User login
Infections in Hospitalized Patients
Supplement Editors:
Susan J. Rehm, MD, and Alpesh N. Amin, MD, MBA
Contents
Infections in hospitalized patients: What is happening and who can help?
Alpesh N. Amin, MD, MBA, and Susan J. Rehm, MD
Impact of community-acquired methicillin-resistant Staphylococcus aureus in the hospital setting
Thomas M. File, Jr., MD
Emerging issues in the management of infections caused by multidrug-resistant gram-negative bacteria
Louis B. Rice, MD
Complicated skin and soft-tissue infections: Diagnostic approach and empiric treatment options
James I. Merlino, MD, and Mark A. Malangoni, MD
Empiric treatment options in the management of complicated intra-abdominal infections
John A. Weigelt, MD
Antibacterial treatment strategies in hospitalized patients: What role for pharmacoeconomics?
Morton P. Goldman, PharmD, BCPS, and Radhika Nair, PhD
Supplement Editors:
Susan J. Rehm, MD, and Alpesh N. Amin, MD, MBA
Contents
Infections in hospitalized patients: What is happening and who can help?
Alpesh N. Amin, MD, MBA, and Susan J. Rehm, MD
Impact of community-acquired methicillin-resistant Staphylococcus aureus in the hospital setting
Thomas M. File, Jr., MD
Emerging issues in the management of infections caused by multidrug-resistant gram-negative bacteria
Louis B. Rice, MD
Complicated skin and soft-tissue infections: Diagnostic approach and empiric treatment options
James I. Merlino, MD, and Mark A. Malangoni, MD
Empiric treatment options in the management of complicated intra-abdominal infections
John A. Weigelt, MD
Antibacterial treatment strategies in hospitalized patients: What role for pharmacoeconomics?
Morton P. Goldman, PharmD, BCPS, and Radhika Nair, PhD
Supplement Editors:
Susan J. Rehm, MD, and Alpesh N. Amin, MD, MBA
Contents
Infections in hospitalized patients: What is happening and who can help?
Alpesh N. Amin, MD, MBA, and Susan J. Rehm, MD
Impact of community-acquired methicillin-resistant Staphylococcus aureus in the hospital setting
Thomas M. File, Jr., MD
Emerging issues in the management of infections caused by multidrug-resistant gram-negative bacteria
Louis B. Rice, MD
Complicated skin and soft-tissue infections: Diagnostic approach and empiric treatment options
James I. Merlino, MD, and Mark A. Malangoni, MD
Empiric treatment options in the management of complicated intra-abdominal infections
John A. Weigelt, MD
Antibacterial treatment strategies in hospitalized patients: What role for pharmacoeconomics?
Morton P. Goldman, PharmD, BCPS, and Radhika Nair, PhD
Atypical antipsychotics: New drugs, new challenges
Medical vs surgical treatment of lumbar disk herniation: Implications for future trials
Modafinil in the treatment of excessive daytime sleepiness
Correction: Obstructive sleep apnea
Revisiting Tanning-Bed Legislation [editorial]
Recently Approved Systemic Therapies for Acne Vulgaris and Rosacea (See Erratum 2007;80:334)
What's Eating You? Saddleback Caterpillar (Acharia stimulea)
Talking to patients about screening colonoscopy—where conversations fall short
- When talking to patients about screening colonoscopy, make clear their risk of colorectal cancer. Also, be sure they know about such commonly overlooked details as insurance/scheduling issues, dietary and medication changes before the procedure, a companion to drive afterward, and possible colonoscopy complications.
- Consider recommending supplemental information sources such as telephone calls, letters, e-mails, Web sites, or videotapes to help patients understand the need for screening colonoscopy.
Abstract
Background A physician’s recommendation is a powerful motivator for a patient to undergo colonoscopy for colorectal cancer screening, yet little is known about how physicians address this topic.
Methods We recruited 30 primary care physicians and physicians-in-training from 4 practices to counsel a “patient,” simulated by a researcher, regarding the need for screening colonoscopy. Audiotapes of the physician-patient encounters were transcribed. Preserving physician anonymity, we assessed each encounter for key informational points, positive or negative message framing, type of numeracy information, and use of colloquial or technical language.
Results Study physicians addressed a mean of 6.7 (standard deviation=1.8) of 13 key informational points. Most physicians (≥80%) discussed the benefits of colorectal cancer screening, the recognition of colonoscopy as a standard exploratory procedure, and the use of sedation. However, few (<20%) addressed the risks of colonoscopy, the nuances of scheduling, or the need for dietary and medication changes. Nearly all physicians (98%) used messages that focused on the positive aspects of screening (gain-framed messages), and many (67%) also used messages that focused on the risk of not screening (loss-framed messages). Numeracy information generally was expressed simply, but half of the physicians used statistical terms. Half used colloquial terms to describe the prep and procedure.
Conclusion Though most physicians used positive, simple terms to describe colonoscopy, they often omitted key information. Correcting for the areas of insufficient information found in our study—perhaps with supplementary educational sources—will help ensure that patients are adequately prepared for colonoscopy.
Colorectal cancer screening has the potential to reduce deaths from colorectal cancer by at least one third.1 Yet only half of eligible patients in the US who are age 50 or older have undergone screening.2 Patients often say they haven’t been screened because their physician didn’t recommend it.3-5
A physician’s recommendation is strongly predictive of whether a patient actually undergoes colorectal cancer screening, even after adjusting for multiple confounders.6-9 Yet several studies have found that, even after the physician has recommended or ordered an endoscopic study of the colon, many patients do not follow through.10-12 Successful completion of screening colonoscopy requires, in part, that a patient understand the need for the procedure and receive sufficient instruction about it. Thus, failure to undergo this test may reflect patient concerns or misunderstandings due to inadequate communication.13,14
In many settings, the primary care physician bears the responsibility for telling the patient about screening colonoscopy because the endoscopist meets the patient only at the time of the procedure. Supplementary educational programs can also play a role. Unfortunately, though, while these materials appear to reduce patient anxiety and increase adherence to screening recommendations,15-17 they are infrequently used.
Looking at physician communication with an eye toward improvement
Our goal in conducting this study was to evaluate the way in which physicians discuss the need for screening colonoscopy with their patients. Using a simulated patient scenario, we wanted to examine 4 dimensions of each discussion: completeness; type of messaging; type of numeracy information (ie, numerical and mathematical data); and use of colloquial vs technical language.
- Completeness reflected the number of key informational points addressed.
- Type of messaging focused on the use of loss- or gain-framed messages, both of which have been linked to increased patient intention to adopt a cancer prevention behavior or test.18-20 Gain-framed counseling emphasizes the positive aspects of screening; loss-framed, the risks of not screening.
- Type of numeracy information. Because poor numeracy skills are thought to impair the accuracy of patients’ perceptions of cancer risk,21 we categorized the type of numeracy information provided by physicians following an approach developed by Ahlers-Schmidt and colleagues.22
- Colloquial vs technical language. Because colonoscopy involves sensitive topics such as the bowels and feces, and because language choices may affect acceptance of care,23 we evaluated physicians’ use of terminology when describing the procedure.
We felt that by looking at these dimensions, we could help physicians to refine screening colonoscopy messages so that conversations with patients could be more clear, complete, and balanced.
Methods
13 key points regarding screening colonoscopy
We reviewed published literature and Internet sources to develop a preliminary list of topics a primary care physician could address when discussing colorectal cancer screening, especially screening colonoscopy. We used NLM Gateway and Medline databases and the following search terms: colonoscopy, patient education, patient instructions, guidelines, physician, colon cancer, counseling, and knowledge. A medical librarian directed the search. Despite having expert assistance, we did not find any publications that offered a peer-reviewed, validated list of topics to guide physicians’ discussions about screening colonoscopy.
We then conducted an Internet search using the terms colon cancer, colon cancer screening, colonoscopy, and colon cancer patient education. We categorized data from identified sites such as the American Gastroenterological Association, Up-to-Date, the American Cancer Society, and the National Library of Medicine, among others, into 13 common topics (TABLE 1). Three points addressed general information about colorectal cancer, and the rest dealt with colonoscopy specifically. A panel of 2 gastroenterologists and 3 internists from the same institution independently judged each item on the list for importance, relevance, and feasibility for discussion. Except for one panelist, all endorsed the need to address the 13 items.
TABLE 1
Percentage of physicians who covered key colorectal cancer screening points
| TOPIC | INFORMATIONAL POINT | PHYSICIANS ADDRESSING TOPIC (N=30), % |
|---|---|---|
| General colorectal prevention | ||
| 1. Standard preventive health care procedure | Recommended* as a standard screening test for those age 50 and older | 83 |
| 2. Value of screening | Can prevent cancer as well as detect cancer at a treatable stage | 83 |
| 3. Risk of colorectal cancer | Prevalence or incidence either nationally or regionally (family history)† | 43 |
| Specifics about colonoscopy | ||
| 4. Anesthesia | Sedation to reduce discomfort; risk information discussed or to be reviewed by anesthetist | 87 |
| 5. Gastrointestinal prep | Use of laxative, usual types used, and what patient can expect | 77 |
| 6. Abnormalities detected by colonoscopy | Finds growths (polyps) or cancer | 76 |
| 7. Description of procedure | Camera at the end of a flexible tube views the entire colon and tiny tweezers at the end sample or remove growths | 70 |
| 8. Follow-up after a negative test | Experts recommend screening after a negative test every 10 years | 67 |
| 9. Patient experience or knowledge‡ | Any personal or family/friend experience with colonoscopy or knowledge about the test | 64 |
| 10. Transportation | Another person must accompany the patient after procedure | 53 |
| 11. Insurance/scheduling | Insurance coverage, who arranges for the procedure, where test is performed | 13 |
| 12. Diet | Diet the day before and day of procedure, importance of hydration | 10 |
| 13. Risk of colonoscopy | Risk of bowel perforation or other complication | 10 |
| 14. Medications | Changes in medications for the procedure | 3 |
| *Recommendation by expert panels need not be specified. Physicians often just say, “We recommend.” | ||
| †Family history not necessary in this study because the patient was said to be at average risk for colorectal cancer. | ||
| ‡Point was not identified originally by the review and excluded from analysis. | ||
Physician sample
Of 135 providers practicing in 2 primary care and 1 geriatrics practice affiliated with the same urban academic medical center, we invited 30 physicians to participate. This sample was chosen to adequately represent female and minority physicians as well as physicians at different levels of training (TABLE 2). The physicians were invited to participate either by e-mail (N=19) or in person (N=11), and all invitees consented. Interviews were conducted alone in the physician’s office or in a practice conference room, and they were audiotaped with the physician’s consent.
Interviews lasted fewer than 15 minutes and did not intrude on patient care time. Study physicians read a vignette of a fictitious 51-year-old African American woman who was an established patient in their practice, without a family history of colon cancer but with arthritis and hypertension. We asked each physician to inform the patient (simulated by the interviewer) about colorectal cancer screening and colonoscopy, as well as the logistics of getting this test. To standardize the interaction, interviewers predefined the patient’s responses to questions. For example, if the physician asked about prior knowledge of colonoscopy, the simulated patient replied that she had none. Study physicians were not prompted in any way and, though not given time restrictions, all were brief and to the point.
TABLE 2
Study physician characteristics
| CHARACTERISTIC | PHYSICIANS WITH CHARACTERISTIC (N=30), % | INFORMATIONAL POINTS ADDRESSED,* MEAN (SD) |
|---|---|---|
| Total | 100 | 6.73 (1.84) |
| Gender | ||
| Female | 66 | 6.70 (1.89) |
| Male | 34 | 6.80 (1.81) |
| Race | ||
| White | 80 | 6.84 (1.80) |
| Non-white | 20 | 6.20 (2.17) |
| Level of training | ||
| Attending | 63 | 6.84 (1.98) |
| Trainee | 37 | 6.54 (1.63) |
| Specialty | ||
| General Internal Medicine | 90 | 6.89 (1.83) |
| Geriatrics | 10 | 5.33 (1.53) |
| * All comparisons P >.05 | ||
Analysis
Interview transcripts were anonymous, identified only by a study number. The 2 study investigators coded transcribed interviews independently as to whether physicians addressed the 13 informational points. Inter-rater concordance in coding was 90%. We also independently evaluated the interviews according to the use of gain- or loss-framed messages (eg, detecting colon polyps early before cancer develops vs colorectal cancer being the second most common cause of cancer death). We independently classified types of numeracy information provided into 15 categories.22 We also independently examined audiotaped transcripts for examples of colloquial terms/slang or technical language. Because we are unaware of a validated approach to characterizing a physician’s language in this manner, we asked a layperson for assistance in identifying colloquial/slang terms.
To determine whether there were predictors of a physician addressing more of the informational points than his or her peers, we examined bivariate associations of the following demographic and professional data: gender, race (white vs non-white), academic advancement (attending vs trainee), and specialty (general internist vs geriatrician).
We analyzed data using the Wilcoxon rank-sum test because the data were not normally distributed. We used SAS Statistical Software (SAS Institute, Cary, NC). The University of Pennsylvania Institutional Review Board approved the study. The project was supported by a grant from the Bach Fund of the Presbyterian Medical Center, University of Pennsylvania.
Results
How did the physicians talk to their patient?
The 30 study physicians were primarily women, one fifth were from under-represented minorities, and one third were either residents or fellows (TABLE 2). Of 13 key informational points endorsed by our physician panel (TABLE 1), the physician-subjects addressed a mean of 6.7 points (range, 3–10). Nearly all physician-subjects discussed the value of colorectal cancer screening, colonoscopy as a standard colorectal screening procedure, and sedation during the procedure. However, fewer than 20% addressed the following topics: insurance/scheduling, dietary changes, medication modification, and risks of colonoscopy. In this small sample, the number of topics mentioned did not differ significantly by physician characteristic (TABLE 2).
Two thirds of the physicians asked the simulated patient about her prior knowledge or experience with colonoscopy. Although this question was not among the original 13 informational points, it helped to guide the discussion by identifying specific preconceptions or prior knowledge of this test. Therefore, this post hoc 14th informational point was added to our list but not considered in our analyses.
Gain-framed messages used more than loss-framed messages
Nearly all physicians used gain-framed messages, and more than half also used loss-framed messages (TABLE 3). Only 1 physician offered only a loss-framed message. Overall, study physicians mentioned less than 2 gain- or loss-framed messages.
- The most common types of gain-framed messages were detecting cancer early, preventing cancer by taking out polyps, and screening at only a 10-year interval if the test result is negative.
- The most common loss-framed messages noted that colorectal cancer was the second most common cause of cancer death and that risk is increased with a family history of this cancer.
TABLE 3
Gain- and loss-framed messages and types of numeracy information used by study physicians
| TYPE OF MESSAGE OR NUMERACY | PHYSICIANS N (%) | OCCURRENCES IN INTERVIEWS, Total N (MEAN AMONG USERS, RANGE) |
|---|---|---|
| Message framing | ||
| Gain-framed | 29 (96) | 56 (1.9, 1–5) |
| Loss-framed | 20 (67) | 31 (1.6, 1–3) |
| Numeracy | ||
| Descriptive terms | 19 (63) | 36 (1.9, 1–3) |
| Statistical terms | 15 (50) | 30 (2.0, 1–5) |
| Temporal terms | 9 (30) | 11 (1.2, 1–2) |
| Proportions | 4 (13) | 5 (1.3, 1–2) |
| Fractions | 3 (10) | 3 (1.0, 1–1) |
Physicians avoided using numbers
Of the 15 types of numeracy information described by Ahlers-Schmit et al, our physicians used only 5. Nineteen physicians (63%) used descriptive terms such as “likely” or “increased,” and 15 (50%) used statistical concepts such as risk and second-most-common cause. Physicians avoided using numbers; 9 (30%) used temporal terms such as “early”; 4 (13%) cited a proportion; and only 3 (10%) used a fraction.
Colloquial language, or was it crude?
While reading the transcripts, we noted that some physicians used colloquial terms that could be regarded as crude. Other terms were probably too technical without an explanation. Some information was simply incorrect. We offer selected quotes to illustrate various types of language used.
About the prep:
- “Getting a colonoscopy is not the most fun experience…you have really bad diarrhea and you just empty out your guts.”
- “It’s basically Liquid Plumber for your bowels.”
- “Bowel prep…is kind of voluminous and associated with kind of massive bowel movements.”
- “Everybody hates the prep and you may be one of those and that’s just that.”
- “Generally you have to be up all night, sometimes, cleaning your bowels out.”
About the procedure:
- “It’s not the most comfortable screening exam in the world.”
- “It’s a test where they stick a lighted tube up your back-side.”
- “The stomach doctors put a camera up your bottom and look at the walls of your colon.”
- “They can go in with a microscope and look around and look at the colon itself.”
- “It’s a painless test.”
Word polyp is used, but not defined
Physicians often employed technical language when describing the pathology detected by colonoscopy. “Polyp” was mentioned by 20 physicians (67%) but rarely defined; “biopsy” by 5 (17%), and “lesion” by 6 (20%). Other technical terms were precancerous, symptomatic, and incapacitated.
Discussion
An informed patient is a willing patient
Our study physicians addressed only half of the 13 informational points, likely reflecting the time constraints of a typical office visit. Primary care physicians appear to expect that either the colonoscopist or other sources of information would fill in the gaps. As reported in several studies, unanswered questions can discourage patients from keeping their scheduled colonoscopy appointment.10,11 In one report of African-American church members, those with adequate knowledge about colorectal cancer screening were more likely to complete screening.24
Wolf and Becker suggested that discussions about cancer screening address 4 broad topics: the probability of developing the cancer, the operating characteristics of the screening test(s), the likelihood that screening will benefit the patient, and potential burdens of the test.25 Instead of a balanced and lengthy discussion, our study physicians generally emphasized the positives such as the value of avoiding colon cancer, the standard nature of this test, and the benefit of being sedated for the procedure. Thus, gain-framed messages about colorectal cancer were the norm for our study physicians.
Half of the physicians also offered loss-framed messages emphasizing the need to avoid the consequences of colorectal cancer and the increased threat associated with a family history of this malignancy. Research in mammography screening suggests that loss-framed messaging may be a more powerful motivator than gain-framed messaging,26 but it is not clear if this observation can be generalized to colorectal cancer screening.
Walking a fine line with the particulars of risk
Our study physicians rarely provided data on the probability of developing colorectal cancer. Physicians may avoid this topic because many patients have difficulty understanding information about the risk of colorectal cancer.11 In support of this approach, Lipkus and colleagues reported that various ways of informing patients about colorectal cancer risk did not affect their intention to be screened.27 Of concern, most of our physicians did not address the common misconception that colorectal cancer screening is unnecessary in the absence of symptoms.28
Overall, the level of numeracy information provided by study physicians required minimal patient understanding of mathematical and statistical concepts. Most information was descriptive, such as colonoscopy being “more thorough” than other tests. Though statistical concepts such as “risk” were often mentioned, few physicians offered probabilities or incidence data. Experts recommend providing such data,25 but Web sites have been criticized for offering excessive numerical cancer risk data.22 Therefore, physicians must walk a fine line between providing adequate information and offering data that require a high level of health numeracy for understanding.
6 key points physicians often overlook
Most physicians failed to mention dietary and medication changes, scheduling/insurance coverage issues, and risk of complications from colonoscopy. Nearly 60% failed to discuss the patient’s risk of colorectal cancer. Almost half did not mention the need for a companion to accompany the patient after the test. Scheduling challenges, in particular, are known to interfere with completing colonoscopy.11
Many neglect to describe the procedure
Thirty percent of physicians failed to describe the procedure itself, so it is not surprising that patients complain they have a poor understanding of test logistics.11,29,30 Denberg and colleagues have reported that mailing an informational brochure about colonoscopy can increase the number who keep their appointment.31
How language choices may affect understanding
Other researchers have identified additional patient barriers to colonoscopy, including fear of pain, concern for modesty, and desire to avoid the bowel prep.11,32 These concerns may be mitigated or heightened by the physician’s language. In our review of transcripts, physicians often used slang or colloquial language to describe the procedure, probably in an attempt to convey information in a familiar way. This language may be viewed as crude and potentially discouraging, but further research is needed to evaluate patient receptiveness to different ways of speaking about sensitive topics.
Additionally, physicians commonly used technical terms such as “polyp” and “biopsy” without explaining them. Technical language may increase racial disparities in adhering to scheduled colonoscopy. In a family medicine clinic, patients from minority groups had particular difficulty understanding medical terms and procedure names.28 Because little time is available for counseling about cancer screening tests, and because patients retain only a limited amount of information about procedures,33 supplementary informational sources are warranted.15-17,31 Options include brochures, telephone calls, letters, e-mails, Web site data, and videotapes, but it is unclear which sources optimally improve patient adherence to screening colonoscopy.34
Study limitations include simulated interaction
There were a number of limitations to this study. First, the investigators “simulated” the patient. Though study physicians were told to act as if they were speaking to a regular patient, they may still have unconsciously modified their usual approach to addressing this topic.
Second, we did not assess the effectiveness of these discussions in motivating actual patients to receive colonoscopy.
Other limitations included the following:
- We did not set a time period for these discussions, so they may have been even more limited in actual practice.
- We studied physicians from a single health care setting wherein colonoscopy appears to be the preferred approach to screen an average risk patient for colorectal cancer. In addition, in this health care system, this test is performed by a gastroenterologist, rather than a primary care physician.
- We did not determine whether patients regard our selected quotes as too colloquial or technical.
- This study did not address the important barrier of a physician forgetting to recommend colorectal cancer screening.35
Further research, next steps
Our study supports the hypothesis that physicians differ widely—but are generally deficient—when informing patients about screening colonoscopy. They generally emphasize the positives of colonoscopy and use terms that are colloquial, avoiding statistical concepts that may be hard for patients to understand. Future studies need to address the effectiveness of these approaches to discussing screening colonoscopy.
Given the central role of the primary care physician in motivating patients to undergo screening colonoscopy in a limited time period, it appears that additional supports are needed to supplement physician discussion about this important preventive care procedure.
Correspondence
Barbara J. Turner MD, MSEd, University of Pennsylvania, 1123 Blockley Hall/6021, 423 Guardian Drive, Philadelphia, PA 19104; [email protected]
1. Ries LA, Wingo PA, Miller DS, et al. The annual report to the nation on the status of cancer, 1973–1997, with a special section on colorectal cancer. Cancer 2000;88:2398-2424.
2. Centers for Disease Control and Prevention (CDC). Colorectal cancer test use among persons aged > or = 50 years—United States, 2001. MMWR Morb Mortal Wkly Rep 2003;52:193-196.
3. Wee CC, McCarthy EP, Phillips RS. Factors associated with colon cancer screening: the role of patient factors and physician counseling. Prev Med 2005;41:23-29.
4. Taylor V, Lessler D, Mertens K, et al. Colorectal cancer screening among African Americans: the importance of physician recommendations. J Natl Med Assoc 2003;95:806-812.
5. Brawarsky P, Brooks DR, Mucci LA, Wood PA. Effect of physician recommendation and patient adherence on rates of colorectal cancer testing. Cancer Detect Prevent 2004;28:260-268.
6. Holt WS, Jr. Factors affecting compliance with screening sigmoidoscopy. J Fam Pract 1991;32:585-589.
7. Brenes GA, Paskett ED. Predictors of stage of adoption for colorectal cancer screening. Prev Med 2000;31:410-416.
8. Myers RE, Turner B, Weinberg D, et al. Impact of a physician-oriented intervention on follow-up in colorectal cancer screening. Prev Med 2004;38:375-381.
9. Brawarsky P, Brooks DR, Mucci LA, Wood PA. Effect of physician recommendation and patient adherence on rates of colorectal cancer testing. Cancer Detect Prev 2004;28:260-268.
10. Turner BJ, Weiner M, Yang C, TenHave T. Predicting adherence to colonoscopy or flexible sigmoidoscopy on the basis of physician appointment-keeping behavior. Ann Intern Med 2004;140:528-532.
11. Denberg TD, Melhado TV, Coombes JM, et al. Predictors of nonadherence to screening colonoscopy. J Gen Intern Med 2005;20:989-995.
12. Kelly RB, Shank JC. Adherence to screening flexible sigmoidoscopy in asymptomatic patients. Med Care 1992;30:1029-1042.
13. Janz NK, Wren PA, Schottenfeld D, Guire KE. Colorectal cancer screening attitudes and behavior: a population-based study. Prev Med 2003;37:627-634.
14. US Preventive Services Task Force. Screening for colorectal cancer: recommendations and rationale. Ann Intern Med 2002;137:129-131.
15. Abuksis G, Mor M, Segal N, et al. A patient education program is cost-effective for preventing failure of endoscopic procedures in a gastroenterology department. Am J Gastroenterol 2001;96:1786-1790.
16. Pignone M, Harris R, Kinsinger L. Videotape-based decision aid for colon cancer screening. A randomized, controlled trial. Ann Intern Med 2000;13:761-769.
17. Wardle J, Williamson S, McCaffery K, et al. Increasing attendance at colorectal cancer screening: testing the efficacy of a mailed, psychoeducational intervention in a community sample of older adults. Health Psychol 2003;22:99-105.
18. Detweiler JB, Bedell BT, Salovey P, et al. Message framing and sunscreen use: gain-framed messages motivate beach-goers. Health Psychol 1999;18:189-196.
19. Banks SM, Salovey P, Greener S, et al. The effects of message framing on mammography utilization. Health Psychol 1995;14:178-184.
20. Rivers SE, Salovey P, Pizarro DA, et al. Message framing and pap test utilization among women attending a community health clinic. J Health Psychol 2005;10:65-77.
21. Davids SL, Schapira MM, McAuliffe TL, Nattinger AB. Predictors of pessimistic breast cancer risk perceptions in a primary care population. J Gen Intern Med 2004;19:310-315.
22. Ahlers-Schmidt CR, Golbeck AL, Paschal AM, et al. Breast cancer counts: numeracy in breast cancer information on the web. J Cancer Educ 2006;21:95-98.
23. Hodgson J, Hughes E, Lambert C. “SLANG”—Sensitive Language and the New Genetics—an exploratory study. J Genet Couns 2005;14:415-421.
24. Katz ML, James AS, Pignone MP, et al. Colorectal cancer screening among African American church members: a qualitative and quantitative study of patient-provider communication. BMC Public Health 2004;4:62.-
25. Wolf AM, Becker DM. Cancer screening and informed patient discussions. Truth and consequences. Arch Intern Med 1996;156:1069-1072.
26. Banks SM, Salovey P, Greener S, et al. The effects of message framing on mammography utilization. Health Psychol 1995;14:178-184.
27. Lipkus IM, Crawford Y, Fenn K, et al. Testing different formats for communicating colorectal cancer risk. J Health Commun 1999;4:311-324.
28. Shokar NK, Vernon SW, Weller SC. Cancer and colorectal cancer: knowledge, beliefs, and screening p of a diverse patient population. Fam Med 2005;37:341-347.
29. Katz ML, Ruzek SB, Miller SM, Legos P. Gender differences in patients needs and concerns to diagnostic tests for possible cancer. J Cancer Educ 2004;19:227-231.
30. Dube CE, Fuller BK, Rosen RK, et al. Men’s experiences of physical exams and cancer screening tests: a qualitative study. Prev Med 2005;40:628-635.
31. Denberg TD, Coombes JM, Byers TE, et al. Effect of a mailed brochure on appointment-keeping for screening colonoscopy: a randomized trial. Ann Intern Med 2006;145:895-900.
32. Harewood GC, Wiersema MJ, Melton LJ, 3rd. A prospective, controlled assessment of factors influencing acceptance of screening colonoscopy. Am J Gastroenterol 2002;97:3186-3194.
33. Godwin Y. Do they listen? A review of information retained by patients following consent for reduction mammoplasty. Br J Plastic Surgery 2000;53:121-125.
34. Greisinger A, Hawley ST, Bettencourt JL, et al. Primary care patients’ understanding of colorectal cancer screening. Cancer Detect Prev 2006;30:67-74.
35. Dulai GS, Farmer MM, Ganz PA, et al. Primary care physician perceptions of barriers to and facilitators of colorectal cancer screening in a managed care setting. Cancer 2004;100:1843-1852.
- When talking to patients about screening colonoscopy, make clear their risk of colorectal cancer. Also, be sure they know about such commonly overlooked details as insurance/scheduling issues, dietary and medication changes before the procedure, a companion to drive afterward, and possible colonoscopy complications.
- Consider recommending supplemental information sources such as telephone calls, letters, e-mails, Web sites, or videotapes to help patients understand the need for screening colonoscopy.
Abstract
Background A physician’s recommendation is a powerful motivator for a patient to undergo colonoscopy for colorectal cancer screening, yet little is known about how physicians address this topic.
Methods We recruited 30 primary care physicians and physicians-in-training from 4 practices to counsel a “patient,” simulated by a researcher, regarding the need for screening colonoscopy. Audiotapes of the physician-patient encounters were transcribed. Preserving physician anonymity, we assessed each encounter for key informational points, positive or negative message framing, type of numeracy information, and use of colloquial or technical language.
Results Study physicians addressed a mean of 6.7 (standard deviation=1.8) of 13 key informational points. Most physicians (≥80%) discussed the benefits of colorectal cancer screening, the recognition of colonoscopy as a standard exploratory procedure, and the use of sedation. However, few (<20%) addressed the risks of colonoscopy, the nuances of scheduling, or the need for dietary and medication changes. Nearly all physicians (98%) used messages that focused on the positive aspects of screening (gain-framed messages), and many (67%) also used messages that focused on the risk of not screening (loss-framed messages). Numeracy information generally was expressed simply, but half of the physicians used statistical terms. Half used colloquial terms to describe the prep and procedure.
Conclusion Though most physicians used positive, simple terms to describe colonoscopy, they often omitted key information. Correcting for the areas of insufficient information found in our study—perhaps with supplementary educational sources—will help ensure that patients are adequately prepared for colonoscopy.
Colorectal cancer screening has the potential to reduce deaths from colorectal cancer by at least one third.1 Yet only half of eligible patients in the US who are age 50 or older have undergone screening.2 Patients often say they haven’t been screened because their physician didn’t recommend it.3-5
A physician’s recommendation is strongly predictive of whether a patient actually undergoes colorectal cancer screening, even after adjusting for multiple confounders.6-9 Yet several studies have found that, even after the physician has recommended or ordered an endoscopic study of the colon, many patients do not follow through.10-12 Successful completion of screening colonoscopy requires, in part, that a patient understand the need for the procedure and receive sufficient instruction about it. Thus, failure to undergo this test may reflect patient concerns or misunderstandings due to inadequate communication.13,14
In many settings, the primary care physician bears the responsibility for telling the patient about screening colonoscopy because the endoscopist meets the patient only at the time of the procedure. Supplementary educational programs can also play a role. Unfortunately, though, while these materials appear to reduce patient anxiety and increase adherence to screening recommendations,15-17 they are infrequently used.
Looking at physician communication with an eye toward improvement
Our goal in conducting this study was to evaluate the way in which physicians discuss the need for screening colonoscopy with their patients. Using a simulated patient scenario, we wanted to examine 4 dimensions of each discussion: completeness; type of messaging; type of numeracy information (ie, numerical and mathematical data); and use of colloquial vs technical language.
- Completeness reflected the number of key informational points addressed.
- Type of messaging focused on the use of loss- or gain-framed messages, both of which have been linked to increased patient intention to adopt a cancer prevention behavior or test.18-20 Gain-framed counseling emphasizes the positive aspects of screening; loss-framed, the risks of not screening.
- Type of numeracy information. Because poor numeracy skills are thought to impair the accuracy of patients’ perceptions of cancer risk,21 we categorized the type of numeracy information provided by physicians following an approach developed by Ahlers-Schmidt and colleagues.22
- Colloquial vs technical language. Because colonoscopy involves sensitive topics such as the bowels and feces, and because language choices may affect acceptance of care,23 we evaluated physicians’ use of terminology when describing the procedure.
We felt that by looking at these dimensions, we could help physicians to refine screening colonoscopy messages so that conversations with patients could be more clear, complete, and balanced.
Methods
13 key points regarding screening colonoscopy
We reviewed published literature and Internet sources to develop a preliminary list of topics a primary care physician could address when discussing colorectal cancer screening, especially screening colonoscopy. We used NLM Gateway and Medline databases and the following search terms: colonoscopy, patient education, patient instructions, guidelines, physician, colon cancer, counseling, and knowledge. A medical librarian directed the search. Despite having expert assistance, we did not find any publications that offered a peer-reviewed, validated list of topics to guide physicians’ discussions about screening colonoscopy.
We then conducted an Internet search using the terms colon cancer, colon cancer screening, colonoscopy, and colon cancer patient education. We categorized data from identified sites such as the American Gastroenterological Association, Up-to-Date, the American Cancer Society, and the National Library of Medicine, among others, into 13 common topics (TABLE 1). Three points addressed general information about colorectal cancer, and the rest dealt with colonoscopy specifically. A panel of 2 gastroenterologists and 3 internists from the same institution independently judged each item on the list for importance, relevance, and feasibility for discussion. Except for one panelist, all endorsed the need to address the 13 items.
TABLE 1
Percentage of physicians who covered key colorectal cancer screening points
| TOPIC | INFORMATIONAL POINT | PHYSICIANS ADDRESSING TOPIC (N=30), % |
|---|---|---|
| General colorectal prevention | ||
| 1. Standard preventive health care procedure | Recommended* as a standard screening test for those age 50 and older | 83 |
| 2. Value of screening | Can prevent cancer as well as detect cancer at a treatable stage | 83 |
| 3. Risk of colorectal cancer | Prevalence or incidence either nationally or regionally (family history)† | 43 |
| Specifics about colonoscopy | ||
| 4. Anesthesia | Sedation to reduce discomfort; risk information discussed or to be reviewed by anesthetist | 87 |
| 5. Gastrointestinal prep | Use of laxative, usual types used, and what patient can expect | 77 |
| 6. Abnormalities detected by colonoscopy | Finds growths (polyps) or cancer | 76 |
| 7. Description of procedure | Camera at the end of a flexible tube views the entire colon and tiny tweezers at the end sample or remove growths | 70 |
| 8. Follow-up after a negative test | Experts recommend screening after a negative test every 10 years | 67 |
| 9. Patient experience or knowledge‡ | Any personal or family/friend experience with colonoscopy or knowledge about the test | 64 |
| 10. Transportation | Another person must accompany the patient after procedure | 53 |
| 11. Insurance/scheduling | Insurance coverage, who arranges for the procedure, where test is performed | 13 |
| 12. Diet | Diet the day before and day of procedure, importance of hydration | 10 |
| 13. Risk of colonoscopy | Risk of bowel perforation or other complication | 10 |
| 14. Medications | Changes in medications for the procedure | 3 |
| *Recommendation by expert panels need not be specified. Physicians often just say, “We recommend.” | ||
| †Family history not necessary in this study because the patient was said to be at average risk for colorectal cancer. | ||
| ‡Point was not identified originally by the review and excluded from analysis. | ||
Physician sample
Of 135 providers practicing in 2 primary care and 1 geriatrics practice affiliated with the same urban academic medical center, we invited 30 physicians to participate. This sample was chosen to adequately represent female and minority physicians as well as physicians at different levels of training (TABLE 2). The physicians were invited to participate either by e-mail (N=19) or in person (N=11), and all invitees consented. Interviews were conducted alone in the physician’s office or in a practice conference room, and they were audiotaped with the physician’s consent.
Interviews lasted fewer than 15 minutes and did not intrude on patient care time. Study physicians read a vignette of a fictitious 51-year-old African American woman who was an established patient in their practice, without a family history of colon cancer but with arthritis and hypertension. We asked each physician to inform the patient (simulated by the interviewer) about colorectal cancer screening and colonoscopy, as well as the logistics of getting this test. To standardize the interaction, interviewers predefined the patient’s responses to questions. For example, if the physician asked about prior knowledge of colonoscopy, the simulated patient replied that she had none. Study physicians were not prompted in any way and, though not given time restrictions, all were brief and to the point.
TABLE 2
Study physician characteristics
| CHARACTERISTIC | PHYSICIANS WITH CHARACTERISTIC (N=30), % | INFORMATIONAL POINTS ADDRESSED,* MEAN (SD) |
|---|---|---|
| Total | 100 | 6.73 (1.84) |
| Gender | ||
| Female | 66 | 6.70 (1.89) |
| Male | 34 | 6.80 (1.81) |
| Race | ||
| White | 80 | 6.84 (1.80) |
| Non-white | 20 | 6.20 (2.17) |
| Level of training | ||
| Attending | 63 | 6.84 (1.98) |
| Trainee | 37 | 6.54 (1.63) |
| Specialty | ||
| General Internal Medicine | 90 | 6.89 (1.83) |
| Geriatrics | 10 | 5.33 (1.53) |
| * All comparisons P >.05 | ||
Analysis
Interview transcripts were anonymous, identified only by a study number. The 2 study investigators coded transcribed interviews independently as to whether physicians addressed the 13 informational points. Inter-rater concordance in coding was 90%. We also independently evaluated the interviews according to the use of gain- or loss-framed messages (eg, detecting colon polyps early before cancer develops vs colorectal cancer being the second most common cause of cancer death). We independently classified types of numeracy information provided into 15 categories.22 We also independently examined audiotaped transcripts for examples of colloquial terms/slang or technical language. Because we are unaware of a validated approach to characterizing a physician’s language in this manner, we asked a layperson for assistance in identifying colloquial/slang terms.
To determine whether there were predictors of a physician addressing more of the informational points than his or her peers, we examined bivariate associations of the following demographic and professional data: gender, race (white vs non-white), academic advancement (attending vs trainee), and specialty (general internist vs geriatrician).
We analyzed data using the Wilcoxon rank-sum test because the data were not normally distributed. We used SAS Statistical Software (SAS Institute, Cary, NC). The University of Pennsylvania Institutional Review Board approved the study. The project was supported by a grant from the Bach Fund of the Presbyterian Medical Center, University of Pennsylvania.
Results
How did the physicians talk to their patient?
The 30 study physicians were primarily women, one fifth were from under-represented minorities, and one third were either residents or fellows (TABLE 2). Of 13 key informational points endorsed by our physician panel (TABLE 1), the physician-subjects addressed a mean of 6.7 points (range, 3–10). Nearly all physician-subjects discussed the value of colorectal cancer screening, colonoscopy as a standard colorectal screening procedure, and sedation during the procedure. However, fewer than 20% addressed the following topics: insurance/scheduling, dietary changes, medication modification, and risks of colonoscopy. In this small sample, the number of topics mentioned did not differ significantly by physician characteristic (TABLE 2).
Two thirds of the physicians asked the simulated patient about her prior knowledge or experience with colonoscopy. Although this question was not among the original 13 informational points, it helped to guide the discussion by identifying specific preconceptions or prior knowledge of this test. Therefore, this post hoc 14th informational point was added to our list but not considered in our analyses.
Gain-framed messages used more than loss-framed messages
Nearly all physicians used gain-framed messages, and more than half also used loss-framed messages (TABLE 3). Only 1 physician offered only a loss-framed message. Overall, study physicians mentioned less than 2 gain- or loss-framed messages.
- The most common types of gain-framed messages were detecting cancer early, preventing cancer by taking out polyps, and screening at only a 10-year interval if the test result is negative.
- The most common loss-framed messages noted that colorectal cancer was the second most common cause of cancer death and that risk is increased with a family history of this cancer.
TABLE 3
Gain- and loss-framed messages and types of numeracy information used by study physicians
| TYPE OF MESSAGE OR NUMERACY | PHYSICIANS N (%) | OCCURRENCES IN INTERVIEWS, Total N (MEAN AMONG USERS, RANGE) |
|---|---|---|
| Message framing | ||
| Gain-framed | 29 (96) | 56 (1.9, 1–5) |
| Loss-framed | 20 (67) | 31 (1.6, 1–3) |
| Numeracy | ||
| Descriptive terms | 19 (63) | 36 (1.9, 1–3) |
| Statistical terms | 15 (50) | 30 (2.0, 1–5) |
| Temporal terms | 9 (30) | 11 (1.2, 1–2) |
| Proportions | 4 (13) | 5 (1.3, 1–2) |
| Fractions | 3 (10) | 3 (1.0, 1–1) |
Physicians avoided using numbers
Of the 15 types of numeracy information described by Ahlers-Schmit et al, our physicians used only 5. Nineteen physicians (63%) used descriptive terms such as “likely” or “increased,” and 15 (50%) used statistical concepts such as risk and second-most-common cause. Physicians avoided using numbers; 9 (30%) used temporal terms such as “early”; 4 (13%) cited a proportion; and only 3 (10%) used a fraction.
Colloquial language, or was it crude?
While reading the transcripts, we noted that some physicians used colloquial terms that could be regarded as crude. Other terms were probably too technical without an explanation. Some information was simply incorrect. We offer selected quotes to illustrate various types of language used.
About the prep:
- “Getting a colonoscopy is not the most fun experience…you have really bad diarrhea and you just empty out your guts.”
- “It’s basically Liquid Plumber for your bowels.”
- “Bowel prep…is kind of voluminous and associated with kind of massive bowel movements.”
- “Everybody hates the prep and you may be one of those and that’s just that.”
- “Generally you have to be up all night, sometimes, cleaning your bowels out.”
About the procedure:
- “It’s not the most comfortable screening exam in the world.”
- “It’s a test where they stick a lighted tube up your back-side.”
- “The stomach doctors put a camera up your bottom and look at the walls of your colon.”
- “They can go in with a microscope and look around and look at the colon itself.”
- “It’s a painless test.”
Word polyp is used, but not defined
Physicians often employed technical language when describing the pathology detected by colonoscopy. “Polyp” was mentioned by 20 physicians (67%) but rarely defined; “biopsy” by 5 (17%), and “lesion” by 6 (20%). Other technical terms were precancerous, symptomatic, and incapacitated.
Discussion
An informed patient is a willing patient
Our study physicians addressed only half of the 13 informational points, likely reflecting the time constraints of a typical office visit. Primary care physicians appear to expect that either the colonoscopist or other sources of information would fill in the gaps. As reported in several studies, unanswered questions can discourage patients from keeping their scheduled colonoscopy appointment.10,11 In one report of African-American church members, those with adequate knowledge about colorectal cancer screening were more likely to complete screening.24
Wolf and Becker suggested that discussions about cancer screening address 4 broad topics: the probability of developing the cancer, the operating characteristics of the screening test(s), the likelihood that screening will benefit the patient, and potential burdens of the test.25 Instead of a balanced and lengthy discussion, our study physicians generally emphasized the positives such as the value of avoiding colon cancer, the standard nature of this test, and the benefit of being sedated for the procedure. Thus, gain-framed messages about colorectal cancer were the norm for our study physicians.
Half of the physicians also offered loss-framed messages emphasizing the need to avoid the consequences of colorectal cancer and the increased threat associated with a family history of this malignancy. Research in mammography screening suggests that loss-framed messaging may be a more powerful motivator than gain-framed messaging,26 but it is not clear if this observation can be generalized to colorectal cancer screening.
Walking a fine line with the particulars of risk
Our study physicians rarely provided data on the probability of developing colorectal cancer. Physicians may avoid this topic because many patients have difficulty understanding information about the risk of colorectal cancer.11 In support of this approach, Lipkus and colleagues reported that various ways of informing patients about colorectal cancer risk did not affect their intention to be screened.27 Of concern, most of our physicians did not address the common misconception that colorectal cancer screening is unnecessary in the absence of symptoms.28
Overall, the level of numeracy information provided by study physicians required minimal patient understanding of mathematical and statistical concepts. Most information was descriptive, such as colonoscopy being “more thorough” than other tests. Though statistical concepts such as “risk” were often mentioned, few physicians offered probabilities or incidence data. Experts recommend providing such data,25 but Web sites have been criticized for offering excessive numerical cancer risk data.22 Therefore, physicians must walk a fine line between providing adequate information and offering data that require a high level of health numeracy for understanding.
6 key points physicians often overlook
Most physicians failed to mention dietary and medication changes, scheduling/insurance coverage issues, and risk of complications from colonoscopy. Nearly 60% failed to discuss the patient’s risk of colorectal cancer. Almost half did not mention the need for a companion to accompany the patient after the test. Scheduling challenges, in particular, are known to interfere with completing colonoscopy.11
Many neglect to describe the procedure
Thirty percent of physicians failed to describe the procedure itself, so it is not surprising that patients complain they have a poor understanding of test logistics.11,29,30 Denberg and colleagues have reported that mailing an informational brochure about colonoscopy can increase the number who keep their appointment.31
How language choices may affect understanding
Other researchers have identified additional patient barriers to colonoscopy, including fear of pain, concern for modesty, and desire to avoid the bowel prep.11,32 These concerns may be mitigated or heightened by the physician’s language. In our review of transcripts, physicians often used slang or colloquial language to describe the procedure, probably in an attempt to convey information in a familiar way. This language may be viewed as crude and potentially discouraging, but further research is needed to evaluate patient receptiveness to different ways of speaking about sensitive topics.
Additionally, physicians commonly used technical terms such as “polyp” and “biopsy” without explaining them. Technical language may increase racial disparities in adhering to scheduled colonoscopy. In a family medicine clinic, patients from minority groups had particular difficulty understanding medical terms and procedure names.28 Because little time is available for counseling about cancer screening tests, and because patients retain only a limited amount of information about procedures,33 supplementary informational sources are warranted.15-17,31 Options include brochures, telephone calls, letters, e-mails, Web site data, and videotapes, but it is unclear which sources optimally improve patient adherence to screening colonoscopy.34
Study limitations include simulated interaction
There were a number of limitations to this study. First, the investigators “simulated” the patient. Though study physicians were told to act as if they were speaking to a regular patient, they may still have unconsciously modified their usual approach to addressing this topic.
Second, we did not assess the effectiveness of these discussions in motivating actual patients to receive colonoscopy.
Other limitations included the following:
- We did not set a time period for these discussions, so they may have been even more limited in actual practice.
- We studied physicians from a single health care setting wherein colonoscopy appears to be the preferred approach to screen an average risk patient for colorectal cancer. In addition, in this health care system, this test is performed by a gastroenterologist, rather than a primary care physician.
- We did not determine whether patients regard our selected quotes as too colloquial or technical.
- This study did not address the important barrier of a physician forgetting to recommend colorectal cancer screening.35
Further research, next steps
Our study supports the hypothesis that physicians differ widely—but are generally deficient—when informing patients about screening colonoscopy. They generally emphasize the positives of colonoscopy and use terms that are colloquial, avoiding statistical concepts that may be hard for patients to understand. Future studies need to address the effectiveness of these approaches to discussing screening colonoscopy.
Given the central role of the primary care physician in motivating patients to undergo screening colonoscopy in a limited time period, it appears that additional supports are needed to supplement physician discussion about this important preventive care procedure.
Correspondence
Barbara J. Turner MD, MSEd, University of Pennsylvania, 1123 Blockley Hall/6021, 423 Guardian Drive, Philadelphia, PA 19104; [email protected]
- When talking to patients about screening colonoscopy, make clear their risk of colorectal cancer. Also, be sure they know about such commonly overlooked details as insurance/scheduling issues, dietary and medication changes before the procedure, a companion to drive afterward, and possible colonoscopy complications.
- Consider recommending supplemental information sources such as telephone calls, letters, e-mails, Web sites, or videotapes to help patients understand the need for screening colonoscopy.
Abstract
Background A physician’s recommendation is a powerful motivator for a patient to undergo colonoscopy for colorectal cancer screening, yet little is known about how physicians address this topic.
Methods We recruited 30 primary care physicians and physicians-in-training from 4 practices to counsel a “patient,” simulated by a researcher, regarding the need for screening colonoscopy. Audiotapes of the physician-patient encounters were transcribed. Preserving physician anonymity, we assessed each encounter for key informational points, positive or negative message framing, type of numeracy information, and use of colloquial or technical language.
Results Study physicians addressed a mean of 6.7 (standard deviation=1.8) of 13 key informational points. Most physicians (≥80%) discussed the benefits of colorectal cancer screening, the recognition of colonoscopy as a standard exploratory procedure, and the use of sedation. However, few (<20%) addressed the risks of colonoscopy, the nuances of scheduling, or the need for dietary and medication changes. Nearly all physicians (98%) used messages that focused on the positive aspects of screening (gain-framed messages), and many (67%) also used messages that focused on the risk of not screening (loss-framed messages). Numeracy information generally was expressed simply, but half of the physicians used statistical terms. Half used colloquial terms to describe the prep and procedure.
Conclusion Though most physicians used positive, simple terms to describe colonoscopy, they often omitted key information. Correcting for the areas of insufficient information found in our study—perhaps with supplementary educational sources—will help ensure that patients are adequately prepared for colonoscopy.
Colorectal cancer screening has the potential to reduce deaths from colorectal cancer by at least one third.1 Yet only half of eligible patients in the US who are age 50 or older have undergone screening.2 Patients often say they haven’t been screened because their physician didn’t recommend it.3-5
A physician’s recommendation is strongly predictive of whether a patient actually undergoes colorectal cancer screening, even after adjusting for multiple confounders.6-9 Yet several studies have found that, even after the physician has recommended or ordered an endoscopic study of the colon, many patients do not follow through.10-12 Successful completion of screening colonoscopy requires, in part, that a patient understand the need for the procedure and receive sufficient instruction about it. Thus, failure to undergo this test may reflect patient concerns or misunderstandings due to inadequate communication.13,14
In many settings, the primary care physician bears the responsibility for telling the patient about screening colonoscopy because the endoscopist meets the patient only at the time of the procedure. Supplementary educational programs can also play a role. Unfortunately, though, while these materials appear to reduce patient anxiety and increase adherence to screening recommendations,15-17 they are infrequently used.
Looking at physician communication with an eye toward improvement
Our goal in conducting this study was to evaluate the way in which physicians discuss the need for screening colonoscopy with their patients. Using a simulated patient scenario, we wanted to examine 4 dimensions of each discussion: completeness; type of messaging; type of numeracy information (ie, numerical and mathematical data); and use of colloquial vs technical language.
- Completeness reflected the number of key informational points addressed.
- Type of messaging focused on the use of loss- or gain-framed messages, both of which have been linked to increased patient intention to adopt a cancer prevention behavior or test.18-20 Gain-framed counseling emphasizes the positive aspects of screening; loss-framed, the risks of not screening.
- Type of numeracy information. Because poor numeracy skills are thought to impair the accuracy of patients’ perceptions of cancer risk,21 we categorized the type of numeracy information provided by physicians following an approach developed by Ahlers-Schmidt and colleagues.22
- Colloquial vs technical language. Because colonoscopy involves sensitive topics such as the bowels and feces, and because language choices may affect acceptance of care,23 we evaluated physicians’ use of terminology when describing the procedure.
We felt that by looking at these dimensions, we could help physicians to refine screening colonoscopy messages so that conversations with patients could be more clear, complete, and balanced.
Methods
13 key points regarding screening colonoscopy
We reviewed published literature and Internet sources to develop a preliminary list of topics a primary care physician could address when discussing colorectal cancer screening, especially screening colonoscopy. We used NLM Gateway and Medline databases and the following search terms: colonoscopy, patient education, patient instructions, guidelines, physician, colon cancer, counseling, and knowledge. A medical librarian directed the search. Despite having expert assistance, we did not find any publications that offered a peer-reviewed, validated list of topics to guide physicians’ discussions about screening colonoscopy.
We then conducted an Internet search using the terms colon cancer, colon cancer screening, colonoscopy, and colon cancer patient education. We categorized data from identified sites such as the American Gastroenterological Association, Up-to-Date, the American Cancer Society, and the National Library of Medicine, among others, into 13 common topics (TABLE 1). Three points addressed general information about colorectal cancer, and the rest dealt with colonoscopy specifically. A panel of 2 gastroenterologists and 3 internists from the same institution independently judged each item on the list for importance, relevance, and feasibility for discussion. Except for one panelist, all endorsed the need to address the 13 items.
TABLE 1
Percentage of physicians who covered key colorectal cancer screening points
| TOPIC | INFORMATIONAL POINT | PHYSICIANS ADDRESSING TOPIC (N=30), % |
|---|---|---|
| General colorectal prevention | ||
| 1. Standard preventive health care procedure | Recommended* as a standard screening test for those age 50 and older | 83 |
| 2. Value of screening | Can prevent cancer as well as detect cancer at a treatable stage | 83 |
| 3. Risk of colorectal cancer | Prevalence or incidence either nationally or regionally (family history)† | 43 |
| Specifics about colonoscopy | ||
| 4. Anesthesia | Sedation to reduce discomfort; risk information discussed or to be reviewed by anesthetist | 87 |
| 5. Gastrointestinal prep | Use of laxative, usual types used, and what patient can expect | 77 |
| 6. Abnormalities detected by colonoscopy | Finds growths (polyps) or cancer | 76 |
| 7. Description of procedure | Camera at the end of a flexible tube views the entire colon and tiny tweezers at the end sample or remove growths | 70 |
| 8. Follow-up after a negative test | Experts recommend screening after a negative test every 10 years | 67 |
| 9. Patient experience or knowledge‡ | Any personal or family/friend experience with colonoscopy or knowledge about the test | 64 |
| 10. Transportation | Another person must accompany the patient after procedure | 53 |
| 11. Insurance/scheduling | Insurance coverage, who arranges for the procedure, where test is performed | 13 |
| 12. Diet | Diet the day before and day of procedure, importance of hydration | 10 |
| 13. Risk of colonoscopy | Risk of bowel perforation or other complication | 10 |
| 14. Medications | Changes in medications for the procedure | 3 |
| *Recommendation by expert panels need not be specified. Physicians often just say, “We recommend.” | ||
| †Family history not necessary in this study because the patient was said to be at average risk for colorectal cancer. | ||
| ‡Point was not identified originally by the review and excluded from analysis. | ||
Physician sample
Of 135 providers practicing in 2 primary care and 1 geriatrics practice affiliated with the same urban academic medical center, we invited 30 physicians to participate. This sample was chosen to adequately represent female and minority physicians as well as physicians at different levels of training (TABLE 2). The physicians were invited to participate either by e-mail (N=19) or in person (N=11), and all invitees consented. Interviews were conducted alone in the physician’s office or in a practice conference room, and they were audiotaped with the physician’s consent.
Interviews lasted fewer than 15 minutes and did not intrude on patient care time. Study physicians read a vignette of a fictitious 51-year-old African American woman who was an established patient in their practice, without a family history of colon cancer but with arthritis and hypertension. We asked each physician to inform the patient (simulated by the interviewer) about colorectal cancer screening and colonoscopy, as well as the logistics of getting this test. To standardize the interaction, interviewers predefined the patient’s responses to questions. For example, if the physician asked about prior knowledge of colonoscopy, the simulated patient replied that she had none. Study physicians were not prompted in any way and, though not given time restrictions, all were brief and to the point.
TABLE 2
Study physician characteristics
| CHARACTERISTIC | PHYSICIANS WITH CHARACTERISTIC (N=30), % | INFORMATIONAL POINTS ADDRESSED,* MEAN (SD) |
|---|---|---|
| Total | 100 | 6.73 (1.84) |
| Gender | ||
| Female | 66 | 6.70 (1.89) |
| Male | 34 | 6.80 (1.81) |
| Race | ||
| White | 80 | 6.84 (1.80) |
| Non-white | 20 | 6.20 (2.17) |
| Level of training | ||
| Attending | 63 | 6.84 (1.98) |
| Trainee | 37 | 6.54 (1.63) |
| Specialty | ||
| General Internal Medicine | 90 | 6.89 (1.83) |
| Geriatrics | 10 | 5.33 (1.53) |
| * All comparisons P >.05 | ||
Analysis
Interview transcripts were anonymous, identified only by a study number. The 2 study investigators coded transcribed interviews independently as to whether physicians addressed the 13 informational points. Inter-rater concordance in coding was 90%. We also independently evaluated the interviews according to the use of gain- or loss-framed messages (eg, detecting colon polyps early before cancer develops vs colorectal cancer being the second most common cause of cancer death). We independently classified types of numeracy information provided into 15 categories.22 We also independently examined audiotaped transcripts for examples of colloquial terms/slang or technical language. Because we are unaware of a validated approach to characterizing a physician’s language in this manner, we asked a layperson for assistance in identifying colloquial/slang terms.
To determine whether there were predictors of a physician addressing more of the informational points than his or her peers, we examined bivariate associations of the following demographic and professional data: gender, race (white vs non-white), academic advancement (attending vs trainee), and specialty (general internist vs geriatrician).
We analyzed data using the Wilcoxon rank-sum test because the data were not normally distributed. We used SAS Statistical Software (SAS Institute, Cary, NC). The University of Pennsylvania Institutional Review Board approved the study. The project was supported by a grant from the Bach Fund of the Presbyterian Medical Center, University of Pennsylvania.
Results
How did the physicians talk to their patient?
The 30 study physicians were primarily women, one fifth were from under-represented minorities, and one third were either residents or fellows (TABLE 2). Of 13 key informational points endorsed by our physician panel (TABLE 1), the physician-subjects addressed a mean of 6.7 points (range, 3–10). Nearly all physician-subjects discussed the value of colorectal cancer screening, colonoscopy as a standard colorectal screening procedure, and sedation during the procedure. However, fewer than 20% addressed the following topics: insurance/scheduling, dietary changes, medication modification, and risks of colonoscopy. In this small sample, the number of topics mentioned did not differ significantly by physician characteristic (TABLE 2).
Two thirds of the physicians asked the simulated patient about her prior knowledge or experience with colonoscopy. Although this question was not among the original 13 informational points, it helped to guide the discussion by identifying specific preconceptions or prior knowledge of this test. Therefore, this post hoc 14th informational point was added to our list but not considered in our analyses.
Gain-framed messages used more than loss-framed messages
Nearly all physicians used gain-framed messages, and more than half also used loss-framed messages (TABLE 3). Only 1 physician offered only a loss-framed message. Overall, study physicians mentioned less than 2 gain- or loss-framed messages.
- The most common types of gain-framed messages were detecting cancer early, preventing cancer by taking out polyps, and screening at only a 10-year interval if the test result is negative.
- The most common loss-framed messages noted that colorectal cancer was the second most common cause of cancer death and that risk is increased with a family history of this cancer.
TABLE 3
Gain- and loss-framed messages and types of numeracy information used by study physicians
| TYPE OF MESSAGE OR NUMERACY | PHYSICIANS N (%) | OCCURRENCES IN INTERVIEWS, Total N (MEAN AMONG USERS, RANGE) |
|---|---|---|
| Message framing | ||
| Gain-framed | 29 (96) | 56 (1.9, 1–5) |
| Loss-framed | 20 (67) | 31 (1.6, 1–3) |
| Numeracy | ||
| Descriptive terms | 19 (63) | 36 (1.9, 1–3) |
| Statistical terms | 15 (50) | 30 (2.0, 1–5) |
| Temporal terms | 9 (30) | 11 (1.2, 1–2) |
| Proportions | 4 (13) | 5 (1.3, 1–2) |
| Fractions | 3 (10) | 3 (1.0, 1–1) |
Physicians avoided using numbers
Of the 15 types of numeracy information described by Ahlers-Schmit et al, our physicians used only 5. Nineteen physicians (63%) used descriptive terms such as “likely” or “increased,” and 15 (50%) used statistical concepts such as risk and second-most-common cause. Physicians avoided using numbers; 9 (30%) used temporal terms such as “early”; 4 (13%) cited a proportion; and only 3 (10%) used a fraction.
Colloquial language, or was it crude?
While reading the transcripts, we noted that some physicians used colloquial terms that could be regarded as crude. Other terms were probably too technical without an explanation. Some information was simply incorrect. We offer selected quotes to illustrate various types of language used.
About the prep:
- “Getting a colonoscopy is not the most fun experience…you have really bad diarrhea and you just empty out your guts.”
- “It’s basically Liquid Plumber for your bowels.”
- “Bowel prep…is kind of voluminous and associated with kind of massive bowel movements.”
- “Everybody hates the prep and you may be one of those and that’s just that.”
- “Generally you have to be up all night, sometimes, cleaning your bowels out.”
About the procedure:
- “It’s not the most comfortable screening exam in the world.”
- “It’s a test where they stick a lighted tube up your back-side.”
- “The stomach doctors put a camera up your bottom and look at the walls of your colon.”
- “They can go in with a microscope and look around and look at the colon itself.”
- “It’s a painless test.”
Word polyp is used, but not defined
Physicians often employed technical language when describing the pathology detected by colonoscopy. “Polyp” was mentioned by 20 physicians (67%) but rarely defined; “biopsy” by 5 (17%), and “lesion” by 6 (20%). Other technical terms were precancerous, symptomatic, and incapacitated.
Discussion
An informed patient is a willing patient
Our study physicians addressed only half of the 13 informational points, likely reflecting the time constraints of a typical office visit. Primary care physicians appear to expect that either the colonoscopist or other sources of information would fill in the gaps. As reported in several studies, unanswered questions can discourage patients from keeping their scheduled colonoscopy appointment.10,11 In one report of African-American church members, those with adequate knowledge about colorectal cancer screening were more likely to complete screening.24
Wolf and Becker suggested that discussions about cancer screening address 4 broad topics: the probability of developing the cancer, the operating characteristics of the screening test(s), the likelihood that screening will benefit the patient, and potential burdens of the test.25 Instead of a balanced and lengthy discussion, our study physicians generally emphasized the positives such as the value of avoiding colon cancer, the standard nature of this test, and the benefit of being sedated for the procedure. Thus, gain-framed messages about colorectal cancer were the norm for our study physicians.
Half of the physicians also offered loss-framed messages emphasizing the need to avoid the consequences of colorectal cancer and the increased threat associated with a family history of this malignancy. Research in mammography screening suggests that loss-framed messaging may be a more powerful motivator than gain-framed messaging,26 but it is not clear if this observation can be generalized to colorectal cancer screening.
Walking a fine line with the particulars of risk
Our study physicians rarely provided data on the probability of developing colorectal cancer. Physicians may avoid this topic because many patients have difficulty understanding information about the risk of colorectal cancer.11 In support of this approach, Lipkus and colleagues reported that various ways of informing patients about colorectal cancer risk did not affect their intention to be screened.27 Of concern, most of our physicians did not address the common misconception that colorectal cancer screening is unnecessary in the absence of symptoms.28
Overall, the level of numeracy information provided by study physicians required minimal patient understanding of mathematical and statistical concepts. Most information was descriptive, such as colonoscopy being “more thorough” than other tests. Though statistical concepts such as “risk” were often mentioned, few physicians offered probabilities or incidence data. Experts recommend providing such data,25 but Web sites have been criticized for offering excessive numerical cancer risk data.22 Therefore, physicians must walk a fine line between providing adequate information and offering data that require a high level of health numeracy for understanding.
6 key points physicians often overlook
Most physicians failed to mention dietary and medication changes, scheduling/insurance coverage issues, and risk of complications from colonoscopy. Nearly 60% failed to discuss the patient’s risk of colorectal cancer. Almost half did not mention the need for a companion to accompany the patient after the test. Scheduling challenges, in particular, are known to interfere with completing colonoscopy.11
Many neglect to describe the procedure
Thirty percent of physicians failed to describe the procedure itself, so it is not surprising that patients complain they have a poor understanding of test logistics.11,29,30 Denberg and colleagues have reported that mailing an informational brochure about colonoscopy can increase the number who keep their appointment.31
How language choices may affect understanding
Other researchers have identified additional patient barriers to colonoscopy, including fear of pain, concern for modesty, and desire to avoid the bowel prep.11,32 These concerns may be mitigated or heightened by the physician’s language. In our review of transcripts, physicians often used slang or colloquial language to describe the procedure, probably in an attempt to convey information in a familiar way. This language may be viewed as crude and potentially discouraging, but further research is needed to evaluate patient receptiveness to different ways of speaking about sensitive topics.
Additionally, physicians commonly used technical terms such as “polyp” and “biopsy” without explaining them. Technical language may increase racial disparities in adhering to scheduled colonoscopy. In a family medicine clinic, patients from minority groups had particular difficulty understanding medical terms and procedure names.28 Because little time is available for counseling about cancer screening tests, and because patients retain only a limited amount of information about procedures,33 supplementary informational sources are warranted.15-17,31 Options include brochures, telephone calls, letters, e-mails, Web site data, and videotapes, but it is unclear which sources optimally improve patient adherence to screening colonoscopy.34
Study limitations include simulated interaction
There were a number of limitations to this study. First, the investigators “simulated” the patient. Though study physicians were told to act as if they were speaking to a regular patient, they may still have unconsciously modified their usual approach to addressing this topic.
Second, we did not assess the effectiveness of these discussions in motivating actual patients to receive colonoscopy.
Other limitations included the following:
- We did not set a time period for these discussions, so they may have been even more limited in actual practice.
- We studied physicians from a single health care setting wherein colonoscopy appears to be the preferred approach to screen an average risk patient for colorectal cancer. In addition, in this health care system, this test is performed by a gastroenterologist, rather than a primary care physician.
- We did not determine whether patients regard our selected quotes as too colloquial or technical.
- This study did not address the important barrier of a physician forgetting to recommend colorectal cancer screening.35
Further research, next steps
Our study supports the hypothesis that physicians differ widely—but are generally deficient—when informing patients about screening colonoscopy. They generally emphasize the positives of colonoscopy and use terms that are colloquial, avoiding statistical concepts that may be hard for patients to understand. Future studies need to address the effectiveness of these approaches to discussing screening colonoscopy.
Given the central role of the primary care physician in motivating patients to undergo screening colonoscopy in a limited time period, it appears that additional supports are needed to supplement physician discussion about this important preventive care procedure.
Correspondence
Barbara J. Turner MD, MSEd, University of Pennsylvania, 1123 Blockley Hall/6021, 423 Guardian Drive, Philadelphia, PA 19104; [email protected]
1. Ries LA, Wingo PA, Miller DS, et al. The annual report to the nation on the status of cancer, 1973–1997, with a special section on colorectal cancer. Cancer 2000;88:2398-2424.
2. Centers for Disease Control and Prevention (CDC). Colorectal cancer test use among persons aged > or = 50 years—United States, 2001. MMWR Morb Mortal Wkly Rep 2003;52:193-196.
3. Wee CC, McCarthy EP, Phillips RS. Factors associated with colon cancer screening: the role of patient factors and physician counseling. Prev Med 2005;41:23-29.
4. Taylor V, Lessler D, Mertens K, et al. Colorectal cancer screening among African Americans: the importance of physician recommendations. J Natl Med Assoc 2003;95:806-812.
5. Brawarsky P, Brooks DR, Mucci LA, Wood PA. Effect of physician recommendation and patient adherence on rates of colorectal cancer testing. Cancer Detect Prevent 2004;28:260-268.
6. Holt WS, Jr. Factors affecting compliance with screening sigmoidoscopy. J Fam Pract 1991;32:585-589.
7. Brenes GA, Paskett ED. Predictors of stage of adoption for colorectal cancer screening. Prev Med 2000;31:410-416.
8. Myers RE, Turner B, Weinberg D, et al. Impact of a physician-oriented intervention on follow-up in colorectal cancer screening. Prev Med 2004;38:375-381.
9. Brawarsky P, Brooks DR, Mucci LA, Wood PA. Effect of physician recommendation and patient adherence on rates of colorectal cancer testing. Cancer Detect Prev 2004;28:260-268.
10. Turner BJ, Weiner M, Yang C, TenHave T. Predicting adherence to colonoscopy or flexible sigmoidoscopy on the basis of physician appointment-keeping behavior. Ann Intern Med 2004;140:528-532.
11. Denberg TD, Melhado TV, Coombes JM, et al. Predictors of nonadherence to screening colonoscopy. J Gen Intern Med 2005;20:989-995.
12. Kelly RB, Shank JC. Adherence to screening flexible sigmoidoscopy in asymptomatic patients. Med Care 1992;30:1029-1042.
13. Janz NK, Wren PA, Schottenfeld D, Guire KE. Colorectal cancer screening attitudes and behavior: a population-based study. Prev Med 2003;37:627-634.
14. US Preventive Services Task Force. Screening for colorectal cancer: recommendations and rationale. Ann Intern Med 2002;137:129-131.
15. Abuksis G, Mor M, Segal N, et al. A patient education program is cost-effective for preventing failure of endoscopic procedures in a gastroenterology department. Am J Gastroenterol 2001;96:1786-1790.
16. Pignone M, Harris R, Kinsinger L. Videotape-based decision aid for colon cancer screening. A randomized, controlled trial. Ann Intern Med 2000;13:761-769.
17. Wardle J, Williamson S, McCaffery K, et al. Increasing attendance at colorectal cancer screening: testing the efficacy of a mailed, psychoeducational intervention in a community sample of older adults. Health Psychol 2003;22:99-105.
18. Detweiler JB, Bedell BT, Salovey P, et al. Message framing and sunscreen use: gain-framed messages motivate beach-goers. Health Psychol 1999;18:189-196.
19. Banks SM, Salovey P, Greener S, et al. The effects of message framing on mammography utilization. Health Psychol 1995;14:178-184.
20. Rivers SE, Salovey P, Pizarro DA, et al. Message framing and pap test utilization among women attending a community health clinic. J Health Psychol 2005;10:65-77.
21. Davids SL, Schapira MM, McAuliffe TL, Nattinger AB. Predictors of pessimistic breast cancer risk perceptions in a primary care population. J Gen Intern Med 2004;19:310-315.
22. Ahlers-Schmidt CR, Golbeck AL, Paschal AM, et al. Breast cancer counts: numeracy in breast cancer information on the web. J Cancer Educ 2006;21:95-98.
23. Hodgson J, Hughes E, Lambert C. “SLANG”—Sensitive Language and the New Genetics—an exploratory study. J Genet Couns 2005;14:415-421.
24. Katz ML, James AS, Pignone MP, et al. Colorectal cancer screening among African American church members: a qualitative and quantitative study of patient-provider communication. BMC Public Health 2004;4:62.-
25. Wolf AM, Becker DM. Cancer screening and informed patient discussions. Truth and consequences. Arch Intern Med 1996;156:1069-1072.
26. Banks SM, Salovey P, Greener S, et al. The effects of message framing on mammography utilization. Health Psychol 1995;14:178-184.
27. Lipkus IM, Crawford Y, Fenn K, et al. Testing different formats for communicating colorectal cancer risk. J Health Commun 1999;4:311-324.
28. Shokar NK, Vernon SW, Weller SC. Cancer and colorectal cancer: knowledge, beliefs, and screening p of a diverse patient population. Fam Med 2005;37:341-347.
29. Katz ML, Ruzek SB, Miller SM, Legos P. Gender differences in patients needs and concerns to diagnostic tests for possible cancer. J Cancer Educ 2004;19:227-231.
30. Dube CE, Fuller BK, Rosen RK, et al. Men’s experiences of physical exams and cancer screening tests: a qualitative study. Prev Med 2005;40:628-635.
31. Denberg TD, Coombes JM, Byers TE, et al. Effect of a mailed brochure on appointment-keeping for screening colonoscopy: a randomized trial. Ann Intern Med 2006;145:895-900.
32. Harewood GC, Wiersema MJ, Melton LJ, 3rd. A prospective, controlled assessment of factors influencing acceptance of screening colonoscopy. Am J Gastroenterol 2002;97:3186-3194.
33. Godwin Y. Do they listen? A review of information retained by patients following consent for reduction mammoplasty. Br J Plastic Surgery 2000;53:121-125.
34. Greisinger A, Hawley ST, Bettencourt JL, et al. Primary care patients’ understanding of colorectal cancer screening. Cancer Detect Prev 2006;30:67-74.
35. Dulai GS, Farmer MM, Ganz PA, et al. Primary care physician perceptions of barriers to and facilitators of colorectal cancer screening in a managed care setting. Cancer 2004;100:1843-1852.
1. Ries LA, Wingo PA, Miller DS, et al. The annual report to the nation on the status of cancer, 1973–1997, with a special section on colorectal cancer. Cancer 2000;88:2398-2424.
2. Centers for Disease Control and Prevention (CDC). Colorectal cancer test use among persons aged > or = 50 years—United States, 2001. MMWR Morb Mortal Wkly Rep 2003;52:193-196.
3. Wee CC, McCarthy EP, Phillips RS. Factors associated with colon cancer screening: the role of patient factors and physician counseling. Prev Med 2005;41:23-29.
4. Taylor V, Lessler D, Mertens K, et al. Colorectal cancer screening among African Americans: the importance of physician recommendations. J Natl Med Assoc 2003;95:806-812.
5. Brawarsky P, Brooks DR, Mucci LA, Wood PA. Effect of physician recommendation and patient adherence on rates of colorectal cancer testing. Cancer Detect Prevent 2004;28:260-268.
6. Holt WS, Jr. Factors affecting compliance with screening sigmoidoscopy. J Fam Pract 1991;32:585-589.
7. Brenes GA, Paskett ED. Predictors of stage of adoption for colorectal cancer screening. Prev Med 2000;31:410-416.
8. Myers RE, Turner B, Weinberg D, et al. Impact of a physician-oriented intervention on follow-up in colorectal cancer screening. Prev Med 2004;38:375-381.
9. Brawarsky P, Brooks DR, Mucci LA, Wood PA. Effect of physician recommendation and patient adherence on rates of colorectal cancer testing. Cancer Detect Prev 2004;28:260-268.
10. Turner BJ, Weiner M, Yang C, TenHave T. Predicting adherence to colonoscopy or flexible sigmoidoscopy on the basis of physician appointment-keeping behavior. Ann Intern Med 2004;140:528-532.
11. Denberg TD, Melhado TV, Coombes JM, et al. Predictors of nonadherence to screening colonoscopy. J Gen Intern Med 2005;20:989-995.
12. Kelly RB, Shank JC. Adherence to screening flexible sigmoidoscopy in asymptomatic patients. Med Care 1992;30:1029-1042.
13. Janz NK, Wren PA, Schottenfeld D, Guire KE. Colorectal cancer screening attitudes and behavior: a population-based study. Prev Med 2003;37:627-634.
14. US Preventive Services Task Force. Screening for colorectal cancer: recommendations and rationale. Ann Intern Med 2002;137:129-131.
15. Abuksis G, Mor M, Segal N, et al. A patient education program is cost-effective for preventing failure of endoscopic procedures in a gastroenterology department. Am J Gastroenterol 2001;96:1786-1790.
16. Pignone M, Harris R, Kinsinger L. Videotape-based decision aid for colon cancer screening. A randomized, controlled trial. Ann Intern Med 2000;13:761-769.
17. Wardle J, Williamson S, McCaffery K, et al. Increasing attendance at colorectal cancer screening: testing the efficacy of a mailed, psychoeducational intervention in a community sample of older adults. Health Psychol 2003;22:99-105.
18. Detweiler JB, Bedell BT, Salovey P, et al. Message framing and sunscreen use: gain-framed messages motivate beach-goers. Health Psychol 1999;18:189-196.
19. Banks SM, Salovey P, Greener S, et al. The effects of message framing on mammography utilization. Health Psychol 1995;14:178-184.
20. Rivers SE, Salovey P, Pizarro DA, et al. Message framing and pap test utilization among women attending a community health clinic. J Health Psychol 2005;10:65-77.
21. Davids SL, Schapira MM, McAuliffe TL, Nattinger AB. Predictors of pessimistic breast cancer risk perceptions in a primary care population. J Gen Intern Med 2004;19:310-315.
22. Ahlers-Schmidt CR, Golbeck AL, Paschal AM, et al. Breast cancer counts: numeracy in breast cancer information on the web. J Cancer Educ 2006;21:95-98.
23. Hodgson J, Hughes E, Lambert C. “SLANG”—Sensitive Language and the New Genetics—an exploratory study. J Genet Couns 2005;14:415-421.
24. Katz ML, James AS, Pignone MP, et al. Colorectal cancer screening among African American church members: a qualitative and quantitative study of patient-provider communication. BMC Public Health 2004;4:62.-
25. Wolf AM, Becker DM. Cancer screening and informed patient discussions. Truth and consequences. Arch Intern Med 1996;156:1069-1072.
26. Banks SM, Salovey P, Greener S, et al. The effects of message framing on mammography utilization. Health Psychol 1995;14:178-184.
27. Lipkus IM, Crawford Y, Fenn K, et al. Testing different formats for communicating colorectal cancer risk. J Health Commun 1999;4:311-324.
28. Shokar NK, Vernon SW, Weller SC. Cancer and colorectal cancer: knowledge, beliefs, and screening p of a diverse patient population. Fam Med 2005;37:341-347.
29. Katz ML, Ruzek SB, Miller SM, Legos P. Gender differences in patients needs and concerns to diagnostic tests for possible cancer. J Cancer Educ 2004;19:227-231.
30. Dube CE, Fuller BK, Rosen RK, et al. Men’s experiences of physical exams and cancer screening tests: a qualitative study. Prev Med 2005;40:628-635.
31. Denberg TD, Coombes JM, Byers TE, et al. Effect of a mailed brochure on appointment-keeping for screening colonoscopy: a randomized trial. Ann Intern Med 2006;145:895-900.
32. Harewood GC, Wiersema MJ, Melton LJ, 3rd. A prospective, controlled assessment of factors influencing acceptance of screening colonoscopy. Am J Gastroenterol 2002;97:3186-3194.
33. Godwin Y. Do they listen? A review of information retained by patients following consent for reduction mammoplasty. Br J Plastic Surgery 2000;53:121-125.
34. Greisinger A, Hawley ST, Bettencourt JL, et al. Primary care patients’ understanding of colorectal cancer screening. Cancer Detect Prev 2006;30:67-74.
35. Dulai GS, Farmer MM, Ganz PA, et al. Primary care physician perceptions of barriers to and facilitators of colorectal cancer screening in a managed care setting. Cancer 2004;100:1843-1852.
A cheaper, faster way to resolve chronic cough
- When evaluating chronic cough, consider a trial of therapy aimed at the most likely presumptive diagnosis for your locality.
- In developing algorithms such as ours, take into account your experiences, patient characteristics, and the available medical equipment.
At the insistence of her family, a woman comes to you complaining of a cough that has lasted several weeks. Many experts would urge a thorough diagnostic investigation, justifying this action with a presumed shorter course of treatment. But is an involved work-up really necessary? Would a quicker, less expensive approach serve the patient just as well? We designed our study to answer these questions.
“Test all, then treat” is expensive
In the management of patients with chronic cough, most algorithms have advocated the approach of “test all, then treat.”1-6 This is an expensive approach and one that delays relief for the patient, though a confirmative diagnosis may decrease the overall duration of treatment. In most cases, however, this approach may be unnecessary. And because few of the underlying disorders are acutely debilitating or rapidly progressive, even misdiagnosis and resultant inappropriate treatment pose little risk to patients.
The less common approach is a sequence of trial-and-error treatments based on a presumptive hierarchy of possible diagnoses.6 The advantage with this strategy is a 3-to 5-fold cost savings.6 And we suspected that the associated length of treatment would be acceptable.
We proposed that the management of patients with chronic cough begin with a presumptive diagnosis, thus simplifying the initial evaluation, keeping costs low, and offering earlier treatment.
We developed an algorithm for the treatment of patients with chronic cough that relies on minimal diagnostic investigations, regardless of the confirmed diagnosis. We evaluated our approach from the perspectives of the presumptive diagnosis and the therapeutic response period.
Methods
Treatment algorithm reflects experience and local resources
Initially, we designed the algorithm to follow findings in the literature on the treatment of patients with chronic cough. We then simplified and modified the algorithm to reflect the experiences of doctors from the pulmonology clinic in our hospital, and to take into account local patient characteristics and available medical equipment and resources.
For this study, we defined chronic cough as a one that lasts more than 4 weeks. (This definition can vary, depending on the source you consult.1) the patients we enrolled had no abnormalities detected on auscultation, chest radiography, or CBC.
Chronic cough can be managed successfully by accurate treatment of the cause, and most specialists report high success rates in treating it.2-4 The 3 most common causes of chronic cough are 1) postnasal drip, 2) asthma, and 3) gastroesophageal reflux.5
Subjects were otherwise healthy
Between January 1 and December 31, 2005, at the internal medicine clinic of Cheju National University Hospital, we enrolled 378 patients whose chief complaint was cough persisting for more than 4 weeks and who had no abnormalities detected on auscultation by a physician, chest radiography (posterior–anterior view and left lateral view), or complete blood cell counts. Each patient had a complete blood count to detect anemia, hematologic disorders, or inflammatory conditions. Current users of angiotensin-converting enzyme (ACE) inhibitors were excluded.
All of the patients we enrolled were adults living in Jeju, Korea, and the mean age was 51 years. One hundred eighty-six (49%) were men. The median reported cough duration was 2 months (range, 1–36 months) (TABLE 1).
We instructed the patients on our algorithmic approach to treating chronic cough and encouraged them to follow the algorithm through to telephone notification of the next visit.
TABLE 1
Characteristics of the 378 enrolled patients
| Men/women | 186/192 (49/51%) |
| Age, years | 51.2±16.12 |
| Cough duration in months, median (range) | 2 (1–36) |
How we determined treatment outcomes
Patients graded their cough severity subjectively at each visit using a visual analogue scale (VAS) from 1 (no cough at all) to 10 (cough severity same as that remembered during first visit to the clinic). We recorded their reports on a questionnaire.
Successful responders were patients who reported a subjective grade of cough severity less than 3. Partial responders and nonresponders were defined, respectively, as those reporting VAS scores from 3 to 6 and more than 6.
We defined the response period as the number of days from enrollment until the next visit in which the patient first reported a VAS score of cough severity less than 3.
Algorithm: Addressing the 3 most common causes of chronic cough
1. Postnasal drip syndrome. Patients first underwent a rhinoscopic examination (FIGURE). When clinicians detected redness or abnormal discharge on the nasal mucosa, they prescribed a 5-day course of antihistamine (10 mg/day ebastine [Ebastel] orally), pseudoephedrine (30 mg 3 times daily, orally), and intranasal corticosteroid (triamcinolone acetonide [Nasacort] 110 mcg twice daily intranasally). Patients without symptoms of rhinitis were referred to the next diagnostic phase.
With completion of the prescribed medication 5 days after the first visit, we graded the severity of cough by questionnaire. Patients in the successful and partial responder categories received a presumptive diagnosis of postnasal drip syndrome, and we asked them to continue using the medication for at least 2 weeks. We had each nonresponder stop the medication.
2. Asthma syndrome. Partial responder and nonresponder patients entered the next diagnostic phase: a methacholine bronchial provocation test (MPT)7 and eosinophil count with induced sputum by hypertonic saline (3% NaCl).8 We defined a positive MPT result as <10 mg/ mL of methacholine causing a 20% fall in FEV1 from baseline (PC20). Patients with more than 3% eosinophils in the induced sputum specimen or with a positive MPT received a 1-week prescription for inhaled budesonide 160 mcg twice daily and inhaled formoterol (Symbicort) 4.5 mcg twice daily. Patients who did not exhibit these asthma indicators were referred to the next step.
At the next visit, we again graded the severity of cough. Patients in the successful and partial responder categories received a presumptive diagnosis of asthma syndrome. We asked successful and partial responders to continue the medication for at least 2 weeks. Those classed as nonresponders were asked to stop their medication. We referred all patients with positive MPT test results to a special clinic for asthma, regardless of responses to this therapeutic trial or eosinophil count in the induced sputum.
3. Reflux syndrome. Partial responders and nonresponders then received a 2-week prescription for a proton pump inhibitor, pantoprazole (Pantoloc), 40 mg orally once daily.9 At the next visit 2 weeks later, we graded the severity of cough. Successful and partial responders were given a presumptive diagnosis of reflux syndrome, but only successful responders were asked to continue the same medication for at least 6 weeks. At the discretion of their physicians, partial and nonresponders underwent other diagnostic investigations, including high-resolution computerized tomography (CT) of the lungs, bronchoscopic examination, sputum smear and culture for acid fast bacilli, sputum culture for ordinary bacteria and fungi, and a serological test for human immunodeficiency virus.
FIGURE
A presumptive-diagnosis algorithm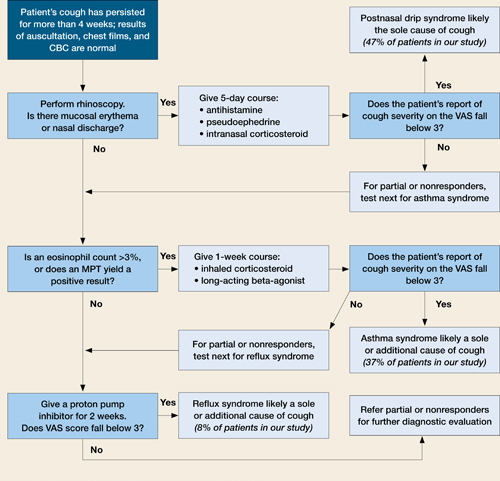
Chronic cough resolved for more than 90% of patients treated according to this algorithm.
MPT, methacholine bronchial provocation test; VAS, visual analog scale.
Results
Presumptive diagnoses
Among 378 patients, 346 (91%) showed erythematous mucosa or abnormal discharge in rhinoscopic examinations and received empiric medication for 5 days. The successful-responder category included 176 patients (47%); 79 (21%) were classed as partial responders, and 255 (67%) received the presumptive diagnosis of postnasal drip syndrome. Among the 346 treated patients, 91 (24% of those enrolled, or 26% of treated) showed no response.
Thirty-two patients with normal rhinoscopic findings and 170 categorized as partial or nonresponders in the first step underwent an MPT and eosinophil count of induced sputum. One hundred forty-four showed positive results and received empiric treatment for 1 week. Among these, 141 were deemed successful responders (37% of enrolled, or 98% of treated), 3 partial responders (1% of enrolled, or 2% of treated), and none were nonresponders.
In all, 61 patients had empiric treatment for reflux syndrome for 2 weeks; 58 had normal findings for both the MPT and sputum eosinophil count, and 3 were classified as partial responders in the previous therapeutic trial. Twenty-nine patients (8% of enrolled, or 47% of treated) were classified as successful responders after 2 weeks (TABLE 2).
TABLE 2
Presumptive diagnoses corresponded to expected frequency (and occasionally co-existed)
| DIAGNOSIS | NO. OF PATIENTS (%)* N=378 |
| Postnasal drip syndrome | 255 (67.5) |
| Asthma syndrome | 144 (38.1) |
| Reflux syndrome | 29 (7.7) |
| CO-EXISTING PATHOLOGIES | 82 (21.7) |
| Postnasal drip syndrome and asthma syndrome | 52 (13.8) |
| Postnasal drip syndrome and reflux syndrome | 7 (1.9) |
| Postnasal drip syndrome and other diagnosis | 20 (5.3) |
| Asthma syndrome and other diagnosis | 3 (0.8) |
| * The percentage of patients under "Diagnosis" does not add up to 100% because some patients had more than one condition, accounted for under "Co-existing pathologies." | |
Therapeutic response period for successful responders
Within 5 days of beginning the course determined by the algorithm (Figure), 176 patients (47%) who received treatment for presumed postnasal drip syndrome experienced resolution of their chronic cough.
Another 141 patients (37%) diagnosed with asthma syndrome (with or without postnasal drip syndrome) reported cough resolution following successful treatment between 7 and 12 days.
Another 29 patients (8%) with re-flux syndrome were successfully treated between 14 and 26 days.
Treatment of chronic cough by the algorithm
After application of the therapeutic algorithm, the chronic cough of 346 patients (92%) resolved. Thirty-two patients (8.5%) underwent other diagnostic investigations.
Final diagnoses after further diagnostic testing
Ten patients reported that they stopped coughing spontaneously while awaiting additional diagnostic investigations. Seven patients had mycobacterial infections confirmed by acid fast bacilli smears or culture of sputum or bronchoscopic washings. Six patients had localized or diffuse bronchiectasis confirmed by high-resolution CT, the results of which were used retrospectively to reassess normal or equivocal findings in the initial diagnostic investigations. Finally, the coughs of 12 patients were judged to be idiopathic or psychogenic.
Discussion
Cough is a symptom not easily assessed objectively. Previous studies measured severity of cough with daily diaries and visual analog scales, which are subjective measurement tools. We, too, used the visual analog scale to measure cough severity and treatment response. We did not pursue a definitive diagnosis of the cause of chronic cough. Rather, our algorithmic approach made presumptive diagnoses that were confirmed or refuted by patients’ successive reports of cough severity in response to treatment.
The logic behind our algorithm
Because studies in Korea have shown that postnasal drip is the most frequent cause of chronic cough, we chose rhinoscopy as the first diagnostic investigation. The second and third steps of our approach investigated asthma syndrome and reflux syndrome, respectively.
We did not take into account whether patients smoked cigarettes. Some investigators rightly point out that smoking might contribute to chronic cough. However, we have not met many smokers willing to quit because of a cough, and our algorithm is designed for practical clinical use. In contrast, patients with chronic cough secondary to ACE inhibitor therapy have readily accepted trials of different antihypertensive medications.
Our assumptions proved true
Patients with any abnormality of the nasal mucosa were treated for postnasal drip syndrome. Though the proportion of abnormal mucosal findings was greater than that reported in previous investigations of the same ethnic subjects, the eventual treatment response showed that the presumptive diagnosis of postnasal drip was equivalent to that in other studies.10,11
Postnasal drip syndrome did indeed turn out to be the most common presumptive cause of cough in our study. However, roughly one third of these patients proved to have an additional presumptive disorder. Previous investigations have also reported dual or multiple pathologies in patients with a chronic cough.11,12
If treatment succeeded at any step in our algorithm, we asked patients to stop taking medication—with the exception of those who had positive results on methacholine bronchial provocation test. Asthma is a chronic inflammatory disorder that needs persistent therapy to prevent exacerbations and declining lung function.13,14 Challenge studies with methacholine or histamine are sensitive tests and provide high negative predictive values for the diagnosis of asthma and cough variant asthma.15,16
What have other studies shown?
The natural course of chronic cough is still in question, primarily because of the heterogeneity of its etiology. The natural course of many common diseases has been investigated, of course, but few studies have focused on duration of symptoms such as cough. Park et al17 investigated the natural course of eosinophilic bronchitis, a common underlying disorder in chronic cough. In a 48-month follow-up of 36 patients diagnosed with eosinophilic bronchitis, 14% experienced recurrence after treatment. And patients with a higher percentage of eosinophils in the sputum had a risk for developing airway hyperresponsiveness.
Ours et al9 reported that, for patients without asthma or postnasal drip, an empiric 2-week trial of high-dose proton pump inhibitors was more reliable and cost effective for chronic cough than was treatment after esophageal manometry or 24 hours dual probe pH monitoring. Besides the expense of manometry and pH monitoring, both procedures are invasive and unavailable in many localities such as ours. Our algorithm supposes, for one thing, minimum availability of medical equipment in many locales.
The algorithm makes sense
Our approach decreased medical expenses and therapeutic response periods. Cough resolved for more than 90% of our patients. This success rate was equivalent to that reported by previous studies, most of which revealed no definitive diagnosis during the therapeutic response period.2-4,18 Half of all patients in our study experienced cough resolution within 5 days, and more than 80% did so within 12 days.
Development of algorithms similar to ours should take into account not just findings in the literature but the experiences of local doctors and available medical equipment and options.
1. Janson C, Chinn S, Jarvis D, Burney P. Determinants of cough in young adults participating in the European Community Respiratory Health Survey. Eur Resp J 2001;18:647-654.
2. Irwin RS, Carrao WM, Pratter MR. Chronic persistent cough in the adult: the spectrum and frequency of causes and successful outcome of specific therapy. Am Rev Respir Dis 1981;123:413-417.
3. Poe RH, Israel RH, Utell MJ, Hall WJ. Chronic cough: bronchoscopy or pulmonary function testing? Am Rev Respir Dis 1982;126:160-162.
4. Irwin RS, Curley FJ, French CL. Chronic cough. The spectrum and frequency of causes, key components of the diagnostic evaluation, and the outcome of specific therapy. Am Rev Respir Dis 1990;141:640-647.
5. Palombini BC, Villanova CA, Araujo E, et al. A pathogenic triad in chronic cough: asthma, postnasal drip syndrome and gastroesophageal reflux disease. Chest 1999;116:279-284.
6. Morice AH, Fontana GA, Sovijarvi ARA, et al. The diagnosis and management of chronic cough. Eur Respir J 2004;24:481-492.
7. Chatham M, Bleecker ER, Norman P, Smith PL, Mason P. A screening test for airways reactivity. An abbreviated methacholine inhalation challenge. Chest 1982;82:15-18.
8. Jang A, Lee J, Park S, et al. Factors influencing the responsiveness to inhaled glucocorticoids in patients with moderate to severe asthma. Korean J Asthma Allergy Clin Immunol 2005;25:175-180.
9. Ours TM, Kavuru MS, Schilz RJ, Richter JE. A prospective evaluation of esophageal testing and a double-blind randomized study of omeprazole in a diagnostic and therapeutic algorithm for chronic cough. Am J Gastroenterol 1999;94:3131-3138.
10. Cho JH, Ryu JS, Lee HL. Chronic cough: the spectrum and the frequency of etiologies. Tuberc Respir Dis 1999;46:555-563.
11. Jeon G, Jang SH, Song HG, et al. Diagnostic performance of routine objective tests and cost-effective approach for chronic cough. Tuberc Respir Dis 2004;57:535-542.
12. Smyrnios NA, Irwin RS, Curley FJ. Chronic cough with a history of excessive sputum production. The spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Chest 1995;108:991-997.
13. Global Initiative for Asthma. Global strategy for asthma management and prevention. NHLBI/WHO workshop report. Bethesda, Md: National Heart, Lung and Blood Institute;2004.
14. James AL, Palmer LJ, Kicic E, et al. Decline in lung function in the Busselton Health Study: the effects of asthma and cigarette smoking. Am J Respir Crit Care Med 2005;171:109-114.
15. Fish JE, Peters SP. Bronchial challenge testing. Middleton’s Allergy Principles and Practice. 6th ed. St Louis, Mo: Mosby, Inc; 2003;657-670.
16. Dicpinigaitis PV. Chronic cough due to asthma: ACCP evidence-based clinical practice guidelines. Chest 2006;129:75S-79S
17. Park JK, Park SW, Lee JH, et al. Evaluation of clinical course in patients with eosinophilic bronchitis: A prospective follow up study. J Asthma Allergy Clin Immunol 2003;23:740-748.
18. Simpson G. Investigation and management of persistent dry cough. Thorax 1999;54:469-470.
- When evaluating chronic cough, consider a trial of therapy aimed at the most likely presumptive diagnosis for your locality.
- In developing algorithms such as ours, take into account your experiences, patient characteristics, and the available medical equipment.
At the insistence of her family, a woman comes to you complaining of a cough that has lasted several weeks. Many experts would urge a thorough diagnostic investigation, justifying this action with a presumed shorter course of treatment. But is an involved work-up really necessary? Would a quicker, less expensive approach serve the patient just as well? We designed our study to answer these questions.
“Test all, then treat” is expensive
In the management of patients with chronic cough, most algorithms have advocated the approach of “test all, then treat.”1-6 This is an expensive approach and one that delays relief for the patient, though a confirmative diagnosis may decrease the overall duration of treatment. In most cases, however, this approach may be unnecessary. And because few of the underlying disorders are acutely debilitating or rapidly progressive, even misdiagnosis and resultant inappropriate treatment pose little risk to patients.
The less common approach is a sequence of trial-and-error treatments based on a presumptive hierarchy of possible diagnoses.6 The advantage with this strategy is a 3-to 5-fold cost savings.6 And we suspected that the associated length of treatment would be acceptable.
We proposed that the management of patients with chronic cough begin with a presumptive diagnosis, thus simplifying the initial evaluation, keeping costs low, and offering earlier treatment.
We developed an algorithm for the treatment of patients with chronic cough that relies on minimal diagnostic investigations, regardless of the confirmed diagnosis. We evaluated our approach from the perspectives of the presumptive diagnosis and the therapeutic response period.
Methods
Treatment algorithm reflects experience and local resources
Initially, we designed the algorithm to follow findings in the literature on the treatment of patients with chronic cough. We then simplified and modified the algorithm to reflect the experiences of doctors from the pulmonology clinic in our hospital, and to take into account local patient characteristics and available medical equipment and resources.
For this study, we defined chronic cough as a one that lasts more than 4 weeks. (This definition can vary, depending on the source you consult.1) the patients we enrolled had no abnormalities detected on auscultation, chest radiography, or CBC.
Chronic cough can be managed successfully by accurate treatment of the cause, and most specialists report high success rates in treating it.2-4 The 3 most common causes of chronic cough are 1) postnasal drip, 2) asthma, and 3) gastroesophageal reflux.5
Subjects were otherwise healthy
Between January 1 and December 31, 2005, at the internal medicine clinic of Cheju National University Hospital, we enrolled 378 patients whose chief complaint was cough persisting for more than 4 weeks and who had no abnormalities detected on auscultation by a physician, chest radiography (posterior–anterior view and left lateral view), or complete blood cell counts. Each patient had a complete blood count to detect anemia, hematologic disorders, or inflammatory conditions. Current users of angiotensin-converting enzyme (ACE) inhibitors were excluded.
All of the patients we enrolled were adults living in Jeju, Korea, and the mean age was 51 years. One hundred eighty-six (49%) were men. The median reported cough duration was 2 months (range, 1–36 months) (TABLE 1).
We instructed the patients on our algorithmic approach to treating chronic cough and encouraged them to follow the algorithm through to telephone notification of the next visit.
TABLE 1
Characteristics of the 378 enrolled patients
| Men/women | 186/192 (49/51%) |
| Age, years | 51.2±16.12 |
| Cough duration in months, median (range) | 2 (1–36) |
How we determined treatment outcomes
Patients graded their cough severity subjectively at each visit using a visual analogue scale (VAS) from 1 (no cough at all) to 10 (cough severity same as that remembered during first visit to the clinic). We recorded their reports on a questionnaire.
Successful responders were patients who reported a subjective grade of cough severity less than 3. Partial responders and nonresponders were defined, respectively, as those reporting VAS scores from 3 to 6 and more than 6.
We defined the response period as the number of days from enrollment until the next visit in which the patient first reported a VAS score of cough severity less than 3.
Algorithm: Addressing the 3 most common causes of chronic cough
1. Postnasal drip syndrome. Patients first underwent a rhinoscopic examination (FIGURE). When clinicians detected redness or abnormal discharge on the nasal mucosa, they prescribed a 5-day course of antihistamine (10 mg/day ebastine [Ebastel] orally), pseudoephedrine (30 mg 3 times daily, orally), and intranasal corticosteroid (triamcinolone acetonide [Nasacort] 110 mcg twice daily intranasally). Patients without symptoms of rhinitis were referred to the next diagnostic phase.
With completion of the prescribed medication 5 days after the first visit, we graded the severity of cough by questionnaire. Patients in the successful and partial responder categories received a presumptive diagnosis of postnasal drip syndrome, and we asked them to continue using the medication for at least 2 weeks. We had each nonresponder stop the medication.
2. Asthma syndrome. Partial responder and nonresponder patients entered the next diagnostic phase: a methacholine bronchial provocation test (MPT)7 and eosinophil count with induced sputum by hypertonic saline (3% NaCl).8 We defined a positive MPT result as <10 mg/ mL of methacholine causing a 20% fall in FEV1 from baseline (PC20). Patients with more than 3% eosinophils in the induced sputum specimen or with a positive MPT received a 1-week prescription for inhaled budesonide 160 mcg twice daily and inhaled formoterol (Symbicort) 4.5 mcg twice daily. Patients who did not exhibit these asthma indicators were referred to the next step.
At the next visit, we again graded the severity of cough. Patients in the successful and partial responder categories received a presumptive diagnosis of asthma syndrome. We asked successful and partial responders to continue the medication for at least 2 weeks. Those classed as nonresponders were asked to stop their medication. We referred all patients with positive MPT test results to a special clinic for asthma, regardless of responses to this therapeutic trial or eosinophil count in the induced sputum.
3. Reflux syndrome. Partial responders and nonresponders then received a 2-week prescription for a proton pump inhibitor, pantoprazole (Pantoloc), 40 mg orally once daily.9 At the next visit 2 weeks later, we graded the severity of cough. Successful and partial responders were given a presumptive diagnosis of reflux syndrome, but only successful responders were asked to continue the same medication for at least 6 weeks. At the discretion of their physicians, partial and nonresponders underwent other diagnostic investigations, including high-resolution computerized tomography (CT) of the lungs, bronchoscopic examination, sputum smear and culture for acid fast bacilli, sputum culture for ordinary bacteria and fungi, and a serological test for human immunodeficiency virus.
FIGURE
A presumptive-diagnosis algorithm
Chronic cough resolved for more than 90% of patients treated according to this algorithm.
MPT, methacholine bronchial provocation test; VAS, visual analog scale.
Results
Presumptive diagnoses
Among 378 patients, 346 (91%) showed erythematous mucosa or abnormal discharge in rhinoscopic examinations and received empiric medication for 5 days. The successful-responder category included 176 patients (47%); 79 (21%) were classed as partial responders, and 255 (67%) received the presumptive diagnosis of postnasal drip syndrome. Among the 346 treated patients, 91 (24% of those enrolled, or 26% of treated) showed no response.
Thirty-two patients with normal rhinoscopic findings and 170 categorized as partial or nonresponders in the first step underwent an MPT and eosinophil count of induced sputum. One hundred forty-four showed positive results and received empiric treatment for 1 week. Among these, 141 were deemed successful responders (37% of enrolled, or 98% of treated), 3 partial responders (1% of enrolled, or 2% of treated), and none were nonresponders.
In all, 61 patients had empiric treatment for reflux syndrome for 2 weeks; 58 had normal findings for both the MPT and sputum eosinophil count, and 3 were classified as partial responders in the previous therapeutic trial. Twenty-nine patients (8% of enrolled, or 47% of treated) were classified as successful responders after 2 weeks (TABLE 2).
TABLE 2
Presumptive diagnoses corresponded to expected frequency (and occasionally co-existed)
| DIAGNOSIS | NO. OF PATIENTS (%)* N=378 |
| Postnasal drip syndrome | 255 (67.5) |
| Asthma syndrome | 144 (38.1) |
| Reflux syndrome | 29 (7.7) |
| CO-EXISTING PATHOLOGIES | 82 (21.7) |
| Postnasal drip syndrome and asthma syndrome | 52 (13.8) |
| Postnasal drip syndrome and reflux syndrome | 7 (1.9) |
| Postnasal drip syndrome and other diagnosis | 20 (5.3) |
| Asthma syndrome and other diagnosis | 3 (0.8) |
| * The percentage of patients under "Diagnosis" does not add up to 100% because some patients had more than one condition, accounted for under "Co-existing pathologies." | |
Therapeutic response period for successful responders
Within 5 days of beginning the course determined by the algorithm (Figure), 176 patients (47%) who received treatment for presumed postnasal drip syndrome experienced resolution of their chronic cough.
Another 141 patients (37%) diagnosed with asthma syndrome (with or without postnasal drip syndrome) reported cough resolution following successful treatment between 7 and 12 days.
Another 29 patients (8%) with re-flux syndrome were successfully treated between 14 and 26 days.
Treatment of chronic cough by the algorithm
After application of the therapeutic algorithm, the chronic cough of 346 patients (92%) resolved. Thirty-two patients (8.5%) underwent other diagnostic investigations.
Final diagnoses after further diagnostic testing
Ten patients reported that they stopped coughing spontaneously while awaiting additional diagnostic investigations. Seven patients had mycobacterial infections confirmed by acid fast bacilli smears or culture of sputum or bronchoscopic washings. Six patients had localized or diffuse bronchiectasis confirmed by high-resolution CT, the results of which were used retrospectively to reassess normal or equivocal findings in the initial diagnostic investigations. Finally, the coughs of 12 patients were judged to be idiopathic or psychogenic.
Discussion
Cough is a symptom not easily assessed objectively. Previous studies measured severity of cough with daily diaries and visual analog scales, which are subjective measurement tools. We, too, used the visual analog scale to measure cough severity and treatment response. We did not pursue a definitive diagnosis of the cause of chronic cough. Rather, our algorithmic approach made presumptive diagnoses that were confirmed or refuted by patients’ successive reports of cough severity in response to treatment.
The logic behind our algorithm
Because studies in Korea have shown that postnasal drip is the most frequent cause of chronic cough, we chose rhinoscopy as the first diagnostic investigation. The second and third steps of our approach investigated asthma syndrome and reflux syndrome, respectively.
We did not take into account whether patients smoked cigarettes. Some investigators rightly point out that smoking might contribute to chronic cough. However, we have not met many smokers willing to quit because of a cough, and our algorithm is designed for practical clinical use. In contrast, patients with chronic cough secondary to ACE inhibitor therapy have readily accepted trials of different antihypertensive medications.
Our assumptions proved true
Patients with any abnormality of the nasal mucosa were treated for postnasal drip syndrome. Though the proportion of abnormal mucosal findings was greater than that reported in previous investigations of the same ethnic subjects, the eventual treatment response showed that the presumptive diagnosis of postnasal drip was equivalent to that in other studies.10,11
Postnasal drip syndrome did indeed turn out to be the most common presumptive cause of cough in our study. However, roughly one third of these patients proved to have an additional presumptive disorder. Previous investigations have also reported dual or multiple pathologies in patients with a chronic cough.11,12
If treatment succeeded at any step in our algorithm, we asked patients to stop taking medication—with the exception of those who had positive results on methacholine bronchial provocation test. Asthma is a chronic inflammatory disorder that needs persistent therapy to prevent exacerbations and declining lung function.13,14 Challenge studies with methacholine or histamine are sensitive tests and provide high negative predictive values for the diagnosis of asthma and cough variant asthma.15,16
What have other studies shown?
The natural course of chronic cough is still in question, primarily because of the heterogeneity of its etiology. The natural course of many common diseases has been investigated, of course, but few studies have focused on duration of symptoms such as cough. Park et al17 investigated the natural course of eosinophilic bronchitis, a common underlying disorder in chronic cough. In a 48-month follow-up of 36 patients diagnosed with eosinophilic bronchitis, 14% experienced recurrence after treatment. And patients with a higher percentage of eosinophils in the sputum had a risk for developing airway hyperresponsiveness.
Ours et al9 reported that, for patients without asthma or postnasal drip, an empiric 2-week trial of high-dose proton pump inhibitors was more reliable and cost effective for chronic cough than was treatment after esophageal manometry or 24 hours dual probe pH monitoring. Besides the expense of manometry and pH monitoring, both procedures are invasive and unavailable in many localities such as ours. Our algorithm supposes, for one thing, minimum availability of medical equipment in many locales.
The algorithm makes sense
Our approach decreased medical expenses and therapeutic response periods. Cough resolved for more than 90% of our patients. This success rate was equivalent to that reported by previous studies, most of which revealed no definitive diagnosis during the therapeutic response period.2-4,18 Half of all patients in our study experienced cough resolution within 5 days, and more than 80% did so within 12 days.
Development of algorithms similar to ours should take into account not just findings in the literature but the experiences of local doctors and available medical equipment and options.
- When evaluating chronic cough, consider a trial of therapy aimed at the most likely presumptive diagnosis for your locality.
- In developing algorithms such as ours, take into account your experiences, patient characteristics, and the available medical equipment.
At the insistence of her family, a woman comes to you complaining of a cough that has lasted several weeks. Many experts would urge a thorough diagnostic investigation, justifying this action with a presumed shorter course of treatment. But is an involved work-up really necessary? Would a quicker, less expensive approach serve the patient just as well? We designed our study to answer these questions.
“Test all, then treat” is expensive
In the management of patients with chronic cough, most algorithms have advocated the approach of “test all, then treat.”1-6 This is an expensive approach and one that delays relief for the patient, though a confirmative diagnosis may decrease the overall duration of treatment. In most cases, however, this approach may be unnecessary. And because few of the underlying disorders are acutely debilitating or rapidly progressive, even misdiagnosis and resultant inappropriate treatment pose little risk to patients.
The less common approach is a sequence of trial-and-error treatments based on a presumptive hierarchy of possible diagnoses.6 The advantage with this strategy is a 3-to 5-fold cost savings.6 And we suspected that the associated length of treatment would be acceptable.
We proposed that the management of patients with chronic cough begin with a presumptive diagnosis, thus simplifying the initial evaluation, keeping costs low, and offering earlier treatment.
We developed an algorithm for the treatment of patients with chronic cough that relies on minimal diagnostic investigations, regardless of the confirmed diagnosis. We evaluated our approach from the perspectives of the presumptive diagnosis and the therapeutic response period.
Methods
Treatment algorithm reflects experience and local resources
Initially, we designed the algorithm to follow findings in the literature on the treatment of patients with chronic cough. We then simplified and modified the algorithm to reflect the experiences of doctors from the pulmonology clinic in our hospital, and to take into account local patient characteristics and available medical equipment and resources.
For this study, we defined chronic cough as a one that lasts more than 4 weeks. (This definition can vary, depending on the source you consult.1) the patients we enrolled had no abnormalities detected on auscultation, chest radiography, or CBC.
Chronic cough can be managed successfully by accurate treatment of the cause, and most specialists report high success rates in treating it.2-4 The 3 most common causes of chronic cough are 1) postnasal drip, 2) asthma, and 3) gastroesophageal reflux.5
Subjects were otherwise healthy
Between January 1 and December 31, 2005, at the internal medicine clinic of Cheju National University Hospital, we enrolled 378 patients whose chief complaint was cough persisting for more than 4 weeks and who had no abnormalities detected on auscultation by a physician, chest radiography (posterior–anterior view and left lateral view), or complete blood cell counts. Each patient had a complete blood count to detect anemia, hematologic disorders, or inflammatory conditions. Current users of angiotensin-converting enzyme (ACE) inhibitors were excluded.
All of the patients we enrolled were adults living in Jeju, Korea, and the mean age was 51 years. One hundred eighty-six (49%) were men. The median reported cough duration was 2 months (range, 1–36 months) (TABLE 1).
We instructed the patients on our algorithmic approach to treating chronic cough and encouraged them to follow the algorithm through to telephone notification of the next visit.
TABLE 1
Characteristics of the 378 enrolled patients
| Men/women | 186/192 (49/51%) |
| Age, years | 51.2±16.12 |
| Cough duration in months, median (range) | 2 (1–36) |
How we determined treatment outcomes
Patients graded their cough severity subjectively at each visit using a visual analogue scale (VAS) from 1 (no cough at all) to 10 (cough severity same as that remembered during first visit to the clinic). We recorded their reports on a questionnaire.
Successful responders were patients who reported a subjective grade of cough severity less than 3. Partial responders and nonresponders were defined, respectively, as those reporting VAS scores from 3 to 6 and more than 6.
We defined the response period as the number of days from enrollment until the next visit in which the patient first reported a VAS score of cough severity less than 3.
Algorithm: Addressing the 3 most common causes of chronic cough
1. Postnasal drip syndrome. Patients first underwent a rhinoscopic examination (FIGURE). When clinicians detected redness or abnormal discharge on the nasal mucosa, they prescribed a 5-day course of antihistamine (10 mg/day ebastine [Ebastel] orally), pseudoephedrine (30 mg 3 times daily, orally), and intranasal corticosteroid (triamcinolone acetonide [Nasacort] 110 mcg twice daily intranasally). Patients without symptoms of rhinitis were referred to the next diagnostic phase.
With completion of the prescribed medication 5 days after the first visit, we graded the severity of cough by questionnaire. Patients in the successful and partial responder categories received a presumptive diagnosis of postnasal drip syndrome, and we asked them to continue using the medication for at least 2 weeks. We had each nonresponder stop the medication.
2. Asthma syndrome. Partial responder and nonresponder patients entered the next diagnostic phase: a methacholine bronchial provocation test (MPT)7 and eosinophil count with induced sputum by hypertonic saline (3% NaCl).8 We defined a positive MPT result as <10 mg/ mL of methacholine causing a 20% fall in FEV1 from baseline (PC20). Patients with more than 3% eosinophils in the induced sputum specimen or with a positive MPT received a 1-week prescription for inhaled budesonide 160 mcg twice daily and inhaled formoterol (Symbicort) 4.5 mcg twice daily. Patients who did not exhibit these asthma indicators were referred to the next step.
At the next visit, we again graded the severity of cough. Patients in the successful and partial responder categories received a presumptive diagnosis of asthma syndrome. We asked successful and partial responders to continue the medication for at least 2 weeks. Those classed as nonresponders were asked to stop their medication. We referred all patients with positive MPT test results to a special clinic for asthma, regardless of responses to this therapeutic trial or eosinophil count in the induced sputum.
3. Reflux syndrome. Partial responders and nonresponders then received a 2-week prescription for a proton pump inhibitor, pantoprazole (Pantoloc), 40 mg orally once daily.9 At the next visit 2 weeks later, we graded the severity of cough. Successful and partial responders were given a presumptive diagnosis of reflux syndrome, but only successful responders were asked to continue the same medication for at least 6 weeks. At the discretion of their physicians, partial and nonresponders underwent other diagnostic investigations, including high-resolution computerized tomography (CT) of the lungs, bronchoscopic examination, sputum smear and culture for acid fast bacilli, sputum culture for ordinary bacteria and fungi, and a serological test for human immunodeficiency virus.
FIGURE
A presumptive-diagnosis algorithm
Chronic cough resolved for more than 90% of patients treated according to this algorithm.
MPT, methacholine bronchial provocation test; VAS, visual analog scale.
Results
Presumptive diagnoses
Among 378 patients, 346 (91%) showed erythematous mucosa or abnormal discharge in rhinoscopic examinations and received empiric medication for 5 days. The successful-responder category included 176 patients (47%); 79 (21%) were classed as partial responders, and 255 (67%) received the presumptive diagnosis of postnasal drip syndrome. Among the 346 treated patients, 91 (24% of those enrolled, or 26% of treated) showed no response.
Thirty-two patients with normal rhinoscopic findings and 170 categorized as partial or nonresponders in the first step underwent an MPT and eosinophil count of induced sputum. One hundred forty-four showed positive results and received empiric treatment for 1 week. Among these, 141 were deemed successful responders (37% of enrolled, or 98% of treated), 3 partial responders (1% of enrolled, or 2% of treated), and none were nonresponders.
In all, 61 patients had empiric treatment for reflux syndrome for 2 weeks; 58 had normal findings for both the MPT and sputum eosinophil count, and 3 were classified as partial responders in the previous therapeutic trial. Twenty-nine patients (8% of enrolled, or 47% of treated) were classified as successful responders after 2 weeks (TABLE 2).
TABLE 2
Presumptive diagnoses corresponded to expected frequency (and occasionally co-existed)
| DIAGNOSIS | NO. OF PATIENTS (%)* N=378 |
| Postnasal drip syndrome | 255 (67.5) |
| Asthma syndrome | 144 (38.1) |
| Reflux syndrome | 29 (7.7) |
| CO-EXISTING PATHOLOGIES | 82 (21.7) |
| Postnasal drip syndrome and asthma syndrome | 52 (13.8) |
| Postnasal drip syndrome and reflux syndrome | 7 (1.9) |
| Postnasal drip syndrome and other diagnosis | 20 (5.3) |
| Asthma syndrome and other diagnosis | 3 (0.8) |
| * The percentage of patients under "Diagnosis" does not add up to 100% because some patients had more than one condition, accounted for under "Co-existing pathologies." | |
Therapeutic response period for successful responders
Within 5 days of beginning the course determined by the algorithm (Figure), 176 patients (47%) who received treatment for presumed postnasal drip syndrome experienced resolution of their chronic cough.
Another 141 patients (37%) diagnosed with asthma syndrome (with or without postnasal drip syndrome) reported cough resolution following successful treatment between 7 and 12 days.
Another 29 patients (8%) with re-flux syndrome were successfully treated between 14 and 26 days.
Treatment of chronic cough by the algorithm
After application of the therapeutic algorithm, the chronic cough of 346 patients (92%) resolved. Thirty-two patients (8.5%) underwent other diagnostic investigations.
Final diagnoses after further diagnostic testing
Ten patients reported that they stopped coughing spontaneously while awaiting additional diagnostic investigations. Seven patients had mycobacterial infections confirmed by acid fast bacilli smears or culture of sputum or bronchoscopic washings. Six patients had localized or diffuse bronchiectasis confirmed by high-resolution CT, the results of which were used retrospectively to reassess normal or equivocal findings in the initial diagnostic investigations. Finally, the coughs of 12 patients were judged to be idiopathic or psychogenic.
Discussion
Cough is a symptom not easily assessed objectively. Previous studies measured severity of cough with daily diaries and visual analog scales, which are subjective measurement tools. We, too, used the visual analog scale to measure cough severity and treatment response. We did not pursue a definitive diagnosis of the cause of chronic cough. Rather, our algorithmic approach made presumptive diagnoses that were confirmed or refuted by patients’ successive reports of cough severity in response to treatment.
The logic behind our algorithm
Because studies in Korea have shown that postnasal drip is the most frequent cause of chronic cough, we chose rhinoscopy as the first diagnostic investigation. The second and third steps of our approach investigated asthma syndrome and reflux syndrome, respectively.
We did not take into account whether patients smoked cigarettes. Some investigators rightly point out that smoking might contribute to chronic cough. However, we have not met many smokers willing to quit because of a cough, and our algorithm is designed for practical clinical use. In contrast, patients with chronic cough secondary to ACE inhibitor therapy have readily accepted trials of different antihypertensive medications.
Our assumptions proved true
Patients with any abnormality of the nasal mucosa were treated for postnasal drip syndrome. Though the proportion of abnormal mucosal findings was greater than that reported in previous investigations of the same ethnic subjects, the eventual treatment response showed that the presumptive diagnosis of postnasal drip was equivalent to that in other studies.10,11
Postnasal drip syndrome did indeed turn out to be the most common presumptive cause of cough in our study. However, roughly one third of these patients proved to have an additional presumptive disorder. Previous investigations have also reported dual or multiple pathologies in patients with a chronic cough.11,12
If treatment succeeded at any step in our algorithm, we asked patients to stop taking medication—with the exception of those who had positive results on methacholine bronchial provocation test. Asthma is a chronic inflammatory disorder that needs persistent therapy to prevent exacerbations and declining lung function.13,14 Challenge studies with methacholine or histamine are sensitive tests and provide high negative predictive values for the diagnosis of asthma and cough variant asthma.15,16
What have other studies shown?
The natural course of chronic cough is still in question, primarily because of the heterogeneity of its etiology. The natural course of many common diseases has been investigated, of course, but few studies have focused on duration of symptoms such as cough. Park et al17 investigated the natural course of eosinophilic bronchitis, a common underlying disorder in chronic cough. In a 48-month follow-up of 36 patients diagnosed with eosinophilic bronchitis, 14% experienced recurrence after treatment. And patients with a higher percentage of eosinophils in the sputum had a risk for developing airway hyperresponsiveness.
Ours et al9 reported that, for patients without asthma or postnasal drip, an empiric 2-week trial of high-dose proton pump inhibitors was more reliable and cost effective for chronic cough than was treatment after esophageal manometry or 24 hours dual probe pH monitoring. Besides the expense of manometry and pH monitoring, both procedures are invasive and unavailable in many localities such as ours. Our algorithm supposes, for one thing, minimum availability of medical equipment in many locales.
The algorithm makes sense
Our approach decreased medical expenses and therapeutic response periods. Cough resolved for more than 90% of our patients. This success rate was equivalent to that reported by previous studies, most of which revealed no definitive diagnosis during the therapeutic response period.2-4,18 Half of all patients in our study experienced cough resolution within 5 days, and more than 80% did so within 12 days.
Development of algorithms similar to ours should take into account not just findings in the literature but the experiences of local doctors and available medical equipment and options.
1. Janson C, Chinn S, Jarvis D, Burney P. Determinants of cough in young adults participating in the European Community Respiratory Health Survey. Eur Resp J 2001;18:647-654.
2. Irwin RS, Carrao WM, Pratter MR. Chronic persistent cough in the adult: the spectrum and frequency of causes and successful outcome of specific therapy. Am Rev Respir Dis 1981;123:413-417.
3. Poe RH, Israel RH, Utell MJ, Hall WJ. Chronic cough: bronchoscopy or pulmonary function testing? Am Rev Respir Dis 1982;126:160-162.
4. Irwin RS, Curley FJ, French CL. Chronic cough. The spectrum and frequency of causes, key components of the diagnostic evaluation, and the outcome of specific therapy. Am Rev Respir Dis 1990;141:640-647.
5. Palombini BC, Villanova CA, Araujo E, et al. A pathogenic triad in chronic cough: asthma, postnasal drip syndrome and gastroesophageal reflux disease. Chest 1999;116:279-284.
6. Morice AH, Fontana GA, Sovijarvi ARA, et al. The diagnosis and management of chronic cough. Eur Respir J 2004;24:481-492.
7. Chatham M, Bleecker ER, Norman P, Smith PL, Mason P. A screening test for airways reactivity. An abbreviated methacholine inhalation challenge. Chest 1982;82:15-18.
8. Jang A, Lee J, Park S, et al. Factors influencing the responsiveness to inhaled glucocorticoids in patients with moderate to severe asthma. Korean J Asthma Allergy Clin Immunol 2005;25:175-180.
9. Ours TM, Kavuru MS, Schilz RJ, Richter JE. A prospective evaluation of esophageal testing and a double-blind randomized study of omeprazole in a diagnostic and therapeutic algorithm for chronic cough. Am J Gastroenterol 1999;94:3131-3138.
10. Cho JH, Ryu JS, Lee HL. Chronic cough: the spectrum and the frequency of etiologies. Tuberc Respir Dis 1999;46:555-563.
11. Jeon G, Jang SH, Song HG, et al. Diagnostic performance of routine objective tests and cost-effective approach for chronic cough. Tuberc Respir Dis 2004;57:535-542.
12. Smyrnios NA, Irwin RS, Curley FJ. Chronic cough with a history of excessive sputum production. The spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Chest 1995;108:991-997.
13. Global Initiative for Asthma. Global strategy for asthma management and prevention. NHLBI/WHO workshop report. Bethesda, Md: National Heart, Lung and Blood Institute;2004.
14. James AL, Palmer LJ, Kicic E, et al. Decline in lung function in the Busselton Health Study: the effects of asthma and cigarette smoking. Am J Respir Crit Care Med 2005;171:109-114.
15. Fish JE, Peters SP. Bronchial challenge testing. Middleton’s Allergy Principles and Practice. 6th ed. St Louis, Mo: Mosby, Inc; 2003;657-670.
16. Dicpinigaitis PV. Chronic cough due to asthma: ACCP evidence-based clinical practice guidelines. Chest 2006;129:75S-79S
17. Park JK, Park SW, Lee JH, et al. Evaluation of clinical course in patients with eosinophilic bronchitis: A prospective follow up study. J Asthma Allergy Clin Immunol 2003;23:740-748.
18. Simpson G. Investigation and management of persistent dry cough. Thorax 1999;54:469-470.
1. Janson C, Chinn S, Jarvis D, Burney P. Determinants of cough in young adults participating in the European Community Respiratory Health Survey. Eur Resp J 2001;18:647-654.
2. Irwin RS, Carrao WM, Pratter MR. Chronic persistent cough in the adult: the spectrum and frequency of causes and successful outcome of specific therapy. Am Rev Respir Dis 1981;123:413-417.
3. Poe RH, Israel RH, Utell MJ, Hall WJ. Chronic cough: bronchoscopy or pulmonary function testing? Am Rev Respir Dis 1982;126:160-162.
4. Irwin RS, Curley FJ, French CL. Chronic cough. The spectrum and frequency of causes, key components of the diagnostic evaluation, and the outcome of specific therapy. Am Rev Respir Dis 1990;141:640-647.
5. Palombini BC, Villanova CA, Araujo E, et al. A pathogenic triad in chronic cough: asthma, postnasal drip syndrome and gastroesophageal reflux disease. Chest 1999;116:279-284.
6. Morice AH, Fontana GA, Sovijarvi ARA, et al. The diagnosis and management of chronic cough. Eur Respir J 2004;24:481-492.
7. Chatham M, Bleecker ER, Norman P, Smith PL, Mason P. A screening test for airways reactivity. An abbreviated methacholine inhalation challenge. Chest 1982;82:15-18.
8. Jang A, Lee J, Park S, et al. Factors influencing the responsiveness to inhaled glucocorticoids in patients with moderate to severe asthma. Korean J Asthma Allergy Clin Immunol 2005;25:175-180.
9. Ours TM, Kavuru MS, Schilz RJ, Richter JE. A prospective evaluation of esophageal testing and a double-blind randomized study of omeprazole in a diagnostic and therapeutic algorithm for chronic cough. Am J Gastroenterol 1999;94:3131-3138.
10. Cho JH, Ryu JS, Lee HL. Chronic cough: the spectrum and the frequency of etiologies. Tuberc Respir Dis 1999;46:555-563.
11. Jeon G, Jang SH, Song HG, et al. Diagnostic performance of routine objective tests and cost-effective approach for chronic cough. Tuberc Respir Dis 2004;57:535-542.
12. Smyrnios NA, Irwin RS, Curley FJ. Chronic cough with a history of excessive sputum production. The spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Chest 1995;108:991-997.
13. Global Initiative for Asthma. Global strategy for asthma management and prevention. NHLBI/WHO workshop report. Bethesda, Md: National Heart, Lung and Blood Institute;2004.
14. James AL, Palmer LJ, Kicic E, et al. Decline in lung function in the Busselton Health Study: the effects of asthma and cigarette smoking. Am J Respir Crit Care Med 2005;171:109-114.
15. Fish JE, Peters SP. Bronchial challenge testing. Middleton’s Allergy Principles and Practice. 6th ed. St Louis, Mo: Mosby, Inc; 2003;657-670.
16. Dicpinigaitis PV. Chronic cough due to asthma: ACCP evidence-based clinical practice guidelines. Chest 2006;129:75S-79S
17. Park JK, Park SW, Lee JH, et al. Evaluation of clinical course in patients with eosinophilic bronchitis: A prospective follow up study. J Asthma Allergy Clin Immunol 2003;23:740-748.
18. Simpson G. Investigation and management of persistent dry cough. Thorax 1999;54:469-470.