User login
Looks Aren’t Everything in Breast Reconstruction
Before-and-after photographs are the stock in trade of house painters, auto repair shops, and, yes, plastic and reconstructive surgeons. But a new study may make the last group pause, since it hints that far more is at play in breast cancer patients’ definition of “successful’’ breast reconstruction surgery than how their breasts appear.
The study from Liverpool, England (J Plast Reconstr Aesthet Surg (2012): doi:10.1016/j.bjps.2012.03.005) sidestepped traditional measures used to evaluate outcomes of aesthetic breast surgery and instead asked open-ended questions of survivors who had undergone reconstruction 1-8 years previously.
What the researchers discovered, not surprisingly, is that reconstruction patients are quite unlike cosmetic surgery patients in fundamental and important ways.

Of particular interest in the initial study cohort of 95 patients were 38 whose subjective evaluations of their surgical results completely contradicted objective ratings of cosmesis, the final appearance of the reconstructed breast(s) by surgeons and surgical nurses.
Incredibly, the association between women’s assessments and objective cosmesis ratings failed even to reach statistical significance.
In a structured data analysis of themes that arose in open-ended interviews with 27 of the survivors, the strongest link to women’s satisfaction with the procedure was the surgeon-patient relationship.
Next came the significance of reconstruction in what patients saw as the “completion of the cancer journey,” the authors wrote. “Patients who focused on this were positive about reconstruction that practitioners had rated negatively.”
A previous study asked patients about scarring, finding a correlation between scarring and dissatisfaction with reconstruction. But scarring wasn’t even a blip on the radar when, quoting from the Liverpool study, “we allowed patients to tell us what mattered to them rather than imposing our preconceptions.”
“It seems that surgeons and patients normally ‘talk different languages’; one technical and the other drawing more from relationships and patients’ sense of how normal they feel and appear and from their sense that reconstruction completes their cancer journey,” the investigators concluded. “In preoperative consultations, surgeons concentrate almost exclusively on the technical and cosmetic aspects of reconstruction: what can be achieved and what complications can occur.”
Of course, women who struggled with complications tended to factor that in to their assessments of their results, even if their final cosmetic outcome was considered by surgeons to be excellent.
Others were disappointed despite what seemed to surgeons to be excellent cosmetic results because, as one said, “I was expecting to feel feminine again, but I don’t, I don’t at all.”
What is perhaps even more interesting is to eavesdrop on the comments of women whose surgeons judged their cosmetic result to be poor.
Said one, “I had a really good relationship with (the surgeon) and I just found it so reassuring to see her. That was part of the whole thing really. She was just so positive, and so, well, just understanding I think … I was really glad that I had chosen that form of reconstruction because I had this regular contact with her.”
Said another, who felt “normal” despite what her surgeon considered to be a poor result: “If I didn’t have it done, I wouldn’t have felt normal at all. It would always remind me of what had happened.”
A highly complex patient-surgeon dance occurs when breast surgery is performed for more than cosmetic reasons, the study found.
One woman, disappointed with the way her reconstructed breast fit in a bra, could not bring herself to voice her concern with the surgeon she credited with saving her life.
“It’s very difficult to come face to face with somebody who says, ‘You’ve had cancer but we can get rid of it,’ and does their best… without seeming ungrateful,” she said, tearfully.
The study concludes with a fascinating discussion about the potential clinical implications of the findings.
Considering the profound influence of the patient-surgeon relationship on these particular patients, the investigators offer a cautionary suggestion to avoid being overly effusive about the cosmetic result they may see. Patients, they explain, may not necessarily share their enthusiasm, if they continue to struggle with the sense that cancer has marred their bodies, their sense of self, or their security in relationships.
“Both patient and surgeon have invested physically and emotionally in the procedure and it is difficult for either to admit to the other that it was “not worth it,” they note.
Women, on the other hand, who appear to be disproportionately pleased with the result of surgery that objectively achieved a poor result may simply be expressing relief and gratitude. “Their apparent satisfaction,” they wrote, “should not excuse poor surgical practice.” Rather, routine assessments of reconstructive practice should be made by objective sources, not simply patient report.
On the other hand, in individual patients, the objective in reconstructive surgery is patient satisfaction, they suggest. An unhappy patient might spur a conscientious surgeon to keep trying, perhaps through repeated procedures, to achieve a better result – a strategy that could be inappropriate and pointless considering that in some cases, “the reason for disappointment with reconstruction include many that the surgeon cannot influence surgically.”
It all suggests that communication between surgeons and reconstruction candidates and patients needs to be deep and candidly honest, informed by the emotional, sexual, and existential meaning the surgery holds.
In a word, it’s complicated.
Betsy Bates Freed, Psych.D., is a clinical psychologist in Santa Barbara, Calif., and a medical journalist.
Before-and-after photographs are the stock in trade of house painters, auto repair shops, and, yes, plastic and reconstructive surgeons. But a new study may make the last group pause, since it hints that far more is at play in breast cancer patients’ definition of “successful’’ breast reconstruction surgery than how their breasts appear.
The study from Liverpool, England (J Plast Reconstr Aesthet Surg (2012): doi:10.1016/j.bjps.2012.03.005) sidestepped traditional measures used to evaluate outcomes of aesthetic breast surgery and instead asked open-ended questions of survivors who had undergone reconstruction 1-8 years previously.
What the researchers discovered, not surprisingly, is that reconstruction patients are quite unlike cosmetic surgery patients in fundamental and important ways.
Of particular interest in the initial study cohort of 95 patients were 38 whose subjective evaluations of their surgical results completely contradicted objective ratings of cosmesis, the final appearance of the reconstructed breast(s) by surgeons and surgical nurses.
Incredibly, the association between women’s assessments and objective cosmesis ratings failed even to reach statistical significance.
In a structured data analysis of themes that arose in open-ended interviews with 27 of the survivors, the strongest link to women’s satisfaction with the procedure was the surgeon-patient relationship.
Next came the significance of reconstruction in what patients saw as the “completion of the cancer journey,” the authors wrote. “Patients who focused on this were positive about reconstruction that practitioners had rated negatively.”
A previous study asked patients about scarring, finding a correlation between scarring and dissatisfaction with reconstruction. But scarring wasn’t even a blip on the radar when, quoting from the Liverpool study, “we allowed patients to tell us what mattered to them rather than imposing our preconceptions.”
“It seems that surgeons and patients normally ‘talk different languages’; one technical and the other drawing more from relationships and patients’ sense of how normal they feel and appear and from their sense that reconstruction completes their cancer journey,” the investigators concluded. “In preoperative consultations, surgeons concentrate almost exclusively on the technical and cosmetic aspects of reconstruction: what can be achieved and what complications can occur.”
Of course, women who struggled with complications tended to factor that in to their assessments of their results, even if their final cosmetic outcome was considered by surgeons to be excellent.
Others were disappointed despite what seemed to surgeons to be excellent cosmetic results because, as one said, “I was expecting to feel feminine again, but I don’t, I don’t at all.”
What is perhaps even more interesting is to eavesdrop on the comments of women whose surgeons judged their cosmetic result to be poor.
Said one, “I had a really good relationship with (the surgeon) and I just found it so reassuring to see her. That was part of the whole thing really. She was just so positive, and so, well, just understanding I think … I was really glad that I had chosen that form of reconstruction because I had this regular contact with her.”
Said another, who felt “normal” despite what her surgeon considered to be a poor result: “If I didn’t have it done, I wouldn’t have felt normal at all. It would always remind me of what had happened.”
A highly complex patient-surgeon dance occurs when breast surgery is performed for more than cosmetic reasons, the study found.
One woman, disappointed with the way her reconstructed breast fit in a bra, could not bring herself to voice her concern with the surgeon she credited with saving her life.
“It’s very difficult to come face to face with somebody who says, ‘You’ve had cancer but we can get rid of it,’ and does their best… without seeming ungrateful,” she said, tearfully.
The study concludes with a fascinating discussion about the potential clinical implications of the findings.
Considering the profound influence of the patient-surgeon relationship on these particular patients, the investigators offer a cautionary suggestion to avoid being overly effusive about the cosmetic result they may see. Patients, they explain, may not necessarily share their enthusiasm, if they continue to struggle with the sense that cancer has marred their bodies, their sense of self, or their security in relationships.
“Both patient and surgeon have invested physically and emotionally in the procedure and it is difficult for either to admit to the other that it was “not worth it,” they note.
Women, on the other hand, who appear to be disproportionately pleased with the result of surgery that objectively achieved a poor result may simply be expressing relief and gratitude. “Their apparent satisfaction,” they wrote, “should not excuse poor surgical practice.” Rather, routine assessments of reconstructive practice should be made by objective sources, not simply patient report.
On the other hand, in individual patients, the objective in reconstructive surgery is patient satisfaction, they suggest. An unhappy patient might spur a conscientious surgeon to keep trying, perhaps through repeated procedures, to achieve a better result – a strategy that could be inappropriate and pointless considering that in some cases, “the reason for disappointment with reconstruction include many that the surgeon cannot influence surgically.”
It all suggests that communication between surgeons and reconstruction candidates and patients needs to be deep and candidly honest, informed by the emotional, sexual, and existential meaning the surgery holds.
In a word, it’s complicated.
Betsy Bates Freed, Psych.D., is a clinical psychologist in Santa Barbara, Calif., and a medical journalist.
Before-and-after photographs are the stock in trade of house painters, auto repair shops, and, yes, plastic and reconstructive surgeons. But a new study may make the last group pause, since it hints that far more is at play in breast cancer patients’ definition of “successful’’ breast reconstruction surgery than how their breasts appear.
The study from Liverpool, England (J Plast Reconstr Aesthet Surg (2012): doi:10.1016/j.bjps.2012.03.005) sidestepped traditional measures used to evaluate outcomes of aesthetic breast surgery and instead asked open-ended questions of survivors who had undergone reconstruction 1-8 years previously.
What the researchers discovered, not surprisingly, is that reconstruction patients are quite unlike cosmetic surgery patients in fundamental and important ways.
Of particular interest in the initial study cohort of 95 patients were 38 whose subjective evaluations of their surgical results completely contradicted objective ratings of cosmesis, the final appearance of the reconstructed breast(s) by surgeons and surgical nurses.
Incredibly, the association between women’s assessments and objective cosmesis ratings failed even to reach statistical significance.
In a structured data analysis of themes that arose in open-ended interviews with 27 of the survivors, the strongest link to women’s satisfaction with the procedure was the surgeon-patient relationship.
Next came the significance of reconstruction in what patients saw as the “completion of the cancer journey,” the authors wrote. “Patients who focused on this were positive about reconstruction that practitioners had rated negatively.”
A previous study asked patients about scarring, finding a correlation between scarring and dissatisfaction with reconstruction. But scarring wasn’t even a blip on the radar when, quoting from the Liverpool study, “we allowed patients to tell us what mattered to them rather than imposing our preconceptions.”
“It seems that surgeons and patients normally ‘talk different languages’; one technical and the other drawing more from relationships and patients’ sense of how normal they feel and appear and from their sense that reconstruction completes their cancer journey,” the investigators concluded. “In preoperative consultations, surgeons concentrate almost exclusively on the technical and cosmetic aspects of reconstruction: what can be achieved and what complications can occur.”
Of course, women who struggled with complications tended to factor that in to their assessments of their results, even if their final cosmetic outcome was considered by surgeons to be excellent.
Others were disappointed despite what seemed to surgeons to be excellent cosmetic results because, as one said, “I was expecting to feel feminine again, but I don’t, I don’t at all.”
What is perhaps even more interesting is to eavesdrop on the comments of women whose surgeons judged their cosmetic result to be poor.
Said one, “I had a really good relationship with (the surgeon) and I just found it so reassuring to see her. That was part of the whole thing really. She was just so positive, and so, well, just understanding I think … I was really glad that I had chosen that form of reconstruction because I had this regular contact with her.”
Said another, who felt “normal” despite what her surgeon considered to be a poor result: “If I didn’t have it done, I wouldn’t have felt normal at all. It would always remind me of what had happened.”
A highly complex patient-surgeon dance occurs when breast surgery is performed for more than cosmetic reasons, the study found.
One woman, disappointed with the way her reconstructed breast fit in a bra, could not bring herself to voice her concern with the surgeon she credited with saving her life.
“It’s very difficult to come face to face with somebody who says, ‘You’ve had cancer but we can get rid of it,’ and does their best… without seeming ungrateful,” she said, tearfully.
The study concludes with a fascinating discussion about the potential clinical implications of the findings.
Considering the profound influence of the patient-surgeon relationship on these particular patients, the investigators offer a cautionary suggestion to avoid being overly effusive about the cosmetic result they may see. Patients, they explain, may not necessarily share their enthusiasm, if they continue to struggle with the sense that cancer has marred their bodies, their sense of self, or their security in relationships.
“Both patient and surgeon have invested physically and emotionally in the procedure and it is difficult for either to admit to the other that it was “not worth it,” they note.
Women, on the other hand, who appear to be disproportionately pleased with the result of surgery that objectively achieved a poor result may simply be expressing relief and gratitude. “Their apparent satisfaction,” they wrote, “should not excuse poor surgical practice.” Rather, routine assessments of reconstructive practice should be made by objective sources, not simply patient report.
On the other hand, in individual patients, the objective in reconstructive surgery is patient satisfaction, they suggest. An unhappy patient might spur a conscientious surgeon to keep trying, perhaps through repeated procedures, to achieve a better result – a strategy that could be inappropriate and pointless considering that in some cases, “the reason for disappointment with reconstruction include many that the surgeon cannot influence surgically.”
It all suggests that communication between surgeons and reconstruction candidates and patients needs to be deep and candidly honest, informed by the emotional, sexual, and existential meaning the surgery holds.
In a word, it’s complicated.
Betsy Bates Freed, Psych.D., is a clinical psychologist in Santa Barbara, Calif., and a medical journalist.
Exploring the Role of Modified-Release Doxycycline in Rosacea

Topics
- Introduction - Exploring the Role of Modified-Release
- Doxycycline in Rosacea
- Comparing Antimicrobial and Anti-Inflammatory Doses of Oral Doxycycline in the Treatment of Rosacea
- Impact of Antibiotic Resistance on Dermatologic Practice
- The Effects of Modified-Release Doxycycline on Quality of Life
- Combining Anti-Inflammatory–Dose Doxycycline With Topical Metronidazole
To view the supplement, click the image above.
Faculty/Faculty Disclosure
Brian Berman, MD, PhD
Voluntary Professor of Dermatology and Cutaneous Surgery
University of Miami, Miller School of Medicine
Co-Director
Center for Clinical and Cosmetic Research, Skin & Cancer Associates, LLP,
Aventura, FL
Dr Berman has received funding for clinical grants from, is an investigator for, and is a consultant to, Galderma Laboratories, L.P.
Copyright © 2012 by Elsevier Inc.
Topics
- Introduction - Exploring the Role of Modified-Release
- Doxycycline in Rosacea
- Comparing Antimicrobial and Anti-Inflammatory Doses of Oral Doxycycline in the Treatment of Rosacea
- Impact of Antibiotic Resistance on Dermatologic Practice
- The Effects of Modified-Release Doxycycline on Quality of Life
- Combining Anti-Inflammatory–Dose Doxycycline With Topical Metronidazole
To view the supplement, click the image above.
Faculty/Faculty Disclosure
Brian Berman, MD, PhD
Voluntary Professor of Dermatology and Cutaneous Surgery
University of Miami, Miller School of Medicine
Co-Director
Center for Clinical and Cosmetic Research, Skin & Cancer Associates, LLP,
Aventura, FL
Dr Berman has received funding for clinical grants from, is an investigator for, and is a consultant to, Galderma Laboratories, L.P.
Copyright © 2012 by Elsevier Inc.
Topics
- Introduction - Exploring the Role of Modified-Release
- Doxycycline in Rosacea
- Comparing Antimicrobial and Anti-Inflammatory Doses of Oral Doxycycline in the Treatment of Rosacea
- Impact of Antibiotic Resistance on Dermatologic Practice
- The Effects of Modified-Release Doxycycline on Quality of Life
- Combining Anti-Inflammatory–Dose Doxycycline With Topical Metronidazole
To view the supplement, click the image above.
Faculty/Faculty Disclosure
Brian Berman, MD, PhD
Voluntary Professor of Dermatology and Cutaneous Surgery
University of Miami, Miller School of Medicine
Co-Director
Center for Clinical and Cosmetic Research, Skin & Cancer Associates, LLP,
Aventura, FL
Dr Berman has received funding for clinical grants from, is an investigator for, and is a consultant to, Galderma Laboratories, L.P.
Copyright © 2012 by Elsevier Inc.
Exploring the Role of Modified-Release Doxycycline in Rosacea

- Introduction - Exploring the Role of Modified-Release
- Doxycycline in Rosacea
- Comparing Antimicrobial and Anti-Inflammatory Doses of Oral Doxycycline in the Treatment of Rosacea
- Impact of Antibiotic Resistance on Dermatologic Practice
- The Effects of Modified-Release Doxycycline on Quality of Life
- Combining Anti-Inflammatory–Dose Doxycycline With Topical Metronidazole
To view the supplement, click the image above.
Faculty/Faculty Disclosure
Brian Berman, MD, PhD
Voluntary Professor of Dermatology and Cutaneous Surgery
University of Miami, Miller School of Medicine Co-Director
Center for Clinical and Cosmetic Research, Skin & Cancer Associates, LLP, Aventura, FL
Copyright (c) 2012 by Elsevier Inc.
- Introduction - Exploring the Role of Modified-Release
- Doxycycline in Rosacea
- Comparing Antimicrobial and Anti-Inflammatory Doses of Oral Doxycycline in the Treatment of Rosacea
- Impact of Antibiotic Resistance on Dermatologic Practice
- The Effects of Modified-Release Doxycycline on Quality of Life
- Combining Anti-Inflammatory–Dose Doxycycline With Topical Metronidazole
To view the supplement, click the image above.
Faculty/Faculty Disclosure
Brian Berman, MD, PhD
Voluntary Professor of Dermatology and Cutaneous Surgery
University of Miami, Miller School of Medicine Co-Director
Center for Clinical and Cosmetic Research, Skin & Cancer Associates, LLP, Aventura, FL
Copyright (c) 2012 by Elsevier Inc.
- Introduction - Exploring the Role of Modified-Release
- Doxycycline in Rosacea
- Comparing Antimicrobial and Anti-Inflammatory Doses of Oral Doxycycline in the Treatment of Rosacea
- Impact of Antibiotic Resistance on Dermatologic Practice
- The Effects of Modified-Release Doxycycline on Quality of Life
- Combining Anti-Inflammatory–Dose Doxycycline With Topical Metronidazole
To view the supplement, click the image above.
Faculty/Faculty Disclosure
Brian Berman, MD, PhD
Voluntary Professor of Dermatology and Cutaneous Surgery
University of Miami, Miller School of Medicine Co-Director
Center for Clinical and Cosmetic Research, Skin & Cancer Associates, LLP, Aventura, FL
Copyright (c) 2012 by Elsevier Inc.

Military Teens Face Unique Mental Health Challenges
"My Story: Blogs by Four Military Teens" is a book that gives voice to military teens by highlighting their feelings and experiences before, during, and after parental deployment. The four youths in "My Story" are fictional, but the stories are real in that the posts are a compilation of real life experiences of military kids.
"Adam" blogs, "My dad is one of the coolest, smartest, bravest men I’ve ever met, but sometimes I just can’t stand being around him. He’s a doctor – a surgeon – and is in the Air Force Reserves. He just returned from a second tour in Iraq, and he sure acts different. After his first tour, it took us some time to get caught up, but just when things got normal again, he got his orders to go back to Iraq. Now he’s finally home (for good?), but he just isn’t the same. He gets mad over the stupidest things and spends most of his time in his bedroom or in front of the computer.
"He’s still in ‘military mode,’ and orders us around way too much. He doesn’t joke around like before, and sometimes just hangs out in the garage by himself. We don’t talk much. I almost liked it better when he was gone. It was a lot quieter and less stressful around the house. Ashley, Lisa, and I just stay out of his way. Derrick is lucky – he’s leaving for college soon."
This book also provides support and education for military teens and preteens by honoring their unique joys and sacrifices, addressing their fears and hopes, and exploring how parental deployment affects their lives.
The book was written by Michelle D. Sherman, Ph.D., and her mother, DeAnne M. Sherman. Together, Dr. Sherman and her mother – a teacher – have written other books for teens, including "Finding My Way: A Teen’s Guide to Living with a Parent Who has Experienced Trauma" (Waco, Tex.: Seeds of Hope Publishers, 2005).
Dr. Sherman is a clinical psychologist at the Oklahoma City VA Medical Center, where she directs its Family Mental Health Program. She has dedicated her career to supporting families affected by mental illness and posttraumatic stress disorder, and has a special interest in the impact of parental mental illness and PTSD on youth.
"Think about the ... challenges facing our military teens," she writes in a guest post on the blog of an organization called Veterans Children. "Their parent(s) may be deployed once, twice, or even multiple times to a war zone. The parent may miss out on important events, such as prom, the school play, the state basketball tournament, and birthdays."
These young people are resilient, Dr. Sherman writes, but some are struggling with increased rates of anxiety, sleeping and behavioral problems, and the use of psychotropics.
"What does this tell us? ...They are affected by their parent’s deployment. We need to listen to them, provide resources, and make services available," writes Dr. Sherman, also is a clinical professor in the department of psychiatry and behavioral sciences at the University of Oklahoma Health Sciences Center and a research affiliate with the South Central Mental Illness Research, Education and Clinical Center (MIRECC).

In her work with veterans and families, Dr. Sherman has developed educational and support programs. Operation Enduring Families is a 5-session family education curriculum for Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) veterans/families, developed with Ursula B. Bowling, Psy.D., and Alan L. Doerman, Psy.D. This program is based on her S.A.F.E (Support and Family Education) program, an 18-session curriculum for those who care about someone with a mental illness/PTSD.
Dr. Sherman has developed an extensive resource list for OEF/OIF service members, and veterans and their families. (See box.) For a complete list, you can e-mail her at [email protected].
This column, "Families in Psychiatry," regularly appears in Clinical Psychiatry News, an Elsevier publication. Dr. Heru is an associate professor of psychiatry at the University of Colorado at Denver, Aurora. She has been a member of the Association of Family Psychiatrists since 2002 and currently serves as the organization’s treasurer. In addition, she is the coauthor of two books on working with families and is the author of numerous articles on this topic.
The following list of books and websites can be used to help military children of all ages cope with parental deployment:
Books
• "After the War Zone: A Practical Guide for Returning Troops and Their Families" (Cambridge, Mass.: Da Capo Press, 2008).
• "Back from the Front: Combat Trauma, Love, and the Family" (Brooklandville, Md.: Sidran Institute Press, 2007).
• "Courage After Fire: Coping Strategies for Returning Soldiers and Their Families" (Berkeley, Calif.: Ulysses Press, 2005).
• "I Miss You!: A Military Kid’s Book About Deployment" (Amherst, N.Y.: Prometheus Books, 2007).
• "Night Catch" (Jamestown, N.D.: Bubble Gum Press, 2005).
• "100 days and 99 nights" (New York: Little, Brown and Co. Books for Young Readers, 2008).
• "Sometimes We Were Brave" (Honesdale, Pa.: Boyds Mills Press, 2010).
• "The Fathers Are Coming Home" (New York: Margaret K. McElderry Books, 2010).
Websites
• "Courage to Care, Courage to Talk About War Injuries," developed by the Center for the Study of Traumatic Stress.
• "Military Child Bill of Rights."
• National Military Family Association.
• Song and video: "The Price of Peace."
• Video (58 minutes): "Returning From the War Zone: A Guide for Families of Military Members," created by the National Center for PTSD.
• SOAR (Student Online Achievement Resources).
• Students at the Center: An Education Resource for Families, the Military, and Schools.
• "Talk, Listen, Connect: Deployments, Homecomings, Changes."
• Veteran Parenting Toolkit, created by the Oklahoma City VA Family Mental Health Program.
• "Welcome Back Parenting: A Guide for Reconnecting Families After Military Deployment."
• DVD: "Young Children on the Homefront: Family Stories, Family, Strengths," developed by the nonprofit organization Zero to Three: National Center for Infants, Toddlers, and Families.
• "Young Heroes: Military Deployment Through the Eyes of Youth."
"My Story: Blogs by Four Military Teens" is a book that gives voice to military teens by highlighting their feelings and experiences before, during, and after parental deployment. The four youths in "My Story" are fictional, but the stories are real in that the posts are a compilation of real life experiences of military kids.
"Adam" blogs, "My dad is one of the coolest, smartest, bravest men I’ve ever met, but sometimes I just can’t stand being around him. He’s a doctor – a surgeon – and is in the Air Force Reserves. He just returned from a second tour in Iraq, and he sure acts different. After his first tour, it took us some time to get caught up, but just when things got normal again, he got his orders to go back to Iraq. Now he’s finally home (for good?), but he just isn’t the same. He gets mad over the stupidest things and spends most of his time in his bedroom or in front of the computer.
"He’s still in ‘military mode,’ and orders us around way too much. He doesn’t joke around like before, and sometimes just hangs out in the garage by himself. We don’t talk much. I almost liked it better when he was gone. It was a lot quieter and less stressful around the house. Ashley, Lisa, and I just stay out of his way. Derrick is lucky – he’s leaving for college soon."
This book also provides support and education for military teens and preteens by honoring their unique joys and sacrifices, addressing their fears and hopes, and exploring how parental deployment affects their lives.
The book was written by Michelle D. Sherman, Ph.D., and her mother, DeAnne M. Sherman. Together, Dr. Sherman and her mother – a teacher – have written other books for teens, including "Finding My Way: A Teen’s Guide to Living with a Parent Who has Experienced Trauma" (Waco, Tex.: Seeds of Hope Publishers, 2005).
Dr. Sherman is a clinical psychologist at the Oklahoma City VA Medical Center, where she directs its Family Mental Health Program. She has dedicated her career to supporting families affected by mental illness and posttraumatic stress disorder, and has a special interest in the impact of parental mental illness and PTSD on youth.
"Think about the ... challenges facing our military teens," she writes in a guest post on the blog of an organization called Veterans Children. "Their parent(s) may be deployed once, twice, or even multiple times to a war zone. The parent may miss out on important events, such as prom, the school play, the state basketball tournament, and birthdays."
These young people are resilient, Dr. Sherman writes, but some are struggling with increased rates of anxiety, sleeping and behavioral problems, and the use of psychotropics.
"What does this tell us? ...They are affected by their parent’s deployment. We need to listen to them, provide resources, and make services available," writes Dr. Sherman, also is a clinical professor in the department of psychiatry and behavioral sciences at the University of Oklahoma Health Sciences Center and a research affiliate with the South Central Mental Illness Research, Education and Clinical Center (MIRECC).
In her work with veterans and families, Dr. Sherman has developed educational and support programs. Operation Enduring Families is a 5-session family education curriculum for Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) veterans/families, developed with Ursula B. Bowling, Psy.D., and Alan L. Doerman, Psy.D. This program is based on her S.A.F.E (Support and Family Education) program, an 18-session curriculum for those who care about someone with a mental illness/PTSD.
Dr. Sherman has developed an extensive resource list for OEF/OIF service members, and veterans and their families. (See box.) For a complete list, you can e-mail her at [email protected].
This column, "Families in Psychiatry," regularly appears in Clinical Psychiatry News, an Elsevier publication. Dr. Heru is an associate professor of psychiatry at the University of Colorado at Denver, Aurora. She has been a member of the Association of Family Psychiatrists since 2002 and currently serves as the organization’s treasurer. In addition, she is the coauthor of two books on working with families and is the author of numerous articles on this topic.
The following list of books and websites can be used to help military children of all ages cope with parental deployment:
Books
• "After the War Zone: A Practical Guide for Returning Troops and Their Families" (Cambridge, Mass.: Da Capo Press, 2008).
• "Back from the Front: Combat Trauma, Love, and the Family" (Brooklandville, Md.: Sidran Institute Press, 2007).
• "Courage After Fire: Coping Strategies for Returning Soldiers and Their Families" (Berkeley, Calif.: Ulysses Press, 2005).
• "I Miss You!: A Military Kid’s Book About Deployment" (Amherst, N.Y.: Prometheus Books, 2007).
• "Night Catch" (Jamestown, N.D.: Bubble Gum Press, 2005).
• "100 days and 99 nights" (New York: Little, Brown and Co. Books for Young Readers, 2008).
• "Sometimes We Were Brave" (Honesdale, Pa.: Boyds Mills Press, 2010).
• "The Fathers Are Coming Home" (New York: Margaret K. McElderry Books, 2010).
Websites
• "Courage to Care, Courage to Talk About War Injuries," developed by the Center for the Study of Traumatic Stress.
• "Military Child Bill of Rights."
• National Military Family Association.
• Song and video: "The Price of Peace."
• Video (58 minutes): "Returning From the War Zone: A Guide for Families of Military Members," created by the National Center for PTSD.
• SOAR (Student Online Achievement Resources).
• Students at the Center: An Education Resource for Families, the Military, and Schools.
• "Talk, Listen, Connect: Deployments, Homecomings, Changes."
• Veteran Parenting Toolkit, created by the Oklahoma City VA Family Mental Health Program.
• "Welcome Back Parenting: A Guide for Reconnecting Families After Military Deployment."
• DVD: "Young Children on the Homefront: Family Stories, Family, Strengths," developed by the nonprofit organization Zero to Three: National Center for Infants, Toddlers, and Families.
• "Young Heroes: Military Deployment Through the Eyes of Youth."
"My Story: Blogs by Four Military Teens" is a book that gives voice to military teens by highlighting their feelings and experiences before, during, and after parental deployment. The four youths in "My Story" are fictional, but the stories are real in that the posts are a compilation of real life experiences of military kids.
"Adam" blogs, "My dad is one of the coolest, smartest, bravest men I’ve ever met, but sometimes I just can’t stand being around him. He’s a doctor – a surgeon – and is in the Air Force Reserves. He just returned from a second tour in Iraq, and he sure acts different. After his first tour, it took us some time to get caught up, but just when things got normal again, he got his orders to go back to Iraq. Now he’s finally home (for good?), but he just isn’t the same. He gets mad over the stupidest things and spends most of his time in his bedroom or in front of the computer.
"He’s still in ‘military mode,’ and orders us around way too much. He doesn’t joke around like before, and sometimes just hangs out in the garage by himself. We don’t talk much. I almost liked it better when he was gone. It was a lot quieter and less stressful around the house. Ashley, Lisa, and I just stay out of his way. Derrick is lucky – he’s leaving for college soon."
This book also provides support and education for military teens and preteens by honoring their unique joys and sacrifices, addressing their fears and hopes, and exploring how parental deployment affects their lives.
The book was written by Michelle D. Sherman, Ph.D., and her mother, DeAnne M. Sherman. Together, Dr. Sherman and her mother – a teacher – have written other books for teens, including "Finding My Way: A Teen’s Guide to Living with a Parent Who has Experienced Trauma" (Waco, Tex.: Seeds of Hope Publishers, 2005).
Dr. Sherman is a clinical psychologist at the Oklahoma City VA Medical Center, where she directs its Family Mental Health Program. She has dedicated her career to supporting families affected by mental illness and posttraumatic stress disorder, and has a special interest in the impact of parental mental illness and PTSD on youth.
"Think about the ... challenges facing our military teens," she writes in a guest post on the blog of an organization called Veterans Children. "Their parent(s) may be deployed once, twice, or even multiple times to a war zone. The parent may miss out on important events, such as prom, the school play, the state basketball tournament, and birthdays."
These young people are resilient, Dr. Sherman writes, but some are struggling with increased rates of anxiety, sleeping and behavioral problems, and the use of psychotropics.
"What does this tell us? ...They are affected by their parent’s deployment. We need to listen to them, provide resources, and make services available," writes Dr. Sherman, also is a clinical professor in the department of psychiatry and behavioral sciences at the University of Oklahoma Health Sciences Center and a research affiliate with the South Central Mental Illness Research, Education and Clinical Center (MIRECC).
In her work with veterans and families, Dr. Sherman has developed educational and support programs. Operation Enduring Families is a 5-session family education curriculum for Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) veterans/families, developed with Ursula B. Bowling, Psy.D., and Alan L. Doerman, Psy.D. This program is based on her S.A.F.E (Support and Family Education) program, an 18-session curriculum for those who care about someone with a mental illness/PTSD.
Dr. Sherman has developed an extensive resource list for OEF/OIF service members, and veterans and their families. (See box.) For a complete list, you can e-mail her at [email protected].
This column, "Families in Psychiatry," regularly appears in Clinical Psychiatry News, an Elsevier publication. Dr. Heru is an associate professor of psychiatry at the University of Colorado at Denver, Aurora. She has been a member of the Association of Family Psychiatrists since 2002 and currently serves as the organization’s treasurer. In addition, she is the coauthor of two books on working with families and is the author of numerous articles on this topic.
The following list of books and websites can be used to help military children of all ages cope with parental deployment:
Books
• "After the War Zone: A Practical Guide for Returning Troops and Their Families" (Cambridge, Mass.: Da Capo Press, 2008).
• "Back from the Front: Combat Trauma, Love, and the Family" (Brooklandville, Md.: Sidran Institute Press, 2007).
• "Courage After Fire: Coping Strategies for Returning Soldiers and Their Families" (Berkeley, Calif.: Ulysses Press, 2005).
• "I Miss You!: A Military Kid’s Book About Deployment" (Amherst, N.Y.: Prometheus Books, 2007).
• "Night Catch" (Jamestown, N.D.: Bubble Gum Press, 2005).
• "100 days and 99 nights" (New York: Little, Brown and Co. Books for Young Readers, 2008).
• "Sometimes We Were Brave" (Honesdale, Pa.: Boyds Mills Press, 2010).
• "The Fathers Are Coming Home" (New York: Margaret K. McElderry Books, 2010).
Websites
• "Courage to Care, Courage to Talk About War Injuries," developed by the Center for the Study of Traumatic Stress.
• "Military Child Bill of Rights."
• National Military Family Association.
• Song and video: "The Price of Peace."
• Video (58 minutes): "Returning From the War Zone: A Guide for Families of Military Members," created by the National Center for PTSD.
• SOAR (Student Online Achievement Resources).
• Students at the Center: An Education Resource for Families, the Military, and Schools.
• "Talk, Listen, Connect: Deployments, Homecomings, Changes."
• Veteran Parenting Toolkit, created by the Oklahoma City VA Family Mental Health Program.
• "Welcome Back Parenting: A Guide for Reconnecting Families After Military Deployment."
• DVD: "Young Children on the Homefront: Family Stories, Family, Strengths," developed by the nonprofit organization Zero to Three: National Center for Infants, Toddlers, and Families.
• "Young Heroes: Military Deployment Through the Eyes of Youth."
Urgent Discharge: What's the Rush?
Rehospitalization within 30 days of an initial acute coronary syndrome or heart failure event has now become a CMS quality measure that will affect overall hospital Medicare payments. It has been appreciated for some time that rehospitalization for these diagnoses has been unacceptably high.
A recent report indicates that a greater percentage of U.S. patients who experienced a STEMI are more likely to be rehospitalized within 30 days, compared with other Western countries (14.5% vs. 9.9%, respectively). That report (JAMA 2012;307:66-74) indicates that the increase is directly related to the shorter length of hospital stay in the United States. Among the 17 countries included in the report, the average duration was shortest in the United States (3 days) and longest in Germany (8 days). Predictors of readmission other than length of stay include the age of the patient and the presence of heart failure. The most interesting part of the story is how we arrived at this state of affairs.
For those of you who were not yet born or are too young to remember when Medicare was passed into law in 1965, I will give you a little history. And for those of you who were around at the time, I will provide a reminder.
As you undoubtedly know, Medicare, in addition to paying physicians’ fees also pays hospital costs. In the period between 1965 and 1983, using a payment system that was defined as "reasonable and allowable costs," Medicare payments to hospitals increased 10-fold, from $3 billion to $37 billion. In consequence, Congress passed a law in 1982 that created a prospective payment system for hospitals using diagnosis-related groups establishing a payment schedule for specific diagnoses, which included acute myocardial infarction and heart failure. With this schedule, hospitals were paid a fixed rate regardless of the number of procedures performed or duration of hospitalization. In order to minimize costs, hospitals accelerated discharges and shortened hospital length of stay. Emergency admissions resulted in urgent discharge.
In order to expedite the process of admission and discharge, hospitalists were hired to accelerate that process since practicing internists and cardiologists were not available to push the paperwork through fast enough to get the patients discharged quickly. Hospitals saw this additional layer of doctors caring for patients as financially profitable. As a result, hospital stays decreased markedly and payments to hospitals decreased by 52% from 1985 to 1990 and by an additional 37% between 1990 and 1995. Everyone seemed to be very happy with this, including the hospitals, Medicare, and doctors. As far as I know, patients were not consulted.
Cardiologists at that time were telling themselves how benign an acute MI is and began doing accelerated discharge after percutaneous coronary intervention. We prided ourselves on how patients could be discharged to home within 24-36 hours, but never actually reached the ultimate goal of a "drive-through PCI." The fact that patients with acute MI and heart failure were frequently readmitted was good business since each admission resulted in further Medicare payments both to the hospital and the doctors. Urging by some physicians to develop plans that could educate patients and develop discharge follow-up systems was met with incredulity by hospital administrators who saw readmission as a revenue source and discharge planning as costly.
It is important to emphasize that readmission not only reflects an important morbidity event, it also carries with it the potential for increased risk of mortality. In the report cited above, one-third of the deaths after hospitalization for a STEMI occurred within the same 30-day post-event period. The recent emphasis on decreasing door-to-balloon time, although effective in shortening that period, has had little effect on the mortality associated with an acute myocardial infarction. It is reasonable to assume that in placing a greater emphasis on insuring that patients are ready to leave the hospital, we can improve mortality and morbidity of both the ACS and heart failure patient. There really is no urgency to discharge patients other than improving the bottom line, and that imperative may no longer be relevant.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
Rehospitalization within 30 days of an initial acute coronary syndrome or heart failure event has now become a CMS quality measure that will affect overall hospital Medicare payments. It has been appreciated for some time that rehospitalization for these diagnoses has been unacceptably high.
A recent report indicates that a greater percentage of U.S. patients who experienced a STEMI are more likely to be rehospitalized within 30 days, compared with other Western countries (14.5% vs. 9.9%, respectively). That report (JAMA 2012;307:66-74) indicates that the increase is directly related to the shorter length of hospital stay in the United States. Among the 17 countries included in the report, the average duration was shortest in the United States (3 days) and longest in Germany (8 days). Predictors of readmission other than length of stay include the age of the patient and the presence of heart failure. The most interesting part of the story is how we arrived at this state of affairs.
For those of you who were not yet born or are too young to remember when Medicare was passed into law in 1965, I will give you a little history. And for those of you who were around at the time, I will provide a reminder.
As you undoubtedly know, Medicare, in addition to paying physicians’ fees also pays hospital costs. In the period between 1965 and 1983, using a payment system that was defined as "reasonable and allowable costs," Medicare payments to hospitals increased 10-fold, from $3 billion to $37 billion. In consequence, Congress passed a law in 1982 that created a prospective payment system for hospitals using diagnosis-related groups establishing a payment schedule for specific diagnoses, which included acute myocardial infarction and heart failure. With this schedule, hospitals were paid a fixed rate regardless of the number of procedures performed or duration of hospitalization. In order to minimize costs, hospitals accelerated discharges and shortened hospital length of stay. Emergency admissions resulted in urgent discharge.
In order to expedite the process of admission and discharge, hospitalists were hired to accelerate that process since practicing internists and cardiologists were not available to push the paperwork through fast enough to get the patients discharged quickly. Hospitals saw this additional layer of doctors caring for patients as financially profitable. As a result, hospital stays decreased markedly and payments to hospitals decreased by 52% from 1985 to 1990 and by an additional 37% between 1990 and 1995. Everyone seemed to be very happy with this, including the hospitals, Medicare, and doctors. As far as I know, patients were not consulted.
Cardiologists at that time were telling themselves how benign an acute MI is and began doing accelerated discharge after percutaneous coronary intervention. We prided ourselves on how patients could be discharged to home within 24-36 hours, but never actually reached the ultimate goal of a "drive-through PCI." The fact that patients with acute MI and heart failure were frequently readmitted was good business since each admission resulted in further Medicare payments both to the hospital and the doctors. Urging by some physicians to develop plans that could educate patients and develop discharge follow-up systems was met with incredulity by hospital administrators who saw readmission as a revenue source and discharge planning as costly.
It is important to emphasize that readmission not only reflects an important morbidity event, it also carries with it the potential for increased risk of mortality. In the report cited above, one-third of the deaths after hospitalization for a STEMI occurred within the same 30-day post-event period. The recent emphasis on decreasing door-to-balloon time, although effective in shortening that period, has had little effect on the mortality associated with an acute myocardial infarction. It is reasonable to assume that in placing a greater emphasis on insuring that patients are ready to leave the hospital, we can improve mortality and morbidity of both the ACS and heart failure patient. There really is no urgency to discharge patients other than improving the bottom line, and that imperative may no longer be relevant.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
Rehospitalization within 30 days of an initial acute coronary syndrome or heart failure event has now become a CMS quality measure that will affect overall hospital Medicare payments. It has been appreciated for some time that rehospitalization for these diagnoses has been unacceptably high.
A recent report indicates that a greater percentage of U.S. patients who experienced a STEMI are more likely to be rehospitalized within 30 days, compared with other Western countries (14.5% vs. 9.9%, respectively). That report (JAMA 2012;307:66-74) indicates that the increase is directly related to the shorter length of hospital stay in the United States. Among the 17 countries included in the report, the average duration was shortest in the United States (3 days) and longest in Germany (8 days). Predictors of readmission other than length of stay include the age of the patient and the presence of heart failure. The most interesting part of the story is how we arrived at this state of affairs.
For those of you who were not yet born or are too young to remember when Medicare was passed into law in 1965, I will give you a little history. And for those of you who were around at the time, I will provide a reminder.
As you undoubtedly know, Medicare, in addition to paying physicians’ fees also pays hospital costs. In the period between 1965 and 1983, using a payment system that was defined as "reasonable and allowable costs," Medicare payments to hospitals increased 10-fold, from $3 billion to $37 billion. In consequence, Congress passed a law in 1982 that created a prospective payment system for hospitals using diagnosis-related groups establishing a payment schedule for specific diagnoses, which included acute myocardial infarction and heart failure. With this schedule, hospitals were paid a fixed rate regardless of the number of procedures performed or duration of hospitalization. In order to minimize costs, hospitals accelerated discharges and shortened hospital length of stay. Emergency admissions resulted in urgent discharge.
In order to expedite the process of admission and discharge, hospitalists were hired to accelerate that process since practicing internists and cardiologists were not available to push the paperwork through fast enough to get the patients discharged quickly. Hospitals saw this additional layer of doctors caring for patients as financially profitable. As a result, hospital stays decreased markedly and payments to hospitals decreased by 52% from 1985 to 1990 and by an additional 37% between 1990 and 1995. Everyone seemed to be very happy with this, including the hospitals, Medicare, and doctors. As far as I know, patients were not consulted.
Cardiologists at that time were telling themselves how benign an acute MI is and began doing accelerated discharge after percutaneous coronary intervention. We prided ourselves on how patients could be discharged to home within 24-36 hours, but never actually reached the ultimate goal of a "drive-through PCI." The fact that patients with acute MI and heart failure were frequently readmitted was good business since each admission resulted in further Medicare payments both to the hospital and the doctors. Urging by some physicians to develop plans that could educate patients and develop discharge follow-up systems was met with incredulity by hospital administrators who saw readmission as a revenue source and discharge planning as costly.
It is important to emphasize that readmission not only reflects an important morbidity event, it also carries with it the potential for increased risk of mortality. In the report cited above, one-third of the deaths after hospitalization for a STEMI occurred within the same 30-day post-event period. The recent emphasis on decreasing door-to-balloon time, although effective in shortening that period, has had little effect on the mortality associated with an acute myocardial infarction. It is reasonable to assume that in placing a greater emphasis on insuring that patients are ready to leave the hospital, we can improve mortality and morbidity of both the ACS and heart failure patient. There really is no urgency to discharge patients other than improving the bottom line, and that imperative may no longer be relevant.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
When Veins Fail, Go to Bone
NATIONAL HARBOR, MD. – When a child needs fluids or drugs but you can’t find a good vein, turn to bone.
Intraosseous (IO) access was pioneered during World War I, and it’s aged well – although peripheral IVs pushed it out of the limelight for several decades. But IO access remains the standard of care in emergency situations where IVs can’t be used, Dr. Angela Ellison said at a meeting sponsored by the American College of Emergency Physicians.

A 1988 review of 33 pediatric cardiac arrests showed that IO is the quickest way to go. Although a successful IO attempt took about 5 minutes, compared with 3 minutes for a peripheral IV, the success rate for an IO placement was much greater – 83% vs. 17%, said Dr. Ellison of the University of Pennsylvania, Philadelphia (Am. J. Emerg. Med. 1988;6:577-9).
"In difficult cases, the investigators recommended that IV attempts be very brief, and if unsuccessful, you should move on to IO right away," she said.
IO access works for children of all sizes, even newborns, she said, and in children with all kinds of emergencies, including shock, trauma, status epilepticus, and severe dehydration. IO access can be established by emergency medical technicians and nurses as well as physicians. With a preprocedural shot of lidocaine, IO catheters can easily be placed in conscious as well as unconscious patients.
For patients who need drugs urgently, IO is superior to IV; animal studies have shown that drugs reach the heart in 10-20 seconds, and there is no need to change the dose from a normal IV concentration.
Technical advances have made IO access easier, she added. "Over the past few decades, we’ve gotten a number of powered devices that have contributed to the rise of IO." Some can be placed in the sternum and others in long bones. Studies have shown that the complication rate is not increased when the needles are placed near a growth plate.
IO access is not for everyone or every bone, however. Contraindications include long bone fracture, vascular injury in the extremity, an overlying skin infection, a burn at the access site, 10 or more previous placements or attempts, and fragile bones (osteogenesis imperfecta or osteoporosis).
For the most part, however, IO access is very safe. Studies conducted in the late 1980s and early 1990s show an overall complication rate of less than 1%. Osteomyelitis occurred in 0.6%, and cellulitis or skin abscess developed in 0.7%. No evidence of bone deformity or growth arrest was seen in long-term follow-up studies.
Dr. Ellison had no financial conflicts.
Intraosseous (IO) access, peripheral IVs, IVs can’t be used, Dr. Angela Ellison, American College of Emergency Physicians, pediatric cardiac arrests, shock, trauma, status epilepticus, severe dehydration, preprocedural shot of lidocaine, IO catheters, IO superior to IV, sternum, long bones, safety of IO
NATIONAL HARBOR, MD. – When a child needs fluids or drugs but you can’t find a good vein, turn to bone.
Intraosseous (IO) access was pioneered during World War I, and it’s aged well – although peripheral IVs pushed it out of the limelight for several decades. But IO access remains the standard of care in emergency situations where IVs can’t be used, Dr. Angela Ellison said at a meeting sponsored by the American College of Emergency Physicians.
A 1988 review of 33 pediatric cardiac arrests showed that IO is the quickest way to go. Although a successful IO attempt took about 5 minutes, compared with 3 minutes for a peripheral IV, the success rate for an IO placement was much greater – 83% vs. 17%, said Dr. Ellison of the University of Pennsylvania, Philadelphia (Am. J. Emerg. Med. 1988;6:577-9).
"In difficult cases, the investigators recommended that IV attempts be very brief, and if unsuccessful, you should move on to IO right away," she said.
IO access works for children of all sizes, even newborns, she said, and in children with all kinds of emergencies, including shock, trauma, status epilepticus, and severe dehydration. IO access can be established by emergency medical technicians and nurses as well as physicians. With a preprocedural shot of lidocaine, IO catheters can easily be placed in conscious as well as unconscious patients.
For patients who need drugs urgently, IO is superior to IV; animal studies have shown that drugs reach the heart in 10-20 seconds, and there is no need to change the dose from a normal IV concentration.
Technical advances have made IO access easier, she added. "Over the past few decades, we’ve gotten a number of powered devices that have contributed to the rise of IO." Some can be placed in the sternum and others in long bones. Studies have shown that the complication rate is not increased when the needles are placed near a growth plate.
IO access is not for everyone or every bone, however. Contraindications include long bone fracture, vascular injury in the extremity, an overlying skin infection, a burn at the access site, 10 or more previous placements or attempts, and fragile bones (osteogenesis imperfecta or osteoporosis).
For the most part, however, IO access is very safe. Studies conducted in the late 1980s and early 1990s show an overall complication rate of less than 1%. Osteomyelitis occurred in 0.6%, and cellulitis or skin abscess developed in 0.7%. No evidence of bone deformity or growth arrest was seen in long-term follow-up studies.
Dr. Ellison had no financial conflicts.
NATIONAL HARBOR, MD. – When a child needs fluids or drugs but you can’t find a good vein, turn to bone.
Intraosseous (IO) access was pioneered during World War I, and it’s aged well – although peripheral IVs pushed it out of the limelight for several decades. But IO access remains the standard of care in emergency situations where IVs can’t be used, Dr. Angela Ellison said at a meeting sponsored by the American College of Emergency Physicians.
A 1988 review of 33 pediatric cardiac arrests showed that IO is the quickest way to go. Although a successful IO attempt took about 5 minutes, compared with 3 minutes for a peripheral IV, the success rate for an IO placement was much greater – 83% vs. 17%, said Dr. Ellison of the University of Pennsylvania, Philadelphia (Am. J. Emerg. Med. 1988;6:577-9).
"In difficult cases, the investigators recommended that IV attempts be very brief, and if unsuccessful, you should move on to IO right away," she said.
IO access works for children of all sizes, even newborns, she said, and in children with all kinds of emergencies, including shock, trauma, status epilepticus, and severe dehydration. IO access can be established by emergency medical technicians and nurses as well as physicians. With a preprocedural shot of lidocaine, IO catheters can easily be placed in conscious as well as unconscious patients.
For patients who need drugs urgently, IO is superior to IV; animal studies have shown that drugs reach the heart in 10-20 seconds, and there is no need to change the dose from a normal IV concentration.
Technical advances have made IO access easier, she added. "Over the past few decades, we’ve gotten a number of powered devices that have contributed to the rise of IO." Some can be placed in the sternum and others in long bones. Studies have shown that the complication rate is not increased when the needles are placed near a growth plate.
IO access is not for everyone or every bone, however. Contraindications include long bone fracture, vascular injury in the extremity, an overlying skin infection, a burn at the access site, 10 or more previous placements or attempts, and fragile bones (osteogenesis imperfecta or osteoporosis).
For the most part, however, IO access is very safe. Studies conducted in the late 1980s and early 1990s show an overall complication rate of less than 1%. Osteomyelitis occurred in 0.6%, and cellulitis or skin abscess developed in 0.7%. No evidence of bone deformity or growth arrest was seen in long-term follow-up studies.
Dr. Ellison had no financial conflicts.
Intraosseous (IO) access, peripheral IVs, IVs can’t be used, Dr. Angela Ellison, American College of Emergency Physicians, pediatric cardiac arrests, shock, trauma, status epilepticus, severe dehydration, preprocedural shot of lidocaine, IO catheters, IO superior to IV, sternum, long bones, safety of IO
Intraosseous (IO) access, peripheral IVs, IVs can’t be used, Dr. Angela Ellison, American College of Emergency Physicians, pediatric cardiac arrests, shock, trauma, status epilepticus, severe dehydration, preprocedural shot of lidocaine, IO catheters, IO superior to IV, sternum, long bones, safety of IO
FROM A MEETING SPONSORED BY THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
Jeffrey Glasheen, New SHM Board Member, Committed to Raising Quality of Care
Although based in an academic hospital program at the University of Colorado Denver, new SHM board member Jeffrey Glasheen, MD, SFHM, does not view himself as representative of only academic hospitalist groups on the board.
"I'd like to say I represent the constituency that cares about the quality, safety, and efficiency of healthcare delivery—and that includes every hospitalist,” says Dr. Glasheen, who has played major roles in developing SHM's Academic Hospitalist Academy and Academic Hospital Medicine Leadership Summit, and now chairs its Academic Committee.
Dr. Glasheen, who recently resigned as physician editor of the The Hospitalist is a senior deputy editor of the Journal of Hospital Medicine and was course director of HM12 in San Diego earlier this month. He intends to "push the envelope" for quality issues in his service on the board. "Quality is the best conceivable care you can provide, and clearly, where we are today is not there yet," he says.
Dr. Glasheen, who is committed to giving hospitalists the skills they need to elevate the quality of hospital care, says that starts with redesigning residency programs and medical school curriculums to teach quality improvement (QI). He believes that payment and healthcare reform will put hospitalists in a great position to serve as their hospitals' quality leaders, "but it's also going to take inspired leadership," he says. Hospitalists and hospitals need to make quality a major priority, which he recognizes is hard to do when groups are understaffed. As such, he hopes to find solutions to HM's pipeline issues—how to fill the hospitalist positions that will be needed in the future.
"I've been blessed in my situation [at my institution] to have an administration that's really supportive of hospital medicine," he says. "Our administration really gets the value equation, and we as hospitalists do, too. But as I travel around the country, I don't always see that."
Although based in an academic hospital program at the University of Colorado Denver, new SHM board member Jeffrey Glasheen, MD, SFHM, does not view himself as representative of only academic hospitalist groups on the board.
"I'd like to say I represent the constituency that cares about the quality, safety, and efficiency of healthcare delivery—and that includes every hospitalist,” says Dr. Glasheen, who has played major roles in developing SHM's Academic Hospitalist Academy and Academic Hospital Medicine Leadership Summit, and now chairs its Academic Committee.
Dr. Glasheen, who recently resigned as physician editor of the The Hospitalist is a senior deputy editor of the Journal of Hospital Medicine and was course director of HM12 in San Diego earlier this month. He intends to "push the envelope" for quality issues in his service on the board. "Quality is the best conceivable care you can provide, and clearly, where we are today is not there yet," he says.
Dr. Glasheen, who is committed to giving hospitalists the skills they need to elevate the quality of hospital care, says that starts with redesigning residency programs and medical school curriculums to teach quality improvement (QI). He believes that payment and healthcare reform will put hospitalists in a great position to serve as their hospitals' quality leaders, "but it's also going to take inspired leadership," he says. Hospitalists and hospitals need to make quality a major priority, which he recognizes is hard to do when groups are understaffed. As such, he hopes to find solutions to HM's pipeline issues—how to fill the hospitalist positions that will be needed in the future.
"I've been blessed in my situation [at my institution] to have an administration that's really supportive of hospital medicine," he says. "Our administration really gets the value equation, and we as hospitalists do, too. But as I travel around the country, I don't always see that."
Although based in an academic hospital program at the University of Colorado Denver, new SHM board member Jeffrey Glasheen, MD, SFHM, does not view himself as representative of only academic hospitalist groups on the board.
"I'd like to say I represent the constituency that cares about the quality, safety, and efficiency of healthcare delivery—and that includes every hospitalist,” says Dr. Glasheen, who has played major roles in developing SHM's Academic Hospitalist Academy and Academic Hospital Medicine Leadership Summit, and now chairs its Academic Committee.
Dr. Glasheen, who recently resigned as physician editor of the The Hospitalist is a senior deputy editor of the Journal of Hospital Medicine and was course director of HM12 in San Diego earlier this month. He intends to "push the envelope" for quality issues in his service on the board. "Quality is the best conceivable care you can provide, and clearly, where we are today is not there yet," he says.
Dr. Glasheen, who is committed to giving hospitalists the skills they need to elevate the quality of hospital care, says that starts with redesigning residency programs and medical school curriculums to teach quality improvement (QI). He believes that payment and healthcare reform will put hospitalists in a great position to serve as their hospitals' quality leaders, "but it's also going to take inspired leadership," he says. Hospitalists and hospitals need to make quality a major priority, which he recognizes is hard to do when groups are understaffed. As such, he hopes to find solutions to HM's pipeline issues—how to fill the hospitalist positions that will be needed in the future.
"I've been blessed in my situation [at my institution] to have an administration that's really supportive of hospital medicine," he says. "Our administration really gets the value equation, and we as hospitalists do, too. But as I travel around the country, I don't always see that."
HM Tool Designed to Pinpoint Program Strengths, Weaknesses
The creators of the first measurement tool for hospitalist programs hope that it becomes a standardized gauge for HM practice performance.
The Greeno-Hawley Hospital Medicine Index, unveiled earlier this month by Cogent HMG, uses a 26-question survey to measure HM group performance in five categories: alignment, performance management, infrastructure, operational processes, and leadership and people. The score will offer HM leaders a perspective on where their group stands in comparison with other hospitalist programs.
"It's meant to be a snapshot in time," says Beth Hawley, MBA, FACHE, Cogent's chief customer experience officer, who helped develop the index with Ron Greeno, MD, MHM, the company's chief medical officer. It is intended to help programs pinpoint the areas on which they need to focus in order to improve their performance, she says.
The index will be formally demonstrated at the American College of Physician Executives meeting April 30 in San Francisco. It will be available online in May.
Hawley says that once programs begin using the index, Cogent can assimilate and review the data to determine whether the tool can serve as a predictive model. Until then, it can be a guidepost for practice improvement for HM leaders who have never before had comparative tools.
"People would sit there thinking they're doing a great job but they only know their little market or their hospital," she says, "and really don’t see the broad picture of where hospital medicine is going and what a hospital medicine program can do for a hospital."
The creators of the first measurement tool for hospitalist programs hope that it becomes a standardized gauge for HM practice performance.
The Greeno-Hawley Hospital Medicine Index, unveiled earlier this month by Cogent HMG, uses a 26-question survey to measure HM group performance in five categories: alignment, performance management, infrastructure, operational processes, and leadership and people. The score will offer HM leaders a perspective on where their group stands in comparison with other hospitalist programs.
"It's meant to be a snapshot in time," says Beth Hawley, MBA, FACHE, Cogent's chief customer experience officer, who helped develop the index with Ron Greeno, MD, MHM, the company's chief medical officer. It is intended to help programs pinpoint the areas on which they need to focus in order to improve their performance, she says.
The index will be formally demonstrated at the American College of Physician Executives meeting April 30 in San Francisco. It will be available online in May.
Hawley says that once programs begin using the index, Cogent can assimilate and review the data to determine whether the tool can serve as a predictive model. Until then, it can be a guidepost for practice improvement for HM leaders who have never before had comparative tools.
"People would sit there thinking they're doing a great job but they only know their little market or their hospital," she says, "and really don’t see the broad picture of where hospital medicine is going and what a hospital medicine program can do for a hospital."
The creators of the first measurement tool for hospitalist programs hope that it becomes a standardized gauge for HM practice performance.
The Greeno-Hawley Hospital Medicine Index, unveiled earlier this month by Cogent HMG, uses a 26-question survey to measure HM group performance in five categories: alignment, performance management, infrastructure, operational processes, and leadership and people. The score will offer HM leaders a perspective on where their group stands in comparison with other hospitalist programs.
"It's meant to be a snapshot in time," says Beth Hawley, MBA, FACHE, Cogent's chief customer experience officer, who helped develop the index with Ron Greeno, MD, MHM, the company's chief medical officer. It is intended to help programs pinpoint the areas on which they need to focus in order to improve their performance, she says.
The index will be formally demonstrated at the American College of Physician Executives meeting April 30 in San Francisco. It will be available online in May.
Hawley says that once programs begin using the index, Cogent can assimilate and review the data to determine whether the tool can serve as a predictive model. Until then, it can be a guidepost for practice improvement for HM leaders who have never before had comparative tools.
"People would sit there thinking they're doing a great job but they only know their little market or their hospital," she says, "and really don’t see the broad picture of where hospital medicine is going and what a hospital medicine program can do for a hospital."
Kids' Deadly Unintentional Injuries Drop 30%
Fewer children died from unintentional injuries between 2000 and 2009, but death rates from suffocation and poisoning increased, according to a report from the Centers for Disease Control and Prevention.
The overall death rate from unintentional injuries among children dropped by nearly 30% during the 10-year period, according to an analysis of national mortality data. There were 9,143 childhood deaths from unintentional injuries in 2009, down from 12,441 in 2000. Yet, that’s about one child death per hour caused by unintentional injury, whether it’s a traffic crash, drowning, poisoning, or fire.

"One child’s death is still one too many," said Ileana Arias, Ph.D., principal deputy director at CDC, in a news conference. "We know most of these events are predictable and preventable."
Traffic crashes were the leading cause of death among children and adolescents (4,564 deaths), followed by suffocation (1,160), drowning (983), poisoning (824), fire/burn (391), and falls (151), according to the report.
Despite a drop in most of the mechanisms, the authors noted the increase in poisoning and suffocation death rates.
There was a 91% increase in poisoning death rate among adolescents aged 15-19 years over the 10-year period. The authors attributed the rise to prescription drug overdoses. Painkillers seem to be replacing marijuana as a gateway drug, said Dr. Arias.
"Strategies to reduce the misuse of prescription drugs include appropriate prescribing, proper storage and disposal, discouraging medication sharing, and state-based prescription drug monitoring programs," the report’s authors wrote (MMWR 2012;61:1-7).
Also, unintentional infant suffocation rates increased 54% between 2000 and 2009. The increase "underscores the importance of safe sleeping environments as recommended by the American Academy of Pediatrics, which includes supine positioning, a firm sleep surface, room-sharing without bed-sharing, and avoiding loose bedding," the investigators noted.
There was nearly a 41% decrease in deaths from traffic crashes during the 10-year-period, which could be due to several factors, including improvements in seat belt use, child safety seat and booster seat use, licensing requirements, and vehicle design, according to the report.
Drowning deaths decreased 28%; deaths from fire/burn decreased 45%, and deaths from accidental falls dropped 19%.
Despite the declines, injury remains the leading cause of death among children in the United States. The nation also ranks worst among all high-income countries when it comes to injury deaths among 0 to 14-year-olds, according to the CDC report, which is the first of its kind to describe trends among 0 to 19-year-olds by mechanism and by state.
Unintentional injury rates varied widely among states, suggesting that "environment, exposure to hazards, and difference in public policy might play a role," the authors wrote. The variation also "demonstrated that it is possible to prevent these injuries," said Dr. Arias. Massachusetts had the lowest unintentional injury death rate (4/100,000), and Mississippi had the highest (25.1/100,000).
The report is based on analysis of national mortality data collected in the CDC’s National Vital Statistics Systems.
The authors said the report has at least two limitations. First, the report is based on death certificate data, which are subject to misclassification errors. In addition, the report is limited to unintentional injury deaths and excludes nonfatal injuries. Thus, it underreports "the total burden from injury on the society and the medical care system."
CDC officials and their partners released the National Action Plan for Child Injury Prevention along with this report, hoping that the plan’s implementation "could result in significant reductions in needless deaths, injuries, and costs associated with injuries among children and adolescents in the United States."
Fewer children died from unintentional injuries between 2000 and 2009, but death rates from suffocation and poisoning increased, according to a report from the Centers for Disease Control and Prevention.
The overall death rate from unintentional injuries among children dropped by nearly 30% during the 10-year period, according to an analysis of national mortality data. There were 9,143 childhood deaths from unintentional injuries in 2009, down from 12,441 in 2000. Yet, that’s about one child death per hour caused by unintentional injury, whether it’s a traffic crash, drowning, poisoning, or fire.
"One child’s death is still one too many," said Ileana Arias, Ph.D., principal deputy director at CDC, in a news conference. "We know most of these events are predictable and preventable."
Traffic crashes were the leading cause of death among children and adolescents (4,564 deaths), followed by suffocation (1,160), drowning (983), poisoning (824), fire/burn (391), and falls (151), according to the report.
Despite a drop in most of the mechanisms, the authors noted the increase in poisoning and suffocation death rates.
There was a 91% increase in poisoning death rate among adolescents aged 15-19 years over the 10-year period. The authors attributed the rise to prescription drug overdoses. Painkillers seem to be replacing marijuana as a gateway drug, said Dr. Arias.
"Strategies to reduce the misuse of prescription drugs include appropriate prescribing, proper storage and disposal, discouraging medication sharing, and state-based prescription drug monitoring programs," the report’s authors wrote (MMWR 2012;61:1-7).
Also, unintentional infant suffocation rates increased 54% between 2000 and 2009. The increase "underscores the importance of safe sleeping environments as recommended by the American Academy of Pediatrics, which includes supine positioning, a firm sleep surface, room-sharing without bed-sharing, and avoiding loose bedding," the investigators noted.
There was nearly a 41% decrease in deaths from traffic crashes during the 10-year-period, which could be due to several factors, including improvements in seat belt use, child safety seat and booster seat use, licensing requirements, and vehicle design, according to the report.
Drowning deaths decreased 28%; deaths from fire/burn decreased 45%, and deaths from accidental falls dropped 19%.
Despite the declines, injury remains the leading cause of death among children in the United States. The nation also ranks worst among all high-income countries when it comes to injury deaths among 0 to 14-year-olds, according to the CDC report, which is the first of its kind to describe trends among 0 to 19-year-olds by mechanism and by state.
Unintentional injury rates varied widely among states, suggesting that "environment, exposure to hazards, and difference in public policy might play a role," the authors wrote. The variation also "demonstrated that it is possible to prevent these injuries," said Dr. Arias. Massachusetts had the lowest unintentional injury death rate (4/100,000), and Mississippi had the highest (25.1/100,000).
The report is based on analysis of national mortality data collected in the CDC’s National Vital Statistics Systems.
The authors said the report has at least two limitations. First, the report is based on death certificate data, which are subject to misclassification errors. In addition, the report is limited to unintentional injury deaths and excludes nonfatal injuries. Thus, it underreports "the total burden from injury on the society and the medical care system."
CDC officials and their partners released the National Action Plan for Child Injury Prevention along with this report, hoping that the plan’s implementation "could result in significant reductions in needless deaths, injuries, and costs associated with injuries among children and adolescents in the United States."
Fewer children died from unintentional injuries between 2000 and 2009, but death rates from suffocation and poisoning increased, according to a report from the Centers for Disease Control and Prevention.
The overall death rate from unintentional injuries among children dropped by nearly 30% during the 10-year period, according to an analysis of national mortality data. There were 9,143 childhood deaths from unintentional injuries in 2009, down from 12,441 in 2000. Yet, that’s about one child death per hour caused by unintentional injury, whether it’s a traffic crash, drowning, poisoning, or fire.
"One child’s death is still one too many," said Ileana Arias, Ph.D., principal deputy director at CDC, in a news conference. "We know most of these events are predictable and preventable."
Traffic crashes were the leading cause of death among children and adolescents (4,564 deaths), followed by suffocation (1,160), drowning (983), poisoning (824), fire/burn (391), and falls (151), according to the report.
Despite a drop in most of the mechanisms, the authors noted the increase in poisoning and suffocation death rates.
There was a 91% increase in poisoning death rate among adolescents aged 15-19 years over the 10-year period. The authors attributed the rise to prescription drug overdoses. Painkillers seem to be replacing marijuana as a gateway drug, said Dr. Arias.
"Strategies to reduce the misuse of prescription drugs include appropriate prescribing, proper storage and disposal, discouraging medication sharing, and state-based prescription drug monitoring programs," the report’s authors wrote (MMWR 2012;61:1-7).
Also, unintentional infant suffocation rates increased 54% between 2000 and 2009. The increase "underscores the importance of safe sleeping environments as recommended by the American Academy of Pediatrics, which includes supine positioning, a firm sleep surface, room-sharing without bed-sharing, and avoiding loose bedding," the investigators noted.
There was nearly a 41% decrease in deaths from traffic crashes during the 10-year-period, which could be due to several factors, including improvements in seat belt use, child safety seat and booster seat use, licensing requirements, and vehicle design, according to the report.
Drowning deaths decreased 28%; deaths from fire/burn decreased 45%, and deaths from accidental falls dropped 19%.
Despite the declines, injury remains the leading cause of death among children in the United States. The nation also ranks worst among all high-income countries when it comes to injury deaths among 0 to 14-year-olds, according to the CDC report, which is the first of its kind to describe trends among 0 to 19-year-olds by mechanism and by state.
Unintentional injury rates varied widely among states, suggesting that "environment, exposure to hazards, and difference in public policy might play a role," the authors wrote. The variation also "demonstrated that it is possible to prevent these injuries," said Dr. Arias. Massachusetts had the lowest unintentional injury death rate (4/100,000), and Mississippi had the highest (25.1/100,000).
The report is based on analysis of national mortality data collected in the CDC’s National Vital Statistics Systems.
The authors said the report has at least two limitations. First, the report is based on death certificate data, which are subject to misclassification errors. In addition, the report is limited to unintentional injury deaths and excludes nonfatal injuries. Thus, it underreports "the total burden from injury on the society and the medical care system."
CDC officials and their partners released the National Action Plan for Child Injury Prevention along with this report, hoping that the plan’s implementation "could result in significant reductions in needless deaths, injuries, and costs associated with injuries among children and adolescents in the United States."
FROM THE CENTERS FOR DISEASE CONTROL AND PREVENTION VITAL SIGNS REPORT
Major Finding: The overall death rate from unintentional injuries among children dropped by nearly 30% during the 10-year period, but death rate from poisoning and suffocation increased in subgroups.
Data Source: Based on analysis of national mortality data collected in the CDC’s National Vital Statistics Systems.
Disclosures: None.

Men, women, and migraine: The role of sex, hormones, obesity, and PTSD
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
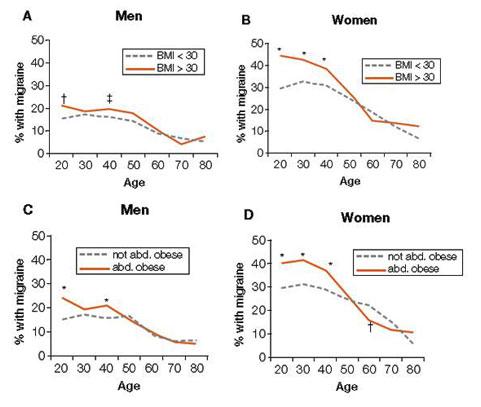
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
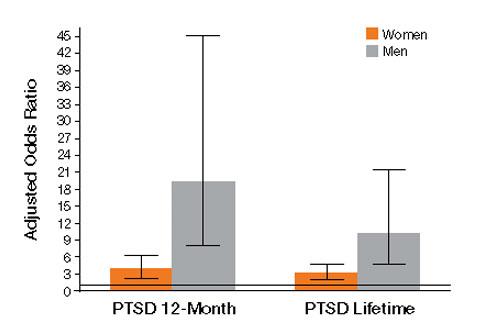
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.