User login
Hospice Heart
When Karie Praszek, MD, a hospitalist at the University of Texas Health Center at Tyler (UTHCT) found out this past fall that she was being considered for the position of medical director of the hospital’s planned hospice inpatient unit, she went home after work and cried. These were tears of happiness because she was finally going to be able to combine her two loves as a physician: hospital medicine and hospice care. “It was like coming full circle,” she explains.
The seven-bed hospice unit at UTHCT opened in partnership with Hospice of East Texas in Tyler in November, following renovations to create more comfortable and spacious rooms. It is one of a growing number of collaborations between hospitals and community hospice programs to provide institutional beds for terminally ill, hospice-enrolled patients in need of short-term inpatient care for symptom management.
In many hospitals, hospitalists are well positioned to provide planning, leadership, hospice referrals, or medical management of hospice units in the hospital. But few of them will follow a path like Dr. Praszek’s to the medical leadership of the hospice unit.
The Needs of End-of-Life Patients
Dr. Praszek’s commitment to the needs of patients facing the end of their lives took her from Texas to Oklahoma to Oregon and back to Texas. She has been a practicing hospitalist at UTHCT since 2004, but medicine wasn’t her first career. In the 1980s, as a computer expert for the U.S. Postal Service, she helped to automate postal facilities. She was well paid, she says, but something was missing in her life.
Wanting to make a meaningful contribution, Dr. Praszek became a volunteer candy striper at a hospital in Dallas. She learned about hospice while assigned to the oncology floor.
“When I started doing hospice care, I fell in love with it, and used volunteer work to hone my skills,” she says. She quit her job and moved to Oklahoma to attend a seminary with a specialized curriculum in death, dying, and grief counseling, all the while volunteering with hospice patients.

“They even trained me to be a certified nurse’s aide,” she says. “I just wanted to do whatever they needed—to do what no one else wanted to do.”
As a volunteer nurse’s aide she cleaned bedpans, changed diapers, and gave bed baths to hospice patients. “I didn’t mind it because it meant I could have more time to talk with the patients,” explains Dr. Praszek.
A turning point came while she was on a hospice wing of a nursing home, working with a patient who had metastatic prostate cancer and was in excruciating pain. “You could hear this gentleman moaning when you entered the building,” she recalls.
The nurses on the unit turned to Dr. Praszek and asked her to call the patient’s physician for an order for more pain medications. “I said, ‘I’m just a volunteer,’ but they told me, ‘You’re our last hope,’ ” recounts Dr. Praszek. “So I called the doctor, and he said he wouldn’t order any more pain medications because he didn’t want the terminally ill patient to become an addict. Then he said, ‘I’m the doctor and you’re not,’ and hung up on me. I thought, well, you so-and-so. I’ll go to medical school instead of nursing school, which I had been considering, so that nobody can ever pull this kind of thing on me again.”
Dr. Praszek completed her pre-med courses, but put off applying because she was afraid that she was too old or not smart enough. Finally, with her husband’s encouragement, she applied to Oregon Health Sciences University and, on her 40th birthday in 1996, received notification of acceptance. Looking for students with significant life experience, the medical school offered Dr. Praszek a full scholarship. She graduated at the head of her class.
After completing her internal medicine residency, she couldn’t find a hospice-related position, but she had learned to appreciate the pace and complexity of hospital medicine. After doing locum tenens (temporary assignments), she landed in the hospitalist position at UTHCT. The 100-bed facility began as a tuberculosis hospital housed in a former U.S. Army base in 1949, and in 1977 it became part of the University of Texas health system.
Today Dr. Praszek heads a three-person hospital medicine department, with another physician and a physician’s assistant and the backup of 10 clinic physicians for after-hours coverage. Her job combines both clinical and administrative responsibilities, including risk assessments, protocol development, and the ethics committee. Roughly 10% of her time is devoted to patients on the hospice unit.

Providing Necessary Care
Hospice is an approach to the care of patients with life-limiting illnesses and their families, emphasizing the relief of pain and other symptoms, maximizing quality of life and support for the emotional and spiritual issues that come up at this time of life. Under the Medicare Hospice Benefit (introduced in 1983) Medicare-certified hospice programs are responsible for providing essentially all of the care needed to manage their enrolled patients, who have a life expectancy of six months or less. Medicare pays the hospice a daily packaged rate for its services—all-inclusive except for attending or consulting physicians, who are able to bill separately. Although the hospice benefit is primarily intended as a service in the patient’s home or other place of residence, such as a nursing home, often terminally ill patients require inpatient care for short periods to bring their medical symptoms under control.
To fill this need, hospice programs can open their own freestanding inpatient facilities, as Hospice of East Texas did with its 28-bed HomePlace, or else contract with a hospital for inpatient beds, as the hospice did with UTHCT. Those involved in planning the hospice unit at UTHCT emphasize that at the rate Medicare pays for inpatient hospice care ($562.69 per day, regionally adjusted), neither partner is likely to derive a profit from it. Instead the unit reflects a true commitment by both to meeting the needs of terminally ill patients in the hospital.
“This hospice unit was the right thing to do,” says UTHCT’s Chief Medical Officer Steven Brown, MD. “It’s an opportunity to educate our medical staff about end-of-life care, introduce the concept of hospice into the hospital, and improve utilization,” by changing the focus of treatment for those who choose the hospice approach.
The unit also provides an opportunity to concentrate palliative care training for nurses on the floor, which includes neuro-restorative and tuberculosis beds as well as non-dedicated hospice beds. Many patients are simultaneously referred to the unit and to Hospice of East Texas, while others may receive hospice care at home at the time of their placement on the unit.
Bring Inpatient Care Closer to Families
Marjorie Ream, CEO of Hospice of East Texas, explains that the origins of the hospice unit at UTHCT are in response to her agency’s family satisfaction surveys. Some families in the northeastern corner of the agency’s 13-county service area said they drove too far to visit loved ones at its HomePlace inpatient facility.
“We looked at our mission statement and started to explore how to make inpatient care available closer to the folks we serve,” says Ream. “I started a dialogue with Dr. Kirk Calhoun, the hospital’s president.”
Coincidentally, Dr. Calhoun had attended a hospital conference where he learned about a collaboration between a public charity hospital and a hospice in Atlanta that had received recognition from the American Hospital Association.
Their first meeting to discuss collaborating was in August 2005, and by November 15 the renovated unit was in operation, with two-room suites large enough to allow the patient’s family members to stay overnight on pullout sofas. Dr. Praszek’s name entered the dialogue after she gave a hospital lecture on end-of-life care and code status. “When we talked with her and she shared her career journey, we could see that she was a logical fit,” explains Ream. “And she really wanted to do this.
“My impression is that Dr. Praszek has a true ‘hospice heart.’ She really understands the interdisciplinary team. She’s an expert clinician, and she understands the differences in treating terminally ill patients. She has a real sense of the patient and family as people,” says Ream. “Nurses love her commitment and enthusiasm and are proud to be her colleagues.”
Dr. Praszek’s first concern is keeping people healthy. “To be a hospitalist on a hospice unit, you have to know how to change your focus from cure to caring,” she says. “It takes someone who is not afraid of confronting their patients’—or their own—mortality. When we first opened the unit, there was a sharp learning curve for physicians in the hospital. But it’s been a pretty smooth transition overall, except for one or two who still have a hard time recognizing when their patient is dying. Most physicians at this institution are learning how to look at the entire lifespan of their patients.”
Dr. Praszek tries to see every patient on the hospice unit each day she is on service. She also works closely with the interdisciplinary team at Hospice of East Texas. Routine care on the unit is provided by hospital staff, while the hospice team provides care management and oversight. Hospice care generally involves fewer intensive medical procedures and more intensive nursing care and comfort measures.
A Deeper Commitment
“My life today is the way it is because I really love my work,” says Dr. Praszek. She brings a lot of it home at night. In fact, Dr. Brown says he occasionally worries about the long hours she works. “But we try to make sure she gets the support she needs.”
“My door is always open,” adds Dr. Praszek. “I’m still learning from the nurses, and I’ve had housekeeping staff give me advice. When they find out my background [as a nurse’s aide], they always say, ‘Oh, that’s why we get along so well.’ ” TH
Larry Beresford wrote about hospitalists who work as administrators in the July issue.
When Karie Praszek, MD, a hospitalist at the University of Texas Health Center at Tyler (UTHCT) found out this past fall that she was being considered for the position of medical director of the hospital’s planned hospice inpatient unit, she went home after work and cried. These were tears of happiness because she was finally going to be able to combine her two loves as a physician: hospital medicine and hospice care. “It was like coming full circle,” she explains.
The seven-bed hospice unit at UTHCT opened in partnership with Hospice of East Texas in Tyler in November, following renovations to create more comfortable and spacious rooms. It is one of a growing number of collaborations between hospitals and community hospice programs to provide institutional beds for terminally ill, hospice-enrolled patients in need of short-term inpatient care for symptom management.
In many hospitals, hospitalists are well positioned to provide planning, leadership, hospice referrals, or medical management of hospice units in the hospital. But few of them will follow a path like Dr. Praszek’s to the medical leadership of the hospice unit.
The Needs of End-of-Life Patients
Dr. Praszek’s commitment to the needs of patients facing the end of their lives took her from Texas to Oklahoma to Oregon and back to Texas. She has been a practicing hospitalist at UTHCT since 2004, but medicine wasn’t her first career. In the 1980s, as a computer expert for the U.S. Postal Service, she helped to automate postal facilities. She was well paid, she says, but something was missing in her life.
Wanting to make a meaningful contribution, Dr. Praszek became a volunteer candy striper at a hospital in Dallas. She learned about hospice while assigned to the oncology floor.
“When I started doing hospice care, I fell in love with it, and used volunteer work to hone my skills,” she says. She quit her job and moved to Oklahoma to attend a seminary with a specialized curriculum in death, dying, and grief counseling, all the while volunteering with hospice patients.
“They even trained me to be a certified nurse’s aide,” she says. “I just wanted to do whatever they needed—to do what no one else wanted to do.”
As a volunteer nurse’s aide she cleaned bedpans, changed diapers, and gave bed baths to hospice patients. “I didn’t mind it because it meant I could have more time to talk with the patients,” explains Dr. Praszek.
A turning point came while she was on a hospice wing of a nursing home, working with a patient who had metastatic prostate cancer and was in excruciating pain. “You could hear this gentleman moaning when you entered the building,” she recalls.
The nurses on the unit turned to Dr. Praszek and asked her to call the patient’s physician for an order for more pain medications. “I said, ‘I’m just a volunteer,’ but they told me, ‘You’re our last hope,’ ” recounts Dr. Praszek. “So I called the doctor, and he said he wouldn’t order any more pain medications because he didn’t want the terminally ill patient to become an addict. Then he said, ‘I’m the doctor and you’re not,’ and hung up on me. I thought, well, you so-and-so. I’ll go to medical school instead of nursing school, which I had been considering, so that nobody can ever pull this kind of thing on me again.”
Dr. Praszek completed her pre-med courses, but put off applying because she was afraid that she was too old or not smart enough. Finally, with her husband’s encouragement, she applied to Oregon Health Sciences University and, on her 40th birthday in 1996, received notification of acceptance. Looking for students with significant life experience, the medical school offered Dr. Praszek a full scholarship. She graduated at the head of her class.
After completing her internal medicine residency, she couldn’t find a hospice-related position, but she had learned to appreciate the pace and complexity of hospital medicine. After doing locum tenens (temporary assignments), she landed in the hospitalist position at UTHCT. The 100-bed facility began as a tuberculosis hospital housed in a former U.S. Army base in 1949, and in 1977 it became part of the University of Texas health system.
Today Dr. Praszek heads a three-person hospital medicine department, with another physician and a physician’s assistant and the backup of 10 clinic physicians for after-hours coverage. Her job combines both clinical and administrative responsibilities, including risk assessments, protocol development, and the ethics committee. Roughly 10% of her time is devoted to patients on the hospice unit.
Providing Necessary Care
Hospice is an approach to the care of patients with life-limiting illnesses and their families, emphasizing the relief of pain and other symptoms, maximizing quality of life and support for the emotional and spiritual issues that come up at this time of life. Under the Medicare Hospice Benefit (introduced in 1983) Medicare-certified hospice programs are responsible for providing essentially all of the care needed to manage their enrolled patients, who have a life expectancy of six months or less. Medicare pays the hospice a daily packaged rate for its services—all-inclusive except for attending or consulting physicians, who are able to bill separately. Although the hospice benefit is primarily intended as a service in the patient’s home or other place of residence, such as a nursing home, often terminally ill patients require inpatient care for short periods to bring their medical symptoms under control.
To fill this need, hospice programs can open their own freestanding inpatient facilities, as Hospice of East Texas did with its 28-bed HomePlace, or else contract with a hospital for inpatient beds, as the hospice did with UTHCT. Those involved in planning the hospice unit at UTHCT emphasize that at the rate Medicare pays for inpatient hospice care ($562.69 per day, regionally adjusted), neither partner is likely to derive a profit from it. Instead the unit reflects a true commitment by both to meeting the needs of terminally ill patients in the hospital.
“This hospice unit was the right thing to do,” says UTHCT’s Chief Medical Officer Steven Brown, MD. “It’s an opportunity to educate our medical staff about end-of-life care, introduce the concept of hospice into the hospital, and improve utilization,” by changing the focus of treatment for those who choose the hospice approach.
The unit also provides an opportunity to concentrate palliative care training for nurses on the floor, which includes neuro-restorative and tuberculosis beds as well as non-dedicated hospice beds. Many patients are simultaneously referred to the unit and to Hospice of East Texas, while others may receive hospice care at home at the time of their placement on the unit.
Bring Inpatient Care Closer to Families
Marjorie Ream, CEO of Hospice of East Texas, explains that the origins of the hospice unit at UTHCT are in response to her agency’s family satisfaction surveys. Some families in the northeastern corner of the agency’s 13-county service area said they drove too far to visit loved ones at its HomePlace inpatient facility.
“We looked at our mission statement and started to explore how to make inpatient care available closer to the folks we serve,” says Ream. “I started a dialogue with Dr. Kirk Calhoun, the hospital’s president.”
Coincidentally, Dr. Calhoun had attended a hospital conference where he learned about a collaboration between a public charity hospital and a hospice in Atlanta that had received recognition from the American Hospital Association.
Their first meeting to discuss collaborating was in August 2005, and by November 15 the renovated unit was in operation, with two-room suites large enough to allow the patient’s family members to stay overnight on pullout sofas. Dr. Praszek’s name entered the dialogue after she gave a hospital lecture on end-of-life care and code status. “When we talked with her and she shared her career journey, we could see that she was a logical fit,” explains Ream. “And she really wanted to do this.
“My impression is that Dr. Praszek has a true ‘hospice heart.’ She really understands the interdisciplinary team. She’s an expert clinician, and she understands the differences in treating terminally ill patients. She has a real sense of the patient and family as people,” says Ream. “Nurses love her commitment and enthusiasm and are proud to be her colleagues.”
Dr. Praszek’s first concern is keeping people healthy. “To be a hospitalist on a hospice unit, you have to know how to change your focus from cure to caring,” she says. “It takes someone who is not afraid of confronting their patients’—or their own—mortality. When we first opened the unit, there was a sharp learning curve for physicians in the hospital. But it’s been a pretty smooth transition overall, except for one or two who still have a hard time recognizing when their patient is dying. Most physicians at this institution are learning how to look at the entire lifespan of their patients.”
Dr. Praszek tries to see every patient on the hospice unit each day she is on service. She also works closely with the interdisciplinary team at Hospice of East Texas. Routine care on the unit is provided by hospital staff, while the hospice team provides care management and oversight. Hospice care generally involves fewer intensive medical procedures and more intensive nursing care and comfort measures.
A Deeper Commitment
“My life today is the way it is because I really love my work,” says Dr. Praszek. She brings a lot of it home at night. In fact, Dr. Brown says he occasionally worries about the long hours she works. “But we try to make sure she gets the support she needs.”
“My door is always open,” adds Dr. Praszek. “I’m still learning from the nurses, and I’ve had housekeeping staff give me advice. When they find out my background [as a nurse’s aide], they always say, ‘Oh, that’s why we get along so well.’ ” TH
Larry Beresford wrote about hospitalists who work as administrators in the July issue.
When Karie Praszek, MD, a hospitalist at the University of Texas Health Center at Tyler (UTHCT) found out this past fall that she was being considered for the position of medical director of the hospital’s planned hospice inpatient unit, she went home after work and cried. These were tears of happiness because she was finally going to be able to combine her two loves as a physician: hospital medicine and hospice care. “It was like coming full circle,” she explains.
The seven-bed hospice unit at UTHCT opened in partnership with Hospice of East Texas in Tyler in November, following renovations to create more comfortable and spacious rooms. It is one of a growing number of collaborations between hospitals and community hospice programs to provide institutional beds for terminally ill, hospice-enrolled patients in need of short-term inpatient care for symptom management.
In many hospitals, hospitalists are well positioned to provide planning, leadership, hospice referrals, or medical management of hospice units in the hospital. But few of them will follow a path like Dr. Praszek’s to the medical leadership of the hospice unit.
The Needs of End-of-Life Patients
Dr. Praszek’s commitment to the needs of patients facing the end of their lives took her from Texas to Oklahoma to Oregon and back to Texas. She has been a practicing hospitalist at UTHCT since 2004, but medicine wasn’t her first career. In the 1980s, as a computer expert for the U.S. Postal Service, she helped to automate postal facilities. She was well paid, she says, but something was missing in her life.
Wanting to make a meaningful contribution, Dr. Praszek became a volunteer candy striper at a hospital in Dallas. She learned about hospice while assigned to the oncology floor.
“When I started doing hospice care, I fell in love with it, and used volunteer work to hone my skills,” she says. She quit her job and moved to Oklahoma to attend a seminary with a specialized curriculum in death, dying, and grief counseling, all the while volunteering with hospice patients.
“They even trained me to be a certified nurse’s aide,” she says. “I just wanted to do whatever they needed—to do what no one else wanted to do.”
As a volunteer nurse’s aide she cleaned bedpans, changed diapers, and gave bed baths to hospice patients. “I didn’t mind it because it meant I could have more time to talk with the patients,” explains Dr. Praszek.
A turning point came while she was on a hospice wing of a nursing home, working with a patient who had metastatic prostate cancer and was in excruciating pain. “You could hear this gentleman moaning when you entered the building,” she recalls.
The nurses on the unit turned to Dr. Praszek and asked her to call the patient’s physician for an order for more pain medications. “I said, ‘I’m just a volunteer,’ but they told me, ‘You’re our last hope,’ ” recounts Dr. Praszek. “So I called the doctor, and he said he wouldn’t order any more pain medications because he didn’t want the terminally ill patient to become an addict. Then he said, ‘I’m the doctor and you’re not,’ and hung up on me. I thought, well, you so-and-so. I’ll go to medical school instead of nursing school, which I had been considering, so that nobody can ever pull this kind of thing on me again.”
Dr. Praszek completed her pre-med courses, but put off applying because she was afraid that she was too old or not smart enough. Finally, with her husband’s encouragement, she applied to Oregon Health Sciences University and, on her 40th birthday in 1996, received notification of acceptance. Looking for students with significant life experience, the medical school offered Dr. Praszek a full scholarship. She graduated at the head of her class.
After completing her internal medicine residency, she couldn’t find a hospice-related position, but she had learned to appreciate the pace and complexity of hospital medicine. After doing locum tenens (temporary assignments), she landed in the hospitalist position at UTHCT. The 100-bed facility began as a tuberculosis hospital housed in a former U.S. Army base in 1949, and in 1977 it became part of the University of Texas health system.
Today Dr. Praszek heads a three-person hospital medicine department, with another physician and a physician’s assistant and the backup of 10 clinic physicians for after-hours coverage. Her job combines both clinical and administrative responsibilities, including risk assessments, protocol development, and the ethics committee. Roughly 10% of her time is devoted to patients on the hospice unit.
Providing Necessary Care
Hospice is an approach to the care of patients with life-limiting illnesses and their families, emphasizing the relief of pain and other symptoms, maximizing quality of life and support for the emotional and spiritual issues that come up at this time of life. Under the Medicare Hospice Benefit (introduced in 1983) Medicare-certified hospice programs are responsible for providing essentially all of the care needed to manage their enrolled patients, who have a life expectancy of six months or less. Medicare pays the hospice a daily packaged rate for its services—all-inclusive except for attending or consulting physicians, who are able to bill separately. Although the hospice benefit is primarily intended as a service in the patient’s home or other place of residence, such as a nursing home, often terminally ill patients require inpatient care for short periods to bring their medical symptoms under control.
To fill this need, hospice programs can open their own freestanding inpatient facilities, as Hospice of East Texas did with its 28-bed HomePlace, or else contract with a hospital for inpatient beds, as the hospice did with UTHCT. Those involved in planning the hospice unit at UTHCT emphasize that at the rate Medicare pays for inpatient hospice care ($562.69 per day, regionally adjusted), neither partner is likely to derive a profit from it. Instead the unit reflects a true commitment by both to meeting the needs of terminally ill patients in the hospital.
“This hospice unit was the right thing to do,” says UTHCT’s Chief Medical Officer Steven Brown, MD. “It’s an opportunity to educate our medical staff about end-of-life care, introduce the concept of hospice into the hospital, and improve utilization,” by changing the focus of treatment for those who choose the hospice approach.
The unit also provides an opportunity to concentrate palliative care training for nurses on the floor, which includes neuro-restorative and tuberculosis beds as well as non-dedicated hospice beds. Many patients are simultaneously referred to the unit and to Hospice of East Texas, while others may receive hospice care at home at the time of their placement on the unit.
Bring Inpatient Care Closer to Families
Marjorie Ream, CEO of Hospice of East Texas, explains that the origins of the hospice unit at UTHCT are in response to her agency’s family satisfaction surveys. Some families in the northeastern corner of the agency’s 13-county service area said they drove too far to visit loved ones at its HomePlace inpatient facility.
“We looked at our mission statement and started to explore how to make inpatient care available closer to the folks we serve,” says Ream. “I started a dialogue with Dr. Kirk Calhoun, the hospital’s president.”
Coincidentally, Dr. Calhoun had attended a hospital conference where he learned about a collaboration between a public charity hospital and a hospice in Atlanta that had received recognition from the American Hospital Association.
Their first meeting to discuss collaborating was in August 2005, and by November 15 the renovated unit was in operation, with two-room suites large enough to allow the patient’s family members to stay overnight on pullout sofas. Dr. Praszek’s name entered the dialogue after she gave a hospital lecture on end-of-life care and code status. “When we talked with her and she shared her career journey, we could see that she was a logical fit,” explains Ream. “And she really wanted to do this.
“My impression is that Dr. Praszek has a true ‘hospice heart.’ She really understands the interdisciplinary team. She’s an expert clinician, and she understands the differences in treating terminally ill patients. She has a real sense of the patient and family as people,” says Ream. “Nurses love her commitment and enthusiasm and are proud to be her colleagues.”
Dr. Praszek’s first concern is keeping people healthy. “To be a hospitalist on a hospice unit, you have to know how to change your focus from cure to caring,” she says. “It takes someone who is not afraid of confronting their patients’—or their own—mortality. When we first opened the unit, there was a sharp learning curve for physicians in the hospital. But it’s been a pretty smooth transition overall, except for one or two who still have a hard time recognizing when their patient is dying. Most physicians at this institution are learning how to look at the entire lifespan of their patients.”
Dr. Praszek tries to see every patient on the hospice unit each day she is on service. She also works closely with the interdisciplinary team at Hospice of East Texas. Routine care on the unit is provided by hospital staff, while the hospice team provides care management and oversight. Hospice care generally involves fewer intensive medical procedures and more intensive nursing care and comfort measures.
A Deeper Commitment
“My life today is the way it is because I really love my work,” says Dr. Praszek. She brings a lot of it home at night. In fact, Dr. Brown says he occasionally worries about the long hours she works. “But we try to make sure she gets the support she needs.”
“My door is always open,” adds Dr. Praszek. “I’m still learning from the nurses, and I’ve had housekeeping staff give me advice. When they find out my background [as a nurse’s aide], they always say, ‘Oh, that’s why we get along so well.’ ” TH
Larry Beresford wrote about hospitalists who work as administrators in the July issue.
Risky Business II: A Whole New Category of Risk
Five years ago, it was clearly recognized that malpractice law associated with hospitalist systems was an emerging phenomenon.1 But today this is rapidly changing, says Linda Greenwald, RN, MS, the editor of Risk Management Publications at the ProMutual Insurance Group, Boston, who keeps an eye on emerging trends related to medical malpractice litigation.
“There’s a whole new category of risk coming up,” she says, “because it’s a whole new specialty that kind of exploded on the scene, and some time needs to be spent defining the role of hospitalists.”
The 2006 winter issue of the company’s newsletter, Perspectives on Clinical Risk Management, was devoted to the subject of hospitalists.2 Patient safety concerns and communication, particularly as they relate to post-discharge communication, were the two overriding issues Greenwald identified connecting malpractice risk and hospitalists. (An upcoming issue of The Hospitalist will address the topic of post-discharge communication.) From her research, Greenwald gathered that hospitalists were considered “like the residents of yore,” expected to “cover the entire house,” to be everything and do everything for everyone.
The newsletter issue advises hospitalists to explain to patients and families who you are and what your role is, and to ask them pointedly whether they have concerns about that. Many patients feel abandoned by their primary care physicians; they don’t understand the new system, and they need to be reassured about the continuity of care. In a larger sense, ProMutual also suggests that institutions provide some type of public forum in their community for the public and providers both, to openly discuss ways to make the hospitalist system work for them all.
—Meg Gaines, JD, LLM
That Dollar Sign
Accumulating evidence shows that some of the contributory causes of rising healthcare-related litigiousness include patients’ higher expectations, poor provider-patient communication, and society’s adversarial legal stance.3
What is really to blame for the rising malpractice costs? “The medical system in our country is grounded in money,” says Meg Gaines, JD, LLM, clinical professor of law at the University of Wisconsin Law School, Madison. “It’s grounded in profit or, at the least, fiscal survival, depending on the institution. … In the bottom line equation, one of the variables is a dollar sign.”
Therefore, she says, anyone working in the hospital needs to recognize that, to a great extent, their working life revolves around that equation.
“The press has made this connection between [the number and amounts of payouts for] lawsuits and rising malpractice costs,” says Professor Gaines. “[It’s not] that there isn’t a connection. But what we do know, and what there is ample research to show, is that malpractice rates are much more linked to the rise and fall of the stock market.”4-10
To an insurance provider, she explains, the premiums are basically a loss leader; that is, a product sold below cost. “They don’t make money on premiums,” says Professor Gaines. “They make money investing premiums. You can see the correlation between rates and stock market performance over time.”
Professor Gaines says that the media has led the public to believe that the high cost of healthcare is due to skyrocketing medical malpractice awards. “Many of the states that put caps on their awards for malpractice torts are doing fine, but so are many states without caps,” she says. “It behooves the press to pit wicked lawyers against angelic doctors, or vice versa,” but it’s a lot more complicated than that. “And that rhetoric takes away from the real point, which is this: Nobody disagrees that too many patients are injured through negligence. But the number of patients injured through documented negligence who actually sue is somewhere between 2%-8%,” which is a very small percentage. Maybe too small.
Bad things happen to good people, and not everybody sues; it’s the people who feel that they’re cared for that tend not to sue. The documentation for this is increasing daily.
“Patients who have good, communicative relationships with their doctors don’t sue,” says Professor Gaines. “We generally don’t sue people we love or who love us.” And that’s a good thing, she speculates. “But it is important for doctors to think about this: So your patients don’t sue you, but you do make mistakes, right? And sometimes you cause injury. So how does that work for you that you have malpractice insurance that covers you for injury that you cause, but your patients won’t sue you because they love you?” she asks. “How do we all sleep at night thinking it’s a good thing that between 92%-98% of people who are injured by our negligence don’t get compensated?”
The Value of Litigation
With respect to the issue of patient safety, says George J. Annas, JD, MPH, Edward R. Utley professor of health law and the chairman of the Department of Health Law, Bioethics, and Human Rights at Boston University School of Public Health, rather than doctors and lawyers viewing each other as “predator and prey,” it would be far more beneficial for them to see each other as “natural allies.”11 He suggests that we recall the intended purpose of litigation and its value for society.
Professor Gaines concurs: “We live in this world where on the medical side people are so litigation-phobic that we really aren’t able to see the value of litigation anymore.” Healthcare itself can be viewed as a patient that might be healthier if required to pay the price of unhealthy practices: namely, failing to engage in communication and safety practices that would reduce error and injury. Shaking up that system might lead to better healthcare.11
In fact, the claim that the malpractice system is fraught with frivolous litigation has been called “overblown” and not substantiated in the literature.12 The malpractice system is effective in separating claims without merit from those with merit and compensating the latter. In an analysis of outcomes and claims costs from 1,452 closed malpractice claims from five liability insurers, “three-quarters of the litigation outcomes were concordant with the merits of the claim.”12
“Some of the most excellent doctors I know have said to me on the QT, ‘I’m sure glad you lawyers are around because if you weren’t I don’t know how we’d ever get rid of the scary doctors.’ ” says Professor Gaines. “And if the rate of malpractice claims for merited negligence “is only 2%-8%,” she says, “we’re probably not doing a great job of it.”
What makes doctors scary to patients? Or, rather, what makes a good doctor? When patients and physicians were both asked this question (pertaining to outpatient physicians), more patients than doctors considered the exchange of health-related information to be an essential aspect of their healthcare. Physicians placed it far lower on their list.13 These kinds of differences in perception may influence the quality of interactions between physicians and patients, the study concluded.
Professor Gaines, who has consulted with hundreds of physicians and nurses in her role as director of the Center for Patient Partnerships at the University of Wisconsin, encourages them to spend time in meaningful communication with their patients. “Their argument usually is: I don’t have time.” she says. “My answer is: You don’t have time not to.”
Communication and Patient Safety Concerns
The needs for superb patient safety and optimal healthcare communication are intertwined. In research on quality of care, patient safety is now specifically named as a factor and is distinguished from effectiveness.4 Malpractice litigation is often pursued when patients experience an adverse outcome coupled with a lack of empathy from and a withholding of essential information by physicians.14 Senators Hillary Clinton (D-NY) and Barack Obama (D-IL) cite documentation for this when they advocate for patient safety to be the centerpiece of medical liability reform.
As careful as hospitalists might be to protect their patients from safety hazards and errors, however, they alone cannot protect themselves and their institutions from wrongdoing or the risk of litigation.
“In hospital care, the challenge is to reform corporate governance to make hospital boards take their responsibility for patient safety at least as seriously as they take the hospital’s financial condition,”11 writes Professor Annas, who’s affiliated with both Boston University’s School of Law and School of Medicine. “Hospitals that do not take specific actions to improve safety should be viewed as negligent and be subject to malpractice lawsuits when a violation of the right to safety results in injury.”
It is also the hospital’s obligation, he says, to maintain a safe environment for healthcare providers. And hospitalists and other providers who “live” in hospitals have an ethical obligation to advance the connection of patient safety and communication in hospital-medicine-led quality improvement as well as whole-hospital initiatives.3,11,15,16 That means that staffing, technologies, and facilities must all be up to par so providers can work with the assurance that available resources will support their efforts to provide the best care for their patients.11
Those objectives were taken on by the University of Michigan (Ann Arbor) in a program launched in 2002 to reduce litigation costs, accelerate provision of compensation to patients, and increase the numbers of patients who are compensated for their injuries. The link between the medical liability environment and patient safety was well illustrated in their results. The program involved three strategic components:
- Acknowledge cases in which a patient was hurt because of medical error and compensate these patients quickly and fairly;
- Aggressively defend cases that the hospital considers to be without merit; and
- Study all adverse events to determine how procedures could be improved.
Whereas the organization had approximately 260 claims and lawsuits pending at any given time prior to August 2001, by August 2005 the number had dropped to 114. The average time from the filing of a claim to its resolution was reduced by 11 months, and annual litigation costs dropped from about $3 million to $1 million.14
This program clearly connected the dots between responsibility, compensation for merited negligence, systems quality improvement, and communication across the board. Senators Rodham Clinton and Obama infused their bill with the sensibility that these humane criteria are particularly important.14 When healthcare providers, administrators, and regulators around the world are being advised that a “post-event communication-cum-mediation framework” is the key national strategy for resolving malpractice disputes,3 the need for empathy, apology, and responsibility are implied. (See “I’m Sorry,” June 2006, p.25.)
“When I talk about patient safety, I imagine hospitalists are particularly attuned to this,” says Professor Gaines, “I am talking about what a physician could do in 15 seconds if every single patient is actively engaged in their [own] care.” It’s a no-brainer and “the easiest thing in the world if patients are invited and made to feel welcome as full members of the team.”
Inattention to little things can cause the risky miscommunications that lead to serious problems, both medically and legally. And yet, says Professor Gaines, the remedy is sometimes as easy as “having an informed patient partner as the final check.”
The Bottom Line for Hospitalists
When asked what she wants to say to hospitalists from her personal experience as a hospital inpatient as well as that of her extensive professional background as a criminal defense lawyer, law professor, and patient advocate, Professor Gaines began with her own expression of empathy. “First, in many ways you’re being asked to do an impossible job,” she says. “And patients like me, critics, and commentators will say, ‘Hey! You’re not doing it as well as you could.’ ”
Hospitalists, she says, might be prone to say, “ ‘Leave me alone. I’m doing the best I can.” You’re doing what may be an untenable job, you’ve got specialists leaning on you from one angle, patients and families … wailing on you from another level, and you’re … stuck in between: a utility player, the one everyone loves to boo off the field when you’re having a bad day.”
On the other hand, she says, “Every day I am carving another little bit of my epitaph, and what it says at the end is of my making. And if you can’t carve in these circumstances, then change them or do something about it. But when the bell tolls for thee, the fact that you worked in a busy hospital and had a bunch of overqualified guys breathing down your neck and under-informed patients blaming you for things that aren’t really your fault—that’s going to be footnote material. Carve out your ground, stand it, and do the job you can be proud of. And nobody and nothing gets you off the hook for that.”
Conclusion
The rising costs of medical malpractice litigation are far more a function of the fluctuations of the economy, among other factors, than of the number and size of malpractice claims payouts. Data show that the vast majority of expenditures that go toward litigation are not due to frivolous claims or unmerited compensation. In fact, litigation may hold value in serving to remind hospitals and providers that the best means of warding off lawsuits is to invest resources in patient safety, including prioritizing communication with patients, families, and colleagues. TH
Andrea Sattinger wrote “Risky Business I” in the Feb. 2006 issue (p. 1).
References
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9S.
- Greenwald L, ed. Hospitalists. Perspectives on Clinical Risk Management. Winter 2006.
- Harold TK. Minimizing medical litigation, part 2. J Med Pract Manage. 2006 Mar-Apr;21(5):257-261.
- Brennan TA, Gawande A, Thomas E, et al. Accidental deaths, saved lives, and improved quality. N Engl J Med. 2005 Sep 29;353(13):1405-1409.
- Brennan TA, Mello MM. Patient safety and medical malpractice: a case study. Ann Intern Med. 2003 Aug 19;139(4):267-273.
- Brennan TA, Sox CM, Burstin HR. Relation between negligent adverse events and the outcomes of medical-malpractice litigation N Engl J Med. 1996 Dec 26;335(26):1963-1967.
- Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991 Feb 7;324(6):370-376.
- Harvard Medical Practice Study. Patients, doctors, and lawyers: medical injury, malpractice litigation, and patient compensation in New York. Report of the Harvard Medical Practice Study to the state of New York. Cambridge, Mass: President and Fellows of Harvard College; 1990: www.nysl.nysed.gov/scandoclinks/OCM21331963.htm. Last accessed July 11, 2006.
- Localio AR, Lawthers AG, Brennan TA et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Mills DH, ed. California Medical Association and California Hospital Association Report on the Medical Insurance Feasibility Study. San Francisco, Calif: Sutter Publications; 1977.
- Annas GJ. The patient's right to safety—improving the quality of care through litigation against hospitals. N Engl J Med. 2006 May 11;354(19):2063-2066.
- Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med. 2006 May 11;354(19):2024-2033.
- Laine C, Davidoff F, Lewis CE, et al. Important elements of outpatient care: a comparison of patients' and physicians' opinions. Ann Intern Med. 1996 Oct 15;125(8):640-645.
- Clinton HR, Obama B. Making patient safety the centerpiece of medical liability reform. N Engl J Med. 2006;354:2205-2208.
- Studdert DM, Mello MM, Brennan TA. Medical malpractice. N Engl J Med. 2004;350:283-292.
- Delbanco TL. Quality of care through the patient's eyes. BMJ. 1996;313:832-833.
Five years ago, it was clearly recognized that malpractice law associated with hospitalist systems was an emerging phenomenon.1 But today this is rapidly changing, says Linda Greenwald, RN, MS, the editor of Risk Management Publications at the ProMutual Insurance Group, Boston, who keeps an eye on emerging trends related to medical malpractice litigation.
“There’s a whole new category of risk coming up,” she says, “because it’s a whole new specialty that kind of exploded on the scene, and some time needs to be spent defining the role of hospitalists.”
The 2006 winter issue of the company’s newsletter, Perspectives on Clinical Risk Management, was devoted to the subject of hospitalists.2 Patient safety concerns and communication, particularly as they relate to post-discharge communication, were the two overriding issues Greenwald identified connecting malpractice risk and hospitalists. (An upcoming issue of The Hospitalist will address the topic of post-discharge communication.) From her research, Greenwald gathered that hospitalists were considered “like the residents of yore,” expected to “cover the entire house,” to be everything and do everything for everyone.
The newsletter issue advises hospitalists to explain to patients and families who you are and what your role is, and to ask them pointedly whether they have concerns about that. Many patients feel abandoned by their primary care physicians; they don’t understand the new system, and they need to be reassured about the continuity of care. In a larger sense, ProMutual also suggests that institutions provide some type of public forum in their community for the public and providers both, to openly discuss ways to make the hospitalist system work for them all.
—Meg Gaines, JD, LLM
That Dollar Sign
Accumulating evidence shows that some of the contributory causes of rising healthcare-related litigiousness include patients’ higher expectations, poor provider-patient communication, and society’s adversarial legal stance.3
What is really to blame for the rising malpractice costs? “The medical system in our country is grounded in money,” says Meg Gaines, JD, LLM, clinical professor of law at the University of Wisconsin Law School, Madison. “It’s grounded in profit or, at the least, fiscal survival, depending on the institution. … In the bottom line equation, one of the variables is a dollar sign.”
Therefore, she says, anyone working in the hospital needs to recognize that, to a great extent, their working life revolves around that equation.
“The press has made this connection between [the number and amounts of payouts for] lawsuits and rising malpractice costs,” says Professor Gaines. “[It’s not] that there isn’t a connection. But what we do know, and what there is ample research to show, is that malpractice rates are much more linked to the rise and fall of the stock market.”4-10
To an insurance provider, she explains, the premiums are basically a loss leader; that is, a product sold below cost. “They don’t make money on premiums,” says Professor Gaines. “They make money investing premiums. You can see the correlation between rates and stock market performance over time.”
Professor Gaines says that the media has led the public to believe that the high cost of healthcare is due to skyrocketing medical malpractice awards. “Many of the states that put caps on their awards for malpractice torts are doing fine, but so are many states without caps,” she says. “It behooves the press to pit wicked lawyers against angelic doctors, or vice versa,” but it’s a lot more complicated than that. “And that rhetoric takes away from the real point, which is this: Nobody disagrees that too many patients are injured through negligence. But the number of patients injured through documented negligence who actually sue is somewhere between 2%-8%,” which is a very small percentage. Maybe too small.
Bad things happen to good people, and not everybody sues; it’s the people who feel that they’re cared for that tend not to sue. The documentation for this is increasing daily.
“Patients who have good, communicative relationships with their doctors don’t sue,” says Professor Gaines. “We generally don’t sue people we love or who love us.” And that’s a good thing, she speculates. “But it is important for doctors to think about this: So your patients don’t sue you, but you do make mistakes, right? And sometimes you cause injury. So how does that work for you that you have malpractice insurance that covers you for injury that you cause, but your patients won’t sue you because they love you?” she asks. “How do we all sleep at night thinking it’s a good thing that between 92%-98% of people who are injured by our negligence don’t get compensated?”
The Value of Litigation
With respect to the issue of patient safety, says George J. Annas, JD, MPH, Edward R. Utley professor of health law and the chairman of the Department of Health Law, Bioethics, and Human Rights at Boston University School of Public Health, rather than doctors and lawyers viewing each other as “predator and prey,” it would be far more beneficial for them to see each other as “natural allies.”11 He suggests that we recall the intended purpose of litigation and its value for society.
Professor Gaines concurs: “We live in this world where on the medical side people are so litigation-phobic that we really aren’t able to see the value of litigation anymore.” Healthcare itself can be viewed as a patient that might be healthier if required to pay the price of unhealthy practices: namely, failing to engage in communication and safety practices that would reduce error and injury. Shaking up that system might lead to better healthcare.11
In fact, the claim that the malpractice system is fraught with frivolous litigation has been called “overblown” and not substantiated in the literature.12 The malpractice system is effective in separating claims without merit from those with merit and compensating the latter. In an analysis of outcomes and claims costs from 1,452 closed malpractice claims from five liability insurers, “three-quarters of the litigation outcomes were concordant with the merits of the claim.”12
“Some of the most excellent doctors I know have said to me on the QT, ‘I’m sure glad you lawyers are around because if you weren’t I don’t know how we’d ever get rid of the scary doctors.’ ” says Professor Gaines. “And if the rate of malpractice claims for merited negligence “is only 2%-8%,” she says, “we’re probably not doing a great job of it.”
What makes doctors scary to patients? Or, rather, what makes a good doctor? When patients and physicians were both asked this question (pertaining to outpatient physicians), more patients than doctors considered the exchange of health-related information to be an essential aspect of their healthcare. Physicians placed it far lower on their list.13 These kinds of differences in perception may influence the quality of interactions between physicians and patients, the study concluded.
Professor Gaines, who has consulted with hundreds of physicians and nurses in her role as director of the Center for Patient Partnerships at the University of Wisconsin, encourages them to spend time in meaningful communication with their patients. “Their argument usually is: I don’t have time.” she says. “My answer is: You don’t have time not to.”
Communication and Patient Safety Concerns
The needs for superb patient safety and optimal healthcare communication are intertwined. In research on quality of care, patient safety is now specifically named as a factor and is distinguished from effectiveness.4 Malpractice litigation is often pursued when patients experience an adverse outcome coupled with a lack of empathy from and a withholding of essential information by physicians.14 Senators Hillary Clinton (D-NY) and Barack Obama (D-IL) cite documentation for this when they advocate for patient safety to be the centerpiece of medical liability reform.
As careful as hospitalists might be to protect their patients from safety hazards and errors, however, they alone cannot protect themselves and their institutions from wrongdoing or the risk of litigation.
“In hospital care, the challenge is to reform corporate governance to make hospital boards take their responsibility for patient safety at least as seriously as they take the hospital’s financial condition,”11 writes Professor Annas, who’s affiliated with both Boston University’s School of Law and School of Medicine. “Hospitals that do not take specific actions to improve safety should be viewed as negligent and be subject to malpractice lawsuits when a violation of the right to safety results in injury.”
It is also the hospital’s obligation, he says, to maintain a safe environment for healthcare providers. And hospitalists and other providers who “live” in hospitals have an ethical obligation to advance the connection of patient safety and communication in hospital-medicine-led quality improvement as well as whole-hospital initiatives.3,11,15,16 That means that staffing, technologies, and facilities must all be up to par so providers can work with the assurance that available resources will support their efforts to provide the best care for their patients.11
Those objectives were taken on by the University of Michigan (Ann Arbor) in a program launched in 2002 to reduce litigation costs, accelerate provision of compensation to patients, and increase the numbers of patients who are compensated for their injuries. The link between the medical liability environment and patient safety was well illustrated in their results. The program involved three strategic components:
- Acknowledge cases in which a patient was hurt because of medical error and compensate these patients quickly and fairly;
- Aggressively defend cases that the hospital considers to be without merit; and
- Study all adverse events to determine how procedures could be improved.
Whereas the organization had approximately 260 claims and lawsuits pending at any given time prior to August 2001, by August 2005 the number had dropped to 114. The average time from the filing of a claim to its resolution was reduced by 11 months, and annual litigation costs dropped from about $3 million to $1 million.14
This program clearly connected the dots between responsibility, compensation for merited negligence, systems quality improvement, and communication across the board. Senators Rodham Clinton and Obama infused their bill with the sensibility that these humane criteria are particularly important.14 When healthcare providers, administrators, and regulators around the world are being advised that a “post-event communication-cum-mediation framework” is the key national strategy for resolving malpractice disputes,3 the need for empathy, apology, and responsibility are implied. (See “I’m Sorry,” June 2006, p.25.)
“When I talk about patient safety, I imagine hospitalists are particularly attuned to this,” says Professor Gaines, “I am talking about what a physician could do in 15 seconds if every single patient is actively engaged in their [own] care.” It’s a no-brainer and “the easiest thing in the world if patients are invited and made to feel welcome as full members of the team.”
Inattention to little things can cause the risky miscommunications that lead to serious problems, both medically and legally. And yet, says Professor Gaines, the remedy is sometimes as easy as “having an informed patient partner as the final check.”
The Bottom Line for Hospitalists
When asked what she wants to say to hospitalists from her personal experience as a hospital inpatient as well as that of her extensive professional background as a criminal defense lawyer, law professor, and patient advocate, Professor Gaines began with her own expression of empathy. “First, in many ways you’re being asked to do an impossible job,” she says. “And patients like me, critics, and commentators will say, ‘Hey! You’re not doing it as well as you could.’ ”
Hospitalists, she says, might be prone to say, “ ‘Leave me alone. I’m doing the best I can.” You’re doing what may be an untenable job, you’ve got specialists leaning on you from one angle, patients and families … wailing on you from another level, and you’re … stuck in between: a utility player, the one everyone loves to boo off the field when you’re having a bad day.”
On the other hand, she says, “Every day I am carving another little bit of my epitaph, and what it says at the end is of my making. And if you can’t carve in these circumstances, then change them or do something about it. But when the bell tolls for thee, the fact that you worked in a busy hospital and had a bunch of overqualified guys breathing down your neck and under-informed patients blaming you for things that aren’t really your fault—that’s going to be footnote material. Carve out your ground, stand it, and do the job you can be proud of. And nobody and nothing gets you off the hook for that.”
Conclusion
The rising costs of medical malpractice litigation are far more a function of the fluctuations of the economy, among other factors, than of the number and size of malpractice claims payouts. Data show that the vast majority of expenditures that go toward litigation are not due to frivolous claims or unmerited compensation. In fact, litigation may hold value in serving to remind hospitals and providers that the best means of warding off lawsuits is to invest resources in patient safety, including prioritizing communication with patients, families, and colleagues. TH
Andrea Sattinger wrote “Risky Business I” in the Feb. 2006 issue (p. 1).
References
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9S.
- Greenwald L, ed. Hospitalists. Perspectives on Clinical Risk Management. Winter 2006.
- Harold TK. Minimizing medical litigation, part 2. J Med Pract Manage. 2006 Mar-Apr;21(5):257-261.
- Brennan TA, Gawande A, Thomas E, et al. Accidental deaths, saved lives, and improved quality. N Engl J Med. 2005 Sep 29;353(13):1405-1409.
- Brennan TA, Mello MM. Patient safety and medical malpractice: a case study. Ann Intern Med. 2003 Aug 19;139(4):267-273.
- Brennan TA, Sox CM, Burstin HR. Relation between negligent adverse events and the outcomes of medical-malpractice litigation N Engl J Med. 1996 Dec 26;335(26):1963-1967.
- Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991 Feb 7;324(6):370-376.
- Harvard Medical Practice Study. Patients, doctors, and lawyers: medical injury, malpractice litigation, and patient compensation in New York. Report of the Harvard Medical Practice Study to the state of New York. Cambridge, Mass: President and Fellows of Harvard College; 1990: www.nysl.nysed.gov/scandoclinks/OCM21331963.htm. Last accessed July 11, 2006.
- Localio AR, Lawthers AG, Brennan TA et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Mills DH, ed. California Medical Association and California Hospital Association Report on the Medical Insurance Feasibility Study. San Francisco, Calif: Sutter Publications; 1977.
- Annas GJ. The patient's right to safety—improving the quality of care through litigation against hospitals. N Engl J Med. 2006 May 11;354(19):2063-2066.
- Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med. 2006 May 11;354(19):2024-2033.
- Laine C, Davidoff F, Lewis CE, et al. Important elements of outpatient care: a comparison of patients' and physicians' opinions. Ann Intern Med. 1996 Oct 15;125(8):640-645.
- Clinton HR, Obama B. Making patient safety the centerpiece of medical liability reform. N Engl J Med. 2006;354:2205-2208.
- Studdert DM, Mello MM, Brennan TA. Medical malpractice. N Engl J Med. 2004;350:283-292.
- Delbanco TL. Quality of care through the patient's eyes. BMJ. 1996;313:832-833.
Five years ago, it was clearly recognized that malpractice law associated with hospitalist systems was an emerging phenomenon.1 But today this is rapidly changing, says Linda Greenwald, RN, MS, the editor of Risk Management Publications at the ProMutual Insurance Group, Boston, who keeps an eye on emerging trends related to medical malpractice litigation.
“There’s a whole new category of risk coming up,” she says, “because it’s a whole new specialty that kind of exploded on the scene, and some time needs to be spent defining the role of hospitalists.”
The 2006 winter issue of the company’s newsletter, Perspectives on Clinical Risk Management, was devoted to the subject of hospitalists.2 Patient safety concerns and communication, particularly as they relate to post-discharge communication, were the two overriding issues Greenwald identified connecting malpractice risk and hospitalists. (An upcoming issue of The Hospitalist will address the topic of post-discharge communication.) From her research, Greenwald gathered that hospitalists were considered “like the residents of yore,” expected to “cover the entire house,” to be everything and do everything for everyone.
The newsletter issue advises hospitalists to explain to patients and families who you are and what your role is, and to ask them pointedly whether they have concerns about that. Many patients feel abandoned by their primary care physicians; they don’t understand the new system, and they need to be reassured about the continuity of care. In a larger sense, ProMutual also suggests that institutions provide some type of public forum in their community for the public and providers both, to openly discuss ways to make the hospitalist system work for them all.
—Meg Gaines, JD, LLM
That Dollar Sign
Accumulating evidence shows that some of the contributory causes of rising healthcare-related litigiousness include patients’ higher expectations, poor provider-patient communication, and society’s adversarial legal stance.3
What is really to blame for the rising malpractice costs? “The medical system in our country is grounded in money,” says Meg Gaines, JD, LLM, clinical professor of law at the University of Wisconsin Law School, Madison. “It’s grounded in profit or, at the least, fiscal survival, depending on the institution. … In the bottom line equation, one of the variables is a dollar sign.”
Therefore, she says, anyone working in the hospital needs to recognize that, to a great extent, their working life revolves around that equation.
“The press has made this connection between [the number and amounts of payouts for] lawsuits and rising malpractice costs,” says Professor Gaines. “[It’s not] that there isn’t a connection. But what we do know, and what there is ample research to show, is that malpractice rates are much more linked to the rise and fall of the stock market.”4-10
To an insurance provider, she explains, the premiums are basically a loss leader; that is, a product sold below cost. “They don’t make money on premiums,” says Professor Gaines. “They make money investing premiums. You can see the correlation between rates and stock market performance over time.”
Professor Gaines says that the media has led the public to believe that the high cost of healthcare is due to skyrocketing medical malpractice awards. “Many of the states that put caps on their awards for malpractice torts are doing fine, but so are many states without caps,” she says. “It behooves the press to pit wicked lawyers against angelic doctors, or vice versa,” but it’s a lot more complicated than that. “And that rhetoric takes away from the real point, which is this: Nobody disagrees that too many patients are injured through negligence. But the number of patients injured through documented negligence who actually sue is somewhere between 2%-8%,” which is a very small percentage. Maybe too small.
Bad things happen to good people, and not everybody sues; it’s the people who feel that they’re cared for that tend not to sue. The documentation for this is increasing daily.
“Patients who have good, communicative relationships with their doctors don’t sue,” says Professor Gaines. “We generally don’t sue people we love or who love us.” And that’s a good thing, she speculates. “But it is important for doctors to think about this: So your patients don’t sue you, but you do make mistakes, right? And sometimes you cause injury. So how does that work for you that you have malpractice insurance that covers you for injury that you cause, but your patients won’t sue you because they love you?” she asks. “How do we all sleep at night thinking it’s a good thing that between 92%-98% of people who are injured by our negligence don’t get compensated?”
The Value of Litigation
With respect to the issue of patient safety, says George J. Annas, JD, MPH, Edward R. Utley professor of health law and the chairman of the Department of Health Law, Bioethics, and Human Rights at Boston University School of Public Health, rather than doctors and lawyers viewing each other as “predator and prey,” it would be far more beneficial for them to see each other as “natural allies.”11 He suggests that we recall the intended purpose of litigation and its value for society.
Professor Gaines concurs: “We live in this world where on the medical side people are so litigation-phobic that we really aren’t able to see the value of litigation anymore.” Healthcare itself can be viewed as a patient that might be healthier if required to pay the price of unhealthy practices: namely, failing to engage in communication and safety practices that would reduce error and injury. Shaking up that system might lead to better healthcare.11
In fact, the claim that the malpractice system is fraught with frivolous litigation has been called “overblown” and not substantiated in the literature.12 The malpractice system is effective in separating claims without merit from those with merit and compensating the latter. In an analysis of outcomes and claims costs from 1,452 closed malpractice claims from five liability insurers, “three-quarters of the litigation outcomes were concordant with the merits of the claim.”12
“Some of the most excellent doctors I know have said to me on the QT, ‘I’m sure glad you lawyers are around because if you weren’t I don’t know how we’d ever get rid of the scary doctors.’ ” says Professor Gaines. “And if the rate of malpractice claims for merited negligence “is only 2%-8%,” she says, “we’re probably not doing a great job of it.”
What makes doctors scary to patients? Or, rather, what makes a good doctor? When patients and physicians were both asked this question (pertaining to outpatient physicians), more patients than doctors considered the exchange of health-related information to be an essential aspect of their healthcare. Physicians placed it far lower on their list.13 These kinds of differences in perception may influence the quality of interactions between physicians and patients, the study concluded.
Professor Gaines, who has consulted with hundreds of physicians and nurses in her role as director of the Center for Patient Partnerships at the University of Wisconsin, encourages them to spend time in meaningful communication with their patients. “Their argument usually is: I don’t have time.” she says. “My answer is: You don’t have time not to.”
Communication and Patient Safety Concerns
The needs for superb patient safety and optimal healthcare communication are intertwined. In research on quality of care, patient safety is now specifically named as a factor and is distinguished from effectiveness.4 Malpractice litigation is often pursued when patients experience an adverse outcome coupled with a lack of empathy from and a withholding of essential information by physicians.14 Senators Hillary Clinton (D-NY) and Barack Obama (D-IL) cite documentation for this when they advocate for patient safety to be the centerpiece of medical liability reform.
As careful as hospitalists might be to protect their patients from safety hazards and errors, however, they alone cannot protect themselves and their institutions from wrongdoing or the risk of litigation.
“In hospital care, the challenge is to reform corporate governance to make hospital boards take their responsibility for patient safety at least as seriously as they take the hospital’s financial condition,”11 writes Professor Annas, who’s affiliated with both Boston University’s School of Law and School of Medicine. “Hospitals that do not take specific actions to improve safety should be viewed as negligent and be subject to malpractice lawsuits when a violation of the right to safety results in injury.”
It is also the hospital’s obligation, he says, to maintain a safe environment for healthcare providers. And hospitalists and other providers who “live” in hospitals have an ethical obligation to advance the connection of patient safety and communication in hospital-medicine-led quality improvement as well as whole-hospital initiatives.3,11,15,16 That means that staffing, technologies, and facilities must all be up to par so providers can work with the assurance that available resources will support their efforts to provide the best care for their patients.11
Those objectives were taken on by the University of Michigan (Ann Arbor) in a program launched in 2002 to reduce litigation costs, accelerate provision of compensation to patients, and increase the numbers of patients who are compensated for their injuries. The link between the medical liability environment and patient safety was well illustrated in their results. The program involved three strategic components:
- Acknowledge cases in which a patient was hurt because of medical error and compensate these patients quickly and fairly;
- Aggressively defend cases that the hospital considers to be without merit; and
- Study all adverse events to determine how procedures could be improved.
Whereas the organization had approximately 260 claims and lawsuits pending at any given time prior to August 2001, by August 2005 the number had dropped to 114. The average time from the filing of a claim to its resolution was reduced by 11 months, and annual litigation costs dropped from about $3 million to $1 million.14
This program clearly connected the dots between responsibility, compensation for merited negligence, systems quality improvement, and communication across the board. Senators Rodham Clinton and Obama infused their bill with the sensibility that these humane criteria are particularly important.14 When healthcare providers, administrators, and regulators around the world are being advised that a “post-event communication-cum-mediation framework” is the key national strategy for resolving malpractice disputes,3 the need for empathy, apology, and responsibility are implied. (See “I’m Sorry,” June 2006, p.25.)
“When I talk about patient safety, I imagine hospitalists are particularly attuned to this,” says Professor Gaines, “I am talking about what a physician could do in 15 seconds if every single patient is actively engaged in their [own] care.” It’s a no-brainer and “the easiest thing in the world if patients are invited and made to feel welcome as full members of the team.”
Inattention to little things can cause the risky miscommunications that lead to serious problems, both medically and legally. And yet, says Professor Gaines, the remedy is sometimes as easy as “having an informed patient partner as the final check.”
The Bottom Line for Hospitalists
When asked what she wants to say to hospitalists from her personal experience as a hospital inpatient as well as that of her extensive professional background as a criminal defense lawyer, law professor, and patient advocate, Professor Gaines began with her own expression of empathy. “First, in many ways you’re being asked to do an impossible job,” she says. “And patients like me, critics, and commentators will say, ‘Hey! You’re not doing it as well as you could.’ ”
Hospitalists, she says, might be prone to say, “ ‘Leave me alone. I’m doing the best I can.” You’re doing what may be an untenable job, you’ve got specialists leaning on you from one angle, patients and families … wailing on you from another level, and you’re … stuck in between: a utility player, the one everyone loves to boo off the field when you’re having a bad day.”
On the other hand, she says, “Every day I am carving another little bit of my epitaph, and what it says at the end is of my making. And if you can’t carve in these circumstances, then change them or do something about it. But when the bell tolls for thee, the fact that you worked in a busy hospital and had a bunch of overqualified guys breathing down your neck and under-informed patients blaming you for things that aren’t really your fault—that’s going to be footnote material. Carve out your ground, stand it, and do the job you can be proud of. And nobody and nothing gets you off the hook for that.”
Conclusion
The rising costs of medical malpractice litigation are far more a function of the fluctuations of the economy, among other factors, than of the number and size of malpractice claims payouts. Data show that the vast majority of expenditures that go toward litigation are not due to frivolous claims or unmerited compensation. In fact, litigation may hold value in serving to remind hospitals and providers that the best means of warding off lawsuits is to invest resources in patient safety, including prioritizing communication with patients, families, and colleagues. TH
Andrea Sattinger wrote “Risky Business I” in the Feb. 2006 issue (p. 1).
References
- Alpers A. Key legal principles for hospitalists. Am J Med. 2001;111:5-9S.
- Greenwald L, ed. Hospitalists. Perspectives on Clinical Risk Management. Winter 2006.
- Harold TK. Minimizing medical litigation, part 2. J Med Pract Manage. 2006 Mar-Apr;21(5):257-261.
- Brennan TA, Gawande A, Thomas E, et al. Accidental deaths, saved lives, and improved quality. N Engl J Med. 2005 Sep 29;353(13):1405-1409.
- Brennan TA, Mello MM. Patient safety and medical malpractice: a case study. Ann Intern Med. 2003 Aug 19;139(4):267-273.
- Brennan TA, Sox CM, Burstin HR. Relation between negligent adverse events and the outcomes of medical-malpractice litigation N Engl J Med. 1996 Dec 26;335(26):1963-1967.
- Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991 Feb 7;324(6):370-376.
- Harvard Medical Practice Study. Patients, doctors, and lawyers: medical injury, malpractice litigation, and patient compensation in New York. Report of the Harvard Medical Practice Study to the state of New York. Cambridge, Mass: President and Fellows of Harvard College; 1990: www.nysl.nysed.gov/scandoclinks/OCM21331963.htm. Last accessed July 11, 2006.
- Localio AR, Lawthers AG, Brennan TA et al. Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. N Engl J Med. 1991 Jul 25;325(4):245-251.
- Mills DH, ed. California Medical Association and California Hospital Association Report on the Medical Insurance Feasibility Study. San Francisco, Calif: Sutter Publications; 1977.
- Annas GJ. The patient's right to safety—improving the quality of care through litigation against hospitals. N Engl J Med. 2006 May 11;354(19):2063-2066.
- Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med. 2006 May 11;354(19):2024-2033.
- Laine C, Davidoff F, Lewis CE, et al. Important elements of outpatient care: a comparison of patients' and physicians' opinions. Ann Intern Med. 1996 Oct 15;125(8):640-645.
- Clinton HR, Obama B. Making patient safety the centerpiece of medical liability reform. N Engl J Med. 2006;354:2205-2208.
- Studdert DM, Mello MM, Brennan TA. Medical malpractice. N Engl J Med. 2004;350:283-292.
- Delbanco TL. Quality of care through the patient's eyes. BMJ. 1996;313:832-833.
Uncertain Prognosis
They’ve already been in the hospital three or four times, and now they’re back,” says Howard Epstein, MD, an internal medicine-trained hospitalist and the medical director of the palliative care program at Regions Hospital, St. Paul, Minn., describing patients who have acute exacerbations of their life-threatening chronic illnesses. “It’s a challenge we face all the time.”
Hospitalists spend a good deal of their time caring for dying patients, and data show that, by many accounts, they do it well.1 But just how near these patients are to death is often uncertain, especially for patients with diagnoses such as advanced heart and lung failure. Despite their slow decline, during any episode in which they are hospitalized, they may indeed die.
“As hospitalists, we encounter these situations regularly, maybe even daily,” wrote Steve Pantilat, MD, SHM past president, in his column in The Hospitalist (July/August 2005, p. 4): “We are the physicians who care for the seriously ill and the dying. The question is not whether we will take care of these patients; rather, when we do, will we be ready and able?”
End of life and palliative care are areas that hospitalists consider important but feel their training is generally inadequate.2 The conversations with patients and families can be challenging and take time, yet the time is worth the investment and they are a critical part of quality care. “We can learn how to conduct these discussions better,” wrote Dr. Pantilat, “and can practice phrases that will help them go more smoothly.”1,3-14 (See “Practice Phrases,” p. 34.)
Is there a difference in the way hospitalists treat those acute exacerbations if they come from or are attempting to return to their homes in the community or in long-term care? Not really, says Dr. Epstein. The exceptions may be in determining what kind of assistance a patient is getting or not getting outside the hospital (e.g., they’ll return home to a “supercaregiver spouse” versus returning to an assisted or skilled nursing facility). A patient in long-term care usually has multiple comorbidities, or their functional state has declined to the point where they need more assistance, palliative care only, or referral to hospice.
When a patient who has chronic obstructive pulmonary disease (COPD) comes in with an acute exacerbation, he says, it’s a good example of when you need to ask those clarifying questions. “If they’re deteriorating and you can paint that broad picture and help them to see that and that they’re going toward some inexorable decline,” says Dr. Epstein, “then they might make different decisions with that information.”
What’s Good in a Good Death?
Phrases such as “good death” and “dying with dignity” bear some interpretation, says Eva Chittenden, MD, a hospitalist with the University of California at San Francisco and a faculty member of its Palliative Care Leadership Center. Most palliative care experts might further define this to mean dying with appropriate respect for who that person is or who that person has been up until this point. A good death, she says, might better be referred to as a death that is “as good as possible.
“People say they want to die at home, but on the other hand, they also want to live forever,” says Dr. Chittenden. The reality is that most people die in acute-care hospitals while receiving invasive therapies.5-6,15 “We want a peaceful death, we want a pain-free death, we want a death where we’re surrounded by our families,” she says, “but at the same time we want to delay that forever. And those two things come into extreme conflict.7,9
“If you have cancer, maybe you don’t want to talk with your oncologist about death and dying because you want them to save your life. So you don’t even want to go there. And then you’re admitted to the hospital you’re told, ‘You’re extremely sick; you have pneumonia, but if we intubate you, we might be able to turn this situation around versus, if we don’t intubate you, you will surely die.’ And people don’t want to make that decision, because they’re not ready to die, even if ideally they’d want to have that good death,” says Dr. Chittenden, noting that not all providers have come to terms with how to use the available medical technology, when to stop using it, and how to talk about prognosis.
Talking about Prognosis
“In no case of serious illness … is predicting the future straightforward or meaningless,” writes Nicholas Christakis, in Death Foretold: Prophecy and Prognosis in Medical Care.16 “Part of the problem is that even formulating, much less communicating, a prediction about death is unpleasant, so physicians are inclined to refrain from it. But when they are able to formulate a prediction and fail to do so, the quality of care that patients receive may suffer.”
According to Dr. Epstein, you have to practice the conversations. “It’s a skill set, just like doing a bedside procedure … something that you have to do over and over and get comfortable doing,” he explains. “And it shocks people out of their seats when they actually hear the ‘D word.’ ” But part of meeting your responsibility to patients and their families requires speaking the truth.
Dr. Epstein says there are numerous resources available to help hospitalists overcome their discomfort and fears about being incorrect about how long the patient has to live. “I think it is OK to also say, ‘Look, I’m not God and I don't have a crystal ball, but I have seen lots of people in your situation and having watched them go through this point in their life, this is my expert opinion … ,’ ” he advises.
This involves telling the patient, “These are your chances of making a full recovery to the point where you might appreciate the quality of life you would have.” You don’t have to give numbers; you can use words such as good, bad, or poor.
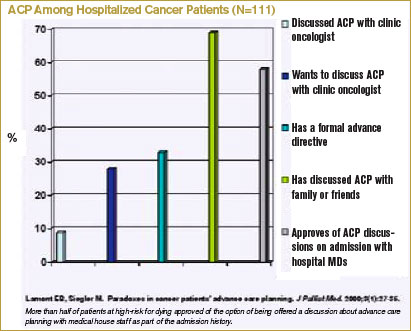
For those with advanced systemic failure, you might discuss prognoses in words that patients can better understand by making a comparison to someone has a cancer diagnosis. For instance, “I’ll say, ‘Your chances for living for a year are about as good as someone living with metastatic lung cancer,’ ” says Dr. Epstein. “I think that’s something that patients grasp a lot easier.”
In addition to the fear of being incorrect in prognosticating, physicians often don’t want their patients to lose hope. “Whereas in truth people are already thinking about these things, and there are studies that show people want their doctors to bring it up,” says Dr. Chittenden.7
A number of these studies were conducted by Dr. Christakis and Elizabeth Lamont, MD, a medical oncologist now practicing at Massachusetts General Hospital Cancer Center and assistant professor of medicine and health care policy at Harvard Medical School.15,17-19 Their findings have shown that doctors’ inaccuracies in their prognoses for terminally ill patients are systematically optimistic and that this may adversely affect the quality of care given to patients near the end of life.17
In their study of 326 patients in five hospices in Chicago, Drs. Christakis and Lamont showed that even if patients with cancer requested survival estimates, doctors would provide a frank estimate only 37% of the time and would provide no estimate, a conscious overestimate, or a conscious underestimate most of the time (63%).18 This, they concluded, may contribute to the observed disparities between physicians’ and patients’ estimates of survival.
Dr. Lamont’s interest in prognosis at end of life and the subject of advanced care planning arose from her experiences as a resident when she was cross-covering the oncology services. “I would be called to see [for example] a 35-year-old woman with widely metastatic breast cancer including brain metastases who was clearly at the end of life,” she says. “She became acutely short of breath, and my concern was that she was having a pulmonary embolism. … I was trying to decide whether to send her to the ICU. I was trying to inform her about the risks of anticoagulation … and I asked, ‘Have you talked about whether or not you’d want to go to the intensive care unit, whether or not you’d want your heart restarted, whether or not you’d want to be put on a ventilator if you couldn’t be breathe on your own; have you talked about these kinds of things with your oncologist?’ [Her answer was,] ‘Oh, no!’ ” Dr. Lamont figured that if she would have these conversations anyway, it would make more sense to have them as part of the admission history and physical. The study she subsequently designed and conducted involved 111 newly admitted patients with cancer whom she interviewed about (among other things) whether they had advanced care preferences (ACP) and whether they had discussed advanced directives with their medical oncologists. Only 9% of patients said that they had advanced directives, although 69% of patients had discussed their ACP with someone else (such as family).19 (See “ACP among Hospitalized Cancer Patients,” below.) However, 58% of patients approved of the option of being offered a discussion about advanced care planning with medical house staff as part of the admission history.
In other words, for the population of patients at high risk for dying during their current hospitalization, more than half would be open to discussing ACP with those whom they do not know well—such as hospitalists.
Advance Care Planning
A study just published in Archives of Internal Medicine suggests that elderly people who suffer from terminal illnesses become increasingly more willing to accept a life-preserving treatment, resulting in further physical disability or more pain if they were already diminished in those domains.20 Terri Fried, MD, an associate professor of internal medicine at Yale, and her colleagues studied 226 older men and women with advanced cancer, congestive heart failure (CHF), or COPD. In the course of in-home interviews conducted over two years, the investigators explored whether the participants would accept life-prolonging treatment if it resulted in one of four diminished health states: mild physical disability, severe physical disability, mental disability, or moderately severe daily pain.
Results showed that the likelihood of a treatment resulting in mild or severe functional disability rating as acceptable increased with each month of participation in the study. More than half of the patients had prepared living wills, and these individuals were more likely to prefer death to disability, but preferences could also change. These findings suggest that even though providers, patients, and families may have already had conversations about advance care planning, a patient’s change in health status might herald the need for a new conversation.
Dr. Lamont says there are two major areas in which hospitalists can politically advocate for changes that could facilitate better advance care planning. The first is to adopt the model proposed in her study, whereby patients are queried regarding advanced directives as part of the admission history.19 Patients for whom this could be added as a new data field would include, for example, those with advanced cancer, metastatic solid tumors, relapsed leukemia, relapsed lymphoma, or with acute exacerbations of illnesses such as CHF or COPD. The second area where hospitalists could advocate for change is national healthcare policy. Like a number of others, Dr. Lamont believes CMS should begin reimbursing for high-quality end-of-life care discussions, the measures of which would be determined at both local and national levels.
Communication Training
“The more hospital medicine training gets incorporated into internal medicine residency,” says Dr. Epstein, “the greater the opportunity to train new hospitalists to have these difficult conversations: how to have a family meeting, to identify the issues, to see if there are any ethical issues involved, any legal issues, and how to negotiate a reasonable plan of care based on the patient’s goals.”2,8,21
In addition to helping with control of physical symptoms, such as pain and nausea control, physicians facilitate decision-making. “We try to address a lot of the existential and reconciliation and legacy issues,” says Dr. Chittenden. Because of the number of situations in which the patient is a woman or man in their 40s or 50s who have young children, she says, “we help the parents come to terms with this and get our child-life specialist involved to help the parents think about how to talk with the kids.”
Because of the growth of the palliative care movement, the training is beginning to improve. “The LCME [Liaison Committee on Medical Education], the licensure group for medical schools, mandates that there be some end-of-life care exposure,” says Dr. Chittenden. “And the ACGME [Accreditation Council for Graduate Medical Education], which licenses the residency programs, strongly suggests that there be opportunities to learn about this. … Slowly but surely we are realizing this needs to happen, but we are far from doing it well.”
What would be ideal? A two-week rotation for residents in a palliative care service? “That would be wonderful,” says Dr. Epstein. “As more palliative care services pop up across the country, the chance of that happening would increase. … And even if you’re not in palliative care and you’re a hospitalist and you do these kinds of things well, the residents should be watching you have those kinds of conversations.”
Explaining that he is paraphrasing Mark Leenay, MD, the former program director at Fairview-University, Minnesota, and the physician who spearheaded the development of a clinical team that comprehensively addresses the multiple aspects of suffering from life-threatening illness, Dr. Epstein says: “I can train anybody to do symptom management in hospice, but how to walk into a room and understand … and negotiate the family dynamics and the patient’s plan of care … to communicate on different levels with different people with … their own agendas, and all the pieces of information … [and different interpretations] … to take it all in and digest it for that meeting and spit it out in a way [in which] everyone can relate and come to some sort of consensus, hopefully, at the end of the meeting? That’s the art. And that takes practice.”
Conclusion
Patients with life-threatening chronic illnesses are often admitted to the hospital multiple times in the course of the period that could be considered the end of life. Important nonmedical issues for hospitalists to address at each new admission include communication regarding prognosis and advance care planning, and addressing existential issues greatly contributes to the quality of care. TH
Resources
- The Hastings Center is involved in bioethics and other issues surrounding end-of-life care (www.thehastingscenter.org/default.asp). The Special Report listed in “References” is downloadable from their Web site.23
- Education in Palliative and End-of-Life Care (EPEC) curriculum (www.epec.net).
- The American Board of Hospice and Palliative Medicine (www.abhpm.org).
- The American Association of Hospice and Palliative Medicine (www.aahpm.org).
- Harvard’s Center for Palliative Care offers courses that emphasize teaching (www.hms.harvard.edu/cdi/pallcare/).
- The Center to Advance Palliative Care (CAPC), Mount Sinai School of Medicine, New York, serves as a resource for hospital-based palliative care program development. CAPC supports six regional Palliative Care Leadership Centers (www.capc.org).
The following Web sites include models for advance directives.
- Five Wishes: www.agingwithdignity.org
- Individual decisions: www.newgrangepress.com
- Respecting choices at end of life: www.gundersenlutheran.com/eolprograms
- Physician orders for life-sustaining treatment: www.polst.org
References
- Auerbach AD, Pantilat SZ. End-of-Life care in a voluntary hospitalist model: effects on communication, processes of care, and patient symptoms. Am J Med. 2004 May 15;116(10):669-675.
- Plauth WH, Pantilat SZ, Wachter RM, et al. Hospitalists' perceptions of their residency training needs: result of a national survey. Am J Med. 2001;111(3):247-254.
- Lo B, Quill TE, Tulsky J. Discussing palliative care with patients. ACP--ASIM End-of-Life Care Consensus Panel. American College of Physicians--American Society of Internal Medicine. Ann Intern Med. 1999 May 4;130(9):744-749.
- Quill TE. Initiating end-of-life discussions with seriously ill patients: addressing the "elephant in the room." JAMA. 2000 Nov 15;284(19):2502-2507.
- Kaufman SR. And a Time to Die: How American Hospitals Shape the End of Life. New York: Scribner; 2005.
- Kaufman SR. A commentary: hospital experience and meaning at the end of life. Gerontologist. 2002 Oct;42 Spec No. 3:34-39.
- Pantilat SZ. End-of-life care for the hospitalized patient. Med Clin North Am. 2002 Jul;86(4):749-770.
- Tulsky JA. Beyond advance directives: importance of communication skills at the end of life. JAMA. 2005 Jul 20;294(3):359-365.
- Heyland DK, Dodek P, Rocker G, et al. What matters most in end-of-life care: perceptions of seriously ill patients and their family members. CMAJ. 2006 Feb 28;174(5):627-633.
- Barbato M. Caring for the dying: the doctor as healer. MJAust. 2003 May 19;178(10):508-509.
- Fallowfield LJ, Jenkins VA, Beveridge HA. Truth may hurt but deceit hurts more: communication in palliative care. Palliat Med. 2002 Jul;16(4):297-303.
- Fins JJ, Miller FG, Acres CA, et al. End-of-life decision-making in the hospital: current practice and future prospects. J Pain Symptom Manage. 1999 Jan;17(1):6-15.
- Kalish RA. Death, grief and caring relationships. Belmont, California: Brooks/Cole; 1985.
- Lynn J, Schuster JL, Kabcenell A. Improving Care for the End of Life: A Sourcebook for Health Care Managers and Clinicians. New York: Oxford University Press; 2000.
- Lamont EB. A demographic and prognostic approach to defining the end of life. J Palliat Med. 2005;8 Suppl 1:S12-21.
- Christakis NA. Death Foretold: Prophecy and Prognosis in Medical Care. Chicago: University of Chicago Press; 2001.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors' prognoses in terminally ill patients: prospective cohort study. BMJ. 2000 Feb;320(7233):469-472.
- Lamont EB, Christakis NA. Prognostic disclosure to patients with cancer near the end of life. Ann Intern Med. 2001 Jun 19; 134 (12):1096-1105.
- Lamont EB, Siegler M. Paradoxes in cancer patients' advance care planning. J Palliat Med. 2000 Spring;3(1):27-35.
- Fried TR, Byers AL, Gallo WT, et al. Prospective study of health status preferences and changes in preferences over time in older adults. Arch Intern Med. 2006 Apr 24;166(8):890-895.
- McPhee SJ, Rabow MW, Pantilat SZ, et al. Finding our way--perspectives on care at the close of life. JAMA. 2000 Nov 15;284(19):2512-2513.
- Solie D. How to Say It to Seniors: Closing the Communication Gap with Our Elders. New York: Prentice Hall Press; 2004.
- Jennings B, Kaebnick GE, Murray TH. Improving End of Life Care: Why Has It Been So Difficult? Hastings Center Special Report. 2005;35.
They’ve already been in the hospital three or four times, and now they’re back,” says Howard Epstein, MD, an internal medicine-trained hospitalist and the medical director of the palliative care program at Regions Hospital, St. Paul, Minn., describing patients who have acute exacerbations of their life-threatening chronic illnesses. “It’s a challenge we face all the time.”
Hospitalists spend a good deal of their time caring for dying patients, and data show that, by many accounts, they do it well.1 But just how near these patients are to death is often uncertain, especially for patients with diagnoses such as advanced heart and lung failure. Despite their slow decline, during any episode in which they are hospitalized, they may indeed die.
“As hospitalists, we encounter these situations regularly, maybe even daily,” wrote Steve Pantilat, MD, SHM past president, in his column in The Hospitalist (July/August 2005, p. 4): “We are the physicians who care for the seriously ill and the dying. The question is not whether we will take care of these patients; rather, when we do, will we be ready and able?”
End of life and palliative care are areas that hospitalists consider important but feel their training is generally inadequate.2 The conversations with patients and families can be challenging and take time, yet the time is worth the investment and they are a critical part of quality care. “We can learn how to conduct these discussions better,” wrote Dr. Pantilat, “and can practice phrases that will help them go more smoothly.”1,3-14 (See “Practice Phrases,” p. 34.)
Is there a difference in the way hospitalists treat those acute exacerbations if they come from or are attempting to return to their homes in the community or in long-term care? Not really, says Dr. Epstein. The exceptions may be in determining what kind of assistance a patient is getting or not getting outside the hospital (e.g., they’ll return home to a “supercaregiver spouse” versus returning to an assisted or skilled nursing facility). A patient in long-term care usually has multiple comorbidities, or their functional state has declined to the point where they need more assistance, palliative care only, or referral to hospice.
When a patient who has chronic obstructive pulmonary disease (COPD) comes in with an acute exacerbation, he says, it’s a good example of when you need to ask those clarifying questions. “If they’re deteriorating and you can paint that broad picture and help them to see that and that they’re going toward some inexorable decline,” says Dr. Epstein, “then they might make different decisions with that information.”
What’s Good in a Good Death?
Phrases such as “good death” and “dying with dignity” bear some interpretation, says Eva Chittenden, MD, a hospitalist with the University of California at San Francisco and a faculty member of its Palliative Care Leadership Center. Most palliative care experts might further define this to mean dying with appropriate respect for who that person is or who that person has been up until this point. A good death, she says, might better be referred to as a death that is “as good as possible.
“People say they want to die at home, but on the other hand, they also want to live forever,” says Dr. Chittenden. The reality is that most people die in acute-care hospitals while receiving invasive therapies.5-6,15 “We want a peaceful death, we want a pain-free death, we want a death where we’re surrounded by our families,” she says, “but at the same time we want to delay that forever. And those two things come into extreme conflict.7,9
“If you have cancer, maybe you don’t want to talk with your oncologist about death and dying because you want them to save your life. So you don’t even want to go there. And then you’re admitted to the hospital you’re told, ‘You’re extremely sick; you have pneumonia, but if we intubate you, we might be able to turn this situation around versus, if we don’t intubate you, you will surely die.’ And people don’t want to make that decision, because they’re not ready to die, even if ideally they’d want to have that good death,” says Dr. Chittenden, noting that not all providers have come to terms with how to use the available medical technology, when to stop using it, and how to talk about prognosis.
Talking about Prognosis
“In no case of serious illness … is predicting the future straightforward or meaningless,” writes Nicholas Christakis, in Death Foretold: Prophecy and Prognosis in Medical Care.16 “Part of the problem is that even formulating, much less communicating, a prediction about death is unpleasant, so physicians are inclined to refrain from it. But when they are able to formulate a prediction and fail to do so, the quality of care that patients receive may suffer.”
According to Dr. Epstein, you have to practice the conversations. “It’s a skill set, just like doing a bedside procedure … something that you have to do over and over and get comfortable doing,” he explains. “And it shocks people out of their seats when they actually hear the ‘D word.’ ” But part of meeting your responsibility to patients and their families requires speaking the truth.
Dr. Epstein says there are numerous resources available to help hospitalists overcome their discomfort and fears about being incorrect about how long the patient has to live. “I think it is OK to also say, ‘Look, I’m not God and I don't have a crystal ball, but I have seen lots of people in your situation and having watched them go through this point in their life, this is my expert opinion … ,’ ” he advises.
This involves telling the patient, “These are your chances of making a full recovery to the point where you might appreciate the quality of life you would have.” You don’t have to give numbers; you can use words such as good, bad, or poor.
For those with advanced systemic failure, you might discuss prognoses in words that patients can better understand by making a comparison to someone has a cancer diagnosis. For instance, “I’ll say, ‘Your chances for living for a year are about as good as someone living with metastatic lung cancer,’ ” says Dr. Epstein. “I think that’s something that patients grasp a lot easier.”
In addition to the fear of being incorrect in prognosticating, physicians often don’t want their patients to lose hope. “Whereas in truth people are already thinking about these things, and there are studies that show people want their doctors to bring it up,” says Dr. Chittenden.7
A number of these studies were conducted by Dr. Christakis and Elizabeth Lamont, MD, a medical oncologist now practicing at Massachusetts General Hospital Cancer Center and assistant professor of medicine and health care policy at Harvard Medical School.15,17-19 Their findings have shown that doctors’ inaccuracies in their prognoses for terminally ill patients are systematically optimistic and that this may adversely affect the quality of care given to patients near the end of life.17
In their study of 326 patients in five hospices in Chicago, Drs. Christakis and Lamont showed that even if patients with cancer requested survival estimates, doctors would provide a frank estimate only 37% of the time and would provide no estimate, a conscious overestimate, or a conscious underestimate most of the time (63%).18 This, they concluded, may contribute to the observed disparities between physicians’ and patients’ estimates of survival.
Dr. Lamont’s interest in prognosis at end of life and the subject of advanced care planning arose from her experiences as a resident when she was cross-covering the oncology services. “I would be called to see [for example] a 35-year-old woman with widely metastatic breast cancer including brain metastases who was clearly at the end of life,” she says. “She became acutely short of breath, and my concern was that she was having a pulmonary embolism. … I was trying to decide whether to send her to the ICU. I was trying to inform her about the risks of anticoagulation … and I asked, ‘Have you talked about whether or not you’d want to go to the intensive care unit, whether or not you’d want your heart restarted, whether or not you’d want to be put on a ventilator if you couldn’t be breathe on your own; have you talked about these kinds of things with your oncologist?’ [Her answer was,] ‘Oh, no!’ ” Dr. Lamont figured that if she would have these conversations anyway, it would make more sense to have them as part of the admission history and physical. The study she subsequently designed and conducted involved 111 newly admitted patients with cancer whom she interviewed about (among other things) whether they had advanced care preferences (ACP) and whether they had discussed advanced directives with their medical oncologists. Only 9% of patients said that they had advanced directives, although 69% of patients had discussed their ACP with someone else (such as family).19 (See “ACP among Hospitalized Cancer Patients,” below.) However, 58% of patients approved of the option of being offered a discussion about advanced care planning with medical house staff as part of the admission history.
In other words, for the population of patients at high risk for dying during their current hospitalization, more than half would be open to discussing ACP with those whom they do not know well—such as hospitalists.
Advance Care Planning
A study just published in Archives of Internal Medicine suggests that elderly people who suffer from terminal illnesses become increasingly more willing to accept a life-preserving treatment, resulting in further physical disability or more pain if they were already diminished in those domains.20 Terri Fried, MD, an associate professor of internal medicine at Yale, and her colleagues studied 226 older men and women with advanced cancer, congestive heart failure (CHF), or COPD. In the course of in-home interviews conducted over two years, the investigators explored whether the participants would accept life-prolonging treatment if it resulted in one of four diminished health states: mild physical disability, severe physical disability, mental disability, or moderately severe daily pain.
Results showed that the likelihood of a treatment resulting in mild or severe functional disability rating as acceptable increased with each month of participation in the study. More than half of the patients had prepared living wills, and these individuals were more likely to prefer death to disability, but preferences could also change. These findings suggest that even though providers, patients, and families may have already had conversations about advance care planning, a patient’s change in health status might herald the need for a new conversation.
Dr. Lamont says there are two major areas in which hospitalists can politically advocate for changes that could facilitate better advance care planning. The first is to adopt the model proposed in her study, whereby patients are queried regarding advanced directives as part of the admission history.19 Patients for whom this could be added as a new data field would include, for example, those with advanced cancer, metastatic solid tumors, relapsed leukemia, relapsed lymphoma, or with acute exacerbations of illnesses such as CHF or COPD. The second area where hospitalists could advocate for change is national healthcare policy. Like a number of others, Dr. Lamont believes CMS should begin reimbursing for high-quality end-of-life care discussions, the measures of which would be determined at both local and national levels.
Communication Training
“The more hospital medicine training gets incorporated into internal medicine residency,” says Dr. Epstein, “the greater the opportunity to train new hospitalists to have these difficult conversations: how to have a family meeting, to identify the issues, to see if there are any ethical issues involved, any legal issues, and how to negotiate a reasonable plan of care based on the patient’s goals.”2,8,21
In addition to helping with control of physical symptoms, such as pain and nausea control, physicians facilitate decision-making. “We try to address a lot of the existential and reconciliation and legacy issues,” says Dr. Chittenden. Because of the number of situations in which the patient is a woman or man in their 40s or 50s who have young children, she says, “we help the parents come to terms with this and get our child-life specialist involved to help the parents think about how to talk with the kids.”
Because of the growth of the palliative care movement, the training is beginning to improve. “The LCME [Liaison Committee on Medical Education], the licensure group for medical schools, mandates that there be some end-of-life care exposure,” says Dr. Chittenden. “And the ACGME [Accreditation Council for Graduate Medical Education], which licenses the residency programs, strongly suggests that there be opportunities to learn about this. … Slowly but surely we are realizing this needs to happen, but we are far from doing it well.”
What would be ideal? A two-week rotation for residents in a palliative care service? “That would be wonderful,” says Dr. Epstein. “As more palliative care services pop up across the country, the chance of that happening would increase. … And even if you’re not in palliative care and you’re a hospitalist and you do these kinds of things well, the residents should be watching you have those kinds of conversations.”
Explaining that he is paraphrasing Mark Leenay, MD, the former program director at Fairview-University, Minnesota, and the physician who spearheaded the development of a clinical team that comprehensively addresses the multiple aspects of suffering from life-threatening illness, Dr. Epstein says: “I can train anybody to do symptom management in hospice, but how to walk into a room and understand … and negotiate the family dynamics and the patient’s plan of care … to communicate on different levels with different people with … their own agendas, and all the pieces of information … [and different interpretations] … to take it all in and digest it for that meeting and spit it out in a way [in which] everyone can relate and come to some sort of consensus, hopefully, at the end of the meeting? That’s the art. And that takes practice.”
Conclusion
Patients with life-threatening chronic illnesses are often admitted to the hospital multiple times in the course of the period that could be considered the end of life. Important nonmedical issues for hospitalists to address at each new admission include communication regarding prognosis and advance care planning, and addressing existential issues greatly contributes to the quality of care. TH
Resources
- The Hastings Center is involved in bioethics and other issues surrounding end-of-life care (www.thehastingscenter.org/default.asp). The Special Report listed in “References” is downloadable from their Web site.23
- Education in Palliative and End-of-Life Care (EPEC) curriculum (www.epec.net).
- The American Board of Hospice and Palliative Medicine (www.abhpm.org).
- The American Association of Hospice and Palliative Medicine (www.aahpm.org).
- Harvard’s Center for Palliative Care offers courses that emphasize teaching (www.hms.harvard.edu/cdi/pallcare/).
- The Center to Advance Palliative Care (CAPC), Mount Sinai School of Medicine, New York, serves as a resource for hospital-based palliative care program development. CAPC supports six regional Palliative Care Leadership Centers (www.capc.org).
The following Web sites include models for advance directives.
- Five Wishes: www.agingwithdignity.org
- Individual decisions: www.newgrangepress.com
- Respecting choices at end of life: www.gundersenlutheran.com/eolprograms
- Physician orders for life-sustaining treatment: www.polst.org
References
- Auerbach AD, Pantilat SZ. End-of-Life care in a voluntary hospitalist model: effects on communication, processes of care, and patient symptoms. Am J Med. 2004 May 15;116(10):669-675.
- Plauth WH, Pantilat SZ, Wachter RM, et al. Hospitalists' perceptions of their residency training needs: result of a national survey. Am J Med. 2001;111(3):247-254.
- Lo B, Quill TE, Tulsky J. Discussing palliative care with patients. ACP--ASIM End-of-Life Care Consensus Panel. American College of Physicians--American Society of Internal Medicine. Ann Intern Med. 1999 May 4;130(9):744-749.
- Quill TE. Initiating end-of-life discussions with seriously ill patients: addressing the "elephant in the room." JAMA. 2000 Nov 15;284(19):2502-2507.
- Kaufman SR. And a Time to Die: How American Hospitals Shape the End of Life. New York: Scribner; 2005.
- Kaufman SR. A commentary: hospital experience and meaning at the end of life. Gerontologist. 2002 Oct;42 Spec No. 3:34-39.
- Pantilat SZ. End-of-life care for the hospitalized patient. Med Clin North Am. 2002 Jul;86(4):749-770.
- Tulsky JA. Beyond advance directives: importance of communication skills at the end of life. JAMA. 2005 Jul 20;294(3):359-365.
- Heyland DK, Dodek P, Rocker G, et al. What matters most in end-of-life care: perceptions of seriously ill patients and their family members. CMAJ. 2006 Feb 28;174(5):627-633.
- Barbato M. Caring for the dying: the doctor as healer. MJAust. 2003 May 19;178(10):508-509.
- Fallowfield LJ, Jenkins VA, Beveridge HA. Truth may hurt but deceit hurts more: communication in palliative care. Palliat Med. 2002 Jul;16(4):297-303.
- Fins JJ, Miller FG, Acres CA, et al. End-of-life decision-making in the hospital: current practice and future prospects. J Pain Symptom Manage. 1999 Jan;17(1):6-15.
- Kalish RA. Death, grief and caring relationships. Belmont, California: Brooks/Cole; 1985.
- Lynn J, Schuster JL, Kabcenell A. Improving Care for the End of Life: A Sourcebook for Health Care Managers and Clinicians. New York: Oxford University Press; 2000.
- Lamont EB. A demographic and prognostic approach to defining the end of life. J Palliat Med. 2005;8 Suppl 1:S12-21.
- Christakis NA. Death Foretold: Prophecy and Prognosis in Medical Care. Chicago: University of Chicago Press; 2001.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors' prognoses in terminally ill patients: prospective cohort study. BMJ. 2000 Feb;320(7233):469-472.
- Lamont EB, Christakis NA. Prognostic disclosure to patients with cancer near the end of life. Ann Intern Med. 2001 Jun 19; 134 (12):1096-1105.
- Lamont EB, Siegler M. Paradoxes in cancer patients' advance care planning. J Palliat Med. 2000 Spring;3(1):27-35.
- Fried TR, Byers AL, Gallo WT, et al. Prospective study of health status preferences and changes in preferences over time in older adults. Arch Intern Med. 2006 Apr 24;166(8):890-895.
- McPhee SJ, Rabow MW, Pantilat SZ, et al. Finding our way--perspectives on care at the close of life. JAMA. 2000 Nov 15;284(19):2512-2513.
- Solie D. How to Say It to Seniors: Closing the Communication Gap with Our Elders. New York: Prentice Hall Press; 2004.
- Jennings B, Kaebnick GE, Murray TH. Improving End of Life Care: Why Has It Been So Difficult? Hastings Center Special Report. 2005;35.
They’ve already been in the hospital three or four times, and now they’re back,” says Howard Epstein, MD, an internal medicine-trained hospitalist and the medical director of the palliative care program at Regions Hospital, St. Paul, Minn., describing patients who have acute exacerbations of their life-threatening chronic illnesses. “It’s a challenge we face all the time.”
Hospitalists spend a good deal of their time caring for dying patients, and data show that, by many accounts, they do it well.1 But just how near these patients are to death is often uncertain, especially for patients with diagnoses such as advanced heart and lung failure. Despite their slow decline, during any episode in which they are hospitalized, they may indeed die.
“As hospitalists, we encounter these situations regularly, maybe even daily,” wrote Steve Pantilat, MD, SHM past president, in his column in The Hospitalist (July/August 2005, p. 4): “We are the physicians who care for the seriously ill and the dying. The question is not whether we will take care of these patients; rather, when we do, will we be ready and able?”
End of life and palliative care are areas that hospitalists consider important but feel their training is generally inadequate.2 The conversations with patients and families can be challenging and take time, yet the time is worth the investment and they are a critical part of quality care. “We can learn how to conduct these discussions better,” wrote Dr. Pantilat, “and can practice phrases that will help them go more smoothly.”1,3-14 (See “Practice Phrases,” p. 34.)
Is there a difference in the way hospitalists treat those acute exacerbations if they come from or are attempting to return to their homes in the community or in long-term care? Not really, says Dr. Epstein. The exceptions may be in determining what kind of assistance a patient is getting or not getting outside the hospital (e.g., they’ll return home to a “supercaregiver spouse” versus returning to an assisted or skilled nursing facility). A patient in long-term care usually has multiple comorbidities, or their functional state has declined to the point where they need more assistance, palliative care only, or referral to hospice.
When a patient who has chronic obstructive pulmonary disease (COPD) comes in with an acute exacerbation, he says, it’s a good example of when you need to ask those clarifying questions. “If they’re deteriorating and you can paint that broad picture and help them to see that and that they’re going toward some inexorable decline,” says Dr. Epstein, “then they might make different decisions with that information.”
What’s Good in a Good Death?
Phrases such as “good death” and “dying with dignity” bear some interpretation, says Eva Chittenden, MD, a hospitalist with the University of California at San Francisco and a faculty member of its Palliative Care Leadership Center. Most palliative care experts might further define this to mean dying with appropriate respect for who that person is or who that person has been up until this point. A good death, she says, might better be referred to as a death that is “as good as possible.
“People say they want to die at home, but on the other hand, they also want to live forever,” says Dr. Chittenden. The reality is that most people die in acute-care hospitals while receiving invasive therapies.5-6,15 “We want a peaceful death, we want a pain-free death, we want a death where we’re surrounded by our families,” she says, “but at the same time we want to delay that forever. And those two things come into extreme conflict.7,9
“If you have cancer, maybe you don’t want to talk with your oncologist about death and dying because you want them to save your life. So you don’t even want to go there. And then you’re admitted to the hospital you’re told, ‘You’re extremely sick; you have pneumonia, but if we intubate you, we might be able to turn this situation around versus, if we don’t intubate you, you will surely die.’ And people don’t want to make that decision, because they’re not ready to die, even if ideally they’d want to have that good death,” says Dr. Chittenden, noting that not all providers have come to terms with how to use the available medical technology, when to stop using it, and how to talk about prognosis.
Talking about Prognosis
“In no case of serious illness … is predicting the future straightforward or meaningless,” writes Nicholas Christakis, in Death Foretold: Prophecy and Prognosis in Medical Care.16 “Part of the problem is that even formulating, much less communicating, a prediction about death is unpleasant, so physicians are inclined to refrain from it. But when they are able to formulate a prediction and fail to do so, the quality of care that patients receive may suffer.”
According to Dr. Epstein, you have to practice the conversations. “It’s a skill set, just like doing a bedside procedure … something that you have to do over and over and get comfortable doing,” he explains. “And it shocks people out of their seats when they actually hear the ‘D word.’ ” But part of meeting your responsibility to patients and their families requires speaking the truth.
Dr. Epstein says there are numerous resources available to help hospitalists overcome their discomfort and fears about being incorrect about how long the patient has to live. “I think it is OK to also say, ‘Look, I’m not God and I don't have a crystal ball, but I have seen lots of people in your situation and having watched them go through this point in their life, this is my expert opinion … ,’ ” he advises.
This involves telling the patient, “These are your chances of making a full recovery to the point where you might appreciate the quality of life you would have.” You don’t have to give numbers; you can use words such as good, bad, or poor.
For those with advanced systemic failure, you might discuss prognoses in words that patients can better understand by making a comparison to someone has a cancer diagnosis. For instance, “I’ll say, ‘Your chances for living for a year are about as good as someone living with metastatic lung cancer,’ ” says Dr. Epstein. “I think that’s something that patients grasp a lot easier.”
In addition to the fear of being incorrect in prognosticating, physicians often don’t want their patients to lose hope. “Whereas in truth people are already thinking about these things, and there are studies that show people want their doctors to bring it up,” says Dr. Chittenden.7
A number of these studies were conducted by Dr. Christakis and Elizabeth Lamont, MD, a medical oncologist now practicing at Massachusetts General Hospital Cancer Center and assistant professor of medicine and health care policy at Harvard Medical School.15,17-19 Their findings have shown that doctors’ inaccuracies in their prognoses for terminally ill patients are systematically optimistic and that this may adversely affect the quality of care given to patients near the end of life.17
In their study of 326 patients in five hospices in Chicago, Drs. Christakis and Lamont showed that even if patients with cancer requested survival estimates, doctors would provide a frank estimate only 37% of the time and would provide no estimate, a conscious overestimate, or a conscious underestimate most of the time (63%).18 This, they concluded, may contribute to the observed disparities between physicians’ and patients’ estimates of survival.
Dr. Lamont’s interest in prognosis at end of life and the subject of advanced care planning arose from her experiences as a resident when she was cross-covering the oncology services. “I would be called to see [for example] a 35-year-old woman with widely metastatic breast cancer including brain metastases who was clearly at the end of life,” she says. “She became acutely short of breath, and my concern was that she was having a pulmonary embolism. … I was trying to decide whether to send her to the ICU. I was trying to inform her about the risks of anticoagulation … and I asked, ‘Have you talked about whether or not you’d want to go to the intensive care unit, whether or not you’d want your heart restarted, whether or not you’d want to be put on a ventilator if you couldn’t be breathe on your own; have you talked about these kinds of things with your oncologist?’ [Her answer was,] ‘Oh, no!’ ” Dr. Lamont figured that if she would have these conversations anyway, it would make more sense to have them as part of the admission history and physical. The study she subsequently designed and conducted involved 111 newly admitted patients with cancer whom she interviewed about (among other things) whether they had advanced care preferences (ACP) and whether they had discussed advanced directives with their medical oncologists. Only 9% of patients said that they had advanced directives, although 69% of patients had discussed their ACP with someone else (such as family).19 (See “ACP among Hospitalized Cancer Patients,” below.) However, 58% of patients approved of the option of being offered a discussion about advanced care planning with medical house staff as part of the admission history.
In other words, for the population of patients at high risk for dying during their current hospitalization, more than half would be open to discussing ACP with those whom they do not know well—such as hospitalists.
Advance Care Planning
A study just published in Archives of Internal Medicine suggests that elderly people who suffer from terminal illnesses become increasingly more willing to accept a life-preserving treatment, resulting in further physical disability or more pain if they were already diminished in those domains.20 Terri Fried, MD, an associate professor of internal medicine at Yale, and her colleagues studied 226 older men and women with advanced cancer, congestive heart failure (CHF), or COPD. In the course of in-home interviews conducted over two years, the investigators explored whether the participants would accept life-prolonging treatment if it resulted in one of four diminished health states: mild physical disability, severe physical disability, mental disability, or moderately severe daily pain.
Results showed that the likelihood of a treatment resulting in mild or severe functional disability rating as acceptable increased with each month of participation in the study. More than half of the patients had prepared living wills, and these individuals were more likely to prefer death to disability, but preferences could also change. These findings suggest that even though providers, patients, and families may have already had conversations about advance care planning, a patient’s change in health status might herald the need for a new conversation.
Dr. Lamont says there are two major areas in which hospitalists can politically advocate for changes that could facilitate better advance care planning. The first is to adopt the model proposed in her study, whereby patients are queried regarding advanced directives as part of the admission history.19 Patients for whom this could be added as a new data field would include, for example, those with advanced cancer, metastatic solid tumors, relapsed leukemia, relapsed lymphoma, or with acute exacerbations of illnesses such as CHF or COPD. The second area where hospitalists could advocate for change is national healthcare policy. Like a number of others, Dr. Lamont believes CMS should begin reimbursing for high-quality end-of-life care discussions, the measures of which would be determined at both local and national levels.
Communication Training
“The more hospital medicine training gets incorporated into internal medicine residency,” says Dr. Epstein, “the greater the opportunity to train new hospitalists to have these difficult conversations: how to have a family meeting, to identify the issues, to see if there are any ethical issues involved, any legal issues, and how to negotiate a reasonable plan of care based on the patient’s goals.”2,8,21
In addition to helping with control of physical symptoms, such as pain and nausea control, physicians facilitate decision-making. “We try to address a lot of the existential and reconciliation and legacy issues,” says Dr. Chittenden. Because of the number of situations in which the patient is a woman or man in their 40s or 50s who have young children, she says, “we help the parents come to terms with this and get our child-life specialist involved to help the parents think about how to talk with the kids.”
Because of the growth of the palliative care movement, the training is beginning to improve. “The LCME [Liaison Committee on Medical Education], the licensure group for medical schools, mandates that there be some end-of-life care exposure,” says Dr. Chittenden. “And the ACGME [Accreditation Council for Graduate Medical Education], which licenses the residency programs, strongly suggests that there be opportunities to learn about this. … Slowly but surely we are realizing this needs to happen, but we are far from doing it well.”
What would be ideal? A two-week rotation for residents in a palliative care service? “That would be wonderful,” says Dr. Epstein. “As more palliative care services pop up across the country, the chance of that happening would increase. … And even if you’re not in palliative care and you’re a hospitalist and you do these kinds of things well, the residents should be watching you have those kinds of conversations.”
Explaining that he is paraphrasing Mark Leenay, MD, the former program director at Fairview-University, Minnesota, and the physician who spearheaded the development of a clinical team that comprehensively addresses the multiple aspects of suffering from life-threatening illness, Dr. Epstein says: “I can train anybody to do symptom management in hospice, but how to walk into a room and understand … and negotiate the family dynamics and the patient’s plan of care … to communicate on different levels with different people with … their own agendas, and all the pieces of information … [and different interpretations] … to take it all in and digest it for that meeting and spit it out in a way [in which] everyone can relate and come to some sort of consensus, hopefully, at the end of the meeting? That’s the art. And that takes practice.”
Conclusion
Patients with life-threatening chronic illnesses are often admitted to the hospital multiple times in the course of the period that could be considered the end of life. Important nonmedical issues for hospitalists to address at each new admission include communication regarding prognosis and advance care planning, and addressing existential issues greatly contributes to the quality of care. TH
Resources
- The Hastings Center is involved in bioethics and other issues surrounding end-of-life care (www.thehastingscenter.org/default.asp). The Special Report listed in “References” is downloadable from their Web site.23
- Education in Palliative and End-of-Life Care (EPEC) curriculum (www.epec.net).
- The American Board of Hospice and Palliative Medicine (www.abhpm.org).
- The American Association of Hospice and Palliative Medicine (www.aahpm.org).
- Harvard’s Center for Palliative Care offers courses that emphasize teaching (www.hms.harvard.edu/cdi/pallcare/).
- The Center to Advance Palliative Care (CAPC), Mount Sinai School of Medicine, New York, serves as a resource for hospital-based palliative care program development. CAPC supports six regional Palliative Care Leadership Centers (www.capc.org).
The following Web sites include models for advance directives.
- Five Wishes: www.agingwithdignity.org
- Individual decisions: www.newgrangepress.com
- Respecting choices at end of life: www.gundersenlutheran.com/eolprograms
- Physician orders for life-sustaining treatment: www.polst.org
References
- Auerbach AD, Pantilat SZ. End-of-Life care in a voluntary hospitalist model: effects on communication, processes of care, and patient symptoms. Am J Med. 2004 May 15;116(10):669-675.
- Plauth WH, Pantilat SZ, Wachter RM, et al. Hospitalists' perceptions of their residency training needs: result of a national survey. Am J Med. 2001;111(3):247-254.
- Lo B, Quill TE, Tulsky J. Discussing palliative care with patients. ACP--ASIM End-of-Life Care Consensus Panel. American College of Physicians--American Society of Internal Medicine. Ann Intern Med. 1999 May 4;130(9):744-749.
- Quill TE. Initiating end-of-life discussions with seriously ill patients: addressing the "elephant in the room." JAMA. 2000 Nov 15;284(19):2502-2507.
- Kaufman SR. And a Time to Die: How American Hospitals Shape the End of Life. New York: Scribner; 2005.
- Kaufman SR. A commentary: hospital experience and meaning at the end of life. Gerontologist. 2002 Oct;42 Spec No. 3:34-39.
- Pantilat SZ. End-of-life care for the hospitalized patient. Med Clin North Am. 2002 Jul;86(4):749-770.
- Tulsky JA. Beyond advance directives: importance of communication skills at the end of life. JAMA. 2005 Jul 20;294(3):359-365.
- Heyland DK, Dodek P, Rocker G, et al. What matters most in end-of-life care: perceptions of seriously ill patients and their family members. CMAJ. 2006 Feb 28;174(5):627-633.
- Barbato M. Caring for the dying: the doctor as healer. MJAust. 2003 May 19;178(10):508-509.
- Fallowfield LJ, Jenkins VA, Beveridge HA. Truth may hurt but deceit hurts more: communication in palliative care. Palliat Med. 2002 Jul;16(4):297-303.
- Fins JJ, Miller FG, Acres CA, et al. End-of-life decision-making in the hospital: current practice and future prospects. J Pain Symptom Manage. 1999 Jan;17(1):6-15.
- Kalish RA. Death, grief and caring relationships. Belmont, California: Brooks/Cole; 1985.
- Lynn J, Schuster JL, Kabcenell A. Improving Care for the End of Life: A Sourcebook for Health Care Managers and Clinicians. New York: Oxford University Press; 2000.
- Lamont EB. A demographic and prognostic approach to defining the end of life. J Palliat Med. 2005;8 Suppl 1:S12-21.
- Christakis NA. Death Foretold: Prophecy and Prognosis in Medical Care. Chicago: University of Chicago Press; 2001.
- Christakis NA, Lamont EB. Extent and determinants of error in doctors' prognoses in terminally ill patients: prospective cohort study. BMJ. 2000 Feb;320(7233):469-472.
- Lamont EB, Christakis NA. Prognostic disclosure to patients with cancer near the end of life. Ann Intern Med. 2001 Jun 19; 134 (12):1096-1105.
- Lamont EB, Siegler M. Paradoxes in cancer patients' advance care planning. J Palliat Med. 2000 Spring;3(1):27-35.
- Fried TR, Byers AL, Gallo WT, et al. Prospective study of health status preferences and changes in preferences over time in older adults. Arch Intern Med. 2006 Apr 24;166(8):890-895.
- McPhee SJ, Rabow MW, Pantilat SZ, et al. Finding our way--perspectives on care at the close of life. JAMA. 2000 Nov 15;284(19):2512-2513.
- Solie D. How to Say It to Seniors: Closing the Communication Gap with Our Elders. New York: Prentice Hall Press; 2004.
- Jennings B, Kaebnick GE, Murray TH. Improving End of Life Care: Why Has It Been So Difficult? Hastings Center Special Report. 2005;35.
Take Research Initiative
Hospitalists should consider the hospital their research laboratory,” says Mark V. Williams, MD, FACP, professor of medicine, director, Emory Hospital Medicine Unit, and editor-in-chief of the Journal of Hospital Medicine. “Just as research scientists consider beakers, pipettes, and spectrometers as some of their research tools, we can consider computerized information databases, chart review, and QI projects the tools we use to figure out how we can best deliver care to patients.”
But what are the best ways for hospitalists to conduct research in their institutions? The challenge, says Jeffrey L. Schnipper, MD, MPH, director of clinical research, Brigham and Women’s/Faulkner Hospitalist Service (Boston), and associate physician, Division of General Medicine at Brigham and Women’s Hospital, is that hospitalists are tied to processes—not single interventions.
“The goal of my research,” says Dr. Schnipper, “is to move beyond ‘I got it to work at my hospital’ to ‘this works, in general, at any hospital.’ The vast majority of my projects are related to inpatient quality improvement. Unfortunately, that is not a ‘blue pill.’ If I prove that my quality improvement method improves diabetes control, you still have a lot of work to do to implement it at your hospital.”
How can hospitalists parlay their natural inclinations to improving systems into research that is publishable and generalizable? Healthcare researchers interviewed for this article maintain that savvy use of tools generated from quality improvement research combined with traditional scientific methods can help busy hospitalists streamline their approach to identifying, designing, and conducting valid research projects with publishable results.
Missions Interlaced
Those interviewed for this article agree that the push for quality improvement dovetails with hospitalists’ mission and approach to patient care. “Hospitalists are very systems-oriented,” says Dr. Schnipper. “They are trying to improve not just the care of their individual patients, but the way the whole system works and runs. Frankly, in any environment in which we work, we have a vested interest in making it run better.”
Hospitalists provide a valuable link in the quality improvement chain, agrees Brent James, MD, executive director of the Institute for Healthcare Delivery Research, at Intermountain Healthcare, an integrated delivery system serving 1.2 million patients in Utah, and a leading QI researcher. “Any time you have a group of people who are trying to deliver coordinated care together, and who rely heavily on being able to support each other as a team, this is just an absolute natural model [for conducting QI studies],” he says.

Dr. James was a member of the Institute of Medicine’s National Roundtable on Quality and its subsequent Committee on Quality of Health Care in America that published Crossing the Quality Chasm in 2001. He also just finished a three-year project with the Hastings Center, Garrison, N.Y., funded by an Agency for Healthcare Research and Quality (AHRQ) grant, to examine the ethics of quality improvement.
“Given the quality chasm,” he says, “there is an ethical obligation for physicians, nurses and health professionals to do quality improvement. It surely shouldn’t be a choice—it’s a way of rigorously learning from your own practice.”
Dr. Williams explains that hospitals will increasingly undertake quality improvement initiatives, not just to improve care delivery in their facilities, but in response to pay-for-performance requirements being set up by the federal government and insurers.
“I strongly believe that hospitalists are going to be seen by many hospital administrators as not only collaborators but the leaders of these initiatives,” says Dr. Williams. “And those initiatives can be a form of research if conducted properly. It does require having sufficient resources from the hospital. I don’t think it’s something you can do on Saturday and Sunday nights.”
Steps to the Research
Dr. James has collaborated with Theodore Speroff, PhD, of the Veterans Affairs Health Services Research Center in Nashville, Tenn., and others on many articles delineating the use of PDSA (plan, do, study, act) methodology—also known as rapid cycle of change methodology—to improve the rigor of quality improvement initiatives.1,2
In a nutshell, says Dr. James, the PDSA model consists of several important steps encompassing a study cycle:
- Establish key clinical processes at your institution that warrant studying, and build an evidence-based best practices guideline. For instance, at Intermountain Healthcare 10% of the system’s processes accounted for 90% of clinicians’ work. Hospitalists pick the most prominent care process (DVT prophylaxis, for example) and build an evidence-based best practice guideline;
- Build best practice guidelines into a workflow format (in the form of standing order sets, data, and decision support) to directly support care at the work flow level;
- Build outcomes data comprising three major sub-categories: medical outcomes, service outcomes, and cost outcomes. Each category is further divided into smaller units. For instance, medical outcomes would include indications for appropriateness, condition-specific complication rates, and achieving therapeutic goals;
- Use electronic medical records to develop a system of decision support that ties together best practices, work flow and outcomes tracking; and
- Build educational materials for patients and for the team of professionals delivering the care.
The beauty of rapid cycle of change methodology, says Dr. James, is that it quickly allows teams to correctly identify worthwhile research projects. The team asks: What is our aim or target? How will we know if the target changes or improves (implying a parallel qualitative or quantitative measurement system)? And finally, what might we change to make things work better? “Rapid cycle” connotes a series of PDSA cycles performed one after another in the context of a measurement system.

Increase the Rigor of Studies
Dr. Schnipper believes that continuous quality improvement methods give researchers a toolkit for conducting successful interventional studies. But to use quality improvement methods (e.g., rapid cycle of change—PDSA—methodology) alone may yield less externally valid study results. For example, he says, using QI methods alone, a researcher might continuously change the intervention (for glucose management, for example), watching the results improve over time. This might be the most effective method for improving glucose control in a specific institution, but this renders results “less generalizable to any other institution. It’s never really a before/after study, much less a concurrent randomized controlled trial,” he says. “Many people believe that if you want to conduct research, you have to ‘hold the intervention still’ for at least a certain amount of time so that it’s describable to other people. You may also decide, in the name of generalizability, not to maximally customize your QI intervention to your institution.”
Dr. Schnipper cites a recent Annals of Internal Medicine study that used a combined methodology. The study, by Fine and colleagues at the University of Pittsburgh in conjunction with the Veterans Affairs Center for Health Equity Research and Promotion, compared three intervention strategies (low, moderate, and high intensity) to improve pneumonia care in emergency departments and assessed the performance in institutions assigned to each strategy.3 The high intensity arm used a continuous quality improvement method, allowing each institution to design an intervention that worked best for it. “It was encouraging to see Annals publish an article of this type,” says Dr. Schnipper. “But the question remains: Is this the best way to publish research, such that it’s most useful for other hospitalists who want to improve care at their institutions? Do you include a 20-page online appendix so other people can see exactly what you did?”
QI methodology, Dr. James concedes, is “inherently an observational study design in the hierarchy of evidence because of the way data is collected.” He maintains that researchers can increase the reliability of quality improvement initiatives “by incorporating prospective non-randomized controlled trials designs, or quasi-experiments, the pinnacle of observational study designs. Staggered implementation, risk adjustment, and case matching can bring a quasi-experimental study design within a hair’s breadth of the same evidence reliability of a full randomized controlled trial.”
Once routine care processes are standardized at an institution, other opportunities for controlled studies will appear. Dr. James cites work done at LDS Hospital, Salt Lake City, Utah, by Allen Morris to produce a best practices guideline for treating acute respiratory distress syndrome (ARDS). Now disseminated via ARDSnet (www.ardsnet.org/clinicalnetwork/; Dublin, Calif.), a national research collaborative, these best practices guidelines are now routine care for ARDS at 16 major academic centers. Because routine care is standardized, says Dr. James, that routine care—with Institutional Review Board (IRB) approval and oversight—can become the control arm for comparing new interventions in additional clinical studies. Also, because researchers do not have to initiate a new control arm, operational overhead for new scientific trials is reduced.
“There are definitely ways in which the two fields [quality improvement and rigorous scientific research] make each other better,” says Dr. Schnipper. For his study of glycemic management of diabetic patients in a non-ICU setting (at press time scheduled to publish in a forthcoming issue of the Journal of Hospital Medicine), Dr. Schnipper and his team conducted rigorous prospective data collection, identifying every diabetic on the general medicine service at the time of admission. Using the APACHE III, the team then assessed each patient’s severity of disease, a known confounder of glucose control in hospitalized diabetics. They conducted a detailed chart review to assess the quality of insulin orders for the diabetic patients. Finally, they used a novel statistical technique (marginal structural models) to remove the confounding by indication that occurs when hyperglycemia results in more intensive insulin therapy. They revealed that better quality insulin orders resulted in better glucose control.
“There’s a lot to be said for designing this research so that it is maximally useful for its consumers—hospitalists and others—who want to improve care in their own hospitals. I think we need to move toward multi-center quality improvement studies. If you can get [an intervention] to work at 10 hospitals, then you’ve gone a long way to say this works, in general. As long as you can answer that question—is there knowledge to be gained—then it’s worth doing a study well, with good methods, and it’s worth publishing.”
In Academia Alone?
Dr. Williams hopes the new emphasis on quality improvement, evidenced in such publications as the AHRQ’s August 2004 technical review, “Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies,” can become a springboard for new areas of research.4 He reports that the Journal of Hospital Medicine has already received article submissions detailing quality improvement initiatives. “We would love to see more,” he says.
It may not always be possible to clear the time for the additional duties of conducting research. Community-based hospitalists do not usually enjoy the same degree of funding and research support infrastructure found in the academic setting. SHM’s “Authoritative Source on the State of the Hospital Medicine Movement” reveals that the majority of hospitalists involved in research are affiliated with universities and medical schools.5 Dr. Williams admits that fitting in research projects can often be a challenge for other busy hospitalists.
“I don’t think it’s something you can just do on nights and weekends. The only way, honestly, that hospitalists can fit research into what they’re doing is if [research] becomes part of their job description,” says Dr. Williams. “And I think the appropriate avenue is through quality improvement initiatives.”
His advice to young hospitalists who want to undertake research projects? Identify existing resources at their institution and find out how they can collaborate with other members of the healthcare team, including nurses and pharmacists.
Community-based hospitalists will most likely benefit, surmises Dr. Schnipper, from emerging initiatives for public reporting and pay for performance, an offshoot of which will yield more useful data sets. “I think they will probably do more collaborative research. Community hospitalists may not have fellowship training in research and protected time to become independent investigators with federal funding,” he says. “What they do have is incredible clinical insight and exact knowledge of the problems in their hospital. I would love to see more academic-community partnerships, where we could do studies in real-world hospitals, not just my ivory tower. Then, we could get some really good, generalizable, multi-center research – which would make everybody happy.” TH
Gretchen Henkel writes regularly for The Hospitalist.
References
- Speroff T, James BC, Nelson EC, et al. Guidelines for appraisal and publication of PDSA quality improvement. Qual Manag Health Care. 2004 Jan-Mar;13(1); 33-39.
- Speroff T, O’Connor GT. Study designs for PDSA quality improvement research. Qual Manag Health Care. 2004 Jan-Mar;13(1);17-32.
- Yealy DM, Auble TE, Stone RA, et al. Effect of increasing the intensity of implementing pneumonia guidelines: a randomized, controlled trial. Ann Intern Med. 2005 Dec 20;143(12):881-894.
- Shojani, KG, McDonald KM, Wachter RM, et al. Closing the quality gap: a critical analysis of quality improvement strategies. Vol. 1, Agency for Healthcare Research and Quality Technical Review; August, 2004. Publication No. 04-0051-1. Available online at www.ahrq.gov/downloads/pub/evidence/pdf/qualgap2/qualgap2.pdf. Last accessed May 30, 2006.
- The Society of Hospital Medicine 2005-2006 Survey. The Authoritative Source on the State of the Hospital Medicine Movement, May, 2006. Philadelphia.
Hospitalists should consider the hospital their research laboratory,” says Mark V. Williams, MD, FACP, professor of medicine, director, Emory Hospital Medicine Unit, and editor-in-chief of the Journal of Hospital Medicine. “Just as research scientists consider beakers, pipettes, and spectrometers as some of their research tools, we can consider computerized information databases, chart review, and QI projects the tools we use to figure out how we can best deliver care to patients.”
But what are the best ways for hospitalists to conduct research in their institutions? The challenge, says Jeffrey L. Schnipper, MD, MPH, director of clinical research, Brigham and Women’s/Faulkner Hospitalist Service (Boston), and associate physician, Division of General Medicine at Brigham and Women’s Hospital, is that hospitalists are tied to processes—not single interventions.
“The goal of my research,” says Dr. Schnipper, “is to move beyond ‘I got it to work at my hospital’ to ‘this works, in general, at any hospital.’ The vast majority of my projects are related to inpatient quality improvement. Unfortunately, that is not a ‘blue pill.’ If I prove that my quality improvement method improves diabetes control, you still have a lot of work to do to implement it at your hospital.”
How can hospitalists parlay their natural inclinations to improving systems into research that is publishable and generalizable? Healthcare researchers interviewed for this article maintain that savvy use of tools generated from quality improvement research combined with traditional scientific methods can help busy hospitalists streamline their approach to identifying, designing, and conducting valid research projects with publishable results.
Missions Interlaced
Those interviewed for this article agree that the push for quality improvement dovetails with hospitalists’ mission and approach to patient care. “Hospitalists are very systems-oriented,” says Dr. Schnipper. “They are trying to improve not just the care of their individual patients, but the way the whole system works and runs. Frankly, in any environment in which we work, we have a vested interest in making it run better.”
Hospitalists provide a valuable link in the quality improvement chain, agrees Brent James, MD, executive director of the Institute for Healthcare Delivery Research, at Intermountain Healthcare, an integrated delivery system serving 1.2 million patients in Utah, and a leading QI researcher. “Any time you have a group of people who are trying to deliver coordinated care together, and who rely heavily on being able to support each other as a team, this is just an absolute natural model [for conducting QI studies],” he says.
Dr. James was a member of the Institute of Medicine’s National Roundtable on Quality and its subsequent Committee on Quality of Health Care in America that published Crossing the Quality Chasm in 2001. He also just finished a three-year project with the Hastings Center, Garrison, N.Y., funded by an Agency for Healthcare Research and Quality (AHRQ) grant, to examine the ethics of quality improvement.
“Given the quality chasm,” he says, “there is an ethical obligation for physicians, nurses and health professionals to do quality improvement. It surely shouldn’t be a choice—it’s a way of rigorously learning from your own practice.”
Dr. Williams explains that hospitals will increasingly undertake quality improvement initiatives, not just to improve care delivery in their facilities, but in response to pay-for-performance requirements being set up by the federal government and insurers.
“I strongly believe that hospitalists are going to be seen by many hospital administrators as not only collaborators but the leaders of these initiatives,” says Dr. Williams. “And those initiatives can be a form of research if conducted properly. It does require having sufficient resources from the hospital. I don’t think it’s something you can do on Saturday and Sunday nights.”
Steps to the Research
Dr. James has collaborated with Theodore Speroff, PhD, of the Veterans Affairs Health Services Research Center in Nashville, Tenn., and others on many articles delineating the use of PDSA (plan, do, study, act) methodology—also known as rapid cycle of change methodology—to improve the rigor of quality improvement initiatives.1,2
In a nutshell, says Dr. James, the PDSA model consists of several important steps encompassing a study cycle:
- Establish key clinical processes at your institution that warrant studying, and build an evidence-based best practices guideline. For instance, at Intermountain Healthcare 10% of the system’s processes accounted for 90% of clinicians’ work. Hospitalists pick the most prominent care process (DVT prophylaxis, for example) and build an evidence-based best practice guideline;
- Build best practice guidelines into a workflow format (in the form of standing order sets, data, and decision support) to directly support care at the work flow level;
- Build outcomes data comprising three major sub-categories: medical outcomes, service outcomes, and cost outcomes. Each category is further divided into smaller units. For instance, medical outcomes would include indications for appropriateness, condition-specific complication rates, and achieving therapeutic goals;
- Use electronic medical records to develop a system of decision support that ties together best practices, work flow and outcomes tracking; and
- Build educational materials for patients and for the team of professionals delivering the care.
The beauty of rapid cycle of change methodology, says Dr. James, is that it quickly allows teams to correctly identify worthwhile research projects. The team asks: What is our aim or target? How will we know if the target changes or improves (implying a parallel qualitative or quantitative measurement system)? And finally, what might we change to make things work better? “Rapid cycle” connotes a series of PDSA cycles performed one after another in the context of a measurement system.
Increase the Rigor of Studies
Dr. Schnipper believes that continuous quality improvement methods give researchers a toolkit for conducting successful interventional studies. But to use quality improvement methods (e.g., rapid cycle of change—PDSA—methodology) alone may yield less externally valid study results. For example, he says, using QI methods alone, a researcher might continuously change the intervention (for glucose management, for example), watching the results improve over time. This might be the most effective method for improving glucose control in a specific institution, but this renders results “less generalizable to any other institution. It’s never really a before/after study, much less a concurrent randomized controlled trial,” he says. “Many people believe that if you want to conduct research, you have to ‘hold the intervention still’ for at least a certain amount of time so that it’s describable to other people. You may also decide, in the name of generalizability, not to maximally customize your QI intervention to your institution.”
Dr. Schnipper cites a recent Annals of Internal Medicine study that used a combined methodology. The study, by Fine and colleagues at the University of Pittsburgh in conjunction with the Veterans Affairs Center for Health Equity Research and Promotion, compared three intervention strategies (low, moderate, and high intensity) to improve pneumonia care in emergency departments and assessed the performance in institutions assigned to each strategy.3 The high intensity arm used a continuous quality improvement method, allowing each institution to design an intervention that worked best for it. “It was encouraging to see Annals publish an article of this type,” says Dr. Schnipper. “But the question remains: Is this the best way to publish research, such that it’s most useful for other hospitalists who want to improve care at their institutions? Do you include a 20-page online appendix so other people can see exactly what you did?”
QI methodology, Dr. James concedes, is “inherently an observational study design in the hierarchy of evidence because of the way data is collected.” He maintains that researchers can increase the reliability of quality improvement initiatives “by incorporating prospective non-randomized controlled trials designs, or quasi-experiments, the pinnacle of observational study designs. Staggered implementation, risk adjustment, and case matching can bring a quasi-experimental study design within a hair’s breadth of the same evidence reliability of a full randomized controlled trial.”
Once routine care processes are standardized at an institution, other opportunities for controlled studies will appear. Dr. James cites work done at LDS Hospital, Salt Lake City, Utah, by Allen Morris to produce a best practices guideline for treating acute respiratory distress syndrome (ARDS). Now disseminated via ARDSnet (www.ardsnet.org/clinicalnetwork/; Dublin, Calif.), a national research collaborative, these best practices guidelines are now routine care for ARDS at 16 major academic centers. Because routine care is standardized, says Dr. James, that routine care—with Institutional Review Board (IRB) approval and oversight—can become the control arm for comparing new interventions in additional clinical studies. Also, because researchers do not have to initiate a new control arm, operational overhead for new scientific trials is reduced.
“There are definitely ways in which the two fields [quality improvement and rigorous scientific research] make each other better,” says Dr. Schnipper. For his study of glycemic management of diabetic patients in a non-ICU setting (at press time scheduled to publish in a forthcoming issue of the Journal of Hospital Medicine), Dr. Schnipper and his team conducted rigorous prospective data collection, identifying every diabetic on the general medicine service at the time of admission. Using the APACHE III, the team then assessed each patient’s severity of disease, a known confounder of glucose control in hospitalized diabetics. They conducted a detailed chart review to assess the quality of insulin orders for the diabetic patients. Finally, they used a novel statistical technique (marginal structural models) to remove the confounding by indication that occurs when hyperglycemia results in more intensive insulin therapy. They revealed that better quality insulin orders resulted in better glucose control.
“There’s a lot to be said for designing this research so that it is maximally useful for its consumers—hospitalists and others—who want to improve care in their own hospitals. I think we need to move toward multi-center quality improvement studies. If you can get [an intervention] to work at 10 hospitals, then you’ve gone a long way to say this works, in general. As long as you can answer that question—is there knowledge to be gained—then it’s worth doing a study well, with good methods, and it’s worth publishing.”
In Academia Alone?
Dr. Williams hopes the new emphasis on quality improvement, evidenced in such publications as the AHRQ’s August 2004 technical review, “Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies,” can become a springboard for new areas of research.4 He reports that the Journal of Hospital Medicine has already received article submissions detailing quality improvement initiatives. “We would love to see more,” he says.
It may not always be possible to clear the time for the additional duties of conducting research. Community-based hospitalists do not usually enjoy the same degree of funding and research support infrastructure found in the academic setting. SHM’s “Authoritative Source on the State of the Hospital Medicine Movement” reveals that the majority of hospitalists involved in research are affiliated with universities and medical schools.5 Dr. Williams admits that fitting in research projects can often be a challenge for other busy hospitalists.
“I don’t think it’s something you can just do on nights and weekends. The only way, honestly, that hospitalists can fit research into what they’re doing is if [research] becomes part of their job description,” says Dr. Williams. “And I think the appropriate avenue is through quality improvement initiatives.”
His advice to young hospitalists who want to undertake research projects? Identify existing resources at their institution and find out how they can collaborate with other members of the healthcare team, including nurses and pharmacists.
Community-based hospitalists will most likely benefit, surmises Dr. Schnipper, from emerging initiatives for public reporting and pay for performance, an offshoot of which will yield more useful data sets. “I think they will probably do more collaborative research. Community hospitalists may not have fellowship training in research and protected time to become independent investigators with federal funding,” he says. “What they do have is incredible clinical insight and exact knowledge of the problems in their hospital. I would love to see more academic-community partnerships, where we could do studies in real-world hospitals, not just my ivory tower. Then, we could get some really good, generalizable, multi-center research – which would make everybody happy.” TH
Gretchen Henkel writes regularly for The Hospitalist.
References
- Speroff T, James BC, Nelson EC, et al. Guidelines for appraisal and publication of PDSA quality improvement. Qual Manag Health Care. 2004 Jan-Mar;13(1); 33-39.
- Speroff T, O’Connor GT. Study designs for PDSA quality improvement research. Qual Manag Health Care. 2004 Jan-Mar;13(1);17-32.
- Yealy DM, Auble TE, Stone RA, et al. Effect of increasing the intensity of implementing pneumonia guidelines: a randomized, controlled trial. Ann Intern Med. 2005 Dec 20;143(12):881-894.
- Shojani, KG, McDonald KM, Wachter RM, et al. Closing the quality gap: a critical analysis of quality improvement strategies. Vol. 1, Agency for Healthcare Research and Quality Technical Review; August, 2004. Publication No. 04-0051-1. Available online at www.ahrq.gov/downloads/pub/evidence/pdf/qualgap2/qualgap2.pdf. Last accessed May 30, 2006.
- The Society of Hospital Medicine 2005-2006 Survey. The Authoritative Source on the State of the Hospital Medicine Movement, May, 2006. Philadelphia.
Hospitalists should consider the hospital their research laboratory,” says Mark V. Williams, MD, FACP, professor of medicine, director, Emory Hospital Medicine Unit, and editor-in-chief of the Journal of Hospital Medicine. “Just as research scientists consider beakers, pipettes, and spectrometers as some of their research tools, we can consider computerized information databases, chart review, and QI projects the tools we use to figure out how we can best deliver care to patients.”
But what are the best ways for hospitalists to conduct research in their institutions? The challenge, says Jeffrey L. Schnipper, MD, MPH, director of clinical research, Brigham and Women’s/Faulkner Hospitalist Service (Boston), and associate physician, Division of General Medicine at Brigham and Women’s Hospital, is that hospitalists are tied to processes—not single interventions.
“The goal of my research,” says Dr. Schnipper, “is to move beyond ‘I got it to work at my hospital’ to ‘this works, in general, at any hospital.’ The vast majority of my projects are related to inpatient quality improvement. Unfortunately, that is not a ‘blue pill.’ If I prove that my quality improvement method improves diabetes control, you still have a lot of work to do to implement it at your hospital.”
How can hospitalists parlay their natural inclinations to improving systems into research that is publishable and generalizable? Healthcare researchers interviewed for this article maintain that savvy use of tools generated from quality improvement research combined with traditional scientific methods can help busy hospitalists streamline their approach to identifying, designing, and conducting valid research projects with publishable results.
Missions Interlaced
Those interviewed for this article agree that the push for quality improvement dovetails with hospitalists’ mission and approach to patient care. “Hospitalists are very systems-oriented,” says Dr. Schnipper. “They are trying to improve not just the care of their individual patients, but the way the whole system works and runs. Frankly, in any environment in which we work, we have a vested interest in making it run better.”
Hospitalists provide a valuable link in the quality improvement chain, agrees Brent James, MD, executive director of the Institute for Healthcare Delivery Research, at Intermountain Healthcare, an integrated delivery system serving 1.2 million patients in Utah, and a leading QI researcher. “Any time you have a group of people who are trying to deliver coordinated care together, and who rely heavily on being able to support each other as a team, this is just an absolute natural model [for conducting QI studies],” he says.
Dr. James was a member of the Institute of Medicine’s National Roundtable on Quality and its subsequent Committee on Quality of Health Care in America that published Crossing the Quality Chasm in 2001. He also just finished a three-year project with the Hastings Center, Garrison, N.Y., funded by an Agency for Healthcare Research and Quality (AHRQ) grant, to examine the ethics of quality improvement.
“Given the quality chasm,” he says, “there is an ethical obligation for physicians, nurses and health professionals to do quality improvement. It surely shouldn’t be a choice—it’s a way of rigorously learning from your own practice.”
Dr. Williams explains that hospitals will increasingly undertake quality improvement initiatives, not just to improve care delivery in their facilities, but in response to pay-for-performance requirements being set up by the federal government and insurers.
“I strongly believe that hospitalists are going to be seen by many hospital administrators as not only collaborators but the leaders of these initiatives,” says Dr. Williams. “And those initiatives can be a form of research if conducted properly. It does require having sufficient resources from the hospital. I don’t think it’s something you can do on Saturday and Sunday nights.”
Steps to the Research
Dr. James has collaborated with Theodore Speroff, PhD, of the Veterans Affairs Health Services Research Center in Nashville, Tenn., and others on many articles delineating the use of PDSA (plan, do, study, act) methodology—also known as rapid cycle of change methodology—to improve the rigor of quality improvement initiatives.1,2
In a nutshell, says Dr. James, the PDSA model consists of several important steps encompassing a study cycle:
- Establish key clinical processes at your institution that warrant studying, and build an evidence-based best practices guideline. For instance, at Intermountain Healthcare 10% of the system’s processes accounted for 90% of clinicians’ work. Hospitalists pick the most prominent care process (DVT prophylaxis, for example) and build an evidence-based best practice guideline;
- Build best practice guidelines into a workflow format (in the form of standing order sets, data, and decision support) to directly support care at the work flow level;
- Build outcomes data comprising three major sub-categories: medical outcomes, service outcomes, and cost outcomes. Each category is further divided into smaller units. For instance, medical outcomes would include indications for appropriateness, condition-specific complication rates, and achieving therapeutic goals;
- Use electronic medical records to develop a system of decision support that ties together best practices, work flow and outcomes tracking; and
- Build educational materials for patients and for the team of professionals delivering the care.
The beauty of rapid cycle of change methodology, says Dr. James, is that it quickly allows teams to correctly identify worthwhile research projects. The team asks: What is our aim or target? How will we know if the target changes or improves (implying a parallel qualitative or quantitative measurement system)? And finally, what might we change to make things work better? “Rapid cycle” connotes a series of PDSA cycles performed one after another in the context of a measurement system.
Increase the Rigor of Studies
Dr. Schnipper believes that continuous quality improvement methods give researchers a toolkit for conducting successful interventional studies. But to use quality improvement methods (e.g., rapid cycle of change—PDSA—methodology) alone may yield less externally valid study results. For example, he says, using QI methods alone, a researcher might continuously change the intervention (for glucose management, for example), watching the results improve over time. This might be the most effective method for improving glucose control in a specific institution, but this renders results “less generalizable to any other institution. It’s never really a before/after study, much less a concurrent randomized controlled trial,” he says. “Many people believe that if you want to conduct research, you have to ‘hold the intervention still’ for at least a certain amount of time so that it’s describable to other people. You may also decide, in the name of generalizability, not to maximally customize your QI intervention to your institution.”
Dr. Schnipper cites a recent Annals of Internal Medicine study that used a combined methodology. The study, by Fine and colleagues at the University of Pittsburgh in conjunction with the Veterans Affairs Center for Health Equity Research and Promotion, compared three intervention strategies (low, moderate, and high intensity) to improve pneumonia care in emergency departments and assessed the performance in institutions assigned to each strategy.3 The high intensity arm used a continuous quality improvement method, allowing each institution to design an intervention that worked best for it. “It was encouraging to see Annals publish an article of this type,” says Dr. Schnipper. “But the question remains: Is this the best way to publish research, such that it’s most useful for other hospitalists who want to improve care at their institutions? Do you include a 20-page online appendix so other people can see exactly what you did?”
QI methodology, Dr. James concedes, is “inherently an observational study design in the hierarchy of evidence because of the way data is collected.” He maintains that researchers can increase the reliability of quality improvement initiatives “by incorporating prospective non-randomized controlled trials designs, or quasi-experiments, the pinnacle of observational study designs. Staggered implementation, risk adjustment, and case matching can bring a quasi-experimental study design within a hair’s breadth of the same evidence reliability of a full randomized controlled trial.”
Once routine care processes are standardized at an institution, other opportunities for controlled studies will appear. Dr. James cites work done at LDS Hospital, Salt Lake City, Utah, by Allen Morris to produce a best practices guideline for treating acute respiratory distress syndrome (ARDS). Now disseminated via ARDSnet (www.ardsnet.org/clinicalnetwork/; Dublin, Calif.), a national research collaborative, these best practices guidelines are now routine care for ARDS at 16 major academic centers. Because routine care is standardized, says Dr. James, that routine care—with Institutional Review Board (IRB) approval and oversight—can become the control arm for comparing new interventions in additional clinical studies. Also, because researchers do not have to initiate a new control arm, operational overhead for new scientific trials is reduced.
“There are definitely ways in which the two fields [quality improvement and rigorous scientific research] make each other better,” says Dr. Schnipper. For his study of glycemic management of diabetic patients in a non-ICU setting (at press time scheduled to publish in a forthcoming issue of the Journal of Hospital Medicine), Dr. Schnipper and his team conducted rigorous prospective data collection, identifying every diabetic on the general medicine service at the time of admission. Using the APACHE III, the team then assessed each patient’s severity of disease, a known confounder of glucose control in hospitalized diabetics. They conducted a detailed chart review to assess the quality of insulin orders for the diabetic patients. Finally, they used a novel statistical technique (marginal structural models) to remove the confounding by indication that occurs when hyperglycemia results in more intensive insulin therapy. They revealed that better quality insulin orders resulted in better glucose control.
“There’s a lot to be said for designing this research so that it is maximally useful for its consumers—hospitalists and others—who want to improve care in their own hospitals. I think we need to move toward multi-center quality improvement studies. If you can get [an intervention] to work at 10 hospitals, then you’ve gone a long way to say this works, in general. As long as you can answer that question—is there knowledge to be gained—then it’s worth doing a study well, with good methods, and it’s worth publishing.”
In Academia Alone?
Dr. Williams hopes the new emphasis on quality improvement, evidenced in such publications as the AHRQ’s August 2004 technical review, “Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies,” can become a springboard for new areas of research.4 He reports that the Journal of Hospital Medicine has already received article submissions detailing quality improvement initiatives. “We would love to see more,” he says.
It may not always be possible to clear the time for the additional duties of conducting research. Community-based hospitalists do not usually enjoy the same degree of funding and research support infrastructure found in the academic setting. SHM’s “Authoritative Source on the State of the Hospital Medicine Movement” reveals that the majority of hospitalists involved in research are affiliated with universities and medical schools.5 Dr. Williams admits that fitting in research projects can often be a challenge for other busy hospitalists.
“I don’t think it’s something you can just do on nights and weekends. The only way, honestly, that hospitalists can fit research into what they’re doing is if [research] becomes part of their job description,” says Dr. Williams. “And I think the appropriate avenue is through quality improvement initiatives.”
His advice to young hospitalists who want to undertake research projects? Identify existing resources at their institution and find out how they can collaborate with other members of the healthcare team, including nurses and pharmacists.
Community-based hospitalists will most likely benefit, surmises Dr. Schnipper, from emerging initiatives for public reporting and pay for performance, an offshoot of which will yield more useful data sets. “I think they will probably do more collaborative research. Community hospitalists may not have fellowship training in research and protected time to become independent investigators with federal funding,” he says. “What they do have is incredible clinical insight and exact knowledge of the problems in their hospital. I would love to see more academic-community partnerships, where we could do studies in real-world hospitals, not just my ivory tower. Then, we could get some really good, generalizable, multi-center research – which would make everybody happy.” TH
Gretchen Henkel writes regularly for The Hospitalist.
References
- Speroff T, James BC, Nelson EC, et al. Guidelines for appraisal and publication of PDSA quality improvement. Qual Manag Health Care. 2004 Jan-Mar;13(1); 33-39.
- Speroff T, O’Connor GT. Study designs for PDSA quality improvement research. Qual Manag Health Care. 2004 Jan-Mar;13(1);17-32.
- Yealy DM, Auble TE, Stone RA, et al. Effect of increasing the intensity of implementing pneumonia guidelines: a randomized, controlled trial. Ann Intern Med. 2005 Dec 20;143(12):881-894.
- Shojani, KG, McDonald KM, Wachter RM, et al. Closing the quality gap: a critical analysis of quality improvement strategies. Vol. 1, Agency for Healthcare Research and Quality Technical Review; August, 2004. Publication No. 04-0051-1. Available online at www.ahrq.gov/downloads/pub/evidence/pdf/qualgap2/qualgap2.pdf. Last accessed May 30, 2006.
- The Society of Hospital Medicine 2005-2006 Survey. The Authoritative Source on the State of the Hospital Medicine Movement, May, 2006. Philadelphia.
To Tube or Not to Tube
The ability to maintain nutrition and hydration is essential when caring for hospitalized older adults. When physicians recognize that long-term nutrition and hydration cannot be maintained through an oral route, percutaneous endoscopic gastrostomy (PEG) tube placement may need to be considered for long-term nutritional support. This decision is often distressing for the patient, family, and physician for several reasons.
First, the significant number of competing benefits, risks, and burdens of long-term enteral feeding that have to be considered can be overwhelming. The second reason is the lack of clinical data regarding outcomes of PEG tubes for many patients. The last and usually most distressing reason in the decision of PEG tube feeding involves the cultural, ethical, and religious beliefs involved in this decision.
For many families and physicians providing nutrition, including enteral nutrition, using a PEG tube symbolizes compassion, love, and care. This is because eating represents one of the most basic of human needs. For some, not providing nutrition with a PEG tube is morally and ethically wrong. Withholding PEG tube placement can be perceived as assisted suicide or murder. Some physicians also fear legal, ethical, or religious misconduct should they decide against tube feeding.
Physicians need not fear the legal consequences of discontinuing life-sustaining treatment if an appropriate decision-making process has been followed.1 An adult patient who has decision-making capacity and is appropriately informed has the right to forego any forms of medical therapy including life-sustaining therapy such as PEG tube feeding.2
Deciding whether or not to recommend PEG tube feeding can be accomplished in a series of steps. The first step is to evaluate the clinical benefits, risks, and burdens of long-term nutrition for the individual patient. The second step involves discussing the patient’s life goals with them and their family. On many occasions, the decision to place a PEG tube will be made by a surrogate decision-maker such as the patient’s spouse or child. Usually discussions about nutrition and hydration by PEG tube will occur between patients, families, and physicians when the overall end-of-life goals are reviewed. A physician’s role includes assisting patients and their families by providing information and a clear recommendation for or against the use of a feeding tube, giving alternative options, and ensuring there is true informed consent prior to feeding tube insertion.
The most frequent indication for long-term PEG tube feeding is a neurological disorder such as a stroke.3 PEG tube feeding has been developed as a practical alternative to parental feeding for patients with a functioning gastrointestinal (GI) tract who lack the ability to take food by mouth. PEG tube feeding is considered a medical intervention and, like any other intervention, has to be considered according to specific patient situations.
Why Are Older Adults at Risk?
With advancing age comes a linear decline in food intake. Involuntary weight loss is common among older adults, especially in those who are chronically ill. Poor caloric intake and weight loss can lead to multiple problems such as muscle wasting, anemia, and depression. There is a strong correlation between weight loss and morbidity and mortality.4 Even with mild weight loss of 5% of their body weight in one month, institutionalized older adults are four times more likely to die within one year.5 Similarly, community-dwelling older adults who have mild weight loss are at a higher risk of death after adjusting for multiple variables.6
Age-related changes can negatively affect the body’s ability to regulate energy intake and puts older adults at risk for negative energy balance.7 Older adults are more likely to have additional medical problems, use more medications, and experience psychosocial issues that can lead to weight loss and poor nutrition.8 Common causes of weight loss in older hospitalized adults include cancer, gastrointestinal disorder, and depression.9
Mechanical problems, such as dysphagia secondary to cerebrovascular accidents or degenerative brain diseases that affect swallowing are frequently encountered in the hospitalized older patient. Also, diseases that affect appetite and feeding increase the risk for negative energy balance such as GI diseases, endocrine diseases, infections, COPD, and others.
Many drugs have been associated with weight loss, especially in frail older adults. Drugs can cause a decrease in appetite, changes in food tastes and adsorption, and increase the body’s metabolism, making the patients unable to meet their caloric needs. Drugs implicated in malnutrition and weight loss in older persons include digoxin, amiodarone, methotrexate, lithium, and amitriptyline (to name a few).
Often the patient has poor oral intake for weeks—even months—prior to hospitalization. The duration of poor intake or weight loss may affect the patient’s prognosis and treatment. The inability to meet the calories needed by mouth can be a potential marker for a serious disease. Social factors such as isolation, poverty, and lack of transportation may also play a role in poor oral intake and even weight loss. Therefore, the mechanisms of poor nutrition or weight loss have to be identified before PEG tube placement is recommended.
The Clinical Case of Mrs. H
Mrs. H is an 88-year-old, 90-pound white woman admitted to the hospital for the third time this year secondary to aspiration pneumonia. She has a significant past medical history of 20-pound weight loss in the past year and advanced Alzheimer’s disease with severe aphasia. Her functional status is poor. She has been unable to walk or feed herself for at least a year.
Situations like this often arise in the acute care setting. The practitioner may ask how much and what kind of care makes sense for someone like Mrs. H with a limited life expectancy. She has advanced dementia with possible dysphasia and aspiration pneumonia that can explain her poor oral intake. In Mrs. H’s case, other factors can cause her poor oral intake, such as medications, malignancy, delirium, and psychosocial issues.
In this case, the first goal is to identify the cause(s) of poor oral intake and weight loss for future treatment and prognosis. Target your diagnostic investigation at the most probable explanation. “Shotgun” investigations have low yields and should be avoided. In Mrs. H’s case, discontinue medications that can affect her oral intake such as anticholinergic drugs if possible.
If Mrs. H can swallow, the next step is to provide frequent, small meals with liquid oral supplements between meals (60 to 90 minutes before meals). Oral protein and energy supplements have been shown to reduce all-cause mortality in older patients.10 You might consider the use of orexigenic medications, but they usually take significant time to work and their benefit in Mrs. H’s case is questionable. If she is diagnosed as depressed, a trial with mirtazapine may help both her depression and weight loss.
Other effective strategies to promote oral intake in older adults involve eliminating dietary restrictions and allowing unlimited intake of favorite foods. However, in Mrs. H’s case, poor intake may not improve due to the acute medical problems of aspiration pneumonia and the severity of her dementia with dysphagia. Often, a short course of tube feeding through a nasogastric tube can be tried until the patient’s acute illness improves. In Mrs. H’s case though, she has received nasogastric nutrition during her two recent hospitalizations, and her clinical situation has continued to worsen.
Mrs. H’s two daughters want to discuss PEG placement to improve her nutritional status. She had a recent modified barium swallowing study that showed dysphagia with high risk for aspiration of solids and liquids.
Mortality is high in patients with severely abnormal swallowing studies.11 The reasons commonly used to start tube feeding—preventing aspiration pneumonia, to improve quality of life, and to improve functional status—have not been proven in patients with severe dementia.12 In addition, PEG tube feeding does not provide survival benefits in this group of patients, either.13 Therefore, carefully consider tube feeding in older adults with advanced dementia. Some authorities even discourage the widespread use of PEG tubes for patients who suffer from advance dementia.12
For Mrs. H, additional resources that can be used to facilitate her care include geriatric or palliative consult services, chaplaincy, or ethics committee consultations. If the decision is made to place a PEG tube, a time-limited trial with functional and cognitive goals can follow. On the other hand, if the decision of not placing a PEG tube is reached, allowing Mrs. H to eat and drink freely—even if aspiration risk is present—is an alternative. Comfort measures independent of the decision can always be provided. Families who decide against PEG tube placement can be expected to second-guess their decision and will need continued team support.
PEG Indications and Benefits
A PEG tube should be considered for older adults who have a functional gastrointestinal tract but are unable to consume sufficient oral intake to meet their nutritional needs. Frequent indications for PEG placement include impaired swallowing associated with neurological conditions such as cerebrovascular accident and neoplastic diseases or trauma of the oropharynx, larynx, and esophagus. Other but infrequent use of PEG tube is for gastric decompression in selected patients with gastrointestinal tract obstruction.
For some older adults, PEG tube feeding can provide long-term enteral nutrition and hydration with low risk for complications. It can also provide psychological benefits for patients and family members. These benefits include helping them to avoid guilt about deciding to withhold non-oral feedings and by providing hope for future clinical improvement.
PEG tubes appear to be beneficial as a nutritional treatment of choice for patients with acute dysphagic stroke and for some older adults with neoplastic diseases of the oropharynx, larynx, and esophagus. PEG tubes appear inappropriate for patients with a rapidly progressing incurable illness. PEG tube feeding has not been proven to improve quality of life, symptoms of thirst, or survival across the population of older adults at the end of life.
Burdens and Risks of PEG Tube Nutrition
Adverse effects of PEG tubes include wound infections, abdominal pain, aspiration, obstruction of the feeding tube, and agitation. After PEG tube feeding begins, some older adults become agitated and attempt to remove the tube. They may even require chemical and physical restraints for behavioral control.14 A nursing home study found that after PEG tube placement, older adults did not experience functional improvement. PEG-related complications occurred in close to 30% of the patients and the one-year mortality rate was 50% after tube placement.15
About a quarter of patients will have a complication, such as tube occlusion, wound infection, pain, aspiration pneumonitis, and peritonitis, after the PEG tube is placed.16 Aspiration occurs frequently after PEG tube placement and can occur in up to half of older patients with feeding tubes regardless of whether nasogastric or gastric tubes are used.14,17 Some predictors of early mortality after PEG tube placement are age (75 and older), diabetes mellitus, low body mass index, low albumin, COPD, confusion, and advanced cancer.18,19
In a study of Medicare beneficiaries following gastrostomy placement, the in-hospital mortality rate was 15.3%, and the one-year mortality rate was close to 60%.19 In patients after dysphagic stroke, the in-hospital mortality and one-year mortality rates were close to 25% and 50%, respectively after PEG tube placement.20 The mortality rate and the rate of complications, however, will mainly depend on the primary disease. For example, Mrs. H has a poor prognosis independent of PEG tube placement. For some older adults, PEG tubes have shown to have more benefits—especially for those with good functional status, and proximal GI obstruction due to cancer.
Conclusion
Many patients come to the hospital with poor oral intake and weight loss. Clinicians, patients, and families should think carefully about the benefits, risks, and burdens of PEG tube use before initiating placement. The goals should be in concert with patients’ previously expressed wishes and values.
Deciding against PEG tube placement and focusing on comfort and palliative care can always play a role in the care of acutely and chronically ill older adults. PEG tube placement remains an ethically complex, emotionally charged, and difficult area for the managing physician, the patient, and the family. Further research is required in this area to assist these individuals in making the most appropriate decision. TH
Dr. Amador works in the Division of Geriatrics University of Texas Medical Center. His work is supported by the Geriatric Academic Career Award 1 K01 HP 00056-01 by the Bureau of Health Professions.
References
- Weir RF, Gostin L. Decisions to abate life-sustaining treatment for nonautonomous patients. Ethical standards and legal liability for physicians after Cruzan. JAMA. 1990 Oct 10;264(14):1846-1853.
- American Thoracic Society Bioethics Task Force. Withholding and withdrawing life-sustaining therapy. Am Rev Respir Dis. 1991 Sept;144: 726-731.
- Nicholson FB, Korman MG, Richardson MA. Percutaneous endoscopic gastrostomy: a review of indications, complications and outcome. J Gastroenterol Hepatol. 2000 Jan;15(1):21-25.
- Sullivan DH, Patch GA, Walls RC, et al. Impact of nutrition status on morbidity and mortality in a select population of geriatric rehabilitation patients. Am J Clin Nutr. 1990 May;51(5):749–758.
- Ryan C, Bryant E, Eleazer P, et al. Unintentional weight loss in long-term care: predictor of mortality in the elderly. South Med J. 1995 Jul;88(7):721-724.
- Newman AB, Yanez D, Harris T et al. Weight change in old age and its association with mortality. J Am Geriatr Soc. 2001;49:1309-1318.
- Morley JE. Anorexia of aging. Am J Clin Nutr. 1997;66:760-773.
- Bouras EP, Lange SM, Scolapio JS. Rational approach to patients with unintentional weight loss. Mayo Clin Proc. 2001;76:923-929.
- Rabinovitz M, Pitlik SD, Leifer M, et al. Unintentional weight loss: a retrospective analysis of 154 cases. Arch Intern Med. 1986;146(1):186-187.
- Milne AC, Potter J, Avenell A. Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Database Syst Rev. 2005 Apr 18;(2):CD003288.
- Cowen ME, Simpson SL, Vettese TE. Survival estimates for patients with abnormal swallowing studies. J Gen Intern Med. 1997 Feb;12(2):88-94.
- Finucane TE, Christmas C, Travis K. Tube feeding in patients with advanced dementia: a review of the evidence. JAMA. 1999 (Oct);282(14):1365-1370.
- Murphy LM, Lipman TO. Percutaneous endoscopic gastrostomy does not prolong survival in patients with dementia. Arch Intern Med. 2003 Jun 9;163 (11):1351-1353.
- Quill T. Utilization of nasogastric feeding tubes in a group of chronically ill, elderly patients in a community hospital. Arch Intern Med. 1989 Sep;149(9):1937-1941.
- Kaw M, Sekas G. Long-term follow-up of consequences of percutaneous endoscopic gastrostomy (PEG) tubes in nursing home patients. Dig Dis Sci. 1994 Apr;39(4):738-743.
- Erdil A, Saka M, Ates Y, et al. Enteral nutrition via percutaneous endoscopic gastrostomy and nutritional status of patients: Five-year prospective study. J Gastroenterol Hepatol. 2005 Jul;20(7):1002-1007.
- Ciocon JO, Silverstone FA, Graver LM, et al. Tube feedings in elderly patients. Arch Intern Med. 1988 Feb;148(2):429-433.
- Mitchell SL, Tetroe JM. Survival after percutaneous endoscopic gastrostomy placement in older persons. J Gerontol A Biol Sci Med Sci. 2000 Dec;55:M735-M739.
- Grant MD, Rudberg MA, Brody JA. Gastrostomy placement and mortality among hospitalized Medicare beneficiaries. JAMA. 1998 Jun 24;279(24):1973-1976.
- James A, Kapur K, Hawthorne AB. Long-term outcome of percutaneous endoscopic gastrostomy feeding in patients with dysphagic stroke. Age and Ageing. 1998 Nov; 27(6):671-676.
The ability to maintain nutrition and hydration is essential when caring for hospitalized older adults. When physicians recognize that long-term nutrition and hydration cannot be maintained through an oral route, percutaneous endoscopic gastrostomy (PEG) tube placement may need to be considered for long-term nutritional support. This decision is often distressing for the patient, family, and physician for several reasons.
First, the significant number of competing benefits, risks, and burdens of long-term enteral feeding that have to be considered can be overwhelming. The second reason is the lack of clinical data regarding outcomes of PEG tubes for many patients. The last and usually most distressing reason in the decision of PEG tube feeding involves the cultural, ethical, and religious beliefs involved in this decision.
For many families and physicians providing nutrition, including enteral nutrition, using a PEG tube symbolizes compassion, love, and care. This is because eating represents one of the most basic of human needs. For some, not providing nutrition with a PEG tube is morally and ethically wrong. Withholding PEG tube placement can be perceived as assisted suicide or murder. Some physicians also fear legal, ethical, or religious misconduct should they decide against tube feeding.
Physicians need not fear the legal consequences of discontinuing life-sustaining treatment if an appropriate decision-making process has been followed.1 An adult patient who has decision-making capacity and is appropriately informed has the right to forego any forms of medical therapy including life-sustaining therapy such as PEG tube feeding.2
Deciding whether or not to recommend PEG tube feeding can be accomplished in a series of steps. The first step is to evaluate the clinical benefits, risks, and burdens of long-term nutrition for the individual patient. The second step involves discussing the patient’s life goals with them and their family. On many occasions, the decision to place a PEG tube will be made by a surrogate decision-maker such as the patient’s spouse or child. Usually discussions about nutrition and hydration by PEG tube will occur between patients, families, and physicians when the overall end-of-life goals are reviewed. A physician’s role includes assisting patients and their families by providing information and a clear recommendation for or against the use of a feeding tube, giving alternative options, and ensuring there is true informed consent prior to feeding tube insertion.
The most frequent indication for long-term PEG tube feeding is a neurological disorder such as a stroke.3 PEG tube feeding has been developed as a practical alternative to parental feeding for patients with a functioning gastrointestinal (GI) tract who lack the ability to take food by mouth. PEG tube feeding is considered a medical intervention and, like any other intervention, has to be considered according to specific patient situations.
Why Are Older Adults at Risk?
With advancing age comes a linear decline in food intake. Involuntary weight loss is common among older adults, especially in those who are chronically ill. Poor caloric intake and weight loss can lead to multiple problems such as muscle wasting, anemia, and depression. There is a strong correlation between weight loss and morbidity and mortality.4 Even with mild weight loss of 5% of their body weight in one month, institutionalized older adults are four times more likely to die within one year.5 Similarly, community-dwelling older adults who have mild weight loss are at a higher risk of death after adjusting for multiple variables.6
Age-related changes can negatively affect the body’s ability to regulate energy intake and puts older adults at risk for negative energy balance.7 Older adults are more likely to have additional medical problems, use more medications, and experience psychosocial issues that can lead to weight loss and poor nutrition.8 Common causes of weight loss in older hospitalized adults include cancer, gastrointestinal disorder, and depression.9
Mechanical problems, such as dysphagia secondary to cerebrovascular accidents or degenerative brain diseases that affect swallowing are frequently encountered in the hospitalized older patient. Also, diseases that affect appetite and feeding increase the risk for negative energy balance such as GI diseases, endocrine diseases, infections, COPD, and others.
Many drugs have been associated with weight loss, especially in frail older adults. Drugs can cause a decrease in appetite, changes in food tastes and adsorption, and increase the body’s metabolism, making the patients unable to meet their caloric needs. Drugs implicated in malnutrition and weight loss in older persons include digoxin, amiodarone, methotrexate, lithium, and amitriptyline (to name a few).
Often the patient has poor oral intake for weeks—even months—prior to hospitalization. The duration of poor intake or weight loss may affect the patient’s prognosis and treatment. The inability to meet the calories needed by mouth can be a potential marker for a serious disease. Social factors such as isolation, poverty, and lack of transportation may also play a role in poor oral intake and even weight loss. Therefore, the mechanisms of poor nutrition or weight loss have to be identified before PEG tube placement is recommended.
The Clinical Case of Mrs. H
Mrs. H is an 88-year-old, 90-pound white woman admitted to the hospital for the third time this year secondary to aspiration pneumonia. She has a significant past medical history of 20-pound weight loss in the past year and advanced Alzheimer’s disease with severe aphasia. Her functional status is poor. She has been unable to walk or feed herself for at least a year.
Situations like this often arise in the acute care setting. The practitioner may ask how much and what kind of care makes sense for someone like Mrs. H with a limited life expectancy. She has advanced dementia with possible dysphasia and aspiration pneumonia that can explain her poor oral intake. In Mrs. H’s case, other factors can cause her poor oral intake, such as medications, malignancy, delirium, and psychosocial issues.
In this case, the first goal is to identify the cause(s) of poor oral intake and weight loss for future treatment and prognosis. Target your diagnostic investigation at the most probable explanation. “Shotgun” investigations have low yields and should be avoided. In Mrs. H’s case, discontinue medications that can affect her oral intake such as anticholinergic drugs if possible.
If Mrs. H can swallow, the next step is to provide frequent, small meals with liquid oral supplements between meals (60 to 90 minutes before meals). Oral protein and energy supplements have been shown to reduce all-cause mortality in older patients.10 You might consider the use of orexigenic medications, but they usually take significant time to work and their benefit in Mrs. H’s case is questionable. If she is diagnosed as depressed, a trial with mirtazapine may help both her depression and weight loss.
Other effective strategies to promote oral intake in older adults involve eliminating dietary restrictions and allowing unlimited intake of favorite foods. However, in Mrs. H’s case, poor intake may not improve due to the acute medical problems of aspiration pneumonia and the severity of her dementia with dysphagia. Often, a short course of tube feeding through a nasogastric tube can be tried until the patient’s acute illness improves. In Mrs. H’s case though, she has received nasogastric nutrition during her two recent hospitalizations, and her clinical situation has continued to worsen.
Mrs. H’s two daughters want to discuss PEG placement to improve her nutritional status. She had a recent modified barium swallowing study that showed dysphagia with high risk for aspiration of solids and liquids.
Mortality is high in patients with severely abnormal swallowing studies.11 The reasons commonly used to start tube feeding—preventing aspiration pneumonia, to improve quality of life, and to improve functional status—have not been proven in patients with severe dementia.12 In addition, PEG tube feeding does not provide survival benefits in this group of patients, either.13 Therefore, carefully consider tube feeding in older adults with advanced dementia. Some authorities even discourage the widespread use of PEG tubes for patients who suffer from advance dementia.12
For Mrs. H, additional resources that can be used to facilitate her care include geriatric or palliative consult services, chaplaincy, or ethics committee consultations. If the decision is made to place a PEG tube, a time-limited trial with functional and cognitive goals can follow. On the other hand, if the decision of not placing a PEG tube is reached, allowing Mrs. H to eat and drink freely—even if aspiration risk is present—is an alternative. Comfort measures independent of the decision can always be provided. Families who decide against PEG tube placement can be expected to second-guess their decision and will need continued team support.
PEG Indications and Benefits
A PEG tube should be considered for older adults who have a functional gastrointestinal tract but are unable to consume sufficient oral intake to meet their nutritional needs. Frequent indications for PEG placement include impaired swallowing associated with neurological conditions such as cerebrovascular accident and neoplastic diseases or trauma of the oropharynx, larynx, and esophagus. Other but infrequent use of PEG tube is for gastric decompression in selected patients with gastrointestinal tract obstruction.
For some older adults, PEG tube feeding can provide long-term enteral nutrition and hydration with low risk for complications. It can also provide psychological benefits for patients and family members. These benefits include helping them to avoid guilt about deciding to withhold non-oral feedings and by providing hope for future clinical improvement.
PEG tubes appear to be beneficial as a nutritional treatment of choice for patients with acute dysphagic stroke and for some older adults with neoplastic diseases of the oropharynx, larynx, and esophagus. PEG tubes appear inappropriate for patients with a rapidly progressing incurable illness. PEG tube feeding has not been proven to improve quality of life, symptoms of thirst, or survival across the population of older adults at the end of life.
Burdens and Risks of PEG Tube Nutrition
Adverse effects of PEG tubes include wound infections, abdominal pain, aspiration, obstruction of the feeding tube, and agitation. After PEG tube feeding begins, some older adults become agitated and attempt to remove the tube. They may even require chemical and physical restraints for behavioral control.14 A nursing home study found that after PEG tube placement, older adults did not experience functional improvement. PEG-related complications occurred in close to 30% of the patients and the one-year mortality rate was 50% after tube placement.15
About a quarter of patients will have a complication, such as tube occlusion, wound infection, pain, aspiration pneumonitis, and peritonitis, after the PEG tube is placed.16 Aspiration occurs frequently after PEG tube placement and can occur in up to half of older patients with feeding tubes regardless of whether nasogastric or gastric tubes are used.14,17 Some predictors of early mortality after PEG tube placement are age (75 and older), diabetes mellitus, low body mass index, low albumin, COPD, confusion, and advanced cancer.18,19
In a study of Medicare beneficiaries following gastrostomy placement, the in-hospital mortality rate was 15.3%, and the one-year mortality rate was close to 60%.19 In patients after dysphagic stroke, the in-hospital mortality and one-year mortality rates were close to 25% and 50%, respectively after PEG tube placement.20 The mortality rate and the rate of complications, however, will mainly depend on the primary disease. For example, Mrs. H has a poor prognosis independent of PEG tube placement. For some older adults, PEG tubes have shown to have more benefits—especially for those with good functional status, and proximal GI obstruction due to cancer.
Conclusion
Many patients come to the hospital with poor oral intake and weight loss. Clinicians, patients, and families should think carefully about the benefits, risks, and burdens of PEG tube use before initiating placement. The goals should be in concert with patients’ previously expressed wishes and values.
Deciding against PEG tube placement and focusing on comfort and palliative care can always play a role in the care of acutely and chronically ill older adults. PEG tube placement remains an ethically complex, emotionally charged, and difficult area for the managing physician, the patient, and the family. Further research is required in this area to assist these individuals in making the most appropriate decision. TH
Dr. Amador works in the Division of Geriatrics University of Texas Medical Center. His work is supported by the Geriatric Academic Career Award 1 K01 HP 00056-01 by the Bureau of Health Professions.
References
- Weir RF, Gostin L. Decisions to abate life-sustaining treatment for nonautonomous patients. Ethical standards and legal liability for physicians after Cruzan. JAMA. 1990 Oct 10;264(14):1846-1853.
- American Thoracic Society Bioethics Task Force. Withholding and withdrawing life-sustaining therapy. Am Rev Respir Dis. 1991 Sept;144: 726-731.
- Nicholson FB, Korman MG, Richardson MA. Percutaneous endoscopic gastrostomy: a review of indications, complications and outcome. J Gastroenterol Hepatol. 2000 Jan;15(1):21-25.
- Sullivan DH, Patch GA, Walls RC, et al. Impact of nutrition status on morbidity and mortality in a select population of geriatric rehabilitation patients. Am J Clin Nutr. 1990 May;51(5):749–758.
- Ryan C, Bryant E, Eleazer P, et al. Unintentional weight loss in long-term care: predictor of mortality in the elderly. South Med J. 1995 Jul;88(7):721-724.
- Newman AB, Yanez D, Harris T et al. Weight change in old age and its association with mortality. J Am Geriatr Soc. 2001;49:1309-1318.
- Morley JE. Anorexia of aging. Am J Clin Nutr. 1997;66:760-773.
- Bouras EP, Lange SM, Scolapio JS. Rational approach to patients with unintentional weight loss. Mayo Clin Proc. 2001;76:923-929.
- Rabinovitz M, Pitlik SD, Leifer M, et al. Unintentional weight loss: a retrospective analysis of 154 cases. Arch Intern Med. 1986;146(1):186-187.
- Milne AC, Potter J, Avenell A. Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Database Syst Rev. 2005 Apr 18;(2):CD003288.
- Cowen ME, Simpson SL, Vettese TE. Survival estimates for patients with abnormal swallowing studies. J Gen Intern Med. 1997 Feb;12(2):88-94.
- Finucane TE, Christmas C, Travis K. Tube feeding in patients with advanced dementia: a review of the evidence. JAMA. 1999 (Oct);282(14):1365-1370.
- Murphy LM, Lipman TO. Percutaneous endoscopic gastrostomy does not prolong survival in patients with dementia. Arch Intern Med. 2003 Jun 9;163 (11):1351-1353.
- Quill T. Utilization of nasogastric feeding tubes in a group of chronically ill, elderly patients in a community hospital. Arch Intern Med. 1989 Sep;149(9):1937-1941.
- Kaw M, Sekas G. Long-term follow-up of consequences of percutaneous endoscopic gastrostomy (PEG) tubes in nursing home patients. Dig Dis Sci. 1994 Apr;39(4):738-743.
- Erdil A, Saka M, Ates Y, et al. Enteral nutrition via percutaneous endoscopic gastrostomy and nutritional status of patients: Five-year prospective study. J Gastroenterol Hepatol. 2005 Jul;20(7):1002-1007.
- Ciocon JO, Silverstone FA, Graver LM, et al. Tube feedings in elderly patients. Arch Intern Med. 1988 Feb;148(2):429-433.
- Mitchell SL, Tetroe JM. Survival after percutaneous endoscopic gastrostomy placement in older persons. J Gerontol A Biol Sci Med Sci. 2000 Dec;55:M735-M739.
- Grant MD, Rudberg MA, Brody JA. Gastrostomy placement and mortality among hospitalized Medicare beneficiaries. JAMA. 1998 Jun 24;279(24):1973-1976.
- James A, Kapur K, Hawthorne AB. Long-term outcome of percutaneous endoscopic gastrostomy feeding in patients with dysphagic stroke. Age and Ageing. 1998 Nov; 27(6):671-676.
The ability to maintain nutrition and hydration is essential when caring for hospitalized older adults. When physicians recognize that long-term nutrition and hydration cannot be maintained through an oral route, percutaneous endoscopic gastrostomy (PEG) tube placement may need to be considered for long-term nutritional support. This decision is often distressing for the patient, family, and physician for several reasons.
First, the significant number of competing benefits, risks, and burdens of long-term enteral feeding that have to be considered can be overwhelming. The second reason is the lack of clinical data regarding outcomes of PEG tubes for many patients. The last and usually most distressing reason in the decision of PEG tube feeding involves the cultural, ethical, and religious beliefs involved in this decision.
For many families and physicians providing nutrition, including enteral nutrition, using a PEG tube symbolizes compassion, love, and care. This is because eating represents one of the most basic of human needs. For some, not providing nutrition with a PEG tube is morally and ethically wrong. Withholding PEG tube placement can be perceived as assisted suicide or murder. Some physicians also fear legal, ethical, or religious misconduct should they decide against tube feeding.
Physicians need not fear the legal consequences of discontinuing life-sustaining treatment if an appropriate decision-making process has been followed.1 An adult patient who has decision-making capacity and is appropriately informed has the right to forego any forms of medical therapy including life-sustaining therapy such as PEG tube feeding.2
Deciding whether or not to recommend PEG tube feeding can be accomplished in a series of steps. The first step is to evaluate the clinical benefits, risks, and burdens of long-term nutrition for the individual patient. The second step involves discussing the patient’s life goals with them and their family. On many occasions, the decision to place a PEG tube will be made by a surrogate decision-maker such as the patient’s spouse or child. Usually discussions about nutrition and hydration by PEG tube will occur between patients, families, and physicians when the overall end-of-life goals are reviewed. A physician’s role includes assisting patients and their families by providing information and a clear recommendation for or against the use of a feeding tube, giving alternative options, and ensuring there is true informed consent prior to feeding tube insertion.
The most frequent indication for long-term PEG tube feeding is a neurological disorder such as a stroke.3 PEG tube feeding has been developed as a practical alternative to parental feeding for patients with a functioning gastrointestinal (GI) tract who lack the ability to take food by mouth. PEG tube feeding is considered a medical intervention and, like any other intervention, has to be considered according to specific patient situations.
Why Are Older Adults at Risk?
With advancing age comes a linear decline in food intake. Involuntary weight loss is common among older adults, especially in those who are chronically ill. Poor caloric intake and weight loss can lead to multiple problems such as muscle wasting, anemia, and depression. There is a strong correlation between weight loss and morbidity and mortality.4 Even with mild weight loss of 5% of their body weight in one month, institutionalized older adults are four times more likely to die within one year.5 Similarly, community-dwelling older adults who have mild weight loss are at a higher risk of death after adjusting for multiple variables.6
Age-related changes can negatively affect the body’s ability to regulate energy intake and puts older adults at risk for negative energy balance.7 Older adults are more likely to have additional medical problems, use more medications, and experience psychosocial issues that can lead to weight loss and poor nutrition.8 Common causes of weight loss in older hospitalized adults include cancer, gastrointestinal disorder, and depression.9
Mechanical problems, such as dysphagia secondary to cerebrovascular accidents or degenerative brain diseases that affect swallowing are frequently encountered in the hospitalized older patient. Also, diseases that affect appetite and feeding increase the risk for negative energy balance such as GI diseases, endocrine diseases, infections, COPD, and others.
Many drugs have been associated with weight loss, especially in frail older adults. Drugs can cause a decrease in appetite, changes in food tastes and adsorption, and increase the body’s metabolism, making the patients unable to meet their caloric needs. Drugs implicated in malnutrition and weight loss in older persons include digoxin, amiodarone, methotrexate, lithium, and amitriptyline (to name a few).
Often the patient has poor oral intake for weeks—even months—prior to hospitalization. The duration of poor intake or weight loss may affect the patient’s prognosis and treatment. The inability to meet the calories needed by mouth can be a potential marker for a serious disease. Social factors such as isolation, poverty, and lack of transportation may also play a role in poor oral intake and even weight loss. Therefore, the mechanisms of poor nutrition or weight loss have to be identified before PEG tube placement is recommended.
The Clinical Case of Mrs. H
Mrs. H is an 88-year-old, 90-pound white woman admitted to the hospital for the third time this year secondary to aspiration pneumonia. She has a significant past medical history of 20-pound weight loss in the past year and advanced Alzheimer’s disease with severe aphasia. Her functional status is poor. She has been unable to walk or feed herself for at least a year.
Situations like this often arise in the acute care setting. The practitioner may ask how much and what kind of care makes sense for someone like Mrs. H with a limited life expectancy. She has advanced dementia with possible dysphasia and aspiration pneumonia that can explain her poor oral intake. In Mrs. H’s case, other factors can cause her poor oral intake, such as medications, malignancy, delirium, and psychosocial issues.
In this case, the first goal is to identify the cause(s) of poor oral intake and weight loss for future treatment and prognosis. Target your diagnostic investigation at the most probable explanation. “Shotgun” investigations have low yields and should be avoided. In Mrs. H’s case, discontinue medications that can affect her oral intake such as anticholinergic drugs if possible.
If Mrs. H can swallow, the next step is to provide frequent, small meals with liquid oral supplements between meals (60 to 90 minutes before meals). Oral protein and energy supplements have been shown to reduce all-cause mortality in older patients.10 You might consider the use of orexigenic medications, but they usually take significant time to work and their benefit in Mrs. H’s case is questionable. If she is diagnosed as depressed, a trial with mirtazapine may help both her depression and weight loss.
Other effective strategies to promote oral intake in older adults involve eliminating dietary restrictions and allowing unlimited intake of favorite foods. However, in Mrs. H’s case, poor intake may not improve due to the acute medical problems of aspiration pneumonia and the severity of her dementia with dysphagia. Often, a short course of tube feeding through a nasogastric tube can be tried until the patient’s acute illness improves. In Mrs. H’s case though, she has received nasogastric nutrition during her two recent hospitalizations, and her clinical situation has continued to worsen.
Mrs. H’s two daughters want to discuss PEG placement to improve her nutritional status. She had a recent modified barium swallowing study that showed dysphagia with high risk for aspiration of solids and liquids.
Mortality is high in patients with severely abnormal swallowing studies.11 The reasons commonly used to start tube feeding—preventing aspiration pneumonia, to improve quality of life, and to improve functional status—have not been proven in patients with severe dementia.12 In addition, PEG tube feeding does not provide survival benefits in this group of patients, either.13 Therefore, carefully consider tube feeding in older adults with advanced dementia. Some authorities even discourage the widespread use of PEG tubes for patients who suffer from advance dementia.12
For Mrs. H, additional resources that can be used to facilitate her care include geriatric or palliative consult services, chaplaincy, or ethics committee consultations. If the decision is made to place a PEG tube, a time-limited trial with functional and cognitive goals can follow. On the other hand, if the decision of not placing a PEG tube is reached, allowing Mrs. H to eat and drink freely—even if aspiration risk is present—is an alternative. Comfort measures independent of the decision can always be provided. Families who decide against PEG tube placement can be expected to second-guess their decision and will need continued team support.
PEG Indications and Benefits
A PEG tube should be considered for older adults who have a functional gastrointestinal tract but are unable to consume sufficient oral intake to meet their nutritional needs. Frequent indications for PEG placement include impaired swallowing associated with neurological conditions such as cerebrovascular accident and neoplastic diseases or trauma of the oropharynx, larynx, and esophagus. Other but infrequent use of PEG tube is for gastric decompression in selected patients with gastrointestinal tract obstruction.
For some older adults, PEG tube feeding can provide long-term enteral nutrition and hydration with low risk for complications. It can also provide psychological benefits for patients and family members. These benefits include helping them to avoid guilt about deciding to withhold non-oral feedings and by providing hope for future clinical improvement.
PEG tubes appear to be beneficial as a nutritional treatment of choice for patients with acute dysphagic stroke and for some older adults with neoplastic diseases of the oropharynx, larynx, and esophagus. PEG tubes appear inappropriate for patients with a rapidly progressing incurable illness. PEG tube feeding has not been proven to improve quality of life, symptoms of thirst, or survival across the population of older adults at the end of life.
Burdens and Risks of PEG Tube Nutrition
Adverse effects of PEG tubes include wound infections, abdominal pain, aspiration, obstruction of the feeding tube, and agitation. After PEG tube feeding begins, some older adults become agitated and attempt to remove the tube. They may even require chemical and physical restraints for behavioral control.14 A nursing home study found that after PEG tube placement, older adults did not experience functional improvement. PEG-related complications occurred in close to 30% of the patients and the one-year mortality rate was 50% after tube placement.15
About a quarter of patients will have a complication, such as tube occlusion, wound infection, pain, aspiration pneumonitis, and peritonitis, after the PEG tube is placed.16 Aspiration occurs frequently after PEG tube placement and can occur in up to half of older patients with feeding tubes regardless of whether nasogastric or gastric tubes are used.14,17 Some predictors of early mortality after PEG tube placement are age (75 and older), diabetes mellitus, low body mass index, low albumin, COPD, confusion, and advanced cancer.18,19
In a study of Medicare beneficiaries following gastrostomy placement, the in-hospital mortality rate was 15.3%, and the one-year mortality rate was close to 60%.19 In patients after dysphagic stroke, the in-hospital mortality and one-year mortality rates were close to 25% and 50%, respectively after PEG tube placement.20 The mortality rate and the rate of complications, however, will mainly depend on the primary disease. For example, Mrs. H has a poor prognosis independent of PEG tube placement. For some older adults, PEG tubes have shown to have more benefits—especially for those with good functional status, and proximal GI obstruction due to cancer.
Conclusion
Many patients come to the hospital with poor oral intake and weight loss. Clinicians, patients, and families should think carefully about the benefits, risks, and burdens of PEG tube use before initiating placement. The goals should be in concert with patients’ previously expressed wishes and values.
Deciding against PEG tube placement and focusing on comfort and palliative care can always play a role in the care of acutely and chronically ill older adults. PEG tube placement remains an ethically complex, emotionally charged, and difficult area for the managing physician, the patient, and the family. Further research is required in this area to assist these individuals in making the most appropriate decision. TH
Dr. Amador works in the Division of Geriatrics University of Texas Medical Center. His work is supported by the Geriatric Academic Career Award 1 K01 HP 00056-01 by the Bureau of Health Professions.
References
- Weir RF, Gostin L. Decisions to abate life-sustaining treatment for nonautonomous patients. Ethical standards and legal liability for physicians after Cruzan. JAMA. 1990 Oct 10;264(14):1846-1853.
- American Thoracic Society Bioethics Task Force. Withholding and withdrawing life-sustaining therapy. Am Rev Respir Dis. 1991 Sept;144: 726-731.
- Nicholson FB, Korman MG, Richardson MA. Percutaneous endoscopic gastrostomy: a review of indications, complications and outcome. J Gastroenterol Hepatol. 2000 Jan;15(1):21-25.
- Sullivan DH, Patch GA, Walls RC, et al. Impact of nutrition status on morbidity and mortality in a select population of geriatric rehabilitation patients. Am J Clin Nutr. 1990 May;51(5):749–758.
- Ryan C, Bryant E, Eleazer P, et al. Unintentional weight loss in long-term care: predictor of mortality in the elderly. South Med J. 1995 Jul;88(7):721-724.
- Newman AB, Yanez D, Harris T et al. Weight change in old age and its association with mortality. J Am Geriatr Soc. 2001;49:1309-1318.
- Morley JE. Anorexia of aging. Am J Clin Nutr. 1997;66:760-773.
- Bouras EP, Lange SM, Scolapio JS. Rational approach to patients with unintentional weight loss. Mayo Clin Proc. 2001;76:923-929.
- Rabinovitz M, Pitlik SD, Leifer M, et al. Unintentional weight loss: a retrospective analysis of 154 cases. Arch Intern Med. 1986;146(1):186-187.
- Milne AC, Potter J, Avenell A. Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Database Syst Rev. 2005 Apr 18;(2):CD003288.
- Cowen ME, Simpson SL, Vettese TE. Survival estimates for patients with abnormal swallowing studies. J Gen Intern Med. 1997 Feb;12(2):88-94.
- Finucane TE, Christmas C, Travis K. Tube feeding in patients with advanced dementia: a review of the evidence. JAMA. 1999 (Oct);282(14):1365-1370.
- Murphy LM, Lipman TO. Percutaneous endoscopic gastrostomy does not prolong survival in patients with dementia. Arch Intern Med. 2003 Jun 9;163 (11):1351-1353.
- Quill T. Utilization of nasogastric feeding tubes in a group of chronically ill, elderly patients in a community hospital. Arch Intern Med. 1989 Sep;149(9):1937-1941.
- Kaw M, Sekas G. Long-term follow-up of consequences of percutaneous endoscopic gastrostomy (PEG) tubes in nursing home patients. Dig Dis Sci. 1994 Apr;39(4):738-743.
- Erdil A, Saka M, Ates Y, et al. Enteral nutrition via percutaneous endoscopic gastrostomy and nutritional status of patients: Five-year prospective study. J Gastroenterol Hepatol. 2005 Jul;20(7):1002-1007.
- Ciocon JO, Silverstone FA, Graver LM, et al. Tube feedings in elderly patients. Arch Intern Med. 1988 Feb;148(2):429-433.
- Mitchell SL, Tetroe JM. Survival after percutaneous endoscopic gastrostomy placement in older persons. J Gerontol A Biol Sci Med Sci. 2000 Dec;55:M735-M739.
- Grant MD, Rudberg MA, Brody JA. Gastrostomy placement and mortality among hospitalized Medicare beneficiaries. JAMA. 1998 Jun 24;279(24):1973-1976.
- James A, Kapur K, Hawthorne AB. Long-term outcome of percutaneous endoscopic gastrostomy feeding in patients with dysphagic stroke. Age and Ageing. 1998 Nov; 27(6):671-676.
Team Rapid
The origin of the RRT can be found in medical emergency teams (METs). METs began in Australia as a result of the realization that earlier intervention could lead to better outcomes.1 In December 2004, in response to persistent problems with patient safety, the Institute for Healthcare Improvement launched its “100,000 Lives Campaign.”2 The Institute’s key plan for saving some of these 100,000 lives was to create RRTs at every participating medical center. Participating facilities would also submit data on mortality.
Olive View-UCLA Medical Center (OV-UCLA) signed on to participate in the campaign, and part of that effort was the creation and implementation of an RRT. We joined a University Health Consortium “Commit to Action” team, which assisted us by providing support as we began the creation and implementation of the RRT. What follows is the story of how we created an RRT.
We chose team members from all disciplines that were to be part of the RRT response—both at and behind the scenes: RNs, nursing administrators, hospital administrators, ICU attendings, house staff, laboratory personnel, nursing educators, radiology technicians, and hospital operators. The group was further organized into specific teams to solve problems and present solutions. At this point we learned our first important lesson: We needed to meet individually with all inpatient department chairs to discuss the effect of RRTs.
Activation and Notification
How would the RRT call be activated—overhead or beeper? Who could call, and what would the indications be? The OV-UCLA activation and notification team decided that the RRT could be activated by any staff member. Criteria, including vital signs, mental status, or simply “concern about the patient,” were created and posted. A telephone line in the ICU (X4415) was dedicated for RRT calls, and all other activation was overhead due to the lack of an adequate beeper system. (Other than code pagers, our beeper system can’t be simultaneously activated, and ancillaries don’t have beepers.)
The primary nurse’s responsibilities included calling the primary team or cross-covering team and obtaining a fingerstick glucose on all patients while waiting for the team. In discussions the primary team, we learned our second important lesson: As we presented the RRT to the hospital staff, everyone was concerned about the primary team. Ensuring that a mechanism for notifying the primary team was in place and reassuring staff that the primary team would be involved emerged as essential tasks. It was also imperative to identify the chain of command.
With this need in mind, we decided the primary team would always be the captain and would, therefore, have the authority to dismiss whomever they wanted from the RRT. An ICU attending was assigned to RRT call as supervision for the ICU resident responder. At OV-UCLA, our attending is not in-house and, to date, has not been called.
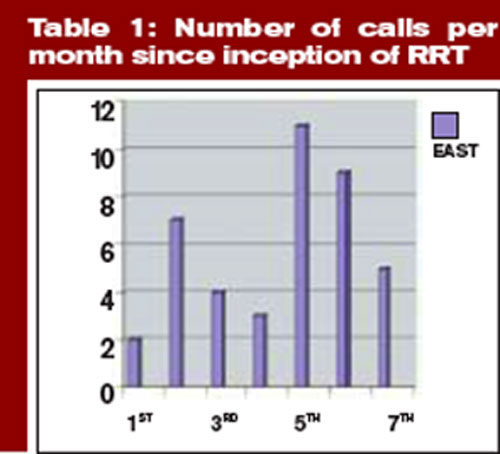
Documentation
The OV-UCLA documentation team was called on to answer the following questions: How would the RRT call be documented? How would medication orders be sent to the pharmacy? How would quality indicators (QI) and data be collected on the calls?
The team’s solution involved creating a one-page, primarily check-based document. The ICU nurse who answered the X4415 telephone in the ICU would begin documentation, which included the time of the call and the chief complaint. When the RRT reached the patient, however, the documentation duties were transferred to the primary RN. All providers were to document on the same page—similar to a code sheet. The RRT nurse and the attending doctor were to check vitals and perform the physical exam, as all information was called out to the documenter.
Medications were to be verbally ordered by the doctor, then read back and verified by the nurses documenting and administering for the RRT. For the most part, medication orders were restricted to what was carried in the RRT bag. The document was eventually copied three times: The original was placed in the chart, one copy was sent to the pharmacy for a record of medication, and the other was saved for QI. The primary team was expected to write a note in the chart’s disposition and time of disposition were to be included in this message.
Equipment
The OV-UCLA equipment team had one important question to answer: What supplies did we need at the bedside?
Although equipment and medications are readily available outside the ICU, the team didn’t want to spend time looking for equipment during an RRT call. “I don’t want a quick RRT call to evolve into a three-hour scavenger hunt,” says one team member.
Because OV-UCLA does not have a 24-hour pharmacist, the group felt it essential to bring medications to the bedside to avoid delays. Our solution to this potential problem was simple. The medication box is prepared by the pharmacy and sealed with one expiration date. Once the box is opened, it is exchanged for a new sealed box. The team chose a rolling duffle to store and transport the supplies, which are compartmentalized into the following sections: infection control, medications, airway and respiratory, IV access and blood draw, and IV start. Medications include respiratory treatments, antibiotics, furosemide, nitroglycerin, metoprolol, heparin and low molecular weight heparin, naloxone, ephedrine, dopamine, glucose, glucagons, and so on. The bag is restocked upon its return to the ICU.
Because of the stress involved in maintaining emergency equipment, we opted to call the supplies a “convenience bag.” This label ensured that only the sealed medication box would require a mandatory check; the rest of the equipment would be monitored on a more informal basis. Because all equipment is available on every floor, and because any RRT call can be converted to a code blue, the team felt that this was reasonable. The committee also purchased a five-pound patient monitor that has a screen for a cardiac tracing, a pulse oximeter, a noninvasive blood pressure monitor, and a temperature probe. This monitor fits easily in a pocket of the duffle.
Education and Publicity
How would staff know to call the RRT? The OV-UCLA team, anticipating that the majority of RRT calls would be activated by the primary RNs, decided that educating all nursing staff was essential.
The hospital nursing education office trained all nurses on all shifts in a short period of time. All nursing staff were taught to use SBAR (situation, background, assessment, and recommendation) communication and to identify early warning signs.1 The importance of recognizing the early warning signs was stressed during the nursing and physician training sessions. Staff were reassured that they didn’t have to know what was wrong with the patient to know that something was wrong and that help was required.
Publicity was accomplished in a variety of ways. The facility purchased pencils in our official color—lime green—that said “Rapid Response Team X4415.” The duffle was wheeled to all nursing stations so that staff could see it. We also ordered custom green-and-white M&M candy (available at www.mms.com) labeled “RRT X4415” to give as a promotional gift when an RRT was called.
Staffing
One last question remained for our team members: Who would respond to the RRT?
The committee felt strongly that an ICU nurse, an ICU resident, and a respiratory therapist should respond. Many physicians on the team did not want a doctor to respond, mostly due to concerns over chain of command. Who would be responsible for decisions made by the RRT? What if an ICU R2 disagreed with a surgery R4? Could they write a “do not call RRT order?” Nursing, on the other hand, wanted physician response; they wanted to be able to stabilize the patient.
Standardized protocols were discussed, but the team felt that the they would unreasonably delay the start. Radiology, which has no code blue response, volunteered to respond to all calls and hand-deliver the film to a computerized viewing system. The lab volunteered to run all RRT labs—designated with a lime green sticker—as quickly as possible.
The medical staff wanted to pilot the RRT, but because we are a small facility (220 beds) and to avoid confusion we launched the RRT for all inpatients. We went live in October 2005. The original plan was to staff an ICU nurse/RRT position. This RRT RN would relieve ICU nurses for breaks to maintain staffing ratios and provide RRT coverage. Because of the omnipresent nursing shortage, however, the RRT position is often pulled and the charge nurse must cover calls. Nurses sign up for RRT overtime and get pulled for patient care duties.
Mock RRT Calls
We performed three RRT drills to determine problem areas. For the first call, we involved a physician who had been vocal about the need for an RRT. The call was for a patient with shortness of breath. Two problems occurred during this drill: The primary team was never called, and there was no overhead page. So a member of our team worked with the hospital operator on our committee and clarified our protocols.
At the second drill, the main problem was documentation. The ICU nurse was so busy documenting that he wasn’t involved with the patient. Because the expertise of the ICU nurse is essential (in fact, there are times when this RN is the most experienced person on the team) we restructured the response so that the primary nurse would document and the ICU nurse was free to provide the hands-on care required.
At the final mock RRT, the major problem was again communication; that is, everyone spoke at once. The team members were encouraged to direct all comments to the team leader and keep any other conversation to a minimum.
A Successful RRT
The following case example, which describes the successful use of our OV-UCLA’s RRT, provides an illuminating look at its effectiveness. In this case, the RRT comprised the ICU nurse, the ICU physician, and the respiratory therapist. The team carried the following equipment: a patient monitor, medications, an IV start, blood sampling tubes, a central line, oxygen masks, and suctioning equipment.
The case began when the primary nurse activated the call. The patient—a 36-year-old HIV-positive male with acute rectal bleeding—was found to have a systolic blood pressure (SBP) reading of 70 and a heart rate of 144. The patient was admitted for anal warts but was noted to have acute bright red blood per rectum. The primary physician team had been called, but had not yet arrived. The primary nurse used the bedside phone to call X4415, and the RRT arrived within three minutes.
Upon arrival, the RRT started a wide bore IV and a central line. The team then called for O-negative blood from the blood bank. The transfusion began seven minutes after the team’s arrival in the patient’s room. The patient was transferred to the ICU and was discharged to the floor the following day.
Results
In four-and-a-half months, we have had 43 calls. The warning signs that precipitated the calls include:
- Respiratory distress: 14 (resulting in eight intubations);
- Cardiac problems: six;
- Altered mental status: four;
- Hypotension: four;
- Post-procedure oversedation: three;
- Vomiting: two;
- Bleeding: two;
- Gastrointestinal: one;
- Mouth bleeding: one;
- Hypoglycemia: one; and
- Unclear etiology: five. TH
Dr. Stein is the medical director, Intensive Care Unit/SDU, at Olive View UCLA Medical Center.
References
- Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. Med J Aust. 2003 Sep 15:179(6):283-287
- The Institute for Healthcare Improvement’s 100,000 Lives Campaign. Available at: www.ihi.org. Last accessed July 10, 2006.
- Leonard MS, Graham S, Taggart B. The human factor: effective teamwork and communication in patient strategy. In: Leonard M, Frankel A, Simmonds T, eds. Achieving safe and reliable health care strategies and solutions. 1st ed. ACHE Management Series; 2004. p.37-65.
- Schein RM, Hazday N, Pena M, et al. Clinical antecedents to in-hospital cardiopulmonary arrests. Chest. 1990;98:1388-1392.
- Franklin C, Matthew J. Developing strategies to prevent-in hospital cardiac arrest: analyzing responses of physicians and nurses in the hours before the event. Crit Care Med. 1994;22(2):244-247.
The origin of the RRT can be found in medical emergency teams (METs). METs began in Australia as a result of the realization that earlier intervention could lead to better outcomes.1 In December 2004, in response to persistent problems with patient safety, the Institute for Healthcare Improvement launched its “100,000 Lives Campaign.”2 The Institute’s key plan for saving some of these 100,000 lives was to create RRTs at every participating medical center. Participating facilities would also submit data on mortality.
Olive View-UCLA Medical Center (OV-UCLA) signed on to participate in the campaign, and part of that effort was the creation and implementation of an RRT. We joined a University Health Consortium “Commit to Action” team, which assisted us by providing support as we began the creation and implementation of the RRT. What follows is the story of how we created an RRT.
We chose team members from all disciplines that were to be part of the RRT response—both at and behind the scenes: RNs, nursing administrators, hospital administrators, ICU attendings, house staff, laboratory personnel, nursing educators, radiology technicians, and hospital operators. The group was further organized into specific teams to solve problems and present solutions. At this point we learned our first important lesson: We needed to meet individually with all inpatient department chairs to discuss the effect of RRTs.
Activation and Notification
How would the RRT call be activated—overhead or beeper? Who could call, and what would the indications be? The OV-UCLA activation and notification team decided that the RRT could be activated by any staff member. Criteria, including vital signs, mental status, or simply “concern about the patient,” were created and posted. A telephone line in the ICU (X4415) was dedicated for RRT calls, and all other activation was overhead due to the lack of an adequate beeper system. (Other than code pagers, our beeper system can’t be simultaneously activated, and ancillaries don’t have beepers.)
The primary nurse’s responsibilities included calling the primary team or cross-covering team and obtaining a fingerstick glucose on all patients while waiting for the team. In discussions the primary team, we learned our second important lesson: As we presented the RRT to the hospital staff, everyone was concerned about the primary team. Ensuring that a mechanism for notifying the primary team was in place and reassuring staff that the primary team would be involved emerged as essential tasks. It was also imperative to identify the chain of command.
With this need in mind, we decided the primary team would always be the captain and would, therefore, have the authority to dismiss whomever they wanted from the RRT. An ICU attending was assigned to RRT call as supervision for the ICU resident responder. At OV-UCLA, our attending is not in-house and, to date, has not been called.
Documentation
The OV-UCLA documentation team was called on to answer the following questions: How would the RRT call be documented? How would medication orders be sent to the pharmacy? How would quality indicators (QI) and data be collected on the calls?
The team’s solution involved creating a one-page, primarily check-based document. The ICU nurse who answered the X4415 telephone in the ICU would begin documentation, which included the time of the call and the chief complaint. When the RRT reached the patient, however, the documentation duties were transferred to the primary RN. All providers were to document on the same page—similar to a code sheet. The RRT nurse and the attending doctor were to check vitals and perform the physical exam, as all information was called out to the documenter.
Medications were to be verbally ordered by the doctor, then read back and verified by the nurses documenting and administering for the RRT. For the most part, medication orders were restricted to what was carried in the RRT bag. The document was eventually copied three times: The original was placed in the chart, one copy was sent to the pharmacy for a record of medication, and the other was saved for QI. The primary team was expected to write a note in the chart’s disposition and time of disposition were to be included in this message.
Equipment
The OV-UCLA equipment team had one important question to answer: What supplies did we need at the bedside?
Although equipment and medications are readily available outside the ICU, the team didn’t want to spend time looking for equipment during an RRT call. “I don’t want a quick RRT call to evolve into a three-hour scavenger hunt,” says one team member.
Because OV-UCLA does not have a 24-hour pharmacist, the group felt it essential to bring medications to the bedside to avoid delays. Our solution to this potential problem was simple. The medication box is prepared by the pharmacy and sealed with one expiration date. Once the box is opened, it is exchanged for a new sealed box. The team chose a rolling duffle to store and transport the supplies, which are compartmentalized into the following sections: infection control, medications, airway and respiratory, IV access and blood draw, and IV start. Medications include respiratory treatments, antibiotics, furosemide, nitroglycerin, metoprolol, heparin and low molecular weight heparin, naloxone, ephedrine, dopamine, glucose, glucagons, and so on. The bag is restocked upon its return to the ICU.
Because of the stress involved in maintaining emergency equipment, we opted to call the supplies a “convenience bag.” This label ensured that only the sealed medication box would require a mandatory check; the rest of the equipment would be monitored on a more informal basis. Because all equipment is available on every floor, and because any RRT call can be converted to a code blue, the team felt that this was reasonable. The committee also purchased a five-pound patient monitor that has a screen for a cardiac tracing, a pulse oximeter, a noninvasive blood pressure monitor, and a temperature probe. This monitor fits easily in a pocket of the duffle.
Education and Publicity
How would staff know to call the RRT? The OV-UCLA team, anticipating that the majority of RRT calls would be activated by the primary RNs, decided that educating all nursing staff was essential.
The hospital nursing education office trained all nurses on all shifts in a short period of time. All nursing staff were taught to use SBAR (situation, background, assessment, and recommendation) communication and to identify early warning signs.1 The importance of recognizing the early warning signs was stressed during the nursing and physician training sessions. Staff were reassured that they didn’t have to know what was wrong with the patient to know that something was wrong and that help was required.
Publicity was accomplished in a variety of ways. The facility purchased pencils in our official color—lime green—that said “Rapid Response Team X4415.” The duffle was wheeled to all nursing stations so that staff could see it. We also ordered custom green-and-white M&M candy (available at www.mms.com) labeled “RRT X4415” to give as a promotional gift when an RRT was called.
Staffing
One last question remained for our team members: Who would respond to the RRT?
The committee felt strongly that an ICU nurse, an ICU resident, and a respiratory therapist should respond. Many physicians on the team did not want a doctor to respond, mostly due to concerns over chain of command. Who would be responsible for decisions made by the RRT? What if an ICU R2 disagreed with a surgery R4? Could they write a “do not call RRT order?” Nursing, on the other hand, wanted physician response; they wanted to be able to stabilize the patient.
Standardized protocols were discussed, but the team felt that the they would unreasonably delay the start. Radiology, which has no code blue response, volunteered to respond to all calls and hand-deliver the film to a computerized viewing system. The lab volunteered to run all RRT labs—designated with a lime green sticker—as quickly as possible.
The medical staff wanted to pilot the RRT, but because we are a small facility (220 beds) and to avoid confusion we launched the RRT for all inpatients. We went live in October 2005. The original plan was to staff an ICU nurse/RRT position. This RRT RN would relieve ICU nurses for breaks to maintain staffing ratios and provide RRT coverage. Because of the omnipresent nursing shortage, however, the RRT position is often pulled and the charge nurse must cover calls. Nurses sign up for RRT overtime and get pulled for patient care duties.
Mock RRT Calls
We performed three RRT drills to determine problem areas. For the first call, we involved a physician who had been vocal about the need for an RRT. The call was for a patient with shortness of breath. Two problems occurred during this drill: The primary team was never called, and there was no overhead page. So a member of our team worked with the hospital operator on our committee and clarified our protocols.
At the second drill, the main problem was documentation. The ICU nurse was so busy documenting that he wasn’t involved with the patient. Because the expertise of the ICU nurse is essential (in fact, there are times when this RN is the most experienced person on the team) we restructured the response so that the primary nurse would document and the ICU nurse was free to provide the hands-on care required.
At the final mock RRT, the major problem was again communication; that is, everyone spoke at once. The team members were encouraged to direct all comments to the team leader and keep any other conversation to a minimum.
A Successful RRT
The following case example, which describes the successful use of our OV-UCLA’s RRT, provides an illuminating look at its effectiveness. In this case, the RRT comprised the ICU nurse, the ICU physician, and the respiratory therapist. The team carried the following equipment: a patient monitor, medications, an IV start, blood sampling tubes, a central line, oxygen masks, and suctioning equipment.
The case began when the primary nurse activated the call. The patient—a 36-year-old HIV-positive male with acute rectal bleeding—was found to have a systolic blood pressure (SBP) reading of 70 and a heart rate of 144. The patient was admitted for anal warts but was noted to have acute bright red blood per rectum. The primary physician team had been called, but had not yet arrived. The primary nurse used the bedside phone to call X4415, and the RRT arrived within three minutes.
Upon arrival, the RRT started a wide bore IV and a central line. The team then called for O-negative blood from the blood bank. The transfusion began seven minutes after the team’s arrival in the patient’s room. The patient was transferred to the ICU and was discharged to the floor the following day.
Results
In four-and-a-half months, we have had 43 calls. The warning signs that precipitated the calls include:
- Respiratory distress: 14 (resulting in eight intubations);
- Cardiac problems: six;
- Altered mental status: four;
- Hypotension: four;
- Post-procedure oversedation: three;
- Vomiting: two;
- Bleeding: two;
- Gastrointestinal: one;
- Mouth bleeding: one;
- Hypoglycemia: one; and
- Unclear etiology: five. TH
Dr. Stein is the medical director, Intensive Care Unit/SDU, at Olive View UCLA Medical Center.
References
- Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. Med J Aust. 2003 Sep 15:179(6):283-287
- The Institute for Healthcare Improvement’s 100,000 Lives Campaign. Available at: www.ihi.org. Last accessed July 10, 2006.
- Leonard MS, Graham S, Taggart B. The human factor: effective teamwork and communication in patient strategy. In: Leonard M, Frankel A, Simmonds T, eds. Achieving safe and reliable health care strategies and solutions. 1st ed. ACHE Management Series; 2004. p.37-65.
- Schein RM, Hazday N, Pena M, et al. Clinical antecedents to in-hospital cardiopulmonary arrests. Chest. 1990;98:1388-1392.
- Franklin C, Matthew J. Developing strategies to prevent-in hospital cardiac arrest: analyzing responses of physicians and nurses in the hours before the event. Crit Care Med. 1994;22(2):244-247.
The origin of the RRT can be found in medical emergency teams (METs). METs began in Australia as a result of the realization that earlier intervention could lead to better outcomes.1 In December 2004, in response to persistent problems with patient safety, the Institute for Healthcare Improvement launched its “100,000 Lives Campaign.”2 The Institute’s key plan for saving some of these 100,000 lives was to create RRTs at every participating medical center. Participating facilities would also submit data on mortality.
Olive View-UCLA Medical Center (OV-UCLA) signed on to participate in the campaign, and part of that effort was the creation and implementation of an RRT. We joined a University Health Consortium “Commit to Action” team, which assisted us by providing support as we began the creation and implementation of the RRT. What follows is the story of how we created an RRT.
We chose team members from all disciplines that were to be part of the RRT response—both at and behind the scenes: RNs, nursing administrators, hospital administrators, ICU attendings, house staff, laboratory personnel, nursing educators, radiology technicians, and hospital operators. The group was further organized into specific teams to solve problems and present solutions. At this point we learned our first important lesson: We needed to meet individually with all inpatient department chairs to discuss the effect of RRTs.
Activation and Notification
How would the RRT call be activated—overhead or beeper? Who could call, and what would the indications be? The OV-UCLA activation and notification team decided that the RRT could be activated by any staff member. Criteria, including vital signs, mental status, or simply “concern about the patient,” were created and posted. A telephone line in the ICU (X4415) was dedicated for RRT calls, and all other activation was overhead due to the lack of an adequate beeper system. (Other than code pagers, our beeper system can’t be simultaneously activated, and ancillaries don’t have beepers.)
The primary nurse’s responsibilities included calling the primary team or cross-covering team and obtaining a fingerstick glucose on all patients while waiting for the team. In discussions the primary team, we learned our second important lesson: As we presented the RRT to the hospital staff, everyone was concerned about the primary team. Ensuring that a mechanism for notifying the primary team was in place and reassuring staff that the primary team would be involved emerged as essential tasks. It was also imperative to identify the chain of command.
With this need in mind, we decided the primary team would always be the captain and would, therefore, have the authority to dismiss whomever they wanted from the RRT. An ICU attending was assigned to RRT call as supervision for the ICU resident responder. At OV-UCLA, our attending is not in-house and, to date, has not been called.
Documentation
The OV-UCLA documentation team was called on to answer the following questions: How would the RRT call be documented? How would medication orders be sent to the pharmacy? How would quality indicators (QI) and data be collected on the calls?
The team’s solution involved creating a one-page, primarily check-based document. The ICU nurse who answered the X4415 telephone in the ICU would begin documentation, which included the time of the call and the chief complaint. When the RRT reached the patient, however, the documentation duties were transferred to the primary RN. All providers were to document on the same page—similar to a code sheet. The RRT nurse and the attending doctor were to check vitals and perform the physical exam, as all information was called out to the documenter.
Medications were to be verbally ordered by the doctor, then read back and verified by the nurses documenting and administering for the RRT. For the most part, medication orders were restricted to what was carried in the RRT bag. The document was eventually copied three times: The original was placed in the chart, one copy was sent to the pharmacy for a record of medication, and the other was saved for QI. The primary team was expected to write a note in the chart’s disposition and time of disposition were to be included in this message.
Equipment
The OV-UCLA equipment team had one important question to answer: What supplies did we need at the bedside?
Although equipment and medications are readily available outside the ICU, the team didn’t want to spend time looking for equipment during an RRT call. “I don’t want a quick RRT call to evolve into a three-hour scavenger hunt,” says one team member.
Because OV-UCLA does not have a 24-hour pharmacist, the group felt it essential to bring medications to the bedside to avoid delays. Our solution to this potential problem was simple. The medication box is prepared by the pharmacy and sealed with one expiration date. Once the box is opened, it is exchanged for a new sealed box. The team chose a rolling duffle to store and transport the supplies, which are compartmentalized into the following sections: infection control, medications, airway and respiratory, IV access and blood draw, and IV start. Medications include respiratory treatments, antibiotics, furosemide, nitroglycerin, metoprolol, heparin and low molecular weight heparin, naloxone, ephedrine, dopamine, glucose, glucagons, and so on. The bag is restocked upon its return to the ICU.
Because of the stress involved in maintaining emergency equipment, we opted to call the supplies a “convenience bag.” This label ensured that only the sealed medication box would require a mandatory check; the rest of the equipment would be monitored on a more informal basis. Because all equipment is available on every floor, and because any RRT call can be converted to a code blue, the team felt that this was reasonable. The committee also purchased a five-pound patient monitor that has a screen for a cardiac tracing, a pulse oximeter, a noninvasive blood pressure monitor, and a temperature probe. This monitor fits easily in a pocket of the duffle.
Education and Publicity
How would staff know to call the RRT? The OV-UCLA team, anticipating that the majority of RRT calls would be activated by the primary RNs, decided that educating all nursing staff was essential.
The hospital nursing education office trained all nurses on all shifts in a short period of time. All nursing staff were taught to use SBAR (situation, background, assessment, and recommendation) communication and to identify early warning signs.1 The importance of recognizing the early warning signs was stressed during the nursing and physician training sessions. Staff were reassured that they didn’t have to know what was wrong with the patient to know that something was wrong and that help was required.
Publicity was accomplished in a variety of ways. The facility purchased pencils in our official color—lime green—that said “Rapid Response Team X4415.” The duffle was wheeled to all nursing stations so that staff could see it. We also ordered custom green-and-white M&M candy (available at www.mms.com) labeled “RRT X4415” to give as a promotional gift when an RRT was called.
Staffing
One last question remained for our team members: Who would respond to the RRT?
The committee felt strongly that an ICU nurse, an ICU resident, and a respiratory therapist should respond. Many physicians on the team did not want a doctor to respond, mostly due to concerns over chain of command. Who would be responsible for decisions made by the RRT? What if an ICU R2 disagreed with a surgery R4? Could they write a “do not call RRT order?” Nursing, on the other hand, wanted physician response; they wanted to be able to stabilize the patient.
Standardized protocols were discussed, but the team felt that the they would unreasonably delay the start. Radiology, which has no code blue response, volunteered to respond to all calls and hand-deliver the film to a computerized viewing system. The lab volunteered to run all RRT labs—designated with a lime green sticker—as quickly as possible.
The medical staff wanted to pilot the RRT, but because we are a small facility (220 beds) and to avoid confusion we launched the RRT for all inpatients. We went live in October 2005. The original plan was to staff an ICU nurse/RRT position. This RRT RN would relieve ICU nurses for breaks to maintain staffing ratios and provide RRT coverage. Because of the omnipresent nursing shortage, however, the RRT position is often pulled and the charge nurse must cover calls. Nurses sign up for RRT overtime and get pulled for patient care duties.
Mock RRT Calls
We performed three RRT drills to determine problem areas. For the first call, we involved a physician who had been vocal about the need for an RRT. The call was for a patient with shortness of breath. Two problems occurred during this drill: The primary team was never called, and there was no overhead page. So a member of our team worked with the hospital operator on our committee and clarified our protocols.
At the second drill, the main problem was documentation. The ICU nurse was so busy documenting that he wasn’t involved with the patient. Because the expertise of the ICU nurse is essential (in fact, there are times when this RN is the most experienced person on the team) we restructured the response so that the primary nurse would document and the ICU nurse was free to provide the hands-on care required.
At the final mock RRT, the major problem was again communication; that is, everyone spoke at once. The team members were encouraged to direct all comments to the team leader and keep any other conversation to a minimum.
A Successful RRT
The following case example, which describes the successful use of our OV-UCLA’s RRT, provides an illuminating look at its effectiveness. In this case, the RRT comprised the ICU nurse, the ICU physician, and the respiratory therapist. The team carried the following equipment: a patient monitor, medications, an IV start, blood sampling tubes, a central line, oxygen masks, and suctioning equipment.
The case began when the primary nurse activated the call. The patient—a 36-year-old HIV-positive male with acute rectal bleeding—was found to have a systolic blood pressure (SBP) reading of 70 and a heart rate of 144. The patient was admitted for anal warts but was noted to have acute bright red blood per rectum. The primary physician team had been called, but had not yet arrived. The primary nurse used the bedside phone to call X4415, and the RRT arrived within three minutes.
Upon arrival, the RRT started a wide bore IV and a central line. The team then called for O-negative blood from the blood bank. The transfusion began seven minutes after the team’s arrival in the patient’s room. The patient was transferred to the ICU and was discharged to the floor the following day.
Results
In four-and-a-half months, we have had 43 calls. The warning signs that precipitated the calls include:
- Respiratory distress: 14 (resulting in eight intubations);
- Cardiac problems: six;
- Altered mental status: four;
- Hypotension: four;
- Post-procedure oversedation: three;
- Vomiting: two;
- Bleeding: two;
- Gastrointestinal: one;
- Mouth bleeding: one;
- Hypoglycemia: one; and
- Unclear etiology: five. TH
Dr. Stein is the medical director, Intensive Care Unit/SDU, at Olive View UCLA Medical Center.
References
- Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. Med J Aust. 2003 Sep 15:179(6):283-287
- The Institute for Healthcare Improvement’s 100,000 Lives Campaign. Available at: www.ihi.org. Last accessed July 10, 2006.
- Leonard MS, Graham S, Taggart B. The human factor: effective teamwork and communication in patient strategy. In: Leonard M, Frankel A, Simmonds T, eds. Achieving safe and reliable health care strategies and solutions. 1st ed. ACHE Management Series; 2004. p.37-65.
- Schein RM, Hazday N, Pena M, et al. Clinical antecedents to in-hospital cardiopulmonary arrests. Chest. 1990;98:1388-1392.
- Franklin C, Matthew J. Developing strategies to prevent-in hospital cardiac arrest: analyzing responses of physicians and nurses in the hours before the event. Crit Care Med. 1994;22(2):244-247.
Doctors of the American Frontier

Discussions of the mid-19th century American physician often conjure up images of the surgeons of the Civil War who tirelessly plied their trade during battle: “During the rest of the night and early morning, he [amputated] arms below the elbow and legs below the knee in less than five minutes. The deep incision … the sweeping cut … pull back the soft parts to expose the bone … saw swiftly.”1
However, in the same period but some thousand miles west, frontier physicians faced similar battle wounds sustained in campaigns against American Indians, as well as a myriad of other duties. Some frontier physicians met these challenges with remarkable ingenuity, while others resorted to treatments later deemed quackery. They often practiced alone in the wilderness without a hospital or colleagues for support.
The first and most obvious task of a military physician on the frontier was to attend to soldiers wounded during battle. The first hurdle was reaching the soldier. In 1874, Surgeon George Miller Sternberg faced daunting challenges in aiding seriously wounded soldiers of General Oliver Otis Howard’s company after a melee with Chief Joseph’s Nez Percé tribe. As dark settled across Clearwater River, Idaho, “Surgeon George Miller Sternberg and an aide crawled out onto the battlefield looking for the wounded. They crept so close to the enemy that they could hear the Indians talking.”1 Dr. Sternberg worked tirelessly throughout the night ligating pulsing arteries and soothing the suffering soldiers with whatever means he had, from opium balls to whiskey. During the course of the evening, an American Indian sentinel spotted Dr. Sternberg’s lantern and shot it out, forcing Dr. Sternberg to continue his treatment in darkness.
In other conflicts, the frontier physician often found himself an active participant in a battle. In the Battle of the Lava Beds fought in Oregon in 1873, Dr. George Martin Kober received a gunshot wound in the arm during the course of the battle. Despite his wound he continued to “treat the wounded before he allowed Dr. Skinner to come to his relief.”1
In the Battle of Bates Creek, fought in the summer of 1874, Dr. Thomas Maghee “was the object of the direct fire of an Indian. Until, laying down his instruments for a moment, he took his carbine and killed the Indian and then returned quietly to his work.”1
When the battle concluded and the soldiers returned to camp, the physicians began to wage a fierce war with disease. Among the plagues that stalked the camps: cholera, scurvy, yellow fever, tuberculosis, and typhoid fever. On one occasion in 1874 cholera struck in the heat of the summer at Fort Riley in Kansas. The pestilence devastated the fort by swiftly taking the lives of dozens of soldiers and compelling a hundred more to desert the fort in fear. One ignorant physician attempted in vain to combat the disease by “burning barrels of pine tar beneath the open windows of the fort hospital.”1
Eventually, Dr. Sternberg conquered the outbreak by implementing a strict disinfection and isolation campaign. In the battle against scurvy, military physicians noted that the typical diet of “meat, white bread, soda biscuits, syrup, lard, and black coffee” was insufficient and often attempted to plant and harvest their own supply of vegetables to treat the vitamin C-deficient soldiers.1
The frontier physician’s duties often expanded outside of the realms of medicine because “by order of the Secretary of War they also studied weather, geography, plants, fauna, Indian customs, and antiquities.”1 In fulfilling these duties, physicians made remarkable contributions to the preservation of the history of the American West, such as Dr. James Kimball’s purchase of the autobiography of Sitting Bull. Indeed, life as a military physician on the American frontier tested the courage, durability, and ingenuity of the early American doctor. TH
John Bois is a second-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Reference
- Dunlop R. Doctors of the American Frontier. Garden City, New York: Doubleday & Company; 1965: 73.
Discussions of the mid-19th century American physician often conjure up images of the surgeons of the Civil War who tirelessly plied their trade during battle: “During the rest of the night and early morning, he [amputated] arms below the elbow and legs below the knee in less than five minutes. The deep incision … the sweeping cut … pull back the soft parts to expose the bone … saw swiftly.”1
However, in the same period but some thousand miles west, frontier physicians faced similar battle wounds sustained in campaigns against American Indians, as well as a myriad of other duties. Some frontier physicians met these challenges with remarkable ingenuity, while others resorted to treatments later deemed quackery. They often practiced alone in the wilderness without a hospital or colleagues for support.
The first and most obvious task of a military physician on the frontier was to attend to soldiers wounded during battle. The first hurdle was reaching the soldier. In 1874, Surgeon George Miller Sternberg faced daunting challenges in aiding seriously wounded soldiers of General Oliver Otis Howard’s company after a melee with Chief Joseph’s Nez Percé tribe. As dark settled across Clearwater River, Idaho, “Surgeon George Miller Sternberg and an aide crawled out onto the battlefield looking for the wounded. They crept so close to the enemy that they could hear the Indians talking.”1 Dr. Sternberg worked tirelessly throughout the night ligating pulsing arteries and soothing the suffering soldiers with whatever means he had, from opium balls to whiskey. During the course of the evening, an American Indian sentinel spotted Dr. Sternberg’s lantern and shot it out, forcing Dr. Sternberg to continue his treatment in darkness.
In other conflicts, the frontier physician often found himself an active participant in a battle. In the Battle of the Lava Beds fought in Oregon in 1873, Dr. George Martin Kober received a gunshot wound in the arm during the course of the battle. Despite his wound he continued to “treat the wounded before he allowed Dr. Skinner to come to his relief.”1
In the Battle of Bates Creek, fought in the summer of 1874, Dr. Thomas Maghee “was the object of the direct fire of an Indian. Until, laying down his instruments for a moment, he took his carbine and killed the Indian and then returned quietly to his work.”1
When the battle concluded and the soldiers returned to camp, the physicians began to wage a fierce war with disease. Among the plagues that stalked the camps: cholera, scurvy, yellow fever, tuberculosis, and typhoid fever. On one occasion in 1874 cholera struck in the heat of the summer at Fort Riley in Kansas. The pestilence devastated the fort by swiftly taking the lives of dozens of soldiers and compelling a hundred more to desert the fort in fear. One ignorant physician attempted in vain to combat the disease by “burning barrels of pine tar beneath the open windows of the fort hospital.”1
Eventually, Dr. Sternberg conquered the outbreak by implementing a strict disinfection and isolation campaign. In the battle against scurvy, military physicians noted that the typical diet of “meat, white bread, soda biscuits, syrup, lard, and black coffee” was insufficient and often attempted to plant and harvest their own supply of vegetables to treat the vitamin C-deficient soldiers.1
The frontier physician’s duties often expanded outside of the realms of medicine because “by order of the Secretary of War they also studied weather, geography, plants, fauna, Indian customs, and antiquities.”1 In fulfilling these duties, physicians made remarkable contributions to the preservation of the history of the American West, such as Dr. James Kimball’s purchase of the autobiography of Sitting Bull. Indeed, life as a military physician on the American frontier tested the courage, durability, and ingenuity of the early American doctor. TH
John Bois is a second-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Reference
- Dunlop R. Doctors of the American Frontier. Garden City, New York: Doubleday & Company; 1965: 73.
Discussions of the mid-19th century American physician often conjure up images of the surgeons of the Civil War who tirelessly plied their trade during battle: “During the rest of the night and early morning, he [amputated] arms below the elbow and legs below the knee in less than five minutes. The deep incision … the sweeping cut … pull back the soft parts to expose the bone … saw swiftly.”1
However, in the same period but some thousand miles west, frontier physicians faced similar battle wounds sustained in campaigns against American Indians, as well as a myriad of other duties. Some frontier physicians met these challenges with remarkable ingenuity, while others resorted to treatments later deemed quackery. They often practiced alone in the wilderness without a hospital or colleagues for support.
The first and most obvious task of a military physician on the frontier was to attend to soldiers wounded during battle. The first hurdle was reaching the soldier. In 1874, Surgeon George Miller Sternberg faced daunting challenges in aiding seriously wounded soldiers of General Oliver Otis Howard’s company after a melee with Chief Joseph’s Nez Percé tribe. As dark settled across Clearwater River, Idaho, “Surgeon George Miller Sternberg and an aide crawled out onto the battlefield looking for the wounded. They crept so close to the enemy that they could hear the Indians talking.”1 Dr. Sternberg worked tirelessly throughout the night ligating pulsing arteries and soothing the suffering soldiers with whatever means he had, from opium balls to whiskey. During the course of the evening, an American Indian sentinel spotted Dr. Sternberg’s lantern and shot it out, forcing Dr. Sternberg to continue his treatment in darkness.
In other conflicts, the frontier physician often found himself an active participant in a battle. In the Battle of the Lava Beds fought in Oregon in 1873, Dr. George Martin Kober received a gunshot wound in the arm during the course of the battle. Despite his wound he continued to “treat the wounded before he allowed Dr. Skinner to come to his relief.”1
In the Battle of Bates Creek, fought in the summer of 1874, Dr. Thomas Maghee “was the object of the direct fire of an Indian. Until, laying down his instruments for a moment, he took his carbine and killed the Indian and then returned quietly to his work.”1
When the battle concluded and the soldiers returned to camp, the physicians began to wage a fierce war with disease. Among the plagues that stalked the camps: cholera, scurvy, yellow fever, tuberculosis, and typhoid fever. On one occasion in 1874 cholera struck in the heat of the summer at Fort Riley in Kansas. The pestilence devastated the fort by swiftly taking the lives of dozens of soldiers and compelling a hundred more to desert the fort in fear. One ignorant physician attempted in vain to combat the disease by “burning barrels of pine tar beneath the open windows of the fort hospital.”1
Eventually, Dr. Sternberg conquered the outbreak by implementing a strict disinfection and isolation campaign. In the battle against scurvy, military physicians noted that the typical diet of “meat, white bread, soda biscuits, syrup, lard, and black coffee” was insufficient and often attempted to plant and harvest their own supply of vegetables to treat the vitamin C-deficient soldiers.1
The frontier physician’s duties often expanded outside of the realms of medicine because “by order of the Secretary of War they also studied weather, geography, plants, fauna, Indian customs, and antiquities.”1 In fulfilling these duties, physicians made remarkable contributions to the preservation of the history of the American West, such as Dr. James Kimball’s purchase of the autobiography of Sitting Bull. Indeed, life as a military physician on the American frontier tested the courage, durability, and ingenuity of the early American doctor. TH
John Bois is a second-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Reference
- Dunlop R. Doctors of the American Frontier. Garden City, New York: Doubleday & Company; 1965: 73.
The Yuk Factor
Despite modern wound treatment and broad-spectrum antibiotic treatment, patients with chronic wounds still exist. The appearance of antibiotic resistant bacteria, such as methicillin-resistant Staphylococcus aureus (MRSA) in the 1980s and ’90s, gave rise to a search for other remedies. One of the remedies that has been rediscovered and subsequently successfully reintroduced is maggot debridement therapy (MDT).1 The fact that more than 100 articles were published on the subject in the past two decades indicates that the use of maggots is making a strong comeback in medicine.2 In January 2004, the U.S. Food and Drug Administration (FDA) issued 510(k)#33391, allowing production and marketing of maggots as a medical device. In this article, we discuss the use of MDT in patients with a chronic wound.
A Long History of Maggot Therapy
MDT has been used in many cultures and has been known for centuries.3 Ambroise Parè is credited as the father of modern MDT. Unfortunately, no evidence can be found of Parè using maggots as a means to clean or heal wounds. The only reference is the often-cited case that occurred in 1557 at the battle of St. Quentin, when Parè observed soldiers whose wounds were covered by maggots. He mainly described the negative effects of the maggots, and, above all, believed they were spontaneously produced by the wound itself, not by the eggs of fly.4
Baron Larey (1766-1842) a famous surgeon in the army of Napoleon Bonaparte, wrote about soldiers who had larvae-infested wounds, but was frustrated that it was difficult to persuade his patients to leave the maggots in place, believing that “they promoted healing without leaving any damage.”5
The first surgeon to use MDT in patients in the hospital was the orthopedic surgeon William Baer. In the 1920s he was faced with a group of untreatable patients with severe osteomyelitis (antibiotics had not yet been discovered). He successfully treated many patients with maggots, and because of his success the therapy became regularly used in the United States.6
By 1934 more than 1,000 surgeons were using maggot therapy. Surgical Maggots were available commercially from Lederle Corporation.7 But with the introduction of antibiotics in the 1940s, the use of maggots dropped off. In the following years, case reports were published only occasionally.

The Negative Image of Maggots
A large problem of MDT is the difficulty of this type of therapy to gain acceptance in the medical community. Maggots are associated with rotting and decay. The image is of filthy, low-life creatures that are ugly and disgusting. Although a nice recent example for the general public is the scene in the movie Gladiator. The main character (played by Russell Crow) is advised to leave the maggots that spontaneously infested a wound on his shoulder in place so that the wound would heal. He leaves them in place and the wound heals without any problem, enabling Crow’s character to fight many battles.
In contrast, in an oral presentation we held recently at a Dutch scientific surgical meeting, a surgical professor in the audience said, “I will never allow those creatures in my ward.”8 This remark shows that widespread use and acceptance of MDT has not yet been reached. It seems there is still much work to do before MDT is generally accepted as a therapeutic method.
Fortunately, the negative image that seems to exist among nurses and physicians does not seem to bother patients.9 We have treated more than 100 patients in our clinic with MDT. All patients to whom we proposed MDT agreed to the therapy. All were allowed to discontinue the therapy whenever they wanted; none did. In a survey of the first 38 MDT-treated patients, 89% agreed to another session of MDT if the surgeon believed it would be beneficial, and 94% of the patients said that they would recommend it to others. This is despite the fact that the therapy was not successful in all patients (there was a below-knee of above the knee amputation-rate of 19% among patients who underwent MDT).10

Indications and Evidence
Indications and contra-indications for maggot therapy are not well defined. Some state that all kind of wounds that contain necrosis or slough can be good candidates for MDT. In our own study of 101 patients with 116 wounds treated with maggots, we had an overall success rate of 67%. (Seventy-eight out of 116 wounds had a beneficial outcome.) However, in 13 patients with septic arthritis, all wounds failed. Success rates where significantly reduced in cases of chronic limb ischemia, visible tendon or bone, and in cases of duration longer than three months before the start of MDT.11
Most physicians who start MDT use it mainly for worst-case scenarios. From our previous studies, it is clear that success rates in those patients are low. After witnessing a few failures, the physician is naturally reluctant to use it again.
What about evidence? Large randomized studies are lacking, although one containing 600 venous ulcer patients was initiated in 2004.12 There have been three randomized studies performed. Wayman, et al., have shown the cost-effectiveness of larval therapy in venous ulcers compared with hydrogel dressing.13 Contreras, et al., could not find a difference between MDT and curettage and topical silver sulfadiazine in patients with venous leg ulcers.14 At the 36th annual meeting of the European Association for the Study of Diabetes, Markevich, et al., reported on a randomized, multicenter, double-blind controlled clinical trial (n=140) for neuropathic diabetic foot lesions compared to conventional treatment. They found a significant higher percentage of granulation tissue after 10 days, compared with the hydrogel group.15 Results from large case-series indicate that MDT works and could even save limbs.2,16-18 The mechanism of action has not been unraveled yet.

Factors Influencing Effectiveness of MDT
Unfortunately, the statement made by Thomas, who said that maggot therapy works by “secreting proteolytic enzymes that break down dead tissue, turning it into a soup, which they then ingest,” still holds.19 It is known that there are mechanical effects, tissue growth effects, that direct killing of bacteria in the alimentary tract of the maggot takes place, and that maggots produce antibacterial factors.2,17,20-31
Although maggots are suitable agents for chronic wound treatment, it is likely that some wounds are more eligible than others for this type of treatment. In our opinion, all wounds that contain gangrenous or necrotic tissue with infection seem to be suited for MDT.32 Success rates of MDT reported in literature vary, but seem to be around 80% to 90%.16,17,33 In our own series, success rate is about 70%.
Patient-selection (case-mix) and method of outcome measurement play essential roles in these percentages. In our opinion, all wounds that contain necrotic tissue can be debrided effectively with MDT. However, if for example wound ischemia is the major etiologic factor, this should also be addressed. In our experience, diabetic foot, venous ulcers, traumatic ulcers, and infections after surgical procedures are all good candidates for MDT.
Absolute contraindications in our opinion are wounds close to large, uncovered blood vessels and wounds that need immediate surgical debridement (e.g., in the case of a septic patient). A relative contraindication is patients with natural of medically induced coagulopathies, but also patient preference could play a role.34 We have had very bad results with infected small joints of the foot; all wounds (n=13) eventually needed a small or large amputation.
Even the technique of application has an effect on outcome. There are two different application techniques: the free-range and the contained technique. The free-range technique is more effective in vitro and in-vivo and has become our standard application technique—not only in the outpatient department, but also in the intra-mural setting.35,36 (Figure 1, p. 16, shows a patient with a necrotic wound on the leg after radiation therapy and a surgical excision for a malignant tumor was performed.) Earlier surgical debridement combined with split skin graft failed. After four applications of maggots, the wound was free of necrosis and could be subsequently closed. (See Figure 2, p. 16.)
The contained technique is used in patients with bleeding tendencies and wounds that do not have enough healthy skin surrounding the wound; in other words, where the covering “cage” needed in case of the free-range technique can’t be applied. (This problem is shown in Figure 3, p. 16: A patient with necrotizing fasciitis of the left upper leg was treated with the contained technique—BiologiQ, Apeldoorn, Netherlands—as there is no proximal skin border. Of course, patient preference plays a role as well in the choice of application technique.37
Wound Clinic
In the Netherlands maggots can be ordered easily and are delivered within 24 hours. We started a wound clinic in 2002. First it was for MDT alone, but now the scope is broader, and we treat chronic wounds with different kind of wound therapies. We have two nurses, one nurse practitioner, one resident-surgeon, and one vascular surgeon who apply the maggots.
Patients do not need to be admitted for MDT. Fifty-nine percent of our patients are treated in the outpatient department. We are able to treat as many as 10 or 15 patients in one session, but MDT-treated patients make up only two or three patients at a time.
We found that after fast, successful biological debridement with MDT we were left with a lot of patients with red, granulating wounds that needed our attention in order to prevent relapses. In our opinion, there are many different treatment methods after MDT. Plaster casting in case of diabetic feet, secondary closure, and split skin grafting are different methods. However, other therapies like VAC-therapy and recently OASIS are promising.
At this time, all patients are prospectively followed after MDT. We are especially interested in patient selection and are now also aiming to find the ideal wound therapy after MDT. TH
Dr. Steenvoorde is a resident surgeon at Rijnland Hospital Leiderdorp, the Netherlands. van Doorn is a nurse-practitioner at Rijnland Hospital Leiderdorp. Jacobi is a senior researcher in the Medical Decision Department at Leiden University Medical Center, in the Netherlands. Dr. Oskam is a vascular surgeon at Rijnland Hospital Leiderdorp.
References
- Beasley WD, Hirst G. Making a meal of MRSA-the role of biosurgery inhospital-acquired infection. J Hosp Infect. 2004;56(1):6-9.
- Jukema GN, Menon AG, Bernards AT. et al. Amputation-sparing treatment by nature: “surgical” maggots revisited. Clin Infect Dis. 2002 Dec 15;35(12):1566-1571.
- Church JC. The traditional use of maggots in wound healing, and the development of larva therapy (biosurgery) in modern medicine. J Altern Complement Med. 1996 Winter;2(4):525-527.
- Coppi C. I dressed your wounds, God healed you—a wounded person’s psychology according to Ambroise Parè. Ostomy Wound Manage. 2005;51:62-64.
- Goldstein HI. Maggots in the treatment of wound and bone infections. J Bone Joint Surg. 1931;13:476-478.
- Baer WS. The treatment of chronic osteomyelitis with the maggot (larva of the blow fly). J Bone Joint Surg. 1931;13:438-475.
- Puckner WA. New and nonofficial remedies, surgical maggots-Lederle. J Am Med Assoc. 1932;98(5):401.
- Steenvoorde P, Doorn Lv, Jacobi CE, et al. Maggot therapy: retrospective study comparing two different application-techniques. (Dutch). Nederlands Tijdschrift voor Heelkunde. 2006;15:86.
- Contreras RJ, Fuentes SA, Karam-Orantes M, et al. Larval debridement therapy in Mexico. Wound Care Canada. 2005;3:42-46.
- Steenvoorde P, Budding TJ, Engeland Av, et al. Maggot therapy and the “yuk factor”: an issue for the patient? Wound Repair Regen. 2005 May-Jun;13(3):350-352.
- Steenvoorde P, Jacobi CA, Doorn Lv, et al. Maggot debridement therapy of infected ulcers: patient and wound factors influencing outcome. Ann Royal Coll Surg Eng. 2006.
- Raynor P, Dumville J, Cullum N. A new clinical trial of the effect of larval therapy. J Tissue Viability. 2004 Jul;14(3):104-105.
- Wayman J, Nirojogi V, Walker A, et al. The cost effectiveness of larval therapy in venous ulcers. J Tissue Viability. 2001 Jan;11(1):51.
- Contreras RJ, Fuentes SA, Arroyo ES, et al. Larval debridement therapy and infection control in venous ulcers: a comparative study. Presented at: the Second World Union of Wound Healing Societies Meeting; July 8-13, 2004.
- Markevich YO, McLeod-Roberts J, Mousley M, et al. Maggot therapy for diabetic neuropathic foot wounds: a randomized study. Presented at: the 36th Annual Meeting of the EASD; September 17-21, 2000. Ref Type: Conference Proceeding.
- Wolff H, Hansson C. Larval therapy—an effective method for ulcer debridement. Clin Exp Dermatol. 2003;28:137.
- Mumcuoglu KY, Ingber A, Gilead L, et al. Maggot therapy for the treatment of intractable wounds. Int J Dermatol. 1999 Aug;38(8):623-627.
- Courtenay M. The use of larval therapy in wound management in the UK. J Wound Care. 1999 Apr;8 (4):177-179.
- Bonn D. Maggot therapy: an alternative for wound infection. Lancet. 2000 Sep 30;356 (9236):1174.
- Robinson W. Stimulation of healing in non-healing wounds. J Bone Joint Surgery. 1935;17:267-271.
- Robinson W. Ammonium bicarbonate secreted by surgical maggots stimulates healing in purulent wounds. Am J Surg. 1940;47:111-115.
- Mumcuoglu KY, Ingber A, Gilead L, et al. Maggot therapy for the treatment of diabetic foot ulcers. Diabetes Care. 1998 Nov;21(11):2030-2031.
- Simmons S. A bactericidal principle in excretions of surgical maggots which destroys important etiological agents of pyogenic infections. J Bacteriol. 1935;30:253-267.
- Simmons S. The bactericidal properties of excretions of the maggot of Lucilia sericata. Bull Entomol Res. 1935;26:559-563.
- Mumcuoglu KY. Clinical applications for maggots in wound care. Am J Clin Dermatol. 2001;2:219-227.
- Armstrong DG, Short B, Martin BR, et al. Maggot therapy in lower extremity hospice wound care. J Am Podiatr Med Assoc. 2005;95(3):254-257.
- Robinson W, Norwood VH. The role of surgical maggots in the disinfection of osteomyelitis and other infected wounds. J Bone Joint Surgery. 1933;15:409-412.
- Robinson W, Norwood VH. Destruction of pyogenic bacteria in the alimentary tract of surgical maggots implanted in infected wounds. J Lab Clin Med. 1933;19:581-585.
- Mumcuoglu KY, Miller J, Mumcuoglu M. et al. Destruction of bacteria in the digestive tract of the maggot of Lucilia sericata (Diptera: Calliphoridae). J Med Entomol. 2001 Mar;38(2):161-166.
- Sherman RA, Hall MJ, Thomas S. Medicinal maggots: an ancient remedy for some contemporary afflictions. Annu Rev Entomol. 2000;45:55-81.
- Prete PE. Growth effects of Phaenicia sericata larval extracts on fibroblasts: mechanism for wound healing by maggot therapy. Life Sci. 1997;60(8):505-510.
- Church JCT, Courtenay M. Maggot debridement therapy for chronic wounds. Int J Low Extrem Wounds. 2002 Jun;1(2):129-134.
- Courtenay M, Church JC, Ryan TJ. Larva therapy in wound management. J R Soc Med. 2000 Feb;93:72-74.
- 34. Steenvoorde P, Oskam J. Bleeding c omplications in patients treated with maggot debridement therapy (MDT). Letter to the editor. IJLEW. 2005;4:57-58.
- Thomas S, Wynn K, Fowler T, et al. The effect of containment on the properties of sterile maggots. Br J Nurs. 2002 Jun;11(12 Suppl):S21-S22, S24, S26 passim.
- Steenvoorde P, Jacobi CE, Oskam J. Maggot debridement therapy: free-range or contained? An in-vivo study. Adv Skin Wound Care. 2005;18:430-435.
- Steenvoorde P, Oskam J. Use of larval therapy to combat infection after breast-conserving surgery. J Wound Care. 2005 May;14(5):212-213.
Despite modern wound treatment and broad-spectrum antibiotic treatment, patients with chronic wounds still exist. The appearance of antibiotic resistant bacteria, such as methicillin-resistant Staphylococcus aureus (MRSA) in the 1980s and ’90s, gave rise to a search for other remedies. One of the remedies that has been rediscovered and subsequently successfully reintroduced is maggot debridement therapy (MDT).1 The fact that more than 100 articles were published on the subject in the past two decades indicates that the use of maggots is making a strong comeback in medicine.2 In January 2004, the U.S. Food and Drug Administration (FDA) issued 510(k)#33391, allowing production and marketing of maggots as a medical device. In this article, we discuss the use of MDT in patients with a chronic wound.
A Long History of Maggot Therapy
MDT has been used in many cultures and has been known for centuries.3 Ambroise Parè is credited as the father of modern MDT. Unfortunately, no evidence can be found of Parè using maggots as a means to clean or heal wounds. The only reference is the often-cited case that occurred in 1557 at the battle of St. Quentin, when Parè observed soldiers whose wounds were covered by maggots. He mainly described the negative effects of the maggots, and, above all, believed they were spontaneously produced by the wound itself, not by the eggs of fly.4
Baron Larey (1766-1842) a famous surgeon in the army of Napoleon Bonaparte, wrote about soldiers who had larvae-infested wounds, but was frustrated that it was difficult to persuade his patients to leave the maggots in place, believing that “they promoted healing without leaving any damage.”5
The first surgeon to use MDT in patients in the hospital was the orthopedic surgeon William Baer. In the 1920s he was faced with a group of untreatable patients with severe osteomyelitis (antibiotics had not yet been discovered). He successfully treated many patients with maggots, and because of his success the therapy became regularly used in the United States.6
By 1934 more than 1,000 surgeons were using maggot therapy. Surgical Maggots were available commercially from Lederle Corporation.7 But with the introduction of antibiotics in the 1940s, the use of maggots dropped off. In the following years, case reports were published only occasionally.
The Negative Image of Maggots
A large problem of MDT is the difficulty of this type of therapy to gain acceptance in the medical community. Maggots are associated with rotting and decay. The image is of filthy, low-life creatures that are ugly and disgusting. Although a nice recent example for the general public is the scene in the movie Gladiator. The main character (played by Russell Crow) is advised to leave the maggots that spontaneously infested a wound on his shoulder in place so that the wound would heal. He leaves them in place and the wound heals without any problem, enabling Crow’s character to fight many battles.
In contrast, in an oral presentation we held recently at a Dutch scientific surgical meeting, a surgical professor in the audience said, “I will never allow those creatures in my ward.”8 This remark shows that widespread use and acceptance of MDT has not yet been reached. It seems there is still much work to do before MDT is generally accepted as a therapeutic method.
Fortunately, the negative image that seems to exist among nurses and physicians does not seem to bother patients.9 We have treated more than 100 patients in our clinic with MDT. All patients to whom we proposed MDT agreed to the therapy. All were allowed to discontinue the therapy whenever they wanted; none did. In a survey of the first 38 MDT-treated patients, 89% agreed to another session of MDT if the surgeon believed it would be beneficial, and 94% of the patients said that they would recommend it to others. This is despite the fact that the therapy was not successful in all patients (there was a below-knee of above the knee amputation-rate of 19% among patients who underwent MDT).10
Indications and Evidence
Indications and contra-indications for maggot therapy are not well defined. Some state that all kind of wounds that contain necrosis or slough can be good candidates for MDT. In our own study of 101 patients with 116 wounds treated with maggots, we had an overall success rate of 67%. (Seventy-eight out of 116 wounds had a beneficial outcome.) However, in 13 patients with septic arthritis, all wounds failed. Success rates where significantly reduced in cases of chronic limb ischemia, visible tendon or bone, and in cases of duration longer than three months before the start of MDT.11
Most physicians who start MDT use it mainly for worst-case scenarios. From our previous studies, it is clear that success rates in those patients are low. After witnessing a few failures, the physician is naturally reluctant to use it again.
What about evidence? Large randomized studies are lacking, although one containing 600 venous ulcer patients was initiated in 2004.12 There have been three randomized studies performed. Wayman, et al., have shown the cost-effectiveness of larval therapy in venous ulcers compared with hydrogel dressing.13 Contreras, et al., could not find a difference between MDT and curettage and topical silver sulfadiazine in patients with venous leg ulcers.14 At the 36th annual meeting of the European Association for the Study of Diabetes, Markevich, et al., reported on a randomized, multicenter, double-blind controlled clinical trial (n=140) for neuropathic diabetic foot lesions compared to conventional treatment. They found a significant higher percentage of granulation tissue after 10 days, compared with the hydrogel group.15 Results from large case-series indicate that MDT works and could even save limbs.2,16-18 The mechanism of action has not been unraveled yet.
Factors Influencing Effectiveness of MDT
Unfortunately, the statement made by Thomas, who said that maggot therapy works by “secreting proteolytic enzymes that break down dead tissue, turning it into a soup, which they then ingest,” still holds.19 It is known that there are mechanical effects, tissue growth effects, that direct killing of bacteria in the alimentary tract of the maggot takes place, and that maggots produce antibacterial factors.2,17,20-31
Although maggots are suitable agents for chronic wound treatment, it is likely that some wounds are more eligible than others for this type of treatment. In our opinion, all wounds that contain gangrenous or necrotic tissue with infection seem to be suited for MDT.32 Success rates of MDT reported in literature vary, but seem to be around 80% to 90%.16,17,33 In our own series, success rate is about 70%.
Patient-selection (case-mix) and method of outcome measurement play essential roles in these percentages. In our opinion, all wounds that contain necrotic tissue can be debrided effectively with MDT. However, if for example wound ischemia is the major etiologic factor, this should also be addressed. In our experience, diabetic foot, venous ulcers, traumatic ulcers, and infections after surgical procedures are all good candidates for MDT.
Absolute contraindications in our opinion are wounds close to large, uncovered blood vessels and wounds that need immediate surgical debridement (e.g., in the case of a septic patient). A relative contraindication is patients with natural of medically induced coagulopathies, but also patient preference could play a role.34 We have had very bad results with infected small joints of the foot; all wounds (n=13) eventually needed a small or large amputation.
Even the technique of application has an effect on outcome. There are two different application techniques: the free-range and the contained technique. The free-range technique is more effective in vitro and in-vivo and has become our standard application technique—not only in the outpatient department, but also in the intra-mural setting.35,36 (Figure 1, p. 16, shows a patient with a necrotic wound on the leg after radiation therapy and a surgical excision for a malignant tumor was performed.) Earlier surgical debridement combined with split skin graft failed. After four applications of maggots, the wound was free of necrosis and could be subsequently closed. (See Figure 2, p. 16.)
The contained technique is used in patients with bleeding tendencies and wounds that do not have enough healthy skin surrounding the wound; in other words, where the covering “cage” needed in case of the free-range technique can’t be applied. (This problem is shown in Figure 3, p. 16: A patient with necrotizing fasciitis of the left upper leg was treated with the contained technique—BiologiQ, Apeldoorn, Netherlands—as there is no proximal skin border. Of course, patient preference plays a role as well in the choice of application technique.37
Wound Clinic
In the Netherlands maggots can be ordered easily and are delivered within 24 hours. We started a wound clinic in 2002. First it was for MDT alone, but now the scope is broader, and we treat chronic wounds with different kind of wound therapies. We have two nurses, one nurse practitioner, one resident-surgeon, and one vascular surgeon who apply the maggots.
Patients do not need to be admitted for MDT. Fifty-nine percent of our patients are treated in the outpatient department. We are able to treat as many as 10 or 15 patients in one session, but MDT-treated patients make up only two or three patients at a time.
We found that after fast, successful biological debridement with MDT we were left with a lot of patients with red, granulating wounds that needed our attention in order to prevent relapses. In our opinion, there are many different treatment methods after MDT. Plaster casting in case of diabetic feet, secondary closure, and split skin grafting are different methods. However, other therapies like VAC-therapy and recently OASIS are promising.
At this time, all patients are prospectively followed after MDT. We are especially interested in patient selection and are now also aiming to find the ideal wound therapy after MDT. TH
Dr. Steenvoorde is a resident surgeon at Rijnland Hospital Leiderdorp, the Netherlands. van Doorn is a nurse-practitioner at Rijnland Hospital Leiderdorp. Jacobi is a senior researcher in the Medical Decision Department at Leiden University Medical Center, in the Netherlands. Dr. Oskam is a vascular surgeon at Rijnland Hospital Leiderdorp.
References
- Beasley WD, Hirst G. Making a meal of MRSA-the role of biosurgery inhospital-acquired infection. J Hosp Infect. 2004;56(1):6-9.
- Jukema GN, Menon AG, Bernards AT. et al. Amputation-sparing treatment by nature: “surgical” maggots revisited. Clin Infect Dis. 2002 Dec 15;35(12):1566-1571.
- Church JC. The traditional use of maggots in wound healing, and the development of larva therapy (biosurgery) in modern medicine. J Altern Complement Med. 1996 Winter;2(4):525-527.
- Coppi C. I dressed your wounds, God healed you—a wounded person’s psychology according to Ambroise Parè. Ostomy Wound Manage. 2005;51:62-64.
- Goldstein HI. Maggots in the treatment of wound and bone infections. J Bone Joint Surg. 1931;13:476-478.
- Baer WS. The treatment of chronic osteomyelitis with the maggot (larva of the blow fly). J Bone Joint Surg. 1931;13:438-475.
- Puckner WA. New and nonofficial remedies, surgical maggots-Lederle. J Am Med Assoc. 1932;98(5):401.
- Steenvoorde P, Doorn Lv, Jacobi CE, et al. Maggot therapy: retrospective study comparing two different application-techniques. (Dutch). Nederlands Tijdschrift voor Heelkunde. 2006;15:86.
- Contreras RJ, Fuentes SA, Karam-Orantes M, et al. Larval debridement therapy in Mexico. Wound Care Canada. 2005;3:42-46.
- Steenvoorde P, Budding TJ, Engeland Av, et al. Maggot therapy and the “yuk factor”: an issue for the patient? Wound Repair Regen. 2005 May-Jun;13(3):350-352.
- Steenvoorde P, Jacobi CA, Doorn Lv, et al. Maggot debridement therapy of infected ulcers: patient and wound factors influencing outcome. Ann Royal Coll Surg Eng. 2006.
- Raynor P, Dumville J, Cullum N. A new clinical trial of the effect of larval therapy. J Tissue Viability. 2004 Jul;14(3):104-105.
- Wayman J, Nirojogi V, Walker A, et al. The cost effectiveness of larval therapy in venous ulcers. J Tissue Viability. 2001 Jan;11(1):51.
- Contreras RJ, Fuentes SA, Arroyo ES, et al. Larval debridement therapy and infection control in venous ulcers: a comparative study. Presented at: the Second World Union of Wound Healing Societies Meeting; July 8-13, 2004.
- Markevich YO, McLeod-Roberts J, Mousley M, et al. Maggot therapy for diabetic neuropathic foot wounds: a randomized study. Presented at: the 36th Annual Meeting of the EASD; September 17-21, 2000. Ref Type: Conference Proceeding.
- Wolff H, Hansson C. Larval therapy—an effective method for ulcer debridement. Clin Exp Dermatol. 2003;28:137.
- Mumcuoglu KY, Ingber A, Gilead L, et al. Maggot therapy for the treatment of intractable wounds. Int J Dermatol. 1999 Aug;38(8):623-627.
- Courtenay M. The use of larval therapy in wound management in the UK. J Wound Care. 1999 Apr;8 (4):177-179.
- Bonn D. Maggot therapy: an alternative for wound infection. Lancet. 2000 Sep 30;356 (9236):1174.
- Robinson W. Stimulation of healing in non-healing wounds. J Bone Joint Surgery. 1935;17:267-271.
- Robinson W. Ammonium bicarbonate secreted by surgical maggots stimulates healing in purulent wounds. Am J Surg. 1940;47:111-115.
- Mumcuoglu KY, Ingber A, Gilead L, et al. Maggot therapy for the treatment of diabetic foot ulcers. Diabetes Care. 1998 Nov;21(11):2030-2031.
- Simmons S. A bactericidal principle in excretions of surgical maggots which destroys important etiological agents of pyogenic infections. J Bacteriol. 1935;30:253-267.
- Simmons S. The bactericidal properties of excretions of the maggot of Lucilia sericata. Bull Entomol Res. 1935;26:559-563.
- Mumcuoglu KY. Clinical applications for maggots in wound care. Am J Clin Dermatol. 2001;2:219-227.
- Armstrong DG, Short B, Martin BR, et al. Maggot therapy in lower extremity hospice wound care. J Am Podiatr Med Assoc. 2005;95(3):254-257.
- Robinson W, Norwood VH. The role of surgical maggots in the disinfection of osteomyelitis and other infected wounds. J Bone Joint Surgery. 1933;15:409-412.
- Robinson W, Norwood VH. Destruction of pyogenic bacteria in the alimentary tract of surgical maggots implanted in infected wounds. J Lab Clin Med. 1933;19:581-585.
- Mumcuoglu KY, Miller J, Mumcuoglu M. et al. Destruction of bacteria in the digestive tract of the maggot of Lucilia sericata (Diptera: Calliphoridae). J Med Entomol. 2001 Mar;38(2):161-166.
- Sherman RA, Hall MJ, Thomas S. Medicinal maggots: an ancient remedy for some contemporary afflictions. Annu Rev Entomol. 2000;45:55-81.
- Prete PE. Growth effects of Phaenicia sericata larval extracts on fibroblasts: mechanism for wound healing by maggot therapy. Life Sci. 1997;60(8):505-510.
- Church JCT, Courtenay M. Maggot debridement therapy for chronic wounds. Int J Low Extrem Wounds. 2002 Jun;1(2):129-134.
- Courtenay M, Church JC, Ryan TJ. Larva therapy in wound management. J R Soc Med. 2000 Feb;93:72-74.
- 34. Steenvoorde P, Oskam J. Bleeding c omplications in patients treated with maggot debridement therapy (MDT). Letter to the editor. IJLEW. 2005;4:57-58.
- Thomas S, Wynn K, Fowler T, et al. The effect of containment on the properties of sterile maggots. Br J Nurs. 2002 Jun;11(12 Suppl):S21-S22, S24, S26 passim.
- Steenvoorde P, Jacobi CE, Oskam J. Maggot debridement therapy: free-range or contained? An in-vivo study. Adv Skin Wound Care. 2005;18:430-435.
- Steenvoorde P, Oskam J. Use of larval therapy to combat infection after breast-conserving surgery. J Wound Care. 2005 May;14(5):212-213.
Despite modern wound treatment and broad-spectrum antibiotic treatment, patients with chronic wounds still exist. The appearance of antibiotic resistant bacteria, such as methicillin-resistant Staphylococcus aureus (MRSA) in the 1980s and ’90s, gave rise to a search for other remedies. One of the remedies that has been rediscovered and subsequently successfully reintroduced is maggot debridement therapy (MDT).1 The fact that more than 100 articles were published on the subject in the past two decades indicates that the use of maggots is making a strong comeback in medicine.2 In January 2004, the U.S. Food and Drug Administration (FDA) issued 510(k)#33391, allowing production and marketing of maggots as a medical device. In this article, we discuss the use of MDT in patients with a chronic wound.
A Long History of Maggot Therapy
MDT has been used in many cultures and has been known for centuries.3 Ambroise Parè is credited as the father of modern MDT. Unfortunately, no evidence can be found of Parè using maggots as a means to clean or heal wounds. The only reference is the often-cited case that occurred in 1557 at the battle of St. Quentin, when Parè observed soldiers whose wounds were covered by maggots. He mainly described the negative effects of the maggots, and, above all, believed they were spontaneously produced by the wound itself, not by the eggs of fly.4
Baron Larey (1766-1842) a famous surgeon in the army of Napoleon Bonaparte, wrote about soldiers who had larvae-infested wounds, but was frustrated that it was difficult to persuade his patients to leave the maggots in place, believing that “they promoted healing without leaving any damage.”5
The first surgeon to use MDT in patients in the hospital was the orthopedic surgeon William Baer. In the 1920s he was faced with a group of untreatable patients with severe osteomyelitis (antibiotics had not yet been discovered). He successfully treated many patients with maggots, and because of his success the therapy became regularly used in the United States.6
By 1934 more than 1,000 surgeons were using maggot therapy. Surgical Maggots were available commercially from Lederle Corporation.7 But with the introduction of antibiotics in the 1940s, the use of maggots dropped off. In the following years, case reports were published only occasionally.
The Negative Image of Maggots
A large problem of MDT is the difficulty of this type of therapy to gain acceptance in the medical community. Maggots are associated with rotting and decay. The image is of filthy, low-life creatures that are ugly and disgusting. Although a nice recent example for the general public is the scene in the movie Gladiator. The main character (played by Russell Crow) is advised to leave the maggots that spontaneously infested a wound on his shoulder in place so that the wound would heal. He leaves them in place and the wound heals without any problem, enabling Crow’s character to fight many battles.
In contrast, in an oral presentation we held recently at a Dutch scientific surgical meeting, a surgical professor in the audience said, “I will never allow those creatures in my ward.”8 This remark shows that widespread use and acceptance of MDT has not yet been reached. It seems there is still much work to do before MDT is generally accepted as a therapeutic method.
Fortunately, the negative image that seems to exist among nurses and physicians does not seem to bother patients.9 We have treated more than 100 patients in our clinic with MDT. All patients to whom we proposed MDT agreed to the therapy. All were allowed to discontinue the therapy whenever they wanted; none did. In a survey of the first 38 MDT-treated patients, 89% agreed to another session of MDT if the surgeon believed it would be beneficial, and 94% of the patients said that they would recommend it to others. This is despite the fact that the therapy was not successful in all patients (there was a below-knee of above the knee amputation-rate of 19% among patients who underwent MDT).10
Indications and Evidence
Indications and contra-indications for maggot therapy are not well defined. Some state that all kind of wounds that contain necrosis or slough can be good candidates for MDT. In our own study of 101 patients with 116 wounds treated with maggots, we had an overall success rate of 67%. (Seventy-eight out of 116 wounds had a beneficial outcome.) However, in 13 patients with septic arthritis, all wounds failed. Success rates where significantly reduced in cases of chronic limb ischemia, visible tendon or bone, and in cases of duration longer than three months before the start of MDT.11
Most physicians who start MDT use it mainly for worst-case scenarios. From our previous studies, it is clear that success rates in those patients are low. After witnessing a few failures, the physician is naturally reluctant to use it again.
What about evidence? Large randomized studies are lacking, although one containing 600 venous ulcer patients was initiated in 2004.12 There have been three randomized studies performed. Wayman, et al., have shown the cost-effectiveness of larval therapy in venous ulcers compared with hydrogel dressing.13 Contreras, et al., could not find a difference between MDT and curettage and topical silver sulfadiazine in patients with venous leg ulcers.14 At the 36th annual meeting of the European Association for the Study of Diabetes, Markevich, et al., reported on a randomized, multicenter, double-blind controlled clinical trial (n=140) for neuropathic diabetic foot lesions compared to conventional treatment. They found a significant higher percentage of granulation tissue after 10 days, compared with the hydrogel group.15 Results from large case-series indicate that MDT works and could even save limbs.2,16-18 The mechanism of action has not been unraveled yet.
Factors Influencing Effectiveness of MDT
Unfortunately, the statement made by Thomas, who said that maggot therapy works by “secreting proteolytic enzymes that break down dead tissue, turning it into a soup, which they then ingest,” still holds.19 It is known that there are mechanical effects, tissue growth effects, that direct killing of bacteria in the alimentary tract of the maggot takes place, and that maggots produce antibacterial factors.2,17,20-31
Although maggots are suitable agents for chronic wound treatment, it is likely that some wounds are more eligible than others for this type of treatment. In our opinion, all wounds that contain gangrenous or necrotic tissue with infection seem to be suited for MDT.32 Success rates of MDT reported in literature vary, but seem to be around 80% to 90%.16,17,33 In our own series, success rate is about 70%.
Patient-selection (case-mix) and method of outcome measurement play essential roles in these percentages. In our opinion, all wounds that contain necrotic tissue can be debrided effectively with MDT. However, if for example wound ischemia is the major etiologic factor, this should also be addressed. In our experience, diabetic foot, venous ulcers, traumatic ulcers, and infections after surgical procedures are all good candidates for MDT.
Absolute contraindications in our opinion are wounds close to large, uncovered blood vessels and wounds that need immediate surgical debridement (e.g., in the case of a septic patient). A relative contraindication is patients with natural of medically induced coagulopathies, but also patient preference could play a role.34 We have had very bad results with infected small joints of the foot; all wounds (n=13) eventually needed a small or large amputation.
Even the technique of application has an effect on outcome. There are two different application techniques: the free-range and the contained technique. The free-range technique is more effective in vitro and in-vivo and has become our standard application technique—not only in the outpatient department, but also in the intra-mural setting.35,36 (Figure 1, p. 16, shows a patient with a necrotic wound on the leg after radiation therapy and a surgical excision for a malignant tumor was performed.) Earlier surgical debridement combined with split skin graft failed. After four applications of maggots, the wound was free of necrosis and could be subsequently closed. (See Figure 2, p. 16.)
The contained technique is used in patients with bleeding tendencies and wounds that do not have enough healthy skin surrounding the wound; in other words, where the covering “cage” needed in case of the free-range technique can’t be applied. (This problem is shown in Figure 3, p. 16: A patient with necrotizing fasciitis of the left upper leg was treated with the contained technique—BiologiQ, Apeldoorn, Netherlands—as there is no proximal skin border. Of course, patient preference plays a role as well in the choice of application technique.37
Wound Clinic
In the Netherlands maggots can be ordered easily and are delivered within 24 hours. We started a wound clinic in 2002. First it was for MDT alone, but now the scope is broader, and we treat chronic wounds with different kind of wound therapies. We have two nurses, one nurse practitioner, one resident-surgeon, and one vascular surgeon who apply the maggots.
Patients do not need to be admitted for MDT. Fifty-nine percent of our patients are treated in the outpatient department. We are able to treat as many as 10 or 15 patients in one session, but MDT-treated patients make up only two or three patients at a time.
We found that after fast, successful biological debridement with MDT we were left with a lot of patients with red, granulating wounds that needed our attention in order to prevent relapses. In our opinion, there are many different treatment methods after MDT. Plaster casting in case of diabetic feet, secondary closure, and split skin grafting are different methods. However, other therapies like VAC-therapy and recently OASIS are promising.
At this time, all patients are prospectively followed after MDT. We are especially interested in patient selection and are now also aiming to find the ideal wound therapy after MDT. TH
Dr. Steenvoorde is a resident surgeon at Rijnland Hospital Leiderdorp, the Netherlands. van Doorn is a nurse-practitioner at Rijnland Hospital Leiderdorp. Jacobi is a senior researcher in the Medical Decision Department at Leiden University Medical Center, in the Netherlands. Dr. Oskam is a vascular surgeon at Rijnland Hospital Leiderdorp.
References
- Beasley WD, Hirst G. Making a meal of MRSA-the role of biosurgery inhospital-acquired infection. J Hosp Infect. 2004;56(1):6-9.
- Jukema GN, Menon AG, Bernards AT. et al. Amputation-sparing treatment by nature: “surgical” maggots revisited. Clin Infect Dis. 2002 Dec 15;35(12):1566-1571.
- Church JC. The traditional use of maggots in wound healing, and the development of larva therapy (biosurgery) in modern medicine. J Altern Complement Med. 1996 Winter;2(4):525-527.
- Coppi C. I dressed your wounds, God healed you—a wounded person’s psychology according to Ambroise Parè. Ostomy Wound Manage. 2005;51:62-64.
- Goldstein HI. Maggots in the treatment of wound and bone infections. J Bone Joint Surg. 1931;13:476-478.
- Baer WS. The treatment of chronic osteomyelitis with the maggot (larva of the blow fly). J Bone Joint Surg. 1931;13:438-475.
- Puckner WA. New and nonofficial remedies, surgical maggots-Lederle. J Am Med Assoc. 1932;98(5):401.
- Steenvoorde P, Doorn Lv, Jacobi CE, et al. Maggot therapy: retrospective study comparing two different application-techniques. (Dutch). Nederlands Tijdschrift voor Heelkunde. 2006;15:86.
- Contreras RJ, Fuentes SA, Karam-Orantes M, et al. Larval debridement therapy in Mexico. Wound Care Canada. 2005;3:42-46.
- Steenvoorde P, Budding TJ, Engeland Av, et al. Maggot therapy and the “yuk factor”: an issue for the patient? Wound Repair Regen. 2005 May-Jun;13(3):350-352.
- Steenvoorde P, Jacobi CA, Doorn Lv, et al. Maggot debridement therapy of infected ulcers: patient and wound factors influencing outcome. Ann Royal Coll Surg Eng. 2006.
- Raynor P, Dumville J, Cullum N. A new clinical trial of the effect of larval therapy. J Tissue Viability. 2004 Jul;14(3):104-105.
- Wayman J, Nirojogi V, Walker A, et al. The cost effectiveness of larval therapy in venous ulcers. J Tissue Viability. 2001 Jan;11(1):51.
- Contreras RJ, Fuentes SA, Arroyo ES, et al. Larval debridement therapy and infection control in venous ulcers: a comparative study. Presented at: the Second World Union of Wound Healing Societies Meeting; July 8-13, 2004.
- Markevich YO, McLeod-Roberts J, Mousley M, et al. Maggot therapy for diabetic neuropathic foot wounds: a randomized study. Presented at: the 36th Annual Meeting of the EASD; September 17-21, 2000. Ref Type: Conference Proceeding.
- Wolff H, Hansson C. Larval therapy—an effective method for ulcer debridement. Clin Exp Dermatol. 2003;28:137.
- Mumcuoglu KY, Ingber A, Gilead L, et al. Maggot therapy for the treatment of intractable wounds. Int J Dermatol. 1999 Aug;38(8):623-627.
- Courtenay M. The use of larval therapy in wound management in the UK. J Wound Care. 1999 Apr;8 (4):177-179.
- Bonn D. Maggot therapy: an alternative for wound infection. Lancet. 2000 Sep 30;356 (9236):1174.
- Robinson W. Stimulation of healing in non-healing wounds. J Bone Joint Surgery. 1935;17:267-271.
- Robinson W. Ammonium bicarbonate secreted by surgical maggots stimulates healing in purulent wounds. Am J Surg. 1940;47:111-115.
- Mumcuoglu KY, Ingber A, Gilead L, et al. Maggot therapy for the treatment of diabetic foot ulcers. Diabetes Care. 1998 Nov;21(11):2030-2031.
- Simmons S. A bactericidal principle in excretions of surgical maggots which destroys important etiological agents of pyogenic infections. J Bacteriol. 1935;30:253-267.
- Simmons S. The bactericidal properties of excretions of the maggot of Lucilia sericata. Bull Entomol Res. 1935;26:559-563.
- Mumcuoglu KY. Clinical applications for maggots in wound care. Am J Clin Dermatol. 2001;2:219-227.
- Armstrong DG, Short B, Martin BR, et al. Maggot therapy in lower extremity hospice wound care. J Am Podiatr Med Assoc. 2005;95(3):254-257.
- Robinson W, Norwood VH. The role of surgical maggots in the disinfection of osteomyelitis and other infected wounds. J Bone Joint Surgery. 1933;15:409-412.
- Robinson W, Norwood VH. Destruction of pyogenic bacteria in the alimentary tract of surgical maggots implanted in infected wounds. J Lab Clin Med. 1933;19:581-585.
- Mumcuoglu KY, Miller J, Mumcuoglu M. et al. Destruction of bacteria in the digestive tract of the maggot of Lucilia sericata (Diptera: Calliphoridae). J Med Entomol. 2001 Mar;38(2):161-166.
- Sherman RA, Hall MJ, Thomas S. Medicinal maggots: an ancient remedy for some contemporary afflictions. Annu Rev Entomol. 2000;45:55-81.
- Prete PE. Growth effects of Phaenicia sericata larval extracts on fibroblasts: mechanism for wound healing by maggot therapy. Life Sci. 1997;60(8):505-510.
- Church JCT, Courtenay M. Maggot debridement therapy for chronic wounds. Int J Low Extrem Wounds. 2002 Jun;1(2):129-134.
- Courtenay M, Church JC, Ryan TJ. Larva therapy in wound management. J R Soc Med. 2000 Feb;93:72-74.
- 34. Steenvoorde P, Oskam J. Bleeding c omplications in patients treated with maggot debridement therapy (MDT). Letter to the editor. IJLEW. 2005;4:57-58.
- Thomas S, Wynn K, Fowler T, et al. The effect of containment on the properties of sterile maggots. Br J Nurs. 2002 Jun;11(12 Suppl):S21-S22, S24, S26 passim.
- Steenvoorde P, Jacobi CE, Oskam J. Maggot debridement therapy: free-range or contained? An in-vivo study. Adv Skin Wound Care. 2005;18:430-435.
- Steenvoorde P, Oskam J. Use of larval therapy to combat infection after breast-conserving surgery. J Wound Care. 2005 May;14(5):212-213.
Pantilat Receives Endowed Chair

Increasingly, hospitals are making palliative care a priority; and more hospitalists are getting involved in providing these services and taking the lead on establishing and facilitating palliative care programs. Among the growing evidence that hospitalists are viewed as key players in the proliferation of hospital palliative care programs is the appointment of Steven Pantilat, MD, associate professor of clinical medicine, to the newly established Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care at the University of California at San Francisco (UCSF).
The chair is the first palliative care chair in the University of California system and only the fifth nationwide. The endowment provides funding for salary support and efforts to build clinical, educational, research, and training components of the UCSF palliative care program. “This chair is important because hospitalists are often the main source of hospital palliative care services,” explains Dr. Pantilat. “Because I am a hospitalist, I understand the needs of these practitioners.”
Numerous Plans, Expectations
Dr. Pantilat has several expectations for what the chair will enable him to accomplish. “We hope to improve palliative care for patients, contribute to the field in terms of research and educational initiatives, and help UC advance in these areas,” he says. “Our main goal is to develop a world-class palliative care program that will advance the field in terms of education, research, and patient care and to provide the highest quality care to patients with life-threatening illness. This will provide seed money to develop educational and research programs that require some early investment when they are just ideas.”
There is a tremendous need for more and better palliative care in the hospital setting. “Patients have many needs, including management of symptoms such as shortness of breath, nausea, and fatigue,” he says. “There isn’t nearly enough research or information on these problems as compared to pain. We need more studies on the best way to treat symptoms.”
Additionally, Dr. Pantilat hopes to add to the body of literature on patient-physician communication, suggesting that hospitalists and other physicians need information about how to communicate sensitive issues such as bad news and how best to support patients and families throughout illnesses and fill their palliative care needs.
“We hope to develop and encourage more education and training on these topics,” he says. Stressing that there already are good educational programs about palliative care topics, Dr. Pantilat notes the need for more instruction specific to the unique needs of hospitalized patients and the hospitalists who care for them.
Create an Interdisciplinary System
“We need systems to provide palliative care. We also need to sensitize everyone who works in the hospital to comfort care issues,” says Dr. Pantilat, adding that there also is a need for programs and systems to ensure that patients and families will get the palliative care they need when they leave the hospital. “We need to work together to create a smooth transition from inpatient to outpatient palliative care. And we need to consider how we, as hospitalists, work with patients in the outpatient setting to ensure that someone is there to take care of them and their needs.”
Many of these needs require widespread education and training. “This grant will allow us to develop more robust and innovative educational efforts that engage ways to teach all team members about palliative care,” says Dr. Pantilat. “This will include projects such as using the Web to teach students.”
Expand the Definition
Dr. Pantilat also hopes to help expand the definition of palliative care and help people understand this as a broad concept of providing interdisciplinary care for people with terminal and chronic diseases. “An important point that we hope to emphasize is that palliative care is not just end-of-life care but something designed to improve life for people with illnesses—particularly chronic illnesses—either through the treatment of the diseases or the symptoms. It is an attempt to alleviate physical, emotional, and psychological suffering and promote the best possible quality of life,” he explains.
Helping people get “past the old limiting idea of palliative care” is another key goal. “A lot of palliative care can be provided while people are pursuing curative care,” explains Dr. Pantilat. “This is an important concept to promote.”
The Hospitalist’s Role
As a hospitalist, Dr. Pantilat also hopes to promote the growing recognition of the importance of hospitalists in palliative care programs: “The beautiful thing is that hospitalists are perfectly poised to handle palliative care programs, and with training they can become palliative care providers.”
The endowed chair reflects the importance of hospitalists in the palliative care field. “Hospitalists will be increasingly important in this area, and I hope to take a leadership role,” he says. While he is pleased and honored to have the chair at UCSF, he is confident that his work will have an impact well beyond his own university. “The chair will bring much recognition to our program but also to the field of palliative care in general and the role of hospitalists nationwide.” TH
Joanne Kaldy writes regularly for The Hospitalist.
Increasingly, hospitals are making palliative care a priority; and more hospitalists are getting involved in providing these services and taking the lead on establishing and facilitating palliative care programs. Among the growing evidence that hospitalists are viewed as key players in the proliferation of hospital palliative care programs is the appointment of Steven Pantilat, MD, associate professor of clinical medicine, to the newly established Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care at the University of California at San Francisco (UCSF).
The chair is the first palliative care chair in the University of California system and only the fifth nationwide. The endowment provides funding for salary support and efforts to build clinical, educational, research, and training components of the UCSF palliative care program. “This chair is important because hospitalists are often the main source of hospital palliative care services,” explains Dr. Pantilat. “Because I am a hospitalist, I understand the needs of these practitioners.”
Numerous Plans, Expectations
Dr. Pantilat has several expectations for what the chair will enable him to accomplish. “We hope to improve palliative care for patients, contribute to the field in terms of research and educational initiatives, and help UC advance in these areas,” he says. “Our main goal is to develop a world-class palliative care program that will advance the field in terms of education, research, and patient care and to provide the highest quality care to patients with life-threatening illness. This will provide seed money to develop educational and research programs that require some early investment when they are just ideas.”
There is a tremendous need for more and better palliative care in the hospital setting. “Patients have many needs, including management of symptoms such as shortness of breath, nausea, and fatigue,” he says. “There isn’t nearly enough research or information on these problems as compared to pain. We need more studies on the best way to treat symptoms.”
Additionally, Dr. Pantilat hopes to add to the body of literature on patient-physician communication, suggesting that hospitalists and other physicians need information about how to communicate sensitive issues such as bad news and how best to support patients and families throughout illnesses and fill their palliative care needs.
“We hope to develop and encourage more education and training on these topics,” he says. Stressing that there already are good educational programs about palliative care topics, Dr. Pantilat notes the need for more instruction specific to the unique needs of hospitalized patients and the hospitalists who care for them.
Create an Interdisciplinary System
“We need systems to provide palliative care. We also need to sensitize everyone who works in the hospital to comfort care issues,” says Dr. Pantilat, adding that there also is a need for programs and systems to ensure that patients and families will get the palliative care they need when they leave the hospital. “We need to work together to create a smooth transition from inpatient to outpatient palliative care. And we need to consider how we, as hospitalists, work with patients in the outpatient setting to ensure that someone is there to take care of them and their needs.”
Many of these needs require widespread education and training. “This grant will allow us to develop more robust and innovative educational efforts that engage ways to teach all team members about palliative care,” says Dr. Pantilat. “This will include projects such as using the Web to teach students.”
Expand the Definition
Dr. Pantilat also hopes to help expand the definition of palliative care and help people understand this as a broad concept of providing interdisciplinary care for people with terminal and chronic diseases. “An important point that we hope to emphasize is that palliative care is not just end-of-life care but something designed to improve life for people with illnesses—particularly chronic illnesses—either through the treatment of the diseases or the symptoms. It is an attempt to alleviate physical, emotional, and psychological suffering and promote the best possible quality of life,” he explains.
Helping people get “past the old limiting idea of palliative care” is another key goal. “A lot of palliative care can be provided while people are pursuing curative care,” explains Dr. Pantilat. “This is an important concept to promote.”
The Hospitalist’s Role
As a hospitalist, Dr. Pantilat also hopes to promote the growing recognition of the importance of hospitalists in palliative care programs: “The beautiful thing is that hospitalists are perfectly poised to handle palliative care programs, and with training they can become palliative care providers.”
The endowed chair reflects the importance of hospitalists in the palliative care field. “Hospitalists will be increasingly important in this area, and I hope to take a leadership role,” he says. While he is pleased and honored to have the chair at UCSF, he is confident that his work will have an impact well beyond his own university. “The chair will bring much recognition to our program but also to the field of palliative care in general and the role of hospitalists nationwide.” TH
Joanne Kaldy writes regularly for The Hospitalist.
Increasingly, hospitals are making palliative care a priority; and more hospitalists are getting involved in providing these services and taking the lead on establishing and facilitating palliative care programs. Among the growing evidence that hospitalists are viewed as key players in the proliferation of hospital palliative care programs is the appointment of Steven Pantilat, MD, associate professor of clinical medicine, to the newly established Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care at the University of California at San Francisco (UCSF).
The chair is the first palliative care chair in the University of California system and only the fifth nationwide. The endowment provides funding for salary support and efforts to build clinical, educational, research, and training components of the UCSF palliative care program. “This chair is important because hospitalists are often the main source of hospital palliative care services,” explains Dr. Pantilat. “Because I am a hospitalist, I understand the needs of these practitioners.”
Numerous Plans, Expectations
Dr. Pantilat has several expectations for what the chair will enable him to accomplish. “We hope to improve palliative care for patients, contribute to the field in terms of research and educational initiatives, and help UC advance in these areas,” he says. “Our main goal is to develop a world-class palliative care program that will advance the field in terms of education, research, and patient care and to provide the highest quality care to patients with life-threatening illness. This will provide seed money to develop educational and research programs that require some early investment when they are just ideas.”
There is a tremendous need for more and better palliative care in the hospital setting. “Patients have many needs, including management of symptoms such as shortness of breath, nausea, and fatigue,” he says. “There isn’t nearly enough research or information on these problems as compared to pain. We need more studies on the best way to treat symptoms.”
Additionally, Dr. Pantilat hopes to add to the body of literature on patient-physician communication, suggesting that hospitalists and other physicians need information about how to communicate sensitive issues such as bad news and how best to support patients and families throughout illnesses and fill their palliative care needs.
“We hope to develop and encourage more education and training on these topics,” he says. Stressing that there already are good educational programs about palliative care topics, Dr. Pantilat notes the need for more instruction specific to the unique needs of hospitalized patients and the hospitalists who care for them.
Create an Interdisciplinary System
“We need systems to provide palliative care. We also need to sensitize everyone who works in the hospital to comfort care issues,” says Dr. Pantilat, adding that there also is a need for programs and systems to ensure that patients and families will get the palliative care they need when they leave the hospital. “We need to work together to create a smooth transition from inpatient to outpatient palliative care. And we need to consider how we, as hospitalists, work with patients in the outpatient setting to ensure that someone is there to take care of them and their needs.”
Many of these needs require widespread education and training. “This grant will allow us to develop more robust and innovative educational efforts that engage ways to teach all team members about palliative care,” says Dr. Pantilat. “This will include projects such as using the Web to teach students.”
Expand the Definition
Dr. Pantilat also hopes to help expand the definition of palliative care and help people understand this as a broad concept of providing interdisciplinary care for people with terminal and chronic diseases. “An important point that we hope to emphasize is that palliative care is not just end-of-life care but something designed to improve life for people with illnesses—particularly chronic illnesses—either through the treatment of the diseases or the symptoms. It is an attempt to alleviate physical, emotional, and psychological suffering and promote the best possible quality of life,” he explains.
Helping people get “past the old limiting idea of palliative care” is another key goal. “A lot of palliative care can be provided while people are pursuing curative care,” explains Dr. Pantilat. “This is an important concept to promote.”
The Hospitalist’s Role
As a hospitalist, Dr. Pantilat also hopes to promote the growing recognition of the importance of hospitalists in palliative care programs: “The beautiful thing is that hospitalists are perfectly poised to handle palliative care programs, and with training they can become palliative care providers.”
The endowed chair reflects the importance of hospitalists in the palliative care field. “Hospitalists will be increasingly important in this area, and I hope to take a leadership role,” he says. While he is pleased and honored to have the chair at UCSF, he is confident that his work will have an impact well beyond his own university. “The chair will bring much recognition to our program but also to the field of palliative care in general and the role of hospitalists nationwide.” TH
Joanne Kaldy writes regularly for The Hospitalist.
Rash Judgement
A 38-year-old, healthy, incarcerated, African-American man presented with a one-and-a-half year history of an eruption in his axillae. The patient stated that the “rash” worsened with sweating but the lesions were otherwise asymptomatic.
Corticosteroid creams, antifungal creams, and oral antibiotics had not led to any improvement. The eruption progressed to involve his trunk, arms, and face. The skin exam showed hyperpigmented, firm plaques with erythematous papules in the axillae. The plaques were also present on the chest, back, and upper extremities. Verrucous papules were noted on the flexural areas of upper extremities as well as tan colored plaques at the lateral canthi of eyes. (See Figures 1-3 this page.)
CBC and serum electrolytes were normal. Lipid panel showed a cholesterol of 593 mg/dL, triglycerides 106 mg/dL, high density lipoprotein of 37 g/dL, low density lipoprotein of 535 mg/dL, and very low density lipoprotein of 21 mg/dL. A biopsy from the axilla and the umbilical area were sent for histologic examination. (See Figure 4 this page.)



What is this patient’s most likely diagnosis?
- Sarcoidosis
- Disseminated xanthomas
- Xanthoma disseminatum
- Erythema elevatum diutinum
- Necrobiosis lipoidica
Discussion
The answer is B: disseminated xanthomas. Punch biopsy from the axilla and shave biopsy from the periumbilical area both revealed localized infiltrates of lipid containing macrophages.
Xanthomas develop due to accumulation of lipid-filled macrophages and suggest an underlying disorder of lipid metabolism. Morbidity and mortality are primarily related to atherosclerosis (e.g., coronary artery disease) and pancreatitis, which occur secondarily to the increased lipid levels rather than the xanthoma itself.
In general, four clinical types of xanthomas exist: tendinous, planar, tuberous, and eruptive. A particular diagnosis cannot necessarily be made on the basis of clinical signs; however, certain types of xanthomas are more characteristic of specific hyperlipidemias. Eruptive xanthomas are found in the setting of primary or secondary hypertriglyeridemia. Tuberous xanthomas have both elevated serum cholesterol and triglycerides. This patient had plane xanthomas and xanthelasma and was especially notable for intertriginous plane xanthomas, which can be pathognomonic for homozygous familial hypercholesterolemia.
This patient’s histology from both the periumbilical area and the axilla depict the characteristic presence of vacuolated macrophages (foamy macrophages) to confirm the diagnosis as disseminated xanthoma.1-3 Sarcoidosis is a chronic idiopathic disorder characterized by noncaseating granulomas that can affect any organ system. Cutaneous sarcoidosis typically presents as asymptomatic, red-brown macules and papules affecting the face, periorbital areas, nasolabial folds, and/or extensor surfaces. Typical sarcoid lesions are characterized by the presence of circumscribed granulomas of epithelioid cells with little or no necrosis. The granulomas are characteristically referred to as “naked” due to the sparse lymphocytic infiltrate at the margins.
This patient’s histologic exam did not reveal any granulomas and localized infiltrates of lipid containing macrophages make the diagnosis of cutaneous sarcoidosis unlikely.4,5
Necrobiosis lipoidica (NL) is a cutaneous disorder that is often, but not always, associated with diabetes mellitus. NL is a disorder of collagen degeneration with a granulomatous response, thickening of blood vessel walls, and fat deposition. Patients usually present with asymptomatic shiny patches that slowly enlarge over months to years. The patient’s main complaint is the unsightly cosmetic appearance of the lesions.
Skin lesions of classic NL begin as 1- to 3-mm well-circumscribed papules or nodules that expand with an active border to become waxy, atrophic, round plaques centrally. Initially, these plaques are red-brown in color but progressively become more yellow and atrophic in appearance. Most cases of NL occur on the pretibial area, but cases have been reported on the face, scalp, trunk, and upper extremities where the diagnosis is more likely to be missed.
Although this patient’s mother had diabetes, his fasting blood glucose was well within normal limits (71 mg/dL). Histologically NL displays sclerotic collagen and obliteration of the bundle pattern, with interstitial and palisaded granulomas that involve the subcutaneous tissue and dermis. Fat containing foam cells are often present.
Although our patient’s biopsy showed fat containing foam cells, it did not have the interstitial granulomas or the sclerotic collagen. In addition, the lack of diabetes makes this diagnosis less likely.6,7
Erythema elevatum diutinum (EED) is a rare type of leukocytoclastic vasculitis characterized by red, purple, brown, or yellow papules, plaques, or nodules. These lesions are usually distributed on the extensor surfaces of the body. The lesions are usually asymptomatic but can be associated occasionally with joint pain. Clinical studies show a preference for the extensor surfaces of the hands, the wrists, the elbows, the ankles, the Achilles’ tendons, the fingers, and the toes. The buttocks, the face, and the ears as well as the palms, the soles, the legs, the forearms, and the genitals may be involved; however, the trunk is usually spared. EED is a type of necrotizing vasculitis.
In its early stages, there are no specific histologic findings that can be used to single out the diagnosis of EED from other leukocytoclastic diseases. Although the distribution and lack of symptomatology in EED is reminiscent of our patient, this patient’s lesions were more often found in the flexural areas rather than extensors. In addition, there was no necrotizing vasculitis on histology, which precludes this rare diagnosis of EED.8
Xanthoma disseminatum (XD) is a rare, benign, proliferative disorder in children and young adults characterized by xanthomatous lesions especially in the flexural folds and eyelids. Although it sounds like a disorder of lipid metabolism, it is actually a histiocytic disorder that is not associated with lipoprotein abnormalities and patients are normolipemic. Histologically, it shows mononuclear phagocyte proliferation with Touton giant cells and CD68 positivity on immunophenotyping. It is unlikely that this patient has XD despite the appropriate clinical presentation because histologically all that is found are foam cells. In addition, the patient had a definite lipoprotein abnormality while XD patients are normolipemic.9 TH
References
- Cruz PD, East C, Bergstresser P. Dermal, subcutaneous, and tendon xanthomas: diagnostic markers for specific lipoprotein disorders. J Am Acad Dermatol 1988 Jul;19(1 pt 1):95-111.
- Massengale WT, Nesbitt LT. Xanthomas. In: Bolognia JL, Jorrizo JL, Rapini RP, eds. Dermatology. Vol. 2. London: Mosby; 2003:1447-1454.
- Parker F. Xanthomas and hyperlipidemias. J Am Acad Dermatol. 1985 Jul;13 (1):1-30.
- Young RJ, 3rd, Gilson RT, Yanase D, et al. Cutaneous sarcoidosis. Int J Dermatol. 2001;40:249-253.
- English JC, Patel PJ, Greer KE. Sarcoidosis. J Am Acad Dermatol. 2001;44:725-743: quiz 744-746.
- Fitzpatrick TB, Johnson R, Wolff K, et al. Genetic, metabolic, endocrine and nutritional diseases. Color Atlas and Synopsis of Clinical Dermatology, Common and Serious Diseases. New York: McGraw-Hill; 2001:415-416.
- Lowitt MH, Dover JS. Necrobiosis lipoidica. J Am Acad Dermatol. 1991; 25:735-748.
- Yiannias JA, el-Azhary RA, Gibson LE. Erythema elevatum diutinum: a clinical and histopathologic study of 13 patients. J Am Acad Dermatol 1992 Jan;26(1):38-44.
- Alexander AS, Turner R, Uniate L, et al. Xanthoma disseminatum: a case report and literature review. Br J Radiol 2005 Feb;78(926):153-157.
A 38-year-old, healthy, incarcerated, African-American man presented with a one-and-a-half year history of an eruption in his axillae. The patient stated that the “rash” worsened with sweating but the lesions were otherwise asymptomatic.
Corticosteroid creams, antifungal creams, and oral antibiotics had not led to any improvement. The eruption progressed to involve his trunk, arms, and face. The skin exam showed hyperpigmented, firm plaques with erythematous papules in the axillae. The plaques were also present on the chest, back, and upper extremities. Verrucous papules were noted on the flexural areas of upper extremities as well as tan colored plaques at the lateral canthi of eyes. (See Figures 1-3 this page.)
CBC and serum electrolytes were normal. Lipid panel showed a cholesterol of 593 mg/dL, triglycerides 106 mg/dL, high density lipoprotein of 37 g/dL, low density lipoprotein of 535 mg/dL, and very low density lipoprotein of 21 mg/dL. A biopsy from the axilla and the umbilical area were sent for histologic examination. (See Figure 4 this page.)
What is this patient’s most likely diagnosis?
- Sarcoidosis
- Disseminated xanthomas
- Xanthoma disseminatum
- Erythema elevatum diutinum
- Necrobiosis lipoidica
Discussion
The answer is B: disseminated xanthomas. Punch biopsy from the axilla and shave biopsy from the periumbilical area both revealed localized infiltrates of lipid containing macrophages.
Xanthomas develop due to accumulation of lipid-filled macrophages and suggest an underlying disorder of lipid metabolism. Morbidity and mortality are primarily related to atherosclerosis (e.g., coronary artery disease) and pancreatitis, which occur secondarily to the increased lipid levels rather than the xanthoma itself.
In general, four clinical types of xanthomas exist: tendinous, planar, tuberous, and eruptive. A particular diagnosis cannot necessarily be made on the basis of clinical signs; however, certain types of xanthomas are more characteristic of specific hyperlipidemias. Eruptive xanthomas are found in the setting of primary or secondary hypertriglyeridemia. Tuberous xanthomas have both elevated serum cholesterol and triglycerides. This patient had plane xanthomas and xanthelasma and was especially notable for intertriginous plane xanthomas, which can be pathognomonic for homozygous familial hypercholesterolemia.
This patient’s histology from both the periumbilical area and the axilla depict the characteristic presence of vacuolated macrophages (foamy macrophages) to confirm the diagnosis as disseminated xanthoma.1-3 Sarcoidosis is a chronic idiopathic disorder characterized by noncaseating granulomas that can affect any organ system. Cutaneous sarcoidosis typically presents as asymptomatic, red-brown macules and papules affecting the face, periorbital areas, nasolabial folds, and/or extensor surfaces. Typical sarcoid lesions are characterized by the presence of circumscribed granulomas of epithelioid cells with little or no necrosis. The granulomas are characteristically referred to as “naked” due to the sparse lymphocytic infiltrate at the margins.
This patient’s histologic exam did not reveal any granulomas and localized infiltrates of lipid containing macrophages make the diagnosis of cutaneous sarcoidosis unlikely.4,5
Necrobiosis lipoidica (NL) is a cutaneous disorder that is often, but not always, associated with diabetes mellitus. NL is a disorder of collagen degeneration with a granulomatous response, thickening of blood vessel walls, and fat deposition. Patients usually present with asymptomatic shiny patches that slowly enlarge over months to years. The patient’s main complaint is the unsightly cosmetic appearance of the lesions.
Skin lesions of classic NL begin as 1- to 3-mm well-circumscribed papules or nodules that expand with an active border to become waxy, atrophic, round plaques centrally. Initially, these plaques are red-brown in color but progressively become more yellow and atrophic in appearance. Most cases of NL occur on the pretibial area, but cases have been reported on the face, scalp, trunk, and upper extremities where the diagnosis is more likely to be missed.
Although this patient’s mother had diabetes, his fasting blood glucose was well within normal limits (71 mg/dL). Histologically NL displays sclerotic collagen and obliteration of the bundle pattern, with interstitial and palisaded granulomas that involve the subcutaneous tissue and dermis. Fat containing foam cells are often present.
Although our patient’s biopsy showed fat containing foam cells, it did not have the interstitial granulomas or the sclerotic collagen. In addition, the lack of diabetes makes this diagnosis less likely.6,7
Erythema elevatum diutinum (EED) is a rare type of leukocytoclastic vasculitis characterized by red, purple, brown, or yellow papules, plaques, or nodules. These lesions are usually distributed on the extensor surfaces of the body. The lesions are usually asymptomatic but can be associated occasionally with joint pain. Clinical studies show a preference for the extensor surfaces of the hands, the wrists, the elbows, the ankles, the Achilles’ tendons, the fingers, and the toes. The buttocks, the face, and the ears as well as the palms, the soles, the legs, the forearms, and the genitals may be involved; however, the trunk is usually spared. EED is a type of necrotizing vasculitis.
In its early stages, there are no specific histologic findings that can be used to single out the diagnosis of EED from other leukocytoclastic diseases. Although the distribution and lack of symptomatology in EED is reminiscent of our patient, this patient’s lesions were more often found in the flexural areas rather than extensors. In addition, there was no necrotizing vasculitis on histology, which precludes this rare diagnosis of EED.8
Xanthoma disseminatum (XD) is a rare, benign, proliferative disorder in children and young adults characterized by xanthomatous lesions especially in the flexural folds and eyelids. Although it sounds like a disorder of lipid metabolism, it is actually a histiocytic disorder that is not associated with lipoprotein abnormalities and patients are normolipemic. Histologically, it shows mononuclear phagocyte proliferation with Touton giant cells and CD68 positivity on immunophenotyping. It is unlikely that this patient has XD despite the appropriate clinical presentation because histologically all that is found are foam cells. In addition, the patient had a definite lipoprotein abnormality while XD patients are normolipemic.9 TH
References
- Cruz PD, East C, Bergstresser P. Dermal, subcutaneous, and tendon xanthomas: diagnostic markers for specific lipoprotein disorders. J Am Acad Dermatol 1988 Jul;19(1 pt 1):95-111.
- Massengale WT, Nesbitt LT. Xanthomas. In: Bolognia JL, Jorrizo JL, Rapini RP, eds. Dermatology. Vol. 2. London: Mosby; 2003:1447-1454.
- Parker F. Xanthomas and hyperlipidemias. J Am Acad Dermatol. 1985 Jul;13 (1):1-30.
- Young RJ, 3rd, Gilson RT, Yanase D, et al. Cutaneous sarcoidosis. Int J Dermatol. 2001;40:249-253.
- English JC, Patel PJ, Greer KE. Sarcoidosis. J Am Acad Dermatol. 2001;44:725-743: quiz 744-746.
- Fitzpatrick TB, Johnson R, Wolff K, et al. Genetic, metabolic, endocrine and nutritional diseases. Color Atlas and Synopsis of Clinical Dermatology, Common and Serious Diseases. New York: McGraw-Hill; 2001:415-416.
- Lowitt MH, Dover JS. Necrobiosis lipoidica. J Am Acad Dermatol. 1991; 25:735-748.
- Yiannias JA, el-Azhary RA, Gibson LE. Erythema elevatum diutinum: a clinical and histopathologic study of 13 patients. J Am Acad Dermatol 1992 Jan;26(1):38-44.
- Alexander AS, Turner R, Uniate L, et al. Xanthoma disseminatum: a case report and literature review. Br J Radiol 2005 Feb;78(926):153-157.
A 38-year-old, healthy, incarcerated, African-American man presented with a one-and-a-half year history of an eruption in his axillae. The patient stated that the “rash” worsened with sweating but the lesions were otherwise asymptomatic.
Corticosteroid creams, antifungal creams, and oral antibiotics had not led to any improvement. The eruption progressed to involve his trunk, arms, and face. The skin exam showed hyperpigmented, firm plaques with erythematous papules in the axillae. The plaques were also present on the chest, back, and upper extremities. Verrucous papules were noted on the flexural areas of upper extremities as well as tan colored plaques at the lateral canthi of eyes. (See Figures 1-3 this page.)
CBC and serum electrolytes were normal. Lipid panel showed a cholesterol of 593 mg/dL, triglycerides 106 mg/dL, high density lipoprotein of 37 g/dL, low density lipoprotein of 535 mg/dL, and very low density lipoprotein of 21 mg/dL. A biopsy from the axilla and the umbilical area were sent for histologic examination. (See Figure 4 this page.)
What is this patient’s most likely diagnosis?
- Sarcoidosis
- Disseminated xanthomas
- Xanthoma disseminatum
- Erythema elevatum diutinum
- Necrobiosis lipoidica
Discussion
The answer is B: disseminated xanthomas. Punch biopsy from the axilla and shave biopsy from the periumbilical area both revealed localized infiltrates of lipid containing macrophages.
Xanthomas develop due to accumulation of lipid-filled macrophages and suggest an underlying disorder of lipid metabolism. Morbidity and mortality are primarily related to atherosclerosis (e.g., coronary artery disease) and pancreatitis, which occur secondarily to the increased lipid levels rather than the xanthoma itself.
In general, four clinical types of xanthomas exist: tendinous, planar, tuberous, and eruptive. A particular diagnosis cannot necessarily be made on the basis of clinical signs; however, certain types of xanthomas are more characteristic of specific hyperlipidemias. Eruptive xanthomas are found in the setting of primary or secondary hypertriglyeridemia. Tuberous xanthomas have both elevated serum cholesterol and triglycerides. This patient had plane xanthomas and xanthelasma and was especially notable for intertriginous plane xanthomas, which can be pathognomonic for homozygous familial hypercholesterolemia.
This patient’s histology from both the periumbilical area and the axilla depict the characteristic presence of vacuolated macrophages (foamy macrophages) to confirm the diagnosis as disseminated xanthoma.1-3 Sarcoidosis is a chronic idiopathic disorder characterized by noncaseating granulomas that can affect any organ system. Cutaneous sarcoidosis typically presents as asymptomatic, red-brown macules and papules affecting the face, periorbital areas, nasolabial folds, and/or extensor surfaces. Typical sarcoid lesions are characterized by the presence of circumscribed granulomas of epithelioid cells with little or no necrosis. The granulomas are characteristically referred to as “naked” due to the sparse lymphocytic infiltrate at the margins.
This patient’s histologic exam did not reveal any granulomas and localized infiltrates of lipid containing macrophages make the diagnosis of cutaneous sarcoidosis unlikely.4,5
Necrobiosis lipoidica (NL) is a cutaneous disorder that is often, but not always, associated with diabetes mellitus. NL is a disorder of collagen degeneration with a granulomatous response, thickening of blood vessel walls, and fat deposition. Patients usually present with asymptomatic shiny patches that slowly enlarge over months to years. The patient’s main complaint is the unsightly cosmetic appearance of the lesions.
Skin lesions of classic NL begin as 1- to 3-mm well-circumscribed papules or nodules that expand with an active border to become waxy, atrophic, round plaques centrally. Initially, these plaques are red-brown in color but progressively become more yellow and atrophic in appearance. Most cases of NL occur on the pretibial area, but cases have been reported on the face, scalp, trunk, and upper extremities where the diagnosis is more likely to be missed.
Although this patient’s mother had diabetes, his fasting blood glucose was well within normal limits (71 mg/dL). Histologically NL displays sclerotic collagen and obliteration of the bundle pattern, with interstitial and palisaded granulomas that involve the subcutaneous tissue and dermis. Fat containing foam cells are often present.
Although our patient’s biopsy showed fat containing foam cells, it did not have the interstitial granulomas or the sclerotic collagen. In addition, the lack of diabetes makes this diagnosis less likely.6,7
Erythema elevatum diutinum (EED) is a rare type of leukocytoclastic vasculitis characterized by red, purple, brown, or yellow papules, plaques, or nodules. These lesions are usually distributed on the extensor surfaces of the body. The lesions are usually asymptomatic but can be associated occasionally with joint pain. Clinical studies show a preference for the extensor surfaces of the hands, the wrists, the elbows, the ankles, the Achilles’ tendons, the fingers, and the toes. The buttocks, the face, and the ears as well as the palms, the soles, the legs, the forearms, and the genitals may be involved; however, the trunk is usually spared. EED is a type of necrotizing vasculitis.
In its early stages, there are no specific histologic findings that can be used to single out the diagnosis of EED from other leukocytoclastic diseases. Although the distribution and lack of symptomatology in EED is reminiscent of our patient, this patient’s lesions were more often found in the flexural areas rather than extensors. In addition, there was no necrotizing vasculitis on histology, which precludes this rare diagnosis of EED.8
Xanthoma disseminatum (XD) is a rare, benign, proliferative disorder in children and young adults characterized by xanthomatous lesions especially in the flexural folds and eyelids. Although it sounds like a disorder of lipid metabolism, it is actually a histiocytic disorder that is not associated with lipoprotein abnormalities and patients are normolipemic. Histologically, it shows mononuclear phagocyte proliferation with Touton giant cells and CD68 positivity on immunophenotyping. It is unlikely that this patient has XD despite the appropriate clinical presentation because histologically all that is found are foam cells. In addition, the patient had a definite lipoprotein abnormality while XD patients are normolipemic.9 TH
References
- Cruz PD, East C, Bergstresser P. Dermal, subcutaneous, and tendon xanthomas: diagnostic markers for specific lipoprotein disorders. J Am Acad Dermatol 1988 Jul;19(1 pt 1):95-111.
- Massengale WT, Nesbitt LT. Xanthomas. In: Bolognia JL, Jorrizo JL, Rapini RP, eds. Dermatology. Vol. 2. London: Mosby; 2003:1447-1454.
- Parker F. Xanthomas and hyperlipidemias. J Am Acad Dermatol. 1985 Jul;13 (1):1-30.
- Young RJ, 3rd, Gilson RT, Yanase D, et al. Cutaneous sarcoidosis. Int J Dermatol. 2001;40:249-253.
- English JC, Patel PJ, Greer KE. Sarcoidosis. J Am Acad Dermatol. 2001;44:725-743: quiz 744-746.
- Fitzpatrick TB, Johnson R, Wolff K, et al. Genetic, metabolic, endocrine and nutritional diseases. Color Atlas and Synopsis of Clinical Dermatology, Common and Serious Diseases. New York: McGraw-Hill; 2001:415-416.
- Lowitt MH, Dover JS. Necrobiosis lipoidica. J Am Acad Dermatol. 1991; 25:735-748.
- Yiannias JA, el-Azhary RA, Gibson LE. Erythema elevatum diutinum: a clinical and histopathologic study of 13 patients. J Am Acad Dermatol 1992 Jan;26(1):38-44.
- Alexander AS, Turner R, Uniate L, et al. Xanthoma disseminatum: a case report and literature review. Br J Radiol 2005 Feb;78(926):153-157.