User login
Comp Close-Up

How hard do hospitalists work and how much are they paid? There are several sources of data to answer this question, and each has its strengths and weaknesses. Because these data influence contract negotiations and compliance with federal regulations, it is worth taking the time to understand the differences in each data set.
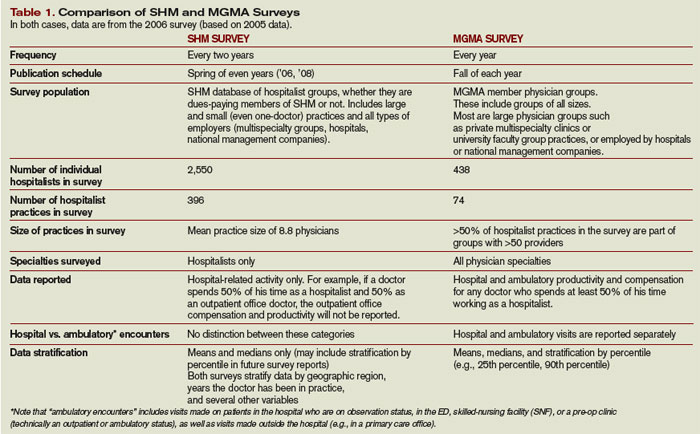
I’ll focus on the two most common sources of data: the biannual SHM survey of hospitalist productivity and compensation (officially titled “The Authoritative Source on the State of Hospital Medicine”), and the Medical Group Management Association’s (MGMA) annual “Physician Compensation and Production Survey.” There are many other surveys that report hospitalist data such as those by the American Medical Group Association (AMGA), Sullivan & Cotter, Hay Group, and others. Each July, Modern Healthcare magazine publishes the average compensation (but no other data) reported for hospitalists and other specialties by each of these organizations and several others (but not the SHM data). It should be easy to find a copy of Modern Healthcare in your hospital administration or library, or on the Internet.
The SHM and MGMA surveys are the most widely used sources of data for hospitalists, and some of their attributes are described in Table 1 (see below).
I should acknowledge my potential conflict of interest and potential for bias in comparing these surveys. This column is in an SHM publication. I’m very active in SHM, and I’m a past chairman and ongoing member of the Benchmarks Committee, which oversees the design and analysis of the SHM survey. And while I am familiar with and regularly review the MGMA survey, I have no other connection to that organization.
Much of the difference between the surveys is a result of the SHM survey being designed specifically for hospitalists in any type of practice setting (e.g., small hospitalist-only groups, as well as hospitalists with huge organizations like a university faculty group practice). In contrast, the MGMA survey is designed for all physician specialties, so a hospitalist answers the same questions as a traditional primary care doctor, plastic surgeon, and obstetrician.
MGMA data can be adversely affected by the inclusion of primary care office-based encounters. One of the principal ways the two surveys differ is how they address ambulatory visits. The MGMA survey reports inpatient and ambulatory visits separately, but “ambulatory” visits include any for a patient who is not a hospital inpatient. By this definition, hospitalists make ambulatory visits, most commonly to hospitalized patients who are on observation status, and also patients seen in an ED, skilled nursing facility, or pre-op clinic. Thus the MGMA survey doesn’t distinguish between ambulatory encounters a hospitalist would generate in the course of serving as a hospitalist, and those generated while that doctor might be serving in a non-hospitalist role such as office-based primary care or urgent care.
The SHM survey doesn’t include—and isn’t contaminated by—office-based primary care or urgent-care visits.
Of the 3,376 total encounters reported in the MGMA survey, 40% (1,351) are ambulatory encounters. Although the SHM survey does not distinguish between hospital and ambulatory encounters, my experience suggests few, if any, hospitalist practices make 40% of their total encounters with patients on observation status, or in an ED, SNF, or pre-op clinic. Thus, many of the ambulatory encounters reported by MGMA might have been office visits, not hospital-related visits.
Additionally, the median internal medicine hospitalist encounters (ambulatory and hospital combined) in the MGMA survey (3,376) is 42% higher than the median total encounters reported for internal medicine hospitalists in SHM’s survey (2,378). Yet the wRVUs reported in the MGMA survey (3,514) are only 8% higher than those reported in the SHM survey (3,256). Thus the calculated average wRVUs per encounter for the MGMA data is only 1.04, compared with 1.37 for the SHM data. An average of 1.04 wRVUs per encounter is very low for hospitalists, when almost all current procedural terminology (CPT) codes a hospitalist uses have a value of one or more wRVUs. Again, this suggests the MGMA data may be significantly influenced by the inclusion of office-based encounters, some of which have wRVUs of less than one. SHM has approached MGMA to discuss this data definition issue in their survey.
Why It Matters
You can use whichever data set best describes your situation. The MGMA has historically shown higher hospitalist salaries and higher workloads than the SHM data. But because the SHM data is the result of a survey customized for hospitalists and less likely than the MGMA data to be contaminated by non-hospital-related visits, the SHM data probably gives a more accurate picture.
Because the MGMA survey has been conducted for many years (far longer than the SHM survey) it has appropriately become one of the most authoritative sources of data on physician compensation for all specialties. Stark II regulations require hospitals to ensure they aren’t paying physicians above the fair market compensation (which could be seen as an inducement to refer patients to the hospital, among other concerns). And it specifically states that the MGMA survey is one of several approved sources of determining what fair market compensation is.
Even though the SHM data is most likely more representative and provides an important benchmark for hospitalists, the MGMA data has “pre-approved” status and thus is potentially safer to use for the specific purpose of determinations of fair market value.
With each iteration, the SHM survey will be adjusted to more specifically capture hospitalist activity; in many cases it is the best data for hospitalists to use in planning and benchmarking. But the MGMA data are still valuable and may be the most appropriate to refer to in contracts.
Note to readers: In May, SHM contacted MGMA regarding their concerns that MGMA survey data was not representative of hospitalists. MGMA responded with a willingness to discuss these issues with SHM. As this story goes to press, SHM and MGMA continue to have a dialogue about maximizing the accuracy of survey data. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
How hard do hospitalists work and how much are they paid? There are several sources of data to answer this question, and each has its strengths and weaknesses. Because these data influence contract negotiations and compliance with federal regulations, it is worth taking the time to understand the differences in each data set.
I’ll focus on the two most common sources of data: the biannual SHM survey of hospitalist productivity and compensation (officially titled “The Authoritative Source on the State of Hospital Medicine”), and the Medical Group Management Association’s (MGMA) annual “Physician Compensation and Production Survey.” There are many other surveys that report hospitalist data such as those by the American Medical Group Association (AMGA), Sullivan & Cotter, Hay Group, and others. Each July, Modern Healthcare magazine publishes the average compensation (but no other data) reported for hospitalists and other specialties by each of these organizations and several others (but not the SHM data). It should be easy to find a copy of Modern Healthcare in your hospital administration or library, or on the Internet.
The SHM and MGMA surveys are the most widely used sources of data for hospitalists, and some of their attributes are described in Table 1 (see below).
I should acknowledge my potential conflict of interest and potential for bias in comparing these surveys. This column is in an SHM publication. I’m very active in SHM, and I’m a past chairman and ongoing member of the Benchmarks Committee, which oversees the design and analysis of the SHM survey. And while I am familiar with and regularly review the MGMA survey, I have no other connection to that organization.
Much of the difference between the surveys is a result of the SHM survey being designed specifically for hospitalists in any type of practice setting (e.g., small hospitalist-only groups, as well as hospitalists with huge organizations like a university faculty group practice). In contrast, the MGMA survey is designed for all physician specialties, so a hospitalist answers the same questions as a traditional primary care doctor, plastic surgeon, and obstetrician.
MGMA data can be adversely affected by the inclusion of primary care office-based encounters. One of the principal ways the two surveys differ is how they address ambulatory visits. The MGMA survey reports inpatient and ambulatory visits separately, but “ambulatory” visits include any for a patient who is not a hospital inpatient. By this definition, hospitalists make ambulatory visits, most commonly to hospitalized patients who are on observation status, and also patients seen in an ED, skilled nursing facility, or pre-op clinic. Thus the MGMA survey doesn’t distinguish between ambulatory encounters a hospitalist would generate in the course of serving as a hospitalist, and those generated while that doctor might be serving in a non-hospitalist role such as office-based primary care or urgent care.
The SHM survey doesn’t include—and isn’t contaminated by—office-based primary care or urgent-care visits.
Of the 3,376 total encounters reported in the MGMA survey, 40% (1,351) are ambulatory encounters. Although the SHM survey does not distinguish between hospital and ambulatory encounters, my experience suggests few, if any, hospitalist practices make 40% of their total encounters with patients on observation status, or in an ED, SNF, or pre-op clinic. Thus, many of the ambulatory encounters reported by MGMA might have been office visits, not hospital-related visits.
Additionally, the median internal medicine hospitalist encounters (ambulatory and hospital combined) in the MGMA survey (3,376) is 42% higher than the median total encounters reported for internal medicine hospitalists in SHM’s survey (2,378). Yet the wRVUs reported in the MGMA survey (3,514) are only 8% higher than those reported in the SHM survey (3,256). Thus the calculated average wRVUs per encounter for the MGMA data is only 1.04, compared with 1.37 for the SHM data. An average of 1.04 wRVUs per encounter is very low for hospitalists, when almost all current procedural terminology (CPT) codes a hospitalist uses have a value of one or more wRVUs. Again, this suggests the MGMA data may be significantly influenced by the inclusion of office-based encounters, some of which have wRVUs of less than one. SHM has approached MGMA to discuss this data definition issue in their survey.
Why It Matters
You can use whichever data set best describes your situation. The MGMA has historically shown higher hospitalist salaries and higher workloads than the SHM data. But because the SHM data is the result of a survey customized for hospitalists and less likely than the MGMA data to be contaminated by non-hospital-related visits, the SHM data probably gives a more accurate picture.
Because the MGMA survey has been conducted for many years (far longer than the SHM survey) it has appropriately become one of the most authoritative sources of data on physician compensation for all specialties. Stark II regulations require hospitals to ensure they aren’t paying physicians above the fair market compensation (which could be seen as an inducement to refer patients to the hospital, among other concerns). And it specifically states that the MGMA survey is one of several approved sources of determining what fair market compensation is.
Even though the SHM data is most likely more representative and provides an important benchmark for hospitalists, the MGMA data has “pre-approved” status and thus is potentially safer to use for the specific purpose of determinations of fair market value.
With each iteration, the SHM survey will be adjusted to more specifically capture hospitalist activity; in many cases it is the best data for hospitalists to use in planning and benchmarking. But the MGMA data are still valuable and may be the most appropriate to refer to in contracts.
Note to readers: In May, SHM contacted MGMA regarding their concerns that MGMA survey data was not representative of hospitalists. MGMA responded with a willingness to discuss these issues with SHM. As this story goes to press, SHM and MGMA continue to have a dialogue about maximizing the accuracy of survey data. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
How hard do hospitalists work and how much are they paid? There are several sources of data to answer this question, and each has its strengths and weaknesses. Because these data influence contract negotiations and compliance with federal regulations, it is worth taking the time to understand the differences in each data set.
I’ll focus on the two most common sources of data: the biannual SHM survey of hospitalist productivity and compensation (officially titled “The Authoritative Source on the State of Hospital Medicine”), and the Medical Group Management Association’s (MGMA) annual “Physician Compensation and Production Survey.” There are many other surveys that report hospitalist data such as those by the American Medical Group Association (AMGA), Sullivan & Cotter, Hay Group, and others. Each July, Modern Healthcare magazine publishes the average compensation (but no other data) reported for hospitalists and other specialties by each of these organizations and several others (but not the SHM data). It should be easy to find a copy of Modern Healthcare in your hospital administration or library, or on the Internet.
The SHM and MGMA surveys are the most widely used sources of data for hospitalists, and some of their attributes are described in Table 1 (see below).
I should acknowledge my potential conflict of interest and potential for bias in comparing these surveys. This column is in an SHM publication. I’m very active in SHM, and I’m a past chairman and ongoing member of the Benchmarks Committee, which oversees the design and analysis of the SHM survey. And while I am familiar with and regularly review the MGMA survey, I have no other connection to that organization.
Much of the difference between the surveys is a result of the SHM survey being designed specifically for hospitalists in any type of practice setting (e.g., small hospitalist-only groups, as well as hospitalists with huge organizations like a university faculty group practice). In contrast, the MGMA survey is designed for all physician specialties, so a hospitalist answers the same questions as a traditional primary care doctor, plastic surgeon, and obstetrician.
MGMA data can be adversely affected by the inclusion of primary care office-based encounters. One of the principal ways the two surveys differ is how they address ambulatory visits. The MGMA survey reports inpatient and ambulatory visits separately, but “ambulatory” visits include any for a patient who is not a hospital inpatient. By this definition, hospitalists make ambulatory visits, most commonly to hospitalized patients who are on observation status, and also patients seen in an ED, skilled nursing facility, or pre-op clinic. Thus the MGMA survey doesn’t distinguish between ambulatory encounters a hospitalist would generate in the course of serving as a hospitalist, and those generated while that doctor might be serving in a non-hospitalist role such as office-based primary care or urgent care.
The SHM survey doesn’t include—and isn’t contaminated by—office-based primary care or urgent-care visits.
Of the 3,376 total encounters reported in the MGMA survey, 40% (1,351) are ambulatory encounters. Although the SHM survey does not distinguish between hospital and ambulatory encounters, my experience suggests few, if any, hospitalist practices make 40% of their total encounters with patients on observation status, or in an ED, SNF, or pre-op clinic. Thus, many of the ambulatory encounters reported by MGMA might have been office visits, not hospital-related visits.
Additionally, the median internal medicine hospitalist encounters (ambulatory and hospital combined) in the MGMA survey (3,376) is 42% higher than the median total encounters reported for internal medicine hospitalists in SHM’s survey (2,378). Yet the wRVUs reported in the MGMA survey (3,514) are only 8% higher than those reported in the SHM survey (3,256). Thus the calculated average wRVUs per encounter for the MGMA data is only 1.04, compared with 1.37 for the SHM data. An average of 1.04 wRVUs per encounter is very low for hospitalists, when almost all current procedural terminology (CPT) codes a hospitalist uses have a value of one or more wRVUs. Again, this suggests the MGMA data may be significantly influenced by the inclusion of office-based encounters, some of which have wRVUs of less than one. SHM has approached MGMA to discuss this data definition issue in their survey.
Why It Matters
You can use whichever data set best describes your situation. The MGMA has historically shown higher hospitalist salaries and higher workloads than the SHM data. But because the SHM data is the result of a survey customized for hospitalists and less likely than the MGMA data to be contaminated by non-hospital-related visits, the SHM data probably gives a more accurate picture.
Because the MGMA survey has been conducted for many years (far longer than the SHM survey) it has appropriately become one of the most authoritative sources of data on physician compensation for all specialties. Stark II regulations require hospitals to ensure they aren’t paying physicians above the fair market compensation (which could be seen as an inducement to refer patients to the hospital, among other concerns). And it specifically states that the MGMA survey is one of several approved sources of determining what fair market compensation is.
Even though the SHM data is most likely more representative and provides an important benchmark for hospitalists, the MGMA data has “pre-approved” status and thus is potentially safer to use for the specific purpose of determinations of fair market value.
With each iteration, the SHM survey will be adjusted to more specifically capture hospitalist activity; in many cases it is the best data for hospitalists to use in planning and benchmarking. But the MGMA data are still valuable and may be the most appropriate to refer to in contracts.
Note to readers: In May, SHM contacted MGMA regarding their concerns that MGMA survey data was not representative of hospitalists. MGMA responded with a willingness to discuss these issues with SHM. As this story goes to press, SHM and MGMA continue to have a dialogue about maximizing the accuracy of survey data. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
In the Literature

Performance Measures and Outcomes for Heart Patients
Fonarow GC, Abraham WT, Albert NM, et al. Association between performance measures and clinical outcomes for patients hospitalized with heart failure. JAMA. 2007 Jan 3;297(1):61-70
As our population ages, more emphasis will be placed on issues surrounding efficient and evidence-based care. Heart failure, which accounted for 3.6 million hospitalizations in 2003 and has an overall prevalence of 5 million, will be at the forefront of public policy. As pay for performance (P4P) and standards of care become increasingly prevalent, the medical community will need to scrutinize the standards by which we are measured.
The American College of Cardiology and the American Heart Association (ACC/AHA) developed guidelines for the treatment and care of patients with heart failure. These measures include heart failure discharge instructions, evaluation of left ventricle (LV) function, angiotensin converting enzyme (ACE) inhibitors or angiotensin II receptor antagonist (ARB) for LV dysfunction, adult smoking cessation counseling, and anticoagulation at discharge for patients with atrial fibrillation. Adherence to these performance measures should be based on evidence.
The authors’ goal was to determine the validity of these guidelines. The Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) registry allowed for the documentation and follow-up of patients adhering to the heart failure guidelines as set forth by the ACC/AHA. The study assessed the relationship between these guidelines and clinical outcomes, including 60- to 90-day mortality and a composite end point of mortality or rehospitalization.
In this study the OPTIMIZE-HF registry was used as the source of prospective data collection. Ten percent of eligible patients were randomly selected from the registry between March 2003 and December 2004 from 91 hospitals. Eligibility for the OPTIMIZE-HF registry included patients 18 and older admitted for worsening heart failure or significant heart failure during their hospital stay. The performance measure of discharge instruction, smoking cessation, and anticoagulation were measured for all eligible patients. Patients with an ejection fraction of 40% or less, or moderate to severe systolic function, were included for the ACE inhibitor/ARB performance measure. One measure not included was treatment with beta-blockers at discharge. The authors included beta-blockers at discharge with metrics similar to those described for ACE/ARB criteria.
The conformity rates and process-outcome links were then determined for the performance measures and beta-blocker treatment as it related to 60- to 90-day mortality/rehospitalization.
The study focused on a random follow-up cohort of 5,791 patients from 91 hospitals. This was similar to the OPTIMIZE-HF cohort of 48,612 patients in 259 hospitals. Demographically, the average cohort’s age was 72, 51% male and 78% white, with 42% of patients diagnosed with ischemic heart disease and 43% with diabetes mellitus. These results were similar to the demographics of the overall OPTIMIZE-HF registry.
Of the eligible patients in the follow-up cohort, 66% (4,010) received complete discharge instructions. Eighty-nine percent of eligible patients (4,664) had their left ventricular function evaluated. For those patients with documented left ventricular systolic dysfunction (2,181), 83% were given an ACE inhibitor or ARB at discharge. Patients who had a diagnosis of atrial fibrillation were discharged with anticoagulation at a rate of 53%, and 72% of patients were counseled on smoking cessation. As compared with ACE inhibitors/ARB, similar results (84%) were seen for beta-blockers at discharge.
Only two of the five ACC/AHA performance measures were predictive of decreasing morbidity and mortality/rehospitalization in unadjusted analysis: patients discharged on ACE inhibitors/ARBs (odds ratio, 0.51; 95% CI 0.34–0.78; P- .002) and smoking cessation counseling. Beta-blockers, not a formal part of the ACC/AHA guidelines, were also a predictor of lower risk of both mortality and rehospitalization (odds ratio, 0.73; 95% CI, 0.55-0.96; P-0.02)
The OPTIMIZE-HF cohort analysis allowed for an opportunity to determine the degree of conformity for the ACC/AHA performance measures. The ACE inhibitors or ARB use at discharge was shown in the OPTIMIZE-HF cohort to have a relative reduction in one-year post discharge mortality by 17% (risk reduction, 0.83; 95% CI, 0.79-0.88) and a trend to lower 60- to 90-days post-discharge mortality and rehospitalization. Although smoking cessation had an early positive correlation, outcomes did not reach statistical significance. The measure of discharge instruction in the current study did not show a benefit on early mortality/rehospitalization in 60- to 90-days post discharge. It is unclear from this study if discharge instructions given to patients were either rushed or discussed in a comprehensive manner. This factor will need clarification and further research.
The measures of discharge instructions, smoking cessation, LV assessment, and anticoagulation for atrial fibrillation have not been examined as effective performance measures prior to this study. These measures were unable to show an independent decrease in 60- to 90-day mortality and rehospitalization.
Patients discharged with beta-blockers showed an association between lower mortality and rehospitalization. This association was found to be stronger than any of the formal ACC/AHA current performance measures.
The ACC/AHA guidelines are becoming standards of care for reporting to agencies such as Centers for Medicare and Medicaid Services or other P4P programs. To allow for improvement of quality, JCAHO and ACC/AHA designed the above criteria to act as a guide for the post discharge care of coronary heart failure patients. Because these criteria are the measures by which hospitals need to report, it will be necessary for data to show validity and a link between the clinical performance measures and improved outcomes.
Of the five measures stated, only ACE inhibitors/ARB at discharge was associated with a decrease in mortality/rehospitalization. Beta-blockers, currently not a performance measure, also showed this trend. Increased scrutiny needs to be part of the criteria for which hospitals and practitioners are being held accountable, and further research validating their effectiveness is warranted.
Risk Indexes for COPD
Niewoehner DE, Lockhnygina Y, Rice K, et al. Risk indexes for exacerbations and hospitalizations due to COPD. Chest. 2007 Jan;131(1):20-28.
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality in the U.S. and continues to increase its numbers annually.
The cornerstone of COPD diagnosis and key predictor of prognosis is a low level of lung function. Another important predictor of morbidity, mortality, and progression of disease is COPD exacerbations.
Unfortunately, the definition of an exacerbation is varied, ranging from an increase in symptoms to COPD-related hospitalizations and death.1 Therefore, prevention of COPD exacerbations is an important management goal. This study focuses on setting a risk model as a clinical management tool, similar to what exists for cardiovascular events or community acquired pneumonia. No previous study has attempted to identify risk factors for exacerbations using prospective data collection and a clearly stated definition of exacerbation.
The study was a parallel-group, randomized, double-blind, placebo-controlled trial in patients with moderate to severe COPD conducted at 26 Veterans Affairs medical centers in the United States. Subjects were 40 or older, with a cigarette smoking history of 10 packs a year or more, a clinical diagnosis of COPD, and a forced expiratory volume [FEV] of 60% or less predicted and 70% or less of the forced vital capacity [FVC].1 Patients were allocated to receive one capsule of tiotropium (18 mg) or placebo for six months.
Of the 1,829 patients selected, 914 were assigned to the tiotropium arm. Patients kept a daily diary, and the investigators collected data by monthly telephone interviews and by site visits at three and six months with spirometry evaluation. They evaluated the association between baseline characteristics, concomitant medications and the study drug and the time to first COPD exacerbation and the time to first hospitalization due to exacerbation. The authors defined an exacerbation as a complex of respiratory symptoms of more than one of the following: cough, sputum, wheezing, dyspnea, or chest tightness with a duration of at least three days requiring treatment with antibiotics and/or systemic corticosteroids and/or hospital admission.
The investigators found that a statistically significant greater risk for both COPD exacerbations and hospitalizations is associated with being of older age, being a noncurrent smoker, having poorer lung function, using home oxygen, visiting the clinic or emergency department more often, either scheduled or unscheduled, being hospitalized for COPD in the prior year, using either antibiotics or systemic steroids for COPD more often in the prior year, and using short-acting beta agonist, inhaled or oral corticosteroid at a baseline rate.
On the other hand, a statistically significant greater risk of only COPD exacerbation was seen in white patients, with presence of productive cough, longer duration of COPD, use of long-acting beta agonist or theophylline at baseline, and presence of any gastrointestinal or hepatobiliary disease. Lower body-mass index and the presence of cardiovascular comorbidity were associated with statistically significant greater risk for only hospitalization due to COPD.
The investigators also confirmed the previous suggestion that chronic cough is an independent predictor of exacerbation. Interestingly, they found that any cardiovascular comorbidity is a strong and independent predictor of hospitalizations due to COPD. It is unclear if cardiovascular disease truly predisposes subjects to COPD hospitalizations or merely represents a misdiagnosis because both diseases have similar symptoms.
Current smokers were identified as having lower risk of exacerbation and hospitalization, probably due to the “healthy smoker” theory—that deteriorating lung function causes the patient to quit smoking.
This study is the first to gather information about predictors of COPD exacerbations in a prospective fashion using a clear definition of exacerbation. The authors developed a model to assess the risk of COPD exacerbations and hospitalizations due to exacerbations in patients with moderate to severe COPD. Moreover, this model can easily be applied to individual patients and reproduced with simple spirometry and a series of questions.
Though this trial had a reasonable level of statistical significance, it is important to mention that the trial was conducted within a single health system (Veterans Affairs medical centers), there were few women in the study, and the eligibility criteria were very specific.
References
- Mannino DM, Watt G, Hole D, et al. The natural history of chronic obstructive pulmonary disease. Eur Respir J. 2006 Mar;27(3):627-643.
Glucose Management in Hospitalized Patients
Leahy JL. Insulin Management of diabetic patients on general medical and surgical floors. Endocr Pract. Jul/Aug 2006;12(Suppl3):86-89.
Although the rationale behind the science for tight control of blood sugar in subsets of hospitalized patient populations is without debate when it comes to the majority of general ward patients, the management of hyperglycemia becomes more of an art. Increasingly we recognize the effect of the relationship between improving glucose management and improving clinical outcomes.
Guidelines for inpatient targeted blood glucose levels exist, but hospitals are moving toward a more individualized approach to subcutaneous insulin protocols for their patients, thus moving beyond the passive sliding scale era.
Institution of an insulin protocol at one such hospital, the University of Vermont, highlights such an approach. The ongoing internal nonrandomized study exemplifies a two-tiered approach initially aimed at expanding the house physician comfort zone to change the culture of hyperglycemic management beyond simply avoiding hypoglycemia to one of an active and—per our current standards—aggressive individualized insulin protocol.
It seems the author envisions a gradual process allowing initial flexibility within the protocol, increasing the intensity of dosing as comfort zones expand. Throughout the process, the principles of determining a patient’s weight-based daily insulin needs are maintained, taking into consideration factors like comorbidities, severity of illness, amount of oral intake, steroid usage, and age. Then, the insulin regimen is physiologically (basal/bolus, basal, continuous) administered according to the route (i.e., total parenteral nutrition) and timing of their nutritional intake.
Adjustments being made to insulin regimens are based on fasting, pre-meal and bedtime glucose as well as the novel approach of bolus insulin after meals with short-acting insulin (i.e., lispro).
Unfortunately although the protocol does perhaps yield itself to being looked at more stringently—in terms of cost effectiveness, improved length of hospital stay, and improved clinical outcomes—the outcome studied here was primarily one of hospitalwide education in advancing the understanding and culture of aggressive individualized insulin protocols. These can often be even more statistically difficult to quantify. As self-reported, improvements were made.
One of the most important aspects of this paper is that it draws attention to the paucity of evidence for improved clinical and monetary outcomes supporting the aggressive hospital management of hyperglycemia in the non-acutely ill patient. Often, the guiding principle is to avoid hypoglycemia. Detailing the specific protocols of one such approach serves as an example for the motivated reader.
Early Switch from IV to Oral Antibiotic in Severe CAP
Oosterheert JJ, Bonten JM, Schneider MME, et al. Effectiveness of early switch from intravenous to oral antibiotics in severe community acquired pneumonia; multicentre randomised trial. BMJ. 2006 Dec 9; 333:1193.
Community acquired pneumonia (CAP) is a common and potentially fatal infection with high healthcare costs. When patients are first admitted to hospitals, antibiotics are usually given intravenously to provide optimal concentrations in the tissues.
The duration of intravenous treatment is an important determinant of length of hospital stay (LOS). The concept of early transition from intravenous to oral antibiotic in the treatment of CAP has been evaluated before, but only in mild to moderately severe disease—and rarely in randomized trials.
This multicenter random controlled trial from five teaching hospitals and two medical centers in the Netherlands enrolled 302 patients in non-intensive care units with severe CAP. The primary outcome was clinical cure and secondary outcome was LOS. The inclusion criteria were adults 18 or older with severe CAP; mean pneumonia severity index of IV-V, new progressive infiltrate on chest X-ray, plus at least two other criteria (cough, sputum production, rectal temperature >38o C or <36.1o C, auscultative findings consistent with pneumonia, leukocytes >109 WBC/L or >15% bands, positive cultures of blob or pleural fluids, CRP three times greater times upper limit of normal).
Exclusion criteria included the need for mechanical ventilation, cystic fibrosis, a history of colonization with gram-negative bacteria due to structural damage to the respiratory tract, malfunction of the digestive tract, life expectancy of less than one month because of underlying disease, infections other than pneumonia that needed antibiotic treatment, and severe immunosuppression (neutropenia [<0.5 109 neutrophils/liter] or a CD4 count< 200/mm3).
Treatment failure was defined as death, still in hospital at day 28 of the study, or clinical deterioration (increase in temperature after initial improvement or the need for mechanical ventilation, switch back to intravenous antibiotics, or readmission for pulmonary reinfection after discharge).
Clinical cure was defined as discharged in good health without signs and symptoms of pneumonia and no treatment failure during follow-up.
The control group comprised 150 subjects who were to receive a standard course of seven days’ intravenous treatment. Meanwhile, 152 subjects were randomized to the early switch group. Baseline characteristics were similar in both groups. More than 80% of patients were in pneumonia severity class IV or V. Most patients received empirical monotherapy with amoxicillin or amoxicillin plus clavulanic acid (n=174; 58%) or a cephalosporin (n=59; 20%), which is in line with Dutch prescribing policies.
The most frequently identified microorganism was S pneumoniae (n=76; 25%). Atypical pathogens were detected in 33 patients (11%). Before day three, 37 patients (12%) were excluded from analysis, leaving 132 patients for analysis in the intervention group and 133 in the control group.
Reasons for exclusion included when the initial diagnosis of CAP was replaced by another diagnosis (n=9), consent was withdrawn (n=11), the protocol was violated (n=4), the patient was admitted to an intensive-care unit for mechanical ventilation (n=6), and the patient died (n=7). After three days of intravenous treatment, 108 of 132 patients (81%) in the intervention group were switched to oral treatment, of whom 102 (94%) received amoxicillin plus clavulanic acid (500+125 mg every eight hours).
In the control group, five patients did not receive intravenous antibiotics for all seven days because of phlebitis associated with intravenous treatment; none of them needed treatment for line-related sepsis. Overall duration of antibiotic treatment was 10.1 days in the intervention group and 9.3 days in the control group (mean difference 0.8 days, 95% confidence interval -0.6 to 2.0).
The duration of intravenous treatment was significantly shorter in the intervention group (mean 3.6 [SD 1.5] versus 7.0 [2.0] days, mean difference 3.4, 2.8 to 3.9). Average time to meet the discharge criteria was 5.2 (2.9) days in the intervention group and 5.7 (3.1) days in the control group (0.5 days -0.3 to 1.2) Total length of hospital stay was 9.6 (5.0) and 11.5 (4.9) days for patients in the intervention group and control group (1.9 days 0.6 to 3.2).
The authors’ findings provide strong evidence that early transition from intravenous to oral antibiotic is also viable in patients with highly graded Pneumonia Severity Index (PSI) CAP, not only in mild to moderately severe disease. This leads to reduced LOS, cost, and possibly reduced risk of line infections and increased patient satisfaction for early discharge.
Note: This study was done with patients suffering straightforward, uncomplicated CAP. The investigators’ findings cannot be applied to patients with other comorbidities like diabetes, COPD, heart failure, or sickle cell, which might require more days on intravenous antibiotic. One might also wonder what impact would have been seen had 37 patients not dropped off, and if another class of oral antibiotic such as quinolones had been used.
Last, the study sample showed S pneumoniae identified in 25% of cases and atypical pathogens to be 11%. What then are the majority of pathogens identified 64% of the time? This would have been another key factor that might have had a great effect on the result.
Although a larger sampling and further risk stratification (to include patients with other comorbidities) are needed, this study makes a valid point for early transition to oral antibiotics in highly graded, uncomplicated CAP. TH
Performance Measures and Outcomes for Heart Patients
Fonarow GC, Abraham WT, Albert NM, et al. Association between performance measures and clinical outcomes for patients hospitalized with heart failure. JAMA. 2007 Jan 3;297(1):61-70
As our population ages, more emphasis will be placed on issues surrounding efficient and evidence-based care. Heart failure, which accounted for 3.6 million hospitalizations in 2003 and has an overall prevalence of 5 million, will be at the forefront of public policy. As pay for performance (P4P) and standards of care become increasingly prevalent, the medical community will need to scrutinize the standards by which we are measured.
The American College of Cardiology and the American Heart Association (ACC/AHA) developed guidelines for the treatment and care of patients with heart failure. These measures include heart failure discharge instructions, evaluation of left ventricle (LV) function, angiotensin converting enzyme (ACE) inhibitors or angiotensin II receptor antagonist (ARB) for LV dysfunction, adult smoking cessation counseling, and anticoagulation at discharge for patients with atrial fibrillation. Adherence to these performance measures should be based on evidence.
The authors’ goal was to determine the validity of these guidelines. The Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) registry allowed for the documentation and follow-up of patients adhering to the heart failure guidelines as set forth by the ACC/AHA. The study assessed the relationship between these guidelines and clinical outcomes, including 60- to 90-day mortality and a composite end point of mortality or rehospitalization.
In this study the OPTIMIZE-HF registry was used as the source of prospective data collection. Ten percent of eligible patients were randomly selected from the registry between March 2003 and December 2004 from 91 hospitals. Eligibility for the OPTIMIZE-HF registry included patients 18 and older admitted for worsening heart failure or significant heart failure during their hospital stay. The performance measure of discharge instruction, smoking cessation, and anticoagulation were measured for all eligible patients. Patients with an ejection fraction of 40% or less, or moderate to severe systolic function, were included for the ACE inhibitor/ARB performance measure. One measure not included was treatment with beta-blockers at discharge. The authors included beta-blockers at discharge with metrics similar to those described for ACE/ARB criteria.
The conformity rates and process-outcome links were then determined for the performance measures and beta-blocker treatment as it related to 60- to 90-day mortality/rehospitalization.
The study focused on a random follow-up cohort of 5,791 patients from 91 hospitals. This was similar to the OPTIMIZE-HF cohort of 48,612 patients in 259 hospitals. Demographically, the average cohort’s age was 72, 51% male and 78% white, with 42% of patients diagnosed with ischemic heart disease and 43% with diabetes mellitus. These results were similar to the demographics of the overall OPTIMIZE-HF registry.
Of the eligible patients in the follow-up cohort, 66% (4,010) received complete discharge instructions. Eighty-nine percent of eligible patients (4,664) had their left ventricular function evaluated. For those patients with documented left ventricular systolic dysfunction (2,181), 83% were given an ACE inhibitor or ARB at discharge. Patients who had a diagnosis of atrial fibrillation were discharged with anticoagulation at a rate of 53%, and 72% of patients were counseled on smoking cessation. As compared with ACE inhibitors/ARB, similar results (84%) were seen for beta-blockers at discharge.
Only two of the five ACC/AHA performance measures were predictive of decreasing morbidity and mortality/rehospitalization in unadjusted analysis: patients discharged on ACE inhibitors/ARBs (odds ratio, 0.51; 95% CI 0.34–0.78; P- .002) and smoking cessation counseling. Beta-blockers, not a formal part of the ACC/AHA guidelines, were also a predictor of lower risk of both mortality and rehospitalization (odds ratio, 0.73; 95% CI, 0.55-0.96; P-0.02)
The OPTIMIZE-HF cohort analysis allowed for an opportunity to determine the degree of conformity for the ACC/AHA performance measures. The ACE inhibitors or ARB use at discharge was shown in the OPTIMIZE-HF cohort to have a relative reduction in one-year post discharge mortality by 17% (risk reduction, 0.83; 95% CI, 0.79-0.88) and a trend to lower 60- to 90-days post-discharge mortality and rehospitalization. Although smoking cessation had an early positive correlation, outcomes did not reach statistical significance. The measure of discharge instruction in the current study did not show a benefit on early mortality/rehospitalization in 60- to 90-days post discharge. It is unclear from this study if discharge instructions given to patients were either rushed or discussed in a comprehensive manner. This factor will need clarification and further research.
The measures of discharge instructions, smoking cessation, LV assessment, and anticoagulation for atrial fibrillation have not been examined as effective performance measures prior to this study. These measures were unable to show an independent decrease in 60- to 90-day mortality and rehospitalization.
Patients discharged with beta-blockers showed an association between lower mortality and rehospitalization. This association was found to be stronger than any of the formal ACC/AHA current performance measures.
The ACC/AHA guidelines are becoming standards of care for reporting to agencies such as Centers for Medicare and Medicaid Services or other P4P programs. To allow for improvement of quality, JCAHO and ACC/AHA designed the above criteria to act as a guide for the post discharge care of coronary heart failure patients. Because these criteria are the measures by which hospitals need to report, it will be necessary for data to show validity and a link between the clinical performance measures and improved outcomes.
Of the five measures stated, only ACE inhibitors/ARB at discharge was associated with a decrease in mortality/rehospitalization. Beta-blockers, currently not a performance measure, also showed this trend. Increased scrutiny needs to be part of the criteria for which hospitals and practitioners are being held accountable, and further research validating their effectiveness is warranted.
Risk Indexes for COPD
Niewoehner DE, Lockhnygina Y, Rice K, et al. Risk indexes for exacerbations and hospitalizations due to COPD. Chest. 2007 Jan;131(1):20-28.
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality in the U.S. and continues to increase its numbers annually.
The cornerstone of COPD diagnosis and key predictor of prognosis is a low level of lung function. Another important predictor of morbidity, mortality, and progression of disease is COPD exacerbations.
Unfortunately, the definition of an exacerbation is varied, ranging from an increase in symptoms to COPD-related hospitalizations and death.1 Therefore, prevention of COPD exacerbations is an important management goal. This study focuses on setting a risk model as a clinical management tool, similar to what exists for cardiovascular events or community acquired pneumonia. No previous study has attempted to identify risk factors for exacerbations using prospective data collection and a clearly stated definition of exacerbation.
The study was a parallel-group, randomized, double-blind, placebo-controlled trial in patients with moderate to severe COPD conducted at 26 Veterans Affairs medical centers in the United States. Subjects were 40 or older, with a cigarette smoking history of 10 packs a year or more, a clinical diagnosis of COPD, and a forced expiratory volume [FEV] of 60% or less predicted and 70% or less of the forced vital capacity [FVC].1 Patients were allocated to receive one capsule of tiotropium (18 mg) or placebo for six months.
Of the 1,829 patients selected, 914 were assigned to the tiotropium arm. Patients kept a daily diary, and the investigators collected data by monthly telephone interviews and by site visits at three and six months with spirometry evaluation. They evaluated the association between baseline characteristics, concomitant medications and the study drug and the time to first COPD exacerbation and the time to first hospitalization due to exacerbation. The authors defined an exacerbation as a complex of respiratory symptoms of more than one of the following: cough, sputum, wheezing, dyspnea, or chest tightness with a duration of at least three days requiring treatment with antibiotics and/or systemic corticosteroids and/or hospital admission.
The investigators found that a statistically significant greater risk for both COPD exacerbations and hospitalizations is associated with being of older age, being a noncurrent smoker, having poorer lung function, using home oxygen, visiting the clinic or emergency department more often, either scheduled or unscheduled, being hospitalized for COPD in the prior year, using either antibiotics or systemic steroids for COPD more often in the prior year, and using short-acting beta agonist, inhaled or oral corticosteroid at a baseline rate.
On the other hand, a statistically significant greater risk of only COPD exacerbation was seen in white patients, with presence of productive cough, longer duration of COPD, use of long-acting beta agonist or theophylline at baseline, and presence of any gastrointestinal or hepatobiliary disease. Lower body-mass index and the presence of cardiovascular comorbidity were associated with statistically significant greater risk for only hospitalization due to COPD.
The investigators also confirmed the previous suggestion that chronic cough is an independent predictor of exacerbation. Interestingly, they found that any cardiovascular comorbidity is a strong and independent predictor of hospitalizations due to COPD. It is unclear if cardiovascular disease truly predisposes subjects to COPD hospitalizations or merely represents a misdiagnosis because both diseases have similar symptoms.
Current smokers were identified as having lower risk of exacerbation and hospitalization, probably due to the “healthy smoker” theory—that deteriorating lung function causes the patient to quit smoking.
This study is the first to gather information about predictors of COPD exacerbations in a prospective fashion using a clear definition of exacerbation. The authors developed a model to assess the risk of COPD exacerbations and hospitalizations due to exacerbations in patients with moderate to severe COPD. Moreover, this model can easily be applied to individual patients and reproduced with simple spirometry and a series of questions.
Though this trial had a reasonable level of statistical significance, it is important to mention that the trial was conducted within a single health system (Veterans Affairs medical centers), there were few women in the study, and the eligibility criteria were very specific.
References
- Mannino DM, Watt G, Hole D, et al. The natural history of chronic obstructive pulmonary disease. Eur Respir J. 2006 Mar;27(3):627-643.
Glucose Management in Hospitalized Patients
Leahy JL. Insulin Management of diabetic patients on general medical and surgical floors. Endocr Pract. Jul/Aug 2006;12(Suppl3):86-89.
Although the rationale behind the science for tight control of blood sugar in subsets of hospitalized patient populations is without debate when it comes to the majority of general ward patients, the management of hyperglycemia becomes more of an art. Increasingly we recognize the effect of the relationship between improving glucose management and improving clinical outcomes.
Guidelines for inpatient targeted blood glucose levels exist, but hospitals are moving toward a more individualized approach to subcutaneous insulin protocols for their patients, thus moving beyond the passive sliding scale era.
Institution of an insulin protocol at one such hospital, the University of Vermont, highlights such an approach. The ongoing internal nonrandomized study exemplifies a two-tiered approach initially aimed at expanding the house physician comfort zone to change the culture of hyperglycemic management beyond simply avoiding hypoglycemia to one of an active and—per our current standards—aggressive individualized insulin protocol.
It seems the author envisions a gradual process allowing initial flexibility within the protocol, increasing the intensity of dosing as comfort zones expand. Throughout the process, the principles of determining a patient’s weight-based daily insulin needs are maintained, taking into consideration factors like comorbidities, severity of illness, amount of oral intake, steroid usage, and age. Then, the insulin regimen is physiologically (basal/bolus, basal, continuous) administered according to the route (i.e., total parenteral nutrition) and timing of their nutritional intake.
Adjustments being made to insulin regimens are based on fasting, pre-meal and bedtime glucose as well as the novel approach of bolus insulin after meals with short-acting insulin (i.e., lispro).
Unfortunately although the protocol does perhaps yield itself to being looked at more stringently—in terms of cost effectiveness, improved length of hospital stay, and improved clinical outcomes—the outcome studied here was primarily one of hospitalwide education in advancing the understanding and culture of aggressive individualized insulin protocols. These can often be even more statistically difficult to quantify. As self-reported, improvements were made.
One of the most important aspects of this paper is that it draws attention to the paucity of evidence for improved clinical and monetary outcomes supporting the aggressive hospital management of hyperglycemia in the non-acutely ill patient. Often, the guiding principle is to avoid hypoglycemia. Detailing the specific protocols of one such approach serves as an example for the motivated reader.
Early Switch from IV to Oral Antibiotic in Severe CAP
Oosterheert JJ, Bonten JM, Schneider MME, et al. Effectiveness of early switch from intravenous to oral antibiotics in severe community acquired pneumonia; multicentre randomised trial. BMJ. 2006 Dec 9; 333:1193.
Community acquired pneumonia (CAP) is a common and potentially fatal infection with high healthcare costs. When patients are first admitted to hospitals, antibiotics are usually given intravenously to provide optimal concentrations in the tissues.
The duration of intravenous treatment is an important determinant of length of hospital stay (LOS). The concept of early transition from intravenous to oral antibiotic in the treatment of CAP has been evaluated before, but only in mild to moderately severe disease—and rarely in randomized trials.
This multicenter random controlled trial from five teaching hospitals and two medical centers in the Netherlands enrolled 302 patients in non-intensive care units with severe CAP. The primary outcome was clinical cure and secondary outcome was LOS. The inclusion criteria were adults 18 or older with severe CAP; mean pneumonia severity index of IV-V, new progressive infiltrate on chest X-ray, plus at least two other criteria (cough, sputum production, rectal temperature >38o C or <36.1o C, auscultative findings consistent with pneumonia, leukocytes >109 WBC/L or >15% bands, positive cultures of blob or pleural fluids, CRP three times greater times upper limit of normal).
Exclusion criteria included the need for mechanical ventilation, cystic fibrosis, a history of colonization with gram-negative bacteria due to structural damage to the respiratory tract, malfunction of the digestive tract, life expectancy of less than one month because of underlying disease, infections other than pneumonia that needed antibiotic treatment, and severe immunosuppression (neutropenia [<0.5 109 neutrophils/liter] or a CD4 count< 200/mm3).
Treatment failure was defined as death, still in hospital at day 28 of the study, or clinical deterioration (increase in temperature after initial improvement or the need for mechanical ventilation, switch back to intravenous antibiotics, or readmission for pulmonary reinfection after discharge).
Clinical cure was defined as discharged in good health without signs and symptoms of pneumonia and no treatment failure during follow-up.
The control group comprised 150 subjects who were to receive a standard course of seven days’ intravenous treatment. Meanwhile, 152 subjects were randomized to the early switch group. Baseline characteristics were similar in both groups. More than 80% of patients were in pneumonia severity class IV or V. Most patients received empirical monotherapy with amoxicillin or amoxicillin plus clavulanic acid (n=174; 58%) or a cephalosporin (n=59; 20%), which is in line with Dutch prescribing policies.
The most frequently identified microorganism was S pneumoniae (n=76; 25%). Atypical pathogens were detected in 33 patients (11%). Before day three, 37 patients (12%) were excluded from analysis, leaving 132 patients for analysis in the intervention group and 133 in the control group.
Reasons for exclusion included when the initial diagnosis of CAP was replaced by another diagnosis (n=9), consent was withdrawn (n=11), the protocol was violated (n=4), the patient was admitted to an intensive-care unit for mechanical ventilation (n=6), and the patient died (n=7). After three days of intravenous treatment, 108 of 132 patients (81%) in the intervention group were switched to oral treatment, of whom 102 (94%) received amoxicillin plus clavulanic acid (500+125 mg every eight hours).
In the control group, five patients did not receive intravenous antibiotics for all seven days because of phlebitis associated with intravenous treatment; none of them needed treatment for line-related sepsis. Overall duration of antibiotic treatment was 10.1 days in the intervention group and 9.3 days in the control group (mean difference 0.8 days, 95% confidence interval -0.6 to 2.0).
The duration of intravenous treatment was significantly shorter in the intervention group (mean 3.6 [SD 1.5] versus 7.0 [2.0] days, mean difference 3.4, 2.8 to 3.9). Average time to meet the discharge criteria was 5.2 (2.9) days in the intervention group and 5.7 (3.1) days in the control group (0.5 days -0.3 to 1.2) Total length of hospital stay was 9.6 (5.0) and 11.5 (4.9) days for patients in the intervention group and control group (1.9 days 0.6 to 3.2).
The authors’ findings provide strong evidence that early transition from intravenous to oral antibiotic is also viable in patients with highly graded Pneumonia Severity Index (PSI) CAP, not only in mild to moderately severe disease. This leads to reduced LOS, cost, and possibly reduced risk of line infections and increased patient satisfaction for early discharge.
Note: This study was done with patients suffering straightforward, uncomplicated CAP. The investigators’ findings cannot be applied to patients with other comorbidities like diabetes, COPD, heart failure, or sickle cell, which might require more days on intravenous antibiotic. One might also wonder what impact would have been seen had 37 patients not dropped off, and if another class of oral antibiotic such as quinolones had been used.
Last, the study sample showed S pneumoniae identified in 25% of cases and atypical pathogens to be 11%. What then are the majority of pathogens identified 64% of the time? This would have been another key factor that might have had a great effect on the result.
Although a larger sampling and further risk stratification (to include patients with other comorbidities) are needed, this study makes a valid point for early transition to oral antibiotics in highly graded, uncomplicated CAP. TH
Performance Measures and Outcomes for Heart Patients
Fonarow GC, Abraham WT, Albert NM, et al. Association between performance measures and clinical outcomes for patients hospitalized with heart failure. JAMA. 2007 Jan 3;297(1):61-70
As our population ages, more emphasis will be placed on issues surrounding efficient and evidence-based care. Heart failure, which accounted for 3.6 million hospitalizations in 2003 and has an overall prevalence of 5 million, will be at the forefront of public policy. As pay for performance (P4P) and standards of care become increasingly prevalent, the medical community will need to scrutinize the standards by which we are measured.
The American College of Cardiology and the American Heart Association (ACC/AHA) developed guidelines for the treatment and care of patients with heart failure. These measures include heart failure discharge instructions, evaluation of left ventricle (LV) function, angiotensin converting enzyme (ACE) inhibitors or angiotensin II receptor antagonist (ARB) for LV dysfunction, adult smoking cessation counseling, and anticoagulation at discharge for patients with atrial fibrillation. Adherence to these performance measures should be based on evidence.
The authors’ goal was to determine the validity of these guidelines. The Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) registry allowed for the documentation and follow-up of patients adhering to the heart failure guidelines as set forth by the ACC/AHA. The study assessed the relationship between these guidelines and clinical outcomes, including 60- to 90-day mortality and a composite end point of mortality or rehospitalization.
In this study the OPTIMIZE-HF registry was used as the source of prospective data collection. Ten percent of eligible patients were randomly selected from the registry between March 2003 and December 2004 from 91 hospitals. Eligibility for the OPTIMIZE-HF registry included patients 18 and older admitted for worsening heart failure or significant heart failure during their hospital stay. The performance measure of discharge instruction, smoking cessation, and anticoagulation were measured for all eligible patients. Patients with an ejection fraction of 40% or less, or moderate to severe systolic function, were included for the ACE inhibitor/ARB performance measure. One measure not included was treatment with beta-blockers at discharge. The authors included beta-blockers at discharge with metrics similar to those described for ACE/ARB criteria.
The conformity rates and process-outcome links were then determined for the performance measures and beta-blocker treatment as it related to 60- to 90-day mortality/rehospitalization.
The study focused on a random follow-up cohort of 5,791 patients from 91 hospitals. This was similar to the OPTIMIZE-HF cohort of 48,612 patients in 259 hospitals. Demographically, the average cohort’s age was 72, 51% male and 78% white, with 42% of patients diagnosed with ischemic heart disease and 43% with diabetes mellitus. These results were similar to the demographics of the overall OPTIMIZE-HF registry.
Of the eligible patients in the follow-up cohort, 66% (4,010) received complete discharge instructions. Eighty-nine percent of eligible patients (4,664) had their left ventricular function evaluated. For those patients with documented left ventricular systolic dysfunction (2,181), 83% were given an ACE inhibitor or ARB at discharge. Patients who had a diagnosis of atrial fibrillation were discharged with anticoagulation at a rate of 53%, and 72% of patients were counseled on smoking cessation. As compared with ACE inhibitors/ARB, similar results (84%) were seen for beta-blockers at discharge.
Only two of the five ACC/AHA performance measures were predictive of decreasing morbidity and mortality/rehospitalization in unadjusted analysis: patients discharged on ACE inhibitors/ARBs (odds ratio, 0.51; 95% CI 0.34–0.78; P- .002) and smoking cessation counseling. Beta-blockers, not a formal part of the ACC/AHA guidelines, were also a predictor of lower risk of both mortality and rehospitalization (odds ratio, 0.73; 95% CI, 0.55-0.96; P-0.02)
The OPTIMIZE-HF cohort analysis allowed for an opportunity to determine the degree of conformity for the ACC/AHA performance measures. The ACE inhibitors or ARB use at discharge was shown in the OPTIMIZE-HF cohort to have a relative reduction in one-year post discharge mortality by 17% (risk reduction, 0.83; 95% CI, 0.79-0.88) and a trend to lower 60- to 90-days post-discharge mortality and rehospitalization. Although smoking cessation had an early positive correlation, outcomes did not reach statistical significance. The measure of discharge instruction in the current study did not show a benefit on early mortality/rehospitalization in 60- to 90-days post discharge. It is unclear from this study if discharge instructions given to patients were either rushed or discussed in a comprehensive manner. This factor will need clarification and further research.
The measures of discharge instructions, smoking cessation, LV assessment, and anticoagulation for atrial fibrillation have not been examined as effective performance measures prior to this study. These measures were unable to show an independent decrease in 60- to 90-day mortality and rehospitalization.
Patients discharged with beta-blockers showed an association between lower mortality and rehospitalization. This association was found to be stronger than any of the formal ACC/AHA current performance measures.
The ACC/AHA guidelines are becoming standards of care for reporting to agencies such as Centers for Medicare and Medicaid Services or other P4P programs. To allow for improvement of quality, JCAHO and ACC/AHA designed the above criteria to act as a guide for the post discharge care of coronary heart failure patients. Because these criteria are the measures by which hospitals need to report, it will be necessary for data to show validity and a link between the clinical performance measures and improved outcomes.
Of the five measures stated, only ACE inhibitors/ARB at discharge was associated with a decrease in mortality/rehospitalization. Beta-blockers, currently not a performance measure, also showed this trend. Increased scrutiny needs to be part of the criteria for which hospitals and practitioners are being held accountable, and further research validating their effectiveness is warranted.
Risk Indexes for COPD
Niewoehner DE, Lockhnygina Y, Rice K, et al. Risk indexes for exacerbations and hospitalizations due to COPD. Chest. 2007 Jan;131(1):20-28.
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality in the U.S. and continues to increase its numbers annually.
The cornerstone of COPD diagnosis and key predictor of prognosis is a low level of lung function. Another important predictor of morbidity, mortality, and progression of disease is COPD exacerbations.
Unfortunately, the definition of an exacerbation is varied, ranging from an increase in symptoms to COPD-related hospitalizations and death.1 Therefore, prevention of COPD exacerbations is an important management goal. This study focuses on setting a risk model as a clinical management tool, similar to what exists for cardiovascular events or community acquired pneumonia. No previous study has attempted to identify risk factors for exacerbations using prospective data collection and a clearly stated definition of exacerbation.
The study was a parallel-group, randomized, double-blind, placebo-controlled trial in patients with moderate to severe COPD conducted at 26 Veterans Affairs medical centers in the United States. Subjects were 40 or older, with a cigarette smoking history of 10 packs a year or more, a clinical diagnosis of COPD, and a forced expiratory volume [FEV] of 60% or less predicted and 70% or less of the forced vital capacity [FVC].1 Patients were allocated to receive one capsule of tiotropium (18 mg) or placebo for six months.
Of the 1,829 patients selected, 914 were assigned to the tiotropium arm. Patients kept a daily diary, and the investigators collected data by monthly telephone interviews and by site visits at three and six months with spirometry evaluation. They evaluated the association between baseline characteristics, concomitant medications and the study drug and the time to first COPD exacerbation and the time to first hospitalization due to exacerbation. The authors defined an exacerbation as a complex of respiratory symptoms of more than one of the following: cough, sputum, wheezing, dyspnea, or chest tightness with a duration of at least three days requiring treatment with antibiotics and/or systemic corticosteroids and/or hospital admission.
The investigators found that a statistically significant greater risk for both COPD exacerbations and hospitalizations is associated with being of older age, being a noncurrent smoker, having poorer lung function, using home oxygen, visiting the clinic or emergency department more often, either scheduled or unscheduled, being hospitalized for COPD in the prior year, using either antibiotics or systemic steroids for COPD more often in the prior year, and using short-acting beta agonist, inhaled or oral corticosteroid at a baseline rate.
On the other hand, a statistically significant greater risk of only COPD exacerbation was seen in white patients, with presence of productive cough, longer duration of COPD, use of long-acting beta agonist or theophylline at baseline, and presence of any gastrointestinal or hepatobiliary disease. Lower body-mass index and the presence of cardiovascular comorbidity were associated with statistically significant greater risk for only hospitalization due to COPD.
The investigators also confirmed the previous suggestion that chronic cough is an independent predictor of exacerbation. Interestingly, they found that any cardiovascular comorbidity is a strong and independent predictor of hospitalizations due to COPD. It is unclear if cardiovascular disease truly predisposes subjects to COPD hospitalizations or merely represents a misdiagnosis because both diseases have similar symptoms.
Current smokers were identified as having lower risk of exacerbation and hospitalization, probably due to the “healthy smoker” theory—that deteriorating lung function causes the patient to quit smoking.
This study is the first to gather information about predictors of COPD exacerbations in a prospective fashion using a clear definition of exacerbation. The authors developed a model to assess the risk of COPD exacerbations and hospitalizations due to exacerbations in patients with moderate to severe COPD. Moreover, this model can easily be applied to individual patients and reproduced with simple spirometry and a series of questions.
Though this trial had a reasonable level of statistical significance, it is important to mention that the trial was conducted within a single health system (Veterans Affairs medical centers), there were few women in the study, and the eligibility criteria were very specific.
References
- Mannino DM, Watt G, Hole D, et al. The natural history of chronic obstructive pulmonary disease. Eur Respir J. 2006 Mar;27(3):627-643.
Glucose Management in Hospitalized Patients
Leahy JL. Insulin Management of diabetic patients on general medical and surgical floors. Endocr Pract. Jul/Aug 2006;12(Suppl3):86-89.
Although the rationale behind the science for tight control of blood sugar in subsets of hospitalized patient populations is without debate when it comes to the majority of general ward patients, the management of hyperglycemia becomes more of an art. Increasingly we recognize the effect of the relationship between improving glucose management and improving clinical outcomes.
Guidelines for inpatient targeted blood glucose levels exist, but hospitals are moving toward a more individualized approach to subcutaneous insulin protocols for their patients, thus moving beyond the passive sliding scale era.
Institution of an insulin protocol at one such hospital, the University of Vermont, highlights such an approach. The ongoing internal nonrandomized study exemplifies a two-tiered approach initially aimed at expanding the house physician comfort zone to change the culture of hyperglycemic management beyond simply avoiding hypoglycemia to one of an active and—per our current standards—aggressive individualized insulin protocol.
It seems the author envisions a gradual process allowing initial flexibility within the protocol, increasing the intensity of dosing as comfort zones expand. Throughout the process, the principles of determining a patient’s weight-based daily insulin needs are maintained, taking into consideration factors like comorbidities, severity of illness, amount of oral intake, steroid usage, and age. Then, the insulin regimen is physiologically (basal/bolus, basal, continuous) administered according to the route (i.e., total parenteral nutrition) and timing of their nutritional intake.
Adjustments being made to insulin regimens are based on fasting, pre-meal and bedtime glucose as well as the novel approach of bolus insulin after meals with short-acting insulin (i.e., lispro).
Unfortunately although the protocol does perhaps yield itself to being looked at more stringently—in terms of cost effectiveness, improved length of hospital stay, and improved clinical outcomes—the outcome studied here was primarily one of hospitalwide education in advancing the understanding and culture of aggressive individualized insulin protocols. These can often be even more statistically difficult to quantify. As self-reported, improvements were made.
One of the most important aspects of this paper is that it draws attention to the paucity of evidence for improved clinical and monetary outcomes supporting the aggressive hospital management of hyperglycemia in the non-acutely ill patient. Often, the guiding principle is to avoid hypoglycemia. Detailing the specific protocols of one such approach serves as an example for the motivated reader.
Early Switch from IV to Oral Antibiotic in Severe CAP
Oosterheert JJ, Bonten JM, Schneider MME, et al. Effectiveness of early switch from intravenous to oral antibiotics in severe community acquired pneumonia; multicentre randomised trial. BMJ. 2006 Dec 9; 333:1193.
Community acquired pneumonia (CAP) is a common and potentially fatal infection with high healthcare costs. When patients are first admitted to hospitals, antibiotics are usually given intravenously to provide optimal concentrations in the tissues.
The duration of intravenous treatment is an important determinant of length of hospital stay (LOS). The concept of early transition from intravenous to oral antibiotic in the treatment of CAP has been evaluated before, but only in mild to moderately severe disease—and rarely in randomized trials.
This multicenter random controlled trial from five teaching hospitals and two medical centers in the Netherlands enrolled 302 patients in non-intensive care units with severe CAP. The primary outcome was clinical cure and secondary outcome was LOS. The inclusion criteria were adults 18 or older with severe CAP; mean pneumonia severity index of IV-V, new progressive infiltrate on chest X-ray, plus at least two other criteria (cough, sputum production, rectal temperature >38o C or <36.1o C, auscultative findings consistent with pneumonia, leukocytes >109 WBC/L or >15% bands, positive cultures of blob or pleural fluids, CRP three times greater times upper limit of normal).
Exclusion criteria included the need for mechanical ventilation, cystic fibrosis, a history of colonization with gram-negative bacteria due to structural damage to the respiratory tract, malfunction of the digestive tract, life expectancy of less than one month because of underlying disease, infections other than pneumonia that needed antibiotic treatment, and severe immunosuppression (neutropenia [<0.5 109 neutrophils/liter] or a CD4 count< 200/mm3).
Treatment failure was defined as death, still in hospital at day 28 of the study, or clinical deterioration (increase in temperature after initial improvement or the need for mechanical ventilation, switch back to intravenous antibiotics, or readmission for pulmonary reinfection after discharge).
Clinical cure was defined as discharged in good health without signs and symptoms of pneumonia and no treatment failure during follow-up.
The control group comprised 150 subjects who were to receive a standard course of seven days’ intravenous treatment. Meanwhile, 152 subjects were randomized to the early switch group. Baseline characteristics were similar in both groups. More than 80% of patients were in pneumonia severity class IV or V. Most patients received empirical monotherapy with amoxicillin or amoxicillin plus clavulanic acid (n=174; 58%) or a cephalosporin (n=59; 20%), which is in line with Dutch prescribing policies.
The most frequently identified microorganism was S pneumoniae (n=76; 25%). Atypical pathogens were detected in 33 patients (11%). Before day three, 37 patients (12%) were excluded from analysis, leaving 132 patients for analysis in the intervention group and 133 in the control group.
Reasons for exclusion included when the initial diagnosis of CAP was replaced by another diagnosis (n=9), consent was withdrawn (n=11), the protocol was violated (n=4), the patient was admitted to an intensive-care unit for mechanical ventilation (n=6), and the patient died (n=7). After three days of intravenous treatment, 108 of 132 patients (81%) in the intervention group were switched to oral treatment, of whom 102 (94%) received amoxicillin plus clavulanic acid (500+125 mg every eight hours).
In the control group, five patients did not receive intravenous antibiotics for all seven days because of phlebitis associated with intravenous treatment; none of them needed treatment for line-related sepsis. Overall duration of antibiotic treatment was 10.1 days in the intervention group and 9.3 days in the control group (mean difference 0.8 days, 95% confidence interval -0.6 to 2.0).
The duration of intravenous treatment was significantly shorter in the intervention group (mean 3.6 [SD 1.5] versus 7.0 [2.0] days, mean difference 3.4, 2.8 to 3.9). Average time to meet the discharge criteria was 5.2 (2.9) days in the intervention group and 5.7 (3.1) days in the control group (0.5 days -0.3 to 1.2) Total length of hospital stay was 9.6 (5.0) and 11.5 (4.9) days for patients in the intervention group and control group (1.9 days 0.6 to 3.2).
The authors’ findings provide strong evidence that early transition from intravenous to oral antibiotic is also viable in patients with highly graded Pneumonia Severity Index (PSI) CAP, not only in mild to moderately severe disease. This leads to reduced LOS, cost, and possibly reduced risk of line infections and increased patient satisfaction for early discharge.
Note: This study was done with patients suffering straightforward, uncomplicated CAP. The investigators’ findings cannot be applied to patients with other comorbidities like diabetes, COPD, heart failure, or sickle cell, which might require more days on intravenous antibiotic. One might also wonder what impact would have been seen had 37 patients not dropped off, and if another class of oral antibiotic such as quinolones had been used.
Last, the study sample showed S pneumoniae identified in 25% of cases and atypical pathogens to be 11%. What then are the majority of pathogens identified 64% of the time? This would have been another key factor that might have had a great effect on the result.
Although a larger sampling and further risk stratification (to include patients with other comorbidities) are needed, this study makes a valid point for early transition to oral antibiotics in highly graded, uncomplicated CAP. TH
Heal the Whole Hurt
Note: This is Part 3 of The Hospitalist’s series on pain and hospital medicine. Part 1 appeared on p. 45 of the April issue, and Part 2 appeared on p. 33 of the June issue.
Hospitalists face demands for pain care every day. Usually, the general pain principles described in the first two articles in this series and the use of a few opioid analgesics with which the hospitalist has become familiar can supply relief.
But what about the more difficult cases in which psychosocial influences or a history of substance abuse complicates the patient’s pain? Perhaps it is a chronic pain case that has never been adequately addressed, or the patient keeps turning up in the emergency department (ED) complaining of out-of-control pain. Other examples of difficult-to-manage pain include complex regional pain syndrome, post-herpetic neuralgia, other neuropathic pains, sickle cell anemia, and patients at high risk of opioid toxicity.
These cases are like a leaky bucket for the hospital—costly, frustrating, unsatisfying to the patient, and prone to bad outcomes, says Jerry Wesch, PhD, director of the pain service for the Alexian Brothers Health System in greater Chicago. “These are the patients who tend to bedevil everybody in the hospital,” he says.
Dealing with such patients is a demanding task.
“You don’t have chronic pain without a psycho-social-spiritual overlay,” adds Scott Fishman, MD, chief of the Division of Pain Medicine at University of California-Davis in Sacramento. “Their emotional lives are deteriorating. They can’t sleep, they’re depressed, and their physical functioning is also deteriorating. There are all kinds of situations that demand use of a full spectrum of bio-psycho-social interventions in addition to opioid analgesics.”
These complex, unresolved cases are likely to have emotional, social, or spiritual manifestations. But what does that mean to a busy hospitalist with a short window of opportunity to address patients’ pain before pointing them toward discharge? A psychologist, social worker, or chaplain may have something to contribute to pain management. Meanwhile, the rest of the caseload is clamoring for the hospitalist’s attention.
Make Pain Management Multidisciplinary
A dizzying array of pain modalities can be brought to bear on complex pain cases. These range from opioid analgesics to a variety of adjuvant non-opioid medications to interventional techniques involving surgery, spinal injections, nerve blocks, nerve stimulation, and nerve destruction techniques.
There are also complementary methodologies (e.g., acupuncture) that have been shown to reduce the volume of narcotics needed for pain control, even though how they work is not well understood.
But how many hospitalists call on acupuncturists, hypnotists, or teachers of guided-imagery meditation for their patients? Many of these techniques are more appropriately initiated in the outpatient setting, but the hospitalist still has a responsibility to make sure “frequent fliers” with complex pain complaints get connected post-discharge to a pain service that can offer long-term relief. The challenge is applying the acute treatment models of the hospital to chronic pain syndromes that are not optimally addressed in crisis mode.
Jonathan Weston, MD, a hospitalist at Penrose Hospital in Colorado Springs, Colo., says these difficult, chronic pain cases are the bane of the hospitalist’s working life. These patients show up at night in the ED saying, “ ‘I’m in so much pain, please don’t send me home,’ ” he says. “The emergency physician puts them on an IV drip and their pain is relieved for the moment, but only one facet of that pain has been addressed.”
The emergency physician—also under caseload pressure— decides the easiest disposition is to admit the patient and dump the problem on the hospitalist. “They’re out of their pain medications at home, and when you call the attending you are told that they are drug seekers,” Dr. Weston relates. “These patients take a lot of energy. They can be manipulative. We can’t do right for them. It’s not satisfying. We don’t want to round on them. The way we hospitalists manage these patients sometimes reflects not only the patient’s personality, but our personality as well.”
Hospitalists don’t just treat these patients’ pain, they also address their suffering, he says.
High-quality pain management is multidisciplinary, Dr. Weston notes, because pain is multifactorial. The hospitalist occupies an important coordinating position and is charged with responsibility for the whole person during that patient’s brief hospital stay. But there are limits to what the hospitalist can accomplish. A palliative care team or an acute pain service can make important contributions to hospitalized patients’ pain. So can social workers, psychologists, pharmacists, and chaplains. But it is the hospitalist’s responsibility to coordinate these pieces of the pain puzzle for patients on service.
In many hospitals, the palliative care service has been set up to consult on pain, suffering, and clarification of treatment goals for patients nearing the end of life. These services vary from institution to institution in terms of whether they prefer to focus on end-of-life issues or are comfortable fielding other kinds of chronic pain questions. Acute pain services equally vary in terms of whether their focus is primarily on surgical pain “interventions” or on a multidisciplinary approach to pain management.
Ideally, Dr. Weston says, a major hospital would have both services available as resources to the hospitalist. Or, if there is only one of them, it should have a broad approach to pain management. Otherwise, it is up to the hospitalist to pull together a virtual pain team to provide a multidisciplinary response to complex pain.
“I am also board certified in hospice and palliative medicine,” Dr. Weston says. “I can use my medical knowledge to try to get the patient comfortable on oral meds so that they can go home. And I can personally make an appointment for them within 48 hours of discharge with their attending physician or a pain specialist. But for too many patients, this connection never happens.”
“Pain management in general is a hard thing to deal with,” adds Lauren Fraser, MD, regional chief of the department of hospital medicine for Kaiser Permanente Colorado in Denver. “It’s frustrating because you want to do the right thing,” she says. “We need first of all to rule out anything we can fix that might be causing the pain. Then we’re dealing with the patient’s quality of life and the disabling effects of pain. Each patient and family has a different need, and when you meet with them one-on-one you’re dealing with all of it.”
Dr. Fraser doesn’t have access to an acute pain service in her current setting, “although we have interventional folks to put in the PCAs and epidurals. We generally are able to get the services we need, although there would be an advantage to having an identified multidisciplinary pain service to provide the coordination.”
A “Pain Hospitalist”
Jerry Wesch, director of the pain program at Alexian Brothers Hospital Network in Arlington Heights, Ill., recently posted a job listing on the Internet seeking a pain management physician. He is looking for a doctor with an interest in comprehensive, interdisciplinary team management of chronic pain who is “able to function as a pain hospitalist.”
Although the details of this new position are still being finalized and a pain hospitalist would function with a different focus than a generalist hospitalist, Wesch suggests the role has important analogies with what hospitalists like Dr. Weston face in coordinating a virtual team of multidisciplinary pain resources.
Wesch is building an inpatient pain service comprising the pain physician, two nurse practitioners, and a part-time psychologist with full-time presence in two Alexian Brothers acute hospitals. This team would work closely with hospitalists, the palliative care service, and ancillary services such as physical therapy and chaplains.
“This should make us ideal collaborators with the hospitalists, who can just walk down the hall and initiate a pain consult,” he explains. “We’re all working toward the same goal, which is to improve efficiency, medical management, quality of care, and patient satisfaction. A good hospitalist is also my best ally in building a multidisciplinary pain service.”
In other settings, however, it will be the hospitalist’s responsibility to build the relationships that bring these pain resources together.
Deb Gordon, RN, MS, FAAN, senior clinical nurse specialist at the University of Wisconsin Medical Center in Madison, also sees herself functioning like a hospitalist in addressing pain issues. “I manage a clinical pain consultation service. I see patients every day,” she says. “I’m also in staff development, helping professionals in the hospital learn to manage pain better, and using quality improvement techniques to take what we know about pain management to support people like hospitalists at the bedside.”
Since 1990, an interdisciplinary quality improvement pain management group has been meeting at the UW medical center to improve the institution’s response to pain patients. Gordon believes pain is a natural target for hospital quality-improvement activities because it touches on the domains of quality identified by groups such as the Institute of Medicine in Washington, D.C., and the Institute for Healthcare Improvement in Cambridge, Mass.
Limits in the Hospital Setting
Even with a vast array of pain modalities, hospitalists face inherent limitations in addressing pain challenges within the hospital, starting with caseload pressures and short lengths of stay. Many of the approaches that might offer long-term solutions to the patient’s chronic pain syndrome belong in the outpatient setting, adds John Massey, MD, president and medical director of Nebraska Pain Consultants in Lincoln.
Dr. Massey sees chronic pain cases that have been refractory to treatment, both at his clinic and as a consultant in the hospital. Inevitably there is a psychological overlay to these cases, he says. That doesn’t mean the patient’s pain isn’t real, but if high doses of analgesics have failed to bring the pain under control, then a different approach is needed—one that includes behavioral techniques and involves the patient not as a passive recipient of treatment, but an active participant in his or her own pain management and coping strategies.
“There are ways to treat, for example, back pain that require finding a specific nerve in the spine responsible for the pain,” says Dr. Massey. “If I can locate that nerve, there are things that I can do, like radio frequency neuro-ablation. But this requires three separate visits to the pain clinic to make an accurate diagnosis. I’m often consulted by hospitalists and there are things I can do to put a finger in the dike. But I try to add another perspective to my discussion with the hospitalist, pointing out that many of the best pain management modalities are done on an outpatient basis.”
What can be achieved in the hospital often is more of a Band-Aid, sometimes even a step backward in terms of the lifestyle changes necessary to get patients out of their passive response to their chronic pain, Dr. Massey says.
The hospitalist’s job is to see what can be done to make patients more comfortable and then send them home with a referral to the pain service, if that is indicated. “I’m happy to help with an intervention in the hospital but, ultimately, we’d like the patient to be less dependent on opioids to treat their pain,” says Dr. Massey. “I know that nothing I can do will really change the situation until I get them out of the hospital and can initiate physical therapy and behavioral interventions.”
There are no shortcuts to permanent pain relief, which can be long, slow, hard work using evidence-based medicine, Dr. Massey says. But it also involves a frank discussion with the patient, which may be hard in the hospital.
“One of the questions we ask patients is: How many times have you visited the emergency room for pain?” says Dr. Massey. “If the answer is more than four in a year, there are likely to be psychological co-morbidities. The challenge for the hospitalist is, ‘How can I arrest this acute pain episode, and then what can I contribute to helping the patient find the help he or she needs to prevent the next episode?’ That means trying to establish rapport and pointing the person to appropriate follow-up pain resources. If you go too hard too fast, the patient may reject what you’re offering. But if you do nothing, you’re facilitating a continued passive approach that doesn’t lead to meaningful solutions.”
Dr. Massey recently saw a woman who had been in the ED 48 times in the previous year for pain that had a major behavioral component. The hospital hired him after the 48th visit to find a different approach to controlling the patient’s pain.
Make Pain a Priority
“My hospitalist group meets regularly to discuss difficult topics, and pain often comes up,” says Stephen Bekanich, MD, hospitalist and palliative care physician at the University of Utah Medical Center in Salt Lake City. “The more you can focus on pain, the more time you spend making it a priority, you are sending a message: This is important to me. You communicate to nurses and other staff that you take pain seriously.”
Dr. Fishman concurs. “Ultimately, it is an issue of priorities and how to prioritize what gets done in the hospital,” he says. “Why would a health professional ever categorize pain relief as a lower priority? We have wandered far from our compassionate mission as doctors when that happens.
“In the real world, when there is no one else to do it, and no pain clinics available, the responsibility for pain management falls on the provider at the front lines, often the emergency physician and the hospitalist. Hospitalists are becoming de facto pain specialists for patients with chronic and terminal conditions. These patients are looking for support, comfort, and redirection. This can also be one of the most rewarding aspects of hospital practice. It really brings you back to the roots of medicine.” TH
Larry Beresford is a regular contributor to The Hospitalist.
Note: This is Part 3 of The Hospitalist’s series on pain and hospital medicine. Part 1 appeared on p. 45 of the April issue, and Part 2 appeared on p. 33 of the June issue.
Hospitalists face demands for pain care every day. Usually, the general pain principles described in the first two articles in this series and the use of a few opioid analgesics with which the hospitalist has become familiar can supply relief.
But what about the more difficult cases in which psychosocial influences or a history of substance abuse complicates the patient’s pain? Perhaps it is a chronic pain case that has never been adequately addressed, or the patient keeps turning up in the emergency department (ED) complaining of out-of-control pain. Other examples of difficult-to-manage pain include complex regional pain syndrome, post-herpetic neuralgia, other neuropathic pains, sickle cell anemia, and patients at high risk of opioid toxicity.
These cases are like a leaky bucket for the hospital—costly, frustrating, unsatisfying to the patient, and prone to bad outcomes, says Jerry Wesch, PhD, director of the pain service for the Alexian Brothers Health System in greater Chicago. “These are the patients who tend to bedevil everybody in the hospital,” he says.
Dealing with such patients is a demanding task.
“You don’t have chronic pain without a psycho-social-spiritual overlay,” adds Scott Fishman, MD, chief of the Division of Pain Medicine at University of California-Davis in Sacramento. “Their emotional lives are deteriorating. They can’t sleep, they’re depressed, and their physical functioning is also deteriorating. There are all kinds of situations that demand use of a full spectrum of bio-psycho-social interventions in addition to opioid analgesics.”
These complex, unresolved cases are likely to have emotional, social, or spiritual manifestations. But what does that mean to a busy hospitalist with a short window of opportunity to address patients’ pain before pointing them toward discharge? A psychologist, social worker, or chaplain may have something to contribute to pain management. Meanwhile, the rest of the caseload is clamoring for the hospitalist’s attention.
Make Pain Management Multidisciplinary
A dizzying array of pain modalities can be brought to bear on complex pain cases. These range from opioid analgesics to a variety of adjuvant non-opioid medications to interventional techniques involving surgery, spinal injections, nerve blocks, nerve stimulation, and nerve destruction techniques.
There are also complementary methodologies (e.g., acupuncture) that have been shown to reduce the volume of narcotics needed for pain control, even though how they work is not well understood.
But how many hospitalists call on acupuncturists, hypnotists, or teachers of guided-imagery meditation for their patients? Many of these techniques are more appropriately initiated in the outpatient setting, but the hospitalist still has a responsibility to make sure “frequent fliers” with complex pain complaints get connected post-discharge to a pain service that can offer long-term relief. The challenge is applying the acute treatment models of the hospital to chronic pain syndromes that are not optimally addressed in crisis mode.
Jonathan Weston, MD, a hospitalist at Penrose Hospital in Colorado Springs, Colo., says these difficult, chronic pain cases are the bane of the hospitalist’s working life. These patients show up at night in the ED saying, “ ‘I’m in so much pain, please don’t send me home,’ ” he says. “The emergency physician puts them on an IV drip and their pain is relieved for the moment, but only one facet of that pain has been addressed.”
The emergency physician—also under caseload pressure— decides the easiest disposition is to admit the patient and dump the problem on the hospitalist. “They’re out of their pain medications at home, and when you call the attending you are told that they are drug seekers,” Dr. Weston relates. “These patients take a lot of energy. They can be manipulative. We can’t do right for them. It’s not satisfying. We don’t want to round on them. The way we hospitalists manage these patients sometimes reflects not only the patient’s personality, but our personality as well.”
Hospitalists don’t just treat these patients’ pain, they also address their suffering, he says.
High-quality pain management is multidisciplinary, Dr. Weston notes, because pain is multifactorial. The hospitalist occupies an important coordinating position and is charged with responsibility for the whole person during that patient’s brief hospital stay. But there are limits to what the hospitalist can accomplish. A palliative care team or an acute pain service can make important contributions to hospitalized patients’ pain. So can social workers, psychologists, pharmacists, and chaplains. But it is the hospitalist’s responsibility to coordinate these pieces of the pain puzzle for patients on service.
In many hospitals, the palliative care service has been set up to consult on pain, suffering, and clarification of treatment goals for patients nearing the end of life. These services vary from institution to institution in terms of whether they prefer to focus on end-of-life issues or are comfortable fielding other kinds of chronic pain questions. Acute pain services equally vary in terms of whether their focus is primarily on surgical pain “interventions” or on a multidisciplinary approach to pain management.
Ideally, Dr. Weston says, a major hospital would have both services available as resources to the hospitalist. Or, if there is only one of them, it should have a broad approach to pain management. Otherwise, it is up to the hospitalist to pull together a virtual pain team to provide a multidisciplinary response to complex pain.
“I am also board certified in hospice and palliative medicine,” Dr. Weston says. “I can use my medical knowledge to try to get the patient comfortable on oral meds so that they can go home. And I can personally make an appointment for them within 48 hours of discharge with their attending physician or a pain specialist. But for too many patients, this connection never happens.”
“Pain management in general is a hard thing to deal with,” adds Lauren Fraser, MD, regional chief of the department of hospital medicine for Kaiser Permanente Colorado in Denver. “It’s frustrating because you want to do the right thing,” she says. “We need first of all to rule out anything we can fix that might be causing the pain. Then we’re dealing with the patient’s quality of life and the disabling effects of pain. Each patient and family has a different need, and when you meet with them one-on-one you’re dealing with all of it.”
Dr. Fraser doesn’t have access to an acute pain service in her current setting, “although we have interventional folks to put in the PCAs and epidurals. We generally are able to get the services we need, although there would be an advantage to having an identified multidisciplinary pain service to provide the coordination.”
A “Pain Hospitalist”
Jerry Wesch, director of the pain program at Alexian Brothers Hospital Network in Arlington Heights, Ill., recently posted a job listing on the Internet seeking a pain management physician. He is looking for a doctor with an interest in comprehensive, interdisciplinary team management of chronic pain who is “able to function as a pain hospitalist.”
Although the details of this new position are still being finalized and a pain hospitalist would function with a different focus than a generalist hospitalist, Wesch suggests the role has important analogies with what hospitalists like Dr. Weston face in coordinating a virtual team of multidisciplinary pain resources.
Wesch is building an inpatient pain service comprising the pain physician, two nurse practitioners, and a part-time psychologist with full-time presence in two Alexian Brothers acute hospitals. This team would work closely with hospitalists, the palliative care service, and ancillary services such as physical therapy and chaplains.
“This should make us ideal collaborators with the hospitalists, who can just walk down the hall and initiate a pain consult,” he explains. “We’re all working toward the same goal, which is to improve efficiency, medical management, quality of care, and patient satisfaction. A good hospitalist is also my best ally in building a multidisciplinary pain service.”
In other settings, however, it will be the hospitalist’s responsibility to build the relationships that bring these pain resources together.
Deb Gordon, RN, MS, FAAN, senior clinical nurse specialist at the University of Wisconsin Medical Center in Madison, also sees herself functioning like a hospitalist in addressing pain issues. “I manage a clinical pain consultation service. I see patients every day,” she says. “I’m also in staff development, helping professionals in the hospital learn to manage pain better, and using quality improvement techniques to take what we know about pain management to support people like hospitalists at the bedside.”
Since 1990, an interdisciplinary quality improvement pain management group has been meeting at the UW medical center to improve the institution’s response to pain patients. Gordon believes pain is a natural target for hospital quality-improvement activities because it touches on the domains of quality identified by groups such as the Institute of Medicine in Washington, D.C., and the Institute for Healthcare Improvement in Cambridge, Mass.
Limits in the Hospital Setting
Even with a vast array of pain modalities, hospitalists face inherent limitations in addressing pain challenges within the hospital, starting with caseload pressures and short lengths of stay. Many of the approaches that might offer long-term solutions to the patient’s chronic pain syndrome belong in the outpatient setting, adds John Massey, MD, president and medical director of Nebraska Pain Consultants in Lincoln.
Dr. Massey sees chronic pain cases that have been refractory to treatment, both at his clinic and as a consultant in the hospital. Inevitably there is a psychological overlay to these cases, he says. That doesn’t mean the patient’s pain isn’t real, but if high doses of analgesics have failed to bring the pain under control, then a different approach is needed—one that includes behavioral techniques and involves the patient not as a passive recipient of treatment, but an active participant in his or her own pain management and coping strategies.
“There are ways to treat, for example, back pain that require finding a specific nerve in the spine responsible for the pain,” says Dr. Massey. “If I can locate that nerve, there are things that I can do, like radio frequency neuro-ablation. But this requires three separate visits to the pain clinic to make an accurate diagnosis. I’m often consulted by hospitalists and there are things I can do to put a finger in the dike. But I try to add another perspective to my discussion with the hospitalist, pointing out that many of the best pain management modalities are done on an outpatient basis.”
What can be achieved in the hospital often is more of a Band-Aid, sometimes even a step backward in terms of the lifestyle changes necessary to get patients out of their passive response to their chronic pain, Dr. Massey says.
The hospitalist’s job is to see what can be done to make patients more comfortable and then send them home with a referral to the pain service, if that is indicated. “I’m happy to help with an intervention in the hospital but, ultimately, we’d like the patient to be less dependent on opioids to treat their pain,” says Dr. Massey. “I know that nothing I can do will really change the situation until I get them out of the hospital and can initiate physical therapy and behavioral interventions.”
There are no shortcuts to permanent pain relief, which can be long, slow, hard work using evidence-based medicine, Dr. Massey says. But it also involves a frank discussion with the patient, which may be hard in the hospital.
“One of the questions we ask patients is: How many times have you visited the emergency room for pain?” says Dr. Massey. “If the answer is more than four in a year, there are likely to be psychological co-morbidities. The challenge for the hospitalist is, ‘How can I arrest this acute pain episode, and then what can I contribute to helping the patient find the help he or she needs to prevent the next episode?’ That means trying to establish rapport and pointing the person to appropriate follow-up pain resources. If you go too hard too fast, the patient may reject what you’re offering. But if you do nothing, you’re facilitating a continued passive approach that doesn’t lead to meaningful solutions.”
Dr. Massey recently saw a woman who had been in the ED 48 times in the previous year for pain that had a major behavioral component. The hospital hired him after the 48th visit to find a different approach to controlling the patient’s pain.
Make Pain a Priority
“My hospitalist group meets regularly to discuss difficult topics, and pain often comes up,” says Stephen Bekanich, MD, hospitalist and palliative care physician at the University of Utah Medical Center in Salt Lake City. “The more you can focus on pain, the more time you spend making it a priority, you are sending a message: This is important to me. You communicate to nurses and other staff that you take pain seriously.”
Dr. Fishman concurs. “Ultimately, it is an issue of priorities and how to prioritize what gets done in the hospital,” he says. “Why would a health professional ever categorize pain relief as a lower priority? We have wandered far from our compassionate mission as doctors when that happens.
“In the real world, when there is no one else to do it, and no pain clinics available, the responsibility for pain management falls on the provider at the front lines, often the emergency physician and the hospitalist. Hospitalists are becoming de facto pain specialists for patients with chronic and terminal conditions. These patients are looking for support, comfort, and redirection. This can also be one of the most rewarding aspects of hospital practice. It really brings you back to the roots of medicine.” TH
Larry Beresford is a regular contributor to The Hospitalist.
Note: This is Part 3 of The Hospitalist’s series on pain and hospital medicine. Part 1 appeared on p. 45 of the April issue, and Part 2 appeared on p. 33 of the June issue.
Hospitalists face demands for pain care every day. Usually, the general pain principles described in the first two articles in this series and the use of a few opioid analgesics with which the hospitalist has become familiar can supply relief.
But what about the more difficult cases in which psychosocial influences or a history of substance abuse complicates the patient’s pain? Perhaps it is a chronic pain case that has never been adequately addressed, or the patient keeps turning up in the emergency department (ED) complaining of out-of-control pain. Other examples of difficult-to-manage pain include complex regional pain syndrome, post-herpetic neuralgia, other neuropathic pains, sickle cell anemia, and patients at high risk of opioid toxicity.
These cases are like a leaky bucket for the hospital—costly, frustrating, unsatisfying to the patient, and prone to bad outcomes, says Jerry Wesch, PhD, director of the pain service for the Alexian Brothers Health System in greater Chicago. “These are the patients who tend to bedevil everybody in the hospital,” he says.
Dealing with such patients is a demanding task.
“You don’t have chronic pain without a psycho-social-spiritual overlay,” adds Scott Fishman, MD, chief of the Division of Pain Medicine at University of California-Davis in Sacramento. “Their emotional lives are deteriorating. They can’t sleep, they’re depressed, and their physical functioning is also deteriorating. There are all kinds of situations that demand use of a full spectrum of bio-psycho-social interventions in addition to opioid analgesics.”
These complex, unresolved cases are likely to have emotional, social, or spiritual manifestations. But what does that mean to a busy hospitalist with a short window of opportunity to address patients’ pain before pointing them toward discharge? A psychologist, social worker, or chaplain may have something to contribute to pain management. Meanwhile, the rest of the caseload is clamoring for the hospitalist’s attention.
Make Pain Management Multidisciplinary
A dizzying array of pain modalities can be brought to bear on complex pain cases. These range from opioid analgesics to a variety of adjuvant non-opioid medications to interventional techniques involving surgery, spinal injections, nerve blocks, nerve stimulation, and nerve destruction techniques.
There are also complementary methodologies (e.g., acupuncture) that have been shown to reduce the volume of narcotics needed for pain control, even though how they work is not well understood.
But how many hospitalists call on acupuncturists, hypnotists, or teachers of guided-imagery meditation for their patients? Many of these techniques are more appropriately initiated in the outpatient setting, but the hospitalist still has a responsibility to make sure “frequent fliers” with complex pain complaints get connected post-discharge to a pain service that can offer long-term relief. The challenge is applying the acute treatment models of the hospital to chronic pain syndromes that are not optimally addressed in crisis mode.
Jonathan Weston, MD, a hospitalist at Penrose Hospital in Colorado Springs, Colo., says these difficult, chronic pain cases are the bane of the hospitalist’s working life. These patients show up at night in the ED saying, “ ‘I’m in so much pain, please don’t send me home,’ ” he says. “The emergency physician puts them on an IV drip and their pain is relieved for the moment, but only one facet of that pain has been addressed.”
The emergency physician—also under caseload pressure— decides the easiest disposition is to admit the patient and dump the problem on the hospitalist. “They’re out of their pain medications at home, and when you call the attending you are told that they are drug seekers,” Dr. Weston relates. “These patients take a lot of energy. They can be manipulative. We can’t do right for them. It’s not satisfying. We don’t want to round on them. The way we hospitalists manage these patients sometimes reflects not only the patient’s personality, but our personality as well.”
Hospitalists don’t just treat these patients’ pain, they also address their suffering, he says.
High-quality pain management is multidisciplinary, Dr. Weston notes, because pain is multifactorial. The hospitalist occupies an important coordinating position and is charged with responsibility for the whole person during that patient’s brief hospital stay. But there are limits to what the hospitalist can accomplish. A palliative care team or an acute pain service can make important contributions to hospitalized patients’ pain. So can social workers, psychologists, pharmacists, and chaplains. But it is the hospitalist’s responsibility to coordinate these pieces of the pain puzzle for patients on service.
In many hospitals, the palliative care service has been set up to consult on pain, suffering, and clarification of treatment goals for patients nearing the end of life. These services vary from institution to institution in terms of whether they prefer to focus on end-of-life issues or are comfortable fielding other kinds of chronic pain questions. Acute pain services equally vary in terms of whether their focus is primarily on surgical pain “interventions” or on a multidisciplinary approach to pain management.
Ideally, Dr. Weston says, a major hospital would have both services available as resources to the hospitalist. Or, if there is only one of them, it should have a broad approach to pain management. Otherwise, it is up to the hospitalist to pull together a virtual pain team to provide a multidisciplinary response to complex pain.
“I am also board certified in hospice and palliative medicine,” Dr. Weston says. “I can use my medical knowledge to try to get the patient comfortable on oral meds so that they can go home. And I can personally make an appointment for them within 48 hours of discharge with their attending physician or a pain specialist. But for too many patients, this connection never happens.”
“Pain management in general is a hard thing to deal with,” adds Lauren Fraser, MD, regional chief of the department of hospital medicine for Kaiser Permanente Colorado in Denver. “It’s frustrating because you want to do the right thing,” she says. “We need first of all to rule out anything we can fix that might be causing the pain. Then we’re dealing with the patient’s quality of life and the disabling effects of pain. Each patient and family has a different need, and when you meet with them one-on-one you’re dealing with all of it.”
Dr. Fraser doesn’t have access to an acute pain service in her current setting, “although we have interventional folks to put in the PCAs and epidurals. We generally are able to get the services we need, although there would be an advantage to having an identified multidisciplinary pain service to provide the coordination.”
A “Pain Hospitalist”
Jerry Wesch, director of the pain program at Alexian Brothers Hospital Network in Arlington Heights, Ill., recently posted a job listing on the Internet seeking a pain management physician. He is looking for a doctor with an interest in comprehensive, interdisciplinary team management of chronic pain who is “able to function as a pain hospitalist.”
Although the details of this new position are still being finalized and a pain hospitalist would function with a different focus than a generalist hospitalist, Wesch suggests the role has important analogies with what hospitalists like Dr. Weston face in coordinating a virtual team of multidisciplinary pain resources.
Wesch is building an inpatient pain service comprising the pain physician, two nurse practitioners, and a part-time psychologist with full-time presence in two Alexian Brothers acute hospitals. This team would work closely with hospitalists, the palliative care service, and ancillary services such as physical therapy and chaplains.
“This should make us ideal collaborators with the hospitalists, who can just walk down the hall and initiate a pain consult,” he explains. “We’re all working toward the same goal, which is to improve efficiency, medical management, quality of care, and patient satisfaction. A good hospitalist is also my best ally in building a multidisciplinary pain service.”
In other settings, however, it will be the hospitalist’s responsibility to build the relationships that bring these pain resources together.
Deb Gordon, RN, MS, FAAN, senior clinical nurse specialist at the University of Wisconsin Medical Center in Madison, also sees herself functioning like a hospitalist in addressing pain issues. “I manage a clinical pain consultation service. I see patients every day,” she says. “I’m also in staff development, helping professionals in the hospital learn to manage pain better, and using quality improvement techniques to take what we know about pain management to support people like hospitalists at the bedside.”
Since 1990, an interdisciplinary quality improvement pain management group has been meeting at the UW medical center to improve the institution’s response to pain patients. Gordon believes pain is a natural target for hospital quality-improvement activities because it touches on the domains of quality identified by groups such as the Institute of Medicine in Washington, D.C., and the Institute for Healthcare Improvement in Cambridge, Mass.
Limits in the Hospital Setting
Even with a vast array of pain modalities, hospitalists face inherent limitations in addressing pain challenges within the hospital, starting with caseload pressures and short lengths of stay. Many of the approaches that might offer long-term solutions to the patient’s chronic pain syndrome belong in the outpatient setting, adds John Massey, MD, president and medical director of Nebraska Pain Consultants in Lincoln.
Dr. Massey sees chronic pain cases that have been refractory to treatment, both at his clinic and as a consultant in the hospital. Inevitably there is a psychological overlay to these cases, he says. That doesn’t mean the patient’s pain isn’t real, but if high doses of analgesics have failed to bring the pain under control, then a different approach is needed—one that includes behavioral techniques and involves the patient not as a passive recipient of treatment, but an active participant in his or her own pain management and coping strategies.
“There are ways to treat, for example, back pain that require finding a specific nerve in the spine responsible for the pain,” says Dr. Massey. “If I can locate that nerve, there are things that I can do, like radio frequency neuro-ablation. But this requires three separate visits to the pain clinic to make an accurate diagnosis. I’m often consulted by hospitalists and there are things I can do to put a finger in the dike. But I try to add another perspective to my discussion with the hospitalist, pointing out that many of the best pain management modalities are done on an outpatient basis.”
What can be achieved in the hospital often is more of a Band-Aid, sometimes even a step backward in terms of the lifestyle changes necessary to get patients out of their passive response to their chronic pain, Dr. Massey says.
The hospitalist’s job is to see what can be done to make patients more comfortable and then send them home with a referral to the pain service, if that is indicated. “I’m happy to help with an intervention in the hospital but, ultimately, we’d like the patient to be less dependent on opioids to treat their pain,” says Dr. Massey. “I know that nothing I can do will really change the situation until I get them out of the hospital and can initiate physical therapy and behavioral interventions.”
There are no shortcuts to permanent pain relief, which can be long, slow, hard work using evidence-based medicine, Dr. Massey says. But it also involves a frank discussion with the patient, which may be hard in the hospital.
“One of the questions we ask patients is: How many times have you visited the emergency room for pain?” says Dr. Massey. “If the answer is more than four in a year, there are likely to be psychological co-morbidities. The challenge for the hospitalist is, ‘How can I arrest this acute pain episode, and then what can I contribute to helping the patient find the help he or she needs to prevent the next episode?’ That means trying to establish rapport and pointing the person to appropriate follow-up pain resources. If you go too hard too fast, the patient may reject what you’re offering. But if you do nothing, you’re facilitating a continued passive approach that doesn’t lead to meaningful solutions.”
Dr. Massey recently saw a woman who had been in the ED 48 times in the previous year for pain that had a major behavioral component. The hospital hired him after the 48th visit to find a different approach to controlling the patient’s pain.
Make Pain a Priority
“My hospitalist group meets regularly to discuss difficult topics, and pain often comes up,” says Stephen Bekanich, MD, hospitalist and palliative care physician at the University of Utah Medical Center in Salt Lake City. “The more you can focus on pain, the more time you spend making it a priority, you are sending a message: This is important to me. You communicate to nurses and other staff that you take pain seriously.”
Dr. Fishman concurs. “Ultimately, it is an issue of priorities and how to prioritize what gets done in the hospital,” he says. “Why would a health professional ever categorize pain relief as a lower priority? We have wandered far from our compassionate mission as doctors when that happens.
“In the real world, when there is no one else to do it, and no pain clinics available, the responsibility for pain management falls on the provider at the front lines, often the emergency physician and the hospitalist. Hospitalists are becoming de facto pain specialists for patients with chronic and terminal conditions. These patients are looking for support, comfort, and redirection. This can also be one of the most rewarding aspects of hospital practice. It really brings you back to the roots of medicine.” TH
Larry Beresford is a regular contributor to The Hospitalist.
Pray With Me
Early in his career, hospitalist Richard Bailey, MD, encountered a widow from the inner city with no family. She was blind, and had been weakened and debilitated by a very challenging hospital course with many iatrogenic complications. “I was first struck, walking into her room,” recalls Dr. Bailey, “that she had a Bible on the table next to her bed. While making conversation, I mentioned this and instinctively asked her if she needed someone to read it to her. She smiled, and asked if I would oblige. I closed the door, sat down, and read her some of her favorite passages. This went on for several days until I went off service.”
Now medical director of Inpatient Care and Hospitalist Services at Saint Clare’s Hospital, a Catholic hospital in Wausau, Wis., Dr. Bailey says he is not an overtly religious person and that his spiritual life is rather private. “But I do like to have that depth of connection with my patients,” he says.
So if a patient or a family member asks him to pray with them, Dr. Bailey does so. “I cannot separate my humanness, which includes spirituality, from my work,” he explains.
When faced with serious or life-threatening medical conditions, patients and their family members are more likely to invoke their faith to cope with the attendant anxieties.
William D. Atchley Jr., MD, medical director of the Division of Hospital Medicine for Sentara Medical Group in Hampton, Va., believes that joining his patients in prayer, when asked, “helps develop a better relationship with the family and patient.”
Many Americans tend to “live in the here and now,” notes Carol R. Taylor, RN, MSN, PhD, director of the Center for Clinical Bioethics at Georgetown University. “They usually do not ask the bigger questions so long as life is good. But when life as we know it is threatened by illness, the bigger questions can become very important: ‘Is there anything beyond the here and now? And if so, where do I stand in relation to that God or higher power?’ ”
Prayer is a common response when patients face perilous medical situations.
“The vast majority of patients who are feeling imperiled due to a severe diagnosis or potential mortality is going to be praying,” says Stephen G. Post, PhD, professor and associate director for educational programs, department of bioethics at Case Western Reserve University, Cleveland. “In a way, you can’t get away from those requests.”
Are hospitalists and their institutions fully equipped to respond to the spiritual aspect of caregiving? Some researchers note that biomedicine often regards faith and spiritual world views as relevant only when they obstruct implementation of scientifically sound medical care.1 Studies have also shown healthcare professionals are less likely than their patients to actively practice a religion.
“There’s very often a mismatch between patients and families who would value that intervention and our comfort in being able to be responsive,” says Dr. Taylor, who is also an assistant professor of nursing.
Dr. Taylor and other bioethicists increasingly urge medical practitioners to include spiritual needs when they take a patient’s history. Timely referrals to chaplaincy services, knowledge of the dominant faiths and ethnic traditions in their hospitals’ catchment areas, and improvement of interpersonal skills can allow hospitalists to compassionately and ethically address their patients’ spiritual concerns.
Need to Do a Better Job
The holistic view of medicine defines health as a multidimensional construct that includes the physical, emotional, and social aspects of the patient. This view should be matched with a holistic approach to healthcare delivery that encompasses patients’ subjective illness experience, says Dr. Post.
Dr. Taylor concedes that the medical community’s recognition of patients’ spiritual needs is growing. And yet, she says, practitioners are not held accountable for delivering spiritual care, “which I think is a failing of healthcare as it is practiced today.”
Many reports have indicated patients are unhappy with the low referral rates to pastoral clinical care, adds Dr. Post.2
Assessment Essential
Incorporate a spiritual-needs assessment when taking each patient’s history upon admittance, the two bioethicists agree. This assessment usually takes the form of questions such as:
- What is your source of strength?
- Is spirituality/religion important to you? (If the patient answers “yes,” proceed to the next question.)
- How would you like us to facilitate your needs?
- Would you like a referral to pastoral care?
Once patients indicate they would like to speak with a chaplain, referral to appropriate clergy trained in pastoral care is essential.
“All physicians need to be respectful of these kinds of appeals,” says Dr. Post. “But they should feel free to make a referral to those who are, in fact, competently trained to deal with this specific area of life.”
While opposed to professional separatism, Dr. Post does argue for keeping “friendly, knee-high white fences” between physicians and pastoral counselors to maintain professional boundaries.3
Marc B. Westle, DO, FACP, president and managing partner of Asheville Hospitalist Group, PA, in North Carolina, agrees with this approach. “As a professional, I completely respect and empathize with the patient’s and the family’s spiritual needs as part of the total care of the patient,” he says. “Just as in other areas where I may not have expertise, I refer to our in-house professionals. We have an excellent chaplaincy service that we involve all the time, on a routine basis.” He says the chaplaincy service at Mission Hospital is in-house 24/7, just as the hospitalists are, and make rounds as the physicians do.
Availability of trained clergy differs from institution to institution, notes Dr. Taylor. She recently visited a metropolitan research institution where the two staff chaplains estimate there are nearly 1,000 daily patient contacts. With this many patients flowing through the facility, the chaplains rely on medical staff to triage patients’ and families’ needs so they can be referred to families who will benefit most from their help. In busy urban hospitals, pastoral coverage may not always be available, and the burden of addressing spiritual requests can fall to the hospital medicine team.
The Comfort Zone
The question of whether to pray with a patient or family member depends on the physician’s comfort with doing so.
- Rule No. 1 when it comes to the question of prayer with/for a patient or family: Clinicians should never proselytize or initiate the prayer. This can constitute a serious breach of professional boundaries.4
- Balancing the need to support patients’ emotional needs while respecting one’s integrity can be difficult. If a physician feels comfortable, it is appropriate to pray with a patient. Or, a physician can offer to sit quietly while a patient prays. If uncomfortable with this scenario, offering to keep the patient in your thoughts is one way to still be supportive while maintaining the integrity of your beliefs.3
“I think most physicians try to be very sensitive to these matters,” says Dr. Post.
Dr. Westle notes he has provided more companionate care (“hugging family and patients, sitting and talking about the good old days”) than spiritual guidance.
“Some patients and families feel supported simply by their doctor or nurse joining in a moment of silence or even holding hands during a spoken prayer,” adds Dr. Taylor. “Some of us are better than others at identifying and responding to spiritual needs. But I do think it’s a shared responsibility. The more people we can engage in identifying and responding to spiritual needs, the better patient, family, and medical team will be served. Hospitalists are in an excellent position to identify those needs because of their everyday contact. And if they simply make the right referrals, they’ve done a really good job.” TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Barnes LL, Plotnikoff GA, Fox K, et al. Spirituality, religion, and pediatrics: intersecting worlds of healing. Pediatrics 2000 Oct;106(4 Suppl):899-908.
- Post SG, Puchalski CM, Larson DB. Physicians and Patient Spirituality: Professional Boundaries, Competency, and Ethics. Ann Intern Med. 2000 April 4;132(7):578-583. Comment in: Ann Intern Med. 2000 Dec 5;133(11):920-1; Ann Intern Med. 2000 Nov 7;133(9):748-9.
- Kwiatkowski K, Arnold B, Barnard D. Physicians and Prayer Requests. Fast Fact and Concept #120. Available at www.eperc.mcw.edu/fastFact/ff_120.htm. Last accessed April 5, 2007.
- Taylor C, Lillis C, LeMone P. Fundamentals of Nursing: The Art and Science of Nursing Care, 5th ed. 2005. Philadelphia: Lippincott, Williams & Wilkins; 2005.
Early in his career, hospitalist Richard Bailey, MD, encountered a widow from the inner city with no family. She was blind, and had been weakened and debilitated by a very challenging hospital course with many iatrogenic complications. “I was first struck, walking into her room,” recalls Dr. Bailey, “that she had a Bible on the table next to her bed. While making conversation, I mentioned this and instinctively asked her if she needed someone to read it to her. She smiled, and asked if I would oblige. I closed the door, sat down, and read her some of her favorite passages. This went on for several days until I went off service.”
Now medical director of Inpatient Care and Hospitalist Services at Saint Clare’s Hospital, a Catholic hospital in Wausau, Wis., Dr. Bailey says he is not an overtly religious person and that his spiritual life is rather private. “But I do like to have that depth of connection with my patients,” he says.
So if a patient or a family member asks him to pray with them, Dr. Bailey does so. “I cannot separate my humanness, which includes spirituality, from my work,” he explains.
When faced with serious or life-threatening medical conditions, patients and their family members are more likely to invoke their faith to cope with the attendant anxieties.
William D. Atchley Jr., MD, medical director of the Division of Hospital Medicine for Sentara Medical Group in Hampton, Va., believes that joining his patients in prayer, when asked, “helps develop a better relationship with the family and patient.”
Many Americans tend to “live in the here and now,” notes Carol R. Taylor, RN, MSN, PhD, director of the Center for Clinical Bioethics at Georgetown University. “They usually do not ask the bigger questions so long as life is good. But when life as we know it is threatened by illness, the bigger questions can become very important: ‘Is there anything beyond the here and now? And if so, where do I stand in relation to that God or higher power?’ ”
Prayer is a common response when patients face perilous medical situations.
“The vast majority of patients who are feeling imperiled due to a severe diagnosis or potential mortality is going to be praying,” says Stephen G. Post, PhD, professor and associate director for educational programs, department of bioethics at Case Western Reserve University, Cleveland. “In a way, you can’t get away from those requests.”
Are hospitalists and their institutions fully equipped to respond to the spiritual aspect of caregiving? Some researchers note that biomedicine often regards faith and spiritual world views as relevant only when they obstruct implementation of scientifically sound medical care.1 Studies have also shown healthcare professionals are less likely than their patients to actively practice a religion.
“There’s very often a mismatch between patients and families who would value that intervention and our comfort in being able to be responsive,” says Dr. Taylor, who is also an assistant professor of nursing.
Dr. Taylor and other bioethicists increasingly urge medical practitioners to include spiritual needs when they take a patient’s history. Timely referrals to chaplaincy services, knowledge of the dominant faiths and ethnic traditions in their hospitals’ catchment areas, and improvement of interpersonal skills can allow hospitalists to compassionately and ethically address their patients’ spiritual concerns.
Need to Do a Better Job
The holistic view of medicine defines health as a multidimensional construct that includes the physical, emotional, and social aspects of the patient. This view should be matched with a holistic approach to healthcare delivery that encompasses patients’ subjective illness experience, says Dr. Post.
Dr. Taylor concedes that the medical community’s recognition of patients’ spiritual needs is growing. And yet, she says, practitioners are not held accountable for delivering spiritual care, “which I think is a failing of healthcare as it is practiced today.”
Many reports have indicated patients are unhappy with the low referral rates to pastoral clinical care, adds Dr. Post.2
Assessment Essential
Incorporate a spiritual-needs assessment when taking each patient’s history upon admittance, the two bioethicists agree. This assessment usually takes the form of questions such as:
- What is your source of strength?
- Is spirituality/religion important to you? (If the patient answers “yes,” proceed to the next question.)
- How would you like us to facilitate your needs?
- Would you like a referral to pastoral care?
Once patients indicate they would like to speak with a chaplain, referral to appropriate clergy trained in pastoral care is essential.
“All physicians need to be respectful of these kinds of appeals,” says Dr. Post. “But they should feel free to make a referral to those who are, in fact, competently trained to deal with this specific area of life.”
While opposed to professional separatism, Dr. Post does argue for keeping “friendly, knee-high white fences” between physicians and pastoral counselors to maintain professional boundaries.3
Marc B. Westle, DO, FACP, president and managing partner of Asheville Hospitalist Group, PA, in North Carolina, agrees with this approach. “As a professional, I completely respect and empathize with the patient’s and the family’s spiritual needs as part of the total care of the patient,” he says. “Just as in other areas where I may not have expertise, I refer to our in-house professionals. We have an excellent chaplaincy service that we involve all the time, on a routine basis.” He says the chaplaincy service at Mission Hospital is in-house 24/7, just as the hospitalists are, and make rounds as the physicians do.
Availability of trained clergy differs from institution to institution, notes Dr. Taylor. She recently visited a metropolitan research institution where the two staff chaplains estimate there are nearly 1,000 daily patient contacts. With this many patients flowing through the facility, the chaplains rely on medical staff to triage patients’ and families’ needs so they can be referred to families who will benefit most from their help. In busy urban hospitals, pastoral coverage may not always be available, and the burden of addressing spiritual requests can fall to the hospital medicine team.
The Comfort Zone
The question of whether to pray with a patient or family member depends on the physician’s comfort with doing so.
- Rule No. 1 when it comes to the question of prayer with/for a patient or family: Clinicians should never proselytize or initiate the prayer. This can constitute a serious breach of professional boundaries.4
- Balancing the need to support patients’ emotional needs while respecting one’s integrity can be difficult. If a physician feels comfortable, it is appropriate to pray with a patient. Or, a physician can offer to sit quietly while a patient prays. If uncomfortable with this scenario, offering to keep the patient in your thoughts is one way to still be supportive while maintaining the integrity of your beliefs.3
“I think most physicians try to be very sensitive to these matters,” says Dr. Post.
Dr. Westle notes he has provided more companionate care (“hugging family and patients, sitting and talking about the good old days”) than spiritual guidance.
“Some patients and families feel supported simply by their doctor or nurse joining in a moment of silence or even holding hands during a spoken prayer,” adds Dr. Taylor. “Some of us are better than others at identifying and responding to spiritual needs. But I do think it’s a shared responsibility. The more people we can engage in identifying and responding to spiritual needs, the better patient, family, and medical team will be served. Hospitalists are in an excellent position to identify those needs because of their everyday contact. And if they simply make the right referrals, they’ve done a really good job.” TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Barnes LL, Plotnikoff GA, Fox K, et al. Spirituality, religion, and pediatrics: intersecting worlds of healing. Pediatrics 2000 Oct;106(4 Suppl):899-908.
- Post SG, Puchalski CM, Larson DB. Physicians and Patient Spirituality: Professional Boundaries, Competency, and Ethics. Ann Intern Med. 2000 April 4;132(7):578-583. Comment in: Ann Intern Med. 2000 Dec 5;133(11):920-1; Ann Intern Med. 2000 Nov 7;133(9):748-9.
- Kwiatkowski K, Arnold B, Barnard D. Physicians and Prayer Requests. Fast Fact and Concept #120. Available at www.eperc.mcw.edu/fastFact/ff_120.htm. Last accessed April 5, 2007.
- Taylor C, Lillis C, LeMone P. Fundamentals of Nursing: The Art and Science of Nursing Care, 5th ed. 2005. Philadelphia: Lippincott, Williams & Wilkins; 2005.
Early in his career, hospitalist Richard Bailey, MD, encountered a widow from the inner city with no family. She was blind, and had been weakened and debilitated by a very challenging hospital course with many iatrogenic complications. “I was first struck, walking into her room,” recalls Dr. Bailey, “that she had a Bible on the table next to her bed. While making conversation, I mentioned this and instinctively asked her if she needed someone to read it to her. She smiled, and asked if I would oblige. I closed the door, sat down, and read her some of her favorite passages. This went on for several days until I went off service.”
Now medical director of Inpatient Care and Hospitalist Services at Saint Clare’s Hospital, a Catholic hospital in Wausau, Wis., Dr. Bailey says he is not an overtly religious person and that his spiritual life is rather private. “But I do like to have that depth of connection with my patients,” he says.
So if a patient or a family member asks him to pray with them, Dr. Bailey does so. “I cannot separate my humanness, which includes spirituality, from my work,” he explains.
When faced with serious or life-threatening medical conditions, patients and their family members are more likely to invoke their faith to cope with the attendant anxieties.
William D. Atchley Jr., MD, medical director of the Division of Hospital Medicine for Sentara Medical Group in Hampton, Va., believes that joining his patients in prayer, when asked, “helps develop a better relationship with the family and patient.”
Many Americans tend to “live in the here and now,” notes Carol R. Taylor, RN, MSN, PhD, director of the Center for Clinical Bioethics at Georgetown University. “They usually do not ask the bigger questions so long as life is good. But when life as we know it is threatened by illness, the bigger questions can become very important: ‘Is there anything beyond the here and now? And if so, where do I stand in relation to that God or higher power?’ ”
Prayer is a common response when patients face perilous medical situations.
“The vast majority of patients who are feeling imperiled due to a severe diagnosis or potential mortality is going to be praying,” says Stephen G. Post, PhD, professor and associate director for educational programs, department of bioethics at Case Western Reserve University, Cleveland. “In a way, you can’t get away from those requests.”
Are hospitalists and their institutions fully equipped to respond to the spiritual aspect of caregiving? Some researchers note that biomedicine often regards faith and spiritual world views as relevant only when they obstruct implementation of scientifically sound medical care.1 Studies have also shown healthcare professionals are less likely than their patients to actively practice a religion.
“There’s very often a mismatch between patients and families who would value that intervention and our comfort in being able to be responsive,” says Dr. Taylor, who is also an assistant professor of nursing.
Dr. Taylor and other bioethicists increasingly urge medical practitioners to include spiritual needs when they take a patient’s history. Timely referrals to chaplaincy services, knowledge of the dominant faiths and ethnic traditions in their hospitals’ catchment areas, and improvement of interpersonal skills can allow hospitalists to compassionately and ethically address their patients’ spiritual concerns.
Need to Do a Better Job
The holistic view of medicine defines health as a multidimensional construct that includes the physical, emotional, and social aspects of the patient. This view should be matched with a holistic approach to healthcare delivery that encompasses patients’ subjective illness experience, says Dr. Post.
Dr. Taylor concedes that the medical community’s recognition of patients’ spiritual needs is growing. And yet, she says, practitioners are not held accountable for delivering spiritual care, “which I think is a failing of healthcare as it is practiced today.”
Many reports have indicated patients are unhappy with the low referral rates to pastoral clinical care, adds Dr. Post.2
Assessment Essential
Incorporate a spiritual-needs assessment when taking each patient’s history upon admittance, the two bioethicists agree. This assessment usually takes the form of questions such as:
- What is your source of strength?
- Is spirituality/religion important to you? (If the patient answers “yes,” proceed to the next question.)
- How would you like us to facilitate your needs?
- Would you like a referral to pastoral care?
Once patients indicate they would like to speak with a chaplain, referral to appropriate clergy trained in pastoral care is essential.
“All physicians need to be respectful of these kinds of appeals,” says Dr. Post. “But they should feel free to make a referral to those who are, in fact, competently trained to deal with this specific area of life.”
While opposed to professional separatism, Dr. Post does argue for keeping “friendly, knee-high white fences” between physicians and pastoral counselors to maintain professional boundaries.3
Marc B. Westle, DO, FACP, president and managing partner of Asheville Hospitalist Group, PA, in North Carolina, agrees with this approach. “As a professional, I completely respect and empathize with the patient’s and the family’s spiritual needs as part of the total care of the patient,” he says. “Just as in other areas where I may not have expertise, I refer to our in-house professionals. We have an excellent chaplaincy service that we involve all the time, on a routine basis.” He says the chaplaincy service at Mission Hospital is in-house 24/7, just as the hospitalists are, and make rounds as the physicians do.
Availability of trained clergy differs from institution to institution, notes Dr. Taylor. She recently visited a metropolitan research institution where the two staff chaplains estimate there are nearly 1,000 daily patient contacts. With this many patients flowing through the facility, the chaplains rely on medical staff to triage patients’ and families’ needs so they can be referred to families who will benefit most from their help. In busy urban hospitals, pastoral coverage may not always be available, and the burden of addressing spiritual requests can fall to the hospital medicine team.
The Comfort Zone
The question of whether to pray with a patient or family member depends on the physician’s comfort with doing so.
- Rule No. 1 when it comes to the question of prayer with/for a patient or family: Clinicians should never proselytize or initiate the prayer. This can constitute a serious breach of professional boundaries.4
- Balancing the need to support patients’ emotional needs while respecting one’s integrity can be difficult. If a physician feels comfortable, it is appropriate to pray with a patient. Or, a physician can offer to sit quietly while a patient prays. If uncomfortable with this scenario, offering to keep the patient in your thoughts is one way to still be supportive while maintaining the integrity of your beliefs.3
“I think most physicians try to be very sensitive to these matters,” says Dr. Post.
Dr. Westle notes he has provided more companionate care (“hugging family and patients, sitting and talking about the good old days”) than spiritual guidance.
“Some patients and families feel supported simply by their doctor or nurse joining in a moment of silence or even holding hands during a spoken prayer,” adds Dr. Taylor. “Some of us are better than others at identifying and responding to spiritual needs. But I do think it’s a shared responsibility. The more people we can engage in identifying and responding to spiritual needs, the better patient, family, and medical team will be served. Hospitalists are in an excellent position to identify those needs because of their everyday contact. And if they simply make the right referrals, they’ve done a really good job.” TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Barnes LL, Plotnikoff GA, Fox K, et al. Spirituality, religion, and pediatrics: intersecting worlds of healing. Pediatrics 2000 Oct;106(4 Suppl):899-908.
- Post SG, Puchalski CM, Larson DB. Physicians and Patient Spirituality: Professional Boundaries, Competency, and Ethics. Ann Intern Med. 2000 April 4;132(7):578-583. Comment in: Ann Intern Med. 2000 Dec 5;133(11):920-1; Ann Intern Med. 2000 Nov 7;133(9):748-9.
- Kwiatkowski K, Arnold B, Barnard D. Physicians and Prayer Requests. Fast Fact and Concept #120. Available at www.eperc.mcw.edu/fastFact/ff_120.htm. Last accessed April 5, 2007.
- Taylor C, Lillis C, LeMone P. Fundamentals of Nursing: The Art and Science of Nursing Care, 5th ed. 2005. Philadelphia: Lippincott, Williams & Wilkins; 2005.
Googling for Diagnoses
Googling—the use of search-engines such as Google—is a new diagnostic tool in the modern clinician’s armamentarium.
A 2006 study published in The British Medical Journal examined how often searching with Google leads physicians to a correct diagnosis.1 The investigators were blinded to the correct diagnoses and compared the results of diagnostic cases published in the 2005 case records of The New England Journal of Medicine (NEJM) with diagnoses made using Google searches. Their results indicated that Google searches revealed the correct diagnosis in 15 of 26 cases, or 58% of the time. (See Table 1, p. 34.)
The limitations of the study are important to recognize when considering how well a Web-searched diagnosis can compare with one made without Web searching.
In some cases, although Google supplied information that approximated the diagnoses made in NEJM, the researchers thought the diagnoses were not specific enough.
For instance, one case for which Google suggested a diagnosis of extrinsic allergic alveolitis was described in the NEJM case record as extrinsic allergic alveolitis caused by Mycobacterium avium, also known as “hot tub lung.” This exemplifies the point that search engines don’t make diagnoses—people do. Expert knowledge is required to choose the best search words and select among the results.
Experts agree that using search engines for a diagnosis is likely to be more effective for conditions with unique symptoms and most useful in a certain class of diagnostic challenges in which clinical experts are at the helm of diagnostic deliberations.1,2
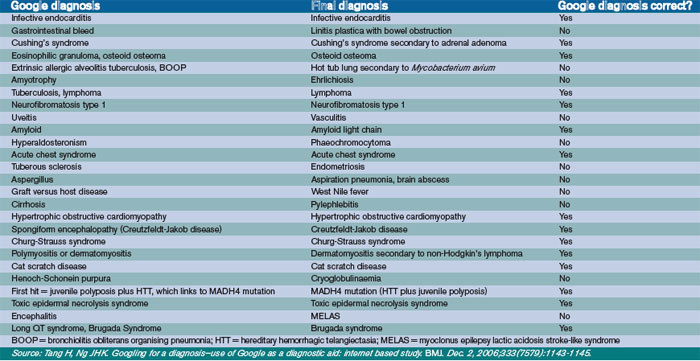
The choice of search engines is important and will increasingly affect accurate diagnoses as the technology develops.
“Hospitalists may utilize [Google] less; they are often working in environments [hospitals] that have ready access to more thoroughly vetted sources such as UpToDate, Medline, or MDConsult,” says Joshua Lee, MD, a hospitalist and medical director of Information Services at the University of California at San Diego. “Within Google there are variations on a theme, such as GoogleScholar, which accesses many of the same academic journals as Medline. Given that they are accessing the same journals, many would feel that searching with GoogleScholar is just as accurate as [searching with] Medline—at least as far as the source material is concerned.”
Search engines offer an impressive volume of new scientific material that is indexed daily. But, current search engines cannot identify differences of meaning in symptoms, drug names, anatomic features, or diagnoses.
“The key drawback to using open Google is that you cannot guarantee that the information comes from peer-reviewed journals,” Dr. Lee says. “When a search with ‘regular’ Google brings back untested medical information that is not peer reviewed, it gets dicey, and thus less reliable.”
Current Web technologies may merely be a first step in creating a much more powerful infrastructure for Web-based diagnostics. The so-called semantic Web will allow computers to process meaning in documentation.3 Two key elements of this revolution are the resource description framework (RDF) and Web ontology language (OWL) technologies. These next-generation search tools are being beta tested and will be freely available within the next decade.
There are a number of caveats to using and trusting information from search-engine investigations. Google stands up much better than other search engines in simple diagnostic searches. Also, diagnostic problems are not solved on a linear scale of difficulty.2 Research and development of the benefits of the semantic Web in clinical practice will help maximize this tool for diagnostics. TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Tang H, Ng JHK. Googling for a diagnosis—use of Google as a diagnostic aid: internet based study. BMJ. 2006 Dec 2;333(7579):1143-1145.
- Gardner M. Diagnosis using search engines. BMJ. 2006 Dec 2;333(7579):1131.
- Berners-Lee T, Hendler J, Lassila O. The semantic web. Sci Am. 2001 May 1;34-43.
When Patients Google for Diagnoses

Even though Tang, et al.,1 cautioned in their study that patients who use Google to find their own diagnosis may find it less efficient and may be less likely than a physician to retrieve the correct diagnosis, organizations such as the Patients Association in the United Kingdom voiced their concerns that the study might encourage the public to self-diagnose. Their primary concern was the lack of regulation of most sites, leading, at best, to some unreliable information.
This view is shared by Art Papier, MD, associate professor of dermatology and medical informatics at the University of Rochester (N.Y.) School of Medicine and Dentistry. Dr. Papier understands the Internet is a powerful and useful tool for gathering information, but it may also be a risk in the hands of people who do not take the time to identify trusted and high-quality sites.
Research shows that most people limit their searches to the one or two first pages of search engine hits they get. Although sites from the National Institutes of Health or the National Library of Medicine, for instance, might appear at the top of a search list, so can commercial sites whose information is of lesser quality and who may be aggressively marketing a product. “The evidence is that many patients do not take the time to differentiate a good and bad site,” says Dr. Papier. “They just use what they get as the [list’s] top sites. That’s a real problem.”
Dr. Papier is hopeful that as the quality of the search engines improve, many of these commercial sites with limited information will no longer appear at the top of the search.
On the other side of the issue, there are some great Web sites with solid information. The ramifications for hospitalists, says Dr. Papier, largely involve counseling patients to consider the reliability of sites they consult and understand that key search words and the capacity to interpret results is something for which a patient ultimately could use the help of a doctor. Hospitalists who distribute a list of the best sites to consult for a particular diagnosis or treatment to patients upon discharge will be contributing the most to their patients’ well-being.
“With hospitalized patients,” says Dr. Papier, “that is, the patient with cancer or heart disease, for instance, the family may find on the Internet a side effect of a medication and bring it to the attention of the provider, who may have been too rushed to think through that side effect or who was unaware.” This is one way families of hospitalized patients have been using the Internet in partnership with physicians.
“Patients and families are Googling [health info] like crazy,” says Dr. Papier. “It’s somewhat random whether they get quality info. It behooves both hospitals and hospitalists to help patients and family members find the quality sites. More and more it is becoming a part of the responsibilities of patient care in the modern era.” —AS
Googling—the use of search-engines such as Google—is a new diagnostic tool in the modern clinician’s armamentarium.
A 2006 study published in The British Medical Journal examined how often searching with Google leads physicians to a correct diagnosis.1 The investigators were blinded to the correct diagnoses and compared the results of diagnostic cases published in the 2005 case records of The New England Journal of Medicine (NEJM) with diagnoses made using Google searches. Their results indicated that Google searches revealed the correct diagnosis in 15 of 26 cases, or 58% of the time. (See Table 1, p. 34.)
The limitations of the study are important to recognize when considering how well a Web-searched diagnosis can compare with one made without Web searching.
In some cases, although Google supplied information that approximated the diagnoses made in NEJM, the researchers thought the diagnoses were not specific enough.
For instance, one case for which Google suggested a diagnosis of extrinsic allergic alveolitis was described in the NEJM case record as extrinsic allergic alveolitis caused by Mycobacterium avium, also known as “hot tub lung.” This exemplifies the point that search engines don’t make diagnoses—people do. Expert knowledge is required to choose the best search words and select among the results.
Experts agree that using search engines for a diagnosis is likely to be more effective for conditions with unique symptoms and most useful in a certain class of diagnostic challenges in which clinical experts are at the helm of diagnostic deliberations.1,2
The choice of search engines is important and will increasingly affect accurate diagnoses as the technology develops.
“Hospitalists may utilize [Google] less; they are often working in environments [hospitals] that have ready access to more thoroughly vetted sources such as UpToDate, Medline, or MDConsult,” says Joshua Lee, MD, a hospitalist and medical director of Information Services at the University of California at San Diego. “Within Google there are variations on a theme, such as GoogleScholar, which accesses many of the same academic journals as Medline. Given that they are accessing the same journals, many would feel that searching with GoogleScholar is just as accurate as [searching with] Medline—at least as far as the source material is concerned.”
Search engines offer an impressive volume of new scientific material that is indexed daily. But, current search engines cannot identify differences of meaning in symptoms, drug names, anatomic features, or diagnoses.
“The key drawback to using open Google is that you cannot guarantee that the information comes from peer-reviewed journals,” Dr. Lee says. “When a search with ‘regular’ Google brings back untested medical information that is not peer reviewed, it gets dicey, and thus less reliable.”
Current Web technologies may merely be a first step in creating a much more powerful infrastructure for Web-based diagnostics. The so-called semantic Web will allow computers to process meaning in documentation.3 Two key elements of this revolution are the resource description framework (RDF) and Web ontology language (OWL) technologies. These next-generation search tools are being beta tested and will be freely available within the next decade.
There are a number of caveats to using and trusting information from search-engine investigations. Google stands up much better than other search engines in simple diagnostic searches. Also, diagnostic problems are not solved on a linear scale of difficulty.2 Research and development of the benefits of the semantic Web in clinical practice will help maximize this tool for diagnostics. TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Tang H, Ng JHK. Googling for a diagnosis—use of Google as a diagnostic aid: internet based study. BMJ. 2006 Dec 2;333(7579):1143-1145.
- Gardner M. Diagnosis using search engines. BMJ. 2006 Dec 2;333(7579):1131.
- Berners-Lee T, Hendler J, Lassila O. The semantic web. Sci Am. 2001 May 1;34-43.
When Patients Google for Diagnoses
Even though Tang, et al.,1 cautioned in their study that patients who use Google to find their own diagnosis may find it less efficient and may be less likely than a physician to retrieve the correct diagnosis, organizations such as the Patients Association in the United Kingdom voiced their concerns that the study might encourage the public to self-diagnose. Their primary concern was the lack of regulation of most sites, leading, at best, to some unreliable information.
This view is shared by Art Papier, MD, associate professor of dermatology and medical informatics at the University of Rochester (N.Y.) School of Medicine and Dentistry. Dr. Papier understands the Internet is a powerful and useful tool for gathering information, but it may also be a risk in the hands of people who do not take the time to identify trusted and high-quality sites.
Research shows that most people limit their searches to the one or two first pages of search engine hits they get. Although sites from the National Institutes of Health or the National Library of Medicine, for instance, might appear at the top of a search list, so can commercial sites whose information is of lesser quality and who may be aggressively marketing a product. “The evidence is that many patients do not take the time to differentiate a good and bad site,” says Dr. Papier. “They just use what they get as the [list’s] top sites. That’s a real problem.”
Dr. Papier is hopeful that as the quality of the search engines improve, many of these commercial sites with limited information will no longer appear at the top of the search.
On the other side of the issue, there are some great Web sites with solid information. The ramifications for hospitalists, says Dr. Papier, largely involve counseling patients to consider the reliability of sites they consult and understand that key search words and the capacity to interpret results is something for which a patient ultimately could use the help of a doctor. Hospitalists who distribute a list of the best sites to consult for a particular diagnosis or treatment to patients upon discharge will be contributing the most to their patients’ well-being.
“With hospitalized patients,” says Dr. Papier, “that is, the patient with cancer or heart disease, for instance, the family may find on the Internet a side effect of a medication and bring it to the attention of the provider, who may have been too rushed to think through that side effect or who was unaware.” This is one way families of hospitalized patients have been using the Internet in partnership with physicians.
“Patients and families are Googling [health info] like crazy,” says Dr. Papier. “It’s somewhat random whether they get quality info. It behooves both hospitals and hospitalists to help patients and family members find the quality sites. More and more it is becoming a part of the responsibilities of patient care in the modern era.” —AS
Googling—the use of search-engines such as Google—is a new diagnostic tool in the modern clinician’s armamentarium.
A 2006 study published in The British Medical Journal examined how often searching with Google leads physicians to a correct diagnosis.1 The investigators were blinded to the correct diagnoses and compared the results of diagnostic cases published in the 2005 case records of The New England Journal of Medicine (NEJM) with diagnoses made using Google searches. Their results indicated that Google searches revealed the correct diagnosis in 15 of 26 cases, or 58% of the time. (See Table 1, p. 34.)
The limitations of the study are important to recognize when considering how well a Web-searched diagnosis can compare with one made without Web searching.
In some cases, although Google supplied information that approximated the diagnoses made in NEJM, the researchers thought the diagnoses were not specific enough.
For instance, one case for which Google suggested a diagnosis of extrinsic allergic alveolitis was described in the NEJM case record as extrinsic allergic alveolitis caused by Mycobacterium avium, also known as “hot tub lung.” This exemplifies the point that search engines don’t make diagnoses—people do. Expert knowledge is required to choose the best search words and select among the results.
Experts agree that using search engines for a diagnosis is likely to be more effective for conditions with unique symptoms and most useful in a certain class of diagnostic challenges in which clinical experts are at the helm of diagnostic deliberations.1,2
The choice of search engines is important and will increasingly affect accurate diagnoses as the technology develops.
“Hospitalists may utilize [Google] less; they are often working in environments [hospitals] that have ready access to more thoroughly vetted sources such as UpToDate, Medline, or MDConsult,” says Joshua Lee, MD, a hospitalist and medical director of Information Services at the University of California at San Diego. “Within Google there are variations on a theme, such as GoogleScholar, which accesses many of the same academic journals as Medline. Given that they are accessing the same journals, many would feel that searching with GoogleScholar is just as accurate as [searching with] Medline—at least as far as the source material is concerned.”
Search engines offer an impressive volume of new scientific material that is indexed daily. But, current search engines cannot identify differences of meaning in symptoms, drug names, anatomic features, or diagnoses.
“The key drawback to using open Google is that you cannot guarantee that the information comes from peer-reviewed journals,” Dr. Lee says. “When a search with ‘regular’ Google brings back untested medical information that is not peer reviewed, it gets dicey, and thus less reliable.”
Current Web technologies may merely be a first step in creating a much more powerful infrastructure for Web-based diagnostics. The so-called semantic Web will allow computers to process meaning in documentation.3 Two key elements of this revolution are the resource description framework (RDF) and Web ontology language (OWL) technologies. These next-generation search tools are being beta tested and will be freely available within the next decade.
There are a number of caveats to using and trusting information from search-engine investigations. Google stands up much better than other search engines in simple diagnostic searches. Also, diagnostic problems are not solved on a linear scale of difficulty.2 Research and development of the benefits of the semantic Web in clinical practice will help maximize this tool for diagnostics. TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Tang H, Ng JHK. Googling for a diagnosis—use of Google as a diagnostic aid: internet based study. BMJ. 2006 Dec 2;333(7579):1143-1145.
- Gardner M. Diagnosis using search engines. BMJ. 2006 Dec 2;333(7579):1131.
- Berners-Lee T, Hendler J, Lassila O. The semantic web. Sci Am. 2001 May 1;34-43.
When Patients Google for Diagnoses
Even though Tang, et al.,1 cautioned in their study that patients who use Google to find their own diagnosis may find it less efficient and may be less likely than a physician to retrieve the correct diagnosis, organizations such as the Patients Association in the United Kingdom voiced their concerns that the study might encourage the public to self-diagnose. Their primary concern was the lack of regulation of most sites, leading, at best, to some unreliable information.
This view is shared by Art Papier, MD, associate professor of dermatology and medical informatics at the University of Rochester (N.Y.) School of Medicine and Dentistry. Dr. Papier understands the Internet is a powerful and useful tool for gathering information, but it may also be a risk in the hands of people who do not take the time to identify trusted and high-quality sites.
Research shows that most people limit their searches to the one or two first pages of search engine hits they get. Although sites from the National Institutes of Health or the National Library of Medicine, for instance, might appear at the top of a search list, so can commercial sites whose information is of lesser quality and who may be aggressively marketing a product. “The evidence is that many patients do not take the time to differentiate a good and bad site,” says Dr. Papier. “They just use what they get as the [list’s] top sites. That’s a real problem.”
Dr. Papier is hopeful that as the quality of the search engines improve, many of these commercial sites with limited information will no longer appear at the top of the search.
On the other side of the issue, there are some great Web sites with solid information. The ramifications for hospitalists, says Dr. Papier, largely involve counseling patients to consider the reliability of sites they consult and understand that key search words and the capacity to interpret results is something for which a patient ultimately could use the help of a doctor. Hospitalists who distribute a list of the best sites to consult for a particular diagnosis or treatment to patients upon discharge will be contributing the most to their patients’ well-being.
“With hospitalized patients,” says Dr. Papier, “that is, the patient with cancer or heart disease, for instance, the family may find on the Internet a side effect of a medication and bring it to the attention of the provider, who may have been too rushed to think through that side effect or who was unaware.” This is one way families of hospitalized patients have been using the Internet in partnership with physicians.
“Patients and families are Googling [health info] like crazy,” says Dr. Papier. “It’s somewhat random whether they get quality info. It behooves both hospitals and hospitalists to help patients and family members find the quality sites. More and more it is becoming a part of the responsibilities of patient care in the modern era.” —AS
The Telehospitalist
The patient was in the ICU at Saint Clare’s Hospital in Wausau, Wis. An intensivist from St. Louis who had been caring for her remotely through telemedicine technology was helping clinicians manage the end-of-life issue for her and her family.
Subjects like this can be difficult for hospitalists, who may not have as much experience with the protocols involved in end-of-life care. But at Saint Clare’s, which offers remote care and monitoring by intensivists and critical-care nurses through an eICU program, critical-care specialists are there to provide continuous care to the hospital’s sickest patients, as well as support for the onsite clinicians in any number of situations involving ICU patient care.
Dellice Dickhaus, MD, medical director for Advanced ICU Care and a practicing intensivist, helps provide remote care around the clock for patients in Saint Clare’s ICU. Advanced ICU Care’s board-certified intensivists and critical-care nurses remotely care for and monitor patients in multiple sites from their operations center, more than 400 miles away in St. Louis. They use telemedicine technology developed by Baltimore, Md., firm VISICU that combines clinical management software with real-time video feeds and patient data, such as labs, vital signs and medications.
In the case of the critically ill patient, while the hospitalist was driving the patient’s care program and taking care of many of the daily issues, Dr. Dickhaus helped manage the end-of-life issue. She was available at the push of a button to talk with relatives and provide information they needed to make decisions about their family member’s care. She discussed the patient’s prognosis and options with the family, and kept the hospitalist on staff apprised of the conversations.
Because Dr. Dickhaus and other clinicians at Advanced ICU Care had been helping manage the patient’s care in the ICU, the patient’s family gained confidence in the remote intensivists, says Dr. Dickhaus.
Demands of an Aging Population
The aging of America will have a tremendous effect on healthcare, particularly regarding care of the critically ill and in managing such areas as pulmonary disease. Consider that more than half of all ICU stays are incurred by patients older than 65. Further, patients older than 65 account for more than two-thirds of all inpatient pulmonary days.
What does this mean for hospitalists? For one, the aging population will create a demand for care that is projected to outpace the supply of intensivists and pulmonologists.1 With fewer of these specialists, hospitalists may be compelled to take on more responsibilities with critically ill patients, leaving less time for other patients. The expectation of healthcare services provided will likely change, possibly growing in scope and complexity. The time it will take to deliver care is also expected to rise. All these are reasons for the growth in telemedicine technologies, with many designed to improve patient care by delivering limited resources where they are needed most.
Continuity of Care
Richard Bailey, MD, medical director of Inpatient Care and Hospitalist Services at Saint Clare’s, says having remote intensivists lets his staff focus on hospital patients outside the ICU.
“One critical patient can tie you up for hours,” Dr. Bailey says. “Advanced ICU Care’s intensivists are hands-on physicians, helping us round on ICU patients, take patient notes, and handle first-line phone calls.”
There is no difference, he says, between having intensivists in St. Louis, for example, versus on-site. “They are more than a microphone and a camera in the ceiling; they are members of our staff,” he says. “We trust them to take care of our patients.”
He explains that remote intensivists are often good at being the “bug in the ear” for hospitalists, helping with treatment recommendations and asking, “Did you remember to … ?” While stabilizing a just-transferred ICU patient in a near-code situation, Dr. Bailey needed immediate access to the patient’s labs. An intensivist in St. Louis was able to look at the labs and recommend treatment.
Preliminary numbers at Saint Clare’s hint at a reduction of one day in ICU length of stay and two days for total hospitalization, notes Dr. Bailey. Figures like these can mean real savings in hospital costs.
Working together, hospitalists and remote intensivists can provide continuity of care as the patient is admitted through the emergency department and brought into the ICU, explains Dr. Bailey.
William D. Atchley Jr., MD, medical director for the Division of Hospital Medicine for Sentara Medical Group in Norfolk, Va., agrees with Dr. Bailey’s view. Dr. Atchley’s group also uses telemedicine technology for the remote care and monitoring of ICU patients. He is also a member of SHM’s Board of Directors.
“This is a true team effort, creating a seamless continuity from the emergency department to the ICU,” says Dr. Atchley. He cites septic shock patients as an example. He is able to start the septic shock protocols with the patient in the ED, and the intensivist will carry the protocols forward with the patient in the ICU. By morning, Dr. Atchley says he knows the patient has received the care needed, which frees him to care for other patients.
Sentara Healthcare, based in Norfolk, Va., was the first hospital system in the nation to implement VISICU’s technology, which allows hospitals to create a systemwide critical-care program. Using the VISICU eICU, the hospital or healthcare system provides the intensivists to staff the program, helping to leverage scarce clinical resources among the system’s ICUs.
Studies have shown that care by intensivists via telemedicine technology improves patient care and safety in the ICU. In a 2004 study, Sentara documented a 27% decrease in overall ICU and hospital mortality.2
Mobile Telemedicine
Advances in telemedicine technology have come a long way. Take remote robotic systems, for instance, which allow physicians to consult with patients, family members, and on-site caregivers while seated in their office, in another wing of the hospital, or at home.
InTouch Health, a Santa Barbara, Calif., company, uses about 100 robotic systems. While seated at a control station, equipped with video capabilities, a microphone, and a joystick, the physician can “drive” the robot into a patient’s room for consultation. The patient can see the doctor’s face on the monitor and—on the other end—the physician has access to patient data and can see the patient through a live video image.
The robotic system provides added ability for intensivists and other specialists to do another evening round on their patients, explains Tim Wright, vice president of strategic marketing for InTouch. A recent study shows that when physicians use robotic telepresence to make rounds in the ICU in response to nursing pages, physician response is significantly faster. Additionally, the study found a reduced length of stay, particularly for patients with subarachnoid hemorrhage and brain trauma, as well as an ICU cost savings of $1.1 million.3
The idea of robotic telepresence is similar to the telemedicine model of care being used in the ICU. Through the robotic system, an intensivist can log in and perform an evening round, updating hospitalists on new patients and issues that may have arisen.
“The beauty is that the intensivist and the hospitalist can be looking at everything together,” Wright says. “The intensivist can provide the specialist knowledge and training, while the hospitalist provides the ongoing care.”
Not Just the ICU
Of course, telemedicine is not limited to the ICU. It is being used for virtually every medical specialty to help provide greater access to care.
Take the University of Texas Medical Branch at Galveston (UTMB), which has used telemedicine technologies since 1994. Its Electronic Health Network (EHN) utilizes telemedicine to help care for the state’s indigent and rural populations, as well as other groups, such as the elderly, prisoners, and even researchers in Antarctica.
One of the fastest-growing services UTMB operates is the telemedicine-based corporate healthcare programs, allowing employees to “see” a primary care physician without leaving work. Companies see this as a way to help control healthcare costs and make preventive care more accessible, notes Glenn Hammack, OD, assistant vice president and executive director of the UTMB Electronic Health Network. He also pegs the application of telemedicine to psychiatry as another growing service and one that illustrates how the technology is being used to help address a shortage of providers, especially in rural and underserved parts of Texas. Like the eICU programs designed to bring scarce intensivist care to ICU patients, UTMB’s services help distribute rare resources, such as child and adolescent psychiatrists who speak Spanish, to patients.
The telemedicine program at UMTB began in 1994 as a way to help provide cost-effective healthcare for inmates in the Texas prison system. Today, the Correctional Managed Care (CMC) department has telemedicine stations in 120 correctional units throughout Texas and accounts for about half of UTMB’s telemedicine program.
The 11 telemedicine studios at UTMB used for patients across the EHN are equipped with live interactive video links that allow the telemedicine physician to see and hear the patient, located at the remote station with a registered health professional on-site. Digital stethoscopes, hand-held cameras, and other electronic medical devices help the physician treat patients. The telemedicine program also utilizes shared electronic medical records, which are critical to its success, says Dr. Hammack.
Telemedicine can also be used between departments within the hospital. Dr. Hammack notes that hospitals have become large and complicated; the journey from one end to another for a test or procedure can be difficult on patients. “Telemedicine offers the ability for face-to-face interaction, and when used within hospital departments, it can bring some humanity of scale back to the increasingly complicated hospital environment,” he says.
Another Vision
Troy Sybert, MD, medical director for CMC Hospital Medicine and a practicing hospitalist at Texas Department of Criminal Justice (TDCJ) Hospital in Galveston, Texas, was hired a year ago to help create a hospitalist program within the prison system. His is the only health facility dedicated to prisoners and located on a medical school campus.
While his six-member team is not engaged in telemedicine, he sees a number of possibilities for CMC hospitalists to utilize telemedicine technology. For one, hospitalists could use their expertise in admissions to help triage patients via telemedicine. The CMC recently created a network of regional hubs similar to ED observation centers but without a 24/7 physician presence. Telemedicine triage could help the system offload the decision to admit and would likely reduce the number of hospital admissions, says Dr. Sybert.
Telemedicine technology could also provide other possibilities in perioperative care for surgery patients at TDCJ Hospital. In partnership with the surgery and anesthesia departments, pre- and post-operative work up and care could be done remotely with the patient back in the unit, promoting shorter lengths of stay and reducing transportation needs. The hospitalists, trained in correctional care, would provide support and coordinate with surgery—especially on the patient’s transition to and from the prison facility.
“The whole concept of telemedicine is to utilize experience from a centralized location,” says Dr. Sybert. “We have a vision for where we might like to go with telemedicine, bringing our hospitalist group’s experience with managed correctional care to prison units throughout the state.”
Whether it is bringing intensivist care to a critically ill patient, providing therapy sessions to patients in rural areas, or delivering the expertise of hospitalists, telemedicine technology is likely to play an ever-increasing role in healthcare. Dr. Hammack believes telemedicine will be used more and more as care providers and administrators find the right balance between technology and touch.
“It can be difficult to figure out how telemedicine can fit into the way hospitals do things. But it can fit in and does so very well. Technologies like these have the promise to provide support and result in better quality of care for patients,” he says.
Donya Hengehold is freelance medical journalist.
References
- Angus DC, Kelley MA, Schmitz RJ, et al. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease. JAMA. 2000 Dec 6;284(21):2762-2770. Comment in JAMA. 2001 Feb 28;285(8):1016-1017; author reply 1018. JAMA. 2001 Feb 28;285(8):1017-1018.
- Breslow MJ, Rosenfeld BA, Doerfler M, et al. Effect of a multiple-site intensive care unit telemedicine program on clinical and economic outcomes: an alternative paradigm for intensivist staffing. Crit Care Med. 2004 Jan;32(1):31-38. Erratum in: Crit Care Med. 2004 Jul;32(7):1632.Comment in: Crit Care Med. 2004 Jan;32(1):287-288. Crit Care Med. 2004 Jan;32(1):288-290.
- Vespa PM, Miller C, Hu X, et al. Intensive care unit robotic telepresence facilitates rapid physician response to unstable patients and decreased cost in neurointensive care. Surg Neurol. 2007 April;67(4):331-337.
The patient was in the ICU at Saint Clare’s Hospital in Wausau, Wis. An intensivist from St. Louis who had been caring for her remotely through telemedicine technology was helping clinicians manage the end-of-life issue for her and her family.
Subjects like this can be difficult for hospitalists, who may not have as much experience with the protocols involved in end-of-life care. But at Saint Clare’s, which offers remote care and monitoring by intensivists and critical-care nurses through an eICU program, critical-care specialists are there to provide continuous care to the hospital’s sickest patients, as well as support for the onsite clinicians in any number of situations involving ICU patient care.
Dellice Dickhaus, MD, medical director for Advanced ICU Care and a practicing intensivist, helps provide remote care around the clock for patients in Saint Clare’s ICU. Advanced ICU Care’s board-certified intensivists and critical-care nurses remotely care for and monitor patients in multiple sites from their operations center, more than 400 miles away in St. Louis. They use telemedicine technology developed by Baltimore, Md., firm VISICU that combines clinical management software with real-time video feeds and patient data, such as labs, vital signs and medications.
In the case of the critically ill patient, while the hospitalist was driving the patient’s care program and taking care of many of the daily issues, Dr. Dickhaus helped manage the end-of-life issue. She was available at the push of a button to talk with relatives and provide information they needed to make decisions about their family member’s care. She discussed the patient’s prognosis and options with the family, and kept the hospitalist on staff apprised of the conversations.
Because Dr. Dickhaus and other clinicians at Advanced ICU Care had been helping manage the patient’s care in the ICU, the patient’s family gained confidence in the remote intensivists, says Dr. Dickhaus.
Demands of an Aging Population
The aging of America will have a tremendous effect on healthcare, particularly regarding care of the critically ill and in managing such areas as pulmonary disease. Consider that more than half of all ICU stays are incurred by patients older than 65. Further, patients older than 65 account for more than two-thirds of all inpatient pulmonary days.
What does this mean for hospitalists? For one, the aging population will create a demand for care that is projected to outpace the supply of intensivists and pulmonologists.1 With fewer of these specialists, hospitalists may be compelled to take on more responsibilities with critically ill patients, leaving less time for other patients. The expectation of healthcare services provided will likely change, possibly growing in scope and complexity. The time it will take to deliver care is also expected to rise. All these are reasons for the growth in telemedicine technologies, with many designed to improve patient care by delivering limited resources where they are needed most.
Continuity of Care
Richard Bailey, MD, medical director of Inpatient Care and Hospitalist Services at Saint Clare’s, says having remote intensivists lets his staff focus on hospital patients outside the ICU.
“One critical patient can tie you up for hours,” Dr. Bailey says. “Advanced ICU Care’s intensivists are hands-on physicians, helping us round on ICU patients, take patient notes, and handle first-line phone calls.”
There is no difference, he says, between having intensivists in St. Louis, for example, versus on-site. “They are more than a microphone and a camera in the ceiling; they are members of our staff,” he says. “We trust them to take care of our patients.”
He explains that remote intensivists are often good at being the “bug in the ear” for hospitalists, helping with treatment recommendations and asking, “Did you remember to … ?” While stabilizing a just-transferred ICU patient in a near-code situation, Dr. Bailey needed immediate access to the patient’s labs. An intensivist in St. Louis was able to look at the labs and recommend treatment.
Preliminary numbers at Saint Clare’s hint at a reduction of one day in ICU length of stay and two days for total hospitalization, notes Dr. Bailey. Figures like these can mean real savings in hospital costs.
Working together, hospitalists and remote intensivists can provide continuity of care as the patient is admitted through the emergency department and brought into the ICU, explains Dr. Bailey.
William D. Atchley Jr., MD, medical director for the Division of Hospital Medicine for Sentara Medical Group in Norfolk, Va., agrees with Dr. Bailey’s view. Dr. Atchley’s group also uses telemedicine technology for the remote care and monitoring of ICU patients. He is also a member of SHM’s Board of Directors.
“This is a true team effort, creating a seamless continuity from the emergency department to the ICU,” says Dr. Atchley. He cites septic shock patients as an example. He is able to start the septic shock protocols with the patient in the ED, and the intensivist will carry the protocols forward with the patient in the ICU. By morning, Dr. Atchley says he knows the patient has received the care needed, which frees him to care for other patients.
Sentara Healthcare, based in Norfolk, Va., was the first hospital system in the nation to implement VISICU’s technology, which allows hospitals to create a systemwide critical-care program. Using the VISICU eICU, the hospital or healthcare system provides the intensivists to staff the program, helping to leverage scarce clinical resources among the system’s ICUs.
Studies have shown that care by intensivists via telemedicine technology improves patient care and safety in the ICU. In a 2004 study, Sentara documented a 27% decrease in overall ICU and hospital mortality.2
Mobile Telemedicine
Advances in telemedicine technology have come a long way. Take remote robotic systems, for instance, which allow physicians to consult with patients, family members, and on-site caregivers while seated in their office, in another wing of the hospital, or at home.
InTouch Health, a Santa Barbara, Calif., company, uses about 100 robotic systems. While seated at a control station, equipped with video capabilities, a microphone, and a joystick, the physician can “drive” the robot into a patient’s room for consultation. The patient can see the doctor’s face on the monitor and—on the other end—the physician has access to patient data and can see the patient through a live video image.
The robotic system provides added ability for intensivists and other specialists to do another evening round on their patients, explains Tim Wright, vice president of strategic marketing for InTouch. A recent study shows that when physicians use robotic telepresence to make rounds in the ICU in response to nursing pages, physician response is significantly faster. Additionally, the study found a reduced length of stay, particularly for patients with subarachnoid hemorrhage and brain trauma, as well as an ICU cost savings of $1.1 million.3
The idea of robotic telepresence is similar to the telemedicine model of care being used in the ICU. Through the robotic system, an intensivist can log in and perform an evening round, updating hospitalists on new patients and issues that may have arisen.
“The beauty is that the intensivist and the hospitalist can be looking at everything together,” Wright says. “The intensivist can provide the specialist knowledge and training, while the hospitalist provides the ongoing care.”
Not Just the ICU
Of course, telemedicine is not limited to the ICU. It is being used for virtually every medical specialty to help provide greater access to care.
Take the University of Texas Medical Branch at Galveston (UTMB), which has used telemedicine technologies since 1994. Its Electronic Health Network (EHN) utilizes telemedicine to help care for the state’s indigent and rural populations, as well as other groups, such as the elderly, prisoners, and even researchers in Antarctica.
One of the fastest-growing services UTMB operates is the telemedicine-based corporate healthcare programs, allowing employees to “see” a primary care physician without leaving work. Companies see this as a way to help control healthcare costs and make preventive care more accessible, notes Glenn Hammack, OD, assistant vice president and executive director of the UTMB Electronic Health Network. He also pegs the application of telemedicine to psychiatry as another growing service and one that illustrates how the technology is being used to help address a shortage of providers, especially in rural and underserved parts of Texas. Like the eICU programs designed to bring scarce intensivist care to ICU patients, UTMB’s services help distribute rare resources, such as child and adolescent psychiatrists who speak Spanish, to patients.
The telemedicine program at UMTB began in 1994 as a way to help provide cost-effective healthcare for inmates in the Texas prison system. Today, the Correctional Managed Care (CMC) department has telemedicine stations in 120 correctional units throughout Texas and accounts for about half of UTMB’s telemedicine program.
The 11 telemedicine studios at UTMB used for patients across the EHN are equipped with live interactive video links that allow the telemedicine physician to see and hear the patient, located at the remote station with a registered health professional on-site. Digital stethoscopes, hand-held cameras, and other electronic medical devices help the physician treat patients. The telemedicine program also utilizes shared electronic medical records, which are critical to its success, says Dr. Hammack.
Telemedicine can also be used between departments within the hospital. Dr. Hammack notes that hospitals have become large and complicated; the journey from one end to another for a test or procedure can be difficult on patients. “Telemedicine offers the ability for face-to-face interaction, and when used within hospital departments, it can bring some humanity of scale back to the increasingly complicated hospital environment,” he says.
Another Vision
Troy Sybert, MD, medical director for CMC Hospital Medicine and a practicing hospitalist at Texas Department of Criminal Justice (TDCJ) Hospital in Galveston, Texas, was hired a year ago to help create a hospitalist program within the prison system. His is the only health facility dedicated to prisoners and located on a medical school campus.
While his six-member team is not engaged in telemedicine, he sees a number of possibilities for CMC hospitalists to utilize telemedicine technology. For one, hospitalists could use their expertise in admissions to help triage patients via telemedicine. The CMC recently created a network of regional hubs similar to ED observation centers but without a 24/7 physician presence. Telemedicine triage could help the system offload the decision to admit and would likely reduce the number of hospital admissions, says Dr. Sybert.
Telemedicine technology could also provide other possibilities in perioperative care for surgery patients at TDCJ Hospital. In partnership with the surgery and anesthesia departments, pre- and post-operative work up and care could be done remotely with the patient back in the unit, promoting shorter lengths of stay and reducing transportation needs. The hospitalists, trained in correctional care, would provide support and coordinate with surgery—especially on the patient’s transition to and from the prison facility.
“The whole concept of telemedicine is to utilize experience from a centralized location,” says Dr. Sybert. “We have a vision for where we might like to go with telemedicine, bringing our hospitalist group’s experience with managed correctional care to prison units throughout the state.”
Whether it is bringing intensivist care to a critically ill patient, providing therapy sessions to patients in rural areas, or delivering the expertise of hospitalists, telemedicine technology is likely to play an ever-increasing role in healthcare. Dr. Hammack believes telemedicine will be used more and more as care providers and administrators find the right balance between technology and touch.
“It can be difficult to figure out how telemedicine can fit into the way hospitals do things. But it can fit in and does so very well. Technologies like these have the promise to provide support and result in better quality of care for patients,” he says.
Donya Hengehold is freelance medical journalist.
References
- Angus DC, Kelley MA, Schmitz RJ, et al. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease. JAMA. 2000 Dec 6;284(21):2762-2770. Comment in JAMA. 2001 Feb 28;285(8):1016-1017; author reply 1018. JAMA. 2001 Feb 28;285(8):1017-1018.
- Breslow MJ, Rosenfeld BA, Doerfler M, et al. Effect of a multiple-site intensive care unit telemedicine program on clinical and economic outcomes: an alternative paradigm for intensivist staffing. Crit Care Med. 2004 Jan;32(1):31-38. Erratum in: Crit Care Med. 2004 Jul;32(7):1632.Comment in: Crit Care Med. 2004 Jan;32(1):287-288. Crit Care Med. 2004 Jan;32(1):288-290.
- Vespa PM, Miller C, Hu X, et al. Intensive care unit robotic telepresence facilitates rapid physician response to unstable patients and decreased cost in neurointensive care. Surg Neurol. 2007 April;67(4):331-337.
The patient was in the ICU at Saint Clare’s Hospital in Wausau, Wis. An intensivist from St. Louis who had been caring for her remotely through telemedicine technology was helping clinicians manage the end-of-life issue for her and her family.
Subjects like this can be difficult for hospitalists, who may not have as much experience with the protocols involved in end-of-life care. But at Saint Clare’s, which offers remote care and monitoring by intensivists and critical-care nurses through an eICU program, critical-care specialists are there to provide continuous care to the hospital’s sickest patients, as well as support for the onsite clinicians in any number of situations involving ICU patient care.
Dellice Dickhaus, MD, medical director for Advanced ICU Care and a practicing intensivist, helps provide remote care around the clock for patients in Saint Clare’s ICU. Advanced ICU Care’s board-certified intensivists and critical-care nurses remotely care for and monitor patients in multiple sites from their operations center, more than 400 miles away in St. Louis. They use telemedicine technology developed by Baltimore, Md., firm VISICU that combines clinical management software with real-time video feeds and patient data, such as labs, vital signs and medications.
In the case of the critically ill patient, while the hospitalist was driving the patient’s care program and taking care of many of the daily issues, Dr. Dickhaus helped manage the end-of-life issue. She was available at the push of a button to talk with relatives and provide information they needed to make decisions about their family member’s care. She discussed the patient’s prognosis and options with the family, and kept the hospitalist on staff apprised of the conversations.
Because Dr. Dickhaus and other clinicians at Advanced ICU Care had been helping manage the patient’s care in the ICU, the patient’s family gained confidence in the remote intensivists, says Dr. Dickhaus.
Demands of an Aging Population
The aging of America will have a tremendous effect on healthcare, particularly regarding care of the critically ill and in managing such areas as pulmonary disease. Consider that more than half of all ICU stays are incurred by patients older than 65. Further, patients older than 65 account for more than two-thirds of all inpatient pulmonary days.
What does this mean for hospitalists? For one, the aging population will create a demand for care that is projected to outpace the supply of intensivists and pulmonologists.1 With fewer of these specialists, hospitalists may be compelled to take on more responsibilities with critically ill patients, leaving less time for other patients. The expectation of healthcare services provided will likely change, possibly growing in scope and complexity. The time it will take to deliver care is also expected to rise. All these are reasons for the growth in telemedicine technologies, with many designed to improve patient care by delivering limited resources where they are needed most.
Continuity of Care
Richard Bailey, MD, medical director of Inpatient Care and Hospitalist Services at Saint Clare’s, says having remote intensivists lets his staff focus on hospital patients outside the ICU.
“One critical patient can tie you up for hours,” Dr. Bailey says. “Advanced ICU Care’s intensivists are hands-on physicians, helping us round on ICU patients, take patient notes, and handle first-line phone calls.”
There is no difference, he says, between having intensivists in St. Louis, for example, versus on-site. “They are more than a microphone and a camera in the ceiling; they are members of our staff,” he says. “We trust them to take care of our patients.”
He explains that remote intensivists are often good at being the “bug in the ear” for hospitalists, helping with treatment recommendations and asking, “Did you remember to … ?” While stabilizing a just-transferred ICU patient in a near-code situation, Dr. Bailey needed immediate access to the patient’s labs. An intensivist in St. Louis was able to look at the labs and recommend treatment.
Preliminary numbers at Saint Clare’s hint at a reduction of one day in ICU length of stay and two days for total hospitalization, notes Dr. Bailey. Figures like these can mean real savings in hospital costs.
Working together, hospitalists and remote intensivists can provide continuity of care as the patient is admitted through the emergency department and brought into the ICU, explains Dr. Bailey.
William D. Atchley Jr., MD, medical director for the Division of Hospital Medicine for Sentara Medical Group in Norfolk, Va., agrees with Dr. Bailey’s view. Dr. Atchley’s group also uses telemedicine technology for the remote care and monitoring of ICU patients. He is also a member of SHM’s Board of Directors.
“This is a true team effort, creating a seamless continuity from the emergency department to the ICU,” says Dr. Atchley. He cites septic shock patients as an example. He is able to start the septic shock protocols with the patient in the ED, and the intensivist will carry the protocols forward with the patient in the ICU. By morning, Dr. Atchley says he knows the patient has received the care needed, which frees him to care for other patients.
Sentara Healthcare, based in Norfolk, Va., was the first hospital system in the nation to implement VISICU’s technology, which allows hospitals to create a systemwide critical-care program. Using the VISICU eICU, the hospital or healthcare system provides the intensivists to staff the program, helping to leverage scarce clinical resources among the system’s ICUs.
Studies have shown that care by intensivists via telemedicine technology improves patient care and safety in the ICU. In a 2004 study, Sentara documented a 27% decrease in overall ICU and hospital mortality.2
Mobile Telemedicine
Advances in telemedicine technology have come a long way. Take remote robotic systems, for instance, which allow physicians to consult with patients, family members, and on-site caregivers while seated in their office, in another wing of the hospital, or at home.
InTouch Health, a Santa Barbara, Calif., company, uses about 100 robotic systems. While seated at a control station, equipped with video capabilities, a microphone, and a joystick, the physician can “drive” the robot into a patient’s room for consultation. The patient can see the doctor’s face on the monitor and—on the other end—the physician has access to patient data and can see the patient through a live video image.
The robotic system provides added ability for intensivists and other specialists to do another evening round on their patients, explains Tim Wright, vice president of strategic marketing for InTouch. A recent study shows that when physicians use robotic telepresence to make rounds in the ICU in response to nursing pages, physician response is significantly faster. Additionally, the study found a reduced length of stay, particularly for patients with subarachnoid hemorrhage and brain trauma, as well as an ICU cost savings of $1.1 million.3
The idea of robotic telepresence is similar to the telemedicine model of care being used in the ICU. Through the robotic system, an intensivist can log in and perform an evening round, updating hospitalists on new patients and issues that may have arisen.
“The beauty is that the intensivist and the hospitalist can be looking at everything together,” Wright says. “The intensivist can provide the specialist knowledge and training, while the hospitalist provides the ongoing care.”
Not Just the ICU
Of course, telemedicine is not limited to the ICU. It is being used for virtually every medical specialty to help provide greater access to care.
Take the University of Texas Medical Branch at Galveston (UTMB), which has used telemedicine technologies since 1994. Its Electronic Health Network (EHN) utilizes telemedicine to help care for the state’s indigent and rural populations, as well as other groups, such as the elderly, prisoners, and even researchers in Antarctica.
One of the fastest-growing services UTMB operates is the telemedicine-based corporate healthcare programs, allowing employees to “see” a primary care physician without leaving work. Companies see this as a way to help control healthcare costs and make preventive care more accessible, notes Glenn Hammack, OD, assistant vice president and executive director of the UTMB Electronic Health Network. He also pegs the application of telemedicine to psychiatry as another growing service and one that illustrates how the technology is being used to help address a shortage of providers, especially in rural and underserved parts of Texas. Like the eICU programs designed to bring scarce intensivist care to ICU patients, UTMB’s services help distribute rare resources, such as child and adolescent psychiatrists who speak Spanish, to patients.
The telemedicine program at UMTB began in 1994 as a way to help provide cost-effective healthcare for inmates in the Texas prison system. Today, the Correctional Managed Care (CMC) department has telemedicine stations in 120 correctional units throughout Texas and accounts for about half of UTMB’s telemedicine program.
The 11 telemedicine studios at UTMB used for patients across the EHN are equipped with live interactive video links that allow the telemedicine physician to see and hear the patient, located at the remote station with a registered health professional on-site. Digital stethoscopes, hand-held cameras, and other electronic medical devices help the physician treat patients. The telemedicine program also utilizes shared electronic medical records, which are critical to its success, says Dr. Hammack.
Telemedicine can also be used between departments within the hospital. Dr. Hammack notes that hospitals have become large and complicated; the journey from one end to another for a test or procedure can be difficult on patients. “Telemedicine offers the ability for face-to-face interaction, and when used within hospital departments, it can bring some humanity of scale back to the increasingly complicated hospital environment,” he says.
Another Vision
Troy Sybert, MD, medical director for CMC Hospital Medicine and a practicing hospitalist at Texas Department of Criminal Justice (TDCJ) Hospital in Galveston, Texas, was hired a year ago to help create a hospitalist program within the prison system. His is the only health facility dedicated to prisoners and located on a medical school campus.
While his six-member team is not engaged in telemedicine, he sees a number of possibilities for CMC hospitalists to utilize telemedicine technology. For one, hospitalists could use their expertise in admissions to help triage patients via telemedicine. The CMC recently created a network of regional hubs similar to ED observation centers but without a 24/7 physician presence. Telemedicine triage could help the system offload the decision to admit and would likely reduce the number of hospital admissions, says Dr. Sybert.
Telemedicine technology could also provide other possibilities in perioperative care for surgery patients at TDCJ Hospital. In partnership with the surgery and anesthesia departments, pre- and post-operative work up and care could be done remotely with the patient back in the unit, promoting shorter lengths of stay and reducing transportation needs. The hospitalists, trained in correctional care, would provide support and coordinate with surgery—especially on the patient’s transition to and from the prison facility.
“The whole concept of telemedicine is to utilize experience from a centralized location,” says Dr. Sybert. “We have a vision for where we might like to go with telemedicine, bringing our hospitalist group’s experience with managed correctional care to prison units throughout the state.”
Whether it is bringing intensivist care to a critically ill patient, providing therapy sessions to patients in rural areas, or delivering the expertise of hospitalists, telemedicine technology is likely to play an ever-increasing role in healthcare. Dr. Hammack believes telemedicine will be used more and more as care providers and administrators find the right balance between technology and touch.
“It can be difficult to figure out how telemedicine can fit into the way hospitals do things. But it can fit in and does so very well. Technologies like these have the promise to provide support and result in better quality of care for patients,” he says.
Donya Hengehold is freelance medical journalist.
References
- Angus DC, Kelley MA, Schmitz RJ, et al. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease. JAMA. 2000 Dec 6;284(21):2762-2770. Comment in JAMA. 2001 Feb 28;285(8):1016-1017; author reply 1018. JAMA. 2001 Feb 28;285(8):1017-1018.
- Breslow MJ, Rosenfeld BA, Doerfler M, et al. Effect of a multiple-site intensive care unit telemedicine program on clinical and economic outcomes: an alternative paradigm for intensivist staffing. Crit Care Med. 2004 Jan;32(1):31-38. Erratum in: Crit Care Med. 2004 Jul;32(7):1632.Comment in: Crit Care Med. 2004 Jan;32(1):287-288. Crit Care Med. 2004 Jan;32(1):288-290.
- Vespa PM, Miller C, Hu X, et al. Intensive care unit robotic telepresence facilitates rapid physician response to unstable patients and decreased cost in neurointensive care. Surg Neurol. 2007 April;67(4):331-337.
AIDS Treatment Evolves
This is the first of a two-part series on care of the HIV/AIDS patient. Part 2 will address the public health and counseling aspects of HIV management, as well as the care of children with HIV.
It’s been a little more than a quarter-century since acquired immune deficiency syndrome (AIDS) was first identified. Since 1981, many facets of our understanding and management of HIV/AIDS have changed.
In some populations, HIV (when well-controlled) has been transformed to a chronic disease state, with few episodes of the AIDS-defining conditions (opportunistic infections, Kaposi’s sarcoma, wasting syndromes) seen in the early years of the epidemic. However, when treating underserved and indigent populations, hospitalists may still encounter the common symptoms of advanced disease in their HIV-positive patients.
What are the common presenting scenarios of HIV/AIDS seen by hospitalists in the current era of highly active antiretroviral therapy (HAART), and how does antiretroviral therapy affect hospitalists’ management of these patients? The Hospitalist recently interviewed HIV/AIDS specialists and practicing hospitalists to learn find out.
The Differential Diagnosis: Think Broadly
The Centers for Disease Control and Prevention estimates 1.04 million to 1.19 million people live with HIV/AIDS in the United States. The CDC also estimates approximately 40,000 people become infected with HIV each year.1
The conditions that bring HIV-positive patients to the hospital run the gamut. There is a broad range of presenting symptoms, noted Sigall K. Bell, MD, the Division of Infectious Diseases and General Medicine at Harvard Medical School and Beth Israel Deaconess Medical Center in Boston. “The differential diagnoses for patients who are HIV-infected—depending on their immunological status—can be dramatically expanded compared to HIV-negative patients,” says Dr. Bell. “For any given presenting symptom, one needs to think about whether the person’s HIV itself, an opportunistic infection secondary to the HIV, or HIV medication effects are playing into potential explanations for the presenting symptoms.”
Even the demographics of the hospital’s catchment area can be associated with patients’ problems. “The types of problems seen in hospitalized HIV-infected patients largely depends on the degree of access to care that people have,” says HIV and infectious disease specialist Harry Hollander, MD, program director for the University of California, San Francisco Internal Medicine Residency Program, and professor of Clinical Medicine at UCSF. In areas where care systems are not robust, explains Dr. Hollander, people admitted to the hospital will most likely have the same problems seen at the beginning of the epidemic.
If hospitalists are practicing in areas with highly developed systems of care and good penetration of care, people with HIV are just as likely to be admitted to the hospital with problems completely unrelated to their HIV status. In the pre-antiretroviral era, according to Dr. Hollander, hospital physicians typically saw three or four common types of presentations in these patients. “My biggest message these days,” he says, “is to think broadly about the problems these patients present with, and to generate parallel thinking about HIV-related causes as well as causes not related to HIV. Many patients with well-controlled HIV are more likely to wind up in the hospital because of other routine medical problems. If you only consider the HIV status, you may be missing other important, related and treatable conditions.”
Thomas Baudendistel, MD, who is associate residency program director at California Pacific Medical Center, a community-based hospital in San Francisco operated by Sutter Health, confirms that as HIV patients are getting healthier, “their immune systems are being kept intact [with CD4 counts in the normal range] for longer periods of time. We don’t see issues of HIV-related conditions in hospitalization as much as we did 20, 10, or even five years ago. The life-threatening opportunistic infections, although still there, have receded as cause for hospitalization. When an HIV patient gets admitted, it’s just as likely to be a noninfectious condition, such as lymphoma, or hematologic complications. Or, the patients may be old enough to have heart disease or COPD.”

Other hospitalists practice in areas where the opposite is true. Aman D. Sabharwal, MD, is associate medical director, Inpatient and Hospitalist Services for Jackson Health Systems and practices primarily at Jackson Memorial Hospital, which serves a large indigent population in south Florida. While he agrees that some HIV patients are being well-managed because of advances in antiretroviral therapy, these are not the patients seen by hospitalists in his group.
“A majority of our HIV-positive patients come in for illnesses or opportunistic infections that are due to their HIV,” he says. “Most of these patients are either noncompliant with their medications or have low CD4 counts. Generally, the acute issue for which they are admitted is generally unrelated to the medication itself—it is probably due more so to the lack of medication.”

Dr. Baudendistel reports that he and fellow hospitalists at California Pacific Medical Center are also seeing more immune reconstitution illness, in which the reconstituted immune system exhibits an “overexuberant” reaction, causing unique presentations. For example, patients with low CD4 counts who have clinically silent infection with Mycobacterium Avium Complex, hepatitis B, or a variety of infectious agents may experience a significant boost in their CD4 count with antiretroviral therapy. The resurgent immune system can then mount a response to these previously quiescent pathogens, causing a flare-up of symptoms.
“If the primary site of occult disease is the lungs, a respiratory exacerbation will occur; if in the liver, as in the example of hepatitis B, a significant hepatitis can ensue,” says Dr. Baudendistel.
Call in Consultants: Keep a Low Threshold
As the management of HIV becomes more sophisticated, hospitalists should frequently consult infectious-disease and consulting pharmacy colleagues. “I think the hospitalist is very well-equipped to deal with the acute illnesses that these patients have,” notes Dr. Hollander. “Most hospitalists feel less comfortable with the details of managing the chronic medical regimen—particularly the antiretroviral drugs, which they don’t have an opportunity to prescribe, manage, and monitor over time.”
Dr. Baudendistel concurs: “As a hospitalist, what I face with these patients—especially if they come in with an illness unrelated to HIV—is trying to figure out how a drug I am thinking of prescribing for their heart disease or kidney failure will impact their HAART therapy. Is there going to be some hidden interaction that I’m not aware of because I don’t deal with those medications every day?”
It is precisely when weighing those questions about chronic therapy when hospitalists would be best served to quickly consider consulting either a primary physician or the appropriate consultant about the details of the medication regimen. “In most cases, you’re going to want to continue that regimen during hospitalization for other intercurrent problems,” he says.
When possible, it’s a good idea for the hospitalist to touch base with the primary HIV provider, says Dr. Bell. “There are sometimes subtleties to the care that are not necessarily transmitted in a faxed document or in information the patient brings to the hospital. Those subtleties—about doses of antiretroviral drugs or changes in regimen—can make big differences.”
Hospitalists should inform themselves of the potentially harmful effects of antiretroviral drugs, as well as the potential harm in stopping them. “It takes an awareness of knowing what the potential problems are to know when to utilize a consultant,” says Dr. Bell. “As doctors, we are appropriately aware of the power of medications, and it’s not uncommon when the clinical picture is unclear for physicians to think, ‘First do no harm—let me stop these medications.’ One has to be aware of the fact that stopping a medication doesn’t happen in a vacuum.”
Nuances of HAART Require Vigilance
“Highly active antiretroviral therapy has resulted in improved immunological status for many HIV-positive patients, but the therapy has also introduced several potential complications and consequences of which hospitalists should be aware,” says Dr. Bell. Most notable among those consequences: the effects of starting and stopping medications.
“It used to be,” says Dr. Baudendistel, “that we would say, ‘The patients are only going to be here in the hospital for a few days; let’s just stop their highly active HIV treatment.’ Now we know that is not a good idea, because stopping treatment can create resistant viruses.”
Dr. Bell explains one such example: Each of the classes of antiretroviral drugs has a different half-life. If a physician stops all antiretroviral therapy at the same time, the nucleoside/nucleotide reverse transcriptase inhibitor (NRTI) may wash out of the system more quickly than does the nonnucleoside reverse transcriptase inhibitor (NNRTI). The result will be NNRTI monotherapy, and drug resistance can occur quickly in that setting, says Dr. Bell. (Note: not all patients are on NNRTIs; some may be on protease inhibitors or fusion inhibitors, which all have potentially adverse events and drug-drug interactions.)
As another example, if a patient has co-infection with hepatitis B, stopping an NRTI with activity against hepatitis B (such as lamivudine or tenofovir), may cause hepatitis to flare up. Finally, several studies now suggest that the long-term consequences of starting and stopping therapy (structured treatment interruptions) are also detrimental.2
Hospitalists can incorporate into their diagnosis and treatment of these patients other management strategies beyond potential drug-drug interactions and consequences of incurring resistance when stopping antiretroviral medication. For instance:

- Screen for other problems that may be attributable to long-term antiretroviral therapy, such as dyslipidemia, diabetes, and osteoporosis if the patient has adhered to HAART.3 Because mounting data suggest an increased incidence of cardiovascular disease, aggressive management of other underlying cardiovascular risk factors is an important part of care.
- Ensure electronic medication orders do not automatically default to inappropriate doses. For instance, ritonavir, a protease inhibitor, is most commonly used as a booster dose and not at full dose—but electronic pharmacy ordering systems may not reflect this current knowledge.
- Raise nursing and physician staff awareness to confirm that HAART doses are not missed (e.g., if a patient is off the floor for extended periods of time). Reconcile medication orders and the medication administration record to ensure all ordered medications are given. For example, if there is a delay in accessing one of the patient’s usual medications, it may be harmful to administer just the other two until the third is available. Alternative arrangements would be required.
- Consider orders allowing patients to use their own supply of medications if the hospital pharmacy is not able to supply the exact drug needed for their specific HAART regimen.
It is also advisable to ask HIV patients about their use of alternative therapies, says Dr. Hollander, because studies have shown that a substantial minority of people with HIV infection do, in fact, take alternative therapies.4 “We also know,” he says, “that some of these therapies cause adverse reactions and toxicities that you would not ordinarily consider, unless you had obtained that history.”
Education, Education, Education
Dr. Bell notes that there is wide variability in adherence to medication and follow-up clinic visits among those infected with HIV. “It’s important for hospitalists to emphasize links to care,” she says. “A hospital visit is an important time to emphasize education, and to make sure that those patients have the appropriate follow-up.”
The role of hospitalist as patient educator takes on more prominence in settings with a larger percentage of more indigent patients. “I think the key is education, education, education,” Dr. Sabharwal asserts.
He and hospitalists in his group make patient counseling a key component in their treatment, from the time they encounter patients until discharge. They emphasize that with today’s therapies, a 60-year-old HIV-positive patient may avoid hospitalization, while those who do not take their medications risk the severe sequelae of AIDS-defining conditions.
“It’s very important that physicians not be in a hurry to go from patient to patient,” he says. “A lot of times what’s lacking is for physicians to take the time to sit down with the patient and go over the severity of the disease in its later stages. We counsel patients every single time.”
Dr. Baudendistel’s counsel to fellow hospitalists is that although they may still be attuned to treating HIV complications, such as PCP or TB, HIV is now a chronic disease. And as such, “It’s not something that the casual generalist can manage independently,” he says. “When I was in training, I was very well-versed in managing HIV disease. With the initial drug treatments and the common opportunistic infections, treatment was pretty straightforward. But now I wouldn’t feel comfortable managing the HIV part of the illness on my own. HIV is a subspecialist disease now, and it is important to have a colleague with HIV expertise with whom they can consult.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- CDC HIV/AIDS Fact Sheet, “A Glance at the HIV/AIDS Epidemic.” January 2007. Available online at http://www.cdc.gov/hiv. Last accessed April 2007.
- Pai NP, Lawrence J, Reingold AL, et al. Structured treatment interruptions (STI) in chronic unsuppressed HIV infection in adults. Cochran Database Syst Rev. 2006 Jul 19;3:CD006148.
- Agins BD, Alexander CS, Bartlett JG. Metabolic Complications of Antiretroviral Therapy. A Guide to Primary Care of People with HIV/AIDS, 2004 Ed. Available online at http://hab.hrsa.gov/tools/primarycareguide. Last accessed May 21, 2007.
- Wutoh AK, Brown CM, Kumoji EK, et al. Antiretroviral adherence and use of alternative therapies among older HIV-infected adults. J Natl Med Assoc. 2001 Jul-Aug;93(7-8):243-250.
This is the first of a two-part series on care of the HIV/AIDS patient. Part 2 will address the public health and counseling aspects of HIV management, as well as the care of children with HIV.
It’s been a little more than a quarter-century since acquired immune deficiency syndrome (AIDS) was first identified. Since 1981, many facets of our understanding and management of HIV/AIDS have changed.
In some populations, HIV (when well-controlled) has been transformed to a chronic disease state, with few episodes of the AIDS-defining conditions (opportunistic infections, Kaposi’s sarcoma, wasting syndromes) seen in the early years of the epidemic. However, when treating underserved and indigent populations, hospitalists may still encounter the common symptoms of advanced disease in their HIV-positive patients.
What are the common presenting scenarios of HIV/AIDS seen by hospitalists in the current era of highly active antiretroviral therapy (HAART), and how does antiretroviral therapy affect hospitalists’ management of these patients? The Hospitalist recently interviewed HIV/AIDS specialists and practicing hospitalists to learn find out.
The Differential Diagnosis: Think Broadly
The Centers for Disease Control and Prevention estimates 1.04 million to 1.19 million people live with HIV/AIDS in the United States. The CDC also estimates approximately 40,000 people become infected with HIV each year.1
The conditions that bring HIV-positive patients to the hospital run the gamut. There is a broad range of presenting symptoms, noted Sigall K. Bell, MD, the Division of Infectious Diseases and General Medicine at Harvard Medical School and Beth Israel Deaconess Medical Center in Boston. “The differential diagnoses for patients who are HIV-infected—depending on their immunological status—can be dramatically expanded compared to HIV-negative patients,” says Dr. Bell. “For any given presenting symptom, one needs to think about whether the person’s HIV itself, an opportunistic infection secondary to the HIV, or HIV medication effects are playing into potential explanations for the presenting symptoms.”
Even the demographics of the hospital’s catchment area can be associated with patients’ problems. “The types of problems seen in hospitalized HIV-infected patients largely depends on the degree of access to care that people have,” says HIV and infectious disease specialist Harry Hollander, MD, program director for the University of California, San Francisco Internal Medicine Residency Program, and professor of Clinical Medicine at UCSF. In areas where care systems are not robust, explains Dr. Hollander, people admitted to the hospital will most likely have the same problems seen at the beginning of the epidemic.
If hospitalists are practicing in areas with highly developed systems of care and good penetration of care, people with HIV are just as likely to be admitted to the hospital with problems completely unrelated to their HIV status. In the pre-antiretroviral era, according to Dr. Hollander, hospital physicians typically saw three or four common types of presentations in these patients. “My biggest message these days,” he says, “is to think broadly about the problems these patients present with, and to generate parallel thinking about HIV-related causes as well as causes not related to HIV. Many patients with well-controlled HIV are more likely to wind up in the hospital because of other routine medical problems. If you only consider the HIV status, you may be missing other important, related and treatable conditions.”
Thomas Baudendistel, MD, who is associate residency program director at California Pacific Medical Center, a community-based hospital in San Francisco operated by Sutter Health, confirms that as HIV patients are getting healthier, “their immune systems are being kept intact [with CD4 counts in the normal range] for longer periods of time. We don’t see issues of HIV-related conditions in hospitalization as much as we did 20, 10, or even five years ago. The life-threatening opportunistic infections, although still there, have receded as cause for hospitalization. When an HIV patient gets admitted, it’s just as likely to be a noninfectious condition, such as lymphoma, or hematologic complications. Or, the patients may be old enough to have heart disease or COPD.”
Other hospitalists practice in areas where the opposite is true. Aman D. Sabharwal, MD, is associate medical director, Inpatient and Hospitalist Services for Jackson Health Systems and practices primarily at Jackson Memorial Hospital, which serves a large indigent population in south Florida. While he agrees that some HIV patients are being well-managed because of advances in antiretroviral therapy, these are not the patients seen by hospitalists in his group.
“A majority of our HIV-positive patients come in for illnesses or opportunistic infections that are due to their HIV,” he says. “Most of these patients are either noncompliant with their medications or have low CD4 counts. Generally, the acute issue for which they are admitted is generally unrelated to the medication itself—it is probably due more so to the lack of medication.”
Dr. Baudendistel reports that he and fellow hospitalists at California Pacific Medical Center are also seeing more immune reconstitution illness, in which the reconstituted immune system exhibits an “overexuberant” reaction, causing unique presentations. For example, patients with low CD4 counts who have clinically silent infection with Mycobacterium Avium Complex, hepatitis B, or a variety of infectious agents may experience a significant boost in their CD4 count with antiretroviral therapy. The resurgent immune system can then mount a response to these previously quiescent pathogens, causing a flare-up of symptoms.
“If the primary site of occult disease is the lungs, a respiratory exacerbation will occur; if in the liver, as in the example of hepatitis B, a significant hepatitis can ensue,” says Dr. Baudendistel.
Call in Consultants: Keep a Low Threshold
As the management of HIV becomes more sophisticated, hospitalists should frequently consult infectious-disease and consulting pharmacy colleagues. “I think the hospitalist is very well-equipped to deal with the acute illnesses that these patients have,” notes Dr. Hollander. “Most hospitalists feel less comfortable with the details of managing the chronic medical regimen—particularly the antiretroviral drugs, which they don’t have an opportunity to prescribe, manage, and monitor over time.”
Dr. Baudendistel concurs: “As a hospitalist, what I face with these patients—especially if they come in with an illness unrelated to HIV—is trying to figure out how a drug I am thinking of prescribing for their heart disease or kidney failure will impact their HAART therapy. Is there going to be some hidden interaction that I’m not aware of because I don’t deal with those medications every day?”
It is precisely when weighing those questions about chronic therapy when hospitalists would be best served to quickly consider consulting either a primary physician or the appropriate consultant about the details of the medication regimen. “In most cases, you’re going to want to continue that regimen during hospitalization for other intercurrent problems,” he says.
When possible, it’s a good idea for the hospitalist to touch base with the primary HIV provider, says Dr. Bell. “There are sometimes subtleties to the care that are not necessarily transmitted in a faxed document or in information the patient brings to the hospital. Those subtleties—about doses of antiretroviral drugs or changes in regimen—can make big differences.”
Hospitalists should inform themselves of the potentially harmful effects of antiretroviral drugs, as well as the potential harm in stopping them. “It takes an awareness of knowing what the potential problems are to know when to utilize a consultant,” says Dr. Bell. “As doctors, we are appropriately aware of the power of medications, and it’s not uncommon when the clinical picture is unclear for physicians to think, ‘First do no harm—let me stop these medications.’ One has to be aware of the fact that stopping a medication doesn’t happen in a vacuum.”
Nuances of HAART Require Vigilance
“Highly active antiretroviral therapy has resulted in improved immunological status for many HIV-positive patients, but the therapy has also introduced several potential complications and consequences of which hospitalists should be aware,” says Dr. Bell. Most notable among those consequences: the effects of starting and stopping medications.
“It used to be,” says Dr. Baudendistel, “that we would say, ‘The patients are only going to be here in the hospital for a few days; let’s just stop their highly active HIV treatment.’ Now we know that is not a good idea, because stopping treatment can create resistant viruses.”
Dr. Bell explains one such example: Each of the classes of antiretroviral drugs has a different half-life. If a physician stops all antiretroviral therapy at the same time, the nucleoside/nucleotide reverse transcriptase inhibitor (NRTI) may wash out of the system more quickly than does the nonnucleoside reverse transcriptase inhibitor (NNRTI). The result will be NNRTI monotherapy, and drug resistance can occur quickly in that setting, says Dr. Bell. (Note: not all patients are on NNRTIs; some may be on protease inhibitors or fusion inhibitors, which all have potentially adverse events and drug-drug interactions.)
As another example, if a patient has co-infection with hepatitis B, stopping an NRTI with activity against hepatitis B (such as lamivudine or tenofovir), may cause hepatitis to flare up. Finally, several studies now suggest that the long-term consequences of starting and stopping therapy (structured treatment interruptions) are also detrimental.2
Hospitalists can incorporate into their diagnosis and treatment of these patients other management strategies beyond potential drug-drug interactions and consequences of incurring resistance when stopping antiretroviral medication. For instance:
- Screen for other problems that may be attributable to long-term antiretroviral therapy, such as dyslipidemia, diabetes, and osteoporosis if the patient has adhered to HAART.3 Because mounting data suggest an increased incidence of cardiovascular disease, aggressive management of other underlying cardiovascular risk factors is an important part of care.
- Ensure electronic medication orders do not automatically default to inappropriate doses. For instance, ritonavir, a protease inhibitor, is most commonly used as a booster dose and not at full dose—but electronic pharmacy ordering systems may not reflect this current knowledge.
- Raise nursing and physician staff awareness to confirm that HAART doses are not missed (e.g., if a patient is off the floor for extended periods of time). Reconcile medication orders and the medication administration record to ensure all ordered medications are given. For example, if there is a delay in accessing one of the patient’s usual medications, it may be harmful to administer just the other two until the third is available. Alternative arrangements would be required.
- Consider orders allowing patients to use their own supply of medications if the hospital pharmacy is not able to supply the exact drug needed for their specific HAART regimen.
It is also advisable to ask HIV patients about their use of alternative therapies, says Dr. Hollander, because studies have shown that a substantial minority of people with HIV infection do, in fact, take alternative therapies.4 “We also know,” he says, “that some of these therapies cause adverse reactions and toxicities that you would not ordinarily consider, unless you had obtained that history.”
Education, Education, Education
Dr. Bell notes that there is wide variability in adherence to medication and follow-up clinic visits among those infected with HIV. “It’s important for hospitalists to emphasize links to care,” she says. “A hospital visit is an important time to emphasize education, and to make sure that those patients have the appropriate follow-up.”
The role of hospitalist as patient educator takes on more prominence in settings with a larger percentage of more indigent patients. “I think the key is education, education, education,” Dr. Sabharwal asserts.
He and hospitalists in his group make patient counseling a key component in their treatment, from the time they encounter patients until discharge. They emphasize that with today’s therapies, a 60-year-old HIV-positive patient may avoid hospitalization, while those who do not take their medications risk the severe sequelae of AIDS-defining conditions.
“It’s very important that physicians not be in a hurry to go from patient to patient,” he says. “A lot of times what’s lacking is for physicians to take the time to sit down with the patient and go over the severity of the disease in its later stages. We counsel patients every single time.”
Dr. Baudendistel’s counsel to fellow hospitalists is that although they may still be attuned to treating HIV complications, such as PCP or TB, HIV is now a chronic disease. And as such, “It’s not something that the casual generalist can manage independently,” he says. “When I was in training, I was very well-versed in managing HIV disease. With the initial drug treatments and the common opportunistic infections, treatment was pretty straightforward. But now I wouldn’t feel comfortable managing the HIV part of the illness on my own. HIV is a subspecialist disease now, and it is important to have a colleague with HIV expertise with whom they can consult.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- CDC HIV/AIDS Fact Sheet, “A Glance at the HIV/AIDS Epidemic.” January 2007. Available online at http://www.cdc.gov/hiv. Last accessed April 2007.
- Pai NP, Lawrence J, Reingold AL, et al. Structured treatment interruptions (STI) in chronic unsuppressed HIV infection in adults. Cochran Database Syst Rev. 2006 Jul 19;3:CD006148.
- Agins BD, Alexander CS, Bartlett JG. Metabolic Complications of Antiretroviral Therapy. A Guide to Primary Care of People with HIV/AIDS, 2004 Ed. Available online at http://hab.hrsa.gov/tools/primarycareguide. Last accessed May 21, 2007.
- Wutoh AK, Brown CM, Kumoji EK, et al. Antiretroviral adherence and use of alternative therapies among older HIV-infected adults. J Natl Med Assoc. 2001 Jul-Aug;93(7-8):243-250.
This is the first of a two-part series on care of the HIV/AIDS patient. Part 2 will address the public health and counseling aspects of HIV management, as well as the care of children with HIV.
It’s been a little more than a quarter-century since acquired immune deficiency syndrome (AIDS) was first identified. Since 1981, many facets of our understanding and management of HIV/AIDS have changed.
In some populations, HIV (when well-controlled) has been transformed to a chronic disease state, with few episodes of the AIDS-defining conditions (opportunistic infections, Kaposi’s sarcoma, wasting syndromes) seen in the early years of the epidemic. However, when treating underserved and indigent populations, hospitalists may still encounter the common symptoms of advanced disease in their HIV-positive patients.
What are the common presenting scenarios of HIV/AIDS seen by hospitalists in the current era of highly active antiretroviral therapy (HAART), and how does antiretroviral therapy affect hospitalists’ management of these patients? The Hospitalist recently interviewed HIV/AIDS specialists and practicing hospitalists to learn find out.
The Differential Diagnosis: Think Broadly
The Centers for Disease Control and Prevention estimates 1.04 million to 1.19 million people live with HIV/AIDS in the United States. The CDC also estimates approximately 40,000 people become infected with HIV each year.1
The conditions that bring HIV-positive patients to the hospital run the gamut. There is a broad range of presenting symptoms, noted Sigall K. Bell, MD, the Division of Infectious Diseases and General Medicine at Harvard Medical School and Beth Israel Deaconess Medical Center in Boston. “The differential diagnoses for patients who are HIV-infected—depending on their immunological status—can be dramatically expanded compared to HIV-negative patients,” says Dr. Bell. “For any given presenting symptom, one needs to think about whether the person’s HIV itself, an opportunistic infection secondary to the HIV, or HIV medication effects are playing into potential explanations for the presenting symptoms.”
Even the demographics of the hospital’s catchment area can be associated with patients’ problems. “The types of problems seen in hospitalized HIV-infected patients largely depends on the degree of access to care that people have,” says HIV and infectious disease specialist Harry Hollander, MD, program director for the University of California, San Francisco Internal Medicine Residency Program, and professor of Clinical Medicine at UCSF. In areas where care systems are not robust, explains Dr. Hollander, people admitted to the hospital will most likely have the same problems seen at the beginning of the epidemic.
If hospitalists are practicing in areas with highly developed systems of care and good penetration of care, people with HIV are just as likely to be admitted to the hospital with problems completely unrelated to their HIV status. In the pre-antiretroviral era, according to Dr. Hollander, hospital physicians typically saw three or four common types of presentations in these patients. “My biggest message these days,” he says, “is to think broadly about the problems these patients present with, and to generate parallel thinking about HIV-related causes as well as causes not related to HIV. Many patients with well-controlled HIV are more likely to wind up in the hospital because of other routine medical problems. If you only consider the HIV status, you may be missing other important, related and treatable conditions.”
Thomas Baudendistel, MD, who is associate residency program director at California Pacific Medical Center, a community-based hospital in San Francisco operated by Sutter Health, confirms that as HIV patients are getting healthier, “their immune systems are being kept intact [with CD4 counts in the normal range] for longer periods of time. We don’t see issues of HIV-related conditions in hospitalization as much as we did 20, 10, or even five years ago. The life-threatening opportunistic infections, although still there, have receded as cause for hospitalization. When an HIV patient gets admitted, it’s just as likely to be a noninfectious condition, such as lymphoma, or hematologic complications. Or, the patients may be old enough to have heart disease or COPD.”
Other hospitalists practice in areas where the opposite is true. Aman D. Sabharwal, MD, is associate medical director, Inpatient and Hospitalist Services for Jackson Health Systems and practices primarily at Jackson Memorial Hospital, which serves a large indigent population in south Florida. While he agrees that some HIV patients are being well-managed because of advances in antiretroviral therapy, these are not the patients seen by hospitalists in his group.
“A majority of our HIV-positive patients come in for illnesses or opportunistic infections that are due to their HIV,” he says. “Most of these patients are either noncompliant with their medications or have low CD4 counts. Generally, the acute issue for which they are admitted is generally unrelated to the medication itself—it is probably due more so to the lack of medication.”
Dr. Baudendistel reports that he and fellow hospitalists at California Pacific Medical Center are also seeing more immune reconstitution illness, in which the reconstituted immune system exhibits an “overexuberant” reaction, causing unique presentations. For example, patients with low CD4 counts who have clinically silent infection with Mycobacterium Avium Complex, hepatitis B, or a variety of infectious agents may experience a significant boost in their CD4 count with antiretroviral therapy. The resurgent immune system can then mount a response to these previously quiescent pathogens, causing a flare-up of symptoms.
“If the primary site of occult disease is the lungs, a respiratory exacerbation will occur; if in the liver, as in the example of hepatitis B, a significant hepatitis can ensue,” says Dr. Baudendistel.
Call in Consultants: Keep a Low Threshold
As the management of HIV becomes more sophisticated, hospitalists should frequently consult infectious-disease and consulting pharmacy colleagues. “I think the hospitalist is very well-equipped to deal with the acute illnesses that these patients have,” notes Dr. Hollander. “Most hospitalists feel less comfortable with the details of managing the chronic medical regimen—particularly the antiretroviral drugs, which they don’t have an opportunity to prescribe, manage, and monitor over time.”
Dr. Baudendistel concurs: “As a hospitalist, what I face with these patients—especially if they come in with an illness unrelated to HIV—is trying to figure out how a drug I am thinking of prescribing for their heart disease or kidney failure will impact their HAART therapy. Is there going to be some hidden interaction that I’m not aware of because I don’t deal with those medications every day?”
It is precisely when weighing those questions about chronic therapy when hospitalists would be best served to quickly consider consulting either a primary physician or the appropriate consultant about the details of the medication regimen. “In most cases, you’re going to want to continue that regimen during hospitalization for other intercurrent problems,” he says.
When possible, it’s a good idea for the hospitalist to touch base with the primary HIV provider, says Dr. Bell. “There are sometimes subtleties to the care that are not necessarily transmitted in a faxed document or in information the patient brings to the hospital. Those subtleties—about doses of antiretroviral drugs or changes in regimen—can make big differences.”
Hospitalists should inform themselves of the potentially harmful effects of antiretroviral drugs, as well as the potential harm in stopping them. “It takes an awareness of knowing what the potential problems are to know when to utilize a consultant,” says Dr. Bell. “As doctors, we are appropriately aware of the power of medications, and it’s not uncommon when the clinical picture is unclear for physicians to think, ‘First do no harm—let me stop these medications.’ One has to be aware of the fact that stopping a medication doesn’t happen in a vacuum.”
Nuances of HAART Require Vigilance
“Highly active antiretroviral therapy has resulted in improved immunological status for many HIV-positive patients, but the therapy has also introduced several potential complications and consequences of which hospitalists should be aware,” says Dr. Bell. Most notable among those consequences: the effects of starting and stopping medications.
“It used to be,” says Dr. Baudendistel, “that we would say, ‘The patients are only going to be here in the hospital for a few days; let’s just stop their highly active HIV treatment.’ Now we know that is not a good idea, because stopping treatment can create resistant viruses.”
Dr. Bell explains one such example: Each of the classes of antiretroviral drugs has a different half-life. If a physician stops all antiretroviral therapy at the same time, the nucleoside/nucleotide reverse transcriptase inhibitor (NRTI) may wash out of the system more quickly than does the nonnucleoside reverse transcriptase inhibitor (NNRTI). The result will be NNRTI monotherapy, and drug resistance can occur quickly in that setting, says Dr. Bell. (Note: not all patients are on NNRTIs; some may be on protease inhibitors or fusion inhibitors, which all have potentially adverse events and drug-drug interactions.)
As another example, if a patient has co-infection with hepatitis B, stopping an NRTI with activity against hepatitis B (such as lamivudine or tenofovir), may cause hepatitis to flare up. Finally, several studies now suggest that the long-term consequences of starting and stopping therapy (structured treatment interruptions) are also detrimental.2
Hospitalists can incorporate into their diagnosis and treatment of these patients other management strategies beyond potential drug-drug interactions and consequences of incurring resistance when stopping antiretroviral medication. For instance:
- Screen for other problems that may be attributable to long-term antiretroviral therapy, such as dyslipidemia, diabetes, and osteoporosis if the patient has adhered to HAART.3 Because mounting data suggest an increased incidence of cardiovascular disease, aggressive management of other underlying cardiovascular risk factors is an important part of care.
- Ensure electronic medication orders do not automatically default to inappropriate doses. For instance, ritonavir, a protease inhibitor, is most commonly used as a booster dose and not at full dose—but electronic pharmacy ordering systems may not reflect this current knowledge.
- Raise nursing and physician staff awareness to confirm that HAART doses are not missed (e.g., if a patient is off the floor for extended periods of time). Reconcile medication orders and the medication administration record to ensure all ordered medications are given. For example, if there is a delay in accessing one of the patient’s usual medications, it may be harmful to administer just the other two until the third is available. Alternative arrangements would be required.
- Consider orders allowing patients to use their own supply of medications if the hospital pharmacy is not able to supply the exact drug needed for their specific HAART regimen.
It is also advisable to ask HIV patients about their use of alternative therapies, says Dr. Hollander, because studies have shown that a substantial minority of people with HIV infection do, in fact, take alternative therapies.4 “We also know,” he says, “that some of these therapies cause adverse reactions and toxicities that you would not ordinarily consider, unless you had obtained that history.”
Education, Education, Education
Dr. Bell notes that there is wide variability in adherence to medication and follow-up clinic visits among those infected with HIV. “It’s important for hospitalists to emphasize links to care,” she says. “A hospital visit is an important time to emphasize education, and to make sure that those patients have the appropriate follow-up.”
The role of hospitalist as patient educator takes on more prominence in settings with a larger percentage of more indigent patients. “I think the key is education, education, education,” Dr. Sabharwal asserts.
He and hospitalists in his group make patient counseling a key component in their treatment, from the time they encounter patients until discharge. They emphasize that with today’s therapies, a 60-year-old HIV-positive patient may avoid hospitalization, while those who do not take their medications risk the severe sequelae of AIDS-defining conditions.
“It’s very important that physicians not be in a hurry to go from patient to patient,” he says. “A lot of times what’s lacking is for physicians to take the time to sit down with the patient and go over the severity of the disease in its later stages. We counsel patients every single time.”
Dr. Baudendistel’s counsel to fellow hospitalists is that although they may still be attuned to treating HIV complications, such as PCP or TB, HIV is now a chronic disease. And as such, “It’s not something that the casual generalist can manage independently,” he says. “When I was in training, I was very well-versed in managing HIV disease. With the initial drug treatments and the common opportunistic infections, treatment was pretty straightforward. But now I wouldn’t feel comfortable managing the HIV part of the illness on my own. HIV is a subspecialist disease now, and it is important to have a colleague with HIV expertise with whom they can consult.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- CDC HIV/AIDS Fact Sheet, “A Glance at the HIV/AIDS Epidemic.” January 2007. Available online at http://www.cdc.gov/hiv. Last accessed April 2007.
- Pai NP, Lawrence J, Reingold AL, et al. Structured treatment interruptions (STI) in chronic unsuppressed HIV infection in adults. Cochran Database Syst Rev. 2006 Jul 19;3:CD006148.
- Agins BD, Alexander CS, Bartlett JG. Metabolic Complications of Antiretroviral Therapy. A Guide to Primary Care of People with HIV/AIDS, 2004 Ed. Available online at http://hab.hrsa.gov/tools/primarycareguide. Last accessed May 21, 2007.
- Wutoh AK, Brown CM, Kumoji EK, et al. Antiretroviral adherence and use of alternative therapies among older HIV-infected adults. J Natl Med Assoc. 2001 Jul-Aug;93(7-8):243-250.
It's a Team Thing
Hospitalization can be risky business for geriatric patients. Americans 65 and older make up 13% of the population but account for 48% of inpatient days of care and 78% of hospital deaths. While in the hospital, patients 75 and older are at high risk for deconditioning and functional decline, medication errors, delirium, and falls.1,2
For geriatric patients not closely monitored, notes geriatrician Don Murphy, MD, co-principal of Senior Care of Colorado, a large primary care geriatrics group in Denver, going to the hospital can be like disappearing into a black hole.
As the U.S. population ages, hospitalists will be caring for an increasing number of geriatric patients. They will have to address patients’ acute medical conditions without compromising their functional status.
The Hospitalist asked several leading geriatricians to identify valuable tools and strategies for delivering comprehensive geriatric care in the hospital. Even in the absence of formal geriatric care units, they say, hospitalists are positioned for adopting the principles of quality geriatric care. Many of those principles align with the central mission of hospital medicine: promoting high-quality, patient-centered care, working as a team, and developing clear lines of communication between the hospitalist and the primary care teams.
A Survey of Interventions
“There’s no question that it’s becoming extraordinarily difficult to do good care,” says John Morley, MD, professor of medicine and chief of the Division of Geriatrics and Endocrinology at Saint Louis University Health Sciences Center in Missouri. “Taking care of an older person in the hospital is a team sport—the physician can’t do it alone.”
It’s clear the team approach is a crucial foundation for interventions that target at-risk geriatric patients, agrees Edgar Pierluissi, MD, associate clinical professor of medicine and medical director of the recently established ACE unit at San Francisco General Hospital. Reducing the incidence of delirium, for instance, cannot be accomplished simply by utilizing a geriatric consultation. Once established, acute confusion can be intractable. “The idea is to try to prevent delirium, and research has shown that single-person types of interventions in these massively impervious-to-change facilities don’t work,” he says.
Clinical trials have demonstrated that interventions, including interdisciplinary and collaborative teams, targeted patient-centered therapies, and comprehensive geriatric assessment can improve outcomes of hospitalization in geriatric patients. Four major interventions include:
- Acute Care for Elders (ACE) units based on interdisciplinary team rounds, discharge planning, and medical review in a prepared environment to foster patient self-care and improve function. Randomized clinical trials have shown ACE units can reduce the length of stay, the risk of nursing home admissions, and the use of physical restraints while improving providers’ satisfaction with patient care.3,4
- The Hospital Elder Life Program (HELP), led by a geriatrics resource nurse, is an intervention designed to reduce the incidence of delirium by adjusting environmental elements, such as dimming lights and keeping the floor quiet at night. HELP also introduces non-pharmacologic interventions, including massages and warm tea at night and promotes mobility and hydration during the day.
- Incidence of delirium is reduced and cost savings are realized using the HELP.5 (Visit http://elderlife.med.yale.edu/public for more information.)
- Geriatric Evaluation and Management (GEM) units also emphasize a multidisciplinary comprehensive approach using geriatrician-led teams. The intervention can reduce long-term costs, while improving physical functioning and general health domains in the SF-36.6
- Use of advanced practice nurses in comprehensive discharge planning interventions, including nursing home visits for older patients with risk factors for poor outcomes post-discharge, has been shown to reduce readmissions.7
Assessment Is the Bottom Line
Robert Palmer, MD, head of the Section of Geriatric Medicine and professor of medicine at Cleveland Clinic Lerner College of Medicine of Case Western Reserve University in Ohio, is known for his work with ACE units. He and his colleagues have tracked patients following discharge and have identified the highest priority issues that should be addressed to avoid deleterious geriatric syndromes in the hospital. Although he advocates what he calls a minimalist approach to conducting a geriatric assessment, Dr. Palmer underlines the idea that it must also be a deliberate and structured approach. Assessing and acting upon key indicators in four to five major domains, he notes, can make a big difference for patients’ hospital trajectories.8 Here are a few domains to consider:
1 Focus on activities of daily living (ADLs). Function and performance of ADLs can predict post-hospital outcome and help the physician prioritize elements of the patient’s trajectory and goals while in the hospital. “If a person was able to independently bathe, dress, toilet, walk, and transfer—from bed to chair, for instance—before the acute illness, then he or she should be able to get back to that point after the illness has been treated,” says Dr. Palmer. The ability to transfer independently is an important predictor of discharge status because if the patient requires assistance to transfer, he or she will need a different level of care upon discharge. The hospitalist should seek information —from the patient, family member or primary caregiver, or primary care physician—about the patient’s ADLs before he or she got sick. Again, recovery of ADLs may be possible if the patient was performing these independently before the acute episode.
2 Cognitive assessments are also key. Dr. Morley places assessment for delirium at the top of his list. Research shows that approximately one third of patients over 70 in the hospital will develop the condition. Delirium, or acute confusion, is also a predictor of decline in ADLs, notes Dr. Palmer. Dr. Morley recommends the use of the Confusion Assessment Method (CAM) because the Mini Mental State Exam can be time-consuming. (A CAM form is available free online as part of SHM’s “Clinical Toolbox for Geriatric Care.” Go to www.hospitalmedicine.org, click on “Resource Center” and then “Geriatric Special Interest Area” to find the Toolbox.) According to Dr. Palmer, the physician should also use common sense when initially examining the patient: Observe whether the patient is confused, distracted, or inappropriate in conversation. If so, the next step is to use the simple Digit Span test: Say a random set of four to five numbers, and ask the patient to repeat them. Inability to do this is consistent with delirium as a cause of cognitive impairment.
For assessing cognitive impairment, Dr. Morley prefers the St. Louis University Mental Status Exam (SLUMS) to the Mini Mental Status Exam. The SLUMS, developed in collaboration with the Department of Veterans Affairs (and available free online at: http://medschool.slu.edu/agingsuccessfully/pdfsurveys/slumsexam_05.pdf) successfully picks up even mild cognitive impairment, according to Dr. Morley. This is important information not just for the hospital trajectory but also for discharge planning: Inability to follow discharge instructions due to cognitive impairment could result in a readmission.
3 Malnutrition is associated with mortality. Dr. Morley uses the four questions of the Simplified Nutrition Assessment Questionnaire (SNAQ), which correlate well with future weight loss and poor outcomes.9
If the SNAQ is positive, the use of a lengthier questionnaire may be warranted. Dr. Palmer suggests that a review of the patient’s comprehensive metabolic panel to judge kidney and liver function and a bedside evaluation using the Subjective Global Assessment (SGA) can yield results just as usable as the more complex and time-consuming textbook nutritional assessments.
4 Mood and affect also play a role in patients’ outcomes. Research has shown that depressed patients have poor outcomes, so physicians should always assess for depression. While the Geriatric Depression Scale (see “Clinical Toolbox for Geriatric Care” on the SHM Web site) can help quantify the extent of the patient’s symptoms, simply asking the patient, “Are you depressed, sad, or blue?” can often elicit enough information about the patient’s psychological status to direct interventions.
5 Mobility is sometimes classified as a stand-alone domain. However, walking and balance may be included in the assessment of ADLs. A patient who can walk independently—even with a cane or a walker—has a good chance to return home, says Dr. Palmer. Requiring another person to help with walking most likely indicates the patient will need short-term rehabilitation in a skilled nursing facility before returning home.
6 Social and living situation are important. The physician must identify the extent and quality of the patient’s support network. If, for instance, a patient has mild dementia but has a network of 10 extended family members who act as caregivers, discharge to home may be possible. If the patient was admitted to the hospital from a nursing home, however, it is most likely he or she will return there.
Revisit Daily Goals
Dr. Palmer advises hospitalists to follow the geriatric assessment with a translation of the information into what he calls a functional trajectory for the patient’s hospital stay. This includes an estimate of the patient’s anticipated length of stay and the expected discharge site. Interventions and consultations from allied health providers will be keyed to the patient’s individualized needs and to the goals of the functional trajectory.
To head off problems, Dr. Palmer advocates consultations from allied health professionals early in the hospital trajectory. For instance, if the patient is having trouble transferring from bed to chair upon admission, a consult with physical therapy may be warranted immediately rather than right before discharge, as is usually the case.
“We should not be depending on physical therapists at the end of hospitalization, when patients are already deconditioned and can’t get out of bed and need to go to a nursing home,” he explains. “The ideal time to bring in the physical therapist or technician is when you’ve identified—on day one—that the patient needs assistance with transfers, so that you can preserve mobility and shorten hospital stay.”
In the same vein, knowing the patient’s living situation will allow involvement of the discharge planner from day one of the hospitalization to plan with the patient or family for the patient’s return to home or to an alternate site. If the patient has been on a complex drug regimen, involving the pharmacist to help straighten out medications can head off potential drug-drug interactions. (SHM’s Geriatric Toolbox also has a list of medications to avoid in geriatric patients.)
It is important to review the functional trajectory on a daily basis. Input from other members of the health team will be invaluable. “Each day you identify barriers to that successful plan of the outcome, and you take care of them one at a time,” says Dr. Palmer. “If the patient is not on track with that daily goal, the team goes back to the drawing board and asks, ‘What are we missing here?’ Then you do a reassessment of ADLs, nutrition, and cognition.”
Hospitalists must also include the patient’s family members and primary caregivers as the patient moves toward discharge, asserts Dr. Morley. Clear, unambiguous written instructions must always be given to the patient or the primary caregiver when the patient leaves the hospital. (You can also find a discharge instruction sheet in SHM’s Toolbox.) If a patient appears to be facing the end of life, the hospitalist should schedule a conference with members of the primary care team, the hospitalist team, and all family stakeholders.
Transportable SKILLS
Some experts maintain that quality care for geriatric patients can be accomplished without a specialized geriatrics unit.
“I never conceived of the ACE intervention as being done exclusively on a unit,” says Dr. Palmer. “The idea was to develop the skills on a unit and then transport those skills to all units.” Although the protocols developed for ACE units are good for teaching, he says the team has been the key.
Dr. Morley agrees: “It’s not the physical part of the ACE unit that works. You must have team interactions. Finding a way to communicate between the different team members is absolutely key to good outcomes.”
Involving healthcare providers from different disciplines only enhances the care of geriatric patients. “Even though hospitalists may not have the depth of knowledge of geriatrics that a geriatrician has, they certainly have the knowledge of acute care medicine that we have, so they can manage the medical problems,” says Dr. Palmer. “What they need to do is think systematically, in a structured way, and to work collaboratively with key players. This only takes a few minutes each day, but more importantly, it saves time. You have fewer phone calls and fewer angry family members when you manage the care in a structured manner, working with a team of health professionals.”
Dr. Morley and his team have developed a form for their ACE unit that allows them to assess a patient’s status and goals in two to three minutes.
Dr. Pierluissi has experienced firsthand the benefits of working as a member of the interdisciplinary team. “Essentially,” he says, working in teams to treat the geriatric patient means there are “more heads in the game, more people trying to work in the patient’s best interest. You [the clinician] really do feel supported, and it makes your day more enjoyable and more productive.” TH
Gretchen Henkel is a medical journalist based in California.
Resources
- Kozak LJ, Hall MJ, Owings MF. Hospitalization fact sheet. In: National Hospital Discharge Survey: 2000 Annual summary with detailed diagnosis and procedure data. Hyattsville, Maryland: National Center for Health Statistics. Vital Health Stat. 2002;13(153).
- Covinsky KE, Palmer RM, Fortinsky RH, et al. Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: increased vulnerability with age. J Am Geriatr Soc. 2003 Apr;51(4):451-458.
- Landefeld CS, Palmer RM, Kresevic DM, et al. A randomized trial of care in a hospital medical unit especially designed to improve the functional outcomes of acutely ill older patients. N Engl J Med. 1995 May;332(20):1338-1344. Comments in: ACP J Club. 1995 Nov-Dec; 123(3):69 and N Engl J Med. 1995 May 18; 332(20):1376-1378.
- Counsell SR, Holder CM, Liebenauer LL, et al. Effects of a multicomponent intervention on functional outcomes and process of care in hospitalized older patients: a randomized controlled trial of acute care for Elders (ACE) in a community hospital. J Am Geriatr Soc. 2000 Dec;48:1572-1581.
- Inouye SK, Bogardus ST Jr, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med. 1999 Mar 4;340(9):669-676. Comments in: N Engl J Med. 1999 Jul 29; 341(5):369-370; author reply 370 and N Engl J Med. 1999 Mar 4; 340(9):720-721.
- Cohen HJ, Feussner JR, Weinberger M, et al. A controlled trial of inpatient and outpatient geriatric evaluation and management. N Engl J Med. 2002 Mar 21;346(12):905-912. Comments in: Curr Surg. 2004 May-Jun;61(3):266-274; N Engl J Med. 2002 Aug 1;347(5):371-373; author reply 371-373 & N Engl J Med. 2002 Mar 21;346(12):874.
- Naylor MD, Brooten DA, Campbell RL, et al. Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial. J Am Geriatr Soc. 2004 May;52(5):675-684. Erratum in J Am Geriatr Soc. 2004 Jul; 52(7):1228. Comment in Evid Based Nurs. 2004 Oct;7(4):116.
- Palmer RM. Acute hospital care of the elderly: making a difference. Caring for the Hospitalized Elderly [special supplement to The Hospitalist]. 2004. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=The_Hospitalist&Template=/CM/ContentDisplay.cfm&ContentFileID=1447. Last accessed March 14, 2007.
- Wilson MM, Thomas DR, Rubenstein LZ, et al. Appetite assessment: simple appetite questionnaire predicts weight loss in community-dwelling adults and nursing home residents. Am J Clin Nutr. 2005 Nov;82(5):1074-1081.
Hospitalization can be risky business for geriatric patients. Americans 65 and older make up 13% of the population but account for 48% of inpatient days of care and 78% of hospital deaths. While in the hospital, patients 75 and older are at high risk for deconditioning and functional decline, medication errors, delirium, and falls.1,2
For geriatric patients not closely monitored, notes geriatrician Don Murphy, MD, co-principal of Senior Care of Colorado, a large primary care geriatrics group in Denver, going to the hospital can be like disappearing into a black hole.
As the U.S. population ages, hospitalists will be caring for an increasing number of geriatric patients. They will have to address patients’ acute medical conditions without compromising their functional status.
The Hospitalist asked several leading geriatricians to identify valuable tools and strategies for delivering comprehensive geriatric care in the hospital. Even in the absence of formal geriatric care units, they say, hospitalists are positioned for adopting the principles of quality geriatric care. Many of those principles align with the central mission of hospital medicine: promoting high-quality, patient-centered care, working as a team, and developing clear lines of communication between the hospitalist and the primary care teams.
A Survey of Interventions
“There’s no question that it’s becoming extraordinarily difficult to do good care,” says John Morley, MD, professor of medicine and chief of the Division of Geriatrics and Endocrinology at Saint Louis University Health Sciences Center in Missouri. “Taking care of an older person in the hospital is a team sport—the physician can’t do it alone.”
It’s clear the team approach is a crucial foundation for interventions that target at-risk geriatric patients, agrees Edgar Pierluissi, MD, associate clinical professor of medicine and medical director of the recently established ACE unit at San Francisco General Hospital. Reducing the incidence of delirium, for instance, cannot be accomplished simply by utilizing a geriatric consultation. Once established, acute confusion can be intractable. “The idea is to try to prevent delirium, and research has shown that single-person types of interventions in these massively impervious-to-change facilities don’t work,” he says.
Clinical trials have demonstrated that interventions, including interdisciplinary and collaborative teams, targeted patient-centered therapies, and comprehensive geriatric assessment can improve outcomes of hospitalization in geriatric patients. Four major interventions include:
- Acute Care for Elders (ACE) units based on interdisciplinary team rounds, discharge planning, and medical review in a prepared environment to foster patient self-care and improve function. Randomized clinical trials have shown ACE units can reduce the length of stay, the risk of nursing home admissions, and the use of physical restraints while improving providers’ satisfaction with patient care.3,4
- The Hospital Elder Life Program (HELP), led by a geriatrics resource nurse, is an intervention designed to reduce the incidence of delirium by adjusting environmental elements, such as dimming lights and keeping the floor quiet at night. HELP also introduces non-pharmacologic interventions, including massages and warm tea at night and promotes mobility and hydration during the day.
- Incidence of delirium is reduced and cost savings are realized using the HELP.5 (Visit http://elderlife.med.yale.edu/public for more information.)
- Geriatric Evaluation and Management (GEM) units also emphasize a multidisciplinary comprehensive approach using geriatrician-led teams. The intervention can reduce long-term costs, while improving physical functioning and general health domains in the SF-36.6
- Use of advanced practice nurses in comprehensive discharge planning interventions, including nursing home visits for older patients with risk factors for poor outcomes post-discharge, has been shown to reduce readmissions.7
Assessment Is the Bottom Line
Robert Palmer, MD, head of the Section of Geriatric Medicine and professor of medicine at Cleveland Clinic Lerner College of Medicine of Case Western Reserve University in Ohio, is known for his work with ACE units. He and his colleagues have tracked patients following discharge and have identified the highest priority issues that should be addressed to avoid deleterious geriatric syndromes in the hospital. Although he advocates what he calls a minimalist approach to conducting a geriatric assessment, Dr. Palmer underlines the idea that it must also be a deliberate and structured approach. Assessing and acting upon key indicators in four to five major domains, he notes, can make a big difference for patients’ hospital trajectories.8 Here are a few domains to consider:
1 Focus on activities of daily living (ADLs). Function and performance of ADLs can predict post-hospital outcome and help the physician prioritize elements of the patient’s trajectory and goals while in the hospital. “If a person was able to independently bathe, dress, toilet, walk, and transfer—from bed to chair, for instance—before the acute illness, then he or she should be able to get back to that point after the illness has been treated,” says Dr. Palmer. The ability to transfer independently is an important predictor of discharge status because if the patient requires assistance to transfer, he or she will need a different level of care upon discharge. The hospitalist should seek information —from the patient, family member or primary caregiver, or primary care physician—about the patient’s ADLs before he or she got sick. Again, recovery of ADLs may be possible if the patient was performing these independently before the acute episode.
2 Cognitive assessments are also key. Dr. Morley places assessment for delirium at the top of his list. Research shows that approximately one third of patients over 70 in the hospital will develop the condition. Delirium, or acute confusion, is also a predictor of decline in ADLs, notes Dr. Palmer. Dr. Morley recommends the use of the Confusion Assessment Method (CAM) because the Mini Mental State Exam can be time-consuming. (A CAM form is available free online as part of SHM’s “Clinical Toolbox for Geriatric Care.” Go to www.hospitalmedicine.org, click on “Resource Center” and then “Geriatric Special Interest Area” to find the Toolbox.) According to Dr. Palmer, the physician should also use common sense when initially examining the patient: Observe whether the patient is confused, distracted, or inappropriate in conversation. If so, the next step is to use the simple Digit Span test: Say a random set of four to five numbers, and ask the patient to repeat them. Inability to do this is consistent with delirium as a cause of cognitive impairment.
For assessing cognitive impairment, Dr. Morley prefers the St. Louis University Mental Status Exam (SLUMS) to the Mini Mental Status Exam. The SLUMS, developed in collaboration with the Department of Veterans Affairs (and available free online at: http://medschool.slu.edu/agingsuccessfully/pdfsurveys/slumsexam_05.pdf) successfully picks up even mild cognitive impairment, according to Dr. Morley. This is important information not just for the hospital trajectory but also for discharge planning: Inability to follow discharge instructions due to cognitive impairment could result in a readmission.
3 Malnutrition is associated with mortality. Dr. Morley uses the four questions of the Simplified Nutrition Assessment Questionnaire (SNAQ), which correlate well with future weight loss and poor outcomes.9
If the SNAQ is positive, the use of a lengthier questionnaire may be warranted. Dr. Palmer suggests that a review of the patient’s comprehensive metabolic panel to judge kidney and liver function and a bedside evaluation using the Subjective Global Assessment (SGA) can yield results just as usable as the more complex and time-consuming textbook nutritional assessments.
4 Mood and affect also play a role in patients’ outcomes. Research has shown that depressed patients have poor outcomes, so physicians should always assess for depression. While the Geriatric Depression Scale (see “Clinical Toolbox for Geriatric Care” on the SHM Web site) can help quantify the extent of the patient’s symptoms, simply asking the patient, “Are you depressed, sad, or blue?” can often elicit enough information about the patient’s psychological status to direct interventions.
5 Mobility is sometimes classified as a stand-alone domain. However, walking and balance may be included in the assessment of ADLs. A patient who can walk independently—even with a cane or a walker—has a good chance to return home, says Dr. Palmer. Requiring another person to help with walking most likely indicates the patient will need short-term rehabilitation in a skilled nursing facility before returning home.
6 Social and living situation are important. The physician must identify the extent and quality of the patient’s support network. If, for instance, a patient has mild dementia but has a network of 10 extended family members who act as caregivers, discharge to home may be possible. If the patient was admitted to the hospital from a nursing home, however, it is most likely he or she will return there.
Revisit Daily Goals
Dr. Palmer advises hospitalists to follow the geriatric assessment with a translation of the information into what he calls a functional trajectory for the patient’s hospital stay. This includes an estimate of the patient’s anticipated length of stay and the expected discharge site. Interventions and consultations from allied health providers will be keyed to the patient’s individualized needs and to the goals of the functional trajectory.
To head off problems, Dr. Palmer advocates consultations from allied health professionals early in the hospital trajectory. For instance, if the patient is having trouble transferring from bed to chair upon admission, a consult with physical therapy may be warranted immediately rather than right before discharge, as is usually the case.
“We should not be depending on physical therapists at the end of hospitalization, when patients are already deconditioned and can’t get out of bed and need to go to a nursing home,” he explains. “The ideal time to bring in the physical therapist or technician is when you’ve identified—on day one—that the patient needs assistance with transfers, so that you can preserve mobility and shorten hospital stay.”
In the same vein, knowing the patient’s living situation will allow involvement of the discharge planner from day one of the hospitalization to plan with the patient or family for the patient’s return to home or to an alternate site. If the patient has been on a complex drug regimen, involving the pharmacist to help straighten out medications can head off potential drug-drug interactions. (SHM’s Geriatric Toolbox also has a list of medications to avoid in geriatric patients.)
It is important to review the functional trajectory on a daily basis. Input from other members of the health team will be invaluable. “Each day you identify barriers to that successful plan of the outcome, and you take care of them one at a time,” says Dr. Palmer. “If the patient is not on track with that daily goal, the team goes back to the drawing board and asks, ‘What are we missing here?’ Then you do a reassessment of ADLs, nutrition, and cognition.”
Hospitalists must also include the patient’s family members and primary caregivers as the patient moves toward discharge, asserts Dr. Morley. Clear, unambiguous written instructions must always be given to the patient or the primary caregiver when the patient leaves the hospital. (You can also find a discharge instruction sheet in SHM’s Toolbox.) If a patient appears to be facing the end of life, the hospitalist should schedule a conference with members of the primary care team, the hospitalist team, and all family stakeholders.
Transportable SKILLS
Some experts maintain that quality care for geriatric patients can be accomplished without a specialized geriatrics unit.
“I never conceived of the ACE intervention as being done exclusively on a unit,” says Dr. Palmer. “The idea was to develop the skills on a unit and then transport those skills to all units.” Although the protocols developed for ACE units are good for teaching, he says the team has been the key.
Dr. Morley agrees: “It’s not the physical part of the ACE unit that works. You must have team interactions. Finding a way to communicate between the different team members is absolutely key to good outcomes.”
Involving healthcare providers from different disciplines only enhances the care of geriatric patients. “Even though hospitalists may not have the depth of knowledge of geriatrics that a geriatrician has, they certainly have the knowledge of acute care medicine that we have, so they can manage the medical problems,” says Dr. Palmer. “What they need to do is think systematically, in a structured way, and to work collaboratively with key players. This only takes a few minutes each day, but more importantly, it saves time. You have fewer phone calls and fewer angry family members when you manage the care in a structured manner, working with a team of health professionals.”
Dr. Morley and his team have developed a form for their ACE unit that allows them to assess a patient’s status and goals in two to three minutes.
Dr. Pierluissi has experienced firsthand the benefits of working as a member of the interdisciplinary team. “Essentially,” he says, working in teams to treat the geriatric patient means there are “more heads in the game, more people trying to work in the patient’s best interest. You [the clinician] really do feel supported, and it makes your day more enjoyable and more productive.” TH
Gretchen Henkel is a medical journalist based in California.
Resources
- Kozak LJ, Hall MJ, Owings MF. Hospitalization fact sheet. In: National Hospital Discharge Survey: 2000 Annual summary with detailed diagnosis and procedure data. Hyattsville, Maryland: National Center for Health Statistics. Vital Health Stat. 2002;13(153).
- Covinsky KE, Palmer RM, Fortinsky RH, et al. Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: increased vulnerability with age. J Am Geriatr Soc. 2003 Apr;51(4):451-458.
- Landefeld CS, Palmer RM, Kresevic DM, et al. A randomized trial of care in a hospital medical unit especially designed to improve the functional outcomes of acutely ill older patients. N Engl J Med. 1995 May;332(20):1338-1344. Comments in: ACP J Club. 1995 Nov-Dec; 123(3):69 and N Engl J Med. 1995 May 18; 332(20):1376-1378.
- Counsell SR, Holder CM, Liebenauer LL, et al. Effects of a multicomponent intervention on functional outcomes and process of care in hospitalized older patients: a randomized controlled trial of acute care for Elders (ACE) in a community hospital. J Am Geriatr Soc. 2000 Dec;48:1572-1581.
- Inouye SK, Bogardus ST Jr, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med. 1999 Mar 4;340(9):669-676. Comments in: N Engl J Med. 1999 Jul 29; 341(5):369-370; author reply 370 and N Engl J Med. 1999 Mar 4; 340(9):720-721.
- Cohen HJ, Feussner JR, Weinberger M, et al. A controlled trial of inpatient and outpatient geriatric evaluation and management. N Engl J Med. 2002 Mar 21;346(12):905-912. Comments in: Curr Surg. 2004 May-Jun;61(3):266-274; N Engl J Med. 2002 Aug 1;347(5):371-373; author reply 371-373 & N Engl J Med. 2002 Mar 21;346(12):874.
- Naylor MD, Brooten DA, Campbell RL, et al. Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial. J Am Geriatr Soc. 2004 May;52(5):675-684. Erratum in J Am Geriatr Soc. 2004 Jul; 52(7):1228. Comment in Evid Based Nurs. 2004 Oct;7(4):116.
- Palmer RM. Acute hospital care of the elderly: making a difference. Caring for the Hospitalized Elderly [special supplement to The Hospitalist]. 2004. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=The_Hospitalist&Template=/CM/ContentDisplay.cfm&ContentFileID=1447. Last accessed March 14, 2007.
- Wilson MM, Thomas DR, Rubenstein LZ, et al. Appetite assessment: simple appetite questionnaire predicts weight loss in community-dwelling adults and nursing home residents. Am J Clin Nutr. 2005 Nov;82(5):1074-1081.
Hospitalization can be risky business for geriatric patients. Americans 65 and older make up 13% of the population but account for 48% of inpatient days of care and 78% of hospital deaths. While in the hospital, patients 75 and older are at high risk for deconditioning and functional decline, medication errors, delirium, and falls.1,2
For geriatric patients not closely monitored, notes geriatrician Don Murphy, MD, co-principal of Senior Care of Colorado, a large primary care geriatrics group in Denver, going to the hospital can be like disappearing into a black hole.
As the U.S. population ages, hospitalists will be caring for an increasing number of geriatric patients. They will have to address patients’ acute medical conditions without compromising their functional status.
The Hospitalist asked several leading geriatricians to identify valuable tools and strategies for delivering comprehensive geriatric care in the hospital. Even in the absence of formal geriatric care units, they say, hospitalists are positioned for adopting the principles of quality geriatric care. Many of those principles align with the central mission of hospital medicine: promoting high-quality, patient-centered care, working as a team, and developing clear lines of communication between the hospitalist and the primary care teams.
A Survey of Interventions
“There’s no question that it’s becoming extraordinarily difficult to do good care,” says John Morley, MD, professor of medicine and chief of the Division of Geriatrics and Endocrinology at Saint Louis University Health Sciences Center in Missouri. “Taking care of an older person in the hospital is a team sport—the physician can’t do it alone.”
It’s clear the team approach is a crucial foundation for interventions that target at-risk geriatric patients, agrees Edgar Pierluissi, MD, associate clinical professor of medicine and medical director of the recently established ACE unit at San Francisco General Hospital. Reducing the incidence of delirium, for instance, cannot be accomplished simply by utilizing a geriatric consultation. Once established, acute confusion can be intractable. “The idea is to try to prevent delirium, and research has shown that single-person types of interventions in these massively impervious-to-change facilities don’t work,” he says.
Clinical trials have demonstrated that interventions, including interdisciplinary and collaborative teams, targeted patient-centered therapies, and comprehensive geriatric assessment can improve outcomes of hospitalization in geriatric patients. Four major interventions include:
- Acute Care for Elders (ACE) units based on interdisciplinary team rounds, discharge planning, and medical review in a prepared environment to foster patient self-care and improve function. Randomized clinical trials have shown ACE units can reduce the length of stay, the risk of nursing home admissions, and the use of physical restraints while improving providers’ satisfaction with patient care.3,4
- The Hospital Elder Life Program (HELP), led by a geriatrics resource nurse, is an intervention designed to reduce the incidence of delirium by adjusting environmental elements, such as dimming lights and keeping the floor quiet at night. HELP also introduces non-pharmacologic interventions, including massages and warm tea at night and promotes mobility and hydration during the day.
- Incidence of delirium is reduced and cost savings are realized using the HELP.5 (Visit http://elderlife.med.yale.edu/public for more information.)
- Geriatric Evaluation and Management (GEM) units also emphasize a multidisciplinary comprehensive approach using geriatrician-led teams. The intervention can reduce long-term costs, while improving physical functioning and general health domains in the SF-36.6
- Use of advanced practice nurses in comprehensive discharge planning interventions, including nursing home visits for older patients with risk factors for poor outcomes post-discharge, has been shown to reduce readmissions.7
Assessment Is the Bottom Line
Robert Palmer, MD, head of the Section of Geriatric Medicine and professor of medicine at Cleveland Clinic Lerner College of Medicine of Case Western Reserve University in Ohio, is known for his work with ACE units. He and his colleagues have tracked patients following discharge and have identified the highest priority issues that should be addressed to avoid deleterious geriatric syndromes in the hospital. Although he advocates what he calls a minimalist approach to conducting a geriatric assessment, Dr. Palmer underlines the idea that it must also be a deliberate and structured approach. Assessing and acting upon key indicators in four to five major domains, he notes, can make a big difference for patients’ hospital trajectories.8 Here are a few domains to consider:
1 Focus on activities of daily living (ADLs). Function and performance of ADLs can predict post-hospital outcome and help the physician prioritize elements of the patient’s trajectory and goals while in the hospital. “If a person was able to independently bathe, dress, toilet, walk, and transfer—from bed to chair, for instance—before the acute illness, then he or she should be able to get back to that point after the illness has been treated,” says Dr. Palmer. The ability to transfer independently is an important predictor of discharge status because if the patient requires assistance to transfer, he or she will need a different level of care upon discharge. The hospitalist should seek information —from the patient, family member or primary caregiver, or primary care physician—about the patient’s ADLs before he or she got sick. Again, recovery of ADLs may be possible if the patient was performing these independently before the acute episode.
2 Cognitive assessments are also key. Dr. Morley places assessment for delirium at the top of his list. Research shows that approximately one third of patients over 70 in the hospital will develop the condition. Delirium, or acute confusion, is also a predictor of decline in ADLs, notes Dr. Palmer. Dr. Morley recommends the use of the Confusion Assessment Method (CAM) because the Mini Mental State Exam can be time-consuming. (A CAM form is available free online as part of SHM’s “Clinical Toolbox for Geriatric Care.” Go to www.hospitalmedicine.org, click on “Resource Center” and then “Geriatric Special Interest Area” to find the Toolbox.) According to Dr. Palmer, the physician should also use common sense when initially examining the patient: Observe whether the patient is confused, distracted, or inappropriate in conversation. If so, the next step is to use the simple Digit Span test: Say a random set of four to five numbers, and ask the patient to repeat them. Inability to do this is consistent with delirium as a cause of cognitive impairment.
For assessing cognitive impairment, Dr. Morley prefers the St. Louis University Mental Status Exam (SLUMS) to the Mini Mental Status Exam. The SLUMS, developed in collaboration with the Department of Veterans Affairs (and available free online at: http://medschool.slu.edu/agingsuccessfully/pdfsurveys/slumsexam_05.pdf) successfully picks up even mild cognitive impairment, according to Dr. Morley. This is important information not just for the hospital trajectory but also for discharge planning: Inability to follow discharge instructions due to cognitive impairment could result in a readmission.
3 Malnutrition is associated with mortality. Dr. Morley uses the four questions of the Simplified Nutrition Assessment Questionnaire (SNAQ), which correlate well with future weight loss and poor outcomes.9
If the SNAQ is positive, the use of a lengthier questionnaire may be warranted. Dr. Palmer suggests that a review of the patient’s comprehensive metabolic panel to judge kidney and liver function and a bedside evaluation using the Subjective Global Assessment (SGA) can yield results just as usable as the more complex and time-consuming textbook nutritional assessments.
4 Mood and affect also play a role in patients’ outcomes. Research has shown that depressed patients have poor outcomes, so physicians should always assess for depression. While the Geriatric Depression Scale (see “Clinical Toolbox for Geriatric Care” on the SHM Web site) can help quantify the extent of the patient’s symptoms, simply asking the patient, “Are you depressed, sad, or blue?” can often elicit enough information about the patient’s psychological status to direct interventions.
5 Mobility is sometimes classified as a stand-alone domain. However, walking and balance may be included in the assessment of ADLs. A patient who can walk independently—even with a cane or a walker—has a good chance to return home, says Dr. Palmer. Requiring another person to help with walking most likely indicates the patient will need short-term rehabilitation in a skilled nursing facility before returning home.
6 Social and living situation are important. The physician must identify the extent and quality of the patient’s support network. If, for instance, a patient has mild dementia but has a network of 10 extended family members who act as caregivers, discharge to home may be possible. If the patient was admitted to the hospital from a nursing home, however, it is most likely he or she will return there.
Revisit Daily Goals
Dr. Palmer advises hospitalists to follow the geriatric assessment with a translation of the information into what he calls a functional trajectory for the patient’s hospital stay. This includes an estimate of the patient’s anticipated length of stay and the expected discharge site. Interventions and consultations from allied health providers will be keyed to the patient’s individualized needs and to the goals of the functional trajectory.
To head off problems, Dr. Palmer advocates consultations from allied health professionals early in the hospital trajectory. For instance, if the patient is having trouble transferring from bed to chair upon admission, a consult with physical therapy may be warranted immediately rather than right before discharge, as is usually the case.
“We should not be depending on physical therapists at the end of hospitalization, when patients are already deconditioned and can’t get out of bed and need to go to a nursing home,” he explains. “The ideal time to bring in the physical therapist or technician is when you’ve identified—on day one—that the patient needs assistance with transfers, so that you can preserve mobility and shorten hospital stay.”
In the same vein, knowing the patient’s living situation will allow involvement of the discharge planner from day one of the hospitalization to plan with the patient or family for the patient’s return to home or to an alternate site. If the patient has been on a complex drug regimen, involving the pharmacist to help straighten out medications can head off potential drug-drug interactions. (SHM’s Geriatric Toolbox also has a list of medications to avoid in geriatric patients.)
It is important to review the functional trajectory on a daily basis. Input from other members of the health team will be invaluable. “Each day you identify barriers to that successful plan of the outcome, and you take care of them one at a time,” says Dr. Palmer. “If the patient is not on track with that daily goal, the team goes back to the drawing board and asks, ‘What are we missing here?’ Then you do a reassessment of ADLs, nutrition, and cognition.”
Hospitalists must also include the patient’s family members and primary caregivers as the patient moves toward discharge, asserts Dr. Morley. Clear, unambiguous written instructions must always be given to the patient or the primary caregiver when the patient leaves the hospital. (You can also find a discharge instruction sheet in SHM’s Toolbox.) If a patient appears to be facing the end of life, the hospitalist should schedule a conference with members of the primary care team, the hospitalist team, and all family stakeholders.
Transportable SKILLS
Some experts maintain that quality care for geriatric patients can be accomplished without a specialized geriatrics unit.
“I never conceived of the ACE intervention as being done exclusively on a unit,” says Dr. Palmer. “The idea was to develop the skills on a unit and then transport those skills to all units.” Although the protocols developed for ACE units are good for teaching, he says the team has been the key.
Dr. Morley agrees: “It’s not the physical part of the ACE unit that works. You must have team interactions. Finding a way to communicate between the different team members is absolutely key to good outcomes.”
Involving healthcare providers from different disciplines only enhances the care of geriatric patients. “Even though hospitalists may not have the depth of knowledge of geriatrics that a geriatrician has, they certainly have the knowledge of acute care medicine that we have, so they can manage the medical problems,” says Dr. Palmer. “What they need to do is think systematically, in a structured way, and to work collaboratively with key players. This only takes a few minutes each day, but more importantly, it saves time. You have fewer phone calls and fewer angry family members when you manage the care in a structured manner, working with a team of health professionals.”
Dr. Morley and his team have developed a form for their ACE unit that allows them to assess a patient’s status and goals in two to three minutes.
Dr. Pierluissi has experienced firsthand the benefits of working as a member of the interdisciplinary team. “Essentially,” he says, working in teams to treat the geriatric patient means there are “more heads in the game, more people trying to work in the patient’s best interest. You [the clinician] really do feel supported, and it makes your day more enjoyable and more productive.” TH
Gretchen Henkel is a medical journalist based in California.
Resources
- Kozak LJ, Hall MJ, Owings MF. Hospitalization fact sheet. In: National Hospital Discharge Survey: 2000 Annual summary with detailed diagnosis and procedure data. Hyattsville, Maryland: National Center for Health Statistics. Vital Health Stat. 2002;13(153).
- Covinsky KE, Palmer RM, Fortinsky RH, et al. Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: increased vulnerability with age. J Am Geriatr Soc. 2003 Apr;51(4):451-458.
- Landefeld CS, Palmer RM, Kresevic DM, et al. A randomized trial of care in a hospital medical unit especially designed to improve the functional outcomes of acutely ill older patients. N Engl J Med. 1995 May;332(20):1338-1344. Comments in: ACP J Club. 1995 Nov-Dec; 123(3):69 and N Engl J Med. 1995 May 18; 332(20):1376-1378.
- Counsell SR, Holder CM, Liebenauer LL, et al. Effects of a multicomponent intervention on functional outcomes and process of care in hospitalized older patients: a randomized controlled trial of acute care for Elders (ACE) in a community hospital. J Am Geriatr Soc. 2000 Dec;48:1572-1581.
- Inouye SK, Bogardus ST Jr, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med. 1999 Mar 4;340(9):669-676. Comments in: N Engl J Med. 1999 Jul 29; 341(5):369-370; author reply 370 and N Engl J Med. 1999 Mar 4; 340(9):720-721.
- Cohen HJ, Feussner JR, Weinberger M, et al. A controlled trial of inpatient and outpatient geriatric evaluation and management. N Engl J Med. 2002 Mar 21;346(12):905-912. Comments in: Curr Surg. 2004 May-Jun;61(3):266-274; N Engl J Med. 2002 Aug 1;347(5):371-373; author reply 371-373 & N Engl J Med. 2002 Mar 21;346(12):874.
- Naylor MD, Brooten DA, Campbell RL, et al. Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial. J Am Geriatr Soc. 2004 May;52(5):675-684. Erratum in J Am Geriatr Soc. 2004 Jul; 52(7):1228. Comment in Evid Based Nurs. 2004 Oct;7(4):116.
- Palmer RM. Acute hospital care of the elderly: making a difference. Caring for the Hospitalized Elderly [special supplement to The Hospitalist]. 2004. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=The_Hospitalist&Template=/CM/ContentDisplay.cfm&ContentFileID=1447. Last accessed March 14, 2007.
- Wilson MM, Thomas DR, Rubenstein LZ, et al. Appetite assessment: simple appetite questionnaire predicts weight loss in community-dwelling adults and nursing home residents. Am J Clin Nutr. 2005 Nov;82(5):1074-1081.
Fall Risk
The problem of falls among older adults has been recognized and studied for many years, including myriad analyses regarding assessment and prevention of falls in this population. The U.S. Census Bureau reported that there were 35.9 million people age 65 and over in the United States as of July 1, 2003. As this population increases, the specific issues pertaining to its members, including falls, must be addressed by hospitalists.
How Big Is the Problem?
The Center for Disease Control and Prevention’s (CDC) National Center for Injury Prevention and Control reports that:
- More than one-third of adults 65 and older fall each year in the United States;
- Falls are the leading cause of injury deaths for older adults;
- In 2003, about 1.8 million people 65 and older were treated in emergency departments for nonfatal falls, and about 460,000 of these patients were hospitalized;
- The rates of fall-related deaths among older adults rose significantly over the past decade;
- Many individuals who fall develop a fear of falling. That may cause them to limit activity, leading to reduced mobility and physical fitness and increasing their risk for additional falls; and
- In 2000, direct medical costs totaled $179 million for fatal falls and $19 billion for nonfatal fall injuries.1
One study exploring the relationship between the mechanism of fall and the pattern and severity of injury in geriatric patients compared with younger patients concluded that falls were the mechanism of injury in 48% of the older patients (those 65 and older) included in the study compared with 7% in the younger group. Further, 32% of falls in the older group resulted in serious injury, while this was true of only 4% of falls in the younger cohort.2
Risk Assessment
When an inpatient in an acute-care hospital falls, a number of negative outcomes can occur, including a longer hospital stay and higher rates of discharge to long-term care.
Falls are associated with higher levels of anxiety and depression and loss of confidence for the patient. They lead to increased costs for patients and hospitals. Feelings of anxiety and/or guilt among staff members may follow. Ultimately, a fall can result in complaints or even litigation from patients or their families.3
Traditional methods of fall risk evaluation may not be effective for assessing the risk of falling for a hospitalized patient, regardless of the reason the patient is hospitalized. The classic risk factors are generally well recognized among physicians and clinical staff and include:
- Age 65 and older;
- A history of falls;
- Cognitive impairment;
- Urinary/fecal incontinence/urgency;
- Balance problems, lower extremity weakness, arthritis;
- Vision problems;
- Use of more than four daily medications or use of psychotropics or narcotics; and
- ETOH.
Acute illness alone accounts for approximately 10% of falls in older adults.4 Many patients suffering or recovering from acute illness may go through a transient period of increased risk for falling that needs to be recognized by physicians and nursing staff.
The impact of pharmacology on a patient’s risk for falling is widely recognized. Patients who take four or more medications are generally considered to be at increased risk. Certain medications, including diuretics, anti-hypertensives, tricyclic antidepressants, sedatives, and hypoglycemics are known to increase an individual’s risk for falling. An October 2004 CDC-funded study by researchers at Johns Hopkins University (Baltimore) concluded that the short-term risk of single and recurring falls may triple within two days after a medication change.5 A patient hospitalized for an acute illness or injury is likely to have had a recent and significant change in the medications he or she is taking, thereby at least temporarily increasing that individual’s risk for falling.
The environmental hazards of the hospital room can’t be overlooked when assessing a patient’s risk for falling. The patient is in an unfamiliar setting—often with informal restraints in place, including IV tubing, feeding tubes, pulse oximeters, and catheters. These obstacles make it more difficult for the patient to maneuver and present opportunities for tripping.
All these things—individually or combined—can increase the chances of falling, even for a patient who at first glance doesn’t appear to be at risk.
Stephen Shaw, MD, medical director of Community Hospitalists in Cleveland, says that while falls assessment tools can be helpful, it would be difficult to outline a foolproof assessment form.
The physician must keep in mind the fact that falls prevention is multifactorial; it may be difficult to attribute the patient’s fall(s) to any single reason. “Any vigorous falls assessment program has to have a comprehensive approach,” he cautions. “Medications, attention to vision limitations, and his or her ability to feel in the dark in their surroundings all have to be taken into consideration.”
The Hospitalist’s Role
When a patient is admitted for injuries resulting from a fall or from an illness that may have been diagnosed as a result of a fall, consider acute conditions first. Also remember that falling is a symptom; understanding why the patient fell is the first step to prevention—both while the patient remains in the hospital and following discharge.
One of the first things the hospitalist must do to reduce patient falls effectively is to study risk assessment and prevention of geriatric falls. A study published in the Journal of Hospital Medicine in January/February 2006 (“Is There a Geriatrician in the House? Geriatric Care Approaches in Hospitalist Programs”) identifies the need for collaboration between hospitalists and geriatricians to better address the issues specific to hospitalized older adults. This collaboration combines the geriatrician’s expertise regarding the elderly patient’s unique needs and considerations with the hospitalist’s expertise regarding specific acute care situations.6
Heidi Wald, MD, MPH, assistant professor, Division of Health Care Policy and Research and General Internal Medicine at the University of Colorado in Denver and primary author of the Journal of Hospital Medicine study, says numerous things can be done to reduce the risk of inpatient falls, beginning with identifying patients at high risk for falling. This can be done by assessing the classic risk factors intrinsic to the patient, while keeping in mind the risk factors that could be mediated by the acute illness.
Risks created by the environment can be fairly easily addressed, according to Dr. Wald. Lower beds as far as they will go, with the wheels locked. Don’t use upper and lower bedrails simultaneously (this reduces the chance of a patient being caught between the two). Cut down on the use of restraints—both formal and informal.
Because many falls result from patients trying to get to the bathroom, Dr. Wald advises scheduled toileting, with the staff regularly assisting the patient to the bathroom. If a patient cannot ambulate to the restroom independently, ensure that a urinal or a bedpan is nearby and readily accessible to the patient.
Dr. Wald also advises utilizing the expertise and skills of those clinicians most familiar with the patient: the nursing staff. The nurses who have daily contact with the patient are in the best position to provide information regarding changes in the patient’s mental status, ability to ambulate, response to medications, compliance, and other factors that may increase the risk for a fall.
“The bottom line of any quality initiative will often fall to the nurses’ assessment,” says Dr. Shaw. “The front-line caregivers for fall assessments are our nurses.”
A Multidisciplinary Approach to Prevention
Drs. Wald and Shaw both stress the importance of a multidisciplinary approach to prevention of falls (both in hospital and following discharge). A patient who has already fallen—or one identified to be at risk for falling—can be offered a great deal of support and guidance pending discharge. And discharge planning can begin literally at admission.
It’s Dr. Shaw’s practice with at-risk patients to involve physical and occupational therapy (as well as social workers) in the patient’s care right from the beginning. Those individuals are then in a position not only to perform a thorough assessment of the patient but also to begin working on ways to reduce the patient’s risk following discharge. As Dr. Shaw points out, the hospitalist has access to resources the patient’s primary-care physician generally does not, and those resources should be utilized to full advantage.
Physical therapy can offer rehabilitative interventions, including transfer, gait, and balance training; strength and range-of-motion exercises; and habituation exercises for vestibular problems. Occupational therapy can offer the patient instruction on simplifying tasks and on performing everyday activities safely. Social workers can assist the patient with finding educational and assistive resources. All disciplines can be involved in home safety evaluations, patient and family education, and the procurement of assistive and adaptive equipment, such as ambulation devices, grab bars, handrails, raised toilet seats, and so on.
When all of these healthcare providers are involved in the patient’s care from the beginning and can coordinate discharge planning as a team, a more well-rounded and comprehensive plan for prevention of falls can be formulated. This team approach also offers a more accurate view of whether the patient is capable of returning home with or without help or if placement in a rehabilitation or long-term care facility may be more appropriate.
Involve the Patient
Once an at-risk patient has been identified, communicate that risk to everyone involved with the patient’s care, including the medical staff, the family, and the patient. “Patients have a certain degree of risk-taking behavior, and they won’t necessarily ask for help,” says Dr. Wald. “Part of that is that they’re not willing to admit that they need help.”
Patients need to be reminded that they are or have recently been sick—that’s why they’re in the hospital in the first place. She says patients and caregivers must be attuned to the fact that as patients begin to feel better and stronger and become more mobile, their risk for falling will go up before it starts to come down.
If a patient remains resistant to asking for or accepting assistance, Dr. Wald suggests finding out what the patient’s barriers are and trying to get around them. “Try to get people to admit that they have a problem,” she advises. “A lot of times, the barriers aren’t rational, so rationalizing isn’t always effective.”
She offers the example of a patient who resists the idea of using a walker. Sometimes simply demonstrating how much more quickly the patient can get around using the walker may do the trick.
Dr. Shaw adds that a certain level of sensitivity is required when approaching a patient who is in denial regarding his or her limitations. It may be necessary to ask a second physician or nurse to lend credibility by explaining to the patient again that he or she may have needs that didn’t exist previously. He cautions, however, that if his patient remains in denial about his or her limitations, he does not hesitate to engage the family. “If the patient is discharged home, it’s going to be the family who will be the policemen and watchdogs,” says Dr. Shaw.
After discharge, following up with the patient can make a big difference in patient compliance. The time following discharge to the home can be confusing for the patient, and he may be overwhelmed with changes in routines, medications, and activities. Dr. Shaw’s organization calls the patient three to four days post-discharge to verify that the patient understands the discharge instructions, to answer questions the patient may have, and to confirm that prescriptions have been filled and that follow-up appointments have been made with the primary-care physician. He notes that although this simple follow-up phone call takes little time and effort, it has improved patient satisfaction immensely.
Quality and Prevention Initiatives
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) 2007 National Patient Safety Goals for hospitals includes the following goal: “Reduce the risk of patient harm resulting from falls” (Goal 9).
The requirement for this goal is the implementation of a fall reduction program, followed by evaluation of the effectiveness of the program. Drs. Wald and Shaw agree that, because of the nature of what they do, hospitalists are in an ideal position to spearhead the movement to assess the reasons a patient may have fallen and the risk for future falls—both in the hospital and following discharge—and to synthesize that data to create comprehensive falls prevention programs in their hospitals.
Because hospitalists are on-site 24 hours a day, seven days a week, they are usually first responders when a patient falls and can best evaluate the reasons for the fall and track outcomes. “We’re in an ideal position to create protocols for what to do once a patient does fall in the hospital and [to] evaluate the fall and the incident,” Dr. Wald says. “This is a great quality improvement project because the data are already being collected.”
Dr. Shaw concurs. “Hospitalists are the quality assessors that are in the trenches,” she says. “The hospitalists are really the clinicians most familiar with the strengths and weaknesses of any institution.” TH
Sheri Polley is a medical journalist based in Pennsylvania.
References
- Centers for Disease Control and Prevention. Falls among older adults: an overview. CDC Web site. Available at: www.cdc.gov/ncipc/factsheets/adultfalls.htm. Last accessed March 13, 2007.
- Sterling DA, O’Connor JA, Bonadies J. Geriatric falls: injury severity is high and disproportionate to mechanism. J Trauma. 2001 Jan;50(1):116-119.
- Oliver D, Daly F, Martin FC, et al. Risk factors and risk assessment tools for falls in hospital in-patients: a systematic review. Age Ageing. 2004 Mar;33(2):122-130.
- Nnodim JO, Alexander NB. Assessing falls in older adults: a comprehensive fall evaluation to reduce fall risk in older adults. Geriatrics. 2005 Oct;60(10):24-28.
- Centers for Disease Control and Prevention. CDC fall prevention activities: research studies. CDC Web site. Available at: www.cdc.gov/ncipc/duip/FallsPreventionActivity.htm. Last accessed March 13, 2007.
- Wald H, Huddleston J, Kramer A. Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs. J Hosp Med. 2006 Jan;1(1):29-35.
The problem of falls among older adults has been recognized and studied for many years, including myriad analyses regarding assessment and prevention of falls in this population. The U.S. Census Bureau reported that there were 35.9 million people age 65 and over in the United States as of July 1, 2003. As this population increases, the specific issues pertaining to its members, including falls, must be addressed by hospitalists.
How Big Is the Problem?
The Center for Disease Control and Prevention’s (CDC) National Center for Injury Prevention and Control reports that:
- More than one-third of adults 65 and older fall each year in the United States;
- Falls are the leading cause of injury deaths for older adults;
- In 2003, about 1.8 million people 65 and older were treated in emergency departments for nonfatal falls, and about 460,000 of these patients were hospitalized;
- The rates of fall-related deaths among older adults rose significantly over the past decade;
- Many individuals who fall develop a fear of falling. That may cause them to limit activity, leading to reduced mobility and physical fitness and increasing their risk for additional falls; and
- In 2000, direct medical costs totaled $179 million for fatal falls and $19 billion for nonfatal fall injuries.1
One study exploring the relationship between the mechanism of fall and the pattern and severity of injury in geriatric patients compared with younger patients concluded that falls were the mechanism of injury in 48% of the older patients (those 65 and older) included in the study compared with 7% in the younger group. Further, 32% of falls in the older group resulted in serious injury, while this was true of only 4% of falls in the younger cohort.2
Risk Assessment
When an inpatient in an acute-care hospital falls, a number of negative outcomes can occur, including a longer hospital stay and higher rates of discharge to long-term care.
Falls are associated with higher levels of anxiety and depression and loss of confidence for the patient. They lead to increased costs for patients and hospitals. Feelings of anxiety and/or guilt among staff members may follow. Ultimately, a fall can result in complaints or even litigation from patients or their families.3
Traditional methods of fall risk evaluation may not be effective for assessing the risk of falling for a hospitalized patient, regardless of the reason the patient is hospitalized. The classic risk factors are generally well recognized among physicians and clinical staff and include:
- Age 65 and older;
- A history of falls;
- Cognitive impairment;
- Urinary/fecal incontinence/urgency;
- Balance problems, lower extremity weakness, arthritis;
- Vision problems;
- Use of more than four daily medications or use of psychotropics or narcotics; and
- ETOH.
Acute illness alone accounts for approximately 10% of falls in older adults.4 Many patients suffering or recovering from acute illness may go through a transient period of increased risk for falling that needs to be recognized by physicians and nursing staff.
The impact of pharmacology on a patient’s risk for falling is widely recognized. Patients who take four or more medications are generally considered to be at increased risk. Certain medications, including diuretics, anti-hypertensives, tricyclic antidepressants, sedatives, and hypoglycemics are known to increase an individual’s risk for falling. An October 2004 CDC-funded study by researchers at Johns Hopkins University (Baltimore) concluded that the short-term risk of single and recurring falls may triple within two days after a medication change.5 A patient hospitalized for an acute illness or injury is likely to have had a recent and significant change in the medications he or she is taking, thereby at least temporarily increasing that individual’s risk for falling.
The environmental hazards of the hospital room can’t be overlooked when assessing a patient’s risk for falling. The patient is in an unfamiliar setting—often with informal restraints in place, including IV tubing, feeding tubes, pulse oximeters, and catheters. These obstacles make it more difficult for the patient to maneuver and present opportunities for tripping.
All these things—individually or combined—can increase the chances of falling, even for a patient who at first glance doesn’t appear to be at risk.
Stephen Shaw, MD, medical director of Community Hospitalists in Cleveland, says that while falls assessment tools can be helpful, it would be difficult to outline a foolproof assessment form.
The physician must keep in mind the fact that falls prevention is multifactorial; it may be difficult to attribute the patient’s fall(s) to any single reason. “Any vigorous falls assessment program has to have a comprehensive approach,” he cautions. “Medications, attention to vision limitations, and his or her ability to feel in the dark in their surroundings all have to be taken into consideration.”
The Hospitalist’s Role
When a patient is admitted for injuries resulting from a fall or from an illness that may have been diagnosed as a result of a fall, consider acute conditions first. Also remember that falling is a symptom; understanding why the patient fell is the first step to prevention—both while the patient remains in the hospital and following discharge.
One of the first things the hospitalist must do to reduce patient falls effectively is to study risk assessment and prevention of geriatric falls. A study published in the Journal of Hospital Medicine in January/February 2006 (“Is There a Geriatrician in the House? Geriatric Care Approaches in Hospitalist Programs”) identifies the need for collaboration between hospitalists and geriatricians to better address the issues specific to hospitalized older adults. This collaboration combines the geriatrician’s expertise regarding the elderly patient’s unique needs and considerations with the hospitalist’s expertise regarding specific acute care situations.6
Heidi Wald, MD, MPH, assistant professor, Division of Health Care Policy and Research and General Internal Medicine at the University of Colorado in Denver and primary author of the Journal of Hospital Medicine study, says numerous things can be done to reduce the risk of inpatient falls, beginning with identifying patients at high risk for falling. This can be done by assessing the classic risk factors intrinsic to the patient, while keeping in mind the risk factors that could be mediated by the acute illness.
Risks created by the environment can be fairly easily addressed, according to Dr. Wald. Lower beds as far as they will go, with the wheels locked. Don’t use upper and lower bedrails simultaneously (this reduces the chance of a patient being caught between the two). Cut down on the use of restraints—both formal and informal.
Because many falls result from patients trying to get to the bathroom, Dr. Wald advises scheduled toileting, with the staff regularly assisting the patient to the bathroom. If a patient cannot ambulate to the restroom independently, ensure that a urinal or a bedpan is nearby and readily accessible to the patient.
Dr. Wald also advises utilizing the expertise and skills of those clinicians most familiar with the patient: the nursing staff. The nurses who have daily contact with the patient are in the best position to provide information regarding changes in the patient’s mental status, ability to ambulate, response to medications, compliance, and other factors that may increase the risk for a fall.
“The bottom line of any quality initiative will often fall to the nurses’ assessment,” says Dr. Shaw. “The front-line caregivers for fall assessments are our nurses.”
A Multidisciplinary Approach to Prevention
Drs. Wald and Shaw both stress the importance of a multidisciplinary approach to prevention of falls (both in hospital and following discharge). A patient who has already fallen—or one identified to be at risk for falling—can be offered a great deal of support and guidance pending discharge. And discharge planning can begin literally at admission.
It’s Dr. Shaw’s practice with at-risk patients to involve physical and occupational therapy (as well as social workers) in the patient’s care right from the beginning. Those individuals are then in a position not only to perform a thorough assessment of the patient but also to begin working on ways to reduce the patient’s risk following discharge. As Dr. Shaw points out, the hospitalist has access to resources the patient’s primary-care physician generally does not, and those resources should be utilized to full advantage.
Physical therapy can offer rehabilitative interventions, including transfer, gait, and balance training; strength and range-of-motion exercises; and habituation exercises for vestibular problems. Occupational therapy can offer the patient instruction on simplifying tasks and on performing everyday activities safely. Social workers can assist the patient with finding educational and assistive resources. All disciplines can be involved in home safety evaluations, patient and family education, and the procurement of assistive and adaptive equipment, such as ambulation devices, grab bars, handrails, raised toilet seats, and so on.
When all of these healthcare providers are involved in the patient’s care from the beginning and can coordinate discharge planning as a team, a more well-rounded and comprehensive plan for prevention of falls can be formulated. This team approach also offers a more accurate view of whether the patient is capable of returning home with or without help or if placement in a rehabilitation or long-term care facility may be more appropriate.
Involve the Patient
Once an at-risk patient has been identified, communicate that risk to everyone involved with the patient’s care, including the medical staff, the family, and the patient. “Patients have a certain degree of risk-taking behavior, and they won’t necessarily ask for help,” says Dr. Wald. “Part of that is that they’re not willing to admit that they need help.”
Patients need to be reminded that they are or have recently been sick—that’s why they’re in the hospital in the first place. She says patients and caregivers must be attuned to the fact that as patients begin to feel better and stronger and become more mobile, their risk for falling will go up before it starts to come down.
If a patient remains resistant to asking for or accepting assistance, Dr. Wald suggests finding out what the patient’s barriers are and trying to get around them. “Try to get people to admit that they have a problem,” she advises. “A lot of times, the barriers aren’t rational, so rationalizing isn’t always effective.”
She offers the example of a patient who resists the idea of using a walker. Sometimes simply demonstrating how much more quickly the patient can get around using the walker may do the trick.
Dr. Shaw adds that a certain level of sensitivity is required when approaching a patient who is in denial regarding his or her limitations. It may be necessary to ask a second physician or nurse to lend credibility by explaining to the patient again that he or she may have needs that didn’t exist previously. He cautions, however, that if his patient remains in denial about his or her limitations, he does not hesitate to engage the family. “If the patient is discharged home, it’s going to be the family who will be the policemen and watchdogs,” says Dr. Shaw.
After discharge, following up with the patient can make a big difference in patient compliance. The time following discharge to the home can be confusing for the patient, and he may be overwhelmed with changes in routines, medications, and activities. Dr. Shaw’s organization calls the patient three to four days post-discharge to verify that the patient understands the discharge instructions, to answer questions the patient may have, and to confirm that prescriptions have been filled and that follow-up appointments have been made with the primary-care physician. He notes that although this simple follow-up phone call takes little time and effort, it has improved patient satisfaction immensely.
Quality and Prevention Initiatives
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) 2007 National Patient Safety Goals for hospitals includes the following goal: “Reduce the risk of patient harm resulting from falls” (Goal 9).
The requirement for this goal is the implementation of a fall reduction program, followed by evaluation of the effectiveness of the program. Drs. Wald and Shaw agree that, because of the nature of what they do, hospitalists are in an ideal position to spearhead the movement to assess the reasons a patient may have fallen and the risk for future falls—both in the hospital and following discharge—and to synthesize that data to create comprehensive falls prevention programs in their hospitals.
Because hospitalists are on-site 24 hours a day, seven days a week, they are usually first responders when a patient falls and can best evaluate the reasons for the fall and track outcomes. “We’re in an ideal position to create protocols for what to do once a patient does fall in the hospital and [to] evaluate the fall and the incident,” Dr. Wald says. “This is a great quality improvement project because the data are already being collected.”
Dr. Shaw concurs. “Hospitalists are the quality assessors that are in the trenches,” she says. “The hospitalists are really the clinicians most familiar with the strengths and weaknesses of any institution.” TH
Sheri Polley is a medical journalist based in Pennsylvania.
References
- Centers for Disease Control and Prevention. Falls among older adults: an overview. CDC Web site. Available at: www.cdc.gov/ncipc/factsheets/adultfalls.htm. Last accessed March 13, 2007.
- Sterling DA, O’Connor JA, Bonadies J. Geriatric falls: injury severity is high and disproportionate to mechanism. J Trauma. 2001 Jan;50(1):116-119.
- Oliver D, Daly F, Martin FC, et al. Risk factors and risk assessment tools for falls in hospital in-patients: a systematic review. Age Ageing. 2004 Mar;33(2):122-130.
- Nnodim JO, Alexander NB. Assessing falls in older adults: a comprehensive fall evaluation to reduce fall risk in older adults. Geriatrics. 2005 Oct;60(10):24-28.
- Centers for Disease Control and Prevention. CDC fall prevention activities: research studies. CDC Web site. Available at: www.cdc.gov/ncipc/duip/FallsPreventionActivity.htm. Last accessed March 13, 2007.
- Wald H, Huddleston J, Kramer A. Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs. J Hosp Med. 2006 Jan;1(1):29-35.
The problem of falls among older adults has been recognized and studied for many years, including myriad analyses regarding assessment and prevention of falls in this population. The U.S. Census Bureau reported that there were 35.9 million people age 65 and over in the United States as of July 1, 2003. As this population increases, the specific issues pertaining to its members, including falls, must be addressed by hospitalists.
How Big Is the Problem?
The Center for Disease Control and Prevention’s (CDC) National Center for Injury Prevention and Control reports that:
- More than one-third of adults 65 and older fall each year in the United States;
- Falls are the leading cause of injury deaths for older adults;
- In 2003, about 1.8 million people 65 and older were treated in emergency departments for nonfatal falls, and about 460,000 of these patients were hospitalized;
- The rates of fall-related deaths among older adults rose significantly over the past decade;
- Many individuals who fall develop a fear of falling. That may cause them to limit activity, leading to reduced mobility and physical fitness and increasing their risk for additional falls; and
- In 2000, direct medical costs totaled $179 million for fatal falls and $19 billion for nonfatal fall injuries.1
One study exploring the relationship between the mechanism of fall and the pattern and severity of injury in geriatric patients compared with younger patients concluded that falls were the mechanism of injury in 48% of the older patients (those 65 and older) included in the study compared with 7% in the younger group. Further, 32% of falls in the older group resulted in serious injury, while this was true of only 4% of falls in the younger cohort.2
Risk Assessment
When an inpatient in an acute-care hospital falls, a number of negative outcomes can occur, including a longer hospital stay and higher rates of discharge to long-term care.
Falls are associated with higher levels of anxiety and depression and loss of confidence for the patient. They lead to increased costs for patients and hospitals. Feelings of anxiety and/or guilt among staff members may follow. Ultimately, a fall can result in complaints or even litigation from patients or their families.3
Traditional methods of fall risk evaluation may not be effective for assessing the risk of falling for a hospitalized patient, regardless of the reason the patient is hospitalized. The classic risk factors are generally well recognized among physicians and clinical staff and include:
- Age 65 and older;
- A history of falls;
- Cognitive impairment;
- Urinary/fecal incontinence/urgency;
- Balance problems, lower extremity weakness, arthritis;
- Vision problems;
- Use of more than four daily medications or use of psychotropics or narcotics; and
- ETOH.
Acute illness alone accounts for approximately 10% of falls in older adults.4 Many patients suffering or recovering from acute illness may go through a transient period of increased risk for falling that needs to be recognized by physicians and nursing staff.
The impact of pharmacology on a patient’s risk for falling is widely recognized. Patients who take four or more medications are generally considered to be at increased risk. Certain medications, including diuretics, anti-hypertensives, tricyclic antidepressants, sedatives, and hypoglycemics are known to increase an individual’s risk for falling. An October 2004 CDC-funded study by researchers at Johns Hopkins University (Baltimore) concluded that the short-term risk of single and recurring falls may triple within two days after a medication change.5 A patient hospitalized for an acute illness or injury is likely to have had a recent and significant change in the medications he or she is taking, thereby at least temporarily increasing that individual’s risk for falling.
The environmental hazards of the hospital room can’t be overlooked when assessing a patient’s risk for falling. The patient is in an unfamiliar setting—often with informal restraints in place, including IV tubing, feeding tubes, pulse oximeters, and catheters. These obstacles make it more difficult for the patient to maneuver and present opportunities for tripping.
All these things—individually or combined—can increase the chances of falling, even for a patient who at first glance doesn’t appear to be at risk.
Stephen Shaw, MD, medical director of Community Hospitalists in Cleveland, says that while falls assessment tools can be helpful, it would be difficult to outline a foolproof assessment form.
The physician must keep in mind the fact that falls prevention is multifactorial; it may be difficult to attribute the patient’s fall(s) to any single reason. “Any vigorous falls assessment program has to have a comprehensive approach,” he cautions. “Medications, attention to vision limitations, and his or her ability to feel in the dark in their surroundings all have to be taken into consideration.”
The Hospitalist’s Role
When a patient is admitted for injuries resulting from a fall or from an illness that may have been diagnosed as a result of a fall, consider acute conditions first. Also remember that falling is a symptom; understanding why the patient fell is the first step to prevention—both while the patient remains in the hospital and following discharge.
One of the first things the hospitalist must do to reduce patient falls effectively is to study risk assessment and prevention of geriatric falls. A study published in the Journal of Hospital Medicine in January/February 2006 (“Is There a Geriatrician in the House? Geriatric Care Approaches in Hospitalist Programs”) identifies the need for collaboration between hospitalists and geriatricians to better address the issues specific to hospitalized older adults. This collaboration combines the geriatrician’s expertise regarding the elderly patient’s unique needs and considerations with the hospitalist’s expertise regarding specific acute care situations.6
Heidi Wald, MD, MPH, assistant professor, Division of Health Care Policy and Research and General Internal Medicine at the University of Colorado in Denver and primary author of the Journal of Hospital Medicine study, says numerous things can be done to reduce the risk of inpatient falls, beginning with identifying patients at high risk for falling. This can be done by assessing the classic risk factors intrinsic to the patient, while keeping in mind the risk factors that could be mediated by the acute illness.
Risks created by the environment can be fairly easily addressed, according to Dr. Wald. Lower beds as far as they will go, with the wheels locked. Don’t use upper and lower bedrails simultaneously (this reduces the chance of a patient being caught between the two). Cut down on the use of restraints—both formal and informal.
Because many falls result from patients trying to get to the bathroom, Dr. Wald advises scheduled toileting, with the staff regularly assisting the patient to the bathroom. If a patient cannot ambulate to the restroom independently, ensure that a urinal or a bedpan is nearby and readily accessible to the patient.
Dr. Wald also advises utilizing the expertise and skills of those clinicians most familiar with the patient: the nursing staff. The nurses who have daily contact with the patient are in the best position to provide information regarding changes in the patient’s mental status, ability to ambulate, response to medications, compliance, and other factors that may increase the risk for a fall.
“The bottom line of any quality initiative will often fall to the nurses’ assessment,” says Dr. Shaw. “The front-line caregivers for fall assessments are our nurses.”
A Multidisciplinary Approach to Prevention
Drs. Wald and Shaw both stress the importance of a multidisciplinary approach to prevention of falls (both in hospital and following discharge). A patient who has already fallen—or one identified to be at risk for falling—can be offered a great deal of support and guidance pending discharge. And discharge planning can begin literally at admission.
It’s Dr. Shaw’s practice with at-risk patients to involve physical and occupational therapy (as well as social workers) in the patient’s care right from the beginning. Those individuals are then in a position not only to perform a thorough assessment of the patient but also to begin working on ways to reduce the patient’s risk following discharge. As Dr. Shaw points out, the hospitalist has access to resources the patient’s primary-care physician generally does not, and those resources should be utilized to full advantage.
Physical therapy can offer rehabilitative interventions, including transfer, gait, and balance training; strength and range-of-motion exercises; and habituation exercises for vestibular problems. Occupational therapy can offer the patient instruction on simplifying tasks and on performing everyday activities safely. Social workers can assist the patient with finding educational and assistive resources. All disciplines can be involved in home safety evaluations, patient and family education, and the procurement of assistive and adaptive equipment, such as ambulation devices, grab bars, handrails, raised toilet seats, and so on.
When all of these healthcare providers are involved in the patient’s care from the beginning and can coordinate discharge planning as a team, a more well-rounded and comprehensive plan for prevention of falls can be formulated. This team approach also offers a more accurate view of whether the patient is capable of returning home with or without help or if placement in a rehabilitation or long-term care facility may be more appropriate.
Involve the Patient
Once an at-risk patient has been identified, communicate that risk to everyone involved with the patient’s care, including the medical staff, the family, and the patient. “Patients have a certain degree of risk-taking behavior, and they won’t necessarily ask for help,” says Dr. Wald. “Part of that is that they’re not willing to admit that they need help.”
Patients need to be reminded that they are or have recently been sick—that’s why they’re in the hospital in the first place. She says patients and caregivers must be attuned to the fact that as patients begin to feel better and stronger and become more mobile, their risk for falling will go up before it starts to come down.
If a patient remains resistant to asking for or accepting assistance, Dr. Wald suggests finding out what the patient’s barriers are and trying to get around them. “Try to get people to admit that they have a problem,” she advises. “A lot of times, the barriers aren’t rational, so rationalizing isn’t always effective.”
She offers the example of a patient who resists the idea of using a walker. Sometimes simply demonstrating how much more quickly the patient can get around using the walker may do the trick.
Dr. Shaw adds that a certain level of sensitivity is required when approaching a patient who is in denial regarding his or her limitations. It may be necessary to ask a second physician or nurse to lend credibility by explaining to the patient again that he or she may have needs that didn’t exist previously. He cautions, however, that if his patient remains in denial about his or her limitations, he does not hesitate to engage the family. “If the patient is discharged home, it’s going to be the family who will be the policemen and watchdogs,” says Dr. Shaw.
After discharge, following up with the patient can make a big difference in patient compliance. The time following discharge to the home can be confusing for the patient, and he may be overwhelmed with changes in routines, medications, and activities. Dr. Shaw’s organization calls the patient three to four days post-discharge to verify that the patient understands the discharge instructions, to answer questions the patient may have, and to confirm that prescriptions have been filled and that follow-up appointments have been made with the primary-care physician. He notes that although this simple follow-up phone call takes little time and effort, it has improved patient satisfaction immensely.
Quality and Prevention Initiatives
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) 2007 National Patient Safety Goals for hospitals includes the following goal: “Reduce the risk of patient harm resulting from falls” (Goal 9).
The requirement for this goal is the implementation of a fall reduction program, followed by evaluation of the effectiveness of the program. Drs. Wald and Shaw agree that, because of the nature of what they do, hospitalists are in an ideal position to spearhead the movement to assess the reasons a patient may have fallen and the risk for future falls—both in the hospital and following discharge—and to synthesize that data to create comprehensive falls prevention programs in their hospitals.
Because hospitalists are on-site 24 hours a day, seven days a week, they are usually first responders when a patient falls and can best evaluate the reasons for the fall and track outcomes. “We’re in an ideal position to create protocols for what to do once a patient does fall in the hospital and [to] evaluate the fall and the incident,” Dr. Wald says. “This is a great quality improvement project because the data are already being collected.”
Dr. Shaw concurs. “Hospitalists are the quality assessors that are in the trenches,” she says. “The hospitalists are really the clinicians most familiar with the strengths and weaknesses of any institution.” TH
Sheri Polley is a medical journalist based in Pennsylvania.
References
- Centers for Disease Control and Prevention. Falls among older adults: an overview. CDC Web site. Available at: www.cdc.gov/ncipc/factsheets/adultfalls.htm. Last accessed March 13, 2007.
- Sterling DA, O’Connor JA, Bonadies J. Geriatric falls: injury severity is high and disproportionate to mechanism. J Trauma. 2001 Jan;50(1):116-119.
- Oliver D, Daly F, Martin FC, et al. Risk factors and risk assessment tools for falls in hospital in-patients: a systematic review. Age Ageing. 2004 Mar;33(2):122-130.
- Nnodim JO, Alexander NB. Assessing falls in older adults: a comprehensive fall evaluation to reduce fall risk in older adults. Geriatrics. 2005 Oct;60(10):24-28.
- Centers for Disease Control and Prevention. CDC fall prevention activities: research studies. CDC Web site. Available at: www.cdc.gov/ncipc/duip/FallsPreventionActivity.htm. Last accessed March 13, 2007.
- Wald H, Huddleston J, Kramer A. Is there a geriatrician in the house? Geriatric care approaches in hospitalist programs. J Hosp Med. 2006 Jan;1(1):29-35.
Action
These days you’re just as likely to find Jeffrey Krebs, MD, FACP, in front of a camera as behind a stethoscope. And his patients are as likely to see him in a movie theater as they are by their hospital beds.
That’s because the San Diego hospitalist has a schedule that allows him to build an acting career without giving up the patient care he loves. But don’t expect to see him playing a physician. The youthful-looking 46-year-old doesn’t match Hollywood’s “Marcus Welby, MD” image. He’s usually only considered for resident or intern roles despite almost two decades of experience working in medicine. “I’ve been a physician for more than 17 years, and yet I don’t look like a doctor, casting directors tell me,” he says.
From Dabbling to Passion
Dr. Krebs has been dabbling in acting since he was a resident, but it wasn’t until he became a hospitalist last year that made his acting passion a priority. He first became interested in acting in 1989 while he interned at Cedars-Sinai Medical Center in Los Angeles. Frequent contact with celebrity patients led to the offer of a role as an extra in the movie “Heart Condition,” (1990) a comedy starring Denzel Washington and Bob Hoskins.
“I thought it would be fun,” Dr. Krebs says. “Because they were filming in a restaurant a couple of miles from the hospital, it was convenient.”
The day he spent on the set in his non-speaking role taught him how things are done in Hollywood. Even though his efforts ended up on the cutting-room floor, the experience sparked a passion for acting that has grown stronger every year.
After completing his internal medicine residency in Los Angeles in 1989, Dr. Krebs moved to San Diego to become a primary care physician at Kaiser Permanente San Diego Medical Center. He found an acting teacher who held classes in San Diego on Sundays and began developing his craft.
Despite the demands of his work as a busy primary care physician, Dr. Krebs has racked up an impressive list of film and TV credits through the years. He was cast as a softball attendant in the martial arts film “3 Ninjas: High Noon at Mega Mountain,” (1998) the last of the “tween” movie “3 Ninjas” series. He played Agent Hans in “The English Job” (2006), a food critic in “Single White Female 2: The Psycho” (2005), a computer programmer in “Form 3254-A” (2005), and a young doctor in “True Vinyl” (2000), a romantic musical movie.
He has also performed in local theater, appearing in “Intrusion,” “Hypocrisy,” “Prelude to a Kiss,” “Apres Opera,” and “Ignoto’s Farewell” in San Diego, where he was often recognized by patients and colleagues.
Time for a Change
But the last-minute demands of an actor have conflicted frequently with his responsibilities as a physician. “I would be cast in a film and then not hear from the casting director for months,” Dr. Krebs explains. “Then the travel department could call one day and tell me I had to be on the out-of-town set in three days. There were times when I had to turn down a role because I won’t put my patients’ health on hold to do a film. I began to realize that if I really wanted to make a go of my acting, I needed to make some changes in my life.”
An opportunity presented itself last year when Kaiser Permanente in San Diego created two nocturnist positions for hospitalists. When Dr. Krebs heard about the positions, he quickly applied. “I thought that was perfect because all the auditions and filming happen during the day, and I could attend them if I worked at night,” he explains.
Dr. Krebs and another physician work 12-hour shifts beginning at 6 p.m. three times a week. For Dr. Krebs it’s Sunday through Tuesday nights. When his shift ends Wednesday morning, he drives the 125 miles from San Diego to his apartment in Los Angeles, catches some sleep, then assumes the role of Hollywood actor.
From Wednesday through Saturday, you might find him auditioning, taking acting classes, filming on location, doing the behind-the-scenes business of an aspiring actor, or attending a Hollywood party to network. On Sunday afternoon, he returns to the hospital in San Diego to begin another round of night shifts.
“Sometimes I can put in a 31-hour day if I have an audition in Los Angeles on Wednesday afternoon after my shift in San Diego Tuesday night,” he says. “Then I’ll be running on adrenaline, but it’s worth it.”
Balanced from the Beginning
A Southern California native, Dr. Krebs grew up near Disneyland, where he played clarinet during the bicentennial parade there in 1976. He knew he wanted to be a doctor when he was 7 years old. His grandfather was an optometrist, and Dr. Krebs spent many of his school holidays talking happily to his grandfather’s office patients.
Dr. Krebs graduated with honors from the University of California at Davis and received a medical degree from the University of California, San Diego, School of Medicine. He has been honored by Kaiser Permanente Medical Group with its Distinguished Service Award, its Everyday Hero Award, and its Primary Care Leadership Recognition Award.
Dr. Krebs says being a physician and an actor creates the perfect balance between his right and left brains: “The analytical side of my brain is satisfied by medicine, and my creative side is satisfied by being able to immerse myself in acting on my days off. It’s a perfect balance for me.”
Patients benefit from this balance, Dr. Krebs believes, because he brings to his job the increased empathy he’s developed as an actor. “My acting has absolutely enhanced my relationships with patients,” he says. “Acting requires developing intense listening skills. I’ve become a much better listener. Acting also requires you to focus on what the other person is saying, and that has helped me really focus on what patients tell me.”
Conversely, being a physician has helped him with his acting.
“Physicians are trained observers. Medicine has helped me become a better observer of people’s mannerisms and what they say about their character,” he explains. “And that training in observation makes me better able to relate to other actors.”
Two different careers also fulfill two different aspects of his personality.
“I’m a bit of a ham, although I don’t ham it up in my acting,” admits Dr. Krebs. “I like being noticed. In acting, it’s all about me, so I’m on the receiving end. But when I’m a physician, it’s never about me; it’s about the patient. So I’m the giver. I like that because it balances my life.”

Win-Win Situation
Dr. Krebs isn’t the only one satisfied with his nocturnist position. It’s also “a win, win, win situation for the hospital,” says Ted Geer, MD, chief of internal medicine at Kaiser Permanente San Diego Medical Center.
“Administratively it’s great because there aren’t as many shifts that have to be covered by other physicians,” Dr. Geer explains. “It’s win-win for patients and the emergency room because we have more physicians who are up all night to help.”
While many hospitalists use their off hours to pursue hobbies, it’s unusual for them to have another profession. “It’s a credit to him that he’s able to have a second career,” says Dr. Geer.
Dr. Krebs is a well-respected clinician and a good internist, according to Dr. Geer. “His skills as an internist make him fit into this role very well,” says Dr. Geer. “He takes very good care of his patients.”
Overlapping Worlds
Dr. Krebs says his medical colleagues get a kick out of his acting career. “Many of their children own the “3 Ninjas” movie. They tell me they have spotted me in the film while watching it with their kids,” he says.
Actors are surprised when they find out about his medical career. Although Dr. Krebs doesn’t volunteer the information that he’s a physician, he’ll tell others in the film industry when asked. “I want to keep my two worlds separate, but I am proud of who I am and what I do as a physician.”
Sometimes those two worlds overlap. When Dr. Krebs was cast in “True Vinyl,” “The casting director asked me what I did in my off hours and, when I said I was a physician, he said, ‘OK, so you’re the doctor in the film.’ ”
For that movie, Dr. Krebs also served as the medical consultant, ensuring the medical scenes were accurate.
Even though he enjoyed the experience, Dr. Krebs doesn’t want to pursue more medical consultant opportunities; acting is his passion. “When I’m on the set, I’m an actor and that’s what I want to be,” he says.
Can Do
It takes a focused, high-energy person to succeed as a physician and an actor. Dr. Krebs keeps his stamina high by making his health a priority. He exercises almost every day, eats right, and surrounds himself with positive people. “I have always been a high-energy person; I’m never depressed and always look at the positive side of any situation,” he says.
He credits his parents with instilling in him an optimistic view of life. “They told us we could be anybody and do anything we wanted,” he recalls. “When I was told that I couldn’t compete at a high level in figure skating and go to medical school, I thought, ‘My parents said I could do anything I wanted and I want to do this,’ so I did.”
It may have been his figure-skating background that gave Dr. Krebs the fearlessness required of a successful actor, according to his manager, Fritz Friedman.
“He’s willing to take chances,” notes Friedman. “It’s a fearsome thing to take those leaps in skating that seem so effortless. The risk he takes, as all actors do, is that he will look foolish. But actors don’t care. They try and hope their bodies will listen to their brains.”
Friedman says Dr. Krebs’ acting style is dramatic and intense: “I think he has capabilities of comedic roles but they haven’t been offered to him yet,” he says. “I think, given the right opportunity, he’d be terrific at that. Jeff has a very strong on-screen presence. When he’s on screen, people focus on him. He’s charismatic.”
And That’s Not All He Does …
In his free time, Dr. Krebs loves to cook, travel, and take photographs. He entertains his friends with a meal made from scratch at least once a month and has hired chefs from local restaurants to teach him advanced cooking techniques. In October, he’s going to Tuscany to indulge all three passions with Italian culinary classes, travel, and photography.
With two careers and many interests, Dr. Krebs sometimes finds it hard to get enough sleep. Although he would like to take singing lessons and French classes, that’s more than he can handle right now. “Sleep has to be a priority so I can continue to make good medical decisions,” he says. And he admits that getting his laundry done “is one of my biggest challenges in life.”
Dr. Krebs recently focused his acting career on film and television, giving up theater. “Acting in plays is harder—if not impossible—with my new life as a nocturnist,” he says. Theater requires months of rehearsals, held in the daytime during the week. But choosing film was an easy choice. “I like watching myself on film so that I can learn from it,” he says.
Dr. Krebs says his favorite roles have been “any in which I can learn something new or develop a new aspect of myself.” In a film to be released this spring, “Half Past Dead II: Justified,” he plays an inmate at a maximum-security prison. “That was a stretch because I had to tap into my inner serial killer. Sometimes the roles that I play are in conflict with who I am,” he explains. “You learn that everyone has every possibility inside of them, and you have to tap into that.”
He does this by developing the back story, which in this case meant creating a character who had done something bad enough to be in Alcatraz. The film’s director called Dr. Krebs recently to praise his efforts.
In March, Dr. Krebs was in Dallas filming “Missionary Man,” starring Dolph Lundgren. It is a Western-style movie involving “revenge and redemption at the end of a gun barrel.” In the film, Dr. Krebs plays Lundgren’s brother; the character’s name was changed to Jeff. “Imagine having a character named after me,” Dr. Krebs exclaims.
The Perfect Combination
What would happen if Dr. Krebs landed a major film role or a long-term television series? Would he give up medicine to become star of the next “ER” or “Grey’s Anatomy”? Not if it meant giving up his medical career, he says.
“It would be very difficult for me to give up medicine completely because I really love being a physician,” Dr. Krebs admits. “I might take a leave for a month or two if a big film opportunity came along. But right now I’m happy with the roles I’m getting that allow me to continue my medical career.”
Dr. Krebs says he could not have been the kind of actor he is and practice the kind of medicine he wants to practice without being a hospitalist, and he’s grateful for the opportunity.
“I’m so happy the hospitalist movement has taken off in the last several years,” he says. “My life is much, much better since I became a hospitalist. I feel like I have it all.” TH
Barbara Dillard is a medical journalist based in Chicago.
These days you’re just as likely to find Jeffrey Krebs, MD, FACP, in front of a camera as behind a stethoscope. And his patients are as likely to see him in a movie theater as they are by their hospital beds.
That’s because the San Diego hospitalist has a schedule that allows him to build an acting career without giving up the patient care he loves. But don’t expect to see him playing a physician. The youthful-looking 46-year-old doesn’t match Hollywood’s “Marcus Welby, MD” image. He’s usually only considered for resident or intern roles despite almost two decades of experience working in medicine. “I’ve been a physician for more than 17 years, and yet I don’t look like a doctor, casting directors tell me,” he says.
From Dabbling to Passion
Dr. Krebs has been dabbling in acting since he was a resident, but it wasn’t until he became a hospitalist last year that made his acting passion a priority. He first became interested in acting in 1989 while he interned at Cedars-Sinai Medical Center in Los Angeles. Frequent contact with celebrity patients led to the offer of a role as an extra in the movie “Heart Condition,” (1990) a comedy starring Denzel Washington and Bob Hoskins.
“I thought it would be fun,” Dr. Krebs says. “Because they were filming in a restaurant a couple of miles from the hospital, it was convenient.”
The day he spent on the set in his non-speaking role taught him how things are done in Hollywood. Even though his efforts ended up on the cutting-room floor, the experience sparked a passion for acting that has grown stronger every year.
After completing his internal medicine residency in Los Angeles in 1989, Dr. Krebs moved to San Diego to become a primary care physician at Kaiser Permanente San Diego Medical Center. He found an acting teacher who held classes in San Diego on Sundays and began developing his craft.
Despite the demands of his work as a busy primary care physician, Dr. Krebs has racked up an impressive list of film and TV credits through the years. He was cast as a softball attendant in the martial arts film “3 Ninjas: High Noon at Mega Mountain,” (1998) the last of the “tween” movie “3 Ninjas” series. He played Agent Hans in “The English Job” (2006), a food critic in “Single White Female 2: The Psycho” (2005), a computer programmer in “Form 3254-A” (2005), and a young doctor in “True Vinyl” (2000), a romantic musical movie.
He has also performed in local theater, appearing in “Intrusion,” “Hypocrisy,” “Prelude to a Kiss,” “Apres Opera,” and “Ignoto’s Farewell” in San Diego, where he was often recognized by patients and colleagues.
Time for a Change
But the last-minute demands of an actor have conflicted frequently with his responsibilities as a physician. “I would be cast in a film and then not hear from the casting director for months,” Dr. Krebs explains. “Then the travel department could call one day and tell me I had to be on the out-of-town set in three days. There were times when I had to turn down a role because I won’t put my patients’ health on hold to do a film. I began to realize that if I really wanted to make a go of my acting, I needed to make some changes in my life.”
An opportunity presented itself last year when Kaiser Permanente in San Diego created two nocturnist positions for hospitalists. When Dr. Krebs heard about the positions, he quickly applied. “I thought that was perfect because all the auditions and filming happen during the day, and I could attend them if I worked at night,” he explains.
Dr. Krebs and another physician work 12-hour shifts beginning at 6 p.m. three times a week. For Dr. Krebs it’s Sunday through Tuesday nights. When his shift ends Wednesday morning, he drives the 125 miles from San Diego to his apartment in Los Angeles, catches some sleep, then assumes the role of Hollywood actor.
From Wednesday through Saturday, you might find him auditioning, taking acting classes, filming on location, doing the behind-the-scenes business of an aspiring actor, or attending a Hollywood party to network. On Sunday afternoon, he returns to the hospital in San Diego to begin another round of night shifts.
“Sometimes I can put in a 31-hour day if I have an audition in Los Angeles on Wednesday afternoon after my shift in San Diego Tuesday night,” he says. “Then I’ll be running on adrenaline, but it’s worth it.”
Balanced from the Beginning
A Southern California native, Dr. Krebs grew up near Disneyland, where he played clarinet during the bicentennial parade there in 1976. He knew he wanted to be a doctor when he was 7 years old. His grandfather was an optometrist, and Dr. Krebs spent many of his school holidays talking happily to his grandfather’s office patients.
Dr. Krebs graduated with honors from the University of California at Davis and received a medical degree from the University of California, San Diego, School of Medicine. He has been honored by Kaiser Permanente Medical Group with its Distinguished Service Award, its Everyday Hero Award, and its Primary Care Leadership Recognition Award.
Dr. Krebs says being a physician and an actor creates the perfect balance between his right and left brains: “The analytical side of my brain is satisfied by medicine, and my creative side is satisfied by being able to immerse myself in acting on my days off. It’s a perfect balance for me.”
Patients benefit from this balance, Dr. Krebs believes, because he brings to his job the increased empathy he’s developed as an actor. “My acting has absolutely enhanced my relationships with patients,” he says. “Acting requires developing intense listening skills. I’ve become a much better listener. Acting also requires you to focus on what the other person is saying, and that has helped me really focus on what patients tell me.”
Conversely, being a physician has helped him with his acting.
“Physicians are trained observers. Medicine has helped me become a better observer of people’s mannerisms and what they say about their character,” he explains. “And that training in observation makes me better able to relate to other actors.”
Two different careers also fulfill two different aspects of his personality.
“I’m a bit of a ham, although I don’t ham it up in my acting,” admits Dr. Krebs. “I like being noticed. In acting, it’s all about me, so I’m on the receiving end. But when I’m a physician, it’s never about me; it’s about the patient. So I’m the giver. I like that because it balances my life.”
Win-Win Situation
Dr. Krebs isn’t the only one satisfied with his nocturnist position. It’s also “a win, win, win situation for the hospital,” says Ted Geer, MD, chief of internal medicine at Kaiser Permanente San Diego Medical Center.
“Administratively it’s great because there aren’t as many shifts that have to be covered by other physicians,” Dr. Geer explains. “It’s win-win for patients and the emergency room because we have more physicians who are up all night to help.”
While many hospitalists use their off hours to pursue hobbies, it’s unusual for them to have another profession. “It’s a credit to him that he’s able to have a second career,” says Dr. Geer.
Dr. Krebs is a well-respected clinician and a good internist, according to Dr. Geer. “His skills as an internist make him fit into this role very well,” says Dr. Geer. “He takes very good care of his patients.”
Overlapping Worlds
Dr. Krebs says his medical colleagues get a kick out of his acting career. “Many of their children own the “3 Ninjas” movie. They tell me they have spotted me in the film while watching it with their kids,” he says.
Actors are surprised when they find out about his medical career. Although Dr. Krebs doesn’t volunteer the information that he’s a physician, he’ll tell others in the film industry when asked. “I want to keep my two worlds separate, but I am proud of who I am and what I do as a physician.”
Sometimes those two worlds overlap. When Dr. Krebs was cast in “True Vinyl,” “The casting director asked me what I did in my off hours and, when I said I was a physician, he said, ‘OK, so you’re the doctor in the film.’ ”
For that movie, Dr. Krebs also served as the medical consultant, ensuring the medical scenes were accurate.
Even though he enjoyed the experience, Dr. Krebs doesn’t want to pursue more medical consultant opportunities; acting is his passion. “When I’m on the set, I’m an actor and that’s what I want to be,” he says.
Can Do
It takes a focused, high-energy person to succeed as a physician and an actor. Dr. Krebs keeps his stamina high by making his health a priority. He exercises almost every day, eats right, and surrounds himself with positive people. “I have always been a high-energy person; I’m never depressed and always look at the positive side of any situation,” he says.
He credits his parents with instilling in him an optimistic view of life. “They told us we could be anybody and do anything we wanted,” he recalls. “When I was told that I couldn’t compete at a high level in figure skating and go to medical school, I thought, ‘My parents said I could do anything I wanted and I want to do this,’ so I did.”
It may have been his figure-skating background that gave Dr. Krebs the fearlessness required of a successful actor, according to his manager, Fritz Friedman.
“He’s willing to take chances,” notes Friedman. “It’s a fearsome thing to take those leaps in skating that seem so effortless. The risk he takes, as all actors do, is that he will look foolish. But actors don’t care. They try and hope their bodies will listen to their brains.”
Friedman says Dr. Krebs’ acting style is dramatic and intense: “I think he has capabilities of comedic roles but they haven’t been offered to him yet,” he says. “I think, given the right opportunity, he’d be terrific at that. Jeff has a very strong on-screen presence. When he’s on screen, people focus on him. He’s charismatic.”
And That’s Not All He Does …
In his free time, Dr. Krebs loves to cook, travel, and take photographs. He entertains his friends with a meal made from scratch at least once a month and has hired chefs from local restaurants to teach him advanced cooking techniques. In October, he’s going to Tuscany to indulge all three passions with Italian culinary classes, travel, and photography.
With two careers and many interests, Dr. Krebs sometimes finds it hard to get enough sleep. Although he would like to take singing lessons and French classes, that’s more than he can handle right now. “Sleep has to be a priority so I can continue to make good medical decisions,” he says. And he admits that getting his laundry done “is one of my biggest challenges in life.”
Dr. Krebs recently focused his acting career on film and television, giving up theater. “Acting in plays is harder—if not impossible—with my new life as a nocturnist,” he says. Theater requires months of rehearsals, held in the daytime during the week. But choosing film was an easy choice. “I like watching myself on film so that I can learn from it,” he says.
Dr. Krebs says his favorite roles have been “any in which I can learn something new or develop a new aspect of myself.” In a film to be released this spring, “Half Past Dead II: Justified,” he plays an inmate at a maximum-security prison. “That was a stretch because I had to tap into my inner serial killer. Sometimes the roles that I play are in conflict with who I am,” he explains. “You learn that everyone has every possibility inside of them, and you have to tap into that.”
He does this by developing the back story, which in this case meant creating a character who had done something bad enough to be in Alcatraz. The film’s director called Dr. Krebs recently to praise his efforts.
In March, Dr. Krebs was in Dallas filming “Missionary Man,” starring Dolph Lundgren. It is a Western-style movie involving “revenge and redemption at the end of a gun barrel.” In the film, Dr. Krebs plays Lundgren’s brother; the character’s name was changed to Jeff. “Imagine having a character named after me,” Dr. Krebs exclaims.
The Perfect Combination
What would happen if Dr. Krebs landed a major film role or a long-term television series? Would he give up medicine to become star of the next “ER” or “Grey’s Anatomy”? Not if it meant giving up his medical career, he says.
“It would be very difficult for me to give up medicine completely because I really love being a physician,” Dr. Krebs admits. “I might take a leave for a month or two if a big film opportunity came along. But right now I’m happy with the roles I’m getting that allow me to continue my medical career.”
Dr. Krebs says he could not have been the kind of actor he is and practice the kind of medicine he wants to practice without being a hospitalist, and he’s grateful for the opportunity.
“I’m so happy the hospitalist movement has taken off in the last several years,” he says. “My life is much, much better since I became a hospitalist. I feel like I have it all.” TH
Barbara Dillard is a medical journalist based in Chicago.
These days you’re just as likely to find Jeffrey Krebs, MD, FACP, in front of a camera as behind a stethoscope. And his patients are as likely to see him in a movie theater as they are by their hospital beds.
That’s because the San Diego hospitalist has a schedule that allows him to build an acting career without giving up the patient care he loves. But don’t expect to see him playing a physician. The youthful-looking 46-year-old doesn’t match Hollywood’s “Marcus Welby, MD” image. He’s usually only considered for resident or intern roles despite almost two decades of experience working in medicine. “I’ve been a physician for more than 17 years, and yet I don’t look like a doctor, casting directors tell me,” he says.
From Dabbling to Passion
Dr. Krebs has been dabbling in acting since he was a resident, but it wasn’t until he became a hospitalist last year that made his acting passion a priority. He first became interested in acting in 1989 while he interned at Cedars-Sinai Medical Center in Los Angeles. Frequent contact with celebrity patients led to the offer of a role as an extra in the movie “Heart Condition,” (1990) a comedy starring Denzel Washington and Bob Hoskins.
“I thought it would be fun,” Dr. Krebs says. “Because they were filming in a restaurant a couple of miles from the hospital, it was convenient.”
The day he spent on the set in his non-speaking role taught him how things are done in Hollywood. Even though his efforts ended up on the cutting-room floor, the experience sparked a passion for acting that has grown stronger every year.
After completing his internal medicine residency in Los Angeles in 1989, Dr. Krebs moved to San Diego to become a primary care physician at Kaiser Permanente San Diego Medical Center. He found an acting teacher who held classes in San Diego on Sundays and began developing his craft.
Despite the demands of his work as a busy primary care physician, Dr. Krebs has racked up an impressive list of film and TV credits through the years. He was cast as a softball attendant in the martial arts film “3 Ninjas: High Noon at Mega Mountain,” (1998) the last of the “tween” movie “3 Ninjas” series. He played Agent Hans in “The English Job” (2006), a food critic in “Single White Female 2: The Psycho” (2005), a computer programmer in “Form 3254-A” (2005), and a young doctor in “True Vinyl” (2000), a romantic musical movie.
He has also performed in local theater, appearing in “Intrusion,” “Hypocrisy,” “Prelude to a Kiss,” “Apres Opera,” and “Ignoto’s Farewell” in San Diego, where he was often recognized by patients and colleagues.
Time for a Change
But the last-minute demands of an actor have conflicted frequently with his responsibilities as a physician. “I would be cast in a film and then not hear from the casting director for months,” Dr. Krebs explains. “Then the travel department could call one day and tell me I had to be on the out-of-town set in three days. There were times when I had to turn down a role because I won’t put my patients’ health on hold to do a film. I began to realize that if I really wanted to make a go of my acting, I needed to make some changes in my life.”
An opportunity presented itself last year when Kaiser Permanente in San Diego created two nocturnist positions for hospitalists. When Dr. Krebs heard about the positions, he quickly applied. “I thought that was perfect because all the auditions and filming happen during the day, and I could attend them if I worked at night,” he explains.
Dr. Krebs and another physician work 12-hour shifts beginning at 6 p.m. three times a week. For Dr. Krebs it’s Sunday through Tuesday nights. When his shift ends Wednesday morning, he drives the 125 miles from San Diego to his apartment in Los Angeles, catches some sleep, then assumes the role of Hollywood actor.
From Wednesday through Saturday, you might find him auditioning, taking acting classes, filming on location, doing the behind-the-scenes business of an aspiring actor, or attending a Hollywood party to network. On Sunday afternoon, he returns to the hospital in San Diego to begin another round of night shifts.
“Sometimes I can put in a 31-hour day if I have an audition in Los Angeles on Wednesday afternoon after my shift in San Diego Tuesday night,” he says. “Then I’ll be running on adrenaline, but it’s worth it.”
Balanced from the Beginning
A Southern California native, Dr. Krebs grew up near Disneyland, where he played clarinet during the bicentennial parade there in 1976. He knew he wanted to be a doctor when he was 7 years old. His grandfather was an optometrist, and Dr. Krebs spent many of his school holidays talking happily to his grandfather’s office patients.
Dr. Krebs graduated with honors from the University of California at Davis and received a medical degree from the University of California, San Diego, School of Medicine. He has been honored by Kaiser Permanente Medical Group with its Distinguished Service Award, its Everyday Hero Award, and its Primary Care Leadership Recognition Award.
Dr. Krebs says being a physician and an actor creates the perfect balance between his right and left brains: “The analytical side of my brain is satisfied by medicine, and my creative side is satisfied by being able to immerse myself in acting on my days off. It’s a perfect balance for me.”
Patients benefit from this balance, Dr. Krebs believes, because he brings to his job the increased empathy he’s developed as an actor. “My acting has absolutely enhanced my relationships with patients,” he says. “Acting requires developing intense listening skills. I’ve become a much better listener. Acting also requires you to focus on what the other person is saying, and that has helped me really focus on what patients tell me.”
Conversely, being a physician has helped him with his acting.
“Physicians are trained observers. Medicine has helped me become a better observer of people’s mannerisms and what they say about their character,” he explains. “And that training in observation makes me better able to relate to other actors.”
Two different careers also fulfill two different aspects of his personality.
“I’m a bit of a ham, although I don’t ham it up in my acting,” admits Dr. Krebs. “I like being noticed. In acting, it’s all about me, so I’m on the receiving end. But when I’m a physician, it’s never about me; it’s about the patient. So I’m the giver. I like that because it balances my life.”
Win-Win Situation
Dr. Krebs isn’t the only one satisfied with his nocturnist position. It’s also “a win, win, win situation for the hospital,” says Ted Geer, MD, chief of internal medicine at Kaiser Permanente San Diego Medical Center.
“Administratively it’s great because there aren’t as many shifts that have to be covered by other physicians,” Dr. Geer explains. “It’s win-win for patients and the emergency room because we have more physicians who are up all night to help.”
While many hospitalists use their off hours to pursue hobbies, it’s unusual for them to have another profession. “It’s a credit to him that he’s able to have a second career,” says Dr. Geer.
Dr. Krebs is a well-respected clinician and a good internist, according to Dr. Geer. “His skills as an internist make him fit into this role very well,” says Dr. Geer. “He takes very good care of his patients.”
Overlapping Worlds
Dr. Krebs says his medical colleagues get a kick out of his acting career. “Many of their children own the “3 Ninjas” movie. They tell me they have spotted me in the film while watching it with their kids,” he says.
Actors are surprised when they find out about his medical career. Although Dr. Krebs doesn’t volunteer the information that he’s a physician, he’ll tell others in the film industry when asked. “I want to keep my two worlds separate, but I am proud of who I am and what I do as a physician.”
Sometimes those two worlds overlap. When Dr. Krebs was cast in “True Vinyl,” “The casting director asked me what I did in my off hours and, when I said I was a physician, he said, ‘OK, so you’re the doctor in the film.’ ”
For that movie, Dr. Krebs also served as the medical consultant, ensuring the medical scenes were accurate.
Even though he enjoyed the experience, Dr. Krebs doesn’t want to pursue more medical consultant opportunities; acting is his passion. “When I’m on the set, I’m an actor and that’s what I want to be,” he says.
Can Do
It takes a focused, high-energy person to succeed as a physician and an actor. Dr. Krebs keeps his stamina high by making his health a priority. He exercises almost every day, eats right, and surrounds himself with positive people. “I have always been a high-energy person; I’m never depressed and always look at the positive side of any situation,” he says.
He credits his parents with instilling in him an optimistic view of life. “They told us we could be anybody and do anything we wanted,” he recalls. “When I was told that I couldn’t compete at a high level in figure skating and go to medical school, I thought, ‘My parents said I could do anything I wanted and I want to do this,’ so I did.”
It may have been his figure-skating background that gave Dr. Krebs the fearlessness required of a successful actor, according to his manager, Fritz Friedman.
“He’s willing to take chances,” notes Friedman. “It’s a fearsome thing to take those leaps in skating that seem so effortless. The risk he takes, as all actors do, is that he will look foolish. But actors don’t care. They try and hope their bodies will listen to their brains.”
Friedman says Dr. Krebs’ acting style is dramatic and intense: “I think he has capabilities of comedic roles but they haven’t been offered to him yet,” he says. “I think, given the right opportunity, he’d be terrific at that. Jeff has a very strong on-screen presence. When he’s on screen, people focus on him. He’s charismatic.”
And That’s Not All He Does …
In his free time, Dr. Krebs loves to cook, travel, and take photographs. He entertains his friends with a meal made from scratch at least once a month and has hired chefs from local restaurants to teach him advanced cooking techniques. In October, he’s going to Tuscany to indulge all three passions with Italian culinary classes, travel, and photography.
With two careers and many interests, Dr. Krebs sometimes finds it hard to get enough sleep. Although he would like to take singing lessons and French classes, that’s more than he can handle right now. “Sleep has to be a priority so I can continue to make good medical decisions,” he says. And he admits that getting his laundry done “is one of my biggest challenges in life.”
Dr. Krebs recently focused his acting career on film and television, giving up theater. “Acting in plays is harder—if not impossible—with my new life as a nocturnist,” he says. Theater requires months of rehearsals, held in the daytime during the week. But choosing film was an easy choice. “I like watching myself on film so that I can learn from it,” he says.
Dr. Krebs says his favorite roles have been “any in which I can learn something new or develop a new aspect of myself.” In a film to be released this spring, “Half Past Dead II: Justified,” he plays an inmate at a maximum-security prison. “That was a stretch because I had to tap into my inner serial killer. Sometimes the roles that I play are in conflict with who I am,” he explains. “You learn that everyone has every possibility inside of them, and you have to tap into that.”
He does this by developing the back story, which in this case meant creating a character who had done something bad enough to be in Alcatraz. The film’s director called Dr. Krebs recently to praise his efforts.
In March, Dr. Krebs was in Dallas filming “Missionary Man,” starring Dolph Lundgren. It is a Western-style movie involving “revenge and redemption at the end of a gun barrel.” In the film, Dr. Krebs plays Lundgren’s brother; the character’s name was changed to Jeff. “Imagine having a character named after me,” Dr. Krebs exclaims.
The Perfect Combination
What would happen if Dr. Krebs landed a major film role or a long-term television series? Would he give up medicine to become star of the next “ER” or “Grey’s Anatomy”? Not if it meant giving up his medical career, he says.
“It would be very difficult for me to give up medicine completely because I really love being a physician,” Dr. Krebs admits. “I might take a leave for a month or two if a big film opportunity came along. But right now I’m happy with the roles I’m getting that allow me to continue my medical career.”
Dr. Krebs says he could not have been the kind of actor he is and practice the kind of medicine he wants to practice without being a hospitalist, and he’s grateful for the opportunity.
“I’m so happy the hospitalist movement has taken off in the last several years,” he says. “My life is much, much better since I became a hospitalist. I feel like I have it all.” TH
Barbara Dillard is a medical journalist based in Chicago.