User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Confidentiality confusion, and who’s at fault for fatal misdiagnosis?
Worker claims therapist disclosed confidential information
Cook County (IL) Circuit Court
A public works employee in Illinois received psychotherapy through his city’s wellness program. After the man left his position, he claimed in court that the treating therapist met with his former co-workers, disclosed his receipt of therapy to them, and told them he was unstable and capable of harming himself or others. The former employee argued that the disclosures violated Illinois law, caused him emotional distress, and made him unable to trust mental health professionals.
The defense denied that the therapist had violated the law or had made any disclosures. Instead, the defense argued that the co-workers—not the therapist—had voiced concern about the plaintiff. The defense maintained that the co-workers were confused about who had discussed the plaintiff, and that the therapist had not discussed him.
- The jury found for the defense.
Dr. Grant’s observations
The courts have recognized and protected the fundamental importance of confidentiality in the therapist/patient relationship.How to avoid ‘foreseeable’ harm,” Current Psychiatry, March 2005, at www.currentpsychiatry.com).
Here, the request for consultation might suggest that an honest error in judgment occurred—the psychiatrist was simply puzzled by the patient’s medical symptoms. Although several doctors failed to diagnose NMS, shouldn’t the psychiatrists have been able to diagnose it?
NMS is a side-effect risk of atypical and conventional neuroleptics,Pearls: Identifying NMS with FEVER,”).
The psychiatrists in this case did not conform to the standard of care, and consulting with another doctor did not absolve them of liability.
Worker claims therapist disclosed confidential information
Cook County (IL) Circuit Court
A public works employee in Illinois received psychotherapy through his city’s wellness program. After the man left his position, he claimed in court that the treating therapist met with his former co-workers, disclosed his receipt of therapy to them, and told them he was unstable and capable of harming himself or others. The former employee argued that the disclosures violated Illinois law, caused him emotional distress, and made him unable to trust mental health professionals.
The defense denied that the therapist had violated the law or had made any disclosures. Instead, the defense argued that the co-workers—not the therapist—had voiced concern about the plaintiff. The defense maintained that the co-workers were confused about who had discussed the plaintiff, and that the therapist had not discussed him.
- The jury found for the defense.
Dr. Grant’s observations
The courts have recognized and protected the fundamental importance of confidentiality in the therapist/patient relationship.How to avoid ‘foreseeable’ harm,” Current Psychiatry, March 2005, at www.currentpsychiatry.com).
Here, the request for consultation might suggest that an honest error in judgment occurred—the psychiatrist was simply puzzled by the patient’s medical symptoms. Although several doctors failed to diagnose NMS, shouldn’t the psychiatrists have been able to diagnose it?
NMS is a side-effect risk of atypical and conventional neuroleptics,Pearls: Identifying NMS with FEVER,”).
The psychiatrists in this case did not conform to the standard of care, and consulting with another doctor did not absolve them of liability.
Worker claims therapist disclosed confidential information
Cook County (IL) Circuit Court
A public works employee in Illinois received psychotherapy through his city’s wellness program. After the man left his position, he claimed in court that the treating therapist met with his former co-workers, disclosed his receipt of therapy to them, and told them he was unstable and capable of harming himself or others. The former employee argued that the disclosures violated Illinois law, caused him emotional distress, and made him unable to trust mental health professionals.
The defense denied that the therapist had violated the law or had made any disclosures. Instead, the defense argued that the co-workers—not the therapist—had voiced concern about the plaintiff. The defense maintained that the co-workers were confused about who had discussed the plaintiff, and that the therapist had not discussed him.
- The jury found for the defense.
Dr. Grant’s observations
The courts have recognized and protected the fundamental importance of confidentiality in the therapist/patient relationship.How to avoid ‘foreseeable’ harm,” Current Psychiatry, March 2005, at www.currentpsychiatry.com).
Here, the request for consultation might suggest that an honest error in judgment occurred—the psychiatrist was simply puzzled by the patient’s medical symptoms. Although several doctors failed to diagnose NMS, shouldn’t the psychiatrists have been able to diagnose it?
NMS is a side-effect risk of atypical and conventional neuroleptics,Pearls: Identifying NMS with FEVER,”).
The psychiatrists in this case did not conform to the standard of care, and consulting with another doctor did not absolve them of liability.
Medications for indigent patients
Dr. Shelley Sellinger’s article “Helping indigent patients obtain medications” (Pearls, Current Psychiatry, April 2005) is helpful for psychiatrists working with patients who lack pharmacy benefits. Not having the information handy or believing the process is too cumbersome may deter some clinicians from using patient assistance programs.
We also suggest the following services:
- www.needymeds.com lists thousands of medications alphabetically (by brand or generic name). Each listing provides complete assistance program information, including the phone number, eligibility criteria, and application form.
- GlaxoSmithKline (GSK) patient assistance program. Simply obtain a brief application by calling 1-866-PATIENT (728-4368) or logging onto www.bridgestoaccess.gsk.com. Fill out the form, then call 1-866-PATIENT to activate the attached coupon. Give the patient the coupon and a 60-day prescription for a GSK medication. The patient can fill the prescription at any pharmacy for a $10 co-payment. GSK then mails you 3-month supplies of the medication for 1 year.
Abigail Kay, MD
Instructor in psychiatry
Rajnish Mago, MD
Assistant professor of psychiatry
Director, mood disorders program
Thomas Jefferson University, Philadelphia, PA
Dr. Shelley Sellinger’s article “Helping indigent patients obtain medications” (Pearls, Current Psychiatry, April 2005) is helpful for psychiatrists working with patients who lack pharmacy benefits. Not having the information handy or believing the process is too cumbersome may deter some clinicians from using patient assistance programs.
We also suggest the following services:
- www.needymeds.com lists thousands of medications alphabetically (by brand or generic name). Each listing provides complete assistance program information, including the phone number, eligibility criteria, and application form.
- GlaxoSmithKline (GSK) patient assistance program. Simply obtain a brief application by calling 1-866-PATIENT (728-4368) or logging onto www.bridgestoaccess.gsk.com. Fill out the form, then call 1-866-PATIENT to activate the attached coupon. Give the patient the coupon and a 60-day prescription for a GSK medication. The patient can fill the prescription at any pharmacy for a $10 co-payment. GSK then mails you 3-month supplies of the medication for 1 year.
Abigail Kay, MD
Instructor in psychiatry
Rajnish Mago, MD
Assistant professor of psychiatry
Director, mood disorders program
Thomas Jefferson University, Philadelphia, PA
Dr. Shelley Sellinger’s article “Helping indigent patients obtain medications” (Pearls, Current Psychiatry, April 2005) is helpful for psychiatrists working with patients who lack pharmacy benefits. Not having the information handy or believing the process is too cumbersome may deter some clinicians from using patient assistance programs.
We also suggest the following services:
- www.needymeds.com lists thousands of medications alphabetically (by brand or generic name). Each listing provides complete assistance program information, including the phone number, eligibility criteria, and application form.
- GlaxoSmithKline (GSK) patient assistance program. Simply obtain a brief application by calling 1-866-PATIENT (728-4368) or logging onto www.bridgestoaccess.gsk.com. Fill out the form, then call 1-866-PATIENT to activate the attached coupon. Give the patient the coupon and a 60-day prescription for a GSK medication. The patient can fill the prescription at any pharmacy for a $10 co-payment. GSK then mails you 3-month supplies of the medication for 1 year.
Abigail Kay, MD
Instructor in psychiatry
Rajnish Mago, MD
Assistant professor of psychiatry
Director, mood disorders program
Thomas Jefferson University, Philadelphia, PA
ADHD or bipolar, but not both
“What’s the best treatment for comorbid ADHD/bipolar mania?” by Drs. Nick C. Patel and Floyd R. Sallee (Current Psychiatry, April 2005) was well-written and offers excellent treatment guidelines. However, the idea that patients can have comorbid bipolar disorder and attention-deficit/hyperactivity disorder (ADHD) is a fallacy.
I challenge any colleague, from the leading expert to the most recent graduate, to present a bona fide case of “comorbid” ADHD/bipolar disorder. I can prove that only one diagnosis is correct because:
- Bipolar disorder is more heritable than other psychiatric illnesses. Many patients labeled as having “comorbid” bipolar disorder and ADHD have parents with bipolar disorder or schizophrenia or are in foster care and their biological parents’ histories are unknown.
- I’ve seen hundreds of patients enter full-blown psychosis after another clinician put them on amphetamines or antidepressants while being treated for ADHD.
- Bipolar disorder can explain any so-called ADHD symptom.
- ADHD does not include moodiness or predatory aggression.
Over 10 years, I have diagnosed three or four patients as having comorbid bipolar disorder and ADHD. After a few years and inpatient treatments, these patients proved the second diagnosis wrong. We can decrease costs and avoid patients’ suffering by refining diagnostic criteria.
Manuel Mota-Castillo, MD, medical director
The Grove Academy, Sanford, FL
and Lake Mary Psychiatric Services
Lake Mary, FL
Drs. Patel and Sallee respond
Dr. Mota-Castillo’s argument is most often stated from the opposite point of view that bipolar symptoms, particularly in patients age <10, are almost indistinguishable from those of ADHD. Our article did not—and cannot—address this controversy.
Because the evidence has been inconclusive, it is unclear if comorbid bipolar disorder and ADHD result from overlapping DSM-IV-TR diagnostic criteria, or whether two concurrent disorders exist. Suffice it to say that ADHD and bipolar disorder have many phenotypes and are both highly—but distinctly—heritable.
Overlapping symptoms may confound clinical diagnosis and result in “false positives” but may not account for most bipolar youths with comorbid ADHD. In one study,1 56% of subjects with both disorders maintained a bipolar disorder diagnosis when overlapping ADHD symptoms were subtracted.
Combination pharmacotherapy is needed because mood stabilizers do not treat attention and neurocognitive problems associated with ADHD. Therefore, a psychostimulant trial may help euthymic bipolar children and adolescents. In a recent placebo-controlled study by Scheffer et al,2 ADHD symptoms—as measured with the Clinical Global Impression of Improvement scale and based upon Conners’ Teachers and Parent Ratings—significantly improved among divalproex sodium responders receiving mixed amphetamine salts.
Dr. Mota-Castillo, however, brings up two important questions:
- Are childhood symptoms that result in ADHD diagnosis a prodromal manifestation of bipolar disorder in some patients? Data from the first 1,000 STEP-BD participants suggest that ADHD may be part of the developmental phenotype of bipolar disorder comorbidity. Participants with mood symptom onset before age 13 had higher rates of comorbid ADHD than did those whose mood symptoms surfaced later on.3
- Do psychostimulants hasten mood disorder onset in a child diagnosed with ADHD who has a high familial risk of a mood disorder? How these agents influence the course of bipolar disorder is unclear. DelBello et al4 reported that psychostimulant exposure may be a stressor in youths at risk for bipolar disorder, may progressively worsen affective symptoms over time, and may lead to earlier mood symptom onset.
Both questions need further exploration as the implications for clinical practice may be tremendous.
Results from numerous independent studies consistently suggest that patients can be diagnosed with comorbid bipolar disorder and ADHD. More research is needed, however, to solve this diagnostic conundrum.
Nick C. Patel, PharmD, PhD
Assistant professor
Departments of pharmacy practice and psychiatry
Floyd R. Sallee, MD, PhD
Professor, department of psychiatry
University of Cincinnati
1. Milberger S, Biederman J, Faraone SV, et al. Attention deficit hyperactivity disorder and comorbid disorders: issues of overlapping symptoms. Am J Psychiatry 1995;152:1793-9.
2. Scheffer RE, Kowatch RA, Carmody T, Rush AJ. Randomized, placebo-controlled trial of mixed amphetamine salts for symptoms of comorbid ADHD in pediatric bipolar disorder after mood stabilization with divalproex sodium. Am J Psychiatry 2005;162:58-64.
3. Perlis RH, Miyahara S, Marangell LB, et al. for the STEP-BD Investigators. Long-term implications of early onset in bipolar disorder: data from the first 1,000 participants in the systematic treatment enhancement program for bipolar disorder (STEP-BD). Biol Psychiatry 2004;55:875-81.
4. DelBello MP, Soutullo CA, Hendricks W, et al. Prior stimulant treatment in adolescents with bipolar disorder: association with age at onset. Bipolar Disord 2001;3:53-7.
“What’s the best treatment for comorbid ADHD/bipolar mania?” by Drs. Nick C. Patel and Floyd R. Sallee (Current Psychiatry, April 2005) was well-written and offers excellent treatment guidelines. However, the idea that patients can have comorbid bipolar disorder and attention-deficit/hyperactivity disorder (ADHD) is a fallacy.
I challenge any colleague, from the leading expert to the most recent graduate, to present a bona fide case of “comorbid” ADHD/bipolar disorder. I can prove that only one diagnosis is correct because:
- Bipolar disorder is more heritable than other psychiatric illnesses. Many patients labeled as having “comorbid” bipolar disorder and ADHD have parents with bipolar disorder or schizophrenia or are in foster care and their biological parents’ histories are unknown.
- I’ve seen hundreds of patients enter full-blown psychosis after another clinician put them on amphetamines or antidepressants while being treated for ADHD.
- Bipolar disorder can explain any so-called ADHD symptom.
- ADHD does not include moodiness or predatory aggression.
Over 10 years, I have diagnosed three or four patients as having comorbid bipolar disorder and ADHD. After a few years and inpatient treatments, these patients proved the second diagnosis wrong. We can decrease costs and avoid patients’ suffering by refining diagnostic criteria.
Manuel Mota-Castillo, MD, medical director
The Grove Academy, Sanford, FL
and Lake Mary Psychiatric Services
Lake Mary, FL
Drs. Patel and Sallee respond
Dr. Mota-Castillo’s argument is most often stated from the opposite point of view that bipolar symptoms, particularly in patients age <10, are almost indistinguishable from those of ADHD. Our article did not—and cannot—address this controversy.
Because the evidence has been inconclusive, it is unclear if comorbid bipolar disorder and ADHD result from overlapping DSM-IV-TR diagnostic criteria, or whether two concurrent disorders exist. Suffice it to say that ADHD and bipolar disorder have many phenotypes and are both highly—but distinctly—heritable.
Overlapping symptoms may confound clinical diagnosis and result in “false positives” but may not account for most bipolar youths with comorbid ADHD. In one study,1 56% of subjects with both disorders maintained a bipolar disorder diagnosis when overlapping ADHD symptoms were subtracted.
Combination pharmacotherapy is needed because mood stabilizers do not treat attention and neurocognitive problems associated with ADHD. Therefore, a psychostimulant trial may help euthymic bipolar children and adolescents. In a recent placebo-controlled study by Scheffer et al,2 ADHD symptoms—as measured with the Clinical Global Impression of Improvement scale and based upon Conners’ Teachers and Parent Ratings—significantly improved among divalproex sodium responders receiving mixed amphetamine salts.
Dr. Mota-Castillo, however, brings up two important questions:
- Are childhood symptoms that result in ADHD diagnosis a prodromal manifestation of bipolar disorder in some patients? Data from the first 1,000 STEP-BD participants suggest that ADHD may be part of the developmental phenotype of bipolar disorder comorbidity. Participants with mood symptom onset before age 13 had higher rates of comorbid ADHD than did those whose mood symptoms surfaced later on.3
- Do psychostimulants hasten mood disorder onset in a child diagnosed with ADHD who has a high familial risk of a mood disorder? How these agents influence the course of bipolar disorder is unclear. DelBello et al4 reported that psychostimulant exposure may be a stressor in youths at risk for bipolar disorder, may progressively worsen affective symptoms over time, and may lead to earlier mood symptom onset.
Both questions need further exploration as the implications for clinical practice may be tremendous.
Results from numerous independent studies consistently suggest that patients can be diagnosed with comorbid bipolar disorder and ADHD. More research is needed, however, to solve this diagnostic conundrum.
Nick C. Patel, PharmD, PhD
Assistant professor
Departments of pharmacy practice and psychiatry
Floyd R. Sallee, MD, PhD
Professor, department of psychiatry
University of Cincinnati
“What’s the best treatment for comorbid ADHD/bipolar mania?” by Drs. Nick C. Patel and Floyd R. Sallee (Current Psychiatry, April 2005) was well-written and offers excellent treatment guidelines. However, the idea that patients can have comorbid bipolar disorder and attention-deficit/hyperactivity disorder (ADHD) is a fallacy.
I challenge any colleague, from the leading expert to the most recent graduate, to present a bona fide case of “comorbid” ADHD/bipolar disorder. I can prove that only one diagnosis is correct because:
- Bipolar disorder is more heritable than other psychiatric illnesses. Many patients labeled as having “comorbid” bipolar disorder and ADHD have parents with bipolar disorder or schizophrenia or are in foster care and their biological parents’ histories are unknown.
- I’ve seen hundreds of patients enter full-blown psychosis after another clinician put them on amphetamines or antidepressants while being treated for ADHD.
- Bipolar disorder can explain any so-called ADHD symptom.
- ADHD does not include moodiness or predatory aggression.
Over 10 years, I have diagnosed three or four patients as having comorbid bipolar disorder and ADHD. After a few years and inpatient treatments, these patients proved the second diagnosis wrong. We can decrease costs and avoid patients’ suffering by refining diagnostic criteria.
Manuel Mota-Castillo, MD, medical director
The Grove Academy, Sanford, FL
and Lake Mary Psychiatric Services
Lake Mary, FL
Drs. Patel and Sallee respond
Dr. Mota-Castillo’s argument is most often stated from the opposite point of view that bipolar symptoms, particularly in patients age <10, are almost indistinguishable from those of ADHD. Our article did not—and cannot—address this controversy.
Because the evidence has been inconclusive, it is unclear if comorbid bipolar disorder and ADHD result from overlapping DSM-IV-TR diagnostic criteria, or whether two concurrent disorders exist. Suffice it to say that ADHD and bipolar disorder have many phenotypes and are both highly—but distinctly—heritable.
Overlapping symptoms may confound clinical diagnosis and result in “false positives” but may not account for most bipolar youths with comorbid ADHD. In one study,1 56% of subjects with both disorders maintained a bipolar disorder diagnosis when overlapping ADHD symptoms were subtracted.
Combination pharmacotherapy is needed because mood stabilizers do not treat attention and neurocognitive problems associated with ADHD. Therefore, a psychostimulant trial may help euthymic bipolar children and adolescents. In a recent placebo-controlled study by Scheffer et al,2 ADHD symptoms—as measured with the Clinical Global Impression of Improvement scale and based upon Conners’ Teachers and Parent Ratings—significantly improved among divalproex sodium responders receiving mixed amphetamine salts.
Dr. Mota-Castillo, however, brings up two important questions:
- Are childhood symptoms that result in ADHD diagnosis a prodromal manifestation of bipolar disorder in some patients? Data from the first 1,000 STEP-BD participants suggest that ADHD may be part of the developmental phenotype of bipolar disorder comorbidity. Participants with mood symptom onset before age 13 had higher rates of comorbid ADHD than did those whose mood symptoms surfaced later on.3
- Do psychostimulants hasten mood disorder onset in a child diagnosed with ADHD who has a high familial risk of a mood disorder? How these agents influence the course of bipolar disorder is unclear. DelBello et al4 reported that psychostimulant exposure may be a stressor in youths at risk for bipolar disorder, may progressively worsen affective symptoms over time, and may lead to earlier mood symptom onset.
Both questions need further exploration as the implications for clinical practice may be tremendous.
Results from numerous independent studies consistently suggest that patients can be diagnosed with comorbid bipolar disorder and ADHD. More research is needed, however, to solve this diagnostic conundrum.
Nick C. Patel, PharmD, PhD
Assistant professor
Departments of pharmacy practice and psychiatry
Floyd R. Sallee, MD, PhD
Professor, department of psychiatry
University of Cincinnati
1. Milberger S, Biederman J, Faraone SV, et al. Attention deficit hyperactivity disorder and comorbid disorders: issues of overlapping symptoms. Am J Psychiatry 1995;152:1793-9.
2. Scheffer RE, Kowatch RA, Carmody T, Rush AJ. Randomized, placebo-controlled trial of mixed amphetamine salts for symptoms of comorbid ADHD in pediatric bipolar disorder after mood stabilization with divalproex sodium. Am J Psychiatry 2005;162:58-64.
3. Perlis RH, Miyahara S, Marangell LB, et al. for the STEP-BD Investigators. Long-term implications of early onset in bipolar disorder: data from the first 1,000 participants in the systematic treatment enhancement program for bipolar disorder (STEP-BD). Biol Psychiatry 2004;55:875-81.
4. DelBello MP, Soutullo CA, Hendricks W, et al. Prior stimulant treatment in adolescents with bipolar disorder: association with age at onset. Bipolar Disord 2001;3:53-7.
1. Milberger S, Biederman J, Faraone SV, et al. Attention deficit hyperactivity disorder and comorbid disorders: issues of overlapping symptoms. Am J Psychiatry 1995;152:1793-9.
2. Scheffer RE, Kowatch RA, Carmody T, Rush AJ. Randomized, placebo-controlled trial of mixed amphetamine salts for symptoms of comorbid ADHD in pediatric bipolar disorder after mood stabilization with divalproex sodium. Am J Psychiatry 2005;162:58-64.
3. Perlis RH, Miyahara S, Marangell LB, et al. for the STEP-BD Investigators. Long-term implications of early onset in bipolar disorder: data from the first 1,000 participants in the systematic treatment enhancement program for bipolar disorder (STEP-BD). Biol Psychiatry 2004;55:875-81.
4. DelBello MP, Soutullo CA, Hendricks W, et al. Prior stimulant treatment in adolescents with bipolar disorder: association with age at onset. Bipolar Disord 2001;3:53-7.
Do ‘black boxes’ make demented patients safer?
Is the FDA being overly zealous with its “black box” warnings? The latest advisory—associating atypical antipsychotics with increased mortality among patients with dementia—joins another black box linking these drugs to potentially fatal diabetes. And, as of October, black boxes warn of “clinical worsening” and “suicidality” associated with using SSRI antidepressants in children and adolescents.
An FDA analysis of 5,111 demented patients in 16 trials found about a 1.6-fold increase in mortality among those receiving atypical antipsychotics. According to the Alzheimer’s Association, the risk of death is “real but small;” 1.5% to 2% of the patients receiving antipsychotics died, compared with 1% of those receiving placebo.
Atypical antipsychotics are useful—at times life-saving—for many agitated elderly patients, and this new labeling should not be used as the basis to withhold these drugs from patients who might benefit from them.
Of course, black boxes are not unique to psychotropics. The COX-2 inhibitor arthritis drugs and others recently have joined more than 200 drugs with these warning labels. What leads the FDA to dichotomize drugs into “black-boxed” or “not black-boxed?” And why do black boxes seem to be proliferating?
I think the reason is that the FDA has been criticized for not doing more to prevent adverse drug events and is feeling the pressure. If someone has an adverse event after taking a black-boxed drug, the FDA can now say something like, “I told you so.” This is, as far as I can tell, the same reason for the Department of Homeland Security’s color-coded terrorism threat levels. One could argue that the much-maligned five-level terror rating system (from green to red) is more rational than the FDA’s two-level system, black or not black.
Congress has been debating whether the terrorism threat system is useful or is unnecessarily alarming the public and making us less safe. We should be asking the same questions about the FDA’s black box system.

James Randolph Hillard, MD
Editor-in-Chief
James Randolph Hillard, MD
Editor-in-Chief
James Randolph Hillard, MD
Editor-in-Chief
Is the FDA being overly zealous with its “black box” warnings? The latest advisory—associating atypical antipsychotics with increased mortality among patients with dementia—joins another black box linking these drugs to potentially fatal diabetes. And, as of October, black boxes warn of “clinical worsening” and “suicidality” associated with using SSRI antidepressants in children and adolescents.
An FDA analysis of 5,111 demented patients in 16 trials found about a 1.6-fold increase in mortality among those receiving atypical antipsychotics. According to the Alzheimer’s Association, the risk of death is “real but small;” 1.5% to 2% of the patients receiving antipsychotics died, compared with 1% of those receiving placebo.
Atypical antipsychotics are useful—at times life-saving—for many agitated elderly patients, and this new labeling should not be used as the basis to withhold these drugs from patients who might benefit from them.
Of course, black boxes are not unique to psychotropics. The COX-2 inhibitor arthritis drugs and others recently have joined more than 200 drugs with these warning labels. What leads the FDA to dichotomize drugs into “black-boxed” or “not black-boxed?” And why do black boxes seem to be proliferating?
I think the reason is that the FDA has been criticized for not doing more to prevent adverse drug events and is feeling the pressure. If someone has an adverse event after taking a black-boxed drug, the FDA can now say something like, “I told you so.” This is, as far as I can tell, the same reason for the Department of Homeland Security’s color-coded terrorism threat levels. One could argue that the much-maligned five-level terror rating system (from green to red) is more rational than the FDA’s two-level system, black or not black.
Congress has been debating whether the terrorism threat system is useful or is unnecessarily alarming the public and making us less safe. We should be asking the same questions about the FDA’s black box system.
Is the FDA being overly zealous with its “black box” warnings? The latest advisory—associating atypical antipsychotics with increased mortality among patients with dementia—joins another black box linking these drugs to potentially fatal diabetes. And, as of October, black boxes warn of “clinical worsening” and “suicidality” associated with using SSRI antidepressants in children and adolescents.
An FDA analysis of 5,111 demented patients in 16 trials found about a 1.6-fold increase in mortality among those receiving atypical antipsychotics. According to the Alzheimer’s Association, the risk of death is “real but small;” 1.5% to 2% of the patients receiving antipsychotics died, compared with 1% of those receiving placebo.
Atypical antipsychotics are useful—at times life-saving—for many agitated elderly patients, and this new labeling should not be used as the basis to withhold these drugs from patients who might benefit from them.
Of course, black boxes are not unique to psychotropics. The COX-2 inhibitor arthritis drugs and others recently have joined more than 200 drugs with these warning labels. What leads the FDA to dichotomize drugs into “black-boxed” or “not black-boxed?” And why do black boxes seem to be proliferating?
I think the reason is that the FDA has been criticized for not doing more to prevent adverse drug events and is feeling the pressure. If someone has an adverse event after taking a black-boxed drug, the FDA can now say something like, “I told you so.” This is, as far as I can tell, the same reason for the Department of Homeland Security’s color-coded terrorism threat levels. One could argue that the much-maligned five-level terror rating system (from green to red) is more rational than the FDA’s two-level system, black or not black.
Congress has been debating whether the terrorism threat system is useful or is unnecessarily alarming the public and making us less safe. We should be asking the same questions about the FDA’s black box system.
Nothing more than feelings?
HISTORY: REPEAT OFFENDER
Mr. V, age 68, was incarcerated for 13 years for two separate pedophilia convictions. During that time, he passed numerous rehabilitative courses. With several years left on his sentence, he was paroled on condition that he undergo a bilateral orchiectomy.
Eight months later, Mr. V complained to his primary care physician that he could not have sex with his girlfriend, even after taking 50 mg of sildenafil, which he had obtained from a friend. He requested testosterone injections to allow him to have intercourse. After consulting an endocrinologist, the physician ordered Mr. V to undergo a psychiatric assessment before receiving testosterone. He was referred to our outpatient clinic.
During our evaluation, Mr. V described both pedophilia incidents. In the first, he had fondled a 14-year-old girl who was a friend of his family. He pled guilty to a charge of inappropriate sexual contact with a minor and was sentenced to 3 years in a state prison for sex offenders.
Less than 2 years after he was paroled, Mr. V said, he fondled his 12-year-old granddaughter. He said his daughter “should have known better” than to leave him home alone with the child. Again he was convicted of illegal sexual relations with a minor and sentenced to 10 years at the state hospital for the criminally insane.
As Mr. V describes his past offenses, we begin feeling tremendously uneasy. Although forthcoming, he blandly denies responsibility for either incident. He acknowledges that society views his actions as wrong, but he never indicates that he believes them to be wrong. At times he tries to normalize his behavior, saying “What man would have acted differently?”
Mr. V is polite and appropriate and promises to abide by our recommendation, yet he sees no reason for us to deny his request and no connection between his criminal record and the nature of his crimes or the terms of his parole. His denial and lack of insight are typical of convicted pedophiles (Box 1).
Most pedophiles are unemployed men ages 30 to 42.1 In one clinical study, 70% of convicted pedophiles reported fewer than 10 victims, and 23% reported 10 to 40 victims.1 Conte et al2 found that the average number of victims per offender may exceed 7.
Poor insight and denial are common among pedophiles. In one study that explored the relationship between denial of hostility and psychopathology, 37 of 82 patients denied the charges against them.3 The study’s authors state that their data “support the contention that alleged sex offenders’ self-reports and their scores on obvious-item hostility inventories are highly suspect and should not be accepted at face value.”
During evaluation, a sex offender who minimizes his psychopathology is less likely to admit to hostility, whereas those who exaggerate psychopathology usually acknowledge more hostility. In one study,3 no offenders who denied charges acknowledged psychopathology, but offenders who denied allegations admitted to less hostility than those who did acknowledge them.
The authors’ observations
Anyone evaluating Mr. V would be inclined to treat or dismiss him, or to suppress his or her feelings to avoid prejudice.
Treat or dismiss. As physicians, we are trained to “First, do no harm.” In this case, however, we must consider who could be harmed by treatment or dismissal.
“First, do no harm” is usually taken to mean “no harm to the patient” but could also be interpreted as “no harm to society.” Even if testosterone treatment did not physically harm Mr. V, activating his sex drive could endanger society by spurring him on to molest another child (Box 2). The treatment could also harm Mr. V by making it easier for him to violate parole.
Although failure to treat Mr. V’s sexual dysfunction would likely pose no harm to society, not assessing him might endanger society by clearing the path toward this treatment.
Sexual abuse of children and adolescents is common but underreported.4
The National Crime Victimization Survey estimates that 110,000 sexual assaults in 1996 involved victims ≤age 12, yet only one-third of these assaults were reported to police.5 Data from law enforcement agencies in 12 states indicate that 67% of victims who reported a sexual assault were age 6
When treating patients such as Mr. V, we must not dismiss our feelings—however uncomfortable or unprofessional they might seem—so that we can manage them appropriately. Don’t be ashamed of your feelings—or at least be aware of your shame.
In such cases, these important steps can minimize the risk of compromising treatment or assessment:
- Be aware of your feelings. Reflecting on countertransference after the session, either alone or with other therapists, can help you recognize your feelings.
- Seek peer supervision when evaluating a patient such as Mr. V to help identify potential “blind spots.”
- Be aware of your limitations. Hubris is among a therapist’s most serious potential pitfalls. We all have strengths and weaknesses and should be mindful of them.
The authors’ observations
We took a passive-neutral stance. Sitting with Mr. V without deciding a course of action gave us time to assess our own reactions and limitations and how they might influence our actions.
CONSULTATION: OTHER OPINIONS
The examining psychiatrist (a psychiatric resident) sought advice from an experienced geriatric psychiatrist, a neuropsychologist, and other residents. We discussed our countertransference toward Mr. V and provided mutual supervision. We then acknowledged that none of us had expertise in treating pedophiles and that treating an unfamiliar mental condition would be unethical.
The authors’ observations
In requesting other opinions, we also weighed these important questions:
Is Mr. V violating parole by requesting testosterone injections and taking (unprescribed) sildenafil? We felt we could not rightfully answer this question, since our expertise in the standard of care for patients such as Mr. V was insufficient and any recommendation would be ill-informed.
Sildenafil use is fairly common among convicted sex offenders, as evidenced by the recent controversy over Medicaid providing the drug to this group (see Related resources).
Assuming the testosterone injections promote intercourse, would they increase Mr. V’s arousal? Hall found that offenders who can voluntarily and completely inhibit sexual arousal are less deviant when not attempting to inhibit arousal than are those who cannot completely inhibit arousal.8
Hall, however, urges clinicians to consider variables that influence sexual response before determining how arousal affects an offender’s behavior. With no objective measure of sexual arousal, it is unclear whether increasing Mr. V’s testosterone would heighten it—and his potential threat to society.
The Abel Assessment of Sexual Interest was devised to determine sexual pathology, but evidence suggests this test is clinically unreliable.
Would enhancing Mr. V’s arousal increase his risk of recidivism? Although some studies have found that castration decreases a sex offender’s sexual activity, evidence suggests that sexual responsiveness after castration varies considerably. Heim found that:
- 31% of castrates could still have intercourse
- rapists are more sexually active than pedophiles after castration
- men ages 46 to 59 experience a greater reduction in sexual behavior than do men age 9
What standard of care applies to Mr. V? Treating pedophilia is difficult and poorly understood. Psychotherapy is considered an adjunct to medication or surgery. Surgical interventions are akin to punishment, whereas medications—well-studied and often augmented with psychotherapy—are associated with high recidivism rates.11,14
Surgery. Orchiectomy is by far the most common surgical intervention. Experimental procedures have targeted stereotaxic ablation of specific parts of the brain, usually the hypothalamus or amygdala, but these techniques have not been adequately studied in humans.11 Even so, testosterone therapy can restore sexual function after castration.10
Medications. Antiandrogens such as medroxy-progesterone acetate (MPA) inhibit intracellular uptake of androgens (such as testosterone) by blocking their binding to the receptor.12 MPA is most frequently used in the United States.
Long-acting analogs of gonadotropin-releasing hormone (GnRH), such as leuprolide, nafarelin, goserelin, and triptorelin, have shown efficacy in early studies.12 These agents down-regulate gonadotroph cells, inducing severe but reversible hypogonadism with few other side effects.
Although decreased libido is a common side effect of selective serotonin reuptake inhibitors (SSRIs), use of these agents to reduce sex drive in convicted pedophiles has not been studied. Because onset of decreased libido with SSRI use is unpredictable, we cannot recommend their use to reduce sex drive in convicted offenders.
Psychotherapy. Power14 nicely outlines the elements of psychotherapy for pedophilia:
- explanation and education
- manipulating the environment
- suggestion, including hypnosis and persuasion
- superficial analysis
- deep-transference analysis
- sublimation.
Stone et al10 draw several germane conclusions:
- Sentencing laws are often unclear or do not take into account scientific research on pedophilia. For example, psychological testing often is not ordered before a treatment is mandated, even though knowing the patient’s psychological profile and the nature of his predilections are crucial to treatment and prognosis.12
- Many laws do not suggest an instrument of implementation. For example, most laws that mandate a patient evaluation do not specify whether a licensed psychiatrist, psychologist, or other clinician should evaluate the patient.
- Many laws directed against pedophilia are punitive in nature. Mandated treatment—or the informed consent that precedes it—is often inadequate,10 and physicians can be held liable in either case. However, we could not determine the liability that could result from enhancing a convicted pedophile’s libido.
REFERRAL: TREATMENT ADVICE
We referred Mr. V back to his primary care physician and advised the doctor to:
- discuss the testosterone treatment request with physicians who treated Mr. V at the state prison
- call our hospital’s attorney to investigate the legal implications of treating Mr. V.
- Sex offenders get Medicaid-paid Viagra. Associated Press May 22, 2005. http://msnbc.msn.com/id/7946129/.
- Conte JR, Wolf S, Smith T. What sexual offenders tell us about prevention strategies. Child Abuse Negl 1989;13:293-301.
- U.S. Department of Justice, Bureau of Justice Statistics. Statistics on sex offenders and victims. www.ojp.usdoj.gov/bjs/abstract/saycrle.htm.
- Goserelin • Zoladex
- Leuprolide • Eligard, others
- Medroxyprogesterone acetate • Depo-Provera, others
- Nafarelin • Synarel
- Sildenafil • Viagra
- Triptorelin • Trelstar Depot
The authors thank Cynthia Meyer, chief librarian, VA Hospital, Fresno, CA, for her help with researching this article.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Elliott M, Browne K, Kilcoyne J. Child sexual abuse prevention: what offenders tell us. J Sex Marital Ther 2002;28:211-8.
2. Conte JR, Wolf S, Smith T. What sexual offenders tell us about prevention strategies. Child Abuse Negl 1989;13:293-301.
3. Wasyliw OE, Grossman LS, Haywood TW. Denial of hostility and psychopathology in the evaluation of child molestation. J Pers Assess 1994;63:185-90.
4. Kempe CH. Sexual abuse, another hidden pediatric problem: the 1977 C. Anderson Aldrich lecture. Pediatrics 1978;62:382-9.
5. Ringel C. Criminal victimization 1996: changes 1995-96 with trends 1993-96. BJS Bulletin, NCJ 165812, November 1997.
6. Snyder HN. Sexual assault of young children as reported to law enforcement: victim, incident, and offender characteristics. U.S. Department of Justice, Office of Justice Programs, Bureau of Justice Statistics, July 2000. Available at: http://www.ojp.usdoj.gov/bjs/cvict_c.htm#relate. Accessed June 3, 2005.
7. Gabbard GO. Psychodynamic psychiatry in clinical practice (3rd ed). Washington, DC: American Psychiatric Press; 2000.
8. Hall GC. Sexual arousal as a function of physiological and cognitive variables in a sexual offender population. Arch Sex Behav 1991;20:359-69.
9. Heim N. Sexual behavior of castrated sex offenders. Arch Sex Behav 1981;10:11-19.
10. Stone TH, Winslade WJ, Klugman CM. Sex offenders, sentencing laws and pharmaceutical treatment: a prescription for failure. Behav Sci Law 2000;18:83-110.
11. Freund K. Therapeutic sex drive reduction. Acta Psychiatr Scand Suppl 1980;287:5-38.
12. Rosler A, Witztum E. Pharmacotherapy of paraphilias in the next millennium. Behav Sci Law 2000;18:43-56.
13. Winslade W, Stone TH, Smith-Bell M, Webb DM. Castrating pedophiles convicted of sex offenses against children: new treatment or old punishment? SMU Law Rev 1998;51:349-411.
14. Power DJ. Paedophilia. Practitioner 1977;218:805-11.
HISTORY: REPEAT OFFENDER
Mr. V, age 68, was incarcerated for 13 years for two separate pedophilia convictions. During that time, he passed numerous rehabilitative courses. With several years left on his sentence, he was paroled on condition that he undergo a bilateral orchiectomy.
Eight months later, Mr. V complained to his primary care physician that he could not have sex with his girlfriend, even after taking 50 mg of sildenafil, which he had obtained from a friend. He requested testosterone injections to allow him to have intercourse. After consulting an endocrinologist, the physician ordered Mr. V to undergo a psychiatric assessment before receiving testosterone. He was referred to our outpatient clinic.
During our evaluation, Mr. V described both pedophilia incidents. In the first, he had fondled a 14-year-old girl who was a friend of his family. He pled guilty to a charge of inappropriate sexual contact with a minor and was sentenced to 3 years in a state prison for sex offenders.
Less than 2 years after he was paroled, Mr. V said, he fondled his 12-year-old granddaughter. He said his daughter “should have known better” than to leave him home alone with the child. Again he was convicted of illegal sexual relations with a minor and sentenced to 10 years at the state hospital for the criminally insane.
As Mr. V describes his past offenses, we begin feeling tremendously uneasy. Although forthcoming, he blandly denies responsibility for either incident. He acknowledges that society views his actions as wrong, but he never indicates that he believes them to be wrong. At times he tries to normalize his behavior, saying “What man would have acted differently?”
Mr. V is polite and appropriate and promises to abide by our recommendation, yet he sees no reason for us to deny his request and no connection between his criminal record and the nature of his crimes or the terms of his parole. His denial and lack of insight are typical of convicted pedophiles (Box 1).
Most pedophiles are unemployed men ages 30 to 42.1 In one clinical study, 70% of convicted pedophiles reported fewer than 10 victims, and 23% reported 10 to 40 victims.1 Conte et al2 found that the average number of victims per offender may exceed 7.
Poor insight and denial are common among pedophiles. In one study that explored the relationship between denial of hostility and psychopathology, 37 of 82 patients denied the charges against them.3 The study’s authors state that their data “support the contention that alleged sex offenders’ self-reports and their scores on obvious-item hostility inventories are highly suspect and should not be accepted at face value.”
During evaluation, a sex offender who minimizes his psychopathology is less likely to admit to hostility, whereas those who exaggerate psychopathology usually acknowledge more hostility. In one study,3 no offenders who denied charges acknowledged psychopathology, but offenders who denied allegations admitted to less hostility than those who did acknowledge them.
The authors’ observations
Anyone evaluating Mr. V would be inclined to treat or dismiss him, or to suppress his or her feelings to avoid prejudice.
Treat or dismiss. As physicians, we are trained to “First, do no harm.” In this case, however, we must consider who could be harmed by treatment or dismissal.
“First, do no harm” is usually taken to mean “no harm to the patient” but could also be interpreted as “no harm to society.” Even if testosterone treatment did not physically harm Mr. V, activating his sex drive could endanger society by spurring him on to molest another child (Box 2). The treatment could also harm Mr. V by making it easier for him to violate parole.
Although failure to treat Mr. V’s sexual dysfunction would likely pose no harm to society, not assessing him might endanger society by clearing the path toward this treatment.
Sexual abuse of children and adolescents is common but underreported.4
The National Crime Victimization Survey estimates that 110,000 sexual assaults in 1996 involved victims ≤age 12, yet only one-third of these assaults were reported to police.5 Data from law enforcement agencies in 12 states indicate that 67% of victims who reported a sexual assault were age 6
When treating patients such as Mr. V, we must not dismiss our feelings—however uncomfortable or unprofessional they might seem—so that we can manage them appropriately. Don’t be ashamed of your feelings—or at least be aware of your shame.
In such cases, these important steps can minimize the risk of compromising treatment or assessment:
- Be aware of your feelings. Reflecting on countertransference after the session, either alone or with other therapists, can help you recognize your feelings.
- Seek peer supervision when evaluating a patient such as Mr. V to help identify potential “blind spots.”
- Be aware of your limitations. Hubris is among a therapist’s most serious potential pitfalls. We all have strengths and weaknesses and should be mindful of them.
The authors’ observations
We took a passive-neutral stance. Sitting with Mr. V without deciding a course of action gave us time to assess our own reactions and limitations and how they might influence our actions.
CONSULTATION: OTHER OPINIONS
The examining psychiatrist (a psychiatric resident) sought advice from an experienced geriatric psychiatrist, a neuropsychologist, and other residents. We discussed our countertransference toward Mr. V and provided mutual supervision. We then acknowledged that none of us had expertise in treating pedophiles and that treating an unfamiliar mental condition would be unethical.
The authors’ observations
In requesting other opinions, we also weighed these important questions:
Is Mr. V violating parole by requesting testosterone injections and taking (unprescribed) sildenafil? We felt we could not rightfully answer this question, since our expertise in the standard of care for patients such as Mr. V was insufficient and any recommendation would be ill-informed.
Sildenafil use is fairly common among convicted sex offenders, as evidenced by the recent controversy over Medicaid providing the drug to this group (see Related resources).
Assuming the testosterone injections promote intercourse, would they increase Mr. V’s arousal? Hall found that offenders who can voluntarily and completely inhibit sexual arousal are less deviant when not attempting to inhibit arousal than are those who cannot completely inhibit arousal.8
Hall, however, urges clinicians to consider variables that influence sexual response before determining how arousal affects an offender’s behavior. With no objective measure of sexual arousal, it is unclear whether increasing Mr. V’s testosterone would heighten it—and his potential threat to society.
The Abel Assessment of Sexual Interest was devised to determine sexual pathology, but evidence suggests this test is clinically unreliable.
Would enhancing Mr. V’s arousal increase his risk of recidivism? Although some studies have found that castration decreases a sex offender’s sexual activity, evidence suggests that sexual responsiveness after castration varies considerably. Heim found that:
- 31% of castrates could still have intercourse
- rapists are more sexually active than pedophiles after castration
- men ages 46 to 59 experience a greater reduction in sexual behavior than do men age 9
What standard of care applies to Mr. V? Treating pedophilia is difficult and poorly understood. Psychotherapy is considered an adjunct to medication or surgery. Surgical interventions are akin to punishment, whereas medications—well-studied and often augmented with psychotherapy—are associated with high recidivism rates.11,14
Surgery. Orchiectomy is by far the most common surgical intervention. Experimental procedures have targeted stereotaxic ablation of specific parts of the brain, usually the hypothalamus or amygdala, but these techniques have not been adequately studied in humans.11 Even so, testosterone therapy can restore sexual function after castration.10
Medications. Antiandrogens such as medroxy-progesterone acetate (MPA) inhibit intracellular uptake of androgens (such as testosterone) by blocking their binding to the receptor.12 MPA is most frequently used in the United States.
Long-acting analogs of gonadotropin-releasing hormone (GnRH), such as leuprolide, nafarelin, goserelin, and triptorelin, have shown efficacy in early studies.12 These agents down-regulate gonadotroph cells, inducing severe but reversible hypogonadism with few other side effects.
Although decreased libido is a common side effect of selective serotonin reuptake inhibitors (SSRIs), use of these agents to reduce sex drive in convicted pedophiles has not been studied. Because onset of decreased libido with SSRI use is unpredictable, we cannot recommend their use to reduce sex drive in convicted offenders.
Psychotherapy. Power14 nicely outlines the elements of psychotherapy for pedophilia:
- explanation and education
- manipulating the environment
- suggestion, including hypnosis and persuasion
- superficial analysis
- deep-transference analysis
- sublimation.
Stone et al10 draw several germane conclusions:
- Sentencing laws are often unclear or do not take into account scientific research on pedophilia. For example, psychological testing often is not ordered before a treatment is mandated, even though knowing the patient’s psychological profile and the nature of his predilections are crucial to treatment and prognosis.12
- Many laws do not suggest an instrument of implementation. For example, most laws that mandate a patient evaluation do not specify whether a licensed psychiatrist, psychologist, or other clinician should evaluate the patient.
- Many laws directed against pedophilia are punitive in nature. Mandated treatment—or the informed consent that precedes it—is often inadequate,10 and physicians can be held liable in either case. However, we could not determine the liability that could result from enhancing a convicted pedophile’s libido.
REFERRAL: TREATMENT ADVICE
We referred Mr. V back to his primary care physician and advised the doctor to:
- discuss the testosterone treatment request with physicians who treated Mr. V at the state prison
- call our hospital’s attorney to investigate the legal implications of treating Mr. V.
- Sex offenders get Medicaid-paid Viagra. Associated Press May 22, 2005. http://msnbc.msn.com/id/7946129/.
- Conte JR, Wolf S, Smith T. What sexual offenders tell us about prevention strategies. Child Abuse Negl 1989;13:293-301.
- U.S. Department of Justice, Bureau of Justice Statistics. Statistics on sex offenders and victims. www.ojp.usdoj.gov/bjs/abstract/saycrle.htm.
- Goserelin • Zoladex
- Leuprolide • Eligard, others
- Medroxyprogesterone acetate • Depo-Provera, others
- Nafarelin • Synarel
- Sildenafil • Viagra
- Triptorelin • Trelstar Depot
The authors thank Cynthia Meyer, chief librarian, VA Hospital, Fresno, CA, for her help with researching this article.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
HISTORY: REPEAT OFFENDER
Mr. V, age 68, was incarcerated for 13 years for two separate pedophilia convictions. During that time, he passed numerous rehabilitative courses. With several years left on his sentence, he was paroled on condition that he undergo a bilateral orchiectomy.
Eight months later, Mr. V complained to his primary care physician that he could not have sex with his girlfriend, even after taking 50 mg of sildenafil, which he had obtained from a friend. He requested testosterone injections to allow him to have intercourse. After consulting an endocrinologist, the physician ordered Mr. V to undergo a psychiatric assessment before receiving testosterone. He was referred to our outpatient clinic.
During our evaluation, Mr. V described both pedophilia incidents. In the first, he had fondled a 14-year-old girl who was a friend of his family. He pled guilty to a charge of inappropriate sexual contact with a minor and was sentenced to 3 years in a state prison for sex offenders.
Less than 2 years after he was paroled, Mr. V said, he fondled his 12-year-old granddaughter. He said his daughter “should have known better” than to leave him home alone with the child. Again he was convicted of illegal sexual relations with a minor and sentenced to 10 years at the state hospital for the criminally insane.
As Mr. V describes his past offenses, we begin feeling tremendously uneasy. Although forthcoming, he blandly denies responsibility for either incident. He acknowledges that society views his actions as wrong, but he never indicates that he believes them to be wrong. At times he tries to normalize his behavior, saying “What man would have acted differently?”
Mr. V is polite and appropriate and promises to abide by our recommendation, yet he sees no reason for us to deny his request and no connection between his criminal record and the nature of his crimes or the terms of his parole. His denial and lack of insight are typical of convicted pedophiles (Box 1).
Most pedophiles are unemployed men ages 30 to 42.1 In one clinical study, 70% of convicted pedophiles reported fewer than 10 victims, and 23% reported 10 to 40 victims.1 Conte et al2 found that the average number of victims per offender may exceed 7.
Poor insight and denial are common among pedophiles. In one study that explored the relationship between denial of hostility and psychopathology, 37 of 82 patients denied the charges against them.3 The study’s authors state that their data “support the contention that alleged sex offenders’ self-reports and their scores on obvious-item hostility inventories are highly suspect and should not be accepted at face value.”
During evaluation, a sex offender who minimizes his psychopathology is less likely to admit to hostility, whereas those who exaggerate psychopathology usually acknowledge more hostility. In one study,3 no offenders who denied charges acknowledged psychopathology, but offenders who denied allegations admitted to less hostility than those who did acknowledge them.
The authors’ observations
Anyone evaluating Mr. V would be inclined to treat or dismiss him, or to suppress his or her feelings to avoid prejudice.
Treat or dismiss. As physicians, we are trained to “First, do no harm.” In this case, however, we must consider who could be harmed by treatment or dismissal.
“First, do no harm” is usually taken to mean “no harm to the patient” but could also be interpreted as “no harm to society.” Even if testosterone treatment did not physically harm Mr. V, activating his sex drive could endanger society by spurring him on to molest another child (Box 2). The treatment could also harm Mr. V by making it easier for him to violate parole.
Although failure to treat Mr. V’s sexual dysfunction would likely pose no harm to society, not assessing him might endanger society by clearing the path toward this treatment.
Sexual abuse of children and adolescents is common but underreported.4
The National Crime Victimization Survey estimates that 110,000 sexual assaults in 1996 involved victims ≤age 12, yet only one-third of these assaults were reported to police.5 Data from law enforcement agencies in 12 states indicate that 67% of victims who reported a sexual assault were age 6
When treating patients such as Mr. V, we must not dismiss our feelings—however uncomfortable or unprofessional they might seem—so that we can manage them appropriately. Don’t be ashamed of your feelings—or at least be aware of your shame.
In such cases, these important steps can minimize the risk of compromising treatment or assessment:
- Be aware of your feelings. Reflecting on countertransference after the session, either alone or with other therapists, can help you recognize your feelings.
- Seek peer supervision when evaluating a patient such as Mr. V to help identify potential “blind spots.”
- Be aware of your limitations. Hubris is among a therapist’s most serious potential pitfalls. We all have strengths and weaknesses and should be mindful of them.
The authors’ observations
We took a passive-neutral stance. Sitting with Mr. V without deciding a course of action gave us time to assess our own reactions and limitations and how they might influence our actions.
CONSULTATION: OTHER OPINIONS
The examining psychiatrist (a psychiatric resident) sought advice from an experienced geriatric psychiatrist, a neuropsychologist, and other residents. We discussed our countertransference toward Mr. V and provided mutual supervision. We then acknowledged that none of us had expertise in treating pedophiles and that treating an unfamiliar mental condition would be unethical.
The authors’ observations
In requesting other opinions, we also weighed these important questions:
Is Mr. V violating parole by requesting testosterone injections and taking (unprescribed) sildenafil? We felt we could not rightfully answer this question, since our expertise in the standard of care for patients such as Mr. V was insufficient and any recommendation would be ill-informed.
Sildenafil use is fairly common among convicted sex offenders, as evidenced by the recent controversy over Medicaid providing the drug to this group (see Related resources).
Assuming the testosterone injections promote intercourse, would they increase Mr. V’s arousal? Hall found that offenders who can voluntarily and completely inhibit sexual arousal are less deviant when not attempting to inhibit arousal than are those who cannot completely inhibit arousal.8
Hall, however, urges clinicians to consider variables that influence sexual response before determining how arousal affects an offender’s behavior. With no objective measure of sexual arousal, it is unclear whether increasing Mr. V’s testosterone would heighten it—and his potential threat to society.
The Abel Assessment of Sexual Interest was devised to determine sexual pathology, but evidence suggests this test is clinically unreliable.
Would enhancing Mr. V’s arousal increase his risk of recidivism? Although some studies have found that castration decreases a sex offender’s sexual activity, evidence suggests that sexual responsiveness after castration varies considerably. Heim found that:
- 31% of castrates could still have intercourse
- rapists are more sexually active than pedophiles after castration
- men ages 46 to 59 experience a greater reduction in sexual behavior than do men age 9
What standard of care applies to Mr. V? Treating pedophilia is difficult and poorly understood. Psychotherapy is considered an adjunct to medication or surgery. Surgical interventions are akin to punishment, whereas medications—well-studied and often augmented with psychotherapy—are associated with high recidivism rates.11,14
Surgery. Orchiectomy is by far the most common surgical intervention. Experimental procedures have targeted stereotaxic ablation of specific parts of the brain, usually the hypothalamus or amygdala, but these techniques have not been adequately studied in humans.11 Even so, testosterone therapy can restore sexual function after castration.10
Medications. Antiandrogens such as medroxy-progesterone acetate (MPA) inhibit intracellular uptake of androgens (such as testosterone) by blocking their binding to the receptor.12 MPA is most frequently used in the United States.
Long-acting analogs of gonadotropin-releasing hormone (GnRH), such as leuprolide, nafarelin, goserelin, and triptorelin, have shown efficacy in early studies.12 These agents down-regulate gonadotroph cells, inducing severe but reversible hypogonadism with few other side effects.
Although decreased libido is a common side effect of selective serotonin reuptake inhibitors (SSRIs), use of these agents to reduce sex drive in convicted pedophiles has not been studied. Because onset of decreased libido with SSRI use is unpredictable, we cannot recommend their use to reduce sex drive in convicted offenders.
Psychotherapy. Power14 nicely outlines the elements of psychotherapy for pedophilia:
- explanation and education
- manipulating the environment
- suggestion, including hypnosis and persuasion
- superficial analysis
- deep-transference analysis
- sublimation.
Stone et al10 draw several germane conclusions:
- Sentencing laws are often unclear or do not take into account scientific research on pedophilia. For example, psychological testing often is not ordered before a treatment is mandated, even though knowing the patient’s psychological profile and the nature of his predilections are crucial to treatment and prognosis.12
- Many laws do not suggest an instrument of implementation. For example, most laws that mandate a patient evaluation do not specify whether a licensed psychiatrist, psychologist, or other clinician should evaluate the patient.
- Many laws directed against pedophilia are punitive in nature. Mandated treatment—or the informed consent that precedes it—is often inadequate,10 and physicians can be held liable in either case. However, we could not determine the liability that could result from enhancing a convicted pedophile’s libido.
REFERRAL: TREATMENT ADVICE
We referred Mr. V back to his primary care physician and advised the doctor to:
- discuss the testosterone treatment request with physicians who treated Mr. V at the state prison
- call our hospital’s attorney to investigate the legal implications of treating Mr. V.
- Sex offenders get Medicaid-paid Viagra. Associated Press May 22, 2005. http://msnbc.msn.com/id/7946129/.
- Conte JR, Wolf S, Smith T. What sexual offenders tell us about prevention strategies. Child Abuse Negl 1989;13:293-301.
- U.S. Department of Justice, Bureau of Justice Statistics. Statistics on sex offenders and victims. www.ojp.usdoj.gov/bjs/abstract/saycrle.htm.
- Goserelin • Zoladex
- Leuprolide • Eligard, others
- Medroxyprogesterone acetate • Depo-Provera, others
- Nafarelin • Synarel
- Sildenafil • Viagra
- Triptorelin • Trelstar Depot
The authors thank Cynthia Meyer, chief librarian, VA Hospital, Fresno, CA, for her help with researching this article.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Elliott M, Browne K, Kilcoyne J. Child sexual abuse prevention: what offenders tell us. J Sex Marital Ther 2002;28:211-8.
2. Conte JR, Wolf S, Smith T. What sexual offenders tell us about prevention strategies. Child Abuse Negl 1989;13:293-301.
3. Wasyliw OE, Grossman LS, Haywood TW. Denial of hostility and psychopathology in the evaluation of child molestation. J Pers Assess 1994;63:185-90.
4. Kempe CH. Sexual abuse, another hidden pediatric problem: the 1977 C. Anderson Aldrich lecture. Pediatrics 1978;62:382-9.
5. Ringel C. Criminal victimization 1996: changes 1995-96 with trends 1993-96. BJS Bulletin, NCJ 165812, November 1997.
6. Snyder HN. Sexual assault of young children as reported to law enforcement: victim, incident, and offender characteristics. U.S. Department of Justice, Office of Justice Programs, Bureau of Justice Statistics, July 2000. Available at: http://www.ojp.usdoj.gov/bjs/cvict_c.htm#relate. Accessed June 3, 2005.
7. Gabbard GO. Psychodynamic psychiatry in clinical practice (3rd ed). Washington, DC: American Psychiatric Press; 2000.
8. Hall GC. Sexual arousal as a function of physiological and cognitive variables in a sexual offender population. Arch Sex Behav 1991;20:359-69.
9. Heim N. Sexual behavior of castrated sex offenders. Arch Sex Behav 1981;10:11-19.
10. Stone TH, Winslade WJ, Klugman CM. Sex offenders, sentencing laws and pharmaceutical treatment: a prescription for failure. Behav Sci Law 2000;18:83-110.
11. Freund K. Therapeutic sex drive reduction. Acta Psychiatr Scand Suppl 1980;287:5-38.
12. Rosler A, Witztum E. Pharmacotherapy of paraphilias in the next millennium. Behav Sci Law 2000;18:43-56.
13. Winslade W, Stone TH, Smith-Bell M, Webb DM. Castrating pedophiles convicted of sex offenses against children: new treatment or old punishment? SMU Law Rev 1998;51:349-411.
14. Power DJ. Paedophilia. Practitioner 1977;218:805-11.
1. Elliott M, Browne K, Kilcoyne J. Child sexual abuse prevention: what offenders tell us. J Sex Marital Ther 2002;28:211-8.
2. Conte JR, Wolf S, Smith T. What sexual offenders tell us about prevention strategies. Child Abuse Negl 1989;13:293-301.
3. Wasyliw OE, Grossman LS, Haywood TW. Denial of hostility and psychopathology in the evaluation of child molestation. J Pers Assess 1994;63:185-90.
4. Kempe CH. Sexual abuse, another hidden pediatric problem: the 1977 C. Anderson Aldrich lecture. Pediatrics 1978;62:382-9.
5. Ringel C. Criminal victimization 1996: changes 1995-96 with trends 1993-96. BJS Bulletin, NCJ 165812, November 1997.
6. Snyder HN. Sexual assault of young children as reported to law enforcement: victim, incident, and offender characteristics. U.S. Department of Justice, Office of Justice Programs, Bureau of Justice Statistics, July 2000. Available at: http://www.ojp.usdoj.gov/bjs/cvict_c.htm#relate. Accessed June 3, 2005.
7. Gabbard GO. Psychodynamic psychiatry in clinical practice (3rd ed). Washington, DC: American Psychiatric Press; 2000.
8. Hall GC. Sexual arousal as a function of physiological and cognitive variables in a sexual offender population. Arch Sex Behav 1991;20:359-69.
9. Heim N. Sexual behavior of castrated sex offenders. Arch Sex Behav 1981;10:11-19.
10. Stone TH, Winslade WJ, Klugman CM. Sex offenders, sentencing laws and pharmaceutical treatment: a prescription for failure. Behav Sci Law 2000;18:83-110.
11. Freund K. Therapeutic sex drive reduction. Acta Psychiatr Scand Suppl 1980;287:5-38.
12. Rosler A, Witztum E. Pharmacotherapy of paraphilias in the next millennium. Behav Sci Law 2000;18:43-56.
13. Winslade W, Stone TH, Smith-Bell M, Webb DM. Castrating pedophiles convicted of sex offenses against children: new treatment or old punishment? SMU Law Rev 1998;51:349-411.
14. Power DJ. Paedophilia. Practitioner 1977;218:805-11.
New Investigators: What makes aripiprazole the ‘different’ antipsychotic
Aripiprazole, the first FDA-approved partial dopamine agonist, causes few side effects when used to treat schizophrenia or acute bipolar mania. This relatively safe profile in approved uses has led clinicians to try aripiprazole for off-label uses as well, though evidence of the drug’s efficacy and safety in other psychiatric conditions is limited (Box 1).1-7 Because this practice may involve unknown risks, this article:
- reviews aripiprazole’s role in correcting dopaminergic dysfunction in patients with schizophrenia
- cites adverse effects reported with aripiprazole use and discusses concerns about its off-label use.
Aripiprazole shows clear efficacy for treating acute mania and schizophrenia’s negative and positive symptoms, but its effectiveness and safety in other psychiatric illnesses is unknown. Even so, it is being used to treat psychotic unipolar and bipolar depression, attention-deficit/hyperactivity disorder, oppositional defiant disorder, and pervasive developmental disorders in childrenand adults.
Dopamine differences. Do not assume that aripiprazole’s safety and effectiveness in treating schizophrenia translates to other psychiatric conditions. Dopamine dysfunction patterns differ in persons with and without schizophrenia; therefore, aripiprazole’s regional and functional selectivity at dopamine receptors—and treatment response and tolerability—is also likely to differ.
Antipsychotic differences. Aripiprazole is unlike other psychotropics and cannot be assumed to have similar therapeutic effects. The agent’s dopamine agonist and antagonist properties hinge on regional dopamine concentrations as well as the drug itself.
Dopaminergic risks in combination. Numerous drugs modulate dopamine function, and switching and combining drugs places patients at unknown risk of dopaminergic side effects with aripiprazole. Adding an antagonist or a low-dose antagonist combination with aripiprazole may increase competition for dopamine receptors and modify its intrinsic activity, depending on the antagonist dosage and regional dopamine concentrations.
Source: References 1-7
DOPAMINE AND SCHIZOPHRENIA
Dopamine neurons arise from two major nuclei in the mesencephalon (midbrain): the substantia nigra and ventral tegmental area (VTA). Neurons from the substantia nigra extend to the basal ganglia via the mesostriatal (nigrostriatal) pathway, which influences extrapyramidal motor function. The VTA sends dopaminergic neurons through mesolimbic and mesocortical pathways.
The basic limbic system includes the cingulate and orbitofrontal gyri, hippocampus, hypothalamus, thalamus, amygdala, medial temporal cortex, and the periaqueductal gray. This system controls emotion, episodic memory, pain, and primitive behaviors such as eating, fighting, sexual desire, and grooming.8 The limbic system is surrounded by cortex, where higher-order sensory, cognitive, and motor processes occur. The VTA links limbic and cortical functions via dopamine.
The tuberoinfundibular pathway, another clinically important dopaminergic route, projects from the hypothalamus to the anterior pituitary gland and regulates prolactin secretion.
Functional dopamine neurotransmission abnormalities in schizophrenia are generally characterized by region, with:
- excessive mesolimbic pathway activity resulting in positive symptoms such as delusions and hallucinations
- mesocortical projection deficits resulting in cognitive and negative symptoms such as impaired memory and attention, emotional blunting, alogia, avolition, and anhedonia.
Dopamine function abnormalities in schizophrenia occur in:
- projections from the substantia nigra to the caudate and putamen in the basal ganglia
- mesolimbic connections to the anterior cingulate, hippocampus, and parahippocampus
- mesocortical projections to the prefrontal cortex.
These dysfunctions contribute to abnormal motor function, perception, attention, memory, volition, emotion, and executive function.9
WHY ARIPIPRAZOLE WAS CREATED
Differences in regional dopamine function and observations of dopamine agonists’ therapeutic effects in schizophrenia10 led to development of partial dopamine agonists such as aripiprazole (Box 2).11,12
Aripiprazole and the investigational agent bifeprunox have complex pharmacologic actions involving numerous neurotransmitters—dopamine, serotonin, and histamine—but are believed to be principally partial agonists at pre- and postsynaptic dopamine receptors. Specifically, aripiprazole decreases hyperdopaminergic states while preserving dopamine function by partial agonism and decreased stimulation of presynaptic regulatory autoreceptors.5
The FDA approved aripiprazole for treating schizophrenia in 2002 and acute bipolar mania in 2004. A dihydroquinolone unrelated to other antipsychotics, it has an active partial agonist metabolite (dehydro-aripiprazole), high affinity for D2 receptors (Figure 1), and partial agonism at dopamine and serotonin receptors.13
Phase III trials are in progress for bifeprunox, a partial dopamine agonist/antagonist and serotonin receptor agonist being investigated for schizophrenia. An FDA decision on its approvability is expected in 2007.
Aripiprazole has approximately 30% intrinsic dopaminergic activity, estimated from studies showing a low incidence of extrapyramidal symptoms (EPS) with dosages up to 30 mg and PET studies showing a therapeutic range of postsynaptic D2 receptor occupancy of 80% to 95%.14 This small intrinsic activity limits excessive stimulation and dopamine receptor blockade.11 It also limits down-regulation of regulatory dopamine autoreceptors and preserves dopaminergic function in pre- and postsynaptic neurons.
The therapeutic window for dopamine receptor agonists (DA) and serotonin-dopamine receptor agonists (SDA) used in schizophrenia is 60% to 80% D2 receptor occupancy in mesostriatal neurons. D2 receptor occupancy and antagonism >80% significantly increases risk of EPS.15 Excessive dosing of high-potency antipsychotics with strong postsynaptic dopamine receptor affinity carries the highest risk of hypodopaminergic side effects, such as cognitive impairment, worsening of negative symptoms, akathisia, Parkinsonism, and hyperprolactinemia.
Aripiprazole’s intrinsic activity allows for higher D2 receptor occupancy with fewer side effects associated with full dopamine receptor antagonism. Clinical implications of this profile are unknown. Dopamine’s role in schizophrenia’s pathophysiology is inferred from knowledge that all effective antipsychotics offer some postsynaptic D2 receptor blockade.
Conventional dopamine receptor agonists (DAs) such as haloperidol and the newer serotonin-dopamine receptor agonists (SDAs) modeled after clozapine are thought to exert clinical effect by blocking D2 and D3 receptors. By contrast, partial dopamine agonists are agonists or antagonists, depending on cell-specific, synaptic dopamine concentrations. DAs and SDAs are competitive, full antagonists at pre- and postsynaptic dopamine receptors, whereas partial dopamine agonists are:
- agonists at presynaptic regulatory autoreceptors and in hypodopaminergic (mesocortical) synapses
- antagonists with small intrinsic activity in hyperdopaminergic (mesolimbic) synapses. Intrinsic activity is a compound’s degree of agonism in proportion to full agonism.
‘Dopamine stabilizers.’ Because of this combination of high-affinity receptor antagonism with preserved intrinsic activity, some call partial dopamine agonists “dopamine stabilizers.”
Source: References 11, 12
FigureAntipsychotics’ D2 receptor binding affinities
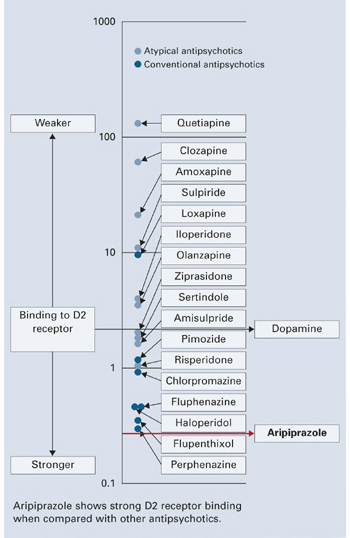
SIDE EFFECTS
Evidence shows fewer side effects with aripiprazole when used to treat schizophrenia and schizoaffective disorder compared with DAs such as haloperidol and SDAs such as risperidone.1,2,4
Dosage-dependent somnolence occurs with aripiprazole; the most common side effects include headache, agitation, anxiety, and insomnia (24.5%, 34.6%, 24%, and 18.6%, respectively).2 continued on page 60 A 10-week, placebo-controlled study using aripiprazole, 2 to 15 mg/d, to treat psychosis in Alzheimer’s dementia showed significantly increased risk of somnolence, accidental injury, and bronchitis (likely caused by aspiration).16
In placebo-controlled trials, aripiprazole, 2 to 30 mg/d, did not increase risk of cardiac, lipid, or prolactin-related side effects2 but showed increased risk of:
- tremor when used at 15 mg/d for up to 26 weeks in chronic schizophrenia, (9% incidence vs 1% with placebo)17
- akathisia when used at mean dosages of 27.9 mg/d to treat acute bipolar mania (11% incidence vs 2%with placebo).3 Aripiprazole also increased akathisia incidence in normal subjects.18
Risk of tardive dyskinesia or hyperglycemia-related adverse events with aripiprazole are unknown. Studies report weight gain of <1 kg (<2.2 lbs) in patients taking aripiprazole, 2 to 30 mg/d. One study found that patients switched from DA and SDA antipsychotics to aripiprazole, 30 mg/d, lost on average 1.5 kg (3.2 lbs) across 8weeks.19
Determining neuroleptic malignant syndrome risk with aripiprazole is difficult; two cases were reported in the premarketing sample.16 One animal study showed diminished catalepsy with chronic aripiprazole use, in contrast to persistent catalepsy with haloperidol.20
A Medline search for aripiprazole in February 2005 found several reports of treatment-emergent side effects, including:
- 3 reports of worsening agitation or psychosis21-23
- 2 reports of EPS24,25
- 1 report of excessive somnolence in a child.26
Adverse effects are probably underrepresented. Clinical deterioration and adverse effects were reported after starting, switching to, or combining aripiprazole with other antipsychotics or serotonergic agents (trazodone, sertraline, or venlafaxine).27,28
This paper by Dr. Mahendra T. Bhati was entered in the 2005 Promising New Investigators competition sponsored by the Neuroleptic Malignant Syndrome Information Service (NMSIS). The theme of this year’s scholarly papers was “New insights on psychotropic drug safety and side effects.”
Current Psychiatry is honored to publish this peer-reviewed, evidence-based article on a clinically important topic for practicing psychiatrists.
NMSIS is dedicated to reducing morbidity and mortality of NMS by improving medical and psychiatric care of patients with heat-related disorders; providing support information for medical professionals, patients and families; and improving scientific understanding of these conditions through research.
Related resources
- Lieberman, J. Aripiprazole. In: Schatzberg, A, Nemeroff, C (eds.) Textbook of Psychopharmacology. Washington DC: American Psychiatric Publishing, 2004:487-494.
- FDA Center for Drug Evaluation and Research. http://www.fda.gov/cder/foi/nda/2002/21-436_Abilify.htm
- Medline Plus Drug Information. http://www.nlm.nih.gov/medlineplus/druginfo/medmaster/a603012.html
Drug brand names
- Aripiprazole •Abilify
- Clozapine • Clozaril
- Haloperidol • Haldol
- Risperidone • Risperdal
- Trazodone • Desyrel
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
This author is supported by grant 2R25MH060490-06 from the National Institute of Mental Health.
1. Kane JM, Carson WH, Saha AR, et al. Efficacy and safety of aripiprazole and haloperidol versus placebo in patients with schizophrenia and schizoaffective disorder. J Clin Psychiatry 2002;63:763-71.
2. Marder SR, McQuade RD, Stock E, et al. Aripiprazole in the treatment of schizophrenia: safety and tolerability in short-term, placebo-controlled trials. Schizophr Res 2003;61:123-36.
3. Keck PE, Jr, Marcus R, Tourkodimitris S, et al. A placebo-controlled, double-blind study of the efficacy and safety of aripiprazole in patients with acute bipolar mania. Am J Psychiatry 2003;160:1651-8.
4. Potkin SG, Saha AR, Kujawa MJ, et al. Aripiprazole, an antipsychotic with a novel mechanism of action, and risperidone vs placebo in patients with schizophrenia and schizoaffective disorder. Arch Gen Psychiatry 2003;60:681-90.
5. Grady MA, Gasperoni TL, Kirkpatrick P. Aripiprazole. Nat Rev Drug Discov 2003;2:427-8.
6. Stigler KA, Posey DJ, McDougle CJ. Aripiprazole for maladaptive behavior in pervasive developmental disorders. J Child Adolesc Psychopharmacol 2004;14:455-63.
7. Tamminga CA. Partial dopamine agonists in the treatment of psychosis. J Neural Transm 2002;109:411-20.
8. Arciniegas DB, Beresford TP. Neuropsychiatry: an Introductory Approach .Cambridge, UK: Cambridge University Press; 2001.
9. Stahl SM. Psychopharmacology of Antipsychotics .London: Martin Dunitz Ltd.; 1999.
10. Tamminga CA, Gotts MD, Thaker GK, et al. Dopamine agonist treatment of schizophrenia with N-propylnorapomorphine. Arch Gen Psychiatry 1986;43:398-402.
11. Grunder G, Carlsson A, Wong D. Mechanism of new antipsychotic medications: occupancy is not just antagonism. Arch Gen Psychiatry 2003;60:974-7.
12. Burris K, Molski T, Xu C, et al. Aripiprazole, a novel antipsychotic, is a high-affinity partial agonist at human dopamine D2 receptors. J Pharmacol Exp Ther 2002;302:381-9.
13. Lieberman J. Dopamine partial agonists: a new class of antipsychotic. CNS Drugs 2004;18:251-67.
14. Yokoi F, Grunder G, Biziere K, et al. Dopamine D2 and D3 receptor occupancy in normal humans treated with the antipsychotic drug aripiprazole (OPC 14597): a study using positron emission tomography and [11C]raclopride. Neuropsychopharmacology 2002;27:248-59.
15. Kapur S, Zipursky R, Jones C, et al. Relationship between dopamine D(2) occupancy, clinical response, and side effects: a double-blind PET study of first-episode schizophrenia. Am J Psychiatry 2000;157:514-20.
16. U.S. Food and Drug Administration. Medwatch online. Available at: http://www.fda.gov/medwatch/SAFETY/2004/abilify_pi.pdf. Accessed June 7, 2004.
17. Pigott T, Carson W, Saha A, et al. Aripiprazole for the prevention of relapse in stabilized patients with chronic schizophrenia: a placebo-controlled 26-week study. J Clin Psychiatry 2003;64:1048-56.
18. Mallikaarjun S, Salazar D, Bramer S. Pharmacokinetics, tolerability, and safety of aripiprazole following multiple oral dosing in normal healthy volunteers. J Clin Pharmacol 2004;44:179-87.
19. Casey D, Carson W, Saha A, et al. Switching patients to aripiprazole from other antipsychotic agents: a multicenter randomized study. Psychopharmacology 2003;166:391-9.
20. Nakai S, Hirose T, Uwahodo Y, et al. Diminished catalepsy and dopamine metabolism distinguish aripiprazole from haloperidol or risperidone. Eur J Pharmacol 2003;472:89-97.
21. Sajbel T, Cheney E, DeQuardo J. Aripiprazole-associated dyskinesia. Ann Pharmacother 2005;39:200-1.
22. Reeves R, Mack J. Worsening schizoaffective disorder with aripiprazole. Am J Psychiatry 2004;161:1308.-
23. Ramaswamy S, Vijay D, William M, et al. Aripiprazole possibly worsens psychosis. Int Clin Psychopharmacol 2004;19:45-8.
24. Mendhekar D. Aripiprazole-induced rabbit syndrome. Aust N Z J Psychiatry 2004;38:561.-
25. Lindsey R, Kaplan D, Koliatsos V, et al. Aripiprazole and extrapyramidal symptoms. J Am Acad Child Adolesc Psychiatry 2003;42:1268-9.
26. Davenport J, McCarthy M, Buck M. Excessive somnolence from aripiprazole in a child. Pharmacotherapy 2004;24:522-5.
27. DeQuardo J. Worsened agitation with aripiprazole: adverse effect of dopamine partial agonism? J Clin Psychiatry 2004;65:132-3.
28. Cohen S, Rulf D, Pies R. Extrapyramidal side effects associated with aripiprazole coprescription in 2 patients. J Clin Psychiatry 2005;66:135-6.
Aripiprazole, the first FDA-approved partial dopamine agonist, causes few side effects when used to treat schizophrenia or acute bipolar mania. This relatively safe profile in approved uses has led clinicians to try aripiprazole for off-label uses as well, though evidence of the drug’s efficacy and safety in other psychiatric conditions is limited (Box 1).1-7 Because this practice may involve unknown risks, this article:
- reviews aripiprazole’s role in correcting dopaminergic dysfunction in patients with schizophrenia
- cites adverse effects reported with aripiprazole use and discusses concerns about its off-label use.
Aripiprazole shows clear efficacy for treating acute mania and schizophrenia’s negative and positive symptoms, but its effectiveness and safety in other psychiatric illnesses is unknown. Even so, it is being used to treat psychotic unipolar and bipolar depression, attention-deficit/hyperactivity disorder, oppositional defiant disorder, and pervasive developmental disorders in childrenand adults.
Dopamine differences. Do not assume that aripiprazole’s safety and effectiveness in treating schizophrenia translates to other psychiatric conditions. Dopamine dysfunction patterns differ in persons with and without schizophrenia; therefore, aripiprazole’s regional and functional selectivity at dopamine receptors—and treatment response and tolerability—is also likely to differ.
Antipsychotic differences. Aripiprazole is unlike other psychotropics and cannot be assumed to have similar therapeutic effects. The agent’s dopamine agonist and antagonist properties hinge on regional dopamine concentrations as well as the drug itself.
Dopaminergic risks in combination. Numerous drugs modulate dopamine function, and switching and combining drugs places patients at unknown risk of dopaminergic side effects with aripiprazole. Adding an antagonist or a low-dose antagonist combination with aripiprazole may increase competition for dopamine receptors and modify its intrinsic activity, depending on the antagonist dosage and regional dopamine concentrations.
Source: References 1-7
DOPAMINE AND SCHIZOPHRENIA
Dopamine neurons arise from two major nuclei in the mesencephalon (midbrain): the substantia nigra and ventral tegmental area (VTA). Neurons from the substantia nigra extend to the basal ganglia via the mesostriatal (nigrostriatal) pathway, which influences extrapyramidal motor function. The VTA sends dopaminergic neurons through mesolimbic and mesocortical pathways.
The basic limbic system includes the cingulate and orbitofrontal gyri, hippocampus, hypothalamus, thalamus, amygdala, medial temporal cortex, and the periaqueductal gray. This system controls emotion, episodic memory, pain, and primitive behaviors such as eating, fighting, sexual desire, and grooming.8 The limbic system is surrounded by cortex, where higher-order sensory, cognitive, and motor processes occur. The VTA links limbic and cortical functions via dopamine.
The tuberoinfundibular pathway, another clinically important dopaminergic route, projects from the hypothalamus to the anterior pituitary gland and regulates prolactin secretion.
Functional dopamine neurotransmission abnormalities in schizophrenia are generally characterized by region, with:
- excessive mesolimbic pathway activity resulting in positive symptoms such as delusions and hallucinations
- mesocortical projection deficits resulting in cognitive and negative symptoms such as impaired memory and attention, emotional blunting, alogia, avolition, and anhedonia.
Dopamine function abnormalities in schizophrenia occur in:
- projections from the substantia nigra to the caudate and putamen in the basal ganglia
- mesolimbic connections to the anterior cingulate, hippocampus, and parahippocampus
- mesocortical projections to the prefrontal cortex.
These dysfunctions contribute to abnormal motor function, perception, attention, memory, volition, emotion, and executive function.9
WHY ARIPIPRAZOLE WAS CREATED
Differences in regional dopamine function and observations of dopamine agonists’ therapeutic effects in schizophrenia10 led to development of partial dopamine agonists such as aripiprazole (Box 2).11,12
Aripiprazole and the investigational agent bifeprunox have complex pharmacologic actions involving numerous neurotransmitters—dopamine, serotonin, and histamine—but are believed to be principally partial agonists at pre- and postsynaptic dopamine receptors. Specifically, aripiprazole decreases hyperdopaminergic states while preserving dopamine function by partial agonism and decreased stimulation of presynaptic regulatory autoreceptors.5
The FDA approved aripiprazole for treating schizophrenia in 2002 and acute bipolar mania in 2004. A dihydroquinolone unrelated to other antipsychotics, it has an active partial agonist metabolite (dehydro-aripiprazole), high affinity for D2 receptors (Figure 1), and partial agonism at dopamine and serotonin receptors.13
Phase III trials are in progress for bifeprunox, a partial dopamine agonist/antagonist and serotonin receptor agonist being investigated for schizophrenia. An FDA decision on its approvability is expected in 2007.
Aripiprazole has approximately 30% intrinsic dopaminergic activity, estimated from studies showing a low incidence of extrapyramidal symptoms (EPS) with dosages up to 30 mg and PET studies showing a therapeutic range of postsynaptic D2 receptor occupancy of 80% to 95%.14 This small intrinsic activity limits excessive stimulation and dopamine receptor blockade.11 It also limits down-regulation of regulatory dopamine autoreceptors and preserves dopaminergic function in pre- and postsynaptic neurons.
The therapeutic window for dopamine receptor agonists (DA) and serotonin-dopamine receptor agonists (SDA) used in schizophrenia is 60% to 80% D2 receptor occupancy in mesostriatal neurons. D2 receptor occupancy and antagonism >80% significantly increases risk of EPS.15 Excessive dosing of high-potency antipsychotics with strong postsynaptic dopamine receptor affinity carries the highest risk of hypodopaminergic side effects, such as cognitive impairment, worsening of negative symptoms, akathisia, Parkinsonism, and hyperprolactinemia.
Aripiprazole’s intrinsic activity allows for higher D2 receptor occupancy with fewer side effects associated with full dopamine receptor antagonism. Clinical implications of this profile are unknown. Dopamine’s role in schizophrenia’s pathophysiology is inferred from knowledge that all effective antipsychotics offer some postsynaptic D2 receptor blockade.
Conventional dopamine receptor agonists (DAs) such as haloperidol and the newer serotonin-dopamine receptor agonists (SDAs) modeled after clozapine are thought to exert clinical effect by blocking D2 and D3 receptors. By contrast, partial dopamine agonists are agonists or antagonists, depending on cell-specific, synaptic dopamine concentrations. DAs and SDAs are competitive, full antagonists at pre- and postsynaptic dopamine receptors, whereas partial dopamine agonists are:
- agonists at presynaptic regulatory autoreceptors and in hypodopaminergic (mesocortical) synapses
- antagonists with small intrinsic activity in hyperdopaminergic (mesolimbic) synapses. Intrinsic activity is a compound’s degree of agonism in proportion to full agonism.
‘Dopamine stabilizers.’ Because of this combination of high-affinity receptor antagonism with preserved intrinsic activity, some call partial dopamine agonists “dopamine stabilizers.”
Source: References 11, 12
FigureAntipsychotics’ D2 receptor binding affinities
SIDE EFFECTS
Evidence shows fewer side effects with aripiprazole when used to treat schizophrenia and schizoaffective disorder compared with DAs such as haloperidol and SDAs such as risperidone.1,2,4
Dosage-dependent somnolence occurs with aripiprazole; the most common side effects include headache, agitation, anxiety, and insomnia (24.5%, 34.6%, 24%, and 18.6%, respectively).2 continued on page 60 A 10-week, placebo-controlled study using aripiprazole, 2 to 15 mg/d, to treat psychosis in Alzheimer’s dementia showed significantly increased risk of somnolence, accidental injury, and bronchitis (likely caused by aspiration).16
In placebo-controlled trials, aripiprazole, 2 to 30 mg/d, did not increase risk of cardiac, lipid, or prolactin-related side effects2 but showed increased risk of:
- tremor when used at 15 mg/d for up to 26 weeks in chronic schizophrenia, (9% incidence vs 1% with placebo)17
- akathisia when used at mean dosages of 27.9 mg/d to treat acute bipolar mania (11% incidence vs 2%with placebo).3 Aripiprazole also increased akathisia incidence in normal subjects.18
Risk of tardive dyskinesia or hyperglycemia-related adverse events with aripiprazole are unknown. Studies report weight gain of <1 kg (<2.2 lbs) in patients taking aripiprazole, 2 to 30 mg/d. One study found that patients switched from DA and SDA antipsychotics to aripiprazole, 30 mg/d, lost on average 1.5 kg (3.2 lbs) across 8weeks.19
Determining neuroleptic malignant syndrome risk with aripiprazole is difficult; two cases were reported in the premarketing sample.16 One animal study showed diminished catalepsy with chronic aripiprazole use, in contrast to persistent catalepsy with haloperidol.20
A Medline search for aripiprazole in February 2005 found several reports of treatment-emergent side effects, including:
- 3 reports of worsening agitation or psychosis21-23
- 2 reports of EPS24,25
- 1 report of excessive somnolence in a child.26
Adverse effects are probably underrepresented. Clinical deterioration and adverse effects were reported after starting, switching to, or combining aripiprazole with other antipsychotics or serotonergic agents (trazodone, sertraline, or venlafaxine).27,28
This paper by Dr. Mahendra T. Bhati was entered in the 2005 Promising New Investigators competition sponsored by the Neuroleptic Malignant Syndrome Information Service (NMSIS). The theme of this year’s scholarly papers was “New insights on psychotropic drug safety and side effects.”
Current Psychiatry is honored to publish this peer-reviewed, evidence-based article on a clinically important topic for practicing psychiatrists.
NMSIS is dedicated to reducing morbidity and mortality of NMS by improving medical and psychiatric care of patients with heat-related disorders; providing support information for medical professionals, patients and families; and improving scientific understanding of these conditions through research.
Related resources
- Lieberman, J. Aripiprazole. In: Schatzberg, A, Nemeroff, C (eds.) Textbook of Psychopharmacology. Washington DC: American Psychiatric Publishing, 2004:487-494.
- FDA Center for Drug Evaluation and Research. http://www.fda.gov/cder/foi/nda/2002/21-436_Abilify.htm
- Medline Plus Drug Information. http://www.nlm.nih.gov/medlineplus/druginfo/medmaster/a603012.html
Drug brand names
- Aripiprazole •Abilify
- Clozapine • Clozaril
- Haloperidol • Haldol
- Risperidone • Risperdal
- Trazodone • Desyrel
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
This author is supported by grant 2R25MH060490-06 from the National Institute of Mental Health.
Aripiprazole, the first FDA-approved partial dopamine agonist, causes few side effects when used to treat schizophrenia or acute bipolar mania. This relatively safe profile in approved uses has led clinicians to try aripiprazole for off-label uses as well, though evidence of the drug’s efficacy and safety in other psychiatric conditions is limited (Box 1).1-7 Because this practice may involve unknown risks, this article:
- reviews aripiprazole’s role in correcting dopaminergic dysfunction in patients with schizophrenia
- cites adverse effects reported with aripiprazole use and discusses concerns about its off-label use.
Aripiprazole shows clear efficacy for treating acute mania and schizophrenia’s negative and positive symptoms, but its effectiveness and safety in other psychiatric illnesses is unknown. Even so, it is being used to treat psychotic unipolar and bipolar depression, attention-deficit/hyperactivity disorder, oppositional defiant disorder, and pervasive developmental disorders in childrenand adults.
Dopamine differences. Do not assume that aripiprazole’s safety and effectiveness in treating schizophrenia translates to other psychiatric conditions. Dopamine dysfunction patterns differ in persons with and without schizophrenia; therefore, aripiprazole’s regional and functional selectivity at dopamine receptors—and treatment response and tolerability—is also likely to differ.
Antipsychotic differences. Aripiprazole is unlike other psychotropics and cannot be assumed to have similar therapeutic effects. The agent’s dopamine agonist and antagonist properties hinge on regional dopamine concentrations as well as the drug itself.
Dopaminergic risks in combination. Numerous drugs modulate dopamine function, and switching and combining drugs places patients at unknown risk of dopaminergic side effects with aripiprazole. Adding an antagonist or a low-dose antagonist combination with aripiprazole may increase competition for dopamine receptors and modify its intrinsic activity, depending on the antagonist dosage and regional dopamine concentrations.
Source: References 1-7
DOPAMINE AND SCHIZOPHRENIA
Dopamine neurons arise from two major nuclei in the mesencephalon (midbrain): the substantia nigra and ventral tegmental area (VTA). Neurons from the substantia nigra extend to the basal ganglia via the mesostriatal (nigrostriatal) pathway, which influences extrapyramidal motor function. The VTA sends dopaminergic neurons through mesolimbic and mesocortical pathways.
The basic limbic system includes the cingulate and orbitofrontal gyri, hippocampus, hypothalamus, thalamus, amygdala, medial temporal cortex, and the periaqueductal gray. This system controls emotion, episodic memory, pain, and primitive behaviors such as eating, fighting, sexual desire, and grooming.8 The limbic system is surrounded by cortex, where higher-order sensory, cognitive, and motor processes occur. The VTA links limbic and cortical functions via dopamine.
The tuberoinfundibular pathway, another clinically important dopaminergic route, projects from the hypothalamus to the anterior pituitary gland and regulates prolactin secretion.
Functional dopamine neurotransmission abnormalities in schizophrenia are generally characterized by region, with:
- excessive mesolimbic pathway activity resulting in positive symptoms such as delusions and hallucinations
- mesocortical projection deficits resulting in cognitive and negative symptoms such as impaired memory and attention, emotional blunting, alogia, avolition, and anhedonia.
Dopamine function abnormalities in schizophrenia occur in:
- projections from the substantia nigra to the caudate and putamen in the basal ganglia
- mesolimbic connections to the anterior cingulate, hippocampus, and parahippocampus
- mesocortical projections to the prefrontal cortex.
These dysfunctions contribute to abnormal motor function, perception, attention, memory, volition, emotion, and executive function.9
WHY ARIPIPRAZOLE WAS CREATED
Differences in regional dopamine function and observations of dopamine agonists’ therapeutic effects in schizophrenia10 led to development of partial dopamine agonists such as aripiprazole (Box 2).11,12
Aripiprazole and the investigational agent bifeprunox have complex pharmacologic actions involving numerous neurotransmitters—dopamine, serotonin, and histamine—but are believed to be principally partial agonists at pre- and postsynaptic dopamine receptors. Specifically, aripiprazole decreases hyperdopaminergic states while preserving dopamine function by partial agonism and decreased stimulation of presynaptic regulatory autoreceptors.5
The FDA approved aripiprazole for treating schizophrenia in 2002 and acute bipolar mania in 2004. A dihydroquinolone unrelated to other antipsychotics, it has an active partial agonist metabolite (dehydro-aripiprazole), high affinity for D2 receptors (Figure 1), and partial agonism at dopamine and serotonin receptors.13
Phase III trials are in progress for bifeprunox, a partial dopamine agonist/antagonist and serotonin receptor agonist being investigated for schizophrenia. An FDA decision on its approvability is expected in 2007.
Aripiprazole has approximately 30% intrinsic dopaminergic activity, estimated from studies showing a low incidence of extrapyramidal symptoms (EPS) with dosages up to 30 mg and PET studies showing a therapeutic range of postsynaptic D2 receptor occupancy of 80% to 95%.14 This small intrinsic activity limits excessive stimulation and dopamine receptor blockade.11 It also limits down-regulation of regulatory dopamine autoreceptors and preserves dopaminergic function in pre- and postsynaptic neurons.
The therapeutic window for dopamine receptor agonists (DA) and serotonin-dopamine receptor agonists (SDA) used in schizophrenia is 60% to 80% D2 receptor occupancy in mesostriatal neurons. D2 receptor occupancy and antagonism >80% significantly increases risk of EPS.15 Excessive dosing of high-potency antipsychotics with strong postsynaptic dopamine receptor affinity carries the highest risk of hypodopaminergic side effects, such as cognitive impairment, worsening of negative symptoms, akathisia, Parkinsonism, and hyperprolactinemia.
Aripiprazole’s intrinsic activity allows for higher D2 receptor occupancy with fewer side effects associated with full dopamine receptor antagonism. Clinical implications of this profile are unknown. Dopamine’s role in schizophrenia’s pathophysiology is inferred from knowledge that all effective antipsychotics offer some postsynaptic D2 receptor blockade.
Conventional dopamine receptor agonists (DAs) such as haloperidol and the newer serotonin-dopamine receptor agonists (SDAs) modeled after clozapine are thought to exert clinical effect by blocking D2 and D3 receptors. By contrast, partial dopamine agonists are agonists or antagonists, depending on cell-specific, synaptic dopamine concentrations. DAs and SDAs are competitive, full antagonists at pre- and postsynaptic dopamine receptors, whereas partial dopamine agonists are:
- agonists at presynaptic regulatory autoreceptors and in hypodopaminergic (mesocortical) synapses
- antagonists with small intrinsic activity in hyperdopaminergic (mesolimbic) synapses. Intrinsic activity is a compound’s degree of agonism in proportion to full agonism.
‘Dopamine stabilizers.’ Because of this combination of high-affinity receptor antagonism with preserved intrinsic activity, some call partial dopamine agonists “dopamine stabilizers.”
Source: References 11, 12
FigureAntipsychotics’ D2 receptor binding affinities
SIDE EFFECTS
Evidence shows fewer side effects with aripiprazole when used to treat schizophrenia and schizoaffective disorder compared with DAs such as haloperidol and SDAs such as risperidone.1,2,4
Dosage-dependent somnolence occurs with aripiprazole; the most common side effects include headache, agitation, anxiety, and insomnia (24.5%, 34.6%, 24%, and 18.6%, respectively).2 continued on page 60 A 10-week, placebo-controlled study using aripiprazole, 2 to 15 mg/d, to treat psychosis in Alzheimer’s dementia showed significantly increased risk of somnolence, accidental injury, and bronchitis (likely caused by aspiration).16
In placebo-controlled trials, aripiprazole, 2 to 30 mg/d, did not increase risk of cardiac, lipid, or prolactin-related side effects2 but showed increased risk of:
- tremor when used at 15 mg/d for up to 26 weeks in chronic schizophrenia, (9% incidence vs 1% with placebo)17
- akathisia when used at mean dosages of 27.9 mg/d to treat acute bipolar mania (11% incidence vs 2%with placebo).3 Aripiprazole also increased akathisia incidence in normal subjects.18
Risk of tardive dyskinesia or hyperglycemia-related adverse events with aripiprazole are unknown. Studies report weight gain of <1 kg (<2.2 lbs) in patients taking aripiprazole, 2 to 30 mg/d. One study found that patients switched from DA and SDA antipsychotics to aripiprazole, 30 mg/d, lost on average 1.5 kg (3.2 lbs) across 8weeks.19
Determining neuroleptic malignant syndrome risk with aripiprazole is difficult; two cases were reported in the premarketing sample.16 One animal study showed diminished catalepsy with chronic aripiprazole use, in contrast to persistent catalepsy with haloperidol.20
A Medline search for aripiprazole in February 2005 found several reports of treatment-emergent side effects, including:
- 3 reports of worsening agitation or psychosis21-23
- 2 reports of EPS24,25
- 1 report of excessive somnolence in a child.26
Adverse effects are probably underrepresented. Clinical deterioration and adverse effects were reported after starting, switching to, or combining aripiprazole with other antipsychotics or serotonergic agents (trazodone, sertraline, or venlafaxine).27,28
This paper by Dr. Mahendra T. Bhati was entered in the 2005 Promising New Investigators competition sponsored by the Neuroleptic Malignant Syndrome Information Service (NMSIS). The theme of this year’s scholarly papers was “New insights on psychotropic drug safety and side effects.”
Current Psychiatry is honored to publish this peer-reviewed, evidence-based article on a clinically important topic for practicing psychiatrists.
NMSIS is dedicated to reducing morbidity and mortality of NMS by improving medical and psychiatric care of patients with heat-related disorders; providing support information for medical professionals, patients and families; and improving scientific understanding of these conditions through research.
Related resources
- Lieberman, J. Aripiprazole. In: Schatzberg, A, Nemeroff, C (eds.) Textbook of Psychopharmacology. Washington DC: American Psychiatric Publishing, 2004:487-494.
- FDA Center for Drug Evaluation and Research. http://www.fda.gov/cder/foi/nda/2002/21-436_Abilify.htm
- Medline Plus Drug Information. http://www.nlm.nih.gov/medlineplus/druginfo/medmaster/a603012.html
Drug brand names
- Aripiprazole •Abilify
- Clozapine • Clozaril
- Haloperidol • Haldol
- Risperidone • Risperdal
- Trazodone • Desyrel
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
This author is supported by grant 2R25MH060490-06 from the National Institute of Mental Health.
1. Kane JM, Carson WH, Saha AR, et al. Efficacy and safety of aripiprazole and haloperidol versus placebo in patients with schizophrenia and schizoaffective disorder. J Clin Psychiatry 2002;63:763-71.
2. Marder SR, McQuade RD, Stock E, et al. Aripiprazole in the treatment of schizophrenia: safety and tolerability in short-term, placebo-controlled trials. Schizophr Res 2003;61:123-36.
3. Keck PE, Jr, Marcus R, Tourkodimitris S, et al. A placebo-controlled, double-blind study of the efficacy and safety of aripiprazole in patients with acute bipolar mania. Am J Psychiatry 2003;160:1651-8.
4. Potkin SG, Saha AR, Kujawa MJ, et al. Aripiprazole, an antipsychotic with a novel mechanism of action, and risperidone vs placebo in patients with schizophrenia and schizoaffective disorder. Arch Gen Psychiatry 2003;60:681-90.
5. Grady MA, Gasperoni TL, Kirkpatrick P. Aripiprazole. Nat Rev Drug Discov 2003;2:427-8.
6. Stigler KA, Posey DJ, McDougle CJ. Aripiprazole for maladaptive behavior in pervasive developmental disorders. J Child Adolesc Psychopharmacol 2004;14:455-63.
7. Tamminga CA. Partial dopamine agonists in the treatment of psychosis. J Neural Transm 2002;109:411-20.
8. Arciniegas DB, Beresford TP. Neuropsychiatry: an Introductory Approach .Cambridge, UK: Cambridge University Press; 2001.
9. Stahl SM. Psychopharmacology of Antipsychotics .London: Martin Dunitz Ltd.; 1999.
10. Tamminga CA, Gotts MD, Thaker GK, et al. Dopamine agonist treatment of schizophrenia with N-propylnorapomorphine. Arch Gen Psychiatry 1986;43:398-402.
11. Grunder G, Carlsson A, Wong D. Mechanism of new antipsychotic medications: occupancy is not just antagonism. Arch Gen Psychiatry 2003;60:974-7.
12. Burris K, Molski T, Xu C, et al. Aripiprazole, a novel antipsychotic, is a high-affinity partial agonist at human dopamine D2 receptors. J Pharmacol Exp Ther 2002;302:381-9.
13. Lieberman J. Dopamine partial agonists: a new class of antipsychotic. CNS Drugs 2004;18:251-67.
14. Yokoi F, Grunder G, Biziere K, et al. Dopamine D2 and D3 receptor occupancy in normal humans treated with the antipsychotic drug aripiprazole (OPC 14597): a study using positron emission tomography and [11C]raclopride. Neuropsychopharmacology 2002;27:248-59.
15. Kapur S, Zipursky R, Jones C, et al. Relationship between dopamine D(2) occupancy, clinical response, and side effects: a double-blind PET study of first-episode schizophrenia. Am J Psychiatry 2000;157:514-20.
16. U.S. Food and Drug Administration. Medwatch online. Available at: http://www.fda.gov/medwatch/SAFETY/2004/abilify_pi.pdf. Accessed June 7, 2004.
17. Pigott T, Carson W, Saha A, et al. Aripiprazole for the prevention of relapse in stabilized patients with chronic schizophrenia: a placebo-controlled 26-week study. J Clin Psychiatry 2003;64:1048-56.
18. Mallikaarjun S, Salazar D, Bramer S. Pharmacokinetics, tolerability, and safety of aripiprazole following multiple oral dosing in normal healthy volunteers. J Clin Pharmacol 2004;44:179-87.
19. Casey D, Carson W, Saha A, et al. Switching patients to aripiprazole from other antipsychotic agents: a multicenter randomized study. Psychopharmacology 2003;166:391-9.
20. Nakai S, Hirose T, Uwahodo Y, et al. Diminished catalepsy and dopamine metabolism distinguish aripiprazole from haloperidol or risperidone. Eur J Pharmacol 2003;472:89-97.
21. Sajbel T, Cheney E, DeQuardo J. Aripiprazole-associated dyskinesia. Ann Pharmacother 2005;39:200-1.
22. Reeves R, Mack J. Worsening schizoaffective disorder with aripiprazole. Am J Psychiatry 2004;161:1308.-
23. Ramaswamy S, Vijay D, William M, et al. Aripiprazole possibly worsens psychosis. Int Clin Psychopharmacol 2004;19:45-8.
24. Mendhekar D. Aripiprazole-induced rabbit syndrome. Aust N Z J Psychiatry 2004;38:561.-
25. Lindsey R, Kaplan D, Koliatsos V, et al. Aripiprazole and extrapyramidal symptoms. J Am Acad Child Adolesc Psychiatry 2003;42:1268-9.
26. Davenport J, McCarthy M, Buck M. Excessive somnolence from aripiprazole in a child. Pharmacotherapy 2004;24:522-5.
27. DeQuardo J. Worsened agitation with aripiprazole: adverse effect of dopamine partial agonism? J Clin Psychiatry 2004;65:132-3.
28. Cohen S, Rulf D, Pies R. Extrapyramidal side effects associated with aripiprazole coprescription in 2 patients. J Clin Psychiatry 2005;66:135-6.
1. Kane JM, Carson WH, Saha AR, et al. Efficacy and safety of aripiprazole and haloperidol versus placebo in patients with schizophrenia and schizoaffective disorder. J Clin Psychiatry 2002;63:763-71.
2. Marder SR, McQuade RD, Stock E, et al. Aripiprazole in the treatment of schizophrenia: safety and tolerability in short-term, placebo-controlled trials. Schizophr Res 2003;61:123-36.
3. Keck PE, Jr, Marcus R, Tourkodimitris S, et al. A placebo-controlled, double-blind study of the efficacy and safety of aripiprazole in patients with acute bipolar mania. Am J Psychiatry 2003;160:1651-8.
4. Potkin SG, Saha AR, Kujawa MJ, et al. Aripiprazole, an antipsychotic with a novel mechanism of action, and risperidone vs placebo in patients with schizophrenia and schizoaffective disorder. Arch Gen Psychiatry 2003;60:681-90.
5. Grady MA, Gasperoni TL, Kirkpatrick P. Aripiprazole. Nat Rev Drug Discov 2003;2:427-8.
6. Stigler KA, Posey DJ, McDougle CJ. Aripiprazole for maladaptive behavior in pervasive developmental disorders. J Child Adolesc Psychopharmacol 2004;14:455-63.
7. Tamminga CA. Partial dopamine agonists in the treatment of psychosis. J Neural Transm 2002;109:411-20.
8. Arciniegas DB, Beresford TP. Neuropsychiatry: an Introductory Approach .Cambridge, UK: Cambridge University Press; 2001.
9. Stahl SM. Psychopharmacology of Antipsychotics .London: Martin Dunitz Ltd.; 1999.
10. Tamminga CA, Gotts MD, Thaker GK, et al. Dopamine agonist treatment of schizophrenia with N-propylnorapomorphine. Arch Gen Psychiatry 1986;43:398-402.
11. Grunder G, Carlsson A, Wong D. Mechanism of new antipsychotic medications: occupancy is not just antagonism. Arch Gen Psychiatry 2003;60:974-7.
12. Burris K, Molski T, Xu C, et al. Aripiprazole, a novel antipsychotic, is a high-affinity partial agonist at human dopamine D2 receptors. J Pharmacol Exp Ther 2002;302:381-9.
13. Lieberman J. Dopamine partial agonists: a new class of antipsychotic. CNS Drugs 2004;18:251-67.
14. Yokoi F, Grunder G, Biziere K, et al. Dopamine D2 and D3 receptor occupancy in normal humans treated with the antipsychotic drug aripiprazole (OPC 14597): a study using positron emission tomography and [11C]raclopride. Neuropsychopharmacology 2002;27:248-59.
15. Kapur S, Zipursky R, Jones C, et al. Relationship between dopamine D(2) occupancy, clinical response, and side effects: a double-blind PET study of first-episode schizophrenia. Am J Psychiatry 2000;157:514-20.
16. U.S. Food and Drug Administration. Medwatch online. Available at: http://www.fda.gov/medwatch/SAFETY/2004/abilify_pi.pdf. Accessed June 7, 2004.
17. Pigott T, Carson W, Saha A, et al. Aripiprazole for the prevention of relapse in stabilized patients with chronic schizophrenia: a placebo-controlled 26-week study. J Clin Psychiatry 2003;64:1048-56.
18. Mallikaarjun S, Salazar D, Bramer S. Pharmacokinetics, tolerability, and safety of aripiprazole following multiple oral dosing in normal healthy volunteers. J Clin Pharmacol 2004;44:179-87.
19. Casey D, Carson W, Saha A, et al. Switching patients to aripiprazole from other antipsychotic agents: a multicenter randomized study. Psychopharmacology 2003;166:391-9.
20. Nakai S, Hirose T, Uwahodo Y, et al. Diminished catalepsy and dopamine metabolism distinguish aripiprazole from haloperidol or risperidone. Eur J Pharmacol 2003;472:89-97.
21. Sajbel T, Cheney E, DeQuardo J. Aripiprazole-associated dyskinesia. Ann Pharmacother 2005;39:200-1.
22. Reeves R, Mack J. Worsening schizoaffective disorder with aripiprazole. Am J Psychiatry 2004;161:1308.-
23. Ramaswamy S, Vijay D, William M, et al. Aripiprazole possibly worsens psychosis. Int Clin Psychopharmacol 2004;19:45-8.
24. Mendhekar D. Aripiprazole-induced rabbit syndrome. Aust N Z J Psychiatry 2004;38:561.-
25. Lindsey R, Kaplan D, Koliatsos V, et al. Aripiprazole and extrapyramidal symptoms. J Am Acad Child Adolesc Psychiatry 2003;42:1268-9.
26. Davenport J, McCarthy M, Buck M. Excessive somnolence from aripiprazole in a child. Pharmacotherapy 2004;24:522-5.
27. DeQuardo J. Worsened agitation with aripiprazole: adverse effect of dopamine partial agonism? J Clin Psychiatry 2004;65:132-3.
28. Cohen S, Rulf D, Pies R. Extrapyramidal side effects associated with aripiprazole coprescription in 2 patients. J Clin Psychiatry 2005;66:135-6.
Is it PANDAS? How to confirm the sore throat/OCD connection
John, age 6, presented for psychiatric evaluation with acute, incapacitating obsessive-compulsive symptoms. For 4 weeks he washed his hands compulsively and had pervasive obsessions about death by choking.
These symptoms had suddenly worsened over 2 days. At first, he washed his hands more than 35 times per day in rituals lasting several minutes each. Then, within 2 weeks, John’s handwashing spontaneously decreased, but his choking fears dramatically increased. He refused all solid foods and continuously sought reassurance from his parents that he would not choke or die.
Approximately 1 week before these symptoms began, John had a sore throat and tested positive via throat culture for group A beta-hemolytic streptococcal infection (GABHS).
Sore throat followed by sudden-onset obsessive-compulsive symptoms or tics in a child such as John suggests a pediatric autoimmune neuropsychiatric disorder associated with streptococcal infection (PANDAS). The association between GABHS infection and these symptoms remains uncertain, as the mechanism by which GABHS infection may cause obsessive-compulsive symptoms and other childhood-onset neuropsychiatric disorders is largely unknown.
Since PANDAS was recognized (Box 1),1-6 some data have emerged on the disorder’s symptoms, course, and prognosis. However:
- diagnostic criteria are not well-defined
- few controlled studies have examined treatment response
- using antibiotics and immunotherapies to treat or prevent PANDAS symptoms remains controversial because of unproven efficacy and potential adverse effects.
To help you diagnose and treat patients with suspected PANDAS, this article examines the limited evidence for the disorder, discusses diagnostic guidelines, and reviews preliminary indications for behavioral and medical treatments.
PANDAS stands for pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections. It describes childhoodonset OCD or tic cases whose onset or worsening appears to be linked to group A beta-hemolytic streptococcal (GABHS) infection.
GABHS antibodies cross-react with the cellular components of the basal ganglia, particularly in the caudate nucleus.1 PANDAS was first recognized in 1987 during an unexpected resurgence of rheumatic fever in the United States.2 Sydenham chorea is thought to occur when GABHS antibodies undergo molecular mimicry and cross-react with epitopes on neurons in the basal ganglia and other brain areas, causing motor and behavioral disruptions.3 Rheumatic fever patients with Sydenham chorea show a high prevalence (up to 70%) of obsessive-compulsive disorder (OCD).4,5
Although individuals with Sydenham chorea appear to be at greatest risk for OCD after GABHS infection, rheumatic fever patients without chorea also appear to be at increased OCD risk.6
CASE REPORT CONTINUED: PANDAS CLUES
John’s sudden-onset compulsive behaviors and obsessive thoughts exemplify the rapid symptom onset often seen in children with PANDAS. His medical records showed a temporal relationship between his streptococcal infection and symptom exacerbations, which his parents confirmed. On examination, we noted choreiform movements when we asked John to extend his hands in a supinated position.
Because this was John’s first documented presentation of PANDAS-like symptoms, an additional episode would provide more convincing support for classifying his OCD as the PANDAS subtype.
DIAGNOSTIC CRITERIA
National Institute of Mental Health (NIMH) diagnostic guidelines for PANDAS,7 initially proposed as working guidelines by Swedo and colleagues,8 are listed in Table 1.
Time between GABHS infection and symptom onset varies, but post-streptococcal diseases generally emerge after a few days to several weeks.9 Because this latent period makes retrospective assessment difficult,10 NIMH guidelines require a prospective link between GABHS infection and at least two OCD/tic symptom episodes.7,8,11 These additional criteria are necessary to avoid misdiagnosing PANDAS in cases when the GABHS infection/OCD connection is spurious.
Table 1
Guidelines for PANDAS diagnosis
| Presence of obsessive-compulsive disorder and/or tic disorder |
| Pediatric symptom onset (age 3 years to puberty) |
| Episodic course of symptom severity |
| Prospectively established association between group A beta-hemolytic streptococcal infection (GABHS)—as shown by positive throat culture and/or elevated anti-GABHS antibody titers and at least 2 separate OCD/tic symptom episodes |
| Association with neurologic abnormalities (motoric hyperactivity or adventitious movements, such as choreiform movements) |
| PANDAS: pediatric autoimmune neuropsychiatric disorders associated with streptococcus |
| Source: References 7, 8, and 11 |
PROSPECTIVE DIAGNOSIS
Neuropsychiatric symptoms. Early PANDAS symptoms are often similar to those of pediatric OCD and tic disorders (Table 2). Notable differences include:
- Sudden onset of obsessive-compulsive or tic behaviors shortly after GABHS infection, as opposed to OCD’s typical insidious course.
- Prepubertal onset (average age 7, as with Tourette’s syndrome7,8), compared with average age 10 of childhood OCD.12
Compulsions reported in PANDAS include germ-related behaviors such as hand washing, hoarding, and excessive toilet hygiene rituals. Most studies show consistent gender differences, with more washing behaviors by girls and more checking behaviors, aggression, and tics among boys.13
Recurrences. PANDAS has an episodic course, and approximately 50% of patients experience recurrences.13 Whether PANDAS remits completely, becomes dormant when neuropsychiatric symptoms are waning, or consistently progresses to a more chronic illness is unclear.
Because young children diagnosed with PANDAS often have repeated, frequent GABHS infections,8 give careful attention to:
- unexplained abdominal pain accompanied by fever
- history of scarlet fever
- brief episodes of tics, OCD, or compulsive urination that remitted
- illness accompanied by sudden onset of OCD or tic-like behaviors
- history of sore throats not severe enough to seek medical attention
- dramatic improvement in behavior/neuropsychiatric symptoms following standard antibiotictherapy for unrelated infection.
Differential diagnosis of OCD, tic disorders, and PANDAS
| Characteristic | OCD | Tourette’s/tic disorders | PANDAS |
|---|---|---|---|
| Typical age of onset | 10 years | 7 years | 7 years |
| Gender relatedness | Slightly higher prevalence in boys than girls before age 15; female-to-male ratio increases after puberty | 2:1 male-to-female ratio | 5:1 male-to-female ratio before age 8; thereafter, boys slightly outnumber girls |
| Course | Typically unremitting, though some episodic cases reported | Peak severity at age 10; 50% of cases remit by late teens | Episodic or sawtooth course; long-term prognosis unknown |
| Involvement of basal ganglia | Strong evidence | Strong evidence | Good evidence |
| GABHS trigger | Reported; cause uncertain | Reported in some cases; cause uncertain | Proposed association |
| Neurologic findings | Increased findings of NSS, including choreiform movements | Increased findings of NSS, including choreiform movements | Choreiform movements |
| GABHS: group A beta-hemolytic streptococcal infection | |||
| NSS: neurologic soft signs | |||
| OCD: obsessive-compulsive disorder | |||
| PANDAS: pediatric autoimmune neuropsychiatric disorders associated with streptococcus | |||
WEIGHING TREATMENT OPTIONS
Antibiotics. Antibiotic treatment of GABHS infection has been thoroughly studied among patients with rheumatic fever. American Heart Association guidelines for preventing rheumatic fever after GABHS infection recommend oral penicillin, 250 mg bid.14 Studies also indicate that using azithromycin, 500 mg once weekly, can protect against GABHS infection but may also increase resistance to macrolide antibiotics.15
Because antibiotic prophylaxis for GABHS infection is effective for rheumatic fever, some researchers have hypothesized that similar treatment would reduce neuropsychiatric symptoms in PANDAS patients.
In a double-blind, randomized, controlled trial, Snider et al16 found significant decreases in GABHS infection and neuropsychiatric symptoms in 23 PANDAS patients who took penicillin (250 mg bid) or azithromycin (250 mg bid on one day of the week) for 12 months.
An earlier study using penicillin for PANDAS prophylaxis was inconclusive. Its design limited more-definitive conclusions by allowing a high rate of antibiotic use during the placebo phase.17
An uncontrolled prospective study by Murphy et al13 documented rapid resolution of primary OCD, tic, and anxiety symptoms after appropriate antibiotic treatment in 12 children with PANDAS. Obsessive-compulsive symptoms remitted 5 to 21 days after patients received penicillin, amoxicillin/clavulanate potassium, or a cephalosporin. Symptoms resolved much more quickly than nonPANDAS obsessive-compulsive and tic disorders usually remit with cognitive-behavioral, habit reversal, and/or drug treatment.18 One-half of patients had at least one OCD recurrence, all documented as GABHS-positive with throat culture or rapid antigen-detection assay.
Recommendation. Obtain a GABHS culture if a child presents with sudden-onset OCD. If positive, treat with a standard course of antibiotics.19 Caution is strongly recommended when using antibiotics in children, as antibiotic-resistant organisms may develop. Collaborate with the child’s pediatrician to ensure that strep infections are treated consistently.
CASE CONTINUED: USING CBT FOR PANDAS
Giving John antibiotics when he had the sore throat might have been a rational choice to manage acute OCD symptoms. However, the scant literature on antibiotic prophylaxis for PANDAS subtype OCD led us to also consider cognitive-behavioral therapy (CBT).
CBT alone or with a selective serotonin reuptake inhibitor (SSRI) is first-line therapy for pediatric OCD.18,20 We hypothesized, therefore, that CBT might also be useful in PANDAS and provided John with five CBT sessions within 1 week, without giving an antibiotic or other medication. [See our study21 for therapy details.]
At baseline, John’s score on the Children’s Yale-Brown Obsessive-Compulsive Scale (CY-BOCS) was 34, indicating severe OCD symptoms, and his score on the Anxiety/Depression subscale of the Child Behavior Checklist (CBCL) was elevated (t = 66). After five CBT sessions, John’s CY-BOCS score decreased by 75% to 8 and his CBCL Anxiety/Depression score decreased into the average range (t = 50).21
Given PANDAS’ fluctuating course, his symptoms could have remitted spontaneously. His symptoms remained in remission 6 months later.
We believe John’s case is the only published description of using CBT alone to treat a patient with PANDAS. Since then, our team has successfully treated several other PANDAS patients using CBT. Based on our experience with trained clinicians, CBT provided an appropriate treatment option for this handful of cases. Controlled trials are needed to establish CBT’s efficacy for treating documented PANDAS.
SSRIs. As stated, CBT alone or with an SSRI is first-line therapy for pediatric OCD, and CBT alone or with an SSRI reduces pediatric OCD symptoms more effectively than antidepressants alone.18 Because no published reports of SSRI use in PANDAS exist, we recommend treating a child with PANDAS as you would any child presenting with OCD and tics:
- For milder cases with recent onset, begin with clinical monitoring for GABHS, without using SSRIs or antibiotics. Early CBT may prevent symptom worsening.
- For more severecases of longer duration, continue with CBT, then consider adding an SSRI.
Immunomodulatory therapies? Immunomodulatory therapies such as IV immunoglobulin (IVIG) and plasma exchange are not appropriate for refractory OCD or tic cases that have no clear GABHS association and a relapsing/remitting course. No studies support using immunomodulatory agents in disorders without an immune-mediated cause.
You might consider these therapies for severe, clearly established PANDAS only when less-invasive treatments (antibiotics, standard OCD therapies) have been ineffective and then only under research protocols and by physicians experienced in giving them.
Immunomodulatory therapies interrupt autoantibodies’ actions on the CNS and have shown moderate (40% to 50%) symptom reduction in some CNS diseases. In the NIMH trial, plasma exchange was better tolerated than IVIG and provided greater symptom relief.22 However, at least one study has shown plasma exchange to be ineffective for chronic OCD.23
USING ANTIBIOTICS FOR PANDAS
Snider and Swedo24 recommend guidelines for treating PANDAS, based on risks of using antibiotics in children, research and clinical experience, and American Academy of Child and Adolescent Psychiatry practice parameters (Box 2).
Elevated streptococcal titers are common in the community population25 and are not necessarily diagnostic of PANDAS. Thus, it is important to demonstrate a change in titer levels (such as a 4-fold dilution rise in antistreptococcal antibody titers 4 to 6 weeks after infection).
In patients with new-onset OCD/tics or recent symptom exacerbation, a positive throat culture provides support that symptoms were triggered by subclinical GABHS infection but does not rule out the possibility that the child is a GABHS carrier.
After streptococcal infections, titers may remain elevated for 6 months to 1 year. Murphy et al25 found persistent elevations in one or more strep titers in patients with dramatically fluctuating neuropsychiatric symptoms, compared with those whose course was inconsistent with PANDAS. It is unclear if these children had undetected, frequent GABHS infections or the elevated titers reflect a chronic immune activation to GABHS.
Assess for GABHS infectionin young children with abrupt-onset, obsessive-compulsive/tic-like behaviors (suspected PANDAS), using a 48-hour throat culture. If positive, promptly give a 10-day course of antibiotics effective for acute GABHS treatment (penicillins, cephalosporins, azithromycin).
Attempt to documenta preceding GABHS infection if neuropsychiatric symptoms began abruptly 4 to 6 weeks ago. Perform a 48-hour throat culture and a blood test for antistreptococcal antibody titers (ASO and anti-DNaseB). Do not give antibiotics unless GABHS culture is positive.
A rising titer 4 to 6 weeks later would suggest a recent infection. A single elevated titer does not adequately support a recent strep infection, as some individuals have elevated titers 6 months or longer after GABHS infection.
Consider prospective assessmentfor GABHS infections in children with episodic symptoms. Obtain throat cultures when neuropsychiatric symptoms return/exacerbate, as even untreated strep infections are usually self-limited.
Reserve antibiotic prophylaxisfor use under research protocols and based on solid evidence of PANDAS diagnosis.
Use immunomodulatory therapiesunder research protocols and only for children with acute, severe symptoms who fit the PANDAS designation.
Source: Reference 24.
- National Institute of Mental Health. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS).http://intramural.nimh.nih.gov/pdn/web.htm.
- Murphy TK, Herbstman, DM, Edge PJ. Infectious trigger in obsessive compulsive and tic disorders. In: Fatemi SH (ed). Infectious etiologies of neuropsychiatric disorders. New York: Taylor & Francis (in press).
- Amoxicillin/potassium clavulanate • Augmentin
- Azithromycin • Zithromax
Michael Larson reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Storch receives grant support from the National Institute of Health and Genentech Inc.
Dr. Murphy receives grant support from the National Institute of Mental Health, Bristol-Myers Squibb Co., and the Tourette Syndrome Association (TSA). She is a speaker for Pfizer, Inc.
1. Snider LA, Swedo SE. PANDAS: current status and directions for research. Mol Psychiatry 2004;9(10):900-7.
2. Hosier DM, Craenen JM, Teske DW, Wheller JJ. Resurgence of acute rheumatic fever. Am J Dis Child 1987;141:730-3.
3. Stollerman GH. Rheumatic fever. Lancet 1997;349:935-42.
4. Swedo S, Leonard HL, Schapiro MB, et al. Sydenham’s chorea: Physical and psychological symptoms of St.Vitus’ dance. Pediatrics 1993;91:706-13.
5. Asbahr FR, Negrao AB, Gentil V, et al. Obsessive-compulsive and related symptoms in children and adolescents with rheumatic fever with and without chorea: A prospective 6-month study. Am J Psychiatry 1998;155:1122-4.
6. Mercadante MT, Busatto GF, Lombroso PJ, et al. The psychiatric symptoms of rheumatic fever. Am J Psychiatry 2000;157:2036-8.
7. National Institute of Mental Health. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections. Available at: http://intramural.nimh.nih.gov/pdn/web.htm. Accessed June 9, 2005.
8. Swedo SE, Leonard HL, Garvey M, et al. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: clinical description of the first 50 cases. Am J Psychiatry 1998;155(2):264-71.
9. Kim SW, Grant JE, Kim SI, et al. A possible association of recurrent streptococcal infections and acute onset of obsessive-compulsive disorder. J Neuropsychiatry Clin Neurosci 2004;16(3):252-60.
10. Garvey MA, Giedd J, Swedo SE. PANDAS: the search for environmental triggers of pediatric neuropsychiatric disorders. Lessons from rheumatic fever. J Child Neurol 1998;13(9):413-23.
11. March JS. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS): implications for clinical practice. Arch Pediatr Adolesc Med 2004;158:927-9.
12. Zohar AH. The epidemiology of obsessive-compulsive disorder in children and adolescents. Child Adolesc Psychiatr Clin N Am 1999;8:445-59.
13. Murphy ML, Pichichero ME. Prospective identification and treatment of children with pediatric autoimmune neuropsychiatric disorder associated with group A streptococcal infection (PANDAS). Arch Pediatr Adolesc Med 2002;156(4):356-61.
14. Dajani A, Taubert K, Ferrieri P, et al. Treatment of acute streptococcal pharyngitis and prevention of rheumatic fever: a statement for health professionals. Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young, the American Heart Association. Pediatrics 1995;96:758-764.
15. Gray GC, McPhate DC, Leinonen M, et al. Weekly oral azithromycin as prophylaxis for agents causing acute respiratory disease. Clin Infect Dis 1998;26:103-10.
16. Snider LA, Lougee L, Slattery M, et al. Antibiotic prophylaxis with azithromycin or penicillin for childhood-onset neuropsychiatric disorders. Biol Psychiatry 2005;57:788-92.
17. Garvey MA, Perlmutter SJ, Allen AJ, et al. A pilot study of penicillin prophylaxis for neuropsychiatric exacerbations triggered by streptococcal infections. Biol Psychiatry 1999;45(12):1564-71.
18. Pediatric OCD Treatment Study (POTS) Team. Cognitive-behavior therapy, sertraline, and their combination for children and adolescents with obsessive-compulsive disorder: the Pediatric OCD Treatment Study (POTS) randomized controlled trial. JAMA 2004;292(16):1969-76.
19. Leonard HL, Swedo SE. Paediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS). Int J Neuropsychopharmacol 2001;4(2):191-8.
20. Snider LA, Swedo SE. Childhood-onset obsessive-compulsive disorder and tic disorders: case report and literature review. J Child Adolesc Psychopharmacol 2003;13(suppl 1):S81-S88.
21. Storch EA, Gerdes AC, Adkins JW, et al. Behavioral treatment of a child with PANDAS. J Am Acad Child Adolesc Psychiatry 2004;43(5):510-11.
22. Nicolson R, Swedo SE, Lenane M, et al. An open trial of plasma exchange in childhood-onset obsessive-compulsive disorder without poststreptococcal exacerbations. J Am Acad Child Adolesc Psychiatry 2000;39(10):1313-5.
23. Perlmutter SJ, Leitman SF, Garvey MA, et al. Therapeutic plasma exchange and intravenous immunoglobulin for obsessive-compulsive disorder and tic disorders in childhood. Lancet 1999;354 (9185):1153-8.
24. Snider LA, Swedo SE. Post-streptococcal autoimmune disorders of the central nervous system. Curr Opin Neurol 2003;16:359-65.
25. Murphy TK, Sajid M, Soto O, et al. Detecting pediatric autoimmune neuropsychiatric disorders associated with streptococcus in children with obsessive-compulsive disorder and tics. Biol Psychiatry 2004;55(1):61-8.
John, age 6, presented for psychiatric evaluation with acute, incapacitating obsessive-compulsive symptoms. For 4 weeks he washed his hands compulsively and had pervasive obsessions about death by choking.
These symptoms had suddenly worsened over 2 days. At first, he washed his hands more than 35 times per day in rituals lasting several minutes each. Then, within 2 weeks, John’s handwashing spontaneously decreased, but his choking fears dramatically increased. He refused all solid foods and continuously sought reassurance from his parents that he would not choke or die.
Approximately 1 week before these symptoms began, John had a sore throat and tested positive via throat culture for group A beta-hemolytic streptococcal infection (GABHS).
Sore throat followed by sudden-onset obsessive-compulsive symptoms or tics in a child such as John suggests a pediatric autoimmune neuropsychiatric disorder associated with streptococcal infection (PANDAS). The association between GABHS infection and these symptoms remains uncertain, as the mechanism by which GABHS infection may cause obsessive-compulsive symptoms and other childhood-onset neuropsychiatric disorders is largely unknown.
Since PANDAS was recognized (Box 1),1-6 some data have emerged on the disorder’s symptoms, course, and prognosis. However:
- diagnostic criteria are not well-defined
- few controlled studies have examined treatment response
- using antibiotics and immunotherapies to treat or prevent PANDAS symptoms remains controversial because of unproven efficacy and potential adverse effects.
To help you diagnose and treat patients with suspected PANDAS, this article examines the limited evidence for the disorder, discusses diagnostic guidelines, and reviews preliminary indications for behavioral and medical treatments.
PANDAS stands for pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections. It describes childhoodonset OCD or tic cases whose onset or worsening appears to be linked to group A beta-hemolytic streptococcal (GABHS) infection.
GABHS antibodies cross-react with the cellular components of the basal ganglia, particularly in the caudate nucleus.1 PANDAS was first recognized in 1987 during an unexpected resurgence of rheumatic fever in the United States.2 Sydenham chorea is thought to occur when GABHS antibodies undergo molecular mimicry and cross-react with epitopes on neurons in the basal ganglia and other brain areas, causing motor and behavioral disruptions.3 Rheumatic fever patients with Sydenham chorea show a high prevalence (up to 70%) of obsessive-compulsive disorder (OCD).4,5
Although individuals with Sydenham chorea appear to be at greatest risk for OCD after GABHS infection, rheumatic fever patients without chorea also appear to be at increased OCD risk.6
CASE REPORT CONTINUED: PANDAS CLUES
John’s sudden-onset compulsive behaviors and obsessive thoughts exemplify the rapid symptom onset often seen in children with PANDAS. His medical records showed a temporal relationship between his streptococcal infection and symptom exacerbations, which his parents confirmed. On examination, we noted choreiform movements when we asked John to extend his hands in a supinated position.
Because this was John’s first documented presentation of PANDAS-like symptoms, an additional episode would provide more convincing support for classifying his OCD as the PANDAS subtype.
DIAGNOSTIC CRITERIA
National Institute of Mental Health (NIMH) diagnostic guidelines for PANDAS,7 initially proposed as working guidelines by Swedo and colleagues,8 are listed in Table 1.
Time between GABHS infection and symptom onset varies, but post-streptococcal diseases generally emerge after a few days to several weeks.9 Because this latent period makes retrospective assessment difficult,10 NIMH guidelines require a prospective link between GABHS infection and at least two OCD/tic symptom episodes.7,8,11 These additional criteria are necessary to avoid misdiagnosing PANDAS in cases when the GABHS infection/OCD connection is spurious.
Table 1
Guidelines for PANDAS diagnosis
| Presence of obsessive-compulsive disorder and/or tic disorder |
| Pediatric symptom onset (age 3 years to puberty) |
| Episodic course of symptom severity |
| Prospectively established association between group A beta-hemolytic streptococcal infection (GABHS)—as shown by positive throat culture and/or elevated anti-GABHS antibody titers and at least 2 separate OCD/tic symptom episodes |
| Association with neurologic abnormalities (motoric hyperactivity or adventitious movements, such as choreiform movements) |
| PANDAS: pediatric autoimmune neuropsychiatric disorders associated with streptococcus |
| Source: References 7, 8, and 11 |
PROSPECTIVE DIAGNOSIS
Neuropsychiatric symptoms. Early PANDAS symptoms are often similar to those of pediatric OCD and tic disorders (Table 2). Notable differences include:
- Sudden onset of obsessive-compulsive or tic behaviors shortly after GABHS infection, as opposed to OCD’s typical insidious course.
- Prepubertal onset (average age 7, as with Tourette’s syndrome7,8), compared with average age 10 of childhood OCD.12
Compulsions reported in PANDAS include germ-related behaviors such as hand washing, hoarding, and excessive toilet hygiene rituals. Most studies show consistent gender differences, with more washing behaviors by girls and more checking behaviors, aggression, and tics among boys.13
Recurrences. PANDAS has an episodic course, and approximately 50% of patients experience recurrences.13 Whether PANDAS remits completely, becomes dormant when neuropsychiatric symptoms are waning, or consistently progresses to a more chronic illness is unclear.
Because young children diagnosed with PANDAS often have repeated, frequent GABHS infections,8 give careful attention to:
- unexplained abdominal pain accompanied by fever
- history of scarlet fever
- brief episodes of tics, OCD, or compulsive urination that remitted
- illness accompanied by sudden onset of OCD or tic-like behaviors
- history of sore throats not severe enough to seek medical attention
- dramatic improvement in behavior/neuropsychiatric symptoms following standard antibiotictherapy for unrelated infection.
Differential diagnosis of OCD, tic disorders, and PANDAS
| Characteristic | OCD | Tourette’s/tic disorders | PANDAS |
|---|---|---|---|
| Typical age of onset | 10 years | 7 years | 7 years |
| Gender relatedness | Slightly higher prevalence in boys than girls before age 15; female-to-male ratio increases after puberty | 2:1 male-to-female ratio | 5:1 male-to-female ratio before age 8; thereafter, boys slightly outnumber girls |
| Course | Typically unremitting, though some episodic cases reported | Peak severity at age 10; 50% of cases remit by late teens | Episodic or sawtooth course; long-term prognosis unknown |
| Involvement of basal ganglia | Strong evidence | Strong evidence | Good evidence |
| GABHS trigger | Reported; cause uncertain | Reported in some cases; cause uncertain | Proposed association |
| Neurologic findings | Increased findings of NSS, including choreiform movements | Increased findings of NSS, including choreiform movements | Choreiform movements |
| GABHS: group A beta-hemolytic streptococcal infection | |||
| NSS: neurologic soft signs | |||
| OCD: obsessive-compulsive disorder | |||
| PANDAS: pediatric autoimmune neuropsychiatric disorders associated with streptococcus | |||
WEIGHING TREATMENT OPTIONS
Antibiotics. Antibiotic treatment of GABHS infection has been thoroughly studied among patients with rheumatic fever. American Heart Association guidelines for preventing rheumatic fever after GABHS infection recommend oral penicillin, 250 mg bid.14 Studies also indicate that using azithromycin, 500 mg once weekly, can protect against GABHS infection but may also increase resistance to macrolide antibiotics.15
Because antibiotic prophylaxis for GABHS infection is effective for rheumatic fever, some researchers have hypothesized that similar treatment would reduce neuropsychiatric symptoms in PANDAS patients.
In a double-blind, randomized, controlled trial, Snider et al16 found significant decreases in GABHS infection and neuropsychiatric symptoms in 23 PANDAS patients who took penicillin (250 mg bid) or azithromycin (250 mg bid on one day of the week) for 12 months.
An earlier study using penicillin for PANDAS prophylaxis was inconclusive. Its design limited more-definitive conclusions by allowing a high rate of antibiotic use during the placebo phase.17
An uncontrolled prospective study by Murphy et al13 documented rapid resolution of primary OCD, tic, and anxiety symptoms after appropriate antibiotic treatment in 12 children with PANDAS. Obsessive-compulsive symptoms remitted 5 to 21 days after patients received penicillin, amoxicillin/clavulanate potassium, or a cephalosporin. Symptoms resolved much more quickly than nonPANDAS obsessive-compulsive and tic disorders usually remit with cognitive-behavioral, habit reversal, and/or drug treatment.18 One-half of patients had at least one OCD recurrence, all documented as GABHS-positive with throat culture or rapid antigen-detection assay.
Recommendation. Obtain a GABHS culture if a child presents with sudden-onset OCD. If positive, treat with a standard course of antibiotics.19 Caution is strongly recommended when using antibiotics in children, as antibiotic-resistant organisms may develop. Collaborate with the child’s pediatrician to ensure that strep infections are treated consistently.
CASE CONTINUED: USING CBT FOR PANDAS
Giving John antibiotics when he had the sore throat might have been a rational choice to manage acute OCD symptoms. However, the scant literature on antibiotic prophylaxis for PANDAS subtype OCD led us to also consider cognitive-behavioral therapy (CBT).
CBT alone or with a selective serotonin reuptake inhibitor (SSRI) is first-line therapy for pediatric OCD.18,20 We hypothesized, therefore, that CBT might also be useful in PANDAS and provided John with five CBT sessions within 1 week, without giving an antibiotic or other medication. [See our study21 for therapy details.]
At baseline, John’s score on the Children’s Yale-Brown Obsessive-Compulsive Scale (CY-BOCS) was 34, indicating severe OCD symptoms, and his score on the Anxiety/Depression subscale of the Child Behavior Checklist (CBCL) was elevated (t = 66). After five CBT sessions, John’s CY-BOCS score decreased by 75% to 8 and his CBCL Anxiety/Depression score decreased into the average range (t = 50).21
Given PANDAS’ fluctuating course, his symptoms could have remitted spontaneously. His symptoms remained in remission 6 months later.
We believe John’s case is the only published description of using CBT alone to treat a patient with PANDAS. Since then, our team has successfully treated several other PANDAS patients using CBT. Based on our experience with trained clinicians, CBT provided an appropriate treatment option for this handful of cases. Controlled trials are needed to establish CBT’s efficacy for treating documented PANDAS.
SSRIs. As stated, CBT alone or with an SSRI is first-line therapy for pediatric OCD, and CBT alone or with an SSRI reduces pediatric OCD symptoms more effectively than antidepressants alone.18 Because no published reports of SSRI use in PANDAS exist, we recommend treating a child with PANDAS as you would any child presenting with OCD and tics:
- For milder cases with recent onset, begin with clinical monitoring for GABHS, without using SSRIs or antibiotics. Early CBT may prevent symptom worsening.
- For more severecases of longer duration, continue with CBT, then consider adding an SSRI.
Immunomodulatory therapies? Immunomodulatory therapies such as IV immunoglobulin (IVIG) and plasma exchange are not appropriate for refractory OCD or tic cases that have no clear GABHS association and a relapsing/remitting course. No studies support using immunomodulatory agents in disorders without an immune-mediated cause.
You might consider these therapies for severe, clearly established PANDAS only when less-invasive treatments (antibiotics, standard OCD therapies) have been ineffective and then only under research protocols and by physicians experienced in giving them.
Immunomodulatory therapies interrupt autoantibodies’ actions on the CNS and have shown moderate (40% to 50%) symptom reduction in some CNS diseases. In the NIMH trial, plasma exchange was better tolerated than IVIG and provided greater symptom relief.22 However, at least one study has shown plasma exchange to be ineffective for chronic OCD.23
USING ANTIBIOTICS FOR PANDAS
Snider and Swedo24 recommend guidelines for treating PANDAS, based on risks of using antibiotics in children, research and clinical experience, and American Academy of Child and Adolescent Psychiatry practice parameters (Box 2).
Elevated streptococcal titers are common in the community population25 and are not necessarily diagnostic of PANDAS. Thus, it is important to demonstrate a change in titer levels (such as a 4-fold dilution rise in antistreptococcal antibody titers 4 to 6 weeks after infection).
In patients with new-onset OCD/tics or recent symptom exacerbation, a positive throat culture provides support that symptoms were triggered by subclinical GABHS infection but does not rule out the possibility that the child is a GABHS carrier.
After streptococcal infections, titers may remain elevated for 6 months to 1 year. Murphy et al25 found persistent elevations in one or more strep titers in patients with dramatically fluctuating neuropsychiatric symptoms, compared with those whose course was inconsistent with PANDAS. It is unclear if these children had undetected, frequent GABHS infections or the elevated titers reflect a chronic immune activation to GABHS.
Assess for GABHS infectionin young children with abrupt-onset, obsessive-compulsive/tic-like behaviors (suspected PANDAS), using a 48-hour throat culture. If positive, promptly give a 10-day course of antibiotics effective for acute GABHS treatment (penicillins, cephalosporins, azithromycin).
Attempt to documenta preceding GABHS infection if neuropsychiatric symptoms began abruptly 4 to 6 weeks ago. Perform a 48-hour throat culture and a blood test for antistreptococcal antibody titers (ASO and anti-DNaseB). Do not give antibiotics unless GABHS culture is positive.
A rising titer 4 to 6 weeks later would suggest a recent infection. A single elevated titer does not adequately support a recent strep infection, as some individuals have elevated titers 6 months or longer after GABHS infection.
Consider prospective assessmentfor GABHS infections in children with episodic symptoms. Obtain throat cultures when neuropsychiatric symptoms return/exacerbate, as even untreated strep infections are usually self-limited.
Reserve antibiotic prophylaxisfor use under research protocols and based on solid evidence of PANDAS diagnosis.
Use immunomodulatory therapiesunder research protocols and only for children with acute, severe symptoms who fit the PANDAS designation.
Source: Reference 24.
- National Institute of Mental Health. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS).http://intramural.nimh.nih.gov/pdn/web.htm.
- Murphy TK, Herbstman, DM, Edge PJ. Infectious trigger in obsessive compulsive and tic disorders. In: Fatemi SH (ed). Infectious etiologies of neuropsychiatric disorders. New York: Taylor & Francis (in press).
- Amoxicillin/potassium clavulanate • Augmentin
- Azithromycin • Zithromax
Michael Larson reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Storch receives grant support from the National Institute of Health and Genentech Inc.
Dr. Murphy receives grant support from the National Institute of Mental Health, Bristol-Myers Squibb Co., and the Tourette Syndrome Association (TSA). She is a speaker for Pfizer, Inc.
John, age 6, presented for psychiatric evaluation with acute, incapacitating obsessive-compulsive symptoms. For 4 weeks he washed his hands compulsively and had pervasive obsessions about death by choking.
These symptoms had suddenly worsened over 2 days. At first, he washed his hands more than 35 times per day in rituals lasting several minutes each. Then, within 2 weeks, John’s handwashing spontaneously decreased, but his choking fears dramatically increased. He refused all solid foods and continuously sought reassurance from his parents that he would not choke or die.
Approximately 1 week before these symptoms began, John had a sore throat and tested positive via throat culture for group A beta-hemolytic streptococcal infection (GABHS).
Sore throat followed by sudden-onset obsessive-compulsive symptoms or tics in a child such as John suggests a pediatric autoimmune neuropsychiatric disorder associated with streptococcal infection (PANDAS). The association between GABHS infection and these symptoms remains uncertain, as the mechanism by which GABHS infection may cause obsessive-compulsive symptoms and other childhood-onset neuropsychiatric disorders is largely unknown.
Since PANDAS was recognized (Box 1),1-6 some data have emerged on the disorder’s symptoms, course, and prognosis. However:
- diagnostic criteria are not well-defined
- few controlled studies have examined treatment response
- using antibiotics and immunotherapies to treat or prevent PANDAS symptoms remains controversial because of unproven efficacy and potential adverse effects.
To help you diagnose and treat patients with suspected PANDAS, this article examines the limited evidence for the disorder, discusses diagnostic guidelines, and reviews preliminary indications for behavioral and medical treatments.
PANDAS stands for pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections. It describes childhoodonset OCD or tic cases whose onset or worsening appears to be linked to group A beta-hemolytic streptococcal (GABHS) infection.
GABHS antibodies cross-react with the cellular components of the basal ganglia, particularly in the caudate nucleus.1 PANDAS was first recognized in 1987 during an unexpected resurgence of rheumatic fever in the United States.2 Sydenham chorea is thought to occur when GABHS antibodies undergo molecular mimicry and cross-react with epitopes on neurons in the basal ganglia and other brain areas, causing motor and behavioral disruptions.3 Rheumatic fever patients with Sydenham chorea show a high prevalence (up to 70%) of obsessive-compulsive disorder (OCD).4,5
Although individuals with Sydenham chorea appear to be at greatest risk for OCD after GABHS infection, rheumatic fever patients without chorea also appear to be at increased OCD risk.6
CASE REPORT CONTINUED: PANDAS CLUES
John’s sudden-onset compulsive behaviors and obsessive thoughts exemplify the rapid symptom onset often seen in children with PANDAS. His medical records showed a temporal relationship between his streptococcal infection and symptom exacerbations, which his parents confirmed. On examination, we noted choreiform movements when we asked John to extend his hands in a supinated position.
Because this was John’s first documented presentation of PANDAS-like symptoms, an additional episode would provide more convincing support for classifying his OCD as the PANDAS subtype.
DIAGNOSTIC CRITERIA
National Institute of Mental Health (NIMH) diagnostic guidelines for PANDAS,7 initially proposed as working guidelines by Swedo and colleagues,8 are listed in Table 1.
Time between GABHS infection and symptom onset varies, but post-streptococcal diseases generally emerge after a few days to several weeks.9 Because this latent period makes retrospective assessment difficult,10 NIMH guidelines require a prospective link between GABHS infection and at least two OCD/tic symptom episodes.7,8,11 These additional criteria are necessary to avoid misdiagnosing PANDAS in cases when the GABHS infection/OCD connection is spurious.
Table 1
Guidelines for PANDAS diagnosis
| Presence of obsessive-compulsive disorder and/or tic disorder |
| Pediatric symptom onset (age 3 years to puberty) |
| Episodic course of symptom severity |
| Prospectively established association between group A beta-hemolytic streptococcal infection (GABHS)—as shown by positive throat culture and/or elevated anti-GABHS antibody titers and at least 2 separate OCD/tic symptom episodes |
| Association with neurologic abnormalities (motoric hyperactivity or adventitious movements, such as choreiform movements) |
| PANDAS: pediatric autoimmune neuropsychiatric disorders associated with streptococcus |
| Source: References 7, 8, and 11 |
PROSPECTIVE DIAGNOSIS
Neuropsychiatric symptoms. Early PANDAS symptoms are often similar to those of pediatric OCD and tic disorders (Table 2). Notable differences include:
- Sudden onset of obsessive-compulsive or tic behaviors shortly after GABHS infection, as opposed to OCD’s typical insidious course.
- Prepubertal onset (average age 7, as with Tourette’s syndrome7,8), compared with average age 10 of childhood OCD.12
Compulsions reported in PANDAS include germ-related behaviors such as hand washing, hoarding, and excessive toilet hygiene rituals. Most studies show consistent gender differences, with more washing behaviors by girls and more checking behaviors, aggression, and tics among boys.13
Recurrences. PANDAS has an episodic course, and approximately 50% of patients experience recurrences.13 Whether PANDAS remits completely, becomes dormant when neuropsychiatric symptoms are waning, or consistently progresses to a more chronic illness is unclear.
Because young children diagnosed with PANDAS often have repeated, frequent GABHS infections,8 give careful attention to:
- unexplained abdominal pain accompanied by fever
- history of scarlet fever
- brief episodes of tics, OCD, or compulsive urination that remitted
- illness accompanied by sudden onset of OCD or tic-like behaviors
- history of sore throats not severe enough to seek medical attention
- dramatic improvement in behavior/neuropsychiatric symptoms following standard antibiotictherapy for unrelated infection.
Differential diagnosis of OCD, tic disorders, and PANDAS
| Characteristic | OCD | Tourette’s/tic disorders | PANDAS |
|---|---|---|---|
| Typical age of onset | 10 years | 7 years | 7 years |
| Gender relatedness | Slightly higher prevalence in boys than girls before age 15; female-to-male ratio increases after puberty | 2:1 male-to-female ratio | 5:1 male-to-female ratio before age 8; thereafter, boys slightly outnumber girls |
| Course | Typically unremitting, though some episodic cases reported | Peak severity at age 10; 50% of cases remit by late teens | Episodic or sawtooth course; long-term prognosis unknown |
| Involvement of basal ganglia | Strong evidence | Strong evidence | Good evidence |
| GABHS trigger | Reported; cause uncertain | Reported in some cases; cause uncertain | Proposed association |
| Neurologic findings | Increased findings of NSS, including choreiform movements | Increased findings of NSS, including choreiform movements | Choreiform movements |
| GABHS: group A beta-hemolytic streptococcal infection | |||
| NSS: neurologic soft signs | |||
| OCD: obsessive-compulsive disorder | |||
| PANDAS: pediatric autoimmune neuropsychiatric disorders associated with streptococcus | |||
WEIGHING TREATMENT OPTIONS
Antibiotics. Antibiotic treatment of GABHS infection has been thoroughly studied among patients with rheumatic fever. American Heart Association guidelines for preventing rheumatic fever after GABHS infection recommend oral penicillin, 250 mg bid.14 Studies also indicate that using azithromycin, 500 mg once weekly, can protect against GABHS infection but may also increase resistance to macrolide antibiotics.15
Because antibiotic prophylaxis for GABHS infection is effective for rheumatic fever, some researchers have hypothesized that similar treatment would reduce neuropsychiatric symptoms in PANDAS patients.
In a double-blind, randomized, controlled trial, Snider et al16 found significant decreases in GABHS infection and neuropsychiatric symptoms in 23 PANDAS patients who took penicillin (250 mg bid) or azithromycin (250 mg bid on one day of the week) for 12 months.
An earlier study using penicillin for PANDAS prophylaxis was inconclusive. Its design limited more-definitive conclusions by allowing a high rate of antibiotic use during the placebo phase.17
An uncontrolled prospective study by Murphy et al13 documented rapid resolution of primary OCD, tic, and anxiety symptoms after appropriate antibiotic treatment in 12 children with PANDAS. Obsessive-compulsive symptoms remitted 5 to 21 days after patients received penicillin, amoxicillin/clavulanate potassium, or a cephalosporin. Symptoms resolved much more quickly than nonPANDAS obsessive-compulsive and tic disorders usually remit with cognitive-behavioral, habit reversal, and/or drug treatment.18 One-half of patients had at least one OCD recurrence, all documented as GABHS-positive with throat culture or rapid antigen-detection assay.
Recommendation. Obtain a GABHS culture if a child presents with sudden-onset OCD. If positive, treat with a standard course of antibiotics.19 Caution is strongly recommended when using antibiotics in children, as antibiotic-resistant organisms may develop. Collaborate with the child’s pediatrician to ensure that strep infections are treated consistently.
CASE CONTINUED: USING CBT FOR PANDAS
Giving John antibiotics when he had the sore throat might have been a rational choice to manage acute OCD symptoms. However, the scant literature on antibiotic prophylaxis for PANDAS subtype OCD led us to also consider cognitive-behavioral therapy (CBT).
CBT alone or with a selective serotonin reuptake inhibitor (SSRI) is first-line therapy for pediatric OCD.18,20 We hypothesized, therefore, that CBT might also be useful in PANDAS and provided John with five CBT sessions within 1 week, without giving an antibiotic or other medication. [See our study21 for therapy details.]
At baseline, John’s score on the Children’s Yale-Brown Obsessive-Compulsive Scale (CY-BOCS) was 34, indicating severe OCD symptoms, and his score on the Anxiety/Depression subscale of the Child Behavior Checklist (CBCL) was elevated (t = 66). After five CBT sessions, John’s CY-BOCS score decreased by 75% to 8 and his CBCL Anxiety/Depression score decreased into the average range (t = 50).21
Given PANDAS’ fluctuating course, his symptoms could have remitted spontaneously. His symptoms remained in remission 6 months later.
We believe John’s case is the only published description of using CBT alone to treat a patient with PANDAS. Since then, our team has successfully treated several other PANDAS patients using CBT. Based on our experience with trained clinicians, CBT provided an appropriate treatment option for this handful of cases. Controlled trials are needed to establish CBT’s efficacy for treating documented PANDAS.
SSRIs. As stated, CBT alone or with an SSRI is first-line therapy for pediatric OCD, and CBT alone or with an SSRI reduces pediatric OCD symptoms more effectively than antidepressants alone.18 Because no published reports of SSRI use in PANDAS exist, we recommend treating a child with PANDAS as you would any child presenting with OCD and tics:
- For milder cases with recent onset, begin with clinical monitoring for GABHS, without using SSRIs or antibiotics. Early CBT may prevent symptom worsening.
- For more severecases of longer duration, continue with CBT, then consider adding an SSRI.
Immunomodulatory therapies? Immunomodulatory therapies such as IV immunoglobulin (IVIG) and plasma exchange are not appropriate for refractory OCD or tic cases that have no clear GABHS association and a relapsing/remitting course. No studies support using immunomodulatory agents in disorders without an immune-mediated cause.
You might consider these therapies for severe, clearly established PANDAS only when less-invasive treatments (antibiotics, standard OCD therapies) have been ineffective and then only under research protocols and by physicians experienced in giving them.
Immunomodulatory therapies interrupt autoantibodies’ actions on the CNS and have shown moderate (40% to 50%) symptom reduction in some CNS diseases. In the NIMH trial, plasma exchange was better tolerated than IVIG and provided greater symptom relief.22 However, at least one study has shown plasma exchange to be ineffective for chronic OCD.23
USING ANTIBIOTICS FOR PANDAS
Snider and Swedo24 recommend guidelines for treating PANDAS, based on risks of using antibiotics in children, research and clinical experience, and American Academy of Child and Adolescent Psychiatry practice parameters (Box 2).
Elevated streptococcal titers are common in the community population25 and are not necessarily diagnostic of PANDAS. Thus, it is important to demonstrate a change in titer levels (such as a 4-fold dilution rise in antistreptococcal antibody titers 4 to 6 weeks after infection).
In patients with new-onset OCD/tics or recent symptom exacerbation, a positive throat culture provides support that symptoms were triggered by subclinical GABHS infection but does not rule out the possibility that the child is a GABHS carrier.
After streptococcal infections, titers may remain elevated for 6 months to 1 year. Murphy et al25 found persistent elevations in one or more strep titers in patients with dramatically fluctuating neuropsychiatric symptoms, compared with those whose course was inconsistent with PANDAS. It is unclear if these children had undetected, frequent GABHS infections or the elevated titers reflect a chronic immune activation to GABHS.
Assess for GABHS infectionin young children with abrupt-onset, obsessive-compulsive/tic-like behaviors (suspected PANDAS), using a 48-hour throat culture. If positive, promptly give a 10-day course of antibiotics effective for acute GABHS treatment (penicillins, cephalosporins, azithromycin).
Attempt to documenta preceding GABHS infection if neuropsychiatric symptoms began abruptly 4 to 6 weeks ago. Perform a 48-hour throat culture and a blood test for antistreptococcal antibody titers (ASO and anti-DNaseB). Do not give antibiotics unless GABHS culture is positive.
A rising titer 4 to 6 weeks later would suggest a recent infection. A single elevated titer does not adequately support a recent strep infection, as some individuals have elevated titers 6 months or longer after GABHS infection.
Consider prospective assessmentfor GABHS infections in children with episodic symptoms. Obtain throat cultures when neuropsychiatric symptoms return/exacerbate, as even untreated strep infections are usually self-limited.
Reserve antibiotic prophylaxisfor use under research protocols and based on solid evidence of PANDAS diagnosis.
Use immunomodulatory therapiesunder research protocols and only for children with acute, severe symptoms who fit the PANDAS designation.
Source: Reference 24.
- National Institute of Mental Health. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS).http://intramural.nimh.nih.gov/pdn/web.htm.
- Murphy TK, Herbstman, DM, Edge PJ. Infectious trigger in obsessive compulsive and tic disorders. In: Fatemi SH (ed). Infectious etiologies of neuropsychiatric disorders. New York: Taylor & Francis (in press).
- Amoxicillin/potassium clavulanate • Augmentin
- Azithromycin • Zithromax
Michael Larson reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Storch receives grant support from the National Institute of Health and Genentech Inc.
Dr. Murphy receives grant support from the National Institute of Mental Health, Bristol-Myers Squibb Co., and the Tourette Syndrome Association (TSA). She is a speaker for Pfizer, Inc.
1. Snider LA, Swedo SE. PANDAS: current status and directions for research. Mol Psychiatry 2004;9(10):900-7.
2. Hosier DM, Craenen JM, Teske DW, Wheller JJ. Resurgence of acute rheumatic fever. Am J Dis Child 1987;141:730-3.
3. Stollerman GH. Rheumatic fever. Lancet 1997;349:935-42.
4. Swedo S, Leonard HL, Schapiro MB, et al. Sydenham’s chorea: Physical and psychological symptoms of St.Vitus’ dance. Pediatrics 1993;91:706-13.
5. Asbahr FR, Negrao AB, Gentil V, et al. Obsessive-compulsive and related symptoms in children and adolescents with rheumatic fever with and without chorea: A prospective 6-month study. Am J Psychiatry 1998;155:1122-4.
6. Mercadante MT, Busatto GF, Lombroso PJ, et al. The psychiatric symptoms of rheumatic fever. Am J Psychiatry 2000;157:2036-8.
7. National Institute of Mental Health. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections. Available at: http://intramural.nimh.nih.gov/pdn/web.htm. Accessed June 9, 2005.
8. Swedo SE, Leonard HL, Garvey M, et al. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: clinical description of the first 50 cases. Am J Psychiatry 1998;155(2):264-71.
9. Kim SW, Grant JE, Kim SI, et al. A possible association of recurrent streptococcal infections and acute onset of obsessive-compulsive disorder. J Neuropsychiatry Clin Neurosci 2004;16(3):252-60.
10. Garvey MA, Giedd J, Swedo SE. PANDAS: the search for environmental triggers of pediatric neuropsychiatric disorders. Lessons from rheumatic fever. J Child Neurol 1998;13(9):413-23.
11. March JS. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS): implications for clinical practice. Arch Pediatr Adolesc Med 2004;158:927-9.
12. Zohar AH. The epidemiology of obsessive-compulsive disorder in children and adolescents. Child Adolesc Psychiatr Clin N Am 1999;8:445-59.
13. Murphy ML, Pichichero ME. Prospective identification and treatment of children with pediatric autoimmune neuropsychiatric disorder associated with group A streptococcal infection (PANDAS). Arch Pediatr Adolesc Med 2002;156(4):356-61.
14. Dajani A, Taubert K, Ferrieri P, et al. Treatment of acute streptococcal pharyngitis and prevention of rheumatic fever: a statement for health professionals. Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young, the American Heart Association. Pediatrics 1995;96:758-764.
15. Gray GC, McPhate DC, Leinonen M, et al. Weekly oral azithromycin as prophylaxis for agents causing acute respiratory disease. Clin Infect Dis 1998;26:103-10.
16. Snider LA, Lougee L, Slattery M, et al. Antibiotic prophylaxis with azithromycin or penicillin for childhood-onset neuropsychiatric disorders. Biol Psychiatry 2005;57:788-92.
17. Garvey MA, Perlmutter SJ, Allen AJ, et al. A pilot study of penicillin prophylaxis for neuropsychiatric exacerbations triggered by streptococcal infections. Biol Psychiatry 1999;45(12):1564-71.
18. Pediatric OCD Treatment Study (POTS) Team. Cognitive-behavior therapy, sertraline, and their combination for children and adolescents with obsessive-compulsive disorder: the Pediatric OCD Treatment Study (POTS) randomized controlled trial. JAMA 2004;292(16):1969-76.
19. Leonard HL, Swedo SE. Paediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS). Int J Neuropsychopharmacol 2001;4(2):191-8.
20. Snider LA, Swedo SE. Childhood-onset obsessive-compulsive disorder and tic disorders: case report and literature review. J Child Adolesc Psychopharmacol 2003;13(suppl 1):S81-S88.
21. Storch EA, Gerdes AC, Adkins JW, et al. Behavioral treatment of a child with PANDAS. J Am Acad Child Adolesc Psychiatry 2004;43(5):510-11.
22. Nicolson R, Swedo SE, Lenane M, et al. An open trial of plasma exchange in childhood-onset obsessive-compulsive disorder without poststreptococcal exacerbations. J Am Acad Child Adolesc Psychiatry 2000;39(10):1313-5.
23. Perlmutter SJ, Leitman SF, Garvey MA, et al. Therapeutic plasma exchange and intravenous immunoglobulin for obsessive-compulsive disorder and tic disorders in childhood. Lancet 1999;354 (9185):1153-8.
24. Snider LA, Swedo SE. Post-streptococcal autoimmune disorders of the central nervous system. Curr Opin Neurol 2003;16:359-65.
25. Murphy TK, Sajid M, Soto O, et al. Detecting pediatric autoimmune neuropsychiatric disorders associated with streptococcus in children with obsessive-compulsive disorder and tics. Biol Psychiatry 2004;55(1):61-8.
1. Snider LA, Swedo SE. PANDAS: current status and directions for research. Mol Psychiatry 2004;9(10):900-7.
2. Hosier DM, Craenen JM, Teske DW, Wheller JJ. Resurgence of acute rheumatic fever. Am J Dis Child 1987;141:730-3.
3. Stollerman GH. Rheumatic fever. Lancet 1997;349:935-42.
4. Swedo S, Leonard HL, Schapiro MB, et al. Sydenham’s chorea: Physical and psychological symptoms of St.Vitus’ dance. Pediatrics 1993;91:706-13.
5. Asbahr FR, Negrao AB, Gentil V, et al. Obsessive-compulsive and related symptoms in children and adolescents with rheumatic fever with and without chorea: A prospective 6-month study. Am J Psychiatry 1998;155:1122-4.
6. Mercadante MT, Busatto GF, Lombroso PJ, et al. The psychiatric symptoms of rheumatic fever. Am J Psychiatry 2000;157:2036-8.
7. National Institute of Mental Health. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections. Available at: http://intramural.nimh.nih.gov/pdn/web.htm. Accessed June 9, 2005.
8. Swedo SE, Leonard HL, Garvey M, et al. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: clinical description of the first 50 cases. Am J Psychiatry 1998;155(2):264-71.
9. Kim SW, Grant JE, Kim SI, et al. A possible association of recurrent streptococcal infections and acute onset of obsessive-compulsive disorder. J Neuropsychiatry Clin Neurosci 2004;16(3):252-60.
10. Garvey MA, Giedd J, Swedo SE. PANDAS: the search for environmental triggers of pediatric neuropsychiatric disorders. Lessons from rheumatic fever. J Child Neurol 1998;13(9):413-23.
11. March JS. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS): implications for clinical practice. Arch Pediatr Adolesc Med 2004;158:927-9.
12. Zohar AH. The epidemiology of obsessive-compulsive disorder in children and adolescents. Child Adolesc Psychiatr Clin N Am 1999;8:445-59.
13. Murphy ML, Pichichero ME. Prospective identification and treatment of children with pediatric autoimmune neuropsychiatric disorder associated with group A streptococcal infection (PANDAS). Arch Pediatr Adolesc Med 2002;156(4):356-61.
14. Dajani A, Taubert K, Ferrieri P, et al. Treatment of acute streptococcal pharyngitis and prevention of rheumatic fever: a statement for health professionals. Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young, the American Heart Association. Pediatrics 1995;96:758-764.
15. Gray GC, McPhate DC, Leinonen M, et al. Weekly oral azithromycin as prophylaxis for agents causing acute respiratory disease. Clin Infect Dis 1998;26:103-10.
16. Snider LA, Lougee L, Slattery M, et al. Antibiotic prophylaxis with azithromycin or penicillin for childhood-onset neuropsychiatric disorders. Biol Psychiatry 2005;57:788-92.
17. Garvey MA, Perlmutter SJ, Allen AJ, et al. A pilot study of penicillin prophylaxis for neuropsychiatric exacerbations triggered by streptococcal infections. Biol Psychiatry 1999;45(12):1564-71.
18. Pediatric OCD Treatment Study (POTS) Team. Cognitive-behavior therapy, sertraline, and their combination for children and adolescents with obsessive-compulsive disorder: the Pediatric OCD Treatment Study (POTS) randomized controlled trial. JAMA 2004;292(16):1969-76.
19. Leonard HL, Swedo SE. Paediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS). Int J Neuropsychopharmacol 2001;4(2):191-8.
20. Snider LA, Swedo SE. Childhood-onset obsessive-compulsive disorder and tic disorders: case report and literature review. J Child Adolesc Psychopharmacol 2003;13(suppl 1):S81-S88.
21. Storch EA, Gerdes AC, Adkins JW, et al. Behavioral treatment of a child with PANDAS. J Am Acad Child Adolesc Psychiatry 2004;43(5):510-11.
22. Nicolson R, Swedo SE, Lenane M, et al. An open trial of plasma exchange in childhood-onset obsessive-compulsive disorder without poststreptococcal exacerbations. J Am Acad Child Adolesc Psychiatry 2000;39(10):1313-5.
23. Perlmutter SJ, Leitman SF, Garvey MA, et al. Therapeutic plasma exchange and intravenous immunoglobulin for obsessive-compulsive disorder and tic disorders in childhood. Lancet 1999;354 (9185):1153-8.
24. Snider LA, Swedo SE. Post-streptococcal autoimmune disorders of the central nervous system. Curr Opin Neurol 2003;16:359-65.
25. Murphy TK, Sajid M, Soto O, et al. Detecting pediatric autoimmune neuropsychiatric disorders associated with streptococcus in children with obsessive-compulsive disorder and tics. Biol Psychiatry 2004;55(1):61-8.
Treatment-resistant psychosis: Are 2 antipsychotics more effective than 1?
Off-label prescribing of two or more antipsychotics for treatment-resistant psychosis carries inherent risks for both schizophrenia patients and their psychiatrists. You can reduce these risks by demonstrating that your patient will benefit more from combining antipsychotics than from monotherapy alternatives.
Until more empiric data become available, clinicians carry the burden of documenting individual patient response to justify combining antipsychotics. This article can help you identify and counsel possible candidates for this therapy, assess the risks and benefits, and defend your treatment choicesif necessary.
What Does ‘Combining’ Mean?
For this discussion, “combining antipsychotics” does not mean simultaneously using two or more antipsychotics to treat psychosis. Rather, it refers to using two or more antipsychotics for long-term control of psychotic symptoms. It does not apply to short-term tactics, such as overlapping antipsychotics when switching between them or combining a parenteral and an oral antipsychotic when treating an acute episode.
How long must a combination be used to qualify as long-term treatment? No standard exists, but a period >6 weeks exceeds normal short-term treatment.
How Safe Are Combinations?
Patient risk. Combination antipsychotics are used to treat 10% to 20% of schizophrenia patients in this country and >90% of those in some Asian countries, such as Japan.1 Statistics on the prevalence of combining antipsychotics seldom:
- distinguish between short- and long-term use
- identify when practitioners use combinations to treat co-existing symptoms such as insomnia, rather than for psychosis.
Clinicians, however, must define safety in terms of risks and benefits. Given that every medication has risks—some (such as allergic reactions) unique to the individual patient—adding another drug to a treatment regimen will always add risk. When considering more than one antipsychotic, ask yourself:
- Do benefits outweigh risks?
- Is a combination the least risky way to achieve these benefits?
How much does a practitioner’s perception of medicolegal risk influence treatment selection? No doubt, comfort level varies greatly. I have frequently met prescribers who use antipsychotic combinations instead of clozapine for fear of being sued should agranulocytosis occur.
Most trials have used criteriafrom the seminal clozapine study to define “treatment resistant” schizophrenia:
- History of poor response to one or more antipsychotics.
- Demonstrated nonresponse to adequate dosage and duration of a nonclozapine antipsychotic before starting clozapine.2
This work defines treatment resistance as persistent positive symptoms despite treatment with ≥2 different antipsychotics other than clozapine.
Newer antipsychotics are different. The original clozapine studies found little likelihood that patients who had not responded to haloperidol would respond to chlorpromazine. Newer-generation antipsychotics are pharmacologically more heterogeneous than the first-generation agents, however, and failure to respond to one might not mean that none of the others will help.
When to start clozapine? Solid evidence is limited, but a consensus panel has recommended starting clozapine after two unsuccessful trials of newer-generation antipsychotics, with the option to try a third antipsychotic (first- or newer-generation) if clinically warranted.3
Symptoms vs function. In clinical practice, defining treatment resistance as persistent positive symptoms may exclude patients impaired by severe negative symptoms and/or disorganized thought processes. The treatment goal is to restore function, not just to reduce psychosis. As treatments evolve, we can expect more emphasis on a recovery model that addresses total patient well-being and combines psychosocial and pharmacologic interventions.
A Practical View
Medical risks. Treating patients with antipsychotic combinations may be associated with medical risks (Table 1). Patients are less likely to adhere to complex medication regimens than to simple ones. Thus, adding a second antipsychotic may decrease adherence to the first antipsychotic and to other medications, such as for hypertension, diabetes, etc.
Increased side-effect risk has been reported with antipsychotic combinations.4 Side effects include those expected from one or both drugs in the combination, especially extrapyramidal effects when conventional antipsychotics are included.4,5 Because the total antipsychotic dosage can be considerably higher than usual in patients receiving combinations,5 some of the increased side effect burden is probably related to high dosing, rather than to the combinations.
Pharmacodynamic or pharmacokinetic interactions or the loss of an agent’s advantages are infrequently reported, perhaps because prescribers are not looking for these effects or do not consider them worth reporting. Of particular concern is tardive dyskinesia (TD), which may develop when conventional antipsychotics are added to agents with very low propensity to cause TD—such as clozapine.
Table 1
Potential risks and benefits of combining antipsychotics
| Medical risks |
| Decreased adherence to multiple medications |
| Increased and/or unexpected side effects |
| Increased potential for undesirable pharmacokinetic or pharmacodynamic interactions |
| Difficulties in making rational dose adjustments |
| Loss of advantages of one of the medications |
| Nonmedical risks |
| Lack of evidence to defend practice in medicolegal cases |
| Increased costs if combining second-generation antipsychotics |
| Increased quality assurance scrutiny and paperwork |
| Medical benefits |
| Reduced symptoms |
| Reduced metabolic side effects (such as partially substituting another atypical antipsychotic for a high clozapine dosage) |
litigation. As noted, some clinicians prefer combining antipsychotics instead of using clozapine because they fear legal action should a patient develop agranulocytosis. In the author’s view, this fear is not well-grounded. Successful lawsuits typically find evidence that the clinician committed errors of omission or commission. In the case of blood monitoring for clozapine-induced neutropenia, the parameters are clear and enforced. You must follow community standards of practice, which provide a strong legal defense.
Administrative scrutiny. Quality assurance programs are increasingly identifying and monitoring antipsychotic combinations—an obvious target by being frequent, lacking a strong evidence base, increasing costs, and raising liability concerns. Typically, such programs discourage antipsychotic combinations and impose administrative hurdles to starting or continuing them.
Gathering data and documenting it in the patient’s medical record—to be discussed later—is key to demonstrating that a combination’s superior efficacy for the individual patient justifies its use.
Medical benefits. Guidelines and algorithms for drug treatment of schizophrenia either omit combination antipsychotics or suggest this strategy when all else has failed.6,7 Lack of evidence for a practice is not the same as evidence against it, however. A combination may be better for some patients than any available antipsychotic monotherapy.
Antipsychotic combinations have been examined in more literature reviews than randomized controlled trials—all of which have addressed augmenting clozapine with another antipsychotic (Table 2).8-12 Augmentation with psychotropics other than a second antipsychotic has most often been tested for negative and cognitive symptoms,4 but some evidence has shown adjunctive anticonvulsants and cognition-enhancing agents to improve positive symptoms.6
Reducing side effects is not directly related to treatment-resistant psychosis, but some articles describe managing clozapine’s metabolic side effects by partially substituting another atypical antipsychotic.11,13
Because clozapine is the treatment of choice for treatment-resistant psychosis, consider tactics that maintain its benefits while reducing its metabolic liabilities. Reducing the clozapine dosage (if feasible) is the first-line approach, but partially substituting another antipsychotic might help if psychotic symptoms return.
Table 2
Results of studies using combination antipsychotic therapy
| Combination | Type of trial | First author | Outcome measures | Results |
|---|---|---|---|---|
| Clozapine/sulpiride* | RCT | Shiloh8 | Positive, negative, and depressive symptoms | Positive |
| Clozapine/risperidone | RCT | Josiassen9 | Positive and negative symptoms | Positive |
| Clozapine/risperidone | RCT | Yagcioglu10 | Positive and negative symptoms | Negative |
| Clozapine/quetiapine | LCS | Reinstein11 | Body weight, serum glucose | Positive |
| Clozapine/amisulpride* | LCS | Agelink12 | Positive and negative symptoms | Positive |
| RCT: randomized controlled trial; LCS: large case series | ||||
| *Sulpiride and amisulpride are not available in the United States. | ||||
Clinical Management Hints
Document, document, document. Crucial to “non-standard” treatments such as combining antipsychotics is using and documenting good medical practices. These include:
- accurately assessing patients
- carefully weighing illness risks vs treatment risks
- talking regularly to patients about their treatment and therapeutic options (Table 3).
Use objective measures. Brief scales to measure psychotic symptoms are being increasingly used in public mental health settings.6 For example, four psychosis items from the Brief Psychiatric Rating Scale (hallucinations, unusual thought content, paranoia, and disorganized thought) can quickly assess and capture much of the variance of the full scale in patients with schizophrenia.14
When properly used, these objective and reliable scales can document clinical change and track illness course across time and providers. Other objective outcome measures can contribute to quality of care and its documentation. For more information, visit the Substance Abuse and Mental Health Services Administration Web site (see Related Resources).
Although it seems obvious that persistent illness is not a good thing, the risks of persistent psychosis vary from patient to patient. Some function relatively well despite ongoing psychotic thoughts, whereas others are terribly impaired, demoralized, and/or suicidal. The rationale for nonstandard treatment such as an antipsychotic combination is to reduce patient suffering and risk and/or to increase function.
Discuss options with patients. Finally, schizophrenia patients (and involved significant others) need to understand and participate in treatment. Ongoing discussion of treatment options is an important part of this process. For example, initially reluctant patients often come to accept clozapine treatment after discussing its risks and benefits with clinicians and other patients who are taking clozapine. Documenting these discussions is as beneficial to the patient and clinician as is documenting symptoms and treatment effects.
Table 3
3 tips for managing risk and medications
| Use objective, quantifiable symptom measures at regular intervals |
| Document patient’s risk of persistent psychosis, based on history |
| Discuss risks and benefits of other treatment options with the patient and/or family at regular intervals |
- How to use medication in a systematic and effective way, as part of the overall treatment for severe mental illness. In: Evidence-based practices: Shaping mental health services toward recovery. Medication management approaches in psychiatry. Substance Abuse and Mental Health Services Administration. U.S. Department of Health and Human Services. http://mentalhealth.samhsa.gov/cmhs/communitysupport/toolkits/medication/.
- Texas Medication Algorithm Project (TMAP). http://www.dshs.state.tx.us/mhprograms/TIMA.shtm.
- Lehman AF, Lieberman JA, Dixon LB, et al. Practice guideline for the treatment of patients with schizophrenia, 2nd ed. Am J Psychiatry 2004;161(suppl):1–56.
- Clozapine • Clozaril
- Haloperidol • Haldol
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Dr. Miller receives research support from or is a consultant or speaker for Abbott Laboratories, Almirall, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb Co., Eli Lilly and Co., Janssen Pharmaceutica, Pfizer Inc., and InforMedix.
1. Miller A, Craig CS. Combination antipsychotics: pros, cons, and questions. Schizophr Bull 2002;28(1):105-9.
2. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry 1988;45(9):789-96.
3. Miller AL, Hall CS, Buchanan RW, et al. The Texas Medication Algorithm Project antipsychotic algorithm for schizophrenia: 2003 update. J Clin Psychiatry 2004;65(4):500-8.
4. Stahl SM, Grady MM. A critical review of atypical antipsychotic utilization: Comparing monotherapy with polypharmacy and augmentation. Curr Med Chem 2004;11(3):313-27.
5. Centorrino F, Goren JL, Hennen J, et al. Multiple versus single antipsychotic agents for hospitalized psychiatric patients: Case-control study of risks versus benefits. Am J Psychiatry 2004;161(4):700-6.
6. Miller AL. Polypharmacy in schizophrenia: science, art, and fiction. Curr Psychosis Ther Rep (in press).
7. Miller AL, Chiles JA, Chiles JK, et al. The Texas Medication Algorithm Project (TMAP) schizophrenia algorithms. J Clin Psychiatry 1999;60(10):649-57.
8. Shiloh R, Zemishlany Z, Aizenberg D, et al. Sulpiride augmentation in people with schizophrenia partially responsive to clozapine. A double-blind, placebo-controlled study. Br J Psychiatry 1997;171:569-73.
9. Josiassen RC, Joseph A, Kohegyi E, et al. Clozapine augmented with risperidone in the treatment of schizophrenia: a randomized, double-blind, placebo-controlled trial. Am J Psychiatry 2005;162(1):130-6.
10. Anil Yagcioglu AE, Kivircik Akdede BB, Turgut TI, et al. A double-blind controlled study of adjunctive treatment with risperidone in schizophrenic patients partially responsive to clozapine: efficacy and safety. J Clin Psychiatry 2005;66(1):63-72.
11. Reinstein MJ, Sirotovskaya LA, Jones LE, et al. Effect of clozapine-quetiapine combination therapy on weight and glycaemic control. Clin Drug Invest 1999;18(2):99-104.
12. Agelink MW, Kavuk I, Ak I. Clozapine with amisulpride for refractory schizophrenia. Am J Psychiatry 2004;161:924-5.
13. Kaye NS. Ziprasidone augmentation of clozapine in 11 patients. J Clin Psychiatry 2003;64(2):215-16.
14. Shores-Wilson K, Biggs MM, Miller AL, et al. Itemized clinician ratings versus global ratings of symptom severity in patients with schizophrenia. Int J Methods Psychiatr Res 2002;11(1):45-53.
Off-label prescribing of two or more antipsychotics for treatment-resistant psychosis carries inherent risks for both schizophrenia patients and their psychiatrists. You can reduce these risks by demonstrating that your patient will benefit more from combining antipsychotics than from monotherapy alternatives.
Until more empiric data become available, clinicians carry the burden of documenting individual patient response to justify combining antipsychotics. This article can help you identify and counsel possible candidates for this therapy, assess the risks and benefits, and defend your treatment choicesif necessary.
What Does ‘Combining’ Mean?
For this discussion, “combining antipsychotics” does not mean simultaneously using two or more antipsychotics to treat psychosis. Rather, it refers to using two or more antipsychotics for long-term control of psychotic symptoms. It does not apply to short-term tactics, such as overlapping antipsychotics when switching between them or combining a parenteral and an oral antipsychotic when treating an acute episode.
How long must a combination be used to qualify as long-term treatment? No standard exists, but a period >6 weeks exceeds normal short-term treatment.
How Safe Are Combinations?
Patient risk. Combination antipsychotics are used to treat 10% to 20% of schizophrenia patients in this country and >90% of those in some Asian countries, such as Japan.1 Statistics on the prevalence of combining antipsychotics seldom:
- distinguish between short- and long-term use
- identify when practitioners use combinations to treat co-existing symptoms such as insomnia, rather than for psychosis.
Clinicians, however, must define safety in terms of risks and benefits. Given that every medication has risks—some (such as allergic reactions) unique to the individual patient—adding another drug to a treatment regimen will always add risk. When considering more than one antipsychotic, ask yourself:
- Do benefits outweigh risks?
- Is a combination the least risky way to achieve these benefits?
How much does a practitioner’s perception of medicolegal risk influence treatment selection? No doubt, comfort level varies greatly. I have frequently met prescribers who use antipsychotic combinations instead of clozapine for fear of being sued should agranulocytosis occur.
Most trials have used criteriafrom the seminal clozapine study to define “treatment resistant” schizophrenia:
- History of poor response to one or more antipsychotics.
- Demonstrated nonresponse to adequate dosage and duration of a nonclozapine antipsychotic before starting clozapine.2
This work defines treatment resistance as persistent positive symptoms despite treatment with ≥2 different antipsychotics other than clozapine.
Newer antipsychotics are different. The original clozapine studies found little likelihood that patients who had not responded to haloperidol would respond to chlorpromazine. Newer-generation antipsychotics are pharmacologically more heterogeneous than the first-generation agents, however, and failure to respond to one might not mean that none of the others will help.
When to start clozapine? Solid evidence is limited, but a consensus panel has recommended starting clozapine after two unsuccessful trials of newer-generation antipsychotics, with the option to try a third antipsychotic (first- or newer-generation) if clinically warranted.3
Symptoms vs function. In clinical practice, defining treatment resistance as persistent positive symptoms may exclude patients impaired by severe negative symptoms and/or disorganized thought processes. The treatment goal is to restore function, not just to reduce psychosis. As treatments evolve, we can expect more emphasis on a recovery model that addresses total patient well-being and combines psychosocial and pharmacologic interventions.
A Practical View
Medical risks. Treating patients with antipsychotic combinations may be associated with medical risks (Table 1). Patients are less likely to adhere to complex medication regimens than to simple ones. Thus, adding a second antipsychotic may decrease adherence to the first antipsychotic and to other medications, such as for hypertension, diabetes, etc.
Increased side-effect risk has been reported with antipsychotic combinations.4 Side effects include those expected from one or both drugs in the combination, especially extrapyramidal effects when conventional antipsychotics are included.4,5 Because the total antipsychotic dosage can be considerably higher than usual in patients receiving combinations,5 some of the increased side effect burden is probably related to high dosing, rather than to the combinations.
Pharmacodynamic or pharmacokinetic interactions or the loss of an agent’s advantages are infrequently reported, perhaps because prescribers are not looking for these effects or do not consider them worth reporting. Of particular concern is tardive dyskinesia (TD), which may develop when conventional antipsychotics are added to agents with very low propensity to cause TD—such as clozapine.
Table 1
Potential risks and benefits of combining antipsychotics
| Medical risks |
| Decreased adherence to multiple medications |
| Increased and/or unexpected side effects |
| Increased potential for undesirable pharmacokinetic or pharmacodynamic interactions |
| Difficulties in making rational dose adjustments |
| Loss of advantages of one of the medications |
| Nonmedical risks |
| Lack of evidence to defend practice in medicolegal cases |
| Increased costs if combining second-generation antipsychotics |
| Increased quality assurance scrutiny and paperwork |
| Medical benefits |
| Reduced symptoms |
| Reduced metabolic side effects (such as partially substituting another atypical antipsychotic for a high clozapine dosage) |
litigation. As noted, some clinicians prefer combining antipsychotics instead of using clozapine because they fear legal action should a patient develop agranulocytosis. In the author’s view, this fear is not well-grounded. Successful lawsuits typically find evidence that the clinician committed errors of omission or commission. In the case of blood monitoring for clozapine-induced neutropenia, the parameters are clear and enforced. You must follow community standards of practice, which provide a strong legal defense.
Administrative scrutiny. Quality assurance programs are increasingly identifying and monitoring antipsychotic combinations—an obvious target by being frequent, lacking a strong evidence base, increasing costs, and raising liability concerns. Typically, such programs discourage antipsychotic combinations and impose administrative hurdles to starting or continuing them.
Gathering data and documenting it in the patient’s medical record—to be discussed later—is key to demonstrating that a combination’s superior efficacy for the individual patient justifies its use.
Medical benefits. Guidelines and algorithms for drug treatment of schizophrenia either omit combination antipsychotics or suggest this strategy when all else has failed.6,7 Lack of evidence for a practice is not the same as evidence against it, however. A combination may be better for some patients than any available antipsychotic monotherapy.
Antipsychotic combinations have been examined in more literature reviews than randomized controlled trials—all of which have addressed augmenting clozapine with another antipsychotic (Table 2).8-12 Augmentation with psychotropics other than a second antipsychotic has most often been tested for negative and cognitive symptoms,4 but some evidence has shown adjunctive anticonvulsants and cognition-enhancing agents to improve positive symptoms.6
Reducing side effects is not directly related to treatment-resistant psychosis, but some articles describe managing clozapine’s metabolic side effects by partially substituting another atypical antipsychotic.11,13
Because clozapine is the treatment of choice for treatment-resistant psychosis, consider tactics that maintain its benefits while reducing its metabolic liabilities. Reducing the clozapine dosage (if feasible) is the first-line approach, but partially substituting another antipsychotic might help if psychotic symptoms return.
Table 2
Results of studies using combination antipsychotic therapy
| Combination | Type of trial | First author | Outcome measures | Results |
|---|---|---|---|---|
| Clozapine/sulpiride* | RCT | Shiloh8 | Positive, negative, and depressive symptoms | Positive |
| Clozapine/risperidone | RCT | Josiassen9 | Positive and negative symptoms | Positive |
| Clozapine/risperidone | RCT | Yagcioglu10 | Positive and negative symptoms | Negative |
| Clozapine/quetiapine | LCS | Reinstein11 | Body weight, serum glucose | Positive |
| Clozapine/amisulpride* | LCS | Agelink12 | Positive and negative symptoms | Positive |
| RCT: randomized controlled trial; LCS: large case series | ||||
| *Sulpiride and amisulpride are not available in the United States. | ||||
Clinical Management Hints
Document, document, document. Crucial to “non-standard” treatments such as combining antipsychotics is using and documenting good medical practices. These include:
- accurately assessing patients
- carefully weighing illness risks vs treatment risks
- talking regularly to patients about their treatment and therapeutic options (Table 3).
Use objective measures. Brief scales to measure psychotic symptoms are being increasingly used in public mental health settings.6 For example, four psychosis items from the Brief Psychiatric Rating Scale (hallucinations, unusual thought content, paranoia, and disorganized thought) can quickly assess and capture much of the variance of the full scale in patients with schizophrenia.14
When properly used, these objective and reliable scales can document clinical change and track illness course across time and providers. Other objective outcome measures can contribute to quality of care and its documentation. For more information, visit the Substance Abuse and Mental Health Services Administration Web site (see Related Resources).
Although it seems obvious that persistent illness is not a good thing, the risks of persistent psychosis vary from patient to patient. Some function relatively well despite ongoing psychotic thoughts, whereas others are terribly impaired, demoralized, and/or suicidal. The rationale for nonstandard treatment such as an antipsychotic combination is to reduce patient suffering and risk and/or to increase function.
Discuss options with patients. Finally, schizophrenia patients (and involved significant others) need to understand and participate in treatment. Ongoing discussion of treatment options is an important part of this process. For example, initially reluctant patients often come to accept clozapine treatment after discussing its risks and benefits with clinicians and other patients who are taking clozapine. Documenting these discussions is as beneficial to the patient and clinician as is documenting symptoms and treatment effects.
Table 3
3 tips for managing risk and medications
| Use objective, quantifiable symptom measures at regular intervals |
| Document patient’s risk of persistent psychosis, based on history |
| Discuss risks and benefits of other treatment options with the patient and/or family at regular intervals |
- How to use medication in a systematic and effective way, as part of the overall treatment for severe mental illness. In: Evidence-based practices: Shaping mental health services toward recovery. Medication management approaches in psychiatry. Substance Abuse and Mental Health Services Administration. U.S. Department of Health and Human Services. http://mentalhealth.samhsa.gov/cmhs/communitysupport/toolkits/medication/.
- Texas Medication Algorithm Project (TMAP). http://www.dshs.state.tx.us/mhprograms/TIMA.shtm.
- Lehman AF, Lieberman JA, Dixon LB, et al. Practice guideline for the treatment of patients with schizophrenia, 2nd ed. Am J Psychiatry 2004;161(suppl):1–56.
- Clozapine • Clozaril
- Haloperidol • Haldol
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Dr. Miller receives research support from or is a consultant or speaker for Abbott Laboratories, Almirall, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb Co., Eli Lilly and Co., Janssen Pharmaceutica, Pfizer Inc., and InforMedix.
Off-label prescribing of two or more antipsychotics for treatment-resistant psychosis carries inherent risks for both schizophrenia patients and their psychiatrists. You can reduce these risks by demonstrating that your patient will benefit more from combining antipsychotics than from monotherapy alternatives.
Until more empiric data become available, clinicians carry the burden of documenting individual patient response to justify combining antipsychotics. This article can help you identify and counsel possible candidates for this therapy, assess the risks and benefits, and defend your treatment choicesif necessary.
What Does ‘Combining’ Mean?
For this discussion, “combining antipsychotics” does not mean simultaneously using two or more antipsychotics to treat psychosis. Rather, it refers to using two or more antipsychotics for long-term control of psychotic symptoms. It does not apply to short-term tactics, such as overlapping antipsychotics when switching between them or combining a parenteral and an oral antipsychotic when treating an acute episode.
How long must a combination be used to qualify as long-term treatment? No standard exists, but a period >6 weeks exceeds normal short-term treatment.
How Safe Are Combinations?
Patient risk. Combination antipsychotics are used to treat 10% to 20% of schizophrenia patients in this country and >90% of those in some Asian countries, such as Japan.1 Statistics on the prevalence of combining antipsychotics seldom:
- distinguish between short- and long-term use
- identify when practitioners use combinations to treat co-existing symptoms such as insomnia, rather than for psychosis.
Clinicians, however, must define safety in terms of risks and benefits. Given that every medication has risks—some (such as allergic reactions) unique to the individual patient—adding another drug to a treatment regimen will always add risk. When considering more than one antipsychotic, ask yourself:
- Do benefits outweigh risks?
- Is a combination the least risky way to achieve these benefits?
How much does a practitioner’s perception of medicolegal risk influence treatment selection? No doubt, comfort level varies greatly. I have frequently met prescribers who use antipsychotic combinations instead of clozapine for fear of being sued should agranulocytosis occur.
Most trials have used criteriafrom the seminal clozapine study to define “treatment resistant” schizophrenia:
- History of poor response to one or more antipsychotics.
- Demonstrated nonresponse to adequate dosage and duration of a nonclozapine antipsychotic before starting clozapine.2
This work defines treatment resistance as persistent positive symptoms despite treatment with ≥2 different antipsychotics other than clozapine.
Newer antipsychotics are different. The original clozapine studies found little likelihood that patients who had not responded to haloperidol would respond to chlorpromazine. Newer-generation antipsychotics are pharmacologically more heterogeneous than the first-generation agents, however, and failure to respond to one might not mean that none of the others will help.
When to start clozapine? Solid evidence is limited, but a consensus panel has recommended starting clozapine after two unsuccessful trials of newer-generation antipsychotics, with the option to try a third antipsychotic (first- or newer-generation) if clinically warranted.3
Symptoms vs function. In clinical practice, defining treatment resistance as persistent positive symptoms may exclude patients impaired by severe negative symptoms and/or disorganized thought processes. The treatment goal is to restore function, not just to reduce psychosis. As treatments evolve, we can expect more emphasis on a recovery model that addresses total patient well-being and combines psychosocial and pharmacologic interventions.
A Practical View
Medical risks. Treating patients with antipsychotic combinations may be associated with medical risks (Table 1). Patients are less likely to adhere to complex medication regimens than to simple ones. Thus, adding a second antipsychotic may decrease adherence to the first antipsychotic and to other medications, such as for hypertension, diabetes, etc.
Increased side-effect risk has been reported with antipsychotic combinations.4 Side effects include those expected from one or both drugs in the combination, especially extrapyramidal effects when conventional antipsychotics are included.4,5 Because the total antipsychotic dosage can be considerably higher than usual in patients receiving combinations,5 some of the increased side effect burden is probably related to high dosing, rather than to the combinations.
Pharmacodynamic or pharmacokinetic interactions or the loss of an agent’s advantages are infrequently reported, perhaps because prescribers are not looking for these effects or do not consider them worth reporting. Of particular concern is tardive dyskinesia (TD), which may develop when conventional antipsychotics are added to agents with very low propensity to cause TD—such as clozapine.
Table 1
Potential risks and benefits of combining antipsychotics
| Medical risks |
| Decreased adherence to multiple medications |
| Increased and/or unexpected side effects |
| Increased potential for undesirable pharmacokinetic or pharmacodynamic interactions |
| Difficulties in making rational dose adjustments |
| Loss of advantages of one of the medications |
| Nonmedical risks |
| Lack of evidence to defend practice in medicolegal cases |
| Increased costs if combining second-generation antipsychotics |
| Increased quality assurance scrutiny and paperwork |
| Medical benefits |
| Reduced symptoms |
| Reduced metabolic side effects (such as partially substituting another atypical antipsychotic for a high clozapine dosage) |
litigation. As noted, some clinicians prefer combining antipsychotics instead of using clozapine because they fear legal action should a patient develop agranulocytosis. In the author’s view, this fear is not well-grounded. Successful lawsuits typically find evidence that the clinician committed errors of omission or commission. In the case of blood monitoring for clozapine-induced neutropenia, the parameters are clear and enforced. You must follow community standards of practice, which provide a strong legal defense.
Administrative scrutiny. Quality assurance programs are increasingly identifying and monitoring antipsychotic combinations—an obvious target by being frequent, lacking a strong evidence base, increasing costs, and raising liability concerns. Typically, such programs discourage antipsychotic combinations and impose administrative hurdles to starting or continuing them.
Gathering data and documenting it in the patient’s medical record—to be discussed later—is key to demonstrating that a combination’s superior efficacy for the individual patient justifies its use.
Medical benefits. Guidelines and algorithms for drug treatment of schizophrenia either omit combination antipsychotics or suggest this strategy when all else has failed.6,7 Lack of evidence for a practice is not the same as evidence against it, however. A combination may be better for some patients than any available antipsychotic monotherapy.
Antipsychotic combinations have been examined in more literature reviews than randomized controlled trials—all of which have addressed augmenting clozapine with another antipsychotic (Table 2).8-12 Augmentation with psychotropics other than a second antipsychotic has most often been tested for negative and cognitive symptoms,4 but some evidence has shown adjunctive anticonvulsants and cognition-enhancing agents to improve positive symptoms.6
Reducing side effects is not directly related to treatment-resistant psychosis, but some articles describe managing clozapine’s metabolic side effects by partially substituting another atypical antipsychotic.11,13
Because clozapine is the treatment of choice for treatment-resistant psychosis, consider tactics that maintain its benefits while reducing its metabolic liabilities. Reducing the clozapine dosage (if feasible) is the first-line approach, but partially substituting another antipsychotic might help if psychotic symptoms return.
Table 2
Results of studies using combination antipsychotic therapy
| Combination | Type of trial | First author | Outcome measures | Results |
|---|---|---|---|---|
| Clozapine/sulpiride* | RCT | Shiloh8 | Positive, negative, and depressive symptoms | Positive |
| Clozapine/risperidone | RCT | Josiassen9 | Positive and negative symptoms | Positive |
| Clozapine/risperidone | RCT | Yagcioglu10 | Positive and negative symptoms | Negative |
| Clozapine/quetiapine | LCS | Reinstein11 | Body weight, serum glucose | Positive |
| Clozapine/amisulpride* | LCS | Agelink12 | Positive and negative symptoms | Positive |
| RCT: randomized controlled trial; LCS: large case series | ||||
| *Sulpiride and amisulpride are not available in the United States. | ||||
Clinical Management Hints
Document, document, document. Crucial to “non-standard” treatments such as combining antipsychotics is using and documenting good medical practices. These include:
- accurately assessing patients
- carefully weighing illness risks vs treatment risks
- talking regularly to patients about their treatment and therapeutic options (Table 3).
Use objective measures. Brief scales to measure psychotic symptoms are being increasingly used in public mental health settings.6 For example, four psychosis items from the Brief Psychiatric Rating Scale (hallucinations, unusual thought content, paranoia, and disorganized thought) can quickly assess and capture much of the variance of the full scale in patients with schizophrenia.14
When properly used, these objective and reliable scales can document clinical change and track illness course across time and providers. Other objective outcome measures can contribute to quality of care and its documentation. For more information, visit the Substance Abuse and Mental Health Services Administration Web site (see Related Resources).
Although it seems obvious that persistent illness is not a good thing, the risks of persistent psychosis vary from patient to patient. Some function relatively well despite ongoing psychotic thoughts, whereas others are terribly impaired, demoralized, and/or suicidal. The rationale for nonstandard treatment such as an antipsychotic combination is to reduce patient suffering and risk and/or to increase function.
Discuss options with patients. Finally, schizophrenia patients (and involved significant others) need to understand and participate in treatment. Ongoing discussion of treatment options is an important part of this process. For example, initially reluctant patients often come to accept clozapine treatment after discussing its risks and benefits with clinicians and other patients who are taking clozapine. Documenting these discussions is as beneficial to the patient and clinician as is documenting symptoms and treatment effects.
Table 3
3 tips for managing risk and medications
| Use objective, quantifiable symptom measures at regular intervals |
| Document patient’s risk of persistent psychosis, based on history |
| Discuss risks and benefits of other treatment options with the patient and/or family at regular intervals |
- How to use medication in a systematic and effective way, as part of the overall treatment for severe mental illness. In: Evidence-based practices: Shaping mental health services toward recovery. Medication management approaches in psychiatry. Substance Abuse and Mental Health Services Administration. U.S. Department of Health and Human Services. http://mentalhealth.samhsa.gov/cmhs/communitysupport/toolkits/medication/.
- Texas Medication Algorithm Project (TMAP). http://www.dshs.state.tx.us/mhprograms/TIMA.shtm.
- Lehman AF, Lieberman JA, Dixon LB, et al. Practice guideline for the treatment of patients with schizophrenia, 2nd ed. Am J Psychiatry 2004;161(suppl):1–56.
- Clozapine • Clozaril
- Haloperidol • Haldol
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Dr. Miller receives research support from or is a consultant or speaker for Abbott Laboratories, Almirall, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb Co., Eli Lilly and Co., Janssen Pharmaceutica, Pfizer Inc., and InforMedix.
1. Miller A, Craig CS. Combination antipsychotics: pros, cons, and questions. Schizophr Bull 2002;28(1):105-9.
2. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry 1988;45(9):789-96.
3. Miller AL, Hall CS, Buchanan RW, et al. The Texas Medication Algorithm Project antipsychotic algorithm for schizophrenia: 2003 update. J Clin Psychiatry 2004;65(4):500-8.
4. Stahl SM, Grady MM. A critical review of atypical antipsychotic utilization: Comparing monotherapy with polypharmacy and augmentation. Curr Med Chem 2004;11(3):313-27.
5. Centorrino F, Goren JL, Hennen J, et al. Multiple versus single antipsychotic agents for hospitalized psychiatric patients: Case-control study of risks versus benefits. Am J Psychiatry 2004;161(4):700-6.
6. Miller AL. Polypharmacy in schizophrenia: science, art, and fiction. Curr Psychosis Ther Rep (in press).
7. Miller AL, Chiles JA, Chiles JK, et al. The Texas Medication Algorithm Project (TMAP) schizophrenia algorithms. J Clin Psychiatry 1999;60(10):649-57.
8. Shiloh R, Zemishlany Z, Aizenberg D, et al. Sulpiride augmentation in people with schizophrenia partially responsive to clozapine. A double-blind, placebo-controlled study. Br J Psychiatry 1997;171:569-73.
9. Josiassen RC, Joseph A, Kohegyi E, et al. Clozapine augmented with risperidone in the treatment of schizophrenia: a randomized, double-blind, placebo-controlled trial. Am J Psychiatry 2005;162(1):130-6.
10. Anil Yagcioglu AE, Kivircik Akdede BB, Turgut TI, et al. A double-blind controlled study of adjunctive treatment with risperidone in schizophrenic patients partially responsive to clozapine: efficacy and safety. J Clin Psychiatry 2005;66(1):63-72.
11. Reinstein MJ, Sirotovskaya LA, Jones LE, et al. Effect of clozapine-quetiapine combination therapy on weight and glycaemic control. Clin Drug Invest 1999;18(2):99-104.
12. Agelink MW, Kavuk I, Ak I. Clozapine with amisulpride for refractory schizophrenia. Am J Psychiatry 2004;161:924-5.
13. Kaye NS. Ziprasidone augmentation of clozapine in 11 patients. J Clin Psychiatry 2003;64(2):215-16.
14. Shores-Wilson K, Biggs MM, Miller AL, et al. Itemized clinician ratings versus global ratings of symptom severity in patients with schizophrenia. Int J Methods Psychiatr Res 2002;11(1):45-53.
1. Miller A, Craig CS. Combination antipsychotics: pros, cons, and questions. Schizophr Bull 2002;28(1):105-9.
2. Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry 1988;45(9):789-96.
3. Miller AL, Hall CS, Buchanan RW, et al. The Texas Medication Algorithm Project antipsychotic algorithm for schizophrenia: 2003 update. J Clin Psychiatry 2004;65(4):500-8.
4. Stahl SM, Grady MM. A critical review of atypical antipsychotic utilization: Comparing monotherapy with polypharmacy and augmentation. Curr Med Chem 2004;11(3):313-27.
5. Centorrino F, Goren JL, Hennen J, et al. Multiple versus single antipsychotic agents for hospitalized psychiatric patients: Case-control study of risks versus benefits. Am J Psychiatry 2004;161(4):700-6.
6. Miller AL. Polypharmacy in schizophrenia: science, art, and fiction. Curr Psychosis Ther Rep (in press).
7. Miller AL, Chiles JA, Chiles JK, et al. The Texas Medication Algorithm Project (TMAP) schizophrenia algorithms. J Clin Psychiatry 1999;60(10):649-57.
8. Shiloh R, Zemishlany Z, Aizenberg D, et al. Sulpiride augmentation in people with schizophrenia partially responsive to clozapine. A double-blind, placebo-controlled study. Br J Psychiatry 1997;171:569-73.
9. Josiassen RC, Joseph A, Kohegyi E, et al. Clozapine augmented with risperidone in the treatment of schizophrenia: a randomized, double-blind, placebo-controlled trial. Am J Psychiatry 2005;162(1):130-6.
10. Anil Yagcioglu AE, Kivircik Akdede BB, Turgut TI, et al. A double-blind controlled study of adjunctive treatment with risperidone in schizophrenic patients partially responsive to clozapine: efficacy and safety. J Clin Psychiatry 2005;66(1):63-72.
11. Reinstein MJ, Sirotovskaya LA, Jones LE, et al. Effect of clozapine-quetiapine combination therapy on weight and glycaemic control. Clin Drug Invest 1999;18(2):99-104.
12. Agelink MW, Kavuk I, Ak I. Clozapine with amisulpride for refractory schizophrenia. Am J Psychiatry 2004;161:924-5.
13. Kaye NS. Ziprasidone augmentation of clozapine in 11 patients. J Clin Psychiatry 2003;64(2):215-16.
14. Shores-Wilson K, Biggs MM, Miller AL, et al. Itemized clinician ratings versus global ratings of symptom severity in patients with schizophrenia. Int J Methods Psychiatr Res 2002;11(1):45-53.
Carbohydrate-deficient transferrin test
Biomarkers can help psychiatrists monitor abstinence and detect relapse in patients with alcohol use disorders. A blood test that measures carbohydrate-deficient transferrin percentage (%CDT) is FDA-approved for detecting heavy drinking (Table 1)1 and has shown effectiveness in several medical and surgical uses.
Table 1
%CDT test: Fast facts
| Brand names: |
| Axis-Shield %CDT, Bio-Rad %CDT TIA, Tina-quant (a) %CDT |
| FDA-approved indication: |
| Testing for excessive alcohol use |
| Manufacturers: |
| Axis-Shield PLC, Bio-Rad Laboratories, Roche Diagnostics |
| Recommended use: |
| Detecting heavy alcohol consumption, monitoring abstinence, and identifying elapse in patients with alcohol use disorders |
| Laboratories that process %CDT results: |
|
HOW %CDT SIGNALS ALCOHOL ABUSE
In 1976, Swedish researchers detected transferrin fractions in the CSF of alcoholic patients but not in nonalcoholics.2 One of these fractions was also present in alcoholics’ serum. This discovery led to the CDT biomarker.
%CDT testing is based on the finding that consuming an average >60 grams of alcohol (about 5 standard drinks) daily for ≥ 2 weeks causes a higher percentage of transferrin—a glycoprotein that transports iron in the blood—to lack its usual carbohydrate content. Transferrin appears in 6 isoforms, and studies have shown that heavy drinking increases three of these—asialo, mono sialo, and disialo transferrin—a state collectively called “carbohydrate-deficient.”
A %CDT reading ≥ 2.6 indicates that a patient may have had on average at least 5 alcoholic drinks daily for ≥ 2 weeks. Because CDT has a short mean half-life (7 to 14 days), readings >2.6 may suggest much heavier drinking at some time before the blood sample was taken.
Microcolumn chromatography separation assays that measure CDT as a percentage of total circulating transferrin have replaced initial CDT assays that used isoelectric focusing separation and immunoassay systems. This advance corrected for individual transferrin level variations.
CLINICAL USE
The %CDT test has shown effectiveness in several medical and surgical uses, including
- screening patients with diseases possibly triggered by alcohol use, such as treatment-resistant hypertension, gastroesophageal reflux disease, or depression
- detecting alcohol-use disorders in hospitalized patients
- screening presurgical and trauma patients to predict alcohol withdrawal syndrome and/or postsurgical complications.3,4
Although no alcohol biomarker alone reliably confirms alcohol abuse/dependence, %CDT can corroborate initial clinical impressions, especially when the patient’s self-report is suspect or information from significant others is not available.
Among biomarkers, %CDT most accurately predicts alcohol withdrawal syndrome in men (mean corpuscular volume [MCV] measurements are more accurate in women).4 During psychiatric consults, the test may help confirm suspected alcohol use in patients admitted to inpatient medical, surgical, or trauma units.
%CDT may also help monitor abstinence when treating an alcohol use disorder. In a major prospective treatment outcome study, %CDT was more sensitive than gamma-glutamyltransferase (GGT) in detecting relapse in male but not female alcoholics.5 Patients who abstained from drinking for 12 weeks showed a 30% decrease in %CDT. Subjects who relapsed during treatment later showed a 60% increase in %CDT, indicating sustained heavy drinking.
%CDT decreased over the first 4 weeks of treatment and continued to decline over time for abstinent patients (Figure). After week 4, %CDT increased again for those who consumed ≥ 5 drinks per day or had a full-blown relapse.5
Together, routine %CDT and GGT testing during treatment and follow-up can help clinicians monitor a patient’s progress and provide accurate reports to courts, child welfare agencies, and programs for impaired professionals. A 30% reduction from baseline in either biomarker indicates abstinence or significantly reduced alcohol consumption, whereas a 30% increase suggests relapse.6 Consider all clinical information in the final analysis, however.
%CDT results also provide an objective basis for discussing relapses with patients. Those who are responding to treatment often welcome %CDT testing as proof they are abstaining from alcohol.
Figure %CDT changes with alcohol use or abstinence
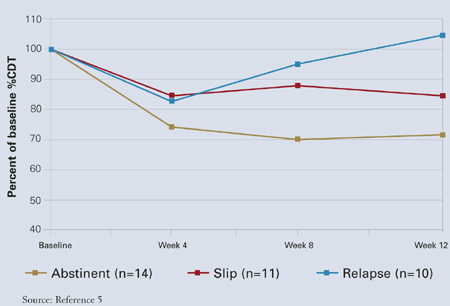
CLINICAL PRACTICALITY
The %CDT test is an immunoassay with ion-exchange column separation followed by turbidimetric measurement. Because the procedure is complex, laboratories generally require 24 to 72 hours to test the sample.
Because the %CDT test is relatively new, pricing, reimbursement rates, and availability are not well established. Pricing will likely vary widely from state to state and among laboratories and insurers. Medicare reimburses approximately $25 for %CDT testing, compared with $10 for GGT testing.
Only select reference laboratories offer %CDT testing, but the test should become more widely available over time (Table 1).
SENSITIVITY AND SPECIFICITY
%CDT test sensitivity is 70% to 90% in male inpatient alcoholics (usually drinking within 4 to 7 days of blood draw), with specificities >90%. Sensitivity is 12% to 40% in general populations—among whom underreporting of drinking may lead to more false positives—and 40% to 60% in outpatient alcoholics.7,8 Specificity, however, remains high—80% to 90%—when sensitivity is reduced.
Overall, %CDT is as sensitive as GGT and more sensitive than other biomarkers, including MCV, aspartate transaminase, and alanine transaminase.9 %CDT is more specific than GGT (92% vs. 75%) and other biomarkers. %CDT appears to be more sensitive in men, whereas GGT is more sensitive in women (Table 2).10
Ample evidence, however, suggests that %CDT and GGT readings together may provide a comprehensive picture of recent alcohol abuse.10 Whereas frequent drinking alters %CDT, GGT signals drinking intensity and is more effective at detecting episodic binge drinking (Table 2). This probably explains why problem drinkers age <20—who typically binge-drink—show little or no change in %CDT.
Table 2
%CDT vs GGT testing for recent alcohol abuse
| %CDT | GGT | |
|---|---|---|
| Advantages |
|
|
| Disadvantages |
|
|
| Cutoff value |
|
|
| %CDT: Carbohydrate-deficient transferrin percentage | ||
| GGT: Gamma-glutamyltransferase | ||
FACTORS THAT ALTER RESULTS
Unlike GGT and MCV, few medical conditions distort %CDT,11 meaning the test is accurate in patients with most medical conditions. Only end-stage liver disease, biliary cirrhosis, and rare genetic transferrin variants alter %CDT.
Women tend to have higher and more-variable CDT values than do men, possibly because of variability in normal transferrin levels, anemia secondary to iron deficiency, pregnancy, use of oral contraceptives, or menopause. %CDT cutoff scores are not gender-specific, however, because percentage rather than absolute CDT is typically measured.
%CDT seems to decrease slightly as body mass index increases, suggesting a small but significant inverse relationship between weight and %CDT. Smoking seems to raise %CDT values slightly. The specifics of and reasons for these relationships are unclear.
Related resources
- Axis-Shield. www.axis-shield.com. Click on “Lab diagnostics,” then “Alcohol-related.”
Disclosure
Dr. Anton is a consultant to Axis-Shield.
Dr. Miller and Ms. Dominick report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Anton RF, Dominick C, Bigelow M, Westby C. CDTect Research Group. Comparison of Bio-Rad %CDT TIA and CDTect as laboratory markers of heavy alcohol use and their relationships with gamma-glutamyltransferase. Clin Chem 2001;47:1769-75.
2. Stibler H, Kjellin KG. Isoelectric focusing and electrophoresis of the CSF proteins on tremor of different origins. J Neurol 1976;30:269-85.
3. Miller PM. Recent developments in alcohol biomarkers: Implications for managing alcohol-sensitive diseases. Resid Staff Physician 2004;50:11-17.
4. Spies CD, Kissner M, Neumann T, et al. Elevated carbohydrate-deficient transferrin predicts prolonged intensive care unit stay in traumatized men. Alcohol Alcohol 1998;33:661-9.
5. Anton RF, Moak DH, Latham P. Carbohydrate-deficient transferrin as an indicator of drinking status during a treatment outcome study. Alcohol Clin Exp Res 1996;20:841-6.
6. Anton RF, Lieber C, Tabakoff B. Carbohydrate-deficient transferrin and gamma-glutamyltransferase for the detection and monitoring of alcohol use: results from a multisite study. Alcohol Clin Exp Res 2002;26:1215-22.
7. Allen JP, Litten RZ, Anton RF, Cross GM. Carbohydrate-deficient transferrin as a measure of immoderate drinking: remaining issues. Alcohol Clin Exp Res 1994;18:799-812.
8. Gronbaek M, Henriksen JH, Becker U. Carbohydrate-deficient transferrin—a valid marker of alcoholism in population studies? Results from the Copenhagen City Heart Study. Alcohol Clin Exp Res 1995;19:457-61.
9. Bell H, Tallaksen CM, Try K, Haug E. Carbohydrate-deficient transferrin and other markers of high alcohol consumption: A study of 502 patients admitted consecutively to a medical department. Alcohol Clin Exp Res 1994;18:1103-8.
10. Conigrave KM, Degenhardt LJ, Whitfield JB, et al. CDT, GGT, and AST as markers of alcohol use: The WHO/ISBRA Collaborative Project. Alcohol Clin Exp Res 2002;26:332-9.
11. Meerkerk GJ, Njoo KH, Bongers IM, et al. The specificity of the CDT assay in general practice: the influence of common chronic diseases and medication on the serum CDT concentration. Alcohol Clin Exp Res 1998;22:908-13.
Biomarkers can help psychiatrists monitor abstinence and detect relapse in patients with alcohol use disorders. A blood test that measures carbohydrate-deficient transferrin percentage (%CDT) is FDA-approved for detecting heavy drinking (Table 1)1 and has shown effectiveness in several medical and surgical uses.
Table 1
%CDT test: Fast facts
| Brand names: |
| Axis-Shield %CDT, Bio-Rad %CDT TIA, Tina-quant (a) %CDT |
| FDA-approved indication: |
| Testing for excessive alcohol use |
| Manufacturers: |
| Axis-Shield PLC, Bio-Rad Laboratories, Roche Diagnostics |
| Recommended use: |
| Detecting heavy alcohol consumption, monitoring abstinence, and identifying elapse in patients with alcohol use disorders |
| Laboratories that process %CDT results: |
|
HOW %CDT SIGNALS ALCOHOL ABUSE
In 1976, Swedish researchers detected transferrin fractions in the CSF of alcoholic patients but not in nonalcoholics.2 One of these fractions was also present in alcoholics’ serum. This discovery led to the CDT biomarker.
%CDT testing is based on the finding that consuming an average >60 grams of alcohol (about 5 standard drinks) daily for ≥ 2 weeks causes a higher percentage of transferrin—a glycoprotein that transports iron in the blood—to lack its usual carbohydrate content. Transferrin appears in 6 isoforms, and studies have shown that heavy drinking increases three of these—asialo, mono sialo, and disialo transferrin—a state collectively called “carbohydrate-deficient.”
A %CDT reading ≥ 2.6 indicates that a patient may have had on average at least 5 alcoholic drinks daily for ≥ 2 weeks. Because CDT has a short mean half-life (7 to 14 days), readings >2.6 may suggest much heavier drinking at some time before the blood sample was taken.
Microcolumn chromatography separation assays that measure CDT as a percentage of total circulating transferrin have replaced initial CDT assays that used isoelectric focusing separation and immunoassay systems. This advance corrected for individual transferrin level variations.
CLINICAL USE
The %CDT test has shown effectiveness in several medical and surgical uses, including
- screening patients with diseases possibly triggered by alcohol use, such as treatment-resistant hypertension, gastroesophageal reflux disease, or depression
- detecting alcohol-use disorders in hospitalized patients
- screening presurgical and trauma patients to predict alcohol withdrawal syndrome and/or postsurgical complications.3,4
Although no alcohol biomarker alone reliably confirms alcohol abuse/dependence, %CDT can corroborate initial clinical impressions, especially when the patient’s self-report is suspect or information from significant others is not available.
Among biomarkers, %CDT most accurately predicts alcohol withdrawal syndrome in men (mean corpuscular volume [MCV] measurements are more accurate in women).4 During psychiatric consults, the test may help confirm suspected alcohol use in patients admitted to inpatient medical, surgical, or trauma units.
%CDT may also help monitor abstinence when treating an alcohol use disorder. In a major prospective treatment outcome study, %CDT was more sensitive than gamma-glutamyltransferase (GGT) in detecting relapse in male but not female alcoholics.5 Patients who abstained from drinking for 12 weeks showed a 30% decrease in %CDT. Subjects who relapsed during treatment later showed a 60% increase in %CDT, indicating sustained heavy drinking.
%CDT decreased over the first 4 weeks of treatment and continued to decline over time for abstinent patients (Figure). After week 4, %CDT increased again for those who consumed ≥ 5 drinks per day or had a full-blown relapse.5
Together, routine %CDT and GGT testing during treatment and follow-up can help clinicians monitor a patient’s progress and provide accurate reports to courts, child welfare agencies, and programs for impaired professionals. A 30% reduction from baseline in either biomarker indicates abstinence or significantly reduced alcohol consumption, whereas a 30% increase suggests relapse.6 Consider all clinical information in the final analysis, however.
%CDT results also provide an objective basis for discussing relapses with patients. Those who are responding to treatment often welcome %CDT testing as proof they are abstaining from alcohol.
Figure %CDT changes with alcohol use or abstinence
CLINICAL PRACTICALITY
The %CDT test is an immunoassay with ion-exchange column separation followed by turbidimetric measurement. Because the procedure is complex, laboratories generally require 24 to 72 hours to test the sample.
Because the %CDT test is relatively new, pricing, reimbursement rates, and availability are not well established. Pricing will likely vary widely from state to state and among laboratories and insurers. Medicare reimburses approximately $25 for %CDT testing, compared with $10 for GGT testing.
Only select reference laboratories offer %CDT testing, but the test should become more widely available over time (Table 1).
SENSITIVITY AND SPECIFICITY
%CDT test sensitivity is 70% to 90% in male inpatient alcoholics (usually drinking within 4 to 7 days of blood draw), with specificities >90%. Sensitivity is 12% to 40% in general populations—among whom underreporting of drinking may lead to more false positives—and 40% to 60% in outpatient alcoholics.7,8 Specificity, however, remains high—80% to 90%—when sensitivity is reduced.
Overall, %CDT is as sensitive as GGT and more sensitive than other biomarkers, including MCV, aspartate transaminase, and alanine transaminase.9 %CDT is more specific than GGT (92% vs. 75%) and other biomarkers. %CDT appears to be more sensitive in men, whereas GGT is more sensitive in women (Table 2).10
Ample evidence, however, suggests that %CDT and GGT readings together may provide a comprehensive picture of recent alcohol abuse.10 Whereas frequent drinking alters %CDT, GGT signals drinking intensity and is more effective at detecting episodic binge drinking (Table 2). This probably explains why problem drinkers age <20—who typically binge-drink—show little or no change in %CDT.
Table 2
%CDT vs GGT testing for recent alcohol abuse
| %CDT | GGT | |
|---|---|---|
| Advantages |
|
|
| Disadvantages |
|
|
| Cutoff value |
|
|
| %CDT: Carbohydrate-deficient transferrin percentage | ||
| GGT: Gamma-glutamyltransferase | ||
FACTORS THAT ALTER RESULTS
Unlike GGT and MCV, few medical conditions distort %CDT,11 meaning the test is accurate in patients with most medical conditions. Only end-stage liver disease, biliary cirrhosis, and rare genetic transferrin variants alter %CDT.
Women tend to have higher and more-variable CDT values than do men, possibly because of variability in normal transferrin levels, anemia secondary to iron deficiency, pregnancy, use of oral contraceptives, or menopause. %CDT cutoff scores are not gender-specific, however, because percentage rather than absolute CDT is typically measured.
%CDT seems to decrease slightly as body mass index increases, suggesting a small but significant inverse relationship between weight and %CDT. Smoking seems to raise %CDT values slightly. The specifics of and reasons for these relationships are unclear.
Related resources
- Axis-Shield. www.axis-shield.com. Click on “Lab diagnostics,” then “Alcohol-related.”
Disclosure
Dr. Anton is a consultant to Axis-Shield.
Dr. Miller and Ms. Dominick report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Biomarkers can help psychiatrists monitor abstinence and detect relapse in patients with alcohol use disorders. A blood test that measures carbohydrate-deficient transferrin percentage (%CDT) is FDA-approved for detecting heavy drinking (Table 1)1 and has shown effectiveness in several medical and surgical uses.
Table 1
%CDT test: Fast facts
| Brand names: |
| Axis-Shield %CDT, Bio-Rad %CDT TIA, Tina-quant (a) %CDT |
| FDA-approved indication: |
| Testing for excessive alcohol use |
| Manufacturers: |
| Axis-Shield PLC, Bio-Rad Laboratories, Roche Diagnostics |
| Recommended use: |
| Detecting heavy alcohol consumption, monitoring abstinence, and identifying elapse in patients with alcohol use disorders |
| Laboratories that process %CDT results: |
|
HOW %CDT SIGNALS ALCOHOL ABUSE
In 1976, Swedish researchers detected transferrin fractions in the CSF of alcoholic patients but not in nonalcoholics.2 One of these fractions was also present in alcoholics’ serum. This discovery led to the CDT biomarker.
%CDT testing is based on the finding that consuming an average >60 grams of alcohol (about 5 standard drinks) daily for ≥ 2 weeks causes a higher percentage of transferrin—a glycoprotein that transports iron in the blood—to lack its usual carbohydrate content. Transferrin appears in 6 isoforms, and studies have shown that heavy drinking increases three of these—asialo, mono sialo, and disialo transferrin—a state collectively called “carbohydrate-deficient.”
A %CDT reading ≥ 2.6 indicates that a patient may have had on average at least 5 alcoholic drinks daily for ≥ 2 weeks. Because CDT has a short mean half-life (7 to 14 days), readings >2.6 may suggest much heavier drinking at some time before the blood sample was taken.
Microcolumn chromatography separation assays that measure CDT as a percentage of total circulating transferrin have replaced initial CDT assays that used isoelectric focusing separation and immunoassay systems. This advance corrected for individual transferrin level variations.
CLINICAL USE
The %CDT test has shown effectiveness in several medical and surgical uses, including
- screening patients with diseases possibly triggered by alcohol use, such as treatment-resistant hypertension, gastroesophageal reflux disease, or depression
- detecting alcohol-use disorders in hospitalized patients
- screening presurgical and trauma patients to predict alcohol withdrawal syndrome and/or postsurgical complications.3,4
Although no alcohol biomarker alone reliably confirms alcohol abuse/dependence, %CDT can corroborate initial clinical impressions, especially when the patient’s self-report is suspect or information from significant others is not available.
Among biomarkers, %CDT most accurately predicts alcohol withdrawal syndrome in men (mean corpuscular volume [MCV] measurements are more accurate in women).4 During psychiatric consults, the test may help confirm suspected alcohol use in patients admitted to inpatient medical, surgical, or trauma units.
%CDT may also help monitor abstinence when treating an alcohol use disorder. In a major prospective treatment outcome study, %CDT was more sensitive than gamma-glutamyltransferase (GGT) in detecting relapse in male but not female alcoholics.5 Patients who abstained from drinking for 12 weeks showed a 30% decrease in %CDT. Subjects who relapsed during treatment later showed a 60% increase in %CDT, indicating sustained heavy drinking.
%CDT decreased over the first 4 weeks of treatment and continued to decline over time for abstinent patients (Figure). After week 4, %CDT increased again for those who consumed ≥ 5 drinks per day or had a full-blown relapse.5
Together, routine %CDT and GGT testing during treatment and follow-up can help clinicians monitor a patient’s progress and provide accurate reports to courts, child welfare agencies, and programs for impaired professionals. A 30% reduction from baseline in either biomarker indicates abstinence or significantly reduced alcohol consumption, whereas a 30% increase suggests relapse.6 Consider all clinical information in the final analysis, however.
%CDT results also provide an objective basis for discussing relapses with patients. Those who are responding to treatment often welcome %CDT testing as proof they are abstaining from alcohol.
Figure %CDT changes with alcohol use or abstinence
CLINICAL PRACTICALITY
The %CDT test is an immunoassay with ion-exchange column separation followed by turbidimetric measurement. Because the procedure is complex, laboratories generally require 24 to 72 hours to test the sample.
Because the %CDT test is relatively new, pricing, reimbursement rates, and availability are not well established. Pricing will likely vary widely from state to state and among laboratories and insurers. Medicare reimburses approximately $25 for %CDT testing, compared with $10 for GGT testing.
Only select reference laboratories offer %CDT testing, but the test should become more widely available over time (Table 1).
SENSITIVITY AND SPECIFICITY
%CDT test sensitivity is 70% to 90% in male inpatient alcoholics (usually drinking within 4 to 7 days of blood draw), with specificities >90%. Sensitivity is 12% to 40% in general populations—among whom underreporting of drinking may lead to more false positives—and 40% to 60% in outpatient alcoholics.7,8 Specificity, however, remains high—80% to 90%—when sensitivity is reduced.
Overall, %CDT is as sensitive as GGT and more sensitive than other biomarkers, including MCV, aspartate transaminase, and alanine transaminase.9 %CDT is more specific than GGT (92% vs. 75%) and other biomarkers. %CDT appears to be more sensitive in men, whereas GGT is more sensitive in women (Table 2).10
Ample evidence, however, suggests that %CDT and GGT readings together may provide a comprehensive picture of recent alcohol abuse.10 Whereas frequent drinking alters %CDT, GGT signals drinking intensity and is more effective at detecting episodic binge drinking (Table 2). This probably explains why problem drinkers age <20—who typically binge-drink—show little or no change in %CDT.
Table 2
%CDT vs GGT testing for recent alcohol abuse
| %CDT | GGT | |
|---|---|---|
| Advantages |
|
|
| Disadvantages |
|
|
| Cutoff value |
|
|
| %CDT: Carbohydrate-deficient transferrin percentage | ||
| GGT: Gamma-glutamyltransferase | ||
FACTORS THAT ALTER RESULTS
Unlike GGT and MCV, few medical conditions distort %CDT,11 meaning the test is accurate in patients with most medical conditions. Only end-stage liver disease, biliary cirrhosis, and rare genetic transferrin variants alter %CDT.
Women tend to have higher and more-variable CDT values than do men, possibly because of variability in normal transferrin levels, anemia secondary to iron deficiency, pregnancy, use of oral contraceptives, or menopause. %CDT cutoff scores are not gender-specific, however, because percentage rather than absolute CDT is typically measured.
%CDT seems to decrease slightly as body mass index increases, suggesting a small but significant inverse relationship between weight and %CDT. Smoking seems to raise %CDT values slightly. The specifics of and reasons for these relationships are unclear.
Related resources
- Axis-Shield. www.axis-shield.com. Click on “Lab diagnostics,” then “Alcohol-related.”
Disclosure
Dr. Anton is a consultant to Axis-Shield.
Dr. Miller and Ms. Dominick report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Anton RF, Dominick C, Bigelow M, Westby C. CDTect Research Group. Comparison of Bio-Rad %CDT TIA and CDTect as laboratory markers of heavy alcohol use and their relationships with gamma-glutamyltransferase. Clin Chem 2001;47:1769-75.
2. Stibler H, Kjellin KG. Isoelectric focusing and electrophoresis of the CSF proteins on tremor of different origins. J Neurol 1976;30:269-85.
3. Miller PM. Recent developments in alcohol biomarkers: Implications for managing alcohol-sensitive diseases. Resid Staff Physician 2004;50:11-17.
4. Spies CD, Kissner M, Neumann T, et al. Elevated carbohydrate-deficient transferrin predicts prolonged intensive care unit stay in traumatized men. Alcohol Alcohol 1998;33:661-9.
5. Anton RF, Moak DH, Latham P. Carbohydrate-deficient transferrin as an indicator of drinking status during a treatment outcome study. Alcohol Clin Exp Res 1996;20:841-6.
6. Anton RF, Lieber C, Tabakoff B. Carbohydrate-deficient transferrin and gamma-glutamyltransferase for the detection and monitoring of alcohol use: results from a multisite study. Alcohol Clin Exp Res 2002;26:1215-22.
7. Allen JP, Litten RZ, Anton RF, Cross GM. Carbohydrate-deficient transferrin as a measure of immoderate drinking: remaining issues. Alcohol Clin Exp Res 1994;18:799-812.
8. Gronbaek M, Henriksen JH, Becker U. Carbohydrate-deficient transferrin—a valid marker of alcoholism in population studies? Results from the Copenhagen City Heart Study. Alcohol Clin Exp Res 1995;19:457-61.
9. Bell H, Tallaksen CM, Try K, Haug E. Carbohydrate-deficient transferrin and other markers of high alcohol consumption: A study of 502 patients admitted consecutively to a medical department. Alcohol Clin Exp Res 1994;18:1103-8.
10. Conigrave KM, Degenhardt LJ, Whitfield JB, et al. CDT, GGT, and AST as markers of alcohol use: The WHO/ISBRA Collaborative Project. Alcohol Clin Exp Res 2002;26:332-9.
11. Meerkerk GJ, Njoo KH, Bongers IM, et al. The specificity of the CDT assay in general practice: the influence of common chronic diseases and medication on the serum CDT concentration. Alcohol Clin Exp Res 1998;22:908-13.
1. Anton RF, Dominick C, Bigelow M, Westby C. CDTect Research Group. Comparison of Bio-Rad %CDT TIA and CDTect as laboratory markers of heavy alcohol use and their relationships with gamma-glutamyltransferase. Clin Chem 2001;47:1769-75.
2. Stibler H, Kjellin KG. Isoelectric focusing and electrophoresis of the CSF proteins on tremor of different origins. J Neurol 1976;30:269-85.
3. Miller PM. Recent developments in alcohol biomarkers: Implications for managing alcohol-sensitive diseases. Resid Staff Physician 2004;50:11-17.
4. Spies CD, Kissner M, Neumann T, et al. Elevated carbohydrate-deficient transferrin predicts prolonged intensive care unit stay in traumatized men. Alcohol Alcohol 1998;33:661-9.
5. Anton RF, Moak DH, Latham P. Carbohydrate-deficient transferrin as an indicator of drinking status during a treatment outcome study. Alcohol Clin Exp Res 1996;20:841-6.
6. Anton RF, Lieber C, Tabakoff B. Carbohydrate-deficient transferrin and gamma-glutamyltransferase for the detection and monitoring of alcohol use: results from a multisite study. Alcohol Clin Exp Res 2002;26:1215-22.
7. Allen JP, Litten RZ, Anton RF, Cross GM. Carbohydrate-deficient transferrin as a measure of immoderate drinking: remaining issues. Alcohol Clin Exp Res 1994;18:799-812.
8. Gronbaek M, Henriksen JH, Becker U. Carbohydrate-deficient transferrin—a valid marker of alcoholism in population studies? Results from the Copenhagen City Heart Study. Alcohol Clin Exp Res 1995;19:457-61.
9. Bell H, Tallaksen CM, Try K, Haug E. Carbohydrate-deficient transferrin and other markers of high alcohol consumption: A study of 502 patients admitted consecutively to a medical department. Alcohol Clin Exp Res 1994;18:1103-8.
10. Conigrave KM, Degenhardt LJ, Whitfield JB, et al. CDT, GGT, and AST as markers of alcohol use: The WHO/ISBRA Collaborative Project. Alcohol Clin Exp Res 2002;26:332-9.
11. Meerkerk GJ, Njoo KH, Bongers IM, et al. The specificity of the CDT assay in general practice: the influence of common chronic diseases and medication on the serum CDT concentration. Alcohol Clin Exp Res 1998;22:908-13.
Homeless, not hopeless: 4 strategies for successful interventions
Treating homeless mentally ill persons in a community-based setting—such as an inpatient medical or psychiatric unit, emergency department, or shelter clinic—requires special clinical adaptations. Four strategies can help achieve a successful intervention.
1. Engage patiently. Many homeless persons view the mental health care system with suspicion and apprehension. Meaningful engagement often develops slowly;1 you could see a patient for weeks or months before he or she accepts treatment. Empathy and persuasion may be your most important therapeutic skills during initial encounters.
2. Assess needs broadly. During the initial evaluation ask about basic needs (safety, food, clothing, and emergency shelter) as well as psychiatric symptoms. Understandably, the homeless patient may place a much higher priority on food and shelter than on mental health services.2
Successful psychiatric treatment will be difficult if the person has no stable access to shelter. Make sure a workable strategy to obtain emergency, transitional, or permanent housing is in place.3 Work closely with the hospital’s social worker or the shelter’s case managers to facilitate this process.
3. Shape interventions pragmatically. To prevent the chaos of a shelter or the street from thwarting even a basic intervention:
- provide psychotropic samples rather than written prescriptions
- simplify dosing regimens to once-daily
- help the patient develop safe storage strategies for medications to prevent theft and exposure. For example, provide pill boxes or blister packs, or request that the shelter’s case manager store pills for the patient.
4. Retain arduously. Don’t expect perfect cooperation. Expect treatment nonadherence, lost or stolen medications, missed appointments, sporadic follow-through with other services, and inconsistency in abstaining from alcohol or other substances of abuse.
Set limits and establish consequences to keep a homeless person in treatment rather than to justify termination. For instance, if the patient repeatedly “loses” her medications, then provide just a few days’ supply at a time. This strategy encourages frequent follow-up and monitoring, which is more effective than discharging the patient for “noncompliance.”
1. Rowe M, Hoge MA, Fisk D. Critical issues in serving people who are homeless and mentally ill. Adm Ment Health 1996;23(6):555-65.
2. Gelberg L, Gallagher TC, Andersen RM, Koegel P. Competing priorities as a barrier to medical care among homeless adults in Los Angeles. Am J Pub Health 1997;87(2):217-20.
3. McQuistion H, Finnerty M, Hirschowitz J, Susser E. Challenges for psychiatry in serving homeless people with psychiatric disorders. Psychiatr Serv 2003;54(5):669-76.
Dr. Christensen is associate professor of psychiatry, University of Florida College Medicine, Jacksonville, and director of the university’s community psychiatry program.
Treating homeless mentally ill persons in a community-based setting—such as an inpatient medical or psychiatric unit, emergency department, or shelter clinic—requires special clinical adaptations. Four strategies can help achieve a successful intervention.
1. Engage patiently. Many homeless persons view the mental health care system with suspicion and apprehension. Meaningful engagement often develops slowly;1 you could see a patient for weeks or months before he or she accepts treatment. Empathy and persuasion may be your most important therapeutic skills during initial encounters.
2. Assess needs broadly. During the initial evaluation ask about basic needs (safety, food, clothing, and emergency shelter) as well as psychiatric symptoms. Understandably, the homeless patient may place a much higher priority on food and shelter than on mental health services.2
Successful psychiatric treatment will be difficult if the person has no stable access to shelter. Make sure a workable strategy to obtain emergency, transitional, or permanent housing is in place.3 Work closely with the hospital’s social worker or the shelter’s case managers to facilitate this process.
3. Shape interventions pragmatically. To prevent the chaos of a shelter or the street from thwarting even a basic intervention:
- provide psychotropic samples rather than written prescriptions
- simplify dosing regimens to once-daily
- help the patient develop safe storage strategies for medications to prevent theft and exposure. For example, provide pill boxes or blister packs, or request that the shelter’s case manager store pills for the patient.
4. Retain arduously. Don’t expect perfect cooperation. Expect treatment nonadherence, lost or stolen medications, missed appointments, sporadic follow-through with other services, and inconsistency in abstaining from alcohol or other substances of abuse.
Set limits and establish consequences to keep a homeless person in treatment rather than to justify termination. For instance, if the patient repeatedly “loses” her medications, then provide just a few days’ supply at a time. This strategy encourages frequent follow-up and monitoring, which is more effective than discharging the patient for “noncompliance.”
Treating homeless mentally ill persons in a community-based setting—such as an inpatient medical or psychiatric unit, emergency department, or shelter clinic—requires special clinical adaptations. Four strategies can help achieve a successful intervention.
1. Engage patiently. Many homeless persons view the mental health care system with suspicion and apprehension. Meaningful engagement often develops slowly;1 you could see a patient for weeks or months before he or she accepts treatment. Empathy and persuasion may be your most important therapeutic skills during initial encounters.
2. Assess needs broadly. During the initial evaluation ask about basic needs (safety, food, clothing, and emergency shelter) as well as psychiatric symptoms. Understandably, the homeless patient may place a much higher priority on food and shelter than on mental health services.2
Successful psychiatric treatment will be difficult if the person has no stable access to shelter. Make sure a workable strategy to obtain emergency, transitional, or permanent housing is in place.3 Work closely with the hospital’s social worker or the shelter’s case managers to facilitate this process.
3. Shape interventions pragmatically. To prevent the chaos of a shelter or the street from thwarting even a basic intervention:
- provide psychotropic samples rather than written prescriptions
- simplify dosing regimens to once-daily
- help the patient develop safe storage strategies for medications to prevent theft and exposure. For example, provide pill boxes or blister packs, or request that the shelter’s case manager store pills for the patient.
4. Retain arduously. Don’t expect perfect cooperation. Expect treatment nonadherence, lost or stolen medications, missed appointments, sporadic follow-through with other services, and inconsistency in abstaining from alcohol or other substances of abuse.
Set limits and establish consequences to keep a homeless person in treatment rather than to justify termination. For instance, if the patient repeatedly “loses” her medications, then provide just a few days’ supply at a time. This strategy encourages frequent follow-up and monitoring, which is more effective than discharging the patient for “noncompliance.”
1. Rowe M, Hoge MA, Fisk D. Critical issues in serving people who are homeless and mentally ill. Adm Ment Health 1996;23(6):555-65.
2. Gelberg L, Gallagher TC, Andersen RM, Koegel P. Competing priorities as a barrier to medical care among homeless adults in Los Angeles. Am J Pub Health 1997;87(2):217-20.
3. McQuistion H, Finnerty M, Hirschowitz J, Susser E. Challenges for psychiatry in serving homeless people with psychiatric disorders. Psychiatr Serv 2003;54(5):669-76.
Dr. Christensen is associate professor of psychiatry, University of Florida College Medicine, Jacksonville, and director of the university’s community psychiatry program.
1. Rowe M, Hoge MA, Fisk D. Critical issues in serving people who are homeless and mentally ill. Adm Ment Health 1996;23(6):555-65.
2. Gelberg L, Gallagher TC, Andersen RM, Koegel P. Competing priorities as a barrier to medical care among homeless adults in Los Angeles. Am J Pub Health 1997;87(2):217-20.
3. McQuistion H, Finnerty M, Hirschowitz J, Susser E. Challenges for psychiatry in serving homeless people with psychiatric disorders. Psychiatr Serv 2003;54(5):669-76.
Dr. Christensen is associate professor of psychiatry, University of Florida College Medicine, Jacksonville, and director of the university’s community psychiatry program.