User login
What's Eating You? Cat Flea (Ctenocephalides felis), Part 1: Clinical Features and Role as a Disease Vector
USPSTF recommendations you may have missed amid the breast cancer controversy
Late in 2009, a change in the recommendations of the US Preventive Services Task Force (USPSTF) brought more public attention to this panel than it had ever experienced before. This publicity centered on revised recommendations on breast cancer screening that pointed out that mammograms benefit a few women under 50, but are also associated with some harms. The Task Force recommended that patients and physicians discuss these potential benefits and harms and make an individual decision about whether to have a mammogram.1
Even though the criticism was loud—and harsh—from some sectors, many professional organizations, including the American Academy of Family Physicians, the American College of Physicians, and the American College of Preventive Medicine, came to the defense of the Task Force and its rigorous, evidence-based methodology.2-4 Both the Journal of the American Medical Association and the Annals of Internal Medicine have since published a series of articles and opinions on the controversy, most of them favorable to the Task Force and its methods.2-9
Lost in all the brouhaha were a number of other, less controversial recommendations that the Task Force made in 2009 (and early 2010). You can find them at www.ahrq.gov/clinic/uspstfix.htm. They are categorized by strength of recommendation (TABLE 1) and listed in TABLES 2 and 3. Family physicians should review the A and B recommendations and try to incorporate those into practice. At the same time, we should avoid services in the D category, as the evidence is strong that they are not effective or cause more harm than benefit. The C and I recommendations leave more discretion for physicians and patients to decide on these interventions based on personal values and risks. A C recommendation means the service can benefit some individuals, but the totality of benefit is small. An I recommendation means that evidence is insufficient to evaluate benefits vs harms.
TABLE 1
US Preventive Services Task Force recommendation categories
| Grade | Definition |
|---|---|
| A | The USPSTF recommends the service. There is high certainty that the net benefit is substantial. |
| B | The USPSTF recommends the service. There is high certainty that the net benefit is moderate or there is moderate certainty that the net benefit is moderate to substantial. |
| C | The USPSTF recommends against routinely providing the service. There may be considerations that support providing the service in an individual patient. There is at least moderate certainty that the net benefit is small. |
| D | The USPSTF recommends against the service. There is moderate or high certainty that the service has no net benefit or that the harms outweigh the benefits. |
| I | The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of the service. Evidence is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined. |
| Source: Agency for Healthcare Research and Quality. US Preventive Services Task Force (USPSTF) ratings. Available at: http://www.uspreventiveservicestaskforce.org/uspstf07/ratingsv2.htm. Accessed September 5, 2013. | |
TABLE 2
USPSTF recommends FOR
| CARDIOVASCULAR DISEASE PREVENTION |
|
| PREGNANCY |
|
| CANCER SCREENING |
|
| DEPRESSION |
|
| OBESITY |
|
TABLE 3
USPSTF recommends AGAINST routinely
|
| USPSTF recommends AGAINST |
|
| USPSTF indicates the evidence is INSUFFICIENT to assess the balance of benefits and harms of |
|
| Source: Agency for Healthcare Research and Quality. Available at: www.ahrq.gov/clinic/uspstfix.htm. Accessed April 2, 2010. |
The A and B recommendations you may have missed
The major additions to the A and B recommendations pertained to the use of aspirin to prevent cardiovascular disease, routine screening for depression in adults and adolescents, and screening for obesity in children ages 6 and older. The other recommendations in these categories were reaffirmations of previous recommendations (asking about smoking and providing smoking cessation guidance to adults and pregnant women, advising folic acid supplementation for women planning or capable of pregnancy, and screening pregnant women for syphilis and hepatitis B virus) and the more controversial recommendation for biennial rather than annual mammography for women ages 50 to 74.
The use of aspirin to prevent myocardial infarction in men ages 45 to 79 and ischemic strokes in women ages 55 to 79 was endorsed if a patient’s risk of these cardiovascular events exceeds the risk of bleeding from regular aspirin use. The Task Force recommendation statement is available athttp://www.ahrq.gov/clinic/uspstf09/aspirincvd/aspcvdrs.htmand provides links to tools for calculating the risk of a myocardial infarction (MI) and ischemic stroke, as well as 2 tables to compare the risks and benefits of aspirin therapy for prevention.
Screening adults for depression is endorsed if “staff-assisted depression care supports” are in place to assure accurate diagnosis, effective treatment, and follow-up. Such support includes the presence of clinical staff members who can assist the primary care provider with care support or coordination, case management, or mental health treatment. The definition can be accessed athttp://www.ahrq.gov/clinic/uspstf09/adultdepression/addeprrs.htm.
One example in the statement describes “a successful study designed for practices without ready access to mental health specialty care, (in which) office staff recruited, screened, and enrolled participants who screened positive for depression before a clinic visit. If the physician confirmed the depression diagnosis, the participant was scheduled for a return visit with the physician and to meet with the nurse specialist in 1 week. The nurse specialist reassessed the patient’s level of depression, discussed treatment options and preferences, and asked the participant to complete a homework assignment. Participants completed up to 8 additional sessions that followed the same pattern, either by phone or in person.”
Screening for major depressive disorder (MDD) in adolescents 12 to 18 years of age is recommended when systems are in place to ensure accurate diagnosis, psychotherapy (cognitive-behavioral or interpersonal), and follow-up. The Task Force addressed screening for MDD only—not for less severe depression. The instruments the group recommended using included the Patient Health Questionnaire for Adolescents (PHQ-A) and the Beck Depression Inventory-Primary Care Version (BDI-PC).
The recommendation for screening for obesity in children ages 6 and older reflects the difficulty in achieving long-term, sustainable weight loss in this group. Effective comprehensive weight-management programs include counseling and other interventions that target both diet and physical activity. Behavioral interventions and parental involvement are also encouraged. Moderate- to high-intensity programs include more than 25 hours of contact with the child and/or the family over a 6-month period; less than this does not result in sustained improvement.
What about the D and I categories?
Two interventions received a D recommendation: Use of aspirin for stroke prevention in women <55 years and for MI prevention in men <45 years, and teaching breast self-examination (BSE) to women. The BSE recommendation has been misinterpreted as recommending against women performing self-breast exams. The recommendation is against formalized teaching of the procedure by physicians, as this leads to increased false positives and no improvement in outcomes when compared to women performing exams on their own.
The list of interventions receiving an I recommendation include some services that are commonly offered in the belief that they are effective. The Task Force is attempting to develop methodologies to decrease the number of interventions that receive an I recommendation. Currently, about 40% of all recommendations end up in this category, and physicians and patients alike could use more guidance on them. This plethora of recommendations made with insufficient evidence reflects the “ready, shoot, aim” philosophy of American medicine. We tend to accept and adopt new interventions before they are proven effective. The I recommendations are valuable reminders that, while many interventions are in common use, we often do not know as much as we should about their benefits and harms.
1. Agency for Healthcare Research and Quality. Screening for breast cancer. Updated December 2009. Available at: www.ahrq.gov/clinic/uspstf/uspsbrca.htm. Accessed March 17, 2010.
2. Woolf SH. The 2009 breast cancer screening recommendations of the US Preventive Services Task Force. JAMA. 2010;303:162-163.
3. Woloshin S, Schwartz LM. The benefits and harms of mammography screening: understanding the trade-offs. JAMA. 2010;303:164-165.
4. Murphy AM. Mammography screening for breast cancer: a view from 2 worlds. JAMA. 2010;303:166-167.
5. Berg WA. Benefits of screening mammography. JAMA. 2010;303:168-169.
6. DeAngelis CF, Fontanarosa PB. US Preventive Services Task Force and breast cancer screening. JAMA. 2010;303:172-173.
7. Editors’ note on the USPSTF recommendation on screening for breast cancer. February 15, 2010. Available at: http://www.annals.org/content/early/2010/02/12/0003-4819-152-8-201004200-00209.full. Accessed April 7, 2010.
8. Begg CB. Comments and response on the USPSTF recommendation on screening for breast cancer. February 15, 2010. Available at: http://www.annals.org/content/early/2010/02/12/0003-4819-152-8-201004200-00203.full. Accessed April 7, 2010.
9. Jorgensen KJ, Gotzsche PC. The background review for the USPSTF recommendation on screening for breast cancer. February 15, 2010. Available at: http://www.annals.org/content/early/2010/02/12/0003-4819-152-8-201004200-00198.full. Accessed April 7, 2010.
Late in 2009, a change in the recommendations of the US Preventive Services Task Force (USPSTF) brought more public attention to this panel than it had ever experienced before. This publicity centered on revised recommendations on breast cancer screening that pointed out that mammograms benefit a few women under 50, but are also associated with some harms. The Task Force recommended that patients and physicians discuss these potential benefits and harms and make an individual decision about whether to have a mammogram.1
Even though the criticism was loud—and harsh—from some sectors, many professional organizations, including the American Academy of Family Physicians, the American College of Physicians, and the American College of Preventive Medicine, came to the defense of the Task Force and its rigorous, evidence-based methodology.2-4 Both the Journal of the American Medical Association and the Annals of Internal Medicine have since published a series of articles and opinions on the controversy, most of them favorable to the Task Force and its methods.2-9
Lost in all the brouhaha were a number of other, less controversial recommendations that the Task Force made in 2009 (and early 2010). You can find them at www.ahrq.gov/clinic/uspstfix.htm. They are categorized by strength of recommendation (TABLE 1) and listed in TABLES 2 and 3. Family physicians should review the A and B recommendations and try to incorporate those into practice. At the same time, we should avoid services in the D category, as the evidence is strong that they are not effective or cause more harm than benefit. The C and I recommendations leave more discretion for physicians and patients to decide on these interventions based on personal values and risks. A C recommendation means the service can benefit some individuals, but the totality of benefit is small. An I recommendation means that evidence is insufficient to evaluate benefits vs harms.
TABLE 1
US Preventive Services Task Force recommendation categories
| Grade | Definition |
|---|---|
| A | The USPSTF recommends the service. There is high certainty that the net benefit is substantial. |
| B | The USPSTF recommends the service. There is high certainty that the net benefit is moderate or there is moderate certainty that the net benefit is moderate to substantial. |
| C | The USPSTF recommends against routinely providing the service. There may be considerations that support providing the service in an individual patient. There is at least moderate certainty that the net benefit is small. |
| D | The USPSTF recommends against the service. There is moderate or high certainty that the service has no net benefit or that the harms outweigh the benefits. |
| I | The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of the service. Evidence is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined. |
| Source: Agency for Healthcare Research and Quality. US Preventive Services Task Force (USPSTF) ratings. Available at: http://www.uspreventiveservicestaskforce.org/uspstf07/ratingsv2.htm. Accessed September 5, 2013. | |
TABLE 2
USPSTF recommends FOR
| CARDIOVASCULAR DISEASE PREVENTION |
|
| PREGNANCY |
|
| CANCER SCREENING |
|
| DEPRESSION |
|
| OBESITY |
|
TABLE 3
USPSTF recommends AGAINST routinely
|
| USPSTF recommends AGAINST |
|
| USPSTF indicates the evidence is INSUFFICIENT to assess the balance of benefits and harms of |
|
| Source: Agency for Healthcare Research and Quality. Available at: www.ahrq.gov/clinic/uspstfix.htm. Accessed April 2, 2010. |
The A and B recommendations you may have missed
The major additions to the A and B recommendations pertained to the use of aspirin to prevent cardiovascular disease, routine screening for depression in adults and adolescents, and screening for obesity in children ages 6 and older. The other recommendations in these categories were reaffirmations of previous recommendations (asking about smoking and providing smoking cessation guidance to adults and pregnant women, advising folic acid supplementation for women planning or capable of pregnancy, and screening pregnant women for syphilis and hepatitis B virus) and the more controversial recommendation for biennial rather than annual mammography for women ages 50 to 74.
The use of aspirin to prevent myocardial infarction in men ages 45 to 79 and ischemic strokes in women ages 55 to 79 was endorsed if a patient’s risk of these cardiovascular events exceeds the risk of bleeding from regular aspirin use. The Task Force recommendation statement is available athttp://www.ahrq.gov/clinic/uspstf09/aspirincvd/aspcvdrs.htmand provides links to tools for calculating the risk of a myocardial infarction (MI) and ischemic stroke, as well as 2 tables to compare the risks and benefits of aspirin therapy for prevention.
Screening adults for depression is endorsed if “staff-assisted depression care supports” are in place to assure accurate diagnosis, effective treatment, and follow-up. Such support includes the presence of clinical staff members who can assist the primary care provider with care support or coordination, case management, or mental health treatment. The definition can be accessed athttp://www.ahrq.gov/clinic/uspstf09/adultdepression/addeprrs.htm.
One example in the statement describes “a successful study designed for practices without ready access to mental health specialty care, (in which) office staff recruited, screened, and enrolled participants who screened positive for depression before a clinic visit. If the physician confirmed the depression diagnosis, the participant was scheduled for a return visit with the physician and to meet with the nurse specialist in 1 week. The nurse specialist reassessed the patient’s level of depression, discussed treatment options and preferences, and asked the participant to complete a homework assignment. Participants completed up to 8 additional sessions that followed the same pattern, either by phone or in person.”
Screening for major depressive disorder (MDD) in adolescents 12 to 18 years of age is recommended when systems are in place to ensure accurate diagnosis, psychotherapy (cognitive-behavioral or interpersonal), and follow-up. The Task Force addressed screening for MDD only—not for less severe depression. The instruments the group recommended using included the Patient Health Questionnaire for Adolescents (PHQ-A) and the Beck Depression Inventory-Primary Care Version (BDI-PC).
The recommendation for screening for obesity in children ages 6 and older reflects the difficulty in achieving long-term, sustainable weight loss in this group. Effective comprehensive weight-management programs include counseling and other interventions that target both diet and physical activity. Behavioral interventions and parental involvement are also encouraged. Moderate- to high-intensity programs include more than 25 hours of contact with the child and/or the family over a 6-month period; less than this does not result in sustained improvement.
What about the D and I categories?
Two interventions received a D recommendation: Use of aspirin for stroke prevention in women <55 years and for MI prevention in men <45 years, and teaching breast self-examination (BSE) to women. The BSE recommendation has been misinterpreted as recommending against women performing self-breast exams. The recommendation is against formalized teaching of the procedure by physicians, as this leads to increased false positives and no improvement in outcomes when compared to women performing exams on their own.
The list of interventions receiving an I recommendation include some services that are commonly offered in the belief that they are effective. The Task Force is attempting to develop methodologies to decrease the number of interventions that receive an I recommendation. Currently, about 40% of all recommendations end up in this category, and physicians and patients alike could use more guidance on them. This plethora of recommendations made with insufficient evidence reflects the “ready, shoot, aim” philosophy of American medicine. We tend to accept and adopt new interventions before they are proven effective. The I recommendations are valuable reminders that, while many interventions are in common use, we often do not know as much as we should about their benefits and harms.
Late in 2009, a change in the recommendations of the US Preventive Services Task Force (USPSTF) brought more public attention to this panel than it had ever experienced before. This publicity centered on revised recommendations on breast cancer screening that pointed out that mammograms benefit a few women under 50, but are also associated with some harms. The Task Force recommended that patients and physicians discuss these potential benefits and harms and make an individual decision about whether to have a mammogram.1
Even though the criticism was loud—and harsh—from some sectors, many professional organizations, including the American Academy of Family Physicians, the American College of Physicians, and the American College of Preventive Medicine, came to the defense of the Task Force and its rigorous, evidence-based methodology.2-4 Both the Journal of the American Medical Association and the Annals of Internal Medicine have since published a series of articles and opinions on the controversy, most of them favorable to the Task Force and its methods.2-9
Lost in all the brouhaha were a number of other, less controversial recommendations that the Task Force made in 2009 (and early 2010). You can find them at www.ahrq.gov/clinic/uspstfix.htm. They are categorized by strength of recommendation (TABLE 1) and listed in TABLES 2 and 3. Family physicians should review the A and B recommendations and try to incorporate those into practice. At the same time, we should avoid services in the D category, as the evidence is strong that they are not effective or cause more harm than benefit. The C and I recommendations leave more discretion for physicians and patients to decide on these interventions based on personal values and risks. A C recommendation means the service can benefit some individuals, but the totality of benefit is small. An I recommendation means that evidence is insufficient to evaluate benefits vs harms.
TABLE 1
US Preventive Services Task Force recommendation categories
| Grade | Definition |
|---|---|
| A | The USPSTF recommends the service. There is high certainty that the net benefit is substantial. |
| B | The USPSTF recommends the service. There is high certainty that the net benefit is moderate or there is moderate certainty that the net benefit is moderate to substantial. |
| C | The USPSTF recommends against routinely providing the service. There may be considerations that support providing the service in an individual patient. There is at least moderate certainty that the net benefit is small. |
| D | The USPSTF recommends against the service. There is moderate or high certainty that the service has no net benefit or that the harms outweigh the benefits. |
| I | The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of the service. Evidence is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined. |
| Source: Agency for Healthcare Research and Quality. US Preventive Services Task Force (USPSTF) ratings. Available at: http://www.uspreventiveservicestaskforce.org/uspstf07/ratingsv2.htm. Accessed September 5, 2013. | |
TABLE 2
USPSTF recommends FOR
| CARDIOVASCULAR DISEASE PREVENTION |
|
| PREGNANCY |
|
| CANCER SCREENING |
|
| DEPRESSION |
|
| OBESITY |
|
TABLE 3
USPSTF recommends AGAINST routinely
|
| USPSTF recommends AGAINST |
|
| USPSTF indicates the evidence is INSUFFICIENT to assess the balance of benefits and harms of |
|
| Source: Agency for Healthcare Research and Quality. Available at: www.ahrq.gov/clinic/uspstfix.htm. Accessed April 2, 2010. |
The A and B recommendations you may have missed
The major additions to the A and B recommendations pertained to the use of aspirin to prevent cardiovascular disease, routine screening for depression in adults and adolescents, and screening for obesity in children ages 6 and older. The other recommendations in these categories were reaffirmations of previous recommendations (asking about smoking and providing smoking cessation guidance to adults and pregnant women, advising folic acid supplementation for women planning or capable of pregnancy, and screening pregnant women for syphilis and hepatitis B virus) and the more controversial recommendation for biennial rather than annual mammography for women ages 50 to 74.
The use of aspirin to prevent myocardial infarction in men ages 45 to 79 and ischemic strokes in women ages 55 to 79 was endorsed if a patient’s risk of these cardiovascular events exceeds the risk of bleeding from regular aspirin use. The Task Force recommendation statement is available athttp://www.ahrq.gov/clinic/uspstf09/aspirincvd/aspcvdrs.htmand provides links to tools for calculating the risk of a myocardial infarction (MI) and ischemic stroke, as well as 2 tables to compare the risks and benefits of aspirin therapy for prevention.
Screening adults for depression is endorsed if “staff-assisted depression care supports” are in place to assure accurate diagnosis, effective treatment, and follow-up. Such support includes the presence of clinical staff members who can assist the primary care provider with care support or coordination, case management, or mental health treatment. The definition can be accessed athttp://www.ahrq.gov/clinic/uspstf09/adultdepression/addeprrs.htm.
One example in the statement describes “a successful study designed for practices without ready access to mental health specialty care, (in which) office staff recruited, screened, and enrolled participants who screened positive for depression before a clinic visit. If the physician confirmed the depression diagnosis, the participant was scheduled for a return visit with the physician and to meet with the nurse specialist in 1 week. The nurse specialist reassessed the patient’s level of depression, discussed treatment options and preferences, and asked the participant to complete a homework assignment. Participants completed up to 8 additional sessions that followed the same pattern, either by phone or in person.”
Screening for major depressive disorder (MDD) in adolescents 12 to 18 years of age is recommended when systems are in place to ensure accurate diagnosis, psychotherapy (cognitive-behavioral or interpersonal), and follow-up. The Task Force addressed screening for MDD only—not for less severe depression. The instruments the group recommended using included the Patient Health Questionnaire for Adolescents (PHQ-A) and the Beck Depression Inventory-Primary Care Version (BDI-PC).
The recommendation for screening for obesity in children ages 6 and older reflects the difficulty in achieving long-term, sustainable weight loss in this group. Effective comprehensive weight-management programs include counseling and other interventions that target both diet and physical activity. Behavioral interventions and parental involvement are also encouraged. Moderate- to high-intensity programs include more than 25 hours of contact with the child and/or the family over a 6-month period; less than this does not result in sustained improvement.
What about the D and I categories?
Two interventions received a D recommendation: Use of aspirin for stroke prevention in women <55 years and for MI prevention in men <45 years, and teaching breast self-examination (BSE) to women. The BSE recommendation has been misinterpreted as recommending against women performing self-breast exams. The recommendation is against formalized teaching of the procedure by physicians, as this leads to increased false positives and no improvement in outcomes when compared to women performing exams on their own.
The list of interventions receiving an I recommendation include some services that are commonly offered in the belief that they are effective. The Task Force is attempting to develop methodologies to decrease the number of interventions that receive an I recommendation. Currently, about 40% of all recommendations end up in this category, and physicians and patients alike could use more guidance on them. This plethora of recommendations made with insufficient evidence reflects the “ready, shoot, aim” philosophy of American medicine. We tend to accept and adopt new interventions before they are proven effective. The I recommendations are valuable reminders that, while many interventions are in common use, we often do not know as much as we should about their benefits and harms.
1. Agency for Healthcare Research and Quality. Screening for breast cancer. Updated December 2009. Available at: www.ahrq.gov/clinic/uspstf/uspsbrca.htm. Accessed March 17, 2010.
2. Woolf SH. The 2009 breast cancer screening recommendations of the US Preventive Services Task Force. JAMA. 2010;303:162-163.
3. Woloshin S, Schwartz LM. The benefits and harms of mammography screening: understanding the trade-offs. JAMA. 2010;303:164-165.
4. Murphy AM. Mammography screening for breast cancer: a view from 2 worlds. JAMA. 2010;303:166-167.
5. Berg WA. Benefits of screening mammography. JAMA. 2010;303:168-169.
6. DeAngelis CF, Fontanarosa PB. US Preventive Services Task Force and breast cancer screening. JAMA. 2010;303:172-173.
7. Editors’ note on the USPSTF recommendation on screening for breast cancer. February 15, 2010. Available at: http://www.annals.org/content/early/2010/02/12/0003-4819-152-8-201004200-00209.full. Accessed April 7, 2010.
8. Begg CB. Comments and response on the USPSTF recommendation on screening for breast cancer. February 15, 2010. Available at: http://www.annals.org/content/early/2010/02/12/0003-4819-152-8-201004200-00203.full. Accessed April 7, 2010.
9. Jorgensen KJ, Gotzsche PC. The background review for the USPSTF recommendation on screening for breast cancer. February 15, 2010. Available at: http://www.annals.org/content/early/2010/02/12/0003-4819-152-8-201004200-00198.full. Accessed April 7, 2010.
1. Agency for Healthcare Research and Quality. Screening for breast cancer. Updated December 2009. Available at: www.ahrq.gov/clinic/uspstf/uspsbrca.htm. Accessed March 17, 2010.
2. Woolf SH. The 2009 breast cancer screening recommendations of the US Preventive Services Task Force. JAMA. 2010;303:162-163.
3. Woloshin S, Schwartz LM. The benefits and harms of mammography screening: understanding the trade-offs. JAMA. 2010;303:164-165.
4. Murphy AM. Mammography screening for breast cancer: a view from 2 worlds. JAMA. 2010;303:166-167.
5. Berg WA. Benefits of screening mammography. JAMA. 2010;303:168-169.
6. DeAngelis CF, Fontanarosa PB. US Preventive Services Task Force and breast cancer screening. JAMA. 2010;303:172-173.
7. Editors’ note on the USPSTF recommendation on screening for breast cancer. February 15, 2010. Available at: http://www.annals.org/content/early/2010/02/12/0003-4819-152-8-201004200-00209.full. Accessed April 7, 2010.
8. Begg CB. Comments and response on the USPSTF recommendation on screening for breast cancer. February 15, 2010. Available at: http://www.annals.org/content/early/2010/02/12/0003-4819-152-8-201004200-00203.full. Accessed April 7, 2010.
9. Jorgensen KJ, Gotzsche PC. The background review for the USPSTF recommendation on screening for breast cancer. February 15, 2010. Available at: http://www.annals.org/content/early/2010/02/12/0003-4819-152-8-201004200-00198.full. Accessed April 7, 2010.
Playing God (part 2)
I am sitting in a Budget car rental lounge waiting for my daughter to arrive from Denver. Tomorrow we will memorialize my mother.
It is interesting to reflect on reader reaction to the editorials I’ve written about my mom’s final year. Some of you lament the resources spent in prolonged ventilator care, repeated hospitalizations, and seemingly futile interventions. And while I can relate to this concern, both my brother and I agreed that following her wishes was what mattered most—all expenses aside.
I recently came across an article on the front page of the Sunday New York Times, about a charismatic leader in palliative care who, when faced with her own metastatic cancer, did everything possible to keep death at bay. Perhaps that should not be surprising. Who is to know what any of us would do when faced with such personal choices? And who better to make such decisions than the patient herself? I remain convinced that predicting the course of severe, even life-threatening illness, is highly chancy. Neither my brother nor I—nor Mom’s physicians—would ever have predicted her lengthy survival.
Other readers share my concern that palliative care remains the exception rather than the rule, and that services such as hospice continue to carry a stigma. A close family friend recently died at a local hospice. Ironically, her final days of inpatient hospice care were deemed unnecessary, and her husband was left with a significant bill. I am sure the peace of mind afforded this friend by the caring, experienced hospice staff was well worth the expense. But it is very disappointing to realize that our health care system is still more prepared to pay for a stint in the ICU than to provide a distraught spouse with the help he so desperately craves. I can’t help but think that this reflects our misplaced values—it’s as if one’s final week is somehow less worthy of support than the previous 75 years.
Over the course of the year, many of you—readers whom I have never met—have provided me with words of encouragement and support. For this, I am indebted. I trust that you—indeed, that all of us who care for patients (and families) at the end of life—will remain dedicated to making their last days as comfortable as possible, in accordance with their wishes.

Jeff Susman, MD
Editor-in-Chief
[email protected]
Jeff Susman, MD
Editor-in-Chief
[email protected]
Jeff Susman, MD
Editor-in-Chief
[email protected]
I am sitting in a Budget car rental lounge waiting for my daughter to arrive from Denver. Tomorrow we will memorialize my mother.
It is interesting to reflect on reader reaction to the editorials I’ve written about my mom’s final year. Some of you lament the resources spent in prolonged ventilator care, repeated hospitalizations, and seemingly futile interventions. And while I can relate to this concern, both my brother and I agreed that following her wishes was what mattered most—all expenses aside.
I recently came across an article on the front page of the Sunday New York Times, about a charismatic leader in palliative care who, when faced with her own metastatic cancer, did everything possible to keep death at bay. Perhaps that should not be surprising. Who is to know what any of us would do when faced with such personal choices? And who better to make such decisions than the patient herself? I remain convinced that predicting the course of severe, even life-threatening illness, is highly chancy. Neither my brother nor I—nor Mom’s physicians—would ever have predicted her lengthy survival.
Other readers share my concern that palliative care remains the exception rather than the rule, and that services such as hospice continue to carry a stigma. A close family friend recently died at a local hospice. Ironically, her final days of inpatient hospice care were deemed unnecessary, and her husband was left with a significant bill. I am sure the peace of mind afforded this friend by the caring, experienced hospice staff was well worth the expense. But it is very disappointing to realize that our health care system is still more prepared to pay for a stint in the ICU than to provide a distraught spouse with the help he so desperately craves. I can’t help but think that this reflects our misplaced values—it’s as if one’s final week is somehow less worthy of support than the previous 75 years.
Over the course of the year, many of you—readers whom I have never met—have provided me with words of encouragement and support. For this, I am indebted. I trust that you—indeed, that all of us who care for patients (and families) at the end of life—will remain dedicated to making their last days as comfortable as possible, in accordance with their wishes.
I am sitting in a Budget car rental lounge waiting for my daughter to arrive from Denver. Tomorrow we will memorialize my mother.
It is interesting to reflect on reader reaction to the editorials I’ve written about my mom’s final year. Some of you lament the resources spent in prolonged ventilator care, repeated hospitalizations, and seemingly futile interventions. And while I can relate to this concern, both my brother and I agreed that following her wishes was what mattered most—all expenses aside.
I recently came across an article on the front page of the Sunday New York Times, about a charismatic leader in palliative care who, when faced with her own metastatic cancer, did everything possible to keep death at bay. Perhaps that should not be surprising. Who is to know what any of us would do when faced with such personal choices? And who better to make such decisions than the patient herself? I remain convinced that predicting the course of severe, even life-threatening illness, is highly chancy. Neither my brother nor I—nor Mom’s physicians—would ever have predicted her lengthy survival.
Other readers share my concern that palliative care remains the exception rather than the rule, and that services such as hospice continue to carry a stigma. A close family friend recently died at a local hospice. Ironically, her final days of inpatient hospice care were deemed unnecessary, and her husband was left with a significant bill. I am sure the peace of mind afforded this friend by the caring, experienced hospice staff was well worth the expense. But it is very disappointing to realize that our health care system is still more prepared to pay for a stint in the ICU than to provide a distraught spouse with the help he so desperately craves. I can’t help but think that this reflects our misplaced values—it’s as if one’s final week is somehow less worthy of support than the previous 75 years.
Over the course of the year, many of you—readers whom I have never met—have provided me with words of encouragement and support. For this, I am indebted. I trust that you—indeed, that all of us who care for patients (and families) at the end of life—will remain dedicated to making their last days as comfortable as possible, in accordance with their wishes.
A look at the long-term safety of an extended-regimen OC
Abstract
Background: Oral contraceptives (OCs) are the most widely used method of reversible contraception. Recent alterations of the standard 28-day regimen have included shortening the traditional hormone-free interval (HFI), supplementing the HFI with low-dose estrogen, or increasing the number of active pills administered, thus extending the time between withdrawal bleeding episodes by a variable number of months. In light of these changes in regimens, clinicians may be seeking evidence that the new regimens are safe and will not result in unexpected adverse events.
Methods: We initiated a long-term extension trial to evaluate the safety of a 91-day extended-regimen OC containing 150 mcg levonorgestrel/30 mcg ethinyl estradiol (EE) for 84 days, followed by 7 days of 10 mcg EE. After participation in a 1-year, open-label, phase 3 contraceptive program, 320 women qualified for enrollment in a multicenter, nonrandomized study of 91-day extended-regimen OCs for up to 3 additional consecutive years; 116 completed the study. We evaluated incidence of reported adverse events (AEs), rates of study discontinuation, and reported bleeding patterns.
Results: Total exposure was equivalent to 8292 28-day cycles. Participants reported no thromboembolic events. Thirty-one (9.7%) women discontinued treatment due to AEs. Unscheduled bleeding and spotting diminished during the course of the trial. Overall rates of study discontinuation and incidence of AEs were consistent with those observed in the phase 3 clinical program.
Conclusion: This study demonstrated that the AE profile of the 91-day extended-regimen OC over 4 years was similar to that seen in the 1-year clinical trials, with no unexpected adverse events.
Two Phase 3 studies assessed a 91-day oral contraceptive (OC) regimen for 1 year—a multicenter, open-label trial that studied safety and efficacy,1 and a multicenter trial that evaluated endometrial safety.2 Results of both studies showed the regimen to be safe, effective, and well tolerated. The regimen: 84 days of combination tablets containing 150 mcg levonorgestrel (LNG) and 30 mcg ethinyl estradiol (EE), followed by 7 days of 10 mcg EE alone instead of placebo to maintain ovarian suppression,3,4 potentially reducing the incidence of intermenstrual bleeding or spotting. To gain longer experience with this regimen, we enrolled selected subjects from both studies in a 3-year extension trial.
Methods
Study design and population
In this nonrandomized, multicenter, open-label extension study, we invited women who had successfully completed 1 year of treatment in either of the Phase 3 trials to participate as part of a convenience sample for an additional 3 years of follow-up. We conducted this study in accordance with ethical guidelines for human subjects and applicable guidelines for good clinical practice.5
Inclusion and exclusion criteria were similar to those used in the Phase 3 studies.1,2 Participants agreed to use the study medication as their primary method of birth control throughout the study. We excluded women who were using a medication that might interfere with the efficacy of OCs, or who had any medical or lifestyle contraindications to OC use (eg, clinically significant abnormal Pap smear; cigarette use if older than 35 years).
We enrolled 320 subjects whose demographic characteristics were similar to those in the earlier Phase 3 trials (TABLE 1).2
TABLE 1
Demographic characteristics of all treated participants (N=320)
| Age at screening, y | |
| Mean (SD) | 28.1 (6.0) |
| Median | 27.5 |
| Min, Max | 18.2, 40.2 |
| Weight, lb | |
| Mean (SD) | 152.3 (37.6) |
| Median | 143.5 |
| Min, Max | 94.0, 360.0 |
| Body mass index, kg/m2 | |
| Mean (SD) | 25.5 (5.8) |
| Median | 24.1 |
| Min, Max | 16.8, 56.5 |
| OC use history, n (%) | |
| Recent user | 225 (70.3%) |
| Prior user | 67 (20.9%) |
| New start | 28 (8.8%) |
| Race, n (%) | |
| African American | 40 (12.5%) |
| Asian | 7 (2.2%) |
| Caucasian | 262 (81.9%) |
| Hispanic | 4 (1.3%) |
| Other | 7 (2.2%) |
| Cigarette use status, n (%) | |
| Nonsmoker | 269 (84.1%) |
| Smoker | 51 (15.9%) |
| OC, oral contraceptive; SD, standard deviation. | |
Regular evaluation of adherence and AEs
Every 3 months at the study site, we assessed adherence with the drug regimen by reviewing participants’ daily diaries and by counting pills in returned used pill packs. We also evaluated subject-reported adverse events (AEs)—side effects, as well as serious adverse events (SAEs) requiring treatment or drug discontinuation—and use of concomitant medications or cigarettes.
Factors in our safety assessment
Our safety analysis included any subject who took at least 1 dose of the study drug. We calculated the incidence rates of subject-reported AEs, overall rates of discontinuation, and cycles of exposure. These included incidence rates of AEs the investigators deemed to be at least “remotely” related to treatment. Safety analyses also included annual changes in laboratory values (complete blood count, serum chemistry, lipid profile, and urinalysis), vital signs, occurrence of pregnancy, and rates of reported bleeding or spotting.
The evaluation included bleeding/spotting that was scheduled—occurring on cycle days 85 through 91 (EE-only tablets)—and unscheduled—intermenstrual or “breakthrough” blood loss occurring on cycle days 1 through 84. We defined bleeding as any vaginal blood loss requiring the use of sanitary protection (pads or tampons); spotting was defined as vaginal blood loss not necessitating sanitary protection.
Statistical analysis
Descriptive statistics included the number of subjects, and the mean, median (where appropriate), standard deviation or standard error of the mean (SE), or minimum and maximum values of patient characteristics. We summarized discrete events using frequencies or percentages. As this study was designed primarily to be observational and to gain further long-term experience with the regimen, we did not conduct formal power analyses and sample size calculations. For contraceptive trials, the US Food and Drug Administration typically requires a minimum exposure of 200 women using the method for 1 year. We also omitted a formal efficacy analysis, as efficacy was established in the Phase 3 clinical program.1
Results
Of the 320 subjects enrolled and treated, 244 (76.3%) completed at least 1 year of treatment; 173 (54.1%) completed at least 2 years of treatment; and 85 (26.6%) completed 3 years of treatment in this extension study, beyond the 1 year completed in the Phase 3 clinical trials (FIGURE). A total of 204 women (63.8%) discontinued treatment; primarily due to personal decisions (26.6%), becoming lost to follow-up (11.3%), and adverse events (9.7%). These discontinuation rates are consistent with those in other long-term studies.6-8
FIGURE
Of the 320 participants enrolled, 116 completed the study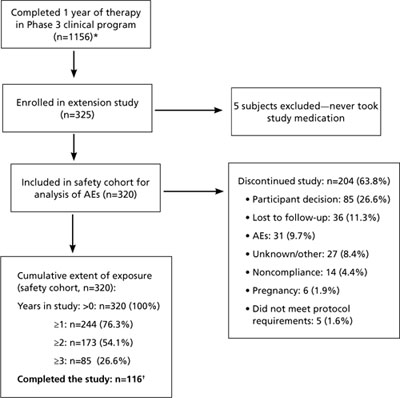
* In the pregnancy prevention study, 979 patients completed 1 year; in the endometrial safety study, 177 completed 1 year. Only 11 of the original 36 sites participated in the extension study, so not all 1156 subjects had the option of enrolling in the extension.
† Not all subjects enrolled at the same time. Thirty-one patients were participating in the study with various durations of exposure when the study was ended. Although they did not complete 3 full years of use, they did participate in the full course of the study that was available to them and were therefore classified as “completers.”
Serious adverse events were few
SAEs were reported by 12 subjects; 3 were possibly related to treatment—spontaneous abortion in a 33-year-old subject, nonthrombotic coronary artery spasm in a 40-year-old subject, and acute cholecystitis in a 37-year old subject. No venous thromboembolic events (VTEs) occurred; however, such events are rare (approximately 7-18 VTEs/100,000 OC users annually9) and would be unlikely in a study of 320 subjects.
Nonurgent adverse events comparable to earlier studies
The most commonly reported treatment-related AEs were headache (9.4%), metrorrhagia (9.1%), increased weight (6.9%), and dysmenorrhea (4.4%), as noted in TABLE 2. The most frequently reported treatment-emergent AEs (ie, regardless of relationship to study medication) were headache (21.9%), upper respiratory tract infection (18.4%), nasopharyngitis (15.0%), sinusitis (12.2%), and back pain (11.6%). A total of 31 subjects (9.7%) discontinued the study due to AEs. The incidence rates of treatment-emergent and treatment-related AEs in this study were not substantially higher than those in the Phase 3 trials.1
TABLE 2
Adverse events attributable to treatment occurred in ≥2% of participants (N=320)
| MedDRA System organ class and preferred term | n (%) |
|---|---|
| Reproductive system and breast disorders Metrorrhagia Dysmenorrhea | 29 (9.1) 14 (4.4) |
| Nervous system disorders Headache | 30 (9.4) |
| Investigations Weight increased | 22 (6.9) |
| Infections and infestations Vulvovaginal mycotic infection Vaginitis, bacterial Fungal infection | 13 (4.1) 9 (2.8) 7 (2.2) |
| Skin and subcutaneous tissue disorders Acne | 7 (2.2) |
| MedDRA, Medical Dictionary for Regulatory Activities. | |
Pregnancies due mostly to nonadherence
We conducted no formal efficacy analyses. Pregnancy was determined by a positive result on a pregnancy test conducted at the study site. Six subjects (1.9%) became pregnant during the study; 4 were noncompliant with the study medication, and 2 became pregnant at least 14 days after completing the study medication. One spontaneous abortion was reported. Among those participants who continued their pregnancies, none reported abnormal outcomes.
Laboratory values changed minimally, if at all
No notable changes occurred in serum chemistry, hematology, or urinalysis values. Specific mean changes from baseline included increases of 5.0 mg/dL for total cholesterol, 2.4 mg/dL for high-density lipoproteins, and 4.0 mg/dL for low-density lipoproteins; and decreases of 5.9 mg/dL for triglycerides and 0.1 g/dL for hemoglobin.
Vital signs remained stable
No notable changes occurred in systolic or diastolic blood pressure, heart rate, or temperature. The increase in mean weight that we observed (10.4 lb) is not unexpected, as the time period of evaluation was as long as 4 years after documentation of the baseline value.
Reported bleeding or spotting diminished over time
Median rates of unscheduled bleeding or spotting declined over the course of the study, from 4 days in 91 during cycle 1 to 1 day in 91 during cycle 11. In most of the 91-day cycles, participants consistently reported a median of 3 days of scheduled (withdrawal) bleeding or spotting.
Discussion
This 3-year study increased our experience with a novel extended-regimen OC to 4 years of continuous use. The results should reassure clinicians who are prescribing extended-regimen OCs that their patients are unlikely to experience side effects that differ significantly from traditional 28-day OC regimens. In other long-term studies of 28-day regimens, the most common AEs were headache, back pain, nausea, pharyngitis, and upper respiratory infection.7,8
Overall rates of study discontinuation and the incidence of AEs (including SAEs and AEs leading to discontinuation) were consistent with those observed in 1-year1,2,10,11 and 2-year6 studies of extended-regimen OCs.
There was no suggestion of increased risk of serious estrogen-related AEs. There were no reports of endometrial abnormalities or hyperplasia, which is consistent with the results of endometrial biopsies in a previous study that compared before- and after-treatment biopsy samples from 63 subjects in the 1-year Phase 3 trial.2
A pharmacokinetic analysis of a similar extended-regimen OC demonstrated that estrogen levels, measured on days 1, 21, 84, and 91 of a 91-day extended-regimen cycle, did not build up over the course of the regimen.12
The risk of thromboembolic disease associated with OCs is not related to the length of use, and a 5-year case-control study found significantly decreasing odds ratios for reports of VTE in OC users over time.13 In this extension study, there were no reported thromboembolic AEs and there was no suggestion of an increased risk of thrombosis with the long-term use of this regimen, although such findings are not unexpected for a small-scale study.
Acknowledgements
The principal investigators and their locations are as follows: Angeli Adamczyk, Paige Brainard (Tucson, Ariz), Ted Anderson, Robert Rosenfeld, Shali Scott (Nashville, Tenn), Matthew Davis (Rochester, NY), William Gibbons, Laurel Stadtmauer (Norfolk, Va), James Lackey (Oklahoma City, Okla), Sooji Lee-Rugh (Arlington, Va), Thomas Littlejohn (Winston-Salem, NC), James Maly (Lincoln, Neb), David Portman (Columbus, Ohio), George Raad (Charlotte, NC), and Mark Shepard (Washington, DC).
CORRESPONDENCE Kathleen Reape, MD, Teva Branded Pharmaceutical Products R&D, Inc., 425 Privet Road, Horsham, PA 19044; Kathleen. [email protected]
1. Anderson FD, Gibbons W, Portman D. Safety and efficacy of an extended-regimen oral contraceptive utilizing continuous low-dose ethinyl estradiol. Contraception. 2006;73:229-234.
2. Anderson FD, Feldman R, Reape KZ. Endometrial effects of a 91-day extended regimen oral contraceptive with low-dose estrogen in place of placebo. Contraception. 2008;77:91-96.
3. Vandever MA, Kuehl TJ, Sulak P, et al. Evaluation of pituitary-ovarian axis suppression with three oral contraceptive regimens. Contraception. 2008;77:162-170.
4. Reape KZ, DiLiberti CE, Hendy CH, et al. Effects on serum hormone levels of low-dose estrogen in place of placebo during the hormone-free interval of an oral contraceptive. Contraception. 2008;77:34-39.
5. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. Available at: http://www.wma.net/en/30publications/10policies/b3/index.html. Accessed April 6, 2010.
6. Anderson FD, Gibbons W, Portman D. Long-term safety of an extended-cycle oral contraceptive (Seasonale): A 2-year multicenter open-label extension trial. Am J Obstet Gynecol. 2006;195:92-96.
7. Zahradnik HP, Hanjalic-Beck A. Efficacy, safety, and sustainability of treatment continuation and results of an oral contraceptive containing 30 mcg ethinyl estradiol and 2 mg chlormadinone acetate, in long-term usage (up to 45 cycles)—an open-label, prospective, noncontrolled, office-based Phase III study. Contraception. 2008;77:337-343.
8. Archer DF, Jensen JT, Johnson JV, et al. Evaluation of a continuous regimen of levonorgestrel/ethinyl estradiol: phase 3 study results. Contraception. 2006;74:439-445.
9. Burkman RT. Venous thromboembolism and oral contraceptives: Current status and clinical implications. Treat Endocrinol. 2002;1:143-147.
10. Anderson FD, Hait H. The Seasonale-301 Study Group. A multicenter, randomized study of an extended cycle oral contraceptive. Contraception. 2003;68:89-96.
11. Anderson FD, Hait H, Hsiu J, et al. Endometrial microstructure after long-term use of a 91-day extended-cycle oral contraceptive regimen. Contraception. 2005;71:55-59.
12. Reape KZ, DiLiberti C. Steady-state pharmacokinetics of an extended-regimen oral contraceptive with continuous estrogen [abstract]. Obstet Gynecol. 2007;109(suppl 4):13S.-
13. Lidegaard O, Edstrom E, Kreiner S. Oral contraceptives and venous thromboembolism: a five-year national case-control study. Contraception. 2002;65:187-196.
Abstract
Background: Oral contraceptives (OCs) are the most widely used method of reversible contraception. Recent alterations of the standard 28-day regimen have included shortening the traditional hormone-free interval (HFI), supplementing the HFI with low-dose estrogen, or increasing the number of active pills administered, thus extending the time between withdrawal bleeding episodes by a variable number of months. In light of these changes in regimens, clinicians may be seeking evidence that the new regimens are safe and will not result in unexpected adverse events.
Methods: We initiated a long-term extension trial to evaluate the safety of a 91-day extended-regimen OC containing 150 mcg levonorgestrel/30 mcg ethinyl estradiol (EE) for 84 days, followed by 7 days of 10 mcg EE. After participation in a 1-year, open-label, phase 3 contraceptive program, 320 women qualified for enrollment in a multicenter, nonrandomized study of 91-day extended-regimen OCs for up to 3 additional consecutive years; 116 completed the study. We evaluated incidence of reported adverse events (AEs), rates of study discontinuation, and reported bleeding patterns.
Results: Total exposure was equivalent to 8292 28-day cycles. Participants reported no thromboembolic events. Thirty-one (9.7%) women discontinued treatment due to AEs. Unscheduled bleeding and spotting diminished during the course of the trial. Overall rates of study discontinuation and incidence of AEs were consistent with those observed in the phase 3 clinical program.
Conclusion: This study demonstrated that the AE profile of the 91-day extended-regimen OC over 4 years was similar to that seen in the 1-year clinical trials, with no unexpected adverse events.
Two Phase 3 studies assessed a 91-day oral contraceptive (OC) regimen for 1 year—a multicenter, open-label trial that studied safety and efficacy,1 and a multicenter trial that evaluated endometrial safety.2 Results of both studies showed the regimen to be safe, effective, and well tolerated. The regimen: 84 days of combination tablets containing 150 mcg levonorgestrel (LNG) and 30 mcg ethinyl estradiol (EE), followed by 7 days of 10 mcg EE alone instead of placebo to maintain ovarian suppression,3,4 potentially reducing the incidence of intermenstrual bleeding or spotting. To gain longer experience with this regimen, we enrolled selected subjects from both studies in a 3-year extension trial.
Methods
Study design and population
In this nonrandomized, multicenter, open-label extension study, we invited women who had successfully completed 1 year of treatment in either of the Phase 3 trials to participate as part of a convenience sample for an additional 3 years of follow-up. We conducted this study in accordance with ethical guidelines for human subjects and applicable guidelines for good clinical practice.5
Inclusion and exclusion criteria were similar to those used in the Phase 3 studies.1,2 Participants agreed to use the study medication as their primary method of birth control throughout the study. We excluded women who were using a medication that might interfere with the efficacy of OCs, or who had any medical or lifestyle contraindications to OC use (eg, clinically significant abnormal Pap smear; cigarette use if older than 35 years).
We enrolled 320 subjects whose demographic characteristics were similar to those in the earlier Phase 3 trials (TABLE 1).2
TABLE 1
Demographic characteristics of all treated participants (N=320)
| Age at screening, y | |
| Mean (SD) | 28.1 (6.0) |
| Median | 27.5 |
| Min, Max | 18.2, 40.2 |
| Weight, lb | |
| Mean (SD) | 152.3 (37.6) |
| Median | 143.5 |
| Min, Max | 94.0, 360.0 |
| Body mass index, kg/m2 | |
| Mean (SD) | 25.5 (5.8) |
| Median | 24.1 |
| Min, Max | 16.8, 56.5 |
| OC use history, n (%) | |
| Recent user | 225 (70.3%) |
| Prior user | 67 (20.9%) |
| New start | 28 (8.8%) |
| Race, n (%) | |
| African American | 40 (12.5%) |
| Asian | 7 (2.2%) |
| Caucasian | 262 (81.9%) |
| Hispanic | 4 (1.3%) |
| Other | 7 (2.2%) |
| Cigarette use status, n (%) | |
| Nonsmoker | 269 (84.1%) |
| Smoker | 51 (15.9%) |
| OC, oral contraceptive; SD, standard deviation. | |
Regular evaluation of adherence and AEs
Every 3 months at the study site, we assessed adherence with the drug regimen by reviewing participants’ daily diaries and by counting pills in returned used pill packs. We also evaluated subject-reported adverse events (AEs)—side effects, as well as serious adverse events (SAEs) requiring treatment or drug discontinuation—and use of concomitant medications or cigarettes.
Factors in our safety assessment
Our safety analysis included any subject who took at least 1 dose of the study drug. We calculated the incidence rates of subject-reported AEs, overall rates of discontinuation, and cycles of exposure. These included incidence rates of AEs the investigators deemed to be at least “remotely” related to treatment. Safety analyses also included annual changes in laboratory values (complete blood count, serum chemistry, lipid profile, and urinalysis), vital signs, occurrence of pregnancy, and rates of reported bleeding or spotting.
The evaluation included bleeding/spotting that was scheduled—occurring on cycle days 85 through 91 (EE-only tablets)—and unscheduled—intermenstrual or “breakthrough” blood loss occurring on cycle days 1 through 84. We defined bleeding as any vaginal blood loss requiring the use of sanitary protection (pads or tampons); spotting was defined as vaginal blood loss not necessitating sanitary protection.
Statistical analysis
Descriptive statistics included the number of subjects, and the mean, median (where appropriate), standard deviation or standard error of the mean (SE), or minimum and maximum values of patient characteristics. We summarized discrete events using frequencies or percentages. As this study was designed primarily to be observational and to gain further long-term experience with the regimen, we did not conduct formal power analyses and sample size calculations. For contraceptive trials, the US Food and Drug Administration typically requires a minimum exposure of 200 women using the method for 1 year. We also omitted a formal efficacy analysis, as efficacy was established in the Phase 3 clinical program.1
Results
Of the 320 subjects enrolled and treated, 244 (76.3%) completed at least 1 year of treatment; 173 (54.1%) completed at least 2 years of treatment; and 85 (26.6%) completed 3 years of treatment in this extension study, beyond the 1 year completed in the Phase 3 clinical trials (FIGURE). A total of 204 women (63.8%) discontinued treatment; primarily due to personal decisions (26.6%), becoming lost to follow-up (11.3%), and adverse events (9.7%). These discontinuation rates are consistent with those in other long-term studies.6-8
FIGURE
Of the 320 participants enrolled, 116 completed the study
* In the pregnancy prevention study, 979 patients completed 1 year; in the endometrial safety study, 177 completed 1 year. Only 11 of the original 36 sites participated in the extension study, so not all 1156 subjects had the option of enrolling in the extension.
† Not all subjects enrolled at the same time. Thirty-one patients were participating in the study with various durations of exposure when the study was ended. Although they did not complete 3 full years of use, they did participate in the full course of the study that was available to them and were therefore classified as “completers.”
Serious adverse events were few
SAEs were reported by 12 subjects; 3 were possibly related to treatment—spontaneous abortion in a 33-year-old subject, nonthrombotic coronary artery spasm in a 40-year-old subject, and acute cholecystitis in a 37-year old subject. No venous thromboembolic events (VTEs) occurred; however, such events are rare (approximately 7-18 VTEs/100,000 OC users annually9) and would be unlikely in a study of 320 subjects.
Nonurgent adverse events comparable to earlier studies
The most commonly reported treatment-related AEs were headache (9.4%), metrorrhagia (9.1%), increased weight (6.9%), and dysmenorrhea (4.4%), as noted in TABLE 2. The most frequently reported treatment-emergent AEs (ie, regardless of relationship to study medication) were headache (21.9%), upper respiratory tract infection (18.4%), nasopharyngitis (15.0%), sinusitis (12.2%), and back pain (11.6%). A total of 31 subjects (9.7%) discontinued the study due to AEs. The incidence rates of treatment-emergent and treatment-related AEs in this study were not substantially higher than those in the Phase 3 trials.1
TABLE 2
Adverse events attributable to treatment occurred in ≥2% of participants (N=320)
| MedDRA System organ class and preferred term | n (%) |
|---|---|
| Reproductive system and breast disorders Metrorrhagia Dysmenorrhea | 29 (9.1) 14 (4.4) |
| Nervous system disorders Headache | 30 (9.4) |
| Investigations Weight increased | 22 (6.9) |
| Infections and infestations Vulvovaginal mycotic infection Vaginitis, bacterial Fungal infection | 13 (4.1) 9 (2.8) 7 (2.2) |
| Skin and subcutaneous tissue disorders Acne | 7 (2.2) |
| MedDRA, Medical Dictionary for Regulatory Activities. | |
Pregnancies due mostly to nonadherence
We conducted no formal efficacy analyses. Pregnancy was determined by a positive result on a pregnancy test conducted at the study site. Six subjects (1.9%) became pregnant during the study; 4 were noncompliant with the study medication, and 2 became pregnant at least 14 days after completing the study medication. One spontaneous abortion was reported. Among those participants who continued their pregnancies, none reported abnormal outcomes.
Laboratory values changed minimally, if at all
No notable changes occurred in serum chemistry, hematology, or urinalysis values. Specific mean changes from baseline included increases of 5.0 mg/dL for total cholesterol, 2.4 mg/dL for high-density lipoproteins, and 4.0 mg/dL for low-density lipoproteins; and decreases of 5.9 mg/dL for triglycerides and 0.1 g/dL for hemoglobin.
Vital signs remained stable
No notable changes occurred in systolic or diastolic blood pressure, heart rate, or temperature. The increase in mean weight that we observed (10.4 lb) is not unexpected, as the time period of evaluation was as long as 4 years after documentation of the baseline value.
Reported bleeding or spotting diminished over time
Median rates of unscheduled bleeding or spotting declined over the course of the study, from 4 days in 91 during cycle 1 to 1 day in 91 during cycle 11. In most of the 91-day cycles, participants consistently reported a median of 3 days of scheduled (withdrawal) bleeding or spotting.
Discussion
This 3-year study increased our experience with a novel extended-regimen OC to 4 years of continuous use. The results should reassure clinicians who are prescribing extended-regimen OCs that their patients are unlikely to experience side effects that differ significantly from traditional 28-day OC regimens. In other long-term studies of 28-day regimens, the most common AEs were headache, back pain, nausea, pharyngitis, and upper respiratory infection.7,8
Overall rates of study discontinuation and the incidence of AEs (including SAEs and AEs leading to discontinuation) were consistent with those observed in 1-year1,2,10,11 and 2-year6 studies of extended-regimen OCs.
There was no suggestion of increased risk of serious estrogen-related AEs. There were no reports of endometrial abnormalities or hyperplasia, which is consistent with the results of endometrial biopsies in a previous study that compared before- and after-treatment biopsy samples from 63 subjects in the 1-year Phase 3 trial.2
A pharmacokinetic analysis of a similar extended-regimen OC demonstrated that estrogen levels, measured on days 1, 21, 84, and 91 of a 91-day extended-regimen cycle, did not build up over the course of the regimen.12
The risk of thromboembolic disease associated with OCs is not related to the length of use, and a 5-year case-control study found significantly decreasing odds ratios for reports of VTE in OC users over time.13 In this extension study, there were no reported thromboembolic AEs and there was no suggestion of an increased risk of thrombosis with the long-term use of this regimen, although such findings are not unexpected for a small-scale study.
Acknowledgements
The principal investigators and their locations are as follows: Angeli Adamczyk, Paige Brainard (Tucson, Ariz), Ted Anderson, Robert Rosenfeld, Shali Scott (Nashville, Tenn), Matthew Davis (Rochester, NY), William Gibbons, Laurel Stadtmauer (Norfolk, Va), James Lackey (Oklahoma City, Okla), Sooji Lee-Rugh (Arlington, Va), Thomas Littlejohn (Winston-Salem, NC), James Maly (Lincoln, Neb), David Portman (Columbus, Ohio), George Raad (Charlotte, NC), and Mark Shepard (Washington, DC).
CORRESPONDENCE Kathleen Reape, MD, Teva Branded Pharmaceutical Products R&D, Inc., 425 Privet Road, Horsham, PA 19044; Kathleen. [email protected]
Abstract
Background: Oral contraceptives (OCs) are the most widely used method of reversible contraception. Recent alterations of the standard 28-day regimen have included shortening the traditional hormone-free interval (HFI), supplementing the HFI with low-dose estrogen, or increasing the number of active pills administered, thus extending the time between withdrawal bleeding episodes by a variable number of months. In light of these changes in regimens, clinicians may be seeking evidence that the new regimens are safe and will not result in unexpected adverse events.
Methods: We initiated a long-term extension trial to evaluate the safety of a 91-day extended-regimen OC containing 150 mcg levonorgestrel/30 mcg ethinyl estradiol (EE) for 84 days, followed by 7 days of 10 mcg EE. After participation in a 1-year, open-label, phase 3 contraceptive program, 320 women qualified for enrollment in a multicenter, nonrandomized study of 91-day extended-regimen OCs for up to 3 additional consecutive years; 116 completed the study. We evaluated incidence of reported adverse events (AEs), rates of study discontinuation, and reported bleeding patterns.
Results: Total exposure was equivalent to 8292 28-day cycles. Participants reported no thromboembolic events. Thirty-one (9.7%) women discontinued treatment due to AEs. Unscheduled bleeding and spotting diminished during the course of the trial. Overall rates of study discontinuation and incidence of AEs were consistent with those observed in the phase 3 clinical program.
Conclusion: This study demonstrated that the AE profile of the 91-day extended-regimen OC over 4 years was similar to that seen in the 1-year clinical trials, with no unexpected adverse events.
Two Phase 3 studies assessed a 91-day oral contraceptive (OC) regimen for 1 year—a multicenter, open-label trial that studied safety and efficacy,1 and a multicenter trial that evaluated endometrial safety.2 Results of both studies showed the regimen to be safe, effective, and well tolerated. The regimen: 84 days of combination tablets containing 150 mcg levonorgestrel (LNG) and 30 mcg ethinyl estradiol (EE), followed by 7 days of 10 mcg EE alone instead of placebo to maintain ovarian suppression,3,4 potentially reducing the incidence of intermenstrual bleeding or spotting. To gain longer experience with this regimen, we enrolled selected subjects from both studies in a 3-year extension trial.
Methods
Study design and population
In this nonrandomized, multicenter, open-label extension study, we invited women who had successfully completed 1 year of treatment in either of the Phase 3 trials to participate as part of a convenience sample for an additional 3 years of follow-up. We conducted this study in accordance with ethical guidelines for human subjects and applicable guidelines for good clinical practice.5
Inclusion and exclusion criteria were similar to those used in the Phase 3 studies.1,2 Participants agreed to use the study medication as their primary method of birth control throughout the study. We excluded women who were using a medication that might interfere with the efficacy of OCs, or who had any medical or lifestyle contraindications to OC use (eg, clinically significant abnormal Pap smear; cigarette use if older than 35 years).
We enrolled 320 subjects whose demographic characteristics were similar to those in the earlier Phase 3 trials (TABLE 1).2
TABLE 1
Demographic characteristics of all treated participants (N=320)
| Age at screening, y | |
| Mean (SD) | 28.1 (6.0) |
| Median | 27.5 |
| Min, Max | 18.2, 40.2 |
| Weight, lb | |
| Mean (SD) | 152.3 (37.6) |
| Median | 143.5 |
| Min, Max | 94.0, 360.0 |
| Body mass index, kg/m2 | |
| Mean (SD) | 25.5 (5.8) |
| Median | 24.1 |
| Min, Max | 16.8, 56.5 |
| OC use history, n (%) | |
| Recent user | 225 (70.3%) |
| Prior user | 67 (20.9%) |
| New start | 28 (8.8%) |
| Race, n (%) | |
| African American | 40 (12.5%) |
| Asian | 7 (2.2%) |
| Caucasian | 262 (81.9%) |
| Hispanic | 4 (1.3%) |
| Other | 7 (2.2%) |
| Cigarette use status, n (%) | |
| Nonsmoker | 269 (84.1%) |
| Smoker | 51 (15.9%) |
| OC, oral contraceptive; SD, standard deviation. | |
Regular evaluation of adherence and AEs
Every 3 months at the study site, we assessed adherence with the drug regimen by reviewing participants’ daily diaries and by counting pills in returned used pill packs. We also evaluated subject-reported adverse events (AEs)—side effects, as well as serious adverse events (SAEs) requiring treatment or drug discontinuation—and use of concomitant medications or cigarettes.
Factors in our safety assessment
Our safety analysis included any subject who took at least 1 dose of the study drug. We calculated the incidence rates of subject-reported AEs, overall rates of discontinuation, and cycles of exposure. These included incidence rates of AEs the investigators deemed to be at least “remotely” related to treatment. Safety analyses also included annual changes in laboratory values (complete blood count, serum chemistry, lipid profile, and urinalysis), vital signs, occurrence of pregnancy, and rates of reported bleeding or spotting.
The evaluation included bleeding/spotting that was scheduled—occurring on cycle days 85 through 91 (EE-only tablets)—and unscheduled—intermenstrual or “breakthrough” blood loss occurring on cycle days 1 through 84. We defined bleeding as any vaginal blood loss requiring the use of sanitary protection (pads or tampons); spotting was defined as vaginal blood loss not necessitating sanitary protection.
Statistical analysis
Descriptive statistics included the number of subjects, and the mean, median (where appropriate), standard deviation or standard error of the mean (SE), or minimum and maximum values of patient characteristics. We summarized discrete events using frequencies or percentages. As this study was designed primarily to be observational and to gain further long-term experience with the regimen, we did not conduct formal power analyses and sample size calculations. For contraceptive trials, the US Food and Drug Administration typically requires a minimum exposure of 200 women using the method for 1 year. We also omitted a formal efficacy analysis, as efficacy was established in the Phase 3 clinical program.1
Results
Of the 320 subjects enrolled and treated, 244 (76.3%) completed at least 1 year of treatment; 173 (54.1%) completed at least 2 years of treatment; and 85 (26.6%) completed 3 years of treatment in this extension study, beyond the 1 year completed in the Phase 3 clinical trials (FIGURE). A total of 204 women (63.8%) discontinued treatment; primarily due to personal decisions (26.6%), becoming lost to follow-up (11.3%), and adverse events (9.7%). These discontinuation rates are consistent with those in other long-term studies.6-8
FIGURE
Of the 320 participants enrolled, 116 completed the study
* In the pregnancy prevention study, 979 patients completed 1 year; in the endometrial safety study, 177 completed 1 year. Only 11 of the original 36 sites participated in the extension study, so not all 1156 subjects had the option of enrolling in the extension.
† Not all subjects enrolled at the same time. Thirty-one patients were participating in the study with various durations of exposure when the study was ended. Although they did not complete 3 full years of use, they did participate in the full course of the study that was available to them and were therefore classified as “completers.”
Serious adverse events were few
SAEs were reported by 12 subjects; 3 were possibly related to treatment—spontaneous abortion in a 33-year-old subject, nonthrombotic coronary artery spasm in a 40-year-old subject, and acute cholecystitis in a 37-year old subject. No venous thromboembolic events (VTEs) occurred; however, such events are rare (approximately 7-18 VTEs/100,000 OC users annually9) and would be unlikely in a study of 320 subjects.
Nonurgent adverse events comparable to earlier studies
The most commonly reported treatment-related AEs were headache (9.4%), metrorrhagia (9.1%), increased weight (6.9%), and dysmenorrhea (4.4%), as noted in TABLE 2. The most frequently reported treatment-emergent AEs (ie, regardless of relationship to study medication) were headache (21.9%), upper respiratory tract infection (18.4%), nasopharyngitis (15.0%), sinusitis (12.2%), and back pain (11.6%). A total of 31 subjects (9.7%) discontinued the study due to AEs. The incidence rates of treatment-emergent and treatment-related AEs in this study were not substantially higher than those in the Phase 3 trials.1
TABLE 2
Adverse events attributable to treatment occurred in ≥2% of participants (N=320)
| MedDRA System organ class and preferred term | n (%) |
|---|---|
| Reproductive system and breast disorders Metrorrhagia Dysmenorrhea | 29 (9.1) 14 (4.4) |
| Nervous system disorders Headache | 30 (9.4) |
| Investigations Weight increased | 22 (6.9) |
| Infections and infestations Vulvovaginal mycotic infection Vaginitis, bacterial Fungal infection | 13 (4.1) 9 (2.8) 7 (2.2) |
| Skin and subcutaneous tissue disorders Acne | 7 (2.2) |
| MedDRA, Medical Dictionary for Regulatory Activities. | |
Pregnancies due mostly to nonadherence
We conducted no formal efficacy analyses. Pregnancy was determined by a positive result on a pregnancy test conducted at the study site. Six subjects (1.9%) became pregnant during the study; 4 were noncompliant with the study medication, and 2 became pregnant at least 14 days after completing the study medication. One spontaneous abortion was reported. Among those participants who continued their pregnancies, none reported abnormal outcomes.
Laboratory values changed minimally, if at all
No notable changes occurred in serum chemistry, hematology, or urinalysis values. Specific mean changes from baseline included increases of 5.0 mg/dL for total cholesterol, 2.4 mg/dL for high-density lipoproteins, and 4.0 mg/dL for low-density lipoproteins; and decreases of 5.9 mg/dL for triglycerides and 0.1 g/dL for hemoglobin.
Vital signs remained stable
No notable changes occurred in systolic or diastolic blood pressure, heart rate, or temperature. The increase in mean weight that we observed (10.4 lb) is not unexpected, as the time period of evaluation was as long as 4 years after documentation of the baseline value.
Reported bleeding or spotting diminished over time
Median rates of unscheduled bleeding or spotting declined over the course of the study, from 4 days in 91 during cycle 1 to 1 day in 91 during cycle 11. In most of the 91-day cycles, participants consistently reported a median of 3 days of scheduled (withdrawal) bleeding or spotting.
Discussion
This 3-year study increased our experience with a novel extended-regimen OC to 4 years of continuous use. The results should reassure clinicians who are prescribing extended-regimen OCs that their patients are unlikely to experience side effects that differ significantly from traditional 28-day OC regimens. In other long-term studies of 28-day regimens, the most common AEs were headache, back pain, nausea, pharyngitis, and upper respiratory infection.7,8
Overall rates of study discontinuation and the incidence of AEs (including SAEs and AEs leading to discontinuation) were consistent with those observed in 1-year1,2,10,11 and 2-year6 studies of extended-regimen OCs.
There was no suggestion of increased risk of serious estrogen-related AEs. There were no reports of endometrial abnormalities or hyperplasia, which is consistent with the results of endometrial biopsies in a previous study that compared before- and after-treatment biopsy samples from 63 subjects in the 1-year Phase 3 trial.2
A pharmacokinetic analysis of a similar extended-regimen OC demonstrated that estrogen levels, measured on days 1, 21, 84, and 91 of a 91-day extended-regimen cycle, did not build up over the course of the regimen.12
The risk of thromboembolic disease associated with OCs is not related to the length of use, and a 5-year case-control study found significantly decreasing odds ratios for reports of VTE in OC users over time.13 In this extension study, there were no reported thromboembolic AEs and there was no suggestion of an increased risk of thrombosis with the long-term use of this regimen, although such findings are not unexpected for a small-scale study.
Acknowledgements
The principal investigators and their locations are as follows: Angeli Adamczyk, Paige Brainard (Tucson, Ariz), Ted Anderson, Robert Rosenfeld, Shali Scott (Nashville, Tenn), Matthew Davis (Rochester, NY), William Gibbons, Laurel Stadtmauer (Norfolk, Va), James Lackey (Oklahoma City, Okla), Sooji Lee-Rugh (Arlington, Va), Thomas Littlejohn (Winston-Salem, NC), James Maly (Lincoln, Neb), David Portman (Columbus, Ohio), George Raad (Charlotte, NC), and Mark Shepard (Washington, DC).
CORRESPONDENCE Kathleen Reape, MD, Teva Branded Pharmaceutical Products R&D, Inc., 425 Privet Road, Horsham, PA 19044; Kathleen. [email protected]
1. Anderson FD, Gibbons W, Portman D. Safety and efficacy of an extended-regimen oral contraceptive utilizing continuous low-dose ethinyl estradiol. Contraception. 2006;73:229-234.
2. Anderson FD, Feldman R, Reape KZ. Endometrial effects of a 91-day extended regimen oral contraceptive with low-dose estrogen in place of placebo. Contraception. 2008;77:91-96.
3. Vandever MA, Kuehl TJ, Sulak P, et al. Evaluation of pituitary-ovarian axis suppression with three oral contraceptive regimens. Contraception. 2008;77:162-170.
4. Reape KZ, DiLiberti CE, Hendy CH, et al. Effects on serum hormone levels of low-dose estrogen in place of placebo during the hormone-free interval of an oral contraceptive. Contraception. 2008;77:34-39.
5. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. Available at: http://www.wma.net/en/30publications/10policies/b3/index.html. Accessed April 6, 2010.
6. Anderson FD, Gibbons W, Portman D. Long-term safety of an extended-cycle oral contraceptive (Seasonale): A 2-year multicenter open-label extension trial. Am J Obstet Gynecol. 2006;195:92-96.
7. Zahradnik HP, Hanjalic-Beck A. Efficacy, safety, and sustainability of treatment continuation and results of an oral contraceptive containing 30 mcg ethinyl estradiol and 2 mg chlormadinone acetate, in long-term usage (up to 45 cycles)—an open-label, prospective, noncontrolled, office-based Phase III study. Contraception. 2008;77:337-343.
8. Archer DF, Jensen JT, Johnson JV, et al. Evaluation of a continuous regimen of levonorgestrel/ethinyl estradiol: phase 3 study results. Contraception. 2006;74:439-445.
9. Burkman RT. Venous thromboembolism and oral contraceptives: Current status and clinical implications. Treat Endocrinol. 2002;1:143-147.
10. Anderson FD, Hait H. The Seasonale-301 Study Group. A multicenter, randomized study of an extended cycle oral contraceptive. Contraception. 2003;68:89-96.
11. Anderson FD, Hait H, Hsiu J, et al. Endometrial microstructure after long-term use of a 91-day extended-cycle oral contraceptive regimen. Contraception. 2005;71:55-59.
12. Reape KZ, DiLiberti C. Steady-state pharmacokinetics of an extended-regimen oral contraceptive with continuous estrogen [abstract]. Obstet Gynecol. 2007;109(suppl 4):13S.-
13. Lidegaard O, Edstrom E, Kreiner S. Oral contraceptives and venous thromboembolism: a five-year national case-control study. Contraception. 2002;65:187-196.
1. Anderson FD, Gibbons W, Portman D. Safety and efficacy of an extended-regimen oral contraceptive utilizing continuous low-dose ethinyl estradiol. Contraception. 2006;73:229-234.
2. Anderson FD, Feldman R, Reape KZ. Endometrial effects of a 91-day extended regimen oral contraceptive with low-dose estrogen in place of placebo. Contraception. 2008;77:91-96.
3. Vandever MA, Kuehl TJ, Sulak P, et al. Evaluation of pituitary-ovarian axis suppression with three oral contraceptive regimens. Contraception. 2008;77:162-170.
4. Reape KZ, DiLiberti CE, Hendy CH, et al. Effects on serum hormone levels of low-dose estrogen in place of placebo during the hormone-free interval of an oral contraceptive. Contraception. 2008;77:34-39.
5. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. Available at: http://www.wma.net/en/30publications/10policies/b3/index.html. Accessed April 6, 2010.
6. Anderson FD, Gibbons W, Portman D. Long-term safety of an extended-cycle oral contraceptive (Seasonale): A 2-year multicenter open-label extension trial. Am J Obstet Gynecol. 2006;195:92-96.
7. Zahradnik HP, Hanjalic-Beck A. Efficacy, safety, and sustainability of treatment continuation and results of an oral contraceptive containing 30 mcg ethinyl estradiol and 2 mg chlormadinone acetate, in long-term usage (up to 45 cycles)—an open-label, prospective, noncontrolled, office-based Phase III study. Contraception. 2008;77:337-343.
8. Archer DF, Jensen JT, Johnson JV, et al. Evaluation of a continuous regimen of levonorgestrel/ethinyl estradiol: phase 3 study results. Contraception. 2006;74:439-445.
9. Burkman RT. Venous thromboembolism and oral contraceptives: Current status and clinical implications. Treat Endocrinol. 2002;1:143-147.
10. Anderson FD, Hait H. The Seasonale-301 Study Group. A multicenter, randomized study of an extended cycle oral contraceptive. Contraception. 2003;68:89-96.
11. Anderson FD, Hait H, Hsiu J, et al. Endometrial microstructure after long-term use of a 91-day extended-cycle oral contraceptive regimen. Contraception. 2005;71:55-59.
12. Reape KZ, DiLiberti C. Steady-state pharmacokinetics of an extended-regimen oral contraceptive with continuous estrogen [abstract]. Obstet Gynecol. 2007;109(suppl 4):13S.-
13. Lidegaard O, Edstrom E, Kreiner S. Oral contraceptives and venous thromboembolism: a five-year national case-control study. Contraception. 2002;65:187-196.
Bedtime battles: When patients act out their dreams
REM sleep behavior disorder (RBD) patients act out their dreams during sleep and could injure themselves or bed partner. In RBD, loss of skeletal muscle atonia during rapid eye movement (REM) sleep allows the patient’s motor activity to reflect dream content. During sleep, patients appear to punch, kick, or choke a bed partner or jump out of bed.
RBD is more common in elderly males and individuals with neurodegenerative disorders of alpha-synuclein accumulation, such as Parkinson’s disease, Lewy body dementia, and multiple system atrophy.1 RBD may be a precursor to these diseases.
Most antidepressants can cause or increase RBD movements.2 RBD also is associated with sedative-hypnotic withdrawal.
Differential diagnosis
When patients report striking out while asleep, differential diagnoses include RBD, periodic limb movement disorder (PLMD), sleepwalking disorder, and restless legs syndrome (RLS). Polysomnography with electromyography may distinguish among these disorders.
PLMD movements are repetitive, stereotyped motions of the foot and leg, and manifest as a repetitive partial flexion of the joints of the great toe, ankle, knee, and occasionally hip. Upper extremity movements are less common. Movements appear similar to myoclonus. Periodic limb movements occur in rhythmic patterns, every 20 to 60 seconds, continuing for 10 minutes to several hours.
Sleepwalking disorder movements occur without an associated dream during non-REM sleep. Individuals with RBD may jump out of bed, but usually don’t walk in their sleep.
RLS movement occurs prior to and in early stages of sleep, whereas in RBD, PLMD, and sleepwalking disorder, motor activity is limited to sleep. Patients perceive unpleasant sensations and an urge to move the feet and legs. Movement temporarily soothes these uncomfortable sensations. Patients are aware of these sensations before sleep; however, RBD patients are not conscious of movements until they wake and find themselves acting out a dream. RLS and PLMD often are comorbid.
Treatment
Clonazepam is most effective for RBD; however, also consider lorazepam, pramipexole, or melatonin. If clinically feasible, consider discontinuing antidepressants because this may decrease movements.3
To reduce risk of injury, recommend sleeping in separate beds, moving objects away from the bed, or padding the headboard and floor. Encourage patients with severe RBD to sleep in a zipped sleeping bag.
1. Salah Uddin ABM, Jarmi T. REM sleep behavior disorder. Available at: http://emedicine.medscape.com/article/1188651-overview. Accessed March 22, 2010.
2. Kaufman DM. Clinical neurology for psychiatrists. 6th ed. Philadelphia, PA: Saunders; 2006.
3. Buysse DJ. Sleep disorders and psychiatry. Arlington, VA: American Psychiatric Publishing, Inc.; 2005.
REM sleep behavior disorder (RBD) patients act out their dreams during sleep and could injure themselves or bed partner. In RBD, loss of skeletal muscle atonia during rapid eye movement (REM) sleep allows the patient’s motor activity to reflect dream content. During sleep, patients appear to punch, kick, or choke a bed partner or jump out of bed.
RBD is more common in elderly males and individuals with neurodegenerative disorders of alpha-synuclein accumulation, such as Parkinson’s disease, Lewy body dementia, and multiple system atrophy.1 RBD may be a precursor to these diseases.
Most antidepressants can cause or increase RBD movements.2 RBD also is associated with sedative-hypnotic withdrawal.
Differential diagnosis
When patients report striking out while asleep, differential diagnoses include RBD, periodic limb movement disorder (PLMD), sleepwalking disorder, and restless legs syndrome (RLS). Polysomnography with electromyography may distinguish among these disorders.
PLMD movements are repetitive, stereotyped motions of the foot and leg, and manifest as a repetitive partial flexion of the joints of the great toe, ankle, knee, and occasionally hip. Upper extremity movements are less common. Movements appear similar to myoclonus. Periodic limb movements occur in rhythmic patterns, every 20 to 60 seconds, continuing for 10 minutes to several hours.
Sleepwalking disorder movements occur without an associated dream during non-REM sleep. Individuals with RBD may jump out of bed, but usually don’t walk in their sleep.
RLS movement occurs prior to and in early stages of sleep, whereas in RBD, PLMD, and sleepwalking disorder, motor activity is limited to sleep. Patients perceive unpleasant sensations and an urge to move the feet and legs. Movement temporarily soothes these uncomfortable sensations. Patients are aware of these sensations before sleep; however, RBD patients are not conscious of movements until they wake and find themselves acting out a dream. RLS and PLMD often are comorbid.
Treatment
Clonazepam is most effective for RBD; however, also consider lorazepam, pramipexole, or melatonin. If clinically feasible, consider discontinuing antidepressants because this may decrease movements.3
To reduce risk of injury, recommend sleeping in separate beds, moving objects away from the bed, or padding the headboard and floor. Encourage patients with severe RBD to sleep in a zipped sleeping bag.
REM sleep behavior disorder (RBD) patients act out their dreams during sleep and could injure themselves or bed partner. In RBD, loss of skeletal muscle atonia during rapid eye movement (REM) sleep allows the patient’s motor activity to reflect dream content. During sleep, patients appear to punch, kick, or choke a bed partner or jump out of bed.
RBD is more common in elderly males and individuals with neurodegenerative disorders of alpha-synuclein accumulation, such as Parkinson’s disease, Lewy body dementia, and multiple system atrophy.1 RBD may be a precursor to these diseases.
Most antidepressants can cause or increase RBD movements.2 RBD also is associated with sedative-hypnotic withdrawal.
Differential diagnosis
When patients report striking out while asleep, differential diagnoses include RBD, periodic limb movement disorder (PLMD), sleepwalking disorder, and restless legs syndrome (RLS). Polysomnography with electromyography may distinguish among these disorders.
PLMD movements are repetitive, stereotyped motions of the foot and leg, and manifest as a repetitive partial flexion of the joints of the great toe, ankle, knee, and occasionally hip. Upper extremity movements are less common. Movements appear similar to myoclonus. Periodic limb movements occur in rhythmic patterns, every 20 to 60 seconds, continuing for 10 minutes to several hours.
Sleepwalking disorder movements occur without an associated dream during non-REM sleep. Individuals with RBD may jump out of bed, but usually don’t walk in their sleep.
RLS movement occurs prior to and in early stages of sleep, whereas in RBD, PLMD, and sleepwalking disorder, motor activity is limited to sleep. Patients perceive unpleasant sensations and an urge to move the feet and legs. Movement temporarily soothes these uncomfortable sensations. Patients are aware of these sensations before sleep; however, RBD patients are not conscious of movements until they wake and find themselves acting out a dream. RLS and PLMD often are comorbid.
Treatment
Clonazepam is most effective for RBD; however, also consider lorazepam, pramipexole, or melatonin. If clinically feasible, consider discontinuing antidepressants because this may decrease movements.3
To reduce risk of injury, recommend sleeping in separate beds, moving objects away from the bed, or padding the headboard and floor. Encourage patients with severe RBD to sleep in a zipped sleeping bag.
1. Salah Uddin ABM, Jarmi T. REM sleep behavior disorder. Available at: http://emedicine.medscape.com/article/1188651-overview. Accessed March 22, 2010.
2. Kaufman DM. Clinical neurology for psychiatrists. 6th ed. Philadelphia, PA: Saunders; 2006.
3. Buysse DJ. Sleep disorders and psychiatry. Arlington, VA: American Psychiatric Publishing, Inc.; 2005.
1. Salah Uddin ABM, Jarmi T. REM sleep behavior disorder. Available at: http://emedicine.medscape.com/article/1188651-overview. Accessed March 22, 2010.
2. Kaufman DM. Clinical neurology for psychiatrists. 6th ed. Philadelphia, PA: Saunders; 2006.
3. Buysse DJ. Sleep disorders and psychiatry. Arlington, VA: American Psychiatric Publishing, Inc.; 2005.
Nighttime anxieties
CASE: Stress and chest pain
A primary care physician refers Mr. J, age 40, to our mental health clinic for evaluation of anxiety symptoms. Almost a decade ago Mr. J presented to his primary care physician with anxiety and panic attacks that included chest pain and shortness of breath. Various pharmacologic treatments, including paroxetine, were only moderately successful until 4 years ago, when Mr. J began nighttime continuous positive airway pressure (CPAP) therapy and pramipexole, 0.25 to 0.5 mg/d, for obstructive sleep apnea (OSA), at which point his anxiety completely resolved.
Mr. J reported no anxiety for many years, but when shortness of breath, palpitations, and chest pain re-emerge, he consults his primary care physician. After a negative workup for myocardial infarction, Mr. J is started on short-term beta-blocker therapy and restarted on paroxetine, 20 mg/d. A sleep medicine specialist repeats polysomnography and makes slight adjustments to Mr. J’s CPAP therapy. Mr. J relocates to our city and his new primary care physician refers Mr. J to our mental health clinic.
In addition to OSA, Mr. J has mild anemia, hyperlipidemia, and vitamin D deficiency. Mr. J was adopted and has no knowledge of his family psychiatric or medical history. His mental status is normal. Mr. J is not obese, exercises regularly, and has slight micrognathia. His current medications include paroxetine, 20 mg/d, modafinil, 200 mg/d, and ergocalciferol, 50,000 units/week for vitamin D deficiency.
Mr. J says he experienced a single panic attack 7 months ago, but none since then. However, he complains of chronic chest pressure and mild intermittent anxiety associated with the stress of his new job and recent relocation.
The authors’ observations
Mr. J’s anxiety resolved fully only after receiving treatment for OSA, which is characterized by episodes of blocked breathing during sleep (Table 1).1 Multiple studies show a significant association between OSA and panic attacks.2-5 In a survey of 301 sleep apnea patients, Edlund et al6 demonstrated that OSA may cause nocturnal panic attacks. Untreated OSA can worsen anxiety symptoms. In a study of 242 OSA patients, those who were not compliant with CPAP therapy had significantly higher anxiety scores as measured on the Hospital Anxiety and Depression Scale.7
OSA treatment options include CPAP, oral appliance, and surgery; weight loss and positional therapy may help. Thyroid function, B12, folate, ferritin, and iron studies, and complete blood count can rule out secondary causes of OSA.
Table 1
Obstructive sleep apnea risk factors, symptoms, and features
| Established risk factors | Obesity, craniofacial abnormalities, upper airway soft tissue abnormalities, male sex |
| Potential risk factors | Heredity, smoking, nasal congestion, diabetes |
| Symptoms | Daytime sleepiness; nonrestorative sleep; witnessed apneas by bed partner; awakening with choking; nocturnal restlessness; insomnia with frequent awakenings; impaired concentration; cognitive deficits; mood changes; morning headaches; vivid, strange, or threatening dreams; gastroesophageal reflux |
| Common features in patients with obstructive sleep apnea | Obesity, large neck circumference, systemic hypertension, hypercapnia, cardiovascular or cerebrovascular disease, cardiac dysrhythmias, narrow or ‘crowded’ airway, pulmonary hypertension, cor pulmonale, polycythemia |
| Source: Reference 1 | |
HISTORY: A succession of diagnoses
Approximately 9 years ago, Mr. J experienced several episodes of waking in the middle of the night from a bad dream with severe shortness of breath and chest pain. He also reported increasing fatigue, anxiety, and stress regarding work, graduate school, and his wife’s recent miscarriage. After negative cardiac workups, his primary care physician diagnosed panic attacks. He referred Mr. J to stress management classes and prescribed clonazepam, 1.5 mg/d, which was discontinued after 2 months.
One week after discontinuing clonazepam, Mr. J experienced chest pain, shortness of breath, and anxiety while awake. A cardiologist ruled out cardiac pathology. Mr. J’s primary care physician prescribed sertraline, 25 mg/d, and propranolol, 60 mg/d and 10 mg as needed, for anxiety.
Shortly after, Mr. J moved to a different city. His new primary care physician discontinued sertraline and propranolol and started paroxetine, titrated to 20 mg/d. A psychiatrist diagnosed Mr. J with panic disorder without agoraphobia, continued paroxetine, and added alprazolam, 1 mg/d as needed. Mr. J’s anxiety symptoms were moderately controlled for several years.
After his son was diagnosed with attention-deficit/hyperactivity disorder (ADHD), Mr. J also was evaluated and found to have ADHD and major depressive disorder, single episode. Mr. J received methylphenidate, 54 mg/d, and paroxetine was titrated to 40 mg/d, with moderate results.
Approximately 6 years before presenting to our clinic, Mr. J reported worsening daytime fatigue, which was treated with modafinil, 200 mg/d. He experienced significant improvement. The next year methylphenidate was switched to amphetamine/dextroamphetamine, then discontinued because of side effects. His physician started Mr. J on atomoxetine, which also was discontinued because of side effects.
Two years later, Mr. J complained of gradual worsening daytime sleepiness. Polysomnography revealed that Mr. J had severe OSA and periodic limb movement disorder. After he began nighttime CPAP and pramipexole, 0.25 to 0.5 mg/d, and continued modafinil, 200 mg/d, his anxiety symptoms completely resolved. Several months later Mr. J’s physician discontinued paroxetine because Mr. J reported it caused mildly decreased concentration.
The authors’ observations
The etiology of Mr. J’s anxiety is unclear; however, he does not meet criteria for:
- panic disorder, because he denies persistent concern about having more attacks or the implications or consequences of panic attacks, or significant change in behavior related to panic attacks (Table 2)8
- generalized anxiety disorder, because between panic attacks Mr. J’s baseline anxiety related to “real-world” stressors is mild, intermittent, and easily controllable8
- substance-induced anxiety disorder, because Mr. J denies using caffeine, tobacco, alcohol, or illicit drugs. Also, for many years he worked for a company that performed random drug screening.
Table 2
Diagnostic criteria for panic disorder without agoraphobia
| A. Both 1 and 2: 1. Recurrent unexpected panic attacks 2. At least one of the attacks has been followed by 1 month (or more) of 1 (or more) of the following: a. Persistent concern about having additional attacks b. Worry about the implications of the attack or its consequences (eg, losing control, having a heart attack, ‘going crazy’) c. A significant change in behavior related to the attacks |
| B. Absence of agoraphobia |
| C. The panic attacks are not due to the direct physiologic effects of a substance (eg, a drug of abuse, a medication) or a general medical condition (eg, hyperthyroidism). |
| D. The panic attacks are not better accounted for by another mental disorder, such as social phobia (eg, occurring on exposure to feared social situations), specific phobia (eg, on exposure to a specific phobic situation), obsessive-compulsive disorder (eg, on exposure to dirt in someone with an obsession about contamination), posttraumatic stress disorder (eg, in response to stimuli associated with a severe stressor), or separation anxiety disorder (eg, in response to being away from home or close relatives). |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Although it is difficult to draw a conclusion from a single case, Mr. J’s dramatic improvement with CPAP warrants speculation about possible etiologic relationships among daytime panic attacks, nighttime panic attacks, and OSA.
According to DSM-IV-TR, a panic attack has a distinct period of intense fear or discomfort (Table 3).8 Recurrent panic attacks can lead to anticipatory anxiety, which is an intense fear and/or dread of having another panic attack.9 According to Steven Reiss’ expectancy theory, anxiety sensitivity—ie, the fear of anxiety or fear of fear—may be a risk factor for panic disorder.10 Therefore, past panic attacks may increase the likelihood of future panic attacks.
Table 3
Diagnostic criteria for panic attack*
A discrete period of intense fear or discomfort, in which 4 (or more) of the following symptoms developed abruptly and reached a peak within 10 minutes:
|
| *Panic attacks occur in the context of several anxiety disorders and cannot be diagnosed as a separate entity |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Mr. J’s panic symptoms may be caused by multiple OSA-induced nocturnal panic attacks. These nighttime panic attacks may predispose him to daytime attacks. It is possible that Mr. J had subclinical panic disorder before developing OSA. In this scenario, his OSA-induced nocturnal panic attacks may have worsened his panic disorder. Unfortunately, we do not know precisely how long Mr. J has had OSA—only that he was diagnosed with the condition 4 years before presenting to our clinic.
Mr. J responded moderately to paroxetine monotherapy but experienced rapid resolution of his panic attacks with a combination of paroxetine and CPAP. CPAP monotherapy sufficiently prevented panic attacks for 4 years. Finally, when Mr. J experienced a single panic attack several months before presenting to our clinic—at the end of a very stressful year—reintroducing paroxetine prevented subsequent attacks. This supports our hypothesis that OSA may predispose or indirectly cause patients to develop daytime panic attacks. Alternately, this case suggests that OSA may cause subclinical panic disorder to present as an acute condition.
We rule out anxiety disorder secondary to a general medical condition (OSA) and diagnose Mr. J with anxiety disorder not otherwise specified.
The authors’ observations
We continue paroxetine at 20 mg/d because it was working fairly well with minimal side effects. The sleep medicine specialist maintained modafinil, 200 mg/d. Laboratory studies—including a comprehensive metabolic panel, complete blood count with differential, and thyroid stimulating hormone—were within normal limits except a fasting blood glucose of 123 mg/dL, for which we referred Mr. J to his primary care physician.
OUTCOME: Discontinue paroxetine?
One month later, Mr. J denies panic attacks, other anxiety symptoms, or other psychiatric symptoms and is sleeping well. However, he reports that his mildly decreased concentration persists and he wants to stop paroxetine.
After discussing the risks and benefits, Mr. J and the treatment team decide to continue paroxetine at 20 mg/d. We cite peer-reviewed literature that recommends continuing antidepressants for at least 1 year and possibly indefinitely after symptom resolution to control panic disorder symptoms.9 In addition, we discuss the lack of studies comparing different lengths of treatment with SSRIs for apparent OSA-induced panic attacks that respond to SSRI/CPAP therapy. Because Mr. J was doing well and experiencing minimal side effects, he feels he would be better served with a longer period of psychopharmacologic treatment.
Six months later, Mr. J says his anxiety symptoms are well controlled and generally unchanged except for an occasional “little flutter” of anxiety every 3 or 4 days that lasts several seconds. For 1 year, he reports no recurrence of panic attacks, compliance with CPAP, and stable OSA.
Related resource
- Saunamäki T, Jehkonen M. Depression and anxiety in obstructive sleep apnea syndrome: a review. Acta Neurol Scand. 2007;116(5):277-288.
Drug brand names
- Alprazolam • Xanax
- Amphetamine/dextroamphetamine • Adderall
- Atomoxetine • Strattera
- Clonazepam • Klonopin
- Ergocalciferol • Calciferol
- Modafinil • Provigil
- Methylphenidate extended release • Concerta
- Paroxetine • Paxil
- Pramipexole • Mirapex
- Propranolol • Inderal
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Strohl K, Basner R, Sanders M, et al. Overview of obstructive sleep apnea in adults. UpToDate Online. May 2009. Available at: http://uptodateonline.com/online/content/topic.do?topicKey=sleepdis/12387&selectedTitle=1~150&source=search_result. Accessed September 1, 2009.
2. Chung SA, Jairam S, Hussain MR, et al. How, what, and why of sleep apnea. Perspectives for primary care physicians. Can Fam Physician. 2002;48:1073-1080.
3. Sharafkhaneh A, Giray N, Richardson P, et al. Association of psychiatric disorders and sleep apnea in a large cohort. Sleep. 2005;28(11):1405-1411.
4. Victor LD. Obstructive sleep apnea. Am Fam Physician. 1999;60(8):2279-2286.
5. Lopes FL, Nardi AE, Nascimento I, et al. Nocturnal panic attacks. Arq Neuropsiquiatr. 2002;60:717-720.
6. Edlund MJ, McNamara ME, Millman RP. Sleep apnea and panic attacks. Compr Psychiatry. 1991;32(2):130-132.
7. Kjelsberg FN, Ruud EA, Stavem K. Predictors of symptoms of anxiety and depression in obstructive sleep apnea. Sleep Med. 2005;6(4):341-346.
8. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000:432,440,476.
9. Strahl N. Clinical study guide for the oral boards in psychiatry. 2nd ed. Arlington, VA: American Psychiatric Publishing, Inc; 2005:244-246.
10. Reiss S. Expectancy model of fear, anxiety, and panic. Clin Psychol Rev. 1991;11:141-153.
CASE: Stress and chest pain
A primary care physician refers Mr. J, age 40, to our mental health clinic for evaluation of anxiety symptoms. Almost a decade ago Mr. J presented to his primary care physician with anxiety and panic attacks that included chest pain and shortness of breath. Various pharmacologic treatments, including paroxetine, were only moderately successful until 4 years ago, when Mr. J began nighttime continuous positive airway pressure (CPAP) therapy and pramipexole, 0.25 to 0.5 mg/d, for obstructive sleep apnea (OSA), at which point his anxiety completely resolved.
Mr. J reported no anxiety for many years, but when shortness of breath, palpitations, and chest pain re-emerge, he consults his primary care physician. After a negative workup for myocardial infarction, Mr. J is started on short-term beta-blocker therapy and restarted on paroxetine, 20 mg/d. A sleep medicine specialist repeats polysomnography and makes slight adjustments to Mr. J’s CPAP therapy. Mr. J relocates to our city and his new primary care physician refers Mr. J to our mental health clinic.
In addition to OSA, Mr. J has mild anemia, hyperlipidemia, and vitamin D deficiency. Mr. J was adopted and has no knowledge of his family psychiatric or medical history. His mental status is normal. Mr. J is not obese, exercises regularly, and has slight micrognathia. His current medications include paroxetine, 20 mg/d, modafinil, 200 mg/d, and ergocalciferol, 50,000 units/week for vitamin D deficiency.
Mr. J says he experienced a single panic attack 7 months ago, but none since then. However, he complains of chronic chest pressure and mild intermittent anxiety associated with the stress of his new job and recent relocation.
The authors’ observations
Mr. J’s anxiety resolved fully only after receiving treatment for OSA, which is characterized by episodes of blocked breathing during sleep (Table 1).1 Multiple studies show a significant association between OSA and panic attacks.2-5 In a survey of 301 sleep apnea patients, Edlund et al6 demonstrated that OSA may cause nocturnal panic attacks. Untreated OSA can worsen anxiety symptoms. In a study of 242 OSA patients, those who were not compliant with CPAP therapy had significantly higher anxiety scores as measured on the Hospital Anxiety and Depression Scale.7
OSA treatment options include CPAP, oral appliance, and surgery; weight loss and positional therapy may help. Thyroid function, B12, folate, ferritin, and iron studies, and complete blood count can rule out secondary causes of OSA.
Table 1
Obstructive sleep apnea risk factors, symptoms, and features
| Established risk factors | Obesity, craniofacial abnormalities, upper airway soft tissue abnormalities, male sex |
| Potential risk factors | Heredity, smoking, nasal congestion, diabetes |
| Symptoms | Daytime sleepiness; nonrestorative sleep; witnessed apneas by bed partner; awakening with choking; nocturnal restlessness; insomnia with frequent awakenings; impaired concentration; cognitive deficits; mood changes; morning headaches; vivid, strange, or threatening dreams; gastroesophageal reflux |
| Common features in patients with obstructive sleep apnea | Obesity, large neck circumference, systemic hypertension, hypercapnia, cardiovascular or cerebrovascular disease, cardiac dysrhythmias, narrow or ‘crowded’ airway, pulmonary hypertension, cor pulmonale, polycythemia |
| Source: Reference 1 | |
HISTORY: A succession of diagnoses
Approximately 9 years ago, Mr. J experienced several episodes of waking in the middle of the night from a bad dream with severe shortness of breath and chest pain. He also reported increasing fatigue, anxiety, and stress regarding work, graduate school, and his wife’s recent miscarriage. After negative cardiac workups, his primary care physician diagnosed panic attacks. He referred Mr. J to stress management classes and prescribed clonazepam, 1.5 mg/d, which was discontinued after 2 months.
One week after discontinuing clonazepam, Mr. J experienced chest pain, shortness of breath, and anxiety while awake. A cardiologist ruled out cardiac pathology. Mr. J’s primary care physician prescribed sertraline, 25 mg/d, and propranolol, 60 mg/d and 10 mg as needed, for anxiety.
Shortly after, Mr. J moved to a different city. His new primary care physician discontinued sertraline and propranolol and started paroxetine, titrated to 20 mg/d. A psychiatrist diagnosed Mr. J with panic disorder without agoraphobia, continued paroxetine, and added alprazolam, 1 mg/d as needed. Mr. J’s anxiety symptoms were moderately controlled for several years.
After his son was diagnosed with attention-deficit/hyperactivity disorder (ADHD), Mr. J also was evaluated and found to have ADHD and major depressive disorder, single episode. Mr. J received methylphenidate, 54 mg/d, and paroxetine was titrated to 40 mg/d, with moderate results.
Approximately 6 years before presenting to our clinic, Mr. J reported worsening daytime fatigue, which was treated with modafinil, 200 mg/d. He experienced significant improvement. The next year methylphenidate was switched to amphetamine/dextroamphetamine, then discontinued because of side effects. His physician started Mr. J on atomoxetine, which also was discontinued because of side effects.
Two years later, Mr. J complained of gradual worsening daytime sleepiness. Polysomnography revealed that Mr. J had severe OSA and periodic limb movement disorder. After he began nighttime CPAP and pramipexole, 0.25 to 0.5 mg/d, and continued modafinil, 200 mg/d, his anxiety symptoms completely resolved. Several months later Mr. J’s physician discontinued paroxetine because Mr. J reported it caused mildly decreased concentration.
The authors’ observations
The etiology of Mr. J’s anxiety is unclear; however, he does not meet criteria for:
- panic disorder, because he denies persistent concern about having more attacks or the implications or consequences of panic attacks, or significant change in behavior related to panic attacks (Table 2)8
- generalized anxiety disorder, because between panic attacks Mr. J’s baseline anxiety related to “real-world” stressors is mild, intermittent, and easily controllable8
- substance-induced anxiety disorder, because Mr. J denies using caffeine, tobacco, alcohol, or illicit drugs. Also, for many years he worked for a company that performed random drug screening.
Table 2
Diagnostic criteria for panic disorder without agoraphobia
| A. Both 1 and 2: 1. Recurrent unexpected panic attacks 2. At least one of the attacks has been followed by 1 month (or more) of 1 (or more) of the following: a. Persistent concern about having additional attacks b. Worry about the implications of the attack or its consequences (eg, losing control, having a heart attack, ‘going crazy’) c. A significant change in behavior related to the attacks |
| B. Absence of agoraphobia |
| C. The panic attacks are not due to the direct physiologic effects of a substance (eg, a drug of abuse, a medication) or a general medical condition (eg, hyperthyroidism). |
| D. The panic attacks are not better accounted for by another mental disorder, such as social phobia (eg, occurring on exposure to feared social situations), specific phobia (eg, on exposure to a specific phobic situation), obsessive-compulsive disorder (eg, on exposure to dirt in someone with an obsession about contamination), posttraumatic stress disorder (eg, in response to stimuli associated with a severe stressor), or separation anxiety disorder (eg, in response to being away from home or close relatives). |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Although it is difficult to draw a conclusion from a single case, Mr. J’s dramatic improvement with CPAP warrants speculation about possible etiologic relationships among daytime panic attacks, nighttime panic attacks, and OSA.
According to DSM-IV-TR, a panic attack has a distinct period of intense fear or discomfort (Table 3).8 Recurrent panic attacks can lead to anticipatory anxiety, which is an intense fear and/or dread of having another panic attack.9 According to Steven Reiss’ expectancy theory, anxiety sensitivity—ie, the fear of anxiety or fear of fear—may be a risk factor for panic disorder.10 Therefore, past panic attacks may increase the likelihood of future panic attacks.
Table 3
Diagnostic criteria for panic attack*
A discrete period of intense fear or discomfort, in which 4 (or more) of the following symptoms developed abruptly and reached a peak within 10 minutes:
|
| *Panic attacks occur in the context of several anxiety disorders and cannot be diagnosed as a separate entity |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Mr. J’s panic symptoms may be caused by multiple OSA-induced nocturnal panic attacks. These nighttime panic attacks may predispose him to daytime attacks. It is possible that Mr. J had subclinical panic disorder before developing OSA. In this scenario, his OSA-induced nocturnal panic attacks may have worsened his panic disorder. Unfortunately, we do not know precisely how long Mr. J has had OSA—only that he was diagnosed with the condition 4 years before presenting to our clinic.
Mr. J responded moderately to paroxetine monotherapy but experienced rapid resolution of his panic attacks with a combination of paroxetine and CPAP. CPAP monotherapy sufficiently prevented panic attacks for 4 years. Finally, when Mr. J experienced a single panic attack several months before presenting to our clinic—at the end of a very stressful year—reintroducing paroxetine prevented subsequent attacks. This supports our hypothesis that OSA may predispose or indirectly cause patients to develop daytime panic attacks. Alternately, this case suggests that OSA may cause subclinical panic disorder to present as an acute condition.
We rule out anxiety disorder secondary to a general medical condition (OSA) and diagnose Mr. J with anxiety disorder not otherwise specified.
The authors’ observations
We continue paroxetine at 20 mg/d because it was working fairly well with minimal side effects. The sleep medicine specialist maintained modafinil, 200 mg/d. Laboratory studies—including a comprehensive metabolic panel, complete blood count with differential, and thyroid stimulating hormone—were within normal limits except a fasting blood glucose of 123 mg/dL, for which we referred Mr. J to his primary care physician.
OUTCOME: Discontinue paroxetine?
One month later, Mr. J denies panic attacks, other anxiety symptoms, or other psychiatric symptoms and is sleeping well. However, he reports that his mildly decreased concentration persists and he wants to stop paroxetine.
After discussing the risks and benefits, Mr. J and the treatment team decide to continue paroxetine at 20 mg/d. We cite peer-reviewed literature that recommends continuing antidepressants for at least 1 year and possibly indefinitely after symptom resolution to control panic disorder symptoms.9 In addition, we discuss the lack of studies comparing different lengths of treatment with SSRIs for apparent OSA-induced panic attacks that respond to SSRI/CPAP therapy. Because Mr. J was doing well and experiencing minimal side effects, he feels he would be better served with a longer period of psychopharmacologic treatment.
Six months later, Mr. J says his anxiety symptoms are well controlled and generally unchanged except for an occasional “little flutter” of anxiety every 3 or 4 days that lasts several seconds. For 1 year, he reports no recurrence of panic attacks, compliance with CPAP, and stable OSA.
Related resource
- Saunamäki T, Jehkonen M. Depression and anxiety in obstructive sleep apnea syndrome: a review. Acta Neurol Scand. 2007;116(5):277-288.
Drug brand names
- Alprazolam • Xanax
- Amphetamine/dextroamphetamine • Adderall
- Atomoxetine • Strattera
- Clonazepam • Klonopin
- Ergocalciferol • Calciferol
- Modafinil • Provigil
- Methylphenidate extended release • Concerta
- Paroxetine • Paxil
- Pramipexole • Mirapex
- Propranolol • Inderal
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Stress and chest pain
A primary care physician refers Mr. J, age 40, to our mental health clinic for evaluation of anxiety symptoms. Almost a decade ago Mr. J presented to his primary care physician with anxiety and panic attacks that included chest pain and shortness of breath. Various pharmacologic treatments, including paroxetine, were only moderately successful until 4 years ago, when Mr. J began nighttime continuous positive airway pressure (CPAP) therapy and pramipexole, 0.25 to 0.5 mg/d, for obstructive sleep apnea (OSA), at which point his anxiety completely resolved.
Mr. J reported no anxiety for many years, but when shortness of breath, palpitations, and chest pain re-emerge, he consults his primary care physician. After a negative workup for myocardial infarction, Mr. J is started on short-term beta-blocker therapy and restarted on paroxetine, 20 mg/d. A sleep medicine specialist repeats polysomnography and makes slight adjustments to Mr. J’s CPAP therapy. Mr. J relocates to our city and his new primary care physician refers Mr. J to our mental health clinic.
In addition to OSA, Mr. J has mild anemia, hyperlipidemia, and vitamin D deficiency. Mr. J was adopted and has no knowledge of his family psychiatric or medical history. His mental status is normal. Mr. J is not obese, exercises regularly, and has slight micrognathia. His current medications include paroxetine, 20 mg/d, modafinil, 200 mg/d, and ergocalciferol, 50,000 units/week for vitamin D deficiency.
Mr. J says he experienced a single panic attack 7 months ago, but none since then. However, he complains of chronic chest pressure and mild intermittent anxiety associated with the stress of his new job and recent relocation.
The authors’ observations
Mr. J’s anxiety resolved fully only after receiving treatment for OSA, which is characterized by episodes of blocked breathing during sleep (Table 1).1 Multiple studies show a significant association between OSA and panic attacks.2-5 In a survey of 301 sleep apnea patients, Edlund et al6 demonstrated that OSA may cause nocturnal panic attacks. Untreated OSA can worsen anxiety symptoms. In a study of 242 OSA patients, those who were not compliant with CPAP therapy had significantly higher anxiety scores as measured on the Hospital Anxiety and Depression Scale.7
OSA treatment options include CPAP, oral appliance, and surgery; weight loss and positional therapy may help. Thyroid function, B12, folate, ferritin, and iron studies, and complete blood count can rule out secondary causes of OSA.
Table 1
Obstructive sleep apnea risk factors, symptoms, and features
| Established risk factors | Obesity, craniofacial abnormalities, upper airway soft tissue abnormalities, male sex |
| Potential risk factors | Heredity, smoking, nasal congestion, diabetes |
| Symptoms | Daytime sleepiness; nonrestorative sleep; witnessed apneas by bed partner; awakening with choking; nocturnal restlessness; insomnia with frequent awakenings; impaired concentration; cognitive deficits; mood changes; morning headaches; vivid, strange, or threatening dreams; gastroesophageal reflux |
| Common features in patients with obstructive sleep apnea | Obesity, large neck circumference, systemic hypertension, hypercapnia, cardiovascular or cerebrovascular disease, cardiac dysrhythmias, narrow or ‘crowded’ airway, pulmonary hypertension, cor pulmonale, polycythemia |
| Source: Reference 1 | |
HISTORY: A succession of diagnoses
Approximately 9 years ago, Mr. J experienced several episodes of waking in the middle of the night from a bad dream with severe shortness of breath and chest pain. He also reported increasing fatigue, anxiety, and stress regarding work, graduate school, and his wife’s recent miscarriage. After negative cardiac workups, his primary care physician diagnosed panic attacks. He referred Mr. J to stress management classes and prescribed clonazepam, 1.5 mg/d, which was discontinued after 2 months.
One week after discontinuing clonazepam, Mr. J experienced chest pain, shortness of breath, and anxiety while awake. A cardiologist ruled out cardiac pathology. Mr. J’s primary care physician prescribed sertraline, 25 mg/d, and propranolol, 60 mg/d and 10 mg as needed, for anxiety.
Shortly after, Mr. J moved to a different city. His new primary care physician discontinued sertraline and propranolol and started paroxetine, titrated to 20 mg/d. A psychiatrist diagnosed Mr. J with panic disorder without agoraphobia, continued paroxetine, and added alprazolam, 1 mg/d as needed. Mr. J’s anxiety symptoms were moderately controlled for several years.
After his son was diagnosed with attention-deficit/hyperactivity disorder (ADHD), Mr. J also was evaluated and found to have ADHD and major depressive disorder, single episode. Mr. J received methylphenidate, 54 mg/d, and paroxetine was titrated to 40 mg/d, with moderate results.
Approximately 6 years before presenting to our clinic, Mr. J reported worsening daytime fatigue, which was treated with modafinil, 200 mg/d. He experienced significant improvement. The next year methylphenidate was switched to amphetamine/dextroamphetamine, then discontinued because of side effects. His physician started Mr. J on atomoxetine, which also was discontinued because of side effects.
Two years later, Mr. J complained of gradual worsening daytime sleepiness. Polysomnography revealed that Mr. J had severe OSA and periodic limb movement disorder. After he began nighttime CPAP and pramipexole, 0.25 to 0.5 mg/d, and continued modafinil, 200 mg/d, his anxiety symptoms completely resolved. Several months later Mr. J’s physician discontinued paroxetine because Mr. J reported it caused mildly decreased concentration.
The authors’ observations
The etiology of Mr. J’s anxiety is unclear; however, he does not meet criteria for:
- panic disorder, because he denies persistent concern about having more attacks or the implications or consequences of panic attacks, or significant change in behavior related to panic attacks (Table 2)8
- generalized anxiety disorder, because between panic attacks Mr. J’s baseline anxiety related to “real-world” stressors is mild, intermittent, and easily controllable8
- substance-induced anxiety disorder, because Mr. J denies using caffeine, tobacco, alcohol, or illicit drugs. Also, for many years he worked for a company that performed random drug screening.
Table 2
Diagnostic criteria for panic disorder without agoraphobia
| A. Both 1 and 2: 1. Recurrent unexpected panic attacks 2. At least one of the attacks has been followed by 1 month (or more) of 1 (or more) of the following: a. Persistent concern about having additional attacks b. Worry about the implications of the attack or its consequences (eg, losing control, having a heart attack, ‘going crazy’) c. A significant change in behavior related to the attacks |
| B. Absence of agoraphobia |
| C. The panic attacks are not due to the direct physiologic effects of a substance (eg, a drug of abuse, a medication) or a general medical condition (eg, hyperthyroidism). |
| D. The panic attacks are not better accounted for by another mental disorder, such as social phobia (eg, occurring on exposure to feared social situations), specific phobia (eg, on exposure to a specific phobic situation), obsessive-compulsive disorder (eg, on exposure to dirt in someone with an obsession about contamination), posttraumatic stress disorder (eg, in response to stimuli associated with a severe stressor), or separation anxiety disorder (eg, in response to being away from home or close relatives). |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Although it is difficult to draw a conclusion from a single case, Mr. J’s dramatic improvement with CPAP warrants speculation about possible etiologic relationships among daytime panic attacks, nighttime panic attacks, and OSA.
According to DSM-IV-TR, a panic attack has a distinct period of intense fear or discomfort (Table 3).8 Recurrent panic attacks can lead to anticipatory anxiety, which is an intense fear and/or dread of having another panic attack.9 According to Steven Reiss’ expectancy theory, anxiety sensitivity—ie, the fear of anxiety or fear of fear—may be a risk factor for panic disorder.10 Therefore, past panic attacks may increase the likelihood of future panic attacks.
Table 3
Diagnostic criteria for panic attack*
A discrete period of intense fear or discomfort, in which 4 (or more) of the following symptoms developed abruptly and reached a peak within 10 minutes:
|
| *Panic attacks occur in the context of several anxiety disorders and cannot be diagnosed as a separate entity |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Mr. J’s panic symptoms may be caused by multiple OSA-induced nocturnal panic attacks. These nighttime panic attacks may predispose him to daytime attacks. It is possible that Mr. J had subclinical panic disorder before developing OSA. In this scenario, his OSA-induced nocturnal panic attacks may have worsened his panic disorder. Unfortunately, we do not know precisely how long Mr. J has had OSA—only that he was diagnosed with the condition 4 years before presenting to our clinic.
Mr. J responded moderately to paroxetine monotherapy but experienced rapid resolution of his panic attacks with a combination of paroxetine and CPAP. CPAP monotherapy sufficiently prevented panic attacks for 4 years. Finally, when Mr. J experienced a single panic attack several months before presenting to our clinic—at the end of a very stressful year—reintroducing paroxetine prevented subsequent attacks. This supports our hypothesis that OSA may predispose or indirectly cause patients to develop daytime panic attacks. Alternately, this case suggests that OSA may cause subclinical panic disorder to present as an acute condition.
We rule out anxiety disorder secondary to a general medical condition (OSA) and diagnose Mr. J with anxiety disorder not otherwise specified.
The authors’ observations
We continue paroxetine at 20 mg/d because it was working fairly well with minimal side effects. The sleep medicine specialist maintained modafinil, 200 mg/d. Laboratory studies—including a comprehensive metabolic panel, complete blood count with differential, and thyroid stimulating hormone—were within normal limits except a fasting blood glucose of 123 mg/dL, for which we referred Mr. J to his primary care physician.
OUTCOME: Discontinue paroxetine?
One month later, Mr. J denies panic attacks, other anxiety symptoms, or other psychiatric symptoms and is sleeping well. However, he reports that his mildly decreased concentration persists and he wants to stop paroxetine.
After discussing the risks and benefits, Mr. J and the treatment team decide to continue paroxetine at 20 mg/d. We cite peer-reviewed literature that recommends continuing antidepressants for at least 1 year and possibly indefinitely after symptom resolution to control panic disorder symptoms.9 In addition, we discuss the lack of studies comparing different lengths of treatment with SSRIs for apparent OSA-induced panic attacks that respond to SSRI/CPAP therapy. Because Mr. J was doing well and experiencing minimal side effects, he feels he would be better served with a longer period of psychopharmacologic treatment.
Six months later, Mr. J says his anxiety symptoms are well controlled and generally unchanged except for an occasional “little flutter” of anxiety every 3 or 4 days that lasts several seconds. For 1 year, he reports no recurrence of panic attacks, compliance with CPAP, and stable OSA.
Related resource
- Saunamäki T, Jehkonen M. Depression and anxiety in obstructive sleep apnea syndrome: a review. Acta Neurol Scand. 2007;116(5):277-288.
Drug brand names
- Alprazolam • Xanax
- Amphetamine/dextroamphetamine • Adderall
- Atomoxetine • Strattera
- Clonazepam • Klonopin
- Ergocalciferol • Calciferol
- Modafinil • Provigil
- Methylphenidate extended release • Concerta
- Paroxetine • Paxil
- Pramipexole • Mirapex
- Propranolol • Inderal
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Strohl K, Basner R, Sanders M, et al. Overview of obstructive sleep apnea in adults. UpToDate Online. May 2009. Available at: http://uptodateonline.com/online/content/topic.do?topicKey=sleepdis/12387&selectedTitle=1~150&source=search_result. Accessed September 1, 2009.
2. Chung SA, Jairam S, Hussain MR, et al. How, what, and why of sleep apnea. Perspectives for primary care physicians. Can Fam Physician. 2002;48:1073-1080.
3. Sharafkhaneh A, Giray N, Richardson P, et al. Association of psychiatric disorders and sleep apnea in a large cohort. Sleep. 2005;28(11):1405-1411.
4. Victor LD. Obstructive sleep apnea. Am Fam Physician. 1999;60(8):2279-2286.
5. Lopes FL, Nardi AE, Nascimento I, et al. Nocturnal panic attacks. Arq Neuropsiquiatr. 2002;60:717-720.
6. Edlund MJ, McNamara ME, Millman RP. Sleep apnea and panic attacks. Compr Psychiatry. 1991;32(2):130-132.
7. Kjelsberg FN, Ruud EA, Stavem K. Predictors of symptoms of anxiety and depression in obstructive sleep apnea. Sleep Med. 2005;6(4):341-346.
8. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000:432,440,476.
9. Strahl N. Clinical study guide for the oral boards in psychiatry. 2nd ed. Arlington, VA: American Psychiatric Publishing, Inc; 2005:244-246.
10. Reiss S. Expectancy model of fear, anxiety, and panic. Clin Psychol Rev. 1991;11:141-153.
1. Strohl K, Basner R, Sanders M, et al. Overview of obstructive sleep apnea in adults. UpToDate Online. May 2009. Available at: http://uptodateonline.com/online/content/topic.do?topicKey=sleepdis/12387&selectedTitle=1~150&source=search_result. Accessed September 1, 2009.
2. Chung SA, Jairam S, Hussain MR, et al. How, what, and why of sleep apnea. Perspectives for primary care physicians. Can Fam Physician. 2002;48:1073-1080.
3. Sharafkhaneh A, Giray N, Richardson P, et al. Association of psychiatric disorders and sleep apnea in a large cohort. Sleep. 2005;28(11):1405-1411.
4. Victor LD. Obstructive sleep apnea. Am Fam Physician. 1999;60(8):2279-2286.
5. Lopes FL, Nardi AE, Nascimento I, et al. Nocturnal panic attacks. Arq Neuropsiquiatr. 2002;60:717-720.
6. Edlund MJ, McNamara ME, Millman RP. Sleep apnea and panic attacks. Compr Psychiatry. 1991;32(2):130-132.
7. Kjelsberg FN, Ruud EA, Stavem K. Predictors of symptoms of anxiety and depression in obstructive sleep apnea. Sleep Med. 2005;6(4):341-346.
8. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000:432,440,476.
9. Strahl N. Clinical study guide for the oral boards in psychiatry. 2nd ed. Arlington, VA: American Psychiatric Publishing, Inc; 2005:244-246.
10. Reiss S. Expectancy model of fear, anxiety, and panic. Clin Psychol Rev. 1991;11:141-153.
Pessary and pelvic floor exercises for incontinence—are two better than one?
Because we will all be seeing more patients with stress urinary incontinence and other urogynecologic issues, it is critical that we keep abreast of the treatment options available—and their relative effectiveness.1
In this exploration of nonsurgical approaches to stress incontinence, Richter and colleagues started with the premise that a combination of instructed pelvic floor exercises and an incontinence pessary would be better than either treatment alone. They (very appropriately) designated the following as primary outcome measures:
- patient-reported improvement
- symptoms of stress incontinence
- patient satisfaction, as measured using validated instruments.
As reported above, combination therapy did not prove to be superior to single-modality intervention. And although behavioral therapy was superior to a pessary at 3 months, by 12 months the modalities were roughly equivalent, and only about half of patients were still using the prescribed therapy: pessary (45%) or pelvic floor exercises (57%).
This is not a real-world study
Most women who have stress incontinence and who select nonsurgical therapy choose only one option—pelvic floor exercises (if very motivated), a vaginal pessary or other device (if not so motivated), or another conservative option such as radiofrequency therapy (if even less motivated). In this study, women enrolled in behavioral therapy paid four visits (at roughly 2-week intervals) to approved “interventionists,” who instructed them in the technique for pelvic floor exercise and explained other skills and strategies to prevent urge and stress incontinence.
Many women find it difficult to attend the four to eight physiotherapy sessions that are necessary for behavioral intervention and are unwilling to devote 1 year to a therapy that they don’t find effective early on. (Physiotherapy is effective but requires a motivated patient.) Other women dislike inserting a vaginal device on a regular basis. 2
What’s more, very safe minimally invasive slings are available that offer more definitive therapy to patients who have stress incontinence. That said, a sling procedure should not be undertaken lightly. Patient selection should be based on preoperative testing, including an assessment of urethral function, for the transobturator sling.3 A retropubic sling requires a greater degree of expertise to tension appropriately but is suitable for a wider range of severity, including intrinsic sphincteric deficiency. The role of single-incision slings is unclear.
Bottom line: individualize care
The authors’ concluding statements are right on the money: “Individualization of care should continue to be the cornerstone of our approach to [stress incontinent] patients.” These women have several effective options available. We should help them make an educated choice based on symptom severity, lifestyle, and willingness to enroll in self-help intervention versus surgical therapy.
Many patients seek to avoid surgery, either because they believe that their stress incontinence is not severe enough to warrant it, or because they are unwilling to take the 6 to 8 weeks of relative inactivity required for the sling to settle in.
In the absence of approved pharmacotherapy for stress incontinence, I tell patients that they 1) can expect their symptoms to become worse over time and 2) should designate a period of time for a trial of conservative therapy—usually, 3 months. If their condition has not improved to their satisfaction over that period, I recommend that they identify a 6-week window during which they can avoid the gym and the golf course, as well as sexual activity, to allow for unstressed healing from a sling procedure.—G. WILLY DAVILA, MD
1. Wu JM, Hundley AF, Fulton RG, Myers ER. Forecasting the prevalence of pelvic floor disorders in US women: 2010 to 2050. Obstet Gynecol. 2009;114(6):1278-1283.
2. Davila GW, Bernier F. Multimodality pelvic physiotherapy treatment of urinary incontinence in adult women. Int Urogynecol J Pelvic Floor Dysfunct. 1995;6(4):187-194.
3. Guerette N, Bena J, Davila GW. Transobturator slings for stress incontinence: using urodynamic parameters to predict outcomes. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(1):97-102.
Because we will all be seeing more patients with stress urinary incontinence and other urogynecologic issues, it is critical that we keep abreast of the treatment options available—and their relative effectiveness.1
In this exploration of nonsurgical approaches to stress incontinence, Richter and colleagues started with the premise that a combination of instructed pelvic floor exercises and an incontinence pessary would be better than either treatment alone. They (very appropriately) designated the following as primary outcome measures:
- patient-reported improvement
- symptoms of stress incontinence
- patient satisfaction, as measured using validated instruments.
As reported above, combination therapy did not prove to be superior to single-modality intervention. And although behavioral therapy was superior to a pessary at 3 months, by 12 months the modalities were roughly equivalent, and only about half of patients were still using the prescribed therapy: pessary (45%) or pelvic floor exercises (57%).
This is not a real-world study
Most women who have stress incontinence and who select nonsurgical therapy choose only one option—pelvic floor exercises (if very motivated), a vaginal pessary or other device (if not so motivated), or another conservative option such as radiofrequency therapy (if even less motivated). In this study, women enrolled in behavioral therapy paid four visits (at roughly 2-week intervals) to approved “interventionists,” who instructed them in the technique for pelvic floor exercise and explained other skills and strategies to prevent urge and stress incontinence.
Many women find it difficult to attend the four to eight physiotherapy sessions that are necessary for behavioral intervention and are unwilling to devote 1 year to a therapy that they don’t find effective early on. (Physiotherapy is effective but requires a motivated patient.) Other women dislike inserting a vaginal device on a regular basis. 2
What’s more, very safe minimally invasive slings are available that offer more definitive therapy to patients who have stress incontinence. That said, a sling procedure should not be undertaken lightly. Patient selection should be based on preoperative testing, including an assessment of urethral function, for the transobturator sling.3 A retropubic sling requires a greater degree of expertise to tension appropriately but is suitable for a wider range of severity, including intrinsic sphincteric deficiency. The role of single-incision slings is unclear.
Bottom line: individualize care
The authors’ concluding statements are right on the money: “Individualization of care should continue to be the cornerstone of our approach to [stress incontinent] patients.” These women have several effective options available. We should help them make an educated choice based on symptom severity, lifestyle, and willingness to enroll in self-help intervention versus surgical therapy.
Many patients seek to avoid surgery, either because they believe that their stress incontinence is not severe enough to warrant it, or because they are unwilling to take the 6 to 8 weeks of relative inactivity required for the sling to settle in.
In the absence of approved pharmacotherapy for stress incontinence, I tell patients that they 1) can expect their symptoms to become worse over time and 2) should designate a period of time for a trial of conservative therapy—usually, 3 months. If their condition has not improved to their satisfaction over that period, I recommend that they identify a 6-week window during which they can avoid the gym and the golf course, as well as sexual activity, to allow for unstressed healing from a sling procedure.—G. WILLY DAVILA, MD
Because we will all be seeing more patients with stress urinary incontinence and other urogynecologic issues, it is critical that we keep abreast of the treatment options available—and their relative effectiveness.1
In this exploration of nonsurgical approaches to stress incontinence, Richter and colleagues started with the premise that a combination of instructed pelvic floor exercises and an incontinence pessary would be better than either treatment alone. They (very appropriately) designated the following as primary outcome measures:
- patient-reported improvement
- symptoms of stress incontinence
- patient satisfaction, as measured using validated instruments.
As reported above, combination therapy did not prove to be superior to single-modality intervention. And although behavioral therapy was superior to a pessary at 3 months, by 12 months the modalities were roughly equivalent, and only about half of patients were still using the prescribed therapy: pessary (45%) or pelvic floor exercises (57%).
This is not a real-world study
Most women who have stress incontinence and who select nonsurgical therapy choose only one option—pelvic floor exercises (if very motivated), a vaginal pessary or other device (if not so motivated), or another conservative option such as radiofrequency therapy (if even less motivated). In this study, women enrolled in behavioral therapy paid four visits (at roughly 2-week intervals) to approved “interventionists,” who instructed them in the technique for pelvic floor exercise and explained other skills and strategies to prevent urge and stress incontinence.
Many women find it difficult to attend the four to eight physiotherapy sessions that are necessary for behavioral intervention and are unwilling to devote 1 year to a therapy that they don’t find effective early on. (Physiotherapy is effective but requires a motivated patient.) Other women dislike inserting a vaginal device on a regular basis. 2
What’s more, very safe minimally invasive slings are available that offer more definitive therapy to patients who have stress incontinence. That said, a sling procedure should not be undertaken lightly. Patient selection should be based on preoperative testing, including an assessment of urethral function, for the transobturator sling.3 A retropubic sling requires a greater degree of expertise to tension appropriately but is suitable for a wider range of severity, including intrinsic sphincteric deficiency. The role of single-incision slings is unclear.
Bottom line: individualize care
The authors’ concluding statements are right on the money: “Individualization of care should continue to be the cornerstone of our approach to [stress incontinent] patients.” These women have several effective options available. We should help them make an educated choice based on symptom severity, lifestyle, and willingness to enroll in self-help intervention versus surgical therapy.
Many patients seek to avoid surgery, either because they believe that their stress incontinence is not severe enough to warrant it, or because they are unwilling to take the 6 to 8 weeks of relative inactivity required for the sling to settle in.
In the absence of approved pharmacotherapy for stress incontinence, I tell patients that they 1) can expect their symptoms to become worse over time and 2) should designate a period of time for a trial of conservative therapy—usually, 3 months. If their condition has not improved to their satisfaction over that period, I recommend that they identify a 6-week window during which they can avoid the gym and the golf course, as well as sexual activity, to allow for unstressed healing from a sling procedure.—G. WILLY DAVILA, MD
1. Wu JM, Hundley AF, Fulton RG, Myers ER. Forecasting the prevalence of pelvic floor disorders in US women: 2010 to 2050. Obstet Gynecol. 2009;114(6):1278-1283.
2. Davila GW, Bernier F. Multimodality pelvic physiotherapy treatment of urinary incontinence in adult women. Int Urogynecol J Pelvic Floor Dysfunct. 1995;6(4):187-194.
3. Guerette N, Bena J, Davila GW. Transobturator slings for stress incontinence: using urodynamic parameters to predict outcomes. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(1):97-102.
1. Wu JM, Hundley AF, Fulton RG, Myers ER. Forecasting the prevalence of pelvic floor disorders in US women: 2010 to 2050. Obstet Gynecol. 2009;114(6):1278-1283.
2. Davila GW, Bernier F. Multimodality pelvic physiotherapy treatment of urinary incontinence in adult women. Int Urogynecol J Pelvic Floor Dysfunct. 1995;6(4):187-194.
3. Guerette N, Bena J, Davila GW. Transobturator slings for stress incontinence: using urodynamic parameters to predict outcomes. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(1):97-102.
The Child With Persistent Fever
Ask about fever duration during your history taking. The main question is how to define “persistent.” If the fever lasts fewer than 5 days and everything else looks fine, most of the time the child will have whatever illness is going around.
If the fever lasts closer to 10 days, and especially if new symptoms appear, it could be a complication of what is going around. Obviously, once you go beyond 10 days, it is a more significant clinical situation. Then we are in the “fever of unknown origin” (FUO) range, which may require a subspecialist evaluation. The current official definition of FUO is fever lasting greater than 3 weeks with no diagnosis after reasonable outpatient or inpatient evaluation. Shorter episodes of unexplained fever are referred to as “fever without a source.” Most of these will resolve spontaneously or evolve into more easily recognized conditions, usually infections.
The best way to proceed really depends on the presentation. The initial evaluation always includes a careful history, physical examination, and screening labs as needed. Start a more thorough evaluation or refer when things are not adding up. How sick does the child look? Are there atypical findings? Remember your training about the typical course of strep throat, mono, or bronchitis—if you see a significant deviation, evaluate the child more thoroughly. Always ask: Do I have a reasonable working diagnosis that I am comfortable with?
Fever is a common symptom and most often is a feature of a routine viral infection. The bigger concern is a serious condition, such as a bloodstream infection; this child needs to get to the emergency room right away. A child with an unusual rash, especially with petechiae and purpura, would need an immediate referral.
Kawasaki disease is another major concern. If you suspect Kawasaki disease, the child needs to be evaluated by a subspecialist. The diagnosis is based on a fever lasting at least 4 or 5 days and associated findings, such as a rash, red strawberry tongue, or very red lips. The patient will need immediate treatment, ideally within 10 days, to minimize the risk for cardiac and coronary inflammation.
Helpful tests include a complete blood count, sedimentation rate, and C-reactive protein assay. Serum chemistries including liver function tests also may be useful. I do a urinalysis and a urine culture because urinary tract infections are common and a common cause of fever. Blood cultures should be considered.
These screening tests can be reassuring. When the clinical evaluation is benign, the white blood cell count is 5,000 cells/mcL with a normal differential; then you can tell the parent to come back in a few days for follow-up. In contrast, if a child with a persistent fever has a white count of 30,000, you really have to be more careful—it could be a sinus infection, pneumonia, or bacteremia. The other extreme, a child with a white blood count of 1,000, also requires more careful evaluation.
The pace of evaluation depends on how ill the child is, any associated findings, and whether one has a diagnosis or not. Time is your ally when the child is not very ill; watchful waiting will often reveal the nature of the problem.
It is important to take a good travel history. We saw a child with malaria last year, and the key to recognition was the history of a recent return from Ghana. Also ask about animal exposures and if anyone else at home is sick. Those can be important clinical clues for diagnosis of a child with prolonged fever.
Consider the time of year. A test that is not useful, but is often obtained, is a Lyme disease test. Lyme is rarely a cause of prolonged fever, especially in winter. Also, sometimes an extensive evaluation for autoimmune disease is performed too early in the diagnostic process. If you do an initial evaluation and do not have a diagnosis, and the fever persists, then you can move on to secondary and tertiary evaluations, such as you would with an FUO. Also, tests for mono are ordered way too often. The diagnosis of mono depends on more than a prolonged fever, and there are some very specific associated features, such as tonsils that look awful, large cervical nodes, and a palpable spleen.
Make sure the fever is real. Sometimes we see a child who reports persistent fever but is afebrile during each clinical visit. In this case, ask the parents how they take the child's temperature. Do they use a thermometer strip, or do they just touch the child and say the child feels warm? There should be some documentation of a persistent fever before you embark on additional, expensive evaluation.
Occasionally I have a child come to see me who is referred with say, 25 days of fever. Does the child really have one prolonged fever? It is more likely two different episodes—a child has illness No. 1, then a break, followed by illness No. 2. Use the history and clinical findings to distinguish between these two scenarios.
Ask about fever duration during your history taking. The main question is how to define “persistent.” If the fever lasts fewer than 5 days and everything else looks fine, most of the time the child will have whatever illness is going around.
If the fever lasts closer to 10 days, and especially if new symptoms appear, it could be a complication of what is going around. Obviously, once you go beyond 10 days, it is a more significant clinical situation. Then we are in the “fever of unknown origin” (FUO) range, which may require a subspecialist evaluation. The current official definition of FUO is fever lasting greater than 3 weeks with no diagnosis after reasonable outpatient or inpatient evaluation. Shorter episodes of unexplained fever are referred to as “fever without a source.” Most of these will resolve spontaneously or evolve into more easily recognized conditions, usually infections.
The best way to proceed really depends on the presentation. The initial evaluation always includes a careful history, physical examination, and screening labs as needed. Start a more thorough evaluation or refer when things are not adding up. How sick does the child look? Are there atypical findings? Remember your training about the typical course of strep throat, mono, or bronchitis—if you see a significant deviation, evaluate the child more thoroughly. Always ask: Do I have a reasonable working diagnosis that I am comfortable with?
Fever is a common symptom and most often is a feature of a routine viral infection. The bigger concern is a serious condition, such as a bloodstream infection; this child needs to get to the emergency room right away. A child with an unusual rash, especially with petechiae and purpura, would need an immediate referral.
Kawasaki disease is another major concern. If you suspect Kawasaki disease, the child needs to be evaluated by a subspecialist. The diagnosis is based on a fever lasting at least 4 or 5 days and associated findings, such as a rash, red strawberry tongue, or very red lips. The patient will need immediate treatment, ideally within 10 days, to minimize the risk for cardiac and coronary inflammation.
Helpful tests include a complete blood count, sedimentation rate, and C-reactive protein assay. Serum chemistries including liver function tests also may be useful. I do a urinalysis and a urine culture because urinary tract infections are common and a common cause of fever. Blood cultures should be considered.
These screening tests can be reassuring. When the clinical evaluation is benign, the white blood cell count is 5,000 cells/mcL with a normal differential; then you can tell the parent to come back in a few days for follow-up. In contrast, if a child with a persistent fever has a white count of 30,000, you really have to be more careful—it could be a sinus infection, pneumonia, or bacteremia. The other extreme, a child with a white blood count of 1,000, also requires more careful evaluation.
The pace of evaluation depends on how ill the child is, any associated findings, and whether one has a diagnosis or not. Time is your ally when the child is not very ill; watchful waiting will often reveal the nature of the problem.
It is important to take a good travel history. We saw a child with malaria last year, and the key to recognition was the history of a recent return from Ghana. Also ask about animal exposures and if anyone else at home is sick. Those can be important clinical clues for diagnosis of a child with prolonged fever.
Consider the time of year. A test that is not useful, but is often obtained, is a Lyme disease test. Lyme is rarely a cause of prolonged fever, especially in winter. Also, sometimes an extensive evaluation for autoimmune disease is performed too early in the diagnostic process. If you do an initial evaluation and do not have a diagnosis, and the fever persists, then you can move on to secondary and tertiary evaluations, such as you would with an FUO. Also, tests for mono are ordered way too often. The diagnosis of mono depends on more than a prolonged fever, and there are some very specific associated features, such as tonsils that look awful, large cervical nodes, and a palpable spleen.
Make sure the fever is real. Sometimes we see a child who reports persistent fever but is afebrile during each clinical visit. In this case, ask the parents how they take the child's temperature. Do they use a thermometer strip, or do they just touch the child and say the child feels warm? There should be some documentation of a persistent fever before you embark on additional, expensive evaluation.
Occasionally I have a child come to see me who is referred with say, 25 days of fever. Does the child really have one prolonged fever? It is more likely two different episodes—a child has illness No. 1, then a break, followed by illness No. 2. Use the history and clinical findings to distinguish between these two scenarios.
Ask about fever duration during your history taking. The main question is how to define “persistent.” If the fever lasts fewer than 5 days and everything else looks fine, most of the time the child will have whatever illness is going around.
If the fever lasts closer to 10 days, and especially if new symptoms appear, it could be a complication of what is going around. Obviously, once you go beyond 10 days, it is a more significant clinical situation. Then we are in the “fever of unknown origin” (FUO) range, which may require a subspecialist evaluation. The current official definition of FUO is fever lasting greater than 3 weeks with no diagnosis after reasonable outpatient or inpatient evaluation. Shorter episodes of unexplained fever are referred to as “fever without a source.” Most of these will resolve spontaneously or evolve into more easily recognized conditions, usually infections.
The best way to proceed really depends on the presentation. The initial evaluation always includes a careful history, physical examination, and screening labs as needed. Start a more thorough evaluation or refer when things are not adding up. How sick does the child look? Are there atypical findings? Remember your training about the typical course of strep throat, mono, or bronchitis—if you see a significant deviation, evaluate the child more thoroughly. Always ask: Do I have a reasonable working diagnosis that I am comfortable with?
Fever is a common symptom and most often is a feature of a routine viral infection. The bigger concern is a serious condition, such as a bloodstream infection; this child needs to get to the emergency room right away. A child with an unusual rash, especially with petechiae and purpura, would need an immediate referral.
Kawasaki disease is another major concern. If you suspect Kawasaki disease, the child needs to be evaluated by a subspecialist. The diagnosis is based on a fever lasting at least 4 or 5 days and associated findings, such as a rash, red strawberry tongue, or very red lips. The patient will need immediate treatment, ideally within 10 days, to minimize the risk for cardiac and coronary inflammation.
Helpful tests include a complete blood count, sedimentation rate, and C-reactive protein assay. Serum chemistries including liver function tests also may be useful. I do a urinalysis and a urine culture because urinary tract infections are common and a common cause of fever. Blood cultures should be considered.
These screening tests can be reassuring. When the clinical evaluation is benign, the white blood cell count is 5,000 cells/mcL with a normal differential; then you can tell the parent to come back in a few days for follow-up. In contrast, if a child with a persistent fever has a white count of 30,000, you really have to be more careful—it could be a sinus infection, pneumonia, or bacteremia. The other extreme, a child with a white blood count of 1,000, also requires more careful evaluation.
The pace of evaluation depends on how ill the child is, any associated findings, and whether one has a diagnosis or not. Time is your ally when the child is not very ill; watchful waiting will often reveal the nature of the problem.
It is important to take a good travel history. We saw a child with malaria last year, and the key to recognition was the history of a recent return from Ghana. Also ask about animal exposures and if anyone else at home is sick. Those can be important clinical clues for diagnosis of a child with prolonged fever.
Consider the time of year. A test that is not useful, but is often obtained, is a Lyme disease test. Lyme is rarely a cause of prolonged fever, especially in winter. Also, sometimes an extensive evaluation for autoimmune disease is performed too early in the diagnostic process. If you do an initial evaluation and do not have a diagnosis, and the fever persists, then you can move on to secondary and tertiary evaluations, such as you would with an FUO. Also, tests for mono are ordered way too often. The diagnosis of mono depends on more than a prolonged fever, and there are some very specific associated features, such as tonsils that look awful, large cervical nodes, and a palpable spleen.
Make sure the fever is real. Sometimes we see a child who reports persistent fever but is afebrile during each clinical visit. In this case, ask the parents how they take the child's temperature. Do they use a thermometer strip, or do they just touch the child and say the child feels warm? There should be some documentation of a persistent fever before you embark on additional, expensive evaluation.
Occasionally I have a child come to see me who is referred with say, 25 days of fever. Does the child really have one prolonged fever? It is more likely two different episodes—a child has illness No. 1, then a break, followed by illness No. 2. Use the history and clinical findings to distinguish between these two scenarios.
BEST PRACTICES IN: The Role of Copay Reduction Programs Within a Physician's Practice.
A supplement to Skin & Allergy News. This supplement was sponsored by Ferndale Laboratories Inc.

- Copay Reduction
- Patient Rebate Programs
- Prescription Abandonment Rates
- Importance of Communication between Providers and their Patients
Faculty/Faculty Disclosure
Joseph S. Eastern, MD
Clinical Associate Professor of Dermatology
Seton Hall UniversitySchool of GraduateMedical Education
South Orange, NJ
Dr. Eastern has a consulting agreement with Abbott Laboratories, Amgen, Inc., Aqua Pharmaceuticals, LLC, Graceway Pharmaceuticals, LLC, Medicis Pharmaceutical Corporation, Promius Pharma, LLC, Stiefel Laboratories, Inc., Quinnova Pharmaceuticals, Inc., and Warner Chilcott; and is a stockholder of Medicis.
Copyright (C) 2010 Elsevier Inc.
A supplement to Skin & Allergy News. This supplement was sponsored by Ferndale Laboratories Inc.
- Copay Reduction
- Patient Rebate Programs
- Prescription Abandonment Rates
- Importance of Communication between Providers and their Patients
Faculty/Faculty Disclosure
Joseph S. Eastern, MD
Clinical Associate Professor of Dermatology
Seton Hall UniversitySchool of GraduateMedical Education
South Orange, NJ
Dr. Eastern has a consulting agreement with Abbott Laboratories, Amgen, Inc., Aqua Pharmaceuticals, LLC, Graceway Pharmaceuticals, LLC, Medicis Pharmaceutical Corporation, Promius Pharma, LLC, Stiefel Laboratories, Inc., Quinnova Pharmaceuticals, Inc., and Warner Chilcott; and is a stockholder of Medicis.
Copyright (C) 2010 Elsevier Inc.
A supplement to Skin & Allergy News. This supplement was sponsored by Ferndale Laboratories Inc.
- Copay Reduction
- Patient Rebate Programs
- Prescription Abandonment Rates
- Importance of Communication between Providers and their Patients
Faculty/Faculty Disclosure
Joseph S. Eastern, MD
Clinical Associate Professor of Dermatology
Seton Hall UniversitySchool of GraduateMedical Education
South Orange, NJ
Dr. Eastern has a consulting agreement with Abbott Laboratories, Amgen, Inc., Aqua Pharmaceuticals, LLC, Graceway Pharmaceuticals, LLC, Medicis Pharmaceutical Corporation, Promius Pharma, LLC, Stiefel Laboratories, Inc., Quinnova Pharmaceuticals, Inc., and Warner Chilcott; and is a stockholder of Medicis.
Copyright (C) 2010 Elsevier Inc.
