User login
PSTF Monitors Quality

In spring 2006 SHM leadership agreed that there was a need to develop a coordinated approach to working with external organizations in the performance and standards quality arena, while collaborating with public policy and educational efforts in this area. To this end, I was hired as the SHM Senior Advisor for Quality Standards and Compliance. At around the same time, leaders from the Public Policy Committee (PPC) and Health Quality Patient Safety (HQPS) Committee joined to form a Performance and Standards Task Force (PSTF).
Purpose of the Task Force
Chaired by Patrick Torcson, MD, the PSTF works with staff to monitor the performance and quality landscape at national organizations charged with the measure development and consensus-building processes, as well as to outreach and develop liaison relationships with other professional medical societies and organizations. Ultimately, the task force wants to create a performance framework unique to and reflective of hospitalists.
Since its inception in the late spring, the PSTF has had several meetings to discuss which organizations SHM should engage with and at what level. In several cases, task force members agreed that an official member liaison should be appointed to serve as SHM’s representative to a particular organization. This serves the purpose of having a clinical expert resource available to staff with regard to the particular activities of each organization, as well as to create a consistent and reliable “SHM face” for a particular organization.
Performance Measures
SHM joined the AMA Physician Consortium for Performance Improvement (PCPI), which works with medical specialty organizations to develop physician-level performance measures. As a new member of the PCPI, SHM submitted feedback during the public comment period on perioperative care measures, the development of which was led by the American College of Surgeons, along with input from other medical specialties. SHM also participated in two expert workgroups this past summer, one on emergency medicine, focusing on treating MI and pneumonia, and another on geriatrics, which focused on falls, urinary incontinence, advanced-care planning as part of end-of-life care, and medication reconciliation as part of care coordination. Both the geriatrics and the emergency medicine measures have been released for public comment. At least through 2006, the PCPI is focusing on measures that fall under the Centers for Medicare and Medicaid Services (CMS) contract and will be included in the Physician Voluntary Reporting Program (PVRP).
The PSTF is actively recruiting leaders to participate in expert workgroups that were convened in November for both outpatient parenteral antimicrobial therapy and anesthesiology topics: perioperative normothermia and critical care. The task force will continue to evaluate the PCPI workgroups to determine which ones it should appoint members to participate in, depending on the topic area.
SHM has also become an organizational member of the National Quality Forum (NQF), a nonprofit organization that Congress, in early July, charged with endorsing consensus-based national standards for measurement and public reporting of healthcare performance data. At around the same time, NQF was seeking nominations for members of the steering committee and technical advisory panels that will oversee the work on the development of new consensus standards for hospital care. This project, sponsored by the Agency for Healthcare Research and Quality (AHRQ), will address patient safety, pediatrics, and inpatient care. The Society hopes to be fully engaged in this initiative.
In mid-October, NQF will hold its 7th Annual Meeting, a National Policy Conference on Quality, at the Grand Hyatt in Washington, D.C. This meeting will feature plenary sessions that focus on issues at the forefront of policy discussions, including incentivizing healthcare quality improvement, the role of policymakers, ways to lead professional and trade associations in improving healthcare quality, and efforts presently underway in the federal government to foster healthcare improvements. Mark Williams, MD, editor in chief of the Journal of Hospital Medicine and SHM member, will attend the policy conference as the SHM representative.
Quality Care Liaisons
In addition to fostering liaisons with organizations like PCPI and NQF, the PSTF has discussed the importance of exploring relationships with other groups, including CMS, the American College of Physicians (ACP), the Ambulatory Quality Care Alliance (AQA), and others engaged in the quality care arena.
In late spring 2006 several SHM members and staff met with CMS to discuss its PVRP in relation to hospitalists. While SHM has endorsed the PVRP, recommending that hospitalists register their intent to report and begin reporting on relevant performance measures to the extent practicable, it is clear that the 16 measures used in the PVRP have limited relevance for hospitalists because most measures used for internal medicine deal with services provided in the ambulatory setting.
Specifically, only two of the 16 measures apply to services billed by hospitalists and those only on a limited basis: aspirin on arrival for myocardial infarction and beta-blocker on arrival for MI have G-codes that can be used with the evaluation and management codes appropriate for hospitalists. In its follow-up letter to CMS staff thanking them for their time, SHM leadership also included recommendations that would expand the current number of PVRP measures that hospitalists could report on from two measures to seven.
SHM has also shared the above quality and performance improvement agenda with the staff of the ACP as well as their quality subcommittee, who have found it to be “well-reasoned and straightforward.” We anticipate having more in-depth discussions with the ACP as our quality agenda evolves.
In August, the Ambulatory Care Quality Alliance (AQA) and the Hospital Quality Alliance (HQA) joined forces to form a Quality Steering Committee in order to better coordinate the promotion of quality measurement, transparency, and improvement in care across hospital and ambulatory care settings. The PSTF is currently pursuing participation in one of the new AQA/HQA workgroups created by the steering committee, which would focus on harmonization of measures across settings.
SHM staff have also reached out to the Society of Critical Care Medicine, the Joint Commission on Accreditation of Healthcare Organizations, and the American Hospital Association to ascertain what these groups are doing in terms of quality and measure development, as well as to see how to align our efforts more closely.
In its work with all of these groups, the task force endeavors to ensure the development of performance measures that more accurately reflect services provided by hospitalists.
2007 Goals
The HQPS has developed a mechanism whereby they review measures proposed by a variety of organizations in order to evaluate which measures are relevant to individual clinicians as compared with institutional measures. It is PSTF’s goal (in conjunction with the HQPS, the PPC, and others) to recommend to the SHM board of directors which physician-level disease-specific measures are relevant to individual hospitalists and to identify where the gaps are. It hopes then to influence the scope of development of care coordination and other hospital-level measures that are in the pipeline, whether working through groups like the PCPI by taking the lead on an expert workgroup, by using the NQF consensus-building process, or by forming other key partnerships with groups like those noted above. It is likely that this work will be accomplished by some combination of these strategies.
Stay tuned for next month’s “SHM Behind the Scenes” by SHM Senior Vice President Joe Miller.
Epstein is the senior advisor for Standards and Compliance at SHM.
2005-2006 Survey Factoid
Use of PAs and NPs in hospital medicine groups
- Thirty percent of all hospital medicine groups (HMGs) employ nurse practitioners (NPs) and physician assistants (PAs).
- Those groups, on average, have 11.2 physicians and 2.8 NPs/PAs. The 70% of groups without NPs/PAs average 7.9 physicians per group.
- The following types of groups are more likely to employ NPs/PAs: academic programs, groups in the eastern U.S., and groups more than 5 years old.
- The frequency with which NPs/PAs perform certain functions in HMGs is summarized in this table:
NP/PA Function - % of HMGs
- Round daily on hospitalized patients - 83%
- Write prescriptions for patients - 82%
- Perform H & Ps upon admission - 77%
- Act as initial responder (consults, admits) - 66%
- Participate in discharge planning - 66%
- Order specialty consultations - 53%
- Assist in teaching students - 33%
- Night or weekend call - 30%
- Post discharge follow-up calls - 20%
- Emergency response; Code Blue - 14%
- Perform invasive procedures - 11%
Source: SHM’s 2005-2006 “Biannual State of the Hospital Medicine Movement” survey.
In spring 2006 SHM leadership agreed that there was a need to develop a coordinated approach to working with external organizations in the performance and standards quality arena, while collaborating with public policy and educational efforts in this area. To this end, I was hired as the SHM Senior Advisor for Quality Standards and Compliance. At around the same time, leaders from the Public Policy Committee (PPC) and Health Quality Patient Safety (HQPS) Committee joined to form a Performance and Standards Task Force (PSTF).
Purpose of the Task Force
Chaired by Patrick Torcson, MD, the PSTF works with staff to monitor the performance and quality landscape at national organizations charged with the measure development and consensus-building processes, as well as to outreach and develop liaison relationships with other professional medical societies and organizations. Ultimately, the task force wants to create a performance framework unique to and reflective of hospitalists.
Since its inception in the late spring, the PSTF has had several meetings to discuss which organizations SHM should engage with and at what level. In several cases, task force members agreed that an official member liaison should be appointed to serve as SHM’s representative to a particular organization. This serves the purpose of having a clinical expert resource available to staff with regard to the particular activities of each organization, as well as to create a consistent and reliable “SHM face” for a particular organization.
Performance Measures
SHM joined the AMA Physician Consortium for Performance Improvement (PCPI), which works with medical specialty organizations to develop physician-level performance measures. As a new member of the PCPI, SHM submitted feedback during the public comment period on perioperative care measures, the development of which was led by the American College of Surgeons, along with input from other medical specialties. SHM also participated in two expert workgroups this past summer, one on emergency medicine, focusing on treating MI and pneumonia, and another on geriatrics, which focused on falls, urinary incontinence, advanced-care planning as part of end-of-life care, and medication reconciliation as part of care coordination. Both the geriatrics and the emergency medicine measures have been released for public comment. At least through 2006, the PCPI is focusing on measures that fall under the Centers for Medicare and Medicaid Services (CMS) contract and will be included in the Physician Voluntary Reporting Program (PVRP).
The PSTF is actively recruiting leaders to participate in expert workgroups that were convened in November for both outpatient parenteral antimicrobial therapy and anesthesiology topics: perioperative normothermia and critical care. The task force will continue to evaluate the PCPI workgroups to determine which ones it should appoint members to participate in, depending on the topic area.
SHM has also become an organizational member of the National Quality Forum (NQF), a nonprofit organization that Congress, in early July, charged with endorsing consensus-based national standards for measurement and public reporting of healthcare performance data. At around the same time, NQF was seeking nominations for members of the steering committee and technical advisory panels that will oversee the work on the development of new consensus standards for hospital care. This project, sponsored by the Agency for Healthcare Research and Quality (AHRQ), will address patient safety, pediatrics, and inpatient care. The Society hopes to be fully engaged in this initiative.
In mid-October, NQF will hold its 7th Annual Meeting, a National Policy Conference on Quality, at the Grand Hyatt in Washington, D.C. This meeting will feature plenary sessions that focus on issues at the forefront of policy discussions, including incentivizing healthcare quality improvement, the role of policymakers, ways to lead professional and trade associations in improving healthcare quality, and efforts presently underway in the federal government to foster healthcare improvements. Mark Williams, MD, editor in chief of the Journal of Hospital Medicine and SHM member, will attend the policy conference as the SHM representative.
Quality Care Liaisons
In addition to fostering liaisons with organizations like PCPI and NQF, the PSTF has discussed the importance of exploring relationships with other groups, including CMS, the American College of Physicians (ACP), the Ambulatory Quality Care Alliance (AQA), and others engaged in the quality care arena.
In late spring 2006 several SHM members and staff met with CMS to discuss its PVRP in relation to hospitalists. While SHM has endorsed the PVRP, recommending that hospitalists register their intent to report and begin reporting on relevant performance measures to the extent practicable, it is clear that the 16 measures used in the PVRP have limited relevance for hospitalists because most measures used for internal medicine deal with services provided in the ambulatory setting.
Specifically, only two of the 16 measures apply to services billed by hospitalists and those only on a limited basis: aspirin on arrival for myocardial infarction and beta-blocker on arrival for MI have G-codes that can be used with the evaluation and management codes appropriate for hospitalists. In its follow-up letter to CMS staff thanking them for their time, SHM leadership also included recommendations that would expand the current number of PVRP measures that hospitalists could report on from two measures to seven.
SHM has also shared the above quality and performance improvement agenda with the staff of the ACP as well as their quality subcommittee, who have found it to be “well-reasoned and straightforward.” We anticipate having more in-depth discussions with the ACP as our quality agenda evolves.
In August, the Ambulatory Care Quality Alliance (AQA) and the Hospital Quality Alliance (HQA) joined forces to form a Quality Steering Committee in order to better coordinate the promotion of quality measurement, transparency, and improvement in care across hospital and ambulatory care settings. The PSTF is currently pursuing participation in one of the new AQA/HQA workgroups created by the steering committee, which would focus on harmonization of measures across settings.
SHM staff have also reached out to the Society of Critical Care Medicine, the Joint Commission on Accreditation of Healthcare Organizations, and the American Hospital Association to ascertain what these groups are doing in terms of quality and measure development, as well as to see how to align our efforts more closely.
In its work with all of these groups, the task force endeavors to ensure the development of performance measures that more accurately reflect services provided by hospitalists.
2007 Goals
The HQPS has developed a mechanism whereby they review measures proposed by a variety of organizations in order to evaluate which measures are relevant to individual clinicians as compared with institutional measures. It is PSTF’s goal (in conjunction with the HQPS, the PPC, and others) to recommend to the SHM board of directors which physician-level disease-specific measures are relevant to individual hospitalists and to identify where the gaps are. It hopes then to influence the scope of development of care coordination and other hospital-level measures that are in the pipeline, whether working through groups like the PCPI by taking the lead on an expert workgroup, by using the NQF consensus-building process, or by forming other key partnerships with groups like those noted above. It is likely that this work will be accomplished by some combination of these strategies.
Stay tuned for next month’s “SHM Behind the Scenes” by SHM Senior Vice President Joe Miller.
Epstein is the senior advisor for Standards and Compliance at SHM.
2005-2006 Survey Factoid
Use of PAs and NPs in hospital medicine groups
- Thirty percent of all hospital medicine groups (HMGs) employ nurse practitioners (NPs) and physician assistants (PAs).
- Those groups, on average, have 11.2 physicians and 2.8 NPs/PAs. The 70% of groups without NPs/PAs average 7.9 physicians per group.
- The following types of groups are more likely to employ NPs/PAs: academic programs, groups in the eastern U.S., and groups more than 5 years old.
- The frequency with which NPs/PAs perform certain functions in HMGs is summarized in this table:
NP/PA Function - % of HMGs
- Round daily on hospitalized patients - 83%
- Write prescriptions for patients - 82%
- Perform H & Ps upon admission - 77%
- Act as initial responder (consults, admits) - 66%
- Participate in discharge planning - 66%
- Order specialty consultations - 53%
- Assist in teaching students - 33%
- Night or weekend call - 30%
- Post discharge follow-up calls - 20%
- Emergency response; Code Blue - 14%
- Perform invasive procedures - 11%
Source: SHM’s 2005-2006 “Biannual State of the Hospital Medicine Movement” survey.
In spring 2006 SHM leadership agreed that there was a need to develop a coordinated approach to working with external organizations in the performance and standards quality arena, while collaborating with public policy and educational efforts in this area. To this end, I was hired as the SHM Senior Advisor for Quality Standards and Compliance. At around the same time, leaders from the Public Policy Committee (PPC) and Health Quality Patient Safety (HQPS) Committee joined to form a Performance and Standards Task Force (PSTF).
Purpose of the Task Force
Chaired by Patrick Torcson, MD, the PSTF works with staff to monitor the performance and quality landscape at national organizations charged with the measure development and consensus-building processes, as well as to outreach and develop liaison relationships with other professional medical societies and organizations. Ultimately, the task force wants to create a performance framework unique to and reflective of hospitalists.
Since its inception in the late spring, the PSTF has had several meetings to discuss which organizations SHM should engage with and at what level. In several cases, task force members agreed that an official member liaison should be appointed to serve as SHM’s representative to a particular organization. This serves the purpose of having a clinical expert resource available to staff with regard to the particular activities of each organization, as well as to create a consistent and reliable “SHM face” for a particular organization.
Performance Measures
SHM joined the AMA Physician Consortium for Performance Improvement (PCPI), which works with medical specialty organizations to develop physician-level performance measures. As a new member of the PCPI, SHM submitted feedback during the public comment period on perioperative care measures, the development of which was led by the American College of Surgeons, along with input from other medical specialties. SHM also participated in two expert workgroups this past summer, one on emergency medicine, focusing on treating MI and pneumonia, and another on geriatrics, which focused on falls, urinary incontinence, advanced-care planning as part of end-of-life care, and medication reconciliation as part of care coordination. Both the geriatrics and the emergency medicine measures have been released for public comment. At least through 2006, the PCPI is focusing on measures that fall under the Centers for Medicare and Medicaid Services (CMS) contract and will be included in the Physician Voluntary Reporting Program (PVRP).
The PSTF is actively recruiting leaders to participate in expert workgroups that were convened in November for both outpatient parenteral antimicrobial therapy and anesthesiology topics: perioperative normothermia and critical care. The task force will continue to evaluate the PCPI workgroups to determine which ones it should appoint members to participate in, depending on the topic area.
SHM has also become an organizational member of the National Quality Forum (NQF), a nonprofit organization that Congress, in early July, charged with endorsing consensus-based national standards for measurement and public reporting of healthcare performance data. At around the same time, NQF was seeking nominations for members of the steering committee and technical advisory panels that will oversee the work on the development of new consensus standards for hospital care. This project, sponsored by the Agency for Healthcare Research and Quality (AHRQ), will address patient safety, pediatrics, and inpatient care. The Society hopes to be fully engaged in this initiative.
In mid-October, NQF will hold its 7th Annual Meeting, a National Policy Conference on Quality, at the Grand Hyatt in Washington, D.C. This meeting will feature plenary sessions that focus on issues at the forefront of policy discussions, including incentivizing healthcare quality improvement, the role of policymakers, ways to lead professional and trade associations in improving healthcare quality, and efforts presently underway in the federal government to foster healthcare improvements. Mark Williams, MD, editor in chief of the Journal of Hospital Medicine and SHM member, will attend the policy conference as the SHM representative.
Quality Care Liaisons
In addition to fostering liaisons with organizations like PCPI and NQF, the PSTF has discussed the importance of exploring relationships with other groups, including CMS, the American College of Physicians (ACP), the Ambulatory Quality Care Alliance (AQA), and others engaged in the quality care arena.
In late spring 2006 several SHM members and staff met with CMS to discuss its PVRP in relation to hospitalists. While SHM has endorsed the PVRP, recommending that hospitalists register their intent to report and begin reporting on relevant performance measures to the extent practicable, it is clear that the 16 measures used in the PVRP have limited relevance for hospitalists because most measures used for internal medicine deal with services provided in the ambulatory setting.
Specifically, only two of the 16 measures apply to services billed by hospitalists and those only on a limited basis: aspirin on arrival for myocardial infarction and beta-blocker on arrival for MI have G-codes that can be used with the evaluation and management codes appropriate for hospitalists. In its follow-up letter to CMS staff thanking them for their time, SHM leadership also included recommendations that would expand the current number of PVRP measures that hospitalists could report on from two measures to seven.
SHM has also shared the above quality and performance improvement agenda with the staff of the ACP as well as their quality subcommittee, who have found it to be “well-reasoned and straightforward.” We anticipate having more in-depth discussions with the ACP as our quality agenda evolves.
In August, the Ambulatory Care Quality Alliance (AQA) and the Hospital Quality Alliance (HQA) joined forces to form a Quality Steering Committee in order to better coordinate the promotion of quality measurement, transparency, and improvement in care across hospital and ambulatory care settings. The PSTF is currently pursuing participation in one of the new AQA/HQA workgroups created by the steering committee, which would focus on harmonization of measures across settings.
SHM staff have also reached out to the Society of Critical Care Medicine, the Joint Commission on Accreditation of Healthcare Organizations, and the American Hospital Association to ascertain what these groups are doing in terms of quality and measure development, as well as to see how to align our efforts more closely.
In its work with all of these groups, the task force endeavors to ensure the development of performance measures that more accurately reflect services provided by hospitalists.
2007 Goals
The HQPS has developed a mechanism whereby they review measures proposed by a variety of organizations in order to evaluate which measures are relevant to individual clinicians as compared with institutional measures. It is PSTF’s goal (in conjunction with the HQPS, the PPC, and others) to recommend to the SHM board of directors which physician-level disease-specific measures are relevant to individual hospitalists and to identify where the gaps are. It hopes then to influence the scope of development of care coordination and other hospital-level measures that are in the pipeline, whether working through groups like the PCPI by taking the lead on an expert workgroup, by using the NQF consensus-building process, or by forming other key partnerships with groups like those noted above. It is likely that this work will be accomplished by some combination of these strategies.
Stay tuned for next month’s “SHM Behind the Scenes” by SHM Senior Vice President Joe Miller.
Epstein is the senior advisor for Standards and Compliance at SHM.
2005-2006 Survey Factoid
Use of PAs and NPs in hospital medicine groups
- Thirty percent of all hospital medicine groups (HMGs) employ nurse practitioners (NPs) and physician assistants (PAs).
- Those groups, on average, have 11.2 physicians and 2.8 NPs/PAs. The 70% of groups without NPs/PAs average 7.9 physicians per group.
- The following types of groups are more likely to employ NPs/PAs: academic programs, groups in the eastern U.S., and groups more than 5 years old.
- The frequency with which NPs/PAs perform certain functions in HMGs is summarized in this table:
NP/PA Function - % of HMGs
- Round daily on hospitalized patients - 83%
- Write prescriptions for patients - 82%
- Perform H & Ps upon admission - 77%
- Act as initial responder (consults, admits) - 66%
- Participate in discharge planning - 66%
- Order specialty consultations - 53%
- Assist in teaching students - 33%
- Night or weekend call - 30%
- Post discharge follow-up calls - 20%
- Emergency response; Code Blue - 14%
- Perform invasive procedures - 11%
Source: SHM’s 2005-2006 “Biannual State of the Hospital Medicine Movement” survey.
Pay Dirt

It’ s easy to find figures on what hospitalists earn these days, but if your own income doesn’t match up, does that mean you’re underpaid? Not necessarily.
The SHM Survey
There are several sources that provide figures on hospitalist income, but SHM offers an accurate, detailed—and the largest representative—picture of what hospitalists earn now. In spring 2006, SHM released its latest comprehensive survey of membership, “The 2005-2006 SHM Survey: The Authoritative Source on the State of the Hospitalist Movement.” The report is based on responses of 396 hospital medicine groups representing more than 2,500 hospitalists. However, Joseph A. Miller, senior vice president of SHM, warns that the survey’s salary figures may skew toward one or more specific demographics.
“In our survey, we have a number of respondents in each cell—academic, pediatric, etc.—as well as a range of geographic areas and other differences,” he says. “Anyone who looks at the metric needs to understand the factors behind it.”
John Nelson, MD, director, hospital practice, Overlake Hospital, Bellevue, Wash., and author of “Practice Management” for The Hospitalist, who has participated in developing and analyzing SHM surveys for years, agrees that the figures in the survey should be used as general guidelines only. “It’s easy to take individual metrics in a vacuum without considering the variables,” he warns.
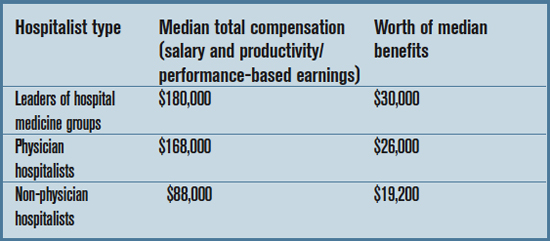
With these caveats in mind, the basic information on hospitalist compensation from the survey breaks down as follows: (table right)
To put these numbers in perspective, the median number of patient encounters per hospitalist was 2,328 per year, and the median number of work RVUs was 3,213.
Both leader- and physician-hospitalists have enjoyed an 8% increase in compensation, as well as an 8% increase in benefits, compared with the 2003-2004 survey. Non-physician hospitalists have seen a whopping increase in median income of 26% since 2003-2004. (Their benefits increased 7%.)
Perhaps the main reason for steadily increasing hospitalist incomes is that demand for hospitalists continues to exceed supply. “I’ve been trying to recruit hospitalists to my group for years,” says Dr. Nelson. “I thought that by 2002 or 2003, the number of available physicians would exceed the demand—but that hasn’t happened. It’s true that the number of doctors interested in hospital medicine has gone up pretty dramatically, but the demand went up even faster.”
By some estimates, says Dr. Nelson, there are two or three open positions for every hospitalist jobseeker.
—John Nelson, MD
Forms of Payment
To break these figures down further, income varies with type of compensation. In other words, how you are paid can influence how much you’re paid. Physician hospitalists who are paid 100% salary had a median income of $150,000. Those who are 100% productivity/performance-based make more money—a median income of $165,000; and those with a mixed-compensation model make the most of all, with a median income of $170,000.
Currently, according to the SHM survey, only 28% of respondents are 100% salary-based and 5% are 100% productivity/performance-based. The remaining majority (67%) is compensated with a combination of the two. Compared to the 2003-2004 SHM survey, the mixed compensation model increased from 47%.
“The portion of hospitalists paid via straight salary or based solely on production has been declining in the last few years,” says Dr. Nelson. “I think [a] low base and high productivity component is ideal, but [a] lower base does impede recruiting even if the total income is very attractive.”
IPC—The Hospitalist Company, one of the largest employers of hospitalists, uses the same combination of base salary and incentives for all physicians, regardless of their level of experience.
“We might change the salary figures slightly for different geographic areas, says Tim Lary, vice president of physician staffing for IPC, “but within our company, the average physician earns a little bit north of $200,000. A large portion earn over $300,000 because of our incentive plan.” That figure includes a base salary of approximately $150,000; the rest is comprised of incentives based on “typical counters” that hospitalists see, according to Lary, including productivity, quality indicators, and compliance.
Lary postulates that compensation is higher at a large organization like IPC because those employers have an infrastructure in place that ensures cost-effectiveness. “We have a 99.9% collection rate because we have a good central business office,” he says. “Small groups don’t have resources like that. We also do a great deal of training in proper coding techniques so that we can bill appropriately.”
A Grain of Salt
Before you barge in to your director’s office and ask for a raise, you should understand that the salaries summarized here have severe limitations and should be seen only as rough guidelines. There are major factors that can boost annual compensation, including:
- A heavy load of on-call, night, or weekend work;
- Employment in a geographic region with a shortage of physicians;
- Employment in a geographic region with higher physician incomes (such as the southeast);
- The type of practice you work for; and
- New practices recruiting hospitalists.
Also keep in mind that compensation totals include all bonuses and incentives received during the year.
Find Your Figure
Hospitalist income—particularly productivity-based income—is also directly affected by workload. Dr. Nelson suggests using the information in the SHM survey to find a rough guideline for productivity and compensation.
“Take the compensation figure from the survey for your region, production type, etc. and take the average production numbers from that same subgroup,” he says. “Then do the math to find the number of dollars per encounter or per RVU, and gauge your own numbers. If you have 25% more encounters, your income should be 25% higher than the average.”
The best rule of thumb for estimating what you should make, says Dr. Nelson, is to aim for five to 15% more than physicians working in traditional practice in your market. Unfortunately, information on what other doctors earn may not be readily available. Some sources (including a few listed in the sidebar to this article) provide information on all physician incomes, but is broken down by region at best. “You have to ask around,” says Dr. Nelson. “And if you’re interviewing, ask what they’re offering—then go and interview at a private practice and ask what they’re offering.”
In other words, there’s no easy way to tell if what you make is exactly on the mark for other hospitalists in your area—unless you ask those other hospitalists. But the SHM survey information should provide enough information to give you an idea. You can view an executive summary of the survey or purchase a complete copy at www.hospitalmedicine.org. TH
Jane Jerrard is the monthly writer for “Career Development.”
It’ s easy to find figures on what hospitalists earn these days, but if your own income doesn’t match up, does that mean you’re underpaid? Not necessarily.
The SHM Survey
There are several sources that provide figures on hospitalist income, but SHM offers an accurate, detailed—and the largest representative—picture of what hospitalists earn now. In spring 2006, SHM released its latest comprehensive survey of membership, “The 2005-2006 SHM Survey: The Authoritative Source on the State of the Hospitalist Movement.” The report is based on responses of 396 hospital medicine groups representing more than 2,500 hospitalists. However, Joseph A. Miller, senior vice president of SHM, warns that the survey’s salary figures may skew toward one or more specific demographics.
“In our survey, we have a number of respondents in each cell—academic, pediatric, etc.—as well as a range of geographic areas and other differences,” he says. “Anyone who looks at the metric needs to understand the factors behind it.”
John Nelson, MD, director, hospital practice, Overlake Hospital, Bellevue, Wash., and author of “Practice Management” for The Hospitalist, who has participated in developing and analyzing SHM surveys for years, agrees that the figures in the survey should be used as general guidelines only. “It’s easy to take individual metrics in a vacuum without considering the variables,” he warns.
With these caveats in mind, the basic information on hospitalist compensation from the survey breaks down as follows: (table right)
To put these numbers in perspective, the median number of patient encounters per hospitalist was 2,328 per year, and the median number of work RVUs was 3,213.
Both leader- and physician-hospitalists have enjoyed an 8% increase in compensation, as well as an 8% increase in benefits, compared with the 2003-2004 survey. Non-physician hospitalists have seen a whopping increase in median income of 26% since 2003-2004. (Their benefits increased 7%.)
Perhaps the main reason for steadily increasing hospitalist incomes is that demand for hospitalists continues to exceed supply. “I’ve been trying to recruit hospitalists to my group for years,” says Dr. Nelson. “I thought that by 2002 or 2003, the number of available physicians would exceed the demand—but that hasn’t happened. It’s true that the number of doctors interested in hospital medicine has gone up pretty dramatically, but the demand went up even faster.”
By some estimates, says Dr. Nelson, there are two or three open positions for every hospitalist jobseeker.
—John Nelson, MD
Forms of Payment
To break these figures down further, income varies with type of compensation. In other words, how you are paid can influence how much you’re paid. Physician hospitalists who are paid 100% salary had a median income of $150,000. Those who are 100% productivity/performance-based make more money—a median income of $165,000; and those with a mixed-compensation model make the most of all, with a median income of $170,000.
Currently, according to the SHM survey, only 28% of respondents are 100% salary-based and 5% are 100% productivity/performance-based. The remaining majority (67%) is compensated with a combination of the two. Compared to the 2003-2004 SHM survey, the mixed compensation model increased from 47%.
“The portion of hospitalists paid via straight salary or based solely on production has been declining in the last few years,” says Dr. Nelson. “I think [a] low base and high productivity component is ideal, but [a] lower base does impede recruiting even if the total income is very attractive.”
IPC—The Hospitalist Company, one of the largest employers of hospitalists, uses the same combination of base salary and incentives for all physicians, regardless of their level of experience.
“We might change the salary figures slightly for different geographic areas, says Tim Lary, vice president of physician staffing for IPC, “but within our company, the average physician earns a little bit north of $200,000. A large portion earn over $300,000 because of our incentive plan.” That figure includes a base salary of approximately $150,000; the rest is comprised of incentives based on “typical counters” that hospitalists see, according to Lary, including productivity, quality indicators, and compliance.
Lary postulates that compensation is higher at a large organization like IPC because those employers have an infrastructure in place that ensures cost-effectiveness. “We have a 99.9% collection rate because we have a good central business office,” he says. “Small groups don’t have resources like that. We also do a great deal of training in proper coding techniques so that we can bill appropriately.”
A Grain of Salt
Before you barge in to your director’s office and ask for a raise, you should understand that the salaries summarized here have severe limitations and should be seen only as rough guidelines. There are major factors that can boost annual compensation, including:
- A heavy load of on-call, night, or weekend work;
- Employment in a geographic region with a shortage of physicians;
- Employment in a geographic region with higher physician incomes (such as the southeast);
- The type of practice you work for; and
- New practices recruiting hospitalists.
Also keep in mind that compensation totals include all bonuses and incentives received during the year.
Find Your Figure
Hospitalist income—particularly productivity-based income—is also directly affected by workload. Dr. Nelson suggests using the information in the SHM survey to find a rough guideline for productivity and compensation.
“Take the compensation figure from the survey for your region, production type, etc. and take the average production numbers from that same subgroup,” he says. “Then do the math to find the number of dollars per encounter or per RVU, and gauge your own numbers. If you have 25% more encounters, your income should be 25% higher than the average.”
The best rule of thumb for estimating what you should make, says Dr. Nelson, is to aim for five to 15% more than physicians working in traditional practice in your market. Unfortunately, information on what other doctors earn may not be readily available. Some sources (including a few listed in the sidebar to this article) provide information on all physician incomes, but is broken down by region at best. “You have to ask around,” says Dr. Nelson. “And if you’re interviewing, ask what they’re offering—then go and interview at a private practice and ask what they’re offering.”
In other words, there’s no easy way to tell if what you make is exactly on the mark for other hospitalists in your area—unless you ask those other hospitalists. But the SHM survey information should provide enough information to give you an idea. You can view an executive summary of the survey or purchase a complete copy at www.hospitalmedicine.org. TH
Jane Jerrard is the monthly writer for “Career Development.”
It’ s easy to find figures on what hospitalists earn these days, but if your own income doesn’t match up, does that mean you’re underpaid? Not necessarily.
The SHM Survey
There are several sources that provide figures on hospitalist income, but SHM offers an accurate, detailed—and the largest representative—picture of what hospitalists earn now. In spring 2006, SHM released its latest comprehensive survey of membership, “The 2005-2006 SHM Survey: The Authoritative Source on the State of the Hospitalist Movement.” The report is based on responses of 396 hospital medicine groups representing more than 2,500 hospitalists. However, Joseph A. Miller, senior vice president of SHM, warns that the survey’s salary figures may skew toward one or more specific demographics.
“In our survey, we have a number of respondents in each cell—academic, pediatric, etc.—as well as a range of geographic areas and other differences,” he says. “Anyone who looks at the metric needs to understand the factors behind it.”
John Nelson, MD, director, hospital practice, Overlake Hospital, Bellevue, Wash., and author of “Practice Management” for The Hospitalist, who has participated in developing and analyzing SHM surveys for years, agrees that the figures in the survey should be used as general guidelines only. “It’s easy to take individual metrics in a vacuum without considering the variables,” he warns.
With these caveats in mind, the basic information on hospitalist compensation from the survey breaks down as follows: (table right)
To put these numbers in perspective, the median number of patient encounters per hospitalist was 2,328 per year, and the median number of work RVUs was 3,213.
Both leader- and physician-hospitalists have enjoyed an 8% increase in compensation, as well as an 8% increase in benefits, compared with the 2003-2004 survey. Non-physician hospitalists have seen a whopping increase in median income of 26% since 2003-2004. (Their benefits increased 7%.)
Perhaps the main reason for steadily increasing hospitalist incomes is that demand for hospitalists continues to exceed supply. “I’ve been trying to recruit hospitalists to my group for years,” says Dr. Nelson. “I thought that by 2002 or 2003, the number of available physicians would exceed the demand—but that hasn’t happened. It’s true that the number of doctors interested in hospital medicine has gone up pretty dramatically, but the demand went up even faster.”
By some estimates, says Dr. Nelson, there are two or three open positions for every hospitalist jobseeker.
—John Nelson, MD
Forms of Payment
To break these figures down further, income varies with type of compensation. In other words, how you are paid can influence how much you’re paid. Physician hospitalists who are paid 100% salary had a median income of $150,000. Those who are 100% productivity/performance-based make more money—a median income of $165,000; and those with a mixed-compensation model make the most of all, with a median income of $170,000.
Currently, according to the SHM survey, only 28% of respondents are 100% salary-based and 5% are 100% productivity/performance-based. The remaining majority (67%) is compensated with a combination of the two. Compared to the 2003-2004 SHM survey, the mixed compensation model increased from 47%.
“The portion of hospitalists paid via straight salary or based solely on production has been declining in the last few years,” says Dr. Nelson. “I think [a] low base and high productivity component is ideal, but [a] lower base does impede recruiting even if the total income is very attractive.”
IPC—The Hospitalist Company, one of the largest employers of hospitalists, uses the same combination of base salary and incentives for all physicians, regardless of their level of experience.
“We might change the salary figures slightly for different geographic areas, says Tim Lary, vice president of physician staffing for IPC, “but within our company, the average physician earns a little bit north of $200,000. A large portion earn over $300,000 because of our incentive plan.” That figure includes a base salary of approximately $150,000; the rest is comprised of incentives based on “typical counters” that hospitalists see, according to Lary, including productivity, quality indicators, and compliance.
Lary postulates that compensation is higher at a large organization like IPC because those employers have an infrastructure in place that ensures cost-effectiveness. “We have a 99.9% collection rate because we have a good central business office,” he says. “Small groups don’t have resources like that. We also do a great deal of training in proper coding techniques so that we can bill appropriately.”
A Grain of Salt
Before you barge in to your director’s office and ask for a raise, you should understand that the salaries summarized here have severe limitations and should be seen only as rough guidelines. There are major factors that can boost annual compensation, including:
- A heavy load of on-call, night, or weekend work;
- Employment in a geographic region with a shortage of physicians;
- Employment in a geographic region with higher physician incomes (such as the southeast);
- The type of practice you work for; and
- New practices recruiting hospitalists.
Also keep in mind that compensation totals include all bonuses and incentives received during the year.
Find Your Figure
Hospitalist income—particularly productivity-based income—is also directly affected by workload. Dr. Nelson suggests using the information in the SHM survey to find a rough guideline for productivity and compensation.
“Take the compensation figure from the survey for your region, production type, etc. and take the average production numbers from that same subgroup,” he says. “Then do the math to find the number of dollars per encounter or per RVU, and gauge your own numbers. If you have 25% more encounters, your income should be 25% higher than the average.”
The best rule of thumb for estimating what you should make, says Dr. Nelson, is to aim for five to 15% more than physicians working in traditional practice in your market. Unfortunately, information on what other doctors earn may not be readily available. Some sources (including a few listed in the sidebar to this article) provide information on all physician incomes, but is broken down by region at best. “You have to ask around,” says Dr. Nelson. “And if you’re interviewing, ask what they’re offering—then go and interview at a private practice and ask what they’re offering.”
In other words, there’s no easy way to tell if what you make is exactly on the mark for other hospitalists in your area—unless you ask those other hospitalists. But the SHM survey information should provide enough information to give you an idea. You can view an executive summary of the survey or purchase a complete copy at www.hospitalmedicine.org. TH
Jane Jerrard is the monthly writer for “Career Development.”
Medicare, Money, and Quality Measures

The federal government—particularly the Centers for Medicare and Medicaid Services (CMS)—is moving faster than anyone thought possible to implement “value-based purchasing,” which ties payment to quality of care and other outcomes. CMS has a congressional mandate to make value-based purchasing a reality by fiscal year 2009.
“As Congress looks at cutting physician payments, they’re very open to alternative payment methods like pay-for-performance,” says Patrick Torcson, MD, MMM, FACP, chair of SHM’s Performance and Standards Task Force, medical director, hospital medicine, St. Tammany Parish Hospital, Covington, La. “There’s tremendous political will behind this.”
Here is an overview of three CMS demonstration programs in various stages that will determine which new payment models may shape your hospital budget—and your salary—in the future.
CMS Gainsharing Demo: An Update
As reported in the October issue of The Hospitalist, CMS has been charged with establishing six three-year gainsharing pilot programs, including two in rural settings, by January 1, 2007.
CMS invited applications for the programs in mid-September, and applications were due by November 17. The six participating hospitals will provide gainsharing payments to physicians who help to save costs. The gainsharing payments will be based on net savings. Each hospital will propose multiple approaches that will both save costs and improve quality and efficiency of care.
“Gainsharing could be a better quality incentive payment model for hospitalists, [but] maybe not for other specialties,” says Dr. Torcson.
New “Gainsharing Plus” Demo—Participation Encouraged!
During Legislative Advocacy Day at the SHM Annual Meeting in Washington, D.C., in May, SHM members personally urged policymakers to broaden the concept of gainsharing and initiate demonstration projects like this that promote physician and hospital collaboration in improving care.
Four months later (in early September) CMS surprised the healthcare community with the announcement of an additional three-year demonstration program that goes beyond the traditional concept of gainsharing—one that will examine whether allowing hospitals to provide financial incentives for physicians to support better care can improve patient outcomes without increasing costs.
“SHM was pleased to hear that CMS was offering this program because we support the development of these payment models,” says Dr. Torcson.
Under the program, known as the Physician-Hospital Collaboration Demonstration (PHCD), hospitals would be paid their usual inpatient rate for the patients’ care but would be allowed to pay physicians a portion of the savings resulting from quality improvement and efficiency initiatives.
In the CMS release announcing this demonstration, former CMS Administrator Mark B. McClellan, MD, PhD, was quoted as saying, “The most costly and intensive physician services are provided in hospitals, yet our payment systems do not support steps by hospitals and doctors to work together to improve care. This demonstration program will support efforts to track and improve the overall episode of patient care, including follow-up and longer-term outcomes.”
The program will begin in 2007, and applications are due by end of business on January 9, 2007. SHM encourages members to explore the possibility of applying for one of the demonstrations with their group and their hospital administrators. Details on the PHCD are available at www.cms.hhs.gov (go to the “Medicare” page and then click the “Demonstration Projects & Evaluation Reports” page. Then click “Medicare Demonstrations).”
Of particular interest is the fact that CMS will allow participating hospitals to set the indicators to be measured. “What they’re asking for are proposals from the hospitals as to what they’ll explore—basing the program on whatever quality indicators the hospital can [use to] measure and demonstrate cost savings,” says Dr. Torcson. “CMS is providing no details regarding specific performance measures.”
Organizations eligible for the PHCD include physician groups, integrated delivery systems (IDSs), and regional coalitions of physician groups. A hospital may be included if it has an affiliation agreement with an eligible physician group. CMS has stated that preference will be given to projects developed and implemented by a consortium of physician groups and their affiliated hospitals. No more than 72 hospitals across all projects will be included in the demonstration.
“This raises the bar that any physician group has to be pretty far along already in measuring quality indicators and performance reporting,” says Dr. Torcson. “It will take a lot of infrastructure to report, measure, [and so on]. I’ll be very impressed with any group that is that far along with performance measurement and reporting. I hope a hospitalist group can be among those that step up and apply.”
Dr. Torcson believes that, while CMS did not specify hospitalists, a hospital medicine group would be uniquely positioned to participate. “Hospitalists are perfect for this,” he emphasizes.
Premier Hospital Demo: Mission Accomplished!
CMS’ first pay-for-performance demonstration program is complete. The Premier Hospital Quality Incentive Demonstration officially ended in September. CMS partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, for the three-year demo. At the end of each of the three years, CMS rewarded the top-performing hospitals with cash bonuses. Performance was based on 33 evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. (The individual measures were compiled into an overall quality score for each clinical condition.)
“I wish all our projects went this well,” said Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS. “We’re absolutely delighted. This program shows the efficacy [of] using pay-for-performance in hospitals.”
According to analysis from Premier, Inc., if every patient in the country with pneumonia, heart bypass, acute myocardial infarction, and hip and knee replacement in 2004 had received most or all (76% to 100%) of a set of widely accepted care processes, it could have resulted in nearly 5,700 fewer deaths, 8,100 fewer complications, 10,000 fewer readmissions, and 750,000 fewer days in the hospital. In addition, hospital costs could have been as much as $1.35 billion lower.
What’s next? Wynn says that CMS is “actively looking at lessons we can use” as the agency prepares a report to be presented to Congress in 2007. “We’ll make a specific recommendation regarding pay-for-performance.”
The Future Is Coming
“Value-based purchasing is here to stay,” says Dr. Torcson. “For the significant amount of money spent on healthcare, you have to see a certain level of quality in return. This hasn’t been so obvious in healthcare. Healthcare is just starting to look like the free market in this regard. There’s a place for both pay-for-performance and gainsharing. The CMS budget is big enough for both.”
SHM is involved in pushing for these changes and wants to prepare members for any new measurement criteria that develop. “We would like for the work of the SHM Performance and Standards Task Force to result in an SHM performance agenda,” says Dr. Torcson. “We want to be able to tell members what to expect when all of these demos become a reality and be able to provide relevant information on designing their programs so that they’re ready.” TH
Jane Jerrard regularly writes “Public Policy.”
The federal government—particularly the Centers for Medicare and Medicaid Services (CMS)—is moving faster than anyone thought possible to implement “value-based purchasing,” which ties payment to quality of care and other outcomes. CMS has a congressional mandate to make value-based purchasing a reality by fiscal year 2009.
“As Congress looks at cutting physician payments, they’re very open to alternative payment methods like pay-for-performance,” says Patrick Torcson, MD, MMM, FACP, chair of SHM’s Performance and Standards Task Force, medical director, hospital medicine, St. Tammany Parish Hospital, Covington, La. “There’s tremendous political will behind this.”
Here is an overview of three CMS demonstration programs in various stages that will determine which new payment models may shape your hospital budget—and your salary—in the future.
CMS Gainsharing Demo: An Update
As reported in the October issue of The Hospitalist, CMS has been charged with establishing six three-year gainsharing pilot programs, including two in rural settings, by January 1, 2007.
CMS invited applications for the programs in mid-September, and applications were due by November 17. The six participating hospitals will provide gainsharing payments to physicians who help to save costs. The gainsharing payments will be based on net savings. Each hospital will propose multiple approaches that will both save costs and improve quality and efficiency of care.
“Gainsharing could be a better quality incentive payment model for hospitalists, [but] maybe not for other specialties,” says Dr. Torcson.
New “Gainsharing Plus” Demo—Participation Encouraged!
During Legislative Advocacy Day at the SHM Annual Meeting in Washington, D.C., in May, SHM members personally urged policymakers to broaden the concept of gainsharing and initiate demonstration projects like this that promote physician and hospital collaboration in improving care.
Four months later (in early September) CMS surprised the healthcare community with the announcement of an additional three-year demonstration program that goes beyond the traditional concept of gainsharing—one that will examine whether allowing hospitals to provide financial incentives for physicians to support better care can improve patient outcomes without increasing costs.
“SHM was pleased to hear that CMS was offering this program because we support the development of these payment models,” says Dr. Torcson.
Under the program, known as the Physician-Hospital Collaboration Demonstration (PHCD), hospitals would be paid their usual inpatient rate for the patients’ care but would be allowed to pay physicians a portion of the savings resulting from quality improvement and efficiency initiatives.
In the CMS release announcing this demonstration, former CMS Administrator Mark B. McClellan, MD, PhD, was quoted as saying, “The most costly and intensive physician services are provided in hospitals, yet our payment systems do not support steps by hospitals and doctors to work together to improve care. This demonstration program will support efforts to track and improve the overall episode of patient care, including follow-up and longer-term outcomes.”
The program will begin in 2007, and applications are due by end of business on January 9, 2007. SHM encourages members to explore the possibility of applying for one of the demonstrations with their group and their hospital administrators. Details on the PHCD are available at www.cms.hhs.gov (go to the “Medicare” page and then click the “Demonstration Projects & Evaluation Reports” page. Then click “Medicare Demonstrations).”
Of particular interest is the fact that CMS will allow participating hospitals to set the indicators to be measured. “What they’re asking for are proposals from the hospitals as to what they’ll explore—basing the program on whatever quality indicators the hospital can [use to] measure and demonstrate cost savings,” says Dr. Torcson. “CMS is providing no details regarding specific performance measures.”
Organizations eligible for the PHCD include physician groups, integrated delivery systems (IDSs), and regional coalitions of physician groups. A hospital may be included if it has an affiliation agreement with an eligible physician group. CMS has stated that preference will be given to projects developed and implemented by a consortium of physician groups and their affiliated hospitals. No more than 72 hospitals across all projects will be included in the demonstration.
“This raises the bar that any physician group has to be pretty far along already in measuring quality indicators and performance reporting,” says Dr. Torcson. “It will take a lot of infrastructure to report, measure, [and so on]. I’ll be very impressed with any group that is that far along with performance measurement and reporting. I hope a hospitalist group can be among those that step up and apply.”
Dr. Torcson believes that, while CMS did not specify hospitalists, a hospital medicine group would be uniquely positioned to participate. “Hospitalists are perfect for this,” he emphasizes.
Premier Hospital Demo: Mission Accomplished!
CMS’ first pay-for-performance demonstration program is complete. The Premier Hospital Quality Incentive Demonstration officially ended in September. CMS partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, for the three-year demo. At the end of each of the three years, CMS rewarded the top-performing hospitals with cash bonuses. Performance was based on 33 evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. (The individual measures were compiled into an overall quality score for each clinical condition.)
“I wish all our projects went this well,” said Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS. “We’re absolutely delighted. This program shows the efficacy [of] using pay-for-performance in hospitals.”
According to analysis from Premier, Inc., if every patient in the country with pneumonia, heart bypass, acute myocardial infarction, and hip and knee replacement in 2004 had received most or all (76% to 100%) of a set of widely accepted care processes, it could have resulted in nearly 5,700 fewer deaths, 8,100 fewer complications, 10,000 fewer readmissions, and 750,000 fewer days in the hospital. In addition, hospital costs could have been as much as $1.35 billion lower.
What’s next? Wynn says that CMS is “actively looking at lessons we can use” as the agency prepares a report to be presented to Congress in 2007. “We’ll make a specific recommendation regarding pay-for-performance.”
The Future Is Coming
“Value-based purchasing is here to stay,” says Dr. Torcson. “For the significant amount of money spent on healthcare, you have to see a certain level of quality in return. This hasn’t been so obvious in healthcare. Healthcare is just starting to look like the free market in this regard. There’s a place for both pay-for-performance and gainsharing. The CMS budget is big enough for both.”
SHM is involved in pushing for these changes and wants to prepare members for any new measurement criteria that develop. “We would like for the work of the SHM Performance and Standards Task Force to result in an SHM performance agenda,” says Dr. Torcson. “We want to be able to tell members what to expect when all of these demos become a reality and be able to provide relevant information on designing their programs so that they’re ready.” TH
Jane Jerrard regularly writes “Public Policy.”
The federal government—particularly the Centers for Medicare and Medicaid Services (CMS)—is moving faster than anyone thought possible to implement “value-based purchasing,” which ties payment to quality of care and other outcomes. CMS has a congressional mandate to make value-based purchasing a reality by fiscal year 2009.
“As Congress looks at cutting physician payments, they’re very open to alternative payment methods like pay-for-performance,” says Patrick Torcson, MD, MMM, FACP, chair of SHM’s Performance and Standards Task Force, medical director, hospital medicine, St. Tammany Parish Hospital, Covington, La. “There’s tremendous political will behind this.”
Here is an overview of three CMS demonstration programs in various stages that will determine which new payment models may shape your hospital budget—and your salary—in the future.
CMS Gainsharing Demo: An Update
As reported in the October issue of The Hospitalist, CMS has been charged with establishing six three-year gainsharing pilot programs, including two in rural settings, by January 1, 2007.
CMS invited applications for the programs in mid-September, and applications were due by November 17. The six participating hospitals will provide gainsharing payments to physicians who help to save costs. The gainsharing payments will be based on net savings. Each hospital will propose multiple approaches that will both save costs and improve quality and efficiency of care.
“Gainsharing could be a better quality incentive payment model for hospitalists, [but] maybe not for other specialties,” says Dr. Torcson.
New “Gainsharing Plus” Demo—Participation Encouraged!
During Legislative Advocacy Day at the SHM Annual Meeting in Washington, D.C., in May, SHM members personally urged policymakers to broaden the concept of gainsharing and initiate demonstration projects like this that promote physician and hospital collaboration in improving care.
Four months later (in early September) CMS surprised the healthcare community with the announcement of an additional three-year demonstration program that goes beyond the traditional concept of gainsharing—one that will examine whether allowing hospitals to provide financial incentives for physicians to support better care can improve patient outcomes without increasing costs.
“SHM was pleased to hear that CMS was offering this program because we support the development of these payment models,” says Dr. Torcson.
Under the program, known as the Physician-Hospital Collaboration Demonstration (PHCD), hospitals would be paid their usual inpatient rate for the patients’ care but would be allowed to pay physicians a portion of the savings resulting from quality improvement and efficiency initiatives.
In the CMS release announcing this demonstration, former CMS Administrator Mark B. McClellan, MD, PhD, was quoted as saying, “The most costly and intensive physician services are provided in hospitals, yet our payment systems do not support steps by hospitals and doctors to work together to improve care. This demonstration program will support efforts to track and improve the overall episode of patient care, including follow-up and longer-term outcomes.”
The program will begin in 2007, and applications are due by end of business on January 9, 2007. SHM encourages members to explore the possibility of applying for one of the demonstrations with their group and their hospital administrators. Details on the PHCD are available at www.cms.hhs.gov (go to the “Medicare” page and then click the “Demonstration Projects & Evaluation Reports” page. Then click “Medicare Demonstrations).”
Of particular interest is the fact that CMS will allow participating hospitals to set the indicators to be measured. “What they’re asking for are proposals from the hospitals as to what they’ll explore—basing the program on whatever quality indicators the hospital can [use to] measure and demonstrate cost savings,” says Dr. Torcson. “CMS is providing no details regarding specific performance measures.”
Organizations eligible for the PHCD include physician groups, integrated delivery systems (IDSs), and regional coalitions of physician groups. A hospital may be included if it has an affiliation agreement with an eligible physician group. CMS has stated that preference will be given to projects developed and implemented by a consortium of physician groups and their affiliated hospitals. No more than 72 hospitals across all projects will be included in the demonstration.
“This raises the bar that any physician group has to be pretty far along already in measuring quality indicators and performance reporting,” says Dr. Torcson. “It will take a lot of infrastructure to report, measure, [and so on]. I’ll be very impressed with any group that is that far along with performance measurement and reporting. I hope a hospitalist group can be among those that step up and apply.”
Dr. Torcson believes that, while CMS did not specify hospitalists, a hospital medicine group would be uniquely positioned to participate. “Hospitalists are perfect for this,” he emphasizes.
Premier Hospital Demo: Mission Accomplished!
CMS’ first pay-for-performance demonstration program is complete. The Premier Hospital Quality Incentive Demonstration officially ended in September. CMS partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, for the three-year demo. At the end of each of the three years, CMS rewarded the top-performing hospitals with cash bonuses. Performance was based on 33 evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. (The individual measures were compiled into an overall quality score for each clinical condition.)
“I wish all our projects went this well,” said Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS. “We’re absolutely delighted. This program shows the efficacy [of] using pay-for-performance in hospitals.”
According to analysis from Premier, Inc., if every patient in the country with pneumonia, heart bypass, acute myocardial infarction, and hip and knee replacement in 2004 had received most or all (76% to 100%) of a set of widely accepted care processes, it could have resulted in nearly 5,700 fewer deaths, 8,100 fewer complications, 10,000 fewer readmissions, and 750,000 fewer days in the hospital. In addition, hospital costs could have been as much as $1.35 billion lower.
What’s next? Wynn says that CMS is “actively looking at lessons we can use” as the agency prepares a report to be presented to Congress in 2007. “We’ll make a specific recommendation regarding pay-for-performance.”
The Future Is Coming
“Value-based purchasing is here to stay,” says Dr. Torcson. “For the significant amount of money spent on healthcare, you have to see a certain level of quality in return. This hasn’t been so obvious in healthcare. Healthcare is just starting to look like the free market in this regard. There’s a place for both pay-for-performance and gainsharing. The CMS budget is big enough for both.”
SHM is involved in pushing for these changes and wants to prepare members for any new measurement criteria that develop. “We would like for the work of the SHM Performance and Standards Task Force to result in an SHM performance agenda,” says Dr. Torcson. “We want to be able to tell members what to expect when all of these demos become a reality and be able to provide relevant information on designing their programs so that they’re ready.” TH
Jane Jerrard regularly writes “Public Policy.”
An Historic Moment for Hospital Medicine

In an historic decision at its October 2006 board meeting, the American Board of Internal Medicine (ABIM) agreed to move forward to develop a process for Focused Recognition of Hospital Medicine through ABIM’s Maintenance of Certification (MOC). This is the first time ABIM has offered focused recognition for any subset of internal medicine. In addition, this brings recognition to the uniqueness of hospitalists, who dedicate their professional careers to managing the care of acutely ill patients and creating a better healthcare delivery process at their local hospitals.
This whole concept started when the SHM Board approved a resolution in February 2004, outlining the need to recognize hospitalists as unique providers of healthcare. At the time, the SHM Board asked SHM staff and leadership to work with existing certifying organizations, such as ABIM, to develop a mechanism for hospitalists to have a formal credential recognizing hospital medicine.
Because more than 80% of hospitalists are initially trained in internal medicine, SHM leadership decided that it made sense to first approach ABIM. At the same time SHM had plans to develop similar solutions for hospitalists who are trained initially as pediatricians, family practitioners, and osteopaths (all of which are certified by boards other than ABIM).
Soon after the 2004 SHM Board meeting, SHM executive staff approached key leaders at ABIM. ABIM held a retreat in 2004 to discuss new models of certification. Later the ABIM Board encouraged meetings with SHM to keep hospital medicine within internal medicine.
In April 2005 ABIM and SHM leadership agreed that recognition of hospitalists initially trained in internal medicine might be achieved by modifying the existing MOC process. At that time the ABIM Board was concerned that any changes to the certification system might fragment the internal medicine community. To its credit the ABIM Board did not let these concerns block the process. ABIM soon convened a range of stakeholders in internal medicine to address these issues.
This group of stakeholders was broadly drawn from the leadership at SHM, the American College of Physicians, the Society of General Internal Medicine, all medical subspecialties, the Alliance for Academic Internal Medicine, the Association of American Medical Colleges, the AMA, the Residency Review Committee, and ABIM itself. These stakeholders met in December 2005, May 2006, and again in September 2006.
In preparation for these meetings SHM had developed its comprehensive Core Competencies in Hospital Medicine that was published as a supplement to the first issue of the Journal of Hospital Medicine (JHM) in February 2006. This was a powerful, tangible set of circumstances for hospital medicine.
When people began questioning what made hospital medicine unique among internal medicine disciplines or what was the substance of hospital medicine, being able to hand them the Core Competencies and to walk them through this thoughtful document was very important. In the same way, establishing our own repository for medical advances in hospital medicine via JHM also supported the development of a new field in internal medicine.
It’s been helpful that other key trends have taken shape in the last few years. The Alliance for Academic Internal Medicine (AAIM), representing the Association of Professors of Medicine (APM) and the Association of Directors of Programs in Internal Medicine (APDIM) and others, worked closely with ACP and the rest of the specialties in internal medicine to redesign the internal medicine residency so that it reflects the current and future practice environment.
Further, throughout healthcare there has been an increasing call for performance standards and quality improvement—all in the context of using resources more efficiently. There has been a movement to reshape healthcare centered on the patient and delivered by teams of health professionals, as well as increasing calls to coordinate care across locales and providers so as to improve patient safety and provide the best care.
In addition, the growth of hospital medicine has accelerated in the last few years. The fact that data not only from SHM but also from the American Hospital Association (AHA) and others show that more than 15,000 hospitalists now practice at more than 2,000 hospitals illustrates that that the size and influence of hospitalists comprise an indisputable trend.
And for many hospitals the driver for developing hospital medicine groups is the need to have on-site health professionals who are committed to changes in quality, systems improvement, patient safety, and efficiency.
Whether you call this a tipping point à la Malcolm Gladwell (The Tipping Point, New York City: Little, Brown and Company; 2000) or a perfect storm, to its credit ABIM—with the support of ACP, AAIM, and others—saw an opportunity to develop meaningful changes to MOC as a means of identifying hospitalists and of motivating the self study and improvement in skills and knowledge so important to meet the demands of healthcare delivery in the 21st century.
Now the hard work begins. In October 2006 the ABIM Board of Directors approved appointment of an ABIM Committee on Hospital Medicine Focused Recognition (HMFR). This work group will make recommendations to the ABIM Board in 2007 regarding the requirements for evidence of proficiency in HMFR in the MOC process as well as recommending policy of how HMFR would relate to the rest of ABIM certification and MOC in internal medicine.
SHM and hospital medicine leaders intend to play a key role in helping ABIM shape the details of the HMFR process so that it’s meaningful to the hospitalists who choose to get HMFR during their MOC—as well as to those who employ hospitalists, the physicians and other health professionals that hospitalists work with, the hospitals we work in, and the patients we care for.
At the same time ABIM must approach the American Board of Medical Specialties (ABMS) because the ABMS will ultimately need to accept the HMFR process before ABIM can put this new process in place. This is a significant hurdle to clear, but the ABIM Board is committed to using its resources and powers of persuasion to make this happen.
Even with the hard work and political battles ahead, it is difficult not to sit back and marvel at how far we have come. Our specialty is just 10 years old, but we now have more than 15,000 practitioners and are on our way to 30,000 or even 40,000. We have our own journal, our own specialty society, our own set of competencies, our own growing national annual meeting, our own textbooks, and a growing number of publications aimed at hospitalists.
Now with the help of ABIM and the blessing of ABMS, there is a serious prospect that the first recognition of hospital medicine in the certification process will become a reality.
Will the first hospitalist claim Hospital Medicine Focused Recognition in 2008 or 2009? The exact date is too difficult to predict. That it will happen and that it will be meaningful is more certain now than it has ever been. To all those who have had the foresight and leadership to make this a reality, we thank you. Now let’s get down to the difficult work of creating a process that will help hospitalists provide the best care to their patients and help them to be leaders of change and improvement at their institutions. TH
Dr. Wellikson has been CEO of SHM since 2000.
In an historic decision at its October 2006 board meeting, the American Board of Internal Medicine (ABIM) agreed to move forward to develop a process for Focused Recognition of Hospital Medicine through ABIM’s Maintenance of Certification (MOC). This is the first time ABIM has offered focused recognition for any subset of internal medicine. In addition, this brings recognition to the uniqueness of hospitalists, who dedicate their professional careers to managing the care of acutely ill patients and creating a better healthcare delivery process at their local hospitals.
This whole concept started when the SHM Board approved a resolution in February 2004, outlining the need to recognize hospitalists as unique providers of healthcare. At the time, the SHM Board asked SHM staff and leadership to work with existing certifying organizations, such as ABIM, to develop a mechanism for hospitalists to have a formal credential recognizing hospital medicine.
Because more than 80% of hospitalists are initially trained in internal medicine, SHM leadership decided that it made sense to first approach ABIM. At the same time SHM had plans to develop similar solutions for hospitalists who are trained initially as pediatricians, family practitioners, and osteopaths (all of which are certified by boards other than ABIM).
Soon after the 2004 SHM Board meeting, SHM executive staff approached key leaders at ABIM. ABIM held a retreat in 2004 to discuss new models of certification. Later the ABIM Board encouraged meetings with SHM to keep hospital medicine within internal medicine.
In April 2005 ABIM and SHM leadership agreed that recognition of hospitalists initially trained in internal medicine might be achieved by modifying the existing MOC process. At that time the ABIM Board was concerned that any changes to the certification system might fragment the internal medicine community. To its credit the ABIM Board did not let these concerns block the process. ABIM soon convened a range of stakeholders in internal medicine to address these issues.
This group of stakeholders was broadly drawn from the leadership at SHM, the American College of Physicians, the Society of General Internal Medicine, all medical subspecialties, the Alliance for Academic Internal Medicine, the Association of American Medical Colleges, the AMA, the Residency Review Committee, and ABIM itself. These stakeholders met in December 2005, May 2006, and again in September 2006.
In preparation for these meetings SHM had developed its comprehensive Core Competencies in Hospital Medicine that was published as a supplement to the first issue of the Journal of Hospital Medicine (JHM) in February 2006. This was a powerful, tangible set of circumstances for hospital medicine.
When people began questioning what made hospital medicine unique among internal medicine disciplines or what was the substance of hospital medicine, being able to hand them the Core Competencies and to walk them through this thoughtful document was very important. In the same way, establishing our own repository for medical advances in hospital medicine via JHM also supported the development of a new field in internal medicine.
It’s been helpful that other key trends have taken shape in the last few years. The Alliance for Academic Internal Medicine (AAIM), representing the Association of Professors of Medicine (APM) and the Association of Directors of Programs in Internal Medicine (APDIM) and others, worked closely with ACP and the rest of the specialties in internal medicine to redesign the internal medicine residency so that it reflects the current and future practice environment.
Further, throughout healthcare there has been an increasing call for performance standards and quality improvement—all in the context of using resources more efficiently. There has been a movement to reshape healthcare centered on the patient and delivered by teams of health professionals, as well as increasing calls to coordinate care across locales and providers so as to improve patient safety and provide the best care.
In addition, the growth of hospital medicine has accelerated in the last few years. The fact that data not only from SHM but also from the American Hospital Association (AHA) and others show that more than 15,000 hospitalists now practice at more than 2,000 hospitals illustrates that that the size and influence of hospitalists comprise an indisputable trend.
And for many hospitals the driver for developing hospital medicine groups is the need to have on-site health professionals who are committed to changes in quality, systems improvement, patient safety, and efficiency.
Whether you call this a tipping point à la Malcolm Gladwell (The Tipping Point, New York City: Little, Brown and Company; 2000) or a perfect storm, to its credit ABIM—with the support of ACP, AAIM, and others—saw an opportunity to develop meaningful changes to MOC as a means of identifying hospitalists and of motivating the self study and improvement in skills and knowledge so important to meet the demands of healthcare delivery in the 21st century.
Now the hard work begins. In October 2006 the ABIM Board of Directors approved appointment of an ABIM Committee on Hospital Medicine Focused Recognition (HMFR). This work group will make recommendations to the ABIM Board in 2007 regarding the requirements for evidence of proficiency in HMFR in the MOC process as well as recommending policy of how HMFR would relate to the rest of ABIM certification and MOC in internal medicine.
SHM and hospital medicine leaders intend to play a key role in helping ABIM shape the details of the HMFR process so that it’s meaningful to the hospitalists who choose to get HMFR during their MOC—as well as to those who employ hospitalists, the physicians and other health professionals that hospitalists work with, the hospitals we work in, and the patients we care for.
At the same time ABIM must approach the American Board of Medical Specialties (ABMS) because the ABMS will ultimately need to accept the HMFR process before ABIM can put this new process in place. This is a significant hurdle to clear, but the ABIM Board is committed to using its resources and powers of persuasion to make this happen.
Even with the hard work and political battles ahead, it is difficult not to sit back and marvel at how far we have come. Our specialty is just 10 years old, but we now have more than 15,000 practitioners and are on our way to 30,000 or even 40,000. We have our own journal, our own specialty society, our own set of competencies, our own growing national annual meeting, our own textbooks, and a growing number of publications aimed at hospitalists.
Now with the help of ABIM and the blessing of ABMS, there is a serious prospect that the first recognition of hospital medicine in the certification process will become a reality.
Will the first hospitalist claim Hospital Medicine Focused Recognition in 2008 or 2009? The exact date is too difficult to predict. That it will happen and that it will be meaningful is more certain now than it has ever been. To all those who have had the foresight and leadership to make this a reality, we thank you. Now let’s get down to the difficult work of creating a process that will help hospitalists provide the best care to their patients and help them to be leaders of change and improvement at their institutions. TH
Dr. Wellikson has been CEO of SHM since 2000.
In an historic decision at its October 2006 board meeting, the American Board of Internal Medicine (ABIM) agreed to move forward to develop a process for Focused Recognition of Hospital Medicine through ABIM’s Maintenance of Certification (MOC). This is the first time ABIM has offered focused recognition for any subset of internal medicine. In addition, this brings recognition to the uniqueness of hospitalists, who dedicate their professional careers to managing the care of acutely ill patients and creating a better healthcare delivery process at their local hospitals.
This whole concept started when the SHM Board approved a resolution in February 2004, outlining the need to recognize hospitalists as unique providers of healthcare. At the time, the SHM Board asked SHM staff and leadership to work with existing certifying organizations, such as ABIM, to develop a mechanism for hospitalists to have a formal credential recognizing hospital medicine.
Because more than 80% of hospitalists are initially trained in internal medicine, SHM leadership decided that it made sense to first approach ABIM. At the same time SHM had plans to develop similar solutions for hospitalists who are trained initially as pediatricians, family practitioners, and osteopaths (all of which are certified by boards other than ABIM).
Soon after the 2004 SHM Board meeting, SHM executive staff approached key leaders at ABIM. ABIM held a retreat in 2004 to discuss new models of certification. Later the ABIM Board encouraged meetings with SHM to keep hospital medicine within internal medicine.
In April 2005 ABIM and SHM leadership agreed that recognition of hospitalists initially trained in internal medicine might be achieved by modifying the existing MOC process. At that time the ABIM Board was concerned that any changes to the certification system might fragment the internal medicine community. To its credit the ABIM Board did not let these concerns block the process. ABIM soon convened a range of stakeholders in internal medicine to address these issues.
This group of stakeholders was broadly drawn from the leadership at SHM, the American College of Physicians, the Society of General Internal Medicine, all medical subspecialties, the Alliance for Academic Internal Medicine, the Association of American Medical Colleges, the AMA, the Residency Review Committee, and ABIM itself. These stakeholders met in December 2005, May 2006, and again in September 2006.
In preparation for these meetings SHM had developed its comprehensive Core Competencies in Hospital Medicine that was published as a supplement to the first issue of the Journal of Hospital Medicine (JHM) in February 2006. This was a powerful, tangible set of circumstances for hospital medicine.
When people began questioning what made hospital medicine unique among internal medicine disciplines or what was the substance of hospital medicine, being able to hand them the Core Competencies and to walk them through this thoughtful document was very important. In the same way, establishing our own repository for medical advances in hospital medicine via JHM also supported the development of a new field in internal medicine.
It’s been helpful that other key trends have taken shape in the last few years. The Alliance for Academic Internal Medicine (AAIM), representing the Association of Professors of Medicine (APM) and the Association of Directors of Programs in Internal Medicine (APDIM) and others, worked closely with ACP and the rest of the specialties in internal medicine to redesign the internal medicine residency so that it reflects the current and future practice environment.
Further, throughout healthcare there has been an increasing call for performance standards and quality improvement—all in the context of using resources more efficiently. There has been a movement to reshape healthcare centered on the patient and delivered by teams of health professionals, as well as increasing calls to coordinate care across locales and providers so as to improve patient safety and provide the best care.
In addition, the growth of hospital medicine has accelerated in the last few years. The fact that data not only from SHM but also from the American Hospital Association (AHA) and others show that more than 15,000 hospitalists now practice at more than 2,000 hospitals illustrates that that the size and influence of hospitalists comprise an indisputable trend.
And for many hospitals the driver for developing hospital medicine groups is the need to have on-site health professionals who are committed to changes in quality, systems improvement, patient safety, and efficiency.
Whether you call this a tipping point à la Malcolm Gladwell (The Tipping Point, New York City: Little, Brown and Company; 2000) or a perfect storm, to its credit ABIM—with the support of ACP, AAIM, and others—saw an opportunity to develop meaningful changes to MOC as a means of identifying hospitalists and of motivating the self study and improvement in skills and knowledge so important to meet the demands of healthcare delivery in the 21st century.
Now the hard work begins. In October 2006 the ABIM Board of Directors approved appointment of an ABIM Committee on Hospital Medicine Focused Recognition (HMFR). This work group will make recommendations to the ABIM Board in 2007 regarding the requirements for evidence of proficiency in HMFR in the MOC process as well as recommending policy of how HMFR would relate to the rest of ABIM certification and MOC in internal medicine.
SHM and hospital medicine leaders intend to play a key role in helping ABIM shape the details of the HMFR process so that it’s meaningful to the hospitalists who choose to get HMFR during their MOC—as well as to those who employ hospitalists, the physicians and other health professionals that hospitalists work with, the hospitals we work in, and the patients we care for.
At the same time ABIM must approach the American Board of Medical Specialties (ABMS) because the ABMS will ultimately need to accept the HMFR process before ABIM can put this new process in place. This is a significant hurdle to clear, but the ABIM Board is committed to using its resources and powers of persuasion to make this happen.
Even with the hard work and political battles ahead, it is difficult not to sit back and marvel at how far we have come. Our specialty is just 10 years old, but we now have more than 15,000 practitioners and are on our way to 30,000 or even 40,000. We have our own journal, our own specialty society, our own set of competencies, our own growing national annual meeting, our own textbooks, and a growing number of publications aimed at hospitalists.
Now with the help of ABIM and the blessing of ABMS, there is a serious prospect that the first recognition of hospital medicine in the certification process will become a reality.
Will the first hospitalist claim Hospital Medicine Focused Recognition in 2008 or 2009? The exact date is too difficult to predict. That it will happen and that it will be meaningful is more certain now than it has ever been. To all those who have had the foresight and leadership to make this a reality, we thank you. Now let’s get down to the difficult work of creating a process that will help hospitalists provide the best care to their patients and help them to be leaders of change and improvement at their institutions. TH
Dr. Wellikson has been CEO of SHM since 2000.
Are You Satisfied?

“(I can’t get no) satisfaction.”—The Rolling Stones
Do you know people who have good health, loving families, a healthy income, and a great house but who are still not satisfied? You may also know some people who seemingly have little to be thankful for, and yet they are very satisfied. There has been a great deal of research on this topic, specifically as it relates to job or career satisfaction. Some assume that the main component of job satisfaction is how much a person is paid. In study after study, however, compensation is never first and is often fourth or lower on the list of items that people identify as the key factors related to their satisfaction. So what are the other factors?
What Stimulates You?
The nature of the work is important. People must find their work stimulating. Everyone finds stimulation at different levels—for some it may involve being technically successful, whether they are reviewing contract language or hanging crown molding. Others find performing a procedure such as a cardiac catheterization or a lumbar puncture highly energizing. Or stimulation—for the master chess player, for example—may be found strictly on a mental level. Whatever the sweet spot, it is important to identify what you find motivating and challenging.
Overstimulating situations, on the other hand, are uncomfortable and dissatisfying. Some individuals thrive in a highly stressful environment, such as air traffic control, that others would find overwhelming.
One of the unique features of being a hospitalist is the need to work collaboratively across many disciplines to achieve results for our patients. The collegiality involved in the team approach can be invigorating and satisfying to many people. For others, it is simply frustrating.
Do You Feel Appreciated?
Recognition for a job well done is something everyone needs. We see this in our co-workers and in children when they try something and are praised for it. We all need recognition for doing a good job day after day. This seemed counterintuitive to me when I first learned about it. Gee whiz, I thought, why do I have to say, “Good job,” when people are just doing what they are supposed to do? It turns out that we all need to be recognized regularly in order to feel that we are valued and needed. It keeps us interested and motivated.
This reminds me of the old joke in which the wife says to her husband of 25 years, “Do you love me?” He replies, “Well, I told you so 15 years ago. Don’t you remember?”
This does not mean we need a financial reward every other day or a big bonus every month. It means that we desire recognition that is meaningful and timely. Studies have shown that unless the recognition is personalized, it can have a negative effect. For instance, if I don’t care for sports, rewarding me with tickets to a baseball game will seem depersonalized and will give me the feeling that no one took the time to know what is important to me.
By the same token, if praise in a public setting makes me uncomfortable, don’t create a reward banquet with great public fanfare. People prize small things like handwritten thank you notes, gift cards for places they like (Starbucks!), or opportunities for educational or other activities. A simple “thank you,” said with enthusiasm, does wonders. Respect is closely tied to recognition. If the hospitalist feels like a glorified resident, the sense of disrespect is pervasive—more on this below.
Are You in Control?
Autonomy and control over your work and work life remain key factors in career satisfaction. This includes having input not only when it comes to the schedule but also, and more importantly, with regard to the processes. Can you participate in design for your group or at the hospital? If you find that all your suggestions fall on deaf ears, then either the work environment needs some adjusting or you are always wrong! Small things can be important here. Just having the flexibility to participate in quality processes or to give input on a protocol creates a feeling of control over your work. Hospitalists who have decisions imposed on them experience a great deal of tension and may, ultimately, resign.
Is there an opportunity for promotion or further learning? An individual who feels boxed in and unable to make career improvements is often dissatisfied. This ties in to the need for challenge and the importance of the nature of the work.
We all have personal challenges that we would like the flexibility to address. You may have childcare or elder care issues. Perhaps you want to train for the next Ironman race. If you are unable to address these personal aspirations and goals, you may feel that you have no control over your life, much less your work life.
Are You Happy at Work?
Work environment—who knew how important this could be? Let’s say you are employed at a large organization, perhaps General Electric. GE controls the environment for all of its employees. The company makes sure that the lighting is adequate. It tries to protect its employees from hostility based on gender, race, or disability. GE controls work assignments, and there is a chain of command for any issue that needs to be addressed.
The hospitalist, as a member of the medical staff, may be in a much different setting. Often, hospitalists work in someone else’s environment. The nurses and physicians with whom they work are generally hired by others. The atmosphere in which they work can be hostile, devoid of respect. There is often no clear chain of command set up to resolve work environment issues. Some facilities are frustrating and challenging to work in, with insufficient translators or inadequate lab or X-ray support. Fellow medical staff members or administrators may not understand how hospitalists differ from other specialists, making the job of the hospitalist more difficult
An individual’s inability to affect the work environment due to the structure of the facility can be detrimental to morale. Are the committees structured so that hospitalists can participate in them and influence the decisions they make? Even seemingly small issues can have a big impact on a hospitalist’s feelings of control and autonomy.
What Do You Earn?
Finally, compensation. Everyone wants a fair wage for a reasonable work effort. It seems simple, but obviously there are tensions here. All things being equal, a person’s income should be competitive and fair. The definition of “fair” is often determined by the marketplace. In the field of hospitalist medicine, there is a great deal of competition for labor, so there are many opportunities to evaluate. But finding the work that is most satisfying involves attaining a combination of the abovementioned characteristics as well as evaluating location.
SHM’s Task Force Examines the Issue
So, what to do? As an organization, SHM has appointed a Career Satisfaction Task Force to study work satisfaction and to design processes that will address this issue specifically for the hospitalist workforce. As I mentioned above, this topic has been studied extensively in various employee environments for many years. Retention of valuable employees is a key component of an organization’s success. This applies to nonmedical as well as to medical fields. The emergency medicine field, for example, has done some work on the challenges specific to their physicians and has some interesting insights. We expect to share the work product of our own task force in the future.
Short-Term Help
But what to do now? If you are a hospitalist leader, ask your group for feedback. Are they finding satisfaction in the areas described above? Find ways to develop control and autonomy for your group. Encourage them to participate in shaping their own careers and futures. Recognize, recognize, recognize. You can’t say “Thank you” or “Good job” too often. Learn how your group members prefer to be recognized and try to personalize what you do for them. Remember this line from The One Minute Manager, by Kenneth Blanchard, PhD, and Spencer Johnson, MD: “Catch them doing something right.” It happens around us all day, but we take performance for granted and fail to praise and recognize.
If you are a hospitalist, help shape your own destiny. Participate, ask questions, and devise solutions. And recognize the nurses, the social worker, and your group leader.
Together we can create career satisfaction and lifelong, fulfilling work. Unlike Mick Jagger, we will then get some satisfaction! TH
Dr. Gorman is the president of SHM.
“(I can’t get no) satisfaction.”—The Rolling Stones
Do you know people who have good health, loving families, a healthy income, and a great house but who are still not satisfied? You may also know some people who seemingly have little to be thankful for, and yet they are very satisfied. There has been a great deal of research on this topic, specifically as it relates to job or career satisfaction. Some assume that the main component of job satisfaction is how much a person is paid. In study after study, however, compensation is never first and is often fourth or lower on the list of items that people identify as the key factors related to their satisfaction. So what are the other factors?
What Stimulates You?
The nature of the work is important. People must find their work stimulating. Everyone finds stimulation at different levels—for some it may involve being technically successful, whether they are reviewing contract language or hanging crown molding. Others find performing a procedure such as a cardiac catheterization or a lumbar puncture highly energizing. Or stimulation—for the master chess player, for example—may be found strictly on a mental level. Whatever the sweet spot, it is important to identify what you find motivating and challenging.
Overstimulating situations, on the other hand, are uncomfortable and dissatisfying. Some individuals thrive in a highly stressful environment, such as air traffic control, that others would find overwhelming.
One of the unique features of being a hospitalist is the need to work collaboratively across many disciplines to achieve results for our patients. The collegiality involved in the team approach can be invigorating and satisfying to many people. For others, it is simply frustrating.
Do You Feel Appreciated?
Recognition for a job well done is something everyone needs. We see this in our co-workers and in children when they try something and are praised for it. We all need recognition for doing a good job day after day. This seemed counterintuitive to me when I first learned about it. Gee whiz, I thought, why do I have to say, “Good job,” when people are just doing what they are supposed to do? It turns out that we all need to be recognized regularly in order to feel that we are valued and needed. It keeps us interested and motivated.
This reminds me of the old joke in which the wife says to her husband of 25 years, “Do you love me?” He replies, “Well, I told you so 15 years ago. Don’t you remember?”
This does not mean we need a financial reward every other day or a big bonus every month. It means that we desire recognition that is meaningful and timely. Studies have shown that unless the recognition is personalized, it can have a negative effect. For instance, if I don’t care for sports, rewarding me with tickets to a baseball game will seem depersonalized and will give me the feeling that no one took the time to know what is important to me.
By the same token, if praise in a public setting makes me uncomfortable, don’t create a reward banquet with great public fanfare. People prize small things like handwritten thank you notes, gift cards for places they like (Starbucks!), or opportunities for educational or other activities. A simple “thank you,” said with enthusiasm, does wonders. Respect is closely tied to recognition. If the hospitalist feels like a glorified resident, the sense of disrespect is pervasive—more on this below.
Are You in Control?
Autonomy and control over your work and work life remain key factors in career satisfaction. This includes having input not only when it comes to the schedule but also, and more importantly, with regard to the processes. Can you participate in design for your group or at the hospital? If you find that all your suggestions fall on deaf ears, then either the work environment needs some adjusting or you are always wrong! Small things can be important here. Just having the flexibility to participate in quality processes or to give input on a protocol creates a feeling of control over your work. Hospitalists who have decisions imposed on them experience a great deal of tension and may, ultimately, resign.
Is there an opportunity for promotion or further learning? An individual who feels boxed in and unable to make career improvements is often dissatisfied. This ties in to the need for challenge and the importance of the nature of the work.
We all have personal challenges that we would like the flexibility to address. You may have childcare or elder care issues. Perhaps you want to train for the next Ironman race. If you are unable to address these personal aspirations and goals, you may feel that you have no control over your life, much less your work life.
Are You Happy at Work?
Work environment—who knew how important this could be? Let’s say you are employed at a large organization, perhaps General Electric. GE controls the environment for all of its employees. The company makes sure that the lighting is adequate. It tries to protect its employees from hostility based on gender, race, or disability. GE controls work assignments, and there is a chain of command for any issue that needs to be addressed.
The hospitalist, as a member of the medical staff, may be in a much different setting. Often, hospitalists work in someone else’s environment. The nurses and physicians with whom they work are generally hired by others. The atmosphere in which they work can be hostile, devoid of respect. There is often no clear chain of command set up to resolve work environment issues. Some facilities are frustrating and challenging to work in, with insufficient translators or inadequate lab or X-ray support. Fellow medical staff members or administrators may not understand how hospitalists differ from other specialists, making the job of the hospitalist more difficult
An individual’s inability to affect the work environment due to the structure of the facility can be detrimental to morale. Are the committees structured so that hospitalists can participate in them and influence the decisions they make? Even seemingly small issues can have a big impact on a hospitalist’s feelings of control and autonomy.
What Do You Earn?
Finally, compensation. Everyone wants a fair wage for a reasonable work effort. It seems simple, but obviously there are tensions here. All things being equal, a person’s income should be competitive and fair. The definition of “fair” is often determined by the marketplace. In the field of hospitalist medicine, there is a great deal of competition for labor, so there are many opportunities to evaluate. But finding the work that is most satisfying involves attaining a combination of the abovementioned characteristics as well as evaluating location.
SHM’s Task Force Examines the Issue
So, what to do? As an organization, SHM has appointed a Career Satisfaction Task Force to study work satisfaction and to design processes that will address this issue specifically for the hospitalist workforce. As I mentioned above, this topic has been studied extensively in various employee environments for many years. Retention of valuable employees is a key component of an organization’s success. This applies to nonmedical as well as to medical fields. The emergency medicine field, for example, has done some work on the challenges specific to their physicians and has some interesting insights. We expect to share the work product of our own task force in the future.
Short-Term Help
But what to do now? If you are a hospitalist leader, ask your group for feedback. Are they finding satisfaction in the areas described above? Find ways to develop control and autonomy for your group. Encourage them to participate in shaping their own careers and futures. Recognize, recognize, recognize. You can’t say “Thank you” or “Good job” too often. Learn how your group members prefer to be recognized and try to personalize what you do for them. Remember this line from The One Minute Manager, by Kenneth Blanchard, PhD, and Spencer Johnson, MD: “Catch them doing something right.” It happens around us all day, but we take performance for granted and fail to praise and recognize.
If you are a hospitalist, help shape your own destiny. Participate, ask questions, and devise solutions. And recognize the nurses, the social worker, and your group leader.
Together we can create career satisfaction and lifelong, fulfilling work. Unlike Mick Jagger, we will then get some satisfaction! TH
Dr. Gorman is the president of SHM.
“(I can’t get no) satisfaction.”—The Rolling Stones
Do you know people who have good health, loving families, a healthy income, and a great house but who are still not satisfied? You may also know some people who seemingly have little to be thankful for, and yet they are very satisfied. There has been a great deal of research on this topic, specifically as it relates to job or career satisfaction. Some assume that the main component of job satisfaction is how much a person is paid. In study after study, however, compensation is never first and is often fourth or lower on the list of items that people identify as the key factors related to their satisfaction. So what are the other factors?
What Stimulates You?
The nature of the work is important. People must find their work stimulating. Everyone finds stimulation at different levels—for some it may involve being technically successful, whether they are reviewing contract language or hanging crown molding. Others find performing a procedure such as a cardiac catheterization or a lumbar puncture highly energizing. Or stimulation—for the master chess player, for example—may be found strictly on a mental level. Whatever the sweet spot, it is important to identify what you find motivating and challenging.
Overstimulating situations, on the other hand, are uncomfortable and dissatisfying. Some individuals thrive in a highly stressful environment, such as air traffic control, that others would find overwhelming.
One of the unique features of being a hospitalist is the need to work collaboratively across many disciplines to achieve results for our patients. The collegiality involved in the team approach can be invigorating and satisfying to many people. For others, it is simply frustrating.
Do You Feel Appreciated?
Recognition for a job well done is something everyone needs. We see this in our co-workers and in children when they try something and are praised for it. We all need recognition for doing a good job day after day. This seemed counterintuitive to me when I first learned about it. Gee whiz, I thought, why do I have to say, “Good job,” when people are just doing what they are supposed to do? It turns out that we all need to be recognized regularly in order to feel that we are valued and needed. It keeps us interested and motivated.
This reminds me of the old joke in which the wife says to her husband of 25 years, “Do you love me?” He replies, “Well, I told you so 15 years ago. Don’t you remember?”
This does not mean we need a financial reward every other day or a big bonus every month. It means that we desire recognition that is meaningful and timely. Studies have shown that unless the recognition is personalized, it can have a negative effect. For instance, if I don’t care for sports, rewarding me with tickets to a baseball game will seem depersonalized and will give me the feeling that no one took the time to know what is important to me.
By the same token, if praise in a public setting makes me uncomfortable, don’t create a reward banquet with great public fanfare. People prize small things like handwritten thank you notes, gift cards for places they like (Starbucks!), or opportunities for educational or other activities. A simple “thank you,” said with enthusiasm, does wonders. Respect is closely tied to recognition. If the hospitalist feels like a glorified resident, the sense of disrespect is pervasive—more on this below.
Are You in Control?
Autonomy and control over your work and work life remain key factors in career satisfaction. This includes having input not only when it comes to the schedule but also, and more importantly, with regard to the processes. Can you participate in design for your group or at the hospital? If you find that all your suggestions fall on deaf ears, then either the work environment needs some adjusting or you are always wrong! Small things can be important here. Just having the flexibility to participate in quality processes or to give input on a protocol creates a feeling of control over your work. Hospitalists who have decisions imposed on them experience a great deal of tension and may, ultimately, resign.
Is there an opportunity for promotion or further learning? An individual who feels boxed in and unable to make career improvements is often dissatisfied. This ties in to the need for challenge and the importance of the nature of the work.
We all have personal challenges that we would like the flexibility to address. You may have childcare or elder care issues. Perhaps you want to train for the next Ironman race. If you are unable to address these personal aspirations and goals, you may feel that you have no control over your life, much less your work life.
Are You Happy at Work?
Work environment—who knew how important this could be? Let’s say you are employed at a large organization, perhaps General Electric. GE controls the environment for all of its employees. The company makes sure that the lighting is adequate. It tries to protect its employees from hostility based on gender, race, or disability. GE controls work assignments, and there is a chain of command for any issue that needs to be addressed.
The hospitalist, as a member of the medical staff, may be in a much different setting. Often, hospitalists work in someone else’s environment. The nurses and physicians with whom they work are generally hired by others. The atmosphere in which they work can be hostile, devoid of respect. There is often no clear chain of command set up to resolve work environment issues. Some facilities are frustrating and challenging to work in, with insufficient translators or inadequate lab or X-ray support. Fellow medical staff members or administrators may not understand how hospitalists differ from other specialists, making the job of the hospitalist more difficult
An individual’s inability to affect the work environment due to the structure of the facility can be detrimental to morale. Are the committees structured so that hospitalists can participate in them and influence the decisions they make? Even seemingly small issues can have a big impact on a hospitalist’s feelings of control and autonomy.
What Do You Earn?
Finally, compensation. Everyone wants a fair wage for a reasonable work effort. It seems simple, but obviously there are tensions here. All things being equal, a person’s income should be competitive and fair. The definition of “fair” is often determined by the marketplace. In the field of hospitalist medicine, there is a great deal of competition for labor, so there are many opportunities to evaluate. But finding the work that is most satisfying involves attaining a combination of the abovementioned characteristics as well as evaluating location.
SHM’s Task Force Examines the Issue
So, what to do? As an organization, SHM has appointed a Career Satisfaction Task Force to study work satisfaction and to design processes that will address this issue specifically for the hospitalist workforce. As I mentioned above, this topic has been studied extensively in various employee environments for many years. Retention of valuable employees is a key component of an organization’s success. This applies to nonmedical as well as to medical fields. The emergency medicine field, for example, has done some work on the challenges specific to their physicians and has some interesting insights. We expect to share the work product of our own task force in the future.
Short-Term Help
But what to do now? If you are a hospitalist leader, ask your group for feedback. Are they finding satisfaction in the areas described above? Find ways to develop control and autonomy for your group. Encourage them to participate in shaping their own careers and futures. Recognize, recognize, recognize. You can’t say “Thank you” or “Good job” too often. Learn how your group members prefer to be recognized and try to personalize what you do for them. Remember this line from The One Minute Manager, by Kenneth Blanchard, PhD, and Spencer Johnson, MD: “Catch them doing something right.” It happens around us all day, but we take performance for granted and fail to praise and recognize.
If you are a hospitalist, help shape your own destiny. Participate, ask questions, and devise solutions. And recognize the nurses, the social worker, and your group leader.
Together we can create career satisfaction and lifelong, fulfilling work. Unlike Mick Jagger, we will then get some satisfaction! TH
Dr. Gorman is the president of SHM.
Here, There, Everywhere
Many primary care physicians welcome the introduction of hospital medicine for its potential to help normalize their schedules, reduce interruptions to their clinic work from hospitalized patients, and moderate after-hours on-call demands. Some have found hospital medicine itself such an attractive option for balancing their schedules between work and personal commitments that they have pursued it as a career.
Internist Doyle Detweiler, MD, started closing down his medical office practice in Newton, Kan., a small town 15 miles north of Wichita, in June of this year so he could become the first full-time hospitalist at 81-bed Newton Medical Center. Pulled between his office practice and the demands of visiting his patients at the hospital, Dr. Detweiler had seen his family life suffer, with limited quality time to spend with his daughters Lilly, 4, and Hannah, 18 months.
“The worst thing was that when I’d go to work, I’d kiss my little girls goodbye and they’d still be bed. When I’d come home and kiss them good night, they’d already be in bed,” he says. “My wife would never know even approximately when I’d be heading home. So it would be difficult for us to plan anything in the evenings.” He also spent a lot of time working on the weekends.
Dr. Detweiler still faces significant time demands in his new job—at least until a second hospitalist can be brought on board later this year. But the move has already produced dividends in terms of shorter and more predictable hours. Generally, he wraps up work shortly after 6 p.m., when the last post-operative case has been admitted, and he has been called back to the hospital only three times in two months for after-hours patient crises.
“One big advantage I can see—once we ultimately get the program rolling—is that I’ll know when I’ll be working and when I’m off and checked out,” he explains. “As a hospitalist, there still will be times when I’m really busy, but it will be easier to plan something like going out for dinner at 7 p.m.”
The Needs of Children—and Parents
The classic juggle of work and home life involves the care of young children, although that is only one of the competing personal demands on doctors’ time. As the proportion of women in medicine has grown, employers have been challenged to find ways to accommodate their staffs’ maternity leaves and child-care responsibilities, while working parents seek to accommodate their children’s swimming lessons, ball games, and ballet classes.
The generation that now dominates hospitalist ranks (average age 37, according to SHM’s “Biannual Survey of the Hospital Medicine Movement”) has little taste for the traditional image of the old-fashioned, male family doctor, essentially available to his patients 24/7. Lifestyle issues are important factors in their career choices.
Other working hospitalists want time to travel or to pursue outside interests. Their hours of work may be shorter and more predictable than for other physicians, but the pace can be intense, with life-and-death situations involving critically ill patients occurring every day. Many of today’s hospitalists also belong to the “sandwich generation,” juggling simultaneous caregiving responsibilities for children and aging parents.
Stacy Walton Goldsholl, MD, of Wilmington, N.C., president of the hospital medicine division of TeamHealth, and member of the SHM Board of Directors, faced an extreme version of these competing demands when starting her new managerial position on January 1, 2006. Pregnant with her second child, Richard, who was born in April, she was also caring for her 65-year-old father, who died of cancer in February.
“It was tough watching my dad, formerly a very robust person, truly the motivating force for my professional success, my moral compass, confidant, and advisor, as he got sicker,” says Dr. Goldsholl. “Some days I’d leave my two-year-old, Aiden, with my husband and go care for my dad, giving him his injection of Lovenox [enoxaparin] or replacing his PCA pump. My mom and I were his primary caregivers at home until we physically couldn’t handle it.”
At that point her father was admitted to a hospice inpatient facility, where she would sit by his bedside with a computer in her lap.
Dr. Goldsholl probably would have needed to take a leave of absence if she had been working as a hospitalist, but her new employers at TeamHealth gave her a lot of flexibility, limiting the number of strategic meetings she had to attend. In general, however, she believes hospitalist shift work is more accommodating to family demands than an administrative position. She returned from maternity leave full time on June 1 and now travels every week for her job; her mother, who lives nearby, fills in as her grandchildren’s nanny. But Dr. Goldsholl’s experience has sparked her interest in exploring sustainability issues for other hospitalists.
“TeamHealth’s leaders told me their turnover rate is about 5 percent for hospitalists, versus an industry average of 19 percent,” says Dr. Goldsholl. “I found that hard to believe, but when I interviewed some of our local medical directors, it turned out to be true. They were all extremely positive about their relationship with our operational infrastructure.
“There’s so much to do and so many opportunities out there, but it must be sustainable,” she continues. “In order to sustain a career, you must be fulfilled personally, which is directly related to your work/life balance.”
When she drilled down into the company’s data, trying to find out why TeamHealth is able to retain its doctors, she found that the hours they work average 7.3% less than the industry as a whole, while their compensation is comparable to others.1
For Daniel Dressler, MD, medical director of the Hospital Medicine Group at Emory Healthcare in Atlanta, Ga., hospital medicine can be a juggling act—as can his committee work for SHM—although he is able to conduct some business from home. “When we do the conference calls for SHM, half of the time I’m home taking care of our kids”—one-year-old twins—often with one of them in his lap.
Dr. Dressler and his wife had been building a new home and working closely with contractors and subcontractors when she discovered she was pregnant last year. The construction project experienced multiple delays. When interviewed in September, the Dresslers were living temporarily with his in-laws and hoping the house would be completed within another month. His wife, a physical therapist, was not working but was looking forward to returning to work.
Dr. Dressler estimates that he puts in a 60-hour workweek, including 30 hours of hospitalist shifts and the rest administrative, teaching, and education. “I don’t recommend building a new house and having kids at the same time,” he says. “Taking care of one-year-old twins is more difficult than anything I do at work. But we have a good time.”
He also tries to squeeze in a basketball game with the medical residents every weekend.
Dr. Dressler’s schedule demands reflect an additional wrinkle in terms of juggling work and family—especially in a relatively new field with huge growth opportunities and an emphasis on changing the healthcare system. Doctors must balance what is truly required to perform the job and satisfy their employers with what they do to satisfy their own standards and expectations, as well as take advantage of opportunities to advance their careers.
“There’s the balance of what’s reasonable for you at this point in your career. It’s a personal decision for everyone—[deciding] what is an adequate amount of time for each of the priorities in your life … what drives you, and what makes you happy in your life,” says Dr. Dressler. “The things that drive me include teaching and advancing the field, which means seizing opportunities to grow with this new and growing field, but hopefully not to the detriment of the rest of my life.”
—Lisa Kettering, MD, medical director, Exempla-St. Joseph Hospital, Denver
A Family-Friendly Practice
Arpana Vidyarthi, MD, an academic hospitalist at the University of California-San Francisco (UCSF), has responsibilities for teaching residents and medical students and additional roles in hospital quality and safety. “It’s a somewhat different role than a shift hospitalist, with different stressors,” she says. “But there are many options out there, and one of the things that makes being a hospitalist attractive to me is the flexibility it offers.”
Dr. Vidyarthi’s husband also has a demanding job. She is able to do some of her own work at home with her two-year-old daughter, Anaiya, but estimates that her nanny puts in a 50-hour week. “I came to UCSF to do a hospitalist fellowship, and this is exactly what I want to do, with tremendous job satisfaction and a varied schedule. Yet I feel stretched all the time,” she says.
Dr. Vidyarthi credits her group practice at UCSF and its head, Robert Wachter, MD, for a supportive and family-friendly working environment. Colleague Adrienne Green, MD, agrees, adding that three of the group’s 24 physician members are pregnant at this time.
Dr. Green’s children are very interested in her work and have visited her at the hospital, which makes the work more real to them. “I’ll tell them about some of my patients who are really sick, and I’ll explain that the reason I’m going to work on the weekend is that I’m helping people get better and get out of the hospital,” says Dr. Green. “When I’m working on a Saturday and my son has a baseball game, I’ll tell him I’ll try to get to the game, but I can’t promise. But when we do have family time, we make it quality time.”
Dr. Wachter explains how he promotes a family-friendly work environment for hospitalists at UCSF: “My overarching management philosophy is that the quality of our program is equal to the quality of the people we’re able to recruit and retain. Thus, an environment that is professionally satisfying, collegiate, fun, and supportive of everyone’s personal and family goals is fundamental.”
Balancing life and work requires some give and take among the members of the group, who cover for each other when needed. It also takes a commitment to staffing in anticipation of predictable future needs for maternity leaves, sabbaticals and the like, rather than waiting for the actual need to arrive.
—Lisa Kettering, MD, medical director, Exempla-St. Joseph Hospital, Denver
Making Good Career Choices
Lisa Kettering, MD, a member of SHM’s Board of Directors, has been a working hospitalist since 1998. Before that she worked in a traditional internal medicine practice. She also believes that hospital medicine offers more flexibility and opportunities for balance, with a full-time hospitalist position roughly comparable to the “part-time” private practice position she once held.
“In private practice, you’re always coming back to phone calls and piles of charts,” says Dr. Kettering. “As a hospitalist, you take care of your business in real time, instead of always playing catch up.”
A year ago, Dr. Kettering assumed medical direction of a practice of nine hospitalists and three intensivists at Exempla-St. Joseph Hospital in Denver, Colo., a position that includes significant clinical duties and requires about 80 hours of her time per week.
“If my children [three sons age 21, 19, and 16] were not almost grown, I could not have accepted this position,” she says. “But this job is my passion. For me, the key to family balance has been a supportive spouse and lots of child care and other supports.”
Dr. Kettering’s sons were born just before or during her medical school and residency, so her long hours have always been part of the equation. “What I gave up [for this career] were aspects of a social life, such as dinners out with our friends and an opportunity to work on my tennis game” and similar hobbies, she says. She has continued to run, a time-efficient form of exercise and stress management. Now that her children are leaving home, there is more time to indulge a love of yoga and Pilates and to resume a more normal social life—although she doesn’t do much cooking.
Don’t be shy about getting help, Dr. Kettering advises. She engages a personal assistant eight hours a week to help with errands such as making travel arrangements, picking up groceries, taking the car in for servicing, or wrapping the birthday presents she buys. “Not that I couldn’t squeeze in a few errands on the way home from work, but it would just be more demands on my time,” she explains.
“I believe I am an optimist, but my advice to young doctors is this: Don’t believe you can do it all,” says Dr. Kettering. “You need to make careful, considered decisions along the way, understanding you do have control over your choices. But there’s no question that you’ll have to give up many things if you choose medicine as a career.”
The biggest recommendation Dr. Kettering offers for future hospitalists is to make career choices based on a passion for the work—not on the flexible hours. Then consider how to make the job work in terms of schedules and the other nuts and bolts of practice, being aware of the varied opportunities that exist.
Although hospital medicine is sometimes described as a young person’s game, Dr. Kettering believes that if it is practiced correctly, with a sustainable work schedule, it doesn’t have to lead to burnout or exhaustion. “My practice is [composed] exclusively of doctors who have chosen hospital medicine as a life’s work—not a stopgap between residency and fellowship,” she says. “We also have a wonderful group of physicians, and there has not been a time when somebody had a family emergency that somebody else didn’t step up to cover.” TH
Larry Beresford is a frequent contributor to The Hospitalist.
Reference
- Compensation by Employment Model, Society of Hospital Medicine Benchmark Survey, 2003.
Many primary care physicians welcome the introduction of hospital medicine for its potential to help normalize their schedules, reduce interruptions to their clinic work from hospitalized patients, and moderate after-hours on-call demands. Some have found hospital medicine itself such an attractive option for balancing their schedules between work and personal commitments that they have pursued it as a career.
Internist Doyle Detweiler, MD, started closing down his medical office practice in Newton, Kan., a small town 15 miles north of Wichita, in June of this year so he could become the first full-time hospitalist at 81-bed Newton Medical Center. Pulled between his office practice and the demands of visiting his patients at the hospital, Dr. Detweiler had seen his family life suffer, with limited quality time to spend with his daughters Lilly, 4, and Hannah, 18 months.
“The worst thing was that when I’d go to work, I’d kiss my little girls goodbye and they’d still be bed. When I’d come home and kiss them good night, they’d already be in bed,” he says. “My wife would never know even approximately when I’d be heading home. So it would be difficult for us to plan anything in the evenings.” He also spent a lot of time working on the weekends.
Dr. Detweiler still faces significant time demands in his new job—at least until a second hospitalist can be brought on board later this year. But the move has already produced dividends in terms of shorter and more predictable hours. Generally, he wraps up work shortly after 6 p.m., when the last post-operative case has been admitted, and he has been called back to the hospital only three times in two months for after-hours patient crises.
“One big advantage I can see—once we ultimately get the program rolling—is that I’ll know when I’ll be working and when I’m off and checked out,” he explains. “As a hospitalist, there still will be times when I’m really busy, but it will be easier to plan something like going out for dinner at 7 p.m.”
The Needs of Children—and Parents
The classic juggle of work and home life involves the care of young children, although that is only one of the competing personal demands on doctors’ time. As the proportion of women in medicine has grown, employers have been challenged to find ways to accommodate their staffs’ maternity leaves and child-care responsibilities, while working parents seek to accommodate their children’s swimming lessons, ball games, and ballet classes.
The generation that now dominates hospitalist ranks (average age 37, according to SHM’s “Biannual Survey of the Hospital Medicine Movement”) has little taste for the traditional image of the old-fashioned, male family doctor, essentially available to his patients 24/7. Lifestyle issues are important factors in their career choices.
Other working hospitalists want time to travel or to pursue outside interests. Their hours of work may be shorter and more predictable than for other physicians, but the pace can be intense, with life-and-death situations involving critically ill patients occurring every day. Many of today’s hospitalists also belong to the “sandwich generation,” juggling simultaneous caregiving responsibilities for children and aging parents.
Stacy Walton Goldsholl, MD, of Wilmington, N.C., president of the hospital medicine division of TeamHealth, and member of the SHM Board of Directors, faced an extreme version of these competing demands when starting her new managerial position on January 1, 2006. Pregnant with her second child, Richard, who was born in April, she was also caring for her 65-year-old father, who died of cancer in February.
“It was tough watching my dad, formerly a very robust person, truly the motivating force for my professional success, my moral compass, confidant, and advisor, as he got sicker,” says Dr. Goldsholl. “Some days I’d leave my two-year-old, Aiden, with my husband and go care for my dad, giving him his injection of Lovenox [enoxaparin] or replacing his PCA pump. My mom and I were his primary caregivers at home until we physically couldn’t handle it.”
At that point her father was admitted to a hospice inpatient facility, where she would sit by his bedside with a computer in her lap.
Dr. Goldsholl probably would have needed to take a leave of absence if she had been working as a hospitalist, but her new employers at TeamHealth gave her a lot of flexibility, limiting the number of strategic meetings she had to attend. In general, however, she believes hospitalist shift work is more accommodating to family demands than an administrative position. She returned from maternity leave full time on June 1 and now travels every week for her job; her mother, who lives nearby, fills in as her grandchildren’s nanny. But Dr. Goldsholl’s experience has sparked her interest in exploring sustainability issues for other hospitalists.
“TeamHealth’s leaders told me their turnover rate is about 5 percent for hospitalists, versus an industry average of 19 percent,” says Dr. Goldsholl. “I found that hard to believe, but when I interviewed some of our local medical directors, it turned out to be true. They were all extremely positive about their relationship with our operational infrastructure.
“There’s so much to do and so many opportunities out there, but it must be sustainable,” she continues. “In order to sustain a career, you must be fulfilled personally, which is directly related to your work/life balance.”
When she drilled down into the company’s data, trying to find out why TeamHealth is able to retain its doctors, she found that the hours they work average 7.3% less than the industry as a whole, while their compensation is comparable to others.1
For Daniel Dressler, MD, medical director of the Hospital Medicine Group at Emory Healthcare in Atlanta, Ga., hospital medicine can be a juggling act—as can his committee work for SHM—although he is able to conduct some business from home. “When we do the conference calls for SHM, half of the time I’m home taking care of our kids”—one-year-old twins—often with one of them in his lap.
Dr. Dressler and his wife had been building a new home and working closely with contractors and subcontractors when she discovered she was pregnant last year. The construction project experienced multiple delays. When interviewed in September, the Dresslers were living temporarily with his in-laws and hoping the house would be completed within another month. His wife, a physical therapist, was not working but was looking forward to returning to work.
Dr. Dressler estimates that he puts in a 60-hour workweek, including 30 hours of hospitalist shifts and the rest administrative, teaching, and education. “I don’t recommend building a new house and having kids at the same time,” he says. “Taking care of one-year-old twins is more difficult than anything I do at work. But we have a good time.”
He also tries to squeeze in a basketball game with the medical residents every weekend.
Dr. Dressler’s schedule demands reflect an additional wrinkle in terms of juggling work and family—especially in a relatively new field with huge growth opportunities and an emphasis on changing the healthcare system. Doctors must balance what is truly required to perform the job and satisfy their employers with what they do to satisfy their own standards and expectations, as well as take advantage of opportunities to advance their careers.
“There’s the balance of what’s reasonable for you at this point in your career. It’s a personal decision for everyone—[deciding] what is an adequate amount of time for each of the priorities in your life … what drives you, and what makes you happy in your life,” says Dr. Dressler. “The things that drive me include teaching and advancing the field, which means seizing opportunities to grow with this new and growing field, but hopefully not to the detriment of the rest of my life.”
—Lisa Kettering, MD, medical director, Exempla-St. Joseph Hospital, Denver
A Family-Friendly Practice
Arpana Vidyarthi, MD, an academic hospitalist at the University of California-San Francisco (UCSF), has responsibilities for teaching residents and medical students and additional roles in hospital quality and safety. “It’s a somewhat different role than a shift hospitalist, with different stressors,” she says. “But there are many options out there, and one of the things that makes being a hospitalist attractive to me is the flexibility it offers.”
Dr. Vidyarthi’s husband also has a demanding job. She is able to do some of her own work at home with her two-year-old daughter, Anaiya, but estimates that her nanny puts in a 50-hour week. “I came to UCSF to do a hospitalist fellowship, and this is exactly what I want to do, with tremendous job satisfaction and a varied schedule. Yet I feel stretched all the time,” she says.
Dr. Vidyarthi credits her group practice at UCSF and its head, Robert Wachter, MD, for a supportive and family-friendly working environment. Colleague Adrienne Green, MD, agrees, adding that three of the group’s 24 physician members are pregnant at this time.
Dr. Green’s children are very interested in her work and have visited her at the hospital, which makes the work more real to them. “I’ll tell them about some of my patients who are really sick, and I’ll explain that the reason I’m going to work on the weekend is that I’m helping people get better and get out of the hospital,” says Dr. Green. “When I’m working on a Saturday and my son has a baseball game, I’ll tell him I’ll try to get to the game, but I can’t promise. But when we do have family time, we make it quality time.”
Dr. Wachter explains how he promotes a family-friendly work environment for hospitalists at UCSF: “My overarching management philosophy is that the quality of our program is equal to the quality of the people we’re able to recruit and retain. Thus, an environment that is professionally satisfying, collegiate, fun, and supportive of everyone’s personal and family goals is fundamental.”
Balancing life and work requires some give and take among the members of the group, who cover for each other when needed. It also takes a commitment to staffing in anticipation of predictable future needs for maternity leaves, sabbaticals and the like, rather than waiting for the actual need to arrive.
—Lisa Kettering, MD, medical director, Exempla-St. Joseph Hospital, Denver
Making Good Career Choices
Lisa Kettering, MD, a member of SHM’s Board of Directors, has been a working hospitalist since 1998. Before that she worked in a traditional internal medicine practice. She also believes that hospital medicine offers more flexibility and opportunities for balance, with a full-time hospitalist position roughly comparable to the “part-time” private practice position she once held.
“In private practice, you’re always coming back to phone calls and piles of charts,” says Dr. Kettering. “As a hospitalist, you take care of your business in real time, instead of always playing catch up.”
A year ago, Dr. Kettering assumed medical direction of a practice of nine hospitalists and three intensivists at Exempla-St. Joseph Hospital in Denver, Colo., a position that includes significant clinical duties and requires about 80 hours of her time per week.
“If my children [three sons age 21, 19, and 16] were not almost grown, I could not have accepted this position,” she says. “But this job is my passion. For me, the key to family balance has been a supportive spouse and lots of child care and other supports.”
Dr. Kettering’s sons were born just before or during her medical school and residency, so her long hours have always been part of the equation. “What I gave up [for this career] were aspects of a social life, such as dinners out with our friends and an opportunity to work on my tennis game” and similar hobbies, she says. She has continued to run, a time-efficient form of exercise and stress management. Now that her children are leaving home, there is more time to indulge a love of yoga and Pilates and to resume a more normal social life—although she doesn’t do much cooking.
Don’t be shy about getting help, Dr. Kettering advises. She engages a personal assistant eight hours a week to help with errands such as making travel arrangements, picking up groceries, taking the car in for servicing, or wrapping the birthday presents she buys. “Not that I couldn’t squeeze in a few errands on the way home from work, but it would just be more demands on my time,” she explains.
“I believe I am an optimist, but my advice to young doctors is this: Don’t believe you can do it all,” says Dr. Kettering. “You need to make careful, considered decisions along the way, understanding you do have control over your choices. But there’s no question that you’ll have to give up many things if you choose medicine as a career.”
The biggest recommendation Dr. Kettering offers for future hospitalists is to make career choices based on a passion for the work—not on the flexible hours. Then consider how to make the job work in terms of schedules and the other nuts and bolts of practice, being aware of the varied opportunities that exist.
Although hospital medicine is sometimes described as a young person’s game, Dr. Kettering believes that if it is practiced correctly, with a sustainable work schedule, it doesn’t have to lead to burnout or exhaustion. “My practice is [composed] exclusively of doctors who have chosen hospital medicine as a life’s work—not a stopgap between residency and fellowship,” she says. “We also have a wonderful group of physicians, and there has not been a time when somebody had a family emergency that somebody else didn’t step up to cover.” TH
Larry Beresford is a frequent contributor to The Hospitalist.
Reference
- Compensation by Employment Model, Society of Hospital Medicine Benchmark Survey, 2003.
Many primary care physicians welcome the introduction of hospital medicine for its potential to help normalize their schedules, reduce interruptions to their clinic work from hospitalized patients, and moderate after-hours on-call demands. Some have found hospital medicine itself such an attractive option for balancing their schedules between work and personal commitments that they have pursued it as a career.
Internist Doyle Detweiler, MD, started closing down his medical office practice in Newton, Kan., a small town 15 miles north of Wichita, in June of this year so he could become the first full-time hospitalist at 81-bed Newton Medical Center. Pulled between his office practice and the demands of visiting his patients at the hospital, Dr. Detweiler had seen his family life suffer, with limited quality time to spend with his daughters Lilly, 4, and Hannah, 18 months.
“The worst thing was that when I’d go to work, I’d kiss my little girls goodbye and they’d still be bed. When I’d come home and kiss them good night, they’d already be in bed,” he says. “My wife would never know even approximately when I’d be heading home. So it would be difficult for us to plan anything in the evenings.” He also spent a lot of time working on the weekends.
Dr. Detweiler still faces significant time demands in his new job—at least until a second hospitalist can be brought on board later this year. But the move has already produced dividends in terms of shorter and more predictable hours. Generally, he wraps up work shortly after 6 p.m., when the last post-operative case has been admitted, and he has been called back to the hospital only three times in two months for after-hours patient crises.
“One big advantage I can see—once we ultimately get the program rolling—is that I’ll know when I’ll be working and when I’m off and checked out,” he explains. “As a hospitalist, there still will be times when I’m really busy, but it will be easier to plan something like going out for dinner at 7 p.m.”
The Needs of Children—and Parents
The classic juggle of work and home life involves the care of young children, although that is only one of the competing personal demands on doctors’ time. As the proportion of women in medicine has grown, employers have been challenged to find ways to accommodate their staffs’ maternity leaves and child-care responsibilities, while working parents seek to accommodate their children’s swimming lessons, ball games, and ballet classes.
The generation that now dominates hospitalist ranks (average age 37, according to SHM’s “Biannual Survey of the Hospital Medicine Movement”) has little taste for the traditional image of the old-fashioned, male family doctor, essentially available to his patients 24/7. Lifestyle issues are important factors in their career choices.
Other working hospitalists want time to travel or to pursue outside interests. Their hours of work may be shorter and more predictable than for other physicians, but the pace can be intense, with life-and-death situations involving critically ill patients occurring every day. Many of today’s hospitalists also belong to the “sandwich generation,” juggling simultaneous caregiving responsibilities for children and aging parents.
Stacy Walton Goldsholl, MD, of Wilmington, N.C., president of the hospital medicine division of TeamHealth, and member of the SHM Board of Directors, faced an extreme version of these competing demands when starting her new managerial position on January 1, 2006. Pregnant with her second child, Richard, who was born in April, she was also caring for her 65-year-old father, who died of cancer in February.
“It was tough watching my dad, formerly a very robust person, truly the motivating force for my professional success, my moral compass, confidant, and advisor, as he got sicker,” says Dr. Goldsholl. “Some days I’d leave my two-year-old, Aiden, with my husband and go care for my dad, giving him his injection of Lovenox [enoxaparin] or replacing his PCA pump. My mom and I were his primary caregivers at home until we physically couldn’t handle it.”
At that point her father was admitted to a hospice inpatient facility, where she would sit by his bedside with a computer in her lap.
Dr. Goldsholl probably would have needed to take a leave of absence if she had been working as a hospitalist, but her new employers at TeamHealth gave her a lot of flexibility, limiting the number of strategic meetings she had to attend. In general, however, she believes hospitalist shift work is more accommodating to family demands than an administrative position. She returned from maternity leave full time on June 1 and now travels every week for her job; her mother, who lives nearby, fills in as her grandchildren’s nanny. But Dr. Goldsholl’s experience has sparked her interest in exploring sustainability issues for other hospitalists.
“TeamHealth’s leaders told me their turnover rate is about 5 percent for hospitalists, versus an industry average of 19 percent,” says Dr. Goldsholl. “I found that hard to believe, but when I interviewed some of our local medical directors, it turned out to be true. They were all extremely positive about their relationship with our operational infrastructure.
“There’s so much to do and so many opportunities out there, but it must be sustainable,” she continues. “In order to sustain a career, you must be fulfilled personally, which is directly related to your work/life balance.”
When she drilled down into the company’s data, trying to find out why TeamHealth is able to retain its doctors, she found that the hours they work average 7.3% less than the industry as a whole, while their compensation is comparable to others.1
For Daniel Dressler, MD, medical director of the Hospital Medicine Group at Emory Healthcare in Atlanta, Ga., hospital medicine can be a juggling act—as can his committee work for SHM—although he is able to conduct some business from home. “When we do the conference calls for SHM, half of the time I’m home taking care of our kids”—one-year-old twins—often with one of them in his lap.
Dr. Dressler and his wife had been building a new home and working closely with contractors and subcontractors when she discovered she was pregnant last year. The construction project experienced multiple delays. When interviewed in September, the Dresslers were living temporarily with his in-laws and hoping the house would be completed within another month. His wife, a physical therapist, was not working but was looking forward to returning to work.
Dr. Dressler estimates that he puts in a 60-hour workweek, including 30 hours of hospitalist shifts and the rest administrative, teaching, and education. “I don’t recommend building a new house and having kids at the same time,” he says. “Taking care of one-year-old twins is more difficult than anything I do at work. But we have a good time.”
He also tries to squeeze in a basketball game with the medical residents every weekend.
Dr. Dressler’s schedule demands reflect an additional wrinkle in terms of juggling work and family—especially in a relatively new field with huge growth opportunities and an emphasis on changing the healthcare system. Doctors must balance what is truly required to perform the job and satisfy their employers with what they do to satisfy their own standards and expectations, as well as take advantage of opportunities to advance their careers.
“There’s the balance of what’s reasonable for you at this point in your career. It’s a personal decision for everyone—[deciding] what is an adequate amount of time for each of the priorities in your life … what drives you, and what makes you happy in your life,” says Dr. Dressler. “The things that drive me include teaching and advancing the field, which means seizing opportunities to grow with this new and growing field, but hopefully not to the detriment of the rest of my life.”
—Lisa Kettering, MD, medical director, Exempla-St. Joseph Hospital, Denver
A Family-Friendly Practice
Arpana Vidyarthi, MD, an academic hospitalist at the University of California-San Francisco (UCSF), has responsibilities for teaching residents and medical students and additional roles in hospital quality and safety. “It’s a somewhat different role than a shift hospitalist, with different stressors,” she says. “But there are many options out there, and one of the things that makes being a hospitalist attractive to me is the flexibility it offers.”
Dr. Vidyarthi’s husband also has a demanding job. She is able to do some of her own work at home with her two-year-old daughter, Anaiya, but estimates that her nanny puts in a 50-hour week. “I came to UCSF to do a hospitalist fellowship, and this is exactly what I want to do, with tremendous job satisfaction and a varied schedule. Yet I feel stretched all the time,” she says.
Dr. Vidyarthi credits her group practice at UCSF and its head, Robert Wachter, MD, for a supportive and family-friendly working environment. Colleague Adrienne Green, MD, agrees, adding that three of the group’s 24 physician members are pregnant at this time.
Dr. Green’s children are very interested in her work and have visited her at the hospital, which makes the work more real to them. “I’ll tell them about some of my patients who are really sick, and I’ll explain that the reason I’m going to work on the weekend is that I’m helping people get better and get out of the hospital,” says Dr. Green. “When I’m working on a Saturday and my son has a baseball game, I’ll tell him I’ll try to get to the game, but I can’t promise. But when we do have family time, we make it quality time.”
Dr. Wachter explains how he promotes a family-friendly work environment for hospitalists at UCSF: “My overarching management philosophy is that the quality of our program is equal to the quality of the people we’re able to recruit and retain. Thus, an environment that is professionally satisfying, collegiate, fun, and supportive of everyone’s personal and family goals is fundamental.”
Balancing life and work requires some give and take among the members of the group, who cover for each other when needed. It also takes a commitment to staffing in anticipation of predictable future needs for maternity leaves, sabbaticals and the like, rather than waiting for the actual need to arrive.
—Lisa Kettering, MD, medical director, Exempla-St. Joseph Hospital, Denver
Making Good Career Choices
Lisa Kettering, MD, a member of SHM’s Board of Directors, has been a working hospitalist since 1998. Before that she worked in a traditional internal medicine practice. She also believes that hospital medicine offers more flexibility and opportunities for balance, with a full-time hospitalist position roughly comparable to the “part-time” private practice position she once held.
“In private practice, you’re always coming back to phone calls and piles of charts,” says Dr. Kettering. “As a hospitalist, you take care of your business in real time, instead of always playing catch up.”
A year ago, Dr. Kettering assumed medical direction of a practice of nine hospitalists and three intensivists at Exempla-St. Joseph Hospital in Denver, Colo., a position that includes significant clinical duties and requires about 80 hours of her time per week.
“If my children [three sons age 21, 19, and 16] were not almost grown, I could not have accepted this position,” she says. “But this job is my passion. For me, the key to family balance has been a supportive spouse and lots of child care and other supports.”
Dr. Kettering’s sons were born just before or during her medical school and residency, so her long hours have always been part of the equation. “What I gave up [for this career] were aspects of a social life, such as dinners out with our friends and an opportunity to work on my tennis game” and similar hobbies, she says. She has continued to run, a time-efficient form of exercise and stress management. Now that her children are leaving home, there is more time to indulge a love of yoga and Pilates and to resume a more normal social life—although she doesn’t do much cooking.
Don’t be shy about getting help, Dr. Kettering advises. She engages a personal assistant eight hours a week to help with errands such as making travel arrangements, picking up groceries, taking the car in for servicing, or wrapping the birthday presents she buys. “Not that I couldn’t squeeze in a few errands on the way home from work, but it would just be more demands on my time,” she explains.
“I believe I am an optimist, but my advice to young doctors is this: Don’t believe you can do it all,” says Dr. Kettering. “You need to make careful, considered decisions along the way, understanding you do have control over your choices. But there’s no question that you’ll have to give up many things if you choose medicine as a career.”
The biggest recommendation Dr. Kettering offers for future hospitalists is to make career choices based on a passion for the work—not on the flexible hours. Then consider how to make the job work in terms of schedules and the other nuts and bolts of practice, being aware of the varied opportunities that exist.
Although hospital medicine is sometimes described as a young person’s game, Dr. Kettering believes that if it is practiced correctly, with a sustainable work schedule, it doesn’t have to lead to burnout or exhaustion. “My practice is [composed] exclusively of doctors who have chosen hospital medicine as a life’s work—not a stopgap between residency and fellowship,” she says. “We also have a wonderful group of physicians, and there has not been a time when somebody had a family emergency that somebody else didn’t step up to cover.” TH
Larry Beresford is a frequent contributor to The Hospitalist.
Reference
- Compensation by Employment Model, Society of Hospital Medicine Benchmark Survey, 2003.
Lead the Change
Modern medicine … certainly as it should be practiced by hospitalists, is the most information-intensive activity that human beings ever engaged in,” says Kenneth W. Kizer, MD, MPH, CEO and chairman of the board of Medsphere Systems Corporation in Aliso Viejo, Calif.
He should know. From his first healthcare-related position in 1969 as a hospital orderly at Stanford University Hospital, he rose to become the Under Secretary for Health in the Department of Veterans Affairs (VA)—the CEO of the largest healthcare system in the nation. He is widely credited as being the chief architect and driving force behind the successful transformation of VA healthcare in the 1990s.
The VA’s 154 hospitals and 875 clinics, which serve 5.4 million patients, have been rated “best in class” by a number of independent groups since it implemented the changes in the 1990s.1 In a study conducted by the Rand Corporation, the VA scored higher compared with the U.S. private sector hospitals in every category except acute care, in which “the numbers ran neck and neck,” says Dr. Kizer. “Where the VA has done much better [than private sector hospitals] is in managing chronic disease and integrating prevention and health maintenance into the acute care program.”
Differences between a VA facility and one in the private sector are mostly “cosmetic and in the financing,” says Dr. Kizer. “The VA takes care of a particular patient population—veterans of military service—but it is a civilian practice that happens to be run by the federal government.”
According to a July 17, 2006, article in BusinessWeek, “The Best Medical Care in the U.S.,” the VA system provides about two-thirds of the care protocols recommended by organizations such as the Agency for Healthcare Research and Quality, compared with 50% provided in private sector hospitals.1 Also, as many as 8% of the prescriptions filled in private sector hospitals contain errors, but the VA’s prescription-related accuracy is greater than 99.997%. In addition, the VA spends an average of $5,000 per patient compared with the national average of $6,300.
Dr. Kizer’s focus on quality improvement at the VA should not be surprising in view of his long-time focus on improving the quality of healthcare. In his mind, an essential element in improving the quality of American healthcare is the widespread adoption of electronic health records (EHR).
When he arrived at his post at the VA in 1994, Dr. Kizer was pleasantly surprised to find advanced automated information management in place. The VA had been working on developing an EHR since 1978. As part Kizer’s transformation of the VA, all of the VA’s information systems were integrated, and VistA (an acronym for Veterans Health Information Systems and Technology Architecture) was launched in 1997. VistA is often the first thing that VA-affiliated hospitalists mention when they are asked what distinguishes VA hospitals from non-VA hospitals.
Key Features and Benefits of the VA
Sanjay Saint, MD, knows a great deal about academically affiliated VAs. He was a resident (July 1993-June 1995) and then chief medical resident at the San Francisco VA (June 1995-June 1996), an affiliate of the University of California at San Francisco. He was also a fellow at the University of Washington-affiliated Seattle VA (July 1996-June 1998), and for more than eight years he has been on the faculty at the University of Michigan as a professor of internal medicine (1998-2006). Dr. Saint is currently a hospitalist at the University of Michigan-affiliated Ann Arbor VA Hospital. He was also recently the acting chief of medicine there for six months (Dec. 2005-May 2006) while the permanent chief was on sabbatical.
The instant availability of the EHR system is a key benefit of practicing in a VA hospital, says Dr. Saint. “It involves not only being able to get up-to-date, relevant patient information at our VA but also the information obtained if the patient has been seen at other VAs.”
“One of the reasons why [the VA’s EHR] is so good is that it is fully integrated,” says Dr. Kizer. “Everything was made to fit together to begin with—in contrast to essentially all commercial products, which have been melded together from pieces that come from a variety of origins. Being fully integrated certainly increases the speed and efficiency of operations. The second reason why VistA is so good is that it was developed by clinicians for clinicians … .”
A key feature operating as part of the EHR is the focus on computer-based provider order entry (CPOE). CPOE can help physicians make correct clinical decisions, says Dr. Saint. He cites the example of a pilot test he and co-workers conducted at the Seattle VA: After 72 hours of urinary catheterization in a patient, an alert reminded physicians to remove the catheter. From that simple type of quality improvement experiment, the data revealed that those patients for whom the reminder had been used had a significantly reduced rate of infection compared with those for whom it had not.
One particularly good, but perhaps underutilized, aspect of the computerized system is the use of care protocols or models that can be used across the VA, says Peter Kaboli, MD, MS, hospitalist at the Iowa City VA Hospital, an affiliate of the University of Iowa. “And we could probably … have more available electronically [that] could be modified for the local care environment,” he says, adding that insulin protocols come to mind first.
Another key EHR feature is an extensive adverse event reporting system, including registering near misses. About 96% of prescriptions and physician orders are entered with the system; in private sector hospitals, the rough estimate is 8%. There is also a bar-coding system for verification of medications and identification of patients. The VA “has done a great job of changing the culture to foster systems-based care and to address errors and adverse patient outcomes straightforward[ly] and deal with them up front.”
Another distinguishing feature of the VA, says Dr. Saint, is its heavy investment in quality improvement and health services research (HSR). The VA has large repositories of administrative and clinical data for performing research with hospitalized patients. Dr. Saint also points out that a lot of the academic centers benefit from having a VA as an affiliate. “The house staff, medical students, and physicians often will be at the VA [and can] see the state-of-the-art electronic medical records and CPOE system and inquire, ‘Why can’t we have that at the university hospital?’ ”
Discharge: Seamless Transition
Dr. Kaboli can point to another advantage for hospital medicine in the VA: a concerted interest in developing hospitalists. Two-thirds of VA medical centers (VAMCs) use hospitalists, and two-thirds of inpatients are cared for by hospitalists. In total, approximately 400 hospitalists are employed by the VA, making it the largest single employer of hospitalists in the United States. Within two years, 75% of VAMCs will use hospitalists.2
Dr. Kaboli has also become well versed on the advantages of the VA’s EHR in the area of patient discharge. The greatest benefit to hospitalists of having a fully integrated medical record with CPOE and all inpatient and outpatient notes available in all the VA facilities across the country, he says, “is the almost seamless transition of these records both from the clinic side to the hospital and from the hospital back to the clinic.”
One “great luxury” of having that integrated system, Dr. Kaboli adds, is that a hospitalist can hand patients their discharge summaries and advise them to pass the information on in the next doctor’s visit. “Even though you’re going to send it via e-mail, [in a] fax, or by mail, you have that as another option to translate that information to other docs,” he explains. Hospitalists can also “alert other providers by making them co-signers to notes so that when it comes into their inbox, they know that a patient was discharged, and they get the discharge summary immediately.”
There is no connection electronically with non-VA providers, however, which is the same situation that exists in any other non-VA healthcare system. “We know [that] a fairly large percentage of veterans receive care, both within and outside the VA, who are what we call co-managed,” says Dr. Kaboli. “If a patient doesn’t live near a VA hospital or clinic, he may have to travel an hour or two, so that person might as well have a local doctor. Without that [EHR system], if [the patient is] speaking to a primary care physician in a local community, [that physician is] up against the same challenges as [someone who works] outside the VA.”
Get on the EHR Bandwagon
“The federal government has a crucial leadership role in promoting a national health information infrastructure,” said Dr. Kizer in his June 17, 2004 testimony to Congress. When asked about that statement, Dr. Saint (who is also director of the VA/University of Michigan Patient Safety Enhancement Program) has one piece of advice for his hospitalist colleagues. “You don’t want perfect to become the enemy of the very good,” he says. “Rather than waiting until there is a national technology information infrastructure, which may be years—if not decades—away, you can at least advocate for change in your own hospital.”
Use the VA as a model, he says. “You don’t have to use the exact same system, but at least you can point to some of the quality advantages that electronic medical records and CPOE can provide. You can also point out some of the advantages that investment in quality improvement and health services research can bring to an organization and say, ‘We can adapt—not necessarily adopt—what the VA has done.’ ”
How can hospitalists best do that? Many publications in the peer-reviewed literature address the quality improvement focus of the VA. There is also a VA Web site that discusses the focus on HSR and development (www1. va.gov/health). A VA-sponsored national health services research and development (HSR&D) meeting, at which investigators from all over the country present their latest findings, is held annually in Washington, D.C., usually in February.
For the young hospitalist who wants to pursue additional training, Dr. Saint says, there are VA-funded fellowships, HSR&D, a quality scholars program, and other career development opportunities within the VA that promote leadership roles both in and outside the VA.
Dr. Kaboli suggests identifying networks of hospitalists within and outside of your own healthcare system that you can work with and learn from. Hospitalists can also collaborate in developing protocols that incorporate local modifications. Also, he suggests, “there are a lot of questions that come up in the day-to-day care of patients. If you have colleagues as interested as you are, as hospitalists, in the quality of care for hospitalized medical patients, you can tap into that passion. The SHM listservs are a great way to connect; one for VA hospitalists has just been organized.
Anyone interested in the OpenVista Electronic Health Record, Medsphere’s commercial product (which, Dr. Kizer says, “is VistA at the core” and is being marketed to hospitals and large clinics) can learn more at www.medsphere.com.
Dr. Kizer says hospitalists will need to understand the needs of future healthcare and help prepare for and welcome it. “For example, performance measurement is an absolute part of the future of healthcare,” he says. “I think, by and large, hospitalists understand that better and are more accepting of that than certainly most docs in private practice.”
He believes hospitalists “can help promote that understanding among their peers and their hospitals and keep moving things forward as opposed to resisting it.” This is just one aspect of the “openness and transparency that we want to see in so many areas,” says Dr. Kizer, and hospitalists can be “pushing for the tools to make it happen. The hospitalists, I would think, should be leading the charge for electronic health records.”
Now and Tomorrow
Dr. Kizer, who is one of nine experts on veterans’ issues named to the newly formed Commission on the Future for America’s Veterans and is board certified in six medical specialties, also has a personal view on the work of hospital medicine. Recently, his wife was hospitalized in the ICU at the University of California at Davis Medical Center for a number of months, and Dr. Kizer says that a succession of hospitalists have served as her principal providers. It’s given him a more intimate view of what matters, beyond strictly clinical care, to patients and their families.
“By and large, I’ve always supported the hospitalist notion,” he says, “because it … supports my view [that] keeping up to date on all the science and technology and running an office practice [at the same time] is just more than you can reasonably expect anyone to do.” What he has especially noticed now, as a family caregiver visiting a hospital, “is that there is tremendous variability in how much [hospitalists] communicate with the patient and his or her family and how they view the episode of care within the context of the family and their community.”
Dr. Kizer, who has studied communications for a long time and in myriad ways, notes that a lot of the hospitalists he has met during this recent experience “think they’re communicating, but they often don’t take the time to determine if they are actually connecting with the family or addressing the issues that are important to the patient and family.”
In the same vein, he agrees that the better the electronic communication systems of a healthcare system—including proficiency in identifying medical errors—the more minutes can be freed up for a physician to pull up a chair and talk with a patient. “It is also a powerful tool to educate and to help inform,” he says. “For example, when [a hospitalist] can just quickly graph out where the patient’s blood pressure … or blood sugars or … creatinine has been, you can use the display of data to quickly educate the patient and/or the family about what has happened and where you need to go. One picture can save you 10 minutes of explaining.”
Conclusion
The VA has taken a lead in addressing the issues that have been brought up over the years by organizations such as the Institute of Medicine and the Institute for Healthcare Improvement. Their integrated electronic health records system can serve as a model for non-VA hospitals. Until there is a national integration of computerized technology, hospitalists can become advocates for improving their own hospital technology systems. “Electronic health records and hospitalists should go hand in glove,” concludes Dr. Kizer. “It’s potentially a great marriage of technology and the human element.” TH
Andrea Sattinger is a regular contributor to The Hospitalist.
References
- Arnst C. The best medical care in the U.S.: How Veterans Affairs transformed itself—and what it means for the rest of us. BusinessWeek online. July 17, 2006. Available at www.businessweek.com/magazine/content/06_29/b3993061.htm?chan=top+news_top+news. Last accessed October 20, 2006.
- Kaboli PJ, Barrett T, Vazirani S, et al. Growth of hospitalists in the Veterans Administration (VA) healthcare system: 1997-2005. Hosp Med. Abstract. 2006;1(S2):1-30.
- Lurie JD, Merrens EJ, Lee J, et al. An approach to hospital quality improvement. Med Clin North Am. 2002 Jul;86(4):825-845.
A Hospitalist Revolutionizes UCSD’s Online Clinical Systems

Josh Lee, MD, is a hospitalist. But Dr. Lee is also a computer geek, and the combination has served him and patient care well.
As medical director of Information Services at the University of California at San Diego (UCSD), Dr. Lee has oversight over all online clinical systems, and that is no small task. With Dr. Lee’s guidance, UCSD is now a leader in the medical informatics movement. With the exception of physician documentation, the system has comprehensive electronic records; that is, some physicians still prefer to “wet-sign” their notes. Lab results at UCSD are 100% electronic, as is order entry for adult inpatients. “We have now completed what we call the entire order life cycle: physician orders, direct integrations through our pharmacy, pharmacy validation, and bar-coded administration at bedside,” he says.
As opposed to the VA’s homegrown EHR, UCSD did what many healthcare systems do: They bought an off-the-shelf product—this one was Invision from Siemens—but UCSD calls their product PCIS, for Patient Care Information Services.
“A lot of people are able to do cool stuff [with medical informatics],” says Dr. Lee, “but they have done it with a proprietary product, so it’s different than VA, where they are using something they have total control over.”
He says many people are now focused on order entry, “but I think the newest area of research and integration [involves the question], how do we communicate key clinical issues and follow-up for discharge?” (See Figure 1, above.) At UCSD Medical Center, these screens can be printed and the pages given directly to the patient upon discharge.) “We have leveraged our electronic system to ensure that, at the moment of discharge, not only is the patient informed about [his or her] care, but it is clear to anybody on our side, or from the side of the receiving physician, what is supposed to happen next.”
As any hospitalist knows, there can be a huge “voltage drop” in this area, as Robert Wachter, MD, professor and associate chairman at UCSF’s Department of Medicine, San Francisco, refers to it. Dr. Wachter is
And the great advantages of the VA’s electronic products are not available to the “99% of American hospitalists who don’t practice in closed systems,” says Dr. Lee.
Because most hospitalists don’t have that advantage, careful and complete discharge communications are imperative. That’s why UCSD built screens that can accommodate the specific information patients need, he says. “It’s different from the classic discharge summary, which is usually a lengthy, unwieldy, dictated document that is mostly [composed] after the patient leaves the hospital. This is done in real time … and these print-outs are immediately available for the patient.”
Before Dr. Lee came to UCSD, he worked with Drs. Jon Lurie, Mark Splaine, and Ed Merrens, all members of the general internal medicine division at Dartmouth-Hitchcock Medical Center in Hanover, N.H.3 As part of the team’s exploration of quality improvement and medical informatics, they particularly looked at how to adapt products to be workflow sensitive.
And one of the most important things Dr. Lee says he would tell his counterparts at other institutions is “to ensure that computerized solutions for safety and documentation are appropriately matched to the work flow.” He thinks that when these initiatives fail it is often due to an underappreciation of the impact that these changes and enhancements have on actual provision of care. “Do those things that are [the] most highly successful, leverage moments that you’re going to do anyway, but then automate it, make it safer, make it more comprehensive,” he says. “That’s my challenge to my colleagues.”—AS
Modern medicine … certainly as it should be practiced by hospitalists, is the most information-intensive activity that human beings ever engaged in,” says Kenneth W. Kizer, MD, MPH, CEO and chairman of the board of Medsphere Systems Corporation in Aliso Viejo, Calif.
He should know. From his first healthcare-related position in 1969 as a hospital orderly at Stanford University Hospital, he rose to become the Under Secretary for Health in the Department of Veterans Affairs (VA)—the CEO of the largest healthcare system in the nation. He is widely credited as being the chief architect and driving force behind the successful transformation of VA healthcare in the 1990s.
The VA’s 154 hospitals and 875 clinics, which serve 5.4 million patients, have been rated “best in class” by a number of independent groups since it implemented the changes in the 1990s.1 In a study conducted by the Rand Corporation, the VA scored higher compared with the U.S. private sector hospitals in every category except acute care, in which “the numbers ran neck and neck,” says Dr. Kizer. “Where the VA has done much better [than private sector hospitals] is in managing chronic disease and integrating prevention and health maintenance into the acute care program.”
Differences between a VA facility and one in the private sector are mostly “cosmetic and in the financing,” says Dr. Kizer. “The VA takes care of a particular patient population—veterans of military service—but it is a civilian practice that happens to be run by the federal government.”
According to a July 17, 2006, article in BusinessWeek, “The Best Medical Care in the U.S.,” the VA system provides about two-thirds of the care protocols recommended by organizations such as the Agency for Healthcare Research and Quality, compared with 50% provided in private sector hospitals.1 Also, as many as 8% of the prescriptions filled in private sector hospitals contain errors, but the VA’s prescription-related accuracy is greater than 99.997%. In addition, the VA spends an average of $5,000 per patient compared with the national average of $6,300.
Dr. Kizer’s focus on quality improvement at the VA should not be surprising in view of his long-time focus on improving the quality of healthcare. In his mind, an essential element in improving the quality of American healthcare is the widespread adoption of electronic health records (EHR).
When he arrived at his post at the VA in 1994, Dr. Kizer was pleasantly surprised to find advanced automated information management in place. The VA had been working on developing an EHR since 1978. As part Kizer’s transformation of the VA, all of the VA’s information systems were integrated, and VistA (an acronym for Veterans Health Information Systems and Technology Architecture) was launched in 1997. VistA is often the first thing that VA-affiliated hospitalists mention when they are asked what distinguishes VA hospitals from non-VA hospitals.
Key Features and Benefits of the VA
Sanjay Saint, MD, knows a great deal about academically affiliated VAs. He was a resident (July 1993-June 1995) and then chief medical resident at the San Francisco VA (June 1995-June 1996), an affiliate of the University of California at San Francisco. He was also a fellow at the University of Washington-affiliated Seattle VA (July 1996-June 1998), and for more than eight years he has been on the faculty at the University of Michigan as a professor of internal medicine (1998-2006). Dr. Saint is currently a hospitalist at the University of Michigan-affiliated Ann Arbor VA Hospital. He was also recently the acting chief of medicine there for six months (Dec. 2005-May 2006) while the permanent chief was on sabbatical.
The instant availability of the EHR system is a key benefit of practicing in a VA hospital, says Dr. Saint. “It involves not only being able to get up-to-date, relevant patient information at our VA but also the information obtained if the patient has been seen at other VAs.”
“One of the reasons why [the VA’s EHR] is so good is that it is fully integrated,” says Dr. Kizer. “Everything was made to fit together to begin with—in contrast to essentially all commercial products, which have been melded together from pieces that come from a variety of origins. Being fully integrated certainly increases the speed and efficiency of operations. The second reason why VistA is so good is that it was developed by clinicians for clinicians … .”
A key feature operating as part of the EHR is the focus on computer-based provider order entry (CPOE). CPOE can help physicians make correct clinical decisions, says Dr. Saint. He cites the example of a pilot test he and co-workers conducted at the Seattle VA: After 72 hours of urinary catheterization in a patient, an alert reminded physicians to remove the catheter. From that simple type of quality improvement experiment, the data revealed that those patients for whom the reminder had been used had a significantly reduced rate of infection compared with those for whom it had not.
One particularly good, but perhaps underutilized, aspect of the computerized system is the use of care protocols or models that can be used across the VA, says Peter Kaboli, MD, MS, hospitalist at the Iowa City VA Hospital, an affiliate of the University of Iowa. “And we could probably … have more available electronically [that] could be modified for the local care environment,” he says, adding that insulin protocols come to mind first.
Another key EHR feature is an extensive adverse event reporting system, including registering near misses. About 96% of prescriptions and physician orders are entered with the system; in private sector hospitals, the rough estimate is 8%. There is also a bar-coding system for verification of medications and identification of patients. The VA “has done a great job of changing the culture to foster systems-based care and to address errors and adverse patient outcomes straightforward[ly] and deal with them up front.”
Another distinguishing feature of the VA, says Dr. Saint, is its heavy investment in quality improvement and health services research (HSR). The VA has large repositories of administrative and clinical data for performing research with hospitalized patients. Dr. Saint also points out that a lot of the academic centers benefit from having a VA as an affiliate. “The house staff, medical students, and physicians often will be at the VA [and can] see the state-of-the-art electronic medical records and CPOE system and inquire, ‘Why can’t we have that at the university hospital?’ ”
Discharge: Seamless Transition
Dr. Kaboli can point to another advantage for hospital medicine in the VA: a concerted interest in developing hospitalists. Two-thirds of VA medical centers (VAMCs) use hospitalists, and two-thirds of inpatients are cared for by hospitalists. In total, approximately 400 hospitalists are employed by the VA, making it the largest single employer of hospitalists in the United States. Within two years, 75% of VAMCs will use hospitalists.2
Dr. Kaboli has also become well versed on the advantages of the VA’s EHR in the area of patient discharge. The greatest benefit to hospitalists of having a fully integrated medical record with CPOE and all inpatient and outpatient notes available in all the VA facilities across the country, he says, “is the almost seamless transition of these records both from the clinic side to the hospital and from the hospital back to the clinic.”
One “great luxury” of having that integrated system, Dr. Kaboli adds, is that a hospitalist can hand patients their discharge summaries and advise them to pass the information on in the next doctor’s visit. “Even though you’re going to send it via e-mail, [in a] fax, or by mail, you have that as another option to translate that information to other docs,” he explains. Hospitalists can also “alert other providers by making them co-signers to notes so that when it comes into their inbox, they know that a patient was discharged, and they get the discharge summary immediately.”
There is no connection electronically with non-VA providers, however, which is the same situation that exists in any other non-VA healthcare system. “We know [that] a fairly large percentage of veterans receive care, both within and outside the VA, who are what we call co-managed,” says Dr. Kaboli. “If a patient doesn’t live near a VA hospital or clinic, he may have to travel an hour or two, so that person might as well have a local doctor. Without that [EHR system], if [the patient is] speaking to a primary care physician in a local community, [that physician is] up against the same challenges as [someone who works] outside the VA.”
Get on the EHR Bandwagon
“The federal government has a crucial leadership role in promoting a national health information infrastructure,” said Dr. Kizer in his June 17, 2004 testimony to Congress. When asked about that statement, Dr. Saint (who is also director of the VA/University of Michigan Patient Safety Enhancement Program) has one piece of advice for his hospitalist colleagues. “You don’t want perfect to become the enemy of the very good,” he says. “Rather than waiting until there is a national technology information infrastructure, which may be years—if not decades—away, you can at least advocate for change in your own hospital.”
Use the VA as a model, he says. “You don’t have to use the exact same system, but at least you can point to some of the quality advantages that electronic medical records and CPOE can provide. You can also point out some of the advantages that investment in quality improvement and health services research can bring to an organization and say, ‘We can adapt—not necessarily adopt—what the VA has done.’ ”
How can hospitalists best do that? Many publications in the peer-reviewed literature address the quality improvement focus of the VA. There is also a VA Web site that discusses the focus on HSR and development (www1. va.gov/health). A VA-sponsored national health services research and development (HSR&D) meeting, at which investigators from all over the country present their latest findings, is held annually in Washington, D.C., usually in February.
For the young hospitalist who wants to pursue additional training, Dr. Saint says, there are VA-funded fellowships, HSR&D, a quality scholars program, and other career development opportunities within the VA that promote leadership roles both in and outside the VA.
Dr. Kaboli suggests identifying networks of hospitalists within and outside of your own healthcare system that you can work with and learn from. Hospitalists can also collaborate in developing protocols that incorporate local modifications. Also, he suggests, “there are a lot of questions that come up in the day-to-day care of patients. If you have colleagues as interested as you are, as hospitalists, in the quality of care for hospitalized medical patients, you can tap into that passion. The SHM listservs are a great way to connect; one for VA hospitalists has just been organized.
Anyone interested in the OpenVista Electronic Health Record, Medsphere’s commercial product (which, Dr. Kizer says, “is VistA at the core” and is being marketed to hospitals and large clinics) can learn more at www.medsphere.com.
Dr. Kizer says hospitalists will need to understand the needs of future healthcare and help prepare for and welcome it. “For example, performance measurement is an absolute part of the future of healthcare,” he says. “I think, by and large, hospitalists understand that better and are more accepting of that than certainly most docs in private practice.”
He believes hospitalists “can help promote that understanding among their peers and their hospitals and keep moving things forward as opposed to resisting it.” This is just one aspect of the “openness and transparency that we want to see in so many areas,” says Dr. Kizer, and hospitalists can be “pushing for the tools to make it happen. The hospitalists, I would think, should be leading the charge for electronic health records.”
Now and Tomorrow
Dr. Kizer, who is one of nine experts on veterans’ issues named to the newly formed Commission on the Future for America’s Veterans and is board certified in six medical specialties, also has a personal view on the work of hospital medicine. Recently, his wife was hospitalized in the ICU at the University of California at Davis Medical Center for a number of months, and Dr. Kizer says that a succession of hospitalists have served as her principal providers. It’s given him a more intimate view of what matters, beyond strictly clinical care, to patients and their families.
“By and large, I’ve always supported the hospitalist notion,” he says, “because it … supports my view [that] keeping up to date on all the science and technology and running an office practice [at the same time] is just more than you can reasonably expect anyone to do.” What he has especially noticed now, as a family caregiver visiting a hospital, “is that there is tremendous variability in how much [hospitalists] communicate with the patient and his or her family and how they view the episode of care within the context of the family and their community.”
Dr. Kizer, who has studied communications for a long time and in myriad ways, notes that a lot of the hospitalists he has met during this recent experience “think they’re communicating, but they often don’t take the time to determine if they are actually connecting with the family or addressing the issues that are important to the patient and family.”
In the same vein, he agrees that the better the electronic communication systems of a healthcare system—including proficiency in identifying medical errors—the more minutes can be freed up for a physician to pull up a chair and talk with a patient. “It is also a powerful tool to educate and to help inform,” he says. “For example, when [a hospitalist] can just quickly graph out where the patient’s blood pressure … or blood sugars or … creatinine has been, you can use the display of data to quickly educate the patient and/or the family about what has happened and where you need to go. One picture can save you 10 minutes of explaining.”
Conclusion
The VA has taken a lead in addressing the issues that have been brought up over the years by organizations such as the Institute of Medicine and the Institute for Healthcare Improvement. Their integrated electronic health records system can serve as a model for non-VA hospitals. Until there is a national integration of computerized technology, hospitalists can become advocates for improving their own hospital technology systems. “Electronic health records and hospitalists should go hand in glove,” concludes Dr. Kizer. “It’s potentially a great marriage of technology and the human element.” TH
Andrea Sattinger is a regular contributor to The Hospitalist.
References
- Arnst C. The best medical care in the U.S.: How Veterans Affairs transformed itself—and what it means for the rest of us. BusinessWeek online. July 17, 2006. Available at www.businessweek.com/magazine/content/06_29/b3993061.htm?chan=top+news_top+news. Last accessed October 20, 2006.
- Kaboli PJ, Barrett T, Vazirani S, et al. Growth of hospitalists in the Veterans Administration (VA) healthcare system: 1997-2005. Hosp Med. Abstract. 2006;1(S2):1-30.
- Lurie JD, Merrens EJ, Lee J, et al. An approach to hospital quality improvement. Med Clin North Am. 2002 Jul;86(4):825-845.
A Hospitalist Revolutionizes UCSD’s Online Clinical Systems
Josh Lee, MD, is a hospitalist. But Dr. Lee is also a computer geek, and the combination has served him and patient care well.
As medical director of Information Services at the University of California at San Diego (UCSD), Dr. Lee has oversight over all online clinical systems, and that is no small task. With Dr. Lee’s guidance, UCSD is now a leader in the medical informatics movement. With the exception of physician documentation, the system has comprehensive electronic records; that is, some physicians still prefer to “wet-sign” their notes. Lab results at UCSD are 100% electronic, as is order entry for adult inpatients. “We have now completed what we call the entire order life cycle: physician orders, direct integrations through our pharmacy, pharmacy validation, and bar-coded administration at bedside,” he says.
As opposed to the VA’s homegrown EHR, UCSD did what many healthcare systems do: They bought an off-the-shelf product—this one was Invision from Siemens—but UCSD calls their product PCIS, for Patient Care Information Services.
“A lot of people are able to do cool stuff [with medical informatics],” says Dr. Lee, “but they have done it with a proprietary product, so it’s different than VA, where they are using something they have total control over.”
He says many people are now focused on order entry, “but I think the newest area of research and integration [involves the question], how do we communicate key clinical issues and follow-up for discharge?” (See Figure 1, above.) At UCSD Medical Center, these screens can be printed and the pages given directly to the patient upon discharge.) “We have leveraged our electronic system to ensure that, at the moment of discharge, not only is the patient informed about [his or her] care, but it is clear to anybody on our side, or from the side of the receiving physician, what is supposed to happen next.”
As any hospitalist knows, there can be a huge “voltage drop” in this area, as Robert Wachter, MD, professor and associate chairman at UCSF’s Department of Medicine, San Francisco, refers to it. Dr. Wachter is
And the great advantages of the VA’s electronic products are not available to the “99% of American hospitalists who don’t practice in closed systems,” says Dr. Lee.
Because most hospitalists don’t have that advantage, careful and complete discharge communications are imperative. That’s why UCSD built screens that can accommodate the specific information patients need, he says. “It’s different from the classic discharge summary, which is usually a lengthy, unwieldy, dictated document that is mostly [composed] after the patient leaves the hospital. This is done in real time … and these print-outs are immediately available for the patient.”
Before Dr. Lee came to UCSD, he worked with Drs. Jon Lurie, Mark Splaine, and Ed Merrens, all members of the general internal medicine division at Dartmouth-Hitchcock Medical Center in Hanover, N.H.3 As part of the team’s exploration of quality improvement and medical informatics, they particularly looked at how to adapt products to be workflow sensitive.
And one of the most important things Dr. Lee says he would tell his counterparts at other institutions is “to ensure that computerized solutions for safety and documentation are appropriately matched to the work flow.” He thinks that when these initiatives fail it is often due to an underappreciation of the impact that these changes and enhancements have on actual provision of care. “Do those things that are [the] most highly successful, leverage moments that you’re going to do anyway, but then automate it, make it safer, make it more comprehensive,” he says. “That’s my challenge to my colleagues.”—AS
Modern medicine … certainly as it should be practiced by hospitalists, is the most information-intensive activity that human beings ever engaged in,” says Kenneth W. Kizer, MD, MPH, CEO and chairman of the board of Medsphere Systems Corporation in Aliso Viejo, Calif.
He should know. From his first healthcare-related position in 1969 as a hospital orderly at Stanford University Hospital, he rose to become the Under Secretary for Health in the Department of Veterans Affairs (VA)—the CEO of the largest healthcare system in the nation. He is widely credited as being the chief architect and driving force behind the successful transformation of VA healthcare in the 1990s.
The VA’s 154 hospitals and 875 clinics, which serve 5.4 million patients, have been rated “best in class” by a number of independent groups since it implemented the changes in the 1990s.1 In a study conducted by the Rand Corporation, the VA scored higher compared with the U.S. private sector hospitals in every category except acute care, in which “the numbers ran neck and neck,” says Dr. Kizer. “Where the VA has done much better [than private sector hospitals] is in managing chronic disease and integrating prevention and health maintenance into the acute care program.”
Differences between a VA facility and one in the private sector are mostly “cosmetic and in the financing,” says Dr. Kizer. “The VA takes care of a particular patient population—veterans of military service—but it is a civilian practice that happens to be run by the federal government.”
According to a July 17, 2006, article in BusinessWeek, “The Best Medical Care in the U.S.,” the VA system provides about two-thirds of the care protocols recommended by organizations such as the Agency for Healthcare Research and Quality, compared with 50% provided in private sector hospitals.1 Also, as many as 8% of the prescriptions filled in private sector hospitals contain errors, but the VA’s prescription-related accuracy is greater than 99.997%. In addition, the VA spends an average of $5,000 per patient compared with the national average of $6,300.
Dr. Kizer’s focus on quality improvement at the VA should not be surprising in view of his long-time focus on improving the quality of healthcare. In his mind, an essential element in improving the quality of American healthcare is the widespread adoption of electronic health records (EHR).
When he arrived at his post at the VA in 1994, Dr. Kizer was pleasantly surprised to find advanced automated information management in place. The VA had been working on developing an EHR since 1978. As part Kizer’s transformation of the VA, all of the VA’s information systems were integrated, and VistA (an acronym for Veterans Health Information Systems and Technology Architecture) was launched in 1997. VistA is often the first thing that VA-affiliated hospitalists mention when they are asked what distinguishes VA hospitals from non-VA hospitals.
Key Features and Benefits of the VA
Sanjay Saint, MD, knows a great deal about academically affiliated VAs. He was a resident (July 1993-June 1995) and then chief medical resident at the San Francisco VA (June 1995-June 1996), an affiliate of the University of California at San Francisco. He was also a fellow at the University of Washington-affiliated Seattle VA (July 1996-June 1998), and for more than eight years he has been on the faculty at the University of Michigan as a professor of internal medicine (1998-2006). Dr. Saint is currently a hospitalist at the University of Michigan-affiliated Ann Arbor VA Hospital. He was also recently the acting chief of medicine there for six months (Dec. 2005-May 2006) while the permanent chief was on sabbatical.
The instant availability of the EHR system is a key benefit of practicing in a VA hospital, says Dr. Saint. “It involves not only being able to get up-to-date, relevant patient information at our VA but also the information obtained if the patient has been seen at other VAs.”
“One of the reasons why [the VA’s EHR] is so good is that it is fully integrated,” says Dr. Kizer. “Everything was made to fit together to begin with—in contrast to essentially all commercial products, which have been melded together from pieces that come from a variety of origins. Being fully integrated certainly increases the speed and efficiency of operations. The second reason why VistA is so good is that it was developed by clinicians for clinicians … .”
A key feature operating as part of the EHR is the focus on computer-based provider order entry (CPOE). CPOE can help physicians make correct clinical decisions, says Dr. Saint. He cites the example of a pilot test he and co-workers conducted at the Seattle VA: After 72 hours of urinary catheterization in a patient, an alert reminded physicians to remove the catheter. From that simple type of quality improvement experiment, the data revealed that those patients for whom the reminder had been used had a significantly reduced rate of infection compared with those for whom it had not.
One particularly good, but perhaps underutilized, aspect of the computerized system is the use of care protocols or models that can be used across the VA, says Peter Kaboli, MD, MS, hospitalist at the Iowa City VA Hospital, an affiliate of the University of Iowa. “And we could probably … have more available electronically [that] could be modified for the local care environment,” he says, adding that insulin protocols come to mind first.
Another key EHR feature is an extensive adverse event reporting system, including registering near misses. About 96% of prescriptions and physician orders are entered with the system; in private sector hospitals, the rough estimate is 8%. There is also a bar-coding system for verification of medications and identification of patients. The VA “has done a great job of changing the culture to foster systems-based care and to address errors and adverse patient outcomes straightforward[ly] and deal with them up front.”
Another distinguishing feature of the VA, says Dr. Saint, is its heavy investment in quality improvement and health services research (HSR). The VA has large repositories of administrative and clinical data for performing research with hospitalized patients. Dr. Saint also points out that a lot of the academic centers benefit from having a VA as an affiliate. “The house staff, medical students, and physicians often will be at the VA [and can] see the state-of-the-art electronic medical records and CPOE system and inquire, ‘Why can’t we have that at the university hospital?’ ”
Discharge: Seamless Transition
Dr. Kaboli can point to another advantage for hospital medicine in the VA: a concerted interest in developing hospitalists. Two-thirds of VA medical centers (VAMCs) use hospitalists, and two-thirds of inpatients are cared for by hospitalists. In total, approximately 400 hospitalists are employed by the VA, making it the largest single employer of hospitalists in the United States. Within two years, 75% of VAMCs will use hospitalists.2
Dr. Kaboli has also become well versed on the advantages of the VA’s EHR in the area of patient discharge. The greatest benefit to hospitalists of having a fully integrated medical record with CPOE and all inpatient and outpatient notes available in all the VA facilities across the country, he says, “is the almost seamless transition of these records both from the clinic side to the hospital and from the hospital back to the clinic.”
One “great luxury” of having that integrated system, Dr. Kaboli adds, is that a hospitalist can hand patients their discharge summaries and advise them to pass the information on in the next doctor’s visit. “Even though you’re going to send it via e-mail, [in a] fax, or by mail, you have that as another option to translate that information to other docs,” he explains. Hospitalists can also “alert other providers by making them co-signers to notes so that when it comes into their inbox, they know that a patient was discharged, and they get the discharge summary immediately.”
There is no connection electronically with non-VA providers, however, which is the same situation that exists in any other non-VA healthcare system. “We know [that] a fairly large percentage of veterans receive care, both within and outside the VA, who are what we call co-managed,” says Dr. Kaboli. “If a patient doesn’t live near a VA hospital or clinic, he may have to travel an hour or two, so that person might as well have a local doctor. Without that [EHR system], if [the patient is] speaking to a primary care physician in a local community, [that physician is] up against the same challenges as [someone who works] outside the VA.”
Get on the EHR Bandwagon
“The federal government has a crucial leadership role in promoting a national health information infrastructure,” said Dr. Kizer in his June 17, 2004 testimony to Congress. When asked about that statement, Dr. Saint (who is also director of the VA/University of Michigan Patient Safety Enhancement Program) has one piece of advice for his hospitalist colleagues. “You don’t want perfect to become the enemy of the very good,” he says. “Rather than waiting until there is a national technology information infrastructure, which may be years—if not decades—away, you can at least advocate for change in your own hospital.”
Use the VA as a model, he says. “You don’t have to use the exact same system, but at least you can point to some of the quality advantages that electronic medical records and CPOE can provide. You can also point out some of the advantages that investment in quality improvement and health services research can bring to an organization and say, ‘We can adapt—not necessarily adopt—what the VA has done.’ ”
How can hospitalists best do that? Many publications in the peer-reviewed literature address the quality improvement focus of the VA. There is also a VA Web site that discusses the focus on HSR and development (www1. va.gov/health). A VA-sponsored national health services research and development (HSR&D) meeting, at which investigators from all over the country present their latest findings, is held annually in Washington, D.C., usually in February.
For the young hospitalist who wants to pursue additional training, Dr. Saint says, there are VA-funded fellowships, HSR&D, a quality scholars program, and other career development opportunities within the VA that promote leadership roles both in and outside the VA.
Dr. Kaboli suggests identifying networks of hospitalists within and outside of your own healthcare system that you can work with and learn from. Hospitalists can also collaborate in developing protocols that incorporate local modifications. Also, he suggests, “there are a lot of questions that come up in the day-to-day care of patients. If you have colleagues as interested as you are, as hospitalists, in the quality of care for hospitalized medical patients, you can tap into that passion. The SHM listservs are a great way to connect; one for VA hospitalists has just been organized.
Anyone interested in the OpenVista Electronic Health Record, Medsphere’s commercial product (which, Dr. Kizer says, “is VistA at the core” and is being marketed to hospitals and large clinics) can learn more at www.medsphere.com.
Dr. Kizer says hospitalists will need to understand the needs of future healthcare and help prepare for and welcome it. “For example, performance measurement is an absolute part of the future of healthcare,” he says. “I think, by and large, hospitalists understand that better and are more accepting of that than certainly most docs in private practice.”
He believes hospitalists “can help promote that understanding among their peers and their hospitals and keep moving things forward as opposed to resisting it.” This is just one aspect of the “openness and transparency that we want to see in so many areas,” says Dr. Kizer, and hospitalists can be “pushing for the tools to make it happen. The hospitalists, I would think, should be leading the charge for electronic health records.”
Now and Tomorrow
Dr. Kizer, who is one of nine experts on veterans’ issues named to the newly formed Commission on the Future for America’s Veterans and is board certified in six medical specialties, also has a personal view on the work of hospital medicine. Recently, his wife was hospitalized in the ICU at the University of California at Davis Medical Center for a number of months, and Dr. Kizer says that a succession of hospitalists have served as her principal providers. It’s given him a more intimate view of what matters, beyond strictly clinical care, to patients and their families.
“By and large, I’ve always supported the hospitalist notion,” he says, “because it … supports my view [that] keeping up to date on all the science and technology and running an office practice [at the same time] is just more than you can reasonably expect anyone to do.” What he has especially noticed now, as a family caregiver visiting a hospital, “is that there is tremendous variability in how much [hospitalists] communicate with the patient and his or her family and how they view the episode of care within the context of the family and their community.”
Dr. Kizer, who has studied communications for a long time and in myriad ways, notes that a lot of the hospitalists he has met during this recent experience “think they’re communicating, but they often don’t take the time to determine if they are actually connecting with the family or addressing the issues that are important to the patient and family.”
In the same vein, he agrees that the better the electronic communication systems of a healthcare system—including proficiency in identifying medical errors—the more minutes can be freed up for a physician to pull up a chair and talk with a patient. “It is also a powerful tool to educate and to help inform,” he says. “For example, when [a hospitalist] can just quickly graph out where the patient’s blood pressure … or blood sugars or … creatinine has been, you can use the display of data to quickly educate the patient and/or the family about what has happened and where you need to go. One picture can save you 10 minutes of explaining.”
Conclusion
The VA has taken a lead in addressing the issues that have been brought up over the years by organizations such as the Institute of Medicine and the Institute for Healthcare Improvement. Their integrated electronic health records system can serve as a model for non-VA hospitals. Until there is a national integration of computerized technology, hospitalists can become advocates for improving their own hospital technology systems. “Electronic health records and hospitalists should go hand in glove,” concludes Dr. Kizer. “It’s potentially a great marriage of technology and the human element.” TH
Andrea Sattinger is a regular contributor to The Hospitalist.
References
- Arnst C. The best medical care in the U.S.: How Veterans Affairs transformed itself—and what it means for the rest of us. BusinessWeek online. July 17, 2006. Available at www.businessweek.com/magazine/content/06_29/b3993061.htm?chan=top+news_top+news. Last accessed October 20, 2006.
- Kaboli PJ, Barrett T, Vazirani S, et al. Growth of hospitalists in the Veterans Administration (VA) healthcare system: 1997-2005. Hosp Med. Abstract. 2006;1(S2):1-30.
- Lurie JD, Merrens EJ, Lee J, et al. An approach to hospital quality improvement. Med Clin North Am. 2002 Jul;86(4):825-845.
A Hospitalist Revolutionizes UCSD’s Online Clinical Systems
Josh Lee, MD, is a hospitalist. But Dr. Lee is also a computer geek, and the combination has served him and patient care well.
As medical director of Information Services at the University of California at San Diego (UCSD), Dr. Lee has oversight over all online clinical systems, and that is no small task. With Dr. Lee’s guidance, UCSD is now a leader in the medical informatics movement. With the exception of physician documentation, the system has comprehensive electronic records; that is, some physicians still prefer to “wet-sign” their notes. Lab results at UCSD are 100% electronic, as is order entry for adult inpatients. “We have now completed what we call the entire order life cycle: physician orders, direct integrations through our pharmacy, pharmacy validation, and bar-coded administration at bedside,” he says.
As opposed to the VA’s homegrown EHR, UCSD did what many healthcare systems do: They bought an off-the-shelf product—this one was Invision from Siemens—but UCSD calls their product PCIS, for Patient Care Information Services.
“A lot of people are able to do cool stuff [with medical informatics],” says Dr. Lee, “but they have done it with a proprietary product, so it’s different than VA, where they are using something they have total control over.”
He says many people are now focused on order entry, “but I think the newest area of research and integration [involves the question], how do we communicate key clinical issues and follow-up for discharge?” (See Figure 1, above.) At UCSD Medical Center, these screens can be printed and the pages given directly to the patient upon discharge.) “We have leveraged our electronic system to ensure that, at the moment of discharge, not only is the patient informed about [his or her] care, but it is clear to anybody on our side, or from the side of the receiving physician, what is supposed to happen next.”
As any hospitalist knows, there can be a huge “voltage drop” in this area, as Robert Wachter, MD, professor and associate chairman at UCSF’s Department of Medicine, San Francisco, refers to it. Dr. Wachter is
And the great advantages of the VA’s electronic products are not available to the “99% of American hospitalists who don’t practice in closed systems,” says Dr. Lee.
Because most hospitalists don’t have that advantage, careful and complete discharge communications are imperative. That’s why UCSD built screens that can accommodate the specific information patients need, he says. “It’s different from the classic discharge summary, which is usually a lengthy, unwieldy, dictated document that is mostly [composed] after the patient leaves the hospital. This is done in real time … and these print-outs are immediately available for the patient.”
Before Dr. Lee came to UCSD, he worked with Drs. Jon Lurie, Mark Splaine, and Ed Merrens, all members of the general internal medicine division at Dartmouth-Hitchcock Medical Center in Hanover, N.H.3 As part of the team’s exploration of quality improvement and medical informatics, they particularly looked at how to adapt products to be workflow sensitive.
And one of the most important things Dr. Lee says he would tell his counterparts at other institutions is “to ensure that computerized solutions for safety and documentation are appropriately matched to the work flow.” He thinks that when these initiatives fail it is often due to an underappreciation of the impact that these changes and enhancements have on actual provision of care. “Do those things that are [the] most highly successful, leverage moments that you’re going to do anyway, but then automate it, make it safer, make it more comprehensive,” he says. “That’s my challenge to my colleagues.”—AS