User login
What I Learned

As I write, I’m fighting the jet stream from Washington, D.C., to Denver, midflight on my return from HM10. I’m 30,000 feet above the ground—literally and figuratively—my mind spinning with the thoughts, ideas, and memories from the largest gathering of hospitalists ever. In the end, 2,500 hospitalists descended on our nation’s capital. Shrouded by the din of healthcare reform, we discussed, deliberated, and discovered what’s new in the clinical, political, and programmatic world of HM. Out of this churn, I learned a lot. Here’s but a small sample.
Smart People = Smart Solutions
I learned that if you put really smart people in a room and give them a problem to grapple with, they come up with really smart solutions. At the inaugural Academic Hospital Medicine Leadership Summit, 100 of the brightest, most influential academic hospitalists convened to tackle the problems facing our field.
The output was an amazing crop of inventive ideas aimed at taming the vexing issues surrounding clinical sustainability, academic viability, and career satisfaction. SHM leadership has heard the cry and promises to work closely with the academic community to transform these smart solutions into future initiatives.
Hospitalists Support Healthcare Reform, Should Collude with Hospitals
I learned that most of us support the recently passed healthcare reform legislation, with a few notable dissenters. In response to a question from the chair of SHM’s Public Policy Committee, the vast majority of attendees at the opening plenary session raised their hands affirmatively in response to the question of whether they support the reform bill. Meanwhile, nearly everyone in the crowd felt it is important that SHM have an opinion regarding the legislation and continue to work closely with Congress to ensure its implementation helps our most important constituent—our patients.
Finally, I learned that Ron Greeno, CMO of Brentwood, Tenn.-based Cogent Healthcare, believes that the development of accountable-care organizations might lead hospitalists to align with hospitals to keep costs down. In fact, he saw this as a welcome, intended consequence. In his opinion, this “collusion” promises to raise the quality of care and reduce waste in the system—a statement that was met with applause from the plenary crowd.
The Healthcare Paradox
I learned that blogs save lives. Paul Levy, CEO of Beth Israel Deaconess Medical Center in Boston, roused the crowd during his keynote address by relating the power of transparency. Bothered by the paradox that the medical profession, comprising the most well-intentioned people in the world, could kill so many people through errors (ranked the No. 4 public health hazard in the U.S.), Levy decided to make his hospital’s struggles public.
On his blog, Running a Hospital (runningahospital.blogspot.com), he took the extraordinary step of publically documenting the rates of harm caused at his medical center for the world to see. Additionally, he set audacious goals to reduce the amount of harm to zero. He encouraged hospital staff to raise issues of safety and efficiency as a way to avoid the workarounds—shortcuts—that ultimately increase variability and reduce quality without addressing the core problem.
In response, the staff swarms the problem to rapidly improve the process and ultimately return the system back to homeostasis. The results of this effort can be viewed at Levy’s hospital’s website (www.bidmc.org/QualityandSafety.aspx).
Which Hill Will You Climb?
I learned that leadership is the ability to help people address problems that make the world better. At a much-anticipated presentation, Peter Pronovost, MD, of Johns Hopkins Hospital in Baltimore related a transformative story from his youth. At a summer camp, each boy was assigned to one of three groups and tasked with climbing a seemingly insurmountable hill. The first camp counselor pummeled the group with overbearing directions, directives, and derision, and in the end the group failed to conquer the hill. The second counselor took a more relaxed approach, giving the group essentially no direction. They, too, failed.
The final counselor offered nothing but the inspiration of how marvelous the view from the top of the hill would be and how they’d all have to pull together and work as a team if they wanted to attain that greatness. Dr. Pronovost was in this last group, and has been summiting insurmountable peaks ever since.
You likely are familiar with Dr. Pronovost’s work on ICU line infections. He elaborated on how he accomplished a rate of zero line infections, first at his hospital and then throughout the entire state of Michigan. The key was an inspiring vision and, once again, removal of workarounds. After compiling a checklist of the five most crucial components of line placement and management, Hopkins personnel discovered they were only compliant with the checklist 30% of the time—mostly due to shortcuts caused by inefficient systems that placed supplies too far from the clinical-care setting. After removing those barriers, the compliance rate went to 70%. It was only after empowering the nursing staff to stop physicians from proceeding with line placement unless the checklist was followed that the team was able to achieve 100% compliance.
Today, patients in the Johns Hopkins cardiovascular unit have not suffered a line infection for 87 consecutive weeks. That’s a hill worth climbing.
Saving Lives and Canine Castaways
I learned that the SHM annual meeting is attracting the highest echelon of clinical speakers. Whether it was Dr. Pronovost speaking about line infections, Dr. Greg Fonarow discussing congestive heart failure, or Dr. John Bartlett presenting on Clostrium difficile infections, HM10 featured world-class speakers.
For example, Dr. Bartlett’s work has defined the C. diff field, and the opportunity to hear him was incredible. I learned from him that severe C. diff infections are on the rise and that recurrences are tougher than ever to treat. I also learned that there are mixed data on whether nurses can detect C. diff based on stool smell alone; that up to 10% of dogs carry C. diff (out of the bed, Hogan and Grady!); and that stool transplants are becoming a quality- and quantity-of-life-saving treatment for those with severe bouts of recurrent C. diff.
To quote Dr. Bartlett, “pathophysiologically, it’s a dream; aesthetically, it sucks.”
Homeward Bound
Finally, I learned that every year, SHM feels more and more like my second family, with the annual meeting its family reunion. I saw tons of friends, made dozens more, and look forward to next year in Dallas.
Mostly, however, I was reminded of the emotional tug of being away from home, the emotive power of a few e-mailed photos of your kids, and how great if feels to turn off your electronic devices and return your folding tray and seat back to the upright and locked position. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
As I write, I’m fighting the jet stream from Washington, D.C., to Denver, midflight on my return from HM10. I’m 30,000 feet above the ground—literally and figuratively—my mind spinning with the thoughts, ideas, and memories from the largest gathering of hospitalists ever. In the end, 2,500 hospitalists descended on our nation’s capital. Shrouded by the din of healthcare reform, we discussed, deliberated, and discovered what’s new in the clinical, political, and programmatic world of HM. Out of this churn, I learned a lot. Here’s but a small sample.
Smart People = Smart Solutions
I learned that if you put really smart people in a room and give them a problem to grapple with, they come up with really smart solutions. At the inaugural Academic Hospital Medicine Leadership Summit, 100 of the brightest, most influential academic hospitalists convened to tackle the problems facing our field.
The output was an amazing crop of inventive ideas aimed at taming the vexing issues surrounding clinical sustainability, academic viability, and career satisfaction. SHM leadership has heard the cry and promises to work closely with the academic community to transform these smart solutions into future initiatives.
Hospitalists Support Healthcare Reform, Should Collude with Hospitals
I learned that most of us support the recently passed healthcare reform legislation, with a few notable dissenters. In response to a question from the chair of SHM’s Public Policy Committee, the vast majority of attendees at the opening plenary session raised their hands affirmatively in response to the question of whether they support the reform bill. Meanwhile, nearly everyone in the crowd felt it is important that SHM have an opinion regarding the legislation and continue to work closely with Congress to ensure its implementation helps our most important constituent—our patients.
Finally, I learned that Ron Greeno, CMO of Brentwood, Tenn.-based Cogent Healthcare, believes that the development of accountable-care organizations might lead hospitalists to align with hospitals to keep costs down. In fact, he saw this as a welcome, intended consequence. In his opinion, this “collusion” promises to raise the quality of care and reduce waste in the system—a statement that was met with applause from the plenary crowd.
The Healthcare Paradox
I learned that blogs save lives. Paul Levy, CEO of Beth Israel Deaconess Medical Center in Boston, roused the crowd during his keynote address by relating the power of transparency. Bothered by the paradox that the medical profession, comprising the most well-intentioned people in the world, could kill so many people through errors (ranked the No. 4 public health hazard in the U.S.), Levy decided to make his hospital’s struggles public.
On his blog, Running a Hospital (runningahospital.blogspot.com), he took the extraordinary step of publically documenting the rates of harm caused at his medical center for the world to see. Additionally, he set audacious goals to reduce the amount of harm to zero. He encouraged hospital staff to raise issues of safety and efficiency as a way to avoid the workarounds—shortcuts—that ultimately increase variability and reduce quality without addressing the core problem.
In response, the staff swarms the problem to rapidly improve the process and ultimately return the system back to homeostasis. The results of this effort can be viewed at Levy’s hospital’s website (www.bidmc.org/QualityandSafety.aspx).
Which Hill Will You Climb?
I learned that leadership is the ability to help people address problems that make the world better. At a much-anticipated presentation, Peter Pronovost, MD, of Johns Hopkins Hospital in Baltimore related a transformative story from his youth. At a summer camp, each boy was assigned to one of three groups and tasked with climbing a seemingly insurmountable hill. The first camp counselor pummeled the group with overbearing directions, directives, and derision, and in the end the group failed to conquer the hill. The second counselor took a more relaxed approach, giving the group essentially no direction. They, too, failed.
The final counselor offered nothing but the inspiration of how marvelous the view from the top of the hill would be and how they’d all have to pull together and work as a team if they wanted to attain that greatness. Dr. Pronovost was in this last group, and has been summiting insurmountable peaks ever since.
You likely are familiar with Dr. Pronovost’s work on ICU line infections. He elaborated on how he accomplished a rate of zero line infections, first at his hospital and then throughout the entire state of Michigan. The key was an inspiring vision and, once again, removal of workarounds. After compiling a checklist of the five most crucial components of line placement and management, Hopkins personnel discovered they were only compliant with the checklist 30% of the time—mostly due to shortcuts caused by inefficient systems that placed supplies too far from the clinical-care setting. After removing those barriers, the compliance rate went to 70%. It was only after empowering the nursing staff to stop physicians from proceeding with line placement unless the checklist was followed that the team was able to achieve 100% compliance.
Today, patients in the Johns Hopkins cardiovascular unit have not suffered a line infection for 87 consecutive weeks. That’s a hill worth climbing.
Saving Lives and Canine Castaways
I learned that the SHM annual meeting is attracting the highest echelon of clinical speakers. Whether it was Dr. Pronovost speaking about line infections, Dr. Greg Fonarow discussing congestive heart failure, or Dr. John Bartlett presenting on Clostrium difficile infections, HM10 featured world-class speakers.
For example, Dr. Bartlett’s work has defined the C. diff field, and the opportunity to hear him was incredible. I learned from him that severe C. diff infections are on the rise and that recurrences are tougher than ever to treat. I also learned that there are mixed data on whether nurses can detect C. diff based on stool smell alone; that up to 10% of dogs carry C. diff (out of the bed, Hogan and Grady!); and that stool transplants are becoming a quality- and quantity-of-life-saving treatment for those with severe bouts of recurrent C. diff.
To quote Dr. Bartlett, “pathophysiologically, it’s a dream; aesthetically, it sucks.”
Homeward Bound
Finally, I learned that every year, SHM feels more and more like my second family, with the annual meeting its family reunion. I saw tons of friends, made dozens more, and look forward to next year in Dallas.
Mostly, however, I was reminded of the emotional tug of being away from home, the emotive power of a few e-mailed photos of your kids, and how great if feels to turn off your electronic devices and return your folding tray and seat back to the upright and locked position. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
As I write, I’m fighting the jet stream from Washington, D.C., to Denver, midflight on my return from HM10. I’m 30,000 feet above the ground—literally and figuratively—my mind spinning with the thoughts, ideas, and memories from the largest gathering of hospitalists ever. In the end, 2,500 hospitalists descended on our nation’s capital. Shrouded by the din of healthcare reform, we discussed, deliberated, and discovered what’s new in the clinical, political, and programmatic world of HM. Out of this churn, I learned a lot. Here’s but a small sample.
Smart People = Smart Solutions
I learned that if you put really smart people in a room and give them a problem to grapple with, they come up with really smart solutions. At the inaugural Academic Hospital Medicine Leadership Summit, 100 of the brightest, most influential academic hospitalists convened to tackle the problems facing our field.
The output was an amazing crop of inventive ideas aimed at taming the vexing issues surrounding clinical sustainability, academic viability, and career satisfaction. SHM leadership has heard the cry and promises to work closely with the academic community to transform these smart solutions into future initiatives.
Hospitalists Support Healthcare Reform, Should Collude with Hospitals
I learned that most of us support the recently passed healthcare reform legislation, with a few notable dissenters. In response to a question from the chair of SHM’s Public Policy Committee, the vast majority of attendees at the opening plenary session raised their hands affirmatively in response to the question of whether they support the reform bill. Meanwhile, nearly everyone in the crowd felt it is important that SHM have an opinion regarding the legislation and continue to work closely with Congress to ensure its implementation helps our most important constituent—our patients.
Finally, I learned that Ron Greeno, CMO of Brentwood, Tenn.-based Cogent Healthcare, believes that the development of accountable-care organizations might lead hospitalists to align with hospitals to keep costs down. In fact, he saw this as a welcome, intended consequence. In his opinion, this “collusion” promises to raise the quality of care and reduce waste in the system—a statement that was met with applause from the plenary crowd.
The Healthcare Paradox
I learned that blogs save lives. Paul Levy, CEO of Beth Israel Deaconess Medical Center in Boston, roused the crowd during his keynote address by relating the power of transparency. Bothered by the paradox that the medical profession, comprising the most well-intentioned people in the world, could kill so many people through errors (ranked the No. 4 public health hazard in the U.S.), Levy decided to make his hospital’s struggles public.
On his blog, Running a Hospital (runningahospital.blogspot.com), he took the extraordinary step of publically documenting the rates of harm caused at his medical center for the world to see. Additionally, he set audacious goals to reduce the amount of harm to zero. He encouraged hospital staff to raise issues of safety and efficiency as a way to avoid the workarounds—shortcuts—that ultimately increase variability and reduce quality without addressing the core problem.
In response, the staff swarms the problem to rapidly improve the process and ultimately return the system back to homeostasis. The results of this effort can be viewed at Levy’s hospital’s website (www.bidmc.org/QualityandSafety.aspx).
Which Hill Will You Climb?
I learned that leadership is the ability to help people address problems that make the world better. At a much-anticipated presentation, Peter Pronovost, MD, of Johns Hopkins Hospital in Baltimore related a transformative story from his youth. At a summer camp, each boy was assigned to one of three groups and tasked with climbing a seemingly insurmountable hill. The first camp counselor pummeled the group with overbearing directions, directives, and derision, and in the end the group failed to conquer the hill. The second counselor took a more relaxed approach, giving the group essentially no direction. They, too, failed.
The final counselor offered nothing but the inspiration of how marvelous the view from the top of the hill would be and how they’d all have to pull together and work as a team if they wanted to attain that greatness. Dr. Pronovost was in this last group, and has been summiting insurmountable peaks ever since.
You likely are familiar with Dr. Pronovost’s work on ICU line infections. He elaborated on how he accomplished a rate of zero line infections, first at his hospital and then throughout the entire state of Michigan. The key was an inspiring vision and, once again, removal of workarounds. After compiling a checklist of the five most crucial components of line placement and management, Hopkins personnel discovered they were only compliant with the checklist 30% of the time—mostly due to shortcuts caused by inefficient systems that placed supplies too far from the clinical-care setting. After removing those barriers, the compliance rate went to 70%. It was only after empowering the nursing staff to stop physicians from proceeding with line placement unless the checklist was followed that the team was able to achieve 100% compliance.
Today, patients in the Johns Hopkins cardiovascular unit have not suffered a line infection for 87 consecutive weeks. That’s a hill worth climbing.
Saving Lives and Canine Castaways
I learned that the SHM annual meeting is attracting the highest echelon of clinical speakers. Whether it was Dr. Pronovost speaking about line infections, Dr. Greg Fonarow discussing congestive heart failure, or Dr. John Bartlett presenting on Clostrium difficile infections, HM10 featured world-class speakers.
For example, Dr. Bartlett’s work has defined the C. diff field, and the opportunity to hear him was incredible. I learned from him that severe C. diff infections are on the rise and that recurrences are tougher than ever to treat. I also learned that there are mixed data on whether nurses can detect C. diff based on stool smell alone; that up to 10% of dogs carry C. diff (out of the bed, Hogan and Grady!); and that stool transplants are becoming a quality- and quantity-of-life-saving treatment for those with severe bouts of recurrent C. diff.
To quote Dr. Bartlett, “pathophysiologically, it’s a dream; aesthetically, it sucks.”
Homeward Bound
Finally, I learned that every year, SHM feels more and more like my second family, with the annual meeting its family reunion. I saw tons of friends, made dozens more, and look forward to next year in Dallas.
Mostly, however, I was reminded of the emotional tug of being away from home, the emotive power of a few e-mailed photos of your kids, and how great if feels to turn off your electronic devices and return your folding tray and seat back to the upright and locked position. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
The Earlier, the Better

Most hospitals work hard to increase the portion of discharges that occur early in the workday and decrease the number that occur in the afternoon or evening. In every case, hospitalists have an important role in making this happen.
In my April 2009 column (“Top O’ the Morning,” p. 53), I wrote about why this is important to hospitals and which strategies hospitalists could adopt. But this is still such a big issue for hospitalists that I thought I would elaborate on a few of the really simple ideas. Your HM group could implement most of the following strategies beginning next week, and you wouldn’t need months of meetings with other hospital departments.
But before I get to the ideas, I want to mention a couple of other things. First, I can’t resist pointing out that giving hospitalists a financial incentive for writing the majority of discharge orders by a certain time in the morning has met with mixed results, despite the fact that some institutions believe this approach is valuable. In the absence of computerized physician order entry (CPOE), it can be really difficult to track exactly when the doctor wrote the discharge order. And, more importantly, a financial incentive might discourage a hospitalist from discharging a patient this afternoon, and they might instead wait to discharge tomorrow morning—adding to length of stay and defeating the goal of the incentive.
It turns out that a lot has been written about throughput; just do an Internet search and pair “throughput” with terms like “hospital,” “hospitalist,” “ED,” etc. Remarkably, I haven’t been able to dig up much material that specifically addresses early-morning discharges, which is an important component of throughput.
Let’s turn our attention to some specific recommendations for increasing morning discharges. Remember, I’ve selected these because they’re easy to implement and won’t require HM groups to negotiate with others at the hospital.
Write “Probable Discharge Tomorrow” Orders
Letting other staff know the anticipated discharge date via an order in the chart typically is more effective than writing the same information in the progress note section of the chart. Although a hospitalist should verbally communicate the anticipated discharge date with the patient’s nurse and discharge planner, it still is worthwhile to write an order, because it increases the chance all, or nearly all, staff (e.g., night nurses) will be aware of the plan and communicate the same message to the family.
Your group could establish a rule or financial incentive, such that all charts will be reviewed after discharge, and a certain portion (e.g., 85%) must have such an order written sometime prior to discharge. It doesn’t always need to be written on the day prior to discharge; instead, an order written on Monday could say “likely discharge on Wednesday or Thursday.” And, of course, there shouldn’t be a requirement that the patient actually be discharged on the day that was forecast.
Prepare the Day Prior
Typically, hospitalized-patient discharges are very time-consuming. Most discharges are complicated by last-minute medical or social loose ends that require attention. Routinely trying to uncover and address these on the evening prior to discharge will ensure that a larger percentage of patients will be discharged—and vacate their room—earlier the next day. Here is what this might look like:
On Tuesday, Dr. Guaraldi is wrapping up most work for the day. He stops by to see his patient, Mr. Schultz, to see if he is improving as expected. Indeed, Mr. Schultz is looking better and probably will be ready for discharge Wednesday morning. So, Dr. Guaraldi talks with Mr. Schultz and calls the patient’s daughter to answer any questions and concerns, ensuring no surprises by the Wednesday-morning discharge. When the daughter asks (as nearly all family members do) what time she should plan to pick up her dad, Dr. Guaraldi can suggest a time based on when he will be able to round in the morning. He also can arrange to have the discharge planning staff alerted if there are more complicated issues (e.g., arranging for professional transport home).
Dr. Guaraldi then dictates the discharge summary, addresses the discharge medicine reconciliation, and writes the prescriptions. In doing so, he might uncover some loose ends and might end up ordering a lab or imaging test to be done in the evening so the results will be available early Wednesday morning and won’t delay the routine discharge.
On Wednesday morning, Dr. Guaraldi rounds on Mr. Schultz early, finds the patient is improving as expected, and writes the discharge order. The whole visit takes only a few minutes, as most of the time-consuming work was completed the prior evening. In fact, because it is a relatively short visit, it is a lot easier for Dr. Guaraldi to arrange to round on Mr. Schultz early in the day (e.g., even on the way to see ICU patients), as the hospital’s chief medical officer is always asking him to do.
I hope this scenario doesn’t sound too difficult. (Another benefit of dictating discharge summaries the evening before discharge is that the typed document should be available the next morning, so the patient can have a copy to take with him at discharge.) Of course, it won’t apply to all patients, such as those patients whose discharges can’t be predicted.
Many hospitalists think arranging for discharge the evening before is impossible because “I’m just too spent at the end of a long day to stay late getting patients ready for discharge tomorrow!” But realize you won’t be doing any more work; you’re rearranging when you do the work. The time you spend arranging for discharge in advance will save you time and stress tomorrow. My own experience is that it is much easier to do all the discharge work the evening before than in the morning when I’m so busy and am being pulled in 10 different directions. Most morning discharge visits are relatively quick and painless, which is really valuable for increasing the efficiency and decreasing the stress of morning rounds.
The alert reader already has figured out there is a pretty big cost to doing the discharge work the evening before. Some patients won’t be able to discharge as planned (e.g., they have a fever overnight) and the preparations will have been in vain. My experience is that such “failed” discharges are reasonably common, but even when they occur, it is usually reasonable to use most of the original prescriptions and discharge summary, with an addendum as required. For example, Dr. Guaraldi could dictate an addendum stating:
“The patient originally was planned for discharge on Wednesday but had a temperature of 38.6 degrees Celsius the night before, so stayed in the hospital for two more days for … ”
Start Rounds Earlier
This strategy might be the most difficult for you and your HM group to arrange, but I propose it because you could do it without having to negotiate with a lot of other departments in the hospital. If your group currently has a day shift that starts at 8 a.m. with a team conference, you could instead start at 7 a.m. Your group could try to shorten the duration of the morning team conference, or eliminate it. Whether the need to get patients discharged early in the day is worth the complexity of rearranging your schedule will depend on the circumstances of your hospital and your group. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Most hospitals work hard to increase the portion of discharges that occur early in the workday and decrease the number that occur in the afternoon or evening. In every case, hospitalists have an important role in making this happen.
In my April 2009 column (“Top O’ the Morning,” p. 53), I wrote about why this is important to hospitals and which strategies hospitalists could adopt. But this is still such a big issue for hospitalists that I thought I would elaborate on a few of the really simple ideas. Your HM group could implement most of the following strategies beginning next week, and you wouldn’t need months of meetings with other hospital departments.
But before I get to the ideas, I want to mention a couple of other things. First, I can’t resist pointing out that giving hospitalists a financial incentive for writing the majority of discharge orders by a certain time in the morning has met with mixed results, despite the fact that some institutions believe this approach is valuable. In the absence of computerized physician order entry (CPOE), it can be really difficult to track exactly when the doctor wrote the discharge order. And, more importantly, a financial incentive might discourage a hospitalist from discharging a patient this afternoon, and they might instead wait to discharge tomorrow morning—adding to length of stay and defeating the goal of the incentive.
It turns out that a lot has been written about throughput; just do an Internet search and pair “throughput” with terms like “hospital,” “hospitalist,” “ED,” etc. Remarkably, I haven’t been able to dig up much material that specifically addresses early-morning discharges, which is an important component of throughput.
Let’s turn our attention to some specific recommendations for increasing morning discharges. Remember, I’ve selected these because they’re easy to implement and won’t require HM groups to negotiate with others at the hospital.
Write “Probable Discharge Tomorrow” Orders
Letting other staff know the anticipated discharge date via an order in the chart typically is more effective than writing the same information in the progress note section of the chart. Although a hospitalist should verbally communicate the anticipated discharge date with the patient’s nurse and discharge planner, it still is worthwhile to write an order, because it increases the chance all, or nearly all, staff (e.g., night nurses) will be aware of the plan and communicate the same message to the family.
Your group could establish a rule or financial incentive, such that all charts will be reviewed after discharge, and a certain portion (e.g., 85%) must have such an order written sometime prior to discharge. It doesn’t always need to be written on the day prior to discharge; instead, an order written on Monday could say “likely discharge on Wednesday or Thursday.” And, of course, there shouldn’t be a requirement that the patient actually be discharged on the day that was forecast.
Prepare the Day Prior
Typically, hospitalized-patient discharges are very time-consuming. Most discharges are complicated by last-minute medical or social loose ends that require attention. Routinely trying to uncover and address these on the evening prior to discharge will ensure that a larger percentage of patients will be discharged—and vacate their room—earlier the next day. Here is what this might look like:
On Tuesday, Dr. Guaraldi is wrapping up most work for the day. He stops by to see his patient, Mr. Schultz, to see if he is improving as expected. Indeed, Mr. Schultz is looking better and probably will be ready for discharge Wednesday morning. So, Dr. Guaraldi talks with Mr. Schultz and calls the patient’s daughter to answer any questions and concerns, ensuring no surprises by the Wednesday-morning discharge. When the daughter asks (as nearly all family members do) what time she should plan to pick up her dad, Dr. Guaraldi can suggest a time based on when he will be able to round in the morning. He also can arrange to have the discharge planning staff alerted if there are more complicated issues (e.g., arranging for professional transport home).
Dr. Guaraldi then dictates the discharge summary, addresses the discharge medicine reconciliation, and writes the prescriptions. In doing so, he might uncover some loose ends and might end up ordering a lab or imaging test to be done in the evening so the results will be available early Wednesday morning and won’t delay the routine discharge.
On Wednesday morning, Dr. Guaraldi rounds on Mr. Schultz early, finds the patient is improving as expected, and writes the discharge order. The whole visit takes only a few minutes, as most of the time-consuming work was completed the prior evening. In fact, because it is a relatively short visit, it is a lot easier for Dr. Guaraldi to arrange to round on Mr. Schultz early in the day (e.g., even on the way to see ICU patients), as the hospital’s chief medical officer is always asking him to do.
I hope this scenario doesn’t sound too difficult. (Another benefit of dictating discharge summaries the evening before discharge is that the typed document should be available the next morning, so the patient can have a copy to take with him at discharge.) Of course, it won’t apply to all patients, such as those patients whose discharges can’t be predicted.
Many hospitalists think arranging for discharge the evening before is impossible because “I’m just too spent at the end of a long day to stay late getting patients ready for discharge tomorrow!” But realize you won’t be doing any more work; you’re rearranging when you do the work. The time you spend arranging for discharge in advance will save you time and stress tomorrow. My own experience is that it is much easier to do all the discharge work the evening before than in the morning when I’m so busy and am being pulled in 10 different directions. Most morning discharge visits are relatively quick and painless, which is really valuable for increasing the efficiency and decreasing the stress of morning rounds.
The alert reader already has figured out there is a pretty big cost to doing the discharge work the evening before. Some patients won’t be able to discharge as planned (e.g., they have a fever overnight) and the preparations will have been in vain. My experience is that such “failed” discharges are reasonably common, but even when they occur, it is usually reasonable to use most of the original prescriptions and discharge summary, with an addendum as required. For example, Dr. Guaraldi could dictate an addendum stating:
“The patient originally was planned for discharge on Wednesday but had a temperature of 38.6 degrees Celsius the night before, so stayed in the hospital for two more days for … ”
Start Rounds Earlier
This strategy might be the most difficult for you and your HM group to arrange, but I propose it because you could do it without having to negotiate with a lot of other departments in the hospital. If your group currently has a day shift that starts at 8 a.m. with a team conference, you could instead start at 7 a.m. Your group could try to shorten the duration of the morning team conference, or eliminate it. Whether the need to get patients discharged early in the day is worth the complexity of rearranging your schedule will depend on the circumstances of your hospital and your group. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Most hospitals work hard to increase the portion of discharges that occur early in the workday and decrease the number that occur in the afternoon or evening. In every case, hospitalists have an important role in making this happen.
In my April 2009 column (“Top O’ the Morning,” p. 53), I wrote about why this is important to hospitals and which strategies hospitalists could adopt. But this is still such a big issue for hospitalists that I thought I would elaborate on a few of the really simple ideas. Your HM group could implement most of the following strategies beginning next week, and you wouldn’t need months of meetings with other hospital departments.
But before I get to the ideas, I want to mention a couple of other things. First, I can’t resist pointing out that giving hospitalists a financial incentive for writing the majority of discharge orders by a certain time in the morning has met with mixed results, despite the fact that some institutions believe this approach is valuable. In the absence of computerized physician order entry (CPOE), it can be really difficult to track exactly when the doctor wrote the discharge order. And, more importantly, a financial incentive might discourage a hospitalist from discharging a patient this afternoon, and they might instead wait to discharge tomorrow morning—adding to length of stay and defeating the goal of the incentive.
It turns out that a lot has been written about throughput; just do an Internet search and pair “throughput” with terms like “hospital,” “hospitalist,” “ED,” etc. Remarkably, I haven’t been able to dig up much material that specifically addresses early-morning discharges, which is an important component of throughput.
Let’s turn our attention to some specific recommendations for increasing morning discharges. Remember, I’ve selected these because they’re easy to implement and won’t require HM groups to negotiate with others at the hospital.
Write “Probable Discharge Tomorrow” Orders
Letting other staff know the anticipated discharge date via an order in the chart typically is more effective than writing the same information in the progress note section of the chart. Although a hospitalist should verbally communicate the anticipated discharge date with the patient’s nurse and discharge planner, it still is worthwhile to write an order, because it increases the chance all, or nearly all, staff (e.g., night nurses) will be aware of the plan and communicate the same message to the family.
Your group could establish a rule or financial incentive, such that all charts will be reviewed after discharge, and a certain portion (e.g., 85%) must have such an order written sometime prior to discharge. It doesn’t always need to be written on the day prior to discharge; instead, an order written on Monday could say “likely discharge on Wednesday or Thursday.” And, of course, there shouldn’t be a requirement that the patient actually be discharged on the day that was forecast.
Prepare the Day Prior
Typically, hospitalized-patient discharges are very time-consuming. Most discharges are complicated by last-minute medical or social loose ends that require attention. Routinely trying to uncover and address these on the evening prior to discharge will ensure that a larger percentage of patients will be discharged—and vacate their room—earlier the next day. Here is what this might look like:
On Tuesday, Dr. Guaraldi is wrapping up most work for the day. He stops by to see his patient, Mr. Schultz, to see if he is improving as expected. Indeed, Mr. Schultz is looking better and probably will be ready for discharge Wednesday morning. So, Dr. Guaraldi talks with Mr. Schultz and calls the patient’s daughter to answer any questions and concerns, ensuring no surprises by the Wednesday-morning discharge. When the daughter asks (as nearly all family members do) what time she should plan to pick up her dad, Dr. Guaraldi can suggest a time based on when he will be able to round in the morning. He also can arrange to have the discharge planning staff alerted if there are more complicated issues (e.g., arranging for professional transport home).
Dr. Guaraldi then dictates the discharge summary, addresses the discharge medicine reconciliation, and writes the prescriptions. In doing so, he might uncover some loose ends and might end up ordering a lab or imaging test to be done in the evening so the results will be available early Wednesday morning and won’t delay the routine discharge.
On Wednesday morning, Dr. Guaraldi rounds on Mr. Schultz early, finds the patient is improving as expected, and writes the discharge order. The whole visit takes only a few minutes, as most of the time-consuming work was completed the prior evening. In fact, because it is a relatively short visit, it is a lot easier for Dr. Guaraldi to arrange to round on Mr. Schultz early in the day (e.g., even on the way to see ICU patients), as the hospital’s chief medical officer is always asking him to do.
I hope this scenario doesn’t sound too difficult. (Another benefit of dictating discharge summaries the evening before discharge is that the typed document should be available the next morning, so the patient can have a copy to take with him at discharge.) Of course, it won’t apply to all patients, such as those patients whose discharges can’t be predicted.
Many hospitalists think arranging for discharge the evening before is impossible because “I’m just too spent at the end of a long day to stay late getting patients ready for discharge tomorrow!” But realize you won’t be doing any more work; you’re rearranging when you do the work. The time you spend arranging for discharge in advance will save you time and stress tomorrow. My own experience is that it is much easier to do all the discharge work the evening before than in the morning when I’m so busy and am being pulled in 10 different directions. Most morning discharge visits are relatively quick and painless, which is really valuable for increasing the efficiency and decreasing the stress of morning rounds.
The alert reader already has figured out there is a pretty big cost to doing the discharge work the evening before. Some patients won’t be able to discharge as planned (e.g., they have a fever overnight) and the preparations will have been in vain. My experience is that such “failed” discharges are reasonably common, but even when they occur, it is usually reasonable to use most of the original prescriptions and discharge summary, with an addendum as required. For example, Dr. Guaraldi could dictate an addendum stating:
“The patient originally was planned for discharge on Wednesday but had a temperature of 38.6 degrees Celsius the night before, so stayed in the hospital for two more days for … ”
Start Rounds Earlier
This strategy might be the most difficult for you and your HM group to arrange, but I propose it because you could do it without having to negotiate with a lot of other departments in the hospital. If your group currently has a day shift that starts at 8 a.m. with a team conference, you could instead start at 7 a.m. Your group could try to shorten the duration of the morning team conference, or eliminate it. Whether the need to get patients discharged early in the day is worth the complexity of rearranging your schedule will depend on the circumstances of your hospital and your group. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Physicians Could Be Eligible to Receive IRS Refund

Physicians Could Be Eligible to Receive IRS Refund
I heard the Internal Revenue Service is going to refund the employment taxes physicians paid when they were residents. Is this true? If so, how do I go about filing for this?
J. Byrne, MD
New YorkRe
Dr. Hospitalist responds: On March 2, the IRS announced that it had “made an administrative determination to accept the position that medical residents are excepted from FICA taxes based on the student exception for tax periods ending before April 1, 2005, when new IRS regulations went into effect.”1 For folks like me, who have a hard time understanding the different numbers on my paycheck, here is an explanation. (I am neither an attorney nor an accountant; for any such counsel, I suggest you visit a professional.)
Federal Insurance Contributions Act, or FICA, taxes are the payroll taxes collected for Medicare and Social Security programs. These taxes fund insurance programs for the elderly, disabled, survivors (Social Security), and for healthcare (Medicare). This tax originated in 1935. Employees and employers are required to make regular contributions to FICA through payroll deductions. For 2010, the FICA tax rate is 7.65% (6.2% for Social Security and 1.45% for Medicare) on gross earnings (earnings before any deductions). The individual contribution limit for the Social Security program is 6.2% of wages up to $106,800 (a $6,621.60 cap per individual). Unlike Social Security, there is no cap on contributions to the Medicare program. Individuals and employers each contribute 1.45% of wages earned (for a total of 2.9%) to fund the Medicare program.
House staff traditionally participate in this government insurance program by contributing FICA taxes. But in the 1990s, employers and individuals began filing FICA refund claims to the IRS based on the student exception (Internal Revenue Code section 3121(b)(10)). It is my understanding that this section of the IRS code exempts students from the FICA tax.
So are house staff recognized as students under the eyes of the law? In the 1998 court case State of Minnesota vs. Apfel, the court opined that University of Minnesota house staff exist for the primary purpose of education, rather than for earning a livelihood. Based on that ruling, the IRS chief counsel issued a memorandum in July 2000 that stated house staff could meet the FICA student exemption if 1) the house staff’s employer is a school, and 2) the house staffer is considered a student by the employer.
So why has it taken so long for the IRS to decide to refund these dollars? Over the past decade, there have been other court cases with conflicting interpretations of the IRS code. In January 2005, the IRS implemented new regulations that did not require house staff to contribute FICA taxes. But this new regulation did nothing about past house-staff contributions. Last year, in another Minnesota case, Mayo Foundation for Medical Education and Research vs. the United States, the court again interpreted the IRS regulations as limiting the student FICA exception to students who are not full-time employees. Despite other ongoing lawsuits, the IRS has decided that individuals who were house staff prior to April 2005 and meet the criteria are excepted from FICA taxes.
So who is eligible to receive these FICA taxes refund? It is my understanding that if you are a house officer who contributed to FICA taxes prior to April 2005, you are eligible for a refund only if you or the institution where you trained filed a claim in a timely fashion. The period of limitation for filing a claim has expired. If you think that you are covered by a claim, the IRS states that you should expect to hear from the institution where you trained about the refund process. You will not be hearing from the IRS directly.
For more information, call 800-919-1703 or visit www.irs.gov/charities and click on “Medical Resident FICA Refund.”
Is the Economy Having a Negative Effect on Hospitalist Jobs?
I will start my senior year as a medical resident in a few months. I am interested in a career as a hospitalist. While I hear that there are a lot of hospitalists out there, one of my friends has been looking for a hospitalist job in the Northeast and has had some difficulty landing a position. Is the problem the area or the economy? Is there anything I can do to make myself a more attractive candidate?
Reza Mohan, MD
Seattle
Dr. Hospitalist responds: Congratul-ations on reaching this stage in your training as a physician; this is the time you can start thinking about your career as a hospitalist. While I understand your desire to land a plum job upon completion of training, I want to encourage you to focus your efforts during your last year of training. Becoming the best doctor possible might be the best preparation to land the ideal HM job.
It is true that since 1996, when the term “hospitalist” was first coined, it has been easy to land HM jobs. The field exploded out of nowhere, and now boasts more than 30,000 hospitalists after little more than a decade. Atlanta, Boston, San Diego, Seattle … hospitalist jobs were plentiful.
While it has been good for physicians looking for jobs, I am not sure it has been ideal for patients. I would argue that the easy availability of jobs has attracted people to our profession who probably are not ideally suited to be hospitalists. From a quality perspective, wouldn’t we be better off if there were more competition for hospitalist jobs? In fact, I am hearing talk from colleagues around the country that there are a few places where it is increasingly more difficult to land a hospitalist job. Seattle and Boston are two such places.
That said, one only has to look at the job ads in the preceding pages of The Hospitalist and the SHM Career Center (www.hospitalmedicine.org/careers) to see that HM jobs are still plentiful in most parts of the country. I would not worry about not being able to land a job as a hospitalist when you finish training. However, you might not be able to find a great job in the city of your choice.
If you are interested in networking, I encourage you to speak with HM physicians at your hospital and in your community. Don’t pass up the opportunity to attend a local SHM chapter meeting or a regional conference; both are great for connecting with hospitalists and hiring managers. Another option is to sign up with an SHM e-mail listserv, so you have the opportunity to participate in online discussions with hospitalists. TH
Reference
- IRS to honor medical resident FICA refund claims. IRS Web site. Available at www.irs.gov/charities/article/ 0,,id=219548,00.html. Published March 2, 2010. Accessed April 14, 2010.
Physicians Could Be Eligible to Receive IRS Refund
I heard the Internal Revenue Service is going to refund the employment taxes physicians paid when they were residents. Is this true? If so, how do I go about filing for this?
J. Byrne, MD
New YorkRe
Dr. Hospitalist responds: On March 2, the IRS announced that it had “made an administrative determination to accept the position that medical residents are excepted from FICA taxes based on the student exception for tax periods ending before April 1, 2005, when new IRS regulations went into effect.”1 For folks like me, who have a hard time understanding the different numbers on my paycheck, here is an explanation. (I am neither an attorney nor an accountant; for any such counsel, I suggest you visit a professional.)
Federal Insurance Contributions Act, or FICA, taxes are the payroll taxes collected for Medicare and Social Security programs. These taxes fund insurance programs for the elderly, disabled, survivors (Social Security), and for healthcare (Medicare). This tax originated in 1935. Employees and employers are required to make regular contributions to FICA through payroll deductions. For 2010, the FICA tax rate is 7.65% (6.2% for Social Security and 1.45% for Medicare) on gross earnings (earnings before any deductions). The individual contribution limit for the Social Security program is 6.2% of wages up to $106,800 (a $6,621.60 cap per individual). Unlike Social Security, there is no cap on contributions to the Medicare program. Individuals and employers each contribute 1.45% of wages earned (for a total of 2.9%) to fund the Medicare program.
House staff traditionally participate in this government insurance program by contributing FICA taxes. But in the 1990s, employers and individuals began filing FICA refund claims to the IRS based on the student exception (Internal Revenue Code section 3121(b)(10)). It is my understanding that this section of the IRS code exempts students from the FICA tax.
So are house staff recognized as students under the eyes of the law? In the 1998 court case State of Minnesota vs. Apfel, the court opined that University of Minnesota house staff exist for the primary purpose of education, rather than for earning a livelihood. Based on that ruling, the IRS chief counsel issued a memorandum in July 2000 that stated house staff could meet the FICA student exemption if 1) the house staff’s employer is a school, and 2) the house staffer is considered a student by the employer.
So why has it taken so long for the IRS to decide to refund these dollars? Over the past decade, there have been other court cases with conflicting interpretations of the IRS code. In January 2005, the IRS implemented new regulations that did not require house staff to contribute FICA taxes. But this new regulation did nothing about past house-staff contributions. Last year, in another Minnesota case, Mayo Foundation for Medical Education and Research vs. the United States, the court again interpreted the IRS regulations as limiting the student FICA exception to students who are not full-time employees. Despite other ongoing lawsuits, the IRS has decided that individuals who were house staff prior to April 2005 and meet the criteria are excepted from FICA taxes.
So who is eligible to receive these FICA taxes refund? It is my understanding that if you are a house officer who contributed to FICA taxes prior to April 2005, you are eligible for a refund only if you or the institution where you trained filed a claim in a timely fashion. The period of limitation for filing a claim has expired. If you think that you are covered by a claim, the IRS states that you should expect to hear from the institution where you trained about the refund process. You will not be hearing from the IRS directly.
For more information, call 800-919-1703 or visit www.irs.gov/charities and click on “Medical Resident FICA Refund.”
Is the Economy Having a Negative Effect on Hospitalist Jobs?
I will start my senior year as a medical resident in a few months. I am interested in a career as a hospitalist. While I hear that there are a lot of hospitalists out there, one of my friends has been looking for a hospitalist job in the Northeast and has had some difficulty landing a position. Is the problem the area or the economy? Is there anything I can do to make myself a more attractive candidate?
Reza Mohan, MD
Seattle
Dr. Hospitalist responds: Congratul-ations on reaching this stage in your training as a physician; this is the time you can start thinking about your career as a hospitalist. While I understand your desire to land a plum job upon completion of training, I want to encourage you to focus your efforts during your last year of training. Becoming the best doctor possible might be the best preparation to land the ideal HM job.
It is true that since 1996, when the term “hospitalist” was first coined, it has been easy to land HM jobs. The field exploded out of nowhere, and now boasts more than 30,000 hospitalists after little more than a decade. Atlanta, Boston, San Diego, Seattle … hospitalist jobs were plentiful.
While it has been good for physicians looking for jobs, I am not sure it has been ideal for patients. I would argue that the easy availability of jobs has attracted people to our profession who probably are not ideally suited to be hospitalists. From a quality perspective, wouldn’t we be better off if there were more competition for hospitalist jobs? In fact, I am hearing talk from colleagues around the country that there are a few places where it is increasingly more difficult to land a hospitalist job. Seattle and Boston are two such places.
That said, one only has to look at the job ads in the preceding pages of The Hospitalist and the SHM Career Center (www.hospitalmedicine.org/careers) to see that HM jobs are still plentiful in most parts of the country. I would not worry about not being able to land a job as a hospitalist when you finish training. However, you might not be able to find a great job in the city of your choice.
If you are interested in networking, I encourage you to speak with HM physicians at your hospital and in your community. Don’t pass up the opportunity to attend a local SHM chapter meeting or a regional conference; both are great for connecting with hospitalists and hiring managers. Another option is to sign up with an SHM e-mail listserv, so you have the opportunity to participate in online discussions with hospitalists. TH
Reference
- IRS to honor medical resident FICA refund claims. IRS Web site. Available at www.irs.gov/charities/article/ 0,,id=219548,00.html. Published March 2, 2010. Accessed April 14, 2010.
Physicians Could Be Eligible to Receive IRS Refund
I heard the Internal Revenue Service is going to refund the employment taxes physicians paid when they were residents. Is this true? If so, how do I go about filing for this?
J. Byrne, MD
New YorkRe
Dr. Hospitalist responds: On March 2, the IRS announced that it had “made an administrative determination to accept the position that medical residents are excepted from FICA taxes based on the student exception for tax periods ending before April 1, 2005, when new IRS regulations went into effect.”1 For folks like me, who have a hard time understanding the different numbers on my paycheck, here is an explanation. (I am neither an attorney nor an accountant; for any such counsel, I suggest you visit a professional.)
Federal Insurance Contributions Act, or FICA, taxes are the payroll taxes collected for Medicare and Social Security programs. These taxes fund insurance programs for the elderly, disabled, survivors (Social Security), and for healthcare (Medicare). This tax originated in 1935. Employees and employers are required to make regular contributions to FICA through payroll deductions. For 2010, the FICA tax rate is 7.65% (6.2% for Social Security and 1.45% for Medicare) on gross earnings (earnings before any deductions). The individual contribution limit for the Social Security program is 6.2% of wages up to $106,800 (a $6,621.60 cap per individual). Unlike Social Security, there is no cap on contributions to the Medicare program. Individuals and employers each contribute 1.45% of wages earned (for a total of 2.9%) to fund the Medicare program.
House staff traditionally participate in this government insurance program by contributing FICA taxes. But in the 1990s, employers and individuals began filing FICA refund claims to the IRS based on the student exception (Internal Revenue Code section 3121(b)(10)). It is my understanding that this section of the IRS code exempts students from the FICA tax.
So are house staff recognized as students under the eyes of the law? In the 1998 court case State of Minnesota vs. Apfel, the court opined that University of Minnesota house staff exist for the primary purpose of education, rather than for earning a livelihood. Based on that ruling, the IRS chief counsel issued a memorandum in July 2000 that stated house staff could meet the FICA student exemption if 1) the house staff’s employer is a school, and 2) the house staffer is considered a student by the employer.
So why has it taken so long for the IRS to decide to refund these dollars? Over the past decade, there have been other court cases with conflicting interpretations of the IRS code. In January 2005, the IRS implemented new regulations that did not require house staff to contribute FICA taxes. But this new regulation did nothing about past house-staff contributions. Last year, in another Minnesota case, Mayo Foundation for Medical Education and Research vs. the United States, the court again interpreted the IRS regulations as limiting the student FICA exception to students who are not full-time employees. Despite other ongoing lawsuits, the IRS has decided that individuals who were house staff prior to April 2005 and meet the criteria are excepted from FICA taxes.
So who is eligible to receive these FICA taxes refund? It is my understanding that if you are a house officer who contributed to FICA taxes prior to April 2005, you are eligible for a refund only if you or the institution where you trained filed a claim in a timely fashion. The period of limitation for filing a claim has expired. If you think that you are covered by a claim, the IRS states that you should expect to hear from the institution where you trained about the refund process. You will not be hearing from the IRS directly.
For more information, call 800-919-1703 or visit www.irs.gov/charities and click on “Medical Resident FICA Refund.”
Is the Economy Having a Negative Effect on Hospitalist Jobs?
I will start my senior year as a medical resident in a few months. I am interested in a career as a hospitalist. While I hear that there are a lot of hospitalists out there, one of my friends has been looking for a hospitalist job in the Northeast and has had some difficulty landing a position. Is the problem the area or the economy? Is there anything I can do to make myself a more attractive candidate?
Reza Mohan, MD
Seattle
Dr. Hospitalist responds: Congratul-ations on reaching this stage in your training as a physician; this is the time you can start thinking about your career as a hospitalist. While I understand your desire to land a plum job upon completion of training, I want to encourage you to focus your efforts during your last year of training. Becoming the best doctor possible might be the best preparation to land the ideal HM job.
It is true that since 1996, when the term “hospitalist” was first coined, it has been easy to land HM jobs. The field exploded out of nowhere, and now boasts more than 30,000 hospitalists after little more than a decade. Atlanta, Boston, San Diego, Seattle … hospitalist jobs were plentiful.
While it has been good for physicians looking for jobs, I am not sure it has been ideal for patients. I would argue that the easy availability of jobs has attracted people to our profession who probably are not ideally suited to be hospitalists. From a quality perspective, wouldn’t we be better off if there were more competition for hospitalist jobs? In fact, I am hearing talk from colleagues around the country that there are a few places where it is increasingly more difficult to land a hospitalist job. Seattle and Boston are two such places.
That said, one only has to look at the job ads in the preceding pages of The Hospitalist and the SHM Career Center (www.hospitalmedicine.org/careers) to see that HM jobs are still plentiful in most parts of the country. I would not worry about not being able to land a job as a hospitalist when you finish training. However, you might not be able to find a great job in the city of your choice.
If you are interested in networking, I encourage you to speak with HM physicians at your hospital and in your community. Don’t pass up the opportunity to attend a local SHM chapter meeting or a regional conference; both are great for connecting with hospitalists and hiring managers. Another option is to sign up with an SHM e-mail listserv, so you have the opportunity to participate in online discussions with hospitalists. TH
Reference
- IRS to honor medical resident FICA refund claims. IRS Web site. Available at www.irs.gov/charities/article/ 0,,id=219548,00.html. Published March 2, 2010. Accessed April 14, 2010.
2010 HM Awards Winners
Awards of Excellence
Award for Excellence in Teamwork in Quality Improvement
The Emory University Hospital Healthcare Team, co-led by Jason Stein, MD, FHM, Carolyn Hill, RN, Laura Phillips, and Dee Cantrell, received the award for excellence in QI teamwork for their groundbreaking work on VTE prophylaxis, a key indicator of hospital quality.
Award for Clinical Excellence
Jennifer Myers, MD, FHM, for leading the “rapid root cause analysis” process that convenes medical error reviews with front-line clinicians and staff.
Award for Excellence in Teaching
Amir Jaffer, MD, FHM

Award for Outstanding Service in Hospital Medicine
Mitchell Wilson, MD, FHM
Award for Excellence in Research
Margaret C. Fang MD, MPH, FHM
Research, Innovation, and Clinical Vignettes Winners
2010 Innovation Poster Winner: Aaron Farberg, BS, Andrew Lin, BS, Latoya Kuhn, MPH, Scott Flanders, MD, SFHM, Christopher Kim, MD, MBA, University of Michigan Medical School, “Dear Doctor: A Tool to Facilitate Patient-Centered Care and Enhance Communication.”
2010 Adult Vignette Winner: Jennie Wei, MD, and Patrick Kneeland, MD, University of California at San Francisco, “A Case of Skin Ulcers and Neutropenia: Definitely Not a Helminth Problem.”
2010 Research Winner: Will Southern, MD, MS, and Julia Arnsten, MD, MPH, Montefiore Medical Center, Bronx, N.Y.: “Increased Mortality and Readmission Among Patients Discharged against Medical Advice.”
2010 Pediatric Vignette Winner: Harry Hoar, MD, Baystate Children’s Hospitalist, Springfield, Mass., “A Teen with Varices: An Uncommon Presentation of a Familiar Disease.”
Researchers Earn First SHM Junior Faculty Development Awards
Two-year, $50,000 commitment bolsters academic pursuits for young hospitalists
By Jason Carris

NATIONAL HARBOR, Md.– Kirsten Kangelaris, MD, and Evan Fieldston, MD, MBA, MSHP, were presented $50,000 Junior Faculty Development Awards at HM10. The first-year awards are part of SHM’s commitment to helping the “generation of new knowledge,” said Scott Flanders, SHM’s outgoing president.
Dr. Kangelaris, a fellow in internal medicine at the University of California at San Francisco, focuses her research on continued clinical and biologic genetic risk-prediction algorithms that will improve the triage and early-management strategies for hospitalized patients with inflammatory illness.

Dr. Fieldston, an assistant professor in pediatrics at the University of Pennsylvania School of Medicine and Children’s Hospital of Philadelphia, plans to use his award to examine the association between dynamic aspects of workload, workforce, and quality of care at children’s hospitals.
SHM also handed out its annual Awards of Excellence (above left) and announced winners from the Research, Innovation, and Clinical Vignette competition (below left). Judges scored more than 400 posters; some of the winning project teams included medical students.
“I am particularly proud to see that we had medical students as award winners,” said Flanders, chief of the hospital medicine division at the University of Michigan Health System in Ann Arbor. “That gives me great hope for the future of HM.”
Awards of Excellence
Award for Excellence in Teamwork in Quality Improvement
The Emory University Hospital Healthcare Team, co-led by Jason Stein, MD, FHM, Carolyn Hill, RN, Laura Phillips, and Dee Cantrell, received the award for excellence in QI teamwork for their groundbreaking work on VTE prophylaxis, a key indicator of hospital quality.
Award for Clinical Excellence
Jennifer Myers, MD, FHM, for leading the “rapid root cause analysis” process that convenes medical error reviews with front-line clinicians and staff.
Award for Excellence in Teaching
Amir Jaffer, MD, FHM
Award for Outstanding Service in Hospital Medicine
Mitchell Wilson, MD, FHM
Award for Excellence in Research
Margaret C. Fang MD, MPH, FHM
Research, Innovation, and Clinical Vignettes Winners
2010 Innovation Poster Winner: Aaron Farberg, BS, Andrew Lin, BS, Latoya Kuhn, MPH, Scott Flanders, MD, SFHM, Christopher Kim, MD, MBA, University of Michigan Medical School, “Dear Doctor: A Tool to Facilitate Patient-Centered Care and Enhance Communication.”
2010 Adult Vignette Winner: Jennie Wei, MD, and Patrick Kneeland, MD, University of California at San Francisco, “A Case of Skin Ulcers and Neutropenia: Definitely Not a Helminth Problem.”
2010 Research Winner: Will Southern, MD, MS, and Julia Arnsten, MD, MPH, Montefiore Medical Center, Bronx, N.Y.: “Increased Mortality and Readmission Among Patients Discharged against Medical Advice.”
2010 Pediatric Vignette Winner: Harry Hoar, MD, Baystate Children’s Hospitalist, Springfield, Mass., “A Teen with Varices: An Uncommon Presentation of a Familiar Disease.”
Researchers Earn First SHM Junior Faculty Development Awards
Two-year, $50,000 commitment bolsters academic pursuits for young hospitalists
By Jason Carris
NATIONAL HARBOR, Md.– Kirsten Kangelaris, MD, and Evan Fieldston, MD, MBA, MSHP, were presented $50,000 Junior Faculty Development Awards at HM10. The first-year awards are part of SHM’s commitment to helping the “generation of new knowledge,” said Scott Flanders, SHM’s outgoing president.
Dr. Kangelaris, a fellow in internal medicine at the University of California at San Francisco, focuses her research on continued clinical and biologic genetic risk-prediction algorithms that will improve the triage and early-management strategies for hospitalized patients with inflammatory illness.
Dr. Fieldston, an assistant professor in pediatrics at the University of Pennsylvania School of Medicine and Children’s Hospital of Philadelphia, plans to use his award to examine the association between dynamic aspects of workload, workforce, and quality of care at children’s hospitals.
SHM also handed out its annual Awards of Excellence (above left) and announced winners from the Research, Innovation, and Clinical Vignette competition (below left). Judges scored more than 400 posters; some of the winning project teams included medical students.
“I am particularly proud to see that we had medical students as award winners,” said Flanders, chief of the hospital medicine division at the University of Michigan Health System in Ann Arbor. “That gives me great hope for the future of HM.”
Awards of Excellence
Award for Excellence in Teamwork in Quality Improvement
The Emory University Hospital Healthcare Team, co-led by Jason Stein, MD, FHM, Carolyn Hill, RN, Laura Phillips, and Dee Cantrell, received the award for excellence in QI teamwork for their groundbreaking work on VTE prophylaxis, a key indicator of hospital quality.
Award for Clinical Excellence
Jennifer Myers, MD, FHM, for leading the “rapid root cause analysis” process that convenes medical error reviews with front-line clinicians and staff.
Award for Excellence in Teaching
Amir Jaffer, MD, FHM
Award for Outstanding Service in Hospital Medicine
Mitchell Wilson, MD, FHM
Award for Excellence in Research
Margaret C. Fang MD, MPH, FHM
Research, Innovation, and Clinical Vignettes Winners
2010 Innovation Poster Winner: Aaron Farberg, BS, Andrew Lin, BS, Latoya Kuhn, MPH, Scott Flanders, MD, SFHM, Christopher Kim, MD, MBA, University of Michigan Medical School, “Dear Doctor: A Tool to Facilitate Patient-Centered Care and Enhance Communication.”
2010 Adult Vignette Winner: Jennie Wei, MD, and Patrick Kneeland, MD, University of California at San Francisco, “A Case of Skin Ulcers and Neutropenia: Definitely Not a Helminth Problem.”
2010 Research Winner: Will Southern, MD, MS, and Julia Arnsten, MD, MPH, Montefiore Medical Center, Bronx, N.Y.: “Increased Mortality and Readmission Among Patients Discharged against Medical Advice.”
2010 Pediatric Vignette Winner: Harry Hoar, MD, Baystate Children’s Hospitalist, Springfield, Mass., “A Teen with Varices: An Uncommon Presentation of a Familiar Disease.”
Researchers Earn First SHM Junior Faculty Development Awards
Two-year, $50,000 commitment bolsters academic pursuits for young hospitalists
By Jason Carris
NATIONAL HARBOR, Md.– Kirsten Kangelaris, MD, and Evan Fieldston, MD, MBA, MSHP, were presented $50,000 Junior Faculty Development Awards at HM10. The first-year awards are part of SHM’s commitment to helping the “generation of new knowledge,” said Scott Flanders, SHM’s outgoing president.
Dr. Kangelaris, a fellow in internal medicine at the University of California at San Francisco, focuses her research on continued clinical and biologic genetic risk-prediction algorithms that will improve the triage and early-management strategies for hospitalized patients with inflammatory illness.
Dr. Fieldston, an assistant professor in pediatrics at the University of Pennsylvania School of Medicine and Children’s Hospital of Philadelphia, plans to use his award to examine the association between dynamic aspects of workload, workforce, and quality of care at children’s hospitals.
SHM also handed out its annual Awards of Excellence (above left) and announced winners from the Research, Innovation, and Clinical Vignette competition (below left). Judges scored more than 400 posters; some of the winning project teams included medical students.
“I am particularly proud to see that we had medical students as award winners,” said Flanders, chief of the hospital medicine division at the University of Michigan Health System in Ann Arbor. “That gives me great hope for the future of HM.”
Historic Gathering
Last month, more than 2,500 hospitalists and experts in HM gathered just outside Washington, D.C., to share the very best the specialty has to offer. The record-setting attendance surpassed the previous record—set at HM09 in Chicago—by more than 20%.
For hospitalists across the country, the meeting provided the perfect venue for continued education, professional development, and networking with friends and colleagues. To SHM CEO Larry Wellikson, MD, FHM, that is exactly what makes the annual meeting important.
“Hospital medicine is growing and evolving at a breakneck pace, and individual hospitalists are expected to keep up on a daily basis,” he says. “Our annual meeting is an opportunity to recognize the leaders in our field and identify the opportunities and challenges on the horizon for hospitalists.”
—Larry Wellikson, MD, SFHM, CEO of SHM
SHM Inducts First Senior Fellows and Masters in Hospital Medicine
The current and future leaders of HM were inducted as Fellows in Hospital Medicine at HM10 (see “Fellows in Hospital Medicine Class of 2010,” p.10). This year, SHM introduced the inaugural class of nearly 200 Senior Fellows in Hospital Medicine (SFHM) and three Masters in Hospital Medicine (MHM).
The three MHM designees—Winthrop F. Whitcomb, MD, MHM, Robert Wachter, MD, MHM, and John Nelson, MD, MHM—were recognized by SHM leadership for the “utmost demonstration of dedication to the field of hospital medicine through significant contributions to the development and maturation of the profession.”
Great Hospital Care? There’s an App for That

Available for iPhone, Windows Mobile, and Palm devices, Hospitalist Connection puts the best in practice-management resources at hospitalists’ fingertips. Each article in Hospitalist Connection is selected by hospitalist Chad Whelan, MD, FHM, who adds his expert commentary on the topic.
“Staying up to date with the latest advances in hospital medicine is a key component of any hospitalist’s job, but they rarely find themselves with time at a desk behind a computer,” Dr. Whelan says. “That’s what makes this combination of format and content so powerful.”
In addition to exclusive content from Dr. Whelan, Hospitalist Connection presents excerpts of articles from the most trusted sources in HM. Topics range from management and care transitions to quality improvement (QI) and patient safety.
Hospitalist Connection is a joint collaboration between SHM and Epocrates, which develops Web-based and mobile applications for the healthcare sector. Epocrates estimates that more than 900,000 healthcare professionals—including 1 in 3 U.S. physicians—use Epocrates products.
The response to the Hospitalist Connection launch has been enthusiastic, according to SHM officials.
“Making great information more accessible empowers hospitalists to truly bring the best to their hospitals and patients,” says Todd Von Deak, SHM vice president and general manager. “We’re thrilled that so many hospitalists have shown such an interest in Hospitalist Connection. This is an extension of our commitment to bring the best resources to hospital medicine and our members.”
“This is a true milestone for the hospital medicine specialty,” said Dr. Wellikson. “The Masters in Hospital Medicine designation is the Hall of Fame of hospital medicine. We are honored to acknowledge Drs. Nelson, Wachter, and Whitcomb. We’re also thrilled to induct hundreds of new Fellows and Senior Fellows into the program. Their demonstrated commitment to improving patient care is one of the hallmarks of hospital medicine.”
The new SFHM designees represent the field’s experienced leaders and the next level of credentialing beyond the original Fellow in Hospital Medicine (FHM). Senior Fellows must have at least five years of HM practice and have been a society member for at least five years.
SHM also inducted 190 new FHM designees. As the second class of Fellows, they join more than 500 other hospitalists who have practiced HM for five years and been a member of SHM for at least three years.
For more information about the SHM Fellowship program, visit www.hospitalmedicine.org/fellows.
Featured Speakers Bring Focus to HM, Healthcare Policy
It’s no coincidence that SHM brought hospitalists to the nation’s capital for the annual meeting. The ongoing public debate over delivering patient care safely, effectively, and efficiently remains at the fore in the nation’s capital.
That was the point driven home by Dr. Wachter in his featured presentation on the final day of the conference. While the recently passed healthcare reform legislation addressed such issues as access to health insurance and costs, the legislation “kicked the can down the road,” he said.
For perspective from a hospital administrator who already has put into practice many of the reform recommendations, HM10 turned to Paul Levy, CEO of Beth Israel Deaconess Medical Center in Boston. Too much attention on political debate could be a distraction, Levy warned. Instead of getting too caught up in national political drama, Levy cautioned, hospitalists would do well to focus on their own practices and identify ways to reduce preventable errors in the hospital.
Levy’s speech was preceded by a panel discussion led by Public Policy Committee Chair Eric Siegal, MD, SFHM, one of the newest members of the SHM board. Leslie Norwalk, a former Centers for Medicare and Medicaid Services (CMS) administrator, participated in the panel and was interviewed later that day by CNN Money about young, healthy individuals and the role they play in reducing health insurance costs.
Hospitalists Bone Up on Career and Clinical Skills
More than 900 hospitalists used the pre-courses at HM10 as an opportunity for continued professional education.
Presented on the day before the formal kickoff of HM10, each pre-course presented an in-depth look at some of the most pressing issues in HM. This year introduced two new pre-courses that characterized the wide range of topics: “Early Career Hospitalist: Skills for Success” and “Essential Neurology for the Hospitalist.”
All told, HM10 was a resounding success that reflected the continued energy and enthusiasm of HM and its impact on healthcare. To SHM Vice President and General Manager Todd Von Deak, that momentum means looking to the future.
“We received great feedback from our attendees this year, and we’re looking forward to using that information to make an even stronger—and record-breaking—annual meeting in Dallas next year,” he said. “See you in 2011!” TH
Brendon Shank is a freelance writer based in Philadelphia.
Last month, more than 2,500 hospitalists and experts in HM gathered just outside Washington, D.C., to share the very best the specialty has to offer. The record-setting attendance surpassed the previous record—set at HM09 in Chicago—by more than 20%.
For hospitalists across the country, the meeting provided the perfect venue for continued education, professional development, and networking with friends and colleagues. To SHM CEO Larry Wellikson, MD, FHM, that is exactly what makes the annual meeting important.
“Hospital medicine is growing and evolving at a breakneck pace, and individual hospitalists are expected to keep up on a daily basis,” he says. “Our annual meeting is an opportunity to recognize the leaders in our field and identify the opportunities and challenges on the horizon for hospitalists.”
—Larry Wellikson, MD, SFHM, CEO of SHM
SHM Inducts First Senior Fellows and Masters in Hospital Medicine
The current and future leaders of HM were inducted as Fellows in Hospital Medicine at HM10 (see “Fellows in Hospital Medicine Class of 2010,” p.10). This year, SHM introduced the inaugural class of nearly 200 Senior Fellows in Hospital Medicine (SFHM) and three Masters in Hospital Medicine (MHM).
The three MHM designees—Winthrop F. Whitcomb, MD, MHM, Robert Wachter, MD, MHM, and John Nelson, MD, MHM—were recognized by SHM leadership for the “utmost demonstration of dedication to the field of hospital medicine through significant contributions to the development and maturation of the profession.”
Great Hospital Care? There’s an App for That
Available for iPhone, Windows Mobile, and Palm devices, Hospitalist Connection puts the best in practice-management resources at hospitalists’ fingertips. Each article in Hospitalist Connection is selected by hospitalist Chad Whelan, MD, FHM, who adds his expert commentary on the topic.
“Staying up to date with the latest advances in hospital medicine is a key component of any hospitalist’s job, but they rarely find themselves with time at a desk behind a computer,” Dr. Whelan says. “That’s what makes this combination of format and content so powerful.”
In addition to exclusive content from Dr. Whelan, Hospitalist Connection presents excerpts of articles from the most trusted sources in HM. Topics range from management and care transitions to quality improvement (QI) and patient safety.
Hospitalist Connection is a joint collaboration between SHM and Epocrates, which develops Web-based and mobile applications for the healthcare sector. Epocrates estimates that more than 900,000 healthcare professionals—including 1 in 3 U.S. physicians—use Epocrates products.
The response to the Hospitalist Connection launch has been enthusiastic, according to SHM officials.
“Making great information more accessible empowers hospitalists to truly bring the best to their hospitals and patients,” says Todd Von Deak, SHM vice president and general manager. “We’re thrilled that so many hospitalists have shown such an interest in Hospitalist Connection. This is an extension of our commitment to bring the best resources to hospital medicine and our members.”
“This is a true milestone for the hospital medicine specialty,” said Dr. Wellikson. “The Masters in Hospital Medicine designation is the Hall of Fame of hospital medicine. We are honored to acknowledge Drs. Nelson, Wachter, and Whitcomb. We’re also thrilled to induct hundreds of new Fellows and Senior Fellows into the program. Their demonstrated commitment to improving patient care is one of the hallmarks of hospital medicine.”
The new SFHM designees represent the field’s experienced leaders and the next level of credentialing beyond the original Fellow in Hospital Medicine (FHM). Senior Fellows must have at least five years of HM practice and have been a society member for at least five years.
SHM also inducted 190 new FHM designees. As the second class of Fellows, they join more than 500 other hospitalists who have practiced HM for five years and been a member of SHM for at least three years.
For more information about the SHM Fellowship program, visit www.hospitalmedicine.org/fellows.
Featured Speakers Bring Focus to HM, Healthcare Policy
It’s no coincidence that SHM brought hospitalists to the nation’s capital for the annual meeting. The ongoing public debate over delivering patient care safely, effectively, and efficiently remains at the fore in the nation’s capital.
That was the point driven home by Dr. Wachter in his featured presentation on the final day of the conference. While the recently passed healthcare reform legislation addressed such issues as access to health insurance and costs, the legislation “kicked the can down the road,” he said.
For perspective from a hospital administrator who already has put into practice many of the reform recommendations, HM10 turned to Paul Levy, CEO of Beth Israel Deaconess Medical Center in Boston. Too much attention on political debate could be a distraction, Levy warned. Instead of getting too caught up in national political drama, Levy cautioned, hospitalists would do well to focus on their own practices and identify ways to reduce preventable errors in the hospital.
Levy’s speech was preceded by a panel discussion led by Public Policy Committee Chair Eric Siegal, MD, SFHM, one of the newest members of the SHM board. Leslie Norwalk, a former Centers for Medicare and Medicaid Services (CMS) administrator, participated in the panel and was interviewed later that day by CNN Money about young, healthy individuals and the role they play in reducing health insurance costs.
Hospitalists Bone Up on Career and Clinical Skills
More than 900 hospitalists used the pre-courses at HM10 as an opportunity for continued professional education.
Presented on the day before the formal kickoff of HM10, each pre-course presented an in-depth look at some of the most pressing issues in HM. This year introduced two new pre-courses that characterized the wide range of topics: “Early Career Hospitalist: Skills for Success” and “Essential Neurology for the Hospitalist.”
All told, HM10 was a resounding success that reflected the continued energy and enthusiasm of HM and its impact on healthcare. To SHM Vice President and General Manager Todd Von Deak, that momentum means looking to the future.
“We received great feedback from our attendees this year, and we’re looking forward to using that information to make an even stronger—and record-breaking—annual meeting in Dallas next year,” he said. “See you in 2011!” TH
Brendon Shank is a freelance writer based in Philadelphia.
Last month, more than 2,500 hospitalists and experts in HM gathered just outside Washington, D.C., to share the very best the specialty has to offer. The record-setting attendance surpassed the previous record—set at HM09 in Chicago—by more than 20%.
For hospitalists across the country, the meeting provided the perfect venue for continued education, professional development, and networking with friends and colleagues. To SHM CEO Larry Wellikson, MD, FHM, that is exactly what makes the annual meeting important.
“Hospital medicine is growing and evolving at a breakneck pace, and individual hospitalists are expected to keep up on a daily basis,” he says. “Our annual meeting is an opportunity to recognize the leaders in our field and identify the opportunities and challenges on the horizon for hospitalists.”
—Larry Wellikson, MD, SFHM, CEO of SHM
SHM Inducts First Senior Fellows and Masters in Hospital Medicine
The current and future leaders of HM were inducted as Fellows in Hospital Medicine at HM10 (see “Fellows in Hospital Medicine Class of 2010,” p.10). This year, SHM introduced the inaugural class of nearly 200 Senior Fellows in Hospital Medicine (SFHM) and three Masters in Hospital Medicine (MHM).
The three MHM designees—Winthrop F. Whitcomb, MD, MHM, Robert Wachter, MD, MHM, and John Nelson, MD, MHM—were recognized by SHM leadership for the “utmost demonstration of dedication to the field of hospital medicine through significant contributions to the development and maturation of the profession.”
Great Hospital Care? There’s an App for That
Available for iPhone, Windows Mobile, and Palm devices, Hospitalist Connection puts the best in practice-management resources at hospitalists’ fingertips. Each article in Hospitalist Connection is selected by hospitalist Chad Whelan, MD, FHM, who adds his expert commentary on the topic.
“Staying up to date with the latest advances in hospital medicine is a key component of any hospitalist’s job, but they rarely find themselves with time at a desk behind a computer,” Dr. Whelan says. “That’s what makes this combination of format and content so powerful.”
In addition to exclusive content from Dr. Whelan, Hospitalist Connection presents excerpts of articles from the most trusted sources in HM. Topics range from management and care transitions to quality improvement (QI) and patient safety.
Hospitalist Connection is a joint collaboration between SHM and Epocrates, which develops Web-based and mobile applications for the healthcare sector. Epocrates estimates that more than 900,000 healthcare professionals—including 1 in 3 U.S. physicians—use Epocrates products.
The response to the Hospitalist Connection launch has been enthusiastic, according to SHM officials.
“Making great information more accessible empowers hospitalists to truly bring the best to their hospitals and patients,” says Todd Von Deak, SHM vice president and general manager. “We’re thrilled that so many hospitalists have shown such an interest in Hospitalist Connection. This is an extension of our commitment to bring the best resources to hospital medicine and our members.”
“This is a true milestone for the hospital medicine specialty,” said Dr. Wellikson. “The Masters in Hospital Medicine designation is the Hall of Fame of hospital medicine. We are honored to acknowledge Drs. Nelson, Wachter, and Whitcomb. We’re also thrilled to induct hundreds of new Fellows and Senior Fellows into the program. Their demonstrated commitment to improving patient care is one of the hallmarks of hospital medicine.”
The new SFHM designees represent the field’s experienced leaders and the next level of credentialing beyond the original Fellow in Hospital Medicine (FHM). Senior Fellows must have at least five years of HM practice and have been a society member for at least five years.
SHM also inducted 190 new FHM designees. As the second class of Fellows, they join more than 500 other hospitalists who have practiced HM for five years and been a member of SHM for at least three years.
For more information about the SHM Fellowship program, visit www.hospitalmedicine.org/fellows.
Featured Speakers Bring Focus to HM, Healthcare Policy
It’s no coincidence that SHM brought hospitalists to the nation’s capital for the annual meeting. The ongoing public debate over delivering patient care safely, effectively, and efficiently remains at the fore in the nation’s capital.
That was the point driven home by Dr. Wachter in his featured presentation on the final day of the conference. While the recently passed healthcare reform legislation addressed such issues as access to health insurance and costs, the legislation “kicked the can down the road,” he said.
For perspective from a hospital administrator who already has put into practice many of the reform recommendations, HM10 turned to Paul Levy, CEO of Beth Israel Deaconess Medical Center in Boston. Too much attention on political debate could be a distraction, Levy warned. Instead of getting too caught up in national political drama, Levy cautioned, hospitalists would do well to focus on their own practices and identify ways to reduce preventable errors in the hospital.
Levy’s speech was preceded by a panel discussion led by Public Policy Committee Chair Eric Siegal, MD, SFHM, one of the newest members of the SHM board. Leslie Norwalk, a former Centers for Medicare and Medicaid Services (CMS) administrator, participated in the panel and was interviewed later that day by CNN Money about young, healthy individuals and the role they play in reducing health insurance costs.
Hospitalists Bone Up on Career and Clinical Skills
More than 900 hospitalists used the pre-courses at HM10 as an opportunity for continued professional education.
Presented on the day before the formal kickoff of HM10, each pre-course presented an in-depth look at some of the most pressing issues in HM. This year introduced two new pre-courses that characterized the wide range of topics: “Early Career Hospitalist: Skills for Success” and “Essential Neurology for the Hospitalist.”
All told, HM10 was a resounding success that reflected the continued energy and enthusiasm of HM and its impact on healthcare. To SHM Vice President and General Manager Todd Von Deak, that momentum means looking to the future.
“We received great feedback from our attendees this year, and we’re looking forward to using that information to make an even stronger—and record-breaking—annual meeting in Dallas next year,” he said. “See you in 2011!” TH
Brendon Shank is a freelance writer based in Philadelphia.
Performance Partnership
With 37,000 individual members and nearly 5,000 hospitals and other provider groups on its roster, the American Hospital Association (AHA) is a major player in national healthcare debates and in shaping policies aimed at improving quality.
John Combes, MD, AHA senior vice president and president and chief operating officer of the association-affiliated Center for Healthcare Governance, serves on several national advisory groups on medical ethics, palliative care, and reducing medication errors.
Among his many duties, he is a principal investigator for a national project aimed at reducing hospital-acquired infections called “On the CUSP: Stop Bloodstream Infections,” sponsored by the Agency for Healthcare Research and Quality (AHRQ). (CUSP is the Comprehensive Unit-based Safety Program, developed by Johns Hopkins University and the Michigan Hospital Association.)
Dr. Combes recently talked with The Hospitalist about the AHA’s vision for healthcare reform, integrated care, and the role of hospitalists in redesigning hospital-based care.
Question: What are the AHA’s biggest priorities over the next year?
Answer: Healthcare reform and making sure that we can increase coverage for patients without insurance. There are 48 million uninsured in this country, and we are very supportive of increasing that coverage to make sure that people have good access to healthcare.
Q: The AHA has stated that “clinical integration holds the promise of greater quality and improved efficiency in delivering patient-centered care.” What’s your vision for clinical integration?
A: What we recognize is that in a reformed delivery system, we have to have a lot of partnerships between hospitals and clinicians—physicians in particular—and between hospitals and other facilities, such as long-term care facilities and post-acute facilities. We need to be able to bring better-coordinated care that meets the patient’s needs, and we need to work with each other to constantly improve that care. So that’s why we’re looking at an integrated delivery system. In our minds, it really means one registration, one bill, one experience for the patient.
Practically speaking, if you look at the healthcare reform legislation … there are pilots in there for accountable-care organizations (ACOs) and other payment reforms. And we’re very interested in making sure that hospitals can participate and take a leadership role in the development of those kinds of new structures.
Q: What role do you expect hospitalists to play in the continued drive for higher quality and more efficient care?
A: I think hospitalists can become a critical partner with the hospital in helping us redesign inpatient care to make it more efficient and effective. Additionally, hospitalists have a key role in engaging and keeping involved the community-based PCP, and making sure that they are considered part of the care team, even though they may not be present in the hospital, since they have the continuing responsibility for the patient.
I think as we look at other models of care delivery, such as the patient-centered medical home, it’s critical that hospitalists really develop some strong relationships and communication networks with those groups as well, so that the care for the patient can become seamless and transitions are not as dangerous as they’ve been in the past, in terms of missed opportunities and missed handoffs.

Q: What are the necessary ingredients for any successful quality incentive payment program?
A: One of our big concerns is that there are lots of regulatory obstacles to true integration, where you can design some of those payment structures in terms of gainsharing and also in terms of payment for high-level-quality performance. One of the concerns of the AHM is to make sure that as we pursue these new models of care that require high levels of integration, we also look at some regulatory relief.
The promise is that if we can integrate the delivery system, we can then get focused on improving care and then rewarding high-quality delivery of care. And that can come through incentive programs or pay-for-performance programs and things of that nature that can be worked out between the hospitals and the physicians.
Q: What can be done to reduce the rates of hospital-acquired infections?
A: The idea of CUSP is that you create teams and a culture on units that will then implement the evidence-based intervention—in this case, eliminating central-line infections.
Hospitalists can play a critical role in helping create that culture of mutual accountability at the team level [and] holding each other accountable to use the evidence-based techniques for, in this case, line insertion, or for any kind of safety intervention. I think eliminating infections is a goal that’s achievable. I think we have come to the understanding over the last five or so years that these complications are avoidable in many, many cases, and that it takes teamwork, communication, and use of evidence-based procedures to get the work done.
Q: What can be done to help reduce preventable hospital readmissions?
A: There are so many things that go into readmissions. And the issue is: What is truly preventable in terms of treatments within the hospital, the coordination of discharge, and aftercare followup? A lot of readmissions are related to social determinants of health. And those have to do with people’s ability to afford their medications, people’s ability to access care, people’s home environment, and things of that nature. It’s going to take an approach by hospitals on those things that are controllable in partnerships with the physicians. But for many, many readmissions, it’s related to other issues that we as a society really have to hold ourselves accountable to.
Q: Some critics have charged that the overuse of medical technology is helping to drive up healthcare costs. Would there be more of a role for hospitals in decision-making about the appropriateness of tests within a model like an ACO?
A: In an ACO, that’s a partnership between hospitals and physicians operating as one entity. So that’s the difference, because there, everybody is aligned to make sure that we deliver the most effective care. There’s going to be much more time spent on physicians ordering the most appropriate technology or treatments for that condition that will deliver value to the patient and to the payor of that care.
But that’s in a totally integrated system. Right now we don’t have that. So where the interests of the physicians may be different from the interests of the hospital and the intentions are not aligned, it’s very hard to get at talking about what’s the most effective care.
Q: Is there a measure that hasn’t received as much attention that you would like to see more focus on to help improve the quality or cost-effectiveness of healthcare?
A: I think the one area that we’re always challenged with—and I think we’ve seen it in the healthcare debate, and I think it’s an appropriate role for us as healthcare providers to pay attention to—is palliative and end-of-life care. I don’t think we’ve done enough work, as a profession, to make sure that we deliver very-high-quality care of patients with chronic and acute catastrophic illnesses.
We need to better understand what the needs of those patients are, to ask them to work with us to set the goals with them, what they want from us.
So I think it’s an opportunity for us to have a real partnership with patients at a critical time in their lives. TH
Bryn Nelson is a freelance medical writer based in Seattle.
With 37,000 individual members and nearly 5,000 hospitals and other provider groups on its roster, the American Hospital Association (AHA) is a major player in national healthcare debates and in shaping policies aimed at improving quality.
John Combes, MD, AHA senior vice president and president and chief operating officer of the association-affiliated Center for Healthcare Governance, serves on several national advisory groups on medical ethics, palliative care, and reducing medication errors.
Among his many duties, he is a principal investigator for a national project aimed at reducing hospital-acquired infections called “On the CUSP: Stop Bloodstream Infections,” sponsored by the Agency for Healthcare Research and Quality (AHRQ). (CUSP is the Comprehensive Unit-based Safety Program, developed by Johns Hopkins University and the Michigan Hospital Association.)
Dr. Combes recently talked with The Hospitalist about the AHA’s vision for healthcare reform, integrated care, and the role of hospitalists in redesigning hospital-based care.
Question: What are the AHA’s biggest priorities over the next year?
Answer: Healthcare reform and making sure that we can increase coverage for patients without insurance. There are 48 million uninsured in this country, and we are very supportive of increasing that coverage to make sure that people have good access to healthcare.
Q: The AHA has stated that “clinical integration holds the promise of greater quality and improved efficiency in delivering patient-centered care.” What’s your vision for clinical integration?
A: What we recognize is that in a reformed delivery system, we have to have a lot of partnerships between hospitals and clinicians—physicians in particular—and between hospitals and other facilities, such as long-term care facilities and post-acute facilities. We need to be able to bring better-coordinated care that meets the patient’s needs, and we need to work with each other to constantly improve that care. So that’s why we’re looking at an integrated delivery system. In our minds, it really means one registration, one bill, one experience for the patient.
Practically speaking, if you look at the healthcare reform legislation … there are pilots in there for accountable-care organizations (ACOs) and other payment reforms. And we’re very interested in making sure that hospitals can participate and take a leadership role in the development of those kinds of new structures.
Q: What role do you expect hospitalists to play in the continued drive for higher quality and more efficient care?
A: I think hospitalists can become a critical partner with the hospital in helping us redesign inpatient care to make it more efficient and effective. Additionally, hospitalists have a key role in engaging and keeping involved the community-based PCP, and making sure that they are considered part of the care team, even though they may not be present in the hospital, since they have the continuing responsibility for the patient.
I think as we look at other models of care delivery, such as the patient-centered medical home, it’s critical that hospitalists really develop some strong relationships and communication networks with those groups as well, so that the care for the patient can become seamless and transitions are not as dangerous as they’ve been in the past, in terms of missed opportunities and missed handoffs.
Q: What are the necessary ingredients for any successful quality incentive payment program?
A: One of our big concerns is that there are lots of regulatory obstacles to true integration, where you can design some of those payment structures in terms of gainsharing and also in terms of payment for high-level-quality performance. One of the concerns of the AHM is to make sure that as we pursue these new models of care that require high levels of integration, we also look at some regulatory relief.
The promise is that if we can integrate the delivery system, we can then get focused on improving care and then rewarding high-quality delivery of care. And that can come through incentive programs or pay-for-performance programs and things of that nature that can be worked out between the hospitals and the physicians.
Q: What can be done to reduce the rates of hospital-acquired infections?
A: The idea of CUSP is that you create teams and a culture on units that will then implement the evidence-based intervention—in this case, eliminating central-line infections.
Hospitalists can play a critical role in helping create that culture of mutual accountability at the team level [and] holding each other accountable to use the evidence-based techniques for, in this case, line insertion, or for any kind of safety intervention. I think eliminating infections is a goal that’s achievable. I think we have come to the understanding over the last five or so years that these complications are avoidable in many, many cases, and that it takes teamwork, communication, and use of evidence-based procedures to get the work done.
Q: What can be done to help reduce preventable hospital readmissions?
A: There are so many things that go into readmissions. And the issue is: What is truly preventable in terms of treatments within the hospital, the coordination of discharge, and aftercare followup? A lot of readmissions are related to social determinants of health. And those have to do with people’s ability to afford their medications, people’s ability to access care, people’s home environment, and things of that nature. It’s going to take an approach by hospitals on those things that are controllable in partnerships with the physicians. But for many, many readmissions, it’s related to other issues that we as a society really have to hold ourselves accountable to.
Q: Some critics have charged that the overuse of medical technology is helping to drive up healthcare costs. Would there be more of a role for hospitals in decision-making about the appropriateness of tests within a model like an ACO?
A: In an ACO, that’s a partnership between hospitals and physicians operating as one entity. So that’s the difference, because there, everybody is aligned to make sure that we deliver the most effective care. There’s going to be much more time spent on physicians ordering the most appropriate technology or treatments for that condition that will deliver value to the patient and to the payor of that care.
But that’s in a totally integrated system. Right now we don’t have that. So where the interests of the physicians may be different from the interests of the hospital and the intentions are not aligned, it’s very hard to get at talking about what’s the most effective care.
Q: Is there a measure that hasn’t received as much attention that you would like to see more focus on to help improve the quality or cost-effectiveness of healthcare?
A: I think the one area that we’re always challenged with—and I think we’ve seen it in the healthcare debate, and I think it’s an appropriate role for us as healthcare providers to pay attention to—is palliative and end-of-life care. I don’t think we’ve done enough work, as a profession, to make sure that we deliver very-high-quality care of patients with chronic and acute catastrophic illnesses.
We need to better understand what the needs of those patients are, to ask them to work with us to set the goals with them, what they want from us.
So I think it’s an opportunity for us to have a real partnership with patients at a critical time in their lives. TH
Bryn Nelson is a freelance medical writer based in Seattle.
With 37,000 individual members and nearly 5,000 hospitals and other provider groups on its roster, the American Hospital Association (AHA) is a major player in national healthcare debates and in shaping policies aimed at improving quality.
John Combes, MD, AHA senior vice president and president and chief operating officer of the association-affiliated Center for Healthcare Governance, serves on several national advisory groups on medical ethics, palliative care, and reducing medication errors.
Among his many duties, he is a principal investigator for a national project aimed at reducing hospital-acquired infections called “On the CUSP: Stop Bloodstream Infections,” sponsored by the Agency for Healthcare Research and Quality (AHRQ). (CUSP is the Comprehensive Unit-based Safety Program, developed by Johns Hopkins University and the Michigan Hospital Association.)
Dr. Combes recently talked with The Hospitalist about the AHA’s vision for healthcare reform, integrated care, and the role of hospitalists in redesigning hospital-based care.
Question: What are the AHA’s biggest priorities over the next year?
Answer: Healthcare reform and making sure that we can increase coverage for patients without insurance. There are 48 million uninsured in this country, and we are very supportive of increasing that coverage to make sure that people have good access to healthcare.
Q: The AHA has stated that “clinical integration holds the promise of greater quality and improved efficiency in delivering patient-centered care.” What’s your vision for clinical integration?
A: What we recognize is that in a reformed delivery system, we have to have a lot of partnerships between hospitals and clinicians—physicians in particular—and between hospitals and other facilities, such as long-term care facilities and post-acute facilities. We need to be able to bring better-coordinated care that meets the patient’s needs, and we need to work with each other to constantly improve that care. So that’s why we’re looking at an integrated delivery system. In our minds, it really means one registration, one bill, one experience for the patient.
Practically speaking, if you look at the healthcare reform legislation … there are pilots in there for accountable-care organizations (ACOs) and other payment reforms. And we’re very interested in making sure that hospitals can participate and take a leadership role in the development of those kinds of new structures.
Q: What role do you expect hospitalists to play in the continued drive for higher quality and more efficient care?
A: I think hospitalists can become a critical partner with the hospital in helping us redesign inpatient care to make it more efficient and effective. Additionally, hospitalists have a key role in engaging and keeping involved the community-based PCP, and making sure that they are considered part of the care team, even though they may not be present in the hospital, since they have the continuing responsibility for the patient.
I think as we look at other models of care delivery, such as the patient-centered medical home, it’s critical that hospitalists really develop some strong relationships and communication networks with those groups as well, so that the care for the patient can become seamless and transitions are not as dangerous as they’ve been in the past, in terms of missed opportunities and missed handoffs.
Q: What are the necessary ingredients for any successful quality incentive payment program?
A: One of our big concerns is that there are lots of regulatory obstacles to true integration, where you can design some of those payment structures in terms of gainsharing and also in terms of payment for high-level-quality performance. One of the concerns of the AHM is to make sure that as we pursue these new models of care that require high levels of integration, we also look at some regulatory relief.
The promise is that if we can integrate the delivery system, we can then get focused on improving care and then rewarding high-quality delivery of care. And that can come through incentive programs or pay-for-performance programs and things of that nature that can be worked out between the hospitals and the physicians.
Q: What can be done to reduce the rates of hospital-acquired infections?
A: The idea of CUSP is that you create teams and a culture on units that will then implement the evidence-based intervention—in this case, eliminating central-line infections.
Hospitalists can play a critical role in helping create that culture of mutual accountability at the team level [and] holding each other accountable to use the evidence-based techniques for, in this case, line insertion, or for any kind of safety intervention. I think eliminating infections is a goal that’s achievable. I think we have come to the understanding over the last five or so years that these complications are avoidable in many, many cases, and that it takes teamwork, communication, and use of evidence-based procedures to get the work done.
Q: What can be done to help reduce preventable hospital readmissions?
A: There are so many things that go into readmissions. And the issue is: What is truly preventable in terms of treatments within the hospital, the coordination of discharge, and aftercare followup? A lot of readmissions are related to social determinants of health. And those have to do with people’s ability to afford their medications, people’s ability to access care, people’s home environment, and things of that nature. It’s going to take an approach by hospitals on those things that are controllable in partnerships with the physicians. But for many, many readmissions, it’s related to other issues that we as a society really have to hold ourselves accountable to.
Q: Some critics have charged that the overuse of medical technology is helping to drive up healthcare costs. Would there be more of a role for hospitals in decision-making about the appropriateness of tests within a model like an ACO?
A: In an ACO, that’s a partnership between hospitals and physicians operating as one entity. So that’s the difference, because there, everybody is aligned to make sure that we deliver the most effective care. There’s going to be much more time spent on physicians ordering the most appropriate technology or treatments for that condition that will deliver value to the patient and to the payor of that care.
But that’s in a totally integrated system. Right now we don’t have that. So where the interests of the physicians may be different from the interests of the hospital and the intentions are not aligned, it’s very hard to get at talking about what’s the most effective care.
Q: Is there a measure that hasn’t received as much attention that you would like to see more focus on to help improve the quality or cost-effectiveness of healthcare?
A: I think the one area that we’re always challenged with—and I think we’ve seen it in the healthcare debate, and I think it’s an appropriate role for us as healthcare providers to pay attention to—is palliative and end-of-life care. I don’t think we’ve done enough work, as a profession, to make sure that we deliver very-high-quality care of patients with chronic and acute catastrophic illnesses.
We need to better understand what the needs of those patients are, to ask them to work with us to set the goals with them, what they want from us.
So I think it’s an opportunity for us to have a real partnership with patients at a critical time in their lives. TH
Bryn Nelson is a freelance medical writer based in Seattle.
Focused Practice in Hospital Medicine
Some in her HM group think Cathleen Ammann, MD, is the guinea pig. Dr. Ammann, the medical director of the hospital medicine division at Wentworth-Douglass Hospital in Dover, N.H., will be one of the first to complete her American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) through the new Focused Practice in Hospital Medicine (FPHM) pathway. Dr. Ammann—and the hospital administration—sees things a little differently.
“Am I the guinea pig or a pioneer?” a hospitalist in Dr. Ammann’s group asked her recently. “I definitely see it as being a pioneer. When you look back in another 10 years, hospital medicine might be a specialty with its own certification. I know it’s a little corny, but I look forward to getting in on that at the ground floor.”
Dr. Ammann is one of about 175 hospitalists who have signed up to recertify through FPHM. Her internal-medicine (IM) certification expires at the end of the year, so she will be taking the recertification exam Oct. 25.
“I hope the test focuses more on what I’m doing … stroke, quality measures,” she says. “Hospitalists know that stuff like the back of our hand. … I think it will work out well for me, but I also think it will be great for our program to have a director who has a Focused Practice in Hospital Medicine. It shows my commitment, and we can hold that up to the rest of the organization and say we really have someone who is concentrated in this field.”
Why Should I Pay Extra?

“We’re actually carving out a new exam,” Dr. Holmboe explains. “The two biggest drivers were the committee for the new test to create the exam and the infrastructure changes to the website.”
Dr. Holmboe also points out that although the test will cost more than a general IM MOC ($1,570), it remains less than a subspecialty MOC.—JC
Dr. Ammann sums up the thinking of many HM leaders who’ve been working with ABIM and the American Board of Medical Specialties to launch the MOC pathway for hospitalists: Not only does a focused practice certification allow the more than 30,000 hospitalists in the U.S. to define themselves as different, it also provides hospitalists an MOC process and secured examination more acutely tailored to their skill sets and daily practice. The new pathway also requires ACLS certification and stresses continued “maintenance of competency,” according to SHM leaders, through a triennial self-evaluation requirement (60 self-evaluation points, with at least 20 points from medical knowledge modules and 40 points from completion of practice performance modules). The traditional IM MOC requires a practice-improvement module (PIM) every 10 years.
“The process will ask diplomates to participate in practice improvement every three years, which will focus on the ongoing need for performance improvement,” says Jeff Wiese, MD, FACP, SFHM, SHM president and chair of the ABIM Hospital Medicine MOC Question Writing Committee. “It will separate out the authentic hospitalist who is representing the goals and virtues that we are espousing as a society, particularly with regards to quality healthcare and safe healthcare. But I also think there are unique benefits for the patient that will be receiving the healthcare, because through this process, I believe, every diplomate will be a better hospitalist as a product of having done it.”
Here’s a brief look at what hospitalists interested in the FPHM MOC can expect:
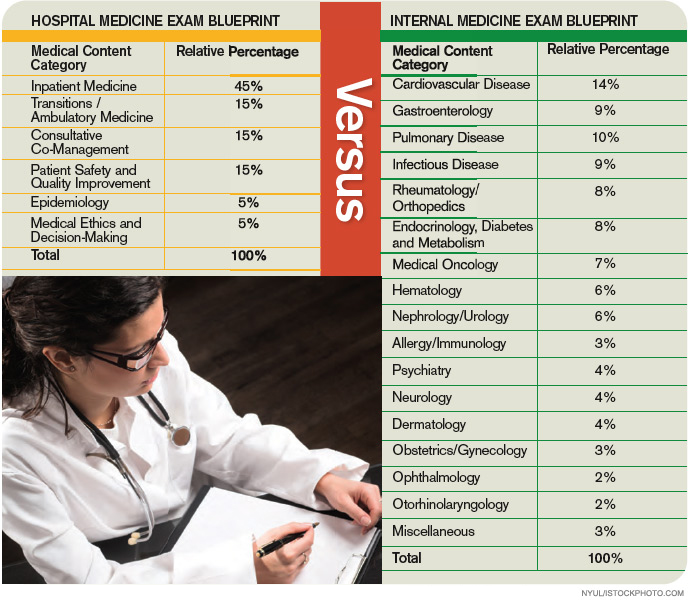
The Process and Timeline
ABIM and SHM began working toward an HM-focused pathway about five years ago, and the two groups announced the FPHM program in September 2009. ABIM is in the process of retooling its website for the new MOC pathway. The entry system—to sign up and begin the MOC’s attestation process—was made public in March. The registration interface for the secure exam opened to the hospitalist community May 1, says Eric Holmboe, MD, ABIM’s chief medical officer.
“Diplomates can signify their interest and start the attestation process, which will allow them to get formal entry into the pathway,” Dr. Holmboe says. “Once they receive the attestation confirmation back, they can start doing the requirements around the medical knowledge and performance and practice requirements. Those are all available on the website. … We’re excited. The first phase of the project is live. This is a brand-new pathway for MOC, and we’re really hopeful people will find it valuable and useful.”
Board recertification is no easy task, and prospective diplomates should organize a plan of attack based upon individual workloads and regular involvement in performance-improvement programs. Some hospitalists will only need six to nine months to complete all the requirements and take the exam; others might take a conservative approach and need one to two years.
“Eighteen months is very reasonable,” Dr. Holmboe says. “Because of the 40-point requirement for the evaluation of performance and practice, that means you have to do the hospital-based PIM or self-directed PIM, or some combination thereof, twice. So if you haven’t been active in QI projects in your hospital, you really need to get going.”
Some hospitalists and HM groups work on quality-improvement (QI) projects regularly. Dr. Ammann plans to use a recent QI project looking at her group’s compliance with antibiotic selection for pneumonia to satisfy one of her required PIMs.

“[The three-year] requirement should be easy for directors because we’re always doing that kind of work anyway,” she says. “We just finished a project where we had to improve our compliance with antibiotic selection. We looked at our processes and found that our pathway wasn’t clear, and it could be interpreted a couple different ways. So our chief of medicine and I just changed the pathway, put it out there, and since then, our compliance has consistently been 100%.
We have two quarters of data, and I’m going to use that for my PIM, which is nice, because it’s done.”
For hospitalists whose certification runs out in 2011 or beyond, Dr. Holmboe suggests the following timeline:
Now through end of 2010
- Register for the Focused Practice in Hospital Medicine MOC pathway on ABIM’ website (www.abim.org/moc/policies. aspx);
- Complete the attestation process;
- Get involved in an appropriate (hospital-based) performance-improvement activity; and
- Complete Update in Hospital Medicine using ABIM or ACP medical education modules.

—Cathleen Ammann, MD, medical director, hospital medicine division, Wentworth-Douglass Hospital, Dover, N.H.
First six months of 2011
- Complete the next yearly Update in HM module;
- Develop a strategy to prepare for the exam, which is given in the fall; and
- Plan and complete your second performance improvement activity.
Second half of 2011
- Prepare for the exam; and
- Pass the exam.
Start Process Now, Start Earning Points
ABIM is encouraging prospective FPHM diplomates to begin working on medical-knowledge modules. Most are designed to “stretch folks and to get them to look things up.”
“ACP, to their credit, also has hospital-based modules,” Dr. Holmboe says. “So if somebody is a dual member, they can certainly use the ACP’s MKSAP (Medical Knowledge Self-Assessment Program) hospital-based modules as well. We’re also working with SHM, looking for areas they might fill in around knowledge and updates—things that could be brought into the program over time.”
In regard to the evaluation and performance modules, ABIM offers three main pathways, including the Hospital-Based PIM, which targets core measure sets like community-acquired pneumonia and congestive heart failure and DVT prophylaxis. “Hospitalists can use those PIMs to start a quality-improvement program, or they can use it to report on one they are working on,” Dr. Holmboe says, adding the Hospital Based PIM’s online module will be redesigned this summer to improve the user experience.
Two other approaches are the Self-Directed PIM and the Accepted Quality Improvement programs. “That would be for hospitalists who may not be working on the core measure sets in the hospital-based PIM, but are still important,” he says. “They can use that module to report on those activities and get the points they need.”
Dr. Holmboe also points out that diplomates do not have to complete all the other requirements before they take the exam. “Some people get confused; you don’t have to cram in the 100 points before the exam,” Dr. Holmboe explains. He notes that the exam can, for example, be taken this year and the remainder of the requirements completed at a later date.
“If it was up to me, you should do a [PIM] every year,” says Larry Wellikson, MD, SFHM, CEO of SHM and one of the architects of the new FPHM pathway. “If you are a real hospitalist, completing a PIM every three years shouldn’t be a big deal. You should be able to say, ‘I’ve looked at 10 things: how I’m doing in pneumonia, how I’m doing in DVT, how I’m doing in glycemic control. This isn’t work for me; it’s part of my workflow.’ It’s like asking a salesman how many sales calls have you made, how many miles have you driven, and how many sales have you closed.”
The Examination
Dr. Wiese, associate dean of Graduate Medical Education and professor of medicine at Tulane University in New Orleans, completed his 10-year MOC in 2008, and he says the process made him “a better physician.” As president of SHM and chair of the FPHM test-writing committee, he envisions that the new MOC pathway will help “ramp up the quality of care for the hospitalized patient.”
“The FPHM MOC process is much more than just a different exam,” he says. “It is true the secure examination will have a lot more hospital-medicine-patient content focus, but not to the exclusion of ambulatory content.”

—Jeff Wiese, SHM president, ABIM Focused Practice in Hospital Medicine Test Writing Committee chair
The content-area blueprint (see “Traditional IM Test vs. Focused Practice in HM Test” below) for the FPHM exam includes 15% of questions in the areas of quality and patient safety, along with another 15% in consultative and comanagement topics. Transitions of care and ambulatory questions make up another 15% of the exam.
“If there is one component of the exam that will [be HM-focused], it’s the questions of the exam that are focusing on the core principles of quality and patient safety,” Dr. Wiese says.
That’s music to the ears of many hospitalists—including Dr. Ammann—who know questions about managing cholesterol aren’t relevant to hospitalists. Dr. Ammann was an office-based physician before becoming a hospitalist in 2005. One year later, she was promoted to director of her group, which includes 14 physicians and two nonphysician providers.
“I was really hoping I would be able to [MOC] through the focused practice in HM,” she says. “I did practice office medicine, so I probably have a little advantage. But I was not looking forward to spending time learning and brushing up on things that I am not doing anymore—not only because I’m not doing it anymore, but it would be a waste of time because I’m not going to be doing it, either.”
One of her hospitalist colleagues is taking the traditional IM pathway to MOC, Dr. Ammann says, because “she doesn’t want to limit her scope.” But that’s not how Dr. Ammann sees the FPHM. She is committed to HM and doesn’t have “any problems kissing office medicine goodbye.”
“I think it will work out well for me, but I also think it will be great for our program to have a director who has a Focused Practice in Hospital Medicine,” she says. “It shows my commitment, and we can hold that up to the rest of the organization and say we really have someone who is concentrated in this field.”
Educational Efforts
Vikas Parekh, MD, FHM, is in his second year as the chair of SHM’s Education Committee, and says the first task at hand is to educate hospitalists about the new FPHM pathway to MOC. The University of Michigan hospitalist says his committee, working with ABIM and SHM staff, is focused on two major educational efforts: developing the SHM strategy to assist hospitalists with the new FPHM MOC pathway, and “fulfilling the needs of hospitalists, in terms of the resources they have for the MOC process.”
“We’ve already started down this route, in terms of developing resources,” Dr. Parekh says. “We’ve done a few things that have been easy. One is the ABIM learning session pre-course at the annual meeting. … It earns you points toward the medical-knowledge component.”
ABIM and ACP are the traditional avenues for medical-knowledge and practice-improvement requirements for the MOC process. SHM and ABIM currently are working to develop medical-knowledge modules in the domains of patient safety and quality improvement, areas most relevant to HM. Dr. Parekh expects those components to be available in early 2011.
“Practice improvement is likely to be our second main effort,” Dr. Parekh says. “SHM has a lot of resources within our resource rooms that have the shell of what you would really need to meet ABIM requirements for a PIM but aren’t quite complete or thorough enough, or have all the bells and whistles that ABIM wants them to have. … We think we can do a much better job focusing the PIMs to hospitalists.”
At a more granular level, Dr. Wellikson envisions a “suite of products” to assist members in the MOC process. “What we are trying to do is develop resources that help people practice better medicine,” he says, “and while we are helping you practice better medicine, you can also use that to prove to [ABIM] that you have done it.
“So if you log onto the website today and downloaded and completed any of those SHM resource rooms, somewhere in the next several months you will be able to click on a form, enter the results, send it to ABIM, and you’ll have satisfied a PIM,” Dr. Wellikson says. “You can do the work today.”
SHM’s Project BOOST (Better Outcomes for Older Adults through Safer Transitions) and Glycemic Control Mentored Implementation programs are prime candidates for Web-based PIMs, according to Dr. Holmboe.
“I think it is still very early, but we are very excited about this,” Dr. Parekh says. “I think a lot of people still have questions about what exactly this mean to me, and why should I recertify through this focused practice as opposed to the traditional general pathway? We hope to change that by making the resources focused to their practice.” TH
Jason Carris is editor of The Hospitalist.

Hospitalists as Test Subjects
Seeing as how the focused-practice pathway for hospitalists is a first of its kind for physician credentialing boards, the ABIM is planning a “fairly significant” research effort tracking participants’ experience, Dr. Holmboe says.
“We’re also going to spend time talking with credentialists and other stakeholders about what value they potentially see having someone participate in this focused-practice pathway,” he says. “The more folks that can do this in the first one or two years, the better, because it will give us an opportunity to learn if the approach makes sense and is providing value to the diplomates, as well as the other stakeholders, such as the hospitals and credentialing agencies.”
Dr. Holmboe also expects ABIM to explore ways to assess teamwork skills in the hospital setting. ABIM is shooting for a mid- to late-summer launch of beta testing, and hospitalists who participate in the pilot program will receive MOC credit.
“It’s an area that, when we were developing the program, came out repeatedly from the leadership of the community—how important teamwork is for this discipline,” he says.
In all, ABIM and hospitalists are blazing new trails in certification testing and fulfillment.
“It’s fair to say the HM community is pioneer in this concept of continuous maintenance of certification, or, if you want to say, maintenance of competence,” Dr. Holmboe says. “That was an initial part of the conversation five years ago. They have really set the table. What we learn from this group will help inform the MOC program.”—JC
Some in her HM group think Cathleen Ammann, MD, is the guinea pig. Dr. Ammann, the medical director of the hospital medicine division at Wentworth-Douglass Hospital in Dover, N.H., will be one of the first to complete her American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) through the new Focused Practice in Hospital Medicine (FPHM) pathway. Dr. Ammann—and the hospital administration—sees things a little differently.
“Am I the guinea pig or a pioneer?” a hospitalist in Dr. Ammann’s group asked her recently. “I definitely see it as being a pioneer. When you look back in another 10 years, hospital medicine might be a specialty with its own certification. I know it’s a little corny, but I look forward to getting in on that at the ground floor.”
Dr. Ammann is one of about 175 hospitalists who have signed up to recertify through FPHM. Her internal-medicine (IM) certification expires at the end of the year, so she will be taking the recertification exam Oct. 25.
“I hope the test focuses more on what I’m doing … stroke, quality measures,” she says. “Hospitalists know that stuff like the back of our hand. … I think it will work out well for me, but I also think it will be great for our program to have a director who has a Focused Practice in Hospital Medicine. It shows my commitment, and we can hold that up to the rest of the organization and say we really have someone who is concentrated in this field.”
Why Should I Pay Extra?
“We’re actually carving out a new exam,” Dr. Holmboe explains. “The two biggest drivers were the committee for the new test to create the exam and the infrastructure changes to the website.”
Dr. Holmboe also points out that although the test will cost more than a general IM MOC ($1,570), it remains less than a subspecialty MOC.—JC
Dr. Ammann sums up the thinking of many HM leaders who’ve been working with ABIM and the American Board of Medical Specialties to launch the MOC pathway for hospitalists: Not only does a focused practice certification allow the more than 30,000 hospitalists in the U.S. to define themselves as different, it also provides hospitalists an MOC process and secured examination more acutely tailored to their skill sets and daily practice. The new pathway also requires ACLS certification and stresses continued “maintenance of competency,” according to SHM leaders, through a triennial self-evaluation requirement (60 self-evaluation points, with at least 20 points from medical knowledge modules and 40 points from completion of practice performance modules). The traditional IM MOC requires a practice-improvement module (PIM) every 10 years.
“The process will ask diplomates to participate in practice improvement every three years, which will focus on the ongoing need for performance improvement,” says Jeff Wiese, MD, FACP, SFHM, SHM president and chair of the ABIM Hospital Medicine MOC Question Writing Committee. “It will separate out the authentic hospitalist who is representing the goals and virtues that we are espousing as a society, particularly with regards to quality healthcare and safe healthcare. But I also think there are unique benefits for the patient that will be receiving the healthcare, because through this process, I believe, every diplomate will be a better hospitalist as a product of having done it.”
Here’s a brief look at what hospitalists interested in the FPHM MOC can expect:
The Process and Timeline
ABIM and SHM began working toward an HM-focused pathway about five years ago, and the two groups announced the FPHM program in September 2009. ABIM is in the process of retooling its website for the new MOC pathway. The entry system—to sign up and begin the MOC’s attestation process—was made public in March. The registration interface for the secure exam opened to the hospitalist community May 1, says Eric Holmboe, MD, ABIM’s chief medical officer.
“Diplomates can signify their interest and start the attestation process, which will allow them to get formal entry into the pathway,” Dr. Holmboe says. “Once they receive the attestation confirmation back, they can start doing the requirements around the medical knowledge and performance and practice requirements. Those are all available on the website. … We’re excited. The first phase of the project is live. This is a brand-new pathway for MOC, and we’re really hopeful people will find it valuable and useful.”
Board recertification is no easy task, and prospective diplomates should organize a plan of attack based upon individual workloads and regular involvement in performance-improvement programs. Some hospitalists will only need six to nine months to complete all the requirements and take the exam; others might take a conservative approach and need one to two years.
“Eighteen months is very reasonable,” Dr. Holmboe says. “Because of the 40-point requirement for the evaluation of performance and practice, that means you have to do the hospital-based PIM or self-directed PIM, or some combination thereof, twice. So if you haven’t been active in QI projects in your hospital, you really need to get going.”
Some hospitalists and HM groups work on quality-improvement (QI) projects regularly. Dr. Ammann plans to use a recent QI project looking at her group’s compliance with antibiotic selection for pneumonia to satisfy one of her required PIMs.
“[The three-year] requirement should be easy for directors because we’re always doing that kind of work anyway,” she says. “We just finished a project where we had to improve our compliance with antibiotic selection. We looked at our processes and found that our pathway wasn’t clear, and it could be interpreted a couple different ways. So our chief of medicine and I just changed the pathway, put it out there, and since then, our compliance has consistently been 100%.
We have two quarters of data, and I’m going to use that for my PIM, which is nice, because it’s done.”
For hospitalists whose certification runs out in 2011 or beyond, Dr. Holmboe suggests the following timeline:
Now through end of 2010
- Register for the Focused Practice in Hospital Medicine MOC pathway on ABIM’ website (www.abim.org/moc/policies. aspx);
- Complete the attestation process;
- Get involved in an appropriate (hospital-based) performance-improvement activity; and
- Complete Update in Hospital Medicine using ABIM or ACP medical education modules.
—Cathleen Ammann, MD, medical director, hospital medicine division, Wentworth-Douglass Hospital, Dover, N.H.
First six months of 2011
- Complete the next yearly Update in HM module;
- Develop a strategy to prepare for the exam, which is given in the fall; and
- Plan and complete your second performance improvement activity.
Second half of 2011
- Prepare for the exam; and
- Pass the exam.
Start Process Now, Start Earning Points
ABIM is encouraging prospective FPHM diplomates to begin working on medical-knowledge modules. Most are designed to “stretch folks and to get them to look things up.”
“ACP, to their credit, also has hospital-based modules,” Dr. Holmboe says. “So if somebody is a dual member, they can certainly use the ACP’s MKSAP (Medical Knowledge Self-Assessment Program) hospital-based modules as well. We’re also working with SHM, looking for areas they might fill in around knowledge and updates—things that could be brought into the program over time.”
In regard to the evaluation and performance modules, ABIM offers three main pathways, including the Hospital-Based PIM, which targets core measure sets like community-acquired pneumonia and congestive heart failure and DVT prophylaxis. “Hospitalists can use those PIMs to start a quality-improvement program, or they can use it to report on one they are working on,” Dr. Holmboe says, adding the Hospital Based PIM’s online module will be redesigned this summer to improve the user experience.
Two other approaches are the Self-Directed PIM and the Accepted Quality Improvement programs. “That would be for hospitalists who may not be working on the core measure sets in the hospital-based PIM, but are still important,” he says. “They can use that module to report on those activities and get the points they need.”
Dr. Holmboe also points out that diplomates do not have to complete all the other requirements before they take the exam. “Some people get confused; you don’t have to cram in the 100 points before the exam,” Dr. Holmboe explains. He notes that the exam can, for example, be taken this year and the remainder of the requirements completed at a later date.
“If it was up to me, you should do a [PIM] every year,” says Larry Wellikson, MD, SFHM, CEO of SHM and one of the architects of the new FPHM pathway. “If you are a real hospitalist, completing a PIM every three years shouldn’t be a big deal. You should be able to say, ‘I’ve looked at 10 things: how I’m doing in pneumonia, how I’m doing in DVT, how I’m doing in glycemic control. This isn’t work for me; it’s part of my workflow.’ It’s like asking a salesman how many sales calls have you made, how many miles have you driven, and how many sales have you closed.”
The Examination
Dr. Wiese, associate dean of Graduate Medical Education and professor of medicine at Tulane University in New Orleans, completed his 10-year MOC in 2008, and he says the process made him “a better physician.” As president of SHM and chair of the FPHM test-writing committee, he envisions that the new MOC pathway will help “ramp up the quality of care for the hospitalized patient.”
“The FPHM MOC process is much more than just a different exam,” he says. “It is true the secure examination will have a lot more hospital-medicine-patient content focus, but not to the exclusion of ambulatory content.”
—Jeff Wiese, SHM president, ABIM Focused Practice in Hospital Medicine Test Writing Committee chair
The content-area blueprint (see “Traditional IM Test vs. Focused Practice in HM Test” below) for the FPHM exam includes 15% of questions in the areas of quality and patient safety, along with another 15% in consultative and comanagement topics. Transitions of care and ambulatory questions make up another 15% of the exam.
“If there is one component of the exam that will [be HM-focused], it’s the questions of the exam that are focusing on the core principles of quality and patient safety,” Dr. Wiese says.
That’s music to the ears of many hospitalists—including Dr. Ammann—who know questions about managing cholesterol aren’t relevant to hospitalists. Dr. Ammann was an office-based physician before becoming a hospitalist in 2005. One year later, she was promoted to director of her group, which includes 14 physicians and two nonphysician providers.
“I was really hoping I would be able to [MOC] through the focused practice in HM,” she says. “I did practice office medicine, so I probably have a little advantage. But I was not looking forward to spending time learning and brushing up on things that I am not doing anymore—not only because I’m not doing it anymore, but it would be a waste of time because I’m not going to be doing it, either.”
One of her hospitalist colleagues is taking the traditional IM pathway to MOC, Dr. Ammann says, because “she doesn’t want to limit her scope.” But that’s not how Dr. Ammann sees the FPHM. She is committed to HM and doesn’t have “any problems kissing office medicine goodbye.”
“I think it will work out well for me, but I also think it will be great for our program to have a director who has a Focused Practice in Hospital Medicine,” she says. “It shows my commitment, and we can hold that up to the rest of the organization and say we really have someone who is concentrated in this field.”
Educational Efforts
Vikas Parekh, MD, FHM, is in his second year as the chair of SHM’s Education Committee, and says the first task at hand is to educate hospitalists about the new FPHM pathway to MOC. The University of Michigan hospitalist says his committee, working with ABIM and SHM staff, is focused on two major educational efforts: developing the SHM strategy to assist hospitalists with the new FPHM MOC pathway, and “fulfilling the needs of hospitalists, in terms of the resources they have for the MOC process.”
“We’ve already started down this route, in terms of developing resources,” Dr. Parekh says. “We’ve done a few things that have been easy. One is the ABIM learning session pre-course at the annual meeting. … It earns you points toward the medical-knowledge component.”
ABIM and ACP are the traditional avenues for medical-knowledge and practice-improvement requirements for the MOC process. SHM and ABIM currently are working to develop medical-knowledge modules in the domains of patient safety and quality improvement, areas most relevant to HM. Dr. Parekh expects those components to be available in early 2011.
“Practice improvement is likely to be our second main effort,” Dr. Parekh says. “SHM has a lot of resources within our resource rooms that have the shell of what you would really need to meet ABIM requirements for a PIM but aren’t quite complete or thorough enough, or have all the bells and whistles that ABIM wants them to have. … We think we can do a much better job focusing the PIMs to hospitalists.”
At a more granular level, Dr. Wellikson envisions a “suite of products” to assist members in the MOC process. “What we are trying to do is develop resources that help people practice better medicine,” he says, “and while we are helping you practice better medicine, you can also use that to prove to [ABIM] that you have done it.
“So if you log onto the website today and downloaded and completed any of those SHM resource rooms, somewhere in the next several months you will be able to click on a form, enter the results, send it to ABIM, and you’ll have satisfied a PIM,” Dr. Wellikson says. “You can do the work today.”
SHM’s Project BOOST (Better Outcomes for Older Adults through Safer Transitions) and Glycemic Control Mentored Implementation programs are prime candidates for Web-based PIMs, according to Dr. Holmboe.
“I think it is still very early, but we are very excited about this,” Dr. Parekh says. “I think a lot of people still have questions about what exactly this mean to me, and why should I recertify through this focused practice as opposed to the traditional general pathway? We hope to change that by making the resources focused to their practice.” TH
Jason Carris is editor of The Hospitalist.
Hospitalists as Test Subjects
Seeing as how the focused-practice pathway for hospitalists is a first of its kind for physician credentialing boards, the ABIM is planning a “fairly significant” research effort tracking participants’ experience, Dr. Holmboe says.
“We’re also going to spend time talking with credentialists and other stakeholders about what value they potentially see having someone participate in this focused-practice pathway,” he says. “The more folks that can do this in the first one or two years, the better, because it will give us an opportunity to learn if the approach makes sense and is providing value to the diplomates, as well as the other stakeholders, such as the hospitals and credentialing agencies.”
Dr. Holmboe also expects ABIM to explore ways to assess teamwork skills in the hospital setting. ABIM is shooting for a mid- to late-summer launch of beta testing, and hospitalists who participate in the pilot program will receive MOC credit.
“It’s an area that, when we were developing the program, came out repeatedly from the leadership of the community—how important teamwork is for this discipline,” he says.
In all, ABIM and hospitalists are blazing new trails in certification testing and fulfillment.
“It’s fair to say the HM community is pioneer in this concept of continuous maintenance of certification, or, if you want to say, maintenance of competence,” Dr. Holmboe says. “That was an initial part of the conversation five years ago. They have really set the table. What we learn from this group will help inform the MOC program.”—JC
Some in her HM group think Cathleen Ammann, MD, is the guinea pig. Dr. Ammann, the medical director of the hospital medicine division at Wentworth-Douglass Hospital in Dover, N.H., will be one of the first to complete her American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) through the new Focused Practice in Hospital Medicine (FPHM) pathway. Dr. Ammann—and the hospital administration—sees things a little differently.
“Am I the guinea pig or a pioneer?” a hospitalist in Dr. Ammann’s group asked her recently. “I definitely see it as being a pioneer. When you look back in another 10 years, hospital medicine might be a specialty with its own certification. I know it’s a little corny, but I look forward to getting in on that at the ground floor.”
Dr. Ammann is one of about 175 hospitalists who have signed up to recertify through FPHM. Her internal-medicine (IM) certification expires at the end of the year, so she will be taking the recertification exam Oct. 25.
“I hope the test focuses more on what I’m doing … stroke, quality measures,” she says. “Hospitalists know that stuff like the back of our hand. … I think it will work out well for me, but I also think it will be great for our program to have a director who has a Focused Practice in Hospital Medicine. It shows my commitment, and we can hold that up to the rest of the organization and say we really have someone who is concentrated in this field.”
Why Should I Pay Extra?
“We’re actually carving out a new exam,” Dr. Holmboe explains. “The two biggest drivers were the committee for the new test to create the exam and the infrastructure changes to the website.”
Dr. Holmboe also points out that although the test will cost more than a general IM MOC ($1,570), it remains less than a subspecialty MOC.—JC
Dr. Ammann sums up the thinking of many HM leaders who’ve been working with ABIM and the American Board of Medical Specialties to launch the MOC pathway for hospitalists: Not only does a focused practice certification allow the more than 30,000 hospitalists in the U.S. to define themselves as different, it also provides hospitalists an MOC process and secured examination more acutely tailored to their skill sets and daily practice. The new pathway also requires ACLS certification and stresses continued “maintenance of competency,” according to SHM leaders, through a triennial self-evaluation requirement (60 self-evaluation points, with at least 20 points from medical knowledge modules and 40 points from completion of practice performance modules). The traditional IM MOC requires a practice-improvement module (PIM) every 10 years.
“The process will ask diplomates to participate in practice improvement every three years, which will focus on the ongoing need for performance improvement,” says Jeff Wiese, MD, FACP, SFHM, SHM president and chair of the ABIM Hospital Medicine MOC Question Writing Committee. “It will separate out the authentic hospitalist who is representing the goals and virtues that we are espousing as a society, particularly with regards to quality healthcare and safe healthcare. But I also think there are unique benefits for the patient that will be receiving the healthcare, because through this process, I believe, every diplomate will be a better hospitalist as a product of having done it.”
Here’s a brief look at what hospitalists interested in the FPHM MOC can expect:
The Process and Timeline
ABIM and SHM began working toward an HM-focused pathway about five years ago, and the two groups announced the FPHM program in September 2009. ABIM is in the process of retooling its website for the new MOC pathway. The entry system—to sign up and begin the MOC’s attestation process—was made public in March. The registration interface for the secure exam opened to the hospitalist community May 1, says Eric Holmboe, MD, ABIM’s chief medical officer.
“Diplomates can signify their interest and start the attestation process, which will allow them to get formal entry into the pathway,” Dr. Holmboe says. “Once they receive the attestation confirmation back, they can start doing the requirements around the medical knowledge and performance and practice requirements. Those are all available on the website. … We’re excited. The first phase of the project is live. This is a brand-new pathway for MOC, and we’re really hopeful people will find it valuable and useful.”
Board recertification is no easy task, and prospective diplomates should organize a plan of attack based upon individual workloads and regular involvement in performance-improvement programs. Some hospitalists will only need six to nine months to complete all the requirements and take the exam; others might take a conservative approach and need one to two years.
“Eighteen months is very reasonable,” Dr. Holmboe says. “Because of the 40-point requirement for the evaluation of performance and practice, that means you have to do the hospital-based PIM or self-directed PIM, or some combination thereof, twice. So if you haven’t been active in QI projects in your hospital, you really need to get going.”
Some hospitalists and HM groups work on quality-improvement (QI) projects regularly. Dr. Ammann plans to use a recent QI project looking at her group’s compliance with antibiotic selection for pneumonia to satisfy one of her required PIMs.
“[The three-year] requirement should be easy for directors because we’re always doing that kind of work anyway,” she says. “We just finished a project where we had to improve our compliance with antibiotic selection. We looked at our processes and found that our pathway wasn’t clear, and it could be interpreted a couple different ways. So our chief of medicine and I just changed the pathway, put it out there, and since then, our compliance has consistently been 100%.
We have two quarters of data, and I’m going to use that for my PIM, which is nice, because it’s done.”
For hospitalists whose certification runs out in 2011 or beyond, Dr. Holmboe suggests the following timeline:
Now through end of 2010
- Register for the Focused Practice in Hospital Medicine MOC pathway on ABIM’ website (www.abim.org/moc/policies. aspx);
- Complete the attestation process;
- Get involved in an appropriate (hospital-based) performance-improvement activity; and
- Complete Update in Hospital Medicine using ABIM or ACP medical education modules.
—Cathleen Ammann, MD, medical director, hospital medicine division, Wentworth-Douglass Hospital, Dover, N.H.
First six months of 2011
- Complete the next yearly Update in HM module;
- Develop a strategy to prepare for the exam, which is given in the fall; and
- Plan and complete your second performance improvement activity.
Second half of 2011
- Prepare for the exam; and
- Pass the exam.
Start Process Now, Start Earning Points
ABIM is encouraging prospective FPHM diplomates to begin working on medical-knowledge modules. Most are designed to “stretch folks and to get them to look things up.”
“ACP, to their credit, also has hospital-based modules,” Dr. Holmboe says. “So if somebody is a dual member, they can certainly use the ACP’s MKSAP (Medical Knowledge Self-Assessment Program) hospital-based modules as well. We’re also working with SHM, looking for areas they might fill in around knowledge and updates—things that could be brought into the program over time.”
In regard to the evaluation and performance modules, ABIM offers three main pathways, including the Hospital-Based PIM, which targets core measure sets like community-acquired pneumonia and congestive heart failure and DVT prophylaxis. “Hospitalists can use those PIMs to start a quality-improvement program, or they can use it to report on one they are working on,” Dr. Holmboe says, adding the Hospital Based PIM’s online module will be redesigned this summer to improve the user experience.
Two other approaches are the Self-Directed PIM and the Accepted Quality Improvement programs. “That would be for hospitalists who may not be working on the core measure sets in the hospital-based PIM, but are still important,” he says. “They can use that module to report on those activities and get the points they need.”
Dr. Holmboe also points out that diplomates do not have to complete all the other requirements before they take the exam. “Some people get confused; you don’t have to cram in the 100 points before the exam,” Dr. Holmboe explains. He notes that the exam can, for example, be taken this year and the remainder of the requirements completed at a later date.
“If it was up to me, you should do a [PIM] every year,” says Larry Wellikson, MD, SFHM, CEO of SHM and one of the architects of the new FPHM pathway. “If you are a real hospitalist, completing a PIM every three years shouldn’t be a big deal. You should be able to say, ‘I’ve looked at 10 things: how I’m doing in pneumonia, how I’m doing in DVT, how I’m doing in glycemic control. This isn’t work for me; it’s part of my workflow.’ It’s like asking a salesman how many sales calls have you made, how many miles have you driven, and how many sales have you closed.”
The Examination
Dr. Wiese, associate dean of Graduate Medical Education and professor of medicine at Tulane University in New Orleans, completed his 10-year MOC in 2008, and he says the process made him “a better physician.” As president of SHM and chair of the FPHM test-writing committee, he envisions that the new MOC pathway will help “ramp up the quality of care for the hospitalized patient.”
“The FPHM MOC process is much more than just a different exam,” he says. “It is true the secure examination will have a lot more hospital-medicine-patient content focus, but not to the exclusion of ambulatory content.”
—Jeff Wiese, SHM president, ABIM Focused Practice in Hospital Medicine Test Writing Committee chair
The content-area blueprint (see “Traditional IM Test vs. Focused Practice in HM Test” below) for the FPHM exam includes 15% of questions in the areas of quality and patient safety, along with another 15% in consultative and comanagement topics. Transitions of care and ambulatory questions make up another 15% of the exam.
“If there is one component of the exam that will [be HM-focused], it’s the questions of the exam that are focusing on the core principles of quality and patient safety,” Dr. Wiese says.
That’s music to the ears of many hospitalists—including Dr. Ammann—who know questions about managing cholesterol aren’t relevant to hospitalists. Dr. Ammann was an office-based physician before becoming a hospitalist in 2005. One year later, she was promoted to director of her group, which includes 14 physicians and two nonphysician providers.
“I was really hoping I would be able to [MOC] through the focused practice in HM,” she says. “I did practice office medicine, so I probably have a little advantage. But I was not looking forward to spending time learning and brushing up on things that I am not doing anymore—not only because I’m not doing it anymore, but it would be a waste of time because I’m not going to be doing it, either.”
One of her hospitalist colleagues is taking the traditional IM pathway to MOC, Dr. Ammann says, because “she doesn’t want to limit her scope.” But that’s not how Dr. Ammann sees the FPHM. She is committed to HM and doesn’t have “any problems kissing office medicine goodbye.”
“I think it will work out well for me, but I also think it will be great for our program to have a director who has a Focused Practice in Hospital Medicine,” she says. “It shows my commitment, and we can hold that up to the rest of the organization and say we really have someone who is concentrated in this field.”
Educational Efforts
Vikas Parekh, MD, FHM, is in his second year as the chair of SHM’s Education Committee, and says the first task at hand is to educate hospitalists about the new FPHM pathway to MOC. The University of Michigan hospitalist says his committee, working with ABIM and SHM staff, is focused on two major educational efforts: developing the SHM strategy to assist hospitalists with the new FPHM MOC pathway, and “fulfilling the needs of hospitalists, in terms of the resources they have for the MOC process.”
“We’ve already started down this route, in terms of developing resources,” Dr. Parekh says. “We’ve done a few things that have been easy. One is the ABIM learning session pre-course at the annual meeting. … It earns you points toward the medical-knowledge component.”
ABIM and ACP are the traditional avenues for medical-knowledge and practice-improvement requirements for the MOC process. SHM and ABIM currently are working to develop medical-knowledge modules in the domains of patient safety and quality improvement, areas most relevant to HM. Dr. Parekh expects those components to be available in early 2011.
“Practice improvement is likely to be our second main effort,” Dr. Parekh says. “SHM has a lot of resources within our resource rooms that have the shell of what you would really need to meet ABIM requirements for a PIM but aren’t quite complete or thorough enough, or have all the bells and whistles that ABIM wants them to have. … We think we can do a much better job focusing the PIMs to hospitalists.”
At a more granular level, Dr. Wellikson envisions a “suite of products” to assist members in the MOC process. “What we are trying to do is develop resources that help people practice better medicine,” he says, “and while we are helping you practice better medicine, you can also use that to prove to [ABIM] that you have done it.
“So if you log onto the website today and downloaded and completed any of those SHM resource rooms, somewhere in the next several months you will be able to click on a form, enter the results, send it to ABIM, and you’ll have satisfied a PIM,” Dr. Wellikson says. “You can do the work today.”
SHM’s Project BOOST (Better Outcomes for Older Adults through Safer Transitions) and Glycemic Control Mentored Implementation programs are prime candidates for Web-based PIMs, according to Dr. Holmboe.
“I think it is still very early, but we are very excited about this,” Dr. Parekh says. “I think a lot of people still have questions about what exactly this mean to me, and why should I recertify through this focused practice as opposed to the traditional general pathway? We hope to change that by making the resources focused to their practice.” TH
Jason Carris is editor of The Hospitalist.
Hospitalists as Test Subjects
Seeing as how the focused-practice pathway for hospitalists is a first of its kind for physician credentialing boards, the ABIM is planning a “fairly significant” research effort tracking participants’ experience, Dr. Holmboe says.
“We’re also going to spend time talking with credentialists and other stakeholders about what value they potentially see having someone participate in this focused-practice pathway,” he says. “The more folks that can do this in the first one or two years, the better, because it will give us an opportunity to learn if the approach makes sense and is providing value to the diplomates, as well as the other stakeholders, such as the hospitals and credentialing agencies.”
Dr. Holmboe also expects ABIM to explore ways to assess teamwork skills in the hospital setting. ABIM is shooting for a mid- to late-summer launch of beta testing, and hospitalists who participate in the pilot program will receive MOC credit.
“It’s an area that, when we were developing the program, came out repeatedly from the leadership of the community—how important teamwork is for this discipline,” he says.
In all, ABIM and hospitalists are blazing new trails in certification testing and fulfillment.
“It’s fair to say the HM community is pioneer in this concept of continuous maintenance of certification, or, if you want to say, maintenance of competence,” Dr. Holmboe says. “That was an initial part of the conversation five years ago. They have really set the table. What we learn from this group will help inform the MOC program.”—JC
Wachter’s World
NATIONAL HARBOR, Md.—Democrats and Republicans have trumpeted that unprecedented changes in the healthcare system are on the way, but the dean of HM cautions that significant change is still years away.
“The reform bill, to my mind, mostly kicked the hard decision for cost, quality, and safety down the road,” said Bob Wachter, MD, MHM, chief of the hospitalist division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco. “All of these issues have been raised, though.”
Dr. Wachter, former SHM president, author of the blog Wachter’s World (www.wachters world.com), and recently named the 10th-most-powerful physician executive in the nation by Modern Healthcare, used his annual HM10 address to paint a cautiously optimistic picture of HM playing a leading role in quality, safety, and innovation in the delivery of healthcare.
“It is a completely open question, whether we will be capable of snapping our fingers and creating a set of incentives or policy drivers that will allow the creation of the next Geisinger [Health System] without waiting 50 years,” Dr. Wachter said. “These cultures take a long time to develop. It’s not just about the [organizational] chart and the way money flows. You have to develop the culture of shared governance.”
In what has become a rite, Dr. Wachter gives the closing address at SHM’s annual meeting. This year’s title: “Use Your Words: Understanding the New Language of Healthcare Reform.” He focused most of his speech on finding the balance between high-quality and low-cost patient care, particularly when viewed through the prism of the “cost curve,” the economic principle that measures benefits against their cost.
Medical care on the “flat part of the curve” equates to tests, procedures, or other engagements that might have prophylactic value but little clinical benefit. From a purely clinical point of view, that is acceptable, but layering in a cost-benefit analysis adds a more objective way of deciding whether the care delivered is “worth the cost,” Dr. Wachter said.
—Bob Wachter, MD, MHM, chief of the hospitalist division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco
“The question is: Where do we want to live on this curve?” he added. “As you spend more money, you may be getting more benefit, but the incremental amount . . . pushes out past the flat part of curve.”
Dr. Wachter boiled his lesson down to two philosophies. In one, the practice of HM means a test, a procedure, or a consult is ordered because the benefits outweigh the risks. In the other, that same episodic treatment is ordered only if every less-expensive option has already been attempted. “These are absolutely fundamental tensions,” he admitted.
But not all that is reform must be contentious, he said. Take the renewed push toward “accountable-care organizations,” in which providers partner and share responsibility for both the quality and cost of healthcare for a specific population of beneficiaries. The healthcare reform bill contains incentives for such a structure, which Dr. Wachter views as the government’s latest attempt to improve care by controlling how much reimbursement physicians and their employers receive.
While other specialists might not be experienced with data-point discussions on cost savings with hospital administrators, HM leaders are all too familiar with the concept, as most have those discussions during annual hospital subsidy negotiations. Correspondingly, those who listened to Dr. Wachter’s advice agreed that there is ample opportunity to lead the charge for quality and safety improvement—and the likely savings to be associated with those changes.
“Let’s be patient for what’s coming around the corner,” said Daniel Dressler, MD, SFHM, director of hospital medicine at Emory University Hospital in Atlanta and an SHM board member. “But let’s not miss the boat.” HM2010
Richard Quinn is a freelance writer based in New Jersey.
NATIONAL HARBOR, Md.—Democrats and Republicans have trumpeted that unprecedented changes in the healthcare system are on the way, but the dean of HM cautions that significant change is still years away.
“The reform bill, to my mind, mostly kicked the hard decision for cost, quality, and safety down the road,” said Bob Wachter, MD, MHM, chief of the hospitalist division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco. “All of these issues have been raised, though.”
Dr. Wachter, former SHM president, author of the blog Wachter’s World (www.wachters world.com), and recently named the 10th-most-powerful physician executive in the nation by Modern Healthcare, used his annual HM10 address to paint a cautiously optimistic picture of HM playing a leading role in quality, safety, and innovation in the delivery of healthcare.
“It is a completely open question, whether we will be capable of snapping our fingers and creating a set of incentives or policy drivers that will allow the creation of the next Geisinger [Health System] without waiting 50 years,” Dr. Wachter said. “These cultures take a long time to develop. It’s not just about the [organizational] chart and the way money flows. You have to develop the culture of shared governance.”
In what has become a rite, Dr. Wachter gives the closing address at SHM’s annual meeting. This year’s title: “Use Your Words: Understanding the New Language of Healthcare Reform.” He focused most of his speech on finding the balance between high-quality and low-cost patient care, particularly when viewed through the prism of the “cost curve,” the economic principle that measures benefits against their cost.
Medical care on the “flat part of the curve” equates to tests, procedures, or other engagements that might have prophylactic value but little clinical benefit. From a purely clinical point of view, that is acceptable, but layering in a cost-benefit analysis adds a more objective way of deciding whether the care delivered is “worth the cost,” Dr. Wachter said.
—Bob Wachter, MD, MHM, chief of the hospitalist division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco
“The question is: Where do we want to live on this curve?” he added. “As you spend more money, you may be getting more benefit, but the incremental amount . . . pushes out past the flat part of curve.”
Dr. Wachter boiled his lesson down to two philosophies. In one, the practice of HM means a test, a procedure, or a consult is ordered because the benefits outweigh the risks. In the other, that same episodic treatment is ordered only if every less-expensive option has already been attempted. “These are absolutely fundamental tensions,” he admitted.
But not all that is reform must be contentious, he said. Take the renewed push toward “accountable-care organizations,” in which providers partner and share responsibility for both the quality and cost of healthcare for a specific population of beneficiaries. The healthcare reform bill contains incentives for such a structure, which Dr. Wachter views as the government’s latest attempt to improve care by controlling how much reimbursement physicians and their employers receive.
While other specialists might not be experienced with data-point discussions on cost savings with hospital administrators, HM leaders are all too familiar with the concept, as most have those discussions during annual hospital subsidy negotiations. Correspondingly, those who listened to Dr. Wachter’s advice agreed that there is ample opportunity to lead the charge for quality and safety improvement—and the likely savings to be associated with those changes.
“Let’s be patient for what’s coming around the corner,” said Daniel Dressler, MD, SFHM, director of hospital medicine at Emory University Hospital in Atlanta and an SHM board member. “But let’s not miss the boat.” HM2010
Richard Quinn is a freelance writer based in New Jersey.
NATIONAL HARBOR, Md.—Democrats and Republicans have trumpeted that unprecedented changes in the healthcare system are on the way, but the dean of HM cautions that significant change is still years away.
“The reform bill, to my mind, mostly kicked the hard decision for cost, quality, and safety down the road,” said Bob Wachter, MD, MHM, chief of the hospitalist division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco. “All of these issues have been raised, though.”
Dr. Wachter, former SHM president, author of the blog Wachter’s World (www.wachters world.com), and recently named the 10th-most-powerful physician executive in the nation by Modern Healthcare, used his annual HM10 address to paint a cautiously optimistic picture of HM playing a leading role in quality, safety, and innovation in the delivery of healthcare.
“It is a completely open question, whether we will be capable of snapping our fingers and creating a set of incentives or policy drivers that will allow the creation of the next Geisinger [Health System] without waiting 50 years,” Dr. Wachter said. “These cultures take a long time to develop. It’s not just about the [organizational] chart and the way money flows. You have to develop the culture of shared governance.”
In what has become a rite, Dr. Wachter gives the closing address at SHM’s annual meeting. This year’s title: “Use Your Words: Understanding the New Language of Healthcare Reform.” He focused most of his speech on finding the balance between high-quality and low-cost patient care, particularly when viewed through the prism of the “cost curve,” the economic principle that measures benefits against their cost.
Medical care on the “flat part of the curve” equates to tests, procedures, or other engagements that might have prophylactic value but little clinical benefit. From a purely clinical point of view, that is acceptable, but layering in a cost-benefit analysis adds a more objective way of deciding whether the care delivered is “worth the cost,” Dr. Wachter said.
—Bob Wachter, MD, MHM, chief of the hospitalist division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco
“The question is: Where do we want to live on this curve?” he added. “As you spend more money, you may be getting more benefit, but the incremental amount . . . pushes out past the flat part of curve.”
Dr. Wachter boiled his lesson down to two philosophies. In one, the practice of HM means a test, a procedure, or a consult is ordered because the benefits outweigh the risks. In the other, that same episodic treatment is ordered only if every less-expensive option has already been attempted. “These are absolutely fundamental tensions,” he admitted.
But not all that is reform must be contentious, he said. Take the renewed push toward “accountable-care organizations,” in which providers partner and share responsibility for both the quality and cost of healthcare for a specific population of beneficiaries. The healthcare reform bill contains incentives for such a structure, which Dr. Wachter views as the government’s latest attempt to improve care by controlling how much reimbursement physicians and their employers receive.
While other specialists might not be experienced with data-point discussions on cost savings with hospital administrators, HM leaders are all too familiar with the concept, as most have those discussions during annual hospital subsidy negotiations. Correspondingly, those who listened to Dr. Wachter’s advice agreed that there is ample opportunity to lead the charge for quality and safety improvement—and the likely savings to be associated with those changes.
“Let’s be patient for what’s coming around the corner,” said Daniel Dressler, MD, SFHM, director of hospital medicine at Emory University Hospital in Atlanta and an SHM board member. “But let’s not miss the boat.” HM2010
Richard Quinn is a freelance writer based in New Jersey.
Special Interests
HOSPITALISTS FROM ALL PARTS OF THE COUNTRY—and a few other countries—discussed a wide swath of topics during a community-based HM special-interest forum at HM10. Issues that were discussed included unit-based rounding, changes to Medicare consult codes, strategies for avoiding “dumps,” and working with specialists.
Two established community hospitalists—SHM co-founders John Nelson, MD, MHM, and Winthrop Whitcomb, MD, MHM—moderated the one-hour session.

Much of the debate centered on defining a hospitalist’s role and relationships with others in the hospital. One hospitalist said he’d noticed significant changes in the 15 years since he began HM practice; however, some issues remain unresolved: Primary-care physicians (PCPs) still know the patients better, and medical specialists still want hospitalists to be their “interns.”
“We have two things to sell: your expertise and your availability. It’s up to your group to determine which one you want to sell,” said Tony Lin, MD, FHM, a hospitalist and chief of the Department of Internal Medicine at Kelsey-Seybold Clinic in Houston. “I don’t think you have to pick one. So I think you have to ask yourself: What does our group want to sell to the specialist? Sometimes you might have to turn them down to make that point.”
Dr. Lin also described a phenomena emerging in the Houston area: independent, one-physician HM groups taking root in community hospitals. “A lot of the surgeons are using them because they are willing to work as the interns and residents, the first people the nurses call at 2 a.m.,” he said. “There is a market for them.”
Dr. Nelson advised community hospitalists to avoid doing “the things that make you appear different from everyone else. Build social connections with specialists; call them by their first name; eat lunch in the cafeteria; and dress professionally.”
•
One community hospitalist spoke of an ethical situation she regularly encounters at her hospital, which contracts with multiple HM groups. Anna Rodriguez, MD, of Chesapeake Hospitalists in Chesapeake, Va., explained that her group’s issue is acutely ill patients who are assigned to one of the other HM group services—which, unlike Dr. Rodriguez’s group, are not responsible for codes or 24/7 patient coverage. So what happens when the “other” group’s patient has a sudden deterioration and the hospital staff calls us to run the rapid response? Dr. Rodriguez asked the group.
Dr. Whitcomb suggested Dr. Rodriguez’s group, which is not contracted to run the code, work to iron that situation out. “Then, that is your job and contractually recognized,” he said.
“We get into the exact same situation in our hospital. We created a hospital medicine section and … established expectations for who responds to codes,” said Dennis Kold, MD, medical director of the hospitalist service Tri-Health in Cincinnati. “If the patient is declining, we will respond to code, but we have it set up where the expectation is that the [attending] will be in to take care of the patient in one hour, or if the patient is admitted overnight to the ICU at 10 p.m., that the [admitting] will be in the ICU to take care of the patient within four hours.” Dr. Kold added that when the attending doesn’t show up in time that penalties are enforced (e.g., taken off the ER call schedule, restriction of hospital privileges).
“If you are not dealing with rapid response, then you are just hurting yourself,” added Edward Rosenfeld, MD, a hospitalist with Lehigh Valley Medical Associates in Allentown, Pa. “You need to do it; that’s your code prevention.”
•
Community hospitalists also discussed bundled payments and the recent changes in Medicare consult codes. “As a hospitalist service, I want to be involved in divvying up the money,” said Dan Allen, MD, a group director in Des Moines, Iowa. “I don’t know where it’s going, but I want to have a seat at the table.”
When asked by Dr. Nelson if they had noticed a significant change in reimbursement due to Medicare’s elimination of consultation codes, few in the room raised their hands. In fact, Dr. Nelson explained, “you can bill initial hospital care instead of initial hospital consult.”
“If done right, you might get paid better,” Dr. Rosenfeld added.
—Jason Carris
Health Information Technology on the Hospitalist Radar
Health information technology (HIT) isn’t for geeks anymore. A year after a mostly tech-savvy room discussed the basics of introducing more IT aspects to HM, nearly three dozen hospitalists clamored for SHM to take advocacy positions on everything from best practices to best vendors.

“SHM could help us all speak the language we need to speak,” said Tosha Wetterneck, MD, MS, a hospitalist with the University of Wisconsin Clinic in Madison. “Visibility, transparency—give us the words.”
Participants in last year’s group focused on the technical side of IT. This year’s attendees talked about the need for SHM to create portals for shared information, message boards to spur interinstitution conversations, and, perhaps, a weekend boot-camp-style course to introduce novices to basic IT information.
“SHM needs to take a stand now,” said Damascene Kurukulasuriya, MD, FACP, CMD, CCD, a hospitalist in perioperative medicine at the University of Missouri Health System in Columbia. “We need to be part of the solution.”
To that end, Kendall Rogers, MD, assistant professor at the University of New Mexico School of Medicine and chair of SHM’s IT Task Force, says the society is making progress. More hospitalists have been encouraged to sign up for the BioMedical Informatics course at the Marine Biology Laboratory in Woods Hole, Mass. The weeklong course is an introduction to the use of computer technologies and information science related to biomedicine and health science, according to the program’s Web site (www.courses.mbl.edu/mi/). The cost of travel, housing, and meals are fully paid for by the National Library of Medicine, making the fellowship even more appealing for cash-strapped hospitals and HM groups. “It’s a hidden program,” Dr. Rogers said.
Dr. Rogers and SHM CEO Larry Wellikson have toured the country meeting with top officials from the largest IT vendors, including Cerner and GE Healthcare. An IT committee has formed, with subcommittees dedicated to policy, quality, and leadership/education. But Bob Lineberger, MD, medical information officer at Durham Regional Hospital in North Carolina, says a nuanced message will take time.
“Our focus is just coming into focus,” Dr. Lineberger conceded. “We do need to come up with a position statement.”
—Richard Quinn
Education in HM: How to Grow Rock Stars and Champions
What skills does a hospitalist need to know to practice well that they didn’t learn in residency? That was the question new SHM President Jeff Weise, MD, SFHM, posed to about 20 hospitalists attending the special-interest forum on educational initiatives at HM10. Led by Dr. Wiese and SHM Education Committee co-chair Vikas Parekh, MD, FHM, the discussion focused on what SHM can do—or perhaps do better—in this capacity.

Dr. Parekh said hospitalists should be experts in quality-improvement (QI) and patient safety, and HM must incorporate that expertise into daily practice. However, he said, SHM’s largest educational focus is the new Focused Practice in Hospital Medicine pathway to American Board of Internal Medicine’s (ABIM) recertification.
In describing the future of this dynamic field, Dr. Weise raised concerns about managing the pipeline of approximately 2,500 new residents turning out each year and the potential for “losing intimacy” among SHM members—which he described as “the curse of being a champion.”
“IT is the only solution,” he added, “and identifying new and better ways of communicating.”
Competency-Based Train-ing (CBT) is critical to the development of new hospitalists, Dr. Wiese explained, as a supplement for what isn’t taught in residency. He posed a question: Should residencies last four or five years to incorporate additional training and career planning? “It’s an MBA paradigm of learning what we do,” he said. “What compels residents to join fellowship programs and earn $50K per year when they can start practicing and earning $150K?”
Educating the membership requires innovation and more than just bench-to-bedside research, Dr. Wiese added. Translational research and best-evidence practices will improve the field. “Five or 10 programs are rock stars,” he said, “but there are 377 that are terrible.”
Future SHM goals include a vision of having hospitalists hold 20% of all Internal Medicine Residency Program Director positions; developing best practices, not unfunded mandates; establishing protected academic time; and encouraging mentorship that positions hospitalists as heroes for the next generation.
An education committee sub-group has been tasked to focus on the recruitment of hospitalists and expose them to the best the society and field have to offer. HM10
—Phaedra Cress
HOSPITALISTS FROM ALL PARTS OF THE COUNTRY—and a few other countries—discussed a wide swath of topics during a community-based HM special-interest forum at HM10. Issues that were discussed included unit-based rounding, changes to Medicare consult codes, strategies for avoiding “dumps,” and working with specialists.
Two established community hospitalists—SHM co-founders John Nelson, MD, MHM, and Winthrop Whitcomb, MD, MHM—moderated the one-hour session.
Much of the debate centered on defining a hospitalist’s role and relationships with others in the hospital. One hospitalist said he’d noticed significant changes in the 15 years since he began HM practice; however, some issues remain unresolved: Primary-care physicians (PCPs) still know the patients better, and medical specialists still want hospitalists to be their “interns.”
“We have two things to sell: your expertise and your availability. It’s up to your group to determine which one you want to sell,” said Tony Lin, MD, FHM, a hospitalist and chief of the Department of Internal Medicine at Kelsey-Seybold Clinic in Houston. “I don’t think you have to pick one. So I think you have to ask yourself: What does our group want to sell to the specialist? Sometimes you might have to turn them down to make that point.”
Dr. Lin also described a phenomena emerging in the Houston area: independent, one-physician HM groups taking root in community hospitals. “A lot of the surgeons are using them because they are willing to work as the interns and residents, the first people the nurses call at 2 a.m.,” he said. “There is a market for them.”
Dr. Nelson advised community hospitalists to avoid doing “the things that make you appear different from everyone else. Build social connections with specialists; call them by their first name; eat lunch in the cafeteria; and dress professionally.”
•
One community hospitalist spoke of an ethical situation she regularly encounters at her hospital, which contracts with multiple HM groups. Anna Rodriguez, MD, of Chesapeake Hospitalists in Chesapeake, Va., explained that her group’s issue is acutely ill patients who are assigned to one of the other HM group services—which, unlike Dr. Rodriguez’s group, are not responsible for codes or 24/7 patient coverage. So what happens when the “other” group’s patient has a sudden deterioration and the hospital staff calls us to run the rapid response? Dr. Rodriguez asked the group.
Dr. Whitcomb suggested Dr. Rodriguez’s group, which is not contracted to run the code, work to iron that situation out. “Then, that is your job and contractually recognized,” he said.
“We get into the exact same situation in our hospital. We created a hospital medicine section and … established expectations for who responds to codes,” said Dennis Kold, MD, medical director of the hospitalist service Tri-Health in Cincinnati. “If the patient is declining, we will respond to code, but we have it set up where the expectation is that the [attending] will be in to take care of the patient in one hour, or if the patient is admitted overnight to the ICU at 10 p.m., that the [admitting] will be in the ICU to take care of the patient within four hours.” Dr. Kold added that when the attending doesn’t show up in time that penalties are enforced (e.g., taken off the ER call schedule, restriction of hospital privileges).
“If you are not dealing with rapid response, then you are just hurting yourself,” added Edward Rosenfeld, MD, a hospitalist with Lehigh Valley Medical Associates in Allentown, Pa. “You need to do it; that’s your code prevention.”
•
Community hospitalists also discussed bundled payments and the recent changes in Medicare consult codes. “As a hospitalist service, I want to be involved in divvying up the money,” said Dan Allen, MD, a group director in Des Moines, Iowa. “I don’t know where it’s going, but I want to have a seat at the table.”
When asked by Dr. Nelson if they had noticed a significant change in reimbursement due to Medicare’s elimination of consultation codes, few in the room raised their hands. In fact, Dr. Nelson explained, “you can bill initial hospital care instead of initial hospital consult.”
“If done right, you might get paid better,” Dr. Rosenfeld added.
—Jason Carris
Health Information Technology on the Hospitalist Radar
Health information technology (HIT) isn’t for geeks anymore. A year after a mostly tech-savvy room discussed the basics of introducing more IT aspects to HM, nearly three dozen hospitalists clamored for SHM to take advocacy positions on everything from best practices to best vendors.
“SHM could help us all speak the language we need to speak,” said Tosha Wetterneck, MD, MS, a hospitalist with the University of Wisconsin Clinic in Madison. “Visibility, transparency—give us the words.”
Participants in last year’s group focused on the technical side of IT. This year’s attendees talked about the need for SHM to create portals for shared information, message boards to spur interinstitution conversations, and, perhaps, a weekend boot-camp-style course to introduce novices to basic IT information.
“SHM needs to take a stand now,” said Damascene Kurukulasuriya, MD, FACP, CMD, CCD, a hospitalist in perioperative medicine at the University of Missouri Health System in Columbia. “We need to be part of the solution.”
To that end, Kendall Rogers, MD, assistant professor at the University of New Mexico School of Medicine and chair of SHM’s IT Task Force, says the society is making progress. More hospitalists have been encouraged to sign up for the BioMedical Informatics course at the Marine Biology Laboratory in Woods Hole, Mass. The weeklong course is an introduction to the use of computer technologies and information science related to biomedicine and health science, according to the program’s Web site (www.courses.mbl.edu/mi/). The cost of travel, housing, and meals are fully paid for by the National Library of Medicine, making the fellowship even more appealing for cash-strapped hospitals and HM groups. “It’s a hidden program,” Dr. Rogers said.
Dr. Rogers and SHM CEO Larry Wellikson have toured the country meeting with top officials from the largest IT vendors, including Cerner and GE Healthcare. An IT committee has formed, with subcommittees dedicated to policy, quality, and leadership/education. But Bob Lineberger, MD, medical information officer at Durham Regional Hospital in North Carolina, says a nuanced message will take time.
“Our focus is just coming into focus,” Dr. Lineberger conceded. “We do need to come up with a position statement.”
—Richard Quinn
Education in HM: How to Grow Rock Stars and Champions
What skills does a hospitalist need to know to practice well that they didn’t learn in residency? That was the question new SHM President Jeff Weise, MD, SFHM, posed to about 20 hospitalists attending the special-interest forum on educational initiatives at HM10. Led by Dr. Wiese and SHM Education Committee co-chair Vikas Parekh, MD, FHM, the discussion focused on what SHM can do—or perhaps do better—in this capacity.
Dr. Parekh said hospitalists should be experts in quality-improvement (QI) and patient safety, and HM must incorporate that expertise into daily practice. However, he said, SHM’s largest educational focus is the new Focused Practice in Hospital Medicine pathway to American Board of Internal Medicine’s (ABIM) recertification.
In describing the future of this dynamic field, Dr. Weise raised concerns about managing the pipeline of approximately 2,500 new residents turning out each year and the potential for “losing intimacy” among SHM members—which he described as “the curse of being a champion.”
“IT is the only solution,” he added, “and identifying new and better ways of communicating.”
Competency-Based Train-ing (CBT) is critical to the development of new hospitalists, Dr. Wiese explained, as a supplement for what isn’t taught in residency. He posed a question: Should residencies last four or five years to incorporate additional training and career planning? “It’s an MBA paradigm of learning what we do,” he said. “What compels residents to join fellowship programs and earn $50K per year when they can start practicing and earning $150K?”
Educating the membership requires innovation and more than just bench-to-bedside research, Dr. Wiese added. Translational research and best-evidence practices will improve the field. “Five or 10 programs are rock stars,” he said, “but there are 377 that are terrible.”
Future SHM goals include a vision of having hospitalists hold 20% of all Internal Medicine Residency Program Director positions; developing best practices, not unfunded mandates; establishing protected academic time; and encouraging mentorship that positions hospitalists as heroes for the next generation.
An education committee sub-group has been tasked to focus on the recruitment of hospitalists and expose them to the best the society and field have to offer. HM10
—Phaedra Cress
HOSPITALISTS FROM ALL PARTS OF THE COUNTRY—and a few other countries—discussed a wide swath of topics during a community-based HM special-interest forum at HM10. Issues that were discussed included unit-based rounding, changes to Medicare consult codes, strategies for avoiding “dumps,” and working with specialists.
Two established community hospitalists—SHM co-founders John Nelson, MD, MHM, and Winthrop Whitcomb, MD, MHM—moderated the one-hour session.
Much of the debate centered on defining a hospitalist’s role and relationships with others in the hospital. One hospitalist said he’d noticed significant changes in the 15 years since he began HM practice; however, some issues remain unresolved: Primary-care physicians (PCPs) still know the patients better, and medical specialists still want hospitalists to be their “interns.”
“We have two things to sell: your expertise and your availability. It’s up to your group to determine which one you want to sell,” said Tony Lin, MD, FHM, a hospitalist and chief of the Department of Internal Medicine at Kelsey-Seybold Clinic in Houston. “I don’t think you have to pick one. So I think you have to ask yourself: What does our group want to sell to the specialist? Sometimes you might have to turn them down to make that point.”
Dr. Lin also described a phenomena emerging in the Houston area: independent, one-physician HM groups taking root in community hospitals. “A lot of the surgeons are using them because they are willing to work as the interns and residents, the first people the nurses call at 2 a.m.,” he said. “There is a market for them.”
Dr. Nelson advised community hospitalists to avoid doing “the things that make you appear different from everyone else. Build social connections with specialists; call them by their first name; eat lunch in the cafeteria; and dress professionally.”
•
One community hospitalist spoke of an ethical situation she regularly encounters at her hospital, which contracts with multiple HM groups. Anna Rodriguez, MD, of Chesapeake Hospitalists in Chesapeake, Va., explained that her group’s issue is acutely ill patients who are assigned to one of the other HM group services—which, unlike Dr. Rodriguez’s group, are not responsible for codes or 24/7 patient coverage. So what happens when the “other” group’s patient has a sudden deterioration and the hospital staff calls us to run the rapid response? Dr. Rodriguez asked the group.
Dr. Whitcomb suggested Dr. Rodriguez’s group, which is not contracted to run the code, work to iron that situation out. “Then, that is your job and contractually recognized,” he said.
“We get into the exact same situation in our hospital. We created a hospital medicine section and … established expectations for who responds to codes,” said Dennis Kold, MD, medical director of the hospitalist service Tri-Health in Cincinnati. “If the patient is declining, we will respond to code, but we have it set up where the expectation is that the [attending] will be in to take care of the patient in one hour, or if the patient is admitted overnight to the ICU at 10 p.m., that the [admitting] will be in the ICU to take care of the patient within four hours.” Dr. Kold added that when the attending doesn’t show up in time that penalties are enforced (e.g., taken off the ER call schedule, restriction of hospital privileges).
“If you are not dealing with rapid response, then you are just hurting yourself,” added Edward Rosenfeld, MD, a hospitalist with Lehigh Valley Medical Associates in Allentown, Pa. “You need to do it; that’s your code prevention.”
•
Community hospitalists also discussed bundled payments and the recent changes in Medicare consult codes. “As a hospitalist service, I want to be involved in divvying up the money,” said Dan Allen, MD, a group director in Des Moines, Iowa. “I don’t know where it’s going, but I want to have a seat at the table.”
When asked by Dr. Nelson if they had noticed a significant change in reimbursement due to Medicare’s elimination of consultation codes, few in the room raised their hands. In fact, Dr. Nelson explained, “you can bill initial hospital care instead of initial hospital consult.”
“If done right, you might get paid better,” Dr. Rosenfeld added.
—Jason Carris
Health Information Technology on the Hospitalist Radar
Health information technology (HIT) isn’t for geeks anymore. A year after a mostly tech-savvy room discussed the basics of introducing more IT aspects to HM, nearly three dozen hospitalists clamored for SHM to take advocacy positions on everything from best practices to best vendors.
“SHM could help us all speak the language we need to speak,” said Tosha Wetterneck, MD, MS, a hospitalist with the University of Wisconsin Clinic in Madison. “Visibility, transparency—give us the words.”
Participants in last year’s group focused on the technical side of IT. This year’s attendees talked about the need for SHM to create portals for shared information, message boards to spur interinstitution conversations, and, perhaps, a weekend boot-camp-style course to introduce novices to basic IT information.
“SHM needs to take a stand now,” said Damascene Kurukulasuriya, MD, FACP, CMD, CCD, a hospitalist in perioperative medicine at the University of Missouri Health System in Columbia. “We need to be part of the solution.”
To that end, Kendall Rogers, MD, assistant professor at the University of New Mexico School of Medicine and chair of SHM’s IT Task Force, says the society is making progress. More hospitalists have been encouraged to sign up for the BioMedical Informatics course at the Marine Biology Laboratory in Woods Hole, Mass. The weeklong course is an introduction to the use of computer technologies and information science related to biomedicine and health science, according to the program’s Web site (www.courses.mbl.edu/mi/). The cost of travel, housing, and meals are fully paid for by the National Library of Medicine, making the fellowship even more appealing for cash-strapped hospitals and HM groups. “It’s a hidden program,” Dr. Rogers said.
Dr. Rogers and SHM CEO Larry Wellikson have toured the country meeting with top officials from the largest IT vendors, including Cerner and GE Healthcare. An IT committee has formed, with subcommittees dedicated to policy, quality, and leadership/education. But Bob Lineberger, MD, medical information officer at Durham Regional Hospital in North Carolina, says a nuanced message will take time.
“Our focus is just coming into focus,” Dr. Lineberger conceded. “We do need to come up with a position statement.”
—Richard Quinn
Education in HM: How to Grow Rock Stars and Champions
What skills does a hospitalist need to know to practice well that they didn’t learn in residency? That was the question new SHM President Jeff Weise, MD, SFHM, posed to about 20 hospitalists attending the special-interest forum on educational initiatives at HM10. Led by Dr. Wiese and SHM Education Committee co-chair Vikas Parekh, MD, FHM, the discussion focused on what SHM can do—or perhaps do better—in this capacity.
Dr. Parekh said hospitalists should be experts in quality-improvement (QI) and patient safety, and HM must incorporate that expertise into daily practice. However, he said, SHM’s largest educational focus is the new Focused Practice in Hospital Medicine pathway to American Board of Internal Medicine’s (ABIM) recertification.
In describing the future of this dynamic field, Dr. Weise raised concerns about managing the pipeline of approximately 2,500 new residents turning out each year and the potential for “losing intimacy” among SHM members—which he described as “the curse of being a champion.”
“IT is the only solution,” he added, “and identifying new and better ways of communicating.”
Competency-Based Train-ing (CBT) is critical to the development of new hospitalists, Dr. Wiese explained, as a supplement for what isn’t taught in residency. He posed a question: Should residencies last four or five years to incorporate additional training and career planning? “It’s an MBA paradigm of learning what we do,” he said. “What compels residents to join fellowship programs and earn $50K per year when they can start practicing and earning $150K?”
Educating the membership requires innovation and more than just bench-to-bedside research, Dr. Wiese added. Translational research and best-evidence practices will improve the field. “Five or 10 programs are rock stars,” he said, “but there are 377 that are terrible.”
Future SHM goals include a vision of having hospitalists hold 20% of all Internal Medicine Residency Program Director positions; developing best practices, not unfunded mandates; establishing protected academic time; and encouraging mentorship that positions hospitalists as heroes for the next generation.
An education committee sub-group has been tasked to focus on the recruitment of hospitalists and expose them to the best the society and field have to offer. HM10
—Phaedra Cress
Jam-Packed & Well Worth It
IT’S 11 MINUTES to 8 o’clock, and the sun is still climbing over the Potomac River just outside the Gaylord National Resort & Convention Center in National Harbor, Md. Day two of SHM’s annual meeting is about to begin.
Hospitalists file into a cavernous ballroom as the day kicks off with a panel discussion on healthcare reform and a speech by that rarest of breed: a popular hospital CEO. The back of the room fills quickly, but front and center, second row—that’s the seat for Nasim Afsarmanesh, MD, director of quality for HM and neurosurgery at Ronald Reagan UCLA Medical Center in Los Angeles.
“If I’m not in the front, I zone out,” she admits.
Dr. Afsarmanesh (who often adds a hyphen to her surname— Afsar-manesh—to help others pronounce it) knows herself and she knows how to plan ahead, from taking notes on her mini-laptop to knowing when to sit up front. And this day in her life is no different. Her schedule is a 12-hour dervish, yet it’s a simple roadmap of how to navigate HM10 and its scores of sessions, speeches, and seminars.



Innovator at Heart
Dr. Afsarmanesh did her residency in 2007 at UCLA. She stayed on to take a faculty position and is now assistant clinical professor of internal medicine (IM) and neurosurgery. Her days are split about 35% clinical practice, 40% on neurology quality issues, and 25% on hospital QI projects. In her free time, she’s an SHM activist and the incoming chair of its Hospital Quality and Patient Safety (HQPS) Committee.
“I get to be an innovator,” she boasts as she picks up a Danish, a chocolate pastry, and a cup of tea following two hours of listening to others talk. “I love that. You can’t really be an innovator when you’re [purely] practicing clinical medicine.”
Innovation requires preparation, though. Dr. Afsarmanesh spends countless hours creating PowerPoint presentations, so she hit a new feature at this year’s meeting: a limited-seating workshop on drawing up effective slides. The presentation is helpful, but she’s partially distracted. “Look up healthcare from talk,” she types as a note to herself for later. She follows that with “Look up Levy’s talk” (a nod to Paul Levy, the well-liked CEO of Beth Israel Deaconess in Boston).
Facial Recognition
The distraction ratchets up as she’s already looking forward to introducing herself to the editorial board of the Journal of Hospital Medicine, where she serves as an assistant editor. There are a few people she’d like to meet in person, so she gracefully sneaks out the side door a few minutes before noon. Handshakes, a box lunch, and a chat with 40 other journal editors ensue for the next hour.
“You can meet people you talk on the phone with for several years,” she says. “You can put a face to the name. That’s important.”
Hobnobbing at a board meeting is only a brief respite, however, before it’s back to professional development. At 1:15, there’s a 60-minute lesson on how to improve care from the patient perspective. Dr. Afsarmanesh, again, is distracted. She’s a first-time presenter in a few minutes, part of a four-woman panel on building a QI educational curriculum for medical students, residents, fellows, faculty, and other healthcare providers.
She scrolls through slides, rehearsing her thoughts. She wonders whether her PowerPoint presentation would have made the grade at this morning’s session.
She is smart enough not to judge her performance too soon—someone in an audience once reached out to her a year later—as she knows the impact of a training session is more than the round of applause at its end.
“You hope that you generate a discussion more than the traditional didactics,” she says. “These meetings are meant to start a discussion and, hopefully, create a network and a community where people can continue to [share ideas and learn from each other]. … I hope that along with some of the content that people take away, the bigger thing is those connections that they make.”
—Nasim Afsarmanesh, MD, director, HM quality initiatives, Ronald Reagan UCLA Medical Center, Los Angeles
Work Never Ends
It’s 4:30 p.m. and Dr. Afsarmanesh still has a sales pitch to rehearse. This time, it’s self-promotion for her soon-to-begin poster presentation: “The ABCs of Hospitalized Patients: A Multi-Disciplinary Checklist for Improving Quality of Patient Care."
After umpteen repetitions of her spiel, the presentation doesn’t win a prize, but, once again, she showcases her attention to detail: A stack of 8.5”x 11” versions of her poster are available for handouts, a feature few others in the competition have.
Some 12 hours into her tour of this massive convention center, the day is coming to a close. But not before SHM CEO Larry Wellikson, MD, SFHM, drops by to say hello.
He points out how strong her research is. Unfortunately, he uses a pen in the process.
“Don’t poke a hole in my poster,” she jokes.
Moments later, it’s back to working the line queued up at her poster. “Hi, would you like to hear about my poster?” HM2010
Richard Quinn is a freelance writer based in New Jersey.
IT’S 11 MINUTES to 8 o’clock, and the sun is still climbing over the Potomac River just outside the Gaylord National Resort & Convention Center in National Harbor, Md. Day two of SHM’s annual meeting is about to begin.
Hospitalists file into a cavernous ballroom as the day kicks off with a panel discussion on healthcare reform and a speech by that rarest of breed: a popular hospital CEO. The back of the room fills quickly, but front and center, second row—that’s the seat for Nasim Afsarmanesh, MD, director of quality for HM and neurosurgery at Ronald Reagan UCLA Medical Center in Los Angeles.
“If I’m not in the front, I zone out,” she admits.
Dr. Afsarmanesh (who often adds a hyphen to her surname— Afsar-manesh—to help others pronounce it) knows herself and she knows how to plan ahead, from taking notes on her mini-laptop to knowing when to sit up front. And this day in her life is no different. Her schedule is a 12-hour dervish, yet it’s a simple roadmap of how to navigate HM10 and its scores of sessions, speeches, and seminars.
Innovator at Heart
Dr. Afsarmanesh did her residency in 2007 at UCLA. She stayed on to take a faculty position and is now assistant clinical professor of internal medicine (IM) and neurosurgery. Her days are split about 35% clinical practice, 40% on neurology quality issues, and 25% on hospital QI projects. In her free time, she’s an SHM activist and the incoming chair of its Hospital Quality and Patient Safety (HQPS) Committee.
“I get to be an innovator,” she boasts as she picks up a Danish, a chocolate pastry, and a cup of tea following two hours of listening to others talk. “I love that. You can’t really be an innovator when you’re [purely] practicing clinical medicine.”
Innovation requires preparation, though. Dr. Afsarmanesh spends countless hours creating PowerPoint presentations, so she hit a new feature at this year’s meeting: a limited-seating workshop on drawing up effective slides. The presentation is helpful, but she’s partially distracted. “Look up healthcare from talk,” she types as a note to herself for later. She follows that with “Look up Levy’s talk” (a nod to Paul Levy, the well-liked CEO of Beth Israel Deaconess in Boston).
Facial Recognition
The distraction ratchets up as she’s already looking forward to introducing herself to the editorial board of the Journal of Hospital Medicine, where she serves as an assistant editor. There are a few people she’d like to meet in person, so she gracefully sneaks out the side door a few minutes before noon. Handshakes, a box lunch, and a chat with 40 other journal editors ensue for the next hour.
“You can meet people you talk on the phone with for several years,” she says. “You can put a face to the name. That’s important.”
Hobnobbing at a board meeting is only a brief respite, however, before it’s back to professional development. At 1:15, there’s a 60-minute lesson on how to improve care from the patient perspective. Dr. Afsarmanesh, again, is distracted. She’s a first-time presenter in a few minutes, part of a four-woman panel on building a QI educational curriculum for medical students, residents, fellows, faculty, and other healthcare providers.
She scrolls through slides, rehearsing her thoughts. She wonders whether her PowerPoint presentation would have made the grade at this morning’s session.
She is smart enough not to judge her performance too soon—someone in an audience once reached out to her a year later—as she knows the impact of a training session is more than the round of applause at its end.
“You hope that you generate a discussion more than the traditional didactics,” she says. “These meetings are meant to start a discussion and, hopefully, create a network and a community where people can continue to [share ideas and learn from each other]. … I hope that along with some of the content that people take away, the bigger thing is those connections that they make.”
—Nasim Afsarmanesh, MD, director, HM quality initiatives, Ronald Reagan UCLA Medical Center, Los Angeles
Work Never Ends
It’s 4:30 p.m. and Dr. Afsarmanesh still has a sales pitch to rehearse. This time, it’s self-promotion for her soon-to-begin poster presentation: “The ABCs of Hospitalized Patients: A Multi-Disciplinary Checklist for Improving Quality of Patient Care."
After umpteen repetitions of her spiel, the presentation doesn’t win a prize, but, once again, she showcases her attention to detail: A stack of 8.5”x 11” versions of her poster are available for handouts, a feature few others in the competition have.
Some 12 hours into her tour of this massive convention center, the day is coming to a close. But not before SHM CEO Larry Wellikson, MD, SFHM, drops by to say hello.
He points out how strong her research is. Unfortunately, he uses a pen in the process.
“Don’t poke a hole in my poster,” she jokes.
Moments later, it’s back to working the line queued up at her poster. “Hi, would you like to hear about my poster?” HM2010
Richard Quinn is a freelance writer based in New Jersey.
IT’S 11 MINUTES to 8 o’clock, and the sun is still climbing over the Potomac River just outside the Gaylord National Resort & Convention Center in National Harbor, Md. Day two of SHM’s annual meeting is about to begin.
Hospitalists file into a cavernous ballroom as the day kicks off with a panel discussion on healthcare reform and a speech by that rarest of breed: a popular hospital CEO. The back of the room fills quickly, but front and center, second row—that’s the seat for Nasim Afsarmanesh, MD, director of quality for HM and neurosurgery at Ronald Reagan UCLA Medical Center in Los Angeles.
“If I’m not in the front, I zone out,” she admits.
Dr. Afsarmanesh (who often adds a hyphen to her surname— Afsar-manesh—to help others pronounce it) knows herself and she knows how to plan ahead, from taking notes on her mini-laptop to knowing when to sit up front. And this day in her life is no different. Her schedule is a 12-hour dervish, yet it’s a simple roadmap of how to navigate HM10 and its scores of sessions, speeches, and seminars.
Innovator at Heart
Dr. Afsarmanesh did her residency in 2007 at UCLA. She stayed on to take a faculty position and is now assistant clinical professor of internal medicine (IM) and neurosurgery. Her days are split about 35% clinical practice, 40% on neurology quality issues, and 25% on hospital QI projects. In her free time, she’s an SHM activist and the incoming chair of its Hospital Quality and Patient Safety (HQPS) Committee.
“I get to be an innovator,” she boasts as she picks up a Danish, a chocolate pastry, and a cup of tea following two hours of listening to others talk. “I love that. You can’t really be an innovator when you’re [purely] practicing clinical medicine.”
Innovation requires preparation, though. Dr. Afsarmanesh spends countless hours creating PowerPoint presentations, so she hit a new feature at this year’s meeting: a limited-seating workshop on drawing up effective slides. The presentation is helpful, but she’s partially distracted. “Look up healthcare from talk,” she types as a note to herself for later. She follows that with “Look up Levy’s talk” (a nod to Paul Levy, the well-liked CEO of Beth Israel Deaconess in Boston).
Facial Recognition
The distraction ratchets up as she’s already looking forward to introducing herself to the editorial board of the Journal of Hospital Medicine, where she serves as an assistant editor. There are a few people she’d like to meet in person, so she gracefully sneaks out the side door a few minutes before noon. Handshakes, a box lunch, and a chat with 40 other journal editors ensue for the next hour.
“You can meet people you talk on the phone with for several years,” she says. “You can put a face to the name. That’s important.”
Hobnobbing at a board meeting is only a brief respite, however, before it’s back to professional development. At 1:15, there’s a 60-minute lesson on how to improve care from the patient perspective. Dr. Afsarmanesh, again, is distracted. She’s a first-time presenter in a few minutes, part of a four-woman panel on building a QI educational curriculum for medical students, residents, fellows, faculty, and other healthcare providers.
She scrolls through slides, rehearsing her thoughts. She wonders whether her PowerPoint presentation would have made the grade at this morning’s session.
She is smart enough not to judge her performance too soon—someone in an audience once reached out to her a year later—as she knows the impact of a training session is more than the round of applause at its end.
“You hope that you generate a discussion more than the traditional didactics,” she says. “These meetings are meant to start a discussion and, hopefully, create a network and a community where people can continue to [share ideas and learn from each other]. … I hope that along with some of the content that people take away, the bigger thing is those connections that they make.”
—Nasim Afsarmanesh, MD, director, HM quality initiatives, Ronald Reagan UCLA Medical Center, Los Angeles
Work Never Ends
It’s 4:30 p.m. and Dr. Afsarmanesh still has a sales pitch to rehearse. This time, it’s self-promotion for her soon-to-begin poster presentation: “The ABCs of Hospitalized Patients: A Multi-Disciplinary Checklist for Improving Quality of Patient Care."
After umpteen repetitions of her spiel, the presentation doesn’t win a prize, but, once again, she showcases her attention to detail: A stack of 8.5”x 11” versions of her poster are available for handouts, a feature few others in the competition have.
Some 12 hours into her tour of this massive convention center, the day is coming to a close. But not before SHM CEO Larry Wellikson, MD, SFHM, drops by to say hello.
He points out how strong her research is. Unfortunately, he uses a pen in the process.
“Don’t poke a hole in my poster,” she jokes.
Moments later, it’s back to working the line queued up at her poster. “Hi, would you like to hear about my poster?” HM2010
Richard Quinn is a freelance writer based in New Jersey.