User login
Zapping Zingers
You know them, you’ve received some, and so have your colleagues: those zinger questions—the tough questions your patients ask that momentarily throw you for a loop. Sometimes they’re simple, other times complex, and their psychological origin can be multifaceted. In any case, responding to zingers requires calm, diplomacy, and tact.
“How you respond to the inevitable zingers depends in large part upon your preparation,” writes Laura Sachs Hills in her Nov/Dec 2005 article in the Journal of Practice Management.1 That preparation, she suggests, is best established using staff training, group work, brainstorming, and role-play scenarios.
Both hospitalists and primary care physicians, writes Bernard Lo, MD, must be prepared for patients to ask difficult questions or make unsettling comments, even about the hospitalist system itself.2 Anticipating the nature of those comments or questions is likely to help the hospitalist respond in the moment.
“I don’t see these so much as zingers as challenging or uncomfortable questions or attempts by patients to assert some control,” says Steven Pantilat, MD, FACP, associate professor of clinical medicine in the Department of Medicine at the University of California, San Francisco, and past president of SHM.
Dr. Pantilat believes that the term “zinger” can imply they are used with malicious intent, yet, he comments, “I’m not sure they are, even if they are an attempt to exert control or challenge the physician. I suspect they arise from fear or other responses.” Below, some of the zingers Dr. Pantilat has dealt with.
How long have you been a doctor? “I’ve now been one long enough not to be flustered by this question, but many hospitalists are young and may be taken aback,” says Dr. Pantilat. “It’s a challenge to the doctor’s authority and expertise.”
Doc, you look so young is a related comment, believes Dr. Pantilat—one that can be interpreted as a compliment or a zinger. “My standard response is always, ‘I’m old enough to take that as a compliment,’ ” he says. “These days I really mean it.”
Vineet Aurora, MD, hospitalist at the University of Chicago Medical Center, says she is sometimes asked, “How old are you?”
“I think it happens to a lot of women who are or look young,” she says. “I usually just state my age, [which is] 32. Often they will say, ‘Oh you look much younger,’ and I take that as a compliment and laugh it off. I think most of the time our patients are just curious. It may also be related to height, and several of us speculate that shorter women may experience this more.”
Ian Jenkins, MD, a hospitalist at the University of California, San Diego, and an associate professor of clinical medicine, shares this zinger: You don't want to order this MRI for my back pain because it’s expensive, so why don’t you just admit it?
His response: “That’s right. We have a certain amount of money to take care of you and the rest of our patients and to do the best job possible. We can’t waste any of it on unnecessary tests or therapies, so you’ve gotten exactly what I would want if I had your back pain—a thorough history and physical exam.”
Here are some zingers from Vijay Rajput, MD, senior hospitalist at Cooper University Hospital, Camden, N.J., associate professor of medicine and program director, Internal Medicine Residency Program, University of Medicine and Dentistry, Robert Wood Johnson Medical School, Piscataway, N.J.º
What’s going on [with my condition]? “Sometimes when I say, ‘I don’t know,’ the patient comes back with, ‘How come you don’t know?’ I usually say, ‘Do you think that we need to know everything in medicine?’ ” says Dr. Rajput. “They usually say, ‘No, not necessarily, but I thought for my condition you might know.’ ”
Dr. Rajput continues, “Sometimes I tell them, ‘Medicine has advanced too fast … many times we [need] more updated knowledge, and sometimes we are not updated … . I would rather update the knowledge and do the right thing for you … than provide you with care with a half-knowledge.’ Most of the people will like and understand that answer.”
Dr. Rajput tells another anecdote: “One time I was rounding with the team on the floor and we all—students, residents, a pharmacy student, and myself—were Asian, [with] three of [us] … born here in the U.S. The patient asked, ‘How come there are too many foreign doctors in this country?’
“That was a zinger,” recalls Dr. Rajput, “and my team thought I [would] pass [on it], but I didn’t. I gave the patient a straight answer with a true explanation. It took a few minutes to explain it in detail.
“I asked him, ‘What is [your] perception?’ He did not have an answer. I explained to him that 25% of [the] doctors [in the U.S.] are not born in this country, and we have a constant need for more doctors. We have proper mechanisms [in place] so that these doctors are trained as well as in American schools and residencies before they start their practice. I also explained the relationships with Educational Commission for Foreign Medical Graduates (ECFMG), National Board of Medical Examiners (NBME), and Council for Graduate Medical Education (ACGME) and said that three out of four of us are U.S.-born and not ‘foreign’ doctors.”
David M. Grace, MD, of The Schumacher Group is a hospitalist practice director in Lafayette, La.; he remembers this zinger: If it’s OK with you, I’d like to stay today and go home tomorrow.
“At least once a week, I have a patient who just doesn’t feel up to going home at the appropriate time of discharge. My response always starts with ‘Why?’ All patients have the right to a safe and stable discharge from the hospital, and it’s important to ensure that no pertinent issues have been overlooked. Is their home support system not ready yet? Is payday tomorrow, and they can’t afford their medicines today? Are they just scared?
“Once I’m satisfied that no occult dangers exist, I sit and discuss the situation with the patient. I first remind them of our discussion … at admission; it’s the same discussion I have with every patient,” says Dr. Grace. “During the admission process, I outline what objectives need to be reached prior to discharge. I emphasize that the role of hospitalization is not to cure the patient but to ‘rectify the problems that require inpatient care’ and allow the convalescence to take place at home.
“Occasionally I have patients [with whom] my first-line strategy doesn’t work, and I move on to plan B. Plan B is where I quote statistics such as, ‘100,000 patients per year die in hospitals due to errors, and on average, each inpatient will have one medication error per day.’ Continuing to stay in the hospital beyond today will shift the risk/benefit ratio to a position where the patient would have additional risk but no additional medical benefit.
“Plan C is rarely used, but it’s in my arsenal,” he says. “I remind the patient that I’m responsible for doing what is medically appropriate, and I reiterate that I understand their concerns, but I cannot commit healthcare fraud by documenting that the patient is not stable for discharge when they are stable. I then shift the decision back to the patient by closing with, ‘We don’t force patients to leave or drag them out of the hospital; however, you need to check with your insurance carrier about whether they will cover the cost of a non-necessary additional hospital day.’ I inform them that the hospital will likely charge the additional day to the patient, and I don’t want to see them get an unexpected bill.”
Another of the zingers Dr. Grace has dealt with: I’m supposed to have test X done as an outpatient, but now that I’m here in the hospital, can we just do it now?
“On days where Lady Luck is shining on me, it’s a test we need to do as part of [the patient’s] acute work-up, and everything works out well. More often than not, it’s a test or procedure unrelated to the admitting diagnoses and one [that] is far more expensive to do as an inpatient, compared with an outpatient study.
“When possible, I’ll explain to the patient that the test they want may not be accurate in the setting of an acute illness, such as the test for lipid levels,” he says. “If the test doesn’t fit into that category, I’ll explain—depending on the request, such as one for an MRI or CT—that they may make it halfway through the test, and the test will need to be aborted because of an acutely sick patient who requires immediate intervention using that piece of equipment, which for the patient would mean that they may need to go through the procedure a second time, or possibly even a third.
“Failing that approach,” he continues, “I often make the insurance company the ‘bad one’ and inform them that their carrier may not pay for the test as an inpatient as it’s not related to their medical illness, and they should check to ensure that the bill won’t be passed on to them. Often the patient, who knows how much of a headache it can be to deal with their insurance company, will drop the request.” TH
Andrea Sattinger writes frequently for The Hospitalist.
References
- Hills LS. How to answer the most common zinger questions. J Med Pract Manage. 2005 Nov-Dec;21(3):153-155.
- Lo B. Ethical and policy implications of hospitalist systems. Am J Med. 2001;111:48-52.
You know them, you’ve received some, and so have your colleagues: those zinger questions—the tough questions your patients ask that momentarily throw you for a loop. Sometimes they’re simple, other times complex, and their psychological origin can be multifaceted. In any case, responding to zingers requires calm, diplomacy, and tact.
“How you respond to the inevitable zingers depends in large part upon your preparation,” writes Laura Sachs Hills in her Nov/Dec 2005 article in the Journal of Practice Management.1 That preparation, she suggests, is best established using staff training, group work, brainstorming, and role-play scenarios.
Both hospitalists and primary care physicians, writes Bernard Lo, MD, must be prepared for patients to ask difficult questions or make unsettling comments, even about the hospitalist system itself.2 Anticipating the nature of those comments or questions is likely to help the hospitalist respond in the moment.
“I don’t see these so much as zingers as challenging or uncomfortable questions or attempts by patients to assert some control,” says Steven Pantilat, MD, FACP, associate professor of clinical medicine in the Department of Medicine at the University of California, San Francisco, and past president of SHM.
Dr. Pantilat believes that the term “zinger” can imply they are used with malicious intent, yet, he comments, “I’m not sure they are, even if they are an attempt to exert control or challenge the physician. I suspect they arise from fear or other responses.” Below, some of the zingers Dr. Pantilat has dealt with.
How long have you been a doctor? “I’ve now been one long enough not to be flustered by this question, but many hospitalists are young and may be taken aback,” says Dr. Pantilat. “It’s a challenge to the doctor’s authority and expertise.”
Doc, you look so young is a related comment, believes Dr. Pantilat—one that can be interpreted as a compliment or a zinger. “My standard response is always, ‘I’m old enough to take that as a compliment,’ ” he says. “These days I really mean it.”
Vineet Aurora, MD, hospitalist at the University of Chicago Medical Center, says she is sometimes asked, “How old are you?”
“I think it happens to a lot of women who are or look young,” she says. “I usually just state my age, [which is] 32. Often they will say, ‘Oh you look much younger,’ and I take that as a compliment and laugh it off. I think most of the time our patients are just curious. It may also be related to height, and several of us speculate that shorter women may experience this more.”
Ian Jenkins, MD, a hospitalist at the University of California, San Diego, and an associate professor of clinical medicine, shares this zinger: You don't want to order this MRI for my back pain because it’s expensive, so why don’t you just admit it?
His response: “That’s right. We have a certain amount of money to take care of you and the rest of our patients and to do the best job possible. We can’t waste any of it on unnecessary tests or therapies, so you’ve gotten exactly what I would want if I had your back pain—a thorough history and physical exam.”
Here are some zingers from Vijay Rajput, MD, senior hospitalist at Cooper University Hospital, Camden, N.J., associate professor of medicine and program director, Internal Medicine Residency Program, University of Medicine and Dentistry, Robert Wood Johnson Medical School, Piscataway, N.J.º
What’s going on [with my condition]? “Sometimes when I say, ‘I don’t know,’ the patient comes back with, ‘How come you don’t know?’ I usually say, ‘Do you think that we need to know everything in medicine?’ ” says Dr. Rajput. “They usually say, ‘No, not necessarily, but I thought for my condition you might know.’ ”
Dr. Rajput continues, “Sometimes I tell them, ‘Medicine has advanced too fast … many times we [need] more updated knowledge, and sometimes we are not updated … . I would rather update the knowledge and do the right thing for you … than provide you with care with a half-knowledge.’ Most of the people will like and understand that answer.”
Dr. Rajput tells another anecdote: “One time I was rounding with the team on the floor and we all—students, residents, a pharmacy student, and myself—were Asian, [with] three of [us] … born here in the U.S. The patient asked, ‘How come there are too many foreign doctors in this country?’
“That was a zinger,” recalls Dr. Rajput, “and my team thought I [would] pass [on it], but I didn’t. I gave the patient a straight answer with a true explanation. It took a few minutes to explain it in detail.
“I asked him, ‘What is [your] perception?’ He did not have an answer. I explained to him that 25% of [the] doctors [in the U.S.] are not born in this country, and we have a constant need for more doctors. We have proper mechanisms [in place] so that these doctors are trained as well as in American schools and residencies before they start their practice. I also explained the relationships with Educational Commission for Foreign Medical Graduates (ECFMG), National Board of Medical Examiners (NBME), and Council for Graduate Medical Education (ACGME) and said that three out of four of us are U.S.-born and not ‘foreign’ doctors.”
David M. Grace, MD, of The Schumacher Group is a hospitalist practice director in Lafayette, La.; he remembers this zinger: If it’s OK with you, I’d like to stay today and go home tomorrow.
“At least once a week, I have a patient who just doesn’t feel up to going home at the appropriate time of discharge. My response always starts with ‘Why?’ All patients have the right to a safe and stable discharge from the hospital, and it’s important to ensure that no pertinent issues have been overlooked. Is their home support system not ready yet? Is payday tomorrow, and they can’t afford their medicines today? Are they just scared?
“Once I’m satisfied that no occult dangers exist, I sit and discuss the situation with the patient. I first remind them of our discussion … at admission; it’s the same discussion I have with every patient,” says Dr. Grace. “During the admission process, I outline what objectives need to be reached prior to discharge. I emphasize that the role of hospitalization is not to cure the patient but to ‘rectify the problems that require inpatient care’ and allow the convalescence to take place at home.
“Occasionally I have patients [with whom] my first-line strategy doesn’t work, and I move on to plan B. Plan B is where I quote statistics such as, ‘100,000 patients per year die in hospitals due to errors, and on average, each inpatient will have one medication error per day.’ Continuing to stay in the hospital beyond today will shift the risk/benefit ratio to a position where the patient would have additional risk but no additional medical benefit.
“Plan C is rarely used, but it’s in my arsenal,” he says. “I remind the patient that I’m responsible for doing what is medically appropriate, and I reiterate that I understand their concerns, but I cannot commit healthcare fraud by documenting that the patient is not stable for discharge when they are stable. I then shift the decision back to the patient by closing with, ‘We don’t force patients to leave or drag them out of the hospital; however, you need to check with your insurance carrier about whether they will cover the cost of a non-necessary additional hospital day.’ I inform them that the hospital will likely charge the additional day to the patient, and I don’t want to see them get an unexpected bill.”
Another of the zingers Dr. Grace has dealt with: I’m supposed to have test X done as an outpatient, but now that I’m here in the hospital, can we just do it now?
“On days where Lady Luck is shining on me, it’s a test we need to do as part of [the patient’s] acute work-up, and everything works out well. More often than not, it’s a test or procedure unrelated to the admitting diagnoses and one [that] is far more expensive to do as an inpatient, compared with an outpatient study.
“When possible, I’ll explain to the patient that the test they want may not be accurate in the setting of an acute illness, such as the test for lipid levels,” he says. “If the test doesn’t fit into that category, I’ll explain—depending on the request, such as one for an MRI or CT—that they may make it halfway through the test, and the test will need to be aborted because of an acutely sick patient who requires immediate intervention using that piece of equipment, which for the patient would mean that they may need to go through the procedure a second time, or possibly even a third.
“Failing that approach,” he continues, “I often make the insurance company the ‘bad one’ and inform them that their carrier may not pay for the test as an inpatient as it’s not related to their medical illness, and they should check to ensure that the bill won’t be passed on to them. Often the patient, who knows how much of a headache it can be to deal with their insurance company, will drop the request.” TH
Andrea Sattinger writes frequently for The Hospitalist.
References
- Hills LS. How to answer the most common zinger questions. J Med Pract Manage. 2005 Nov-Dec;21(3):153-155.
- Lo B. Ethical and policy implications of hospitalist systems. Am J Med. 2001;111:48-52.
You know them, you’ve received some, and so have your colleagues: those zinger questions—the tough questions your patients ask that momentarily throw you for a loop. Sometimes they’re simple, other times complex, and their psychological origin can be multifaceted. In any case, responding to zingers requires calm, diplomacy, and tact.
“How you respond to the inevitable zingers depends in large part upon your preparation,” writes Laura Sachs Hills in her Nov/Dec 2005 article in the Journal of Practice Management.1 That preparation, she suggests, is best established using staff training, group work, brainstorming, and role-play scenarios.
Both hospitalists and primary care physicians, writes Bernard Lo, MD, must be prepared for patients to ask difficult questions or make unsettling comments, even about the hospitalist system itself.2 Anticipating the nature of those comments or questions is likely to help the hospitalist respond in the moment.
“I don’t see these so much as zingers as challenging or uncomfortable questions or attempts by patients to assert some control,” says Steven Pantilat, MD, FACP, associate professor of clinical medicine in the Department of Medicine at the University of California, San Francisco, and past president of SHM.
Dr. Pantilat believes that the term “zinger” can imply they are used with malicious intent, yet, he comments, “I’m not sure they are, even if they are an attempt to exert control or challenge the physician. I suspect they arise from fear or other responses.” Below, some of the zingers Dr. Pantilat has dealt with.
How long have you been a doctor? “I’ve now been one long enough not to be flustered by this question, but many hospitalists are young and may be taken aback,” says Dr. Pantilat. “It’s a challenge to the doctor’s authority and expertise.”
Doc, you look so young is a related comment, believes Dr. Pantilat—one that can be interpreted as a compliment or a zinger. “My standard response is always, ‘I’m old enough to take that as a compliment,’ ” he says. “These days I really mean it.”
Vineet Aurora, MD, hospitalist at the University of Chicago Medical Center, says she is sometimes asked, “How old are you?”
“I think it happens to a lot of women who are or look young,” she says. “I usually just state my age, [which is] 32. Often they will say, ‘Oh you look much younger,’ and I take that as a compliment and laugh it off. I think most of the time our patients are just curious. It may also be related to height, and several of us speculate that shorter women may experience this more.”
Ian Jenkins, MD, a hospitalist at the University of California, San Diego, and an associate professor of clinical medicine, shares this zinger: You don't want to order this MRI for my back pain because it’s expensive, so why don’t you just admit it?
His response: “That’s right. We have a certain amount of money to take care of you and the rest of our patients and to do the best job possible. We can’t waste any of it on unnecessary tests or therapies, so you’ve gotten exactly what I would want if I had your back pain—a thorough history and physical exam.”
Here are some zingers from Vijay Rajput, MD, senior hospitalist at Cooper University Hospital, Camden, N.J., associate professor of medicine and program director, Internal Medicine Residency Program, University of Medicine and Dentistry, Robert Wood Johnson Medical School, Piscataway, N.J.º
What’s going on [with my condition]? “Sometimes when I say, ‘I don’t know,’ the patient comes back with, ‘How come you don’t know?’ I usually say, ‘Do you think that we need to know everything in medicine?’ ” says Dr. Rajput. “They usually say, ‘No, not necessarily, but I thought for my condition you might know.’ ”
Dr. Rajput continues, “Sometimes I tell them, ‘Medicine has advanced too fast … many times we [need] more updated knowledge, and sometimes we are not updated … . I would rather update the knowledge and do the right thing for you … than provide you with care with a half-knowledge.’ Most of the people will like and understand that answer.”
Dr. Rajput tells another anecdote: “One time I was rounding with the team on the floor and we all—students, residents, a pharmacy student, and myself—were Asian, [with] three of [us] … born here in the U.S. The patient asked, ‘How come there are too many foreign doctors in this country?’
“That was a zinger,” recalls Dr. Rajput, “and my team thought I [would] pass [on it], but I didn’t. I gave the patient a straight answer with a true explanation. It took a few minutes to explain it in detail.
“I asked him, ‘What is [your] perception?’ He did not have an answer. I explained to him that 25% of [the] doctors [in the U.S.] are not born in this country, and we have a constant need for more doctors. We have proper mechanisms [in place] so that these doctors are trained as well as in American schools and residencies before they start their practice. I also explained the relationships with Educational Commission for Foreign Medical Graduates (ECFMG), National Board of Medical Examiners (NBME), and Council for Graduate Medical Education (ACGME) and said that three out of four of us are U.S.-born and not ‘foreign’ doctors.”
David M. Grace, MD, of The Schumacher Group is a hospitalist practice director in Lafayette, La.; he remembers this zinger: If it’s OK with you, I’d like to stay today and go home tomorrow.
“At least once a week, I have a patient who just doesn’t feel up to going home at the appropriate time of discharge. My response always starts with ‘Why?’ All patients have the right to a safe and stable discharge from the hospital, and it’s important to ensure that no pertinent issues have been overlooked. Is their home support system not ready yet? Is payday tomorrow, and they can’t afford their medicines today? Are they just scared?
“Once I’m satisfied that no occult dangers exist, I sit and discuss the situation with the patient. I first remind them of our discussion … at admission; it’s the same discussion I have with every patient,” says Dr. Grace. “During the admission process, I outline what objectives need to be reached prior to discharge. I emphasize that the role of hospitalization is not to cure the patient but to ‘rectify the problems that require inpatient care’ and allow the convalescence to take place at home.
“Occasionally I have patients [with whom] my first-line strategy doesn’t work, and I move on to plan B. Plan B is where I quote statistics such as, ‘100,000 patients per year die in hospitals due to errors, and on average, each inpatient will have one medication error per day.’ Continuing to stay in the hospital beyond today will shift the risk/benefit ratio to a position where the patient would have additional risk but no additional medical benefit.
“Plan C is rarely used, but it’s in my arsenal,” he says. “I remind the patient that I’m responsible for doing what is medically appropriate, and I reiterate that I understand their concerns, but I cannot commit healthcare fraud by documenting that the patient is not stable for discharge when they are stable. I then shift the decision back to the patient by closing with, ‘We don’t force patients to leave or drag them out of the hospital; however, you need to check with your insurance carrier about whether they will cover the cost of a non-necessary additional hospital day.’ I inform them that the hospital will likely charge the additional day to the patient, and I don’t want to see them get an unexpected bill.”
Another of the zingers Dr. Grace has dealt with: I’m supposed to have test X done as an outpatient, but now that I’m here in the hospital, can we just do it now?
“On days where Lady Luck is shining on me, it’s a test we need to do as part of [the patient’s] acute work-up, and everything works out well. More often than not, it’s a test or procedure unrelated to the admitting diagnoses and one [that] is far more expensive to do as an inpatient, compared with an outpatient study.
“When possible, I’ll explain to the patient that the test they want may not be accurate in the setting of an acute illness, such as the test for lipid levels,” he says. “If the test doesn’t fit into that category, I’ll explain—depending on the request, such as one for an MRI or CT—that they may make it halfway through the test, and the test will need to be aborted because of an acutely sick patient who requires immediate intervention using that piece of equipment, which for the patient would mean that they may need to go through the procedure a second time, or possibly even a third.
“Failing that approach,” he continues, “I often make the insurance company the ‘bad one’ and inform them that their carrier may not pay for the test as an inpatient as it’s not related to their medical illness, and they should check to ensure that the bill won’t be passed on to them. Often the patient, who knows how much of a headache it can be to deal with their insurance company, will drop the request.” TH
Andrea Sattinger writes frequently for The Hospitalist.
References
- Hills LS. How to answer the most common zinger questions. J Med Pract Manage. 2005 Nov-Dec;21(3):153-155.
- Lo B. Ethical and policy implications of hospitalist systems. Am J Med. 2001;111:48-52.
A Pregnant Pause
As most of us are aware, medical education is a long-term endeavor. Medical schools provide students with the informational foundation and thinking skills necessary to be a doctor. Residency forges the knowledge into a usable skill set that builds the final product: a clinician. Like a hand-thrown pot being placed in the kiln to achieve the final step—that is, hardening with a lustrous glaze—newly graduated medical students take their place in residency programs to gain the experience necessary to practice medicine. It is a system that has worked for generations.
It has worked—but at a price. Many older physicians “put in their dues” at a cost of brutal working hours—often exceeding 120 hours per week—with no patient volume caps, no days off, and absolutely no regard for the resident’s home life or family. In recent years, changes have been made in residency programs to limit the hours worked per week and the number of patients a physician in training is expected to admit and cover; primarily, these changes have been imposed on institutions to address issues of patient safety. It may be time to take a fresh look at residency programs and develop creative work plans that accommodate the changing needs of physicians and twenty-first century medicine.1
What has changed? Everything. The patients changed, the doctors changed, our society changed, and the knowledge base changed; literally, nothing remained static. Increasing demand for patient participation in medical decision-making, increasing requirements for medical documentation, and increasing demand for proof of quality performance while concomitantly paring back the working hours permitted per resident have stressed a rigid system to its breaking point. Creative ideas, such as having residents admit to a single hospital floor, are new innovations to adapt quality teaching to the required 80-hour week.1
Additionally, in the past 25 to 30 years, medicine changed from a “man’s career” to a near gender-neutral profession. In 1970, about 7% of physicians were women. By 1980, women accounted for 11.6% of the workforce, and in 2004, women physicians comprised more than 26% of the total.2 With medical school matriculants numbering women and men at near parity—women have made up 45% to 49% of medical school classes since 1999—it is reasonable to assume that the percentage of women physicians will continue to rise annually.3 This process, the feminization of medicine, has created new needs and demands that have not traditionally been identified.4
As previously noted, medical education and training constitute a long-term process that extends into an individual’s later 20s and 30s. Deferred life issues such as marriage and children can wait only so long, and for women the biological clock imposes an earlier time frame than the one for men. Women often want to start a family before the end of their residency training. The traditional residency system was not designed to support multiple extended absences. In most residency programs—77% of programs in one study—maternity absences are handled by requiring the other residents to pick up the slack, an obviously less than happy arrangement.5,6 In the same survey, 83% of residency programs acknowledged that maternity leave had a significant effect on scheduling, despite the fact that 80% of programs had a maternity policy in place.5
It is time for innovative thinking for residency training. New plans must accommodate system needs as well as individual needs and must retain the teaching function necessary to develop the required clinical skills. This can be done, but it requires planning and flexibility. Most residency programs have a maternity policy.5 This policy defines the length of time allotted for maternity leave—free leave, or time off with no make-up requirement. Some programs, such as the one at the University of California at San Francisco, have incorporated a flexible option to accommodate longer absences using flexible make-up time.7
As early as 1989 the National Health Service in the United Kingdom proposed a part-time option in residency training to encourage women physicians to pursue careers in hospital medicine.8 In response to increasing numbers of women physicians, flexible part-time specialty training programs are now generally available in the United Kingdom.9
Developing a functional part-time residency option requires planning ahead and setting aside several residency slots to be paired as half-time equivalents. Training programs want upfront information; they want to have some idea of how many residents plan to start a family during residency years so that they can anticipate the numbers needed for clinical coverage. One would hope that open communication on this issue would not imply discrimination in hiring and that the information would be used to estimate the hiring needs of the program and to accommodate shared practices.
Obviously, some residents who anticipate using the part-time option may later choose not to have children at that time, while others who did not plan to do so may become pregnant. Because of this variability and the inherent concern of discrimination on the basis of the request, it is preferable for residency programs to build in half-time residency slots based on the need experienced in prior years. Once this program is viewed as a standard option, women with young children—or those who anticipate pregnancy during residency—may well request one of the part-time slots to accommodate their needs.
Flexible—part-time—residency programs have the downside of extending the length of training. Although most residents do not relish the idea of a longer residency, for individuals with family commitments this is a welcome option. The extended residency is a benefit if it allows completion of a training program that might otherwise be impossible.
Of women physicians with children in 1988, 22% had a child before finishing residency, and 54% had at least one child by the time they had completed a fellowship.10 I would guess that those percentages are significantly higher with newer data. All residency programs with young women physicians should anticipate pregnancy-leave time. Without a clear plan to cover the clinical workload during these absences, one can predict anger and resentment among the residents who are expected to cover the extra work.11 If the cross-coverage plan for maternity leave is haphazard and only created as the need arises, fellow residents tend to feel that the burden of work is allocated capriciously. If allowed to persist, the resulting frustration damages the program’s collegiality and may result in a view of women as a risk to the best function of the department.6 This consequence damages both the departmental image and the status of women in medicine.
Proactive departmental planning for maternity leave and potentially reduced work hours for women with small children in residency training should be a priority and should be well defined prior to the employment of new residents. Any plan needs to include options, including a brief, fixed maternity leave and a more extended leave with obligations for time payback or flexible extension of the residency with reduced work hours per week. A leave plan must also include the number of weeks a resident can be absent in a year, in two years, and for the duration of the residency, while still fulfilling requirements for board eligibility. Likewise, to ensure a fundamental knowledge base, rotations that must be successfully completed should be clearly enumerated as part of the policy. As a corollary, paternity policy should also be specifically delineated.
Even residents who don’t utilize the flexible option residency like the idea that it is available if needed and believe that having a policy in place is desirable.7 Maintaining a positive espirit de corps in a residency training program is vital to the smooth functioning of the program and also mentors residents on the benefits of collegiality for a lifetime of practice. Developing a well-thought-out and equitable plan for maternity, health, or family leave during residency training is as essential as figuring out how to teach medicine to residents in an 80-hour week—and it can be done. TH
Dr. Brezina is a hospitalist at Durham Regional Medical Hospital in Durham, N.C., and a member of the consulting clinical faculty at Duke University, Durham, N.C.
References
- Croasdale M. Redesigning Residency: new models for internal medicine programs. American Medical News. October 23/30, 2006;Professional issues:10.
- Smart DR. Table 1: Physicians by gender. In: Smart, DR. Physician Characteristics and Distribution in the U.S., 2006 Edition. American Medical Association; 2006.
- AAMC: Data Warehouse: Applicant Matriculant File by sex, 1995-2006. Association of American Medical Colleges Web site. Available at: www.aamc.org/data/facts/2005/2005summary.htm. Last accessed November 29, 2006.
- Levinson W, Lurie N. When most doctors are women: what lies ahead? Ann Intern Med. 2004 Sep 21;141(6):471-474.
- Davis JL, Baillie S, Hodgson CS, et al. Maternity leave: existing policies in obstetrics and gynecology residency programs. Obstet Gynecol. 2001 Dec;98(6):1093-1098.
- Tamburrino MB, Evans CL, Campbell NB, et al. Physician pregnancy: male and female colleagues’ attitudes. J Am Med Womens Assoc. 1992 May-Jun;47(3):82-84.
- Kamei RK, Chen HC, Loeser H. Residency is not a race: our ten-year experience with a flexible schedule residency training option. Acad Med. 2004 May;79(5):447-452.
- Warren VJ, Wakeford RE. ‘We’d like to have a family’—young women doctors’ opinions of maternity leave and part-time training. J R Soc Med. 1989 Sep;82(9):528-531.
- Maingay J, Goldberg I. Flexible training opportunities in the European Union. Med Educ. 1998 Sep;32(5):543-548.
- Sinal S, Weavil P, Camp MG. Survey of women physicians on issues relating to pregnancy during a medical career. J Med Educ. 1988 Jul;63(7):531-538.
- Finch SJ. Pregnancy during residency: a literature review. Acad Med. 2003 Apr;78(4):418-428.
As most of us are aware, medical education is a long-term endeavor. Medical schools provide students with the informational foundation and thinking skills necessary to be a doctor. Residency forges the knowledge into a usable skill set that builds the final product: a clinician. Like a hand-thrown pot being placed in the kiln to achieve the final step—that is, hardening with a lustrous glaze—newly graduated medical students take their place in residency programs to gain the experience necessary to practice medicine. It is a system that has worked for generations.
It has worked—but at a price. Many older physicians “put in their dues” at a cost of brutal working hours—often exceeding 120 hours per week—with no patient volume caps, no days off, and absolutely no regard for the resident’s home life or family. In recent years, changes have been made in residency programs to limit the hours worked per week and the number of patients a physician in training is expected to admit and cover; primarily, these changes have been imposed on institutions to address issues of patient safety. It may be time to take a fresh look at residency programs and develop creative work plans that accommodate the changing needs of physicians and twenty-first century medicine.1
What has changed? Everything. The patients changed, the doctors changed, our society changed, and the knowledge base changed; literally, nothing remained static. Increasing demand for patient participation in medical decision-making, increasing requirements for medical documentation, and increasing demand for proof of quality performance while concomitantly paring back the working hours permitted per resident have stressed a rigid system to its breaking point. Creative ideas, such as having residents admit to a single hospital floor, are new innovations to adapt quality teaching to the required 80-hour week.1
Additionally, in the past 25 to 30 years, medicine changed from a “man’s career” to a near gender-neutral profession. In 1970, about 7% of physicians were women. By 1980, women accounted for 11.6% of the workforce, and in 2004, women physicians comprised more than 26% of the total.2 With medical school matriculants numbering women and men at near parity—women have made up 45% to 49% of medical school classes since 1999—it is reasonable to assume that the percentage of women physicians will continue to rise annually.3 This process, the feminization of medicine, has created new needs and demands that have not traditionally been identified.4
As previously noted, medical education and training constitute a long-term process that extends into an individual’s later 20s and 30s. Deferred life issues such as marriage and children can wait only so long, and for women the biological clock imposes an earlier time frame than the one for men. Women often want to start a family before the end of their residency training. The traditional residency system was not designed to support multiple extended absences. In most residency programs—77% of programs in one study—maternity absences are handled by requiring the other residents to pick up the slack, an obviously less than happy arrangement.5,6 In the same survey, 83% of residency programs acknowledged that maternity leave had a significant effect on scheduling, despite the fact that 80% of programs had a maternity policy in place.5
It is time for innovative thinking for residency training. New plans must accommodate system needs as well as individual needs and must retain the teaching function necessary to develop the required clinical skills. This can be done, but it requires planning and flexibility. Most residency programs have a maternity policy.5 This policy defines the length of time allotted for maternity leave—free leave, or time off with no make-up requirement. Some programs, such as the one at the University of California at San Francisco, have incorporated a flexible option to accommodate longer absences using flexible make-up time.7
As early as 1989 the National Health Service in the United Kingdom proposed a part-time option in residency training to encourage women physicians to pursue careers in hospital medicine.8 In response to increasing numbers of women physicians, flexible part-time specialty training programs are now generally available in the United Kingdom.9
Developing a functional part-time residency option requires planning ahead and setting aside several residency slots to be paired as half-time equivalents. Training programs want upfront information; they want to have some idea of how many residents plan to start a family during residency years so that they can anticipate the numbers needed for clinical coverage. One would hope that open communication on this issue would not imply discrimination in hiring and that the information would be used to estimate the hiring needs of the program and to accommodate shared practices.
Obviously, some residents who anticipate using the part-time option may later choose not to have children at that time, while others who did not plan to do so may become pregnant. Because of this variability and the inherent concern of discrimination on the basis of the request, it is preferable for residency programs to build in half-time residency slots based on the need experienced in prior years. Once this program is viewed as a standard option, women with young children—or those who anticipate pregnancy during residency—may well request one of the part-time slots to accommodate their needs.
Flexible—part-time—residency programs have the downside of extending the length of training. Although most residents do not relish the idea of a longer residency, for individuals with family commitments this is a welcome option. The extended residency is a benefit if it allows completion of a training program that might otherwise be impossible.
Of women physicians with children in 1988, 22% had a child before finishing residency, and 54% had at least one child by the time they had completed a fellowship.10 I would guess that those percentages are significantly higher with newer data. All residency programs with young women physicians should anticipate pregnancy-leave time. Without a clear plan to cover the clinical workload during these absences, one can predict anger and resentment among the residents who are expected to cover the extra work.11 If the cross-coverage plan for maternity leave is haphazard and only created as the need arises, fellow residents tend to feel that the burden of work is allocated capriciously. If allowed to persist, the resulting frustration damages the program’s collegiality and may result in a view of women as a risk to the best function of the department.6 This consequence damages both the departmental image and the status of women in medicine.
Proactive departmental planning for maternity leave and potentially reduced work hours for women with small children in residency training should be a priority and should be well defined prior to the employment of new residents. Any plan needs to include options, including a brief, fixed maternity leave and a more extended leave with obligations for time payback or flexible extension of the residency with reduced work hours per week. A leave plan must also include the number of weeks a resident can be absent in a year, in two years, and for the duration of the residency, while still fulfilling requirements for board eligibility. Likewise, to ensure a fundamental knowledge base, rotations that must be successfully completed should be clearly enumerated as part of the policy. As a corollary, paternity policy should also be specifically delineated.
Even residents who don’t utilize the flexible option residency like the idea that it is available if needed and believe that having a policy in place is desirable.7 Maintaining a positive espirit de corps in a residency training program is vital to the smooth functioning of the program and also mentors residents on the benefits of collegiality for a lifetime of practice. Developing a well-thought-out and equitable plan for maternity, health, or family leave during residency training is as essential as figuring out how to teach medicine to residents in an 80-hour week—and it can be done. TH
Dr. Brezina is a hospitalist at Durham Regional Medical Hospital in Durham, N.C., and a member of the consulting clinical faculty at Duke University, Durham, N.C.
References
- Croasdale M. Redesigning Residency: new models for internal medicine programs. American Medical News. October 23/30, 2006;Professional issues:10.
- Smart DR. Table 1: Physicians by gender. In: Smart, DR. Physician Characteristics and Distribution in the U.S., 2006 Edition. American Medical Association; 2006.
- AAMC: Data Warehouse: Applicant Matriculant File by sex, 1995-2006. Association of American Medical Colleges Web site. Available at: www.aamc.org/data/facts/2005/2005summary.htm. Last accessed November 29, 2006.
- Levinson W, Lurie N. When most doctors are women: what lies ahead? Ann Intern Med. 2004 Sep 21;141(6):471-474.
- Davis JL, Baillie S, Hodgson CS, et al. Maternity leave: existing policies in obstetrics and gynecology residency programs. Obstet Gynecol. 2001 Dec;98(6):1093-1098.
- Tamburrino MB, Evans CL, Campbell NB, et al. Physician pregnancy: male and female colleagues’ attitudes. J Am Med Womens Assoc. 1992 May-Jun;47(3):82-84.
- Kamei RK, Chen HC, Loeser H. Residency is not a race: our ten-year experience with a flexible schedule residency training option. Acad Med. 2004 May;79(5):447-452.
- Warren VJ, Wakeford RE. ‘We’d like to have a family’—young women doctors’ opinions of maternity leave and part-time training. J R Soc Med. 1989 Sep;82(9):528-531.
- Maingay J, Goldberg I. Flexible training opportunities in the European Union. Med Educ. 1998 Sep;32(5):543-548.
- Sinal S, Weavil P, Camp MG. Survey of women physicians on issues relating to pregnancy during a medical career. J Med Educ. 1988 Jul;63(7):531-538.
- Finch SJ. Pregnancy during residency: a literature review. Acad Med. 2003 Apr;78(4):418-428.
As most of us are aware, medical education is a long-term endeavor. Medical schools provide students with the informational foundation and thinking skills necessary to be a doctor. Residency forges the knowledge into a usable skill set that builds the final product: a clinician. Like a hand-thrown pot being placed in the kiln to achieve the final step—that is, hardening with a lustrous glaze—newly graduated medical students take their place in residency programs to gain the experience necessary to practice medicine. It is a system that has worked for generations.
It has worked—but at a price. Many older physicians “put in their dues” at a cost of brutal working hours—often exceeding 120 hours per week—with no patient volume caps, no days off, and absolutely no regard for the resident’s home life or family. In recent years, changes have been made in residency programs to limit the hours worked per week and the number of patients a physician in training is expected to admit and cover; primarily, these changes have been imposed on institutions to address issues of patient safety. It may be time to take a fresh look at residency programs and develop creative work plans that accommodate the changing needs of physicians and twenty-first century medicine.1
What has changed? Everything. The patients changed, the doctors changed, our society changed, and the knowledge base changed; literally, nothing remained static. Increasing demand for patient participation in medical decision-making, increasing requirements for medical documentation, and increasing demand for proof of quality performance while concomitantly paring back the working hours permitted per resident have stressed a rigid system to its breaking point. Creative ideas, such as having residents admit to a single hospital floor, are new innovations to adapt quality teaching to the required 80-hour week.1
Additionally, in the past 25 to 30 years, medicine changed from a “man’s career” to a near gender-neutral profession. In 1970, about 7% of physicians were women. By 1980, women accounted for 11.6% of the workforce, and in 2004, women physicians comprised more than 26% of the total.2 With medical school matriculants numbering women and men at near parity—women have made up 45% to 49% of medical school classes since 1999—it is reasonable to assume that the percentage of women physicians will continue to rise annually.3 This process, the feminization of medicine, has created new needs and demands that have not traditionally been identified.4
As previously noted, medical education and training constitute a long-term process that extends into an individual’s later 20s and 30s. Deferred life issues such as marriage and children can wait only so long, and for women the biological clock imposes an earlier time frame than the one for men. Women often want to start a family before the end of their residency training. The traditional residency system was not designed to support multiple extended absences. In most residency programs—77% of programs in one study—maternity absences are handled by requiring the other residents to pick up the slack, an obviously less than happy arrangement.5,6 In the same survey, 83% of residency programs acknowledged that maternity leave had a significant effect on scheduling, despite the fact that 80% of programs had a maternity policy in place.5
It is time for innovative thinking for residency training. New plans must accommodate system needs as well as individual needs and must retain the teaching function necessary to develop the required clinical skills. This can be done, but it requires planning and flexibility. Most residency programs have a maternity policy.5 This policy defines the length of time allotted for maternity leave—free leave, or time off with no make-up requirement. Some programs, such as the one at the University of California at San Francisco, have incorporated a flexible option to accommodate longer absences using flexible make-up time.7
As early as 1989 the National Health Service in the United Kingdom proposed a part-time option in residency training to encourage women physicians to pursue careers in hospital medicine.8 In response to increasing numbers of women physicians, flexible part-time specialty training programs are now generally available in the United Kingdom.9
Developing a functional part-time residency option requires planning ahead and setting aside several residency slots to be paired as half-time equivalents. Training programs want upfront information; they want to have some idea of how many residents plan to start a family during residency years so that they can anticipate the numbers needed for clinical coverage. One would hope that open communication on this issue would not imply discrimination in hiring and that the information would be used to estimate the hiring needs of the program and to accommodate shared practices.
Obviously, some residents who anticipate using the part-time option may later choose not to have children at that time, while others who did not plan to do so may become pregnant. Because of this variability and the inherent concern of discrimination on the basis of the request, it is preferable for residency programs to build in half-time residency slots based on the need experienced in prior years. Once this program is viewed as a standard option, women with young children—or those who anticipate pregnancy during residency—may well request one of the part-time slots to accommodate their needs.
Flexible—part-time—residency programs have the downside of extending the length of training. Although most residents do not relish the idea of a longer residency, for individuals with family commitments this is a welcome option. The extended residency is a benefit if it allows completion of a training program that might otherwise be impossible.
Of women physicians with children in 1988, 22% had a child before finishing residency, and 54% had at least one child by the time they had completed a fellowship.10 I would guess that those percentages are significantly higher with newer data. All residency programs with young women physicians should anticipate pregnancy-leave time. Without a clear plan to cover the clinical workload during these absences, one can predict anger and resentment among the residents who are expected to cover the extra work.11 If the cross-coverage plan for maternity leave is haphazard and only created as the need arises, fellow residents tend to feel that the burden of work is allocated capriciously. If allowed to persist, the resulting frustration damages the program’s collegiality and may result in a view of women as a risk to the best function of the department.6 This consequence damages both the departmental image and the status of women in medicine.
Proactive departmental planning for maternity leave and potentially reduced work hours for women with small children in residency training should be a priority and should be well defined prior to the employment of new residents. Any plan needs to include options, including a brief, fixed maternity leave and a more extended leave with obligations for time payback or flexible extension of the residency with reduced work hours per week. A leave plan must also include the number of weeks a resident can be absent in a year, in two years, and for the duration of the residency, while still fulfilling requirements for board eligibility. Likewise, to ensure a fundamental knowledge base, rotations that must be successfully completed should be clearly enumerated as part of the policy. As a corollary, paternity policy should also be specifically delineated.
Even residents who don’t utilize the flexible option residency like the idea that it is available if needed and believe that having a policy in place is desirable.7 Maintaining a positive espirit de corps in a residency training program is vital to the smooth functioning of the program and also mentors residents on the benefits of collegiality for a lifetime of practice. Developing a well-thought-out and equitable plan for maternity, health, or family leave during residency training is as essential as figuring out how to teach medicine to residents in an 80-hour week—and it can be done. TH
Dr. Brezina is a hospitalist at Durham Regional Medical Hospital in Durham, N.C., and a member of the consulting clinical faculty at Duke University, Durham, N.C.
References
- Croasdale M. Redesigning Residency: new models for internal medicine programs. American Medical News. October 23/30, 2006;Professional issues:10.
- Smart DR. Table 1: Physicians by gender. In: Smart, DR. Physician Characteristics and Distribution in the U.S., 2006 Edition. American Medical Association; 2006.
- AAMC: Data Warehouse: Applicant Matriculant File by sex, 1995-2006. Association of American Medical Colleges Web site. Available at: www.aamc.org/data/facts/2005/2005summary.htm. Last accessed November 29, 2006.
- Levinson W, Lurie N. When most doctors are women: what lies ahead? Ann Intern Med. 2004 Sep 21;141(6):471-474.
- Davis JL, Baillie S, Hodgson CS, et al. Maternity leave: existing policies in obstetrics and gynecology residency programs. Obstet Gynecol. 2001 Dec;98(6):1093-1098.
- Tamburrino MB, Evans CL, Campbell NB, et al. Physician pregnancy: male and female colleagues’ attitudes. J Am Med Womens Assoc. 1992 May-Jun;47(3):82-84.
- Kamei RK, Chen HC, Loeser H. Residency is not a race: our ten-year experience with a flexible schedule residency training option. Acad Med. 2004 May;79(5):447-452.
- Warren VJ, Wakeford RE. ‘We’d like to have a family’—young women doctors’ opinions of maternity leave and part-time training. J R Soc Med. 1989 Sep;82(9):528-531.
- Maingay J, Goldberg I. Flexible training opportunities in the European Union. Med Educ. 1998 Sep;32(5):543-548.
- Sinal S, Weavil P, Camp MG. Survey of women physicians on issues relating to pregnancy during a medical career. J Med Educ. 1988 Jul;63(7):531-538.
- Finch SJ. Pregnancy during residency: a literature review. Acad Med. 2003 Apr;78(4):418-428.
Train the Teacher

If you work at a teaching institution, an important part of your career track may be teaching residents the work of hospitalists. “Within academia, there are two major tracks: research[er] and clinical educator,” says Sanjay Saint, MD, MPH, hospitalist and professor of internal medicine at the Ann Arbor Veterans Affairs Medical Center and the University of Michigan Medical School, Ann Arbor. “We’re promoted based on our clinical work and on education evaluations; it’s helpful when we’re being reviewed if we’re seen as good teachers by our students.”
How are your teaching skills? How much thought and effort do you put into how you train your students? Do you take steps to improve your methods?
“Most of us have to work at being good teachers,” admits Dr. Saint. “We watch excellent teachers and learn as we go.” What follows is the advice of one excellent teacher.
Teachers: Champions for Hospital Medicine
Jeffrey Wiese, MD, FACP, is an SHM board member and associate professor of medicine at Tulane University Health Sciences Center in New Orleans, where he also serves as associate chairman of medicine, director of the Tulane Internal Medicine Residency Program, and associate director of student programs, internal medicine. “From an [SHM] board perspective, it’s been my agenda to better situate hospitalists as teachers,” he says.
One reason he’s committed to boosting the number of hospitalist-teachers is that Dr. Wiese believes the specialty is a perfect match for imparting knowledge. “Hospitalists are better instructors primarily because of their greater accessibility for supervision,” he says. “Because of the number of things they do and the consistent repetition with which they do them, they also have a better familiarity with what students need to know and how to do it.”
Another reason that hospitalists are excellent choices to train residents: “Hospitalists work at improving hospital systems and focus on quality of care,” says Dr. Wiese. “What better group of people to teach the systems of care and practice-based learning competencies?”
Coaching Versus Teaching
The basis of Dr. Wiese’s theory of teaching is that you should think and act as a coach—not a teacher. “A teacher is responsible for disseminating knowledge to his pupils; a coach is responsible for the performance of his pupils,” explains Dr. Wiese. “With a coach, the success of the job is contingent on the performance of the player—in this case, the student or resident.”
The coaching theory goes deeper than that distinction. “Components of coaching include [the following]: You have to teach the necessary skill, but you have to motivate the person to want to do it right, create a vision of how they’re going to do it, anticipate and prepare them for potential obstacles that might stand in the way of their performance, and provide feedback and evaluation when they do it,” says Dr. Wiese. “A football coach wouldn’t just tell you how to throw a ball. He would teach you the skill and then watch you do it, while providing feedback on your performance. He would tell you what the opposing team might do to oppose your performance of that skill and prepare you to overcome that opposition. And then he would instill a motivation such that you wanted to perform the skill well.”
Dr. Saint, who is familiar with Dr. Wiese’s theory, says, “I like the metaphor of coaching because a coach tries to make you better at what you’re learning. A coach may use techniques that make you uncomfortable at the time, but if you look back after a couple of years, you’ll be thankful that he pushed you.”
Another aspect of coaching that fits neatly into today’s clinical learning is the team aspect. “Medicine is no longer an individual event,” explains Dr. Wiese. “It’s a team activity, where the best patient care is provided by a team of healthcare professionals from doctors to nurses to physical therapists and others. Teaching the mentality of playing as part of a team will help residents perform better in this environment as they advance in their careers.”
Teaching in a “Vacum”
“I use the mnemonic VACUM [to describe coaching],” says Dr. Wiese. VACUM stands for:
- Visualization: To pique interest in a topic or procedure, start by asking students to visualize themselves using the skill. Repeatedly ask them how they think they will put the skill to use.
“Get the person to picture herself with a patient,” urges Dr. Wiese. This step both hooks learners at the beginning of a session and helps teach them the skill.
- Anticipation: If you’re an experienced teacher and know your students well, you know where they will struggle in the learning process. “Think about the common pitfalls,” says Dr. Wiese. “Alert the student to where she will get confused or make mistakes and spend time preparing the student for how she can avoid the pitfall. For example, if you’re teaching them about putting in a central line, tell them, ‘You [might] not think about the patient’s bleeding risk prior to procedure. Make sure you know his INR [international normalized ratio] and platelet count prior to starting the procedure.’ ”
- Content: “This is where most teachers go awry,” warns Dr. Wiese. “Medical educators try to teach too much, and students try to learn too much. Not every detail in a topic needs to be discussed. It’s far better to sacrifice details to preserve time to ensure that students have mastered the fundamental concepts of a disease or skill. They can pick up the details later—focus on what they need to know.”
How do you know what to focus on? “The guidelines of what students must learn during their internal medicine clerkship are voluminous,” says Dr. Wiese. “Find those that you think have utility in your practice or utility to the students. The best strategy is to stick to the fundamentals. With this strategy, they will walk away with the critical components that will empower them to pick up the details during subsequent teaching sessions.”
- Utility: “This goes with content,” says Dr. Wiese. “Teach them skills that they can utilize. Remember, utility varies from student to student. A student heading into a future career in orthopedics will find greater utility in learning about pre-operative care and management of atrial fibrillation than she will with a discourse on lupus.”
- Motivation: Motivation includes three subcategories. “Students or residents have to know that the coach is on their side,” says Dr. Wiese. One way to do this is to learn their names—and use them frequently. You should also use physical contact to show your support.
“Give a pat on the shoulder, or shake someone’s hand,” he advises. “If you’re in a classroom, move around the room. Show that you’re accessible.” Finally, find people’s hooks—that is, what interests them.
So how do you know you’ve become a good teacher? “The ultimate goal of coaching is successful student performance—not awards or approbation. The measure of your success is defined by seeing your students months or even years later, doing right by a patient because of what you taught them to do,” says Dr. Wiese. “Focus on that goal, and everything else will fall into place.” TH
Jane Jerrard regularly writes “Career Development.”
If you work at a teaching institution, an important part of your career track may be teaching residents the work of hospitalists. “Within academia, there are two major tracks: research[er] and clinical educator,” says Sanjay Saint, MD, MPH, hospitalist and professor of internal medicine at the Ann Arbor Veterans Affairs Medical Center and the University of Michigan Medical School, Ann Arbor. “We’re promoted based on our clinical work and on education evaluations; it’s helpful when we’re being reviewed if we’re seen as good teachers by our students.”
How are your teaching skills? How much thought and effort do you put into how you train your students? Do you take steps to improve your methods?
“Most of us have to work at being good teachers,” admits Dr. Saint. “We watch excellent teachers and learn as we go.” What follows is the advice of one excellent teacher.
Teachers: Champions for Hospital Medicine
Jeffrey Wiese, MD, FACP, is an SHM board member and associate professor of medicine at Tulane University Health Sciences Center in New Orleans, where he also serves as associate chairman of medicine, director of the Tulane Internal Medicine Residency Program, and associate director of student programs, internal medicine. “From an [SHM] board perspective, it’s been my agenda to better situate hospitalists as teachers,” he says.
One reason he’s committed to boosting the number of hospitalist-teachers is that Dr. Wiese believes the specialty is a perfect match for imparting knowledge. “Hospitalists are better instructors primarily because of their greater accessibility for supervision,” he says. “Because of the number of things they do and the consistent repetition with which they do them, they also have a better familiarity with what students need to know and how to do it.”
Another reason that hospitalists are excellent choices to train residents: “Hospitalists work at improving hospital systems and focus on quality of care,” says Dr. Wiese. “What better group of people to teach the systems of care and practice-based learning competencies?”
Coaching Versus Teaching
The basis of Dr. Wiese’s theory of teaching is that you should think and act as a coach—not a teacher. “A teacher is responsible for disseminating knowledge to his pupils; a coach is responsible for the performance of his pupils,” explains Dr. Wiese. “With a coach, the success of the job is contingent on the performance of the player—in this case, the student or resident.”
The coaching theory goes deeper than that distinction. “Components of coaching include [the following]: You have to teach the necessary skill, but you have to motivate the person to want to do it right, create a vision of how they’re going to do it, anticipate and prepare them for potential obstacles that might stand in the way of their performance, and provide feedback and evaluation when they do it,” says Dr. Wiese. “A football coach wouldn’t just tell you how to throw a ball. He would teach you the skill and then watch you do it, while providing feedback on your performance. He would tell you what the opposing team might do to oppose your performance of that skill and prepare you to overcome that opposition. And then he would instill a motivation such that you wanted to perform the skill well.”
Dr. Saint, who is familiar with Dr. Wiese’s theory, says, “I like the metaphor of coaching because a coach tries to make you better at what you’re learning. A coach may use techniques that make you uncomfortable at the time, but if you look back after a couple of years, you’ll be thankful that he pushed you.”
Another aspect of coaching that fits neatly into today’s clinical learning is the team aspect. “Medicine is no longer an individual event,” explains Dr. Wiese. “It’s a team activity, where the best patient care is provided by a team of healthcare professionals from doctors to nurses to physical therapists and others. Teaching the mentality of playing as part of a team will help residents perform better in this environment as they advance in their careers.”
Teaching in a “Vacum”
“I use the mnemonic VACUM [to describe coaching],” says Dr. Wiese. VACUM stands for:
- Visualization: To pique interest in a topic or procedure, start by asking students to visualize themselves using the skill. Repeatedly ask them how they think they will put the skill to use.
“Get the person to picture herself with a patient,” urges Dr. Wiese. This step both hooks learners at the beginning of a session and helps teach them the skill.
- Anticipation: If you’re an experienced teacher and know your students well, you know where they will struggle in the learning process. “Think about the common pitfalls,” says Dr. Wiese. “Alert the student to where she will get confused or make mistakes and spend time preparing the student for how she can avoid the pitfall. For example, if you’re teaching them about putting in a central line, tell them, ‘You [might] not think about the patient’s bleeding risk prior to procedure. Make sure you know his INR [international normalized ratio] and platelet count prior to starting the procedure.’ ”
- Content: “This is where most teachers go awry,” warns Dr. Wiese. “Medical educators try to teach too much, and students try to learn too much. Not every detail in a topic needs to be discussed. It’s far better to sacrifice details to preserve time to ensure that students have mastered the fundamental concepts of a disease or skill. They can pick up the details later—focus on what they need to know.”
How do you know what to focus on? “The guidelines of what students must learn during their internal medicine clerkship are voluminous,” says Dr. Wiese. “Find those that you think have utility in your practice or utility to the students. The best strategy is to stick to the fundamentals. With this strategy, they will walk away with the critical components that will empower them to pick up the details during subsequent teaching sessions.”
- Utility: “This goes with content,” says Dr. Wiese. “Teach them skills that they can utilize. Remember, utility varies from student to student. A student heading into a future career in orthopedics will find greater utility in learning about pre-operative care and management of atrial fibrillation than she will with a discourse on lupus.”
- Motivation: Motivation includes three subcategories. “Students or residents have to know that the coach is on their side,” says Dr. Wiese. One way to do this is to learn their names—and use them frequently. You should also use physical contact to show your support.
“Give a pat on the shoulder, or shake someone’s hand,” he advises. “If you’re in a classroom, move around the room. Show that you’re accessible.” Finally, find people’s hooks—that is, what interests them.
So how do you know you’ve become a good teacher? “The ultimate goal of coaching is successful student performance—not awards or approbation. The measure of your success is defined by seeing your students months or even years later, doing right by a patient because of what you taught them to do,” says Dr. Wiese. “Focus on that goal, and everything else will fall into place.” TH
Jane Jerrard regularly writes “Career Development.”
If you work at a teaching institution, an important part of your career track may be teaching residents the work of hospitalists. “Within academia, there are two major tracks: research[er] and clinical educator,” says Sanjay Saint, MD, MPH, hospitalist and professor of internal medicine at the Ann Arbor Veterans Affairs Medical Center and the University of Michigan Medical School, Ann Arbor. “We’re promoted based on our clinical work and on education evaluations; it’s helpful when we’re being reviewed if we’re seen as good teachers by our students.”
How are your teaching skills? How much thought and effort do you put into how you train your students? Do you take steps to improve your methods?
“Most of us have to work at being good teachers,” admits Dr. Saint. “We watch excellent teachers and learn as we go.” What follows is the advice of one excellent teacher.
Teachers: Champions for Hospital Medicine
Jeffrey Wiese, MD, FACP, is an SHM board member and associate professor of medicine at Tulane University Health Sciences Center in New Orleans, where he also serves as associate chairman of medicine, director of the Tulane Internal Medicine Residency Program, and associate director of student programs, internal medicine. “From an [SHM] board perspective, it’s been my agenda to better situate hospitalists as teachers,” he says.
One reason he’s committed to boosting the number of hospitalist-teachers is that Dr. Wiese believes the specialty is a perfect match for imparting knowledge. “Hospitalists are better instructors primarily because of their greater accessibility for supervision,” he says. “Because of the number of things they do and the consistent repetition with which they do them, they also have a better familiarity with what students need to know and how to do it.”
Another reason that hospitalists are excellent choices to train residents: “Hospitalists work at improving hospital systems and focus on quality of care,” says Dr. Wiese. “What better group of people to teach the systems of care and practice-based learning competencies?”
Coaching Versus Teaching
The basis of Dr. Wiese’s theory of teaching is that you should think and act as a coach—not a teacher. “A teacher is responsible for disseminating knowledge to his pupils; a coach is responsible for the performance of his pupils,” explains Dr. Wiese. “With a coach, the success of the job is contingent on the performance of the player—in this case, the student or resident.”
The coaching theory goes deeper than that distinction. “Components of coaching include [the following]: You have to teach the necessary skill, but you have to motivate the person to want to do it right, create a vision of how they’re going to do it, anticipate and prepare them for potential obstacles that might stand in the way of their performance, and provide feedback and evaluation when they do it,” says Dr. Wiese. “A football coach wouldn’t just tell you how to throw a ball. He would teach you the skill and then watch you do it, while providing feedback on your performance. He would tell you what the opposing team might do to oppose your performance of that skill and prepare you to overcome that opposition. And then he would instill a motivation such that you wanted to perform the skill well.”
Dr. Saint, who is familiar with Dr. Wiese’s theory, says, “I like the metaphor of coaching because a coach tries to make you better at what you’re learning. A coach may use techniques that make you uncomfortable at the time, but if you look back after a couple of years, you’ll be thankful that he pushed you.”
Another aspect of coaching that fits neatly into today’s clinical learning is the team aspect. “Medicine is no longer an individual event,” explains Dr. Wiese. “It’s a team activity, where the best patient care is provided by a team of healthcare professionals from doctors to nurses to physical therapists and others. Teaching the mentality of playing as part of a team will help residents perform better in this environment as they advance in their careers.”
Teaching in a “Vacum”
“I use the mnemonic VACUM [to describe coaching],” says Dr. Wiese. VACUM stands for:
- Visualization: To pique interest in a topic or procedure, start by asking students to visualize themselves using the skill. Repeatedly ask them how they think they will put the skill to use.
“Get the person to picture herself with a patient,” urges Dr. Wiese. This step both hooks learners at the beginning of a session and helps teach them the skill.
- Anticipation: If you’re an experienced teacher and know your students well, you know where they will struggle in the learning process. “Think about the common pitfalls,” says Dr. Wiese. “Alert the student to where she will get confused or make mistakes and spend time preparing the student for how she can avoid the pitfall. For example, if you’re teaching them about putting in a central line, tell them, ‘You [might] not think about the patient’s bleeding risk prior to procedure. Make sure you know his INR [international normalized ratio] and platelet count prior to starting the procedure.’ ”
- Content: “This is where most teachers go awry,” warns Dr. Wiese. “Medical educators try to teach too much, and students try to learn too much. Not every detail in a topic needs to be discussed. It’s far better to sacrifice details to preserve time to ensure that students have mastered the fundamental concepts of a disease or skill. They can pick up the details later—focus on what they need to know.”
How do you know what to focus on? “The guidelines of what students must learn during their internal medicine clerkship are voluminous,” says Dr. Wiese. “Find those that you think have utility in your practice or utility to the students. The best strategy is to stick to the fundamentals. With this strategy, they will walk away with the critical components that will empower them to pick up the details during subsequent teaching sessions.”
- Utility: “This goes with content,” says Dr. Wiese. “Teach them skills that they can utilize. Remember, utility varies from student to student. A student heading into a future career in orthopedics will find greater utility in learning about pre-operative care and management of atrial fibrillation than she will with a discourse on lupus.”
- Motivation: Motivation includes three subcategories. “Students or residents have to know that the coach is on their side,” says Dr. Wiese. One way to do this is to learn their names—and use them frequently. You should also use physical contact to show your support.
“Give a pat on the shoulder, or shake someone’s hand,” he advises. “If you’re in a classroom, move around the room. Show that you’re accessible.” Finally, find people’s hooks—that is, what interests them.
So how do you know you’ve become a good teacher? “The ultimate goal of coaching is successful student performance—not awards or approbation. The measure of your success is defined by seeing your students months or even years later, doing right by a patient because of what you taught them to do,” says Dr. Wiese. “Focus on that goal, and everything else will fall into place.” TH
Jane Jerrard regularly writes “Career Development.”
How to Stay Out of Litigation

We’ve defended physicians involved in lawsuits for more than a decade. After representing dozens of physicians, nurses, and other healthcare professionals, we can say one thing for certain: No one likes to get sued.
Good physicians struggle with the litigation process. Even when their care has been absolutely appropriate, many doctors experience great anxiety when they are accused of having negligently injured a patient. Because they have trained so hard to gain their expertise, many of our clients have found that a lawsuit strikes at them personally as well as professionally. At the end of the day, lawsuits cause stress, take physicians away from their personal lives, and often lead to serious financial and professional consequences.
Therefore, one of the questions that we most often receive is, “How can a physician avoid lawsuits?”
Top 10 Ways to Stay Out of Litigation
1) Good documentation: Often, in a lawsuit, plaintiffs’ attorneys will tell the jury the old adage, “If it’s not in the record, it didn’t happen.” What everyone who has practiced medicine knows, however, is that many things don’t make it to the chart. Physicians don’t have the time to recount their conversations with patients verbatim. What we want to see in the chart are the following:
- A description of the information provided by the patient that factored into your diagnoses or treatment decisions;
- A description of the physical findings or laboratory results that factored into your diagnoses and treatment decisions;
- A discussion of why you made a particular decision;
- A discussion of the course of treatment you selected; and
- A discussion of your anticipated follow-up.
Of these elements, we most often fail to see a discussion of why you made a particular decision, and this is a crucial piece of the record. As you know, physicians often have a broad range of treatment choices. Including information about why you selected a particular course of treatment—in light of the available data—makes the record more understandable to the jury. A good chart lays out more than just the physician’s actions. A good chart is so complete that another physician could assume care for the patient tomorrow, easily understanding both the course of treatment and why you chose it.
2) Good communication: In his book Blink, Malcolm Gladwell describes something defense lawyers have known for many years: That the quality of the care does not determine whether or not a physician gets sued. There are many instances in which a physician who makes a mistake that causes an injury manages to avoid litigation. There are also many instances in which a physician’s care is appropriate, but the patient sues the physician after a recognized complication. What makes the difference?
More often than not, the determining factor in whether or not a physician is sued is the patient’s perception of whether or not the physician cared about her. In situations in which patients leave the physician’s office believing that the physician listened carefully to their complaints, spent the time to explain the course of treatment, and genuinely cared about them as people, we don’t see as many lawsuits. If a physician explains why a complication occurred—not just that it occurred—and appears empathetic to the patient, she has less of a motivation to sue. Conversely, if the patient feels like the physician sees her as a commodity or didn’t take the time to understand her complaints, the risk of litigation goes up.
One of the most important aspects of good communication is adequate informed consent. Remember, informed consent is a dialogue—not a lecture. It requires physicians to discuss:
- The substantial risks of the treatment;
- The benefits of the treatment; and
- The alternatives to the treatment. Sometimes it’s difficult to determine the substantial risks because a patient and a physician may view the magnitude of a particular risk differently. Our rule of thumb is that any risks associated with serious long-term sequelae, such as permanent impairment, must be discussed, even if the probability of the risk occurring is remote.
3) Good consultation: Many hospitalists do not have long-term relationships with their patients. After a course of hospital treatment, the patient will return to her regular physician. A common breakdown occurs when the consultation between the hospitalist and the regular physician is inadequate.
On the front end, the hospitalist who receives a patient should take the opportunity, if possible, to consult with the regular physician about any ongoing course of treatment. Unfortunately, patients are not always accurate medical historians and may not fully appreciate their conditions or courses of treatment. Consulting with the regular physician helps to eliminate the possibility that an important aspect of the patient’s history or condition is overlooked.
On the back end, when the regular physician resumes care of the patient, he should be able to reinforce the course of hospital care and provide an additional layer of education about why the hospitalist made certain treatment decisions. Of course, the regular physician can serve in this role only if the hospitalist has taken the opportunity to inform the regular physician about the course of care.
4) Accurate representations: We are seeing more cases in which physicians are being sued for alleged misrepresentations to patients.
For example, each of you has probably seen an ad in which a Lasik provider advertises that the procedure is “20/20 or it’s free.” A patient may be able to allege that this advertisement is a guarantee that the procedure will result in 20/20 vision, but no medical provider should guarantee a successful outcome. Each human body reacts differently to treatment, and there is no physician who has not seen an unexpected outcome. Providing patients with unrealistic expectations about their outcomes can lead to lawsuits, even if a physician has obtained a signed informed consent detailing the risks involved.
The situation is even worse when the physician misrepresents his experience. We have defended cases in which physicians have told patients that they had performed a procedure hundreds of times, when that representation was not accurate. One of the greatest assets available to physicians in litigation is their advanced training and professional experience, but that asset becomes worthless if a physician gives the jury a reason to doubt his credibility. Once the jury believes that a physician has misrepresented his experience, he loses the ability to credibly explain his treatment decisions.
5) HMO-directed medicine: It’s no secret that many patients are dissatisfied with their managed care plans. In the abstract, patients understand that rising healthcare costs have caused insurers to limit care, but they are unwilling to view their own situations objectively. They believe that they are entitled to unlimited medical resources. When the HMO tells patients “no,” they have a tendency to transfer their frustrations to their physicians.
The coverage provided by the HMO is a contractual matter between the patient and the insurer. At the end of the day, the treating physician does not control the patient’s eligibility for certain types of care. What the treating physician cannot overlook, however, is that the physician-patient relationship is a personal one that exists independently of the insurance relationship. The standards of professional care require a physician to inform patients of all treatment options—even if the physician believes that the HMO is unlikely to authorize some of them. Ultimately, even if the cost of a treatment option would be prohibitive, a physician must remember that the patient has a right to be informed and to make her own decisions. Physicians should also be receptive to advocating on a patient’s behalf about the reasonableness or necessity of care.
6) Attend to the patient: Few things are harder to explain to a jury than a physician’s failure to personally attend to a patient. The reality is that physicians may receive information over the telephone or through an intermediary’s relay, and they often have to use these means of communication. The risk is that a physician will miss a detail that he would have seen if he had personally examined the patient.
Err on the side of caution. If your differential diagnosis includes a potentially serious condition and your ability to rule out that condition might be influenced by physical findings, arrange to see the patient in person. If the situation does not allow for a face-to-face appointment, instruct the patient to seek medical care through an emergency department or another provider.
Having been there, we can say that there is nothing more difficult for a physician than to have to admit, at deposition, “I wish I had seen the patient personally.”
7) Adequate discharge instructions: Another reality of modern medical practice is that patients often leave the hospital before their course of healing is complete. Patients may leave the hospital shortly after surgery or while still affected by an illness. Even when the treatment in the hospital has been appropriate, we regularly see cases arising from the physician’s discharge instructions. Patients allege that they did not receive enough information to allow them to recognize the onset of potentially serious complications. To prevent confusion, discharge instructions should address all areas of potential concern, including pain, wound care, and signs of infection. The instructions should also include information regarding whom to contact if questions arise and should instruct the patient to return if she experiences a change in condition.
8) Be prepared to deal with misinformation: Technology is wonderful. This morning, we typed the term “diabetes mellitus” into the Google search engine. It returned more than 7.3 million references. Within 30 seconds, we located the “final cure for diabetes,” which was compounded from banana, bitter melon, licorice extract, and cayenne pepper (among other things). While this might cure diabetes, we have our doubts; however, we will leave the debate to more scientific minds.
The problem is that sick people often become desperate people—particularly when fighting diseases like cancer, AIDS, and Alzheimer’s. They are likely to be vulnerable to misinformation and might be inclined to pursue courses of action that could actually harm them. Physicians must realize that they will regularly deal with patients who have unrealistic expectations of the medical system. The only way physicians can combat misinformation is by providing better information. Physicians need to be prepared to educate patients who have unsuccessfully tried to educate themselves. Part of that education can be verbal, but physicians should consider directing patients to reliable resources that they can explore after leaving the hospital.
Patients are also bombarded by advertisements for prescription medications, all of which are designed to persuade them to take an active role in requesting particular prescriptions. The problem is that the physician is responsible for selecting an appropriate medication. Physicians have to be able to explain why an advertised medication may not be the best choice under the circumstances, no matter what the TV commercial said.
9) Take responsibility: Everyone makes mistakes. No physician is perfect, nor is it fair to expect perfection from those who deal with the intricate machinery of the human body. A culture of fear, however, has caused many physicians to believe that they should not admit their mistakes. Our experience shows that recognizing and responding to mistakes is a far better course of action than trying to pretend they didn’t exist.
Taking responsibility doesn’t mean admitting that you were negligent. It does mean acknowledging a complication when it occurs and assisting the patient in minimizing the consequences. Sometimes this will result in transferring the patient to another physician. At other times, the physician may have to pay to correct the mistake. Many medical malpractice insurance carriers now have programs targeted at promptly recognizing and reacting to unexpected outcomes. These insurers realize that the best time to correct a bad situation is within hours or days of its occurrence. Enlist the help of your insurer or hospital risk manager. If patients feel like their physicians are trying to minimize a situation, hoping mistakenly that it will go away, it becomes much more difficult to avoid litigation.
10) Don’t compromise your integrity: Physicians are professionals. Whether it’s fair or not, jurors hold physicians to a higher standard of conduct. They expect more of doctors. They expect doctors to “do the right thing.” Consequently, jurors tend to punish physicians who place their personal interests above their patients’ interests. Federal law already prohibits physicians from engaging in many forms of self-dealing, such as investing in certain businesses or receiving kickbacks for medical care. But there are many lawful forms of conduct that might cause a jury to question why a physician chose a particular course of action.
Recent medical literature demonstrates that pharmaceutical manufacturers direct 90% of an estimated $21 billion annual marketing budget at physicians, including the sponsorship of an estimated 300,000 annual education events. This amounts to approximately $13,000 per physician annually. Because of concerns that even small inducements might have an unwanted effect upon physician independence, the Stanford Medical Center recently announced a new policy prohibiting physicians from accepting free drug samples or even small gifts from pharmaceutical sales representatives. Prominent newspapers have been running stories about the “free lunches” physicians receive.
We’re not suggesting that physicians spurn pharmaceutical sales representatives or that they avoid legal business opportunities. We caution you, however, that smart plaintiffs’ attorneys are sensitive to any indications that a physician has allowed his interests to influence a patient’s treatment. Don’t put yourself in a position where a jury could reasonably question whether or not you had your patient’s best interests in mind.
Unfortunately, even if a physician observes all of these precautions, a patient still might file a lawsuit. If you sense a real potential for litigation, contact your insurance company and provide notice of a potential claim. This will help ensure that your insurance coverage is available if a lawsuit is filed. It also allows the insurance company to retain an attorney to assist you. The next time we write, we’ll provide our top tips for winning a lawsuit once it occurs. TH
Patrick O’Rourke is the managing associate university counsel for the University of Colorado’s litigation office. Kari M. Hershey, JD, practices health law in Colorado.
We’ve defended physicians involved in lawsuits for more than a decade. After representing dozens of physicians, nurses, and other healthcare professionals, we can say one thing for certain: No one likes to get sued.
Good physicians struggle with the litigation process. Even when their care has been absolutely appropriate, many doctors experience great anxiety when they are accused of having negligently injured a patient. Because they have trained so hard to gain their expertise, many of our clients have found that a lawsuit strikes at them personally as well as professionally. At the end of the day, lawsuits cause stress, take physicians away from their personal lives, and often lead to serious financial and professional consequences.
Therefore, one of the questions that we most often receive is, “How can a physician avoid lawsuits?”
Top 10 Ways to Stay Out of Litigation
1) Good documentation: Often, in a lawsuit, plaintiffs’ attorneys will tell the jury the old adage, “If it’s not in the record, it didn’t happen.” What everyone who has practiced medicine knows, however, is that many things don’t make it to the chart. Physicians don’t have the time to recount their conversations with patients verbatim. What we want to see in the chart are the following:
- A description of the information provided by the patient that factored into your diagnoses or treatment decisions;
- A description of the physical findings or laboratory results that factored into your diagnoses and treatment decisions;
- A discussion of why you made a particular decision;
- A discussion of the course of treatment you selected; and
- A discussion of your anticipated follow-up.
Of these elements, we most often fail to see a discussion of why you made a particular decision, and this is a crucial piece of the record. As you know, physicians often have a broad range of treatment choices. Including information about why you selected a particular course of treatment—in light of the available data—makes the record more understandable to the jury. A good chart lays out more than just the physician’s actions. A good chart is so complete that another physician could assume care for the patient tomorrow, easily understanding both the course of treatment and why you chose it.
2) Good communication: In his book Blink, Malcolm Gladwell describes something defense lawyers have known for many years: That the quality of the care does not determine whether or not a physician gets sued. There are many instances in which a physician who makes a mistake that causes an injury manages to avoid litigation. There are also many instances in which a physician’s care is appropriate, but the patient sues the physician after a recognized complication. What makes the difference?
More often than not, the determining factor in whether or not a physician is sued is the patient’s perception of whether or not the physician cared about her. In situations in which patients leave the physician’s office believing that the physician listened carefully to their complaints, spent the time to explain the course of treatment, and genuinely cared about them as people, we don’t see as many lawsuits. If a physician explains why a complication occurred—not just that it occurred—and appears empathetic to the patient, she has less of a motivation to sue. Conversely, if the patient feels like the physician sees her as a commodity or didn’t take the time to understand her complaints, the risk of litigation goes up.
One of the most important aspects of good communication is adequate informed consent. Remember, informed consent is a dialogue—not a lecture. It requires physicians to discuss:
- The substantial risks of the treatment;
- The benefits of the treatment; and
- The alternatives to the treatment. Sometimes it’s difficult to determine the substantial risks because a patient and a physician may view the magnitude of a particular risk differently. Our rule of thumb is that any risks associated with serious long-term sequelae, such as permanent impairment, must be discussed, even if the probability of the risk occurring is remote.
3) Good consultation: Many hospitalists do not have long-term relationships with their patients. After a course of hospital treatment, the patient will return to her regular physician. A common breakdown occurs when the consultation between the hospitalist and the regular physician is inadequate.
On the front end, the hospitalist who receives a patient should take the opportunity, if possible, to consult with the regular physician about any ongoing course of treatment. Unfortunately, patients are not always accurate medical historians and may not fully appreciate their conditions or courses of treatment. Consulting with the regular physician helps to eliminate the possibility that an important aspect of the patient’s history or condition is overlooked.
On the back end, when the regular physician resumes care of the patient, he should be able to reinforce the course of hospital care and provide an additional layer of education about why the hospitalist made certain treatment decisions. Of course, the regular physician can serve in this role only if the hospitalist has taken the opportunity to inform the regular physician about the course of care.
4) Accurate representations: We are seeing more cases in which physicians are being sued for alleged misrepresentations to patients.
For example, each of you has probably seen an ad in which a Lasik provider advertises that the procedure is “20/20 or it’s free.” A patient may be able to allege that this advertisement is a guarantee that the procedure will result in 20/20 vision, but no medical provider should guarantee a successful outcome. Each human body reacts differently to treatment, and there is no physician who has not seen an unexpected outcome. Providing patients with unrealistic expectations about their outcomes can lead to lawsuits, even if a physician has obtained a signed informed consent detailing the risks involved.
The situation is even worse when the physician misrepresents his experience. We have defended cases in which physicians have told patients that they had performed a procedure hundreds of times, when that representation was not accurate. One of the greatest assets available to physicians in litigation is their advanced training and professional experience, but that asset becomes worthless if a physician gives the jury a reason to doubt his credibility. Once the jury believes that a physician has misrepresented his experience, he loses the ability to credibly explain his treatment decisions.
5) HMO-directed medicine: It’s no secret that many patients are dissatisfied with their managed care plans. In the abstract, patients understand that rising healthcare costs have caused insurers to limit care, but they are unwilling to view their own situations objectively. They believe that they are entitled to unlimited medical resources. When the HMO tells patients “no,” they have a tendency to transfer their frustrations to their physicians.
The coverage provided by the HMO is a contractual matter between the patient and the insurer. At the end of the day, the treating physician does not control the patient’s eligibility for certain types of care. What the treating physician cannot overlook, however, is that the physician-patient relationship is a personal one that exists independently of the insurance relationship. The standards of professional care require a physician to inform patients of all treatment options—even if the physician believes that the HMO is unlikely to authorize some of them. Ultimately, even if the cost of a treatment option would be prohibitive, a physician must remember that the patient has a right to be informed and to make her own decisions. Physicians should also be receptive to advocating on a patient’s behalf about the reasonableness or necessity of care.
6) Attend to the patient: Few things are harder to explain to a jury than a physician’s failure to personally attend to a patient. The reality is that physicians may receive information over the telephone or through an intermediary’s relay, and they often have to use these means of communication. The risk is that a physician will miss a detail that he would have seen if he had personally examined the patient.
Err on the side of caution. If your differential diagnosis includes a potentially serious condition and your ability to rule out that condition might be influenced by physical findings, arrange to see the patient in person. If the situation does not allow for a face-to-face appointment, instruct the patient to seek medical care through an emergency department or another provider.
Having been there, we can say that there is nothing more difficult for a physician than to have to admit, at deposition, “I wish I had seen the patient personally.”
7) Adequate discharge instructions: Another reality of modern medical practice is that patients often leave the hospital before their course of healing is complete. Patients may leave the hospital shortly after surgery or while still affected by an illness. Even when the treatment in the hospital has been appropriate, we regularly see cases arising from the physician’s discharge instructions. Patients allege that they did not receive enough information to allow them to recognize the onset of potentially serious complications. To prevent confusion, discharge instructions should address all areas of potential concern, including pain, wound care, and signs of infection. The instructions should also include information regarding whom to contact if questions arise and should instruct the patient to return if she experiences a change in condition.
8) Be prepared to deal with misinformation: Technology is wonderful. This morning, we typed the term “diabetes mellitus” into the Google search engine. It returned more than 7.3 million references. Within 30 seconds, we located the “final cure for diabetes,” which was compounded from banana, bitter melon, licorice extract, and cayenne pepper (among other things). While this might cure diabetes, we have our doubts; however, we will leave the debate to more scientific minds.
The problem is that sick people often become desperate people—particularly when fighting diseases like cancer, AIDS, and Alzheimer’s. They are likely to be vulnerable to misinformation and might be inclined to pursue courses of action that could actually harm them. Physicians must realize that they will regularly deal with patients who have unrealistic expectations of the medical system. The only way physicians can combat misinformation is by providing better information. Physicians need to be prepared to educate patients who have unsuccessfully tried to educate themselves. Part of that education can be verbal, but physicians should consider directing patients to reliable resources that they can explore after leaving the hospital.
Patients are also bombarded by advertisements for prescription medications, all of which are designed to persuade them to take an active role in requesting particular prescriptions. The problem is that the physician is responsible for selecting an appropriate medication. Physicians have to be able to explain why an advertised medication may not be the best choice under the circumstances, no matter what the TV commercial said.
9) Take responsibility: Everyone makes mistakes. No physician is perfect, nor is it fair to expect perfection from those who deal with the intricate machinery of the human body. A culture of fear, however, has caused many physicians to believe that they should not admit their mistakes. Our experience shows that recognizing and responding to mistakes is a far better course of action than trying to pretend they didn’t exist.
Taking responsibility doesn’t mean admitting that you were negligent. It does mean acknowledging a complication when it occurs and assisting the patient in minimizing the consequences. Sometimes this will result in transferring the patient to another physician. At other times, the physician may have to pay to correct the mistake. Many medical malpractice insurance carriers now have programs targeted at promptly recognizing and reacting to unexpected outcomes. These insurers realize that the best time to correct a bad situation is within hours or days of its occurrence. Enlist the help of your insurer or hospital risk manager. If patients feel like their physicians are trying to minimize a situation, hoping mistakenly that it will go away, it becomes much more difficult to avoid litigation.
10) Don’t compromise your integrity: Physicians are professionals. Whether it’s fair or not, jurors hold physicians to a higher standard of conduct. They expect more of doctors. They expect doctors to “do the right thing.” Consequently, jurors tend to punish physicians who place their personal interests above their patients’ interests. Federal law already prohibits physicians from engaging in many forms of self-dealing, such as investing in certain businesses or receiving kickbacks for medical care. But there are many lawful forms of conduct that might cause a jury to question why a physician chose a particular course of action.
Recent medical literature demonstrates that pharmaceutical manufacturers direct 90% of an estimated $21 billion annual marketing budget at physicians, including the sponsorship of an estimated 300,000 annual education events. This amounts to approximately $13,000 per physician annually. Because of concerns that even small inducements might have an unwanted effect upon physician independence, the Stanford Medical Center recently announced a new policy prohibiting physicians from accepting free drug samples or even small gifts from pharmaceutical sales representatives. Prominent newspapers have been running stories about the “free lunches” physicians receive.
We’re not suggesting that physicians spurn pharmaceutical sales representatives or that they avoid legal business opportunities. We caution you, however, that smart plaintiffs’ attorneys are sensitive to any indications that a physician has allowed his interests to influence a patient’s treatment. Don’t put yourself in a position where a jury could reasonably question whether or not you had your patient’s best interests in mind.
Unfortunately, even if a physician observes all of these precautions, a patient still might file a lawsuit. If you sense a real potential for litigation, contact your insurance company and provide notice of a potential claim. This will help ensure that your insurance coverage is available if a lawsuit is filed. It also allows the insurance company to retain an attorney to assist you. The next time we write, we’ll provide our top tips for winning a lawsuit once it occurs. TH
Patrick O’Rourke is the managing associate university counsel for the University of Colorado’s litigation office. Kari M. Hershey, JD, practices health law in Colorado.
We’ve defended physicians involved in lawsuits for more than a decade. After representing dozens of physicians, nurses, and other healthcare professionals, we can say one thing for certain: No one likes to get sued.
Good physicians struggle with the litigation process. Even when their care has been absolutely appropriate, many doctors experience great anxiety when they are accused of having negligently injured a patient. Because they have trained so hard to gain their expertise, many of our clients have found that a lawsuit strikes at them personally as well as professionally. At the end of the day, lawsuits cause stress, take physicians away from their personal lives, and often lead to serious financial and professional consequences.
Therefore, one of the questions that we most often receive is, “How can a physician avoid lawsuits?”
Top 10 Ways to Stay Out of Litigation
1) Good documentation: Often, in a lawsuit, plaintiffs’ attorneys will tell the jury the old adage, “If it’s not in the record, it didn’t happen.” What everyone who has practiced medicine knows, however, is that many things don’t make it to the chart. Physicians don’t have the time to recount their conversations with patients verbatim. What we want to see in the chart are the following:
- A description of the information provided by the patient that factored into your diagnoses or treatment decisions;
- A description of the physical findings or laboratory results that factored into your diagnoses and treatment decisions;
- A discussion of why you made a particular decision;
- A discussion of the course of treatment you selected; and
- A discussion of your anticipated follow-up.
Of these elements, we most often fail to see a discussion of why you made a particular decision, and this is a crucial piece of the record. As you know, physicians often have a broad range of treatment choices. Including information about why you selected a particular course of treatment—in light of the available data—makes the record more understandable to the jury. A good chart lays out more than just the physician’s actions. A good chart is so complete that another physician could assume care for the patient tomorrow, easily understanding both the course of treatment and why you chose it.
2) Good communication: In his book Blink, Malcolm Gladwell describes something defense lawyers have known for many years: That the quality of the care does not determine whether or not a physician gets sued. There are many instances in which a physician who makes a mistake that causes an injury manages to avoid litigation. There are also many instances in which a physician’s care is appropriate, but the patient sues the physician after a recognized complication. What makes the difference?
More often than not, the determining factor in whether or not a physician is sued is the patient’s perception of whether or not the physician cared about her. In situations in which patients leave the physician’s office believing that the physician listened carefully to their complaints, spent the time to explain the course of treatment, and genuinely cared about them as people, we don’t see as many lawsuits. If a physician explains why a complication occurred—not just that it occurred—and appears empathetic to the patient, she has less of a motivation to sue. Conversely, if the patient feels like the physician sees her as a commodity or didn’t take the time to understand her complaints, the risk of litigation goes up.
One of the most important aspects of good communication is adequate informed consent. Remember, informed consent is a dialogue—not a lecture. It requires physicians to discuss:
- The substantial risks of the treatment;
- The benefits of the treatment; and
- The alternatives to the treatment. Sometimes it’s difficult to determine the substantial risks because a patient and a physician may view the magnitude of a particular risk differently. Our rule of thumb is that any risks associated with serious long-term sequelae, such as permanent impairment, must be discussed, even if the probability of the risk occurring is remote.
3) Good consultation: Many hospitalists do not have long-term relationships with their patients. After a course of hospital treatment, the patient will return to her regular physician. A common breakdown occurs when the consultation between the hospitalist and the regular physician is inadequate.
On the front end, the hospitalist who receives a patient should take the opportunity, if possible, to consult with the regular physician about any ongoing course of treatment. Unfortunately, patients are not always accurate medical historians and may not fully appreciate their conditions or courses of treatment. Consulting with the regular physician helps to eliminate the possibility that an important aspect of the patient’s history or condition is overlooked.
On the back end, when the regular physician resumes care of the patient, he should be able to reinforce the course of hospital care and provide an additional layer of education about why the hospitalist made certain treatment decisions. Of course, the regular physician can serve in this role only if the hospitalist has taken the opportunity to inform the regular physician about the course of care.
4) Accurate representations: We are seeing more cases in which physicians are being sued for alleged misrepresentations to patients.
For example, each of you has probably seen an ad in which a Lasik provider advertises that the procedure is “20/20 or it’s free.” A patient may be able to allege that this advertisement is a guarantee that the procedure will result in 20/20 vision, but no medical provider should guarantee a successful outcome. Each human body reacts differently to treatment, and there is no physician who has not seen an unexpected outcome. Providing patients with unrealistic expectations about their outcomes can lead to lawsuits, even if a physician has obtained a signed informed consent detailing the risks involved.
The situation is even worse when the physician misrepresents his experience. We have defended cases in which physicians have told patients that they had performed a procedure hundreds of times, when that representation was not accurate. One of the greatest assets available to physicians in litigation is their advanced training and professional experience, but that asset becomes worthless if a physician gives the jury a reason to doubt his credibility. Once the jury believes that a physician has misrepresented his experience, he loses the ability to credibly explain his treatment decisions.
5) HMO-directed medicine: It’s no secret that many patients are dissatisfied with their managed care plans. In the abstract, patients understand that rising healthcare costs have caused insurers to limit care, but they are unwilling to view their own situations objectively. They believe that they are entitled to unlimited medical resources. When the HMO tells patients “no,” they have a tendency to transfer their frustrations to their physicians.
The coverage provided by the HMO is a contractual matter between the patient and the insurer. At the end of the day, the treating physician does not control the patient’s eligibility for certain types of care. What the treating physician cannot overlook, however, is that the physician-patient relationship is a personal one that exists independently of the insurance relationship. The standards of professional care require a physician to inform patients of all treatment options—even if the physician believes that the HMO is unlikely to authorize some of them. Ultimately, even if the cost of a treatment option would be prohibitive, a physician must remember that the patient has a right to be informed and to make her own decisions. Physicians should also be receptive to advocating on a patient’s behalf about the reasonableness or necessity of care.
6) Attend to the patient: Few things are harder to explain to a jury than a physician’s failure to personally attend to a patient. The reality is that physicians may receive information over the telephone or through an intermediary’s relay, and they often have to use these means of communication. The risk is that a physician will miss a detail that he would have seen if he had personally examined the patient.
Err on the side of caution. If your differential diagnosis includes a potentially serious condition and your ability to rule out that condition might be influenced by physical findings, arrange to see the patient in person. If the situation does not allow for a face-to-face appointment, instruct the patient to seek medical care through an emergency department or another provider.
Having been there, we can say that there is nothing more difficult for a physician than to have to admit, at deposition, “I wish I had seen the patient personally.”
7) Adequate discharge instructions: Another reality of modern medical practice is that patients often leave the hospital before their course of healing is complete. Patients may leave the hospital shortly after surgery or while still affected by an illness. Even when the treatment in the hospital has been appropriate, we regularly see cases arising from the physician’s discharge instructions. Patients allege that they did not receive enough information to allow them to recognize the onset of potentially serious complications. To prevent confusion, discharge instructions should address all areas of potential concern, including pain, wound care, and signs of infection. The instructions should also include information regarding whom to contact if questions arise and should instruct the patient to return if she experiences a change in condition.
8) Be prepared to deal with misinformation: Technology is wonderful. This morning, we typed the term “diabetes mellitus” into the Google search engine. It returned more than 7.3 million references. Within 30 seconds, we located the “final cure for diabetes,” which was compounded from banana, bitter melon, licorice extract, and cayenne pepper (among other things). While this might cure diabetes, we have our doubts; however, we will leave the debate to more scientific minds.
The problem is that sick people often become desperate people—particularly when fighting diseases like cancer, AIDS, and Alzheimer’s. They are likely to be vulnerable to misinformation and might be inclined to pursue courses of action that could actually harm them. Physicians must realize that they will regularly deal with patients who have unrealistic expectations of the medical system. The only way physicians can combat misinformation is by providing better information. Physicians need to be prepared to educate patients who have unsuccessfully tried to educate themselves. Part of that education can be verbal, but physicians should consider directing patients to reliable resources that they can explore after leaving the hospital.
Patients are also bombarded by advertisements for prescription medications, all of which are designed to persuade them to take an active role in requesting particular prescriptions. The problem is that the physician is responsible for selecting an appropriate medication. Physicians have to be able to explain why an advertised medication may not be the best choice under the circumstances, no matter what the TV commercial said.
9) Take responsibility: Everyone makes mistakes. No physician is perfect, nor is it fair to expect perfection from those who deal with the intricate machinery of the human body. A culture of fear, however, has caused many physicians to believe that they should not admit their mistakes. Our experience shows that recognizing and responding to mistakes is a far better course of action than trying to pretend they didn’t exist.
Taking responsibility doesn’t mean admitting that you were negligent. It does mean acknowledging a complication when it occurs and assisting the patient in minimizing the consequences. Sometimes this will result in transferring the patient to another physician. At other times, the physician may have to pay to correct the mistake. Many medical malpractice insurance carriers now have programs targeted at promptly recognizing and reacting to unexpected outcomes. These insurers realize that the best time to correct a bad situation is within hours or days of its occurrence. Enlist the help of your insurer or hospital risk manager. If patients feel like their physicians are trying to minimize a situation, hoping mistakenly that it will go away, it becomes much more difficult to avoid litigation.
10) Don’t compromise your integrity: Physicians are professionals. Whether it’s fair or not, jurors hold physicians to a higher standard of conduct. They expect more of doctors. They expect doctors to “do the right thing.” Consequently, jurors tend to punish physicians who place their personal interests above their patients’ interests. Federal law already prohibits physicians from engaging in many forms of self-dealing, such as investing in certain businesses or receiving kickbacks for medical care. But there are many lawful forms of conduct that might cause a jury to question why a physician chose a particular course of action.
Recent medical literature demonstrates that pharmaceutical manufacturers direct 90% of an estimated $21 billion annual marketing budget at physicians, including the sponsorship of an estimated 300,000 annual education events. This amounts to approximately $13,000 per physician annually. Because of concerns that even small inducements might have an unwanted effect upon physician independence, the Stanford Medical Center recently announced a new policy prohibiting physicians from accepting free drug samples or even small gifts from pharmaceutical sales representatives. Prominent newspapers have been running stories about the “free lunches” physicians receive.
We’re not suggesting that physicians spurn pharmaceutical sales representatives or that they avoid legal business opportunities. We caution you, however, that smart plaintiffs’ attorneys are sensitive to any indications that a physician has allowed his interests to influence a patient’s treatment. Don’t put yourself in a position where a jury could reasonably question whether or not you had your patient’s best interests in mind.
Unfortunately, even if a physician observes all of these precautions, a patient still might file a lawsuit. If you sense a real potential for litigation, contact your insurance company and provide notice of a potential claim. This will help ensure that your insurance coverage is available if a lawsuit is filed. It also allows the insurance company to retain an attorney to assist you. The next time we write, we’ll provide our top tips for winning a lawsuit once it occurs. TH
Patrick O’Rourke is the managing associate university counsel for the University of Colorado’s litigation office. Kari M. Hershey, JD, practices health law in Colorado.
BIAS in Medicine
I definitely think there may be some biases on the part of hospitalists,” says Ashish Boghani, MD, chief of the hospitalist service at Highland Hospital, Rochester, N.Y. As a young physician, he noticed some bias in his own thoughts and behaviors.
“But as I got more and more experienced,” he says, “if I was told by another provider that someone was a difficult patient, I left that outside the door. When I go into a patient’s room the first time, I start fresh—no matter what I read on the chart or heard from any staff or colleagues. … And it usually turns out that once you approach it like that … the situation turns out differently.”
In other words, if a physician doesn’t approach a patient with the bias of someone else’s interpretation, that patient will not necessarily be perceived as difficult. What about a physician’s own biases?
Personal Biases
“A lot of a hospitalists’ interactions with patients are colored by our own experiences,” says Bilal Ahmed, MD, associate program director for the residency program and associate professor of clinical medicine, University of Rochester School of Medicine. For example, “when physicians see a patient who has COPD or cancer and is smoking,” he says, “there may be this thought at the back of their minds that this is something they brought upon themselves. [In that case] the empathy that you feel for that person may go down just a notch, which is a very human response.”
Dr. Ahmed often discusses remaining nonjudgmental with his residents. “But it is not that easy to always practice it, so it kind of creeps back in,” he says.
In particular, biases against obese patients are common and have been shown to affect a physician’s practice style. Research published in 2005 demonstrated that with regard to obese patients, poorer physical health, a lower level of education, and a lower income level were significantly associated with the doctor spending more time on technical tasks during primary care medical encounters, rather than engaging in educational interactions with these patients that encouraged health.1, 2
In a study of 62 severely overweight and 29 normal weight adolescents, satisfaction with affective aspects of the patient-physician relationship was negatively correlated with body mass index score.3 And although these were studies involving primary care, a physician’s specialty is irrelevant when it comes to these very human responses, says Howard Beckman, MD, clinical professor of internal medicine and family medicine at the University of Rochester School of Medicine and Dentistry.
In the once- or twice-monthly conversations Dr. Ahmed holds with his residents about the topic of obesity, “we look at the social, cultural, genetic, metabolic, and other components so we can understand that it is not just that the person is eating a lot,” he explains. “It’s multifactorial, and [there is] a complex set of facts that leads a person to be where they are.”
What’s Behind Bias?
“The areas where we judge other people may be just the areas where we are doing these things ourselves,” says Dr. Beckman. “Part of why we are the way we are with certain patients is that we fear that we may be like that person, and we want to blame them to let ourselves off the hook.”
Many types of patients may trigger an individual physician’s dislike or aversion, including passive patients, patients who smoke, overweight patients, depressed patients, patients who abuse various substances, non-adherent patients, whiny patients, passive-aggressive patients, and elderly patients.
“The movement in medicine is for insightful reflection about what the physician brings into the room,” says Dr. Beckman.
When he comes across a patient he does not like, Dr. Beckman asks, “This is someone I could not like, but do I want to not like them?” At that point, he is ready to make a conscious decision either to change his attitude or behavior or to seek a solution that protects patient care.
Insightfulness into the physician’s own history and family of origin is a cornerstone of the work being done by a number of physicians at the University of Rochester, including Dr. Beckman, an expert in physician-patient communication and the medical director for the Rochester Individual Practice Association (RIPA). For instance, was the hospitalist’s mother overly passive or his father an alcoholic?
Dr. Beckman addressed bias recently when he rewrote a chapter on difficult patients for a new edition of a behavioral medicine textbook.4 “One belief is that there are difficult patients; there is something about them that’s difficult,” says Dr. Beckman. “And in some cases that may be true. But what [investigators have now] recognized is that people who are difficult for one doctor [may] not [be] difficult for another doctor. And so it would appear that the variable is not the patient, but rather it’s the doctor.”
When this phenomenon was examined to a greater extent, “they tended to find that the type of person that the doctor doesn’t like, they’ve often seen before … usually in their family,” he explains.
Is Reflection the Answer?
Dr. Beckman believes it is the obligation of medical schools to help practitioners understand their own strengths and weaknesses, including their biases. He and a number of colleagues have just received a grant to study teaching the practice of such mindfulness to physicians. The study will investigate whether that education will ultimately affect a doctor’s cost of care. Essentially, Dr. Beckman says, it comes down to a question: Does knowing more about yourself change the way you practice?
At Strong Memorial Hospital in Rochester, N.Y., where Andrew Rudmann, MD, is chief of a hospital medicine division that includes 17 faculty members and 40 midlevel practitioners, physicians have not formally discussed having negative feelings toward their patients. But, “I think hospitalists would do well to reflect on their feelings about these issues,” says Dr. Rudmann, who is also associate director of the internal medicine residency program at Strong.
Reflection on what physicians bring to their medical encounters should take into account what Dr. Beckman calls “the three big pieces” of how humans work together in a medical encounter: “What is happening to the patient before the doctor walks into room, what is happening to the doctor before he walks into the room, and what happens in the room.” TH
Andrea Sattinger also writes about “vintage bugs” in this issue.
References
- Bertakis KD, Azari R. The impact of obesity on primary care visits. Obes Res. 2005 Sep;13(9):1615-1623.
- Robinson BE, Gjerdingen DK, Houge DR. Obesity: a move from traditional to more patient-oriented management. J Am Board Fam Pract. 1995 Mar-Apr;8(2):99-108.
- Cohen ML, Tanofsky-Kraff M, Young-Hyman D, et al. Weight and its relationship to adolescent perceptions of their providers (WRAP): a qualitative and quantitative assessment of teen weight-related preferences and concerns. J Adolesc Health. 2005;37:163.
- Beckman H. Difficult Patients. In: Feldman MD, Christensen JF, eds. Behavioral Medicine in Primary Care: A Practical Guide. New York: McGraw-Hill Medical; 2003:23-32.
I definitely think there may be some biases on the part of hospitalists,” says Ashish Boghani, MD, chief of the hospitalist service at Highland Hospital, Rochester, N.Y. As a young physician, he noticed some bias in his own thoughts and behaviors.
“But as I got more and more experienced,” he says, “if I was told by another provider that someone was a difficult patient, I left that outside the door. When I go into a patient’s room the first time, I start fresh—no matter what I read on the chart or heard from any staff or colleagues. … And it usually turns out that once you approach it like that … the situation turns out differently.”
In other words, if a physician doesn’t approach a patient with the bias of someone else’s interpretation, that patient will not necessarily be perceived as difficult. What about a physician’s own biases?
Personal Biases
“A lot of a hospitalists’ interactions with patients are colored by our own experiences,” says Bilal Ahmed, MD, associate program director for the residency program and associate professor of clinical medicine, University of Rochester School of Medicine. For example, “when physicians see a patient who has COPD or cancer and is smoking,” he says, “there may be this thought at the back of their minds that this is something they brought upon themselves. [In that case] the empathy that you feel for that person may go down just a notch, which is a very human response.”
Dr. Ahmed often discusses remaining nonjudgmental with his residents. “But it is not that easy to always practice it, so it kind of creeps back in,” he says.
In particular, biases against obese patients are common and have been shown to affect a physician’s practice style. Research published in 2005 demonstrated that with regard to obese patients, poorer physical health, a lower level of education, and a lower income level were significantly associated with the doctor spending more time on technical tasks during primary care medical encounters, rather than engaging in educational interactions with these patients that encouraged health.1, 2
In a study of 62 severely overweight and 29 normal weight adolescents, satisfaction with affective aspects of the patient-physician relationship was negatively correlated with body mass index score.3 And although these were studies involving primary care, a physician’s specialty is irrelevant when it comes to these very human responses, says Howard Beckman, MD, clinical professor of internal medicine and family medicine at the University of Rochester School of Medicine and Dentistry.
In the once- or twice-monthly conversations Dr. Ahmed holds with his residents about the topic of obesity, “we look at the social, cultural, genetic, metabolic, and other components so we can understand that it is not just that the person is eating a lot,” he explains. “It’s multifactorial, and [there is] a complex set of facts that leads a person to be where they are.”
What’s Behind Bias?
“The areas where we judge other people may be just the areas where we are doing these things ourselves,” says Dr. Beckman. “Part of why we are the way we are with certain patients is that we fear that we may be like that person, and we want to blame them to let ourselves off the hook.”
Many types of patients may trigger an individual physician’s dislike or aversion, including passive patients, patients who smoke, overweight patients, depressed patients, patients who abuse various substances, non-adherent patients, whiny patients, passive-aggressive patients, and elderly patients.
“The movement in medicine is for insightful reflection about what the physician brings into the room,” says Dr. Beckman.
When he comes across a patient he does not like, Dr. Beckman asks, “This is someone I could not like, but do I want to not like them?” At that point, he is ready to make a conscious decision either to change his attitude or behavior or to seek a solution that protects patient care.
Insightfulness into the physician’s own history and family of origin is a cornerstone of the work being done by a number of physicians at the University of Rochester, including Dr. Beckman, an expert in physician-patient communication and the medical director for the Rochester Individual Practice Association (RIPA). For instance, was the hospitalist’s mother overly passive or his father an alcoholic?
Dr. Beckman addressed bias recently when he rewrote a chapter on difficult patients for a new edition of a behavioral medicine textbook.4 “One belief is that there are difficult patients; there is something about them that’s difficult,” says Dr. Beckman. “And in some cases that may be true. But what [investigators have now] recognized is that people who are difficult for one doctor [may] not [be] difficult for another doctor. And so it would appear that the variable is not the patient, but rather it’s the doctor.”
When this phenomenon was examined to a greater extent, “they tended to find that the type of person that the doctor doesn’t like, they’ve often seen before … usually in their family,” he explains.
Is Reflection the Answer?
Dr. Beckman believes it is the obligation of medical schools to help practitioners understand their own strengths and weaknesses, including their biases. He and a number of colleagues have just received a grant to study teaching the practice of such mindfulness to physicians. The study will investigate whether that education will ultimately affect a doctor’s cost of care. Essentially, Dr. Beckman says, it comes down to a question: Does knowing more about yourself change the way you practice?
At Strong Memorial Hospital in Rochester, N.Y., where Andrew Rudmann, MD, is chief of a hospital medicine division that includes 17 faculty members and 40 midlevel practitioners, physicians have not formally discussed having negative feelings toward their patients. But, “I think hospitalists would do well to reflect on their feelings about these issues,” says Dr. Rudmann, who is also associate director of the internal medicine residency program at Strong.
Reflection on what physicians bring to their medical encounters should take into account what Dr. Beckman calls “the three big pieces” of how humans work together in a medical encounter: “What is happening to the patient before the doctor walks into room, what is happening to the doctor before he walks into the room, and what happens in the room.” TH
Andrea Sattinger also writes about “vintage bugs” in this issue.
References
- Bertakis KD, Azari R. The impact of obesity on primary care visits. Obes Res. 2005 Sep;13(9):1615-1623.
- Robinson BE, Gjerdingen DK, Houge DR. Obesity: a move from traditional to more patient-oriented management. J Am Board Fam Pract. 1995 Mar-Apr;8(2):99-108.
- Cohen ML, Tanofsky-Kraff M, Young-Hyman D, et al. Weight and its relationship to adolescent perceptions of their providers (WRAP): a qualitative and quantitative assessment of teen weight-related preferences and concerns. J Adolesc Health. 2005;37:163.
- Beckman H. Difficult Patients. In: Feldman MD, Christensen JF, eds. Behavioral Medicine in Primary Care: A Practical Guide. New York: McGraw-Hill Medical; 2003:23-32.
I definitely think there may be some biases on the part of hospitalists,” says Ashish Boghani, MD, chief of the hospitalist service at Highland Hospital, Rochester, N.Y. As a young physician, he noticed some bias in his own thoughts and behaviors.
“But as I got more and more experienced,” he says, “if I was told by another provider that someone was a difficult patient, I left that outside the door. When I go into a patient’s room the first time, I start fresh—no matter what I read on the chart or heard from any staff or colleagues. … And it usually turns out that once you approach it like that … the situation turns out differently.”
In other words, if a physician doesn’t approach a patient with the bias of someone else’s interpretation, that patient will not necessarily be perceived as difficult. What about a physician’s own biases?
Personal Biases
“A lot of a hospitalists’ interactions with patients are colored by our own experiences,” says Bilal Ahmed, MD, associate program director for the residency program and associate professor of clinical medicine, University of Rochester School of Medicine. For example, “when physicians see a patient who has COPD or cancer and is smoking,” he says, “there may be this thought at the back of their minds that this is something they brought upon themselves. [In that case] the empathy that you feel for that person may go down just a notch, which is a very human response.”
Dr. Ahmed often discusses remaining nonjudgmental with his residents. “But it is not that easy to always practice it, so it kind of creeps back in,” he says.
In particular, biases against obese patients are common and have been shown to affect a physician’s practice style. Research published in 2005 demonstrated that with regard to obese patients, poorer physical health, a lower level of education, and a lower income level were significantly associated with the doctor spending more time on technical tasks during primary care medical encounters, rather than engaging in educational interactions with these patients that encouraged health.1, 2
In a study of 62 severely overweight and 29 normal weight adolescents, satisfaction with affective aspects of the patient-physician relationship was negatively correlated with body mass index score.3 And although these were studies involving primary care, a physician’s specialty is irrelevant when it comes to these very human responses, says Howard Beckman, MD, clinical professor of internal medicine and family medicine at the University of Rochester School of Medicine and Dentistry.
In the once- or twice-monthly conversations Dr. Ahmed holds with his residents about the topic of obesity, “we look at the social, cultural, genetic, metabolic, and other components so we can understand that it is not just that the person is eating a lot,” he explains. “It’s multifactorial, and [there is] a complex set of facts that leads a person to be where they are.”
What’s Behind Bias?
“The areas where we judge other people may be just the areas where we are doing these things ourselves,” says Dr. Beckman. “Part of why we are the way we are with certain patients is that we fear that we may be like that person, and we want to blame them to let ourselves off the hook.”
Many types of patients may trigger an individual physician’s dislike or aversion, including passive patients, patients who smoke, overweight patients, depressed patients, patients who abuse various substances, non-adherent patients, whiny patients, passive-aggressive patients, and elderly patients.
“The movement in medicine is for insightful reflection about what the physician brings into the room,” says Dr. Beckman.
When he comes across a patient he does not like, Dr. Beckman asks, “This is someone I could not like, but do I want to not like them?” At that point, he is ready to make a conscious decision either to change his attitude or behavior or to seek a solution that protects patient care.
Insightfulness into the physician’s own history and family of origin is a cornerstone of the work being done by a number of physicians at the University of Rochester, including Dr. Beckman, an expert in physician-patient communication and the medical director for the Rochester Individual Practice Association (RIPA). For instance, was the hospitalist’s mother overly passive or his father an alcoholic?
Dr. Beckman addressed bias recently when he rewrote a chapter on difficult patients for a new edition of a behavioral medicine textbook.4 “One belief is that there are difficult patients; there is something about them that’s difficult,” says Dr. Beckman. “And in some cases that may be true. But what [investigators have now] recognized is that people who are difficult for one doctor [may] not [be] difficult for another doctor. And so it would appear that the variable is not the patient, but rather it’s the doctor.”
When this phenomenon was examined to a greater extent, “they tended to find that the type of person that the doctor doesn’t like, they’ve often seen before … usually in their family,” he explains.
Is Reflection the Answer?
Dr. Beckman believes it is the obligation of medical schools to help practitioners understand their own strengths and weaknesses, including their biases. He and a number of colleagues have just received a grant to study teaching the practice of such mindfulness to physicians. The study will investigate whether that education will ultimately affect a doctor’s cost of care. Essentially, Dr. Beckman says, it comes down to a question: Does knowing more about yourself change the way you practice?
At Strong Memorial Hospital in Rochester, N.Y., where Andrew Rudmann, MD, is chief of a hospital medicine division that includes 17 faculty members and 40 midlevel practitioners, physicians have not formally discussed having negative feelings toward their patients. But, “I think hospitalists would do well to reflect on their feelings about these issues,” says Dr. Rudmann, who is also associate director of the internal medicine residency program at Strong.
Reflection on what physicians bring to their medical encounters should take into account what Dr. Beckman calls “the three big pieces” of how humans work together in a medical encounter: “What is happening to the patient before the doctor walks into room, what is happening to the doctor before he walks into the room, and what happens in the room.” TH
Andrea Sattinger also writes about “vintage bugs” in this issue.
References
- Bertakis KD, Azari R. The impact of obesity on primary care visits. Obes Res. 2005 Sep;13(9):1615-1623.
- Robinson BE, Gjerdingen DK, Houge DR. Obesity: a move from traditional to more patient-oriented management. J Am Board Fam Pract. 1995 Mar-Apr;8(2):99-108.
- Cohen ML, Tanofsky-Kraff M, Young-Hyman D, et al. Weight and its relationship to adolescent perceptions of their providers (WRAP): a qualitative and quantitative assessment of teen weight-related preferences and concerns. J Adolesc Health. 2005;37:163.
- Beckman H. Difficult Patients. In: Feldman MD, Christensen JF, eds. Behavioral Medicine in Primary Care: A Practical Guide. New York: McGraw-Hill Medical; 2003:23-32.
A Look inside Healthcare Transparency

One of the many trends in healthcare today is a move toward making specific quality and pricing information available to the public.
“When you’re buying a car, you can easily compare quality, features, and prices to make an educated guess,” points out Eric Siegal, MD, regional medical director, Cogent Healthcare, Madison, Wis., and chair of SHM’s Public Policy Committee. “In contrast, healthcare is completely opaque. People choose a doctor or a hospital—sometimes for a surgery that’s life threatening—by word of mouth or [based on] proximity. How do you make it possible to choose based on quality of care and on price?”
Known as healthcare transparency, this trend is driven by multiple sources. “The [CMS] Hospital Compare initiative was a first step in this, as were the Leapfrog initiative and the IHI [Institute for Health Improvement] Collaborative,” says Dr. Siegal. “In fact, the government is a little late to the game, but they’re quickly closing the gap.”
Mandate from the President
On August 22, 2006, President George W. Bush signed an executive order requiring key federal agencies to collect information about the quality and cost of the healthcare they provide and to share that data with each another—and with beneficiaries. Agencies included in the order are the Department of Health and Human Services (HHS), the Department of Defense (DoD), the Department of Veterans Affairs (VA), and the Office of Personnel Management (OPM).
The executive order directs these four agencies to work with the private sector and other government agencies to develop programs to measure quality of care. They were required by Jan. 1, 2007, to identify practices that promote high quality care and to compile information on the prices they pay for common services available to their members. Ultimately, the executive order calls for combining that data in a comprehensive source on providers’ quality and prices; this information will then be available to consumers.
President Bush has said that his order sends a message to healthcare providers that “in order to do business with the federal government, you’ve got to show us your prices.” The new requirements for transparency will affect healthcare providers across the country because treating about one-quarter of Americans covered by health insurance entails “doing business with the federal government.” That one-quarter includes Medicare beneficiaries, health insurance beneficiaries at the DoD and the VA, and federal employees. (The order clearly states that the directive does not apply to state-administered or -funded programs.)
House Legislation: Make Prices Public
Comprehensive pricing transparency may also be required on a state level. On Sept. 13, 2006, Representative Michael Burgess (R-Texas) introduced the Health Care Price Transparency Act of 2006 in the House. This American Hospital Association (AHA)-supported legislation would require states to publicly report hospital charges for specific inpatient and outpatient services and would require insurers to give patients, on request, an estimate of their expected out-of-pocket expenses.
—Eric Siegal, MD
The bill would also require the Agency for Healthcare Research and Quality to study what type of healthcare price information consumers would find useful and how that information could be made available in a timely, understandable form.
Thirty-two states already require hospitals to report pricing information, and six more are voluntarily doing so, but this legislation would likely change the information that hospitals and other providers are gathering and providing.
At press time, the legislation had been referred to the House Subcommittee on Health.
How Transparency Will Roll Out
While the House legislation is in limbo, the executive order will have an immediate effect on healthcare, starting this year. The quality measures to be included in reporting will be developed from private and government sources, including local providers, employers, and health plans and insurers.
After the data are gathered and the information technology (IT) infrastructure is set up, consumers will be able to access specific information on pricing and quality of services performed by doctors, hospitals, and other healthcare providers. This information may be available through a variety of sources, including insurance companies, employers, and Medicare-sponsored Web sites.
One of the keys to success will be in the collaboration among the agencies involved. “There’s a keen understanding among the major players that if everyone does their own thing, we’ll have chaos,” says Dr. Siegal. “There has to be a significant degree of harmonization [among] physician measures, hospital measures, inpatient measures, and outpatient measures.”
Where Hospitalists Fit in
Will healthcare transparency affect hospitalists? “It’s already impacting hospitalists,” says Dr. Siegal. “Not on pricing, but on quality reporting. The good news is that hospitalists may be the single best-prepared group of physicians [for transparency] because we’re already doing it. The question will be, as it becomes more pervasive, will it be done in a way that is thoughtful, measured, and practical?”
Hospitals are likely to look to their hospitalists to ensure that their quality measurements are competitive. Dr. Siegal explains, “Hospitals looking to improve quality will be most effective in getting results from the physicians whose financial incentives are aligned with theirs.”
However, additional—or more public—quality indicators will not necessarily create a huge source of income for hospital medicine. “The low-hanging fruit won’t be the patients that hospitalists see; it will be elective surgical cases,” predicts Dr. Siegal. “Those are cleanly defined procedures, with bundled payments and predictable outcomes, where a hospital can understand what happens and what’s included. Then they can say, ‘Why do we charge 20% more for a total elective hip [surgery] than the hospital down the road?’ ”
As transparency is rolled out in U.S. hospitals and healthcare systems, hospitalists will look good. “Hospitalists already live in a quality reporting world, more so than other doctors,” says Dr. Siegal. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
One of the many trends in healthcare today is a move toward making specific quality and pricing information available to the public.
“When you’re buying a car, you can easily compare quality, features, and prices to make an educated guess,” points out Eric Siegal, MD, regional medical director, Cogent Healthcare, Madison, Wis., and chair of SHM’s Public Policy Committee. “In contrast, healthcare is completely opaque. People choose a doctor or a hospital—sometimes for a surgery that’s life threatening—by word of mouth or [based on] proximity. How do you make it possible to choose based on quality of care and on price?”
Known as healthcare transparency, this trend is driven by multiple sources. “The [CMS] Hospital Compare initiative was a first step in this, as were the Leapfrog initiative and the IHI [Institute for Health Improvement] Collaborative,” says Dr. Siegal. “In fact, the government is a little late to the game, but they’re quickly closing the gap.”
Mandate from the President
On August 22, 2006, President George W. Bush signed an executive order requiring key federal agencies to collect information about the quality and cost of the healthcare they provide and to share that data with each another—and with beneficiaries. Agencies included in the order are the Department of Health and Human Services (HHS), the Department of Defense (DoD), the Department of Veterans Affairs (VA), and the Office of Personnel Management (OPM).
The executive order directs these four agencies to work with the private sector and other government agencies to develop programs to measure quality of care. They were required by Jan. 1, 2007, to identify practices that promote high quality care and to compile information on the prices they pay for common services available to their members. Ultimately, the executive order calls for combining that data in a comprehensive source on providers’ quality and prices; this information will then be available to consumers.
President Bush has said that his order sends a message to healthcare providers that “in order to do business with the federal government, you’ve got to show us your prices.” The new requirements for transparency will affect healthcare providers across the country because treating about one-quarter of Americans covered by health insurance entails “doing business with the federal government.” That one-quarter includes Medicare beneficiaries, health insurance beneficiaries at the DoD and the VA, and federal employees. (The order clearly states that the directive does not apply to state-administered or -funded programs.)
House Legislation: Make Prices Public
Comprehensive pricing transparency may also be required on a state level. On Sept. 13, 2006, Representative Michael Burgess (R-Texas) introduced the Health Care Price Transparency Act of 2006 in the House. This American Hospital Association (AHA)-supported legislation would require states to publicly report hospital charges for specific inpatient and outpatient services and would require insurers to give patients, on request, an estimate of their expected out-of-pocket expenses.
—Eric Siegal, MD
The bill would also require the Agency for Healthcare Research and Quality to study what type of healthcare price information consumers would find useful and how that information could be made available in a timely, understandable form.
Thirty-two states already require hospitals to report pricing information, and six more are voluntarily doing so, but this legislation would likely change the information that hospitals and other providers are gathering and providing.
At press time, the legislation had been referred to the House Subcommittee on Health.
How Transparency Will Roll Out
While the House legislation is in limbo, the executive order will have an immediate effect on healthcare, starting this year. The quality measures to be included in reporting will be developed from private and government sources, including local providers, employers, and health plans and insurers.
After the data are gathered and the information technology (IT) infrastructure is set up, consumers will be able to access specific information on pricing and quality of services performed by doctors, hospitals, and other healthcare providers. This information may be available through a variety of sources, including insurance companies, employers, and Medicare-sponsored Web sites.
One of the keys to success will be in the collaboration among the agencies involved. “There’s a keen understanding among the major players that if everyone does their own thing, we’ll have chaos,” says Dr. Siegal. “There has to be a significant degree of harmonization [among] physician measures, hospital measures, inpatient measures, and outpatient measures.”
Where Hospitalists Fit in
Will healthcare transparency affect hospitalists? “It’s already impacting hospitalists,” says Dr. Siegal. “Not on pricing, but on quality reporting. The good news is that hospitalists may be the single best-prepared group of physicians [for transparency] because we’re already doing it. The question will be, as it becomes more pervasive, will it be done in a way that is thoughtful, measured, and practical?”
Hospitals are likely to look to their hospitalists to ensure that their quality measurements are competitive. Dr. Siegal explains, “Hospitals looking to improve quality will be most effective in getting results from the physicians whose financial incentives are aligned with theirs.”
However, additional—or more public—quality indicators will not necessarily create a huge source of income for hospital medicine. “The low-hanging fruit won’t be the patients that hospitalists see; it will be elective surgical cases,” predicts Dr. Siegal. “Those are cleanly defined procedures, with bundled payments and predictable outcomes, where a hospital can understand what happens and what’s included. Then they can say, ‘Why do we charge 20% more for a total elective hip [surgery] than the hospital down the road?’ ”
As transparency is rolled out in U.S. hospitals and healthcare systems, hospitalists will look good. “Hospitalists already live in a quality reporting world, more so than other doctors,” says Dr. Siegal. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
One of the many trends in healthcare today is a move toward making specific quality and pricing information available to the public.
“When you’re buying a car, you can easily compare quality, features, and prices to make an educated guess,” points out Eric Siegal, MD, regional medical director, Cogent Healthcare, Madison, Wis., and chair of SHM’s Public Policy Committee. “In contrast, healthcare is completely opaque. People choose a doctor or a hospital—sometimes for a surgery that’s life threatening—by word of mouth or [based on] proximity. How do you make it possible to choose based on quality of care and on price?”
Known as healthcare transparency, this trend is driven by multiple sources. “The [CMS] Hospital Compare initiative was a first step in this, as were the Leapfrog initiative and the IHI [Institute for Health Improvement] Collaborative,” says Dr. Siegal. “In fact, the government is a little late to the game, but they’re quickly closing the gap.”
Mandate from the President
On August 22, 2006, President George W. Bush signed an executive order requiring key federal agencies to collect information about the quality and cost of the healthcare they provide and to share that data with each another—and with beneficiaries. Agencies included in the order are the Department of Health and Human Services (HHS), the Department of Defense (DoD), the Department of Veterans Affairs (VA), and the Office of Personnel Management (OPM).
The executive order directs these four agencies to work with the private sector and other government agencies to develop programs to measure quality of care. They were required by Jan. 1, 2007, to identify practices that promote high quality care and to compile information on the prices they pay for common services available to their members. Ultimately, the executive order calls for combining that data in a comprehensive source on providers’ quality and prices; this information will then be available to consumers.
President Bush has said that his order sends a message to healthcare providers that “in order to do business with the federal government, you’ve got to show us your prices.” The new requirements for transparency will affect healthcare providers across the country because treating about one-quarter of Americans covered by health insurance entails “doing business with the federal government.” That one-quarter includes Medicare beneficiaries, health insurance beneficiaries at the DoD and the VA, and federal employees. (The order clearly states that the directive does not apply to state-administered or -funded programs.)
House Legislation: Make Prices Public
Comprehensive pricing transparency may also be required on a state level. On Sept. 13, 2006, Representative Michael Burgess (R-Texas) introduced the Health Care Price Transparency Act of 2006 in the House. This American Hospital Association (AHA)-supported legislation would require states to publicly report hospital charges for specific inpatient and outpatient services and would require insurers to give patients, on request, an estimate of their expected out-of-pocket expenses.
—Eric Siegal, MD
The bill would also require the Agency for Healthcare Research and Quality to study what type of healthcare price information consumers would find useful and how that information could be made available in a timely, understandable form.
Thirty-two states already require hospitals to report pricing information, and six more are voluntarily doing so, but this legislation would likely change the information that hospitals and other providers are gathering and providing.
At press time, the legislation had been referred to the House Subcommittee on Health.
How Transparency Will Roll Out
While the House legislation is in limbo, the executive order will have an immediate effect on healthcare, starting this year. The quality measures to be included in reporting will be developed from private and government sources, including local providers, employers, and health plans and insurers.
After the data are gathered and the information technology (IT) infrastructure is set up, consumers will be able to access specific information on pricing and quality of services performed by doctors, hospitals, and other healthcare providers. This information may be available through a variety of sources, including insurance companies, employers, and Medicare-sponsored Web sites.
One of the keys to success will be in the collaboration among the agencies involved. “There’s a keen understanding among the major players that if everyone does their own thing, we’ll have chaos,” says Dr. Siegal. “There has to be a significant degree of harmonization [among] physician measures, hospital measures, inpatient measures, and outpatient measures.”
Where Hospitalists Fit in
Will healthcare transparency affect hospitalists? “It’s already impacting hospitalists,” says Dr. Siegal. “Not on pricing, but on quality reporting. The good news is that hospitalists may be the single best-prepared group of physicians [for transparency] because we’re already doing it. The question will be, as it becomes more pervasive, will it be done in a way that is thoughtful, measured, and practical?”
Hospitals are likely to look to their hospitalists to ensure that their quality measurements are competitive. Dr. Siegal explains, “Hospitals looking to improve quality will be most effective in getting results from the physicians whose financial incentives are aligned with theirs.”
However, additional—or more public—quality indicators will not necessarily create a huge source of income for hospital medicine. “The low-hanging fruit won’t be the patients that hospitalists see; it will be elective surgical cases,” predicts Dr. Siegal. “Those are cleanly defined procedures, with bundled payments and predictable outcomes, where a hospital can understand what happens and what’s included. Then they can say, ‘Why do we charge 20% more for a total elective hip [surgery] than the hospital down the road?’ ”
As transparency is rolled out in U.S. hospitals and healthcare systems, hospitalists will look good. “Hospitalists already live in a quality reporting world, more so than other doctors,” says Dr. Siegal. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
Register Now for February’s SHM Leadership Academy

SHM’s Level I Leadership Academy is back. If you were unable to register for the sold-out September Academy, now is your chance. This semi-annual course will be held during the week of February 26–March 1, 2007, at the Gaylord Palms Resort and Convention Center in Orlando, Fla. This course gives attendees hands-on experience and a unique opportunity to learn from the best in the field. All previous Level I academies have sold out weeks in advance, so reserve your spot today by visiting www.hospitalmedicine.org for more information.
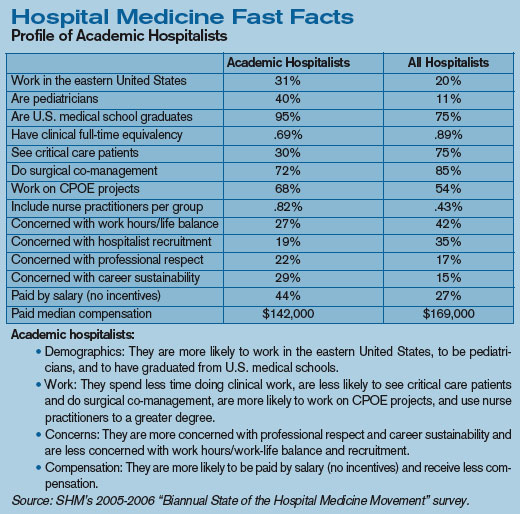
ASHP Foundation Launches New Hospital Pharmacist-Hospitalist Team Research Grant
Foundation seeks to encourage collaborative studies of VTE prevention
Venous thromboembolism (VTE) is a significant cause of morbidity and mortality in hospitals. It mostly affects patients with primary medical conditions; those who have had surgery for gynecologic, orthopedic, urologic, and vascular conditions; and those receiving care in critical care settings.
The American Society of Health-System Pharmacists (ASHP) Research and Education Foundation has created a new grant program sponsored by the Sanofi Aventis Group to support multidisciplinary research studies conducted by hospital pharmacists and hospitalists to prevent and treat VTE in hospitalized patients.
“Because the focus of a hospitalist is providing quality medical care for hospitalized patients and the unique medical problems that they may face as a result of being hospitalized, the ASHP Foundation felt it was important to offer hospital pharmacists an opportunity to partner with this group of physicians,” says Daniel J. Cobaugh, PharmD, FAACT, DABAT, ASHP Foundation director of research. “We wanted to focus the research grant on a major patient care issue that can be effectively addressed through hospital pharmacist-hospitalist collaborations. We believe this collaborative approach will have far-reaching implications for improving patient care and patient safety.”
“The hospital of the future will be based on patient-centered care, with measurable quality outcomes and delivered by teams of health professionals,” explains Larry Wellikson, MD, FACP, SHM CEO. “This collaborative process with hospital-based pharmacists and hospitalists working together to improve VTE care is just the kind of interdisciplinary teamwork that can serve as a beacon to lead us to a better future.”
Applications should emphasize the following:
- Project objectives that address health services research related to the prevention and treatment of VTE;
- Sound research methods that support the study objectives;
- Interdisciplinary collaboration between hospital pharmacists and hospitalist physicians;
- The potential for findings to be replicated in other healthcare facilities; and
- Prudent use of grant funds.
Potential areas of research focus include the use of appropriate interventions to prevent VTE, optimization and monitoring of therapies used for VTE, ensuring continuity of care, provision of literacy-sensitive education to patients and caregivers, and health professional education.
Applications and detailed instructions for the Hospital Pharmacist-Hospitalist Collaboration: VTE Prevention and Treatment Team Grant is available on the ASHP Foundation Web site at www.ashpfoundation.org. The deadline for completed applications is March 1.
SHM Launches New Grassroots Advocacy Tool
Grassroots involvement by SHM members is critical to our ability to influence health policy in Washington. That is why SHM has launched a powerful new advocacy tool designed to help you communicate quickly and effectively with your congressional representatives. Capwiz·XC, located in the “Advocacy” section of our Web site, enables you to take action on any issue important to hospital medicine by sending personalized communications to your elected officials.
Advocacy doesn’t have to require a big time commitment. Communicating with your representatives in Congress now takes just a few minutes at SHM’s Legislative Action Center. You can send an e-mail whenever it is convenient for you, and our action alerts contain sample text for you to use and personalize as desired. Physician payment reform, quality improvement, palliative care, and funding levels for the National Institutes of Health and the Agency for Healthcare Research and Quality are just a few of the many issues before the 110th Congress. You can help influence the debate, improve patient care, and increase the visibility of hospitalists by making your voice heard through Capwiz.
Capwiz has many other features that will help keep you informed and educated about the legislative process. These include an interactive map to help you find your elected officials. Simply enter your ZIP code or click on your state to find out who your elected officials are. From there, you can easily select one of the listed state or congressional officials to see the full legislative biography page. Each bio page includes direct links you can use to contact the legislator, look up his or her key votes, and find staff contact information. You’ll also find a plethora of information about each elected representative, including:
- Office term;
- Co-sponsorship status;
- Contact information;
- Party affiliation;
- Political background;
- Committee(s); and
- PAC contributions.
Are you interested in looking up a piece of legislation recently mentioned in the news? Or do you want to monitor the various bills that will affect issues important to your practice? The “Legislative Action Center” in the “Advocacy” section contains “Issues and Legislation” to help you to stay on top of current legislation affecting healthcare. Keep track of any bill’s name, summary, co-sponsor(s), and key votes, while also monitoring SHM’s position on the legislation.
SHM is pleased to provide you with the opportunity to become more familiar with the political process and actively participate in influencing the policies that affect hospitalists and their patients. Capwiz contains up-to-the-minute legislative data and online tools to enable you to make a difference in the political process. Please visit our Legislative Action Center today at www.hospitalmedicine.org. TH
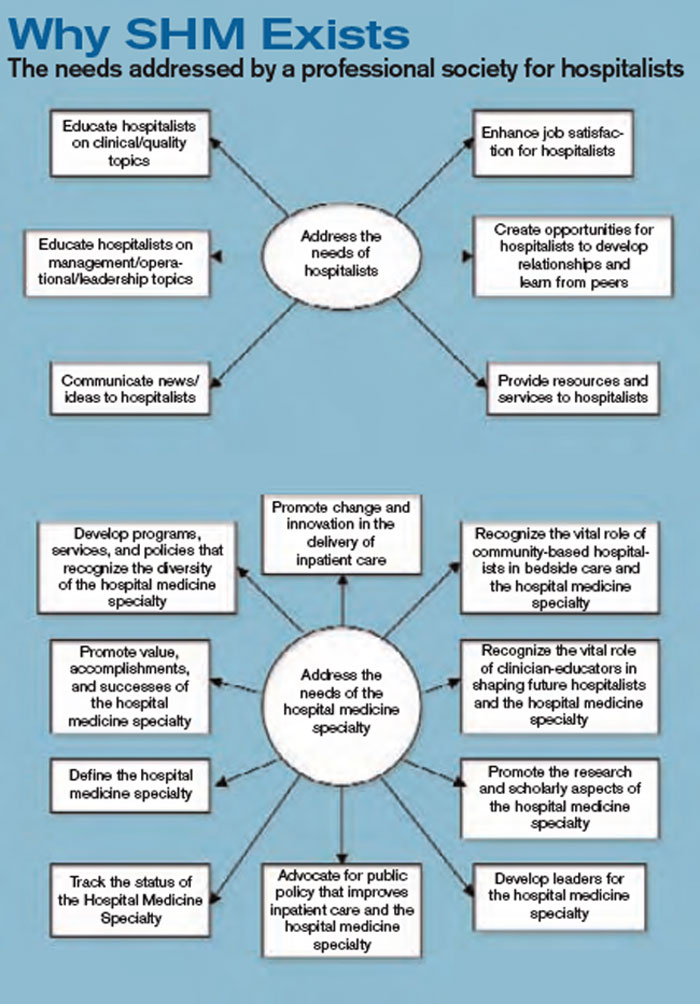
A response to the needs:
Products and Initiatives
- Annual Awards
- Antimicrobial Resistance Resource Room
- Career Center
- Chapters
- Coding and Documentation Precourse
- Collaboration with IHI and Other Organizations
- Core Competencies
- Credentialing by ABIM
- Dashboard White Paper
- Discharge Planning Checklist
- DVT Awareness Campaign
- DVT Mentored Implementation
- e-Newsletter
- Geriatric Resource Room
- Glycemic Control Resource Room
- Heart Failure Resource Room
- Journal of Hospital Medicine
- Leadership Academies
- Legislative Action Day
- Letters to Congress
- List Serves
- Mentoring
- Practice Management Precourse
- Productivity and Compensation Survey
- Public Policy White Paper
- Quality Precourse
- Research Grants
- Resource Rooms
- RIV Competition
- SEPs Workshop
- Stroke Resource Room
- Survey Collaboration with AHA
- The Hospitalist
- Value Added White Paper
- VTE Resource Room
- Web site
A response to the needs:
Committees and Task Forces
- Annual Meeting Committee
- Awards Committee
- Benchmarks Committee
- Board of Directors
- Career Satisfaction Task Force
- Certification Task Force
- Curriculum Task Force
- Education Committee
- Ethics Committee
- Executive Committee of the Board of Directors
- Executive Review Committee
- Family Practice Task Force
- Finance Committee of the Board of Directors
- Hospital Quality and Patient Safety Committee
- Heart Failure Award Task Force
- Leadership Committee
- Membership Committee
- Nominations Committee
- Non Physician Provider Committee
- Palliative Care Task Force
- Pediatric Committee
- Pediatric Core Curriculum Task Force
- Performance and Standards Task Force
- Public Policy Committee
- Research Committee
- Resource Room Oversight Committee
- Research, Innovation, and Clinical Vignettes Committee
- Women in Hospital Medicine
- Young Physicians Committee TH
SHM’s Level I Leadership Academy is back. If you were unable to register for the sold-out September Academy, now is your chance. This semi-annual course will be held during the week of February 26–March 1, 2007, at the Gaylord Palms Resort and Convention Center in Orlando, Fla. This course gives attendees hands-on experience and a unique opportunity to learn from the best in the field. All previous Level I academies have sold out weeks in advance, so reserve your spot today by visiting www.hospitalmedicine.org for more information.
ASHP Foundation Launches New Hospital Pharmacist-Hospitalist Team Research Grant
Foundation seeks to encourage collaborative studies of VTE prevention
Venous thromboembolism (VTE) is a significant cause of morbidity and mortality in hospitals. It mostly affects patients with primary medical conditions; those who have had surgery for gynecologic, orthopedic, urologic, and vascular conditions; and those receiving care in critical care settings.
The American Society of Health-System Pharmacists (ASHP) Research and Education Foundation has created a new grant program sponsored by the Sanofi Aventis Group to support multidisciplinary research studies conducted by hospital pharmacists and hospitalists to prevent and treat VTE in hospitalized patients.
“Because the focus of a hospitalist is providing quality medical care for hospitalized patients and the unique medical problems that they may face as a result of being hospitalized, the ASHP Foundation felt it was important to offer hospital pharmacists an opportunity to partner with this group of physicians,” says Daniel J. Cobaugh, PharmD, FAACT, DABAT, ASHP Foundation director of research. “We wanted to focus the research grant on a major patient care issue that can be effectively addressed through hospital pharmacist-hospitalist collaborations. We believe this collaborative approach will have far-reaching implications for improving patient care and patient safety.”
“The hospital of the future will be based on patient-centered care, with measurable quality outcomes and delivered by teams of health professionals,” explains Larry Wellikson, MD, FACP, SHM CEO. “This collaborative process with hospital-based pharmacists and hospitalists working together to improve VTE care is just the kind of interdisciplinary teamwork that can serve as a beacon to lead us to a better future.”
Applications should emphasize the following:
- Project objectives that address health services research related to the prevention and treatment of VTE;
- Sound research methods that support the study objectives;
- Interdisciplinary collaboration between hospital pharmacists and hospitalist physicians;
- The potential for findings to be replicated in other healthcare facilities; and
- Prudent use of grant funds.
Potential areas of research focus include the use of appropriate interventions to prevent VTE, optimization and monitoring of therapies used for VTE, ensuring continuity of care, provision of literacy-sensitive education to patients and caregivers, and health professional education.
Applications and detailed instructions for the Hospital Pharmacist-Hospitalist Collaboration: VTE Prevention and Treatment Team Grant is available on the ASHP Foundation Web site at www.ashpfoundation.org. The deadline for completed applications is March 1.
SHM Launches New Grassroots Advocacy Tool
Grassroots involvement by SHM members is critical to our ability to influence health policy in Washington. That is why SHM has launched a powerful new advocacy tool designed to help you communicate quickly and effectively with your congressional representatives. Capwiz·XC, located in the “Advocacy” section of our Web site, enables you to take action on any issue important to hospital medicine by sending personalized communications to your elected officials.
Advocacy doesn’t have to require a big time commitment. Communicating with your representatives in Congress now takes just a few minutes at SHM’s Legislative Action Center. You can send an e-mail whenever it is convenient for you, and our action alerts contain sample text for you to use and personalize as desired. Physician payment reform, quality improvement, palliative care, and funding levels for the National Institutes of Health and the Agency for Healthcare Research and Quality are just a few of the many issues before the 110th Congress. You can help influence the debate, improve patient care, and increase the visibility of hospitalists by making your voice heard through Capwiz.
Capwiz has many other features that will help keep you informed and educated about the legislative process. These include an interactive map to help you find your elected officials. Simply enter your ZIP code or click on your state to find out who your elected officials are. From there, you can easily select one of the listed state or congressional officials to see the full legislative biography page. Each bio page includes direct links you can use to contact the legislator, look up his or her key votes, and find staff contact information. You’ll also find a plethora of information about each elected representative, including:
- Office term;
- Co-sponsorship status;
- Contact information;
- Party affiliation;
- Political background;
- Committee(s); and
- PAC contributions.
Are you interested in looking up a piece of legislation recently mentioned in the news? Or do you want to monitor the various bills that will affect issues important to your practice? The “Legislative Action Center” in the “Advocacy” section contains “Issues and Legislation” to help you to stay on top of current legislation affecting healthcare. Keep track of any bill’s name, summary, co-sponsor(s), and key votes, while also monitoring SHM’s position on the legislation.
SHM is pleased to provide you with the opportunity to become more familiar with the political process and actively participate in influencing the policies that affect hospitalists and their patients. Capwiz contains up-to-the-minute legislative data and online tools to enable you to make a difference in the political process. Please visit our Legislative Action Center today at www.hospitalmedicine.org. TH
A response to the needs:
Products and Initiatives
- Annual Awards
- Antimicrobial Resistance Resource Room
- Career Center
- Chapters
- Coding and Documentation Precourse
- Collaboration with IHI and Other Organizations
- Core Competencies
- Credentialing by ABIM
- Dashboard White Paper
- Discharge Planning Checklist
- DVT Awareness Campaign
- DVT Mentored Implementation
- e-Newsletter
- Geriatric Resource Room
- Glycemic Control Resource Room
- Heart Failure Resource Room
- Journal of Hospital Medicine
- Leadership Academies
- Legislative Action Day
- Letters to Congress
- List Serves
- Mentoring
- Practice Management Precourse
- Productivity and Compensation Survey
- Public Policy White Paper
- Quality Precourse
- Research Grants
- Resource Rooms
- RIV Competition
- SEPs Workshop
- Stroke Resource Room
- Survey Collaboration with AHA
- The Hospitalist
- Value Added White Paper
- VTE Resource Room
- Web site
A response to the needs:
Committees and Task Forces
- Annual Meeting Committee
- Awards Committee
- Benchmarks Committee
- Board of Directors
- Career Satisfaction Task Force
- Certification Task Force
- Curriculum Task Force
- Education Committee
- Ethics Committee
- Executive Committee of the Board of Directors
- Executive Review Committee
- Family Practice Task Force
- Finance Committee of the Board of Directors
- Hospital Quality and Patient Safety Committee
- Heart Failure Award Task Force
- Leadership Committee
- Membership Committee
- Nominations Committee
- Non Physician Provider Committee
- Palliative Care Task Force
- Pediatric Committee
- Pediatric Core Curriculum Task Force
- Performance and Standards Task Force
- Public Policy Committee
- Research Committee
- Resource Room Oversight Committee
- Research, Innovation, and Clinical Vignettes Committee
- Women in Hospital Medicine
- Young Physicians Committee TH
SHM’s Level I Leadership Academy is back. If you were unable to register for the sold-out September Academy, now is your chance. This semi-annual course will be held during the week of February 26–March 1, 2007, at the Gaylord Palms Resort and Convention Center in Orlando, Fla. This course gives attendees hands-on experience and a unique opportunity to learn from the best in the field. All previous Level I academies have sold out weeks in advance, so reserve your spot today by visiting www.hospitalmedicine.org for more information.
ASHP Foundation Launches New Hospital Pharmacist-Hospitalist Team Research Grant
Foundation seeks to encourage collaborative studies of VTE prevention
Venous thromboembolism (VTE) is a significant cause of morbidity and mortality in hospitals. It mostly affects patients with primary medical conditions; those who have had surgery for gynecologic, orthopedic, urologic, and vascular conditions; and those receiving care in critical care settings.
The American Society of Health-System Pharmacists (ASHP) Research and Education Foundation has created a new grant program sponsored by the Sanofi Aventis Group to support multidisciplinary research studies conducted by hospital pharmacists and hospitalists to prevent and treat VTE in hospitalized patients.
“Because the focus of a hospitalist is providing quality medical care for hospitalized patients and the unique medical problems that they may face as a result of being hospitalized, the ASHP Foundation felt it was important to offer hospital pharmacists an opportunity to partner with this group of physicians,” says Daniel J. Cobaugh, PharmD, FAACT, DABAT, ASHP Foundation director of research. “We wanted to focus the research grant on a major patient care issue that can be effectively addressed through hospital pharmacist-hospitalist collaborations. We believe this collaborative approach will have far-reaching implications for improving patient care and patient safety.”
“The hospital of the future will be based on patient-centered care, with measurable quality outcomes and delivered by teams of health professionals,” explains Larry Wellikson, MD, FACP, SHM CEO. “This collaborative process with hospital-based pharmacists and hospitalists working together to improve VTE care is just the kind of interdisciplinary teamwork that can serve as a beacon to lead us to a better future.”
Applications should emphasize the following:
- Project objectives that address health services research related to the prevention and treatment of VTE;
- Sound research methods that support the study objectives;
- Interdisciplinary collaboration between hospital pharmacists and hospitalist physicians;
- The potential for findings to be replicated in other healthcare facilities; and
- Prudent use of grant funds.
Potential areas of research focus include the use of appropriate interventions to prevent VTE, optimization and monitoring of therapies used for VTE, ensuring continuity of care, provision of literacy-sensitive education to patients and caregivers, and health professional education.
Applications and detailed instructions for the Hospital Pharmacist-Hospitalist Collaboration: VTE Prevention and Treatment Team Grant is available on the ASHP Foundation Web site at www.ashpfoundation.org. The deadline for completed applications is March 1.
SHM Launches New Grassroots Advocacy Tool
Grassroots involvement by SHM members is critical to our ability to influence health policy in Washington. That is why SHM has launched a powerful new advocacy tool designed to help you communicate quickly and effectively with your congressional representatives. Capwiz·XC, located in the “Advocacy” section of our Web site, enables you to take action on any issue important to hospital medicine by sending personalized communications to your elected officials.
Advocacy doesn’t have to require a big time commitment. Communicating with your representatives in Congress now takes just a few minutes at SHM’s Legislative Action Center. You can send an e-mail whenever it is convenient for you, and our action alerts contain sample text for you to use and personalize as desired. Physician payment reform, quality improvement, palliative care, and funding levels for the National Institutes of Health and the Agency for Healthcare Research and Quality are just a few of the many issues before the 110th Congress. You can help influence the debate, improve patient care, and increase the visibility of hospitalists by making your voice heard through Capwiz.
Capwiz has many other features that will help keep you informed and educated about the legislative process. These include an interactive map to help you find your elected officials. Simply enter your ZIP code or click on your state to find out who your elected officials are. From there, you can easily select one of the listed state or congressional officials to see the full legislative biography page. Each bio page includes direct links you can use to contact the legislator, look up his or her key votes, and find staff contact information. You’ll also find a plethora of information about each elected representative, including:
- Office term;
- Co-sponsorship status;
- Contact information;
- Party affiliation;
- Political background;
- Committee(s); and
- PAC contributions.
Are you interested in looking up a piece of legislation recently mentioned in the news? Or do you want to monitor the various bills that will affect issues important to your practice? The “Legislative Action Center” in the “Advocacy” section contains “Issues and Legislation” to help you to stay on top of current legislation affecting healthcare. Keep track of any bill’s name, summary, co-sponsor(s), and key votes, while also monitoring SHM’s position on the legislation.
SHM is pleased to provide you with the opportunity to become more familiar with the political process and actively participate in influencing the policies that affect hospitalists and their patients. Capwiz contains up-to-the-minute legislative data and online tools to enable you to make a difference in the political process. Please visit our Legislative Action Center today at www.hospitalmedicine.org. TH
A response to the needs:
Products and Initiatives
- Annual Awards
- Antimicrobial Resistance Resource Room
- Career Center
- Chapters
- Coding and Documentation Precourse
- Collaboration with IHI and Other Organizations
- Core Competencies
- Credentialing by ABIM
- Dashboard White Paper
- Discharge Planning Checklist
- DVT Awareness Campaign
- DVT Mentored Implementation
- e-Newsletter
- Geriatric Resource Room
- Glycemic Control Resource Room
- Heart Failure Resource Room
- Journal of Hospital Medicine
- Leadership Academies
- Legislative Action Day
- Letters to Congress
- List Serves
- Mentoring
- Practice Management Precourse
- Productivity and Compensation Survey
- Public Policy White Paper
- Quality Precourse
- Research Grants
- Resource Rooms
- RIV Competition
- SEPs Workshop
- Stroke Resource Room
- Survey Collaboration with AHA
- The Hospitalist
- Value Added White Paper
- VTE Resource Room
- Web site
A response to the needs:
Committees and Task Forces
- Annual Meeting Committee
- Awards Committee
- Benchmarks Committee
- Board of Directors
- Career Satisfaction Task Force
- Certification Task Force
- Curriculum Task Force
- Education Committee
- Ethics Committee
- Executive Committee of the Board of Directors
- Executive Review Committee
- Family Practice Task Force
- Finance Committee of the Board of Directors
- Hospital Quality and Patient Safety Committee
- Heart Failure Award Task Force
- Leadership Committee
- Membership Committee
- Nominations Committee
- Non Physician Provider Committee
- Palliative Care Task Force
- Pediatric Committee
- Pediatric Core Curriculum Task Force
- Performance and Standards Task Force
- Public Policy Committee
- Research Committee
- Resource Room Oversight Committee
- Research, Innovation, and Clinical Vignettes Committee
- Women in Hospital Medicine
- Young Physicians Committee TH
A Case of Pruritis Rash

History of Present Illness
A55-year-old male presented with a one and one-half week history of a sore throat, shortness of breath on exertion, ankle edema, and arthralgias that began in the ankles and subsequently spread to involve the elbows and wrists.
He had also developed a pruritic eruption involving the lower extremities, which consisted of erythematous palpable purpuric lesions and patches with superficial and central necrosis and ulceration, as well as a large 4-cm bulla of the right lateral ankle. (See Figures 1 and 2, below.) Other skin findings included petechiae of the palms and multiple ulcerations of the hard palate. Laboratory evaluation demonstrated c-ANCA antibody positivity (1:512), a proteinase 3 antibody level of greater than 100 U/ml, and a creatinine of 1.0mg/dl. TH

What is the most appropriate treatment for this condition?
- Prednisone;
- Azathioprine;
- Cyclophosphamide;
- Prednisone combined with cyclophosphamide; or
- Vancomycin combined with rifampin
Discussion
The answer is D: Wegener’s granulomatosis (WG) is a chronic granulomatous inflammatory response of unknown etiology that usually presents with the classic triad of systemic vasculitis, necrotizing granulomatous inflammation of the upper and lower respiratory tracts, and glomerulonephritis. The generalized or classic form of WG can progress rapidly to cause irreversible organ dysfunction and death. Although the pathogenesis remains unknown, it is felt that WG may result from an exaggerated cell-mediated response to an unknown antigen.1

The average age of onset for WG is 45.2 years, with 63.5% of patients male and 91% Caucasian.2 A WG diagnosis can be very difficult, and elements of the classic triad may not all be present initially. Pulmonary infiltrates or nodules are seen via chest X-ray or CT scan in just less than half of patients as an early manifestation of WG.
Occasionally WG presents with skin lesions (13%) or oral ulcers (6%), however, 40% of patients eventually develop skin involvement consisting of painful subcutaneous nodules, papules, vesicles or bullae, petechiae, palpable purpura, and pyoderma gangrenosum-like lesions.3 Histologic evaluation of these skin lesions reveals non-specific perivascular lymphocytic inflammation, leukocytoclastic vasculitis-like changes, palisading granulomas, and granulomatous vasculitis; however, it is rare to see granulomatous vasculitis or palisading necrotizing granulomas in skin specimens.4,5
WG can also affect the eyes, heart, respiratory system, nervous system, kidneys, and joints.6 The upper respiratory tract is involved in the majority of patients, and symptoms reflecting otitis, epistaxis, rhinorrhea, or sinusitis are common and may be the first manifestation of disease. When mucosal necrotizing granulomas occur, they can result in the typical saddle nose deformity seen in patients with WG. Lower respiratory tract involvement is also common and can present with cough, dyspnea, chest pain, and hemoptysis.1
Patients with WG usually have a positive c-ANCA, however this is not specific for WG and may also indicate Churg-Strauss Syndrome and microscopic polyarteritis. The median survival of patients with untreated WG is five months, and corticosteroids used alone do not change this median survival. When corticosteroids are combined with cytotoxic agents, such as cyclophosphamide, the prognosis significantly improves in greater than 90% of patients, with a 75% remission rate, and an 87% survival of patients followed from six months to 24 years.3 TH
References
- Hannon CW, Swerlick RA. Vasculitis. In: Bolognia JL, Jorizzo JL, Rapini RP, et al, eds. Dermatology. Vol 1. New York: Elsevier Limited; 2003: 393-395.
- Cotch MF, Hoffman GS, Yerg DE, et al. The epidemiology of Wegener’s granulomatosis. Estimates of the five-year period prevalence, annual mortality, and geographic disease distribution from population-based data sources. Arthritis Rheum. 1996 Jan;39(1):87-92.
- Hoffman GS, Kerr GS, Leavitt RY, et al. Wegener granulomatosis: an analysis of 158 patients. [see comments]. Ann Int Med. 1992;116:488-498.
- Hu CH, O’Loughlin S, Winkelmann RK. Cutaneous manifestations of Wegener granulomatosis. Arch Dermatol. 1997;113(2):175-182.
- Lie JT. Wegener’s granulomatosis: histological documentation of common and uncommon manifestations in 216 patients. Vasa. 1997;26:261-270.
- Yi ES, Colby TV. Wegener’s granulomatosis. Semin Diagn Pathol. 2001 Feb;18(1):34-46.
History of Present Illness
A55-year-old male presented with a one and one-half week history of a sore throat, shortness of breath on exertion, ankle edema, and arthralgias that began in the ankles and subsequently spread to involve the elbows and wrists.
He had also developed a pruritic eruption involving the lower extremities, which consisted of erythematous palpable purpuric lesions and patches with superficial and central necrosis and ulceration, as well as a large 4-cm bulla of the right lateral ankle. (See Figures 1 and 2, below.) Other skin findings included petechiae of the palms and multiple ulcerations of the hard palate. Laboratory evaluation demonstrated c-ANCA antibody positivity (1:512), a proteinase 3 antibody level of greater than 100 U/ml, and a creatinine of 1.0mg/dl. TH
What is the most appropriate treatment for this condition?
- Prednisone;
- Azathioprine;
- Cyclophosphamide;
- Prednisone combined with cyclophosphamide; or
- Vancomycin combined with rifampin
Discussion
The answer is D: Wegener’s granulomatosis (WG) is a chronic granulomatous inflammatory response of unknown etiology that usually presents with the classic triad of systemic vasculitis, necrotizing granulomatous inflammation of the upper and lower respiratory tracts, and glomerulonephritis. The generalized or classic form of WG can progress rapidly to cause irreversible organ dysfunction and death. Although the pathogenesis remains unknown, it is felt that WG may result from an exaggerated cell-mediated response to an unknown antigen.1
The average age of onset for WG is 45.2 years, with 63.5% of patients male and 91% Caucasian.2 A WG diagnosis can be very difficult, and elements of the classic triad may not all be present initially. Pulmonary infiltrates or nodules are seen via chest X-ray or CT scan in just less than half of patients as an early manifestation of WG.
Occasionally WG presents with skin lesions (13%) or oral ulcers (6%), however, 40% of patients eventually develop skin involvement consisting of painful subcutaneous nodules, papules, vesicles or bullae, petechiae, palpable purpura, and pyoderma gangrenosum-like lesions.3 Histologic evaluation of these skin lesions reveals non-specific perivascular lymphocytic inflammation, leukocytoclastic vasculitis-like changes, palisading granulomas, and granulomatous vasculitis; however, it is rare to see granulomatous vasculitis or palisading necrotizing granulomas in skin specimens.4,5
WG can also affect the eyes, heart, respiratory system, nervous system, kidneys, and joints.6 The upper respiratory tract is involved in the majority of patients, and symptoms reflecting otitis, epistaxis, rhinorrhea, or sinusitis are common and may be the first manifestation of disease. When mucosal necrotizing granulomas occur, they can result in the typical saddle nose deformity seen in patients with WG. Lower respiratory tract involvement is also common and can present with cough, dyspnea, chest pain, and hemoptysis.1
Patients with WG usually have a positive c-ANCA, however this is not specific for WG and may also indicate Churg-Strauss Syndrome and microscopic polyarteritis. The median survival of patients with untreated WG is five months, and corticosteroids used alone do not change this median survival. When corticosteroids are combined with cytotoxic agents, such as cyclophosphamide, the prognosis significantly improves in greater than 90% of patients, with a 75% remission rate, and an 87% survival of patients followed from six months to 24 years.3 TH
References
- Hannon CW, Swerlick RA. Vasculitis. In: Bolognia JL, Jorizzo JL, Rapini RP, et al, eds. Dermatology. Vol 1. New York: Elsevier Limited; 2003: 393-395.
- Cotch MF, Hoffman GS, Yerg DE, et al. The epidemiology of Wegener’s granulomatosis. Estimates of the five-year period prevalence, annual mortality, and geographic disease distribution from population-based data sources. Arthritis Rheum. 1996 Jan;39(1):87-92.
- Hoffman GS, Kerr GS, Leavitt RY, et al. Wegener granulomatosis: an analysis of 158 patients. [see comments]. Ann Int Med. 1992;116:488-498.
- Hu CH, O’Loughlin S, Winkelmann RK. Cutaneous manifestations of Wegener granulomatosis. Arch Dermatol. 1997;113(2):175-182.
- Lie JT. Wegener’s granulomatosis: histological documentation of common and uncommon manifestations in 216 patients. Vasa. 1997;26:261-270.
- Yi ES, Colby TV. Wegener’s granulomatosis. Semin Diagn Pathol. 2001 Feb;18(1):34-46.
History of Present Illness
A55-year-old male presented with a one and one-half week history of a sore throat, shortness of breath on exertion, ankle edema, and arthralgias that began in the ankles and subsequently spread to involve the elbows and wrists.
He had also developed a pruritic eruption involving the lower extremities, which consisted of erythematous palpable purpuric lesions and patches with superficial and central necrosis and ulceration, as well as a large 4-cm bulla of the right lateral ankle. (See Figures 1 and 2, below.) Other skin findings included petechiae of the palms and multiple ulcerations of the hard palate. Laboratory evaluation demonstrated c-ANCA antibody positivity (1:512), a proteinase 3 antibody level of greater than 100 U/ml, and a creatinine of 1.0mg/dl. TH
What is the most appropriate treatment for this condition?
- Prednisone;
- Azathioprine;
- Cyclophosphamide;
- Prednisone combined with cyclophosphamide; or
- Vancomycin combined with rifampin
Discussion
The answer is D: Wegener’s granulomatosis (WG) is a chronic granulomatous inflammatory response of unknown etiology that usually presents with the classic triad of systemic vasculitis, necrotizing granulomatous inflammation of the upper and lower respiratory tracts, and glomerulonephritis. The generalized or classic form of WG can progress rapidly to cause irreversible organ dysfunction and death. Although the pathogenesis remains unknown, it is felt that WG may result from an exaggerated cell-mediated response to an unknown antigen.1
The average age of onset for WG is 45.2 years, with 63.5% of patients male and 91% Caucasian.2 A WG diagnosis can be very difficult, and elements of the classic triad may not all be present initially. Pulmonary infiltrates or nodules are seen via chest X-ray or CT scan in just less than half of patients as an early manifestation of WG.
Occasionally WG presents with skin lesions (13%) or oral ulcers (6%), however, 40% of patients eventually develop skin involvement consisting of painful subcutaneous nodules, papules, vesicles or bullae, petechiae, palpable purpura, and pyoderma gangrenosum-like lesions.3 Histologic evaluation of these skin lesions reveals non-specific perivascular lymphocytic inflammation, leukocytoclastic vasculitis-like changes, palisading granulomas, and granulomatous vasculitis; however, it is rare to see granulomatous vasculitis or palisading necrotizing granulomas in skin specimens.4,5
WG can also affect the eyes, heart, respiratory system, nervous system, kidneys, and joints.6 The upper respiratory tract is involved in the majority of patients, and symptoms reflecting otitis, epistaxis, rhinorrhea, or sinusitis are common and may be the first manifestation of disease. When mucosal necrotizing granulomas occur, they can result in the typical saddle nose deformity seen in patients with WG. Lower respiratory tract involvement is also common and can present with cough, dyspnea, chest pain, and hemoptysis.1
Patients with WG usually have a positive c-ANCA, however this is not specific for WG and may also indicate Churg-Strauss Syndrome and microscopic polyarteritis. The median survival of patients with untreated WG is five months, and corticosteroids used alone do not change this median survival. When corticosteroids are combined with cytotoxic agents, such as cyclophosphamide, the prognosis significantly improves in greater than 90% of patients, with a 75% remission rate, and an 87% survival of patients followed from six months to 24 years.3 TH
References
- Hannon CW, Swerlick RA. Vasculitis. In: Bolognia JL, Jorizzo JL, Rapini RP, et al, eds. Dermatology. Vol 1. New York: Elsevier Limited; 2003: 393-395.
- Cotch MF, Hoffman GS, Yerg DE, et al. The epidemiology of Wegener’s granulomatosis. Estimates of the five-year period prevalence, annual mortality, and geographic disease distribution from population-based data sources. Arthritis Rheum. 1996 Jan;39(1):87-92.
- Hoffman GS, Kerr GS, Leavitt RY, et al. Wegener granulomatosis: an analysis of 158 patients. [see comments]. Ann Int Med. 1992;116:488-498.
- Hu CH, O’Loughlin S, Winkelmann RK. Cutaneous manifestations of Wegener granulomatosis. Arch Dermatol. 1997;113(2):175-182.
- Lie JT. Wegener’s granulomatosis: histological documentation of common and uncommon manifestations in 216 patients. Vasa. 1997;26:261-270.
- Yi ES, Colby TV. Wegener’s granulomatosis. Semin Diagn Pathol. 2001 Feb;18(1):34-46.
JHM Accepted for Indexing in MEDLINE
In December the Journal of Hospital Medicine (JHM, the peer-reviewed sister publication of The Hospitalist) was selected for indexing and inclusion in the National Library of Medicine’s MEDLINE (Medical Literature Analysis and Retrieval System Online). MEDLINE is a bibliographic database that contains 13 million references to journal articles in medicine, nursing, dentistry, veterinary medicine, healthcare systems, and preclinical sciences. It’s the primary component of PubMed, part of the Entrez series of databases provided by the Library’s National Center for Biotechnology Information (NCBI).
“The Journal’s acceptance is a profound recognition that hospital medicine has developed its own sphere of medical knowledge and that hospitalists are making a significant impact on our modern healthcare delivery system,” says Larry Wellikson, MD, FACP, SHM CEO.
JHM, an official SHM publication, debuted in February 2006 and is the premier forum for peer-reviewed research articles and evidence-based reviews in the specialty of hospital medicine. For more information about JHM, visit www.interscience.wiley.com/journal/jhm.
In December the Journal of Hospital Medicine (JHM, the peer-reviewed sister publication of The Hospitalist) was selected for indexing and inclusion in the National Library of Medicine’s MEDLINE (Medical Literature Analysis and Retrieval System Online). MEDLINE is a bibliographic database that contains 13 million references to journal articles in medicine, nursing, dentistry, veterinary medicine, healthcare systems, and preclinical sciences. It’s the primary component of PubMed, part of the Entrez series of databases provided by the Library’s National Center for Biotechnology Information (NCBI).
“The Journal’s acceptance is a profound recognition that hospital medicine has developed its own sphere of medical knowledge and that hospitalists are making a significant impact on our modern healthcare delivery system,” says Larry Wellikson, MD, FACP, SHM CEO.
JHM, an official SHM publication, debuted in February 2006 and is the premier forum for peer-reviewed research articles and evidence-based reviews in the specialty of hospital medicine. For more information about JHM, visit www.interscience.wiley.com/journal/jhm.
In December the Journal of Hospital Medicine (JHM, the peer-reviewed sister publication of The Hospitalist) was selected for indexing and inclusion in the National Library of Medicine’s MEDLINE (Medical Literature Analysis and Retrieval System Online). MEDLINE is a bibliographic database that contains 13 million references to journal articles in medicine, nursing, dentistry, veterinary medicine, healthcare systems, and preclinical sciences. It’s the primary component of PubMed, part of the Entrez series of databases provided by the Library’s National Center for Biotechnology Information (NCBI).
“The Journal’s acceptance is a profound recognition that hospital medicine has developed its own sphere of medical knowledge and that hospitalists are making a significant impact on our modern healthcare delivery system,” says Larry Wellikson, MD, FACP, SHM CEO.
JHM, an official SHM publication, debuted in February 2006 and is the premier forum for peer-reviewed research articles and evidence-based reviews in the specialty of hospital medicine. For more information about JHM, visit www.interscience.wiley.com/journal/jhm.
A Stake in the Sand
Productivity and compensation benchmarks can be useful when negotiating with hospital administrators for increased reimbursements and support resources, when recruiting hospitalists, and when conducting self-evaluations. For many of these processes, hospitalists—and, indeed, hospital administrators—turn to the information contained in the voluminous SHM 2005-2006 Survey, “The Authoritative Source on the State of the Hospital Medicine Movement.” (See “For More Information,” p. 32.)
With a response rate of 26%, the survey represents some 2,550 hospitalists across the nation, and its variables present a more comprehensive aerial view of hospital medicine than did previous surveys. But on the ground and in the trenches, hospital medicine groups must be careful to look at the survey’s metrics with a discerning eye.
When applying the survey metrics to one’s own practice, there can be benefits as well as pitfalls, cautions Joe Miller, SHM senior vice president and principal analyst of the survey data. He emphasizes the great variation among hospital medicine groups and warns against looking at survey medians as representing a “typical” hospital medicine practice.
“When you’ve seen one hospital medicine group, you’ve seen one hospital medicine group,” he quips. In several recent conversations, hospital medicine group leaders and SHM leaders involved in compiling the survey discussed the survey’s strengths and limitations as a benchmarking tool.
Healthy to Negotiate
According to the survey 97% of hospitalist programs receive some type of financial support. “Virtually every program in the country is challenged to defend the amount of money [they receive] or to negotiate for support dollars,” says Miller, who believes that negotiation can be a healthy dynamic. “There is a sense of equality of both sides of the table, a mutual respect between hospitalists and the hospital.” In the process of such negotiations, it will be important not to pin one’s position entirely to the survey metrics.
John Nelson, MD, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., a consultant for hospitalist practices with Nelson/Flores Associates, a columnist for The Hospitalist (“Practice Management”), and a co-founder and past president of SHM, believes that some hospitalists mistakenly view the survey as SHM’s position on what a hospitalist should make. “The survey is the best information we have about what hospitalists do make—there is no better source—but it’s still a survey.”
Using compensation medians as yardsticks for actual salaries and compensation packages is analogous to “learning the average weight of an American and deciding that’s what we all should weigh—and that’s a big mistake,” he says. “If you hold up the survey as the governing document, then each party will use it to their advantage.”
Because the survey is regarded as the most authoritative existing source on hospitalists’ compensation and productivity, it nevertheless ends up being used as a benchmark, says Robin L. Dauterive, assistant director of the clinical hospitalist service at Massachusetts General Hospital in Boston.
“Whenever I’m preparing billings reports or dashboard measures—anything that shows my group’s workload—sooner or later, I always have to include something in there that states, ‘This is what other people are doing,’ ” says Dauterive. “It’s something that you can’t get away from, unfortunately, in medicine.”
She realizes that the survey does not purport to set any national standards, and yet, “all administrations want comparisons.” Dr. Nelson has also noted this phenomenon with the survey. In the absence of additional guidance, hospital executives and hospitalists often find that they’re just arguing about the survey. “And that’s unfortunate,” he says. “It means they’ve lost sight of the unique attributes of a given practice that might support higher or lower incomes and higher or lower workloads.”
View in Context
Hospitalists reading the survey for the first time might first seek to analyze the metrics regarding billings and collections. Here it is especially important not to view the reported numbers in isolation, says Dr. Nelson. For instance, to learn how a hospitalist’s annual gross charges (billings) compare with others across the country (question 12 of the Individual Hospitalist questionnaire—p. 87, Appendix 2), details on pages 251 and 252 supply pertinent variables. For instance, in comparing the four regions of the country, Table 056-A shows that the median annual gross charges for physicians in the south are highest, at $354,000. Hospitalists compensated by a 100% incentive method report higher charges per year ($392,000) than those who are on a 100% salary or a mix of the two methods of payment. Turning to Table 056-B, on page 252 of the published survey, hospitalists can find annual gross charges according to practitioner type, specialty, and employment model. Hospitalists should not stop their reading there, however, as a comparison of others’ annual gross collections might give a more complete picture.
Still, the SHM Survey does not reference all possible explanatory variables. Collections can be influenced by location and payer mix. Hospitalists practicing in a large urban hospital are likely to see more indigent patients for whom the hospital is not reimbursed. A careful reading of the survey should include the questionnaire and the tables supporting chapter conclusions, and the reader must recognize the survey’s limitations.
Apples to Oranges
IPC–The Hospitalist Company participates in the SHM survey and also uses it as a recruitment tool, reports IPC Vice President of Physician Staffing Timothy Lary. “We look at the income averages, and we’re able to demonstrate how our averages are, for the most part, higher than the averages,” he explains. “We also look at the survey from an internal viewpoint, but oftentimes you are comparing apples to oranges.”
Like individual hospitalists, hospital medicine group leaders seek comparisons when they read the survey. For her part, Dr. Dauterive has found the data on starting salaries for new hospitalists useful. For example, page 259, detailed table 060-A on hospitalists’ compensation by category and total, breaks out median yearly income by years as a hospitalist, from less than a year to six or more years. (Many of the detailed “A” tables in Chapter 8 on compensation include the “years as a hospitalist” category.) Dr. Dauterive praises the wealth of data in the survey, pointing to examples of the many variables she was surprised to learn. One of those factors was that 48% of surveyed hospitalist programs were at non-teaching hospitals. (See page 7 of the survey, Executive Summary, “Teaching status of affiliated hospital.”)
Those interviewed for this article agree that productivity data are probably more telling about the day-to-day clinical realities for hospitalists. Productivity metrics figure prominently in Dr. Dauterive’s uses for the survey. Accordingly, the annual number of billable patient encounters seen by the hospitalist (Table 58-B, page 256) and the annual number of work relative value units (RVUs) worked by the hospitalist (Table 59-B, page 258) caught her interest.
Still, Dr. Dauterive found herself wanting more data to shed light on those numbers. In negotiations for resources with hospital administrators, Dr. Dauterive would like to be able to pinpoint the reasons behind reported numbers of clinical encounters seen by the hospitalist. If the median number of billable patient encounters seen by the hospitalist in a teaching service was 1,668 (based on 107 responses; page 256, Detailed Table 058-B), what were some of the influences on this number? What was the acuity level of patients? Did the hospitalist have group resources, such as physician extenders, to help with patient admissions and rounds?
“For groups that have low lengths of stay, it would be important for me to know why,” she says. “Did they have extra supports? Do their [doctors] use Palm Pilots? You don’t always know from looking at the numbers how to apply them, make the connection, and justify the resources you’re trying to achieve,” she says.
No Perfect Measure
The ideal survey for Dr. Dauterive would include specific structured models, providing links between categories so that she could compare characteristics that more closely align with her group’s situation.
“Our program is very mixed, so it would be helpful for me to know how work RVUs were being reported,” she says. Pointing to results showing higher productivity (work RVUs) in practices compensated by 100% incentive (Table 060-A, page 259 of the survey), Dr. Dauterive wonders what factors drive these results. While the 100% incentive might appear to be the most important factor, perhaps these groups also have physician extenders or are located in a geographic location that boosts their productivity.
“I’m in a nonprofit hospital, in a clinical hospitalist service, and I want to be able to approach the administration and say, ‘If you want us to see the most patients, these are the kinds of services that see the most patients,’ ”says Dr. Dauterive. “But, if you are more interested in physician retention and work/life, then these are the characteristics of those successful programs.”
This level of detail can be difficult to interpolate from the survey, agrees Dr. Nelson. Patient acuity, for instance, is not specifically queried in the survey questionnaire. “I agree, in the ideal world, this is all information that you would want to know,” he says. Answers to the following questions could help refine product metrics:
- Does your group have teaching responsibilities for residents?
- Do you take a lot of calls from home, or do you have a separate night shift?
- Do you cover more than one physical hospital on the same day?
- Does your group do more than the typical amount of committee and administrative work?
“All these factors,” notes Dr. Nelson, “would influence productivity. There is no perfect way to know the answer to any of those things.” And, he adds, the survey already comprises 292 pages, including numerous detailed tables of data. To include all pertinent variables would entail a longer questionnaire, which might affect the response rate.
Healthcare Delivery Is Local
In his consultations with hospitalist groups, Dr. Nelson always emphasizes that the survey is “a starting point” and not the goal of what hospitalists should make. He favors adjunctive methods for benchmarking practices: “I think that when you’re benchmarking your practice, it’s as important to gather as much local and regional data as you can—in addition to the SHM survey.” He tries to network with other Seattle hospitalist programs to learn about their patterns of work hours, patient loads, and the like.
Thomas Baudendistel, MD, FACP, associate program director of the Internal Medicine Residency Program at Sutter Health’s California Pacific Medical Center in San Francisco, notes that regional markets differ widely. The healthcare market in the Northern California Bay area is very different from the one in Los Angeles in terms of financial remuneration and incentivization.
“The survey,” he says, “gives a global gestalt of the regional flavor of hospital medicine” and reveals general ballpark medians that can be a good starting point for practice benchmarking. “I think what our administration [at California Pacific Medical Center] wants to see is our data compared to the people across the street and down the road, because that’s a closer comparison in terms of payer mix and insurance reimbursements.”
IPC’s Lary agrees. “When I compete, I don’t compete against people across the country; I compete with people across the street,” he says. “As large as IPC is, we realize that healthcare is delivered locally. What we try to do [with the survey] is take the information and, to the best or our ability, figure out how it applies to our individual settings and [to the] different markets that we are in.”
A Stake in the Sand
“I think the benchmarks we have in the survey are just a piece of information—[the survey] is a context, it’s a stake in the sand,” concludes Miller. “We do have variations by type of program, by size of hospital, by geographic location, by size of program. There are numbers for each one of those, and you can clue in as to what some of the more important variations are. We could list probably 25 to 50 variables that would affect hospitalists’ productivity in one way or the other—and that’s not taking into account the individual styles of hospitalists.”
For instance, some hospitalists want to work and earn as much money as possible, while others are searching for a work/life balance that will allow them time with their families.
The survey, says Lary, supplies a piece of information in a complex puzzle about a highly variable profession. “There are so many different ways this business is being conducted right now,” he says. “One medical community may be willing to subsidize a hospital medicine program, and another may not be willing.”
Hospitalists’ professional goals vary widely as well. As far as Dr. Nelson is concerned, the bottom line for hospitalists is to structure independent practices tailored to fit their goals. This means that hospitalists are connected to the economic consequences of their staffing and workload decisions. In that way, he says, rather than approaching administrators about hiring more physicians, the practice itself can decide whether it is worth the decrease in individual hospitalists’ incomes to hire another doctor.
Because their specialty is still evolving, hospitalists will find themselves educating their clients about the profession’s services and advantages. And for that process, the survey can be a helpful adjunct. Miller agrees that the use of the survey requires a certain amount of interpolation on the part of hospitalist leaders. They should be careful, he emphasizes, not to lose sight of the individuality of their own practices.
“If you hold up the survey as the governing document when you negotiate with your hospital, then each party will use it to their advantage,” says Dr. Nelson. “This can push you towards being ‘average’ when that might not be appropriate for your practice.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
Productivity and compensation benchmarks can be useful when negotiating with hospital administrators for increased reimbursements and support resources, when recruiting hospitalists, and when conducting self-evaluations. For many of these processes, hospitalists—and, indeed, hospital administrators—turn to the information contained in the voluminous SHM 2005-2006 Survey, “The Authoritative Source on the State of the Hospital Medicine Movement.” (See “For More Information,” p. 32.)
With a response rate of 26%, the survey represents some 2,550 hospitalists across the nation, and its variables present a more comprehensive aerial view of hospital medicine than did previous surveys. But on the ground and in the trenches, hospital medicine groups must be careful to look at the survey’s metrics with a discerning eye.
When applying the survey metrics to one’s own practice, there can be benefits as well as pitfalls, cautions Joe Miller, SHM senior vice president and principal analyst of the survey data. He emphasizes the great variation among hospital medicine groups and warns against looking at survey medians as representing a “typical” hospital medicine practice.
“When you’ve seen one hospital medicine group, you’ve seen one hospital medicine group,” he quips. In several recent conversations, hospital medicine group leaders and SHM leaders involved in compiling the survey discussed the survey’s strengths and limitations as a benchmarking tool.
Healthy to Negotiate
According to the survey 97% of hospitalist programs receive some type of financial support. “Virtually every program in the country is challenged to defend the amount of money [they receive] or to negotiate for support dollars,” says Miller, who believes that negotiation can be a healthy dynamic. “There is a sense of equality of both sides of the table, a mutual respect between hospitalists and the hospital.” In the process of such negotiations, it will be important not to pin one’s position entirely to the survey metrics.
John Nelson, MD, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., a consultant for hospitalist practices with Nelson/Flores Associates, a columnist for The Hospitalist (“Practice Management”), and a co-founder and past president of SHM, believes that some hospitalists mistakenly view the survey as SHM’s position on what a hospitalist should make. “The survey is the best information we have about what hospitalists do make—there is no better source—but it’s still a survey.”
Using compensation medians as yardsticks for actual salaries and compensation packages is analogous to “learning the average weight of an American and deciding that’s what we all should weigh—and that’s a big mistake,” he says. “If you hold up the survey as the governing document, then each party will use it to their advantage.”
Because the survey is regarded as the most authoritative existing source on hospitalists’ compensation and productivity, it nevertheless ends up being used as a benchmark, says Robin L. Dauterive, assistant director of the clinical hospitalist service at Massachusetts General Hospital in Boston.
“Whenever I’m preparing billings reports or dashboard measures—anything that shows my group’s workload—sooner or later, I always have to include something in there that states, ‘This is what other people are doing,’ ” says Dauterive. “It’s something that you can’t get away from, unfortunately, in medicine.”
She realizes that the survey does not purport to set any national standards, and yet, “all administrations want comparisons.” Dr. Nelson has also noted this phenomenon with the survey. In the absence of additional guidance, hospital executives and hospitalists often find that they’re just arguing about the survey. “And that’s unfortunate,” he says. “It means they’ve lost sight of the unique attributes of a given practice that might support higher or lower incomes and higher or lower workloads.”
View in Context
Hospitalists reading the survey for the first time might first seek to analyze the metrics regarding billings and collections. Here it is especially important not to view the reported numbers in isolation, says Dr. Nelson. For instance, to learn how a hospitalist’s annual gross charges (billings) compare with others across the country (question 12 of the Individual Hospitalist questionnaire—p. 87, Appendix 2), details on pages 251 and 252 supply pertinent variables. For instance, in comparing the four regions of the country, Table 056-A shows that the median annual gross charges for physicians in the south are highest, at $354,000. Hospitalists compensated by a 100% incentive method report higher charges per year ($392,000) than those who are on a 100% salary or a mix of the two methods of payment. Turning to Table 056-B, on page 252 of the published survey, hospitalists can find annual gross charges according to practitioner type, specialty, and employment model. Hospitalists should not stop their reading there, however, as a comparison of others’ annual gross collections might give a more complete picture.
Still, the SHM Survey does not reference all possible explanatory variables. Collections can be influenced by location and payer mix. Hospitalists practicing in a large urban hospital are likely to see more indigent patients for whom the hospital is not reimbursed. A careful reading of the survey should include the questionnaire and the tables supporting chapter conclusions, and the reader must recognize the survey’s limitations.
Apples to Oranges
IPC–The Hospitalist Company participates in the SHM survey and also uses it as a recruitment tool, reports IPC Vice President of Physician Staffing Timothy Lary. “We look at the income averages, and we’re able to demonstrate how our averages are, for the most part, higher than the averages,” he explains. “We also look at the survey from an internal viewpoint, but oftentimes you are comparing apples to oranges.”
Like individual hospitalists, hospital medicine group leaders seek comparisons when they read the survey. For her part, Dr. Dauterive has found the data on starting salaries for new hospitalists useful. For example, page 259, detailed table 060-A on hospitalists’ compensation by category and total, breaks out median yearly income by years as a hospitalist, from less than a year to six or more years. (Many of the detailed “A” tables in Chapter 8 on compensation include the “years as a hospitalist” category.) Dr. Dauterive praises the wealth of data in the survey, pointing to examples of the many variables she was surprised to learn. One of those factors was that 48% of surveyed hospitalist programs were at non-teaching hospitals. (See page 7 of the survey, Executive Summary, “Teaching status of affiliated hospital.”)
Those interviewed for this article agree that productivity data are probably more telling about the day-to-day clinical realities for hospitalists. Productivity metrics figure prominently in Dr. Dauterive’s uses for the survey. Accordingly, the annual number of billable patient encounters seen by the hospitalist (Table 58-B, page 256) and the annual number of work relative value units (RVUs) worked by the hospitalist (Table 59-B, page 258) caught her interest.
Still, Dr. Dauterive found herself wanting more data to shed light on those numbers. In negotiations for resources with hospital administrators, Dr. Dauterive would like to be able to pinpoint the reasons behind reported numbers of clinical encounters seen by the hospitalist. If the median number of billable patient encounters seen by the hospitalist in a teaching service was 1,668 (based on 107 responses; page 256, Detailed Table 058-B), what were some of the influences on this number? What was the acuity level of patients? Did the hospitalist have group resources, such as physician extenders, to help with patient admissions and rounds?
“For groups that have low lengths of stay, it would be important for me to know why,” she says. “Did they have extra supports? Do their [doctors] use Palm Pilots? You don’t always know from looking at the numbers how to apply them, make the connection, and justify the resources you’re trying to achieve,” she says.
No Perfect Measure
The ideal survey for Dr. Dauterive would include specific structured models, providing links between categories so that she could compare characteristics that more closely align with her group’s situation.
“Our program is very mixed, so it would be helpful for me to know how work RVUs were being reported,” she says. Pointing to results showing higher productivity (work RVUs) in practices compensated by 100% incentive (Table 060-A, page 259 of the survey), Dr. Dauterive wonders what factors drive these results. While the 100% incentive might appear to be the most important factor, perhaps these groups also have physician extenders or are located in a geographic location that boosts their productivity.
“I’m in a nonprofit hospital, in a clinical hospitalist service, and I want to be able to approach the administration and say, ‘If you want us to see the most patients, these are the kinds of services that see the most patients,’ ”says Dr. Dauterive. “But, if you are more interested in physician retention and work/life, then these are the characteristics of those successful programs.”
This level of detail can be difficult to interpolate from the survey, agrees Dr. Nelson. Patient acuity, for instance, is not specifically queried in the survey questionnaire. “I agree, in the ideal world, this is all information that you would want to know,” he says. Answers to the following questions could help refine product metrics:
- Does your group have teaching responsibilities for residents?
- Do you take a lot of calls from home, or do you have a separate night shift?
- Do you cover more than one physical hospital on the same day?
- Does your group do more than the typical amount of committee and administrative work?
“All these factors,” notes Dr. Nelson, “would influence productivity. There is no perfect way to know the answer to any of those things.” And, he adds, the survey already comprises 292 pages, including numerous detailed tables of data. To include all pertinent variables would entail a longer questionnaire, which might affect the response rate.
Healthcare Delivery Is Local
In his consultations with hospitalist groups, Dr. Nelson always emphasizes that the survey is “a starting point” and not the goal of what hospitalists should make. He favors adjunctive methods for benchmarking practices: “I think that when you’re benchmarking your practice, it’s as important to gather as much local and regional data as you can—in addition to the SHM survey.” He tries to network with other Seattle hospitalist programs to learn about their patterns of work hours, patient loads, and the like.
Thomas Baudendistel, MD, FACP, associate program director of the Internal Medicine Residency Program at Sutter Health’s California Pacific Medical Center in San Francisco, notes that regional markets differ widely. The healthcare market in the Northern California Bay area is very different from the one in Los Angeles in terms of financial remuneration and incentivization.
“The survey,” he says, “gives a global gestalt of the regional flavor of hospital medicine” and reveals general ballpark medians that can be a good starting point for practice benchmarking. “I think what our administration [at California Pacific Medical Center] wants to see is our data compared to the people across the street and down the road, because that’s a closer comparison in terms of payer mix and insurance reimbursements.”
IPC’s Lary agrees. “When I compete, I don’t compete against people across the country; I compete with people across the street,” he says. “As large as IPC is, we realize that healthcare is delivered locally. What we try to do [with the survey] is take the information and, to the best or our ability, figure out how it applies to our individual settings and [to the] different markets that we are in.”
A Stake in the Sand
“I think the benchmarks we have in the survey are just a piece of information—[the survey] is a context, it’s a stake in the sand,” concludes Miller. “We do have variations by type of program, by size of hospital, by geographic location, by size of program. There are numbers for each one of those, and you can clue in as to what some of the more important variations are. We could list probably 25 to 50 variables that would affect hospitalists’ productivity in one way or the other—and that’s not taking into account the individual styles of hospitalists.”
For instance, some hospitalists want to work and earn as much money as possible, while others are searching for a work/life balance that will allow them time with their families.
The survey, says Lary, supplies a piece of information in a complex puzzle about a highly variable profession. “There are so many different ways this business is being conducted right now,” he says. “One medical community may be willing to subsidize a hospital medicine program, and another may not be willing.”
Hospitalists’ professional goals vary widely as well. As far as Dr. Nelson is concerned, the bottom line for hospitalists is to structure independent practices tailored to fit their goals. This means that hospitalists are connected to the economic consequences of their staffing and workload decisions. In that way, he says, rather than approaching administrators about hiring more physicians, the practice itself can decide whether it is worth the decrease in individual hospitalists’ incomes to hire another doctor.
Because their specialty is still evolving, hospitalists will find themselves educating their clients about the profession’s services and advantages. And for that process, the survey can be a helpful adjunct. Miller agrees that the use of the survey requires a certain amount of interpolation on the part of hospitalist leaders. They should be careful, he emphasizes, not to lose sight of the individuality of their own practices.
“If you hold up the survey as the governing document when you negotiate with your hospital, then each party will use it to their advantage,” says Dr. Nelson. “This can push you towards being ‘average’ when that might not be appropriate for your practice.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
Productivity and compensation benchmarks can be useful when negotiating with hospital administrators for increased reimbursements and support resources, when recruiting hospitalists, and when conducting self-evaluations. For many of these processes, hospitalists—and, indeed, hospital administrators—turn to the information contained in the voluminous SHM 2005-2006 Survey, “The Authoritative Source on the State of the Hospital Medicine Movement.” (See “For More Information,” p. 32.)
With a response rate of 26%, the survey represents some 2,550 hospitalists across the nation, and its variables present a more comprehensive aerial view of hospital medicine than did previous surveys. But on the ground and in the trenches, hospital medicine groups must be careful to look at the survey’s metrics with a discerning eye.
When applying the survey metrics to one’s own practice, there can be benefits as well as pitfalls, cautions Joe Miller, SHM senior vice president and principal analyst of the survey data. He emphasizes the great variation among hospital medicine groups and warns against looking at survey medians as representing a “typical” hospital medicine practice.
“When you’ve seen one hospital medicine group, you’ve seen one hospital medicine group,” he quips. In several recent conversations, hospital medicine group leaders and SHM leaders involved in compiling the survey discussed the survey’s strengths and limitations as a benchmarking tool.
Healthy to Negotiate
According to the survey 97% of hospitalist programs receive some type of financial support. “Virtually every program in the country is challenged to defend the amount of money [they receive] or to negotiate for support dollars,” says Miller, who believes that negotiation can be a healthy dynamic. “There is a sense of equality of both sides of the table, a mutual respect between hospitalists and the hospital.” In the process of such negotiations, it will be important not to pin one’s position entirely to the survey metrics.
John Nelson, MD, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., a consultant for hospitalist practices with Nelson/Flores Associates, a columnist for The Hospitalist (“Practice Management”), and a co-founder and past president of SHM, believes that some hospitalists mistakenly view the survey as SHM’s position on what a hospitalist should make. “The survey is the best information we have about what hospitalists do make—there is no better source—but it’s still a survey.”
Using compensation medians as yardsticks for actual salaries and compensation packages is analogous to “learning the average weight of an American and deciding that’s what we all should weigh—and that’s a big mistake,” he says. “If you hold up the survey as the governing document, then each party will use it to their advantage.”
Because the survey is regarded as the most authoritative existing source on hospitalists’ compensation and productivity, it nevertheless ends up being used as a benchmark, says Robin L. Dauterive, assistant director of the clinical hospitalist service at Massachusetts General Hospital in Boston.
“Whenever I’m preparing billings reports or dashboard measures—anything that shows my group’s workload—sooner or later, I always have to include something in there that states, ‘This is what other people are doing,’ ” says Dauterive. “It’s something that you can’t get away from, unfortunately, in medicine.”
She realizes that the survey does not purport to set any national standards, and yet, “all administrations want comparisons.” Dr. Nelson has also noted this phenomenon with the survey. In the absence of additional guidance, hospital executives and hospitalists often find that they’re just arguing about the survey. “And that’s unfortunate,” he says. “It means they’ve lost sight of the unique attributes of a given practice that might support higher or lower incomes and higher or lower workloads.”
View in Context
Hospitalists reading the survey for the first time might first seek to analyze the metrics regarding billings and collections. Here it is especially important not to view the reported numbers in isolation, says Dr. Nelson. For instance, to learn how a hospitalist’s annual gross charges (billings) compare with others across the country (question 12 of the Individual Hospitalist questionnaire—p. 87, Appendix 2), details on pages 251 and 252 supply pertinent variables. For instance, in comparing the four regions of the country, Table 056-A shows that the median annual gross charges for physicians in the south are highest, at $354,000. Hospitalists compensated by a 100% incentive method report higher charges per year ($392,000) than those who are on a 100% salary or a mix of the two methods of payment. Turning to Table 056-B, on page 252 of the published survey, hospitalists can find annual gross charges according to practitioner type, specialty, and employment model. Hospitalists should not stop their reading there, however, as a comparison of others’ annual gross collections might give a more complete picture.
Still, the SHM Survey does not reference all possible explanatory variables. Collections can be influenced by location and payer mix. Hospitalists practicing in a large urban hospital are likely to see more indigent patients for whom the hospital is not reimbursed. A careful reading of the survey should include the questionnaire and the tables supporting chapter conclusions, and the reader must recognize the survey’s limitations.
Apples to Oranges
IPC–The Hospitalist Company participates in the SHM survey and also uses it as a recruitment tool, reports IPC Vice President of Physician Staffing Timothy Lary. “We look at the income averages, and we’re able to demonstrate how our averages are, for the most part, higher than the averages,” he explains. “We also look at the survey from an internal viewpoint, but oftentimes you are comparing apples to oranges.”
Like individual hospitalists, hospital medicine group leaders seek comparisons when they read the survey. For her part, Dr. Dauterive has found the data on starting salaries for new hospitalists useful. For example, page 259, detailed table 060-A on hospitalists’ compensation by category and total, breaks out median yearly income by years as a hospitalist, from less than a year to six or more years. (Many of the detailed “A” tables in Chapter 8 on compensation include the “years as a hospitalist” category.) Dr. Dauterive praises the wealth of data in the survey, pointing to examples of the many variables she was surprised to learn. One of those factors was that 48% of surveyed hospitalist programs were at non-teaching hospitals. (See page 7 of the survey, Executive Summary, “Teaching status of affiliated hospital.”)
Those interviewed for this article agree that productivity data are probably more telling about the day-to-day clinical realities for hospitalists. Productivity metrics figure prominently in Dr. Dauterive’s uses for the survey. Accordingly, the annual number of billable patient encounters seen by the hospitalist (Table 58-B, page 256) and the annual number of work relative value units (RVUs) worked by the hospitalist (Table 59-B, page 258) caught her interest.
Still, Dr. Dauterive found herself wanting more data to shed light on those numbers. In negotiations for resources with hospital administrators, Dr. Dauterive would like to be able to pinpoint the reasons behind reported numbers of clinical encounters seen by the hospitalist. If the median number of billable patient encounters seen by the hospitalist in a teaching service was 1,668 (based on 107 responses; page 256, Detailed Table 058-B), what were some of the influences on this number? What was the acuity level of patients? Did the hospitalist have group resources, such as physician extenders, to help with patient admissions and rounds?
“For groups that have low lengths of stay, it would be important for me to know why,” she says. “Did they have extra supports? Do their [doctors] use Palm Pilots? You don’t always know from looking at the numbers how to apply them, make the connection, and justify the resources you’re trying to achieve,” she says.
No Perfect Measure
The ideal survey for Dr. Dauterive would include specific structured models, providing links between categories so that she could compare characteristics that more closely align with her group’s situation.
“Our program is very mixed, so it would be helpful for me to know how work RVUs were being reported,” she says. Pointing to results showing higher productivity (work RVUs) in practices compensated by 100% incentive (Table 060-A, page 259 of the survey), Dr. Dauterive wonders what factors drive these results. While the 100% incentive might appear to be the most important factor, perhaps these groups also have physician extenders or are located in a geographic location that boosts their productivity.
“I’m in a nonprofit hospital, in a clinical hospitalist service, and I want to be able to approach the administration and say, ‘If you want us to see the most patients, these are the kinds of services that see the most patients,’ ”says Dr. Dauterive. “But, if you are more interested in physician retention and work/life, then these are the characteristics of those successful programs.”
This level of detail can be difficult to interpolate from the survey, agrees Dr. Nelson. Patient acuity, for instance, is not specifically queried in the survey questionnaire. “I agree, in the ideal world, this is all information that you would want to know,” he says. Answers to the following questions could help refine product metrics:
- Does your group have teaching responsibilities for residents?
- Do you take a lot of calls from home, or do you have a separate night shift?
- Do you cover more than one physical hospital on the same day?
- Does your group do more than the typical amount of committee and administrative work?
“All these factors,” notes Dr. Nelson, “would influence productivity. There is no perfect way to know the answer to any of those things.” And, he adds, the survey already comprises 292 pages, including numerous detailed tables of data. To include all pertinent variables would entail a longer questionnaire, which might affect the response rate.
Healthcare Delivery Is Local
In his consultations with hospitalist groups, Dr. Nelson always emphasizes that the survey is “a starting point” and not the goal of what hospitalists should make. He favors adjunctive methods for benchmarking practices: “I think that when you’re benchmarking your practice, it’s as important to gather as much local and regional data as you can—in addition to the SHM survey.” He tries to network with other Seattle hospitalist programs to learn about their patterns of work hours, patient loads, and the like.
Thomas Baudendistel, MD, FACP, associate program director of the Internal Medicine Residency Program at Sutter Health’s California Pacific Medical Center in San Francisco, notes that regional markets differ widely. The healthcare market in the Northern California Bay area is very different from the one in Los Angeles in terms of financial remuneration and incentivization.
“The survey,” he says, “gives a global gestalt of the regional flavor of hospital medicine” and reveals general ballpark medians that can be a good starting point for practice benchmarking. “I think what our administration [at California Pacific Medical Center] wants to see is our data compared to the people across the street and down the road, because that’s a closer comparison in terms of payer mix and insurance reimbursements.”
IPC’s Lary agrees. “When I compete, I don’t compete against people across the country; I compete with people across the street,” he says. “As large as IPC is, we realize that healthcare is delivered locally. What we try to do [with the survey] is take the information and, to the best or our ability, figure out how it applies to our individual settings and [to the] different markets that we are in.”
A Stake in the Sand
“I think the benchmarks we have in the survey are just a piece of information—[the survey] is a context, it’s a stake in the sand,” concludes Miller. “We do have variations by type of program, by size of hospital, by geographic location, by size of program. There are numbers for each one of those, and you can clue in as to what some of the more important variations are. We could list probably 25 to 50 variables that would affect hospitalists’ productivity in one way or the other—and that’s not taking into account the individual styles of hospitalists.”
For instance, some hospitalists want to work and earn as much money as possible, while others are searching for a work/life balance that will allow them time with their families.
The survey, says Lary, supplies a piece of information in a complex puzzle about a highly variable profession. “There are so many different ways this business is being conducted right now,” he says. “One medical community may be willing to subsidize a hospital medicine program, and another may not be willing.”
Hospitalists’ professional goals vary widely as well. As far as Dr. Nelson is concerned, the bottom line for hospitalists is to structure independent practices tailored to fit their goals. This means that hospitalists are connected to the economic consequences of their staffing and workload decisions. In that way, he says, rather than approaching administrators about hiring more physicians, the practice itself can decide whether it is worth the decrease in individual hospitalists’ incomes to hire another doctor.
Because their specialty is still evolving, hospitalists will find themselves educating their clients about the profession’s services and advantages. And for that process, the survey can be a helpful adjunct. Miller agrees that the use of the survey requires a certain amount of interpolation on the part of hospitalist leaders. They should be careful, he emphasizes, not to lose sight of the individuality of their own practices.
“If you hold up the survey as the governing document when you negotiate with your hospital, then each party will use it to their advantage,” says Dr. Nelson. “This can push you towards being ‘average’ when that might not be appropriate for your practice.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.