User login
Hospital Medicine 2007

This year marks the 10-year anniversary of Robert Wachter’s coining of the term “hospitalist,” as well as the celebration of the decade-old SHM. The celebration culminates in a stellar annual meeting that epitomizes the growth of hospital medicine.
The SHM Annual Meeting attendance has grown from just a handful of participants to more than 1,200 expected at the 2007 Annual Meeting. More importantly, as the role of hospitalists has changed from primarily focusing on providing care to the hospitalized patient to serving as the leader of quality improvement, a key staff educator, and a facilitator of care transitions, so have their educational needs. Thus, the annual meeting has evolved in order to provide an educational experience that has relevance on a practical level.
The SHM 2007 Annual Meeting Committee (AMC), led by Course Director Chad Whelan, MD, challenged itself to develop a program that will meet the needs of a diverse audience that includes community-based and academic-based hospitalists; research-oriented and clinician-focused seasoned veteran physicians and early career hospitalists; as well as pediatric, geriatric, and family practice hospitalists. Such an effort begins with the big picture: What is happening in the environment that will impact healthcare today and in the future?
The answer is found in the role of information technology, and SHM will welcome two renowned speakers to provide current and future perspectives. David Brailer, MD, PhD, the first National Coordinator for Health Information Technology (2004-2006), will examine the forces driving health information technology and how technology affects pressures on the quality and cost of care. Jonathan Perlin, MD, PhD, chief medical officer and senior vice president for Quality for Hospital Corporation of America, will look to healthcare’s challenges and opportunities in the decade ahead, with a focus on health IT and performance and the role of hospital medicine as it relates to care improvement.
The 2007 Annual Meeting will again feature Robert Wachter, MD, as the keynote speaker in the closing plenary session. Dr. Wachter is sure to entertain as he examines “The Hospitalist Movement a Decade Later: Life as a Swiss Army Knife.”
The goal of a broad-based program will be achieved through separate breakout sessions and workshops, divided into seven tracks. Though the format is similar to other years, the 2007 program has some new twists. One clinical track focuses on “Things You Didn’t Learn in Medical School,” and a palliative care track has been added. Relevant sessions have been selected using the Core Competencies in Hospital Medicine and collaborating with SHM’s committees, which serve the interests of all of the groups.
The connection between the program and SHM’s committees will be strong. The committees will focus their efforts on topics and goals that are important to our members. The AMC solicits ideas for breakout sessions from the committees; it also profiles the output of a committee that has significance to attendees in their daily responsibilities.
Suggestions from the committees have resulted in a combination of pertinent and innovative sessions. Here are just a few to whet your appetite for the complete program:
- A workshop jointly planned by the Hospital Quality and Patient Safety (HQPS) and Education Committees, designed to obtain input and consensus on SHM-developed communication and hand-off standards;
- An Academic Track, intended to appeal to those hospitalists focused on teaching, quality improvement, research, and growing a hospital medicine program;
- A workshop, proposed by the Career Satisfaction Task Force, that addresses relevant career issues from the leaders’ and hospitalists’ perspectives;
- A Quality Track defined by the HQPS Committee that, in addition to the consensus-building workshop, features medication reconciliation and Toyota Methods sessions;
- A Pediatric Track, designed to address the needs of our fastest growing member segment, features a range of clinical and leadership topics, including electronic health records, the prevention of the transmission of infectious agents, and the utilization of dashboards to improve care;
- The work of the Benchmarks Committee will be profiled in a session that will demonstrate how to use key performance metrics to improve hospital medicine and the care of the hospitalized patient;
- The Public Policy Committee has recommended a pay-for-performance (P4P) breakout session, because P4P has been identified as an important issue in hospital medicine;
- A Palliative Care Track, proposed and developed by the Palliative Care Task Force, includes relevant topics such as pain management, the ethical and legal considerations of palliative care, and communications skills; and
- A visiting professor, Stephan Fihn, MD, MPH, will conduct poster rounds, lead a workshop, and participate in “Breakfast with Leaders in Hospital Medicine.”
The Annual Meeting Committee focused on identifying faculty members who can share their experience and expertise in an entertaining and elucidating way. We anticipate that you will enjoy presentations by experts new to the SHM Annual Meeting, as well as return engagements by past faculty.
Letters
Correction

On p. 6 of the January 2007 issue the “Profile of Academic Hospitalists” contained errors inadvertently introduced in the editing process.
Line 4 of the table should read: “Clinical Full Time Equivalency—Academic Hospitalists .69, All Hospitalists .89.”
Line 8 of the table should read “Nurse Practitioners Per Group—Academic Hospitalists .82, All Hospitalists .43.”
The SHM Annual Meeting traditionally offers networking opportunities with more than 1,100 hospitalists. Special Interest Forums provide each attendee not only with a unique occasion to meet with hospitalists who share similar interests but also with the venue to express their opinions on a national level. SHM utilizes the input to change and grow the organization and hospital medicine. Planned Special Interest Forums include:
- Research;
- Community-based hospitalists;
- Pediatric hospitalists;
- Medical directors and leadership;
- Family practice hospitalists;
- Geriatric hospitalists;
- Nurse practitioners and physician assistants;
- Women in hospital medicine;
- Early career hospitalists;
- Education;
- Curriculum/fellowship;
- Public policy; and
- History of medicine.
Other networking mainstays of the Annual Meeting, including the Research, Innovations, and Clinical Vignettes Competition; Exhibits; President’s Lunch; and Town Meeting, will again be featured. Satellite symposia are planned, as well as the following pre-courses:
- Inpatient Coding and Documentation: Getting Paid What You Deserve;
- Best Practices in Managing a Hospital Medicine Program;
- Critical Care Medicine for the Hospitalist;
- Perioperative Medicine for the Hospitalist; and
- High Impact Quality Improvement: How to Ensure a Successful Project.
Additionally, a PICC Line Placement for Pediatric and Adult Hospitalists pre-course is being proposed by the Pediatrics Committee.
As you can see, 2007 Annual Meeting will present variety and choice; there is something for everyone. Don’t miss this premier educational event for hospitalists and the opportunity to be a part of the hospital medicine movement. The SHM 2007 Annual Meeting will be held at the Gaylord Texan Resort and Convention Center outside Dallas on May 24 and 25, with pre-courses held on May 23. Visit the SHM Web site at www.hospitalmedicine.org/hospitalmedicine2007 for complete program details or to register online. You may also register by calling SHM at (800) 843-3360. Come to Texas and help us celebrate 10 years of improving the quality of healthcare!
SHM: BEHIND THE SCENES
Resolutions
By Tina Budnitz, MPH

This is the time of year when many New Year’s resolutions dissolve. In some cases, people set unrealistic goals. Others lack the tools to succeed or live in an environment that makes change too difficult. In 2006 I resolved to start running each morning before work. I have the determination and the physical ability to meet this goal. Disarming the house alarm at 5 a.m., however, awakens my two toddlers. And detaching two toddlers from my legs proves to be quite a challenge. It also turns out that my tolerance for cold weather is low, while my ability to forgive a missed run is high.
Sustaining quality improvement initiatives at the hospital is lot like sustaining New Year’s resolutions. The best of intentions are often thwarted by a lack of time, resources, or energy to change the system, as well as by those within the system who resist change. For example, SHM members tell me that attempting to introduce a new discharge planning process feels a lot like trying to run through the hospital with two toddlers hanging on to your legs. SHM strives to support hospitalists in their resolutions to implement positive change in the hospital.
My role at SHM is to lead the development of programs, tool kits, and support mechanisms that will enable you, our members, to implement and sustain local quality improvement efforts.
SHM currently supports members in their efforts to improve outcomes for patients with heart failure, stroke, or diabetes; we work to prevent venous thromboembolism (VTE) and hospital-acquired blood-stream infections. We also support members in their efforts to improve the discharge process for older adults, thereby reducing readmission rates and adverse drug events while improving communications with receiving physicians.
We support members in their efforts to implement, evaluate, and sustain QI initiatives using a variety of methodologies. We offer symposia, workshops, and a full-day Annual Meeting Pre-Course on quality improvement; we also provide Leadership Academy Level I and Level II and networking opportunities for members and their mentors. We’ve designed Web-based clinical tool kits around specific disease states and special patient populations. We offer Web-based resource rooms to guide members from start to finish through a new local QI initiative. We have funded demonstration projects to pilot new approaches and tools for use in discharge planning, along with innovative research to improve care for heart failure patients. And we’ve only just begun.
Researching the Approach
For each QI area we address, an advisory board is recruited to represent the best available experts, organizations, and multidisciplinary professionals. For example, the Discharge Planning for Older Adults Advisory Board includes representatives from the American Geriatrics Society (AGS), the Institute for Healthcare Improvement (IHI), the Agency for Healthcare Research and Quality (AHRQ), the Society of General Internal Medicine (SGIM), the Case Management Society of America (CMSA), the National Quality Forum (NQF), and the Association for Health-System Pharmacists (AHSP), in addition to nationally renowned leaders in care transitions, geriatrics, nursing, patient literacy, and pharmacy.
Each Advisory Board conducts a needs assessment and a review of the literature to examine interventions and approaches. The board identifies existing “gaps” in clinical tools and guidelines. Finally, the Advisory Board determines specific, measurable targets for a hospitalist-led intervention and suggests the evidence-based approach(es) that should be most effective.
Implementing an Intervention: Where the Rubber Meets the Road
As I pointed out earlier, resolving what should be done and getting it done are two very different things. In most cases, few people debate the need for the intervention—reducing the incidence of inpatient VTEs, for example—or the validity of the proposed intervention. The challenge arises in changing the system of care so that the intervention becomes the new standard of care. Therefore, after the Advisory Board has determined the aims and intervention(s), SHM develops a “workbook,” a step-by-step field guide for hospitalists that walks them through the process of building a project team, establishing project aims and key metrics, obtaining institutional support, planning the intervention, launching the intervention, measuring impact, and sustaining system improvements.
The workbooks are posted in the SHM Resource Rooms along with other key resources, including slide sets, bedside teaching tools, patient education literature, CME modules, reviews of key literature, interactive “Ask the Expert” discussion boards, and improvement reports detailing the strategies, successes, and setbacks of other institutions. SHM currently offers resource rooms for Preventing VTE, Heart Failure, Stroke, Discharge Planning for the Elderly, Glycemic Control, and Antimicrobial Resistance. To access the resource rooms, visit our Web site at www.hospitalmedicine.org.
Training Leaders
SHM offers its members diverse training opportunities designed to accommodate the range of knowledge, expertise, and resources available at local institutions. The resource rooms and workbooks described above are made freely available to everyone. At the 2007 SHM Annual Meeting, we will offer a quality pre-course for hands-on training to lead a QI initiative for discharge planning, VTE prevention, or glycemic control.
For SHM members who desire additional support, SHM is developing “Mentored Implementation” and “On-Site Consulting” programs. The Mentored Implementation Program provides enrolled sites with all of the tools described above and an additional yearlong training program conducted via monthly conference calls with SHM mentors and/or one-day training programs. The On-Site Consulting Program surveys an institution’s resources and infrastructure. The SHM consultant team reviews the assessment with the site. Following this assessment, the consultant team visits the site to meet with hospital administrators, QI teams, and others to further assess the site and to help build internal support for the QI initiative. Following the visit, each site receives a customized report detailing recommendations and strategies to advance specific local QI initiatives.
SHM recently launched a Mentored Implementation and On-Site Consulting Program for VTE (known as the SHM VTE Collaborative). Similar programs are scheduled to launch for discharge planning this spring. In the coming years, we hope to add training programs in several other key patient safety areas.
Additionally, SHM is engaged in a strategic planning process to determine how best to attract the highest caliber medical students into hospital medicine and to mentor, train, and retain the next generation of leaders.
In summary, I hope the range of training opportunities and educational programs, the depth of SHM tool kits, and the scope of patient safety initiatives are meeting your needs to plan, implement, evaluate, and sustain positive change at your institution. If you are interested in learning more about SHM QI programs or have suggestions on how we might improve them to better meet your needs, please e-mail me at [email protected].
And, in case you were wondering, I’m making progress on my resolution to run. This year my resolution has the support of my department chairs (Jacob, five; Noah, two), with better-defined outcomes (run three times a week for more than 40 minutes each time), and a better tool kit (gloves, ear muffs). In the planning stage, I addressed my biggest barrier (leave the alarm off) and built a support team (my neighbor joins me).
If you see me at the annual meeting, please let me know how your resolutions are working to prevent DVT or to improve the discharge process, glycemic control, or heart failure care. Or better yet, submit those stories to me to share with members in our “Improvement Stories” or resource rooms Web site areas or in print via The Hospitalist or Journal of Hospital Medicine.
Budnitz is senior advisor, quality initiatives, for SHM.
This year marks the 10-year anniversary of Robert Wachter’s coining of the term “hospitalist,” as well as the celebration of the decade-old SHM. The celebration culminates in a stellar annual meeting that epitomizes the growth of hospital medicine.
The SHM Annual Meeting attendance has grown from just a handful of participants to more than 1,200 expected at the 2007 Annual Meeting. More importantly, as the role of hospitalists has changed from primarily focusing on providing care to the hospitalized patient to serving as the leader of quality improvement, a key staff educator, and a facilitator of care transitions, so have their educational needs. Thus, the annual meeting has evolved in order to provide an educational experience that has relevance on a practical level.
The SHM 2007 Annual Meeting Committee (AMC), led by Course Director Chad Whelan, MD, challenged itself to develop a program that will meet the needs of a diverse audience that includes community-based and academic-based hospitalists; research-oriented and clinician-focused seasoned veteran physicians and early career hospitalists; as well as pediatric, geriatric, and family practice hospitalists. Such an effort begins with the big picture: What is happening in the environment that will impact healthcare today and in the future?
The answer is found in the role of information technology, and SHM will welcome two renowned speakers to provide current and future perspectives. David Brailer, MD, PhD, the first National Coordinator for Health Information Technology (2004-2006), will examine the forces driving health information technology and how technology affects pressures on the quality and cost of care. Jonathan Perlin, MD, PhD, chief medical officer and senior vice president for Quality for Hospital Corporation of America, will look to healthcare’s challenges and opportunities in the decade ahead, with a focus on health IT and performance and the role of hospital medicine as it relates to care improvement.
The 2007 Annual Meeting will again feature Robert Wachter, MD, as the keynote speaker in the closing plenary session. Dr. Wachter is sure to entertain as he examines “The Hospitalist Movement a Decade Later: Life as a Swiss Army Knife.”
The goal of a broad-based program will be achieved through separate breakout sessions and workshops, divided into seven tracks. Though the format is similar to other years, the 2007 program has some new twists. One clinical track focuses on “Things You Didn’t Learn in Medical School,” and a palliative care track has been added. Relevant sessions have been selected using the Core Competencies in Hospital Medicine and collaborating with SHM’s committees, which serve the interests of all of the groups.
The connection between the program and SHM’s committees will be strong. The committees will focus their efforts on topics and goals that are important to our members. The AMC solicits ideas for breakout sessions from the committees; it also profiles the output of a committee that has significance to attendees in their daily responsibilities.
Suggestions from the committees have resulted in a combination of pertinent and innovative sessions. Here are just a few to whet your appetite for the complete program:
- A workshop jointly planned by the Hospital Quality and Patient Safety (HQPS) and Education Committees, designed to obtain input and consensus on SHM-developed communication and hand-off standards;
- An Academic Track, intended to appeal to those hospitalists focused on teaching, quality improvement, research, and growing a hospital medicine program;
- A workshop, proposed by the Career Satisfaction Task Force, that addresses relevant career issues from the leaders’ and hospitalists’ perspectives;
- A Quality Track defined by the HQPS Committee that, in addition to the consensus-building workshop, features medication reconciliation and Toyota Methods sessions;
- A Pediatric Track, designed to address the needs of our fastest growing member segment, features a range of clinical and leadership topics, including electronic health records, the prevention of the transmission of infectious agents, and the utilization of dashboards to improve care;
- The work of the Benchmarks Committee will be profiled in a session that will demonstrate how to use key performance metrics to improve hospital medicine and the care of the hospitalized patient;
- The Public Policy Committee has recommended a pay-for-performance (P4P) breakout session, because P4P has been identified as an important issue in hospital medicine;
- A Palliative Care Track, proposed and developed by the Palliative Care Task Force, includes relevant topics such as pain management, the ethical and legal considerations of palliative care, and communications skills; and
- A visiting professor, Stephan Fihn, MD, MPH, will conduct poster rounds, lead a workshop, and participate in “Breakfast with Leaders in Hospital Medicine.”
The Annual Meeting Committee focused on identifying faculty members who can share their experience and expertise in an entertaining and elucidating way. We anticipate that you will enjoy presentations by experts new to the SHM Annual Meeting, as well as return engagements by past faculty.
Letters
Correction
On p. 6 of the January 2007 issue the “Profile of Academic Hospitalists” contained errors inadvertently introduced in the editing process.
Line 4 of the table should read: “Clinical Full Time Equivalency—Academic Hospitalists .69, All Hospitalists .89.”
Line 8 of the table should read “Nurse Practitioners Per Group—Academic Hospitalists .82, All Hospitalists .43.”
The SHM Annual Meeting traditionally offers networking opportunities with more than 1,100 hospitalists. Special Interest Forums provide each attendee not only with a unique occasion to meet with hospitalists who share similar interests but also with the venue to express their opinions on a national level. SHM utilizes the input to change and grow the organization and hospital medicine. Planned Special Interest Forums include:
- Research;
- Community-based hospitalists;
- Pediatric hospitalists;
- Medical directors and leadership;
- Family practice hospitalists;
- Geriatric hospitalists;
- Nurse practitioners and physician assistants;
- Women in hospital medicine;
- Early career hospitalists;
- Education;
- Curriculum/fellowship;
- Public policy; and
- History of medicine.
Other networking mainstays of the Annual Meeting, including the Research, Innovations, and Clinical Vignettes Competition; Exhibits; President’s Lunch; and Town Meeting, will again be featured. Satellite symposia are planned, as well as the following pre-courses:
- Inpatient Coding and Documentation: Getting Paid What You Deserve;
- Best Practices in Managing a Hospital Medicine Program;
- Critical Care Medicine for the Hospitalist;
- Perioperative Medicine for the Hospitalist; and
- High Impact Quality Improvement: How to Ensure a Successful Project.
Additionally, a PICC Line Placement for Pediatric and Adult Hospitalists pre-course is being proposed by the Pediatrics Committee.
As you can see, 2007 Annual Meeting will present variety and choice; there is something for everyone. Don’t miss this premier educational event for hospitalists and the opportunity to be a part of the hospital medicine movement. The SHM 2007 Annual Meeting will be held at the Gaylord Texan Resort and Convention Center outside Dallas on May 24 and 25, with pre-courses held on May 23. Visit the SHM Web site at www.hospitalmedicine.org/hospitalmedicine2007 for complete program details or to register online. You may also register by calling SHM at (800) 843-3360. Come to Texas and help us celebrate 10 years of improving the quality of healthcare!
SHM: BEHIND THE SCENES
Resolutions
By Tina Budnitz, MPH
This is the time of year when many New Year’s resolutions dissolve. In some cases, people set unrealistic goals. Others lack the tools to succeed or live in an environment that makes change too difficult. In 2006 I resolved to start running each morning before work. I have the determination and the physical ability to meet this goal. Disarming the house alarm at 5 a.m., however, awakens my two toddlers. And detaching two toddlers from my legs proves to be quite a challenge. It also turns out that my tolerance for cold weather is low, while my ability to forgive a missed run is high.
Sustaining quality improvement initiatives at the hospital is lot like sustaining New Year’s resolutions. The best of intentions are often thwarted by a lack of time, resources, or energy to change the system, as well as by those within the system who resist change. For example, SHM members tell me that attempting to introduce a new discharge planning process feels a lot like trying to run through the hospital with two toddlers hanging on to your legs. SHM strives to support hospitalists in their resolutions to implement positive change in the hospital.
My role at SHM is to lead the development of programs, tool kits, and support mechanisms that will enable you, our members, to implement and sustain local quality improvement efforts.
SHM currently supports members in their efforts to improve outcomes for patients with heart failure, stroke, or diabetes; we work to prevent venous thromboembolism (VTE) and hospital-acquired blood-stream infections. We also support members in their efforts to improve the discharge process for older adults, thereby reducing readmission rates and adverse drug events while improving communications with receiving physicians.
We support members in their efforts to implement, evaluate, and sustain QI initiatives using a variety of methodologies. We offer symposia, workshops, and a full-day Annual Meeting Pre-Course on quality improvement; we also provide Leadership Academy Level I and Level II and networking opportunities for members and their mentors. We’ve designed Web-based clinical tool kits around specific disease states and special patient populations. We offer Web-based resource rooms to guide members from start to finish through a new local QI initiative. We have funded demonstration projects to pilot new approaches and tools for use in discharge planning, along with innovative research to improve care for heart failure patients. And we’ve only just begun.
Researching the Approach
For each QI area we address, an advisory board is recruited to represent the best available experts, organizations, and multidisciplinary professionals. For example, the Discharge Planning for Older Adults Advisory Board includes representatives from the American Geriatrics Society (AGS), the Institute for Healthcare Improvement (IHI), the Agency for Healthcare Research and Quality (AHRQ), the Society of General Internal Medicine (SGIM), the Case Management Society of America (CMSA), the National Quality Forum (NQF), and the Association for Health-System Pharmacists (AHSP), in addition to nationally renowned leaders in care transitions, geriatrics, nursing, patient literacy, and pharmacy.
Each Advisory Board conducts a needs assessment and a review of the literature to examine interventions and approaches. The board identifies existing “gaps” in clinical tools and guidelines. Finally, the Advisory Board determines specific, measurable targets for a hospitalist-led intervention and suggests the evidence-based approach(es) that should be most effective.
Implementing an Intervention: Where the Rubber Meets the Road
As I pointed out earlier, resolving what should be done and getting it done are two very different things. In most cases, few people debate the need for the intervention—reducing the incidence of inpatient VTEs, for example—or the validity of the proposed intervention. The challenge arises in changing the system of care so that the intervention becomes the new standard of care. Therefore, after the Advisory Board has determined the aims and intervention(s), SHM develops a “workbook,” a step-by-step field guide for hospitalists that walks them through the process of building a project team, establishing project aims and key metrics, obtaining institutional support, planning the intervention, launching the intervention, measuring impact, and sustaining system improvements.
The workbooks are posted in the SHM Resource Rooms along with other key resources, including slide sets, bedside teaching tools, patient education literature, CME modules, reviews of key literature, interactive “Ask the Expert” discussion boards, and improvement reports detailing the strategies, successes, and setbacks of other institutions. SHM currently offers resource rooms for Preventing VTE, Heart Failure, Stroke, Discharge Planning for the Elderly, Glycemic Control, and Antimicrobial Resistance. To access the resource rooms, visit our Web site at www.hospitalmedicine.org.
Training Leaders
SHM offers its members diverse training opportunities designed to accommodate the range of knowledge, expertise, and resources available at local institutions. The resource rooms and workbooks described above are made freely available to everyone. At the 2007 SHM Annual Meeting, we will offer a quality pre-course for hands-on training to lead a QI initiative for discharge planning, VTE prevention, or glycemic control.
For SHM members who desire additional support, SHM is developing “Mentored Implementation” and “On-Site Consulting” programs. The Mentored Implementation Program provides enrolled sites with all of the tools described above and an additional yearlong training program conducted via monthly conference calls with SHM mentors and/or one-day training programs. The On-Site Consulting Program surveys an institution’s resources and infrastructure. The SHM consultant team reviews the assessment with the site. Following this assessment, the consultant team visits the site to meet with hospital administrators, QI teams, and others to further assess the site and to help build internal support for the QI initiative. Following the visit, each site receives a customized report detailing recommendations and strategies to advance specific local QI initiatives.
SHM recently launched a Mentored Implementation and On-Site Consulting Program for VTE (known as the SHM VTE Collaborative). Similar programs are scheduled to launch for discharge planning this spring. In the coming years, we hope to add training programs in several other key patient safety areas.
Additionally, SHM is engaged in a strategic planning process to determine how best to attract the highest caliber medical students into hospital medicine and to mentor, train, and retain the next generation of leaders.
In summary, I hope the range of training opportunities and educational programs, the depth of SHM tool kits, and the scope of patient safety initiatives are meeting your needs to plan, implement, evaluate, and sustain positive change at your institution. If you are interested in learning more about SHM QI programs or have suggestions on how we might improve them to better meet your needs, please e-mail me at [email protected].
And, in case you were wondering, I’m making progress on my resolution to run. This year my resolution has the support of my department chairs (Jacob, five; Noah, two), with better-defined outcomes (run three times a week for more than 40 minutes each time), and a better tool kit (gloves, ear muffs). In the planning stage, I addressed my biggest barrier (leave the alarm off) and built a support team (my neighbor joins me).
If you see me at the annual meeting, please let me know how your resolutions are working to prevent DVT or to improve the discharge process, glycemic control, or heart failure care. Or better yet, submit those stories to me to share with members in our “Improvement Stories” or resource rooms Web site areas or in print via The Hospitalist or Journal of Hospital Medicine.
Budnitz is senior advisor, quality initiatives, for SHM.
This year marks the 10-year anniversary of Robert Wachter’s coining of the term “hospitalist,” as well as the celebration of the decade-old SHM. The celebration culminates in a stellar annual meeting that epitomizes the growth of hospital medicine.
The SHM Annual Meeting attendance has grown from just a handful of participants to more than 1,200 expected at the 2007 Annual Meeting. More importantly, as the role of hospitalists has changed from primarily focusing on providing care to the hospitalized patient to serving as the leader of quality improvement, a key staff educator, and a facilitator of care transitions, so have their educational needs. Thus, the annual meeting has evolved in order to provide an educational experience that has relevance on a practical level.
The SHM 2007 Annual Meeting Committee (AMC), led by Course Director Chad Whelan, MD, challenged itself to develop a program that will meet the needs of a diverse audience that includes community-based and academic-based hospitalists; research-oriented and clinician-focused seasoned veteran physicians and early career hospitalists; as well as pediatric, geriatric, and family practice hospitalists. Such an effort begins with the big picture: What is happening in the environment that will impact healthcare today and in the future?
The answer is found in the role of information technology, and SHM will welcome two renowned speakers to provide current and future perspectives. David Brailer, MD, PhD, the first National Coordinator for Health Information Technology (2004-2006), will examine the forces driving health information technology and how technology affects pressures on the quality and cost of care. Jonathan Perlin, MD, PhD, chief medical officer and senior vice president for Quality for Hospital Corporation of America, will look to healthcare’s challenges and opportunities in the decade ahead, with a focus on health IT and performance and the role of hospital medicine as it relates to care improvement.
The 2007 Annual Meeting will again feature Robert Wachter, MD, as the keynote speaker in the closing plenary session. Dr. Wachter is sure to entertain as he examines “The Hospitalist Movement a Decade Later: Life as a Swiss Army Knife.”
The goal of a broad-based program will be achieved through separate breakout sessions and workshops, divided into seven tracks. Though the format is similar to other years, the 2007 program has some new twists. One clinical track focuses on “Things You Didn’t Learn in Medical School,” and a palliative care track has been added. Relevant sessions have been selected using the Core Competencies in Hospital Medicine and collaborating with SHM’s committees, which serve the interests of all of the groups.
The connection between the program and SHM’s committees will be strong. The committees will focus their efforts on topics and goals that are important to our members. The AMC solicits ideas for breakout sessions from the committees; it also profiles the output of a committee that has significance to attendees in their daily responsibilities.
Suggestions from the committees have resulted in a combination of pertinent and innovative sessions. Here are just a few to whet your appetite for the complete program:
- A workshop jointly planned by the Hospital Quality and Patient Safety (HQPS) and Education Committees, designed to obtain input and consensus on SHM-developed communication and hand-off standards;
- An Academic Track, intended to appeal to those hospitalists focused on teaching, quality improvement, research, and growing a hospital medicine program;
- A workshop, proposed by the Career Satisfaction Task Force, that addresses relevant career issues from the leaders’ and hospitalists’ perspectives;
- A Quality Track defined by the HQPS Committee that, in addition to the consensus-building workshop, features medication reconciliation and Toyota Methods sessions;
- A Pediatric Track, designed to address the needs of our fastest growing member segment, features a range of clinical and leadership topics, including electronic health records, the prevention of the transmission of infectious agents, and the utilization of dashboards to improve care;
- The work of the Benchmarks Committee will be profiled in a session that will demonstrate how to use key performance metrics to improve hospital medicine and the care of the hospitalized patient;
- The Public Policy Committee has recommended a pay-for-performance (P4P) breakout session, because P4P has been identified as an important issue in hospital medicine;
- A Palliative Care Track, proposed and developed by the Palliative Care Task Force, includes relevant topics such as pain management, the ethical and legal considerations of palliative care, and communications skills; and
- A visiting professor, Stephan Fihn, MD, MPH, will conduct poster rounds, lead a workshop, and participate in “Breakfast with Leaders in Hospital Medicine.”
The Annual Meeting Committee focused on identifying faculty members who can share their experience and expertise in an entertaining and elucidating way. We anticipate that you will enjoy presentations by experts new to the SHM Annual Meeting, as well as return engagements by past faculty.
Letters
Correction
On p. 6 of the January 2007 issue the “Profile of Academic Hospitalists” contained errors inadvertently introduced in the editing process.
Line 4 of the table should read: “Clinical Full Time Equivalency—Academic Hospitalists .69, All Hospitalists .89.”
Line 8 of the table should read “Nurse Practitioners Per Group—Academic Hospitalists .82, All Hospitalists .43.”
The SHM Annual Meeting traditionally offers networking opportunities with more than 1,100 hospitalists. Special Interest Forums provide each attendee not only with a unique occasion to meet with hospitalists who share similar interests but also with the venue to express their opinions on a national level. SHM utilizes the input to change and grow the organization and hospital medicine. Planned Special Interest Forums include:
- Research;
- Community-based hospitalists;
- Pediatric hospitalists;
- Medical directors and leadership;
- Family practice hospitalists;
- Geriatric hospitalists;
- Nurse practitioners and physician assistants;
- Women in hospital medicine;
- Early career hospitalists;
- Education;
- Curriculum/fellowship;
- Public policy; and
- History of medicine.
Other networking mainstays of the Annual Meeting, including the Research, Innovations, and Clinical Vignettes Competition; Exhibits; President’s Lunch; and Town Meeting, will again be featured. Satellite symposia are planned, as well as the following pre-courses:
- Inpatient Coding and Documentation: Getting Paid What You Deserve;
- Best Practices in Managing a Hospital Medicine Program;
- Critical Care Medicine for the Hospitalist;
- Perioperative Medicine for the Hospitalist; and
- High Impact Quality Improvement: How to Ensure a Successful Project.
Additionally, a PICC Line Placement for Pediatric and Adult Hospitalists pre-course is being proposed by the Pediatrics Committee.
As you can see, 2007 Annual Meeting will present variety and choice; there is something for everyone. Don’t miss this premier educational event for hospitalists and the opportunity to be a part of the hospital medicine movement. The SHM 2007 Annual Meeting will be held at the Gaylord Texan Resort and Convention Center outside Dallas on May 24 and 25, with pre-courses held on May 23. Visit the SHM Web site at www.hospitalmedicine.org/hospitalmedicine2007 for complete program details or to register online. You may also register by calling SHM at (800) 843-3360. Come to Texas and help us celebrate 10 years of improving the quality of healthcare!
SHM: BEHIND THE SCENES
Resolutions
By Tina Budnitz, MPH
This is the time of year when many New Year’s resolutions dissolve. In some cases, people set unrealistic goals. Others lack the tools to succeed or live in an environment that makes change too difficult. In 2006 I resolved to start running each morning before work. I have the determination and the physical ability to meet this goal. Disarming the house alarm at 5 a.m., however, awakens my two toddlers. And detaching two toddlers from my legs proves to be quite a challenge. It also turns out that my tolerance for cold weather is low, while my ability to forgive a missed run is high.
Sustaining quality improvement initiatives at the hospital is lot like sustaining New Year’s resolutions. The best of intentions are often thwarted by a lack of time, resources, or energy to change the system, as well as by those within the system who resist change. For example, SHM members tell me that attempting to introduce a new discharge planning process feels a lot like trying to run through the hospital with two toddlers hanging on to your legs. SHM strives to support hospitalists in their resolutions to implement positive change in the hospital.
My role at SHM is to lead the development of programs, tool kits, and support mechanisms that will enable you, our members, to implement and sustain local quality improvement efforts.
SHM currently supports members in their efforts to improve outcomes for patients with heart failure, stroke, or diabetes; we work to prevent venous thromboembolism (VTE) and hospital-acquired blood-stream infections. We also support members in their efforts to improve the discharge process for older adults, thereby reducing readmission rates and adverse drug events while improving communications with receiving physicians.
We support members in their efforts to implement, evaluate, and sustain QI initiatives using a variety of methodologies. We offer symposia, workshops, and a full-day Annual Meeting Pre-Course on quality improvement; we also provide Leadership Academy Level I and Level II and networking opportunities for members and their mentors. We’ve designed Web-based clinical tool kits around specific disease states and special patient populations. We offer Web-based resource rooms to guide members from start to finish through a new local QI initiative. We have funded demonstration projects to pilot new approaches and tools for use in discharge planning, along with innovative research to improve care for heart failure patients. And we’ve only just begun.
Researching the Approach
For each QI area we address, an advisory board is recruited to represent the best available experts, organizations, and multidisciplinary professionals. For example, the Discharge Planning for Older Adults Advisory Board includes representatives from the American Geriatrics Society (AGS), the Institute for Healthcare Improvement (IHI), the Agency for Healthcare Research and Quality (AHRQ), the Society of General Internal Medicine (SGIM), the Case Management Society of America (CMSA), the National Quality Forum (NQF), and the Association for Health-System Pharmacists (AHSP), in addition to nationally renowned leaders in care transitions, geriatrics, nursing, patient literacy, and pharmacy.
Each Advisory Board conducts a needs assessment and a review of the literature to examine interventions and approaches. The board identifies existing “gaps” in clinical tools and guidelines. Finally, the Advisory Board determines specific, measurable targets for a hospitalist-led intervention and suggests the evidence-based approach(es) that should be most effective.
Implementing an Intervention: Where the Rubber Meets the Road
As I pointed out earlier, resolving what should be done and getting it done are two very different things. In most cases, few people debate the need for the intervention—reducing the incidence of inpatient VTEs, for example—or the validity of the proposed intervention. The challenge arises in changing the system of care so that the intervention becomes the new standard of care. Therefore, after the Advisory Board has determined the aims and intervention(s), SHM develops a “workbook,” a step-by-step field guide for hospitalists that walks them through the process of building a project team, establishing project aims and key metrics, obtaining institutional support, planning the intervention, launching the intervention, measuring impact, and sustaining system improvements.
The workbooks are posted in the SHM Resource Rooms along with other key resources, including slide sets, bedside teaching tools, patient education literature, CME modules, reviews of key literature, interactive “Ask the Expert” discussion boards, and improvement reports detailing the strategies, successes, and setbacks of other institutions. SHM currently offers resource rooms for Preventing VTE, Heart Failure, Stroke, Discharge Planning for the Elderly, Glycemic Control, and Antimicrobial Resistance. To access the resource rooms, visit our Web site at www.hospitalmedicine.org.
Training Leaders
SHM offers its members diverse training opportunities designed to accommodate the range of knowledge, expertise, and resources available at local institutions. The resource rooms and workbooks described above are made freely available to everyone. At the 2007 SHM Annual Meeting, we will offer a quality pre-course for hands-on training to lead a QI initiative for discharge planning, VTE prevention, or glycemic control.
For SHM members who desire additional support, SHM is developing “Mentored Implementation” and “On-Site Consulting” programs. The Mentored Implementation Program provides enrolled sites with all of the tools described above and an additional yearlong training program conducted via monthly conference calls with SHM mentors and/or one-day training programs. The On-Site Consulting Program surveys an institution’s resources and infrastructure. The SHM consultant team reviews the assessment with the site. Following this assessment, the consultant team visits the site to meet with hospital administrators, QI teams, and others to further assess the site and to help build internal support for the QI initiative. Following the visit, each site receives a customized report detailing recommendations and strategies to advance specific local QI initiatives.
SHM recently launched a Mentored Implementation and On-Site Consulting Program for VTE (known as the SHM VTE Collaborative). Similar programs are scheduled to launch for discharge planning this spring. In the coming years, we hope to add training programs in several other key patient safety areas.
Additionally, SHM is engaged in a strategic planning process to determine how best to attract the highest caliber medical students into hospital medicine and to mentor, train, and retain the next generation of leaders.
In summary, I hope the range of training opportunities and educational programs, the depth of SHM tool kits, and the scope of patient safety initiatives are meeting your needs to plan, implement, evaluate, and sustain positive change at your institution. If you are interested in learning more about SHM QI programs or have suggestions on how we might improve them to better meet your needs, please e-mail me at [email protected].
And, in case you were wondering, I’m making progress on my resolution to run. This year my resolution has the support of my department chairs (Jacob, five; Noah, two), with better-defined outcomes (run three times a week for more than 40 minutes each time), and a better tool kit (gloves, ear muffs). In the planning stage, I addressed my biggest barrier (leave the alarm off) and built a support team (my neighbor joins me).
If you see me at the annual meeting, please let me know how your resolutions are working to prevent DVT or to improve the discharge process, glycemic control, or heart failure care. Or better yet, submit those stories to me to share with members in our “Improvement Stories” or resource rooms Web site areas or in print via The Hospitalist or Journal of Hospital Medicine.
Budnitz is senior advisor, quality initiatives, for SHM.
Face the Future

We need not be afraid of the future, for the future will be in our own hands.
—Thomas E. Dewey
Your SHM board recently spent some time on the most comprehensive strategic planning that we have undertaken. Our last strategic planning meeting was almost three years ago. It is reassuring to review those minutes and see that we have accomplished a number of things that we set out to do. We have:
- Enhanced our chapters by making more resources and staff assistance available to them;
- Expanded our leadership training offerings;
- Established relationships with other organizations, such as the American Hospital Association, the Joint Commission on Accreditation of Healthcare Organizations, the Society of Critical Care Medicine, and many others; and
- Explored a credential for the hospitalist that distinguishes our work from other practitioners.
Planning to Plan
In these exciting times, however, we decided it was important to stop and take stock to either confirm that we are on the right track or adjust our direction. To prepare for the meeting, we hired an outside facilitator. We invited all board members and our staff from Philadelphia. Our staff has grown from several people to more than 20. They are a diverse group with a tremendous amount of talent. Their perspective and input remain crucial to our success.
We included some of our key committee chairs as well. These individuals have regular contact with other agencies, our members, and their employees. We surveyed our membership and hospitalist leaders to determine their perspective on the dilemmas that they face. We interviewed 13 “futurists” to obtain their opinions about key trends that will affect hospitalists, including:
- The current environment for hospitalists;
- The implications of future trends in patient populations;
- The regulatory and political environment;
- The competitive forces; and
- Advancements in science, technology, and pharmaceuticals.
Bang for the Buck
The SHM board, when surveyed, expressed a strong interest in better understanding SHM’s customer groups, what they value, and what we can offer to them. We conduct many activities and support many projects through our staff, our volunteer leadership, and our members. We need to know if we are spending our resources in a way that optimizes our impact on our members and our field. Each participant spent two to three hours reviewing materials in preparation for the meeting.
When we gathered for two days, our facilitator worked us hard. We began by reviewing what we are doing and checking that against the needs and directions identified by our members and others. We then attempted to prioritize new initiatives so that we could focus on “bang for the buck.”
As we continued the process of refining our findings and designing our action plans, a few things become apparent. Among them:
- There is and will continue to be a shortage of qualified hospitalists;
- The demands of an aging population, in conjunction with the expectations of healthcare givers, will be a source of pressure;
- It will take more time to deliver care to our incoming group of patients than it did for their grandparents;
- The technology and options that are available continue to expand, as does the need to stay abreast of ongoing changes; and
- There will be more medical information to absorb and more to communicate and organize.
As this pressure increases, the facilities’ search for solutions to the impact on cost will increase. In addition, the transparency of hospital results, as well as pay for performance, will drive a desire to improve quality results. The process improvement changes that will be needed cannot be accomplished without a committed medical staff. Hospitalists are uniquely positioned to take on this role. Thus, the demands on hospitalists for participation and leadership will increase.
Labor Shortage a Key Issue
It appears from our membership survey that the labor shortage is a key worry. Because we have no control over demand and we expect demand to increase, we will need to be creative about impacting supply. SHM may be able to address this issue. One approach is to increase supply in the following ways:
1. Design programs that attract individuals who want to be hospitalists into the primary residencies for hospitalists: internal medicine, pediatrics, and family medicine.
An example:
- Influencing training programs and educators to develop positive experiences for residents.
2. Create a model that includes nursing and physician assistants, as well as others, who can extend physicians’ capabilities
Another approach is to improve retention, a goal that might be accomplished by:
- Educating hospitals on their roles in creating a good working environment with excellent support systems for their hospitalists;
- Training group leaders to manage their programs for success;
- Creating alternative delivery models that enhance the physician lifestyle and practice experience; and
- Training individuals to matching their career goals with the right program.
Leadership Gap
Our members and their leaders seem to feel adequately prepared for clinical decision-making to deliver high quality care, but they see a gap when it comes to how they are equipped to provide leadership in a number of areas. These areas include transitions and coordination of care, resource utilization, and collaboration with multidisciplinary teams. SHM can respond to this need with training and mentoring. Perhaps we can also influence training programs and their curriculum.
Caring for the Uninsured
As many of you experience, hospitalists are increasingly called on to provide care for those without funds. When caring for the uninsured, physicians experience special challenges that create job dissatisfaction and affect the sustainability of the practice. In many cases, hospitals are willing to pay for this care because they are required by government regulation to provide it. As they see their profit margins erode, however, they are reluctant to compensate this work. It is important for SHM to be positioned to participate in these discussions as the payment and care of the uninsured gets increasing attention. Our public policy committee will continue to try to identify our best opportunities to impact this issue. How their mission will change is unclear, but this issue continues to be identified by our members as an important one.
This article only touches briefly on the many topics that SHM continues to explore as we try to see the future and take it into our hands. TH
Dr. Gorman is the president of SHM.
We need not be afraid of the future, for the future will be in our own hands.
—Thomas E. Dewey
Your SHM board recently spent some time on the most comprehensive strategic planning that we have undertaken. Our last strategic planning meeting was almost three years ago. It is reassuring to review those minutes and see that we have accomplished a number of things that we set out to do. We have:
- Enhanced our chapters by making more resources and staff assistance available to them;
- Expanded our leadership training offerings;
- Established relationships with other organizations, such as the American Hospital Association, the Joint Commission on Accreditation of Healthcare Organizations, the Society of Critical Care Medicine, and many others; and
- Explored a credential for the hospitalist that distinguishes our work from other practitioners.
Planning to Plan
In these exciting times, however, we decided it was important to stop and take stock to either confirm that we are on the right track or adjust our direction. To prepare for the meeting, we hired an outside facilitator. We invited all board members and our staff from Philadelphia. Our staff has grown from several people to more than 20. They are a diverse group with a tremendous amount of talent. Their perspective and input remain crucial to our success.
We included some of our key committee chairs as well. These individuals have regular contact with other agencies, our members, and their employees. We surveyed our membership and hospitalist leaders to determine their perspective on the dilemmas that they face. We interviewed 13 “futurists” to obtain their opinions about key trends that will affect hospitalists, including:
- The current environment for hospitalists;
- The implications of future trends in patient populations;
- The regulatory and political environment;
- The competitive forces; and
- Advancements in science, technology, and pharmaceuticals.
Bang for the Buck
The SHM board, when surveyed, expressed a strong interest in better understanding SHM’s customer groups, what they value, and what we can offer to them. We conduct many activities and support many projects through our staff, our volunteer leadership, and our members. We need to know if we are spending our resources in a way that optimizes our impact on our members and our field. Each participant spent two to three hours reviewing materials in preparation for the meeting.
When we gathered for two days, our facilitator worked us hard. We began by reviewing what we are doing and checking that against the needs and directions identified by our members and others. We then attempted to prioritize new initiatives so that we could focus on “bang for the buck.”
As we continued the process of refining our findings and designing our action plans, a few things become apparent. Among them:
- There is and will continue to be a shortage of qualified hospitalists;
- The demands of an aging population, in conjunction with the expectations of healthcare givers, will be a source of pressure;
- It will take more time to deliver care to our incoming group of patients than it did for their grandparents;
- The technology and options that are available continue to expand, as does the need to stay abreast of ongoing changes; and
- There will be more medical information to absorb and more to communicate and organize.
As this pressure increases, the facilities’ search for solutions to the impact on cost will increase. In addition, the transparency of hospital results, as well as pay for performance, will drive a desire to improve quality results. The process improvement changes that will be needed cannot be accomplished without a committed medical staff. Hospitalists are uniquely positioned to take on this role. Thus, the demands on hospitalists for participation and leadership will increase.
Labor Shortage a Key Issue
It appears from our membership survey that the labor shortage is a key worry. Because we have no control over demand and we expect demand to increase, we will need to be creative about impacting supply. SHM may be able to address this issue. One approach is to increase supply in the following ways:
1. Design programs that attract individuals who want to be hospitalists into the primary residencies for hospitalists: internal medicine, pediatrics, and family medicine.
An example:
- Influencing training programs and educators to develop positive experiences for residents.
2. Create a model that includes nursing and physician assistants, as well as others, who can extend physicians’ capabilities
Another approach is to improve retention, a goal that might be accomplished by:
- Educating hospitals on their roles in creating a good working environment with excellent support systems for their hospitalists;
- Training group leaders to manage their programs for success;
- Creating alternative delivery models that enhance the physician lifestyle and practice experience; and
- Training individuals to matching their career goals with the right program.
Leadership Gap
Our members and their leaders seem to feel adequately prepared for clinical decision-making to deliver high quality care, but they see a gap when it comes to how they are equipped to provide leadership in a number of areas. These areas include transitions and coordination of care, resource utilization, and collaboration with multidisciplinary teams. SHM can respond to this need with training and mentoring. Perhaps we can also influence training programs and their curriculum.
Caring for the Uninsured
As many of you experience, hospitalists are increasingly called on to provide care for those without funds. When caring for the uninsured, physicians experience special challenges that create job dissatisfaction and affect the sustainability of the practice. In many cases, hospitals are willing to pay for this care because they are required by government regulation to provide it. As they see their profit margins erode, however, they are reluctant to compensate this work. It is important for SHM to be positioned to participate in these discussions as the payment and care of the uninsured gets increasing attention. Our public policy committee will continue to try to identify our best opportunities to impact this issue. How their mission will change is unclear, but this issue continues to be identified by our members as an important one.
This article only touches briefly on the many topics that SHM continues to explore as we try to see the future and take it into our hands. TH
Dr. Gorman is the president of SHM.
We need not be afraid of the future, for the future will be in our own hands.
—Thomas E. Dewey
Your SHM board recently spent some time on the most comprehensive strategic planning that we have undertaken. Our last strategic planning meeting was almost three years ago. It is reassuring to review those minutes and see that we have accomplished a number of things that we set out to do. We have:
- Enhanced our chapters by making more resources and staff assistance available to them;
- Expanded our leadership training offerings;
- Established relationships with other organizations, such as the American Hospital Association, the Joint Commission on Accreditation of Healthcare Organizations, the Society of Critical Care Medicine, and many others; and
- Explored a credential for the hospitalist that distinguishes our work from other practitioners.
Planning to Plan
In these exciting times, however, we decided it was important to stop and take stock to either confirm that we are on the right track or adjust our direction. To prepare for the meeting, we hired an outside facilitator. We invited all board members and our staff from Philadelphia. Our staff has grown from several people to more than 20. They are a diverse group with a tremendous amount of talent. Their perspective and input remain crucial to our success.
We included some of our key committee chairs as well. These individuals have regular contact with other agencies, our members, and their employees. We surveyed our membership and hospitalist leaders to determine their perspective on the dilemmas that they face. We interviewed 13 “futurists” to obtain their opinions about key trends that will affect hospitalists, including:
- The current environment for hospitalists;
- The implications of future trends in patient populations;
- The regulatory and political environment;
- The competitive forces; and
- Advancements in science, technology, and pharmaceuticals.
Bang for the Buck
The SHM board, when surveyed, expressed a strong interest in better understanding SHM’s customer groups, what they value, and what we can offer to them. We conduct many activities and support many projects through our staff, our volunteer leadership, and our members. We need to know if we are spending our resources in a way that optimizes our impact on our members and our field. Each participant spent two to three hours reviewing materials in preparation for the meeting.
When we gathered for two days, our facilitator worked us hard. We began by reviewing what we are doing and checking that against the needs and directions identified by our members and others. We then attempted to prioritize new initiatives so that we could focus on “bang for the buck.”
As we continued the process of refining our findings and designing our action plans, a few things become apparent. Among them:
- There is and will continue to be a shortage of qualified hospitalists;
- The demands of an aging population, in conjunction with the expectations of healthcare givers, will be a source of pressure;
- It will take more time to deliver care to our incoming group of patients than it did for their grandparents;
- The technology and options that are available continue to expand, as does the need to stay abreast of ongoing changes; and
- There will be more medical information to absorb and more to communicate and organize.
As this pressure increases, the facilities’ search for solutions to the impact on cost will increase. In addition, the transparency of hospital results, as well as pay for performance, will drive a desire to improve quality results. The process improvement changes that will be needed cannot be accomplished without a committed medical staff. Hospitalists are uniquely positioned to take on this role. Thus, the demands on hospitalists for participation and leadership will increase.
Labor Shortage a Key Issue
It appears from our membership survey that the labor shortage is a key worry. Because we have no control over demand and we expect demand to increase, we will need to be creative about impacting supply. SHM may be able to address this issue. One approach is to increase supply in the following ways:
1. Design programs that attract individuals who want to be hospitalists into the primary residencies for hospitalists: internal medicine, pediatrics, and family medicine.
An example:
- Influencing training programs and educators to develop positive experiences for residents.
2. Create a model that includes nursing and physician assistants, as well as others, who can extend physicians’ capabilities
Another approach is to improve retention, a goal that might be accomplished by:
- Educating hospitals on their roles in creating a good working environment with excellent support systems for their hospitalists;
- Training group leaders to manage their programs for success;
- Creating alternative delivery models that enhance the physician lifestyle and practice experience; and
- Training individuals to matching their career goals with the right program.
Leadership Gap
Our members and their leaders seem to feel adequately prepared for clinical decision-making to deliver high quality care, but they see a gap when it comes to how they are equipped to provide leadership in a number of areas. These areas include transitions and coordination of care, resource utilization, and collaboration with multidisciplinary teams. SHM can respond to this need with training and mentoring. Perhaps we can also influence training programs and their curriculum.
Caring for the Uninsured
As many of you experience, hospitalists are increasingly called on to provide care for those without funds. When caring for the uninsured, physicians experience special challenges that create job dissatisfaction and affect the sustainability of the practice. In many cases, hospitals are willing to pay for this care because they are required by government regulation to provide it. As they see their profit margins erode, however, they are reluctant to compensate this work. It is important for SHM to be positioned to participate in these discussions as the payment and care of the uninsured gets increasing attention. Our public policy committee will continue to try to identify our best opportunities to impact this issue. How their mission will change is unclear, but this issue continues to be identified by our members as an important one.
This article only touches briefly on the many topics that SHM continues to explore as we try to see the future and take it into our hands. TH
Dr. Gorman is the president of SHM.
TH NewsAlerts
Hospitalists Prone to Evidence-Based Treatments
Researchers from Harvard Medical School (Boston) and other institutions surveyed 213 pediatric hospitalists and a random sample of 352 community pediatricians. They found that, overall, the hospitalist group showed greater adherence to evidence-based therapies and tests for common pediatric illnesses in hospitalized patients, and relied less on those therapies and tests of unproven benefits.
Hourly Rounding Pays Off
According to a study by the Studer Group (Gulf Breeze, Fl.) and the Alliance for Health Care Research, having nurses round every hour results in an average 8.9-point increase in patient satisfaction, a 50% decrease in patient falls, a reduction in the use of call lights, and an undocumented improvement in clinical outcomes.
SHM Makes Acute Heart Failure a High Priority

SHM, supported in part by funding from Scios, Inc., will undertake a major outreach campaign on quality improvement related to acute heart failure. These initiatives will focus on the “front end” of the acutely decompensated heart failure patient admission, beginning with early diagnosis and aggressive treatment and intervention including emergency department and observation unit care to optimize outcomes.
“Hospitalists manage a significant number of heart failure patients across the hospital continuum,” says Larry Wellikson, MD, CEO of SHM. “Our goal is to improve heart failure care by disseminating the necessary tools and knowledge to hospitalists.”
Google as Diagnostic Tool
The popular Web site Google (Mountain View, Calif.) can help physicians with diagnoses, according to researchers from Princess Alexandria Hospital in Brisbane, Australia. The team “googled” symptoms of 26 mystery cases, and a Web search resulted in a correct diagnosis for 15 of them. The researchers call Google a useful aid for physicians.
SHM Participates in IHI Campaign
When the Institute for Healthcare Improvement (IHI) introduced its “5 Million Lives” campaign recently, SHM was one of the few organizations asked to speak about their part in the campaign.
“We are ready … and could not be more enthusiastic about participating in this landmark campaign,” said Russell Holman, M.D., SHM’s president-elect.
A Winning Team Reaps Rewards
Caritas Good Samaritan Medical Center in Brockton, Mass., and hospital medicine provider Cogent Healthcare (Irvine, Calif.) collaborated to achieve quality of care goals that earned the facility pay-for-performance bonuses from major commercial payers. Cogent used best practices that also helped reduce length of stay and unnecessary re-admissions, and improve patient and physician satisfaction.
A Prevalence of Persistent Pain
The “Health United States 2006” report issued by the National Center for Health Statistics (Hyattsville, Md.) finds a prevalence of pain in the U.S. One in four adults reported a daylong bout of pain in the last month, and one in 10 say they’ve suffered pain for at least a year.

Palliative Medicine Now Official Subspecialty
The American Board of Medical Specialties (ABMS) will establish a subspecialty certificate in Hospice and Palliative Medicine. “[This certification] affirms the concept that specialized knowledge and skills must be learned to care for the increasingly complex-care needs of the dying and their families,” says David Weissman, MD, FACP, editor-in-chief of the Journal of Palliative Medicine.
Busy Shifts Put Elderly Admissions at Risk
Older patients admitted during busy hospital shifts may have a greater mortality rate, according to a study by the University of California San Francisco’s Moffitt-Long Hospital. The retrospective cohort analysis included 5,742 adults admitted to the general medicine service and intensive care unit without cardiovascular, neurologic, or cancer- related primary diagnoses. TH
Hospitalists Prone to Evidence-Based Treatments
Researchers from Harvard Medical School (Boston) and other institutions surveyed 213 pediatric hospitalists and a random sample of 352 community pediatricians. They found that, overall, the hospitalist group showed greater adherence to evidence-based therapies and tests for common pediatric illnesses in hospitalized patients, and relied less on those therapies and tests of unproven benefits.
Hourly Rounding Pays Off
According to a study by the Studer Group (Gulf Breeze, Fl.) and the Alliance for Health Care Research, having nurses round every hour results in an average 8.9-point increase in patient satisfaction, a 50% decrease in patient falls, a reduction in the use of call lights, and an undocumented improvement in clinical outcomes.
SHM Makes Acute Heart Failure a High Priority
SHM, supported in part by funding from Scios, Inc., will undertake a major outreach campaign on quality improvement related to acute heart failure. These initiatives will focus on the “front end” of the acutely decompensated heart failure patient admission, beginning with early diagnosis and aggressive treatment and intervention including emergency department and observation unit care to optimize outcomes.
“Hospitalists manage a significant number of heart failure patients across the hospital continuum,” says Larry Wellikson, MD, CEO of SHM. “Our goal is to improve heart failure care by disseminating the necessary tools and knowledge to hospitalists.”
Google as Diagnostic Tool
The popular Web site Google (Mountain View, Calif.) can help physicians with diagnoses, according to researchers from Princess Alexandria Hospital in Brisbane, Australia. The team “googled” symptoms of 26 mystery cases, and a Web search resulted in a correct diagnosis for 15 of them. The researchers call Google a useful aid for physicians.
SHM Participates in IHI Campaign
When the Institute for Healthcare Improvement (IHI) introduced its “5 Million Lives” campaign recently, SHM was one of the few organizations asked to speak about their part in the campaign.
“We are ready … and could not be more enthusiastic about participating in this landmark campaign,” said Russell Holman, M.D., SHM’s president-elect.
A Winning Team Reaps Rewards
Caritas Good Samaritan Medical Center in Brockton, Mass., and hospital medicine provider Cogent Healthcare (Irvine, Calif.) collaborated to achieve quality of care goals that earned the facility pay-for-performance bonuses from major commercial payers. Cogent used best practices that also helped reduce length of stay and unnecessary re-admissions, and improve patient and physician satisfaction.
A Prevalence of Persistent Pain
The “Health United States 2006” report issued by the National Center for Health Statistics (Hyattsville, Md.) finds a prevalence of pain in the U.S. One in four adults reported a daylong bout of pain in the last month, and one in 10 say they’ve suffered pain for at least a year.
Palliative Medicine Now Official Subspecialty
The American Board of Medical Specialties (ABMS) will establish a subspecialty certificate in Hospice and Palliative Medicine. “[This certification] affirms the concept that specialized knowledge and skills must be learned to care for the increasingly complex-care needs of the dying and their families,” says David Weissman, MD, FACP, editor-in-chief of the Journal of Palliative Medicine.
Busy Shifts Put Elderly Admissions at Risk
Older patients admitted during busy hospital shifts may have a greater mortality rate, according to a study by the University of California San Francisco’s Moffitt-Long Hospital. The retrospective cohort analysis included 5,742 adults admitted to the general medicine service and intensive care unit without cardiovascular, neurologic, or cancer- related primary diagnoses. TH
Hospitalists Prone to Evidence-Based Treatments
Researchers from Harvard Medical School (Boston) and other institutions surveyed 213 pediatric hospitalists and a random sample of 352 community pediatricians. They found that, overall, the hospitalist group showed greater adherence to evidence-based therapies and tests for common pediatric illnesses in hospitalized patients, and relied less on those therapies and tests of unproven benefits.
Hourly Rounding Pays Off
According to a study by the Studer Group (Gulf Breeze, Fl.) and the Alliance for Health Care Research, having nurses round every hour results in an average 8.9-point increase in patient satisfaction, a 50% decrease in patient falls, a reduction in the use of call lights, and an undocumented improvement in clinical outcomes.
SHM Makes Acute Heart Failure a High Priority
SHM, supported in part by funding from Scios, Inc., will undertake a major outreach campaign on quality improvement related to acute heart failure. These initiatives will focus on the “front end” of the acutely decompensated heart failure patient admission, beginning with early diagnosis and aggressive treatment and intervention including emergency department and observation unit care to optimize outcomes.
“Hospitalists manage a significant number of heart failure patients across the hospital continuum,” says Larry Wellikson, MD, CEO of SHM. “Our goal is to improve heart failure care by disseminating the necessary tools and knowledge to hospitalists.”
Google as Diagnostic Tool
The popular Web site Google (Mountain View, Calif.) can help physicians with diagnoses, according to researchers from Princess Alexandria Hospital in Brisbane, Australia. The team “googled” symptoms of 26 mystery cases, and a Web search resulted in a correct diagnosis for 15 of them. The researchers call Google a useful aid for physicians.
SHM Participates in IHI Campaign
When the Institute for Healthcare Improvement (IHI) introduced its “5 Million Lives” campaign recently, SHM was one of the few organizations asked to speak about their part in the campaign.
“We are ready … and could not be more enthusiastic about participating in this landmark campaign,” said Russell Holman, M.D., SHM’s president-elect.
A Winning Team Reaps Rewards
Caritas Good Samaritan Medical Center in Brockton, Mass., and hospital medicine provider Cogent Healthcare (Irvine, Calif.) collaborated to achieve quality of care goals that earned the facility pay-for-performance bonuses from major commercial payers. Cogent used best practices that also helped reduce length of stay and unnecessary re-admissions, and improve patient and physician satisfaction.
A Prevalence of Persistent Pain
The “Health United States 2006” report issued by the National Center for Health Statistics (Hyattsville, Md.) finds a prevalence of pain in the U.S. One in four adults reported a daylong bout of pain in the last month, and one in 10 say they’ve suffered pain for at least a year.
Palliative Medicine Now Official Subspecialty
The American Board of Medical Specialties (ABMS) will establish a subspecialty certificate in Hospice and Palliative Medicine. “[This certification] affirms the concept that specialized knowledge and skills must be learned to care for the increasingly complex-care needs of the dying and their families,” says David Weissman, MD, FACP, editor-in-chief of the Journal of Palliative Medicine.
Busy Shifts Put Elderly Admissions at Risk
Older patients admitted during busy hospital shifts may have a greater mortality rate, according to a study by the University of California San Francisco’s Moffitt-Long Hospital. The retrospective cohort analysis included 5,742 adults admitted to the general medicine service and intensive care unit without cardiovascular, neurologic, or cancer- related primary diagnoses. TH
Proceedings of the Heart-Brain Summit
Supplement Editor:
Marc S. Penn, MD, PhD
Contents
Introduction
Heart-brain medicine: Where we go from here and why
Marc S. Penn, MD, PhD, Cleveland Clinic, Cleveland, Ohio, and Earl E. Bakken, DSc (hon), Medtronic, Inc., Minneapolis, Minnesota, and North Hawaii Community Hospital, Kamuela, Hawaii
Opening remarks
The dream behind the summit
Earl E. Bakken, DSc (hon), Medtronic, Inc., Minneapolis, Minnesota, and North Hawaii Community Hospital, Kamuela, Hawaii
Keynote address
'Voodoo' death revisited: The modern lessons of neurocardiology
Martin A. Samuels, MD, DSc (hon), Brigham and Women's Hospital, Boston, Massachusetts
The broken heart syndrome
Ilan S. Wittstein, MD, Johns Hopkins University School of Medicine, Baltimore, Maryland
Brain imaging in cardiovascular disease: State of the art
Michael Phillips, MD, Cleveland Clinic, Cleveland, Ohio
Cortical control of the heart
Stephen Oppenheimer, MD, PhD, Sentient Medical Systems, Cockeysville, Maryland
Neurological mechanisms of chest pain and cardiac disease
Robert D. Foreman, PhD, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma
Hypertension in sleep apnea: The role of the sympathetic pathway
Diana L. Kunze, PhD; David Kline, PhD; and Angelina Ramirez-Navarro, PhD, MetroHealth Medical Center and Case Western Reserve University, Cleveland, Ohio
Inflammation: Implications for understanding the heart-brain connection
Mehdi H. Shishehbor, DO; Carlos Alves, MD; and Vivek Rajagopal, MD, Cleveland Clinic, Cleveland, Ohio
The anti-ischemic effects of electrical neurostimulation in the heart
Jessica de Vries, MD, University of Groningen, The Netherlands; Robert D. Foreman, PhD, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma; and Mike J.L. DeJongste, MD, PhD, University of Groningen, The Netherlands
The little brain on the heart
J. Andrew Armour, MD, PhD, Hôpital du Sacré-Coeur and Université de Montréal, Montréal, Québec, Canada
Open heart surgery and cognitive decline
Mark F. Newman, MD, Duke University Medical Center, Durham, North Carolina
The heart and the brain within the broader context of wellness
Michael O’Donnell, PhD, MBA, MPH, Cleveland Clinic, Cleveland, Ohio
The heart-brain interaction during emotionally provoked myocardial ischemia: Implications of cortical hyperactivation in CAD and gender interactions
Robert Soufer, MD, Yale University, New Haven, Connecticut, and Matthew M. Burg, PhD, Yale University, New Haven, Connecticut, and Columbia University, New York, New York
Depression and heart disease
François Lespérance, MD, Montréal Heart Institute, and Nancy Frasure-Smith, PhD, McGill University and Montréal Heart Institute, Montréal, Québec, Canada
Sick at heart: The pathophysiology of negative emotions
Laura D. Kubzansky, PhD, MPH, Harvard School of Public Health, Boston, Massachusetts
Role of the brain in ventricular fibrillation and hypertension: From animal models to early human studies
James E. Skinner, PhD, Vicor Technologies, Inc., Boca Raton, Florida
New paradigms in heart-brain medicine: Nonlinear physiology, state-dependent proteomics
James E. Skinner, PhD, Vicor Technologies, Inc., Boca Raton, Florida
Subarachnoid hemorrhage: A model for heart-brain interactions
J. Javier Provencio, MD, Cleveland Clinic, Cleveland, Ohio
Cardiac denervation in patients with Parkinson disease
David S. Goldstein, MD, PhD, National Institutes of Health, Bethesda, Maryland
Aging and the brain renin-angiotensin system: Insights from studies in transgenic rats
Debra I. Diz, PhD; Sherry O. Kasper, PhD; Atsushi Sakima, MD; and Carlos M. Ferrario, MD, Wake Forest University School of Medicine, Winston-Salem, North Carolina
Contextual cardiology: What modern medicine can learn from ancient Hawaiian wisdom
Paul Pearsall, PhD, University of Hawaii at Manoa and Hawaii State Consortium for Integrative Medicine, Honolulu, Hawaii
Cardiocerebral resuscitation: The optimal approach to cardiac arrest
Gordon A. Ewy, MD, University of Arizona College of Medicine, Tucson, Arizona
Heart transplantation: A magnified model of heart-brain interactions
Mohamad H. Yamani, MD, and Randall C. Starling, MD, MPH, Cleveland Clinic, Cleveland, Ohio
Patent foramen ovale and migraine
Gian Paolo Anzola, MD, S. Orsola Hospital FBF, Brescia, Italy
Patent foramen ovale and stroke: To close or not to close?
Anthony J. Furlan, MD, Cleveland Clinic, Cleveland, Ohio
Sudden unexplained death in epilepsy: The role of the heart
Stephan U. Schuele, MD, Cleveland Clinic, Cleveland, Ohio, and Northwestern University, Chicago, Illinois; Peter Widdess-Walsh, MD, Adriana Bermeo, MD, and Hans O. Lüders, MD, PhD, Cleveland Clinic, Cleveland, Ohio
Hydrocephalus and the heart: Interactions of the first and third circulations
Mark Luciano, MD, PhD, and Stephen Dombrowski, PhD, Cleveland Clinic, Cleveland, Ohio
Cognitive impairment in chronic heart failure
Cathy A. Sila, MD, Cleveland Clinic, Cleveland, Ohio
Cardiac events and brain injury: Ethical implications
Paul J. Ford, PhD, Cleveland Clinic, Cleveland, Ohio
Supplement Editor:
Marc S. Penn, MD, PhD
Contents
Introduction
Heart-brain medicine: Where we go from here and why
Marc S. Penn, MD, PhD, Cleveland Clinic, Cleveland, Ohio, and Earl E. Bakken, DSc (hon), Medtronic, Inc., Minneapolis, Minnesota, and North Hawaii Community Hospital, Kamuela, Hawaii
Opening remarks
The dream behind the summit
Earl E. Bakken, DSc (hon), Medtronic, Inc., Minneapolis, Minnesota, and North Hawaii Community Hospital, Kamuela, Hawaii
Keynote address
'Voodoo' death revisited: The modern lessons of neurocardiology
Martin A. Samuels, MD, DSc (hon), Brigham and Women's Hospital, Boston, Massachusetts
The broken heart syndrome
Ilan S. Wittstein, MD, Johns Hopkins University School of Medicine, Baltimore, Maryland
Brain imaging in cardiovascular disease: State of the art
Michael Phillips, MD, Cleveland Clinic, Cleveland, Ohio
Cortical control of the heart
Stephen Oppenheimer, MD, PhD, Sentient Medical Systems, Cockeysville, Maryland
Neurological mechanisms of chest pain and cardiac disease
Robert D. Foreman, PhD, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma
Hypertension in sleep apnea: The role of the sympathetic pathway
Diana L. Kunze, PhD; David Kline, PhD; and Angelina Ramirez-Navarro, PhD, MetroHealth Medical Center and Case Western Reserve University, Cleveland, Ohio
Inflammation: Implications for understanding the heart-brain connection
Mehdi H. Shishehbor, DO; Carlos Alves, MD; and Vivek Rajagopal, MD, Cleveland Clinic, Cleveland, Ohio
The anti-ischemic effects of electrical neurostimulation in the heart
Jessica de Vries, MD, University of Groningen, The Netherlands; Robert D. Foreman, PhD, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma; and Mike J.L. DeJongste, MD, PhD, University of Groningen, The Netherlands
The little brain on the heart
J. Andrew Armour, MD, PhD, Hôpital du Sacré-Coeur and Université de Montréal, Montréal, Québec, Canada
Open heart surgery and cognitive decline
Mark F. Newman, MD, Duke University Medical Center, Durham, North Carolina
The heart and the brain within the broader context of wellness
Michael O’Donnell, PhD, MBA, MPH, Cleveland Clinic, Cleveland, Ohio
The heart-brain interaction during emotionally provoked myocardial ischemia: Implications of cortical hyperactivation in CAD and gender interactions
Robert Soufer, MD, Yale University, New Haven, Connecticut, and Matthew M. Burg, PhD, Yale University, New Haven, Connecticut, and Columbia University, New York, New York
Depression and heart disease
François Lespérance, MD, Montréal Heart Institute, and Nancy Frasure-Smith, PhD, McGill University and Montréal Heart Institute, Montréal, Québec, Canada
Sick at heart: The pathophysiology of negative emotions
Laura D. Kubzansky, PhD, MPH, Harvard School of Public Health, Boston, Massachusetts
Role of the brain in ventricular fibrillation and hypertension: From animal models to early human studies
James E. Skinner, PhD, Vicor Technologies, Inc., Boca Raton, Florida
New paradigms in heart-brain medicine: Nonlinear physiology, state-dependent proteomics
James E. Skinner, PhD, Vicor Technologies, Inc., Boca Raton, Florida
Subarachnoid hemorrhage: A model for heart-brain interactions
J. Javier Provencio, MD, Cleveland Clinic, Cleveland, Ohio
Cardiac denervation in patients with Parkinson disease
David S. Goldstein, MD, PhD, National Institutes of Health, Bethesda, Maryland
Aging and the brain renin-angiotensin system: Insights from studies in transgenic rats
Debra I. Diz, PhD; Sherry O. Kasper, PhD; Atsushi Sakima, MD; and Carlos M. Ferrario, MD, Wake Forest University School of Medicine, Winston-Salem, North Carolina
Contextual cardiology: What modern medicine can learn from ancient Hawaiian wisdom
Paul Pearsall, PhD, University of Hawaii at Manoa and Hawaii State Consortium for Integrative Medicine, Honolulu, Hawaii
Cardiocerebral resuscitation: The optimal approach to cardiac arrest
Gordon A. Ewy, MD, University of Arizona College of Medicine, Tucson, Arizona
Heart transplantation: A magnified model of heart-brain interactions
Mohamad H. Yamani, MD, and Randall C. Starling, MD, MPH, Cleveland Clinic, Cleveland, Ohio
Patent foramen ovale and migraine
Gian Paolo Anzola, MD, S. Orsola Hospital FBF, Brescia, Italy
Patent foramen ovale and stroke: To close or not to close?
Anthony J. Furlan, MD, Cleveland Clinic, Cleveland, Ohio
Sudden unexplained death in epilepsy: The role of the heart
Stephan U. Schuele, MD, Cleveland Clinic, Cleveland, Ohio, and Northwestern University, Chicago, Illinois; Peter Widdess-Walsh, MD, Adriana Bermeo, MD, and Hans O. Lüders, MD, PhD, Cleveland Clinic, Cleveland, Ohio
Hydrocephalus and the heart: Interactions of the first and third circulations
Mark Luciano, MD, PhD, and Stephen Dombrowski, PhD, Cleveland Clinic, Cleveland, Ohio
Cognitive impairment in chronic heart failure
Cathy A. Sila, MD, Cleveland Clinic, Cleveland, Ohio
Cardiac events and brain injury: Ethical implications
Paul J. Ford, PhD, Cleveland Clinic, Cleveland, Ohio
Supplement Editor:
Marc S. Penn, MD, PhD
Contents
Introduction
Heart-brain medicine: Where we go from here and why
Marc S. Penn, MD, PhD, Cleveland Clinic, Cleveland, Ohio, and Earl E. Bakken, DSc (hon), Medtronic, Inc., Minneapolis, Minnesota, and North Hawaii Community Hospital, Kamuela, Hawaii
Opening remarks
The dream behind the summit
Earl E. Bakken, DSc (hon), Medtronic, Inc., Minneapolis, Minnesota, and North Hawaii Community Hospital, Kamuela, Hawaii
Keynote address
'Voodoo' death revisited: The modern lessons of neurocardiology
Martin A. Samuels, MD, DSc (hon), Brigham and Women's Hospital, Boston, Massachusetts
The broken heart syndrome
Ilan S. Wittstein, MD, Johns Hopkins University School of Medicine, Baltimore, Maryland
Brain imaging in cardiovascular disease: State of the art
Michael Phillips, MD, Cleveland Clinic, Cleveland, Ohio
Cortical control of the heart
Stephen Oppenheimer, MD, PhD, Sentient Medical Systems, Cockeysville, Maryland
Neurological mechanisms of chest pain and cardiac disease
Robert D. Foreman, PhD, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma
Hypertension in sleep apnea: The role of the sympathetic pathway
Diana L. Kunze, PhD; David Kline, PhD; and Angelina Ramirez-Navarro, PhD, MetroHealth Medical Center and Case Western Reserve University, Cleveland, Ohio
Inflammation: Implications for understanding the heart-brain connection
Mehdi H. Shishehbor, DO; Carlos Alves, MD; and Vivek Rajagopal, MD, Cleveland Clinic, Cleveland, Ohio
The anti-ischemic effects of electrical neurostimulation in the heart
Jessica de Vries, MD, University of Groningen, The Netherlands; Robert D. Foreman, PhD, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma; and Mike J.L. DeJongste, MD, PhD, University of Groningen, The Netherlands
The little brain on the heart
J. Andrew Armour, MD, PhD, Hôpital du Sacré-Coeur and Université de Montréal, Montréal, Québec, Canada
Open heart surgery and cognitive decline
Mark F. Newman, MD, Duke University Medical Center, Durham, North Carolina
The heart and the brain within the broader context of wellness
Michael O’Donnell, PhD, MBA, MPH, Cleveland Clinic, Cleveland, Ohio
The heart-brain interaction during emotionally provoked myocardial ischemia: Implications of cortical hyperactivation in CAD and gender interactions
Robert Soufer, MD, Yale University, New Haven, Connecticut, and Matthew M. Burg, PhD, Yale University, New Haven, Connecticut, and Columbia University, New York, New York
Depression and heart disease
François Lespérance, MD, Montréal Heart Institute, and Nancy Frasure-Smith, PhD, McGill University and Montréal Heart Institute, Montréal, Québec, Canada
Sick at heart: The pathophysiology of negative emotions
Laura D. Kubzansky, PhD, MPH, Harvard School of Public Health, Boston, Massachusetts
Role of the brain in ventricular fibrillation and hypertension: From animal models to early human studies
James E. Skinner, PhD, Vicor Technologies, Inc., Boca Raton, Florida
New paradigms in heart-brain medicine: Nonlinear physiology, state-dependent proteomics
James E. Skinner, PhD, Vicor Technologies, Inc., Boca Raton, Florida
Subarachnoid hemorrhage: A model for heart-brain interactions
J. Javier Provencio, MD, Cleveland Clinic, Cleveland, Ohio
Cardiac denervation in patients with Parkinson disease
David S. Goldstein, MD, PhD, National Institutes of Health, Bethesda, Maryland
Aging and the brain renin-angiotensin system: Insights from studies in transgenic rats
Debra I. Diz, PhD; Sherry O. Kasper, PhD; Atsushi Sakima, MD; and Carlos M. Ferrario, MD, Wake Forest University School of Medicine, Winston-Salem, North Carolina
Contextual cardiology: What modern medicine can learn from ancient Hawaiian wisdom
Paul Pearsall, PhD, University of Hawaii at Manoa and Hawaii State Consortium for Integrative Medicine, Honolulu, Hawaii
Cardiocerebral resuscitation: The optimal approach to cardiac arrest
Gordon A. Ewy, MD, University of Arizona College of Medicine, Tucson, Arizona
Heart transplantation: A magnified model of heart-brain interactions
Mohamad H. Yamani, MD, and Randall C. Starling, MD, MPH, Cleveland Clinic, Cleveland, Ohio
Patent foramen ovale and migraine
Gian Paolo Anzola, MD, S. Orsola Hospital FBF, Brescia, Italy
Patent foramen ovale and stroke: To close or not to close?
Anthony J. Furlan, MD, Cleveland Clinic, Cleveland, Ohio
Sudden unexplained death in epilepsy: The role of the heart
Stephan U. Schuele, MD, Cleveland Clinic, Cleveland, Ohio, and Northwestern University, Chicago, Illinois; Peter Widdess-Walsh, MD, Adriana Bermeo, MD, and Hans O. Lüders, MD, PhD, Cleveland Clinic, Cleveland, Ohio
Hydrocephalus and the heart: Interactions of the first and third circulations
Mark Luciano, MD, PhD, and Stephen Dombrowski, PhD, Cleveland Clinic, Cleveland, Ohio
Cognitive impairment in chronic heart failure
Cathy A. Sila, MD, Cleveland Clinic, Cleveland, Ohio
Cardiac events and brain injury: Ethical implications
Paul J. Ford, PhD, Cleveland Clinic, Cleveland, Ohio
The dream behind the summit
Pediatric Hospitalist Comanagement
As the field of pediatric hospital medicine has emerged, so too has evidence that hospitalist management of pediatric medical patients in the tertiary‐care setting is associated with decreased length of stay (LOS).13 The American Academy of Pediatrics Committee on Hospital Care has recommended hospitalist consultation for pediatric surgical patients being managed by adult surgeons.4 In one survey of pediatric hospitalists, 66% of community hospitalists and 47% of academic hospitalists reported comanaging surgical patients.5 However, little work has been published on the effect of hospitalist comanagement of pediatric surgical patients.
Since June 2000 patients undergoing spinal fusion surgery at the Children's Hospital in Denver, Colorado have been screened by a spine nurse for medical complexity. Medically complex patients undergoing preoperative multispecialty evaluation and their perioperative care are coordinated by the spine nurse.6 Introduction of a general pediatric hospitalist to aid with pre‐ and perioperative management of the most complicated patients in December 2004 provided us with an opportunity to study hospitalist comanagement of medically complex pediatric patients undergoing spine fusion surgery.
Our objectives were (1) to describe comanagement activities and (2) to determine the association of hospitalist comanagement on LOS following spinal fusion surgery. We hypothesized that by addressing a variety of pre‐ and perioperative medical issues, hospitalist comanagement would be associated with a decreased LOS for medically complex pediatric patients undergoing spinal fusion surgery.
METHODS
Design and Population
A retrospective analysis of the orthopedic surgeons' log at the Children's Hospital in Denver, Colorado, a tertiary‐care academic pediatric hospital serving the Rocky Mountain region, was performed. Patients included were those underwent their first episode of spinal fusion surgery between July 1, 2000, and October 1, 2005 (n = 759); exclusion criteria included diagnoses of spondylolisthesis or spondylolysis. The study was approved by the Colorado Multiple Institutional Review Board and exempted from ongoing review, and informed consent was not required.
Intervention: Pre‐ and Perioperative High‐Risk Pathway
Since June 2000 medically complex patients undergoing spinal fusion surgery at the Children's Hospital in Denver, Colorado have been referred by either the orthopedic surgeon or the rehabilitation physician to the spine surgery nurse. This nurse, an RN, BSN with more than a decade of experience with spinal fusion patients, then coordinates preoperative multispecialty evaluation (Fig. 1, column 2). Patients are seen by a pulmonologist pre‐operatively, and undergo pulmonary function tests, chest radiograph, venous blood gas, and, at times, a polysomnogram and electrocardiography. A cardiology consult is obtained for patients with muscle disease. Gastroenterology and neurology may be consulted if there are significant feeding and/or neurological issues that the primary care physician needs assistance addressing preoperatively. Shortly before the scheduled surgery, the patient is evaluated at a discharge planning meeting by a nutritionist, respiratory therapist, physical therapist, social worker (at times), and the spinal surgery nurse for discharge equipment planning. Immediately before surgery, in addition to teaching, surgical consent and a surgical history and physical are obtained, as well as laboratory studies that include a complete blood cell count, type, and cross, coagulation studies, and spine radiographs.5 Medically complex patients are managed in the intensive care unit for at least 24 hours after surgery. In addition, standardized order sets developed in 2001 and edited in July 2005 are used to streamline management of the intensive care unit and the orthopedic ward.

Since December 2004, a hospitalist has aided pre‐ and perioperative evaluation and management (Fig. 1, column 3). The patients seen and comanaged by the hospitalist have been those who have significant medical issues in addition to neuromuscular disease, including multiple medications, seizure disorders, nutritional concerns, and/or significant social concerns. Whereas patients with a multitude of different diagnoses were referred to the spinal surgery nurse for a variety of reasons, patients comanaged by hospitalists were generally children with multiple medical conditions who had neuromuscular scoliosis.
Data Sources
The primary data source used was the surgeons' log. The surgeons' log is a record of patients undergoing spinal fusion surgery maintained concurrently by 2 individuals (the spine surgery nurse and her assistant). From January 2000 on, patient data were manually input into an Excel spreadsheet regularly and were cross‐referenced weekly with the surgery schedule. Data entered include: patient name, medical record number, date of surgery, date of discharge (from hospital admission information), underlying diagnosis, type of procedure, primary surgeon (from operative and/or discharge summaries), and LOS (calculated from dates of discharge and surgery). If either underlying diagnosis or type of procedure needed clarification, the spine surgery nurse discussed it with the primary surgeon. We verified the completeness of the surgeons' log for first spinal fusion surgeries by cross‐referencing with billing records; of 572 surgeries performed by 5 surgeons, 571 were recorded (99.8%) in the surgeons' log.
To perform the descriptive analysis of hospitalist activities, the first author (T.S.) performed a retrospective review of the charts of patients she had seen in her role as hospitalist from December 1, 2004, to October 1, 2005. Prepared in advance was a checklist of pre‐ and perioperative activities, modeled on prior work reporting clinical activities.7 Activities either mentioned in the daily progress note or ordered were recorded as completed and entered into an Excel spreadsheet.
Data Collection
The outcome measure was LOS, log‐transformed for analyses. Covariates included were: patient age, underlying diagnosis, procedure type, and surgeon. Underlying diagnoses were subdivided on the basis of the manually input Excel spreadsheet entries into 5 categories: idiopathic, congenital, neuromuscular, osteogenic, and other. The major diagnoses in the idiopathic category were infantile, juvenile, and adolescent idiopathic scoliosis; in the congenital category were congenital scoliosis, congenital kyphoscoliosis; in the neuromuscular category were cerebral palsy, Duchenne's muscular dystrophy, spina bifida, brain injury, spinal cord injury, and chromosomal anomalies; and in the osteogenic category were Scheuermann's kyphosis, trauma, tumor, kyphoscoliosis, and bone disease. Procedures were subdivided according to the manually input Excel spreadsheet entries into 3 categories: posterior only, anterior/ posterior, and anterior spinal fusion only.
After our initial analysis demonstrated a decline in LOS after December 2004 in both idiopathic and neuromuscular patients, we asked the orthopedic surgeons and spine surgery nurse to determine cointerventions that may have occurred around December 2004. We attempted to contact each surgeon who performed surgery during the study period and asked, What changes did you make on or around November 2004 in your management of spinal fusion patients? We received e‐mail and verbal responses from the spine surgery nurse and from 6 surgeons who had performed 646 of the procedures (78%) over the study period.
Increased use of intrathecal morphine was raised as a possible confounding cointervention. To characterize use of intrathecal morphine, we reviewed the charts of all the patients categorized as idiopathic or neuromuscular patients who underwent surgery after December 2004 and a random sample of 20% of these patients who underwent surgery before December 2004.
Analyses
All quantitative analyses (ie, those of the surgeons' log) were performed in a blinded manner, whereas the chart review was not blinded. Univariate analyses of hospitalist activities and univariate and bivariate analyses of the surgeons' log were performed using SAS 9.1. Mean LOS after log back‐transformation along with 95% confidence interval is reported. The chi square test of equality of variance was used to analyze whether the variances differed.
The multifaceted approach to the care of spinal fusion patients is a tiered approach, with 3 major patient groups (Fig. 1): (1) patients with scoliosis, generally idiopathic, and no or minimal medical conditions, who receive care by the usual pathway and do not receive care by the high‐risk pathway or do not have a hospitalist; (2) patients with scoliosis with any underlying diagnosis and some medical conditions, who receive care by high‐risk pathway; and (3) patients with scoliosis, usually neuromuscular scoliosis, and multiple medical conditions, who receive care by the high‐risk pathway and have hospitalist comanagement. Because of selection bias in the receipt of hospitalist comanagement (ie, the most complicated patients), we cannot reasonably compare hospitalist patients to nonhospitalist patients after December 2004. Instead, we compared all neuromuscular patients before and after hospitalist comanagement with a control group of idiopathic patients.
Initial examination of mean monthly LOS from June 2000 to October 2005 (Fig. 2) suggested a possible decline in both mean LOS and variability in LOS after December 2004, when hospitalist comanagement was initiated. To determine the trend in LOS over time before and after December 2004, we performed a mixed‐effects piecewise Poisson regression, adjusting for patient covariates (patient age, underlying diagnosis, procedure type, and intrathecal morphine [for idiopathic and neuromuscular patients]) and clustering by surgeon (as a random effect). We used the model to estimate 2 slopes to represent the linear trend before and after December 2004 (when hospitalist comanagement started). After regression modeling generated beta coefficients for each covariate, the average covariates were entered into the model to generate an average adjusted LOS as shown in Figure 3.
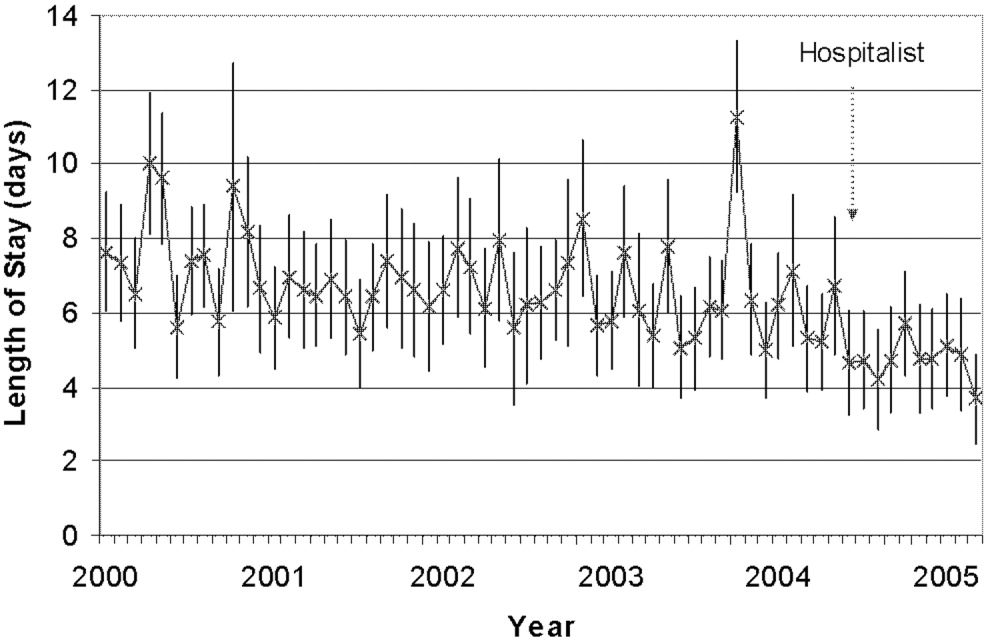
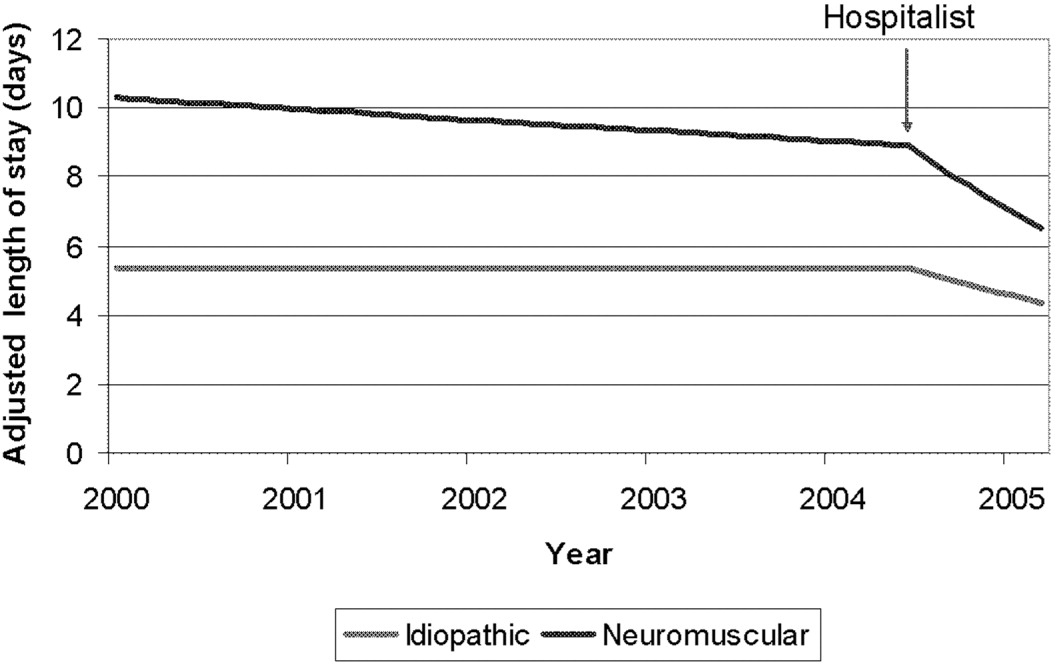
RESULTS
A total of 759 patients underwent initial spinal fusion surgery between July 1, 2000, and October 1, 2005644 before and 115 after December 2004, when hospitalist involvement started. After December 2004, 12% (14 of 115) of all spinal fusion surgery patients were comanaged by a hospitalist. Most comanaged patients (14 of 15, 93%) had neuromuscular scoliosis, and comanaged patients represented 37% (13 of 35) of all neuromuscular patients (Table 1). Over the course of the study, the number of more invasive and complicated anterior/posterior spinal fusion surgeries declined, whereas the number of posterior spinal fusion surgeries increased significantly because of the introduction of new technology (data not shown).
| LOS Days (95% CI) | ||||
|---|---|---|---|---|
| All Surgeries | Preintervention (July 2000December 2004) | Postintervention (December 2004September 2005) | Hospitalist Comanaged (December 2004September 2005) | |
| ||||
| Number of surgeries | 759 | 644 | 115 | 14* |
| Age (years), mean (SD) | 13.6 (3.4) | 13.7 (3.4) | 13.1 (3.4) | 12.6 (4.0) |
| Diagnosis | ||||
| Idiopathic | 328 (43%) | 277 (43%) | 51 (44%) | 1 (7%) |
| Neuromuscular | 247 (32%) | 212 (33%) | 35 (30%) | 13 (93%) |
| Congenital | 66 (9%) | 55 (8%) | 11 (10%) | |
| Osteogenic | 96 (13%) | 81 (13%) | 15 (13%) | |
| Other | 22 (3%) | 19 (3%) | 3 (3%) | |
| Procedure | ||||
| Posterior | 470 (62%) | 365 (57%) | 105 (91%) | 13 (93%) |
| Ant/post | 227 (30%) | 217 (34%) | 10 (8%) | 1 (7%) |
| Anterior | 62 (8%) | 62 (9%) | ||
| Intrathecal morphine use | ||||
| Idiopathic | 30/50 (60%) | 45/51 (88%) | 0 (0%) | |
| Neuromuscular | 10/42 (24%) | 21/35 (62%) | 5/13 (38%) | |
The 15 patients seen by the hospitalist received a total of 60 visits by the hospitalist. The hospitalist saw 9 patients preoperatively. Of the 15 patients comanaged in the hospital, 5 (33%) were seen once, 8 (53%) were seen between 2 and 5 times, and 2 (14%) were seen more than 10 times. Patients were seen both in the ICU and on the surgical ward. Among the patients seen preoperatively, the hospitalist recommended nutritional interventions for 5 patients (33%), bowel regimens for 4 patients (27%), and preoperative hospitalization for 1 patient for 5 days to optimize nutritional intake, address reflux, and modify bowel regimen, as well as facilitate multispecialty evaluation. Postoperative involvement generally addressed a variety of issues, but 20% of patients had no changes in their management (Table 2).
| Hospitalist Activity | Number of Patients (%) (n = 15) |
|---|---|
| |
| Care coordination | |
| Updated family | 11 (73%) |
| Coordinated discharge | 8 (53%) |
| Updated PCP | 7 (47%) |
| Transfer facilitated | 4 (27%) |
| Consulted pulmonary | 3 (20%) |
| Consulted GI | 2 (13%) |
| Type of recommendation | |
| Home medications reviewed | 14 (93%) |
| Nutritional (ie, feed changes) | 11 (73%) |
| Pain medications reviewed | 11 (73%) |
| Bowel regimen | 10 (67%) |
| New medical issues* | 10 (67%) |
| Pain medications modified | 9 (60%) |
| Foley removed | 7 (46%) |
| Unnecessary medication removed | 6 (40%) |
| Central line removed | 4 (27%) |
| No changes in management | 3 (20%) |
| TPN | 2 (13%) |
| Harmful medications removed | 0 (0%) |
Initial examination of mean monthly LOS from June 2000 to October 2005 suggested a possible decline in both mean LOS and variability in LOS after hospitalist comanagement was initiated (Fig. 2). Mean LOS for all initial spinal fusion surgeries decreased from 6.5 days (95% CI: 6.26.7) to 4.8 days (95% CI: 4.55.1) after December 2004. The standard deviation in LOS for all initial spinal fusion surgeries decreased from 1.64 to 1.39 days (P < .0001; Table 3). In the 52 months prior to hospitalist comanagement, there was no change in adjusted LOS over time (slope = 0.009 days/month, P = .3997). After December 2004, there was a significant decline in average adjusted LOS (slope = 0.2 days/month; P < .0001).
| Before Hospitalist 7/0012/04 n=644 | After Hospitalist After 12/04 n=115 | p value | |
|---|---|---|---|
| LOS Days (95% CI) | |||
| All Initial Spinal Fusion Surgeries | 6.5 (6.26.7) | 4.8 (4.55.1) | |
| Idiopathic | 5.2 (5.05.4) | 4.1(3.94.4) | |
| Neuromuscular | 8.6 (8.09.2) | 6.25 (5.56.9) | |
| Standard Deviation Days | |||
| All Initial Spinal Fusion Surgeries | 1.64 | 1.39 | <0.0001 |
| Idiopathic | 1.35 | 1.26 | 0.03 |
| Neuromuscular | 1.70 | 1.41 | 0.002 |
Mean and adjusted LOS of patients in the 2 main diagnostic categories, idiopathic and neuromuscular scoliosis, decreased. The absolute mean LOS decreased more for neuromuscular patients (8.6 days [95% CI: 8.09.2] to 6.2 days [95% CI: 5.56.9]) than for idiopathic patients (5.2 days [95% CI: 5.05.4] to 4.1 days [95% CI: 3.94.4]). The standard deviation in LOS decreased more for the neuromuscular patients, from 1.70 to 1.41 days (P = .002), as shown in Table 3. In the 52 months prior to hospitalist comanagement, there was no change in adjusted LOS over time (neuromuscular slope = 0.024 to 0.027 days/month, P = .49; idiopathic slope = 0.0005 days/month, P = .96). After December 2004, there was a significant decline in average adjusted LOS (neuromuscular slope = 0.23 to 0.31 days/month, P = .0075; idiopathic slope = 0.10 to 0.12 days/month; P = .0007), as demonstrated in Figure 3. A survey of the orthopedic surgical staff demonstrated no known specific changes in surgical or postoperative management initiated around December 2004 other than intrathecal morphine use. Some surgeons performed fewer surgeries, particularly of idiopathic patients.
DISCUSSION
The introduction of hospitalist comanagement to ongoing multispecialty evaluation for medically complex spinal fusion surgery patients was associated with a decrease in mean LOS among all patients undergoing initial spinal fusion surgery. A greater magnitude of decline in LOS was seen among children with neuromuscular scoliosis, who were often comanaged, than among children with idiopathic scoliosis, who were rarely comanaged. Variability in LOS also decreased following initiation of hospitalist comanagement, particularly in the more complex patients. The decreases in LOS persisted after adjustment for patient age, diagnosis, procedure type, intrathecal morphine use, and surgeon. This study provides support for the hypothesis that selective hospitalist comanagement of pediatric surgical patients in the tertiary‐care setting is associated with decreased LOS and decreased variability in LOS.
Analysis of a nationally representative data set demonstrated that 4504 children with idiopathic scoliosis and 1570 children with neuromuscular scoliosis underwent spinal fusion surgery in the United States in 2000.8 The average LOS for children with neuromuscular scoliosis was 9.2 days versus 6.1 days for those with idiopathic scoliosis. The LOS of both our patient populations, those before hospitalist comanagement and those after hospitalist comanagement, was less than the national estimates. Multidisciplinary management strategies with or without hospitalist comanagement may be associated with decreases in LOS for neuromuscular scoliosis patients undergoing spinal fusion surgery.
The hospitalist performed a variety of activities in comanaging the medically complex pediatric orthopedic patients. Hospitalist comanagement may have been associated with reduction in LOS for several reasons: preoperative prevention of medical problems, early postoperative identification of and intervention on medical complications, improved coordination of care, or simply consistency of postoperative medical care.
These findings are consistent with the pediatric nonsurgical literature, which suggests that hospitalist management of pediatric medical patients in the tertiary‐care setting is associated with decreased LOS.13 Hospitalist comanagement of adult orthopedic patients has been better studied than has been comanagement of pediatric patients. Elderly patients undergoing elective hip or knee arthroplasty were randomized to hospitalist care versus traditional orthopedic care after surgery. Both sets of patients were managed by the same nursing staff according to standardized care pathways. The mean LOS did not differ between the 2 groups, but the adjusted LOS was lower in the group that received hospitalist care.9 When the same center examined outcomes in hip fracture patients before and after implementation of a hospitalist care model, there was a decrease in LOS and no change in readmission or deaths.10 As in these studies, spinal fusion surgery management is highly standardized in our center. Nonetheless, hospitalist comanagement still was associated with a decreased LOS.
This study found a decline in LOS among all patients undergoing spinal fusion surgery, even among children with idiopathic scoliosis, of whom only 1 was comanaged. This finding may suggest hospitalist comanagement had a global, or indirect, effect on the management of all postoperative patients. However, the time‐series design could have been biased by a cointervention implemented at the same time as hospitalist care. Some surgeons performed fewer surgeries on their idiopathic patients over the course of the study; however, we adjusted for that surgeon in our analysis. Intrathecal morphine use is the only known change in postoperative management that may have affected care starting in December 2004; we also adjusted for intrathecal morphine use in our analysis. There may be other changes of which we are unaware. Nonetheless, the decline in LOS seen in the idiopathic population was exceeded by the decline in LOS in the comanaged neuromuscular population.
Unlike earlier reported studies, which examined hospitalist management among pediatric medical patients, this study did not assess complications (such as pneumonia, respiratory failure, urinary tract infection, gastric ulcers, pathologic fractures, poor wound healing, nutritional compromise, and readmission),7, 11, 12 costs, or patient and provider satisfaction with hospitalist comanagement.13 This assessment is critical to defining the value of these services to patients and providers. In addition, because we did not collect information on severity of disability, we were unable to control for disability. These are other covariates and outcomes of interest that should be assessed in future studies. Furthermore, there was potential bias introduced by having the lead author both conducting the study and performing the intervention; this was minimized by having different individuals responsible for primary data collection and having the analyses performed in a blinded fashion. In addition, although this study provided promising initial evidence that selective hospitalist comanagement along with multispecialty evaluation of spinal fusion surgery patients may lead to a significant decrease in LOS, this evidence needs to be replicated in other surgical patient populations and hospital settings. Ideally, the impact of hospitalist comanagement should be more fully evaluated in a randomized controlled trial. Hospitalist comanagement is a promising technique for improving the care of children undergoing spinal fusion surgery, particularly those with complex medical conditions.
Acknowledgements
The authors acknowledge the contributions of Heidi Gullord of University Physician, Incorporated, for assistance with obtaining billing records. We also appreciate the ongoing input of the Children's Hospital Department of Epidemiology, including Lorna Dyk, BSN, MBA; Michael Rannie, RN, MS; Meghan Birkholz, MSPH; and Michael Kahn, MD, PhD. We appreciate the willingness of the Department of Orthopedics to cooperate with this study, including (but not limited to) Mark Erickson, MD; Frank Chang, MD; and Gaia Georgopoulos, MD. In addition, we acknowledge the ongoing efforts of the care providers involved in the High Risk Pathway at the Children's Hospital, including Carol Page, PT; Alice Radic, PTA; Sarah Hack Baltazar, RD; Monte Leidholm, RRT; Cloy Vaneman, RRT; Gail Shattuck, MSW; and Lynn Katz, MSW, as well as the Divisions of Pulmonary Medicine and Intensive Care of the Department of Pediatrics. We also thank Heather Ramey, BS, BA, for her assistance with organizing the multispecialty evaluation of patients undergoing surgery. We also appreciate the efforts of the fellows and faculty of the Primary Care Research Fellowship and appreciate their assistance in crafting this research.
- ,.Evaluation of a pediatric hospitalist service: impact on length of stay and hospital charges.Pediatrics.2000;105:478–484.
- ,,, et al.Impact of a health maintenance organization hospitalist system in academic pediatrics.Pediatrics.2002;110:720–728.
- ,,,.Evaluation of a staff‐only hospitalist system in a tertiary care, academic children's hospital.Pediatrics.2004;114:1545–1549.
- and theCommittee on Hospital Care.Physicians' roles in coordinating care of hospitalized children.Pediatrics.2003;111:707–709.
- and.Differences in work environment, responsibilities, and training need between community hospital and academic center hospitalists. E‐PAS2006:59:4128.3.
- ,.Development and implementation of a spine fusion high risk pathway. 5th Annual Pre‐Brandon Carrell Pediatric Orthopaedic Symposium for Nursing and Allied Healthcare Professionals, Texas Scottish Rite Hospital for Children, Dallas, Texas, June 26,2003.
- ,,,.Reducing delirium after hip fracture: a randomized trial.J Am Geriatr Soc.2001;49:516–522.
- ,,, et al.Spinal fusion in children with idiopathic and neuromuscular scoliosis: what's the difference?J Pediatr Orthop.2006;26(2):216–220.
- ,,, et al.Medical and surgical comanagement after elective hip and knee arthroplasty.Ann Intern Med.2004;141:28–38.
- ,,, et al.Effects of a hospitalist model on elderly patients with hip fracture.Arch Intern Med2005;165:796–801.
- ,,, et al.Factors predicting post‐operative complications following spinal fusion in children with cerebral palsy.J Spinal Disord.1999;12:297–305.
- ,,, et al.Neuromuscular scoliosis: clinical evaluation pre‐ and post‐operative.J Pediatr Orthop..2000;9(4):217–220.
As the field of pediatric hospital medicine has emerged, so too has evidence that hospitalist management of pediatric medical patients in the tertiary‐care setting is associated with decreased length of stay (LOS).13 The American Academy of Pediatrics Committee on Hospital Care has recommended hospitalist consultation for pediatric surgical patients being managed by adult surgeons.4 In one survey of pediatric hospitalists, 66% of community hospitalists and 47% of academic hospitalists reported comanaging surgical patients.5 However, little work has been published on the effect of hospitalist comanagement of pediatric surgical patients.
Since June 2000 patients undergoing spinal fusion surgery at the Children's Hospital in Denver, Colorado have been screened by a spine nurse for medical complexity. Medically complex patients undergoing preoperative multispecialty evaluation and their perioperative care are coordinated by the spine nurse.6 Introduction of a general pediatric hospitalist to aid with pre‐ and perioperative management of the most complicated patients in December 2004 provided us with an opportunity to study hospitalist comanagement of medically complex pediatric patients undergoing spine fusion surgery.
Our objectives were (1) to describe comanagement activities and (2) to determine the association of hospitalist comanagement on LOS following spinal fusion surgery. We hypothesized that by addressing a variety of pre‐ and perioperative medical issues, hospitalist comanagement would be associated with a decreased LOS for medically complex pediatric patients undergoing spinal fusion surgery.
METHODS
Design and Population
A retrospective analysis of the orthopedic surgeons' log at the Children's Hospital in Denver, Colorado, a tertiary‐care academic pediatric hospital serving the Rocky Mountain region, was performed. Patients included were those underwent their first episode of spinal fusion surgery between July 1, 2000, and October 1, 2005 (n = 759); exclusion criteria included diagnoses of spondylolisthesis or spondylolysis. The study was approved by the Colorado Multiple Institutional Review Board and exempted from ongoing review, and informed consent was not required.
Intervention: Pre‐ and Perioperative High‐Risk Pathway
Since June 2000 medically complex patients undergoing spinal fusion surgery at the Children's Hospital in Denver, Colorado have been referred by either the orthopedic surgeon or the rehabilitation physician to the spine surgery nurse. This nurse, an RN, BSN with more than a decade of experience with spinal fusion patients, then coordinates preoperative multispecialty evaluation (Fig. 1, column 2). Patients are seen by a pulmonologist pre‐operatively, and undergo pulmonary function tests, chest radiograph, venous blood gas, and, at times, a polysomnogram and electrocardiography. A cardiology consult is obtained for patients with muscle disease. Gastroenterology and neurology may be consulted if there are significant feeding and/or neurological issues that the primary care physician needs assistance addressing preoperatively. Shortly before the scheduled surgery, the patient is evaluated at a discharge planning meeting by a nutritionist, respiratory therapist, physical therapist, social worker (at times), and the spinal surgery nurse for discharge equipment planning. Immediately before surgery, in addition to teaching, surgical consent and a surgical history and physical are obtained, as well as laboratory studies that include a complete blood cell count, type, and cross, coagulation studies, and spine radiographs.5 Medically complex patients are managed in the intensive care unit for at least 24 hours after surgery. In addition, standardized order sets developed in 2001 and edited in July 2005 are used to streamline management of the intensive care unit and the orthopedic ward.
Since December 2004, a hospitalist has aided pre‐ and perioperative evaluation and management (Fig. 1, column 3). The patients seen and comanaged by the hospitalist have been those who have significant medical issues in addition to neuromuscular disease, including multiple medications, seizure disorders, nutritional concerns, and/or significant social concerns. Whereas patients with a multitude of different diagnoses were referred to the spinal surgery nurse for a variety of reasons, patients comanaged by hospitalists were generally children with multiple medical conditions who had neuromuscular scoliosis.
Data Sources
The primary data source used was the surgeons' log. The surgeons' log is a record of patients undergoing spinal fusion surgery maintained concurrently by 2 individuals (the spine surgery nurse and her assistant). From January 2000 on, patient data were manually input into an Excel spreadsheet regularly and were cross‐referenced weekly with the surgery schedule. Data entered include: patient name, medical record number, date of surgery, date of discharge (from hospital admission information), underlying diagnosis, type of procedure, primary surgeon (from operative and/or discharge summaries), and LOS (calculated from dates of discharge and surgery). If either underlying diagnosis or type of procedure needed clarification, the spine surgery nurse discussed it with the primary surgeon. We verified the completeness of the surgeons' log for first spinal fusion surgeries by cross‐referencing with billing records; of 572 surgeries performed by 5 surgeons, 571 were recorded (99.8%) in the surgeons' log.
To perform the descriptive analysis of hospitalist activities, the first author (T.S.) performed a retrospective review of the charts of patients she had seen in her role as hospitalist from December 1, 2004, to October 1, 2005. Prepared in advance was a checklist of pre‐ and perioperative activities, modeled on prior work reporting clinical activities.7 Activities either mentioned in the daily progress note or ordered were recorded as completed and entered into an Excel spreadsheet.
Data Collection
The outcome measure was LOS, log‐transformed for analyses. Covariates included were: patient age, underlying diagnosis, procedure type, and surgeon. Underlying diagnoses were subdivided on the basis of the manually input Excel spreadsheet entries into 5 categories: idiopathic, congenital, neuromuscular, osteogenic, and other. The major diagnoses in the idiopathic category were infantile, juvenile, and adolescent idiopathic scoliosis; in the congenital category were congenital scoliosis, congenital kyphoscoliosis; in the neuromuscular category were cerebral palsy, Duchenne's muscular dystrophy, spina bifida, brain injury, spinal cord injury, and chromosomal anomalies; and in the osteogenic category were Scheuermann's kyphosis, trauma, tumor, kyphoscoliosis, and bone disease. Procedures were subdivided according to the manually input Excel spreadsheet entries into 3 categories: posterior only, anterior/ posterior, and anterior spinal fusion only.
After our initial analysis demonstrated a decline in LOS after December 2004 in both idiopathic and neuromuscular patients, we asked the orthopedic surgeons and spine surgery nurse to determine cointerventions that may have occurred around December 2004. We attempted to contact each surgeon who performed surgery during the study period and asked, What changes did you make on or around November 2004 in your management of spinal fusion patients? We received e‐mail and verbal responses from the spine surgery nurse and from 6 surgeons who had performed 646 of the procedures (78%) over the study period.
Increased use of intrathecal morphine was raised as a possible confounding cointervention. To characterize use of intrathecal morphine, we reviewed the charts of all the patients categorized as idiopathic or neuromuscular patients who underwent surgery after December 2004 and a random sample of 20% of these patients who underwent surgery before December 2004.
Analyses
All quantitative analyses (ie, those of the surgeons' log) were performed in a blinded manner, whereas the chart review was not blinded. Univariate analyses of hospitalist activities and univariate and bivariate analyses of the surgeons' log were performed using SAS 9.1. Mean LOS after log back‐transformation along with 95% confidence interval is reported. The chi square test of equality of variance was used to analyze whether the variances differed.
The multifaceted approach to the care of spinal fusion patients is a tiered approach, with 3 major patient groups (Fig. 1): (1) patients with scoliosis, generally idiopathic, and no or minimal medical conditions, who receive care by the usual pathway and do not receive care by the high‐risk pathway or do not have a hospitalist; (2) patients with scoliosis with any underlying diagnosis and some medical conditions, who receive care by high‐risk pathway; and (3) patients with scoliosis, usually neuromuscular scoliosis, and multiple medical conditions, who receive care by the high‐risk pathway and have hospitalist comanagement. Because of selection bias in the receipt of hospitalist comanagement (ie, the most complicated patients), we cannot reasonably compare hospitalist patients to nonhospitalist patients after December 2004. Instead, we compared all neuromuscular patients before and after hospitalist comanagement with a control group of idiopathic patients.
Initial examination of mean monthly LOS from June 2000 to October 2005 (Fig. 2) suggested a possible decline in both mean LOS and variability in LOS after December 2004, when hospitalist comanagement was initiated. To determine the trend in LOS over time before and after December 2004, we performed a mixed‐effects piecewise Poisson regression, adjusting for patient covariates (patient age, underlying diagnosis, procedure type, and intrathecal morphine [for idiopathic and neuromuscular patients]) and clustering by surgeon (as a random effect). We used the model to estimate 2 slopes to represent the linear trend before and after December 2004 (when hospitalist comanagement started). After regression modeling generated beta coefficients for each covariate, the average covariates were entered into the model to generate an average adjusted LOS as shown in Figure 3.
RESULTS
A total of 759 patients underwent initial spinal fusion surgery between July 1, 2000, and October 1, 2005644 before and 115 after December 2004, when hospitalist involvement started. After December 2004, 12% (14 of 115) of all spinal fusion surgery patients were comanaged by a hospitalist. Most comanaged patients (14 of 15, 93%) had neuromuscular scoliosis, and comanaged patients represented 37% (13 of 35) of all neuromuscular patients (Table 1). Over the course of the study, the number of more invasive and complicated anterior/posterior spinal fusion surgeries declined, whereas the number of posterior spinal fusion surgeries increased significantly because of the introduction of new technology (data not shown).
| LOS Days (95% CI) | ||||
|---|---|---|---|---|
| All Surgeries | Preintervention (July 2000December 2004) | Postintervention (December 2004September 2005) | Hospitalist Comanaged (December 2004September 2005) | |
| ||||
| Number of surgeries | 759 | 644 | 115 | 14* |
| Age (years), mean (SD) | 13.6 (3.4) | 13.7 (3.4) | 13.1 (3.4) | 12.6 (4.0) |
| Diagnosis | ||||
| Idiopathic | 328 (43%) | 277 (43%) | 51 (44%) | 1 (7%) |
| Neuromuscular | 247 (32%) | 212 (33%) | 35 (30%) | 13 (93%) |
| Congenital | 66 (9%) | 55 (8%) | 11 (10%) | |
| Osteogenic | 96 (13%) | 81 (13%) | 15 (13%) | |
| Other | 22 (3%) | 19 (3%) | 3 (3%) | |
| Procedure | ||||
| Posterior | 470 (62%) | 365 (57%) | 105 (91%) | 13 (93%) |
| Ant/post | 227 (30%) | 217 (34%) | 10 (8%) | 1 (7%) |
| Anterior | 62 (8%) | 62 (9%) | ||
| Intrathecal morphine use | ||||
| Idiopathic | 30/50 (60%) | 45/51 (88%) | 0 (0%) | |
| Neuromuscular | 10/42 (24%) | 21/35 (62%) | 5/13 (38%) | |
The 15 patients seen by the hospitalist received a total of 60 visits by the hospitalist. The hospitalist saw 9 patients preoperatively. Of the 15 patients comanaged in the hospital, 5 (33%) were seen once, 8 (53%) were seen between 2 and 5 times, and 2 (14%) were seen more than 10 times. Patients were seen both in the ICU and on the surgical ward. Among the patients seen preoperatively, the hospitalist recommended nutritional interventions for 5 patients (33%), bowel regimens for 4 patients (27%), and preoperative hospitalization for 1 patient for 5 days to optimize nutritional intake, address reflux, and modify bowel regimen, as well as facilitate multispecialty evaluation. Postoperative involvement generally addressed a variety of issues, but 20% of patients had no changes in their management (Table 2).
| Hospitalist Activity | Number of Patients (%) (n = 15) |
|---|---|
| |
| Care coordination | |
| Updated family | 11 (73%) |
| Coordinated discharge | 8 (53%) |
| Updated PCP | 7 (47%) |
| Transfer facilitated | 4 (27%) |
| Consulted pulmonary | 3 (20%) |
| Consulted GI | 2 (13%) |
| Type of recommendation | |
| Home medications reviewed | 14 (93%) |
| Nutritional (ie, feed changes) | 11 (73%) |
| Pain medications reviewed | 11 (73%) |
| Bowel regimen | 10 (67%) |
| New medical issues* | 10 (67%) |
| Pain medications modified | 9 (60%) |
| Foley removed | 7 (46%) |
| Unnecessary medication removed | 6 (40%) |
| Central line removed | 4 (27%) |
| No changes in management | 3 (20%) |
| TPN | 2 (13%) |
| Harmful medications removed | 0 (0%) |
Initial examination of mean monthly LOS from June 2000 to October 2005 suggested a possible decline in both mean LOS and variability in LOS after hospitalist comanagement was initiated (Fig. 2). Mean LOS for all initial spinal fusion surgeries decreased from 6.5 days (95% CI: 6.26.7) to 4.8 days (95% CI: 4.55.1) after December 2004. The standard deviation in LOS for all initial spinal fusion surgeries decreased from 1.64 to 1.39 days (P < .0001; Table 3). In the 52 months prior to hospitalist comanagement, there was no change in adjusted LOS over time (slope = 0.009 days/month, P = .3997). After December 2004, there was a significant decline in average adjusted LOS (slope = 0.2 days/month; P < .0001).
| Before Hospitalist 7/0012/04 n=644 | After Hospitalist After 12/04 n=115 | p value | |
|---|---|---|---|
| LOS Days (95% CI) | |||
| All Initial Spinal Fusion Surgeries | 6.5 (6.26.7) | 4.8 (4.55.1) | |
| Idiopathic | 5.2 (5.05.4) | 4.1(3.94.4) | |
| Neuromuscular | 8.6 (8.09.2) | 6.25 (5.56.9) | |
| Standard Deviation Days | |||
| All Initial Spinal Fusion Surgeries | 1.64 | 1.39 | <0.0001 |
| Idiopathic | 1.35 | 1.26 | 0.03 |
| Neuromuscular | 1.70 | 1.41 | 0.002 |
Mean and adjusted LOS of patients in the 2 main diagnostic categories, idiopathic and neuromuscular scoliosis, decreased. The absolute mean LOS decreased more for neuromuscular patients (8.6 days [95% CI: 8.09.2] to 6.2 days [95% CI: 5.56.9]) than for idiopathic patients (5.2 days [95% CI: 5.05.4] to 4.1 days [95% CI: 3.94.4]). The standard deviation in LOS decreased more for the neuromuscular patients, from 1.70 to 1.41 days (P = .002), as shown in Table 3. In the 52 months prior to hospitalist comanagement, there was no change in adjusted LOS over time (neuromuscular slope = 0.024 to 0.027 days/month, P = .49; idiopathic slope = 0.0005 days/month, P = .96). After December 2004, there was a significant decline in average adjusted LOS (neuromuscular slope = 0.23 to 0.31 days/month, P = .0075; idiopathic slope = 0.10 to 0.12 days/month; P = .0007), as demonstrated in Figure 3. A survey of the orthopedic surgical staff demonstrated no known specific changes in surgical or postoperative management initiated around December 2004 other than intrathecal morphine use. Some surgeons performed fewer surgeries, particularly of idiopathic patients.
DISCUSSION
The introduction of hospitalist comanagement to ongoing multispecialty evaluation for medically complex spinal fusion surgery patients was associated with a decrease in mean LOS among all patients undergoing initial spinal fusion surgery. A greater magnitude of decline in LOS was seen among children with neuromuscular scoliosis, who were often comanaged, than among children with idiopathic scoliosis, who were rarely comanaged. Variability in LOS also decreased following initiation of hospitalist comanagement, particularly in the more complex patients. The decreases in LOS persisted after adjustment for patient age, diagnosis, procedure type, intrathecal morphine use, and surgeon. This study provides support for the hypothesis that selective hospitalist comanagement of pediatric surgical patients in the tertiary‐care setting is associated with decreased LOS and decreased variability in LOS.
Analysis of a nationally representative data set demonstrated that 4504 children with idiopathic scoliosis and 1570 children with neuromuscular scoliosis underwent spinal fusion surgery in the United States in 2000.8 The average LOS for children with neuromuscular scoliosis was 9.2 days versus 6.1 days for those with idiopathic scoliosis. The LOS of both our patient populations, those before hospitalist comanagement and those after hospitalist comanagement, was less than the national estimates. Multidisciplinary management strategies with or without hospitalist comanagement may be associated with decreases in LOS for neuromuscular scoliosis patients undergoing spinal fusion surgery.
The hospitalist performed a variety of activities in comanaging the medically complex pediatric orthopedic patients. Hospitalist comanagement may have been associated with reduction in LOS for several reasons: preoperative prevention of medical problems, early postoperative identification of and intervention on medical complications, improved coordination of care, or simply consistency of postoperative medical care.
These findings are consistent with the pediatric nonsurgical literature, which suggests that hospitalist management of pediatric medical patients in the tertiary‐care setting is associated with decreased LOS.13 Hospitalist comanagement of adult orthopedic patients has been better studied than has been comanagement of pediatric patients. Elderly patients undergoing elective hip or knee arthroplasty were randomized to hospitalist care versus traditional orthopedic care after surgery. Both sets of patients were managed by the same nursing staff according to standardized care pathways. The mean LOS did not differ between the 2 groups, but the adjusted LOS was lower in the group that received hospitalist care.9 When the same center examined outcomes in hip fracture patients before and after implementation of a hospitalist care model, there was a decrease in LOS and no change in readmission or deaths.10 As in these studies, spinal fusion surgery management is highly standardized in our center. Nonetheless, hospitalist comanagement still was associated with a decreased LOS.
This study found a decline in LOS among all patients undergoing spinal fusion surgery, even among children with idiopathic scoliosis, of whom only 1 was comanaged. This finding may suggest hospitalist comanagement had a global, or indirect, effect on the management of all postoperative patients. However, the time‐series design could have been biased by a cointervention implemented at the same time as hospitalist care. Some surgeons performed fewer surgeries on their idiopathic patients over the course of the study; however, we adjusted for that surgeon in our analysis. Intrathecal morphine use is the only known change in postoperative management that may have affected care starting in December 2004; we also adjusted for intrathecal morphine use in our analysis. There may be other changes of which we are unaware. Nonetheless, the decline in LOS seen in the idiopathic population was exceeded by the decline in LOS in the comanaged neuromuscular population.
Unlike earlier reported studies, which examined hospitalist management among pediatric medical patients, this study did not assess complications (such as pneumonia, respiratory failure, urinary tract infection, gastric ulcers, pathologic fractures, poor wound healing, nutritional compromise, and readmission),7, 11, 12 costs, or patient and provider satisfaction with hospitalist comanagement.13 This assessment is critical to defining the value of these services to patients and providers. In addition, because we did not collect information on severity of disability, we were unable to control for disability. These are other covariates and outcomes of interest that should be assessed in future studies. Furthermore, there was potential bias introduced by having the lead author both conducting the study and performing the intervention; this was minimized by having different individuals responsible for primary data collection and having the analyses performed in a blinded fashion. In addition, although this study provided promising initial evidence that selective hospitalist comanagement along with multispecialty evaluation of spinal fusion surgery patients may lead to a significant decrease in LOS, this evidence needs to be replicated in other surgical patient populations and hospital settings. Ideally, the impact of hospitalist comanagement should be more fully evaluated in a randomized controlled trial. Hospitalist comanagement is a promising technique for improving the care of children undergoing spinal fusion surgery, particularly those with complex medical conditions.
Acknowledgements
The authors acknowledge the contributions of Heidi Gullord of University Physician, Incorporated, for assistance with obtaining billing records. We also appreciate the ongoing input of the Children's Hospital Department of Epidemiology, including Lorna Dyk, BSN, MBA; Michael Rannie, RN, MS; Meghan Birkholz, MSPH; and Michael Kahn, MD, PhD. We appreciate the willingness of the Department of Orthopedics to cooperate with this study, including (but not limited to) Mark Erickson, MD; Frank Chang, MD; and Gaia Georgopoulos, MD. In addition, we acknowledge the ongoing efforts of the care providers involved in the High Risk Pathway at the Children's Hospital, including Carol Page, PT; Alice Radic, PTA; Sarah Hack Baltazar, RD; Monte Leidholm, RRT; Cloy Vaneman, RRT; Gail Shattuck, MSW; and Lynn Katz, MSW, as well as the Divisions of Pulmonary Medicine and Intensive Care of the Department of Pediatrics. We also thank Heather Ramey, BS, BA, for her assistance with organizing the multispecialty evaluation of patients undergoing surgery. We also appreciate the efforts of the fellows and faculty of the Primary Care Research Fellowship and appreciate their assistance in crafting this research.
As the field of pediatric hospital medicine has emerged, so too has evidence that hospitalist management of pediatric medical patients in the tertiary‐care setting is associated with decreased length of stay (LOS).13 The American Academy of Pediatrics Committee on Hospital Care has recommended hospitalist consultation for pediatric surgical patients being managed by adult surgeons.4 In one survey of pediatric hospitalists, 66% of community hospitalists and 47% of academic hospitalists reported comanaging surgical patients.5 However, little work has been published on the effect of hospitalist comanagement of pediatric surgical patients.
Since June 2000 patients undergoing spinal fusion surgery at the Children's Hospital in Denver, Colorado have been screened by a spine nurse for medical complexity. Medically complex patients undergoing preoperative multispecialty evaluation and their perioperative care are coordinated by the spine nurse.6 Introduction of a general pediatric hospitalist to aid with pre‐ and perioperative management of the most complicated patients in December 2004 provided us with an opportunity to study hospitalist comanagement of medically complex pediatric patients undergoing spine fusion surgery.
Our objectives were (1) to describe comanagement activities and (2) to determine the association of hospitalist comanagement on LOS following spinal fusion surgery. We hypothesized that by addressing a variety of pre‐ and perioperative medical issues, hospitalist comanagement would be associated with a decreased LOS for medically complex pediatric patients undergoing spinal fusion surgery.
METHODS
Design and Population
A retrospective analysis of the orthopedic surgeons' log at the Children's Hospital in Denver, Colorado, a tertiary‐care academic pediatric hospital serving the Rocky Mountain region, was performed. Patients included were those underwent their first episode of spinal fusion surgery between July 1, 2000, and October 1, 2005 (n = 759); exclusion criteria included diagnoses of spondylolisthesis or spondylolysis. The study was approved by the Colorado Multiple Institutional Review Board and exempted from ongoing review, and informed consent was not required.
Intervention: Pre‐ and Perioperative High‐Risk Pathway
Since June 2000 medically complex patients undergoing spinal fusion surgery at the Children's Hospital in Denver, Colorado have been referred by either the orthopedic surgeon or the rehabilitation physician to the spine surgery nurse. This nurse, an RN, BSN with more than a decade of experience with spinal fusion patients, then coordinates preoperative multispecialty evaluation (Fig. 1, column 2). Patients are seen by a pulmonologist pre‐operatively, and undergo pulmonary function tests, chest radiograph, venous blood gas, and, at times, a polysomnogram and electrocardiography. A cardiology consult is obtained for patients with muscle disease. Gastroenterology and neurology may be consulted if there are significant feeding and/or neurological issues that the primary care physician needs assistance addressing preoperatively. Shortly before the scheduled surgery, the patient is evaluated at a discharge planning meeting by a nutritionist, respiratory therapist, physical therapist, social worker (at times), and the spinal surgery nurse for discharge equipment planning. Immediately before surgery, in addition to teaching, surgical consent and a surgical history and physical are obtained, as well as laboratory studies that include a complete blood cell count, type, and cross, coagulation studies, and spine radiographs.5 Medically complex patients are managed in the intensive care unit for at least 24 hours after surgery. In addition, standardized order sets developed in 2001 and edited in July 2005 are used to streamline management of the intensive care unit and the orthopedic ward.
Since December 2004, a hospitalist has aided pre‐ and perioperative evaluation and management (Fig. 1, column 3). The patients seen and comanaged by the hospitalist have been those who have significant medical issues in addition to neuromuscular disease, including multiple medications, seizure disorders, nutritional concerns, and/or significant social concerns. Whereas patients with a multitude of different diagnoses were referred to the spinal surgery nurse for a variety of reasons, patients comanaged by hospitalists were generally children with multiple medical conditions who had neuromuscular scoliosis.
Data Sources
The primary data source used was the surgeons' log. The surgeons' log is a record of patients undergoing spinal fusion surgery maintained concurrently by 2 individuals (the spine surgery nurse and her assistant). From January 2000 on, patient data were manually input into an Excel spreadsheet regularly and were cross‐referenced weekly with the surgery schedule. Data entered include: patient name, medical record number, date of surgery, date of discharge (from hospital admission information), underlying diagnosis, type of procedure, primary surgeon (from operative and/or discharge summaries), and LOS (calculated from dates of discharge and surgery). If either underlying diagnosis or type of procedure needed clarification, the spine surgery nurse discussed it with the primary surgeon. We verified the completeness of the surgeons' log for first spinal fusion surgeries by cross‐referencing with billing records; of 572 surgeries performed by 5 surgeons, 571 were recorded (99.8%) in the surgeons' log.
To perform the descriptive analysis of hospitalist activities, the first author (T.S.) performed a retrospective review of the charts of patients she had seen in her role as hospitalist from December 1, 2004, to October 1, 2005. Prepared in advance was a checklist of pre‐ and perioperative activities, modeled on prior work reporting clinical activities.7 Activities either mentioned in the daily progress note or ordered were recorded as completed and entered into an Excel spreadsheet.
Data Collection
The outcome measure was LOS, log‐transformed for analyses. Covariates included were: patient age, underlying diagnosis, procedure type, and surgeon. Underlying diagnoses were subdivided on the basis of the manually input Excel spreadsheet entries into 5 categories: idiopathic, congenital, neuromuscular, osteogenic, and other. The major diagnoses in the idiopathic category were infantile, juvenile, and adolescent idiopathic scoliosis; in the congenital category were congenital scoliosis, congenital kyphoscoliosis; in the neuromuscular category were cerebral palsy, Duchenne's muscular dystrophy, spina bifida, brain injury, spinal cord injury, and chromosomal anomalies; and in the osteogenic category were Scheuermann's kyphosis, trauma, tumor, kyphoscoliosis, and bone disease. Procedures were subdivided according to the manually input Excel spreadsheet entries into 3 categories: posterior only, anterior/ posterior, and anterior spinal fusion only.
After our initial analysis demonstrated a decline in LOS after December 2004 in both idiopathic and neuromuscular patients, we asked the orthopedic surgeons and spine surgery nurse to determine cointerventions that may have occurred around December 2004. We attempted to contact each surgeon who performed surgery during the study period and asked, What changes did you make on or around November 2004 in your management of spinal fusion patients? We received e‐mail and verbal responses from the spine surgery nurse and from 6 surgeons who had performed 646 of the procedures (78%) over the study period.
Increased use of intrathecal morphine was raised as a possible confounding cointervention. To characterize use of intrathecal morphine, we reviewed the charts of all the patients categorized as idiopathic or neuromuscular patients who underwent surgery after December 2004 and a random sample of 20% of these patients who underwent surgery before December 2004.
Analyses
All quantitative analyses (ie, those of the surgeons' log) were performed in a blinded manner, whereas the chart review was not blinded. Univariate analyses of hospitalist activities and univariate and bivariate analyses of the surgeons' log were performed using SAS 9.1. Mean LOS after log back‐transformation along with 95% confidence interval is reported. The chi square test of equality of variance was used to analyze whether the variances differed.
The multifaceted approach to the care of spinal fusion patients is a tiered approach, with 3 major patient groups (Fig. 1): (1) patients with scoliosis, generally idiopathic, and no or minimal medical conditions, who receive care by the usual pathway and do not receive care by the high‐risk pathway or do not have a hospitalist; (2) patients with scoliosis with any underlying diagnosis and some medical conditions, who receive care by high‐risk pathway; and (3) patients with scoliosis, usually neuromuscular scoliosis, and multiple medical conditions, who receive care by the high‐risk pathway and have hospitalist comanagement. Because of selection bias in the receipt of hospitalist comanagement (ie, the most complicated patients), we cannot reasonably compare hospitalist patients to nonhospitalist patients after December 2004. Instead, we compared all neuromuscular patients before and after hospitalist comanagement with a control group of idiopathic patients.
Initial examination of mean monthly LOS from June 2000 to October 2005 (Fig. 2) suggested a possible decline in both mean LOS and variability in LOS after December 2004, when hospitalist comanagement was initiated. To determine the trend in LOS over time before and after December 2004, we performed a mixed‐effects piecewise Poisson regression, adjusting for patient covariates (patient age, underlying diagnosis, procedure type, and intrathecal morphine [for idiopathic and neuromuscular patients]) and clustering by surgeon (as a random effect). We used the model to estimate 2 slopes to represent the linear trend before and after December 2004 (when hospitalist comanagement started). After regression modeling generated beta coefficients for each covariate, the average covariates were entered into the model to generate an average adjusted LOS as shown in Figure 3.
RESULTS
A total of 759 patients underwent initial spinal fusion surgery between July 1, 2000, and October 1, 2005644 before and 115 after December 2004, when hospitalist involvement started. After December 2004, 12% (14 of 115) of all spinal fusion surgery patients were comanaged by a hospitalist. Most comanaged patients (14 of 15, 93%) had neuromuscular scoliosis, and comanaged patients represented 37% (13 of 35) of all neuromuscular patients (Table 1). Over the course of the study, the number of more invasive and complicated anterior/posterior spinal fusion surgeries declined, whereas the number of posterior spinal fusion surgeries increased significantly because of the introduction of new technology (data not shown).
| LOS Days (95% CI) | ||||
|---|---|---|---|---|
| All Surgeries | Preintervention (July 2000December 2004) | Postintervention (December 2004September 2005) | Hospitalist Comanaged (December 2004September 2005) | |
| ||||
| Number of surgeries | 759 | 644 | 115 | 14* |
| Age (years), mean (SD) | 13.6 (3.4) | 13.7 (3.4) | 13.1 (3.4) | 12.6 (4.0) |
| Diagnosis | ||||
| Idiopathic | 328 (43%) | 277 (43%) | 51 (44%) | 1 (7%) |
| Neuromuscular | 247 (32%) | 212 (33%) | 35 (30%) | 13 (93%) |
| Congenital | 66 (9%) | 55 (8%) | 11 (10%) | |
| Osteogenic | 96 (13%) | 81 (13%) | 15 (13%) | |
| Other | 22 (3%) | 19 (3%) | 3 (3%) | |
| Procedure | ||||
| Posterior | 470 (62%) | 365 (57%) | 105 (91%) | 13 (93%) |
| Ant/post | 227 (30%) | 217 (34%) | 10 (8%) | 1 (7%) |
| Anterior | 62 (8%) | 62 (9%) | ||
| Intrathecal morphine use | ||||
| Idiopathic | 30/50 (60%) | 45/51 (88%) | 0 (0%) | |
| Neuromuscular | 10/42 (24%) | 21/35 (62%) | 5/13 (38%) | |
The 15 patients seen by the hospitalist received a total of 60 visits by the hospitalist. The hospitalist saw 9 patients preoperatively. Of the 15 patients comanaged in the hospital, 5 (33%) were seen once, 8 (53%) were seen between 2 and 5 times, and 2 (14%) were seen more than 10 times. Patients were seen both in the ICU and on the surgical ward. Among the patients seen preoperatively, the hospitalist recommended nutritional interventions for 5 patients (33%), bowel regimens for 4 patients (27%), and preoperative hospitalization for 1 patient for 5 days to optimize nutritional intake, address reflux, and modify bowel regimen, as well as facilitate multispecialty evaluation. Postoperative involvement generally addressed a variety of issues, but 20% of patients had no changes in their management (Table 2).
| Hospitalist Activity | Number of Patients (%) (n = 15) |
|---|---|
| |
| Care coordination | |
| Updated family | 11 (73%) |
| Coordinated discharge | 8 (53%) |
| Updated PCP | 7 (47%) |
| Transfer facilitated | 4 (27%) |
| Consulted pulmonary | 3 (20%) |
| Consulted GI | 2 (13%) |
| Type of recommendation | |
| Home medications reviewed | 14 (93%) |
| Nutritional (ie, feed changes) | 11 (73%) |
| Pain medications reviewed | 11 (73%) |
| Bowel regimen | 10 (67%) |
| New medical issues* | 10 (67%) |
| Pain medications modified | 9 (60%) |
| Foley removed | 7 (46%) |
| Unnecessary medication removed | 6 (40%) |
| Central line removed | 4 (27%) |
| No changes in management | 3 (20%) |
| TPN | 2 (13%) |
| Harmful medications removed | 0 (0%) |
Initial examination of mean monthly LOS from June 2000 to October 2005 suggested a possible decline in both mean LOS and variability in LOS after hospitalist comanagement was initiated (Fig. 2). Mean LOS for all initial spinal fusion surgeries decreased from 6.5 days (95% CI: 6.26.7) to 4.8 days (95% CI: 4.55.1) after December 2004. The standard deviation in LOS for all initial spinal fusion surgeries decreased from 1.64 to 1.39 days (P < .0001; Table 3). In the 52 months prior to hospitalist comanagement, there was no change in adjusted LOS over time (slope = 0.009 days/month, P = .3997). After December 2004, there was a significant decline in average adjusted LOS (slope = 0.2 days/month; P < .0001).
| Before Hospitalist 7/0012/04 n=644 | After Hospitalist After 12/04 n=115 | p value | |
|---|---|---|---|
| LOS Days (95% CI) | |||
| All Initial Spinal Fusion Surgeries | 6.5 (6.26.7) | 4.8 (4.55.1) | |
| Idiopathic | 5.2 (5.05.4) | 4.1(3.94.4) | |
| Neuromuscular | 8.6 (8.09.2) | 6.25 (5.56.9) | |
| Standard Deviation Days | |||
| All Initial Spinal Fusion Surgeries | 1.64 | 1.39 | <0.0001 |
| Idiopathic | 1.35 | 1.26 | 0.03 |
| Neuromuscular | 1.70 | 1.41 | 0.002 |
Mean and adjusted LOS of patients in the 2 main diagnostic categories, idiopathic and neuromuscular scoliosis, decreased. The absolute mean LOS decreased more for neuromuscular patients (8.6 days [95% CI: 8.09.2] to 6.2 days [95% CI: 5.56.9]) than for idiopathic patients (5.2 days [95% CI: 5.05.4] to 4.1 days [95% CI: 3.94.4]). The standard deviation in LOS decreased more for the neuromuscular patients, from 1.70 to 1.41 days (P = .002), as shown in Table 3. In the 52 months prior to hospitalist comanagement, there was no change in adjusted LOS over time (neuromuscular slope = 0.024 to 0.027 days/month, P = .49; idiopathic slope = 0.0005 days/month, P = .96). After December 2004, there was a significant decline in average adjusted LOS (neuromuscular slope = 0.23 to 0.31 days/month, P = .0075; idiopathic slope = 0.10 to 0.12 days/month; P = .0007), as demonstrated in Figure 3. A survey of the orthopedic surgical staff demonstrated no known specific changes in surgical or postoperative management initiated around December 2004 other than intrathecal morphine use. Some surgeons performed fewer surgeries, particularly of idiopathic patients.
DISCUSSION
The introduction of hospitalist comanagement to ongoing multispecialty evaluation for medically complex spinal fusion surgery patients was associated with a decrease in mean LOS among all patients undergoing initial spinal fusion surgery. A greater magnitude of decline in LOS was seen among children with neuromuscular scoliosis, who were often comanaged, than among children with idiopathic scoliosis, who were rarely comanaged. Variability in LOS also decreased following initiation of hospitalist comanagement, particularly in the more complex patients. The decreases in LOS persisted after adjustment for patient age, diagnosis, procedure type, intrathecal morphine use, and surgeon. This study provides support for the hypothesis that selective hospitalist comanagement of pediatric surgical patients in the tertiary‐care setting is associated with decreased LOS and decreased variability in LOS.
Analysis of a nationally representative data set demonstrated that 4504 children with idiopathic scoliosis and 1570 children with neuromuscular scoliosis underwent spinal fusion surgery in the United States in 2000.8 The average LOS for children with neuromuscular scoliosis was 9.2 days versus 6.1 days for those with idiopathic scoliosis. The LOS of both our patient populations, those before hospitalist comanagement and those after hospitalist comanagement, was less than the national estimates. Multidisciplinary management strategies with or without hospitalist comanagement may be associated with decreases in LOS for neuromuscular scoliosis patients undergoing spinal fusion surgery.
The hospitalist performed a variety of activities in comanaging the medically complex pediatric orthopedic patients. Hospitalist comanagement may have been associated with reduction in LOS for several reasons: preoperative prevention of medical problems, early postoperative identification of and intervention on medical complications, improved coordination of care, or simply consistency of postoperative medical care.
These findings are consistent with the pediatric nonsurgical literature, which suggests that hospitalist management of pediatric medical patients in the tertiary‐care setting is associated with decreased LOS.13 Hospitalist comanagement of adult orthopedic patients has been better studied than has been comanagement of pediatric patients. Elderly patients undergoing elective hip or knee arthroplasty were randomized to hospitalist care versus traditional orthopedic care after surgery. Both sets of patients were managed by the same nursing staff according to standardized care pathways. The mean LOS did not differ between the 2 groups, but the adjusted LOS was lower in the group that received hospitalist care.9 When the same center examined outcomes in hip fracture patients before and after implementation of a hospitalist care model, there was a decrease in LOS and no change in readmission or deaths.10 As in these studies, spinal fusion surgery management is highly standardized in our center. Nonetheless, hospitalist comanagement still was associated with a decreased LOS.
This study found a decline in LOS among all patients undergoing spinal fusion surgery, even among children with idiopathic scoliosis, of whom only 1 was comanaged. This finding may suggest hospitalist comanagement had a global, or indirect, effect on the management of all postoperative patients. However, the time‐series design could have been biased by a cointervention implemented at the same time as hospitalist care. Some surgeons performed fewer surgeries on their idiopathic patients over the course of the study; however, we adjusted for that surgeon in our analysis. Intrathecal morphine use is the only known change in postoperative management that may have affected care starting in December 2004; we also adjusted for intrathecal morphine use in our analysis. There may be other changes of which we are unaware. Nonetheless, the decline in LOS seen in the idiopathic population was exceeded by the decline in LOS in the comanaged neuromuscular population.
Unlike earlier reported studies, which examined hospitalist management among pediatric medical patients, this study did not assess complications (such as pneumonia, respiratory failure, urinary tract infection, gastric ulcers, pathologic fractures, poor wound healing, nutritional compromise, and readmission),7, 11, 12 costs, or patient and provider satisfaction with hospitalist comanagement.13 This assessment is critical to defining the value of these services to patients and providers. In addition, because we did not collect information on severity of disability, we were unable to control for disability. These are other covariates and outcomes of interest that should be assessed in future studies. Furthermore, there was potential bias introduced by having the lead author both conducting the study and performing the intervention; this was minimized by having different individuals responsible for primary data collection and having the analyses performed in a blinded fashion. In addition, although this study provided promising initial evidence that selective hospitalist comanagement along with multispecialty evaluation of spinal fusion surgery patients may lead to a significant decrease in LOS, this evidence needs to be replicated in other surgical patient populations and hospital settings. Ideally, the impact of hospitalist comanagement should be more fully evaluated in a randomized controlled trial. Hospitalist comanagement is a promising technique for improving the care of children undergoing spinal fusion surgery, particularly those with complex medical conditions.
Acknowledgements
The authors acknowledge the contributions of Heidi Gullord of University Physician, Incorporated, for assistance with obtaining billing records. We also appreciate the ongoing input of the Children's Hospital Department of Epidemiology, including Lorna Dyk, BSN, MBA; Michael Rannie, RN, MS; Meghan Birkholz, MSPH; and Michael Kahn, MD, PhD. We appreciate the willingness of the Department of Orthopedics to cooperate with this study, including (but not limited to) Mark Erickson, MD; Frank Chang, MD; and Gaia Georgopoulos, MD. In addition, we acknowledge the ongoing efforts of the care providers involved in the High Risk Pathway at the Children's Hospital, including Carol Page, PT; Alice Radic, PTA; Sarah Hack Baltazar, RD; Monte Leidholm, RRT; Cloy Vaneman, RRT; Gail Shattuck, MSW; and Lynn Katz, MSW, as well as the Divisions of Pulmonary Medicine and Intensive Care of the Department of Pediatrics. We also thank Heather Ramey, BS, BA, for her assistance with organizing the multispecialty evaluation of patients undergoing surgery. We also appreciate the efforts of the fellows and faculty of the Primary Care Research Fellowship and appreciate their assistance in crafting this research.
- ,.Evaluation of a pediatric hospitalist service: impact on length of stay and hospital charges.Pediatrics.2000;105:478–484.
- ,,, et al.Impact of a health maintenance organization hospitalist system in academic pediatrics.Pediatrics.2002;110:720–728.
- ,,,.Evaluation of a staff‐only hospitalist system in a tertiary care, academic children's hospital.Pediatrics.2004;114:1545–1549.
- and theCommittee on Hospital Care.Physicians' roles in coordinating care of hospitalized children.Pediatrics.2003;111:707–709.
- and.Differences in work environment, responsibilities, and training need between community hospital and academic center hospitalists. E‐PAS2006:59:4128.3.
- ,.Development and implementation of a spine fusion high risk pathway. 5th Annual Pre‐Brandon Carrell Pediatric Orthopaedic Symposium for Nursing and Allied Healthcare Professionals, Texas Scottish Rite Hospital for Children, Dallas, Texas, June 26,2003.
- ,,,.Reducing delirium after hip fracture: a randomized trial.J Am Geriatr Soc.2001;49:516–522.
- ,,, et al.Spinal fusion in children with idiopathic and neuromuscular scoliosis: what's the difference?J Pediatr Orthop.2006;26(2):216–220.
- ,,, et al.Medical and surgical comanagement after elective hip and knee arthroplasty.Ann Intern Med.2004;141:28–38.
- ,,, et al.Effects of a hospitalist model on elderly patients with hip fracture.Arch Intern Med2005;165:796–801.
- ,,, et al.Factors predicting post‐operative complications following spinal fusion in children with cerebral palsy.J Spinal Disord.1999;12:297–305.
- ,,, et al.Neuromuscular scoliosis: clinical evaluation pre‐ and post‐operative.J Pediatr Orthop..2000;9(4):217–220.
- ,.Evaluation of a pediatric hospitalist service: impact on length of stay and hospital charges.Pediatrics.2000;105:478–484.
- ,,, et al.Impact of a health maintenance organization hospitalist system in academic pediatrics.Pediatrics.2002;110:720–728.
- ,,,.Evaluation of a staff‐only hospitalist system in a tertiary care, academic children's hospital.Pediatrics.2004;114:1545–1549.
- and theCommittee on Hospital Care.Physicians' roles in coordinating care of hospitalized children.Pediatrics.2003;111:707–709.
- and.Differences in work environment, responsibilities, and training need between community hospital and academic center hospitalists. E‐PAS2006:59:4128.3.
- ,.Development and implementation of a spine fusion high risk pathway. 5th Annual Pre‐Brandon Carrell Pediatric Orthopaedic Symposium for Nursing and Allied Healthcare Professionals, Texas Scottish Rite Hospital for Children, Dallas, Texas, June 26,2003.
- ,,,.Reducing delirium after hip fracture: a randomized trial.J Am Geriatr Soc.2001;49:516–522.
- ,,, et al.Spinal fusion in children with idiopathic and neuromuscular scoliosis: what's the difference?J Pediatr Orthop.2006;26(2):216–220.
- ,,, et al.Medical and surgical comanagement after elective hip and knee arthroplasty.Ann Intern Med.2004;141:28–38.
- ,,, et al.Effects of a hospitalist model on elderly patients with hip fracture.Arch Intern Med2005;165:796–801.
- ,,, et al.Factors predicting post‐operative complications following spinal fusion in children with cerebral palsy.J Spinal Disord.1999;12:297–305.
- ,,, et al.Neuromuscular scoliosis: clinical evaluation pre‐ and post‐operative.J Pediatr Orthop..2000;9(4):217–220.
Copyright © 2007 Society of Hospital Medicine
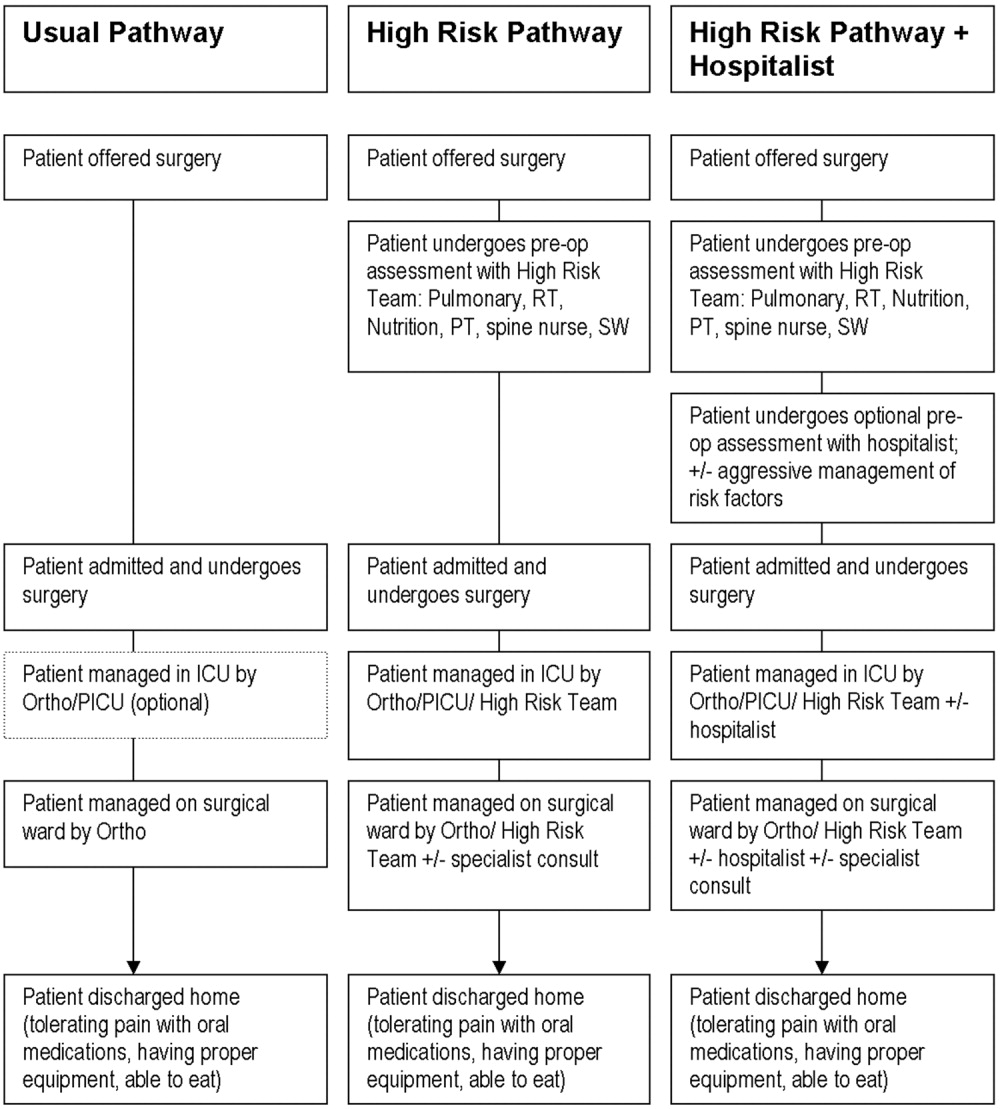
Discharge Appointments
Dicharge of a patient from the hospital is a complicated, interprofessional endeavor.1, 2 Several institutions report that discharge is one of the least satisfying elements of the patient's hospital experience.35 Recent evidence suggests that a poorly planned or disorganized discharge may compromise patient safety in the period soon after dismissal.6 Several initiatives have been aimed at improving patient satisfaction and safety related to discharge.710
In 2000 the Mayo Clinic (Rochester, Minnesota) Department of Internal Medicine leadership established a goal to improve patient satisfaction with the hospital dismissal process. Patient focus group data suggested that uncertainty about the anticipated date and time of discharge causes frustration to some patients and families.
We hypothesized that an appointment to leave the hospital might be practicable. We joined an Institute for Healthcare Improvement collaborative (Improving Flow Through Acute Care Settings, 1 of 6 Improvement Action Network [IMPACT] Learning and Innovation Communities) aimed at scheduling discharge appointments (DAs). The collaborating members deemed that, although the ideal DA is set at least a day in advance, a same‐day DA is also desirable for both patient satisfaction and staff task organization in pursuit of a high‐quality discharge.
METHODS
This project was approved by the Mayo Foundation Institutional Review Board. We tested the following hypotheses:
It is possible to make and display DAs in various care units.
Most DAs can be scheduled a day before dismissal.
Most DA patients depart on time.
Setting
Mayo Clinic in Rochester, Minnesota, is a tertiary academic medical center with 2 hospitals (Saint Marys and Rochester Methodist) that house a total of 1951 licensed beds in 76 care units.
The preliminary study displaying DAs was carried out in the Innovation and Quality (IQ) Unit of Saint Marys Hospital, a 23‐bed general medical care unit that supports both resident and nonresident services. Traditionally, primary services usually consist of an attending physician and house officer physicians (junior and senior residents). Less commonly, primary services consist of an attending physician and either a nurse‐practitioner or a physician assistant.
The design pilot took place between August 2 and December 24, 2003. The subsequent, larger study of applicability took place across 8 care units (including the IQ Unit) between December 28, 2003, and April 25, 2004.
Preliminary Work: Design Pilot
We designed bedside dry‐erase wall displays and mounted them in the rooms in plain view of patients and their families and caregivers. Pilot testing of DA scheduling was done on a general medical care unit from August 2 to December 24, 2003. To optimize the process for scheduling a DA, our team developed 21 small tests to change the dismissal process through plan, do, study, and act cycles.11
The recommended process was that as soon as an organized discharge could be reasonably envisioned, the primary service provider would discuss with the patient, family, and primary nurse (and a social service worker, if involved) the anticipated discharge day. A member of the primary service was to handwrite (with a marker) the anticipated day on the specially designed bedside dry‐erase board (Fig. 1) in view of the patient. The same primary service prescribers could amend this anticipated day (or time) by repeating the process of consultation and discussion as needed. The time of the DA could be written on the DA board (or amended) by either a member of the primary service or the primary care nurse.
Each morning, the primary care nurse transmitted the DA board data to the admission, discharge, and transfer log kept at the unit secretary desk (in which the actual discharge time has always been routinely recorded by the unit secretary).
Adoption of DA Scheduling in Other Care Units
Several meetings were held with 7 other patient care unit leaders about adopting the protocol. These units, both medical and surgical, were selected according to 3 criteria: (1) prior participation in unit‐level continuous improvement work, (2) current or recent work in any aspect of the discharge process, and (3) a reputation for having innovative nursing leadership and staff.
Data Acquisition and Analysis
Data were collected daily from each participating unit's admission, discharge, and transfer log: both the actual time of departure and the DA, if one had been scheduled. For each DA patient, the DA time was compared with the actual departure time.
RESULTS
During the 4‐month study of discharges across 8 care units, 1256 of 2046 patients (61%) received a DA; 576 of the DAs (46%) were scheduled at least 1 day in advance (Table 1). Among patients with a DA, 752 were discharged on time (60%), and only 240 (19%) were tardy.
| Unit | DAs | Departure time of patients compared with DA | |||||
|---|---|---|---|---|---|---|---|
| No. | Type of unit | No. of patients | Patients with DAs, n (%) | DAs scheduled ϵ 1 day ahead, n (%) | On time, n (%)a | Early, n (%) | Late, n (%) |
| |||||||
| 1 | Neurology/neurosurgery | 525 | 270 (51) | 0 (0) | 175 (65) | 44 (16) | 51 (19) |
| 2 | Surgery (mixed) | 481 | 325 (68) | 289 (89) | 166 (51) | 101 (31) | 58 (18) |
| 3 | General internal medicine (IQ Unit) | 466 | 243 (52) | 35 (14) | 132 (54) | 50 (21) | 61 (25) |
| 4 | Neurology/neurosurgery | 267 | 189 (71) | 40 (21) | 119 (63) | 41 (22) | 29 (15) |
| 5 | Vascular surgery | 201 | 127 (63) | 127 (100) | 90 (71) | 12 (9) | 25 (20) |
| 6 | Psychiatry | 46 | 42 (91) | 42 (100) | 28 (67) | 9 (21) | 5 (12) |
| 7 | Orthopedic surgeryelective | 38 | 38 (100) | 22 (58) | 24 (63) | 3 (8) | 11 (29) |
| 8 | Orthopedic surgerytrauma | 22 | 22 (100) | 21 (95) | 18 (82) | 4 (18) | 0 (0) |
| Total | 2046 | 1256 (61) | 576 (46) | 752 (60) | 264 (21) | 240 (19) | |
DISCUSSION
In response to patient focus group feedback, we designed a tool and a process by which a DA could be made and posted at bedside. Among 2046 patients discharged from 8 care units over 4 months, 61% (1256) had a posted, in‐room DA. Almost half the patients with DAs (46%) had a DA scheduled at least 1 calendar day ahead. Remarkably, among patients with a DA, fewer than 20% were discharged tardily. In‐room posting of DAs across a spectrum of care units appears to be practicable, even in the face of extant diagnostic or therapeutic uncertainty.
This was an initial test‐of‐concept project and an exploratory trial. The limitations are: (1) satisfaction (patient, family, nurse, and physician) was not tested with any validated survey instrument, (2) length of stay was not studied, (3) reasons for variable DA success among care units were not ascertained, and (4) resource use was not measured.
Anecdotal information from a postdischarge phone survey indicated that patients seemed appreciative of a DA. The survey data were not included in this article because the survey tool was not a validated instrument and the interviewer (a coauthor) was not blinded to the hypothesis and was therefore subject to bias. No negative comments were received through informal real‐time feedback from patients and family during the making and posting of DAs, and encouraging comments were common.
Physician participation in posting the DA appeared to be key, and the unavoidable dialogue about the clinical rationale for a chosen date seemed welcome. A telling anecdote came from a patient who did not have a DA board: I didn't get the same treatment as my roommate with the [DA] board. The other doctors talked with [him] more about discharge. I wish my team would have done this more with me.
We cannot be certain of the reasons for the care unit disparity in setting and meeting DAs. We speculate that the level of staff enthusiasm for DAs explains the variation rather than patient population characteristics. Further, we cannot explain why 39% of the patients did not receive a DA. Physician feedback was generally, but not uniformly, positive. Negative comments that might explain DA omissions include: (1) patients already are informed and awarethe tool is superfluous; (2) the day of discharge is unknowable in advance; and (3) patients or family members will hold us to it or be upset if the DA is changed.
We expected that diagnostic uncertainty might pose challenges to providing DAs. When primary service providers were reassured that DAs could be amended, this concern was reduced (but not eliminated). It seemed useful for providers to envision the earliest day of discharge by assuming that the results of a pending key test or consultation would be favorable. Frequency of DA modification was not studied. DAs were amended, however, and patients (to our knowledge) seemed unperturbedperhaps because of an almost unavoidable discussion of the clinical rationale because the act of posting the DA occurred in full view of (and in partnership with) the patient.
A trend toward discharge earlier in the day was observed (data not shown). Theoretically, such a trend offers the potential to improve inpatient flow, in part by discharging patients before morning surgical cases are completed.
Although we had many favorable comments about DAs from patients, family members, and nurses, satisfaction of patients, families, and staff members deserves formal study. Further, it is not known whether unused DA boards might contribute to patient dissatisfaction. Any effect that the display of DAs may have on the length of stay also may be a topic worthy of future study.
CONCLUSIONS
Patients and their families sometimes desire more communication about the anticipated day and time of hospital discharge. We designed a process for making a tentative DA and a tool by which the DA could be posted at the bedside. The results of this study suggest that (1) despite some uncertainty it is possible to schedule and post DAs in‐room in various care units and in various settings, (2) DAs were made at least a day ahead of time in almost half the DA discharges, and (3) most DA discharges were characterized by on‐time departure. In addition, patient, family, and nursing satisfaction (in relation to the DA) warrants further investigation.
Acknowledgements
We acknowledge the valuable insights and collaboration of our colleagues Deborah R. Fischer, Steven L. Bahnemann, Matthew Skelton, MD, Lauri J. Dahl, Pamela O. Johnson, MSN, Debra A. Hernke, MSN, Susan L. Stirn, MSN, Barbara R. Spurrier, Ryan R. Armbruster, Todd J. Bille, and Donna K. Lawson of the Mayo Clinic and Mayo Foundation.
- ,,, et al.Learning from patients: a discharge planning improvement project.Jt Comm J Qual Improv.1996;22:311–22.
- ,,,,,, et al.Payer‐hospital collaboration to improve patient satisfaction with hospital discharge.Jt Comm J Qual Improv.1996;22:336–344.
- ,,,,,.How was your hospital stay? Patients' reports about their care in Canadian hospitals.CMAJ.1994;150:1813–1822.
- .A hospitalization from hell: a patient's perspective on quality.Ann Intern Med.2003;138:33–39.
- ,,.Predictors of elder and family caregiver satisfaction with discharge planning.J Cardiovasc Nurs.2000;14:76–87.
- ,,,,.The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138:161–167.
- ,,, et al.Patient callback program: a quality improvement, customer service, and marketing tool.J Health Care Mark.1993;13:60–65.
- ,,,.Effects of a medical team coordinator on length of hospital stay.CMAJ.1992;146:511–515.
- ,.Discharge planning from hospital to home.Cochrane Database Syst Rev.2000;4:CD000313.
- ,,,.Continuity of care and patient outcomes after hospital discharge.J Gen Intern Med.2004;19:624–631.
- Institute for Healthcare Improvement. Cambridge, UK: Institute for Healthcare Improvement. Available from: http://www.ihi.org/IHI/Topics/Improvement/ImprovementMethods/HowToImprove/testingchanges.htm. Accessed July 28,2006.
Dicharge of a patient from the hospital is a complicated, interprofessional endeavor.1, 2 Several institutions report that discharge is one of the least satisfying elements of the patient's hospital experience.35 Recent evidence suggests that a poorly planned or disorganized discharge may compromise patient safety in the period soon after dismissal.6 Several initiatives have been aimed at improving patient satisfaction and safety related to discharge.710
In 2000 the Mayo Clinic (Rochester, Minnesota) Department of Internal Medicine leadership established a goal to improve patient satisfaction with the hospital dismissal process. Patient focus group data suggested that uncertainty about the anticipated date and time of discharge causes frustration to some patients and families.
We hypothesized that an appointment to leave the hospital might be practicable. We joined an Institute for Healthcare Improvement collaborative (Improving Flow Through Acute Care Settings, 1 of 6 Improvement Action Network [IMPACT] Learning and Innovation Communities) aimed at scheduling discharge appointments (DAs). The collaborating members deemed that, although the ideal DA is set at least a day in advance, a same‐day DA is also desirable for both patient satisfaction and staff task organization in pursuit of a high‐quality discharge.
METHODS
This project was approved by the Mayo Foundation Institutional Review Board. We tested the following hypotheses:
It is possible to make and display DAs in various care units.
Most DAs can be scheduled a day before dismissal.
Most DA patients depart on time.
Setting
Mayo Clinic in Rochester, Minnesota, is a tertiary academic medical center with 2 hospitals (Saint Marys and Rochester Methodist) that house a total of 1951 licensed beds in 76 care units.
The preliminary study displaying DAs was carried out in the Innovation and Quality (IQ) Unit of Saint Marys Hospital, a 23‐bed general medical care unit that supports both resident and nonresident services. Traditionally, primary services usually consist of an attending physician and house officer physicians (junior and senior residents). Less commonly, primary services consist of an attending physician and either a nurse‐practitioner or a physician assistant.
The design pilot took place between August 2 and December 24, 2003. The subsequent, larger study of applicability took place across 8 care units (including the IQ Unit) between December 28, 2003, and April 25, 2004.
Preliminary Work: Design Pilot
We designed bedside dry‐erase wall displays and mounted them in the rooms in plain view of patients and their families and caregivers. Pilot testing of DA scheduling was done on a general medical care unit from August 2 to December 24, 2003. To optimize the process for scheduling a DA, our team developed 21 small tests to change the dismissal process through plan, do, study, and act cycles.11
The recommended process was that as soon as an organized discharge could be reasonably envisioned, the primary service provider would discuss with the patient, family, and primary nurse (and a social service worker, if involved) the anticipated discharge day. A member of the primary service was to handwrite (with a marker) the anticipated day on the specially designed bedside dry‐erase board (Fig. 1) in view of the patient. The same primary service prescribers could amend this anticipated day (or time) by repeating the process of consultation and discussion as needed. The time of the DA could be written on the DA board (or amended) by either a member of the primary service or the primary care nurse.
Each morning, the primary care nurse transmitted the DA board data to the admission, discharge, and transfer log kept at the unit secretary desk (in which the actual discharge time has always been routinely recorded by the unit secretary).
Adoption of DA Scheduling in Other Care Units
Several meetings were held with 7 other patient care unit leaders about adopting the protocol. These units, both medical and surgical, were selected according to 3 criteria: (1) prior participation in unit‐level continuous improvement work, (2) current or recent work in any aspect of the discharge process, and (3) a reputation for having innovative nursing leadership and staff.
Data Acquisition and Analysis
Data were collected daily from each participating unit's admission, discharge, and transfer log: both the actual time of departure and the DA, if one had been scheduled. For each DA patient, the DA time was compared with the actual departure time.
RESULTS
During the 4‐month study of discharges across 8 care units, 1256 of 2046 patients (61%) received a DA; 576 of the DAs (46%) were scheduled at least 1 day in advance (Table 1). Among patients with a DA, 752 were discharged on time (60%), and only 240 (19%) were tardy.
| Unit | DAs | Departure time of patients compared with DA | |||||
|---|---|---|---|---|---|---|---|
| No. | Type of unit | No. of patients | Patients with DAs, n (%) | DAs scheduled ϵ 1 day ahead, n (%) | On time, n (%)a | Early, n (%) | Late, n (%) |
| |||||||
| 1 | Neurology/neurosurgery | 525 | 270 (51) | 0 (0) | 175 (65) | 44 (16) | 51 (19) |
| 2 | Surgery (mixed) | 481 | 325 (68) | 289 (89) | 166 (51) | 101 (31) | 58 (18) |
| 3 | General internal medicine (IQ Unit) | 466 | 243 (52) | 35 (14) | 132 (54) | 50 (21) | 61 (25) |
| 4 | Neurology/neurosurgery | 267 | 189 (71) | 40 (21) | 119 (63) | 41 (22) | 29 (15) |
| 5 | Vascular surgery | 201 | 127 (63) | 127 (100) | 90 (71) | 12 (9) | 25 (20) |
| 6 | Psychiatry | 46 | 42 (91) | 42 (100) | 28 (67) | 9 (21) | 5 (12) |
| 7 | Orthopedic surgeryelective | 38 | 38 (100) | 22 (58) | 24 (63) | 3 (8) | 11 (29) |
| 8 | Orthopedic surgerytrauma | 22 | 22 (100) | 21 (95) | 18 (82) | 4 (18) | 0 (0) |
| Total | 2046 | 1256 (61) | 576 (46) | 752 (60) | 264 (21) | 240 (19) | |
DISCUSSION
In response to patient focus group feedback, we designed a tool and a process by which a DA could be made and posted at bedside. Among 2046 patients discharged from 8 care units over 4 months, 61% (1256) had a posted, in‐room DA. Almost half the patients with DAs (46%) had a DA scheduled at least 1 calendar day ahead. Remarkably, among patients with a DA, fewer than 20% were discharged tardily. In‐room posting of DAs across a spectrum of care units appears to be practicable, even in the face of extant diagnostic or therapeutic uncertainty.
This was an initial test‐of‐concept project and an exploratory trial. The limitations are: (1) satisfaction (patient, family, nurse, and physician) was not tested with any validated survey instrument, (2) length of stay was not studied, (3) reasons for variable DA success among care units were not ascertained, and (4) resource use was not measured.
Anecdotal information from a postdischarge phone survey indicated that patients seemed appreciative of a DA. The survey data were not included in this article because the survey tool was not a validated instrument and the interviewer (a coauthor) was not blinded to the hypothesis and was therefore subject to bias. No negative comments were received through informal real‐time feedback from patients and family during the making and posting of DAs, and encouraging comments were common.
Physician participation in posting the DA appeared to be key, and the unavoidable dialogue about the clinical rationale for a chosen date seemed welcome. A telling anecdote came from a patient who did not have a DA board: I didn't get the same treatment as my roommate with the [DA] board. The other doctors talked with [him] more about discharge. I wish my team would have done this more with me.
We cannot be certain of the reasons for the care unit disparity in setting and meeting DAs. We speculate that the level of staff enthusiasm for DAs explains the variation rather than patient population characteristics. Further, we cannot explain why 39% of the patients did not receive a DA. Physician feedback was generally, but not uniformly, positive. Negative comments that might explain DA omissions include: (1) patients already are informed and awarethe tool is superfluous; (2) the day of discharge is unknowable in advance; and (3) patients or family members will hold us to it or be upset if the DA is changed.
We expected that diagnostic uncertainty might pose challenges to providing DAs. When primary service providers were reassured that DAs could be amended, this concern was reduced (but not eliminated). It seemed useful for providers to envision the earliest day of discharge by assuming that the results of a pending key test or consultation would be favorable. Frequency of DA modification was not studied. DAs were amended, however, and patients (to our knowledge) seemed unperturbedperhaps because of an almost unavoidable discussion of the clinical rationale because the act of posting the DA occurred in full view of (and in partnership with) the patient.
A trend toward discharge earlier in the day was observed (data not shown). Theoretically, such a trend offers the potential to improve inpatient flow, in part by discharging patients before morning surgical cases are completed.
Although we had many favorable comments about DAs from patients, family members, and nurses, satisfaction of patients, families, and staff members deserves formal study. Further, it is not known whether unused DA boards might contribute to patient dissatisfaction. Any effect that the display of DAs may have on the length of stay also may be a topic worthy of future study.
CONCLUSIONS
Patients and their families sometimes desire more communication about the anticipated day and time of hospital discharge. We designed a process for making a tentative DA and a tool by which the DA could be posted at the bedside. The results of this study suggest that (1) despite some uncertainty it is possible to schedule and post DAs in‐room in various care units and in various settings, (2) DAs were made at least a day ahead of time in almost half the DA discharges, and (3) most DA discharges were characterized by on‐time departure. In addition, patient, family, and nursing satisfaction (in relation to the DA) warrants further investigation.
Acknowledgements
We acknowledge the valuable insights and collaboration of our colleagues Deborah R. Fischer, Steven L. Bahnemann, Matthew Skelton, MD, Lauri J. Dahl, Pamela O. Johnson, MSN, Debra A. Hernke, MSN, Susan L. Stirn, MSN, Barbara R. Spurrier, Ryan R. Armbruster, Todd J. Bille, and Donna K. Lawson of the Mayo Clinic and Mayo Foundation.
Dicharge of a patient from the hospital is a complicated, interprofessional endeavor.1, 2 Several institutions report that discharge is one of the least satisfying elements of the patient's hospital experience.35 Recent evidence suggests that a poorly planned or disorganized discharge may compromise patient safety in the period soon after dismissal.6 Several initiatives have been aimed at improving patient satisfaction and safety related to discharge.710
In 2000 the Mayo Clinic (Rochester, Minnesota) Department of Internal Medicine leadership established a goal to improve patient satisfaction with the hospital dismissal process. Patient focus group data suggested that uncertainty about the anticipated date and time of discharge causes frustration to some patients and families.
We hypothesized that an appointment to leave the hospital might be practicable. We joined an Institute for Healthcare Improvement collaborative (Improving Flow Through Acute Care Settings, 1 of 6 Improvement Action Network [IMPACT] Learning and Innovation Communities) aimed at scheduling discharge appointments (DAs). The collaborating members deemed that, although the ideal DA is set at least a day in advance, a same‐day DA is also desirable for both patient satisfaction and staff task organization in pursuit of a high‐quality discharge.
METHODS
This project was approved by the Mayo Foundation Institutional Review Board. We tested the following hypotheses:
It is possible to make and display DAs in various care units.
Most DAs can be scheduled a day before dismissal.
Most DA patients depart on time.
Setting
Mayo Clinic in Rochester, Minnesota, is a tertiary academic medical center with 2 hospitals (Saint Marys and Rochester Methodist) that house a total of 1951 licensed beds in 76 care units.
The preliminary study displaying DAs was carried out in the Innovation and Quality (IQ) Unit of Saint Marys Hospital, a 23‐bed general medical care unit that supports both resident and nonresident services. Traditionally, primary services usually consist of an attending physician and house officer physicians (junior and senior residents). Less commonly, primary services consist of an attending physician and either a nurse‐practitioner or a physician assistant.
The design pilot took place between August 2 and December 24, 2003. The subsequent, larger study of applicability took place across 8 care units (including the IQ Unit) between December 28, 2003, and April 25, 2004.
Preliminary Work: Design Pilot
We designed bedside dry‐erase wall displays and mounted them in the rooms in plain view of patients and their families and caregivers. Pilot testing of DA scheduling was done on a general medical care unit from August 2 to December 24, 2003. To optimize the process for scheduling a DA, our team developed 21 small tests to change the dismissal process through plan, do, study, and act cycles.11
The recommended process was that as soon as an organized discharge could be reasonably envisioned, the primary service provider would discuss with the patient, family, and primary nurse (and a social service worker, if involved) the anticipated discharge day. A member of the primary service was to handwrite (with a marker) the anticipated day on the specially designed bedside dry‐erase board (Fig. 1) in view of the patient. The same primary service prescribers could amend this anticipated day (or time) by repeating the process of consultation and discussion as needed. The time of the DA could be written on the DA board (or amended) by either a member of the primary service or the primary care nurse.
Each morning, the primary care nurse transmitted the DA board data to the admission, discharge, and transfer log kept at the unit secretary desk (in which the actual discharge time has always been routinely recorded by the unit secretary).
Adoption of DA Scheduling in Other Care Units
Several meetings were held with 7 other patient care unit leaders about adopting the protocol. These units, both medical and surgical, were selected according to 3 criteria: (1) prior participation in unit‐level continuous improvement work, (2) current or recent work in any aspect of the discharge process, and (3) a reputation for having innovative nursing leadership and staff.
Data Acquisition and Analysis
Data were collected daily from each participating unit's admission, discharge, and transfer log: both the actual time of departure and the DA, if one had been scheduled. For each DA patient, the DA time was compared with the actual departure time.
RESULTS
During the 4‐month study of discharges across 8 care units, 1256 of 2046 patients (61%) received a DA; 576 of the DAs (46%) were scheduled at least 1 day in advance (Table 1). Among patients with a DA, 752 were discharged on time (60%), and only 240 (19%) were tardy.
| Unit | DAs | Departure time of patients compared with DA | |||||
|---|---|---|---|---|---|---|---|
| No. | Type of unit | No. of patients | Patients with DAs, n (%) | DAs scheduled ϵ 1 day ahead, n (%) | On time, n (%)a | Early, n (%) | Late, n (%) |
| |||||||
| 1 | Neurology/neurosurgery | 525 | 270 (51) | 0 (0) | 175 (65) | 44 (16) | 51 (19) |
| 2 | Surgery (mixed) | 481 | 325 (68) | 289 (89) | 166 (51) | 101 (31) | 58 (18) |
| 3 | General internal medicine (IQ Unit) | 466 | 243 (52) | 35 (14) | 132 (54) | 50 (21) | 61 (25) |
| 4 | Neurology/neurosurgery | 267 | 189 (71) | 40 (21) | 119 (63) | 41 (22) | 29 (15) |
| 5 | Vascular surgery | 201 | 127 (63) | 127 (100) | 90 (71) | 12 (9) | 25 (20) |
| 6 | Psychiatry | 46 | 42 (91) | 42 (100) | 28 (67) | 9 (21) | 5 (12) |
| 7 | Orthopedic surgeryelective | 38 | 38 (100) | 22 (58) | 24 (63) | 3 (8) | 11 (29) |
| 8 | Orthopedic surgerytrauma | 22 | 22 (100) | 21 (95) | 18 (82) | 4 (18) | 0 (0) |
| Total | 2046 | 1256 (61) | 576 (46) | 752 (60) | 264 (21) | 240 (19) | |
DISCUSSION
In response to patient focus group feedback, we designed a tool and a process by which a DA could be made and posted at bedside. Among 2046 patients discharged from 8 care units over 4 months, 61% (1256) had a posted, in‐room DA. Almost half the patients with DAs (46%) had a DA scheduled at least 1 calendar day ahead. Remarkably, among patients with a DA, fewer than 20% were discharged tardily. In‐room posting of DAs across a spectrum of care units appears to be practicable, even in the face of extant diagnostic or therapeutic uncertainty.
This was an initial test‐of‐concept project and an exploratory trial. The limitations are: (1) satisfaction (patient, family, nurse, and physician) was not tested with any validated survey instrument, (2) length of stay was not studied, (3) reasons for variable DA success among care units were not ascertained, and (4) resource use was not measured.
Anecdotal information from a postdischarge phone survey indicated that patients seemed appreciative of a DA. The survey data were not included in this article because the survey tool was not a validated instrument and the interviewer (a coauthor) was not blinded to the hypothesis and was therefore subject to bias. No negative comments were received through informal real‐time feedback from patients and family during the making and posting of DAs, and encouraging comments were common.
Physician participation in posting the DA appeared to be key, and the unavoidable dialogue about the clinical rationale for a chosen date seemed welcome. A telling anecdote came from a patient who did not have a DA board: I didn't get the same treatment as my roommate with the [DA] board. The other doctors talked with [him] more about discharge. I wish my team would have done this more with me.
We cannot be certain of the reasons for the care unit disparity in setting and meeting DAs. We speculate that the level of staff enthusiasm for DAs explains the variation rather than patient population characteristics. Further, we cannot explain why 39% of the patients did not receive a DA. Physician feedback was generally, but not uniformly, positive. Negative comments that might explain DA omissions include: (1) patients already are informed and awarethe tool is superfluous; (2) the day of discharge is unknowable in advance; and (3) patients or family members will hold us to it or be upset if the DA is changed.
We expected that diagnostic uncertainty might pose challenges to providing DAs. When primary service providers were reassured that DAs could be amended, this concern was reduced (but not eliminated). It seemed useful for providers to envision the earliest day of discharge by assuming that the results of a pending key test or consultation would be favorable. Frequency of DA modification was not studied. DAs were amended, however, and patients (to our knowledge) seemed unperturbedperhaps because of an almost unavoidable discussion of the clinical rationale because the act of posting the DA occurred in full view of (and in partnership with) the patient.
A trend toward discharge earlier in the day was observed (data not shown). Theoretically, such a trend offers the potential to improve inpatient flow, in part by discharging patients before morning surgical cases are completed.
Although we had many favorable comments about DAs from patients, family members, and nurses, satisfaction of patients, families, and staff members deserves formal study. Further, it is not known whether unused DA boards might contribute to patient dissatisfaction. Any effect that the display of DAs may have on the length of stay also may be a topic worthy of future study.
CONCLUSIONS
Patients and their families sometimes desire more communication about the anticipated day and time of hospital discharge. We designed a process for making a tentative DA and a tool by which the DA could be posted at the bedside. The results of this study suggest that (1) despite some uncertainty it is possible to schedule and post DAs in‐room in various care units and in various settings, (2) DAs were made at least a day ahead of time in almost half the DA discharges, and (3) most DA discharges were characterized by on‐time departure. In addition, patient, family, and nursing satisfaction (in relation to the DA) warrants further investigation.
Acknowledgements
We acknowledge the valuable insights and collaboration of our colleagues Deborah R. Fischer, Steven L. Bahnemann, Matthew Skelton, MD, Lauri J. Dahl, Pamela O. Johnson, MSN, Debra A. Hernke, MSN, Susan L. Stirn, MSN, Barbara R. Spurrier, Ryan R. Armbruster, Todd J. Bille, and Donna K. Lawson of the Mayo Clinic and Mayo Foundation.
- ,,, et al.Learning from patients: a discharge planning improvement project.Jt Comm J Qual Improv.1996;22:311–22.
- ,,,,,, et al.Payer‐hospital collaboration to improve patient satisfaction with hospital discharge.Jt Comm J Qual Improv.1996;22:336–344.
- ,,,,,.How was your hospital stay? Patients' reports about their care in Canadian hospitals.CMAJ.1994;150:1813–1822.
- .A hospitalization from hell: a patient's perspective on quality.Ann Intern Med.2003;138:33–39.
- ,,.Predictors of elder and family caregiver satisfaction with discharge planning.J Cardiovasc Nurs.2000;14:76–87.
- ,,,,.The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138:161–167.
- ,,, et al.Patient callback program: a quality improvement, customer service, and marketing tool.J Health Care Mark.1993;13:60–65.
- ,,,.Effects of a medical team coordinator on length of hospital stay.CMAJ.1992;146:511–515.
- ,.Discharge planning from hospital to home.Cochrane Database Syst Rev.2000;4:CD000313.
- ,,,.Continuity of care and patient outcomes after hospital discharge.J Gen Intern Med.2004;19:624–631.
- Institute for Healthcare Improvement. Cambridge, UK: Institute for Healthcare Improvement. Available from: http://www.ihi.org/IHI/Topics/Improvement/ImprovementMethods/HowToImprove/testingchanges.htm. Accessed July 28,2006.
- ,,, et al.Learning from patients: a discharge planning improvement project.Jt Comm J Qual Improv.1996;22:311–22.
- ,,,,,, et al.Payer‐hospital collaboration to improve patient satisfaction with hospital discharge.Jt Comm J Qual Improv.1996;22:336–344.
- ,,,,,.How was your hospital stay? Patients' reports about their care in Canadian hospitals.CMAJ.1994;150:1813–1822.
- .A hospitalization from hell: a patient's perspective on quality.Ann Intern Med.2003;138:33–39.
- ,,.Predictors of elder and family caregiver satisfaction with discharge planning.J Cardiovasc Nurs.2000;14:76–87.
- ,,,,.The incidence and severity of adverse events affecting patients after discharge from the hospital.Ann Intern Med.2003;138:161–167.
- ,,, et al.Patient callback program: a quality improvement, customer service, and marketing tool.J Health Care Mark.1993;13:60–65.
- ,,,.Effects of a medical team coordinator on length of hospital stay.CMAJ.1992;146:511–515.
- ,.Discharge planning from hospital to home.Cochrane Database Syst Rev.2000;4:CD000313.
- ,,,.Continuity of care and patient outcomes after hospital discharge.J Gen Intern Med.2004;19:624–631.
- Institute for Healthcare Improvement. Cambridge, UK: Institute for Healthcare Improvement. Available from: http://www.ihi.org/IHI/Topics/Improvement/ImprovementMethods/HowToImprove/testingchanges.htm. Accessed July 28,2006.
Copyright © 2007 Society of Hospital Medicine
Medical Student Evaluation of Hospitalist and Nonhospitalist Faculty
In 1996 Wachter and Goldman anticipated the emergence of hospitalists,1 physicians who are responsible for the care of hospitalized patients in place of their primary care physicians. The number of physicians who identify themselves as hospitalists has grown rapidly since 1996 and is currently estimated to be 10,00012,000, with the potential to reach as high as 30,000 in the next decade.2 This growth includes academic medical centers. In surveys of chairs of internal medicine and pediatric departments, 50% have hospitalists employed at their institutions.3, 4
Hospitalists in academic institutions are playing an increasingly prominent role in the medical education of both residents and medical students. The implications of adopting a hospitalist model on medical education has been discussed.57 Despite such concerns as fragmented continuity of care; decreased exposure to primary care physicians, subspecialists and physician‐scientists; reduced autonomy; and fewer educational opportunities to observe the natural histories of illnesses because of improved efficiency,57 the overall impact of hospitalists on medical and resident education has generally been favorable.818 Internal medicine residents have rated the teaching skills of hospitalists comparable to traditional academic physicians,8, 9 and believe the addition of hospitalists has contributed to an improved educational experience.10, 11, 14 In addition, a survey of third‐year medical students at a single academic teaching hospital concluded that hospitalists were able to provide at least as positive an educational experience during their inpatient medicine rotations as highly rated nonhospitalist teaching faculty.13
The role of hospitalists as educators in pediatrics has been studied much less. Pediatric resident satisfaction has improved in institutions that have used a hospitalist model.1618 In another study, hospitalists were rated by pediatric residents as more effective teachers than nonhospitalists.15 Because we are unaware of any study that has evaluated hospitalists in the education of medical students during their inpatient pediatric rotation, the purpose of our study was to compare hospitalist and nonhospitalist faculty on the educational experience of third‐year medical students during the inpatient portion of their pediatric clerkships at a single university children's hospital.
METHODS
Study Design
We conducted a retrospective study using evaluations of third‐year medical students comparing hospitalist and nonhospitalist faculty during the inpatient portions of their pediatrics clerkships at a single academic children's hospital over a 15‐month period (July 1999September 2000).
Setting and Sample
We conducted our study at Penn State Children's Hospital (PSCH), a 120‐bed tertiary‐care facility within the 504‐bed Hershey Medical Center, the main teaching hospital affiliated with the Penn State College of Medicine, Hershey, Pennsylvania. The pediatric hospitalist program commenced on July 1, 1999, and during the 15‐month study period the hospitalist staff consisted of 2 physicians who attended a total of 8 months, whereas the nonhospitalist staff consisted of 4 academic general pediatricians and 4 academic pediatric subspecialists who attended the remaining 7 months.
The inpatient clinical responsibilities of both groups of physicians during each month were similar. Both groups of physicians conducted daily rounds with a team that included a senior resident (postgraduate year 3), 2 to 4 interns (postgraduate year 1), 1 acting intern (fourth‐year medical student), and 2 to 4 third‐year medical students. This team was responsible for all admissions to the general pediatrics service, which averages 100 admissions per month. Both the hospitalists and nonhospitalists had outpatient responsibilities during the time they served as inpatient attendings.
During the 15‐month study period, 131 students completed their third‐year pediatrics clerkships. Students at the Penn State College of Medicine may complete their pediatrics clerkship at PSCH or at one of several alternative sites. Because of variability in the structure of the rotation from site to site, it was considered valid only to analyze evaluations completed by students who rotated at PSCH. Sixty‐seven students rotated at PSCH during the study period. Students spent 3 weeks of the 6‐week rotation on the inpatient general pediatrics service. The remaining 3 weeks occurred in multiple outpatient pediatric practice settings and in the newborn nursery. During the 3 weeks the students spent on the inpatient service they did not have outpatient clinic responsibilities, so they did not interact with either the hospitalists or nonhospitalists in the outpatient setting. At the end of the rotation, students were asked to rate the effectiveness of the faculty as teachers, pediatricians, and student advocates and overall on a 4‐point scale (1 = inadequate; 2 = adequate; 3 = very good; 4 = excellent). Students were also asked to evaluate 7 components of the clerkship on the same 4‐point scale (Table 1). Finally, students were asked to provide additional written comments in an unstructured format.
| Evaluation item | Hospitalist mean score (32 evaluations) | Nonhospitalist mean score (35 evaluations) | P value | No. of evaluations rated adequate or inadequate (%)b | |
|---|---|---|---|---|---|
| Hospitalist | Nonhospitalist | ||||
| |||||
| Effectiveness as teacherc | 3.87 | 2.91 | < .001a | 1 (2.9) | 13 (40.6) |
| Effectiveness as pediatriciand | 3.94 | 3.25 | < .001a | 0 (0.0) | 5 (15.6) |
| Effectiveness as student advocatee | 3.76 | 2.97 | < .001a | 2 (5.7) | 13 (40.6) |
| Overall evaluation | 3.93 | 3.06 | < .001a | 0 (0.0) | 10 (31.3) |
| Ward rounds | 3.15 | 2.58 | < .006a | 5 (15.6) | 12 (37.5) |
| Morning report | 3.16 | 3.14 | 0.923 | ||
| Sick newborn | 2.79 | 2.60 | 0.518 | ||
| Well newborn | 2.89 | 3.13 | 0.211 | ||
| Outpatient department clinics | 2.96 | 3.06 | 0.425 | ||
| Private physician's office | 2.97 | 3.01 | 0.794 | ||
| Noon conference | 3.03 | 3.13 | 0.512 | ||
After reviewing the literature concerning faculty evaluation forms and their components, an evaluation form was created for students to indicate their reactions to clerkship components. All the medical students' faculty evaluations were anonymous, and the faculty was not able to review student evaluations prior to assigning grades. Students were required to turn in an evaluation at the end of their rotations. The study was limited to 15 months, as the format of the evaluation form was changed after September 2000 and the general pediatrics service was in the process of transitioning to an exclusively hospitalist‐run service, thereby limiting the number of nonhospitalists available as a comparison group. Demographic characteristics of the hospitalist and nonhospitalist faculty were collected from a faculty database. The study was approved by the Penn State Milton S. Hershey Medical Center's Institutional Review Board.
Statistics and Analysis
For all questions, a Wilcoxon rank sum test was used to evaluate whether the responses for nonhospitalists were different than those for hospitalists. Differences in response by group whose 2‐tailed P values were less than .05 were considered statistically significant. All analyses were performed using the SAS statistical software, version 8.2 (SAS Institute Inc., Cary, NC).
RESULTS
All 67 of the students who completed a pediatrics clerkship at PSCH returned evaluation forms, which were the data for further analysis. Thirty‐five students rotated with the hospitalist faculty, and 32 students rotated with the nonhospitalist faculty. There were no significant demographic differences between the hospitalist and nonhospitalist faculty in age, sex, academic rank, specialty, and years since completing training (Table 2). All the hospitalist faculty fulfilled the definition of a hospitalist,2 whereas none of the physicians in the nonhospitalist group did.
| Characteristic | Hospitalists (n = 2) | Nonhospitalists (n = 8) | P value |
|---|---|---|---|
| Age, mean (range) | 36.0 (3141) | 46.5 (3063) | 0.30 |
| Male/Female | 1/1 | 6/2 | 0.95 |
| Academic rank | |||
| Instructor | 0 | 1 | |
| Assistant professor | 2 | 3 | |
| Associate professor | 0 | 0 | 0.56 |
| Professor | 0 | 4 | |
| Specialty | |||
| General pediatrics | 1 | 4 | |
| Nephrology | 1 | 1 | |
| Genetics | 0 | 1 | 0.95 |
| Infectious ciseases | 0 | 1 | |
| Rheumatology | 0 | 1 | |
| Years since training, mean (range) | 4.0 (08) | 13.8 (030) | 0.43 |
The hospitalists were rated significantly higher than the nonhospitalist faculty in all 4 of the attending characteristics measured (Table 1): teaching effectiveness (3.87 vs. 2.91; P < .0001), effectiveness as a pediatrician (3.94 vs. 3.25; P < .001), student advocacy effectiveness (3.76 vs. 2.97; P < .0001), and overall evaluation (3.93 vs. 3.06; P < .001).
Analysis of specific aspects of the rotation showed the only feature that hospitalists were rated significantly higher on was quality of ward rounds (3.15 vs. 2.58, P < .006). There was no significant difference between the hospitalists and nonhospitalists on features that were not specifically part of the inpatient rotation, including various conferences, outpatient clinics, and newborn care (Table 1).
DISCUSSION
Our study demonstrates that pediatric hospitalists had a positive impact on the overall educational experience of third‐year medical students during the inpatient portions of their pediatrics clerkships. Hospitalists were rated more favorably than nonhospitalists as teachers, as pediatricians, as student advocates, and overall. Medical students also rated the value of ward rounds more favorably when hospitalists conducted them. In addition, higher percentages of nonhospitalists than hospitalists were rated as adequate or inadequate for the above items. When other aspects of the clerkship were analyzed, there were no statistically significant differences between the students who rotated with hospitalists and the students who rotated with nonhospitalists. This suggests that the higher scores for hospitalists were specifically related to their interactions with students, rather than with an overall more positive view of the rotation.
It has been suggested that forces promoting the use of hospitalists in adult medicine are even more persuasive in the pediatric population, as the difference in severity of illness between the inpatient and outpatient setting is greater, and the average pediatrician has less experience than the average internist in managing hospitalized patients.19 In a recent systematic review of the literature, Landrigan et al.20 reported that 6 of 7 studies demonstrated hospitalist systems had decreased hospital length of stay compared to systems in which a primary pediatrician served as the physician of record. This improved efficiency, if combined with the pressure to see more patients while trying to balance teaching and research demands, may have a negative impact on the quality of medical education.
Several factors may have contributed to the students' satisfaction with hospitalists. Studies have demonstrated that students rate clinical teachers more favorably with whom they have greater involvement.21 Hospitalists may be more likely to spend time on the inpatient wards given that is the primary site of their clinical activity. This increased presence may have contributed to more favorable evaluations for the hospitalist faculty, whereas the additional outpatient workload for nonhospitalist faculty may have reduced inpatient teaching opportunities, accounting for their lower teaching score. Included in the pediatrician category was the attribute of being a role model. In a study by Wright et al.,22 spending more than 25% of the time or 25 or more hours per week teaching and conducting rounds was independently associated with being considered an excellent role model. Again, the increased availability of the hospitalists on the inpatient wards may have led to more teaching opportunities, contributing to their higher score.
Our study had several limitations. First, it was a retrospective study conducted at a single institution with only 2 hospitalists. Although there were not statistical significant demographic differences between the 2 groups, this may simply reflect the small size of the sample in our study; therefore, the results may not be applicable to other academic institutions. Second, we retrospectively analyzed an evaluation form that had not been validated or specifically designed to compare 2 physician groups. Third, there were multiple statements in each category that students were asked to consider before scoring each attending on the parameters measured. Although hospitalists were rated higher in each category, there may have been individual characteristics within each category for which the nonhospitalist faculty performed better. Fourth, although hospitalists received higher average ratings than nonhospitalist faculty from third‐year medical students, it is important to emphasize this study measured students' attitudes and beliefs not specific educational outcomes. However, even though we cannot rule out the possibility that potentially confounding factors such as the personality of an attending physician influenced the results, prior studies have demonstrated that medical students make sophisticated judgments about teaching in the clinical setting.23, 24 It is unlikely that hospitalists at our institution were specifically selected to attend more months on a new inpatient service because they had a history of having more favorable teaching qualities because 1 of the 2 hospitalists had just finished residency training, and there were no significant demographic differences between the 2 groups. In a study examining trainee satisfaction in an internal medicine rotation 4 years after adoption of a hospitalist model, where nonhospitalist faculty attended based on their own interest and inpatient skill rather than as a requirement, Hauer et al.14 reported that trainees experienced more effective teaching and a more satisfying inpatient rotation when supervised by hospitalists. This suggests that hospitalists may possess or develop a specific inpatient knowledge base and teaching acumen over time that distinguishes them from nonhospitalists. There is evidence of accumulated experience leading to improved outcomes in the clinical setting for HIV infection,25 various surgical procedures,26 and hospitalist systems.27
In conclusion, this is the first study to evaluate the performance of hospitalists in the setting of a third‐year medical student pediatrics clerkship. Although third‐year medical students rate hospitalists at least as highly as nonhospitalist faculty, further studies are needed to reproduce this finding. In addition to the increased time spent on the wards with students and increased experience in caring for hospitalized patients, further studies should also examine the role that communication plays in clinical teaching. Also, the recent development of core competencies in hospital medicine28 may lead to the development of educational outcomes that can be objectively measured.
Acknowledgements
The authors thank David Mauger, PhD, from the Department of Health Evaluation Sciences at the Penn State College of Medicine for providing statistical analysis of the survey results.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- Society of Hospital Medicine. Frequently asked questions. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=FAQs75:S34–6.
- ,,,,,.Pediatric hospitalists in Canada and the United States: a survey of pediatric academic department chairs.Ambul Pediatr.2001;1:338–339.
- .The impact of hospitalists on medical education and the academic health system.Ann Intern Med.1999;130:364–367.
- ,.The role of hospitalists in medical education.Am J Med.1999;107:305–309.
- ,.Implications of the hospitalist model for medical students' education.Acad. Med.2001;76:324–330.
- ,,,,.Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education.JAMA.1998;279:1560–1565.
- ,,, et al.Hospitalists as teachers: how do they compare to subspecialty and general medicine faculty.J Gen Intern Med.2004;19:8–15.
- ,,,,.Assessing the value of hospitalists to academic health centers: Brigham and Women's Hospital and Harvard Medical School.Am J Med.1999;106:134–137.
- ,,,,,.Resident satisfaction on an academic hospitalist service: time to teach.Am J Med.2002;112:597–601.
- ,,,,,,.The positive impact of initiation of hospitalist clinician educators: resource utilization and medical resident education.J Gen Intern Med.2004;19:293–301.
- ,,,.Medical student evaluation of the quality of hospitalist and nonhospitalist teaching faculty on inpatient medicine rotations.Acad Med.2004;79:78–82.
- ,,,,.Effects of hospitalist attending physicians on trainee satisfaction with teaching and with internal medicine rotations.Arch Intern Med.2004;164:1866–1871.
- ,,,,,.Effect of a pediatric hospitalist system on housestaff education and experience.Arch Pediatr Adolesc Med.2002;156:877–883.
- .Employing hospitalists to improve residents' inpatient learning.Acad Med.2001;76:556.
- ,,.Establishing a pediatric hospitalist program at an academic medical center.Clin Pediatr.2000;39:221–227.
- ,,,,,.Restructuring an academic pediatric inpatient service using concepts developed by hospitalists.Clin Pediatr.2001;40:653–660.
- ,.The hospitalist movement and its implications for the care of hospitalized children.Pediatrics.1999;103:473–477.
- ,,,.Pediatric hospitalists: a systematic review of the literature.Pediatrics.2006;117:1736–1744.
- ,,.Factors affecting ratings of clinical teachers by medical students and residents.J Med Educ.1987;62:1–7.
- ,,,,.Attributes of excellent attending‐physician role models.N Engl J Med.1998;339:1986–1993.
- ,.Evaluation of clinical instructors by third‐year medical students.Acad Med.1989;64:159–164.
- ,,.Clinical tutor evaluation: a 5‐year study by students on an in‐patient service and residents in an ambulatory care clinic.Med Educ.1993;27:48–53.
- ,,,,,.Physicians' experience with the acquired immunodeficiency syndrome as a factor in patients' survival.N Engl J Med.1996;334:701–706.
- ,,,.Hospital Volume, Physician Volume, and Patient Outcomes: Assessing the Evidence. Ann Arbor, MI: Health Administration Perspectives;1990.
- ,,, et al.Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;137:866–874.
- ,,,,, eds.The core competencies in hospital medicine: a framework for curriculum development by the Society of Hospital Medicine.J Hosp Med.2006;1(S1):1–67.
In 1996 Wachter and Goldman anticipated the emergence of hospitalists,1 physicians who are responsible for the care of hospitalized patients in place of their primary care physicians. The number of physicians who identify themselves as hospitalists has grown rapidly since 1996 and is currently estimated to be 10,00012,000, with the potential to reach as high as 30,000 in the next decade.2 This growth includes academic medical centers. In surveys of chairs of internal medicine and pediatric departments, 50% have hospitalists employed at their institutions.3, 4
Hospitalists in academic institutions are playing an increasingly prominent role in the medical education of both residents and medical students. The implications of adopting a hospitalist model on medical education has been discussed.57 Despite such concerns as fragmented continuity of care; decreased exposure to primary care physicians, subspecialists and physician‐scientists; reduced autonomy; and fewer educational opportunities to observe the natural histories of illnesses because of improved efficiency,57 the overall impact of hospitalists on medical and resident education has generally been favorable.818 Internal medicine residents have rated the teaching skills of hospitalists comparable to traditional academic physicians,8, 9 and believe the addition of hospitalists has contributed to an improved educational experience.10, 11, 14 In addition, a survey of third‐year medical students at a single academic teaching hospital concluded that hospitalists were able to provide at least as positive an educational experience during their inpatient medicine rotations as highly rated nonhospitalist teaching faculty.13
The role of hospitalists as educators in pediatrics has been studied much less. Pediatric resident satisfaction has improved in institutions that have used a hospitalist model.1618 In another study, hospitalists were rated by pediatric residents as more effective teachers than nonhospitalists.15 Because we are unaware of any study that has evaluated hospitalists in the education of medical students during their inpatient pediatric rotation, the purpose of our study was to compare hospitalist and nonhospitalist faculty on the educational experience of third‐year medical students during the inpatient portion of their pediatric clerkships at a single university children's hospital.
METHODS
Study Design
We conducted a retrospective study using evaluations of third‐year medical students comparing hospitalist and nonhospitalist faculty during the inpatient portions of their pediatrics clerkships at a single academic children's hospital over a 15‐month period (July 1999September 2000).
Setting and Sample
We conducted our study at Penn State Children's Hospital (PSCH), a 120‐bed tertiary‐care facility within the 504‐bed Hershey Medical Center, the main teaching hospital affiliated with the Penn State College of Medicine, Hershey, Pennsylvania. The pediatric hospitalist program commenced on July 1, 1999, and during the 15‐month study period the hospitalist staff consisted of 2 physicians who attended a total of 8 months, whereas the nonhospitalist staff consisted of 4 academic general pediatricians and 4 academic pediatric subspecialists who attended the remaining 7 months.
The inpatient clinical responsibilities of both groups of physicians during each month were similar. Both groups of physicians conducted daily rounds with a team that included a senior resident (postgraduate year 3), 2 to 4 interns (postgraduate year 1), 1 acting intern (fourth‐year medical student), and 2 to 4 third‐year medical students. This team was responsible for all admissions to the general pediatrics service, which averages 100 admissions per month. Both the hospitalists and nonhospitalists had outpatient responsibilities during the time they served as inpatient attendings.
During the 15‐month study period, 131 students completed their third‐year pediatrics clerkships. Students at the Penn State College of Medicine may complete their pediatrics clerkship at PSCH or at one of several alternative sites. Because of variability in the structure of the rotation from site to site, it was considered valid only to analyze evaluations completed by students who rotated at PSCH. Sixty‐seven students rotated at PSCH during the study period. Students spent 3 weeks of the 6‐week rotation on the inpatient general pediatrics service. The remaining 3 weeks occurred in multiple outpatient pediatric practice settings and in the newborn nursery. During the 3 weeks the students spent on the inpatient service they did not have outpatient clinic responsibilities, so they did not interact with either the hospitalists or nonhospitalists in the outpatient setting. At the end of the rotation, students were asked to rate the effectiveness of the faculty as teachers, pediatricians, and student advocates and overall on a 4‐point scale (1 = inadequate; 2 = adequate; 3 = very good; 4 = excellent). Students were also asked to evaluate 7 components of the clerkship on the same 4‐point scale (Table 1). Finally, students were asked to provide additional written comments in an unstructured format.
| Evaluation item | Hospitalist mean score (32 evaluations) | Nonhospitalist mean score (35 evaluations) | P value | No. of evaluations rated adequate or inadequate (%)b | |
|---|---|---|---|---|---|
| Hospitalist | Nonhospitalist | ||||
| |||||
| Effectiveness as teacherc | 3.87 | 2.91 | < .001a | 1 (2.9) | 13 (40.6) |
| Effectiveness as pediatriciand | 3.94 | 3.25 | < .001a | 0 (0.0) | 5 (15.6) |
| Effectiveness as student advocatee | 3.76 | 2.97 | < .001a | 2 (5.7) | 13 (40.6) |
| Overall evaluation | 3.93 | 3.06 | < .001a | 0 (0.0) | 10 (31.3) |
| Ward rounds | 3.15 | 2.58 | < .006a | 5 (15.6) | 12 (37.5) |
| Morning report | 3.16 | 3.14 | 0.923 | ||
| Sick newborn | 2.79 | 2.60 | 0.518 | ||
| Well newborn | 2.89 | 3.13 | 0.211 | ||
| Outpatient department clinics | 2.96 | 3.06 | 0.425 | ||
| Private physician's office | 2.97 | 3.01 | 0.794 | ||
| Noon conference | 3.03 | 3.13 | 0.512 | ||
After reviewing the literature concerning faculty evaluation forms and their components, an evaluation form was created for students to indicate their reactions to clerkship components. All the medical students' faculty evaluations were anonymous, and the faculty was not able to review student evaluations prior to assigning grades. Students were required to turn in an evaluation at the end of their rotations. The study was limited to 15 months, as the format of the evaluation form was changed after September 2000 and the general pediatrics service was in the process of transitioning to an exclusively hospitalist‐run service, thereby limiting the number of nonhospitalists available as a comparison group. Demographic characteristics of the hospitalist and nonhospitalist faculty were collected from a faculty database. The study was approved by the Penn State Milton S. Hershey Medical Center's Institutional Review Board.
Statistics and Analysis
For all questions, a Wilcoxon rank sum test was used to evaluate whether the responses for nonhospitalists were different than those for hospitalists. Differences in response by group whose 2‐tailed P values were less than .05 were considered statistically significant. All analyses were performed using the SAS statistical software, version 8.2 (SAS Institute Inc., Cary, NC).
RESULTS
All 67 of the students who completed a pediatrics clerkship at PSCH returned evaluation forms, which were the data for further analysis. Thirty‐five students rotated with the hospitalist faculty, and 32 students rotated with the nonhospitalist faculty. There were no significant demographic differences between the hospitalist and nonhospitalist faculty in age, sex, academic rank, specialty, and years since completing training (Table 2). All the hospitalist faculty fulfilled the definition of a hospitalist,2 whereas none of the physicians in the nonhospitalist group did.
| Characteristic | Hospitalists (n = 2) | Nonhospitalists (n = 8) | P value |
|---|---|---|---|
| Age, mean (range) | 36.0 (3141) | 46.5 (3063) | 0.30 |
| Male/Female | 1/1 | 6/2 | 0.95 |
| Academic rank | |||
| Instructor | 0 | 1 | |
| Assistant professor | 2 | 3 | |
| Associate professor | 0 | 0 | 0.56 |
| Professor | 0 | 4 | |
| Specialty | |||
| General pediatrics | 1 | 4 | |
| Nephrology | 1 | 1 | |
| Genetics | 0 | 1 | 0.95 |
| Infectious ciseases | 0 | 1 | |
| Rheumatology | 0 | 1 | |
| Years since training, mean (range) | 4.0 (08) | 13.8 (030) | 0.43 |
The hospitalists were rated significantly higher than the nonhospitalist faculty in all 4 of the attending characteristics measured (Table 1): teaching effectiveness (3.87 vs. 2.91; P < .0001), effectiveness as a pediatrician (3.94 vs. 3.25; P < .001), student advocacy effectiveness (3.76 vs. 2.97; P < .0001), and overall evaluation (3.93 vs. 3.06; P < .001).
Analysis of specific aspects of the rotation showed the only feature that hospitalists were rated significantly higher on was quality of ward rounds (3.15 vs. 2.58, P < .006). There was no significant difference between the hospitalists and nonhospitalists on features that were not specifically part of the inpatient rotation, including various conferences, outpatient clinics, and newborn care (Table 1).
DISCUSSION
Our study demonstrates that pediatric hospitalists had a positive impact on the overall educational experience of third‐year medical students during the inpatient portions of their pediatrics clerkships. Hospitalists were rated more favorably than nonhospitalists as teachers, as pediatricians, as student advocates, and overall. Medical students also rated the value of ward rounds more favorably when hospitalists conducted them. In addition, higher percentages of nonhospitalists than hospitalists were rated as adequate or inadequate for the above items. When other aspects of the clerkship were analyzed, there were no statistically significant differences between the students who rotated with hospitalists and the students who rotated with nonhospitalists. This suggests that the higher scores for hospitalists were specifically related to their interactions with students, rather than with an overall more positive view of the rotation.
It has been suggested that forces promoting the use of hospitalists in adult medicine are even more persuasive in the pediatric population, as the difference in severity of illness between the inpatient and outpatient setting is greater, and the average pediatrician has less experience than the average internist in managing hospitalized patients.19 In a recent systematic review of the literature, Landrigan et al.20 reported that 6 of 7 studies demonstrated hospitalist systems had decreased hospital length of stay compared to systems in which a primary pediatrician served as the physician of record. This improved efficiency, if combined with the pressure to see more patients while trying to balance teaching and research demands, may have a negative impact on the quality of medical education.
Several factors may have contributed to the students' satisfaction with hospitalists. Studies have demonstrated that students rate clinical teachers more favorably with whom they have greater involvement.21 Hospitalists may be more likely to spend time on the inpatient wards given that is the primary site of their clinical activity. This increased presence may have contributed to more favorable evaluations for the hospitalist faculty, whereas the additional outpatient workload for nonhospitalist faculty may have reduced inpatient teaching opportunities, accounting for their lower teaching score. Included in the pediatrician category was the attribute of being a role model. In a study by Wright et al.,22 spending more than 25% of the time or 25 or more hours per week teaching and conducting rounds was independently associated with being considered an excellent role model. Again, the increased availability of the hospitalists on the inpatient wards may have led to more teaching opportunities, contributing to their higher score.
Our study had several limitations. First, it was a retrospective study conducted at a single institution with only 2 hospitalists. Although there were not statistical significant demographic differences between the 2 groups, this may simply reflect the small size of the sample in our study; therefore, the results may not be applicable to other academic institutions. Second, we retrospectively analyzed an evaluation form that had not been validated or specifically designed to compare 2 physician groups. Third, there were multiple statements in each category that students were asked to consider before scoring each attending on the parameters measured. Although hospitalists were rated higher in each category, there may have been individual characteristics within each category for which the nonhospitalist faculty performed better. Fourth, although hospitalists received higher average ratings than nonhospitalist faculty from third‐year medical students, it is important to emphasize this study measured students' attitudes and beliefs not specific educational outcomes. However, even though we cannot rule out the possibility that potentially confounding factors such as the personality of an attending physician influenced the results, prior studies have demonstrated that medical students make sophisticated judgments about teaching in the clinical setting.23, 24 It is unlikely that hospitalists at our institution were specifically selected to attend more months on a new inpatient service because they had a history of having more favorable teaching qualities because 1 of the 2 hospitalists had just finished residency training, and there were no significant demographic differences between the 2 groups. In a study examining trainee satisfaction in an internal medicine rotation 4 years after adoption of a hospitalist model, where nonhospitalist faculty attended based on their own interest and inpatient skill rather than as a requirement, Hauer et al.14 reported that trainees experienced more effective teaching and a more satisfying inpatient rotation when supervised by hospitalists. This suggests that hospitalists may possess or develop a specific inpatient knowledge base and teaching acumen over time that distinguishes them from nonhospitalists. There is evidence of accumulated experience leading to improved outcomes in the clinical setting for HIV infection,25 various surgical procedures,26 and hospitalist systems.27
In conclusion, this is the first study to evaluate the performance of hospitalists in the setting of a third‐year medical student pediatrics clerkship. Although third‐year medical students rate hospitalists at least as highly as nonhospitalist faculty, further studies are needed to reproduce this finding. In addition to the increased time spent on the wards with students and increased experience in caring for hospitalized patients, further studies should also examine the role that communication plays in clinical teaching. Also, the recent development of core competencies in hospital medicine28 may lead to the development of educational outcomes that can be objectively measured.
Acknowledgements
The authors thank David Mauger, PhD, from the Department of Health Evaluation Sciences at the Penn State College of Medicine for providing statistical analysis of the survey results.
In 1996 Wachter and Goldman anticipated the emergence of hospitalists,1 physicians who are responsible for the care of hospitalized patients in place of their primary care physicians. The number of physicians who identify themselves as hospitalists has grown rapidly since 1996 and is currently estimated to be 10,00012,000, with the potential to reach as high as 30,000 in the next decade.2 This growth includes academic medical centers. In surveys of chairs of internal medicine and pediatric departments, 50% have hospitalists employed at their institutions.3, 4
Hospitalists in academic institutions are playing an increasingly prominent role in the medical education of both residents and medical students. The implications of adopting a hospitalist model on medical education has been discussed.57 Despite such concerns as fragmented continuity of care; decreased exposure to primary care physicians, subspecialists and physician‐scientists; reduced autonomy; and fewer educational opportunities to observe the natural histories of illnesses because of improved efficiency,57 the overall impact of hospitalists on medical and resident education has generally been favorable.818 Internal medicine residents have rated the teaching skills of hospitalists comparable to traditional academic physicians,8, 9 and believe the addition of hospitalists has contributed to an improved educational experience.10, 11, 14 In addition, a survey of third‐year medical students at a single academic teaching hospital concluded that hospitalists were able to provide at least as positive an educational experience during their inpatient medicine rotations as highly rated nonhospitalist teaching faculty.13
The role of hospitalists as educators in pediatrics has been studied much less. Pediatric resident satisfaction has improved in institutions that have used a hospitalist model.1618 In another study, hospitalists were rated by pediatric residents as more effective teachers than nonhospitalists.15 Because we are unaware of any study that has evaluated hospitalists in the education of medical students during their inpatient pediatric rotation, the purpose of our study was to compare hospitalist and nonhospitalist faculty on the educational experience of third‐year medical students during the inpatient portion of their pediatric clerkships at a single university children's hospital.
METHODS
Study Design
We conducted a retrospective study using evaluations of third‐year medical students comparing hospitalist and nonhospitalist faculty during the inpatient portions of their pediatrics clerkships at a single academic children's hospital over a 15‐month period (July 1999September 2000).
Setting and Sample
We conducted our study at Penn State Children's Hospital (PSCH), a 120‐bed tertiary‐care facility within the 504‐bed Hershey Medical Center, the main teaching hospital affiliated with the Penn State College of Medicine, Hershey, Pennsylvania. The pediatric hospitalist program commenced on July 1, 1999, and during the 15‐month study period the hospitalist staff consisted of 2 physicians who attended a total of 8 months, whereas the nonhospitalist staff consisted of 4 academic general pediatricians and 4 academic pediatric subspecialists who attended the remaining 7 months.
The inpatient clinical responsibilities of both groups of physicians during each month were similar. Both groups of physicians conducted daily rounds with a team that included a senior resident (postgraduate year 3), 2 to 4 interns (postgraduate year 1), 1 acting intern (fourth‐year medical student), and 2 to 4 third‐year medical students. This team was responsible for all admissions to the general pediatrics service, which averages 100 admissions per month. Both the hospitalists and nonhospitalists had outpatient responsibilities during the time they served as inpatient attendings.
During the 15‐month study period, 131 students completed their third‐year pediatrics clerkships. Students at the Penn State College of Medicine may complete their pediatrics clerkship at PSCH or at one of several alternative sites. Because of variability in the structure of the rotation from site to site, it was considered valid only to analyze evaluations completed by students who rotated at PSCH. Sixty‐seven students rotated at PSCH during the study period. Students spent 3 weeks of the 6‐week rotation on the inpatient general pediatrics service. The remaining 3 weeks occurred in multiple outpatient pediatric practice settings and in the newborn nursery. During the 3 weeks the students spent on the inpatient service they did not have outpatient clinic responsibilities, so they did not interact with either the hospitalists or nonhospitalists in the outpatient setting. At the end of the rotation, students were asked to rate the effectiveness of the faculty as teachers, pediatricians, and student advocates and overall on a 4‐point scale (1 = inadequate; 2 = adequate; 3 = very good; 4 = excellent). Students were also asked to evaluate 7 components of the clerkship on the same 4‐point scale (Table 1). Finally, students were asked to provide additional written comments in an unstructured format.
| Evaluation item | Hospitalist mean score (32 evaluations) | Nonhospitalist mean score (35 evaluations) | P value | No. of evaluations rated adequate or inadequate (%)b | |
|---|---|---|---|---|---|
| Hospitalist | Nonhospitalist | ||||
| |||||
| Effectiveness as teacherc | 3.87 | 2.91 | < .001a | 1 (2.9) | 13 (40.6) |
| Effectiveness as pediatriciand | 3.94 | 3.25 | < .001a | 0 (0.0) | 5 (15.6) |
| Effectiveness as student advocatee | 3.76 | 2.97 | < .001a | 2 (5.7) | 13 (40.6) |
| Overall evaluation | 3.93 | 3.06 | < .001a | 0 (0.0) | 10 (31.3) |
| Ward rounds | 3.15 | 2.58 | < .006a | 5 (15.6) | 12 (37.5) |
| Morning report | 3.16 | 3.14 | 0.923 | ||
| Sick newborn | 2.79 | 2.60 | 0.518 | ||
| Well newborn | 2.89 | 3.13 | 0.211 | ||
| Outpatient department clinics | 2.96 | 3.06 | 0.425 | ||
| Private physician's office | 2.97 | 3.01 | 0.794 | ||
| Noon conference | 3.03 | 3.13 | 0.512 | ||
After reviewing the literature concerning faculty evaluation forms and their components, an evaluation form was created for students to indicate their reactions to clerkship components. All the medical students' faculty evaluations were anonymous, and the faculty was not able to review student evaluations prior to assigning grades. Students were required to turn in an evaluation at the end of their rotations. The study was limited to 15 months, as the format of the evaluation form was changed after September 2000 and the general pediatrics service was in the process of transitioning to an exclusively hospitalist‐run service, thereby limiting the number of nonhospitalists available as a comparison group. Demographic characteristics of the hospitalist and nonhospitalist faculty were collected from a faculty database. The study was approved by the Penn State Milton S. Hershey Medical Center's Institutional Review Board.
Statistics and Analysis
For all questions, a Wilcoxon rank sum test was used to evaluate whether the responses for nonhospitalists were different than those for hospitalists. Differences in response by group whose 2‐tailed P values were less than .05 were considered statistically significant. All analyses were performed using the SAS statistical software, version 8.2 (SAS Institute Inc., Cary, NC).
RESULTS
All 67 of the students who completed a pediatrics clerkship at PSCH returned evaluation forms, which were the data for further analysis. Thirty‐five students rotated with the hospitalist faculty, and 32 students rotated with the nonhospitalist faculty. There were no significant demographic differences between the hospitalist and nonhospitalist faculty in age, sex, academic rank, specialty, and years since completing training (Table 2). All the hospitalist faculty fulfilled the definition of a hospitalist,2 whereas none of the physicians in the nonhospitalist group did.
| Characteristic | Hospitalists (n = 2) | Nonhospitalists (n = 8) | P value |
|---|---|---|---|
| Age, mean (range) | 36.0 (3141) | 46.5 (3063) | 0.30 |
| Male/Female | 1/1 | 6/2 | 0.95 |
| Academic rank | |||
| Instructor | 0 | 1 | |
| Assistant professor | 2 | 3 | |
| Associate professor | 0 | 0 | 0.56 |
| Professor | 0 | 4 | |
| Specialty | |||
| General pediatrics | 1 | 4 | |
| Nephrology | 1 | 1 | |
| Genetics | 0 | 1 | 0.95 |
| Infectious ciseases | 0 | 1 | |
| Rheumatology | 0 | 1 | |
| Years since training, mean (range) | 4.0 (08) | 13.8 (030) | 0.43 |
The hospitalists were rated significantly higher than the nonhospitalist faculty in all 4 of the attending characteristics measured (Table 1): teaching effectiveness (3.87 vs. 2.91; P < .0001), effectiveness as a pediatrician (3.94 vs. 3.25; P < .001), student advocacy effectiveness (3.76 vs. 2.97; P < .0001), and overall evaluation (3.93 vs. 3.06; P < .001).
Analysis of specific aspects of the rotation showed the only feature that hospitalists were rated significantly higher on was quality of ward rounds (3.15 vs. 2.58, P < .006). There was no significant difference between the hospitalists and nonhospitalists on features that were not specifically part of the inpatient rotation, including various conferences, outpatient clinics, and newborn care (Table 1).
DISCUSSION
Our study demonstrates that pediatric hospitalists had a positive impact on the overall educational experience of third‐year medical students during the inpatient portions of their pediatrics clerkships. Hospitalists were rated more favorably than nonhospitalists as teachers, as pediatricians, as student advocates, and overall. Medical students also rated the value of ward rounds more favorably when hospitalists conducted them. In addition, higher percentages of nonhospitalists than hospitalists were rated as adequate or inadequate for the above items. When other aspects of the clerkship were analyzed, there were no statistically significant differences between the students who rotated with hospitalists and the students who rotated with nonhospitalists. This suggests that the higher scores for hospitalists were specifically related to their interactions with students, rather than with an overall more positive view of the rotation.
It has been suggested that forces promoting the use of hospitalists in adult medicine are even more persuasive in the pediatric population, as the difference in severity of illness between the inpatient and outpatient setting is greater, and the average pediatrician has less experience than the average internist in managing hospitalized patients.19 In a recent systematic review of the literature, Landrigan et al.20 reported that 6 of 7 studies demonstrated hospitalist systems had decreased hospital length of stay compared to systems in which a primary pediatrician served as the physician of record. This improved efficiency, if combined with the pressure to see more patients while trying to balance teaching and research demands, may have a negative impact on the quality of medical education.
Several factors may have contributed to the students' satisfaction with hospitalists. Studies have demonstrated that students rate clinical teachers more favorably with whom they have greater involvement.21 Hospitalists may be more likely to spend time on the inpatient wards given that is the primary site of their clinical activity. This increased presence may have contributed to more favorable evaluations for the hospitalist faculty, whereas the additional outpatient workload for nonhospitalist faculty may have reduced inpatient teaching opportunities, accounting for their lower teaching score. Included in the pediatrician category was the attribute of being a role model. In a study by Wright et al.,22 spending more than 25% of the time or 25 or more hours per week teaching and conducting rounds was independently associated with being considered an excellent role model. Again, the increased availability of the hospitalists on the inpatient wards may have led to more teaching opportunities, contributing to their higher score.
Our study had several limitations. First, it was a retrospective study conducted at a single institution with only 2 hospitalists. Although there were not statistical significant demographic differences between the 2 groups, this may simply reflect the small size of the sample in our study; therefore, the results may not be applicable to other academic institutions. Second, we retrospectively analyzed an evaluation form that had not been validated or specifically designed to compare 2 physician groups. Third, there were multiple statements in each category that students were asked to consider before scoring each attending on the parameters measured. Although hospitalists were rated higher in each category, there may have been individual characteristics within each category for which the nonhospitalist faculty performed better. Fourth, although hospitalists received higher average ratings than nonhospitalist faculty from third‐year medical students, it is important to emphasize this study measured students' attitudes and beliefs not specific educational outcomes. However, even though we cannot rule out the possibility that potentially confounding factors such as the personality of an attending physician influenced the results, prior studies have demonstrated that medical students make sophisticated judgments about teaching in the clinical setting.23, 24 It is unlikely that hospitalists at our institution were specifically selected to attend more months on a new inpatient service because they had a history of having more favorable teaching qualities because 1 of the 2 hospitalists had just finished residency training, and there were no significant demographic differences between the 2 groups. In a study examining trainee satisfaction in an internal medicine rotation 4 years after adoption of a hospitalist model, where nonhospitalist faculty attended based on their own interest and inpatient skill rather than as a requirement, Hauer et al.14 reported that trainees experienced more effective teaching and a more satisfying inpatient rotation when supervised by hospitalists. This suggests that hospitalists may possess or develop a specific inpatient knowledge base and teaching acumen over time that distinguishes them from nonhospitalists. There is evidence of accumulated experience leading to improved outcomes in the clinical setting for HIV infection,25 various surgical procedures,26 and hospitalist systems.27
In conclusion, this is the first study to evaluate the performance of hospitalists in the setting of a third‐year medical student pediatrics clerkship. Although third‐year medical students rate hospitalists at least as highly as nonhospitalist faculty, further studies are needed to reproduce this finding. In addition to the increased time spent on the wards with students and increased experience in caring for hospitalized patients, further studies should also examine the role that communication plays in clinical teaching. Also, the recent development of core competencies in hospital medicine28 may lead to the development of educational outcomes that can be objectively measured.
Acknowledgements
The authors thank David Mauger, PhD, from the Department of Health Evaluation Sciences at the Penn State College of Medicine for providing statistical analysis of the survey results.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- Society of Hospital Medicine. Frequently asked questions. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=FAQs75:S34–6.
- ,,,,,.Pediatric hospitalists in Canada and the United States: a survey of pediatric academic department chairs.Ambul Pediatr.2001;1:338–339.
- .The impact of hospitalists on medical education and the academic health system.Ann Intern Med.1999;130:364–367.
- ,.The role of hospitalists in medical education.Am J Med.1999;107:305–309.
- ,.Implications of the hospitalist model for medical students' education.Acad. Med.2001;76:324–330.
- ,,,,.Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education.JAMA.1998;279:1560–1565.
- ,,, et al.Hospitalists as teachers: how do they compare to subspecialty and general medicine faculty.J Gen Intern Med.2004;19:8–15.
- ,,,,.Assessing the value of hospitalists to academic health centers: Brigham and Women's Hospital and Harvard Medical School.Am J Med.1999;106:134–137.
- ,,,,,.Resident satisfaction on an academic hospitalist service: time to teach.Am J Med.2002;112:597–601.
- ,,,,,,.The positive impact of initiation of hospitalist clinician educators: resource utilization and medical resident education.J Gen Intern Med.2004;19:293–301.
- ,,,.Medical student evaluation of the quality of hospitalist and nonhospitalist teaching faculty on inpatient medicine rotations.Acad Med.2004;79:78–82.
- ,,,,.Effects of hospitalist attending physicians on trainee satisfaction with teaching and with internal medicine rotations.Arch Intern Med.2004;164:1866–1871.
- ,,,,,.Effect of a pediatric hospitalist system on housestaff education and experience.Arch Pediatr Adolesc Med.2002;156:877–883.
- .Employing hospitalists to improve residents' inpatient learning.Acad Med.2001;76:556.
- ,,.Establishing a pediatric hospitalist program at an academic medical center.Clin Pediatr.2000;39:221–227.
- ,,,,,.Restructuring an academic pediatric inpatient service using concepts developed by hospitalists.Clin Pediatr.2001;40:653–660.
- ,.The hospitalist movement and its implications for the care of hospitalized children.Pediatrics.1999;103:473–477.
- ,,,.Pediatric hospitalists: a systematic review of the literature.Pediatrics.2006;117:1736–1744.
- ,,.Factors affecting ratings of clinical teachers by medical students and residents.J Med Educ.1987;62:1–7.
- ,,,,.Attributes of excellent attending‐physician role models.N Engl J Med.1998;339:1986–1993.
- ,.Evaluation of clinical instructors by third‐year medical students.Acad Med.1989;64:159–164.
- ,,.Clinical tutor evaluation: a 5‐year study by students on an in‐patient service and residents in an ambulatory care clinic.Med Educ.1993;27:48–53.
- ,,,,,.Physicians' experience with the acquired immunodeficiency syndrome as a factor in patients' survival.N Engl J Med.1996;334:701–706.
- ,,,.Hospital Volume, Physician Volume, and Patient Outcomes: Assessing the Evidence. Ann Arbor, MI: Health Administration Perspectives;1990.
- ,,, et al.Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;137:866–874.
- ,,,,, eds.The core competencies in hospital medicine: a framework for curriculum development by the Society of Hospital Medicine.J Hosp Med.2006;1(S1):1–67.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- Society of Hospital Medicine. Frequently asked questions. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=FAQs75:S34–6.
- ,,,,,.Pediatric hospitalists in Canada and the United States: a survey of pediatric academic department chairs.Ambul Pediatr.2001;1:338–339.
- .The impact of hospitalists on medical education and the academic health system.Ann Intern Med.1999;130:364–367.
- ,.The role of hospitalists in medical education.Am J Med.1999;107:305–309.
- ,.Implications of the hospitalist model for medical students' education.Acad. Med.2001;76:324–330.
- ,,,,.Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education.JAMA.1998;279:1560–1565.
- ,,, et al.Hospitalists as teachers: how do they compare to subspecialty and general medicine faculty.J Gen Intern Med.2004;19:8–15.
- ,,,,.Assessing the value of hospitalists to academic health centers: Brigham and Women's Hospital and Harvard Medical School.Am J Med.1999;106:134–137.
- ,,,,,.Resident satisfaction on an academic hospitalist service: time to teach.Am J Med.2002;112:597–601.
- ,,,,,,.The positive impact of initiation of hospitalist clinician educators: resource utilization and medical resident education.J Gen Intern Med.2004;19:293–301.
- ,,,.Medical student evaluation of the quality of hospitalist and nonhospitalist teaching faculty on inpatient medicine rotations.Acad Med.2004;79:78–82.
- ,,,,.Effects of hospitalist attending physicians on trainee satisfaction with teaching and with internal medicine rotations.Arch Intern Med.2004;164:1866–1871.
- ,,,,,.Effect of a pediatric hospitalist system on housestaff education and experience.Arch Pediatr Adolesc Med.2002;156:877–883.
- .Employing hospitalists to improve residents' inpatient learning.Acad Med.2001;76:556.
- ,,.Establishing a pediatric hospitalist program at an academic medical center.Clin Pediatr.2000;39:221–227.
- ,,,,,.Restructuring an academic pediatric inpatient service using concepts developed by hospitalists.Clin Pediatr.2001;40:653–660.
- ,.The hospitalist movement and its implications for the care of hospitalized children.Pediatrics.1999;103:473–477.
- ,,,.Pediatric hospitalists: a systematic review of the literature.Pediatrics.2006;117:1736–1744.
- ,,.Factors affecting ratings of clinical teachers by medical students and residents.J Med Educ.1987;62:1–7.
- ,,,,.Attributes of excellent attending‐physician role models.N Engl J Med.1998;339:1986–1993.
- ,.Evaluation of clinical instructors by third‐year medical students.Acad Med.1989;64:159–164.
- ,,.Clinical tutor evaluation: a 5‐year study by students on an in‐patient service and residents in an ambulatory care clinic.Med Educ.1993;27:48–53.
- ,,,,,.Physicians' experience with the acquired immunodeficiency syndrome as a factor in patients' survival.N Engl J Med.1996;334:701–706.
- ,,,.Hospital Volume, Physician Volume, and Patient Outcomes: Assessing the Evidence. Ann Arbor, MI: Health Administration Perspectives;1990.
- ,,, et al.Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;137:866–874.
- ,,,,, eds.The core competencies in hospital medicine: a framework for curriculum development by the Society of Hospital Medicine.J Hosp Med.2006;1(S1):1–67.
Copyright © 2007 Society of Hospital Medicine
A new home awaits the hospitalist
In this issue of the Journal of Hospital Medicine, Simon et al.1 provide the first report of pediatric hospitalist comanagement of patients undergoing spinal fusion surgery. In this retrospective cohort study, 14 of 115 patients were comanaged by a pediatric hospitalist. The primary outcomes of the study were length of stay and variability in length of stay. Prior to the initiation of hospitalist comanagement service, all patients were managed preoperatively by a spine surgery nurse and aided by medical subspecialists and other allied health professionals (nutritionists, respiratory therapists, physical therapists, social workers). After the intervention, patients with the most complex medical disease were assigned to comanagement by a pediatric hospitalist. When compared to a historical control of patients with similar medical complexity but not comanaged by hospitalists, the length of stay was reduced by 2.4 days (8.6 vs. 6.2 days). The variability in mean length of stay was also reduced.
This study follows on the heels of 3 important studies addressing the utility of hospitalists in the comanagement of surgical patients. The HOT (Hospitalist Orthopedic Team) trial was a randomized controlled trial assessing the effect of hospitalists on the management of patients undergoing elective hip and knee arthroplasty.2 There was no effect on length of stay or patient outcomes, though the comanagement model did decrease minor postoperative medical complications and improve physician and nurse satisfaction. Macpherson et al. conducted a retrospective trial where an internist joined a cardiothoracic surgery service at a tertiary‐care center.3 They found a decrease in overall mortality and resource utilization such as labs testing and consultations. There was significant reduction in the length of stay and number of x‐rays performed. The third study, by Jaffer et al.,4 showed that an outpatient, preoperative evaluation clinic staffed by hospitalists at a large tertiary‐care center provides a practical model for managing preoperative patients and may be associated with a low rate of postoperative pulmonary complications.
The study by Simon et al. in this issue of the journal has limitations. It is a retrospective cohort trial, and like all such study designs, the validity of the results is subject to confounding. Severity of patient medical disease, intraoperative complications, and advances in surgical technique are examples. While the authors did everything possible to minimize the effect of confounding, it remains a limitation of the study. The study also enrolled only 14 patients in the comanagement group, and this limited any stratification or subgroup analysis to offset known confounders. Patients assigned to the hospitalist comanagement service were by design more medically complex than other spinal fusion patients, and generalizing the results of this trial to all spinal fusion patients may not be possible.
From the study's limitations, however, comes great insight into the role of the hospitalist in surgical comanagement. It is clear from the aforementioned studies that there is a role for the hospitalist in comanagement of surgical patients. While the evidence is conflicting, there are scenarios in which comanagement improves efficiency and quality of care. Yet it is also possible that hospitalist comanagement is not ideal for all surgical patients. The HOT trial did not show benefits in length‐of‐stay reduction or patient mortality because the patients were homogenous in their complexity and pre‐ and postoperative care was protocol driven. Length of stay was limited by accessibility of rehabilitation facilities after discharge and not the efficiency of medical care in the hospital. The study in this issue of the Journal of Hospital Medicine selectively included patients with the highest complexity of medical disease, and there was a reduction in length of stay. Both trials suggest that the greatest potential benefit for augmenting efficiency and outcomes with hospitalist comanagement may be predicated on the complexity of the patients involved and the surgical system through which they will receive care.
The next step in assessing hospitalist comanagement should not be a hunt‐and‐peck exercise to stumble on the surgical procedures that show benefit from comanagement. Rather, the prudent next step is to follow the lead of Simon et al. and others3, 4 in trying to identify those surgical patients who represent the greatest medical complexity or have the most variability in their preoperative and postoperative medical care. These are the patients for whom the hospitalist can effect the greatest benefit and the services for which the hospitalist can best augment efficiency. High‐risk procedures, patients with multiple comorbitities or elevated preoperative risks, and surgical procedures without defined pre‐ and postoperative protocols would appear to be the ideal candidates for hospitalist comanagement.
As the discussion of hospital comanagement progresses, it is important to recognize comanagement as a paradigm shift. Surgical comanagement is not merely medical consultation. To be successful, the role of the hospitalist in comanaging surgical patients must be clearly defined as advancing postoperative care as much as it is in assessing preoperative risk. As a comanager, a hospitalist must actively manage preexisting and newly developed medical issues rather than just make recommendations for the surgical team.
The hospitalist must also be more than a discharge coordinator postoperatively; investing in hospitalists merely for discharge planning is a poor use of resources both from a financial and an opportunity‐cost perspective. The paradigm of comanagement is not foreign, however, and hospitalists are likely to prosper by learning from the experience of our nephrology and hepatology colleagues, who have successfully found collaborative roles in improving patient care on renal and liver transplant services. The success of these services is due to the precisely defined roles for the internist and the surgeon and because the complexity of the patient being managed warrants continuity of expert consultation.
There is great potential for the hospitalist in surgical comanagement. In less than a decade, the focus of hospital‐based medical care has shifted from staffing a shift to improving the quality of the system through which patients traverse the hospital. The lessons hospitalists have learned in quality improvement and in augmenting systems of care are perfectly suited for application to surgical services. Hospitalist comanagement is right not only because it may offer improvement in a surgical patient's medical care, but also for the augmentation of quality improvement in surgical services that have yet to reap the benefits that have defined the excellence of hospitalist medicine. The next step is to embark on the road of prudent prospective research: identifying the patients, and the procedures, that have the greatest opportunity for improvement by hospitalist comanagement. And at the end of that road will be a new home for the hospitalist, assuming the role of the quality‐advocate for all aspects of hospital care: pediatric, medical, and surgical patients.
- ,,,,.Pediatric co‐management of spine fusion surgery patients.J Hosp Med.2007;2:23–30.
- ,,, et al.;Hospitalist‐Orthopedic Team Trial Investigators.Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial.Ann Intern Med.2004;141(1):28–38.
- ,,,,.An internist joins the surgery service: does comanagement make a difference?J Gen Intern Med.1994;9:440–444.
- ,,, et al.Postoperative pulmonary complications: experience with an outpatient pre‐operative assessment program.J Clin Outcomes Manag.2005;12:505–510.
In this issue of the Journal of Hospital Medicine, Simon et al.1 provide the first report of pediatric hospitalist comanagement of patients undergoing spinal fusion surgery. In this retrospective cohort study, 14 of 115 patients were comanaged by a pediatric hospitalist. The primary outcomes of the study were length of stay and variability in length of stay. Prior to the initiation of hospitalist comanagement service, all patients were managed preoperatively by a spine surgery nurse and aided by medical subspecialists and other allied health professionals (nutritionists, respiratory therapists, physical therapists, social workers). After the intervention, patients with the most complex medical disease were assigned to comanagement by a pediatric hospitalist. When compared to a historical control of patients with similar medical complexity but not comanaged by hospitalists, the length of stay was reduced by 2.4 days (8.6 vs. 6.2 days). The variability in mean length of stay was also reduced.
This study follows on the heels of 3 important studies addressing the utility of hospitalists in the comanagement of surgical patients. The HOT (Hospitalist Orthopedic Team) trial was a randomized controlled trial assessing the effect of hospitalists on the management of patients undergoing elective hip and knee arthroplasty.2 There was no effect on length of stay or patient outcomes, though the comanagement model did decrease minor postoperative medical complications and improve physician and nurse satisfaction. Macpherson et al. conducted a retrospective trial where an internist joined a cardiothoracic surgery service at a tertiary‐care center.3 They found a decrease in overall mortality and resource utilization such as labs testing and consultations. There was significant reduction in the length of stay and number of x‐rays performed. The third study, by Jaffer et al.,4 showed that an outpatient, preoperative evaluation clinic staffed by hospitalists at a large tertiary‐care center provides a practical model for managing preoperative patients and may be associated with a low rate of postoperative pulmonary complications.
The study by Simon et al. in this issue of the journal has limitations. It is a retrospective cohort trial, and like all such study designs, the validity of the results is subject to confounding. Severity of patient medical disease, intraoperative complications, and advances in surgical technique are examples. While the authors did everything possible to minimize the effect of confounding, it remains a limitation of the study. The study also enrolled only 14 patients in the comanagement group, and this limited any stratification or subgroup analysis to offset known confounders. Patients assigned to the hospitalist comanagement service were by design more medically complex than other spinal fusion patients, and generalizing the results of this trial to all spinal fusion patients may not be possible.
From the study's limitations, however, comes great insight into the role of the hospitalist in surgical comanagement. It is clear from the aforementioned studies that there is a role for the hospitalist in comanagement of surgical patients. While the evidence is conflicting, there are scenarios in which comanagement improves efficiency and quality of care. Yet it is also possible that hospitalist comanagement is not ideal for all surgical patients. The HOT trial did not show benefits in length‐of‐stay reduction or patient mortality because the patients were homogenous in their complexity and pre‐ and postoperative care was protocol driven. Length of stay was limited by accessibility of rehabilitation facilities after discharge and not the efficiency of medical care in the hospital. The study in this issue of the Journal of Hospital Medicine selectively included patients with the highest complexity of medical disease, and there was a reduction in length of stay. Both trials suggest that the greatest potential benefit for augmenting efficiency and outcomes with hospitalist comanagement may be predicated on the complexity of the patients involved and the surgical system through which they will receive care.
The next step in assessing hospitalist comanagement should not be a hunt‐and‐peck exercise to stumble on the surgical procedures that show benefit from comanagement. Rather, the prudent next step is to follow the lead of Simon et al. and others3, 4 in trying to identify those surgical patients who represent the greatest medical complexity or have the most variability in their preoperative and postoperative medical care. These are the patients for whom the hospitalist can effect the greatest benefit and the services for which the hospitalist can best augment efficiency. High‐risk procedures, patients with multiple comorbitities or elevated preoperative risks, and surgical procedures without defined pre‐ and postoperative protocols would appear to be the ideal candidates for hospitalist comanagement.
As the discussion of hospital comanagement progresses, it is important to recognize comanagement as a paradigm shift. Surgical comanagement is not merely medical consultation. To be successful, the role of the hospitalist in comanaging surgical patients must be clearly defined as advancing postoperative care as much as it is in assessing preoperative risk. As a comanager, a hospitalist must actively manage preexisting and newly developed medical issues rather than just make recommendations for the surgical team.
The hospitalist must also be more than a discharge coordinator postoperatively; investing in hospitalists merely for discharge planning is a poor use of resources both from a financial and an opportunity‐cost perspective. The paradigm of comanagement is not foreign, however, and hospitalists are likely to prosper by learning from the experience of our nephrology and hepatology colleagues, who have successfully found collaborative roles in improving patient care on renal and liver transplant services. The success of these services is due to the precisely defined roles for the internist and the surgeon and because the complexity of the patient being managed warrants continuity of expert consultation.
There is great potential for the hospitalist in surgical comanagement. In less than a decade, the focus of hospital‐based medical care has shifted from staffing a shift to improving the quality of the system through which patients traverse the hospital. The lessons hospitalists have learned in quality improvement and in augmenting systems of care are perfectly suited for application to surgical services. Hospitalist comanagement is right not only because it may offer improvement in a surgical patient's medical care, but also for the augmentation of quality improvement in surgical services that have yet to reap the benefits that have defined the excellence of hospitalist medicine. The next step is to embark on the road of prudent prospective research: identifying the patients, and the procedures, that have the greatest opportunity for improvement by hospitalist comanagement. And at the end of that road will be a new home for the hospitalist, assuming the role of the quality‐advocate for all aspects of hospital care: pediatric, medical, and surgical patients.
In this issue of the Journal of Hospital Medicine, Simon et al.1 provide the first report of pediatric hospitalist comanagement of patients undergoing spinal fusion surgery. In this retrospective cohort study, 14 of 115 patients were comanaged by a pediatric hospitalist. The primary outcomes of the study were length of stay and variability in length of stay. Prior to the initiation of hospitalist comanagement service, all patients were managed preoperatively by a spine surgery nurse and aided by medical subspecialists and other allied health professionals (nutritionists, respiratory therapists, physical therapists, social workers). After the intervention, patients with the most complex medical disease were assigned to comanagement by a pediatric hospitalist. When compared to a historical control of patients with similar medical complexity but not comanaged by hospitalists, the length of stay was reduced by 2.4 days (8.6 vs. 6.2 days). The variability in mean length of stay was also reduced.
This study follows on the heels of 3 important studies addressing the utility of hospitalists in the comanagement of surgical patients. The HOT (Hospitalist Orthopedic Team) trial was a randomized controlled trial assessing the effect of hospitalists on the management of patients undergoing elective hip and knee arthroplasty.2 There was no effect on length of stay or patient outcomes, though the comanagement model did decrease minor postoperative medical complications and improve physician and nurse satisfaction. Macpherson et al. conducted a retrospective trial where an internist joined a cardiothoracic surgery service at a tertiary‐care center.3 They found a decrease in overall mortality and resource utilization such as labs testing and consultations. There was significant reduction in the length of stay and number of x‐rays performed. The third study, by Jaffer et al.,4 showed that an outpatient, preoperative evaluation clinic staffed by hospitalists at a large tertiary‐care center provides a practical model for managing preoperative patients and may be associated with a low rate of postoperative pulmonary complications.
The study by Simon et al. in this issue of the journal has limitations. It is a retrospective cohort trial, and like all such study designs, the validity of the results is subject to confounding. Severity of patient medical disease, intraoperative complications, and advances in surgical technique are examples. While the authors did everything possible to minimize the effect of confounding, it remains a limitation of the study. The study also enrolled only 14 patients in the comanagement group, and this limited any stratification or subgroup analysis to offset known confounders. Patients assigned to the hospitalist comanagement service were by design more medically complex than other spinal fusion patients, and generalizing the results of this trial to all spinal fusion patients may not be possible.
From the study's limitations, however, comes great insight into the role of the hospitalist in surgical comanagement. It is clear from the aforementioned studies that there is a role for the hospitalist in comanagement of surgical patients. While the evidence is conflicting, there are scenarios in which comanagement improves efficiency and quality of care. Yet it is also possible that hospitalist comanagement is not ideal for all surgical patients. The HOT trial did not show benefits in length‐of‐stay reduction or patient mortality because the patients were homogenous in their complexity and pre‐ and postoperative care was protocol driven. Length of stay was limited by accessibility of rehabilitation facilities after discharge and not the efficiency of medical care in the hospital. The study in this issue of the Journal of Hospital Medicine selectively included patients with the highest complexity of medical disease, and there was a reduction in length of stay. Both trials suggest that the greatest potential benefit for augmenting efficiency and outcomes with hospitalist comanagement may be predicated on the complexity of the patients involved and the surgical system through which they will receive care.
The next step in assessing hospitalist comanagement should not be a hunt‐and‐peck exercise to stumble on the surgical procedures that show benefit from comanagement. Rather, the prudent next step is to follow the lead of Simon et al. and others3, 4 in trying to identify those surgical patients who represent the greatest medical complexity or have the most variability in their preoperative and postoperative medical care. These are the patients for whom the hospitalist can effect the greatest benefit and the services for which the hospitalist can best augment efficiency. High‐risk procedures, patients with multiple comorbitities or elevated preoperative risks, and surgical procedures without defined pre‐ and postoperative protocols would appear to be the ideal candidates for hospitalist comanagement.
As the discussion of hospital comanagement progresses, it is important to recognize comanagement as a paradigm shift. Surgical comanagement is not merely medical consultation. To be successful, the role of the hospitalist in comanaging surgical patients must be clearly defined as advancing postoperative care as much as it is in assessing preoperative risk. As a comanager, a hospitalist must actively manage preexisting and newly developed medical issues rather than just make recommendations for the surgical team.
The hospitalist must also be more than a discharge coordinator postoperatively; investing in hospitalists merely for discharge planning is a poor use of resources both from a financial and an opportunity‐cost perspective. The paradigm of comanagement is not foreign, however, and hospitalists are likely to prosper by learning from the experience of our nephrology and hepatology colleagues, who have successfully found collaborative roles in improving patient care on renal and liver transplant services. The success of these services is due to the precisely defined roles for the internist and the surgeon and because the complexity of the patient being managed warrants continuity of expert consultation.
There is great potential for the hospitalist in surgical comanagement. In less than a decade, the focus of hospital‐based medical care has shifted from staffing a shift to improving the quality of the system through which patients traverse the hospital. The lessons hospitalists have learned in quality improvement and in augmenting systems of care are perfectly suited for application to surgical services. Hospitalist comanagement is right not only because it may offer improvement in a surgical patient's medical care, but also for the augmentation of quality improvement in surgical services that have yet to reap the benefits that have defined the excellence of hospitalist medicine. The next step is to embark on the road of prudent prospective research: identifying the patients, and the procedures, that have the greatest opportunity for improvement by hospitalist comanagement. And at the end of that road will be a new home for the hospitalist, assuming the role of the quality‐advocate for all aspects of hospital care: pediatric, medical, and surgical patients.
- ,,,,.Pediatric co‐management of spine fusion surgery patients.J Hosp Med.2007;2:23–30.
- ,,, et al.;Hospitalist‐Orthopedic Team Trial Investigators.Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial.Ann Intern Med.2004;141(1):28–38.
- ,,,,.An internist joins the surgery service: does comanagement make a difference?J Gen Intern Med.1994;9:440–444.
- ,,, et al.Postoperative pulmonary complications: experience with an outpatient pre‐operative assessment program.J Clin Outcomes Manag.2005;12:505–510.
- ,,,,.Pediatric co‐management of spine fusion surgery patients.J Hosp Med.2007;2:23–30.
- ,,, et al.;Hospitalist‐Orthopedic Team Trial Investigators.Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial.Ann Intern Med.2004;141(1):28–38.
- ,,,,.An internist joins the surgery service: does comanagement make a difference?J Gen Intern Med.1994;9:440–444.
- ,,, et al.Postoperative pulmonary complications: experience with an outpatient pre‐operative assessment program.J Clin Outcomes Manag.2005;12:505–510.
Editorial
One year of the Journal of Hospital Medicine is done, and we now embark on our second with this first issue of volume 2. Before moving on, I heartily thank all the authors who contributed their manuscripts to the Journal of Hospital Medicine (JHM), bravely investing in this new academic periodical. A remarkable 284 manuscripts have been submitted since we first opened the JHM Web site, 197 of them during 2006. This clearly reflects the robust demand by hospitalists and their colleagues for original research and relevant clinical reviews about our evolving specialty of hospital medicine. I probably should not be surprised that this demand exists among the 15,000‐plus hospitalists in America and the 6000‐plus members of the Society of Hospital Medicine. Regardless, I am ineffably humbled by the enthusiasm and energy of all the contributors.
Understandably, this volume of submissions, exceeding our projections by nearly 50%, required yeoman's work by our associate editors and reviewers. On page 55 we list the 203 reviewers who donated their time and acumen to assure the quality of our publication. Many reviewed more than 4 articles during the year. Our associate editors deserve particular appreciation and gratitude for their willingness to donate extraordinary amounts of time and effort to ensure the success of JHMVincent Chang from Boston Children's Hospital, Scott Flanders from the University of Michigan, Karen Hauer from the University of California, San Francisco, Jean Kutner from the University of Colorado, James Pile from Cleveland MetroHealth, and Kaveh Shojania from the University of Ottawa. Additionally, the energetic assistant editors have supported them and me with frequent reviews, article submissions, and creative ideas for improving the journal. Finally, our auspicious editorial board has proffered sage guidance, and many of its members have also submitted manuscripts and participated in reviewing articles.
Moving forward we expect continued growth, as both the submitted articles and demand for the journal are being recognized. At 7:29 a.m. on November 30, 2006, Vickie Thaw (Vice President and Publisher, John Wiley & Sons, Inc.) called me to report that the National Library of Medicine validated all our efforts. The Journal of Hospital Medicine had been selected for indexing and inclusion in the National Library of Medicine's MEDLINE (Medical Literature Analysis and Retrieval System Online). The primary component of PubMed, MEDLINE is a bibliographic database containing approximately 13 million references to journal articles on medicine, nursing, dentistry, veterinary medicine, health care systems, and preclinical sciences dating to the mid‐1960s. With this approval, hospital medicine has achieved another milestone in its evolution into a new specialty.
We now hope to respond to the robust interest in clinical materials as well as to continue publication of original research. To achieve our aim of increasing the amount of clinically relevant content for practicing hospitalists, authors are encouraged to submit to JHM case reports, clinical updates, and clinical images that convey novel or underappreciated teaching points. Teaching points may be purely clinical and may focus on clinical pearls or unusual presentations of well‐known diseases, although submission of straightforward presentations of rare diseases is discouraged. Alternatively, manuscripts may involve succinct case‐based descriptions of innovations, quality improvementrelated issues, or medical errors. Submitted case reports should be less than 800 words and should contain a maximum of 5 references and no more than 1 table or figure. Case reports should not include an abstract. Submission of the case report and review type should be avoided. Instead, we seek formal clinical updates of no more than 2000 words that present important aspects of a case along with new research findings and citations from the literature that change what has historically been the standard of delivery of care. Finally, we continue to seek cases most appropriate for the Hospital Images Dx section, edited by Paul Aronowitz. They should be submitted with that designation and have fewer than 150 words. These 3 categories are identified on our Manuscript Central website (
Again, thanks to all of you for making the launch of the Journal of Hospital Medicine an unqualified success. We look forward to your continued participation as we grow as the premier journal for the specialty of hospital medicine.
P.S. Sadly, one of our superstar associate editors, Kaveh Shojania, is stepping aside, and we sincerely express thanks for his terrific contributions. We welcome suggestions for an alternative to fulfill his responsibilities.
One year of the Journal of Hospital Medicine is done, and we now embark on our second with this first issue of volume 2. Before moving on, I heartily thank all the authors who contributed their manuscripts to the Journal of Hospital Medicine (JHM), bravely investing in this new academic periodical. A remarkable 284 manuscripts have been submitted since we first opened the JHM Web site, 197 of them during 2006. This clearly reflects the robust demand by hospitalists and their colleagues for original research and relevant clinical reviews about our evolving specialty of hospital medicine. I probably should not be surprised that this demand exists among the 15,000‐plus hospitalists in America and the 6000‐plus members of the Society of Hospital Medicine. Regardless, I am ineffably humbled by the enthusiasm and energy of all the contributors.
Understandably, this volume of submissions, exceeding our projections by nearly 50%, required yeoman's work by our associate editors and reviewers. On page 55 we list the 203 reviewers who donated their time and acumen to assure the quality of our publication. Many reviewed more than 4 articles during the year. Our associate editors deserve particular appreciation and gratitude for their willingness to donate extraordinary amounts of time and effort to ensure the success of JHMVincent Chang from Boston Children's Hospital, Scott Flanders from the University of Michigan, Karen Hauer from the University of California, San Francisco, Jean Kutner from the University of Colorado, James Pile from Cleveland MetroHealth, and Kaveh Shojania from the University of Ottawa. Additionally, the energetic assistant editors have supported them and me with frequent reviews, article submissions, and creative ideas for improving the journal. Finally, our auspicious editorial board has proffered sage guidance, and many of its members have also submitted manuscripts and participated in reviewing articles.
Moving forward we expect continued growth, as both the submitted articles and demand for the journal are being recognized. At 7:29 a.m. on November 30, 2006, Vickie Thaw (Vice President and Publisher, John Wiley & Sons, Inc.) called me to report that the National Library of Medicine validated all our efforts. The Journal of Hospital Medicine had been selected for indexing and inclusion in the National Library of Medicine's MEDLINE (Medical Literature Analysis and Retrieval System Online). The primary component of PubMed, MEDLINE is a bibliographic database containing approximately 13 million references to journal articles on medicine, nursing, dentistry, veterinary medicine, health care systems, and preclinical sciences dating to the mid‐1960s. With this approval, hospital medicine has achieved another milestone in its evolution into a new specialty.
We now hope to respond to the robust interest in clinical materials as well as to continue publication of original research. To achieve our aim of increasing the amount of clinically relevant content for practicing hospitalists, authors are encouraged to submit to JHM case reports, clinical updates, and clinical images that convey novel or underappreciated teaching points. Teaching points may be purely clinical and may focus on clinical pearls or unusual presentations of well‐known diseases, although submission of straightforward presentations of rare diseases is discouraged. Alternatively, manuscripts may involve succinct case‐based descriptions of innovations, quality improvementrelated issues, or medical errors. Submitted case reports should be less than 800 words and should contain a maximum of 5 references and no more than 1 table or figure. Case reports should not include an abstract. Submission of the case report and review type should be avoided. Instead, we seek formal clinical updates of no more than 2000 words that present important aspects of a case along with new research findings and citations from the literature that change what has historically been the standard of delivery of care. Finally, we continue to seek cases most appropriate for the Hospital Images Dx section, edited by Paul Aronowitz. They should be submitted with that designation and have fewer than 150 words. These 3 categories are identified on our Manuscript Central website (
Again, thanks to all of you for making the launch of the Journal of Hospital Medicine an unqualified success. We look forward to your continued participation as we grow as the premier journal for the specialty of hospital medicine.
P.S. Sadly, one of our superstar associate editors, Kaveh Shojania, is stepping aside, and we sincerely express thanks for his terrific contributions. We welcome suggestions for an alternative to fulfill his responsibilities.
One year of the Journal of Hospital Medicine is done, and we now embark on our second with this first issue of volume 2. Before moving on, I heartily thank all the authors who contributed their manuscripts to the Journal of Hospital Medicine (JHM), bravely investing in this new academic periodical. A remarkable 284 manuscripts have been submitted since we first opened the JHM Web site, 197 of them during 2006. This clearly reflects the robust demand by hospitalists and their colleagues for original research and relevant clinical reviews about our evolving specialty of hospital medicine. I probably should not be surprised that this demand exists among the 15,000‐plus hospitalists in America and the 6000‐plus members of the Society of Hospital Medicine. Regardless, I am ineffably humbled by the enthusiasm and energy of all the contributors.
Understandably, this volume of submissions, exceeding our projections by nearly 50%, required yeoman's work by our associate editors and reviewers. On page 55 we list the 203 reviewers who donated their time and acumen to assure the quality of our publication. Many reviewed more than 4 articles during the year. Our associate editors deserve particular appreciation and gratitude for their willingness to donate extraordinary amounts of time and effort to ensure the success of JHMVincent Chang from Boston Children's Hospital, Scott Flanders from the University of Michigan, Karen Hauer from the University of California, San Francisco, Jean Kutner from the University of Colorado, James Pile from Cleveland MetroHealth, and Kaveh Shojania from the University of Ottawa. Additionally, the energetic assistant editors have supported them and me with frequent reviews, article submissions, and creative ideas for improving the journal. Finally, our auspicious editorial board has proffered sage guidance, and many of its members have also submitted manuscripts and participated in reviewing articles.
Moving forward we expect continued growth, as both the submitted articles and demand for the journal are being recognized. At 7:29 a.m. on November 30, 2006, Vickie Thaw (Vice President and Publisher, John Wiley & Sons, Inc.) called me to report that the National Library of Medicine validated all our efforts. The Journal of Hospital Medicine had been selected for indexing and inclusion in the National Library of Medicine's MEDLINE (Medical Literature Analysis and Retrieval System Online). The primary component of PubMed, MEDLINE is a bibliographic database containing approximately 13 million references to journal articles on medicine, nursing, dentistry, veterinary medicine, health care systems, and preclinical sciences dating to the mid‐1960s. With this approval, hospital medicine has achieved another milestone in its evolution into a new specialty.
We now hope to respond to the robust interest in clinical materials as well as to continue publication of original research. To achieve our aim of increasing the amount of clinically relevant content for practicing hospitalists, authors are encouraged to submit to JHM case reports, clinical updates, and clinical images that convey novel or underappreciated teaching points. Teaching points may be purely clinical and may focus on clinical pearls or unusual presentations of well‐known diseases, although submission of straightforward presentations of rare diseases is discouraged. Alternatively, manuscripts may involve succinct case‐based descriptions of innovations, quality improvementrelated issues, or medical errors. Submitted case reports should be less than 800 words and should contain a maximum of 5 references and no more than 1 table or figure. Case reports should not include an abstract. Submission of the case report and review type should be avoided. Instead, we seek formal clinical updates of no more than 2000 words that present important aspects of a case along with new research findings and citations from the literature that change what has historically been the standard of delivery of care. Finally, we continue to seek cases most appropriate for the Hospital Images Dx section, edited by Paul Aronowitz. They should be submitted with that designation and have fewer than 150 words. These 3 categories are identified on our Manuscript Central website (
Again, thanks to all of you for making the launch of the Journal of Hospital Medicine an unqualified success. We look forward to your continued participation as we grow as the premier journal for the specialty of hospital medicine.
P.S. Sadly, one of our superstar associate editors, Kaveh Shojania, is stepping aside, and we sincerely express thanks for his terrific contributions. We welcome suggestions for an alternative to fulfill his responsibilities.