User login
Radiotherapy After Breast Cancer Surgery: Don't Wait
Grand Rounds: Woman, 80, With Hallucinations and Tremors
An 80-year-old Mandarin-speaking Chinese woman was referred to a mental health outpatient clinic for evaluation and treatment. The patient had a history of mild depression, for which she had been treated for many years with sertraline.
Five years earlier at age 75, the patient had been evaluated by a psychiatrist after she began to experience psychotic symptoms, including frequent repetitive auditory hallucinations of people counting, alternating with music from her childhood. At that time, she also had persecutory paranoid thoughts and delusional thinking that she was receiving messages in Mandarin while watching American TV programs. Initially, her only cognitive disturbance was an inability to differentiate among numbers on a calendar or a telephone keypad. No reports of memory problems were noted. Although the patient acknowledged auditory hallucinations, she denied experiencing command auditory hallucinations or hallucinations of other forms. The patient had no history of suicide attempts and denied suicidal or homicidal ideation. She had no history of psychiatric hospitalization.
The psychiatrist made a diagnosis of major depressive disorder with psychotic features, not otherwise specified1 and prescribed sertraline 50 mg/d. The patient was also started on risperidone 0.25 mg/d for management of her psychotic symptoms, with the dosage gradually increased to 2.0 mg/d over five years. While taking this combination, the patient experienced stable mood and fewer paranoid thoughts, although her auditory hallucinations continued.
Two months before the current visit, the patient moved into a retirement living facility, and she reported having adapted well to the new setting. She was sleeping well and had a good appetite. Her BMI was within normal range.
The patient described herself as a single parent for nearly 40 years, raising one daughter. Formerly high functioning, she had held a full-time clerical job until age 70. She appeared well-groomed, polite but anxious, and oriented to time, person, and place. Her speech was normal, her thought processes were coherent, and her mood was stable. However, her affect was constricted; she acknowledged auditory hallucinations, which impaired her thought content. The patient reported feeling increased anxiety prior to any nonroutine activity, such as a doctor’s appointment; this, she said, would cause insomnia, leaving her to pace in her room.
During the examination, fine tremors on upper and lower extremities were noted. The patient’s Abnormal Involuntary Movement Scale (AIMS) score2 was 13, which placed her in the highest risk category for antipsychotic-induced dopamine-blockade extrapyramidal symptoms (EPS). The patient was found to be negative for tardive dyskinesia, with no abnormal facial movements. She was aware of the tremors in her limbs and said she felt bothered by them.
The patient had an unsteady gait and used a four-point walker. Her Mini-Mental State Exam (MMSE) score3 was 28/30, which was normal for her age and education level (high school completed).
Apart from the described symptoms, the patient was healthy for her age and had no other medical diagnosis. Her vital signs were within normal range. The medical work-up to rule out other causes of dementia yielded negative results. Lab values were normal, including electrolyte levels and thyroid tests. The patient’s hearing test showed age-related hearing loss of full range, not limited to high pitch. She was able to engage in a meaningful conversation at a normal volume. Clinically, however, it was concerning to observe the possible signs of EPS and the relatively high risperidone dosage, considering the patient’s advanced age.
After the meeting with the patient, a treatment plan was created to 1) gradually reduce the dosage of antipsychotic medication, and 2) refer her to a neurologist for a complete work-up to rule out underlying neurologic disorders, such as dementia. Risperidone was tapered by increments of 0.25 mg/d every three to four weeks; throughout this process, the patient was closely monitored by the nursing staff at the retirement living facility. Monthly appointments were scheduled at the outpatient mental health clinic for evaluation and medication management.
Two months after the initial mental health clinic visit, the patient’s condition was pronounced stable on the current regimen of sertraline 50 mg/d and risperidone 1.0 mg/d. She was later seen by a neurologist, who made a diagnosis of Parkinson’s disease and placed her on carbidopa-levodopa (1 1/2 tablets, 25/100 mg, tid). The patient’s auditory hallucinations continued with the same intensity as at baseline, but fewer tremors were noted in her extremities. By six months into the tapering process (with risperidone reduced at that time to 0.25 mg/d and carbidopa-levodopa to 25/100 mg tid), the patient had begun to experience dissipation of the tremors, and her AIMS score2 was 0. She was able to replace her four-point walker with a cane.
One year after her initial visit to the mental health clinic, the patient’s neurologist suggested replacing risperidone with quetiapine (12.5 mg/d) for its improved tolerability and lower adverse effect profile.4 She continued to take sertraline and carbidopa-levodopa.
Improvement of symptoms was noted following the switch. After one month on the revised regimen, the patient reported that the number of auditory hallucinations persisted, but that their intensity had decreased dramatically. She had a brighter affect and appeared to feel uplifted and more energetic. She became involved in the social activities offered at the retirement living facility and the mental health clinic. She also maintained a steady gait without her cane. According to the patient’s daughter, her mother was at her best psychological state since the onset of psychotic symptoms six years earlier. The pharmacologic regimen had reached its maximum benefit.
At a mental health appointment at the outpatient clinic 18 months after her initial visit there, it was evident that the patient’s auditory hallucinations persisted as a major stressor. She began to complain about other residents in her facility. She said she disliked the resident with whom she shared meals, and she claimed that other residents often spit on the floor in front of her room. The nursing staff did not confirm these incidents, which they considered a delusion despite the patient’s “evidence” (the tissues she said she had used to clean up).
Additionally, a new theme had emerged in the patient’s auditory hallucinations. She reported hearing a male voice that announced changes in meal times. Although she knew there was no public address system in her room or in the hallway, the “announcement” was so convincing that she would go to the dining room and once there, realize that nothing had changed. She seemed to drift between reality and her hallucinations/delusions. According to her daughter, the patient’s independent and reserved personality forced her to internalize her stressors—in this case, her frustration about the other residents—which fed into her hallucinations and delusions.
In response to her worsening psychotic symptoms, the patient’s provider increased her quetiapine dosage from 12.5 mg/d to 25 mg/d. Her MMSE score3 at this visit was 25/30.
Two months later, the patient exhibited increasing symptoms of paranoia, delusions, and auditory hallucinations. She continued to respond to the “broadcast” messages about meal times, and she voiced her frustrations to others who spoke Mandarin. She became agitated in response to out-of-the-ordinary events. When her alarm clock battery ran out, for example, she insisted that “a man’s voice” kept reminding her to replace the battery; in response, she placed the alarm clock in the refrigerator, later explaining, “Now I don’t need to worry about it.”
Her cognitive status began to show obvious, progressive deterioration, with an MMSE score3 of 22/30 at this visit—a significant reduction from previous scores. Worsening of her short-term memory became apparent when she had difficulty playing bingo and was unable to remember her appointment or the current date. She became upset when others corrected her.
In a review of the trends in this patient’s clinical presentation, it became increasingly evident to the patient’s mental health care providers that she had Lewy body dementia.
DISCUSSION
Dementia with Lewy bodies (DLB), a progressive disease, is the second most common cause of neurodegenerative dementia after Alzheimer’s disease.5-7 It is estimated that DLB accounts for 20% of US cases of dementia (ie, about 800,000 patients).8,9 Although public awareness of DLB is on the rise, the disorder is still underrecognized and underdiagnosed because its clinical manifestations so closely resemble those of Alzheimer’s disease, Parkinson’s disease, and psychosis.10,11
Clinical symptoms of DLB include progressive cognitive decline, cognitive fluctuation, EPS, and parkinsonism; hallucinations involving all five senses, particularly sight; delusions; REM sleep disturbance, with or without vivid and frightening dreams; changes in mood and behavior; impaired judgment and insight; and autonomic dysfunction, such as orthostatic hypotension and carotid-sinus hypersensitivity.5,11-15
The symptoms of DLB are caused by the accumulations of Lewy bodies, that is, deposits of alpha-synuclein protein in the nuclei of neurons. Lewy bodies destroy neurons over time, resulting in the destruction of dopaminergic and acetylcholinergic pathways from the brain stem to areas of the cerebral cortex associated with cognition and motor functions.4,5,16
DLB is a spectrum disorder; it often coexists with Parkinson’s disease or Alzheimer’s disease, as Lewy bodies are also found in patients with these illnesses.7 This poses a challenge for formulating a differential diagnosis, particularly in patients with fluctuating cognition,10 and for attempting to establish disease prevalence.
Diagnosis
Currently, a conclusive diagnosis of DLB can be confirmed only through postmortem autopsy, although use of medial temporal lobe volume (via structural MRI) and regional blood flow (via single photon emission CT [SPECT] tracers) is being investigated.17
The diagnosis of DLB is currently based on the presenting clinical symptoms and the exclusion of other medical conditions whose symptoms mimic those of DLB.7 The screening assessment may include a neurologic/psychiatric assessment (MMSE, psychiatric evaluation, and interviews with family members or caretakers), neuroimaging such as MRI to rule out other organic causes, and laboratory evaluation to rule out potentially reversible causes of dementia, including electrolyte imbalance, vitamin deficiency (specifically vitamin B12), anemia, thyroid dysfunction, and kidney or liver impairment.18
The American Psychiatric Assocation1 categorizes DLB under “Dementia Due to Other General Medical Conditions” (294.1x). The World Health Organization19 includes it among “Other specified degenerative diseases of the nervous system” (G31.8).
Treatment
Lewy body dementia is an irreversible neurologic degenerative disorder. Treatment for DLB comprises symptom management, primarily through pharmacology; however, the response to medication is highly individualized. Treatment includes management of the following symptoms:
Cognitive impairment. Cholinesterase inhibitors, such as rivastigmine (3 to 12 mg/d), donepezil (10 mg/d), or galantamine (titrated up to 12 mg bid),20-23 improve attention and behavior and reduce apathy, anxiety, delusions, and hallucinations. As cognitive impairment worsens, memantine (10 mg bid) may be effective.24 The potential for anticholinergic adverse effects requires close monitoring in patients taking these agents.
Parkinsonian symptoms. Medications indicated for Parkinson’s disease and syndrome, such as carbidopa-levodopa (25/100 mg tid), can be effective; dosage may be slowly titrated upward as tolerated and if needed for symptom management.25,26 The dopaminergic effect of antiparkinson medications may intensify the psychotic symptoms and worsen the REM sleep pattern. In this case, a low-dose atypical antipsychotic is suggested27,28 (see below).
Psychotic symptoms. An atypical antipsychotic agent, such as quetiapine (12.5 mg), risperidone (0.25 mg), olanzapine (2.5 mg), ziprasidone (20 mg), aripiprazole (2 mg), or paliperidone (1.5 mg), may be used. Because of the DLB-associated risk of neuroleptic sensitivity, atypical antipsychotic agents should be initiated at a low dose with slow upward titration17,26,29; quetiapine appears less likely than risperidone or olanzapine to cause neuroleptic sensitivity or to trigger EPS.4 For Asian patients, who often respond to lower doses of these medications (and are more easily affected by associated adverse effects), Chen et al30 recommend a starting dose of about one-half the recommended dose.
Depression. An SSRI antidepressant with relatively simple pharmacologic properties and moderate half-life may be used to manage symptoms of depression.26,31,32 Long–half-life SSRIs (eg, fluoxetine) should be avoided in elderly patients; in response to SNRIs (serotonin-norepinephrine reuptake inhibitors), these patients may experience elevated blood pressures and pulses, with subsequent morbidity.33
REM sleep disturbances. Clonazepam (0.25 mg), melatonin (3.0 mg), or quetiapine (12.5 mg) may be administered at bedtime.34
Important Lessons
In general, providers should consider the benefits and risks of any pharmacologic treatment and avoid polypharmacy, if possible. Family and caretakers should be included in the treatment planning, with a focus on prioritizing and managing the most debilitating symptoms or dysfunctions that prompt concerns for safety.
For optimal homeostasis, some DLB patients may require joint pharmacologic modalities that appear counterintuitive—for example, an antiparkinsonism (dopaminergic) agent for parkinsonian symptoms or neuroleptic-induced EPS, versus an antipsychotic (eg, a dopamine antagonist) to treat profound hallucinations.26
As the response to treatment for DLB is highly individualized, it is essential to titrate and augment with care.
CONCLUSION
In DLB, as with other dementing illnesses, the onset of symptoms can be gradual and insidious, posing a great challenge to the clinician who seeks to confirm the diagnosis. In the illness’s early stages, the clinician may have to treat targeted symptoms and adjust the treatment plan once signs of the pathologic origins emerge.
It is critical to understand the mechanisms of psychotropic medications and targeted neurotransmitters when evaluating treatment for DLB. Titrating or augmenting these medications in elderly patients requires the clinician to follow a principle of start low and go slow, making only one change at a time.
It is always helpful to include family members in the patient’s care and to gather information on previous history, personality traits, family history, and cultural components. It is also important to communicate with other specialists to implement collaborative care.
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed (text revision). Washington, DC: American Psychiatric Association; 2000:167.
2. National Institute of Mental Health. Abnormal Involuntary Movement Scale (AIMS). www.atlantapsychia try.com/forms/AIMS.pdf. Accessed May 20, 2010.
3. Mini–Mental State Examination. www.nmaging .state.nm.us/pdf_files/Mini_Mental_Status_Exam.pdf. Accessed May 20, 2010.
4. Baskys A. Lewy body dementia: the litmus test for neuroleptic sensitivity and extrapyramidal symptoms. J Clin Psychiatry. 2004;65 suppl 11:16-22.
5. Weisman D, McKeith I. Dementia with Lewy bodies. Semin Neurol. 2007;27(1):42-47.
6. McKeith IG. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the Consortium on DLB International Workshop. J Alzheimers Dis. 2006;9(3 suppl):417-423.
7. McKeith IG, Galasko D, Kosaka K, et al. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the Consortium on DLB International Workshop. Neurology. 1996;47(5):1113-1124.
8. Hill C, Reiss N. Lewy body dementia (2008). www.mentalhelp.net/poc/view_doc.php?type=doc& id=13151&cn=231. Accessed May 20, 2010.
9. Lewy Body Dementia Association, Inc. Lewy body dementia: current issues in diagnosis and treatment. www.lewybodydementia.org. Accessed May 20, 2010.
10. Varanese S, Perfetti B, Monaco D, et al. Fluctuating cognition and different cognitive and behavioural profiles in Parkinson’s disease with dementia: comparison of dementia with Lewy bodies and Alzheimer’s disease. J Neurol. 2010 Jan 22. [Epub ahead of print]
11. Kurita A, Murakami M, Takagi S, et al. Visual hallucinations and altered visual information processing in Parkinson disease and dementia with Lewy bodies. Mov Disorder. 2010;25(2):167-171.
12. Gagnon JF, Postuma RB, Mazza S, et al. Rapid-eye-movement sleep behaviour disorder and neurodegenerative diseases. Lancet Neurol. 2006;5(5):424-432.
13. Dodel R, Csoti I, Ebersbach G, et al. Lewy body dementia and Parkinson’s disease with dementia. J Neurol. 2008;255 suppl 5:39-47.
14. Sonnesyn H, Nilsen DW, Rongve A, et al. High prevalence of orthostatic hypotension in mild dementia. Dement Geriatr Cogn Disord. 2009;28(4):307-313.
15. Kenny RA, Shaw FE, O’Brien JT, et al. Carotid sinus syndrome is common in dementia with Lewy bodies and correlates with deep white matter lesions. J Neurol Neurosurg Psychiatry. 2004;75(7):966-971.
16. Hickey C, Chisholm T, Passmore MJ, et al. Differentiating the dementias: revisiting synucleinopathies and tauopathies. Curr Alzheimer Res. 2008;5(1):52-60.
17. McKeith IG, Burn DJ, Ballard CG, et al. Dementia with Lewy bodies. Semin Clin Neuropsychiatry. 2003; 8(1):46-57.
18. Bird TD, Miller BL. Dementia. In: Fauci AS, Braunwald E, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine. 17th ed. New York, NY: McGraw Hill Medical; 2008:2536-2549.
19. World Health Organization. International Classification of Diseases (ICD), Version 2007. Chapter VI: Diseases of the Central Nervous System. http://apps.who.int/classifications/apps/icd/icd10online/index.htm?kg00.htm+. Accessed May 20, 2010.
20. McKeith I, Del Ser T, Spano P, et al. Efficacy of rivastigmine in dementia with Lewy bodies: a randomised, double-blind, placebo-controlled international study. Lancet. 2000;356(9247):2031-2036.
21. Emre M, Cummings JL, Lane RM. Rivastigmine in dementia associated with Parkinson’s disease and Alzheimer’s disease: similarities and differences. J Alzheimers Dis. 2007;11(4):509-519.
22. Lam B, Hollingdrake E, Kennedy JL, et al. Cholinesterase inhibitors in Alzheimer’s disease and Lewy body spectrum disorders: the emerging pharmacogenetic story. Hum Genomics. 2009;4(2):91-106.
23. Wild R, Pettit T, Burns A. Cholinesterase inhibitors for dementia with Lewy bodies. Cochrane Database Syst Rev. 2003;(3):CD003672.
24. Aarsland D, Ballard C, Walker Z, et al. Memantine in patients with Parkinson’s disease dementia or dementia with Lewy bodies: a double-blind, placebo-controlled, multicentre trial. Lancet Neurol. 2009;8(7):613-618.
25. Merck & Co., Inc. Sinemet® CR (carbidopa-levodopa) sustained-release tablets. http://packageinserts.bms.com/pi/pi_sinemet_cr.pdf. Accessed May 20, 2010.
26. Fernandez HH, Wu CK, Ott BR. Pharmacotherapy of dementia with Lewy bodies. Expert Opin Pharmacother. 2003;4(11):2027-2037.
27. Kato K, Wada T, Kawakatsu S, Otani K. Improvement of both psychotic symptoms and Parkinsonism in a case of dementia with Lewy bodies by the combination therapy of risperidone and L-DOPA. Prog Neuropsychopharmacol Biol Psychiatry. 2002;26(1):201-203.
28. Yamauchi K, Takehisa M, Tsuno M, et al. Levodopa improved rapid eye movement sleep behavior disorder with diffuse Lewy body disease. Gen Hosp Psychiatry. 2003;25(2):140-142.
29. Stahl SM. The Prescriber’s Guide: Stahl’s Essential Psychopharmacology. Cambridge University Press; 2006:459.
30. Chen JP, Barron C, Lin KM, Chung H. Prescribing medication for Asians with mental disorders. West J Med. 2002;176(4):271-275.
31. Sink KM, Holden KF, Yaffe K. Pharmacological treatment of neuropsychiatric symptoms of dementia: a review of the evidence. JAMA. 2005;293(5):596-608.
32. Pollock BG, Mulsant BH, Rosen J, et al. Comparison of citalopram, perphenazine, and placebo for the acute treatment of psychosis and behavioral disturbances in hospitalized, demented patients. Am J Psychiatry. 2002;159(3):460-465.
33. Schwab W, Messinger-Rapport B, Franco K. Psychiatric symptoms of dementia: treatable, but no silver bullet. Cleve Clin J Med. 2009;76(3):167-174.
34. Gagnon JF, Postuma RB, Montplaisir J. Update on the pharmacology of REM sleep behavior disorder. Neurology. 2006;67(5):742-747
An 80-year-old Mandarin-speaking Chinese woman was referred to a mental health outpatient clinic for evaluation and treatment. The patient had a history of mild depression, for which she had been treated for many years with sertraline.
Five years earlier at age 75, the patient had been evaluated by a psychiatrist after she began to experience psychotic symptoms, including frequent repetitive auditory hallucinations of people counting, alternating with music from her childhood. At that time, she also had persecutory paranoid thoughts and delusional thinking that she was receiving messages in Mandarin while watching American TV programs. Initially, her only cognitive disturbance was an inability to differentiate among numbers on a calendar or a telephone keypad. No reports of memory problems were noted. Although the patient acknowledged auditory hallucinations, she denied experiencing command auditory hallucinations or hallucinations of other forms. The patient had no history of suicide attempts and denied suicidal or homicidal ideation. She had no history of psychiatric hospitalization.
The psychiatrist made a diagnosis of major depressive disorder with psychotic features, not otherwise specified1 and prescribed sertraline 50 mg/d. The patient was also started on risperidone 0.25 mg/d for management of her psychotic symptoms, with the dosage gradually increased to 2.0 mg/d over five years. While taking this combination, the patient experienced stable mood and fewer paranoid thoughts, although her auditory hallucinations continued.
Two months before the current visit, the patient moved into a retirement living facility, and she reported having adapted well to the new setting. She was sleeping well and had a good appetite. Her BMI was within normal range.
The patient described herself as a single parent for nearly 40 years, raising one daughter. Formerly high functioning, she had held a full-time clerical job until age 70. She appeared well-groomed, polite but anxious, and oriented to time, person, and place. Her speech was normal, her thought processes were coherent, and her mood was stable. However, her affect was constricted; she acknowledged auditory hallucinations, which impaired her thought content. The patient reported feeling increased anxiety prior to any nonroutine activity, such as a doctor’s appointment; this, she said, would cause insomnia, leaving her to pace in her room.
During the examination, fine tremors on upper and lower extremities were noted. The patient’s Abnormal Involuntary Movement Scale (AIMS) score2 was 13, which placed her in the highest risk category for antipsychotic-induced dopamine-blockade extrapyramidal symptoms (EPS). The patient was found to be negative for tardive dyskinesia, with no abnormal facial movements. She was aware of the tremors in her limbs and said she felt bothered by them.
The patient had an unsteady gait and used a four-point walker. Her Mini-Mental State Exam (MMSE) score3 was 28/30, which was normal for her age and education level (high school completed).
Apart from the described symptoms, the patient was healthy for her age and had no other medical diagnosis. Her vital signs were within normal range. The medical work-up to rule out other causes of dementia yielded negative results. Lab values were normal, including electrolyte levels and thyroid tests. The patient’s hearing test showed age-related hearing loss of full range, not limited to high pitch. She was able to engage in a meaningful conversation at a normal volume. Clinically, however, it was concerning to observe the possible signs of EPS and the relatively high risperidone dosage, considering the patient’s advanced age.
After the meeting with the patient, a treatment plan was created to 1) gradually reduce the dosage of antipsychotic medication, and 2) refer her to a neurologist for a complete work-up to rule out underlying neurologic disorders, such as dementia. Risperidone was tapered by increments of 0.25 mg/d every three to four weeks; throughout this process, the patient was closely monitored by the nursing staff at the retirement living facility. Monthly appointments were scheduled at the outpatient mental health clinic for evaluation and medication management.
Two months after the initial mental health clinic visit, the patient’s condition was pronounced stable on the current regimen of sertraline 50 mg/d and risperidone 1.0 mg/d. She was later seen by a neurologist, who made a diagnosis of Parkinson’s disease and placed her on carbidopa-levodopa (1 1/2 tablets, 25/100 mg, tid). The patient’s auditory hallucinations continued with the same intensity as at baseline, but fewer tremors were noted in her extremities. By six months into the tapering process (with risperidone reduced at that time to 0.25 mg/d and carbidopa-levodopa to 25/100 mg tid), the patient had begun to experience dissipation of the tremors, and her AIMS score2 was 0. She was able to replace her four-point walker with a cane.
One year after her initial visit to the mental health clinic, the patient’s neurologist suggested replacing risperidone with quetiapine (12.5 mg/d) for its improved tolerability and lower adverse effect profile.4 She continued to take sertraline and carbidopa-levodopa.
Improvement of symptoms was noted following the switch. After one month on the revised regimen, the patient reported that the number of auditory hallucinations persisted, but that their intensity had decreased dramatically. She had a brighter affect and appeared to feel uplifted and more energetic. She became involved in the social activities offered at the retirement living facility and the mental health clinic. She also maintained a steady gait without her cane. According to the patient’s daughter, her mother was at her best psychological state since the onset of psychotic symptoms six years earlier. The pharmacologic regimen had reached its maximum benefit.
At a mental health appointment at the outpatient clinic 18 months after her initial visit there, it was evident that the patient’s auditory hallucinations persisted as a major stressor. She began to complain about other residents in her facility. She said she disliked the resident with whom she shared meals, and she claimed that other residents often spit on the floor in front of her room. The nursing staff did not confirm these incidents, which they considered a delusion despite the patient’s “evidence” (the tissues she said she had used to clean up).
Additionally, a new theme had emerged in the patient’s auditory hallucinations. She reported hearing a male voice that announced changes in meal times. Although she knew there was no public address system in her room or in the hallway, the “announcement” was so convincing that she would go to the dining room and once there, realize that nothing had changed. She seemed to drift between reality and her hallucinations/delusions. According to her daughter, the patient’s independent and reserved personality forced her to internalize her stressors—in this case, her frustration about the other residents—which fed into her hallucinations and delusions.
In response to her worsening psychotic symptoms, the patient’s provider increased her quetiapine dosage from 12.5 mg/d to 25 mg/d. Her MMSE score3 at this visit was 25/30.
Two months later, the patient exhibited increasing symptoms of paranoia, delusions, and auditory hallucinations. She continued to respond to the “broadcast” messages about meal times, and she voiced her frustrations to others who spoke Mandarin. She became agitated in response to out-of-the-ordinary events. When her alarm clock battery ran out, for example, she insisted that “a man’s voice” kept reminding her to replace the battery; in response, she placed the alarm clock in the refrigerator, later explaining, “Now I don’t need to worry about it.”
Her cognitive status began to show obvious, progressive deterioration, with an MMSE score3 of 22/30 at this visit—a significant reduction from previous scores. Worsening of her short-term memory became apparent when she had difficulty playing bingo and was unable to remember her appointment or the current date. She became upset when others corrected her.
In a review of the trends in this patient’s clinical presentation, it became increasingly evident to the patient’s mental health care providers that she had Lewy body dementia.
DISCUSSION
Dementia with Lewy bodies (DLB), a progressive disease, is the second most common cause of neurodegenerative dementia after Alzheimer’s disease.5-7 It is estimated that DLB accounts for 20% of US cases of dementia (ie, about 800,000 patients).8,9 Although public awareness of DLB is on the rise, the disorder is still underrecognized and underdiagnosed because its clinical manifestations so closely resemble those of Alzheimer’s disease, Parkinson’s disease, and psychosis.10,11
Clinical symptoms of DLB include progressive cognitive decline, cognitive fluctuation, EPS, and parkinsonism; hallucinations involving all five senses, particularly sight; delusions; REM sleep disturbance, with or without vivid and frightening dreams; changes in mood and behavior; impaired judgment and insight; and autonomic dysfunction, such as orthostatic hypotension and carotid-sinus hypersensitivity.5,11-15
The symptoms of DLB are caused by the accumulations of Lewy bodies, that is, deposits of alpha-synuclein protein in the nuclei of neurons. Lewy bodies destroy neurons over time, resulting in the destruction of dopaminergic and acetylcholinergic pathways from the brain stem to areas of the cerebral cortex associated with cognition and motor functions.4,5,16
DLB is a spectrum disorder; it often coexists with Parkinson’s disease or Alzheimer’s disease, as Lewy bodies are also found in patients with these illnesses.7 This poses a challenge for formulating a differential diagnosis, particularly in patients with fluctuating cognition,10 and for attempting to establish disease prevalence.
Diagnosis
Currently, a conclusive diagnosis of DLB can be confirmed only through postmortem autopsy, although use of medial temporal lobe volume (via structural MRI) and regional blood flow (via single photon emission CT [SPECT] tracers) is being investigated.17
The diagnosis of DLB is currently based on the presenting clinical symptoms and the exclusion of other medical conditions whose symptoms mimic those of DLB.7 The screening assessment may include a neurologic/psychiatric assessment (MMSE, psychiatric evaluation, and interviews with family members or caretakers), neuroimaging such as MRI to rule out other organic causes, and laboratory evaluation to rule out potentially reversible causes of dementia, including electrolyte imbalance, vitamin deficiency (specifically vitamin B12), anemia, thyroid dysfunction, and kidney or liver impairment.18
The American Psychiatric Assocation1 categorizes DLB under “Dementia Due to Other General Medical Conditions” (294.1x). The World Health Organization19 includes it among “Other specified degenerative diseases of the nervous system” (G31.8).
Treatment
Lewy body dementia is an irreversible neurologic degenerative disorder. Treatment for DLB comprises symptom management, primarily through pharmacology; however, the response to medication is highly individualized. Treatment includes management of the following symptoms:
Cognitive impairment. Cholinesterase inhibitors, such as rivastigmine (3 to 12 mg/d), donepezil (10 mg/d), or galantamine (titrated up to 12 mg bid),20-23 improve attention and behavior and reduce apathy, anxiety, delusions, and hallucinations. As cognitive impairment worsens, memantine (10 mg bid) may be effective.24 The potential for anticholinergic adverse effects requires close monitoring in patients taking these agents.
Parkinsonian symptoms. Medications indicated for Parkinson’s disease and syndrome, such as carbidopa-levodopa (25/100 mg tid), can be effective; dosage may be slowly titrated upward as tolerated and if needed for symptom management.25,26 The dopaminergic effect of antiparkinson medications may intensify the psychotic symptoms and worsen the REM sleep pattern. In this case, a low-dose atypical antipsychotic is suggested27,28 (see below).
Psychotic symptoms. An atypical antipsychotic agent, such as quetiapine (12.5 mg), risperidone (0.25 mg), olanzapine (2.5 mg), ziprasidone (20 mg), aripiprazole (2 mg), or paliperidone (1.5 mg), may be used. Because of the DLB-associated risk of neuroleptic sensitivity, atypical antipsychotic agents should be initiated at a low dose with slow upward titration17,26,29; quetiapine appears less likely than risperidone or olanzapine to cause neuroleptic sensitivity or to trigger EPS.4 For Asian patients, who often respond to lower doses of these medications (and are more easily affected by associated adverse effects), Chen et al30 recommend a starting dose of about one-half the recommended dose.
Depression. An SSRI antidepressant with relatively simple pharmacologic properties and moderate half-life may be used to manage symptoms of depression.26,31,32 Long–half-life SSRIs (eg, fluoxetine) should be avoided in elderly patients; in response to SNRIs (serotonin-norepinephrine reuptake inhibitors), these patients may experience elevated blood pressures and pulses, with subsequent morbidity.33
REM sleep disturbances. Clonazepam (0.25 mg), melatonin (3.0 mg), or quetiapine (12.5 mg) may be administered at bedtime.34
Important Lessons
In general, providers should consider the benefits and risks of any pharmacologic treatment and avoid polypharmacy, if possible. Family and caretakers should be included in the treatment planning, with a focus on prioritizing and managing the most debilitating symptoms or dysfunctions that prompt concerns for safety.
For optimal homeostasis, some DLB patients may require joint pharmacologic modalities that appear counterintuitive—for example, an antiparkinsonism (dopaminergic) agent for parkinsonian symptoms or neuroleptic-induced EPS, versus an antipsychotic (eg, a dopamine antagonist) to treat profound hallucinations.26
As the response to treatment for DLB is highly individualized, it is essential to titrate and augment with care.
CONCLUSION
In DLB, as with other dementing illnesses, the onset of symptoms can be gradual and insidious, posing a great challenge to the clinician who seeks to confirm the diagnosis. In the illness’s early stages, the clinician may have to treat targeted symptoms and adjust the treatment plan once signs of the pathologic origins emerge.
It is critical to understand the mechanisms of psychotropic medications and targeted neurotransmitters when evaluating treatment for DLB. Titrating or augmenting these medications in elderly patients requires the clinician to follow a principle of start low and go slow, making only one change at a time.
It is always helpful to include family members in the patient’s care and to gather information on previous history, personality traits, family history, and cultural components. It is also important to communicate with other specialists to implement collaborative care.
An 80-year-old Mandarin-speaking Chinese woman was referred to a mental health outpatient clinic for evaluation and treatment. The patient had a history of mild depression, for which she had been treated for many years with sertraline.
Five years earlier at age 75, the patient had been evaluated by a psychiatrist after she began to experience psychotic symptoms, including frequent repetitive auditory hallucinations of people counting, alternating with music from her childhood. At that time, she also had persecutory paranoid thoughts and delusional thinking that she was receiving messages in Mandarin while watching American TV programs. Initially, her only cognitive disturbance was an inability to differentiate among numbers on a calendar or a telephone keypad. No reports of memory problems were noted. Although the patient acknowledged auditory hallucinations, she denied experiencing command auditory hallucinations or hallucinations of other forms. The patient had no history of suicide attempts and denied suicidal or homicidal ideation. She had no history of psychiatric hospitalization.
The psychiatrist made a diagnosis of major depressive disorder with psychotic features, not otherwise specified1 and prescribed sertraline 50 mg/d. The patient was also started on risperidone 0.25 mg/d for management of her psychotic symptoms, with the dosage gradually increased to 2.0 mg/d over five years. While taking this combination, the patient experienced stable mood and fewer paranoid thoughts, although her auditory hallucinations continued.
Two months before the current visit, the patient moved into a retirement living facility, and she reported having adapted well to the new setting. She was sleeping well and had a good appetite. Her BMI was within normal range.
The patient described herself as a single parent for nearly 40 years, raising one daughter. Formerly high functioning, she had held a full-time clerical job until age 70. She appeared well-groomed, polite but anxious, and oriented to time, person, and place. Her speech was normal, her thought processes were coherent, and her mood was stable. However, her affect was constricted; she acknowledged auditory hallucinations, which impaired her thought content. The patient reported feeling increased anxiety prior to any nonroutine activity, such as a doctor’s appointment; this, she said, would cause insomnia, leaving her to pace in her room.
During the examination, fine tremors on upper and lower extremities were noted. The patient’s Abnormal Involuntary Movement Scale (AIMS) score2 was 13, which placed her in the highest risk category for antipsychotic-induced dopamine-blockade extrapyramidal symptoms (EPS). The patient was found to be negative for tardive dyskinesia, with no abnormal facial movements. She was aware of the tremors in her limbs and said she felt bothered by them.
The patient had an unsteady gait and used a four-point walker. Her Mini-Mental State Exam (MMSE) score3 was 28/30, which was normal for her age and education level (high school completed).
Apart from the described symptoms, the patient was healthy for her age and had no other medical diagnosis. Her vital signs were within normal range. The medical work-up to rule out other causes of dementia yielded negative results. Lab values were normal, including electrolyte levels and thyroid tests. The patient’s hearing test showed age-related hearing loss of full range, not limited to high pitch. She was able to engage in a meaningful conversation at a normal volume. Clinically, however, it was concerning to observe the possible signs of EPS and the relatively high risperidone dosage, considering the patient’s advanced age.
After the meeting with the patient, a treatment plan was created to 1) gradually reduce the dosage of antipsychotic medication, and 2) refer her to a neurologist for a complete work-up to rule out underlying neurologic disorders, such as dementia. Risperidone was tapered by increments of 0.25 mg/d every three to four weeks; throughout this process, the patient was closely monitored by the nursing staff at the retirement living facility. Monthly appointments were scheduled at the outpatient mental health clinic for evaluation and medication management.
Two months after the initial mental health clinic visit, the patient’s condition was pronounced stable on the current regimen of sertraline 50 mg/d and risperidone 1.0 mg/d. She was later seen by a neurologist, who made a diagnosis of Parkinson’s disease and placed her on carbidopa-levodopa (1 1/2 tablets, 25/100 mg, tid). The patient’s auditory hallucinations continued with the same intensity as at baseline, but fewer tremors were noted in her extremities. By six months into the tapering process (with risperidone reduced at that time to 0.25 mg/d and carbidopa-levodopa to 25/100 mg tid), the patient had begun to experience dissipation of the tremors, and her AIMS score2 was 0. She was able to replace her four-point walker with a cane.
One year after her initial visit to the mental health clinic, the patient’s neurologist suggested replacing risperidone with quetiapine (12.5 mg/d) for its improved tolerability and lower adverse effect profile.4 She continued to take sertraline and carbidopa-levodopa.
Improvement of symptoms was noted following the switch. After one month on the revised regimen, the patient reported that the number of auditory hallucinations persisted, but that their intensity had decreased dramatically. She had a brighter affect and appeared to feel uplifted and more energetic. She became involved in the social activities offered at the retirement living facility and the mental health clinic. She also maintained a steady gait without her cane. According to the patient’s daughter, her mother was at her best psychological state since the onset of psychotic symptoms six years earlier. The pharmacologic regimen had reached its maximum benefit.
At a mental health appointment at the outpatient clinic 18 months after her initial visit there, it was evident that the patient’s auditory hallucinations persisted as a major stressor. She began to complain about other residents in her facility. She said she disliked the resident with whom she shared meals, and she claimed that other residents often spit on the floor in front of her room. The nursing staff did not confirm these incidents, which they considered a delusion despite the patient’s “evidence” (the tissues she said she had used to clean up).
Additionally, a new theme had emerged in the patient’s auditory hallucinations. She reported hearing a male voice that announced changes in meal times. Although she knew there was no public address system in her room or in the hallway, the “announcement” was so convincing that she would go to the dining room and once there, realize that nothing had changed. She seemed to drift between reality and her hallucinations/delusions. According to her daughter, the patient’s independent and reserved personality forced her to internalize her stressors—in this case, her frustration about the other residents—which fed into her hallucinations and delusions.
In response to her worsening psychotic symptoms, the patient’s provider increased her quetiapine dosage from 12.5 mg/d to 25 mg/d. Her MMSE score3 at this visit was 25/30.
Two months later, the patient exhibited increasing symptoms of paranoia, delusions, and auditory hallucinations. She continued to respond to the “broadcast” messages about meal times, and she voiced her frustrations to others who spoke Mandarin. She became agitated in response to out-of-the-ordinary events. When her alarm clock battery ran out, for example, she insisted that “a man’s voice” kept reminding her to replace the battery; in response, she placed the alarm clock in the refrigerator, later explaining, “Now I don’t need to worry about it.”
Her cognitive status began to show obvious, progressive deterioration, with an MMSE score3 of 22/30 at this visit—a significant reduction from previous scores. Worsening of her short-term memory became apparent when she had difficulty playing bingo and was unable to remember her appointment or the current date. She became upset when others corrected her.
In a review of the trends in this patient’s clinical presentation, it became increasingly evident to the patient’s mental health care providers that she had Lewy body dementia.
DISCUSSION
Dementia with Lewy bodies (DLB), a progressive disease, is the second most common cause of neurodegenerative dementia after Alzheimer’s disease.5-7 It is estimated that DLB accounts for 20% of US cases of dementia (ie, about 800,000 patients).8,9 Although public awareness of DLB is on the rise, the disorder is still underrecognized and underdiagnosed because its clinical manifestations so closely resemble those of Alzheimer’s disease, Parkinson’s disease, and psychosis.10,11
Clinical symptoms of DLB include progressive cognitive decline, cognitive fluctuation, EPS, and parkinsonism; hallucinations involving all five senses, particularly sight; delusions; REM sleep disturbance, with or without vivid and frightening dreams; changes in mood and behavior; impaired judgment and insight; and autonomic dysfunction, such as orthostatic hypotension and carotid-sinus hypersensitivity.5,11-15
The symptoms of DLB are caused by the accumulations of Lewy bodies, that is, deposits of alpha-synuclein protein in the nuclei of neurons. Lewy bodies destroy neurons over time, resulting in the destruction of dopaminergic and acetylcholinergic pathways from the brain stem to areas of the cerebral cortex associated with cognition and motor functions.4,5,16
DLB is a spectrum disorder; it often coexists with Parkinson’s disease or Alzheimer’s disease, as Lewy bodies are also found in patients with these illnesses.7 This poses a challenge for formulating a differential diagnosis, particularly in patients with fluctuating cognition,10 and for attempting to establish disease prevalence.
Diagnosis
Currently, a conclusive diagnosis of DLB can be confirmed only through postmortem autopsy, although use of medial temporal lobe volume (via structural MRI) and regional blood flow (via single photon emission CT [SPECT] tracers) is being investigated.17
The diagnosis of DLB is currently based on the presenting clinical symptoms and the exclusion of other medical conditions whose symptoms mimic those of DLB.7 The screening assessment may include a neurologic/psychiatric assessment (MMSE, psychiatric evaluation, and interviews with family members or caretakers), neuroimaging such as MRI to rule out other organic causes, and laboratory evaluation to rule out potentially reversible causes of dementia, including electrolyte imbalance, vitamin deficiency (specifically vitamin B12), anemia, thyroid dysfunction, and kidney or liver impairment.18
The American Psychiatric Assocation1 categorizes DLB under “Dementia Due to Other General Medical Conditions” (294.1x). The World Health Organization19 includes it among “Other specified degenerative diseases of the nervous system” (G31.8).
Treatment
Lewy body dementia is an irreversible neurologic degenerative disorder. Treatment for DLB comprises symptom management, primarily through pharmacology; however, the response to medication is highly individualized. Treatment includes management of the following symptoms:
Cognitive impairment. Cholinesterase inhibitors, such as rivastigmine (3 to 12 mg/d), donepezil (10 mg/d), or galantamine (titrated up to 12 mg bid),20-23 improve attention and behavior and reduce apathy, anxiety, delusions, and hallucinations. As cognitive impairment worsens, memantine (10 mg bid) may be effective.24 The potential for anticholinergic adverse effects requires close monitoring in patients taking these agents.
Parkinsonian symptoms. Medications indicated for Parkinson’s disease and syndrome, such as carbidopa-levodopa (25/100 mg tid), can be effective; dosage may be slowly titrated upward as tolerated and if needed for symptom management.25,26 The dopaminergic effect of antiparkinson medications may intensify the psychotic symptoms and worsen the REM sleep pattern. In this case, a low-dose atypical antipsychotic is suggested27,28 (see below).
Psychotic symptoms. An atypical antipsychotic agent, such as quetiapine (12.5 mg), risperidone (0.25 mg), olanzapine (2.5 mg), ziprasidone (20 mg), aripiprazole (2 mg), or paliperidone (1.5 mg), may be used. Because of the DLB-associated risk of neuroleptic sensitivity, atypical antipsychotic agents should be initiated at a low dose with slow upward titration17,26,29; quetiapine appears less likely than risperidone or olanzapine to cause neuroleptic sensitivity or to trigger EPS.4 For Asian patients, who often respond to lower doses of these medications (and are more easily affected by associated adverse effects), Chen et al30 recommend a starting dose of about one-half the recommended dose.
Depression. An SSRI antidepressant with relatively simple pharmacologic properties and moderate half-life may be used to manage symptoms of depression.26,31,32 Long–half-life SSRIs (eg, fluoxetine) should be avoided in elderly patients; in response to SNRIs (serotonin-norepinephrine reuptake inhibitors), these patients may experience elevated blood pressures and pulses, with subsequent morbidity.33
REM sleep disturbances. Clonazepam (0.25 mg), melatonin (3.0 mg), or quetiapine (12.5 mg) may be administered at bedtime.34
Important Lessons
In general, providers should consider the benefits and risks of any pharmacologic treatment and avoid polypharmacy, if possible. Family and caretakers should be included in the treatment planning, with a focus on prioritizing and managing the most debilitating symptoms or dysfunctions that prompt concerns for safety.
For optimal homeostasis, some DLB patients may require joint pharmacologic modalities that appear counterintuitive—for example, an antiparkinsonism (dopaminergic) agent for parkinsonian symptoms or neuroleptic-induced EPS, versus an antipsychotic (eg, a dopamine antagonist) to treat profound hallucinations.26
As the response to treatment for DLB is highly individualized, it is essential to titrate and augment with care.
CONCLUSION
In DLB, as with other dementing illnesses, the onset of symptoms can be gradual and insidious, posing a great challenge to the clinician who seeks to confirm the diagnosis. In the illness’s early stages, the clinician may have to treat targeted symptoms and adjust the treatment plan once signs of the pathologic origins emerge.
It is critical to understand the mechanisms of psychotropic medications and targeted neurotransmitters when evaluating treatment for DLB. Titrating or augmenting these medications in elderly patients requires the clinician to follow a principle of start low and go slow, making only one change at a time.
It is always helpful to include family members in the patient’s care and to gather information on previous history, personality traits, family history, and cultural components. It is also important to communicate with other specialists to implement collaborative care.
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed (text revision). Washington, DC: American Psychiatric Association; 2000:167.
2. National Institute of Mental Health. Abnormal Involuntary Movement Scale (AIMS). www.atlantapsychia try.com/forms/AIMS.pdf. Accessed May 20, 2010.
3. Mini–Mental State Examination. www.nmaging .state.nm.us/pdf_files/Mini_Mental_Status_Exam.pdf. Accessed May 20, 2010.
4. Baskys A. Lewy body dementia: the litmus test for neuroleptic sensitivity and extrapyramidal symptoms. J Clin Psychiatry. 2004;65 suppl 11:16-22.
5. Weisman D, McKeith I. Dementia with Lewy bodies. Semin Neurol. 2007;27(1):42-47.
6. McKeith IG. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the Consortium on DLB International Workshop. J Alzheimers Dis. 2006;9(3 suppl):417-423.
7. McKeith IG, Galasko D, Kosaka K, et al. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the Consortium on DLB International Workshop. Neurology. 1996;47(5):1113-1124.
8. Hill C, Reiss N. Lewy body dementia (2008). www.mentalhelp.net/poc/view_doc.php?type=doc& id=13151&cn=231. Accessed May 20, 2010.
9. Lewy Body Dementia Association, Inc. Lewy body dementia: current issues in diagnosis and treatment. www.lewybodydementia.org. Accessed May 20, 2010.
10. Varanese S, Perfetti B, Monaco D, et al. Fluctuating cognition and different cognitive and behavioural profiles in Parkinson’s disease with dementia: comparison of dementia with Lewy bodies and Alzheimer’s disease. J Neurol. 2010 Jan 22. [Epub ahead of print]
11. Kurita A, Murakami M, Takagi S, et al. Visual hallucinations and altered visual information processing in Parkinson disease and dementia with Lewy bodies. Mov Disorder. 2010;25(2):167-171.
12. Gagnon JF, Postuma RB, Mazza S, et al. Rapid-eye-movement sleep behaviour disorder and neurodegenerative diseases. Lancet Neurol. 2006;5(5):424-432.
13. Dodel R, Csoti I, Ebersbach G, et al. Lewy body dementia and Parkinson’s disease with dementia. J Neurol. 2008;255 suppl 5:39-47.
14. Sonnesyn H, Nilsen DW, Rongve A, et al. High prevalence of orthostatic hypotension in mild dementia. Dement Geriatr Cogn Disord. 2009;28(4):307-313.
15. Kenny RA, Shaw FE, O’Brien JT, et al. Carotid sinus syndrome is common in dementia with Lewy bodies and correlates with deep white matter lesions. J Neurol Neurosurg Psychiatry. 2004;75(7):966-971.
16. Hickey C, Chisholm T, Passmore MJ, et al. Differentiating the dementias: revisiting synucleinopathies and tauopathies. Curr Alzheimer Res. 2008;5(1):52-60.
17. McKeith IG, Burn DJ, Ballard CG, et al. Dementia with Lewy bodies. Semin Clin Neuropsychiatry. 2003; 8(1):46-57.
18. Bird TD, Miller BL. Dementia. In: Fauci AS, Braunwald E, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine. 17th ed. New York, NY: McGraw Hill Medical; 2008:2536-2549.
19. World Health Organization. International Classification of Diseases (ICD), Version 2007. Chapter VI: Diseases of the Central Nervous System. http://apps.who.int/classifications/apps/icd/icd10online/index.htm?kg00.htm+. Accessed May 20, 2010.
20. McKeith I, Del Ser T, Spano P, et al. Efficacy of rivastigmine in dementia with Lewy bodies: a randomised, double-blind, placebo-controlled international study. Lancet. 2000;356(9247):2031-2036.
21. Emre M, Cummings JL, Lane RM. Rivastigmine in dementia associated with Parkinson’s disease and Alzheimer’s disease: similarities and differences. J Alzheimers Dis. 2007;11(4):509-519.
22. Lam B, Hollingdrake E, Kennedy JL, et al. Cholinesterase inhibitors in Alzheimer’s disease and Lewy body spectrum disorders: the emerging pharmacogenetic story. Hum Genomics. 2009;4(2):91-106.
23. Wild R, Pettit T, Burns A. Cholinesterase inhibitors for dementia with Lewy bodies. Cochrane Database Syst Rev. 2003;(3):CD003672.
24. Aarsland D, Ballard C, Walker Z, et al. Memantine in patients with Parkinson’s disease dementia or dementia with Lewy bodies: a double-blind, placebo-controlled, multicentre trial. Lancet Neurol. 2009;8(7):613-618.
25. Merck & Co., Inc. Sinemet® CR (carbidopa-levodopa) sustained-release tablets. http://packageinserts.bms.com/pi/pi_sinemet_cr.pdf. Accessed May 20, 2010.
26. Fernandez HH, Wu CK, Ott BR. Pharmacotherapy of dementia with Lewy bodies. Expert Opin Pharmacother. 2003;4(11):2027-2037.
27. Kato K, Wada T, Kawakatsu S, Otani K. Improvement of both psychotic symptoms and Parkinsonism in a case of dementia with Lewy bodies by the combination therapy of risperidone and L-DOPA. Prog Neuropsychopharmacol Biol Psychiatry. 2002;26(1):201-203.
28. Yamauchi K, Takehisa M, Tsuno M, et al. Levodopa improved rapid eye movement sleep behavior disorder with diffuse Lewy body disease. Gen Hosp Psychiatry. 2003;25(2):140-142.
29. Stahl SM. The Prescriber’s Guide: Stahl’s Essential Psychopharmacology. Cambridge University Press; 2006:459.
30. Chen JP, Barron C, Lin KM, Chung H. Prescribing medication for Asians with mental disorders. West J Med. 2002;176(4):271-275.
31. Sink KM, Holden KF, Yaffe K. Pharmacological treatment of neuropsychiatric symptoms of dementia: a review of the evidence. JAMA. 2005;293(5):596-608.
32. Pollock BG, Mulsant BH, Rosen J, et al. Comparison of citalopram, perphenazine, and placebo for the acute treatment of psychosis and behavioral disturbances in hospitalized, demented patients. Am J Psychiatry. 2002;159(3):460-465.
33. Schwab W, Messinger-Rapport B, Franco K. Psychiatric symptoms of dementia: treatable, but no silver bullet. Cleve Clin J Med. 2009;76(3):167-174.
34. Gagnon JF, Postuma RB, Montplaisir J. Update on the pharmacology of REM sleep behavior disorder. Neurology. 2006;67(5):742-747
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed (text revision). Washington, DC: American Psychiatric Association; 2000:167.
2. National Institute of Mental Health. Abnormal Involuntary Movement Scale (AIMS). www.atlantapsychia try.com/forms/AIMS.pdf. Accessed May 20, 2010.
3. Mini–Mental State Examination. www.nmaging .state.nm.us/pdf_files/Mini_Mental_Status_Exam.pdf. Accessed May 20, 2010.
4. Baskys A. Lewy body dementia: the litmus test for neuroleptic sensitivity and extrapyramidal symptoms. J Clin Psychiatry. 2004;65 suppl 11:16-22.
5. Weisman D, McKeith I. Dementia with Lewy bodies. Semin Neurol. 2007;27(1):42-47.
6. McKeith IG. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the Consortium on DLB International Workshop. J Alzheimers Dis. 2006;9(3 suppl):417-423.
7. McKeith IG, Galasko D, Kosaka K, et al. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the Consortium on DLB International Workshop. Neurology. 1996;47(5):1113-1124.
8. Hill C, Reiss N. Lewy body dementia (2008). www.mentalhelp.net/poc/view_doc.php?type=doc& id=13151&cn=231. Accessed May 20, 2010.
9. Lewy Body Dementia Association, Inc. Lewy body dementia: current issues in diagnosis and treatment. www.lewybodydementia.org. Accessed May 20, 2010.
10. Varanese S, Perfetti B, Monaco D, et al. Fluctuating cognition and different cognitive and behavioural profiles in Parkinson’s disease with dementia: comparison of dementia with Lewy bodies and Alzheimer’s disease. J Neurol. 2010 Jan 22. [Epub ahead of print]
11. Kurita A, Murakami M, Takagi S, et al. Visual hallucinations and altered visual information processing in Parkinson disease and dementia with Lewy bodies. Mov Disorder. 2010;25(2):167-171.
12. Gagnon JF, Postuma RB, Mazza S, et al. Rapid-eye-movement sleep behaviour disorder and neurodegenerative diseases. Lancet Neurol. 2006;5(5):424-432.
13. Dodel R, Csoti I, Ebersbach G, et al. Lewy body dementia and Parkinson’s disease with dementia. J Neurol. 2008;255 suppl 5:39-47.
14. Sonnesyn H, Nilsen DW, Rongve A, et al. High prevalence of orthostatic hypotension in mild dementia. Dement Geriatr Cogn Disord. 2009;28(4):307-313.
15. Kenny RA, Shaw FE, O’Brien JT, et al. Carotid sinus syndrome is common in dementia with Lewy bodies and correlates with deep white matter lesions. J Neurol Neurosurg Psychiatry. 2004;75(7):966-971.
16. Hickey C, Chisholm T, Passmore MJ, et al. Differentiating the dementias: revisiting synucleinopathies and tauopathies. Curr Alzheimer Res. 2008;5(1):52-60.
17. McKeith IG, Burn DJ, Ballard CG, et al. Dementia with Lewy bodies. Semin Clin Neuropsychiatry. 2003; 8(1):46-57.
18. Bird TD, Miller BL. Dementia. In: Fauci AS, Braunwald E, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine. 17th ed. New York, NY: McGraw Hill Medical; 2008:2536-2549.
19. World Health Organization. International Classification of Diseases (ICD), Version 2007. Chapter VI: Diseases of the Central Nervous System. http://apps.who.int/classifications/apps/icd/icd10online/index.htm?kg00.htm+. Accessed May 20, 2010.
20. McKeith I, Del Ser T, Spano P, et al. Efficacy of rivastigmine in dementia with Lewy bodies: a randomised, double-blind, placebo-controlled international study. Lancet. 2000;356(9247):2031-2036.
21. Emre M, Cummings JL, Lane RM. Rivastigmine in dementia associated with Parkinson’s disease and Alzheimer’s disease: similarities and differences. J Alzheimers Dis. 2007;11(4):509-519.
22. Lam B, Hollingdrake E, Kennedy JL, et al. Cholinesterase inhibitors in Alzheimer’s disease and Lewy body spectrum disorders: the emerging pharmacogenetic story. Hum Genomics. 2009;4(2):91-106.
23. Wild R, Pettit T, Burns A. Cholinesterase inhibitors for dementia with Lewy bodies. Cochrane Database Syst Rev. 2003;(3):CD003672.
24. Aarsland D, Ballard C, Walker Z, et al. Memantine in patients with Parkinson’s disease dementia or dementia with Lewy bodies: a double-blind, placebo-controlled, multicentre trial. Lancet Neurol. 2009;8(7):613-618.
25. Merck & Co., Inc. Sinemet® CR (carbidopa-levodopa) sustained-release tablets. http://packageinserts.bms.com/pi/pi_sinemet_cr.pdf. Accessed May 20, 2010.
26. Fernandez HH, Wu CK, Ott BR. Pharmacotherapy of dementia with Lewy bodies. Expert Opin Pharmacother. 2003;4(11):2027-2037.
27. Kato K, Wada T, Kawakatsu S, Otani K. Improvement of both psychotic symptoms and Parkinsonism in a case of dementia with Lewy bodies by the combination therapy of risperidone and L-DOPA. Prog Neuropsychopharmacol Biol Psychiatry. 2002;26(1):201-203.
28. Yamauchi K, Takehisa M, Tsuno M, et al. Levodopa improved rapid eye movement sleep behavior disorder with diffuse Lewy body disease. Gen Hosp Psychiatry. 2003;25(2):140-142.
29. Stahl SM. The Prescriber’s Guide: Stahl’s Essential Psychopharmacology. Cambridge University Press; 2006:459.
30. Chen JP, Barron C, Lin KM, Chung H. Prescribing medication for Asians with mental disorders. West J Med. 2002;176(4):271-275.
31. Sink KM, Holden KF, Yaffe K. Pharmacological treatment of neuropsychiatric symptoms of dementia: a review of the evidence. JAMA. 2005;293(5):596-608.
32. Pollock BG, Mulsant BH, Rosen J, et al. Comparison of citalopram, perphenazine, and placebo for the acute treatment of psychosis and behavioral disturbances in hospitalized, demented patients. Am J Psychiatry. 2002;159(3):460-465.
33. Schwab W, Messinger-Rapport B, Franco K. Psychiatric symptoms of dementia: treatable, but no silver bullet. Cleve Clin J Med. 2009;76(3):167-174.
34. Gagnon JF, Postuma RB, Montplaisir J. Update on the pharmacology of REM sleep behavior disorder. Neurology. 2006;67(5):742-747
Two-Layer Repair of a Chronic Patellar Tendon Rupture: A Novel Technique and Literature Review
Vesiculopustular Eruption in a Neonate With Trisomy 21 Syndrome as a Clue of Transient Myeloproliferative Disorders
What's Eating You? Cat Flea (Ctenocephalides felis), Part 2: Prevention and Control
Successfully navigating the 15-minute ‘med check’
How to reduce malpractice risk with better documentation.
Tips to make documentation easier, faster, and more satisfying” (Current Psychiatry, February 2008), I discussed documentation techniques at length. Table 3 reprints principles that may be especially helpful in practices that consist primarily of med checks.
Table 3
Keys to better documentation
| Technique | Benefits |
|---|---|
| Time and date your notes | After an adverse event, establish when you saw the patient, recorded findings, wrote orders, reviewed lab results, or discussed problems with others can make a big difference in how your care is viewed |
| Sooner is better | Charting completed long after an adverse event occurred is vulnerable to accusations of fabrication |
| Brief quotes | Verbatim statements (‘I’ve never considered suicide’) quickly convey key factors in your therapeutic decision |
| Dictate or use speech recognition software | You speak faster than you write allowing you to document more |
| Provide handouts | Patients often do not remember or understand much of medication instructions doctors tell them |
| Use rating scales | Record more information in a scientifically validated format |
| Try macros and templates | These reduce documentation time and help you remember to cover everything you should |
| Source: Adapted from reference 18 | |
Acknowledgment
Thanks to James Knoll IV, MD for his helpful input on this article.
1. Mojtabai R, Olfson M. National trends in psychotherapy by office-based psychiatrists. Arch Gen Psychiatry. 2008;65:962-970.
2. Lewis MH, Gohagan JK, Merenstein DJ. The locality rule and the physician’s dilemma: local medical practices vs the national standard of care. JAMA. 2007;297(23):2633-2637.
3. Gabbard GO. Deconstructing the “med check.” Psychiatric Times. September 3, 2009. Available at: http://www.psychiatrictimes.com/display/article/10168/1444238. Accessed April 28, 2010.
4. Pies RW. Psychiatrists, physicians, and the prescriptive bond. Psychiatric Times. April 16, 2010. Available at: http://www.psychiatrictimes.com/blog/couchincrisis/content/article/10168/1555057. Accessed April 28, 2010.
5. Carlat DJ. Unhinged: the trouble with psychiatry—a doctor’s revelations about a profession in crisis. New York, NY: Free Press; 2010.
6. Nemeroff CB. The myth of the med check in psychopharmacology. Presented at: Presidential Symposium, Annual Meeting of the American Psychiatric Association; May 7, 2008; Washington, DC.
7. Rush W, Gochfeli L, Minkov K, et al. Medication visits: visit time and quality—the connection. Compliance Watch. 2009;2(2):13-15.
8. Fine P. Psychodynamic psychiatry in community settings. J Am Acad Psychoanal Dyn Psychiatry. 2007;35:431-441.
9. Sherman C. Don’t forget therapeutic skills even during a “med check.” Clinical Psychiatry News. 2002;30(7):390.-Available at: http://findarticles.com/p/articles/mi_hb4345/is_7_30/ai_n28933329. Accessed April 28, 2010.
10. Ackerman SJ, Hilsenroth MJ. A review of therapist characteristics and techniques positively impacting the therapeutic alliance. Clinical Psychology Rev. 2003;23:1-33.
11. Guggenheim FG. Prime time: maximizing the therapeutic experience—a primer for psychiatric clinicians. New York, NY: Routledge; 2009.
12. Saks ER. The center cannot hold: my journey through madness. New York, NY: Hyperion; 2007.
13. Pincus HA, Tanielian TL, Marcus SC, et al. Prescribing trends in psychotropic medications: primary care, psychiatry, and other medical specialties. JAMA. 1998;279(7):526-531.
14. Harman JS, Veazie PJ, Lyness JM. Primary care physician office visits for depression by older Americans. J Gen Intern Med. 2006;21:926-930.
15. Chen LM, Farwell WR, Jha AK. Primary care visit duration and quality: does good care take longer? Arch Intern Med. 2009;169:1866-1872.
16. Gilchrist VJ, Stange KC, Flocke SA, et al. A comparison of the National Ambulatory Medical Care Survey (NAMCS) measurement approach with direct observation of outpatient visits. Med Care. 2004;42(3):276-280.
17. Moffic HS. Make the most of the “15-minute med-check.” Current Psychiatry. 2006;5(9):116.-
18. Mossman D. Tips to make documentation easier, faster, and more satisfying. Current Psychiatry. 2008;7(2):84-86.

Douglas Mossman, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and adjunct professor of clinical psychiatry and training director for the forensic psychiatry fellowship, University of Cincinnati College of Medicine.
Douglas Mossman, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and adjunct professor of clinical psychiatry and training director for the forensic psychiatry fellowship, University of Cincinnati College of Medicine.
Douglas Mossman, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and adjunct professor of clinical psychiatry and training director for the forensic psychiatry fellowship, University of Cincinnati College of Medicine.
How to reduce malpractice risk with better documentation.
Tips to make documentation easier, faster, and more satisfying” (Current Psychiatry, February 2008), I discussed documentation techniques at length. Table 3 reprints principles that may be especially helpful in practices that consist primarily of med checks.
Table 3
Keys to better documentation
| Technique | Benefits |
|---|---|
| Time and date your notes | After an adverse event, establish when you saw the patient, recorded findings, wrote orders, reviewed lab results, or discussed problems with others can make a big difference in how your care is viewed |
| Sooner is better | Charting completed long after an adverse event occurred is vulnerable to accusations of fabrication |
| Brief quotes | Verbatim statements (‘I’ve never considered suicide’) quickly convey key factors in your therapeutic decision |
| Dictate or use speech recognition software | You speak faster than you write allowing you to document more |
| Provide handouts | Patients often do not remember or understand much of medication instructions doctors tell them |
| Use rating scales | Record more information in a scientifically validated format |
| Try macros and templates | These reduce documentation time and help you remember to cover everything you should |
| Source: Adapted from reference 18 | |
Acknowledgment
Thanks to James Knoll IV, MD for his helpful input on this article.
How to reduce malpractice risk with better documentation.
Tips to make documentation easier, faster, and more satisfying” (Current Psychiatry, February 2008), I discussed documentation techniques at length. Table 3 reprints principles that may be especially helpful in practices that consist primarily of med checks.
Table 3
Keys to better documentation
| Technique | Benefits |
|---|---|
| Time and date your notes | After an adverse event, establish when you saw the patient, recorded findings, wrote orders, reviewed lab results, or discussed problems with others can make a big difference in how your care is viewed |
| Sooner is better | Charting completed long after an adverse event occurred is vulnerable to accusations of fabrication |
| Brief quotes | Verbatim statements (‘I’ve never considered suicide’) quickly convey key factors in your therapeutic decision |
| Dictate or use speech recognition software | You speak faster than you write allowing you to document more |
| Provide handouts | Patients often do not remember or understand much of medication instructions doctors tell them |
| Use rating scales | Record more information in a scientifically validated format |
| Try macros and templates | These reduce documentation time and help you remember to cover everything you should |
| Source: Adapted from reference 18 | |
Acknowledgment
Thanks to James Knoll IV, MD for his helpful input on this article.
1. Mojtabai R, Olfson M. National trends in psychotherapy by office-based psychiatrists. Arch Gen Psychiatry. 2008;65:962-970.
2. Lewis MH, Gohagan JK, Merenstein DJ. The locality rule and the physician’s dilemma: local medical practices vs the national standard of care. JAMA. 2007;297(23):2633-2637.
3. Gabbard GO. Deconstructing the “med check.” Psychiatric Times. September 3, 2009. Available at: http://www.psychiatrictimes.com/display/article/10168/1444238. Accessed April 28, 2010.
4. Pies RW. Psychiatrists, physicians, and the prescriptive bond. Psychiatric Times. April 16, 2010. Available at: http://www.psychiatrictimes.com/blog/couchincrisis/content/article/10168/1555057. Accessed April 28, 2010.
5. Carlat DJ. Unhinged: the trouble with psychiatry—a doctor’s revelations about a profession in crisis. New York, NY: Free Press; 2010.
6. Nemeroff CB. The myth of the med check in psychopharmacology. Presented at: Presidential Symposium, Annual Meeting of the American Psychiatric Association; May 7, 2008; Washington, DC.
7. Rush W, Gochfeli L, Minkov K, et al. Medication visits: visit time and quality—the connection. Compliance Watch. 2009;2(2):13-15.
8. Fine P. Psychodynamic psychiatry in community settings. J Am Acad Psychoanal Dyn Psychiatry. 2007;35:431-441.
9. Sherman C. Don’t forget therapeutic skills even during a “med check.” Clinical Psychiatry News. 2002;30(7):390.-Available at: http://findarticles.com/p/articles/mi_hb4345/is_7_30/ai_n28933329. Accessed April 28, 2010.
10. Ackerman SJ, Hilsenroth MJ. A review of therapist characteristics and techniques positively impacting the therapeutic alliance. Clinical Psychology Rev. 2003;23:1-33.
11. Guggenheim FG. Prime time: maximizing the therapeutic experience—a primer for psychiatric clinicians. New York, NY: Routledge; 2009.
12. Saks ER. The center cannot hold: my journey through madness. New York, NY: Hyperion; 2007.
13. Pincus HA, Tanielian TL, Marcus SC, et al. Prescribing trends in psychotropic medications: primary care, psychiatry, and other medical specialties. JAMA. 1998;279(7):526-531.
14. Harman JS, Veazie PJ, Lyness JM. Primary care physician office visits for depression by older Americans. J Gen Intern Med. 2006;21:926-930.
15. Chen LM, Farwell WR, Jha AK. Primary care visit duration and quality: does good care take longer? Arch Intern Med. 2009;169:1866-1872.
16. Gilchrist VJ, Stange KC, Flocke SA, et al. A comparison of the National Ambulatory Medical Care Survey (NAMCS) measurement approach with direct observation of outpatient visits. Med Care. 2004;42(3):276-280.
17. Moffic HS. Make the most of the “15-minute med-check.” Current Psychiatry. 2006;5(9):116.-
18. Mossman D. Tips to make documentation easier, faster, and more satisfying. Current Psychiatry. 2008;7(2):84-86.
1. Mojtabai R, Olfson M. National trends in psychotherapy by office-based psychiatrists. Arch Gen Psychiatry. 2008;65:962-970.
2. Lewis MH, Gohagan JK, Merenstein DJ. The locality rule and the physician’s dilemma: local medical practices vs the national standard of care. JAMA. 2007;297(23):2633-2637.
3. Gabbard GO. Deconstructing the “med check.” Psychiatric Times. September 3, 2009. Available at: http://www.psychiatrictimes.com/display/article/10168/1444238. Accessed April 28, 2010.
4. Pies RW. Psychiatrists, physicians, and the prescriptive bond. Psychiatric Times. April 16, 2010. Available at: http://www.psychiatrictimes.com/blog/couchincrisis/content/article/10168/1555057. Accessed April 28, 2010.
5. Carlat DJ. Unhinged: the trouble with psychiatry—a doctor’s revelations about a profession in crisis. New York, NY: Free Press; 2010.
6. Nemeroff CB. The myth of the med check in psychopharmacology. Presented at: Presidential Symposium, Annual Meeting of the American Psychiatric Association; May 7, 2008; Washington, DC.
7. Rush W, Gochfeli L, Minkov K, et al. Medication visits: visit time and quality—the connection. Compliance Watch. 2009;2(2):13-15.
8. Fine P. Psychodynamic psychiatry in community settings. J Am Acad Psychoanal Dyn Psychiatry. 2007;35:431-441.
9. Sherman C. Don’t forget therapeutic skills even during a “med check.” Clinical Psychiatry News. 2002;30(7):390.-Available at: http://findarticles.com/p/articles/mi_hb4345/is_7_30/ai_n28933329. Accessed April 28, 2010.
10. Ackerman SJ, Hilsenroth MJ. A review of therapist characteristics and techniques positively impacting the therapeutic alliance. Clinical Psychology Rev. 2003;23:1-33.
11. Guggenheim FG. Prime time: maximizing the therapeutic experience—a primer for psychiatric clinicians. New York, NY: Routledge; 2009.
12. Saks ER. The center cannot hold: my journey through madness. New York, NY: Hyperion; 2007.
13. Pincus HA, Tanielian TL, Marcus SC, et al. Prescribing trends in psychotropic medications: primary care, psychiatry, and other medical specialties. JAMA. 1998;279(7):526-531.
14. Harman JS, Veazie PJ, Lyness JM. Primary care physician office visits for depression by older Americans. J Gen Intern Med. 2006;21:926-930.
15. Chen LM, Farwell WR, Jha AK. Primary care visit duration and quality: does good care take longer? Arch Intern Med. 2009;169:1866-1872.
16. Gilchrist VJ, Stange KC, Flocke SA, et al. A comparison of the National Ambulatory Medical Care Survey (NAMCS) measurement approach with direct observation of outpatient visits. Med Care. 2004;42(3):276-280.
17. Moffic HS. Make the most of the “15-minute med-check.” Current Psychiatry. 2006;5(9):116.-
18. Mossman D. Tips to make documentation easier, faster, and more satisfying. Current Psychiatry. 2008;7(2):84-86.
The manipulative self-harmer
CASE: Self-destructive behaviors
After being acquitted of 4 counts of second-degree forgery for writing checks from her mother’s bank account, Ms. L, age 52, is sent to the state hospital for a forensic examination to determine competency. Two years later she is granted conditional release from the hospital, transferred to our not-for-profit community mental health center, and enrolled in an intensive inpatient treatment program to monitor forensic patients. She is legally required to comply with treatment recommendations.
At admission, Ms. L is diagnosed with major depression, recurrent, and borderline personality disorder (BPD). She has no history of antisocial behavior or criminal acts other than forging checks and has never spent time in prison, which makes it unlikely she has co morbid antisocial personality disorder (Table 1).1
Over the next 5 years Ms. L tests limits with the treatment team and acts out by engaging in self-harming behaviors. In 1 instance, she cuts her forearm deeply, stuffs the wound with mayonnaise and paper towels, and wraps her arm with a bandage. She wears a long-sleeved shirt to hide her wound, which is not discovered until a severe infection develops.
Ms. L has difficulty with coping skills and interpersonal relationships. She approaches others with ambivalence and mistrust and consistently expects them to demean or take advantage of her. Ms. L is manipulative, at times injuring herself after perceived wrongdoings by staff. For example, after her therapist reschedules a meeting because of an emergency, Ms. L pours scalding water on her foot.
Table 1
Cluster B personality disorders: Differential diagnosis
| Diagnosis | Features |
|---|---|
| Borderline personality disorder | Self-destructiveness, angry disruptions in close relationships, and chronic feelings of deep emptiness and loneliness |
| Histrionic personality disorder | Attention seeking, manipulative behavior, and rapidly shifting emotions |
| Antisocial personality disorder | Manipulative to gain profit, power, or other material gratification |
| Source: Reference 1 | |
The authors’ observations
Ms. L consistently displays 3 common constructs of BPD:
- primitive defense mechanisms
- identity diffusion
- generally intact reality testing.2
Defense mechanisms are psychological attempts to deal with intrapsychic stress. Splitting—vacillating between extremes of idealization and devaluation—is a fundamental primitive defense mechanism that is the root of BPD.2 Identity diffusion causes confusion about life goals and values and feelings of boredom and emptiness. This internal world leads a patient to have the same perception of the external world, which explains many symptoms of BPD, such as rapidly shifting moods, intense anger, lack of clear sense of self, fear of abandonment, and unstable and intense interpersonal relationships.2
Early in treatment, Ms. L had difficulty breaking a cycle of self-defeating behavior, such as destroying personal items, trying to hang herself, and gluing an ear plug in her ear. During an argument with a staff member, Ms. L punched a wall and fractured her left hand. BPD patients sometimes will “up the ante” when acting out. For example, one of our patients claimed to have planted a bomb in an elementary school and another swallowed inedible objects, including spoons, forks, and butter knives. In Ms. L’s case, we addressed her self-harm behavior by helping her:
- develop less destructive coping skills such as drawing or painting
- identify irrational thoughts that contribute to self harm.
HISTORY: Troubled past
Raised by her biologic parents, Ms. L met all developmental milestones. She denies a history of childhood abuse but reports experiencing “depression and memory loss” and relationship problems with her parents during adolescence. As a child she often missed school because she “did not want anyone to know what a disgusting person I was” and “I should have my head cut open and cut into little pieces for thinking such mean thoughts.” Ms. L dropped out of school in the twelfth grade but obtained her general educational development certificate.
Notes and letters Ms. L wrote while in treatment consistently refer to her negative self-image. Ms. L writes that she feels she does not deserve to “be a part of this world,” is “never good enough for anyone,” and “should be thrown away with the garbage.”
Ms. L vacillates between desiring a closer relationship with her parents, especially her mother, and wanting to “cut them out of my life for good.” She has minimal contact with her older sister. Ms. L is divorced and has 2 adult sons. She was involved sporadically in her sons’ lives when they were children, but now has no contact with them.
BPD and crime
Ms. L is enrolled in the “911 program,” which monitors individuals who have been found not guilty by reason of mental defect. Individuals with BPD often are convicted of serious and violent crimes, which may be because of BPD features such as interpersonal hostility and self-harm. Impulsivity, substance abuse, and parental neglect—all of which are associated with BPD—can increase risk of criminality.3 There is no evidence to suggest a direct link between BPD and criminality; however, over-representation of BPD in prison populations suggest that in severe cases it may increase criminogenic risk.1,3
TREATMENT: Worsened depression
When Ms. L arrives at our facility, her medication regimen includes fluoxetine, 80 mg/d, risperidone, 2 mg/d, and buspirone, 20 mg/d. Risperidone and buspirone are discontinued because of perceived lack of efficacy. Venlafaxine XR is added and titrated to 300 mg/d, and Ms. L receives lorazepam, 1 and 2 mg as needed. However, lorazepam carries risks because impulsivity and impaired judgment—which are common in BPD—can lead to dependence and abuse. We feel that in a supervised setting the risks can be managed.
Recently, staff witnessed Ms. L experiencing an episode that appeared to be a grand mal seizure. After Ms. L is evaluated at the local emergency room, her EEG is normal, but a neurologic consult recommends discontinuing fluoxetine or venlafaxine XR because they may have contributed to the seizure. We taper and discontinue venlafaxine XR but Ms. L complains bitterly that she is getting increasingly depressed. On several occasions she attempts to pit team members against each other.
Ms. L falls, injures her back, and begins to abuse opiates. After her prescription runs out, she obtains more from an intellectually limited patient in her treatment program. Ms. L says she is getting more depressed, threatens suicide, and is placed in a more restrictive in-patient setting. We consider adding pregabalin to address her pain and help with anxiety and impulse control but the consulting neurologist prescribes carbamazepine, 400 mg/d, and her pain improves.5,6
The authors’ observations
BPD treatment primarily is psychotherapeutic and emphasizes skill building (Table 2) with focused, symptom-targeted pharmacotherapy as indicated.4 Pharmacotherapy typically targets 3 domains:
- affective dysregulation
- impulsive-behavioral dyscontrol symptoms
- cognitive-perceptual symptoms.
Patients with prominent anxiety may benefit from benzodiazepines, although research on these agents for BPD is limited. Recent studies show efficacy with fluoxetine, olanzapine, or a combination of both,7 and divalproex.8 Preliminary data supports the use of topiramate, quetiapine, risperidone, ziprasidone, lamotrigine, and clonidine (Table 3).9-14 A recent review and meta-analysis showed efficacy with topira-mate, lamotrigine, valproate, aripiprazole, and olanzapine.15
For Ms. L, we restart venlafaxine at a lower dose of 50 mg/d and titrate it to 150 mg/d, which is still lower than her previous dose of 300 mg/d. She has no recurrence of seizures and her depression improves.
Table 2
Features of psychotherapeutic modalities for BPD
| Description | Mode of treatment | Skills taught | |
|---|---|---|---|
| Dialectical behavior therapy | Manualized, time-limited, cognitive-behavioral approach based on the biosocial theory of BPD | Individual therapy, group skills training, telephone contact, and therapist consultation | Core mindfulness skills, interpersonal effectiveness skills, emotion modulation skills, and distress tolerance skills |
| Systems Training for Emotional Predictability and Problem Solving | Manual-based, group treatment that includes a systems component to train family members, friends, and significant others | 20-week basic skills group and a 1-year, twice-monthly advanced group program; utilizes a classroom ‘seminar’ format | Awareness of illness, emotion management skills, and behavior management skills |
| BPD: borderline personality disorder | |||
Table 3
Pharmacotherapy for BPD: What the evidence says
| Study | Design | Results |
|---|---|---|
| Hollander et al, 20039 | 96 patients with Cluster B personality disorders randomized to divalproex or placebo for 12 weeks | Divalproex was superior to placebo in treating impulsive aggression, irritability, and global severity |
| Hilger et al, 200310 | Case report of 2 women with BPD and severe self-mutilation receiving quetiapine monotherapy | Quetiapine resulted in a marked improvement of impulsive behavior and overall level of function |
| Rizvi, 200211 | Case report of a 14-year-old female with borderline personality traits admitted to an inpatient facility for suicide attempt, impulsive behavior, and mood lability. Lamotrigine was started at 25 mg/d and titrated to 200 mg/d. At admission, she was receiving clonazepam, valproic acid, quetiapine, and fluoxetine, which were tapered and discontinued | Over 6 months of inpatient treatment, suicidal behavior and ideation diminished and impulse control and mood lability improved; continued improvement at 1-year follow up |
| Rocca et al, 200212 | 15 BPD outpatients with aggressive behavior given risperidone (mean dose 3.27 mg/d) in an 8-week open-label study | Risperidone produced a significant reduction in aggression based on AQ scores, reduction in depressive symptoms, and an increase in energy and global functioning |
| Philipsen et al, 200413 | 14 women with BPD given oral clonidine, 75 and 150 µg, while experiencing strong aversive inner tension and urge to commit self-injury | Clonidine significantly decreased aversive inner tension, dissociative symptoms, and urge to commit self-injury as measured by self rated scales |
| Pascual et al, 200414 | A 2-week open-label study of 10 females and 2 males presenting to psychiatric emergency service for self-injurious behavior, aggression/hostility, loss of impulse control, and severe anxiety/depressive symptoms received IM ziprasidone, 20 mg, followed by flexible oral dosing between 40 mg/d and 160 mg/d | 9 patients who completed the study showed statistically significant improvements on CGI-S, HAM-D-17, HAM-A, BPRS, and BIS |
| AQ: Aggression Questionnaire; BIS: Barratt Impulsiveness Scale; BPD: borderline personality disorder; BPRS: Brief Psychiatric Rating Scale; CGI-S: Clinical Global Impressions-Severity of Illness; HAM-A: Hamilton Anxiety Rating scale; HAM-D-17: 17-item Hamilton Depression Rating scale | ||
OUTCOME: Some improvement
Ms. L has no dramatic suicidal gestures for 3 years. Although she continues to engage in self-injurious behaviors, the intensity and frequency are reduced and she does not inflict any serious injury for 18 months. Her mood and behavior continue to oscillate; she is relatively calm and satisfied 1 week, angry and assaultive the next. This stormy course is expected given her BPD diagnosis.
Initially, Ms. L resided in a locked residential unit and was minimally compliant with treatment recommendations and unit policies. As treatment progressed she moved to a different locked unit and eventually to an apartment. Recently, she was placed in a more restrictive setting because her hostile and self-destructive behavior escalated.
The authors’ observations
Ms. L is no different from most Axis II Cluster B disordered patients. During treatment she shows improvement by refraining from self-destructive behaviors for up to 18 months, but she then briefly reverts back to maladaptive behaviors. Ms. L resides in a very structured treatment setting. It is not clear if the gains she made in treatment would have been possible if she was living on her own in the community.
One year after finishing the court-mandated “911 program,” Ms. L lives in the community, draws and paints quite well, attends weekly individual and group therapy, and refrains from self-mutilation. She still experiences volatile moods, but can handle them without inflicting self injury.
Related resources
- Oldham JM. Guideline watch: practice guideline for the treatment of patients with borderline personality disorder. Arlington, VA: American Psychiatric Association; 2005. www.psychiatryonline.com/content.aspx?aID=148722.
- Koenigsberg HW, Kernberg OF, Stone MH, et al. Borderline patients: extending the limits of treatability. New York, NY: Basic Books; 2000.
Drug brand names
- Aripiprazole • Abilify
- Buspirone • Buspar
- Carbamazepine • Tegretol
- Clonidine • Catapres
- Divalproex • Depakote
- Fluoxetine • Prozac
- Fluoxetine-olanzapine • Symbyax
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Pregabalin • Lyrica
- Risperidone • Risperdal
- Topiramate • Topamax
- Valproic acid • Depakene
- Venlafaxine XR • Effexor XR
- Ziprasidone • Geodon
Disclosures
Dr. Hashmi is on the speakers bureau for AstraZeneca, Eli Lilly and Company, and Janssen.
Dr. Vowell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Diagnostic and statistical manual of mental disorders, 4th ed, text revision. Washington, DC: American Psychiatric Association; 2000.
2. Koenigsberg HW, Kernberg OF, Stone MH, et al. Borderline patients: extending the limits of treatability. New York, NY: Basic Books; 2000.
3. Nee C, Farman S. Female prisoners with borderline personality disorder: some promising treatment developments. Crim Behav Ment Health. 2005;15:2-16.
4. Oldham JM, Bender DS, Skodol AE, et al. Testing an APA practice guideline: symptom-targeted medication utilization for patients with borderline personality disorder. J Psychiatr Pract. 2004;10:156-161.
5. American Psychiatric Association Practice Guidelines. Practice guideline for the treatment of patients with borderline personality disorder. Am J Psychiatry. 2001;158(suppl 10):1-52.
6. Yatham LN. Newer anticonvulsants in the treatment of bipolar disorder. J Clin Psychiatry. 2004;65(suppl 10):28-35.
7. Rinne T, van den Brink W, Wouters L, et al. SSRI treatment of borderline personality disorder: a randomized, placebo-controlled clinical trial for female patients with borderline personality disorder. Am J Psychiatry. 2002;159(12):2048-2054.
8. Zanarini MC, Frankenburg FR, Parachini EA. A preliminary, randomized trial of fluoxetine, olanzapine, and the olanzapine-fluoxetine combination in women with borderline personality disorder. J Clin Psychiatry. 2004;65(7):903-907.
9. Hollander E, Tracy KA, Swann AC, et al. Divalproex in the treatment of impulsive aggression: efficacy in cluster B personality disorders. Neuropsychopharmacology. 2003;28(6):1186-1197.
10. Hilger E, Barnas C, Kasper S. Quetiapine in the treatment of borderline personality disorder. World J Biol Psychiatry. 2003;4(1):42-44.
11. Rizvi ST. Lamotrigine and borderline personality disorder. J Child Adolesc Psychopharmacol. 2002;12(4):365-366.
12. Rocca P, Marchiaro L, Cocuzza E, et al. Treatment of borderline personality disorder with risperidone. J Clin Psychiatry. 2002;63(3):241-244.
13. Philipsen A, Richter H, Schmahl C, et al. Clonidine in acute aversive inner tension and self-injurious behavior in female patients with borderline personality disorder. J Clin Psychiatry. 2004;65(10):1414-1419.
14. Pascual JC, Oller S, Soler J, et al. Ziprasidone in the acute treatment of borderline personality disorder in psychiatric emergency services. J Clin Psychiatry. 2004;65(9):1281-1282.
15. Lieb K, Völlm B, Rücker G, et al. Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials. Br J Psychiatry. 2010;196(1):4-12.
CASE: Self-destructive behaviors
After being acquitted of 4 counts of second-degree forgery for writing checks from her mother’s bank account, Ms. L, age 52, is sent to the state hospital for a forensic examination to determine competency. Two years later she is granted conditional release from the hospital, transferred to our not-for-profit community mental health center, and enrolled in an intensive inpatient treatment program to monitor forensic patients. She is legally required to comply with treatment recommendations.
At admission, Ms. L is diagnosed with major depression, recurrent, and borderline personality disorder (BPD). She has no history of antisocial behavior or criminal acts other than forging checks and has never spent time in prison, which makes it unlikely she has co morbid antisocial personality disorder (Table 1).1
Over the next 5 years Ms. L tests limits with the treatment team and acts out by engaging in self-harming behaviors. In 1 instance, she cuts her forearm deeply, stuffs the wound with mayonnaise and paper towels, and wraps her arm with a bandage. She wears a long-sleeved shirt to hide her wound, which is not discovered until a severe infection develops.
Ms. L has difficulty with coping skills and interpersonal relationships. She approaches others with ambivalence and mistrust and consistently expects them to demean or take advantage of her. Ms. L is manipulative, at times injuring herself after perceived wrongdoings by staff. For example, after her therapist reschedules a meeting because of an emergency, Ms. L pours scalding water on her foot.
Table 1
Cluster B personality disorders: Differential diagnosis
| Diagnosis | Features |
|---|---|
| Borderline personality disorder | Self-destructiveness, angry disruptions in close relationships, and chronic feelings of deep emptiness and loneliness |
| Histrionic personality disorder | Attention seeking, manipulative behavior, and rapidly shifting emotions |
| Antisocial personality disorder | Manipulative to gain profit, power, or other material gratification |
| Source: Reference 1 | |
The authors’ observations
Ms. L consistently displays 3 common constructs of BPD:
- primitive defense mechanisms
- identity diffusion
- generally intact reality testing.2
Defense mechanisms are psychological attempts to deal with intrapsychic stress. Splitting—vacillating between extremes of idealization and devaluation—is a fundamental primitive defense mechanism that is the root of BPD.2 Identity diffusion causes confusion about life goals and values and feelings of boredom and emptiness. This internal world leads a patient to have the same perception of the external world, which explains many symptoms of BPD, such as rapidly shifting moods, intense anger, lack of clear sense of self, fear of abandonment, and unstable and intense interpersonal relationships.2
Early in treatment, Ms. L had difficulty breaking a cycle of self-defeating behavior, such as destroying personal items, trying to hang herself, and gluing an ear plug in her ear. During an argument with a staff member, Ms. L punched a wall and fractured her left hand. BPD patients sometimes will “up the ante” when acting out. For example, one of our patients claimed to have planted a bomb in an elementary school and another swallowed inedible objects, including spoons, forks, and butter knives. In Ms. L’s case, we addressed her self-harm behavior by helping her:
- develop less destructive coping skills such as drawing or painting
- identify irrational thoughts that contribute to self harm.
HISTORY: Troubled past
Raised by her biologic parents, Ms. L met all developmental milestones. She denies a history of childhood abuse but reports experiencing “depression and memory loss” and relationship problems with her parents during adolescence. As a child she often missed school because she “did not want anyone to know what a disgusting person I was” and “I should have my head cut open and cut into little pieces for thinking such mean thoughts.” Ms. L dropped out of school in the twelfth grade but obtained her general educational development certificate.
Notes and letters Ms. L wrote while in treatment consistently refer to her negative self-image. Ms. L writes that she feels she does not deserve to “be a part of this world,” is “never good enough for anyone,” and “should be thrown away with the garbage.”
Ms. L vacillates between desiring a closer relationship with her parents, especially her mother, and wanting to “cut them out of my life for good.” She has minimal contact with her older sister. Ms. L is divorced and has 2 adult sons. She was involved sporadically in her sons’ lives when they were children, but now has no contact with them.
BPD and crime
Ms. L is enrolled in the “911 program,” which monitors individuals who have been found not guilty by reason of mental defect. Individuals with BPD often are convicted of serious and violent crimes, which may be because of BPD features such as interpersonal hostility and self-harm. Impulsivity, substance abuse, and parental neglect—all of which are associated with BPD—can increase risk of criminality.3 There is no evidence to suggest a direct link between BPD and criminality; however, over-representation of BPD in prison populations suggest that in severe cases it may increase criminogenic risk.1,3
TREATMENT: Worsened depression
When Ms. L arrives at our facility, her medication regimen includes fluoxetine, 80 mg/d, risperidone, 2 mg/d, and buspirone, 20 mg/d. Risperidone and buspirone are discontinued because of perceived lack of efficacy. Venlafaxine XR is added and titrated to 300 mg/d, and Ms. L receives lorazepam, 1 and 2 mg as needed. However, lorazepam carries risks because impulsivity and impaired judgment—which are common in BPD—can lead to dependence and abuse. We feel that in a supervised setting the risks can be managed.
Recently, staff witnessed Ms. L experiencing an episode that appeared to be a grand mal seizure. After Ms. L is evaluated at the local emergency room, her EEG is normal, but a neurologic consult recommends discontinuing fluoxetine or venlafaxine XR because they may have contributed to the seizure. We taper and discontinue venlafaxine XR but Ms. L complains bitterly that she is getting increasingly depressed. On several occasions she attempts to pit team members against each other.
Ms. L falls, injures her back, and begins to abuse opiates. After her prescription runs out, she obtains more from an intellectually limited patient in her treatment program. Ms. L says she is getting more depressed, threatens suicide, and is placed in a more restrictive in-patient setting. We consider adding pregabalin to address her pain and help with anxiety and impulse control but the consulting neurologist prescribes carbamazepine, 400 mg/d, and her pain improves.5,6
The authors’ observations
BPD treatment primarily is psychotherapeutic and emphasizes skill building (Table 2) with focused, symptom-targeted pharmacotherapy as indicated.4 Pharmacotherapy typically targets 3 domains:
- affective dysregulation
- impulsive-behavioral dyscontrol symptoms
- cognitive-perceptual symptoms.
Patients with prominent anxiety may benefit from benzodiazepines, although research on these agents for BPD is limited. Recent studies show efficacy with fluoxetine, olanzapine, or a combination of both,7 and divalproex.8 Preliminary data supports the use of topiramate, quetiapine, risperidone, ziprasidone, lamotrigine, and clonidine (Table 3).9-14 A recent review and meta-analysis showed efficacy with topira-mate, lamotrigine, valproate, aripiprazole, and olanzapine.15
For Ms. L, we restart venlafaxine at a lower dose of 50 mg/d and titrate it to 150 mg/d, which is still lower than her previous dose of 300 mg/d. She has no recurrence of seizures and her depression improves.
Table 2
Features of psychotherapeutic modalities for BPD
| Description | Mode of treatment | Skills taught | |
|---|---|---|---|
| Dialectical behavior therapy | Manualized, time-limited, cognitive-behavioral approach based on the biosocial theory of BPD | Individual therapy, group skills training, telephone contact, and therapist consultation | Core mindfulness skills, interpersonal effectiveness skills, emotion modulation skills, and distress tolerance skills |
| Systems Training for Emotional Predictability and Problem Solving | Manual-based, group treatment that includes a systems component to train family members, friends, and significant others | 20-week basic skills group and a 1-year, twice-monthly advanced group program; utilizes a classroom ‘seminar’ format | Awareness of illness, emotion management skills, and behavior management skills |
| BPD: borderline personality disorder | |||
Table 3
Pharmacotherapy for BPD: What the evidence says
| Study | Design | Results |
|---|---|---|
| Hollander et al, 20039 | 96 patients with Cluster B personality disorders randomized to divalproex or placebo for 12 weeks | Divalproex was superior to placebo in treating impulsive aggression, irritability, and global severity |
| Hilger et al, 200310 | Case report of 2 women with BPD and severe self-mutilation receiving quetiapine monotherapy | Quetiapine resulted in a marked improvement of impulsive behavior and overall level of function |
| Rizvi, 200211 | Case report of a 14-year-old female with borderline personality traits admitted to an inpatient facility for suicide attempt, impulsive behavior, and mood lability. Lamotrigine was started at 25 mg/d and titrated to 200 mg/d. At admission, she was receiving clonazepam, valproic acid, quetiapine, and fluoxetine, which were tapered and discontinued | Over 6 months of inpatient treatment, suicidal behavior and ideation diminished and impulse control and mood lability improved; continued improvement at 1-year follow up |
| Rocca et al, 200212 | 15 BPD outpatients with aggressive behavior given risperidone (mean dose 3.27 mg/d) in an 8-week open-label study | Risperidone produced a significant reduction in aggression based on AQ scores, reduction in depressive symptoms, and an increase in energy and global functioning |
| Philipsen et al, 200413 | 14 women with BPD given oral clonidine, 75 and 150 µg, while experiencing strong aversive inner tension and urge to commit self-injury | Clonidine significantly decreased aversive inner tension, dissociative symptoms, and urge to commit self-injury as measured by self rated scales |
| Pascual et al, 200414 | A 2-week open-label study of 10 females and 2 males presenting to psychiatric emergency service for self-injurious behavior, aggression/hostility, loss of impulse control, and severe anxiety/depressive symptoms received IM ziprasidone, 20 mg, followed by flexible oral dosing between 40 mg/d and 160 mg/d | 9 patients who completed the study showed statistically significant improvements on CGI-S, HAM-D-17, HAM-A, BPRS, and BIS |
| AQ: Aggression Questionnaire; BIS: Barratt Impulsiveness Scale; BPD: borderline personality disorder; BPRS: Brief Psychiatric Rating Scale; CGI-S: Clinical Global Impressions-Severity of Illness; HAM-A: Hamilton Anxiety Rating scale; HAM-D-17: 17-item Hamilton Depression Rating scale | ||
OUTCOME: Some improvement
Ms. L has no dramatic suicidal gestures for 3 years. Although she continues to engage in self-injurious behaviors, the intensity and frequency are reduced and she does not inflict any serious injury for 18 months. Her mood and behavior continue to oscillate; she is relatively calm and satisfied 1 week, angry and assaultive the next. This stormy course is expected given her BPD diagnosis.
Initially, Ms. L resided in a locked residential unit and was minimally compliant with treatment recommendations and unit policies. As treatment progressed she moved to a different locked unit and eventually to an apartment. Recently, she was placed in a more restrictive setting because her hostile and self-destructive behavior escalated.
The authors’ observations
Ms. L is no different from most Axis II Cluster B disordered patients. During treatment she shows improvement by refraining from self-destructive behaviors for up to 18 months, but she then briefly reverts back to maladaptive behaviors. Ms. L resides in a very structured treatment setting. It is not clear if the gains she made in treatment would have been possible if she was living on her own in the community.
One year after finishing the court-mandated “911 program,” Ms. L lives in the community, draws and paints quite well, attends weekly individual and group therapy, and refrains from self-mutilation. She still experiences volatile moods, but can handle them without inflicting self injury.
Related resources
- Oldham JM. Guideline watch: practice guideline for the treatment of patients with borderline personality disorder. Arlington, VA: American Psychiatric Association; 2005. www.psychiatryonline.com/content.aspx?aID=148722.
- Koenigsberg HW, Kernberg OF, Stone MH, et al. Borderline patients: extending the limits of treatability. New York, NY: Basic Books; 2000.
Drug brand names
- Aripiprazole • Abilify
- Buspirone • Buspar
- Carbamazepine • Tegretol
- Clonidine • Catapres
- Divalproex • Depakote
- Fluoxetine • Prozac
- Fluoxetine-olanzapine • Symbyax
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Pregabalin • Lyrica
- Risperidone • Risperdal
- Topiramate • Topamax
- Valproic acid • Depakene
- Venlafaxine XR • Effexor XR
- Ziprasidone • Geodon
Disclosures
Dr. Hashmi is on the speakers bureau for AstraZeneca, Eli Lilly and Company, and Janssen.
Dr. Vowell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Self-destructive behaviors
After being acquitted of 4 counts of second-degree forgery for writing checks from her mother’s bank account, Ms. L, age 52, is sent to the state hospital for a forensic examination to determine competency. Two years later she is granted conditional release from the hospital, transferred to our not-for-profit community mental health center, and enrolled in an intensive inpatient treatment program to monitor forensic patients. She is legally required to comply with treatment recommendations.
At admission, Ms. L is diagnosed with major depression, recurrent, and borderline personality disorder (BPD). She has no history of antisocial behavior or criminal acts other than forging checks and has never spent time in prison, which makes it unlikely she has co morbid antisocial personality disorder (Table 1).1
Over the next 5 years Ms. L tests limits with the treatment team and acts out by engaging in self-harming behaviors. In 1 instance, she cuts her forearm deeply, stuffs the wound with mayonnaise and paper towels, and wraps her arm with a bandage. She wears a long-sleeved shirt to hide her wound, which is not discovered until a severe infection develops.
Ms. L has difficulty with coping skills and interpersonal relationships. She approaches others with ambivalence and mistrust and consistently expects them to demean or take advantage of her. Ms. L is manipulative, at times injuring herself after perceived wrongdoings by staff. For example, after her therapist reschedules a meeting because of an emergency, Ms. L pours scalding water on her foot.
Table 1
Cluster B personality disorders: Differential diagnosis
| Diagnosis | Features |
|---|---|
| Borderline personality disorder | Self-destructiveness, angry disruptions in close relationships, and chronic feelings of deep emptiness and loneliness |
| Histrionic personality disorder | Attention seeking, manipulative behavior, and rapidly shifting emotions |
| Antisocial personality disorder | Manipulative to gain profit, power, or other material gratification |
| Source: Reference 1 | |
The authors’ observations
Ms. L consistently displays 3 common constructs of BPD:
- primitive defense mechanisms
- identity diffusion
- generally intact reality testing.2
Defense mechanisms are psychological attempts to deal with intrapsychic stress. Splitting—vacillating between extremes of idealization and devaluation—is a fundamental primitive defense mechanism that is the root of BPD.2 Identity diffusion causes confusion about life goals and values and feelings of boredom and emptiness. This internal world leads a patient to have the same perception of the external world, which explains many symptoms of BPD, such as rapidly shifting moods, intense anger, lack of clear sense of self, fear of abandonment, and unstable and intense interpersonal relationships.2
Early in treatment, Ms. L had difficulty breaking a cycle of self-defeating behavior, such as destroying personal items, trying to hang herself, and gluing an ear plug in her ear. During an argument with a staff member, Ms. L punched a wall and fractured her left hand. BPD patients sometimes will “up the ante” when acting out. For example, one of our patients claimed to have planted a bomb in an elementary school and another swallowed inedible objects, including spoons, forks, and butter knives. In Ms. L’s case, we addressed her self-harm behavior by helping her:
- develop less destructive coping skills such as drawing or painting
- identify irrational thoughts that contribute to self harm.
HISTORY: Troubled past
Raised by her biologic parents, Ms. L met all developmental milestones. She denies a history of childhood abuse but reports experiencing “depression and memory loss” and relationship problems with her parents during adolescence. As a child she often missed school because she “did not want anyone to know what a disgusting person I was” and “I should have my head cut open and cut into little pieces for thinking such mean thoughts.” Ms. L dropped out of school in the twelfth grade but obtained her general educational development certificate.
Notes and letters Ms. L wrote while in treatment consistently refer to her negative self-image. Ms. L writes that she feels she does not deserve to “be a part of this world,” is “never good enough for anyone,” and “should be thrown away with the garbage.”
Ms. L vacillates between desiring a closer relationship with her parents, especially her mother, and wanting to “cut them out of my life for good.” She has minimal contact with her older sister. Ms. L is divorced and has 2 adult sons. She was involved sporadically in her sons’ lives when they were children, but now has no contact with them.
BPD and crime
Ms. L is enrolled in the “911 program,” which monitors individuals who have been found not guilty by reason of mental defect. Individuals with BPD often are convicted of serious and violent crimes, which may be because of BPD features such as interpersonal hostility and self-harm. Impulsivity, substance abuse, and parental neglect—all of which are associated with BPD—can increase risk of criminality.3 There is no evidence to suggest a direct link between BPD and criminality; however, over-representation of BPD in prison populations suggest that in severe cases it may increase criminogenic risk.1,3
TREATMENT: Worsened depression
When Ms. L arrives at our facility, her medication regimen includes fluoxetine, 80 mg/d, risperidone, 2 mg/d, and buspirone, 20 mg/d. Risperidone and buspirone are discontinued because of perceived lack of efficacy. Venlafaxine XR is added and titrated to 300 mg/d, and Ms. L receives lorazepam, 1 and 2 mg as needed. However, lorazepam carries risks because impulsivity and impaired judgment—which are common in BPD—can lead to dependence and abuse. We feel that in a supervised setting the risks can be managed.
Recently, staff witnessed Ms. L experiencing an episode that appeared to be a grand mal seizure. After Ms. L is evaluated at the local emergency room, her EEG is normal, but a neurologic consult recommends discontinuing fluoxetine or venlafaxine XR because they may have contributed to the seizure. We taper and discontinue venlafaxine XR but Ms. L complains bitterly that she is getting increasingly depressed. On several occasions she attempts to pit team members against each other.
Ms. L falls, injures her back, and begins to abuse opiates. After her prescription runs out, she obtains more from an intellectually limited patient in her treatment program. Ms. L says she is getting more depressed, threatens suicide, and is placed in a more restrictive in-patient setting. We consider adding pregabalin to address her pain and help with anxiety and impulse control but the consulting neurologist prescribes carbamazepine, 400 mg/d, and her pain improves.5,6
The authors’ observations
BPD treatment primarily is psychotherapeutic and emphasizes skill building (Table 2) with focused, symptom-targeted pharmacotherapy as indicated.4 Pharmacotherapy typically targets 3 domains:
- affective dysregulation
- impulsive-behavioral dyscontrol symptoms
- cognitive-perceptual symptoms.
Patients with prominent anxiety may benefit from benzodiazepines, although research on these agents for BPD is limited. Recent studies show efficacy with fluoxetine, olanzapine, or a combination of both,7 and divalproex.8 Preliminary data supports the use of topiramate, quetiapine, risperidone, ziprasidone, lamotrigine, and clonidine (Table 3).9-14 A recent review and meta-analysis showed efficacy with topira-mate, lamotrigine, valproate, aripiprazole, and olanzapine.15
For Ms. L, we restart venlafaxine at a lower dose of 50 mg/d and titrate it to 150 mg/d, which is still lower than her previous dose of 300 mg/d. She has no recurrence of seizures and her depression improves.
Table 2
Features of psychotherapeutic modalities for BPD
| Description | Mode of treatment | Skills taught | |
|---|---|---|---|
| Dialectical behavior therapy | Manualized, time-limited, cognitive-behavioral approach based on the biosocial theory of BPD | Individual therapy, group skills training, telephone contact, and therapist consultation | Core mindfulness skills, interpersonal effectiveness skills, emotion modulation skills, and distress tolerance skills |
| Systems Training for Emotional Predictability and Problem Solving | Manual-based, group treatment that includes a systems component to train family members, friends, and significant others | 20-week basic skills group and a 1-year, twice-monthly advanced group program; utilizes a classroom ‘seminar’ format | Awareness of illness, emotion management skills, and behavior management skills |
| BPD: borderline personality disorder | |||
Table 3
Pharmacotherapy for BPD: What the evidence says
| Study | Design | Results |
|---|---|---|
| Hollander et al, 20039 | 96 patients with Cluster B personality disorders randomized to divalproex or placebo for 12 weeks | Divalproex was superior to placebo in treating impulsive aggression, irritability, and global severity |
| Hilger et al, 200310 | Case report of 2 women with BPD and severe self-mutilation receiving quetiapine monotherapy | Quetiapine resulted in a marked improvement of impulsive behavior and overall level of function |
| Rizvi, 200211 | Case report of a 14-year-old female with borderline personality traits admitted to an inpatient facility for suicide attempt, impulsive behavior, and mood lability. Lamotrigine was started at 25 mg/d and titrated to 200 mg/d. At admission, she was receiving clonazepam, valproic acid, quetiapine, and fluoxetine, which were tapered and discontinued | Over 6 months of inpatient treatment, suicidal behavior and ideation diminished and impulse control and mood lability improved; continued improvement at 1-year follow up |
| Rocca et al, 200212 | 15 BPD outpatients with aggressive behavior given risperidone (mean dose 3.27 mg/d) in an 8-week open-label study | Risperidone produced a significant reduction in aggression based on AQ scores, reduction in depressive symptoms, and an increase in energy and global functioning |
| Philipsen et al, 200413 | 14 women with BPD given oral clonidine, 75 and 150 µg, while experiencing strong aversive inner tension and urge to commit self-injury | Clonidine significantly decreased aversive inner tension, dissociative symptoms, and urge to commit self-injury as measured by self rated scales |
| Pascual et al, 200414 | A 2-week open-label study of 10 females and 2 males presenting to psychiatric emergency service for self-injurious behavior, aggression/hostility, loss of impulse control, and severe anxiety/depressive symptoms received IM ziprasidone, 20 mg, followed by flexible oral dosing between 40 mg/d and 160 mg/d | 9 patients who completed the study showed statistically significant improvements on CGI-S, HAM-D-17, HAM-A, BPRS, and BIS |
| AQ: Aggression Questionnaire; BIS: Barratt Impulsiveness Scale; BPD: borderline personality disorder; BPRS: Brief Psychiatric Rating Scale; CGI-S: Clinical Global Impressions-Severity of Illness; HAM-A: Hamilton Anxiety Rating scale; HAM-D-17: 17-item Hamilton Depression Rating scale | ||
OUTCOME: Some improvement
Ms. L has no dramatic suicidal gestures for 3 years. Although she continues to engage in self-injurious behaviors, the intensity and frequency are reduced and she does not inflict any serious injury for 18 months. Her mood and behavior continue to oscillate; she is relatively calm and satisfied 1 week, angry and assaultive the next. This stormy course is expected given her BPD diagnosis.
Initially, Ms. L resided in a locked residential unit and was minimally compliant with treatment recommendations and unit policies. As treatment progressed she moved to a different locked unit and eventually to an apartment. Recently, she was placed in a more restrictive setting because her hostile and self-destructive behavior escalated.
The authors’ observations
Ms. L is no different from most Axis II Cluster B disordered patients. During treatment she shows improvement by refraining from self-destructive behaviors for up to 18 months, but she then briefly reverts back to maladaptive behaviors. Ms. L resides in a very structured treatment setting. It is not clear if the gains she made in treatment would have been possible if she was living on her own in the community.
One year after finishing the court-mandated “911 program,” Ms. L lives in the community, draws and paints quite well, attends weekly individual and group therapy, and refrains from self-mutilation. She still experiences volatile moods, but can handle them without inflicting self injury.
Related resources
- Oldham JM. Guideline watch: practice guideline for the treatment of patients with borderline personality disorder. Arlington, VA: American Psychiatric Association; 2005. www.psychiatryonline.com/content.aspx?aID=148722.
- Koenigsberg HW, Kernberg OF, Stone MH, et al. Borderline patients: extending the limits of treatability. New York, NY: Basic Books; 2000.
Drug brand names
- Aripiprazole • Abilify
- Buspirone • Buspar
- Carbamazepine • Tegretol
- Clonidine • Catapres
- Divalproex • Depakote
- Fluoxetine • Prozac
- Fluoxetine-olanzapine • Symbyax
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Pregabalin • Lyrica
- Risperidone • Risperdal
- Topiramate • Topamax
- Valproic acid • Depakene
- Venlafaxine XR • Effexor XR
- Ziprasidone • Geodon
Disclosures
Dr. Hashmi is on the speakers bureau for AstraZeneca, Eli Lilly and Company, and Janssen.
Dr. Vowell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Diagnostic and statistical manual of mental disorders, 4th ed, text revision. Washington, DC: American Psychiatric Association; 2000.
2. Koenigsberg HW, Kernberg OF, Stone MH, et al. Borderline patients: extending the limits of treatability. New York, NY: Basic Books; 2000.
3. Nee C, Farman S. Female prisoners with borderline personality disorder: some promising treatment developments. Crim Behav Ment Health. 2005;15:2-16.
4. Oldham JM, Bender DS, Skodol AE, et al. Testing an APA practice guideline: symptom-targeted medication utilization for patients with borderline personality disorder. J Psychiatr Pract. 2004;10:156-161.
5. American Psychiatric Association Practice Guidelines. Practice guideline for the treatment of patients with borderline personality disorder. Am J Psychiatry. 2001;158(suppl 10):1-52.
6. Yatham LN. Newer anticonvulsants in the treatment of bipolar disorder. J Clin Psychiatry. 2004;65(suppl 10):28-35.
7. Rinne T, van den Brink W, Wouters L, et al. SSRI treatment of borderline personality disorder: a randomized, placebo-controlled clinical trial for female patients with borderline personality disorder. Am J Psychiatry. 2002;159(12):2048-2054.
8. Zanarini MC, Frankenburg FR, Parachini EA. A preliminary, randomized trial of fluoxetine, olanzapine, and the olanzapine-fluoxetine combination in women with borderline personality disorder. J Clin Psychiatry. 2004;65(7):903-907.
9. Hollander E, Tracy KA, Swann AC, et al. Divalproex in the treatment of impulsive aggression: efficacy in cluster B personality disorders. Neuropsychopharmacology. 2003;28(6):1186-1197.
10. Hilger E, Barnas C, Kasper S. Quetiapine in the treatment of borderline personality disorder. World J Biol Psychiatry. 2003;4(1):42-44.
11. Rizvi ST. Lamotrigine and borderline personality disorder. J Child Adolesc Psychopharmacol. 2002;12(4):365-366.
12. Rocca P, Marchiaro L, Cocuzza E, et al. Treatment of borderline personality disorder with risperidone. J Clin Psychiatry. 2002;63(3):241-244.
13. Philipsen A, Richter H, Schmahl C, et al. Clonidine in acute aversive inner tension and self-injurious behavior in female patients with borderline personality disorder. J Clin Psychiatry. 2004;65(10):1414-1419.
14. Pascual JC, Oller S, Soler J, et al. Ziprasidone in the acute treatment of borderline personality disorder in psychiatric emergency services. J Clin Psychiatry. 2004;65(9):1281-1282.
15. Lieb K, Völlm B, Rücker G, et al. Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials. Br J Psychiatry. 2010;196(1):4-12.
1. Diagnostic and statistical manual of mental disorders, 4th ed, text revision. Washington, DC: American Psychiatric Association; 2000.
2. Koenigsberg HW, Kernberg OF, Stone MH, et al. Borderline patients: extending the limits of treatability. New York, NY: Basic Books; 2000.
3. Nee C, Farman S. Female prisoners with borderline personality disorder: some promising treatment developments. Crim Behav Ment Health. 2005;15:2-16.
4. Oldham JM, Bender DS, Skodol AE, et al. Testing an APA practice guideline: symptom-targeted medication utilization for patients with borderline personality disorder. J Psychiatr Pract. 2004;10:156-161.
5. American Psychiatric Association Practice Guidelines. Practice guideline for the treatment of patients with borderline personality disorder. Am J Psychiatry. 2001;158(suppl 10):1-52.
6. Yatham LN. Newer anticonvulsants in the treatment of bipolar disorder. J Clin Psychiatry. 2004;65(suppl 10):28-35.
7. Rinne T, van den Brink W, Wouters L, et al. SSRI treatment of borderline personality disorder: a randomized, placebo-controlled clinical trial for female patients with borderline personality disorder. Am J Psychiatry. 2002;159(12):2048-2054.
8. Zanarini MC, Frankenburg FR, Parachini EA. A preliminary, randomized trial of fluoxetine, olanzapine, and the olanzapine-fluoxetine combination in women with borderline personality disorder. J Clin Psychiatry. 2004;65(7):903-907.
9. Hollander E, Tracy KA, Swann AC, et al. Divalproex in the treatment of impulsive aggression: efficacy in cluster B personality disorders. Neuropsychopharmacology. 2003;28(6):1186-1197.
10. Hilger E, Barnas C, Kasper S. Quetiapine in the treatment of borderline personality disorder. World J Biol Psychiatry. 2003;4(1):42-44.
11. Rizvi ST. Lamotrigine and borderline personality disorder. J Child Adolesc Psychopharmacol. 2002;12(4):365-366.
12. Rocca P, Marchiaro L, Cocuzza E, et al. Treatment of borderline personality disorder with risperidone. J Clin Psychiatry. 2002;63(3):241-244.
13. Philipsen A, Richter H, Schmahl C, et al. Clonidine in acute aversive inner tension and self-injurious behavior in female patients with borderline personality disorder. J Clin Psychiatry. 2004;65(10):1414-1419.
14. Pascual JC, Oller S, Soler J, et al. Ziprasidone in the acute treatment of borderline personality disorder in psychiatric emergency services. J Clin Psychiatry. 2004;65(9):1281-1282.
15. Lieb K, Völlm B, Rücker G, et al. Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials. Br J Psychiatry. 2010;196(1):4-12.
Lowering risk of Alzheimer’s disease
Pharmacologic treatments for Alzheimer’s disease (AD) may improve symptoms but have not been shown to prevent AD onset. Primary prevention therefore remains the goal. Although preventing AD by managing risk factors such as age or genetics is beyond our control (Box 1), we can do something about other factors.
This article summarizes the findings of many studies that address AD prevention and includes an online-only bibliography for readers seeking an in-depth review. The evidence does not support a firm recommendation for any specific form of primary prevention and has revealed hazards associated with estrogen therapy and nonsteroidal anti-inflammatory drugs (Box 2). Most important, it suggests that you could reduce your patients’ risk of developing AD by routinely supporting their mental, physical, and social health.
The potential benefits of modifying an individual’s AD risk factors likely will depend on his or her genetic makeup, environment, and lifestyle. Even so, counseling patients to exercise more and improve their diets—such as by eating more fish, fruits, and vegetables and less saturated fat—might help protect the brain. Your ongoing efforts to manage hypertension, hypercholesterolemia, and diabetes also may reduce their AD risk.
Age remains the strongest risk factor for dementia, particularly for Alzheimer’s disease (AD).a The risk of developing AD doubles every 5 years after age 65 and approaches 50% after age 85.b
Family history is a risk factor for AD, although true familial AD accounts for <5% of cases.c When diseases show a familial pattern, either genetics, environmental factors, or both may play a role. Patients with a first-degree relative with dementia have a 10% to 30% increased risk of developing the disorder.d
Genetic factors play a role in both early-onset and late-onset AD. Early-onset AD (before age 65) accounts for 6% to 7% of cases.e From this small pool of patients, only 13% exhibit clear autosomal dominant transmission over >1 generation.f Three gene mutations have been associated with early-onset AD:
- 30% to 70% are in the presenilin-1 gene
- 10% to 15% are in the amyloid precursor protein gene
- <5% are in the presenilin-2 gene.g,h
For late-onset AD (after age 65), the strongest evidence for a genetic risk factor exists for the epsilon 4 allele of the apolipoprotein E gene (APOE e4).i This genotype has been linked to the development of AD and possibly to vascular dementia.j,k In contrast, the epsilon 2 allele of APOE may exert a protective effect in AD.l APOE e3, the most common allele, appears to play a neutral role in the development of AD.
References
a. Evans DA. The epidemiology of dementia and Alzheimer’s disease: an evolving field. J Am Geriatr Soc. 1996;44:1482-1483.
b. Jorm AF, Jolley D. The incidence of dementia: a meta-analysis. Neurology. 1998;51:728-733.
c. van Duijn CM, Clayton D, Chandra V, et al. Familial aggregation of Alzheimer’s disease and related disorders: a collaborative re-analysis of case-control studies. EURODEM Risk Factors Research Group. Int J Epidemiol. 1991;20(suppl 2):S13-S20.
d. Chang JB, Wang PN, Chen WT, et al. ApoE epsilon4 allele is associated with incidental hallucinations and delusions in patients with AD. Neurology. 2004;63:1105-1107.
e. Sleegers K, Roks G, Theuns J, et al. Familial clustering and genetic risk for dementia in a genetically isolated Dutch population. Brain. 2004;127:1641-1649.
f. Schoenberg BS, Anderson DW, Haerer AF. Severe dementia. Prevalence and clinical features in a biracial US population. Arch Neurol. 1985;42:740-743.
g. Hsiung GY, Sadovnick AD. Genetics and dementia: risk factors, diagnosis and management. Alzheimers Dement. 2007;3:418-427.
h. GeneTests database. Available at: http://www.genetests.org. Accessed March 19, 2010.
i. Li H, Wetten S, Li L, et al. Candidate single-nucleotide polymorphisms from a genomewide association study of Alzheimer disease. Arch Neurol. 2008;65:45-53.
j. Graff-Radford NR, Green RC, Go RC, et al. Association between apolipoprotein E genotype and Alzheimer disease in African American subjects. Arch Neurol. 2002;59:594-600.
k. Slooter AJ, Cruts M, Hofman A, et al. The impact of APOE on myocardial infarction, stroke, and dementia: the Rotterdam Study. Neurology. 2004;62:1196-1198.
l. Tiraboschi P, Hansen LA, Masliah E, et al. Impact of APOE genotype on neuropathologic and neurochemical markers of Alzheimer disease. Neurology. 2004;62:1977-1983.
Estrogen. Before the Women’s Health Initiative (WHI) study, various trials of the effects of estrogen therapy on the development of Alzheimer’s disease (AD) in women age ≥65 showed inconsistent results. In the randomized, placebo-controlled WHI Memory Study, conjugated equine estrogen, 0.625 mg/d, plus medroxyprogesterone acetate, 2.5 mg/d, did not prevent mild cognitive impairment or improve global cognitive function and was associated with an increased risk for probable dementia.a Based on this evidence, conjugated equine estrogen with or without medroxyprogesterone is not recommended as therapy to protect cognitive function in older women.
NSAID therapy. Cytokine-mediated inflammation may play a role in neurodegenerative disorders and cognitive impairment in the elderly. Nonsteroidal anti-inflammatory drugs (NSAIDs), including cyclooxygenase-2 (COX-2) inhibitors, have been studied for a possible protective effect against AD and cognitive decline,b possibly by lowering amyloidogenic proteins.c A 1-year randomized controlled trial by the Alzheimer’s Disease Cooperative Consortium found no significant differences in cognition scores of patients treated with once-daily rofecoxib, 25 mg, or twice-daily naproxen sodium, 220 mg, when compared with placebo.d Similarly, naproxen and celecoxib did not prevent AD in the randomized, controlled Alzheimer’s Disease Anti-inflammatory Prevention Trial (ADAPT).e Rofecoxib has been withdrawn from the market, and celecoxib labeling carries a warning of potential for increased risk of cardiovascular events and life-threatening gastrointestinal bleeding associated with its use.
NSAIDs and COX-2 inhibitors are not recommended for the treatment or prevention of dementia or cognitive impairment. Their use for AD prevention is not supported by randomized clinical trialsd,e and they may have serious adverse effects.
References
a. Shumaker SA, Legault C, Kuller L, et al. Conjugated equine estrogens and incidence of probable dementia and mild cognitive impairment in postmenopausal women: Women’s Health Initiative Memory Study. JAMA. 2004;291:2947-2958.
b. Szekely CA, Breitner JC, Fitzpatrick AL, et al. NSAID use and dementia risk in the Cardiovascular Health Study: role of APOE and NSAID type. Neurology. 2008;70:17-24.
c. Weggen S, Eriksen JL, Das P, et al. A subset of NSAIDs lower amyloidogenic Abeta42 independently of cyclooxygenase activity. Nature. 2001;414:212-216.
d. Aisen PS, Schafer KA, Grundman M, et al. Effects of rofecoxib or naproxen vs placebo on Alzheimer disease progression: a randomized controlled trial. JAMA. 2003;289(21):2819-2826.
e. ADAPT Research Group, Martin BK, Szekely C, Brandt J, et al. Cognitive function over time in the Alzheimer’s Disease Anti-inflammatory Prevention Trial (ADAPT): results of a randomized, controlled trial of naproxen and celecoxib. Arch Neurol. 2008;65(7):896-905.
Cardiovascular risk factors
The risk of developing AD or vascular dementia appears to be increased by conditions that damage the heart or blood vessels. Recent evidence suggests that successfully managing cardiovascular risk factors may decrease the likelihood of dementia in later life.
Hypertension is associated with a higher risk of AD and all-cause dementia. Curiously, some studies have shown that low blood pressure also increases dementia risk, suggesting a U-shaped relationship between blood pressure and cognitive decline. Systolic hypertension in midlife may be associated with dementia 20 years later.
One might assume that antihypertensive therapy would help prevent dementia, but the data are conflicting. The Systolic Hypertension in Europe (SYST-EUR) study1 showed a 53% reduction in vascular dementia or mixed dementia among patients receiving antihypertensive medication and a 60% reduction in AD. Similarly, the PROGRESS2 clinical trial of prevention of recurrent stroke by antihypertensive treatment reported a 34% reduction in a composite measure of cognitive impairment and dementia. On the other hand, cognitive function neither improved nor worsened in the Hypertension in the Very Elderly Trial (HYVET-COG),3 whether patients received blood pressure treatment or placebo.
Hyperlipidemia. Lipid metabolism likely is an important pathway in amyloid beta-protein deposition, tau phosphorylation, and disruption of synaptic plasticity and neurodegenerative endpoints. Cognitive decline and incident dementia have been associated with higher dietary intake of saturated fats, partially hydrogenated unsaturated fatty acids (trans fats), and cholesterol. Not all studies have found this association, however. This could be because serum cholesterol levels may decrease in early dementia, limiting the ability to detect an effect of hypercholesterolemia on dementia risk when measurements are made later in life.
Using statins (3-hydroxy-3-methylglutaryl–coenzyme A reductase inhibitors) to treat hypercholesterolemia has been hypothesized to impede large vessel atherosclerosis and its consequences and to trigger metabolic effects in the brain related to AD pathogenesis. Mechanisms by which statins might help prevent dementia include:
- a direct association between amyloid processing and cholesterol in the brain
- an indirect effect by decreasing the risk of stroke, as even small cerebral infarcts worsen AD severity.
Nonrandomized epidemiologic studies such as the Cardiovascular Health Study4 and MRC/BHF Heart Protection Study5 suggested that statin treatment might reduce the incidence of dementia, the degree of age-related cognitive decline, and AD’s neuropathologic burden. Large, randomized, controlled trials have not supported these observations, however. Statins failed to reduce the incidence of dementia in:
- the Heart Protection Study, testing simvastatin for 5 years in 20,536 subjects age 40 to 805
- the 3-year Preventive Study of Pravastatin in the Elderly at Risk (PROSPER) of 5,800 subjects.6
Similarly, patients receiving adjunctive atorvastatin or placebo showed no significant differences in cognition assessments after 72 weeks in the Lipitor’s Effect in Alzheimer’s Dementia (LEADe) study. This trial enrolled 640 subjects age 50 to 90 with mild-to-moderate dementia who were treated with donepezil.7 A recent Cochrane review concluded that high serum cholesterol may contribute to the development of AD and vascular dementia, but lowering cholesterol levels with statins does not prevent these problems.8
Diabetes mellitus. Diabetes and cognitive decline are closely associated. Diabetes is associated with a 50% to 100% increase in risk of AD and dementia overall and a 100% to 150% increased risk of vascular dementia. The mechanism by which diabetes increases dementia risk is uncertain but does not appear to be mediated entirely through vascular disease. High and low insulin levels may increase the risk of dementia, independent of diabetes and blood glucose. Increased peripheral insulin levels are associated with reduced brain atrophy and cognitive impairment in patients with early AD, suggesting a role for insulin signaling in AD pathophysiology. A possible relationship between insulin and beta amyloid metabolism is being studied.
Elevated postprandial plasma glucose has been associated with accelerated declines in cognitive performance.9 An inverse correlation has been noted between some cognitive measures and hemoglobin A1C levels.10 It is not clear that treating diabetes reduces the risk of dementia. In addition, in the prospective, population-based Rotterdam study, elderly patients with type 2 diabetes treated with insulin had the highest incidence of dementia.11
Tobacco smoke directly affects neuronal function, integrity, and survival. Chronic smoking has been linked to decreased global cerebral blood flow, accelerated cerebral atrophy, and ventricular enlargement.
Some studies suggest an increased risk of dementia in middle-aged and elderly smokers, possibly through a cerebrovascular mechanism such as stroke. Other studies found no association between smoking and dementia risk, and 1 suggested that nicotine may protect against AD by reducing senile plaque formation. Any protective effect of smoking would be offset by increased risks of lung cancer, chronic obstructive pulmonary disease, and vascular dementia.
The apolipoprotein E epsilon 4 (APOE e4) gene may explain, at least in part, the conflicting results of these studies. In 2 population-based cohorts,12,13 smoking was associated with memory decline in patients without, but not with, the APOE e4 genotype.
Dietary factors
Antioxidants. The brains of patients with AD contain elevated levels of endogenous antioxidants. In vitro studies show exogenous antioxidants can reduce the toxicity of beta-amyloid in brain tissue of persons with AD. These findings have led to interest in assessing the role of dietary antioxidants such as vitamins E and C for AD prevention.
High-dose alpha-tocopherol (vitamin E, 2,000 IU/d) may slow disease progression in patients with AD, but this association is not consistently found. Furthermore, a meta-analysis of 19 randomized controlled trials (RCTs) totaling >135,000 patients found an association between vitamin E doses >400 IU/d and increased all-cause mortality.14 High-dose vitamin E supplementation for primary or secondary prevention of AD may be dangerous and is not recommended.
The lack of consistent efficacy data for vitamin C in preventing or treating AD may discourage its routine use for this purpose.15
Homocysteine is a risk factor for stroke and heart disease. It also could play a role in vascular dementia through its association with large- and small-vessel disease.
Low folate and hyperhomocysteinemia have been associated with dementia or cognitive impairment, although a cause-effect relationship is not clear. In non-demented elderly populations, plasma homocysteine is inversely associated with poor performance in tests of global cognitive function, particularly in measures of psychomotor speed.
In a recent double-blind RCT, folic acid supplementation for 3 years significantly improved domains of cognitive function that tend to decline with age, especially information processing and sensorimotor speed.16 No other good evidence, however, has shown that homocysteine-lowering therapy using folic acid or other vitamin B supplements improves cognitive function or prevents cognitive decline.
Fish and omega-3 fatty acids. High total fat, saturated fat, and total cholesterol intake increases the risk for incident dementia. In epidemiologic studies, low omega-3 fatty acid serum levels have been linked to increased dementia risk.
Fish consumption may be beneficial in reducing the risk of dementia or cognitive decline. A prospective study of 815 elderly persons found 60% less risk of developing AD in those who ate ≥1 fish meal per week, compared with those who rarely or never ate fish.17 In the Framingham study, individuals who at baseline were in the top quartile of docosahexaenoic acid consumption had lower dementia rates over 9 years of follow-up.18 Results from cross-sectional and longitudinal studies have been inconsistent; some have shown that high intake of n-3 polyunsaturated fatty acids is associated with less cognitive decline,19 whereas others have not.20
Although we cannot offer unequivocal advice regarding seafood or omega-3 fatty acid intake for primary prevention of dementia without evidence from RCTs, these uncontrolled studies show promise.
Mediterranean diet (MeDi) components include abundant fruits and vegetables, fish or shellfish at least twice weekly, very limited red meat, olive oil or canola oil instead of butter or margarine, tree nuts such as walnuts or pecans, red wine in moderation, and using herbs and spices instead of salt to season food. High adherence to the MeDi has been associated with a significantly lower risk for incident AD. The MeDi may affect the risk of developing AD21 as well as subsequent disease course, with a possible dose-response relationship in lower mortality.22
Eating fruits and vegetables has been associated with improved cognitive performance22 and decreased incident dementia in elderly subjects.18
Alcohol. A U-shaped relationship exists between alcohol consumption and dementia risk. High alcohol intake is associated with clinical problem drinking and alcoholism and can lead to cognitive decline. Conversely, moderate wine consumption (250 to 500 mL/d) may be protective—compared with more or less than this amount—and is associated with approximately 50% less risk of dementia.
Alcohol use may increase the risk of dementia in persons carrying the APOE e4 allele, according to the population-based Cardiovascular Risk Factors, Aging and Dementia (CAIDE) study from Sweden.23 After an average 21 years of follow-up of 1,449 individuals, researchers found that environmental factors—such as physical inactivity, dietary fat intake, alcohol consumption, and smoking at midlife—were associated with an increased risk of dementia at age 65 to 79 in APOE e4 carriers compared with noncarriers. The study also found that physical inactivity, dietary fat intake, and smoking at midlife increase AD risk, especially among APOE e4 carriers.
In the absence of evidence from RCTs, we cannot recommend alcohol to reduce the risk of AD.
Lifestyle and activity
Three components of lifestyle—social, mental, and physical activity—are inversely associated with the risk for dementia, AD, and cognitive impairment.
Physical exercise has been thought to enhance brain neurotrophic factor and modify apoptosis. Exercise can deter stroke and microvascular disease and improve regional cerebral blood flow. In the Cardiovascular Health Study, participants who expended the highest quartile of energy had a lower risk of all-cause dementia and AD compared with participants who expended the lowest quartile of energy.24
Mental and social activity. Epidemiologic studies have shown associations between higher educational achievement and other socioeconomic factors and reduced AD risk. Advanced education is believed to represent a cognitive reserve that delays presentation of AD’s effects on memory and cognitive function, rather than providing a protective effect against accumulation of AD pathology. Higher-educated individuals appear to experience a somewhat more rapid rate of cognitive decline when AD does become apparent, perhaps because they have accumulated a greater degree of AD pathology at that point compared with less-educated persons.
Among 117 persons with dementia in the Bronx Aging Study, each additional year of formal education delayed the time of accelerated decline by 0.21 years. After accelerated decline began, each year of additional formal education was associated with a slightly faster rate of memory decline.25
The longitudinal, population-based Kungsholmen Project in Stockholm, Sweden, found an association between daily mentally stimulating activities and decreased risk of all-cause dementia.26 Similarly, higher levels of leisure activity were linked to reduced risk of all-cause dementia in a longitudinal study of 1,772 persons age ≥65 living in Manhattan, NY.27 In a randomized, single-controlled study of the long-term effects of cognitive training, elderly individuals from 6 U.S. cities showed sustained improvement in specific cognitive performance up to 5 years after training sessions began, including memory, reasoning, and speed of processing.28
It seems reasonable to encourage older patients to maintain or increase physical, cognitive, and leisure activities as well as social interaction. These interventions can improve the quality of life and lower the risk of depression, which may be a response to cognitive decline or an independent risk factor for dementia (Box 3). The Table lists “brain exercises” you can suggest to patients to increase their mental and social activity.
Head trauma. The Multi-Institutional Research in Alzheimer’s Genetic Epidemiology (MIRAGE) project found an association between AD risk and a history of head trauma, especially in persons with APOE e4 alleles.29 Conversely, the Rotterdam Study showed no change in dementia risk for persons with a history of head trauma.30
Even in the absence of conclusive evidence supporting AD prevention, protecting the head by buckling seat belts while driving, wearing helmets when participating in sports, and “fall-proofing” the home is recommended.
Depression often occurs before or as a coexisting condition with Alzheimer’s disease (AD).a Although depression has been considered a response to cognitive decline or an early manifestation of dementia,b it also could be an independent risk factor.c,d
The pathologic mechanism linking depression and subsequent dementia is not well understood. Hypotheses include an indirect neurotoxic effect of depression mediated by cortisol-induced hippocampal atrophy or lowered brain-derived neurotrophic factor levels.e Depression and dementia might share genetic links, although a cohort study of 404 individuals with AD detected no association between apolipoprotein E genotypes or alleles and depressive symptoms.f
References
a. Lupien SJ, Nair NP, Brière S, et al. Increased cortisol levels and impaired cognition in human aging: implication for depression and dementia in later life. Rev Neurosci. 1999;10(2):117-139.
b. Preuss UW, Siafarikas N, Petrucci M, et al. Depressive disorders in dementia and mild cognitive impairments: is comorbidity a cause or a risk factor? Fortschr Neurol Psychiatr. 2009;77:399-406.
c. Green RC, Cupples LA, Kurz A, et al. Depression as a risk factor for Alzheimer disease: the MIRAGE Study. Arch Neurol. 2003;60(5):753-759.
d. Ownby RL, Crocco E, Acevedo A, et al. Depression and risk for Alzheimer’s disease: systematic review, meta-analysis, and metaregression analysis. Arch Gen Psychiatry. 2006;63(5):530-538.
e. Meeks TW, Ropacki SA, Jeste DV. The neurobiology of neuropsychiatric syndromes in dementia. Curr Opin Psychiatry. 2006;19(6):581-586.
f. Craig D, Hart DJ, McIlroy SP, et al. Association analysis of apolipoprotein E genotype and risk of depressive symptoms in Alzheimer’s disease. Dement Geriatr Cogn Disord. 2005;19(2-3):154-157.
Table
Brain exercises to suggest to patients
| Learn something new (how to play a musical instrument, a foreign language, or a new hobby) |
| Play memory games |
| Practice using the opposite hand to perform tasks you usually do with your dominant hand |
| Read, especially challenging material |
| Join a book discussion group |
| Write; if not a book or article, write a diary, letters, or emails or start your memoirs |
| Do crossword, Sudoku, or jigsaw puzzles |
| Play board games, card games, and other strategy games |
| Debate or discuss topics |
Related resource
- For an extensive bibliography of literature on Alzheimer’s disease risk factors and prevention, see this article at CurrentPsychiatry.com.
Drug brand names
- Atorvastatin • Lipitor
- Celecoxib • Celebrex
- Donepezil • Aricept
- Medroxyprogesterone • Provera
- Pravastatin • Pravachol
- Rofecoxib • Vioxx
- Simvastatin • Zocor
Disclosures
Dr. Bassil reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Grossberg receives research/grant support from and is a consultant to Bristol-Myers Squibb, Forest Pharmaceuticals, Novartis, Pfizer Inc., and Wyeth Pharmaceuticals. He also receives research/grant support from Baxter.
1. Forette F, Seux ML, Staessen JA, et al. The prevention of dementia with antihypertensive treatment: new evidence from the systolic hypertension in Europe (Syst-Eur) study. Arch Intern Med. 2002;162:2046-2052.
2. Tzourio C, Anderson C, Chapman N, et al. Effects of blood pressure lowering with perindopril and indapamide therapy on dementia and cognitive decline in patients with cerebrovascular disease. Arch Intern Med. 2003;163:1069-1075.
3. Peters R, Beckett N, Forette F. Incident dementia and blood pressure lowering in the Hypertension in the Very Elderly Trial cognitive function assessment (HYVET-COG). Lancet Neurol. 2008;7(8):683-689.
4. Rea TD, Breitner JC, Psaty BM, et al. Statin use and the risk of incident dementia: the Cardiovascular Health Study. Arch Neurol. 2005;62:1047-1051.
5. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002;360:7-22.
6. Kulbertus H, Scheen AJ. [The PROSPER Study (PROspective study of pravastatin in the elderly at risk)]. Rev Med Liege. 2002;57(12):809-813.
7. Feldman HH, Doody RS, Kivipelto M, et al. Randomized controlled trial of atorvastatin in mild to moderate Alzheimer disease: LEADe. Neurology. 2010;74(12):956-964.
8. McGuinness B, Bullock R, Craig D, et al. Statins for the treatment of Alzheimer’s disease and dementia (protocol). Cochrane Database Syst Rev. 2009;1:CD007514.-
9. Abbatecola AM, Rizzo MR, Barbieri M, et al. Postprandial plasmaglucose excursions and cognitive functioning in aged type 2 diabetics. Neurology. 2006;67:235-240.
10. Munshi M, Grande L, Hayes M, et al. Cognitive dysfunction is associated with poor diabetes control in older adults. Diabetes Care. 2006;29:1794-1799.
11. Ott A, Stolk RP, van Harskamp F, et al. Diabetes mellitus and the risk of dementia. The Rotterdam study. Neurology. 1999;53:1937-1942.
12. Reitz C, Luchsinger J, Tang MX, et al. Effect of smoking and time on cognitive function in the elderly without dementia. Neurology. 2005;65:870-875.
13. Reitz C, den Heijer T, van Duijn C, et al. Relation between smoking and risk of dementia and Alzheimer disease: the Rotterdam Study. Neurology. 2007;69:998-1005.
14. Miller ER, III, Pastor-Barriuso R, Dalal D, et al. Meta-analysis: high-dosage vitamin E supplementation may increase all-cause mortality. Ann Intern Med. 2005;142(1):37-46.
15. Boothby LA, Doering PL. Vitamin C and vitamin E for Alzheimer’s disease. Ann Pharmacother. 2005;39(12):2073-2080.
16. Durga J, van Boxtel MP, Schouten EG, et al. Effect of 3-year folic acid supplementation on cognitive function in older adults in the FACIT trial: a randomised, double blind, controlled trial. Lancet. 2007;369:208-216.
17. Morris MC, Evans DA, Bienias JL, et al. Consumption of fish and n-3 fatty acids and risk of incident Alzheimer disease. Arch Neurol. 2003;60:940-946.
18. Schaefer EJ, Bongard V, Beiser AS, et al. Plasma phosphatidylcholine docosahexaenoic acid content and risk of dementia and Alzheimer disease: the Framingham Heart Study. Arch Neurol. 2006;63:1545-1550.
19. Kalmijn S, Launer LJ, Ott A, et al. Dietary fat intake and the risk of incident dementia in the Rotterdam Study. Ann Neurol. 1997;42:776-782.
20. van Gelder BM, Tijhuis M, Kalmijn S, et al. Fish consumption, n-3 fatty acids, and subsequent 5-y cognitive decline in elderly men: the Zutphen Elderly Study. Am J Clin Nutr. 2007;85:1142-1147.
21. Solfrizzi V, Capurso C, Panza F. Adherence to a Mediterranean dietary pattern and risk of Alzheimer’s disease. Ann Neurol. 2006;60:620.-
22. Scarmeas N, Luchsinger JA, Mayeux R, et al. Mediterranean diet and Alzheimer disease mortality. Neurology. 2007;69(11):1084-1093.
23. Kivipelto M, Rovio S, Ngandu T, et al. Apolipoprotein E epsilon4 magnifies lifestyle risks for dementia: a population-based study. J Cell Mol Med. 2008;12(6B):2762-2771.
24. Podewils LJ, Guallar E, Kuller LH, et al. Physical activity, APOE genotype and dementia risk: findings from the Cardiovascular Health Cognition Study. Am J Epidemiol. 2005;161:639-651.
25. Hall CB, Derby C, LeValley A, et al. Education delays accelerated decline on a memory test in persons who develop dementia. Neurology. 2007;69:1657-1664.
26. Wang HX, Karp A, Winblad B, et al. Late-life engagement in social and leisure activities is associated with a decreased risk of dementia: a longitudinal study from the Kungsholmen Project. Am J Epidemiol. 2002;155:1081-1087.
27. Scarmeas N, Levy G, Tang MX, et al. Influence of leisure activity on the incidence of Alzheimer’s disease. Neurology. 2001;57:2236-2242.
28. Willis SL, Tennstedt SL, Marsiske M, et al. Long-term effects of cognitive training on everyday functional outcomes in older adults. JAMA. 2006;296:2805-2814.
29. Guo Z, Cupples LA, Kurz A, et al. Head injury and the risk of AD in the MIRAGE study. Neurology. 2000;54:1316-1323.
30. Ruitenberg A, van Swieten JC, Witteman JC, et al. Alcohol consumption and risk of dementia: the Rotterdam Study. Lancet. 2002;359:281-286.
Pharmacologic treatments for Alzheimer’s disease (AD) may improve symptoms but have not been shown to prevent AD onset. Primary prevention therefore remains the goal. Although preventing AD by managing risk factors such as age or genetics is beyond our control (Box 1), we can do something about other factors.
This article summarizes the findings of many studies that address AD prevention and includes an online-only bibliography for readers seeking an in-depth review. The evidence does not support a firm recommendation for any specific form of primary prevention and has revealed hazards associated with estrogen therapy and nonsteroidal anti-inflammatory drugs (Box 2). Most important, it suggests that you could reduce your patients’ risk of developing AD by routinely supporting their mental, physical, and social health.
The potential benefits of modifying an individual’s AD risk factors likely will depend on his or her genetic makeup, environment, and lifestyle. Even so, counseling patients to exercise more and improve their diets—such as by eating more fish, fruits, and vegetables and less saturated fat—might help protect the brain. Your ongoing efforts to manage hypertension, hypercholesterolemia, and diabetes also may reduce their AD risk.
Age remains the strongest risk factor for dementia, particularly for Alzheimer’s disease (AD).a The risk of developing AD doubles every 5 years after age 65 and approaches 50% after age 85.b
Family history is a risk factor for AD, although true familial AD accounts for <5% of cases.c When diseases show a familial pattern, either genetics, environmental factors, or both may play a role. Patients with a first-degree relative with dementia have a 10% to 30% increased risk of developing the disorder.d
Genetic factors play a role in both early-onset and late-onset AD. Early-onset AD (before age 65) accounts for 6% to 7% of cases.e From this small pool of patients, only 13% exhibit clear autosomal dominant transmission over >1 generation.f Three gene mutations have been associated with early-onset AD:
- 30% to 70% are in the presenilin-1 gene
- 10% to 15% are in the amyloid precursor protein gene
- <5% are in the presenilin-2 gene.g,h
For late-onset AD (after age 65), the strongest evidence for a genetic risk factor exists for the epsilon 4 allele of the apolipoprotein E gene (APOE e4).i This genotype has been linked to the development of AD and possibly to vascular dementia.j,k In contrast, the epsilon 2 allele of APOE may exert a protective effect in AD.l APOE e3, the most common allele, appears to play a neutral role in the development of AD.
References
a. Evans DA. The epidemiology of dementia and Alzheimer’s disease: an evolving field. J Am Geriatr Soc. 1996;44:1482-1483.
b. Jorm AF, Jolley D. The incidence of dementia: a meta-analysis. Neurology. 1998;51:728-733.
c. van Duijn CM, Clayton D, Chandra V, et al. Familial aggregation of Alzheimer’s disease and related disorders: a collaborative re-analysis of case-control studies. EURODEM Risk Factors Research Group. Int J Epidemiol. 1991;20(suppl 2):S13-S20.
d. Chang JB, Wang PN, Chen WT, et al. ApoE epsilon4 allele is associated with incidental hallucinations and delusions in patients with AD. Neurology. 2004;63:1105-1107.
e. Sleegers K, Roks G, Theuns J, et al. Familial clustering and genetic risk for dementia in a genetically isolated Dutch population. Brain. 2004;127:1641-1649.
f. Schoenberg BS, Anderson DW, Haerer AF. Severe dementia. Prevalence and clinical features in a biracial US population. Arch Neurol. 1985;42:740-743.
g. Hsiung GY, Sadovnick AD. Genetics and dementia: risk factors, diagnosis and management. Alzheimers Dement. 2007;3:418-427.
h. GeneTests database. Available at: http://www.genetests.org. Accessed March 19, 2010.
i. Li H, Wetten S, Li L, et al. Candidate single-nucleotide polymorphisms from a genomewide association study of Alzheimer disease. Arch Neurol. 2008;65:45-53.
j. Graff-Radford NR, Green RC, Go RC, et al. Association between apolipoprotein E genotype and Alzheimer disease in African American subjects. Arch Neurol. 2002;59:594-600.
k. Slooter AJ, Cruts M, Hofman A, et al. The impact of APOE on myocardial infarction, stroke, and dementia: the Rotterdam Study. Neurology. 2004;62:1196-1198.
l. Tiraboschi P, Hansen LA, Masliah E, et al. Impact of APOE genotype on neuropathologic and neurochemical markers of Alzheimer disease. Neurology. 2004;62:1977-1983.
Estrogen. Before the Women’s Health Initiative (WHI) study, various trials of the effects of estrogen therapy on the development of Alzheimer’s disease (AD) in women age ≥65 showed inconsistent results. In the randomized, placebo-controlled WHI Memory Study, conjugated equine estrogen, 0.625 mg/d, plus medroxyprogesterone acetate, 2.5 mg/d, did not prevent mild cognitive impairment or improve global cognitive function and was associated with an increased risk for probable dementia.a Based on this evidence, conjugated equine estrogen with or without medroxyprogesterone is not recommended as therapy to protect cognitive function in older women.
NSAID therapy. Cytokine-mediated inflammation may play a role in neurodegenerative disorders and cognitive impairment in the elderly. Nonsteroidal anti-inflammatory drugs (NSAIDs), including cyclooxygenase-2 (COX-2) inhibitors, have been studied for a possible protective effect against AD and cognitive decline,b possibly by lowering amyloidogenic proteins.c A 1-year randomized controlled trial by the Alzheimer’s Disease Cooperative Consortium found no significant differences in cognition scores of patients treated with once-daily rofecoxib, 25 mg, or twice-daily naproxen sodium, 220 mg, when compared with placebo.d Similarly, naproxen and celecoxib did not prevent AD in the randomized, controlled Alzheimer’s Disease Anti-inflammatory Prevention Trial (ADAPT).e Rofecoxib has been withdrawn from the market, and celecoxib labeling carries a warning of potential for increased risk of cardiovascular events and life-threatening gastrointestinal bleeding associated with its use.
NSAIDs and COX-2 inhibitors are not recommended for the treatment or prevention of dementia or cognitive impairment. Their use for AD prevention is not supported by randomized clinical trialsd,e and they may have serious adverse effects.
References
a. Shumaker SA, Legault C, Kuller L, et al. Conjugated equine estrogens and incidence of probable dementia and mild cognitive impairment in postmenopausal women: Women’s Health Initiative Memory Study. JAMA. 2004;291:2947-2958.
b. Szekely CA, Breitner JC, Fitzpatrick AL, et al. NSAID use and dementia risk in the Cardiovascular Health Study: role of APOE and NSAID type. Neurology. 2008;70:17-24.
c. Weggen S, Eriksen JL, Das P, et al. A subset of NSAIDs lower amyloidogenic Abeta42 independently of cyclooxygenase activity. Nature. 2001;414:212-216.
d. Aisen PS, Schafer KA, Grundman M, et al. Effects of rofecoxib or naproxen vs placebo on Alzheimer disease progression: a randomized controlled trial. JAMA. 2003;289(21):2819-2826.
e. ADAPT Research Group, Martin BK, Szekely C, Brandt J, et al. Cognitive function over time in the Alzheimer’s Disease Anti-inflammatory Prevention Trial (ADAPT): results of a randomized, controlled trial of naproxen and celecoxib. Arch Neurol. 2008;65(7):896-905.
Cardiovascular risk factors
The risk of developing AD or vascular dementia appears to be increased by conditions that damage the heart or blood vessels. Recent evidence suggests that successfully managing cardiovascular risk factors may decrease the likelihood of dementia in later life.
Hypertension is associated with a higher risk of AD and all-cause dementia. Curiously, some studies have shown that low blood pressure also increases dementia risk, suggesting a U-shaped relationship between blood pressure and cognitive decline. Systolic hypertension in midlife may be associated with dementia 20 years later.
One might assume that antihypertensive therapy would help prevent dementia, but the data are conflicting. The Systolic Hypertension in Europe (SYST-EUR) study1 showed a 53% reduction in vascular dementia or mixed dementia among patients receiving antihypertensive medication and a 60% reduction in AD. Similarly, the PROGRESS2 clinical trial of prevention of recurrent stroke by antihypertensive treatment reported a 34% reduction in a composite measure of cognitive impairment and dementia. On the other hand, cognitive function neither improved nor worsened in the Hypertension in the Very Elderly Trial (HYVET-COG),3 whether patients received blood pressure treatment or placebo.
Hyperlipidemia. Lipid metabolism likely is an important pathway in amyloid beta-protein deposition, tau phosphorylation, and disruption of synaptic plasticity and neurodegenerative endpoints. Cognitive decline and incident dementia have been associated with higher dietary intake of saturated fats, partially hydrogenated unsaturated fatty acids (trans fats), and cholesterol. Not all studies have found this association, however. This could be because serum cholesterol levels may decrease in early dementia, limiting the ability to detect an effect of hypercholesterolemia on dementia risk when measurements are made later in life.
Using statins (3-hydroxy-3-methylglutaryl–coenzyme A reductase inhibitors) to treat hypercholesterolemia has been hypothesized to impede large vessel atherosclerosis and its consequences and to trigger metabolic effects in the brain related to AD pathogenesis. Mechanisms by which statins might help prevent dementia include:
- a direct association between amyloid processing and cholesterol in the brain
- an indirect effect by decreasing the risk of stroke, as even small cerebral infarcts worsen AD severity.
Nonrandomized epidemiologic studies such as the Cardiovascular Health Study4 and MRC/BHF Heart Protection Study5 suggested that statin treatment might reduce the incidence of dementia, the degree of age-related cognitive decline, and AD’s neuropathologic burden. Large, randomized, controlled trials have not supported these observations, however. Statins failed to reduce the incidence of dementia in:
- the Heart Protection Study, testing simvastatin for 5 years in 20,536 subjects age 40 to 805
- the 3-year Preventive Study of Pravastatin in the Elderly at Risk (PROSPER) of 5,800 subjects.6
Similarly, patients receiving adjunctive atorvastatin or placebo showed no significant differences in cognition assessments after 72 weeks in the Lipitor’s Effect in Alzheimer’s Dementia (LEADe) study. This trial enrolled 640 subjects age 50 to 90 with mild-to-moderate dementia who were treated with donepezil.7 A recent Cochrane review concluded that high serum cholesterol may contribute to the development of AD and vascular dementia, but lowering cholesterol levels with statins does not prevent these problems.8
Diabetes mellitus. Diabetes and cognitive decline are closely associated. Diabetes is associated with a 50% to 100% increase in risk of AD and dementia overall and a 100% to 150% increased risk of vascular dementia. The mechanism by which diabetes increases dementia risk is uncertain but does not appear to be mediated entirely through vascular disease. High and low insulin levels may increase the risk of dementia, independent of diabetes and blood glucose. Increased peripheral insulin levels are associated with reduced brain atrophy and cognitive impairment in patients with early AD, suggesting a role for insulin signaling in AD pathophysiology. A possible relationship between insulin and beta amyloid metabolism is being studied.
Elevated postprandial plasma glucose has been associated with accelerated declines in cognitive performance.9 An inverse correlation has been noted between some cognitive measures and hemoglobin A1C levels.10 It is not clear that treating diabetes reduces the risk of dementia. In addition, in the prospective, population-based Rotterdam study, elderly patients with type 2 diabetes treated with insulin had the highest incidence of dementia.11
Tobacco smoke directly affects neuronal function, integrity, and survival. Chronic smoking has been linked to decreased global cerebral blood flow, accelerated cerebral atrophy, and ventricular enlargement.
Some studies suggest an increased risk of dementia in middle-aged and elderly smokers, possibly through a cerebrovascular mechanism such as stroke. Other studies found no association between smoking and dementia risk, and 1 suggested that nicotine may protect against AD by reducing senile plaque formation. Any protective effect of smoking would be offset by increased risks of lung cancer, chronic obstructive pulmonary disease, and vascular dementia.
The apolipoprotein E epsilon 4 (APOE e4) gene may explain, at least in part, the conflicting results of these studies. In 2 population-based cohorts,12,13 smoking was associated with memory decline in patients without, but not with, the APOE e4 genotype.
Dietary factors
Antioxidants. The brains of patients with AD contain elevated levels of endogenous antioxidants. In vitro studies show exogenous antioxidants can reduce the toxicity of beta-amyloid in brain tissue of persons with AD. These findings have led to interest in assessing the role of dietary antioxidants such as vitamins E and C for AD prevention.
High-dose alpha-tocopherol (vitamin E, 2,000 IU/d) may slow disease progression in patients with AD, but this association is not consistently found. Furthermore, a meta-analysis of 19 randomized controlled trials (RCTs) totaling >135,000 patients found an association between vitamin E doses >400 IU/d and increased all-cause mortality.14 High-dose vitamin E supplementation for primary or secondary prevention of AD may be dangerous and is not recommended.
The lack of consistent efficacy data for vitamin C in preventing or treating AD may discourage its routine use for this purpose.15
Homocysteine is a risk factor for stroke and heart disease. It also could play a role in vascular dementia through its association with large- and small-vessel disease.
Low folate and hyperhomocysteinemia have been associated with dementia or cognitive impairment, although a cause-effect relationship is not clear. In non-demented elderly populations, plasma homocysteine is inversely associated with poor performance in tests of global cognitive function, particularly in measures of psychomotor speed.
In a recent double-blind RCT, folic acid supplementation for 3 years significantly improved domains of cognitive function that tend to decline with age, especially information processing and sensorimotor speed.16 No other good evidence, however, has shown that homocysteine-lowering therapy using folic acid or other vitamin B supplements improves cognitive function or prevents cognitive decline.
Fish and omega-3 fatty acids. High total fat, saturated fat, and total cholesterol intake increases the risk for incident dementia. In epidemiologic studies, low omega-3 fatty acid serum levels have been linked to increased dementia risk.
Fish consumption may be beneficial in reducing the risk of dementia or cognitive decline. A prospective study of 815 elderly persons found 60% less risk of developing AD in those who ate ≥1 fish meal per week, compared with those who rarely or never ate fish.17 In the Framingham study, individuals who at baseline were in the top quartile of docosahexaenoic acid consumption had lower dementia rates over 9 years of follow-up.18 Results from cross-sectional and longitudinal studies have been inconsistent; some have shown that high intake of n-3 polyunsaturated fatty acids is associated with less cognitive decline,19 whereas others have not.20
Although we cannot offer unequivocal advice regarding seafood or omega-3 fatty acid intake for primary prevention of dementia without evidence from RCTs, these uncontrolled studies show promise.
Mediterranean diet (MeDi) components include abundant fruits and vegetables, fish or shellfish at least twice weekly, very limited red meat, olive oil or canola oil instead of butter or margarine, tree nuts such as walnuts or pecans, red wine in moderation, and using herbs and spices instead of salt to season food. High adherence to the MeDi has been associated with a significantly lower risk for incident AD. The MeDi may affect the risk of developing AD21 as well as subsequent disease course, with a possible dose-response relationship in lower mortality.22
Eating fruits and vegetables has been associated with improved cognitive performance22 and decreased incident dementia in elderly subjects.18
Alcohol. A U-shaped relationship exists between alcohol consumption and dementia risk. High alcohol intake is associated with clinical problem drinking and alcoholism and can lead to cognitive decline. Conversely, moderate wine consumption (250 to 500 mL/d) may be protective—compared with more or less than this amount—and is associated with approximately 50% less risk of dementia.
Alcohol use may increase the risk of dementia in persons carrying the APOE e4 allele, according to the population-based Cardiovascular Risk Factors, Aging and Dementia (CAIDE) study from Sweden.23 After an average 21 years of follow-up of 1,449 individuals, researchers found that environmental factors—such as physical inactivity, dietary fat intake, alcohol consumption, and smoking at midlife—were associated with an increased risk of dementia at age 65 to 79 in APOE e4 carriers compared with noncarriers. The study also found that physical inactivity, dietary fat intake, and smoking at midlife increase AD risk, especially among APOE e4 carriers.
In the absence of evidence from RCTs, we cannot recommend alcohol to reduce the risk of AD.
Lifestyle and activity
Three components of lifestyle—social, mental, and physical activity—are inversely associated with the risk for dementia, AD, and cognitive impairment.
Physical exercise has been thought to enhance brain neurotrophic factor and modify apoptosis. Exercise can deter stroke and microvascular disease and improve regional cerebral blood flow. In the Cardiovascular Health Study, participants who expended the highest quartile of energy had a lower risk of all-cause dementia and AD compared with participants who expended the lowest quartile of energy.24
Mental and social activity. Epidemiologic studies have shown associations between higher educational achievement and other socioeconomic factors and reduced AD risk. Advanced education is believed to represent a cognitive reserve that delays presentation of AD’s effects on memory and cognitive function, rather than providing a protective effect against accumulation of AD pathology. Higher-educated individuals appear to experience a somewhat more rapid rate of cognitive decline when AD does become apparent, perhaps because they have accumulated a greater degree of AD pathology at that point compared with less-educated persons.
Among 117 persons with dementia in the Bronx Aging Study, each additional year of formal education delayed the time of accelerated decline by 0.21 years. After accelerated decline began, each year of additional formal education was associated with a slightly faster rate of memory decline.25
The longitudinal, population-based Kungsholmen Project in Stockholm, Sweden, found an association between daily mentally stimulating activities and decreased risk of all-cause dementia.26 Similarly, higher levels of leisure activity were linked to reduced risk of all-cause dementia in a longitudinal study of 1,772 persons age ≥65 living in Manhattan, NY.27 In a randomized, single-controlled study of the long-term effects of cognitive training, elderly individuals from 6 U.S. cities showed sustained improvement in specific cognitive performance up to 5 years after training sessions began, including memory, reasoning, and speed of processing.28
It seems reasonable to encourage older patients to maintain or increase physical, cognitive, and leisure activities as well as social interaction. These interventions can improve the quality of life and lower the risk of depression, which may be a response to cognitive decline or an independent risk factor for dementia (Box 3). The Table lists “brain exercises” you can suggest to patients to increase their mental and social activity.
Head trauma. The Multi-Institutional Research in Alzheimer’s Genetic Epidemiology (MIRAGE) project found an association between AD risk and a history of head trauma, especially in persons with APOE e4 alleles.29 Conversely, the Rotterdam Study showed no change in dementia risk for persons with a history of head trauma.30
Even in the absence of conclusive evidence supporting AD prevention, protecting the head by buckling seat belts while driving, wearing helmets when participating in sports, and “fall-proofing” the home is recommended.
Depression often occurs before or as a coexisting condition with Alzheimer’s disease (AD).a Although depression has been considered a response to cognitive decline or an early manifestation of dementia,b it also could be an independent risk factor.c,d
The pathologic mechanism linking depression and subsequent dementia is not well understood. Hypotheses include an indirect neurotoxic effect of depression mediated by cortisol-induced hippocampal atrophy or lowered brain-derived neurotrophic factor levels.e Depression and dementia might share genetic links, although a cohort study of 404 individuals with AD detected no association between apolipoprotein E genotypes or alleles and depressive symptoms.f
References
a. Lupien SJ, Nair NP, Brière S, et al. Increased cortisol levels and impaired cognition in human aging: implication for depression and dementia in later life. Rev Neurosci. 1999;10(2):117-139.
b. Preuss UW, Siafarikas N, Petrucci M, et al. Depressive disorders in dementia and mild cognitive impairments: is comorbidity a cause or a risk factor? Fortschr Neurol Psychiatr. 2009;77:399-406.
c. Green RC, Cupples LA, Kurz A, et al. Depression as a risk factor for Alzheimer disease: the MIRAGE Study. Arch Neurol. 2003;60(5):753-759.
d. Ownby RL, Crocco E, Acevedo A, et al. Depression and risk for Alzheimer’s disease: systematic review, meta-analysis, and metaregression analysis. Arch Gen Psychiatry. 2006;63(5):530-538.
e. Meeks TW, Ropacki SA, Jeste DV. The neurobiology of neuropsychiatric syndromes in dementia. Curr Opin Psychiatry. 2006;19(6):581-586.
f. Craig D, Hart DJ, McIlroy SP, et al. Association analysis of apolipoprotein E genotype and risk of depressive symptoms in Alzheimer’s disease. Dement Geriatr Cogn Disord. 2005;19(2-3):154-157.
Table
Brain exercises to suggest to patients
| Learn something new (how to play a musical instrument, a foreign language, or a new hobby) |
| Play memory games |
| Practice using the opposite hand to perform tasks you usually do with your dominant hand |
| Read, especially challenging material |
| Join a book discussion group |
| Write; if not a book or article, write a diary, letters, or emails or start your memoirs |
| Do crossword, Sudoku, or jigsaw puzzles |
| Play board games, card games, and other strategy games |
| Debate or discuss topics |
Related resource
- For an extensive bibliography of literature on Alzheimer’s disease risk factors and prevention, see this article at CurrentPsychiatry.com.
Drug brand names
- Atorvastatin • Lipitor
- Celecoxib • Celebrex
- Donepezil • Aricept
- Medroxyprogesterone • Provera
- Pravastatin • Pravachol
- Rofecoxib • Vioxx
- Simvastatin • Zocor
Disclosures
Dr. Bassil reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Grossberg receives research/grant support from and is a consultant to Bristol-Myers Squibb, Forest Pharmaceuticals, Novartis, Pfizer Inc., and Wyeth Pharmaceuticals. He also receives research/grant support from Baxter.
Pharmacologic treatments for Alzheimer’s disease (AD) may improve symptoms but have not been shown to prevent AD onset. Primary prevention therefore remains the goal. Although preventing AD by managing risk factors such as age or genetics is beyond our control (Box 1), we can do something about other factors.
This article summarizes the findings of many studies that address AD prevention and includes an online-only bibliography for readers seeking an in-depth review. The evidence does not support a firm recommendation for any specific form of primary prevention and has revealed hazards associated with estrogen therapy and nonsteroidal anti-inflammatory drugs (Box 2). Most important, it suggests that you could reduce your patients’ risk of developing AD by routinely supporting their mental, physical, and social health.
The potential benefits of modifying an individual’s AD risk factors likely will depend on his or her genetic makeup, environment, and lifestyle. Even so, counseling patients to exercise more and improve their diets—such as by eating more fish, fruits, and vegetables and less saturated fat—might help protect the brain. Your ongoing efforts to manage hypertension, hypercholesterolemia, and diabetes also may reduce their AD risk.
Age remains the strongest risk factor for dementia, particularly for Alzheimer’s disease (AD).a The risk of developing AD doubles every 5 years after age 65 and approaches 50% after age 85.b
Family history is a risk factor for AD, although true familial AD accounts for <5% of cases.c When diseases show a familial pattern, either genetics, environmental factors, or both may play a role. Patients with a first-degree relative with dementia have a 10% to 30% increased risk of developing the disorder.d
Genetic factors play a role in both early-onset and late-onset AD. Early-onset AD (before age 65) accounts for 6% to 7% of cases.e From this small pool of patients, only 13% exhibit clear autosomal dominant transmission over >1 generation.f Three gene mutations have been associated with early-onset AD:
- 30% to 70% are in the presenilin-1 gene
- 10% to 15% are in the amyloid precursor protein gene
- <5% are in the presenilin-2 gene.g,h
For late-onset AD (after age 65), the strongest evidence for a genetic risk factor exists for the epsilon 4 allele of the apolipoprotein E gene (APOE e4).i This genotype has been linked to the development of AD and possibly to vascular dementia.j,k In contrast, the epsilon 2 allele of APOE may exert a protective effect in AD.l APOE e3, the most common allele, appears to play a neutral role in the development of AD.
References
a. Evans DA. The epidemiology of dementia and Alzheimer’s disease: an evolving field. J Am Geriatr Soc. 1996;44:1482-1483.
b. Jorm AF, Jolley D. The incidence of dementia: a meta-analysis. Neurology. 1998;51:728-733.
c. van Duijn CM, Clayton D, Chandra V, et al. Familial aggregation of Alzheimer’s disease and related disorders: a collaborative re-analysis of case-control studies. EURODEM Risk Factors Research Group. Int J Epidemiol. 1991;20(suppl 2):S13-S20.
d. Chang JB, Wang PN, Chen WT, et al. ApoE epsilon4 allele is associated with incidental hallucinations and delusions in patients with AD. Neurology. 2004;63:1105-1107.
e. Sleegers K, Roks G, Theuns J, et al. Familial clustering and genetic risk for dementia in a genetically isolated Dutch population. Brain. 2004;127:1641-1649.
f. Schoenberg BS, Anderson DW, Haerer AF. Severe dementia. Prevalence and clinical features in a biracial US population. Arch Neurol. 1985;42:740-743.
g. Hsiung GY, Sadovnick AD. Genetics and dementia: risk factors, diagnosis and management. Alzheimers Dement. 2007;3:418-427.
h. GeneTests database. Available at: http://www.genetests.org. Accessed March 19, 2010.
i. Li H, Wetten S, Li L, et al. Candidate single-nucleotide polymorphisms from a genomewide association study of Alzheimer disease. Arch Neurol. 2008;65:45-53.
j. Graff-Radford NR, Green RC, Go RC, et al. Association between apolipoprotein E genotype and Alzheimer disease in African American subjects. Arch Neurol. 2002;59:594-600.
k. Slooter AJ, Cruts M, Hofman A, et al. The impact of APOE on myocardial infarction, stroke, and dementia: the Rotterdam Study. Neurology. 2004;62:1196-1198.
l. Tiraboschi P, Hansen LA, Masliah E, et al. Impact of APOE genotype on neuropathologic and neurochemical markers of Alzheimer disease. Neurology. 2004;62:1977-1983.
Estrogen. Before the Women’s Health Initiative (WHI) study, various trials of the effects of estrogen therapy on the development of Alzheimer’s disease (AD) in women age ≥65 showed inconsistent results. In the randomized, placebo-controlled WHI Memory Study, conjugated equine estrogen, 0.625 mg/d, plus medroxyprogesterone acetate, 2.5 mg/d, did not prevent mild cognitive impairment or improve global cognitive function and was associated with an increased risk for probable dementia.a Based on this evidence, conjugated equine estrogen with or without medroxyprogesterone is not recommended as therapy to protect cognitive function in older women.
NSAID therapy. Cytokine-mediated inflammation may play a role in neurodegenerative disorders and cognitive impairment in the elderly. Nonsteroidal anti-inflammatory drugs (NSAIDs), including cyclooxygenase-2 (COX-2) inhibitors, have been studied for a possible protective effect against AD and cognitive decline,b possibly by lowering amyloidogenic proteins.c A 1-year randomized controlled trial by the Alzheimer’s Disease Cooperative Consortium found no significant differences in cognition scores of patients treated with once-daily rofecoxib, 25 mg, or twice-daily naproxen sodium, 220 mg, when compared with placebo.d Similarly, naproxen and celecoxib did not prevent AD in the randomized, controlled Alzheimer’s Disease Anti-inflammatory Prevention Trial (ADAPT).e Rofecoxib has been withdrawn from the market, and celecoxib labeling carries a warning of potential for increased risk of cardiovascular events and life-threatening gastrointestinal bleeding associated with its use.
NSAIDs and COX-2 inhibitors are not recommended for the treatment or prevention of dementia or cognitive impairment. Their use for AD prevention is not supported by randomized clinical trialsd,e and they may have serious adverse effects.
References
a. Shumaker SA, Legault C, Kuller L, et al. Conjugated equine estrogens and incidence of probable dementia and mild cognitive impairment in postmenopausal women: Women’s Health Initiative Memory Study. JAMA. 2004;291:2947-2958.
b. Szekely CA, Breitner JC, Fitzpatrick AL, et al. NSAID use and dementia risk in the Cardiovascular Health Study: role of APOE and NSAID type. Neurology. 2008;70:17-24.
c. Weggen S, Eriksen JL, Das P, et al. A subset of NSAIDs lower amyloidogenic Abeta42 independently of cyclooxygenase activity. Nature. 2001;414:212-216.
d. Aisen PS, Schafer KA, Grundman M, et al. Effects of rofecoxib or naproxen vs placebo on Alzheimer disease progression: a randomized controlled trial. JAMA. 2003;289(21):2819-2826.
e. ADAPT Research Group, Martin BK, Szekely C, Brandt J, et al. Cognitive function over time in the Alzheimer’s Disease Anti-inflammatory Prevention Trial (ADAPT): results of a randomized, controlled trial of naproxen and celecoxib. Arch Neurol. 2008;65(7):896-905.
Cardiovascular risk factors
The risk of developing AD or vascular dementia appears to be increased by conditions that damage the heart or blood vessels. Recent evidence suggests that successfully managing cardiovascular risk factors may decrease the likelihood of dementia in later life.
Hypertension is associated with a higher risk of AD and all-cause dementia. Curiously, some studies have shown that low blood pressure also increases dementia risk, suggesting a U-shaped relationship between blood pressure and cognitive decline. Systolic hypertension in midlife may be associated with dementia 20 years later.
One might assume that antihypertensive therapy would help prevent dementia, but the data are conflicting. The Systolic Hypertension in Europe (SYST-EUR) study1 showed a 53% reduction in vascular dementia or mixed dementia among patients receiving antihypertensive medication and a 60% reduction in AD. Similarly, the PROGRESS2 clinical trial of prevention of recurrent stroke by antihypertensive treatment reported a 34% reduction in a composite measure of cognitive impairment and dementia. On the other hand, cognitive function neither improved nor worsened in the Hypertension in the Very Elderly Trial (HYVET-COG),3 whether patients received blood pressure treatment or placebo.
Hyperlipidemia. Lipid metabolism likely is an important pathway in amyloid beta-protein deposition, tau phosphorylation, and disruption of synaptic plasticity and neurodegenerative endpoints. Cognitive decline and incident dementia have been associated with higher dietary intake of saturated fats, partially hydrogenated unsaturated fatty acids (trans fats), and cholesterol. Not all studies have found this association, however. This could be because serum cholesterol levels may decrease in early dementia, limiting the ability to detect an effect of hypercholesterolemia on dementia risk when measurements are made later in life.
Using statins (3-hydroxy-3-methylglutaryl–coenzyme A reductase inhibitors) to treat hypercholesterolemia has been hypothesized to impede large vessel atherosclerosis and its consequences and to trigger metabolic effects in the brain related to AD pathogenesis. Mechanisms by which statins might help prevent dementia include:
- a direct association between amyloid processing and cholesterol in the brain
- an indirect effect by decreasing the risk of stroke, as even small cerebral infarcts worsen AD severity.
Nonrandomized epidemiologic studies such as the Cardiovascular Health Study4 and MRC/BHF Heart Protection Study5 suggested that statin treatment might reduce the incidence of dementia, the degree of age-related cognitive decline, and AD’s neuropathologic burden. Large, randomized, controlled trials have not supported these observations, however. Statins failed to reduce the incidence of dementia in:
- the Heart Protection Study, testing simvastatin for 5 years in 20,536 subjects age 40 to 805
- the 3-year Preventive Study of Pravastatin in the Elderly at Risk (PROSPER) of 5,800 subjects.6
Similarly, patients receiving adjunctive atorvastatin or placebo showed no significant differences in cognition assessments after 72 weeks in the Lipitor’s Effect in Alzheimer’s Dementia (LEADe) study. This trial enrolled 640 subjects age 50 to 90 with mild-to-moderate dementia who were treated with donepezil.7 A recent Cochrane review concluded that high serum cholesterol may contribute to the development of AD and vascular dementia, but lowering cholesterol levels with statins does not prevent these problems.8
Diabetes mellitus. Diabetes and cognitive decline are closely associated. Diabetes is associated with a 50% to 100% increase in risk of AD and dementia overall and a 100% to 150% increased risk of vascular dementia. The mechanism by which diabetes increases dementia risk is uncertain but does not appear to be mediated entirely through vascular disease. High and low insulin levels may increase the risk of dementia, independent of diabetes and blood glucose. Increased peripheral insulin levels are associated with reduced brain atrophy and cognitive impairment in patients with early AD, suggesting a role for insulin signaling in AD pathophysiology. A possible relationship between insulin and beta amyloid metabolism is being studied.
Elevated postprandial plasma glucose has been associated with accelerated declines in cognitive performance.9 An inverse correlation has been noted between some cognitive measures and hemoglobin A1C levels.10 It is not clear that treating diabetes reduces the risk of dementia. In addition, in the prospective, population-based Rotterdam study, elderly patients with type 2 diabetes treated with insulin had the highest incidence of dementia.11
Tobacco smoke directly affects neuronal function, integrity, and survival. Chronic smoking has been linked to decreased global cerebral blood flow, accelerated cerebral atrophy, and ventricular enlargement.
Some studies suggest an increased risk of dementia in middle-aged and elderly smokers, possibly through a cerebrovascular mechanism such as stroke. Other studies found no association between smoking and dementia risk, and 1 suggested that nicotine may protect against AD by reducing senile plaque formation. Any protective effect of smoking would be offset by increased risks of lung cancer, chronic obstructive pulmonary disease, and vascular dementia.
The apolipoprotein E epsilon 4 (APOE e4) gene may explain, at least in part, the conflicting results of these studies. In 2 population-based cohorts,12,13 smoking was associated with memory decline in patients without, but not with, the APOE e4 genotype.
Dietary factors
Antioxidants. The brains of patients with AD contain elevated levels of endogenous antioxidants. In vitro studies show exogenous antioxidants can reduce the toxicity of beta-amyloid in brain tissue of persons with AD. These findings have led to interest in assessing the role of dietary antioxidants such as vitamins E and C for AD prevention.
High-dose alpha-tocopherol (vitamin E, 2,000 IU/d) may slow disease progression in patients with AD, but this association is not consistently found. Furthermore, a meta-analysis of 19 randomized controlled trials (RCTs) totaling >135,000 patients found an association between vitamin E doses >400 IU/d and increased all-cause mortality.14 High-dose vitamin E supplementation for primary or secondary prevention of AD may be dangerous and is not recommended.
The lack of consistent efficacy data for vitamin C in preventing or treating AD may discourage its routine use for this purpose.15
Homocysteine is a risk factor for stroke and heart disease. It also could play a role in vascular dementia through its association with large- and small-vessel disease.
Low folate and hyperhomocysteinemia have been associated with dementia or cognitive impairment, although a cause-effect relationship is not clear. In non-demented elderly populations, plasma homocysteine is inversely associated with poor performance in tests of global cognitive function, particularly in measures of psychomotor speed.
In a recent double-blind RCT, folic acid supplementation for 3 years significantly improved domains of cognitive function that tend to decline with age, especially information processing and sensorimotor speed.16 No other good evidence, however, has shown that homocysteine-lowering therapy using folic acid or other vitamin B supplements improves cognitive function or prevents cognitive decline.
Fish and omega-3 fatty acids. High total fat, saturated fat, and total cholesterol intake increases the risk for incident dementia. In epidemiologic studies, low omega-3 fatty acid serum levels have been linked to increased dementia risk.
Fish consumption may be beneficial in reducing the risk of dementia or cognitive decline. A prospective study of 815 elderly persons found 60% less risk of developing AD in those who ate ≥1 fish meal per week, compared with those who rarely or never ate fish.17 In the Framingham study, individuals who at baseline were in the top quartile of docosahexaenoic acid consumption had lower dementia rates over 9 years of follow-up.18 Results from cross-sectional and longitudinal studies have been inconsistent; some have shown that high intake of n-3 polyunsaturated fatty acids is associated with less cognitive decline,19 whereas others have not.20
Although we cannot offer unequivocal advice regarding seafood or omega-3 fatty acid intake for primary prevention of dementia without evidence from RCTs, these uncontrolled studies show promise.
Mediterranean diet (MeDi) components include abundant fruits and vegetables, fish or shellfish at least twice weekly, very limited red meat, olive oil or canola oil instead of butter or margarine, tree nuts such as walnuts or pecans, red wine in moderation, and using herbs and spices instead of salt to season food. High adherence to the MeDi has been associated with a significantly lower risk for incident AD. The MeDi may affect the risk of developing AD21 as well as subsequent disease course, with a possible dose-response relationship in lower mortality.22
Eating fruits and vegetables has been associated with improved cognitive performance22 and decreased incident dementia in elderly subjects.18
Alcohol. A U-shaped relationship exists between alcohol consumption and dementia risk. High alcohol intake is associated with clinical problem drinking and alcoholism and can lead to cognitive decline. Conversely, moderate wine consumption (250 to 500 mL/d) may be protective—compared with more or less than this amount—and is associated with approximately 50% less risk of dementia.
Alcohol use may increase the risk of dementia in persons carrying the APOE e4 allele, according to the population-based Cardiovascular Risk Factors, Aging and Dementia (CAIDE) study from Sweden.23 After an average 21 years of follow-up of 1,449 individuals, researchers found that environmental factors—such as physical inactivity, dietary fat intake, alcohol consumption, and smoking at midlife—were associated with an increased risk of dementia at age 65 to 79 in APOE e4 carriers compared with noncarriers. The study also found that physical inactivity, dietary fat intake, and smoking at midlife increase AD risk, especially among APOE e4 carriers.
In the absence of evidence from RCTs, we cannot recommend alcohol to reduce the risk of AD.
Lifestyle and activity
Three components of lifestyle—social, mental, and physical activity—are inversely associated with the risk for dementia, AD, and cognitive impairment.
Physical exercise has been thought to enhance brain neurotrophic factor and modify apoptosis. Exercise can deter stroke and microvascular disease and improve regional cerebral blood flow. In the Cardiovascular Health Study, participants who expended the highest quartile of energy had a lower risk of all-cause dementia and AD compared with participants who expended the lowest quartile of energy.24
Mental and social activity. Epidemiologic studies have shown associations between higher educational achievement and other socioeconomic factors and reduced AD risk. Advanced education is believed to represent a cognitive reserve that delays presentation of AD’s effects on memory and cognitive function, rather than providing a protective effect against accumulation of AD pathology. Higher-educated individuals appear to experience a somewhat more rapid rate of cognitive decline when AD does become apparent, perhaps because they have accumulated a greater degree of AD pathology at that point compared with less-educated persons.
Among 117 persons with dementia in the Bronx Aging Study, each additional year of formal education delayed the time of accelerated decline by 0.21 years. After accelerated decline began, each year of additional formal education was associated with a slightly faster rate of memory decline.25
The longitudinal, population-based Kungsholmen Project in Stockholm, Sweden, found an association between daily mentally stimulating activities and decreased risk of all-cause dementia.26 Similarly, higher levels of leisure activity were linked to reduced risk of all-cause dementia in a longitudinal study of 1,772 persons age ≥65 living in Manhattan, NY.27 In a randomized, single-controlled study of the long-term effects of cognitive training, elderly individuals from 6 U.S. cities showed sustained improvement in specific cognitive performance up to 5 years after training sessions began, including memory, reasoning, and speed of processing.28
It seems reasonable to encourage older patients to maintain or increase physical, cognitive, and leisure activities as well as social interaction. These interventions can improve the quality of life and lower the risk of depression, which may be a response to cognitive decline or an independent risk factor for dementia (Box 3). The Table lists “brain exercises” you can suggest to patients to increase their mental and social activity.
Head trauma. The Multi-Institutional Research in Alzheimer’s Genetic Epidemiology (MIRAGE) project found an association between AD risk and a history of head trauma, especially in persons with APOE e4 alleles.29 Conversely, the Rotterdam Study showed no change in dementia risk for persons with a history of head trauma.30
Even in the absence of conclusive evidence supporting AD prevention, protecting the head by buckling seat belts while driving, wearing helmets when participating in sports, and “fall-proofing” the home is recommended.
Depression often occurs before or as a coexisting condition with Alzheimer’s disease (AD).a Although depression has been considered a response to cognitive decline or an early manifestation of dementia,b it also could be an independent risk factor.c,d
The pathologic mechanism linking depression and subsequent dementia is not well understood. Hypotheses include an indirect neurotoxic effect of depression mediated by cortisol-induced hippocampal atrophy or lowered brain-derived neurotrophic factor levels.e Depression and dementia might share genetic links, although a cohort study of 404 individuals with AD detected no association between apolipoprotein E genotypes or alleles and depressive symptoms.f
References
a. Lupien SJ, Nair NP, Brière S, et al. Increased cortisol levels and impaired cognition in human aging: implication for depression and dementia in later life. Rev Neurosci. 1999;10(2):117-139.
b. Preuss UW, Siafarikas N, Petrucci M, et al. Depressive disorders in dementia and mild cognitive impairments: is comorbidity a cause or a risk factor? Fortschr Neurol Psychiatr. 2009;77:399-406.
c. Green RC, Cupples LA, Kurz A, et al. Depression as a risk factor for Alzheimer disease: the MIRAGE Study. Arch Neurol. 2003;60(5):753-759.
d. Ownby RL, Crocco E, Acevedo A, et al. Depression and risk for Alzheimer’s disease: systematic review, meta-analysis, and metaregression analysis. Arch Gen Psychiatry. 2006;63(5):530-538.
e. Meeks TW, Ropacki SA, Jeste DV. The neurobiology of neuropsychiatric syndromes in dementia. Curr Opin Psychiatry. 2006;19(6):581-586.
f. Craig D, Hart DJ, McIlroy SP, et al. Association analysis of apolipoprotein E genotype and risk of depressive symptoms in Alzheimer’s disease. Dement Geriatr Cogn Disord. 2005;19(2-3):154-157.
Table
Brain exercises to suggest to patients
| Learn something new (how to play a musical instrument, a foreign language, or a new hobby) |
| Play memory games |
| Practice using the opposite hand to perform tasks you usually do with your dominant hand |
| Read, especially challenging material |
| Join a book discussion group |
| Write; if not a book or article, write a diary, letters, or emails or start your memoirs |
| Do crossword, Sudoku, or jigsaw puzzles |
| Play board games, card games, and other strategy games |
| Debate or discuss topics |
Related resource
- For an extensive bibliography of literature on Alzheimer’s disease risk factors and prevention, see this article at CurrentPsychiatry.com.
Drug brand names
- Atorvastatin • Lipitor
- Celecoxib • Celebrex
- Donepezil • Aricept
- Medroxyprogesterone • Provera
- Pravastatin • Pravachol
- Rofecoxib • Vioxx
- Simvastatin • Zocor
Disclosures
Dr. Bassil reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Grossberg receives research/grant support from and is a consultant to Bristol-Myers Squibb, Forest Pharmaceuticals, Novartis, Pfizer Inc., and Wyeth Pharmaceuticals. He also receives research/grant support from Baxter.
1. Forette F, Seux ML, Staessen JA, et al. The prevention of dementia with antihypertensive treatment: new evidence from the systolic hypertension in Europe (Syst-Eur) study. Arch Intern Med. 2002;162:2046-2052.
2. Tzourio C, Anderson C, Chapman N, et al. Effects of blood pressure lowering with perindopril and indapamide therapy on dementia and cognitive decline in patients with cerebrovascular disease. Arch Intern Med. 2003;163:1069-1075.
3. Peters R, Beckett N, Forette F. Incident dementia and blood pressure lowering in the Hypertension in the Very Elderly Trial cognitive function assessment (HYVET-COG). Lancet Neurol. 2008;7(8):683-689.
4. Rea TD, Breitner JC, Psaty BM, et al. Statin use and the risk of incident dementia: the Cardiovascular Health Study. Arch Neurol. 2005;62:1047-1051.
5. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002;360:7-22.
6. Kulbertus H, Scheen AJ. [The PROSPER Study (PROspective study of pravastatin in the elderly at risk)]. Rev Med Liege. 2002;57(12):809-813.
7. Feldman HH, Doody RS, Kivipelto M, et al. Randomized controlled trial of atorvastatin in mild to moderate Alzheimer disease: LEADe. Neurology. 2010;74(12):956-964.
8. McGuinness B, Bullock R, Craig D, et al. Statins for the treatment of Alzheimer’s disease and dementia (protocol). Cochrane Database Syst Rev. 2009;1:CD007514.-
9. Abbatecola AM, Rizzo MR, Barbieri M, et al. Postprandial plasmaglucose excursions and cognitive functioning in aged type 2 diabetics. Neurology. 2006;67:235-240.
10. Munshi M, Grande L, Hayes M, et al. Cognitive dysfunction is associated with poor diabetes control in older adults. Diabetes Care. 2006;29:1794-1799.
11. Ott A, Stolk RP, van Harskamp F, et al. Diabetes mellitus and the risk of dementia. The Rotterdam study. Neurology. 1999;53:1937-1942.
12. Reitz C, Luchsinger J, Tang MX, et al. Effect of smoking and time on cognitive function in the elderly without dementia. Neurology. 2005;65:870-875.
13. Reitz C, den Heijer T, van Duijn C, et al. Relation between smoking and risk of dementia and Alzheimer disease: the Rotterdam Study. Neurology. 2007;69:998-1005.
14. Miller ER, III, Pastor-Barriuso R, Dalal D, et al. Meta-analysis: high-dosage vitamin E supplementation may increase all-cause mortality. Ann Intern Med. 2005;142(1):37-46.
15. Boothby LA, Doering PL. Vitamin C and vitamin E for Alzheimer’s disease. Ann Pharmacother. 2005;39(12):2073-2080.
16. Durga J, van Boxtel MP, Schouten EG, et al. Effect of 3-year folic acid supplementation on cognitive function in older adults in the FACIT trial: a randomised, double blind, controlled trial. Lancet. 2007;369:208-216.
17. Morris MC, Evans DA, Bienias JL, et al. Consumption of fish and n-3 fatty acids and risk of incident Alzheimer disease. Arch Neurol. 2003;60:940-946.
18. Schaefer EJ, Bongard V, Beiser AS, et al. Plasma phosphatidylcholine docosahexaenoic acid content and risk of dementia and Alzheimer disease: the Framingham Heart Study. Arch Neurol. 2006;63:1545-1550.
19. Kalmijn S, Launer LJ, Ott A, et al. Dietary fat intake and the risk of incident dementia in the Rotterdam Study. Ann Neurol. 1997;42:776-782.
20. van Gelder BM, Tijhuis M, Kalmijn S, et al. Fish consumption, n-3 fatty acids, and subsequent 5-y cognitive decline in elderly men: the Zutphen Elderly Study. Am J Clin Nutr. 2007;85:1142-1147.
21. Solfrizzi V, Capurso C, Panza F. Adherence to a Mediterranean dietary pattern and risk of Alzheimer’s disease. Ann Neurol. 2006;60:620.-
22. Scarmeas N, Luchsinger JA, Mayeux R, et al. Mediterranean diet and Alzheimer disease mortality. Neurology. 2007;69(11):1084-1093.
23. Kivipelto M, Rovio S, Ngandu T, et al. Apolipoprotein E epsilon4 magnifies lifestyle risks for dementia: a population-based study. J Cell Mol Med. 2008;12(6B):2762-2771.
24. Podewils LJ, Guallar E, Kuller LH, et al. Physical activity, APOE genotype and dementia risk: findings from the Cardiovascular Health Cognition Study. Am J Epidemiol. 2005;161:639-651.
25. Hall CB, Derby C, LeValley A, et al. Education delays accelerated decline on a memory test in persons who develop dementia. Neurology. 2007;69:1657-1664.
26. Wang HX, Karp A, Winblad B, et al. Late-life engagement in social and leisure activities is associated with a decreased risk of dementia: a longitudinal study from the Kungsholmen Project. Am J Epidemiol. 2002;155:1081-1087.
27. Scarmeas N, Levy G, Tang MX, et al. Influence of leisure activity on the incidence of Alzheimer’s disease. Neurology. 2001;57:2236-2242.
28. Willis SL, Tennstedt SL, Marsiske M, et al. Long-term effects of cognitive training on everyday functional outcomes in older adults. JAMA. 2006;296:2805-2814.
29. Guo Z, Cupples LA, Kurz A, et al. Head injury and the risk of AD in the MIRAGE study. Neurology. 2000;54:1316-1323.
30. Ruitenberg A, van Swieten JC, Witteman JC, et al. Alcohol consumption and risk of dementia: the Rotterdam Study. Lancet. 2002;359:281-286.
1. Forette F, Seux ML, Staessen JA, et al. The prevention of dementia with antihypertensive treatment: new evidence from the systolic hypertension in Europe (Syst-Eur) study. Arch Intern Med. 2002;162:2046-2052.
2. Tzourio C, Anderson C, Chapman N, et al. Effects of blood pressure lowering with perindopril and indapamide therapy on dementia and cognitive decline in patients with cerebrovascular disease. Arch Intern Med. 2003;163:1069-1075.
3. Peters R, Beckett N, Forette F. Incident dementia and blood pressure lowering in the Hypertension in the Very Elderly Trial cognitive function assessment (HYVET-COG). Lancet Neurol. 2008;7(8):683-689.
4. Rea TD, Breitner JC, Psaty BM, et al. Statin use and the risk of incident dementia: the Cardiovascular Health Study. Arch Neurol. 2005;62:1047-1051.
5. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002;360:7-22.
6. Kulbertus H, Scheen AJ. [The PROSPER Study (PROspective study of pravastatin in the elderly at risk)]. Rev Med Liege. 2002;57(12):809-813.
7. Feldman HH, Doody RS, Kivipelto M, et al. Randomized controlled trial of atorvastatin in mild to moderate Alzheimer disease: LEADe. Neurology. 2010;74(12):956-964.
8. McGuinness B, Bullock R, Craig D, et al. Statins for the treatment of Alzheimer’s disease and dementia (protocol). Cochrane Database Syst Rev. 2009;1:CD007514.-
9. Abbatecola AM, Rizzo MR, Barbieri M, et al. Postprandial plasmaglucose excursions and cognitive functioning in aged type 2 diabetics. Neurology. 2006;67:235-240.
10. Munshi M, Grande L, Hayes M, et al. Cognitive dysfunction is associated with poor diabetes control in older adults. Diabetes Care. 2006;29:1794-1799.
11. Ott A, Stolk RP, van Harskamp F, et al. Diabetes mellitus and the risk of dementia. The Rotterdam study. Neurology. 1999;53:1937-1942.
12. Reitz C, Luchsinger J, Tang MX, et al. Effect of smoking and time on cognitive function in the elderly without dementia. Neurology. 2005;65:870-875.
13. Reitz C, den Heijer T, van Duijn C, et al. Relation between smoking and risk of dementia and Alzheimer disease: the Rotterdam Study. Neurology. 2007;69:998-1005.
14. Miller ER, III, Pastor-Barriuso R, Dalal D, et al. Meta-analysis: high-dosage vitamin E supplementation may increase all-cause mortality. Ann Intern Med. 2005;142(1):37-46.
15. Boothby LA, Doering PL. Vitamin C and vitamin E for Alzheimer’s disease. Ann Pharmacother. 2005;39(12):2073-2080.
16. Durga J, van Boxtel MP, Schouten EG, et al. Effect of 3-year folic acid supplementation on cognitive function in older adults in the FACIT trial: a randomised, double blind, controlled trial. Lancet. 2007;369:208-216.
17. Morris MC, Evans DA, Bienias JL, et al. Consumption of fish and n-3 fatty acids and risk of incident Alzheimer disease. Arch Neurol. 2003;60:940-946.
18. Schaefer EJ, Bongard V, Beiser AS, et al. Plasma phosphatidylcholine docosahexaenoic acid content and risk of dementia and Alzheimer disease: the Framingham Heart Study. Arch Neurol. 2006;63:1545-1550.
19. Kalmijn S, Launer LJ, Ott A, et al. Dietary fat intake and the risk of incident dementia in the Rotterdam Study. Ann Neurol. 1997;42:776-782.
20. van Gelder BM, Tijhuis M, Kalmijn S, et al. Fish consumption, n-3 fatty acids, and subsequent 5-y cognitive decline in elderly men: the Zutphen Elderly Study. Am J Clin Nutr. 2007;85:1142-1147.
21. Solfrizzi V, Capurso C, Panza F. Adherence to a Mediterranean dietary pattern and risk of Alzheimer’s disease. Ann Neurol. 2006;60:620.-
22. Scarmeas N, Luchsinger JA, Mayeux R, et al. Mediterranean diet and Alzheimer disease mortality. Neurology. 2007;69(11):1084-1093.
23. Kivipelto M, Rovio S, Ngandu T, et al. Apolipoprotein E epsilon4 magnifies lifestyle risks for dementia: a population-based study. J Cell Mol Med. 2008;12(6B):2762-2771.
24. Podewils LJ, Guallar E, Kuller LH, et al. Physical activity, APOE genotype and dementia risk: findings from the Cardiovascular Health Cognition Study. Am J Epidemiol. 2005;161:639-651.
25. Hall CB, Derby C, LeValley A, et al. Education delays accelerated decline on a memory test in persons who develop dementia. Neurology. 2007;69:1657-1664.
26. Wang HX, Karp A, Winblad B, et al. Late-life engagement in social and leisure activities is associated with a decreased risk of dementia: a longitudinal study from the Kungsholmen Project. Am J Epidemiol. 2002;155:1081-1087.
27. Scarmeas N, Levy G, Tang MX, et al. Influence of leisure activity on the incidence of Alzheimer’s disease. Neurology. 2001;57:2236-2242.
28. Willis SL, Tennstedt SL, Marsiske M, et al. Long-term effects of cognitive training on everyday functional outcomes in older adults. JAMA. 2006;296:2805-2814.
29. Guo Z, Cupples LA, Kurz A, et al. Head injury and the risk of AD in the MIRAGE study. Neurology. 2000;54:1316-1323.
30. Ruitenberg A, van Swieten JC, Witteman JC, et al. Alcohol consumption and risk of dementia: the Rotterdam Study. Lancet. 2002;359:281-286.
A better future for baby: Stemming the tide of fetal alcohol syndrome
Screen all females of childbearing age for alcohol use with standardized screening instruments such as TWEAK, T-ACE, or AUDIT. A
Use brief, in-office interventions to decrease alcohol consumption and increase effective contraception in sexually active women. Involve a supportive adult of the patient’s choosing where possible. A
Advise pregnant patients that complete abstinence from alcohol is safest. B
Refer a child who meets FAS referral criteria for multi-disciplinary evaluations as early as possible. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Family physicians who care for infants and young children are often asked to diagnose growth lags and failure to meet parents’ expectations for reaching developmental milestones: Why isn’t my child gaining weight? Why isn’t he talking? The other kids in the day-care center ride tricycles—why can’t he? Will he catch up? My mother thinks he’s funny looking. Do you?
Simple reassurance is all that most of these worried families need. But for families with children whose growth or developmental milestones are sufficiently outside the usual parameters, more than reassurance is called for. As you consider whether the lags that worry parents are signs of a serious disability, it’s important to make a place for fetal alcohol syndrome (FAS) in your differential.
FAS, a congenital disorder caused by alcohol exposure during pregnancy, is characterized by growth deficiency before and after birth, distinctive facial features, and central nervous system (CNS) dysfunctions. The cognitive and developmental effects of FAS persist throughout life and are severe enough to limit employment and independent living.1,2
A spectrum of severity. FAS is the most severe expression of prenatal alcohol exposure. The term fetal alcohol spectrum disorders (FASD) is a nondiagnostic umbrella term that includes FAS as well as ARND (alcohol-related neurobehavioral disorder) and ARBD (alcohol-related birth defects). Children with ARND and ARBD fail to meet the full FAS diagnostic criteria but still exhibit the negative effects of gestational alcohol exposure. Centers for Disease Control and Prevention (CDC) diagnostic criteria for FAS are summarized in TABLE 1. Studies by the CDC have reported FAS prevalence rates from 0.2 to 1.5 cases per 1000 live births, with a higher prevalence among minority (Native American and African American) and impoverished groups.1
An opportunity—and a challenge. As a family physician, you have a unique opportunity to modify the impact of FAS by recognizing the disorder in infancy or early childhood, actively engineering appropriate referrals, and supporting families in the difficult task of parenting a child with disabilities. Correctly diagnosing a child with FAS before age 6 can have a protective influence, decreasing the odds that he or she will suffer severe secondary disabilities in adolescence and adulthood. You can also help prevent FAS by screening for potentially harmful drinking patterns and helping sexually active female patients decrease alcohol consumption and use contraception successfully.
Providing these supportive and preventive services can be challenging. A recent survey of pediatricians revealed that only 34% felt prepared to manage and coordinate the treatment of children with FASD, and only 13% routinely counseled adolescent patients about the risks of drinking and pregnancy.3 Th is article will help you surmount the difficulties these tasks present and perform vital functions for alcohol-affected families you may encounter in your practice.
TABLE 1
Diagnostic criteria for fetal alcohol syndrome
Facial dysmorphia
| ≤10th percentile for age and racial norms Score of 4 or 5 on lip-philtrum guide* Score of 4 or 5 on lip-philtrum guide* |
| Growth problems | <10th percentile for age, sex, gestational age, racial norms in height or weight, prenatally or postnatally |
| CNS abnormalities | Any structural abnormality (head circumference <10% of age norm or clinically significant brain abnormalities observable through imaging); neurological abnormality not due to postnatal insult or fever; or functional abnormality demonstrated by cognitive performance less than expected for age, schooling, or family circumstances. An individual could meet the CNS abnormality criteria for a FAS diagnosis through a structural abnormality, yet not demonstrate detectable functional deficits. |
| CNS, central nervous system. | |
| *The lip-philtrum guide is available at http://depts.washington.edu/fasdpn/htmls/lip-philtrum-guides.htm. | |
| Source: Centers for Disease Control and Prevention. Fetal Alcohol Syndrome: Guidelines for Referral and Diagnosis. 2005. Available at www.cdc.gov/ncbddd/fasd/documents/FAS_guidelines_accessible.pdf. Accessed April 10, 2010. | |
The place to start: Spotting mothers at risk
Recognizing an infant with FAS starts by asking the baby’s mother about her pattern of drinking while she was pregnant. Most studies on the effects of gestational exposure to alcohol have emphasized moderate to high levels of exposure. In 1 study, children who were exposed to binge drinking were 1.7 times as likely to have IQ scores in the mentally retarded range and 2.5 times more likely to have clinically significant levels of delinquent behavior.4 Binge drinking is defined by the National Institute of Alcohol Abuse and Alcoholism as a pattern of drinking that brings blood alcohol concentration to 0.8% or above, which typically happens in women who consume 4 or more drinks in a period of about 2 hours.5
But a pregnant woman doesn’t have to be a binge drinker to put her fetus at risk. Even low levels of prenatal alcohol use—as low as 1 drink per week—have been associated with adverse behavioral changes in children, including increased aggressive behaviors documented at school age.6,7 The research documenting effects at these low levels has led the American Academy of Pediatrics (AAP) and the American Congress of Obstetricians and Gynecologists (ACOG) to recommend total abstinence from alcohol throughout pregnancy.8,9 Patterns of “at risk” drinking for women include binge drinking or persistent regular use (>7 drinks in 1 week). If a mother provides a history of that level of prenatal exposure, her child should be referred for multidisciplinary evaluation at an FAS center, even in the absence of the characteristic facial features.1
The face of FAS
Without a history of prenatal alcohol exposure, the cardinal features of facial dysmorphia (short palpebral fissures, smooth philtrum, and thin vermillion border) plus deficits in height and weight are the main physical findings of FAS. Evaluating height and weight percentiles is a routine part of well-child care, requiring minimal training. Height or weight or both at or below the 10th percentile, adjusted for age, sex, gestational age, and race or ethnicity, meet part of the CDC diagnostic criteria for FAS, but must be accompanied by at least 1 of the typical facial features associated with FAS to meet referral guidelines.1 The diagnostic guidelines are more restrictive, requiring all 3 facial features to meet the threshold for an FAS diagnosis, vs another diagnosis, such as alcohol-related neurodevelopmental disorders (TABLE 1).
Learning to measure faces. Examining a child for the facial characteristics of FAS requires a set of skills that can be learned in a relatively short time, with moderate interrater reliability when compared with dysmorphologists, according to 1 study.10
Tools for measuring. Palpebral fissure length (PFL) can be measured with a clear plastic ruler pressed onto the child’s cheek to determine the distance from the endocanthion to the exocanthion while the child is gazing upward.11 To meet the CDC criteria for FAS, this distance should be at or below the 10th percentile compared to norms. The shape of the lips and the nature of the philtrum are then compared to preestablished comparison photographs available on the University of Washington Lip-Philtrum Guides (see URL that follows).12 The vermillion border and the philtrum must both receive a rank of 4 or 5 to meet FAS criteria.11
Changes in the clinical presentation of fetal alcohol syndrome (FAS) occur across the lifespan. Clinicians searching for an explanation of an older child’s difficulties may need to reconsider a possible diagnosis of FAS, even if the facial features are less recognizable.
Preschool children with FAS may display a delay in early language acquisition and the beginnings of attention problems and hyperactivity. School-age children may have difficulty remembering material even when they have gone over it many times. They may lack social perception skills, be hyperactive, and show cognitive delays. Mathematics is often an area of severe delay, and sleep problems can persist.1
Teens and adults with FAS often have a wide range of secondary disabilities: disrupted schooling, inappropriate sexual behavior, mental health problems, aggression, trouble with the law, confinement in jail or as inpatients in psychiatric or substance abuse treatment facilities, alcohol and drug problems, and failure or inability to live independently at an appropriate age. They may have trouble finding a job and keeping one. More than 90% of patients with FAS exhibit mental health problems, with attention problems appearing in early childhood and persisting, and depression appearing in adolescence and adulthod.15
Tools available online for physicians include Lip-Philtrum Guides (www.depts.washington.edu/fasdpn/htmls/lip-philtrum-guides.htm) and an instructional video depicting PFL measurement techniques (www.depts.washington.edu/fasdpn/htmls/photo-face.htm), both from the University of Washington FAS Diagnostic and Prevention Network. In addition, a physical evaluation summary form, with reference data for PFL in Caucasian, black, and Hispanic children, is available at http://www.fas.academicedge.com/documents/phyevaln.pdf.
The Astley-Clarren criteria. The 4-digit diagnostic code developed by Astley and Clarren for diagnosis of FAS and employed at some FAS referral centers uses very strict criteria.13 Centers using these criteria define “abnormal” as ≥2 standard deviations below the mean or its equivalent, ≤2.5th percentile.13 Th is applies to the 3 facial features and CNS dysfunction (low IQ, eg). If all 3 facial features are identified in the Astley-Clarren system as abnormal (PFL ≤2.5th percentile, lip philtrum 5, vermillion 5), the sensitivity of the facial features is 100% and specificity is 99.8% for a diagnosis of FAS.13
The CDC criteria, developed with increased surveillance by providers as a goal, uses relaxed criteria of ≤10th percentile of PFL and 4 or 5 on the philtrum/vermillion border guide to identify abnormal facial features and <10th percentile in CNS dysfunctions. Sensitivity and specificity data for those CDC criteria are not available.1
CNS abnormalities may be noted early enough to trigger a referral for complete evaluation, but must be present in some degree to confirm a diagnosis of FAS. Abnormalities may include microcephaly with head circumference below the 10th percentile; clinically significant brain abnormalities observable through imaging, especially a small or absent corpus callosum; and functional deficits in any of a multitude of domains. In an infant, these deficits may be expressed in global developmental delays, sleep cycle problems, poor muscle tone, and feeding problems with poor suck and texture aversion.1
Evaluation may not confirm the diagnosis. Children referred for more extensive evaluation may or may not be confirmed to have FAS. In 2 demographically similar counties in New York state, only 5% of children initially identified in 1 county (10 of 208) and 13% (53 of 420) of children in the other county were confirmed to have FAS.12 The FAS diagnosis is complicated and the CNS and growth deficiencies may not be expressed until a later age.14 (See “Fetal alcohol syndrome across the lifespan”1,15)
Providers may feel reluctant to alarm or stigmatize families when they are unsure of the diagnosis, but the long-term benefit of confirming the diagnosis early on may be significant for the child and family. The case on page 341 (Tanya) illustrates the complexity of diagnosing FASD.
The encouraging news for family physicians is that the odds of escaping adverse life outcomes are increased 2- to 4-fold by receiving a diagnosis of FAS before age 6 and by being raised in a stable environment.16 Early diagnosis can be protective by helping with eligibility requirements for support services and by opening the door to medical management of FAS-associated conditions such as ADHD and depression. In addition, the diagnosis can alert family physicians to the family’s need for help with ongoing problems with alcohol use. The case on page 341 (Brianna) illustrates the complex secondary problems a teen with FAS may face.
Putting families in touch with resources
Multidisciplinary FAS teams may include physicians (a geneticist or developmental pediatrician), psychologists, speech pathologists, educational specialists, social workers, and occupational therapists. These groups typically have in-depth intake and evaluation processes, including neurodiagnostic studies that help clarify the cognitive and functional domains that are affected.
You can locate the nearest FAS evaluation team and other resources for providers and families on the National and State Resource Directory for the National Organization on Fetal Alcohol Syndrome. Go to www.nofas.org, click on Resources, then on National and State Resources Directory in the box on the left side of the page. There may be a waiting list for evaluation, but under Part C of the Individuals with Disabilities Education Act (IDEA), FAS is considered a “presumptive eligibility” diagnosis. Presumptive diagnoses allow children under age 3 at risk of later developmental delay to be served without meeting particular eligibility criteria.1 Physicians may refer these children for developmental assessment services and early intervention services while waiting for the more complete FAS evaluation.
After the age of 3, children and families are referred to preschool programs for children with disabilities that are administered through IDEA Part B, with no “presumptive eligibility” diagnoses. Eligibility for educational services under this program is entirely based on functional criteria.
Your best bet: Prevention
The key to preventing FAS is to find out whether your patient’s drinking patterns and contraceptive habits put her at risk for an alcohol-exposed pregnancy. Make it routine practice to ask women, in a way that encourages honest reporting, about both of these aspects of their lives. The US Preventive Services Task Force recommends screening and counseling intervention in primary care settings to reduce alcohol misuse in adults, including pregnant women.17 The case on page 341 (Clarice) illustrates how screening and brief intervention can be used to prevent alcohol-exposed pregnancy.
TANYA
Possible, though unconfirmed, FAS
This 1-month-old African American girl was admitted to the hospital with stridor, possible cardiorespiratory issues, and failure to thrive. She exhibited microcephaly, poor suck, floppy overall muscle tone, and small palpebral fissure lengths. The respiratory noise was attributed to tracheomalacia, secondary to her poor muscle tone.
An initial magnetic resonance imaging of the brain showed an almost complete absence of the corpus callosum. Obviously at risk for future delays, Tanya was referred for early childhood development intervention. By the age of 5½, she was within her peer group’s normal range in fine motor, gross motor, and speech skills. She was removed from her mother’s care for neglect and later placed in an extended family adoption.
Her initial evaluation took place before the widespread publication of fetal alcohol syndrome (FAS) criteria, and she was not referred for more specific FAS evaluation, as she would have been had she been seen more recently. Tanya has been lost to long-term follow-up from her initial medical home, but her mother returned to the same practice for a subsequent pregnancy and was screened as a problem drinker.
BRIANNA
Facing severe secondary disabilities
This 16-year-old Caucasian girl entered foster care for the second time because her first placement could not deal with her complex behavioral issues. Her mother committed suicide last year, and her father is in an alcohol rehabilitation program. No pregnancy history is available.
The social service agency supervising Brianna’s care decided not to return her to her father’s home. She made a suicidal gesture, her behavior is sometimes violent, and she has been diagnosed with attention deficit hyperactivity disorder (ADHD). She is being treated for depression, requiring multiple medications.
Brianna’s life has been difficult. Before she was 2 years old, she underwent surgery for a ventricular septal defect. Although her cardiac repair was successful, she remains significantly underweight, <3rd percentile on the growth curve. Because she is an adolescent, her facial features are less distinctive for FAS, but she appears to have a smooth philtrum and thin vermillion. Her learning disabilities are significant enough that she has been held back a grade and requires an individualized education plan.
It may be too late to help provide any assistance to Brianna, who is already experiencing severe secondary disabilities. But if a diagnosis of FAS (or alcohol-related neurobehavioral disorder) can be made, even at this point in her life, provisions may be made within the foster care system for transitional housing and emphasis on life skills training, rather than simply allowing her to “age out” of the system when she turns 18.
CLARICE
Preventing an alcohol-exposed pregnancy
Clarice is an 18-year-old, college-bound woman who came in for a pre-college health maintenance examination. She reported being sexually active and was using effective contraception only intermittently. On the TWEAK questionnaire, she said the most she has had to drink on a single occasion was 6 drinks, noted that she had never passed out and had not had any problems associated with drinking. The only worry she connected with drinking was a fear of gaining weight.
Clarice met the criteria for “at risk” drinking (TABLE 3). She was a candidate for a brief intervention, including information on the hazards of alcohol-exposed pregnancy and on effective contraceptive practices. We scheduled a telephone follow-up and checkup in 6 months.
* Drawn from the author’s case files. Names have been changed to protect patient privacy.
Screening should include simple quantity and frequency questions developed by the National Institute on Alcohol Abuse to clarify a patient’s current drinking patterns. The questions include the numbers of days per week of any drinking, the average number of drinks per day, and the maximum number of drinks consumed in 1 day during the past month. Determining that a woman drinks more than 7 drinks per week has a 29% sensitivity, but a 90% specificity for identifying lifetime risk of alcohol abuse or dependence.18
Other tools include TWEAK (Tolerance, Worry, Eye-opener, Amnesia, (K)Cut down), T-ACE (Tolerance, Annoyed, Cut down, Eye opener), and AUDIT (Alcohol Use Disorder Identification Test). They are detailed below and available online at Project Cork. Go to www.projectcork.org, and click on “clinical tools.”
The 5-item TWEAK tool (TABLE 2) appears to be the optimal screening questionnaire for identifying women in racially mixed populations with heavy drinking or alcohol abuse and dependence, but a score of 2 points should be the threshold for identifying female problem drinkers.19,20 Using the lower cutoff of 2, the sensitivity of TWEAK is in the 87% to 91% range for women, with a specificity of 77% to 90%.18
The T-ACE tool is a set of 4 questions, with the question addressing tolerance weighted more heavily than the others. With a score of 2 or more, the sensitivity of T-ACE is 70% to 88%; the specificity is 79% to 85%.18
The AUDIT tool is a self-administered screen that consists of a series of 10 questions that are each scored on a scale of 0 to 4. The maximum score is 40. A score of 2 indicates some harmful use of alcohol, but a score of 8 or more has a sensitivity of 59% to 66%, with a specificity of 93% to 97% in women.18
TABLE 2
TWEAK your patients for alcohol use
| Tolerance: How many drinks does it take for you to: | Score |
| 2 points for ≥3 drinks 2 points for ≥5 drinks |
| Worry about drinking | |
| Have your friends or relatives worried about your drinking in the past year? | 1 point for Yes |
| Eye-opener | |
| Do you sometimes take a drink in the morning when you first get up? | 1 point for Yes |
| Amnesia | |
| Are there times when you drink and afterwards can’t remember what you said or did? | 1 point for Yes |
| (K)Cut down | |
| Do you sometimes feel the need to cut down on your drinking? | 1 point for Yes |
| Scoring: ≥3 points is considered positive for alcoholism/heavy drinking. Thresholds differ for screening different populations, and a score of ≥2 points should be used as the threshold for identifying female problem drinkers. | |
| Source: Chan AW, et al. Alcohol Clin Exp Res. 1993.19 | |
When your patient is at risk
Brief interventions are recommended for nonpregnant and pregnant women who have exhibited a pattern of at-risk or problem drinking.21TABLE 3 summarizes patterns of drinking in women, from not drinking at all through various degrees of risk to alcohol dependency. Referral to an addiction specialist is recommended for women with alcohol dependence.
Brief interventions for alcohol abuse can be single-session encounters from 5 to 15 minutes’ duration, or multi-contact brief sessions, including possible phone follow-up contacts. Project TrEAT (Trial for Early Alcohol Treatment) provided two 15-minute sessions with the primary care physician (either a family physician or internist in community-based practice) scheduled 1 month apart, with nurse follow-up phone calls 2 weeks after each appointment.22
TABLE 3
Drinking patterns in women
Abstainer
|
Low-risk drinking
|
At-risk drinking
|
Problem drinking
|
Alcohol-dependent drinking: Maladaptive patterns of alcohol use leading to clinically significant impairment manifested by 3 or more of the following, occurring at any time during the same 12-month period:
|
| Source: Training program for medical students and other health professionals on fetal alcohol syndrome. Presented by the Midwest Regional Fetal Alcohol Syndrome Training Center; March 18, 2005; St. Louis, Mo. |
Patients received general information regarding adverse effects of alcohol and the prevalence of problem drinking, in addition to tools to help them identify drinking triggers and track their consumption. The patient and physician developed a “drinking agreement” in the form of a rescription. Men and non pregnant women were included in this study.
Women reduced their alcohol use by 47% and their frequency of binge drinking by 56%, as noted at a 6-month follow-up, with changes well maintained at 12 months. The reductions for female patients were actually slightly higher than for male participants.22
Chang and colleagues provided a 25-minute single session brief intervention to pregnant women who had screened positive on the T-ACE questionnaire with a score of 2 or more, and were identified as being at risk for prenatal alcohol use.23 Participants were randomly assigned to the intervention group or a control group. Both the control group and the brief intervention group decreased their use of alcohol after enrolling in the study and undergoing the initial detailed assessment.
For women who were heavier drinkers, the brief interventions for prenatal alcohol use were statistically more effective in reducing their frequency of alcohol consumption, vs the initial assessment alone. In addition, the effects of the brief intervention were significantly enhanced when a support partner of the woman’s choice also participated.23
The Project Choices Intervention Research Group studied an intervention that included 4 sessions of motivational interviewing regarding alcohol habits, and a contraception counseling session.24 Study participants were recruited from 6 community-based settings with high proportions of women at risk for an alcohol-exposed pregnancy, including a jail and 2 drug and alcohol treatment centers. Among the 143 women who completed the 6-month follow-up, 68.5% were no longer at risk of having an alcohol-exposed pregnancy.
These participants successfully lowered their risk by reducing alcohol use only (12.9%), adopting appropriate contraception use only (23.1%), or by changing both risk factors (32.9%). Even if all the study participants who were lost to follow-up were assumed to have been unsuccessful at eliminating their risk of alcohol-exposed pregnancy, more than half of the women (51.6%) successfully changed.24
Take advantage of opportunities
FAS is the most severe consequence of alcohol-exposed pregnancy, leaving the affected child with a lifelong disability. As a family physician, you have access to easy-touse, cost-effective clinical tools to screen for at-risk drinking behaviors and have sufficient rapport with your patients to encourage effective contraceptive practices. You also have effective tools for helping patients reduce their alcohol consumption.
Within the context of your long-term relationships with patients, you can provide brief interventions that include factual information and opportunities for goal setting. You can assist families with an FAS child to access services, manage medically related complications, and plan for special education and vocational skills training.
Recognition that 1 child in a family is affected by prenatal alcohol exposure gives you another window of opportunity to address the underlying substance use issues in the mother and the family, increasing the odds that future pregnancies will not be alcohol exposed.
CORRESPONDENCE Mary C. Boyce, MD, Wesley Family Medicine Residency, 850 N. Hillside, Wichita, KS 67214; [email protected]
1. Centers for Disease Control and Prevention. Fetal Alcohol Syndrome: Guidelines for Referral and Diagnosis. 2005. Available at: www.cdc.gov/ncbddd/fasd/documents/FAS_guidelines_accessible.pdf. Accessed April 10, 2010.
2. Spohr HL, Williams J, Steinhausen HC. Fetal alcohol spectrum disorders in young adulthood. J Pediatr. 2007;150:175-179.
3. Gahagan S, Sharpe TT, Brimacombe M, et al. Pediatricians’ knowledge, training, and experience in the care of children with fetal alcohol syndrome. Pediatrics. 2006;118:e657-e668.
4. Bailey BN, Delaney-Black V, Covington CY, et al. Prenatal exposure to binge drinking and cognitive and behavioral outcomes at age 7 years. Am J Obstet Gynecol. 2004;191:1037-1043.
5. CDC. Alcohol and public health/binge drinking. Quick stats. Available at: www.cdc.gov/alcohol/quickstats/binge_drinking.htm. Accessed April 21, 2010.
6. Sood B, Delaney-Black V, Covington C, et al. Prenatal alcohol exposure and childhood behavior at age 6 to 7 years: I. Doseresponse effect. Pediatrics. 2001;108:E34.-
7. Sokol RJ, Delaney-Black V, Nordstrom B. Fetal alcohol spectrum disorder. JAMA. 2003;290:2996-2999.
8. American Congress of Obstetricians and Gynecologists. ACOG Education Pamphlet AP170: Tobacco, alcohol, drugs, and pregnancy. Available at www.acog.org/publications/patient_education/bp170.cfm. Accessed May 3, 2010.
9. Committee on Substance Abuse and Committee on Children With Disabilities. Fetal alcohol syndrome and alcohol-related neurodevelopmental disorders. Pediatrics. 2000;106:358-361.
10. Jones KL, Robinson LK, Bakhireva LN, et al. Accuracy of the diagnosis of physical features of fetal alcohol syndrome by pediatricians after specialized training. Pediatrics. 2006;118:e1734-e1738.
11. University of Washington Fetal Alcohol Syndrome Diagnostic and Prevention Network. FAS facial photography and measurement instruction. Available at: www.depts.washington.edu/fasdpn/htmls/photo-face.htm. Accessed April 21,2010.
12. University of Washington Fetal Alcohol Syndrome Diagnostic and Prevention Network. Lip philtrum guides. Available at: www.depts.washington.edu/fasdpn/htmls/lip-philtrum-guides.htm. Accessed April 21, 2010.
13. Astley S. Comparison of the 4-digit diagnostic code and the Hoyme diagnostic guidelines for fetal alcohol spectrum disorder. Pediatrics. 2006;188:1532-1545.
14. Druschel CM, Fox DJ. Issues in estimating the prevalence of fetal alcohol syndrome: examination of 2 counties in New York State. Pediatrics. 2007;119:e384-e390.
15. Streissguth AP, Barr HM, Kogan J, et al. Understanding the occurrence of secondary disabilities in clients with fetal alcohol syndrome (FAS) and fetal alcohol effects (FAE). Final Report to the Centers for Disease Control and Prevention. Technical report no. 96-06. Seattle, WA: University of Washington, Fetal Alcohol and Drug Unit; 1996.
16. Streissguth AP, Bookstein FL, Barr H, et al. Risk factors for adverse life outcomes in fetal alcohol syndrome and fetal alcohol effects. J Dev Behav Pediatr. 2004;25:228-238.
17. US Preventive Services Task Force. Screening and behavioral interventions in primary care to reduce alcohol misuse: recommendation statement, April 2004. Available at: www.ahrq.gov/clinic/3rduspstf/alcohol/alcomisrs.htm. Accessed April 10, 2010.
18. Bradley KA, Boyd-Wickizer J, Powell SH, et al. Alcohol screening questionnaires in women: a critical review. JAMA. 1998;20:166-171.
19. Chan AW, Pristach EA, Welte JW, et al. Use of the TWEAK test in screening for alcoholism/heavy drinking in three populations. Alcohol Clin Exp Res. 1993;17:1188-1192.
20. Russell M, Bigler L. Screening for alcohol-related problems in an outpatient obstetric-gynecologic clinic. Am J Obstet Gynecol. 1979;134:4-12.
21. National Institute on Alcohol Abuse and Alcoholism. Helping patients who drink too much: a clinician’s guide. Updated January 2007. Available at: http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/clinicians_guide.htm. Accessed April 21, 2010.
22. Fleming MF, Barry KL, Manwell LB, et al. Brief physician advice for problem alcohol drinkers. JAMA. 1997;277:1039-1045.
23. Chang G, McNamara TK, Orav J, et al. Brief interventions for prenatal alcohol use: a randomized trial. Obstet Gynecol. 2005;105:991-998.
24. The Project Choices Intervention Research Group. Reducing the risk of alcohol-exposed pregnancies: a study of motivational intervention in community settings. Pediatrics. 2003;111:1131-1135.
Screen all females of childbearing age for alcohol use with standardized screening instruments such as TWEAK, T-ACE, or AUDIT. A
Use brief, in-office interventions to decrease alcohol consumption and increase effective contraception in sexually active women. Involve a supportive adult of the patient’s choosing where possible. A
Advise pregnant patients that complete abstinence from alcohol is safest. B
Refer a child who meets FAS referral criteria for multi-disciplinary evaluations as early as possible. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Family physicians who care for infants and young children are often asked to diagnose growth lags and failure to meet parents’ expectations for reaching developmental milestones: Why isn’t my child gaining weight? Why isn’t he talking? The other kids in the day-care center ride tricycles—why can’t he? Will he catch up? My mother thinks he’s funny looking. Do you?
Simple reassurance is all that most of these worried families need. But for families with children whose growth or developmental milestones are sufficiently outside the usual parameters, more than reassurance is called for. As you consider whether the lags that worry parents are signs of a serious disability, it’s important to make a place for fetal alcohol syndrome (FAS) in your differential.
FAS, a congenital disorder caused by alcohol exposure during pregnancy, is characterized by growth deficiency before and after birth, distinctive facial features, and central nervous system (CNS) dysfunctions. The cognitive and developmental effects of FAS persist throughout life and are severe enough to limit employment and independent living.1,2
A spectrum of severity. FAS is the most severe expression of prenatal alcohol exposure. The term fetal alcohol spectrum disorders (FASD) is a nondiagnostic umbrella term that includes FAS as well as ARND (alcohol-related neurobehavioral disorder) and ARBD (alcohol-related birth defects). Children with ARND and ARBD fail to meet the full FAS diagnostic criteria but still exhibit the negative effects of gestational alcohol exposure. Centers for Disease Control and Prevention (CDC) diagnostic criteria for FAS are summarized in TABLE 1. Studies by the CDC have reported FAS prevalence rates from 0.2 to 1.5 cases per 1000 live births, with a higher prevalence among minority (Native American and African American) and impoverished groups.1
An opportunity—and a challenge. As a family physician, you have a unique opportunity to modify the impact of FAS by recognizing the disorder in infancy or early childhood, actively engineering appropriate referrals, and supporting families in the difficult task of parenting a child with disabilities. Correctly diagnosing a child with FAS before age 6 can have a protective influence, decreasing the odds that he or she will suffer severe secondary disabilities in adolescence and adulthood. You can also help prevent FAS by screening for potentially harmful drinking patterns and helping sexually active female patients decrease alcohol consumption and use contraception successfully.
Providing these supportive and preventive services can be challenging. A recent survey of pediatricians revealed that only 34% felt prepared to manage and coordinate the treatment of children with FASD, and only 13% routinely counseled adolescent patients about the risks of drinking and pregnancy.3 Th is article will help you surmount the difficulties these tasks present and perform vital functions for alcohol-affected families you may encounter in your practice.
TABLE 1
Diagnostic criteria for fetal alcohol syndrome
Facial dysmorphia
| ≤10th percentile for age and racial norms Score of 4 or 5 on lip-philtrum guide* Score of 4 or 5 on lip-philtrum guide* |
| Growth problems | <10th percentile for age, sex, gestational age, racial norms in height or weight, prenatally or postnatally |
| CNS abnormalities | Any structural abnormality (head circumference <10% of age norm or clinically significant brain abnormalities observable through imaging); neurological abnormality not due to postnatal insult or fever; or functional abnormality demonstrated by cognitive performance less than expected for age, schooling, or family circumstances. An individual could meet the CNS abnormality criteria for a FAS diagnosis through a structural abnormality, yet not demonstrate detectable functional deficits. |
| CNS, central nervous system. | |
| *The lip-philtrum guide is available at http://depts.washington.edu/fasdpn/htmls/lip-philtrum-guides.htm. | |
| Source: Centers for Disease Control and Prevention. Fetal Alcohol Syndrome: Guidelines for Referral and Diagnosis. 2005. Available at www.cdc.gov/ncbddd/fasd/documents/FAS_guidelines_accessible.pdf. Accessed April 10, 2010. | |
The place to start: Spotting mothers at risk
Recognizing an infant with FAS starts by asking the baby’s mother about her pattern of drinking while she was pregnant. Most studies on the effects of gestational exposure to alcohol have emphasized moderate to high levels of exposure. In 1 study, children who were exposed to binge drinking were 1.7 times as likely to have IQ scores in the mentally retarded range and 2.5 times more likely to have clinically significant levels of delinquent behavior.4 Binge drinking is defined by the National Institute of Alcohol Abuse and Alcoholism as a pattern of drinking that brings blood alcohol concentration to 0.8% or above, which typically happens in women who consume 4 or more drinks in a period of about 2 hours.5
But a pregnant woman doesn’t have to be a binge drinker to put her fetus at risk. Even low levels of prenatal alcohol use—as low as 1 drink per week—have been associated with adverse behavioral changes in children, including increased aggressive behaviors documented at school age.6,7 The research documenting effects at these low levels has led the American Academy of Pediatrics (AAP) and the American Congress of Obstetricians and Gynecologists (ACOG) to recommend total abstinence from alcohol throughout pregnancy.8,9 Patterns of “at risk” drinking for women include binge drinking or persistent regular use (>7 drinks in 1 week). If a mother provides a history of that level of prenatal exposure, her child should be referred for multidisciplinary evaluation at an FAS center, even in the absence of the characteristic facial features.1
The face of FAS
Without a history of prenatal alcohol exposure, the cardinal features of facial dysmorphia (short palpebral fissures, smooth philtrum, and thin vermillion border) plus deficits in height and weight are the main physical findings of FAS. Evaluating height and weight percentiles is a routine part of well-child care, requiring minimal training. Height or weight or both at or below the 10th percentile, adjusted for age, sex, gestational age, and race or ethnicity, meet part of the CDC diagnostic criteria for FAS, but must be accompanied by at least 1 of the typical facial features associated with FAS to meet referral guidelines.1 The diagnostic guidelines are more restrictive, requiring all 3 facial features to meet the threshold for an FAS diagnosis, vs another diagnosis, such as alcohol-related neurodevelopmental disorders (TABLE 1).
Learning to measure faces. Examining a child for the facial characteristics of FAS requires a set of skills that can be learned in a relatively short time, with moderate interrater reliability when compared with dysmorphologists, according to 1 study.10
Tools for measuring. Palpebral fissure length (PFL) can be measured with a clear plastic ruler pressed onto the child’s cheek to determine the distance from the endocanthion to the exocanthion while the child is gazing upward.11 To meet the CDC criteria for FAS, this distance should be at or below the 10th percentile compared to norms. The shape of the lips and the nature of the philtrum are then compared to preestablished comparison photographs available on the University of Washington Lip-Philtrum Guides (see URL that follows).12 The vermillion border and the philtrum must both receive a rank of 4 or 5 to meet FAS criteria.11
Changes in the clinical presentation of fetal alcohol syndrome (FAS) occur across the lifespan. Clinicians searching for an explanation of an older child’s difficulties may need to reconsider a possible diagnosis of FAS, even if the facial features are less recognizable.
Preschool children with FAS may display a delay in early language acquisition and the beginnings of attention problems and hyperactivity. School-age children may have difficulty remembering material even when they have gone over it many times. They may lack social perception skills, be hyperactive, and show cognitive delays. Mathematics is often an area of severe delay, and sleep problems can persist.1
Teens and adults with FAS often have a wide range of secondary disabilities: disrupted schooling, inappropriate sexual behavior, mental health problems, aggression, trouble with the law, confinement in jail or as inpatients in psychiatric or substance abuse treatment facilities, alcohol and drug problems, and failure or inability to live independently at an appropriate age. They may have trouble finding a job and keeping one. More than 90% of patients with FAS exhibit mental health problems, with attention problems appearing in early childhood and persisting, and depression appearing in adolescence and adulthod.15
Tools available online for physicians include Lip-Philtrum Guides (www.depts.washington.edu/fasdpn/htmls/lip-philtrum-guides.htm) and an instructional video depicting PFL measurement techniques (www.depts.washington.edu/fasdpn/htmls/photo-face.htm), both from the University of Washington FAS Diagnostic and Prevention Network. In addition, a physical evaluation summary form, with reference data for PFL in Caucasian, black, and Hispanic children, is available at http://www.fas.academicedge.com/documents/phyevaln.pdf.
The Astley-Clarren criteria. The 4-digit diagnostic code developed by Astley and Clarren for diagnosis of FAS and employed at some FAS referral centers uses very strict criteria.13 Centers using these criteria define “abnormal” as ≥2 standard deviations below the mean or its equivalent, ≤2.5th percentile.13 Th is applies to the 3 facial features and CNS dysfunction (low IQ, eg). If all 3 facial features are identified in the Astley-Clarren system as abnormal (PFL ≤2.5th percentile, lip philtrum 5, vermillion 5), the sensitivity of the facial features is 100% and specificity is 99.8% for a diagnosis of FAS.13
The CDC criteria, developed with increased surveillance by providers as a goal, uses relaxed criteria of ≤10th percentile of PFL and 4 or 5 on the philtrum/vermillion border guide to identify abnormal facial features and <10th percentile in CNS dysfunctions. Sensitivity and specificity data for those CDC criteria are not available.1
CNS abnormalities may be noted early enough to trigger a referral for complete evaluation, but must be present in some degree to confirm a diagnosis of FAS. Abnormalities may include microcephaly with head circumference below the 10th percentile; clinically significant brain abnormalities observable through imaging, especially a small or absent corpus callosum; and functional deficits in any of a multitude of domains. In an infant, these deficits may be expressed in global developmental delays, sleep cycle problems, poor muscle tone, and feeding problems with poor suck and texture aversion.1
Evaluation may not confirm the diagnosis. Children referred for more extensive evaluation may or may not be confirmed to have FAS. In 2 demographically similar counties in New York state, only 5% of children initially identified in 1 county (10 of 208) and 13% (53 of 420) of children in the other county were confirmed to have FAS.12 The FAS diagnosis is complicated and the CNS and growth deficiencies may not be expressed until a later age.14 (See “Fetal alcohol syndrome across the lifespan”1,15)
Providers may feel reluctant to alarm or stigmatize families when they are unsure of the diagnosis, but the long-term benefit of confirming the diagnosis early on may be significant for the child and family. The case on page 341 (Tanya) illustrates the complexity of diagnosing FASD.
The encouraging news for family physicians is that the odds of escaping adverse life outcomes are increased 2- to 4-fold by receiving a diagnosis of FAS before age 6 and by being raised in a stable environment.16 Early diagnosis can be protective by helping with eligibility requirements for support services and by opening the door to medical management of FAS-associated conditions such as ADHD and depression. In addition, the diagnosis can alert family physicians to the family’s need for help with ongoing problems with alcohol use. The case on page 341 (Brianna) illustrates the complex secondary problems a teen with FAS may face.
Putting families in touch with resources
Multidisciplinary FAS teams may include physicians (a geneticist or developmental pediatrician), psychologists, speech pathologists, educational specialists, social workers, and occupational therapists. These groups typically have in-depth intake and evaluation processes, including neurodiagnostic studies that help clarify the cognitive and functional domains that are affected.
You can locate the nearest FAS evaluation team and other resources for providers and families on the National and State Resource Directory for the National Organization on Fetal Alcohol Syndrome. Go to www.nofas.org, click on Resources, then on National and State Resources Directory in the box on the left side of the page. There may be a waiting list for evaluation, but under Part C of the Individuals with Disabilities Education Act (IDEA), FAS is considered a “presumptive eligibility” diagnosis. Presumptive diagnoses allow children under age 3 at risk of later developmental delay to be served without meeting particular eligibility criteria.1 Physicians may refer these children for developmental assessment services and early intervention services while waiting for the more complete FAS evaluation.
After the age of 3, children and families are referred to preschool programs for children with disabilities that are administered through IDEA Part B, with no “presumptive eligibility” diagnoses. Eligibility for educational services under this program is entirely based on functional criteria.
Your best bet: Prevention
The key to preventing FAS is to find out whether your patient’s drinking patterns and contraceptive habits put her at risk for an alcohol-exposed pregnancy. Make it routine practice to ask women, in a way that encourages honest reporting, about both of these aspects of their lives. The US Preventive Services Task Force recommends screening and counseling intervention in primary care settings to reduce alcohol misuse in adults, including pregnant women.17 The case on page 341 (Clarice) illustrates how screening and brief intervention can be used to prevent alcohol-exposed pregnancy.
TANYA
Possible, though unconfirmed, FAS
This 1-month-old African American girl was admitted to the hospital with stridor, possible cardiorespiratory issues, and failure to thrive. She exhibited microcephaly, poor suck, floppy overall muscle tone, and small palpebral fissure lengths. The respiratory noise was attributed to tracheomalacia, secondary to her poor muscle tone.
An initial magnetic resonance imaging of the brain showed an almost complete absence of the corpus callosum. Obviously at risk for future delays, Tanya was referred for early childhood development intervention. By the age of 5½, she was within her peer group’s normal range in fine motor, gross motor, and speech skills. She was removed from her mother’s care for neglect and later placed in an extended family adoption.
Her initial evaluation took place before the widespread publication of fetal alcohol syndrome (FAS) criteria, and she was not referred for more specific FAS evaluation, as she would have been had she been seen more recently. Tanya has been lost to long-term follow-up from her initial medical home, but her mother returned to the same practice for a subsequent pregnancy and was screened as a problem drinker.
BRIANNA
Facing severe secondary disabilities
This 16-year-old Caucasian girl entered foster care for the second time because her first placement could not deal with her complex behavioral issues. Her mother committed suicide last year, and her father is in an alcohol rehabilitation program. No pregnancy history is available.
The social service agency supervising Brianna’s care decided not to return her to her father’s home. She made a suicidal gesture, her behavior is sometimes violent, and she has been diagnosed with attention deficit hyperactivity disorder (ADHD). She is being treated for depression, requiring multiple medications.
Brianna’s life has been difficult. Before she was 2 years old, she underwent surgery for a ventricular septal defect. Although her cardiac repair was successful, she remains significantly underweight, <3rd percentile on the growth curve. Because she is an adolescent, her facial features are less distinctive for FAS, but she appears to have a smooth philtrum and thin vermillion. Her learning disabilities are significant enough that she has been held back a grade and requires an individualized education plan.
It may be too late to help provide any assistance to Brianna, who is already experiencing severe secondary disabilities. But if a diagnosis of FAS (or alcohol-related neurobehavioral disorder) can be made, even at this point in her life, provisions may be made within the foster care system for transitional housing and emphasis on life skills training, rather than simply allowing her to “age out” of the system when she turns 18.
CLARICE
Preventing an alcohol-exposed pregnancy
Clarice is an 18-year-old, college-bound woman who came in for a pre-college health maintenance examination. She reported being sexually active and was using effective contraception only intermittently. On the TWEAK questionnaire, she said the most she has had to drink on a single occasion was 6 drinks, noted that she had never passed out and had not had any problems associated with drinking. The only worry she connected with drinking was a fear of gaining weight.
Clarice met the criteria for “at risk” drinking (TABLE 3). She was a candidate for a brief intervention, including information on the hazards of alcohol-exposed pregnancy and on effective contraceptive practices. We scheduled a telephone follow-up and checkup in 6 months.
* Drawn from the author’s case files. Names have been changed to protect patient privacy.
Screening should include simple quantity and frequency questions developed by the National Institute on Alcohol Abuse to clarify a patient’s current drinking patterns. The questions include the numbers of days per week of any drinking, the average number of drinks per day, and the maximum number of drinks consumed in 1 day during the past month. Determining that a woman drinks more than 7 drinks per week has a 29% sensitivity, but a 90% specificity for identifying lifetime risk of alcohol abuse or dependence.18
Other tools include TWEAK (Tolerance, Worry, Eye-opener, Amnesia, (K)Cut down), T-ACE (Tolerance, Annoyed, Cut down, Eye opener), and AUDIT (Alcohol Use Disorder Identification Test). They are detailed below and available online at Project Cork. Go to www.projectcork.org, and click on “clinical tools.”
The 5-item TWEAK tool (TABLE 2) appears to be the optimal screening questionnaire for identifying women in racially mixed populations with heavy drinking or alcohol abuse and dependence, but a score of 2 points should be the threshold for identifying female problem drinkers.19,20 Using the lower cutoff of 2, the sensitivity of TWEAK is in the 87% to 91% range for women, with a specificity of 77% to 90%.18
The T-ACE tool is a set of 4 questions, with the question addressing tolerance weighted more heavily than the others. With a score of 2 or more, the sensitivity of T-ACE is 70% to 88%; the specificity is 79% to 85%.18
The AUDIT tool is a self-administered screen that consists of a series of 10 questions that are each scored on a scale of 0 to 4. The maximum score is 40. A score of 2 indicates some harmful use of alcohol, but a score of 8 or more has a sensitivity of 59% to 66%, with a specificity of 93% to 97% in women.18
TABLE 2
TWEAK your patients for alcohol use
| Tolerance: How many drinks does it take for you to: | Score |
| 2 points for ≥3 drinks 2 points for ≥5 drinks |
| Worry about drinking | |
| Have your friends or relatives worried about your drinking in the past year? | 1 point for Yes |
| Eye-opener | |
| Do you sometimes take a drink in the morning when you first get up? | 1 point for Yes |
| Amnesia | |
| Are there times when you drink and afterwards can’t remember what you said or did? | 1 point for Yes |
| (K)Cut down | |
| Do you sometimes feel the need to cut down on your drinking? | 1 point for Yes |
| Scoring: ≥3 points is considered positive for alcoholism/heavy drinking. Thresholds differ for screening different populations, and a score of ≥2 points should be used as the threshold for identifying female problem drinkers. | |
| Source: Chan AW, et al. Alcohol Clin Exp Res. 1993.19 | |
When your patient is at risk
Brief interventions are recommended for nonpregnant and pregnant women who have exhibited a pattern of at-risk or problem drinking.21TABLE 3 summarizes patterns of drinking in women, from not drinking at all through various degrees of risk to alcohol dependency. Referral to an addiction specialist is recommended for women with alcohol dependence.
Brief interventions for alcohol abuse can be single-session encounters from 5 to 15 minutes’ duration, or multi-contact brief sessions, including possible phone follow-up contacts. Project TrEAT (Trial for Early Alcohol Treatment) provided two 15-minute sessions with the primary care physician (either a family physician or internist in community-based practice) scheduled 1 month apart, with nurse follow-up phone calls 2 weeks after each appointment.22
TABLE 3
Drinking patterns in women
Abstainer
|
Low-risk drinking
|
At-risk drinking
|
Problem drinking
|
Alcohol-dependent drinking: Maladaptive patterns of alcohol use leading to clinically significant impairment manifested by 3 or more of the following, occurring at any time during the same 12-month period:
|
| Source: Training program for medical students and other health professionals on fetal alcohol syndrome. Presented by the Midwest Regional Fetal Alcohol Syndrome Training Center; March 18, 2005; St. Louis, Mo. |
Patients received general information regarding adverse effects of alcohol and the prevalence of problem drinking, in addition to tools to help them identify drinking triggers and track their consumption. The patient and physician developed a “drinking agreement” in the form of a rescription. Men and non pregnant women were included in this study.
Women reduced their alcohol use by 47% and their frequency of binge drinking by 56%, as noted at a 6-month follow-up, with changes well maintained at 12 months. The reductions for female patients were actually slightly higher than for male participants.22
Chang and colleagues provided a 25-minute single session brief intervention to pregnant women who had screened positive on the T-ACE questionnaire with a score of 2 or more, and were identified as being at risk for prenatal alcohol use.23 Participants were randomly assigned to the intervention group or a control group. Both the control group and the brief intervention group decreased their use of alcohol after enrolling in the study and undergoing the initial detailed assessment.
For women who were heavier drinkers, the brief interventions for prenatal alcohol use were statistically more effective in reducing their frequency of alcohol consumption, vs the initial assessment alone. In addition, the effects of the brief intervention were significantly enhanced when a support partner of the woman’s choice also participated.23
The Project Choices Intervention Research Group studied an intervention that included 4 sessions of motivational interviewing regarding alcohol habits, and a contraception counseling session.24 Study participants were recruited from 6 community-based settings with high proportions of women at risk for an alcohol-exposed pregnancy, including a jail and 2 drug and alcohol treatment centers. Among the 143 women who completed the 6-month follow-up, 68.5% were no longer at risk of having an alcohol-exposed pregnancy.
These participants successfully lowered their risk by reducing alcohol use only (12.9%), adopting appropriate contraception use only (23.1%), or by changing both risk factors (32.9%). Even if all the study participants who were lost to follow-up were assumed to have been unsuccessful at eliminating their risk of alcohol-exposed pregnancy, more than half of the women (51.6%) successfully changed.24
Take advantage of opportunities
FAS is the most severe consequence of alcohol-exposed pregnancy, leaving the affected child with a lifelong disability. As a family physician, you have access to easy-touse, cost-effective clinical tools to screen for at-risk drinking behaviors and have sufficient rapport with your patients to encourage effective contraceptive practices. You also have effective tools for helping patients reduce their alcohol consumption.
Within the context of your long-term relationships with patients, you can provide brief interventions that include factual information and opportunities for goal setting. You can assist families with an FAS child to access services, manage medically related complications, and plan for special education and vocational skills training.
Recognition that 1 child in a family is affected by prenatal alcohol exposure gives you another window of opportunity to address the underlying substance use issues in the mother and the family, increasing the odds that future pregnancies will not be alcohol exposed.
CORRESPONDENCE Mary C. Boyce, MD, Wesley Family Medicine Residency, 850 N. Hillside, Wichita, KS 67214; [email protected]
Screen all females of childbearing age for alcohol use with standardized screening instruments such as TWEAK, T-ACE, or AUDIT. A
Use brief, in-office interventions to decrease alcohol consumption and increase effective contraception in sexually active women. Involve a supportive adult of the patient’s choosing where possible. A
Advise pregnant patients that complete abstinence from alcohol is safest. B
Refer a child who meets FAS referral criteria for multi-disciplinary evaluations as early as possible. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Family physicians who care for infants and young children are often asked to diagnose growth lags and failure to meet parents’ expectations for reaching developmental milestones: Why isn’t my child gaining weight? Why isn’t he talking? The other kids in the day-care center ride tricycles—why can’t he? Will he catch up? My mother thinks he’s funny looking. Do you?
Simple reassurance is all that most of these worried families need. But for families with children whose growth or developmental milestones are sufficiently outside the usual parameters, more than reassurance is called for. As you consider whether the lags that worry parents are signs of a serious disability, it’s important to make a place for fetal alcohol syndrome (FAS) in your differential.
FAS, a congenital disorder caused by alcohol exposure during pregnancy, is characterized by growth deficiency before and after birth, distinctive facial features, and central nervous system (CNS) dysfunctions. The cognitive and developmental effects of FAS persist throughout life and are severe enough to limit employment and independent living.1,2
A spectrum of severity. FAS is the most severe expression of prenatal alcohol exposure. The term fetal alcohol spectrum disorders (FASD) is a nondiagnostic umbrella term that includes FAS as well as ARND (alcohol-related neurobehavioral disorder) and ARBD (alcohol-related birth defects). Children with ARND and ARBD fail to meet the full FAS diagnostic criteria but still exhibit the negative effects of gestational alcohol exposure. Centers for Disease Control and Prevention (CDC) diagnostic criteria for FAS are summarized in TABLE 1. Studies by the CDC have reported FAS prevalence rates from 0.2 to 1.5 cases per 1000 live births, with a higher prevalence among minority (Native American and African American) and impoverished groups.1
An opportunity—and a challenge. As a family physician, you have a unique opportunity to modify the impact of FAS by recognizing the disorder in infancy or early childhood, actively engineering appropriate referrals, and supporting families in the difficult task of parenting a child with disabilities. Correctly diagnosing a child with FAS before age 6 can have a protective influence, decreasing the odds that he or she will suffer severe secondary disabilities in adolescence and adulthood. You can also help prevent FAS by screening for potentially harmful drinking patterns and helping sexually active female patients decrease alcohol consumption and use contraception successfully.
Providing these supportive and preventive services can be challenging. A recent survey of pediatricians revealed that only 34% felt prepared to manage and coordinate the treatment of children with FASD, and only 13% routinely counseled adolescent patients about the risks of drinking and pregnancy.3 Th is article will help you surmount the difficulties these tasks present and perform vital functions for alcohol-affected families you may encounter in your practice.
TABLE 1
Diagnostic criteria for fetal alcohol syndrome
Facial dysmorphia
| ≤10th percentile for age and racial norms Score of 4 or 5 on lip-philtrum guide* Score of 4 or 5 on lip-philtrum guide* |
| Growth problems | <10th percentile for age, sex, gestational age, racial norms in height or weight, prenatally or postnatally |
| CNS abnormalities | Any structural abnormality (head circumference <10% of age norm or clinically significant brain abnormalities observable through imaging); neurological abnormality not due to postnatal insult or fever; or functional abnormality demonstrated by cognitive performance less than expected for age, schooling, or family circumstances. An individual could meet the CNS abnormality criteria for a FAS diagnosis through a structural abnormality, yet not demonstrate detectable functional deficits. |
| CNS, central nervous system. | |
| *The lip-philtrum guide is available at http://depts.washington.edu/fasdpn/htmls/lip-philtrum-guides.htm. | |
| Source: Centers for Disease Control and Prevention. Fetal Alcohol Syndrome: Guidelines for Referral and Diagnosis. 2005. Available at www.cdc.gov/ncbddd/fasd/documents/FAS_guidelines_accessible.pdf. Accessed April 10, 2010. | |
The place to start: Spotting mothers at risk
Recognizing an infant with FAS starts by asking the baby’s mother about her pattern of drinking while she was pregnant. Most studies on the effects of gestational exposure to alcohol have emphasized moderate to high levels of exposure. In 1 study, children who were exposed to binge drinking were 1.7 times as likely to have IQ scores in the mentally retarded range and 2.5 times more likely to have clinically significant levels of delinquent behavior.4 Binge drinking is defined by the National Institute of Alcohol Abuse and Alcoholism as a pattern of drinking that brings blood alcohol concentration to 0.8% or above, which typically happens in women who consume 4 or more drinks in a period of about 2 hours.5
But a pregnant woman doesn’t have to be a binge drinker to put her fetus at risk. Even low levels of prenatal alcohol use—as low as 1 drink per week—have been associated with adverse behavioral changes in children, including increased aggressive behaviors documented at school age.6,7 The research documenting effects at these low levels has led the American Academy of Pediatrics (AAP) and the American Congress of Obstetricians and Gynecologists (ACOG) to recommend total abstinence from alcohol throughout pregnancy.8,9 Patterns of “at risk” drinking for women include binge drinking or persistent regular use (>7 drinks in 1 week). If a mother provides a history of that level of prenatal exposure, her child should be referred for multidisciplinary evaluation at an FAS center, even in the absence of the characteristic facial features.1
The face of FAS
Without a history of prenatal alcohol exposure, the cardinal features of facial dysmorphia (short palpebral fissures, smooth philtrum, and thin vermillion border) plus deficits in height and weight are the main physical findings of FAS. Evaluating height and weight percentiles is a routine part of well-child care, requiring minimal training. Height or weight or both at or below the 10th percentile, adjusted for age, sex, gestational age, and race or ethnicity, meet part of the CDC diagnostic criteria for FAS, but must be accompanied by at least 1 of the typical facial features associated with FAS to meet referral guidelines.1 The diagnostic guidelines are more restrictive, requiring all 3 facial features to meet the threshold for an FAS diagnosis, vs another diagnosis, such as alcohol-related neurodevelopmental disorders (TABLE 1).
Learning to measure faces. Examining a child for the facial characteristics of FAS requires a set of skills that can be learned in a relatively short time, with moderate interrater reliability when compared with dysmorphologists, according to 1 study.10
Tools for measuring. Palpebral fissure length (PFL) can be measured with a clear plastic ruler pressed onto the child’s cheek to determine the distance from the endocanthion to the exocanthion while the child is gazing upward.11 To meet the CDC criteria for FAS, this distance should be at or below the 10th percentile compared to norms. The shape of the lips and the nature of the philtrum are then compared to preestablished comparison photographs available on the University of Washington Lip-Philtrum Guides (see URL that follows).12 The vermillion border and the philtrum must both receive a rank of 4 or 5 to meet FAS criteria.11
Changes in the clinical presentation of fetal alcohol syndrome (FAS) occur across the lifespan. Clinicians searching for an explanation of an older child’s difficulties may need to reconsider a possible diagnosis of FAS, even if the facial features are less recognizable.
Preschool children with FAS may display a delay in early language acquisition and the beginnings of attention problems and hyperactivity. School-age children may have difficulty remembering material even when they have gone over it many times. They may lack social perception skills, be hyperactive, and show cognitive delays. Mathematics is often an area of severe delay, and sleep problems can persist.1
Teens and adults with FAS often have a wide range of secondary disabilities: disrupted schooling, inappropriate sexual behavior, mental health problems, aggression, trouble with the law, confinement in jail or as inpatients in psychiatric or substance abuse treatment facilities, alcohol and drug problems, and failure or inability to live independently at an appropriate age. They may have trouble finding a job and keeping one. More than 90% of patients with FAS exhibit mental health problems, with attention problems appearing in early childhood and persisting, and depression appearing in adolescence and adulthod.15
Tools available online for physicians include Lip-Philtrum Guides (www.depts.washington.edu/fasdpn/htmls/lip-philtrum-guides.htm) and an instructional video depicting PFL measurement techniques (www.depts.washington.edu/fasdpn/htmls/photo-face.htm), both from the University of Washington FAS Diagnostic and Prevention Network. In addition, a physical evaluation summary form, with reference data for PFL in Caucasian, black, and Hispanic children, is available at http://www.fas.academicedge.com/documents/phyevaln.pdf.
The Astley-Clarren criteria. The 4-digit diagnostic code developed by Astley and Clarren for diagnosis of FAS and employed at some FAS referral centers uses very strict criteria.13 Centers using these criteria define “abnormal” as ≥2 standard deviations below the mean or its equivalent, ≤2.5th percentile.13 Th is applies to the 3 facial features and CNS dysfunction (low IQ, eg). If all 3 facial features are identified in the Astley-Clarren system as abnormal (PFL ≤2.5th percentile, lip philtrum 5, vermillion 5), the sensitivity of the facial features is 100% and specificity is 99.8% for a diagnosis of FAS.13
The CDC criteria, developed with increased surveillance by providers as a goal, uses relaxed criteria of ≤10th percentile of PFL and 4 or 5 on the philtrum/vermillion border guide to identify abnormal facial features and <10th percentile in CNS dysfunctions. Sensitivity and specificity data for those CDC criteria are not available.1
CNS abnormalities may be noted early enough to trigger a referral for complete evaluation, but must be present in some degree to confirm a diagnosis of FAS. Abnormalities may include microcephaly with head circumference below the 10th percentile; clinically significant brain abnormalities observable through imaging, especially a small or absent corpus callosum; and functional deficits in any of a multitude of domains. In an infant, these deficits may be expressed in global developmental delays, sleep cycle problems, poor muscle tone, and feeding problems with poor suck and texture aversion.1
Evaluation may not confirm the diagnosis. Children referred for more extensive evaluation may or may not be confirmed to have FAS. In 2 demographically similar counties in New York state, only 5% of children initially identified in 1 county (10 of 208) and 13% (53 of 420) of children in the other county were confirmed to have FAS.12 The FAS diagnosis is complicated and the CNS and growth deficiencies may not be expressed until a later age.14 (See “Fetal alcohol syndrome across the lifespan”1,15)
Providers may feel reluctant to alarm or stigmatize families when they are unsure of the diagnosis, but the long-term benefit of confirming the diagnosis early on may be significant for the child and family. The case on page 341 (Tanya) illustrates the complexity of diagnosing FASD.
The encouraging news for family physicians is that the odds of escaping adverse life outcomes are increased 2- to 4-fold by receiving a diagnosis of FAS before age 6 and by being raised in a stable environment.16 Early diagnosis can be protective by helping with eligibility requirements for support services and by opening the door to medical management of FAS-associated conditions such as ADHD and depression. In addition, the diagnosis can alert family physicians to the family’s need for help with ongoing problems with alcohol use. The case on page 341 (Brianna) illustrates the complex secondary problems a teen with FAS may face.
Putting families in touch with resources
Multidisciplinary FAS teams may include physicians (a geneticist or developmental pediatrician), psychologists, speech pathologists, educational specialists, social workers, and occupational therapists. These groups typically have in-depth intake and evaluation processes, including neurodiagnostic studies that help clarify the cognitive and functional domains that are affected.
You can locate the nearest FAS evaluation team and other resources for providers and families on the National and State Resource Directory for the National Organization on Fetal Alcohol Syndrome. Go to www.nofas.org, click on Resources, then on National and State Resources Directory in the box on the left side of the page. There may be a waiting list for evaluation, but under Part C of the Individuals with Disabilities Education Act (IDEA), FAS is considered a “presumptive eligibility” diagnosis. Presumptive diagnoses allow children under age 3 at risk of later developmental delay to be served without meeting particular eligibility criteria.1 Physicians may refer these children for developmental assessment services and early intervention services while waiting for the more complete FAS evaluation.
After the age of 3, children and families are referred to preschool programs for children with disabilities that are administered through IDEA Part B, with no “presumptive eligibility” diagnoses. Eligibility for educational services under this program is entirely based on functional criteria.
Your best bet: Prevention
The key to preventing FAS is to find out whether your patient’s drinking patterns and contraceptive habits put her at risk for an alcohol-exposed pregnancy. Make it routine practice to ask women, in a way that encourages honest reporting, about both of these aspects of their lives. The US Preventive Services Task Force recommends screening and counseling intervention in primary care settings to reduce alcohol misuse in adults, including pregnant women.17 The case on page 341 (Clarice) illustrates how screening and brief intervention can be used to prevent alcohol-exposed pregnancy.
TANYA
Possible, though unconfirmed, FAS
This 1-month-old African American girl was admitted to the hospital with stridor, possible cardiorespiratory issues, and failure to thrive. She exhibited microcephaly, poor suck, floppy overall muscle tone, and small palpebral fissure lengths. The respiratory noise was attributed to tracheomalacia, secondary to her poor muscle tone.
An initial magnetic resonance imaging of the brain showed an almost complete absence of the corpus callosum. Obviously at risk for future delays, Tanya was referred for early childhood development intervention. By the age of 5½, she was within her peer group’s normal range in fine motor, gross motor, and speech skills. She was removed from her mother’s care for neglect and later placed in an extended family adoption.
Her initial evaluation took place before the widespread publication of fetal alcohol syndrome (FAS) criteria, and she was not referred for more specific FAS evaluation, as she would have been had she been seen more recently. Tanya has been lost to long-term follow-up from her initial medical home, but her mother returned to the same practice for a subsequent pregnancy and was screened as a problem drinker.
BRIANNA
Facing severe secondary disabilities
This 16-year-old Caucasian girl entered foster care for the second time because her first placement could not deal with her complex behavioral issues. Her mother committed suicide last year, and her father is in an alcohol rehabilitation program. No pregnancy history is available.
The social service agency supervising Brianna’s care decided not to return her to her father’s home. She made a suicidal gesture, her behavior is sometimes violent, and she has been diagnosed with attention deficit hyperactivity disorder (ADHD). She is being treated for depression, requiring multiple medications.
Brianna’s life has been difficult. Before she was 2 years old, she underwent surgery for a ventricular septal defect. Although her cardiac repair was successful, she remains significantly underweight, <3rd percentile on the growth curve. Because she is an adolescent, her facial features are less distinctive for FAS, but she appears to have a smooth philtrum and thin vermillion. Her learning disabilities are significant enough that she has been held back a grade and requires an individualized education plan.
It may be too late to help provide any assistance to Brianna, who is already experiencing severe secondary disabilities. But if a diagnosis of FAS (or alcohol-related neurobehavioral disorder) can be made, even at this point in her life, provisions may be made within the foster care system for transitional housing and emphasis on life skills training, rather than simply allowing her to “age out” of the system when she turns 18.
CLARICE
Preventing an alcohol-exposed pregnancy
Clarice is an 18-year-old, college-bound woman who came in for a pre-college health maintenance examination. She reported being sexually active and was using effective contraception only intermittently. On the TWEAK questionnaire, she said the most she has had to drink on a single occasion was 6 drinks, noted that she had never passed out and had not had any problems associated with drinking. The only worry she connected with drinking was a fear of gaining weight.
Clarice met the criteria for “at risk” drinking (TABLE 3). She was a candidate for a brief intervention, including information on the hazards of alcohol-exposed pregnancy and on effective contraceptive practices. We scheduled a telephone follow-up and checkup in 6 months.
* Drawn from the author’s case files. Names have been changed to protect patient privacy.
Screening should include simple quantity and frequency questions developed by the National Institute on Alcohol Abuse to clarify a patient’s current drinking patterns. The questions include the numbers of days per week of any drinking, the average number of drinks per day, and the maximum number of drinks consumed in 1 day during the past month. Determining that a woman drinks more than 7 drinks per week has a 29% sensitivity, but a 90% specificity for identifying lifetime risk of alcohol abuse or dependence.18
Other tools include TWEAK (Tolerance, Worry, Eye-opener, Amnesia, (K)Cut down), T-ACE (Tolerance, Annoyed, Cut down, Eye opener), and AUDIT (Alcohol Use Disorder Identification Test). They are detailed below and available online at Project Cork. Go to www.projectcork.org, and click on “clinical tools.”
The 5-item TWEAK tool (TABLE 2) appears to be the optimal screening questionnaire for identifying women in racially mixed populations with heavy drinking or alcohol abuse and dependence, but a score of 2 points should be the threshold for identifying female problem drinkers.19,20 Using the lower cutoff of 2, the sensitivity of TWEAK is in the 87% to 91% range for women, with a specificity of 77% to 90%.18
The T-ACE tool is a set of 4 questions, with the question addressing tolerance weighted more heavily than the others. With a score of 2 or more, the sensitivity of T-ACE is 70% to 88%; the specificity is 79% to 85%.18
The AUDIT tool is a self-administered screen that consists of a series of 10 questions that are each scored on a scale of 0 to 4. The maximum score is 40. A score of 2 indicates some harmful use of alcohol, but a score of 8 or more has a sensitivity of 59% to 66%, with a specificity of 93% to 97% in women.18
TABLE 2
TWEAK your patients for alcohol use
| Tolerance: How many drinks does it take for you to: | Score |
| 2 points for ≥3 drinks 2 points for ≥5 drinks |
| Worry about drinking | |
| Have your friends or relatives worried about your drinking in the past year? | 1 point for Yes |
| Eye-opener | |
| Do you sometimes take a drink in the morning when you first get up? | 1 point for Yes |
| Amnesia | |
| Are there times when you drink and afterwards can’t remember what you said or did? | 1 point for Yes |
| (K)Cut down | |
| Do you sometimes feel the need to cut down on your drinking? | 1 point for Yes |
| Scoring: ≥3 points is considered positive for alcoholism/heavy drinking. Thresholds differ for screening different populations, and a score of ≥2 points should be used as the threshold for identifying female problem drinkers. | |
| Source: Chan AW, et al. Alcohol Clin Exp Res. 1993.19 | |
When your patient is at risk
Brief interventions are recommended for nonpregnant and pregnant women who have exhibited a pattern of at-risk or problem drinking.21TABLE 3 summarizes patterns of drinking in women, from not drinking at all through various degrees of risk to alcohol dependency. Referral to an addiction specialist is recommended for women with alcohol dependence.
Brief interventions for alcohol abuse can be single-session encounters from 5 to 15 minutes’ duration, or multi-contact brief sessions, including possible phone follow-up contacts. Project TrEAT (Trial for Early Alcohol Treatment) provided two 15-minute sessions with the primary care physician (either a family physician or internist in community-based practice) scheduled 1 month apart, with nurse follow-up phone calls 2 weeks after each appointment.22
TABLE 3
Drinking patterns in women
Abstainer
|
Low-risk drinking
|
At-risk drinking
|
Problem drinking
|
Alcohol-dependent drinking: Maladaptive patterns of alcohol use leading to clinically significant impairment manifested by 3 or more of the following, occurring at any time during the same 12-month period:
|
| Source: Training program for medical students and other health professionals on fetal alcohol syndrome. Presented by the Midwest Regional Fetal Alcohol Syndrome Training Center; March 18, 2005; St. Louis, Mo. |
Patients received general information regarding adverse effects of alcohol and the prevalence of problem drinking, in addition to tools to help them identify drinking triggers and track their consumption. The patient and physician developed a “drinking agreement” in the form of a rescription. Men and non pregnant women were included in this study.
Women reduced their alcohol use by 47% and their frequency of binge drinking by 56%, as noted at a 6-month follow-up, with changes well maintained at 12 months. The reductions for female patients were actually slightly higher than for male participants.22
Chang and colleagues provided a 25-minute single session brief intervention to pregnant women who had screened positive on the T-ACE questionnaire with a score of 2 or more, and were identified as being at risk for prenatal alcohol use.23 Participants were randomly assigned to the intervention group or a control group. Both the control group and the brief intervention group decreased their use of alcohol after enrolling in the study and undergoing the initial detailed assessment.
For women who were heavier drinkers, the brief interventions for prenatal alcohol use were statistically more effective in reducing their frequency of alcohol consumption, vs the initial assessment alone. In addition, the effects of the brief intervention were significantly enhanced when a support partner of the woman’s choice also participated.23
The Project Choices Intervention Research Group studied an intervention that included 4 sessions of motivational interviewing regarding alcohol habits, and a contraception counseling session.24 Study participants were recruited from 6 community-based settings with high proportions of women at risk for an alcohol-exposed pregnancy, including a jail and 2 drug and alcohol treatment centers. Among the 143 women who completed the 6-month follow-up, 68.5% were no longer at risk of having an alcohol-exposed pregnancy.
These participants successfully lowered their risk by reducing alcohol use only (12.9%), adopting appropriate contraception use only (23.1%), or by changing both risk factors (32.9%). Even if all the study participants who were lost to follow-up were assumed to have been unsuccessful at eliminating their risk of alcohol-exposed pregnancy, more than half of the women (51.6%) successfully changed.24
Take advantage of opportunities
FAS is the most severe consequence of alcohol-exposed pregnancy, leaving the affected child with a lifelong disability. As a family physician, you have access to easy-touse, cost-effective clinical tools to screen for at-risk drinking behaviors and have sufficient rapport with your patients to encourage effective contraceptive practices. You also have effective tools for helping patients reduce their alcohol consumption.
Within the context of your long-term relationships with patients, you can provide brief interventions that include factual information and opportunities for goal setting. You can assist families with an FAS child to access services, manage medically related complications, and plan for special education and vocational skills training.
Recognition that 1 child in a family is affected by prenatal alcohol exposure gives you another window of opportunity to address the underlying substance use issues in the mother and the family, increasing the odds that future pregnancies will not be alcohol exposed.
CORRESPONDENCE Mary C. Boyce, MD, Wesley Family Medicine Residency, 850 N. Hillside, Wichita, KS 67214; [email protected]
1. Centers for Disease Control and Prevention. Fetal Alcohol Syndrome: Guidelines for Referral and Diagnosis. 2005. Available at: www.cdc.gov/ncbddd/fasd/documents/FAS_guidelines_accessible.pdf. Accessed April 10, 2010.
2. Spohr HL, Williams J, Steinhausen HC. Fetal alcohol spectrum disorders in young adulthood. J Pediatr. 2007;150:175-179.
3. Gahagan S, Sharpe TT, Brimacombe M, et al. Pediatricians’ knowledge, training, and experience in the care of children with fetal alcohol syndrome. Pediatrics. 2006;118:e657-e668.
4. Bailey BN, Delaney-Black V, Covington CY, et al. Prenatal exposure to binge drinking and cognitive and behavioral outcomes at age 7 years. Am J Obstet Gynecol. 2004;191:1037-1043.
5. CDC. Alcohol and public health/binge drinking. Quick stats. Available at: www.cdc.gov/alcohol/quickstats/binge_drinking.htm. Accessed April 21, 2010.
6. Sood B, Delaney-Black V, Covington C, et al. Prenatal alcohol exposure and childhood behavior at age 6 to 7 years: I. Doseresponse effect. Pediatrics. 2001;108:E34.-
7. Sokol RJ, Delaney-Black V, Nordstrom B. Fetal alcohol spectrum disorder. JAMA. 2003;290:2996-2999.
8. American Congress of Obstetricians and Gynecologists. ACOG Education Pamphlet AP170: Tobacco, alcohol, drugs, and pregnancy. Available at www.acog.org/publications/patient_education/bp170.cfm. Accessed May 3, 2010.
9. Committee on Substance Abuse and Committee on Children With Disabilities. Fetal alcohol syndrome and alcohol-related neurodevelopmental disorders. Pediatrics. 2000;106:358-361.
10. Jones KL, Robinson LK, Bakhireva LN, et al. Accuracy of the diagnosis of physical features of fetal alcohol syndrome by pediatricians after specialized training. Pediatrics. 2006;118:e1734-e1738.
11. University of Washington Fetal Alcohol Syndrome Diagnostic and Prevention Network. FAS facial photography and measurement instruction. Available at: www.depts.washington.edu/fasdpn/htmls/photo-face.htm. Accessed April 21,2010.
12. University of Washington Fetal Alcohol Syndrome Diagnostic and Prevention Network. Lip philtrum guides. Available at: www.depts.washington.edu/fasdpn/htmls/lip-philtrum-guides.htm. Accessed April 21, 2010.
13. Astley S. Comparison of the 4-digit diagnostic code and the Hoyme diagnostic guidelines for fetal alcohol spectrum disorder. Pediatrics. 2006;188:1532-1545.
14. Druschel CM, Fox DJ. Issues in estimating the prevalence of fetal alcohol syndrome: examination of 2 counties in New York State. Pediatrics. 2007;119:e384-e390.
15. Streissguth AP, Barr HM, Kogan J, et al. Understanding the occurrence of secondary disabilities in clients with fetal alcohol syndrome (FAS) and fetal alcohol effects (FAE). Final Report to the Centers for Disease Control and Prevention. Technical report no. 96-06. Seattle, WA: University of Washington, Fetal Alcohol and Drug Unit; 1996.
16. Streissguth AP, Bookstein FL, Barr H, et al. Risk factors for adverse life outcomes in fetal alcohol syndrome and fetal alcohol effects. J Dev Behav Pediatr. 2004;25:228-238.
17. US Preventive Services Task Force. Screening and behavioral interventions in primary care to reduce alcohol misuse: recommendation statement, April 2004. Available at: www.ahrq.gov/clinic/3rduspstf/alcohol/alcomisrs.htm. Accessed April 10, 2010.
18. Bradley KA, Boyd-Wickizer J, Powell SH, et al. Alcohol screening questionnaires in women: a critical review. JAMA. 1998;20:166-171.
19. Chan AW, Pristach EA, Welte JW, et al. Use of the TWEAK test in screening for alcoholism/heavy drinking in three populations. Alcohol Clin Exp Res. 1993;17:1188-1192.
20. Russell M, Bigler L. Screening for alcohol-related problems in an outpatient obstetric-gynecologic clinic. Am J Obstet Gynecol. 1979;134:4-12.
21. National Institute on Alcohol Abuse and Alcoholism. Helping patients who drink too much: a clinician’s guide. Updated January 2007. Available at: http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/clinicians_guide.htm. Accessed April 21, 2010.
22. Fleming MF, Barry KL, Manwell LB, et al. Brief physician advice for problem alcohol drinkers. JAMA. 1997;277:1039-1045.
23. Chang G, McNamara TK, Orav J, et al. Brief interventions for prenatal alcohol use: a randomized trial. Obstet Gynecol. 2005;105:991-998.
24. The Project Choices Intervention Research Group. Reducing the risk of alcohol-exposed pregnancies: a study of motivational intervention in community settings. Pediatrics. 2003;111:1131-1135.
1. Centers for Disease Control and Prevention. Fetal Alcohol Syndrome: Guidelines for Referral and Diagnosis. 2005. Available at: www.cdc.gov/ncbddd/fasd/documents/FAS_guidelines_accessible.pdf. Accessed April 10, 2010.
2. Spohr HL, Williams J, Steinhausen HC. Fetal alcohol spectrum disorders in young adulthood. J Pediatr. 2007;150:175-179.
3. Gahagan S, Sharpe TT, Brimacombe M, et al. Pediatricians’ knowledge, training, and experience in the care of children with fetal alcohol syndrome. Pediatrics. 2006;118:e657-e668.
4. Bailey BN, Delaney-Black V, Covington CY, et al. Prenatal exposure to binge drinking and cognitive and behavioral outcomes at age 7 years. Am J Obstet Gynecol. 2004;191:1037-1043.
5. CDC. Alcohol and public health/binge drinking. Quick stats. Available at: www.cdc.gov/alcohol/quickstats/binge_drinking.htm. Accessed April 21, 2010.
6. Sood B, Delaney-Black V, Covington C, et al. Prenatal alcohol exposure and childhood behavior at age 6 to 7 years: I. Doseresponse effect. Pediatrics. 2001;108:E34.-
7. Sokol RJ, Delaney-Black V, Nordstrom B. Fetal alcohol spectrum disorder. JAMA. 2003;290:2996-2999.
8. American Congress of Obstetricians and Gynecologists. ACOG Education Pamphlet AP170: Tobacco, alcohol, drugs, and pregnancy. Available at www.acog.org/publications/patient_education/bp170.cfm. Accessed May 3, 2010.
9. Committee on Substance Abuse and Committee on Children With Disabilities. Fetal alcohol syndrome and alcohol-related neurodevelopmental disorders. Pediatrics. 2000;106:358-361.
10. Jones KL, Robinson LK, Bakhireva LN, et al. Accuracy of the diagnosis of physical features of fetal alcohol syndrome by pediatricians after specialized training. Pediatrics. 2006;118:e1734-e1738.
11. University of Washington Fetal Alcohol Syndrome Diagnostic and Prevention Network. FAS facial photography and measurement instruction. Available at: www.depts.washington.edu/fasdpn/htmls/photo-face.htm. Accessed April 21,2010.
12. University of Washington Fetal Alcohol Syndrome Diagnostic and Prevention Network. Lip philtrum guides. Available at: www.depts.washington.edu/fasdpn/htmls/lip-philtrum-guides.htm. Accessed April 21, 2010.
13. Astley S. Comparison of the 4-digit diagnostic code and the Hoyme diagnostic guidelines for fetal alcohol spectrum disorder. Pediatrics. 2006;188:1532-1545.
14. Druschel CM, Fox DJ. Issues in estimating the prevalence of fetal alcohol syndrome: examination of 2 counties in New York State. Pediatrics. 2007;119:e384-e390.
15. Streissguth AP, Barr HM, Kogan J, et al. Understanding the occurrence of secondary disabilities in clients with fetal alcohol syndrome (FAS) and fetal alcohol effects (FAE). Final Report to the Centers for Disease Control and Prevention. Technical report no. 96-06. Seattle, WA: University of Washington, Fetal Alcohol and Drug Unit; 1996.
16. Streissguth AP, Bookstein FL, Barr H, et al. Risk factors for adverse life outcomes in fetal alcohol syndrome and fetal alcohol effects. J Dev Behav Pediatr. 2004;25:228-238.
17. US Preventive Services Task Force. Screening and behavioral interventions in primary care to reduce alcohol misuse: recommendation statement, April 2004. Available at: www.ahrq.gov/clinic/3rduspstf/alcohol/alcomisrs.htm. Accessed April 10, 2010.
18. Bradley KA, Boyd-Wickizer J, Powell SH, et al. Alcohol screening questionnaires in women: a critical review. JAMA. 1998;20:166-171.
19. Chan AW, Pristach EA, Welte JW, et al. Use of the TWEAK test in screening for alcoholism/heavy drinking in three populations. Alcohol Clin Exp Res. 1993;17:1188-1192.
20. Russell M, Bigler L. Screening for alcohol-related problems in an outpatient obstetric-gynecologic clinic. Am J Obstet Gynecol. 1979;134:4-12.
21. National Institute on Alcohol Abuse and Alcoholism. Helping patients who drink too much: a clinician’s guide. Updated January 2007. Available at: http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/clinicians_guide.htm. Accessed April 21, 2010.
22. Fleming MF, Barry KL, Manwell LB, et al. Brief physician advice for problem alcohol drinkers. JAMA. 1997;277:1039-1045.
23. Chang G, McNamara TK, Orav J, et al. Brief interventions for prenatal alcohol use: a randomized trial. Obstet Gynecol. 2005;105:991-998.
24. The Project Choices Intervention Research Group. Reducing the risk of alcohol-exposed pregnancies: a study of motivational intervention in community settings. Pediatrics. 2003;111:1131-1135.
An algorithm for the treatment of chronic testicular pain
Order ultrasound of the scrotum and testes to evaluate chronic testicular pain, with color Doppler to identify areas of hypervascularity. C
Treat suspected epididymitis with empiric coverage for chlamydia with either a 10-day regimen of doxycycline (100 mg twice daily) or a single dose (1 g) of azithromycin; treat suspected gonorrhea with a single intramuscular injection (125 mg) of ceftriaxone. A
Do not treat small epididymal cysts that do not correlate with testicular pain; larger, painful cysts can be aspirated, injected with a sclerosing agent, or surgically excised. C
Consider surgical options only after medical and conservative therapies have failed to alleviate chronic testicular pain. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Vincent B, a 33-year-old executive, visits his family physician for an evaluation of chronic orchialgia. Although his testicular pain has waxed and waned for several years, it has recently worsened, making it increasingly difficult for him to exercise or to sit for extended periods of time. In fact, this visit was prompted by a lengthy meeting during which he developed a “dull ache” that did not let up until he left the meeting and walked around.
CASE 2 Jason H, a 42-year-old married father of 3 who had a vasectomy 2 years ago, has had progressively worsening testicular pain ever since. He also has occasional pain after ejaculation, but no known hematospermia. Recently, the pain has become so bad that it limits both his physical and sexual activities and is having a negative effect on his relationship with his wife. Jason is sexually monogamous, has no significant medical history, and takes no prescription medications.
These 2 cases are based on actual patients we have seen in our practices. If Vincent and Jason (not their real names) were your patients, how would you initiate a work-up for testicular pain? What treatments would you offer? And at what point would you consider a referral to a urologist?
Chronic orchialgia is a complex urogenital focal pain syndrome in which neurogenic inflammation is the principal mediator. This debilitating condition is associated with substantial anxiety and frustration, and is characterized by intermittent or constant unilateral or bilateral testicular pain, occurring for at least 3 months, that has a significant negative impact on activities of daily living and physical activity.1
A variety of procedural and surgical options may help to minimize or alleviate chronic orchialgia. But which approach is best? There are no evidence-based guidelines for the treatment of this condition, and no randomized controlled trials to demonstrate the superiority of 1 modality over another. All diagnostic and treatment recommendations are based on expert opinion derived from small cohort studies.
With that in mind, we conducted a systematic review of the literature evaluating medical and surgical therapies for chronic testicular pain—and developed an algorithm (FIGURE 1), along with the text and TABLE that follow, for family physicians (FPs) to use as a guide.
FIGURE 1
Chronic orchialgia: A diagnosis and treatment algorithm1,3,4,6,10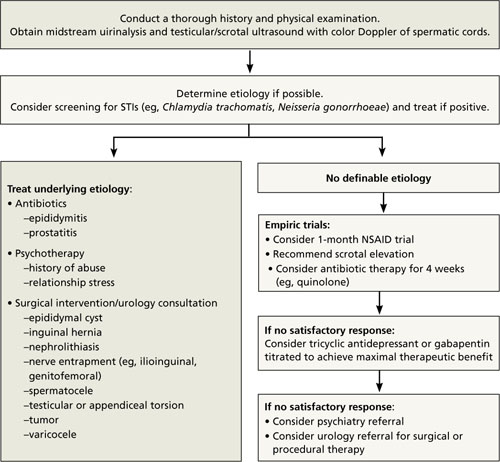
NSAID, nonsteroidal anti-inflammatory drug; STIs, sexually transmitted infections.
CASE 1 Vincent B
Over the last few years, Vincent has had similar episodes of bilateral testicular pain. He denies any history of direct trauma to the testicles, and he works out regularly by lifting weights and running. When the pain becomes unbearable, he takes acetaminophen or ibuprofen and takes a few days off from exercising, which provides modest—but temporary—relief.
Vincent reports that he has had about a dozen lifetime sexual partners and had chlamydia over a decade ago as a college student. He is currently engaged and sexually monogamous, and tested negative for Chlamydia trachomatis, Neisseria gonorrhoeae, hepatitis, syphilis, and human immunodeficiency virus (HIV) at his annual health maintenance examination last month. Shortly before that, Vincent was treated empirically for epididymitis with a 4-week course of ciprofloxacin, with no significant improvement in symptoms. He has no significant past medical history, denies depression, and takes no prescription medications.
Physical examination reveals mild to moderate diffuse tenderness to palpation throughout the scrotum, including both testicles and spermatic cords. There is no erythema of the scrotum. Nor are there any palpable scrotal masses, varicoceles, or hydroceles; testicular, scrotal, or penile lesions; inguinal masses; or lymph nodes. His urethral meatus is patent. The prostate is smooth, nonnodular, and non-tender. The remainder of the physical exam is unremarkable.
Determining a cause can be a challenge
There are numerous possible causes of testicular pain (TABLE), including an inguinal hernia, torsion of the testicle, trauma, and a history of chlamydia or gonorrhea, to name a few.
TABLE
Causes of acute and chronic orchialgia1,3,4
Acute
|
Chronic
|
Chronic testicular pain can also be psychogenic, often relating to a history of sexual abuse or relationship stress. One study examining comorbid psychological conditions in men with chronic orchialgia identified a somatization disorder in 56% of the patients, nongenital chronic pain syndromes in 50%, and major depression or chemical dependency in 27%.2 Overall, however, estimates suggest that in about 25% of patients with chronic orchialgia, no identifiable etiology is found. 1
Establish a baseline with a physical exam
Conduct a physical examination of the scrotum, testes, spermatic cords, penis, inguinal region, and prostate as a baseline measurement in a patient who presents with chronic orchialgia.3,4 An initial urinalysis should be performed to rule out infection or identify microscopic hematuria, which may prompt a more targeted work-up and therapeutic plan. Take a thorough medical and psychosocial/ sexual history, as well.
Order an ultrasound of the scrotum and testes, the accepted gold standard to highlight structural abnormalities of the testicles. The addition of color Doppler makes it possible to find areas of hypervascularity, an indication of inflammation in the testicle and epididymis (FIGURES 2A AND B).
FIGURE 2
Well-circumscribed extratesticular mass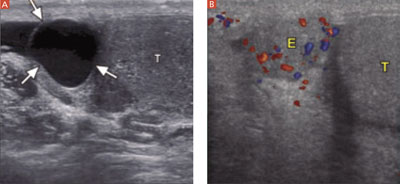
In the image at left, ultrasound reveals an anechoic mass (arrows), representing either an epididymal cyst or spermatocele, superior to the testicle (T). A color Doppler image (right) reveals increased vascularity to the epididymis (E), as compared with the testicle.
Epididymal cysts are common findings on scrotal ultrasound; they are frequently incidental, but may relate to the patient’s pain, depending on the size of the cyst. Smaller cysts that do not correlate with pain do not require treatment. Larger, painful cysts can be treated with aspiration or injection with a sclerosing agent—or with surgical excision, which offers the highest potential cure rate.3,4 A computed tomography (CT) scan without contrast is the best way to find genitourinary system calculi, which could be the source of referred renal pain to the groin and scrotum. A contrast-enhanced CT is best to evaluate for solid renal masses.
Start with the most conservative treatment
In the absence of any findings that require surgical intervention, start conservatively.
Initiate a trial of nonsteroidal anti-inflammatory drugs (NSAIDs) for at least 1 month. Although this is the standard first-line treatment, NSAIDs have been shown to help only a small percentage of patients with chronic orchialgia, and only on a short-term basis.1,3,4
Recommend scrotal elevation with supportive undergarments to decrease venous congestion. Tell the patient, too, that modifying his seated posture to avoid scrotal pressure may alleviate pain and poses no discernible risk of worsening orchialgia.5
Treat suspected STIs. The Centers for Disease Control and Prevention report that in men 14 to 35 years of age, epididymitis is most commonly caused by chlamydia or gonorrhea.6 In males younger than 14 or older than 35, epididymitis is most commonly caused by urinary coliform pathogens, including Eschericia coli.
If epididymitis is suspected to be due to chlamydia or gonorrhea, treatment should include either doxycycline 100 mg orally twice daily for 10 days or a single dose of azithromycin 1 g orally (for chlamydia eradication) and a single dose of ceftriaxone 125 mg intramuscularly (for gonorrhea eradication).6,7 If coliform bacteria is suspected, order a standard dose of a quinolone (eg, ciprofloxacin or levofloxacin 500 mg/d) for 10 days.6 For refractory cases, treatment with a standard dose of a quinolone for 4 weeks is recommended.6
It is generally reasonable to treat most patients empirically for suspected epididymitis with antibiotics if no other identifiable etiology can be determined. Multiple antibiotic treatments should be avoided, however, in the absence of either an identifiable urogenital infection or ultrasound findings consistent with epididymitis (eg, congestion and enlargement). Antibiotics have not been shown to decrease the severity of chronic orchialgia and their use, unless clearly indicated, may lead to drug resistance.3
Consider a tricyclic antidepressant or gabapentin
Both tricyclic antidepressants (TCAs) and gabapentin have demonstrated benefit in the treatment of chronic pelvic and neuropathic pain.8,9 Doses should be titrated to achieve a maximal therapeutic benefit while avoiding anticholinergic and neurologic side effects.
A cohort study using a multidisciplinary team consisting of a psychologist, an anesthetist, a physiotherapist, and an occupational therapist found >50% symptomatic improvement in 62% of men with chronic orchialgia treated with gabapentin up to 1800 mg per day, and 67% of men treated with nortriptyline up to 150 mg per day.10
However, a subgroup of patients who reported postvasectomy testicular pain did not achieve a 50% symptomatic improvement rate with either TCA or gabapentin therapy.
CASE 1 Vincent B
The FP reassured Vincent that his physical examination was normal and recommended a 1-month trial of ibuprofen (600 mg every 6 hours), and regular use of supportive briefs. Since the patient had been treated with antibiotics in the past with no change in symptoms—and because he was thought to be at low risk for an STI—the physician did not prescribe another empiric trial of antibiotics. He did send the patient for an ultrasound evaluation of the scrotum and testes, which revealed only a 0.5 × 0.4 × 0.6-cm right epididymal cyst that was not palpable on examination.
The patient returned after 1 month, noting that his symptoms had neither improved nor worsened. The FP suggested that he stop taking the ibuprofen and begin a trial of gabapentin 100 mg daily, titrating up to 3 times daily for the first month, then to 300 mg 3 times daily in the second month.
When he returned 3 months later, Vincent reported that his symptoms had improved by about 50%. He has since been able to increase both the intensity and frequency of physical activity. Vincent is not interested in further increasing the dose of gabapentin and declined a referral to a urologist for consideration of procedural and surgical therapeutic options, but agreed to follow up as needed if his testicular pain worsened.
Postvasectomy pain is not unusual
Several years after a vasectomy, the diameter of a man’s ejaculatory ducts often doubles in size to counteract the increase in fluid pressure.11 The specific cause of long-term post-vasectomy pain syndrome, or congestive epididymitis, is unknown, but has been reported in 5% to 43% of men who have undergone this procedure.12-14 Sperm granulomas or spermatoceles represent the body’s effort to spare the testicle from damage secondary to increasing fluid pressure. While these granulomas are benign lesions, their presence may predispose a man to postvasectomy pain syndrome.15-17
CASE 2 Jason H
Two months before Jason’s visit to the FP, his testicular pain had become so excrutiating that he went to the ED seeking treatment. He was given an ultrasound with color Doppler and found to have postvasectomy surgical changes consistent with bilateral spermatoceles, but no evidence of epididymitis or a mass. Before leaving the ED, Jason received ceftriaxone (125 mg IM) as gonorrhea prophylaxis. He was discharged home with prophylactic antibiotics for chlamydia, as well as ibuprofen. He was advised to avoid strenuous physical activity and told to follow-up with his FP if his symptoms did not improve.
During several months of conservative medical therapy, including trials of NSAIDs, quinolone antibiotics, TCAs, and gabapentin, Jason did not experience any significant pain relief. He was frustrated by the dull, aching pain in his scrotum that continued to limit his physical and sexual activities.
Finally, the FP recommended a urologic consultation.
Consider these minimally invasive procedures
When conservative medical management fails, minimally invasive techniques are the next step. There are 2 commonly used procedures, both of which can be performed by a urologist in an outpatient setting.
Spermatic cord blocks with lidocaine and methylprednisolone have been shown to provide relief for weeks up to several months in small case studies, and may be repeated at intervals of several months if modest relief is achieved.18,19
Transrectal ultrasound-guided periprostatic anesthetic injections, another microinvasive option, offers minimal risk and may provide some short-term relief. However, data on long-term benefit and resolution of pain and disability are lacking.20
Consider surgery only after all else fails
If all medical and conservative therapies have been tried and the patient continues to have debilitating pain, surgical options should be considered. Because current surgical therapies are not always effective and are not reversible (and research on the various options is limited), it is important to initiate a detailed discussion with the patient. Such conversations should be held in consultation with a urologist.
Highlight risks and benefits and provide realistic expectations of short- and long-term postsurgical outcomes. It is also important to address psychological factors and social stressors that often contribute to chronic pelvic pain syndromes, which can improve long-term outcomes regardless of the chosen treatment. For this reason, a referral to a psychiatrist may be indicated.
Microsurgical denervation of the spermatic cord. Removal of the afferent nerve stimulus to the testicle is believed to result in the downregulation of the peripheral and central nervous systems, so the patient no longer has the perception of testicular pain. Several small trials have yielded favorable symptomatic pain relief scores in up to 71% of patients, with reported adverse outcomes including rare testicular atrophy—but no complaints of hypoesthesia or hyperesthesia of the scrotum, penile shaft, inguinal, or medial thigh skin.21,22 This treatment should be considered only in patients who have experienced a significant degree of temporary relief from spermatic cord injection.
Epididymectomy is recommended only when pain is localized to the epididymis, as this is a testicle-sparing procedure. Unilateral or bilateral epididymectomy is a viable option for the treatment of chronic orchialgia related to postvasectomy pain syndrome or chronic epididymitis. Reports highlighting symptomatic improvement based on small case series range from 43% to 74%, with the highest success rate found during a 5½-year follow-up.23-25 In 1 study, 90% of patients reported that they were satisfied with their choice to undergo the procedure.25
Vasectomy reversal (vasovasostomy) and inguinal or scrotal orchiectomy should be considered only after all other treatment modalities have failed. Vasovasostomy has the potential to restore fertility in up to 98% of cases,26 which may or may not be desirable. One study of men who experienced post-vasectomy pain syndrome and underwent microsurgical vasovasostomy found that after nearly 2½ years, 84% experienced complete pain resolution.27
The goal of orchiectomy is to relieve orchialgia by releasing the entrapped ipsilateral genitofemoral and/or ilioinguinal nerves. One study determined that 90% of men who underwent unilateral epididymectomy for chronic orchialgia required an orchiectomy to resolve pain.1 Another study found that 80% of patients continued to suffer both short- and long-term debilitating orchialgia postorchiectomy.28
CASE 2 Jason H
Jason saw a urologist, who initially offered him bilateral spermatic cord blocks. They provided Jason with moderate symptom relief on most days of the week and allowed him to increase his physical and sexual activities. Three months later, Jason went back to the urologist for evaluation because he felt that the effects of the spermatic cord blocks had worn off. In the next 6 months, he had 2 additional bilateral blocks.
Nearly a year after a series of spermatic cord blocks, most of it spent in persistent discomfort, Jason returned to his FP with a request for narcotic pain medication. The FP tried to be supportive, but told Jason that chronic narcotic therapy was not an ideal choice—and referred him back to the urologist to discuss surgical options.
The urologist recommended a bilateral epididymectomy and the patient, who was desperate to obtain some pain relief and now regretted undergoing a vasectomy, agreed. Within the first few weeks after his surgery, he noticed a reduction in pain, and he slowly increased his physical activity. A year later, Jason reported only minimal testicular and scrotal discomfort that did not limit his physical or sexual activities—and he continues to be pleased with the outcome of his treatment.
CORRESPONDENCE Joel J. Heidelbaugh, MD, FAAFP, Ypsilanti Health Center, 200 Arnet, Suite 200, Ypsilanti, MI 48198; [email protected]
1. Davis B, Noble MJ, Weigel JD, et al. Analysis and management of chronic testicular pain. J Urol. 1990;143:936-939.
2. Schover LR. Psychological factors in men with genital pain. Cleve Clin J Med. 1990;57:697-700.
3. Masarani M, Cox R. Th e aetiology, pathophysiology and management of chronic orchialgia. Br J Urol Int. 2003;91:435-437.
4. Granitsiotis P, Kirk D. Chronic testicular pain: an overview. Eur Urol. 2004;45:430-436.
5. Coogan CL. Painful scrotum. In: Myers JA, Millikan KW, Sacla-rides TJ, eds. Common Surgical Diseases. New York: Springer; 2008:293-295.
6. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2006. MMWR Morb Mortal Wkly Rep. 2006;55(RR-11):1-94.
7. Newman LM, Moran JS, Workowski KA. Update on the management of gonorrhea in adults in the United States. Clin Infect Dis. 2007;44(suppl 3):S84-S101.
8. Wiffen PJ, McQuay HJ, Rees J, et al. Gabapentin for acute and chronic pain. Cochrane Database Syst Rev. 2005;(3):CD005452.-
9. American College of Obstetricians and Gynecologists. Chronic pelvic pain. ACOG Practice Bulletin No. 51. Obstet Gynecol. 2004;103:589-605.
10. Sinclair AM, Miller B, Lee LK. Chronic orchialgia: consider gabapentin or nortriptyline before considering surgery. Int J Urol. 2007;14:622-625.
11. Jarow JP, Budin RE, Dym M, et al. Quantitative pathologic changes in the human testis after vasectomy. N Engl J Med. 1985;313:1252-1256.
12. Choe J, Kirkemo A. Questionnaire-based outcomes study of nononcological post-vasectomy complications. J Urol. 1996;155:1284-1286.
13. McMahon A, Buckley J, Taylor A, et al. Chronic testicular pain following vasectomy. Br J Urol. 1992;69:188-191.
14. Ahmed I, Rasheed S, White C, et al. Th e incidence of post-vasectomy chronic testicular pain and the role of nerve stripping (denervation) of the spermatic cord in its management. Br J Urol. 1997;79:269-270.
15. Christiansen CG, Sandlow JI. Testicular pain following vasectomy: a review of postvasectomy pain syndrome. J Androl. 2003;24:293-298.
16. Shapiro EI, Silber SJ. Open-ended vasectomy, sperm granuloma, and postvasectomy orchialgia. Fertil Steril. 1979;32:546-550.
17. Taxy JB, Marshall FF, Erlickman RJ. Vasectomy: subclinical pathologic changes. Am J Surg Pathol. 1981;5:767-772.
18. Fuchs E. Cord block anesthesia for scrotal surgery. J Urol. 1982;128:718-719.
19. Issa M, Hsiao K, Bassel Y, et al. Spermatic cord anesthesia block for scrotal procedures in the outpatient clinic setting. J Urol. 2004;172:2358-2361.
20. Zorn B, Rauchenwald M, Steers WD. Periprostatic injection of local anesthesia for relief of chronic orchialgia. J Urol. 1994;151:411,A735.-
21. Levine LA, Matkov TG, Lubenow TR. Microsurgical denervation of the spermatic cord: a surgical alternative in the treatment of chronic orchialgia. J Urol. 1996;155:1005-1007.
22. Strom KH, Levine LA. Microsurgical denervation of the spermatic cord for chronic orchialgia: long-term results from a single center. J Urol. 2008;180:949-953.
23. Padmore DE, Norman RW, Millard OH. Analyses of indications for and outcomes of epdidymectomy. J Urol. 1996;156:95-96.
24. West AF, Leung HY, Powell PH. Epididymectomy is an effective treatment for scrotal pain after vasectomy. Br J Urol Int. 2000;85:1097-1099.
25. Siu W, Ohl DA, Schuster TG. Long-term follow-up after epididymectomy for chronic epidiymal pain. Urology. 2007;70:333-336.
26. Patel SR, Sigman M. Comparison of outcomes of vasovasostomy performed in the convoluted and straight vas deferens. J Urol. 2008;179:256-259.
27. Myers SA, Mershon CE, Fuchs EF. Vasectomy reversal for treatment of the post-vasectomy pain syndrome. J Urol. 1997;157:518-520.
28. Costabile RA, Hahn M, McLeod DG. Chronic orchialgia in the pain prone patient: the clinical perspective. J Urol. 1991;146:1571-1574.
| Testicular pain treatment tips |
Joel J. Heidelbaugh, MD, FAAFP
Departments of Family Medicine , Urology, University of Michigan Medical School, Ann Arbor
[email protected]
Mikel Llanes, MD
Department of Family Medicine, University of Michigan Medical School, Ann Arbor
William J. Weadock, MD
Radiology, University of Michigan Medical School, Ann Arbor
The authors reported no potential conflict of interest relevant to this article.
| Testicular pain treatment tips |
Joel J. Heidelbaugh, MD, FAAFP
Departments of Family Medicine , Urology, University of Michigan Medical School, Ann Arbor
[email protected]
Mikel Llanes, MD
Department of Family Medicine, University of Michigan Medical School, Ann Arbor
William J. Weadock, MD
Radiology, University of Michigan Medical School, Ann Arbor
The authors reported no potential conflict of interest relevant to this article.
| Testicular pain treatment tips |
Joel J. Heidelbaugh, MD, FAAFP
Departments of Family Medicine , Urology, University of Michigan Medical School, Ann Arbor
[email protected]
Mikel Llanes, MD
Department of Family Medicine, University of Michigan Medical School, Ann Arbor
William J. Weadock, MD
Radiology, University of Michigan Medical School, Ann Arbor
The authors reported no potential conflict of interest relevant to this article.
Order ultrasound of the scrotum and testes to evaluate chronic testicular pain, with color Doppler to identify areas of hypervascularity. C
Treat suspected epididymitis with empiric coverage for chlamydia with either a 10-day regimen of doxycycline (100 mg twice daily) or a single dose (1 g) of azithromycin; treat suspected gonorrhea with a single intramuscular injection (125 mg) of ceftriaxone. A
Do not treat small epididymal cysts that do not correlate with testicular pain; larger, painful cysts can be aspirated, injected with a sclerosing agent, or surgically excised. C
Consider surgical options only after medical and conservative therapies have failed to alleviate chronic testicular pain. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Vincent B, a 33-year-old executive, visits his family physician for an evaluation of chronic orchialgia. Although his testicular pain has waxed and waned for several years, it has recently worsened, making it increasingly difficult for him to exercise or to sit for extended periods of time. In fact, this visit was prompted by a lengthy meeting during which he developed a “dull ache” that did not let up until he left the meeting and walked around.
CASE 2 Jason H, a 42-year-old married father of 3 who had a vasectomy 2 years ago, has had progressively worsening testicular pain ever since. He also has occasional pain after ejaculation, but no known hematospermia. Recently, the pain has become so bad that it limits both his physical and sexual activities and is having a negative effect on his relationship with his wife. Jason is sexually monogamous, has no significant medical history, and takes no prescription medications.
These 2 cases are based on actual patients we have seen in our practices. If Vincent and Jason (not their real names) were your patients, how would you initiate a work-up for testicular pain? What treatments would you offer? And at what point would you consider a referral to a urologist?
Chronic orchialgia is a complex urogenital focal pain syndrome in which neurogenic inflammation is the principal mediator. This debilitating condition is associated with substantial anxiety and frustration, and is characterized by intermittent or constant unilateral or bilateral testicular pain, occurring for at least 3 months, that has a significant negative impact on activities of daily living and physical activity.1
A variety of procedural and surgical options may help to minimize or alleviate chronic orchialgia. But which approach is best? There are no evidence-based guidelines for the treatment of this condition, and no randomized controlled trials to demonstrate the superiority of 1 modality over another. All diagnostic and treatment recommendations are based on expert opinion derived from small cohort studies.
With that in mind, we conducted a systematic review of the literature evaluating medical and surgical therapies for chronic testicular pain—and developed an algorithm (FIGURE 1), along with the text and TABLE that follow, for family physicians (FPs) to use as a guide.
FIGURE 1
Chronic orchialgia: A diagnosis and treatment algorithm1,3,4,6,10
NSAID, nonsteroidal anti-inflammatory drug; STIs, sexually transmitted infections.
CASE 1 Vincent B
Over the last few years, Vincent has had similar episodes of bilateral testicular pain. He denies any history of direct trauma to the testicles, and he works out regularly by lifting weights and running. When the pain becomes unbearable, he takes acetaminophen or ibuprofen and takes a few days off from exercising, which provides modest—but temporary—relief.
Vincent reports that he has had about a dozen lifetime sexual partners and had chlamydia over a decade ago as a college student. He is currently engaged and sexually monogamous, and tested negative for Chlamydia trachomatis, Neisseria gonorrhoeae, hepatitis, syphilis, and human immunodeficiency virus (HIV) at his annual health maintenance examination last month. Shortly before that, Vincent was treated empirically for epididymitis with a 4-week course of ciprofloxacin, with no significant improvement in symptoms. He has no significant past medical history, denies depression, and takes no prescription medications.
Physical examination reveals mild to moderate diffuse tenderness to palpation throughout the scrotum, including both testicles and spermatic cords. There is no erythema of the scrotum. Nor are there any palpable scrotal masses, varicoceles, or hydroceles; testicular, scrotal, or penile lesions; inguinal masses; or lymph nodes. His urethral meatus is patent. The prostate is smooth, nonnodular, and non-tender. The remainder of the physical exam is unremarkable.
Determining a cause can be a challenge
There are numerous possible causes of testicular pain (TABLE), including an inguinal hernia, torsion of the testicle, trauma, and a history of chlamydia or gonorrhea, to name a few.
TABLE
Causes of acute and chronic orchialgia1,3,4
Acute
|
Chronic
|
Chronic testicular pain can also be psychogenic, often relating to a history of sexual abuse or relationship stress. One study examining comorbid psychological conditions in men with chronic orchialgia identified a somatization disorder in 56% of the patients, nongenital chronic pain syndromes in 50%, and major depression or chemical dependency in 27%.2 Overall, however, estimates suggest that in about 25% of patients with chronic orchialgia, no identifiable etiology is found. 1
Establish a baseline with a physical exam
Conduct a physical examination of the scrotum, testes, spermatic cords, penis, inguinal region, and prostate as a baseline measurement in a patient who presents with chronic orchialgia.3,4 An initial urinalysis should be performed to rule out infection or identify microscopic hematuria, which may prompt a more targeted work-up and therapeutic plan. Take a thorough medical and psychosocial/ sexual history, as well.
Order an ultrasound of the scrotum and testes, the accepted gold standard to highlight structural abnormalities of the testicles. The addition of color Doppler makes it possible to find areas of hypervascularity, an indication of inflammation in the testicle and epididymis (FIGURES 2A AND B).
FIGURE 2
Well-circumscribed extratesticular mass
In the image at left, ultrasound reveals an anechoic mass (arrows), representing either an epididymal cyst or spermatocele, superior to the testicle (T). A color Doppler image (right) reveals increased vascularity to the epididymis (E), as compared with the testicle.
Epididymal cysts are common findings on scrotal ultrasound; they are frequently incidental, but may relate to the patient’s pain, depending on the size of the cyst. Smaller cysts that do not correlate with pain do not require treatment. Larger, painful cysts can be treated with aspiration or injection with a sclerosing agent—or with surgical excision, which offers the highest potential cure rate.3,4 A computed tomography (CT) scan without contrast is the best way to find genitourinary system calculi, which could be the source of referred renal pain to the groin and scrotum. A contrast-enhanced CT is best to evaluate for solid renal masses.
Start with the most conservative treatment
In the absence of any findings that require surgical intervention, start conservatively.
Initiate a trial of nonsteroidal anti-inflammatory drugs (NSAIDs) for at least 1 month. Although this is the standard first-line treatment, NSAIDs have been shown to help only a small percentage of patients with chronic orchialgia, and only on a short-term basis.1,3,4
Recommend scrotal elevation with supportive undergarments to decrease venous congestion. Tell the patient, too, that modifying his seated posture to avoid scrotal pressure may alleviate pain and poses no discernible risk of worsening orchialgia.5
Treat suspected STIs. The Centers for Disease Control and Prevention report that in men 14 to 35 years of age, epididymitis is most commonly caused by chlamydia or gonorrhea.6 In males younger than 14 or older than 35, epididymitis is most commonly caused by urinary coliform pathogens, including Eschericia coli.
If epididymitis is suspected to be due to chlamydia or gonorrhea, treatment should include either doxycycline 100 mg orally twice daily for 10 days or a single dose of azithromycin 1 g orally (for chlamydia eradication) and a single dose of ceftriaxone 125 mg intramuscularly (for gonorrhea eradication).6,7 If coliform bacteria is suspected, order a standard dose of a quinolone (eg, ciprofloxacin or levofloxacin 500 mg/d) for 10 days.6 For refractory cases, treatment with a standard dose of a quinolone for 4 weeks is recommended.6
It is generally reasonable to treat most patients empirically for suspected epididymitis with antibiotics if no other identifiable etiology can be determined. Multiple antibiotic treatments should be avoided, however, in the absence of either an identifiable urogenital infection or ultrasound findings consistent with epididymitis (eg, congestion and enlargement). Antibiotics have not been shown to decrease the severity of chronic orchialgia and their use, unless clearly indicated, may lead to drug resistance.3
Consider a tricyclic antidepressant or gabapentin
Both tricyclic antidepressants (TCAs) and gabapentin have demonstrated benefit in the treatment of chronic pelvic and neuropathic pain.8,9 Doses should be titrated to achieve a maximal therapeutic benefit while avoiding anticholinergic and neurologic side effects.
A cohort study using a multidisciplinary team consisting of a psychologist, an anesthetist, a physiotherapist, and an occupational therapist found >50% symptomatic improvement in 62% of men with chronic orchialgia treated with gabapentin up to 1800 mg per day, and 67% of men treated with nortriptyline up to 150 mg per day.10
However, a subgroup of patients who reported postvasectomy testicular pain did not achieve a 50% symptomatic improvement rate with either TCA or gabapentin therapy.
CASE 1 Vincent B
The FP reassured Vincent that his physical examination was normal and recommended a 1-month trial of ibuprofen (600 mg every 6 hours), and regular use of supportive briefs. Since the patient had been treated with antibiotics in the past with no change in symptoms—and because he was thought to be at low risk for an STI—the physician did not prescribe another empiric trial of antibiotics. He did send the patient for an ultrasound evaluation of the scrotum and testes, which revealed only a 0.5 × 0.4 × 0.6-cm right epididymal cyst that was not palpable on examination.
The patient returned after 1 month, noting that his symptoms had neither improved nor worsened. The FP suggested that he stop taking the ibuprofen and begin a trial of gabapentin 100 mg daily, titrating up to 3 times daily for the first month, then to 300 mg 3 times daily in the second month.
When he returned 3 months later, Vincent reported that his symptoms had improved by about 50%. He has since been able to increase both the intensity and frequency of physical activity. Vincent is not interested in further increasing the dose of gabapentin and declined a referral to a urologist for consideration of procedural and surgical therapeutic options, but agreed to follow up as needed if his testicular pain worsened.
Postvasectomy pain is not unusual
Several years after a vasectomy, the diameter of a man’s ejaculatory ducts often doubles in size to counteract the increase in fluid pressure.11 The specific cause of long-term post-vasectomy pain syndrome, or congestive epididymitis, is unknown, but has been reported in 5% to 43% of men who have undergone this procedure.12-14 Sperm granulomas or spermatoceles represent the body’s effort to spare the testicle from damage secondary to increasing fluid pressure. While these granulomas are benign lesions, their presence may predispose a man to postvasectomy pain syndrome.15-17
CASE 2 Jason H
Two months before Jason’s visit to the FP, his testicular pain had become so excrutiating that he went to the ED seeking treatment. He was given an ultrasound with color Doppler and found to have postvasectomy surgical changes consistent with bilateral spermatoceles, but no evidence of epididymitis or a mass. Before leaving the ED, Jason received ceftriaxone (125 mg IM) as gonorrhea prophylaxis. He was discharged home with prophylactic antibiotics for chlamydia, as well as ibuprofen. He was advised to avoid strenuous physical activity and told to follow-up with his FP if his symptoms did not improve.
During several months of conservative medical therapy, including trials of NSAIDs, quinolone antibiotics, TCAs, and gabapentin, Jason did not experience any significant pain relief. He was frustrated by the dull, aching pain in his scrotum that continued to limit his physical and sexual activities.
Finally, the FP recommended a urologic consultation.
Consider these minimally invasive procedures
When conservative medical management fails, minimally invasive techniques are the next step. There are 2 commonly used procedures, both of which can be performed by a urologist in an outpatient setting.
Spermatic cord blocks with lidocaine and methylprednisolone have been shown to provide relief for weeks up to several months in small case studies, and may be repeated at intervals of several months if modest relief is achieved.18,19
Transrectal ultrasound-guided periprostatic anesthetic injections, another microinvasive option, offers minimal risk and may provide some short-term relief. However, data on long-term benefit and resolution of pain and disability are lacking.20
Consider surgery only after all else fails
If all medical and conservative therapies have been tried and the patient continues to have debilitating pain, surgical options should be considered. Because current surgical therapies are not always effective and are not reversible (and research on the various options is limited), it is important to initiate a detailed discussion with the patient. Such conversations should be held in consultation with a urologist.
Highlight risks and benefits and provide realistic expectations of short- and long-term postsurgical outcomes. It is also important to address psychological factors and social stressors that often contribute to chronic pelvic pain syndromes, which can improve long-term outcomes regardless of the chosen treatment. For this reason, a referral to a psychiatrist may be indicated.
Microsurgical denervation of the spermatic cord. Removal of the afferent nerve stimulus to the testicle is believed to result in the downregulation of the peripheral and central nervous systems, so the patient no longer has the perception of testicular pain. Several small trials have yielded favorable symptomatic pain relief scores in up to 71% of patients, with reported adverse outcomes including rare testicular atrophy—but no complaints of hypoesthesia or hyperesthesia of the scrotum, penile shaft, inguinal, or medial thigh skin.21,22 This treatment should be considered only in patients who have experienced a significant degree of temporary relief from spermatic cord injection.
Epididymectomy is recommended only when pain is localized to the epididymis, as this is a testicle-sparing procedure. Unilateral or bilateral epididymectomy is a viable option for the treatment of chronic orchialgia related to postvasectomy pain syndrome or chronic epididymitis. Reports highlighting symptomatic improvement based on small case series range from 43% to 74%, with the highest success rate found during a 5½-year follow-up.23-25 In 1 study, 90% of patients reported that they were satisfied with their choice to undergo the procedure.25
Vasectomy reversal (vasovasostomy) and inguinal or scrotal orchiectomy should be considered only after all other treatment modalities have failed. Vasovasostomy has the potential to restore fertility in up to 98% of cases,26 which may or may not be desirable. One study of men who experienced post-vasectomy pain syndrome and underwent microsurgical vasovasostomy found that after nearly 2½ years, 84% experienced complete pain resolution.27
The goal of orchiectomy is to relieve orchialgia by releasing the entrapped ipsilateral genitofemoral and/or ilioinguinal nerves. One study determined that 90% of men who underwent unilateral epididymectomy for chronic orchialgia required an orchiectomy to resolve pain.1 Another study found that 80% of patients continued to suffer both short- and long-term debilitating orchialgia postorchiectomy.28
CASE 2 Jason H
Jason saw a urologist, who initially offered him bilateral spermatic cord blocks. They provided Jason with moderate symptom relief on most days of the week and allowed him to increase his physical and sexual activities. Three months later, Jason went back to the urologist for evaluation because he felt that the effects of the spermatic cord blocks had worn off. In the next 6 months, he had 2 additional bilateral blocks.
Nearly a year after a series of spermatic cord blocks, most of it spent in persistent discomfort, Jason returned to his FP with a request for narcotic pain medication. The FP tried to be supportive, but told Jason that chronic narcotic therapy was not an ideal choice—and referred him back to the urologist to discuss surgical options.
The urologist recommended a bilateral epididymectomy and the patient, who was desperate to obtain some pain relief and now regretted undergoing a vasectomy, agreed. Within the first few weeks after his surgery, he noticed a reduction in pain, and he slowly increased his physical activity. A year later, Jason reported only minimal testicular and scrotal discomfort that did not limit his physical or sexual activities—and he continues to be pleased with the outcome of his treatment.
CORRESPONDENCE Joel J. Heidelbaugh, MD, FAAFP, Ypsilanti Health Center, 200 Arnet, Suite 200, Ypsilanti, MI 48198; [email protected]
Order ultrasound of the scrotum and testes to evaluate chronic testicular pain, with color Doppler to identify areas of hypervascularity. C
Treat suspected epididymitis with empiric coverage for chlamydia with either a 10-day regimen of doxycycline (100 mg twice daily) or a single dose (1 g) of azithromycin; treat suspected gonorrhea with a single intramuscular injection (125 mg) of ceftriaxone. A
Do not treat small epididymal cysts that do not correlate with testicular pain; larger, painful cysts can be aspirated, injected with a sclerosing agent, or surgically excised. C
Consider surgical options only after medical and conservative therapies have failed to alleviate chronic testicular pain. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Vincent B, a 33-year-old executive, visits his family physician for an evaluation of chronic orchialgia. Although his testicular pain has waxed and waned for several years, it has recently worsened, making it increasingly difficult for him to exercise or to sit for extended periods of time. In fact, this visit was prompted by a lengthy meeting during which he developed a “dull ache” that did not let up until he left the meeting and walked around.
CASE 2 Jason H, a 42-year-old married father of 3 who had a vasectomy 2 years ago, has had progressively worsening testicular pain ever since. He also has occasional pain after ejaculation, but no known hematospermia. Recently, the pain has become so bad that it limits both his physical and sexual activities and is having a negative effect on his relationship with his wife. Jason is sexually monogamous, has no significant medical history, and takes no prescription medications.
These 2 cases are based on actual patients we have seen in our practices. If Vincent and Jason (not their real names) were your patients, how would you initiate a work-up for testicular pain? What treatments would you offer? And at what point would you consider a referral to a urologist?
Chronic orchialgia is a complex urogenital focal pain syndrome in which neurogenic inflammation is the principal mediator. This debilitating condition is associated with substantial anxiety and frustration, and is characterized by intermittent or constant unilateral or bilateral testicular pain, occurring for at least 3 months, that has a significant negative impact on activities of daily living and physical activity.1
A variety of procedural and surgical options may help to minimize or alleviate chronic orchialgia. But which approach is best? There are no evidence-based guidelines for the treatment of this condition, and no randomized controlled trials to demonstrate the superiority of 1 modality over another. All diagnostic and treatment recommendations are based on expert opinion derived from small cohort studies.
With that in mind, we conducted a systematic review of the literature evaluating medical and surgical therapies for chronic testicular pain—and developed an algorithm (FIGURE 1), along with the text and TABLE that follow, for family physicians (FPs) to use as a guide.
FIGURE 1
Chronic orchialgia: A diagnosis and treatment algorithm1,3,4,6,10
NSAID, nonsteroidal anti-inflammatory drug; STIs, sexually transmitted infections.
CASE 1 Vincent B
Over the last few years, Vincent has had similar episodes of bilateral testicular pain. He denies any history of direct trauma to the testicles, and he works out regularly by lifting weights and running. When the pain becomes unbearable, he takes acetaminophen or ibuprofen and takes a few days off from exercising, which provides modest—but temporary—relief.
Vincent reports that he has had about a dozen lifetime sexual partners and had chlamydia over a decade ago as a college student. He is currently engaged and sexually monogamous, and tested negative for Chlamydia trachomatis, Neisseria gonorrhoeae, hepatitis, syphilis, and human immunodeficiency virus (HIV) at his annual health maintenance examination last month. Shortly before that, Vincent was treated empirically for epididymitis with a 4-week course of ciprofloxacin, with no significant improvement in symptoms. He has no significant past medical history, denies depression, and takes no prescription medications.
Physical examination reveals mild to moderate diffuse tenderness to palpation throughout the scrotum, including both testicles and spermatic cords. There is no erythema of the scrotum. Nor are there any palpable scrotal masses, varicoceles, or hydroceles; testicular, scrotal, or penile lesions; inguinal masses; or lymph nodes. His urethral meatus is patent. The prostate is smooth, nonnodular, and non-tender. The remainder of the physical exam is unremarkable.
Determining a cause can be a challenge
There are numerous possible causes of testicular pain (TABLE), including an inguinal hernia, torsion of the testicle, trauma, and a history of chlamydia or gonorrhea, to name a few.
TABLE
Causes of acute and chronic orchialgia1,3,4
Acute
|
Chronic
|
Chronic testicular pain can also be psychogenic, often relating to a history of sexual abuse or relationship stress. One study examining comorbid psychological conditions in men with chronic orchialgia identified a somatization disorder in 56% of the patients, nongenital chronic pain syndromes in 50%, and major depression or chemical dependency in 27%.2 Overall, however, estimates suggest that in about 25% of patients with chronic orchialgia, no identifiable etiology is found. 1
Establish a baseline with a physical exam
Conduct a physical examination of the scrotum, testes, spermatic cords, penis, inguinal region, and prostate as a baseline measurement in a patient who presents with chronic orchialgia.3,4 An initial urinalysis should be performed to rule out infection or identify microscopic hematuria, which may prompt a more targeted work-up and therapeutic plan. Take a thorough medical and psychosocial/ sexual history, as well.
Order an ultrasound of the scrotum and testes, the accepted gold standard to highlight structural abnormalities of the testicles. The addition of color Doppler makes it possible to find areas of hypervascularity, an indication of inflammation in the testicle and epididymis (FIGURES 2A AND B).
FIGURE 2
Well-circumscribed extratesticular mass
In the image at left, ultrasound reveals an anechoic mass (arrows), representing either an epididymal cyst or spermatocele, superior to the testicle (T). A color Doppler image (right) reveals increased vascularity to the epididymis (E), as compared with the testicle.
Epididymal cysts are common findings on scrotal ultrasound; they are frequently incidental, but may relate to the patient’s pain, depending on the size of the cyst. Smaller cysts that do not correlate with pain do not require treatment. Larger, painful cysts can be treated with aspiration or injection with a sclerosing agent—or with surgical excision, which offers the highest potential cure rate.3,4 A computed tomography (CT) scan without contrast is the best way to find genitourinary system calculi, which could be the source of referred renal pain to the groin and scrotum. A contrast-enhanced CT is best to evaluate for solid renal masses.
Start with the most conservative treatment
In the absence of any findings that require surgical intervention, start conservatively.
Initiate a trial of nonsteroidal anti-inflammatory drugs (NSAIDs) for at least 1 month. Although this is the standard first-line treatment, NSAIDs have been shown to help only a small percentage of patients with chronic orchialgia, and only on a short-term basis.1,3,4
Recommend scrotal elevation with supportive undergarments to decrease venous congestion. Tell the patient, too, that modifying his seated posture to avoid scrotal pressure may alleviate pain and poses no discernible risk of worsening orchialgia.5
Treat suspected STIs. The Centers for Disease Control and Prevention report that in men 14 to 35 years of age, epididymitis is most commonly caused by chlamydia or gonorrhea.6 In males younger than 14 or older than 35, epididymitis is most commonly caused by urinary coliform pathogens, including Eschericia coli.
If epididymitis is suspected to be due to chlamydia or gonorrhea, treatment should include either doxycycline 100 mg orally twice daily for 10 days or a single dose of azithromycin 1 g orally (for chlamydia eradication) and a single dose of ceftriaxone 125 mg intramuscularly (for gonorrhea eradication).6,7 If coliform bacteria is suspected, order a standard dose of a quinolone (eg, ciprofloxacin or levofloxacin 500 mg/d) for 10 days.6 For refractory cases, treatment with a standard dose of a quinolone for 4 weeks is recommended.6
It is generally reasonable to treat most patients empirically for suspected epididymitis with antibiotics if no other identifiable etiology can be determined. Multiple antibiotic treatments should be avoided, however, in the absence of either an identifiable urogenital infection or ultrasound findings consistent with epididymitis (eg, congestion and enlargement). Antibiotics have not been shown to decrease the severity of chronic orchialgia and their use, unless clearly indicated, may lead to drug resistance.3
Consider a tricyclic antidepressant or gabapentin
Both tricyclic antidepressants (TCAs) and gabapentin have demonstrated benefit in the treatment of chronic pelvic and neuropathic pain.8,9 Doses should be titrated to achieve a maximal therapeutic benefit while avoiding anticholinergic and neurologic side effects.
A cohort study using a multidisciplinary team consisting of a psychologist, an anesthetist, a physiotherapist, and an occupational therapist found >50% symptomatic improvement in 62% of men with chronic orchialgia treated with gabapentin up to 1800 mg per day, and 67% of men treated with nortriptyline up to 150 mg per day.10
However, a subgroup of patients who reported postvasectomy testicular pain did not achieve a 50% symptomatic improvement rate with either TCA or gabapentin therapy.
CASE 1 Vincent B
The FP reassured Vincent that his physical examination was normal and recommended a 1-month trial of ibuprofen (600 mg every 6 hours), and regular use of supportive briefs. Since the patient had been treated with antibiotics in the past with no change in symptoms—and because he was thought to be at low risk for an STI—the physician did not prescribe another empiric trial of antibiotics. He did send the patient for an ultrasound evaluation of the scrotum and testes, which revealed only a 0.5 × 0.4 × 0.6-cm right epididymal cyst that was not palpable on examination.
The patient returned after 1 month, noting that his symptoms had neither improved nor worsened. The FP suggested that he stop taking the ibuprofen and begin a trial of gabapentin 100 mg daily, titrating up to 3 times daily for the first month, then to 300 mg 3 times daily in the second month.
When he returned 3 months later, Vincent reported that his symptoms had improved by about 50%. He has since been able to increase both the intensity and frequency of physical activity. Vincent is not interested in further increasing the dose of gabapentin and declined a referral to a urologist for consideration of procedural and surgical therapeutic options, but agreed to follow up as needed if his testicular pain worsened.
Postvasectomy pain is not unusual
Several years after a vasectomy, the diameter of a man’s ejaculatory ducts often doubles in size to counteract the increase in fluid pressure.11 The specific cause of long-term post-vasectomy pain syndrome, or congestive epididymitis, is unknown, but has been reported in 5% to 43% of men who have undergone this procedure.12-14 Sperm granulomas or spermatoceles represent the body’s effort to spare the testicle from damage secondary to increasing fluid pressure. While these granulomas are benign lesions, their presence may predispose a man to postvasectomy pain syndrome.15-17
CASE 2 Jason H
Two months before Jason’s visit to the FP, his testicular pain had become so excrutiating that he went to the ED seeking treatment. He was given an ultrasound with color Doppler and found to have postvasectomy surgical changes consistent with bilateral spermatoceles, but no evidence of epididymitis or a mass. Before leaving the ED, Jason received ceftriaxone (125 mg IM) as gonorrhea prophylaxis. He was discharged home with prophylactic antibiotics for chlamydia, as well as ibuprofen. He was advised to avoid strenuous physical activity and told to follow-up with his FP if his symptoms did not improve.
During several months of conservative medical therapy, including trials of NSAIDs, quinolone antibiotics, TCAs, and gabapentin, Jason did not experience any significant pain relief. He was frustrated by the dull, aching pain in his scrotum that continued to limit his physical and sexual activities.
Finally, the FP recommended a urologic consultation.
Consider these minimally invasive procedures
When conservative medical management fails, minimally invasive techniques are the next step. There are 2 commonly used procedures, both of which can be performed by a urologist in an outpatient setting.
Spermatic cord blocks with lidocaine and methylprednisolone have been shown to provide relief for weeks up to several months in small case studies, and may be repeated at intervals of several months if modest relief is achieved.18,19
Transrectal ultrasound-guided periprostatic anesthetic injections, another microinvasive option, offers minimal risk and may provide some short-term relief. However, data on long-term benefit and resolution of pain and disability are lacking.20
Consider surgery only after all else fails
If all medical and conservative therapies have been tried and the patient continues to have debilitating pain, surgical options should be considered. Because current surgical therapies are not always effective and are not reversible (and research on the various options is limited), it is important to initiate a detailed discussion with the patient. Such conversations should be held in consultation with a urologist.
Highlight risks and benefits and provide realistic expectations of short- and long-term postsurgical outcomes. It is also important to address psychological factors and social stressors that often contribute to chronic pelvic pain syndromes, which can improve long-term outcomes regardless of the chosen treatment. For this reason, a referral to a psychiatrist may be indicated.
Microsurgical denervation of the spermatic cord. Removal of the afferent nerve stimulus to the testicle is believed to result in the downregulation of the peripheral and central nervous systems, so the patient no longer has the perception of testicular pain. Several small trials have yielded favorable symptomatic pain relief scores in up to 71% of patients, with reported adverse outcomes including rare testicular atrophy—but no complaints of hypoesthesia or hyperesthesia of the scrotum, penile shaft, inguinal, or medial thigh skin.21,22 This treatment should be considered only in patients who have experienced a significant degree of temporary relief from spermatic cord injection.
Epididymectomy is recommended only when pain is localized to the epididymis, as this is a testicle-sparing procedure. Unilateral or bilateral epididymectomy is a viable option for the treatment of chronic orchialgia related to postvasectomy pain syndrome or chronic epididymitis. Reports highlighting symptomatic improvement based on small case series range from 43% to 74%, with the highest success rate found during a 5½-year follow-up.23-25 In 1 study, 90% of patients reported that they were satisfied with their choice to undergo the procedure.25
Vasectomy reversal (vasovasostomy) and inguinal or scrotal orchiectomy should be considered only after all other treatment modalities have failed. Vasovasostomy has the potential to restore fertility in up to 98% of cases,26 which may or may not be desirable. One study of men who experienced post-vasectomy pain syndrome and underwent microsurgical vasovasostomy found that after nearly 2½ years, 84% experienced complete pain resolution.27
The goal of orchiectomy is to relieve orchialgia by releasing the entrapped ipsilateral genitofemoral and/or ilioinguinal nerves. One study determined that 90% of men who underwent unilateral epididymectomy for chronic orchialgia required an orchiectomy to resolve pain.1 Another study found that 80% of patients continued to suffer both short- and long-term debilitating orchialgia postorchiectomy.28
CASE 2 Jason H
Jason saw a urologist, who initially offered him bilateral spermatic cord blocks. They provided Jason with moderate symptom relief on most days of the week and allowed him to increase his physical and sexual activities. Three months later, Jason went back to the urologist for evaluation because he felt that the effects of the spermatic cord blocks had worn off. In the next 6 months, he had 2 additional bilateral blocks.
Nearly a year after a series of spermatic cord blocks, most of it spent in persistent discomfort, Jason returned to his FP with a request for narcotic pain medication. The FP tried to be supportive, but told Jason that chronic narcotic therapy was not an ideal choice—and referred him back to the urologist to discuss surgical options.
The urologist recommended a bilateral epididymectomy and the patient, who was desperate to obtain some pain relief and now regretted undergoing a vasectomy, agreed. Within the first few weeks after his surgery, he noticed a reduction in pain, and he slowly increased his physical activity. A year later, Jason reported only minimal testicular and scrotal discomfort that did not limit his physical or sexual activities—and he continues to be pleased with the outcome of his treatment.
CORRESPONDENCE Joel J. Heidelbaugh, MD, FAAFP, Ypsilanti Health Center, 200 Arnet, Suite 200, Ypsilanti, MI 48198; [email protected]
1. Davis B, Noble MJ, Weigel JD, et al. Analysis and management of chronic testicular pain. J Urol. 1990;143:936-939.
2. Schover LR. Psychological factors in men with genital pain. Cleve Clin J Med. 1990;57:697-700.
3. Masarani M, Cox R. Th e aetiology, pathophysiology and management of chronic orchialgia. Br J Urol Int. 2003;91:435-437.
4. Granitsiotis P, Kirk D. Chronic testicular pain: an overview. Eur Urol. 2004;45:430-436.
5. Coogan CL. Painful scrotum. In: Myers JA, Millikan KW, Sacla-rides TJ, eds. Common Surgical Diseases. New York: Springer; 2008:293-295.
6. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2006. MMWR Morb Mortal Wkly Rep. 2006;55(RR-11):1-94.
7. Newman LM, Moran JS, Workowski KA. Update on the management of gonorrhea in adults in the United States. Clin Infect Dis. 2007;44(suppl 3):S84-S101.
8. Wiffen PJ, McQuay HJ, Rees J, et al. Gabapentin for acute and chronic pain. Cochrane Database Syst Rev. 2005;(3):CD005452.-
9. American College of Obstetricians and Gynecologists. Chronic pelvic pain. ACOG Practice Bulletin No. 51. Obstet Gynecol. 2004;103:589-605.
10. Sinclair AM, Miller B, Lee LK. Chronic orchialgia: consider gabapentin or nortriptyline before considering surgery. Int J Urol. 2007;14:622-625.
11. Jarow JP, Budin RE, Dym M, et al. Quantitative pathologic changes in the human testis after vasectomy. N Engl J Med. 1985;313:1252-1256.
12. Choe J, Kirkemo A. Questionnaire-based outcomes study of nononcological post-vasectomy complications. J Urol. 1996;155:1284-1286.
13. McMahon A, Buckley J, Taylor A, et al. Chronic testicular pain following vasectomy. Br J Urol. 1992;69:188-191.
14. Ahmed I, Rasheed S, White C, et al. Th e incidence of post-vasectomy chronic testicular pain and the role of nerve stripping (denervation) of the spermatic cord in its management. Br J Urol. 1997;79:269-270.
15. Christiansen CG, Sandlow JI. Testicular pain following vasectomy: a review of postvasectomy pain syndrome. J Androl. 2003;24:293-298.
16. Shapiro EI, Silber SJ. Open-ended vasectomy, sperm granuloma, and postvasectomy orchialgia. Fertil Steril. 1979;32:546-550.
17. Taxy JB, Marshall FF, Erlickman RJ. Vasectomy: subclinical pathologic changes. Am J Surg Pathol. 1981;5:767-772.
18. Fuchs E. Cord block anesthesia for scrotal surgery. J Urol. 1982;128:718-719.
19. Issa M, Hsiao K, Bassel Y, et al. Spermatic cord anesthesia block for scrotal procedures in the outpatient clinic setting. J Urol. 2004;172:2358-2361.
20. Zorn B, Rauchenwald M, Steers WD. Periprostatic injection of local anesthesia for relief of chronic orchialgia. J Urol. 1994;151:411,A735.-
21. Levine LA, Matkov TG, Lubenow TR. Microsurgical denervation of the spermatic cord: a surgical alternative in the treatment of chronic orchialgia. J Urol. 1996;155:1005-1007.
22. Strom KH, Levine LA. Microsurgical denervation of the spermatic cord for chronic orchialgia: long-term results from a single center. J Urol. 2008;180:949-953.
23. Padmore DE, Norman RW, Millard OH. Analyses of indications for and outcomes of epdidymectomy. J Urol. 1996;156:95-96.
24. West AF, Leung HY, Powell PH. Epididymectomy is an effective treatment for scrotal pain after vasectomy. Br J Urol Int. 2000;85:1097-1099.
25. Siu W, Ohl DA, Schuster TG. Long-term follow-up after epididymectomy for chronic epidiymal pain. Urology. 2007;70:333-336.
26. Patel SR, Sigman M. Comparison of outcomes of vasovasostomy performed in the convoluted and straight vas deferens. J Urol. 2008;179:256-259.
27. Myers SA, Mershon CE, Fuchs EF. Vasectomy reversal for treatment of the post-vasectomy pain syndrome. J Urol. 1997;157:518-520.
28. Costabile RA, Hahn M, McLeod DG. Chronic orchialgia in the pain prone patient: the clinical perspective. J Urol. 1991;146:1571-1574.
1. Davis B, Noble MJ, Weigel JD, et al. Analysis and management of chronic testicular pain. J Urol. 1990;143:936-939.
2. Schover LR. Psychological factors in men with genital pain. Cleve Clin J Med. 1990;57:697-700.
3. Masarani M, Cox R. Th e aetiology, pathophysiology and management of chronic orchialgia. Br J Urol Int. 2003;91:435-437.
4. Granitsiotis P, Kirk D. Chronic testicular pain: an overview. Eur Urol. 2004;45:430-436.
5. Coogan CL. Painful scrotum. In: Myers JA, Millikan KW, Sacla-rides TJ, eds. Common Surgical Diseases. New York: Springer; 2008:293-295.
6. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2006. MMWR Morb Mortal Wkly Rep. 2006;55(RR-11):1-94.
7. Newman LM, Moran JS, Workowski KA. Update on the management of gonorrhea in adults in the United States. Clin Infect Dis. 2007;44(suppl 3):S84-S101.
8. Wiffen PJ, McQuay HJ, Rees J, et al. Gabapentin for acute and chronic pain. Cochrane Database Syst Rev. 2005;(3):CD005452.-
9. American College of Obstetricians and Gynecologists. Chronic pelvic pain. ACOG Practice Bulletin No. 51. Obstet Gynecol. 2004;103:589-605.
10. Sinclair AM, Miller B, Lee LK. Chronic orchialgia: consider gabapentin or nortriptyline before considering surgery. Int J Urol. 2007;14:622-625.
11. Jarow JP, Budin RE, Dym M, et al. Quantitative pathologic changes in the human testis after vasectomy. N Engl J Med. 1985;313:1252-1256.
12. Choe J, Kirkemo A. Questionnaire-based outcomes study of nononcological post-vasectomy complications. J Urol. 1996;155:1284-1286.
13. McMahon A, Buckley J, Taylor A, et al. Chronic testicular pain following vasectomy. Br J Urol. 1992;69:188-191.
14. Ahmed I, Rasheed S, White C, et al. Th e incidence of post-vasectomy chronic testicular pain and the role of nerve stripping (denervation) of the spermatic cord in its management. Br J Urol. 1997;79:269-270.
15. Christiansen CG, Sandlow JI. Testicular pain following vasectomy: a review of postvasectomy pain syndrome. J Androl. 2003;24:293-298.
16. Shapiro EI, Silber SJ. Open-ended vasectomy, sperm granuloma, and postvasectomy orchialgia. Fertil Steril. 1979;32:546-550.
17. Taxy JB, Marshall FF, Erlickman RJ. Vasectomy: subclinical pathologic changes. Am J Surg Pathol. 1981;5:767-772.
18. Fuchs E. Cord block anesthesia for scrotal surgery. J Urol. 1982;128:718-719.
19. Issa M, Hsiao K, Bassel Y, et al. Spermatic cord anesthesia block for scrotal procedures in the outpatient clinic setting. J Urol. 2004;172:2358-2361.
20. Zorn B, Rauchenwald M, Steers WD. Periprostatic injection of local anesthesia for relief of chronic orchialgia. J Urol. 1994;151:411,A735.-
21. Levine LA, Matkov TG, Lubenow TR. Microsurgical denervation of the spermatic cord: a surgical alternative in the treatment of chronic orchialgia. J Urol. 1996;155:1005-1007.
22. Strom KH, Levine LA. Microsurgical denervation of the spermatic cord for chronic orchialgia: long-term results from a single center. J Urol. 2008;180:949-953.
23. Padmore DE, Norman RW, Millard OH. Analyses of indications for and outcomes of epdidymectomy. J Urol. 1996;156:95-96.
24. West AF, Leung HY, Powell PH. Epididymectomy is an effective treatment for scrotal pain after vasectomy. Br J Urol Int. 2000;85:1097-1099.
25. Siu W, Ohl DA, Schuster TG. Long-term follow-up after epididymectomy for chronic epidiymal pain. Urology. 2007;70:333-336.
26. Patel SR, Sigman M. Comparison of outcomes of vasovasostomy performed in the convoluted and straight vas deferens. J Urol. 2008;179:256-259.
27. Myers SA, Mershon CE, Fuchs EF. Vasectomy reversal for treatment of the post-vasectomy pain syndrome. J Urol. 1997;157:518-520.
28. Costabile RA, Hahn M, McLeod DG. Chronic orchialgia in the pain prone patient: the clinical perspective. J Urol. 1991;146:1571-1574.