User login
HbA1c cutpoint predicts pediatric T1DM within a year
ORLANDO – Among children with genetic risks for type 1 diabetes and autoantibodies against pancreatic islet cells, a hemoglobin A1c at or above 5.6% strongly predicts the onset of type 1 diabetes within a year, according to investigators from The Environmental Determinants of Diabetes in the Young (TEDDY) study.

The risk is even greater if other factors – age at A1c test, month of A1c test, continent of residence, and the z-score for one antibody in particular, IA2A, a tyrosine phosphatase antigen protein – are taken into account, with an area under the curve (AUC) of about 0.97. The study team is developing an online risk calculator for clinicians so they can simply plug in the numbers.
But the 5.6% cutpoint works well even by itself, with an AUC of about 0.86. Among the children with genetic risk factors and islet cell autoantibodies who hit that mark in the study, the median time to diagnosis of type 1 diabetes mellitus (T1DM) was 7.1 months.
The point of the work is to catch disease onset early to prevent children from going into diabetic ketoacidosis.
The ultimate goal of TEDDY is to identify infectious agents, dietary factors, and other environmental agents that either trigger or protect against T1DM in genetically susceptible children, to develop strategies to prevent, delay, or even reverse T1DM. For more than a decade, the consortium has been following more than 8,000 children who screened positive at birth for genetic anomalies in the human leukocyte antigen region on their 6th chromosome, a major risk factor for T1DM. The team is following them to find out what puts them over the edge; A1c seems to be key.
Catching the disease early is a goal. Until now, the TEDDY team has used the development of pancreatic islet cell autoantibodies to trigger oral glucose tolerance tests (OGTTs) every 6 months.
The problem is that islet antibodies “are great at saying that you are going to get diabetes but not when. We have kids who have been multiple antibody positive now for 6, 7, 8 years” but who still haven’t developed T1DM. In the meantime, their parents have been dragging them in for OGTTs every 6 months for years, said lead investigator and TEDDY study coordinator Michael Killian, of the Pacific Northwest Research Institute, Seattle.
With the A1c cutpoint, it should be safe to hold off on direct glycemic surveillance until A1c levels reach 5.6%, and even safer when the full risk prediction model with 1A2A z-scores and other factors are available. Once children hit the parameters, it’s near certain they will develop T1DM within a year, so the findings should reduce the number of OGTT tests to just two or three. In the end, “we’ll get better compliance” with testing and still “catch these kids early,” Mr. Killian said at the annual scientific sessions of the American Diabetes Association.
Rare is the newborn who is screened for diabetes risk at birth, and even rarer is the child who is followed for autoantibodies. If the findings hold out, however, such early action could be the future.
“We envision a time” when newborns are screened for T1DM risk and followed for autoantibodies. Glycemic surveillance will kick in if they hit A1c levels of 5.6%, said William Hagopian, MD, PhD, clinical associate professor at the University of Washington, Seattle, and a TEDDY principal investigator.
Among the 8,000-plus children followed, 456 had persistent islet autoantibodies and at least three A1c tests in the prior 12 months; 104 progressed to T1DM and 352 did not. The mean age to islet autoantibody seroconversion was 43 months, and mean age to T1DM diagnosis was 73 months. The team ran a receiver operating curve analysis to identify the optimum A1c cutpoint, 5.6%.
The month of testing mattered, because “glycemia is higher in the winter, lower in the summer, and insulin sensitivity is lower in the winter, and higher in the summer,” Dr. Hagopian said. It probably has something to do with what the stresses of early human evolution bred into the genes.
The IA2A autoantibody z-score is the only number that will be cumbersome to plug into the upcoming online risk calculator. It’s the number of standard deviations off your reference lab’s mean. “You have to talk to the lab that does your IA2As to know what the standard deviation is,” Dr. Hagopian said.
The investigators had no disclosures. TEDDY is supported by the National Institutes of Health, among other entities.
SOURCE: Killian M et al. ADA 2018, Abstract 162-LB
ORLANDO – Among children with genetic risks for type 1 diabetes and autoantibodies against pancreatic islet cells, a hemoglobin A1c at or above 5.6% strongly predicts the onset of type 1 diabetes within a year, according to investigators from The Environmental Determinants of Diabetes in the Young (TEDDY) study.
The risk is even greater if other factors – age at A1c test, month of A1c test, continent of residence, and the z-score for one antibody in particular, IA2A, a tyrosine phosphatase antigen protein – are taken into account, with an area under the curve (AUC) of about 0.97. The study team is developing an online risk calculator for clinicians so they can simply plug in the numbers.
But the 5.6% cutpoint works well even by itself, with an AUC of about 0.86. Among the children with genetic risk factors and islet cell autoantibodies who hit that mark in the study, the median time to diagnosis of type 1 diabetes mellitus (T1DM) was 7.1 months.
The point of the work is to catch disease onset early to prevent children from going into diabetic ketoacidosis.
The ultimate goal of TEDDY is to identify infectious agents, dietary factors, and other environmental agents that either trigger or protect against T1DM in genetically susceptible children, to develop strategies to prevent, delay, or even reverse T1DM. For more than a decade, the consortium has been following more than 8,000 children who screened positive at birth for genetic anomalies in the human leukocyte antigen region on their 6th chromosome, a major risk factor for T1DM. The team is following them to find out what puts them over the edge; A1c seems to be key.
Catching the disease early is a goal. Until now, the TEDDY team has used the development of pancreatic islet cell autoantibodies to trigger oral glucose tolerance tests (OGTTs) every 6 months.
The problem is that islet antibodies “are great at saying that you are going to get diabetes but not when. We have kids who have been multiple antibody positive now for 6, 7, 8 years” but who still haven’t developed T1DM. In the meantime, their parents have been dragging them in for OGTTs every 6 months for years, said lead investigator and TEDDY study coordinator Michael Killian, of the Pacific Northwest Research Institute, Seattle.
With the A1c cutpoint, it should be safe to hold off on direct glycemic surveillance until A1c levels reach 5.6%, and even safer when the full risk prediction model with 1A2A z-scores and other factors are available. Once children hit the parameters, it’s near certain they will develop T1DM within a year, so the findings should reduce the number of OGTT tests to just two or three. In the end, “we’ll get better compliance” with testing and still “catch these kids early,” Mr. Killian said at the annual scientific sessions of the American Diabetes Association.
Rare is the newborn who is screened for diabetes risk at birth, and even rarer is the child who is followed for autoantibodies. If the findings hold out, however, such early action could be the future.
“We envision a time” when newborns are screened for T1DM risk and followed for autoantibodies. Glycemic surveillance will kick in if they hit A1c levels of 5.6%, said William Hagopian, MD, PhD, clinical associate professor at the University of Washington, Seattle, and a TEDDY principal investigator.
Among the 8,000-plus children followed, 456 had persistent islet autoantibodies and at least three A1c tests in the prior 12 months; 104 progressed to T1DM and 352 did not. The mean age to islet autoantibody seroconversion was 43 months, and mean age to T1DM diagnosis was 73 months. The team ran a receiver operating curve analysis to identify the optimum A1c cutpoint, 5.6%.
The month of testing mattered, because “glycemia is higher in the winter, lower in the summer, and insulin sensitivity is lower in the winter, and higher in the summer,” Dr. Hagopian said. It probably has something to do with what the stresses of early human evolution bred into the genes.
The IA2A autoantibody z-score is the only number that will be cumbersome to plug into the upcoming online risk calculator. It’s the number of standard deviations off your reference lab’s mean. “You have to talk to the lab that does your IA2As to know what the standard deviation is,” Dr. Hagopian said.
The investigators had no disclosures. TEDDY is supported by the National Institutes of Health, among other entities.
SOURCE: Killian M et al. ADA 2018, Abstract 162-LB
ORLANDO – Among children with genetic risks for type 1 diabetes and autoantibodies against pancreatic islet cells, a hemoglobin A1c at or above 5.6% strongly predicts the onset of type 1 diabetes within a year, according to investigators from The Environmental Determinants of Diabetes in the Young (TEDDY) study.
The risk is even greater if other factors – age at A1c test, month of A1c test, continent of residence, and the z-score for one antibody in particular, IA2A, a tyrosine phosphatase antigen protein – are taken into account, with an area under the curve (AUC) of about 0.97. The study team is developing an online risk calculator for clinicians so they can simply plug in the numbers.
But the 5.6% cutpoint works well even by itself, with an AUC of about 0.86. Among the children with genetic risk factors and islet cell autoantibodies who hit that mark in the study, the median time to diagnosis of type 1 diabetes mellitus (T1DM) was 7.1 months.
The point of the work is to catch disease onset early to prevent children from going into diabetic ketoacidosis.
The ultimate goal of TEDDY is to identify infectious agents, dietary factors, and other environmental agents that either trigger or protect against T1DM in genetically susceptible children, to develop strategies to prevent, delay, or even reverse T1DM. For more than a decade, the consortium has been following more than 8,000 children who screened positive at birth for genetic anomalies in the human leukocyte antigen region on their 6th chromosome, a major risk factor for T1DM. The team is following them to find out what puts them over the edge; A1c seems to be key.
Catching the disease early is a goal. Until now, the TEDDY team has used the development of pancreatic islet cell autoantibodies to trigger oral glucose tolerance tests (OGTTs) every 6 months.
The problem is that islet antibodies “are great at saying that you are going to get diabetes but not when. We have kids who have been multiple antibody positive now for 6, 7, 8 years” but who still haven’t developed T1DM. In the meantime, their parents have been dragging them in for OGTTs every 6 months for years, said lead investigator and TEDDY study coordinator Michael Killian, of the Pacific Northwest Research Institute, Seattle.
With the A1c cutpoint, it should be safe to hold off on direct glycemic surveillance until A1c levels reach 5.6%, and even safer when the full risk prediction model with 1A2A z-scores and other factors are available. Once children hit the parameters, it’s near certain they will develop T1DM within a year, so the findings should reduce the number of OGTT tests to just two or three. In the end, “we’ll get better compliance” with testing and still “catch these kids early,” Mr. Killian said at the annual scientific sessions of the American Diabetes Association.
Rare is the newborn who is screened for diabetes risk at birth, and even rarer is the child who is followed for autoantibodies. If the findings hold out, however, such early action could be the future.
“We envision a time” when newborns are screened for T1DM risk and followed for autoantibodies. Glycemic surveillance will kick in if they hit A1c levels of 5.6%, said William Hagopian, MD, PhD, clinical associate professor at the University of Washington, Seattle, and a TEDDY principal investigator.
Among the 8,000-plus children followed, 456 had persistent islet autoantibodies and at least three A1c tests in the prior 12 months; 104 progressed to T1DM and 352 did not. The mean age to islet autoantibody seroconversion was 43 months, and mean age to T1DM diagnosis was 73 months. The team ran a receiver operating curve analysis to identify the optimum A1c cutpoint, 5.6%.
The month of testing mattered, because “glycemia is higher in the winter, lower in the summer, and insulin sensitivity is lower in the winter, and higher in the summer,” Dr. Hagopian said. It probably has something to do with what the stresses of early human evolution bred into the genes.
The IA2A autoantibody z-score is the only number that will be cumbersome to plug into the upcoming online risk calculator. It’s the number of standard deviations off your reference lab’s mean. “You have to talk to the lab that does your IA2As to know what the standard deviation is,” Dr. Hagopian said.
The investigators had no disclosures. TEDDY is supported by the National Institutes of Health, among other entities.
SOURCE: Killian M et al. ADA 2018, Abstract 162-LB
FROM ADA 2018
Key clinical point: Among children with genetic risks for type 1 diabetes and autoantibodies against pancreatic islet cells, a hemoglobin A1c at or above 5.6% strongly predicts the onset of type 1 diabetes within a year.
Major finding: Among the children with genetic risk factors and islet cell autoantibodies who hit that mark, the median time to diagnosis was 7.1 months.
Study details: The findings are from more than 400 children in The Environmental Determinants of Diabetes in the Young (TEDDY) cohort.
Disclosures: The investigators had no disclosures. TEDDY is supported by the National Institutes of Health, among other entities.
Source: Killian M et al. ADA 2018, Abstract 162-LB.
Endocrinologists clash over routine CGM during pregnancy
ORLANDO – Diabetes and pregnancy aren’t a good mix, but what about pregnancy and continuous glucose monitors (CGMs)? In a polite but pointed debate, two endocrinologists used each other’s studies as evidence to support their opposing perspectives about routine GCM use by diabetic women during pregnancy.

“This topic shouldn’t really be debated because the evidence is clear” in favor of CGM, said Denice S. Feig, MD, MSc, FRCPC, of the University of Toronto and Mt. Sinai Hospital, also in Toronto, in a presentation at the annual scientific sessions of the American Diabetes Association.
However, Elisabeth R. Mathiesen, MD, DMSc, of Rigshospitalet in Copenhagen, rebutted. She said her own research suggests CGM use may lead to larger babies and more premature births, convincing her to “say no to uncritical use of CGM in pregnancy.”
At issue: What is the best routine treatment for diabetic women before, during, and after pregnancy? As the American Diabetes Association noted in its 2018 Standards of Medical Care in Diabetes report, “specific risks of uncontrolled diabetes in pregnancy include spontaneous abortion, fetal anomalies, preeclampsia, fetal demise, macrosomia, neonatal hypoglycemia, and neonatal hyperbilirubinemia, among others. In addition, diabetes in pregnancy may increase the risk of obesity and type 2 diabetes [mellitus] in offspring later in life.”
In her presentation, Dr. Feig pointed to a 2017 study she led that examined the effectiveness of continuous, real-time CGM on women with type 1 diabetes mellitus who were pregnant or planning to become pregnant (Lancet. 2017 Nov 25;390(10110):2347-2359).
“The study, in effect, was two parallel, randomized trials, one in those who planned pregnancy and one in those who were pregnant,” Dr. Feig said.
Participants, aged 18-40 years, from 31 hospitals in seven European and North American nations, had to have hemoglobin A1c levels greater than or equal to 6.5% during pregnancy or greater than or equal to 7% while planning pregnancy to be included in the study.
“We had a run-in phase to make sure they were able and willing to wear the CGM. Then we had 215 women in the pregnancy arm and 110 in the prepregnancy group randomized to real-time continuous CGM or standard care,” Dr. Feig said. The study ran for 34 weeks in the pregnant patients and for 24 weeks or until conception in the other women.
According to Dr. Feig, 70% of pregnant participants used CGM devices for more than 75% of the time. Compared with the control group, HbA1c levels in those who used CGM fell by 0.19% (P = .0207). The researchers also reported that women in the CGM group spent 100 more minutes a day within the glucose target range.
No differences in outcomes such as gestational age at delivery and rate of preterm delivery was found, although incidence of large-for-gestational-age infants, hypoglycemia requiring dextrose infusion, and neonatal ICU admission were lower in the CGM group to a statistically significant degree. “The numbers needed to treat were very small at six to eight women to reduce one of these events,” said Dr. Feig, who added that the numbers suggest the potential for cost savings.
Whatever the case, she said, “what price would you place on your baby avoiding a prolonged stay in the NICU? I think [it’s] priceless.”
She added that 80% of participants reported having trouble with the devices, which she attributed to the technology being old.
As for the planned pregnancy group, the study noted that “it did not have sufficient power to detect the magnitude of differences that were significant in the pregnancy trial.”
However, Dr. Feig said the study showed a trend toward lower HbA1c levels among CGM users in this population in which “tight glycemic control is absolutely paramount,” and that other studies also provide evidence supporting CGM use through the breastfeeding period.
Dr. Feig also pointed to a similar 2013 study coauthored by Dr. Mathiesen, her debate opponent. Dr. Feig said its findings are weakened because participants used CGM intermittently. She also pointed to the low participation (64%) in CGM by women assigned to a CGM group. (Diabetes Care. 2013 Jul;36[7]:1877-83)
In that study, researchers assigned 123 Danish women with type 1 diabetes mellitus and 31 women with type 2 diabetes mellitus to use real-time CGM for 6 days at various points in pregnancy or to only engage in routine care (including self-monitored plasma glucose seven times daily).
Researchers found no difference in HbA1c levels at 33 weeks between the groups, and they found similar rates of severe hypoglycemia and perinatal outcomes such as large-for-gestational-age infants.

These results, Dr. Mathiesen said, make her skeptical of a blanket recommendation to use CGM in pregnancy. Women aren’t eager to upload their glucose readings, making it difficult for doctors to make adjustments. “My women are Vikings. They come from Denmark,” she said, but “even these women don’t upload their glucose data between visits. ... I rarely have women who upload their data and look at their curves themselves. I think that’s a major disadvantage.”
Dr. Mathiesen also pointed to Dr. Feig’s study and noted that many women used CGM less than 75% of the time. In addition, 80% reported problems with the technology. “I’ve seen lots of skin problems with sensors. One lady used CGM during pregnancy; 4 years later, during another pregnancy, she showed me the mark of her sensor.”
Finally, the cost of CGM use is high considering the ongoing expense of the devices and the nurse time needed to upload data in the clinic. “As a rough estimate, the cost of CGM use in about 20 women during their pregnancies is the cost of the salary for one nurse per year,” she said.
Dr. Feig reported speaking fees from Medtronic, which provided CGM devices at reduced cost to her trial. Dr. Mathiesen reported research funding from the Novo Nordisk Foundation and speaker fees from Novo Nordisk, Lilly, AstraZeneca, and Sanofi-Aventis.
ORLANDO – Diabetes and pregnancy aren’t a good mix, but what about pregnancy and continuous glucose monitors (CGMs)? In a polite but pointed debate, two endocrinologists used each other’s studies as evidence to support their opposing perspectives about routine GCM use by diabetic women during pregnancy.
“This topic shouldn’t really be debated because the evidence is clear” in favor of CGM, said Denice S. Feig, MD, MSc, FRCPC, of the University of Toronto and Mt. Sinai Hospital, also in Toronto, in a presentation at the annual scientific sessions of the American Diabetes Association.
However, Elisabeth R. Mathiesen, MD, DMSc, of Rigshospitalet in Copenhagen, rebutted. She said her own research suggests CGM use may lead to larger babies and more premature births, convincing her to “say no to uncritical use of CGM in pregnancy.”
At issue: What is the best routine treatment for diabetic women before, during, and after pregnancy? As the American Diabetes Association noted in its 2018 Standards of Medical Care in Diabetes report, “specific risks of uncontrolled diabetes in pregnancy include spontaneous abortion, fetal anomalies, preeclampsia, fetal demise, macrosomia, neonatal hypoglycemia, and neonatal hyperbilirubinemia, among others. In addition, diabetes in pregnancy may increase the risk of obesity and type 2 diabetes [mellitus] in offspring later in life.”
In her presentation, Dr. Feig pointed to a 2017 study she led that examined the effectiveness of continuous, real-time CGM on women with type 1 diabetes mellitus who were pregnant or planning to become pregnant (Lancet. 2017 Nov 25;390(10110):2347-2359).
“The study, in effect, was two parallel, randomized trials, one in those who planned pregnancy and one in those who were pregnant,” Dr. Feig said.
Participants, aged 18-40 years, from 31 hospitals in seven European and North American nations, had to have hemoglobin A1c levels greater than or equal to 6.5% during pregnancy or greater than or equal to 7% while planning pregnancy to be included in the study.
“We had a run-in phase to make sure they were able and willing to wear the CGM. Then we had 215 women in the pregnancy arm and 110 in the prepregnancy group randomized to real-time continuous CGM or standard care,” Dr. Feig said. The study ran for 34 weeks in the pregnant patients and for 24 weeks or until conception in the other women.
According to Dr. Feig, 70% of pregnant participants used CGM devices for more than 75% of the time. Compared with the control group, HbA1c levels in those who used CGM fell by 0.19% (P = .0207). The researchers also reported that women in the CGM group spent 100 more minutes a day within the glucose target range.
No differences in outcomes such as gestational age at delivery and rate of preterm delivery was found, although incidence of large-for-gestational-age infants, hypoglycemia requiring dextrose infusion, and neonatal ICU admission were lower in the CGM group to a statistically significant degree. “The numbers needed to treat were very small at six to eight women to reduce one of these events,” said Dr. Feig, who added that the numbers suggest the potential for cost savings.
Whatever the case, she said, “what price would you place on your baby avoiding a prolonged stay in the NICU? I think [it’s] priceless.”
She added that 80% of participants reported having trouble with the devices, which she attributed to the technology being old.
As for the planned pregnancy group, the study noted that “it did not have sufficient power to detect the magnitude of differences that were significant in the pregnancy trial.”
However, Dr. Feig said the study showed a trend toward lower HbA1c levels among CGM users in this population in which “tight glycemic control is absolutely paramount,” and that other studies also provide evidence supporting CGM use through the breastfeeding period.
Dr. Feig also pointed to a similar 2013 study coauthored by Dr. Mathiesen, her debate opponent. Dr. Feig said its findings are weakened because participants used CGM intermittently. She also pointed to the low participation (64%) in CGM by women assigned to a CGM group. (Diabetes Care. 2013 Jul;36[7]:1877-83)
In that study, researchers assigned 123 Danish women with type 1 diabetes mellitus and 31 women with type 2 diabetes mellitus to use real-time CGM for 6 days at various points in pregnancy or to only engage in routine care (including self-monitored plasma glucose seven times daily).
Researchers found no difference in HbA1c levels at 33 weeks between the groups, and they found similar rates of severe hypoglycemia and perinatal outcomes such as large-for-gestational-age infants.
These results, Dr. Mathiesen said, make her skeptical of a blanket recommendation to use CGM in pregnancy. Women aren’t eager to upload their glucose readings, making it difficult for doctors to make adjustments. “My women are Vikings. They come from Denmark,” she said, but “even these women don’t upload their glucose data between visits. ... I rarely have women who upload their data and look at their curves themselves. I think that’s a major disadvantage.”
Dr. Mathiesen also pointed to Dr. Feig’s study and noted that many women used CGM less than 75% of the time. In addition, 80% reported problems with the technology. “I’ve seen lots of skin problems with sensors. One lady used CGM during pregnancy; 4 years later, during another pregnancy, she showed me the mark of her sensor.”
Finally, the cost of CGM use is high considering the ongoing expense of the devices and the nurse time needed to upload data in the clinic. “As a rough estimate, the cost of CGM use in about 20 women during their pregnancies is the cost of the salary for one nurse per year,” she said.
Dr. Feig reported speaking fees from Medtronic, which provided CGM devices at reduced cost to her trial. Dr. Mathiesen reported research funding from the Novo Nordisk Foundation and speaker fees from Novo Nordisk, Lilly, AstraZeneca, and Sanofi-Aventis.
ORLANDO – Diabetes and pregnancy aren’t a good mix, but what about pregnancy and continuous glucose monitors (CGMs)? In a polite but pointed debate, two endocrinologists used each other’s studies as evidence to support their opposing perspectives about routine GCM use by diabetic women during pregnancy.
“This topic shouldn’t really be debated because the evidence is clear” in favor of CGM, said Denice S. Feig, MD, MSc, FRCPC, of the University of Toronto and Mt. Sinai Hospital, also in Toronto, in a presentation at the annual scientific sessions of the American Diabetes Association.
However, Elisabeth R. Mathiesen, MD, DMSc, of Rigshospitalet in Copenhagen, rebutted. She said her own research suggests CGM use may lead to larger babies and more premature births, convincing her to “say no to uncritical use of CGM in pregnancy.”
At issue: What is the best routine treatment for diabetic women before, during, and after pregnancy? As the American Diabetes Association noted in its 2018 Standards of Medical Care in Diabetes report, “specific risks of uncontrolled diabetes in pregnancy include spontaneous abortion, fetal anomalies, preeclampsia, fetal demise, macrosomia, neonatal hypoglycemia, and neonatal hyperbilirubinemia, among others. In addition, diabetes in pregnancy may increase the risk of obesity and type 2 diabetes [mellitus] in offspring later in life.”
In her presentation, Dr. Feig pointed to a 2017 study she led that examined the effectiveness of continuous, real-time CGM on women with type 1 diabetes mellitus who were pregnant or planning to become pregnant (Lancet. 2017 Nov 25;390(10110):2347-2359).
“The study, in effect, was two parallel, randomized trials, one in those who planned pregnancy and one in those who were pregnant,” Dr. Feig said.
Participants, aged 18-40 years, from 31 hospitals in seven European and North American nations, had to have hemoglobin A1c levels greater than or equal to 6.5% during pregnancy or greater than or equal to 7% while planning pregnancy to be included in the study.
“We had a run-in phase to make sure they were able and willing to wear the CGM. Then we had 215 women in the pregnancy arm and 110 in the prepregnancy group randomized to real-time continuous CGM or standard care,” Dr. Feig said. The study ran for 34 weeks in the pregnant patients and for 24 weeks or until conception in the other women.
According to Dr. Feig, 70% of pregnant participants used CGM devices for more than 75% of the time. Compared with the control group, HbA1c levels in those who used CGM fell by 0.19% (P = .0207). The researchers also reported that women in the CGM group spent 100 more minutes a day within the glucose target range.
No differences in outcomes such as gestational age at delivery and rate of preterm delivery was found, although incidence of large-for-gestational-age infants, hypoglycemia requiring dextrose infusion, and neonatal ICU admission were lower in the CGM group to a statistically significant degree. “The numbers needed to treat were very small at six to eight women to reduce one of these events,” said Dr. Feig, who added that the numbers suggest the potential for cost savings.
Whatever the case, she said, “what price would you place on your baby avoiding a prolonged stay in the NICU? I think [it’s] priceless.”
She added that 80% of participants reported having trouble with the devices, which she attributed to the technology being old.
As for the planned pregnancy group, the study noted that “it did not have sufficient power to detect the magnitude of differences that were significant in the pregnancy trial.”
However, Dr. Feig said the study showed a trend toward lower HbA1c levels among CGM users in this population in which “tight glycemic control is absolutely paramount,” and that other studies also provide evidence supporting CGM use through the breastfeeding period.
Dr. Feig also pointed to a similar 2013 study coauthored by Dr. Mathiesen, her debate opponent. Dr. Feig said its findings are weakened because participants used CGM intermittently. She also pointed to the low participation (64%) in CGM by women assigned to a CGM group. (Diabetes Care. 2013 Jul;36[7]:1877-83)
In that study, researchers assigned 123 Danish women with type 1 diabetes mellitus and 31 women with type 2 diabetes mellitus to use real-time CGM for 6 days at various points in pregnancy or to only engage in routine care (including self-monitored plasma glucose seven times daily).
Researchers found no difference in HbA1c levels at 33 weeks between the groups, and they found similar rates of severe hypoglycemia and perinatal outcomes such as large-for-gestational-age infants.
These results, Dr. Mathiesen said, make her skeptical of a blanket recommendation to use CGM in pregnancy. Women aren’t eager to upload their glucose readings, making it difficult for doctors to make adjustments. “My women are Vikings. They come from Denmark,” she said, but “even these women don’t upload their glucose data between visits. ... I rarely have women who upload their data and look at their curves themselves. I think that’s a major disadvantage.”
Dr. Mathiesen also pointed to Dr. Feig’s study and noted that many women used CGM less than 75% of the time. In addition, 80% reported problems with the technology. “I’ve seen lots of skin problems with sensors. One lady used CGM during pregnancy; 4 years later, during another pregnancy, she showed me the mark of her sensor.”
Finally, the cost of CGM use is high considering the ongoing expense of the devices and the nurse time needed to upload data in the clinic. “As a rough estimate, the cost of CGM use in about 20 women during their pregnancies is the cost of the salary for one nurse per year,” she said.
Dr. Feig reported speaking fees from Medtronic, which provided CGM devices at reduced cost to her trial. Dr. Mathiesen reported research funding from the Novo Nordisk Foundation and speaker fees from Novo Nordisk, Lilly, AstraZeneca, and Sanofi-Aventis.
EXPERT ANALYSIS FROM ADA 2018
NAFLD less common, more severe in black children
ORLANDO – according to a review of 503 adolescents at the Yale University pediatric obesity clinic in New Haven, Conn.

As childhood obesity rates have climbed – the prevalence is now estimated to be around 20% – there’s been a corresponding increase in pediatric NAFLD, but it’s not very well characterized in children, and “there are many gaps in our knowledge,” said Nicola Santoro, MD, PhD, an assistant professor of pediatric endocrinology at Yale, and senior author of the review.
The goal of the work was to begin to plug the gaps. The children had baseline abdominal MRIs to quantify their hepatic fat content, along with oral glucose tolerance tests and genotyping for three single nucleotide polymorphisms (SNPs) strongly associated with the condition (PNPLA3 rs738409, GCKR rs1260326, and TM6SF2 rs58542926). MRI and metabolic testing were repeated at a mean of 2.27 years in 133 children.
The subjects were 13 years old on average, with a mean body mass index z-score of 2.52; 191 were white, 134 black, and 178 Hispanic. NAFLD was defined as a hepatic fat content of at least 5.5%.
The prevalence of fatty liver was 41.6% but ranged widely by ethnicity, with NAFLD diagnosed in 60% of Hispanic, 43% of white, but only 16% of black children. Among all three groups, prevalence was higher among boys.
Although NAFLD was least common among black children, when it was present, it was worse. Black children with NAFLD, compared with others, had the highest fasting glucose and 2-hour glucose levels; the highest insulin and C-peptide levels, and the highest hemoglobin A1c, despite similar age and gender distribution across the groups.
The findings translated to a higher prevalence of prediabetes and type 2 diabetes mellitus (66.6%), compared with white (24.4%) and Hispanic children (31.1%) with NAFLD.
Among 76 children who didn’t have NAFLD at baseline, 17 were diagnosed with the condition at follow-up. Progressors, compared with nonprogressors, showed higher baseline C-peptide levels (about 1,250 pmol/L versus 1,000 pmol/L) and greater weight gain (increase, versus a loss of, about 0.1 point on body mass index z-scores). Black children were the least likely to progress to NAFLD.
Increasing BMI z-score, higher baseline fasting C-peptide levels, and nonblack race strongly predicted progression (area under the curve = 0.887). The risk of progression was even higher when a NAFLD SNP was on board (AUC equal to or greater than 0.96).
Of 57 children with NAFLD at baseline, 13 didn’t meet the definition at follow-up, but regression turned out to be harder to predict. Regressors showed lower intrahepatic fat fractions at baseline (about 10% versus 20%), and a lowering of BMI z-scores at follow-up. Adding SNPs didn’t improve the model (AUC = 0.756).
As in adults, weight loss is the single most important factor to reverse NAFLD. “Even if you lose only a few kilos, fatty liver can go away. The liver cleans up pretty easily, but if you keep your weight, or you gain even a little bit, the disease keeps progressing,” Dr. Santoro said at the annual scientific sessions of the American Diabetes Association.
The investigators didn’t have any disclosures. The work was funded by the National Institutes of Health.
*This story was updated on 7/20/2018.
SOURCE: Trico D et al. ADA 2018, Abstract 313-OR.
ORLANDO – according to a review of 503 adolescents at the Yale University pediatric obesity clinic in New Haven, Conn.
As childhood obesity rates have climbed – the prevalence is now estimated to be around 20% – there’s been a corresponding increase in pediatric NAFLD, but it’s not very well characterized in children, and “there are many gaps in our knowledge,” said Nicola Santoro, MD, PhD, an assistant professor of pediatric endocrinology at Yale, and senior author of the review.
The goal of the work was to begin to plug the gaps. The children had baseline abdominal MRIs to quantify their hepatic fat content, along with oral glucose tolerance tests and genotyping for three single nucleotide polymorphisms (SNPs) strongly associated with the condition (PNPLA3 rs738409, GCKR rs1260326, and TM6SF2 rs58542926). MRI and metabolic testing were repeated at a mean of 2.27 years in 133 children.
The subjects were 13 years old on average, with a mean body mass index z-score of 2.52; 191 were white, 134 black, and 178 Hispanic. NAFLD was defined as a hepatic fat content of at least 5.5%.
The prevalence of fatty liver was 41.6% but ranged widely by ethnicity, with NAFLD diagnosed in 60% of Hispanic, 43% of white, but only 16% of black children. Among all three groups, prevalence was higher among boys.
Although NAFLD was least common among black children, when it was present, it was worse. Black children with NAFLD, compared with others, had the highest fasting glucose and 2-hour glucose levels; the highest insulin and C-peptide levels, and the highest hemoglobin A1c, despite similar age and gender distribution across the groups.
The findings translated to a higher prevalence of prediabetes and type 2 diabetes mellitus (66.6%), compared with white (24.4%) and Hispanic children (31.1%) with NAFLD.
Among 76 children who didn’t have NAFLD at baseline, 17 were diagnosed with the condition at follow-up. Progressors, compared with nonprogressors, showed higher baseline C-peptide levels (about 1,250 pmol/L versus 1,000 pmol/L) and greater weight gain (increase, versus a loss of, about 0.1 point on body mass index z-scores). Black children were the least likely to progress to NAFLD.
Increasing BMI z-score, higher baseline fasting C-peptide levels, and nonblack race strongly predicted progression (area under the curve = 0.887). The risk of progression was even higher when a NAFLD SNP was on board (AUC equal to or greater than 0.96).
Of 57 children with NAFLD at baseline, 13 didn’t meet the definition at follow-up, but regression turned out to be harder to predict. Regressors showed lower intrahepatic fat fractions at baseline (about 10% versus 20%), and a lowering of BMI z-scores at follow-up. Adding SNPs didn’t improve the model (AUC = 0.756).
As in adults, weight loss is the single most important factor to reverse NAFLD. “Even if you lose only a few kilos, fatty liver can go away. The liver cleans up pretty easily, but if you keep your weight, or you gain even a little bit, the disease keeps progressing,” Dr. Santoro said at the annual scientific sessions of the American Diabetes Association.
The investigators didn’t have any disclosures. The work was funded by the National Institutes of Health.
*This story was updated on 7/20/2018.
SOURCE: Trico D et al. ADA 2018, Abstract 313-OR.
ORLANDO – according to a review of 503 adolescents at the Yale University pediatric obesity clinic in New Haven, Conn.
As childhood obesity rates have climbed – the prevalence is now estimated to be around 20% – there’s been a corresponding increase in pediatric NAFLD, but it’s not very well characterized in children, and “there are many gaps in our knowledge,” said Nicola Santoro, MD, PhD, an assistant professor of pediatric endocrinology at Yale, and senior author of the review.
The goal of the work was to begin to plug the gaps. The children had baseline abdominal MRIs to quantify their hepatic fat content, along with oral glucose tolerance tests and genotyping for three single nucleotide polymorphisms (SNPs) strongly associated with the condition (PNPLA3 rs738409, GCKR rs1260326, and TM6SF2 rs58542926). MRI and metabolic testing were repeated at a mean of 2.27 years in 133 children.
The subjects were 13 years old on average, with a mean body mass index z-score of 2.52; 191 were white, 134 black, and 178 Hispanic. NAFLD was defined as a hepatic fat content of at least 5.5%.
The prevalence of fatty liver was 41.6% but ranged widely by ethnicity, with NAFLD diagnosed in 60% of Hispanic, 43% of white, but only 16% of black children. Among all three groups, prevalence was higher among boys.
Although NAFLD was least common among black children, when it was present, it was worse. Black children with NAFLD, compared with others, had the highest fasting glucose and 2-hour glucose levels; the highest insulin and C-peptide levels, and the highest hemoglobin A1c, despite similar age and gender distribution across the groups.
The findings translated to a higher prevalence of prediabetes and type 2 diabetes mellitus (66.6%), compared with white (24.4%) and Hispanic children (31.1%) with NAFLD.
Among 76 children who didn’t have NAFLD at baseline, 17 were diagnosed with the condition at follow-up. Progressors, compared with nonprogressors, showed higher baseline C-peptide levels (about 1,250 pmol/L versus 1,000 pmol/L) and greater weight gain (increase, versus a loss of, about 0.1 point on body mass index z-scores). Black children were the least likely to progress to NAFLD.
Increasing BMI z-score, higher baseline fasting C-peptide levels, and nonblack race strongly predicted progression (area under the curve = 0.887). The risk of progression was even higher when a NAFLD SNP was on board (AUC equal to or greater than 0.96).
Of 57 children with NAFLD at baseline, 13 didn’t meet the definition at follow-up, but regression turned out to be harder to predict. Regressors showed lower intrahepatic fat fractions at baseline (about 10% versus 20%), and a lowering of BMI z-scores at follow-up. Adding SNPs didn’t improve the model (AUC = 0.756).
As in adults, weight loss is the single most important factor to reverse NAFLD. “Even if you lose only a few kilos, fatty liver can go away. The liver cleans up pretty easily, but if you keep your weight, or you gain even a little bit, the disease keeps progressing,” Dr. Santoro said at the annual scientific sessions of the American Diabetes Association.
The investigators didn’t have any disclosures. The work was funded by the National Institutes of Health.
*This story was updated on 7/20/2018.
SOURCE: Trico D et al. ADA 2018, Abstract 313-OR.
REPORTING FROM ADA 2018
Key clinical point: Obese black children are less likely than others to develop non-alcoholic fatty liver disease, but more likely to suffer its consequences if they do.
Major finding: Black children with NAFLD had a higher prevalence of prediabetes and type 2 diabetes (66.6%), compared with white (24.4%) and Hispanic children (31.1%).
Study details: Review of 503 obese adolescents
Disclosures: The investigators didn’t have any disclosures. The work was funded by the National Institutes of Health.
Source: Trico D et al. ADA 2018, Abstract 313-OR.
Trial data suggest beneficial class effects of SGLT2 inhibitors, including dapagliflozin
ORLANDO – a post hoc analysis of data from the EXSCEL trial suggested.
The findings are consistent with those from published cardiovascular outcomes trials (CVOTs) of sodium-glucose transporter 2 (SGLT2) inhibitors other than dapagliflozin, real-world data, and findings from non-CVOTs of dapagliflozin, Lindsay Clegg, PhD, reported in a late-breaking poster at the annual scientific sessions of the American Diabetes Association.
In EXSCEL – a CVOT of once-weekly treatment with the glucagonlike peptide–1 receptor agonist exenatide added to usual care in patients with type 2 diabetes mellitus – 10% of patients took an SGLT2 inhibitor, and about half of those took dapagliflozin. For the current analysis, the effects of all SGLT2 inhibitors and dapagliflozin alone were evaluated in EXSCEL patients who received placebo.
“Just looking at that placebo data, we wanted to ask what the impact of SGLT2 inhibition was on the adjudicated cardiovascular events, as well as all-cause death and eGFR [estimated glomerular filtration rate] in this population,” Dr. Clegg, a postdoctoral fellow with the AstraZeneca Quantitative Clinical Pharmacology Group in Gaithersburg, Md., said in an interview.
In two propensity-matched cohorts, including a cohort of 709 SGLT2 inhibitor users and a cohort of 709 non-SGLT2 inhibitor users, SGLT2 inhibitors and dapagliflozin alone were found to numerically decrease the major adverse cardiac event (MACE) hazard ratio, and SGLT2 inhibitors significantly reduced all-cause mortality risk, she explained.
MACE events – a composite endpoint of cardiovascular death, nonfatal MI, or nonfatal stroke – occurred in 28 versus 44 patients in the SGLT2 and non-SGLT2 inhibitor groups, respectively (event rate per 100 patient-years, 3.41 vs. 4.45; adjusted HR, 0.79). Dr. Clegg noted that this hazard ratio is “very consistent with what has been seen in the CVOTs for [the SGLT2 inhibitors] empagliflozin and canagliflozin in literature.”
The corresponding figures for dapagliflozin were 11 versus 22 events (event rate per 100 patient-years, 2.69 vs. 4.54; aHR, 0.55).
“So those weren’t statistically significant, but those point estimates were very similar to literature,” she said.
All-cause mortality events occurred in 14 versus 37 patients in the SGLT2 and non-SGLT2 inhibitor groups, respectively (event rate per 100 patient-years, 1.61 vs. 3.34; aHR, 0.50), and in 7 versus 13 dapagliflozin patients within these groups, respectively (event rate per 100 patient-years, 1.62 vs. 2.42; aHR, 0.66).
The overall SGLT2 inhibitor all-cause mortality findings were very similar to what was seen in CVD-REAL, a real-world evidence trial which looked at cardiovascular outcomes in new users of SGLT-2 inhibitors, and the differences were statistically significant for the treatment effect.
“For dapagliflozin, the numbers were pretty similar as well. Not statistically significant, because the number of subjects was smaller, but similar,” Dr. Clegg said.
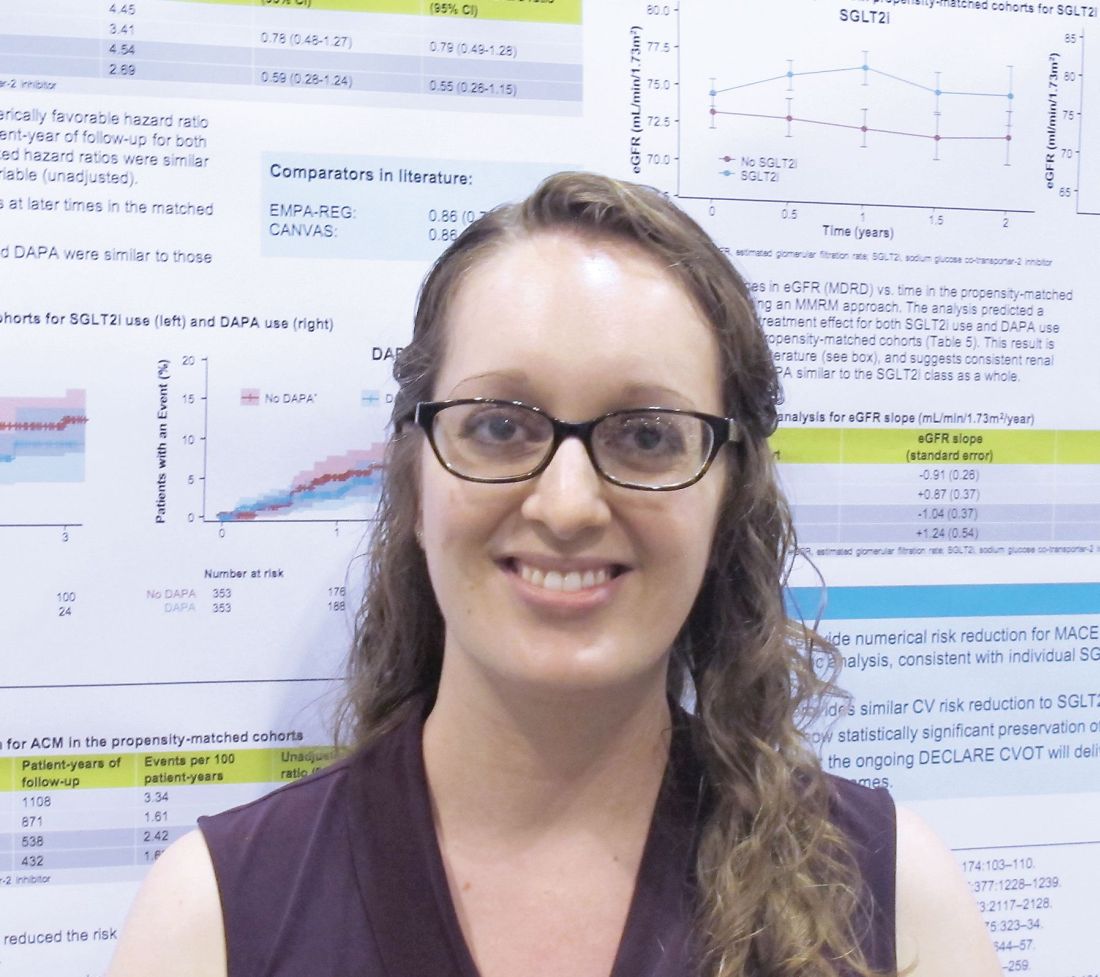
“On eGFR looking at renal function ... subjects not using an SGLT2 inhibitor had about a 1 mL/min per year decline, which is what we would expect for this population. At baseline the median eGFR was about 80, so it’s a fairly healthy population, because exenatide isn’t used in people with poor renal function,” she explained.
The effects of SGLT2 inhibitors overall, and dapagliflozin alone, were associated with the statistically significant increase in the eGFR slope over time – an outcome that the Food and Drug Administration now recognizes as a surrogate endpoint for renal outcomes, she added. “And again, that’s very consistent with what was seen for [the SGLT2 inhibitor empagliflozin] in the literature.”
Empagliflozin and canagliflozin (another SGLT2 inhibitor) have been shown to reduce MACE, all-cause mortality, and renal events in CVOTs, and real-world evidence suggests a class effect benefit, but dapagliflozin CVOT data have not yet been published.
“Overall this was a nice dataset where we had these adjudicated events to look at outcomes with SGLT2 inhibitors and with [dapagliflozin] specifically, and what we see is very encouraging and suggestive of a class effect,” she concluded, noting that findings from the ongoing phase 3 DECLARE-TIMI58 dapagliflozin CVOT should be released later this year.
Dr. Clegg is employed by AstraZeneca. She reported having no other disclosures.
SOURCE: Clegg L et al. ADA 2018, Abstract 130-LB.
ORLANDO – a post hoc analysis of data from the EXSCEL trial suggested.
The findings are consistent with those from published cardiovascular outcomes trials (CVOTs) of sodium-glucose transporter 2 (SGLT2) inhibitors other than dapagliflozin, real-world data, and findings from non-CVOTs of dapagliflozin, Lindsay Clegg, PhD, reported in a late-breaking poster at the annual scientific sessions of the American Diabetes Association.
In EXSCEL – a CVOT of once-weekly treatment with the glucagonlike peptide–1 receptor agonist exenatide added to usual care in patients with type 2 diabetes mellitus – 10% of patients took an SGLT2 inhibitor, and about half of those took dapagliflozin. For the current analysis, the effects of all SGLT2 inhibitors and dapagliflozin alone were evaluated in EXSCEL patients who received placebo.
“Just looking at that placebo data, we wanted to ask what the impact of SGLT2 inhibition was on the adjudicated cardiovascular events, as well as all-cause death and eGFR [estimated glomerular filtration rate] in this population,” Dr. Clegg, a postdoctoral fellow with the AstraZeneca Quantitative Clinical Pharmacology Group in Gaithersburg, Md., said in an interview.
In two propensity-matched cohorts, including a cohort of 709 SGLT2 inhibitor users and a cohort of 709 non-SGLT2 inhibitor users, SGLT2 inhibitors and dapagliflozin alone were found to numerically decrease the major adverse cardiac event (MACE) hazard ratio, and SGLT2 inhibitors significantly reduced all-cause mortality risk, she explained.
MACE events – a composite endpoint of cardiovascular death, nonfatal MI, or nonfatal stroke – occurred in 28 versus 44 patients in the SGLT2 and non-SGLT2 inhibitor groups, respectively (event rate per 100 patient-years, 3.41 vs. 4.45; adjusted HR, 0.79). Dr. Clegg noted that this hazard ratio is “very consistent with what has been seen in the CVOTs for [the SGLT2 inhibitors] empagliflozin and canagliflozin in literature.”
The corresponding figures for dapagliflozin were 11 versus 22 events (event rate per 100 patient-years, 2.69 vs. 4.54; aHR, 0.55).
“So those weren’t statistically significant, but those point estimates were very similar to literature,” she said.
All-cause mortality events occurred in 14 versus 37 patients in the SGLT2 and non-SGLT2 inhibitor groups, respectively (event rate per 100 patient-years, 1.61 vs. 3.34; aHR, 0.50), and in 7 versus 13 dapagliflozin patients within these groups, respectively (event rate per 100 patient-years, 1.62 vs. 2.42; aHR, 0.66).
The overall SGLT2 inhibitor all-cause mortality findings were very similar to what was seen in CVD-REAL, a real-world evidence trial which looked at cardiovascular outcomes in new users of SGLT-2 inhibitors, and the differences were statistically significant for the treatment effect.
“For dapagliflozin, the numbers were pretty similar as well. Not statistically significant, because the number of subjects was smaller, but similar,” Dr. Clegg said.
“On eGFR looking at renal function ... subjects not using an SGLT2 inhibitor had about a 1 mL/min per year decline, which is what we would expect for this population. At baseline the median eGFR was about 80, so it’s a fairly healthy population, because exenatide isn’t used in people with poor renal function,” she explained.
The effects of SGLT2 inhibitors overall, and dapagliflozin alone, were associated with the statistically significant increase in the eGFR slope over time – an outcome that the Food and Drug Administration now recognizes as a surrogate endpoint for renal outcomes, she added. “And again, that’s very consistent with what was seen for [the SGLT2 inhibitor empagliflozin] in the literature.”
Empagliflozin and canagliflozin (another SGLT2 inhibitor) have been shown to reduce MACE, all-cause mortality, and renal events in CVOTs, and real-world evidence suggests a class effect benefit, but dapagliflozin CVOT data have not yet been published.
“Overall this was a nice dataset where we had these adjudicated events to look at outcomes with SGLT2 inhibitors and with [dapagliflozin] specifically, and what we see is very encouraging and suggestive of a class effect,” she concluded, noting that findings from the ongoing phase 3 DECLARE-TIMI58 dapagliflozin CVOT should be released later this year.
Dr. Clegg is employed by AstraZeneca. She reported having no other disclosures.
SOURCE: Clegg L et al. ADA 2018, Abstract 130-LB.
ORLANDO – a post hoc analysis of data from the EXSCEL trial suggested.
The findings are consistent with those from published cardiovascular outcomes trials (CVOTs) of sodium-glucose transporter 2 (SGLT2) inhibitors other than dapagliflozin, real-world data, and findings from non-CVOTs of dapagliflozin, Lindsay Clegg, PhD, reported in a late-breaking poster at the annual scientific sessions of the American Diabetes Association.
In EXSCEL – a CVOT of once-weekly treatment with the glucagonlike peptide–1 receptor agonist exenatide added to usual care in patients with type 2 diabetes mellitus – 10% of patients took an SGLT2 inhibitor, and about half of those took dapagliflozin. For the current analysis, the effects of all SGLT2 inhibitors and dapagliflozin alone were evaluated in EXSCEL patients who received placebo.
“Just looking at that placebo data, we wanted to ask what the impact of SGLT2 inhibition was on the adjudicated cardiovascular events, as well as all-cause death and eGFR [estimated glomerular filtration rate] in this population,” Dr. Clegg, a postdoctoral fellow with the AstraZeneca Quantitative Clinical Pharmacology Group in Gaithersburg, Md., said in an interview.
In two propensity-matched cohorts, including a cohort of 709 SGLT2 inhibitor users and a cohort of 709 non-SGLT2 inhibitor users, SGLT2 inhibitors and dapagliflozin alone were found to numerically decrease the major adverse cardiac event (MACE) hazard ratio, and SGLT2 inhibitors significantly reduced all-cause mortality risk, she explained.
MACE events – a composite endpoint of cardiovascular death, nonfatal MI, or nonfatal stroke – occurred in 28 versus 44 patients in the SGLT2 and non-SGLT2 inhibitor groups, respectively (event rate per 100 patient-years, 3.41 vs. 4.45; adjusted HR, 0.79). Dr. Clegg noted that this hazard ratio is “very consistent with what has been seen in the CVOTs for [the SGLT2 inhibitors] empagliflozin and canagliflozin in literature.”
The corresponding figures for dapagliflozin were 11 versus 22 events (event rate per 100 patient-years, 2.69 vs. 4.54; aHR, 0.55).
“So those weren’t statistically significant, but those point estimates were very similar to literature,” she said.
All-cause mortality events occurred in 14 versus 37 patients in the SGLT2 and non-SGLT2 inhibitor groups, respectively (event rate per 100 patient-years, 1.61 vs. 3.34; aHR, 0.50), and in 7 versus 13 dapagliflozin patients within these groups, respectively (event rate per 100 patient-years, 1.62 vs. 2.42; aHR, 0.66).
The overall SGLT2 inhibitor all-cause mortality findings were very similar to what was seen in CVD-REAL, a real-world evidence trial which looked at cardiovascular outcomes in new users of SGLT-2 inhibitors, and the differences were statistically significant for the treatment effect.
“For dapagliflozin, the numbers were pretty similar as well. Not statistically significant, because the number of subjects was smaller, but similar,” Dr. Clegg said.
“On eGFR looking at renal function ... subjects not using an SGLT2 inhibitor had about a 1 mL/min per year decline, which is what we would expect for this population. At baseline the median eGFR was about 80, so it’s a fairly healthy population, because exenatide isn’t used in people with poor renal function,” she explained.
The effects of SGLT2 inhibitors overall, and dapagliflozin alone, were associated with the statistically significant increase in the eGFR slope over time – an outcome that the Food and Drug Administration now recognizes as a surrogate endpoint for renal outcomes, she added. “And again, that’s very consistent with what was seen for [the SGLT2 inhibitor empagliflozin] in the literature.”
Empagliflozin and canagliflozin (another SGLT2 inhibitor) have been shown to reduce MACE, all-cause mortality, and renal events in CVOTs, and real-world evidence suggests a class effect benefit, but dapagliflozin CVOT data have not yet been published.
“Overall this was a nice dataset where we had these adjudicated events to look at outcomes with SGLT2 inhibitors and with [dapagliflozin] specifically, and what we see is very encouraging and suggestive of a class effect,” she concluded, noting that findings from the ongoing phase 3 DECLARE-TIMI58 dapagliflozin CVOT should be released later this year.
Dr. Clegg is employed by AstraZeneca. She reported having no other disclosures.
SOURCE: Clegg L et al. ADA 2018, Abstract 130-LB.
REPORTING FROM ADA 2018
Key clinical point: Sodium-glucose transporter 2 inhibitors, including dapagliflozin, have beneficial class effects on major adverse cardiac events, all-cause mortality, and renal function.
Major finding: MACE occurred in 28 versus 44 patients in the SGLT2 and non-SGLT2 inhibitor groups, respectively (adjusted hazard ratio, 0.79).
Study details: A post hoc analysis of data from 1,418 EXSCEL trial subjects.
Disclosures: Dr. Clegg is employed by AstraZeneca. She reported having no other disclosures.
Source: Clegg L et al. ADA 2018, Abstract 130-LB.
CVD-REAL 2: Lower mortality, CV risks with SGLT-2i vs. DPP-4i treatment in T2DM
ORLANDO – according to findings from the CVD-REAL 2 study.
CVD-REAL 2 is a real-world, observational cohort study involving the analysis of health records for two matched cohorts of patients with T2DM from 12 countries across the globe, including 181,620 SGLT-2 inhibitor recipients and 181,620 DPP-4 inhibitor recipients who were newly initiated on their respective treatments between December 2012 and November 2017. The respective rates of all-cause death were 0.83 and 1.33 per 100 patient-years (4,768 events; hazard ratio, 0.51), Shun Kohsaka, MD, of Keio University School of Medicine, Tokyo, and his colleagues reported in a late-breaking poster at the annual scientific sessions of the American Diabetes Association.
“HRs for all-cause death consistently favored SGLT-2 inhibitor vs. DPP-4 inhibitor in each country,” the investigators noted. “Directionally, the same results were observed in other cardiovascular outcomes, including [hospitalization for heart failure (HHF)], and the composite of all-cause death or HHF but modestly for [myocardial infarction] and stroke.”
The rates of hospitalization for heart failure per 100 patient-years were 0.80 and 1.08 in the SGLT-2 inhibitor and DPP-4 inhibitor groups (3,875 events; HR, 0.68), and for HHF plus all-cause death, they were 1.55 and 2.22 per 100 patient-years (7,807 events; HR, 0.67), respectively. The rates of myocardial infarction in the groups, respectively, were 0.53 and 0.58 per 100 patient-years (2,298 events; HR, 0.90), and for stroke, they were 0.82 and 0.99 per 100 patient-years (3,747 events; HR, 0.84), the investigators reported.
Study subjects in both cohorts had a mean age of 58 years, and 30% and 29% in the SGLT-2 inhibitor and DPP-4 inhibitor groups, respectively, had established cardiovascular disease. Only those newly initiated on either an SGLT-2 inhibitor or DPP-4 inhibitor were selected from each data source; fixed-dose combinations were allowed as long as there was no use of either drug during the year prior to enrollment.
In the SGLT-2 inhibitor cohort, most exposures (60.1%) were to dapagliflozin, followed by canagliflozin (23.8%) and empagliflozin (12.1%). The remaining exposures were to ipragliflozin, tofogliflozin, or luseogliflozin (0.3-2.8%). In the DPP-4 inhibitor group, most exposures (49.7%) were to sitagliptin, 18.9% were to linagliptin, 10.4% were to saxagliptin, and the remaining exposures were to alogliptin, gemigliptin, teneligliptin, anagliptin, evogliptin, and trelagliptin (0.1%-4.7%).
Those in the SGLT-2 inhibitor group were followed for a mean of 439 days, and those in the DPP-4 inhibitor group were followed for a mean of 446 days.
“The results were consistent across the subgroups of patients with and without established [cardiovascular disease], favoring SGLT-2 inhibitor vs. DPP-4 inhibitor for all outcomes,” they noted.
Both DPP-4 inhibitors and SGLT2 inhibitors are widely used in T2DM, and although clinical trials demonstrated lower risk of cardiovascular events with SGLT-2 inhibitors and a neutral effect on cardiovascular events with DPP-4 inhibitors, large comparative studies are lacking, the investigators explained.
Though limited by the possibility of residual, unmeasured confounding, as well as by a lack of mortality data in Japan and Singapore apart from the inpatient setting, the findings of this “large, contemporary analysis of real-world administrative data” are complementary to those from previous observational studies and clinical trials, they concluded, noting that “SGLT-2 inhibitor experience in real-world practice is still relatively short and longer-term follow-up is required to examine whether effects are sustained over time.”
The CVD-REAL studies are sponsored by AstraZeneca. Dr. Kohsaka reported receiving research support from Bayer Yakuhin and Daiichi Sankyo and serving on the speaker’s bureau for Bayer Yakuhin and Bristol-Myers Squibb.
SOURCE: Kohsaka S et al. ADA 2018, Abstract 124-LB.
ORLANDO – according to findings from the CVD-REAL 2 study.
CVD-REAL 2 is a real-world, observational cohort study involving the analysis of health records for two matched cohorts of patients with T2DM from 12 countries across the globe, including 181,620 SGLT-2 inhibitor recipients and 181,620 DPP-4 inhibitor recipients who were newly initiated on their respective treatments between December 2012 and November 2017. The respective rates of all-cause death were 0.83 and 1.33 per 100 patient-years (4,768 events; hazard ratio, 0.51), Shun Kohsaka, MD, of Keio University School of Medicine, Tokyo, and his colleagues reported in a late-breaking poster at the annual scientific sessions of the American Diabetes Association.
“HRs for all-cause death consistently favored SGLT-2 inhibitor vs. DPP-4 inhibitor in each country,” the investigators noted. “Directionally, the same results were observed in other cardiovascular outcomes, including [hospitalization for heart failure (HHF)], and the composite of all-cause death or HHF but modestly for [myocardial infarction] and stroke.”
The rates of hospitalization for heart failure per 100 patient-years were 0.80 and 1.08 in the SGLT-2 inhibitor and DPP-4 inhibitor groups (3,875 events; HR, 0.68), and for HHF plus all-cause death, they were 1.55 and 2.22 per 100 patient-years (7,807 events; HR, 0.67), respectively. The rates of myocardial infarction in the groups, respectively, were 0.53 and 0.58 per 100 patient-years (2,298 events; HR, 0.90), and for stroke, they were 0.82 and 0.99 per 100 patient-years (3,747 events; HR, 0.84), the investigators reported.
Study subjects in both cohorts had a mean age of 58 years, and 30% and 29% in the SGLT-2 inhibitor and DPP-4 inhibitor groups, respectively, had established cardiovascular disease. Only those newly initiated on either an SGLT-2 inhibitor or DPP-4 inhibitor were selected from each data source; fixed-dose combinations were allowed as long as there was no use of either drug during the year prior to enrollment.
In the SGLT-2 inhibitor cohort, most exposures (60.1%) were to dapagliflozin, followed by canagliflozin (23.8%) and empagliflozin (12.1%). The remaining exposures were to ipragliflozin, tofogliflozin, or luseogliflozin (0.3-2.8%). In the DPP-4 inhibitor group, most exposures (49.7%) were to sitagliptin, 18.9% were to linagliptin, 10.4% were to saxagliptin, and the remaining exposures were to alogliptin, gemigliptin, teneligliptin, anagliptin, evogliptin, and trelagliptin (0.1%-4.7%).
Those in the SGLT-2 inhibitor group were followed for a mean of 439 days, and those in the DPP-4 inhibitor group were followed for a mean of 446 days.
“The results were consistent across the subgroups of patients with and without established [cardiovascular disease], favoring SGLT-2 inhibitor vs. DPP-4 inhibitor for all outcomes,” they noted.
Both DPP-4 inhibitors and SGLT2 inhibitors are widely used in T2DM, and although clinical trials demonstrated lower risk of cardiovascular events with SGLT-2 inhibitors and a neutral effect on cardiovascular events with DPP-4 inhibitors, large comparative studies are lacking, the investigators explained.
Though limited by the possibility of residual, unmeasured confounding, as well as by a lack of mortality data in Japan and Singapore apart from the inpatient setting, the findings of this “large, contemporary analysis of real-world administrative data” are complementary to those from previous observational studies and clinical trials, they concluded, noting that “SGLT-2 inhibitor experience in real-world practice is still relatively short and longer-term follow-up is required to examine whether effects are sustained over time.”
The CVD-REAL studies are sponsored by AstraZeneca. Dr. Kohsaka reported receiving research support from Bayer Yakuhin and Daiichi Sankyo and serving on the speaker’s bureau for Bayer Yakuhin and Bristol-Myers Squibb.
SOURCE: Kohsaka S et al. ADA 2018, Abstract 124-LB.
ORLANDO – according to findings from the CVD-REAL 2 study.
CVD-REAL 2 is a real-world, observational cohort study involving the analysis of health records for two matched cohorts of patients with T2DM from 12 countries across the globe, including 181,620 SGLT-2 inhibitor recipients and 181,620 DPP-4 inhibitor recipients who were newly initiated on their respective treatments between December 2012 and November 2017. The respective rates of all-cause death were 0.83 and 1.33 per 100 patient-years (4,768 events; hazard ratio, 0.51), Shun Kohsaka, MD, of Keio University School of Medicine, Tokyo, and his colleagues reported in a late-breaking poster at the annual scientific sessions of the American Diabetes Association.
“HRs for all-cause death consistently favored SGLT-2 inhibitor vs. DPP-4 inhibitor in each country,” the investigators noted. “Directionally, the same results were observed in other cardiovascular outcomes, including [hospitalization for heart failure (HHF)], and the composite of all-cause death or HHF but modestly for [myocardial infarction] and stroke.”
The rates of hospitalization for heart failure per 100 patient-years were 0.80 and 1.08 in the SGLT-2 inhibitor and DPP-4 inhibitor groups (3,875 events; HR, 0.68), and for HHF plus all-cause death, they were 1.55 and 2.22 per 100 patient-years (7,807 events; HR, 0.67), respectively. The rates of myocardial infarction in the groups, respectively, were 0.53 and 0.58 per 100 patient-years (2,298 events; HR, 0.90), and for stroke, they were 0.82 and 0.99 per 100 patient-years (3,747 events; HR, 0.84), the investigators reported.
Study subjects in both cohorts had a mean age of 58 years, and 30% and 29% in the SGLT-2 inhibitor and DPP-4 inhibitor groups, respectively, had established cardiovascular disease. Only those newly initiated on either an SGLT-2 inhibitor or DPP-4 inhibitor were selected from each data source; fixed-dose combinations were allowed as long as there was no use of either drug during the year prior to enrollment.
In the SGLT-2 inhibitor cohort, most exposures (60.1%) were to dapagliflozin, followed by canagliflozin (23.8%) and empagliflozin (12.1%). The remaining exposures were to ipragliflozin, tofogliflozin, or luseogliflozin (0.3-2.8%). In the DPP-4 inhibitor group, most exposures (49.7%) were to sitagliptin, 18.9% were to linagliptin, 10.4% were to saxagliptin, and the remaining exposures were to alogliptin, gemigliptin, teneligliptin, anagliptin, evogliptin, and trelagliptin (0.1%-4.7%).
Those in the SGLT-2 inhibitor group were followed for a mean of 439 days, and those in the DPP-4 inhibitor group were followed for a mean of 446 days.
“The results were consistent across the subgroups of patients with and without established [cardiovascular disease], favoring SGLT-2 inhibitor vs. DPP-4 inhibitor for all outcomes,” they noted.
Both DPP-4 inhibitors and SGLT2 inhibitors are widely used in T2DM, and although clinical trials demonstrated lower risk of cardiovascular events with SGLT-2 inhibitors and a neutral effect on cardiovascular events with DPP-4 inhibitors, large comparative studies are lacking, the investigators explained.
Though limited by the possibility of residual, unmeasured confounding, as well as by a lack of mortality data in Japan and Singapore apart from the inpatient setting, the findings of this “large, contemporary analysis of real-world administrative data” are complementary to those from previous observational studies and clinical trials, they concluded, noting that “SGLT-2 inhibitor experience in real-world practice is still relatively short and longer-term follow-up is required to examine whether effects are sustained over time.”
The CVD-REAL studies are sponsored by AstraZeneca. Dr. Kohsaka reported receiving research support from Bayer Yakuhin and Daiichi Sankyo and serving on the speaker’s bureau for Bayer Yakuhin and Bristol-Myers Squibb.
SOURCE: Kohsaka S et al. ADA 2018, Abstract 124-LB.
REPORTING FROM ADA 2018
Key clinical point: SGLT-2 inhibitor treatment is associated with significantly lower risks of death, CV events, and stroke in T2DM, compared with DPP-4 inhibitor treatment.
Major finding: The rates of all-cause death in the SGLT-2 inhibitor and DPP-4 inhibitor groups, respectively, were 0.83 and 1.33 per 100 patient-years (4,768 events; hazard ratio, 0.51).
Study details: A multinational, observational cohort study of more than 360,000 subjects.
Disclosures: The CVD-REAL studies are sponsored by AstraZeneca. Dr. Kohsaka reported receiving research support from Bayer Yakuhin and Daiichi Sankyo and serving on the speaker’s bureau for Bayer Yakuhin and Bristol-Myers Squibb.
Source: Kohsaka S et al. ADA 2018, Abstract 124-LB.
Special care advised for HIV-infected patients with diabetes
ORLANDO – Research suggests that HIV-positive people who take the latest generations of AIDS medications are living almost as long as everyone else. But they still face special medical challenges, and an endocrinologist urged colleagues to adjust their approaches to diabetes in these patients.
said Todd T. Brown, MD, PhD, of Johns Hopkins Medicine, Baltimore, in a presentation at the annual scientific sessions of the American Diabetes Association.
It’s not just a matter of subbing in an alternate drug here or there. When it comes to diabetes, patients with HIV require significant adjustments to diagnosis and treatment, Dr. Brown said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
In terms of diagnosis, treatment guidelines approved by the Infectious Diseases Society of America and ADA recommend that all HIV-positive patients be tested for diabetes before they begin taking antiretroviral therapy. Then, the guidelines suggest, they should be tested 4-6 weeks after initiation of therapy, and every 6-12 months going forward.
“It’s a bit of overkill to go every 6 months,” said Dr. Brown, who prefers an annual testing approach. He added that research has suggested that the 2-hour postload glucose test is more sensitive than the fasting glucose test in some HIV-positive populations. However, he believes that it’s generally fine to give a fasting glucose test before initiation of therapy – and on an annual basis afterward – rather than the more cumbersome postload test.
Still, he said, the postload test may be appropriate in a patient with impaired glucose tolerance “if you really want to make the diagnosis, and especially if you’ll change your treatment based on it.”
Ongoing treatment of HIV-positive patients also presents unique challenges, he said. For one, antiretroviral therapy seems to affect glucose metabolism and body fat, he said, and findings from a 2016 study suggest HIV-positive people who begin antiretroviral therapy face a higher risk of developing diabetes after weight gain (J Acquir Immune Defic Syndr. 2016 Oct 1;73[2]:228-36).
One option is to switch patients to integrase inhibitors, but findings from a 2017 study suggested that this may also lead to more weight gain, Dr. Brown said.
“This has been an evolving story,” he said. “The clinical consequences of this are unclear. This is a topic that’s being hotly investigated now in the HIV health world” (JAIDS. 2017 Dec 15;76[5]:527-31).
As for other diabetes management issues, Dr. Brown noted that hemoglobin A1c tests appear to underestimate glycemia in HIV-infected patients. He suggested that goal HbA1c levels should be lower in diabetic patients with HIV, especially those with CD4+ counts under 500 cells /mm3 and/or mean cell volume over 100 fL.
Research suggests that lifestyle changes seem to work well in HIV-positive patients, he said, and metformin is the ideal first-line drug treatment just as in the HIV-negative population. “It’s a good drug. We all love it,” he said. “It may improve lipohypertrophy and coronary plaque.”
He added that proteinuria and neuropathy are more common in HIV-positive patients with diabetes. He said levels of neuropathy and nephropathy could be related to AIDS drugs.
On the medication front, Dr. Brown cautioned about certain drugs in HIV-positive patients: The HIV drug dolutegravir increases metformin concentrations by about 80%, he said, and there are concerns about bone and cardiac health in HIV-positive patients who take the diabetes medications known as thiazolidinediones (glitazones).
He added that there are sparse data about the use of several types of diabetes drugs – DPP IV inhibitors, GLP-1 receptor agonists, and SGLT2 inhibitors – in HIV-positive patients.
Dr. Brown discloses consulting for Gilead Sciences, ViiV, BMS, Merck, Theratechnologies, and EMD Serono.
ORLANDO – Research suggests that HIV-positive people who take the latest generations of AIDS medications are living almost as long as everyone else. But they still face special medical challenges, and an endocrinologist urged colleagues to adjust their approaches to diabetes in these patients.
said Todd T. Brown, MD, PhD, of Johns Hopkins Medicine, Baltimore, in a presentation at the annual scientific sessions of the American Diabetes Association.
It’s not just a matter of subbing in an alternate drug here or there. When it comes to diabetes, patients with HIV require significant adjustments to diagnosis and treatment, Dr. Brown said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
In terms of diagnosis, treatment guidelines approved by the Infectious Diseases Society of America and ADA recommend that all HIV-positive patients be tested for diabetes before they begin taking antiretroviral therapy. Then, the guidelines suggest, they should be tested 4-6 weeks after initiation of therapy, and every 6-12 months going forward.
“It’s a bit of overkill to go every 6 months,” said Dr. Brown, who prefers an annual testing approach. He added that research has suggested that the 2-hour postload glucose test is more sensitive than the fasting glucose test in some HIV-positive populations. However, he believes that it’s generally fine to give a fasting glucose test before initiation of therapy – and on an annual basis afterward – rather than the more cumbersome postload test.
Still, he said, the postload test may be appropriate in a patient with impaired glucose tolerance “if you really want to make the diagnosis, and especially if you’ll change your treatment based on it.”
Ongoing treatment of HIV-positive patients also presents unique challenges, he said. For one, antiretroviral therapy seems to affect glucose metabolism and body fat, he said, and findings from a 2016 study suggest HIV-positive people who begin antiretroviral therapy face a higher risk of developing diabetes after weight gain (J Acquir Immune Defic Syndr. 2016 Oct 1;73[2]:228-36).
One option is to switch patients to integrase inhibitors, but findings from a 2017 study suggested that this may also lead to more weight gain, Dr. Brown said.
“This has been an evolving story,” he said. “The clinical consequences of this are unclear. This is a topic that’s being hotly investigated now in the HIV health world” (JAIDS. 2017 Dec 15;76[5]:527-31).
As for other diabetes management issues, Dr. Brown noted that hemoglobin A1c tests appear to underestimate glycemia in HIV-infected patients. He suggested that goal HbA1c levels should be lower in diabetic patients with HIV, especially those with CD4+ counts under 500 cells /mm3 and/or mean cell volume over 100 fL.
Research suggests that lifestyle changes seem to work well in HIV-positive patients, he said, and metformin is the ideal first-line drug treatment just as in the HIV-negative population. “It’s a good drug. We all love it,” he said. “It may improve lipohypertrophy and coronary plaque.”
He added that proteinuria and neuropathy are more common in HIV-positive patients with diabetes. He said levels of neuropathy and nephropathy could be related to AIDS drugs.
On the medication front, Dr. Brown cautioned about certain drugs in HIV-positive patients: The HIV drug dolutegravir increases metformin concentrations by about 80%, he said, and there are concerns about bone and cardiac health in HIV-positive patients who take the diabetes medications known as thiazolidinediones (glitazones).
He added that there are sparse data about the use of several types of diabetes drugs – DPP IV inhibitors, GLP-1 receptor agonists, and SGLT2 inhibitors – in HIV-positive patients.
Dr. Brown discloses consulting for Gilead Sciences, ViiV, BMS, Merck, Theratechnologies, and EMD Serono.
ORLANDO – Research suggests that HIV-positive people who take the latest generations of AIDS medications are living almost as long as everyone else. But they still face special medical challenges, and an endocrinologist urged colleagues to adjust their approaches to diabetes in these patients.
said Todd T. Brown, MD, PhD, of Johns Hopkins Medicine, Baltimore, in a presentation at the annual scientific sessions of the American Diabetes Association.
It’s not just a matter of subbing in an alternate drug here or there. When it comes to diabetes, patients with HIV require significant adjustments to diagnosis and treatment, Dr. Brown said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
In terms of diagnosis, treatment guidelines approved by the Infectious Diseases Society of America and ADA recommend that all HIV-positive patients be tested for diabetes before they begin taking antiretroviral therapy. Then, the guidelines suggest, they should be tested 4-6 weeks after initiation of therapy, and every 6-12 months going forward.
“It’s a bit of overkill to go every 6 months,” said Dr. Brown, who prefers an annual testing approach. He added that research has suggested that the 2-hour postload glucose test is more sensitive than the fasting glucose test in some HIV-positive populations. However, he believes that it’s generally fine to give a fasting glucose test before initiation of therapy – and on an annual basis afterward – rather than the more cumbersome postload test.
Still, he said, the postload test may be appropriate in a patient with impaired glucose tolerance “if you really want to make the diagnosis, and especially if you’ll change your treatment based on it.”
Ongoing treatment of HIV-positive patients also presents unique challenges, he said. For one, antiretroviral therapy seems to affect glucose metabolism and body fat, he said, and findings from a 2016 study suggest HIV-positive people who begin antiretroviral therapy face a higher risk of developing diabetes after weight gain (J Acquir Immune Defic Syndr. 2016 Oct 1;73[2]:228-36).
One option is to switch patients to integrase inhibitors, but findings from a 2017 study suggested that this may also lead to more weight gain, Dr. Brown said.
“This has been an evolving story,” he said. “The clinical consequences of this are unclear. This is a topic that’s being hotly investigated now in the HIV health world” (JAIDS. 2017 Dec 15;76[5]:527-31).
As for other diabetes management issues, Dr. Brown noted that hemoglobin A1c tests appear to underestimate glycemia in HIV-infected patients. He suggested that goal HbA1c levels should be lower in diabetic patients with HIV, especially those with CD4+ counts under 500 cells /mm3 and/or mean cell volume over 100 fL.
Research suggests that lifestyle changes seem to work well in HIV-positive patients, he said, and metformin is the ideal first-line drug treatment just as in the HIV-negative population. “It’s a good drug. We all love it,” he said. “It may improve lipohypertrophy and coronary plaque.”
He added that proteinuria and neuropathy are more common in HIV-positive patients with diabetes. He said levels of neuropathy and nephropathy could be related to AIDS drugs.
On the medication front, Dr. Brown cautioned about certain drugs in HIV-positive patients: The HIV drug dolutegravir increases metformin concentrations by about 80%, he said, and there are concerns about bone and cardiac health in HIV-positive patients who take the diabetes medications known as thiazolidinediones (glitazones).
He added that there are sparse data about the use of several types of diabetes drugs – DPP IV inhibitors, GLP-1 receptor agonists, and SGLT2 inhibitors – in HIV-positive patients.
Dr. Brown discloses consulting for Gilead Sciences, ViiV, BMS, Merck, Theratechnologies, and EMD Serono.
EXPERT ANALYSIS FROM ADA 2018
Closed-loop insulin control for T2DM is feasible in hospital setting
ORLANDO – (T2DM).
The findings, released at the annual scientific sessions of the American Diabetes Association and via simultaneous publication in The New England Journal of Medicine, don’t examine cost or clinical outcomes. However, “our results suggest this new technology might be another approach to manage in-patient hypoglycemia in a safe and effective way, lead author Lia Bally, MD, PhD, of the division of endocrinology, diabetes, and clinical nutrition, Bern (Switzerland ) University Hospital, said in an interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
For the open-label trial, the researchers recruited 136 adults with T2DM under noncritical care at two hospitals (one in the England and the other in Switzerland). Some patients had undergone surgery, Dr. Bally said, and some others were being treated for systemic infections. Comorbidities were significantly more severe in the closed-loop group, and 43% had sepsis.
All of the subjects required subcutaneous insulin therapy.
From 2016 to 2017, patients were randomly assigned to receive normal subcutaneous insulin therapy (n = 70) or closed-loop insulin delivery (n = 66).
It took about 15 minutes to perform the procedure to implement the closed-loop insulin delivery system, Dr. Bally said. It featured a subcutaneous cannula inserted into the abdomen, a continuous glucose monitor (a device also used in the control group), and a trial insulin pump.
This was not a hybrid system, and it did not include prandial insulin boluses or input of the timing and carbohydrate content of meals. One reason behind the choice to adopt a fully automated system was to relieve the burden on both health care professionals and patients, coauthor Hood Thabit, PhD, of Wellcome Trust–MRC Institute of Metabolic Science, the Manchester Academic Health Science Center, and University of Manchester, said in an interview.
For up to 15 days or until discharge, researchers tracked how much of the time sensor glucose measurements were in a target range of 100 mg/dL to 180 mg/dL.
In the closed-loop group, glucose measurements were in the target range 66 mg/dL ± 17% of the time compared to 42 mg/dL ± 17% in the control group, a difference of 24 mg/dL ± 3% (95% confidence interval, 19-30; P less than .001).
For the closed-loop group, the average glucose level was 154 mg/dL, and it was 188 mg/dL in the control group (P less than .001).
The researchers didn’t find a statistically significant difference between the groups in duration of hypoglycemia or amount of insulin delivered.
None of the patients suffered from severe hypoglycemia or clinically significant hyperglycemia with ketonemia.
There were 18 incidents of clinically significant hyperglycemia events (capillary glucose levels of more than 360 mg/dL) in the closed-loop group, compared with 41 such events in the control group. (P = .03)
Three patients in each group had adverse trial-related device effects.
Of 62 patients in the closed-loop group who completed the trial, 87% reported being pleased by their glucose levels, and all but one reported being happy to have their levels monitored automatically. All 62 patients said they’d recommend the system to others.
Going forward, the researchers hope to launch a multicenter trial that will examine clinical outcomes such as postoperative complications, infections, mortality, and glucose control after hospital discharge, according to Dr. Bally.
The study was supported by Diabetes UK, the Swiss National Science Foundation, the European Foundation for the Study of Diabetes, the JDRF, the National Institute for Health Research Cambridge Biomedical Research Center, and a Wellcome Strategic Award. Abbott Diabetes Care supplied equipment and guidance regarding connectivity, and representatives reviewed the manuscript before submission.
Dr. Bally reported funding from the University Hospital Bern, University of Bern and the Swiss Diabetes Foundation. Dr. Thabit reported no disclosures. Other authors report no disclosures or various disclosures.
SOURCE: Bally L et al. ADA 2018 Abstract 350-OR. Published simultaneously in The New England Journal of Medicine. June 25, 2018
ORLANDO – (T2DM).
The findings, released at the annual scientific sessions of the American Diabetes Association and via simultaneous publication in The New England Journal of Medicine, don’t examine cost or clinical outcomes. However, “our results suggest this new technology might be another approach to manage in-patient hypoglycemia in a safe and effective way, lead author Lia Bally, MD, PhD, of the division of endocrinology, diabetes, and clinical nutrition, Bern (Switzerland ) University Hospital, said in an interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
For the open-label trial, the researchers recruited 136 adults with T2DM under noncritical care at two hospitals (one in the England and the other in Switzerland). Some patients had undergone surgery, Dr. Bally said, and some others were being treated for systemic infections. Comorbidities were significantly more severe in the closed-loop group, and 43% had sepsis.
All of the subjects required subcutaneous insulin therapy.
From 2016 to 2017, patients were randomly assigned to receive normal subcutaneous insulin therapy (n = 70) or closed-loop insulin delivery (n = 66).
It took about 15 minutes to perform the procedure to implement the closed-loop insulin delivery system, Dr. Bally said. It featured a subcutaneous cannula inserted into the abdomen, a continuous glucose monitor (a device also used in the control group), and a trial insulin pump.
This was not a hybrid system, and it did not include prandial insulin boluses or input of the timing and carbohydrate content of meals. One reason behind the choice to adopt a fully automated system was to relieve the burden on both health care professionals and patients, coauthor Hood Thabit, PhD, of Wellcome Trust–MRC Institute of Metabolic Science, the Manchester Academic Health Science Center, and University of Manchester, said in an interview.
For up to 15 days or until discharge, researchers tracked how much of the time sensor glucose measurements were in a target range of 100 mg/dL to 180 mg/dL.
In the closed-loop group, glucose measurements were in the target range 66 mg/dL ± 17% of the time compared to 42 mg/dL ± 17% in the control group, a difference of 24 mg/dL ± 3% (95% confidence interval, 19-30; P less than .001).
For the closed-loop group, the average glucose level was 154 mg/dL, and it was 188 mg/dL in the control group (P less than .001).
The researchers didn’t find a statistically significant difference between the groups in duration of hypoglycemia or amount of insulin delivered.
None of the patients suffered from severe hypoglycemia or clinically significant hyperglycemia with ketonemia.
There were 18 incidents of clinically significant hyperglycemia events (capillary glucose levels of more than 360 mg/dL) in the closed-loop group, compared with 41 such events in the control group. (P = .03)
Three patients in each group had adverse trial-related device effects.
Of 62 patients in the closed-loop group who completed the trial, 87% reported being pleased by their glucose levels, and all but one reported being happy to have their levels monitored automatically. All 62 patients said they’d recommend the system to others.
Going forward, the researchers hope to launch a multicenter trial that will examine clinical outcomes such as postoperative complications, infections, mortality, and glucose control after hospital discharge, according to Dr. Bally.
The study was supported by Diabetes UK, the Swiss National Science Foundation, the European Foundation for the Study of Diabetes, the JDRF, the National Institute for Health Research Cambridge Biomedical Research Center, and a Wellcome Strategic Award. Abbott Diabetes Care supplied equipment and guidance regarding connectivity, and representatives reviewed the manuscript before submission.
Dr. Bally reported funding from the University Hospital Bern, University of Bern and the Swiss Diabetes Foundation. Dr. Thabit reported no disclosures. Other authors report no disclosures or various disclosures.
SOURCE: Bally L et al. ADA 2018 Abstract 350-OR. Published simultaneously in The New England Journal of Medicine. June 25, 2018
ORLANDO – (T2DM).
The findings, released at the annual scientific sessions of the American Diabetes Association and via simultaneous publication in The New England Journal of Medicine, don’t examine cost or clinical outcomes. However, “our results suggest this new technology might be another approach to manage in-patient hypoglycemia in a safe and effective way, lead author Lia Bally, MD, PhD, of the division of endocrinology, diabetes, and clinical nutrition, Bern (Switzerland ) University Hospital, said in an interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
For the open-label trial, the researchers recruited 136 adults with T2DM under noncritical care at two hospitals (one in the England and the other in Switzerland). Some patients had undergone surgery, Dr. Bally said, and some others were being treated for systemic infections. Comorbidities were significantly more severe in the closed-loop group, and 43% had sepsis.
All of the subjects required subcutaneous insulin therapy.
From 2016 to 2017, patients were randomly assigned to receive normal subcutaneous insulin therapy (n = 70) or closed-loop insulin delivery (n = 66).
It took about 15 minutes to perform the procedure to implement the closed-loop insulin delivery system, Dr. Bally said. It featured a subcutaneous cannula inserted into the abdomen, a continuous glucose monitor (a device also used in the control group), and a trial insulin pump.
This was not a hybrid system, and it did not include prandial insulin boluses or input of the timing and carbohydrate content of meals. One reason behind the choice to adopt a fully automated system was to relieve the burden on both health care professionals and patients, coauthor Hood Thabit, PhD, of Wellcome Trust–MRC Institute of Metabolic Science, the Manchester Academic Health Science Center, and University of Manchester, said in an interview.
For up to 15 days or until discharge, researchers tracked how much of the time sensor glucose measurements were in a target range of 100 mg/dL to 180 mg/dL.
In the closed-loop group, glucose measurements were in the target range 66 mg/dL ± 17% of the time compared to 42 mg/dL ± 17% in the control group, a difference of 24 mg/dL ± 3% (95% confidence interval, 19-30; P less than .001).
For the closed-loop group, the average glucose level was 154 mg/dL, and it was 188 mg/dL in the control group (P less than .001).
The researchers didn’t find a statistically significant difference between the groups in duration of hypoglycemia or amount of insulin delivered.
None of the patients suffered from severe hypoglycemia or clinically significant hyperglycemia with ketonemia.
There were 18 incidents of clinically significant hyperglycemia events (capillary glucose levels of more than 360 mg/dL) in the closed-loop group, compared with 41 such events in the control group. (P = .03)
Three patients in each group had adverse trial-related device effects.
Of 62 patients in the closed-loop group who completed the trial, 87% reported being pleased by their glucose levels, and all but one reported being happy to have their levels monitored automatically. All 62 patients said they’d recommend the system to others.
Going forward, the researchers hope to launch a multicenter trial that will examine clinical outcomes such as postoperative complications, infections, mortality, and glucose control after hospital discharge, according to Dr. Bally.
The study was supported by Diabetes UK, the Swiss National Science Foundation, the European Foundation for the Study of Diabetes, the JDRF, the National Institute for Health Research Cambridge Biomedical Research Center, and a Wellcome Strategic Award. Abbott Diabetes Care supplied equipment and guidance regarding connectivity, and representatives reviewed the manuscript before submission.
Dr. Bally reported funding from the University Hospital Bern, University of Bern and the Swiss Diabetes Foundation. Dr. Thabit reported no disclosures. Other authors report no disclosures or various disclosures.
SOURCE: Bally L et al. ADA 2018 Abstract 350-OR. Published simultaneously in The New England Journal of Medicine. June 25, 2018
REPORTING FROM ADA 2018
Key clinical point: Use of an automated closed-loop insulin delivery system may be feasible in the noncritical hospital setting.
Major finding: In the closed-loop group, glucose measurements were in the target range 66 mg/dL ± 17% of the time compared with 42 mg/dL ± 17% in the control group, a difference of 24 mg/dL ± 3% (95% CI, 19-30; P less than .001).
Study details: Randomized, open-label, two-center trial of 136 inpatients with type 2 diabetes mellitus assigned to either standard subcutaneous insulin therapy or closed-loop insulin delivery for 15 days or until discharge.
Disclosures: The study was supported by Diabetes UK, the Swiss National Science Foundation, the European Foundation for the Study of Diabetes, the JDRF, the National Institute for Health Research Cambridge Biomedical Research Center, and a Wellcome Strategic Award. Abbott Diabetes Care supplied equipment and guidance regarding connectivity, and representatives reviewed the manuscript before submission. The researchers reported no disclosures or various disclosures.
Source: Bally L et al. ADA 2018 Abstract 350-OR.

Meet the rare diabetes diagnosis that thrills patients
ORLANDO – Liana K. Billings, MD, an endocrinologist at the University of Chicago and the NorthShore University HealthSystem in Skokie, Ill., loves the thrill of letting patients know they have a rare kind of diabetes. “Once you do this once, you don’t want to stop,” she told colleagues in a presentation at the annual scientific sessions of the American Diabetes Association.

Yes, it’s true: There’s a diabetes diagnosis that spawns good feelings like delight and relief. The cause for celebration is a condition known as monogenetic diabetes, also known as maturity-onset diabetes of the young (MODY) if it develops after the neonatal period.
“The reason that getting a diagnosis of MODY can be a ‘good’ diagnosis is because the three most common forms of MODY have gene-specific treatments that typically improve patients’ glycemic control and are less onerous than the treatments patients were previously receiving when they were thought to have type 1 or type 2 diabetes,” explained Miriam S. Udler, MD, PhD, of Massachusetts General Hospital and Harvard Medical School, Boston, in an interview.
Dr. Udler and Dr. Billings spoke to colleagues about monogenetic diabetes in their presentation at the ADA meeting.
Research has suggested that 1%-4% of people with diabetes have the monogenetic form, in which the condition is caused by changes in a single gene. A 2017 British study of 1,407 patients with diabetes reported that “the minimum prevalence of monogenic diabetes is 3.6% of patients diagnosed at age 30 years or younger.”
The study, which tested a screening regimen, also turned up 17 new diagnoses of monogenetic diabetes among the 1,407 patients, doubling the total. The findings reflect an apparent fact about monogenetic diabetes: Physicians often don’t look for it, even though a diagnosis can be a godsend – especially for those who were previously diagnosed with type 1 or type 2 and placed on treatment regimens that are unnecessary at best and harmful at worst. (Diabetes Care. 2017 Aug;40[8]: 1017-25)
Patients with the MODY variant in the GCK gene, for example, “can generally stop all medications because they are not at risk for clinically significant complications of diabetes,” Dr. Udler said. “Patients with HNF1A and HNF4A variants can often be switched from insulin injections to ... a sulfonylurea, which is easier to take than insulin injections, and patients generally have better glycemic control after switching to pills.”
Unfortunately for doctors and patients, it can be complicated and costly to test for monogenetic diabetes. But screening tools are available to help physicians make choices about whether to launch testing in the first place, according to Dr. Udler and Dr. Billings.
There are two forms of monogenetic diabetes – neonatal diabetes, which is diagnosed by age 6-9 months, and MODY, which is typically diagnosed in those aged between 10 and 25 years, noted Dr. Billings.
Reasons to suspect MODY include early onset of diabetes (under 35 years), a family history of diabetes, a lack of obesity, and negative islet-cell antibodies, she said.
Obese patients may also have the condition: A 2017 American study of 488 overweight and obese children and adolescents diagnosed with type 2 diabetes found that 4.5% actually had monogenetic diabetes. (Genet Med. 2018 Jun;20[6]:583-90).
Once a physician suspects MODY, physicians may consult the University of Exeter’s risk calculator. It provides guidance about whether a test is a good idea. Dr. Billings cautioned, however, that the value of a calculator’s estimate of risk is not all-encompassing. “You should never use the calculator by itself as a reason to not pursue your intuition,” she said.
Dr. Udler noted that the University of Exeter calculator has important limitations, such as its reliance on specific genes, its lack of consideration of family history outside of parents, and its reliance on the experiences of white European patients.
As for tests, the University of Chicago and the University of Exeter both offer free genetic testing for neonatal diabetes, Dr. Billings said in her presentation.
Monogenetic diabetes tests in older children and adults are not free. However, Dr. Udler said the tests are often covered by insurance companies whether done for one or more genes.
At least one company offers a direct-to-consumer monogenetic diabetes test, according to Dr. Udler, but she recommended against it, especially in light of a curious online notice that says the test isn’t intended to be diagnostic. “I’m not sure what this would be useful for then,” she said.
For her part, Dr. Billings cautioned that test results may be inconclusive, and tests may offer different answers. She also recommended referring patients to genetic counseling.
Dr. Udler reported a board member/advisory panel relationship with Encompass Bioscience. Dr. Billings reported relationships with Novo Nordisk, Sanofi, and Dexcom.
ORLANDO – Liana K. Billings, MD, an endocrinologist at the University of Chicago and the NorthShore University HealthSystem in Skokie, Ill., loves the thrill of letting patients know they have a rare kind of diabetes. “Once you do this once, you don’t want to stop,” she told colleagues in a presentation at the annual scientific sessions of the American Diabetes Association.
Yes, it’s true: There’s a diabetes diagnosis that spawns good feelings like delight and relief. The cause for celebration is a condition known as monogenetic diabetes, also known as maturity-onset diabetes of the young (MODY) if it develops after the neonatal period.
“The reason that getting a diagnosis of MODY can be a ‘good’ diagnosis is because the three most common forms of MODY have gene-specific treatments that typically improve patients’ glycemic control and are less onerous than the treatments patients were previously receiving when they were thought to have type 1 or type 2 diabetes,” explained Miriam S. Udler, MD, PhD, of Massachusetts General Hospital and Harvard Medical School, Boston, in an interview.
Dr. Udler and Dr. Billings spoke to colleagues about monogenetic diabetes in their presentation at the ADA meeting.
Research has suggested that 1%-4% of people with diabetes have the monogenetic form, in which the condition is caused by changes in a single gene. A 2017 British study of 1,407 patients with diabetes reported that “the minimum prevalence of monogenic diabetes is 3.6% of patients diagnosed at age 30 years or younger.”
The study, which tested a screening regimen, also turned up 17 new diagnoses of monogenetic diabetes among the 1,407 patients, doubling the total. The findings reflect an apparent fact about monogenetic diabetes: Physicians often don’t look for it, even though a diagnosis can be a godsend – especially for those who were previously diagnosed with type 1 or type 2 and placed on treatment regimens that are unnecessary at best and harmful at worst. (Diabetes Care. 2017 Aug;40[8]: 1017-25)
Patients with the MODY variant in the GCK gene, for example, “can generally stop all medications because they are not at risk for clinically significant complications of diabetes,” Dr. Udler said. “Patients with HNF1A and HNF4A variants can often be switched from insulin injections to ... a sulfonylurea, which is easier to take than insulin injections, and patients generally have better glycemic control after switching to pills.”
Unfortunately for doctors and patients, it can be complicated and costly to test for monogenetic diabetes. But screening tools are available to help physicians make choices about whether to launch testing in the first place, according to Dr. Udler and Dr. Billings.
There are two forms of monogenetic diabetes – neonatal diabetes, which is diagnosed by age 6-9 months, and MODY, which is typically diagnosed in those aged between 10 and 25 years, noted Dr. Billings.
Reasons to suspect MODY include early onset of diabetes (under 35 years), a family history of diabetes, a lack of obesity, and negative islet-cell antibodies, she said.
Obese patients may also have the condition: A 2017 American study of 488 overweight and obese children and adolescents diagnosed with type 2 diabetes found that 4.5% actually had monogenetic diabetes. (Genet Med. 2018 Jun;20[6]:583-90).
Once a physician suspects MODY, physicians may consult the University of Exeter’s risk calculator. It provides guidance about whether a test is a good idea. Dr. Billings cautioned, however, that the value of a calculator’s estimate of risk is not all-encompassing. “You should never use the calculator by itself as a reason to not pursue your intuition,” she said.
Dr. Udler noted that the University of Exeter calculator has important limitations, such as its reliance on specific genes, its lack of consideration of family history outside of parents, and its reliance on the experiences of white European patients.
As for tests, the University of Chicago and the University of Exeter both offer free genetic testing for neonatal diabetes, Dr. Billings said in her presentation.
Monogenetic diabetes tests in older children and adults are not free. However, Dr. Udler said the tests are often covered by insurance companies whether done for one or more genes.
At least one company offers a direct-to-consumer monogenetic diabetes test, according to Dr. Udler, but she recommended against it, especially in light of a curious online notice that says the test isn’t intended to be diagnostic. “I’m not sure what this would be useful for then,” she said.
For her part, Dr. Billings cautioned that test results may be inconclusive, and tests may offer different answers. She also recommended referring patients to genetic counseling.
Dr. Udler reported a board member/advisory panel relationship with Encompass Bioscience. Dr. Billings reported relationships with Novo Nordisk, Sanofi, and Dexcom.
ORLANDO – Liana K. Billings, MD, an endocrinologist at the University of Chicago and the NorthShore University HealthSystem in Skokie, Ill., loves the thrill of letting patients know they have a rare kind of diabetes. “Once you do this once, you don’t want to stop,” she told colleagues in a presentation at the annual scientific sessions of the American Diabetes Association.
Yes, it’s true: There’s a diabetes diagnosis that spawns good feelings like delight and relief. The cause for celebration is a condition known as monogenetic diabetes, also known as maturity-onset diabetes of the young (MODY) if it develops after the neonatal period.
“The reason that getting a diagnosis of MODY can be a ‘good’ diagnosis is because the three most common forms of MODY have gene-specific treatments that typically improve patients’ glycemic control and are less onerous than the treatments patients were previously receiving when they were thought to have type 1 or type 2 diabetes,” explained Miriam S. Udler, MD, PhD, of Massachusetts General Hospital and Harvard Medical School, Boston, in an interview.
Dr. Udler and Dr. Billings spoke to colleagues about monogenetic diabetes in their presentation at the ADA meeting.
Research has suggested that 1%-4% of people with diabetes have the monogenetic form, in which the condition is caused by changes in a single gene. A 2017 British study of 1,407 patients with diabetes reported that “the minimum prevalence of monogenic diabetes is 3.6% of patients diagnosed at age 30 years or younger.”
The study, which tested a screening regimen, also turned up 17 new diagnoses of monogenetic diabetes among the 1,407 patients, doubling the total. The findings reflect an apparent fact about monogenetic diabetes: Physicians often don’t look for it, even though a diagnosis can be a godsend – especially for those who were previously diagnosed with type 1 or type 2 and placed on treatment regimens that are unnecessary at best and harmful at worst. (Diabetes Care. 2017 Aug;40[8]: 1017-25)
Patients with the MODY variant in the GCK gene, for example, “can generally stop all medications because they are not at risk for clinically significant complications of diabetes,” Dr. Udler said. “Patients with HNF1A and HNF4A variants can often be switched from insulin injections to ... a sulfonylurea, which is easier to take than insulin injections, and patients generally have better glycemic control after switching to pills.”
Unfortunately for doctors and patients, it can be complicated and costly to test for monogenetic diabetes. But screening tools are available to help physicians make choices about whether to launch testing in the first place, according to Dr. Udler and Dr. Billings.
There are two forms of monogenetic diabetes – neonatal diabetes, which is diagnosed by age 6-9 months, and MODY, which is typically diagnosed in those aged between 10 and 25 years, noted Dr. Billings.
Reasons to suspect MODY include early onset of diabetes (under 35 years), a family history of diabetes, a lack of obesity, and negative islet-cell antibodies, she said.
Obese patients may also have the condition: A 2017 American study of 488 overweight and obese children and adolescents diagnosed with type 2 diabetes found that 4.5% actually had monogenetic diabetes. (Genet Med. 2018 Jun;20[6]:583-90).
Once a physician suspects MODY, physicians may consult the University of Exeter’s risk calculator. It provides guidance about whether a test is a good idea. Dr. Billings cautioned, however, that the value of a calculator’s estimate of risk is not all-encompassing. “You should never use the calculator by itself as a reason to not pursue your intuition,” she said.
Dr. Udler noted that the University of Exeter calculator has important limitations, such as its reliance on specific genes, its lack of consideration of family history outside of parents, and its reliance on the experiences of white European patients.
As for tests, the University of Chicago and the University of Exeter both offer free genetic testing for neonatal diabetes, Dr. Billings said in her presentation.
Monogenetic diabetes tests in older children and adults are not free. However, Dr. Udler said the tests are often covered by insurance companies whether done for one or more genes.
At least one company offers a direct-to-consumer monogenetic diabetes test, according to Dr. Udler, but she recommended against it, especially in light of a curious online notice that says the test isn’t intended to be diagnostic. “I’m not sure what this would be useful for then,” she said.
For her part, Dr. Billings cautioned that test results may be inconclusive, and tests may offer different answers. She also recommended referring patients to genetic counseling.
Dr. Udler reported a board member/advisory panel relationship with Encompass Bioscience. Dr. Billings reported relationships with Novo Nordisk, Sanofi, and Dexcom.
EXPERT ANALYSIS FROM ADA 2018
RISE: Insulin glargine, metformin offer no beta cell function benefit in youth
ORLANDO – in the pediatric medication portion of the Restoring Insulin Secretion (RISE) study.
The treatments, including either metformin for 12 months in 47 participants or insulin glargine for 3 months followed by metformin for 9 months in 44 participants, were not associated with improvement in beta cell function at 12 months, compared with baseline, according to reports from members of the RISE Consortium at the annual scientific sessions of the American Diabetes Association.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Furthermore, measures of beta cell function worsened in both groups at 15-month follow-up, and the same was true for participants with impaired glucose tolerance only; the outcomes in that subset of patients were similar to the entire group, including patients with early T2DM.
“Beta cell failure progressed despite that intervention, and though both [metformin and insulin glargine] were effective for lowering glucose – and metformin for lowering weight ... it had nothing to do with the natural history of the disease, and that’s really quite disappointing,” John B. Buse, MD, said in a video interview.
But that’s not to say the findings weren’t of value.
“The exciting bit was our greater understanding of what’s different about diabetes in youth, and basically [the findings] showed that, both in the setting of impaired glucose tolerance and early diabetes, youth have more insulin resistance than adults, they have relatively more well-preserved beta cell function – they’re secreting more insulin at both impaired glucose tolerance and diabetes, and they have lesser hepatic insulin clearance,” said Dr. Buse, professor, chief of the division of endocrinology, and director of the Diabetes Center at the University of North Carolina, Chapel Hill.
Dr. Buse provided invited commentary on the findings at the ADA scientific sessions and elaborated on those comments in this interview, noting that, in addition to identifying important differences between children and adults with impaired glucose tolerance and diabetes, the RISE study demonstrated that the numerous challenges associated with conducting a major study involving children with impaired glucose tolerance or T2DM can be overcome.
“It’s a really heartwarming story,” he said of the efforts and successes of the RISE investigators in completing the pediatric medication portion of the study. “It at least gives us hope that, even if we haven’t found a cure for type 2 diabetes in children, we at least know we can do the studies.”
Dr. Buse also provided his take on what the future holds for both parts of the RISE study (findings from the adult medication and adult surgery portions are expected to be reported within the next year) and for other studies in children and youth with diabetes; he noted that the current findings and successes in enrolling and completing the pediatric portion of the study highlight multiple opportunities for future research.
Dr. Buse reported financial relationships with Adocia, AstraZeneca, Dexcom, Elcelyx, Eli Lilly, Fractyl Laboratories, Intarcia Therapeutics, Lexicon Pharmaceuticals, Metavention, NovaTarg Therapeutics, Novo Nordisk, Sanofi, VTV Therapeutics, Boehringer Ingelheim, Johnson & Johnson Services, Theracos, Shenzhen Hightide Biopharmaceutical, National Heart Lung and Blood Institute, National Center for Advancing Translational Sciences, National Institute of Diabetes and Digestive and Kidney Diseases, American Diabetes Association, Patient-Centered Outcomes Research Institute, and the National Institute of Environmental Health Sciences.
ORLANDO – in the pediatric medication portion of the Restoring Insulin Secretion (RISE) study.
The treatments, including either metformin for 12 months in 47 participants or insulin glargine for 3 months followed by metformin for 9 months in 44 participants, were not associated with improvement in beta cell function at 12 months, compared with baseline, according to reports from members of the RISE Consortium at the annual scientific sessions of the American Diabetes Association.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Furthermore, measures of beta cell function worsened in both groups at 15-month follow-up, and the same was true for participants with impaired glucose tolerance only; the outcomes in that subset of patients were similar to the entire group, including patients with early T2DM.
“Beta cell failure progressed despite that intervention, and though both [metformin and insulin glargine] were effective for lowering glucose – and metformin for lowering weight ... it had nothing to do with the natural history of the disease, and that’s really quite disappointing,” John B. Buse, MD, said in a video interview.
But that’s not to say the findings weren’t of value.
“The exciting bit was our greater understanding of what’s different about diabetes in youth, and basically [the findings] showed that, both in the setting of impaired glucose tolerance and early diabetes, youth have more insulin resistance than adults, they have relatively more well-preserved beta cell function – they’re secreting more insulin at both impaired glucose tolerance and diabetes, and they have lesser hepatic insulin clearance,” said Dr. Buse, professor, chief of the division of endocrinology, and director of the Diabetes Center at the University of North Carolina, Chapel Hill.
Dr. Buse provided invited commentary on the findings at the ADA scientific sessions and elaborated on those comments in this interview, noting that, in addition to identifying important differences between children and adults with impaired glucose tolerance and diabetes, the RISE study demonstrated that the numerous challenges associated with conducting a major study involving children with impaired glucose tolerance or T2DM can be overcome.
“It’s a really heartwarming story,” he said of the efforts and successes of the RISE investigators in completing the pediatric medication portion of the study. “It at least gives us hope that, even if we haven’t found a cure for type 2 diabetes in children, we at least know we can do the studies.”
Dr. Buse also provided his take on what the future holds for both parts of the RISE study (findings from the adult medication and adult surgery portions are expected to be reported within the next year) and for other studies in children and youth with diabetes; he noted that the current findings and successes in enrolling and completing the pediatric portion of the study highlight multiple opportunities for future research.
Dr. Buse reported financial relationships with Adocia, AstraZeneca, Dexcom, Elcelyx, Eli Lilly, Fractyl Laboratories, Intarcia Therapeutics, Lexicon Pharmaceuticals, Metavention, NovaTarg Therapeutics, Novo Nordisk, Sanofi, VTV Therapeutics, Boehringer Ingelheim, Johnson & Johnson Services, Theracos, Shenzhen Hightide Biopharmaceutical, National Heart Lung and Blood Institute, National Center for Advancing Translational Sciences, National Institute of Diabetes and Digestive and Kidney Diseases, American Diabetes Association, Patient-Centered Outcomes Research Institute, and the National Institute of Environmental Health Sciences.
ORLANDO – in the pediatric medication portion of the Restoring Insulin Secretion (RISE) study.
The treatments, including either metformin for 12 months in 47 participants or insulin glargine for 3 months followed by metformin for 9 months in 44 participants, were not associated with improvement in beta cell function at 12 months, compared with baseline, according to reports from members of the RISE Consortium at the annual scientific sessions of the American Diabetes Association.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Furthermore, measures of beta cell function worsened in both groups at 15-month follow-up, and the same was true for participants with impaired glucose tolerance only; the outcomes in that subset of patients were similar to the entire group, including patients with early T2DM.
“Beta cell failure progressed despite that intervention, and though both [metformin and insulin glargine] were effective for lowering glucose – and metformin for lowering weight ... it had nothing to do with the natural history of the disease, and that’s really quite disappointing,” John B. Buse, MD, said in a video interview.
But that’s not to say the findings weren’t of value.
“The exciting bit was our greater understanding of what’s different about diabetes in youth, and basically [the findings] showed that, both in the setting of impaired glucose tolerance and early diabetes, youth have more insulin resistance than adults, they have relatively more well-preserved beta cell function – they’re secreting more insulin at both impaired glucose tolerance and diabetes, and they have lesser hepatic insulin clearance,” said Dr. Buse, professor, chief of the division of endocrinology, and director of the Diabetes Center at the University of North Carolina, Chapel Hill.
Dr. Buse provided invited commentary on the findings at the ADA scientific sessions and elaborated on those comments in this interview, noting that, in addition to identifying important differences between children and adults with impaired glucose tolerance and diabetes, the RISE study demonstrated that the numerous challenges associated with conducting a major study involving children with impaired glucose tolerance or T2DM can be overcome.
“It’s a really heartwarming story,” he said of the efforts and successes of the RISE investigators in completing the pediatric medication portion of the study. “It at least gives us hope that, even if we haven’t found a cure for type 2 diabetes in children, we at least know we can do the studies.”
Dr. Buse also provided his take on what the future holds for both parts of the RISE study (findings from the adult medication and adult surgery portions are expected to be reported within the next year) and for other studies in children and youth with diabetes; he noted that the current findings and successes in enrolling and completing the pediatric portion of the study highlight multiple opportunities for future research.
Dr. Buse reported financial relationships with Adocia, AstraZeneca, Dexcom, Elcelyx, Eli Lilly, Fractyl Laboratories, Intarcia Therapeutics, Lexicon Pharmaceuticals, Metavention, NovaTarg Therapeutics, Novo Nordisk, Sanofi, VTV Therapeutics, Boehringer Ingelheim, Johnson & Johnson Services, Theracos, Shenzhen Hightide Biopharmaceutical, National Heart Lung and Blood Institute, National Center for Advancing Translational Sciences, National Institute of Diabetes and Digestive and Kidney Diseases, American Diabetes Association, Patient-Centered Outcomes Research Institute, and the National Institute of Environmental Health Sciences.
EXPERT ANALYSIS AT ADA 2018

CANVAS data: Canagliflozin generally well tolerated up to 6.5 years
ORLANDO – according to the latest safety data from the CANVAS (Canagliflozin Cardiovascular Assessment Study) program.
CANVAS included two studies (CANVAS and CANVAS-R) involving a total of 10,142 patients, which established the superiority of canagliflozin (Invokana) over placebo for reducing the risk of a three-point major adverse cardiac event endpoint, including cardiovascular death, nonfatal MI, and nonfatal stroke. The sodium-glucose cotransporter-2 (SGLT2) inhibitor also improved other cardiovascular outcomes.
For the current analysis, outcomes in the CANVAS participants were compared with those from a general population of 8,114 patients with type 2 diabetes mellitus (T2DM) who participated in 12 non-CANVAS studies of canagliflozin. As previously reported, the risks for fracture or amputation were novel safety findings associated with canagliflozin in the CANVAS program and, in the current analysis, the incidence of fractures per 1,000 patient-years in CANVAS was 15.4 vs. 11.9 with treatment vs. placebo, whereas no significant difference was seen in the non-CANVAS studies (incidence rate of 11.8 vs. 10.8 per 1,000 patient-years for treatment vs. placebo), Priscilla Hollander, MD, reported at the annual meeting of the American Diabetes Association.
Of note, when the CANVAS and CANVAS-R studies were compared, the imbalance was seen only in CANVAS (incidence rates of 16.9 vs. 10.9 for treatment vs. placebo [hazard ratio, 1.55], compared with incidence rates of 11.3 and 13.2 , respectively, in CANVAS-R [HR, 0.86]), said Dr. Hollander, Baylor Scott & White Endocrine Center in Dallas.
“Ongoing analyses are trying to determine why there is a difference between the two studies,” she noted.
For the novel safety finding of increased amputation risk with canagliflozin, an excess of three events per 1,000 patient years was seen in both CANVAS (incidence of 6.3 vs. 3.4; HR, 1.97) and CANVAS-R (incidence of 5.9 vs. 2.8; HR, 2.12). No difference in risk was seen among the non-CANVAS population (incidence of 0.5 and 2.2 with treatment vs. placebo; HR, 0.23).
“Amputations were primarily at the level of the toe or the metatarsal. Patients with a history of amputation or peripheral vascular disease had the highest risk of amputation,” she said, adding that this was true in both treatment and placebo groups.
“Again, ongoing analyses are being done to look at the mechanism in this regard,” she said.
For safety outcomes known to be related to the mechanism of SGLT2 inhibition, including osmotic diuresis, volume depletion, and genital mycotic infection (GMI), similar differences between canagliflozin and placebo groups were seen in the CANVAS and non-CANVAS studies at 6.5 years, Dr. Hollander said.
Hazard ratios in the canagliflozin vs. placebo groups for the CANVAS and non-CANVAS studies, respectively, were 2.80 and 2.66 for osmotic diuresis, 1.44 and 1.35 for volume depletion, 4.37 and 4.32 for female GMI, and 3.76 and 6.26 for male GMI.
No imbalances were observed in other AEs of interest – including hypoglycemia, urinary tract infections, or hypersensitivity reactions – in either the CANVAS or the non-CANVAS studies.
“The point estimate for [diabetic ketoacidosis] was 2.3, but with very wide confidence intervals due to a very low number of events, so it really did not reach significance,” Dr. Hollander noted. “Again, due to the mechanism of action of canagliflozin, and the warning for acute kidney injury on the label, renal adverse events were also of interest, but there was no imbalance observed in the renal-related AEs between the CANVAS program and the non-CANVAS program.”
A closer look at renal-related adverse events (AEs) of interest in the CANVAS program only (not in comparison with the non-CANVAS findings) also showed no significant difference with canagliflozin vs. placebo in blood creatinine increase, blood urea increase, glomerular filtration rate decrease, acute kidney injury, renal impairment, renal failure, oliguria, acute prerenal failure, hypercreatininemia, nephritis, or prerenal failure, she said.
Furthermore, although hyperkalemia is noted as a risk with canagliflozin in patients with moderate renal impairment who are taking medications that interfere with potassium excretion, no significant differences were observed between the treatment and placebo groups over 6.5 years in the CANVAS program, she added, noting that “this was also supported by the lack of imbalance between the laboratory changes for serum potassium in the two groups.”
There also were no differences seen between the treatment and placebo groups in the rates of all serious AEs or in the rates of AEs leading to discontinuation, she said.
Canagliflozin has been generally well tolerated in both placebo-controlled trials and trials in which the SGLT2 inhibitor was compared with other active treatments. The non-CANVAS studies used for comparison in the current analysis included phase 3/4 canagliflozin clinical development program studies lasting up to 104 weeks and involving a general T2DM patient population, Dr. Hollander noted.
The CANVAS program, which was launched in 2009, included patients with T2DM and established cardiovascular disease or high cardiovascular disease risk who received a 2-week placebo run-in followed by placebo or either 100- or 300-mg doses of canagliflozin. CANVAS participants had hemoglobin A1c of 7%-10.5%; estimated glomerular filtration rate of 30 mL/min per 1.72m2 or greater; age of 30 years or greater plus a history of a prior cardiovascular event, or age of 50 years or greater with at least 2 cardiovascular risk factors, including diabetes for 10 years or more; systolic blood pressure greater than 140 mm Hg on at least one medication; current smoking status; micro- or macroalbuminuria; and an HDL cholesterol level less than 1 mmol/L.
The current analysis provides the longest-term safety data to date for the program, Dr. Hollander said.
The CANVAS Program is sponsored by Janssen Research & Development. Dr. Hollander is an advisory panel member for Eli Lilly, Merck, and Novo Nordisk.
SOURCE: Hollander P et al. ADA 2018, Abstract 259-OR.
ORLANDO – according to the latest safety data from the CANVAS (Canagliflozin Cardiovascular Assessment Study) program.
CANVAS included two studies (CANVAS and CANVAS-R) involving a total of 10,142 patients, which established the superiority of canagliflozin (Invokana) over placebo for reducing the risk of a three-point major adverse cardiac event endpoint, including cardiovascular death, nonfatal MI, and nonfatal stroke. The sodium-glucose cotransporter-2 (SGLT2) inhibitor also improved other cardiovascular outcomes.
For the current analysis, outcomes in the CANVAS participants were compared with those from a general population of 8,114 patients with type 2 diabetes mellitus (T2DM) who participated in 12 non-CANVAS studies of canagliflozin. As previously reported, the risks for fracture or amputation were novel safety findings associated with canagliflozin in the CANVAS program and, in the current analysis, the incidence of fractures per 1,000 patient-years in CANVAS was 15.4 vs. 11.9 with treatment vs. placebo, whereas no significant difference was seen in the non-CANVAS studies (incidence rate of 11.8 vs. 10.8 per 1,000 patient-years for treatment vs. placebo), Priscilla Hollander, MD, reported at the annual meeting of the American Diabetes Association.
Of note, when the CANVAS and CANVAS-R studies were compared, the imbalance was seen only in CANVAS (incidence rates of 16.9 vs. 10.9 for treatment vs. placebo [hazard ratio, 1.55], compared with incidence rates of 11.3 and 13.2 , respectively, in CANVAS-R [HR, 0.86]), said Dr. Hollander, Baylor Scott & White Endocrine Center in Dallas.
“Ongoing analyses are trying to determine why there is a difference between the two studies,” she noted.
For the novel safety finding of increased amputation risk with canagliflozin, an excess of three events per 1,000 patient years was seen in both CANVAS (incidence of 6.3 vs. 3.4; HR, 1.97) and CANVAS-R (incidence of 5.9 vs. 2.8; HR, 2.12). No difference in risk was seen among the non-CANVAS population (incidence of 0.5 and 2.2 with treatment vs. placebo; HR, 0.23).
“Amputations were primarily at the level of the toe or the metatarsal. Patients with a history of amputation or peripheral vascular disease had the highest risk of amputation,” she said, adding that this was true in both treatment and placebo groups.
“Again, ongoing analyses are being done to look at the mechanism in this regard,” she said.
For safety outcomes known to be related to the mechanism of SGLT2 inhibition, including osmotic diuresis, volume depletion, and genital mycotic infection (GMI), similar differences between canagliflozin and placebo groups were seen in the CANVAS and non-CANVAS studies at 6.5 years, Dr. Hollander said.
Hazard ratios in the canagliflozin vs. placebo groups for the CANVAS and non-CANVAS studies, respectively, were 2.80 and 2.66 for osmotic diuresis, 1.44 and 1.35 for volume depletion, 4.37 and 4.32 for female GMI, and 3.76 and 6.26 for male GMI.
No imbalances were observed in other AEs of interest – including hypoglycemia, urinary tract infections, or hypersensitivity reactions – in either the CANVAS or the non-CANVAS studies.
“The point estimate for [diabetic ketoacidosis] was 2.3, but with very wide confidence intervals due to a very low number of events, so it really did not reach significance,” Dr. Hollander noted. “Again, due to the mechanism of action of canagliflozin, and the warning for acute kidney injury on the label, renal adverse events were also of interest, but there was no imbalance observed in the renal-related AEs between the CANVAS program and the non-CANVAS program.”
A closer look at renal-related adverse events (AEs) of interest in the CANVAS program only (not in comparison with the non-CANVAS findings) also showed no significant difference with canagliflozin vs. placebo in blood creatinine increase, blood urea increase, glomerular filtration rate decrease, acute kidney injury, renal impairment, renal failure, oliguria, acute prerenal failure, hypercreatininemia, nephritis, or prerenal failure, she said.
Furthermore, although hyperkalemia is noted as a risk with canagliflozin in patients with moderate renal impairment who are taking medications that interfere with potassium excretion, no significant differences were observed between the treatment and placebo groups over 6.5 years in the CANVAS program, she added, noting that “this was also supported by the lack of imbalance between the laboratory changes for serum potassium in the two groups.”
There also were no differences seen between the treatment and placebo groups in the rates of all serious AEs or in the rates of AEs leading to discontinuation, she said.
Canagliflozin has been generally well tolerated in both placebo-controlled trials and trials in which the SGLT2 inhibitor was compared with other active treatments. The non-CANVAS studies used for comparison in the current analysis included phase 3/4 canagliflozin clinical development program studies lasting up to 104 weeks and involving a general T2DM patient population, Dr. Hollander noted.
The CANVAS program, which was launched in 2009, included patients with T2DM and established cardiovascular disease or high cardiovascular disease risk who received a 2-week placebo run-in followed by placebo or either 100- or 300-mg doses of canagliflozin. CANVAS participants had hemoglobin A1c of 7%-10.5%; estimated glomerular filtration rate of 30 mL/min per 1.72m2 or greater; age of 30 years or greater plus a history of a prior cardiovascular event, or age of 50 years or greater with at least 2 cardiovascular risk factors, including diabetes for 10 years or more; systolic blood pressure greater than 140 mm Hg on at least one medication; current smoking status; micro- or macroalbuminuria; and an HDL cholesterol level less than 1 mmol/L.
The current analysis provides the longest-term safety data to date for the program, Dr. Hollander said.
The CANVAS Program is sponsored by Janssen Research & Development. Dr. Hollander is an advisory panel member for Eli Lilly, Merck, and Novo Nordisk.
SOURCE: Hollander P et al. ADA 2018, Abstract 259-OR.
ORLANDO – according to the latest safety data from the CANVAS (Canagliflozin Cardiovascular Assessment Study) program.
CANVAS included two studies (CANVAS and CANVAS-R) involving a total of 10,142 patients, which established the superiority of canagliflozin (Invokana) over placebo for reducing the risk of a three-point major adverse cardiac event endpoint, including cardiovascular death, nonfatal MI, and nonfatal stroke. The sodium-glucose cotransporter-2 (SGLT2) inhibitor also improved other cardiovascular outcomes.
For the current analysis, outcomes in the CANVAS participants were compared with those from a general population of 8,114 patients with type 2 diabetes mellitus (T2DM) who participated in 12 non-CANVAS studies of canagliflozin. As previously reported, the risks for fracture or amputation were novel safety findings associated with canagliflozin in the CANVAS program and, in the current analysis, the incidence of fractures per 1,000 patient-years in CANVAS was 15.4 vs. 11.9 with treatment vs. placebo, whereas no significant difference was seen in the non-CANVAS studies (incidence rate of 11.8 vs. 10.8 per 1,000 patient-years for treatment vs. placebo), Priscilla Hollander, MD, reported at the annual meeting of the American Diabetes Association.
Of note, when the CANVAS and CANVAS-R studies were compared, the imbalance was seen only in CANVAS (incidence rates of 16.9 vs. 10.9 for treatment vs. placebo [hazard ratio, 1.55], compared with incidence rates of 11.3 and 13.2 , respectively, in CANVAS-R [HR, 0.86]), said Dr. Hollander, Baylor Scott & White Endocrine Center in Dallas.
“Ongoing analyses are trying to determine why there is a difference between the two studies,” she noted.
For the novel safety finding of increased amputation risk with canagliflozin, an excess of three events per 1,000 patient years was seen in both CANVAS (incidence of 6.3 vs. 3.4; HR, 1.97) and CANVAS-R (incidence of 5.9 vs. 2.8; HR, 2.12). No difference in risk was seen among the non-CANVAS population (incidence of 0.5 and 2.2 with treatment vs. placebo; HR, 0.23).
“Amputations were primarily at the level of the toe or the metatarsal. Patients with a history of amputation or peripheral vascular disease had the highest risk of amputation,” she said, adding that this was true in both treatment and placebo groups.
“Again, ongoing analyses are being done to look at the mechanism in this regard,” she said.
For safety outcomes known to be related to the mechanism of SGLT2 inhibition, including osmotic diuresis, volume depletion, and genital mycotic infection (GMI), similar differences between canagliflozin and placebo groups were seen in the CANVAS and non-CANVAS studies at 6.5 years, Dr. Hollander said.
Hazard ratios in the canagliflozin vs. placebo groups for the CANVAS and non-CANVAS studies, respectively, were 2.80 and 2.66 for osmotic diuresis, 1.44 and 1.35 for volume depletion, 4.37 and 4.32 for female GMI, and 3.76 and 6.26 for male GMI.
No imbalances were observed in other AEs of interest – including hypoglycemia, urinary tract infections, or hypersensitivity reactions – in either the CANVAS or the non-CANVAS studies.
“The point estimate for [diabetic ketoacidosis] was 2.3, but with very wide confidence intervals due to a very low number of events, so it really did not reach significance,” Dr. Hollander noted. “Again, due to the mechanism of action of canagliflozin, and the warning for acute kidney injury on the label, renal adverse events were also of interest, but there was no imbalance observed in the renal-related AEs between the CANVAS program and the non-CANVAS program.”
A closer look at renal-related adverse events (AEs) of interest in the CANVAS program only (not in comparison with the non-CANVAS findings) also showed no significant difference with canagliflozin vs. placebo in blood creatinine increase, blood urea increase, glomerular filtration rate decrease, acute kidney injury, renal impairment, renal failure, oliguria, acute prerenal failure, hypercreatininemia, nephritis, or prerenal failure, she said.
Furthermore, although hyperkalemia is noted as a risk with canagliflozin in patients with moderate renal impairment who are taking medications that interfere with potassium excretion, no significant differences were observed between the treatment and placebo groups over 6.5 years in the CANVAS program, she added, noting that “this was also supported by the lack of imbalance between the laboratory changes for serum potassium in the two groups.”
There also were no differences seen between the treatment and placebo groups in the rates of all serious AEs or in the rates of AEs leading to discontinuation, she said.
Canagliflozin has been generally well tolerated in both placebo-controlled trials and trials in which the SGLT2 inhibitor was compared with other active treatments. The non-CANVAS studies used for comparison in the current analysis included phase 3/4 canagliflozin clinical development program studies lasting up to 104 weeks and involving a general T2DM patient population, Dr. Hollander noted.
The CANVAS program, which was launched in 2009, included patients with T2DM and established cardiovascular disease or high cardiovascular disease risk who received a 2-week placebo run-in followed by placebo or either 100- or 300-mg doses of canagliflozin. CANVAS participants had hemoglobin A1c of 7%-10.5%; estimated glomerular filtration rate of 30 mL/min per 1.72m2 or greater; age of 30 years or greater plus a history of a prior cardiovascular event, or age of 50 years or greater with at least 2 cardiovascular risk factors, including diabetes for 10 years or more; systolic blood pressure greater than 140 mm Hg on at least one medication; current smoking status; micro- or macroalbuminuria; and an HDL cholesterol level less than 1 mmol/L.
The current analysis provides the longest-term safety data to date for the program, Dr. Hollander said.
The CANVAS Program is sponsored by Janssen Research & Development. Dr. Hollander is an advisory panel member for Eli Lilly, Merck, and Novo Nordisk.
SOURCE: Hollander P et al. ADA 2018, Abstract 259-OR.
REPORTING FROM ADA 2018
Key clinical point: Canagliflozin is generally well tolerated for up to 6.5 years in patients with T2DM and high CV risk.
Major finding: Similar differences between canagliflozin and placebo groups for outcomes related to the mechanism of SGLT2 inhibition were seen in the CANVAS and non-CANVAS studies at 6.5 years.
Study details: A comparison of safety outcomes in 10,142 patients in CANVAS and 8,114 patients in non-CANVAS studies.
Disclosures: The CANVAS Program is sponsored by Janssen Research & Development. Dr. Hollander is an advisory panel member for Eli Lilly, Merck, and Novo Nordisk.
Source: Hollander P et al. ADA 2018 Abstract 259-OR.