User login
11 Steps to a Successful Transition
A65-lb., 25-year-old, male cerebral palsy (CP) patient with pneumonia arrives at your Children’s Hospital via ambulance. Although chronologically this patient is an adult, in many ways he’s still a child, and the parents told the paramedics that they’ve always taken their son to Children’s. You’ve been the treating physician during the patient’s frequent hospital stays. Is Children’s Hospital still the best destination for this patient? Will the family’s insurance still cover an admission at Children’s?
During the hospital stay, the patient has complications. He has to be intubated. IV antibiotics need to be continued for a course after hospital discharge. A long recovery is expected. Is it time for the family to consider discharge to a long-term care facility rather than home? Are there any long-term care facilities in the area that accept young adult CP patients?
As the treating pediatric hospitalist, what is your role in helping this patient and his family transition from pediatric care to an adult-care medical home?
Introduction
Approximately 8.6 million children in the United States age 10–17 have a disability, according to the Adolescent Health Transition Project, which is housed at the Center on Human Development and Disability (CHDD) at the University of Washington, Seattle. Of these, 16% (or 1.4 million) experience limitations in their activities and will likely have difficulty making the transition to adult healthcare.1
Given enough time in the profession, every pediatric hospitalist will face the challenge of transitioning patients from child-centered to adult-oriented healthcare systems. The good news: Medical advances have made it increasingly possible for children who once would have died in childhood to survive into adulthood.
Example: One in 2,500 children is born with cystic fibrosis (CF); however, with the recent, unprecedented increase in the success of diagnosis and treatment modalities for the pulmonary component of CF, the estimated median survival age for those born in the 1990s is now 40.2 As of the year 2004, 41.8% of the 22,301 patients with CF were 18 or older.3 In fact, each year nearly 500,000 children with special healthcare needs reach adulthood, and 90% of children with a chronic illness and/or disability now survive to adulthood.4,5
The bad news: Many physicians whose practices focus on adults aren’t familiar with disease processes, such as CF, that have historically been considered pediatric illnesses.
For patients with chronic physical and medical conditions—particularly for those who are medically fragile and/or technology-dependent—the transition can prove especially difficult. And pediatric hospitalists in children’s hospitals face different challenges than those in facilities that admit patients of all ages. One thing remains the same, though, the goal: to provide uninterrupted, coordinated, developmentally appropriate healthcare.
Why Transition?
There are several good reasons for patients to be transitioned from pediatric care to adult care. First, as patients age medical issues develop that are beyond the sphere of pediatricians. In CF, for example, diabetes and biliary tract problems occur with greater frequency in adults. However, because so few CF patients historically survived to adulthood, few physicians who care for adults learned about the disease. Thus, the pediatricians who cared for CF patients continued to do so, leading to situations in which 30- and 40-year-olds have been hospitalized with children. But is that truly appropriate?
Adult patients may have high blood pressure, gynecologic issues, osteoporosis, or other problems the pediatrician may not be prepared to deal with. Example: A primary care pediatrician has been the “medical home” for a small, cerebral palsy patient since she was 10. She’s now 25. If she presents with a breast mass, will the pediatrician pick up on the condition adequately? Will they know where to send the patient?
“Adult providers know those systems better,” says Brett Pickering, MD, director of the Special Needs Clinic at San Diego’s UCSD Medical Center, Department of Pediatrics.
The adult patient has different emotional needs than the pediatric patient, and the pediatric hospitalist may not be in tune with adult needs. “Pediatricians do a lot of handholding,” says Dr. Pickering. “Adult providers are more matter of fact.”
Age restrictions on admissions, insurance, and funding issues also affect transition. For example, funding under the Social Security Act’s Title V Children with Special Health Care Needs typically ends at 21 despite a patient’s education or employment status.
Given these factors, what is the appropriate age to transition care from a pediatric floor or facility to an adult-oriented unit? According to the American Academy of Pediatrics, the responsibility of pediatrics continues through age 21, but there’s no hard-and-fast rule.
Challenges
The transition to adult-care facilities is typically a lengthy process involving multiple specialties and possibly joint care during a transition period—and a process that should ideally be coordinated by the patient’s primary care pediatrician. But hospitalists know that circumstances are typically far from ideal.
First, during a transition, the patient may feel abandoned by the medical team they’ve known for most of their lives. It takes time to develop trust and confidence in a new doctor. In this respect, pediatric hospitalists in facilities that care for patients of all ages have an advantage over hospitalists in children’s hospitals. They can call on their adult-care colleagues in other areas of the hospital for consultations and transfer care over time.
“The pediatric hospitalist must make bridges with their adult colleagues who are comfortable [with the issues] and willing to take on this patient population,” says Dr. Pickering.
Second, parents may feel an emotional dependency on the pediatric team and can feel threatened by the adult environment as they lose some control. To the parents, the patient will always be their child, Dr. Pickering notes.
Third, pediatric hospitalists may be reluctant to let go, particularly if they feel adult services are inferior to those they have provided, which brings us to the fourth major challenge: To whom do you transition care?
Many adult healthcare providers receive only limited training in disorders associated with pediatrics (e.g., CF, spina bifida). The Cystic Fibrosis Foundation is leading the way in educating physicians in what have historically been considered pediatric problems. In the 1980s, the foundation launched an educational program to train physicians already involved in adult pulmonary care in CF. Unfortunately, education in other areas has lagged. And finding a physician with both an interest in and knowledge of such disorders can prove challenging.
“It’s incumbent on our adult colleagues to take these patients on, but they need training,” says Dr. Pickering. “Long-term issues require long-term solutions.
How do you jazz people up to take care of this population?” she asks. Physicians must have at least a little bit of desire to learn about these special patient populations, but academic institutions also need to identify core knowledge and skills and make them part of training and certification requirements for primary care residents and physicians in practice. Continuing medical education for physicians, nurses, and allied healthcare professionals should include drug dosing, medical complications seen in transition populations, and related developmental, psychosocial, and behavioral issues.
Steps to a Successful Transition
So what should hospitalists do? In an April 2005 presentation at the SHM Annual Meeting, Joseph M. Geskey, DO, assistant professor of pediatrics and medicine, and director of inpatient pediatrics at Penn State College of Medicine, Hershey, Penn., recommended that pediatric hospitalists take the following steps:
- Identify the key aspects of transition;
- Bring stakeholders together;
- Identify transitional needs;
- Identify and provide resources;
- Create an audit and evaluation process;
- Decide who will hand off care of these patients when they are admitted to the hospital (the hospitalist or the disease-specific specialist);
- Create an up-to-date medical summary that is portable and accessible. It should include important historic information, such as diagnostic data, procedures, operations, and medications;
- Upon patient discharge, include specific instructions on who to call if the patient develops a problem after leaving the hospital;
- Create a working group in your area that represents pediatric and adult hospitalists to examine transition issues in the hospitalized patient; and
- Facilitate effective communication between patients and their families, primary care physicians and specialists; and
- Know when to transfer care to a center with more expertise in caring for specific conditions.
Conclusion
Just as every patient is different and every patient’s circumstances are unique, every transition needs to be individualized. “It’s hard to set policy,” says Dr. Pickering. Open, direct communication, specific discharge instructions, an up-to-date medical summary and knowledge of the adult resources in your area can make any transition a success. TH
Keri Losavio regularly writes for “Pediatric Special Section.”
References
- Adolescent Health Transition Project, Center on Human Development and Disability (CHDD) at the University of Washington, Seattle. Available at http://depts.washington.edu/healthtr/Providers/intro.htm. Last accessed January 16, 2006.
- Bufi PL. Cystic fibrosis: therapeutic options for co-management. Available at www.thorne.com/altmedrev/fulltext/cystic.html. Last accessed January 16, 2006.
- Cystic Fibrosis Foundation: 2004 Patient Registry Report. Available at www.cff.org/living_with_cf/. Last accessed Jan. 26, 2006
- Newacheck PW, Taylor WR. Childhood chronic illness: prevalence, severity, and impact. Am J Pub Health. 1992;82(3):364-371.
- Committee on Children with Disabilities and Committee on Adolescence, American Academy of Pediatrics. Transition of care provided for adolescents with special health care needs. Pediatrics. 1996;98(6):1203–1206.
Pediatric Special Section
In the Literature
By Mary Ann Queen, MD, and Amita Amonker, MD
Utilization of a Clinical Pathway Improves Care for Bronchiolitis
Cheney J, Barber S, Altamirano L, et al. A Clinical Pathway for Bronchiolitis is Effective in Reducing Readmission Rates. J Pediatr. 2005;147(5):622-626.
Bronchiolitis is the most common respiratory illness in infants that results in hospitalization. Many hospitals have developed clinical pathways to assist clinicians in managing this common infection; however, the effectiveness of such pathways has not been fully studied. Of those clinical practice guidelines analyzed, varying results have been identified.
To determine the effectiveness of a bronchiolitis pathway, this study compared infants managed prospectively using a pathway protocol with a retrospective analysis of infants managed without a pathway. Infants from a tertiary care children’s hospital and three regional hospitals were enrolled prospectively from May 2000 to August 2001. (One must note this study was completed in Australia, hence the difference from the typical Northern Hemisphere winter months.) The historical control group was admitted between May 1998 and August 1999 at the same four institutions. Two-hundred-twenty-nine patients admitted with bronchiolitis were treated using the pathway protocol. These patients were compared with 207 randomly selected control patients who were admitted prior to the institution of the bronchiolitis pathway. All patients were less than 12 months of age with their first episode of wheezing necessitating hospitalization.
These particular guidelines were developed and used to promote consistency of nursing management during a separate study on bronchiolitis. The pathway included an initial admission assessment. It also stated parameters for initiating and stopping both oxygen therapy and intravenous fluid therapy along with discharge guidelines.
The authors found no significant difference in length of stay or time in oxygen. Fifteen infants (7.2%) in the control group required readmission within two weeks of discharge compared with two infants (0.9%) in the pathway group (p=.001). Of the control group 33.8% received intravenous fluids (IVFs) compared with 19.2% of the pathway infants (p=.001). There was also greater steroid use in the control group but no difference in antibiotic usage. Specific data regarding steroids and antibiotics is not included.
The clinical pathway appears a useful tool for discharge planning with a decreased incidence of hospital readmission when specific discharge goals are utilized. The authors also reported a decreased use of IVFs in the pathway group. This was attributed to having specific parameters (O2 required, RR>60/min or inadequate oral feeding) for when to initiate them. It is unclear from the article whether meeting a single parameter or all three parameters triggered the initiation of IVFs.
The authors also point out the limitation of using a historical control given annual variations in severity sometimes seen with bronchiolitis. They attempted to minimize this by collecting data for each group over two consecutive winters.
Preprinted Paper Orders Reduce Medication Errors
Kozer E, Scolnik D, MacPherson A, et al. Using a preprinted order sheet to reduce prescription errors in a pediatric emergency department: A randomized, controlled trial. Pediatrics. 2005(116):1299-1302.
Medical errors, including medication errors, are common and are written about with increasing frequency in the lay press. Accreditation bodies and individual hospitals are striving for ways to decrease these errors. In some instances potential solutions include purchasing new computer systems for electronic physician order entry. This study looks at whether implementing a preprinted paper order sheet can decrease the incidence of medication errors in a pediatric ED.
This randomized, prospective study occurred during 18 days in July 2001 with nine days randomly assigned into each arm. The first arm used the hospital’s regular blank order sheets for all medication orders. The second arm used the experimental preprinted order sheet. This sheet required the staff to specify the dose, weight-adjusted dose, total daily dose, route of administration, and frequency for each medication ordered. Two medical students entered the data into a database that included information about patients’ demographics, diagnosis, acuity, details on the prescribing physician, the form used, and all medications prescribed and given to the patient. This information was subsequently reviewed by two blinded pediatric emergency physicians who determined if an error occurred and, if so, the degree of the error.
During the study period there were 2,157 visits to the ED with 95.4% charts available for review. Seven-hundred-ninety-five medications were prescribed with 376 ordered on the new form. Drug errors were identified in 68 (16.6%) orders when the regular form was used and in 37 (9.8%) orders on the new form. There was one severe error and 13 significant errors using the new form and 36 significant errors on the regular form. The new form was associated with a twofold decrease in the risk for a medication error even after accounting for the level of training of the ordering practitioner. There was an even greater reduction in the risk for a severe or significant error.
The literature has shown that computerized physician order entry can reduce the number of medication errors in the inpatient setting; however, it is not available in many hospitals and its effectiveness has not been shown in EDs. The authors point out that most medications ordered in the ED are prepared and given by nurses. The benefits of a computerized system in this setting is unclear.
This study occurred over an 18-day period with the new form only used for nine days outside of an earlier pilot period. One could speculate that the novelty of the form encouraged the physicians to examine orders more carefully, leading to decreased errors. It is unknown if the decrease in errors would be sustained over time.
Also important to note is that the definition of an error was limited to a mistake in dose, interval between doses, dose unit, and/or route. Errors such as legibility, medication allergy, or drug interactions are not discussed. However, as hospitals strive to implement technologies aimed at reducing errors this simple, economical solution may be of benefit.
No Association between Kawasaki Disease and Adenovirus
Shike H, Shimizu C, Kanegaye J, et al. Adenovirus, adeno-associated virus and Kawasaki disease. Pediatr Infect Dis J. 2005;24:1011-1014.
Kawasaki disease is a self-limited acute vasculitis of children with a suspected infectious etiology and defined seasonality. In an attempt to find a clue for a possible infectious cause of Kawasaki disease this study examined the seasonality of different viruses. The study recognized a similar bimodal seasonality for some serotypes of adenovirus. Adenovirus accounts for 5%-10% of respiratory tract infections in children and can mimic the clinical manifestations and laboratory abnormalities seen in Kawasaki disease.
This study postulated that infection with a non-cultivatable adenovirus or antecedent adenovirus infection might be a trigger for Kawasaki disease. The study analyzed patient samples using polymerase chain reaction primers for all 51 adenovirus serotypes, viral culture, and neutralization assay for the most common adenovirus serotypes. This study also investigated possible involvement of adeno-associated viruses (AAVs), because AAVs depend on helper viruses, such as adenovirus.
Kawasaki disease patients were enrolled during a 25-month period from February 2002 to February 2004 at Children’s Hospital and Health Center in San Diego. Illness day one was defined as the first day of fever. Clinical samples used in this study were collected within the first 14 days of fever onset and before intravenous immunoglobulin (IVIG) therapy.
Nasopharyngeal swabs were cultured for adenovirus. Standard adenoviral neutralization assays for the five most common serotypes were performed with the use of patient sera. Sera with a titer of 1/10 or greater were scored as positive. At least two clinical samples from each patient, including throat swabs, sera or urine, were tested by quantitative polymerase chain reaction (PCR) for adenovirus and AAV.
Nasopharyngeal viral cultures were collected before IVIG administration on illness day three—14 from 70 Kawasaki disease patients. Of the 70 patients, 52 patients fulfilled four of the five classic criteria or three of the five criteria with abnormal coronary arteries by echocardiogram. Of the remaining 18 patients with atypical Kawasaki disease, six had coronary artery abnormalities. Overall, seven patients had coronary artery aneurysms and 22 patients had coronary artery dilatation. Viral cultures were negative in 66 of the 70 Kawasaki disease patients. The viral isolates in four patients were respiratory syncytial (one), parainfluenza virus 3 (one) and adenovirus (two). Therefore adenovirus culture was negative in 97% of patients.
Fifteen Kawasaki disease patients with negative adenovirus cultures were evaluated by PCR assay on at least two clinical samples. Fourteen patients had a negative PCR result. The throat swab from one patient collected on illness day seven contained 800 adenovirus genome copies.
Results of the adenovirus neutralization assays from 26 Kawasaki disease patients revealed that neutralization titers against any of the five most common adenovirus serotypes were undetectable in four of 26 patients.
None of the 36 samples from the same 15 acute Kawasaki disease patients described for the PCR assay was positive for AAV.
This study concluded that despite the striking similarities between Kawasaki disease and adenovirus infection there is no evidence to suggest a link between the two.
Epidemiology and Clinical Description of Severe, Multifocal Staphylococcus aureus Infection
Miles F, Voss L, Segedin E, et al. Review of Staphylococcus aureus infections requiring admission to a paediatric intensive care unit. Arch Dis Child. 2005;90(12):1274-1278.
Staphylococcus aureus is a recognized cause of multifocal infection with a high mortality rate. Children with community acquired S. aureus bacteremia (SAB) have higher frequencies of unknown foci compared with hospital-acquired SAB. Those children with S. aureus sepsis (SAS) presenting to the pediatric intensive care unit tend to have multisystemic disease—either by direct invasion or toxin production—before the diagnosis is made and treatment is initiated.
This study evaluates the clinical features and mortality from SAS in those children who required intensive care management. A retrospective review of clinical notes from all children with SAS admitted from October 1993 to April 2004 to the PICU in Auckland Children’s Hospital in New Zealand was undertaken. Children coded for SAS were identified from the PICU database.
All clinical notes were reviewed by one investigator using a standardized questionnaire that sought information on patient demographics, clinical findings, investigations, microbiology, and management in the PICU. Cases were included if blood or an isolate from a site that is normally sterile was positive for S. aureus. Hospital-acquired infection was defined by an isolate obtained at least 48 hours after hospital admission; community acquired infection was defined by an isolate obtained within 48 hours of admission.
Fifty-eight patients were identified with SAS over the 10-year study period; 55 were community acquired. Children with staphylococcal illness comprised 1% of all admission to the PICU. Musculoskeletal symptoms (79%) dominated presentation rather than isolated pneumonia (10%). An aggressive search for foci and surgical drainage of infective foci was required in 50% of children.
Most children (67%) either presented with multiple site involvement or secondary sites developed during their hospital stay. These pathologies included pneumonia, septic arthritis, osteomyelitis, and soft tissue involvement (cellulitis, fasciitis, abscess). A transthoracic echocardiogram detected valve abnormalities in only 5% of children, and these children were known to have pre-existing cardiac lesions. Few children (12%) presenting with methicillin-resistant S. aureus (MRSA) had community-acquired infection. The median length of stay in the PICU was three (mean 5.8, range one-44) days. Mortality due to SAS was 8.6%. Ten children had significant morbidity after discharge; these morbidities included renal failure requiring dialysis (three), an ongoing oxygen requirement at three months follow-up (two), and problems relating to limb movement and function (eight). Two children with epidural abscesses were paraplegic.
Community-acquired SAS affects healthy children, is multifocal, and has a high morbidity and mortality. It is imperative to look for sites of dissemination and to drain and debride foci. Routine echocardiography had a low yield in the absence of pre-existing cardiac lesions, persisting fever, or persisting bacteremia.
Long-Term Outcomes for Childhood Headache
Brna P, Dooley J, Gordon K Dewan T. The prognosis of childhood headache. Arch Pediatr Adolesc Med. 2005;159(12):1157-1160.
Headaches affect most children and rank third among illness-related causes of school absenteeism. Although the short-term outcome for most children appears favorable, few studies have reported long-term outcome. The objective of this study was to evaluate the long-term prognosis of childhood headaches 20 years after initial diagnosis in a cohort of Atlantic Canadian children who had headaches diagnosed in 1983.
Ninety-five patients with headaches who consulted one of the authors in 1983 were subsequently studied in 1993. The 77 patients contacted in 1993 were followed up in 2003. A standard telephone interview was used. Data were collected regarding headache symptoms, severity, frequency, treatment, and precipitants. Headache severity was simply classified as mild, moderate, or severe.
Sixty (78%) of 77 patients responded (60 of the 95 in the original cohort). At 20 years 16 (27%) were headache free, 20 (33%) had tension-type headaches, 10 (17%) had migraine, 14 (23%) had migraine and tension-type headaches. Having more than one headache type was more than at diagnosis or initial follow-up, and headache type varied across time. Of those who had headaches at follow-up, 80% (35/44) described their headaches as moderate or severe, although improvement in headaches was reported by 29 (66%). Tension-type headaches were more likely than migraine to resolve. During the month before follow-up, non-prescription medications were used by six (14%). However, 20 (45%) felt that non-pharmacological methods were most effective. Medication use increased during the 10 years since the last follow-up. No patient used selective serotonin receptor agonists.
This study concluded that 20 years after the diagnosis of pediatric headache, most patients continue to have headache, although the headache classification often changed across time. Most patients report moderate or severe headache and increasingly choose to care for their headaches pharmacologically. TH
A65-lb., 25-year-old, male cerebral palsy (CP) patient with pneumonia arrives at your Children’s Hospital via ambulance. Although chronologically this patient is an adult, in many ways he’s still a child, and the parents told the paramedics that they’ve always taken their son to Children’s. You’ve been the treating physician during the patient’s frequent hospital stays. Is Children’s Hospital still the best destination for this patient? Will the family’s insurance still cover an admission at Children’s?
During the hospital stay, the patient has complications. He has to be intubated. IV antibiotics need to be continued for a course after hospital discharge. A long recovery is expected. Is it time for the family to consider discharge to a long-term care facility rather than home? Are there any long-term care facilities in the area that accept young adult CP patients?
As the treating pediatric hospitalist, what is your role in helping this patient and his family transition from pediatric care to an adult-care medical home?
Introduction
Approximately 8.6 million children in the United States age 10–17 have a disability, according to the Adolescent Health Transition Project, which is housed at the Center on Human Development and Disability (CHDD) at the University of Washington, Seattle. Of these, 16% (or 1.4 million) experience limitations in their activities and will likely have difficulty making the transition to adult healthcare.1
Given enough time in the profession, every pediatric hospitalist will face the challenge of transitioning patients from child-centered to adult-oriented healthcare systems. The good news: Medical advances have made it increasingly possible for children who once would have died in childhood to survive into adulthood.
Example: One in 2,500 children is born with cystic fibrosis (CF); however, with the recent, unprecedented increase in the success of diagnosis and treatment modalities for the pulmonary component of CF, the estimated median survival age for those born in the 1990s is now 40.2 As of the year 2004, 41.8% of the 22,301 patients with CF were 18 or older.3 In fact, each year nearly 500,000 children with special healthcare needs reach adulthood, and 90% of children with a chronic illness and/or disability now survive to adulthood.4,5
The bad news: Many physicians whose practices focus on adults aren’t familiar with disease processes, such as CF, that have historically been considered pediatric illnesses.
For patients with chronic physical and medical conditions—particularly for those who are medically fragile and/or technology-dependent—the transition can prove especially difficult. And pediatric hospitalists in children’s hospitals face different challenges than those in facilities that admit patients of all ages. One thing remains the same, though, the goal: to provide uninterrupted, coordinated, developmentally appropriate healthcare.
Why Transition?
There are several good reasons for patients to be transitioned from pediatric care to adult care. First, as patients age medical issues develop that are beyond the sphere of pediatricians. In CF, for example, diabetes and biliary tract problems occur with greater frequency in adults. However, because so few CF patients historically survived to adulthood, few physicians who care for adults learned about the disease. Thus, the pediatricians who cared for CF patients continued to do so, leading to situations in which 30- and 40-year-olds have been hospitalized with children. But is that truly appropriate?
Adult patients may have high blood pressure, gynecologic issues, osteoporosis, or other problems the pediatrician may not be prepared to deal with. Example: A primary care pediatrician has been the “medical home” for a small, cerebral palsy patient since she was 10. She’s now 25. If she presents with a breast mass, will the pediatrician pick up on the condition adequately? Will they know where to send the patient?
“Adult providers know those systems better,” says Brett Pickering, MD, director of the Special Needs Clinic at San Diego’s UCSD Medical Center, Department of Pediatrics.
The adult patient has different emotional needs than the pediatric patient, and the pediatric hospitalist may not be in tune with adult needs. “Pediatricians do a lot of handholding,” says Dr. Pickering. “Adult providers are more matter of fact.”
Age restrictions on admissions, insurance, and funding issues also affect transition. For example, funding under the Social Security Act’s Title V Children with Special Health Care Needs typically ends at 21 despite a patient’s education or employment status.
Given these factors, what is the appropriate age to transition care from a pediatric floor or facility to an adult-oriented unit? According to the American Academy of Pediatrics, the responsibility of pediatrics continues through age 21, but there’s no hard-and-fast rule.
Challenges
The transition to adult-care facilities is typically a lengthy process involving multiple specialties and possibly joint care during a transition period—and a process that should ideally be coordinated by the patient’s primary care pediatrician. But hospitalists know that circumstances are typically far from ideal.
First, during a transition, the patient may feel abandoned by the medical team they’ve known for most of their lives. It takes time to develop trust and confidence in a new doctor. In this respect, pediatric hospitalists in facilities that care for patients of all ages have an advantage over hospitalists in children’s hospitals. They can call on their adult-care colleagues in other areas of the hospital for consultations and transfer care over time.
“The pediatric hospitalist must make bridges with their adult colleagues who are comfortable [with the issues] and willing to take on this patient population,” says Dr. Pickering.
Second, parents may feel an emotional dependency on the pediatric team and can feel threatened by the adult environment as they lose some control. To the parents, the patient will always be their child, Dr. Pickering notes.
Third, pediatric hospitalists may be reluctant to let go, particularly if they feel adult services are inferior to those they have provided, which brings us to the fourth major challenge: To whom do you transition care?
Many adult healthcare providers receive only limited training in disorders associated with pediatrics (e.g., CF, spina bifida). The Cystic Fibrosis Foundation is leading the way in educating physicians in what have historically been considered pediatric problems. In the 1980s, the foundation launched an educational program to train physicians already involved in adult pulmonary care in CF. Unfortunately, education in other areas has lagged. And finding a physician with both an interest in and knowledge of such disorders can prove challenging.
“It’s incumbent on our adult colleagues to take these patients on, but they need training,” says Dr. Pickering. “Long-term issues require long-term solutions.
How do you jazz people up to take care of this population?” she asks. Physicians must have at least a little bit of desire to learn about these special patient populations, but academic institutions also need to identify core knowledge and skills and make them part of training and certification requirements for primary care residents and physicians in practice. Continuing medical education for physicians, nurses, and allied healthcare professionals should include drug dosing, medical complications seen in transition populations, and related developmental, psychosocial, and behavioral issues.
Steps to a Successful Transition
So what should hospitalists do? In an April 2005 presentation at the SHM Annual Meeting, Joseph M. Geskey, DO, assistant professor of pediatrics and medicine, and director of inpatient pediatrics at Penn State College of Medicine, Hershey, Penn., recommended that pediatric hospitalists take the following steps:
- Identify the key aspects of transition;
- Bring stakeholders together;
- Identify transitional needs;
- Identify and provide resources;
- Create an audit and evaluation process;
- Decide who will hand off care of these patients when they are admitted to the hospital (the hospitalist or the disease-specific specialist);
- Create an up-to-date medical summary that is portable and accessible. It should include important historic information, such as diagnostic data, procedures, operations, and medications;
- Upon patient discharge, include specific instructions on who to call if the patient develops a problem after leaving the hospital;
- Create a working group in your area that represents pediatric and adult hospitalists to examine transition issues in the hospitalized patient; and
- Facilitate effective communication between patients and their families, primary care physicians and specialists; and
- Know when to transfer care to a center with more expertise in caring for specific conditions.
Conclusion
Just as every patient is different and every patient’s circumstances are unique, every transition needs to be individualized. “It’s hard to set policy,” says Dr. Pickering. Open, direct communication, specific discharge instructions, an up-to-date medical summary and knowledge of the adult resources in your area can make any transition a success. TH
Keri Losavio regularly writes for “Pediatric Special Section.”
References
- Adolescent Health Transition Project, Center on Human Development and Disability (CHDD) at the University of Washington, Seattle. Available at http://depts.washington.edu/healthtr/Providers/intro.htm. Last accessed January 16, 2006.
- Bufi PL. Cystic fibrosis: therapeutic options for co-management. Available at www.thorne.com/altmedrev/fulltext/cystic.html. Last accessed January 16, 2006.
- Cystic Fibrosis Foundation: 2004 Patient Registry Report. Available at www.cff.org/living_with_cf/. Last accessed Jan. 26, 2006
- Newacheck PW, Taylor WR. Childhood chronic illness: prevalence, severity, and impact. Am J Pub Health. 1992;82(3):364-371.
- Committee on Children with Disabilities and Committee on Adolescence, American Academy of Pediatrics. Transition of care provided for adolescents with special health care needs. Pediatrics. 1996;98(6):1203–1206.
Pediatric Special Section
In the Literature
By Mary Ann Queen, MD, and Amita Amonker, MD
Utilization of a Clinical Pathway Improves Care for Bronchiolitis
Cheney J, Barber S, Altamirano L, et al. A Clinical Pathway for Bronchiolitis is Effective in Reducing Readmission Rates. J Pediatr. 2005;147(5):622-626.
Bronchiolitis is the most common respiratory illness in infants that results in hospitalization. Many hospitals have developed clinical pathways to assist clinicians in managing this common infection; however, the effectiveness of such pathways has not been fully studied. Of those clinical practice guidelines analyzed, varying results have been identified.
To determine the effectiveness of a bronchiolitis pathway, this study compared infants managed prospectively using a pathway protocol with a retrospective analysis of infants managed without a pathway. Infants from a tertiary care children’s hospital and three regional hospitals were enrolled prospectively from May 2000 to August 2001. (One must note this study was completed in Australia, hence the difference from the typical Northern Hemisphere winter months.) The historical control group was admitted between May 1998 and August 1999 at the same four institutions. Two-hundred-twenty-nine patients admitted with bronchiolitis were treated using the pathway protocol. These patients were compared with 207 randomly selected control patients who were admitted prior to the institution of the bronchiolitis pathway. All patients were less than 12 months of age with their first episode of wheezing necessitating hospitalization.
These particular guidelines were developed and used to promote consistency of nursing management during a separate study on bronchiolitis. The pathway included an initial admission assessment. It also stated parameters for initiating and stopping both oxygen therapy and intravenous fluid therapy along with discharge guidelines.
The authors found no significant difference in length of stay or time in oxygen. Fifteen infants (7.2%) in the control group required readmission within two weeks of discharge compared with two infants (0.9%) in the pathway group (p=.001). Of the control group 33.8% received intravenous fluids (IVFs) compared with 19.2% of the pathway infants (p=.001). There was also greater steroid use in the control group but no difference in antibiotic usage. Specific data regarding steroids and antibiotics is not included.
The clinical pathway appears a useful tool for discharge planning with a decreased incidence of hospital readmission when specific discharge goals are utilized. The authors also reported a decreased use of IVFs in the pathway group. This was attributed to having specific parameters (O2 required, RR>60/min or inadequate oral feeding) for when to initiate them. It is unclear from the article whether meeting a single parameter or all three parameters triggered the initiation of IVFs.
The authors also point out the limitation of using a historical control given annual variations in severity sometimes seen with bronchiolitis. They attempted to minimize this by collecting data for each group over two consecutive winters.
Preprinted Paper Orders Reduce Medication Errors
Kozer E, Scolnik D, MacPherson A, et al. Using a preprinted order sheet to reduce prescription errors in a pediatric emergency department: A randomized, controlled trial. Pediatrics. 2005(116):1299-1302.
Medical errors, including medication errors, are common and are written about with increasing frequency in the lay press. Accreditation bodies and individual hospitals are striving for ways to decrease these errors. In some instances potential solutions include purchasing new computer systems for electronic physician order entry. This study looks at whether implementing a preprinted paper order sheet can decrease the incidence of medication errors in a pediatric ED.
This randomized, prospective study occurred during 18 days in July 2001 with nine days randomly assigned into each arm. The first arm used the hospital’s regular blank order sheets for all medication orders. The second arm used the experimental preprinted order sheet. This sheet required the staff to specify the dose, weight-adjusted dose, total daily dose, route of administration, and frequency for each medication ordered. Two medical students entered the data into a database that included information about patients’ demographics, diagnosis, acuity, details on the prescribing physician, the form used, and all medications prescribed and given to the patient. This information was subsequently reviewed by two blinded pediatric emergency physicians who determined if an error occurred and, if so, the degree of the error.
During the study period there were 2,157 visits to the ED with 95.4% charts available for review. Seven-hundred-ninety-five medications were prescribed with 376 ordered on the new form. Drug errors were identified in 68 (16.6%) orders when the regular form was used and in 37 (9.8%) orders on the new form. There was one severe error and 13 significant errors using the new form and 36 significant errors on the regular form. The new form was associated with a twofold decrease in the risk for a medication error even after accounting for the level of training of the ordering practitioner. There was an even greater reduction in the risk for a severe or significant error.
The literature has shown that computerized physician order entry can reduce the number of medication errors in the inpatient setting; however, it is not available in many hospitals and its effectiveness has not been shown in EDs. The authors point out that most medications ordered in the ED are prepared and given by nurses. The benefits of a computerized system in this setting is unclear.
This study occurred over an 18-day period with the new form only used for nine days outside of an earlier pilot period. One could speculate that the novelty of the form encouraged the physicians to examine orders more carefully, leading to decreased errors. It is unknown if the decrease in errors would be sustained over time.
Also important to note is that the definition of an error was limited to a mistake in dose, interval between doses, dose unit, and/or route. Errors such as legibility, medication allergy, or drug interactions are not discussed. However, as hospitals strive to implement technologies aimed at reducing errors this simple, economical solution may be of benefit.
No Association between Kawasaki Disease and Adenovirus
Shike H, Shimizu C, Kanegaye J, et al. Adenovirus, adeno-associated virus and Kawasaki disease. Pediatr Infect Dis J. 2005;24:1011-1014.
Kawasaki disease is a self-limited acute vasculitis of children with a suspected infectious etiology and defined seasonality. In an attempt to find a clue for a possible infectious cause of Kawasaki disease this study examined the seasonality of different viruses. The study recognized a similar bimodal seasonality for some serotypes of adenovirus. Adenovirus accounts for 5%-10% of respiratory tract infections in children and can mimic the clinical manifestations and laboratory abnormalities seen in Kawasaki disease.
This study postulated that infection with a non-cultivatable adenovirus or antecedent adenovirus infection might be a trigger for Kawasaki disease. The study analyzed patient samples using polymerase chain reaction primers for all 51 adenovirus serotypes, viral culture, and neutralization assay for the most common adenovirus serotypes. This study also investigated possible involvement of adeno-associated viruses (AAVs), because AAVs depend on helper viruses, such as adenovirus.
Kawasaki disease patients were enrolled during a 25-month period from February 2002 to February 2004 at Children’s Hospital and Health Center in San Diego. Illness day one was defined as the first day of fever. Clinical samples used in this study were collected within the first 14 days of fever onset and before intravenous immunoglobulin (IVIG) therapy.
Nasopharyngeal swabs were cultured for adenovirus. Standard adenoviral neutralization assays for the five most common serotypes were performed with the use of patient sera. Sera with a titer of 1/10 or greater were scored as positive. At least two clinical samples from each patient, including throat swabs, sera or urine, were tested by quantitative polymerase chain reaction (PCR) for adenovirus and AAV.
Nasopharyngeal viral cultures were collected before IVIG administration on illness day three—14 from 70 Kawasaki disease patients. Of the 70 patients, 52 patients fulfilled four of the five classic criteria or three of the five criteria with abnormal coronary arteries by echocardiogram. Of the remaining 18 patients with atypical Kawasaki disease, six had coronary artery abnormalities. Overall, seven patients had coronary artery aneurysms and 22 patients had coronary artery dilatation. Viral cultures were negative in 66 of the 70 Kawasaki disease patients. The viral isolates in four patients were respiratory syncytial (one), parainfluenza virus 3 (one) and adenovirus (two). Therefore adenovirus culture was negative in 97% of patients.
Fifteen Kawasaki disease patients with negative adenovirus cultures were evaluated by PCR assay on at least two clinical samples. Fourteen patients had a negative PCR result. The throat swab from one patient collected on illness day seven contained 800 adenovirus genome copies.
Results of the adenovirus neutralization assays from 26 Kawasaki disease patients revealed that neutralization titers against any of the five most common adenovirus serotypes were undetectable in four of 26 patients.
None of the 36 samples from the same 15 acute Kawasaki disease patients described for the PCR assay was positive for AAV.
This study concluded that despite the striking similarities between Kawasaki disease and adenovirus infection there is no evidence to suggest a link between the two.
Epidemiology and Clinical Description of Severe, Multifocal Staphylococcus aureus Infection
Miles F, Voss L, Segedin E, et al. Review of Staphylococcus aureus infections requiring admission to a paediatric intensive care unit. Arch Dis Child. 2005;90(12):1274-1278.
Staphylococcus aureus is a recognized cause of multifocal infection with a high mortality rate. Children with community acquired S. aureus bacteremia (SAB) have higher frequencies of unknown foci compared with hospital-acquired SAB. Those children with S. aureus sepsis (SAS) presenting to the pediatric intensive care unit tend to have multisystemic disease—either by direct invasion or toxin production—before the diagnosis is made and treatment is initiated.
This study evaluates the clinical features and mortality from SAS in those children who required intensive care management. A retrospective review of clinical notes from all children with SAS admitted from October 1993 to April 2004 to the PICU in Auckland Children’s Hospital in New Zealand was undertaken. Children coded for SAS were identified from the PICU database.
All clinical notes were reviewed by one investigator using a standardized questionnaire that sought information on patient demographics, clinical findings, investigations, microbiology, and management in the PICU. Cases were included if blood or an isolate from a site that is normally sterile was positive for S. aureus. Hospital-acquired infection was defined by an isolate obtained at least 48 hours after hospital admission; community acquired infection was defined by an isolate obtained within 48 hours of admission.
Fifty-eight patients were identified with SAS over the 10-year study period; 55 were community acquired. Children with staphylococcal illness comprised 1% of all admission to the PICU. Musculoskeletal symptoms (79%) dominated presentation rather than isolated pneumonia (10%). An aggressive search for foci and surgical drainage of infective foci was required in 50% of children.
Most children (67%) either presented with multiple site involvement or secondary sites developed during their hospital stay. These pathologies included pneumonia, septic arthritis, osteomyelitis, and soft tissue involvement (cellulitis, fasciitis, abscess). A transthoracic echocardiogram detected valve abnormalities in only 5% of children, and these children were known to have pre-existing cardiac lesions. Few children (12%) presenting with methicillin-resistant S. aureus (MRSA) had community-acquired infection. The median length of stay in the PICU was three (mean 5.8, range one-44) days. Mortality due to SAS was 8.6%. Ten children had significant morbidity after discharge; these morbidities included renal failure requiring dialysis (three), an ongoing oxygen requirement at three months follow-up (two), and problems relating to limb movement and function (eight). Two children with epidural abscesses were paraplegic.
Community-acquired SAS affects healthy children, is multifocal, and has a high morbidity and mortality. It is imperative to look for sites of dissemination and to drain and debride foci. Routine echocardiography had a low yield in the absence of pre-existing cardiac lesions, persisting fever, or persisting bacteremia.
Long-Term Outcomes for Childhood Headache
Brna P, Dooley J, Gordon K Dewan T. The prognosis of childhood headache. Arch Pediatr Adolesc Med. 2005;159(12):1157-1160.
Headaches affect most children and rank third among illness-related causes of school absenteeism. Although the short-term outcome for most children appears favorable, few studies have reported long-term outcome. The objective of this study was to evaluate the long-term prognosis of childhood headaches 20 years after initial diagnosis in a cohort of Atlantic Canadian children who had headaches diagnosed in 1983.
Ninety-five patients with headaches who consulted one of the authors in 1983 were subsequently studied in 1993. The 77 patients contacted in 1993 were followed up in 2003. A standard telephone interview was used. Data were collected regarding headache symptoms, severity, frequency, treatment, and precipitants. Headache severity was simply classified as mild, moderate, or severe.
Sixty (78%) of 77 patients responded (60 of the 95 in the original cohort). At 20 years 16 (27%) were headache free, 20 (33%) had tension-type headaches, 10 (17%) had migraine, 14 (23%) had migraine and tension-type headaches. Having more than one headache type was more than at diagnosis or initial follow-up, and headache type varied across time. Of those who had headaches at follow-up, 80% (35/44) described their headaches as moderate or severe, although improvement in headaches was reported by 29 (66%). Tension-type headaches were more likely than migraine to resolve. During the month before follow-up, non-prescription medications were used by six (14%). However, 20 (45%) felt that non-pharmacological methods were most effective. Medication use increased during the 10 years since the last follow-up. No patient used selective serotonin receptor agonists.
This study concluded that 20 years after the diagnosis of pediatric headache, most patients continue to have headache, although the headache classification often changed across time. Most patients report moderate or severe headache and increasingly choose to care for their headaches pharmacologically. TH
A65-lb., 25-year-old, male cerebral palsy (CP) patient with pneumonia arrives at your Children’s Hospital via ambulance. Although chronologically this patient is an adult, in many ways he’s still a child, and the parents told the paramedics that they’ve always taken their son to Children’s. You’ve been the treating physician during the patient’s frequent hospital stays. Is Children’s Hospital still the best destination for this patient? Will the family’s insurance still cover an admission at Children’s?
During the hospital stay, the patient has complications. He has to be intubated. IV antibiotics need to be continued for a course after hospital discharge. A long recovery is expected. Is it time for the family to consider discharge to a long-term care facility rather than home? Are there any long-term care facilities in the area that accept young adult CP patients?
As the treating pediatric hospitalist, what is your role in helping this patient and his family transition from pediatric care to an adult-care medical home?
Introduction
Approximately 8.6 million children in the United States age 10–17 have a disability, according to the Adolescent Health Transition Project, which is housed at the Center on Human Development and Disability (CHDD) at the University of Washington, Seattle. Of these, 16% (or 1.4 million) experience limitations in their activities and will likely have difficulty making the transition to adult healthcare.1
Given enough time in the profession, every pediatric hospitalist will face the challenge of transitioning patients from child-centered to adult-oriented healthcare systems. The good news: Medical advances have made it increasingly possible for children who once would have died in childhood to survive into adulthood.
Example: One in 2,500 children is born with cystic fibrosis (CF); however, with the recent, unprecedented increase in the success of diagnosis and treatment modalities for the pulmonary component of CF, the estimated median survival age for those born in the 1990s is now 40.2 As of the year 2004, 41.8% of the 22,301 patients with CF were 18 or older.3 In fact, each year nearly 500,000 children with special healthcare needs reach adulthood, and 90% of children with a chronic illness and/or disability now survive to adulthood.4,5
The bad news: Many physicians whose practices focus on adults aren’t familiar with disease processes, such as CF, that have historically been considered pediatric illnesses.
For patients with chronic physical and medical conditions—particularly for those who are medically fragile and/or technology-dependent—the transition can prove especially difficult. And pediatric hospitalists in children’s hospitals face different challenges than those in facilities that admit patients of all ages. One thing remains the same, though, the goal: to provide uninterrupted, coordinated, developmentally appropriate healthcare.
Why Transition?
There are several good reasons for patients to be transitioned from pediatric care to adult care. First, as patients age medical issues develop that are beyond the sphere of pediatricians. In CF, for example, diabetes and biliary tract problems occur with greater frequency in adults. However, because so few CF patients historically survived to adulthood, few physicians who care for adults learned about the disease. Thus, the pediatricians who cared for CF patients continued to do so, leading to situations in which 30- and 40-year-olds have been hospitalized with children. But is that truly appropriate?
Adult patients may have high blood pressure, gynecologic issues, osteoporosis, or other problems the pediatrician may not be prepared to deal with. Example: A primary care pediatrician has been the “medical home” for a small, cerebral palsy patient since she was 10. She’s now 25. If she presents with a breast mass, will the pediatrician pick up on the condition adequately? Will they know where to send the patient?
“Adult providers know those systems better,” says Brett Pickering, MD, director of the Special Needs Clinic at San Diego’s UCSD Medical Center, Department of Pediatrics.
The adult patient has different emotional needs than the pediatric patient, and the pediatric hospitalist may not be in tune with adult needs. “Pediatricians do a lot of handholding,” says Dr. Pickering. “Adult providers are more matter of fact.”
Age restrictions on admissions, insurance, and funding issues also affect transition. For example, funding under the Social Security Act’s Title V Children with Special Health Care Needs typically ends at 21 despite a patient’s education or employment status.
Given these factors, what is the appropriate age to transition care from a pediatric floor or facility to an adult-oriented unit? According to the American Academy of Pediatrics, the responsibility of pediatrics continues through age 21, but there’s no hard-and-fast rule.
Challenges
The transition to adult-care facilities is typically a lengthy process involving multiple specialties and possibly joint care during a transition period—and a process that should ideally be coordinated by the patient’s primary care pediatrician. But hospitalists know that circumstances are typically far from ideal.
First, during a transition, the patient may feel abandoned by the medical team they’ve known for most of their lives. It takes time to develop trust and confidence in a new doctor. In this respect, pediatric hospitalists in facilities that care for patients of all ages have an advantage over hospitalists in children’s hospitals. They can call on their adult-care colleagues in other areas of the hospital for consultations and transfer care over time.
“The pediatric hospitalist must make bridges with their adult colleagues who are comfortable [with the issues] and willing to take on this patient population,” says Dr. Pickering.
Second, parents may feel an emotional dependency on the pediatric team and can feel threatened by the adult environment as they lose some control. To the parents, the patient will always be their child, Dr. Pickering notes.
Third, pediatric hospitalists may be reluctant to let go, particularly if they feel adult services are inferior to those they have provided, which brings us to the fourth major challenge: To whom do you transition care?
Many adult healthcare providers receive only limited training in disorders associated with pediatrics (e.g., CF, spina bifida). The Cystic Fibrosis Foundation is leading the way in educating physicians in what have historically been considered pediatric problems. In the 1980s, the foundation launched an educational program to train physicians already involved in adult pulmonary care in CF. Unfortunately, education in other areas has lagged. And finding a physician with both an interest in and knowledge of such disorders can prove challenging.
“It’s incumbent on our adult colleagues to take these patients on, but they need training,” says Dr. Pickering. “Long-term issues require long-term solutions.
How do you jazz people up to take care of this population?” she asks. Physicians must have at least a little bit of desire to learn about these special patient populations, but academic institutions also need to identify core knowledge and skills and make them part of training and certification requirements for primary care residents and physicians in practice. Continuing medical education for physicians, nurses, and allied healthcare professionals should include drug dosing, medical complications seen in transition populations, and related developmental, psychosocial, and behavioral issues.
Steps to a Successful Transition
So what should hospitalists do? In an April 2005 presentation at the SHM Annual Meeting, Joseph M. Geskey, DO, assistant professor of pediatrics and medicine, and director of inpatient pediatrics at Penn State College of Medicine, Hershey, Penn., recommended that pediatric hospitalists take the following steps:
- Identify the key aspects of transition;
- Bring stakeholders together;
- Identify transitional needs;
- Identify and provide resources;
- Create an audit and evaluation process;
- Decide who will hand off care of these patients when they are admitted to the hospital (the hospitalist or the disease-specific specialist);
- Create an up-to-date medical summary that is portable and accessible. It should include important historic information, such as diagnostic data, procedures, operations, and medications;
- Upon patient discharge, include specific instructions on who to call if the patient develops a problem after leaving the hospital;
- Create a working group in your area that represents pediatric and adult hospitalists to examine transition issues in the hospitalized patient; and
- Facilitate effective communication between patients and their families, primary care physicians and specialists; and
- Know when to transfer care to a center with more expertise in caring for specific conditions.
Conclusion
Just as every patient is different and every patient’s circumstances are unique, every transition needs to be individualized. “It’s hard to set policy,” says Dr. Pickering. Open, direct communication, specific discharge instructions, an up-to-date medical summary and knowledge of the adult resources in your area can make any transition a success. TH
Keri Losavio regularly writes for “Pediatric Special Section.”
References
- Adolescent Health Transition Project, Center on Human Development and Disability (CHDD) at the University of Washington, Seattle. Available at http://depts.washington.edu/healthtr/Providers/intro.htm. Last accessed January 16, 2006.
- Bufi PL. Cystic fibrosis: therapeutic options for co-management. Available at www.thorne.com/altmedrev/fulltext/cystic.html. Last accessed January 16, 2006.
- Cystic Fibrosis Foundation: 2004 Patient Registry Report. Available at www.cff.org/living_with_cf/. Last accessed Jan. 26, 2006
- Newacheck PW, Taylor WR. Childhood chronic illness: prevalence, severity, and impact. Am J Pub Health. 1992;82(3):364-371.
- Committee on Children with Disabilities and Committee on Adolescence, American Academy of Pediatrics. Transition of care provided for adolescents with special health care needs. Pediatrics. 1996;98(6):1203–1206.
Pediatric Special Section
In the Literature
By Mary Ann Queen, MD, and Amita Amonker, MD
Utilization of a Clinical Pathway Improves Care for Bronchiolitis
Cheney J, Barber S, Altamirano L, et al. A Clinical Pathway for Bronchiolitis is Effective in Reducing Readmission Rates. J Pediatr. 2005;147(5):622-626.
Bronchiolitis is the most common respiratory illness in infants that results in hospitalization. Many hospitals have developed clinical pathways to assist clinicians in managing this common infection; however, the effectiveness of such pathways has not been fully studied. Of those clinical practice guidelines analyzed, varying results have been identified.
To determine the effectiveness of a bronchiolitis pathway, this study compared infants managed prospectively using a pathway protocol with a retrospective analysis of infants managed without a pathway. Infants from a tertiary care children’s hospital and three regional hospitals were enrolled prospectively from May 2000 to August 2001. (One must note this study was completed in Australia, hence the difference from the typical Northern Hemisphere winter months.) The historical control group was admitted between May 1998 and August 1999 at the same four institutions. Two-hundred-twenty-nine patients admitted with bronchiolitis were treated using the pathway protocol. These patients were compared with 207 randomly selected control patients who were admitted prior to the institution of the bronchiolitis pathway. All patients were less than 12 months of age with their first episode of wheezing necessitating hospitalization.
These particular guidelines were developed and used to promote consistency of nursing management during a separate study on bronchiolitis. The pathway included an initial admission assessment. It also stated parameters for initiating and stopping both oxygen therapy and intravenous fluid therapy along with discharge guidelines.
The authors found no significant difference in length of stay or time in oxygen. Fifteen infants (7.2%) in the control group required readmission within two weeks of discharge compared with two infants (0.9%) in the pathway group (p=.001). Of the control group 33.8% received intravenous fluids (IVFs) compared with 19.2% of the pathway infants (p=.001). There was also greater steroid use in the control group but no difference in antibiotic usage. Specific data regarding steroids and antibiotics is not included.
The clinical pathway appears a useful tool for discharge planning with a decreased incidence of hospital readmission when specific discharge goals are utilized. The authors also reported a decreased use of IVFs in the pathway group. This was attributed to having specific parameters (O2 required, RR>60/min or inadequate oral feeding) for when to initiate them. It is unclear from the article whether meeting a single parameter or all three parameters triggered the initiation of IVFs.
The authors also point out the limitation of using a historical control given annual variations in severity sometimes seen with bronchiolitis. They attempted to minimize this by collecting data for each group over two consecutive winters.
Preprinted Paper Orders Reduce Medication Errors
Kozer E, Scolnik D, MacPherson A, et al. Using a preprinted order sheet to reduce prescription errors in a pediatric emergency department: A randomized, controlled trial. Pediatrics. 2005(116):1299-1302.
Medical errors, including medication errors, are common and are written about with increasing frequency in the lay press. Accreditation bodies and individual hospitals are striving for ways to decrease these errors. In some instances potential solutions include purchasing new computer systems for electronic physician order entry. This study looks at whether implementing a preprinted paper order sheet can decrease the incidence of medication errors in a pediatric ED.
This randomized, prospective study occurred during 18 days in July 2001 with nine days randomly assigned into each arm. The first arm used the hospital’s regular blank order sheets for all medication orders. The second arm used the experimental preprinted order sheet. This sheet required the staff to specify the dose, weight-adjusted dose, total daily dose, route of administration, and frequency for each medication ordered. Two medical students entered the data into a database that included information about patients’ demographics, diagnosis, acuity, details on the prescribing physician, the form used, and all medications prescribed and given to the patient. This information was subsequently reviewed by two blinded pediatric emergency physicians who determined if an error occurred and, if so, the degree of the error.
During the study period there were 2,157 visits to the ED with 95.4% charts available for review. Seven-hundred-ninety-five medications were prescribed with 376 ordered on the new form. Drug errors were identified in 68 (16.6%) orders when the regular form was used and in 37 (9.8%) orders on the new form. There was one severe error and 13 significant errors using the new form and 36 significant errors on the regular form. The new form was associated with a twofold decrease in the risk for a medication error even after accounting for the level of training of the ordering practitioner. There was an even greater reduction in the risk for a severe or significant error.
The literature has shown that computerized physician order entry can reduce the number of medication errors in the inpatient setting; however, it is not available in many hospitals and its effectiveness has not been shown in EDs. The authors point out that most medications ordered in the ED are prepared and given by nurses. The benefits of a computerized system in this setting is unclear.
This study occurred over an 18-day period with the new form only used for nine days outside of an earlier pilot period. One could speculate that the novelty of the form encouraged the physicians to examine orders more carefully, leading to decreased errors. It is unknown if the decrease in errors would be sustained over time.
Also important to note is that the definition of an error was limited to a mistake in dose, interval between doses, dose unit, and/or route. Errors such as legibility, medication allergy, or drug interactions are not discussed. However, as hospitals strive to implement technologies aimed at reducing errors this simple, economical solution may be of benefit.
No Association between Kawasaki Disease and Adenovirus
Shike H, Shimizu C, Kanegaye J, et al. Adenovirus, adeno-associated virus and Kawasaki disease. Pediatr Infect Dis J. 2005;24:1011-1014.
Kawasaki disease is a self-limited acute vasculitis of children with a suspected infectious etiology and defined seasonality. In an attempt to find a clue for a possible infectious cause of Kawasaki disease this study examined the seasonality of different viruses. The study recognized a similar bimodal seasonality for some serotypes of adenovirus. Adenovirus accounts for 5%-10% of respiratory tract infections in children and can mimic the clinical manifestations and laboratory abnormalities seen in Kawasaki disease.
This study postulated that infection with a non-cultivatable adenovirus or antecedent adenovirus infection might be a trigger for Kawasaki disease. The study analyzed patient samples using polymerase chain reaction primers for all 51 adenovirus serotypes, viral culture, and neutralization assay for the most common adenovirus serotypes. This study also investigated possible involvement of adeno-associated viruses (AAVs), because AAVs depend on helper viruses, such as adenovirus.
Kawasaki disease patients were enrolled during a 25-month period from February 2002 to February 2004 at Children’s Hospital and Health Center in San Diego. Illness day one was defined as the first day of fever. Clinical samples used in this study were collected within the first 14 days of fever onset and before intravenous immunoglobulin (IVIG) therapy.
Nasopharyngeal swabs were cultured for adenovirus. Standard adenoviral neutralization assays for the five most common serotypes were performed with the use of patient sera. Sera with a titer of 1/10 or greater were scored as positive. At least two clinical samples from each patient, including throat swabs, sera or urine, were tested by quantitative polymerase chain reaction (PCR) for adenovirus and AAV.
Nasopharyngeal viral cultures were collected before IVIG administration on illness day three—14 from 70 Kawasaki disease patients. Of the 70 patients, 52 patients fulfilled four of the five classic criteria or three of the five criteria with abnormal coronary arteries by echocardiogram. Of the remaining 18 patients with atypical Kawasaki disease, six had coronary artery abnormalities. Overall, seven patients had coronary artery aneurysms and 22 patients had coronary artery dilatation. Viral cultures were negative in 66 of the 70 Kawasaki disease patients. The viral isolates in four patients were respiratory syncytial (one), parainfluenza virus 3 (one) and adenovirus (two). Therefore adenovirus culture was negative in 97% of patients.
Fifteen Kawasaki disease patients with negative adenovirus cultures were evaluated by PCR assay on at least two clinical samples. Fourteen patients had a negative PCR result. The throat swab from one patient collected on illness day seven contained 800 adenovirus genome copies.
Results of the adenovirus neutralization assays from 26 Kawasaki disease patients revealed that neutralization titers against any of the five most common adenovirus serotypes were undetectable in four of 26 patients.
None of the 36 samples from the same 15 acute Kawasaki disease patients described for the PCR assay was positive for AAV.
This study concluded that despite the striking similarities between Kawasaki disease and adenovirus infection there is no evidence to suggest a link between the two.
Epidemiology and Clinical Description of Severe, Multifocal Staphylococcus aureus Infection
Miles F, Voss L, Segedin E, et al. Review of Staphylococcus aureus infections requiring admission to a paediatric intensive care unit. Arch Dis Child. 2005;90(12):1274-1278.
Staphylococcus aureus is a recognized cause of multifocal infection with a high mortality rate. Children with community acquired S. aureus bacteremia (SAB) have higher frequencies of unknown foci compared with hospital-acquired SAB. Those children with S. aureus sepsis (SAS) presenting to the pediatric intensive care unit tend to have multisystemic disease—either by direct invasion or toxin production—before the diagnosis is made and treatment is initiated.
This study evaluates the clinical features and mortality from SAS in those children who required intensive care management. A retrospective review of clinical notes from all children with SAS admitted from October 1993 to April 2004 to the PICU in Auckland Children’s Hospital in New Zealand was undertaken. Children coded for SAS were identified from the PICU database.
All clinical notes were reviewed by one investigator using a standardized questionnaire that sought information on patient demographics, clinical findings, investigations, microbiology, and management in the PICU. Cases were included if blood or an isolate from a site that is normally sterile was positive for S. aureus. Hospital-acquired infection was defined by an isolate obtained at least 48 hours after hospital admission; community acquired infection was defined by an isolate obtained within 48 hours of admission.
Fifty-eight patients were identified with SAS over the 10-year study period; 55 were community acquired. Children with staphylococcal illness comprised 1% of all admission to the PICU. Musculoskeletal symptoms (79%) dominated presentation rather than isolated pneumonia (10%). An aggressive search for foci and surgical drainage of infective foci was required in 50% of children.
Most children (67%) either presented with multiple site involvement or secondary sites developed during their hospital stay. These pathologies included pneumonia, septic arthritis, osteomyelitis, and soft tissue involvement (cellulitis, fasciitis, abscess). A transthoracic echocardiogram detected valve abnormalities in only 5% of children, and these children were known to have pre-existing cardiac lesions. Few children (12%) presenting with methicillin-resistant S. aureus (MRSA) had community-acquired infection. The median length of stay in the PICU was three (mean 5.8, range one-44) days. Mortality due to SAS was 8.6%. Ten children had significant morbidity after discharge; these morbidities included renal failure requiring dialysis (three), an ongoing oxygen requirement at three months follow-up (two), and problems relating to limb movement and function (eight). Two children with epidural abscesses were paraplegic.
Community-acquired SAS affects healthy children, is multifocal, and has a high morbidity and mortality. It is imperative to look for sites of dissemination and to drain and debride foci. Routine echocardiography had a low yield in the absence of pre-existing cardiac lesions, persisting fever, or persisting bacteremia.
Long-Term Outcomes for Childhood Headache
Brna P, Dooley J, Gordon K Dewan T. The prognosis of childhood headache. Arch Pediatr Adolesc Med. 2005;159(12):1157-1160.
Headaches affect most children and rank third among illness-related causes of school absenteeism. Although the short-term outcome for most children appears favorable, few studies have reported long-term outcome. The objective of this study was to evaluate the long-term prognosis of childhood headaches 20 years after initial diagnosis in a cohort of Atlantic Canadian children who had headaches diagnosed in 1983.
Ninety-five patients with headaches who consulted one of the authors in 1983 were subsequently studied in 1993. The 77 patients contacted in 1993 were followed up in 2003. A standard telephone interview was used. Data were collected regarding headache symptoms, severity, frequency, treatment, and precipitants. Headache severity was simply classified as mild, moderate, or severe.
Sixty (78%) of 77 patients responded (60 of the 95 in the original cohort). At 20 years 16 (27%) were headache free, 20 (33%) had tension-type headaches, 10 (17%) had migraine, 14 (23%) had migraine and tension-type headaches. Having more than one headache type was more than at diagnosis or initial follow-up, and headache type varied across time. Of those who had headaches at follow-up, 80% (35/44) described their headaches as moderate or severe, although improvement in headaches was reported by 29 (66%). Tension-type headaches were more likely than migraine to resolve. During the month before follow-up, non-prescription medications were used by six (14%). However, 20 (45%) felt that non-pharmacological methods were most effective. Medication use increased during the 10 years since the last follow-up. No patient used selective serotonin receptor agonists.
This study concluded that 20 years after the diagnosis of pediatric headache, most patients continue to have headache, although the headache classification often changed across time. Most patients report moderate or severe headache and increasingly choose to care for their headaches pharmacologically. TH
Hospitalist Burnout
Long hours, extreme dedication to their work, and an overload of responsibility can make physicians more prone to burnout than other professionals. And hospitalists are no exception because they may experience more causes of burnout than other types of physicians.
Here are some basic facts about burnout among physicians, how to determine if you are burning out, and what to do about it.
Facts about Physician Burnout
In her presentation “Burnout and Hospitalists” at the 2005 SHM Annual Meeting in Chicago, Tosha Wetterneck, MD, hospitalist and assistant professor of medicine at University of Wisconsin (Madison), defined physician burnout as “erosion of engagement with the job.” The components of this erosion can include emotional exhaustion, depersonalization (distancing yourself from your job), and reduced personal accomplishment.
“Burnout,” said Dr. Wetterneck in her presentation, “is caused by work overload and time pressure, as well as role ambiguity, lack of job resources or support, severity of patient problems, and lack of reciprocity from patients.” Other factors include a perceived loss of control and rapid changes on the job.
Hospitalists in particular may be prone to burnout because they work under high expectations—their own as well as others’—to provide better outcomes. A 1999 study by the National Association of Inpatient Physicians (SHM’s former name) revealed a 13% burnout rate among hospitalists, with an additional 25% at risk for burnout. That may sound high, but emergency and critical care physicians experience burnout rates of up to 60%.
What to Do about Burnout
Lidia Schapira, MD, an oncologist at Massachusetts General Hospital, Boston, has written and spoken on the subject of physician burnout.
“It’s a real phenomenon,” she explains, “and in part it reflects an exaggerated commitment to work. But a professional who loves what they do—if they have support—can [experience] enthusiasm rather than burnout.”
Without support from their organization or colleagues, a physician can become overwhelmed by the long hours and responsibilities of work, among other stressors. Here are Dr. Schapira’s steps for dealing with burnout:
1. Recognize it: “The symptoms [of burnout] are very similar to depression,” she points out. “One way to distinguish between burnout and depression is to take a little holiday from work. If your symptoms are connected to work, you’ll feel better. If you feel equally bad on vacation, you probably suffer from depression.”
2. Address your stressors: If you realize you are burned out, your next step should be to make a list of on-the-job stressors and prioritize them. Then tackle them one at a time. “You have to identify the things that are most stressful to you and make changes,” says Dr. Schapira. “For example, if your schedule is overloaded, find a way to build in breaks for food or fresh air.”
If there are specific parts of the job that are “horrible” for you, she says, try to delegate them to someone else on your team. By delegating or swapping tasks with others, you may be able to eliminate your burnout—and possibly theirs as well. Another important factor is having an ally. “Find someone on your team who you can talk to,” advises Dr. Schapira. “Chat with your colleagues about your problems.”
3. Work for organizational change: Hospitalists can talk to their administrators and colleagues about easy changes that can eliminate stressors, such as a change to the schedule, improved communications or additional secretarial help to ease the burden.
“Point out that a change may lead to more productivity,” suggests Dr. Schapira. “There’s a far better likelihood of having your changes accepted.” To help ensure that your employer is willing to make some changes, point out that burnout in general is associated with turnover and absenteeism, lower productivity, and stress-related health outcomes including alcohol and drug abuse.
Find a Good Fit
One key to avoiding burnout is to make sure you find an employer you can be happy with.
“There are as many different styles of management as there are hospitalist groups,” says Michael-Anthony Williams, MD, president of Inpatient Services, PC, in Denver. “It’s important that the doctors in a group share values and have the same goal. There’s no right answer.”
Dr. Schapira agrees. “There needs to be a good fit between the physician and the workplace,” she says. “If you’re the only person constantly upset by the system, maybe you’re not working in the right place.”
Dr. Williams, a co-presenter with Dr. Wetterneck in Chicago, outlined how his hospital medicine group has combated burnout by hiring physicians who seem likely to be a good fit. Dr. Williams realized that the hospitalists at Inpatient Services value time off over monetary gain.
“Our group is not motivated by finances,” he explains. “The salaries aren’t as high here, and Denver attracts physicians who aren’t seeking a lot of money.” Therefore Inpatient Services provides more time off. “Everyone gets one vacation request each month,” [per person] says Dr. Williams. “Day-to-day, the job is very unpredictable. So we try to give people control over their schedule.”
Burnout is a serious emotional condition that can lead some hospitalists and other physicians to seek a change in career—or lead them to substance abuse or other problems. The good news is that identifying it in the first place and then advocating to change workplace conditions can overcome it. TH
Long hours, extreme dedication to their work, and an overload of responsibility can make physicians more prone to burnout than other professionals. And hospitalists are no exception because they may experience more causes of burnout than other types of physicians.
Here are some basic facts about burnout among physicians, how to determine if you are burning out, and what to do about it.
Facts about Physician Burnout
In her presentation “Burnout and Hospitalists” at the 2005 SHM Annual Meeting in Chicago, Tosha Wetterneck, MD, hospitalist and assistant professor of medicine at University of Wisconsin (Madison), defined physician burnout as “erosion of engagement with the job.” The components of this erosion can include emotional exhaustion, depersonalization (distancing yourself from your job), and reduced personal accomplishment.
“Burnout,” said Dr. Wetterneck in her presentation, “is caused by work overload and time pressure, as well as role ambiguity, lack of job resources or support, severity of patient problems, and lack of reciprocity from patients.” Other factors include a perceived loss of control and rapid changes on the job.
Hospitalists in particular may be prone to burnout because they work under high expectations—their own as well as others’—to provide better outcomes. A 1999 study by the National Association of Inpatient Physicians (SHM’s former name) revealed a 13% burnout rate among hospitalists, with an additional 25% at risk for burnout. That may sound high, but emergency and critical care physicians experience burnout rates of up to 60%.
What to Do about Burnout
Lidia Schapira, MD, an oncologist at Massachusetts General Hospital, Boston, has written and spoken on the subject of physician burnout.
“It’s a real phenomenon,” she explains, “and in part it reflects an exaggerated commitment to work. But a professional who loves what they do—if they have support—can [experience] enthusiasm rather than burnout.”
Without support from their organization or colleagues, a physician can become overwhelmed by the long hours and responsibilities of work, among other stressors. Here are Dr. Schapira’s steps for dealing with burnout:
1. Recognize it: “The symptoms [of burnout] are very similar to depression,” she points out. “One way to distinguish between burnout and depression is to take a little holiday from work. If your symptoms are connected to work, you’ll feel better. If you feel equally bad on vacation, you probably suffer from depression.”
2. Address your stressors: If you realize you are burned out, your next step should be to make a list of on-the-job stressors and prioritize them. Then tackle them one at a time. “You have to identify the things that are most stressful to you and make changes,” says Dr. Schapira. “For example, if your schedule is overloaded, find a way to build in breaks for food or fresh air.”
If there are specific parts of the job that are “horrible” for you, she says, try to delegate them to someone else on your team. By delegating or swapping tasks with others, you may be able to eliminate your burnout—and possibly theirs as well. Another important factor is having an ally. “Find someone on your team who you can talk to,” advises Dr. Schapira. “Chat with your colleagues about your problems.”
3. Work for organizational change: Hospitalists can talk to their administrators and colleagues about easy changes that can eliminate stressors, such as a change to the schedule, improved communications or additional secretarial help to ease the burden.
“Point out that a change may lead to more productivity,” suggests Dr. Schapira. “There’s a far better likelihood of having your changes accepted.” To help ensure that your employer is willing to make some changes, point out that burnout in general is associated with turnover and absenteeism, lower productivity, and stress-related health outcomes including alcohol and drug abuse.
Find a Good Fit
One key to avoiding burnout is to make sure you find an employer you can be happy with.
“There are as many different styles of management as there are hospitalist groups,” says Michael-Anthony Williams, MD, president of Inpatient Services, PC, in Denver. “It’s important that the doctors in a group share values and have the same goal. There’s no right answer.”
Dr. Schapira agrees. “There needs to be a good fit between the physician and the workplace,” she says. “If you’re the only person constantly upset by the system, maybe you’re not working in the right place.”
Dr. Williams, a co-presenter with Dr. Wetterneck in Chicago, outlined how his hospital medicine group has combated burnout by hiring physicians who seem likely to be a good fit. Dr. Williams realized that the hospitalists at Inpatient Services value time off over monetary gain.
“Our group is not motivated by finances,” he explains. “The salaries aren’t as high here, and Denver attracts physicians who aren’t seeking a lot of money.” Therefore Inpatient Services provides more time off. “Everyone gets one vacation request each month,” [per person] says Dr. Williams. “Day-to-day, the job is very unpredictable. So we try to give people control over their schedule.”
Burnout is a serious emotional condition that can lead some hospitalists and other physicians to seek a change in career—or lead them to substance abuse or other problems. The good news is that identifying it in the first place and then advocating to change workplace conditions can overcome it. TH
Long hours, extreme dedication to their work, and an overload of responsibility can make physicians more prone to burnout than other professionals. And hospitalists are no exception because they may experience more causes of burnout than other types of physicians.
Here are some basic facts about burnout among physicians, how to determine if you are burning out, and what to do about it.
Facts about Physician Burnout
In her presentation “Burnout and Hospitalists” at the 2005 SHM Annual Meeting in Chicago, Tosha Wetterneck, MD, hospitalist and assistant professor of medicine at University of Wisconsin (Madison), defined physician burnout as “erosion of engagement with the job.” The components of this erosion can include emotional exhaustion, depersonalization (distancing yourself from your job), and reduced personal accomplishment.
“Burnout,” said Dr. Wetterneck in her presentation, “is caused by work overload and time pressure, as well as role ambiguity, lack of job resources or support, severity of patient problems, and lack of reciprocity from patients.” Other factors include a perceived loss of control and rapid changes on the job.
Hospitalists in particular may be prone to burnout because they work under high expectations—their own as well as others’—to provide better outcomes. A 1999 study by the National Association of Inpatient Physicians (SHM’s former name) revealed a 13% burnout rate among hospitalists, with an additional 25% at risk for burnout. That may sound high, but emergency and critical care physicians experience burnout rates of up to 60%.
What to Do about Burnout
Lidia Schapira, MD, an oncologist at Massachusetts General Hospital, Boston, has written and spoken on the subject of physician burnout.
“It’s a real phenomenon,” she explains, “and in part it reflects an exaggerated commitment to work. But a professional who loves what they do—if they have support—can [experience] enthusiasm rather than burnout.”
Without support from their organization or colleagues, a physician can become overwhelmed by the long hours and responsibilities of work, among other stressors. Here are Dr. Schapira’s steps for dealing with burnout:
1. Recognize it: “The symptoms [of burnout] are very similar to depression,” she points out. “One way to distinguish between burnout and depression is to take a little holiday from work. If your symptoms are connected to work, you’ll feel better. If you feel equally bad on vacation, you probably suffer from depression.”
2. Address your stressors: If you realize you are burned out, your next step should be to make a list of on-the-job stressors and prioritize them. Then tackle them one at a time. “You have to identify the things that are most stressful to you and make changes,” says Dr. Schapira. “For example, if your schedule is overloaded, find a way to build in breaks for food or fresh air.”
If there are specific parts of the job that are “horrible” for you, she says, try to delegate them to someone else on your team. By delegating or swapping tasks with others, you may be able to eliminate your burnout—and possibly theirs as well. Another important factor is having an ally. “Find someone on your team who you can talk to,” advises Dr. Schapira. “Chat with your colleagues about your problems.”
3. Work for organizational change: Hospitalists can talk to their administrators and colleagues about easy changes that can eliminate stressors, such as a change to the schedule, improved communications or additional secretarial help to ease the burden.
“Point out that a change may lead to more productivity,” suggests Dr. Schapira. “There’s a far better likelihood of having your changes accepted.” To help ensure that your employer is willing to make some changes, point out that burnout in general is associated with turnover and absenteeism, lower productivity, and stress-related health outcomes including alcohol and drug abuse.
Find a Good Fit
One key to avoiding burnout is to make sure you find an employer you can be happy with.
“There are as many different styles of management as there are hospitalist groups,” says Michael-Anthony Williams, MD, president of Inpatient Services, PC, in Denver. “It’s important that the doctors in a group share values and have the same goal. There’s no right answer.”
Dr. Schapira agrees. “There needs to be a good fit between the physician and the workplace,” she says. “If you’re the only person constantly upset by the system, maybe you’re not working in the right place.”
Dr. Williams, a co-presenter with Dr. Wetterneck in Chicago, outlined how his hospital medicine group has combated burnout by hiring physicians who seem likely to be a good fit. Dr. Williams realized that the hospitalists at Inpatient Services value time off over monetary gain.
“Our group is not motivated by finances,” he explains. “The salaries aren’t as high here, and Denver attracts physicians who aren’t seeking a lot of money.” Therefore Inpatient Services provides more time off. “Everyone gets one vacation request each month,” [per person] says Dr. Williams. “Day-to-day, the job is very unpredictable. So we try to give people control over their schedule.”
Burnout is a serious emotional condition that can lead some hospitalists and other physicians to seek a change in career—or lead them to substance abuse or other problems. The good news is that identifying it in the first place and then advocating to change workplace conditions can overcome it. TH
Survey Responses Exceed Goal
The Benchmarks Committee has completed the data accumulation portion of the SHM 2005-2006 Productivity and Compensation Survey. As you might recall, we set a goal of 400 group respondents. With a final push for responses in early December, we exceeded our target. The responses were invaluable in making this survey a worthwhile effort and a credible reflection of the national hospitalist movement.
The Benchmarks Committee would like to specially thank those who attempted to complete the survey online and gave us feedback on this process. We had a few glitches with the online survey, and thanks to these folks and their communication we learned a few valuable lessons regarding this electronic process. We were able to intervene immediately and re-direct folks to the written survey. We’ll apply these lessons to the electronic component of future surveys as well.
Over the next few months we will be analyzing the data in preparation for presentation of the results to be offered up initially at the SHM Annual Meeting in Washington, D.C., the first week in May. (Visit www.hospitalmedicine.org under “Upcoming Events” to register.) Additionally, results will be available to survey participants online later in the year following the national presentation.
On a different note, the committee continues to work on the Hospitalist Dashboard Project. We are creating a dashboard that deals with metrics in the categories of resource utilization, clinical quality, productivity, and satisfaction.
Subsequently, we have worked through a Delphi process to whittle a long list of possible metrics down to 10 key metrics. These have been divided among the committee members, who will use an agreed-upon outline to write a brief description of the metric, how it is measured, and how it can be utilized to manage a hospitalist practice. The final product will be a white paper made available to the SHM membership.
How to Develop a Hospital-Based Palliative Care Program
Why your hospital needs such a program and how to create it
By Eva H. Chittenden, MD, and the SHM Palliative Care Task Force
Palliative care consists of medical care focused on the relief of suffering for patients living with chronic, advanced illness and it also helps their families. It is offered at any stage of disease, concurrently with all other appropriate medical treatment.
Palliative care providers treat the many physical symptoms that patients experience, including pain, dyspnea, nausea, and delirium. In addition, providers assist patients and families with complex medical decision-making, and attend to patients’ and families’ spiritual and psychosocial needs. Physicians work closely with an interdisciplinary team of nurses, chaplains, social workers, and pharmacists. Care continues beyond the point of death, with phone calls and consolation letters, as well as bereavement services.
Arguments for inpatient Palliative Care
The clinical imperative: We need better quality of care for people with serious and complex illness. The multicenter SUPPORT study, published in JAMA in 1995, looked at more than 9,000 hospitalized patients with life-threatening illness and demonstrated significant problems with pain and symptom control and with patient-doctor communication.1 Of the patients who died, more than 50% had moderate to severe pain more than half the time during the last three days of their lives. Of patients preferring do-not-resuscitate status, less than 50% of their physicians were aware of their wishes.
In another study, Nelson, et al. documented that more than half of cancer patients receiving intensive care had moderate to severe pain, anxiety, thirst, and hunger, and that 75% had moderate to severe discomfort of some kind.2 These studies have been a wake-up call to clinicians and hospitals across the country.
Patient and Family Preferences
Family members—especially women—shoulder most of the care of patients with serious illness. A minority of caregivers are over age 65 themselves and in ill health. When asked what they want from the medical system, family caregivers ask for help with transportation and personal care of their loved one at home, and for better home nursing support. They want 24/7 access to providers, better communication with their doctors, and to be remembered and contacted after the death of their family member.3-5 Caregiving itself has been shown to increase likelihood of premature mortality and lead to financial crisis.6
In the SUPPORT study, one-third of families lost most of their savings due to illness.7 Patients want pain and symptom control, avoidance of inappropriate prolongation of the dying process, and relief of burdens on family.8 Palliative care programs, both inpatient and ambulatory, can help provide families with needed services and improve communication at all levels.
The Demographic Argument
Hospitals need palliative care to effectively treat the growing numbers of people with serious, advanced, and complex illness. By 2030, the number of people over age 85 will double to almost 10 million.9 Many of these patients will have multiple chronic conditions, making their care complicated and expensive. And for many chronic conditions, including heart and lung disease, diabetes, and hypertension, death is not predictable.
Therefore, people need better care throughout the multiyear course of advanced illness. And while the Medicare Hospice Benefit is helpful for care of the dying (defined as people with six months or less to live) we need additional approaches for the much larger number of patients with chronic, progressive illness, years to live, continued benefit from disease-modifying therapy, and obvious palliative care needs.
The Educational Imperative
Hospitals are the site of training for most clinicians. Researchers have documented significant deficits in palliative care knowledge, skills, and attitudes among medical students, residents, and practicing physicians. Medical school and residency curricula, although improving, offer relatively little teaching in palliative care principles and practice.10,11
In 2000 the Liaison Committee on Medical Education mandated that medical school curricula include “important aspects of … end-of-life-care.” That same year the Accreditation Council for Graduate Medical Education encouraged internal medicine training programs to provide instruction in the principles of palliative care. Inpatient palliative care programs could provide much of this teaching through medical student and resident rotations, informal teaching during the consultation process, and through workshops and grand rounds.
The Financial Argument
Medical costs are rising exponentially due to multiple factors, including effective yet expensive new technologies and an expanding elderly population with more chronic conditions. Under the current Diagnosis Related Group (DRG) system, long, high-intensity hospital stays are causing a fiscal crisis for hospitals. The hospital and insurer of the future will have to work together to learn how to treat serious and complex illness efficiently and in the most cost-effective manner possible. Palliative care programs have the potential to ease this looming crisis through decreasing length of stay, both in the ICU and on the floors, and decreasing direct costs, including radiology, pharmacy, and laboratory costs. Researchers are beginning to document the positive fiscal impacts in rigorous studies.
Palliative Care: The Bottom Line
Palliative care teams have demonstrated improvement in pain and other symptom scores, in patient and family satisfaction with care, and in patient-provider communication. In addition, they have improved compliance with Joint Commission on Accreditation of Healthcare Organizations (JCAHO) quality measures. They have had these positive effects while simultaneously showing decreases in length of stay and costs. As a result, many programs have gained significant financial and administrative support from their hospitals.
Hospitalists and Palliative Care
Many hospitalist groups have found that building and staffing a palliative care consultation team is an important addition to their portfolio of services, further solidifying their value in the eyes of their hospital administration. The professional fee revenues are one more funding source, and palliative care is a critical service the group can provide the institution to improve the quality of care, improve patient satisfaction, and decrease costs.
The work involved in starting a program, including needs assessment, internal marketing, building a financial case, and developing a staffing model, is similar to that done when starting a hospitalist program. Hospitalists are ideally positioned to start palliative care services because they have already built relationships with key administrators and opinion leaders, and they understand the institution’s method for evaluating financial data, and how to access outcome and satisfaction data.
What Hospitalists Gain
By leading and staffing palliative care programs, hospitalists gain visibility and respect from colleagues, and improve their patients’ quality of care and their hospital’s financial bottom line. Clinically palliative care adds variety and depth to the work life of hospitalists and allows them to work with a rich interdisciplinary team. Although hospitalists should obtain additional training, they already possess the building blocks to provide excellent palliative care, such as skillfully leading family conferences and treating complex symptoms. When wearing the palliative care “hat,” providers have the luxury of spending more time at a patient’s bedside discussing what is truly important to the patient and his or her loved ones. The work is meaningful and rewarding.
Obtaining the Tools to Start a Program
The Center to Advance Palliative Care (CAPC), funded by the Robert Wood Johnson Foundation, is dedicated to advancing inpatient palliative care programs through their Web site (www.capc.org) and through their manual, “A Guide to Building a Hospital-Based Palliative Care Program,” available for purchase on its Web site.
In addition, CAPC sponsors the six national Palliative Care Leadership Centers (PCLCs) that each hold two-day, hands-on workshops on the nuts and bolts of starting inpatient palliative care programs, followed by a year of personalized mentoring by phone. The University of California, San Francisco’s PCLC, which is tailored specifically to hospitalists, will hold its last workshop in April 2006. For more information, visit www.capc.org/palliative-care-leadership-initiative.
At the upcoming SHM Annual Meeting in May, the Palliative Care Taskforce will present a workshop, “The Basic Why and How to Develop a Hospital-Based Palliative Care Program.”
Obtaining the Clinical Expertise
There are numerous opportunities for hospitalists to gain clinical expertise in palliative care, including Web-based and written materials and CME courses. Highlights include the Education in Palliative and End of Life Care programs; courses and study guides through the American Association of Hospice and Palliative Medicine, as well as Fast Facts (one-page synopses of relevant palliative care concepts that can be made into handouts or downloaded to one’s PDA). For more information on these resources and others, visit www.capc.org/palliative-care-professional-development/Education_Material_for _Professionals.
In addition, on Thursday, May 4, at 1:20, there will be a breakout session on pain management at the SHM Annual Meeting.
Hospitalists and other physicians can get certified in Hospice and Palliative Medicine by documenting relevant clinical experience and sitting for a qualifying exam. The American Board of Hospice and Palliative Medicine will administer its last exam in November 2006 (final application deadline is May 31, 2006). In September 2006 the field of Hospice and Palliative Medicine is expected to win American Board of Medical Specialties’ (ABMS) recognition as a subspecialty. After that the ABMS will take over administration of the exams. There will likely be a grandfathering period with the ABMS in which relevant clinical experience can substitute for completion of an ACGME-approved palliative care fellowship. For more information, visit the AAHPM Web site at www.abhpm.org/gfxc_100.aspx.
Summary/Conclusions
Inpatient palliative care programs benefit patients, hospitalists, and hospitals alike. Hospitalists are in the perfect position to lead the next generation of inpatient palliative care programs. Currently, about 20% of hospitals in the United States have programs. With the help of hospitalists, the percentage can increase significantly.
Special thanks to Diane Meier, MD, whose work inspired and informed this article.
References
- A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatment. The SUPPORT Principal Investigators. JAMA. 1995;274:1591-1598.
- Nelson JE, Meier DE, Oei EJ, et al. Self-reported
- symptom experience of critically ill cancer patients receiving intensive care. Crit Care Med. 2001;29 (2):277-282.
- Emanuel EJ, Fairclough DL, Slutsman J, et al. Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients. N Engl J Med. 1999;341 (13):956-963.
- Emanuel EJ, Fairclough DL, Slutsman J, et al. Understanding economic and other burdens of terminal Illness: the experience of patients and their caregivers. Ann Intern Med. 2000;132(6):451-459.
- Tolle et al. The Oregon report card: Improving care of the dying. 1999. Available at www.ohsu.edu/ethics/barriers2.pdf. Last accessed Feb. 3, 2006.
- Schulz R, Beach SR. Caregiving as a risk factor for mortality: the caregiver health effects study. JAMA. 1999;282 (23):2215-2219.
- Covinsky KE, Goldman L, Cook EF, et al. The impact of serious illness on patients’ families. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. JAMA. 1994;272:1839-1844.
- Singer PA, Martin DK, Kelner M. Quality end-of-life care: patients’ perspectives. JAMA. 1999;281(2):163-168.
- U.S. Interim Projections by Age, Sex, Race, and Hispanic Origin. Table 2a. US Census Bureau/CDC. 2002. Available at www.census.gov/ipc/www/usinterimproj/. Last accessed Feb. 3, 2006.
- Meier DE, Morrison RS, Cassel CK. Improving palliative care. Ann Intern Med. 1997;127:225-230.
- Billings JA, Block S. Palliative care in undergraduate medical education. Status report and future directions. JAMA. 1997;278:733-738.
Update:
New Hospitalist Productivity & Compensation Data
Survey results to be presented at 2006 SHM Annual Meeting
By the end of the data collection period in December 2005 approximately 400 hospital medicine programs had submitted responses for SHM’s 2005-2006 Hospitalist Productivity and Compensation Survey—a 35% increase from 2003. In addition to salary and production trends, this year’s survey should provide new insights into hospitalist responsibilities, the concerns of hospitalist program leaders, night coverage arrangements, and the use of nurse practitioners and physician assistants.
SHM thanks the program leaders who completed the comprehensive survey questionnaire. The following participants were randomly selected to receive awards:
- Danny Moore, MD, of Gilmore Memorial Hospital (Amory, Miss.) received a complimentary registration at the SHM Leadership Academy; and
- Four hospitalists received complimentary registration to the SHM Annual Meeting: Adrienne L. Bennett, MD, PhD, Ohio State University College of Medicine (Columbus, Ohio); Jasvinder S. Dhillon, St. Mary’s Hospital PICU Pediatric Hospitalist Program (Richmond, Va.); Howard Dubin, MD, Inpatient Medical Services of Bristol Hospital (Cheshire, Conn.); and Sujith Sundararaj MD, Signature Healthcare Solutions (Chicago).
The results of the 2005-2006 Hospitalist Productivity and Compensation Survey will be presented for the first time on Thursday, May 4 at 8:10 a.m. at the SHM Annual Meeting. A panel representing different perspectives within hospital medicine will react to the data. The panelists—SHM co-founder John Nelson, MD, President-Elect Mary Jo Gorman, MD, and Past-President Bob Wachter, MD—will represent hospital-employed practices, private groups, and academic programs, respectively. A report of the survey results will be available to survey participants for free. SHM members will be able to purchase the report at a discounted price. TH
The Benchmarks Committee has completed the data accumulation portion of the SHM 2005-2006 Productivity and Compensation Survey. As you might recall, we set a goal of 400 group respondents. With a final push for responses in early December, we exceeded our target. The responses were invaluable in making this survey a worthwhile effort and a credible reflection of the national hospitalist movement.
The Benchmarks Committee would like to specially thank those who attempted to complete the survey online and gave us feedback on this process. We had a few glitches with the online survey, and thanks to these folks and their communication we learned a few valuable lessons regarding this electronic process. We were able to intervene immediately and re-direct folks to the written survey. We’ll apply these lessons to the electronic component of future surveys as well.
Over the next few months we will be analyzing the data in preparation for presentation of the results to be offered up initially at the SHM Annual Meeting in Washington, D.C., the first week in May. (Visit www.hospitalmedicine.org under “Upcoming Events” to register.) Additionally, results will be available to survey participants online later in the year following the national presentation.
On a different note, the committee continues to work on the Hospitalist Dashboard Project. We are creating a dashboard that deals with metrics in the categories of resource utilization, clinical quality, productivity, and satisfaction.
Subsequently, we have worked through a Delphi process to whittle a long list of possible metrics down to 10 key metrics. These have been divided among the committee members, who will use an agreed-upon outline to write a brief description of the metric, how it is measured, and how it can be utilized to manage a hospitalist practice. The final product will be a white paper made available to the SHM membership.
How to Develop a Hospital-Based Palliative Care Program
Why your hospital needs such a program and how to create it
By Eva H. Chittenden, MD, and the SHM Palliative Care Task Force
Palliative care consists of medical care focused on the relief of suffering for patients living with chronic, advanced illness and it also helps their families. It is offered at any stage of disease, concurrently with all other appropriate medical treatment.
Palliative care providers treat the many physical symptoms that patients experience, including pain, dyspnea, nausea, and delirium. In addition, providers assist patients and families with complex medical decision-making, and attend to patients’ and families’ spiritual and psychosocial needs. Physicians work closely with an interdisciplinary team of nurses, chaplains, social workers, and pharmacists. Care continues beyond the point of death, with phone calls and consolation letters, as well as bereavement services.
Arguments for inpatient Palliative Care
The clinical imperative: We need better quality of care for people with serious and complex illness. The multicenter SUPPORT study, published in JAMA in 1995, looked at more than 9,000 hospitalized patients with life-threatening illness and demonstrated significant problems with pain and symptom control and with patient-doctor communication.1 Of the patients who died, more than 50% had moderate to severe pain more than half the time during the last three days of their lives. Of patients preferring do-not-resuscitate status, less than 50% of their physicians were aware of their wishes.
In another study, Nelson, et al. documented that more than half of cancer patients receiving intensive care had moderate to severe pain, anxiety, thirst, and hunger, and that 75% had moderate to severe discomfort of some kind.2 These studies have been a wake-up call to clinicians and hospitals across the country.
Patient and Family Preferences
Family members—especially women—shoulder most of the care of patients with serious illness. A minority of caregivers are over age 65 themselves and in ill health. When asked what they want from the medical system, family caregivers ask for help with transportation and personal care of their loved one at home, and for better home nursing support. They want 24/7 access to providers, better communication with their doctors, and to be remembered and contacted after the death of their family member.3-5 Caregiving itself has been shown to increase likelihood of premature mortality and lead to financial crisis.6
In the SUPPORT study, one-third of families lost most of their savings due to illness.7 Patients want pain and symptom control, avoidance of inappropriate prolongation of the dying process, and relief of burdens on family.8 Palliative care programs, both inpatient and ambulatory, can help provide families with needed services and improve communication at all levels.
The Demographic Argument
Hospitals need palliative care to effectively treat the growing numbers of people with serious, advanced, and complex illness. By 2030, the number of people over age 85 will double to almost 10 million.9 Many of these patients will have multiple chronic conditions, making their care complicated and expensive. And for many chronic conditions, including heart and lung disease, diabetes, and hypertension, death is not predictable.
Therefore, people need better care throughout the multiyear course of advanced illness. And while the Medicare Hospice Benefit is helpful for care of the dying (defined as people with six months or less to live) we need additional approaches for the much larger number of patients with chronic, progressive illness, years to live, continued benefit from disease-modifying therapy, and obvious palliative care needs.
The Educational Imperative
Hospitals are the site of training for most clinicians. Researchers have documented significant deficits in palliative care knowledge, skills, and attitudes among medical students, residents, and practicing physicians. Medical school and residency curricula, although improving, offer relatively little teaching in palliative care principles and practice.10,11
In 2000 the Liaison Committee on Medical Education mandated that medical school curricula include “important aspects of … end-of-life-care.” That same year the Accreditation Council for Graduate Medical Education encouraged internal medicine training programs to provide instruction in the principles of palliative care. Inpatient palliative care programs could provide much of this teaching through medical student and resident rotations, informal teaching during the consultation process, and through workshops and grand rounds.
The Financial Argument
Medical costs are rising exponentially due to multiple factors, including effective yet expensive new technologies and an expanding elderly population with more chronic conditions. Under the current Diagnosis Related Group (DRG) system, long, high-intensity hospital stays are causing a fiscal crisis for hospitals. The hospital and insurer of the future will have to work together to learn how to treat serious and complex illness efficiently and in the most cost-effective manner possible. Palliative care programs have the potential to ease this looming crisis through decreasing length of stay, both in the ICU and on the floors, and decreasing direct costs, including radiology, pharmacy, and laboratory costs. Researchers are beginning to document the positive fiscal impacts in rigorous studies.
Palliative Care: The Bottom Line
Palliative care teams have demonstrated improvement in pain and other symptom scores, in patient and family satisfaction with care, and in patient-provider communication. In addition, they have improved compliance with Joint Commission on Accreditation of Healthcare Organizations (JCAHO) quality measures. They have had these positive effects while simultaneously showing decreases in length of stay and costs. As a result, many programs have gained significant financial and administrative support from their hospitals.
Hospitalists and Palliative Care
Many hospitalist groups have found that building and staffing a palliative care consultation team is an important addition to their portfolio of services, further solidifying their value in the eyes of their hospital administration. The professional fee revenues are one more funding source, and palliative care is a critical service the group can provide the institution to improve the quality of care, improve patient satisfaction, and decrease costs.
The work involved in starting a program, including needs assessment, internal marketing, building a financial case, and developing a staffing model, is similar to that done when starting a hospitalist program. Hospitalists are ideally positioned to start palliative care services because they have already built relationships with key administrators and opinion leaders, and they understand the institution’s method for evaluating financial data, and how to access outcome and satisfaction data.
What Hospitalists Gain
By leading and staffing palliative care programs, hospitalists gain visibility and respect from colleagues, and improve their patients’ quality of care and their hospital’s financial bottom line. Clinically palliative care adds variety and depth to the work life of hospitalists and allows them to work with a rich interdisciplinary team. Although hospitalists should obtain additional training, they already possess the building blocks to provide excellent palliative care, such as skillfully leading family conferences and treating complex symptoms. When wearing the palliative care “hat,” providers have the luxury of spending more time at a patient’s bedside discussing what is truly important to the patient and his or her loved ones. The work is meaningful and rewarding.
Obtaining the Tools to Start a Program
The Center to Advance Palliative Care (CAPC), funded by the Robert Wood Johnson Foundation, is dedicated to advancing inpatient palliative care programs through their Web site (www.capc.org) and through their manual, “A Guide to Building a Hospital-Based Palliative Care Program,” available for purchase on its Web site.
In addition, CAPC sponsors the six national Palliative Care Leadership Centers (PCLCs) that each hold two-day, hands-on workshops on the nuts and bolts of starting inpatient palliative care programs, followed by a year of personalized mentoring by phone. The University of California, San Francisco’s PCLC, which is tailored specifically to hospitalists, will hold its last workshop in April 2006. For more information, visit www.capc.org/palliative-care-leadership-initiative.
At the upcoming SHM Annual Meeting in May, the Palliative Care Taskforce will present a workshop, “The Basic Why and How to Develop a Hospital-Based Palliative Care Program.”
Obtaining the Clinical Expertise
There are numerous opportunities for hospitalists to gain clinical expertise in palliative care, including Web-based and written materials and CME courses. Highlights include the Education in Palliative and End of Life Care programs; courses and study guides through the American Association of Hospice and Palliative Medicine, as well as Fast Facts (one-page synopses of relevant palliative care concepts that can be made into handouts or downloaded to one’s PDA). For more information on these resources and others, visit www.capc.org/palliative-care-professional-development/Education_Material_for _Professionals.
In addition, on Thursday, May 4, at 1:20, there will be a breakout session on pain management at the SHM Annual Meeting.
Hospitalists and other physicians can get certified in Hospice and Palliative Medicine by documenting relevant clinical experience and sitting for a qualifying exam. The American Board of Hospice and Palliative Medicine will administer its last exam in November 2006 (final application deadline is May 31, 2006). In September 2006 the field of Hospice and Palliative Medicine is expected to win American Board of Medical Specialties’ (ABMS) recognition as a subspecialty. After that the ABMS will take over administration of the exams. There will likely be a grandfathering period with the ABMS in which relevant clinical experience can substitute for completion of an ACGME-approved palliative care fellowship. For more information, visit the AAHPM Web site at www.abhpm.org/gfxc_100.aspx.
Summary/Conclusions
Inpatient palliative care programs benefit patients, hospitalists, and hospitals alike. Hospitalists are in the perfect position to lead the next generation of inpatient palliative care programs. Currently, about 20% of hospitals in the United States have programs. With the help of hospitalists, the percentage can increase significantly.
Special thanks to Diane Meier, MD, whose work inspired and informed this article.
References
- A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatment. The SUPPORT Principal Investigators. JAMA. 1995;274:1591-1598.
- Nelson JE, Meier DE, Oei EJ, et al. Self-reported
- symptom experience of critically ill cancer patients receiving intensive care. Crit Care Med. 2001;29 (2):277-282.
- Emanuel EJ, Fairclough DL, Slutsman J, et al. Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients. N Engl J Med. 1999;341 (13):956-963.
- Emanuel EJ, Fairclough DL, Slutsman J, et al. Understanding economic and other burdens of terminal Illness: the experience of patients and their caregivers. Ann Intern Med. 2000;132(6):451-459.
- Tolle et al. The Oregon report card: Improving care of the dying. 1999. Available at www.ohsu.edu/ethics/barriers2.pdf. Last accessed Feb. 3, 2006.
- Schulz R, Beach SR. Caregiving as a risk factor for mortality: the caregiver health effects study. JAMA. 1999;282 (23):2215-2219.
- Covinsky KE, Goldman L, Cook EF, et al. The impact of serious illness on patients’ families. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. JAMA. 1994;272:1839-1844.
- Singer PA, Martin DK, Kelner M. Quality end-of-life care: patients’ perspectives. JAMA. 1999;281(2):163-168.
- U.S. Interim Projections by Age, Sex, Race, and Hispanic Origin. Table 2a. US Census Bureau/CDC. 2002. Available at www.census.gov/ipc/www/usinterimproj/. Last accessed Feb. 3, 2006.
- Meier DE, Morrison RS, Cassel CK. Improving palliative care. Ann Intern Med. 1997;127:225-230.
- Billings JA, Block S. Palliative care in undergraduate medical education. Status report and future directions. JAMA. 1997;278:733-738.
Update:
New Hospitalist Productivity & Compensation Data
Survey results to be presented at 2006 SHM Annual Meeting
By the end of the data collection period in December 2005 approximately 400 hospital medicine programs had submitted responses for SHM’s 2005-2006 Hospitalist Productivity and Compensation Survey—a 35% increase from 2003. In addition to salary and production trends, this year’s survey should provide new insights into hospitalist responsibilities, the concerns of hospitalist program leaders, night coverage arrangements, and the use of nurse practitioners and physician assistants.
SHM thanks the program leaders who completed the comprehensive survey questionnaire. The following participants were randomly selected to receive awards:
- Danny Moore, MD, of Gilmore Memorial Hospital (Amory, Miss.) received a complimentary registration at the SHM Leadership Academy; and
- Four hospitalists received complimentary registration to the SHM Annual Meeting: Adrienne L. Bennett, MD, PhD, Ohio State University College of Medicine (Columbus, Ohio); Jasvinder S. Dhillon, St. Mary’s Hospital PICU Pediatric Hospitalist Program (Richmond, Va.); Howard Dubin, MD, Inpatient Medical Services of Bristol Hospital (Cheshire, Conn.); and Sujith Sundararaj MD, Signature Healthcare Solutions (Chicago).
The results of the 2005-2006 Hospitalist Productivity and Compensation Survey will be presented for the first time on Thursday, May 4 at 8:10 a.m. at the SHM Annual Meeting. A panel representing different perspectives within hospital medicine will react to the data. The panelists—SHM co-founder John Nelson, MD, President-Elect Mary Jo Gorman, MD, and Past-President Bob Wachter, MD—will represent hospital-employed practices, private groups, and academic programs, respectively. A report of the survey results will be available to survey participants for free. SHM members will be able to purchase the report at a discounted price. TH
The Benchmarks Committee has completed the data accumulation portion of the SHM 2005-2006 Productivity and Compensation Survey. As you might recall, we set a goal of 400 group respondents. With a final push for responses in early December, we exceeded our target. The responses were invaluable in making this survey a worthwhile effort and a credible reflection of the national hospitalist movement.
The Benchmarks Committee would like to specially thank those who attempted to complete the survey online and gave us feedback on this process. We had a few glitches with the online survey, and thanks to these folks and their communication we learned a few valuable lessons regarding this electronic process. We were able to intervene immediately and re-direct folks to the written survey. We’ll apply these lessons to the electronic component of future surveys as well.
Over the next few months we will be analyzing the data in preparation for presentation of the results to be offered up initially at the SHM Annual Meeting in Washington, D.C., the first week in May. (Visit www.hospitalmedicine.org under “Upcoming Events” to register.) Additionally, results will be available to survey participants online later in the year following the national presentation.
On a different note, the committee continues to work on the Hospitalist Dashboard Project. We are creating a dashboard that deals with metrics in the categories of resource utilization, clinical quality, productivity, and satisfaction.
Subsequently, we have worked through a Delphi process to whittle a long list of possible metrics down to 10 key metrics. These have been divided among the committee members, who will use an agreed-upon outline to write a brief description of the metric, how it is measured, and how it can be utilized to manage a hospitalist practice. The final product will be a white paper made available to the SHM membership.
How to Develop a Hospital-Based Palliative Care Program
Why your hospital needs such a program and how to create it
By Eva H. Chittenden, MD, and the SHM Palliative Care Task Force
Palliative care consists of medical care focused on the relief of suffering for patients living with chronic, advanced illness and it also helps their families. It is offered at any stage of disease, concurrently with all other appropriate medical treatment.
Palliative care providers treat the many physical symptoms that patients experience, including pain, dyspnea, nausea, and delirium. In addition, providers assist patients and families with complex medical decision-making, and attend to patients’ and families’ spiritual and psychosocial needs. Physicians work closely with an interdisciplinary team of nurses, chaplains, social workers, and pharmacists. Care continues beyond the point of death, with phone calls and consolation letters, as well as bereavement services.
Arguments for inpatient Palliative Care
The clinical imperative: We need better quality of care for people with serious and complex illness. The multicenter SUPPORT study, published in JAMA in 1995, looked at more than 9,000 hospitalized patients with life-threatening illness and demonstrated significant problems with pain and symptom control and with patient-doctor communication.1 Of the patients who died, more than 50% had moderate to severe pain more than half the time during the last three days of their lives. Of patients preferring do-not-resuscitate status, less than 50% of their physicians were aware of their wishes.
In another study, Nelson, et al. documented that more than half of cancer patients receiving intensive care had moderate to severe pain, anxiety, thirst, and hunger, and that 75% had moderate to severe discomfort of some kind.2 These studies have been a wake-up call to clinicians and hospitals across the country.
Patient and Family Preferences
Family members—especially women—shoulder most of the care of patients with serious illness. A minority of caregivers are over age 65 themselves and in ill health. When asked what they want from the medical system, family caregivers ask for help with transportation and personal care of their loved one at home, and for better home nursing support. They want 24/7 access to providers, better communication with their doctors, and to be remembered and contacted after the death of their family member.3-5 Caregiving itself has been shown to increase likelihood of premature mortality and lead to financial crisis.6
In the SUPPORT study, one-third of families lost most of their savings due to illness.7 Patients want pain and symptom control, avoidance of inappropriate prolongation of the dying process, and relief of burdens on family.8 Palliative care programs, both inpatient and ambulatory, can help provide families with needed services and improve communication at all levels.
The Demographic Argument
Hospitals need palliative care to effectively treat the growing numbers of people with serious, advanced, and complex illness. By 2030, the number of people over age 85 will double to almost 10 million.9 Many of these patients will have multiple chronic conditions, making their care complicated and expensive. And for many chronic conditions, including heart and lung disease, diabetes, and hypertension, death is not predictable.
Therefore, people need better care throughout the multiyear course of advanced illness. And while the Medicare Hospice Benefit is helpful for care of the dying (defined as people with six months or less to live) we need additional approaches for the much larger number of patients with chronic, progressive illness, years to live, continued benefit from disease-modifying therapy, and obvious palliative care needs.
The Educational Imperative
Hospitals are the site of training for most clinicians. Researchers have documented significant deficits in palliative care knowledge, skills, and attitudes among medical students, residents, and practicing physicians. Medical school and residency curricula, although improving, offer relatively little teaching in palliative care principles and practice.10,11
In 2000 the Liaison Committee on Medical Education mandated that medical school curricula include “important aspects of … end-of-life-care.” That same year the Accreditation Council for Graduate Medical Education encouraged internal medicine training programs to provide instruction in the principles of palliative care. Inpatient palliative care programs could provide much of this teaching through medical student and resident rotations, informal teaching during the consultation process, and through workshops and grand rounds.
The Financial Argument
Medical costs are rising exponentially due to multiple factors, including effective yet expensive new technologies and an expanding elderly population with more chronic conditions. Under the current Diagnosis Related Group (DRG) system, long, high-intensity hospital stays are causing a fiscal crisis for hospitals. The hospital and insurer of the future will have to work together to learn how to treat serious and complex illness efficiently and in the most cost-effective manner possible. Palliative care programs have the potential to ease this looming crisis through decreasing length of stay, both in the ICU and on the floors, and decreasing direct costs, including radiology, pharmacy, and laboratory costs. Researchers are beginning to document the positive fiscal impacts in rigorous studies.
Palliative Care: The Bottom Line
Palliative care teams have demonstrated improvement in pain and other symptom scores, in patient and family satisfaction with care, and in patient-provider communication. In addition, they have improved compliance with Joint Commission on Accreditation of Healthcare Organizations (JCAHO) quality measures. They have had these positive effects while simultaneously showing decreases in length of stay and costs. As a result, many programs have gained significant financial and administrative support from their hospitals.
Hospitalists and Palliative Care
Many hospitalist groups have found that building and staffing a palliative care consultation team is an important addition to their portfolio of services, further solidifying their value in the eyes of their hospital administration. The professional fee revenues are one more funding source, and palliative care is a critical service the group can provide the institution to improve the quality of care, improve patient satisfaction, and decrease costs.
The work involved in starting a program, including needs assessment, internal marketing, building a financial case, and developing a staffing model, is similar to that done when starting a hospitalist program. Hospitalists are ideally positioned to start palliative care services because they have already built relationships with key administrators and opinion leaders, and they understand the institution’s method for evaluating financial data, and how to access outcome and satisfaction data.
What Hospitalists Gain
By leading and staffing palliative care programs, hospitalists gain visibility and respect from colleagues, and improve their patients’ quality of care and their hospital’s financial bottom line. Clinically palliative care adds variety and depth to the work life of hospitalists and allows them to work with a rich interdisciplinary team. Although hospitalists should obtain additional training, they already possess the building blocks to provide excellent palliative care, such as skillfully leading family conferences and treating complex symptoms. When wearing the palliative care “hat,” providers have the luxury of spending more time at a patient’s bedside discussing what is truly important to the patient and his or her loved ones. The work is meaningful and rewarding.
Obtaining the Tools to Start a Program
The Center to Advance Palliative Care (CAPC), funded by the Robert Wood Johnson Foundation, is dedicated to advancing inpatient palliative care programs through their Web site (www.capc.org) and through their manual, “A Guide to Building a Hospital-Based Palliative Care Program,” available for purchase on its Web site.
In addition, CAPC sponsors the six national Palliative Care Leadership Centers (PCLCs) that each hold two-day, hands-on workshops on the nuts and bolts of starting inpatient palliative care programs, followed by a year of personalized mentoring by phone. The University of California, San Francisco’s PCLC, which is tailored specifically to hospitalists, will hold its last workshop in April 2006. For more information, visit www.capc.org/palliative-care-leadership-initiative.
At the upcoming SHM Annual Meeting in May, the Palliative Care Taskforce will present a workshop, “The Basic Why and How to Develop a Hospital-Based Palliative Care Program.”
Obtaining the Clinical Expertise
There are numerous opportunities for hospitalists to gain clinical expertise in palliative care, including Web-based and written materials and CME courses. Highlights include the Education in Palliative and End of Life Care programs; courses and study guides through the American Association of Hospice and Palliative Medicine, as well as Fast Facts (one-page synopses of relevant palliative care concepts that can be made into handouts or downloaded to one’s PDA). For more information on these resources and others, visit www.capc.org/palliative-care-professional-development/Education_Material_for _Professionals.
In addition, on Thursday, May 4, at 1:20, there will be a breakout session on pain management at the SHM Annual Meeting.
Hospitalists and other physicians can get certified in Hospice and Palliative Medicine by documenting relevant clinical experience and sitting for a qualifying exam. The American Board of Hospice and Palliative Medicine will administer its last exam in November 2006 (final application deadline is May 31, 2006). In September 2006 the field of Hospice and Palliative Medicine is expected to win American Board of Medical Specialties’ (ABMS) recognition as a subspecialty. After that the ABMS will take over administration of the exams. There will likely be a grandfathering period with the ABMS in which relevant clinical experience can substitute for completion of an ACGME-approved palliative care fellowship. For more information, visit the AAHPM Web site at www.abhpm.org/gfxc_100.aspx.
Summary/Conclusions
Inpatient palliative care programs benefit patients, hospitalists, and hospitals alike. Hospitalists are in the perfect position to lead the next generation of inpatient palliative care programs. Currently, about 20% of hospitals in the United States have programs. With the help of hospitalists, the percentage can increase significantly.
Special thanks to Diane Meier, MD, whose work inspired and informed this article.
References
- A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatment. The SUPPORT Principal Investigators. JAMA. 1995;274:1591-1598.
- Nelson JE, Meier DE, Oei EJ, et al. Self-reported
- symptom experience of critically ill cancer patients receiving intensive care. Crit Care Med. 2001;29 (2):277-282.
- Emanuel EJ, Fairclough DL, Slutsman J, et al. Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients. N Engl J Med. 1999;341 (13):956-963.
- Emanuel EJ, Fairclough DL, Slutsman J, et al. Understanding economic and other burdens of terminal Illness: the experience of patients and their caregivers. Ann Intern Med. 2000;132(6):451-459.
- Tolle et al. The Oregon report card: Improving care of the dying. 1999. Available at www.ohsu.edu/ethics/barriers2.pdf. Last accessed Feb. 3, 2006.
- Schulz R, Beach SR. Caregiving as a risk factor for mortality: the caregiver health effects study. JAMA. 1999;282 (23):2215-2219.
- Covinsky KE, Goldman L, Cook EF, et al. The impact of serious illness on patients’ families. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. JAMA. 1994;272:1839-1844.
- Singer PA, Martin DK, Kelner M. Quality end-of-life care: patients’ perspectives. JAMA. 1999;281(2):163-168.
- U.S. Interim Projections by Age, Sex, Race, and Hispanic Origin. Table 2a. US Census Bureau/CDC. 2002. Available at www.census.gov/ipc/www/usinterimproj/. Last accessed Feb. 3, 2006.
- Meier DE, Morrison RS, Cassel CK. Improving palliative care. Ann Intern Med. 1997;127:225-230.
- Billings JA, Block S. Palliative care in undergraduate medical education. Status report and future directions. JAMA. 1997;278:733-738.
Update:
New Hospitalist Productivity & Compensation Data
Survey results to be presented at 2006 SHM Annual Meeting
By the end of the data collection period in December 2005 approximately 400 hospital medicine programs had submitted responses for SHM’s 2005-2006 Hospitalist Productivity and Compensation Survey—a 35% increase from 2003. In addition to salary and production trends, this year’s survey should provide new insights into hospitalist responsibilities, the concerns of hospitalist program leaders, night coverage arrangements, and the use of nurse practitioners and physician assistants.
SHM thanks the program leaders who completed the comprehensive survey questionnaire. The following participants were randomly selected to receive awards:
- Danny Moore, MD, of Gilmore Memorial Hospital (Amory, Miss.) received a complimentary registration at the SHM Leadership Academy; and
- Four hospitalists received complimentary registration to the SHM Annual Meeting: Adrienne L. Bennett, MD, PhD, Ohio State University College of Medicine (Columbus, Ohio); Jasvinder S. Dhillon, St. Mary’s Hospital PICU Pediatric Hospitalist Program (Richmond, Va.); Howard Dubin, MD, Inpatient Medical Services of Bristol Hospital (Cheshire, Conn.); and Sujith Sundararaj MD, Signature Healthcare Solutions (Chicago).
The results of the 2005-2006 Hospitalist Productivity and Compensation Survey will be presented for the first time on Thursday, May 4 at 8:10 a.m. at the SHM Annual Meeting. A panel representing different perspectives within hospital medicine will react to the data. The panelists—SHM co-founder John Nelson, MD, President-Elect Mary Jo Gorman, MD, and Past-President Bob Wachter, MD—will represent hospital-employed practices, private groups, and academic programs, respectively. A report of the survey results will be available to survey participants for free. SHM members will be able to purchase the report at a discounted price. TH
Medicare Pays for Performance
The future of a Medicare-sponsored pay-for-performance model for hospitals rests on a three-year trial involving 268 hospitals and millions of dollars in bonuses.
The Centers for Medicare and Medicaid Services (CMS) has partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, to undertake The Premier Hospital Quality Incentive Demonstration Project. Premier was selected for this demonstration project because each of its hospital members has a database system in place that allows tracking and reporting of data for 34 quality measures.
“This is the only [pay-for-performance project] for hospitals at this time,” says Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS.
The project began in October 2003. At the end of each of the three years of the trial, top-performing hospitals are rewarded with cash bonuses from CMS. Performance is based on multiple evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. The individual measures are compiled into an overall quality score for each clinical condition.
“The administration is extremely interested in pay for performance in general, and very pleased with the project,” says Wynn. “The administrator is interested in expanding pay for performance to other hospitals, but exact details on this are not available.”
Money Matters
The pay structure of the project rewards those Premier hospitals that rank highest for each quality measure: Hospitals that rank in the top 20% of quality for the five general clinical areas receive a bonus. Those in the top 10% for each of the quality measures will receive a 2% bonus of their Medicare payments for the measured condition; hospitals in the top 20% will receive a 1% bonus.
In the first year of the project, Medicare spent approximately $8.9 million in incentive bonuses, and bonuses per hospital ranged from $847,000 to $900,000. This money comes, in part, from savings earned by improved outcomes, including shorter hospital stays and fewer readmissions.
Overall, though, participants seem to believe that the real payoff is not in dollars, but in improved quality of care as well as public recognition of their outcomes. (CMS has agreed not to reveal the names of the 130 lowest-performing hospitals, but the top performers are enjoying positive publicity.)
“Quality is the key motivator,” says Bill M. Hazelwood, MD, FCCP, McLeod Regional Medical Center, Florence, S.C. “Money doesn’t do anything for me—I’m sure my administrators think differently. But our efforts have paid off in lives saved and in people getting home quicker.”
Winning Ways
Hackensack University Medical Center (N.J.) and McLeod Regional Medical Center each scored in the top 20% for all five clinical conditions. Hackensack earned the largest total bonus for the first year, receiving $848,000. A hospitalist from each of these institutions shares insights into their success.
Gerard A. Burns, MD, MBA, director of medical informatics at Hackensack University Medical Center, explains that meeting the quality measures set by Medicare for the project was not new. “Some are process measures like giving aspirin, and some are outcome measures, like our mortality rates,” he says. “Many are tried and true, and not totally foreign to all hospitals. We’ve seen these things before.”
A few of the measures require no additional work from staff. “Some are automatically calculated by the Premier databases,” says Dr. Burns. “There’s no data collection involved in some of these.”
Every week or month, each hospital downloads all of the coded data. The facility also receives results on how they are doing. “We get quarterly reports to see where we’re doing well and where we’re not doing well,” says Dr. Burns. “We may see too many re-admits, and ask, ‘What’s going on?’ We’ll take a closer look. Each time is a great opportunity to improve our scores.”
Many, if not most, of the participating hospitals saw immediate improvements for multiple quality measures. The problem is that now that the project is in its last year, it’s more difficult to find ways to improve.
“The big push from here on out is fine-tuning and finding new areas for improvement,” says Dr. Hazelwood. “We hope to plug in new information and improve outcomes. And, by its nature, we’ll have to increase the number of protocols. They help us in the hustle and bustle of daily practice.”
How Hospitalists Help
In a handful of top-ranked hospitals, hospitalists play an active role in helping to meet the quality measures.
“Our hospitalists contribute in three ways,” says Dr. Burns. “We have five full-time hospitalists in the emergency department to assist our ED physicians and admitting physicians. They use specific disease order sets with built-in processes for medications, etc. Using a hospitalist to assist or write these orders is one more layer on the team to ensure we do the right thing.”
In addition, hospitalists at Hackensack are often included in new multidisciplinary team rounds. “We have multidisciplinary teams of a physician—sometimes a hospitalist—along with a nurse manager, a case manager, a social worker, a nutritionist, and sometimes a pharmacist,” explains Dr. Burns. “The team discusses each patient and tries to facilitate the physician’s plan of care. They may have to bring in a coding person to help figure out the coding rules.”
And having hospitalists involved with patients admitted without primary care physicians is “a tremendous help,” according to Dr. Burns, “because they really focus on our care measures. And each month, we have new residents come in, and the hospitalists train them on the project.”
As for McLeod Regional Medical Center, Dr. Hazelwood says, “Hospitalists are big admitters to the hospital—especially for those unassigned patients. And like other physicians, we are involved in various physician-led committees that develop our protocol for change.”
Are top-ranking hospitals sharing their bonus earnings with participating hospitalists and other physicians? “As far as I know, that has not happened, and it will not happen,” says Charles Riccobono, MD, chairman of the Performance Improvement Department at Hackensack. “I would hope that [bonus] money will filter down to support other quality projects, but I don’t know if the funds have been earmarked for anything specific.”
The Future Impact
The outcome of The Premier Hospital Quality Incentive Demonstration Project will shape any pay-for-performance guidelines that Medicare sets for hospitals around the country, including new or revised protocols and data collection hospital-wide. Final information will be available soon after the project ends this fall. Meanwhile, all data collected on the quality measures is available on the CMS Web site at www.cms.hhs.gov/HospitalQualityInits/35_HospitalPremier.asp. TH
The future of a Medicare-sponsored pay-for-performance model for hospitals rests on a three-year trial involving 268 hospitals and millions of dollars in bonuses.
The Centers for Medicare and Medicaid Services (CMS) has partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, to undertake The Premier Hospital Quality Incentive Demonstration Project. Premier was selected for this demonstration project because each of its hospital members has a database system in place that allows tracking and reporting of data for 34 quality measures.
“This is the only [pay-for-performance project] for hospitals at this time,” says Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS.
The project began in October 2003. At the end of each of the three years of the trial, top-performing hospitals are rewarded with cash bonuses from CMS. Performance is based on multiple evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. The individual measures are compiled into an overall quality score for each clinical condition.
“The administration is extremely interested in pay for performance in general, and very pleased with the project,” says Wynn. “The administrator is interested in expanding pay for performance to other hospitals, but exact details on this are not available.”
Money Matters
The pay structure of the project rewards those Premier hospitals that rank highest for each quality measure: Hospitals that rank in the top 20% of quality for the five general clinical areas receive a bonus. Those in the top 10% for each of the quality measures will receive a 2% bonus of their Medicare payments for the measured condition; hospitals in the top 20% will receive a 1% bonus.
In the first year of the project, Medicare spent approximately $8.9 million in incentive bonuses, and bonuses per hospital ranged from $847,000 to $900,000. This money comes, in part, from savings earned by improved outcomes, including shorter hospital stays and fewer readmissions.
Overall, though, participants seem to believe that the real payoff is not in dollars, but in improved quality of care as well as public recognition of their outcomes. (CMS has agreed not to reveal the names of the 130 lowest-performing hospitals, but the top performers are enjoying positive publicity.)
“Quality is the key motivator,” says Bill M. Hazelwood, MD, FCCP, McLeod Regional Medical Center, Florence, S.C. “Money doesn’t do anything for me—I’m sure my administrators think differently. But our efforts have paid off in lives saved and in people getting home quicker.”
Winning Ways
Hackensack University Medical Center (N.J.) and McLeod Regional Medical Center each scored in the top 20% for all five clinical conditions. Hackensack earned the largest total bonus for the first year, receiving $848,000. A hospitalist from each of these institutions shares insights into their success.
Gerard A. Burns, MD, MBA, director of medical informatics at Hackensack University Medical Center, explains that meeting the quality measures set by Medicare for the project was not new. “Some are process measures like giving aspirin, and some are outcome measures, like our mortality rates,” he says. “Many are tried and true, and not totally foreign to all hospitals. We’ve seen these things before.”
A few of the measures require no additional work from staff. “Some are automatically calculated by the Premier databases,” says Dr. Burns. “There’s no data collection involved in some of these.”
Every week or month, each hospital downloads all of the coded data. The facility also receives results on how they are doing. “We get quarterly reports to see where we’re doing well and where we’re not doing well,” says Dr. Burns. “We may see too many re-admits, and ask, ‘What’s going on?’ We’ll take a closer look. Each time is a great opportunity to improve our scores.”
Many, if not most, of the participating hospitals saw immediate improvements for multiple quality measures. The problem is that now that the project is in its last year, it’s more difficult to find ways to improve.
“The big push from here on out is fine-tuning and finding new areas for improvement,” says Dr. Hazelwood. “We hope to plug in new information and improve outcomes. And, by its nature, we’ll have to increase the number of protocols. They help us in the hustle and bustle of daily practice.”
How Hospitalists Help
In a handful of top-ranked hospitals, hospitalists play an active role in helping to meet the quality measures.
“Our hospitalists contribute in three ways,” says Dr. Burns. “We have five full-time hospitalists in the emergency department to assist our ED physicians and admitting physicians. They use specific disease order sets with built-in processes for medications, etc. Using a hospitalist to assist or write these orders is one more layer on the team to ensure we do the right thing.”
In addition, hospitalists at Hackensack are often included in new multidisciplinary team rounds. “We have multidisciplinary teams of a physician—sometimes a hospitalist—along with a nurse manager, a case manager, a social worker, a nutritionist, and sometimes a pharmacist,” explains Dr. Burns. “The team discusses each patient and tries to facilitate the physician’s plan of care. They may have to bring in a coding person to help figure out the coding rules.”
And having hospitalists involved with patients admitted without primary care physicians is “a tremendous help,” according to Dr. Burns, “because they really focus on our care measures. And each month, we have new residents come in, and the hospitalists train them on the project.”
As for McLeod Regional Medical Center, Dr. Hazelwood says, “Hospitalists are big admitters to the hospital—especially for those unassigned patients. And like other physicians, we are involved in various physician-led committees that develop our protocol for change.”
Are top-ranking hospitals sharing their bonus earnings with participating hospitalists and other physicians? “As far as I know, that has not happened, and it will not happen,” says Charles Riccobono, MD, chairman of the Performance Improvement Department at Hackensack. “I would hope that [bonus] money will filter down to support other quality projects, but I don’t know if the funds have been earmarked for anything specific.”
The Future Impact
The outcome of The Premier Hospital Quality Incentive Demonstration Project will shape any pay-for-performance guidelines that Medicare sets for hospitals around the country, including new or revised protocols and data collection hospital-wide. Final information will be available soon after the project ends this fall. Meanwhile, all data collected on the quality measures is available on the CMS Web site at www.cms.hhs.gov/HospitalQualityInits/35_HospitalPremier.asp. TH
The future of a Medicare-sponsored pay-for-performance model for hospitals rests on a three-year trial involving 268 hospitals and millions of dollars in bonuses.
The Centers for Medicare and Medicaid Services (CMS) has partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, to undertake The Premier Hospital Quality Incentive Demonstration Project. Premier was selected for this demonstration project because each of its hospital members has a database system in place that allows tracking and reporting of data for 34 quality measures.
“This is the only [pay-for-performance project] for hospitals at this time,” says Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS.
The project began in October 2003. At the end of each of the three years of the trial, top-performing hospitals are rewarded with cash bonuses from CMS. Performance is based on multiple evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. The individual measures are compiled into an overall quality score for each clinical condition.
“The administration is extremely interested in pay for performance in general, and very pleased with the project,” says Wynn. “The administrator is interested in expanding pay for performance to other hospitals, but exact details on this are not available.”
Money Matters
The pay structure of the project rewards those Premier hospitals that rank highest for each quality measure: Hospitals that rank in the top 20% of quality for the five general clinical areas receive a bonus. Those in the top 10% for each of the quality measures will receive a 2% bonus of their Medicare payments for the measured condition; hospitals in the top 20% will receive a 1% bonus.
In the first year of the project, Medicare spent approximately $8.9 million in incentive bonuses, and bonuses per hospital ranged from $847,000 to $900,000. This money comes, in part, from savings earned by improved outcomes, including shorter hospital stays and fewer readmissions.
Overall, though, participants seem to believe that the real payoff is not in dollars, but in improved quality of care as well as public recognition of their outcomes. (CMS has agreed not to reveal the names of the 130 lowest-performing hospitals, but the top performers are enjoying positive publicity.)
“Quality is the key motivator,” says Bill M. Hazelwood, MD, FCCP, McLeod Regional Medical Center, Florence, S.C. “Money doesn’t do anything for me—I’m sure my administrators think differently. But our efforts have paid off in lives saved and in people getting home quicker.”
Winning Ways
Hackensack University Medical Center (N.J.) and McLeod Regional Medical Center each scored in the top 20% for all five clinical conditions. Hackensack earned the largest total bonus for the first year, receiving $848,000. A hospitalist from each of these institutions shares insights into their success.
Gerard A. Burns, MD, MBA, director of medical informatics at Hackensack University Medical Center, explains that meeting the quality measures set by Medicare for the project was not new. “Some are process measures like giving aspirin, and some are outcome measures, like our mortality rates,” he says. “Many are tried and true, and not totally foreign to all hospitals. We’ve seen these things before.”
A few of the measures require no additional work from staff. “Some are automatically calculated by the Premier databases,” says Dr. Burns. “There’s no data collection involved in some of these.”
Every week or month, each hospital downloads all of the coded data. The facility also receives results on how they are doing. “We get quarterly reports to see where we’re doing well and where we’re not doing well,” says Dr. Burns. “We may see too many re-admits, and ask, ‘What’s going on?’ We’ll take a closer look. Each time is a great opportunity to improve our scores.”
Many, if not most, of the participating hospitals saw immediate improvements for multiple quality measures. The problem is that now that the project is in its last year, it’s more difficult to find ways to improve.
“The big push from here on out is fine-tuning and finding new areas for improvement,” says Dr. Hazelwood. “We hope to plug in new information and improve outcomes. And, by its nature, we’ll have to increase the number of protocols. They help us in the hustle and bustle of daily practice.”
How Hospitalists Help
In a handful of top-ranked hospitals, hospitalists play an active role in helping to meet the quality measures.
“Our hospitalists contribute in three ways,” says Dr. Burns. “We have five full-time hospitalists in the emergency department to assist our ED physicians and admitting physicians. They use specific disease order sets with built-in processes for medications, etc. Using a hospitalist to assist or write these orders is one more layer on the team to ensure we do the right thing.”
In addition, hospitalists at Hackensack are often included in new multidisciplinary team rounds. “We have multidisciplinary teams of a physician—sometimes a hospitalist—along with a nurse manager, a case manager, a social worker, a nutritionist, and sometimes a pharmacist,” explains Dr. Burns. “The team discusses each patient and tries to facilitate the physician’s plan of care. They may have to bring in a coding person to help figure out the coding rules.”
And having hospitalists involved with patients admitted without primary care physicians is “a tremendous help,” according to Dr. Burns, “because they really focus on our care measures. And each month, we have new residents come in, and the hospitalists train them on the project.”
As for McLeod Regional Medical Center, Dr. Hazelwood says, “Hospitalists are big admitters to the hospital—especially for those unassigned patients. And like other physicians, we are involved in various physician-led committees that develop our protocol for change.”
Are top-ranking hospitals sharing their bonus earnings with participating hospitalists and other physicians? “As far as I know, that has not happened, and it will not happen,” says Charles Riccobono, MD, chairman of the Performance Improvement Department at Hackensack. “I would hope that [bonus] money will filter down to support other quality projects, but I don’t know if the funds have been earmarked for anything specific.”
The Future Impact
The outcome of The Premier Hospital Quality Incentive Demonstration Project will shape any pay-for-performance guidelines that Medicare sets for hospitals around the country, including new or revised protocols and data collection hospital-wide. Final information will be available soon after the project ends this fall. Meanwhile, all data collected on the quality measures is available on the CMS Web site at www.cms.hhs.gov/HospitalQualityInits/35_HospitalPremier.asp. TH
An Historic Puzzler
This month in “Flashback:” a medical mystery and competition. This following is an actual case described by Theodore Tronchin. Dr. Tronchin routinely made diagnoses without seeing patients and based on descriptions of signs and symptoms included in patients’ letters. This makes this month’s written diagnosis “contest” all the more relevant.
Review Dr. Tronchin’s case below and see if you can make the diagnosis based on the information provided. E-mail your diagnosis to Physician Editor Jamie Newman at [email protected]. The deadline is Tuesday, April 4. We’ll select a winner at random and publish their response in a future issue of The Hospitalist.

The Case
You move to Paris in 1752 to practice medicine. You are consulted on the following case:
A 42-year-old man complains of abdominal pain. Four weeks prior to this visit he noted a gradual onset of diffuse cramping abdominal pain. The illness began with a sensation of generalized weakness, cold sweats, and nausea. He had several episodes of emesis. He was constipated, and his stool was occasionally streaked with blood. He had increased thirst and mild dysuria. He also had a mild, nonproductive cough.
Subsequently, he noted a mild tremor of his hands and occasional difficulty focusing his eyes. In the past few days, he had experienced weakness in his knees and arms (noticeable when he tried to stand from a sitting position) with a mild tingling in his feet but no loss of sensation.
The patient reports no unusual childhood illnesses and has been inoculated against smallpox. He was seen by another provider several weeks ago for gonorrhea. He does not drink alcohol excessively and both of his parents died in a carriage accident.
On exam the patient appeared pale, weak, and tremulous. His pulse was slightly weak but regular. He experienced some soreness to his mouth and gums without loss of teeth. His breath was slightly fetid, his teeth were intact, the gums were tender, and the tongue was coated whitish green. His abdomen was bloated but not tender. His grip was weak as were his legs, though they seemed intact to sensation.
What is your diagnosis? TH
This month in “Flashback:” a medical mystery and competition. This following is an actual case described by Theodore Tronchin. Dr. Tronchin routinely made diagnoses without seeing patients and based on descriptions of signs and symptoms included in patients’ letters. This makes this month’s written diagnosis “contest” all the more relevant.
Review Dr. Tronchin’s case below and see if you can make the diagnosis based on the information provided. E-mail your diagnosis to Physician Editor Jamie Newman at [email protected]. The deadline is Tuesday, April 4. We’ll select a winner at random and publish their response in a future issue of The Hospitalist.
The Case
You move to Paris in 1752 to practice medicine. You are consulted on the following case:
A 42-year-old man complains of abdominal pain. Four weeks prior to this visit he noted a gradual onset of diffuse cramping abdominal pain. The illness began with a sensation of generalized weakness, cold sweats, and nausea. He had several episodes of emesis. He was constipated, and his stool was occasionally streaked with blood. He had increased thirst and mild dysuria. He also had a mild, nonproductive cough.
Subsequently, he noted a mild tremor of his hands and occasional difficulty focusing his eyes. In the past few days, he had experienced weakness in his knees and arms (noticeable when he tried to stand from a sitting position) with a mild tingling in his feet but no loss of sensation.
The patient reports no unusual childhood illnesses and has been inoculated against smallpox. He was seen by another provider several weeks ago for gonorrhea. He does not drink alcohol excessively and both of his parents died in a carriage accident.
On exam the patient appeared pale, weak, and tremulous. His pulse was slightly weak but regular. He experienced some soreness to his mouth and gums without loss of teeth. His breath was slightly fetid, his teeth were intact, the gums were tender, and the tongue was coated whitish green. His abdomen was bloated but not tender. His grip was weak as were his legs, though they seemed intact to sensation.
What is your diagnosis? TH
This month in “Flashback:” a medical mystery and competition. This following is an actual case described by Theodore Tronchin. Dr. Tronchin routinely made diagnoses without seeing patients and based on descriptions of signs and symptoms included in patients’ letters. This makes this month’s written diagnosis “contest” all the more relevant.
Review Dr. Tronchin’s case below and see if you can make the diagnosis based on the information provided. E-mail your diagnosis to Physician Editor Jamie Newman at [email protected]. The deadline is Tuesday, April 4. We’ll select a winner at random and publish their response in a future issue of The Hospitalist.
The Case
You move to Paris in 1752 to practice medicine. You are consulted on the following case:
A 42-year-old man complains of abdominal pain. Four weeks prior to this visit he noted a gradual onset of diffuse cramping abdominal pain. The illness began with a sensation of generalized weakness, cold sweats, and nausea. He had several episodes of emesis. He was constipated, and his stool was occasionally streaked with blood. He had increased thirst and mild dysuria. He also had a mild, nonproductive cough.
Subsequently, he noted a mild tremor of his hands and occasional difficulty focusing his eyes. In the past few days, he had experienced weakness in his knees and arms (noticeable when he tried to stand from a sitting position) with a mild tingling in his feet but no loss of sensation.
The patient reports no unusual childhood illnesses and has been inoculated against smallpox. He was seen by another provider several weeks ago for gonorrhea. He does not drink alcohol excessively and both of his parents died in a carriage accident.
On exam the patient appeared pale, weak, and tremulous. His pulse was slightly weak but regular. He experienced some soreness to his mouth and gums without loss of teeth. His breath was slightly fetid, his teeth were intact, the gums were tender, and the tongue was coated whitish green. His abdomen was bloated but not tender. His grip was weak as were his legs, though they seemed intact to sensation.
What is your diagnosis? TH
A Case of Shortness of Breath, Abdominal Pain, and Hematuria
A48-year-old male presents with three weeks of worsening shortness of breath and pleuritic chest discomfort. A week before the onset of these symptoms, he noticed increasing fatigue, weight loss, abdominal discomfort, and persistent hematuria He was otherwise healthy and was taking no medications.
Physical examination reveals a tachypneic yet hemodynamically stable patient, with left upper quadrant fullness. CT chest and abdomen, reveal the following (see right).
You suspect that this finding is secondary to an extrapulmonary process. What unifying diagnosis most likely accounts for these findings? What is your diagnosis?
- Antiphospholipid syndrome
- Antithrombin III deficiency
- Renal cell carcinoma
- Protein C deficiency
- Prostate carcinoma
Discussion
The answer is C: Renal cell carcinoma (RCC) with caval extension causing PE; this suggests that the PE was due to tumor thrombus. The photo on p. 8 shows areas of increased attenuation in the prominent right and left pulmonary arteries, consistent with a saddle pulmonary embolism. An MRI of the abdomen (see photo above) reveals a large left renal mass extending to Gerota’s fascia and into the left renal vein, protruding slightly into the inferior vena cava (IVC).
The MRI demonstrates an occlusive thrombus in the left renal vein with propagation into the inferior vena cava. The patient underwent a left radical nephrectomy, an inferior vena cava thrombectomy, and a saddle embolectomy. Histological examination of the mass and thrombus confirmed the diagnosis. He had an uneventful recovery and was discharged from the hospital.
RCC accounts for approximately 80% of all primary renal neoplasms, and commonly is termed the “internist’s tumor.” Hematuria is the most common symptom. It is accompanied by flank pain and a palpable abdominal mass in less than 15% of cases.1 Diagnosis of RCC is often made late due to delayed clinical presentation and 20% of patients have metastatic disease at initial diagnosis.2 PE due to tumor thrombus as an initial manifestation of RCC is rare, but is a well-recognized entity leading to dyspnea, pleuritic chest pain, hypoxemia, and—in severe cases—acute cor pulmonale with hemodynamic failure.3-5

Staging CT is required in patients with suspected RCC, and MRI is needed, with transesophageal echocardiography used adjunctively, to evaluate cephalic thrombus extension when indicated.6 IVC tumor thrombus occurs in 4%-10% of all cases, most often originating in the renal vein and extending cranially, subsequently propagating to the lungs.7 Survival in local non-metastatic disease with IVC thrombus is no different whether renal vein extension occurs or not, and ranges from 40%-69%, following surgical resection and thrombectomy.8 In those with distant metastases who require venal caval thrombectomy, five-year survivals range from 0%-12.5%.2
The first case of successful removal of a PE secondary to RCC was documented in 1977.1 The goal of surgery is tumor resection and prevention of recurrent embolic events. It is the only effective means of improving survival in the presence of intravascular tumor. Preoperative anticoagulation may be warranted in patients who present with PE, but should be discontinued following definitive surgical treatment secondary to increased risks of hemorrhage.8 TH
References
- Daughtry JD, Stewart BH, Golding LAR, Groves LK. Pulmonary embolus presenting as the initial manifestation of renal cell carcinoma. Ann Thorac Surg. 1977;24:178-181.
- Goetzl MA, Goluboff ET, Murphy AM, et al. A contemporary evaluation of cytoreductive nephrectomy with tumor thrombus: morbidity and long term survival. Urol Oncol. 2004; 22:182-187.
- Kubota H, Furuse A, Kotsuka Y, et al. Successful management of massive pulmonary tumor embolism from renal cell carcinoma. Ann Thorac Surg. 1996;61:708-710.
- Gayer G, Mini S, Olchovsky D, et al. Pulmonary embolism—the initial manifestation of renal cell carcinoma in a young woman. Emerg Radiol. 2003;10:43-45.
- Eggener SE, Dalton DP. Bilateral pulmonary artery tumour emboli from renal carcinoma. Lancet Oncol. 2004;5:173.
- Tsuji Y, Goto A, Hara I, et al. Renal cell carcinoma with extension of tumor thrombus into vena cava: Surgical strategy and prognosis. J Vasc Surg. 2001;33:789-796.
- Zisman A, Pantuck AJ, Chao DH, et al. Renal cell carcinoma with tumor thrombus: is cytoreductive nephrectomy for advanced disease associated with an increased complication rate? J Urol. 2002;168:962-967.
- Nesbitt JC, Soltero ER, Dinney CPN, et al. Surgical management of renal cell carcinoma with inferior vena cava tumor thrombus. Ann Thorac Surg. 1997;63:1592-1600.
A48-year-old male presents with three weeks of worsening shortness of breath and pleuritic chest discomfort. A week before the onset of these symptoms, he noticed increasing fatigue, weight loss, abdominal discomfort, and persistent hematuria He was otherwise healthy and was taking no medications.
Physical examination reveals a tachypneic yet hemodynamically stable patient, with left upper quadrant fullness. CT chest and abdomen, reveal the following (see right).
You suspect that this finding is secondary to an extrapulmonary process. What unifying diagnosis most likely accounts for these findings? What is your diagnosis?
- Antiphospholipid syndrome
- Antithrombin III deficiency
- Renal cell carcinoma
- Protein C deficiency
- Prostate carcinoma
Discussion
The answer is C: Renal cell carcinoma (RCC) with caval extension causing PE; this suggests that the PE was due to tumor thrombus. The photo on p. 8 shows areas of increased attenuation in the prominent right and left pulmonary arteries, consistent with a saddle pulmonary embolism. An MRI of the abdomen (see photo above) reveals a large left renal mass extending to Gerota’s fascia and into the left renal vein, protruding slightly into the inferior vena cava (IVC).
The MRI demonstrates an occlusive thrombus in the left renal vein with propagation into the inferior vena cava. The patient underwent a left radical nephrectomy, an inferior vena cava thrombectomy, and a saddle embolectomy. Histological examination of the mass and thrombus confirmed the diagnosis. He had an uneventful recovery and was discharged from the hospital.
RCC accounts for approximately 80% of all primary renal neoplasms, and commonly is termed the “internist’s tumor.” Hematuria is the most common symptom. It is accompanied by flank pain and a palpable abdominal mass in less than 15% of cases.1 Diagnosis of RCC is often made late due to delayed clinical presentation and 20% of patients have metastatic disease at initial diagnosis.2 PE due to tumor thrombus as an initial manifestation of RCC is rare, but is a well-recognized entity leading to dyspnea, pleuritic chest pain, hypoxemia, and—in severe cases—acute cor pulmonale with hemodynamic failure.3-5
Staging CT is required in patients with suspected RCC, and MRI is needed, with transesophageal echocardiography used adjunctively, to evaluate cephalic thrombus extension when indicated.6 IVC tumor thrombus occurs in 4%-10% of all cases, most often originating in the renal vein and extending cranially, subsequently propagating to the lungs.7 Survival in local non-metastatic disease with IVC thrombus is no different whether renal vein extension occurs or not, and ranges from 40%-69%, following surgical resection and thrombectomy.8 In those with distant metastases who require venal caval thrombectomy, five-year survivals range from 0%-12.5%.2
The first case of successful removal of a PE secondary to RCC was documented in 1977.1 The goal of surgery is tumor resection and prevention of recurrent embolic events. It is the only effective means of improving survival in the presence of intravascular tumor. Preoperative anticoagulation may be warranted in patients who present with PE, but should be discontinued following definitive surgical treatment secondary to increased risks of hemorrhage.8 TH
References
- Daughtry JD, Stewart BH, Golding LAR, Groves LK. Pulmonary embolus presenting as the initial manifestation of renal cell carcinoma. Ann Thorac Surg. 1977;24:178-181.
- Goetzl MA, Goluboff ET, Murphy AM, et al. A contemporary evaluation of cytoreductive nephrectomy with tumor thrombus: morbidity and long term survival. Urol Oncol. 2004; 22:182-187.
- Kubota H, Furuse A, Kotsuka Y, et al. Successful management of massive pulmonary tumor embolism from renal cell carcinoma. Ann Thorac Surg. 1996;61:708-710.
- Gayer G, Mini S, Olchovsky D, et al. Pulmonary embolism—the initial manifestation of renal cell carcinoma in a young woman. Emerg Radiol. 2003;10:43-45.
- Eggener SE, Dalton DP. Bilateral pulmonary artery tumour emboli from renal carcinoma. Lancet Oncol. 2004;5:173.
- Tsuji Y, Goto A, Hara I, et al. Renal cell carcinoma with extension of tumor thrombus into vena cava: Surgical strategy and prognosis. J Vasc Surg. 2001;33:789-796.
- Zisman A, Pantuck AJ, Chao DH, et al. Renal cell carcinoma with tumor thrombus: is cytoreductive nephrectomy for advanced disease associated with an increased complication rate? J Urol. 2002;168:962-967.
- Nesbitt JC, Soltero ER, Dinney CPN, et al. Surgical management of renal cell carcinoma with inferior vena cava tumor thrombus. Ann Thorac Surg. 1997;63:1592-1600.
A48-year-old male presents with three weeks of worsening shortness of breath and pleuritic chest discomfort. A week before the onset of these symptoms, he noticed increasing fatigue, weight loss, abdominal discomfort, and persistent hematuria He was otherwise healthy and was taking no medications.
Physical examination reveals a tachypneic yet hemodynamically stable patient, with left upper quadrant fullness. CT chest and abdomen, reveal the following (see right).
You suspect that this finding is secondary to an extrapulmonary process. What unifying diagnosis most likely accounts for these findings? What is your diagnosis?
- Antiphospholipid syndrome
- Antithrombin III deficiency
- Renal cell carcinoma
- Protein C deficiency
- Prostate carcinoma
Discussion
The answer is C: Renal cell carcinoma (RCC) with caval extension causing PE; this suggests that the PE was due to tumor thrombus. The photo on p. 8 shows areas of increased attenuation in the prominent right and left pulmonary arteries, consistent with a saddle pulmonary embolism. An MRI of the abdomen (see photo above) reveals a large left renal mass extending to Gerota’s fascia and into the left renal vein, protruding slightly into the inferior vena cava (IVC).
The MRI demonstrates an occlusive thrombus in the left renal vein with propagation into the inferior vena cava. The patient underwent a left radical nephrectomy, an inferior vena cava thrombectomy, and a saddle embolectomy. Histological examination of the mass and thrombus confirmed the diagnosis. He had an uneventful recovery and was discharged from the hospital.
RCC accounts for approximately 80% of all primary renal neoplasms, and commonly is termed the “internist’s tumor.” Hematuria is the most common symptom. It is accompanied by flank pain and a palpable abdominal mass in less than 15% of cases.1 Diagnosis of RCC is often made late due to delayed clinical presentation and 20% of patients have metastatic disease at initial diagnosis.2 PE due to tumor thrombus as an initial manifestation of RCC is rare, but is a well-recognized entity leading to dyspnea, pleuritic chest pain, hypoxemia, and—in severe cases—acute cor pulmonale with hemodynamic failure.3-5
Staging CT is required in patients with suspected RCC, and MRI is needed, with transesophageal echocardiography used adjunctively, to evaluate cephalic thrombus extension when indicated.6 IVC tumor thrombus occurs in 4%-10% of all cases, most often originating in the renal vein and extending cranially, subsequently propagating to the lungs.7 Survival in local non-metastatic disease with IVC thrombus is no different whether renal vein extension occurs or not, and ranges from 40%-69%, following surgical resection and thrombectomy.8 In those with distant metastases who require venal caval thrombectomy, five-year survivals range from 0%-12.5%.2
The first case of successful removal of a PE secondary to RCC was documented in 1977.1 The goal of surgery is tumor resection and prevention of recurrent embolic events. It is the only effective means of improving survival in the presence of intravascular tumor. Preoperative anticoagulation may be warranted in patients who present with PE, but should be discontinued following definitive surgical treatment secondary to increased risks of hemorrhage.8 TH
References
- Daughtry JD, Stewart BH, Golding LAR, Groves LK. Pulmonary embolus presenting as the initial manifestation of renal cell carcinoma. Ann Thorac Surg. 1977;24:178-181.
- Goetzl MA, Goluboff ET, Murphy AM, et al. A contemporary evaluation of cytoreductive nephrectomy with tumor thrombus: morbidity and long term survival. Urol Oncol. 2004; 22:182-187.
- Kubota H, Furuse A, Kotsuka Y, et al. Successful management of massive pulmonary tumor embolism from renal cell carcinoma. Ann Thorac Surg. 1996;61:708-710.
- Gayer G, Mini S, Olchovsky D, et al. Pulmonary embolism—the initial manifestation of renal cell carcinoma in a young woman. Emerg Radiol. 2003;10:43-45.
- Eggener SE, Dalton DP. Bilateral pulmonary artery tumour emboli from renal carcinoma. Lancet Oncol. 2004;5:173.
- Tsuji Y, Goto A, Hara I, et al. Renal cell carcinoma with extension of tumor thrombus into vena cava: Surgical strategy and prognosis. J Vasc Surg. 2001;33:789-796.
- Zisman A, Pantuck AJ, Chao DH, et al. Renal cell carcinoma with tumor thrombus: is cytoreductive nephrectomy for advanced disease associated with an increased complication rate? J Urol. 2002;168:962-967.
- Nesbitt JC, Soltero ER, Dinney CPN, et al. Surgical management of renal cell carcinoma with inferior vena cava tumor thrombus. Ann Thorac Surg. 1997;63:1592-1600.
Critical Coalition

March is an important month for SHM. It is DVT Awareness Month, and once again SHM is leading a coalition of almost 40 organizations to raise the understanding of this disease. DVT causes complications that kill more people every year than AIDS and breast cancer combined. This coalition includes the American College of Physicians, the American Public Health Association, the American College of Chest Physicians, the American Society of Health System Pharmacists, the American Association of Critical Care Nurses, and many more.
The goals of the coalition are to use our knowledge and influence to inform not only the public at large, but health professionals as well. And if our success in 2005 is any measure, the DVT Awareness campaign has really had an impact.
Last year more than 400 million people saw on TV or read our message in magazines and newspapers. Utilizing the compelling story of our national spokesperson, Melanie Bloom, a mother of three girls who lost her young, athletic NBC war-correspondent husband, David, to a fatal pulmonary embolism (PE), our message was seen on “Larry King Live” on CNN, on the “Jane Pauley Show,” on “Access Hollywood,” and in Ladies Home Journal.
Often Melanie was accompanied by hospitalists such as Frank Michota, MD, the head of the Hospital Medicine Division at Cleveland Clinic. Dr. Michota answered the clinical questions in the interviews. Who can forget when Larry King turned to Dr. Michota and asked, “Are you a cardiologist?”
“No, Larry, I am a hospitalist,” said Dr. Michota.
And when Larry King asked “What is a hospitalist?” Dr. Michota spread the gospel according to hospital medicine to a nationwide audience.
Later in the year a billboard on Rockefeller Center in New York City proclaimed the DVT Awareness message along with the SHM logo. If you can make it there, you can make it anywhere.
But this campaign isn’t just about TV appearances and magazine articles. This is about using awareness to save lives. And save lives we did. More than a thousand letters and e-mails were sent to the coalition in 2005 from patients and family members with personal stories of how exposure to our campaign led them to go to their doctors or show up in an ED. They were treated early for DVT—before they developed a potentially fatal PE. They credit the DVT Awareness Campaign with saving their lives.
In 2006 SHM is back at the head of the coalition. In January at the National Press Club, I was fortunate enough to help roll out the details of our 2006 campaign. Joining me on the dais were Dr. Michota; Geno Merli, MD, from Jefferson Medical College and a frequent speaker at SHM meetings; and Sam Goldhaber, MD, from Harvard’s Brigham and Women’s in Boston.
This year we have set a goal of further engaging the public by telling our patients’ stories, by forming patient affinity groups, by providing the tools for health professionals to provide the best care for DVT and PE, and by continuing to use the media to spread our message.
SHM has a robust set of educational and quality improvement tools in the DVT Resource Room on the SHM Web site at www.hospitalmedicine.org under the “Quality/Patient Safety” tab. There hospitalists can find an SHM DVT workbook to help measure their performance and improve their outcomes. At the SHM 2006 Annual Meeting on May 3, from 8 a.m. to 5:30 p.m., SHM will host a precourse on quality improvement, and one of the key conditions is DVT. SHM hopes to raise funds for future demonstration projects to improve patient outcomes in DVT and even to set up skilled mentors who can help hospitalists trying to affect change at their hospitals for the first time.
SHM is a young, enthusiastic organization that lacks the cynicism of entrenchment. We actually do believe with some help and support we can make quality matter, even without pay for performance and before regulated performance standards.
We see the DVT Awareness Coalition as a template for SHM’s call to action. It involves participation across the continuum involving other physicians, nurses, pharmacists, and patients. It is proactive and targeted with not only improving public knowledge, but recognizing that maybe not every doctor and nurse knows all the latest information, either. It is focused on making a tangible difference, not just writing a white paper or a guideline and declaring victory. It is about saving lives in 2005 and again in 2006. It is about multiplying the efforts of SHM by the multiple of the number of hospitals that now have hospitalists.
There is much promise to hospital medicine. Some see this as a future play with only a foundation being built today. There are surely many great things ahead for hospital medicine as we grow to more than 30,000 hospitalists at virtually every hospital in America. There are many skills left for us to learn. But hospitalists and SHM are making a difference today. We are not doing it alone, but through teamwork and coalition-building. We are proud to be a partner in the DVT Awareness Coalition and we are glad to provide leadership when asked. The payoff is in the lives we have saved and the lives we have changed for the better. TH
Dr. Wellikson has been CEO of SHM since 2000.
March is an important month for SHM. It is DVT Awareness Month, and once again SHM is leading a coalition of almost 40 organizations to raise the understanding of this disease. DVT causes complications that kill more people every year than AIDS and breast cancer combined. This coalition includes the American College of Physicians, the American Public Health Association, the American College of Chest Physicians, the American Society of Health System Pharmacists, the American Association of Critical Care Nurses, and many more.
The goals of the coalition are to use our knowledge and influence to inform not only the public at large, but health professionals as well. And if our success in 2005 is any measure, the DVT Awareness campaign has really had an impact.
Last year more than 400 million people saw on TV or read our message in magazines and newspapers. Utilizing the compelling story of our national spokesperson, Melanie Bloom, a mother of three girls who lost her young, athletic NBC war-correspondent husband, David, to a fatal pulmonary embolism (PE), our message was seen on “Larry King Live” on CNN, on the “Jane Pauley Show,” on “Access Hollywood,” and in Ladies Home Journal.
Often Melanie was accompanied by hospitalists such as Frank Michota, MD, the head of the Hospital Medicine Division at Cleveland Clinic. Dr. Michota answered the clinical questions in the interviews. Who can forget when Larry King turned to Dr. Michota and asked, “Are you a cardiologist?”
“No, Larry, I am a hospitalist,” said Dr. Michota.
And when Larry King asked “What is a hospitalist?” Dr. Michota spread the gospel according to hospital medicine to a nationwide audience.
Later in the year a billboard on Rockefeller Center in New York City proclaimed the DVT Awareness message along with the SHM logo. If you can make it there, you can make it anywhere.
But this campaign isn’t just about TV appearances and magazine articles. This is about using awareness to save lives. And save lives we did. More than a thousand letters and e-mails were sent to the coalition in 2005 from patients and family members with personal stories of how exposure to our campaign led them to go to their doctors or show up in an ED. They were treated early for DVT—before they developed a potentially fatal PE. They credit the DVT Awareness Campaign with saving their lives.
In 2006 SHM is back at the head of the coalition. In January at the National Press Club, I was fortunate enough to help roll out the details of our 2006 campaign. Joining me on the dais were Dr. Michota; Geno Merli, MD, from Jefferson Medical College and a frequent speaker at SHM meetings; and Sam Goldhaber, MD, from Harvard’s Brigham and Women’s in Boston.
This year we have set a goal of further engaging the public by telling our patients’ stories, by forming patient affinity groups, by providing the tools for health professionals to provide the best care for DVT and PE, and by continuing to use the media to spread our message.
SHM has a robust set of educational and quality improvement tools in the DVT Resource Room on the SHM Web site at www.hospitalmedicine.org under the “Quality/Patient Safety” tab. There hospitalists can find an SHM DVT workbook to help measure their performance and improve their outcomes. At the SHM 2006 Annual Meeting on May 3, from 8 a.m. to 5:30 p.m., SHM will host a precourse on quality improvement, and one of the key conditions is DVT. SHM hopes to raise funds for future demonstration projects to improve patient outcomes in DVT and even to set up skilled mentors who can help hospitalists trying to affect change at their hospitals for the first time.
SHM is a young, enthusiastic organization that lacks the cynicism of entrenchment. We actually do believe with some help and support we can make quality matter, even without pay for performance and before regulated performance standards.
We see the DVT Awareness Coalition as a template for SHM’s call to action. It involves participation across the continuum involving other physicians, nurses, pharmacists, and patients. It is proactive and targeted with not only improving public knowledge, but recognizing that maybe not every doctor and nurse knows all the latest information, either. It is focused on making a tangible difference, not just writing a white paper or a guideline and declaring victory. It is about saving lives in 2005 and again in 2006. It is about multiplying the efforts of SHM by the multiple of the number of hospitals that now have hospitalists.
There is much promise to hospital medicine. Some see this as a future play with only a foundation being built today. There are surely many great things ahead for hospital medicine as we grow to more than 30,000 hospitalists at virtually every hospital in America. There are many skills left for us to learn. But hospitalists and SHM are making a difference today. We are not doing it alone, but through teamwork and coalition-building. We are proud to be a partner in the DVT Awareness Coalition and we are glad to provide leadership when asked. The payoff is in the lives we have saved and the lives we have changed for the better. TH
Dr. Wellikson has been CEO of SHM since 2000.
March is an important month for SHM. It is DVT Awareness Month, and once again SHM is leading a coalition of almost 40 organizations to raise the understanding of this disease. DVT causes complications that kill more people every year than AIDS and breast cancer combined. This coalition includes the American College of Physicians, the American Public Health Association, the American College of Chest Physicians, the American Society of Health System Pharmacists, the American Association of Critical Care Nurses, and many more.
The goals of the coalition are to use our knowledge and influence to inform not only the public at large, but health professionals as well. And if our success in 2005 is any measure, the DVT Awareness campaign has really had an impact.
Last year more than 400 million people saw on TV or read our message in magazines and newspapers. Utilizing the compelling story of our national spokesperson, Melanie Bloom, a mother of three girls who lost her young, athletic NBC war-correspondent husband, David, to a fatal pulmonary embolism (PE), our message was seen on “Larry King Live” on CNN, on the “Jane Pauley Show,” on “Access Hollywood,” and in Ladies Home Journal.
Often Melanie was accompanied by hospitalists such as Frank Michota, MD, the head of the Hospital Medicine Division at Cleveland Clinic. Dr. Michota answered the clinical questions in the interviews. Who can forget when Larry King turned to Dr. Michota and asked, “Are you a cardiologist?”
“No, Larry, I am a hospitalist,” said Dr. Michota.
And when Larry King asked “What is a hospitalist?” Dr. Michota spread the gospel according to hospital medicine to a nationwide audience.
Later in the year a billboard on Rockefeller Center in New York City proclaimed the DVT Awareness message along with the SHM logo. If you can make it there, you can make it anywhere.
But this campaign isn’t just about TV appearances and magazine articles. This is about using awareness to save lives. And save lives we did. More than a thousand letters and e-mails were sent to the coalition in 2005 from patients and family members with personal stories of how exposure to our campaign led them to go to their doctors or show up in an ED. They were treated early for DVT—before they developed a potentially fatal PE. They credit the DVT Awareness Campaign with saving their lives.
In 2006 SHM is back at the head of the coalition. In January at the National Press Club, I was fortunate enough to help roll out the details of our 2006 campaign. Joining me on the dais were Dr. Michota; Geno Merli, MD, from Jefferson Medical College and a frequent speaker at SHM meetings; and Sam Goldhaber, MD, from Harvard’s Brigham and Women’s in Boston.
This year we have set a goal of further engaging the public by telling our patients’ stories, by forming patient affinity groups, by providing the tools for health professionals to provide the best care for DVT and PE, and by continuing to use the media to spread our message.
SHM has a robust set of educational and quality improvement tools in the DVT Resource Room on the SHM Web site at www.hospitalmedicine.org under the “Quality/Patient Safety” tab. There hospitalists can find an SHM DVT workbook to help measure their performance and improve their outcomes. At the SHM 2006 Annual Meeting on May 3, from 8 a.m. to 5:30 p.m., SHM will host a precourse on quality improvement, and one of the key conditions is DVT. SHM hopes to raise funds for future demonstration projects to improve patient outcomes in DVT and even to set up skilled mentors who can help hospitalists trying to affect change at their hospitals for the first time.
SHM is a young, enthusiastic organization that lacks the cynicism of entrenchment. We actually do believe with some help and support we can make quality matter, even without pay for performance and before regulated performance standards.
We see the DVT Awareness Coalition as a template for SHM’s call to action. It involves participation across the continuum involving other physicians, nurses, pharmacists, and patients. It is proactive and targeted with not only improving public knowledge, but recognizing that maybe not every doctor and nurse knows all the latest information, either. It is focused on making a tangible difference, not just writing a white paper or a guideline and declaring victory. It is about saving lives in 2005 and again in 2006. It is about multiplying the efforts of SHM by the multiple of the number of hospitals that now have hospitalists.
There is much promise to hospital medicine. Some see this as a future play with only a foundation being built today. There are surely many great things ahead for hospital medicine as we grow to more than 30,000 hospitalists at virtually every hospital in America. There are many skills left for us to learn. But hospitalists and SHM are making a difference today. We are not doing it alone, but through teamwork and coalition-building. We are proud to be a partner in the DVT Awareness Coalition and we are glad to provide leadership when asked. The payoff is in the lives we have saved and the lives we have changed for the better. TH
Dr. Wellikson has been CEO of SHM since 2000.
A Landmark Event

In February we experienced a landmark in the development of the field of hospital medicine with the publication of the premiere issue of the Journal of Hospital Medicine (JHM). The debut of JHM demonstrates that hospital medicine is maturing as a field and—even more importantly—that it is developing as a new field with specific issues relevant to its practice.
It is difficult to overestimate the critical role that our journal will play in the growth of our field. The content for the inaugural issue of JHM reflects the depth and breadth of hospital medicine—community acquired pneumonia, palliative care, gastrointestinal bleeding, geriatrics, and a patient’s perspective on hospital care. The many authors who submitted their manuscripts took a leap of faith that our journal would be a respected and widely read vehicle for disseminating their hard work. This leap is even greater given that JHM is not yet listed in PubMed. Nonetheless these authors believe that JHM will thrive, be well read, and influence practice and patient care.
I agree because I know the talent of hospitalists and the potential of our field. The first issue of JHM also included a supplement devoted to the core competencies in hospital medicine. These core competencies represent another milestone in the growth of our field. With the core competencies we have outlined the specific knowledge, skills, and attitudes that define who we are and what we do.
Bringing a journal from concept to reality takes a Herculean effort by many people. I especially want to thank Mark Williams, MD, editor of JHM, for his leadership and grand vision for JHM that reflects our society and field so well. I also want to thank the associate editors and editorial board for giving their time, energy, and expertise to our journal.
I want to share my gratitude and appreciation for Larry Wellikson, MD, the CEO of SHM, who took an idea and mandate presented by the SHM Board of Directors and “operationalized” it in the most effective way. Finally, I want to thank Vickie Thaw, associate publisher at John Wiley & Sons, and her publishing team who have been such great partners in this endeavor.
Growth in Research at the SHM
Papers published in JHM represent only the tip of the iceberg of research in hospital medicine. This year we had 176 abstracts submitted for presentation at our annual meeting in May. These abstracts in research, innovations, and vignettes reflect the enthusiasm, interest, and dedication of many hospitalists. I am always impressed as I read the abstracts and wander through the poster session at the amount of work and creativity represented.
What is even more impressive about these abstracts is that they reflect the breadth of hospital medicine—adult medicine and pediatrics; academic and community hospitals; clinical work and administration; internal medicine, family practice, and pediatrics; disease-specific treatments; and system approaches to care. This year for the first time we will publish the abstracts in a supplement to both The Hospitalist and JHM. All hospitalists who have an abstract accepted for the meeting will be able to cite their work. The supplement marks another advance for our society and field.
I hope that many of you who have submitted abstracts will consider turning them into manuscripts and submitting to JHM. Abstracts whet the appetite to know more, and papers provide the details to improve care.
The Importance of Pursuing Research at SHM
These efforts are critical to our field and represent one visible way that SHM pursues research. SHM must pursue research because it helps define our field. We must ensure that the questions asked are relevant to hospital medicine and that the interventions tested and solutions advocated reflect the real world.
While we welcome anyone to pursue research in hospital medicine and how to improve the care of hospitalized patients, we must ensure that hospitalists play a key role in conducting this research. Research conducted by non-hospitalists may advocate for unrealistic interventions or result in research that is not representative of our field. As the organization that represents hospitalists, SHM can also ensure that research asks the right questions and finds practical solutions with real-world applicability.
For example, SHM should promote:
- Research about best practices, innovations in care delivery, and implementation of known beneficial treatments;
- New approaches to system issues, including error reduction, inpatient-outpatient communication, information systems and transitions; and
- Clinical trials of common inpatient conditions, such as pneumonia and acute decompensated heart failure.
By playing a central role in research, SHM can also advocate for community-based initiatives that ensure research occurs where the majority of patients are cared for.
If we fail to lead in research someone else will, and others will be able to define best practices in hospital medicine. We should not let others define hospital medicine. We took a critical step in defining our field by developing and publishing the core competencies in hospital medicine. Research will be another important way for us to delineate our field. Finally, if SHM does not pursue research we risk losing our academic credentials as a society and a field. Ultimately it will be difficult to succeed as a field and specialty if we do not succeed in academic centers because that is where students and residents—the hospitalists of tomorrow—choose their careers. Hospitalists are great teachers and role models for students and residents. However, in order to ensure that the role models and teachers flourish, we need to pursue research so hospital medicine remains a legitimate part of the academic mission.
SHM Research Initiatives
Although JHM may be the most visible sign of research at SHM, it is not the only one. Research projects directly sponsored by SHM include a demonstration project evaluating interventions to improve care of patients with heart failure, a planned survey of hospitalist involvement in managing heart failure in the emergency department and observation units, and a project to develop and evaluate a tool kit to support discharge planning for elders.
I am especially proud that each of these projects involves community and academic hospitalist programs. The SHM Research Committee, chaired by Andy Auerbach, MD, has played a key role in defining a vision for research at the SHM, and I thank Dr. Auerbach and the committee for their efforts and guidance. I am also delighted that SHM recently hired Kathleen Kerr as a senior advisor for research. Kerr’s extensive experience with hospitalists, quality improvement, and research at the University of California, San Francisco, makes her the ideal person to help spearhead this important initiative at SHM. Taken together we have a strong foundation for our research initiative and ensuring that SHM plays a key role in helping to define and shepherd research in hospital medicine.
The Future of Research at SHM
As difficult as it is to publish the first issue of a new journal, the real challenge will be to publish the second issue and beyond. Sustaining the quality and breadth reflected in the first issue will take the combined efforts of the entire editorial staff at JHM, all hospitalists, and all others interested in improving the care of hospitalized patients.
The good news is that, as reflected in our abstract submissions, there is a deep pool of good work in hospital medicine to write about and publish. The other good news is that our field is one in which many of the best innovations and much of the important research comes from community settings and not just academic centers. In fact our strength in research comes from the fact that we can draw from both academic and community programs to create new, “generalizable” knowledge. An even greater strength is when these programs collaborate to take advantage of the best that each has to offer to research.
I encourage each of us to think about the work we are doing and to think about what innovative, creative, or successful program should be shared and implore each of us to submit our work to JHM. Help make JHM the best source for innovation and best practices in hospital medicine. Help shape JHM into the best possible journal it can be—the one you open right away and read through because it is so relevant to your practice.
As our field grows we will look back on this moment as a critical landmark in the development of our field. Hold on to your first issue: It may be a valuable collector’s item when volume 50 is being published and JHM is one of the world’s leading journals. What practices will we look back on and laugh at? What practices will have survived years of scrutiny? What will our field look like? Only time will tell. Read JHM to find out. TH
SHM President Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
In February we experienced a landmark in the development of the field of hospital medicine with the publication of the premiere issue of the Journal of Hospital Medicine (JHM). The debut of JHM demonstrates that hospital medicine is maturing as a field and—even more importantly—that it is developing as a new field with specific issues relevant to its practice.
It is difficult to overestimate the critical role that our journal will play in the growth of our field. The content for the inaugural issue of JHM reflects the depth and breadth of hospital medicine—community acquired pneumonia, palliative care, gastrointestinal bleeding, geriatrics, and a patient’s perspective on hospital care. The many authors who submitted their manuscripts took a leap of faith that our journal would be a respected and widely read vehicle for disseminating their hard work. This leap is even greater given that JHM is not yet listed in PubMed. Nonetheless these authors believe that JHM will thrive, be well read, and influence practice and patient care.
I agree because I know the talent of hospitalists and the potential of our field. The first issue of JHM also included a supplement devoted to the core competencies in hospital medicine. These core competencies represent another milestone in the growth of our field. With the core competencies we have outlined the specific knowledge, skills, and attitudes that define who we are and what we do.
Bringing a journal from concept to reality takes a Herculean effort by many people. I especially want to thank Mark Williams, MD, editor of JHM, for his leadership and grand vision for JHM that reflects our society and field so well. I also want to thank the associate editors and editorial board for giving their time, energy, and expertise to our journal.
I want to share my gratitude and appreciation for Larry Wellikson, MD, the CEO of SHM, who took an idea and mandate presented by the SHM Board of Directors and “operationalized” it in the most effective way. Finally, I want to thank Vickie Thaw, associate publisher at John Wiley & Sons, and her publishing team who have been such great partners in this endeavor.
Growth in Research at the SHM
Papers published in JHM represent only the tip of the iceberg of research in hospital medicine. This year we had 176 abstracts submitted for presentation at our annual meeting in May. These abstracts in research, innovations, and vignettes reflect the enthusiasm, interest, and dedication of many hospitalists. I am always impressed as I read the abstracts and wander through the poster session at the amount of work and creativity represented.
What is even more impressive about these abstracts is that they reflect the breadth of hospital medicine—adult medicine and pediatrics; academic and community hospitals; clinical work and administration; internal medicine, family practice, and pediatrics; disease-specific treatments; and system approaches to care. This year for the first time we will publish the abstracts in a supplement to both The Hospitalist and JHM. All hospitalists who have an abstract accepted for the meeting will be able to cite their work. The supplement marks another advance for our society and field.
I hope that many of you who have submitted abstracts will consider turning them into manuscripts and submitting to JHM. Abstracts whet the appetite to know more, and papers provide the details to improve care.
The Importance of Pursuing Research at SHM
These efforts are critical to our field and represent one visible way that SHM pursues research. SHM must pursue research because it helps define our field. We must ensure that the questions asked are relevant to hospital medicine and that the interventions tested and solutions advocated reflect the real world.
While we welcome anyone to pursue research in hospital medicine and how to improve the care of hospitalized patients, we must ensure that hospitalists play a key role in conducting this research. Research conducted by non-hospitalists may advocate for unrealistic interventions or result in research that is not representative of our field. As the organization that represents hospitalists, SHM can also ensure that research asks the right questions and finds practical solutions with real-world applicability.
For example, SHM should promote:
- Research about best practices, innovations in care delivery, and implementation of known beneficial treatments;
- New approaches to system issues, including error reduction, inpatient-outpatient communication, information systems and transitions; and
- Clinical trials of common inpatient conditions, such as pneumonia and acute decompensated heart failure.
By playing a central role in research, SHM can also advocate for community-based initiatives that ensure research occurs where the majority of patients are cared for.
If we fail to lead in research someone else will, and others will be able to define best practices in hospital medicine. We should not let others define hospital medicine. We took a critical step in defining our field by developing and publishing the core competencies in hospital medicine. Research will be another important way for us to delineate our field. Finally, if SHM does not pursue research we risk losing our academic credentials as a society and a field. Ultimately it will be difficult to succeed as a field and specialty if we do not succeed in academic centers because that is where students and residents—the hospitalists of tomorrow—choose their careers. Hospitalists are great teachers and role models for students and residents. However, in order to ensure that the role models and teachers flourish, we need to pursue research so hospital medicine remains a legitimate part of the academic mission.
SHM Research Initiatives
Although JHM may be the most visible sign of research at SHM, it is not the only one. Research projects directly sponsored by SHM include a demonstration project evaluating interventions to improve care of patients with heart failure, a planned survey of hospitalist involvement in managing heart failure in the emergency department and observation units, and a project to develop and evaluate a tool kit to support discharge planning for elders.
I am especially proud that each of these projects involves community and academic hospitalist programs. The SHM Research Committee, chaired by Andy Auerbach, MD, has played a key role in defining a vision for research at the SHM, and I thank Dr. Auerbach and the committee for their efforts and guidance. I am also delighted that SHM recently hired Kathleen Kerr as a senior advisor for research. Kerr’s extensive experience with hospitalists, quality improvement, and research at the University of California, San Francisco, makes her the ideal person to help spearhead this important initiative at SHM. Taken together we have a strong foundation for our research initiative and ensuring that SHM plays a key role in helping to define and shepherd research in hospital medicine.
The Future of Research at SHM
As difficult as it is to publish the first issue of a new journal, the real challenge will be to publish the second issue and beyond. Sustaining the quality and breadth reflected in the first issue will take the combined efforts of the entire editorial staff at JHM, all hospitalists, and all others interested in improving the care of hospitalized patients.
The good news is that, as reflected in our abstract submissions, there is a deep pool of good work in hospital medicine to write about and publish. The other good news is that our field is one in which many of the best innovations and much of the important research comes from community settings and not just academic centers. In fact our strength in research comes from the fact that we can draw from both academic and community programs to create new, “generalizable” knowledge. An even greater strength is when these programs collaborate to take advantage of the best that each has to offer to research.
I encourage each of us to think about the work we are doing and to think about what innovative, creative, or successful program should be shared and implore each of us to submit our work to JHM. Help make JHM the best source for innovation and best practices in hospital medicine. Help shape JHM into the best possible journal it can be—the one you open right away and read through because it is so relevant to your practice.
As our field grows we will look back on this moment as a critical landmark in the development of our field. Hold on to your first issue: It may be a valuable collector’s item when volume 50 is being published and JHM is one of the world’s leading journals. What practices will we look back on and laugh at? What practices will have survived years of scrutiny? What will our field look like? Only time will tell. Read JHM to find out. TH
SHM President Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
In February we experienced a landmark in the development of the field of hospital medicine with the publication of the premiere issue of the Journal of Hospital Medicine (JHM). The debut of JHM demonstrates that hospital medicine is maturing as a field and—even more importantly—that it is developing as a new field with specific issues relevant to its practice.
It is difficult to overestimate the critical role that our journal will play in the growth of our field. The content for the inaugural issue of JHM reflects the depth and breadth of hospital medicine—community acquired pneumonia, palliative care, gastrointestinal bleeding, geriatrics, and a patient’s perspective on hospital care. The many authors who submitted their manuscripts took a leap of faith that our journal would be a respected and widely read vehicle for disseminating their hard work. This leap is even greater given that JHM is not yet listed in PubMed. Nonetheless these authors believe that JHM will thrive, be well read, and influence practice and patient care.
I agree because I know the talent of hospitalists and the potential of our field. The first issue of JHM also included a supplement devoted to the core competencies in hospital medicine. These core competencies represent another milestone in the growth of our field. With the core competencies we have outlined the specific knowledge, skills, and attitudes that define who we are and what we do.
Bringing a journal from concept to reality takes a Herculean effort by many people. I especially want to thank Mark Williams, MD, editor of JHM, for his leadership and grand vision for JHM that reflects our society and field so well. I also want to thank the associate editors and editorial board for giving their time, energy, and expertise to our journal.
I want to share my gratitude and appreciation for Larry Wellikson, MD, the CEO of SHM, who took an idea and mandate presented by the SHM Board of Directors and “operationalized” it in the most effective way. Finally, I want to thank Vickie Thaw, associate publisher at John Wiley & Sons, and her publishing team who have been such great partners in this endeavor.
Growth in Research at the SHM
Papers published in JHM represent only the tip of the iceberg of research in hospital medicine. This year we had 176 abstracts submitted for presentation at our annual meeting in May. These abstracts in research, innovations, and vignettes reflect the enthusiasm, interest, and dedication of many hospitalists. I am always impressed as I read the abstracts and wander through the poster session at the amount of work and creativity represented.
What is even more impressive about these abstracts is that they reflect the breadth of hospital medicine—adult medicine and pediatrics; academic and community hospitals; clinical work and administration; internal medicine, family practice, and pediatrics; disease-specific treatments; and system approaches to care. This year for the first time we will publish the abstracts in a supplement to both The Hospitalist and JHM. All hospitalists who have an abstract accepted for the meeting will be able to cite their work. The supplement marks another advance for our society and field.
I hope that many of you who have submitted abstracts will consider turning them into manuscripts and submitting to JHM. Abstracts whet the appetite to know more, and papers provide the details to improve care.
The Importance of Pursuing Research at SHM
These efforts are critical to our field and represent one visible way that SHM pursues research. SHM must pursue research because it helps define our field. We must ensure that the questions asked are relevant to hospital medicine and that the interventions tested and solutions advocated reflect the real world.
While we welcome anyone to pursue research in hospital medicine and how to improve the care of hospitalized patients, we must ensure that hospitalists play a key role in conducting this research. Research conducted by non-hospitalists may advocate for unrealistic interventions or result in research that is not representative of our field. As the organization that represents hospitalists, SHM can also ensure that research asks the right questions and finds practical solutions with real-world applicability.
For example, SHM should promote:
- Research about best practices, innovations in care delivery, and implementation of known beneficial treatments;
- New approaches to system issues, including error reduction, inpatient-outpatient communication, information systems and transitions; and
- Clinical trials of common inpatient conditions, such as pneumonia and acute decompensated heart failure.
By playing a central role in research, SHM can also advocate for community-based initiatives that ensure research occurs where the majority of patients are cared for.
If we fail to lead in research someone else will, and others will be able to define best practices in hospital medicine. We should not let others define hospital medicine. We took a critical step in defining our field by developing and publishing the core competencies in hospital medicine. Research will be another important way for us to delineate our field. Finally, if SHM does not pursue research we risk losing our academic credentials as a society and a field. Ultimately it will be difficult to succeed as a field and specialty if we do not succeed in academic centers because that is where students and residents—the hospitalists of tomorrow—choose their careers. Hospitalists are great teachers and role models for students and residents. However, in order to ensure that the role models and teachers flourish, we need to pursue research so hospital medicine remains a legitimate part of the academic mission.
SHM Research Initiatives
Although JHM may be the most visible sign of research at SHM, it is not the only one. Research projects directly sponsored by SHM include a demonstration project evaluating interventions to improve care of patients with heart failure, a planned survey of hospitalist involvement in managing heart failure in the emergency department and observation units, and a project to develop and evaluate a tool kit to support discharge planning for elders.
I am especially proud that each of these projects involves community and academic hospitalist programs. The SHM Research Committee, chaired by Andy Auerbach, MD, has played a key role in defining a vision for research at the SHM, and I thank Dr. Auerbach and the committee for their efforts and guidance. I am also delighted that SHM recently hired Kathleen Kerr as a senior advisor for research. Kerr’s extensive experience with hospitalists, quality improvement, and research at the University of California, San Francisco, makes her the ideal person to help spearhead this important initiative at SHM. Taken together we have a strong foundation for our research initiative and ensuring that SHM plays a key role in helping to define and shepherd research in hospital medicine.
The Future of Research at SHM
As difficult as it is to publish the first issue of a new journal, the real challenge will be to publish the second issue and beyond. Sustaining the quality and breadth reflected in the first issue will take the combined efforts of the entire editorial staff at JHM, all hospitalists, and all others interested in improving the care of hospitalized patients.
The good news is that, as reflected in our abstract submissions, there is a deep pool of good work in hospital medicine to write about and publish. The other good news is that our field is one in which many of the best innovations and much of the important research comes from community settings and not just academic centers. In fact our strength in research comes from the fact that we can draw from both academic and community programs to create new, “generalizable” knowledge. An even greater strength is when these programs collaborate to take advantage of the best that each has to offer to research.
I encourage each of us to think about the work we are doing and to think about what innovative, creative, or successful program should be shared and implore each of us to submit our work to JHM. Help make JHM the best source for innovation and best practices in hospital medicine. Help shape JHM into the best possible journal it can be—the one you open right away and read through because it is so relevant to your practice.
As our field grows we will look back on this moment as a critical landmark in the development of our field. Hold on to your first issue: It may be a valuable collector’s item when volume 50 is being published and JHM is one of the world’s leading journals. What practices will we look back on and laugh at? What practices will have survived years of scrutiny? What will our field look like? Only time will tell. Read JHM to find out. TH
SHM President Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
The Gender Factor
In 1980 women physicians represented 11.6% of all U.S. physicians. In 2003 they represented 26% of the total physician population.1 Drawing from the ranks of internal medicine and pediatrics, in which women physicians represent 41.8% and 65.6% of all residents, hospital medicine will likely reap the benefits of these increasing numbers.2 Indeed, hospital medicine appears to offer many advantages for women: an intrinsically collaborative working environment, flexible work hours, and the opportunity to participate in forming the structure for a new specialty. But do enough opportunities for advancement exist in this relatively young specialty?
The Hospitalist recently talked with women hospitalists, SHM leadership, and a researcher on gender discrimination in academic medicine. All shared their perceptions about how hospital medicine fares regarding inclusion of women—both in the ranks and in leadership positions.
A Career that Works
“As a woman hospitalist, I’ve had many opportunities to advocate for patient safety and quality being the primary guiding principle in reorganizing care,” says Lakshmi Halasyamani, MD, associate chair, Department of Internal Medicine and an academic hospitalist at St. Joseph Mercy Hospital, Ann Arbor, Mich. “I think as women we do juggle a lot of responsibilities, but I think those skills probably uniquely position us to be very effective in managing groups and being members and leaders of teams.”
As a mother of two young children, Dr. Halasyamani enjoys the flexibility of her current position. “I have a very busy life, but I make sure I have time to do the other parts of my life because those will never come back to me. Today, I went to my daughter’s school and helped her class with some of their math problems, and I chair a multicultural committee at her school as well.”
She finds that she brings the same type of organizational skills to both her working and family life. “Whether it’s preparing for a school assembly or preparing for a patient safety committee meeting,” explains Dr. Halasyamani, “there just isn’t time to focus on what is not important or to come unprepared. Every minute is incredibly precious.”
Like Dr. Halasyamani, Sheri Chernetsky Tejedor, MD, a clinical instructor of medicine at Emory University School of Medicine in Atlanta, has also been able to carve out a clinical and academic track that suits her present needs for family time. Under a supportive supervisor, Mark Williams, MD, FACP, professor of medicine and director, Emory Hospital Medicine Unit, and editor of the Journal of Hospital Medicine, Dr. Tejedor has worked part time as a hospitalist in a nearby community hospital; has worked in academia, including writing and research in quality improvement; and essentially has been a full-time mother when she is home. “I haven’t felt that any doors have closed, and the only ones that have closed are ones that I’ve closed myself—just accepting that I can’t do everything,” says Dr. Tejedor.
According to the AMA, 62.6% of all women physicians fall within the specialties of internal medicine, pediatrics, family medicine, obstetrics/gynecology, psychiatry, and anesthesiology.1 That is one reason the numbers of women in hospital medicine are also increasing, says Larry Wellikson, MD, FACP, CEO of SHM.
“Because hospitalists come from the ranks of pediatricians and internists, as those specialties attract more women, I think they will also find hospital medicine very attractive as they are looking for their career choice,” says Dr. Wellikson.

—Lakshmi Halasyamani, MD
Approaching Parity?
Although SHM does not currently keep statistics on percentages of women in the organization, many hospitalist services point to increasing numbers of women in their departments. For instance, SHM Past President Robert Wachter, MD, FACP, director of the hospitalist group at the University of California, San Francisco, reports that 57% (12 out of 21) of the hospitalists in his group are women. This majority does not stem from deliberate recruiting on his part.
“My goal here has been to recruit and retain the best people. I couldn’t care less whether they are women or men,” says Dr. Wachter. “I would begin to care if we were so skewed in one direction or the other that it might indicate that we weren’t providing a positive environment for either women or men. But our group has grown organically and it has just turned out that we’ve ended up with more women than men.”
Leadership Opportunities in Medicine
While overall increases in the numbers of women physicians can be seen as a hopeful sign, these percentages may mask the reality for women trying to achieve parity in leadership roles. In fact, the percentages of women in leadership positions in academic medicine remain low: For example, only 11% of department chairs in medical schools are women, and 10% of medical school deans are women.1
A higher percentage of women in a particular specialty does not necessarily translate into better advancement opportunities, according to statistician Arlene S. Ash, PhD, a research professor in the Department of General Internal Medicine at the Boston University School of Medicine. “Sadly,” she says, “the main thing you can predict about a specialty with more women is that it will be less well-paid overall.”
Many committee assignments and semi-leadership positions in the academic medicine arena are informally awarded, and they often go to men. “Often these are innocent decisions,” explains Dr. Ash. “The positions carry perks, and perhaps some regular funding, and can be stepping stones to later promotion, but they usually go to the person who pops into the mind of the administrator making the decision.”
It takes “incredible vigilance,” says Dr. Ash, “to see your way past the prejudiced lens with which we all, having grown up in this society, view the relative value of men’s and women’s contributions.”
To achieve more parity for women, Dr. Ash believes it’s necessary to more closely scrutinize and to set standards for leadership selection processes. Currently, she explains, “There is no comprehensive attempt to cast a wide net, to consider all who might be appropriate, and to ensure a non-sexist, non-biased process for choosing people to get such positions. Even in departments with more than 50% women, and even where the problem is recognized, most of these ‘gateway’ opportunities still go to guys.”
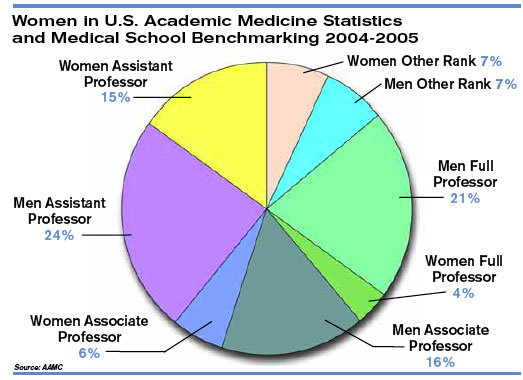
Hospitalists Breaking the Mold?
Those interviewed believe hospital medicine, as a new specialty, may have a chance to break the traditional molds established by more entrenched medical school specialties.
“We’re inventing this entire thing [the hospital medicine specialty] as we go along, so we have not had time to develop an ‘old boys’ network,’” quips Dr. Wachter. “The hope is that if you start a field now, it will not develop along those lines. As we look at those holding leadership roles at individual hospitals and in the society, you find that talented people rise to the top. If you start with a neutral playing field without the tradition and history of the smoke-filled room, it turns out that people sort out on their skills and their interests.”
“I think hospital medicine is a very accessible profession for women on a number of levels,” says Dr. Wellikson. “This is a young, growing, evolving field—as opposed to some of the more static fields in medicine, like orthopedics or thoracic surgery. One of the hallmarks of hospital medicine is creating true teams of health professionals. Women come in as equals, with good ideas, and I think this is mirrored on the SHM Board.”
Currently, four of the 12 SHM board members are women; Jean Huddleston, MD, of the Mayo Clinic is a past president; and the incoming president, Mary Jo Gorman, MD, of IPC, is also a woman. “We [the Society of Hospital Medicine] are very much an open tent,” remarks Dr. Wellikson.
According to Sylvia Cheney McKean, MD, FACP, medical director of the Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston, there are pros and cons to hospital medicine being a new specialty.
“In some ways, because [hospital medicine] is a new specialty, women may have been given the opportunity to lead hospitalist programs because early hospitalist services—at least initially—were viewed as experimental,” she says. “Many hospital leaders hired hospitalists to function as ‘super residents’ rather than as leaders. So, therefore, academic institutions didn’t really feel that they had much to lose by hiring women versus men, and many hospitalist leaders—male and female—found themselves functioning as middle managers without necessarily having much input into their job descriptions.
“Even in 2006 some physician administrators hire hospitalists with the expectation that turnover is inevitable as physicians advance to other specialties,” continues Dr. McKean. “Hospital administrators and residency directors may not understand the evolving role of hospitalists as change agents in the hospital setting and may not recognize that hospitalists offer special expertise in addition to on-site availability. So it’s a two-edged sword. A lot of hospital medicine programs, because they have not only young physician leaders, but also proportionately more female physician leaders, may find that they really cannot have the same amount of clout as other established specialties within the department of medicine hierarchy.”
Dr. Halasyamani believes that the male hierarchy may be changing. In hospital medicine, she notes, “because the emphasis in inpatient care delivery is so team focused, the leaders in hospital medicine who are able to best meet those goals and have those skills are really the ones who are being given the most opportunity. If the structures within organizations are very hierarchical, then care delivery ends up looking that way. But if the leadership and decision-making structures are more collaborative, then I think care reflects that.”
At her institution, Dr. Halasyamani has had numerous opportunities to help build some of those new structures. For example, in the past year, she helped form an institutional quality and patient safety collaborative practice team, which she chaired jointly with the head of nursing. The team “brings together people who touch the patient; they identify the barriers in delivering the type of care that we want to be proud of every time, and to help solve those problems.”
Possible Pitfalls
Can hospital medicine, in fact, succeed in developing new leadership paradigms? Much will depend on consciously constructing new systems for nurturing talent and leaders. “You really have to think through your mechanisms for recognizing and rewarding achievement and ask if those mechanisms encourage the behaviors you want to encourage, or do they disadvantage people who do the work that you most want done?” says Dr. Ash.
For example, she says, the collaborative nature of hospital medicine can create problems with career advancement. “To do something meaningful, you may need to involve 20 people on a five-year project,” she explains. “How do you ensure that those people don’t get punished for choosing that work?”
Dr. Ash, together with Boston University colleague Phyllis L. Carr, MD, and Linda Pololi, MD, from Brandeis University (the principal investigator) has started a Josiah Macy Jr. Foundation-funded project to “try to change the culture of academic medicine so that it will better encourage and reward collaborative research,” she says. “This change should benefit the entire academic enterprise—although its immediate goal is to make a common career track for women more viable.
“I want to fix a generic problem about the failure to reward certain kinds of highly desirable activities,” says Dr. Ash. “The current reward system hurts women more than men, but I’m not the slightest bit unhappy—it would be a wonderful thing, actually—for men who do collaborative research to also get the career benefits they deserve.”
Advice for Leaders and Women
Are opportunities for women hospitalists improving? Dr. McKean thinks that “hierarchies exist in hospitals, where surgeons are more powerful than physicians in the department of medicine, which has its own internal hierarchy. I see many more women interviewing for internal medicine slots. And, you could say, that’s great, it’s equalizing out. But I wonder if all it’s going to mean is that the pay scale will go down. I think that’s a real consideration. What we’re seeing now is that the starting salary for physician assistants in the hospital may be more than the starting salary for some physicians in primary care. Adding more women [to a specialty] may not change inequalities. The key is adding more women in the highest leadership positions.”
“The whole process of growing talent needs to be done in a take-control sort of way,” says Dr. Ash. There is a predictable, ongoing need to fill leadership positions, she notes, and “not enough good thought about how to systematically reach out to the entire potential talent pool.”
“Mentorship is very important,” emphasizes Dr. McKean. Her own career as a physician was characterized early on, she says, by a lack of support and mentorship. Twenty-five years later, she hopes things are beginning to change and hospital medicine may in fact set the standard for other specialties for both male and female physicians.
“Medicine is always going to be unpredictable,” she continues. “It will always be stressful. There will be acutely ill patients, and people will return [to the hospital] with unanticipated problems. You cannot change this reality. But you can change how things are structured. The more the Society of Hospital Medicine can give people the tools to identify modifiable risk factors in their own practices, help leaders of the hospitalist services analyze what works and what doesn’t work, and allow for as much diversity as possible within each service, I think that a career in hospital medicine will be sustainable and extremely satisfying, and that people will get promoted. They will find different niches in which they are expert.”
To that end, with Win Whitcomb, MD (SHM co-founder), Dr. McKean approached the SHM to charge a task force to identify what makes for a long and satisfying career in hospital medicine and to develop practice standards. The job-person fit is important, and she advises young women hospitalists to take a look at themselves, define what is important, and then “tailor a schedule around that. If it is important to you to be teaching residents, for example, then you need to be in an academic program. If it is more important to have time off, and to work shifts, then you might want to work at a community hospital. There are a lot of different models,” she says “so you have to look at yourself and your husband and the other issues you have to grapple with in addition to your career.”
Above all Dr. McKean urges women (as well as men) to be receptive to advocates or mentors within their organizations.
Going Forward
Overall, Dr. Wachter sees “the nature of the field [of hospital medicine] as one that involves a lot of collaboration and multidisciplinary work seems to draw a certain kind of person. The kind of person who is most happy and successful in our field is one who likes working closely with nurses, physical therapists, social workers, and hospital administrators, and recognizes that the quality of care and patients’ outcomes are going to be, in large part, dependent on how well that team functions.”
Many younger women and men hospitalists are finding that the job-person fit contributes to a fulfilling work/life balance.
“I chose this field because I was interested in inpatient care,” says Dr. Tejedor, and the flexibility offered by her institution has reinforced that choice. “This [hospital medicine] is a great way to have the best of everything.” TH
Writer Gretchen Henkel is based in California.
References
- Women in Medicine Statistics. Prepared by the Women Physicians Congress from Physician Characteristics and Distribution in the US, 2005 ed., Chicago. AMA Press. Available at www.ama-assn.org/ama1/pub/upload/mm/19/wimstats2005.pdf. Last accessed January 9, 2005.
- Table 2. Distribution of Residents by Specialty, 1994 Compared to 2004. Women in U.S. Academic Medicine: Statistics and Medical School Benchmarking, 2004-2005. Association of American Medical Colleges; page 12. Available at www.aamc.org/members/wim/statistics/stats05/wimstats2005.pdf. Last accessed January 9, 2005.
In 1980 women physicians represented 11.6% of all U.S. physicians. In 2003 they represented 26% of the total physician population.1 Drawing from the ranks of internal medicine and pediatrics, in which women physicians represent 41.8% and 65.6% of all residents, hospital medicine will likely reap the benefits of these increasing numbers.2 Indeed, hospital medicine appears to offer many advantages for women: an intrinsically collaborative working environment, flexible work hours, and the opportunity to participate in forming the structure for a new specialty. But do enough opportunities for advancement exist in this relatively young specialty?
The Hospitalist recently talked with women hospitalists, SHM leadership, and a researcher on gender discrimination in academic medicine. All shared their perceptions about how hospital medicine fares regarding inclusion of women—both in the ranks and in leadership positions.
A Career that Works
“As a woman hospitalist, I’ve had many opportunities to advocate for patient safety and quality being the primary guiding principle in reorganizing care,” says Lakshmi Halasyamani, MD, associate chair, Department of Internal Medicine and an academic hospitalist at St. Joseph Mercy Hospital, Ann Arbor, Mich. “I think as women we do juggle a lot of responsibilities, but I think those skills probably uniquely position us to be very effective in managing groups and being members and leaders of teams.”
As a mother of two young children, Dr. Halasyamani enjoys the flexibility of her current position. “I have a very busy life, but I make sure I have time to do the other parts of my life because those will never come back to me. Today, I went to my daughter’s school and helped her class with some of their math problems, and I chair a multicultural committee at her school as well.”
She finds that she brings the same type of organizational skills to both her working and family life. “Whether it’s preparing for a school assembly or preparing for a patient safety committee meeting,” explains Dr. Halasyamani, “there just isn’t time to focus on what is not important or to come unprepared. Every minute is incredibly precious.”
Like Dr. Halasyamani, Sheri Chernetsky Tejedor, MD, a clinical instructor of medicine at Emory University School of Medicine in Atlanta, has also been able to carve out a clinical and academic track that suits her present needs for family time. Under a supportive supervisor, Mark Williams, MD, FACP, professor of medicine and director, Emory Hospital Medicine Unit, and editor of the Journal of Hospital Medicine, Dr. Tejedor has worked part time as a hospitalist in a nearby community hospital; has worked in academia, including writing and research in quality improvement; and essentially has been a full-time mother when she is home. “I haven’t felt that any doors have closed, and the only ones that have closed are ones that I’ve closed myself—just accepting that I can’t do everything,” says Dr. Tejedor.
According to the AMA, 62.6% of all women physicians fall within the specialties of internal medicine, pediatrics, family medicine, obstetrics/gynecology, psychiatry, and anesthesiology.1 That is one reason the numbers of women in hospital medicine are also increasing, says Larry Wellikson, MD, FACP, CEO of SHM.
“Because hospitalists come from the ranks of pediatricians and internists, as those specialties attract more women, I think they will also find hospital medicine very attractive as they are looking for their career choice,” says Dr. Wellikson.
—Lakshmi Halasyamani, MD
Approaching Parity?
Although SHM does not currently keep statistics on percentages of women in the organization, many hospitalist services point to increasing numbers of women in their departments. For instance, SHM Past President Robert Wachter, MD, FACP, director of the hospitalist group at the University of California, San Francisco, reports that 57% (12 out of 21) of the hospitalists in his group are women. This majority does not stem from deliberate recruiting on his part.
“My goal here has been to recruit and retain the best people. I couldn’t care less whether they are women or men,” says Dr. Wachter. “I would begin to care if we were so skewed in one direction or the other that it might indicate that we weren’t providing a positive environment for either women or men. But our group has grown organically and it has just turned out that we’ve ended up with more women than men.”
Leadership Opportunities in Medicine
While overall increases in the numbers of women physicians can be seen as a hopeful sign, these percentages may mask the reality for women trying to achieve parity in leadership roles. In fact, the percentages of women in leadership positions in academic medicine remain low: For example, only 11% of department chairs in medical schools are women, and 10% of medical school deans are women.1
A higher percentage of women in a particular specialty does not necessarily translate into better advancement opportunities, according to statistician Arlene S. Ash, PhD, a research professor in the Department of General Internal Medicine at the Boston University School of Medicine. “Sadly,” she says, “the main thing you can predict about a specialty with more women is that it will be less well-paid overall.”
Many committee assignments and semi-leadership positions in the academic medicine arena are informally awarded, and they often go to men. “Often these are innocent decisions,” explains Dr. Ash. “The positions carry perks, and perhaps some regular funding, and can be stepping stones to later promotion, but they usually go to the person who pops into the mind of the administrator making the decision.”
It takes “incredible vigilance,” says Dr. Ash, “to see your way past the prejudiced lens with which we all, having grown up in this society, view the relative value of men’s and women’s contributions.”
To achieve more parity for women, Dr. Ash believes it’s necessary to more closely scrutinize and to set standards for leadership selection processes. Currently, she explains, “There is no comprehensive attempt to cast a wide net, to consider all who might be appropriate, and to ensure a non-sexist, non-biased process for choosing people to get such positions. Even in departments with more than 50% women, and even where the problem is recognized, most of these ‘gateway’ opportunities still go to guys.”
Hospitalists Breaking the Mold?
Those interviewed believe hospital medicine, as a new specialty, may have a chance to break the traditional molds established by more entrenched medical school specialties.
“We’re inventing this entire thing [the hospital medicine specialty] as we go along, so we have not had time to develop an ‘old boys’ network,’” quips Dr. Wachter. “The hope is that if you start a field now, it will not develop along those lines. As we look at those holding leadership roles at individual hospitals and in the society, you find that talented people rise to the top. If you start with a neutral playing field without the tradition and history of the smoke-filled room, it turns out that people sort out on their skills and their interests.”
“I think hospital medicine is a very accessible profession for women on a number of levels,” says Dr. Wellikson. “This is a young, growing, evolving field—as opposed to some of the more static fields in medicine, like orthopedics or thoracic surgery. One of the hallmarks of hospital medicine is creating true teams of health professionals. Women come in as equals, with good ideas, and I think this is mirrored on the SHM Board.”
Currently, four of the 12 SHM board members are women; Jean Huddleston, MD, of the Mayo Clinic is a past president; and the incoming president, Mary Jo Gorman, MD, of IPC, is also a woman. “We [the Society of Hospital Medicine] are very much an open tent,” remarks Dr. Wellikson.
According to Sylvia Cheney McKean, MD, FACP, medical director of the Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston, there are pros and cons to hospital medicine being a new specialty.
“In some ways, because [hospital medicine] is a new specialty, women may have been given the opportunity to lead hospitalist programs because early hospitalist services—at least initially—were viewed as experimental,” she says. “Many hospital leaders hired hospitalists to function as ‘super residents’ rather than as leaders. So, therefore, academic institutions didn’t really feel that they had much to lose by hiring women versus men, and many hospitalist leaders—male and female—found themselves functioning as middle managers without necessarily having much input into their job descriptions.
“Even in 2006 some physician administrators hire hospitalists with the expectation that turnover is inevitable as physicians advance to other specialties,” continues Dr. McKean. “Hospital administrators and residency directors may not understand the evolving role of hospitalists as change agents in the hospital setting and may not recognize that hospitalists offer special expertise in addition to on-site availability. So it’s a two-edged sword. A lot of hospital medicine programs, because they have not only young physician leaders, but also proportionately more female physician leaders, may find that they really cannot have the same amount of clout as other established specialties within the department of medicine hierarchy.”
Dr. Halasyamani believes that the male hierarchy may be changing. In hospital medicine, she notes, “because the emphasis in inpatient care delivery is so team focused, the leaders in hospital medicine who are able to best meet those goals and have those skills are really the ones who are being given the most opportunity. If the structures within organizations are very hierarchical, then care delivery ends up looking that way. But if the leadership and decision-making structures are more collaborative, then I think care reflects that.”
At her institution, Dr. Halasyamani has had numerous opportunities to help build some of those new structures. For example, in the past year, she helped form an institutional quality and patient safety collaborative practice team, which she chaired jointly with the head of nursing. The team “brings together people who touch the patient; they identify the barriers in delivering the type of care that we want to be proud of every time, and to help solve those problems.”
Possible Pitfalls
Can hospital medicine, in fact, succeed in developing new leadership paradigms? Much will depend on consciously constructing new systems for nurturing talent and leaders. “You really have to think through your mechanisms for recognizing and rewarding achievement and ask if those mechanisms encourage the behaviors you want to encourage, or do they disadvantage people who do the work that you most want done?” says Dr. Ash.
For example, she says, the collaborative nature of hospital medicine can create problems with career advancement. “To do something meaningful, you may need to involve 20 people on a five-year project,” she explains. “How do you ensure that those people don’t get punished for choosing that work?”
Dr. Ash, together with Boston University colleague Phyllis L. Carr, MD, and Linda Pololi, MD, from Brandeis University (the principal investigator) has started a Josiah Macy Jr. Foundation-funded project to “try to change the culture of academic medicine so that it will better encourage and reward collaborative research,” she says. “This change should benefit the entire academic enterprise—although its immediate goal is to make a common career track for women more viable.
“I want to fix a generic problem about the failure to reward certain kinds of highly desirable activities,” says Dr. Ash. “The current reward system hurts women more than men, but I’m not the slightest bit unhappy—it would be a wonderful thing, actually—for men who do collaborative research to also get the career benefits they deserve.”
Advice for Leaders and Women
Are opportunities for women hospitalists improving? Dr. McKean thinks that “hierarchies exist in hospitals, where surgeons are more powerful than physicians in the department of medicine, which has its own internal hierarchy. I see many more women interviewing for internal medicine slots. And, you could say, that’s great, it’s equalizing out. But I wonder if all it’s going to mean is that the pay scale will go down. I think that’s a real consideration. What we’re seeing now is that the starting salary for physician assistants in the hospital may be more than the starting salary for some physicians in primary care. Adding more women [to a specialty] may not change inequalities. The key is adding more women in the highest leadership positions.”
“The whole process of growing talent needs to be done in a take-control sort of way,” says Dr. Ash. There is a predictable, ongoing need to fill leadership positions, she notes, and “not enough good thought about how to systematically reach out to the entire potential talent pool.”
“Mentorship is very important,” emphasizes Dr. McKean. Her own career as a physician was characterized early on, she says, by a lack of support and mentorship. Twenty-five years later, she hopes things are beginning to change and hospital medicine may in fact set the standard for other specialties for both male and female physicians.
“Medicine is always going to be unpredictable,” she continues. “It will always be stressful. There will be acutely ill patients, and people will return [to the hospital] with unanticipated problems. You cannot change this reality. But you can change how things are structured. The more the Society of Hospital Medicine can give people the tools to identify modifiable risk factors in their own practices, help leaders of the hospitalist services analyze what works and what doesn’t work, and allow for as much diversity as possible within each service, I think that a career in hospital medicine will be sustainable and extremely satisfying, and that people will get promoted. They will find different niches in which they are expert.”
To that end, with Win Whitcomb, MD (SHM co-founder), Dr. McKean approached the SHM to charge a task force to identify what makes for a long and satisfying career in hospital medicine and to develop practice standards. The job-person fit is important, and she advises young women hospitalists to take a look at themselves, define what is important, and then “tailor a schedule around that. If it is important to you to be teaching residents, for example, then you need to be in an academic program. If it is more important to have time off, and to work shifts, then you might want to work at a community hospital. There are a lot of different models,” she says “so you have to look at yourself and your husband and the other issues you have to grapple with in addition to your career.”
Above all Dr. McKean urges women (as well as men) to be receptive to advocates or mentors within their organizations.
Going Forward
Overall, Dr. Wachter sees “the nature of the field [of hospital medicine] as one that involves a lot of collaboration and multidisciplinary work seems to draw a certain kind of person. The kind of person who is most happy and successful in our field is one who likes working closely with nurses, physical therapists, social workers, and hospital administrators, and recognizes that the quality of care and patients’ outcomes are going to be, in large part, dependent on how well that team functions.”
Many younger women and men hospitalists are finding that the job-person fit contributes to a fulfilling work/life balance.
“I chose this field because I was interested in inpatient care,” says Dr. Tejedor, and the flexibility offered by her institution has reinforced that choice. “This [hospital medicine] is a great way to have the best of everything.” TH
Writer Gretchen Henkel is based in California.
References
- Women in Medicine Statistics. Prepared by the Women Physicians Congress from Physician Characteristics and Distribution in the US, 2005 ed., Chicago. AMA Press. Available at www.ama-assn.org/ama1/pub/upload/mm/19/wimstats2005.pdf. Last accessed January 9, 2005.
- Table 2. Distribution of Residents by Specialty, 1994 Compared to 2004. Women in U.S. Academic Medicine: Statistics and Medical School Benchmarking, 2004-2005. Association of American Medical Colleges; page 12. Available at www.aamc.org/members/wim/statistics/stats05/wimstats2005.pdf. Last accessed January 9, 2005.
In 1980 women physicians represented 11.6% of all U.S. physicians. In 2003 they represented 26% of the total physician population.1 Drawing from the ranks of internal medicine and pediatrics, in which women physicians represent 41.8% and 65.6% of all residents, hospital medicine will likely reap the benefits of these increasing numbers.2 Indeed, hospital medicine appears to offer many advantages for women: an intrinsically collaborative working environment, flexible work hours, and the opportunity to participate in forming the structure for a new specialty. But do enough opportunities for advancement exist in this relatively young specialty?
The Hospitalist recently talked with women hospitalists, SHM leadership, and a researcher on gender discrimination in academic medicine. All shared their perceptions about how hospital medicine fares regarding inclusion of women—both in the ranks and in leadership positions.
A Career that Works
“As a woman hospitalist, I’ve had many opportunities to advocate for patient safety and quality being the primary guiding principle in reorganizing care,” says Lakshmi Halasyamani, MD, associate chair, Department of Internal Medicine and an academic hospitalist at St. Joseph Mercy Hospital, Ann Arbor, Mich. “I think as women we do juggle a lot of responsibilities, but I think those skills probably uniquely position us to be very effective in managing groups and being members and leaders of teams.”
As a mother of two young children, Dr. Halasyamani enjoys the flexibility of her current position. “I have a very busy life, but I make sure I have time to do the other parts of my life because those will never come back to me. Today, I went to my daughter’s school and helped her class with some of their math problems, and I chair a multicultural committee at her school as well.”
She finds that she brings the same type of organizational skills to both her working and family life. “Whether it’s preparing for a school assembly or preparing for a patient safety committee meeting,” explains Dr. Halasyamani, “there just isn’t time to focus on what is not important or to come unprepared. Every minute is incredibly precious.”
Like Dr. Halasyamani, Sheri Chernetsky Tejedor, MD, a clinical instructor of medicine at Emory University School of Medicine in Atlanta, has also been able to carve out a clinical and academic track that suits her present needs for family time. Under a supportive supervisor, Mark Williams, MD, FACP, professor of medicine and director, Emory Hospital Medicine Unit, and editor of the Journal of Hospital Medicine, Dr. Tejedor has worked part time as a hospitalist in a nearby community hospital; has worked in academia, including writing and research in quality improvement; and essentially has been a full-time mother when she is home. “I haven’t felt that any doors have closed, and the only ones that have closed are ones that I’ve closed myself—just accepting that I can’t do everything,” says Dr. Tejedor.
According to the AMA, 62.6% of all women physicians fall within the specialties of internal medicine, pediatrics, family medicine, obstetrics/gynecology, psychiatry, and anesthesiology.1 That is one reason the numbers of women in hospital medicine are also increasing, says Larry Wellikson, MD, FACP, CEO of SHM.
“Because hospitalists come from the ranks of pediatricians and internists, as those specialties attract more women, I think they will also find hospital medicine very attractive as they are looking for their career choice,” says Dr. Wellikson.
—Lakshmi Halasyamani, MD
Approaching Parity?
Although SHM does not currently keep statistics on percentages of women in the organization, many hospitalist services point to increasing numbers of women in their departments. For instance, SHM Past President Robert Wachter, MD, FACP, director of the hospitalist group at the University of California, San Francisco, reports that 57% (12 out of 21) of the hospitalists in his group are women. This majority does not stem from deliberate recruiting on his part.
“My goal here has been to recruit and retain the best people. I couldn’t care less whether they are women or men,” says Dr. Wachter. “I would begin to care if we were so skewed in one direction or the other that it might indicate that we weren’t providing a positive environment for either women or men. But our group has grown organically and it has just turned out that we’ve ended up with more women than men.”
Leadership Opportunities in Medicine
While overall increases in the numbers of women physicians can be seen as a hopeful sign, these percentages may mask the reality for women trying to achieve parity in leadership roles. In fact, the percentages of women in leadership positions in academic medicine remain low: For example, only 11% of department chairs in medical schools are women, and 10% of medical school deans are women.1
A higher percentage of women in a particular specialty does not necessarily translate into better advancement opportunities, according to statistician Arlene S. Ash, PhD, a research professor in the Department of General Internal Medicine at the Boston University School of Medicine. “Sadly,” she says, “the main thing you can predict about a specialty with more women is that it will be less well-paid overall.”
Many committee assignments and semi-leadership positions in the academic medicine arena are informally awarded, and they often go to men. “Often these are innocent decisions,” explains Dr. Ash. “The positions carry perks, and perhaps some regular funding, and can be stepping stones to later promotion, but they usually go to the person who pops into the mind of the administrator making the decision.”
It takes “incredible vigilance,” says Dr. Ash, “to see your way past the prejudiced lens with which we all, having grown up in this society, view the relative value of men’s and women’s contributions.”
To achieve more parity for women, Dr. Ash believes it’s necessary to more closely scrutinize and to set standards for leadership selection processes. Currently, she explains, “There is no comprehensive attempt to cast a wide net, to consider all who might be appropriate, and to ensure a non-sexist, non-biased process for choosing people to get such positions. Even in departments with more than 50% women, and even where the problem is recognized, most of these ‘gateway’ opportunities still go to guys.”
Hospitalists Breaking the Mold?
Those interviewed believe hospital medicine, as a new specialty, may have a chance to break the traditional molds established by more entrenched medical school specialties.
“We’re inventing this entire thing [the hospital medicine specialty] as we go along, so we have not had time to develop an ‘old boys’ network,’” quips Dr. Wachter. “The hope is that if you start a field now, it will not develop along those lines. As we look at those holding leadership roles at individual hospitals and in the society, you find that talented people rise to the top. If you start with a neutral playing field without the tradition and history of the smoke-filled room, it turns out that people sort out on their skills and their interests.”
“I think hospital medicine is a very accessible profession for women on a number of levels,” says Dr. Wellikson. “This is a young, growing, evolving field—as opposed to some of the more static fields in medicine, like orthopedics or thoracic surgery. One of the hallmarks of hospital medicine is creating true teams of health professionals. Women come in as equals, with good ideas, and I think this is mirrored on the SHM Board.”
Currently, four of the 12 SHM board members are women; Jean Huddleston, MD, of the Mayo Clinic is a past president; and the incoming president, Mary Jo Gorman, MD, of IPC, is also a woman. “We [the Society of Hospital Medicine] are very much an open tent,” remarks Dr. Wellikson.
According to Sylvia Cheney McKean, MD, FACP, medical director of the Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston, there are pros and cons to hospital medicine being a new specialty.
“In some ways, because [hospital medicine] is a new specialty, women may have been given the opportunity to lead hospitalist programs because early hospitalist services—at least initially—were viewed as experimental,” she says. “Many hospital leaders hired hospitalists to function as ‘super residents’ rather than as leaders. So, therefore, academic institutions didn’t really feel that they had much to lose by hiring women versus men, and many hospitalist leaders—male and female—found themselves functioning as middle managers without necessarily having much input into their job descriptions.
“Even in 2006 some physician administrators hire hospitalists with the expectation that turnover is inevitable as physicians advance to other specialties,” continues Dr. McKean. “Hospital administrators and residency directors may not understand the evolving role of hospitalists as change agents in the hospital setting and may not recognize that hospitalists offer special expertise in addition to on-site availability. So it’s a two-edged sword. A lot of hospital medicine programs, because they have not only young physician leaders, but also proportionately more female physician leaders, may find that they really cannot have the same amount of clout as other established specialties within the department of medicine hierarchy.”
Dr. Halasyamani believes that the male hierarchy may be changing. In hospital medicine, she notes, “because the emphasis in inpatient care delivery is so team focused, the leaders in hospital medicine who are able to best meet those goals and have those skills are really the ones who are being given the most opportunity. If the structures within organizations are very hierarchical, then care delivery ends up looking that way. But if the leadership and decision-making structures are more collaborative, then I think care reflects that.”
At her institution, Dr. Halasyamani has had numerous opportunities to help build some of those new structures. For example, in the past year, she helped form an institutional quality and patient safety collaborative practice team, which she chaired jointly with the head of nursing. The team “brings together people who touch the patient; they identify the barriers in delivering the type of care that we want to be proud of every time, and to help solve those problems.”
Possible Pitfalls
Can hospital medicine, in fact, succeed in developing new leadership paradigms? Much will depend on consciously constructing new systems for nurturing talent and leaders. “You really have to think through your mechanisms for recognizing and rewarding achievement and ask if those mechanisms encourage the behaviors you want to encourage, or do they disadvantage people who do the work that you most want done?” says Dr. Ash.
For example, she says, the collaborative nature of hospital medicine can create problems with career advancement. “To do something meaningful, you may need to involve 20 people on a five-year project,” she explains. “How do you ensure that those people don’t get punished for choosing that work?”
Dr. Ash, together with Boston University colleague Phyllis L. Carr, MD, and Linda Pololi, MD, from Brandeis University (the principal investigator) has started a Josiah Macy Jr. Foundation-funded project to “try to change the culture of academic medicine so that it will better encourage and reward collaborative research,” she says. “This change should benefit the entire academic enterprise—although its immediate goal is to make a common career track for women more viable.
“I want to fix a generic problem about the failure to reward certain kinds of highly desirable activities,” says Dr. Ash. “The current reward system hurts women more than men, but I’m not the slightest bit unhappy—it would be a wonderful thing, actually—for men who do collaborative research to also get the career benefits they deserve.”
Advice for Leaders and Women
Are opportunities for women hospitalists improving? Dr. McKean thinks that “hierarchies exist in hospitals, where surgeons are more powerful than physicians in the department of medicine, which has its own internal hierarchy. I see many more women interviewing for internal medicine slots. And, you could say, that’s great, it’s equalizing out. But I wonder if all it’s going to mean is that the pay scale will go down. I think that’s a real consideration. What we’re seeing now is that the starting salary for physician assistants in the hospital may be more than the starting salary for some physicians in primary care. Adding more women [to a specialty] may not change inequalities. The key is adding more women in the highest leadership positions.”
“The whole process of growing talent needs to be done in a take-control sort of way,” says Dr. Ash. There is a predictable, ongoing need to fill leadership positions, she notes, and “not enough good thought about how to systematically reach out to the entire potential talent pool.”
“Mentorship is very important,” emphasizes Dr. McKean. Her own career as a physician was characterized early on, she says, by a lack of support and mentorship. Twenty-five years later, she hopes things are beginning to change and hospital medicine may in fact set the standard for other specialties for both male and female physicians.
“Medicine is always going to be unpredictable,” she continues. “It will always be stressful. There will be acutely ill patients, and people will return [to the hospital] with unanticipated problems. You cannot change this reality. But you can change how things are structured. The more the Society of Hospital Medicine can give people the tools to identify modifiable risk factors in their own practices, help leaders of the hospitalist services analyze what works and what doesn’t work, and allow for as much diversity as possible within each service, I think that a career in hospital medicine will be sustainable and extremely satisfying, and that people will get promoted. They will find different niches in which they are expert.”
To that end, with Win Whitcomb, MD (SHM co-founder), Dr. McKean approached the SHM to charge a task force to identify what makes for a long and satisfying career in hospital medicine and to develop practice standards. The job-person fit is important, and she advises young women hospitalists to take a look at themselves, define what is important, and then “tailor a schedule around that. If it is important to you to be teaching residents, for example, then you need to be in an academic program. If it is more important to have time off, and to work shifts, then you might want to work at a community hospital. There are a lot of different models,” she says “so you have to look at yourself and your husband and the other issues you have to grapple with in addition to your career.”
Above all Dr. McKean urges women (as well as men) to be receptive to advocates or mentors within their organizations.
Going Forward
Overall, Dr. Wachter sees “the nature of the field [of hospital medicine] as one that involves a lot of collaboration and multidisciplinary work seems to draw a certain kind of person. The kind of person who is most happy and successful in our field is one who likes working closely with nurses, physical therapists, social workers, and hospital administrators, and recognizes that the quality of care and patients’ outcomes are going to be, in large part, dependent on how well that team functions.”
Many younger women and men hospitalists are finding that the job-person fit contributes to a fulfilling work/life balance.
“I chose this field because I was interested in inpatient care,” says Dr. Tejedor, and the flexibility offered by her institution has reinforced that choice. “This [hospital medicine] is a great way to have the best of everything.” TH
Writer Gretchen Henkel is based in California.
References
- Women in Medicine Statistics. Prepared by the Women Physicians Congress from Physician Characteristics and Distribution in the US, 2005 ed., Chicago. AMA Press. Available at www.ama-assn.org/ama1/pub/upload/mm/19/wimstats2005.pdf. Last accessed January 9, 2005.
- Table 2. Distribution of Residents by Specialty, 1994 Compared to 2004. Women in U.S. Academic Medicine: Statistics and Medical School Benchmarking, 2004-2005. Association of American Medical Colleges; page 12. Available at www.aamc.org/members/wim/statistics/stats05/wimstats2005.pdf. Last accessed January 9, 2005.
Proceedings of the Perioperative Medicine Summit

Summit Co-Directors and Co-Editors:
Amir K. Jaffer, MD, and Franklin A. Michota, Jr., MD
Contents
Foreword: Why perioperative medicine matters more than ever
Amir K. Jaffer, MD, and Franklin A. Michota, Jr., MD, Cleveland Clinic Foundation, Cleveland, OH
The preoperative evaluation and use of laboratory testing
Franklin A. Michota, Jr., MD, Cleveland Clinic Foundation, Cleveland, OH
The surgical burden: How to prevent a crisis in perioperative medicine
Michael F. Roizen, MD, Cleveland Clinic Foundation, Cleveland, OH
Anesthetics and anesthesia techniques: Impact on perioperative management and postoperative outcomes
Brian M. Parker, MD, Cleveland Clinic Foundation, Cleveland, OH
Cardiac risk stratification before noncardiac surgery
Steven L. Cohn, MD, FACP, SUNY Downstate Medical Center, Brooklyn, NY
Perioperative cardiac risk reduction: Doing it right
Andrew D. Auerbach, MD, MPH, University of California, San Francisco, CA
Quality measurement: Who is measuring outcomes and what are patients being told?
Walter G. Maurer, MD, and Christopher J. Hebert, MD, Cleveland Clinic Foundation, Cleveland, OH
Preoperative pulmonary evaluation: Identifying and reducing risks for pulmonary complications
Gerald W. Smetana, MD, Beth Israel Deaconess Medicine Center and Harvard Medical School, Boston, MA
Antibiotic prophylaxis against postoperative wound infections
Steven M. Gordon, MD, Cleveland Clinic Foundation, Cleveland, OH
Managing perioperative risk in the hip fracture patient
Wael K. Barsoum, MD; Robert Helfand, MD; Viktor Krebs, MD; and Christopher Whinney, MD, Cleveland Clinic Foundation, Cleveland, OH
Perioperative management of the bariatric surgery patient: Focus on cardiac and anesthesia considerations
Bipan Chand, MD; David Gugliotti, MD; Philip Schauer, MD; and Karen Steckner, MD, Cleveland Clinic Foundation, Cleveland, OH
Ambulatory anesthesia: Preventing perioperative and postoperative complications
Raymond G. Borkowski, MD, Cleveland Clinic Foundation, Cleveland, OH
Evaluating postoperative fever: A focused approach
James C. Pile, MD, MetroHealth Medical Center, Cleveland, OH
Septic shock in the postoperative patient: Three important management decisions
Ali Jahan, MD, Cleveland Clinic Foundation, Cleveland, OH
Optimizing postoperative pain management
R. Michael Ritchey, MD, Cleveland Clinic Foundation, Cleveland, OH
Nutritional issues in the surgical patient
Douglas L. Seidner, MD, Cleveland Clinic Foundation, Cleveland, OH
Perioperative medication management: A case-based review of general principles
Wael Saber, MD, Cleveland Clinic Foundation, Cleveland, OH
Preventing venous thromboembolism in surgical patients
Franklin A. Michota, Jr., MD, Cleveland Clinic Foundation, Cleveland, OH
Perioperative management of diabetes mellitus: How should we act on the limited evidence?
Byron J. Hoogwerf, MD, Cleveland Clinic Foundation, Cleveland, OH
Anticoagulation management strategies for patients on warfarin who need surgery
Amir K. Jaffer, MD, FHM, Cleveland Clinic Foundation, Cleveland, OH
Perioperative care of the elderly patient
Robert M. Palmer, MD, Cleveland Clinic Foundation, Cleveland, OH
Optimizing the preoperative evaluation of patients with aortic stenosis or congestive heart failure prior to noncardiac surgery
Curtis M. Rimmerman, MD, MBA, Cleveland Clinic Foundation, Cleveland, OH
Minimizing perioperative complications in patients with renal insufficiency
Martin J. Schreiber, Jr., MD, Cleveland Clinic Foundation, Cleveland, OH
Summit Co-Directors and Co-Editors:
Amir K. Jaffer, MD, and Franklin A. Michota, Jr., MD
Contents
Foreword: Why perioperative medicine matters more than ever
Amir K. Jaffer, MD, and Franklin A. Michota, Jr., MD, Cleveland Clinic Foundation, Cleveland, OH
The preoperative evaluation and use of laboratory testing
Franklin A. Michota, Jr., MD, Cleveland Clinic Foundation, Cleveland, OH
The surgical burden: How to prevent a crisis in perioperative medicine
Michael F. Roizen, MD, Cleveland Clinic Foundation, Cleveland, OH
Anesthetics and anesthesia techniques: Impact on perioperative management and postoperative outcomes
Brian M. Parker, MD, Cleveland Clinic Foundation, Cleveland, OH
Cardiac risk stratification before noncardiac surgery
Steven L. Cohn, MD, FACP, SUNY Downstate Medical Center, Brooklyn, NY
Perioperative cardiac risk reduction: Doing it right
Andrew D. Auerbach, MD, MPH, University of California, San Francisco, CA
Quality measurement: Who is measuring outcomes and what are patients being told?
Walter G. Maurer, MD, and Christopher J. Hebert, MD, Cleveland Clinic Foundation, Cleveland, OH
Preoperative pulmonary evaluation: Identifying and reducing risks for pulmonary complications
Gerald W. Smetana, MD, Beth Israel Deaconess Medicine Center and Harvard Medical School, Boston, MA
Antibiotic prophylaxis against postoperative wound infections
Steven M. Gordon, MD, Cleveland Clinic Foundation, Cleveland, OH
Managing perioperative risk in the hip fracture patient
Wael K. Barsoum, MD; Robert Helfand, MD; Viktor Krebs, MD; and Christopher Whinney, MD, Cleveland Clinic Foundation, Cleveland, OH
Perioperative management of the bariatric surgery patient: Focus on cardiac and anesthesia considerations
Bipan Chand, MD; David Gugliotti, MD; Philip Schauer, MD; and Karen Steckner, MD, Cleveland Clinic Foundation, Cleveland, OH
Ambulatory anesthesia: Preventing perioperative and postoperative complications
Raymond G. Borkowski, MD, Cleveland Clinic Foundation, Cleveland, OH
Evaluating postoperative fever: A focused approach
James C. Pile, MD, MetroHealth Medical Center, Cleveland, OH
Septic shock in the postoperative patient: Three important management decisions
Ali Jahan, MD, Cleveland Clinic Foundation, Cleveland, OH
Optimizing postoperative pain management
R. Michael Ritchey, MD, Cleveland Clinic Foundation, Cleveland, OH
Nutritional issues in the surgical patient
Douglas L. Seidner, MD, Cleveland Clinic Foundation, Cleveland, OH
Perioperative medication management: A case-based review of general principles
Wael Saber, MD, Cleveland Clinic Foundation, Cleveland, OH
Preventing venous thromboembolism in surgical patients
Franklin A. Michota, Jr., MD, Cleveland Clinic Foundation, Cleveland, OH
Perioperative management of diabetes mellitus: How should we act on the limited evidence?
Byron J. Hoogwerf, MD, Cleveland Clinic Foundation, Cleveland, OH
Anticoagulation management strategies for patients on warfarin who need surgery
Amir K. Jaffer, MD, FHM, Cleveland Clinic Foundation, Cleveland, OH
Perioperative care of the elderly patient
Robert M. Palmer, MD, Cleveland Clinic Foundation, Cleveland, OH
Optimizing the preoperative evaluation of patients with aortic stenosis or congestive heart failure prior to noncardiac surgery
Curtis M. Rimmerman, MD, MBA, Cleveland Clinic Foundation, Cleveland, OH
Minimizing perioperative complications in patients with renal insufficiency
Martin J. Schreiber, Jr., MD, Cleveland Clinic Foundation, Cleveland, OH
Summit Co-Directors and Co-Editors:
Amir K. Jaffer, MD, and Franklin A. Michota, Jr., MD
Contents
Foreword: Why perioperative medicine matters more than ever
Amir K. Jaffer, MD, and Franklin A. Michota, Jr., MD, Cleveland Clinic Foundation, Cleveland, OH
The preoperative evaluation and use of laboratory testing
Franklin A. Michota, Jr., MD, Cleveland Clinic Foundation, Cleveland, OH
The surgical burden: How to prevent a crisis in perioperative medicine
Michael F. Roizen, MD, Cleveland Clinic Foundation, Cleveland, OH
Anesthetics and anesthesia techniques: Impact on perioperative management and postoperative outcomes
Brian M. Parker, MD, Cleveland Clinic Foundation, Cleveland, OH
Cardiac risk stratification before noncardiac surgery
Steven L. Cohn, MD, FACP, SUNY Downstate Medical Center, Brooklyn, NY
Perioperative cardiac risk reduction: Doing it right
Andrew D. Auerbach, MD, MPH, University of California, San Francisco, CA
Quality measurement: Who is measuring outcomes and what are patients being told?
Walter G. Maurer, MD, and Christopher J. Hebert, MD, Cleveland Clinic Foundation, Cleveland, OH
Preoperative pulmonary evaluation: Identifying and reducing risks for pulmonary complications
Gerald W. Smetana, MD, Beth Israel Deaconess Medicine Center and Harvard Medical School, Boston, MA
Antibiotic prophylaxis against postoperative wound infections
Steven M. Gordon, MD, Cleveland Clinic Foundation, Cleveland, OH
Managing perioperative risk in the hip fracture patient
Wael K. Barsoum, MD; Robert Helfand, MD; Viktor Krebs, MD; and Christopher Whinney, MD, Cleveland Clinic Foundation, Cleveland, OH
Perioperative management of the bariatric surgery patient: Focus on cardiac and anesthesia considerations
Bipan Chand, MD; David Gugliotti, MD; Philip Schauer, MD; and Karen Steckner, MD, Cleveland Clinic Foundation, Cleveland, OH
Ambulatory anesthesia: Preventing perioperative and postoperative complications
Raymond G. Borkowski, MD, Cleveland Clinic Foundation, Cleveland, OH
Evaluating postoperative fever: A focused approach
James C. Pile, MD, MetroHealth Medical Center, Cleveland, OH
Septic shock in the postoperative patient: Three important management decisions
Ali Jahan, MD, Cleveland Clinic Foundation, Cleveland, OH
Optimizing postoperative pain management
R. Michael Ritchey, MD, Cleveland Clinic Foundation, Cleveland, OH
Nutritional issues in the surgical patient
Douglas L. Seidner, MD, Cleveland Clinic Foundation, Cleveland, OH
Perioperative medication management: A case-based review of general principles
Wael Saber, MD, Cleveland Clinic Foundation, Cleveland, OH
Preventing venous thromboembolism in surgical patients
Franklin A. Michota, Jr., MD, Cleveland Clinic Foundation, Cleveland, OH
Perioperative management of diabetes mellitus: How should we act on the limited evidence?
Byron J. Hoogwerf, MD, Cleveland Clinic Foundation, Cleveland, OH
Anticoagulation management strategies for patients on warfarin who need surgery
Amir K. Jaffer, MD, FHM, Cleveland Clinic Foundation, Cleveland, OH
Perioperative care of the elderly patient
Robert M. Palmer, MD, Cleveland Clinic Foundation, Cleveland, OH
Optimizing the preoperative evaluation of patients with aortic stenosis or congestive heart failure prior to noncardiac surgery
Curtis M. Rimmerman, MD, MBA, Cleveland Clinic Foundation, Cleveland, OH
Minimizing perioperative complications in patients with renal insufficiency
Martin J. Schreiber, Jr., MD, Cleveland Clinic Foundation, Cleveland, OH