User login
Shift Perspectives
The shifts worked by a hospital medicine group can reflect its values or simply ensure adequate coverage. Either way, the shifts your group assigns can play a significant role in recruiting new hospitalists and retaining those you have. And there may be more scheduling options than you have considered.
The Most Attractive Shift Debunked
Many new hospitalists seek as much time off as possible, and there are plenty of groups catering to that desire. “Most physicians prefer time off, and seven on, seven off is attractive in recruiting new people to your practice—but it strikes me as a poisonous way to work,” says John Nelson, MD, co-founder of SHM, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., and author of the “Practice Management” column in The Hospitalist. Dr. Nelson acts as a consultant to hospitalist practices around the country and has written articles and given presentations on the topic of scheduling for hospital medicine groups.
Dr. Nelson understands the attractions of working seven on, seven off—particularly for young physicians. “Even seven on is not as bad as being an intern; it’s easier than they were used to in their residency,” he says. “But I worry this schedule might increase burnout and resentment of work. It’s asystole/diastole lifestyle and may not be a healthy way to organize your life or your career.”
An Alternative Scheduling Idea
Dr. Nelson has his own unique ideas of how a group’s shift assignments should work to ensure better coverage and keep hospitalists happy. His ideas are not just theories—his own group lives and works by a flexible arrangement.
Their schedule is partly dictated by a desire to keep the physicians happy and healthy. “I believe a constant mix of work and the rest of your life is best,” says Dr. Nelson. “You shouldn’t have to put the rest of your life into the seven days that you’re off.”
So Dr. Nelson’s practice allows considerable flexibility to each physician, but ensures that any given workday is shorter than 12 hours. “I think it’s better not to have a rigidly repeating schedule,” he explains.
Dr. Nelson’s group uses pagers to ensure a hospitalist is always available during coverage hours, but they don’t adhere to a strict schedule. “So many groups work specified shifts, whether it’s 10 or 12 hours, and I think there’s a better idea,” he says. “If everyone has to punch a clock, it interferes with flexibility. I would not tell doctors when to start or stop.”
Of course, as a group, someone has to be available for emergencies all the time, and physicians may need to start daily rounds to write most discharge orders by a certain time. “I have a pager on by 7 a.m., but nothing says I have to be in the hospital by 7 a.m.,” says Dr. Nelson. “It’s often in my interest to start rounding earlier than 7 a.m. so that I can finish earlier or have time for a break later in the day.”
Greater Flexibility = Better Coverage
Another benefit to moving to shorter, more flexible days is ensuring adequate coverage. “Rigidly defined shifts almost never precisely match the day’s workload,” points out Dr. Nelson. Therefore, his practice boosts staffing to cover busy periods. “My recommendation is to intentionally overstaff for the average day’s workload. When it’s busy, everyone can pitch in and work an extra one or two hours.”
If it’s not busy, one or more doctors may leave early. “This is nimble and responsive to the day-to-day workload,” says Dr. Nelson.
To move from a seven on, seven off schedule to this model, Dr. Nelson recommends that every doctor in the practice work 30 to 40 more days annually. A seven on, seven off schedule would have a physician work 182.5 days per year; if you decrease the hours per day and boost the number of working days to 220 a year, your physicians will be working the same number of hours, but in shorter days—even if the practice workload stays the same and each individual doctor’s annual productivity stays the same.
“It’s more realistic to work more days when they’re not so grueling,” says Dr. Nelson. “Plus, you have a built-in capacity to meet a sudden increase in workload. Imagine an eight-man group, where four doctors each work 12-hour shifts. Now imagine that instead of four, you get a fifth doctor to show up every day. [You can get this fifth doctor without adding staff if each doctor works more days annually.] When a day is unpredictably busy, the physicians won’t be absolutely overwhelmed. If it’s not busy, you can send someone home early. You get a lot more flexibility.”
For a hospital medicine group, implementing a flexible schedule such as this generally requires payment for production, which ties individual physicians into the economic health of their group. Compensation matches workload, allowing individual physicians to work to their values—more money or more free time.
“I think it’s better to pay on production,” says Dr. Nelson. “That way each person has the opportunity to choose. If one values money, he can volunteer to stay and work more and make more money. Each works to their own sweet spot, whereas a seven on, seven off schedule with rigidly defined shifts forces everyone to do the same thing.”
Physicians working on a flexible schedule still need to get their work finished each day, but they have more autonomy in how and when they get it done. “Doctors who work fast can go home early; physicians can decide for themselves the right balance for spending time each patient,” says Dr. Nelson. “As long as they understand there are economic consequences … and act with reasonableness. In our group, we get the work done. There’s no official start or stop time. Each of us chooses an individual work style. There are boundaries; the work needs to be done. There are costs as well, but I believe this system is healthy and liberating.” TH
Jane Jerrard regularly writes “Career Development.”
The shifts worked by a hospital medicine group can reflect its values or simply ensure adequate coverage. Either way, the shifts your group assigns can play a significant role in recruiting new hospitalists and retaining those you have. And there may be more scheduling options than you have considered.
The Most Attractive Shift Debunked
Many new hospitalists seek as much time off as possible, and there are plenty of groups catering to that desire. “Most physicians prefer time off, and seven on, seven off is attractive in recruiting new people to your practice—but it strikes me as a poisonous way to work,” says John Nelson, MD, co-founder of SHM, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., and author of the “Practice Management” column in The Hospitalist. Dr. Nelson acts as a consultant to hospitalist practices around the country and has written articles and given presentations on the topic of scheduling for hospital medicine groups.
Dr. Nelson understands the attractions of working seven on, seven off—particularly for young physicians. “Even seven on is not as bad as being an intern; it’s easier than they were used to in their residency,” he says. “But I worry this schedule might increase burnout and resentment of work. It’s asystole/diastole lifestyle and may not be a healthy way to organize your life or your career.”
An Alternative Scheduling Idea
Dr. Nelson has his own unique ideas of how a group’s shift assignments should work to ensure better coverage and keep hospitalists happy. His ideas are not just theories—his own group lives and works by a flexible arrangement.
Their schedule is partly dictated by a desire to keep the physicians happy and healthy. “I believe a constant mix of work and the rest of your life is best,” says Dr. Nelson. “You shouldn’t have to put the rest of your life into the seven days that you’re off.”
So Dr. Nelson’s practice allows considerable flexibility to each physician, but ensures that any given workday is shorter than 12 hours. “I think it’s better not to have a rigidly repeating schedule,” he explains.
Dr. Nelson’s group uses pagers to ensure a hospitalist is always available during coverage hours, but they don’t adhere to a strict schedule. “So many groups work specified shifts, whether it’s 10 or 12 hours, and I think there’s a better idea,” he says. “If everyone has to punch a clock, it interferes with flexibility. I would not tell doctors when to start or stop.”
Of course, as a group, someone has to be available for emergencies all the time, and physicians may need to start daily rounds to write most discharge orders by a certain time. “I have a pager on by 7 a.m., but nothing says I have to be in the hospital by 7 a.m.,” says Dr. Nelson. “It’s often in my interest to start rounding earlier than 7 a.m. so that I can finish earlier or have time for a break later in the day.”
Greater Flexibility = Better Coverage
Another benefit to moving to shorter, more flexible days is ensuring adequate coverage. “Rigidly defined shifts almost never precisely match the day’s workload,” points out Dr. Nelson. Therefore, his practice boosts staffing to cover busy periods. “My recommendation is to intentionally overstaff for the average day’s workload. When it’s busy, everyone can pitch in and work an extra one or two hours.”
If it’s not busy, one or more doctors may leave early. “This is nimble and responsive to the day-to-day workload,” says Dr. Nelson.
To move from a seven on, seven off schedule to this model, Dr. Nelson recommends that every doctor in the practice work 30 to 40 more days annually. A seven on, seven off schedule would have a physician work 182.5 days per year; if you decrease the hours per day and boost the number of working days to 220 a year, your physicians will be working the same number of hours, but in shorter days—even if the practice workload stays the same and each individual doctor’s annual productivity stays the same.
“It’s more realistic to work more days when they’re not so grueling,” says Dr. Nelson. “Plus, you have a built-in capacity to meet a sudden increase in workload. Imagine an eight-man group, where four doctors each work 12-hour shifts. Now imagine that instead of four, you get a fifth doctor to show up every day. [You can get this fifth doctor without adding staff if each doctor works more days annually.] When a day is unpredictably busy, the physicians won’t be absolutely overwhelmed. If it’s not busy, you can send someone home early. You get a lot more flexibility.”
For a hospital medicine group, implementing a flexible schedule such as this generally requires payment for production, which ties individual physicians into the economic health of their group. Compensation matches workload, allowing individual physicians to work to their values—more money or more free time.
“I think it’s better to pay on production,” says Dr. Nelson. “That way each person has the opportunity to choose. If one values money, he can volunteer to stay and work more and make more money. Each works to their own sweet spot, whereas a seven on, seven off schedule with rigidly defined shifts forces everyone to do the same thing.”
Physicians working on a flexible schedule still need to get their work finished each day, but they have more autonomy in how and when they get it done. “Doctors who work fast can go home early; physicians can decide for themselves the right balance for spending time each patient,” says Dr. Nelson. “As long as they understand there are economic consequences … and act with reasonableness. In our group, we get the work done. There’s no official start or stop time. Each of us chooses an individual work style. There are boundaries; the work needs to be done. There are costs as well, but I believe this system is healthy and liberating.” TH
Jane Jerrard regularly writes “Career Development.”
The shifts worked by a hospital medicine group can reflect its values or simply ensure adequate coverage. Either way, the shifts your group assigns can play a significant role in recruiting new hospitalists and retaining those you have. And there may be more scheduling options than you have considered.
The Most Attractive Shift Debunked
Many new hospitalists seek as much time off as possible, and there are plenty of groups catering to that desire. “Most physicians prefer time off, and seven on, seven off is attractive in recruiting new people to your practice—but it strikes me as a poisonous way to work,” says John Nelson, MD, co-founder of SHM, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., and author of the “Practice Management” column in The Hospitalist. Dr. Nelson acts as a consultant to hospitalist practices around the country and has written articles and given presentations on the topic of scheduling for hospital medicine groups.
Dr. Nelson understands the attractions of working seven on, seven off—particularly for young physicians. “Even seven on is not as bad as being an intern; it’s easier than they were used to in their residency,” he says. “But I worry this schedule might increase burnout and resentment of work. It’s asystole/diastole lifestyle and may not be a healthy way to organize your life or your career.”
An Alternative Scheduling Idea
Dr. Nelson has his own unique ideas of how a group’s shift assignments should work to ensure better coverage and keep hospitalists happy. His ideas are not just theories—his own group lives and works by a flexible arrangement.
Their schedule is partly dictated by a desire to keep the physicians happy and healthy. “I believe a constant mix of work and the rest of your life is best,” says Dr. Nelson. “You shouldn’t have to put the rest of your life into the seven days that you’re off.”
So Dr. Nelson’s practice allows considerable flexibility to each physician, but ensures that any given workday is shorter than 12 hours. “I think it’s better not to have a rigidly repeating schedule,” he explains.
Dr. Nelson’s group uses pagers to ensure a hospitalist is always available during coverage hours, but they don’t adhere to a strict schedule. “So many groups work specified shifts, whether it’s 10 or 12 hours, and I think there’s a better idea,” he says. “If everyone has to punch a clock, it interferes with flexibility. I would not tell doctors when to start or stop.”
Of course, as a group, someone has to be available for emergencies all the time, and physicians may need to start daily rounds to write most discharge orders by a certain time. “I have a pager on by 7 a.m., but nothing says I have to be in the hospital by 7 a.m.,” says Dr. Nelson. “It’s often in my interest to start rounding earlier than 7 a.m. so that I can finish earlier or have time for a break later in the day.”
Greater Flexibility = Better Coverage
Another benefit to moving to shorter, more flexible days is ensuring adequate coverage. “Rigidly defined shifts almost never precisely match the day’s workload,” points out Dr. Nelson. Therefore, his practice boosts staffing to cover busy periods. “My recommendation is to intentionally overstaff for the average day’s workload. When it’s busy, everyone can pitch in and work an extra one or two hours.”
If it’s not busy, one or more doctors may leave early. “This is nimble and responsive to the day-to-day workload,” says Dr. Nelson.
To move from a seven on, seven off schedule to this model, Dr. Nelson recommends that every doctor in the practice work 30 to 40 more days annually. A seven on, seven off schedule would have a physician work 182.5 days per year; if you decrease the hours per day and boost the number of working days to 220 a year, your physicians will be working the same number of hours, but in shorter days—even if the practice workload stays the same and each individual doctor’s annual productivity stays the same.
“It’s more realistic to work more days when they’re not so grueling,” says Dr. Nelson. “Plus, you have a built-in capacity to meet a sudden increase in workload. Imagine an eight-man group, where four doctors each work 12-hour shifts. Now imagine that instead of four, you get a fifth doctor to show up every day. [You can get this fifth doctor without adding staff if each doctor works more days annually.] When a day is unpredictably busy, the physicians won’t be absolutely overwhelmed. If it’s not busy, you can send someone home early. You get a lot more flexibility.”
For a hospital medicine group, implementing a flexible schedule such as this generally requires payment for production, which ties individual physicians into the economic health of their group. Compensation matches workload, allowing individual physicians to work to their values—more money or more free time.
“I think it’s better to pay on production,” says Dr. Nelson. “That way each person has the opportunity to choose. If one values money, he can volunteer to stay and work more and make more money. Each works to their own sweet spot, whereas a seven on, seven off schedule with rigidly defined shifts forces everyone to do the same thing.”
Physicians working on a flexible schedule still need to get their work finished each day, but they have more autonomy in how and when they get it done. “Doctors who work fast can go home early; physicians can decide for themselves the right balance for spending time each patient,” says Dr. Nelson. “As long as they understand there are economic consequences … and act with reasonableness. In our group, we get the work done. There’s no official start or stop time. Each of us chooses an individual work style. There are boundaries; the work needs to be done. There are costs as well, but I believe this system is healthy and liberating.” TH
Jane Jerrard regularly writes “Career Development.”
SHM Surveys Revisited
The Benchmarks Committee has had a busy 2006 so far. Many thanks to the 400-plus hospital medicine groups that completed the 2005-06 SHM survey, “The Authoritative Source on the State of Hospital Medicine,” as well as those of you who participated in the follow-up survey to clarify questions around additional revenue or supplements to program income.
We had some behind-the-scenes work on the survey. After the first pass of data analysis, it became clear that there was something amiss with the responses pertaining to the supplemental income questions. Only 47% of programs reported that they received additional income from hospitals or other sources. This seemed incompatible with what we know about current payment rates for fee-for-service work. A quick discussion took place among the committee and we decided to resurvey the group with more precise questions on exactly how finances flow into a program. As you have seen, the additional results bore out our suspicions. With the revised survey tool, 97% of the programs (when re-queried) reported receiving income above and beyond fees from direct patient care.
It was a Herculean task of digesting and formatting the data into usable form. SHM Senior Vice President Joe Miller deserves many thanks for poring through the data and creating something that all of you can use to better your programs.
Now, a few words about the recent annual meeting in Washington, DC: The work of the Benchmarks Committee was highlighted by SHM CEO Larry Wellikson, MD, in a plenary session on the first day of the meeting. An insightful panel discussion followed in which panel members Bob Wachter, MD (representing academic hospital medicine), Mary Jo Gorman, MD (corporate hospital medicine), and John Nelson, MD (community hospital medicine) gave some insightful commentary on the results of the survey and then fielded questions from the audience.
In between sessions at the conference, the committee held its annual face-to-face meeting and discussed plans for the year.
Under the guidance and editorial excellence of committee member Leslie Flores, the Benchmarks Committee continues to make strong progress with the dashboard project. As you may recall, this project will document and describe 10 commonly used dashboard metrics, including sample reports. There are plans for this material to be published as a supplement to The Hospitalist later this year.
The committee discussed the type of surveys conducted by SHM. A recommendation came out of our meeting to change from large-scale, all-encompassing, biannual surveys to smaller annual surveys. The annual survey would alternate its focus every other year between evaluating individuals’ productivity and compensation, and the characteristics of hospital medicine groups. Each survey would also have the flexibility to address specific timely questions that might focus on a specific research or hot topic of the day. The goal is to get our first trial survey out by the end of 2006, which would focus on group characteristics.
Lastly, a big thank you to our outgoing chairperson, Teresa Jones. Her hard work and organizational skills are going to be a tough act to follow.
Dr. Kealey is chair of SHM’s Benchmarks Committee
Advocacy Day Educates Lawmakers about Hospital Medicine
By Eric Siegal, MD
As reported in the SHM Meeting Reporter (see July The Hospitalist, supplement 1), SHM’s first Legislative Advocacy Day was an overwhelming success. More than 70 members from 29 states visited Capitol Hill on May 3 to educate lawmakers and their staffs about hospital medicine and SHM’s proposals to improve the quality of care in our nation’s hospitals.
Advocacy Day participants attended a morning briefing that covered procedural tips on how to have a successful meeting and the health issues currently before Congress—and SHM’s positions—before leaving for previously scheduled appointments on Capitol Hill.
Once there, hospitalists took time to educate legislators and their staff members about the fastest growing medical specialty in the United States, and then turned to SHM’s recommendations for improving the quality, safety, and cost-effectiveness of inpatient medical care.
Among the issues discussed with lawmakers: the need for more funding for the Agency for Healthcare Research and Quality (AHRQ); SHM support for federal initiatives to measure resource use and improve quality, including a CMS demonstration project to assess the contributions of hospital medicine programs to improve patient care and more efficient management of hospital resources; and the importance of gainsharing demonstration projects that focus on inpatient medical services such as those provided by hospital medicine programs.
More than 130 appointments were scheduled with House and Senate offices, many with members of Congress who sit on the key health committees with jurisdiction over Medicare as well as on committees responsible for determining funding levels for the National Institutes of Health, the CDC, and the Agency for Healthcare Research and Quality.
SHM encourages those of you who participated in Advocacy Day to thank the lawmakers and staff with whom you visited (view the sample thank-you letter and instructions online at www.hospitalmedicine.org under “Advocacy & Policy”).
Advocacy Day opened doors to congressional offices; follow-up from SHM members will keep hospital medicine’s issues before lawmakers as they vote on legislation of importance to our specialty. The more SHM members interact with members of Congress and their staff, the louder our voices and the more effective our messages. Advocacy Day is just the beginning of regular contact by hospitalists with their elected representatives in Washington.
A New Way to Get Everything SHM
SHM has launched the SHM Store, a new Internet-based marketplace that will redefine the way SHM educational products and apparel are distributed. The online store will be a convenient option for hectic lifestyles because it will be open 24 hours a day and can be accessed from anywhere there is an Internet connection.
The SHM Store is user-friendly and allows you to easily and quickly purchase the quality products and apparel that you have come to expect from SHM. Apparel and accessories include men’s and women’s wind jackets, golf shirts, scrub tops, baseball caps, and lapel pins—all with the SHM logo.
You’ll also find the most up-to-date educational materials from SHM. The 2005-2006 results of the SHM survey, “The Authoritative Source on the State of Hospital Medicine,” can be ordered in CD and print format. The Practice Management Course CD with binder is also available. This combination package includes all of the materials distributed at an onsite presentation of the course. And, last but not least, get your very own copy or additional copies of The Core Competencies in Hospital Medicine: A Framework For Curriculum Development.
The ordering process is simple. Access the SHM Store at www.hospitalmedicine.org/shmstore or navigate from www.hospitalmedicine.org and click on SHM Store. The store allows you to browse available products and descriptions. When you see something you want, select the quantity you’d like to purchase and add the items to your shopping cart. Once you have completed your shopping trip, click “Check Out.” A confirmation of your transaction will be sent to your e-mail inbox and your products will be shipped to your attention.
It’s that easy. Make sure you go online to browse the new SHM Store. If you have any questions or would like to learn more about the SHM Store, contact SHM at CustomerService@hospitalmedicine. org.
SHM, Health Groups Urge House to Boost Discretionary Funding
SHM joined more than 800 health, education, and labor organizations in writing a May 8 letter to the House leadership. Organized by the Coalition for Health Funding and the Committee on Education Funding, the letter calls on Congress to add $7 billion to the budget in discretionary funding for health, education, and labor programs. It asks lawmakers to ensure that the final allocation for the House and Senate Labor, Health and Human Services, Education Appropriations Subcommittees reflects a $7 billion increase above the President’s request for these critically important programs in FY 2007.
“While our organizations represent a wide array of domestic priorities,” the letter states, “we are united in our effort to advance the bipartisan goal of adding $7 billion in discretionary funding for health, education, labor enforcement, job training, and social services programs as the budget process moves forward. On behalf of our millions of constituents, we strongly urge you to provide at least $7 billion in additional federal support to restore funding levels to FY 2005. This is essential to sustain the well-being and prosperity of our nation.”
Agencies whose funding could be boosted by the additional spending called for in the coalition letter include the Agency for Healthcare Research and Quality, the National Institutes of Health, and the Centers for Disease Control and Prevention.
For full coverage of May 2006 advocacy and policy news, visit www.hospitalmedicine.org. TH
Dr. Siegal is chair of SHM’s Public Policy Committee.
SHM: BEHIND THE SCENES
Education and Quality Initiatives: SHM’s Heart and Soul
By Geri Barnes

This month’s SHM staff article highlights the department responsible for SHM’s education and quality initiatives. While my fellow senior managers may disagree, I believe that we are the heart and soul of SHM in meeting members’ needs. So important is this organizational focus that the Education Committee, chaired by Preetha Basaviah, MD, has its own mission, which parallels and provides detail to the organizational mission of promoting excellence in the practice of hospital medicine. And the Hospital Quality and Patient Safety Committee, chaired by Mahalakshmi Halasyamani, MD, is one of the most dynamic and prolific of SHM’s committees.
We know that members join SHM for the opportunity to effect change and network with colleagues. Equally strong is the quest for educational resources that will facilitate their efforts in improving quality inpatient care. SHM’s education plan focuses and organizes our energy on developing those resources.
SHM’s resources come in many forms. The most visible is our annual meeting. By all accounts, the 2006 annual meeting was extremely successful. It was our largest meeting to date, with almost 1,200 attendees, 99% of whom were members. That number represents more than 21% of our total membership. I wonder how many other organizations can boast of such a high percentage of member attendance at their annual meeting. The attendees actively participated in the educational sessions and the Research, Innovations, and Clinical Vignettes poster session, visited the exhibits, and networked during breaks and social events. To enhance the educational experience, we created a password-protected Web site where registrants could access the handouts for sessions they planned to attend. Because of the value of these materials, we are currently determining ways to utilize the handouts to expand our educational resources.
For several years, SHM has presented the Leadership Academy and “Best Practices in Managing a Hospital Medicine Program” course. These courses are so popular that they have become a mainstay of SHM educational programs and are offered on an annual basis. In September we will present the first Level II Leadership Academy designed to build upon and expand Leadership Academy I. Additionally, “Fundamentals in Billing and Coding” a pre-course to the University of California San Francisco “Management of the Hospitalized Patient” course will be offered in October for the first time. This outgrowth of the Best Practices course was identified as a need by attendees and other members. We anticipate that we will continue to offer these important programs for many years to come.
While we reach a significant number of hospitalists and other healthcare providers through our annual meeting and other face-to-face meetings, we reach many more through other educational and quality improvement efforts. Hospitalists, in their unique role as providers responsible for the general medical care of hospitalized patients, find themselves filling roles as key players and drivers of institutional quality improvement. To aid them in this effort, we’ve developed Web-based resource rooms designed to facilitate the implementation of a quality improvement program for specific disease state/clinical condition, including antimicrobial resistance, stroke, venous thromboembolism, and heart failure. Resource rooms on glycemic control and discharge planning are currently under development.
For most resource rooms, the key is the QI Workbook, a resource built on proven principles of quality improvement, personal experiences, and evidence-based medicine. Resources in addition to the workbook include slide sets that can be used in training sessions, “Teaching Pearls,” patient education resources, and clinical tools in the form of algorithms, order sets, and discharge planning sheets. Most of the resource rooms have online CME programs and each room has a well-developed bibliography.
What will likely prove to be SHM’s most far-reaching resource is The Core Competencies in Hospital Medicine: A Framework For Curriculum Development. Published earlier this year as a supplement to the Journal of Hospital Medicine, the Core Competencies provides a structure for professional and curricular development based on a shared understanding of the essential knowledge, skills, and attitudes expected of physicians working as hospitalists. While the target audience is the directors of hospitalist programs and fellowships and residency programs (and medical school internal medicine clerkships), imagine the number of people reached when the Core Competencies touch hospitalist students across the board. Additionally, the Core Competencies are the focal point for every educational and quality improvement initiative that we undertake. This document will continue to drive the content of each annual meeting, provide direction for the organization, and help us prioritize the development of resources rooms and other educational and quality improvement resources.
SHM is lucky to have partners who understand the importance of hospitalists as key members of the multidisciplinary team and the army that will lead the charge in implementing protocols to improve patient care. From foundations and sister associations, to government and industry, we partner with organizations that appreciate the role that hospitalists play in improving the healthcare system. The partnerships have led to the development of toolkits, resource rooms, CME modules, and other important resources. New initiatives soon to be launched are mentored implementation programs and demonstration projects that will provide us with increased knowledge of how our resources are used and identify areas in which they can be improved.
What is required on a staff level to make this happen? A commitment to do whatever it takes to get the job done. Six of us are equally dedicated to leading, managing, and supporting these efforts. In addition to me, staff members Tina Budnitz, Erica Pearson, Joy Wittnebert, Lillian Higgins, and Theresa Jones chart new ground and are actively engaged in a dynamic learning process on a daily basis. But it is our members and experts that drive this process, and we are grateful for their patience and guidance.
The Education and Quality Initiatives staff members do not work in a vacuum in the national office. We have the support and brainpower of the rest of the staff, with whom we collaborate daily. Membership and marketing, information technology, and business operations staff all play a role in our success.
What makes the national office run as a well-oiled machine? Next month you’ll hear from Steve Poitras, director, Business Operations, who is instrumental in making that happen.
Barnes is director, Education & Quality Initiatives, for SHM.
The Benchmarks Committee has had a busy 2006 so far. Many thanks to the 400-plus hospital medicine groups that completed the 2005-06 SHM survey, “The Authoritative Source on the State of Hospital Medicine,” as well as those of you who participated in the follow-up survey to clarify questions around additional revenue or supplements to program income.
We had some behind-the-scenes work on the survey. After the first pass of data analysis, it became clear that there was something amiss with the responses pertaining to the supplemental income questions. Only 47% of programs reported that they received additional income from hospitals or other sources. This seemed incompatible with what we know about current payment rates for fee-for-service work. A quick discussion took place among the committee and we decided to resurvey the group with more precise questions on exactly how finances flow into a program. As you have seen, the additional results bore out our suspicions. With the revised survey tool, 97% of the programs (when re-queried) reported receiving income above and beyond fees from direct patient care.
It was a Herculean task of digesting and formatting the data into usable form. SHM Senior Vice President Joe Miller deserves many thanks for poring through the data and creating something that all of you can use to better your programs.
Now, a few words about the recent annual meeting in Washington, DC: The work of the Benchmarks Committee was highlighted by SHM CEO Larry Wellikson, MD, in a plenary session on the first day of the meeting. An insightful panel discussion followed in which panel members Bob Wachter, MD (representing academic hospital medicine), Mary Jo Gorman, MD (corporate hospital medicine), and John Nelson, MD (community hospital medicine) gave some insightful commentary on the results of the survey and then fielded questions from the audience.
In between sessions at the conference, the committee held its annual face-to-face meeting and discussed plans for the year.
Under the guidance and editorial excellence of committee member Leslie Flores, the Benchmarks Committee continues to make strong progress with the dashboard project. As you may recall, this project will document and describe 10 commonly used dashboard metrics, including sample reports. There are plans for this material to be published as a supplement to The Hospitalist later this year.
The committee discussed the type of surveys conducted by SHM. A recommendation came out of our meeting to change from large-scale, all-encompassing, biannual surveys to smaller annual surveys. The annual survey would alternate its focus every other year between evaluating individuals’ productivity and compensation, and the characteristics of hospital medicine groups. Each survey would also have the flexibility to address specific timely questions that might focus on a specific research or hot topic of the day. The goal is to get our first trial survey out by the end of 2006, which would focus on group characteristics.
Lastly, a big thank you to our outgoing chairperson, Teresa Jones. Her hard work and organizational skills are going to be a tough act to follow.
Dr. Kealey is chair of SHM’s Benchmarks Committee
Advocacy Day Educates Lawmakers about Hospital Medicine
By Eric Siegal, MD
As reported in the SHM Meeting Reporter (see July The Hospitalist, supplement 1), SHM’s first Legislative Advocacy Day was an overwhelming success. More than 70 members from 29 states visited Capitol Hill on May 3 to educate lawmakers and their staffs about hospital medicine and SHM’s proposals to improve the quality of care in our nation’s hospitals.
Advocacy Day participants attended a morning briefing that covered procedural tips on how to have a successful meeting and the health issues currently before Congress—and SHM’s positions—before leaving for previously scheduled appointments on Capitol Hill.
Once there, hospitalists took time to educate legislators and their staff members about the fastest growing medical specialty in the United States, and then turned to SHM’s recommendations for improving the quality, safety, and cost-effectiveness of inpatient medical care.
Among the issues discussed with lawmakers: the need for more funding for the Agency for Healthcare Research and Quality (AHRQ); SHM support for federal initiatives to measure resource use and improve quality, including a CMS demonstration project to assess the contributions of hospital medicine programs to improve patient care and more efficient management of hospital resources; and the importance of gainsharing demonstration projects that focus on inpatient medical services such as those provided by hospital medicine programs.
More than 130 appointments were scheduled with House and Senate offices, many with members of Congress who sit on the key health committees with jurisdiction over Medicare as well as on committees responsible for determining funding levels for the National Institutes of Health, the CDC, and the Agency for Healthcare Research and Quality.
SHM encourages those of you who participated in Advocacy Day to thank the lawmakers and staff with whom you visited (view the sample thank-you letter and instructions online at www.hospitalmedicine.org under “Advocacy & Policy”).
Advocacy Day opened doors to congressional offices; follow-up from SHM members will keep hospital medicine’s issues before lawmakers as they vote on legislation of importance to our specialty. The more SHM members interact with members of Congress and their staff, the louder our voices and the more effective our messages. Advocacy Day is just the beginning of regular contact by hospitalists with their elected representatives in Washington.
A New Way to Get Everything SHM
SHM has launched the SHM Store, a new Internet-based marketplace that will redefine the way SHM educational products and apparel are distributed. The online store will be a convenient option for hectic lifestyles because it will be open 24 hours a day and can be accessed from anywhere there is an Internet connection.
The SHM Store is user-friendly and allows you to easily and quickly purchase the quality products and apparel that you have come to expect from SHM. Apparel and accessories include men’s and women’s wind jackets, golf shirts, scrub tops, baseball caps, and lapel pins—all with the SHM logo.
You’ll also find the most up-to-date educational materials from SHM. The 2005-2006 results of the SHM survey, “The Authoritative Source on the State of Hospital Medicine,” can be ordered in CD and print format. The Practice Management Course CD with binder is also available. This combination package includes all of the materials distributed at an onsite presentation of the course. And, last but not least, get your very own copy or additional copies of The Core Competencies in Hospital Medicine: A Framework For Curriculum Development.
The ordering process is simple. Access the SHM Store at www.hospitalmedicine.org/shmstore or navigate from www.hospitalmedicine.org and click on SHM Store. The store allows you to browse available products and descriptions. When you see something you want, select the quantity you’d like to purchase and add the items to your shopping cart. Once you have completed your shopping trip, click “Check Out.” A confirmation of your transaction will be sent to your e-mail inbox and your products will be shipped to your attention.
It’s that easy. Make sure you go online to browse the new SHM Store. If you have any questions or would like to learn more about the SHM Store, contact SHM at CustomerService@hospitalmedicine. org.
SHM, Health Groups Urge House to Boost Discretionary Funding
SHM joined more than 800 health, education, and labor organizations in writing a May 8 letter to the House leadership. Organized by the Coalition for Health Funding and the Committee on Education Funding, the letter calls on Congress to add $7 billion to the budget in discretionary funding for health, education, and labor programs. It asks lawmakers to ensure that the final allocation for the House and Senate Labor, Health and Human Services, Education Appropriations Subcommittees reflects a $7 billion increase above the President’s request for these critically important programs in FY 2007.
“While our organizations represent a wide array of domestic priorities,” the letter states, “we are united in our effort to advance the bipartisan goal of adding $7 billion in discretionary funding for health, education, labor enforcement, job training, and social services programs as the budget process moves forward. On behalf of our millions of constituents, we strongly urge you to provide at least $7 billion in additional federal support to restore funding levels to FY 2005. This is essential to sustain the well-being and prosperity of our nation.”
Agencies whose funding could be boosted by the additional spending called for in the coalition letter include the Agency for Healthcare Research and Quality, the National Institutes of Health, and the Centers for Disease Control and Prevention.
For full coverage of May 2006 advocacy and policy news, visit www.hospitalmedicine.org. TH
Dr. Siegal is chair of SHM’s Public Policy Committee.
SHM: BEHIND THE SCENES
Education and Quality Initiatives: SHM’s Heart and Soul
By Geri Barnes
This month’s SHM staff article highlights the department responsible for SHM’s education and quality initiatives. While my fellow senior managers may disagree, I believe that we are the heart and soul of SHM in meeting members’ needs. So important is this organizational focus that the Education Committee, chaired by Preetha Basaviah, MD, has its own mission, which parallels and provides detail to the organizational mission of promoting excellence in the practice of hospital medicine. And the Hospital Quality and Patient Safety Committee, chaired by Mahalakshmi Halasyamani, MD, is one of the most dynamic and prolific of SHM’s committees.
We know that members join SHM for the opportunity to effect change and network with colleagues. Equally strong is the quest for educational resources that will facilitate their efforts in improving quality inpatient care. SHM’s education plan focuses and organizes our energy on developing those resources.
SHM’s resources come in many forms. The most visible is our annual meeting. By all accounts, the 2006 annual meeting was extremely successful. It was our largest meeting to date, with almost 1,200 attendees, 99% of whom were members. That number represents more than 21% of our total membership. I wonder how many other organizations can boast of such a high percentage of member attendance at their annual meeting. The attendees actively participated in the educational sessions and the Research, Innovations, and Clinical Vignettes poster session, visited the exhibits, and networked during breaks and social events. To enhance the educational experience, we created a password-protected Web site where registrants could access the handouts for sessions they planned to attend. Because of the value of these materials, we are currently determining ways to utilize the handouts to expand our educational resources.
For several years, SHM has presented the Leadership Academy and “Best Practices in Managing a Hospital Medicine Program” course. These courses are so popular that they have become a mainstay of SHM educational programs and are offered on an annual basis. In September we will present the first Level II Leadership Academy designed to build upon and expand Leadership Academy I. Additionally, “Fundamentals in Billing and Coding” a pre-course to the University of California San Francisco “Management of the Hospitalized Patient” course will be offered in October for the first time. This outgrowth of the Best Practices course was identified as a need by attendees and other members. We anticipate that we will continue to offer these important programs for many years to come.
While we reach a significant number of hospitalists and other healthcare providers through our annual meeting and other face-to-face meetings, we reach many more through other educational and quality improvement efforts. Hospitalists, in their unique role as providers responsible for the general medical care of hospitalized patients, find themselves filling roles as key players and drivers of institutional quality improvement. To aid them in this effort, we’ve developed Web-based resource rooms designed to facilitate the implementation of a quality improvement program for specific disease state/clinical condition, including antimicrobial resistance, stroke, venous thromboembolism, and heart failure. Resource rooms on glycemic control and discharge planning are currently under development.
For most resource rooms, the key is the QI Workbook, a resource built on proven principles of quality improvement, personal experiences, and evidence-based medicine. Resources in addition to the workbook include slide sets that can be used in training sessions, “Teaching Pearls,” patient education resources, and clinical tools in the form of algorithms, order sets, and discharge planning sheets. Most of the resource rooms have online CME programs and each room has a well-developed bibliography.
What will likely prove to be SHM’s most far-reaching resource is The Core Competencies in Hospital Medicine: A Framework For Curriculum Development. Published earlier this year as a supplement to the Journal of Hospital Medicine, the Core Competencies provides a structure for professional and curricular development based on a shared understanding of the essential knowledge, skills, and attitudes expected of physicians working as hospitalists. While the target audience is the directors of hospitalist programs and fellowships and residency programs (and medical school internal medicine clerkships), imagine the number of people reached when the Core Competencies touch hospitalist students across the board. Additionally, the Core Competencies are the focal point for every educational and quality improvement initiative that we undertake. This document will continue to drive the content of each annual meeting, provide direction for the organization, and help us prioritize the development of resources rooms and other educational and quality improvement resources.
SHM is lucky to have partners who understand the importance of hospitalists as key members of the multidisciplinary team and the army that will lead the charge in implementing protocols to improve patient care. From foundations and sister associations, to government and industry, we partner with organizations that appreciate the role that hospitalists play in improving the healthcare system. The partnerships have led to the development of toolkits, resource rooms, CME modules, and other important resources. New initiatives soon to be launched are mentored implementation programs and demonstration projects that will provide us with increased knowledge of how our resources are used and identify areas in which they can be improved.
What is required on a staff level to make this happen? A commitment to do whatever it takes to get the job done. Six of us are equally dedicated to leading, managing, and supporting these efforts. In addition to me, staff members Tina Budnitz, Erica Pearson, Joy Wittnebert, Lillian Higgins, and Theresa Jones chart new ground and are actively engaged in a dynamic learning process on a daily basis. But it is our members and experts that drive this process, and we are grateful for their patience and guidance.
The Education and Quality Initiatives staff members do not work in a vacuum in the national office. We have the support and brainpower of the rest of the staff, with whom we collaborate daily. Membership and marketing, information technology, and business operations staff all play a role in our success.
What makes the national office run as a well-oiled machine? Next month you’ll hear from Steve Poitras, director, Business Operations, who is instrumental in making that happen.
Barnes is director, Education & Quality Initiatives, for SHM.
The Benchmarks Committee has had a busy 2006 so far. Many thanks to the 400-plus hospital medicine groups that completed the 2005-06 SHM survey, “The Authoritative Source on the State of Hospital Medicine,” as well as those of you who participated in the follow-up survey to clarify questions around additional revenue or supplements to program income.
We had some behind-the-scenes work on the survey. After the first pass of data analysis, it became clear that there was something amiss with the responses pertaining to the supplemental income questions. Only 47% of programs reported that they received additional income from hospitals or other sources. This seemed incompatible with what we know about current payment rates for fee-for-service work. A quick discussion took place among the committee and we decided to resurvey the group with more precise questions on exactly how finances flow into a program. As you have seen, the additional results bore out our suspicions. With the revised survey tool, 97% of the programs (when re-queried) reported receiving income above and beyond fees from direct patient care.
It was a Herculean task of digesting and formatting the data into usable form. SHM Senior Vice President Joe Miller deserves many thanks for poring through the data and creating something that all of you can use to better your programs.
Now, a few words about the recent annual meeting in Washington, DC: The work of the Benchmarks Committee was highlighted by SHM CEO Larry Wellikson, MD, in a plenary session on the first day of the meeting. An insightful panel discussion followed in which panel members Bob Wachter, MD (representing academic hospital medicine), Mary Jo Gorman, MD (corporate hospital medicine), and John Nelson, MD (community hospital medicine) gave some insightful commentary on the results of the survey and then fielded questions from the audience.
In between sessions at the conference, the committee held its annual face-to-face meeting and discussed plans for the year.
Under the guidance and editorial excellence of committee member Leslie Flores, the Benchmarks Committee continues to make strong progress with the dashboard project. As you may recall, this project will document and describe 10 commonly used dashboard metrics, including sample reports. There are plans for this material to be published as a supplement to The Hospitalist later this year.
The committee discussed the type of surveys conducted by SHM. A recommendation came out of our meeting to change from large-scale, all-encompassing, biannual surveys to smaller annual surveys. The annual survey would alternate its focus every other year between evaluating individuals’ productivity and compensation, and the characteristics of hospital medicine groups. Each survey would also have the flexibility to address specific timely questions that might focus on a specific research or hot topic of the day. The goal is to get our first trial survey out by the end of 2006, which would focus on group characteristics.
Lastly, a big thank you to our outgoing chairperson, Teresa Jones. Her hard work and organizational skills are going to be a tough act to follow.
Dr. Kealey is chair of SHM’s Benchmarks Committee
Advocacy Day Educates Lawmakers about Hospital Medicine
By Eric Siegal, MD
As reported in the SHM Meeting Reporter (see July The Hospitalist, supplement 1), SHM’s first Legislative Advocacy Day was an overwhelming success. More than 70 members from 29 states visited Capitol Hill on May 3 to educate lawmakers and their staffs about hospital medicine and SHM’s proposals to improve the quality of care in our nation’s hospitals.
Advocacy Day participants attended a morning briefing that covered procedural tips on how to have a successful meeting and the health issues currently before Congress—and SHM’s positions—before leaving for previously scheduled appointments on Capitol Hill.
Once there, hospitalists took time to educate legislators and their staff members about the fastest growing medical specialty in the United States, and then turned to SHM’s recommendations for improving the quality, safety, and cost-effectiveness of inpatient medical care.
Among the issues discussed with lawmakers: the need for more funding for the Agency for Healthcare Research and Quality (AHRQ); SHM support for federal initiatives to measure resource use and improve quality, including a CMS demonstration project to assess the contributions of hospital medicine programs to improve patient care and more efficient management of hospital resources; and the importance of gainsharing demonstration projects that focus on inpatient medical services such as those provided by hospital medicine programs.
More than 130 appointments were scheduled with House and Senate offices, many with members of Congress who sit on the key health committees with jurisdiction over Medicare as well as on committees responsible for determining funding levels for the National Institutes of Health, the CDC, and the Agency for Healthcare Research and Quality.
SHM encourages those of you who participated in Advocacy Day to thank the lawmakers and staff with whom you visited (view the sample thank-you letter and instructions online at www.hospitalmedicine.org under “Advocacy & Policy”).
Advocacy Day opened doors to congressional offices; follow-up from SHM members will keep hospital medicine’s issues before lawmakers as they vote on legislation of importance to our specialty. The more SHM members interact with members of Congress and their staff, the louder our voices and the more effective our messages. Advocacy Day is just the beginning of regular contact by hospitalists with their elected representatives in Washington.
A New Way to Get Everything SHM
SHM has launched the SHM Store, a new Internet-based marketplace that will redefine the way SHM educational products and apparel are distributed. The online store will be a convenient option for hectic lifestyles because it will be open 24 hours a day and can be accessed from anywhere there is an Internet connection.
The SHM Store is user-friendly and allows you to easily and quickly purchase the quality products and apparel that you have come to expect from SHM. Apparel and accessories include men’s and women’s wind jackets, golf shirts, scrub tops, baseball caps, and lapel pins—all with the SHM logo.
You’ll also find the most up-to-date educational materials from SHM. The 2005-2006 results of the SHM survey, “The Authoritative Source on the State of Hospital Medicine,” can be ordered in CD and print format. The Practice Management Course CD with binder is also available. This combination package includes all of the materials distributed at an onsite presentation of the course. And, last but not least, get your very own copy or additional copies of The Core Competencies in Hospital Medicine: A Framework For Curriculum Development.
The ordering process is simple. Access the SHM Store at www.hospitalmedicine.org/shmstore or navigate from www.hospitalmedicine.org and click on SHM Store. The store allows you to browse available products and descriptions. When you see something you want, select the quantity you’d like to purchase and add the items to your shopping cart. Once you have completed your shopping trip, click “Check Out.” A confirmation of your transaction will be sent to your e-mail inbox and your products will be shipped to your attention.
It’s that easy. Make sure you go online to browse the new SHM Store. If you have any questions or would like to learn more about the SHM Store, contact SHM at CustomerService@hospitalmedicine. org.
SHM, Health Groups Urge House to Boost Discretionary Funding
SHM joined more than 800 health, education, and labor organizations in writing a May 8 letter to the House leadership. Organized by the Coalition for Health Funding and the Committee on Education Funding, the letter calls on Congress to add $7 billion to the budget in discretionary funding for health, education, and labor programs. It asks lawmakers to ensure that the final allocation for the House and Senate Labor, Health and Human Services, Education Appropriations Subcommittees reflects a $7 billion increase above the President’s request for these critically important programs in FY 2007.
“While our organizations represent a wide array of domestic priorities,” the letter states, “we are united in our effort to advance the bipartisan goal of adding $7 billion in discretionary funding for health, education, labor enforcement, job training, and social services programs as the budget process moves forward. On behalf of our millions of constituents, we strongly urge you to provide at least $7 billion in additional federal support to restore funding levels to FY 2005. This is essential to sustain the well-being and prosperity of our nation.”
Agencies whose funding could be boosted by the additional spending called for in the coalition letter include the Agency for Healthcare Research and Quality, the National Institutes of Health, and the Centers for Disease Control and Prevention.
For full coverage of May 2006 advocacy and policy news, visit www.hospitalmedicine.org. TH
Dr. Siegal is chair of SHM’s Public Policy Committee.
SHM: BEHIND THE SCENES
Education and Quality Initiatives: SHM’s Heart and Soul
By Geri Barnes
This month’s SHM staff article highlights the department responsible for SHM’s education and quality initiatives. While my fellow senior managers may disagree, I believe that we are the heart and soul of SHM in meeting members’ needs. So important is this organizational focus that the Education Committee, chaired by Preetha Basaviah, MD, has its own mission, which parallels and provides detail to the organizational mission of promoting excellence in the practice of hospital medicine. And the Hospital Quality and Patient Safety Committee, chaired by Mahalakshmi Halasyamani, MD, is one of the most dynamic and prolific of SHM’s committees.
We know that members join SHM for the opportunity to effect change and network with colleagues. Equally strong is the quest for educational resources that will facilitate their efforts in improving quality inpatient care. SHM’s education plan focuses and organizes our energy on developing those resources.
SHM’s resources come in many forms. The most visible is our annual meeting. By all accounts, the 2006 annual meeting was extremely successful. It was our largest meeting to date, with almost 1,200 attendees, 99% of whom were members. That number represents more than 21% of our total membership. I wonder how many other organizations can boast of such a high percentage of member attendance at their annual meeting. The attendees actively participated in the educational sessions and the Research, Innovations, and Clinical Vignettes poster session, visited the exhibits, and networked during breaks and social events. To enhance the educational experience, we created a password-protected Web site where registrants could access the handouts for sessions they planned to attend. Because of the value of these materials, we are currently determining ways to utilize the handouts to expand our educational resources.
For several years, SHM has presented the Leadership Academy and “Best Practices in Managing a Hospital Medicine Program” course. These courses are so popular that they have become a mainstay of SHM educational programs and are offered on an annual basis. In September we will present the first Level II Leadership Academy designed to build upon and expand Leadership Academy I. Additionally, “Fundamentals in Billing and Coding” a pre-course to the University of California San Francisco “Management of the Hospitalized Patient” course will be offered in October for the first time. This outgrowth of the Best Practices course was identified as a need by attendees and other members. We anticipate that we will continue to offer these important programs for many years to come.
While we reach a significant number of hospitalists and other healthcare providers through our annual meeting and other face-to-face meetings, we reach many more through other educational and quality improvement efforts. Hospitalists, in their unique role as providers responsible for the general medical care of hospitalized patients, find themselves filling roles as key players and drivers of institutional quality improvement. To aid them in this effort, we’ve developed Web-based resource rooms designed to facilitate the implementation of a quality improvement program for specific disease state/clinical condition, including antimicrobial resistance, stroke, venous thromboembolism, and heart failure. Resource rooms on glycemic control and discharge planning are currently under development.
For most resource rooms, the key is the QI Workbook, a resource built on proven principles of quality improvement, personal experiences, and evidence-based medicine. Resources in addition to the workbook include slide sets that can be used in training sessions, “Teaching Pearls,” patient education resources, and clinical tools in the form of algorithms, order sets, and discharge planning sheets. Most of the resource rooms have online CME programs and each room has a well-developed bibliography.
What will likely prove to be SHM’s most far-reaching resource is The Core Competencies in Hospital Medicine: A Framework For Curriculum Development. Published earlier this year as a supplement to the Journal of Hospital Medicine, the Core Competencies provides a structure for professional and curricular development based on a shared understanding of the essential knowledge, skills, and attitudes expected of physicians working as hospitalists. While the target audience is the directors of hospitalist programs and fellowships and residency programs (and medical school internal medicine clerkships), imagine the number of people reached when the Core Competencies touch hospitalist students across the board. Additionally, the Core Competencies are the focal point for every educational and quality improvement initiative that we undertake. This document will continue to drive the content of each annual meeting, provide direction for the organization, and help us prioritize the development of resources rooms and other educational and quality improvement resources.
SHM is lucky to have partners who understand the importance of hospitalists as key members of the multidisciplinary team and the army that will lead the charge in implementing protocols to improve patient care. From foundations and sister associations, to government and industry, we partner with organizations that appreciate the role that hospitalists play in improving the healthcare system. The partnerships have led to the development of toolkits, resource rooms, CME modules, and other important resources. New initiatives soon to be launched are mentored implementation programs and demonstration projects that will provide us with increased knowledge of how our resources are used and identify areas in which they can be improved.
What is required on a staff level to make this happen? A commitment to do whatever it takes to get the job done. Six of us are equally dedicated to leading, managing, and supporting these efforts. In addition to me, staff members Tina Budnitz, Erica Pearson, Joy Wittnebert, Lillian Higgins, and Theresa Jones chart new ground and are actively engaged in a dynamic learning process on a daily basis. But it is our members and experts that drive this process, and we are grateful for their patience and guidance.
The Education and Quality Initiatives staff members do not work in a vacuum in the national office. We have the support and brainpower of the rest of the staff, with whom we collaborate daily. Membership and marketing, information technology, and business operations staff all play a role in our success.
What makes the national office run as a well-oiled machine? Next month you’ll hear from Steve Poitras, director, Business Operations, who is instrumental in making that happen.
Barnes is director, Education & Quality Initiatives, for SHM.
Virus Alerts
CDC Urges Awareness of Measles in Americans Returning from Germany
By Alfred Valles, resident, internal medicine, Mayo Clinic College of Medicine
The Centers for Disease Control and Prevention (CDC) has issued an alert urging American travelers to remain aware of the possibility of measles exposure. Many Americans have traveled to and from Germany for the World Cup soccer championship games. Three of the twelve hosting cities—Cologne, Dortmund, and Gelsenkirchen—are of particular concern, given the recent measles outbreaks that have been reported in those cities and their surrounding areas.
Since January 1 of this year, some 1,200 cases have been identified in or near these cities. American travelers were undoubtedly among the large crowds of people gathered to pay homage to their favorite sport, and many others will visit Germany on vacation or business, making transmission of this respiratory droplet-born pathogen a very real threat.
The CDC recommends the following precautions:
- Travelers who plan to go to Germany should check their immunization records and visit their doctors if they are not immune to measles or are not sure they are.
- People returning from Germany, especially those who went to see the World Cup, should see a healthcare provider if they develop the symptoms of measles, including a fever, a raised rash that begins on the face and spreads to the arms and legs, a cough, red eyes, or a runny nose.
- People with these symptoms should limit their contact with others.
- Clinicians seeing patients with these symptoms should inquire about travel history and immunization status.
This warning is not to be taken lightly. Approximately two of every 1,000 patients infected with measles will die of the disease. Complications such as encephalitis are of particular concern for those who are malnourished or immunosuppressed.
Remember, live virus measles vaccine given within 72 hours of exposure may prevent the disease, while immune globulin given up to six days after exposure may prevent complications of measles in those who are at risk, including pregnant women, people with weak immune systems, and children.
The World cup can be dangerous, even for non-players. For more information about the measles outbreak and travel precautions, visit www.cdc.gov.
Lymphocytic Choriomeningitis Virus: Facts and Prevention
By the Special Pathogens Branch, CDC
In May 2005, the CDC investigated a cluster of lymphocytic choriomeningitis virus (LCMV) illnesses in four solid organ transplant recipients from a common donor, three of whom died. The source of the LCMV was traced to a hamster that had recently been acquired by a member of the donor’s household. It was subsequently determined that several LCMV-infected pet rodents had originated from a single distributor, who may have distributed other infected rodents to pet stores in the northeastern and midwestern United States.1 However, the risk of contracting LCMV from rodent exposure is not limited only to this outbreak, nor is the danger confined only to patients undergoing organ transplant.
Clinicians need to be familiar with LCMV because of its potential to cause meningitis, its teratogenicity, and the risk that it may bring about serious disease in immunocompromised individuals.
LCMV is normally carried by wild house mice, but can be transmitted to laboratory and pet rodents at breeding facilities, in pet stores, and in homes. Humans become infected in one of the following ways:
- Through direct contact with the secretions or excretions of infected rodents;
- By inhalation of dust or droplets containing LCMV from rodents;
- As a result of transplacental spread from an infected pregnant woman to her fetus; and
- By receipt of an organ transplant from an infected donor.2
Among those tested, about 5% have shown serologic evidence of previous infection with LCMV.3,4 In healthy adults, LCMV is typically a nonspecific viral syndrome sometimes followed by aseptic meningitis or other neurologic signs. Patients with weakened immune systems can suffer severe, possibly fatal systemic illness.2,5 Maternal infection with LCMV during pregnancy can result in spontaneous abortion or early neonatal death, as well as in defects similar to those of other congenital infections such as toxoplasmosis and cytomegalovirus (“TORCH” infections).6-10 The proportion of developmental defects caused by LCMV is not known.
Clinicians should consider LCMV in the differential diagnosis of patients with aseptic meningitis; in cases of fetal demise or congenital defects, including congenital hydrocephalus, chorioretinitis, blindness, or mental retardation; or in recent transplant recipients who present with signs of post-transplant infection. A detailed rodent exposure history should be taken. Contact your state health department or Special Pathogens Branch, CDC (404-639-1510), for information about testing for LCMV.
Currently, there is no specific treatment for LCMV infection other than supportive care. Ribavirin inhibits LCMV multiplication in laboratory experiments but has not been tested in clinical trials.
Clinicians should counsel their patients about the risks of contracting LCMV from laboratory, pet, and wild rodents. Wild mice in the home should be controlled and removed promptly. Immunocompromised individuals and women who are pregnant or planning to become pregnant should avoid any contact with wild or pet rodents, their excretions, and their nesting materials. While a woman is pregnant, pet rodents should be housed outside the home or in a separate part of the home where other individuals can care for the pets and clean their cages. Counseling a woman already exposed to rodents during pregnancy can be challenging; for assistance, contact your state health department.
Further information about LCMV infection and its prevention, including management and prevention of rodent infestation in the home, is available from Special Pathogens Branch, CDC, at www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/lcmv.htm. For more information about diseases commonly carried by rodents, please visit www.cdc.gov/rodents. TH
References
- Centers for Disease Control and Prevention. Update: interim guidance for minimizing risk for human lymphocytic choriomeningitis virus infection associated with pet rodents. MMWR. Aug 19, 2005;54(32):799-801.
- Fischer SA, Graham MB, Kuehnert MJ, et al. Transmission of lymphocytic choriomeningitis virus by organ transplantation. N Engl J Med. 2006;354(21):2235-2249.
- Childs JE, Glass GE, Ksiazek TG, et al. Human-rodent contact and infection with lymphocytic choriomeningitis and Seoul viruses in an inner-city population. Am J Trop Med Hyg. 1991 Feb;44(2):117–121.
- Park JY, Peters CJ, Rollin PE, et al. Age distribution of lymphocytic choriomeningitis virus serum antibody in Birmingham, Alabama: evidence of a decreased risk of infection. Am J Trop Med Hyg. 1997 Jul;57(1):37–41.
- Horton J, Hotchin JE, Olson KB, et al. The effects of MP virus infection in lymphoma. Cancer Res. 1971 Aug;31(8):1066–1068.
- Barton LL, Mets MB. Congenital lymphocytic choriomeningitis virus infection: decade of rediscovery. Clin Infect Dis. 2001 Aug 1;33(3):370–374.
- Barton LL, Mets MB, Beauchamp CL. Lymphocytic choriomeningitis virus: emerging fetal teratogen. Am J Obstet Gynecol. 2002 Dec ;187(6):1715–1716.
- Wright R, Johnson D, Neumann M, et al. Congenital lymphocytic choriomeningitis virus syndrome: a disease that mimics congenital toxoplasmosis or cytomegalovirus infection. Pediatrics. 1997 Jul;100(1):E9.
- Ford-Jones EL, Ryan G . Implications for the fetus of maternal infections in pregnancy. In: Cohen J, Powderly WG, eds. Infectious Diseases, 2nd ed. New York, NY: Mosby; 2004: 709–723.
- Greenhow TL, Weintrub PS. Your diagnosis, please. Neonate with hydrocephalus. Pediatr Infect Dis J. 2003 Dec;22(12):1099, 1111–1112.
CDC Urges Awareness of Measles in Americans Returning from Germany
By Alfred Valles, resident, internal medicine, Mayo Clinic College of Medicine
The Centers for Disease Control and Prevention (CDC) has issued an alert urging American travelers to remain aware of the possibility of measles exposure. Many Americans have traveled to and from Germany for the World Cup soccer championship games. Three of the twelve hosting cities—Cologne, Dortmund, and Gelsenkirchen—are of particular concern, given the recent measles outbreaks that have been reported in those cities and their surrounding areas.
Since January 1 of this year, some 1,200 cases have been identified in or near these cities. American travelers were undoubtedly among the large crowds of people gathered to pay homage to their favorite sport, and many others will visit Germany on vacation or business, making transmission of this respiratory droplet-born pathogen a very real threat.
The CDC recommends the following precautions:
- Travelers who plan to go to Germany should check their immunization records and visit their doctors if they are not immune to measles or are not sure they are.
- People returning from Germany, especially those who went to see the World Cup, should see a healthcare provider if they develop the symptoms of measles, including a fever, a raised rash that begins on the face and spreads to the arms and legs, a cough, red eyes, or a runny nose.
- People with these symptoms should limit their contact with others.
- Clinicians seeing patients with these symptoms should inquire about travel history and immunization status.
This warning is not to be taken lightly. Approximately two of every 1,000 patients infected with measles will die of the disease. Complications such as encephalitis are of particular concern for those who are malnourished or immunosuppressed.
Remember, live virus measles vaccine given within 72 hours of exposure may prevent the disease, while immune globulin given up to six days after exposure may prevent complications of measles in those who are at risk, including pregnant women, people with weak immune systems, and children.
The World cup can be dangerous, even for non-players. For more information about the measles outbreak and travel precautions, visit www.cdc.gov.
Lymphocytic Choriomeningitis Virus: Facts and Prevention
By the Special Pathogens Branch, CDC
In May 2005, the CDC investigated a cluster of lymphocytic choriomeningitis virus (LCMV) illnesses in four solid organ transplant recipients from a common donor, three of whom died. The source of the LCMV was traced to a hamster that had recently been acquired by a member of the donor’s household. It was subsequently determined that several LCMV-infected pet rodents had originated from a single distributor, who may have distributed other infected rodents to pet stores in the northeastern and midwestern United States.1 However, the risk of contracting LCMV from rodent exposure is not limited only to this outbreak, nor is the danger confined only to patients undergoing organ transplant.
Clinicians need to be familiar with LCMV because of its potential to cause meningitis, its teratogenicity, and the risk that it may bring about serious disease in immunocompromised individuals.
LCMV is normally carried by wild house mice, but can be transmitted to laboratory and pet rodents at breeding facilities, in pet stores, and in homes. Humans become infected in one of the following ways:
- Through direct contact with the secretions or excretions of infected rodents;
- By inhalation of dust or droplets containing LCMV from rodents;
- As a result of transplacental spread from an infected pregnant woman to her fetus; and
- By receipt of an organ transplant from an infected donor.2
Among those tested, about 5% have shown serologic evidence of previous infection with LCMV.3,4 In healthy adults, LCMV is typically a nonspecific viral syndrome sometimes followed by aseptic meningitis or other neurologic signs. Patients with weakened immune systems can suffer severe, possibly fatal systemic illness.2,5 Maternal infection with LCMV during pregnancy can result in spontaneous abortion or early neonatal death, as well as in defects similar to those of other congenital infections such as toxoplasmosis and cytomegalovirus (“TORCH” infections).6-10 The proportion of developmental defects caused by LCMV is not known.
Clinicians should consider LCMV in the differential diagnosis of patients with aseptic meningitis; in cases of fetal demise or congenital defects, including congenital hydrocephalus, chorioretinitis, blindness, or mental retardation; or in recent transplant recipients who present with signs of post-transplant infection. A detailed rodent exposure history should be taken. Contact your state health department or Special Pathogens Branch, CDC (404-639-1510), for information about testing for LCMV.
Currently, there is no specific treatment for LCMV infection other than supportive care. Ribavirin inhibits LCMV multiplication in laboratory experiments but has not been tested in clinical trials.
Clinicians should counsel their patients about the risks of contracting LCMV from laboratory, pet, and wild rodents. Wild mice in the home should be controlled and removed promptly. Immunocompromised individuals and women who are pregnant or planning to become pregnant should avoid any contact with wild or pet rodents, their excretions, and their nesting materials. While a woman is pregnant, pet rodents should be housed outside the home or in a separate part of the home where other individuals can care for the pets and clean their cages. Counseling a woman already exposed to rodents during pregnancy can be challenging; for assistance, contact your state health department.
Further information about LCMV infection and its prevention, including management and prevention of rodent infestation in the home, is available from Special Pathogens Branch, CDC, at www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/lcmv.htm. For more information about diseases commonly carried by rodents, please visit www.cdc.gov/rodents. TH
References
- Centers for Disease Control and Prevention. Update: interim guidance for minimizing risk for human lymphocytic choriomeningitis virus infection associated with pet rodents. MMWR. Aug 19, 2005;54(32):799-801.
- Fischer SA, Graham MB, Kuehnert MJ, et al. Transmission of lymphocytic choriomeningitis virus by organ transplantation. N Engl J Med. 2006;354(21):2235-2249.
- Childs JE, Glass GE, Ksiazek TG, et al. Human-rodent contact and infection with lymphocytic choriomeningitis and Seoul viruses in an inner-city population. Am J Trop Med Hyg. 1991 Feb;44(2):117–121.
- Park JY, Peters CJ, Rollin PE, et al. Age distribution of lymphocytic choriomeningitis virus serum antibody in Birmingham, Alabama: evidence of a decreased risk of infection. Am J Trop Med Hyg. 1997 Jul;57(1):37–41.
- Horton J, Hotchin JE, Olson KB, et al. The effects of MP virus infection in lymphoma. Cancer Res. 1971 Aug;31(8):1066–1068.
- Barton LL, Mets MB. Congenital lymphocytic choriomeningitis virus infection: decade of rediscovery. Clin Infect Dis. 2001 Aug 1;33(3):370–374.
- Barton LL, Mets MB, Beauchamp CL. Lymphocytic choriomeningitis virus: emerging fetal teratogen. Am J Obstet Gynecol. 2002 Dec ;187(6):1715–1716.
- Wright R, Johnson D, Neumann M, et al. Congenital lymphocytic choriomeningitis virus syndrome: a disease that mimics congenital toxoplasmosis or cytomegalovirus infection. Pediatrics. 1997 Jul;100(1):E9.
- Ford-Jones EL, Ryan G . Implications for the fetus of maternal infections in pregnancy. In: Cohen J, Powderly WG, eds. Infectious Diseases, 2nd ed. New York, NY: Mosby; 2004: 709–723.
- Greenhow TL, Weintrub PS. Your diagnosis, please. Neonate with hydrocephalus. Pediatr Infect Dis J. 2003 Dec;22(12):1099, 1111–1112.
CDC Urges Awareness of Measles in Americans Returning from Germany
By Alfred Valles, resident, internal medicine, Mayo Clinic College of Medicine
The Centers for Disease Control and Prevention (CDC) has issued an alert urging American travelers to remain aware of the possibility of measles exposure. Many Americans have traveled to and from Germany for the World Cup soccer championship games. Three of the twelve hosting cities—Cologne, Dortmund, and Gelsenkirchen—are of particular concern, given the recent measles outbreaks that have been reported in those cities and their surrounding areas.
Since January 1 of this year, some 1,200 cases have been identified in or near these cities. American travelers were undoubtedly among the large crowds of people gathered to pay homage to their favorite sport, and many others will visit Germany on vacation or business, making transmission of this respiratory droplet-born pathogen a very real threat.
The CDC recommends the following precautions:
- Travelers who plan to go to Germany should check their immunization records and visit their doctors if they are not immune to measles or are not sure they are.
- People returning from Germany, especially those who went to see the World Cup, should see a healthcare provider if they develop the symptoms of measles, including a fever, a raised rash that begins on the face and spreads to the arms and legs, a cough, red eyes, or a runny nose.
- People with these symptoms should limit their contact with others.
- Clinicians seeing patients with these symptoms should inquire about travel history and immunization status.
This warning is not to be taken lightly. Approximately two of every 1,000 patients infected with measles will die of the disease. Complications such as encephalitis are of particular concern for those who are malnourished or immunosuppressed.
Remember, live virus measles vaccine given within 72 hours of exposure may prevent the disease, while immune globulin given up to six days after exposure may prevent complications of measles in those who are at risk, including pregnant women, people with weak immune systems, and children.
The World cup can be dangerous, even for non-players. For more information about the measles outbreak and travel precautions, visit www.cdc.gov.
Lymphocytic Choriomeningitis Virus: Facts and Prevention
By the Special Pathogens Branch, CDC
In May 2005, the CDC investigated a cluster of lymphocytic choriomeningitis virus (LCMV) illnesses in four solid organ transplant recipients from a common donor, three of whom died. The source of the LCMV was traced to a hamster that had recently been acquired by a member of the donor’s household. It was subsequently determined that several LCMV-infected pet rodents had originated from a single distributor, who may have distributed other infected rodents to pet stores in the northeastern and midwestern United States.1 However, the risk of contracting LCMV from rodent exposure is not limited only to this outbreak, nor is the danger confined only to patients undergoing organ transplant.
Clinicians need to be familiar with LCMV because of its potential to cause meningitis, its teratogenicity, and the risk that it may bring about serious disease in immunocompromised individuals.
LCMV is normally carried by wild house mice, but can be transmitted to laboratory and pet rodents at breeding facilities, in pet stores, and in homes. Humans become infected in one of the following ways:
- Through direct contact with the secretions or excretions of infected rodents;
- By inhalation of dust or droplets containing LCMV from rodents;
- As a result of transplacental spread from an infected pregnant woman to her fetus; and
- By receipt of an organ transplant from an infected donor.2
Among those tested, about 5% have shown serologic evidence of previous infection with LCMV.3,4 In healthy adults, LCMV is typically a nonspecific viral syndrome sometimes followed by aseptic meningitis or other neurologic signs. Patients with weakened immune systems can suffer severe, possibly fatal systemic illness.2,5 Maternal infection with LCMV during pregnancy can result in spontaneous abortion or early neonatal death, as well as in defects similar to those of other congenital infections such as toxoplasmosis and cytomegalovirus (“TORCH” infections).6-10 The proportion of developmental defects caused by LCMV is not known.
Clinicians should consider LCMV in the differential diagnosis of patients with aseptic meningitis; in cases of fetal demise or congenital defects, including congenital hydrocephalus, chorioretinitis, blindness, or mental retardation; or in recent transplant recipients who present with signs of post-transplant infection. A detailed rodent exposure history should be taken. Contact your state health department or Special Pathogens Branch, CDC (404-639-1510), for information about testing for LCMV.
Currently, there is no specific treatment for LCMV infection other than supportive care. Ribavirin inhibits LCMV multiplication in laboratory experiments but has not been tested in clinical trials.
Clinicians should counsel their patients about the risks of contracting LCMV from laboratory, pet, and wild rodents. Wild mice in the home should be controlled and removed promptly. Immunocompromised individuals and women who are pregnant or planning to become pregnant should avoid any contact with wild or pet rodents, their excretions, and their nesting materials. While a woman is pregnant, pet rodents should be housed outside the home or in a separate part of the home where other individuals can care for the pets and clean their cages. Counseling a woman already exposed to rodents during pregnancy can be challenging; for assistance, contact your state health department.
Further information about LCMV infection and its prevention, including management and prevention of rodent infestation in the home, is available from Special Pathogens Branch, CDC, at www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/lcmv.htm. For more information about diseases commonly carried by rodents, please visit www.cdc.gov/rodents. TH
References
- Centers for Disease Control and Prevention. Update: interim guidance for minimizing risk for human lymphocytic choriomeningitis virus infection associated with pet rodents. MMWR. Aug 19, 2005;54(32):799-801.
- Fischer SA, Graham MB, Kuehnert MJ, et al. Transmission of lymphocytic choriomeningitis virus by organ transplantation. N Engl J Med. 2006;354(21):2235-2249.
- Childs JE, Glass GE, Ksiazek TG, et al. Human-rodent contact and infection with lymphocytic choriomeningitis and Seoul viruses in an inner-city population. Am J Trop Med Hyg. 1991 Feb;44(2):117–121.
- Park JY, Peters CJ, Rollin PE, et al. Age distribution of lymphocytic choriomeningitis virus serum antibody in Birmingham, Alabama: evidence of a decreased risk of infection. Am J Trop Med Hyg. 1997 Jul;57(1):37–41.
- Horton J, Hotchin JE, Olson KB, et al. The effects of MP virus infection in lymphoma. Cancer Res. 1971 Aug;31(8):1066–1068.
- Barton LL, Mets MB. Congenital lymphocytic choriomeningitis virus infection: decade of rediscovery. Clin Infect Dis. 2001 Aug 1;33(3):370–374.
- Barton LL, Mets MB, Beauchamp CL. Lymphocytic choriomeningitis virus: emerging fetal teratogen. Am J Obstet Gynecol. 2002 Dec ;187(6):1715–1716.
- Wright R, Johnson D, Neumann M, et al. Congenital lymphocytic choriomeningitis virus syndrome: a disease that mimics congenital toxoplasmosis or cytomegalovirus infection. Pediatrics. 1997 Jul;100(1):E9.
- Ford-Jones EL, Ryan G . Implications for the fetus of maternal infections in pregnancy. In: Cohen J, Powderly WG, eds. Infectious Diseases, 2nd ed. New York, NY: Mosby; 2004: 709–723.
- Greenhow TL, Weintrub PS. Your diagnosis, please. Neonate with hydrocephalus. Pediatr Infect Dis J. 2003 Dec;22(12):1099, 1111–1112.
The Reality of Today

SHM has been working with JCAHO on its Hospital of the Future Roundtable. JCAHO has brought together an interesting international group made up of leaders representing hospital administrators, architects, social behaviorists, nurses, pharmacists, physicians, economists, government, technology experts, and others with a stake in the evolution of the hospital as an institution.
At our recent meeting in Chicago we discussed some aspects of the economics of hospitals that I thought would be worth sharing with the hospital medicine audience.
Right now many hospitals are actually in a good economic position. For the past 12 months hospitals have had an operating margin of 3.6% with a total margin of more than 6%. A number of factors have favored the hospital’s bottom line in recent years. There has been hospital consolidation with the closing of some hospitals. Managed care’s tightening of revenue forced hospitals in the 1990s to examine their operations and many hospitals became more efficient. This reduced hospital size and forced changes in staffing and other parts of the expense equation. Now that managed care has loosened its grip on the fees paid to hospitals, revenues have risen faster than costs, especially on the commercial side. There has actually been an increase of 8.6% in revenue to hospitals in the past year.
The dark side of this equation is that while many hospitals have benefited, some hospitals continue to run in the red because of geography (inner city, rural), and patient mix. This gap between haves and have-nots is increasing. The specter of more Americans without insurance coverage (or undercovered) also raises the burden of undercompensated care on hospitals in general.
Competition and Transparency
Recently, some people have been talking about trying to make true competition work in healthcare. One step in creating a marketplace is to have price and cost transparency. The thought is if the users of healthcare (patients) and the buyers of healthcare (businesses and government) could see each hospital’s charges, then people would make their decisions armed with information like they have when buying a car or a house.
Unfortunately that is not how the healthcare marketplace (if you can call it that) operates. The reality is that the government (as Medicare and Medicaid) sets price levels fairly arbitrarily and very often below the actual cost of delivering the services. You also have to throw into the mix all the care hospitals provide to patients without any insurance coverage or means to pay for their care. This leads to cost shifting to the tune that hospitals now expect private insurers to pay 122% of costs just to balance the CMS shortfall. Price transparency makes it more difficult to cost shift because a hospital would set its “price,” but would that be the price for Medicare, for Medicaid, for the “Blues” (Blue Cross/Blue Shield) as well?
Now that employers are cost shifting to their employees with larger co-pays and basically offering a fixed benefit and asking the workers to pick up more of the health tab, it is even harder for hospitals to cost shift to the private commercial side (i.e., people under 65 with insurance).
Hospital Disaggregation
The good old Marcus Welby, MD-era hospital as the total community resource that takes the profitable and the needy is eroding. Specialty hospitals have sprung up to siphon some of the best revenue sources and help physicians get on the facility side of the equation. Many of the most lucrative outpatient modalities (e.g., surgicenters, imaging) have moved off campus and out of the hospital’s domain. And there sits the full-service hospital left with many of the responsibilities and a disproportionate share of expense, but with less of the high-ticket revenue.
Populations Demographics
Our population is getting older, but aging baby boomers will account for only about a 10% increase in healthcare spending. The bigger problem is that as the population ages a greater proportion of healthcare spending shifts from private to public (i.e., from the Blues to Medicare). There is already a problem in cost shifting as I mentioned above with Medicare and Medicaid paying <95% of healthcare costs. You can’t make up those losses with volume. It’s predicted that more than 65% of hospital funding will come from the government by 2025. How can a hospital survive with those dynamics?
There are only three options. Faced with decreasing revenues, hospitals can further reduce expenses. With much of the fat already trimmed this is a daunting proposition. Second, the hospital can cost shift and ask a greater percentage from the private insurer. This will be difficult with price transparency and a greater portion of the bill being paid by the patient. Third, we can all pray that the government will increase its reimbursement; unlikely, when it’s such a fight just to not be cut each year.
Need to Add Capacity
With the aging population and the increasing acuity of hospitalized patients, changes need to occur in the hospital’s physical plant. Recent surveys have shown that more than 85% of hospitals plan to add or change their capacity. While this is significant in Florida, Arizona, Nevada, and other places faced with population migrations, in other places this is driven by the need to expand the emergency department, add telemetry beds, and expand the ICU.
This is further complicated by the movement of well-heeled (and well-insured) populations to the suburbs with the hospitals following them and leaving disturbing realities for the older inner city in their wake.
Technology Is Your Friend
New advances are more than gadgetry gone wild. When best deployed these 21st-century advances can lead to better outcomes, safer hospitals, and actually make economic sense. The problem: Where can hospitals go to find out just which technology to use? At many hospitals these decisions are made by committees with less than perfect knowledge in a rapidly evolving market. Once the technology is chosen, the implementation can be disruptive more than helpful, especially in the short run, and the processes of care can be thrown off course. Sometimes this can have convulsive results such as in the failed implementation of CPOE at Cedars Sinai Hospital in Los Angeles.
And whether it is new technology or the adding of capacity, just where will the hospitals get the capital to pay for all this investment in the future? Not from Medicare and Medicaid, not from big business, and not from the out-of-pocket dollars of their patients.
This is the reality of today flavored with best guesses for the future. From this vantage point will arise the ideas of how to shape the hospital of the future. This is the world tomorrow’s hospitalists will inhabit. We need to understand how this will shape resource availability, hospital design, the commitment to quality improvement and accountability, and the environment in which hospitalists will work and our patients will receive care.
Once we understand what will shape the hospital of the future, hospitalists can be better prepared to be active partners in the shaping the new reality. TH
Dr. Wellikson has been CEO of SHM since 2000.
SHM has been working with JCAHO on its Hospital of the Future Roundtable. JCAHO has brought together an interesting international group made up of leaders representing hospital administrators, architects, social behaviorists, nurses, pharmacists, physicians, economists, government, technology experts, and others with a stake in the evolution of the hospital as an institution.
At our recent meeting in Chicago we discussed some aspects of the economics of hospitals that I thought would be worth sharing with the hospital medicine audience.
Right now many hospitals are actually in a good economic position. For the past 12 months hospitals have had an operating margin of 3.6% with a total margin of more than 6%. A number of factors have favored the hospital’s bottom line in recent years. There has been hospital consolidation with the closing of some hospitals. Managed care’s tightening of revenue forced hospitals in the 1990s to examine their operations and many hospitals became more efficient. This reduced hospital size and forced changes in staffing and other parts of the expense equation. Now that managed care has loosened its grip on the fees paid to hospitals, revenues have risen faster than costs, especially on the commercial side. There has actually been an increase of 8.6% in revenue to hospitals in the past year.
The dark side of this equation is that while many hospitals have benefited, some hospitals continue to run in the red because of geography (inner city, rural), and patient mix. This gap between haves and have-nots is increasing. The specter of more Americans without insurance coverage (or undercovered) also raises the burden of undercompensated care on hospitals in general.
Competition and Transparency
Recently, some people have been talking about trying to make true competition work in healthcare. One step in creating a marketplace is to have price and cost transparency. The thought is if the users of healthcare (patients) and the buyers of healthcare (businesses and government) could see each hospital’s charges, then people would make their decisions armed with information like they have when buying a car or a house.
Unfortunately that is not how the healthcare marketplace (if you can call it that) operates. The reality is that the government (as Medicare and Medicaid) sets price levels fairly arbitrarily and very often below the actual cost of delivering the services. You also have to throw into the mix all the care hospitals provide to patients without any insurance coverage or means to pay for their care. This leads to cost shifting to the tune that hospitals now expect private insurers to pay 122% of costs just to balance the CMS shortfall. Price transparency makes it more difficult to cost shift because a hospital would set its “price,” but would that be the price for Medicare, for Medicaid, for the “Blues” (Blue Cross/Blue Shield) as well?
Now that employers are cost shifting to their employees with larger co-pays and basically offering a fixed benefit and asking the workers to pick up more of the health tab, it is even harder for hospitals to cost shift to the private commercial side (i.e., people under 65 with insurance).
Hospital Disaggregation
The good old Marcus Welby, MD-era hospital as the total community resource that takes the profitable and the needy is eroding. Specialty hospitals have sprung up to siphon some of the best revenue sources and help physicians get on the facility side of the equation. Many of the most lucrative outpatient modalities (e.g., surgicenters, imaging) have moved off campus and out of the hospital’s domain. And there sits the full-service hospital left with many of the responsibilities and a disproportionate share of expense, but with less of the high-ticket revenue.
Populations Demographics
Our population is getting older, but aging baby boomers will account for only about a 10% increase in healthcare spending. The bigger problem is that as the population ages a greater proportion of healthcare spending shifts from private to public (i.e., from the Blues to Medicare). There is already a problem in cost shifting as I mentioned above with Medicare and Medicaid paying <95% of healthcare costs. You can’t make up those losses with volume. It’s predicted that more than 65% of hospital funding will come from the government by 2025. How can a hospital survive with those dynamics?
There are only three options. Faced with decreasing revenues, hospitals can further reduce expenses. With much of the fat already trimmed this is a daunting proposition. Second, the hospital can cost shift and ask a greater percentage from the private insurer. This will be difficult with price transparency and a greater portion of the bill being paid by the patient. Third, we can all pray that the government will increase its reimbursement; unlikely, when it’s such a fight just to not be cut each year.
Need to Add Capacity
With the aging population and the increasing acuity of hospitalized patients, changes need to occur in the hospital’s physical plant. Recent surveys have shown that more than 85% of hospitals plan to add or change their capacity. While this is significant in Florida, Arizona, Nevada, and other places faced with population migrations, in other places this is driven by the need to expand the emergency department, add telemetry beds, and expand the ICU.
This is further complicated by the movement of well-heeled (and well-insured) populations to the suburbs with the hospitals following them and leaving disturbing realities for the older inner city in their wake.
Technology Is Your Friend
New advances are more than gadgetry gone wild. When best deployed these 21st-century advances can lead to better outcomes, safer hospitals, and actually make economic sense. The problem: Where can hospitals go to find out just which technology to use? At many hospitals these decisions are made by committees with less than perfect knowledge in a rapidly evolving market. Once the technology is chosen, the implementation can be disruptive more than helpful, especially in the short run, and the processes of care can be thrown off course. Sometimes this can have convulsive results such as in the failed implementation of CPOE at Cedars Sinai Hospital in Los Angeles.
And whether it is new technology or the adding of capacity, just where will the hospitals get the capital to pay for all this investment in the future? Not from Medicare and Medicaid, not from big business, and not from the out-of-pocket dollars of their patients.
This is the reality of today flavored with best guesses for the future. From this vantage point will arise the ideas of how to shape the hospital of the future. This is the world tomorrow’s hospitalists will inhabit. We need to understand how this will shape resource availability, hospital design, the commitment to quality improvement and accountability, and the environment in which hospitalists will work and our patients will receive care.
Once we understand what will shape the hospital of the future, hospitalists can be better prepared to be active partners in the shaping the new reality. TH
Dr. Wellikson has been CEO of SHM since 2000.
SHM has been working with JCAHO on its Hospital of the Future Roundtable. JCAHO has brought together an interesting international group made up of leaders representing hospital administrators, architects, social behaviorists, nurses, pharmacists, physicians, economists, government, technology experts, and others with a stake in the evolution of the hospital as an institution.
At our recent meeting in Chicago we discussed some aspects of the economics of hospitals that I thought would be worth sharing with the hospital medicine audience.
Right now many hospitals are actually in a good economic position. For the past 12 months hospitals have had an operating margin of 3.6% with a total margin of more than 6%. A number of factors have favored the hospital’s bottom line in recent years. There has been hospital consolidation with the closing of some hospitals. Managed care’s tightening of revenue forced hospitals in the 1990s to examine their operations and many hospitals became more efficient. This reduced hospital size and forced changes in staffing and other parts of the expense equation. Now that managed care has loosened its grip on the fees paid to hospitals, revenues have risen faster than costs, especially on the commercial side. There has actually been an increase of 8.6% in revenue to hospitals in the past year.
The dark side of this equation is that while many hospitals have benefited, some hospitals continue to run in the red because of geography (inner city, rural), and patient mix. This gap between haves and have-nots is increasing. The specter of more Americans without insurance coverage (or undercovered) also raises the burden of undercompensated care on hospitals in general.
Competition and Transparency
Recently, some people have been talking about trying to make true competition work in healthcare. One step in creating a marketplace is to have price and cost transparency. The thought is if the users of healthcare (patients) and the buyers of healthcare (businesses and government) could see each hospital’s charges, then people would make their decisions armed with information like they have when buying a car or a house.
Unfortunately that is not how the healthcare marketplace (if you can call it that) operates. The reality is that the government (as Medicare and Medicaid) sets price levels fairly arbitrarily and very often below the actual cost of delivering the services. You also have to throw into the mix all the care hospitals provide to patients without any insurance coverage or means to pay for their care. This leads to cost shifting to the tune that hospitals now expect private insurers to pay 122% of costs just to balance the CMS shortfall. Price transparency makes it more difficult to cost shift because a hospital would set its “price,” but would that be the price for Medicare, for Medicaid, for the “Blues” (Blue Cross/Blue Shield) as well?
Now that employers are cost shifting to their employees with larger co-pays and basically offering a fixed benefit and asking the workers to pick up more of the health tab, it is even harder for hospitals to cost shift to the private commercial side (i.e., people under 65 with insurance).
Hospital Disaggregation
The good old Marcus Welby, MD-era hospital as the total community resource that takes the profitable and the needy is eroding. Specialty hospitals have sprung up to siphon some of the best revenue sources and help physicians get on the facility side of the equation. Many of the most lucrative outpatient modalities (e.g., surgicenters, imaging) have moved off campus and out of the hospital’s domain. And there sits the full-service hospital left with many of the responsibilities and a disproportionate share of expense, but with less of the high-ticket revenue.
Populations Demographics
Our population is getting older, but aging baby boomers will account for only about a 10% increase in healthcare spending. The bigger problem is that as the population ages a greater proportion of healthcare spending shifts from private to public (i.e., from the Blues to Medicare). There is already a problem in cost shifting as I mentioned above with Medicare and Medicaid paying <95% of healthcare costs. You can’t make up those losses with volume. It’s predicted that more than 65% of hospital funding will come from the government by 2025. How can a hospital survive with those dynamics?
There are only three options. Faced with decreasing revenues, hospitals can further reduce expenses. With much of the fat already trimmed this is a daunting proposition. Second, the hospital can cost shift and ask a greater percentage from the private insurer. This will be difficult with price transparency and a greater portion of the bill being paid by the patient. Third, we can all pray that the government will increase its reimbursement; unlikely, when it’s such a fight just to not be cut each year.
Need to Add Capacity
With the aging population and the increasing acuity of hospitalized patients, changes need to occur in the hospital’s physical plant. Recent surveys have shown that more than 85% of hospitals plan to add or change their capacity. While this is significant in Florida, Arizona, Nevada, and other places faced with population migrations, in other places this is driven by the need to expand the emergency department, add telemetry beds, and expand the ICU.
This is further complicated by the movement of well-heeled (and well-insured) populations to the suburbs with the hospitals following them and leaving disturbing realities for the older inner city in their wake.
Technology Is Your Friend
New advances are more than gadgetry gone wild. When best deployed these 21st-century advances can lead to better outcomes, safer hospitals, and actually make economic sense. The problem: Where can hospitals go to find out just which technology to use? At many hospitals these decisions are made by committees with less than perfect knowledge in a rapidly evolving market. Once the technology is chosen, the implementation can be disruptive more than helpful, especially in the short run, and the processes of care can be thrown off course. Sometimes this can have convulsive results such as in the failed implementation of CPOE at Cedars Sinai Hospital in Los Angeles.
And whether it is new technology or the adding of capacity, just where will the hospitals get the capital to pay for all this investment in the future? Not from Medicare and Medicaid, not from big business, and not from the out-of-pocket dollars of their patients.
This is the reality of today flavored with best guesses for the future. From this vantage point will arise the ideas of how to shape the hospital of the future. This is the world tomorrow’s hospitalists will inhabit. We need to understand how this will shape resource availability, hospital design, the commitment to quality improvement and accountability, and the environment in which hospitalists will work and our patients will receive care.
Once we understand what will shape the hospital of the future, hospitalists can be better prepared to be active partners in the shaping the new reality. TH
Dr. Wellikson has been CEO of SHM since 2000.
Tough Negotiations Avert B.C. Hospitalist Walkout
Two weeks of intense talks between hospitalists and government officials resulted in an 11th-hour compromise on June 29th in British Columbia, one day before hospitalists’ contracts were set to expire. Throughout the month of June, the B.C. hospitalists had threatened to move back to community practice if the Ministry of Health (MOH) did not offer a contract that recognized the value of their work. The hospitalists contended that low payment schedules and staffing levels were seriously undermining staff retention and recruiting—as well as patient safety. During the dispute, MOH officials had been equally adamant about their position. The province’s Minister of Health, George Abbott, said that the salaries were fair, and that the government would not be “held for ransom on this issue.”
Hospitalists believed that failure to reach agreement would have left many hospitals scrambling to provide coverage for hospitalized patients.
Wayne DeMott, MD, is a hospitalist at Royal Jubilee Hospital in Victoria, B.C., and chief negotiator for the British Columbia Medical Association’s Section of Hospitalist Medicine.
Hospitalists in B.C., he says, “are in a position to … severely compromise many functions of most major hospitals in this province. If an agreement had not been reached, we were quite prepared to stand up and take our leave.”
The June 29 compromise established a one-year period to re-examine workload issues and clarify funding models. If hospitalists are not satisfied at the six-month mark with the provisions to address ongoing funding, workload, recruitment and retention issues, they can give six months’ notice.
Roots of the Dispute
The majority of primary care in British Columbia has traditionally been provided by general practitioners. According to David Wilton, MD, one of the directors of the Vancouver Hospitalist Society, a nonprofit society that contracts with Vancouver General Hospital and the University of British Columbia Hospital (overseen by the Vancouver Coastal Health Authority), and a core negotiator for B.C. hospitalists at the talks, “the economic model for hospital care faltered through the late ’80s and early ’90s, and general practitioners started giving up their hospital privileges and focusing on their community-based practices.”
To fill the gap, many hospitals in the more populated urban areas started hospitalist programs, which evolved through the late ’90s and grew quickly after the year 2000. One of the largest health authorities in the province—the Fraser Health Authority—serves approximately 1.3 million people on the B.C. mainland, runs 12 hospitals, and now has 110 hospitalists working for that health authority alone. Most (85%-90%) Canadian hospitalists are trained in family practice medicine, as opposed to internal medicine.
In some ways, B.C. hospitalists have been victims of their own success. As programs grew and as house staff became aware of hospitalists’ skill sets and expertise, many shifted their work burdens to the hospitalist services, says Dr. Wilton. The workload climbed exponentially, but appreciation of hospitalists’ value-added services on the part of MOH officials did not keep pace with the workload. The result, explains Dr. Wilton, was a kind of disconnect between the intense nature of hospitalists’ services and their compensation and staffing structures.
“In British Columbia the local hospital administrators saw the efficiencies that we were bringing to the system,” explains Dr. Wilton. “They saw the improved quality of care and the fact that we were able to step in, be flexible, and help specialists in various areas and fill the gaps of care. But we hadn’t yet broken through to the higher levels of the provincial Ministry of Health. They didn’t fully recognize the value that we were bringing to the healthcare system and the fact that hospitalists are the cornerstone of the acute care system now.”
Mike Morris, MD, president of the Section of Hospital Medicine, agrees with this characterization. A hospitalist at Nanaimo Regional General Hospital (part of the Vancouver Island Health Authority), Dr. Morris believes that most of the health authorities, which administer the region’s hospitals, appreciate hospitalists’ value. “They know how much we help the patient flow and problems in the emergency room,” he says. Emergency department crowding has been a huge problem in British Columbia, due to lack of hospital beds and a dearth of long-term-care beds. “Hospitalists are able to come in and safely discharge people on a timely basis, and help the flow through the emergency department. That’s one of our biggest values to the hospital. We think that the family physicians coming into the hospital are platinum doctors because they’re keeping up with the rapid changes in hospital medicine. And we feel that they are being highly undervalued.”
On average, hospitalists were making $111 an hour (Canadian dollars, equating to about $98 U.S. dollars at the July 12 exchange rate). According to Dr. Wilton, the hospitalists contended that their earning potential was at least equivalent to that of a lower-intensity Monday-Friday community-based general practice. At the negotiations, they valued their services at $135/hour. If the government was unwilling to value hospitalists’ compensation appropriately, they warned they could easily return to a community-based practice model.
Payment Not the Only Issue
The province of British Columbia is divided into six health authorities, five of which have active hospitalist programs. Overarching compensation frameworks for all physicians are established through negotiations between the British Columbia Medical Association (BCMA) and the MOH. Individual health authorities then negotiate specific terms of compensation and workload expectations with physicians. There is considerable variation between health authorities (and indeed throughout each of the Canadian provinces) regarding hospitalists’ workload models, such as the number of expected patient encounters per shift and compensation packages.
The BCMA had recently completed contract renewal negotiations involving the entire physician body in British Columbia and the government on April 1, resulting in a new six-year Letter of Agreement that hospitalists maintained did not address their needs.
“The way we saw [the Letter of Agreement] being interpreted,” says Dr. Wilton, “was that the base rate for calculating our advances going forward was going to be between 10% and 25% less than what we were currently earning. Part of our goal was to get a wage that is consistent with the complexity and intensity of our work. I think that, in the eyes of the government, they were seeing our work and our value more in the range of the less-intense community-based general practice work. We wanted to shift that focus more towards the intensity of the acute care setting, where we think we’re more comparable to emergency medicine and internal medicine specialists.”
Dr. DeMott adds, “The workload model is a very important aspect of what we do. It isn’t only what you are paid, it is what you are being asked to do for what you’re being paid. Workload expectations have tremendous implications for the health of this career path in the future, the ability to recruit into this career path, and the ability to retain people, so that they do not become burnt out or personally destroyed.”
Views of the Dispute
B.C. hospitalists decided to hire their own attorney (the Vancouver firm of Tevlin Gleadle) and a press relations person to take their dispute public. Margaret MacDiarmid, MD, is president of the BCMA and has her own family practice in the Kootenays region eight hours east/southeast of Vancouver on the British Columbian mainland. “We [the BCMA] were very keen to assist, if we could, in the resolution of the conflict, and we were calling them about that,” she explains. “But we felt we had to operate within the Letter of Agreement that we had just signed, which I think is reasonable. So we did not play any active role in the final resolution.”
Assistant Deputy Minister for Medical Services Stephen Brown, PhD, the MOH official who oversees physician compensation, admits that the issue of the threatened walkout was “a bit of a surprise” to him because the government had just signed the Letter of Agreement with the BCMA. He became engaged with the health authorities and the hospitalists, “trying to understand how we got to where we were when we had just signed an agreement.”
Although hospitalists felt the Letter of Agreement did not address their concerns, Brown did not characterize the talks with the various stakeholders as negotiations. “I acknowledged that we were trying to understand the issues they were presenting and how we could address those issues within the context of the BCMA-government negotiated agreement,” he said during a telephone interview.
“Over the period of a couple weeks of dialogue, we got to a tentative agreement—which hopefully will now translate into contracts over the next week—that is within the framework of the Agreement.”
Goals Accomplished
Key figures involved in the talks expressed satisfaction with some of the goals achieved. Dr. Wilton reflects that the dispute has resulted in more public awareness of the presence of hospitalists and more awareness of hospitalists’ value within the BCMA. Most importantly, he says, “we sat across the table from some of the senior administrators in the Ministry of Health and were able to educate them about the values that hospitalists can bring to the system. We’re hoping that by having the opportunity to educate them, they will take a more proactive and organized approach to supporting the hospitalist model of care and utilizing it to its full potential.”
“I wasn’t thrilled that we were in this situation,” says Brown. “But the positive that’s come out of it is that I think we’ve got a platform, we’ve got a dialogue, and we have committed to work with them over the next six months to look at workload and see if we can get some level of consistency on that.”
Brown indicated that he had acquired more understanding of how hospitalists’ roles have evolved in the province and the difficulties they encounter to provide quality care. “The reality of what we found was that regions had developed hospitalist services in slightly different ways, with slightly different compensation arrangements,” he noted. “I hope what we have just done is we have now created the same platform for all the hospitalists across the province. They’re going to have a contract that looks similar and dialogue is now underway with the HAs [health authorities] about the range of services that hospitalists will provide. So I think that’s an opportunity as well, over the next six months now, to clean that up.”
While hospitalists gained some traction on the development of new workload standards, they did not fully accomplish their financial goals, the two key negotiators said. According to Dr. DeMott, “We became lost in a complex political and economic struggle that involved all of the doctors in the province. The doctors had recently ratified an agreement that left us completely out in the cold. In the end, we had to comply with the essential terms of that [BCMA-negotiated Letter of Agreement].”
To have insisted on the hospitalists’ financial goals, he says, would have injured too many programs, and—if they had walked off the job—ultimately would have compromised patient care. “In the end,” says Dr. DeMott, “we acquiesced and came up with a compromise that should work for the short term.”
Parallels with the United States?
Many of those interviewed for this article observed that hospitalist programs in British Columbia are still evolving, and that U.S. hospitalist programs are probably five years ahead in terms of established program models. Dr. DeMott praises the pioneering work done by SHM: “We look to you for guidance, and we really do appreciate the SHM advancement that is moving the hospitalist profession along.”
As negotiators for the Section of Hospital Medicine during the talks, Dr. DeMott says that his team used the surveys and studies that SHM has pioneered about the value-added contributions of hospitalists to increase awareness with the MOH, the government of British Columbia, and the BCMA about hospitalists’ roles. Dr. Morris notes that B.C. hospitalists, taking the lead from SHM, are now developing their core competencies.
William D. Atchley, Jr., MD, FACP, medical director of Peninsula Inpatient Care Specialists at Sentara Careplex Hospital in Hampton, Va., is a long-time member of the SHM board of directors. He has followed the growth of hospitalists in Canada, and applauds the efforts of those like Echo-Marie Enns, MD, who served as a National Association of Inpatient Physicians (NAIP) Canadian chapter president in Calgary. He has also conducted surveys of Canadian hospitalists. He doubts that a parallel strike situation could develop here in the United States.
“Their situation is unique to Canada,” he says. “From SHM’s perspective, we have always acted as an advocate for hospitalists in Canada and offered whatever we have learned here in the United States to help facilitate their movement. They are still in the process of explaining what a hospitalist is, and explaining to their national medical societies about what hospitalists can do. Their ability to get the message across is just going to take some time.”
Summing up their accomplishments thus far, Dr. DeMott says, “We considered this disagreement a defining moment for hospitalists in this province and quite possibly for [Canada]. We’re not there yet, but we put ourselves on the map. There will likely be another battle on the horizon for us, but hopefully one colored by a much greater appreciation of the expertise we bring to the acute care arena.” TH
Gretchen Henkel writes regularly for The Hospitalist.
Two weeks of intense talks between hospitalists and government officials resulted in an 11th-hour compromise on June 29th in British Columbia, one day before hospitalists’ contracts were set to expire. Throughout the month of June, the B.C. hospitalists had threatened to move back to community practice if the Ministry of Health (MOH) did not offer a contract that recognized the value of their work. The hospitalists contended that low payment schedules and staffing levels were seriously undermining staff retention and recruiting—as well as patient safety. During the dispute, MOH officials had been equally adamant about their position. The province’s Minister of Health, George Abbott, said that the salaries were fair, and that the government would not be “held for ransom on this issue.”
Hospitalists believed that failure to reach agreement would have left many hospitals scrambling to provide coverage for hospitalized patients.
Wayne DeMott, MD, is a hospitalist at Royal Jubilee Hospital in Victoria, B.C., and chief negotiator for the British Columbia Medical Association’s Section of Hospitalist Medicine.
Hospitalists in B.C., he says, “are in a position to … severely compromise many functions of most major hospitals in this province. If an agreement had not been reached, we were quite prepared to stand up and take our leave.”
The June 29 compromise established a one-year period to re-examine workload issues and clarify funding models. If hospitalists are not satisfied at the six-month mark with the provisions to address ongoing funding, workload, recruitment and retention issues, they can give six months’ notice.
Roots of the Dispute
The majority of primary care in British Columbia has traditionally been provided by general practitioners. According to David Wilton, MD, one of the directors of the Vancouver Hospitalist Society, a nonprofit society that contracts with Vancouver General Hospital and the University of British Columbia Hospital (overseen by the Vancouver Coastal Health Authority), and a core negotiator for B.C. hospitalists at the talks, “the economic model for hospital care faltered through the late ’80s and early ’90s, and general practitioners started giving up their hospital privileges and focusing on their community-based practices.”
To fill the gap, many hospitals in the more populated urban areas started hospitalist programs, which evolved through the late ’90s and grew quickly after the year 2000. One of the largest health authorities in the province—the Fraser Health Authority—serves approximately 1.3 million people on the B.C. mainland, runs 12 hospitals, and now has 110 hospitalists working for that health authority alone. Most (85%-90%) Canadian hospitalists are trained in family practice medicine, as opposed to internal medicine.
In some ways, B.C. hospitalists have been victims of their own success. As programs grew and as house staff became aware of hospitalists’ skill sets and expertise, many shifted their work burdens to the hospitalist services, says Dr. Wilton. The workload climbed exponentially, but appreciation of hospitalists’ value-added services on the part of MOH officials did not keep pace with the workload. The result, explains Dr. Wilton, was a kind of disconnect between the intense nature of hospitalists’ services and their compensation and staffing structures.
“In British Columbia the local hospital administrators saw the efficiencies that we were bringing to the system,” explains Dr. Wilton. “They saw the improved quality of care and the fact that we were able to step in, be flexible, and help specialists in various areas and fill the gaps of care. But we hadn’t yet broken through to the higher levels of the provincial Ministry of Health. They didn’t fully recognize the value that we were bringing to the healthcare system and the fact that hospitalists are the cornerstone of the acute care system now.”
Mike Morris, MD, president of the Section of Hospital Medicine, agrees with this characterization. A hospitalist at Nanaimo Regional General Hospital (part of the Vancouver Island Health Authority), Dr. Morris believes that most of the health authorities, which administer the region’s hospitals, appreciate hospitalists’ value. “They know how much we help the patient flow and problems in the emergency room,” he says. Emergency department crowding has been a huge problem in British Columbia, due to lack of hospital beds and a dearth of long-term-care beds. “Hospitalists are able to come in and safely discharge people on a timely basis, and help the flow through the emergency department. That’s one of our biggest values to the hospital. We think that the family physicians coming into the hospital are platinum doctors because they’re keeping up with the rapid changes in hospital medicine. And we feel that they are being highly undervalued.”
On average, hospitalists were making $111 an hour (Canadian dollars, equating to about $98 U.S. dollars at the July 12 exchange rate). According to Dr. Wilton, the hospitalists contended that their earning potential was at least equivalent to that of a lower-intensity Monday-Friday community-based general practice. At the negotiations, they valued their services at $135/hour. If the government was unwilling to value hospitalists’ compensation appropriately, they warned they could easily return to a community-based practice model.
Payment Not the Only Issue
The province of British Columbia is divided into six health authorities, five of which have active hospitalist programs. Overarching compensation frameworks for all physicians are established through negotiations between the British Columbia Medical Association (BCMA) and the MOH. Individual health authorities then negotiate specific terms of compensation and workload expectations with physicians. There is considerable variation between health authorities (and indeed throughout each of the Canadian provinces) regarding hospitalists’ workload models, such as the number of expected patient encounters per shift and compensation packages.
The BCMA had recently completed contract renewal negotiations involving the entire physician body in British Columbia and the government on April 1, resulting in a new six-year Letter of Agreement that hospitalists maintained did not address their needs.
“The way we saw [the Letter of Agreement] being interpreted,” says Dr. Wilton, “was that the base rate for calculating our advances going forward was going to be between 10% and 25% less than what we were currently earning. Part of our goal was to get a wage that is consistent with the complexity and intensity of our work. I think that, in the eyes of the government, they were seeing our work and our value more in the range of the less-intense community-based general practice work. We wanted to shift that focus more towards the intensity of the acute care setting, where we think we’re more comparable to emergency medicine and internal medicine specialists.”
Dr. DeMott adds, “The workload model is a very important aspect of what we do. It isn’t only what you are paid, it is what you are being asked to do for what you’re being paid. Workload expectations have tremendous implications for the health of this career path in the future, the ability to recruit into this career path, and the ability to retain people, so that they do not become burnt out or personally destroyed.”
Views of the Dispute
B.C. hospitalists decided to hire their own attorney (the Vancouver firm of Tevlin Gleadle) and a press relations person to take their dispute public. Margaret MacDiarmid, MD, is president of the BCMA and has her own family practice in the Kootenays region eight hours east/southeast of Vancouver on the British Columbian mainland. “We [the BCMA] were very keen to assist, if we could, in the resolution of the conflict, and we were calling them about that,” she explains. “But we felt we had to operate within the Letter of Agreement that we had just signed, which I think is reasonable. So we did not play any active role in the final resolution.”
Assistant Deputy Minister for Medical Services Stephen Brown, PhD, the MOH official who oversees physician compensation, admits that the issue of the threatened walkout was “a bit of a surprise” to him because the government had just signed the Letter of Agreement with the BCMA. He became engaged with the health authorities and the hospitalists, “trying to understand how we got to where we were when we had just signed an agreement.”
Although hospitalists felt the Letter of Agreement did not address their concerns, Brown did not characterize the talks with the various stakeholders as negotiations. “I acknowledged that we were trying to understand the issues they were presenting and how we could address those issues within the context of the BCMA-government negotiated agreement,” he said during a telephone interview.
“Over the period of a couple weeks of dialogue, we got to a tentative agreement—which hopefully will now translate into contracts over the next week—that is within the framework of the Agreement.”
Goals Accomplished
Key figures involved in the talks expressed satisfaction with some of the goals achieved. Dr. Wilton reflects that the dispute has resulted in more public awareness of the presence of hospitalists and more awareness of hospitalists’ value within the BCMA. Most importantly, he says, “we sat across the table from some of the senior administrators in the Ministry of Health and were able to educate them about the values that hospitalists can bring to the system. We’re hoping that by having the opportunity to educate them, they will take a more proactive and organized approach to supporting the hospitalist model of care and utilizing it to its full potential.”
“I wasn’t thrilled that we were in this situation,” says Brown. “But the positive that’s come out of it is that I think we’ve got a platform, we’ve got a dialogue, and we have committed to work with them over the next six months to look at workload and see if we can get some level of consistency on that.”
Brown indicated that he had acquired more understanding of how hospitalists’ roles have evolved in the province and the difficulties they encounter to provide quality care. “The reality of what we found was that regions had developed hospitalist services in slightly different ways, with slightly different compensation arrangements,” he noted. “I hope what we have just done is we have now created the same platform for all the hospitalists across the province. They’re going to have a contract that looks similar and dialogue is now underway with the HAs [health authorities] about the range of services that hospitalists will provide. So I think that’s an opportunity as well, over the next six months now, to clean that up.”
While hospitalists gained some traction on the development of new workload standards, they did not fully accomplish their financial goals, the two key negotiators said. According to Dr. DeMott, “We became lost in a complex political and economic struggle that involved all of the doctors in the province. The doctors had recently ratified an agreement that left us completely out in the cold. In the end, we had to comply with the essential terms of that [BCMA-negotiated Letter of Agreement].”
To have insisted on the hospitalists’ financial goals, he says, would have injured too many programs, and—if they had walked off the job—ultimately would have compromised patient care. “In the end,” says Dr. DeMott, “we acquiesced and came up with a compromise that should work for the short term.”
Parallels with the United States?
Many of those interviewed for this article observed that hospitalist programs in British Columbia are still evolving, and that U.S. hospitalist programs are probably five years ahead in terms of established program models. Dr. DeMott praises the pioneering work done by SHM: “We look to you for guidance, and we really do appreciate the SHM advancement that is moving the hospitalist profession along.”
As negotiators for the Section of Hospital Medicine during the talks, Dr. DeMott says that his team used the surveys and studies that SHM has pioneered about the value-added contributions of hospitalists to increase awareness with the MOH, the government of British Columbia, and the BCMA about hospitalists’ roles. Dr. Morris notes that B.C. hospitalists, taking the lead from SHM, are now developing their core competencies.
William D. Atchley, Jr., MD, FACP, medical director of Peninsula Inpatient Care Specialists at Sentara Careplex Hospital in Hampton, Va., is a long-time member of the SHM board of directors. He has followed the growth of hospitalists in Canada, and applauds the efforts of those like Echo-Marie Enns, MD, who served as a National Association of Inpatient Physicians (NAIP) Canadian chapter president in Calgary. He has also conducted surveys of Canadian hospitalists. He doubts that a parallel strike situation could develop here in the United States.
“Their situation is unique to Canada,” he says. “From SHM’s perspective, we have always acted as an advocate for hospitalists in Canada and offered whatever we have learned here in the United States to help facilitate their movement. They are still in the process of explaining what a hospitalist is, and explaining to their national medical societies about what hospitalists can do. Their ability to get the message across is just going to take some time.”
Summing up their accomplishments thus far, Dr. DeMott says, “We considered this disagreement a defining moment for hospitalists in this province and quite possibly for [Canada]. We’re not there yet, but we put ourselves on the map. There will likely be another battle on the horizon for us, but hopefully one colored by a much greater appreciation of the expertise we bring to the acute care arena.” TH
Gretchen Henkel writes regularly for The Hospitalist.
Two weeks of intense talks between hospitalists and government officials resulted in an 11th-hour compromise on June 29th in British Columbia, one day before hospitalists’ contracts were set to expire. Throughout the month of June, the B.C. hospitalists had threatened to move back to community practice if the Ministry of Health (MOH) did not offer a contract that recognized the value of their work. The hospitalists contended that low payment schedules and staffing levels were seriously undermining staff retention and recruiting—as well as patient safety. During the dispute, MOH officials had been equally adamant about their position. The province’s Minister of Health, George Abbott, said that the salaries were fair, and that the government would not be “held for ransom on this issue.”
Hospitalists believed that failure to reach agreement would have left many hospitals scrambling to provide coverage for hospitalized patients.
Wayne DeMott, MD, is a hospitalist at Royal Jubilee Hospital in Victoria, B.C., and chief negotiator for the British Columbia Medical Association’s Section of Hospitalist Medicine.
Hospitalists in B.C., he says, “are in a position to … severely compromise many functions of most major hospitals in this province. If an agreement had not been reached, we were quite prepared to stand up and take our leave.”
The June 29 compromise established a one-year period to re-examine workload issues and clarify funding models. If hospitalists are not satisfied at the six-month mark with the provisions to address ongoing funding, workload, recruitment and retention issues, they can give six months’ notice.
Roots of the Dispute
The majority of primary care in British Columbia has traditionally been provided by general practitioners. According to David Wilton, MD, one of the directors of the Vancouver Hospitalist Society, a nonprofit society that contracts with Vancouver General Hospital and the University of British Columbia Hospital (overseen by the Vancouver Coastal Health Authority), and a core negotiator for B.C. hospitalists at the talks, “the economic model for hospital care faltered through the late ’80s and early ’90s, and general practitioners started giving up their hospital privileges and focusing on their community-based practices.”
To fill the gap, many hospitals in the more populated urban areas started hospitalist programs, which evolved through the late ’90s and grew quickly after the year 2000. One of the largest health authorities in the province—the Fraser Health Authority—serves approximately 1.3 million people on the B.C. mainland, runs 12 hospitals, and now has 110 hospitalists working for that health authority alone. Most (85%-90%) Canadian hospitalists are trained in family practice medicine, as opposed to internal medicine.
In some ways, B.C. hospitalists have been victims of their own success. As programs grew and as house staff became aware of hospitalists’ skill sets and expertise, many shifted their work burdens to the hospitalist services, says Dr. Wilton. The workload climbed exponentially, but appreciation of hospitalists’ value-added services on the part of MOH officials did not keep pace with the workload. The result, explains Dr. Wilton, was a kind of disconnect between the intense nature of hospitalists’ services and their compensation and staffing structures.
“In British Columbia the local hospital administrators saw the efficiencies that we were bringing to the system,” explains Dr. Wilton. “They saw the improved quality of care and the fact that we were able to step in, be flexible, and help specialists in various areas and fill the gaps of care. But we hadn’t yet broken through to the higher levels of the provincial Ministry of Health. They didn’t fully recognize the value that we were bringing to the healthcare system and the fact that hospitalists are the cornerstone of the acute care system now.”
Mike Morris, MD, president of the Section of Hospital Medicine, agrees with this characterization. A hospitalist at Nanaimo Regional General Hospital (part of the Vancouver Island Health Authority), Dr. Morris believes that most of the health authorities, which administer the region’s hospitals, appreciate hospitalists’ value. “They know how much we help the patient flow and problems in the emergency room,” he says. Emergency department crowding has been a huge problem in British Columbia, due to lack of hospital beds and a dearth of long-term-care beds. “Hospitalists are able to come in and safely discharge people on a timely basis, and help the flow through the emergency department. That’s one of our biggest values to the hospital. We think that the family physicians coming into the hospital are platinum doctors because they’re keeping up with the rapid changes in hospital medicine. And we feel that they are being highly undervalued.”
On average, hospitalists were making $111 an hour (Canadian dollars, equating to about $98 U.S. dollars at the July 12 exchange rate). According to Dr. Wilton, the hospitalists contended that their earning potential was at least equivalent to that of a lower-intensity Monday-Friday community-based general practice. At the negotiations, they valued their services at $135/hour. If the government was unwilling to value hospitalists’ compensation appropriately, they warned they could easily return to a community-based practice model.
Payment Not the Only Issue
The province of British Columbia is divided into six health authorities, five of which have active hospitalist programs. Overarching compensation frameworks for all physicians are established through negotiations between the British Columbia Medical Association (BCMA) and the MOH. Individual health authorities then negotiate specific terms of compensation and workload expectations with physicians. There is considerable variation between health authorities (and indeed throughout each of the Canadian provinces) regarding hospitalists’ workload models, such as the number of expected patient encounters per shift and compensation packages.
The BCMA had recently completed contract renewal negotiations involving the entire physician body in British Columbia and the government on April 1, resulting in a new six-year Letter of Agreement that hospitalists maintained did not address their needs.
“The way we saw [the Letter of Agreement] being interpreted,” says Dr. Wilton, “was that the base rate for calculating our advances going forward was going to be between 10% and 25% less than what we were currently earning. Part of our goal was to get a wage that is consistent with the complexity and intensity of our work. I think that, in the eyes of the government, they were seeing our work and our value more in the range of the less-intense community-based general practice work. We wanted to shift that focus more towards the intensity of the acute care setting, where we think we’re more comparable to emergency medicine and internal medicine specialists.”
Dr. DeMott adds, “The workload model is a very important aspect of what we do. It isn’t only what you are paid, it is what you are being asked to do for what you’re being paid. Workload expectations have tremendous implications for the health of this career path in the future, the ability to recruit into this career path, and the ability to retain people, so that they do not become burnt out or personally destroyed.”
Views of the Dispute
B.C. hospitalists decided to hire their own attorney (the Vancouver firm of Tevlin Gleadle) and a press relations person to take their dispute public. Margaret MacDiarmid, MD, is president of the BCMA and has her own family practice in the Kootenays region eight hours east/southeast of Vancouver on the British Columbian mainland. “We [the BCMA] were very keen to assist, if we could, in the resolution of the conflict, and we were calling them about that,” she explains. “But we felt we had to operate within the Letter of Agreement that we had just signed, which I think is reasonable. So we did not play any active role in the final resolution.”
Assistant Deputy Minister for Medical Services Stephen Brown, PhD, the MOH official who oversees physician compensation, admits that the issue of the threatened walkout was “a bit of a surprise” to him because the government had just signed the Letter of Agreement with the BCMA. He became engaged with the health authorities and the hospitalists, “trying to understand how we got to where we were when we had just signed an agreement.”
Although hospitalists felt the Letter of Agreement did not address their concerns, Brown did not characterize the talks with the various stakeholders as negotiations. “I acknowledged that we were trying to understand the issues they were presenting and how we could address those issues within the context of the BCMA-government negotiated agreement,” he said during a telephone interview.
“Over the period of a couple weeks of dialogue, we got to a tentative agreement—which hopefully will now translate into contracts over the next week—that is within the framework of the Agreement.”
Goals Accomplished
Key figures involved in the talks expressed satisfaction with some of the goals achieved. Dr. Wilton reflects that the dispute has resulted in more public awareness of the presence of hospitalists and more awareness of hospitalists’ value within the BCMA. Most importantly, he says, “we sat across the table from some of the senior administrators in the Ministry of Health and were able to educate them about the values that hospitalists can bring to the system. We’re hoping that by having the opportunity to educate them, they will take a more proactive and organized approach to supporting the hospitalist model of care and utilizing it to its full potential.”
“I wasn’t thrilled that we were in this situation,” says Brown. “But the positive that’s come out of it is that I think we’ve got a platform, we’ve got a dialogue, and we have committed to work with them over the next six months to look at workload and see if we can get some level of consistency on that.”
Brown indicated that he had acquired more understanding of how hospitalists’ roles have evolved in the province and the difficulties they encounter to provide quality care. “The reality of what we found was that regions had developed hospitalist services in slightly different ways, with slightly different compensation arrangements,” he noted. “I hope what we have just done is we have now created the same platform for all the hospitalists across the province. They’re going to have a contract that looks similar and dialogue is now underway with the HAs [health authorities] about the range of services that hospitalists will provide. So I think that’s an opportunity as well, over the next six months now, to clean that up.”
While hospitalists gained some traction on the development of new workload standards, they did not fully accomplish their financial goals, the two key negotiators said. According to Dr. DeMott, “We became lost in a complex political and economic struggle that involved all of the doctors in the province. The doctors had recently ratified an agreement that left us completely out in the cold. In the end, we had to comply with the essential terms of that [BCMA-negotiated Letter of Agreement].”
To have insisted on the hospitalists’ financial goals, he says, would have injured too many programs, and—if they had walked off the job—ultimately would have compromised patient care. “In the end,” says Dr. DeMott, “we acquiesced and came up with a compromise that should work for the short term.”
Parallels with the United States?
Many of those interviewed for this article observed that hospitalist programs in British Columbia are still evolving, and that U.S. hospitalist programs are probably five years ahead in terms of established program models. Dr. DeMott praises the pioneering work done by SHM: “We look to you for guidance, and we really do appreciate the SHM advancement that is moving the hospitalist profession along.”
As negotiators for the Section of Hospital Medicine during the talks, Dr. DeMott says that his team used the surveys and studies that SHM has pioneered about the value-added contributions of hospitalists to increase awareness with the MOH, the government of British Columbia, and the BCMA about hospitalists’ roles. Dr. Morris notes that B.C. hospitalists, taking the lead from SHM, are now developing their core competencies.
William D. Atchley, Jr., MD, FACP, medical director of Peninsula Inpatient Care Specialists at Sentara Careplex Hospital in Hampton, Va., is a long-time member of the SHM board of directors. He has followed the growth of hospitalists in Canada, and applauds the efforts of those like Echo-Marie Enns, MD, who served as a National Association of Inpatient Physicians (NAIP) Canadian chapter president in Calgary. He has also conducted surveys of Canadian hospitalists. He doubts that a parallel strike situation could develop here in the United States.
“Their situation is unique to Canada,” he says. “From SHM’s perspective, we have always acted as an advocate for hospitalists in Canada and offered whatever we have learned here in the United States to help facilitate their movement. They are still in the process of explaining what a hospitalist is, and explaining to their national medical societies about what hospitalists can do. Their ability to get the message across is just going to take some time.”
Summing up their accomplishments thus far, Dr. DeMott says, “We considered this disagreement a defining moment for hospitalists in this province and quite possibly for [Canada]. We’re not there yet, but we put ourselves on the map. There will likely be another battle on the horizon for us, but hopefully one colored by a much greater appreciation of the expertise we bring to the acute care arena.” TH
Gretchen Henkel writes regularly for The Hospitalist.
The Coming Windfall
In June the Centers for Medicare and Medicaid Services (CMS) issued a notice proposing changes to the Medicare Physician Fee Schedule (MPFS) that, if enacted, would significantly increase Medicare payments to hospitalists for many services routinely performed. Because many private health plans use the Medicare-approved RVUs for their own fee schedules, it is anticipated that hospitalists will likely see payment increases for their non-Medicare services as well.
The changes, which will take effect in January 2007 if enacted, reflect the recommendations of the Relative Value Update Committee (RUC) of the American Medical Association, along with input from SHM. At this point, however, they are only proposed changes that CMS could modify based on input from affected groups and Congress. SHM will continue to urge CMS to implement the proposed changes and we encourage all hospitalists and other interested individuals to send a letter to CMS indicating support for the proposed changes. (See “How to Show Your Support,” p. 15.) CMS is accepting comments on the rule until August 21, with the final ruling expected in November.
The suggested revisions—the largest ever proposed for services related to patient evaluation and management—are designed to improve the accuracy of payments to physicians for the services they furnish to Medicare beneficiaries. The proposed notice includes substantial increases for “evaluation and management” services (that is, time and effort that physicians spend with patients in evaluating their condition and advising and assisting them in managing their health).
The proposed notice addresses two components of physician payments under the MPFS:
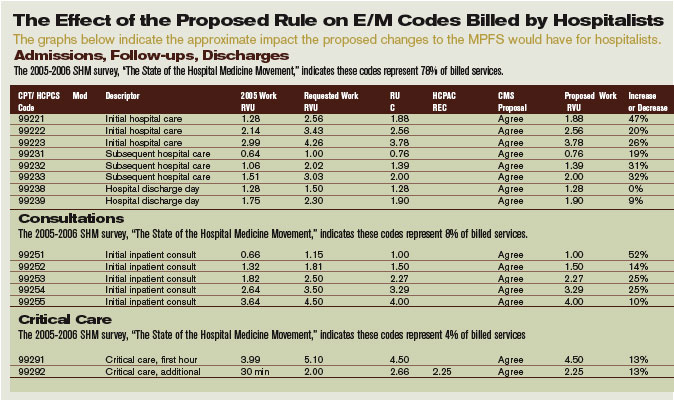
- A comprehensive review of physician work RVUs; and
- A proposed change in the methodology for calculating practice expenses.
“Medicare law requires CMS to assess the accuracy of the work relative values it assigns to physician-services every five years,” says SHM CEO Larry Wellikson, MD. “SHM, on behalf of our members, participated in a coalition of internal medicine groups, led by the American College of Physicians, which provided survey data and other evidence to the RUC to show that many services were undervalued compared to other physician services and that it was essential that their work RVUs be increased.”
Consistent with the RUC’s recommendations, CMS is proposing the largest increase in the work RVUs assigned to office and hospital visits and consultations since Medicare implemented its physician fee schedule in 1992. Many of these reflect double-digit increases for codes commonly billed by hospitalists:
- The work RVU for initial hospital care (CPT code 99221) would increase by 47%;
- The work RVU for subsequent hospital care (CPT code 99232) would increase by 31%; and
- The work RVU for subsequent hospital care (CPT code 99233) would increase by 32%.
“It’s time to increase Medicare’s payment rates for physicians to spend time with their patients,” says CMS Administrator Mark McClellan, MD, PhD. “We expect that improved payments for evaluation and management services will result in better outcomes because physicians will get financial support for giving patients the help they need to manage illnesses more effectively.”
While Medicare payments to each hospitalist won’t increase by the same percentages listed in the above examples, 2007 Medicare payments for many evaluation and management services would increase significantly, assuming continuation of the current 2006 dollar conversion factor. (See “The Effect of the Proposed Rule on E/M Codes Billed by Hospitalists,” above.)
Changes in physician work RVUs affect approximately 55% of the total RVUs (the rest are determined by changes in practice expense and medical liability RVUs), so the increase in work RVUs will determine more than half of the total payments per service.
Further, by law CMS must offset the total increases in work RVUs from the five-year review with a separate budget neutrality adjustment so that 2007 expenditures are roughly equal to their 2006 level. The agency is estimating that the proposed changes to the work RVUs would cost Medicare approximately $4 billion. To achieve budget neutrality, CMS is proposing to reduce the work RVU for each service by 10%.
Overall, the proposed notice revises work RVUs for more than 400 services to better reflect the work and time required of a physician in furnishing the service, which can include not just procedures performed but also the services involved in evaluating a patient’s condition, and determining a course of treatment (known as “evaluation and management” services).
Work RVUs account for approximately $35 billion in MPFS payments, representing more than 50% of overall Medicare payments under the fee schedule. TH
SHM encourages hospitalists and others to send a letter to CMS indicating support for the proposed changes.
In June the Centers for Medicare and Medicaid Services (CMS) issued a notice proposing changes to the Medicare Physician Fee Schedule (MPFS) that, if enacted, would significantly increase Medicare payments to hospitalists for many services routinely performed. Because many private health plans use the Medicare-approved RVUs for their own fee schedules, it is anticipated that hospitalists will likely see payment increases for their non-Medicare services as well.
The changes, which will take effect in January 2007 if enacted, reflect the recommendations of the Relative Value Update Committee (RUC) of the American Medical Association, along with input from SHM. At this point, however, they are only proposed changes that CMS could modify based on input from affected groups and Congress. SHM will continue to urge CMS to implement the proposed changes and we encourage all hospitalists and other interested individuals to send a letter to CMS indicating support for the proposed changes. (See “How to Show Your Support,” p. 15.) CMS is accepting comments on the rule until August 21, with the final ruling expected in November.
The suggested revisions—the largest ever proposed for services related to patient evaluation and management—are designed to improve the accuracy of payments to physicians for the services they furnish to Medicare beneficiaries. The proposed notice includes substantial increases for “evaluation and management” services (that is, time and effort that physicians spend with patients in evaluating their condition and advising and assisting them in managing their health).
The proposed notice addresses two components of physician payments under the MPFS:
- A comprehensive review of physician work RVUs; and
- A proposed change in the methodology for calculating practice expenses.
“Medicare law requires CMS to assess the accuracy of the work relative values it assigns to physician-services every five years,” says SHM CEO Larry Wellikson, MD. “SHM, on behalf of our members, participated in a coalition of internal medicine groups, led by the American College of Physicians, which provided survey data and other evidence to the RUC to show that many services were undervalued compared to other physician services and that it was essential that their work RVUs be increased.”
Consistent with the RUC’s recommendations, CMS is proposing the largest increase in the work RVUs assigned to office and hospital visits and consultations since Medicare implemented its physician fee schedule in 1992. Many of these reflect double-digit increases for codes commonly billed by hospitalists:
- The work RVU for initial hospital care (CPT code 99221) would increase by 47%;
- The work RVU for subsequent hospital care (CPT code 99232) would increase by 31%; and
- The work RVU for subsequent hospital care (CPT code 99233) would increase by 32%.
“It’s time to increase Medicare’s payment rates for physicians to spend time with their patients,” says CMS Administrator Mark McClellan, MD, PhD. “We expect that improved payments for evaluation and management services will result in better outcomes because physicians will get financial support for giving patients the help they need to manage illnesses more effectively.”
While Medicare payments to each hospitalist won’t increase by the same percentages listed in the above examples, 2007 Medicare payments for many evaluation and management services would increase significantly, assuming continuation of the current 2006 dollar conversion factor. (See “The Effect of the Proposed Rule on E/M Codes Billed by Hospitalists,” above.)
Changes in physician work RVUs affect approximately 55% of the total RVUs (the rest are determined by changes in practice expense and medical liability RVUs), so the increase in work RVUs will determine more than half of the total payments per service.
Further, by law CMS must offset the total increases in work RVUs from the five-year review with a separate budget neutrality adjustment so that 2007 expenditures are roughly equal to their 2006 level. The agency is estimating that the proposed changes to the work RVUs would cost Medicare approximately $4 billion. To achieve budget neutrality, CMS is proposing to reduce the work RVU for each service by 10%.
Overall, the proposed notice revises work RVUs for more than 400 services to better reflect the work and time required of a physician in furnishing the service, which can include not just procedures performed but also the services involved in evaluating a patient’s condition, and determining a course of treatment (known as “evaluation and management” services).
Work RVUs account for approximately $35 billion in MPFS payments, representing more than 50% of overall Medicare payments under the fee schedule. TH
SHM encourages hospitalists and others to send a letter to CMS indicating support for the proposed changes.
In June the Centers for Medicare and Medicaid Services (CMS) issued a notice proposing changes to the Medicare Physician Fee Schedule (MPFS) that, if enacted, would significantly increase Medicare payments to hospitalists for many services routinely performed. Because many private health plans use the Medicare-approved RVUs for their own fee schedules, it is anticipated that hospitalists will likely see payment increases for their non-Medicare services as well.
The changes, which will take effect in January 2007 if enacted, reflect the recommendations of the Relative Value Update Committee (RUC) of the American Medical Association, along with input from SHM. At this point, however, they are only proposed changes that CMS could modify based on input from affected groups and Congress. SHM will continue to urge CMS to implement the proposed changes and we encourage all hospitalists and other interested individuals to send a letter to CMS indicating support for the proposed changes. (See “How to Show Your Support,” p. 15.) CMS is accepting comments on the rule until August 21, with the final ruling expected in November.
The suggested revisions—the largest ever proposed for services related to patient evaluation and management—are designed to improve the accuracy of payments to physicians for the services they furnish to Medicare beneficiaries. The proposed notice includes substantial increases for “evaluation and management” services (that is, time and effort that physicians spend with patients in evaluating their condition and advising and assisting them in managing their health).
The proposed notice addresses two components of physician payments under the MPFS:
- A comprehensive review of physician work RVUs; and
- A proposed change in the methodology for calculating practice expenses.
“Medicare law requires CMS to assess the accuracy of the work relative values it assigns to physician-services every five years,” says SHM CEO Larry Wellikson, MD. “SHM, on behalf of our members, participated in a coalition of internal medicine groups, led by the American College of Physicians, which provided survey data and other evidence to the RUC to show that many services were undervalued compared to other physician services and that it was essential that their work RVUs be increased.”
Consistent with the RUC’s recommendations, CMS is proposing the largest increase in the work RVUs assigned to office and hospital visits and consultations since Medicare implemented its physician fee schedule in 1992. Many of these reflect double-digit increases for codes commonly billed by hospitalists:
- The work RVU for initial hospital care (CPT code 99221) would increase by 47%;
- The work RVU for subsequent hospital care (CPT code 99232) would increase by 31%; and
- The work RVU for subsequent hospital care (CPT code 99233) would increase by 32%.
“It’s time to increase Medicare’s payment rates for physicians to spend time with their patients,” says CMS Administrator Mark McClellan, MD, PhD. “We expect that improved payments for evaluation and management services will result in better outcomes because physicians will get financial support for giving patients the help they need to manage illnesses more effectively.”
While Medicare payments to each hospitalist won’t increase by the same percentages listed in the above examples, 2007 Medicare payments for many evaluation and management services would increase significantly, assuming continuation of the current 2006 dollar conversion factor. (See “The Effect of the Proposed Rule on E/M Codes Billed by Hospitalists,” above.)
Changes in physician work RVUs affect approximately 55% of the total RVUs (the rest are determined by changes in practice expense and medical liability RVUs), so the increase in work RVUs will determine more than half of the total payments per service.
Further, by law CMS must offset the total increases in work RVUs from the five-year review with a separate budget neutrality adjustment so that 2007 expenditures are roughly equal to their 2006 level. The agency is estimating that the proposed changes to the work RVUs would cost Medicare approximately $4 billion. To achieve budget neutrality, CMS is proposing to reduce the work RVU for each service by 10%.
Overall, the proposed notice revises work RVUs for more than 400 services to better reflect the work and time required of a physician in furnishing the service, which can include not just procedures performed but also the services involved in evaluating a patient’s condition, and determining a course of treatment (known as “evaluation and management” services).
Work RVUs account for approximately $35 billion in MPFS payments, representing more than 50% of overall Medicare payments under the fee schedule. TH
SHM encourages hospitalists and others to send a letter to CMS indicating support for the proposed changes.
Clinical approach to patients with neuropathic pain
Lung Cancer Gender Gap
Aquatic Antagonists: Stingray Injury
ECT wipes out 30 years of memories
Woman loses 30 years of memories after electroconvulsive therapy
Richland County (SC) Circuit Court
A 55-year old woman with a history of depression underwent successful electroconvulsive therapy (ECT) after her husband and father died. Six months later she became depressed, and a new psychiatrist referred her to his partner for additional ECT treatments.
The partner administered outpatient ECT at a hospital daily for 10 days. The referring psychiatrist wrote in the patient’s chart that the patient experienced memory loss and severe cognitive problems during the initial ECT regimen but did not report this development to his partner and allegedly encouraged the patient to continue ECT.
After the second round of ECT treatments, the patient suffered brain damage and lost all her memories from the past 30 years—including the births of her children and her job skills—leaving her unable to work.
In court, the patient claimed ECT should be administered no more than three times a week, and the referring psychiatrist should have told his partner about the patient’s memory problems.
- The case was settled for $18,000
Dr. Grant’s observations
Although this case concerns ECT, the claim is based on negligence—that is, the psychiatrist did not fulfill his duty to care for the patient. The negligence claim focused on how the treatment was implemented, not whether ECT was appropriate for this woman’s depression.
ECT’s response rate ranges from 50% to 60%1 among patients who did not respond to one or more antidepressant trials. Symptomatic improvement usually is faster with ECT than with pharmacotherapy2 when ECT is administered three times per week. Mortality rates with ECT are similar to those associated with minor surgery.1
In addition to being an effective and safe treatment for depression, ECT rarely is a basis for malpractice. One study found that only 4 (0.2%) of 1,700 psychiatric malpractice claims filed between 1984 and 1990 concerned ECT’s side effects, complications, or appropriateness.3 Few patients who receive ECT file a malpractice claim because most are satisfied with the treatment; approximately 80% of ECT patients say they would consent to ECT again.4,5 In fact, one might consider withholding ECT from severely depressed patients grounds for malpractice.
Although safe and effective, ECT could present health risks that you need to discuss with patients. In particular, cognitive problems such as delirium and impaired attention and memory may result.1
Cognitive impairment risk in ect
ECT’s more severe cognitive side effects stem from:
- bilateral electrode placement
- sine wave stimulation
- suprathreshold stimulus intensity
- administration >3 times per week
- large numbers of treatments, usually >20 in an acute treatment course
- some medications, such as lithium carbonate and anticholinergics6
- pre-existing neurologic diseases such as Alzheimer’s or Parkinson’s disease.1
The magnitude of retrograde amnesia often is greatest immediately after treatment. Patients are more likely to forget public information such as current events than personal information.10 The effects usually subside over time, and older memories are more likely to be recovered than more recent ones. ECT can cause permanent memory loss, particularly after bilateral electrode placement, suprathreshold stimulus intensity, sine wave stimulation, or large numbers of treatments—usually more than 20.
Ensuring adequate informed consent when delivering ECT or before referring a patient for treatment can help prevent a malpractice claim. Although specific requirements for ECT consent vary by jurisdiction, follow these general principles:1
- Provide the patient adequate information. Explain the reasons for ECT, describe the procedure including choice of stimulus electrode placement, offer alternative treatments, and explain the risks, benefits, anticipated number of treatments, relapse risk, and need for continuing treatment.
- Make sure the patient is capable of understanding and acting reasonably on this information and knows he or she can refuse treatment at any time.
- Tell the patient that a successful outcome is not guaranteed.
- Describe the likelihood and potential severity of major risks associated with ECT, including mortality, cardiovascular and CNS problems, and minor side effects such as headache, muscle aches, or nausea.
- Be sure the patient understands that consent is voluntary and can be withdrawn. The patient should know that he or she is also consenting to emergency treatment.
- Tell patients about possible behavioral restrictions—such as needing a friend or family member to monitor the patient or not being able to drive a car—that may be necessary during evaluation, treatment, and recuperation.
Although ECT might impair memory, it can improve neuropsychological domains such as global cognitive status and measures of general intelligence.11 Also, there is no evidence that ECT causes lasting problems in executive functioning, abstract reasoning, creativity, semantic memory, implicit memory, or skill acquisition or retention. Long-term negative effects on ability to learn and retain new information are unlikely.1
Avoiding an ect related malpractice claim
To reduce the possibility of a malpractice claim after ECT:
- Inform the patient about the risk of cognitive side effects as part of the informed consent process (Box).
- Assess the patient’s orientation and memory functions before and throughout ECT. In the above case, the referring psychiatrist had a duty to inform the psychiatrist administering ECT about the patient’s memory problems and recommend decreasing or discontinuing ECT.
- Consider a patient’s mood state, which may influence how ECT patients rate their memory.12 Ask about symptoms of depression. Patients with cognitive complaints such as subjective memory loss are more likely than those without such problems to have depression symptoms.1
- Do not administer ECT more than 3 times per week. No evidence supports more frequent use, and daily ECT may increase cognitive problems.1 The psychiatrist in the above case was negligent in providing a treatment frequency with no scientific support or medical rationale.
- Verify that the physician is qualified to perform ECT. Hospitals must ensure ECT quality and safety and should have a written plan for providing and maintaining ECT privileges.
- Involve the family when appropriate. Family members often care for patients during outpatient ECT. Give patients and family members literature describing ECT. Allow them time to consider the procedure, then schedule an appointment to answer questions.
1. American Psychiatric Association. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging, 2nd ed. Washington, DC: American Psychiatric Publishing; 2001.
2. Nobler MS, Sackeim HA, Moeller JR, et al. Quantifying the speed of symptomatic improvement with electroconvulsive therapy: comparison of alternative statistical methods. Convuls Ther 1997;13:208-21.
3. Slawson P. Psychiatric malpractice and ECT: a review of 1,700 claims. Convuls Ther 1991;7:255-61.
4. Freeman CP, Cheshire KE. Attitude studies on electroconvulsive therapy. Convuls Ther. 1986;2:31-42.
5. Pettinati HM, Tanburello TA, Ruetsch CR, et al. Patient attitudes toward electroconvulsive therapy. Psychopharmacol Bull. 1994;30:471-5.
6. Small JG, Kellams JJ, Milstein V, et al. Complications with electroconvulsive treatment combined with lithium. Biol Psychiatry 1980;15:103-12.
7. Sobin C, Sackeim HA, Prudic J, et al. Predictors of retrograde amnesia following ECT. Am J Psychiatry 1995;152:995-1001.
8. Donahue JC. Electroconvulsive therapy and memory loss: anatomy of a debate. J ECT 2000;16:133-43.
9. Sackeim HA. Memory and ECT: from polarization to reconciliation. J ECT 2000;16:87-96.
10. Lisanby SH, Maddox JH, Prudic J, et al. The effects of electroconvulsive therapy on memory of autobiographical and public events. Arch Gen Psychiatry 2000;57:581-90.
11. Sackeim HA, Prudic J, Devanand DP, et al. Effects of stimulus intensity and electrode placement on the efficacy and cognitive effects of electroconvulsive therapy. N Engl J Med 1993;328:839-46.
12. Coleman EA, Sackeim HA, Prudic J, et al. Subjective memory complaints before and after electroconvulsive therapy. Biol Psychiatry 1996;39:346-56.
Woman loses 30 years of memories after electroconvulsive therapy
Richland County (SC) Circuit Court
A 55-year old woman with a history of depression underwent successful electroconvulsive therapy (ECT) after her husband and father died. Six months later she became depressed, and a new psychiatrist referred her to his partner for additional ECT treatments.
The partner administered outpatient ECT at a hospital daily for 10 days. The referring psychiatrist wrote in the patient’s chart that the patient experienced memory loss and severe cognitive problems during the initial ECT regimen but did not report this development to his partner and allegedly encouraged the patient to continue ECT.
After the second round of ECT treatments, the patient suffered brain damage and lost all her memories from the past 30 years—including the births of her children and her job skills—leaving her unable to work.
In court, the patient claimed ECT should be administered no more than three times a week, and the referring psychiatrist should have told his partner about the patient’s memory problems.
- The case was settled for $18,000
Dr. Grant’s observations
Although this case concerns ECT, the claim is based on negligence—that is, the psychiatrist did not fulfill his duty to care for the patient. The negligence claim focused on how the treatment was implemented, not whether ECT was appropriate for this woman’s depression.
ECT’s response rate ranges from 50% to 60%1 among patients who did not respond to one or more antidepressant trials. Symptomatic improvement usually is faster with ECT than with pharmacotherapy2 when ECT is administered three times per week. Mortality rates with ECT are similar to those associated with minor surgery.1
In addition to being an effective and safe treatment for depression, ECT rarely is a basis for malpractice. One study found that only 4 (0.2%) of 1,700 psychiatric malpractice claims filed between 1984 and 1990 concerned ECT’s side effects, complications, or appropriateness.3 Few patients who receive ECT file a malpractice claim because most are satisfied with the treatment; approximately 80% of ECT patients say they would consent to ECT again.4,5 In fact, one might consider withholding ECT from severely depressed patients grounds for malpractice.
Although safe and effective, ECT could present health risks that you need to discuss with patients. In particular, cognitive problems such as delirium and impaired attention and memory may result.1
Cognitive impairment risk in ect
ECT’s more severe cognitive side effects stem from:
- bilateral electrode placement
- sine wave stimulation
- suprathreshold stimulus intensity
- administration >3 times per week
- large numbers of treatments, usually >20 in an acute treatment course
- some medications, such as lithium carbonate and anticholinergics6
- pre-existing neurologic diseases such as Alzheimer’s or Parkinson’s disease.1
The magnitude of retrograde amnesia often is greatest immediately after treatment. Patients are more likely to forget public information such as current events than personal information.10 The effects usually subside over time, and older memories are more likely to be recovered than more recent ones. ECT can cause permanent memory loss, particularly after bilateral electrode placement, suprathreshold stimulus intensity, sine wave stimulation, or large numbers of treatments—usually more than 20.
Ensuring adequate informed consent when delivering ECT or before referring a patient for treatment can help prevent a malpractice claim. Although specific requirements for ECT consent vary by jurisdiction, follow these general principles:1
- Provide the patient adequate information. Explain the reasons for ECT, describe the procedure including choice of stimulus electrode placement, offer alternative treatments, and explain the risks, benefits, anticipated number of treatments, relapse risk, and need for continuing treatment.
- Make sure the patient is capable of understanding and acting reasonably on this information and knows he or she can refuse treatment at any time.
- Tell the patient that a successful outcome is not guaranteed.
- Describe the likelihood and potential severity of major risks associated with ECT, including mortality, cardiovascular and CNS problems, and minor side effects such as headache, muscle aches, or nausea.
- Be sure the patient understands that consent is voluntary and can be withdrawn. The patient should know that he or she is also consenting to emergency treatment.
- Tell patients about possible behavioral restrictions—such as needing a friend or family member to monitor the patient or not being able to drive a car—that may be necessary during evaluation, treatment, and recuperation.
Although ECT might impair memory, it can improve neuropsychological domains such as global cognitive status and measures of general intelligence.11 Also, there is no evidence that ECT causes lasting problems in executive functioning, abstract reasoning, creativity, semantic memory, implicit memory, or skill acquisition or retention. Long-term negative effects on ability to learn and retain new information are unlikely.1
Avoiding an ect related malpractice claim
To reduce the possibility of a malpractice claim after ECT:
- Inform the patient about the risk of cognitive side effects as part of the informed consent process (Box).
- Assess the patient’s orientation and memory functions before and throughout ECT. In the above case, the referring psychiatrist had a duty to inform the psychiatrist administering ECT about the patient’s memory problems and recommend decreasing or discontinuing ECT.
- Consider a patient’s mood state, which may influence how ECT patients rate their memory.12 Ask about symptoms of depression. Patients with cognitive complaints such as subjective memory loss are more likely than those without such problems to have depression symptoms.1
- Do not administer ECT more than 3 times per week. No evidence supports more frequent use, and daily ECT may increase cognitive problems.1 The psychiatrist in the above case was negligent in providing a treatment frequency with no scientific support or medical rationale.
- Verify that the physician is qualified to perform ECT. Hospitals must ensure ECT quality and safety and should have a written plan for providing and maintaining ECT privileges.
- Involve the family when appropriate. Family members often care for patients during outpatient ECT. Give patients and family members literature describing ECT. Allow them time to consider the procedure, then schedule an appointment to answer questions.
Woman loses 30 years of memories after electroconvulsive therapy
Richland County (SC) Circuit Court
A 55-year old woman with a history of depression underwent successful electroconvulsive therapy (ECT) after her husband and father died. Six months later she became depressed, and a new psychiatrist referred her to his partner for additional ECT treatments.
The partner administered outpatient ECT at a hospital daily for 10 days. The referring psychiatrist wrote in the patient’s chart that the patient experienced memory loss and severe cognitive problems during the initial ECT regimen but did not report this development to his partner and allegedly encouraged the patient to continue ECT.
After the second round of ECT treatments, the patient suffered brain damage and lost all her memories from the past 30 years—including the births of her children and her job skills—leaving her unable to work.
In court, the patient claimed ECT should be administered no more than three times a week, and the referring psychiatrist should have told his partner about the patient’s memory problems.
- The case was settled for $18,000
Dr. Grant’s observations
Although this case concerns ECT, the claim is based on negligence—that is, the psychiatrist did not fulfill his duty to care for the patient. The negligence claim focused on how the treatment was implemented, not whether ECT was appropriate for this woman’s depression.
ECT’s response rate ranges from 50% to 60%1 among patients who did not respond to one or more antidepressant trials. Symptomatic improvement usually is faster with ECT than with pharmacotherapy2 when ECT is administered three times per week. Mortality rates with ECT are similar to those associated with minor surgery.1
In addition to being an effective and safe treatment for depression, ECT rarely is a basis for malpractice. One study found that only 4 (0.2%) of 1,700 psychiatric malpractice claims filed between 1984 and 1990 concerned ECT’s side effects, complications, or appropriateness.3 Few patients who receive ECT file a malpractice claim because most are satisfied with the treatment; approximately 80% of ECT patients say they would consent to ECT again.4,5 In fact, one might consider withholding ECT from severely depressed patients grounds for malpractice.
Although safe and effective, ECT could present health risks that you need to discuss with patients. In particular, cognitive problems such as delirium and impaired attention and memory may result.1
Cognitive impairment risk in ect
ECT’s more severe cognitive side effects stem from:
- bilateral electrode placement
- sine wave stimulation
- suprathreshold stimulus intensity
- administration >3 times per week
- large numbers of treatments, usually >20 in an acute treatment course
- some medications, such as lithium carbonate and anticholinergics6
- pre-existing neurologic diseases such as Alzheimer’s or Parkinson’s disease.1
The magnitude of retrograde amnesia often is greatest immediately after treatment. Patients are more likely to forget public information such as current events than personal information.10 The effects usually subside over time, and older memories are more likely to be recovered than more recent ones. ECT can cause permanent memory loss, particularly after bilateral electrode placement, suprathreshold stimulus intensity, sine wave stimulation, or large numbers of treatments—usually more than 20.
Ensuring adequate informed consent when delivering ECT or before referring a patient for treatment can help prevent a malpractice claim. Although specific requirements for ECT consent vary by jurisdiction, follow these general principles:1
- Provide the patient adequate information. Explain the reasons for ECT, describe the procedure including choice of stimulus electrode placement, offer alternative treatments, and explain the risks, benefits, anticipated number of treatments, relapse risk, and need for continuing treatment.
- Make sure the patient is capable of understanding and acting reasonably on this information and knows he or she can refuse treatment at any time.
- Tell the patient that a successful outcome is not guaranteed.
- Describe the likelihood and potential severity of major risks associated with ECT, including mortality, cardiovascular and CNS problems, and minor side effects such as headache, muscle aches, or nausea.
- Be sure the patient understands that consent is voluntary and can be withdrawn. The patient should know that he or she is also consenting to emergency treatment.
- Tell patients about possible behavioral restrictions—such as needing a friend or family member to monitor the patient or not being able to drive a car—that may be necessary during evaluation, treatment, and recuperation.
Although ECT might impair memory, it can improve neuropsychological domains such as global cognitive status and measures of general intelligence.11 Also, there is no evidence that ECT causes lasting problems in executive functioning, abstract reasoning, creativity, semantic memory, implicit memory, or skill acquisition or retention. Long-term negative effects on ability to learn and retain new information are unlikely.1
Avoiding an ect related malpractice claim
To reduce the possibility of a malpractice claim after ECT:
- Inform the patient about the risk of cognitive side effects as part of the informed consent process (Box).
- Assess the patient’s orientation and memory functions before and throughout ECT. In the above case, the referring psychiatrist had a duty to inform the psychiatrist administering ECT about the patient’s memory problems and recommend decreasing or discontinuing ECT.
- Consider a patient’s mood state, which may influence how ECT patients rate their memory.12 Ask about symptoms of depression. Patients with cognitive complaints such as subjective memory loss are more likely than those without such problems to have depression symptoms.1
- Do not administer ECT more than 3 times per week. No evidence supports more frequent use, and daily ECT may increase cognitive problems.1 The psychiatrist in the above case was negligent in providing a treatment frequency with no scientific support or medical rationale.
- Verify that the physician is qualified to perform ECT. Hospitals must ensure ECT quality and safety and should have a written plan for providing and maintaining ECT privileges.
- Involve the family when appropriate. Family members often care for patients during outpatient ECT. Give patients and family members literature describing ECT. Allow them time to consider the procedure, then schedule an appointment to answer questions.
1. American Psychiatric Association. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging, 2nd ed. Washington, DC: American Psychiatric Publishing; 2001.
2. Nobler MS, Sackeim HA, Moeller JR, et al. Quantifying the speed of symptomatic improvement with electroconvulsive therapy: comparison of alternative statistical methods. Convuls Ther 1997;13:208-21.
3. Slawson P. Psychiatric malpractice and ECT: a review of 1,700 claims. Convuls Ther 1991;7:255-61.
4. Freeman CP, Cheshire KE. Attitude studies on electroconvulsive therapy. Convuls Ther. 1986;2:31-42.
5. Pettinati HM, Tanburello TA, Ruetsch CR, et al. Patient attitudes toward electroconvulsive therapy. Psychopharmacol Bull. 1994;30:471-5.
6. Small JG, Kellams JJ, Milstein V, et al. Complications with electroconvulsive treatment combined with lithium. Biol Psychiatry 1980;15:103-12.
7. Sobin C, Sackeim HA, Prudic J, et al. Predictors of retrograde amnesia following ECT. Am J Psychiatry 1995;152:995-1001.
8. Donahue JC. Electroconvulsive therapy and memory loss: anatomy of a debate. J ECT 2000;16:133-43.
9. Sackeim HA. Memory and ECT: from polarization to reconciliation. J ECT 2000;16:87-96.
10. Lisanby SH, Maddox JH, Prudic J, et al. The effects of electroconvulsive therapy on memory of autobiographical and public events. Arch Gen Psychiatry 2000;57:581-90.
11. Sackeim HA, Prudic J, Devanand DP, et al. Effects of stimulus intensity and electrode placement on the efficacy and cognitive effects of electroconvulsive therapy. N Engl J Med 1993;328:839-46.
12. Coleman EA, Sackeim HA, Prudic J, et al. Subjective memory complaints before and after electroconvulsive therapy. Biol Psychiatry 1996;39:346-56.
1. American Psychiatric Association. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging, 2nd ed. Washington, DC: American Psychiatric Publishing; 2001.
2. Nobler MS, Sackeim HA, Moeller JR, et al. Quantifying the speed of symptomatic improvement with electroconvulsive therapy: comparison of alternative statistical methods. Convuls Ther 1997;13:208-21.
3. Slawson P. Psychiatric malpractice and ECT: a review of 1,700 claims. Convuls Ther 1991;7:255-61.
4. Freeman CP, Cheshire KE. Attitude studies on electroconvulsive therapy. Convuls Ther. 1986;2:31-42.
5. Pettinati HM, Tanburello TA, Ruetsch CR, et al. Patient attitudes toward electroconvulsive therapy. Psychopharmacol Bull. 1994;30:471-5.
6. Small JG, Kellams JJ, Milstein V, et al. Complications with electroconvulsive treatment combined with lithium. Biol Psychiatry 1980;15:103-12.
7. Sobin C, Sackeim HA, Prudic J, et al. Predictors of retrograde amnesia following ECT. Am J Psychiatry 1995;152:995-1001.
8. Donahue JC. Electroconvulsive therapy and memory loss: anatomy of a debate. J ECT 2000;16:133-43.
9. Sackeim HA. Memory and ECT: from polarization to reconciliation. J ECT 2000;16:87-96.
10. Lisanby SH, Maddox JH, Prudic J, et al. The effects of electroconvulsive therapy on memory of autobiographical and public events. Arch Gen Psychiatry 2000;57:581-90.
11. Sackeim HA, Prudic J, Devanand DP, et al. Effects of stimulus intensity and electrode placement on the efficacy and cognitive effects of electroconvulsive therapy. N Engl J Med 1993;328:839-46.
12. Coleman EA, Sackeim HA, Prudic J, et al. Subjective memory complaints before and after electroconvulsive therapy. Biol Psychiatry 1996;39:346-56.