User login
Newman's Handy Dandy Admit Note

(Circle the appropriate answers.)
HISTORY OF PRESENT ILLNESS
This (0-109)-year-old (Asian, Black, Caucasian, Aleutian, Venusian) (male, female, other) presents with a (1, 7, 100)-(second, minute, day, year, century) history of (pain, swelling, itching, enlargement) of the (arm, chest, scrotum, uvula, pineal gland). (She/He/It) rates it as (11, 12, 20) out of 10. It is aggravated by (breathing, thinking, hang gliding, vigorous dancing, ennui) and alleviated by (acetaminophen, chocolate, high-dose morphine).
PAST MEDICAL HISTORY
Diabetes, hypertension, pineal insufficiency, Kluver-Bucy syndrome, rectal prolapse, Chagas disease, visceral larval migrans, ichthyosis, all of the above
PAST SURGICAL HISTORY
- Transplant of the (heart, kidney, pancreas, amygdala, pineal gland)
- ORIF of (humerus, femur, rear axle)
- Hemorrhoidectomy, cholecystectomy, pancreatectomy, cerumen removal, all of the above
ALLERGIES
(Penicillin, sulfa, every known drug in existence except Demerol)
CURRENT MEDICATION
- Insulin, metformin, Gila monster venom
- Alpha blocker, calcium blocker, beta blocker, blocker blocker
- Amoxicillin, “gorillacillin,” maggot extract, “mickeymycin”
- SSRI, MAOI, TRIAD, ECT, DOA
- (Thyroid, adrenal, pineal) gland extract
FAMILY HISTORY
Adopted, old age, some kind of cancer
SOCIAL HISTORY
- Alcohol: (teetotaler, tippler, boozer, lush, no alcohol—only beer)—multiply by 10
- Smoking: (never; three packs a day; not tobacco; old stogies I have found, short but not too big around)
- Drugs: (Is this confidential?, Freon, whatever I can get my hands on)
- Employment: (meter maid, sewer maintenance worker, JCAHO auditor, forensic proctologist, hospitologist)
REVIEW OF SYMPTOMS
- (Chest pain, more chest pain, even more chest pain), (rectal, urinary, salivary) incontinence, (ears itch with urination, nose runs with defecation, small bugs crawling out of my skin), (short of breath, short of patience)
- Stool is (sticky, floating, malodorous, frequent, shaped like the Statue of Liberty)
- Double vision, tunnel vision, television, hyperacusis, hearing loss, could you repeat that?, halitosis, dysgeusia, dysphonia, “datphonia”
- Abdominal (pain, cramping, crunches)
PHYSICAL EXAM
- BP (0, 90, 140, 230, 290)/(0, 3, 90, 160)
- Pulse (absent, irregularly irregularly irregular, tachycardic, tacky dresser) rate (0, 3, 84, 112, 190, 280)
- Temperature (32.2, 36.8, 25 minutes at 450—baste often)
- Normocephalic/atraumatic, bullet-headed, pointy-headed, hatchet in skull
- Eyes (PERRLA, anisocoria, bloodshot, pinpoint dude)
- Fundus exam (never can see them, cotton wool spots, cotton candy)
- Ears (present, “hyperceruminic,” absent)
- Mouth (macroglossia, foot in mouth, black hairy tongue, halitotic, skin of the teeth, wooden teeth)
- Neck (supple without adenopathy, thick, multiple hickies, red)
- Lungs (clear to auscultation and percussion—OK, I never really percussed; Velcro rales; egophonic; wheezy)
- Heart (systolic, 5/6, even a medical student can hear) murmur (no, pericardial, aye there’s the) rub
- Abdomen (scaphoid, pendulous, six-pack); bowel sounds (absent—was that you?)
- Umbilicus (surgically absent, Sister Mary Joseph nodule, high lint content)
- Extremities (extreme, all six present, night-clubbing)
NEURO EXAM
- Reflexes (cremaster positive, anal wink intact)
- Mentation (alert and oriented x3, catatonic, dogatonic)
- Psychiatric (appropriate, psychotic, truly weird, bipolar, tripolar)
- Skin (present, hideous thing growing on the patient’s face)
LABORATORY FINDINGS
Results of (CBC, ionized calcium, “citrulated ceruloplasmin,” complement levels, insult levels, saliva electrophoresis, urinary zinc level, melatonin level, and protein Q) all markedly abnormal.
IMAGING
(CAT scan, PET scan, DOG scan, plain film, complex film, KUB, IVP, XYZ, molybdenum scan, Afghaniscan)—all suggest need for further imaging.
ASSESSMENT AND PLAN
- “Hyperlabemia:” Likely iatrogenic etiology, or not. Correct with supplemental lab results.
- Pain: Source unclear but probably malingering. Treat with excessive narcotics, thereby causing problems 3 and 4 (see below).
- Bowel obstruction: Discontinue narcotics. Place (NG tube, rectal tube, boob tube, multiple consults).
- Altered mental status: Baseline worsened by narcotics. Give benzodiazepines, antipsychotics, antihistamine, more narcotics; then intubate.
- Discharge planning: The patient is a rock and will be on service forever.
- Abnormal imaging: Perform further scans.
- Code status: (Full code, no code, Morse code)
- Pineal: Gland abnormal—consult the pineal gland service TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
(Circle the appropriate answers.)
HISTORY OF PRESENT ILLNESS
This (0-109)-year-old (Asian, Black, Caucasian, Aleutian, Venusian) (male, female, other) presents with a (1, 7, 100)-(second, minute, day, year, century) history of (pain, swelling, itching, enlargement) of the (arm, chest, scrotum, uvula, pineal gland). (She/He/It) rates it as (11, 12, 20) out of 10. It is aggravated by (breathing, thinking, hang gliding, vigorous dancing, ennui) and alleviated by (acetaminophen, chocolate, high-dose morphine).
PAST MEDICAL HISTORY
Diabetes, hypertension, pineal insufficiency, Kluver-Bucy syndrome, rectal prolapse, Chagas disease, visceral larval migrans, ichthyosis, all of the above
PAST SURGICAL HISTORY
- Transplant of the (heart, kidney, pancreas, amygdala, pineal gland)
- ORIF of (humerus, femur, rear axle)
- Hemorrhoidectomy, cholecystectomy, pancreatectomy, cerumen removal, all of the above
ALLERGIES
(Penicillin, sulfa, every known drug in existence except Demerol)
CURRENT MEDICATION
- Insulin, metformin, Gila monster venom
- Alpha blocker, calcium blocker, beta blocker, blocker blocker
- Amoxicillin, “gorillacillin,” maggot extract, “mickeymycin”
- SSRI, MAOI, TRIAD, ECT, DOA
- (Thyroid, adrenal, pineal) gland extract
FAMILY HISTORY
Adopted, old age, some kind of cancer
SOCIAL HISTORY
- Alcohol: (teetotaler, tippler, boozer, lush, no alcohol—only beer)—multiply by 10
- Smoking: (never; three packs a day; not tobacco; old stogies I have found, short but not too big around)
- Drugs: (Is this confidential?, Freon, whatever I can get my hands on)
- Employment: (meter maid, sewer maintenance worker, JCAHO auditor, forensic proctologist, hospitologist)
REVIEW OF SYMPTOMS
- (Chest pain, more chest pain, even more chest pain), (rectal, urinary, salivary) incontinence, (ears itch with urination, nose runs with defecation, small bugs crawling out of my skin), (short of breath, short of patience)
- Stool is (sticky, floating, malodorous, frequent, shaped like the Statue of Liberty)
- Double vision, tunnel vision, television, hyperacusis, hearing loss, could you repeat that?, halitosis, dysgeusia, dysphonia, “datphonia”
- Abdominal (pain, cramping, crunches)
PHYSICAL EXAM
- BP (0, 90, 140, 230, 290)/(0, 3, 90, 160)
- Pulse (absent, irregularly irregularly irregular, tachycardic, tacky dresser) rate (0, 3, 84, 112, 190, 280)
- Temperature (32.2, 36.8, 25 minutes at 450—baste often)
- Normocephalic/atraumatic, bullet-headed, pointy-headed, hatchet in skull
- Eyes (PERRLA, anisocoria, bloodshot, pinpoint dude)
- Fundus exam (never can see them, cotton wool spots, cotton candy)
- Ears (present, “hyperceruminic,” absent)
- Mouth (macroglossia, foot in mouth, black hairy tongue, halitotic, skin of the teeth, wooden teeth)
- Neck (supple without adenopathy, thick, multiple hickies, red)
- Lungs (clear to auscultation and percussion—OK, I never really percussed; Velcro rales; egophonic; wheezy)
- Heart (systolic, 5/6, even a medical student can hear) murmur (no, pericardial, aye there’s the) rub
- Abdomen (scaphoid, pendulous, six-pack); bowel sounds (absent—was that you?)
- Umbilicus (surgically absent, Sister Mary Joseph nodule, high lint content)
- Extremities (extreme, all six present, night-clubbing)
NEURO EXAM
- Reflexes (cremaster positive, anal wink intact)
- Mentation (alert and oriented x3, catatonic, dogatonic)
- Psychiatric (appropriate, psychotic, truly weird, bipolar, tripolar)
- Skin (present, hideous thing growing on the patient’s face)
LABORATORY FINDINGS
Results of (CBC, ionized calcium, “citrulated ceruloplasmin,” complement levels, insult levels, saliva electrophoresis, urinary zinc level, melatonin level, and protein Q) all markedly abnormal.
IMAGING
(CAT scan, PET scan, DOG scan, plain film, complex film, KUB, IVP, XYZ, molybdenum scan, Afghaniscan)—all suggest need for further imaging.
ASSESSMENT AND PLAN
- “Hyperlabemia:” Likely iatrogenic etiology, or not. Correct with supplemental lab results.
- Pain: Source unclear but probably malingering. Treat with excessive narcotics, thereby causing problems 3 and 4 (see below).
- Bowel obstruction: Discontinue narcotics. Place (NG tube, rectal tube, boob tube, multiple consults).
- Altered mental status: Baseline worsened by narcotics. Give benzodiazepines, antipsychotics, antihistamine, more narcotics; then intubate.
- Discharge planning: The patient is a rock and will be on service forever.
- Abnormal imaging: Perform further scans.
- Code status: (Full code, no code, Morse code)
- Pineal: Gland abnormal—consult the pineal gland service TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
(Circle the appropriate answers.)
HISTORY OF PRESENT ILLNESS
This (0-109)-year-old (Asian, Black, Caucasian, Aleutian, Venusian) (male, female, other) presents with a (1, 7, 100)-(second, minute, day, year, century) history of (pain, swelling, itching, enlargement) of the (arm, chest, scrotum, uvula, pineal gland). (She/He/It) rates it as (11, 12, 20) out of 10. It is aggravated by (breathing, thinking, hang gliding, vigorous dancing, ennui) and alleviated by (acetaminophen, chocolate, high-dose morphine).
PAST MEDICAL HISTORY
Diabetes, hypertension, pineal insufficiency, Kluver-Bucy syndrome, rectal prolapse, Chagas disease, visceral larval migrans, ichthyosis, all of the above
PAST SURGICAL HISTORY
- Transplant of the (heart, kidney, pancreas, amygdala, pineal gland)
- ORIF of (humerus, femur, rear axle)
- Hemorrhoidectomy, cholecystectomy, pancreatectomy, cerumen removal, all of the above
ALLERGIES
(Penicillin, sulfa, every known drug in existence except Demerol)
CURRENT MEDICATION
- Insulin, metformin, Gila monster venom
- Alpha blocker, calcium blocker, beta blocker, blocker blocker
- Amoxicillin, “gorillacillin,” maggot extract, “mickeymycin”
- SSRI, MAOI, TRIAD, ECT, DOA
- (Thyroid, adrenal, pineal) gland extract
FAMILY HISTORY
Adopted, old age, some kind of cancer
SOCIAL HISTORY
- Alcohol: (teetotaler, tippler, boozer, lush, no alcohol—only beer)—multiply by 10
- Smoking: (never; three packs a day; not tobacco; old stogies I have found, short but not too big around)
- Drugs: (Is this confidential?, Freon, whatever I can get my hands on)
- Employment: (meter maid, sewer maintenance worker, JCAHO auditor, forensic proctologist, hospitologist)
REVIEW OF SYMPTOMS
- (Chest pain, more chest pain, even more chest pain), (rectal, urinary, salivary) incontinence, (ears itch with urination, nose runs with defecation, small bugs crawling out of my skin), (short of breath, short of patience)
- Stool is (sticky, floating, malodorous, frequent, shaped like the Statue of Liberty)
- Double vision, tunnel vision, television, hyperacusis, hearing loss, could you repeat that?, halitosis, dysgeusia, dysphonia, “datphonia”
- Abdominal (pain, cramping, crunches)
PHYSICAL EXAM
- BP (0, 90, 140, 230, 290)/(0, 3, 90, 160)
- Pulse (absent, irregularly irregularly irregular, tachycardic, tacky dresser) rate (0, 3, 84, 112, 190, 280)
- Temperature (32.2, 36.8, 25 minutes at 450—baste often)
- Normocephalic/atraumatic, bullet-headed, pointy-headed, hatchet in skull
- Eyes (PERRLA, anisocoria, bloodshot, pinpoint dude)
- Fundus exam (never can see them, cotton wool spots, cotton candy)
- Ears (present, “hyperceruminic,” absent)
- Mouth (macroglossia, foot in mouth, black hairy tongue, halitotic, skin of the teeth, wooden teeth)
- Neck (supple without adenopathy, thick, multiple hickies, red)
- Lungs (clear to auscultation and percussion—OK, I never really percussed; Velcro rales; egophonic; wheezy)
- Heart (systolic, 5/6, even a medical student can hear) murmur (no, pericardial, aye there’s the) rub
- Abdomen (scaphoid, pendulous, six-pack); bowel sounds (absent—was that you?)
- Umbilicus (surgically absent, Sister Mary Joseph nodule, high lint content)
- Extremities (extreme, all six present, night-clubbing)
NEURO EXAM
- Reflexes (cremaster positive, anal wink intact)
- Mentation (alert and oriented x3, catatonic, dogatonic)
- Psychiatric (appropriate, psychotic, truly weird, bipolar, tripolar)
- Skin (present, hideous thing growing on the patient’s face)
LABORATORY FINDINGS
Results of (CBC, ionized calcium, “citrulated ceruloplasmin,” complement levels, insult levels, saliva electrophoresis, urinary zinc level, melatonin level, and protein Q) all markedly abnormal.
IMAGING
(CAT scan, PET scan, DOG scan, plain film, complex film, KUB, IVP, XYZ, molybdenum scan, Afghaniscan)—all suggest need for further imaging.
ASSESSMENT AND PLAN
- “Hyperlabemia:” Likely iatrogenic etiology, or not. Correct with supplemental lab results.
- Pain: Source unclear but probably malingering. Treat with excessive narcotics, thereby causing problems 3 and 4 (see below).
- Bowel obstruction: Discontinue narcotics. Place (NG tube, rectal tube, boob tube, multiple consults).
- Altered mental status: Baseline worsened by narcotics. Give benzodiazepines, antipsychotics, antihistamine, more narcotics; then intubate.
- Discharge planning: The patient is a rock and will be on service forever.
- Abnormal imaging: Perform further scans.
- Code status: (Full code, no code, Morse code)
- Pineal: Gland abnormal—consult the pineal gland service TH
Jamie Newman, MD, FACP, is the physician editor of The Hospitalist, consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
The First Catheterization

It was very painful. I felt that I had planted an apple orchard and other men who had gathered the harvest stood at the wall, laughing at me.” Dr. Werner Forssmann said these words toward the end of his life on his unexpected scientific exile after having laid the foundations of modern cardiology.
Pacemaker Insertion, angioplasty, and valve repair might now be impossible without the daring of Dr. Forssmann, whose humble roots set into sharp relief the depth of his accomplishments.
Leading physicians in turn-of-the-century Europe said that investigation and treatment of conditions affecting the heart were anathema to mainstream medical society; the heart was off-limits. In 1896 Sir Stephen Paget went so far as to say that “no new method, and no new discovery, can overcome the natural difficulties that attend a wound of the heart.”
Enter Dr. Forssmann. Raised by in Berlin by his mother in a middle-class household after his father was killed in WWI, this young surgeon in training broached a bold idea with his surgeon-mentor Dr. Richard Schneider, a friend of the Forssmann family, in summer 1929.
Far from fantasy, Dr. Forssmann’s inspiration to perform what is now called cardiac catheterization came from a sketch in his physiology textbook depicting a long, thin tube being placed into a horse’s jugular vein and guided into the animal’s heart with balloon-assisted measurements of intracardiac pressures. Dr. Forssmann proposed to reach the heart of man—not through the jugular, but through the veins in the crease of the arm, which was more accessible
But how would this experiment happen? Dr. Forssmann elicited the help of Gerda Ditzen, a surgical nurse at Auguste Viktoria Home (Hospital), Eberswalde, near Berlin. In a month, Dr. Forssmann had convinced her to be his first human guinea pig. Dr. Forssmann, unbeknownst to Ditzen, planned on experimenting on himself. She held the keys to the closet, which was needed to obtain a long enough catheter.
As nurse Ditzen was strapped to the surgical table in the small operating room, sweating from both excitement and the sweltering
heat, Dr. Forssmann walked the distance of the OR and began his self-experimentation. With an incision in his left elbow crease, Dr. Forssmann identified the predominant vein and inserted the 65-cm-long ureteral tube into his arm, feeling progressive painless warmth as the tube coursed along. He had determined this was the only tube thin and long enough to safely and adequately reach the endocardium. However he still needed her help to conceal the tube hanging out of his arm. They went—tube in place—to the fluoroscopic X-ray facility, where images were obtained in the hospital basement.
The initial X-ray clearly indicated that the tube had not yet reached its destination. Dr. Forssmann forced the tube farther, resisting at one point the overwhelming urge to cough when the tube collided against his vein. When the tube was shown to be in the right auricle Dr. Forssmann had the technician snap the picture, finally obtaining the proof that he needed. Dr. Forssmann uneventfully removed the tube.
The real incident involved in this daring experiment was to come: Dr. Forssmann had to face the reactions—not only of his mentor Dr. Schneider, but also the medical community. The majority was ostensibly displeased with his methods, rationale, and approach, believing them too dangerous. After repeated self-experiments, Dr. Forssmann learned that his self-cath procedure could be safely performed; he submitted his findings with fluoroscopic proof to the German medical community at large. At least one prior researcher, the surgeon Ernst Unger, repudiated Dr. Forssmann’s claim, saying he had done the same thing many years earlier, but without hard evidence to back his claim.
Despite the rising tide of opposition to his findings, Dr. Forssmann pushed on. His subsequent experiments with rabbits and dogs (and ultimately himself) proved that catheterization angiography could not be achieved with simply sodium iodide. He developed the use of groin catheterization to reach the inferior vena cava through the femoral veins. Dr. Forssmann’s further experiments in aortography proved unfruitful. By this time, he had decided to stop his self-experimentation, having reached his limits with exploration. Instead he decided to seek work as a local urologist in a small German farming community.
In 1956, Forssmann was awarded the Nobel Prize in Medicine, which he shared with André Cournand, MD, and Dickinson W. Richards, MD, who were affiliated with Columbia University, New York City. When offered a job to head a German cardiovascular institute, Dr. Forssmann declined, citing his lack of knowledge about advancements in the field since his last self-experimentation in 1935. TH
Reference
- Altman, Lawrence K. Who Goes First: The Story of Self-Experimentation in Medicine. New York: Random House; 1987.
Historic Puzzler ANSWER: ”The Root of the Problem“
The answer to our third puzzler
By Jamie Newman, MD, FACP
There were several correct answers to the Historic Puzzler #3 (September, p. 10), but the best family effort award goes to Juan Solis, MD, a former hospitalist who now runs a private practice in internal medicine/geriatrics in Ohio, and his sisters—Rosa A. Solis, MD, a hospitalist in Binghamton, N.Y., and Regina A. Solis-Pastor, MD, a dermatologist.
Juan was showing off his name in The Hospitalist to his sisters when Regina pointed out Puzzler #3. Rather serendipitously she remembered seeing what we described on cable TV in the Philippines.
The captain of the expedition was James Cook, the naturalist was George Forster, and the root was kava kava. Juan looked up the herb and found the possible offending chemical component to be pipermethystine—seemingly found more on the leaves and stems of the plant than on the root itself. Neuro-ophthalmologic side effects include weakness, lack of coordination, lethargy, and change in mental status—even Parkinsonism. Dermatologic manifestations include xerosis (parchment-like, mosaic) and leprous ulcers. TH
Puzzler Special Recognition

And the best track record to date award goes to Collin Kroen, MD, of the Cleveland Clinic, the only one to solve all three puzzlers! Bijo Chacko, MD, the hospitalist program medical director at Central Brooklyn Medical Group, N.Y., and Alberto Burgos-Tiburcio, MD, Caritas Carney Hospital, Dorchester, Mass., are two for three.
So if you see a scaly, wild-eyed Polynesian lurching down the beach, have no fears, they may have been dipping into the coconut bowl once too often.—JN
It was very painful. I felt that I had planted an apple orchard and other men who had gathered the harvest stood at the wall, laughing at me.” Dr. Werner Forssmann said these words toward the end of his life on his unexpected scientific exile after having laid the foundations of modern cardiology.
Pacemaker Insertion, angioplasty, and valve repair might now be impossible without the daring of Dr. Forssmann, whose humble roots set into sharp relief the depth of his accomplishments.
Leading physicians in turn-of-the-century Europe said that investigation and treatment of conditions affecting the heart were anathema to mainstream medical society; the heart was off-limits. In 1896 Sir Stephen Paget went so far as to say that “no new method, and no new discovery, can overcome the natural difficulties that attend a wound of the heart.”
Enter Dr. Forssmann. Raised by in Berlin by his mother in a middle-class household after his father was killed in WWI, this young surgeon in training broached a bold idea with his surgeon-mentor Dr. Richard Schneider, a friend of the Forssmann family, in summer 1929.
Far from fantasy, Dr. Forssmann’s inspiration to perform what is now called cardiac catheterization came from a sketch in his physiology textbook depicting a long, thin tube being placed into a horse’s jugular vein and guided into the animal’s heart with balloon-assisted measurements of intracardiac pressures. Dr. Forssmann proposed to reach the heart of man—not through the jugular, but through the veins in the crease of the arm, which was more accessible
But how would this experiment happen? Dr. Forssmann elicited the help of Gerda Ditzen, a surgical nurse at Auguste Viktoria Home (Hospital), Eberswalde, near Berlin. In a month, Dr. Forssmann had convinced her to be his first human guinea pig. Dr. Forssmann, unbeknownst to Ditzen, planned on experimenting on himself. She held the keys to the closet, which was needed to obtain a long enough catheter.
As nurse Ditzen was strapped to the surgical table in the small operating room, sweating from both excitement and the sweltering
heat, Dr. Forssmann walked the distance of the OR and began his self-experimentation. With an incision in his left elbow crease, Dr. Forssmann identified the predominant vein and inserted the 65-cm-long ureteral tube into his arm, feeling progressive painless warmth as the tube coursed along. He had determined this was the only tube thin and long enough to safely and adequately reach the endocardium. However he still needed her help to conceal the tube hanging out of his arm. They went—tube in place—to the fluoroscopic X-ray facility, where images were obtained in the hospital basement.
The initial X-ray clearly indicated that the tube had not yet reached its destination. Dr. Forssmann forced the tube farther, resisting at one point the overwhelming urge to cough when the tube collided against his vein. When the tube was shown to be in the right auricle Dr. Forssmann had the technician snap the picture, finally obtaining the proof that he needed. Dr. Forssmann uneventfully removed the tube.
The real incident involved in this daring experiment was to come: Dr. Forssmann had to face the reactions—not only of his mentor Dr. Schneider, but also the medical community. The majority was ostensibly displeased with his methods, rationale, and approach, believing them too dangerous. After repeated self-experiments, Dr. Forssmann learned that his self-cath procedure could be safely performed; he submitted his findings with fluoroscopic proof to the German medical community at large. At least one prior researcher, the surgeon Ernst Unger, repudiated Dr. Forssmann’s claim, saying he had done the same thing many years earlier, but without hard evidence to back his claim.
Despite the rising tide of opposition to his findings, Dr. Forssmann pushed on. His subsequent experiments with rabbits and dogs (and ultimately himself) proved that catheterization angiography could not be achieved with simply sodium iodide. He developed the use of groin catheterization to reach the inferior vena cava through the femoral veins. Dr. Forssmann’s further experiments in aortography proved unfruitful. By this time, he had decided to stop his self-experimentation, having reached his limits with exploration. Instead he decided to seek work as a local urologist in a small German farming community.
In 1956, Forssmann was awarded the Nobel Prize in Medicine, which he shared with André Cournand, MD, and Dickinson W. Richards, MD, who were affiliated with Columbia University, New York City. When offered a job to head a German cardiovascular institute, Dr. Forssmann declined, citing his lack of knowledge about advancements in the field since his last self-experimentation in 1935. TH
Reference
- Altman, Lawrence K. Who Goes First: The Story of Self-Experimentation in Medicine. New York: Random House; 1987.
Historic Puzzler ANSWER: ”The Root of the Problem“
The answer to our third puzzler
By Jamie Newman, MD, FACP
There were several correct answers to the Historic Puzzler #3 (September, p. 10), but the best family effort award goes to Juan Solis, MD, a former hospitalist who now runs a private practice in internal medicine/geriatrics in Ohio, and his sisters—Rosa A. Solis, MD, a hospitalist in Binghamton, N.Y., and Regina A. Solis-Pastor, MD, a dermatologist.
Juan was showing off his name in The Hospitalist to his sisters when Regina pointed out Puzzler #3. Rather serendipitously she remembered seeing what we described on cable TV in the Philippines.
The captain of the expedition was James Cook, the naturalist was George Forster, and the root was kava kava. Juan looked up the herb and found the possible offending chemical component to be pipermethystine—seemingly found more on the leaves and stems of the plant than on the root itself. Neuro-ophthalmologic side effects include weakness, lack of coordination, lethargy, and change in mental status—even Parkinsonism. Dermatologic manifestations include xerosis (parchment-like, mosaic) and leprous ulcers. TH
Puzzler Special Recognition
And the best track record to date award goes to Collin Kroen, MD, of the Cleveland Clinic, the only one to solve all three puzzlers! Bijo Chacko, MD, the hospitalist program medical director at Central Brooklyn Medical Group, N.Y., and Alberto Burgos-Tiburcio, MD, Caritas Carney Hospital, Dorchester, Mass., are two for three.
So if you see a scaly, wild-eyed Polynesian lurching down the beach, have no fears, they may have been dipping into the coconut bowl once too often.—JN
It was very painful. I felt that I had planted an apple orchard and other men who had gathered the harvest stood at the wall, laughing at me.” Dr. Werner Forssmann said these words toward the end of his life on his unexpected scientific exile after having laid the foundations of modern cardiology.
Pacemaker Insertion, angioplasty, and valve repair might now be impossible without the daring of Dr. Forssmann, whose humble roots set into sharp relief the depth of his accomplishments.
Leading physicians in turn-of-the-century Europe said that investigation and treatment of conditions affecting the heart were anathema to mainstream medical society; the heart was off-limits. In 1896 Sir Stephen Paget went so far as to say that “no new method, and no new discovery, can overcome the natural difficulties that attend a wound of the heart.”
Enter Dr. Forssmann. Raised by in Berlin by his mother in a middle-class household after his father was killed in WWI, this young surgeon in training broached a bold idea with his surgeon-mentor Dr. Richard Schneider, a friend of the Forssmann family, in summer 1929.
Far from fantasy, Dr. Forssmann’s inspiration to perform what is now called cardiac catheterization came from a sketch in his physiology textbook depicting a long, thin tube being placed into a horse’s jugular vein and guided into the animal’s heart with balloon-assisted measurements of intracardiac pressures. Dr. Forssmann proposed to reach the heart of man—not through the jugular, but through the veins in the crease of the arm, which was more accessible
But how would this experiment happen? Dr. Forssmann elicited the help of Gerda Ditzen, a surgical nurse at Auguste Viktoria Home (Hospital), Eberswalde, near Berlin. In a month, Dr. Forssmann had convinced her to be his first human guinea pig. Dr. Forssmann, unbeknownst to Ditzen, planned on experimenting on himself. She held the keys to the closet, which was needed to obtain a long enough catheter.
As nurse Ditzen was strapped to the surgical table in the small operating room, sweating from both excitement and the sweltering
heat, Dr. Forssmann walked the distance of the OR and began his self-experimentation. With an incision in his left elbow crease, Dr. Forssmann identified the predominant vein and inserted the 65-cm-long ureteral tube into his arm, feeling progressive painless warmth as the tube coursed along. He had determined this was the only tube thin and long enough to safely and adequately reach the endocardium. However he still needed her help to conceal the tube hanging out of his arm. They went—tube in place—to the fluoroscopic X-ray facility, where images were obtained in the hospital basement.
The initial X-ray clearly indicated that the tube had not yet reached its destination. Dr. Forssmann forced the tube farther, resisting at one point the overwhelming urge to cough when the tube collided against his vein. When the tube was shown to be in the right auricle Dr. Forssmann had the technician snap the picture, finally obtaining the proof that he needed. Dr. Forssmann uneventfully removed the tube.
The real incident involved in this daring experiment was to come: Dr. Forssmann had to face the reactions—not only of his mentor Dr. Schneider, but also the medical community. The majority was ostensibly displeased with his methods, rationale, and approach, believing them too dangerous. After repeated self-experiments, Dr. Forssmann learned that his self-cath procedure could be safely performed; he submitted his findings with fluoroscopic proof to the German medical community at large. At least one prior researcher, the surgeon Ernst Unger, repudiated Dr. Forssmann’s claim, saying he had done the same thing many years earlier, but without hard evidence to back his claim.
Despite the rising tide of opposition to his findings, Dr. Forssmann pushed on. His subsequent experiments with rabbits and dogs (and ultimately himself) proved that catheterization angiography could not be achieved with simply sodium iodide. He developed the use of groin catheterization to reach the inferior vena cava through the femoral veins. Dr. Forssmann’s further experiments in aortography proved unfruitful. By this time, he had decided to stop his self-experimentation, having reached his limits with exploration. Instead he decided to seek work as a local urologist in a small German farming community.
In 1956, Forssmann was awarded the Nobel Prize in Medicine, which he shared with André Cournand, MD, and Dickinson W. Richards, MD, who were affiliated with Columbia University, New York City. When offered a job to head a German cardiovascular institute, Dr. Forssmann declined, citing his lack of knowledge about advancements in the field since his last self-experimentation in 1935. TH
Reference
- Altman, Lawrence K. Who Goes First: The Story of Self-Experimentation in Medicine. New York: Random House; 1987.
Historic Puzzler ANSWER: ”The Root of the Problem“
The answer to our third puzzler
By Jamie Newman, MD, FACP
There were several correct answers to the Historic Puzzler #3 (September, p. 10), but the best family effort award goes to Juan Solis, MD, a former hospitalist who now runs a private practice in internal medicine/geriatrics in Ohio, and his sisters—Rosa A. Solis, MD, a hospitalist in Binghamton, N.Y., and Regina A. Solis-Pastor, MD, a dermatologist.
Juan was showing off his name in The Hospitalist to his sisters when Regina pointed out Puzzler #3. Rather serendipitously she remembered seeing what we described on cable TV in the Philippines.
The captain of the expedition was James Cook, the naturalist was George Forster, and the root was kava kava. Juan looked up the herb and found the possible offending chemical component to be pipermethystine—seemingly found more on the leaves and stems of the plant than on the root itself. Neuro-ophthalmologic side effects include weakness, lack of coordination, lethargy, and change in mental status—even Parkinsonism. Dermatologic manifestations include xerosis (parchment-like, mosaic) and leprous ulcers. TH
Puzzler Special Recognition
And the best track record to date award goes to Collin Kroen, MD, of the Cleveland Clinic, the only one to solve all three puzzlers! Bijo Chacko, MD, the hospitalist program medical director at Central Brooklyn Medical Group, N.Y., and Alberto Burgos-Tiburcio, MD, Caritas Carney Hospital, Dorchester, Mass., are two for three.
So if you see a scaly, wild-eyed Polynesian lurching down the beach, have no fears, they may have been dipping into the coconut bowl once too often.—JN
In the Literature

Semi-Recumbent Position to Prevent Ventilator-Associated Pneumonia: Is It Possible?
By Joseph Ming Wah Li, MD
Van Nieuwenhoven CA, Vandenbroucke-Grauls C, van Tiel FH, et al. Feasibility and effects of the semirecumbent position to prevent ventilator-associated pneumonia: a randomized study. Crit Care Med. 2006 Feb;34(2):396-402.
Ventilator-associated pneumonia (VAP) is a cause of significant morbidity and mortality among mechanically ventilated patients. Studies with radioactive-labeled enteral feeds have demonstrated an increased frequency of endotracheal aspiration of gastric contents in supine patients. The CDC guidelines for prevention of nosocomial pneumonia advise placement of mechanically ventilated patients in a semi-recumbent position as a VAP prevention measure.
Only one previous study, by Drakulovic and colleagues, has assessed this strategy to prevent VAP.1 That study demonstrated a 75% decrease in the incidence of VAP. But van Nieuwenhoven and colleagues raised two important questions about the findings from the previous study: First, the Drakulovic study placed control patients in a horizontal (zero degrees) position, which is not the standard of care in most ICUs. Most patients are placed at 10 degrees, and this position is elevated as patients are weaned. Second, the Drakulovic study measured patients only once daily but did not monitor their body positions in between the daily measurements.
Dr. van Nieuwenhoven and colleagues set out to determine whether it is feasible to keep mechanically ventilated patients in a semi-recumbent position on a continual basis and whether this measure would prevent VAP. This was a prospective multi-centered trial in which mechanically ventilated patients were randomly assigned to the semi-recumbent position with a target backrest elevation of 45 degrees or standard of care (supine position) with a backrest elevation of 10 degrees. They used a transducer with a pendulum, which was placed on the bed frame to measure the backrest elevation every 60 seconds for up to seven days. They calculated a mean degree of elevation for each patient daily. Nurses always respected the patient’s request for positioning, but a dedicated research nurse restored backrest position to the randomized position whenever possible.
Baseline characteristics for both groups were similar. For the supine (control) group, average elevations were 9.8 degrees on day one and 16.1 degrees on day seven. For the semi-recumbent group, average elevations were 28.1 degrees on day one and 22.6 degrees on day seven. There were no significant differences in numbers of patients who developed VAP in either group.
This study suggests that, despite the use of dedicated research nurses to maintain positioning, it may not be possible to keep patients’ backrests elevated to 45 degrees. Keeping patients’ backrests at an elevation of nearly 30 degrees does not appear to prevent VAP more than keeping patients’ backrests at 10 degrees, the present standard of care.
Reference
- Drakulovic MB, Torres A, Bauer TT, et al. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet. 1999;354(9193):1851-1858.
Bar Codes in Medicine: An Opportunity for Quality Improvement
By Alex Carbo, MD
Poon EG, Cina JL, Churchill W, et al. Medication dispensing errors and potential adverse drug events before and after implementing bar code technology in the pharmacy. Ann Intern Med. 2006;145:426-434.
Medication errors and adverse drug events (ADEs) have received much attention in the literature; the use of health information technology to mitigate these errors and ADEs has now been proposed in many areas of healthcare. In an effort to decrease medication-dispensing errors, the U.S. Food and Drug Administration (FDA) mandated bar code use for all medications in hospitals, beginning in April 2006. While this technology has been extensively studied in other industries, there is little data describing its effects in the healthcare system.
Poon and colleagues set out to evaluate whether implementation of bar code technology reduced dispensing errors and the ADEs that might be caused by these miscalculations. In a before-and-after evaluation, they studied more than 350,000 dispensed medication doses in an academic medical center between February 2003 and September 2004.
During the bar code conversion process, the hospital pharmacy built a dedicated repackaging center, which was responsible for affixing a bar code to every dose of medication. These medications were then dispensed in three different configurations: two configurations required staff to verify all doses at least once using bar code scanning, and the third configuration—for commonly dispensed medications that could not be accommodated in a standard carousel machine because of their size or need for refrigeration—required scanning only one dose from each batch.
The authors found a 93% to 96% relative reduction in the incidence of target dispensing errors (P<0.001) and an 86% to 97% relative reduction in the incidence of potential ADEs (P<0.001) in the two configurations that required staff to verify all doses by scanning. The greatest reductions were seen in wrong medication errors (56%), wrong strength/dose errors (71%), wrong formulation errors (90%), and expired medication errors (100%).
In the configuration that did not require scanning of every dose, however, there was a 60% relative reduction in the incidence of target dispensing errors (P<0.001), but a 2.4-fold increase in the incidence of target potential ADEs. This included new errors attributable to wrong strength and wrong medication dispensing.
In light of the FDA’s mandate regarding bar codes, it seems that every hospital has the opportunity to improve patient safety and decrease medication error rates with the use of bar code technology. This study suggests that in order to achieve this benefit these systems should be designed to ensure that every medication dose is verified by scanning during the dispensing process.
Evaluation of a Guideline to Guide Resuscitation
By Cindy Lien, MD
Morrison LJ, Visentin LM, Kiss A, et al. Validation of a rule for termination of resuscitation in out-of-hospital cardiac arrest. N Engl J Med. 2006 Aug 3;355(5):478-487.
The survival rate of patients with out-of-hospital cardiac arrest is very low. Thus, guidelines have been developed for termination of resuscitation for those patients who have had no response to advanced cardiac life support provided by emergency medical service (EMS) personnel. Similar guidelines have not yet been developed, however, for situations in which patients receive basic life support from emergency workers trained in the use of an automated external cardiac defibrillator. Patients with little potential for survival are routinely transported to emergency departments, at significant cost to the healthcare system.
Morrison and colleagues present results from the Termination of Resuscitation (TOR) study, a prospective evaluation of a clinical prediction rule for the termination of basic life support by emergency medical personnel trained in the use of automated external defibrillators. The clinical prediction rule, previously developed in a retrospective review of case records from a large urban EMS system, recommends termination of resuscitation if there is no return of spontaneous circulation, no shock administered, and no witness of the arrest by EMS personnel.
In the current study, the authors obtained follow-up data for 1,240 adult patients in Ontario, Canada, who had suffered an arrest of presumed cardiac cause and were subsequently transported to the emergency department after resuscitative efforts. Twenty-four EMS systems participated in the study. The study found that only 0.5% of the patients for whom the clinical prediction rule recommended termination survived (four out of 776 patients). Of the 1,240 total study patients, 41 (3%) survived. The clinical prediction rule recommended continuation of resuscitative efforts for 37 of these 41 patients, resulting in a specificity of 90.2%. The positive predictive value for death was calculated to be 99.5% when termination was recommended.
The TOR trial also determined whether the addition of other criteria to the original prediction rule could further refine the specificity and positive predictive value. They found that the addition to the criteria of a response time greater than eight minutes increased the positive predictive value and specificity to 99.7% and 97.6%, respectively. When the variable “not witnessed by bystander” was added to the clinical prediction rule, both the positive predictive value and specificity increased to 100%. In other words, no patients survived if they had had a completely unwitnessed arrest, no return of spontaneous circulation, and no shocks delivered.
This study identifies a subpopulation of patients with presumed cardiac arrest for whom termination of resuscitative efforts in the field appears reasonable. The authors note that a survival rate of 1% or less has been suggested in past literature as reflective of medical futility. The TOR investigators acknowledge that their study took place before the 2005 AHA Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care were released and that their study protocols were consistent with the 2000 resuscitation guidelines. In light of this information, continued validity testing of the clinical prediction rule under the 2005 AHA protocols is needed.
Nonetheless, it is quite impressive that use of their clinical prediction rule would have resulted in transportation of only 37% of patients (464 of 1,240), rather than 100% of patients, as is currently the practice. If the guidelines described in this article are to be implemented, further studies are necessary to address the training of EMS personnel, who would carry responsibility for terminating resuscitation and notifying families of patients’ deaths.
Prevention of Ventilator-Associated Pneumonia
By Diane Sliwka, MD
Koeman M, van der Ven AJ, Hak E, et al. Oral decontamination with chlorhexidine reduces the incidence of ventilator-associated pneumonia. Am J Respir Crit Care Med. 2006 Jun;173(12):1348-1355. Epub 2006 Apr 7.
Ventilator-associated pneumonia (VAP) is an important nosocomial source of morbidity and mortality. The use of prophylactic antimicrobials to decrease VAP raises concern for antimicrobial resistance. This study evaluates the topical antiseptic chlorhexidine (CHX) as an alternative prophylactic intervention for VAP. CHX has previously been shown to decrease VAP in cardiac surgical patients, but has not been studied in higher risk, long-term-ventilated patients. Because CHX works better for gram-positive organisms, the combination of colistin and CHX (COL + CHX) was also studied for improved gram-negative coverage.
This multi-center, randomized, double-blind, placebo-controlled trial enrolled 385 adult patients. Patients who were expected to be intubated for longer than 48 hours were randomized to 3 arms: CHX alone, CHX + COL, and placebo. Exclusion criteria included known preadmission immunocompromised state, pregnancy, and physical limitation to oral application. Pneumonia was defined by clinical decision-making, which was later confirmed by three blinded intensivists’ reviews of the case records and supported by daily clinical pulmonary infection scores.
The primary endpoint of VAP was diagnosed in 52 of 385 patients: 18% placebo, 13% CHX, and 10% CHX + COL. Rate of VAP in the two treatment groups was lower than placebo and reached statistical significance when compared to placebo. The daily hazard ratio for CHX versus placebo was .352 (95% CI .160, .791); for CHX + COL versus placebo, it was .454 (95% CI .224, .925), showing a 65% and 55% reduction in the rate of pneumonia development. Multivariate analysis of variables such as gender, pulmonary admission diagnosis, colonization at time of admission, and antimicrobial use on admission did not affect the data.
The secondary endpoint of endotracheal colonization was evaluated by a twice-weekly endotracheal culture. There was no statistically significant difference in colonization among the three groups in the first (days 1-4) or third (days 9-12) time frames. During the second time frame (days 5-8), there was a statistically significant decrease in colonization for the CHX + COL treatment group when compared to both placebo (16% versus 40% p<.007) and to CHX (16% versus 38%, p<.011); this decrease is thought to be due to gram-negative coverage by COL.
The secondary endpoint of oropharyngeal colonization was evaluated for 87% of all patient days. CHX and CHX + COL were similarly effective for gram-positive bacteria when compared to placebo, with 30% and 27% reduction in rates of colonization, respectively: HR 0.695 for CHX (95% CI, 0.606, 0.796; p < 0.001) and 0.732 (95% CI, 0.640, 0.838; p < 0.001) for CHX + COL. The CHX + COL combination was more effective for gram-negative bacteria: daily HR .534 (95% CI, 0.455, 0.626; p <0.001) alone with a 47% reduction in gram-negative colonization compared to CHX.
No difference was seen in ICU mortality, duration of mechanical ventilation, or duration of ICU stay. One adverse event (tongue swelling) occurred in the CHX + COL group.
Limitations of the study include the following:
- Daily assessments on all patients were not performed;
- The placebo group had more males and more infections on admission than the other two groups, raising the question of randomization error;
- Clinical versus quantitative diagnosis of pneumonia may overestimate VAP in this study;
- It is not known how many patients were not enrolled in the study due to short anticipated ventilator times, but who later had prolonged ventilations; and
- The lack of effect on ventilator time, ICU length of stay, and mortality raises the question of the significance of these findings.
Despite these limitations, the low cost of these treatments, minimal adverse events, low risk of promoting significant antimicrobial resistance, and the finding of decreased VAP and bacterial colonization risk shown in this study support the potential benefit of topical decontamination with CHX and COL in conjunction with other measures of VAP prevention. TH
Reference
- De Riso AJ II, Ladowski JS, Dillon TA, et al. Chlorhexidine gluconate 0.12% oral rinse reduces the incidence of total nosocomial respiratory infection and nonprophylactic systemic antibiotic use in patients undergoing heart surgery. Chest. 1996;109:1556-1561.
Semi-Recumbent Position to Prevent Ventilator-Associated Pneumonia: Is It Possible?
By Joseph Ming Wah Li, MD
Van Nieuwenhoven CA, Vandenbroucke-Grauls C, van Tiel FH, et al. Feasibility and effects of the semirecumbent position to prevent ventilator-associated pneumonia: a randomized study. Crit Care Med. 2006 Feb;34(2):396-402.
Ventilator-associated pneumonia (VAP) is a cause of significant morbidity and mortality among mechanically ventilated patients. Studies with radioactive-labeled enteral feeds have demonstrated an increased frequency of endotracheal aspiration of gastric contents in supine patients. The CDC guidelines for prevention of nosocomial pneumonia advise placement of mechanically ventilated patients in a semi-recumbent position as a VAP prevention measure.
Only one previous study, by Drakulovic and colleagues, has assessed this strategy to prevent VAP.1 That study demonstrated a 75% decrease in the incidence of VAP. But van Nieuwenhoven and colleagues raised two important questions about the findings from the previous study: First, the Drakulovic study placed control patients in a horizontal (zero degrees) position, which is not the standard of care in most ICUs. Most patients are placed at 10 degrees, and this position is elevated as patients are weaned. Second, the Drakulovic study measured patients only once daily but did not monitor their body positions in between the daily measurements.
Dr. van Nieuwenhoven and colleagues set out to determine whether it is feasible to keep mechanically ventilated patients in a semi-recumbent position on a continual basis and whether this measure would prevent VAP. This was a prospective multi-centered trial in which mechanically ventilated patients were randomly assigned to the semi-recumbent position with a target backrest elevation of 45 degrees or standard of care (supine position) with a backrest elevation of 10 degrees. They used a transducer with a pendulum, which was placed on the bed frame to measure the backrest elevation every 60 seconds for up to seven days. They calculated a mean degree of elevation for each patient daily. Nurses always respected the patient’s request for positioning, but a dedicated research nurse restored backrest position to the randomized position whenever possible.
Baseline characteristics for both groups were similar. For the supine (control) group, average elevations were 9.8 degrees on day one and 16.1 degrees on day seven. For the semi-recumbent group, average elevations were 28.1 degrees on day one and 22.6 degrees on day seven. There were no significant differences in numbers of patients who developed VAP in either group.
This study suggests that, despite the use of dedicated research nurses to maintain positioning, it may not be possible to keep patients’ backrests elevated to 45 degrees. Keeping patients’ backrests at an elevation of nearly 30 degrees does not appear to prevent VAP more than keeping patients’ backrests at 10 degrees, the present standard of care.
Reference
- Drakulovic MB, Torres A, Bauer TT, et al. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet. 1999;354(9193):1851-1858.
Bar Codes in Medicine: An Opportunity for Quality Improvement
By Alex Carbo, MD
Poon EG, Cina JL, Churchill W, et al. Medication dispensing errors and potential adverse drug events before and after implementing bar code technology in the pharmacy. Ann Intern Med. 2006;145:426-434.
Medication errors and adverse drug events (ADEs) have received much attention in the literature; the use of health information technology to mitigate these errors and ADEs has now been proposed in many areas of healthcare. In an effort to decrease medication-dispensing errors, the U.S. Food and Drug Administration (FDA) mandated bar code use for all medications in hospitals, beginning in April 2006. While this technology has been extensively studied in other industries, there is little data describing its effects in the healthcare system.
Poon and colleagues set out to evaluate whether implementation of bar code technology reduced dispensing errors and the ADEs that might be caused by these miscalculations. In a before-and-after evaluation, they studied more than 350,000 dispensed medication doses in an academic medical center between February 2003 and September 2004.
During the bar code conversion process, the hospital pharmacy built a dedicated repackaging center, which was responsible for affixing a bar code to every dose of medication. These medications were then dispensed in three different configurations: two configurations required staff to verify all doses at least once using bar code scanning, and the third configuration—for commonly dispensed medications that could not be accommodated in a standard carousel machine because of their size or need for refrigeration—required scanning only one dose from each batch.
The authors found a 93% to 96% relative reduction in the incidence of target dispensing errors (P<0.001) and an 86% to 97% relative reduction in the incidence of potential ADEs (P<0.001) in the two configurations that required staff to verify all doses by scanning. The greatest reductions were seen in wrong medication errors (56%), wrong strength/dose errors (71%), wrong formulation errors (90%), and expired medication errors (100%).
In the configuration that did not require scanning of every dose, however, there was a 60% relative reduction in the incidence of target dispensing errors (P<0.001), but a 2.4-fold increase in the incidence of target potential ADEs. This included new errors attributable to wrong strength and wrong medication dispensing.
In light of the FDA’s mandate regarding bar codes, it seems that every hospital has the opportunity to improve patient safety and decrease medication error rates with the use of bar code technology. This study suggests that in order to achieve this benefit these systems should be designed to ensure that every medication dose is verified by scanning during the dispensing process.
Evaluation of a Guideline to Guide Resuscitation
By Cindy Lien, MD
Morrison LJ, Visentin LM, Kiss A, et al. Validation of a rule for termination of resuscitation in out-of-hospital cardiac arrest. N Engl J Med. 2006 Aug 3;355(5):478-487.
The survival rate of patients with out-of-hospital cardiac arrest is very low. Thus, guidelines have been developed for termination of resuscitation for those patients who have had no response to advanced cardiac life support provided by emergency medical service (EMS) personnel. Similar guidelines have not yet been developed, however, for situations in which patients receive basic life support from emergency workers trained in the use of an automated external cardiac defibrillator. Patients with little potential for survival are routinely transported to emergency departments, at significant cost to the healthcare system.
Morrison and colleagues present results from the Termination of Resuscitation (TOR) study, a prospective evaluation of a clinical prediction rule for the termination of basic life support by emergency medical personnel trained in the use of automated external defibrillators. The clinical prediction rule, previously developed in a retrospective review of case records from a large urban EMS system, recommends termination of resuscitation if there is no return of spontaneous circulation, no shock administered, and no witness of the arrest by EMS personnel.
In the current study, the authors obtained follow-up data for 1,240 adult patients in Ontario, Canada, who had suffered an arrest of presumed cardiac cause and were subsequently transported to the emergency department after resuscitative efforts. Twenty-four EMS systems participated in the study. The study found that only 0.5% of the patients for whom the clinical prediction rule recommended termination survived (four out of 776 patients). Of the 1,240 total study patients, 41 (3%) survived. The clinical prediction rule recommended continuation of resuscitative efforts for 37 of these 41 patients, resulting in a specificity of 90.2%. The positive predictive value for death was calculated to be 99.5% when termination was recommended.
The TOR trial also determined whether the addition of other criteria to the original prediction rule could further refine the specificity and positive predictive value. They found that the addition to the criteria of a response time greater than eight minutes increased the positive predictive value and specificity to 99.7% and 97.6%, respectively. When the variable “not witnessed by bystander” was added to the clinical prediction rule, both the positive predictive value and specificity increased to 100%. In other words, no patients survived if they had had a completely unwitnessed arrest, no return of spontaneous circulation, and no shocks delivered.
This study identifies a subpopulation of patients with presumed cardiac arrest for whom termination of resuscitative efforts in the field appears reasonable. The authors note that a survival rate of 1% or less has been suggested in past literature as reflective of medical futility. The TOR investigators acknowledge that their study took place before the 2005 AHA Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care were released and that their study protocols were consistent with the 2000 resuscitation guidelines. In light of this information, continued validity testing of the clinical prediction rule under the 2005 AHA protocols is needed.
Nonetheless, it is quite impressive that use of their clinical prediction rule would have resulted in transportation of only 37% of patients (464 of 1,240), rather than 100% of patients, as is currently the practice. If the guidelines described in this article are to be implemented, further studies are necessary to address the training of EMS personnel, who would carry responsibility for terminating resuscitation and notifying families of patients’ deaths.
Prevention of Ventilator-Associated Pneumonia
By Diane Sliwka, MD
Koeman M, van der Ven AJ, Hak E, et al. Oral decontamination with chlorhexidine reduces the incidence of ventilator-associated pneumonia. Am J Respir Crit Care Med. 2006 Jun;173(12):1348-1355. Epub 2006 Apr 7.
Ventilator-associated pneumonia (VAP) is an important nosocomial source of morbidity and mortality. The use of prophylactic antimicrobials to decrease VAP raises concern for antimicrobial resistance. This study evaluates the topical antiseptic chlorhexidine (CHX) as an alternative prophylactic intervention for VAP. CHX has previously been shown to decrease VAP in cardiac surgical patients, but has not been studied in higher risk, long-term-ventilated patients. Because CHX works better for gram-positive organisms, the combination of colistin and CHX (COL + CHX) was also studied for improved gram-negative coverage.
This multi-center, randomized, double-blind, placebo-controlled trial enrolled 385 adult patients. Patients who were expected to be intubated for longer than 48 hours were randomized to 3 arms: CHX alone, CHX + COL, and placebo. Exclusion criteria included known preadmission immunocompromised state, pregnancy, and physical limitation to oral application. Pneumonia was defined by clinical decision-making, which was later confirmed by three blinded intensivists’ reviews of the case records and supported by daily clinical pulmonary infection scores.
The primary endpoint of VAP was diagnosed in 52 of 385 patients: 18% placebo, 13% CHX, and 10% CHX + COL. Rate of VAP in the two treatment groups was lower than placebo and reached statistical significance when compared to placebo. The daily hazard ratio for CHX versus placebo was .352 (95% CI .160, .791); for CHX + COL versus placebo, it was .454 (95% CI .224, .925), showing a 65% and 55% reduction in the rate of pneumonia development. Multivariate analysis of variables such as gender, pulmonary admission diagnosis, colonization at time of admission, and antimicrobial use on admission did not affect the data.
The secondary endpoint of endotracheal colonization was evaluated by a twice-weekly endotracheal culture. There was no statistically significant difference in colonization among the three groups in the first (days 1-4) or third (days 9-12) time frames. During the second time frame (days 5-8), there was a statistically significant decrease in colonization for the CHX + COL treatment group when compared to both placebo (16% versus 40% p<.007) and to CHX (16% versus 38%, p<.011); this decrease is thought to be due to gram-negative coverage by COL.
The secondary endpoint of oropharyngeal colonization was evaluated for 87% of all patient days. CHX and CHX + COL were similarly effective for gram-positive bacteria when compared to placebo, with 30% and 27% reduction in rates of colonization, respectively: HR 0.695 for CHX (95% CI, 0.606, 0.796; p < 0.001) and 0.732 (95% CI, 0.640, 0.838; p < 0.001) for CHX + COL. The CHX + COL combination was more effective for gram-negative bacteria: daily HR .534 (95% CI, 0.455, 0.626; p <0.001) alone with a 47% reduction in gram-negative colonization compared to CHX.
No difference was seen in ICU mortality, duration of mechanical ventilation, or duration of ICU stay. One adverse event (tongue swelling) occurred in the CHX + COL group.
Limitations of the study include the following:
- Daily assessments on all patients were not performed;
- The placebo group had more males and more infections on admission than the other two groups, raising the question of randomization error;
- Clinical versus quantitative diagnosis of pneumonia may overestimate VAP in this study;
- It is not known how many patients were not enrolled in the study due to short anticipated ventilator times, but who later had prolonged ventilations; and
- The lack of effect on ventilator time, ICU length of stay, and mortality raises the question of the significance of these findings.
Despite these limitations, the low cost of these treatments, minimal adverse events, low risk of promoting significant antimicrobial resistance, and the finding of decreased VAP and bacterial colonization risk shown in this study support the potential benefit of topical decontamination with CHX and COL in conjunction with other measures of VAP prevention. TH
Reference
- De Riso AJ II, Ladowski JS, Dillon TA, et al. Chlorhexidine gluconate 0.12% oral rinse reduces the incidence of total nosocomial respiratory infection and nonprophylactic systemic antibiotic use in patients undergoing heart surgery. Chest. 1996;109:1556-1561.
Semi-Recumbent Position to Prevent Ventilator-Associated Pneumonia: Is It Possible?
By Joseph Ming Wah Li, MD
Van Nieuwenhoven CA, Vandenbroucke-Grauls C, van Tiel FH, et al. Feasibility and effects of the semirecumbent position to prevent ventilator-associated pneumonia: a randomized study. Crit Care Med. 2006 Feb;34(2):396-402.
Ventilator-associated pneumonia (VAP) is a cause of significant morbidity and mortality among mechanically ventilated patients. Studies with radioactive-labeled enteral feeds have demonstrated an increased frequency of endotracheal aspiration of gastric contents in supine patients. The CDC guidelines for prevention of nosocomial pneumonia advise placement of mechanically ventilated patients in a semi-recumbent position as a VAP prevention measure.
Only one previous study, by Drakulovic and colleagues, has assessed this strategy to prevent VAP.1 That study demonstrated a 75% decrease in the incidence of VAP. But van Nieuwenhoven and colleagues raised two important questions about the findings from the previous study: First, the Drakulovic study placed control patients in a horizontal (zero degrees) position, which is not the standard of care in most ICUs. Most patients are placed at 10 degrees, and this position is elevated as patients are weaned. Second, the Drakulovic study measured patients only once daily but did not monitor their body positions in between the daily measurements.
Dr. van Nieuwenhoven and colleagues set out to determine whether it is feasible to keep mechanically ventilated patients in a semi-recumbent position on a continual basis and whether this measure would prevent VAP. This was a prospective multi-centered trial in which mechanically ventilated patients were randomly assigned to the semi-recumbent position with a target backrest elevation of 45 degrees or standard of care (supine position) with a backrest elevation of 10 degrees. They used a transducer with a pendulum, which was placed on the bed frame to measure the backrest elevation every 60 seconds for up to seven days. They calculated a mean degree of elevation for each patient daily. Nurses always respected the patient’s request for positioning, but a dedicated research nurse restored backrest position to the randomized position whenever possible.
Baseline characteristics for both groups were similar. For the supine (control) group, average elevations were 9.8 degrees on day one and 16.1 degrees on day seven. For the semi-recumbent group, average elevations were 28.1 degrees on day one and 22.6 degrees on day seven. There were no significant differences in numbers of patients who developed VAP in either group.
This study suggests that, despite the use of dedicated research nurses to maintain positioning, it may not be possible to keep patients’ backrests elevated to 45 degrees. Keeping patients’ backrests at an elevation of nearly 30 degrees does not appear to prevent VAP more than keeping patients’ backrests at 10 degrees, the present standard of care.
Reference
- Drakulovic MB, Torres A, Bauer TT, et al. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet. 1999;354(9193):1851-1858.
Bar Codes in Medicine: An Opportunity for Quality Improvement
By Alex Carbo, MD
Poon EG, Cina JL, Churchill W, et al. Medication dispensing errors and potential adverse drug events before and after implementing bar code technology in the pharmacy. Ann Intern Med. 2006;145:426-434.
Medication errors and adverse drug events (ADEs) have received much attention in the literature; the use of health information technology to mitigate these errors and ADEs has now been proposed in many areas of healthcare. In an effort to decrease medication-dispensing errors, the U.S. Food and Drug Administration (FDA) mandated bar code use for all medications in hospitals, beginning in April 2006. While this technology has been extensively studied in other industries, there is little data describing its effects in the healthcare system.
Poon and colleagues set out to evaluate whether implementation of bar code technology reduced dispensing errors and the ADEs that might be caused by these miscalculations. In a before-and-after evaluation, they studied more than 350,000 dispensed medication doses in an academic medical center between February 2003 and September 2004.
During the bar code conversion process, the hospital pharmacy built a dedicated repackaging center, which was responsible for affixing a bar code to every dose of medication. These medications were then dispensed in three different configurations: two configurations required staff to verify all doses at least once using bar code scanning, and the third configuration—for commonly dispensed medications that could not be accommodated in a standard carousel machine because of their size or need for refrigeration—required scanning only one dose from each batch.
The authors found a 93% to 96% relative reduction in the incidence of target dispensing errors (P<0.001) and an 86% to 97% relative reduction in the incidence of potential ADEs (P<0.001) in the two configurations that required staff to verify all doses by scanning. The greatest reductions were seen in wrong medication errors (56%), wrong strength/dose errors (71%), wrong formulation errors (90%), and expired medication errors (100%).
In the configuration that did not require scanning of every dose, however, there was a 60% relative reduction in the incidence of target dispensing errors (P<0.001), but a 2.4-fold increase in the incidence of target potential ADEs. This included new errors attributable to wrong strength and wrong medication dispensing.
In light of the FDA’s mandate regarding bar codes, it seems that every hospital has the opportunity to improve patient safety and decrease medication error rates with the use of bar code technology. This study suggests that in order to achieve this benefit these systems should be designed to ensure that every medication dose is verified by scanning during the dispensing process.
Evaluation of a Guideline to Guide Resuscitation
By Cindy Lien, MD
Morrison LJ, Visentin LM, Kiss A, et al. Validation of a rule for termination of resuscitation in out-of-hospital cardiac arrest. N Engl J Med. 2006 Aug 3;355(5):478-487.
The survival rate of patients with out-of-hospital cardiac arrest is very low. Thus, guidelines have been developed for termination of resuscitation for those patients who have had no response to advanced cardiac life support provided by emergency medical service (EMS) personnel. Similar guidelines have not yet been developed, however, for situations in which patients receive basic life support from emergency workers trained in the use of an automated external cardiac defibrillator. Patients with little potential for survival are routinely transported to emergency departments, at significant cost to the healthcare system.
Morrison and colleagues present results from the Termination of Resuscitation (TOR) study, a prospective evaluation of a clinical prediction rule for the termination of basic life support by emergency medical personnel trained in the use of automated external defibrillators. The clinical prediction rule, previously developed in a retrospective review of case records from a large urban EMS system, recommends termination of resuscitation if there is no return of spontaneous circulation, no shock administered, and no witness of the arrest by EMS personnel.
In the current study, the authors obtained follow-up data for 1,240 adult patients in Ontario, Canada, who had suffered an arrest of presumed cardiac cause and were subsequently transported to the emergency department after resuscitative efforts. Twenty-four EMS systems participated in the study. The study found that only 0.5% of the patients for whom the clinical prediction rule recommended termination survived (four out of 776 patients). Of the 1,240 total study patients, 41 (3%) survived. The clinical prediction rule recommended continuation of resuscitative efforts for 37 of these 41 patients, resulting in a specificity of 90.2%. The positive predictive value for death was calculated to be 99.5% when termination was recommended.
The TOR trial also determined whether the addition of other criteria to the original prediction rule could further refine the specificity and positive predictive value. They found that the addition to the criteria of a response time greater than eight minutes increased the positive predictive value and specificity to 99.7% and 97.6%, respectively. When the variable “not witnessed by bystander” was added to the clinical prediction rule, both the positive predictive value and specificity increased to 100%. In other words, no patients survived if they had had a completely unwitnessed arrest, no return of spontaneous circulation, and no shocks delivered.
This study identifies a subpopulation of patients with presumed cardiac arrest for whom termination of resuscitative efforts in the field appears reasonable. The authors note that a survival rate of 1% or less has been suggested in past literature as reflective of medical futility. The TOR investigators acknowledge that their study took place before the 2005 AHA Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care were released and that their study protocols were consistent with the 2000 resuscitation guidelines. In light of this information, continued validity testing of the clinical prediction rule under the 2005 AHA protocols is needed.
Nonetheless, it is quite impressive that use of their clinical prediction rule would have resulted in transportation of only 37% of patients (464 of 1,240), rather than 100% of patients, as is currently the practice. If the guidelines described in this article are to be implemented, further studies are necessary to address the training of EMS personnel, who would carry responsibility for terminating resuscitation and notifying families of patients’ deaths.
Prevention of Ventilator-Associated Pneumonia
By Diane Sliwka, MD
Koeman M, van der Ven AJ, Hak E, et al. Oral decontamination with chlorhexidine reduces the incidence of ventilator-associated pneumonia. Am J Respir Crit Care Med. 2006 Jun;173(12):1348-1355. Epub 2006 Apr 7.
Ventilator-associated pneumonia (VAP) is an important nosocomial source of morbidity and mortality. The use of prophylactic antimicrobials to decrease VAP raises concern for antimicrobial resistance. This study evaluates the topical antiseptic chlorhexidine (CHX) as an alternative prophylactic intervention for VAP. CHX has previously been shown to decrease VAP in cardiac surgical patients, but has not been studied in higher risk, long-term-ventilated patients. Because CHX works better for gram-positive organisms, the combination of colistin and CHX (COL + CHX) was also studied for improved gram-negative coverage.
This multi-center, randomized, double-blind, placebo-controlled trial enrolled 385 adult patients. Patients who were expected to be intubated for longer than 48 hours were randomized to 3 arms: CHX alone, CHX + COL, and placebo. Exclusion criteria included known preadmission immunocompromised state, pregnancy, and physical limitation to oral application. Pneumonia was defined by clinical decision-making, which was later confirmed by three blinded intensivists’ reviews of the case records and supported by daily clinical pulmonary infection scores.
The primary endpoint of VAP was diagnosed in 52 of 385 patients: 18% placebo, 13% CHX, and 10% CHX + COL. Rate of VAP in the two treatment groups was lower than placebo and reached statistical significance when compared to placebo. The daily hazard ratio for CHX versus placebo was .352 (95% CI .160, .791); for CHX + COL versus placebo, it was .454 (95% CI .224, .925), showing a 65% and 55% reduction in the rate of pneumonia development. Multivariate analysis of variables such as gender, pulmonary admission diagnosis, colonization at time of admission, and antimicrobial use on admission did not affect the data.
The secondary endpoint of endotracheal colonization was evaluated by a twice-weekly endotracheal culture. There was no statistically significant difference in colonization among the three groups in the first (days 1-4) or third (days 9-12) time frames. During the second time frame (days 5-8), there was a statistically significant decrease in colonization for the CHX + COL treatment group when compared to both placebo (16% versus 40% p<.007) and to CHX (16% versus 38%, p<.011); this decrease is thought to be due to gram-negative coverage by COL.
The secondary endpoint of oropharyngeal colonization was evaluated for 87% of all patient days. CHX and CHX + COL were similarly effective for gram-positive bacteria when compared to placebo, with 30% and 27% reduction in rates of colonization, respectively: HR 0.695 for CHX (95% CI, 0.606, 0.796; p < 0.001) and 0.732 (95% CI, 0.640, 0.838; p < 0.001) for CHX + COL. The CHX + COL combination was more effective for gram-negative bacteria: daily HR .534 (95% CI, 0.455, 0.626; p <0.001) alone with a 47% reduction in gram-negative colonization compared to CHX.
No difference was seen in ICU mortality, duration of mechanical ventilation, or duration of ICU stay. One adverse event (tongue swelling) occurred in the CHX + COL group.
Limitations of the study include the following:
- Daily assessments on all patients were not performed;
- The placebo group had more males and more infections on admission than the other two groups, raising the question of randomization error;
- Clinical versus quantitative diagnosis of pneumonia may overestimate VAP in this study;
- It is not known how many patients were not enrolled in the study due to short anticipated ventilator times, but who later had prolonged ventilations; and
- The lack of effect on ventilator time, ICU length of stay, and mortality raises the question of the significance of these findings.
Despite these limitations, the low cost of these treatments, minimal adverse events, low risk of promoting significant antimicrobial resistance, and the finding of decreased VAP and bacterial colonization risk shown in this study support the potential benefit of topical decontamination with CHX and COL in conjunction with other measures of VAP prevention. TH
Reference
- De Riso AJ II, Ladowski JS, Dillon TA, et al. Chlorhexidine gluconate 0.12% oral rinse reduces the incidence of total nosocomial respiratory infection and nonprophylactic systemic antibiotic use in patients undergoing heart surgery. Chest. 1996;109:1556-1561.
Protocol Pilot
Evidence from randomized controlled trials and historical series convincingly demonstrates that tight glycemic control in the critical care setting reduces mortality, length of hospital stay, and other morbidities.1-6 Several protocols targeting a range of glucoses have been published.7-10 We modified a protocol used at the University of Washington (Seattle) that targeted glucoses of 80-180 mg/dl to aim for a tighter glycemic goal range of 80-110 mg/dl and effectively lowered blood glucoses in our intensive care unit (ICU) with a low rate of hypoglycemia.9 We share here our protocol and results over the past year.
Methods
Column protocols have the advantage of accommodating rates of insulin infusion adjustment to the individual patient’s degree of insulin resistance. If glucoses are not falling appropriately using one column, a protocol is followed to move to a more aggressive column. If glucoses fall precipitously, a similar process guides the nurse to a less aggressive column. The column format avoids the need for nurses to do calculations, which reduces the possibility of error.
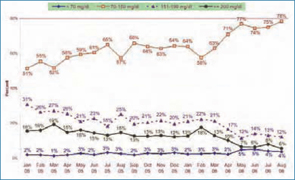
In August 2005, in our ICU, we piloted a four-column protocol used at the University of Washington. This protocol was designed with an initial target glucose range of 80-180 mg/dl, and during our pilot it did not work well because we were targeting a glucose range of 80-110 mg/dl. Our ICU nursing staff at Southwest Washington Medical Center (SWMC), Vancouver, preferred to revise the column format rather than switch to a different type of protocol such as the Portland Protocol. We therefore created a new six-column protocol targeting the 80-110 mg/dl glucose range. (See Figure 1, above.)
In creating this protocol, we reviewed infusion rates in an unpublished Oregon Health and Sciences University (OHSU), Portland, six-column protocol and the Georgia Hospital Association, Marietta, 10-column protocol.11,12 Our current version includes new glucose ranges of 70-89 mg/dl, 90-99 mg/dl, and 100-109 mg/dl to allow for more rate adjustments within the overall target range, while our previous version had only one glucose category of 70-109 mg/dl within the target range.
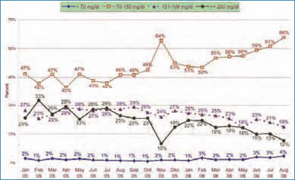
Nursing feedback also led us to modify criteria for moving to the right (more aggressive) column as follows: If blood glucose is lower than 200, algorithm failure is defined as glucose outside of goal range and not decreased since previous reading; if blood glucose is greater than or equal to 200, algorithm failure is defined as glucose outside of goal range and has not decreased by at least 60 mg/dl within one hour. The longest interval we allow between glucometer checks for stable patients is two hours. Automatic triggers for implementing the protocol include two consecutive glucoses over 140 mg/dl or a single glucose over 180 mg/dl.
Our revised protocol succeeded when we intensified nursing education, solicited frequent nursing feedback, and organized the procedure so that ICU nurse managers drove the process with a responsive physician/pharmacist team.
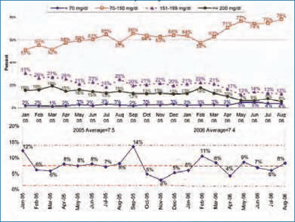
Results
In March 2006 we instituted the revised six-column insulin infusion protocol in our ICU. The percent of glucometer readings in the ICU between 70-150 mg/dl increased from 58% in February 2006 to 78% in August of 2006. (See Figure 2, above.) In our cardiac care unit (CCU), where an older, non-column insulin infusion protocol continued to be used, glucoses went from 50% in the 70-150 mg/dl range in February 2006 to 61% in that range in July 2006. When we began the six-column ICU insulin infusion protocol in the CCU in August 2006, 66% of glucoses were in the 70-150 range. (See Figure 3, p. 43.)
The percentage of glucoses below 70 mg/dl increased from 2%-3% using the four-column protocol to 4%-5% using the six-column protocol, as the percentage of glucoses between 70-150 mg/dl rose above 70%.
The main complaint from nurses relates to the need for frequent (hourly to twice hourly) glucose monitoring, which was also a complaint with earlier protocols in our institution.
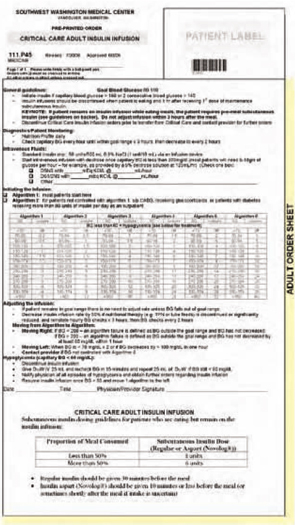
Discussion
These results compare favorably with those achieved by acknowledged leaders in critical care glycemic control in the United States.13 We have achieved them with the use of a safe column protocol that our critical care nurses are now comfortable using. The hypoglycemia rates with our protocol have been lower than those seen in some other published protocols. The Berghe protocol, for example, reported 5% of patients experiencing glucoses lower than or equal to 40 mg/dl, while our protocol resulted in 4%-5% of glucose values lower than 70 mg/dl.
Mortality rates in our ICU have fallen from 14% in September 2005 to 11% in February 2006 to 8% in August 2006. Although this decline in mortality has occurred over the range of time in which we have improved glycemic control in our ICU, multiple other mortality reduction initiatives, any or all of which could account for the decline, occurred simultaneously in our hospital; in addition, mortality rates were falling before the introduction of the new insulin infusion protocol.
Head-to-head comparisons of existing protocols, using agreed upon glucometrics such as time-to-goal range and degree of glycemic variability, are needed.14 Testing new protocols, including proactive insulin infusion adjustments at the time of administration of known caloric loads—such as antibiotics delivered as a bolus in D5W solution—or at the time of initiation of high dose steroids or epinephrine drips, may be a means to keep a higher percentage of blood sugars in range. Ultimately, continuous blood sensing devices with closed loop insulin infusion responses are desired.
For now, our protocol offers a user-friendly means of getting a high percentage of critical care patients into a reasonable glycemic range with a low risk of hypoglycemia. Others are free to use and/or modify it. TH
The authors work at Southwest Washington Medical Center, Vancouver, Wash.
References
- van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001 Nov 8;345(19):1359-1367.
- Malmberg K, Norhammar A, Wedel H, et al. Glycometabolic state at admission: important risk marker of mortality in conventionally treated patients with diabetes mellitus and acute myocardial infarction: long-term results from the Diabetes and Insulin-Glucose Infusion in Acute Myocardial Infarction (DIGAMI) study. Circulation. 1999;99:2626-2632.
- Furnary AP, Wu Y, Bookin SO. Clinical effects of hyperglycemia in the cardiac surgery population: the Portland diabetic project. Endocr Pract. 2006 Mar-Apr;12 Suppl 3:22-26.
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006 Feb 2;354(5):449-461.
- Krinsley JS. Effect of an intensive glucose management protocol on the mortality of critically ill adult patients. Mayo Clin Proc. 2004 Aug;79(8):992-1000.
- Pittas AG, Siegel RD, Lau J. Insulin therapy for critically ill hospitalized patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2004 Oct 11;164(18):2005-2011.
- Goldberg PA. Memoirs of a root canal salesman: the successful implementation of a hospital-wide intravenous insulin infusion protocol. Endocr Pract. 2006;12 Suppl 3:79-85.
- Markovitz LJ, Weichmann RJ, Harris N, et al. Description and evaluation of a glycemic management protocol for patients with diabetes undergoing heart surgery. Endocr Pract. 2002 Jan-Feb;8(1):10-18.
- Ku SY, Sayre CA, Hirsch IB, et al. New insulin infusion protocol improves blood glucose control in hospitalized patients without increasing hypoglycemia. Jt Comm J Qual Patient Saf. 2005 Mar;31(3):141-147.
- Furnary AP, Wu Y, Bookin SO. Effect of hyperglycemia and continuous intravenous insulin infusions on outcomes of cardiac surgical procedures: the Portland Diabetic Project. Endocr Pract. 2004 Mar-Apr;10 Suppl 2:21-33.
- In a written communication from Andy Ahmann, MD, OHSU, in 2006.
- Georgia Hospital Association Diabetes Protocols. Chart 6b. Available at: www.adaendo.com/GHA/index.html. Accessed October 29, 2006.
- In a written communication from Terry Clemmer, MD, director, Critical Care Medicine, LDS Hospital, Salt Lake City, Utah, in October 2006.
- Braithwaite SS, Godara H, Song HJ, et al. No patient left behind: evaluation and design of intravenous insulin infusion algorithms. Endocr Pract. 2006 Jul-Aug;12 Suppl 3:72-78.
Evidence from randomized controlled trials and historical series convincingly demonstrates that tight glycemic control in the critical care setting reduces mortality, length of hospital stay, and other morbidities.1-6 Several protocols targeting a range of glucoses have been published.7-10 We modified a protocol used at the University of Washington (Seattle) that targeted glucoses of 80-180 mg/dl to aim for a tighter glycemic goal range of 80-110 mg/dl and effectively lowered blood glucoses in our intensive care unit (ICU) with a low rate of hypoglycemia.9 We share here our protocol and results over the past year.
Methods
Column protocols have the advantage of accommodating rates of insulin infusion adjustment to the individual patient’s degree of insulin resistance. If glucoses are not falling appropriately using one column, a protocol is followed to move to a more aggressive column. If glucoses fall precipitously, a similar process guides the nurse to a less aggressive column. The column format avoids the need for nurses to do calculations, which reduces the possibility of error.
In August 2005, in our ICU, we piloted a four-column protocol used at the University of Washington. This protocol was designed with an initial target glucose range of 80-180 mg/dl, and during our pilot it did not work well because we were targeting a glucose range of 80-110 mg/dl. Our ICU nursing staff at Southwest Washington Medical Center (SWMC), Vancouver, preferred to revise the column format rather than switch to a different type of protocol such as the Portland Protocol. We therefore created a new six-column protocol targeting the 80-110 mg/dl glucose range. (See Figure 1, above.)
In creating this protocol, we reviewed infusion rates in an unpublished Oregon Health and Sciences University (OHSU), Portland, six-column protocol and the Georgia Hospital Association, Marietta, 10-column protocol.11,12 Our current version includes new glucose ranges of 70-89 mg/dl, 90-99 mg/dl, and 100-109 mg/dl to allow for more rate adjustments within the overall target range, while our previous version had only one glucose category of 70-109 mg/dl within the target range.
Nursing feedback also led us to modify criteria for moving to the right (more aggressive) column as follows: If blood glucose is lower than 200, algorithm failure is defined as glucose outside of goal range and not decreased since previous reading; if blood glucose is greater than or equal to 200, algorithm failure is defined as glucose outside of goal range and has not decreased by at least 60 mg/dl within one hour. The longest interval we allow between glucometer checks for stable patients is two hours. Automatic triggers for implementing the protocol include two consecutive glucoses over 140 mg/dl or a single glucose over 180 mg/dl.
Our revised protocol succeeded when we intensified nursing education, solicited frequent nursing feedback, and organized the procedure so that ICU nurse managers drove the process with a responsive physician/pharmacist team.
Results
In March 2006 we instituted the revised six-column insulin infusion protocol in our ICU. The percent of glucometer readings in the ICU between 70-150 mg/dl increased from 58% in February 2006 to 78% in August of 2006. (See Figure 2, above.) In our cardiac care unit (CCU), where an older, non-column insulin infusion protocol continued to be used, glucoses went from 50% in the 70-150 mg/dl range in February 2006 to 61% in that range in July 2006. When we began the six-column ICU insulin infusion protocol in the CCU in August 2006, 66% of glucoses were in the 70-150 range. (See Figure 3, p. 43.)
The percentage of glucoses below 70 mg/dl increased from 2%-3% using the four-column protocol to 4%-5% using the six-column protocol, as the percentage of glucoses between 70-150 mg/dl rose above 70%.
The main complaint from nurses relates to the need for frequent (hourly to twice hourly) glucose monitoring, which was also a complaint with earlier protocols in our institution.
Discussion
These results compare favorably with those achieved by acknowledged leaders in critical care glycemic control in the United States.13 We have achieved them with the use of a safe column protocol that our critical care nurses are now comfortable using. The hypoglycemia rates with our protocol have been lower than those seen in some other published protocols. The Berghe protocol, for example, reported 5% of patients experiencing glucoses lower than or equal to 40 mg/dl, while our protocol resulted in 4%-5% of glucose values lower than 70 mg/dl.
Mortality rates in our ICU have fallen from 14% in September 2005 to 11% in February 2006 to 8% in August 2006. Although this decline in mortality has occurred over the range of time in which we have improved glycemic control in our ICU, multiple other mortality reduction initiatives, any or all of which could account for the decline, occurred simultaneously in our hospital; in addition, mortality rates were falling before the introduction of the new insulin infusion protocol.
Head-to-head comparisons of existing protocols, using agreed upon glucometrics such as time-to-goal range and degree of glycemic variability, are needed.14 Testing new protocols, including proactive insulin infusion adjustments at the time of administration of known caloric loads—such as antibiotics delivered as a bolus in D5W solution—or at the time of initiation of high dose steroids or epinephrine drips, may be a means to keep a higher percentage of blood sugars in range. Ultimately, continuous blood sensing devices with closed loop insulin infusion responses are desired.
For now, our protocol offers a user-friendly means of getting a high percentage of critical care patients into a reasonable glycemic range with a low risk of hypoglycemia. Others are free to use and/or modify it. TH
The authors work at Southwest Washington Medical Center, Vancouver, Wash.
References
- van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001 Nov 8;345(19):1359-1367.
- Malmberg K, Norhammar A, Wedel H, et al. Glycometabolic state at admission: important risk marker of mortality in conventionally treated patients with diabetes mellitus and acute myocardial infarction: long-term results from the Diabetes and Insulin-Glucose Infusion in Acute Myocardial Infarction (DIGAMI) study. Circulation. 1999;99:2626-2632.
- Furnary AP, Wu Y, Bookin SO. Clinical effects of hyperglycemia in the cardiac surgery population: the Portland diabetic project. Endocr Pract. 2006 Mar-Apr;12 Suppl 3:22-26.
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006 Feb 2;354(5):449-461.
- Krinsley JS. Effect of an intensive glucose management protocol on the mortality of critically ill adult patients. Mayo Clin Proc. 2004 Aug;79(8):992-1000.
- Pittas AG, Siegel RD, Lau J. Insulin therapy for critically ill hospitalized patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2004 Oct 11;164(18):2005-2011.
- Goldberg PA. Memoirs of a root canal salesman: the successful implementation of a hospital-wide intravenous insulin infusion protocol. Endocr Pract. 2006;12 Suppl 3:79-85.
- Markovitz LJ, Weichmann RJ, Harris N, et al. Description and evaluation of a glycemic management protocol for patients with diabetes undergoing heart surgery. Endocr Pract. 2002 Jan-Feb;8(1):10-18.
- Ku SY, Sayre CA, Hirsch IB, et al. New insulin infusion protocol improves blood glucose control in hospitalized patients without increasing hypoglycemia. Jt Comm J Qual Patient Saf. 2005 Mar;31(3):141-147.
- Furnary AP, Wu Y, Bookin SO. Effect of hyperglycemia and continuous intravenous insulin infusions on outcomes of cardiac surgical procedures: the Portland Diabetic Project. Endocr Pract. 2004 Mar-Apr;10 Suppl 2:21-33.
- In a written communication from Andy Ahmann, MD, OHSU, in 2006.
- Georgia Hospital Association Diabetes Protocols. Chart 6b. Available at: www.adaendo.com/GHA/index.html. Accessed October 29, 2006.
- In a written communication from Terry Clemmer, MD, director, Critical Care Medicine, LDS Hospital, Salt Lake City, Utah, in October 2006.
- Braithwaite SS, Godara H, Song HJ, et al. No patient left behind: evaluation and design of intravenous insulin infusion algorithms. Endocr Pract. 2006 Jul-Aug;12 Suppl 3:72-78.
Evidence from randomized controlled trials and historical series convincingly demonstrates that tight glycemic control in the critical care setting reduces mortality, length of hospital stay, and other morbidities.1-6 Several protocols targeting a range of glucoses have been published.7-10 We modified a protocol used at the University of Washington (Seattle) that targeted glucoses of 80-180 mg/dl to aim for a tighter glycemic goal range of 80-110 mg/dl and effectively lowered blood glucoses in our intensive care unit (ICU) with a low rate of hypoglycemia.9 We share here our protocol and results over the past year.
Methods
Column protocols have the advantage of accommodating rates of insulin infusion adjustment to the individual patient’s degree of insulin resistance. If glucoses are not falling appropriately using one column, a protocol is followed to move to a more aggressive column. If glucoses fall precipitously, a similar process guides the nurse to a less aggressive column. The column format avoids the need for nurses to do calculations, which reduces the possibility of error.
In August 2005, in our ICU, we piloted a four-column protocol used at the University of Washington. This protocol was designed with an initial target glucose range of 80-180 mg/dl, and during our pilot it did not work well because we were targeting a glucose range of 80-110 mg/dl. Our ICU nursing staff at Southwest Washington Medical Center (SWMC), Vancouver, preferred to revise the column format rather than switch to a different type of protocol such as the Portland Protocol. We therefore created a new six-column protocol targeting the 80-110 mg/dl glucose range. (See Figure 1, above.)
In creating this protocol, we reviewed infusion rates in an unpublished Oregon Health and Sciences University (OHSU), Portland, six-column protocol and the Georgia Hospital Association, Marietta, 10-column protocol.11,12 Our current version includes new glucose ranges of 70-89 mg/dl, 90-99 mg/dl, and 100-109 mg/dl to allow for more rate adjustments within the overall target range, while our previous version had only one glucose category of 70-109 mg/dl within the target range.
Nursing feedback also led us to modify criteria for moving to the right (more aggressive) column as follows: If blood glucose is lower than 200, algorithm failure is defined as glucose outside of goal range and not decreased since previous reading; if blood glucose is greater than or equal to 200, algorithm failure is defined as glucose outside of goal range and has not decreased by at least 60 mg/dl within one hour. The longest interval we allow between glucometer checks for stable patients is two hours. Automatic triggers for implementing the protocol include two consecutive glucoses over 140 mg/dl or a single glucose over 180 mg/dl.
Our revised protocol succeeded when we intensified nursing education, solicited frequent nursing feedback, and organized the procedure so that ICU nurse managers drove the process with a responsive physician/pharmacist team.
Results
In March 2006 we instituted the revised six-column insulin infusion protocol in our ICU. The percent of glucometer readings in the ICU between 70-150 mg/dl increased from 58% in February 2006 to 78% in August of 2006. (See Figure 2, above.) In our cardiac care unit (CCU), where an older, non-column insulin infusion protocol continued to be used, glucoses went from 50% in the 70-150 mg/dl range in February 2006 to 61% in that range in July 2006. When we began the six-column ICU insulin infusion protocol in the CCU in August 2006, 66% of glucoses were in the 70-150 range. (See Figure 3, p. 43.)
The percentage of glucoses below 70 mg/dl increased from 2%-3% using the four-column protocol to 4%-5% using the six-column protocol, as the percentage of glucoses between 70-150 mg/dl rose above 70%.
The main complaint from nurses relates to the need for frequent (hourly to twice hourly) glucose monitoring, which was also a complaint with earlier protocols in our institution.
Discussion
These results compare favorably with those achieved by acknowledged leaders in critical care glycemic control in the United States.13 We have achieved them with the use of a safe column protocol that our critical care nurses are now comfortable using. The hypoglycemia rates with our protocol have been lower than those seen in some other published protocols. The Berghe protocol, for example, reported 5% of patients experiencing glucoses lower than or equal to 40 mg/dl, while our protocol resulted in 4%-5% of glucose values lower than 70 mg/dl.
Mortality rates in our ICU have fallen from 14% in September 2005 to 11% in February 2006 to 8% in August 2006. Although this decline in mortality has occurred over the range of time in which we have improved glycemic control in our ICU, multiple other mortality reduction initiatives, any or all of which could account for the decline, occurred simultaneously in our hospital; in addition, mortality rates were falling before the introduction of the new insulin infusion protocol.
Head-to-head comparisons of existing protocols, using agreed upon glucometrics such as time-to-goal range and degree of glycemic variability, are needed.14 Testing new protocols, including proactive insulin infusion adjustments at the time of administration of known caloric loads—such as antibiotics delivered as a bolus in D5W solution—or at the time of initiation of high dose steroids or epinephrine drips, may be a means to keep a higher percentage of blood sugars in range. Ultimately, continuous blood sensing devices with closed loop insulin infusion responses are desired.
For now, our protocol offers a user-friendly means of getting a high percentage of critical care patients into a reasonable glycemic range with a low risk of hypoglycemia. Others are free to use and/or modify it. TH
The authors work at Southwest Washington Medical Center, Vancouver, Wash.
References
- van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001 Nov 8;345(19):1359-1367.
- Malmberg K, Norhammar A, Wedel H, et al. Glycometabolic state at admission: important risk marker of mortality in conventionally treated patients with diabetes mellitus and acute myocardial infarction: long-term results from the Diabetes and Insulin-Glucose Infusion in Acute Myocardial Infarction (DIGAMI) study. Circulation. 1999;99:2626-2632.
- Furnary AP, Wu Y, Bookin SO. Clinical effects of hyperglycemia in the cardiac surgery population: the Portland diabetic project. Endocr Pract. 2006 Mar-Apr;12 Suppl 3:22-26.
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006 Feb 2;354(5):449-461.
- Krinsley JS. Effect of an intensive glucose management protocol on the mortality of critically ill adult patients. Mayo Clin Proc. 2004 Aug;79(8):992-1000.
- Pittas AG, Siegel RD, Lau J. Insulin therapy for critically ill hospitalized patients: a meta-analysis of randomized controlled trials. Arch Intern Med. 2004 Oct 11;164(18):2005-2011.
- Goldberg PA. Memoirs of a root canal salesman: the successful implementation of a hospital-wide intravenous insulin infusion protocol. Endocr Pract. 2006;12 Suppl 3:79-85.
- Markovitz LJ, Weichmann RJ, Harris N, et al. Description and evaluation of a glycemic management protocol for patients with diabetes undergoing heart surgery. Endocr Pract. 2002 Jan-Feb;8(1):10-18.
- Ku SY, Sayre CA, Hirsch IB, et al. New insulin infusion protocol improves blood glucose control in hospitalized patients without increasing hypoglycemia. Jt Comm J Qual Patient Saf. 2005 Mar;31(3):141-147.
- Furnary AP, Wu Y, Bookin SO. Effect of hyperglycemia and continuous intravenous insulin infusions on outcomes of cardiac surgical procedures: the Portland Diabetic Project. Endocr Pract. 2004 Mar-Apr;10 Suppl 2:21-33.
- In a written communication from Andy Ahmann, MD, OHSU, in 2006.
- Georgia Hospital Association Diabetes Protocols. Chart 6b. Available at: www.adaendo.com/GHA/index.html. Accessed October 29, 2006.
- In a written communication from Terry Clemmer, MD, director, Critical Care Medicine, LDS Hospital, Salt Lake City, Utah, in October 2006.
- Braithwaite SS, Godara H, Song HJ, et al. No patient left behind: evaluation and design of intravenous insulin infusion algorithms. Endocr Pract. 2006 Jul-Aug;12 Suppl 3:72-78.
Focus on Family

Many physicians see being a hospitalist as an opportunity to focus on direct patient care. For Mary Ottolini, MD, it is a way to have it all. Every day, she cares for patients at Children’s National Medical Center in Washington, D.C., teaches at Children’s and at George Washington University School of Medicine in Washington, D.C., serves on a variety of committees and in numerous organizations, and works as a department head.
Early Start, Full Day
“It’s just another typical, crazy day,” says Dr. Ottolini, division chief of the hospitalist division and director of pediatric medical student education at Children’s National Medical Center and professor of pediatrics at George Washington, as she walks briskly down the hall at 9 a.m. on her way to radiology rounds. Her day actually starts at about 7 a.m., when she sees overnight admissions and addresses any urgent problems that require her attention. By 9 a.m., her day is in full swing.
During radiology rounds she and her team, which consists of residents, interns, and third-year medical students, review films from the previous day with the radiologist. The group addresses issues such as what additional tests might be useful. Sometimes they try to determine whether a condition is the result of an illness or injury.
Leaving radiology, Dr. Ottolini and her team head to the ward for patient rounds. As they walk to the first room, they pass cheerful murals featuring cartoon characters and several paintings and drawings created by children. A third-year resident leads the rounds, filling the group in on each patient’s condition and progress. Dr. Ottolini conducts the physical exams and talks to family members when they are present. When she offers her thoughts and comments to the group, the students listen attentively and take notes as she talks.
At one point, the team has to send for a translator for a non-English speaking family. Dr. Ottolini explains that this is common. In fact, Children’s has translators readily available who speak several common languages, including Spanish, French, and Japanese. Additionally, they have access to individuals who speak just about any language that arises.
Despite the ready availability of translators, these family discussions can be challenging. “When we have the translator, we are trying to balance efficiency with effective family communication,” explains Dr. Ottolini. “The translator adds a time factor because everything has to be repeated, and then there’s a lag time when we are looking at each other and waiting for the translation. It works, but it adds a layer of complexity to the situation, especially when you are trying to teach trainees while addressing parental concerns.”
—Mary Ottolini, MD, division chief, Hospitalist Division, and director of pediatric medical student education, Children’s National Medical Center, Washington, D.C.
Family Matters
Family communication is an important part of Dr. Ottolini’s daily activities. Because she doesn’t have a previous relationship with the patient or family, Dr. Ottolini faces the task of establishing rapport quickly—often in the midst of a crisis. “Especially when the child is seriously ill, it can be challenging to establish a level of trust,” she says. “For me, it’s a matter of trying to put myself in the parents’ shoes.”
Dr. Ottolini has also gained insights from being on the other side of the doctor-patient relationship. “I had an amazing relationship with a doctor who helped me tremendously, and I think of that,” she says. “Part of it is listening and trying to understand what is concerning the family the most. Sometimes, this is not what we think is the greatest concern. If we can get past what’s troubling them, it helps to move the care plan forward and establish a trusting relationship.
“There is no substitute for spending time with the family and getting to know them a little,” she continues. “It is important to understand how the illness is affecting the family’s routines, and helping to resolve these issues is useful as well.”
Dr. Ottolini’s concern for the family is evident in her interactions with them. She speaks with them gently, asks questions, and listens compassionately. Occasionally, Dr. Ottolini will schedule a family conference to address family concerns or other issues. “Family meetings are based on patient complexity—when there is multi-organ system involvement,” she says. “Sometimes, if the parents’ long-term expectations for their child’s prognosis are unrealistic, we want to have a meeting so that they can hear—from different sub-specialists involved—our rationale for what we are recommending— and [so that we can] clarify issues they don’t understand.”
Another level of concern involves families with limited resources. For example, “We have many recent immigrants for whom navigating the system is challenging,” says Dr. Ottolini. “We help them ensure that their child gets the best possible care, and we work to address work schedules and other issues.”
First and foremost, she and her team are patient and family advocates. “If we think it is important or necessary, we will keep a child here even if the insurance company says no,” she says.

Busy Afternoons, Late Days
By 1 p.m., Dr. Ottolini’s day is far from over. Her afternoon is filled with a variety of activities. In addition to seeing new patients, she spends time on billing and administrative activities, holds teaching sessions with medical students and residents at bedside and in the classroom, and writes notes.
“I still write my notes by hand,” she says. “However, this will be computerized in a year or so. When I finish with all of my clinical work and teaching responsibilities, I can catch up on administrative responsibilities or work on one of my research projects.”
Currently she is studying “ways to best conduct rounds and ensure that residents and students can take the information they get and put it all together to clinically problem solve and to see the big picture.”
Committee work is a big part of Dr. Ottolini’s work life. In addition to serving on several hospital committees, she also serves on the George Washington University faculty senate. Elsewhere, she is involved in several national organizations, including SHM.
Talking with families isn’t the only communication activity that takes Dr. Ottolini’s time. She works hard to keep referring physicians informed and to ensure they are involved in the patient’s care as necessary.
“We keep the patient’s pediatrician in the loop as much as possible. We make sure he or she understands how the disease process was managed, what new diagnoses arose, what prescription changes there were, and what follow-up is recommended,” Dr. Ottolini says. She especially wants to involve the pediatrician when a patient is critically ill or when the family is upset or in crisis. “Having a family voice to talk to helps the family feel as if they are getting support from someone they trust,” she explains. “This can be very reassuring for them.”
Dr. Ottolini encourages her students to appreciate the role and involvement of the pediatrician in a hospitalized patient’s care. “I try to make sure that residents and students have some sense of what it is like to be on the other side of things,” she offers. “I encourage them to think about how they would like to be treated if they were the pediatrician.”
Some physicians choose to become hospitalists because they want to spend the majority of their time on direct patient care. While Dr. Ottolini takes great satisfaction from this part of her work, it currently comprises only 30% of her professional time. Forty percent of her time involves medical education and research, which Dr. Ottolini greatly enjoys; administrative activities take up the remaining 30% of her time.
Many hospitalists appreciate the opportunities they have to teach, and Dr. Ottolini is no exception. She proudly observes that several physicians she has taught or mentored have become hospitalists: “For me, this is one of the most satisfying things.”
Admit and Discharge Issues
Dr. Ottolini has some involvement with admission and discharge issues. These decisions are simplified by the involvement of an expert team, however. For example, “We have case managers on rounds with us, and this helps them understand nuances of what we are doing that may not be exclusive in the notes and why it may be important for a patient to stay or appropriate for him or her to be discharged,” she says. “We look at patients’ criteria for discharge and anticipate, [on] the day before, any potential delays that could affect their release—such as getting tests performed and results back.”
Discharge planning is key. “We plan ahead for discharge and communicate goals to the family—such as getting the child off oxygen, getting cultures finalized, and so on,” says Dr. Ottolini. “We assign a discharge time the day before and make sure that the discharge summary, all necessary paperwork, and prescriptions are ready to go.”
For Dr. Ottolini, involvement in admission is limited. “The majority of our patients come through the emergency department,” she says. “However, we do admit patients coming in from the community, and we have input with community physicians if it’s not a clear-cut decision.”
The length of stay (LOS) for the nearly 300 beds in the hospital varies based on the patient’s condition. The average LOS for patients in the short-stay unit is three days. Facility-wide, the average LOS ranges from three to five days.
Challenges, Frustrations, Rewards, and Successes
“Challenges—such as dealing with very ill children who are not going to survive and addressing social situations where children are abused—also are rewarding, [and] we know we have worked in the best interest of the children,” says Dr. Ottolini. She and her team have the satisfaction of knowing they did everything they could to protect their patients, provide them with excellent care, and maximize their quality of life.
Dr. Ottolini says that she faces many of the same frustrations as others who work in a large organization. “With medically fragile children, a lot of coordination and communication needs to take place,” she says. “Sometimes, when lines of communication break down, you think something is happening when it isn’t. For example, after you have prepared a patient for an MRI, you find out that he or she has been bumped because of a more urgent situation. This frustrates the family and affects all of us.”
Pride of a Seasoned Hospitalist
A hospitalist since 1992, Dr. Ottolini is proud to have the title. She enjoys the teamwork she experiences on a daily basis, and even the challenges she experiences bring her tremendous professional and personal satisfaction.
While she sees herself as a generalist, Dr. Ottolini says her work “has enabled me to become especially good at those diagnoses we see a lot of—such as infectious disease problems and dehydration and fluid imbalance.”
An area in which Dr. Ottolini has become something of an expert is one that she would rather not have to see. “Sometimes we are lucky and see no abuse and neglect cases. The majority of the time, there is at least one admitted in a two-week period,” she says. “Out of necessity, I have learned quite a bit about abuse and neglect and caring for children who are abused and neglected. And, in presenting testimony on various cases, I have learned a bit about the court system.”
Helping students deal with this difficult reality is an important part of her teaching and mentoring activities. “From a clinical viewpoint, I help my students understand how to evaluate patients and look for red flags suggesting abuse or neglect,” she says. “However, it also is important for them to consider abuse in terms of different problems.”
Dr. Ottolini teaches her students “not to be closed-minded and not to be prejudiced concerning patients’ socieoeconomic status. They need to understand that abuse and neglect don’t just happen to poor children.”
From a personal standpoint, “we really need to focus on caring for children and not focus on who’s to blame. We want to work in a therapeutic relationship with parents as well as the child,” explains Dr. Ottolini. “It is not for us to figure out who is responsible for the abuse or neglect but to care for the child and work with the parent who is there. It is our job to make it clear to the police when abuse has occurred. Then we make sure that the situation to which the child is being sent when he or she leaves the hospital is reasonable and safe.”
A Happy Hospitalist
Dr. Ottolini rushes down the hall to see a patient as two residents hurry to keep up with her. They pepper her with questions as they walk, and she answers between glances at the chart in front of her. The smile on her face makes it clear that she is enjoying every minute of her “busy, crazy day.” TH
Joanne Kaldy writes regularly for The Hospitalist.
Many physicians see being a hospitalist as an opportunity to focus on direct patient care. For Mary Ottolini, MD, it is a way to have it all. Every day, she cares for patients at Children’s National Medical Center in Washington, D.C., teaches at Children’s and at George Washington University School of Medicine in Washington, D.C., serves on a variety of committees and in numerous organizations, and works as a department head.
Early Start, Full Day
“It’s just another typical, crazy day,” says Dr. Ottolini, division chief of the hospitalist division and director of pediatric medical student education at Children’s National Medical Center and professor of pediatrics at George Washington, as she walks briskly down the hall at 9 a.m. on her way to radiology rounds. Her day actually starts at about 7 a.m., when she sees overnight admissions and addresses any urgent problems that require her attention. By 9 a.m., her day is in full swing.
During radiology rounds she and her team, which consists of residents, interns, and third-year medical students, review films from the previous day with the radiologist. The group addresses issues such as what additional tests might be useful. Sometimes they try to determine whether a condition is the result of an illness or injury.
Leaving radiology, Dr. Ottolini and her team head to the ward for patient rounds. As they walk to the first room, they pass cheerful murals featuring cartoon characters and several paintings and drawings created by children. A third-year resident leads the rounds, filling the group in on each patient’s condition and progress. Dr. Ottolini conducts the physical exams and talks to family members when they are present. When she offers her thoughts and comments to the group, the students listen attentively and take notes as she talks.
At one point, the team has to send for a translator for a non-English speaking family. Dr. Ottolini explains that this is common. In fact, Children’s has translators readily available who speak several common languages, including Spanish, French, and Japanese. Additionally, they have access to individuals who speak just about any language that arises.
Despite the ready availability of translators, these family discussions can be challenging. “When we have the translator, we are trying to balance efficiency with effective family communication,” explains Dr. Ottolini. “The translator adds a time factor because everything has to be repeated, and then there’s a lag time when we are looking at each other and waiting for the translation. It works, but it adds a layer of complexity to the situation, especially when you are trying to teach trainees while addressing parental concerns.”
—Mary Ottolini, MD, division chief, Hospitalist Division, and director of pediatric medical student education, Children’s National Medical Center, Washington, D.C.
Family Matters
Family communication is an important part of Dr. Ottolini’s daily activities. Because she doesn’t have a previous relationship with the patient or family, Dr. Ottolini faces the task of establishing rapport quickly—often in the midst of a crisis. “Especially when the child is seriously ill, it can be challenging to establish a level of trust,” she says. “For me, it’s a matter of trying to put myself in the parents’ shoes.”
Dr. Ottolini has also gained insights from being on the other side of the doctor-patient relationship. “I had an amazing relationship with a doctor who helped me tremendously, and I think of that,” she says. “Part of it is listening and trying to understand what is concerning the family the most. Sometimes, this is not what we think is the greatest concern. If we can get past what’s troubling them, it helps to move the care plan forward and establish a trusting relationship.
“There is no substitute for spending time with the family and getting to know them a little,” she continues. “It is important to understand how the illness is affecting the family’s routines, and helping to resolve these issues is useful as well.”
Dr. Ottolini’s concern for the family is evident in her interactions with them. She speaks with them gently, asks questions, and listens compassionately. Occasionally, Dr. Ottolini will schedule a family conference to address family concerns or other issues. “Family meetings are based on patient complexity—when there is multi-organ system involvement,” she says. “Sometimes, if the parents’ long-term expectations for their child’s prognosis are unrealistic, we want to have a meeting so that they can hear—from different sub-specialists involved—our rationale for what we are recommending— and [so that we can] clarify issues they don’t understand.”
Another level of concern involves families with limited resources. For example, “We have many recent immigrants for whom navigating the system is challenging,” says Dr. Ottolini. “We help them ensure that their child gets the best possible care, and we work to address work schedules and other issues.”
First and foremost, she and her team are patient and family advocates. “If we think it is important or necessary, we will keep a child here even if the insurance company says no,” she says.
Busy Afternoons, Late Days
By 1 p.m., Dr. Ottolini’s day is far from over. Her afternoon is filled with a variety of activities. In addition to seeing new patients, she spends time on billing and administrative activities, holds teaching sessions with medical students and residents at bedside and in the classroom, and writes notes.
“I still write my notes by hand,” she says. “However, this will be computerized in a year or so. When I finish with all of my clinical work and teaching responsibilities, I can catch up on administrative responsibilities or work on one of my research projects.”
Currently she is studying “ways to best conduct rounds and ensure that residents and students can take the information they get and put it all together to clinically problem solve and to see the big picture.”
Committee work is a big part of Dr. Ottolini’s work life. In addition to serving on several hospital committees, she also serves on the George Washington University faculty senate. Elsewhere, she is involved in several national organizations, including SHM.
Talking with families isn’t the only communication activity that takes Dr. Ottolini’s time. She works hard to keep referring physicians informed and to ensure they are involved in the patient’s care as necessary.
“We keep the patient’s pediatrician in the loop as much as possible. We make sure he or she understands how the disease process was managed, what new diagnoses arose, what prescription changes there were, and what follow-up is recommended,” Dr. Ottolini says. She especially wants to involve the pediatrician when a patient is critically ill or when the family is upset or in crisis. “Having a family voice to talk to helps the family feel as if they are getting support from someone they trust,” she explains. “This can be very reassuring for them.”
Dr. Ottolini encourages her students to appreciate the role and involvement of the pediatrician in a hospitalized patient’s care. “I try to make sure that residents and students have some sense of what it is like to be on the other side of things,” she offers. “I encourage them to think about how they would like to be treated if they were the pediatrician.”
Some physicians choose to become hospitalists because they want to spend the majority of their time on direct patient care. While Dr. Ottolini takes great satisfaction from this part of her work, it currently comprises only 30% of her professional time. Forty percent of her time involves medical education and research, which Dr. Ottolini greatly enjoys; administrative activities take up the remaining 30% of her time.
Many hospitalists appreciate the opportunities they have to teach, and Dr. Ottolini is no exception. She proudly observes that several physicians she has taught or mentored have become hospitalists: “For me, this is one of the most satisfying things.”
Admit and Discharge Issues
Dr. Ottolini has some involvement with admission and discharge issues. These decisions are simplified by the involvement of an expert team, however. For example, “We have case managers on rounds with us, and this helps them understand nuances of what we are doing that may not be exclusive in the notes and why it may be important for a patient to stay or appropriate for him or her to be discharged,” she says. “We look at patients’ criteria for discharge and anticipate, [on] the day before, any potential delays that could affect their release—such as getting tests performed and results back.”
Discharge planning is key. “We plan ahead for discharge and communicate goals to the family—such as getting the child off oxygen, getting cultures finalized, and so on,” says Dr. Ottolini. “We assign a discharge time the day before and make sure that the discharge summary, all necessary paperwork, and prescriptions are ready to go.”
For Dr. Ottolini, involvement in admission is limited. “The majority of our patients come through the emergency department,” she says. “However, we do admit patients coming in from the community, and we have input with community physicians if it’s not a clear-cut decision.”
The length of stay (LOS) for the nearly 300 beds in the hospital varies based on the patient’s condition. The average LOS for patients in the short-stay unit is three days. Facility-wide, the average LOS ranges from three to five days.
Challenges, Frustrations, Rewards, and Successes
“Challenges—such as dealing with very ill children who are not going to survive and addressing social situations where children are abused—also are rewarding, [and] we know we have worked in the best interest of the children,” says Dr. Ottolini. She and her team have the satisfaction of knowing they did everything they could to protect their patients, provide them with excellent care, and maximize their quality of life.
Dr. Ottolini says that she faces many of the same frustrations as others who work in a large organization. “With medically fragile children, a lot of coordination and communication needs to take place,” she says. “Sometimes, when lines of communication break down, you think something is happening when it isn’t. For example, after you have prepared a patient for an MRI, you find out that he or she has been bumped because of a more urgent situation. This frustrates the family and affects all of us.”
Pride of a Seasoned Hospitalist
A hospitalist since 1992, Dr. Ottolini is proud to have the title. She enjoys the teamwork she experiences on a daily basis, and even the challenges she experiences bring her tremendous professional and personal satisfaction.
While she sees herself as a generalist, Dr. Ottolini says her work “has enabled me to become especially good at those diagnoses we see a lot of—such as infectious disease problems and dehydration and fluid imbalance.”
An area in which Dr. Ottolini has become something of an expert is one that she would rather not have to see. “Sometimes we are lucky and see no abuse and neglect cases. The majority of the time, there is at least one admitted in a two-week period,” she says. “Out of necessity, I have learned quite a bit about abuse and neglect and caring for children who are abused and neglected. And, in presenting testimony on various cases, I have learned a bit about the court system.”
Helping students deal with this difficult reality is an important part of her teaching and mentoring activities. “From a clinical viewpoint, I help my students understand how to evaluate patients and look for red flags suggesting abuse or neglect,” she says. “However, it also is important for them to consider abuse in terms of different problems.”
Dr. Ottolini teaches her students “not to be closed-minded and not to be prejudiced concerning patients’ socieoeconomic status. They need to understand that abuse and neglect don’t just happen to poor children.”
From a personal standpoint, “we really need to focus on caring for children and not focus on who’s to blame. We want to work in a therapeutic relationship with parents as well as the child,” explains Dr. Ottolini. “It is not for us to figure out who is responsible for the abuse or neglect but to care for the child and work with the parent who is there. It is our job to make it clear to the police when abuse has occurred. Then we make sure that the situation to which the child is being sent when he or she leaves the hospital is reasonable and safe.”
A Happy Hospitalist
Dr. Ottolini rushes down the hall to see a patient as two residents hurry to keep up with her. They pepper her with questions as they walk, and she answers between glances at the chart in front of her. The smile on her face makes it clear that she is enjoying every minute of her “busy, crazy day.” TH
Joanne Kaldy writes regularly for The Hospitalist.
Many physicians see being a hospitalist as an opportunity to focus on direct patient care. For Mary Ottolini, MD, it is a way to have it all. Every day, she cares for patients at Children’s National Medical Center in Washington, D.C., teaches at Children’s and at George Washington University School of Medicine in Washington, D.C., serves on a variety of committees and in numerous organizations, and works as a department head.
Early Start, Full Day
“It’s just another typical, crazy day,” says Dr. Ottolini, division chief of the hospitalist division and director of pediatric medical student education at Children’s National Medical Center and professor of pediatrics at George Washington, as she walks briskly down the hall at 9 a.m. on her way to radiology rounds. Her day actually starts at about 7 a.m., when she sees overnight admissions and addresses any urgent problems that require her attention. By 9 a.m., her day is in full swing.
During radiology rounds she and her team, which consists of residents, interns, and third-year medical students, review films from the previous day with the radiologist. The group addresses issues such as what additional tests might be useful. Sometimes they try to determine whether a condition is the result of an illness or injury.
Leaving radiology, Dr. Ottolini and her team head to the ward for patient rounds. As they walk to the first room, they pass cheerful murals featuring cartoon characters and several paintings and drawings created by children. A third-year resident leads the rounds, filling the group in on each patient’s condition and progress. Dr. Ottolini conducts the physical exams and talks to family members when they are present. When she offers her thoughts and comments to the group, the students listen attentively and take notes as she talks.
At one point, the team has to send for a translator for a non-English speaking family. Dr. Ottolini explains that this is common. In fact, Children’s has translators readily available who speak several common languages, including Spanish, French, and Japanese. Additionally, they have access to individuals who speak just about any language that arises.
Despite the ready availability of translators, these family discussions can be challenging. “When we have the translator, we are trying to balance efficiency with effective family communication,” explains Dr. Ottolini. “The translator adds a time factor because everything has to be repeated, and then there’s a lag time when we are looking at each other and waiting for the translation. It works, but it adds a layer of complexity to the situation, especially when you are trying to teach trainees while addressing parental concerns.”
—Mary Ottolini, MD, division chief, Hospitalist Division, and director of pediatric medical student education, Children’s National Medical Center, Washington, D.C.
Family Matters
Family communication is an important part of Dr. Ottolini’s daily activities. Because she doesn’t have a previous relationship with the patient or family, Dr. Ottolini faces the task of establishing rapport quickly—often in the midst of a crisis. “Especially when the child is seriously ill, it can be challenging to establish a level of trust,” she says. “For me, it’s a matter of trying to put myself in the parents’ shoes.”
Dr. Ottolini has also gained insights from being on the other side of the doctor-patient relationship. “I had an amazing relationship with a doctor who helped me tremendously, and I think of that,” she says. “Part of it is listening and trying to understand what is concerning the family the most. Sometimes, this is not what we think is the greatest concern. If we can get past what’s troubling them, it helps to move the care plan forward and establish a trusting relationship.
“There is no substitute for spending time with the family and getting to know them a little,” she continues. “It is important to understand how the illness is affecting the family’s routines, and helping to resolve these issues is useful as well.”
Dr. Ottolini’s concern for the family is evident in her interactions with them. She speaks with them gently, asks questions, and listens compassionately. Occasionally, Dr. Ottolini will schedule a family conference to address family concerns or other issues. “Family meetings are based on patient complexity—when there is multi-organ system involvement,” she says. “Sometimes, if the parents’ long-term expectations for their child’s prognosis are unrealistic, we want to have a meeting so that they can hear—from different sub-specialists involved—our rationale for what we are recommending— and [so that we can] clarify issues they don’t understand.”
Another level of concern involves families with limited resources. For example, “We have many recent immigrants for whom navigating the system is challenging,” says Dr. Ottolini. “We help them ensure that their child gets the best possible care, and we work to address work schedules and other issues.”
First and foremost, she and her team are patient and family advocates. “If we think it is important or necessary, we will keep a child here even if the insurance company says no,” she says.
Busy Afternoons, Late Days
By 1 p.m., Dr. Ottolini’s day is far from over. Her afternoon is filled with a variety of activities. In addition to seeing new patients, she spends time on billing and administrative activities, holds teaching sessions with medical students and residents at bedside and in the classroom, and writes notes.
“I still write my notes by hand,” she says. “However, this will be computerized in a year or so. When I finish with all of my clinical work and teaching responsibilities, I can catch up on administrative responsibilities or work on one of my research projects.”
Currently she is studying “ways to best conduct rounds and ensure that residents and students can take the information they get and put it all together to clinically problem solve and to see the big picture.”
Committee work is a big part of Dr. Ottolini’s work life. In addition to serving on several hospital committees, she also serves on the George Washington University faculty senate. Elsewhere, she is involved in several national organizations, including SHM.
Talking with families isn’t the only communication activity that takes Dr. Ottolini’s time. She works hard to keep referring physicians informed and to ensure they are involved in the patient’s care as necessary.
“We keep the patient’s pediatrician in the loop as much as possible. We make sure he or she understands how the disease process was managed, what new diagnoses arose, what prescription changes there were, and what follow-up is recommended,” Dr. Ottolini says. She especially wants to involve the pediatrician when a patient is critically ill or when the family is upset or in crisis. “Having a family voice to talk to helps the family feel as if they are getting support from someone they trust,” she explains. “This can be very reassuring for them.”
Dr. Ottolini encourages her students to appreciate the role and involvement of the pediatrician in a hospitalized patient’s care. “I try to make sure that residents and students have some sense of what it is like to be on the other side of things,” she offers. “I encourage them to think about how they would like to be treated if they were the pediatrician.”
Some physicians choose to become hospitalists because they want to spend the majority of their time on direct patient care. While Dr. Ottolini takes great satisfaction from this part of her work, it currently comprises only 30% of her professional time. Forty percent of her time involves medical education and research, which Dr. Ottolini greatly enjoys; administrative activities take up the remaining 30% of her time.
Many hospitalists appreciate the opportunities they have to teach, and Dr. Ottolini is no exception. She proudly observes that several physicians she has taught or mentored have become hospitalists: “For me, this is one of the most satisfying things.”
Admit and Discharge Issues
Dr. Ottolini has some involvement with admission and discharge issues. These decisions are simplified by the involvement of an expert team, however. For example, “We have case managers on rounds with us, and this helps them understand nuances of what we are doing that may not be exclusive in the notes and why it may be important for a patient to stay or appropriate for him or her to be discharged,” she says. “We look at patients’ criteria for discharge and anticipate, [on] the day before, any potential delays that could affect their release—such as getting tests performed and results back.”
Discharge planning is key. “We plan ahead for discharge and communicate goals to the family—such as getting the child off oxygen, getting cultures finalized, and so on,” says Dr. Ottolini. “We assign a discharge time the day before and make sure that the discharge summary, all necessary paperwork, and prescriptions are ready to go.”
For Dr. Ottolini, involvement in admission is limited. “The majority of our patients come through the emergency department,” she says. “However, we do admit patients coming in from the community, and we have input with community physicians if it’s not a clear-cut decision.”
The length of stay (LOS) for the nearly 300 beds in the hospital varies based on the patient’s condition. The average LOS for patients in the short-stay unit is three days. Facility-wide, the average LOS ranges from three to five days.
Challenges, Frustrations, Rewards, and Successes
“Challenges—such as dealing with very ill children who are not going to survive and addressing social situations where children are abused—also are rewarding, [and] we know we have worked in the best interest of the children,” says Dr. Ottolini. She and her team have the satisfaction of knowing they did everything they could to protect their patients, provide them with excellent care, and maximize their quality of life.
Dr. Ottolini says that she faces many of the same frustrations as others who work in a large organization. “With medically fragile children, a lot of coordination and communication needs to take place,” she says. “Sometimes, when lines of communication break down, you think something is happening when it isn’t. For example, after you have prepared a patient for an MRI, you find out that he or she has been bumped because of a more urgent situation. This frustrates the family and affects all of us.”
Pride of a Seasoned Hospitalist
A hospitalist since 1992, Dr. Ottolini is proud to have the title. She enjoys the teamwork she experiences on a daily basis, and even the challenges she experiences bring her tremendous professional and personal satisfaction.
While she sees herself as a generalist, Dr. Ottolini says her work “has enabled me to become especially good at those diagnoses we see a lot of—such as infectious disease problems and dehydration and fluid imbalance.”
An area in which Dr. Ottolini has become something of an expert is one that she would rather not have to see. “Sometimes we are lucky and see no abuse and neglect cases. The majority of the time, there is at least one admitted in a two-week period,” she says. “Out of necessity, I have learned quite a bit about abuse and neglect and caring for children who are abused and neglected. And, in presenting testimony on various cases, I have learned a bit about the court system.”
Helping students deal with this difficult reality is an important part of her teaching and mentoring activities. “From a clinical viewpoint, I help my students understand how to evaluate patients and look for red flags suggesting abuse or neglect,” she says. “However, it also is important for them to consider abuse in terms of different problems.”
Dr. Ottolini teaches her students “not to be closed-minded and not to be prejudiced concerning patients’ socieoeconomic status. They need to understand that abuse and neglect don’t just happen to poor children.”
From a personal standpoint, “we really need to focus on caring for children and not focus on who’s to blame. We want to work in a therapeutic relationship with parents as well as the child,” explains Dr. Ottolini. “It is not for us to figure out who is responsible for the abuse or neglect but to care for the child and work with the parent who is there. It is our job to make it clear to the police when abuse has occurred. Then we make sure that the situation to which the child is being sent when he or she leaves the hospital is reasonable and safe.”
A Happy Hospitalist
Dr. Ottolini rushes down the hall to see a patient as two residents hurry to keep up with her. They pepper her with questions as they walk, and she answers between glances at the chart in front of her. The smile on her face makes it clear that she is enjoying every minute of her “busy, crazy day.” TH
Joanne Kaldy writes regularly for The Hospitalist.
Why Do Hospitalist Programs Risk Failure?
The purported benefits of hospital medicine, including reduced lengths of stay, cost savings and quality improvement for the hospital, and higher satisfaction for primary care physicians and patients, have been widely discussed. But are these positive outcomes always ensured when a hospital or a medical group decides to start a hospitalist program?
If the program is launched without adequate planning, a viable business plan, sufficient staffing, or other basic components of any successful business enterprise, the results may disappoint. The program may not deliver desired outcomes in terms of quality or cost savings. Hospitalist staff may become disillusioned, overworked, or burned out and then leave. The program might even fail, which is doubly problematic once physicians and hospital administrators have gotten used to the advantages of having hospitalist coverage in their facility.
What Not to Do … and How to Fix It
A hospitalist service started by Lewis-Gale Clinic, a multi-specialty medical group in Salem, Va., and practicing at 521-bed Lewis-Gale Medical Center, experienced serious problems after its launch in 1997.
“Our program initially wasn’t a true hospitalist program per se, but more like a service provided to internists in the medical group,” says Harsukh Patolia, MD, the hospitalist program’s medical director. “I was the first person hired. I made it clear that I wanted to be a hospitalist. But there were not many models available for us to base our program on.”
Demand was great from clinic physicians, who no longer had time to see their patients at the hospital, says Dr. Patolia. Three additional hospitalists were hired, but by 1999, one had left and the others were stressed out and overworked. “We were working very hard,” he says. But the program was dependent on locum tenens physicians to fill shifts, and quality was starting to suffer. “I’m not sure we were on the brink of failure, but there was a lot of dissatisfaction.”
Jon Ness, then the medical group’s administrator, identified a problem with the hospitalist service soon after he started work in Salem in 1999. “My sense was that both the hospital and medical staff really wanted the program and didn’t want to see it fail. But they didn’t understand why we were having so many challenges with it,” he says. “The first thing we did was a thorough clinical and administrative review of the program. The more information I collected, the more concerned I got.”
Recognizing that there wasn’t enough expertise within the organization to sort out the problems, Ness contacted Colorado Springs, Colo., consultant Roger Heroux of Hospitalist Management Resources, LLC. Additionally, he approached Lewis-Gale Medical Center’s new CEO, James Thweatt, who also realized that there was a problem with the program.
“If they hadn’t come to me, I would have gone to them with my recommendation for a consultant,” adds Thweatt. Basically, there were serious lacks in terms of logistical support for the service, of clarity in its strategic goals, and of authority for the practice’s leadership, while its relationship with the rest of the clinic was also deteriorating.
“With the changing face of healthcare, a viable hospitalist program was a necessity,” Thweatt says. He also had to satisfy the demands of physicians—not only those belonging to the group practice but also independent primary care practitioners in the community—or else they might take their patients to a competing hospital.
Ness and Heroux surveyed physicians about their needs and desires for the program, visiting a number of key physicians in their offices. Another challenge they handled was to negotiate a contract with the hospital for the hospitalists’ services, including a subsidy to reflect their 24/7 coverage in the hospital. Then they needed to agree on appropriate quality and financial performance measures by which to gauge the program’s success.
“With Roger’s help, we all got smarter about what a true hospitalist program was,” says Ness. “What I discovered was that a hospitalist program is no different than any other significant business venture. It needs its own goals, leadership, and overarching business plan. You can’t just put it in place and assume that you’ll be successful. It requires just as much discipline, rigor, and hard work as other businesses.”
Practice Management Tasks
A comprehensive list of why some hospitalist programs risk failure, including problems with recruitment, retention, scheduling, compensation, communication with primary physicians, buy-in, marketing, data analysis, financial performance, and return on investment for the hospital, would closely track with the content of any hospitalist practice management course. One such course, “Best Practices in Managing a Hospital Medicine Program,” sponsored by SHM and presented at UCSF’s Management of the Hospitalized Patient meeting in San Francisco on October 11 by some of the field’s top consultants and practice leaders, covered these topics.
Heroux was on the UCSF faculty, and he presented his model of the Fourth Generation hospitalist practice that has evolved from a simple rounding model with daily assignments of outpatient physicians, a rotational model with one-week assignments of outpatient physicians, and a group of dedicated hospitalists who lack administrative support. The Fourth Generation hospitalist program is a sustainable, dedicated program that enjoys full clinical and administrative support, including a practice manager and a case manager.
Such a practice provides dedicated 24-hour coverage with realistic staffing ratios, employs effective practice leadership, is strategically aligned with the hospital and medical community, and utilizes a financial management system and data sets for benchmarking of key performance measures demonstrating its value. Without these components in place, Heroux says, the hospitalist program risks serious dysfunction and eventual failure.
Reflecting on his work with Lewis-Gale and other clients, Heroux believes it is important to be disciplined and deliberate about evaluating the real need for a hospitalist service in the community. “Talk to your medical staff. Find out what they want and need from the service. Then prioritize those needs because you can’t do everything at once, and build your business plan on how you’ll meet the identified priorities. Let them drive your staffing patterns and your cost savings targets,” he says. “And make your program data-driven from the start.”
When Heroux started working with Lewis-Gale, they had none of these components. “They were trying to meet the needs without the infrastructure, and that is how they got into trouble,” he says.
Why are some hospitalist programs launched without this kind of support or the business planning that would be de rigueur for any hospital launching a new imaging center or outpatient surgery center? Perhaps the lack of capital investment on equipment for a hospitalist service leads to a casual attitude about doing the needed homework. Or else misconceptions blind hospital administrators to the real complexities and financial implications of a hospitalist program.
“I think there is a mentality sometimes that says, ‘Hey, we’re good managers, we can do this,’ ” suggests Heroux. “Sometimes they don’t know what they don’t know. Many times they don’t want to spend the time and money or get the help [they need] to do it right.”
Do Your Homework
Bruce Becker, MD, a family practice physician and chief medical officer at Medical Center Hospital in Odessa, Texas, spent two years helping his institution do its homework and gathering support within the medical community before the hospital’s board of directors approved a plan for a hospitalist program in July 2006.
“We started exploring a hospitalist program two years ago,” says Dr. Becker. A national company made a proposal to the hospital to develop a turnkey program. “We also attempted to work with private physicians and with the local medical school but couldn’t come to an agreement at that time.”
When the board was first approached with a $100,000 proposal for a consultant’s study, it had the usual concerns about return on investment and volume of demand, Dr. Becker says. But the biggest barrier to the new service was an attitude within the local medical community that hospitalists would disrupt continuity of care and longstanding relationships between physicians and their patients. To address this discomfort, “we decided to go step by step with our consultant—polling the medical staff, administration and board members,” says Dr. Becker. Their responses suggested that sufficient demand existed.
Dr. Becker asked a physician he knew who had set up a hospitalist program in another community to speak to the hospital board. He and several colleagues attended an SHM conference to learn more about the basics of operating a program. Eventually, the board approved a request for proposals (RFP), which was sent to seven potential contractors, both local groups and national companies.
“What we were going through was an educational process,” explains Dr. Becker. “I could see a visible change taking place on the faces of board members. Two years ago, they weren’t ready, and if I had tried to push it, they would have said no. Now they are ready, and our medical staff is much more accepting.” Hospitalists are now being interviewed for the new program, with a projected launch date of July 2007.
The Importance of Leadership
Winthrop Whitcomb, MD, a practicing hospitalist at Mercy Medical Center in Springfield, Mass., and co-founder of SHM, believes the absence of strong practice leadership by someone with leadership and management skills who is based on site and devoted to hospital medicine is the number one reason why hospitalist programs fail. He tells the story of a hospitalist program started by a multi-specialty group that assigned as its medical director a primary care physician who had a busy office practice.
“That leader wasn’t able to have much contact with the group or the day-in, day-out challenges of its growing caseload,” relates Dr. Whitcomb. “The hospitalists began to get demoralized, feeling that no one was advocating for them.” A consultant recommended hiring an on-site leader for the program. The next medical director had some knowledge of medical management and hospital medicine but was only one-quarter-time dedicated to the hospitalist program. Problems of morale, turnover, and service quality continued.
“The leader instituted a few good things, including an incentive-based compensation program, but ultimately was ineffective and unable to develop the staff’s trust,” says Dr. Whitcomb. “I could tell that story over and over again. To put it another way, a lot of the pitfalls can be overcome with a good, strong leader.” Often, programs such as the one he describes flounder but continue to limp along for years, until a good leader comes along to place the program on a stronger footing.
In other cases, a new hospitalist program might be launched with just one physician and limited coverage, with plans to grow from there. “That’s fine, as long as that person you’re starting with is serving in a leadership capacity as well as seeing patients. It’s hard to find a good leader. But you will need somebody who is driving the bus in fairly short order,” says Dr. Whitcomb.
Growth Pains and Other Common Problems
John Nelson, MD, a hospitalist and consultant in Bellevue, Wash., co-founder of SHM, and columnist for The Hospitalist, points out some other common causes of hospitalist program collapse, including the failure to appreciate how rapidly the program will grow or to have a plan for how to deal with growth. “It doesn’t take a year to reach your projections,” he advises. “Suddenly, you’ve got a bigger caseload than the original doctors can handle. They get overwhelmed and burned out and then leave.”
If the hospitalists feel no ownership or personal investment in the practice’s success, they may develop a kind of civil service mentality about the job instead of a customer service mindset, says Dr. Nelson. Combine that with a straight salary instead of productivity incentives, and they may lack the necessary commitment to the program’s quality and growth.
“I also work as a consultant to help other hospitals start hospitalist practices. I’ve had a lot of experience with programs that never got off the ground,” he says. In one case, staff did an analysis to find out how much it would cost to support the program and then decided not to go forward. In that case, the hospital was reimbursed more on per diems than diagnosis-related groups, so reduced lengths of stay would not have benefited the facility.
In other cases, hospitals have not gone forward because of local medical politics or unfounded suspicions about hospital medicine. The dominant local multi-specialty group may insist on operating the hospitalist program itself, refusing to let anyone else do it. But the group makes unrealistic assumptions about workload or else wants to charge the same high overhead rate to the hospitalists that its clinic doctors pay, which is not feasible for a hospitalist program.
“I came to my current position because of a medical group that wanted to control the hospital medicine practice,” says Dr. Nelson. “But then they got busy and exhausted and wanted to quit being hospitalists. At that point, the hospital administrator panicked.”
Learn from Success
Thweatt believes that the hospitalist program at Lewis-Gale Medical Center, which now directly employs the hospitalists, is doing well, with seven full-time dedicated hospitalists. “Not that it’s always easy, but it’s no different than running any other business. If this program went away tomorrow, I think I’d be tarred and feathered by the medical staff,” he quips.
Dr. Patolia adds that the program has a compensation structure based entirely on productivity and a schedule that ensures 24-hour coverage. “We work as a team, and we depend on each other so much. We’re all committed people who want to be hospitalists,” he says. “Right now, I love being a hospitalist to such a degree that I can’t imagine doing anything else.”
Recently, a senior vice president from the hospital’s parent company, Hospital Corporation of America (HCA), visited Lewis-Gale to learn how to replicate its successful hospitalist program in all HCA hospitals.
Jon Ness, now chief operating officer of Billings Clinic in Billings, Mont., says one of the first things he did in his new job was to develop a hospitalist program. “I brought in Roger Heroux to do the evaluation,” he says. The process followed a familiar checklist: defining program goals, lining up clinic and hospital support, assessing manpower needs, and developing a data support system.
The Billings program was launched in January 2006 and today employs six full-time hospitalists. In contrast to the early days at Lewis-Gale, however, “we started out with a strong, deep business plan.”
For more information on the Fourth Generation hospitalist practice, contact Roger Heroux, Partner, Hospitalist Management Resources, LLC, 5490 Creighton Ct., Colorado Springs, CO 80918, 719/331-7119, or [email protected]. Visit the Society of Hospital Medicine Web site (www.hospitalmedicine.org) for information on practice management courses and other educational resources, including audiotapes of “Best Practices in Managing a Hospital Medicine Program.” TH
Larry Beresford is a regular contributor to The Hospitalist.
The purported benefits of hospital medicine, including reduced lengths of stay, cost savings and quality improvement for the hospital, and higher satisfaction for primary care physicians and patients, have been widely discussed. But are these positive outcomes always ensured when a hospital or a medical group decides to start a hospitalist program?
If the program is launched without adequate planning, a viable business plan, sufficient staffing, or other basic components of any successful business enterprise, the results may disappoint. The program may not deliver desired outcomes in terms of quality or cost savings. Hospitalist staff may become disillusioned, overworked, or burned out and then leave. The program might even fail, which is doubly problematic once physicians and hospital administrators have gotten used to the advantages of having hospitalist coverage in their facility.
What Not to Do … and How to Fix It
A hospitalist service started by Lewis-Gale Clinic, a multi-specialty medical group in Salem, Va., and practicing at 521-bed Lewis-Gale Medical Center, experienced serious problems after its launch in 1997.
“Our program initially wasn’t a true hospitalist program per se, but more like a service provided to internists in the medical group,” says Harsukh Patolia, MD, the hospitalist program’s medical director. “I was the first person hired. I made it clear that I wanted to be a hospitalist. But there were not many models available for us to base our program on.”
Demand was great from clinic physicians, who no longer had time to see their patients at the hospital, says Dr. Patolia. Three additional hospitalists were hired, but by 1999, one had left and the others were stressed out and overworked. “We were working very hard,” he says. But the program was dependent on locum tenens physicians to fill shifts, and quality was starting to suffer. “I’m not sure we were on the brink of failure, but there was a lot of dissatisfaction.”
Jon Ness, then the medical group’s administrator, identified a problem with the hospitalist service soon after he started work in Salem in 1999. “My sense was that both the hospital and medical staff really wanted the program and didn’t want to see it fail. But they didn’t understand why we were having so many challenges with it,” he says. “The first thing we did was a thorough clinical and administrative review of the program. The more information I collected, the more concerned I got.”
Recognizing that there wasn’t enough expertise within the organization to sort out the problems, Ness contacted Colorado Springs, Colo., consultant Roger Heroux of Hospitalist Management Resources, LLC. Additionally, he approached Lewis-Gale Medical Center’s new CEO, James Thweatt, who also realized that there was a problem with the program.
“If they hadn’t come to me, I would have gone to them with my recommendation for a consultant,” adds Thweatt. Basically, there were serious lacks in terms of logistical support for the service, of clarity in its strategic goals, and of authority for the practice’s leadership, while its relationship with the rest of the clinic was also deteriorating.
“With the changing face of healthcare, a viable hospitalist program was a necessity,” Thweatt says. He also had to satisfy the demands of physicians—not only those belonging to the group practice but also independent primary care practitioners in the community—or else they might take their patients to a competing hospital.
Ness and Heroux surveyed physicians about their needs and desires for the program, visiting a number of key physicians in their offices. Another challenge they handled was to negotiate a contract with the hospital for the hospitalists’ services, including a subsidy to reflect their 24/7 coverage in the hospital. Then they needed to agree on appropriate quality and financial performance measures by which to gauge the program’s success.
“With Roger’s help, we all got smarter about what a true hospitalist program was,” says Ness. “What I discovered was that a hospitalist program is no different than any other significant business venture. It needs its own goals, leadership, and overarching business plan. You can’t just put it in place and assume that you’ll be successful. It requires just as much discipline, rigor, and hard work as other businesses.”
Practice Management Tasks
A comprehensive list of why some hospitalist programs risk failure, including problems with recruitment, retention, scheduling, compensation, communication with primary physicians, buy-in, marketing, data analysis, financial performance, and return on investment for the hospital, would closely track with the content of any hospitalist practice management course. One such course, “Best Practices in Managing a Hospital Medicine Program,” sponsored by SHM and presented at UCSF’s Management of the Hospitalized Patient meeting in San Francisco on October 11 by some of the field’s top consultants and practice leaders, covered these topics.
Heroux was on the UCSF faculty, and he presented his model of the Fourth Generation hospitalist practice that has evolved from a simple rounding model with daily assignments of outpatient physicians, a rotational model with one-week assignments of outpatient physicians, and a group of dedicated hospitalists who lack administrative support. The Fourth Generation hospitalist program is a sustainable, dedicated program that enjoys full clinical and administrative support, including a practice manager and a case manager.
Such a practice provides dedicated 24-hour coverage with realistic staffing ratios, employs effective practice leadership, is strategically aligned with the hospital and medical community, and utilizes a financial management system and data sets for benchmarking of key performance measures demonstrating its value. Without these components in place, Heroux says, the hospitalist program risks serious dysfunction and eventual failure.
Reflecting on his work with Lewis-Gale and other clients, Heroux believes it is important to be disciplined and deliberate about evaluating the real need for a hospitalist service in the community. “Talk to your medical staff. Find out what they want and need from the service. Then prioritize those needs because you can’t do everything at once, and build your business plan on how you’ll meet the identified priorities. Let them drive your staffing patterns and your cost savings targets,” he says. “And make your program data-driven from the start.”
When Heroux started working with Lewis-Gale, they had none of these components. “They were trying to meet the needs without the infrastructure, and that is how they got into trouble,” he says.
Why are some hospitalist programs launched without this kind of support or the business planning that would be de rigueur for any hospital launching a new imaging center or outpatient surgery center? Perhaps the lack of capital investment on equipment for a hospitalist service leads to a casual attitude about doing the needed homework. Or else misconceptions blind hospital administrators to the real complexities and financial implications of a hospitalist program.
“I think there is a mentality sometimes that says, ‘Hey, we’re good managers, we can do this,’ ” suggests Heroux. “Sometimes they don’t know what they don’t know. Many times they don’t want to spend the time and money or get the help [they need] to do it right.”
Do Your Homework
Bruce Becker, MD, a family practice physician and chief medical officer at Medical Center Hospital in Odessa, Texas, spent two years helping his institution do its homework and gathering support within the medical community before the hospital’s board of directors approved a plan for a hospitalist program in July 2006.
“We started exploring a hospitalist program two years ago,” says Dr. Becker. A national company made a proposal to the hospital to develop a turnkey program. “We also attempted to work with private physicians and with the local medical school but couldn’t come to an agreement at that time.”
When the board was first approached with a $100,000 proposal for a consultant’s study, it had the usual concerns about return on investment and volume of demand, Dr. Becker says. But the biggest barrier to the new service was an attitude within the local medical community that hospitalists would disrupt continuity of care and longstanding relationships between physicians and their patients. To address this discomfort, “we decided to go step by step with our consultant—polling the medical staff, administration and board members,” says Dr. Becker. Their responses suggested that sufficient demand existed.
Dr. Becker asked a physician he knew who had set up a hospitalist program in another community to speak to the hospital board. He and several colleagues attended an SHM conference to learn more about the basics of operating a program. Eventually, the board approved a request for proposals (RFP), which was sent to seven potential contractors, both local groups and national companies.
“What we were going through was an educational process,” explains Dr. Becker. “I could see a visible change taking place on the faces of board members. Two years ago, they weren’t ready, and if I had tried to push it, they would have said no. Now they are ready, and our medical staff is much more accepting.” Hospitalists are now being interviewed for the new program, with a projected launch date of July 2007.
The Importance of Leadership
Winthrop Whitcomb, MD, a practicing hospitalist at Mercy Medical Center in Springfield, Mass., and co-founder of SHM, believes the absence of strong practice leadership by someone with leadership and management skills who is based on site and devoted to hospital medicine is the number one reason why hospitalist programs fail. He tells the story of a hospitalist program started by a multi-specialty group that assigned as its medical director a primary care physician who had a busy office practice.
“That leader wasn’t able to have much contact with the group or the day-in, day-out challenges of its growing caseload,” relates Dr. Whitcomb. “The hospitalists began to get demoralized, feeling that no one was advocating for them.” A consultant recommended hiring an on-site leader for the program. The next medical director had some knowledge of medical management and hospital medicine but was only one-quarter-time dedicated to the hospitalist program. Problems of morale, turnover, and service quality continued.
“The leader instituted a few good things, including an incentive-based compensation program, but ultimately was ineffective and unable to develop the staff’s trust,” says Dr. Whitcomb. “I could tell that story over and over again. To put it another way, a lot of the pitfalls can be overcome with a good, strong leader.” Often, programs such as the one he describes flounder but continue to limp along for years, until a good leader comes along to place the program on a stronger footing.
In other cases, a new hospitalist program might be launched with just one physician and limited coverage, with plans to grow from there. “That’s fine, as long as that person you’re starting with is serving in a leadership capacity as well as seeing patients. It’s hard to find a good leader. But you will need somebody who is driving the bus in fairly short order,” says Dr. Whitcomb.
Growth Pains and Other Common Problems
John Nelson, MD, a hospitalist and consultant in Bellevue, Wash., co-founder of SHM, and columnist for The Hospitalist, points out some other common causes of hospitalist program collapse, including the failure to appreciate how rapidly the program will grow or to have a plan for how to deal with growth. “It doesn’t take a year to reach your projections,” he advises. “Suddenly, you’ve got a bigger caseload than the original doctors can handle. They get overwhelmed and burned out and then leave.”
If the hospitalists feel no ownership or personal investment in the practice’s success, they may develop a kind of civil service mentality about the job instead of a customer service mindset, says Dr. Nelson. Combine that with a straight salary instead of productivity incentives, and they may lack the necessary commitment to the program’s quality and growth.
“I also work as a consultant to help other hospitals start hospitalist practices. I’ve had a lot of experience with programs that never got off the ground,” he says. In one case, staff did an analysis to find out how much it would cost to support the program and then decided not to go forward. In that case, the hospital was reimbursed more on per diems than diagnosis-related groups, so reduced lengths of stay would not have benefited the facility.
In other cases, hospitals have not gone forward because of local medical politics or unfounded suspicions about hospital medicine. The dominant local multi-specialty group may insist on operating the hospitalist program itself, refusing to let anyone else do it. But the group makes unrealistic assumptions about workload or else wants to charge the same high overhead rate to the hospitalists that its clinic doctors pay, which is not feasible for a hospitalist program.
“I came to my current position because of a medical group that wanted to control the hospital medicine practice,” says Dr. Nelson. “But then they got busy and exhausted and wanted to quit being hospitalists. At that point, the hospital administrator panicked.”
Learn from Success
Thweatt believes that the hospitalist program at Lewis-Gale Medical Center, which now directly employs the hospitalists, is doing well, with seven full-time dedicated hospitalists. “Not that it’s always easy, but it’s no different than running any other business. If this program went away tomorrow, I think I’d be tarred and feathered by the medical staff,” he quips.
Dr. Patolia adds that the program has a compensation structure based entirely on productivity and a schedule that ensures 24-hour coverage. “We work as a team, and we depend on each other so much. We’re all committed people who want to be hospitalists,” he says. “Right now, I love being a hospitalist to such a degree that I can’t imagine doing anything else.”
Recently, a senior vice president from the hospital’s parent company, Hospital Corporation of America (HCA), visited Lewis-Gale to learn how to replicate its successful hospitalist program in all HCA hospitals.
Jon Ness, now chief operating officer of Billings Clinic in Billings, Mont., says one of the first things he did in his new job was to develop a hospitalist program. “I brought in Roger Heroux to do the evaluation,” he says. The process followed a familiar checklist: defining program goals, lining up clinic and hospital support, assessing manpower needs, and developing a data support system.
The Billings program was launched in January 2006 and today employs six full-time hospitalists. In contrast to the early days at Lewis-Gale, however, “we started out with a strong, deep business plan.”
For more information on the Fourth Generation hospitalist practice, contact Roger Heroux, Partner, Hospitalist Management Resources, LLC, 5490 Creighton Ct., Colorado Springs, CO 80918, 719/331-7119, or [email protected]. Visit the Society of Hospital Medicine Web site (www.hospitalmedicine.org) for information on practice management courses and other educational resources, including audiotapes of “Best Practices in Managing a Hospital Medicine Program.” TH
Larry Beresford is a regular contributor to The Hospitalist.
The purported benefits of hospital medicine, including reduced lengths of stay, cost savings and quality improvement for the hospital, and higher satisfaction for primary care physicians and patients, have been widely discussed. But are these positive outcomes always ensured when a hospital or a medical group decides to start a hospitalist program?
If the program is launched without adequate planning, a viable business plan, sufficient staffing, or other basic components of any successful business enterprise, the results may disappoint. The program may not deliver desired outcomes in terms of quality or cost savings. Hospitalist staff may become disillusioned, overworked, or burned out and then leave. The program might even fail, which is doubly problematic once physicians and hospital administrators have gotten used to the advantages of having hospitalist coverage in their facility.
What Not to Do … and How to Fix It
A hospitalist service started by Lewis-Gale Clinic, a multi-specialty medical group in Salem, Va., and practicing at 521-bed Lewis-Gale Medical Center, experienced serious problems after its launch in 1997.
“Our program initially wasn’t a true hospitalist program per se, but more like a service provided to internists in the medical group,” says Harsukh Patolia, MD, the hospitalist program’s medical director. “I was the first person hired. I made it clear that I wanted to be a hospitalist. But there were not many models available for us to base our program on.”
Demand was great from clinic physicians, who no longer had time to see their patients at the hospital, says Dr. Patolia. Three additional hospitalists were hired, but by 1999, one had left and the others were stressed out and overworked. “We were working very hard,” he says. But the program was dependent on locum tenens physicians to fill shifts, and quality was starting to suffer. “I’m not sure we were on the brink of failure, but there was a lot of dissatisfaction.”
Jon Ness, then the medical group’s administrator, identified a problem with the hospitalist service soon after he started work in Salem in 1999. “My sense was that both the hospital and medical staff really wanted the program and didn’t want to see it fail. But they didn’t understand why we were having so many challenges with it,” he says. “The first thing we did was a thorough clinical and administrative review of the program. The more information I collected, the more concerned I got.”
Recognizing that there wasn’t enough expertise within the organization to sort out the problems, Ness contacted Colorado Springs, Colo., consultant Roger Heroux of Hospitalist Management Resources, LLC. Additionally, he approached Lewis-Gale Medical Center’s new CEO, James Thweatt, who also realized that there was a problem with the program.
“If they hadn’t come to me, I would have gone to them with my recommendation for a consultant,” adds Thweatt. Basically, there were serious lacks in terms of logistical support for the service, of clarity in its strategic goals, and of authority for the practice’s leadership, while its relationship with the rest of the clinic was also deteriorating.
“With the changing face of healthcare, a viable hospitalist program was a necessity,” Thweatt says. He also had to satisfy the demands of physicians—not only those belonging to the group practice but also independent primary care practitioners in the community—or else they might take their patients to a competing hospital.
Ness and Heroux surveyed physicians about their needs and desires for the program, visiting a number of key physicians in their offices. Another challenge they handled was to negotiate a contract with the hospital for the hospitalists’ services, including a subsidy to reflect their 24/7 coverage in the hospital. Then they needed to agree on appropriate quality and financial performance measures by which to gauge the program’s success.
“With Roger’s help, we all got smarter about what a true hospitalist program was,” says Ness. “What I discovered was that a hospitalist program is no different than any other significant business venture. It needs its own goals, leadership, and overarching business plan. You can’t just put it in place and assume that you’ll be successful. It requires just as much discipline, rigor, and hard work as other businesses.”
Practice Management Tasks
A comprehensive list of why some hospitalist programs risk failure, including problems with recruitment, retention, scheduling, compensation, communication with primary physicians, buy-in, marketing, data analysis, financial performance, and return on investment for the hospital, would closely track with the content of any hospitalist practice management course. One such course, “Best Practices in Managing a Hospital Medicine Program,” sponsored by SHM and presented at UCSF’s Management of the Hospitalized Patient meeting in San Francisco on October 11 by some of the field’s top consultants and practice leaders, covered these topics.
Heroux was on the UCSF faculty, and he presented his model of the Fourth Generation hospitalist practice that has evolved from a simple rounding model with daily assignments of outpatient physicians, a rotational model with one-week assignments of outpatient physicians, and a group of dedicated hospitalists who lack administrative support. The Fourth Generation hospitalist program is a sustainable, dedicated program that enjoys full clinical and administrative support, including a practice manager and a case manager.
Such a practice provides dedicated 24-hour coverage with realistic staffing ratios, employs effective practice leadership, is strategically aligned with the hospital and medical community, and utilizes a financial management system and data sets for benchmarking of key performance measures demonstrating its value. Without these components in place, Heroux says, the hospitalist program risks serious dysfunction and eventual failure.
Reflecting on his work with Lewis-Gale and other clients, Heroux believes it is important to be disciplined and deliberate about evaluating the real need for a hospitalist service in the community. “Talk to your medical staff. Find out what they want and need from the service. Then prioritize those needs because you can’t do everything at once, and build your business plan on how you’ll meet the identified priorities. Let them drive your staffing patterns and your cost savings targets,” he says. “And make your program data-driven from the start.”
When Heroux started working with Lewis-Gale, they had none of these components. “They were trying to meet the needs without the infrastructure, and that is how they got into trouble,” he says.
Why are some hospitalist programs launched without this kind of support or the business planning that would be de rigueur for any hospital launching a new imaging center or outpatient surgery center? Perhaps the lack of capital investment on equipment for a hospitalist service leads to a casual attitude about doing the needed homework. Or else misconceptions blind hospital administrators to the real complexities and financial implications of a hospitalist program.
“I think there is a mentality sometimes that says, ‘Hey, we’re good managers, we can do this,’ ” suggests Heroux. “Sometimes they don’t know what they don’t know. Many times they don’t want to spend the time and money or get the help [they need] to do it right.”
Do Your Homework
Bruce Becker, MD, a family practice physician and chief medical officer at Medical Center Hospital in Odessa, Texas, spent two years helping his institution do its homework and gathering support within the medical community before the hospital’s board of directors approved a plan for a hospitalist program in July 2006.
“We started exploring a hospitalist program two years ago,” says Dr. Becker. A national company made a proposal to the hospital to develop a turnkey program. “We also attempted to work with private physicians and with the local medical school but couldn’t come to an agreement at that time.”
When the board was first approached with a $100,000 proposal for a consultant’s study, it had the usual concerns about return on investment and volume of demand, Dr. Becker says. But the biggest barrier to the new service was an attitude within the local medical community that hospitalists would disrupt continuity of care and longstanding relationships between physicians and their patients. To address this discomfort, “we decided to go step by step with our consultant—polling the medical staff, administration and board members,” says Dr. Becker. Their responses suggested that sufficient demand existed.
Dr. Becker asked a physician he knew who had set up a hospitalist program in another community to speak to the hospital board. He and several colleagues attended an SHM conference to learn more about the basics of operating a program. Eventually, the board approved a request for proposals (RFP), which was sent to seven potential contractors, both local groups and national companies.
“What we were going through was an educational process,” explains Dr. Becker. “I could see a visible change taking place on the faces of board members. Two years ago, they weren’t ready, and if I had tried to push it, they would have said no. Now they are ready, and our medical staff is much more accepting.” Hospitalists are now being interviewed for the new program, with a projected launch date of July 2007.
The Importance of Leadership
Winthrop Whitcomb, MD, a practicing hospitalist at Mercy Medical Center in Springfield, Mass., and co-founder of SHM, believes the absence of strong practice leadership by someone with leadership and management skills who is based on site and devoted to hospital medicine is the number one reason why hospitalist programs fail. He tells the story of a hospitalist program started by a multi-specialty group that assigned as its medical director a primary care physician who had a busy office practice.
“That leader wasn’t able to have much contact with the group or the day-in, day-out challenges of its growing caseload,” relates Dr. Whitcomb. “The hospitalists began to get demoralized, feeling that no one was advocating for them.” A consultant recommended hiring an on-site leader for the program. The next medical director had some knowledge of medical management and hospital medicine but was only one-quarter-time dedicated to the hospitalist program. Problems of morale, turnover, and service quality continued.
“The leader instituted a few good things, including an incentive-based compensation program, but ultimately was ineffective and unable to develop the staff’s trust,” says Dr. Whitcomb. “I could tell that story over and over again. To put it another way, a lot of the pitfalls can be overcome with a good, strong leader.” Often, programs such as the one he describes flounder but continue to limp along for years, until a good leader comes along to place the program on a stronger footing.
In other cases, a new hospitalist program might be launched with just one physician and limited coverage, with plans to grow from there. “That’s fine, as long as that person you’re starting with is serving in a leadership capacity as well as seeing patients. It’s hard to find a good leader. But you will need somebody who is driving the bus in fairly short order,” says Dr. Whitcomb.
Growth Pains and Other Common Problems
John Nelson, MD, a hospitalist and consultant in Bellevue, Wash., co-founder of SHM, and columnist for The Hospitalist, points out some other common causes of hospitalist program collapse, including the failure to appreciate how rapidly the program will grow or to have a plan for how to deal with growth. “It doesn’t take a year to reach your projections,” he advises. “Suddenly, you’ve got a bigger caseload than the original doctors can handle. They get overwhelmed and burned out and then leave.”
If the hospitalists feel no ownership or personal investment in the practice’s success, they may develop a kind of civil service mentality about the job instead of a customer service mindset, says Dr. Nelson. Combine that with a straight salary instead of productivity incentives, and they may lack the necessary commitment to the program’s quality and growth.
“I also work as a consultant to help other hospitals start hospitalist practices. I’ve had a lot of experience with programs that never got off the ground,” he says. In one case, staff did an analysis to find out how much it would cost to support the program and then decided not to go forward. In that case, the hospital was reimbursed more on per diems than diagnosis-related groups, so reduced lengths of stay would not have benefited the facility.
In other cases, hospitals have not gone forward because of local medical politics or unfounded suspicions about hospital medicine. The dominant local multi-specialty group may insist on operating the hospitalist program itself, refusing to let anyone else do it. But the group makes unrealistic assumptions about workload or else wants to charge the same high overhead rate to the hospitalists that its clinic doctors pay, which is not feasible for a hospitalist program.
“I came to my current position because of a medical group that wanted to control the hospital medicine practice,” says Dr. Nelson. “But then they got busy and exhausted and wanted to quit being hospitalists. At that point, the hospital administrator panicked.”
Learn from Success
Thweatt believes that the hospitalist program at Lewis-Gale Medical Center, which now directly employs the hospitalists, is doing well, with seven full-time dedicated hospitalists. “Not that it’s always easy, but it’s no different than running any other business. If this program went away tomorrow, I think I’d be tarred and feathered by the medical staff,” he quips.
Dr. Patolia adds that the program has a compensation structure based entirely on productivity and a schedule that ensures 24-hour coverage. “We work as a team, and we depend on each other so much. We’re all committed people who want to be hospitalists,” he says. “Right now, I love being a hospitalist to such a degree that I can’t imagine doing anything else.”
Recently, a senior vice president from the hospital’s parent company, Hospital Corporation of America (HCA), visited Lewis-Gale to learn how to replicate its successful hospitalist program in all HCA hospitals.
Jon Ness, now chief operating officer of Billings Clinic in Billings, Mont., says one of the first things he did in his new job was to develop a hospitalist program. “I brought in Roger Heroux to do the evaluation,” he says. The process followed a familiar checklist: defining program goals, lining up clinic and hospital support, assessing manpower needs, and developing a data support system.
The Billings program was launched in January 2006 and today employs six full-time hospitalists. In contrast to the early days at Lewis-Gale, however, “we started out with a strong, deep business plan.”
For more information on the Fourth Generation hospitalist practice, contact Roger Heroux, Partner, Hospitalist Management Resources, LLC, 5490 Creighton Ct., Colorado Springs, CO 80918, 719/331-7119, or [email protected]. Visit the Society of Hospital Medicine Web site (www.hospitalmedicine.org) for information on practice management courses and other educational resources, including audiotapes of “Best Practices in Managing a Hospital Medicine Program.” TH
Larry Beresford is a regular contributor to The Hospitalist.
Smoking Out Meth Use
With methamphetamine use spreading across the country like a flu epidemic, hospitalists see more meth addicts and deal increasingly with the physical and psychiatric conditions common in these individuals. In overcoming the challenges and frustrations of working with these patients, hospitalists in regions where meth use is rampant have become experts of sorts, and they have messages for their colleagues nationwide: Learn our lessons, because you could be next.
The Meth Evolution
Methamphetamine has become popular for obvious reasons. The drug is cheap, and because it is manufactured using common and easily obtained ingredients, it is accessible anywhere.
The meth epidemic is not a new phenomenon. It started in the 1970s in the American heartland—Iowa and parts of Missouri. Since then, it has spread from West to East—hitting California and Hawaii in the ’80s and moving to Southeastern states such as Georgia and South Carolina in the late ’90s.
According to Richard A. Rawson, PhD, associate director and professor-in-residence for the Integrated Substance Abuse Programs at the Semel Institute for Neuroscience and Human Behavior in the David Geffen School of Medicine at the University of California at Los Angeles, “The spread of meth in the U.S. looks much like that of an infectious disease. It has spread in a very systematic way.”
It is a particular problem in rural communities, where it’s easily accessible and cheap. In fact, Dr. Rawson suggests that the drug doesn’t really present a major problem in urban areas—with the exception of cities that have a concentration of gay men. “Meth use in this population is a unique phenomenon that doesn’t follow the same homogenous spread from west to east,” he says.
Compounding this problem is the fact that HIV and sexually transmitted diseases often accompany meth use. “The drug is uniquely connected to sexual behavior because it increases sex drive, sexual performance, and pleasure,” observes Dr. Rawson. At the same time, hepatitis C is a broad concern in communities in which users inject the drug instead of smoking it. In fact, he says, about 50% of meth injectors are hepatitis-C-positive.
Meth Addicts: Routine for Some Hospitalists
For those hospitalists who see many meth users, working with these patients is fairly routine. As Emory University, Atlanta, assistant professor of medicine and hospitalist J. Allen Garner, MD, says, “As many as 30% of the patients I deal with on any given day are addicted to something—cocaine, alcohol, meth. I can’t say it’s a greater burden than anything else.”
Establishing rapport with these patients can be challenging. “Some say, ‘I’m really strung out and need help.’ Many come in with some physical complaint and don’t tell me that they’re high on meth and haven’t slept for 72 hours,” says Dr. Garner. “Basically, this has to do with the denial that goes along with chemical dependency.
Even patients who readily admit that they have a problem are often in denial about the depth of their addiction. “They’ll say that they have it under control, that they only did it once, or that someone slipped them the drug—all ‘party lines’ that take the heat off of them,” he says.
Gaining the trust of meth addicts is a major challenge, “because the drug produces paranoia, agitation, and nervousness,” says Dr. Rawson, noting that “quick urine tests” can be used to identify meth users, and drug use shows up for hours. These tests are great because they only cost $5-$10 each.
Many meth patients come into the hospital because of a physical ailment. “They present with chest pain, palpitations, and/or shortness of breath, although these conditions clear up pretty quickly,” says Dr. Garner.
Tip-offs that the problem might be drug related include poor hygiene, disheveled appearance, and edgy, antsy behavior. Additionally, says Dr. Rawson, “Weight loss, skin sores and scabs, dental disorders, nervous behavior, and paranoid ideation are blue-ribbon signs of meth use. In places where users inject meth, look for needle marks. In regions where users smoke meth, pulmonary disease and coughing are common.”
In the patients Dr. Garner sees, meth’s lasting effects affect their physical health less than their mental health and quality of life. “Meth deteriorates them to the point that they can’t work, and they detach themselves from family, friends, and society as a whole,” he explains. “They require a lot of deep-seated [psychiatric] therapy to deal with multiple issues.”
While most of the meth users Dr. Garner sees are poorly educated and come from the working class, meth is increasingly popular among college students and professionals. In fact, he says, “I know of several doctors for whom meth was the drug of choice.” It is important for hospitalists to remember that addiction knows no socioeconomic boundaries. Many clinicians view meth addicts in an unsympathetic light and as people who have caused their own problems. This is a barrier that needs to be overcome, stresses Dr. Garner.
What Hospitalists Can Do
Meth users often aren’t even admitted to the hospital. “Treatment is mostly supportive. There is no drug you can give them to bring them down,” says Dr. Garner. “Withdrawal is a terrible thing—a sensation like Satan is crawling up their chest. We give them valium, but they basically have to weather it out.”
Even if the hospitalist addresses the physical effects and discusses treatment options with the meth user, it’s common for these patients to go back to their drug use when they leave the hospital. “Because meth doesn’t have life-threatening withdrawal symptoms—although you feel like you’re going to die—it’s easy for them to keep going back and using. Detox centers generally won’t touch these people,” says Dr. Garner. As a result, many patients end up in a catch-22, repeatedly going back to meth use.
While Dr. Garner does everything he can to help these patients, “they already are slaves to the drug by the time I see them,” he says. “Meth is highly addictive, and many people get hooked after using it just once or twice.”
This lack of available treatment for meth addicts is one of the greatest frustrations Dr. Garner faces as a hospitalist. “We keep putting resources into catching addicts as criminals and not getting them treatment and help before they become burdens on society,” he says.
He is pleased to note that this is changing in some states. “A few of the courts in our locale are starting to incorporate treatment programs through the court systems,” he explains.
Meth and Youth
While meth has become a popular drug among all age groups, “very few teens end up in the hospital because of meth,” says Wendy Wright, MD, a hospitalist at Rady Children’s Hospital in San Diego. “If kids are high on meth, they generally aren’t admitted when they are coming down. And, unlike many adults, they don’t have physical or medical issues that require hospitalization,” she explains. “Kids tolerate meth really well from the physical standpoint. We don’t see the arrhythmias or heart attacks that we see in adult addicts.”
When teen addicts do come in with medical conditions, Dr. Wright suggests, hospitalists often see problems such as skin or urinary tract infections. Teen meth users more frequently come to the hospital with psychiatric problems. “They have paranoid delusions, and some are fairly aggressive,” says Dr. Wright.
While hospitalists dealing with teens face the usual challenge of establishing rapport quickly, Dr. Wright observes that teens tend to be much more open than adults about their drug use. “They are pretty up front; they tell me right off the bat what drugs they use,” she says. “Of course I’m mostly seeing kids [who] aren’t living in an upper-class environment, and they’re not trying to hide things from their parents. The kids I see are streetwise and no nonsense. They have a sense of what their medical needs are and think nothing of asking for HIV or STD testing.”
Because of their youth and general good physical health, teens don’t necessarily create a burden for the hospitals and professionals who care for them. The biggest burden of meth-using teenagers, she suggests, “has to do with social issues. These kids often don’t grow into productive adults. They also have a lot of mental health issues such as bipolar disorder or severe depression, and these are the biggest burdens on the community as a whole. We also see a lot of chlamydia and gonorrhea in our kids.”
Although Dr. Wright strictly sees young patients, she acknowledges intergenerational meth use in families. Her facility sees many children who are brought into protective custody because their parents are meth users and unfit to care for them.
“These kids end up staying in the system, which is a bad place for them to be,” says Dr. Wright. “They grow up with a lot of insecurities and mental health issues, and many go on to be users themselves. While she sees many kids whose grandmothers and mothers are addicts, she believes the problem is situational and not hereditary. Nonetheless, “We’re not sure how to break this cycle,” she says.
Some kids are hospitalized because they are hurt or sick as a result of being in an unsafe environment where parents are meth users. These children are often malnourished or sick because of neglect.
Helping Hospitalists Manage Meth
It helps hospitalists if their facility has clear protocols for handling meth intoxication. “It is especially good to establish a procedure in the emergency department,” advises Dr. Rawson. He stresses that these procedures should address ways to de-escalate aggressive behavior. There are also clinical training techniques and brief interventions used to treat alcoholics that can be useful for dealing with meth addicts. These interventions involve efforts to change behaviors. Specifically, helping patients understand that their substance abuse is putting them at risk and encouraging them to reduce or stop their drug use altogether. The elements of brief interventions for substance abuse have been summarized in the acronym “FRAMES,” which stands for feedback, responsibility, advice, menu of options, empathy, and self-efficacy.
“These tools can help get people to talk about their meth problem[s] and deal with [them],” says Dr. Rawson. “Some of these brief interventions can be amazing in terms of deferring further drug use.”
Burdens of Meth
What hospitalists see in their meth-using patients depends on the maturity of the problem in their community. “In communities where the problem is newer, you are likely to see younger users and fewer physical problems,” says Dr. Rawson.
In areas where the problem has existed for years, hospitalists can expect to see older addicts with physical problems that range from heart conditions to widespread tooth decay (a condition known as “meth mouth”). The longer a community has had a meth problem, the more likely the epidemic is placing a financial burden on the healthcare system.
Dr. Garner urges his colleagues to learn about meth. “A couple of years ago, this was a nonexistent problem,” he says. “Now it has reached crisis proportions in many communities.”
Gina DiRenzo-Coffey, MD, director of inpatient pediatrics and a pediatric hospitalist at Alegent Health/Bergan Mercy Medical Center in Omaha, Neb., agrees: “You can lull yourself into believing that this can’t happen in your community. But no one has been able to stop meth use [among members of their community], and it keeps spreading. It is our job to learn everything we can about this drug and help meth addicts as much as we can.” TH
Joanne Kaldy also writes about a day in the life of a pediatric hospitalist in this issue.
With methamphetamine use spreading across the country like a flu epidemic, hospitalists see more meth addicts and deal increasingly with the physical and psychiatric conditions common in these individuals. In overcoming the challenges and frustrations of working with these patients, hospitalists in regions where meth use is rampant have become experts of sorts, and they have messages for their colleagues nationwide: Learn our lessons, because you could be next.
The Meth Evolution
Methamphetamine has become popular for obvious reasons. The drug is cheap, and because it is manufactured using common and easily obtained ingredients, it is accessible anywhere.
The meth epidemic is not a new phenomenon. It started in the 1970s in the American heartland—Iowa and parts of Missouri. Since then, it has spread from West to East—hitting California and Hawaii in the ’80s and moving to Southeastern states such as Georgia and South Carolina in the late ’90s.
According to Richard A. Rawson, PhD, associate director and professor-in-residence for the Integrated Substance Abuse Programs at the Semel Institute for Neuroscience and Human Behavior in the David Geffen School of Medicine at the University of California at Los Angeles, “The spread of meth in the U.S. looks much like that of an infectious disease. It has spread in a very systematic way.”
It is a particular problem in rural communities, where it’s easily accessible and cheap. In fact, Dr. Rawson suggests that the drug doesn’t really present a major problem in urban areas—with the exception of cities that have a concentration of gay men. “Meth use in this population is a unique phenomenon that doesn’t follow the same homogenous spread from west to east,” he says.
Compounding this problem is the fact that HIV and sexually transmitted diseases often accompany meth use. “The drug is uniquely connected to sexual behavior because it increases sex drive, sexual performance, and pleasure,” observes Dr. Rawson. At the same time, hepatitis C is a broad concern in communities in which users inject the drug instead of smoking it. In fact, he says, about 50% of meth injectors are hepatitis-C-positive.
Meth Addicts: Routine for Some Hospitalists
For those hospitalists who see many meth users, working with these patients is fairly routine. As Emory University, Atlanta, assistant professor of medicine and hospitalist J. Allen Garner, MD, says, “As many as 30% of the patients I deal with on any given day are addicted to something—cocaine, alcohol, meth. I can’t say it’s a greater burden than anything else.”
Establishing rapport with these patients can be challenging. “Some say, ‘I’m really strung out and need help.’ Many come in with some physical complaint and don’t tell me that they’re high on meth and haven’t slept for 72 hours,” says Dr. Garner. “Basically, this has to do with the denial that goes along with chemical dependency.
Even patients who readily admit that they have a problem are often in denial about the depth of their addiction. “They’ll say that they have it under control, that they only did it once, or that someone slipped them the drug—all ‘party lines’ that take the heat off of them,” he says.
Gaining the trust of meth addicts is a major challenge, “because the drug produces paranoia, agitation, and nervousness,” says Dr. Rawson, noting that “quick urine tests” can be used to identify meth users, and drug use shows up for hours. These tests are great because they only cost $5-$10 each.
Many meth patients come into the hospital because of a physical ailment. “They present with chest pain, palpitations, and/or shortness of breath, although these conditions clear up pretty quickly,” says Dr. Garner.
Tip-offs that the problem might be drug related include poor hygiene, disheveled appearance, and edgy, antsy behavior. Additionally, says Dr. Rawson, “Weight loss, skin sores and scabs, dental disorders, nervous behavior, and paranoid ideation are blue-ribbon signs of meth use. In places where users inject meth, look for needle marks. In regions where users smoke meth, pulmonary disease and coughing are common.”
In the patients Dr. Garner sees, meth’s lasting effects affect their physical health less than their mental health and quality of life. “Meth deteriorates them to the point that they can’t work, and they detach themselves from family, friends, and society as a whole,” he explains. “They require a lot of deep-seated [psychiatric] therapy to deal with multiple issues.”
While most of the meth users Dr. Garner sees are poorly educated and come from the working class, meth is increasingly popular among college students and professionals. In fact, he says, “I know of several doctors for whom meth was the drug of choice.” It is important for hospitalists to remember that addiction knows no socioeconomic boundaries. Many clinicians view meth addicts in an unsympathetic light and as people who have caused their own problems. This is a barrier that needs to be overcome, stresses Dr. Garner.
What Hospitalists Can Do
Meth users often aren’t even admitted to the hospital. “Treatment is mostly supportive. There is no drug you can give them to bring them down,” says Dr. Garner. “Withdrawal is a terrible thing—a sensation like Satan is crawling up their chest. We give them valium, but they basically have to weather it out.”
Even if the hospitalist addresses the physical effects and discusses treatment options with the meth user, it’s common for these patients to go back to their drug use when they leave the hospital. “Because meth doesn’t have life-threatening withdrawal symptoms—although you feel like you’re going to die—it’s easy for them to keep going back and using. Detox centers generally won’t touch these people,” says Dr. Garner. As a result, many patients end up in a catch-22, repeatedly going back to meth use.
While Dr. Garner does everything he can to help these patients, “they already are slaves to the drug by the time I see them,” he says. “Meth is highly addictive, and many people get hooked after using it just once or twice.”
This lack of available treatment for meth addicts is one of the greatest frustrations Dr. Garner faces as a hospitalist. “We keep putting resources into catching addicts as criminals and not getting them treatment and help before they become burdens on society,” he says.
He is pleased to note that this is changing in some states. “A few of the courts in our locale are starting to incorporate treatment programs through the court systems,” he explains.
Meth and Youth
While meth has become a popular drug among all age groups, “very few teens end up in the hospital because of meth,” says Wendy Wright, MD, a hospitalist at Rady Children’s Hospital in San Diego. “If kids are high on meth, they generally aren’t admitted when they are coming down. And, unlike many adults, they don’t have physical or medical issues that require hospitalization,” she explains. “Kids tolerate meth really well from the physical standpoint. We don’t see the arrhythmias or heart attacks that we see in adult addicts.”
When teen addicts do come in with medical conditions, Dr. Wright suggests, hospitalists often see problems such as skin or urinary tract infections. Teen meth users more frequently come to the hospital with psychiatric problems. “They have paranoid delusions, and some are fairly aggressive,” says Dr. Wright.
While hospitalists dealing with teens face the usual challenge of establishing rapport quickly, Dr. Wright observes that teens tend to be much more open than adults about their drug use. “They are pretty up front; they tell me right off the bat what drugs they use,” she says. “Of course I’m mostly seeing kids [who] aren’t living in an upper-class environment, and they’re not trying to hide things from their parents. The kids I see are streetwise and no nonsense. They have a sense of what their medical needs are and think nothing of asking for HIV or STD testing.”
Because of their youth and general good physical health, teens don’t necessarily create a burden for the hospitals and professionals who care for them. The biggest burden of meth-using teenagers, she suggests, “has to do with social issues. These kids often don’t grow into productive adults. They also have a lot of mental health issues such as bipolar disorder or severe depression, and these are the biggest burdens on the community as a whole. We also see a lot of chlamydia and gonorrhea in our kids.”
Although Dr. Wright strictly sees young patients, she acknowledges intergenerational meth use in families. Her facility sees many children who are brought into protective custody because their parents are meth users and unfit to care for them.
“These kids end up staying in the system, which is a bad place for them to be,” says Dr. Wright. “They grow up with a lot of insecurities and mental health issues, and many go on to be users themselves. While she sees many kids whose grandmothers and mothers are addicts, she believes the problem is situational and not hereditary. Nonetheless, “We’re not sure how to break this cycle,” she says.
Some kids are hospitalized because they are hurt or sick as a result of being in an unsafe environment where parents are meth users. These children are often malnourished or sick because of neglect.
Helping Hospitalists Manage Meth
It helps hospitalists if their facility has clear protocols for handling meth intoxication. “It is especially good to establish a procedure in the emergency department,” advises Dr. Rawson. He stresses that these procedures should address ways to de-escalate aggressive behavior. There are also clinical training techniques and brief interventions used to treat alcoholics that can be useful for dealing with meth addicts. These interventions involve efforts to change behaviors. Specifically, helping patients understand that their substance abuse is putting them at risk and encouraging them to reduce or stop their drug use altogether. The elements of brief interventions for substance abuse have been summarized in the acronym “FRAMES,” which stands for feedback, responsibility, advice, menu of options, empathy, and self-efficacy.
“These tools can help get people to talk about their meth problem[s] and deal with [them],” says Dr. Rawson. “Some of these brief interventions can be amazing in terms of deferring further drug use.”
Burdens of Meth
What hospitalists see in their meth-using patients depends on the maturity of the problem in their community. “In communities where the problem is newer, you are likely to see younger users and fewer physical problems,” says Dr. Rawson.
In areas where the problem has existed for years, hospitalists can expect to see older addicts with physical problems that range from heart conditions to widespread tooth decay (a condition known as “meth mouth”). The longer a community has had a meth problem, the more likely the epidemic is placing a financial burden on the healthcare system.
Dr. Garner urges his colleagues to learn about meth. “A couple of years ago, this was a nonexistent problem,” he says. “Now it has reached crisis proportions in many communities.”
Gina DiRenzo-Coffey, MD, director of inpatient pediatrics and a pediatric hospitalist at Alegent Health/Bergan Mercy Medical Center in Omaha, Neb., agrees: “You can lull yourself into believing that this can’t happen in your community. But no one has been able to stop meth use [among members of their community], and it keeps spreading. It is our job to learn everything we can about this drug and help meth addicts as much as we can.” TH
Joanne Kaldy also writes about a day in the life of a pediatric hospitalist in this issue.
With methamphetamine use spreading across the country like a flu epidemic, hospitalists see more meth addicts and deal increasingly with the physical and psychiatric conditions common in these individuals. In overcoming the challenges and frustrations of working with these patients, hospitalists in regions where meth use is rampant have become experts of sorts, and they have messages for their colleagues nationwide: Learn our lessons, because you could be next.
The Meth Evolution
Methamphetamine has become popular for obvious reasons. The drug is cheap, and because it is manufactured using common and easily obtained ingredients, it is accessible anywhere.
The meth epidemic is not a new phenomenon. It started in the 1970s in the American heartland—Iowa and parts of Missouri. Since then, it has spread from West to East—hitting California and Hawaii in the ’80s and moving to Southeastern states such as Georgia and South Carolina in the late ’90s.
According to Richard A. Rawson, PhD, associate director and professor-in-residence for the Integrated Substance Abuse Programs at the Semel Institute for Neuroscience and Human Behavior in the David Geffen School of Medicine at the University of California at Los Angeles, “The spread of meth in the U.S. looks much like that of an infectious disease. It has spread in a very systematic way.”
It is a particular problem in rural communities, where it’s easily accessible and cheap. In fact, Dr. Rawson suggests that the drug doesn’t really present a major problem in urban areas—with the exception of cities that have a concentration of gay men. “Meth use in this population is a unique phenomenon that doesn’t follow the same homogenous spread from west to east,” he says.
Compounding this problem is the fact that HIV and sexually transmitted diseases often accompany meth use. “The drug is uniquely connected to sexual behavior because it increases sex drive, sexual performance, and pleasure,” observes Dr. Rawson. At the same time, hepatitis C is a broad concern in communities in which users inject the drug instead of smoking it. In fact, he says, about 50% of meth injectors are hepatitis-C-positive.
Meth Addicts: Routine for Some Hospitalists
For those hospitalists who see many meth users, working with these patients is fairly routine. As Emory University, Atlanta, assistant professor of medicine and hospitalist J. Allen Garner, MD, says, “As many as 30% of the patients I deal with on any given day are addicted to something—cocaine, alcohol, meth. I can’t say it’s a greater burden than anything else.”
Establishing rapport with these patients can be challenging. “Some say, ‘I’m really strung out and need help.’ Many come in with some physical complaint and don’t tell me that they’re high on meth and haven’t slept for 72 hours,” says Dr. Garner. “Basically, this has to do with the denial that goes along with chemical dependency.
Even patients who readily admit that they have a problem are often in denial about the depth of their addiction. “They’ll say that they have it under control, that they only did it once, or that someone slipped them the drug—all ‘party lines’ that take the heat off of them,” he says.
Gaining the trust of meth addicts is a major challenge, “because the drug produces paranoia, agitation, and nervousness,” says Dr. Rawson, noting that “quick urine tests” can be used to identify meth users, and drug use shows up for hours. These tests are great because they only cost $5-$10 each.
Many meth patients come into the hospital because of a physical ailment. “They present with chest pain, palpitations, and/or shortness of breath, although these conditions clear up pretty quickly,” says Dr. Garner.
Tip-offs that the problem might be drug related include poor hygiene, disheveled appearance, and edgy, antsy behavior. Additionally, says Dr. Rawson, “Weight loss, skin sores and scabs, dental disorders, nervous behavior, and paranoid ideation are blue-ribbon signs of meth use. In places where users inject meth, look for needle marks. In regions where users smoke meth, pulmonary disease and coughing are common.”
In the patients Dr. Garner sees, meth’s lasting effects affect their physical health less than their mental health and quality of life. “Meth deteriorates them to the point that they can’t work, and they detach themselves from family, friends, and society as a whole,” he explains. “They require a lot of deep-seated [psychiatric] therapy to deal with multiple issues.”
While most of the meth users Dr. Garner sees are poorly educated and come from the working class, meth is increasingly popular among college students and professionals. In fact, he says, “I know of several doctors for whom meth was the drug of choice.” It is important for hospitalists to remember that addiction knows no socioeconomic boundaries. Many clinicians view meth addicts in an unsympathetic light and as people who have caused their own problems. This is a barrier that needs to be overcome, stresses Dr. Garner.
What Hospitalists Can Do
Meth users often aren’t even admitted to the hospital. “Treatment is mostly supportive. There is no drug you can give them to bring them down,” says Dr. Garner. “Withdrawal is a terrible thing—a sensation like Satan is crawling up their chest. We give them valium, but they basically have to weather it out.”
Even if the hospitalist addresses the physical effects and discusses treatment options with the meth user, it’s common for these patients to go back to their drug use when they leave the hospital. “Because meth doesn’t have life-threatening withdrawal symptoms—although you feel like you’re going to die—it’s easy for them to keep going back and using. Detox centers generally won’t touch these people,” says Dr. Garner. As a result, many patients end up in a catch-22, repeatedly going back to meth use.
While Dr. Garner does everything he can to help these patients, “they already are slaves to the drug by the time I see them,” he says. “Meth is highly addictive, and many people get hooked after using it just once or twice.”
This lack of available treatment for meth addicts is one of the greatest frustrations Dr. Garner faces as a hospitalist. “We keep putting resources into catching addicts as criminals and not getting them treatment and help before they become burdens on society,” he says.
He is pleased to note that this is changing in some states. “A few of the courts in our locale are starting to incorporate treatment programs through the court systems,” he explains.
Meth and Youth
While meth has become a popular drug among all age groups, “very few teens end up in the hospital because of meth,” says Wendy Wright, MD, a hospitalist at Rady Children’s Hospital in San Diego. “If kids are high on meth, they generally aren’t admitted when they are coming down. And, unlike many adults, they don’t have physical or medical issues that require hospitalization,” she explains. “Kids tolerate meth really well from the physical standpoint. We don’t see the arrhythmias or heart attacks that we see in adult addicts.”
When teen addicts do come in with medical conditions, Dr. Wright suggests, hospitalists often see problems such as skin or urinary tract infections. Teen meth users more frequently come to the hospital with psychiatric problems. “They have paranoid delusions, and some are fairly aggressive,” says Dr. Wright.
While hospitalists dealing with teens face the usual challenge of establishing rapport quickly, Dr. Wright observes that teens tend to be much more open than adults about their drug use. “They are pretty up front; they tell me right off the bat what drugs they use,” she says. “Of course I’m mostly seeing kids [who] aren’t living in an upper-class environment, and they’re not trying to hide things from their parents. The kids I see are streetwise and no nonsense. They have a sense of what their medical needs are and think nothing of asking for HIV or STD testing.”
Because of their youth and general good physical health, teens don’t necessarily create a burden for the hospitals and professionals who care for them. The biggest burden of meth-using teenagers, she suggests, “has to do with social issues. These kids often don’t grow into productive adults. They also have a lot of mental health issues such as bipolar disorder or severe depression, and these are the biggest burdens on the community as a whole. We also see a lot of chlamydia and gonorrhea in our kids.”
Although Dr. Wright strictly sees young patients, she acknowledges intergenerational meth use in families. Her facility sees many children who are brought into protective custody because their parents are meth users and unfit to care for them.
“These kids end up staying in the system, which is a bad place for them to be,” says Dr. Wright. “They grow up with a lot of insecurities and mental health issues, and many go on to be users themselves. While she sees many kids whose grandmothers and mothers are addicts, she believes the problem is situational and not hereditary. Nonetheless, “We’re not sure how to break this cycle,” she says.
Some kids are hospitalized because they are hurt or sick as a result of being in an unsafe environment where parents are meth users. These children are often malnourished or sick because of neglect.
Helping Hospitalists Manage Meth
It helps hospitalists if their facility has clear protocols for handling meth intoxication. “It is especially good to establish a procedure in the emergency department,” advises Dr. Rawson. He stresses that these procedures should address ways to de-escalate aggressive behavior. There are also clinical training techniques and brief interventions used to treat alcoholics that can be useful for dealing with meth addicts. These interventions involve efforts to change behaviors. Specifically, helping patients understand that their substance abuse is putting them at risk and encouraging them to reduce or stop their drug use altogether. The elements of brief interventions for substance abuse have been summarized in the acronym “FRAMES,” which stands for feedback, responsibility, advice, menu of options, empathy, and self-efficacy.
“These tools can help get people to talk about their meth problem[s] and deal with [them],” says Dr. Rawson. “Some of these brief interventions can be amazing in terms of deferring further drug use.”
Burdens of Meth
What hospitalists see in their meth-using patients depends on the maturity of the problem in their community. “In communities where the problem is newer, you are likely to see younger users and fewer physical problems,” says Dr. Rawson.
In areas where the problem has existed for years, hospitalists can expect to see older addicts with physical problems that range from heart conditions to widespread tooth decay (a condition known as “meth mouth”). The longer a community has had a meth problem, the more likely the epidemic is placing a financial burden on the healthcare system.
Dr. Garner urges his colleagues to learn about meth. “A couple of years ago, this was a nonexistent problem,” he says. “Now it has reached crisis proportions in many communities.”
Gina DiRenzo-Coffey, MD, director of inpatient pediatrics and a pediatric hospitalist at Alegent Health/Bergan Mercy Medical Center in Omaha, Neb., agrees: “You can lull yourself into believing that this can’t happen in your community. But no one has been able to stop meth use [among members of their community], and it keeps spreading. It is our job to learn everything we can about this drug and help meth addicts as much as we can.” TH
Joanne Kaldy also writes about a day in the life of a pediatric hospitalist in this issue.
X-Ray Has Left the Building
Medical outsourcing is a growing trend in American hospitals, driven by shortages of on-call radiologists and intensivists, economic pressures, and advances in telemedicine. Hospitalists will likely encounter—if they haven’t already—outsourced services that range from off-site medical transcription and language interpreters to long-distance radiology and, increasingly, electronic intensivist services.1 What are the implications for quality patient care and collegial interface when hospitals contract with outsourced providers? What are the advantages, possible disadvantages, and opportunities for hospitalists as teleradiology and eICUs become facts of life?
A Variety of Configurations
According to Rick Wade, senior vice president for strategic communications for the American Hospital Association (Chicago), it’s difficult to quantify the extent to which outsourcing is currently being used in U.S. hospitals. VISICU, Inc., a leader in the provision of eICU services, currently has 150 client hospitals. Eight hospitalists contacted at community and university hospitals in Colo., Fla., Maine, Minn., Ga. and N.M. reported that they were not directly involved with outsourcing other than with transcription services.
Robert M. Wachter, MD, professor and associate chairman, Department of Medicine, and chief of the Medical Service at the University of California at San Francisco (UCSF), whose “Perspective” piece on medical outsourcing appeared in the February 16 New England Journal of Medicine, is intrigued by the implications of outsourcing trends for medicine: “I think medicine has been peculiarly insulated from [the globalization of services], and it’s just very interesting and exciting—and troubling as well.”1
Off-Site X-Ray Reads Common
According to the American College of Radiology, teleradiology has become a fixture in most practices and hospitals.2,3 Some institutions have retained their own radiologists, who take advantage of teleradiology by reading digitized radiographs and CT scans from home instead of within the hospital building. A shortage of radiologists has led others to contract with off-site providers of teleradiology services. Those who provide services at night are sometimes called “nighthawk” companies.1 Outsourcing of radiology, Dr. Wachter believes, is a logical step due to technological advances, though he admits that visiting the radiology department in his hospital often yields educational and collegial opportunities that online X-ray reading does not.
At Saint Clare’s Hospital in Weston/Wasau, Wis., a new, 107-bed state-of-the-art facility built by Ministry Health Care, Richard Bailey, MD, is medical director of Inpatient Care and Hospitalist Services. Radiology and other ancillary specialist services are provided by the Diagnostic and Treatment Center (DTC), jointly owned by Ministry Health Care and the Marshfield Clinic. The DTC, through a relationship with a radiology group in Hawaii, provides night coverage for full reads of radiographs and scans from 5 p.m. to 5 a.m. The interactions are virtually seamless, according to Dr. Bailey. “We don’t even notice they’re in Hawaii” when conferring with radiologists on the phone, he reports.
Off-site radiology also created an opportunity for his hospitalist group, Dr. Bailey says. Saint Clare’s hospitalist group provides supervision of contrast administration when needed during night and weekend coverage times. “This is one more way our hospitalist program supports the hospital and provides value beyond just seeing patients,” he says.
Overseas Outsourcing a ‘Hot Button’
Using an overseas teleradiology company provides many advantages, says Sunita Maheshwari, MD, a consulting pediatric cardiologist and director of Teleradiology Solutions, a four-year-old teleradiology company located in Bangalore, India. The company’s radiologists do mostly preliminary night-reads but also do final-reads on approximately 20% of their cases. If contrast must be administered for an imaging study at the client hospital, a local tech, emergency department physician, or resident usually handles the procedure, with the Teleradiology Solutions radiologist in constant voice contact.
“The time zone advantage is huge,” says Dr. Maheshwari. With the 12.5-hour time difference between the United States and India, Teleradiology Solutions’ radiologists work regular day shifts and are able to cover 10-20 hospitals simultaneously, depending on how busy their client hospitals are.
“You don’t have to have one radiologist who stays up all night to be able to read two CT scans and one X-ray, who will [then] be groggy the next morning for his [or her] regular day shift,” she says. It makes a lot of sense from the standpoint of human resource efficiency to not waste several nights of several doctors covering multiple hospitals.” Dr. Maheshwari reports that American hospital staff are often pleasantly surprised to find a “cheerful, awake” radiologist on the other end of the phone line.
Despite these benefits, however, Dr. Maheshwari and her colleagues have noticed a political backlash stemming from the outsourcing of U.S. jobs to Asia that colors Americans’ reactions to overseas teleradiology. In her company’s first two years, some physicians questioned the company’s level of quality and lashed out because it is located in India, reports Dr. Maheshwari.
“Our work speaks for itself,” she says. “We have not lost a client, and, in fact, our hospitals have managed to grow because they have been able to take their radiologists off the night shift, and they take on more day work.”
Like several overseas teleradiology companies, Teleradiology Solutions retains a staff of U.S.-trained radiologists and goes through the same licensing and credentialing (they are JCAHO-accredited) as American companies.
The company now has 40 U.S. hospitals as clients and includes in its client mix some remote hospitals in India and Singapore, where the Ministry of Health is experiencing a similar shortage of radiologists.
Filling an ICU Gap
Shortages of specialists—and federal mandates to improve access to care—have spurred the growth of telemedicine in remote rural areas. Wade notes that multi-hospital systems are now installing remote electronic ICU care programs, where intensivists simultaneously monitor ICU patients in several hospitals from a central location. Preliminary studies have demonstrated both improved clinical outcomes and heightened hospital performance with programs such as VISICU Inc.’s eCare Manager software, which features built-in online decision support, adverse events alerts, and outcomes tracking. One 2004 study documented a 27% reduction in severity-adjusted hospital mortality for ICU patients, a 17% reduction in ICU length of stay, and a savings of $2,150 per patient, even after accounting for initial capital outlays to install the eICU system.4
SHM President Mary Jo Gorman, MD, MBA, is now chief executive officer for Advanced ICU Care, headquartered in St. Louis, Mo. Using VISICU’s patented software platform, the new company currently contracts with two community-based Midwestern hospitals to deliver real-time intensivist rounding and decision-making support.
Saint Clare’s Hospital, located in north central Wisconsin, was opened by Ministry Health Care in October 2005 with the intention of creating a tertiary referral center, says Dr. Bailey. To be competitive in the market, the hospital needed to provide a full-service intensive care unit. He explains, “[Unfortunately,] we are in an area that is suffering from the same kind of recruitment drought in pulmonary and critical care medicine as everyone else—and ours is accentuated because we are not in a large city, and we are not a teaching hospital.”
Advanced ICU proved a good fit for addressing the hospital’s ICU needs. The hospital “went live” with eICU in January and no longer has to send patients to sister hospitals with on-site intensivist coverage, says Dr. Bailey. Saint Clare’s staff intensivist works regular day shifts, and the hospitalist group co-manages the ICU with Advanced ICU’s staff the rest of the time, providing 24/7 coverage. ICU mortality, after adjusting for Acute Physiology and Chronic Health Evaluation (APACHE) scores and other severity indices, is also below predicted numbers.
Patient and Staff Acceptance
Does the notion of real-time video surveillance coupled with real-time data feeds on vital signs, lab work, and medications present problems for patients or staff? Patients are “very accepting and feel it’s an extra sort of security” knowing that Advanced ICU intensivists are on the job, says Dr. Gorman: “One patient referred to us as a ‘guardian angel’ looking over them.
“The nursing staff has been extremely accepting because it reduces their stress about making a determination of whether to interrupt the attending doctor during his office hours or at night,” she continues. “We’re really a partner to the local medical staff. We all know that to reduce medical errors, the bedside caregiver needs to recognize the problem, be able to contact somebody, address the problem, and then see if that intervention is the right one for the problem described. With eICU, you just move past all of those points of failure to get the patient right to the doctor in a very timely manner.”
Janet Pestle, RN, MSN, director of the Cardiovascular Program at SSM Health Care’s St. Mary’s Hospital and Medical Center in Jefferson City, Mo., echoes Dr. Gorman’s assessment. Encountering the same intensivist drought as other hospitals outside of metropolitan areas, St. Mary’s also contracted with Advanced ICU.
“I’d have a fist fight if I ever wanted to take [the eICU] away from the nurses and staff on the night shift,” declares Pestle. “I think there is definitely some guilt associated with healthcare workers having to wake up a doctor who may have been working all day. They love being able to push a button and have a physician there.”
Dr. Bailey believes the eICU offers many advantages for Saint Clare’s six-member hospitalist group. Although hospitalists have a large presence in the ICU, “ … we shouldn’t expect them to be intensivists,” he insists. “Given that the typical hospitalist is very young, I was concerned about setting up hospitalists for failure by not giving them the resources to help them provide high quality care and to be successful.”
Partnering with Advanced ICU has also helped recruitment of younger hospitalists, he says, noting that hospitalists have chosen Saint Clare’s over other hospitals because of the eICU presence. “Our hospitalists get very concerned about being pulled in too many directions,” says Dr. Bailey. “Advanced ICU frees up our hospitalists, giving them a high degree of comfort and confidence that they can handle multiple cases at once.”
To ensure continuity between the ICU and the medical floor, all admissions are still handled by the hospitalists. The eCare Manager software used by Advanced ICU also provides another layer of attention to quality indicators, with built-in decision support and alerts.
Outsourcing Opens the Box
Dr. Bailey visited Advanced ICU’s command center and was impressed with the frequency with which the company’s intensivists were virtually “rounding” on Saint Clare’s patients. “It’s very exciting if you think about it,” he says. “Intensivists in Missouri can talk with a radiologist in Hawaii about a patient in Wisconsin. This is certainly improving our quality of care.”
“The eICU is really mind-blowing,” agrees Dr. Wachter. Once services are no longer located in the building, “there’s not much difference between 30 miles and 10,000 miles away, and this just opens up the box in some very interesting ways.” Service providers operating from different countries under different sets of laws and value systems, he notes in his New England Journal of Medicine article, can, however, “create opportunities for new kinds of mischief.”
Asked for an example of this, he explains that his institution’s initial foray into medical outsourcing was a bit of a cautionary tale. Unbeknownst to UCSF, their domestic medical transcription company sub-contracted with a transcription company in Pakistan. Administrators discovered this fact when a Pakistani transcriptionist contacted the university, threatening to put all the medical records she had transcribed on the Web if she did not get a raise. This would have constituted a breach of HIPAA and would have created multiple liability issues for UCSF. Contractors dealing with the medical center now have to guarantee, in writing, that they will use only domestic subcontractors, says Dr. Wachter.
Future Directions
Because of the “high-touch” nature of hospital medicine, Dr. Wachter does not think that hospitalists’ services are feasible candidates for outsourcing.
“I guess one could conceive of a robotic hospitalist running around the building being controlled by a joystick in Singapore, but that’s science fiction and not a real risk,” he quips.
Still, relationships with specialists such as radiologists and intensivists may more likely be formed over the telephone, through video conferencing, and in online interactions—phenomena with which younger physicians may be much more comfortable.
Dr. Maheshwari, who, like the company’s founder Arjun Kalyanpur, MD, trained at Yale University in New Haven, Conn., expects that Teleradiology Solution’s business will continue to grow and that, over time, “the world will truly be flat—hopefully!”
Wade admits that the need for outsourced services is not going to diminish. “Our need to be able to harness technology to provide [a high] level of intensive care to patients, no matter where they are, is going to be very strong,” he says. “So I think we will see more of this [outsourcing]. But I also think we’ll see a much greater emphasis on trying to train new physicians. Outsourcing is part of the same phenomenon as medical tourism. Hospitals that go this route are going to have a responsibility to demand high-quality physicians, demand Joint Commission certification, and demand to know the background and training of these [outsourced] physicians, because the patients and families are going to have questions. That’s part of the doctor-patient relationship that the hospital is going to create.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- Wachter RM. The “dis-location” of U.S. medicine – the implications of medical outsourcing. N Engl J Med. 2006; 354(7):661-665.
- Larson DB, Cypel YS, Forman HP, et al. A comprehensive portrait of teleradiology in radiology practices: results from the American College of Radiology’s 1999 Survey. AJR Am J Roentgenol. 2005 Jul;185(1):24-35.
- Dimmick SL, Ignatova KD. The diffusion of a medical innovation: where teleradiology is and where it is going. J Telemed Telecare. 2006;12 Suppl 2:S51-58.
- Breslow MJ, Rosenfeld BA, Doerfler M, et al. Effect of a multiple-site intensive care unit telemedicine program on clinical and economic outcomes: an alternative paradigm for intensivist staffing. Crit Care Med. 2004 Jan;32(1):31-38.
Medical outsourcing is a growing trend in American hospitals, driven by shortages of on-call radiologists and intensivists, economic pressures, and advances in telemedicine. Hospitalists will likely encounter—if they haven’t already—outsourced services that range from off-site medical transcription and language interpreters to long-distance radiology and, increasingly, electronic intensivist services.1 What are the implications for quality patient care and collegial interface when hospitals contract with outsourced providers? What are the advantages, possible disadvantages, and opportunities for hospitalists as teleradiology and eICUs become facts of life?
A Variety of Configurations
According to Rick Wade, senior vice president for strategic communications for the American Hospital Association (Chicago), it’s difficult to quantify the extent to which outsourcing is currently being used in U.S. hospitals. VISICU, Inc., a leader in the provision of eICU services, currently has 150 client hospitals. Eight hospitalists contacted at community and university hospitals in Colo., Fla., Maine, Minn., Ga. and N.M. reported that they were not directly involved with outsourcing other than with transcription services.
Robert M. Wachter, MD, professor and associate chairman, Department of Medicine, and chief of the Medical Service at the University of California at San Francisco (UCSF), whose “Perspective” piece on medical outsourcing appeared in the February 16 New England Journal of Medicine, is intrigued by the implications of outsourcing trends for medicine: “I think medicine has been peculiarly insulated from [the globalization of services], and it’s just very interesting and exciting—and troubling as well.”1
Off-Site X-Ray Reads Common
According to the American College of Radiology, teleradiology has become a fixture in most practices and hospitals.2,3 Some institutions have retained their own radiologists, who take advantage of teleradiology by reading digitized radiographs and CT scans from home instead of within the hospital building. A shortage of radiologists has led others to contract with off-site providers of teleradiology services. Those who provide services at night are sometimes called “nighthawk” companies.1 Outsourcing of radiology, Dr. Wachter believes, is a logical step due to technological advances, though he admits that visiting the radiology department in his hospital often yields educational and collegial opportunities that online X-ray reading does not.
At Saint Clare’s Hospital in Weston/Wasau, Wis., a new, 107-bed state-of-the-art facility built by Ministry Health Care, Richard Bailey, MD, is medical director of Inpatient Care and Hospitalist Services. Radiology and other ancillary specialist services are provided by the Diagnostic and Treatment Center (DTC), jointly owned by Ministry Health Care and the Marshfield Clinic. The DTC, through a relationship with a radiology group in Hawaii, provides night coverage for full reads of radiographs and scans from 5 p.m. to 5 a.m. The interactions are virtually seamless, according to Dr. Bailey. “We don’t even notice they’re in Hawaii” when conferring with radiologists on the phone, he reports.
Off-site radiology also created an opportunity for his hospitalist group, Dr. Bailey says. Saint Clare’s hospitalist group provides supervision of contrast administration when needed during night and weekend coverage times. “This is one more way our hospitalist program supports the hospital and provides value beyond just seeing patients,” he says.
Overseas Outsourcing a ‘Hot Button’
Using an overseas teleradiology company provides many advantages, says Sunita Maheshwari, MD, a consulting pediatric cardiologist and director of Teleradiology Solutions, a four-year-old teleradiology company located in Bangalore, India. The company’s radiologists do mostly preliminary night-reads but also do final-reads on approximately 20% of their cases. If contrast must be administered for an imaging study at the client hospital, a local tech, emergency department physician, or resident usually handles the procedure, with the Teleradiology Solutions radiologist in constant voice contact.
“The time zone advantage is huge,” says Dr. Maheshwari. With the 12.5-hour time difference between the United States and India, Teleradiology Solutions’ radiologists work regular day shifts and are able to cover 10-20 hospitals simultaneously, depending on how busy their client hospitals are.
“You don’t have to have one radiologist who stays up all night to be able to read two CT scans and one X-ray, who will [then] be groggy the next morning for his [or her] regular day shift,” she says. It makes a lot of sense from the standpoint of human resource efficiency to not waste several nights of several doctors covering multiple hospitals.” Dr. Maheshwari reports that American hospital staff are often pleasantly surprised to find a “cheerful, awake” radiologist on the other end of the phone line.
Despite these benefits, however, Dr. Maheshwari and her colleagues have noticed a political backlash stemming from the outsourcing of U.S. jobs to Asia that colors Americans’ reactions to overseas teleradiology. In her company’s first two years, some physicians questioned the company’s level of quality and lashed out because it is located in India, reports Dr. Maheshwari.
“Our work speaks for itself,” she says. “We have not lost a client, and, in fact, our hospitals have managed to grow because they have been able to take their radiologists off the night shift, and they take on more day work.”
Like several overseas teleradiology companies, Teleradiology Solutions retains a staff of U.S.-trained radiologists and goes through the same licensing and credentialing (they are JCAHO-accredited) as American companies.
The company now has 40 U.S. hospitals as clients and includes in its client mix some remote hospitals in India and Singapore, where the Ministry of Health is experiencing a similar shortage of radiologists.
Filling an ICU Gap
Shortages of specialists—and federal mandates to improve access to care—have spurred the growth of telemedicine in remote rural areas. Wade notes that multi-hospital systems are now installing remote electronic ICU care programs, where intensivists simultaneously monitor ICU patients in several hospitals from a central location. Preliminary studies have demonstrated both improved clinical outcomes and heightened hospital performance with programs such as VISICU Inc.’s eCare Manager software, which features built-in online decision support, adverse events alerts, and outcomes tracking. One 2004 study documented a 27% reduction in severity-adjusted hospital mortality for ICU patients, a 17% reduction in ICU length of stay, and a savings of $2,150 per patient, even after accounting for initial capital outlays to install the eICU system.4
SHM President Mary Jo Gorman, MD, MBA, is now chief executive officer for Advanced ICU Care, headquartered in St. Louis, Mo. Using VISICU’s patented software platform, the new company currently contracts with two community-based Midwestern hospitals to deliver real-time intensivist rounding and decision-making support.
Saint Clare’s Hospital, located in north central Wisconsin, was opened by Ministry Health Care in October 2005 with the intention of creating a tertiary referral center, says Dr. Bailey. To be competitive in the market, the hospital needed to provide a full-service intensive care unit. He explains, “[Unfortunately,] we are in an area that is suffering from the same kind of recruitment drought in pulmonary and critical care medicine as everyone else—and ours is accentuated because we are not in a large city, and we are not a teaching hospital.”
Advanced ICU proved a good fit for addressing the hospital’s ICU needs. The hospital “went live” with eICU in January and no longer has to send patients to sister hospitals with on-site intensivist coverage, says Dr. Bailey. Saint Clare’s staff intensivist works regular day shifts, and the hospitalist group co-manages the ICU with Advanced ICU’s staff the rest of the time, providing 24/7 coverage. ICU mortality, after adjusting for Acute Physiology and Chronic Health Evaluation (APACHE) scores and other severity indices, is also below predicted numbers.
Patient and Staff Acceptance
Does the notion of real-time video surveillance coupled with real-time data feeds on vital signs, lab work, and medications present problems for patients or staff? Patients are “very accepting and feel it’s an extra sort of security” knowing that Advanced ICU intensivists are on the job, says Dr. Gorman: “One patient referred to us as a ‘guardian angel’ looking over them.
“The nursing staff has been extremely accepting because it reduces their stress about making a determination of whether to interrupt the attending doctor during his office hours or at night,” she continues. “We’re really a partner to the local medical staff. We all know that to reduce medical errors, the bedside caregiver needs to recognize the problem, be able to contact somebody, address the problem, and then see if that intervention is the right one for the problem described. With eICU, you just move past all of those points of failure to get the patient right to the doctor in a very timely manner.”
Janet Pestle, RN, MSN, director of the Cardiovascular Program at SSM Health Care’s St. Mary’s Hospital and Medical Center in Jefferson City, Mo., echoes Dr. Gorman’s assessment. Encountering the same intensivist drought as other hospitals outside of metropolitan areas, St. Mary’s also contracted with Advanced ICU.
“I’d have a fist fight if I ever wanted to take [the eICU] away from the nurses and staff on the night shift,” declares Pestle. “I think there is definitely some guilt associated with healthcare workers having to wake up a doctor who may have been working all day. They love being able to push a button and have a physician there.”
Dr. Bailey believes the eICU offers many advantages for Saint Clare’s six-member hospitalist group. Although hospitalists have a large presence in the ICU, “ … we shouldn’t expect them to be intensivists,” he insists. “Given that the typical hospitalist is very young, I was concerned about setting up hospitalists for failure by not giving them the resources to help them provide high quality care and to be successful.”
Partnering with Advanced ICU has also helped recruitment of younger hospitalists, he says, noting that hospitalists have chosen Saint Clare’s over other hospitals because of the eICU presence. “Our hospitalists get very concerned about being pulled in too many directions,” says Dr. Bailey. “Advanced ICU frees up our hospitalists, giving them a high degree of comfort and confidence that they can handle multiple cases at once.”
To ensure continuity between the ICU and the medical floor, all admissions are still handled by the hospitalists. The eCare Manager software used by Advanced ICU also provides another layer of attention to quality indicators, with built-in decision support and alerts.
Outsourcing Opens the Box
Dr. Bailey visited Advanced ICU’s command center and was impressed with the frequency with which the company’s intensivists were virtually “rounding” on Saint Clare’s patients. “It’s very exciting if you think about it,” he says. “Intensivists in Missouri can talk with a radiologist in Hawaii about a patient in Wisconsin. This is certainly improving our quality of care.”
“The eICU is really mind-blowing,” agrees Dr. Wachter. Once services are no longer located in the building, “there’s not much difference between 30 miles and 10,000 miles away, and this just opens up the box in some very interesting ways.” Service providers operating from different countries under different sets of laws and value systems, he notes in his New England Journal of Medicine article, can, however, “create opportunities for new kinds of mischief.”
Asked for an example of this, he explains that his institution’s initial foray into medical outsourcing was a bit of a cautionary tale. Unbeknownst to UCSF, their domestic medical transcription company sub-contracted with a transcription company in Pakistan. Administrators discovered this fact when a Pakistani transcriptionist contacted the university, threatening to put all the medical records she had transcribed on the Web if she did not get a raise. This would have constituted a breach of HIPAA and would have created multiple liability issues for UCSF. Contractors dealing with the medical center now have to guarantee, in writing, that they will use only domestic subcontractors, says Dr. Wachter.
Future Directions
Because of the “high-touch” nature of hospital medicine, Dr. Wachter does not think that hospitalists’ services are feasible candidates for outsourcing.
“I guess one could conceive of a robotic hospitalist running around the building being controlled by a joystick in Singapore, but that’s science fiction and not a real risk,” he quips.
Still, relationships with specialists such as radiologists and intensivists may more likely be formed over the telephone, through video conferencing, and in online interactions—phenomena with which younger physicians may be much more comfortable.
Dr. Maheshwari, who, like the company’s founder Arjun Kalyanpur, MD, trained at Yale University in New Haven, Conn., expects that Teleradiology Solution’s business will continue to grow and that, over time, “the world will truly be flat—hopefully!”
Wade admits that the need for outsourced services is not going to diminish. “Our need to be able to harness technology to provide [a high] level of intensive care to patients, no matter where they are, is going to be very strong,” he says. “So I think we will see more of this [outsourcing]. But I also think we’ll see a much greater emphasis on trying to train new physicians. Outsourcing is part of the same phenomenon as medical tourism. Hospitals that go this route are going to have a responsibility to demand high-quality physicians, demand Joint Commission certification, and demand to know the background and training of these [outsourced] physicians, because the patients and families are going to have questions. That’s part of the doctor-patient relationship that the hospital is going to create.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- Wachter RM. The “dis-location” of U.S. medicine – the implications of medical outsourcing. N Engl J Med. 2006; 354(7):661-665.
- Larson DB, Cypel YS, Forman HP, et al. A comprehensive portrait of teleradiology in radiology practices: results from the American College of Radiology’s 1999 Survey. AJR Am J Roentgenol. 2005 Jul;185(1):24-35.
- Dimmick SL, Ignatova KD. The diffusion of a medical innovation: where teleradiology is and where it is going. J Telemed Telecare. 2006;12 Suppl 2:S51-58.
- Breslow MJ, Rosenfeld BA, Doerfler M, et al. Effect of a multiple-site intensive care unit telemedicine program on clinical and economic outcomes: an alternative paradigm for intensivist staffing. Crit Care Med. 2004 Jan;32(1):31-38.
Medical outsourcing is a growing trend in American hospitals, driven by shortages of on-call radiologists and intensivists, economic pressures, and advances in telemedicine. Hospitalists will likely encounter—if they haven’t already—outsourced services that range from off-site medical transcription and language interpreters to long-distance radiology and, increasingly, electronic intensivist services.1 What are the implications for quality patient care and collegial interface when hospitals contract with outsourced providers? What are the advantages, possible disadvantages, and opportunities for hospitalists as teleradiology and eICUs become facts of life?
A Variety of Configurations
According to Rick Wade, senior vice president for strategic communications for the American Hospital Association (Chicago), it’s difficult to quantify the extent to which outsourcing is currently being used in U.S. hospitals. VISICU, Inc., a leader in the provision of eICU services, currently has 150 client hospitals. Eight hospitalists contacted at community and university hospitals in Colo., Fla., Maine, Minn., Ga. and N.M. reported that they were not directly involved with outsourcing other than with transcription services.
Robert M. Wachter, MD, professor and associate chairman, Department of Medicine, and chief of the Medical Service at the University of California at San Francisco (UCSF), whose “Perspective” piece on medical outsourcing appeared in the February 16 New England Journal of Medicine, is intrigued by the implications of outsourcing trends for medicine: “I think medicine has been peculiarly insulated from [the globalization of services], and it’s just very interesting and exciting—and troubling as well.”1
Off-Site X-Ray Reads Common
According to the American College of Radiology, teleradiology has become a fixture in most practices and hospitals.2,3 Some institutions have retained their own radiologists, who take advantage of teleradiology by reading digitized radiographs and CT scans from home instead of within the hospital building. A shortage of radiologists has led others to contract with off-site providers of teleradiology services. Those who provide services at night are sometimes called “nighthawk” companies.1 Outsourcing of radiology, Dr. Wachter believes, is a logical step due to technological advances, though he admits that visiting the radiology department in his hospital often yields educational and collegial opportunities that online X-ray reading does not.
At Saint Clare’s Hospital in Weston/Wasau, Wis., a new, 107-bed state-of-the-art facility built by Ministry Health Care, Richard Bailey, MD, is medical director of Inpatient Care and Hospitalist Services. Radiology and other ancillary specialist services are provided by the Diagnostic and Treatment Center (DTC), jointly owned by Ministry Health Care and the Marshfield Clinic. The DTC, through a relationship with a radiology group in Hawaii, provides night coverage for full reads of radiographs and scans from 5 p.m. to 5 a.m. The interactions are virtually seamless, according to Dr. Bailey. “We don’t even notice they’re in Hawaii” when conferring with radiologists on the phone, he reports.
Off-site radiology also created an opportunity for his hospitalist group, Dr. Bailey says. Saint Clare’s hospitalist group provides supervision of contrast administration when needed during night and weekend coverage times. “This is one more way our hospitalist program supports the hospital and provides value beyond just seeing patients,” he says.
Overseas Outsourcing a ‘Hot Button’
Using an overseas teleradiology company provides many advantages, says Sunita Maheshwari, MD, a consulting pediatric cardiologist and director of Teleradiology Solutions, a four-year-old teleradiology company located in Bangalore, India. The company’s radiologists do mostly preliminary night-reads but also do final-reads on approximately 20% of their cases. If contrast must be administered for an imaging study at the client hospital, a local tech, emergency department physician, or resident usually handles the procedure, with the Teleradiology Solutions radiologist in constant voice contact.
“The time zone advantage is huge,” says Dr. Maheshwari. With the 12.5-hour time difference between the United States and India, Teleradiology Solutions’ radiologists work regular day shifts and are able to cover 10-20 hospitals simultaneously, depending on how busy their client hospitals are.
“You don’t have to have one radiologist who stays up all night to be able to read two CT scans and one X-ray, who will [then] be groggy the next morning for his [or her] regular day shift,” she says. It makes a lot of sense from the standpoint of human resource efficiency to not waste several nights of several doctors covering multiple hospitals.” Dr. Maheshwari reports that American hospital staff are often pleasantly surprised to find a “cheerful, awake” radiologist on the other end of the phone line.
Despite these benefits, however, Dr. Maheshwari and her colleagues have noticed a political backlash stemming from the outsourcing of U.S. jobs to Asia that colors Americans’ reactions to overseas teleradiology. In her company’s first two years, some physicians questioned the company’s level of quality and lashed out because it is located in India, reports Dr. Maheshwari.
“Our work speaks for itself,” she says. “We have not lost a client, and, in fact, our hospitals have managed to grow because they have been able to take their radiologists off the night shift, and they take on more day work.”
Like several overseas teleradiology companies, Teleradiology Solutions retains a staff of U.S.-trained radiologists and goes through the same licensing and credentialing (they are JCAHO-accredited) as American companies.
The company now has 40 U.S. hospitals as clients and includes in its client mix some remote hospitals in India and Singapore, where the Ministry of Health is experiencing a similar shortage of radiologists.
Filling an ICU Gap
Shortages of specialists—and federal mandates to improve access to care—have spurred the growth of telemedicine in remote rural areas. Wade notes that multi-hospital systems are now installing remote electronic ICU care programs, where intensivists simultaneously monitor ICU patients in several hospitals from a central location. Preliminary studies have demonstrated both improved clinical outcomes and heightened hospital performance with programs such as VISICU Inc.’s eCare Manager software, which features built-in online decision support, adverse events alerts, and outcomes tracking. One 2004 study documented a 27% reduction in severity-adjusted hospital mortality for ICU patients, a 17% reduction in ICU length of stay, and a savings of $2,150 per patient, even after accounting for initial capital outlays to install the eICU system.4
SHM President Mary Jo Gorman, MD, MBA, is now chief executive officer for Advanced ICU Care, headquartered in St. Louis, Mo. Using VISICU’s patented software platform, the new company currently contracts with two community-based Midwestern hospitals to deliver real-time intensivist rounding and decision-making support.
Saint Clare’s Hospital, located in north central Wisconsin, was opened by Ministry Health Care in October 2005 with the intention of creating a tertiary referral center, says Dr. Bailey. To be competitive in the market, the hospital needed to provide a full-service intensive care unit. He explains, “[Unfortunately,] we are in an area that is suffering from the same kind of recruitment drought in pulmonary and critical care medicine as everyone else—and ours is accentuated because we are not in a large city, and we are not a teaching hospital.”
Advanced ICU proved a good fit for addressing the hospital’s ICU needs. The hospital “went live” with eICU in January and no longer has to send patients to sister hospitals with on-site intensivist coverage, says Dr. Bailey. Saint Clare’s staff intensivist works regular day shifts, and the hospitalist group co-manages the ICU with Advanced ICU’s staff the rest of the time, providing 24/7 coverage. ICU mortality, after adjusting for Acute Physiology and Chronic Health Evaluation (APACHE) scores and other severity indices, is also below predicted numbers.
Patient and Staff Acceptance
Does the notion of real-time video surveillance coupled with real-time data feeds on vital signs, lab work, and medications present problems for patients or staff? Patients are “very accepting and feel it’s an extra sort of security” knowing that Advanced ICU intensivists are on the job, says Dr. Gorman: “One patient referred to us as a ‘guardian angel’ looking over them.
“The nursing staff has been extremely accepting because it reduces their stress about making a determination of whether to interrupt the attending doctor during his office hours or at night,” she continues. “We’re really a partner to the local medical staff. We all know that to reduce medical errors, the bedside caregiver needs to recognize the problem, be able to contact somebody, address the problem, and then see if that intervention is the right one for the problem described. With eICU, you just move past all of those points of failure to get the patient right to the doctor in a very timely manner.”
Janet Pestle, RN, MSN, director of the Cardiovascular Program at SSM Health Care’s St. Mary’s Hospital and Medical Center in Jefferson City, Mo., echoes Dr. Gorman’s assessment. Encountering the same intensivist drought as other hospitals outside of metropolitan areas, St. Mary’s also contracted with Advanced ICU.
“I’d have a fist fight if I ever wanted to take [the eICU] away from the nurses and staff on the night shift,” declares Pestle. “I think there is definitely some guilt associated with healthcare workers having to wake up a doctor who may have been working all day. They love being able to push a button and have a physician there.”
Dr. Bailey believes the eICU offers many advantages for Saint Clare’s six-member hospitalist group. Although hospitalists have a large presence in the ICU, “ … we shouldn’t expect them to be intensivists,” he insists. “Given that the typical hospitalist is very young, I was concerned about setting up hospitalists for failure by not giving them the resources to help them provide high quality care and to be successful.”
Partnering with Advanced ICU has also helped recruitment of younger hospitalists, he says, noting that hospitalists have chosen Saint Clare’s over other hospitals because of the eICU presence. “Our hospitalists get very concerned about being pulled in too many directions,” says Dr. Bailey. “Advanced ICU frees up our hospitalists, giving them a high degree of comfort and confidence that they can handle multiple cases at once.”
To ensure continuity between the ICU and the medical floor, all admissions are still handled by the hospitalists. The eCare Manager software used by Advanced ICU also provides another layer of attention to quality indicators, with built-in decision support and alerts.
Outsourcing Opens the Box
Dr. Bailey visited Advanced ICU’s command center and was impressed with the frequency with which the company’s intensivists were virtually “rounding” on Saint Clare’s patients. “It’s very exciting if you think about it,” he says. “Intensivists in Missouri can talk with a radiologist in Hawaii about a patient in Wisconsin. This is certainly improving our quality of care.”
“The eICU is really mind-blowing,” agrees Dr. Wachter. Once services are no longer located in the building, “there’s not much difference between 30 miles and 10,000 miles away, and this just opens up the box in some very interesting ways.” Service providers operating from different countries under different sets of laws and value systems, he notes in his New England Journal of Medicine article, can, however, “create opportunities for new kinds of mischief.”
Asked for an example of this, he explains that his institution’s initial foray into medical outsourcing was a bit of a cautionary tale. Unbeknownst to UCSF, their domestic medical transcription company sub-contracted with a transcription company in Pakistan. Administrators discovered this fact when a Pakistani transcriptionist contacted the university, threatening to put all the medical records she had transcribed on the Web if she did not get a raise. This would have constituted a breach of HIPAA and would have created multiple liability issues for UCSF. Contractors dealing with the medical center now have to guarantee, in writing, that they will use only domestic subcontractors, says Dr. Wachter.
Future Directions
Because of the “high-touch” nature of hospital medicine, Dr. Wachter does not think that hospitalists’ services are feasible candidates for outsourcing.
“I guess one could conceive of a robotic hospitalist running around the building being controlled by a joystick in Singapore, but that’s science fiction and not a real risk,” he quips.
Still, relationships with specialists such as radiologists and intensivists may more likely be formed over the telephone, through video conferencing, and in online interactions—phenomena with which younger physicians may be much more comfortable.
Dr. Maheshwari, who, like the company’s founder Arjun Kalyanpur, MD, trained at Yale University in New Haven, Conn., expects that Teleradiology Solution’s business will continue to grow and that, over time, “the world will truly be flat—hopefully!”
Wade admits that the need for outsourced services is not going to diminish. “Our need to be able to harness technology to provide [a high] level of intensive care to patients, no matter where they are, is going to be very strong,” he says. “So I think we will see more of this [outsourcing]. But I also think we’ll see a much greater emphasis on trying to train new physicians. Outsourcing is part of the same phenomenon as medical tourism. Hospitals that go this route are going to have a responsibility to demand high-quality physicians, demand Joint Commission certification, and demand to know the background and training of these [outsourced] physicians, because the patients and families are going to have questions. That’s part of the doctor-patient relationship that the hospital is going to create.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- Wachter RM. The “dis-location” of U.S. medicine – the implications of medical outsourcing. N Engl J Med. 2006; 354(7):661-665.
- Larson DB, Cypel YS, Forman HP, et al. A comprehensive portrait of teleradiology in radiology practices: results from the American College of Radiology’s 1999 Survey. AJR Am J Roentgenol. 2005 Jul;185(1):24-35.
- Dimmick SL, Ignatova KD. The diffusion of a medical innovation: where teleradiology is and where it is going. J Telemed Telecare. 2006;12 Suppl 2:S51-58.
- Breslow MJ, Rosenfeld BA, Doerfler M, et al. Effect of a multiple-site intensive care unit telemedicine program on clinical and economic outcomes: an alternative paradigm for intensivist staffing. Crit Care Med. 2004 Jan;32(1):31-38.
Perilious Prescriptions
Medication-related errors jeopardize patient safety and commonly result in otherwise unnecessary hospitalizations. Approximately 7% of hospital admissions result from drug-related errors, of which 59% are considered preventable.1 It is estimated that adverse drug events affect 2% to 5% of hospitalized patients.2,3 These errors result in increased hospital costs of $4,700 per admission, or about $2 billion annually for U.S. hospitals.2 Calculations indicate that in the nursing home, for each dollar spent on a medication, there is another $1.33 spent on healthcare resources for the treatment of a drug-related morbidity or mortality.
Unfortunately, older folks are particularly susceptible to medication-related problems. Age-associated changes in body composition and physiology, multiple comorbidities, and—last but not least—polypharmacy, are contributing factors. In the United States, patients older than 65 fill an average of 12 prescriptions per year, compared with five fills for patients between ages 25 and 40. In addition, the use of nonprescription medications is more common in the elderly. This opens up the possibility of increased drug-drug or drug-herbal interactions.
Depending on the healthcare setting, as well as the criteria that define inappropriate medication use, studies alert us that between 7% and 21% of ambulatory older folks receive at least one potentially inappropriate medication.4,5 About 60% of nursing home residents, and a staggering 92% of frail elderly hospitalized veterans, receive at least one potentially inappropriate medication.6,7 The consequences of inappropriate drug use in the elderly can be significant. Weakness, resulting in loss of independence and falls that end in bone fractures, is only one possible negative consequence. Between 10% and 20% of the elderly are hospitalized as a result of receiving these inappropriate medications.8,9
Screening Inappropriate Medication
So, what are inappropriate medications for the elderly? Overly simplified, they include any medication that has a greater potential for doing more harm than good. In 1991, Beers and colleagues published criteria for screening inappropriate medication use in elderly patients.10 The authors reviewed the literature and identified 14 nationally recognized authorities in the fields of geriatric pharmacology, epidemiology, geriatrics, and long-term care. Among these experts, consensus was reached on a list of inappropriate medications for elderly nursing home residents. The list was intended to identify medications that should be avoided except under unusual circumstances. The experts also developed criteria for optimal doses, frequencies, and duration of use for these medications.
Since 1991, the criteria have been updated twice (in 1997 and 2002) to include ambulatory elderly. The 2002 Beers list included 48 inappropriate drugs or medication classes, regardless of diagnosis or conditions.11 Because drug-disease interactions in the elderly are increasingly recognized, the 2003 Beers list also included inappropriate medications or medication classes for 20 medical conditions. The consensus panel of experts identified 66 inappropriate drugs with adverse outcomes of potentially high severity. The authors stated specifically that the criteria were not meant to regulate practice to the point at which they would supersede the clinical judgment and assessment of the medical practitioner.
Drug-Drug Interaction
Based on Beers’ criteria for inappropriate prescribing, a literature review of studies conducted between 1992 and 1999 found that between 14% and 23% of the elderly filled a prescription for one or more drugs on the Beers list.12 Long-acting benzodiazepines, dipyridamole, propoxyphene, and amitriptyline were among the most frequently prescribed inappropriate medications.
Cardiovascular and psychotropic drugs are most commonly involved in drug-drug interactions. The most common adverse effects are acute renal failure, hypotension, and neuropsychological presentations such as delirium. Risk factors predisposing to adverse reactions are using multiple medications, receiving care from several prescribing clinicians, and filling prescriptions at more than one pharmacy. Physicians should also be vigilant for drug-herbal interactions.
Drug-Disease Interaction
Another phenomenon responsible for adverse drug events is a drug-disease interaction. For example, renal failure or hepatic insufficiency can interfere with detoxification and excretion; ascites can alter the volume of distribution of hydrophilic drugs, while obesity has an altering effect on lipophilic drugs. Patients with advanced cognitive impairment may have increased sensitivity or paradoxical reactions to drugs with central nervous system or anticholinergic activities.
Optimal Prescribing
As with safety, effective drug therapy for older people is also far from optimal. Optimal drug prescribing should aim for a balance between overprescribing and underprescribing while keeping a safe environment in mind (i.e., monitoring for adverse drug reactions and reducing medication errors). More than 50% of outpatient prescriptions are without indication, while necessary drugs are withheld in the cases of about 55% of elderly outpatients and 25% of hospitalized elderly patients.13
Overprescribing refers not only to the use of multiple medications but also implies a lack of appropriateness in selection, dosing, or use of the medication. For example, the term “prescribing cascade” refers to adding a new medication to treat symptoms of an adverse drug event that is mistakenly assumed to be a separate new diagnosis. Potential consequences of overprescribing include adverse drug events, drug-drug interactions, decreased quality of life, and unnecessary costs. Common factors connected to overprescribing include, but are not limited to, advanced age, multiple comorbidities, multiple prescribers, poor record-keeping, and failure for healthcare providers to thoroughly review a patient’s medication regimen.
Underprescribing of medications to older people is also of concern. Underprescribing results from efforts to avoid complex medication regimens, fear for adverse events, problems with patient adherence to medications, and economic barriers. Underprescribing can result from the notion that older folks will not benefit from medications intended for primary or secondary prevention or for aggressive management of chronic conditions (e.g., angiotensin-converting enzyme inhibitors and beta blockers prescribed for congestive heart failure and after a myocardial infarction).
New Prescribing Initiatives
There have been new initiatives to emphasize optimal prescribing. The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) mandates medication reconciliation across inpatient and outpatient practices. In 1999, the Centers for Medicare and Medicaid Services (CMS) expanded the drug use review policy for nursing home certification. Using specific criteria, surveyors and pharmacists must assess resident records for potentially inappropriate medication exposures and associated adverse drug reactions. The “Assessing Care for Vulnerable Elders” (ACOVE) initiative implemented use of quality indicators for prescribing appropriate medications, documentation, education, and medication monitoring. The White House Conference on Aging, held in December 2005, also addressed medication management issues in its resolution entitled “Optimize Medication Management Programs.”
Prescribing Principles
There are a few principles for prescribing that the clinician can keep in mind while caring for the older person. When starting therapy, the basic principle should be to start low and go slow. New complaints or worsening of an existing condition after a drug has been introduced should be scrutinized for the possibility of a drug-induced problem. When choosing treatment for a new medical condition, always consider non-pharmacologic approaches first.
Overprescribing can also be prevented by regularly reviewing a patient’s medication list each time a new medication is started or changed. It is important to know what other providers have prescribed and where prescriptions were filled. It is essential to maintain accurate records. In this regard, the use of electronic medical records can be both an advantage and a disadvantage. Inaccurate drug lists can be self-perpetuating when providers simply copy and paste these sections of the medical records. It is best if the patient can bring all medications, including those purchased over the counter, to the visit. Discontinue any medications that are deemed to be unnecessary after review.
A Few Final Suggestions
For many reasons, patient compliance and adherence can be problematic in older patients.14 Patients often don’t admit not taking their medications as directed. If nonadherence is suspected, the care provider should consider the patient’s financial, cognitive, and functional status, as well as the patient’s beliefs about and understanding of the medications and disease. A simple regimen (such as once daily dosing) and a caregiver who is involved in overseeing medication management are helpful. Medication trays or drug calendars are handy tools. Many older folks may need the reassurance regarding safety that additional education or reinforcement can provide.
Regardless of the steps the physician takes to ensure safe prescribing for the elderly, provider-patient communication is of utmost importance. TH
Dr. Egger works in General Internal Medicine, Section Hospital Medicine, at the Mayo Clinic in Rochester, Minn.
References
- Winterstein AG, Sauer BC, Hepler CD, et al. Preventable drug-related hospital admissions. Ann Pharmacother. 2002;36(7-8):1238-1248.
- Kohn L, Corrigan J, Donaldson M, eds. To Err Is Human: Building a Safer Health System. Committee on Quality of Health Care in America, Institute of Medicine. Washington, D.C.: National Academies Press; 2000.
- Bond CA, Raehl CL, Franke T. Medication errors in United States hospitals. Pharmacotherapy. 2001 Sep;21(9):1023-1036.
- Goulding MR. Inappropriate medication prescribing for elderly ambulatory care patients. Arch Intern Med. 2004 Feb;164(3):305-312.
- Zhan C, Sangl J, Bierman AS, et al. Potentially inappropriate medication use in the community-dwelling elderly: findings from the 1996 Medical Expenditure Panel Survey. JAMA. 2001 Dec 12;286(22):2823-2829.
- Cooper JW. Probable adverse drug reactions in a rural geriatric nursing home population: a four-year study. J Am Geriatr Soc. 1996 Feb;44(2):194-197.
- Hanlon JT, Artz MB, Pieper CF, et al. Inappropriate medication use among frail elderly inpatients. Ann Pharmacother. 2004 Jan;38(1):9-14.
- Beard K. Adverse reactions as a cause of hospital admission in the aged. Drugs Aging. 1992 Jul-Aug;2(4):356-367.
- Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998 Apr 15;279(15):1200-1205.
- Beers MH, Ouslander JG, Rollingher I, et al. Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA Division of Geriatric Medicine. Arch Intern Med. 1991 Sep;151(9):1825-1832.
- Fick DM, Cooper JW, Wade WE, et al. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts. Arch Intern Med. 2003 Dec 8-22;163(22):2716-2724.
- Aparasu RR, Mort JR. Inappropriate prescribing for the elderly: beers criteria-based review. Ann Pharmacother. 2000 Mar;34(3):338-346.
- Hanlon JT, Schmader KE, Ruby CM, et al. Suboptimal prescribing in older inpatients and outpatients. J Am Geriatr Soc. 2001 Feb;49(2):200-209.
- Moisan J, Gaudet M, Gregoire JP, et al. Non-compliance with drug treatment and reading difficulties with regard to prescription labelling among seniors. Gerontology. 2002 Jan-Feb;48(1):44-51.
Medication-related errors jeopardize patient safety and commonly result in otherwise unnecessary hospitalizations. Approximately 7% of hospital admissions result from drug-related errors, of which 59% are considered preventable.1 It is estimated that adverse drug events affect 2% to 5% of hospitalized patients.2,3 These errors result in increased hospital costs of $4,700 per admission, or about $2 billion annually for U.S. hospitals.2 Calculations indicate that in the nursing home, for each dollar spent on a medication, there is another $1.33 spent on healthcare resources for the treatment of a drug-related morbidity or mortality.
Unfortunately, older folks are particularly susceptible to medication-related problems. Age-associated changes in body composition and physiology, multiple comorbidities, and—last but not least—polypharmacy, are contributing factors. In the United States, patients older than 65 fill an average of 12 prescriptions per year, compared with five fills for patients between ages 25 and 40. In addition, the use of nonprescription medications is more common in the elderly. This opens up the possibility of increased drug-drug or drug-herbal interactions.
Depending on the healthcare setting, as well as the criteria that define inappropriate medication use, studies alert us that between 7% and 21% of ambulatory older folks receive at least one potentially inappropriate medication.4,5 About 60% of nursing home residents, and a staggering 92% of frail elderly hospitalized veterans, receive at least one potentially inappropriate medication.6,7 The consequences of inappropriate drug use in the elderly can be significant. Weakness, resulting in loss of independence and falls that end in bone fractures, is only one possible negative consequence. Between 10% and 20% of the elderly are hospitalized as a result of receiving these inappropriate medications.8,9
Screening Inappropriate Medication
So, what are inappropriate medications for the elderly? Overly simplified, they include any medication that has a greater potential for doing more harm than good. In 1991, Beers and colleagues published criteria for screening inappropriate medication use in elderly patients.10 The authors reviewed the literature and identified 14 nationally recognized authorities in the fields of geriatric pharmacology, epidemiology, geriatrics, and long-term care. Among these experts, consensus was reached on a list of inappropriate medications for elderly nursing home residents. The list was intended to identify medications that should be avoided except under unusual circumstances. The experts also developed criteria for optimal doses, frequencies, and duration of use for these medications.
Since 1991, the criteria have been updated twice (in 1997 and 2002) to include ambulatory elderly. The 2002 Beers list included 48 inappropriate drugs or medication classes, regardless of diagnosis or conditions.11 Because drug-disease interactions in the elderly are increasingly recognized, the 2003 Beers list also included inappropriate medications or medication classes for 20 medical conditions. The consensus panel of experts identified 66 inappropriate drugs with adverse outcomes of potentially high severity. The authors stated specifically that the criteria were not meant to regulate practice to the point at which they would supersede the clinical judgment and assessment of the medical practitioner.
Drug-Drug Interaction
Based on Beers’ criteria for inappropriate prescribing, a literature review of studies conducted between 1992 and 1999 found that between 14% and 23% of the elderly filled a prescription for one or more drugs on the Beers list.12 Long-acting benzodiazepines, dipyridamole, propoxyphene, and amitriptyline were among the most frequently prescribed inappropriate medications.
Cardiovascular and psychotropic drugs are most commonly involved in drug-drug interactions. The most common adverse effects are acute renal failure, hypotension, and neuropsychological presentations such as delirium. Risk factors predisposing to adverse reactions are using multiple medications, receiving care from several prescribing clinicians, and filling prescriptions at more than one pharmacy. Physicians should also be vigilant for drug-herbal interactions.
Drug-Disease Interaction
Another phenomenon responsible for adverse drug events is a drug-disease interaction. For example, renal failure or hepatic insufficiency can interfere with detoxification and excretion; ascites can alter the volume of distribution of hydrophilic drugs, while obesity has an altering effect on lipophilic drugs. Patients with advanced cognitive impairment may have increased sensitivity or paradoxical reactions to drugs with central nervous system or anticholinergic activities.
Optimal Prescribing
As with safety, effective drug therapy for older people is also far from optimal. Optimal drug prescribing should aim for a balance between overprescribing and underprescribing while keeping a safe environment in mind (i.e., monitoring for adverse drug reactions and reducing medication errors). More than 50% of outpatient prescriptions are without indication, while necessary drugs are withheld in the cases of about 55% of elderly outpatients and 25% of hospitalized elderly patients.13
Overprescribing refers not only to the use of multiple medications but also implies a lack of appropriateness in selection, dosing, or use of the medication. For example, the term “prescribing cascade” refers to adding a new medication to treat symptoms of an adverse drug event that is mistakenly assumed to be a separate new diagnosis. Potential consequences of overprescribing include adverse drug events, drug-drug interactions, decreased quality of life, and unnecessary costs. Common factors connected to overprescribing include, but are not limited to, advanced age, multiple comorbidities, multiple prescribers, poor record-keeping, and failure for healthcare providers to thoroughly review a patient’s medication regimen.
Underprescribing of medications to older people is also of concern. Underprescribing results from efforts to avoid complex medication regimens, fear for adverse events, problems with patient adherence to medications, and economic barriers. Underprescribing can result from the notion that older folks will not benefit from medications intended for primary or secondary prevention or for aggressive management of chronic conditions (e.g., angiotensin-converting enzyme inhibitors and beta blockers prescribed for congestive heart failure and after a myocardial infarction).
New Prescribing Initiatives
There have been new initiatives to emphasize optimal prescribing. The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) mandates medication reconciliation across inpatient and outpatient practices. In 1999, the Centers for Medicare and Medicaid Services (CMS) expanded the drug use review policy for nursing home certification. Using specific criteria, surveyors and pharmacists must assess resident records for potentially inappropriate medication exposures and associated adverse drug reactions. The “Assessing Care for Vulnerable Elders” (ACOVE) initiative implemented use of quality indicators for prescribing appropriate medications, documentation, education, and medication monitoring. The White House Conference on Aging, held in December 2005, also addressed medication management issues in its resolution entitled “Optimize Medication Management Programs.”
Prescribing Principles
There are a few principles for prescribing that the clinician can keep in mind while caring for the older person. When starting therapy, the basic principle should be to start low and go slow. New complaints or worsening of an existing condition after a drug has been introduced should be scrutinized for the possibility of a drug-induced problem. When choosing treatment for a new medical condition, always consider non-pharmacologic approaches first.
Overprescribing can also be prevented by regularly reviewing a patient’s medication list each time a new medication is started or changed. It is important to know what other providers have prescribed and where prescriptions were filled. It is essential to maintain accurate records. In this regard, the use of electronic medical records can be both an advantage and a disadvantage. Inaccurate drug lists can be self-perpetuating when providers simply copy and paste these sections of the medical records. It is best if the patient can bring all medications, including those purchased over the counter, to the visit. Discontinue any medications that are deemed to be unnecessary after review.
A Few Final Suggestions
For many reasons, patient compliance and adherence can be problematic in older patients.14 Patients often don’t admit not taking their medications as directed. If nonadherence is suspected, the care provider should consider the patient’s financial, cognitive, and functional status, as well as the patient’s beliefs about and understanding of the medications and disease. A simple regimen (such as once daily dosing) and a caregiver who is involved in overseeing medication management are helpful. Medication trays or drug calendars are handy tools. Many older folks may need the reassurance regarding safety that additional education or reinforcement can provide.
Regardless of the steps the physician takes to ensure safe prescribing for the elderly, provider-patient communication is of utmost importance. TH
Dr. Egger works in General Internal Medicine, Section Hospital Medicine, at the Mayo Clinic in Rochester, Minn.
References
- Winterstein AG, Sauer BC, Hepler CD, et al. Preventable drug-related hospital admissions. Ann Pharmacother. 2002;36(7-8):1238-1248.
- Kohn L, Corrigan J, Donaldson M, eds. To Err Is Human: Building a Safer Health System. Committee on Quality of Health Care in America, Institute of Medicine. Washington, D.C.: National Academies Press; 2000.
- Bond CA, Raehl CL, Franke T. Medication errors in United States hospitals. Pharmacotherapy. 2001 Sep;21(9):1023-1036.
- Goulding MR. Inappropriate medication prescribing for elderly ambulatory care patients. Arch Intern Med. 2004 Feb;164(3):305-312.
- Zhan C, Sangl J, Bierman AS, et al. Potentially inappropriate medication use in the community-dwelling elderly: findings from the 1996 Medical Expenditure Panel Survey. JAMA. 2001 Dec 12;286(22):2823-2829.
- Cooper JW. Probable adverse drug reactions in a rural geriatric nursing home population: a four-year study. J Am Geriatr Soc. 1996 Feb;44(2):194-197.
- Hanlon JT, Artz MB, Pieper CF, et al. Inappropriate medication use among frail elderly inpatients. Ann Pharmacother. 2004 Jan;38(1):9-14.
- Beard K. Adverse reactions as a cause of hospital admission in the aged. Drugs Aging. 1992 Jul-Aug;2(4):356-367.
- Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998 Apr 15;279(15):1200-1205.
- Beers MH, Ouslander JG, Rollingher I, et al. Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA Division of Geriatric Medicine. Arch Intern Med. 1991 Sep;151(9):1825-1832.
- Fick DM, Cooper JW, Wade WE, et al. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts. Arch Intern Med. 2003 Dec 8-22;163(22):2716-2724.
- Aparasu RR, Mort JR. Inappropriate prescribing for the elderly: beers criteria-based review. Ann Pharmacother. 2000 Mar;34(3):338-346.
- Hanlon JT, Schmader KE, Ruby CM, et al. Suboptimal prescribing in older inpatients and outpatients. J Am Geriatr Soc. 2001 Feb;49(2):200-209.
- Moisan J, Gaudet M, Gregoire JP, et al. Non-compliance with drug treatment and reading difficulties with regard to prescription labelling among seniors. Gerontology. 2002 Jan-Feb;48(1):44-51.
Medication-related errors jeopardize patient safety and commonly result in otherwise unnecessary hospitalizations. Approximately 7% of hospital admissions result from drug-related errors, of which 59% are considered preventable.1 It is estimated that adverse drug events affect 2% to 5% of hospitalized patients.2,3 These errors result in increased hospital costs of $4,700 per admission, or about $2 billion annually for U.S. hospitals.2 Calculations indicate that in the nursing home, for each dollar spent on a medication, there is another $1.33 spent on healthcare resources for the treatment of a drug-related morbidity or mortality.
Unfortunately, older folks are particularly susceptible to medication-related problems. Age-associated changes in body composition and physiology, multiple comorbidities, and—last but not least—polypharmacy, are contributing factors. In the United States, patients older than 65 fill an average of 12 prescriptions per year, compared with five fills for patients between ages 25 and 40. In addition, the use of nonprescription medications is more common in the elderly. This opens up the possibility of increased drug-drug or drug-herbal interactions.
Depending on the healthcare setting, as well as the criteria that define inappropriate medication use, studies alert us that between 7% and 21% of ambulatory older folks receive at least one potentially inappropriate medication.4,5 About 60% of nursing home residents, and a staggering 92% of frail elderly hospitalized veterans, receive at least one potentially inappropriate medication.6,7 The consequences of inappropriate drug use in the elderly can be significant. Weakness, resulting in loss of independence and falls that end in bone fractures, is only one possible negative consequence. Between 10% and 20% of the elderly are hospitalized as a result of receiving these inappropriate medications.8,9
Screening Inappropriate Medication
So, what are inappropriate medications for the elderly? Overly simplified, they include any medication that has a greater potential for doing more harm than good. In 1991, Beers and colleagues published criteria for screening inappropriate medication use in elderly patients.10 The authors reviewed the literature and identified 14 nationally recognized authorities in the fields of geriatric pharmacology, epidemiology, geriatrics, and long-term care. Among these experts, consensus was reached on a list of inappropriate medications for elderly nursing home residents. The list was intended to identify medications that should be avoided except under unusual circumstances. The experts also developed criteria for optimal doses, frequencies, and duration of use for these medications.
Since 1991, the criteria have been updated twice (in 1997 and 2002) to include ambulatory elderly. The 2002 Beers list included 48 inappropriate drugs or medication classes, regardless of diagnosis or conditions.11 Because drug-disease interactions in the elderly are increasingly recognized, the 2003 Beers list also included inappropriate medications or medication classes for 20 medical conditions. The consensus panel of experts identified 66 inappropriate drugs with adverse outcomes of potentially high severity. The authors stated specifically that the criteria were not meant to regulate practice to the point at which they would supersede the clinical judgment and assessment of the medical practitioner.
Drug-Drug Interaction
Based on Beers’ criteria for inappropriate prescribing, a literature review of studies conducted between 1992 and 1999 found that between 14% and 23% of the elderly filled a prescription for one or more drugs on the Beers list.12 Long-acting benzodiazepines, dipyridamole, propoxyphene, and amitriptyline were among the most frequently prescribed inappropriate medications.
Cardiovascular and psychotropic drugs are most commonly involved in drug-drug interactions. The most common adverse effects are acute renal failure, hypotension, and neuropsychological presentations such as delirium. Risk factors predisposing to adverse reactions are using multiple medications, receiving care from several prescribing clinicians, and filling prescriptions at more than one pharmacy. Physicians should also be vigilant for drug-herbal interactions.
Drug-Disease Interaction
Another phenomenon responsible for adverse drug events is a drug-disease interaction. For example, renal failure or hepatic insufficiency can interfere with detoxification and excretion; ascites can alter the volume of distribution of hydrophilic drugs, while obesity has an altering effect on lipophilic drugs. Patients with advanced cognitive impairment may have increased sensitivity or paradoxical reactions to drugs with central nervous system or anticholinergic activities.
Optimal Prescribing
As with safety, effective drug therapy for older people is also far from optimal. Optimal drug prescribing should aim for a balance between overprescribing and underprescribing while keeping a safe environment in mind (i.e., monitoring for adverse drug reactions and reducing medication errors). More than 50% of outpatient prescriptions are without indication, while necessary drugs are withheld in the cases of about 55% of elderly outpatients and 25% of hospitalized elderly patients.13
Overprescribing refers not only to the use of multiple medications but also implies a lack of appropriateness in selection, dosing, or use of the medication. For example, the term “prescribing cascade” refers to adding a new medication to treat symptoms of an adverse drug event that is mistakenly assumed to be a separate new diagnosis. Potential consequences of overprescribing include adverse drug events, drug-drug interactions, decreased quality of life, and unnecessary costs. Common factors connected to overprescribing include, but are not limited to, advanced age, multiple comorbidities, multiple prescribers, poor record-keeping, and failure for healthcare providers to thoroughly review a patient’s medication regimen.
Underprescribing of medications to older people is also of concern. Underprescribing results from efforts to avoid complex medication regimens, fear for adverse events, problems with patient adherence to medications, and economic barriers. Underprescribing can result from the notion that older folks will not benefit from medications intended for primary or secondary prevention or for aggressive management of chronic conditions (e.g., angiotensin-converting enzyme inhibitors and beta blockers prescribed for congestive heart failure and after a myocardial infarction).
New Prescribing Initiatives
There have been new initiatives to emphasize optimal prescribing. The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) mandates medication reconciliation across inpatient and outpatient practices. In 1999, the Centers for Medicare and Medicaid Services (CMS) expanded the drug use review policy for nursing home certification. Using specific criteria, surveyors and pharmacists must assess resident records for potentially inappropriate medication exposures and associated adverse drug reactions. The “Assessing Care for Vulnerable Elders” (ACOVE) initiative implemented use of quality indicators for prescribing appropriate medications, documentation, education, and medication monitoring. The White House Conference on Aging, held in December 2005, also addressed medication management issues in its resolution entitled “Optimize Medication Management Programs.”
Prescribing Principles
There are a few principles for prescribing that the clinician can keep in mind while caring for the older person. When starting therapy, the basic principle should be to start low and go slow. New complaints or worsening of an existing condition after a drug has been introduced should be scrutinized for the possibility of a drug-induced problem. When choosing treatment for a new medical condition, always consider non-pharmacologic approaches first.
Overprescribing can also be prevented by regularly reviewing a patient’s medication list each time a new medication is started or changed. It is important to know what other providers have prescribed and where prescriptions were filled. It is essential to maintain accurate records. In this regard, the use of electronic medical records can be both an advantage and a disadvantage. Inaccurate drug lists can be self-perpetuating when providers simply copy and paste these sections of the medical records. It is best if the patient can bring all medications, including those purchased over the counter, to the visit. Discontinue any medications that are deemed to be unnecessary after review.
A Few Final Suggestions
For many reasons, patient compliance and adherence can be problematic in older patients.14 Patients often don’t admit not taking their medications as directed. If nonadherence is suspected, the care provider should consider the patient’s financial, cognitive, and functional status, as well as the patient’s beliefs about and understanding of the medications and disease. A simple regimen (such as once daily dosing) and a caregiver who is involved in overseeing medication management are helpful. Medication trays or drug calendars are handy tools. Many older folks may need the reassurance regarding safety that additional education or reinforcement can provide.
Regardless of the steps the physician takes to ensure safe prescribing for the elderly, provider-patient communication is of utmost importance. TH
Dr. Egger works in General Internal Medicine, Section Hospital Medicine, at the Mayo Clinic in Rochester, Minn.
References
- Winterstein AG, Sauer BC, Hepler CD, et al. Preventable drug-related hospital admissions. Ann Pharmacother. 2002;36(7-8):1238-1248.
- Kohn L, Corrigan J, Donaldson M, eds. To Err Is Human: Building a Safer Health System. Committee on Quality of Health Care in America, Institute of Medicine. Washington, D.C.: National Academies Press; 2000.
- Bond CA, Raehl CL, Franke T. Medication errors in United States hospitals. Pharmacotherapy. 2001 Sep;21(9):1023-1036.
- Goulding MR. Inappropriate medication prescribing for elderly ambulatory care patients. Arch Intern Med. 2004 Feb;164(3):305-312.
- Zhan C, Sangl J, Bierman AS, et al. Potentially inappropriate medication use in the community-dwelling elderly: findings from the 1996 Medical Expenditure Panel Survey. JAMA. 2001 Dec 12;286(22):2823-2829.
- Cooper JW. Probable adverse drug reactions in a rural geriatric nursing home population: a four-year study. J Am Geriatr Soc. 1996 Feb;44(2):194-197.
- Hanlon JT, Artz MB, Pieper CF, et al. Inappropriate medication use among frail elderly inpatients. Ann Pharmacother. 2004 Jan;38(1):9-14.
- Beard K. Adverse reactions as a cause of hospital admission in the aged. Drugs Aging. 1992 Jul-Aug;2(4):356-367.
- Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998 Apr 15;279(15):1200-1205.
- Beers MH, Ouslander JG, Rollingher I, et al. Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA Division of Geriatric Medicine. Arch Intern Med. 1991 Sep;151(9):1825-1832.
- Fick DM, Cooper JW, Wade WE, et al. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts. Arch Intern Med. 2003 Dec 8-22;163(22):2716-2724.
- Aparasu RR, Mort JR. Inappropriate prescribing for the elderly: beers criteria-based review. Ann Pharmacother. 2000 Mar;34(3):338-346.
- Hanlon JT, Schmader KE, Ruby CM, et al. Suboptimal prescribing in older inpatients and outpatients. J Am Geriatr Soc. 2001 Feb;49(2):200-209.
- Moisan J, Gaudet M, Gregoire JP, et al. Non-compliance with drug treatment and reading difficulties with regard to prescription labelling among seniors. Gerontology. 2002 Jan-Feb;48(1):44-51.
An Intense Rash

A32-year-old white male with Down syndrome was initially admitted with fever, cough, and productive sputum. He was started on appropriate antibiotics, but soon became hypoxic and developed respiratory failure requiring mechanical ventilation. The patient developed acute respiratory distress syndrome (ARDS) and eventually had a tracheostomy. On day 10, while in the intensive care unit, the patient developed multiple 1-2 mL clear vesicular eruptions with no surrounding erythema or edema. These were primarily distributed on the chest; the patient’s face was clear. TH
In dealing with this new eruption, the physician should have:
- Lowered the ambient room temperature and otherwise continued the current management.
- Performed a Tzanck smear, isolated the patient, and started acyclovir IV for presumed disseminated herpes zoster.
- Discontinued current antibiotics due to the drug reaction.
- Performed a skin biopsy for hematoxylin and eosin (H&E) stain as well as immunofluorescence for suspected primary early bullous disease (i.e., bullous pemphigoid).
- Started amphotericin.
Discussion
The correct answer is A: The physician should have lowered the ambient room temperature and continued the current management.
This patient had developed miliaria crystallina, a transient disorder of occluded sweat glands that usually results from excessive exposure to heat and humidity. Miliaria, also known as sweat rash, defines a group of disorders exhibiting eccrine gland obstruction with leakage and retention of sweat at different levels in the skin. The clinical presentation of miliaria is related to the depth of this obstruction and occurs in three main forms: miliaria crystallina, miliaria rubra, and miliaria profunda.1
Of the three variants, eccrine obstruction in miliaria crystallina occurs most superficially, at either the distal duct or pore, and drives sweat vesiculation into the stratum corneum of the epidermis.1 It is characterized by diffuse eruptions of non-inflamed, translucent vesicles of one to two millimeters, typically forming in crops on the trunk of the body. The tiny blisters have been likened to beads of sweat and are extremely fragile, rupturing spontaneously or with light friction.
Clinically, miliaria crystallina is an asymptomatic and self-limited disorder. It often occurs during the summer months and in tropical climates after prolonged exposure to heat and humidity. It is thought that overhydration of corneocytes from excessive sweating predisposes the eccrine duct to obstruction. This may be compounded by any form of occlusion, like clothing or bedding, that traps moisture and impedes the evaporation of sweat.2 Other risk factors include persistent fevers, neonate age less than two weeks, secondary to eccrine duct immaturity, and drugs such as isotretinoin and bethanechol.3,4,5
In the case of this 32-year-old male with respiratory failure, the characteristic eruption of miliaria crystallina developed on day 10 of intensive care. After lowering the ambient temperature of the patient’s room and adding the benefit of a circulatory fan, the vesicles resolved within two to three days. As this example demonstrates, the treatment of miliaria crystallina is straightforward and consists of drying the skin and preventing sweating for several days by keeping the patient in a cool, air-conditioned environment. Eventually, the keratinous plug will be shed, and normal sweating will resume.
In the literature, there is only one published report documenting two distinct cases of miliaria crystallina in the intensive care setting. At the time of onset, these two patients had been in the ICU for slightly over two weeks, and both were receiving treatment with multiple neuroautonomic agents, including—but not limited to—clonidine, a beta blocker, and opiates for pain. The innervation of eccrine glands is under sympathetic control mostly through the postsynaptic release of acetylcholine but also via adrenergic stimulation of contractile myoepithelia. While temperature and humidity are carefully regulated in most intensive care facilities, significant sweating may result from eccrine stimulation by neuroautonomic medications with intrinsic sympathomimetic activity.6 Combined with prolonged immobility, this sweating may create the perfect environment for eccrine duct obstruction and the development of miliaria crystallina.
Incidence in the intensive care setting has not been studied, but miliaria crystallina probably occurs much more frequently than it is reported. The ability to recognize the characteristic eruptions may prevent the hospitalist who encounters it from ordering unnecessary consults or diagnostics, and knowledge of its risk factors will aid both in treatment and in prevention. TH
References
- Wenzel FG, Horn TD. Nonneoplastic disorders of the eccrine glands. J Am Acad Dermatol. 1998 Jan;38(1):1–20.
- Sperling L. Chapter 3: Skin Diseases Associated with Excessive Heat, Humidity, and Sunlight. In: Textbook of Military Dermatology. Washington, D.C.: Office of The Surgeon General at TMM Publications; 1994:39-54. Available at: www.bordeninstitute.army.mil/derm/default_index.htm. Last accessed: September 8, 2006.
- Haas N, Henz BM, Weigel H. Congenital miliaria crystallina. J Am Acad Dermatol. 2002 Nov;47(5 Suppl):S270–272.
- Gupta AK, Ellis CN, Madison KC, et al. Miliaria crystallina occurring in a patient treated with isotretinoin. Cutis. 1986 Oct;38(4):275–276.
- Rochmis PG, Koplon BS. Iatrogenic miliaria crystallina due to bethanechol. Arch Dermatol. 1967 May;95(9):499–500.
- Haas N, Martens F, Henz BM. Miliaria crystallina in an intensive care setting. Clin Exp Dermatol. 2004 Jan;29 (1):32-34.
A32-year-old white male with Down syndrome was initially admitted with fever, cough, and productive sputum. He was started on appropriate antibiotics, but soon became hypoxic and developed respiratory failure requiring mechanical ventilation. The patient developed acute respiratory distress syndrome (ARDS) and eventually had a tracheostomy. On day 10, while in the intensive care unit, the patient developed multiple 1-2 mL clear vesicular eruptions with no surrounding erythema or edema. These were primarily distributed on the chest; the patient’s face was clear. TH
In dealing with this new eruption, the physician should have:
- Lowered the ambient room temperature and otherwise continued the current management.
- Performed a Tzanck smear, isolated the patient, and started acyclovir IV for presumed disseminated herpes zoster.
- Discontinued current antibiotics due to the drug reaction.
- Performed a skin biopsy for hematoxylin and eosin (H&E) stain as well as immunofluorescence for suspected primary early bullous disease (i.e., bullous pemphigoid).
- Started amphotericin.
Discussion
The correct answer is A: The physician should have lowered the ambient room temperature and continued the current management.
This patient had developed miliaria crystallina, a transient disorder of occluded sweat glands that usually results from excessive exposure to heat and humidity. Miliaria, also known as sweat rash, defines a group of disorders exhibiting eccrine gland obstruction with leakage and retention of sweat at different levels in the skin. The clinical presentation of miliaria is related to the depth of this obstruction and occurs in three main forms: miliaria crystallina, miliaria rubra, and miliaria profunda.1
Of the three variants, eccrine obstruction in miliaria crystallina occurs most superficially, at either the distal duct or pore, and drives sweat vesiculation into the stratum corneum of the epidermis.1 It is characterized by diffuse eruptions of non-inflamed, translucent vesicles of one to two millimeters, typically forming in crops on the trunk of the body. The tiny blisters have been likened to beads of sweat and are extremely fragile, rupturing spontaneously or with light friction.
Clinically, miliaria crystallina is an asymptomatic and self-limited disorder. It often occurs during the summer months and in tropical climates after prolonged exposure to heat and humidity. It is thought that overhydration of corneocytes from excessive sweating predisposes the eccrine duct to obstruction. This may be compounded by any form of occlusion, like clothing or bedding, that traps moisture and impedes the evaporation of sweat.2 Other risk factors include persistent fevers, neonate age less than two weeks, secondary to eccrine duct immaturity, and drugs such as isotretinoin and bethanechol.3,4,5
In the case of this 32-year-old male with respiratory failure, the characteristic eruption of miliaria crystallina developed on day 10 of intensive care. After lowering the ambient temperature of the patient’s room and adding the benefit of a circulatory fan, the vesicles resolved within two to three days. As this example demonstrates, the treatment of miliaria crystallina is straightforward and consists of drying the skin and preventing sweating for several days by keeping the patient in a cool, air-conditioned environment. Eventually, the keratinous plug will be shed, and normal sweating will resume.
In the literature, there is only one published report documenting two distinct cases of miliaria crystallina in the intensive care setting. At the time of onset, these two patients had been in the ICU for slightly over two weeks, and both were receiving treatment with multiple neuroautonomic agents, including—but not limited to—clonidine, a beta blocker, and opiates for pain. The innervation of eccrine glands is under sympathetic control mostly through the postsynaptic release of acetylcholine but also via adrenergic stimulation of contractile myoepithelia. While temperature and humidity are carefully regulated in most intensive care facilities, significant sweating may result from eccrine stimulation by neuroautonomic medications with intrinsic sympathomimetic activity.6 Combined with prolonged immobility, this sweating may create the perfect environment for eccrine duct obstruction and the development of miliaria crystallina.
Incidence in the intensive care setting has not been studied, but miliaria crystallina probably occurs much more frequently than it is reported. The ability to recognize the characteristic eruptions may prevent the hospitalist who encounters it from ordering unnecessary consults or diagnostics, and knowledge of its risk factors will aid both in treatment and in prevention. TH
References
- Wenzel FG, Horn TD. Nonneoplastic disorders of the eccrine glands. J Am Acad Dermatol. 1998 Jan;38(1):1–20.
- Sperling L. Chapter 3: Skin Diseases Associated with Excessive Heat, Humidity, and Sunlight. In: Textbook of Military Dermatology. Washington, D.C.: Office of The Surgeon General at TMM Publications; 1994:39-54. Available at: www.bordeninstitute.army.mil/derm/default_index.htm. Last accessed: September 8, 2006.
- Haas N, Henz BM, Weigel H. Congenital miliaria crystallina. J Am Acad Dermatol. 2002 Nov;47(5 Suppl):S270–272.
- Gupta AK, Ellis CN, Madison KC, et al. Miliaria crystallina occurring in a patient treated with isotretinoin. Cutis. 1986 Oct;38(4):275–276.
- Rochmis PG, Koplon BS. Iatrogenic miliaria crystallina due to bethanechol. Arch Dermatol. 1967 May;95(9):499–500.
- Haas N, Martens F, Henz BM. Miliaria crystallina in an intensive care setting. Clin Exp Dermatol. 2004 Jan;29 (1):32-34.
A32-year-old white male with Down syndrome was initially admitted with fever, cough, and productive sputum. He was started on appropriate antibiotics, but soon became hypoxic and developed respiratory failure requiring mechanical ventilation. The patient developed acute respiratory distress syndrome (ARDS) and eventually had a tracheostomy. On day 10, while in the intensive care unit, the patient developed multiple 1-2 mL clear vesicular eruptions with no surrounding erythema or edema. These were primarily distributed on the chest; the patient’s face was clear. TH
In dealing with this new eruption, the physician should have:
- Lowered the ambient room temperature and otherwise continued the current management.
- Performed a Tzanck smear, isolated the patient, and started acyclovir IV for presumed disseminated herpes zoster.
- Discontinued current antibiotics due to the drug reaction.
- Performed a skin biopsy for hematoxylin and eosin (H&E) stain as well as immunofluorescence for suspected primary early bullous disease (i.e., bullous pemphigoid).
- Started amphotericin.
Discussion
The correct answer is A: The physician should have lowered the ambient room temperature and continued the current management.
This patient had developed miliaria crystallina, a transient disorder of occluded sweat glands that usually results from excessive exposure to heat and humidity. Miliaria, also known as sweat rash, defines a group of disorders exhibiting eccrine gland obstruction with leakage and retention of sweat at different levels in the skin. The clinical presentation of miliaria is related to the depth of this obstruction and occurs in three main forms: miliaria crystallina, miliaria rubra, and miliaria profunda.1
Of the three variants, eccrine obstruction in miliaria crystallina occurs most superficially, at either the distal duct or pore, and drives sweat vesiculation into the stratum corneum of the epidermis.1 It is characterized by diffuse eruptions of non-inflamed, translucent vesicles of one to two millimeters, typically forming in crops on the trunk of the body. The tiny blisters have been likened to beads of sweat and are extremely fragile, rupturing spontaneously or with light friction.
Clinically, miliaria crystallina is an asymptomatic and self-limited disorder. It often occurs during the summer months and in tropical climates after prolonged exposure to heat and humidity. It is thought that overhydration of corneocytes from excessive sweating predisposes the eccrine duct to obstruction. This may be compounded by any form of occlusion, like clothing or bedding, that traps moisture and impedes the evaporation of sweat.2 Other risk factors include persistent fevers, neonate age less than two weeks, secondary to eccrine duct immaturity, and drugs such as isotretinoin and bethanechol.3,4,5
In the case of this 32-year-old male with respiratory failure, the characteristic eruption of miliaria crystallina developed on day 10 of intensive care. After lowering the ambient temperature of the patient’s room and adding the benefit of a circulatory fan, the vesicles resolved within two to three days. As this example demonstrates, the treatment of miliaria crystallina is straightforward and consists of drying the skin and preventing sweating for several days by keeping the patient in a cool, air-conditioned environment. Eventually, the keratinous plug will be shed, and normal sweating will resume.
In the literature, there is only one published report documenting two distinct cases of miliaria crystallina in the intensive care setting. At the time of onset, these two patients had been in the ICU for slightly over two weeks, and both were receiving treatment with multiple neuroautonomic agents, including—but not limited to—clonidine, a beta blocker, and opiates for pain. The innervation of eccrine glands is under sympathetic control mostly through the postsynaptic release of acetylcholine but also via adrenergic stimulation of contractile myoepithelia. While temperature and humidity are carefully regulated in most intensive care facilities, significant sweating may result from eccrine stimulation by neuroautonomic medications with intrinsic sympathomimetic activity.6 Combined with prolonged immobility, this sweating may create the perfect environment for eccrine duct obstruction and the development of miliaria crystallina.
Incidence in the intensive care setting has not been studied, but miliaria crystallina probably occurs much more frequently than it is reported. The ability to recognize the characteristic eruptions may prevent the hospitalist who encounters it from ordering unnecessary consults or diagnostics, and knowledge of its risk factors will aid both in treatment and in prevention. TH
References
- Wenzel FG, Horn TD. Nonneoplastic disorders of the eccrine glands. J Am Acad Dermatol. 1998 Jan;38(1):1–20.
- Sperling L. Chapter 3: Skin Diseases Associated with Excessive Heat, Humidity, and Sunlight. In: Textbook of Military Dermatology. Washington, D.C.: Office of The Surgeon General at TMM Publications; 1994:39-54. Available at: www.bordeninstitute.army.mil/derm/default_index.htm. Last accessed: September 8, 2006.
- Haas N, Henz BM, Weigel H. Congenital miliaria crystallina. J Am Acad Dermatol. 2002 Nov;47(5 Suppl):S270–272.
- Gupta AK, Ellis CN, Madison KC, et al. Miliaria crystallina occurring in a patient treated with isotretinoin. Cutis. 1986 Oct;38(4):275–276.
- Rochmis PG, Koplon BS. Iatrogenic miliaria crystallina due to bethanechol. Arch Dermatol. 1967 May;95(9):499–500.
- Haas N, Martens F, Henz BM. Miliaria crystallina in an intensive care setting. Clin Exp Dermatol. 2004 Jan;29 (1):32-34.