-female transsexuals who are attracted to women, both sexes, or neither sex than among those attracted only to men.16
Gender identity fluidity. Clinicians have recorded fluidity in gender identity (sense of masculinity or femininity) and sexual orientation (the sex to which one is attracted). Sexologists have tried to create scales that gauge these changes.
The Kinsey Heterosexual-Homosexual Rating Scale17 is based on Kinsey’s theory that men are not strictly heterosexual or homosexual. Scores between 0 and 6 indicate some degree of both (Table).
The Benjamin Gender Disorientation Scale, which measures gender identity variations, recognizes variability of gender dysphoria expression and underscores the difficulty of classifying patients who—like Mr. C—present with varied symptoms. The scale is available at www.wpath.org.
I did not administer the Kinsey or Benjamin scales to Mr. C. Although his case shows how innate sense of masculinity or femininity can vary among patients with gender dysphoria, his presentation has been stable, albeit unusual.
Mr. C’s symptoms. Mr. C shows autogynephilic features. He lacks the schizoid’s emotional inertness and his gender presentation is static, though dramatic. He appears to meet criteria for GID and transvestism, autogynephilic variant.
Schizoid and other personality disorders are associated with unusual sexual fantasies. Mr. C lacks primary schizoid features, such as flattened affectivity and indifference to close relationships.
Table
Kinsey Heterosexual-Homosexual Rating Scale
| Score | Indicates… |
|---|---|
| 0 | Exclusively heterosexual |
| 1 | Predominantly heterosexual, incidentally homosexual |
| 2 | Predominantly heterosexual, more than incidentally homosexual |
| 3 | Equally heterosexual and homosexual |
| 4 | Predominantly homosexual, more than incidentally heterosexual |
| 5 | Predominantly homosexual, incidentally heterosexual |
| 6 | Exclusively homosexual |
| Source: Reference 17. Reprinted by permission of The Kinsey Institute for Research in Sex, Gender, and Reproduction, Inc., Indiana University, Bloomington. | |
The author’s observations
Mr. C is a poor candidate for hormone therapy or gender reassignment surgery because of his circumscribed desire to live as a woman at home. Also, sexual gratification is his primary motivation for wanting to develop breasts.
Treating gender dysphoria
Serotonergic agents such as fluoxetine have shown effectiveness for treating paraphilias and nonparaphilic sexual addiction in case reports.18,19
Behavioral techniques, however, might have a more definite impact on gender dysphoria. Marks19 reported a 4-year remission of transsexualism in a patient after comorbid OCD improved with self-exposure therapy.
Psychotherapy will not resolve gender identity disorder but can promote a stable lifestyle and improve the patient’s chances for success in relationships, education, work, and gender identity expression.20 Psychotherapy can also help determine patients’ readiness for sexual reassignment surgery.
Treatment: learning to accept
I refer Mr. C back to his primary psychiatrist, who adds aripiprazole, 5 mg/d, to address grandiosity and hypomania that emerged months after my initial evaluation.
I also refer Mr. C to a gender disorder specialist for psychotherapy directed at examining his history, understanding his dilemmas, and identifying unrealistic ideas and maladaptive behaviors. The therapist has been teaching Mr. C coping skills and educating him on gender disorders and normal gender variations in activities and interests. He has been attending weekly sessions for 4 months.
To address his resentment over trying to look manly, I assure him that he doesn’t need to assume additional “masculine” behaviors and attitudes, and that his height and features make him appear masculine.
- World Professional Association for Transgender Health, formerly the Harry Benjamin International Gender Dysphoria Association (offers links to transgender resources, gender programs, and sexologists). www.hbigda.org.
- Divalproex sodium • Depakote
- Fluoxetine • Prozac
- Paroxetine • Paxil
Dr. Martin reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
History: normal on paper
Mr. C, age 65, presents to an endocrinologist complaining of hot flashes and low libido. Initial testing shows low male testosterone, but a repeat test shows normal levels. No medical cause is found for his symptoms.
“My testosterone might be normal on paper,” Mr. C tells the endocrinologist, “but I’m not. I think I’m a woman.”
Mr. C requests referral to a female psychiatrist because he feels more comfortable discussing sexual issues with a woman. The endocrinologist refers him to me for evaluation.
Over 7 years, Mr. C’s other psychiatrist—a man—has been treating him for obsessive-compulsive disorder (OCD), anxiety disorder, and bipolar disorder type II. Mr. C takes paroxetine, 60 mg/d, for depressive symptoms and was taking divalproex, 1,500 mg/d, to stabilize his mood. He recently stopped divalproex because it was causing nausea and sedation.
During our initial visit, Mr. C says he’s “through pretending to be a man.” He says he first questioned his sexual identity in early childhood, when he sometimes dressed in his mother’s clothes for play. As an adult, he mostly cross-dresses in lingerie; he wears a woman’s tank top in public once or twice weekly underneath his polo dress shirt. Fifteen years ago, he suffered anorexia and bulimia while trying to look as svelte as a woman.
At 6 feet, 2 inches with good muscle tone and short, wavy black hair, Mr. C looks strikingly masculine. Now retired, he served in the Air Force and later worked as a commercial pilot and in construction. In private, however, he prefers gardening and cooking over sports and cars.
Mr. C is married but seldom has sexual intercourse with women. He gains sexual fulfillment by visualizing himself as a woman having sex with other women or with himself as a man. He denies interest in male-male sex.
The patient has been masturbating since age 5, mostly by rubbing his scrotum against a swing set pole he still keeps in his utility shed. He often tucks his penis to mimic female genitalia and makes believe his rectum is a vagina.
- Transsexualism
- Pure transvestism (having a firm gender identity but becoming sexually aroused by cross-dressing)
- Dual-role transvestism (cross-dressing solely to experience temporary membership in the opposite sex)
- Stress-related cross-dressing
- Men who desire penectomy or castration but no other gender-reassignment interventions
- Congenital intersex conditions, such as hermaphrodism
Mr. C’s Mini-Mental State Examination score of 30 indicates no underlying dementia. He shows stable affect with no evidence of derailment, paranoia, thought blocking, or auditory hallucinations.
Medical examination results are normal. Negative urine toxicology screen rules out substance abuse, and negative rapid plasma reagin rules out syphilis. Testosterone is not rechecked because levels were normal 2 days before.
The author’s observations
I suspect gender dysphoria, which describes a heterogeneous group of persons who express varying degrees of distress with their anatomic sex and sometimes desire secondary opposite-gender sexual characteristics (Box).
Sexual identity in gender dysphoria is often fluid. Symptoms might suggest transvestism, then evolve to transsexualism. Recognizing this heterogeneity and fluidity is crucial to diagnosis and treatment.
Primary transsexualism. The term “transsexualism” describes persons who want to live and be accepted within the opposite sex.1 The transsexual identity persists for ≥ 2 years and is not caused by another mental disorder or intersexed condition. Fetishism is classically absent and cross-dressing is not sexually gratifying. Most transsexuals want surgical and hormone treatment to make their bodies as congruent as possible with the preferred sex.
In 1994, DSM-IV recognized that some late-onset transsexuals showed features of comorbid transvestism and were sexually aroused by female dress and behaviors. Gender identity disorder (GID) replaced the term “transsexualism” and includes these individuals. A secondary diagnosis of transvestism is applied.
Secondary transsexualism. Case reports2 describe psychosis-induced transsexual desires in patients with schizophrenia. Gender dysphoria improved as their schizophrenia symptoms lessened.
The relationship between transsexualism and schizophrenia has been debated. Hyde and Kenna3 view transsexualism as a schizophrenia spectrum disorder, whereas sexologists consider transsexualism and schizophrenia distinct syndromes that can occur simultaneously.
Affective disorders might also alter contentment with gender role, but the relationship is unclear. Case reports of patients with bipolar disorder suggest that gender dysphoria intensity fluctuates with affective excursions.4 O’Gorman,5 however, described a bipolar patient whose gender dysphoria was mitigated during manic episodes.
Paraphilias are sexual disorders with recurrent intense urges and fantasies that do not follow normative arousal patterns and can diminish capacity for sexual intimacy.6 Manifestations include exhibitionism, fetishism, frotteurism, pedophilia, masochism/sadism, voyeurism, and transvestic fetishism.
Dividing transsexualism and pure transvestism paraphilia into discrete categories is simplistic, as transvestites can develop secondary components of transsexualism. Hoenig and Kenna7 assert that transsexualism—though not an anomalous erotic preference—is almost always preceded by transvestism or accompanied by cross-gender fetishism.
Nonparaphilic sexual addiction—included in DSM-IV-TR as sexual disorder not otherwise specified—describes culturally acceptable sexual interests and behaviors that are frequent or intense enough to reduce capacity for sexual intimacy. Such behaviors include compulsive masturbation, repetitive promiscuity, and dependence on anonymous sexual encounters.
An addiction model conceptualizes paraphilia as a form of pleasure seeking that has become habitual and self-destructive. Treatment involves directing patients to 12-step groups patterned after Alcoholics Anonymous.
Other models place paraphilias and related disorders within the OCD spectrum.8-13 Persons with OCD often are obsessed with sexual content and might grapple with religious and moral concerns about sexual issues. They typically consider their symptoms intrusive or senseless. Selective serotonin reuptake inhibitors—the standard medication for OCD—might alleviate paraphilia, but results are mixed.14
Mr. C’s symptoms. Mr. C shows features of GID and transvestism. His strong, persistent cross-gender identification and sense of inappropriateness with being a man indicate GID. His recurrent sexual urges and fantasies and impaired capacity for sexual intimacy suggest a paraphilia or transvestism.
The significance of Mr. C’s comorbid bipolar disorder and OCD is unclear. Both appeared controlled, but the potential for mania-induced hypersexuality cannot be ignored.
Diagnosing gender dysphoria
A thorough medical, psychiatric, and sexual history can reveal sexual identity symptoms’ source.
Consider a medical cause. Your medical workup may include a genital exam to check for irregularities such as hermaphrodism that can compound questions of sexual identity, and karyotyping to probe chromosomal anomalies, such as mosaicism or chimerism.
Consider schizophrenia or bipolar disorder, as mania or psychosis can cause aberrant sexual behavior. In gender-dysphoric patients with either disorder, treating the psychiatric comorbidity might alleviate the dysphoria. Watch for fluctuations in gender dysphoria intensity when you treat other psychopathologies.
Take a thorough sexual history. Being matter-of-fact while discussing unusual sexual acts will help the patient “open up” about his sexual problems. Ask him if he:
- showed gender-atypical behavior as a child, which can predict transsexualism or homosexuality has engaged in heterosexual, homosexual, or abnormal sexual acts; ask about frequency and preference
- is married or has a girlfriend. If so, are they getting along? How often do they have sex?
- cross-dresses. Does his partner cross-dress as well and, if so, do they cross-dress for sexual gratification or to identify with the opposite gender? Has this response changed over time? Where and how often do they cross-dress?
- is achieving sexual gratification. If so, how?
- has sexual fantasies involving breast-feeding, giving birth, or forced feminization through gender-changing surgeries or other means
- “tucks” his penis, urinates sitting down, or mimics other stereotypical feminine behavior.
The answers will uncover a motivation behind these behaviors, which is key to diagnosis. Sexual gratification as a motive suggests paraphilia, whereas a desire to live as a woman points to transsexualism. Because of the myriad presentations, multiple patient visits are necessary for a specific diagnosis.
Diagnosis: ‘i enjoy womanhood, but…’
I diagnose gender dysphoria, but because Mr. C’s mood is euthymic, I cannot discern how his mood instability might affect his dysphoria. His sexual fantasies are mood-congruent and evoke no shame.
Mr. C then states that he adamantly opposes living outwardly as a woman, and fears that an overt sex change would destroy his marriage and other relationships. Even so, he desires hormone therapy and surgical breast implants so he can more closely mimic physical womanhood and make masturbation more pleasurable. He says he would flatten his breasts with gauze while in public so he can continue to look like a man.
Though comfortable with his sexual fantasies, Mr. C laments that presenting himself as an “alpha male” drains his psychic energy.
The author’s observations
Mr. C meets criteria for GID and transvestism. Some transvestites also meet criteria for autogynephilia and report erotic arousal upon seeing oneself as a woman. Character pathology, specifically sexual fantasies associated with schizoid personality, might also contribute to unusual gender presentation. Sexologists also propose fluidity in gender identification across populations and over a person’s life span.
Autogynephilia—by which a man becomes sexually aroused by imagining or seeing himself as a woman15—usually is associated with transvestism. Autogynephiles often have sexual fantasies of possessing female anatomical structures, engaging in feminine behaviors, or performing female bodily functions such as lactation, menstruation, or childbirth.
Autogynephilia may be a misdirected heterosexuality and is more prevalent among male-to-female transsexuals who are attracted to women, both sexes, or neither sex than among those attracted only to men.16
Gender identity fluidity. Clinicians have recorded fluidity in gender identity (sense of masculinity or femininity) and sexual orientation (the sex to which one is attracted). Sexologists have tried to create scales that gauge these changes.
The Kinsey Heterosexual-Homosexual Rating Scale17 is based on Kinsey’s theory that men are not strictly heterosexual or homosexual. Scores between 0 and 6 indicate some degree of both (Table).
The Benjamin Gender Disorientation Scale, which measures gender identity variations, recognizes variability of gender dysphoria expression and underscores the difficulty of classifying patients who—like Mr. C—present with varied symptoms. The scale is available at www.wpath.org.
I did not administer the Kinsey or Benjamin scales to Mr. C. Although his case shows how innate sense of masculinity or femininity can vary among patients with gender dysphoria, his presentation has been stable, albeit unusual.
Mr. C’s symptoms. Mr. C shows autogynephilic features. He lacks the schizoid’s emotional inertness and his gender presentation is static, though dramatic. He appears to meet criteria for GID and transvestism, autogynephilic variant.
Schizoid and other personality disorders are associated with unusual sexual fantasies. Mr. C lacks primary schizoid features, such as flattened affectivity and indifference to close relationships.
Table
Kinsey Heterosexual-Homosexual Rating Scale
| Score | Indicates… |
|---|---|
| 0 | Exclusively heterosexual |
| 1 | Predominantly heterosexual, incidentally homosexual |
| 2 | Predominantly heterosexual, more than incidentally homosexual |
| 3 | Equally heterosexual and homosexual |
| 4 | Predominantly homosexual, more than incidentally heterosexual |
| 5 | Predominantly homosexual, incidentally heterosexual |
| 6 | Exclusively homosexual |
| Source: Reference 17. Reprinted by permission of The Kinsey Institute for Research in Sex, Gender, and Reproduction, Inc., Indiana University, Bloomington. | |
The author’s observations
Mr. C is a poor candidate for hormone therapy or gender reassignment surgery because of his circumscribed desire to live as a woman at home. Also, sexual gratification is his primary motivation for wanting to develop breasts.
Treating gender dysphoria
Serotonergic agents such as fluoxetine have shown effectiveness for treating paraphilias and nonparaphilic sexual addiction in case reports.18,19
Behavioral techniques, however, might have a more definite impact on gender dysphoria. Marks19 reported a 4-year remission of transsexualism in a patient after comorbid OCD improved with self-exposure therapy.
Psychotherapy will not resolve gender identity disorder but can promote a stable lifestyle and improve the patient’s chances for success in relationships, education, work, and gender identity expression.20 Psychotherapy can also help determine patients’ readiness for sexual reassignment surgery.
Treatment: learning to accept
I refer Mr. C back to his primary psychiatrist, who adds aripiprazole, 5 mg/d, to address grandiosity and hypomania that emerged months after my initial evaluation.
I also refer Mr. C to a gender disorder specialist for psychotherapy directed at examining his history, understanding his dilemmas, and identifying unrealistic ideas and maladaptive behaviors. The therapist has been teaching Mr. C coping skills and educating him on gender disorders and normal gender variations in activities and interests. He has been attending weekly sessions for 4 months.
To address his resentment over trying to look manly, I assure him that he doesn’t need to assume additional “masculine” behaviors and attitudes, and that his height and features make him appear masculine.
- World Professional Association for Transgender Health, formerly the Harry Benjamin International Gender Dysphoria Association (offers links to transgender resources, gender programs, and sexologists). www.hbigda.org.
- Divalproex sodium • Depakote
- Fluoxetine • Prozac
- Paroxetine • Paxil
Dr. Martin reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Mental and behavioral disorders, diagnostic criteria for research. In: The ICD-10 classification of mental and behavioural disorders: diagnostic criteria for research. Geneva: World Health Organization; 1993.
2. Caldwell C, Keshavan MS. Schizophrenia with secondary transsexualism. Can J Psychiatry 1991;36:300-1.
3. Hyde C, Kenna JC. A male MZ twin pair, concordant for transsexualism, discordant for schizophrenia. Acta Psychiatr Scand 1977;56:265-75.
4. Habermeyer E, Kamps I, Kawohl W. A case of bipolar psychosis and transsexualism. Psychopathology 2003;36:168-70.
5. O’Gorman EC. The effect of psychosis on gender identity. Br J Psychiatry 1980;136:314-5.
6. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000:566-76.
7. Hoenig J, Kenna JC. The nosolgical position of transsexualism. Arch Sex Behav 1974;3:273-87.
8. Jenike MA. Obsessive-compulsive and related disorders: a hidden epidemic. N Engl J Med 1989;24;321:539-41.
9. Stein DJ, Hollander E. The spectrum of obsessive-compulsive related disorders. In: Hollander E, ed. The obsessive-compulsive related disorders. Washington, DC: American Psychiatric Publishing. In press.
10. Hollander E. Serotonergic drugs and the treatment of disorders related to obsessive-compulsive disorder. In: Pato MT, Zohar J, eds. Current treatments of obsessive-compulsive disorder. Washington, DC: American Psychiatric Publishing; 1991:173-92.
11. Quadland MC. Compulsive sexual behavior: definition of a problem and an approach to treatment. J Sex Marital Ther 1985;11:121-32.
12. Coleman E. Sexual compulsivity: definition, etiology, and treatment considerations. In: Coleman E, ed. Chemical dependency and intimacy dysfunction. New York: Haworth Press; 1988.
13. Anthony DT, Hollander E. Sexual compulsions. In: Hollander E, ed. The obsessive-compulsive related disorders. Washington, DC: American Psychiatric Publishing. In press.
14. Perilstein RD, Lipper S, Friedman LJ. Three cases of paraphilias responsive to fluoxetine treatment. J Clin Psychiatry 1991;52:169-70.
15. Blanchard R. Nonmonotonic relation of autogynephilia and heterosexual attraction. J Abnorm Psychol 1992;101:271-6.
16. Hirschfeld M. Sexual anomalies. New York: Emerson Books; 1948.
17. Kinsey AC, Pomeroy WB, Martin CE. Sexual behavior in the human male. Philadelphia: WB Saunders; 1948;636-59.
18. Kafka MP. Successful antidepressant treatment of nonparaphilic sexual addictions and paraphilias in men. J Clin Psychiatry 1991;52:60-5.
19. Marks IM, Mataix-Cols D. Four-year remission of transsexualism after comorbid obsessive-compulsive disorder improved with self-exposure therapy. Case report. Br J Psychiatry 1997;171:389-90.
20. Harry Benjamin International Gender Dysphoria Association’s Standards of Care for Gender Identity Disorders. Int J Transgenderism 2001; 5(1). Available at: http://www.symposion.com/ijt/index.htm. Accessed November 3, 2006.
1. Mental and behavioral disorders, diagnostic criteria for research. In: The ICD-10 classification of mental and behavioural disorders: diagnostic criteria for research. Geneva: World Health Organization; 1993.
2. Caldwell C, Keshavan MS. Schizophrenia with secondary transsexualism. Can J Psychiatry 1991;36:300-1.
3. Hyde C, Kenna JC. A male MZ twin pair, concordant for transsexualism, discordant for schizophrenia. Acta Psychiatr Scand 1977;56:265-75.
4. Habermeyer E, Kamps I, Kawohl W. A case of bipolar psychosis and transsexualism. Psychopathology 2003;36:168-70.
5. O’Gorman EC. The effect of psychosis on gender identity. Br J Psychiatry 1980;136:314-5.
6. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000:566-76.
7. Hoenig J, Kenna JC. The nosolgical position of transsexualism. Arch Sex Behav 1974;3:273-87.
8. Jenike MA. Obsessive-compulsive and related disorders: a hidden epidemic. N Engl J Med 1989;24;321:539-41.
9. Stein DJ, Hollander E. The spectrum of obsessive-compulsive related disorders. In: Hollander E, ed. The obsessive-compulsive related disorders. Washington, DC: American Psychiatric Publishing. In press.
10. Hollander E. Serotonergic drugs and the treatment of disorders related to obsessive-compulsive disorder. In: Pato MT, Zohar J, eds. Current treatments of obsessive-compulsive disorder. Washington, DC: American Psychiatric Publishing; 1991:173-92.
11. Quadland MC. Compulsive sexual behavior: definition of a problem and an approach to treatment. J Sex Marital Ther 1985;11:121-32.
12. Coleman E. Sexual compulsivity: definition, etiology, and treatment considerations. In: Coleman E, ed. Chemical dependency and intimacy dysfunction. New York: Haworth Press; 1988.
13. Anthony DT, Hollander E. Sexual compulsions. In: Hollander E, ed. The obsessive-compulsive related disorders. Washington, DC: American Psychiatric Publishing. In press.
14. Perilstein RD, Lipper S, Friedman LJ. Three cases of paraphilias responsive to fluoxetine treatment. J Clin Psychiatry 1991;52:169-70.
15. Blanchard R. Nonmonotonic relation of autogynephilia and heterosexual attraction. J Abnorm Psychol 1992;101:271-6.
16. Hirschfeld M. Sexual anomalies. New York: Emerson Books; 1948.
17. Kinsey AC, Pomeroy WB, Martin CE. Sexual behavior in the human male. Philadelphia: WB Saunders; 1948;636-59.
18. Kafka MP. Successful antidepressant treatment of nonparaphilic sexual addictions and paraphilias in men. J Clin Psychiatry 1991;52:60-5.
19. Marks IM, Mataix-Cols D. Four-year remission of transsexualism after comorbid obsessive-compulsive disorder improved with self-exposure therapy. Case report. Br J Psychiatry 1997;171:389-90.
20. Harry Benjamin International Gender Dysphoria Association’s Standards of Care for Gender Identity Disorders. Int J Transgenderism 2001; 5(1). Available at: http://www.symposion.com/ijt/index.htm. Accessed November 3, 2006.
Struggling not to nap: Causes of daytime sleepiness
Poor energy, hypersomnia, amotivation, irritability, and frustration can suggest depression or other psychiatric disorders to busy primary care physicians. As a result, psychiatrists often are referred patients with excessive daytime sleepiness (EDS) caused by undiagnosed primary sleep disorders.
Physicians may miss obstructive sleep apnea (OSA), restless legs syndrome, circadian rhythm disorders, or narcolepsy because:
- many have little training in sleep disorders and limited time to diagnose them1
- patients do not report sleepiness or recognize it as a legitimate medical concern
- definitive diagnostic tests are expensive and usually are not ordered.
Psychiatrists, therefore, need a clear understanding of the EDS differential diagnosis to determine whether a patient’s behavioral symptoms are a sleep or psychiatric issue.
How likely are you to doze off or fall asleep in the following situations, in contrast to feeling just tired? This refers to your usual way of life in recent times. Even if you have not done some of these things recently, try to work out how each situation would affect you now. Use the scale below to choose the most appropriate number for each situation:
0 no chance of dozing
1 slight chance of dozing
2 moderate chance of dozing
3 high chance of dozing
Chance of dozing Situation
Sitting and reading
Watching TV
Sitting inactive in a public place (such as in a theater or a meeting)
As a passenger in a car for an hour without a break
Lying down to rest in the afternoon when circumstances permit
Sitting and talking to someone
Sitting quietly after a lunch without alcohol
In a car, while stopped for a few minutes in traffic
Scoring key
1 to 6 Getting enough sleep
7 to 8 Average
>8 Seek a sleep specialist’s advice without delay
Assessing the sleepy patient
Sleepiness is an inability to stay awake at appropriate times. Fatigue, by comparison, does not involve sleepiness but very low energy associated with wakefulness. In general, sleepy patients get transient relief from napping, whereas fatigued patients report they cannot fall asleep.
Untreated EDS results in compromised quality of life, reduced productivity, and public safety concerns such as falling asleep while driving.2 Sleep complaints fall into three major categories:
- EDS
- insomnia (marked by distress because of poor sleep, but usually with minimal EDS)
- unusual nocturnal behaviors (ranging from arm waving to violent behaviors.
When you evaluate a patient with sleep complaints, valuable sources of data include observation, questionnaires, and screening devices. The most important may be common sense.
Observation. Observe the patient in the waiting room or office before starting the interview. Did he or she nod off while waiting to see you? Pay attention to anyone who appears sleepy—even those who deny having trouble staying awake. Over time, sleepy patients can lose their perspective on alertness. Some have had EDS so long that they no longer recall what it is like to feel fully awake.
Collateral history often is important because family members probably have observed the sleeping patient. The bed partner can provide information about snoring, irregular breathing, leg kicks, unplanned naps, and strained interpersonal relationships because of EDS. For the patient without a bed partner, consider interviewing a travel companion.
Questionnaires. Few useful screening tests exist for sleepiness; most are neither reliable nor valid. One of the better questionnaires—the Epworth Sleepiness Scale (Box 1)—helps confirm the presence of sleepiness with a score >8, differentiating the inability to stay awake from fatigue. This brief questionnaire also provides a useful measure of sleepiness severity.3
The Epworth scale’s value is limited because its questions of specific time and context might not represent a patient’s experiences. Additional validated surveys include the Pittsburgh Sleep Quality Inventory and several for sleep apnea.4
Screening. Electroencephalographic (EEG) monitoring can accurately measure the patient’s degree of sleep disruption. This information is key to understanding if a patient’s EDS is caused by a physiologic condition that prevents quality nocturnal sleep.
None of the widely used screening devices that assess leg kicks indicate the presence of possible periodic limb movements.
Overnight pulse oximetry has been used to screen for sleep-disordered breathing5 but also has limitations:
- Most pulse oximeters do not provide information about sleep stage or body position.
- Patients with sleep-disordered breathing can lack adequate oxygen desaturations but have frequent EEG arousals related to sleep issues. Because EEG data are not collected during arousals, pulse oximetry would generate a false-negative result in this scenario, which occurs most often in female and thin patients.
- Oximetry provides only oxygen saturation data and possibly heart rate, whereas other physiologic processes such as body movement or sleep architecture can be disrupted repetitively during sleep.
Common sense. The most productive tools for detecting sleep disorders are intuition and common sense. The Figure suggests sequential questions that might uncover specific sleep disorders. Then the decision whether to refer the patient to a sleep disorder center for diagnostic testing depends on the type of sleep disorder you detect.
Nasal continuous positive airway pressure
(CPAP) should be started in an observed setting so that the clinician can determine the optimal amount of positive pressure needed to keep the upper airway patent.
For some patients, CPAP is started in the second half of a “split-night” sleep study after a diagnosis of obstructive sleep apnea (OSA) is made. Other patients return a second night for a nasal CPAP trial. Those with severe OSA might notice improved sleep quality and reduced EDS after only a few hours of CPAP use. Some wish to start CPAP treatment immediately.
Advances in masks and equipment have improved patient adherence to CPAP. Innovations include auto-titrating machines, in which the pressure level can be varied depending on sleep state or body position. Many machines include a data microchip that allows the clinician to determine duration of usage, then use that information to counsel the patient about adherence, if necessary.
Patient education also can promote CPAP adherence. When patients are first told they might need to sleep each night wearing a nasal mask, they often voice well-founded concerns about comfort, claustrophobia, or sexual activity.
Obtaining the support of the bed partner by welcoming her or him to all appointments, including educational activities, is optimal. The bed partner’s concerns about the patient’s excessive snoring or apneas probably were the impetus for the appointment in the first place.
Medication. Some patients benefit from 1 to 2 weeks of a sleeping medication such as zolpidem or trazodone while they acclimate to using nasal CPAP.
Figure The sleepy patient: Possible medical and psychiatric explanations
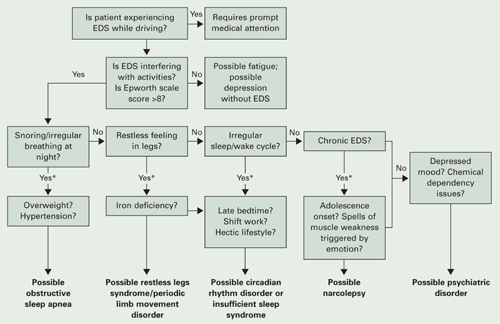
* Supportive factors: Persuasive if present, but if absent do not exclude possible conditions
Obstructive sleep apnea
Because OSA affects at least 4% of men and 2% of women,6 you are virtually assured of seeing undiagnosed patients. OSA is caused by repeated collapse of the soft tissues surrounding the upper airway, decreasing airflow that is restored when the patient briefly awakens. Patients develop EDS because sleep is fragmented by frequent arousals.
Obese patients, because of their body habitus, are at higher risk for OSA than patients at normal weight. Carefully screen patients for OSA if they develop weight problems while taking psychotropics, such as antipsychotics.
Alcohol or sedatives used at bedtime can aggravate OSA. These substances promote muscle relaxation and increase the arousal threshold so that patients do not awaken readily when apneas occur.
Long-term complications of untreated OSA include sleepiness leading to accidents, hypertension, cerebrovascular disease, and progressive obesity. Data also associate OSA with cardiovascular complications such as arrhythmias, congestive heart failure, and myocardial infarction.7
Physical examination focuses on detecting:
- nasal obstruction (have patient sniff separately through each nostril)
- large neck
- crowded oropharynx (low-hanging palate, reddened uvula, enlarged tonsils, large tongue relative to oropharynx diameter)
- jaw structure (particularly a small, retrognathic mandible).
Sleep studies. Referral for nocturnal polysomnography might be the next step. A comprehensive sleep study collects data about respiratory, cardiovascular, and muscle activity at night, as well as the sounds the patient makes—such as snoring or coughing—when asleep. EEG monitoring also is performed. OSA may be diagnosed if repeated episodes of reduced airflow and oxygen desaturation (arousals) are observed as brief shifts in EEG frequency.
Treatment. First-line interventions for the patient with OSA include:
- no alcohol 1 to 2 hours before bedtime
- sleeping on the side instead of the back
- weight loss (ideally with exercise)
- nasal sprays for allergies.
If first-line treatments are ineffective, nasal continuous positive airway pressure (CPAP) works well for most patients who adhere to the regimen.8 CPAP requires the patient to wear a nasal mask that delivers room air, splinting open the nasopharynx and upper airway (Box 2).
Surgical options. The most common surgeries for OSA are uvulopalatopharyngoplasty and laser-assisted uvulopalatoplasty. Others include tongue reduction and mandibular advancement.
The response rate to surgery averages 50%, depending on patient characteristics and procedure.9 Positive outcomes are most likely for thin patients with obvious upper airway obstruction, including deviated nasal septum, large tonsils, low-hanging palate, and large uvula. Postsurgical complications include nasal regurgitation, voice change, pain, bleeding, infection, tongue numbness, and snoring without apnea (silent apnea).
Oral appliances open the oropharynx by moving the mandible and tongue out of way. Patients with mild to moderate OSA accept these devices well. Evidence suggests that oral appliances improve sleep and reduce EDS more effectively than nasal CPAP and are preferred by patients.10
Oral devices have drawbacks, however. In most settings, their effectiveness cannot be observed during a “split-night” laboratory sleep study because the patient has not yet purchased the device. Also, multiple visits sometimes are required to custom-fit the appliance; this can pose a hardship for patients who live a distance from the provider.
Restless legs syndrome
Patients with restless legs syndrome (RLS) typically report a restless, painful feeling in the limbs that occurs in the evening and at night, disrupting sleep. This condition—which affects 10% of the population—is associated with aging, blood loss, anemia, peripheral neuropathies, and pregnancy.11 Onset can occur in childhood, and in some cases there is a familial tendency.
Most patients with RLS have periodic limb movements (repetitive leg jerks or twitches). The clinical significance of periodic limb movements with no subjective disagreeable feelings in the limbs is controversial, and these cases usually are not treated.
The history usually confirms RLS. Order sleep studies only if you suspect a coexisting sleep problem or the diagnosis is unclear.
A suspected mechanism of restless legs is dopamine deficiency. Low serum ferritin levels have been associated with RLS—presumably because iron is a cofactor necessary for dopamine synthesis12—and may be diagnostically helpful.
The most common technique is to ask the patient to establish a consistent awakening time and a regular bedtime. Initially this could be unconventional by societal standards—such as bedtime at 5 AM and arising at 2 PM. After this pattern is in place, the patient gradually shifts the timing by 1 hour per day. Most patients find it easier to delay rather than advance the bedtime until it conforms to the desired time.
Reinforce this new sleep pattern with a structured daytime schedule that includes predictable mealtimes, regular exercise, social activities, and possibly bright light exposure. Provide reinforcement in the morning for patients with delayed sleep phase disorder and in the evening for advanced sleep phase disorder. These interventions take time and discipline.
Another approach is for the patient to skip sleep one night and, in a sleep-deprived state, establish a new bedtime at the desired time. Use the same modalities listed above to reinforce (“entrain”) this schedule; otherwise the patient will slip back into the previous abnormal sleep-wake rhythm.
Treatment can include iron repletion when indicated. Medications include dopaminergic agents, most notably pramipexole and levodopa/carbidopa. Other options include gabapentin, benzodiazepines, and narcotics.
Antidepressants have been suspected to worsen restless legs syndrome, but definitive studies are lacking.13
Circadian rhythm disorders
Instead of compromising the quality or quantity of sleep, circadian rhythm disorders cause sleep to occur at inappropriate times. These disorders are most common in adolescents and young adults.
Delayed sleep phase disorder—a persistent pattern of staying up late and “sleeping in”—is most common. Careful assessment will reveal that the patient is getting adequate sleep but at a socially unacceptable time, sometimes to the extreme that his or her nights and days are reversed.
Patients’ reluctance to acknowledge the severity of this problem can lead to inaccurate sleep diaries and interviews. A portable wrist actigraph can provide data about limb movement and is more objective than self-reports.
Delayed sleep phase disorder is highly comorbid with depressive disorders.14 The cause of this syndrome is unclear, but light exposure, social patterns, psychological issues, and possibly a genetic substrate are known to contribute.
Advanced sleep phase disorder—a less common circadian rhythm disorder—also can cause EDS. Patients have an inappropriately early time of sleep onset and then are fully awake in the middle of the night. A large family with a severe form of this disorder was found to have an abnormality on chromosome 2.15
Treatment. Relatively few treatments are effective for circadian rhythm disorders. Some patients elect not to pursue therapy, instead fitting activities around their unconventional sleep schedules.
Individuals with delayed sleep phase who cannot arrange their lives around their sleep schedules are at risk for poor early morning performance because of sleepiness. Their internal circadian clocks can be gradually readjusted with phototherapy or gradual shifting of the major sleep period (Box 3). Stimulants usually are not used, but hypnotics can sometimes help these patients fall asleep earlier.
Insufficient sleep syndrome
People attempting to “burn the candle at both ends” are at risk for developing insufficient sleep syndrome.16 In our 24/7 society, people trying to make do with less than the required 7.5 hours sleep per night may adversely affect their health. The problem is compounded for shift workers because of the difficulty in obtaining sufficient quality sleep during daylight hours.
Many patients do not seek treatment for fatigue or sleepiness because they are aware of their lifestyle choices. Still, they might develop psychological symptoms such as irritability, mood swings, and strained interpersonal relationships. These symptoms can prompt patients to request treatment.
Take a careful history that includes discussing the patient’s daily and weekly schedule. Avoid psychostimulants; instead, address the nonnegotiable need to get adequate sleep and challenge the patient to prioritize his or her activities around a full night’s sleep.
When to consider narcolepsy
Narcolepsy is a CNS disease characterized by abnormal regulation of REM sleep. EDS—the cardinal symptom—is often associated with cataplexy (75%), sleep paralysis (50%), vivid dreams, and insomnia, all of which interfere with REM phenomena. Narcolepsy affects 0.05% of the U.S. population and can lead to severe occupational, educational, and family disruption.
When you obtain a history that suggests narcolepsy, use the history, a sleep diary, or wrist actigraphy to document whether the patient is getting adequate sleep, with a consistent sleep/wake cycle. Next, consider referring the patient for polysomnography, primarily to rule out other causes of EDS such as sleep-disordered breathing. In some cases, REM latency on the overnight sleep study will be <20 minutes after sleep onset, which supports the diagnosis of narcolepsy.
A multiple sleep latency test (MSLT)—a diagnostic session in which the patient takes 4 to 5 daytime naps—is performed the following day. Narcolepsy is confirmed if the patient has a mean initial sleep latency of <10 minutes during these naps plus at least two REM episodes within 15 minutes after sleep onset.
The 4 most appropriate indications for an urgent sleep evaluation are:
- difficulty staying alert while driving
- nocturnal cardiac arrhythmias
- frequent observed apneas
- excessive daytime sleepiness (EDS) leading to academic or occupational problems.
Insurance companies usually cover a specialty sleep evaluation, particularly if the referring physician documents a suspicion of sleep-disordered breathing or EDS that jeopardizes safe driving.
Most patients with narcolepsy and cataplexy have undetectable cerebrospinal fluid levels of a neuropeptide called hypocretin or orexin.17 Hypocretin/orexin replacement therapy is a theoretical possibility, but for now treatment includes a combination of optimal sleep hygiene, psychostimulants, antidepressants, and hypnotics.
Other causes of EDS
EDS can also be caused by unrecognized alcohol dependence, inappropriate or excessive medication use, and depressive disorders. Overnight sleep studies are seldom indicated unless patients endorse the symptoms in the Figure.
Before pursuing polysomnography or an MSLT (Box 4), eliminate medications that might confound the results, such as:
- antidepressants, which alter the timing and duration of REM sleep
- sedating medications, which modify initial sleep latency and sleep efficiency and potentially aggravate sleep disordered breathing.
Initial REM latency provides a potential biologic marker of major depression but is used more often in research than in clinical psychiatry.
Primary insomnia is the distressing inability to sleep at night or nap during the day. It suggests a hyperarousal state—the opposite of EDS.18 In rare cases, however, patients who cannot sleep at night also have EDS. When evaluated, they typically endorse at least one symptom in the Figure. Sleep studies occasionally reveal OSA or restless legs syndrome.
Treating a patient with chronic insomnia may require several trials of behavioral interventions or sedating medications before you make a referral to a sleep disorder center. Patients can struggle with unrecognized primary sleep disorders for years, and many are given empiric trials of stimulating antidepressants. Antidepressants are unlikely to cause harm, but they might complicate diagnostic testing.
When you confirm coexisting depression and a primary sleep disorder, treatments that separately target each condition provide optimal management of the sleepy patient.
Medications to enhance wakefulness
Wake-promoting agents are a treatment option when EDS is contributing to compromised functioning. These drugs are no substitute for thoughtful evaluation of hypersomnolence, however. When you diagnose OSA or restless legs syndrome, first try treatments that target these conditions. If residual sleepiness persists, then consider augmenting with stimulating medications.
Modafinil is FDA-approved for residual sleepiness in patients with OSA and for shift work sleep disorder, a condition of circadian misalignment from frequent schedule changes. Evidence does not support its use for other circadian rhythm disorders, such as delayed sleep phase disorder.
Low-dose modafinil (such as 100 to 200 mg/d) is well tolerated, but its therapeutic effect as augmentation is modest.19 Increasing the dosage to >200 mg usually does not increase alertness.
Caffeine. Some patients report benefit from caffeine used in moderation and only in the morning. This practice is acceptable as long as patients do not use excessive amounts or experience insomnia, exacerbation of anxiety, or tachycardia.
Psychostimulants such as methylphenidate and amphetamines are less well-studied than modafinil for treating EDS in patients without narcolepsy. Monitor carefully for insomnia, exacerbation of anxiety, tachycardia, or hypertension and to prevent overuse of these habituating agents.
Related resources
- National Sleep Foundation. www.sleepfoundation.org.
- American Academy of Sleep Medicine. www.aasmnet.org.
- American Sleep Apnea Association. www.sleepapnea.org.
- Restless Legs Syndrome Foundation. www.rls.org.
- Association for the Study of Light Therapy and Biological Rhythms. www.sltbr.org.
Drug brand names
- Carbidopa/levodopa • Sinemet
- Gabapentin • Neurontin
- Modafinil • Provigil
- Pramipexole • Mirapex
- Trazodone • Desyrel
- Zolpidem • Ambien
Disclosure
Dr. Krahn reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
Dr. Krahn published the original version this article in the January 2002 issue of Current Psychiatry and has updated it for this issue.
1. Punjabi N, Haponik E. Ask about daytime sleepiness. J Amer Geriatr Soc 2000;48:228-9.
2. Ronald J, Delaive K, Roos L, et al. Health care utilization in the 10 years prior to diagnosis in obstructive sleep apnea syndrome patients. Sleep 1999;22(2):225-9.
3. Johns M. A new method for measuring daytime sleepiness: The Epworth Sleepiness Scale. Sleep 1991;14(6):540-5.
4. Rowley J, Aboussouan L, Badr M. The use of clinical prediction formulas in the evaluation of obstructive sleep apnea. Sleep 2000;23:929-38.
5. Yamashiro Y, Kryger M. Nocturnal oximetry: Is it a screening tool for sleep disorders? Sleep 1995;18:167-71.
6. Morrell M, Finn L, Kim H, et al. Sleep fragmentation, awake blood pressure, and sleep-disordered breathing in a population-based study. Am J Respir Critical Care Med 2000;162(6):2091-6.
7. Roux F, D’Ambrosio C, Mohsenin V. Sleep-related breathing disorders and cardiovascular disease. Am J Med. 2000;108:396-402.
8. Engleman H, Martin S, Deary I, Douglas N. Effect of continuous positive airway pressure treatment on daytime function in sleep apnoea/hypopnoea syndrome. Lancet 1994;343(8897):572-5.
9. Lojander J, Maasilta P, Partinen M, et al. Nasal-CPAP, surgery, and conservative management for treatment of obstructive sleep apnea syndrome. A randomized study. Chest. 1996;110(1):114-9.
10. Mehta A, Qian J, Petocz P, et al. A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am J Respir Critical Care Med 2001;163(6):1457-61.
11. Chesson A, Wise M, Davila D, et al. Practice parameters for the treatment of restless legs syndrome and periodic limb movement disorder. An American Academy of Sleep Medicine Report. Standards of Practice Committee of the American Academy of Sleep Medicine. Sleep 1999;22(7):961-8.
12. Phillips B, Young T, Finn L, et al. Epidemiology of restless legs symptoms in adults. Arch Intern Med 2000;160(14):2137-41.
13. Thorpy M, Ehrenberg B, Hening W, et al. Restless legs syndrome: Detection and management in primary care. Amer Fam Phys 2000;62:108-14.
14. Regestein Q, Monk T. Delayed sleep phase syndrome: A review of its clinical aspects. Am J Psychiatry 1995;152:602-8.
15. Toh K, Jones C, He Y, et al. An hPer2 phosphorylation site mutation in familial advanced sleep phase syndrome. Science 2001;291(5506):1040-3.
16. Yoshikawa N, Suzuki S, Ishimoto T, et al. A case of insufficient sleep syndrome. Psychiatry Clin Neuro 1998;52(2):200-1.
17. Nishino S, Ripley B, Overeem S, et al. Hypocretin (orexin) deficiency in human narcolepsy. Lancet. 2000;355:39-40.
18. Hauri P, Esther M. Insomnia. Mayo Clin Proc 1990;65:869-82.
19. Schwartz JR. Modafinil: new indications for wake promotion. Expert Opin Pharmacother 2005;6(1):115-29.
Poor energy, hypersomnia, amotivation, irritability, and frustration can suggest depression or other psychiatric disorders to busy primary care physicians. As a result, psychiatrists often are referred patients with excessive daytime sleepiness (EDS) caused by undiagnosed primary sleep disorders.
Physicians may miss obstructive sleep apnea (OSA), restless legs syndrome, circadian rhythm disorders, or narcolepsy because:
- many have little training in sleep disorders and limited time to diagnose them1
- patients do not report sleepiness or recognize it as a legitimate medical concern
- definitive diagnostic tests are expensive and usually are not ordered.
Psychiatrists, therefore, need a clear understanding of the EDS differential diagnosis to determine whether a patient’s behavioral symptoms are a sleep or psychiatric issue.
How likely are you to doze off or fall asleep in the following situations, in contrast to feeling just tired? This refers to your usual way of life in recent times. Even if you have not done some of these things recently, try to work out how each situation would affect you now. Use the scale below to choose the most appropriate number for each situation:
0 no chance of dozing
1 slight chance of dozing
2 moderate chance of dozing
3 high chance of dozing
Chance of dozing Situation
Sitting and reading
Watching TV
Sitting inactive in a public place (such as in a theater or a meeting)
As a passenger in a car for an hour without a break
Lying down to rest in the afternoon when circumstances permit
Sitting and talking to someone
Sitting quietly after a lunch without alcohol
In a car, while stopped for a few minutes in traffic
Scoring key
1 to 6 Getting enough sleep
7 to 8 Average
>8 Seek a sleep specialist’s advice without delay
Assessing the sleepy patient
Sleepiness is an inability to stay awake at appropriate times. Fatigue, by comparison, does not involve sleepiness but very low energy associated with wakefulness. In general, sleepy patients get transient relief from napping, whereas fatigued patients report they cannot fall asleep.
Untreated EDS results in compromised quality of life, reduced productivity, and public safety concerns such as falling asleep while driving.2 Sleep complaints fall into three major categories:
- EDS
- insomnia (marked by distress because of poor sleep, but usually with minimal EDS)
- unusual nocturnal behaviors (ranging from arm waving to violent behaviors.
When you evaluate a patient with sleep complaints, valuable sources of data include observation, questionnaires, and screening devices. The most important may be common sense.
Observation. Observe the patient in the waiting room or office before starting the interview. Did he or she nod off while waiting to see you? Pay attention to anyone who appears sleepy—even those who deny having trouble staying awake. Over time, sleepy patients can lose their perspective on alertness. Some have had EDS so long that they no longer recall what it is like to feel fully awake.
Collateral history often is important because family members probably have observed the sleeping patient. The bed partner can provide information about snoring, irregular breathing, leg kicks, unplanned naps, and strained interpersonal relationships because of EDS. For the patient without a bed partner, consider interviewing a travel companion.
Questionnaires. Few useful screening tests exist for sleepiness; most are neither reliable nor valid. One of the better questionnaires—the Epworth Sleepiness Scale (Box 1)—helps confirm the presence of sleepiness with a score >8, differentiating the inability to stay awake from fatigue. This brief questionnaire also provides a useful measure of sleepiness severity.3
The Epworth scale’s value is limited because its questions of specific time and context might not represent a patient’s experiences. Additional validated surveys include the Pittsburgh Sleep Quality Inventory and several for sleep apnea.4
Screening. Electroencephalographic (EEG) monitoring can accurately measure the patient’s degree of sleep disruption. This information is key to understanding if a patient’s EDS is caused by a physiologic condition that prevents quality nocturnal sleep.
None of the widely used screening devices that assess leg kicks indicate the presence of possible periodic limb movements.
Overnight pulse oximetry has been used to screen for sleep-disordered breathing5 but also has limitations:
- Most pulse oximeters do not provide information about sleep stage or body position.
- Patients with sleep-disordered breathing can lack adequate oxygen desaturations but have frequent EEG arousals related to sleep issues. Because EEG data are not collected during arousals, pulse oximetry would generate a false-negative result in this scenario, which occurs most often in female and thin patients.
- Oximetry provides only oxygen saturation data and possibly heart rate, whereas other physiologic processes such as body movement or sleep architecture can be disrupted repetitively during sleep.
Common sense. The most productive tools for detecting sleep disorders are intuition and common sense. The Figure suggests sequential questions that might uncover specific sleep disorders. Then the decision whether to refer the patient to a sleep disorder center for diagnostic testing depends on the type of sleep disorder you detect.
Nasal continuous positive airway pressure
(CPAP) should be started in an observed setting so that the clinician can determine the optimal amount of positive pressure needed to keep the upper airway patent.
For some patients, CPAP is started in the second half of a “split-night” sleep study after a diagnosis of obstructive sleep apnea (OSA) is made. Other patients return a second night for a nasal CPAP trial. Those with severe OSA might notice improved sleep quality and reduced EDS after only a few hours of CPAP use. Some wish to start CPAP treatment immediately.
Advances in masks and equipment have improved patient adherence to CPAP. Innovations include auto-titrating machines, in which the pressure level can be varied depending on sleep state or body position. Many machines include a data microchip that allows the clinician to determine duration of usage, then use that information to counsel the patient about adherence, if necessary.
Patient education also can promote CPAP adherence. When patients are first told they might need to sleep each night wearing a nasal mask, they often voice well-founded concerns about comfort, claustrophobia, or sexual activity.
Obtaining the support of the bed partner by welcoming her or him to all appointments, including educational activities, is optimal. The bed partner’s concerns about the patient’s excessive snoring or apneas probably were the impetus for the appointment in the first place.
Medication. Some patients benefit from 1 to 2 weeks of a sleeping medication such as zolpidem or trazodone while they acclimate to using nasal CPAP.
Figure The sleepy patient: Possible medical and psychiatric explanations
* Supportive factors: Persuasive if present, but if absent do not exclude possible conditions
Obstructive sleep apnea
Because OSA affects at least 4% of men and 2% of women,6 you are virtually assured of seeing undiagnosed patients. OSA is caused by repeated collapse of the soft tissues surrounding the upper airway, decreasing airflow that is restored when the patient briefly awakens. Patients develop EDS because sleep is fragmented by frequent arousals.
Obese patients, because of their body habitus, are at higher risk for OSA than patients at normal weight. Carefully screen patients for OSA if they develop weight problems while taking psychotropics, such as antipsychotics.
Alcohol or sedatives used at bedtime can aggravate OSA. These substances promote muscle relaxation and increase the arousal threshold so that patients do not awaken readily when apneas occur.
Long-term complications of untreated OSA include sleepiness leading to accidents, hypertension, cerebrovascular disease, and progressive obesity. Data also associate OSA with cardiovascular complications such as arrhythmias, congestive heart failure, and myocardial infarction.7
Physical examination focuses on detecting:
- nasal obstruction (have patient sniff separately through each nostril)
- large neck
- crowded oropharynx (low-hanging palate, reddened uvula, enlarged tonsils, large tongue relative to oropharynx diameter)
- jaw structure (particularly a small, retrognathic mandible).
Sleep studies. Referral for nocturnal polysomnography might be the next step. A comprehensive sleep study collects data about respiratory, cardiovascular, and muscle activity at night, as well as the sounds the patient makes—such as snoring or coughing—when asleep. EEG monitoring also is performed. OSA may be diagnosed if repeated episodes of reduced airflow and oxygen desaturation (arousals) are observed as brief shifts in EEG frequency.
Treatment. First-line interventions for the patient with OSA include:
- no alcohol 1 to 2 hours before bedtime
- sleeping on the side instead of the back
- weight loss (ideally with exercise)
- nasal sprays for allergies.
If first-line treatments are ineffective, nasal continuous positive airway pressure (CPAP) works well for most patients who adhere to the regimen.8 CPAP requires the patient to wear a nasal mask that delivers room air, splinting open the nasopharynx and upper airway (Box 2).
Surgical options. The most common surgeries for OSA are uvulopalatopharyngoplasty and laser-assisted uvulopalatoplasty. Others include tongue reduction and mandibular advancement.
The response rate to surgery averages 50%, depending on patient characteristics and procedure.9 Positive outcomes are most likely for thin patients with obvious upper airway obstruction, including deviated nasal septum, large tonsils, low-hanging palate, and large uvula. Postsurgical complications include nasal regurgitation, voice change, pain, bleeding, infection, tongue numbness, and snoring without apnea (silent apnea).
Oral appliances open the oropharynx by moving the mandible and tongue out of way. Patients with mild to moderate OSA accept these devices well. Evidence suggests that oral appliances improve sleep and reduce EDS more effectively than nasal CPAP and are preferred by patients.10
Oral devices have drawbacks, however. In most settings, their effectiveness cannot be observed during a “split-night” laboratory sleep study because the patient has not yet purchased the device. Also, multiple visits sometimes are required to custom-fit the appliance; this can pose a hardship for patients who live a distance from the provider.
Restless legs syndrome
Patients with restless legs syndrome (RLS) typically report a restless, painful feeling in the limbs that occurs in the evening and at night, disrupting sleep. This condition—which affects 10% of the population—is associated with aging, blood loss, anemia, peripheral neuropathies, and pregnancy.11 Onset can occur in childhood, and in some cases there is a familial tendency.
Most patients with RLS have periodic limb movements (repetitive leg jerks or twitches). The clinical significance of periodic limb movements with no subjective disagreeable feelings in the limbs is controversial, and these cases usually are not treated.
The history usually confirms RLS. Order sleep studies only if you suspect a coexisting sleep problem or the diagnosis is unclear.
A suspected mechanism of restless legs is dopamine deficiency. Low serum ferritin levels have been associated with RLS—presumably because iron is a cofactor necessary for dopamine synthesis12—and may be diagnostically helpful.
The most common technique is to ask the patient to establish a consistent awakening time and a regular bedtime. Initially this could be unconventional by societal standards—such as bedtime at 5 AM and arising at 2 PM. After this pattern is in place, the patient gradually shifts the timing by 1 hour per day. Most patients find it easier to delay rather than advance the bedtime until it conforms to the desired time.
Reinforce this new sleep pattern with a structured daytime schedule that includes predictable mealtimes, regular exercise, social activities, and possibly bright light exposure. Provide reinforcement in the morning for patients with delayed sleep phase disorder and in the evening for advanced sleep phase disorder. These interventions take time and discipline.
Another approach is for the patient to skip sleep one night and, in a sleep-deprived state, establish a new bedtime at the desired time. Use the same modalities listed above to reinforce (“entrain”) this schedule; otherwise the patient will slip back into the previous abnormal sleep-wake rhythm.
Treatment can include iron repletion when indicated. Medications include dopaminergic agents, most notably pramipexole and levodopa/carbidopa. Other options include gabapentin, benzodiazepines, and narcotics.
Antidepressants have been suspected to worsen restless legs syndrome, but definitive studies are lacking.13
Circadian rhythm disorders
Instead of compromising the quality or quantity of sleep, circadian rhythm disorders cause sleep to occur at inappropriate times. These disorders are most common in adolescents and young adults.
Delayed sleep phase disorder—a persistent pattern of staying up late and “sleeping in”—is most common. Careful assessment will reveal that the patient is getting adequate sleep but at a socially unacceptable time, sometimes to the extreme that his or her nights and days are reversed.
Patients’ reluctance to acknowledge the severity of this problem can lead to inaccurate sleep diaries and interviews. A portable wrist actigraph can provide data about limb movement and is more objective than self-reports.
Delayed sleep phase disorder is highly comorbid with depressive disorders.14 The cause of this syndrome is unclear, but light exposure, social patterns, psychological issues, and possibly a genetic substrate are known to contribute.
Advanced sleep phase disorder—a less common circadian rhythm disorder—also can cause EDS. Patients have an inappropriately early time of sleep onset and then are fully awake in the middle of the night. A large family with a severe form of this disorder was found to have an abnormality on chromosome 2.15
Treatment. Relatively few treatments are effective for circadian rhythm disorders. Some patients elect not to pursue therapy, instead fitting activities around their unconventional sleep schedules.
Individuals with delayed sleep phase who cannot arrange their lives around their sleep schedules are at risk for poor early morning performance because of sleepiness. Their internal circadian clocks can be gradually readjusted with phototherapy or gradual shifting of the major sleep period (Box 3). Stimulants usually are not used, but hypnotics can sometimes help these patients fall asleep earlier.
Insufficient sleep syndrome
People attempting to “burn the candle at both ends” are at risk for developing insufficient sleep syndrome.16 In our 24/7 society, people trying to make do with less than the required 7.5 hours sleep per night may adversely affect their health. The problem is compounded for shift workers because of the difficulty in obtaining sufficient quality sleep during daylight hours.
Many patients do not seek treatment for fatigue or sleepiness because they are aware of their lifestyle choices. Still, they might develop psychological symptoms such as irritability, mood swings, and strained interpersonal relationships. These symptoms can prompt patients to request treatment.
Take a careful history that includes discussing the patient’s daily and weekly schedule. Avoid psychostimulants; instead, address the nonnegotiable need to get adequate sleep and challenge the patient to prioritize his or her activities around a full night’s sleep.
When to consider narcolepsy
Narcolepsy is a CNS disease characterized by abnormal regulation of REM sleep. EDS—the cardinal symptom—is often associated with cataplexy (75%), sleep paralysis (50%), vivid dreams, and insomnia, all of which interfere with REM phenomena. Narcolepsy affects 0.05% of the U.S. population and can lead to severe occupational, educational, and family disruption.
When you obtain a history that suggests narcolepsy, use the history, a sleep diary, or wrist actigraphy to document whether the patient is getting adequate sleep, with a consistent sleep/wake cycle. Next, consider referring the patient for polysomnography, primarily to rule out other causes of EDS such as sleep-disordered breathing. In some cases, REM latency on the overnight sleep study will be <20 minutes after sleep onset, which supports the diagnosis of narcolepsy.
A multiple sleep latency test (MSLT)—a diagnostic session in which the patient takes 4 to 5 daytime naps—is performed the following day. Narcolepsy is confirmed if the patient has a mean initial sleep latency of <10 minutes during these naps plus at least two REM episodes within 15 minutes after sleep onset.
The 4 most appropriate indications for an urgent sleep evaluation are:
- difficulty staying alert while driving
- nocturnal cardiac arrhythmias
- frequent observed apneas
- excessive daytime sleepiness (EDS) leading to academic or occupational problems.
Insurance companies usually cover a specialty sleep evaluation, particularly if the referring physician documents a suspicion of sleep-disordered breathing or EDS that jeopardizes safe driving.
Most patients with narcolepsy and cataplexy have undetectable cerebrospinal fluid levels of a neuropeptide called hypocretin or orexin.17 Hypocretin/orexin replacement therapy is a theoretical possibility, but for now treatment includes a combination of optimal sleep hygiene, psychostimulants, antidepressants, and hypnotics.
Other causes of EDS
EDS can also be caused by unrecognized alcohol dependence, inappropriate or excessive medication use, and depressive disorders. Overnight sleep studies are seldom indicated unless patients endorse the symptoms in the Figure.
Before pursuing polysomnography or an MSLT (Box 4), eliminate medications that might confound the results, such as:
- antidepressants, which alter the timing and duration of REM sleep
- sedating medications, which modify initial sleep latency and sleep efficiency and potentially aggravate sleep disordered breathing.
Initial REM latency provides a potential biologic marker of major depression but is used more often in research than in clinical psychiatry.
Primary insomnia is the distressing inability to sleep at night or nap during the day. It suggests a hyperarousal state—the opposite of EDS.18 In rare cases, however, patients who cannot sleep at night also have EDS. When evaluated, they typically endorse at least one symptom in the Figure. Sleep studies occasionally reveal OSA or restless legs syndrome.
Treating a patient with chronic insomnia may require several trials of behavioral interventions or sedating medications before you make a referral to a sleep disorder center. Patients can struggle with unrecognized primary sleep disorders for years, and many are given empiric trials of stimulating antidepressants. Antidepressants are unlikely to cause harm, but they might complicate diagnostic testing.
When you confirm coexisting depression and a primary sleep disorder, treatments that separately target each condition provide optimal management of the sleepy patient.
Medications to enhance wakefulness
Wake-promoting agents are a treatment option when EDS is contributing to compromised functioning. These drugs are no substitute for thoughtful evaluation of hypersomnolence, however. When you diagnose OSA or restless legs syndrome, first try treatments that target these conditions. If residual sleepiness persists, then consider augmenting with stimulating medications.
Modafinil is FDA-approved for residual sleepiness in patients with OSA and for shift work sleep disorder, a condition of circadian misalignment from frequent schedule changes. Evidence does not support its use for other circadian rhythm disorders, such as delayed sleep phase disorder.
Low-dose modafinil (such as 100 to 200 mg/d) is well tolerated, but its therapeutic effect as augmentation is modest.19 Increasing the dosage to >200 mg usually does not increase alertness.
Caffeine. Some patients report benefit from caffeine used in moderation and only in the morning. This practice is acceptable as long as patients do not use excessive amounts or experience insomnia, exacerbation of anxiety, or tachycardia.
Psychostimulants such as methylphenidate and amphetamines are less well-studied than modafinil for treating EDS in patients without narcolepsy. Monitor carefully for insomnia, exacerbation of anxiety, tachycardia, or hypertension and to prevent overuse of these habituating agents.
Related resources
- National Sleep Foundation. www.sleepfoundation.org.
- American Academy of Sleep Medicine. www.aasmnet.org.
- American Sleep Apnea Association. www.sleepapnea.org.
- Restless Legs Syndrome Foundation. www.rls.org.
- Association for the Study of Light Therapy and Biological Rhythms. www.sltbr.org.
Drug brand names
- Carbidopa/levodopa • Sinemet
- Gabapentin • Neurontin
- Modafinil • Provigil
- Pramipexole • Mirapex
- Trazodone • Desyrel
- Zolpidem • Ambien
Disclosure
Dr. Krahn reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
Dr. Krahn published the original version this article in the January 2002 issue of Current Psychiatry and has updated it for this issue.
Poor energy, hypersomnia, amotivation, irritability, and frustration can suggest depression or other psychiatric disorders to busy primary care physicians. As a result, psychiatrists often are referred patients with excessive daytime sleepiness (EDS) caused by undiagnosed primary sleep disorders.
Physicians may miss obstructive sleep apnea (OSA), restless legs syndrome, circadian rhythm disorders, or narcolepsy because:
- many have little training in sleep disorders and limited time to diagnose them1
- patients do not report sleepiness or recognize it as a legitimate medical concern
- definitive diagnostic tests are expensive and usually are not ordered.
Psychiatrists, therefore, need a clear understanding of the EDS differential diagnosis to determine whether a patient’s behavioral symptoms are a sleep or psychiatric issue.
How likely are you to doze off or fall asleep in the following situations, in contrast to feeling just tired? This refers to your usual way of life in recent times. Even if you have not done some of these things recently, try to work out how each situation would affect you now. Use the scale below to choose the most appropriate number for each situation:
0 no chance of dozing
1 slight chance of dozing
2 moderate chance of dozing
3 high chance of dozing
Chance of dozing Situation
Sitting and reading
Watching TV
Sitting inactive in a public place (such as in a theater or a meeting)
As a passenger in a car for an hour without a break
Lying down to rest in the afternoon when circumstances permit
Sitting and talking to someone
Sitting quietly after a lunch without alcohol
In a car, while stopped for a few minutes in traffic
Scoring key
1 to 6 Getting enough sleep
7 to 8 Average
>8 Seek a sleep specialist’s advice without delay
Assessing the sleepy patient
Sleepiness is an inability to stay awake at appropriate times. Fatigue, by comparison, does not involve sleepiness but very low energy associated with wakefulness. In general, sleepy patients get transient relief from napping, whereas fatigued patients report they cannot fall asleep.
Untreated EDS results in compromised quality of life, reduced productivity, and public safety concerns such as falling asleep while driving.2 Sleep complaints fall into three major categories:
- EDS
- insomnia (marked by distress because of poor sleep, but usually with minimal EDS)
- unusual nocturnal behaviors (ranging from arm waving to violent behaviors.
When you evaluate a patient with sleep complaints, valuable sources of data include observation, questionnaires, and screening devices. The most important may be common sense.
Observation. Observe the patient in the waiting room or office before starting the interview. Did he or she nod off while waiting to see you? Pay attention to anyone who appears sleepy—even those who deny having trouble staying awake. Over time, sleepy patients can lose their perspective on alertness. Some have had EDS so long that they no longer recall what it is like to feel fully awake.
Collateral history often is important because family members probably have observed the sleeping patient. The bed partner can provide information about snoring, irregular breathing, leg kicks, unplanned naps, and strained interpersonal relationships because of EDS. For the patient without a bed partner, consider interviewing a travel companion.
Questionnaires. Few useful screening tests exist for sleepiness; most are neither reliable nor valid. One of the better questionnaires—the Epworth Sleepiness Scale (Box 1)—helps confirm the presence of sleepiness with a score >8, differentiating the inability to stay awake from fatigue. This brief questionnaire also provides a useful measure of sleepiness severity.3
The Epworth scale’s value is limited because its questions of specific time and context might not represent a patient’s experiences. Additional validated surveys include the Pittsburgh Sleep Quality Inventory and several for sleep apnea.4
Screening. Electroencephalographic (EEG) monitoring can accurately measure the patient’s degree of sleep disruption. This information is key to understanding if a patient’s EDS is caused by a physiologic condition that prevents quality nocturnal sleep.
None of the widely used screening devices that assess leg kicks indicate the presence of possible periodic limb movements.
Overnight pulse oximetry has been used to screen for sleep-disordered breathing5 but also has limitations:
- Most pulse oximeters do not provide information about sleep stage or body position.
- Patients with sleep-disordered breathing can lack adequate oxygen desaturations but have frequent EEG arousals related to sleep issues. Because EEG data are not collected during arousals, pulse oximetry would generate a false-negative result in this scenario, which occurs most often in female and thin patients.
- Oximetry provides only oxygen saturation data and possibly heart rate, whereas other physiologic processes such as body movement or sleep architecture can be disrupted repetitively during sleep.
Common sense. The most productive tools for detecting sleep disorders are intuition and common sense. The Figure suggests sequential questions that might uncover specific sleep disorders. Then the decision whether to refer the patient to a sleep disorder center for diagnostic testing depends on the type of sleep disorder you detect.
Nasal continuous positive airway pressure
(CPAP) should be started in an observed setting so that the clinician can determine the optimal amount of positive pressure needed to keep the upper airway patent.
For some patients, CPAP is started in the second half of a “split-night” sleep study after a diagnosis of obstructive sleep apnea (OSA) is made. Other patients return a second night for a nasal CPAP trial. Those with severe OSA might notice improved sleep quality and reduced EDS after only a few hours of CPAP use. Some wish to start CPAP treatment immediately.
Advances in masks and equipment have improved patient adherence to CPAP. Innovations include auto-titrating machines, in which the pressure level can be varied depending on sleep state or body position. Many machines include a data microchip that allows the clinician to determine duration of usage, then use that information to counsel the patient about adherence, if necessary.
Patient education also can promote CPAP adherence. When patients are first told they might need to sleep each night wearing a nasal mask, they often voice well-founded concerns about comfort, claustrophobia, or sexual activity.
Obtaining the support of the bed partner by welcoming her or him to all appointments, including educational activities, is optimal. The bed partner’s concerns about the patient’s excessive snoring or apneas probably were the impetus for the appointment in the first place.
Medication. Some patients benefit from 1 to 2 weeks of a sleeping medication such as zolpidem or trazodone while they acclimate to using nasal CPAP.
Figure The sleepy patient: Possible medical and psychiatric explanations
* Supportive factors: Persuasive if present, but if absent do not exclude possible conditions
Obstructive sleep apnea
Because OSA affects at least 4% of men and 2% of women,6 you are virtually assured of seeing undiagnosed patients. OSA is caused by repeated collapse of the soft tissues surrounding the upper airway, decreasing airflow that is restored when the patient briefly awakens. Patients develop EDS because sleep is fragmented by frequent arousals.
Obese patients, because of their body habitus, are at higher risk for OSA than patients at normal weight. Carefully screen patients for OSA if they develop weight problems while taking psychotropics, such as antipsychotics.
Alcohol or sedatives used at bedtime can aggravate OSA. These substances promote muscle relaxation and increase the arousal threshold so that patients do not awaken readily when apneas occur.
Long-term complications of untreated OSA include sleepiness leading to accidents, hypertension, cerebrovascular disease, and progressive obesity. Data also associate OSA with cardiovascular complications such as arrhythmias, congestive heart failure, and myocardial infarction.7
Physical examination focuses on detecting:
- nasal obstruction (have patient sniff separately through each nostril)
- large neck
- crowded oropharynx (low-hanging palate, reddened uvula, enlarged tonsils, large tongue relative to oropharynx diameter)
- jaw structure (particularly a small, retrognathic mandible).
Sleep studies. Referral for nocturnal polysomnography might be the next step. A comprehensive sleep study collects data about respiratory, cardiovascular, and muscle activity at night, as well as the sounds the patient makes—such as snoring or coughing—when asleep. EEG monitoring also is performed. OSA may be diagnosed if repeated episodes of reduced airflow and oxygen desaturation (arousals) are observed as brief shifts in EEG frequency.
Treatment. First-line interventions for the patient with OSA include:
- no alcohol 1 to 2 hours before bedtime
- sleeping on the side instead of the back
- weight loss (ideally with exercise)
- nasal sprays for allergies.
If first-line treatments are ineffective, nasal continuous positive airway pressure (CPAP) works well for most patients who adhere to the regimen.8 CPAP requires the patient to wear a nasal mask that delivers room air, splinting open the nasopharynx and upper airway (Box 2).
Surgical options. The most common surgeries for OSA are uvulopalatopharyngoplasty and laser-assisted uvulopalatoplasty. Others include tongue reduction and mandibular advancement.
The response rate to surgery averages 50%, depending on patient characteristics and procedure.9 Positive outcomes are most likely for thin patients with obvious upper airway obstruction, including deviated nasal septum, large tonsils, low-hanging palate, and large uvula. Postsurgical complications include nasal regurgitation, voice change, pain, bleeding, infection, tongue numbness, and snoring without apnea (silent apnea).
Oral appliances open the oropharynx by moving the mandible and tongue out of way. Patients with mild to moderate OSA accept these devices well. Evidence suggests that oral appliances improve sleep and reduce EDS more effectively than nasal CPAP and are preferred by patients.10
Oral devices have drawbacks, however. In most settings, their effectiveness cannot be observed during a “split-night” laboratory sleep study because the patient has not yet purchased the device. Also, multiple visits sometimes are required to custom-fit the appliance; this can pose a hardship for patients who live a distance from the provider.
Restless legs syndrome
Patients with restless legs syndrome (RLS) typically report a restless, painful feeling in the limbs that occurs in the evening and at night, disrupting sleep. This condition—which affects 10% of the population—is associated with aging, blood loss, anemia, peripheral neuropathies, and pregnancy.11 Onset can occur in childhood, and in some cases there is a familial tendency.
Most patients with RLS have periodic limb movements (repetitive leg jerks or twitches). The clinical significance of periodic limb movements with no subjective disagreeable feelings in the limbs is controversial, and these cases usually are not treated.
The history usually confirms RLS. Order sleep studies only if you suspect a coexisting sleep problem or the diagnosis is unclear.
A suspected mechanism of restless legs is dopamine deficiency. Low serum ferritin levels have been associated with RLS—presumably because iron is a cofactor necessary for dopamine synthesis12—and may be diagnostically helpful.
The most common technique is to ask the patient to establish a consistent awakening time and a regular bedtime. Initially this could be unconventional by societal standards—such as bedtime at 5 AM and arising at 2 PM. After this pattern is in place, the patient gradually shifts the timing by 1 hour per day. Most patients find it easier to delay rather than advance the bedtime until it conforms to the desired time.
Reinforce this new sleep pattern with a structured daytime schedule that includes predictable mealtimes, regular exercise, social activities, and possibly bright light exposure. Provide reinforcement in the morning for patients with delayed sleep phase disorder and in the evening for advanced sleep phase disorder. These interventions take time and discipline.
Another approach is for the patient to skip sleep one night and, in a sleep-deprived state, establish a new bedtime at the desired time. Use the same modalities listed above to reinforce (“entrain”) this schedule; otherwise the patient will slip back into the previous abnormal sleep-wake rhythm.
Treatment can include iron repletion when indicated. Medications include dopaminergic agents, most notably pramipexole and levodopa/carbidopa. Other options include gabapentin, benzodiazepines, and narcotics.
Antidepressants have been suspected to worsen restless legs syndrome, but definitive studies are lacking.13
Circadian rhythm disorders
Instead of compromising the quality or quantity of sleep, circadian rhythm disorders cause sleep to occur at inappropriate times. These disorders are most common in adolescents and young adults.
Delayed sleep phase disorder—a persistent pattern of staying up late and “sleeping in”—is most common. Careful assessment will reveal that the patient is getting adequate sleep but at a socially unacceptable time, sometimes to the extreme that his or her nights and days are reversed.
Patients’ reluctance to acknowledge the severity of this problem can lead to inaccurate sleep diaries and interviews. A portable wrist actigraph can provide data about limb movement and is more objective than self-reports.
Delayed sleep phase disorder is highly comorbid with depressive disorders.14 The cause of this syndrome is unclear, but light exposure, social patterns, psychological issues, and possibly a genetic substrate are known to contribute.
Advanced sleep phase disorder—a less common circadian rhythm disorder—also can cause EDS. Patients have an inappropriately early time of sleep onset and then are fully awake in the middle of the night. A large family with a severe form of this disorder was found to have an abnormality on chromosome 2.15
Treatment. Relatively few treatments are effective for circadian rhythm disorders. Some patients elect not to pursue therapy, instead fitting activities around their unconventional sleep schedules.
Individuals with delayed sleep phase who cannot arrange their lives around their sleep schedules are at risk for poor early morning performance because of sleepiness. Their internal circadian clocks can be gradually readjusted with phototherapy or gradual shifting of the major sleep period (Box 3). Stimulants usually are not used, but hypnotics can sometimes help these patients fall asleep earlier.
Insufficient sleep syndrome
People attempting to “burn the candle at both ends” are at risk for developing insufficient sleep syndrome.16 In our 24/7 society, people trying to make do with less than the required 7.5 hours sleep per night may adversely affect their health. The problem is compounded for shift workers because of the difficulty in obtaining sufficient quality sleep during daylight hours.
Many patients do not seek treatment for fatigue or sleepiness because they are aware of their lifestyle choices. Still, they might develop psychological symptoms such as irritability, mood swings, and strained interpersonal relationships. These symptoms can prompt patients to request treatment.
Take a careful history that includes discussing the patient’s daily and weekly schedule. Avoid psychostimulants; instead, address the nonnegotiable need to get adequate sleep and challenge the patient to prioritize his or her activities around a full night’s sleep.
When to consider narcolepsy
Narcolepsy is a CNS disease characterized by abnormal regulation of REM sleep. EDS—the cardinal symptom—is often associated with cataplexy (75%), sleep paralysis (50%), vivid dreams, and insomnia, all of which interfere with REM phenomena. Narcolepsy affects 0.05% of the U.S. population and can lead to severe occupational, educational, and family disruption.
When you obtain a history that suggests narcolepsy, use the history, a sleep diary, or wrist actigraphy to document whether the patient is getting adequate sleep, with a consistent sleep/wake cycle. Next, consider referring the patient for polysomnography, primarily to rule out other causes of EDS such as sleep-disordered breathing. In some cases, REM latency on the overnight sleep study will be <20 minutes after sleep onset, which supports the diagnosis of narcolepsy.
A multiple sleep latency test (MSLT)—a diagnostic session in which the patient takes 4 to 5 daytime naps—is performed the following day. Narcolepsy is confirmed if the patient has a mean initial sleep latency of <10 minutes during these naps plus at least two REM episodes within 15 minutes after sleep onset.
The 4 most appropriate indications for an urgent sleep evaluation are:
- difficulty staying alert while driving
- nocturnal cardiac arrhythmias
- frequent observed apneas
- excessive daytime sleepiness (EDS) leading to academic or occupational problems.
Insurance companies usually cover a specialty sleep evaluation, particularly if the referring physician documents a suspicion of sleep-disordered breathing or EDS that jeopardizes safe driving.
Most patients with narcolepsy and cataplexy have undetectable cerebrospinal fluid levels of a neuropeptide called hypocretin or orexin.17 Hypocretin/orexin replacement therapy is a theoretical possibility, but for now treatment includes a combination of optimal sleep hygiene, psychostimulants, antidepressants, and hypnotics.
Other causes of EDS
EDS can also be caused by unrecognized alcohol dependence, inappropriate or excessive medication use, and depressive disorders. Overnight sleep studies are seldom indicated unless patients endorse the symptoms in the Figure.
Before pursuing polysomnography or an MSLT (Box 4), eliminate medications that might confound the results, such as:
- antidepressants, which alter the timing and duration of REM sleep
- sedating medications, which modify initial sleep latency and sleep efficiency and potentially aggravate sleep disordered breathing.
Initial REM latency provides a potential biologic marker of major depression but is used more often in research than in clinical psychiatry.
Primary insomnia is the distressing inability to sleep at night or nap during the day. It suggests a hyperarousal state—the opposite of EDS.18 In rare cases, however, patients who cannot sleep at night also have EDS. When evaluated, they typically endorse at least one symptom in the Figure. Sleep studies occasionally reveal OSA or restless legs syndrome.
Treating a patient with chronic insomnia may require several trials of behavioral interventions or sedating medications before you make a referral to a sleep disorder center. Patients can struggle with unrecognized primary sleep disorders for years, and many are given empiric trials of stimulating antidepressants. Antidepressants are unlikely to cause harm, but they might complicate diagnostic testing.
When you confirm coexisting depression and a primary sleep disorder, treatments that separately target each condition provide optimal management of the sleepy patient.
Medications to enhance wakefulness
Wake-promoting agents are a treatment option when EDS is contributing to compromised functioning. These drugs are no substitute for thoughtful evaluation of hypersomnolence, however. When you diagnose OSA or restless legs syndrome, first try treatments that target these conditions. If residual sleepiness persists, then consider augmenting with stimulating medications.
Modafinil is FDA-approved for residual sleepiness in patients with OSA and for shift work sleep disorder, a condition of circadian misalignment from frequent schedule changes. Evidence does not support its use for other circadian rhythm disorders, such as delayed sleep phase disorder.
Low-dose modafinil (such as 100 to 200 mg/d) is well tolerated, but its therapeutic effect as augmentation is modest.19 Increasing the dosage to >200 mg usually does not increase alertness.
Caffeine. Some patients report benefit from caffeine used in moderation and only in the morning. This practice is acceptable as long as patients do not use excessive amounts or experience insomnia, exacerbation of anxiety, or tachycardia.
Psychostimulants such as methylphenidate and amphetamines are less well-studied than modafinil for treating EDS in patients without narcolepsy. Monitor carefully for insomnia, exacerbation of anxiety, tachycardia, or hypertension and to prevent overuse of these habituating agents.
Related resources
- National Sleep Foundation. www.sleepfoundation.org.
- American Academy of Sleep Medicine. www.aasmnet.org.
- American Sleep Apnea Association. www.sleepapnea.org.
- Restless Legs Syndrome Foundation. www.rls.org.
- Association for the Study of Light Therapy and Biological Rhythms. www.sltbr.org.
Drug brand names
- Carbidopa/levodopa • Sinemet
- Gabapentin • Neurontin
- Modafinil • Provigil
- Pramipexole • Mirapex
- Trazodone • Desyrel
- Zolpidem • Ambien
Disclosure
Dr. Krahn reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
Dr. Krahn published the original version this article in the January 2002 issue of Current Psychiatry and has updated it for this issue.
1. Punjabi N, Haponik E. Ask about daytime sleepiness. J Amer Geriatr Soc 2000;48:228-9.
2. Ronald J, Delaive K, Roos L, et al. Health care utilization in the 10 years prior to diagnosis in obstructive sleep apnea syndrome patients. Sleep 1999;22(2):225-9.
3. Johns M. A new method for measuring daytime sleepiness: The Epworth Sleepiness Scale. Sleep 1991;14(6):540-5.
4. Rowley J, Aboussouan L, Badr M. The use of clinical prediction formulas in the evaluation of obstructive sleep apnea. Sleep 2000;23:929-38.
5. Yamashiro Y, Kryger M. Nocturnal oximetry: Is it a screening tool for sleep disorders? Sleep 1995;18:167-71.
6. Morrell M, Finn L, Kim H, et al. Sleep fragmentation, awake blood pressure, and sleep-disordered breathing in a population-based study. Am J Respir Critical Care Med 2000;162(6):2091-6.
7. Roux F, D’Ambrosio C, Mohsenin V. Sleep-related breathing disorders and cardiovascular disease. Am J Med. 2000;108:396-402.
8. Engleman H, Martin S, Deary I, Douglas N. Effect of continuous positive airway pressure treatment on daytime function in sleep apnoea/hypopnoea syndrome. Lancet 1994;343(8897):572-5.
9. Lojander J, Maasilta P, Partinen M, et al. Nasal-CPAP, surgery, and conservative management for treatment of obstructive sleep apnea syndrome. A randomized study. Chest. 1996;110(1):114-9.
10. Mehta A, Qian J, Petocz P, et al. A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am J Respir Critical Care Med 2001;163(6):1457-61.
11. Chesson A, Wise M, Davila D, et al. Practice parameters for the treatment of restless legs syndrome and periodic limb movement disorder. An American Academy of Sleep Medicine Report. Standards of Practice Committee of the American Academy of Sleep Medicine. Sleep 1999;22(7):961-8.
12. Phillips B, Young T, Finn L, et al. Epidemiology of restless legs symptoms in adults. Arch Intern Med 2000;160(14):2137-41.
13. Thorpy M, Ehrenberg B, Hening W, et al. Restless legs syndrome: Detection and management in primary care. Amer Fam Phys 2000;62:108-14.
14. Regestein Q, Monk T. Delayed sleep phase syndrome: A review of its clinical aspects. Am J Psychiatry 1995;152:602-8.
15. Toh K, Jones C, He Y, et al. An hPer2 phosphorylation site mutation in familial advanced sleep phase syndrome. Science 2001;291(5506):1040-3.
16. Yoshikawa N, Suzuki S, Ishimoto T, et al. A case of insufficient sleep syndrome. Psychiatry Clin Neuro 1998;52(2):200-1.
17. Nishino S, Ripley B, Overeem S, et al. Hypocretin (orexin) deficiency in human narcolepsy. Lancet. 2000;355:39-40.
18. Hauri P, Esther M. Insomnia. Mayo Clin Proc 1990;65:869-82.
19. Schwartz JR. Modafinil: new indications for wake promotion. Expert Opin Pharmacother 2005;6(1):115-29.
1. Punjabi N, Haponik E. Ask about daytime sleepiness. J Amer Geriatr Soc 2000;48:228-9.
2. Ronald J, Delaive K, Roos L, et al. Health care utilization in the 10 years prior to diagnosis in obstructive sleep apnea syndrome patients. Sleep 1999;22(2):225-9.
3. Johns M. A new method for measuring daytime sleepiness: The Epworth Sleepiness Scale. Sleep 1991;14(6):540-5.
4. Rowley J, Aboussouan L, Badr M. The use of clinical prediction formulas in the evaluation of obstructive sleep apnea. Sleep 2000;23:929-38.
5. Yamashiro Y, Kryger M. Nocturnal oximetry: Is it a screening tool for sleep disorders? Sleep 1995;18:167-71.
6. Morrell M, Finn L, Kim H, et al. Sleep fragmentation, awake blood pressure, and sleep-disordered breathing in a population-based study. Am J Respir Critical Care Med 2000;162(6):2091-6.
7. Roux F, D’Ambrosio C, Mohsenin V. Sleep-related breathing disorders and cardiovascular disease. Am J Med. 2000;108:396-402.
8. Engleman H, Martin S, Deary I, Douglas N. Effect of continuous positive airway pressure treatment on daytime function in sleep apnoea/hypopnoea syndrome. Lancet 1994;343(8897):572-5.
9. Lojander J, Maasilta P, Partinen M, et al. Nasal-CPAP, surgery, and conservative management for treatment of obstructive sleep apnea syndrome. A randomized study. Chest. 1996;110(1):114-9.
10. Mehta A, Qian J, Petocz P, et al. A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am J Respir Critical Care Med 2001;163(6):1457-61.
11. Chesson A, Wise M, Davila D, et al. Practice parameters for the treatment of restless legs syndrome and periodic limb movement disorder. An American Academy of Sleep Medicine Report. Standards of Practice Committee of the American Academy of Sleep Medicine. Sleep 1999;22(7):961-8.
12. Phillips B, Young T, Finn L, et al. Epidemiology of restless legs symptoms in adults. Arch Intern Med 2000;160(14):2137-41.
13. Thorpy M, Ehrenberg B, Hening W, et al. Restless legs syndrome: Detection and management in primary care. Amer Fam Phys 2000;62:108-14.
14. Regestein Q, Monk T. Delayed sleep phase syndrome: A review of its clinical aspects. Am J Psychiatry 1995;152:602-8.
15. Toh K, Jones C, He Y, et al. An hPer2 phosphorylation site mutation in familial advanced sleep phase syndrome. Science 2001;291(5506):1040-3.
16. Yoshikawa N, Suzuki S, Ishimoto T, et al. A case of insufficient sleep syndrome. Psychiatry Clin Neuro 1998;52(2):200-1.
17. Nishino S, Ripley B, Overeem S, et al. Hypocretin (orexin) deficiency in human narcolepsy. Lancet. 2000;355:39-40.
18. Hauri P, Esther M. Insomnia. Mayo Clin Proc 1990;65:869-82.
19. Schwartz JR. Modafinil: new indications for wake promotion. Expert Opin Pharmacother 2005;6(1):115-29.