User login
HM13 Session Analysis: Things Hospitalists Do for No Reason
I attended an excellent presentation by Hopkins' Leonard Feldman, MD, FAAP, FACP, SFHM, that challenged some of our practices, most notably unnecessary diagnostic tests that cost the hundreds of billions of dollars per year. Dr. Feldman focused on the evaluation of syncope, seizure prophylaxis for brain tumors, adjusting serum potassium levels in STEMI, and GI prophylaxis outside of the ICU.
Here are the key takeways for hospitalists:
- Using carotid Doppler for the evaluation of syncope adds no value in unveiling the etiology. Even if used in a high-risk group with cardiovascular disease, Doppler is helpful in determining the etiology only in the presence of focal neurological symptoms or carotid bruits. On the other hand, checking orthostatics is very helpful and inexpensive, providing an etiology about 25% to 30% of the time.
- There is no benefit of a 7-day peri-operative seizure prophylaxis in patients undergoing resection for a brain tumor (Wu et al, Journal of Neurosurgery, April 2013). The number of seizures within 30 days was actually slightly higher in the group of patients, who had received prophylaxis.
Watch a 2-minute video clip of Bob Wachter's HM13 keynote address
- In the past, medical societies have published guidelines for target serum potassium levels. These had been developed in the setting of STEMI and date back quite a while, before beta-blockers or reperfusion therapies were utilized in the acute management of STEMI. Target potassium levels of >4.0 or even between 4.5 and 5.5 had been recommended. Review of the literature did not find evidence to support this, but rather suggests that a target range of 3.5 to 4.5 is advisable.
- Hospitalized patients are frequently placed on proton-pump inhibitors (PPI) or H2-blockers for GI prophylaxis. Is there any benefit of this practice outside of the ICU? According to a study by Herzig et al (Archives of Internal Medicine, June 2011) clinically significant GI bleeding occurred in 0.18% of patients without prophylaxis compared to 0.26% with prophylaxis. To look at it from a different angle: The number needed to treat to prevent 1 episode of clinically significant GI bleeding was 834, whereas the number needed to harm was 553 for C. diff and 111 for hospital-acquired pneumonia. According to these data, there is no benefit and, if anything, harm done by providing GI prophylaxis to hospitalized patients outside of the ICU.
This is just a small sample of all the things we do. The results should motivate us to look for many other things we may do for no reason in our daily practice. TH
Dr. Suehler is a hospitalist at Mercy Hospital, Allina Health, in Minneapolis, and Team Hospitalist member.
I attended an excellent presentation by Hopkins' Leonard Feldman, MD, FAAP, FACP, SFHM, that challenged some of our practices, most notably unnecessary diagnostic tests that cost the hundreds of billions of dollars per year. Dr. Feldman focused on the evaluation of syncope, seizure prophylaxis for brain tumors, adjusting serum potassium levels in STEMI, and GI prophylaxis outside of the ICU.
Here are the key takeways for hospitalists:
- Using carotid Doppler for the evaluation of syncope adds no value in unveiling the etiology. Even if used in a high-risk group with cardiovascular disease, Doppler is helpful in determining the etiology only in the presence of focal neurological symptoms or carotid bruits. On the other hand, checking orthostatics is very helpful and inexpensive, providing an etiology about 25% to 30% of the time.
- There is no benefit of a 7-day peri-operative seizure prophylaxis in patients undergoing resection for a brain tumor (Wu et al, Journal of Neurosurgery, April 2013). The number of seizures within 30 days was actually slightly higher in the group of patients, who had received prophylaxis.
Watch a 2-minute video clip of Bob Wachter's HM13 keynote address
- In the past, medical societies have published guidelines for target serum potassium levels. These had been developed in the setting of STEMI and date back quite a while, before beta-blockers or reperfusion therapies were utilized in the acute management of STEMI. Target potassium levels of >4.0 or even between 4.5 and 5.5 had been recommended. Review of the literature did not find evidence to support this, but rather suggests that a target range of 3.5 to 4.5 is advisable.
- Hospitalized patients are frequently placed on proton-pump inhibitors (PPI) or H2-blockers for GI prophylaxis. Is there any benefit of this practice outside of the ICU? According to a study by Herzig et al (Archives of Internal Medicine, June 2011) clinically significant GI bleeding occurred in 0.18% of patients without prophylaxis compared to 0.26% with prophylaxis. To look at it from a different angle: The number needed to treat to prevent 1 episode of clinically significant GI bleeding was 834, whereas the number needed to harm was 553 for C. diff and 111 for hospital-acquired pneumonia. According to these data, there is no benefit and, if anything, harm done by providing GI prophylaxis to hospitalized patients outside of the ICU.
This is just a small sample of all the things we do. The results should motivate us to look for many other things we may do for no reason in our daily practice. TH
Dr. Suehler is a hospitalist at Mercy Hospital, Allina Health, in Minneapolis, and Team Hospitalist member.
I attended an excellent presentation by Hopkins' Leonard Feldman, MD, FAAP, FACP, SFHM, that challenged some of our practices, most notably unnecessary diagnostic tests that cost the hundreds of billions of dollars per year. Dr. Feldman focused on the evaluation of syncope, seizure prophylaxis for brain tumors, adjusting serum potassium levels in STEMI, and GI prophylaxis outside of the ICU.
Here are the key takeways for hospitalists:
- Using carotid Doppler for the evaluation of syncope adds no value in unveiling the etiology. Even if used in a high-risk group with cardiovascular disease, Doppler is helpful in determining the etiology only in the presence of focal neurological symptoms or carotid bruits. On the other hand, checking orthostatics is very helpful and inexpensive, providing an etiology about 25% to 30% of the time.
- There is no benefit of a 7-day peri-operative seizure prophylaxis in patients undergoing resection for a brain tumor (Wu et al, Journal of Neurosurgery, April 2013). The number of seizures within 30 days was actually slightly higher in the group of patients, who had received prophylaxis.
Watch a 2-minute video clip of Bob Wachter's HM13 keynote address
- In the past, medical societies have published guidelines for target serum potassium levels. These had been developed in the setting of STEMI and date back quite a while, before beta-blockers or reperfusion therapies were utilized in the acute management of STEMI. Target potassium levels of >4.0 or even between 4.5 and 5.5 had been recommended. Review of the literature did not find evidence to support this, but rather suggests that a target range of 3.5 to 4.5 is advisable.
- Hospitalized patients are frequently placed on proton-pump inhibitors (PPI) or H2-blockers for GI prophylaxis. Is there any benefit of this practice outside of the ICU? According to a study by Herzig et al (Archives of Internal Medicine, June 2011) clinically significant GI bleeding occurred in 0.18% of patients without prophylaxis compared to 0.26% with prophylaxis. To look at it from a different angle: The number needed to treat to prevent 1 episode of clinically significant GI bleeding was 834, whereas the number needed to harm was 553 for C. diff and 111 for hospital-acquired pneumonia. According to these data, there is no benefit and, if anything, harm done by providing GI prophylaxis to hospitalized patients outside of the ICU.
This is just a small sample of all the things we do. The results should motivate us to look for many other things we may do for no reason in our daily practice. TH
Dr. Suehler is a hospitalist at Mercy Hospital, Allina Health, in Minneapolis, and Team Hospitalist member.
HM13 Session Analysis: Success Stories: How to Integrate NPs and PAs into a Hospitalist Practice
I attended the HM13 breakout session “Success Stories: How to Integrate NPs and PAs into a Hospitalist Practice,” which featured Timothy Capstack, MD, a hospitalist at Maryland Inpatient Care Specialists, James Levy, a physician assistant/hospitalist at Hospitalists of Northern Michigan, Kaine Brown, MD, a hospitalist at Tift Regional Medical Center, and Justin Psaila, MD, a hospitalist at St. Luke’s University Hospital and Health Network. Judging from the attendance, this is a very relevant topic. It seems every group is looking to hire NP/PAs, and most want to learn how to successfully incorporate them into a hospitalist practice.
Dr. Psaila explained the first key to success is hiring “beyond the basics,” meaning that it is not enough to be a good clinician, you must also hire a good fit to your practice culture. Additionally, NPs/PAs need to be part of a team they can rely on. He said critical-thinking skills are a much better asset for an NP/PA than technical procedural skills.
Levy agreed, and noted successful integration starts with getting the “right people on the bus.” HM groups should develop a thoughtful, consistent hiring process—and be willing to cut loose a provider if they are not a good fit. He also thinks it is important to have a lead NP/PA, so new hires know where to turn.
Dr. Brown found successful integration when his group turned to NP/PAs to run the post-discharge transition clinic. His group’s NP/PAs are helping reduce readmissions, improve patient/provider communication, and supporting the social and emotional needs of patients.
Watch a 2-minute video clip of Bob Wachter's HM13 keynote address
Dr. Capstack agreed that HM groups have to “hire right.” Hospitalist NP/PAs need to communicate well and be a team player, but also “know what they don’t know.” If the skill set is right, and you create a culture of collaboration, he said success is guaranteed.
All of the presenters agreed NP/PAs in hospital medicine are here to stay, and that they can be an asset to any HM group. TH
Tracy Cardin is a nurse practitioner in the Section of Hospital Medicine at the University of Chicago.
I attended the HM13 breakout session “Success Stories: How to Integrate NPs and PAs into a Hospitalist Practice,” which featured Timothy Capstack, MD, a hospitalist at Maryland Inpatient Care Specialists, James Levy, a physician assistant/hospitalist at Hospitalists of Northern Michigan, Kaine Brown, MD, a hospitalist at Tift Regional Medical Center, and Justin Psaila, MD, a hospitalist at St. Luke’s University Hospital and Health Network. Judging from the attendance, this is a very relevant topic. It seems every group is looking to hire NP/PAs, and most want to learn how to successfully incorporate them into a hospitalist practice.
Dr. Psaila explained the first key to success is hiring “beyond the basics,” meaning that it is not enough to be a good clinician, you must also hire a good fit to your practice culture. Additionally, NPs/PAs need to be part of a team they can rely on. He said critical-thinking skills are a much better asset for an NP/PA than technical procedural skills.
Levy agreed, and noted successful integration starts with getting the “right people on the bus.” HM groups should develop a thoughtful, consistent hiring process—and be willing to cut loose a provider if they are not a good fit. He also thinks it is important to have a lead NP/PA, so new hires know where to turn.
Dr. Brown found successful integration when his group turned to NP/PAs to run the post-discharge transition clinic. His group’s NP/PAs are helping reduce readmissions, improve patient/provider communication, and supporting the social and emotional needs of patients.
Watch a 2-minute video clip of Bob Wachter's HM13 keynote address
Dr. Capstack agreed that HM groups have to “hire right.” Hospitalist NP/PAs need to communicate well and be a team player, but also “know what they don’t know.” If the skill set is right, and you create a culture of collaboration, he said success is guaranteed.
All of the presenters agreed NP/PAs in hospital medicine are here to stay, and that they can be an asset to any HM group. TH
Tracy Cardin is a nurse practitioner in the Section of Hospital Medicine at the University of Chicago.
I attended the HM13 breakout session “Success Stories: How to Integrate NPs and PAs into a Hospitalist Practice,” which featured Timothy Capstack, MD, a hospitalist at Maryland Inpatient Care Specialists, James Levy, a physician assistant/hospitalist at Hospitalists of Northern Michigan, Kaine Brown, MD, a hospitalist at Tift Regional Medical Center, and Justin Psaila, MD, a hospitalist at St. Luke’s University Hospital and Health Network. Judging from the attendance, this is a very relevant topic. It seems every group is looking to hire NP/PAs, and most want to learn how to successfully incorporate them into a hospitalist practice.
Dr. Psaila explained the first key to success is hiring “beyond the basics,” meaning that it is not enough to be a good clinician, you must also hire a good fit to your practice culture. Additionally, NPs/PAs need to be part of a team they can rely on. He said critical-thinking skills are a much better asset for an NP/PA than technical procedural skills.
Levy agreed, and noted successful integration starts with getting the “right people on the bus.” HM groups should develop a thoughtful, consistent hiring process—and be willing to cut loose a provider if they are not a good fit. He also thinks it is important to have a lead NP/PA, so new hires know where to turn.
Dr. Brown found successful integration when his group turned to NP/PAs to run the post-discharge transition clinic. His group’s NP/PAs are helping reduce readmissions, improve patient/provider communication, and supporting the social and emotional needs of patients.
Watch a 2-minute video clip of Bob Wachter's HM13 keynote address
Dr. Capstack agreed that HM groups have to “hire right.” Hospitalist NP/PAs need to communicate well and be a team player, but also “know what they don’t know.” If the skill set is right, and you create a culture of collaboration, he said success is guaranteed.
All of the presenters agreed NP/PAs in hospital medicine are here to stay, and that they can be an asset to any HM group. TH
Tracy Cardin is a nurse practitioner in the Section of Hospital Medicine at the University of Chicago.
The Heart of the Matter
A 52 year‐old male presented to the emergency department with a 2‐month history of a sensation of fluttering in his chest and rapid heartbeat. The symptoms occurred episodically 6 to 8 times per day and lasted 15 to 60 minutes without associated chest pain, lightheadedness, or syncope. Over the past 2 weeks, he also began to experience dyspnea with minimal exertion.
These symptoms strongly hint at a cardiac dysrhythmia. Premature atrial and ventricular beats are frequent causes of palpitations in outpatients; however, the associated dyspnea on exertion indicates a more serious etiology. The 2‐month duration and absence of more severe sequelae up until now are points against life‐threatening ventricular tachycardia. A supraventricular arrhythmia would be most likely, especially atrial fibrillation, atrial flutter, atrioventricular nodal re‐entrant (AVNRT) or atrioventricular re‐entrant tachycardia (AVRT).
Evaluation should proceed along 2 parallel paths: to diagnose the specific type of arrhythmia and to uncover predisposing conditions. Etiologies of supraventricular arrhythmias include hypertensive heart disease, other structural heart disease including cardiomyopathy, pulmonary disease (eg, chronic obstructive pulmonary disease, pulmonary hypertension, or pulmonary embolism), pericardial disease, hyperthyroidism, sympathomimetic drug use, and in the case of AVRT, an underlying accessory pathway.
The patient's past medical history included hyperlipidemia. Two years prior, his electrocardiogram (ECG) at the time of a health insurance screening had demonstrated sinus rhythm with Q waves in leads III and aVF, and T wave inversions in the inferolateral and anterior leads. An exercise treadmill thallium test at that time demonstrated an area of reversibility in the inferior wall of the left ventricle and a normal ejection fraction. Coronary angiography revealed focal inferior and apical hypokinesis, with frequent premature ventricular contractions (PVCs) and normal coronary arteries.
These prior studies reveal an underlying cardiomyopathy. An ischemic etiology is less likely in the face of normal‐appearing coronary arteries, and he lacks a history of hypertension. Hypertrophic and restrictive cardiomyopathies are possibilities, and tachycardia‐induced cardiomyopathy is an uncommon cause to consider. The pattern of wall‐motion abnormalities is not classic for the Takotsubo phenomenon of apical ballooning, which is typically transient, related to stress, and more common in women. Frequent PVCs are associated with an increased risk of sudden death. I would inquire about illicit drug use and family history of sudden death or cardiac disease.
The patient was a married Caucasian male who reported significant stress related to his career at a software company. He drank 4 glasses of red wine weekly and never smoked cigarettes. He last used cocaine 30 years previously and denied ever using intravenous drugs. Prior to this illness he exercised regularly and traveled frequently to Europe, China, and Japan. He had no family history of cardiac disease or sudden cardiac death. On review of systems, he endorsed a dry cough for 3 weeks without fever, chills, or sweats, and he denied rashes or joint pains. Medications included aspirin, metoprolol, ezetimibe/simvastatin, fish oil, vitamin E, saw palmetto, glucosamine, chondroitin, and a multivitamin.
His remote cocaine use may have predisposed him to cardiomyopathy and hints at ongoing unacknowledged use, but otherwise the additional history is not helpful.
On physical examination, the patient appeared ill. His heart rate was 86 beats per minute, blood pressure 114/67 mm Hg, temperature 36.4C, respiratory rate 18 breaths per minute, and oxygen saturation was 95% while breathing ambient air. There was no conjunctival erythema or pallor, and the oropharynx was moist. The jugular venous pressure (JVP) was not elevated. The heart rhythm was irregular, with a variable intensity of the first heart sound; there were no murmurs or gallops. The apical impulse was normal. The lungs were clear to auscultation. The abdomen was soft, nontender, and nondistended without hepatosplenomegaly. The extremities were without clubbing, cyanosis, or edema. There was no joint swelling. Neurological examination was normal.
In this ill‐appearing patient with 2 months of palpitations, dry cough, and dyspnea on exertion, 2 diagnostic possibilities leap to the front: primary cardiac disease or a primary pulmonary disorder producing a cardiac arrhythmia. The normal JVP, apical impulse, clear lungs, and absence of edema indicate he does not have decompensated heart failure. However, based on prior studies that demonstrated structural heart disease, a cardiac etiology remains more probable. An oxygen saturation of 95% is not normal in a 52‐year‐old nonsmoker and needs to be investigated.
The white blood cell count was 10,000/mm3 with a normal differential, hemoglobin was 15 g/dL, and platelets were 250,000/mm3. Chemistries including sodium, potassium, chloride, bicarbonate, blood urea nitrogen, creatinine, glucose, calcium, magnesium, total protein, albumin, liver enzymes, and troponin‐I were all normal.
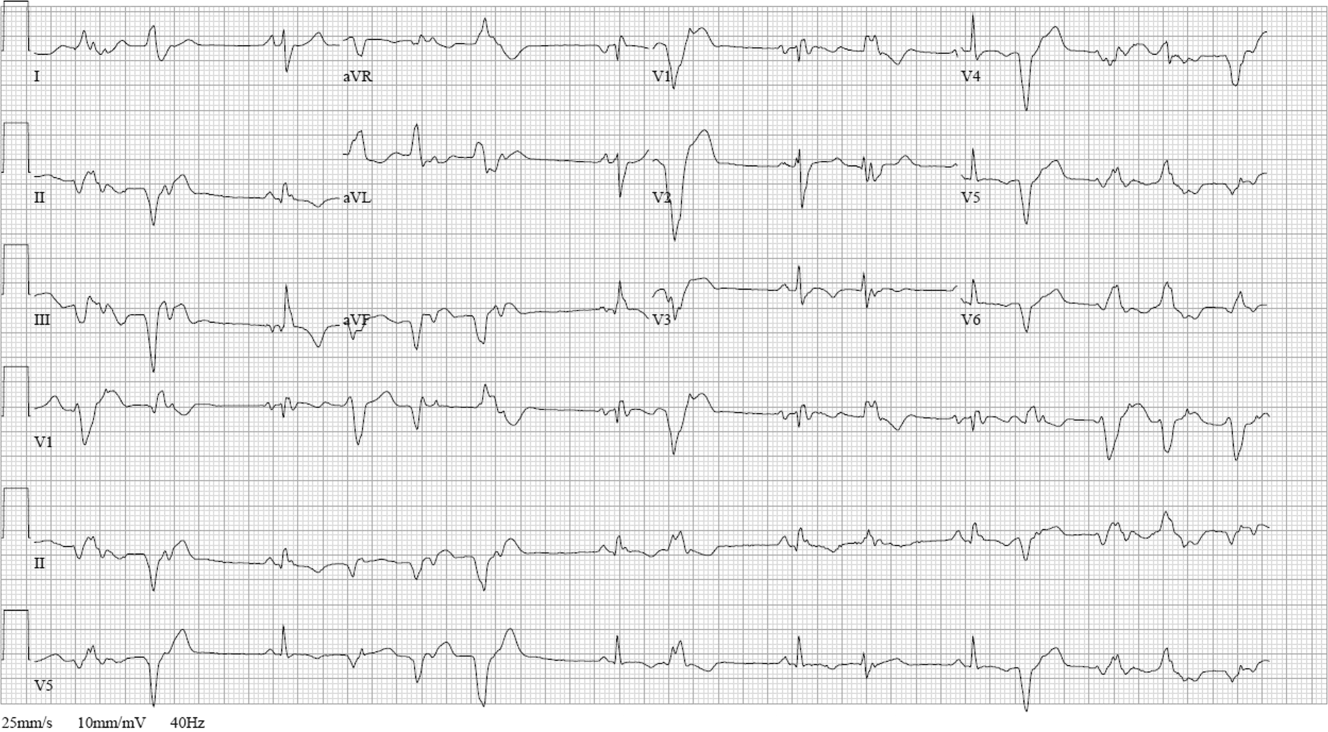
ECG (Figure 11) demonstrated sinus rhythm with an incomplete right bundle branch block, right axis deviation, low voltage, premature atrial contractions, and frequent multiform PVCs with couplets and triplets. Chest radiographs (Figure 22) demonstrated bilateral pleural effusions and a borderline enlarged cardiac silhouette.

The review of systems, physical exam, and laboratory tests provided no evidence of widespread systemic disease, promoting the hypothesis that a primary cardiac or pulmonary disorder is responsible for this patient's illness. The markedly abnormal ECG with conduction disturbance and ventricular ectopy provide further evidence of cardiomyopathy. Cardiomyopathies can be categorized as restrictive, dilated, hypertrophic, arrhythmogenic right ventricular, and miscellaneous causes. Transthoracic echocardiogram is the next key diagnostic test.
The patient was admitted to the hospital. Over the first 24 hours, serial ECGs and telemetry demonstrated runs of ventricular tachycardia at a rate of 169 beats per minute, frequent multiform PVCs, bifascicular block, and runs of supraventricular tachycardia.
Transthoracic echocardiogram showed right and left atrial enlargement, 2+ mitral regurgitation, an estimated right ventricular peak pressure of 35 mm Hg, severe left ventricular global hypokinesis with ejection fraction of 20% to 25%, and moderate right ventricular global hypokinesis. Oral amiodarone was administered, and subsequently an internal cardiac defibrillator (ICD) was placed.
I suspect the pulmonary hypertension and mitral regurgitation are consequences of left ventricular impairment, and therefore are not useful diagnostic clues. By contrast, the presence of severe biventricular failure narrows the diagnostic possibilities considerably. I would attempt to obtain the prior coronary angiography films to confirm the presence of normal coronary arteries. In the absence of coronary artery disease, biventricular failure suggests an advanced infiltrative or dilated cardiomyopathy, because hypertrophic cardiomyopathies are less likely to impair the right ventricle this profoundly.
Causes of restrictive cardiomyopathy in adults include amyloidosis, hemochromatosis, sarcoidosis, and the hypereosinophilic syndrome. Dilated cardiomyopathy may arise from antecedent myocarditis from numerous viruses including parvovirus B19, human herpesvirus 6, coxsackievirus, influenza, human immunodeficiency virus (HIV), or from other infections such as Chagas and Lyme disease, toxins (including alcohol and cocaine), autoimmune disease, hypothyroidism, peripartum, genetic causes, nutritional deficiency, or may be idiopathic.
I would check for antibodies to HIV, serum thyrotropin, transferrin saturation, and ferritin, test for serum and urine light chains (looking for evidence of AL amyloid), and obtain a toxicology screen. I would also obtain a computed tomography (CT) scan of the chest to look for supportive evidence of sarcoidosis in this mildly hypoxic patient.
Prior coronary angiography films were unobtainable. Repeat cardiac catheterization demonstrated normal coronary arteries, mildly enlarged left ventricle with ejection fraction of 35%. The mean right atrial, right ventricular end‐diastolic, and left ventricular end‐diastolic pressures were equal at 11 mm Hg, pulmonary capillary wedge pressure was 8 mm Hg. Serologies for coxsackie B, HIV, syphilis, cytomegalovirus, Epstein‐Barr virus, and hepatitis B and C were negative. A purified protein derivative was placed and was nonreactive 48 hours later. Erythrocyte sedimentation rate, C‐reactive protein, antinuclear antibodies, rheumatoid factor, and antibodies to citrullinated peptide were negative. Serum angiotensin‐converting enzyme (ACE) level was normal, lysozyme was elevated at 27 g/mL (normal range, 917), and interleukin (IL)6 was elevated at 27 pg/mL (normal range, 05). Serum protein electrophoresis, serum thyrotropin, transferrin saturation, and ferritin were normal.
The finding of equalization of diastolic pressures at catheterization suggests either constrictive or restrictive physiology; pressure measurements alone cannot distinguish the 2. In the absence of an obvious etiology of constrictive pericarditis (eg, tuberculosis, prior radiation therapy, or cardiac surgery), I remain concerned about infiltrative diseases. Normal iron studies rule out hemochromatosis, and the absence of peripheral eosinophilia removes hypereosinophilic syndrome as a diagnostic consideration. Sarcoidosis can definitely manifest with conduction block as well as biventricular failure, as can amyloidosis. By the time cardiac involvement manifests in sarcoidosis, pulmonary disease is often present, although it may be subclinical. Chest radiography and serum ACE levels are neither sensitive nor specific for screening for pulmonary sarcoidosis. Lysozyme and IL‐6 levels may be elevated in sarcoid, but these too are not specific.
Cardiac involvement in amyloidosis is typically due to AL amyloid light chain deposition associated with a plasma cell dyscrasia. I would expect evidence of organ involvement elsewhere, such as the liver, intestinal tract, tongue, peripheral nerves, or kidneys, none of which are evident in this man. Furthermore, lung involvement in amyloidosis is much less common than in sarcoid. If chest CT fails to demonstrate evidence of sarcoidosis, assays for light chains in the serum and urine might be warranted, as serum protein electrophoresis may fail to detect the abnormal paraprotein.
Chest CT demonstrated bronchial thickening and peribronchovascular bundle ground‐glass opacification, predominantly in the apical lobes with diffuse nodules, and mediastinal lymphadenopathy.
Taken together with the rest of this patient's illness, the CT findings are highly suspicious for sarcoidosis. Biopsy confirmation is essential prior to initiating immunosuppressive therapy. Endomyocardial biopsy and transbronchial biopsy would both be reasonable options; I would discuss these possibilities with pulmonary and cardiology consultants.
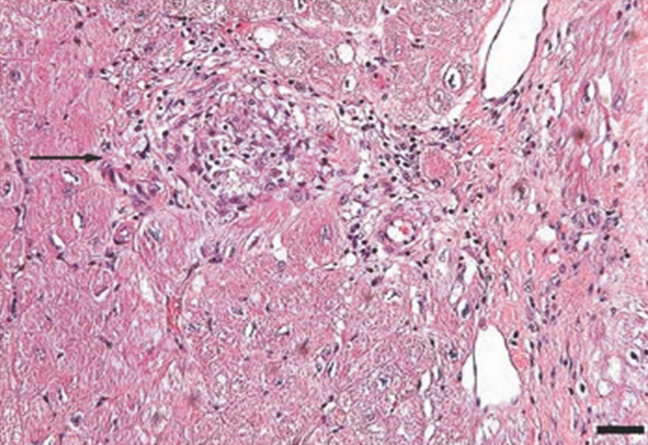
An endomyocardial biopsy was performed. The results (Figure 33) revealed the presence of noncaseating granulomas. A diagnosis of cardiac and pulmonary sarcoidosis was made, and treatment with corticosteroids was initiated. At follow‐up 3 years later, he was stable with New York Heart Association class II symptoms and an ejection fraction of 40% to 45%.
DISCUSSION
In outpatient medical practice, up to 16% of individuals report palpitations.[1] In 1 study, primary cardiac disorders accounted for 43% of palpitations, and clinically significant arrhythmias were found in 19% of patients.[2] A history of cardiac disease substantially raises the probability of an arrhythmic etiology of palpitations; over 90% of cases of palpitations in patients with prior cardiac disease are due to arrhythmias.[3]
In patients with palpitations, the history and physical examination do not reliably differentiate patients with significant arrhythmias from those without arrhythmias or those with benign arrhythmias (PVCs and sinus tachycardia). In a recent systematic review, palpitations awakening patients from sleep or occurring while at work, or a known history of cardiac disease, modestly increase the probability of a cardiac arrhythmia, with positive likelihood ratios of 2.03 to 2.29. On the other hand, palpitations lasting 5 minutes and a known history of panic disorder make an arrhythmia much less likely. Interestingly, palpitations associated with a regular rapid‐pounding sensation in the neck (as opposed to neck fullness) substantially increase the probability of AVNRT with an impressive likelihood ratio of 177.[3]
Sarcoidosis is a rare cause of palpitations and arrhythmias. Most commonly seen in young and middle‐aged adults, sarcoidosis is a disorder of unknown cause characterized by the formation of granulomas in multiple organs. Cardiac involvement is detected in 20% to 30% of sarcoidosis patients at autopsy, but only 5% of patients have clinically significant cardiac involvement.[4] Cardiac involvement can be the presenting and lone feature of sarcoidosis or may occur later in a patient with multisystem disease.
Within the heart, sarcoid granulomas are most abundant in the myocardium of the left ventricular free wall followed by the interventricular septum, right ventricle, and atria. The diffuse cardiac involvement explains the protean clinical and electrocardiographic manifestations seen in cardiac sarcoid. Symptoms of cardiac disease include palpitations, syncope, sudden death, or heart failure. The most common ECG manifestations are heart blocks of all types, followed by ventricular arrhythmias and then supraventricular arrhythmias, the latter attributed to secondary atrial enlargement or direct atrial infiltration by granuloma.[5]
The diagnosis of sarcoidosis is challenging. Presenting clinical features, physical exam, routine laboratory tests, ECG, and echocardiography are neither sensitive nor specific. Among the noninvasive tests, serum ACE has been commonly used, but its low sensitivity ranging from 60% to 77%[6, 7, 8] and 50% specificity[8] limit its usefulness in the diagnosis of sarcoid. IL‐6 and lysozyme are other serum markers sometimes obtained in cases of suspected sarcoid, but they too lack adequate sensitivity and specificity to be useful diagnostic tools.[8, 9]
When available, cardiac magnetic resonance imaging (MRI) can enhance clinicians' ability to diagnose cardiac sarcoidosis. It demonstrates zones of thinning and segmental myocardial wall motion abnormalities with increased signal intensity, more pronounced on T2‐weighted images due to inflammation and granulomatous edema. One study reported 100% sensitivity and 78% specificity of MRI in diagnosing cardiac sarcoid.[10]
Because of the limitations of noninvasive tests, tissue biopsy is necessary to diagnose sarcoidosis. If an accessible extracardiac site, such as an enlarged lymph node or skin lesion, is unavailable, a more invasive biopsy is recommended. Transbronchial biopsy is an option if there is obvious thoracic disease. Another alternative is to obtain a 18‐fluorodeoxyglucose positron emission tomography (18FDG‐PET) scan to identify hypermetabolic granulomas, which can be targeted for biopsy. For cardiac sarcoidosis, endomyocardial biopsy is often performed. This procedure is generally quite safe, with severe complications such as right ventricular perforation occurring in fewer than 1% of procedures.[11] However, the patchy nature of heart involvement in sarcoidosis results in a sensitivity as low as 20%.[12] Despite its low yield, according to guidelines from the American College of Cardiology and the American Heart Association, patients with unexplained heart failure of 3 months' duration associated with heart block or ventricular arrhythmias have a class I indication for endomyocardial biopsy.[11]
The prognosis of sarcoidosis is generally favorable, with fewer than 5% of patients dying from the disease. Although the impact of cardiac involvement is poorly established, the available literature indicate a worse prognosis for patients with symptomatic heart disease due to sarcoidosis. In 1 series, over half of 19 patients with cardiac involvement were either dead or required an ICD or pacemaker within 2 years of detection, as opposed to none of 82 sarcoid patients without clinically apparent cardiac involvement.[13]
The mainstay of treatment of cardiac sarcoidosis is corticosteroids, which may halt disease progression and improve survival, but do not reduce the incidence of ventricular arrhythmias. Initially, 1 mg/kg doses of prednisone dose are administered daily. Patients should be reassessed for response to treatment, and repeat ejection fraction measurement by echocardiogram should be obtained if symptoms worsen. The use of serial serum ACE levels to monitor disease activity is controversial. For patients responding to prednisone, the dose can be tapered over a period of 6 months to a maintenance daily dose of 10 to 15 mg, with a goal of eventually stopping therapy if disease is quiescent.[14] For patients who do not respond to glucocorticoids or who experience intolerable side effects, other immunosuppressive agents have been tried with reported success based on limited data. Options include methotrexate, azathioprine, hydroxychloroquine, cyclophosphamide, and infliximab.[5] Treatment of asymptomatic or minimally symptomatic patients with corticosteroids remains controversial.[14]
Adjunctive treatments are often necessary in cardiac sarcoidosis. Permanent pacemaker implantation is indicated if there is complete atrioventricular block or other high‐grade conduction system disease. Survivors of sudden cardiac death, individuals with refractory ventricular arrhythmias, and those with severely impaired systolic function are candidates for ICDs.[15] Catheter radiofrequency ablation may be effective in patients with ventricular tachyarrhythmias.[16]
Cardiac sarcoidosis is important to suspect in a patient with unexplained cardiomyopathy associated with conduction blocks or tachyarrhythmias because it is potentially reversible. Diagnosis can be elusive, as noninvasive tests lack sufficient sensitivity and specificity to establish the presence or absence of the disorder. Biopsy of affected organs is essential to identify the noncaseating granulomas that characterize the disease. When no extracardiac target exists, clinicians may need an endomyocardial biopsy to get to the heart of the matter.
CLINICAL TEACHING POINTS
- A history of cardiac disease substantially raises the possibility of an arrhythmic etiology of palpitations.
- Cardiac involvement in sarcoidosis can be asymptomatic or include conduction blocks, supraventricular and ventricular tachyarrhythmias, or cardiomyopathy.
- Cardiac sarcoid can be an elusive diagnosis to establish, because both noninvasive tests and endomyocardial biopsy demonstrate low sensitivity.
- Cardiac sarcoidosis portends a worse prognosis than sarcoid in general, but is a potentially reversible condition that therefore warrants an aggressive approach to establishing a diagnosis.
Acknowledgments
The authors thank Ellen Killebrew, MD, for help with the formal interpretation of the admission ECG.
Disclosures
Dr. Baudendistel is a former Deputy Editor and CME Editor of the Journal of Hospital Medicine, a position he ended in 2011. He received a stipend of less than $2000 for this work in 2010 and 2011. The authors are not aware of any conflicts of interest related to this article. The initial oral part of this presentation was presented at the University of California Davis Grand Rounds on August 16, 2010.
- , , , . Predictors of persistent palpitations and continued medical utilization. J Fam Pract. 1996;42:465–472.
- , . Evaluation and outcomes of patients with palpitations. Am J Med. 1996;100:138–148.
- , , , , . Does this patient with palpitations have a cardiac arrhythmia? JAMA. 2009;302:2135–2143.
- , . Myocardial sarcoidosis in forensic medicine. Am J Forensic Med Pathol. 1999;20:52–56.
- , , , et al. Cardiac sarcoidosis. Am Heart J. 2009;157:9–21.
- , , . Sarcoidosis. N Engl J Med. 2007;357:2153–2165.
- , . An angiotensin‐converting enzyme (ACE) inhibitor in human serum. Increased sensitivity of the serum ACE assay for detecting active sarcoidosis. Chest. 1986;90:869–875.
- , , , et al. Comparative evaluation of serum markers in pulmonary sarcoidosis. Chest. 2010;137:1391–1397.
- , , . Cardiac sarcoidosis: cytokine patterns in the course of the disease. Arch Pathol Lab Med. 2003;127:1207–1210.
- , , , et al. Evaluation of the accuracy of gadolinium‐enhanced cardiovascular magnetic resonance in the diagnosis of cardiac sarcoidosis. J Am Coll Cardiol. 2005;45:1683–1690.
- , , . Current status of endomyocardial biopsy. Mayo Clin Proc. 2011;86:1095–1102.
- , , , , , . Histologic diagnostic rate of cardiac sarcoidosis: evaluation of endomyocardial biopsies. Am Heart J. 1999;138:299–302.
- , , , et al. Cardiac involvement in patients with pulmonary sarcoidosis assessed at two university medical centers in the Netherlands. Chest. 2005;128(1):30–35.
- , , , et al. Prognostic determinants of long‐term survival in Japanese patients with cardiac sarcoidosis treated with prednisone. Am J Cardiol. 2001;88:1006–1010.
- , , , . The automated implantable cardiac defibrillator. Prophylaxis in cardiac sarcoidosis. Chest. 1994;106:1603–1607.
- , , , et al. Ventricular tachycardia in cardiac sarcoidosis controlled by radiofrequency catheter ablation. Intern Med. 2011;50:1201–1206.
A 52 year‐old male presented to the emergency department with a 2‐month history of a sensation of fluttering in his chest and rapid heartbeat. The symptoms occurred episodically 6 to 8 times per day and lasted 15 to 60 minutes without associated chest pain, lightheadedness, or syncope. Over the past 2 weeks, he also began to experience dyspnea with minimal exertion.
These symptoms strongly hint at a cardiac dysrhythmia. Premature atrial and ventricular beats are frequent causes of palpitations in outpatients; however, the associated dyspnea on exertion indicates a more serious etiology. The 2‐month duration and absence of more severe sequelae up until now are points against life‐threatening ventricular tachycardia. A supraventricular arrhythmia would be most likely, especially atrial fibrillation, atrial flutter, atrioventricular nodal re‐entrant (AVNRT) or atrioventricular re‐entrant tachycardia (AVRT).
Evaluation should proceed along 2 parallel paths: to diagnose the specific type of arrhythmia and to uncover predisposing conditions. Etiologies of supraventricular arrhythmias include hypertensive heart disease, other structural heart disease including cardiomyopathy, pulmonary disease (eg, chronic obstructive pulmonary disease, pulmonary hypertension, or pulmonary embolism), pericardial disease, hyperthyroidism, sympathomimetic drug use, and in the case of AVRT, an underlying accessory pathway.
The patient's past medical history included hyperlipidemia. Two years prior, his electrocardiogram (ECG) at the time of a health insurance screening had demonstrated sinus rhythm with Q waves in leads III and aVF, and T wave inversions in the inferolateral and anterior leads. An exercise treadmill thallium test at that time demonstrated an area of reversibility in the inferior wall of the left ventricle and a normal ejection fraction. Coronary angiography revealed focal inferior and apical hypokinesis, with frequent premature ventricular contractions (PVCs) and normal coronary arteries.
These prior studies reveal an underlying cardiomyopathy. An ischemic etiology is less likely in the face of normal‐appearing coronary arteries, and he lacks a history of hypertension. Hypertrophic and restrictive cardiomyopathies are possibilities, and tachycardia‐induced cardiomyopathy is an uncommon cause to consider. The pattern of wall‐motion abnormalities is not classic for the Takotsubo phenomenon of apical ballooning, which is typically transient, related to stress, and more common in women. Frequent PVCs are associated with an increased risk of sudden death. I would inquire about illicit drug use and family history of sudden death or cardiac disease.
The patient was a married Caucasian male who reported significant stress related to his career at a software company. He drank 4 glasses of red wine weekly and never smoked cigarettes. He last used cocaine 30 years previously and denied ever using intravenous drugs. Prior to this illness he exercised regularly and traveled frequently to Europe, China, and Japan. He had no family history of cardiac disease or sudden cardiac death. On review of systems, he endorsed a dry cough for 3 weeks without fever, chills, or sweats, and he denied rashes or joint pains. Medications included aspirin, metoprolol, ezetimibe/simvastatin, fish oil, vitamin E, saw palmetto, glucosamine, chondroitin, and a multivitamin.
His remote cocaine use may have predisposed him to cardiomyopathy and hints at ongoing unacknowledged use, but otherwise the additional history is not helpful.
On physical examination, the patient appeared ill. His heart rate was 86 beats per minute, blood pressure 114/67 mm Hg, temperature 36.4C, respiratory rate 18 breaths per minute, and oxygen saturation was 95% while breathing ambient air. There was no conjunctival erythema or pallor, and the oropharynx was moist. The jugular venous pressure (JVP) was not elevated. The heart rhythm was irregular, with a variable intensity of the first heart sound; there were no murmurs or gallops. The apical impulse was normal. The lungs were clear to auscultation. The abdomen was soft, nontender, and nondistended without hepatosplenomegaly. The extremities were without clubbing, cyanosis, or edema. There was no joint swelling. Neurological examination was normal.
In this ill‐appearing patient with 2 months of palpitations, dry cough, and dyspnea on exertion, 2 diagnostic possibilities leap to the front: primary cardiac disease or a primary pulmonary disorder producing a cardiac arrhythmia. The normal JVP, apical impulse, clear lungs, and absence of edema indicate he does not have decompensated heart failure. However, based on prior studies that demonstrated structural heart disease, a cardiac etiology remains more probable. An oxygen saturation of 95% is not normal in a 52‐year‐old nonsmoker and needs to be investigated.
The white blood cell count was 10,000/mm3 with a normal differential, hemoglobin was 15 g/dL, and platelets were 250,000/mm3. Chemistries including sodium, potassium, chloride, bicarbonate, blood urea nitrogen, creatinine, glucose, calcium, magnesium, total protein, albumin, liver enzymes, and troponin‐I were all normal.
ECG (Figure 11) demonstrated sinus rhythm with an incomplete right bundle branch block, right axis deviation, low voltage, premature atrial contractions, and frequent multiform PVCs with couplets and triplets. Chest radiographs (Figure 22) demonstrated bilateral pleural effusions and a borderline enlarged cardiac silhouette.
The review of systems, physical exam, and laboratory tests provided no evidence of widespread systemic disease, promoting the hypothesis that a primary cardiac or pulmonary disorder is responsible for this patient's illness. The markedly abnormal ECG with conduction disturbance and ventricular ectopy provide further evidence of cardiomyopathy. Cardiomyopathies can be categorized as restrictive, dilated, hypertrophic, arrhythmogenic right ventricular, and miscellaneous causes. Transthoracic echocardiogram is the next key diagnostic test.
The patient was admitted to the hospital. Over the first 24 hours, serial ECGs and telemetry demonstrated runs of ventricular tachycardia at a rate of 169 beats per minute, frequent multiform PVCs, bifascicular block, and runs of supraventricular tachycardia.
Transthoracic echocardiogram showed right and left atrial enlargement, 2+ mitral regurgitation, an estimated right ventricular peak pressure of 35 mm Hg, severe left ventricular global hypokinesis with ejection fraction of 20% to 25%, and moderate right ventricular global hypokinesis. Oral amiodarone was administered, and subsequently an internal cardiac defibrillator (ICD) was placed.
I suspect the pulmonary hypertension and mitral regurgitation are consequences of left ventricular impairment, and therefore are not useful diagnostic clues. By contrast, the presence of severe biventricular failure narrows the diagnostic possibilities considerably. I would attempt to obtain the prior coronary angiography films to confirm the presence of normal coronary arteries. In the absence of coronary artery disease, biventricular failure suggests an advanced infiltrative or dilated cardiomyopathy, because hypertrophic cardiomyopathies are less likely to impair the right ventricle this profoundly.
Causes of restrictive cardiomyopathy in adults include amyloidosis, hemochromatosis, sarcoidosis, and the hypereosinophilic syndrome. Dilated cardiomyopathy may arise from antecedent myocarditis from numerous viruses including parvovirus B19, human herpesvirus 6, coxsackievirus, influenza, human immunodeficiency virus (HIV), or from other infections such as Chagas and Lyme disease, toxins (including alcohol and cocaine), autoimmune disease, hypothyroidism, peripartum, genetic causes, nutritional deficiency, or may be idiopathic.
I would check for antibodies to HIV, serum thyrotropin, transferrin saturation, and ferritin, test for serum and urine light chains (looking for evidence of AL amyloid), and obtain a toxicology screen. I would also obtain a computed tomography (CT) scan of the chest to look for supportive evidence of sarcoidosis in this mildly hypoxic patient.
Prior coronary angiography films were unobtainable. Repeat cardiac catheterization demonstrated normal coronary arteries, mildly enlarged left ventricle with ejection fraction of 35%. The mean right atrial, right ventricular end‐diastolic, and left ventricular end‐diastolic pressures were equal at 11 mm Hg, pulmonary capillary wedge pressure was 8 mm Hg. Serologies for coxsackie B, HIV, syphilis, cytomegalovirus, Epstein‐Barr virus, and hepatitis B and C were negative. A purified protein derivative was placed and was nonreactive 48 hours later. Erythrocyte sedimentation rate, C‐reactive protein, antinuclear antibodies, rheumatoid factor, and antibodies to citrullinated peptide were negative. Serum angiotensin‐converting enzyme (ACE) level was normal, lysozyme was elevated at 27 g/mL (normal range, 917), and interleukin (IL)6 was elevated at 27 pg/mL (normal range, 05). Serum protein electrophoresis, serum thyrotropin, transferrin saturation, and ferritin were normal.
The finding of equalization of diastolic pressures at catheterization suggests either constrictive or restrictive physiology; pressure measurements alone cannot distinguish the 2. In the absence of an obvious etiology of constrictive pericarditis (eg, tuberculosis, prior radiation therapy, or cardiac surgery), I remain concerned about infiltrative diseases. Normal iron studies rule out hemochromatosis, and the absence of peripheral eosinophilia removes hypereosinophilic syndrome as a diagnostic consideration. Sarcoidosis can definitely manifest with conduction block as well as biventricular failure, as can amyloidosis. By the time cardiac involvement manifests in sarcoidosis, pulmonary disease is often present, although it may be subclinical. Chest radiography and serum ACE levels are neither sensitive nor specific for screening for pulmonary sarcoidosis. Lysozyme and IL‐6 levels may be elevated in sarcoid, but these too are not specific.
Cardiac involvement in amyloidosis is typically due to AL amyloid light chain deposition associated with a plasma cell dyscrasia. I would expect evidence of organ involvement elsewhere, such as the liver, intestinal tract, tongue, peripheral nerves, or kidneys, none of which are evident in this man. Furthermore, lung involvement in amyloidosis is much less common than in sarcoid. If chest CT fails to demonstrate evidence of sarcoidosis, assays for light chains in the serum and urine might be warranted, as serum protein electrophoresis may fail to detect the abnormal paraprotein.
Chest CT demonstrated bronchial thickening and peribronchovascular bundle ground‐glass opacification, predominantly in the apical lobes with diffuse nodules, and mediastinal lymphadenopathy.
Taken together with the rest of this patient's illness, the CT findings are highly suspicious for sarcoidosis. Biopsy confirmation is essential prior to initiating immunosuppressive therapy. Endomyocardial biopsy and transbronchial biopsy would both be reasonable options; I would discuss these possibilities with pulmonary and cardiology consultants.
An endomyocardial biopsy was performed. The results (Figure 33) revealed the presence of noncaseating granulomas. A diagnosis of cardiac and pulmonary sarcoidosis was made, and treatment with corticosteroids was initiated. At follow‐up 3 years later, he was stable with New York Heart Association class II symptoms and an ejection fraction of 40% to 45%.
DISCUSSION
In outpatient medical practice, up to 16% of individuals report palpitations.[1] In 1 study, primary cardiac disorders accounted for 43% of palpitations, and clinically significant arrhythmias were found in 19% of patients.[2] A history of cardiac disease substantially raises the probability of an arrhythmic etiology of palpitations; over 90% of cases of palpitations in patients with prior cardiac disease are due to arrhythmias.[3]
In patients with palpitations, the history and physical examination do not reliably differentiate patients with significant arrhythmias from those without arrhythmias or those with benign arrhythmias (PVCs and sinus tachycardia). In a recent systematic review, palpitations awakening patients from sleep or occurring while at work, or a known history of cardiac disease, modestly increase the probability of a cardiac arrhythmia, with positive likelihood ratios of 2.03 to 2.29. On the other hand, palpitations lasting 5 minutes and a known history of panic disorder make an arrhythmia much less likely. Interestingly, palpitations associated with a regular rapid‐pounding sensation in the neck (as opposed to neck fullness) substantially increase the probability of AVNRT with an impressive likelihood ratio of 177.[3]
Sarcoidosis is a rare cause of palpitations and arrhythmias. Most commonly seen in young and middle‐aged adults, sarcoidosis is a disorder of unknown cause characterized by the formation of granulomas in multiple organs. Cardiac involvement is detected in 20% to 30% of sarcoidosis patients at autopsy, but only 5% of patients have clinically significant cardiac involvement.[4] Cardiac involvement can be the presenting and lone feature of sarcoidosis or may occur later in a patient with multisystem disease.
Within the heart, sarcoid granulomas are most abundant in the myocardium of the left ventricular free wall followed by the interventricular septum, right ventricle, and atria. The diffuse cardiac involvement explains the protean clinical and electrocardiographic manifestations seen in cardiac sarcoid. Symptoms of cardiac disease include palpitations, syncope, sudden death, or heart failure. The most common ECG manifestations are heart blocks of all types, followed by ventricular arrhythmias and then supraventricular arrhythmias, the latter attributed to secondary atrial enlargement or direct atrial infiltration by granuloma.[5]
The diagnosis of sarcoidosis is challenging. Presenting clinical features, physical exam, routine laboratory tests, ECG, and echocardiography are neither sensitive nor specific. Among the noninvasive tests, serum ACE has been commonly used, but its low sensitivity ranging from 60% to 77%[6, 7, 8] and 50% specificity[8] limit its usefulness in the diagnosis of sarcoid. IL‐6 and lysozyme are other serum markers sometimes obtained in cases of suspected sarcoid, but they too lack adequate sensitivity and specificity to be useful diagnostic tools.[8, 9]
When available, cardiac magnetic resonance imaging (MRI) can enhance clinicians' ability to diagnose cardiac sarcoidosis. It demonstrates zones of thinning and segmental myocardial wall motion abnormalities with increased signal intensity, more pronounced on T2‐weighted images due to inflammation and granulomatous edema. One study reported 100% sensitivity and 78% specificity of MRI in diagnosing cardiac sarcoid.[10]
Because of the limitations of noninvasive tests, tissue biopsy is necessary to diagnose sarcoidosis. If an accessible extracardiac site, such as an enlarged lymph node or skin lesion, is unavailable, a more invasive biopsy is recommended. Transbronchial biopsy is an option if there is obvious thoracic disease. Another alternative is to obtain a 18‐fluorodeoxyglucose positron emission tomography (18FDG‐PET) scan to identify hypermetabolic granulomas, which can be targeted for biopsy. For cardiac sarcoidosis, endomyocardial biopsy is often performed. This procedure is generally quite safe, with severe complications such as right ventricular perforation occurring in fewer than 1% of procedures.[11] However, the patchy nature of heart involvement in sarcoidosis results in a sensitivity as low as 20%.[12] Despite its low yield, according to guidelines from the American College of Cardiology and the American Heart Association, patients with unexplained heart failure of 3 months' duration associated with heart block or ventricular arrhythmias have a class I indication for endomyocardial biopsy.[11]
The prognosis of sarcoidosis is generally favorable, with fewer than 5% of patients dying from the disease. Although the impact of cardiac involvement is poorly established, the available literature indicate a worse prognosis for patients with symptomatic heart disease due to sarcoidosis. In 1 series, over half of 19 patients with cardiac involvement were either dead or required an ICD or pacemaker within 2 years of detection, as opposed to none of 82 sarcoid patients without clinically apparent cardiac involvement.[13]
The mainstay of treatment of cardiac sarcoidosis is corticosteroids, which may halt disease progression and improve survival, but do not reduce the incidence of ventricular arrhythmias. Initially, 1 mg/kg doses of prednisone dose are administered daily. Patients should be reassessed for response to treatment, and repeat ejection fraction measurement by echocardiogram should be obtained if symptoms worsen. The use of serial serum ACE levels to monitor disease activity is controversial. For patients responding to prednisone, the dose can be tapered over a period of 6 months to a maintenance daily dose of 10 to 15 mg, with a goal of eventually stopping therapy if disease is quiescent.[14] For patients who do not respond to glucocorticoids or who experience intolerable side effects, other immunosuppressive agents have been tried with reported success based on limited data. Options include methotrexate, azathioprine, hydroxychloroquine, cyclophosphamide, and infliximab.[5] Treatment of asymptomatic or minimally symptomatic patients with corticosteroids remains controversial.[14]
Adjunctive treatments are often necessary in cardiac sarcoidosis. Permanent pacemaker implantation is indicated if there is complete atrioventricular block or other high‐grade conduction system disease. Survivors of sudden cardiac death, individuals with refractory ventricular arrhythmias, and those with severely impaired systolic function are candidates for ICDs.[15] Catheter radiofrequency ablation may be effective in patients with ventricular tachyarrhythmias.[16]
Cardiac sarcoidosis is important to suspect in a patient with unexplained cardiomyopathy associated with conduction blocks or tachyarrhythmias because it is potentially reversible. Diagnosis can be elusive, as noninvasive tests lack sufficient sensitivity and specificity to establish the presence or absence of the disorder. Biopsy of affected organs is essential to identify the noncaseating granulomas that characterize the disease. When no extracardiac target exists, clinicians may need an endomyocardial biopsy to get to the heart of the matter.
CLINICAL TEACHING POINTS
- A history of cardiac disease substantially raises the possibility of an arrhythmic etiology of palpitations.
- Cardiac involvement in sarcoidosis can be asymptomatic or include conduction blocks, supraventricular and ventricular tachyarrhythmias, or cardiomyopathy.
- Cardiac sarcoid can be an elusive diagnosis to establish, because both noninvasive tests and endomyocardial biopsy demonstrate low sensitivity.
- Cardiac sarcoidosis portends a worse prognosis than sarcoid in general, but is a potentially reversible condition that therefore warrants an aggressive approach to establishing a diagnosis.
Acknowledgments
The authors thank Ellen Killebrew, MD, for help with the formal interpretation of the admission ECG.
Disclosures
Dr. Baudendistel is a former Deputy Editor and CME Editor of the Journal of Hospital Medicine, a position he ended in 2011. He received a stipend of less than $2000 for this work in 2010 and 2011. The authors are not aware of any conflicts of interest related to this article. The initial oral part of this presentation was presented at the University of California Davis Grand Rounds on August 16, 2010.
A 52 year‐old male presented to the emergency department with a 2‐month history of a sensation of fluttering in his chest and rapid heartbeat. The symptoms occurred episodically 6 to 8 times per day and lasted 15 to 60 minutes without associated chest pain, lightheadedness, or syncope. Over the past 2 weeks, he also began to experience dyspnea with minimal exertion.
These symptoms strongly hint at a cardiac dysrhythmia. Premature atrial and ventricular beats are frequent causes of palpitations in outpatients; however, the associated dyspnea on exertion indicates a more serious etiology. The 2‐month duration and absence of more severe sequelae up until now are points against life‐threatening ventricular tachycardia. A supraventricular arrhythmia would be most likely, especially atrial fibrillation, atrial flutter, atrioventricular nodal re‐entrant (AVNRT) or atrioventricular re‐entrant tachycardia (AVRT).
Evaluation should proceed along 2 parallel paths: to diagnose the specific type of arrhythmia and to uncover predisposing conditions. Etiologies of supraventricular arrhythmias include hypertensive heart disease, other structural heart disease including cardiomyopathy, pulmonary disease (eg, chronic obstructive pulmonary disease, pulmonary hypertension, or pulmonary embolism), pericardial disease, hyperthyroidism, sympathomimetic drug use, and in the case of AVRT, an underlying accessory pathway.
The patient's past medical history included hyperlipidemia. Two years prior, his electrocardiogram (ECG) at the time of a health insurance screening had demonstrated sinus rhythm with Q waves in leads III and aVF, and T wave inversions in the inferolateral and anterior leads. An exercise treadmill thallium test at that time demonstrated an area of reversibility in the inferior wall of the left ventricle and a normal ejection fraction. Coronary angiography revealed focal inferior and apical hypokinesis, with frequent premature ventricular contractions (PVCs) and normal coronary arteries.
These prior studies reveal an underlying cardiomyopathy. An ischemic etiology is less likely in the face of normal‐appearing coronary arteries, and he lacks a history of hypertension. Hypertrophic and restrictive cardiomyopathies are possibilities, and tachycardia‐induced cardiomyopathy is an uncommon cause to consider. The pattern of wall‐motion abnormalities is not classic for the Takotsubo phenomenon of apical ballooning, which is typically transient, related to stress, and more common in women. Frequent PVCs are associated with an increased risk of sudden death. I would inquire about illicit drug use and family history of sudden death or cardiac disease.
The patient was a married Caucasian male who reported significant stress related to his career at a software company. He drank 4 glasses of red wine weekly and never smoked cigarettes. He last used cocaine 30 years previously and denied ever using intravenous drugs. Prior to this illness he exercised regularly and traveled frequently to Europe, China, and Japan. He had no family history of cardiac disease or sudden cardiac death. On review of systems, he endorsed a dry cough for 3 weeks without fever, chills, or sweats, and he denied rashes or joint pains. Medications included aspirin, metoprolol, ezetimibe/simvastatin, fish oil, vitamin E, saw palmetto, glucosamine, chondroitin, and a multivitamin.
His remote cocaine use may have predisposed him to cardiomyopathy and hints at ongoing unacknowledged use, but otherwise the additional history is not helpful.
On physical examination, the patient appeared ill. His heart rate was 86 beats per minute, blood pressure 114/67 mm Hg, temperature 36.4C, respiratory rate 18 breaths per minute, and oxygen saturation was 95% while breathing ambient air. There was no conjunctival erythema or pallor, and the oropharynx was moist. The jugular venous pressure (JVP) was not elevated. The heart rhythm was irregular, with a variable intensity of the first heart sound; there were no murmurs or gallops. The apical impulse was normal. The lungs were clear to auscultation. The abdomen was soft, nontender, and nondistended without hepatosplenomegaly. The extremities were without clubbing, cyanosis, or edema. There was no joint swelling. Neurological examination was normal.
In this ill‐appearing patient with 2 months of palpitations, dry cough, and dyspnea on exertion, 2 diagnostic possibilities leap to the front: primary cardiac disease or a primary pulmonary disorder producing a cardiac arrhythmia. The normal JVP, apical impulse, clear lungs, and absence of edema indicate he does not have decompensated heart failure. However, based on prior studies that demonstrated structural heart disease, a cardiac etiology remains more probable. An oxygen saturation of 95% is not normal in a 52‐year‐old nonsmoker and needs to be investigated.
The white blood cell count was 10,000/mm3 with a normal differential, hemoglobin was 15 g/dL, and platelets were 250,000/mm3. Chemistries including sodium, potassium, chloride, bicarbonate, blood urea nitrogen, creatinine, glucose, calcium, magnesium, total protein, albumin, liver enzymes, and troponin‐I were all normal.
ECG (Figure 11) demonstrated sinus rhythm with an incomplete right bundle branch block, right axis deviation, low voltage, premature atrial contractions, and frequent multiform PVCs with couplets and triplets. Chest radiographs (Figure 22) demonstrated bilateral pleural effusions and a borderline enlarged cardiac silhouette.
The review of systems, physical exam, and laboratory tests provided no evidence of widespread systemic disease, promoting the hypothesis that a primary cardiac or pulmonary disorder is responsible for this patient's illness. The markedly abnormal ECG with conduction disturbance and ventricular ectopy provide further evidence of cardiomyopathy. Cardiomyopathies can be categorized as restrictive, dilated, hypertrophic, arrhythmogenic right ventricular, and miscellaneous causes. Transthoracic echocardiogram is the next key diagnostic test.
The patient was admitted to the hospital. Over the first 24 hours, serial ECGs and telemetry demonstrated runs of ventricular tachycardia at a rate of 169 beats per minute, frequent multiform PVCs, bifascicular block, and runs of supraventricular tachycardia.
Transthoracic echocardiogram showed right and left atrial enlargement, 2+ mitral regurgitation, an estimated right ventricular peak pressure of 35 mm Hg, severe left ventricular global hypokinesis with ejection fraction of 20% to 25%, and moderate right ventricular global hypokinesis. Oral amiodarone was administered, and subsequently an internal cardiac defibrillator (ICD) was placed.
I suspect the pulmonary hypertension and mitral regurgitation are consequences of left ventricular impairment, and therefore are not useful diagnostic clues. By contrast, the presence of severe biventricular failure narrows the diagnostic possibilities considerably. I would attempt to obtain the prior coronary angiography films to confirm the presence of normal coronary arteries. In the absence of coronary artery disease, biventricular failure suggests an advanced infiltrative or dilated cardiomyopathy, because hypertrophic cardiomyopathies are less likely to impair the right ventricle this profoundly.
Causes of restrictive cardiomyopathy in adults include amyloidosis, hemochromatosis, sarcoidosis, and the hypereosinophilic syndrome. Dilated cardiomyopathy may arise from antecedent myocarditis from numerous viruses including parvovirus B19, human herpesvirus 6, coxsackievirus, influenza, human immunodeficiency virus (HIV), or from other infections such as Chagas and Lyme disease, toxins (including alcohol and cocaine), autoimmune disease, hypothyroidism, peripartum, genetic causes, nutritional deficiency, or may be idiopathic.
I would check for antibodies to HIV, serum thyrotropin, transferrin saturation, and ferritin, test for serum and urine light chains (looking for evidence of AL amyloid), and obtain a toxicology screen. I would also obtain a computed tomography (CT) scan of the chest to look for supportive evidence of sarcoidosis in this mildly hypoxic patient.
Prior coronary angiography films were unobtainable. Repeat cardiac catheterization demonstrated normal coronary arteries, mildly enlarged left ventricle with ejection fraction of 35%. The mean right atrial, right ventricular end‐diastolic, and left ventricular end‐diastolic pressures were equal at 11 mm Hg, pulmonary capillary wedge pressure was 8 mm Hg. Serologies for coxsackie B, HIV, syphilis, cytomegalovirus, Epstein‐Barr virus, and hepatitis B and C were negative. A purified protein derivative was placed and was nonreactive 48 hours later. Erythrocyte sedimentation rate, C‐reactive protein, antinuclear antibodies, rheumatoid factor, and antibodies to citrullinated peptide were negative. Serum angiotensin‐converting enzyme (ACE) level was normal, lysozyme was elevated at 27 g/mL (normal range, 917), and interleukin (IL)6 was elevated at 27 pg/mL (normal range, 05). Serum protein electrophoresis, serum thyrotropin, transferrin saturation, and ferritin were normal.
The finding of equalization of diastolic pressures at catheterization suggests either constrictive or restrictive physiology; pressure measurements alone cannot distinguish the 2. In the absence of an obvious etiology of constrictive pericarditis (eg, tuberculosis, prior radiation therapy, or cardiac surgery), I remain concerned about infiltrative diseases. Normal iron studies rule out hemochromatosis, and the absence of peripheral eosinophilia removes hypereosinophilic syndrome as a diagnostic consideration. Sarcoidosis can definitely manifest with conduction block as well as biventricular failure, as can amyloidosis. By the time cardiac involvement manifests in sarcoidosis, pulmonary disease is often present, although it may be subclinical. Chest radiography and serum ACE levels are neither sensitive nor specific for screening for pulmonary sarcoidosis. Lysozyme and IL‐6 levels may be elevated in sarcoid, but these too are not specific.
Cardiac involvement in amyloidosis is typically due to AL amyloid light chain deposition associated with a plasma cell dyscrasia. I would expect evidence of organ involvement elsewhere, such as the liver, intestinal tract, tongue, peripheral nerves, or kidneys, none of which are evident in this man. Furthermore, lung involvement in amyloidosis is much less common than in sarcoid. If chest CT fails to demonstrate evidence of sarcoidosis, assays for light chains in the serum and urine might be warranted, as serum protein electrophoresis may fail to detect the abnormal paraprotein.
Chest CT demonstrated bronchial thickening and peribronchovascular bundle ground‐glass opacification, predominantly in the apical lobes with diffuse nodules, and mediastinal lymphadenopathy.
Taken together with the rest of this patient's illness, the CT findings are highly suspicious for sarcoidosis. Biopsy confirmation is essential prior to initiating immunosuppressive therapy. Endomyocardial biopsy and transbronchial biopsy would both be reasonable options; I would discuss these possibilities with pulmonary and cardiology consultants.
An endomyocardial biopsy was performed. The results (Figure 33) revealed the presence of noncaseating granulomas. A diagnosis of cardiac and pulmonary sarcoidosis was made, and treatment with corticosteroids was initiated. At follow‐up 3 years later, he was stable with New York Heart Association class II symptoms and an ejection fraction of 40% to 45%.
DISCUSSION
In outpatient medical practice, up to 16% of individuals report palpitations.[1] In 1 study, primary cardiac disorders accounted for 43% of palpitations, and clinically significant arrhythmias were found in 19% of patients.[2] A history of cardiac disease substantially raises the probability of an arrhythmic etiology of palpitations; over 90% of cases of palpitations in patients with prior cardiac disease are due to arrhythmias.[3]
In patients with palpitations, the history and physical examination do not reliably differentiate patients with significant arrhythmias from those without arrhythmias or those with benign arrhythmias (PVCs and sinus tachycardia). In a recent systematic review, palpitations awakening patients from sleep or occurring while at work, or a known history of cardiac disease, modestly increase the probability of a cardiac arrhythmia, with positive likelihood ratios of 2.03 to 2.29. On the other hand, palpitations lasting 5 minutes and a known history of panic disorder make an arrhythmia much less likely. Interestingly, palpitations associated with a regular rapid‐pounding sensation in the neck (as opposed to neck fullness) substantially increase the probability of AVNRT with an impressive likelihood ratio of 177.[3]
Sarcoidosis is a rare cause of palpitations and arrhythmias. Most commonly seen in young and middle‐aged adults, sarcoidosis is a disorder of unknown cause characterized by the formation of granulomas in multiple organs. Cardiac involvement is detected in 20% to 30% of sarcoidosis patients at autopsy, but only 5% of patients have clinically significant cardiac involvement.[4] Cardiac involvement can be the presenting and lone feature of sarcoidosis or may occur later in a patient with multisystem disease.
Within the heart, sarcoid granulomas are most abundant in the myocardium of the left ventricular free wall followed by the interventricular septum, right ventricle, and atria. The diffuse cardiac involvement explains the protean clinical and electrocardiographic manifestations seen in cardiac sarcoid. Symptoms of cardiac disease include palpitations, syncope, sudden death, or heart failure. The most common ECG manifestations are heart blocks of all types, followed by ventricular arrhythmias and then supraventricular arrhythmias, the latter attributed to secondary atrial enlargement or direct atrial infiltration by granuloma.[5]
The diagnosis of sarcoidosis is challenging. Presenting clinical features, physical exam, routine laboratory tests, ECG, and echocardiography are neither sensitive nor specific. Among the noninvasive tests, serum ACE has been commonly used, but its low sensitivity ranging from 60% to 77%[6, 7, 8] and 50% specificity[8] limit its usefulness in the diagnosis of sarcoid. IL‐6 and lysozyme are other serum markers sometimes obtained in cases of suspected sarcoid, but they too lack adequate sensitivity and specificity to be useful diagnostic tools.[8, 9]
When available, cardiac magnetic resonance imaging (MRI) can enhance clinicians' ability to diagnose cardiac sarcoidosis. It demonstrates zones of thinning and segmental myocardial wall motion abnormalities with increased signal intensity, more pronounced on T2‐weighted images due to inflammation and granulomatous edema. One study reported 100% sensitivity and 78% specificity of MRI in diagnosing cardiac sarcoid.[10]
Because of the limitations of noninvasive tests, tissue biopsy is necessary to diagnose sarcoidosis. If an accessible extracardiac site, such as an enlarged lymph node or skin lesion, is unavailable, a more invasive biopsy is recommended. Transbronchial biopsy is an option if there is obvious thoracic disease. Another alternative is to obtain a 18‐fluorodeoxyglucose positron emission tomography (18FDG‐PET) scan to identify hypermetabolic granulomas, which can be targeted for biopsy. For cardiac sarcoidosis, endomyocardial biopsy is often performed. This procedure is generally quite safe, with severe complications such as right ventricular perforation occurring in fewer than 1% of procedures.[11] However, the patchy nature of heart involvement in sarcoidosis results in a sensitivity as low as 20%.[12] Despite its low yield, according to guidelines from the American College of Cardiology and the American Heart Association, patients with unexplained heart failure of 3 months' duration associated with heart block or ventricular arrhythmias have a class I indication for endomyocardial biopsy.[11]
The prognosis of sarcoidosis is generally favorable, with fewer than 5% of patients dying from the disease. Although the impact of cardiac involvement is poorly established, the available literature indicate a worse prognosis for patients with symptomatic heart disease due to sarcoidosis. In 1 series, over half of 19 patients with cardiac involvement were either dead or required an ICD or pacemaker within 2 years of detection, as opposed to none of 82 sarcoid patients without clinically apparent cardiac involvement.[13]
The mainstay of treatment of cardiac sarcoidosis is corticosteroids, which may halt disease progression and improve survival, but do not reduce the incidence of ventricular arrhythmias. Initially, 1 mg/kg doses of prednisone dose are administered daily. Patients should be reassessed for response to treatment, and repeat ejection fraction measurement by echocardiogram should be obtained if symptoms worsen. The use of serial serum ACE levels to monitor disease activity is controversial. For patients responding to prednisone, the dose can be tapered over a period of 6 months to a maintenance daily dose of 10 to 15 mg, with a goal of eventually stopping therapy if disease is quiescent.[14] For patients who do not respond to glucocorticoids or who experience intolerable side effects, other immunosuppressive agents have been tried with reported success based on limited data. Options include methotrexate, azathioprine, hydroxychloroquine, cyclophosphamide, and infliximab.[5] Treatment of asymptomatic or minimally symptomatic patients with corticosteroids remains controversial.[14]
Adjunctive treatments are often necessary in cardiac sarcoidosis. Permanent pacemaker implantation is indicated if there is complete atrioventricular block or other high‐grade conduction system disease. Survivors of sudden cardiac death, individuals with refractory ventricular arrhythmias, and those with severely impaired systolic function are candidates for ICDs.[15] Catheter radiofrequency ablation may be effective in patients with ventricular tachyarrhythmias.[16]
Cardiac sarcoidosis is important to suspect in a patient with unexplained cardiomyopathy associated with conduction blocks or tachyarrhythmias because it is potentially reversible. Diagnosis can be elusive, as noninvasive tests lack sufficient sensitivity and specificity to establish the presence or absence of the disorder. Biopsy of affected organs is essential to identify the noncaseating granulomas that characterize the disease. When no extracardiac target exists, clinicians may need an endomyocardial biopsy to get to the heart of the matter.
CLINICAL TEACHING POINTS
- A history of cardiac disease substantially raises the possibility of an arrhythmic etiology of palpitations.
- Cardiac involvement in sarcoidosis can be asymptomatic or include conduction blocks, supraventricular and ventricular tachyarrhythmias, or cardiomyopathy.
- Cardiac sarcoid can be an elusive diagnosis to establish, because both noninvasive tests and endomyocardial biopsy demonstrate low sensitivity.
- Cardiac sarcoidosis portends a worse prognosis than sarcoid in general, but is a potentially reversible condition that therefore warrants an aggressive approach to establishing a diagnosis.
Acknowledgments
The authors thank Ellen Killebrew, MD, for help with the formal interpretation of the admission ECG.
Disclosures
Dr. Baudendistel is a former Deputy Editor and CME Editor of the Journal of Hospital Medicine, a position he ended in 2011. He received a stipend of less than $2000 for this work in 2010 and 2011. The authors are not aware of any conflicts of interest related to this article. The initial oral part of this presentation was presented at the University of California Davis Grand Rounds on August 16, 2010.
- , , , . Predictors of persistent palpitations and continued medical utilization. J Fam Pract. 1996;42:465–472.
- , . Evaluation and outcomes of patients with palpitations. Am J Med. 1996;100:138–148.
- , , , , . Does this patient with palpitations have a cardiac arrhythmia? JAMA. 2009;302:2135–2143.
- , . Myocardial sarcoidosis in forensic medicine. Am J Forensic Med Pathol. 1999;20:52–56.
- , , , et al. Cardiac sarcoidosis. Am Heart J. 2009;157:9–21.
- , , . Sarcoidosis. N Engl J Med. 2007;357:2153–2165.
- , . An angiotensin‐converting enzyme (ACE) inhibitor in human serum. Increased sensitivity of the serum ACE assay for detecting active sarcoidosis. Chest. 1986;90:869–875.
- , , , et al. Comparative evaluation of serum markers in pulmonary sarcoidosis. Chest. 2010;137:1391–1397.
- , , . Cardiac sarcoidosis: cytokine patterns in the course of the disease. Arch Pathol Lab Med. 2003;127:1207–1210.
- , , , et al. Evaluation of the accuracy of gadolinium‐enhanced cardiovascular magnetic resonance in the diagnosis of cardiac sarcoidosis. J Am Coll Cardiol. 2005;45:1683–1690.
- , , . Current status of endomyocardial biopsy. Mayo Clin Proc. 2011;86:1095–1102.
- , , , , , . Histologic diagnostic rate of cardiac sarcoidosis: evaluation of endomyocardial biopsies. Am Heart J. 1999;138:299–302.
- , , , et al. Cardiac involvement in patients with pulmonary sarcoidosis assessed at two university medical centers in the Netherlands. Chest. 2005;128(1):30–35.
- , , , et al. Prognostic determinants of long‐term survival in Japanese patients with cardiac sarcoidosis treated with prednisone. Am J Cardiol. 2001;88:1006–1010.
- , , , . The automated implantable cardiac defibrillator. Prophylaxis in cardiac sarcoidosis. Chest. 1994;106:1603–1607.
- , , , et al. Ventricular tachycardia in cardiac sarcoidosis controlled by radiofrequency catheter ablation. Intern Med. 2011;50:1201–1206.
- , , , . Predictors of persistent palpitations and continued medical utilization. J Fam Pract. 1996;42:465–472.
- , . Evaluation and outcomes of patients with palpitations. Am J Med. 1996;100:138–148.
- , , , , . Does this patient with palpitations have a cardiac arrhythmia? JAMA. 2009;302:2135–2143.
- , . Myocardial sarcoidosis in forensic medicine. Am J Forensic Med Pathol. 1999;20:52–56.
- , , , et al. Cardiac sarcoidosis. Am Heart J. 2009;157:9–21.
- , , . Sarcoidosis. N Engl J Med. 2007;357:2153–2165.
- , . An angiotensin‐converting enzyme (ACE) inhibitor in human serum. Increased sensitivity of the serum ACE assay for detecting active sarcoidosis. Chest. 1986;90:869–875.
- , , , et al. Comparative evaluation of serum markers in pulmonary sarcoidosis. Chest. 2010;137:1391–1397.
- , , . Cardiac sarcoidosis: cytokine patterns in the course of the disease. Arch Pathol Lab Med. 2003;127:1207–1210.
- , , , et al. Evaluation of the accuracy of gadolinium‐enhanced cardiovascular magnetic resonance in the diagnosis of cardiac sarcoidosis. J Am Coll Cardiol. 2005;45:1683–1690.
- , , . Current status of endomyocardial biopsy. Mayo Clin Proc. 2011;86:1095–1102.
- , , , , , . Histologic diagnostic rate of cardiac sarcoidosis: evaluation of endomyocardial biopsies. Am Heart J. 1999;138:299–302.
- , , , et al. Cardiac involvement in patients with pulmonary sarcoidosis assessed at two university medical centers in the Netherlands. Chest. 2005;128(1):30–35.
- , , , et al. Prognostic determinants of long‐term survival in Japanese patients with cardiac sarcoidosis treated with prednisone. Am J Cardiol. 2001;88:1006–1010.
- , , , . The automated implantable cardiac defibrillator. Prophylaxis in cardiac sarcoidosis. Chest. 1994;106:1603–1607.
- , , , et al. Ventricular tachycardia in cardiac sarcoidosis controlled by radiofrequency catheter ablation. Intern Med. 2011;50:1201–1206.
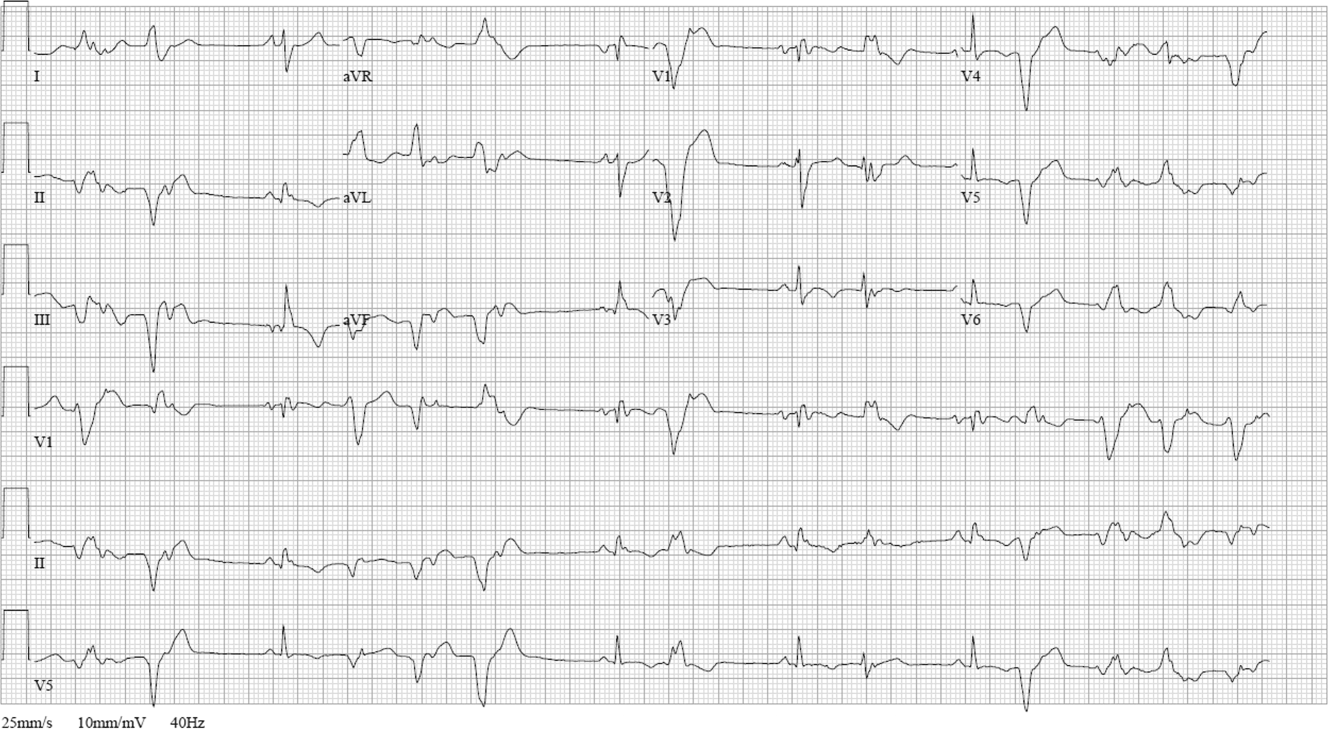
Wachter Sees Bright Future for Hospital Medicine

He believes HM's reputation as "generalists able to solve all kinds of problems" means the specialty is poised to adapt and thrive, he told a crowded ballroom at HM13's final keynote address yesterday at the Gaylord National Resort & Convention Center.
The annual plenary session was the effective wrap-up of SHM's four-day annual meeting, which drew some 2,700 attendees.
"We will morph into what is needed," he said. "That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists…we will fill new niches."
Watch a 2-minute video excerpt from Dr. Wachter's HM13 keynote address
What Dr. Wachter does not want to see is that the field grows "fat and happy" as it is now firmly entrenched in the U.S. healthcare delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs, and, ultimately, improve the patient experience.
"You can't survive and thrive in a world with the kinds of pressures that we have to improve performance, if you do business the same old way," he added. "It's no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care."
He believes HM's reputation as "generalists able to solve all kinds of problems" means the specialty is poised to adapt and thrive, he told a crowded ballroom at HM13's final keynote address yesterday at the Gaylord National Resort & Convention Center.
The annual plenary session was the effective wrap-up of SHM's four-day annual meeting, which drew some 2,700 attendees.
"We will morph into what is needed," he said. "That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists…we will fill new niches."
Watch a 2-minute video excerpt from Dr. Wachter's HM13 keynote address
What Dr. Wachter does not want to see is that the field grows "fat and happy" as it is now firmly entrenched in the U.S. healthcare delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs, and, ultimately, improve the patient experience.
"You can't survive and thrive in a world with the kinds of pressures that we have to improve performance, if you do business the same old way," he added. "It's no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care."
He believes HM's reputation as "generalists able to solve all kinds of problems" means the specialty is poised to adapt and thrive, he told a crowded ballroom at HM13's final keynote address yesterday at the Gaylord National Resort & Convention Center.
The annual plenary session was the effective wrap-up of SHM's four-day annual meeting, which drew some 2,700 attendees.
"We will morph into what is needed," he said. "That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists…we will fill new niches."
Watch a 2-minute video excerpt from Dr. Wachter's HM13 keynote address
What Dr. Wachter does not want to see is that the field grows "fat and happy" as it is now firmly entrenched in the U.S. healthcare delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs, and, ultimately, improve the patient experience.
"You can't survive and thrive in a world with the kinds of pressures that we have to improve performance, if you do business the same old way," he added. "It's no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care."
Is Post-Acute-Care In Your Future?
NATIONAL HARBOR, Md.—Hospitalists' growing attention to the "post-acute-care space" is driven in part by high rates of 30-day readmissions for patients who get discharged to skilled nursing facilities (SNF)—1 in 4 Medicare patients, according to government estimates. The rate is 1 in 3 for heart-failure patients.
But post-acute care also is "a great place to change your career trajectory and have an immediate impact on the quality of care," Jerome Wilborn, MD, national medical director for post acute services for IPC The Hospitalist Company, said Sunday at HM13.
Dr. Wilborn made that transition and now is part of an IPC medical group in Ann Arbor, Mich., that works with 85 long-term-care facilities. “A lot of our post-acute providers do very well on professional billing,” he noted.
Hospitalists may be able to divide their practices between the acute and post-acute worlds, especially for facilities in close proximity. However, Dr. Wilborn noted that IPC prefers dedicated post-acute providers.
Watch a 2-minute video clip of Bob Wachter's HM13 keynote address
Hospitalists entering the post-acute world need to understand that these patients generally are very sick, although without access to the plethora of medical monitoring equipment that hospitalists take for granted. And sick patients need in-person medical attention, Dr. Wilborn said. Another key to success is regular, scheduled presence to develop institutional bonding with the facility, its staff and its culture. IPC physicians, especially if they take on the role of facility medical director, are expected to visit the facility at least three times a week.
SHM established a post-acute care task force and is surveying its members on their involvement and interest in this realm. For information or to participate in the survey, email SHM senior vice president Joseph Miller.
NATIONAL HARBOR, Md.—Hospitalists' growing attention to the "post-acute-care space" is driven in part by high rates of 30-day readmissions for patients who get discharged to skilled nursing facilities (SNF)—1 in 4 Medicare patients, according to government estimates. The rate is 1 in 3 for heart-failure patients.
But post-acute care also is "a great place to change your career trajectory and have an immediate impact on the quality of care," Jerome Wilborn, MD, national medical director for post acute services for IPC The Hospitalist Company, said Sunday at HM13.
Dr. Wilborn made that transition and now is part of an IPC medical group in Ann Arbor, Mich., that works with 85 long-term-care facilities. “A lot of our post-acute providers do very well on professional billing,” he noted.
Hospitalists may be able to divide their practices between the acute and post-acute worlds, especially for facilities in close proximity. However, Dr. Wilborn noted that IPC prefers dedicated post-acute providers.
Watch a 2-minute video clip of Bob Wachter's HM13 keynote address
Hospitalists entering the post-acute world need to understand that these patients generally are very sick, although without access to the plethora of medical monitoring equipment that hospitalists take for granted. And sick patients need in-person medical attention, Dr. Wilborn said. Another key to success is regular, scheduled presence to develop institutional bonding with the facility, its staff and its culture. IPC physicians, especially if they take on the role of facility medical director, are expected to visit the facility at least three times a week.
SHM established a post-acute care task force and is surveying its members on their involvement and interest in this realm. For information or to participate in the survey, email SHM senior vice president Joseph Miller.
NATIONAL HARBOR, Md.—Hospitalists' growing attention to the "post-acute-care space" is driven in part by high rates of 30-day readmissions for patients who get discharged to skilled nursing facilities (SNF)—1 in 4 Medicare patients, according to government estimates. The rate is 1 in 3 for heart-failure patients.
But post-acute care also is "a great place to change your career trajectory and have an immediate impact on the quality of care," Jerome Wilborn, MD, national medical director for post acute services for IPC The Hospitalist Company, said Sunday at HM13.
Dr. Wilborn made that transition and now is part of an IPC medical group in Ann Arbor, Mich., that works with 85 long-term-care facilities. “A lot of our post-acute providers do very well on professional billing,” he noted.
Hospitalists may be able to divide their practices between the acute and post-acute worlds, especially for facilities in close proximity. However, Dr. Wilborn noted that IPC prefers dedicated post-acute providers.
Watch a 2-minute video clip of Bob Wachter's HM13 keynote address
Hospitalists entering the post-acute world need to understand that these patients generally are very sick, although without access to the plethora of medical monitoring equipment that hospitalists take for granted. And sick patients need in-person medical attention, Dr. Wilborn said. Another key to success is regular, scheduled presence to develop institutional bonding with the facility, its staff and its culture. IPC physicians, especially if they take on the role of facility medical director, are expected to visit the facility at least three times a week.
SHM established a post-acute care task force and is surveying its members on their involvement and interest in this realm. For information or to participate in the survey, email SHM senior vice president Joseph Miller.
Low vitamin D level may up risk for IBD flares
ORLANDO – Vitamin D may protect patients with inflammatory bowel disease from more serious disease flare-ups, investigators reported at the annual Digestive Disease Week.
Among 3,217 patients followed for a median of 8 years, those with Crohn’s disease who had the lowest levels of plasma 25-hydroxyvitamin D had a nearly twofold risk for surgery and double the risk for hospitalization related to IBD, compared with patients who had higher vitamin D levels.
A similar relationship was seen between vitamin D levels and risk of surgery and hospitalization among patients with ulcerative colitis (UC), reported Dr. Ashwin Ananthakrishnan of Massachusetts General Hospital in Boston.

Tellingly, patients with Crohn’s disease (CD) who had initially low vitamin D levels that normalized during the study had significant reductions in their risk of surgery and hospitalization compared with patients whose vitamin D levels did not improve over time. In addition, patients with both CD and UC who normalized their vitamin D status during the study had significantly lower levels of the inflammatory marker C-reactive protein, the investigators found.
"There’s considerable evidence that supports a role for vitamin D in inflammatory bowel diseases," Dr. Ananthakrishnan said.
He noted that high vitamin D levels were associated with a reduced risk for CD in a prior study performed by his group (Gastroenterology 2012;142:482-9), and a second study showed that polymorphisms in the vitamin D receptor were associated with a risk of both CD and UC (Gut 2000;47:211-4).
Although vitamin D levels have been weakly associated with IBD exacerbations in retrospective studies, stronger evidence for the potential anti-inflammatory role of vitamin D has been hard to come by, partly because of researchers’ inability to determine vitamin D status before clinical outcomes such as surgery or hospitalization, Dr. Ananthakrishnan said.
He and colleagues prospectively followed all members of an IBD cohort treated at Massachusetts General Hospital and Brigham and Women’s Hospital, Boston, who had a least one measured plasma 25(OH)D level before a first IBD-related surgery and/or hospitalization (the primary outcome; median C-reactive protein was a secondary outcome).
The researchers found that 16% of all patients had disease-related surgery, and 40% were hospitalized during the follow-up period.
A third of all patients (32%) were considered to be vitamin D deficient, defined as having a plasma 25(OH)D level below 20 ng/mL, and 28% were deemed to be vitamin D insufficient (20-30 ng/mL). The remaining 40% had sufficient vitamin D levels of 30 ng/mL and higher.
When the investigators controlled for age, sex, race, Charlson score (non-IBD comorbidity), disease-related complications, medication, vitamin D supplementation, and season of 25(OH)D measurement, analysis showed that patients with CD who had plasma vitamin D levels below 20 ng/mL had odds ratios of 1.76 for surgery and 2.07 for IBD-related hospitalization.
Similarly, for patients with UC and low vitamin D levels, the odds ratios for surgery and hospitalization were 1.70 and 2.26, respectively.
Overall, 76% of patients in the study with CD who had initial vitamin D levels below 30 ng/mL had subsequent normalization of their D values, as did 80% of those with ulcerative colitis.
In adjusted analysis, patients with CD had a nearly 50% reduction in the risk of surgery (odds ratio, 0.56) and a nearly 25% reduction in the risk of hospitalization (OR, 0.78), compared with patients whose vitamin D levels never corrected to the normal range. Patients with UC also had reductions in risk for both surgery and hospitalization, but these reductions were not significant.
In addition, patients with CD and UC who had vitamin D that normalized over the course of the study had significantly lower C-reactive protein levels than did those who remained vitamin D deficient (–5. 2 mg/L, P = .002).
The study was supported by grants and awards from the American Gastroenterological Association, the IBD Working Group, the Broad Foundation, and the National Institutes of Health. Dr. Ananthakrishnan reported having no financial disclosures.
ORLANDO – Vitamin D may protect patients with inflammatory bowel disease from more serious disease flare-ups, investigators reported at the annual Digestive Disease Week.
Among 3,217 patients followed for a median of 8 years, those with Crohn’s disease who had the lowest levels of plasma 25-hydroxyvitamin D had a nearly twofold risk for surgery and double the risk for hospitalization related to IBD, compared with patients who had higher vitamin D levels.
A similar relationship was seen between vitamin D levels and risk of surgery and hospitalization among patients with ulcerative colitis (UC), reported Dr. Ashwin Ananthakrishnan of Massachusetts General Hospital in Boston.
Tellingly, patients with Crohn’s disease (CD) who had initially low vitamin D levels that normalized during the study had significant reductions in their risk of surgery and hospitalization compared with patients whose vitamin D levels did not improve over time. In addition, patients with both CD and UC who normalized their vitamin D status during the study had significantly lower levels of the inflammatory marker C-reactive protein, the investigators found.
"There’s considerable evidence that supports a role for vitamin D in inflammatory bowel diseases," Dr. Ananthakrishnan said.
He noted that high vitamin D levels were associated with a reduced risk for CD in a prior study performed by his group (Gastroenterology 2012;142:482-9), and a second study showed that polymorphisms in the vitamin D receptor were associated with a risk of both CD and UC (Gut 2000;47:211-4).
Although vitamin D levels have been weakly associated with IBD exacerbations in retrospective studies, stronger evidence for the potential anti-inflammatory role of vitamin D has been hard to come by, partly because of researchers’ inability to determine vitamin D status before clinical outcomes such as surgery or hospitalization, Dr. Ananthakrishnan said.
He and colleagues prospectively followed all members of an IBD cohort treated at Massachusetts General Hospital and Brigham and Women’s Hospital, Boston, who had a least one measured plasma 25(OH)D level before a first IBD-related surgery and/or hospitalization (the primary outcome; median C-reactive protein was a secondary outcome).
The researchers found that 16% of all patients had disease-related surgery, and 40% were hospitalized during the follow-up period.
A third of all patients (32%) were considered to be vitamin D deficient, defined as having a plasma 25(OH)D level below 20 ng/mL, and 28% were deemed to be vitamin D insufficient (20-30 ng/mL). The remaining 40% had sufficient vitamin D levels of 30 ng/mL and higher.
When the investigators controlled for age, sex, race, Charlson score (non-IBD comorbidity), disease-related complications, medication, vitamin D supplementation, and season of 25(OH)D measurement, analysis showed that patients with CD who had plasma vitamin D levels below 20 ng/mL had odds ratios of 1.76 for surgery and 2.07 for IBD-related hospitalization.
Similarly, for patients with UC and low vitamin D levels, the odds ratios for surgery and hospitalization were 1.70 and 2.26, respectively.
Overall, 76% of patients in the study with CD who had initial vitamin D levels below 30 ng/mL had subsequent normalization of their D values, as did 80% of those with ulcerative colitis.
In adjusted analysis, patients with CD had a nearly 50% reduction in the risk of surgery (odds ratio, 0.56) and a nearly 25% reduction in the risk of hospitalization (OR, 0.78), compared with patients whose vitamin D levels never corrected to the normal range. Patients with UC also had reductions in risk for both surgery and hospitalization, but these reductions were not significant.
In addition, patients with CD and UC who had vitamin D that normalized over the course of the study had significantly lower C-reactive protein levels than did those who remained vitamin D deficient (–5. 2 mg/L, P = .002).
The study was supported by grants and awards from the American Gastroenterological Association, the IBD Working Group, the Broad Foundation, and the National Institutes of Health. Dr. Ananthakrishnan reported having no financial disclosures.
ORLANDO – Vitamin D may protect patients with inflammatory bowel disease from more serious disease flare-ups, investigators reported at the annual Digestive Disease Week.
Among 3,217 patients followed for a median of 8 years, those with Crohn’s disease who had the lowest levels of plasma 25-hydroxyvitamin D had a nearly twofold risk for surgery and double the risk for hospitalization related to IBD, compared with patients who had higher vitamin D levels.
A similar relationship was seen between vitamin D levels and risk of surgery and hospitalization among patients with ulcerative colitis (UC), reported Dr. Ashwin Ananthakrishnan of Massachusetts General Hospital in Boston.
Tellingly, patients with Crohn’s disease (CD) who had initially low vitamin D levels that normalized during the study had significant reductions in their risk of surgery and hospitalization compared with patients whose vitamin D levels did not improve over time. In addition, patients with both CD and UC who normalized their vitamin D status during the study had significantly lower levels of the inflammatory marker C-reactive protein, the investigators found.
"There’s considerable evidence that supports a role for vitamin D in inflammatory bowel diseases," Dr. Ananthakrishnan said.
He noted that high vitamin D levels were associated with a reduced risk for CD in a prior study performed by his group (Gastroenterology 2012;142:482-9), and a second study showed that polymorphisms in the vitamin D receptor were associated with a risk of both CD and UC (Gut 2000;47:211-4).
Although vitamin D levels have been weakly associated with IBD exacerbations in retrospective studies, stronger evidence for the potential anti-inflammatory role of vitamin D has been hard to come by, partly because of researchers’ inability to determine vitamin D status before clinical outcomes such as surgery or hospitalization, Dr. Ananthakrishnan said.
He and colleagues prospectively followed all members of an IBD cohort treated at Massachusetts General Hospital and Brigham and Women’s Hospital, Boston, who had a least one measured plasma 25(OH)D level before a first IBD-related surgery and/or hospitalization (the primary outcome; median C-reactive protein was a secondary outcome).
The researchers found that 16% of all patients had disease-related surgery, and 40% were hospitalized during the follow-up period.
A third of all patients (32%) were considered to be vitamin D deficient, defined as having a plasma 25(OH)D level below 20 ng/mL, and 28% were deemed to be vitamin D insufficient (20-30 ng/mL). The remaining 40% had sufficient vitamin D levels of 30 ng/mL and higher.
When the investigators controlled for age, sex, race, Charlson score (non-IBD comorbidity), disease-related complications, medication, vitamin D supplementation, and season of 25(OH)D measurement, analysis showed that patients with CD who had plasma vitamin D levels below 20 ng/mL had odds ratios of 1.76 for surgery and 2.07 for IBD-related hospitalization.
Similarly, for patients with UC and low vitamin D levels, the odds ratios for surgery and hospitalization were 1.70 and 2.26, respectively.
Overall, 76% of patients in the study with CD who had initial vitamin D levels below 30 ng/mL had subsequent normalization of their D values, as did 80% of those with ulcerative colitis.
In adjusted analysis, patients with CD had a nearly 50% reduction in the risk of surgery (odds ratio, 0.56) and a nearly 25% reduction in the risk of hospitalization (OR, 0.78), compared with patients whose vitamin D levels never corrected to the normal range. Patients with UC also had reductions in risk for both surgery and hospitalization, but these reductions were not significant.
In addition, patients with CD and UC who had vitamin D that normalized over the course of the study had significantly lower C-reactive protein levels than did those who remained vitamin D deficient (–5. 2 mg/L, P = .002).
The study was supported by grants and awards from the American Gastroenterological Association, the IBD Working Group, the Broad Foundation, and the National Institutes of Health. Dr. Ananthakrishnan reported having no financial disclosures.
AT DDW 2013
Major finding: In all, 32% of patients with Crohn’s disease who had plasma vitamin D below 20 ng/mL had IBD-related surgery, compared with 13% of those with normal vitamin D levels.
Data source: Prospective cohort study using electronic medical records of 3,217 patients with irritable bowel disease.
Disclosures: The study was supported by grants/awards from the American Gastroenterological Association, the IBD Working Group, the Broad Foundation, and the National Institutes of Health. Dr. Ananthakrishnan reported having no financial disclosures.

Hospitalist Pioneer Says Cost Equation Is Shifting in Ever-Changing Healthcare Paradigm
SHM Looking for a Few Good (Future) Hospitalists
NATIONAL HARBOR, MD–New SHM president Eric Howell, MD, SFHM, set a concrete goal for his one-year term he began yesterday at HM13: double the society's number of student and housestaff members from 500 to 1,000.
He then immediately recruited the first member of the 2014 class: his younger sister.
Lesley Sutherland, a third-year medical student at the University of Maryland in College Park, Md., had been debating whether to go into family medicine versus internal medicine. That decision seems a moot point now, after her big brother pulled her onstage and inducted her into SHM before a packed ballroom at the Gaylord National Resort & Convention Center.
"For our specialty to be just as powerful, and just as important, and thrive just as much in the next 16 years as it has in the past 16 years, we are going to need high-quality recruits and a lot of them," said Dr. Howell, chief of hospital medicine at Johns Hopkins Bayview Medical Center in Baltimore, Md. "I know exactly where we're going to get them."
Check out today's HM13 video exclusive: Channeling Osler, Pioneer in Bedside Exams
Dr. Howell said recruiting medical students and housestaff—an initiative he calls the "Challenge of 2014"—is important to the future of hospital medicine. The marketing pitch to those would-be hospitalists is as simple as touting the work-life balance that has helped to boost the specialty's ranks to some 40,000 practitioners, and imparting the sense of pride and ownership that hospitalists take in their institutions.
"If you consider the hospital the house, then we are house owners and not renters," he added. "We're not waiting for two weeks to rotate off service and go to our real research job. We’re not coming in early in the morning and leaving for our actual office. We live in that professional house and we want to make the best house we can." TH
NATIONAL HARBOR, MD–New SHM president Eric Howell, MD, SFHM, set a concrete goal for his one-year term he began yesterday at HM13: double the society's number of student and housestaff members from 500 to 1,000.
He then immediately recruited the first member of the 2014 class: his younger sister.
Lesley Sutherland, a third-year medical student at the University of Maryland in College Park, Md., had been debating whether to go into family medicine versus internal medicine. That decision seems a moot point now, after her big brother pulled her onstage and inducted her into SHM before a packed ballroom at the Gaylord National Resort & Convention Center.
"For our specialty to be just as powerful, and just as important, and thrive just as much in the next 16 years as it has in the past 16 years, we are going to need high-quality recruits and a lot of them," said Dr. Howell, chief of hospital medicine at Johns Hopkins Bayview Medical Center in Baltimore, Md. "I know exactly where we're going to get them."
Check out today's HM13 video exclusive: Channeling Osler, Pioneer in Bedside Exams
Dr. Howell said recruiting medical students and housestaff—an initiative he calls the "Challenge of 2014"—is important to the future of hospital medicine. The marketing pitch to those would-be hospitalists is as simple as touting the work-life balance that has helped to boost the specialty's ranks to some 40,000 practitioners, and imparting the sense of pride and ownership that hospitalists take in their institutions.
"If you consider the hospital the house, then we are house owners and not renters," he added. "We're not waiting for two weeks to rotate off service and go to our real research job. We’re not coming in early in the morning and leaving for our actual office. We live in that professional house and we want to make the best house we can." TH
NATIONAL HARBOR, MD–New SHM president Eric Howell, MD, SFHM, set a concrete goal for his one-year term he began yesterday at HM13: double the society's number of student and housestaff members from 500 to 1,000.
He then immediately recruited the first member of the 2014 class: his younger sister.
Lesley Sutherland, a third-year medical student at the University of Maryland in College Park, Md., had been debating whether to go into family medicine versus internal medicine. That decision seems a moot point now, after her big brother pulled her onstage and inducted her into SHM before a packed ballroom at the Gaylord National Resort & Convention Center.
"For our specialty to be just as powerful, and just as important, and thrive just as much in the next 16 years as it has in the past 16 years, we are going to need high-quality recruits and a lot of them," said Dr. Howell, chief of hospital medicine at Johns Hopkins Bayview Medical Center in Baltimore, Md. "I know exactly where we're going to get them."
Check out today's HM13 video exclusive: Channeling Osler, Pioneer in Bedside Exams
Dr. Howell said recruiting medical students and housestaff—an initiative he calls the "Challenge of 2014"—is important to the future of hospital medicine. The marketing pitch to those would-be hospitalists is as simple as touting the work-life balance that has helped to boost the specialty's ranks to some 40,000 practitioners, and imparting the sense of pride and ownership that hospitalists take in their institutions.
"If you consider the hospital the house, then we are house owners and not renters," he added. "We're not waiting for two weeks to rotate off service and go to our real research job. We’re not coming in early in the morning and leaving for our actual office. We live in that professional house and we want to make the best house we can." TH
Technology Is King at HM13 RIV Competition
NATIONAL HARBOR, MD—As fast as the annual Research, Innovation, and Clinical Vignette competition is growing, research abstracts focused on technology applications for quality improvement and patient safety are growing nearly as quickly.
One good example on display Saturday during the HM13 oral presentations was research that documented Internet use by re-hospitalized patients from S. Ryan Greysen, MD, MHS, MA, of the Division of Hospital Medicine at the University of California at San Francisco. Dr. Greysen and colleagues found that two-thirds of re-hospitalized patients had Internet access at home and half had looked up health information within the past year, but most did not use the Internet to communicate with PCPs, or to manage medical appointments or prescriptions—three core tasks in helping to avoid readmissions.
One patient told the researchers he went home with a nebulizer but could not recall instructions given in the hospital for its use. “But he used YouTube to find an instructional video,” Dr. Greysen said. “We need to tailor online patient resources to focus on post-discharge tasks.”
HM13 VIDEO EXCLUSIVE: Hospitalists practice physical exam skills, learn to teach them better
More than 800 abstracts were submitted and nearly 600 were accepted for HM13. And technology applications for improving hospital care are more popular than ever, said Eduard Vasilevskis, MD, hospitalist at Vanderbilt University in Nashville, Tenn., and co-chair of SHM’s research abstracts judging committee. “What’s increasingly apparent is that people are trying to harness the electronic health record (EHR) for research,” Dr. Vasilevskis added.
HM13 Research, Innovations, and Clinical Vignettes Competition WINNERS
RESEARCH: "Comparison of Palliative Care Consultation Services in California Hospitals Between 2007 and 2011”
By Steven Pantilat, MD, David O’Riordan, PhD, University of California at San Francisco
INNOVATIONS: “SEPTRIS: Improving Sepsis Recognition and Management Through a Mobile Educational Game”
By Lisa Shieh, Eileen Pummer, J. Tsui, B. Tobin, J. Leung, M. Strehlow, W. Daines, P. Maggio, K. Hooper, Stanford Hospital, Stanford, Calif.
ADULT VIGNETTE: “Something Fishy in Dixie”
By Leslie Anne Cassidy, Sarah Lofgren, MD, Praneetha Thulasi, MD, Laurence Beer, MD, Daniel Dressler, MD, MSc, Emory University School of Medicine, Atlanta
PEDIATRIC VIGNETTE: "You Can’t Handle the Truth: Another Cause of Headache with Neurologic Deficits”
By Richard Bloomfield, MD, Eric Edwards, MD, University of North Carolina School of Medicine, Chapel Hill, N.C.
NATIONAL HARBOR, MD—As fast as the annual Research, Innovation, and Clinical Vignette competition is growing, research abstracts focused on technology applications for quality improvement and patient safety are growing nearly as quickly.
One good example on display Saturday during the HM13 oral presentations was research that documented Internet use by re-hospitalized patients from S. Ryan Greysen, MD, MHS, MA, of the Division of Hospital Medicine at the University of California at San Francisco. Dr. Greysen and colleagues found that two-thirds of re-hospitalized patients had Internet access at home and half had looked up health information within the past year, but most did not use the Internet to communicate with PCPs, or to manage medical appointments or prescriptions—three core tasks in helping to avoid readmissions.
One patient told the researchers he went home with a nebulizer but could not recall instructions given in the hospital for its use. “But he used YouTube to find an instructional video,” Dr. Greysen said. “We need to tailor online patient resources to focus on post-discharge tasks.”
HM13 VIDEO EXCLUSIVE: Hospitalists practice physical exam skills, learn to teach them better
More than 800 abstracts were submitted and nearly 600 were accepted for HM13. And technology applications for improving hospital care are more popular than ever, said Eduard Vasilevskis, MD, hospitalist at Vanderbilt University in Nashville, Tenn., and co-chair of SHM’s research abstracts judging committee. “What’s increasingly apparent is that people are trying to harness the electronic health record (EHR) for research,” Dr. Vasilevskis added.
HM13 Research, Innovations, and Clinical Vignettes Competition WINNERS
RESEARCH: "Comparison of Palliative Care Consultation Services in California Hospitals Between 2007 and 2011”
By Steven Pantilat, MD, David O’Riordan, PhD, University of California at San Francisco
INNOVATIONS: “SEPTRIS: Improving Sepsis Recognition and Management Through a Mobile Educational Game”
By Lisa Shieh, Eileen Pummer, J. Tsui, B. Tobin, J. Leung, M. Strehlow, W. Daines, P. Maggio, K. Hooper, Stanford Hospital, Stanford, Calif.
ADULT VIGNETTE: “Something Fishy in Dixie”
By Leslie Anne Cassidy, Sarah Lofgren, MD, Praneetha Thulasi, MD, Laurence Beer, MD, Daniel Dressler, MD, MSc, Emory University School of Medicine, Atlanta
PEDIATRIC VIGNETTE: "You Can’t Handle the Truth: Another Cause of Headache with Neurologic Deficits”
By Richard Bloomfield, MD, Eric Edwards, MD, University of North Carolina School of Medicine, Chapel Hill, N.C.
NATIONAL HARBOR, MD—As fast as the annual Research, Innovation, and Clinical Vignette competition is growing, research abstracts focused on technology applications for quality improvement and patient safety are growing nearly as quickly.
One good example on display Saturday during the HM13 oral presentations was research that documented Internet use by re-hospitalized patients from S. Ryan Greysen, MD, MHS, MA, of the Division of Hospital Medicine at the University of California at San Francisco. Dr. Greysen and colleagues found that two-thirds of re-hospitalized patients had Internet access at home and half had looked up health information within the past year, but most did not use the Internet to communicate with PCPs, or to manage medical appointments or prescriptions—three core tasks in helping to avoid readmissions.
One patient told the researchers he went home with a nebulizer but could not recall instructions given in the hospital for its use. “But he used YouTube to find an instructional video,” Dr. Greysen said. “We need to tailor online patient resources to focus on post-discharge tasks.”
HM13 VIDEO EXCLUSIVE: Hospitalists practice physical exam skills, learn to teach them better
More than 800 abstracts were submitted and nearly 600 were accepted for HM13. And technology applications for improving hospital care are more popular than ever, said Eduard Vasilevskis, MD, hospitalist at Vanderbilt University in Nashville, Tenn., and co-chair of SHM’s research abstracts judging committee. “What’s increasingly apparent is that people are trying to harness the electronic health record (EHR) for research,” Dr. Vasilevskis added.
HM13 Research, Innovations, and Clinical Vignettes Competition WINNERS
RESEARCH: "Comparison of Palliative Care Consultation Services in California Hospitals Between 2007 and 2011”
By Steven Pantilat, MD, David O’Riordan, PhD, University of California at San Francisco
INNOVATIONS: “SEPTRIS: Improving Sepsis Recognition and Management Through a Mobile Educational Game”
By Lisa Shieh, Eileen Pummer, J. Tsui, B. Tobin, J. Leung, M. Strehlow, W. Daines, P. Maggio, K. Hooper, Stanford Hospital, Stanford, Calif.
ADULT VIGNETTE: “Something Fishy in Dixie”
By Leslie Anne Cassidy, Sarah Lofgren, MD, Praneetha Thulasi, MD, Laurence Beer, MD, Daniel Dressler, MD, MSc, Emory University School of Medicine, Atlanta
PEDIATRIC VIGNETTE: "You Can’t Handle the Truth: Another Cause of Headache with Neurologic Deficits”
By Richard Bloomfield, MD, Eric Edwards, MD, University of North Carolina School of Medicine, Chapel Hill, N.C.
HM13 Session Analysis: Pneumonia Update
Scott Flanders, MD, SFHM, director of the hospitalist program at the University of Michigan in Ann Arbor set out to answer three key questions in “rapid-fire” format during the “Pneumonia Update” at HM13.
- Is procalcitonin ready for “prime time” in determining community-acquired pneumonia (CAP) treatment duration?
- What is the utility of diagnostic testing in CAP patients?
- How do you decide which pneumonia patients need broad-spectrum antibiotic coverage?
It turns out that lots of other countries follow procalcitonin levels as a marker of inflammation during CAP treatment. A 2012 Archives of Internal Medicine article notes that U.S. compliance with measuring procalcitonin levels is less than 40%, and monitoring these levels can help diagnosis and guide treatment and the duration of treatment. Procalcitonin is released in the blood in response to bacterial infection. It rises within four hours of infection (earlier than other markers such as CRP and ESR.) The degree and rate of rise is associated with severity; the rate of decline is associated with resolution. Numerous studies show that when providers correlate CAP treatment with procalcitonin levels there is a safe reduction in antibiotic days.
Dr. Flanders also examined the utility of diagnostic tests. In general, CAP outcomes are unchanged and management rarely is impacted by sputum collection. Within the ICU setting it is recommended to get sputum cultures, as it may have a role in healthcare-associated pneumonia, especially if a patient has a history of drug-resistant organisms.
With regard to blood culture analysis, only 4% to 7% of blood cultures are positive in CAP, with many of them being false positives. False positive cultures lead to a 50% increase in charges, and increase length of stay by 65%. A 2004 American Journal of Respiratory and Critical Care Medicine article recommends targeted blood culture screen that correctly detect 90% of bacteremia with 40% fewer cultures. It recommends that patients who are at risk for bacteremia (those with prior antibiotics, WBC count greater than 20, systolic BP less than 90, history of liver disease, temperature greater than 40 degrees or less than 35 degrees celsius, elevated BUN greater than 30, sodium less than 130, pulse greater than 125) be given a point for each risk factor. Those with no risk and no prior antibiotics were deemed safe to forgo cultures. Those with one risk factor, with prior antibiotics were recommended to get one set of cultures. Those with more than one risk factor were recommended to receive two sets of cultures.
Pneumococcal urinary antigen was evaluated. It is noted to have great specificity, but lousy sensitivity. Patients with bacteremia might have false negative results. In general, the antigen might be appropriate in non-severe cases if it will help you narrow therapy. But it shouldn’t be ordered if it is not going to change therapy.
Dr. Flanders also noted that urinary legionella antigen is 80% sensitive for legionella.
Answering the question about the need for broad-spectrum antibiotics, it was thought that any patient receiving home care or home wound care, goes to a dialysis center, lives in a NH or LTC facility would need broad-spectrum antibiotics for HCAP. But Dr. Flanders states it may be a case of doing too much too fast. He recommends patients that reside in nursing homes or who receive home care be treated as a CAP, as the risk of drug-resistant organisms isn’t actually that high in that group. But if a patient had previous admission to the hospital, he recommends treatment for HCAP.
Strong risk factors for resistant organisms include prior hospitalization in past 90 days, LTAC/SNF patients if they have had prior antibiotics and have poor functional status, critically-ill patients, or those with prior MRSA/pseudomonal infections. The data for nursing home patients, home health or home wound care or dialysis patients is less clear. TH
Tracy Cardin is a nurse practitioner in the section of hospital medicine at University of Chicago.
Scott Flanders, MD, SFHM, director of the hospitalist program at the University of Michigan in Ann Arbor set out to answer three key questions in “rapid-fire” format during the “Pneumonia Update” at HM13.
- Is procalcitonin ready for “prime time” in determining community-acquired pneumonia (CAP) treatment duration?
- What is the utility of diagnostic testing in CAP patients?
- How do you decide which pneumonia patients need broad-spectrum antibiotic coverage?
It turns out that lots of other countries follow procalcitonin levels as a marker of inflammation during CAP treatment. A 2012 Archives of Internal Medicine article notes that U.S. compliance with measuring procalcitonin levels is less than 40%, and monitoring these levels can help diagnosis and guide treatment and the duration of treatment. Procalcitonin is released in the blood in response to bacterial infection. It rises within four hours of infection (earlier than other markers such as CRP and ESR.) The degree and rate of rise is associated with severity; the rate of decline is associated with resolution. Numerous studies show that when providers correlate CAP treatment with procalcitonin levels there is a safe reduction in antibiotic days.
Dr. Flanders also examined the utility of diagnostic tests. In general, CAP outcomes are unchanged and management rarely is impacted by sputum collection. Within the ICU setting it is recommended to get sputum cultures, as it may have a role in healthcare-associated pneumonia, especially if a patient has a history of drug-resistant organisms.
With regard to blood culture analysis, only 4% to 7% of blood cultures are positive in CAP, with many of them being false positives. False positive cultures lead to a 50% increase in charges, and increase length of stay by 65%. A 2004 American Journal of Respiratory and Critical Care Medicine article recommends targeted blood culture screen that correctly detect 90% of bacteremia with 40% fewer cultures. It recommends that patients who are at risk for bacteremia (those with prior antibiotics, WBC count greater than 20, systolic BP less than 90, history of liver disease, temperature greater than 40 degrees or less than 35 degrees celsius, elevated BUN greater than 30, sodium less than 130, pulse greater than 125) be given a point for each risk factor. Those with no risk and no prior antibiotics were deemed safe to forgo cultures. Those with one risk factor, with prior antibiotics were recommended to get one set of cultures. Those with more than one risk factor were recommended to receive two sets of cultures.
Pneumococcal urinary antigen was evaluated. It is noted to have great specificity, but lousy sensitivity. Patients with bacteremia might have false negative results. In general, the antigen might be appropriate in non-severe cases if it will help you narrow therapy. But it shouldn’t be ordered if it is not going to change therapy.
Dr. Flanders also noted that urinary legionella antigen is 80% sensitive for legionella.
Answering the question about the need for broad-spectrum antibiotics, it was thought that any patient receiving home care or home wound care, goes to a dialysis center, lives in a NH or LTC facility would need broad-spectrum antibiotics for HCAP. But Dr. Flanders states it may be a case of doing too much too fast. He recommends patients that reside in nursing homes or who receive home care be treated as a CAP, as the risk of drug-resistant organisms isn’t actually that high in that group. But if a patient had previous admission to the hospital, he recommends treatment for HCAP.
Strong risk factors for resistant organisms include prior hospitalization in past 90 days, LTAC/SNF patients if they have had prior antibiotics and have poor functional status, critically-ill patients, or those with prior MRSA/pseudomonal infections. The data for nursing home patients, home health or home wound care or dialysis patients is less clear. TH
Tracy Cardin is a nurse practitioner in the section of hospital medicine at University of Chicago.
Scott Flanders, MD, SFHM, director of the hospitalist program at the University of Michigan in Ann Arbor set out to answer three key questions in “rapid-fire” format during the “Pneumonia Update” at HM13.
- Is procalcitonin ready for “prime time” in determining community-acquired pneumonia (CAP) treatment duration?
- What is the utility of diagnostic testing in CAP patients?
- How do you decide which pneumonia patients need broad-spectrum antibiotic coverage?
It turns out that lots of other countries follow procalcitonin levels as a marker of inflammation during CAP treatment. A 2012 Archives of Internal Medicine article notes that U.S. compliance with measuring procalcitonin levels is less than 40%, and monitoring these levels can help diagnosis and guide treatment and the duration of treatment. Procalcitonin is released in the blood in response to bacterial infection. It rises within four hours of infection (earlier than other markers such as CRP and ESR.) The degree and rate of rise is associated with severity; the rate of decline is associated with resolution. Numerous studies show that when providers correlate CAP treatment with procalcitonin levels there is a safe reduction in antibiotic days.
Dr. Flanders also examined the utility of diagnostic tests. In general, CAP outcomes are unchanged and management rarely is impacted by sputum collection. Within the ICU setting it is recommended to get sputum cultures, as it may have a role in healthcare-associated pneumonia, especially if a patient has a history of drug-resistant organisms.
With regard to blood culture analysis, only 4% to 7% of blood cultures are positive in CAP, with many of them being false positives. False positive cultures lead to a 50% increase in charges, and increase length of stay by 65%. A 2004 American Journal of Respiratory and Critical Care Medicine article recommends targeted blood culture screen that correctly detect 90% of bacteremia with 40% fewer cultures. It recommends that patients who are at risk for bacteremia (those with prior antibiotics, WBC count greater than 20, systolic BP less than 90, history of liver disease, temperature greater than 40 degrees or less than 35 degrees celsius, elevated BUN greater than 30, sodium less than 130, pulse greater than 125) be given a point for each risk factor. Those with no risk and no prior antibiotics were deemed safe to forgo cultures. Those with one risk factor, with prior antibiotics were recommended to get one set of cultures. Those with more than one risk factor were recommended to receive two sets of cultures.
Pneumococcal urinary antigen was evaluated. It is noted to have great specificity, but lousy sensitivity. Patients with bacteremia might have false negative results. In general, the antigen might be appropriate in non-severe cases if it will help you narrow therapy. But it shouldn’t be ordered if it is not going to change therapy.
Dr. Flanders also noted that urinary legionella antigen is 80% sensitive for legionella.
Answering the question about the need for broad-spectrum antibiotics, it was thought that any patient receiving home care or home wound care, goes to a dialysis center, lives in a NH or LTC facility would need broad-spectrum antibiotics for HCAP. But Dr. Flanders states it may be a case of doing too much too fast. He recommends patients that reside in nursing homes or who receive home care be treated as a CAP, as the risk of drug-resistant organisms isn’t actually that high in that group. But if a patient had previous admission to the hospital, he recommends treatment for HCAP.
Strong risk factors for resistant organisms include prior hospitalization in past 90 days, LTAC/SNF patients if they have had prior antibiotics and have poor functional status, critically-ill patients, or those with prior MRSA/pseudomonal infections. The data for nursing home patients, home health or home wound care or dialysis patients is less clear. TH
Tracy Cardin is a nurse practitioner in the section of hospital medicine at University of Chicago.