User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Informative and relevant
The January 2005 issue of Current psychiatry is the best collection of informative and relevant articles I have ever read in a professional journal.
You should be commended for the selection of topics and for publishing such useful, detailed information. I am impressed with the quality of writing and your knowledge of what we in the field need.
Please accept my heartfelt gratitude and my hope for your continued standard of excellence.
Margaret Wicks, RN, CNS
West Palm Beach, FL
The January 2005 issue of Current psychiatry is the best collection of informative and relevant articles I have ever read in a professional journal.
You should be commended for the selection of topics and for publishing such useful, detailed information. I am impressed with the quality of writing and your knowledge of what we in the field need.
Please accept my heartfelt gratitude and my hope for your continued standard of excellence.
Margaret Wicks, RN, CNS
West Palm Beach, FL
The January 2005 issue of Current psychiatry is the best collection of informative and relevant articles I have ever read in a professional journal.
You should be commended for the selection of topics and for publishing such useful, detailed information. I am impressed with the quality of writing and your knowledge of what we in the field need.
Please accept my heartfelt gratitude and my hope for your continued standard of excellence.
Margaret Wicks, RN, CNS
West Palm Beach, FL
Forcing hoarders to conquer clutter
Drs. Jamie Feusner and Sanjaya Saxena offer valuable strategies for treating compulsive hoarding disorder (Current Psychiatry, March 2005),
Encouraging these patients to regularly have visitors over to their houses also can be extremely therapeutic. This approach works on several levels:
- Patients would be embarrassed to have company see a messy home, so they will clean frantically before the visit.
- To avoid future all-night clean-ups, they will be motivated to prevent clutter from accumulating day-to-day.
- Social interaction with visitors provides support that reduces some causes of hoarding.
These visits force patients to be accountable and confront denial, much as Alcoholics Anonymous does for patients with alcohol use disorders. Even if the clutter is displaced to closets—as is often the case—it is still a major step forward. This approach requires a strong therapeutic alliance, but patients will receive positive reinforcement that sustains their progress.
Isaac Steven Herschkopf, MD
Clinical instructor
Department of psychiatry
New York University School of Medicine
New York, NY
Drs. Jamie Feusner and Sanjaya Saxena offer valuable strategies for treating compulsive hoarding disorder (Current Psychiatry, March 2005),
Encouraging these patients to regularly have visitors over to their houses also can be extremely therapeutic. This approach works on several levels:
- Patients would be embarrassed to have company see a messy home, so they will clean frantically before the visit.
- To avoid future all-night clean-ups, they will be motivated to prevent clutter from accumulating day-to-day.
- Social interaction with visitors provides support that reduces some causes of hoarding.
These visits force patients to be accountable and confront denial, much as Alcoholics Anonymous does for patients with alcohol use disorders. Even if the clutter is displaced to closets—as is often the case—it is still a major step forward. This approach requires a strong therapeutic alliance, but patients will receive positive reinforcement that sustains their progress.
Isaac Steven Herschkopf, MD
Clinical instructor
Department of psychiatry
New York University School of Medicine
New York, NY
Drs. Jamie Feusner and Sanjaya Saxena offer valuable strategies for treating compulsive hoarding disorder (Current Psychiatry, March 2005),
Encouraging these patients to regularly have visitors over to their houses also can be extremely therapeutic. This approach works on several levels:
- Patients would be embarrassed to have company see a messy home, so they will clean frantically before the visit.
- To avoid future all-night clean-ups, they will be motivated to prevent clutter from accumulating day-to-day.
- Social interaction with visitors provides support that reduces some causes of hoarding.
These visits force patients to be accountable and confront denial, much as Alcoholics Anonymous does for patients with alcohol use disorders. Even if the clutter is displaced to closets—as is often the case—it is still a major step forward. This approach requires a strong therapeutic alliance, but patients will receive positive reinforcement that sustains their progress.
Isaac Steven Herschkopf, MD
Clinical instructor
Department of psychiatry
New York University School of Medicine
New York, NY
Dialectical behavior therapy to help ‘borderline’ patients
I would like to clarify several points in our article on using dialectical behavior therapy to treat patients with borderline personality disorder (Current Psychiatry, April 2005).
The reader is given the impression that a training program involving 2 weeks of didactic training plus some months of consultation is sufficient to practice the treatment competently. Although 2 weeks of intensive training may be a useful first step, providing competent treatment requires using that knowledge and continuing to develop skill as a therapist over time.
Table 2 (problem-solving strategies) includes structural strategies, which are neither acceptance nor problem-solving strategies, but rather serve to organize treatment.
Irreverence was misidentified as an acceptance strategy in Table 3 (acceptance strategies). Irreverence is used primarily to present novel stimuli to which the patient must respond; in this way, it is primarily a change strategy. Also in Table 3:
- Dialectical strategies defy being clearly acceptance or problem-solving tools. To the degree that these strategies highlight tensions, they serve to push the patient toward change.
- Case management can be both an acceptance and problem-solving strategy. It is acceptance when the therapist accepts that patients’ situations are such that they cannot effectively act on their own behalf and that the therapist must intervene. It is problem-solving when the therapist coaches patients to intervene on their own behalf.
Anthony P. DuBose, PsyD
President & CEO, DBT Center of Seattle, PLLC
I would like to clarify several points in our article on using dialectical behavior therapy to treat patients with borderline personality disorder (Current Psychiatry, April 2005).
The reader is given the impression that a training program involving 2 weeks of didactic training plus some months of consultation is sufficient to practice the treatment competently. Although 2 weeks of intensive training may be a useful first step, providing competent treatment requires using that knowledge and continuing to develop skill as a therapist over time.
Table 2 (problem-solving strategies) includes structural strategies, which are neither acceptance nor problem-solving strategies, but rather serve to organize treatment.
Irreverence was misidentified as an acceptance strategy in Table 3 (acceptance strategies). Irreverence is used primarily to present novel stimuli to which the patient must respond; in this way, it is primarily a change strategy. Also in Table 3:
- Dialectical strategies defy being clearly acceptance or problem-solving tools. To the degree that these strategies highlight tensions, they serve to push the patient toward change.
- Case management can be both an acceptance and problem-solving strategy. It is acceptance when the therapist accepts that patients’ situations are such that they cannot effectively act on their own behalf and that the therapist must intervene. It is problem-solving when the therapist coaches patients to intervene on their own behalf.
Anthony P. DuBose, PsyD
President & CEO, DBT Center of Seattle, PLLC
I would like to clarify several points in our article on using dialectical behavior therapy to treat patients with borderline personality disorder (Current Psychiatry, April 2005).
The reader is given the impression that a training program involving 2 weeks of didactic training plus some months of consultation is sufficient to practice the treatment competently. Although 2 weeks of intensive training may be a useful first step, providing competent treatment requires using that knowledge and continuing to develop skill as a therapist over time.
Table 2 (problem-solving strategies) includes structural strategies, which are neither acceptance nor problem-solving strategies, but rather serve to organize treatment.
Irreverence was misidentified as an acceptance strategy in Table 3 (acceptance strategies). Irreverence is used primarily to present novel stimuli to which the patient must respond; in this way, it is primarily a change strategy. Also in Table 3:
- Dialectical strategies defy being clearly acceptance or problem-solving tools. To the degree that these strategies highlight tensions, they serve to push the patient toward change.
- Case management can be both an acceptance and problem-solving strategy. It is acceptance when the therapist accepts that patients’ situations are such that they cannot effectively act on their own behalf and that the therapist must intervene. It is problem-solving when the therapist coaches patients to intervene on their own behalf.
Anthony P. DuBose, PsyD
President & CEO, DBT Center of Seattle, PLLC
Too much ‘evidence-based’ medicine?
The American Psychiatric Association, National Alliance for the Mentally Ill, and National Mental Health Association recently warned against relying on “effectiveness research.”
How can anyone warn against effectiveness research? Isn’t that like warning against mom or apple pie? (Well, I guess psychiatrists and nutritionists have warned us about mom and apple pie.) But shouldn’t we aspire to practice evidence-based medicine?
These organizations, of course, are warning against a trend to rely solely on “evidence-based” research. Appropriate research should inform our therapy choices, but an approach that lacks double-blind, placebo-controlled studies is not necessarily ineffective. Parachutes are not considered ineffective, though no properly controlled trials have compared outcomes of users versus nonusers jumping from planes (see “Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomized controlled trials.” British Medical Journal 2003;327:1459-61).
Concerned that some insurers are paying for only the cheapest medications unless “evidence-based” proof shows a more-expensive treatment to be significantly better, the APA/NAMI/NMHA stated: “True evidence-based approaches marry all available and appropriate scientific research with clinical experience to ensure treatments lead to the best possible outcomes. Implementing public policies based solely on one of these elements without the other is not an evidence-based approach.”
We at Current Psychiatry agree. The marriage of clinical data with clinical experience is what this journal is all about.

James Randolph Hillard, MD
James Randolph Hillard, MD
James Randolph Hillard, MD
The American Psychiatric Association, National Alliance for the Mentally Ill, and National Mental Health Association recently warned against relying on “effectiveness research.”
How can anyone warn against effectiveness research? Isn’t that like warning against mom or apple pie? (Well, I guess psychiatrists and nutritionists have warned us about mom and apple pie.) But shouldn’t we aspire to practice evidence-based medicine?
These organizations, of course, are warning against a trend to rely solely on “evidence-based” research. Appropriate research should inform our therapy choices, but an approach that lacks double-blind, placebo-controlled studies is not necessarily ineffective. Parachutes are not considered ineffective, though no properly controlled trials have compared outcomes of users versus nonusers jumping from planes (see “Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomized controlled trials.” British Medical Journal 2003;327:1459-61).
Concerned that some insurers are paying for only the cheapest medications unless “evidence-based” proof shows a more-expensive treatment to be significantly better, the APA/NAMI/NMHA stated: “True evidence-based approaches marry all available and appropriate scientific research with clinical experience to ensure treatments lead to the best possible outcomes. Implementing public policies based solely on one of these elements without the other is not an evidence-based approach.”
We at Current Psychiatry agree. The marriage of clinical data with clinical experience is what this journal is all about.
The American Psychiatric Association, National Alliance for the Mentally Ill, and National Mental Health Association recently warned against relying on “effectiveness research.”
How can anyone warn against effectiveness research? Isn’t that like warning against mom or apple pie? (Well, I guess psychiatrists and nutritionists have warned us about mom and apple pie.) But shouldn’t we aspire to practice evidence-based medicine?
These organizations, of course, are warning against a trend to rely solely on “evidence-based” research. Appropriate research should inform our therapy choices, but an approach that lacks double-blind, placebo-controlled studies is not necessarily ineffective. Parachutes are not considered ineffective, though no properly controlled trials have compared outcomes of users versus nonusers jumping from planes (see “Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomized controlled trials.” British Medical Journal 2003;327:1459-61).
Concerned that some insurers are paying for only the cheapest medications unless “evidence-based” proof shows a more-expensive treatment to be significantly better, the APA/NAMI/NMHA stated: “True evidence-based approaches marry all available and appropriate scientific research with clinical experience to ensure treatments lead to the best possible outcomes. Implementing public policies based solely on one of these elements without the other is not an evidence-based approach.”
We at Current Psychiatry agree. The marriage of clinical data with clinical experience is what this journal is all about.
A suicidal injection obsession
HISTORY: TIRED OF LIVING
Mr. F, age 43, presents to the emergency room with complications of type 2 diabetes mellitus: blurry vision, increased urination, fatigue, and polydipsia. Blood glucose is 676 mg/dL.
The patient flees during treatment—possibly to attempt suicide—but returns 36 hours later, noticeably disoriented. He is readmitted to the ER, where he tells staff he is considering suicide and plans to self-inject a lethal substance. The ER staff refers him to the psychiatry service.
Mr. F also complains of shortness of breath after minimal exertion, aching joints throughout his body, and intense pain in his right great toe. He has been sleeping 12 to 20 hours daily, yet has trouble sleeping at night. He persistently feels fatigued, hopeless, and helpless. He says his suicidal urges have become more intense over 2 months, but he fears he will lose his computer repair job if he is admitted. He also shows difficulties with short-term memory. We admit him for observation.
Mental status examination suggests that Mr. F is generally withdrawn. Eye contact is poor and he is quiet and evasive, possibly signaling paranoia. He spends most of his stay watching television. His thought process is linear, and he thinks constantly of suicide. During the Mini-Mental State Examination, he gives the incorrect date and county. He misses two other items on recall but gets them correct with prompts.
A mild intention tremor distorts his handwriting. He has trouble keeping his balance during the Romberg test, and his gait is mildly ataxic. Ophthalmology consult suggests that diabetic retinopathy and optic disc cupping secondary to glaucoma may be blurring his vision.
Mr. F is taking no medications but had previously used insulin twice a day, and his outpatient doctor insists he should go back on insulin. He smokes 1 pack of cigarettes per day, drinks alcohol moderately (one to two drinks/day), and does not abuse illicit drugs.
The authors’ observations
Mr. F’s depressed mood, hopelessness, concentration problems, psychomotor retardation, and suicidal thoughts suggest major depressive disorder. Depression or a delirium secondary to diabetes may account for his referential ideas.
FURTHER HISTORY: ONE SHOT AT SATISFACTION
Over the following week, Mr. F becomes more talkative as the psychiatry staff develops a therapeutic rapport. He tells his treatment team that he feels urges to self-inject liquids he finds in his hospital room, such as shower gel and beverages.
Mr. F tells us that approximately 2 years ago, he tried to kill himself by swallowing boric acid. After 6 weeks in intensive care, the poison’s physical effects resolved and he no longer appeared suicidal. The staff at that time prepared to discharge Mr. F when, while left alone in his room, he dislodged a wall-mounted sphygmomanometer, disassembled it, and broke open the mercury tube. He then injected about 3 mL of mercury into his intravenous port and swallowed another 3 mL.
A nurse who checked on Mr. F minutes after the incident did not notice the sphygmomanometer was missing. He showed the broken device to the nurse, saying, “Look what I did.” When the nurse asked why, he responded, “I was just sitting here alone and saw the thing on the wall. I thought to myself, I can do this.”
The hospital viewed the episode as another suicide attempt. Staff immediately began chelation therapy with dimercaprol, 10 mg/kg every 8 hours for 5 days, then 10 mg/kg every 12 hours for 2 weeks. Within 24 hours of ingesting mercury, Mr. F developed shortness of breath, tachycardia (104 BPM), a fever (101.8°F), and had GI complaints. Increased blood urea nitrogen, increased creatinine, and decreased urination suggested declining renal function. He developed a pruritic rash over his back and mild skin loss on his soles.
Mr. F’s mercury levels were 20.8 mg/dL (serum) and 216 mg/dL (urine) 36 hours after ingestation, and 24.8 mg/dL (serum) and 397 mg/dL (urine) after chelation. Serum mercury >5 mg/dL is usually symptomatic.
Approximately 72 hours after the incident, most pulmonary, renal, and dermal manifestations of mercury toxicity began to improve. Mr. F was discharged after 21 days. He was diagnosed with major depression and started on sertraline, 150 mg/d.
‘The best feeling.’ Two years later, Mr. F tells us he has attempted suicide at least six times. Diffuse metallic foreign bodies throughout his lung vasculature and a 9.6 mg/dL serum mercury reading confirm he has injected mercury. His painful toe is x-rayed to check for mercury deposits, but he ultimately is diagnosed with gout.
During our evaluation, Mr. F admits that “the calmest, best feeling I have ever had” was while injecting mercury, yet he fears the incident has caused permanent physical and mental damage. He describes his desire to self-inject liquids as “impulses” triggered by twice-daily subcutaneous insulin use. For this reason, he has stopped taking insulin against his doctor’s advice.
The authors’ observations
Mr. F’s mental status changes and serum mercury suggest mercury poisoning. He shows numerous heavy-metal poisoning symptoms (Box 1) as well as erethism, a malaise that can result from heavy-metal exposure.2
The patient insists that insulin shots bring on self-injection urges, but his impulsive and repetitive suicidal behavior, dysphoria, and transient paranoia suggest borderline personality disorder. His impulses may reflect a subtle, long-term personality change caused by mercury’s neurotoxic effects.1 Or they could be akin to cutting behaviors shown by some patients with personality disorders, particularly borderline personality disorder.
We ruled out substance abuse disorder, as Mr. F’s mercury ingestion was not premeditated, he has no history of illicit drug use, and intravenous elemental mercury is not psychoactive.
- Emotional lability
- Excessive shyness
- Headaches
- Hearing loss
- Insomnia
- Irritability
- Lack of ambition
- Lack of sexual desire
- Loss of confidence
- Memory loss
- Nervousness
- Neuromuscular changes (including weakness, muscle atrophy, muscle twitching)
- Performance deficits in cognitive function tests
- Polyneuropathy
- Tremor of hands
- Visual field defects
Source: Reference 1
Elemental mercury found in thermometers, lamps, and dental amalgams slowly ionizes in the blood stream before crossing the blood-brain barrier. Mercury and carbon form toxic “organic” compounds, including methylmercury (found in the environment), phenylmercury (used in some commercial products), and dimethylmercury (found in solid waste sites).
Because mercury’s half-life is 60 days, it dissipates slowly, can accumulate with chronic exposure, and stays in the blood stream long after high-dose exposure.3
Serum mercury >5 mg/dL can cause subtle, enduring neurotoxic effects, including tremor, dizziness, shortness of breath, blurry vision, decreased visual fields, depression, memory loss, and irritability.3 Serum mercury rarely exceeds 1.5 mg/dL without direct exposure.
Irritability, depressive symptoms, and renal manifestations emerge when urine mercury reaches 200 to 1,000 mg/dL. Renal, respiratory, and GI effects are seen at 1,000 to 2,000 mg/dL.
Means of exposure. Vapor inhalation is the most common means of elemental mercury exposure.3 Elemental mercury used in manufacturing vaporizes at room temperature.
Orally ingested elemental mercury is poorly absorbed from the GI tract, mostly passes unabsorbed, and is toxic only at high doses. Injected elemental mercury is poorly absorbed but can cause mechanical and immunologic effects. The psychiatric literature describes some 200 cases of mercury self-injection4-8 but offers little information on cognitive effects or long-term follow-up.
Consider heavy-metal poisoning in the differential diagnosis of patients with depressive symptoms. Ask about risk factors for environmental mercury exposure, including use of folk medicines, some cosmetics, over-the-counter nasal sprays, ophthalmic solutions, skin-lightening creams, daily fish consumption (particularly tuna or swordfish), living in a house painted with latex paint, or continuous exposure at work (Box 2).
Also ask if the patient or a household member recently ingested mercury or handled a broken thermometer. Liquid mercury on clothing and in bodily fluids may cause secondary contamination, whereas mercury vapor cannot.
Order serum mercury testing if you suspect chronic exposure. Refer patients with serum mercury ≥ 1.5 mg/dL to their primary care physicians and to a poison control center for evaluation and possible chelation. Refer patients with acute mercury exposure symptoms to the ER.
Consuming or using certain products or working in some industries increases mercury exposure risk. Mercury-containing products include:
Over-the-counter herbal remedies imported from China, Hong Kong, Haiti, and Cuba.9
Older, larger marine animals, including tuna, shark, or swordfish from mercury-contaminated waters.10,11
Vaccines and medications. Small amounts of thimerosal (ethylmercury sodium salt) were used as a preservative in some vaccines.12 Some antiseptics, eye drops, eye ointments, nasal sprays, skin-lightening creams, and gamma globulin contain mercury.
Dental amalgams are approximately 50% mercury. Each amalgam releases roughly 10 mg/d of mercury; chewing gum or grinding teeth may increase exposure.13 Some suggest removing the fillings, but this can increase mercury exposure if done incorrectly.1
Household goods, including latex paint made before 1990 and broken thermometers.3,14
Other environmental exposure, such as from burning coal, water treatment facilities, landfills, and mercury-containing fungicides.
Occupations that carry a high risk of mercury exposure include:3
Manufacturing
Batteries, cosmetics, explosives, paint/pigments, fluorescent lamps, ink, mercury vapor lamps, pharmaceuticals, switches, and rectifiers
Skilled trades
Plumbing, chlorine and caustic soda production, electroplating, felt-making, leather tanning, grinding machine operators, paper millers
Medical
Dental and medical laboratory personnel
Service industries
Hazardous-waste site personnel, painters, pesticide/fungicide production/application
Mining/processing
Cinnabar, gold, silver, copper, or zinc; metallurgy
The authors’ observations
Antidepressants generally will not reduce depression, irritability, personality changes, or apathy secondary to mercury poisoning. We have found that a psychostimulant such as methylphenidate, starting at 10 mg bid and titrating to therapeutic effect, can help treat mercury-related apathy.
We did not give Mr. F a psychostimulant, however, fearing it would worsen his impulsive behavior and disordered sleep. Also, more effectively managing Mr. F’s diabetes should improve his depression.
DISCHARGE: CHELATION CHALLENGE
Mr. F’s suicidal thoughts continued intermittently. Chelation was tried again with succimer, 1,000 mg tid for 5 days and bid for 5 more days, but the agent caused severe nausea without significantly decreasing serum mercury. He declined outpatient chelation.
After 2 weeks, Mr. F denied suicidal thoughts and said he felt physically better. He was discharged on venlafaxine, 300 mg/d, for his depressive symptoms; and metformin, 1,000 mg/d, glipizide, 10 mg bid, and rosiglitazone, 4 mg/d, to control his blood glucose. We arranged for medication management at a community mental health center. Mr. F was also told to visit the hospital’s outpatient clinic for endocrine follow-up but has not returned for 18 months.
Related resources
- Agency for Toxic Substances and Disease Registry. Information about toxic substances in the environment and diseases they may cause. www.atsdr.cdc.gov.
- Dimercaprol • BAL in Oil
- Glipizide • Glucotrol
- Metformin • Glucophage
- Methylphenidate • Ritalin, Concerta
- Rosiglitazone • Avandia
- Sertraline • Zoloft
- Succimer • Chemet
- Venlafaxine • Effexor
Dr. Matthews is an American Psychiatric Association Bristol-Myers Squibb Co. fellow in public and community psychiatry.
Dr. Hauser receives research/grant support from GlaxoSmithKline, Hoffman LaRoche, and AstraZeneca Pharmaceuticals. He is a speaker for Abbott Laboratories, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb Co., GlaxoSmithKline, and Janssen Pharmaceuticals.
1. Agency for Toxic Substances and Disease Registry. Toxicological profile for mercury, March 1999. Available at: http://www.atsdr.cdc.gov/toxprofiles/tp46.html. Accessed May 4, 2005.
2. Clarkson TW, Magos L, Myers GJ. The toxicology of mercury—current exposures and clinical manifestations. N Engl J Med 2003;349:1731-7.
3. Mercury toxicity. Agency for Toxic Substance and Disease Registry. Am Fam Physician 1992;46:1731-41.
4. Manoukian SV, Wenger NK. Mercury in the heart. Am J Cardiol 1991;67:317-8.
5. Maniatis V, Zois G, Stringaris K. IV mercury self-injection: CT imaging. AJR Am J Roentgenol 1997;169:1197-8.
6. McFee RB, Caraccio TR. Intravenous mercury injection and ingestion: clinical manifestations and management. J Toxicol Clin Toxicol 2001;39:733-8.
7. Shareeff M, Bhat YM, Adabala R, Raoof S. Shortness of breath after suicide attempt. Chest 2000;118:837-8.
8. Torres-Alanis O, Garza-Ocanas L, Pineyro-Lopez A. Intravenous self-administration of metallic mercury: report of a case with a 5-year follow-up. J Toxicol Clin Toxicol 1997;35:83-7.
9. Li AM, Chan MH, Leung TF, et al. Mercury intoxication presenting with tics. Arch Dis Child 2000;83:74-5.
10. Dewailly E, Ayotte P, Bruneau S, et al. Exposure of the Inuit population of Nunavik (Arctic Quebec) to lead and mercury. Arch Environ Health 2001;56:350-7.
11. Stephenson J. FDA warns on mercury in tuna. JAMA 2004;291:171.
12. Dantzig PI. A new cutaneous sign of mercury poisoning. Ann Intern Med 2003;139:78-80.
13. Fitzpatrick M. Heavy metal. Lancet 2003;361:1664.-
14. From the Centers for Disease Control. Acute, chronic poisoning, residential exposures to elemental mercury—Michigan, 1989-1990. JAMA 1991;266:196.-
HISTORY: TIRED OF LIVING
Mr. F, age 43, presents to the emergency room with complications of type 2 diabetes mellitus: blurry vision, increased urination, fatigue, and polydipsia. Blood glucose is 676 mg/dL.
The patient flees during treatment—possibly to attempt suicide—but returns 36 hours later, noticeably disoriented. He is readmitted to the ER, where he tells staff he is considering suicide and plans to self-inject a lethal substance. The ER staff refers him to the psychiatry service.
Mr. F also complains of shortness of breath after minimal exertion, aching joints throughout his body, and intense pain in his right great toe. He has been sleeping 12 to 20 hours daily, yet has trouble sleeping at night. He persistently feels fatigued, hopeless, and helpless. He says his suicidal urges have become more intense over 2 months, but he fears he will lose his computer repair job if he is admitted. He also shows difficulties with short-term memory. We admit him for observation.
Mental status examination suggests that Mr. F is generally withdrawn. Eye contact is poor and he is quiet and evasive, possibly signaling paranoia. He spends most of his stay watching television. His thought process is linear, and he thinks constantly of suicide. During the Mini-Mental State Examination, he gives the incorrect date and county. He misses two other items on recall but gets them correct with prompts.
A mild intention tremor distorts his handwriting. He has trouble keeping his balance during the Romberg test, and his gait is mildly ataxic. Ophthalmology consult suggests that diabetic retinopathy and optic disc cupping secondary to glaucoma may be blurring his vision.
Mr. F is taking no medications but had previously used insulin twice a day, and his outpatient doctor insists he should go back on insulin. He smokes 1 pack of cigarettes per day, drinks alcohol moderately (one to two drinks/day), and does not abuse illicit drugs.
The authors’ observations
Mr. F’s depressed mood, hopelessness, concentration problems, psychomotor retardation, and suicidal thoughts suggest major depressive disorder. Depression or a delirium secondary to diabetes may account for his referential ideas.
FURTHER HISTORY: ONE SHOT AT SATISFACTION
Over the following week, Mr. F becomes more talkative as the psychiatry staff develops a therapeutic rapport. He tells his treatment team that he feels urges to self-inject liquids he finds in his hospital room, such as shower gel and beverages.
Mr. F tells us that approximately 2 years ago, he tried to kill himself by swallowing boric acid. After 6 weeks in intensive care, the poison’s physical effects resolved and he no longer appeared suicidal. The staff at that time prepared to discharge Mr. F when, while left alone in his room, he dislodged a wall-mounted sphygmomanometer, disassembled it, and broke open the mercury tube. He then injected about 3 mL of mercury into his intravenous port and swallowed another 3 mL.
A nurse who checked on Mr. F minutes after the incident did not notice the sphygmomanometer was missing. He showed the broken device to the nurse, saying, “Look what I did.” When the nurse asked why, he responded, “I was just sitting here alone and saw the thing on the wall. I thought to myself, I can do this.”
The hospital viewed the episode as another suicide attempt. Staff immediately began chelation therapy with dimercaprol, 10 mg/kg every 8 hours for 5 days, then 10 mg/kg every 12 hours for 2 weeks. Within 24 hours of ingesting mercury, Mr. F developed shortness of breath, tachycardia (104 BPM), a fever (101.8°F), and had GI complaints. Increased blood urea nitrogen, increased creatinine, and decreased urination suggested declining renal function. He developed a pruritic rash over his back and mild skin loss on his soles.
Mr. F’s mercury levels were 20.8 mg/dL (serum) and 216 mg/dL (urine) 36 hours after ingestation, and 24.8 mg/dL (serum) and 397 mg/dL (urine) after chelation. Serum mercury >5 mg/dL is usually symptomatic.
Approximately 72 hours after the incident, most pulmonary, renal, and dermal manifestations of mercury toxicity began to improve. Mr. F was discharged after 21 days. He was diagnosed with major depression and started on sertraline, 150 mg/d.
‘The best feeling.’ Two years later, Mr. F tells us he has attempted suicide at least six times. Diffuse metallic foreign bodies throughout his lung vasculature and a 9.6 mg/dL serum mercury reading confirm he has injected mercury. His painful toe is x-rayed to check for mercury deposits, but he ultimately is diagnosed with gout.
During our evaluation, Mr. F admits that “the calmest, best feeling I have ever had” was while injecting mercury, yet he fears the incident has caused permanent physical and mental damage. He describes his desire to self-inject liquids as “impulses” triggered by twice-daily subcutaneous insulin use. For this reason, he has stopped taking insulin against his doctor’s advice.
The authors’ observations
Mr. F’s mental status changes and serum mercury suggest mercury poisoning. He shows numerous heavy-metal poisoning symptoms (Box 1) as well as erethism, a malaise that can result from heavy-metal exposure.2
The patient insists that insulin shots bring on self-injection urges, but his impulsive and repetitive suicidal behavior, dysphoria, and transient paranoia suggest borderline personality disorder. His impulses may reflect a subtle, long-term personality change caused by mercury’s neurotoxic effects.1 Or they could be akin to cutting behaviors shown by some patients with personality disorders, particularly borderline personality disorder.
We ruled out substance abuse disorder, as Mr. F’s mercury ingestion was not premeditated, he has no history of illicit drug use, and intravenous elemental mercury is not psychoactive.
- Emotional lability
- Excessive shyness
- Headaches
- Hearing loss
- Insomnia
- Irritability
- Lack of ambition
- Lack of sexual desire
- Loss of confidence
- Memory loss
- Nervousness
- Neuromuscular changes (including weakness, muscle atrophy, muscle twitching)
- Performance deficits in cognitive function tests
- Polyneuropathy
- Tremor of hands
- Visual field defects
Source: Reference 1
Elemental mercury found in thermometers, lamps, and dental amalgams slowly ionizes in the blood stream before crossing the blood-brain barrier. Mercury and carbon form toxic “organic” compounds, including methylmercury (found in the environment), phenylmercury (used in some commercial products), and dimethylmercury (found in solid waste sites).
Because mercury’s half-life is 60 days, it dissipates slowly, can accumulate with chronic exposure, and stays in the blood stream long after high-dose exposure.3
Serum mercury >5 mg/dL can cause subtle, enduring neurotoxic effects, including tremor, dizziness, shortness of breath, blurry vision, decreased visual fields, depression, memory loss, and irritability.3 Serum mercury rarely exceeds 1.5 mg/dL without direct exposure.
Irritability, depressive symptoms, and renal manifestations emerge when urine mercury reaches 200 to 1,000 mg/dL. Renal, respiratory, and GI effects are seen at 1,000 to 2,000 mg/dL.
Means of exposure. Vapor inhalation is the most common means of elemental mercury exposure.3 Elemental mercury used in manufacturing vaporizes at room temperature.
Orally ingested elemental mercury is poorly absorbed from the GI tract, mostly passes unabsorbed, and is toxic only at high doses. Injected elemental mercury is poorly absorbed but can cause mechanical and immunologic effects. The psychiatric literature describes some 200 cases of mercury self-injection4-8 but offers little information on cognitive effects or long-term follow-up.
Consider heavy-metal poisoning in the differential diagnosis of patients with depressive symptoms. Ask about risk factors for environmental mercury exposure, including use of folk medicines, some cosmetics, over-the-counter nasal sprays, ophthalmic solutions, skin-lightening creams, daily fish consumption (particularly tuna or swordfish), living in a house painted with latex paint, or continuous exposure at work (Box 2).
Also ask if the patient or a household member recently ingested mercury or handled a broken thermometer. Liquid mercury on clothing and in bodily fluids may cause secondary contamination, whereas mercury vapor cannot.
Order serum mercury testing if you suspect chronic exposure. Refer patients with serum mercury ≥ 1.5 mg/dL to their primary care physicians and to a poison control center for evaluation and possible chelation. Refer patients with acute mercury exposure symptoms to the ER.
Consuming or using certain products or working in some industries increases mercury exposure risk. Mercury-containing products include:
Over-the-counter herbal remedies imported from China, Hong Kong, Haiti, and Cuba.9
Older, larger marine animals, including tuna, shark, or swordfish from mercury-contaminated waters.10,11
Vaccines and medications. Small amounts of thimerosal (ethylmercury sodium salt) were used as a preservative in some vaccines.12 Some antiseptics, eye drops, eye ointments, nasal sprays, skin-lightening creams, and gamma globulin contain mercury.
Dental amalgams are approximately 50% mercury. Each amalgam releases roughly 10 mg/d of mercury; chewing gum or grinding teeth may increase exposure.13 Some suggest removing the fillings, but this can increase mercury exposure if done incorrectly.1
Household goods, including latex paint made before 1990 and broken thermometers.3,14
Other environmental exposure, such as from burning coal, water treatment facilities, landfills, and mercury-containing fungicides.
Occupations that carry a high risk of mercury exposure include:3
Manufacturing
Batteries, cosmetics, explosives, paint/pigments, fluorescent lamps, ink, mercury vapor lamps, pharmaceuticals, switches, and rectifiers
Skilled trades
Plumbing, chlorine and caustic soda production, electroplating, felt-making, leather tanning, grinding machine operators, paper millers
Medical
Dental and medical laboratory personnel
Service industries
Hazardous-waste site personnel, painters, pesticide/fungicide production/application
Mining/processing
Cinnabar, gold, silver, copper, or zinc; metallurgy
The authors’ observations
Antidepressants generally will not reduce depression, irritability, personality changes, or apathy secondary to mercury poisoning. We have found that a psychostimulant such as methylphenidate, starting at 10 mg bid and titrating to therapeutic effect, can help treat mercury-related apathy.
We did not give Mr. F a psychostimulant, however, fearing it would worsen his impulsive behavior and disordered sleep. Also, more effectively managing Mr. F’s diabetes should improve his depression.
DISCHARGE: CHELATION CHALLENGE
Mr. F’s suicidal thoughts continued intermittently. Chelation was tried again with succimer, 1,000 mg tid for 5 days and bid for 5 more days, but the agent caused severe nausea without significantly decreasing serum mercury. He declined outpatient chelation.
After 2 weeks, Mr. F denied suicidal thoughts and said he felt physically better. He was discharged on venlafaxine, 300 mg/d, for his depressive symptoms; and metformin, 1,000 mg/d, glipizide, 10 mg bid, and rosiglitazone, 4 mg/d, to control his blood glucose. We arranged for medication management at a community mental health center. Mr. F was also told to visit the hospital’s outpatient clinic for endocrine follow-up but has not returned for 18 months.
Related resources
- Agency for Toxic Substances and Disease Registry. Information about toxic substances in the environment and diseases they may cause. www.atsdr.cdc.gov.
- Dimercaprol • BAL in Oil
- Glipizide • Glucotrol
- Metformin • Glucophage
- Methylphenidate • Ritalin, Concerta
- Rosiglitazone • Avandia
- Sertraline • Zoloft
- Succimer • Chemet
- Venlafaxine • Effexor
Dr. Matthews is an American Psychiatric Association Bristol-Myers Squibb Co. fellow in public and community psychiatry.
Dr. Hauser receives research/grant support from GlaxoSmithKline, Hoffman LaRoche, and AstraZeneca Pharmaceuticals. He is a speaker for Abbott Laboratories, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb Co., GlaxoSmithKline, and Janssen Pharmaceuticals.
HISTORY: TIRED OF LIVING
Mr. F, age 43, presents to the emergency room with complications of type 2 diabetes mellitus: blurry vision, increased urination, fatigue, and polydipsia. Blood glucose is 676 mg/dL.
The patient flees during treatment—possibly to attempt suicide—but returns 36 hours later, noticeably disoriented. He is readmitted to the ER, where he tells staff he is considering suicide and plans to self-inject a lethal substance. The ER staff refers him to the psychiatry service.
Mr. F also complains of shortness of breath after minimal exertion, aching joints throughout his body, and intense pain in his right great toe. He has been sleeping 12 to 20 hours daily, yet has trouble sleeping at night. He persistently feels fatigued, hopeless, and helpless. He says his suicidal urges have become more intense over 2 months, but he fears he will lose his computer repair job if he is admitted. He also shows difficulties with short-term memory. We admit him for observation.
Mental status examination suggests that Mr. F is generally withdrawn. Eye contact is poor and he is quiet and evasive, possibly signaling paranoia. He spends most of his stay watching television. His thought process is linear, and he thinks constantly of suicide. During the Mini-Mental State Examination, he gives the incorrect date and county. He misses two other items on recall but gets them correct with prompts.
A mild intention tremor distorts his handwriting. He has trouble keeping his balance during the Romberg test, and his gait is mildly ataxic. Ophthalmology consult suggests that diabetic retinopathy and optic disc cupping secondary to glaucoma may be blurring his vision.
Mr. F is taking no medications but had previously used insulin twice a day, and his outpatient doctor insists he should go back on insulin. He smokes 1 pack of cigarettes per day, drinks alcohol moderately (one to two drinks/day), and does not abuse illicit drugs.
The authors’ observations
Mr. F’s depressed mood, hopelessness, concentration problems, psychomotor retardation, and suicidal thoughts suggest major depressive disorder. Depression or a delirium secondary to diabetes may account for his referential ideas.
FURTHER HISTORY: ONE SHOT AT SATISFACTION
Over the following week, Mr. F becomes more talkative as the psychiatry staff develops a therapeutic rapport. He tells his treatment team that he feels urges to self-inject liquids he finds in his hospital room, such as shower gel and beverages.
Mr. F tells us that approximately 2 years ago, he tried to kill himself by swallowing boric acid. After 6 weeks in intensive care, the poison’s physical effects resolved and he no longer appeared suicidal. The staff at that time prepared to discharge Mr. F when, while left alone in his room, he dislodged a wall-mounted sphygmomanometer, disassembled it, and broke open the mercury tube. He then injected about 3 mL of mercury into his intravenous port and swallowed another 3 mL.
A nurse who checked on Mr. F minutes after the incident did not notice the sphygmomanometer was missing. He showed the broken device to the nurse, saying, “Look what I did.” When the nurse asked why, he responded, “I was just sitting here alone and saw the thing on the wall. I thought to myself, I can do this.”
The hospital viewed the episode as another suicide attempt. Staff immediately began chelation therapy with dimercaprol, 10 mg/kg every 8 hours for 5 days, then 10 mg/kg every 12 hours for 2 weeks. Within 24 hours of ingesting mercury, Mr. F developed shortness of breath, tachycardia (104 BPM), a fever (101.8°F), and had GI complaints. Increased blood urea nitrogen, increased creatinine, and decreased urination suggested declining renal function. He developed a pruritic rash over his back and mild skin loss on his soles.
Mr. F’s mercury levels were 20.8 mg/dL (serum) and 216 mg/dL (urine) 36 hours after ingestation, and 24.8 mg/dL (serum) and 397 mg/dL (urine) after chelation. Serum mercury >5 mg/dL is usually symptomatic.
Approximately 72 hours after the incident, most pulmonary, renal, and dermal manifestations of mercury toxicity began to improve. Mr. F was discharged after 21 days. He was diagnosed with major depression and started on sertraline, 150 mg/d.
‘The best feeling.’ Two years later, Mr. F tells us he has attempted suicide at least six times. Diffuse metallic foreign bodies throughout his lung vasculature and a 9.6 mg/dL serum mercury reading confirm he has injected mercury. His painful toe is x-rayed to check for mercury deposits, but he ultimately is diagnosed with gout.
During our evaluation, Mr. F admits that “the calmest, best feeling I have ever had” was while injecting mercury, yet he fears the incident has caused permanent physical and mental damage. He describes his desire to self-inject liquids as “impulses” triggered by twice-daily subcutaneous insulin use. For this reason, he has stopped taking insulin against his doctor’s advice.
The authors’ observations
Mr. F’s mental status changes and serum mercury suggest mercury poisoning. He shows numerous heavy-metal poisoning symptoms (Box 1) as well as erethism, a malaise that can result from heavy-metal exposure.2
The patient insists that insulin shots bring on self-injection urges, but his impulsive and repetitive suicidal behavior, dysphoria, and transient paranoia suggest borderline personality disorder. His impulses may reflect a subtle, long-term personality change caused by mercury’s neurotoxic effects.1 Or they could be akin to cutting behaviors shown by some patients with personality disorders, particularly borderline personality disorder.
We ruled out substance abuse disorder, as Mr. F’s mercury ingestion was not premeditated, he has no history of illicit drug use, and intravenous elemental mercury is not psychoactive.
- Emotional lability
- Excessive shyness
- Headaches
- Hearing loss
- Insomnia
- Irritability
- Lack of ambition
- Lack of sexual desire
- Loss of confidence
- Memory loss
- Nervousness
- Neuromuscular changes (including weakness, muscle atrophy, muscle twitching)
- Performance deficits in cognitive function tests
- Polyneuropathy
- Tremor of hands
- Visual field defects
Source: Reference 1
Elemental mercury found in thermometers, lamps, and dental amalgams slowly ionizes in the blood stream before crossing the blood-brain barrier. Mercury and carbon form toxic “organic” compounds, including methylmercury (found in the environment), phenylmercury (used in some commercial products), and dimethylmercury (found in solid waste sites).
Because mercury’s half-life is 60 days, it dissipates slowly, can accumulate with chronic exposure, and stays in the blood stream long after high-dose exposure.3
Serum mercury >5 mg/dL can cause subtle, enduring neurotoxic effects, including tremor, dizziness, shortness of breath, blurry vision, decreased visual fields, depression, memory loss, and irritability.3 Serum mercury rarely exceeds 1.5 mg/dL without direct exposure.
Irritability, depressive symptoms, and renal manifestations emerge when urine mercury reaches 200 to 1,000 mg/dL. Renal, respiratory, and GI effects are seen at 1,000 to 2,000 mg/dL.
Means of exposure. Vapor inhalation is the most common means of elemental mercury exposure.3 Elemental mercury used in manufacturing vaporizes at room temperature.
Orally ingested elemental mercury is poorly absorbed from the GI tract, mostly passes unabsorbed, and is toxic only at high doses. Injected elemental mercury is poorly absorbed but can cause mechanical and immunologic effects. The psychiatric literature describes some 200 cases of mercury self-injection4-8 but offers little information on cognitive effects or long-term follow-up.
Consider heavy-metal poisoning in the differential diagnosis of patients with depressive symptoms. Ask about risk factors for environmental mercury exposure, including use of folk medicines, some cosmetics, over-the-counter nasal sprays, ophthalmic solutions, skin-lightening creams, daily fish consumption (particularly tuna or swordfish), living in a house painted with latex paint, or continuous exposure at work (Box 2).
Also ask if the patient or a household member recently ingested mercury or handled a broken thermometer. Liquid mercury on clothing and in bodily fluids may cause secondary contamination, whereas mercury vapor cannot.
Order serum mercury testing if you suspect chronic exposure. Refer patients with serum mercury ≥ 1.5 mg/dL to their primary care physicians and to a poison control center for evaluation and possible chelation. Refer patients with acute mercury exposure symptoms to the ER.
Consuming or using certain products or working in some industries increases mercury exposure risk. Mercury-containing products include:
Over-the-counter herbal remedies imported from China, Hong Kong, Haiti, and Cuba.9
Older, larger marine animals, including tuna, shark, or swordfish from mercury-contaminated waters.10,11
Vaccines and medications. Small amounts of thimerosal (ethylmercury sodium salt) were used as a preservative in some vaccines.12 Some antiseptics, eye drops, eye ointments, nasal sprays, skin-lightening creams, and gamma globulin contain mercury.
Dental amalgams are approximately 50% mercury. Each amalgam releases roughly 10 mg/d of mercury; chewing gum or grinding teeth may increase exposure.13 Some suggest removing the fillings, but this can increase mercury exposure if done incorrectly.1
Household goods, including latex paint made before 1990 and broken thermometers.3,14
Other environmental exposure, such as from burning coal, water treatment facilities, landfills, and mercury-containing fungicides.
Occupations that carry a high risk of mercury exposure include:3
Manufacturing
Batteries, cosmetics, explosives, paint/pigments, fluorescent lamps, ink, mercury vapor lamps, pharmaceuticals, switches, and rectifiers
Skilled trades
Plumbing, chlorine and caustic soda production, electroplating, felt-making, leather tanning, grinding machine operators, paper millers
Medical
Dental and medical laboratory personnel
Service industries
Hazardous-waste site personnel, painters, pesticide/fungicide production/application
Mining/processing
Cinnabar, gold, silver, copper, or zinc; metallurgy
The authors’ observations
Antidepressants generally will not reduce depression, irritability, personality changes, or apathy secondary to mercury poisoning. We have found that a psychostimulant such as methylphenidate, starting at 10 mg bid and titrating to therapeutic effect, can help treat mercury-related apathy.
We did not give Mr. F a psychostimulant, however, fearing it would worsen his impulsive behavior and disordered sleep. Also, more effectively managing Mr. F’s diabetes should improve his depression.
DISCHARGE: CHELATION CHALLENGE
Mr. F’s suicidal thoughts continued intermittently. Chelation was tried again with succimer, 1,000 mg tid for 5 days and bid for 5 more days, but the agent caused severe nausea without significantly decreasing serum mercury. He declined outpatient chelation.
After 2 weeks, Mr. F denied suicidal thoughts and said he felt physically better. He was discharged on venlafaxine, 300 mg/d, for his depressive symptoms; and metformin, 1,000 mg/d, glipizide, 10 mg bid, and rosiglitazone, 4 mg/d, to control his blood glucose. We arranged for medication management at a community mental health center. Mr. F was also told to visit the hospital’s outpatient clinic for endocrine follow-up but has not returned for 18 months.
Related resources
- Agency for Toxic Substances and Disease Registry. Information about toxic substances in the environment and diseases they may cause. www.atsdr.cdc.gov.
- Dimercaprol • BAL in Oil
- Glipizide • Glucotrol
- Metformin • Glucophage
- Methylphenidate • Ritalin, Concerta
- Rosiglitazone • Avandia
- Sertraline • Zoloft
- Succimer • Chemet
- Venlafaxine • Effexor
Dr. Matthews is an American Psychiatric Association Bristol-Myers Squibb Co. fellow in public and community psychiatry.
Dr. Hauser receives research/grant support from GlaxoSmithKline, Hoffman LaRoche, and AstraZeneca Pharmaceuticals. He is a speaker for Abbott Laboratories, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb Co., GlaxoSmithKline, and Janssen Pharmaceuticals.
1. Agency for Toxic Substances and Disease Registry. Toxicological profile for mercury, March 1999. Available at: http://www.atsdr.cdc.gov/toxprofiles/tp46.html. Accessed May 4, 2005.
2. Clarkson TW, Magos L, Myers GJ. The toxicology of mercury—current exposures and clinical manifestations. N Engl J Med 2003;349:1731-7.
3. Mercury toxicity. Agency for Toxic Substance and Disease Registry. Am Fam Physician 1992;46:1731-41.
4. Manoukian SV, Wenger NK. Mercury in the heart. Am J Cardiol 1991;67:317-8.
5. Maniatis V, Zois G, Stringaris K. IV mercury self-injection: CT imaging. AJR Am J Roentgenol 1997;169:1197-8.
6. McFee RB, Caraccio TR. Intravenous mercury injection and ingestion: clinical manifestations and management. J Toxicol Clin Toxicol 2001;39:733-8.
7. Shareeff M, Bhat YM, Adabala R, Raoof S. Shortness of breath after suicide attempt. Chest 2000;118:837-8.
8. Torres-Alanis O, Garza-Ocanas L, Pineyro-Lopez A. Intravenous self-administration of metallic mercury: report of a case with a 5-year follow-up. J Toxicol Clin Toxicol 1997;35:83-7.
9. Li AM, Chan MH, Leung TF, et al. Mercury intoxication presenting with tics. Arch Dis Child 2000;83:74-5.
10. Dewailly E, Ayotte P, Bruneau S, et al. Exposure of the Inuit population of Nunavik (Arctic Quebec) to lead and mercury. Arch Environ Health 2001;56:350-7.
11. Stephenson J. FDA warns on mercury in tuna. JAMA 2004;291:171.
12. Dantzig PI. A new cutaneous sign of mercury poisoning. Ann Intern Med 2003;139:78-80.
13. Fitzpatrick M. Heavy metal. Lancet 2003;361:1664.-
14. From the Centers for Disease Control. Acute, chronic poisoning, residential exposures to elemental mercury—Michigan, 1989-1990. JAMA 1991;266:196.-
1. Agency for Toxic Substances and Disease Registry. Toxicological profile for mercury, March 1999. Available at: http://www.atsdr.cdc.gov/toxprofiles/tp46.html. Accessed May 4, 2005.
2. Clarkson TW, Magos L, Myers GJ. The toxicology of mercury—current exposures and clinical manifestations. N Engl J Med 2003;349:1731-7.
3. Mercury toxicity. Agency for Toxic Substance and Disease Registry. Am Fam Physician 1992;46:1731-41.
4. Manoukian SV, Wenger NK. Mercury in the heart. Am J Cardiol 1991;67:317-8.
5. Maniatis V, Zois G, Stringaris K. IV mercury self-injection: CT imaging. AJR Am J Roentgenol 1997;169:1197-8.
6. McFee RB, Caraccio TR. Intravenous mercury injection and ingestion: clinical manifestations and management. J Toxicol Clin Toxicol 2001;39:733-8.
7. Shareeff M, Bhat YM, Adabala R, Raoof S. Shortness of breath after suicide attempt. Chest 2000;118:837-8.
8. Torres-Alanis O, Garza-Ocanas L, Pineyro-Lopez A. Intravenous self-administration of metallic mercury: report of a case with a 5-year follow-up. J Toxicol Clin Toxicol 1997;35:83-7.
9. Li AM, Chan MH, Leung TF, et al. Mercury intoxication presenting with tics. Arch Dis Child 2000;83:74-5.
10. Dewailly E, Ayotte P, Bruneau S, et al. Exposure of the Inuit population of Nunavik (Arctic Quebec) to lead and mercury. Arch Environ Health 2001;56:350-7.
11. Stephenson J. FDA warns on mercury in tuna. JAMA 2004;291:171.
12. Dantzig PI. A new cutaneous sign of mercury poisoning. Ann Intern Med 2003;139:78-80.
13. Fitzpatrick M. Heavy metal. Lancet 2003;361:1664.-
14. From the Centers for Disease Control. Acute, chronic poisoning, residential exposures to elemental mercury—Michigan, 1989-1990. JAMA 1991;266:196.-
Psychological testing: Use do-it-yourself tools or refer?
Mr. A, age 38, presents with severe anxiety symptoms that suggest generalized anxiety disorder (GAD). You wish to confirm the diagnosis before starting medication, measure treatment response, and provide documentation to Mr. A’s managed care company.
Miss B, age 73, complains of memory and organization problems. Her history of transient ischemic attacks suggests vascular dementia, but the gradual symptom onset suggests Alzheimer’s dementia. You need to clarify the diagnosis.
Informed use of psychological testing can help you plan treatment by clarifying the causes, diagnosis, and prognosis of patients’ symptoms. With hundreds of instruments available, we offer an overview to help you quickly choose appropriate in-office tools or refer for more-intensive testing.
QUICK BUT IMPERFECT
Checklists and rating scales can quickly gauge a personality trait such as impulsivity or target symptom such as anxiety, using a numerical list of words or statements:
- A checklist’s response format is dichotomous (typically yes/no).
- Rating scales offer greater options, such as a 4-point scale for measuring symptoms as 0 (not present), 1 (mild), 2 (moderate), 3 (severe).
Some checklists/rating scales can assess more than one disorder or target symptom. These wide-band instruments—often called inventories or schedules—tend to be lengthy (1 to 2 hours), often require an interview, and generally require specialized training to administer.1-4
Pros. Two attributes make checklist/rating scales popular in clinical practice: their convenience, and managed care’s quest for documentation of service need, quality of care, cost-effectiveness, and symptom reduction.5 Brief, accurate, efficient checklists/rating scales can help you give managed care firms the documentation they require to authorize continued treatment—whether psychotherapy or medication monitoring.
Cons. Many checklists/rating scales are psychometrically weak, with low reliability and unproven validity. Some are lengthy or have other traits that diminish their clinical value (Table 1).
Table 1
Pros and cons of checklists/rating scales
| Pros |
|
| Cons |
|
LONGER AND MORE DETAILED
Objective tests typically contain true/false questions for which responses are reported as percentiles or standard scores. Examples are the Minnesota Multiphasic Personality Inventory (MMPI-2), used to clarify axis I diagnoses, and Millon Clinical Multiaxial Inventory (MCMI-III), chiefly used to assess personality disorders. Objective tests’ ability to assess a wide band of psychopathology can help you evaluate patients with complex differential diagnoses.6
Projective tests are unstructured instruments developed to detect covert psychosis and pathologic conflicts/impulses. Patients respond to ambiguous stimuli (inkblots, pictures, incomplete sentences) that are assumed to function as a screen onto which a person projects his or her conflicts and issues.3
Useful projective tests include the Rorschach ink blot test, Thematic Apperception Test (TAT) of interpersonal relationships, and several sentence-completion tests. The Rorschach can take 1 to 2 hours to administer and score and requires years to master. The Rotter Incomplete Sentences Blank (2nd ed) (RISB) is well-constructed; available in high school, college, and adult forms; and can help clarify major conflicts.3
Projective tests’ psychometric properties have been questioned, but the Rorschach is considered useful in detecting subtle psychoses.6
Neuropsychological tests can identify and localize brain injury. Board-certified neuropsychologists (with 2 years’ postdoctoral training) use them to assess traumatic brain injury, evaluate post-stroke syndromes or early dementia, and differentiate dementia and depression.7 These tests also have litigation and forensic applications, such as assessing competence or malingering.
Some neuropsychologists use a comprehensive instrument such as the Halstead-Reitan Neuropsychological Test Battery, which evaluates memory, abstract thought, language, sensory-motor integration, imperception, and motor dexterity. Others may select specific instruments to answer a referring psychiatrist’s question.
CHOOSING AN INSTRUMENT
Medical reference librarians can help research specific instruments and choose useful testing tools. We also recommend Corcoran and Fischer’s Measures for Clinical Practice,8 which provides practical information on administration, advantages, and disadvantages of instruments that:
- are used in clinical practice
- provide data on psychometric properties
- take
- are rapidly scored
- provide information on symptom severity
- can be used to document change.
Table 2
Commonly used checklists/rating scales for adult assessment
| Disorder/target symptom | Commonly used scales |
|---|---|
| Anger | Anger, Irritability and Assault Questionnaire (AIAQ) |
| Anxiety | |
| Phobias | Fear Questionnaire (FQ) |
| GAD | Beck Anxiety Inventory (BAI) |
| OCD | Yale-Brown Obsessive Compulsive Scale (Y-BOCS) |
| PTSD | Posttraumatic Stress Diagnostic Scale (PDS) |
| Bipolar disorder | Young Mania Rating Scale (YMRS) |
| Depression | Beck Depression Inventory (BDI) |
| Zung Self-rating Depression Scale (SDS) | |
| Eating disorders | Eating Disorders Inventory-2 |
| Family issues | Family Assessment Device (FAD) |
| Impulse control | Barratt Impulsiveness Scale, Version II (BIS-II) |
| Pain | McGill Pain Questionnaire (MPQ) |
| Personality disorders | Millon Clinical Multiaxial Inventory (MCMI-III) |
| Psychosis | Brief Psychiatric Rating Scale (BPRS) |
| Manchester Scale | |
| Sexuality | Sexual Interaction Inventory (SII) |
| Sleep | Sleep Disorder Questionnaire (SDQ) |
| Suicide risk | Beck Scale for Suicide Ideation (BSS) |
| GAD: Generalized anxiety disorder | |
| OCD: Obsessive-compulsive disorder | |
| PTSD: Posttraumatic stress disorder | |
Common checklists/rating scales for geriatric assessment
| Disorder/target symptom | Commonly used scales |
|---|---|
| Cognitive status | Mini-Mental State Examination (MMSE) |
| Neurobehavioral Cognitive Status Examination (Cognistat) | |
| Dementia Rating Scale | |
| Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) | |
| Caregiver stress | Caregiver’s Burden Scale (CBS) |
| Death concerns | Concern About Death-Dying (CADD) and Coping (C) checklist |
| Depression | Geriatric Depression Scale (GDS) |
Common checklists/rating scales for child and adolescent assessment
| Disorder/target symptom | Commonly used scales |
|---|---|
| Anxiety | Multidimensional Anxiety Scale for Children (MASC) |
| Assertiveness | Assertiveness Scale for Adolescents (ASA) |
| Conduct | Child Behavior Checklist (CBCL) |
| Depression | Children’s Depression Self Rating Scale (CDRS) |
| Drug/alcohol risk | CAGE Questionnaire |
| Michigan Alcohol Screening Test (MAST) | |
| Impulsivity | Impulsivity Scale (IS) |
| PTSD | Child Report of Posttraumatic Symptoms (CROPS) |
| Reaction to divorce | Children’s Belief About Parental Divorce Scale (CBAPS) |
| Self-esteem | Rosenberg Self-Esteem Scale (RSE) |
| Suicide risk | Multi-Attitude Suicide Tendency Scale (MAST) |
| Test anxiety | Children’s Cognitive Assessment Questionnaire (CCAQ) |
| PTSD: Posttraumatic stress disorder | |
IN-OFFICE TESTING VS REFERRAL
You could use in-office testing to diagnose Mr. A’s anxiety symptoms and provide documentation to his managed care company. For Miss B’s memory problems, we recommend referral for psychological testing.
Mr. A completes the 21-item Beck Anxiety Inventory (BAI) in your office. You select the BAI because it is psychometrically sound, brief (about 10 minutes to complete and score), and easily understood. Results can be readily used for feedback to patients or third-party payers.
Mr. A’s score of 19 is consistent with GAD and justifies a medication trial. The BAI provides information about his experience of anxiety (subjective vs. somatic) that can guide psychotherapy. You plan to repeat the BAI over time to monitor treatment.
Miss B would benefit from referral to a neuropsychologist, as screening tools do not reliably differentiate among the dementias. The neuropsychologist will likely use all or part of the Halstead-Reitan Neuropsychological Test Battery to localize any ischemic-related brain injury and clarify the diagnosis. This test also can provide data to stage her dementia and help you and her family with care decisions.
PSYCHOLOGIST REFERRAL
When referring patients for psychological testing, we recommend that you tell the psychologist what information you need and let him or her select the tests. Relying on their expertise can save time and yield a report that targets the referral question.
Three cases follow that illustrate types of referral questions doctoral-level psychologists can help answer with appropriately chosen tests:
WHAT EXPLAINS TREATMENT RESISTANCE?
Mr. C, age 43, presents with mixed anxiety and depression. He complains of insomnia, fatigue, tightness in the chest, and trembling hands. You give him the Beck Depression Inventory (BDI) and Beck Anxiety Inventory (BAI), which show mild depression/anxiety. You prescribe fluoxetine, 20 mg/d, and 8 weeks later his symptoms are unchanged. The patient is demanding, critical, and has a pattern of interpersonal difficulty. You suspect a personality disorder is complicating treatment.
In this case, the MMPI-2 and MCMI-III would be useful to clarify diagnosis. The MMPI-2 gauges anxiety (state anxiety, phobias, social anxiety and posttraumatic stress disorder), and depression. The MCMI-III was developed to assess axis II diagnoses and has scales to assess each personality disorder. These tests provide information about psychological-mindedness, treatment resistance, and characteristics that can guide psychotherapy.
DRUGS, PSYCHOSIS, OR BIPOLAR DISORDER?
Mr. D’s parents report that their 20-year-old is isolating himself in his room, is not sleeping, and has grandiose beliefs of special powers and knowledge. He has no psychiatric history. Because these symptoms could suggest numerous psychopathologies, you would like help with the differential diagnosis.
Mr. D’s symptoms could suggest drug abuse, schizophrenia, psychotic depression, or bipolar disorder. The psychologist might use the MMPI-2 to assess drug abuse, depression, mania, and psychosis. The relative elevation of each scale could be clinically useful; if scales gauging psychosis and depression are both elevated, psychotic depression is likely, whereas an elevation chiefly on the mania scale would point to bipolar disorder.
The Rorschach test could assess psychotic process. The MMPI-2 could be repeated in a few months to gauge treatment response.
IS THIS EARLY ALZHEIMER’S DISEASE?
Mr. E, age 78, presents with mild memory and word-finding deficits and complains of fatigue, loss of appetite, and anhedonia. Physical exam and lab tests are unremarkable, and you suspect early Alzheimer’s dementia and depression. You wish to confirm the diagnosis to decide whether to start a cholinesterase inhibitor, antidepressant, or other medication. You also wish to document change over time.
An in-office depression checklist would be appropriate for Mr. E. The 30-item, self-rated Geriatric Depression Scale is psychometrically sound and can be completed in 15 to 20 minutes.
Referral is recommended for dementia screening with an tool such as the Neurobehavioral Cognitive Status Examination (Cognistat) or Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). The Mini-Mental State Examination (MMSE) is used for in-office screening of cognitive deficits but lacks sensitivity to detect mild decline. Cognistat or RBANS are less influenced by the patient’s education level and are more sensitive than the MMSE to early dementia.
All three instruments are brief enough to repeat as needed to document change.
Related resources
- Corcoran K, Fischer J. Measures for clinical practice, vols. 1 and 2. New York: Free Press; 2000.
- Maruish ME (ed). The use of psychological testing for treatment planning and outcomes assessment. Mahwah, NJ: Lawrence Erlbaum Associates; 1999.
- Rush AJ, Pincus HJ, First MB, et al. (eds). Handbook of psychiatric measures. Washington, DC: American Psychiatric Association; 2000.
- American Psychological Association. FAQ/Finding information about psychological tests. http://www.apa.org/science/faq-findtests.html.
- Fluoxetine • Prozac
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Maruish ME (ed) The use of psychological testing for treatment planning and outcomes assessment. Mahwah, NJ: Lawrence Erlbaum Associates; 1999.
2. Sajatovic M, Ramirez LF. Rating scales in mental health. Hudson, OH: Lexi-Comp; 2003.
3. Aiken LR. Assessment of adult personality. New York: Springer; 1997.
4. Rush AJ, Pincus HJ, First MB, et al (eds). Handbook of Psychiatric Measures. Washington, DC: American Psychiatric Association; 2000.
5. Belar CD. Psychological assessment in capitated care. In: Butcher JN (ed). Personality assessment in managed care: Using the MMPI-2 in treatment planning. New York: Oxford Press; 1997;13:80.-
6. Adams RL, Culbertson JL. Personality assessment: adults and children. In: Sadock BJ, Sadock VA (eds). Comprehensive textbook of psychiatry, vol. 1 (7th ed). Baltimore: Lippincott Williams & Wilkins; 2000;702:21.-
7. Swanda RM, Haaland KY, La Rue A. Clinical neuropsychology and intellectual assessment of adults. In: Sadock BJ, Sadock VA (eds). Comprehensive textbook of psychiatry, vol. 1 (7th ed). Baltimore: Lippincott Williams & Wilkins; 2000;689:701.-
8. Corcoran K, Fischer J. Measures for clinical practice, vols 1 and 2. New York: Free Press; 2000.
9. Blacker D. Psychiatric rating scales. In: Sadock BJ, Sadock VA (eds). Comprehensive textbook of psychiatry, vol. 1 (7th ed). Baltimore: Lippincott Williams & Wilkins; 2000;755-83.
Mr. A, age 38, presents with severe anxiety symptoms that suggest generalized anxiety disorder (GAD). You wish to confirm the diagnosis before starting medication, measure treatment response, and provide documentation to Mr. A’s managed care company.
Miss B, age 73, complains of memory and organization problems. Her history of transient ischemic attacks suggests vascular dementia, but the gradual symptom onset suggests Alzheimer’s dementia. You need to clarify the diagnosis.
Informed use of psychological testing can help you plan treatment by clarifying the causes, diagnosis, and prognosis of patients’ symptoms. With hundreds of instruments available, we offer an overview to help you quickly choose appropriate in-office tools or refer for more-intensive testing.
QUICK BUT IMPERFECT
Checklists and rating scales can quickly gauge a personality trait such as impulsivity or target symptom such as anxiety, using a numerical list of words or statements:
- A checklist’s response format is dichotomous (typically yes/no).
- Rating scales offer greater options, such as a 4-point scale for measuring symptoms as 0 (not present), 1 (mild), 2 (moderate), 3 (severe).
Some checklists/rating scales can assess more than one disorder or target symptom. These wide-band instruments—often called inventories or schedules—tend to be lengthy (1 to 2 hours), often require an interview, and generally require specialized training to administer.1-4
Pros. Two attributes make checklist/rating scales popular in clinical practice: their convenience, and managed care’s quest for documentation of service need, quality of care, cost-effectiveness, and symptom reduction.5 Brief, accurate, efficient checklists/rating scales can help you give managed care firms the documentation they require to authorize continued treatment—whether psychotherapy or medication monitoring.
Cons. Many checklists/rating scales are psychometrically weak, with low reliability and unproven validity. Some are lengthy or have other traits that diminish their clinical value (Table 1).
Table 1
Pros and cons of checklists/rating scales
| Pros |
|
| Cons |
|
LONGER AND MORE DETAILED
Objective tests typically contain true/false questions for which responses are reported as percentiles or standard scores. Examples are the Minnesota Multiphasic Personality Inventory (MMPI-2), used to clarify axis I diagnoses, and Millon Clinical Multiaxial Inventory (MCMI-III), chiefly used to assess personality disorders. Objective tests’ ability to assess a wide band of psychopathology can help you evaluate patients with complex differential diagnoses.6
Projective tests are unstructured instruments developed to detect covert psychosis and pathologic conflicts/impulses. Patients respond to ambiguous stimuli (inkblots, pictures, incomplete sentences) that are assumed to function as a screen onto which a person projects his or her conflicts and issues.3
Useful projective tests include the Rorschach ink blot test, Thematic Apperception Test (TAT) of interpersonal relationships, and several sentence-completion tests. The Rorschach can take 1 to 2 hours to administer and score and requires years to master. The Rotter Incomplete Sentences Blank (2nd ed) (RISB) is well-constructed; available in high school, college, and adult forms; and can help clarify major conflicts.3
Projective tests’ psychometric properties have been questioned, but the Rorschach is considered useful in detecting subtle psychoses.6
Neuropsychological tests can identify and localize brain injury. Board-certified neuropsychologists (with 2 years’ postdoctoral training) use them to assess traumatic brain injury, evaluate post-stroke syndromes or early dementia, and differentiate dementia and depression.7 These tests also have litigation and forensic applications, such as assessing competence or malingering.
Some neuropsychologists use a comprehensive instrument such as the Halstead-Reitan Neuropsychological Test Battery, which evaluates memory, abstract thought, language, sensory-motor integration, imperception, and motor dexterity. Others may select specific instruments to answer a referring psychiatrist’s question.
CHOOSING AN INSTRUMENT
Medical reference librarians can help research specific instruments and choose useful testing tools. We also recommend Corcoran and Fischer’s Measures for Clinical Practice,8 which provides practical information on administration, advantages, and disadvantages of instruments that:
- are used in clinical practice
- provide data on psychometric properties
- take
- are rapidly scored
- provide information on symptom severity
- can be used to document change.
Table 2
Commonly used checklists/rating scales for adult assessment
| Disorder/target symptom | Commonly used scales |
|---|---|
| Anger | Anger, Irritability and Assault Questionnaire (AIAQ) |
| Anxiety | |
| Phobias | Fear Questionnaire (FQ) |
| GAD | Beck Anxiety Inventory (BAI) |
| OCD | Yale-Brown Obsessive Compulsive Scale (Y-BOCS) |
| PTSD | Posttraumatic Stress Diagnostic Scale (PDS) |
| Bipolar disorder | Young Mania Rating Scale (YMRS) |
| Depression | Beck Depression Inventory (BDI) |
| Zung Self-rating Depression Scale (SDS) | |
| Eating disorders | Eating Disorders Inventory-2 |
| Family issues | Family Assessment Device (FAD) |
| Impulse control | Barratt Impulsiveness Scale, Version II (BIS-II) |
| Pain | McGill Pain Questionnaire (MPQ) |
| Personality disorders | Millon Clinical Multiaxial Inventory (MCMI-III) |
| Psychosis | Brief Psychiatric Rating Scale (BPRS) |
| Manchester Scale | |
| Sexuality | Sexual Interaction Inventory (SII) |
| Sleep | Sleep Disorder Questionnaire (SDQ) |
| Suicide risk | Beck Scale for Suicide Ideation (BSS) |
| GAD: Generalized anxiety disorder | |
| OCD: Obsessive-compulsive disorder | |
| PTSD: Posttraumatic stress disorder | |
Common checklists/rating scales for geriatric assessment
| Disorder/target symptom | Commonly used scales |
|---|---|
| Cognitive status | Mini-Mental State Examination (MMSE) |
| Neurobehavioral Cognitive Status Examination (Cognistat) | |
| Dementia Rating Scale | |
| Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) | |
| Caregiver stress | Caregiver’s Burden Scale (CBS) |
| Death concerns | Concern About Death-Dying (CADD) and Coping (C) checklist |
| Depression | Geriatric Depression Scale (GDS) |
Common checklists/rating scales for child and adolescent assessment
| Disorder/target symptom | Commonly used scales |
|---|---|
| Anxiety | Multidimensional Anxiety Scale for Children (MASC) |
| Assertiveness | Assertiveness Scale for Adolescents (ASA) |
| Conduct | Child Behavior Checklist (CBCL) |
| Depression | Children’s Depression Self Rating Scale (CDRS) |
| Drug/alcohol risk | CAGE Questionnaire |
| Michigan Alcohol Screening Test (MAST) | |
| Impulsivity | Impulsivity Scale (IS) |
| PTSD | Child Report of Posttraumatic Symptoms (CROPS) |
| Reaction to divorce | Children’s Belief About Parental Divorce Scale (CBAPS) |
| Self-esteem | Rosenberg Self-Esteem Scale (RSE) |
| Suicide risk | Multi-Attitude Suicide Tendency Scale (MAST) |
| Test anxiety | Children’s Cognitive Assessment Questionnaire (CCAQ) |
| PTSD: Posttraumatic stress disorder | |
IN-OFFICE TESTING VS REFERRAL
You could use in-office testing to diagnose Mr. A’s anxiety symptoms and provide documentation to his managed care company. For Miss B’s memory problems, we recommend referral for psychological testing.
Mr. A completes the 21-item Beck Anxiety Inventory (BAI) in your office. You select the BAI because it is psychometrically sound, brief (about 10 minutes to complete and score), and easily understood. Results can be readily used for feedback to patients or third-party payers.
Mr. A’s score of 19 is consistent with GAD and justifies a medication trial. The BAI provides information about his experience of anxiety (subjective vs. somatic) that can guide psychotherapy. You plan to repeat the BAI over time to monitor treatment.
Miss B would benefit from referral to a neuropsychologist, as screening tools do not reliably differentiate among the dementias. The neuropsychologist will likely use all or part of the Halstead-Reitan Neuropsychological Test Battery to localize any ischemic-related brain injury and clarify the diagnosis. This test also can provide data to stage her dementia and help you and her family with care decisions.
PSYCHOLOGIST REFERRAL
When referring patients for psychological testing, we recommend that you tell the psychologist what information you need and let him or her select the tests. Relying on their expertise can save time and yield a report that targets the referral question.
Three cases follow that illustrate types of referral questions doctoral-level psychologists can help answer with appropriately chosen tests:
WHAT EXPLAINS TREATMENT RESISTANCE?
Mr. C, age 43, presents with mixed anxiety and depression. He complains of insomnia, fatigue, tightness in the chest, and trembling hands. You give him the Beck Depression Inventory (BDI) and Beck Anxiety Inventory (BAI), which show mild depression/anxiety. You prescribe fluoxetine, 20 mg/d, and 8 weeks later his symptoms are unchanged. The patient is demanding, critical, and has a pattern of interpersonal difficulty. You suspect a personality disorder is complicating treatment.
In this case, the MMPI-2 and MCMI-III would be useful to clarify diagnosis. The MMPI-2 gauges anxiety (state anxiety, phobias, social anxiety and posttraumatic stress disorder), and depression. The MCMI-III was developed to assess axis II diagnoses and has scales to assess each personality disorder. These tests provide information about psychological-mindedness, treatment resistance, and characteristics that can guide psychotherapy.
DRUGS, PSYCHOSIS, OR BIPOLAR DISORDER?
Mr. D’s parents report that their 20-year-old is isolating himself in his room, is not sleeping, and has grandiose beliefs of special powers and knowledge. He has no psychiatric history. Because these symptoms could suggest numerous psychopathologies, you would like help with the differential diagnosis.
Mr. D’s symptoms could suggest drug abuse, schizophrenia, psychotic depression, or bipolar disorder. The psychologist might use the MMPI-2 to assess drug abuse, depression, mania, and psychosis. The relative elevation of each scale could be clinically useful; if scales gauging psychosis and depression are both elevated, psychotic depression is likely, whereas an elevation chiefly on the mania scale would point to bipolar disorder.
The Rorschach test could assess psychotic process. The MMPI-2 could be repeated in a few months to gauge treatment response.
IS THIS EARLY ALZHEIMER’S DISEASE?
Mr. E, age 78, presents with mild memory and word-finding deficits and complains of fatigue, loss of appetite, and anhedonia. Physical exam and lab tests are unremarkable, and you suspect early Alzheimer’s dementia and depression. You wish to confirm the diagnosis to decide whether to start a cholinesterase inhibitor, antidepressant, or other medication. You also wish to document change over time.
An in-office depression checklist would be appropriate for Mr. E. The 30-item, self-rated Geriatric Depression Scale is psychometrically sound and can be completed in 15 to 20 minutes.
Referral is recommended for dementia screening with an tool such as the Neurobehavioral Cognitive Status Examination (Cognistat) or Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). The Mini-Mental State Examination (MMSE) is used for in-office screening of cognitive deficits but lacks sensitivity to detect mild decline. Cognistat or RBANS are less influenced by the patient’s education level and are more sensitive than the MMSE to early dementia.
All three instruments are brief enough to repeat as needed to document change.
Related resources
- Corcoran K, Fischer J. Measures for clinical practice, vols. 1 and 2. New York: Free Press; 2000.
- Maruish ME (ed). The use of psychological testing for treatment planning and outcomes assessment. Mahwah, NJ: Lawrence Erlbaum Associates; 1999.
- Rush AJ, Pincus HJ, First MB, et al. (eds). Handbook of psychiatric measures. Washington, DC: American Psychiatric Association; 2000.
- American Psychological Association. FAQ/Finding information about psychological tests. http://www.apa.org/science/faq-findtests.html.
- Fluoxetine • Prozac
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mr. A, age 38, presents with severe anxiety symptoms that suggest generalized anxiety disorder (GAD). You wish to confirm the diagnosis before starting medication, measure treatment response, and provide documentation to Mr. A’s managed care company.
Miss B, age 73, complains of memory and organization problems. Her history of transient ischemic attacks suggests vascular dementia, but the gradual symptom onset suggests Alzheimer’s dementia. You need to clarify the diagnosis.
Informed use of psychological testing can help you plan treatment by clarifying the causes, diagnosis, and prognosis of patients’ symptoms. With hundreds of instruments available, we offer an overview to help you quickly choose appropriate in-office tools or refer for more-intensive testing.
QUICK BUT IMPERFECT
Checklists and rating scales can quickly gauge a personality trait such as impulsivity or target symptom such as anxiety, using a numerical list of words or statements:
- A checklist’s response format is dichotomous (typically yes/no).
- Rating scales offer greater options, such as a 4-point scale for measuring symptoms as 0 (not present), 1 (mild), 2 (moderate), 3 (severe).
Some checklists/rating scales can assess more than one disorder or target symptom. These wide-band instruments—often called inventories or schedules—tend to be lengthy (1 to 2 hours), often require an interview, and generally require specialized training to administer.1-4
Pros. Two attributes make checklist/rating scales popular in clinical practice: their convenience, and managed care’s quest for documentation of service need, quality of care, cost-effectiveness, and symptom reduction.5 Brief, accurate, efficient checklists/rating scales can help you give managed care firms the documentation they require to authorize continued treatment—whether psychotherapy or medication monitoring.
Cons. Many checklists/rating scales are psychometrically weak, with low reliability and unproven validity. Some are lengthy or have other traits that diminish their clinical value (Table 1).
Table 1
Pros and cons of checklists/rating scales
| Pros |
|
| Cons |
|
LONGER AND MORE DETAILED
Objective tests typically contain true/false questions for which responses are reported as percentiles or standard scores. Examples are the Minnesota Multiphasic Personality Inventory (MMPI-2), used to clarify axis I diagnoses, and Millon Clinical Multiaxial Inventory (MCMI-III), chiefly used to assess personality disorders. Objective tests’ ability to assess a wide band of psychopathology can help you evaluate patients with complex differential diagnoses.6
Projective tests are unstructured instruments developed to detect covert psychosis and pathologic conflicts/impulses. Patients respond to ambiguous stimuli (inkblots, pictures, incomplete sentences) that are assumed to function as a screen onto which a person projects his or her conflicts and issues.3
Useful projective tests include the Rorschach ink blot test, Thematic Apperception Test (TAT) of interpersonal relationships, and several sentence-completion tests. The Rorschach can take 1 to 2 hours to administer and score and requires years to master. The Rotter Incomplete Sentences Blank (2nd ed) (RISB) is well-constructed; available in high school, college, and adult forms; and can help clarify major conflicts.3
Projective tests’ psychometric properties have been questioned, but the Rorschach is considered useful in detecting subtle psychoses.6
Neuropsychological tests can identify and localize brain injury. Board-certified neuropsychologists (with 2 years’ postdoctoral training) use them to assess traumatic brain injury, evaluate post-stroke syndromes or early dementia, and differentiate dementia and depression.7 These tests also have litigation and forensic applications, such as assessing competence or malingering.
Some neuropsychologists use a comprehensive instrument such as the Halstead-Reitan Neuropsychological Test Battery, which evaluates memory, abstract thought, language, sensory-motor integration, imperception, and motor dexterity. Others may select specific instruments to answer a referring psychiatrist’s question.
CHOOSING AN INSTRUMENT
Medical reference librarians can help research specific instruments and choose useful testing tools. We also recommend Corcoran and Fischer’s Measures for Clinical Practice,8 which provides practical information on administration, advantages, and disadvantages of instruments that:
- are used in clinical practice
- provide data on psychometric properties
- take
- are rapidly scored
- provide information on symptom severity
- can be used to document change.
Table 2
Commonly used checklists/rating scales for adult assessment
| Disorder/target symptom | Commonly used scales |
|---|---|
| Anger | Anger, Irritability and Assault Questionnaire (AIAQ) |
| Anxiety | |
| Phobias | Fear Questionnaire (FQ) |
| GAD | Beck Anxiety Inventory (BAI) |
| OCD | Yale-Brown Obsessive Compulsive Scale (Y-BOCS) |
| PTSD | Posttraumatic Stress Diagnostic Scale (PDS) |
| Bipolar disorder | Young Mania Rating Scale (YMRS) |
| Depression | Beck Depression Inventory (BDI) |
| Zung Self-rating Depression Scale (SDS) | |
| Eating disorders | Eating Disorders Inventory-2 |
| Family issues | Family Assessment Device (FAD) |
| Impulse control | Barratt Impulsiveness Scale, Version II (BIS-II) |
| Pain | McGill Pain Questionnaire (MPQ) |
| Personality disorders | Millon Clinical Multiaxial Inventory (MCMI-III) |
| Psychosis | Brief Psychiatric Rating Scale (BPRS) |
| Manchester Scale | |
| Sexuality | Sexual Interaction Inventory (SII) |
| Sleep | Sleep Disorder Questionnaire (SDQ) |
| Suicide risk | Beck Scale for Suicide Ideation (BSS) |
| GAD: Generalized anxiety disorder | |
| OCD: Obsessive-compulsive disorder | |
| PTSD: Posttraumatic stress disorder | |
Common checklists/rating scales for geriatric assessment
| Disorder/target symptom | Commonly used scales |
|---|---|
| Cognitive status | Mini-Mental State Examination (MMSE) |
| Neurobehavioral Cognitive Status Examination (Cognistat) | |
| Dementia Rating Scale | |
| Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) | |
| Caregiver stress | Caregiver’s Burden Scale (CBS) |
| Death concerns | Concern About Death-Dying (CADD) and Coping (C) checklist |
| Depression | Geriatric Depression Scale (GDS) |
Common checklists/rating scales for child and adolescent assessment
| Disorder/target symptom | Commonly used scales |
|---|---|
| Anxiety | Multidimensional Anxiety Scale for Children (MASC) |
| Assertiveness | Assertiveness Scale for Adolescents (ASA) |
| Conduct | Child Behavior Checklist (CBCL) |
| Depression | Children’s Depression Self Rating Scale (CDRS) |
| Drug/alcohol risk | CAGE Questionnaire |
| Michigan Alcohol Screening Test (MAST) | |
| Impulsivity | Impulsivity Scale (IS) |
| PTSD | Child Report of Posttraumatic Symptoms (CROPS) |
| Reaction to divorce | Children’s Belief About Parental Divorce Scale (CBAPS) |
| Self-esteem | Rosenberg Self-Esteem Scale (RSE) |
| Suicide risk | Multi-Attitude Suicide Tendency Scale (MAST) |
| Test anxiety | Children’s Cognitive Assessment Questionnaire (CCAQ) |
| PTSD: Posttraumatic stress disorder | |
IN-OFFICE TESTING VS REFERRAL
You could use in-office testing to diagnose Mr. A’s anxiety symptoms and provide documentation to his managed care company. For Miss B’s memory problems, we recommend referral for psychological testing.
Mr. A completes the 21-item Beck Anxiety Inventory (BAI) in your office. You select the BAI because it is psychometrically sound, brief (about 10 minutes to complete and score), and easily understood. Results can be readily used for feedback to patients or third-party payers.
Mr. A’s score of 19 is consistent with GAD and justifies a medication trial. The BAI provides information about his experience of anxiety (subjective vs. somatic) that can guide psychotherapy. You plan to repeat the BAI over time to monitor treatment.
Miss B would benefit from referral to a neuropsychologist, as screening tools do not reliably differentiate among the dementias. The neuropsychologist will likely use all or part of the Halstead-Reitan Neuropsychological Test Battery to localize any ischemic-related brain injury and clarify the diagnosis. This test also can provide data to stage her dementia and help you and her family with care decisions.
PSYCHOLOGIST REFERRAL
When referring patients for psychological testing, we recommend that you tell the psychologist what information you need and let him or her select the tests. Relying on their expertise can save time and yield a report that targets the referral question.
Three cases follow that illustrate types of referral questions doctoral-level psychologists can help answer with appropriately chosen tests:
WHAT EXPLAINS TREATMENT RESISTANCE?
Mr. C, age 43, presents with mixed anxiety and depression. He complains of insomnia, fatigue, tightness in the chest, and trembling hands. You give him the Beck Depression Inventory (BDI) and Beck Anxiety Inventory (BAI), which show mild depression/anxiety. You prescribe fluoxetine, 20 mg/d, and 8 weeks later his symptoms are unchanged. The patient is demanding, critical, and has a pattern of interpersonal difficulty. You suspect a personality disorder is complicating treatment.
In this case, the MMPI-2 and MCMI-III would be useful to clarify diagnosis. The MMPI-2 gauges anxiety (state anxiety, phobias, social anxiety and posttraumatic stress disorder), and depression. The MCMI-III was developed to assess axis II diagnoses and has scales to assess each personality disorder. These tests provide information about psychological-mindedness, treatment resistance, and characteristics that can guide psychotherapy.
DRUGS, PSYCHOSIS, OR BIPOLAR DISORDER?
Mr. D’s parents report that their 20-year-old is isolating himself in his room, is not sleeping, and has grandiose beliefs of special powers and knowledge. He has no psychiatric history. Because these symptoms could suggest numerous psychopathologies, you would like help with the differential diagnosis.
Mr. D’s symptoms could suggest drug abuse, schizophrenia, psychotic depression, or bipolar disorder. The psychologist might use the MMPI-2 to assess drug abuse, depression, mania, and psychosis. The relative elevation of each scale could be clinically useful; if scales gauging psychosis and depression are both elevated, psychotic depression is likely, whereas an elevation chiefly on the mania scale would point to bipolar disorder.
The Rorschach test could assess psychotic process. The MMPI-2 could be repeated in a few months to gauge treatment response.
IS THIS EARLY ALZHEIMER’S DISEASE?
Mr. E, age 78, presents with mild memory and word-finding deficits and complains of fatigue, loss of appetite, and anhedonia. Physical exam and lab tests are unremarkable, and you suspect early Alzheimer’s dementia and depression. You wish to confirm the diagnosis to decide whether to start a cholinesterase inhibitor, antidepressant, or other medication. You also wish to document change over time.
An in-office depression checklist would be appropriate for Mr. E. The 30-item, self-rated Geriatric Depression Scale is psychometrically sound and can be completed in 15 to 20 minutes.
Referral is recommended for dementia screening with an tool such as the Neurobehavioral Cognitive Status Examination (Cognistat) or Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). The Mini-Mental State Examination (MMSE) is used for in-office screening of cognitive deficits but lacks sensitivity to detect mild decline. Cognistat or RBANS are less influenced by the patient’s education level and are more sensitive than the MMSE to early dementia.
All three instruments are brief enough to repeat as needed to document change.
Related resources
- Corcoran K, Fischer J. Measures for clinical practice, vols. 1 and 2. New York: Free Press; 2000.
- Maruish ME (ed). The use of psychological testing for treatment planning and outcomes assessment. Mahwah, NJ: Lawrence Erlbaum Associates; 1999.
- Rush AJ, Pincus HJ, First MB, et al. (eds). Handbook of psychiatric measures. Washington, DC: American Psychiatric Association; 2000.
- American Psychological Association. FAQ/Finding information about psychological tests. http://www.apa.org/science/faq-findtests.html.
- Fluoxetine • Prozac
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Maruish ME (ed) The use of psychological testing for treatment planning and outcomes assessment. Mahwah, NJ: Lawrence Erlbaum Associates; 1999.
2. Sajatovic M, Ramirez LF. Rating scales in mental health. Hudson, OH: Lexi-Comp; 2003.
3. Aiken LR. Assessment of adult personality. New York: Springer; 1997.
4. Rush AJ, Pincus HJ, First MB, et al (eds). Handbook of Psychiatric Measures. Washington, DC: American Psychiatric Association; 2000.
5. Belar CD. Psychological assessment in capitated care. In: Butcher JN (ed). Personality assessment in managed care: Using the MMPI-2 in treatment planning. New York: Oxford Press; 1997;13:80.-
6. Adams RL, Culbertson JL. Personality assessment: adults and children. In: Sadock BJ, Sadock VA (eds). Comprehensive textbook of psychiatry, vol. 1 (7th ed). Baltimore: Lippincott Williams & Wilkins; 2000;702:21.-
7. Swanda RM, Haaland KY, La Rue A. Clinical neuropsychology and intellectual assessment of adults. In: Sadock BJ, Sadock VA (eds). Comprehensive textbook of psychiatry, vol. 1 (7th ed). Baltimore: Lippincott Williams & Wilkins; 2000;689:701.-
8. Corcoran K, Fischer J. Measures for clinical practice, vols 1 and 2. New York: Free Press; 2000.
9. Blacker D. Psychiatric rating scales. In: Sadock BJ, Sadock VA (eds). Comprehensive textbook of psychiatry, vol. 1 (7th ed). Baltimore: Lippincott Williams & Wilkins; 2000;755-83.
1. Maruish ME (ed) The use of psychological testing for treatment planning and outcomes assessment. Mahwah, NJ: Lawrence Erlbaum Associates; 1999.
2. Sajatovic M, Ramirez LF. Rating scales in mental health. Hudson, OH: Lexi-Comp; 2003.
3. Aiken LR. Assessment of adult personality. New York: Springer; 1997.
4. Rush AJ, Pincus HJ, First MB, et al (eds). Handbook of Psychiatric Measures. Washington, DC: American Psychiatric Association; 2000.
5. Belar CD. Psychological assessment in capitated care. In: Butcher JN (ed). Personality assessment in managed care: Using the MMPI-2 in treatment planning. New York: Oxford Press; 1997;13:80.-
6. Adams RL, Culbertson JL. Personality assessment: adults and children. In: Sadock BJ, Sadock VA (eds). Comprehensive textbook of psychiatry, vol. 1 (7th ed). Baltimore: Lippincott Williams & Wilkins; 2000;702:21.-
7. Swanda RM, Haaland KY, La Rue A. Clinical neuropsychology and intellectual assessment of adults. In: Sadock BJ, Sadock VA (eds). Comprehensive textbook of psychiatry, vol. 1 (7th ed). Baltimore: Lippincott Williams & Wilkins; 2000;689:701.-
8. Corcoran K, Fischer J. Measures for clinical practice, vols 1 and 2. New York: Free Press; 2000.
9. Blacker D. Psychiatric rating scales. In: Sadock BJ, Sadock VA (eds). Comprehensive textbook of psychiatry, vol. 1 (7th ed). Baltimore: Lippincott Williams & Wilkins; 2000;755-83.
Perimenopausal depression? Ask how she’s sleeping
Trying to treat depression or anxiety in a midlife woman without asking how she’s sleeping may doom your treatment plan. Asking about sleep addresses issues that affect her quality of life and can provide valuable insight into effective interventions.
Psychiatric, psychosocial, and medical problems can disturb sleep during perimenopause.1 To help you diagnose and treat both mood disorders and insomnia, this article:
- describes how irregular hormone levels and psychosocial changes are linked to perimenopausal mood and sleep disorders
- offers evidence-based strategies for hormone replacement therapy (HRT), antidepressants, hypnotics, and psychotherapy.
DEPRESSION AND INSOMNIA AT MIDLIFE
Sixty-five percent of women seeking outpatient treatment for depression report disturbed sleep.2 Even mild anxiety and depression can undermine sleep quality, whereas insomnia can precede other symptoms of an evolving major depression.
Depressive disorders affect up to 29% of perimenopausal women (depending on the assessment tool used), compared with 8% to 12% of premenopausal women. Menopausal symptoms—hot flashes, poor sleep, memory problems—and not using HRT are associated with depression.3
Causes of midlife depression. Gonadal hormone changes have been implicated as a cause of increased depression in midlife women; declines in serum estradiol and testosterone are inversely associated with depression.4 The natural menopause transition (perimenopause) begins during the mid-40s, persists to the early 50s, and lasts an average 2 to 9 years. Estradiol produced by the ovary becomes erratic then decreases. Follicle-stimulating hormone (FSH) and luteinizing hormone (LH) serum levels increase, then plateau and serve as laboratory markers of menopause.5
Sociodemographic factors also may contribute to depression, anxiety, and insomnia. A midlife woman may experience role transitions—such as children leaving home and aging parents needing care. She may be adapting to her or her spouse’s retirement or to the loss of her partner by divorce or death. She may be grappling with her own aging and questions about mortality and life purpose.
In the workup, consider medical factors that may worsen sleep problems, such as hot flashes, sleep apnea, thyroid disease, urinary frequency, chronic pain, restless leg syndrome, caffeine use, sedentary lifestyle, and primary insomnia. Some women lose sleep from a bed partner’s snoring or movement (“spousal arousal”). Stimulating drugs such as theophylline can also play a role.
SLEEP CHANGES AT PERIMENOPAUSE
Sleep changes are among the most common physical and psychological experiences healthy women describe during perimenopause:
- 100 consecutive women surveyed at a menopause clinic reported fatigue (91%), hot flashes (80%), insomnia and early awakenings (77%), and depression (65%).6
- Sleep problems were reported by >50% of 203 women interviewed for the Decisions at Menopause Study (DAMES).7
- Difficulty sleeping across 2 weeks was reported by 38% of a multiethnic population of 12,603 women ages 40 to 55.8
Sleep problems occur more often during perimenopause than earlier in life. In a clinic sample of 521 women, Owens et al1 found insomnia in 33% to 36% of those in premenopause and in 44% to 61% of women during perimenopause. In the total sample of healthy middle-aged women, 42% had sleep complaints, including:
- initial insomnia: 49%
- middle insomnia: 92%
- early morning awakening: 59%.
No association? Individuals experience sleep quality subjectively, and these assessments may not match those obtained objectively. The Wisconsin Sleep Cohort Study,9 for example, found no association between menopause and diminished sleep quality in polysomnographic studies of 589 community-dwelling women. Even so, the peri- and postmenopausal women in the study reported less sleep satisfaction than premenopausal women did.
Most clinicians agree that a woman’s subjective experience of sleep is clinically relevant. Thus, rule out underlying sleep disorders before you attribute a midlife woman’s depressive signs and symptoms primarily to menopause.10
Treatment. Combination therapy may be useful, depending on the patient’s psychiatric and medical comorbidities (Algorithm).
TREATING PERIMENOPAUSAL DEPRESSION
HRT. Before the Women’s Health Initiative (WHI),10 guidelines recommended HRT for a first depressive episode during perimenopause and antidepressants for severe depressive symptoms and for women with a history of depression.11 This practice changed when the WHI found risks of thromboembolism, breast cancer, stroke, and coronary artery disease that increased over time with HRT.
HRT remains a short-term treatment option but is no longer considered the first or only approach to mood symptoms at perimenopause. Discuss with your patient potential benefits of short-term HRT for a first episode of depression—especially if she has vasomotor symptoms—versus potential risks.
Antidepressants can improve perimenopausal depression, but few studies have tested these agents’ effects on sleep. To reduce treatment-associated insomnia:
- select a relatively sedating antidepressant such as mirtazapine
- accept some insomnia for 3 to 4 weeks, until a stimulating antidepressant has had a full ffect on mood and its associated side effects would be expected to resolve
- or augment the antidepressant with a hypnotic such as zolpidem, zaleplon, eszopiclone, or trazodone.
When choosing therapy, consider patient factors and insomnia severity. For example, mirtazapine is typically associated with weight gain, so consider other options for overweight patients. Those with severe insomnia may prefer not to wait 3 to 4 weeks for improved sleep. With hypnotics, consider cost, any coexisting chemical dependency, and potential for morning hangover.
Psychotherapy can help perimenopausal patients accept aging, evaluate relationships, and examine their roles in the lives of more-dependent parents and less-dependent children.
HOT FLASHES AND INSOMNIA
Persistent hot flashes that disturb sleep may cause depression.12 They can wake a perimenopausal woman repeatedly (Figure 1). The awakenings may be brief—90% last <3 minutes—but a severely affected woman can lose an hour of sleep in a night.13 Even after a hot flash resolves, other factors such as anxiety may keep her awake.
Up to 85% of perimenopausal women experience hot flashes, especially during the first year after menses cease. Hot flashes persist for 5 years after menopause in 25% of women and indefinitely in a minority (Box ).14
Estrogen deficiency is thought to cause hot flashes via decreased serotonin synthesis and up-regulated 5HT2A receptors—the mediators of heat loss. As a result, a woman’s thermoregulatory zone narrows during perimenopause, reducing her tolerance for core body temperature changes. The thermoregulatory nucleus resides in the medial preoptic area of the anterior hypothalamus.
A hot flash begins with facial warmth when core temperatures exceed the thermoregulatory line. Heat spreads to the chest, often accompanied by flushing, diaphoresis, and headache. A woman may feel agitated, irritable, and distressed.
CNS noradrenergic activity may initiate hot flashes. Freedman et al13 compared the effects of IV clonidine (an alpha2 adrenergic agonist) plus yohimbine (an alpha2 adrenergic antagonist) or placebo in menopausal women with or without vasomotor symptoms. Among 9 symptomatic women, 6 experienced hot flashes when given yohimbine, and none did with placebo. No hot flashes occurred in asymptomatic women. Clonidine increased the duration of peripheral heating needed to trigger a hot flash and reduced the number of hot flashes in symptomatic women, compared with baseline.
Risk factors for nocturnal hot flashes include surgical menopause, Caucasian versus Asian ethnicity, lack of exercise, and nicotine use.8 Women suffering anxiety and stress also are at increased risk.15
HOT-FLASH THERAPIES
Placebo-controlled trials of hot flash therapies have found efficacies from 85% for HRT to 25% for placebo, vitamin E, black cohosh, soy, and behavioral therapy (Figure 2).16 Most trials were not designed to test the link between hot flashes and sleep, and many enrolled cancer patients not experiencing natural menopause. With the 25% placeboresponse rate, some therapies’ efficacy is unclear.
HRT can reduce nocturnal hot flash frequency. In a polysomnographic study,17 21 postmenopausal women received 6 months of conjugated estrogens, 0.625 mg/d, with medroxyprogesterone, 5 mg/d, or micronized progesterone, 200 mg/d. Sleep efficiency improved by 8% in women receiving micronized progesterone but was unchanged with medroxyprogesterone. Even so, both groups reported improved sleep quality and duration, with decreased awakenings.
The Wisconsin Sleep Cohort Study9 found that HRT was not associated with improved sleep, as measured by polysomnography. Even so, the women in that study noted subjective sleep improvement with HRT.
Antidepressants. Venlafaxine, 75 mg/d, and fluoxetine, 20 mg/d, have shown benefit in reducing hot flashes,18 presumably by increasing CNS serotonin. As mentioned, however, many antidepressants can cause insomnia, and few studies have examined this problem.
Gabapentin has been effective for patients with hot flashes.19 This agent, which increases GABA levels and may modestly increase slow-wave sleep—can improve conditions that disrupt sleep, including restless legs syndrome and chronic pain. It is well-tolerated, even at 900 mg/d, and is more-sedating than most serotonergic antidepressants.
Hypnotics. Surprisingly little evidence addresses hypnotics’ role in managing insomnia caused by hot flashes. No data have been published on the role of benzodiazepines or the benzodiazepine receptor agonists (zolpidem, zaleplon, and eszopiclone). In my experience, benzodiazepine receptor agonists improve sleep quality compromised by multiple factors, including hot flashes.
Soy and black cohosh. Isoflavones in soy may be estrogen receptor modulators. Twelve randomized, controlled trials of soy or soy extracts have shown a modest benefit for hot flashes.20
Black cohosh extracts, 8 mg/d, were given to 80 postmenopausal women in a randomized, double-blind, placebo-controlled trial (RCT). Hot flashes in those receiving black cohosh decreased from 4.9 to 0.7 daily, compared with reductions of 5.2 to 3.2 in women receiving estrogen and 5.1 to 3.1 in those receiving placebo.21 As a result, the National Institutes of Health is funding a 12-month, RCT to determine whether black cohosh reduces hot flash frequency and intensity.
Alternative agents are widely used and warrant study. Those shown to be safe can be used alone or with other therapies, but advise the patient that these agents may not be effective. Relaxation and exercise may decrease hot flashes,22 although some outcomes have been similar to a placebo response.
SLEEP APNEA AT PERIMENOPAUSE
Obstructive sleep apnea (OSA), although more common in men than women, appears to increase during perimenopause. Women with untreated OSA are twice as likely as men to be treated for depression, less likely to report excessive daytime sleepiness and snoring, and more likely to present with depression, anxiety, and morning headache.
Bixler et al23 interviewed 12,219 women and 4,364 men ages 20 to 100 and conducted 1-night sleep studies in 1,000 women and 741 men. OSA rates were 3.9% in men, 0.6% in premenopausal women, 2.7% in postmenopausal women not taking HRT, and 0.5% in postmenopausal women taking HRT.
The risk of sleep-disordered breathing is lower during early menopause and peaks at approximately age 65. Declining hormones likely play a role; progesterone increases ventilatory drive, and estrogen increases ventilatory centers’ sensitivity to progesterone’s stimulant effect. In small studies, exogenous progesterone has shown a slight effect in improving OSA.24
OSA’s transient, repetitive upper airway collapse increases inspiratory effort and may cause hypoxemia. Repeated arousals can lead to prolonged awakenings and unrefreshing sleep. Snoring and increased body mass index are strongly associated factors, although the Wisconsin Sleep Cohort Study10 showed an increase in sleep apnea in perimenopausal women that was unrelated to increased body mass index.
Obesity may not explain the increase in obstructive sleep apnea at perimenopause (Figure 3),28 although body fat distribution does change with aging. Women at perimenopause are likely to develop abdominal weight distribution.
Figure 3 Increased OSA in postmenopausal women is unrelated to obesity (BMI >32)
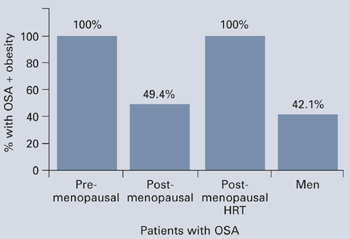
Obstructive sleep apnea (OSA) in 1,000 women and 741 men was associated exclusively with obesity in premenopausal women and postmenopausal women using HRT, but nearly one-half of the postmenopausal women with OSA were not obese.
Source: Adapted from reference 23.Treatment. In the Sleep Heart Health Study25 of 2,852 women age 50 or older, HRT users had one-half the apnea prevalence of nonusers (6% vs 14%). HRT users were less likely to awaken at night and to get inadequate sleep. Snoring rates were similar (25% for HRT users, 23% for nonusers).
Nasal continuous positive airway pressure (CPAP) is the mainstay of apnea treatment, although some women appear to have difficulty accepting CPAP.26 Weight loss and moderate exercise can help manage weight and improve sleep quality by increasing slow-wave sleep. Regular exercise also may improve depressed mood.
Related resources
- American College of Obstetricians and Gynecologists. www.acog.org
- The North American Menopause Society. www.menopause.org
Drug brand names
- Conjugated estrogens • Premarin
- Eszopiclone • Lunesta
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Medroxyprogesterone • Provera
- Micronized progesterone • Prometrium
- Mirtazapine • Remeron
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Zaleplon • Sonata
- Zolpidem • Ambien
Disclosures
Dr. Krahn reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Owens JF, Matthews KA. Sleep disturbance in healthy middle-aged women. Maturitas 1998;30:41-50.
2. Perlis ML, Giles DE, Buysse DJ, et al. Self-reported sleep disturbance as a prodromal symptom in recurrent depression. J Affect Disord 1997;42(2-3):209-12.
3. Bromberger JT, Assmann SF, Avis NE, et al. Persistent mood symptoms in a multiethnic community cohort of pre- and perimenopausal women. Am J Epidemiol 2003;158:347-56.
4. Sherwin BB. Changes in sexual behavior as a function of plasma sex steroid levels in post-menopausal women. Maturitas 1985;7(3):225-33.
5. Brizendine L. Minding menopause. Psychotropics vs estrogen: What you need to know now. Current Psychiatry 2003;2(10):12-31.
6. Anderson E, Hamburger S, Liu JH, Rebar RW. Characteristics of menopausal women seeking assistance. Am J Obstet Gynecol 1987;156(2):428-33.
7. Obermeyer CM, Reynolds RF, Price K, Abraham A. Therapeutic decisions for menopause: results of the DAMES project in central Massachusetts. Menopause 2004;11(4):456-65.
8. Kravitz HM, Ganz PA, Bromberger J, et al. Sleep difficulty in women at midlife: a community survey of sleep and the menopausal transition. Menopause 2003;10(1):19-28.
9. Young T, Rabago D, Zgierska A, et al. Objective and subjective sleep quality in premenopausal, perimenopausal, and postmenopausal women in the Wisconsin Sleep Cohort Study. Sleep 2003;26(6):667-72.
10. Wassertheil-Smoller S, Shumaker S, Ockene J, et al. Depression and cardiovascular sequelae in postmenopausal women. Arch Intern Med 2004;164:289-98.
11. Altshuler LL, Cohen LS, Moline ML, et al. The expert consensus guideline series. Treatment of depression in women. Postgrad Med 2001;March:1-107.
12. Krystal AD. Insomnia in women. Clin Cornerstone 2003;5(3):41-50.
13. Freedman RR. Physiology of hot flashes. Am J Hum Biol 2001;13(4):453-64.
14. Freedman RR, Woodward S, Sabharwal SC. A2-adrenergic mechanism in menopausal hot flushes. Obstet Gynecol 1990;76(4):573-8.
15. Miller AG, Li RM. Measuring hot flashes: summary of a NIH workshop. Mayo Clin Proc 2004;79:777-81.
16. Joffe H, Soares CN, Cohen LS. Assessment and treatment of hot flushes and menopausal mood disturbance. Psychiatr Clin North Am 2003 Sep;26(3):563-80.
17. Montplaisir J, Lorrain J, Denesle R, Petit D. Sleep in menopause: differential effects of two forms of hormone replacement therapy. Menopause 2001;8(1):10-16.
18. Loprinzi CL, Sloan JA, Perez EA, et al. Phase III evaluation of fluoxetine for treatment of hot flashes. J Clin Oncol 2002;20:1578-83.
19. Guttoso T, Jr, Kurlan R, McDermott MP, Kieburtz K. Gabapentin’s effects on hot flashes in postmenopausal women: a randomized controlled trial. Obstet Gynecol 2003;101:337-45.
20. Kessel B, Kronenberg F. The role of complementary and alternative medicine in management of menopausal symptoms. Endocrinol Metab Clin North Am 2004;33:717-39.
21. National Institutes of Health. National Center for Complementary and Alternative Medicine. Office of Dietary Supplements. Questions and answers about black cohosh and the symptoms of menopause. Available at: http://ods.od.nih.gov/factsheets/blackcohosh.asp. Accessed May 9, 2005.
22. Ivarsson T, Spetz AC, Hammar M. Physical exercise and vasomotor symptoms in postmenopausal women. Mauritas 1998;29:139-46.
23. Bixler EO, Vgontzas AN, Lin HM, et al. Prevalence of sleep-disordered breathing in women: effects of gender. Am J Respir Crit Care Med 2001;163:608-13.
24. Block AJ, Wynne JW, Boysen PG, et al. Menopause, medroxyprogesterone and breathing during sleep. Am J Med 1981;70:506-10.
25. Shahar E, Redline S, Young T, et al. Hormone replacement therapy and sleep-disordered breathing. Am J Respir Crit Care Med 2003;167:1186-92.
26. McArdle N, Devereux G, Heidarnejad H, et al. Long-term use of CPAP therapy for sleep apnea/hypopnea syndrome. Am J Respir Crit. Care Med 1999;159:1108-14.
Trying to treat depression or anxiety in a midlife woman without asking how she’s sleeping may doom your treatment plan. Asking about sleep addresses issues that affect her quality of life and can provide valuable insight into effective interventions.
Psychiatric, psychosocial, and medical problems can disturb sleep during perimenopause.1 To help you diagnose and treat both mood disorders and insomnia, this article:
- describes how irregular hormone levels and psychosocial changes are linked to perimenopausal mood and sleep disorders
- offers evidence-based strategies for hormone replacement therapy (HRT), antidepressants, hypnotics, and psychotherapy.
DEPRESSION AND INSOMNIA AT MIDLIFE
Sixty-five percent of women seeking outpatient treatment for depression report disturbed sleep.2 Even mild anxiety and depression can undermine sleep quality, whereas insomnia can precede other symptoms of an evolving major depression.
Depressive disorders affect up to 29% of perimenopausal women (depending on the assessment tool used), compared with 8% to 12% of premenopausal women. Menopausal symptoms—hot flashes, poor sleep, memory problems—and not using HRT are associated with depression.3
Causes of midlife depression. Gonadal hormone changes have been implicated as a cause of increased depression in midlife women; declines in serum estradiol and testosterone are inversely associated with depression.4 The natural menopause transition (perimenopause) begins during the mid-40s, persists to the early 50s, and lasts an average 2 to 9 years. Estradiol produced by the ovary becomes erratic then decreases. Follicle-stimulating hormone (FSH) and luteinizing hormone (LH) serum levels increase, then plateau and serve as laboratory markers of menopause.5
Sociodemographic factors also may contribute to depression, anxiety, and insomnia. A midlife woman may experience role transitions—such as children leaving home and aging parents needing care. She may be adapting to her or her spouse’s retirement or to the loss of her partner by divorce or death. She may be grappling with her own aging and questions about mortality and life purpose.
In the workup, consider medical factors that may worsen sleep problems, such as hot flashes, sleep apnea, thyroid disease, urinary frequency, chronic pain, restless leg syndrome, caffeine use, sedentary lifestyle, and primary insomnia. Some women lose sleep from a bed partner’s snoring or movement (“spousal arousal”). Stimulating drugs such as theophylline can also play a role.
SLEEP CHANGES AT PERIMENOPAUSE
Sleep changes are among the most common physical and psychological experiences healthy women describe during perimenopause:
- 100 consecutive women surveyed at a menopause clinic reported fatigue (91%), hot flashes (80%), insomnia and early awakenings (77%), and depression (65%).6
- Sleep problems were reported by >50% of 203 women interviewed for the Decisions at Menopause Study (DAMES).7
- Difficulty sleeping across 2 weeks was reported by 38% of a multiethnic population of 12,603 women ages 40 to 55.8
Sleep problems occur more often during perimenopause than earlier in life. In a clinic sample of 521 women, Owens et al1 found insomnia in 33% to 36% of those in premenopause and in 44% to 61% of women during perimenopause. In the total sample of healthy middle-aged women, 42% had sleep complaints, including:
- initial insomnia: 49%
- middle insomnia: 92%
- early morning awakening: 59%.
No association? Individuals experience sleep quality subjectively, and these assessments may not match those obtained objectively. The Wisconsin Sleep Cohort Study,9 for example, found no association between menopause and diminished sleep quality in polysomnographic studies of 589 community-dwelling women. Even so, the peri- and postmenopausal women in the study reported less sleep satisfaction than premenopausal women did.
Most clinicians agree that a woman’s subjective experience of sleep is clinically relevant. Thus, rule out underlying sleep disorders before you attribute a midlife woman’s depressive signs and symptoms primarily to menopause.10
Treatment. Combination therapy may be useful, depending on the patient’s psychiatric and medical comorbidities (Algorithm).
TREATING PERIMENOPAUSAL DEPRESSION
HRT. Before the Women’s Health Initiative (WHI),10 guidelines recommended HRT for a first depressive episode during perimenopause and antidepressants for severe depressive symptoms and for women with a history of depression.11 This practice changed when the WHI found risks of thromboembolism, breast cancer, stroke, and coronary artery disease that increased over time with HRT.
HRT remains a short-term treatment option but is no longer considered the first or only approach to mood symptoms at perimenopause. Discuss with your patient potential benefits of short-term HRT for a first episode of depression—especially if she has vasomotor symptoms—versus potential risks.
Antidepressants can improve perimenopausal depression, but few studies have tested these agents’ effects on sleep. To reduce treatment-associated insomnia:
- select a relatively sedating antidepressant such as mirtazapine
- accept some insomnia for 3 to 4 weeks, until a stimulating antidepressant has had a full ffect on mood and its associated side effects would be expected to resolve
- or augment the antidepressant with a hypnotic such as zolpidem, zaleplon, eszopiclone, or trazodone.
When choosing therapy, consider patient factors and insomnia severity. For example, mirtazapine is typically associated with weight gain, so consider other options for overweight patients. Those with severe insomnia may prefer not to wait 3 to 4 weeks for improved sleep. With hypnotics, consider cost, any coexisting chemical dependency, and potential for morning hangover.
Psychotherapy can help perimenopausal patients accept aging, evaluate relationships, and examine their roles in the lives of more-dependent parents and less-dependent children.
HOT FLASHES AND INSOMNIA
Persistent hot flashes that disturb sleep may cause depression.12 They can wake a perimenopausal woman repeatedly (Figure 1). The awakenings may be brief—90% last <3 minutes—but a severely affected woman can lose an hour of sleep in a night.13 Even after a hot flash resolves, other factors such as anxiety may keep her awake.
Up to 85% of perimenopausal women experience hot flashes, especially during the first year after menses cease. Hot flashes persist for 5 years after menopause in 25% of women and indefinitely in a minority (Box ).14
Estrogen deficiency is thought to cause hot flashes via decreased serotonin synthesis and up-regulated 5HT2A receptors—the mediators of heat loss. As a result, a woman’s thermoregulatory zone narrows during perimenopause, reducing her tolerance for core body temperature changes. The thermoregulatory nucleus resides in the medial preoptic area of the anterior hypothalamus.
A hot flash begins with facial warmth when core temperatures exceed the thermoregulatory line. Heat spreads to the chest, often accompanied by flushing, diaphoresis, and headache. A woman may feel agitated, irritable, and distressed.
CNS noradrenergic activity may initiate hot flashes. Freedman et al13 compared the effects of IV clonidine (an alpha2 adrenergic agonist) plus yohimbine (an alpha2 adrenergic antagonist) or placebo in menopausal women with or without vasomotor symptoms. Among 9 symptomatic women, 6 experienced hot flashes when given yohimbine, and none did with placebo. No hot flashes occurred in asymptomatic women. Clonidine increased the duration of peripheral heating needed to trigger a hot flash and reduced the number of hot flashes in symptomatic women, compared with baseline.
Risk factors for nocturnal hot flashes include surgical menopause, Caucasian versus Asian ethnicity, lack of exercise, and nicotine use.8 Women suffering anxiety and stress also are at increased risk.15
HOT-FLASH THERAPIES
Placebo-controlled trials of hot flash therapies have found efficacies from 85% for HRT to 25% for placebo, vitamin E, black cohosh, soy, and behavioral therapy (Figure 2).16 Most trials were not designed to test the link between hot flashes and sleep, and many enrolled cancer patients not experiencing natural menopause. With the 25% placeboresponse rate, some therapies’ efficacy is unclear.
HRT can reduce nocturnal hot flash frequency. In a polysomnographic study,17 21 postmenopausal women received 6 months of conjugated estrogens, 0.625 mg/d, with medroxyprogesterone, 5 mg/d, or micronized progesterone, 200 mg/d. Sleep efficiency improved by 8% in women receiving micronized progesterone but was unchanged with medroxyprogesterone. Even so, both groups reported improved sleep quality and duration, with decreased awakenings.
The Wisconsin Sleep Cohort Study9 found that HRT was not associated with improved sleep, as measured by polysomnography. Even so, the women in that study noted subjective sleep improvement with HRT.
Antidepressants. Venlafaxine, 75 mg/d, and fluoxetine, 20 mg/d, have shown benefit in reducing hot flashes,18 presumably by increasing CNS serotonin. As mentioned, however, many antidepressants can cause insomnia, and few studies have examined this problem.
Gabapentin has been effective for patients with hot flashes.19 This agent, which increases GABA levels and may modestly increase slow-wave sleep—can improve conditions that disrupt sleep, including restless legs syndrome and chronic pain. It is well-tolerated, even at 900 mg/d, and is more-sedating than most serotonergic antidepressants.
Hypnotics. Surprisingly little evidence addresses hypnotics’ role in managing insomnia caused by hot flashes. No data have been published on the role of benzodiazepines or the benzodiazepine receptor agonists (zolpidem, zaleplon, and eszopiclone). In my experience, benzodiazepine receptor agonists improve sleep quality compromised by multiple factors, including hot flashes.
Soy and black cohosh. Isoflavones in soy may be estrogen receptor modulators. Twelve randomized, controlled trials of soy or soy extracts have shown a modest benefit for hot flashes.20
Black cohosh extracts, 8 mg/d, were given to 80 postmenopausal women in a randomized, double-blind, placebo-controlled trial (RCT). Hot flashes in those receiving black cohosh decreased from 4.9 to 0.7 daily, compared with reductions of 5.2 to 3.2 in women receiving estrogen and 5.1 to 3.1 in those receiving placebo.21 As a result, the National Institutes of Health is funding a 12-month, RCT to determine whether black cohosh reduces hot flash frequency and intensity.
Alternative agents are widely used and warrant study. Those shown to be safe can be used alone or with other therapies, but advise the patient that these agents may not be effective. Relaxation and exercise may decrease hot flashes,22 although some outcomes have been similar to a placebo response.
SLEEP APNEA AT PERIMENOPAUSE
Obstructive sleep apnea (OSA), although more common in men than women, appears to increase during perimenopause. Women with untreated OSA are twice as likely as men to be treated for depression, less likely to report excessive daytime sleepiness and snoring, and more likely to present with depression, anxiety, and morning headache.
Bixler et al23 interviewed 12,219 women and 4,364 men ages 20 to 100 and conducted 1-night sleep studies in 1,000 women and 741 men. OSA rates were 3.9% in men, 0.6% in premenopausal women, 2.7% in postmenopausal women not taking HRT, and 0.5% in postmenopausal women taking HRT.
The risk of sleep-disordered breathing is lower during early menopause and peaks at approximately age 65. Declining hormones likely play a role; progesterone increases ventilatory drive, and estrogen increases ventilatory centers’ sensitivity to progesterone’s stimulant effect. In small studies, exogenous progesterone has shown a slight effect in improving OSA.24
OSA’s transient, repetitive upper airway collapse increases inspiratory effort and may cause hypoxemia. Repeated arousals can lead to prolonged awakenings and unrefreshing sleep. Snoring and increased body mass index are strongly associated factors, although the Wisconsin Sleep Cohort Study10 showed an increase in sleep apnea in perimenopausal women that was unrelated to increased body mass index.
Obesity may not explain the increase in obstructive sleep apnea at perimenopause (Figure 3),28 although body fat distribution does change with aging. Women at perimenopause are likely to develop abdominal weight distribution.
Figure 3 Increased OSA in postmenopausal women is unrelated to obesity (BMI >32)
Obstructive sleep apnea (OSA) in 1,000 women and 741 men was associated exclusively with obesity in premenopausal women and postmenopausal women using HRT, but nearly one-half of the postmenopausal women with OSA were not obese.
Source: Adapted from reference 23.Treatment. In the Sleep Heart Health Study25 of 2,852 women age 50 or older, HRT users had one-half the apnea prevalence of nonusers (6% vs 14%). HRT users were less likely to awaken at night and to get inadequate sleep. Snoring rates were similar (25% for HRT users, 23% for nonusers).
Nasal continuous positive airway pressure (CPAP) is the mainstay of apnea treatment, although some women appear to have difficulty accepting CPAP.26 Weight loss and moderate exercise can help manage weight and improve sleep quality by increasing slow-wave sleep. Regular exercise also may improve depressed mood.
Related resources
- American College of Obstetricians and Gynecologists. www.acog.org
- The North American Menopause Society. www.menopause.org
Drug brand names
- Conjugated estrogens • Premarin
- Eszopiclone • Lunesta
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Medroxyprogesterone • Provera
- Micronized progesterone • Prometrium
- Mirtazapine • Remeron
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Zaleplon • Sonata
- Zolpidem • Ambien
Disclosures
Dr. Krahn reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Trying to treat depression or anxiety in a midlife woman without asking how she’s sleeping may doom your treatment plan. Asking about sleep addresses issues that affect her quality of life and can provide valuable insight into effective interventions.
Psychiatric, psychosocial, and medical problems can disturb sleep during perimenopause.1 To help you diagnose and treat both mood disorders and insomnia, this article:
- describes how irregular hormone levels and psychosocial changes are linked to perimenopausal mood and sleep disorders
- offers evidence-based strategies for hormone replacement therapy (HRT), antidepressants, hypnotics, and psychotherapy.
DEPRESSION AND INSOMNIA AT MIDLIFE
Sixty-five percent of women seeking outpatient treatment for depression report disturbed sleep.2 Even mild anxiety and depression can undermine sleep quality, whereas insomnia can precede other symptoms of an evolving major depression.
Depressive disorders affect up to 29% of perimenopausal women (depending on the assessment tool used), compared with 8% to 12% of premenopausal women. Menopausal symptoms—hot flashes, poor sleep, memory problems—and not using HRT are associated with depression.3
Causes of midlife depression. Gonadal hormone changes have been implicated as a cause of increased depression in midlife women; declines in serum estradiol and testosterone are inversely associated with depression.4 The natural menopause transition (perimenopause) begins during the mid-40s, persists to the early 50s, and lasts an average 2 to 9 years. Estradiol produced by the ovary becomes erratic then decreases. Follicle-stimulating hormone (FSH) and luteinizing hormone (LH) serum levels increase, then plateau and serve as laboratory markers of menopause.5
Sociodemographic factors also may contribute to depression, anxiety, and insomnia. A midlife woman may experience role transitions—such as children leaving home and aging parents needing care. She may be adapting to her or her spouse’s retirement or to the loss of her partner by divorce or death. She may be grappling with her own aging and questions about mortality and life purpose.
In the workup, consider medical factors that may worsen sleep problems, such as hot flashes, sleep apnea, thyroid disease, urinary frequency, chronic pain, restless leg syndrome, caffeine use, sedentary lifestyle, and primary insomnia. Some women lose sleep from a bed partner’s snoring or movement (“spousal arousal”). Stimulating drugs such as theophylline can also play a role.
SLEEP CHANGES AT PERIMENOPAUSE
Sleep changes are among the most common physical and psychological experiences healthy women describe during perimenopause:
- 100 consecutive women surveyed at a menopause clinic reported fatigue (91%), hot flashes (80%), insomnia and early awakenings (77%), and depression (65%).6
- Sleep problems were reported by >50% of 203 women interviewed for the Decisions at Menopause Study (DAMES).7
- Difficulty sleeping across 2 weeks was reported by 38% of a multiethnic population of 12,603 women ages 40 to 55.8
Sleep problems occur more often during perimenopause than earlier in life. In a clinic sample of 521 women, Owens et al1 found insomnia in 33% to 36% of those in premenopause and in 44% to 61% of women during perimenopause. In the total sample of healthy middle-aged women, 42% had sleep complaints, including:
- initial insomnia: 49%
- middle insomnia: 92%
- early morning awakening: 59%.
No association? Individuals experience sleep quality subjectively, and these assessments may not match those obtained objectively. The Wisconsin Sleep Cohort Study,9 for example, found no association between menopause and diminished sleep quality in polysomnographic studies of 589 community-dwelling women. Even so, the peri- and postmenopausal women in the study reported less sleep satisfaction than premenopausal women did.
Most clinicians agree that a woman’s subjective experience of sleep is clinically relevant. Thus, rule out underlying sleep disorders before you attribute a midlife woman’s depressive signs and symptoms primarily to menopause.10
Treatment. Combination therapy may be useful, depending on the patient’s psychiatric and medical comorbidities (Algorithm).
TREATING PERIMENOPAUSAL DEPRESSION
HRT. Before the Women’s Health Initiative (WHI),10 guidelines recommended HRT for a first depressive episode during perimenopause and antidepressants for severe depressive symptoms and for women with a history of depression.11 This practice changed when the WHI found risks of thromboembolism, breast cancer, stroke, and coronary artery disease that increased over time with HRT.
HRT remains a short-term treatment option but is no longer considered the first or only approach to mood symptoms at perimenopause. Discuss with your patient potential benefits of short-term HRT for a first episode of depression—especially if she has vasomotor symptoms—versus potential risks.
Antidepressants can improve perimenopausal depression, but few studies have tested these agents’ effects on sleep. To reduce treatment-associated insomnia:
- select a relatively sedating antidepressant such as mirtazapine
- accept some insomnia for 3 to 4 weeks, until a stimulating antidepressant has had a full ffect on mood and its associated side effects would be expected to resolve
- or augment the antidepressant with a hypnotic such as zolpidem, zaleplon, eszopiclone, or trazodone.
When choosing therapy, consider patient factors and insomnia severity. For example, mirtazapine is typically associated with weight gain, so consider other options for overweight patients. Those with severe insomnia may prefer not to wait 3 to 4 weeks for improved sleep. With hypnotics, consider cost, any coexisting chemical dependency, and potential for morning hangover.
Psychotherapy can help perimenopausal patients accept aging, evaluate relationships, and examine their roles in the lives of more-dependent parents and less-dependent children.
HOT FLASHES AND INSOMNIA
Persistent hot flashes that disturb sleep may cause depression.12 They can wake a perimenopausal woman repeatedly (Figure 1). The awakenings may be brief—90% last <3 minutes—but a severely affected woman can lose an hour of sleep in a night.13 Even after a hot flash resolves, other factors such as anxiety may keep her awake.
Up to 85% of perimenopausal women experience hot flashes, especially during the first year after menses cease. Hot flashes persist for 5 years after menopause in 25% of women and indefinitely in a minority (Box ).14
Estrogen deficiency is thought to cause hot flashes via decreased serotonin synthesis and up-regulated 5HT2A receptors—the mediators of heat loss. As a result, a woman’s thermoregulatory zone narrows during perimenopause, reducing her tolerance for core body temperature changes. The thermoregulatory nucleus resides in the medial preoptic area of the anterior hypothalamus.
A hot flash begins with facial warmth when core temperatures exceed the thermoregulatory line. Heat spreads to the chest, often accompanied by flushing, diaphoresis, and headache. A woman may feel agitated, irritable, and distressed.
CNS noradrenergic activity may initiate hot flashes. Freedman et al13 compared the effects of IV clonidine (an alpha2 adrenergic agonist) plus yohimbine (an alpha2 adrenergic antagonist) or placebo in menopausal women with or without vasomotor symptoms. Among 9 symptomatic women, 6 experienced hot flashes when given yohimbine, and none did with placebo. No hot flashes occurred in asymptomatic women. Clonidine increased the duration of peripheral heating needed to trigger a hot flash and reduced the number of hot flashes in symptomatic women, compared with baseline.
Risk factors for nocturnal hot flashes include surgical menopause, Caucasian versus Asian ethnicity, lack of exercise, and nicotine use.8 Women suffering anxiety and stress also are at increased risk.15
HOT-FLASH THERAPIES
Placebo-controlled trials of hot flash therapies have found efficacies from 85% for HRT to 25% for placebo, vitamin E, black cohosh, soy, and behavioral therapy (Figure 2).16 Most trials were not designed to test the link between hot flashes and sleep, and many enrolled cancer patients not experiencing natural menopause. With the 25% placeboresponse rate, some therapies’ efficacy is unclear.
HRT can reduce nocturnal hot flash frequency. In a polysomnographic study,17 21 postmenopausal women received 6 months of conjugated estrogens, 0.625 mg/d, with medroxyprogesterone, 5 mg/d, or micronized progesterone, 200 mg/d. Sleep efficiency improved by 8% in women receiving micronized progesterone but was unchanged with medroxyprogesterone. Even so, both groups reported improved sleep quality and duration, with decreased awakenings.
The Wisconsin Sleep Cohort Study9 found that HRT was not associated with improved sleep, as measured by polysomnography. Even so, the women in that study noted subjective sleep improvement with HRT.
Antidepressants. Venlafaxine, 75 mg/d, and fluoxetine, 20 mg/d, have shown benefit in reducing hot flashes,18 presumably by increasing CNS serotonin. As mentioned, however, many antidepressants can cause insomnia, and few studies have examined this problem.
Gabapentin has been effective for patients with hot flashes.19 This agent, which increases GABA levels and may modestly increase slow-wave sleep—can improve conditions that disrupt sleep, including restless legs syndrome and chronic pain. It is well-tolerated, even at 900 mg/d, and is more-sedating than most serotonergic antidepressants.
Hypnotics. Surprisingly little evidence addresses hypnotics’ role in managing insomnia caused by hot flashes. No data have been published on the role of benzodiazepines or the benzodiazepine receptor agonists (zolpidem, zaleplon, and eszopiclone). In my experience, benzodiazepine receptor agonists improve sleep quality compromised by multiple factors, including hot flashes.
Soy and black cohosh. Isoflavones in soy may be estrogen receptor modulators. Twelve randomized, controlled trials of soy or soy extracts have shown a modest benefit for hot flashes.20
Black cohosh extracts, 8 mg/d, were given to 80 postmenopausal women in a randomized, double-blind, placebo-controlled trial (RCT). Hot flashes in those receiving black cohosh decreased from 4.9 to 0.7 daily, compared with reductions of 5.2 to 3.2 in women receiving estrogen and 5.1 to 3.1 in those receiving placebo.21 As a result, the National Institutes of Health is funding a 12-month, RCT to determine whether black cohosh reduces hot flash frequency and intensity.
Alternative agents are widely used and warrant study. Those shown to be safe can be used alone or with other therapies, but advise the patient that these agents may not be effective. Relaxation and exercise may decrease hot flashes,22 although some outcomes have been similar to a placebo response.
SLEEP APNEA AT PERIMENOPAUSE
Obstructive sleep apnea (OSA), although more common in men than women, appears to increase during perimenopause. Women with untreated OSA are twice as likely as men to be treated for depression, less likely to report excessive daytime sleepiness and snoring, and more likely to present with depression, anxiety, and morning headache.
Bixler et al23 interviewed 12,219 women and 4,364 men ages 20 to 100 and conducted 1-night sleep studies in 1,000 women and 741 men. OSA rates were 3.9% in men, 0.6% in premenopausal women, 2.7% in postmenopausal women not taking HRT, and 0.5% in postmenopausal women taking HRT.
The risk of sleep-disordered breathing is lower during early menopause and peaks at approximately age 65. Declining hormones likely play a role; progesterone increases ventilatory drive, and estrogen increases ventilatory centers’ sensitivity to progesterone’s stimulant effect. In small studies, exogenous progesterone has shown a slight effect in improving OSA.24
OSA’s transient, repetitive upper airway collapse increases inspiratory effort and may cause hypoxemia. Repeated arousals can lead to prolonged awakenings and unrefreshing sleep. Snoring and increased body mass index are strongly associated factors, although the Wisconsin Sleep Cohort Study10 showed an increase in sleep apnea in perimenopausal women that was unrelated to increased body mass index.
Obesity may not explain the increase in obstructive sleep apnea at perimenopause (Figure 3),28 although body fat distribution does change with aging. Women at perimenopause are likely to develop abdominal weight distribution.
Figure 3 Increased OSA in postmenopausal women is unrelated to obesity (BMI >32)
Obstructive sleep apnea (OSA) in 1,000 women and 741 men was associated exclusively with obesity in premenopausal women and postmenopausal women using HRT, but nearly one-half of the postmenopausal women with OSA were not obese.
Source: Adapted from reference 23.Treatment. In the Sleep Heart Health Study25 of 2,852 women age 50 or older, HRT users had one-half the apnea prevalence of nonusers (6% vs 14%). HRT users were less likely to awaken at night and to get inadequate sleep. Snoring rates were similar (25% for HRT users, 23% for nonusers).
Nasal continuous positive airway pressure (CPAP) is the mainstay of apnea treatment, although some women appear to have difficulty accepting CPAP.26 Weight loss and moderate exercise can help manage weight and improve sleep quality by increasing slow-wave sleep. Regular exercise also may improve depressed mood.
Related resources
- American College of Obstetricians and Gynecologists. www.acog.org
- The North American Menopause Society. www.menopause.org
Drug brand names
- Conjugated estrogens • Premarin
- Eszopiclone • Lunesta
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Medroxyprogesterone • Provera
- Micronized progesterone • Prometrium
- Mirtazapine • Remeron
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Zaleplon • Sonata
- Zolpidem • Ambien
Disclosures
Dr. Krahn reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Owens JF, Matthews KA. Sleep disturbance in healthy middle-aged women. Maturitas 1998;30:41-50.
2. Perlis ML, Giles DE, Buysse DJ, et al. Self-reported sleep disturbance as a prodromal symptom in recurrent depression. J Affect Disord 1997;42(2-3):209-12.
3. Bromberger JT, Assmann SF, Avis NE, et al. Persistent mood symptoms in a multiethnic community cohort of pre- and perimenopausal women. Am J Epidemiol 2003;158:347-56.
4. Sherwin BB. Changes in sexual behavior as a function of plasma sex steroid levels in post-menopausal women. Maturitas 1985;7(3):225-33.
5. Brizendine L. Minding menopause. Psychotropics vs estrogen: What you need to know now. Current Psychiatry 2003;2(10):12-31.
6. Anderson E, Hamburger S, Liu JH, Rebar RW. Characteristics of menopausal women seeking assistance. Am J Obstet Gynecol 1987;156(2):428-33.
7. Obermeyer CM, Reynolds RF, Price K, Abraham A. Therapeutic decisions for menopause: results of the DAMES project in central Massachusetts. Menopause 2004;11(4):456-65.
8. Kravitz HM, Ganz PA, Bromberger J, et al. Sleep difficulty in women at midlife: a community survey of sleep and the menopausal transition. Menopause 2003;10(1):19-28.
9. Young T, Rabago D, Zgierska A, et al. Objective and subjective sleep quality in premenopausal, perimenopausal, and postmenopausal women in the Wisconsin Sleep Cohort Study. Sleep 2003;26(6):667-72.
10. Wassertheil-Smoller S, Shumaker S, Ockene J, et al. Depression and cardiovascular sequelae in postmenopausal women. Arch Intern Med 2004;164:289-98.
11. Altshuler LL, Cohen LS, Moline ML, et al. The expert consensus guideline series. Treatment of depression in women. Postgrad Med 2001;March:1-107.
12. Krystal AD. Insomnia in women. Clin Cornerstone 2003;5(3):41-50.
13. Freedman RR. Physiology of hot flashes. Am J Hum Biol 2001;13(4):453-64.
14. Freedman RR, Woodward S, Sabharwal SC. A2-adrenergic mechanism in menopausal hot flushes. Obstet Gynecol 1990;76(4):573-8.
15. Miller AG, Li RM. Measuring hot flashes: summary of a NIH workshop. Mayo Clin Proc 2004;79:777-81.
16. Joffe H, Soares CN, Cohen LS. Assessment and treatment of hot flushes and menopausal mood disturbance. Psychiatr Clin North Am 2003 Sep;26(3):563-80.
17. Montplaisir J, Lorrain J, Denesle R, Petit D. Sleep in menopause: differential effects of two forms of hormone replacement therapy. Menopause 2001;8(1):10-16.
18. Loprinzi CL, Sloan JA, Perez EA, et al. Phase III evaluation of fluoxetine for treatment of hot flashes. J Clin Oncol 2002;20:1578-83.
19. Guttoso T, Jr, Kurlan R, McDermott MP, Kieburtz K. Gabapentin’s effects on hot flashes in postmenopausal women: a randomized controlled trial. Obstet Gynecol 2003;101:337-45.
20. Kessel B, Kronenberg F. The role of complementary and alternative medicine in management of menopausal symptoms. Endocrinol Metab Clin North Am 2004;33:717-39.
21. National Institutes of Health. National Center for Complementary and Alternative Medicine. Office of Dietary Supplements. Questions and answers about black cohosh and the symptoms of menopause. Available at: http://ods.od.nih.gov/factsheets/blackcohosh.asp. Accessed May 9, 2005.
22. Ivarsson T, Spetz AC, Hammar M. Physical exercise and vasomotor symptoms in postmenopausal women. Mauritas 1998;29:139-46.
23. Bixler EO, Vgontzas AN, Lin HM, et al. Prevalence of sleep-disordered breathing in women: effects of gender. Am J Respir Crit Care Med 2001;163:608-13.
24. Block AJ, Wynne JW, Boysen PG, et al. Menopause, medroxyprogesterone and breathing during sleep. Am J Med 1981;70:506-10.
25. Shahar E, Redline S, Young T, et al. Hormone replacement therapy and sleep-disordered breathing. Am J Respir Crit Care Med 2003;167:1186-92.
26. McArdle N, Devereux G, Heidarnejad H, et al. Long-term use of CPAP therapy for sleep apnea/hypopnea syndrome. Am J Respir Crit. Care Med 1999;159:1108-14.
1. Owens JF, Matthews KA. Sleep disturbance in healthy middle-aged women. Maturitas 1998;30:41-50.
2. Perlis ML, Giles DE, Buysse DJ, et al. Self-reported sleep disturbance as a prodromal symptom in recurrent depression. J Affect Disord 1997;42(2-3):209-12.
3. Bromberger JT, Assmann SF, Avis NE, et al. Persistent mood symptoms in a multiethnic community cohort of pre- and perimenopausal women. Am J Epidemiol 2003;158:347-56.
4. Sherwin BB. Changes in sexual behavior as a function of plasma sex steroid levels in post-menopausal women. Maturitas 1985;7(3):225-33.
5. Brizendine L. Minding menopause. Psychotropics vs estrogen: What you need to know now. Current Psychiatry 2003;2(10):12-31.
6. Anderson E, Hamburger S, Liu JH, Rebar RW. Characteristics of menopausal women seeking assistance. Am J Obstet Gynecol 1987;156(2):428-33.
7. Obermeyer CM, Reynolds RF, Price K, Abraham A. Therapeutic decisions for menopause: results of the DAMES project in central Massachusetts. Menopause 2004;11(4):456-65.
8. Kravitz HM, Ganz PA, Bromberger J, et al. Sleep difficulty in women at midlife: a community survey of sleep and the menopausal transition. Menopause 2003;10(1):19-28.
9. Young T, Rabago D, Zgierska A, et al. Objective and subjective sleep quality in premenopausal, perimenopausal, and postmenopausal women in the Wisconsin Sleep Cohort Study. Sleep 2003;26(6):667-72.
10. Wassertheil-Smoller S, Shumaker S, Ockene J, et al. Depression and cardiovascular sequelae in postmenopausal women. Arch Intern Med 2004;164:289-98.
11. Altshuler LL, Cohen LS, Moline ML, et al. The expert consensus guideline series. Treatment of depression in women. Postgrad Med 2001;March:1-107.
12. Krystal AD. Insomnia in women. Clin Cornerstone 2003;5(3):41-50.
13. Freedman RR. Physiology of hot flashes. Am J Hum Biol 2001;13(4):453-64.
14. Freedman RR, Woodward S, Sabharwal SC. A2-adrenergic mechanism in menopausal hot flushes. Obstet Gynecol 1990;76(4):573-8.
15. Miller AG, Li RM. Measuring hot flashes: summary of a NIH workshop. Mayo Clin Proc 2004;79:777-81.
16. Joffe H, Soares CN, Cohen LS. Assessment and treatment of hot flushes and menopausal mood disturbance. Psychiatr Clin North Am 2003 Sep;26(3):563-80.
17. Montplaisir J, Lorrain J, Denesle R, Petit D. Sleep in menopause: differential effects of two forms of hormone replacement therapy. Menopause 2001;8(1):10-16.
18. Loprinzi CL, Sloan JA, Perez EA, et al. Phase III evaluation of fluoxetine for treatment of hot flashes. J Clin Oncol 2002;20:1578-83.
19. Guttoso T, Jr, Kurlan R, McDermott MP, Kieburtz K. Gabapentin’s effects on hot flashes in postmenopausal women: a randomized controlled trial. Obstet Gynecol 2003;101:337-45.
20. Kessel B, Kronenberg F. The role of complementary and alternative medicine in management of menopausal symptoms. Endocrinol Metab Clin North Am 2004;33:717-39.
21. National Institutes of Health. National Center for Complementary and Alternative Medicine. Office of Dietary Supplements. Questions and answers about black cohosh and the symptoms of menopause. Available at: http://ods.od.nih.gov/factsheets/blackcohosh.asp. Accessed May 9, 2005.
22. Ivarsson T, Spetz AC, Hammar M. Physical exercise and vasomotor symptoms in postmenopausal women. Mauritas 1998;29:139-46.
23. Bixler EO, Vgontzas AN, Lin HM, et al. Prevalence of sleep-disordered breathing in women: effects of gender. Am J Respir Crit Care Med 2001;163:608-13.
24. Block AJ, Wynne JW, Boysen PG, et al. Menopause, medroxyprogesterone and breathing during sleep. Am J Med 1981;70:506-10.
25. Shahar E, Redline S, Young T, et al. Hormone replacement therapy and sleep-disordered breathing. Am J Respir Crit Care Med 2003;167:1186-92.
26. McArdle N, Devereux G, Heidarnejad H, et al. Long-term use of CPAP therapy for sleep apnea/hypopnea syndrome. Am J Respir Crit. Care Med 1999;159:1108-14.
Performance anxiety: How to ease stage fright
The violin is slippery in my grasp. I hear the thud of my foot tapping, but the tempo feels wrong. I’m aware of my chest pounding, a lump in my throat, and heat rising from my face. Everyone is watching me, waiting for me to make a mistake.
Why can’t I stop my hand from trembling? I can only watch as the bow jumps noisily across the strings. I should have practiced more. My mind goes blank, and I miss the page turn.
Silence. I blink, and the lights blind me as the applause comes, thankfully, and I exhale and run off the stage as the curtain closes.
Well-known performing artists—Sir Laurence Olivier, Kim Basinger, Peter O’Toole, Richard Burton, Barbra Streisand, and Luciano Pavarotti —have described bouts with acute stage fright. Performance anxiety can occur with acting, singing, or playing a musical instrument, and with nonartistic performances such as public speaking, oral examinations, competing in sporting events, sexual activity, using public restrooms, or being watched while doing a task such as surgery, eating, or writing.2
Like social phobia, performance anxiety probably develops in accomplished artists and not-so-famous individuals because of a mélange of genetic factors, innate temperament, parental influences, conditioning events, and cognitive influences.3
NORMAL VS. ABNORMAL FEAR
Performance anxiety is characterized by persisting, distressful apprehension about—or actual impairment of—performance skills to a degree unwarranted by the individual’s aptitude, training, and preparation.1 Not all performance anxiety qualifies as a mental disorder; for example, though 85% of the population experiences discomfort about public speaking,4 this anxiety does not impair most people’s ability to function.
Mild to moderate anxiety is normal and motivating in performances.5 However, anxiety’s effect on performance does not follow a bell-shaped curve, wherein moderate anxiety promotes optimal performance.6 Instead, a catastrophic model is more accurate: increasing anxiety is helpful until a certain threshold is reached, then performance plunges.7
Diagnostic criteria. DSM-IV-TR describes performance anxiety as a form of social phobia (or social anxiety disorder) characterized by marked and persistent fear of social or performance situations in which embarrassment or humiliation might occur. Approximately 13% of adults experience social phobia,8 and about 2% suffer from severe discrete performance anxiety.9
Performance anxiety does not completely overlap with social phobia, however. Test-taking anxiety and writer’s block, which can occur in a nonpublic context, do not fit neatly into the social phobia category.2 Thus, some performance anxiety forms are better grouped as another type of anxiety disorder, such as specific phobia (Figure).
Figure Performance anxiety features overlap with other anxieties
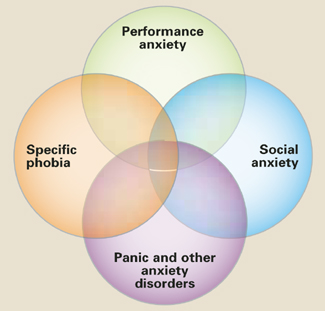
Performance anxiety is not easy to categorize. It is situational anxiety that occurs in a public context and overlaps with but does not entirely match diagnostic criteria for specific phobia, social anxiety, or panic disorder and generalized anxiety.
DIFFERENTIAL DIAGNOSIS
Social anxiety? Ask the patient about all situations that provoke anxiety to differentiate between:
- discrete performance anxiety (1 or 2 performance situations that provoke anxiety)
- and generalized social anxiety (3 or more situations that provoke anxiety).9
Individuals with “trait” anxiety may exhibit innate shyness and are considered to have generalized social phobia. Those with “state” anxiety experience anxiety in specific situations or circumstances and are more aptly described as having discrete performance anxiety.10 Whereas persons with social phobia may avoid the feared activity without inner conflict, those with performance anxiety are committed to performing the activity and are distressed when unable to perform.9
Specific phobia? A specific phobia is a circumscribed fear of a specific object, situation, or activity from which a grim outcome is feared. Specific phobia usually has no performance aspect or fear of embarrassment or failure.
Some clinicians consider certain performance anxieties—such as writer’s block, test-taking anxiety, paruresis, and even fear about sexual performance—to be specific phobias. Because performance anxieties and phobias share some cognitive and behavioral components, their treatments are similar and use of medication is controversial.
General medical condition? Perform or refer the patient for a thorough medical evaluation before you diagnose performance anxiety, as endocrine, cardiovascular, respiratory, and circulatory abnormalities can mimic or exacerbate anxiety disorders. Also consider substance abuse or withdrawal as possible causes of anxiety.
PATIENT EVALUATION
Family history. Individuals with social anxiety often report a family history of generalized social anxiety, panic disorder, or major depressive disorder.3 Similar findings seem plausible for persons with discrete performance anxiety, although comparable family history data have not been reported.
Cognitive symptoms. Four cognitive distortions are common in persons with social phobia (Table 1).11 These negative thoughts are presumably the same for performance anxiety, at least when it is a sub-type of social phobia.
Somatic symptoms. Persons with performance anxiety tend to have heightened awareness of hyperadrenergic arousal symptoms (Table 2), sometimes in all body systems. Symptoms may resemble those of a panic attack.
Behavioral symptoms. Behavioral symptoms include stuttering, mumbling, trembling voice, yawning, biting nails or lips, gritting jaw, poor eye contact, shuffling or tapping feet, unnatural or rigid postures or movements, warming up too fast or too slowly, wearing excessive makeup, or smiling abnormally. A performer may forget to carry out a routine task such as blinking, moistening lips, or turning a page of music.
These behaviors may perpetuate and reinforce anxiety by eliciting negative reactions from an audience and fulfilling the performer’s pessimistic expectations. The therapist can identify these maladaptive behaviors and target them for treatment.
Table 1
4 cognitive distortions that underlie performance anxiety
|
Table 2
Somatic symptoms of performance anxiety
| Bodily system | Symptoms |
|---|---|
| Autonomic | Blushing, diaphoresis, dry mouth |
| GI, urologic | Urinary or bowel urgency, GI discomfort |
| Cardiovascular | Tachycardia, palpitations |
| Neuromuscular | Muscle tension, tremor, paralysis |
PSYCHIATRIC COMORBIDITY
About one-third of individuals with performance anxiety have psychiatric comorbidities.9 Most common are other anxiety disorders, specifically the generalized form of social phobia, generalized anxiety disorder, panic disorder, or specific phobia.12 Mood disorders are less common. We also recommend monitoring for eating disorders because some performing artists are driven to maintain high physical appearance standards.
Personality disorder comorbidities with performance anxiety have not been studied. Some experts believe that avoidant personality and social phobia are the same conditions expressed to varying degrees on a continuum.13 Other personality disorders to consider include schizoid, paranoid, and obsessive-compulsive personalities.
Alcohol and substance use disorders are highly comorbid with performance anxiety. Alcohol use decreases public speaking anxiety,14 and approximately 6% of orchestral musicians use alcohol before a performance.15 For comparison, approximately 16% of patients who present for treatment of generalized anxiety disorder abuse alcohol, often as an attempt to self-medicate.16
TREATMENT PLANNING
Just as performance anxiety’s diagnostic classification may vary, so may treatment. Pharmacologic interventions and psychotherapy for social and specific phobias are similar. Some clinicians favor a multimodal approach addressing behavior, affect, sensation, imagery, cognition, interpersonal relationships, and biological factors.9
The performing arts community is competitive, and individuals may have differing standards about what treatments are acceptable. Some may view using medications as “cheating” or an admission of professional failure. A performer may feel medication gives an unfair advantage, that respect would be lost if others found out, or that taking medication before performing is similar to steroid use by athletes.17,18
Medication vs. psychotherapy. Medication can help diminish anxiety’s physical symptoms, but certain psychotherapies rely on these somatic symptoms for effective treatment and extinguishing of responses. Concurrent use of medications and psychotherapy for social phobia is common in everyday practice, although some studies find the combination no more effective than either treatment alone.11 Symptoms appear less likely to return after cognitive-behavioral therapy (CBT) ends than after medication is discontinued.16
Discuss treatment options with the patient. A patient who feels unable to perform without medication may develop psychological dependency. Conversely, a patient may not be able to afford the full course of psychotherapy needed for positive results. For performing artists, longer visits that incorporate medication management with psychotherapy may be more successful than brief, symptom-targeted visits.
MEDICATION MANAGEMENT
All medication use for performance anxiety is off-label. The most common choices are short-acting agents such as beta blockers or benzodiazepines (Table 3).
Table 3
Medications used to treat performance anxiety*
| Medication | Typical dosage | Possible side effects |
|---|---|---|
| Beta blockers | Medical: sedation, fatigue, dizziness, ataxia, nausea, sexual dysfunction Psychiatric:insomnia, nightmares, depression Contraindications: heart failure, bradycardia, breathing difficulties, hypotension | |
| Propranolol | 10 to 40 mg | |
| Nadolol | 20 to 120 mg | |
| Atenolol | 50 to 100 mg | |
| Benzodiazepines | Performance decrement, amnesia, sedation, discontinuation symptoms, tolerance, abuse potential | |
| Clonazepam | 0.25 to 0.5 mg | |
| Lorazepam | 0.5 to 1 mg | |
| * Off-label use; taken as-needed approximately 1 hour before performance | ||
Beta blockers can relieve autonomic and somatic symptoms such as tachycardia, tremor, and stuttering when used in low doses as needed for mild to moderate circumscribed performance anxiety.16,19 Propranolol, 10 mg about 1 hour before the performance, is most often prescribed.
Before prescribing a beta blocker, evaluate the patient’s medical history and cardiovascular status, including blood pressure and pulse. Have the patient try a test dose before the first live performance to check for side effects and tolerability (Table 3).16,19
Benzodiazepines have been used to treat social anxiety, but controlled studies have not reliably addressed their efficacy in performance anxiety. Advise the patient to abstain from alcohol when taking these medications (Table 3).
PSYCHOTHERAPY OPTIONS
CBT with components of exposure and retraining can ameliorate performance anxiety.10,20
Many performers forgo normal childhood social experiences to hone their talents, at times sacrificing sound coping skills.17 CBT’s goal is to help them reduce negative biases and restructure cognitive processes to function better at whatever task is at hand. This involves teaching them to:
- recognize pessimistic thoughts that occur before, during, and after performances
- challenge the accuracy of these thoughts
- replace them with rational, helpful thoughts based on the assimilated information.11
Exposure therapy can help individuals face feared activities so that counter-conditioning through habituation and extinction can safely occur. Useful strategies include imagination, role play, confrontation, videotaping, and homework assignments.11
Experiencing anxiety is a component of exposure therapy. Thus, some clinicians avoid using concomitant medication that might decrease anxiety’s physical symptoms and interfere with the exposure process.21
Relaxation training can help the patient recognize and respond to autonomic and physical arousal during a performance.11 For example, progressive muscle relaxation can be practiced first in session and then as homework.
Social skills training can help patients identify and change anxiety behaviors that cause negative audience reactions. Tools to help direct the patient towards more appropriate behaviors include modeling, behavior rehearsal, corrective feedback, social reinforcement, and homework assignments such as videotaping performances.11 For public speaking anxiety, vocal and physical skills training10 and computerized virtual reality courses can help.4
Interpersonal therapy may be useful, based on the premise that performance anxiety occurs within a social and interpersonal context.22
Related resources
- Toastmasters for public speaking. http://www.toastmasters.com
- Anxiety Disorders Association of America. http://www.adaa.org
- Social Anxiety Association. http://www.socialphobia.org
Drug brand names
- Atenolol • Tenormin
- Clonazepam • Klonopin
- Lorazepam • Ativan
- Nadolol • Corgard
- Propranolol • Inderal
Disclosure
Dr. Kelly reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Saveanu receives research support from Pfizer Inc. and is a consultant and speaker for Pfizer Inc. and GlaxoSmithKline.
1. Salmon PG. A psychological perspective on musical performance anxiety: a review of the literature. Med Prob Perform Artists 1900;51(1):2-11.
2. Beatty M. Situational and predispositional correlates of public speaking anxiety. Commun Ed 1998;37:28-39.
3. Ollendick TH, Hirshfeld-Becker DR. The developmental psychopathology of social anxiety disorder. Biol Psychiatry 2002;51(1):44-58.
4. Harris SR, Kemmerling RL, North MM. Brief virtual reality therapy for public speaking anxiety. Cyberpsychol Behav 2002;5(6):543-50.
5. Rafferty BD, Smith RE, Ptacek JT. Facilitating and debilitating trait anxiety, situational anxiety, and coping with an anticipated stressor: a process analysis. J Pers Soc Psychol 1997;72:892-906.
6. Yerkes RM, Dodson JD. The relation of strength of stimulus to rapidity of habit formation. J Comp Neurol Psychol 1908;18:459-482.
7. Hardy L, Parfitt G. A catastrophic model of anxiety and performance. Br J Psychol 1991;82:163-78.
8. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry 1994;51(1):8-19.
9. Powell D. Treating individuals with debilitating performance anxiety: an introduction. J Clin Psychol 2004;60(8):801-8.
10. Merritt L, Richards A, Davis P. Performance anxiety: loss of the spoken edge. J Voice 2001;15(2):257-69.
11. Heimberg RG. Cognitive-behavioral therapy for social anxiety disorder: current status and future directions. Biol Psychiatry 2002;51:101-8.
12. Brown TA, Barlow DH. Comorbidities among anxiety disorders: implications for treatment and DSM-IV. J Consult Clin Psychol 1992;60(6):835-44.
13. Schneier FR, Johnson J, Hornig CD, et al. Social phobia: comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry 1992;49:282-8.
14. Abrams K, Kushner M, Medina K, Voight A. Self-administration of alcohol before and after a public speaking challenge by individuals with social phobias. Psychol Addict Behav 2002;16(1):121-8.
15. Maran AGD. Performing arts medicine. Br J Sports Med 1998;32(1):5.-
16. Bruce TJ, Saeed SA. Social anxiety disorder: a common, underrecognized mental disorder. Am Fam Physician 1999;60(8):2311-22.
17. Ostwald PF, Baron BC, Byl NM, Wilson FR. Performing arts medicine. West J Med 1994;160:48-52.
18. Slomka J. Playing with propranolol. Hastings Cent Rep 1992;22(4):13-18.
19. Blanco C, Antia SX, Liebowitz MR. Pharmacotherapy of social anxiety disorder. Biol Psychiatry 2002;51:109-20.
20. Rodebaugh TL, Chambless DL. Cognitive therapy for performance anxiety. J Clin Psychol 2004;60(8):809-20.
21. Birk L. Pharmacotherapy for performance anxiety disorders: occasionally useful but typically contraindicated. J Clin Psychol: In Session 2004;60(8):867-79.
22. Lipsitz JD, Markowitz JC, Cherry S, Fyer AJ. Open trial of interpersonal psychotherapy for the treatment of social phobia. Am J Psychiatry 1999;156(11):1814-6.
The violin is slippery in my grasp. I hear the thud of my foot tapping, but the tempo feels wrong. I’m aware of my chest pounding, a lump in my throat, and heat rising from my face. Everyone is watching me, waiting for me to make a mistake.
Why can’t I stop my hand from trembling? I can only watch as the bow jumps noisily across the strings. I should have practiced more. My mind goes blank, and I miss the page turn.
Silence. I blink, and the lights blind me as the applause comes, thankfully, and I exhale and run off the stage as the curtain closes.
Well-known performing artists—Sir Laurence Olivier, Kim Basinger, Peter O’Toole, Richard Burton, Barbra Streisand, and Luciano Pavarotti —have described bouts with acute stage fright. Performance anxiety can occur with acting, singing, or playing a musical instrument, and with nonartistic performances such as public speaking, oral examinations, competing in sporting events, sexual activity, using public restrooms, or being watched while doing a task such as surgery, eating, or writing.2
Like social phobia, performance anxiety probably develops in accomplished artists and not-so-famous individuals because of a mélange of genetic factors, innate temperament, parental influences, conditioning events, and cognitive influences.3
NORMAL VS. ABNORMAL FEAR
Performance anxiety is characterized by persisting, distressful apprehension about—or actual impairment of—performance skills to a degree unwarranted by the individual’s aptitude, training, and preparation.1 Not all performance anxiety qualifies as a mental disorder; for example, though 85% of the population experiences discomfort about public speaking,4 this anxiety does not impair most people’s ability to function.
Mild to moderate anxiety is normal and motivating in performances.5 However, anxiety’s effect on performance does not follow a bell-shaped curve, wherein moderate anxiety promotes optimal performance.6 Instead, a catastrophic model is more accurate: increasing anxiety is helpful until a certain threshold is reached, then performance plunges.7
Diagnostic criteria. DSM-IV-TR describes performance anxiety as a form of social phobia (or social anxiety disorder) characterized by marked and persistent fear of social or performance situations in which embarrassment or humiliation might occur. Approximately 13% of adults experience social phobia,8 and about 2% suffer from severe discrete performance anxiety.9
Performance anxiety does not completely overlap with social phobia, however. Test-taking anxiety and writer’s block, which can occur in a nonpublic context, do not fit neatly into the social phobia category.2 Thus, some performance anxiety forms are better grouped as another type of anxiety disorder, such as specific phobia (Figure).
Figure Performance anxiety features overlap with other anxieties
Performance anxiety is not easy to categorize. It is situational anxiety that occurs in a public context and overlaps with but does not entirely match diagnostic criteria for specific phobia, social anxiety, or panic disorder and generalized anxiety.
DIFFERENTIAL DIAGNOSIS
Social anxiety? Ask the patient about all situations that provoke anxiety to differentiate between:
- discrete performance anxiety (1 or 2 performance situations that provoke anxiety)
- and generalized social anxiety (3 or more situations that provoke anxiety).9
Individuals with “trait” anxiety may exhibit innate shyness and are considered to have generalized social phobia. Those with “state” anxiety experience anxiety in specific situations or circumstances and are more aptly described as having discrete performance anxiety.10 Whereas persons with social phobia may avoid the feared activity without inner conflict, those with performance anxiety are committed to performing the activity and are distressed when unable to perform.9
Specific phobia? A specific phobia is a circumscribed fear of a specific object, situation, or activity from which a grim outcome is feared. Specific phobia usually has no performance aspect or fear of embarrassment or failure.
Some clinicians consider certain performance anxieties—such as writer’s block, test-taking anxiety, paruresis, and even fear about sexual performance—to be specific phobias. Because performance anxieties and phobias share some cognitive and behavioral components, their treatments are similar and use of medication is controversial.
General medical condition? Perform or refer the patient for a thorough medical evaluation before you diagnose performance anxiety, as endocrine, cardiovascular, respiratory, and circulatory abnormalities can mimic or exacerbate anxiety disorders. Also consider substance abuse or withdrawal as possible causes of anxiety.
PATIENT EVALUATION
Family history. Individuals with social anxiety often report a family history of generalized social anxiety, panic disorder, or major depressive disorder.3 Similar findings seem plausible for persons with discrete performance anxiety, although comparable family history data have not been reported.
Cognitive symptoms. Four cognitive distortions are common in persons with social phobia (Table 1).11 These negative thoughts are presumably the same for performance anxiety, at least when it is a sub-type of social phobia.
Somatic symptoms. Persons with performance anxiety tend to have heightened awareness of hyperadrenergic arousal symptoms (Table 2), sometimes in all body systems. Symptoms may resemble those of a panic attack.
Behavioral symptoms. Behavioral symptoms include stuttering, mumbling, trembling voice, yawning, biting nails or lips, gritting jaw, poor eye contact, shuffling or tapping feet, unnatural or rigid postures or movements, warming up too fast or too slowly, wearing excessive makeup, or smiling abnormally. A performer may forget to carry out a routine task such as blinking, moistening lips, or turning a page of music.
These behaviors may perpetuate and reinforce anxiety by eliciting negative reactions from an audience and fulfilling the performer’s pessimistic expectations. The therapist can identify these maladaptive behaviors and target them for treatment.
Table 1
4 cognitive distortions that underlie performance anxiety
|
Table 2
Somatic symptoms of performance anxiety
| Bodily system | Symptoms |
|---|---|
| Autonomic | Blushing, diaphoresis, dry mouth |
| GI, urologic | Urinary or bowel urgency, GI discomfort |
| Cardiovascular | Tachycardia, palpitations |
| Neuromuscular | Muscle tension, tremor, paralysis |
PSYCHIATRIC COMORBIDITY
About one-third of individuals with performance anxiety have psychiatric comorbidities.9 Most common are other anxiety disorders, specifically the generalized form of social phobia, generalized anxiety disorder, panic disorder, or specific phobia.12 Mood disorders are less common. We also recommend monitoring for eating disorders because some performing artists are driven to maintain high physical appearance standards.
Personality disorder comorbidities with performance anxiety have not been studied. Some experts believe that avoidant personality and social phobia are the same conditions expressed to varying degrees on a continuum.13 Other personality disorders to consider include schizoid, paranoid, and obsessive-compulsive personalities.
Alcohol and substance use disorders are highly comorbid with performance anxiety. Alcohol use decreases public speaking anxiety,14 and approximately 6% of orchestral musicians use alcohol before a performance.15 For comparison, approximately 16% of patients who present for treatment of generalized anxiety disorder abuse alcohol, often as an attempt to self-medicate.16
TREATMENT PLANNING
Just as performance anxiety’s diagnostic classification may vary, so may treatment. Pharmacologic interventions and psychotherapy for social and specific phobias are similar. Some clinicians favor a multimodal approach addressing behavior, affect, sensation, imagery, cognition, interpersonal relationships, and biological factors.9
The performing arts community is competitive, and individuals may have differing standards about what treatments are acceptable. Some may view using medications as “cheating” or an admission of professional failure. A performer may feel medication gives an unfair advantage, that respect would be lost if others found out, or that taking medication before performing is similar to steroid use by athletes.17,18
Medication vs. psychotherapy. Medication can help diminish anxiety’s physical symptoms, but certain psychotherapies rely on these somatic symptoms for effective treatment and extinguishing of responses. Concurrent use of medications and psychotherapy for social phobia is common in everyday practice, although some studies find the combination no more effective than either treatment alone.11 Symptoms appear less likely to return after cognitive-behavioral therapy (CBT) ends than after medication is discontinued.16
Discuss treatment options with the patient. A patient who feels unable to perform without medication may develop psychological dependency. Conversely, a patient may not be able to afford the full course of psychotherapy needed for positive results. For performing artists, longer visits that incorporate medication management with psychotherapy may be more successful than brief, symptom-targeted visits.
MEDICATION MANAGEMENT
All medication use for performance anxiety is off-label. The most common choices are short-acting agents such as beta blockers or benzodiazepines (Table 3).
Table 3
Medications used to treat performance anxiety*
| Medication | Typical dosage | Possible side effects |
|---|---|---|
| Beta blockers | Medical: sedation, fatigue, dizziness, ataxia, nausea, sexual dysfunction Psychiatric:insomnia, nightmares, depression Contraindications: heart failure, bradycardia, breathing difficulties, hypotension | |
| Propranolol | 10 to 40 mg | |
| Nadolol | 20 to 120 mg | |
| Atenolol | 50 to 100 mg | |
| Benzodiazepines | Performance decrement, amnesia, sedation, discontinuation symptoms, tolerance, abuse potential | |
| Clonazepam | 0.25 to 0.5 mg | |
| Lorazepam | 0.5 to 1 mg | |
| * Off-label use; taken as-needed approximately 1 hour before performance | ||
Beta blockers can relieve autonomic and somatic symptoms such as tachycardia, tremor, and stuttering when used in low doses as needed for mild to moderate circumscribed performance anxiety.16,19 Propranolol, 10 mg about 1 hour before the performance, is most often prescribed.
Before prescribing a beta blocker, evaluate the patient’s medical history and cardiovascular status, including blood pressure and pulse. Have the patient try a test dose before the first live performance to check for side effects and tolerability (Table 3).16,19
Benzodiazepines have been used to treat social anxiety, but controlled studies have not reliably addressed their efficacy in performance anxiety. Advise the patient to abstain from alcohol when taking these medications (Table 3).
PSYCHOTHERAPY OPTIONS
CBT with components of exposure and retraining can ameliorate performance anxiety.10,20
Many performers forgo normal childhood social experiences to hone their talents, at times sacrificing sound coping skills.17 CBT’s goal is to help them reduce negative biases and restructure cognitive processes to function better at whatever task is at hand. This involves teaching them to:
- recognize pessimistic thoughts that occur before, during, and after performances
- challenge the accuracy of these thoughts
- replace them with rational, helpful thoughts based on the assimilated information.11
Exposure therapy can help individuals face feared activities so that counter-conditioning through habituation and extinction can safely occur. Useful strategies include imagination, role play, confrontation, videotaping, and homework assignments.11
Experiencing anxiety is a component of exposure therapy. Thus, some clinicians avoid using concomitant medication that might decrease anxiety’s physical symptoms and interfere with the exposure process.21
Relaxation training can help the patient recognize and respond to autonomic and physical arousal during a performance.11 For example, progressive muscle relaxation can be practiced first in session and then as homework.
Social skills training can help patients identify and change anxiety behaviors that cause negative audience reactions. Tools to help direct the patient towards more appropriate behaviors include modeling, behavior rehearsal, corrective feedback, social reinforcement, and homework assignments such as videotaping performances.11 For public speaking anxiety, vocal and physical skills training10 and computerized virtual reality courses can help.4
Interpersonal therapy may be useful, based on the premise that performance anxiety occurs within a social and interpersonal context.22
Related resources
- Toastmasters for public speaking. http://www.toastmasters.com
- Anxiety Disorders Association of America. http://www.adaa.org
- Social Anxiety Association. http://www.socialphobia.org
Drug brand names
- Atenolol • Tenormin
- Clonazepam • Klonopin
- Lorazepam • Ativan
- Nadolol • Corgard
- Propranolol • Inderal
Disclosure
Dr. Kelly reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Saveanu receives research support from Pfizer Inc. and is a consultant and speaker for Pfizer Inc. and GlaxoSmithKline.
The violin is slippery in my grasp. I hear the thud of my foot tapping, but the tempo feels wrong. I’m aware of my chest pounding, a lump in my throat, and heat rising from my face. Everyone is watching me, waiting for me to make a mistake.
Why can’t I stop my hand from trembling? I can only watch as the bow jumps noisily across the strings. I should have practiced more. My mind goes blank, and I miss the page turn.
Silence. I blink, and the lights blind me as the applause comes, thankfully, and I exhale and run off the stage as the curtain closes.
Well-known performing artists—Sir Laurence Olivier, Kim Basinger, Peter O’Toole, Richard Burton, Barbra Streisand, and Luciano Pavarotti —have described bouts with acute stage fright. Performance anxiety can occur with acting, singing, or playing a musical instrument, and with nonartistic performances such as public speaking, oral examinations, competing in sporting events, sexual activity, using public restrooms, or being watched while doing a task such as surgery, eating, or writing.2
Like social phobia, performance anxiety probably develops in accomplished artists and not-so-famous individuals because of a mélange of genetic factors, innate temperament, parental influences, conditioning events, and cognitive influences.3
NORMAL VS. ABNORMAL FEAR
Performance anxiety is characterized by persisting, distressful apprehension about—or actual impairment of—performance skills to a degree unwarranted by the individual’s aptitude, training, and preparation.1 Not all performance anxiety qualifies as a mental disorder; for example, though 85% of the population experiences discomfort about public speaking,4 this anxiety does not impair most people’s ability to function.
Mild to moderate anxiety is normal and motivating in performances.5 However, anxiety’s effect on performance does not follow a bell-shaped curve, wherein moderate anxiety promotes optimal performance.6 Instead, a catastrophic model is more accurate: increasing anxiety is helpful until a certain threshold is reached, then performance plunges.7
Diagnostic criteria. DSM-IV-TR describes performance anxiety as a form of social phobia (or social anxiety disorder) characterized by marked and persistent fear of social or performance situations in which embarrassment or humiliation might occur. Approximately 13% of adults experience social phobia,8 and about 2% suffer from severe discrete performance anxiety.9
Performance anxiety does not completely overlap with social phobia, however. Test-taking anxiety and writer’s block, which can occur in a nonpublic context, do not fit neatly into the social phobia category.2 Thus, some performance anxiety forms are better grouped as another type of anxiety disorder, such as specific phobia (Figure).
Figure Performance anxiety features overlap with other anxieties
Performance anxiety is not easy to categorize. It is situational anxiety that occurs in a public context and overlaps with but does not entirely match diagnostic criteria for specific phobia, social anxiety, or panic disorder and generalized anxiety.
DIFFERENTIAL DIAGNOSIS
Social anxiety? Ask the patient about all situations that provoke anxiety to differentiate between:
- discrete performance anxiety (1 or 2 performance situations that provoke anxiety)
- and generalized social anxiety (3 or more situations that provoke anxiety).9
Individuals with “trait” anxiety may exhibit innate shyness and are considered to have generalized social phobia. Those with “state” anxiety experience anxiety in specific situations or circumstances and are more aptly described as having discrete performance anxiety.10 Whereas persons with social phobia may avoid the feared activity without inner conflict, those with performance anxiety are committed to performing the activity and are distressed when unable to perform.9
Specific phobia? A specific phobia is a circumscribed fear of a specific object, situation, or activity from which a grim outcome is feared. Specific phobia usually has no performance aspect or fear of embarrassment or failure.
Some clinicians consider certain performance anxieties—such as writer’s block, test-taking anxiety, paruresis, and even fear about sexual performance—to be specific phobias. Because performance anxieties and phobias share some cognitive and behavioral components, their treatments are similar and use of medication is controversial.
General medical condition? Perform or refer the patient for a thorough medical evaluation before you diagnose performance anxiety, as endocrine, cardiovascular, respiratory, and circulatory abnormalities can mimic or exacerbate anxiety disorders. Also consider substance abuse or withdrawal as possible causes of anxiety.
PATIENT EVALUATION
Family history. Individuals with social anxiety often report a family history of generalized social anxiety, panic disorder, or major depressive disorder.3 Similar findings seem plausible for persons with discrete performance anxiety, although comparable family history data have not been reported.
Cognitive symptoms. Four cognitive distortions are common in persons with social phobia (Table 1).11 These negative thoughts are presumably the same for performance anxiety, at least when it is a sub-type of social phobia.
Somatic symptoms. Persons with performance anxiety tend to have heightened awareness of hyperadrenergic arousal symptoms (Table 2), sometimes in all body systems. Symptoms may resemble those of a panic attack.
Behavioral symptoms. Behavioral symptoms include stuttering, mumbling, trembling voice, yawning, biting nails or lips, gritting jaw, poor eye contact, shuffling or tapping feet, unnatural or rigid postures or movements, warming up too fast or too slowly, wearing excessive makeup, or smiling abnormally. A performer may forget to carry out a routine task such as blinking, moistening lips, or turning a page of music.
These behaviors may perpetuate and reinforce anxiety by eliciting negative reactions from an audience and fulfilling the performer’s pessimistic expectations. The therapist can identify these maladaptive behaviors and target them for treatment.
Table 1
4 cognitive distortions that underlie performance anxiety
|
Table 2
Somatic symptoms of performance anxiety
| Bodily system | Symptoms |
|---|---|
| Autonomic | Blushing, diaphoresis, dry mouth |
| GI, urologic | Urinary or bowel urgency, GI discomfort |
| Cardiovascular | Tachycardia, palpitations |
| Neuromuscular | Muscle tension, tremor, paralysis |
PSYCHIATRIC COMORBIDITY
About one-third of individuals with performance anxiety have psychiatric comorbidities.9 Most common are other anxiety disorders, specifically the generalized form of social phobia, generalized anxiety disorder, panic disorder, or specific phobia.12 Mood disorders are less common. We also recommend monitoring for eating disorders because some performing artists are driven to maintain high physical appearance standards.
Personality disorder comorbidities with performance anxiety have not been studied. Some experts believe that avoidant personality and social phobia are the same conditions expressed to varying degrees on a continuum.13 Other personality disorders to consider include schizoid, paranoid, and obsessive-compulsive personalities.
Alcohol and substance use disorders are highly comorbid with performance anxiety. Alcohol use decreases public speaking anxiety,14 and approximately 6% of orchestral musicians use alcohol before a performance.15 For comparison, approximately 16% of patients who present for treatment of generalized anxiety disorder abuse alcohol, often as an attempt to self-medicate.16
TREATMENT PLANNING
Just as performance anxiety’s diagnostic classification may vary, so may treatment. Pharmacologic interventions and psychotherapy for social and specific phobias are similar. Some clinicians favor a multimodal approach addressing behavior, affect, sensation, imagery, cognition, interpersonal relationships, and biological factors.9
The performing arts community is competitive, and individuals may have differing standards about what treatments are acceptable. Some may view using medications as “cheating” or an admission of professional failure. A performer may feel medication gives an unfair advantage, that respect would be lost if others found out, or that taking medication before performing is similar to steroid use by athletes.17,18
Medication vs. psychotherapy. Medication can help diminish anxiety’s physical symptoms, but certain psychotherapies rely on these somatic symptoms for effective treatment and extinguishing of responses. Concurrent use of medications and psychotherapy for social phobia is common in everyday practice, although some studies find the combination no more effective than either treatment alone.11 Symptoms appear less likely to return after cognitive-behavioral therapy (CBT) ends than after medication is discontinued.16
Discuss treatment options with the patient. A patient who feels unable to perform without medication may develop psychological dependency. Conversely, a patient may not be able to afford the full course of psychotherapy needed for positive results. For performing artists, longer visits that incorporate medication management with psychotherapy may be more successful than brief, symptom-targeted visits.
MEDICATION MANAGEMENT
All medication use for performance anxiety is off-label. The most common choices are short-acting agents such as beta blockers or benzodiazepines (Table 3).
Table 3
Medications used to treat performance anxiety*
| Medication | Typical dosage | Possible side effects |
|---|---|---|
| Beta blockers | Medical: sedation, fatigue, dizziness, ataxia, nausea, sexual dysfunction Psychiatric:insomnia, nightmares, depression Contraindications: heart failure, bradycardia, breathing difficulties, hypotension | |
| Propranolol | 10 to 40 mg | |
| Nadolol | 20 to 120 mg | |
| Atenolol | 50 to 100 mg | |
| Benzodiazepines | Performance decrement, amnesia, sedation, discontinuation symptoms, tolerance, abuse potential | |
| Clonazepam | 0.25 to 0.5 mg | |
| Lorazepam | 0.5 to 1 mg | |
| * Off-label use; taken as-needed approximately 1 hour before performance | ||
Beta blockers can relieve autonomic and somatic symptoms such as tachycardia, tremor, and stuttering when used in low doses as needed for mild to moderate circumscribed performance anxiety.16,19 Propranolol, 10 mg about 1 hour before the performance, is most often prescribed.
Before prescribing a beta blocker, evaluate the patient’s medical history and cardiovascular status, including blood pressure and pulse. Have the patient try a test dose before the first live performance to check for side effects and tolerability (Table 3).16,19
Benzodiazepines have been used to treat social anxiety, but controlled studies have not reliably addressed their efficacy in performance anxiety. Advise the patient to abstain from alcohol when taking these medications (Table 3).
PSYCHOTHERAPY OPTIONS
CBT with components of exposure and retraining can ameliorate performance anxiety.10,20
Many performers forgo normal childhood social experiences to hone their talents, at times sacrificing sound coping skills.17 CBT’s goal is to help them reduce negative biases and restructure cognitive processes to function better at whatever task is at hand. This involves teaching them to:
- recognize pessimistic thoughts that occur before, during, and after performances
- challenge the accuracy of these thoughts
- replace them with rational, helpful thoughts based on the assimilated information.11
Exposure therapy can help individuals face feared activities so that counter-conditioning through habituation and extinction can safely occur. Useful strategies include imagination, role play, confrontation, videotaping, and homework assignments.11
Experiencing anxiety is a component of exposure therapy. Thus, some clinicians avoid using concomitant medication that might decrease anxiety’s physical symptoms and interfere with the exposure process.21
Relaxation training can help the patient recognize and respond to autonomic and physical arousal during a performance.11 For example, progressive muscle relaxation can be practiced first in session and then as homework.
Social skills training can help patients identify and change anxiety behaviors that cause negative audience reactions. Tools to help direct the patient towards more appropriate behaviors include modeling, behavior rehearsal, corrective feedback, social reinforcement, and homework assignments such as videotaping performances.11 For public speaking anxiety, vocal and physical skills training10 and computerized virtual reality courses can help.4
Interpersonal therapy may be useful, based on the premise that performance anxiety occurs within a social and interpersonal context.22
Related resources
- Toastmasters for public speaking. http://www.toastmasters.com
- Anxiety Disorders Association of America. http://www.adaa.org
- Social Anxiety Association. http://www.socialphobia.org
Drug brand names
- Atenolol • Tenormin
- Clonazepam • Klonopin
- Lorazepam • Ativan
- Nadolol • Corgard
- Propranolol • Inderal
Disclosure
Dr. Kelly reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Saveanu receives research support from Pfizer Inc. and is a consultant and speaker for Pfizer Inc. and GlaxoSmithKline.
1. Salmon PG. A psychological perspective on musical performance anxiety: a review of the literature. Med Prob Perform Artists 1900;51(1):2-11.
2. Beatty M. Situational and predispositional correlates of public speaking anxiety. Commun Ed 1998;37:28-39.
3. Ollendick TH, Hirshfeld-Becker DR. The developmental psychopathology of social anxiety disorder. Biol Psychiatry 2002;51(1):44-58.
4. Harris SR, Kemmerling RL, North MM. Brief virtual reality therapy for public speaking anxiety. Cyberpsychol Behav 2002;5(6):543-50.
5. Rafferty BD, Smith RE, Ptacek JT. Facilitating and debilitating trait anxiety, situational anxiety, and coping with an anticipated stressor: a process analysis. J Pers Soc Psychol 1997;72:892-906.
6. Yerkes RM, Dodson JD. The relation of strength of stimulus to rapidity of habit formation. J Comp Neurol Psychol 1908;18:459-482.
7. Hardy L, Parfitt G. A catastrophic model of anxiety and performance. Br J Psychol 1991;82:163-78.
8. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry 1994;51(1):8-19.
9. Powell D. Treating individuals with debilitating performance anxiety: an introduction. J Clin Psychol 2004;60(8):801-8.
10. Merritt L, Richards A, Davis P. Performance anxiety: loss of the spoken edge. J Voice 2001;15(2):257-69.
11. Heimberg RG. Cognitive-behavioral therapy for social anxiety disorder: current status and future directions. Biol Psychiatry 2002;51:101-8.
12. Brown TA, Barlow DH. Comorbidities among anxiety disorders: implications for treatment and DSM-IV. J Consult Clin Psychol 1992;60(6):835-44.
13. Schneier FR, Johnson J, Hornig CD, et al. Social phobia: comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry 1992;49:282-8.
14. Abrams K, Kushner M, Medina K, Voight A. Self-administration of alcohol before and after a public speaking challenge by individuals with social phobias. Psychol Addict Behav 2002;16(1):121-8.
15. Maran AGD. Performing arts medicine. Br J Sports Med 1998;32(1):5.-
16. Bruce TJ, Saeed SA. Social anxiety disorder: a common, underrecognized mental disorder. Am Fam Physician 1999;60(8):2311-22.
17. Ostwald PF, Baron BC, Byl NM, Wilson FR. Performing arts medicine. West J Med 1994;160:48-52.
18. Slomka J. Playing with propranolol. Hastings Cent Rep 1992;22(4):13-18.
19. Blanco C, Antia SX, Liebowitz MR. Pharmacotherapy of social anxiety disorder. Biol Psychiatry 2002;51:109-20.
20. Rodebaugh TL, Chambless DL. Cognitive therapy for performance anxiety. J Clin Psychol 2004;60(8):809-20.
21. Birk L. Pharmacotherapy for performance anxiety disorders: occasionally useful but typically contraindicated. J Clin Psychol: In Session 2004;60(8):867-79.
22. Lipsitz JD, Markowitz JC, Cherry S, Fyer AJ. Open trial of interpersonal psychotherapy for the treatment of social phobia. Am J Psychiatry 1999;156(11):1814-6.
1. Salmon PG. A psychological perspective on musical performance anxiety: a review of the literature. Med Prob Perform Artists 1900;51(1):2-11.
2. Beatty M. Situational and predispositional correlates of public speaking anxiety. Commun Ed 1998;37:28-39.
3. Ollendick TH, Hirshfeld-Becker DR. The developmental psychopathology of social anxiety disorder. Biol Psychiatry 2002;51(1):44-58.
4. Harris SR, Kemmerling RL, North MM. Brief virtual reality therapy for public speaking anxiety. Cyberpsychol Behav 2002;5(6):543-50.
5. Rafferty BD, Smith RE, Ptacek JT. Facilitating and debilitating trait anxiety, situational anxiety, and coping with an anticipated stressor: a process analysis. J Pers Soc Psychol 1997;72:892-906.
6. Yerkes RM, Dodson JD. The relation of strength of stimulus to rapidity of habit formation. J Comp Neurol Psychol 1908;18:459-482.
7. Hardy L, Parfitt G. A catastrophic model of anxiety and performance. Br J Psychol 1991;82:163-78.
8. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry 1994;51(1):8-19.
9. Powell D. Treating individuals with debilitating performance anxiety: an introduction. J Clin Psychol 2004;60(8):801-8.
10. Merritt L, Richards A, Davis P. Performance anxiety: loss of the spoken edge. J Voice 2001;15(2):257-69.
11. Heimberg RG. Cognitive-behavioral therapy for social anxiety disorder: current status and future directions. Biol Psychiatry 2002;51:101-8.
12. Brown TA, Barlow DH. Comorbidities among anxiety disorders: implications for treatment and DSM-IV. J Consult Clin Psychol 1992;60(6):835-44.
13. Schneier FR, Johnson J, Hornig CD, et al. Social phobia: comorbidity and morbidity in an epidemiologic sample. Arch Gen Psychiatry 1992;49:282-8.
14. Abrams K, Kushner M, Medina K, Voight A. Self-administration of alcohol before and after a public speaking challenge by individuals with social phobias. Psychol Addict Behav 2002;16(1):121-8.
15. Maran AGD. Performing arts medicine. Br J Sports Med 1998;32(1):5.-
16. Bruce TJ, Saeed SA. Social anxiety disorder: a common, underrecognized mental disorder. Am Fam Physician 1999;60(8):2311-22.
17. Ostwald PF, Baron BC, Byl NM, Wilson FR. Performing arts medicine. West J Med 1994;160:48-52.
18. Slomka J. Playing with propranolol. Hastings Cent Rep 1992;22(4):13-18.
19. Blanco C, Antia SX, Liebowitz MR. Pharmacotherapy of social anxiety disorder. Biol Psychiatry 2002;51:109-20.
20. Rodebaugh TL, Chambless DL. Cognitive therapy for performance anxiety. J Clin Psychol 2004;60(8):809-20.
21. Birk L. Pharmacotherapy for performance anxiety disorders: occasionally useful but typically contraindicated. J Clin Psychol: In Session 2004;60(8):867-79.
22. Lipsitz JD, Markowitz JC, Cherry S, Fyer AJ. Open trial of interpersonal psychotherapy for the treatment of social phobia. Am J Psychiatry 1999;156(11):1814-6.
Drug-drug interactions: Avoid serious adverse events with mood stabilizers
Drug-drug interactions (DDIs) can be viewed as physiologic combat wherein a “perpetrator” drug affects a “victim” drug’s pharmacokinetics or pharmacodynamics. Your challenge is to deter that interaction in patients taking two or more medications.
This article—first in a series—discusses polypharmacy risk factors that increase the likelihood of detrimental DDIs, then focuses on DDIs in patients taking mood stabilizers for bipolar disorder. We also offer practical tips to reduce DDI risk. Future articles will discuss DDI risks with antidepressants, antipsychotics, and anxiolytics.
To predict DDIs, you need to know psychotropics’ mechanism of action, metabolism, and effects on cytochrome P-450 (CYP) enzymes. Our discussion is not exhaustive because the data base is massive and new interactions continue to be discovered. Our aim is to equip you to anticipate and prevent DDIs when prescribing.
WHAT ARE ADVERSE DDIs?
An adverse event (AE) is any undesirable experience that occurs when a patient uses a medical product, whether or not the product caused the event. The FDA says an “undesirable experience” may be:
- an unfavorable and unintended symptom or sign
- an abnormal lab or radiographic finding
- a disease that is temporarily associated with the medical product.
An AE becomes “serious” (an SAE) when its duration, intensity, and/or frequency leads to death, a life-threatening condition, initial or prolonged hospitalization, disability, or congenital anomaly. Reporting is voluntary, but we strongly recommend that you report all SAEs to the FDA.
These definitions can help you confirm that a patient has experienced an SAE, but the task becomes more complicated when you try to attribute an SAE to a drug interaction. In the absence of an FDA definition, we assert that DDIs are responsible for SAEs when a perpetrator drug affects the pharmacokinetics or pharmacodynamics of a victim drug and exacerbates a known untoward event of the victim drug (Box 1).1-5 Which drug is the perpetrator and which is the victim is not always clear, and sometimes a medication—such as carbamazepine—can be both at once.
More than 100,000 possible detrimental DDIs have been documented in medical literature and pharmaceutical company data. This number is likely to grow with increased scrutiny, as
DDIs cause morbidity, mortality, and increased health care costs. More than 106,000 Americans die each year from properly prescribed, correctly taken medications. Polypharmacy is associated with extended hospital stays, and using >6 drugs is an independent predictor of death. DDIs contribute to the cause of death in acute overdoses and can be responsible for false-positive suicide diagnoses.
In clinical practice, DDI-associated toxicity may be mistaken for a new disease process, or a disease may be incorrectly perceived as progressing when a medication is rendered ineffective.
Source: References 1-5
RISKS OF POLYPHARMACY
Individuals with psychiatric illnesses are at particular risk for DDIs (Box 2). Patients seen by psychiatrists, for example, are six times more likely than patients seen by primary care physicians to be taking multiple medications.6
Polypharmacy increases the risk of adverse events, nonadherence, medication errors, and drug interactions.7 FDA’s MedWatch Web site lists more than 630 DDI warnings.8 The more medications a patient is taking, the greater the risk for detrimental DDIs and cumulative toxicity,9 which often lead to DDI-induced AEs.10
A study of DDIs in 5,125 mostly older outpatients11 found that:
- 1,594 (31%) had at least one interacting drug combination (average 1.6)
- subjects with one or more DDIs were taking an average 8.1 drugs, compared with 5.2 drugs in those without DDIs—a significant difference
- 155 (3%) had interactions of “major clinical significance.”
- Although drug interactions are responsible for only 3.8% of emergency department visits, patients with DDIs are usually admitted to the hospital.13
- Preventable drug interactions cause approximately one-third of all AEs in hospitalized patients and account for one-half of all AE costs.14
Symptom-based prescribing. Patients with psychiatric illness are often prescribed >1 medication to manage symptoms and signs, rather than a single medication targeting a specific psychiatric disorder.
Multiple prescribers. Patients with anxiety and depressive disorders may see multiple providers, which increases the risk for polypharmacy, drug-drug interactions, and adverse events.
Medical comorbidity. Persons with psychiatric illness are at increased risk for concomitant medical illness, and persons with medical illness are at increased risk for psychiatric illness.
Psychiatric comorbidity. Persons with one psychiatric illness are at increased risk for other psychiatric illnesses.
Source: Adapted from reference 6.
HOW TO MINIMIZE DDI RISK
Use the acronym “LISTEN” (Table 1) to minimize DDI risk in patients taking combination therapies.16 The 6 steps in LISTEN can help you determine which drug or drugs you may discontinue before adding another.
We also recommend that you monitor therapeutic and toxic effects by checking serum drug levels, especially for drugs with a low therapeutic index. Lithium, for example, requires close mentoring of plasma concentration every 2 to 6 months and during dosage adjustments to avoid toxicity.17 Therapeutic drug monitoring has been shown to prevent adverse events from DDIs.16 For added safety, encourage patents to purchase all medications at one pharmacy and to enroll in that pharmacy’s DDI monitoring program.18
Keep in mind that systemic conditions may require a dosage change:
- Increased volume of distribution, as in patients who gain weight or total water volume, requires higher doses to maintain a constant therapeutic effect.
- Reduced clearance, as in patients with decreased renal or hepatic function, will likely require lower doses to prevent toxicity.19
LISTEN: 6 tips to minimize DDI risk
| L | Listeach drug’s name and dosage in the patient’s chart and in a note given to the patient. |
| I | Each drug should have a clear indication and well-defined therapeutic goal; discontinue any drug not achieving its goal |
| S | Make the regimen as simple as possible, with once- or twice-daily dosing. |
| T | When possible, treat multiple symptoms with a single drug, rather than multiple symptoms with multiple drugs |
| E | Educatepatients about polypharmacy, DDIs, and adverse events; assess all medications—including vitamins, minerals, herbs, dietary supplements, nonprescription products—and address potential DDIs |
| N | Avoid prescribing medications with a narrow therapeutic window. |
DDIsWITH MOOD STABILIZERS
Diagnoses of schizophrenia, anxiety disorders, and affective disorders are major risk factors for polypharmacy.20 DDIs are a particular concern in patients with bipolar disorder, given their complex treatment regimens.21
Interactions occur with the most commonly prescribed bipolar medications, including lithium and anticonvulsants (Table 2).17.21-25 Although atypical antipsychotics are also considered mood stabilizers in bipolar disorder, we will discuss their potential DDIs in a future article.
Table 2
Some drug-drug interactions with mood stabilizers
| Mood stabilizer | Drug interactions |
|---|---|
| Carbamazepine | ↑plasma clomipramine, phenytoin, primidone |
| ↑risk of neurotoxic side effects and confusional states with lithium | |
| Alters thyroid function with anticonvulsants | |
| ↓anticoagulant concentrations and↑bleeding risk | |
| ↓oral contraceptive reliability; can cause false-negative pregnancy tests | |
| ↑metabolism and may ↓efficacy of cancer chemotherapy (docetaxel, estrogens, paclitaxel, progesterone, cyclophosphamide) | |
| ↑aprepitant, granisetron metabolism and ↓efficacy | |
| ↑glipizide, tolbutamide metabolism | |
| Lithium | NSAIDs (ibuprofen, indomethacin, piroxicam) and COX-2 inhibitors ↑plasma lithium |
| ACE inhibitors ↑plasma lithium | |
| Calcium channel blockers and carbamazepine ↑lithium neurotoxicity | |
| SSRIs ↑diarrhea, confusion, tremor, dizziness, and agitation | |
| Acetazolamide, urea, xanthine preparations, alkalinizing agents such as sodium bicarbonate ↓plasma lithium | |
| Metronidazole ↑lithium toxicity | |
| Encephalopathic syndrome possible with haloperidol | |
| Lamotrigine | ↑concentration of carbamazepine’s epoxide metabolite |
| Carbamazepine, phenytoin, phenobarbital ↓plasma lamotrigine 40% to 50% | |
| ↑plasma sertraline | |
| ↓plasma valproic acid 25%; valproic acid doubles plasma lamotrigine and ↑rash risk | |
| Topiramate | ↑valproic acid concentrations 11%; valproic acid ↓plasma topiramate 14% |
| ↑plasma phenytoin up to 25%; phenytoin, carbamazepine ↓plasma topiramate by 40% to 48% | |
| ↓digoxin bioavailability | |
| ↓oral contraceptive efficacy | |
| Valproic acid | ↑plasma phenobarbital, primidone |
| ↓phenytoin clearance, volume distribution and ↑breakthrough seizure risk | |
| ↑serum concentration of antiepileptics, such as lamotrigine; absence status possible with clonazepam | |
| ↑= Increases ↓= Decreases | |
| ACE = angiotensin-converting enzyme; COX = cyclooxygenase | |
| NSAIDs = nonsteroidal anti-inflammatory drugs; SSRIs = selective serotonin reuptake inhibitors | |
| Source: References 17, 21-25 | |
LITHIUM: TOXICITY RISK
Lithium is excreted via the kidneys, so be cautious when using lithium in patients taking diuretics.17,22 Drugs that can lower serum lithium concentrations by increasing urinary lithium excretion include acetazolamide, urea, xanthine preparations, and alkalinizing agents such as sodium bicarbonate.17
Combining lithium with selective serotonin reuptake inhibitors can cause diarrhea, confusion, tremor, dizziness, and agitation.17 An encephalopathic syndrome has occurred in a few patients treated with lithium plus haloperidol.
Monitor lithium levels closely when bipolar patients start or stop nonsteroidal anti-inflammatory drugs (NSAIDs). Nonprescription ibuprofen can cause serious and even life-threatening serum lithium elevations by affecting lithium’s rate of tubular reabsorption.26 Indomethacin, piroxicam, and selective cyclooxygenase-2 (COX-2) inhibitors also increase plasma lithium concentrations.25
For patients taking lithium with heart drugs, angiotensin-converting enzyme (ACE) inhibitors may increase plasma lithium levels,17 and calcium channel blockers may increase the neurotoxicity risk.17,22 Using the anti-infective metronidazole with lithium may provoke lithium toxicity.
VALPROIC ACID: MONITOR CLEARANCE
Drugs that affect the expression of hepatic enzymes—especially glucuronosyltransferase—may increase clearance of valproic acid and its derivatives. Phenytoin, carbamazepine, or phenobarbital, for example, can double valproic acid clearance.
On the other hand, drugs that inhibit CYP-450 (such as antidepressants) have little effect on valproic acid concentration. Valproate can decrease plasma clearance of amitriptyline, so consider monitoring this tricyclic’s blood levels in patients also taking valproate.17
Because valproic acid can increase serum phenobarbital, monitor barbiturate concentrations when using these two drugs. A similar interaction occurs with primidone, which is metabolized into a barbiturate. Breakthrough seizures may occur with phenytoin, as valproic acid can reduce phenytoin clearance and apparent volume distribution by 25%.22
Using valproic acid with clonazepam may produce absence status in patients with a history of absence-type seizures.17 Valproic acid also displaces diazepam from its plasma albumin binding sites and inhibits its metabolism.
Concomitant use of valproic acid can increase serum concentrations of other antiepileptic drugs. For example, lamotrigine levels may double,24 and felbamate’s peak concentration may increase and require dosage reduction. Valproic acid may also interact with nonpsychiatric medications:
- Subtherapeutic valproic acid levels have been reported when co-administered with the antibiotic meropenem.
- In patients with HIV infection, valproic acid can decrease clearance of the antiretroviral zidovudine by 38%.
- Patients receiving rifampin for tuberculosis may need a dosage adjustment, as oral rifampin’s clearance can increase 40% with concomitant valproic acid.
CARBAMAZEPINE: SELF-INDUCER
Metabolized by CYP 3A4, carbamazepine may induce its own metabolism as well as the CYP 3A4 isoenzyme. Therefore inhibitors and inducers of CYP 3A4 may affect carbamazepine plasma levels.
Carbamazepine can increase plasma levels of other psychotropics including clomipramine, phenytoin, and primidone.17,22 When used with lithium, it may increase the risk of neurotoxic side effects and confusion.23 It can alter thyroid function when used with other anticonvulsants.
For bipolar patients with diabetes, carbamazepine can cause hyperglycemia by inducing the metabolism of oral sulfonylureas such as glipizide and tolbutamide. In women, carbamazepine decreases the reliability of oral contraceptives17 and can cause false-negative pregnancy tests.24
For cancer patients, concurrent carbamazepine may induce metabolism of chemotherapy drugs such as docetaxel, estrogens, paclitaxel, progesterone, and cyclophosphamide, decreasing their efficacy.21 It can increase metabolism of aprepitant and granisetron—used to treat chemotherapy-related nausea—reducing plasma concentrations and possibly efficacy. Carbamazepine’s additive dopamine blockade can increase the risk of extrapyramidal symptoms when used with docetaxel or the antiemetic/antivertigo agents chlorpromazine, metoclopramide, or prochlorperazine.
Carbamazepine increases elimination of some cardiovascular drugs and may decrease the effect of antiarrhythmics such as lidocaine and quinidine; calcium channel blockers such as amlodipine, nifedipine, felodipine, nisoldipine, diltiazem, and verapamil; the beta blocker propranolol; and the vasodilator bosetan.21 Carbamazepine also reduces anticoagulant concentrations, and breakthrough bleeding has been reported.
(See "Out of the Pipeline−extended−release carbamazepine" for a listing of drugs that interact with this agent.)
OTHER ANTICONVULSANTS
Lamotrigine. Some concomitant CNS medications—such as carbamazepine, phenytoin or phenobarbital—reduce lamotrigine serum concentrations by as much as 50%.17 This substantial reduction may give the impression that the patient is not responding to therapeutic lamotrigine doses.
Patients taking lamotrigine with carbamazepine may be at greater risk for dizziness, diplopia, ataxia, and blurred vision because of increased serum concentration of carbamazepine’s epoxide metabolite. Valproic acid doubles lamotrigine serum concentration and increases the risk of rash, whereas lamotrigine decreases valproic acid concentration by 25%.17 Lamotrigine’s manufacturer offers special starting kits for patients taking carbamazepine or valproic acid.
Sertraline increases plasma lamotrigine concentration—but to a lesser extent than does valproic acid17 —and no dosage adjustment is needed.
Topiramate. Concomitant carbamazepine or phenytoin reduces topiramate concentration by 40% to 48%, whereas topiramate increases phenytoin concentration up to 25%. Similarly, valproic acid reduces topiramate’s concentration by 14%, while at the same time valproic acid concentration increases by 11%.17
Topiramate slightly decreases digoxin’s bioavailability and the efficacy of estrogenic oral contraceptives.17,22
Related resources
- Cytochrome P-450 interaction checker. www.drug-interaction.com.
- FDA-reported drug-drug interactions. http://vm.cfsan.fda.gov/~lrd/fdinter.html.
- Psychiatric drug interactions. www.preskorn.com.
- FDA definitions Adverse event: http://www.fda.gov/cder/guidance/iche2a.pdf. Serious adverse event: http://www.fda.gov/medwatch/report/DESK/advevnt.htm.
- Aprepitant • Emend
- Bosentan • Tracleer
- Carbamazepine • Tegretol, others
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil, others
- Clonazepam • Klonopin
- Cyclophosphamide • Cytoxan, Neosar
- Diazepam • Valium
- Diltiazem • Cardizem, others
- Docetaxel • Taxotere
- Felbamate • Felbatol
- Felodipine • Plendil
- Granisetron • Kytril
- Glipizide • Glucotrol
- Haloperidol • Haldol
- Indomethacin • Indocin
- Lamotrigine • Lamictal
- Meropenem • Merrem
- Metoclopramide • Reglan
- Metronidazole • Flagyl
- Nifedipine • Adalat, Procardia
- Nisoldipine • Sular
- Paclitaxel • Taxol, others
- Phenobarbital • Solfoton
- Phenytoin • Dilantin
- Piroxicam • Feldene
- Primidone • Mysoline
- Prochlorperazine • Compazine
- Propranolol • Inderal
- Rifampin • Rifadin
- Sertraline • Zoloft
- Tolbutamide • Orinase
- Topiramate • Topamax
- Valproic acid • Depakote
- Verapamil • Calan, others
- Zidovudine • Retrovir
Dr. Ramadan and Dr. Werder report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Preskorn has received grants or has been a consultant or speaker for Abbott Laboratories, AstraZeneca, Boehringer-Ingelheim, Bristol-Myers Squibb Co., Merck & Co., Eisai Inc., Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, Johnson & Johnson, Novartis Pharmaceuticals, Organon, Otsuka America Pharmaceutical Inc., Pfizer Inc., Solvay Pharmaceuticals, Sanofi-Aventis, and Wyeth.
1. Langdorf MI, Fox JC, Marwah RS, et al. Physician versus computer knowledge of potential drug interactions in the emergency department. Acad Emerg Med 2000;7:1321-9.
2. Lazarou J, Pomeranz BH, Cory PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA 1998;279(15):1200-5.
3. Incalzi RA, Gemma A, Capparella O, et al. Predicting mortality and length of stay of geriatric patients in an acute care general hospital. J Gerontol 1992;47(2):M35-9.
4. Preskorn SH. Fatal drug-drug interaction as a differential consideration in apparent suicide. J Psychiatr Pract 2002;8(4):233-8.
5. Peterson JF, Bates D. Preventable medication errors: identifying and eliminating serious drug interactions. J Am Pharm Assoc (Wash) 2001;41(2):159-60.
6. Nichol MB, Stimmel GL, Lange SC. Factors predicting the use of multiple psychotropic medications. J Clin Psychiatry 1995;2:60-6.
7. Ananth J, Parameswaran S, Gunatilake S. Antipsychotic polypharmacy. Curr Pharm Des 2004;10(18):2231-8.
8. Medwatch Web site. Food and Drug Administration. Search for Drug-drug interactions. Available at: http://www.fda.gov/med-watch/index.html. Accessed March 31, 2005.
9. Rascati K. Drug utilization review of concomitant use of specific serotonin reuptake inhibitors or clomipramine and antianxiety/sleep medications. Clin Ther 1995;17:786-90.
10. Tanaka E, Hisawa S. Clinically significant pharmacokinetic drug interactions with psychoactive drugs: antidepressants and antipsychotics and the cytochrome P450 system. J Clin Pharm Ther 1999;24:7-16.
11. Bergendal L, Friberg A, Schaffrath A. Potential drug-drug interactions in 5,125 mostly elderly outpatients in Gothenburg, Sweden. Pharm World Sci 1995;17(5):152-7.
12. De Las Cuevas C, Sanz EJ. Polypharmacy in psychiatric practice in the Canary Islands. BMC Psychiatry 2004;4(1):18.-
13. Raschetti R, Morgutti M, Menniti Ippolito F, et al. Suspected adverse drug events requiring emergency department visits or hospital admissions. Eur J Clin Pharmacol 1999;54:959-63.
14. Bates DW, Spell N, Cullen DJ, et al. The costs of adverse drug events in hospitalized patients. JAMA 1997;277:307-11.
15. Frye MA, Ketter TA, Leverich GS, et al. The increasing use of polypharmacotherapy for refractory mood disorders: 22 years of study. J Clin Psychiatry 2000;1:9-15.
16. Werder SF, Preskorn SH. Managing polypharmacy: walking the fine line between help and harm. Current Psychiatry 2003;2(2):24-36.
17. Physicians’ Desk Reference (59th ed). Montvale, NJ: Thomson PDR; 2005.
18. Sandson NB. Exploring drug interaction in psychiatry. Psychiatric times 2004;May:42-8.
19. Todi SK, Hartmann RA. Pharmacologic principles. In: Civetta JM, Taylor RW, Kirby RR, (eds). Critical care (3rd ed). Philadelphia: Lippincott-Raven Publishers; 1997;485-8.
20. Shapiro LE, Shear NH. Drug interactions: Proteins, pumps, and P-450s. J Am Acad Dermatol 2002;47:467-84.
21. Keck PE, Jr, Dewan N, Nasrallah HA. Bipolar disorder: the clinician’s guide to pharmacotherapy for patients with co-occurring medical conditions. Current Psychiatry 2005;4(Feb)(suppl):1-51.
22. Sadock BJ, Sadock VA. Kaplan and Sadock’s pocket handbook of psychiatric drug treatment (3rd ed). Philadelphia: Lippincott Williams & Wilkins; 2001;144-5,178-83,256-7.
23. Shukla S, Godwin CD, Long LE, Miller MG. Lithium-carbamazepine neurotoxicity and risk factors. Am J Psychiatry 1984;141:1604-6.
24. Licht RW, Vestergaard P, Kessing LV, et al. Psychopharmacological treatment with lithium and antiepileptic drugs: suggested guidelines from the Danish Psychiatric Association and the Child and Adolescent Psychiatric Association in Denmark. Acta Psychiatr Scand Suppl 2003;(419):1-22.
25. Phelan KM, Mosholder AD, Lu S. Lithium interaction with the cyclooxygenase 2 inhibitors rofecoxib and celecoxib and other nonsteroidal anti-inflammatory drugs. J Clin Psychiatry 2003;64:1328-34.
26. Ragheb M, Ban TA, Buchanan D, Frolich JC. Interaction of indomethacin and ibuprofen with lithium in manic patients under steady-state lithium level. J Clin Psychiatry 1980;11:397-8.
Drug-drug interactions (DDIs) can be viewed as physiologic combat wherein a “perpetrator” drug affects a “victim” drug’s pharmacokinetics or pharmacodynamics. Your challenge is to deter that interaction in patients taking two or more medications.
This article—first in a series—discusses polypharmacy risk factors that increase the likelihood of detrimental DDIs, then focuses on DDIs in patients taking mood stabilizers for bipolar disorder. We also offer practical tips to reduce DDI risk. Future articles will discuss DDI risks with antidepressants, antipsychotics, and anxiolytics.
To predict DDIs, you need to know psychotropics’ mechanism of action, metabolism, and effects on cytochrome P-450 (CYP) enzymes. Our discussion is not exhaustive because the data base is massive and new interactions continue to be discovered. Our aim is to equip you to anticipate and prevent DDIs when prescribing.
WHAT ARE ADVERSE DDIs?
An adverse event (AE) is any undesirable experience that occurs when a patient uses a medical product, whether or not the product caused the event. The FDA says an “undesirable experience” may be:
- an unfavorable and unintended symptom or sign
- an abnormal lab or radiographic finding
- a disease that is temporarily associated with the medical product.
An AE becomes “serious” (an SAE) when its duration, intensity, and/or frequency leads to death, a life-threatening condition, initial or prolonged hospitalization, disability, or congenital anomaly. Reporting is voluntary, but we strongly recommend that you report all SAEs to the FDA.
These definitions can help you confirm that a patient has experienced an SAE, but the task becomes more complicated when you try to attribute an SAE to a drug interaction. In the absence of an FDA definition, we assert that DDIs are responsible for SAEs when a perpetrator drug affects the pharmacokinetics or pharmacodynamics of a victim drug and exacerbates a known untoward event of the victim drug (Box 1).1-5 Which drug is the perpetrator and which is the victim is not always clear, and sometimes a medication—such as carbamazepine—can be both at once.
More than 100,000 possible detrimental DDIs have been documented in medical literature and pharmaceutical company data. This number is likely to grow with increased scrutiny, as
DDIs cause morbidity, mortality, and increased health care costs. More than 106,000 Americans die each year from properly prescribed, correctly taken medications. Polypharmacy is associated with extended hospital stays, and using >6 drugs is an independent predictor of death. DDIs contribute to the cause of death in acute overdoses and can be responsible for false-positive suicide diagnoses.
In clinical practice, DDI-associated toxicity may be mistaken for a new disease process, or a disease may be incorrectly perceived as progressing when a medication is rendered ineffective.
Source: References 1-5
RISKS OF POLYPHARMACY
Individuals with psychiatric illnesses are at particular risk for DDIs (Box 2). Patients seen by psychiatrists, for example, are six times more likely than patients seen by primary care physicians to be taking multiple medications.6
Polypharmacy increases the risk of adverse events, nonadherence, medication errors, and drug interactions.7 FDA’s MedWatch Web site lists more than 630 DDI warnings.8 The more medications a patient is taking, the greater the risk for detrimental DDIs and cumulative toxicity,9 which often lead to DDI-induced AEs.10
A study of DDIs in 5,125 mostly older outpatients11 found that:
- 1,594 (31%) had at least one interacting drug combination (average 1.6)
- subjects with one or more DDIs were taking an average 8.1 drugs, compared with 5.2 drugs in those without DDIs—a significant difference
- 155 (3%) had interactions of “major clinical significance.”
- Although drug interactions are responsible for only 3.8% of emergency department visits, patients with DDIs are usually admitted to the hospital.13
- Preventable drug interactions cause approximately one-third of all AEs in hospitalized patients and account for one-half of all AE costs.14
Symptom-based prescribing. Patients with psychiatric illness are often prescribed >1 medication to manage symptoms and signs, rather than a single medication targeting a specific psychiatric disorder.
Multiple prescribers. Patients with anxiety and depressive disorders may see multiple providers, which increases the risk for polypharmacy, drug-drug interactions, and adverse events.
Medical comorbidity. Persons with psychiatric illness are at increased risk for concomitant medical illness, and persons with medical illness are at increased risk for psychiatric illness.
Psychiatric comorbidity. Persons with one psychiatric illness are at increased risk for other psychiatric illnesses.
Source: Adapted from reference 6.
HOW TO MINIMIZE DDI RISK
Use the acronym “LISTEN” (Table 1) to minimize DDI risk in patients taking combination therapies.16 The 6 steps in LISTEN can help you determine which drug or drugs you may discontinue before adding another.
We also recommend that you monitor therapeutic and toxic effects by checking serum drug levels, especially for drugs with a low therapeutic index. Lithium, for example, requires close mentoring of plasma concentration every 2 to 6 months and during dosage adjustments to avoid toxicity.17 Therapeutic drug monitoring has been shown to prevent adverse events from DDIs.16 For added safety, encourage patents to purchase all medications at one pharmacy and to enroll in that pharmacy’s DDI monitoring program.18
Keep in mind that systemic conditions may require a dosage change:
- Increased volume of distribution, as in patients who gain weight or total water volume, requires higher doses to maintain a constant therapeutic effect.
- Reduced clearance, as in patients with decreased renal or hepatic function, will likely require lower doses to prevent toxicity.19
LISTEN: 6 tips to minimize DDI risk
| L | Listeach drug’s name and dosage in the patient’s chart and in a note given to the patient. |
| I | Each drug should have a clear indication and well-defined therapeutic goal; discontinue any drug not achieving its goal |
| S | Make the regimen as simple as possible, with once- or twice-daily dosing. |
| T | When possible, treat multiple symptoms with a single drug, rather than multiple symptoms with multiple drugs |
| E | Educatepatients about polypharmacy, DDIs, and adverse events; assess all medications—including vitamins, minerals, herbs, dietary supplements, nonprescription products—and address potential DDIs |
| N | Avoid prescribing medications with a narrow therapeutic window. |
DDIsWITH MOOD STABILIZERS
Diagnoses of schizophrenia, anxiety disorders, and affective disorders are major risk factors for polypharmacy.20 DDIs are a particular concern in patients with bipolar disorder, given their complex treatment regimens.21
Interactions occur with the most commonly prescribed bipolar medications, including lithium and anticonvulsants (Table 2).17.21-25 Although atypical antipsychotics are also considered mood stabilizers in bipolar disorder, we will discuss their potential DDIs in a future article.
Table 2
Some drug-drug interactions with mood stabilizers
| Mood stabilizer | Drug interactions |
|---|---|
| Carbamazepine | ↑plasma clomipramine, phenytoin, primidone |
| ↑risk of neurotoxic side effects and confusional states with lithium | |
| Alters thyroid function with anticonvulsants | |
| ↓anticoagulant concentrations and↑bleeding risk | |
| ↓oral contraceptive reliability; can cause false-negative pregnancy tests | |
| ↑metabolism and may ↓efficacy of cancer chemotherapy (docetaxel, estrogens, paclitaxel, progesterone, cyclophosphamide) | |
| ↑aprepitant, granisetron metabolism and ↓efficacy | |
| ↑glipizide, tolbutamide metabolism | |
| Lithium | NSAIDs (ibuprofen, indomethacin, piroxicam) and COX-2 inhibitors ↑plasma lithium |
| ACE inhibitors ↑plasma lithium | |
| Calcium channel blockers and carbamazepine ↑lithium neurotoxicity | |
| SSRIs ↑diarrhea, confusion, tremor, dizziness, and agitation | |
| Acetazolamide, urea, xanthine preparations, alkalinizing agents such as sodium bicarbonate ↓plasma lithium | |
| Metronidazole ↑lithium toxicity | |
| Encephalopathic syndrome possible with haloperidol | |
| Lamotrigine | ↑concentration of carbamazepine’s epoxide metabolite |
| Carbamazepine, phenytoin, phenobarbital ↓plasma lamotrigine 40% to 50% | |
| ↑plasma sertraline | |
| ↓plasma valproic acid 25%; valproic acid doubles plasma lamotrigine and ↑rash risk | |
| Topiramate | ↑valproic acid concentrations 11%; valproic acid ↓plasma topiramate 14% |
| ↑plasma phenytoin up to 25%; phenytoin, carbamazepine ↓plasma topiramate by 40% to 48% | |
| ↓digoxin bioavailability | |
| ↓oral contraceptive efficacy | |
| Valproic acid | ↑plasma phenobarbital, primidone |
| ↓phenytoin clearance, volume distribution and ↑breakthrough seizure risk | |
| ↑serum concentration of antiepileptics, such as lamotrigine; absence status possible with clonazepam | |
| ↑= Increases ↓= Decreases | |
| ACE = angiotensin-converting enzyme; COX = cyclooxygenase | |
| NSAIDs = nonsteroidal anti-inflammatory drugs; SSRIs = selective serotonin reuptake inhibitors | |
| Source: References 17, 21-25 | |
LITHIUM: TOXICITY RISK
Lithium is excreted via the kidneys, so be cautious when using lithium in patients taking diuretics.17,22 Drugs that can lower serum lithium concentrations by increasing urinary lithium excretion include acetazolamide, urea, xanthine preparations, and alkalinizing agents such as sodium bicarbonate.17
Combining lithium with selective serotonin reuptake inhibitors can cause diarrhea, confusion, tremor, dizziness, and agitation.17 An encephalopathic syndrome has occurred in a few patients treated with lithium plus haloperidol.
Monitor lithium levels closely when bipolar patients start or stop nonsteroidal anti-inflammatory drugs (NSAIDs). Nonprescription ibuprofen can cause serious and even life-threatening serum lithium elevations by affecting lithium’s rate of tubular reabsorption.26 Indomethacin, piroxicam, and selective cyclooxygenase-2 (COX-2) inhibitors also increase plasma lithium concentrations.25
For patients taking lithium with heart drugs, angiotensin-converting enzyme (ACE) inhibitors may increase plasma lithium levels,17 and calcium channel blockers may increase the neurotoxicity risk.17,22 Using the anti-infective metronidazole with lithium may provoke lithium toxicity.
VALPROIC ACID: MONITOR CLEARANCE
Drugs that affect the expression of hepatic enzymes—especially glucuronosyltransferase—may increase clearance of valproic acid and its derivatives. Phenytoin, carbamazepine, or phenobarbital, for example, can double valproic acid clearance.
On the other hand, drugs that inhibit CYP-450 (such as antidepressants) have little effect on valproic acid concentration. Valproate can decrease plasma clearance of amitriptyline, so consider monitoring this tricyclic’s blood levels in patients also taking valproate.17
Because valproic acid can increase serum phenobarbital, monitor barbiturate concentrations when using these two drugs. A similar interaction occurs with primidone, which is metabolized into a barbiturate. Breakthrough seizures may occur with phenytoin, as valproic acid can reduce phenytoin clearance and apparent volume distribution by 25%.22
Using valproic acid with clonazepam may produce absence status in patients with a history of absence-type seizures.17 Valproic acid also displaces diazepam from its plasma albumin binding sites and inhibits its metabolism.
Concomitant use of valproic acid can increase serum concentrations of other antiepileptic drugs. For example, lamotrigine levels may double,24 and felbamate’s peak concentration may increase and require dosage reduction. Valproic acid may also interact with nonpsychiatric medications:
- Subtherapeutic valproic acid levels have been reported when co-administered with the antibiotic meropenem.
- In patients with HIV infection, valproic acid can decrease clearance of the antiretroviral zidovudine by 38%.
- Patients receiving rifampin for tuberculosis may need a dosage adjustment, as oral rifampin’s clearance can increase 40% with concomitant valproic acid.
CARBAMAZEPINE: SELF-INDUCER
Metabolized by CYP 3A4, carbamazepine may induce its own metabolism as well as the CYP 3A4 isoenzyme. Therefore inhibitors and inducers of CYP 3A4 may affect carbamazepine plasma levels.
Carbamazepine can increase plasma levels of other psychotropics including clomipramine, phenytoin, and primidone.17,22 When used with lithium, it may increase the risk of neurotoxic side effects and confusion.23 It can alter thyroid function when used with other anticonvulsants.
For bipolar patients with diabetes, carbamazepine can cause hyperglycemia by inducing the metabolism of oral sulfonylureas such as glipizide and tolbutamide. In women, carbamazepine decreases the reliability of oral contraceptives17 and can cause false-negative pregnancy tests.24
For cancer patients, concurrent carbamazepine may induce metabolism of chemotherapy drugs such as docetaxel, estrogens, paclitaxel, progesterone, and cyclophosphamide, decreasing their efficacy.21 It can increase metabolism of aprepitant and granisetron—used to treat chemotherapy-related nausea—reducing plasma concentrations and possibly efficacy. Carbamazepine’s additive dopamine blockade can increase the risk of extrapyramidal symptoms when used with docetaxel or the antiemetic/antivertigo agents chlorpromazine, metoclopramide, or prochlorperazine.
Carbamazepine increases elimination of some cardiovascular drugs and may decrease the effect of antiarrhythmics such as lidocaine and quinidine; calcium channel blockers such as amlodipine, nifedipine, felodipine, nisoldipine, diltiazem, and verapamil; the beta blocker propranolol; and the vasodilator bosetan.21 Carbamazepine also reduces anticoagulant concentrations, and breakthrough bleeding has been reported.
(See "Out of the Pipeline−extended−release carbamazepine" for a listing of drugs that interact with this agent.)
OTHER ANTICONVULSANTS
Lamotrigine. Some concomitant CNS medications—such as carbamazepine, phenytoin or phenobarbital—reduce lamotrigine serum concentrations by as much as 50%.17 This substantial reduction may give the impression that the patient is not responding to therapeutic lamotrigine doses.
Patients taking lamotrigine with carbamazepine may be at greater risk for dizziness, diplopia, ataxia, and blurred vision because of increased serum concentration of carbamazepine’s epoxide metabolite. Valproic acid doubles lamotrigine serum concentration and increases the risk of rash, whereas lamotrigine decreases valproic acid concentration by 25%.17 Lamotrigine’s manufacturer offers special starting kits for patients taking carbamazepine or valproic acid.
Sertraline increases plasma lamotrigine concentration—but to a lesser extent than does valproic acid17 —and no dosage adjustment is needed.
Topiramate. Concomitant carbamazepine or phenytoin reduces topiramate concentration by 40% to 48%, whereas topiramate increases phenytoin concentration up to 25%. Similarly, valproic acid reduces topiramate’s concentration by 14%, while at the same time valproic acid concentration increases by 11%.17
Topiramate slightly decreases digoxin’s bioavailability and the efficacy of estrogenic oral contraceptives.17,22
Related resources
- Cytochrome P-450 interaction checker. www.drug-interaction.com.
- FDA-reported drug-drug interactions. http://vm.cfsan.fda.gov/~lrd/fdinter.html.
- Psychiatric drug interactions. www.preskorn.com.
- FDA definitions Adverse event: http://www.fda.gov/cder/guidance/iche2a.pdf. Serious adverse event: http://www.fda.gov/medwatch/report/DESK/advevnt.htm.
- Aprepitant • Emend
- Bosentan • Tracleer
- Carbamazepine • Tegretol, others
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil, others
- Clonazepam • Klonopin
- Cyclophosphamide • Cytoxan, Neosar
- Diazepam • Valium
- Diltiazem • Cardizem, others
- Docetaxel • Taxotere
- Felbamate • Felbatol
- Felodipine • Plendil
- Granisetron • Kytril
- Glipizide • Glucotrol
- Haloperidol • Haldol
- Indomethacin • Indocin
- Lamotrigine • Lamictal
- Meropenem • Merrem
- Metoclopramide • Reglan
- Metronidazole • Flagyl
- Nifedipine • Adalat, Procardia
- Nisoldipine • Sular
- Paclitaxel • Taxol, others
- Phenobarbital • Solfoton
- Phenytoin • Dilantin
- Piroxicam • Feldene
- Primidone • Mysoline
- Prochlorperazine • Compazine
- Propranolol • Inderal
- Rifampin • Rifadin
- Sertraline • Zoloft
- Tolbutamide • Orinase
- Topiramate • Topamax
- Valproic acid • Depakote
- Verapamil • Calan, others
- Zidovudine • Retrovir
Dr. Ramadan and Dr. Werder report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Preskorn has received grants or has been a consultant or speaker for Abbott Laboratories, AstraZeneca, Boehringer-Ingelheim, Bristol-Myers Squibb Co., Merck & Co., Eisai Inc., Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, Johnson & Johnson, Novartis Pharmaceuticals, Organon, Otsuka America Pharmaceutical Inc., Pfizer Inc., Solvay Pharmaceuticals, Sanofi-Aventis, and Wyeth.
Drug-drug interactions (DDIs) can be viewed as physiologic combat wherein a “perpetrator” drug affects a “victim” drug’s pharmacokinetics or pharmacodynamics. Your challenge is to deter that interaction in patients taking two or more medications.
This article—first in a series—discusses polypharmacy risk factors that increase the likelihood of detrimental DDIs, then focuses on DDIs in patients taking mood stabilizers for bipolar disorder. We also offer practical tips to reduce DDI risk. Future articles will discuss DDI risks with antidepressants, antipsychotics, and anxiolytics.
To predict DDIs, you need to know psychotropics’ mechanism of action, metabolism, and effects on cytochrome P-450 (CYP) enzymes. Our discussion is not exhaustive because the data base is massive and new interactions continue to be discovered. Our aim is to equip you to anticipate and prevent DDIs when prescribing.
WHAT ARE ADVERSE DDIs?
An adverse event (AE) is any undesirable experience that occurs when a patient uses a medical product, whether or not the product caused the event. The FDA says an “undesirable experience” may be:
- an unfavorable and unintended symptom or sign
- an abnormal lab or radiographic finding
- a disease that is temporarily associated with the medical product.
An AE becomes “serious” (an SAE) when its duration, intensity, and/or frequency leads to death, a life-threatening condition, initial or prolonged hospitalization, disability, or congenital anomaly. Reporting is voluntary, but we strongly recommend that you report all SAEs to the FDA.
These definitions can help you confirm that a patient has experienced an SAE, but the task becomes more complicated when you try to attribute an SAE to a drug interaction. In the absence of an FDA definition, we assert that DDIs are responsible for SAEs when a perpetrator drug affects the pharmacokinetics or pharmacodynamics of a victim drug and exacerbates a known untoward event of the victim drug (Box 1).1-5 Which drug is the perpetrator and which is the victim is not always clear, and sometimes a medication—such as carbamazepine—can be both at once.
More than 100,000 possible detrimental DDIs have been documented in medical literature and pharmaceutical company data. This number is likely to grow with increased scrutiny, as
DDIs cause morbidity, mortality, and increased health care costs. More than 106,000 Americans die each year from properly prescribed, correctly taken medications. Polypharmacy is associated with extended hospital stays, and using >6 drugs is an independent predictor of death. DDIs contribute to the cause of death in acute overdoses and can be responsible for false-positive suicide diagnoses.
In clinical practice, DDI-associated toxicity may be mistaken for a new disease process, or a disease may be incorrectly perceived as progressing when a medication is rendered ineffective.
Source: References 1-5
RISKS OF POLYPHARMACY
Individuals with psychiatric illnesses are at particular risk for DDIs (Box 2). Patients seen by psychiatrists, for example, are six times more likely than patients seen by primary care physicians to be taking multiple medications.6
Polypharmacy increases the risk of adverse events, nonadherence, medication errors, and drug interactions.7 FDA’s MedWatch Web site lists more than 630 DDI warnings.8 The more medications a patient is taking, the greater the risk for detrimental DDIs and cumulative toxicity,9 which often lead to DDI-induced AEs.10
A study of DDIs in 5,125 mostly older outpatients11 found that:
- 1,594 (31%) had at least one interacting drug combination (average 1.6)
- subjects with one or more DDIs were taking an average 8.1 drugs, compared with 5.2 drugs in those without DDIs—a significant difference
- 155 (3%) had interactions of “major clinical significance.”
- Although drug interactions are responsible for only 3.8% of emergency department visits, patients with DDIs are usually admitted to the hospital.13
- Preventable drug interactions cause approximately one-third of all AEs in hospitalized patients and account for one-half of all AE costs.14
Symptom-based prescribing. Patients with psychiatric illness are often prescribed >1 medication to manage symptoms and signs, rather than a single medication targeting a specific psychiatric disorder.
Multiple prescribers. Patients with anxiety and depressive disorders may see multiple providers, which increases the risk for polypharmacy, drug-drug interactions, and adverse events.
Medical comorbidity. Persons with psychiatric illness are at increased risk for concomitant medical illness, and persons with medical illness are at increased risk for psychiatric illness.
Psychiatric comorbidity. Persons with one psychiatric illness are at increased risk for other psychiatric illnesses.
Source: Adapted from reference 6.
HOW TO MINIMIZE DDI RISK
Use the acronym “LISTEN” (Table 1) to minimize DDI risk in patients taking combination therapies.16 The 6 steps in LISTEN can help you determine which drug or drugs you may discontinue before adding another.
We also recommend that you monitor therapeutic and toxic effects by checking serum drug levels, especially for drugs with a low therapeutic index. Lithium, for example, requires close mentoring of plasma concentration every 2 to 6 months and during dosage adjustments to avoid toxicity.17 Therapeutic drug monitoring has been shown to prevent adverse events from DDIs.16 For added safety, encourage patents to purchase all medications at one pharmacy and to enroll in that pharmacy’s DDI monitoring program.18
Keep in mind that systemic conditions may require a dosage change:
- Increased volume of distribution, as in patients who gain weight or total water volume, requires higher doses to maintain a constant therapeutic effect.
- Reduced clearance, as in patients with decreased renal or hepatic function, will likely require lower doses to prevent toxicity.19
LISTEN: 6 tips to minimize DDI risk
| L | Listeach drug’s name and dosage in the patient’s chart and in a note given to the patient. |
| I | Each drug should have a clear indication and well-defined therapeutic goal; discontinue any drug not achieving its goal |
| S | Make the regimen as simple as possible, with once- or twice-daily dosing. |
| T | When possible, treat multiple symptoms with a single drug, rather than multiple symptoms with multiple drugs |
| E | Educatepatients about polypharmacy, DDIs, and adverse events; assess all medications—including vitamins, minerals, herbs, dietary supplements, nonprescription products—and address potential DDIs |
| N | Avoid prescribing medications with a narrow therapeutic window. |
DDIsWITH MOOD STABILIZERS
Diagnoses of schizophrenia, anxiety disorders, and affective disorders are major risk factors for polypharmacy.20 DDIs are a particular concern in patients with bipolar disorder, given their complex treatment regimens.21
Interactions occur with the most commonly prescribed bipolar medications, including lithium and anticonvulsants (Table 2).17.21-25 Although atypical antipsychotics are also considered mood stabilizers in bipolar disorder, we will discuss their potential DDIs in a future article.
Table 2
Some drug-drug interactions with mood stabilizers
| Mood stabilizer | Drug interactions |
|---|---|
| Carbamazepine | ↑plasma clomipramine, phenytoin, primidone |
| ↑risk of neurotoxic side effects and confusional states with lithium | |
| Alters thyroid function with anticonvulsants | |
| ↓anticoagulant concentrations and↑bleeding risk | |
| ↓oral contraceptive reliability; can cause false-negative pregnancy tests | |
| ↑metabolism and may ↓efficacy of cancer chemotherapy (docetaxel, estrogens, paclitaxel, progesterone, cyclophosphamide) | |
| ↑aprepitant, granisetron metabolism and ↓efficacy | |
| ↑glipizide, tolbutamide metabolism | |
| Lithium | NSAIDs (ibuprofen, indomethacin, piroxicam) and COX-2 inhibitors ↑plasma lithium |
| ACE inhibitors ↑plasma lithium | |
| Calcium channel blockers and carbamazepine ↑lithium neurotoxicity | |
| SSRIs ↑diarrhea, confusion, tremor, dizziness, and agitation | |
| Acetazolamide, urea, xanthine preparations, alkalinizing agents such as sodium bicarbonate ↓plasma lithium | |
| Metronidazole ↑lithium toxicity | |
| Encephalopathic syndrome possible with haloperidol | |
| Lamotrigine | ↑concentration of carbamazepine’s epoxide metabolite |
| Carbamazepine, phenytoin, phenobarbital ↓plasma lamotrigine 40% to 50% | |
| ↑plasma sertraline | |
| ↓plasma valproic acid 25%; valproic acid doubles plasma lamotrigine and ↑rash risk | |
| Topiramate | ↑valproic acid concentrations 11%; valproic acid ↓plasma topiramate 14% |
| ↑plasma phenytoin up to 25%; phenytoin, carbamazepine ↓plasma topiramate by 40% to 48% | |
| ↓digoxin bioavailability | |
| ↓oral contraceptive efficacy | |
| Valproic acid | ↑plasma phenobarbital, primidone |
| ↓phenytoin clearance, volume distribution and ↑breakthrough seizure risk | |
| ↑serum concentration of antiepileptics, such as lamotrigine; absence status possible with clonazepam | |
| ↑= Increases ↓= Decreases | |
| ACE = angiotensin-converting enzyme; COX = cyclooxygenase | |
| NSAIDs = nonsteroidal anti-inflammatory drugs; SSRIs = selective serotonin reuptake inhibitors | |
| Source: References 17, 21-25 | |
LITHIUM: TOXICITY RISK
Lithium is excreted via the kidneys, so be cautious when using lithium in patients taking diuretics.17,22 Drugs that can lower serum lithium concentrations by increasing urinary lithium excretion include acetazolamide, urea, xanthine preparations, and alkalinizing agents such as sodium bicarbonate.17
Combining lithium with selective serotonin reuptake inhibitors can cause diarrhea, confusion, tremor, dizziness, and agitation.17 An encephalopathic syndrome has occurred in a few patients treated with lithium plus haloperidol.
Monitor lithium levels closely when bipolar patients start or stop nonsteroidal anti-inflammatory drugs (NSAIDs). Nonprescription ibuprofen can cause serious and even life-threatening serum lithium elevations by affecting lithium’s rate of tubular reabsorption.26 Indomethacin, piroxicam, and selective cyclooxygenase-2 (COX-2) inhibitors also increase plasma lithium concentrations.25
For patients taking lithium with heart drugs, angiotensin-converting enzyme (ACE) inhibitors may increase plasma lithium levels,17 and calcium channel blockers may increase the neurotoxicity risk.17,22 Using the anti-infective metronidazole with lithium may provoke lithium toxicity.
VALPROIC ACID: MONITOR CLEARANCE
Drugs that affect the expression of hepatic enzymes—especially glucuronosyltransferase—may increase clearance of valproic acid and its derivatives. Phenytoin, carbamazepine, or phenobarbital, for example, can double valproic acid clearance.
On the other hand, drugs that inhibit CYP-450 (such as antidepressants) have little effect on valproic acid concentration. Valproate can decrease plasma clearance of amitriptyline, so consider monitoring this tricyclic’s blood levels in patients also taking valproate.17
Because valproic acid can increase serum phenobarbital, monitor barbiturate concentrations when using these two drugs. A similar interaction occurs with primidone, which is metabolized into a barbiturate. Breakthrough seizures may occur with phenytoin, as valproic acid can reduce phenytoin clearance and apparent volume distribution by 25%.22
Using valproic acid with clonazepam may produce absence status in patients with a history of absence-type seizures.17 Valproic acid also displaces diazepam from its plasma albumin binding sites and inhibits its metabolism.
Concomitant use of valproic acid can increase serum concentrations of other antiepileptic drugs. For example, lamotrigine levels may double,24 and felbamate’s peak concentration may increase and require dosage reduction. Valproic acid may also interact with nonpsychiatric medications:
- Subtherapeutic valproic acid levels have been reported when co-administered with the antibiotic meropenem.
- In patients with HIV infection, valproic acid can decrease clearance of the antiretroviral zidovudine by 38%.
- Patients receiving rifampin for tuberculosis may need a dosage adjustment, as oral rifampin’s clearance can increase 40% with concomitant valproic acid.
CARBAMAZEPINE: SELF-INDUCER
Metabolized by CYP 3A4, carbamazepine may induce its own metabolism as well as the CYP 3A4 isoenzyme. Therefore inhibitors and inducers of CYP 3A4 may affect carbamazepine plasma levels.
Carbamazepine can increase plasma levels of other psychotropics including clomipramine, phenytoin, and primidone.17,22 When used with lithium, it may increase the risk of neurotoxic side effects and confusion.23 It can alter thyroid function when used with other anticonvulsants.
For bipolar patients with diabetes, carbamazepine can cause hyperglycemia by inducing the metabolism of oral sulfonylureas such as glipizide and tolbutamide. In women, carbamazepine decreases the reliability of oral contraceptives17 and can cause false-negative pregnancy tests.24
For cancer patients, concurrent carbamazepine may induce metabolism of chemotherapy drugs such as docetaxel, estrogens, paclitaxel, progesterone, and cyclophosphamide, decreasing their efficacy.21 It can increase metabolism of aprepitant and granisetron—used to treat chemotherapy-related nausea—reducing plasma concentrations and possibly efficacy. Carbamazepine’s additive dopamine blockade can increase the risk of extrapyramidal symptoms when used with docetaxel or the antiemetic/antivertigo agents chlorpromazine, metoclopramide, or prochlorperazine.
Carbamazepine increases elimination of some cardiovascular drugs and may decrease the effect of antiarrhythmics such as lidocaine and quinidine; calcium channel blockers such as amlodipine, nifedipine, felodipine, nisoldipine, diltiazem, and verapamil; the beta blocker propranolol; and the vasodilator bosetan.21 Carbamazepine also reduces anticoagulant concentrations, and breakthrough bleeding has been reported.
(See "Out of the Pipeline−extended−release carbamazepine" for a listing of drugs that interact with this agent.)
OTHER ANTICONVULSANTS
Lamotrigine. Some concomitant CNS medications—such as carbamazepine, phenytoin or phenobarbital—reduce lamotrigine serum concentrations by as much as 50%.17 This substantial reduction may give the impression that the patient is not responding to therapeutic lamotrigine doses.
Patients taking lamotrigine with carbamazepine may be at greater risk for dizziness, diplopia, ataxia, and blurred vision because of increased serum concentration of carbamazepine’s epoxide metabolite. Valproic acid doubles lamotrigine serum concentration and increases the risk of rash, whereas lamotrigine decreases valproic acid concentration by 25%.17 Lamotrigine’s manufacturer offers special starting kits for patients taking carbamazepine or valproic acid.
Sertraline increases plasma lamotrigine concentration—but to a lesser extent than does valproic acid17 —and no dosage adjustment is needed.
Topiramate. Concomitant carbamazepine or phenytoin reduces topiramate concentration by 40% to 48%, whereas topiramate increases phenytoin concentration up to 25%. Similarly, valproic acid reduces topiramate’s concentration by 14%, while at the same time valproic acid concentration increases by 11%.17
Topiramate slightly decreases digoxin’s bioavailability and the efficacy of estrogenic oral contraceptives.17,22
Related resources
- Cytochrome P-450 interaction checker. www.drug-interaction.com.
- FDA-reported drug-drug interactions. http://vm.cfsan.fda.gov/~lrd/fdinter.html.
- Psychiatric drug interactions. www.preskorn.com.
- FDA definitions Adverse event: http://www.fda.gov/cder/guidance/iche2a.pdf. Serious adverse event: http://www.fda.gov/medwatch/report/DESK/advevnt.htm.
- Aprepitant • Emend
- Bosentan • Tracleer
- Carbamazepine • Tegretol, others
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil, others
- Clonazepam • Klonopin
- Cyclophosphamide • Cytoxan, Neosar
- Diazepam • Valium
- Diltiazem • Cardizem, others
- Docetaxel • Taxotere
- Felbamate • Felbatol
- Felodipine • Plendil
- Granisetron • Kytril
- Glipizide • Glucotrol
- Haloperidol • Haldol
- Indomethacin • Indocin
- Lamotrigine • Lamictal
- Meropenem • Merrem
- Metoclopramide • Reglan
- Metronidazole • Flagyl
- Nifedipine • Adalat, Procardia
- Nisoldipine • Sular
- Paclitaxel • Taxol, others
- Phenobarbital • Solfoton
- Phenytoin • Dilantin
- Piroxicam • Feldene
- Primidone • Mysoline
- Prochlorperazine • Compazine
- Propranolol • Inderal
- Rifampin • Rifadin
- Sertraline • Zoloft
- Tolbutamide • Orinase
- Topiramate • Topamax
- Valproic acid • Depakote
- Verapamil • Calan, others
- Zidovudine • Retrovir
Dr. Ramadan and Dr. Werder report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Preskorn has received grants or has been a consultant or speaker for Abbott Laboratories, AstraZeneca, Boehringer-Ingelheim, Bristol-Myers Squibb Co., Merck & Co., Eisai Inc., Eli Lilly and Co., GlaxoSmithKline, Janssen Pharmaceutica, Johnson & Johnson, Novartis Pharmaceuticals, Organon, Otsuka America Pharmaceutical Inc., Pfizer Inc., Solvay Pharmaceuticals, Sanofi-Aventis, and Wyeth.
1. Langdorf MI, Fox JC, Marwah RS, et al. Physician versus computer knowledge of potential drug interactions in the emergency department. Acad Emerg Med 2000;7:1321-9.
2. Lazarou J, Pomeranz BH, Cory PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA 1998;279(15):1200-5.
3. Incalzi RA, Gemma A, Capparella O, et al. Predicting mortality and length of stay of geriatric patients in an acute care general hospital. J Gerontol 1992;47(2):M35-9.
4. Preskorn SH. Fatal drug-drug interaction as a differential consideration in apparent suicide. J Psychiatr Pract 2002;8(4):233-8.
5. Peterson JF, Bates D. Preventable medication errors: identifying and eliminating serious drug interactions. J Am Pharm Assoc (Wash) 2001;41(2):159-60.
6. Nichol MB, Stimmel GL, Lange SC. Factors predicting the use of multiple psychotropic medications. J Clin Psychiatry 1995;2:60-6.
7. Ananth J, Parameswaran S, Gunatilake S. Antipsychotic polypharmacy. Curr Pharm Des 2004;10(18):2231-8.
8. Medwatch Web site. Food and Drug Administration. Search for Drug-drug interactions. Available at: http://www.fda.gov/med-watch/index.html. Accessed March 31, 2005.
9. Rascati K. Drug utilization review of concomitant use of specific serotonin reuptake inhibitors or clomipramine and antianxiety/sleep medications. Clin Ther 1995;17:786-90.
10. Tanaka E, Hisawa S. Clinically significant pharmacokinetic drug interactions with psychoactive drugs: antidepressants and antipsychotics and the cytochrome P450 system. J Clin Pharm Ther 1999;24:7-16.
11. Bergendal L, Friberg A, Schaffrath A. Potential drug-drug interactions in 5,125 mostly elderly outpatients in Gothenburg, Sweden. Pharm World Sci 1995;17(5):152-7.
12. De Las Cuevas C, Sanz EJ. Polypharmacy in psychiatric practice in the Canary Islands. BMC Psychiatry 2004;4(1):18.-
13. Raschetti R, Morgutti M, Menniti Ippolito F, et al. Suspected adverse drug events requiring emergency department visits or hospital admissions. Eur J Clin Pharmacol 1999;54:959-63.
14. Bates DW, Spell N, Cullen DJ, et al. The costs of adverse drug events in hospitalized patients. JAMA 1997;277:307-11.
15. Frye MA, Ketter TA, Leverich GS, et al. The increasing use of polypharmacotherapy for refractory mood disorders: 22 years of study. J Clin Psychiatry 2000;1:9-15.
16. Werder SF, Preskorn SH. Managing polypharmacy: walking the fine line between help and harm. Current Psychiatry 2003;2(2):24-36.
17. Physicians’ Desk Reference (59th ed). Montvale, NJ: Thomson PDR; 2005.
18. Sandson NB. Exploring drug interaction in psychiatry. Psychiatric times 2004;May:42-8.
19. Todi SK, Hartmann RA. Pharmacologic principles. In: Civetta JM, Taylor RW, Kirby RR, (eds). Critical care (3rd ed). Philadelphia: Lippincott-Raven Publishers; 1997;485-8.
20. Shapiro LE, Shear NH. Drug interactions: Proteins, pumps, and P-450s. J Am Acad Dermatol 2002;47:467-84.
21. Keck PE, Jr, Dewan N, Nasrallah HA. Bipolar disorder: the clinician’s guide to pharmacotherapy for patients with co-occurring medical conditions. Current Psychiatry 2005;4(Feb)(suppl):1-51.
22. Sadock BJ, Sadock VA. Kaplan and Sadock’s pocket handbook of psychiatric drug treatment (3rd ed). Philadelphia: Lippincott Williams & Wilkins; 2001;144-5,178-83,256-7.
23. Shukla S, Godwin CD, Long LE, Miller MG. Lithium-carbamazepine neurotoxicity and risk factors. Am J Psychiatry 1984;141:1604-6.
24. Licht RW, Vestergaard P, Kessing LV, et al. Psychopharmacological treatment with lithium and antiepileptic drugs: suggested guidelines from the Danish Psychiatric Association and the Child and Adolescent Psychiatric Association in Denmark. Acta Psychiatr Scand Suppl 2003;(419):1-22.
25. Phelan KM, Mosholder AD, Lu S. Lithium interaction with the cyclooxygenase 2 inhibitors rofecoxib and celecoxib and other nonsteroidal anti-inflammatory drugs. J Clin Psychiatry 2003;64:1328-34.
26. Ragheb M, Ban TA, Buchanan D, Frolich JC. Interaction of indomethacin and ibuprofen with lithium in manic patients under steady-state lithium level. J Clin Psychiatry 1980;11:397-8.
1. Langdorf MI, Fox JC, Marwah RS, et al. Physician versus computer knowledge of potential drug interactions in the emergency department. Acad Emerg Med 2000;7:1321-9.
2. Lazarou J, Pomeranz BH, Cory PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA 1998;279(15):1200-5.
3. Incalzi RA, Gemma A, Capparella O, et al. Predicting mortality and length of stay of geriatric patients in an acute care general hospital. J Gerontol 1992;47(2):M35-9.
4. Preskorn SH. Fatal drug-drug interaction as a differential consideration in apparent suicide. J Psychiatr Pract 2002;8(4):233-8.
5. Peterson JF, Bates D. Preventable medication errors: identifying and eliminating serious drug interactions. J Am Pharm Assoc (Wash) 2001;41(2):159-60.
6. Nichol MB, Stimmel GL, Lange SC. Factors predicting the use of multiple psychotropic medications. J Clin Psychiatry 1995;2:60-6.
7. Ananth J, Parameswaran S, Gunatilake S. Antipsychotic polypharmacy. Curr Pharm Des 2004;10(18):2231-8.
8. Medwatch Web site. Food and Drug Administration. Search for Drug-drug interactions. Available at: http://www.fda.gov/med-watch/index.html. Accessed March 31, 2005.
9. Rascati K. Drug utilization review of concomitant use of specific serotonin reuptake inhibitors or clomipramine and antianxiety/sleep medications. Clin Ther 1995;17:786-90.
10. Tanaka E, Hisawa S. Clinically significant pharmacokinetic drug interactions with psychoactive drugs: antidepressants and antipsychotics and the cytochrome P450 system. J Clin Pharm Ther 1999;24:7-16.
11. Bergendal L, Friberg A, Schaffrath A. Potential drug-drug interactions in 5,125 mostly elderly outpatients in Gothenburg, Sweden. Pharm World Sci 1995;17(5):152-7.
12. De Las Cuevas C, Sanz EJ. Polypharmacy in psychiatric practice in the Canary Islands. BMC Psychiatry 2004;4(1):18.-
13. Raschetti R, Morgutti M, Menniti Ippolito F, et al. Suspected adverse drug events requiring emergency department visits or hospital admissions. Eur J Clin Pharmacol 1999;54:959-63.
14. Bates DW, Spell N, Cullen DJ, et al. The costs of adverse drug events in hospitalized patients. JAMA 1997;277:307-11.
15. Frye MA, Ketter TA, Leverich GS, et al. The increasing use of polypharmacotherapy for refractory mood disorders: 22 years of study. J Clin Psychiatry 2000;1:9-15.
16. Werder SF, Preskorn SH. Managing polypharmacy: walking the fine line between help and harm. Current Psychiatry 2003;2(2):24-36.
17. Physicians’ Desk Reference (59th ed). Montvale, NJ: Thomson PDR; 2005.
18. Sandson NB. Exploring drug interaction in psychiatry. Psychiatric times 2004;May:42-8.
19. Todi SK, Hartmann RA. Pharmacologic principles. In: Civetta JM, Taylor RW, Kirby RR, (eds). Critical care (3rd ed). Philadelphia: Lippincott-Raven Publishers; 1997;485-8.
20. Shapiro LE, Shear NH. Drug interactions: Proteins, pumps, and P-450s. J Am Acad Dermatol 2002;47:467-84.
21. Keck PE, Jr, Dewan N, Nasrallah HA. Bipolar disorder: the clinician’s guide to pharmacotherapy for patients with co-occurring medical conditions. Current Psychiatry 2005;4(Feb)(suppl):1-51.
22. Sadock BJ, Sadock VA. Kaplan and Sadock’s pocket handbook of psychiatric drug treatment (3rd ed). Philadelphia: Lippincott Williams & Wilkins; 2001;144-5,178-83,256-7.
23. Shukla S, Godwin CD, Long LE, Miller MG. Lithium-carbamazepine neurotoxicity and risk factors. Am J Psychiatry 1984;141:1604-6.
24. Licht RW, Vestergaard P, Kessing LV, et al. Psychopharmacological treatment with lithium and antiepileptic drugs: suggested guidelines from the Danish Psychiatric Association and the Child and Adolescent Psychiatric Association in Denmark. Acta Psychiatr Scand Suppl 2003;(419):1-22.
25. Phelan KM, Mosholder AD, Lu S. Lithium interaction with the cyclooxygenase 2 inhibitors rofecoxib and celecoxib and other nonsteroidal anti-inflammatory drugs. J Clin Psychiatry 2003;64:1328-34.
26. Ragheb M, Ban TA, Buchanan D, Frolich JC. Interaction of indomethacin and ibuprofen with lithium in manic patients under steady-state lithium level. J Clin Psychiatry 1980;11:397-8.
Data backup: Don’t wait for the next crash
We know backing up data is important yet few of us do it consistently, either because we don’t think of it or cannot spare the time. Also, because today’s computers are less expensive and more reliable than before, many doctors think a system crash “can’t happen to me.”
Don’t wait for a power surge or hard drive failure to obliterate your crucial files or documents. This article describes numerous ways to back up and store data, each with different features. Your needs will determine which method is best for you.
HARD DRIVE FAILURE
Hard drives, which store information on platters via electrical charges, are vulnerable. They are rated with a mean time between failure (MTBF),1 which indicates how long on average a hard drive will work before it fails. Although the average MTBF is 50 years, electrical discharges such as power surges or lightning storms can force failure much sooner.
Viruses—if programmed to do so—can also corrupt hard drives. Most viruses propagate to another computer, using your computer as a host.
Companies such as Dataleach can recover information from your hard drive, but recovery may take days.
BASIC BACKUP TOOLS
CD-ROM-burning programs such as Nero Burning ROM are one way to back up data. Most computers purchased within the last 2 years have a built-in CD-ROM burner—a device that reads and creates CD-ROMs—along with CD-burning software.
Keep in mind the size of the disk you are using. CD-ROMs have a maximum capacity of 700 megabytes, but file location information consumes about 10 megabytes. A DVD-ROM can hold 4.7 gigabytes, almost 7 times the capacity of a CD-ROM.
Also consider expense. Recordable CDs on average cost 25 cents per disk. Recordable DVDs are more expensive (between 50 cents and $1 per disk depending on quantity purchased) but could save you money if you’re storing several gigabytes of data. The average cost per 100 megabytes of backup is 3.6 cents with CDs and 1.5 cents with DVDs.
Avoid rewriteable CD and DVDs—disks that can be erased and used again. Although such a disk may minimize backup costs, another computer may be unable to read it.
Alternate storage devices offer varying speeds and capacities. For example, a portable USB flash drive may be useful for storing less than 2 gigabytes. If you need more capacity, external USB hard drives can store up to 80 gigabytes. You can download or store a file within seconds with either device if it has a USB 2.0 transfer speed rating.
Zip drives, which can hold 750 megabytes, were once popular but have become less useful because they lack speed. Tape backup systems are extremely fast and can hold 130 gigabytes, but these devices are expensive and used more for large-scale business server backup.
‘WHICH FILES SHOULD I BACK UP?’
Obviously, you should back up electronic medical and billing records as well as documents created in your Microsoft Office suite.
Don’t ignore other critical information sources, such as Web browser bookmarks and e-mails, but remember that your mail, address book, and account information may be stored in different places depending on your e-mail program.
If you use a recordable CD or DVD, you must determine one by one which directories and files to archive. Nero has an easy-to-use “wizard” that guides you through this process. Nero also lets you automate backup: You would no loner have to remember to do it. Backing up e-mail and browser-bookmarked sites will be difficult, however, unless you know where they are kept.
Products such as Genie Backup Home Manager and NovaBACKUP have built-in search/inventory capability and back up to CDs or DVDs. Also, once the first backup is created, these programs can determine if the files have changed. Thus, subsequent backups will duplicate only files or modifications created since the previous backup. Specialized back-up programs also encrypt information and compress data to conserve space.
SCHEDULING DATA BACKUP
If you don’t create a schedule for backup, chances are it will never get done.
Ideally, you should back up data daily at a set time, such as at noon or closing.
Many psychiatrists, however, probably need a longer interval depending on how long backup takes (anywhere from 5 to 20 minutes depending on volume of data) and whether the information is critical. Also, a file cannot be duplicated while in use, as two computer programs cannot share a file in order to protect the data.
STORING BACKUP
After creating your backup:
- keep the backup and the software used to create it at another location in case of fire or theft
- test with your staff the process of restoring the information to the original hard drive, so that you will learn how to do it and how long it takes to get your computers running.
ALTERNATIVE BACKUP METHODS
If you have broadband Internet access via DSL or cable modem, consider using online backup services offered by Connected or Xdrive. Your data will be safe once you’ve downloaded and installed their software, designated files, and determined backup frequency. These online services also store the data at a remote site in case of fire or theft. Some physicians, however, may feel uncomfortable keeping data on another server for security reasons.
The Mirra Personal Server, an alternative to off-site backup, can be connected to one computer or a network and can back up one or all computers. This server can also synchronize files between computers and allow access to them over the Internet.
For real-time backup, a RAID array2 (redundant array of inexpensive drives) is your only choice. With RAID level 1, two hard drives record simultaneously. When one drive fails, another continues to work and has the information. A RAID array requires a specialized drive controller card, which costs around $150, or specialized software.3 Controller cards are widely available on the Internet (use search terms “Mac Raid controller” or “PC raid controller”), and raid arrays are available for any platform.
THE FUTURE
As multimedia become integrated into medical records and software programs create more information, physicians will need more storage space. New storage technologies such as the HD-DVD and Blu-Ray4 offer up to 25 to 30 gigabytes per disc. Similar to the VHS-Betamax wars of the 1980s, manufacturers are vying to make these high-density storage devices the future storage standard. Also, perpendicular recording technology is increasing hard drive storage capacity.5
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
(accessed April 22, 2005 )
1. Webopedia: What is MTBF? Available at: http://www.webopedia.com/TERM/M/MTBF.html.
2. ACITS open VMS services: Introduction to RAID technology. Available at: http://www.utexas.edu/cc/vms/about/raid.html.
3. The PC Guide: RAID. Available at: http://www.pcguide.com/ref/hdd/perf/raid/index.htm.
4. Wikipedia: HD-DVD. Available at: http://en.wikipedia.org/wiki/HD-DVD.
5. Dahl E. PC drive reaches 500 GB. PC World ‘News & Trends,’ May 2005. Available at: http://www.pcworld.com/news/article/0,aid,120102,00.asp.
We know backing up data is important yet few of us do it consistently, either because we don’t think of it or cannot spare the time. Also, because today’s computers are less expensive and more reliable than before, many doctors think a system crash “can’t happen to me.”
Don’t wait for a power surge or hard drive failure to obliterate your crucial files or documents. This article describes numerous ways to back up and store data, each with different features. Your needs will determine which method is best for you.
HARD DRIVE FAILURE
Hard drives, which store information on platters via electrical charges, are vulnerable. They are rated with a mean time between failure (MTBF),1 which indicates how long on average a hard drive will work before it fails. Although the average MTBF is 50 years, electrical discharges such as power surges or lightning storms can force failure much sooner.
Viruses—if programmed to do so—can also corrupt hard drives. Most viruses propagate to another computer, using your computer as a host.
Companies such as Dataleach can recover information from your hard drive, but recovery may take days.
BASIC BACKUP TOOLS
CD-ROM-burning programs such as Nero Burning ROM are one way to back up data. Most computers purchased within the last 2 years have a built-in CD-ROM burner—a device that reads and creates CD-ROMs—along with CD-burning software.
Keep in mind the size of the disk you are using. CD-ROMs have a maximum capacity of 700 megabytes, but file location information consumes about 10 megabytes. A DVD-ROM can hold 4.7 gigabytes, almost 7 times the capacity of a CD-ROM.
Also consider expense. Recordable CDs on average cost 25 cents per disk. Recordable DVDs are more expensive (between 50 cents and $1 per disk depending on quantity purchased) but could save you money if you’re storing several gigabytes of data. The average cost per 100 megabytes of backup is 3.6 cents with CDs and 1.5 cents with DVDs.
Avoid rewriteable CD and DVDs—disks that can be erased and used again. Although such a disk may minimize backup costs, another computer may be unable to read it.
Alternate storage devices offer varying speeds and capacities. For example, a portable USB flash drive may be useful for storing less than 2 gigabytes. If you need more capacity, external USB hard drives can store up to 80 gigabytes. You can download or store a file within seconds with either device if it has a USB 2.0 transfer speed rating.
Zip drives, which can hold 750 megabytes, were once popular but have become less useful because they lack speed. Tape backup systems are extremely fast and can hold 130 gigabytes, but these devices are expensive and used more for large-scale business server backup.
‘WHICH FILES SHOULD I BACK UP?’
Obviously, you should back up electronic medical and billing records as well as documents created in your Microsoft Office suite.
Don’t ignore other critical information sources, such as Web browser bookmarks and e-mails, but remember that your mail, address book, and account information may be stored in different places depending on your e-mail program.
If you use a recordable CD or DVD, you must determine one by one which directories and files to archive. Nero has an easy-to-use “wizard” that guides you through this process. Nero also lets you automate backup: You would no loner have to remember to do it. Backing up e-mail and browser-bookmarked sites will be difficult, however, unless you know where they are kept.
Products such as Genie Backup Home Manager and NovaBACKUP have built-in search/inventory capability and back up to CDs or DVDs. Also, once the first backup is created, these programs can determine if the files have changed. Thus, subsequent backups will duplicate only files or modifications created since the previous backup. Specialized back-up programs also encrypt information and compress data to conserve space.
SCHEDULING DATA BACKUP
If you don’t create a schedule for backup, chances are it will never get done.
Ideally, you should back up data daily at a set time, such as at noon or closing.
Many psychiatrists, however, probably need a longer interval depending on how long backup takes (anywhere from 5 to 20 minutes depending on volume of data) and whether the information is critical. Also, a file cannot be duplicated while in use, as two computer programs cannot share a file in order to protect the data.
STORING BACKUP
After creating your backup:
- keep the backup and the software used to create it at another location in case of fire or theft
- test with your staff the process of restoring the information to the original hard drive, so that you will learn how to do it and how long it takes to get your computers running.
ALTERNATIVE BACKUP METHODS
If you have broadband Internet access via DSL or cable modem, consider using online backup services offered by Connected or Xdrive. Your data will be safe once you’ve downloaded and installed their software, designated files, and determined backup frequency. These online services also store the data at a remote site in case of fire or theft. Some physicians, however, may feel uncomfortable keeping data on another server for security reasons.
The Mirra Personal Server, an alternative to off-site backup, can be connected to one computer or a network and can back up one or all computers. This server can also synchronize files between computers and allow access to them over the Internet.
For real-time backup, a RAID array2 (redundant array of inexpensive drives) is your only choice. With RAID level 1, two hard drives record simultaneously. When one drive fails, another continues to work and has the information. A RAID array requires a specialized drive controller card, which costs around $150, or specialized software.3 Controller cards are widely available on the Internet (use search terms “Mac Raid controller” or “PC raid controller”), and raid arrays are available for any platform.
THE FUTURE
As multimedia become integrated into medical records and software programs create more information, physicians will need more storage space. New storage technologies such as the HD-DVD and Blu-Ray4 offer up to 25 to 30 gigabytes per disc. Similar to the VHS-Betamax wars of the 1980s, manufacturers are vying to make these high-density storage devices the future storage standard. Also, perpendicular recording technology is increasing hard drive storage capacity.5
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
We know backing up data is important yet few of us do it consistently, either because we don’t think of it or cannot spare the time. Also, because today’s computers are less expensive and more reliable than before, many doctors think a system crash “can’t happen to me.”
Don’t wait for a power surge or hard drive failure to obliterate your crucial files or documents. This article describes numerous ways to back up and store data, each with different features. Your needs will determine which method is best for you.
HARD DRIVE FAILURE
Hard drives, which store information on platters via electrical charges, are vulnerable. They are rated with a mean time between failure (MTBF),1 which indicates how long on average a hard drive will work before it fails. Although the average MTBF is 50 years, electrical discharges such as power surges or lightning storms can force failure much sooner.
Viruses—if programmed to do so—can also corrupt hard drives. Most viruses propagate to another computer, using your computer as a host.
Companies such as Dataleach can recover information from your hard drive, but recovery may take days.
BASIC BACKUP TOOLS
CD-ROM-burning programs such as Nero Burning ROM are one way to back up data. Most computers purchased within the last 2 years have a built-in CD-ROM burner—a device that reads and creates CD-ROMs—along with CD-burning software.
Keep in mind the size of the disk you are using. CD-ROMs have a maximum capacity of 700 megabytes, but file location information consumes about 10 megabytes. A DVD-ROM can hold 4.7 gigabytes, almost 7 times the capacity of a CD-ROM.
Also consider expense. Recordable CDs on average cost 25 cents per disk. Recordable DVDs are more expensive (between 50 cents and $1 per disk depending on quantity purchased) but could save you money if you’re storing several gigabytes of data. The average cost per 100 megabytes of backup is 3.6 cents with CDs and 1.5 cents with DVDs.
Avoid rewriteable CD and DVDs—disks that can be erased and used again. Although such a disk may minimize backup costs, another computer may be unable to read it.
Alternate storage devices offer varying speeds and capacities. For example, a portable USB flash drive may be useful for storing less than 2 gigabytes. If you need more capacity, external USB hard drives can store up to 80 gigabytes. You can download or store a file within seconds with either device if it has a USB 2.0 transfer speed rating.
Zip drives, which can hold 750 megabytes, were once popular but have become less useful because they lack speed. Tape backup systems are extremely fast and can hold 130 gigabytes, but these devices are expensive and used more for large-scale business server backup.
‘WHICH FILES SHOULD I BACK UP?’
Obviously, you should back up electronic medical and billing records as well as documents created in your Microsoft Office suite.
Don’t ignore other critical information sources, such as Web browser bookmarks and e-mails, but remember that your mail, address book, and account information may be stored in different places depending on your e-mail program.
If you use a recordable CD or DVD, you must determine one by one which directories and files to archive. Nero has an easy-to-use “wizard” that guides you through this process. Nero also lets you automate backup: You would no loner have to remember to do it. Backing up e-mail and browser-bookmarked sites will be difficult, however, unless you know where they are kept.
Products such as Genie Backup Home Manager and NovaBACKUP have built-in search/inventory capability and back up to CDs or DVDs. Also, once the first backup is created, these programs can determine if the files have changed. Thus, subsequent backups will duplicate only files or modifications created since the previous backup. Specialized back-up programs also encrypt information and compress data to conserve space.
SCHEDULING DATA BACKUP
If you don’t create a schedule for backup, chances are it will never get done.
Ideally, you should back up data daily at a set time, such as at noon or closing.
Many psychiatrists, however, probably need a longer interval depending on how long backup takes (anywhere from 5 to 20 minutes depending on volume of data) and whether the information is critical. Also, a file cannot be duplicated while in use, as two computer programs cannot share a file in order to protect the data.
STORING BACKUP
After creating your backup:
- keep the backup and the software used to create it at another location in case of fire or theft
- test with your staff the process of restoring the information to the original hard drive, so that you will learn how to do it and how long it takes to get your computers running.
ALTERNATIVE BACKUP METHODS
If you have broadband Internet access via DSL or cable modem, consider using online backup services offered by Connected or Xdrive. Your data will be safe once you’ve downloaded and installed their software, designated files, and determined backup frequency. These online services also store the data at a remote site in case of fire or theft. Some physicians, however, may feel uncomfortable keeping data on another server for security reasons.
The Mirra Personal Server, an alternative to off-site backup, can be connected to one computer or a network and can back up one or all computers. This server can also synchronize files between computers and allow access to them over the Internet.
For real-time backup, a RAID array2 (redundant array of inexpensive drives) is your only choice. With RAID level 1, two hard drives record simultaneously. When one drive fails, another continues to work and has the information. A RAID array requires a specialized drive controller card, which costs around $150, or specialized software.3 Controller cards are widely available on the Internet (use search terms “Mac Raid controller” or “PC raid controller”), and raid arrays are available for any platform.
THE FUTURE
As multimedia become integrated into medical records and software programs create more information, physicians will need more storage space. New storage technologies such as the HD-DVD and Blu-Ray4 offer up to 25 to 30 gigabytes per disc. Similar to the VHS-Betamax wars of the 1980s, manufacturers are vying to make these high-density storage devices the future storage standard. Also, perpendicular recording technology is increasing hard drive storage capacity.5
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
(accessed April 22, 2005 )
1. Webopedia: What is MTBF? Available at: http://www.webopedia.com/TERM/M/MTBF.html.
2. ACITS open VMS services: Introduction to RAID technology. Available at: http://www.utexas.edu/cc/vms/about/raid.html.
3. The PC Guide: RAID. Available at: http://www.pcguide.com/ref/hdd/perf/raid/index.htm.
4. Wikipedia: HD-DVD. Available at: http://en.wikipedia.org/wiki/HD-DVD.
5. Dahl E. PC drive reaches 500 GB. PC World ‘News & Trends,’ May 2005. Available at: http://www.pcworld.com/news/article/0,aid,120102,00.asp.
(accessed April 22, 2005 )
1. Webopedia: What is MTBF? Available at: http://www.webopedia.com/TERM/M/MTBF.html.
2. ACITS open VMS services: Introduction to RAID technology. Available at: http://www.utexas.edu/cc/vms/about/raid.html.
3. The PC Guide: RAID. Available at: http://www.pcguide.com/ref/hdd/perf/raid/index.htm.
4. Wikipedia: HD-DVD. Available at: http://en.wikipedia.org/wiki/HD-DVD.
5. Dahl E. PC drive reaches 500 GB. PC World ‘News & Trends,’ May 2005. Available at: http://www.pcworld.com/news/article/0,aid,120102,00.asp.