User login
Cost, Frequency of Emergency Department Revisits Evaluated
Clinical question: What is the cost and frequency of ED revisits within three days and 30 days?
Background: ED revisits lead to a financial and resource utilization burden on the medical system. The costs and rates of these return visits are unknown and limited in characterization.
Study design: Observational study.
Setting: Six states, using Healthcare Cost and Utilization Project databases.
Synopsis: An observational study examined data from 2006-2010 across six states to determine cost and frequency of ED revisits within a 30-day period from initial ED treatment and discharge. The study examined revisit rates within the first three days of discharge, as well as the 30 days following discharge from the initial presentation.
Three-day revisit rates were 8.2%, with 29% resulting in admission; 32% of the revisits took place at a different institution.
The 30-day revisit rate was 19.9%, with 28% resulting in admission. The most common diagnoses were skin and soft tissue infections (23.9%) and abdominal pain (9.7%). The vast majority of revisits (89%) resulted in the same diagnosis as the first encounter.
Cost of the revisits was more difficult to assess, because only one of six states had full data (Florida); the cost data was extrapolated for the other states involved. In Florida, three-day revisit costs accounted for 30.3% of all primary visit costs. Thirty-day revisit costs were 118% of all primary ED visits costs within that time period.
There was not always an indication of whether the revisit was due to a planned revisit, worsening of symptoms, or inadequate initial treatment, however, leaving the evaluation of cost and revisit burden incomplete.
Bottom line: Initial evaluation of ED revisits shows that rates and cost are significant, though the nature of the revisits remains underevaluated. Preliminary data demonstrate that ED revisits are a significant cost to the healthcare system, though the number of preventable revisits remains unknown.
Citation: Duseja R, Bardach NS, Lin GA, et al. Revisit rates and associated costs after and emergency department encounter. Ann Intern Med. 2015;162(11):750-756.
Clinical question: What is the cost and frequency of ED revisits within three days and 30 days?
Background: ED revisits lead to a financial and resource utilization burden on the medical system. The costs and rates of these return visits are unknown and limited in characterization.
Study design: Observational study.
Setting: Six states, using Healthcare Cost and Utilization Project databases.
Synopsis: An observational study examined data from 2006-2010 across six states to determine cost and frequency of ED revisits within a 30-day period from initial ED treatment and discharge. The study examined revisit rates within the first three days of discharge, as well as the 30 days following discharge from the initial presentation.
Three-day revisit rates were 8.2%, with 29% resulting in admission; 32% of the revisits took place at a different institution.
The 30-day revisit rate was 19.9%, with 28% resulting in admission. The most common diagnoses were skin and soft tissue infections (23.9%) and abdominal pain (9.7%). The vast majority of revisits (89%) resulted in the same diagnosis as the first encounter.
Cost of the revisits was more difficult to assess, because only one of six states had full data (Florida); the cost data was extrapolated for the other states involved. In Florida, three-day revisit costs accounted for 30.3% of all primary visit costs. Thirty-day revisit costs were 118% of all primary ED visits costs within that time period.
There was not always an indication of whether the revisit was due to a planned revisit, worsening of symptoms, or inadequate initial treatment, however, leaving the evaluation of cost and revisit burden incomplete.
Bottom line: Initial evaluation of ED revisits shows that rates and cost are significant, though the nature of the revisits remains underevaluated. Preliminary data demonstrate that ED revisits are a significant cost to the healthcare system, though the number of preventable revisits remains unknown.
Citation: Duseja R, Bardach NS, Lin GA, et al. Revisit rates and associated costs after and emergency department encounter. Ann Intern Med. 2015;162(11):750-756.
Clinical question: What is the cost and frequency of ED revisits within three days and 30 days?
Background: ED revisits lead to a financial and resource utilization burden on the medical system. The costs and rates of these return visits are unknown and limited in characterization.
Study design: Observational study.
Setting: Six states, using Healthcare Cost and Utilization Project databases.
Synopsis: An observational study examined data from 2006-2010 across six states to determine cost and frequency of ED revisits within a 30-day period from initial ED treatment and discharge. The study examined revisit rates within the first three days of discharge, as well as the 30 days following discharge from the initial presentation.
Three-day revisit rates were 8.2%, with 29% resulting in admission; 32% of the revisits took place at a different institution.
The 30-day revisit rate was 19.9%, with 28% resulting in admission. The most common diagnoses were skin and soft tissue infections (23.9%) and abdominal pain (9.7%). The vast majority of revisits (89%) resulted in the same diagnosis as the first encounter.
Cost of the revisits was more difficult to assess, because only one of six states had full data (Florida); the cost data was extrapolated for the other states involved. In Florida, three-day revisit costs accounted for 30.3% of all primary visit costs. Thirty-day revisit costs were 118% of all primary ED visits costs within that time period.
There was not always an indication of whether the revisit was due to a planned revisit, worsening of symptoms, or inadequate initial treatment, however, leaving the evaluation of cost and revisit burden incomplete.
Bottom line: Initial evaluation of ED revisits shows that rates and cost are significant, though the nature of the revisits remains underevaluated. Preliminary data demonstrate that ED revisits are a significant cost to the healthcare system, though the number of preventable revisits remains unknown.
Citation: Duseja R, Bardach NS, Lin GA, et al. Revisit rates and associated costs after and emergency department encounter. Ann Intern Med. 2015;162(11):750-756.
Early, Late Hospital Readmission Factors Differ
Clinical question: What are the differences between factors associated with early (zero to seven days after discharge) and late (eight to 30 days after discharge) readmission?
Background: Thirty-day readmission rates are a quality metric; however, recent evidence challenges the notion that readmissions represent unnecessary and preventable healthcare use. It remains unclear whether the 30-day window post-discharge represents a homogenous period or if there are factors that contribute to readmission during that time.
Study design: Retrospective, single-center, cohort study.
Setting: Large, urban teaching hospital.
Synopsis: Based on 13,355 admissions representing 8,078 patients over a two-year period, the overall readmission rate was 19.7%, with 7.8% early (zero to seven days post-discharge) readmissions, and 11.9% late (eight to 30 days post-discharge) readmissions. Variables were categorized as indicators of acute illness burden, chronic illness burden, patient care process factors, and social determinants of health.
Several markers of acute illness burden were associated with early readmission only. Some markers of chronic illness burden were associated with late readmissions only (e.g. hemodialysis), while others were associated with readmissions throughout the 30-day period. Worse social determinants of health increased odds of readmission in both periods.
The single-center study was able to examine detailed clinical variables; however, this approach limited the generalizability of the the results.
Bottom line: Policies to reduce 30-day readmissions should reflect the different risk factors at play across that time frame.
Citation: Graham KL, Wilker EH, Howell MD, Davis RB, Marcantonio ER. Differences between early and late readmissions among patients: A cohort study. Ann Intern Med. 2015;162(11):741-749.
Clinical question: What are the differences between factors associated with early (zero to seven days after discharge) and late (eight to 30 days after discharge) readmission?
Background: Thirty-day readmission rates are a quality metric; however, recent evidence challenges the notion that readmissions represent unnecessary and preventable healthcare use. It remains unclear whether the 30-day window post-discharge represents a homogenous period or if there are factors that contribute to readmission during that time.
Study design: Retrospective, single-center, cohort study.
Setting: Large, urban teaching hospital.
Synopsis: Based on 13,355 admissions representing 8,078 patients over a two-year period, the overall readmission rate was 19.7%, with 7.8% early (zero to seven days post-discharge) readmissions, and 11.9% late (eight to 30 days post-discharge) readmissions. Variables were categorized as indicators of acute illness burden, chronic illness burden, patient care process factors, and social determinants of health.
Several markers of acute illness burden were associated with early readmission only. Some markers of chronic illness burden were associated with late readmissions only (e.g. hemodialysis), while others were associated with readmissions throughout the 30-day period. Worse social determinants of health increased odds of readmission in both periods.
The single-center study was able to examine detailed clinical variables; however, this approach limited the generalizability of the the results.
Bottom line: Policies to reduce 30-day readmissions should reflect the different risk factors at play across that time frame.
Citation: Graham KL, Wilker EH, Howell MD, Davis RB, Marcantonio ER. Differences between early and late readmissions among patients: A cohort study. Ann Intern Med. 2015;162(11):741-749.
Clinical question: What are the differences between factors associated with early (zero to seven days after discharge) and late (eight to 30 days after discharge) readmission?
Background: Thirty-day readmission rates are a quality metric; however, recent evidence challenges the notion that readmissions represent unnecessary and preventable healthcare use. It remains unclear whether the 30-day window post-discharge represents a homogenous period or if there are factors that contribute to readmission during that time.
Study design: Retrospective, single-center, cohort study.
Setting: Large, urban teaching hospital.
Synopsis: Based on 13,355 admissions representing 8,078 patients over a two-year period, the overall readmission rate was 19.7%, with 7.8% early (zero to seven days post-discharge) readmissions, and 11.9% late (eight to 30 days post-discharge) readmissions. Variables were categorized as indicators of acute illness burden, chronic illness burden, patient care process factors, and social determinants of health.
Several markers of acute illness burden were associated with early readmission only. Some markers of chronic illness burden were associated with late readmissions only (e.g. hemodialysis), while others were associated with readmissions throughout the 30-day period. Worse social determinants of health increased odds of readmission in both periods.
The single-center study was able to examine detailed clinical variables; however, this approach limited the generalizability of the the results.
Bottom line: Policies to reduce 30-day readmissions should reflect the different risk factors at play across that time frame.
Citation: Graham KL, Wilker EH, Howell MD, Davis RB, Marcantonio ER. Differences between early and late readmissions among patients: A cohort study. Ann Intern Med. 2015;162(11):741-749.
Patient Adherence to Pharmacological Thromboprophylaxis Improves with Interventions
Clinical question: How can patient adherence to pharmacological thromboprophylaxis be improved?
Background: Prior studies suggest that the hospital-wide prevalence of nonadministration of VTE thromboprophylaxis orders ranges from 5% to 13%, with patient refusal listed as the most common reason for nonadministration.
Study design: Quasi-experimental, pre-post intervention, with intervention and control units.
Setting: Academic medical center in Philadelphia.
Synopsis: Researchers identified 20,208 admissions for the study; 8,293 (41%) admissions occurred prior to the intervention and 11,915 (59%) after. The three-part intervention, which was composed of (1) standardized nurse response to patient refusal, (2) integration of daily assessment of VTE into rounds, and (3) regular audit with feedback, resulted in a decrease in nonadministration rates during the intervention. Rates continued to decline in the 21-month follow-up period.
After the intervention, the rate of missed doses of pharmacological thromboprophylaxis decreased from 24.7% to 14.7% (P<0.01). This was due to a decrease in patient refusal from 18.3% to 9.4% (P<0.01).
Although there was a decrease in the missed doses of thromboprophylaxis, there was no statistically significant change in the rate of hospital-associated VTE.
Bottom line: A multifaceted intervention resulted in a decrease in the proportion of missed and refused doses of pharmacological VTE thromboprophylaxis, but this was not associated with a statistically significant change in VTE rates.
Citation: Baillie CA, Guevara JP, Boston RC, Hecht TE. A unit-based intervention aimed at improving patient adherence to pharmacological thromboprophylaxis [published online ahead of print June 2, 2015]. BMJ Qual Saf. doi:10.1136/bmjqs-2015-003992.
Clinical question: How can patient adherence to pharmacological thromboprophylaxis be improved?
Background: Prior studies suggest that the hospital-wide prevalence of nonadministration of VTE thromboprophylaxis orders ranges from 5% to 13%, with patient refusal listed as the most common reason for nonadministration.
Study design: Quasi-experimental, pre-post intervention, with intervention and control units.
Setting: Academic medical center in Philadelphia.
Synopsis: Researchers identified 20,208 admissions for the study; 8,293 (41%) admissions occurred prior to the intervention and 11,915 (59%) after. The three-part intervention, which was composed of (1) standardized nurse response to patient refusal, (2) integration of daily assessment of VTE into rounds, and (3) regular audit with feedback, resulted in a decrease in nonadministration rates during the intervention. Rates continued to decline in the 21-month follow-up period.
After the intervention, the rate of missed doses of pharmacological thromboprophylaxis decreased from 24.7% to 14.7% (P<0.01). This was due to a decrease in patient refusal from 18.3% to 9.4% (P<0.01).
Although there was a decrease in the missed doses of thromboprophylaxis, there was no statistically significant change in the rate of hospital-associated VTE.
Bottom line: A multifaceted intervention resulted in a decrease in the proportion of missed and refused doses of pharmacological VTE thromboprophylaxis, but this was not associated with a statistically significant change in VTE rates.
Citation: Baillie CA, Guevara JP, Boston RC, Hecht TE. A unit-based intervention aimed at improving patient adherence to pharmacological thromboprophylaxis [published online ahead of print June 2, 2015]. BMJ Qual Saf. doi:10.1136/bmjqs-2015-003992.
Clinical question: How can patient adherence to pharmacological thromboprophylaxis be improved?
Background: Prior studies suggest that the hospital-wide prevalence of nonadministration of VTE thromboprophylaxis orders ranges from 5% to 13%, with patient refusal listed as the most common reason for nonadministration.
Study design: Quasi-experimental, pre-post intervention, with intervention and control units.
Setting: Academic medical center in Philadelphia.
Synopsis: Researchers identified 20,208 admissions for the study; 8,293 (41%) admissions occurred prior to the intervention and 11,915 (59%) after. The three-part intervention, which was composed of (1) standardized nurse response to patient refusal, (2) integration of daily assessment of VTE into rounds, and (3) regular audit with feedback, resulted in a decrease in nonadministration rates during the intervention. Rates continued to decline in the 21-month follow-up period.
After the intervention, the rate of missed doses of pharmacological thromboprophylaxis decreased from 24.7% to 14.7% (P<0.01). This was due to a decrease in patient refusal from 18.3% to 9.4% (P<0.01).
Although there was a decrease in the missed doses of thromboprophylaxis, there was no statistically significant change in the rate of hospital-associated VTE.
Bottom line: A multifaceted intervention resulted in a decrease in the proportion of missed and refused doses of pharmacological VTE thromboprophylaxis, but this was not associated with a statistically significant change in VTE rates.
Citation: Baillie CA, Guevara JP, Boston RC, Hecht TE. A unit-based intervention aimed at improving patient adherence to pharmacological thromboprophylaxis [published online ahead of print June 2, 2015]. BMJ Qual Saf. doi:10.1136/bmjqs-2015-003992.
Mortality Risk in Patients Older than 75 Presenting with Non-ST-Elevation Acute Coronary Syndrome
Clinical question: Is there a score that will predict the mortality rate in elderly patients presenting with a non-ST-elevation myocardial infarction (NSTEMI)?
Background: Although they represent only 9% of patients in clinical trials, patients over the age of 75 make up one third of patients with NSTEMI, accounting for more than half of NSTEMI-related mortality.
Study design: Retrospective cohort analysis for score calculator design, with prospective cohort validation.
Setting: The retrospective cohort was derived from a meta-analysis of 55 papers. The prospective validation arm used a cohort of patients from a randomized multicenter Italian trial.
Synopsis: The authors developed and validated a mortality predictor for patients 75 and older who present with an NSTEMI. The calculator: hemoglobin less than 10 g/dl (two points), elevated troponin levels, ECG ischemic changes, estimated glomerular filtration rate (eGFR) less than 45, previous vascular event (one point each two). The calculator predicted probabilities of death in one year ranging from 2% (score of zero) to 75% (score of six). The calculator allowed stratification into low (score: zero to one), intermediate (score: two), or high (score: three or greater) risk. High-risk patients appeared to benefit from intervention with significantly reduced risk for mortality (odds ratio 0.44).
Bottom line: A simple risk calculator stratifies elderly patients into low, intermediate, or high risk to predict mortality from NSTEMI. High-risk patients appear to achieve a mortality benefit from intervention.
Citation: Angeli F, Cavallini C, Verdecchia P, et al. A risk score for predicting 1-year mortality in patients ≥75 years of age presenting with non-ST-elevation acute coronary syndrome. Am J Cardiol. 2015;116(2):208-213.
Clinical question: Is there a score that will predict the mortality rate in elderly patients presenting with a non-ST-elevation myocardial infarction (NSTEMI)?
Background: Although they represent only 9% of patients in clinical trials, patients over the age of 75 make up one third of patients with NSTEMI, accounting for more than half of NSTEMI-related mortality.
Study design: Retrospective cohort analysis for score calculator design, with prospective cohort validation.
Setting: The retrospective cohort was derived from a meta-analysis of 55 papers. The prospective validation arm used a cohort of patients from a randomized multicenter Italian trial.
Synopsis: The authors developed and validated a mortality predictor for patients 75 and older who present with an NSTEMI. The calculator: hemoglobin less than 10 g/dl (two points), elevated troponin levels, ECG ischemic changes, estimated glomerular filtration rate (eGFR) less than 45, previous vascular event (one point each two). The calculator predicted probabilities of death in one year ranging from 2% (score of zero) to 75% (score of six). The calculator allowed stratification into low (score: zero to one), intermediate (score: two), or high (score: three or greater) risk. High-risk patients appeared to benefit from intervention with significantly reduced risk for mortality (odds ratio 0.44).
Bottom line: A simple risk calculator stratifies elderly patients into low, intermediate, or high risk to predict mortality from NSTEMI. High-risk patients appear to achieve a mortality benefit from intervention.
Citation: Angeli F, Cavallini C, Verdecchia P, et al. A risk score for predicting 1-year mortality in patients ≥75 years of age presenting with non-ST-elevation acute coronary syndrome. Am J Cardiol. 2015;116(2):208-213.
Clinical question: Is there a score that will predict the mortality rate in elderly patients presenting with a non-ST-elevation myocardial infarction (NSTEMI)?
Background: Although they represent only 9% of patients in clinical trials, patients over the age of 75 make up one third of patients with NSTEMI, accounting for more than half of NSTEMI-related mortality.
Study design: Retrospective cohort analysis for score calculator design, with prospective cohort validation.
Setting: The retrospective cohort was derived from a meta-analysis of 55 papers. The prospective validation arm used a cohort of patients from a randomized multicenter Italian trial.
Synopsis: The authors developed and validated a mortality predictor for patients 75 and older who present with an NSTEMI. The calculator: hemoglobin less than 10 g/dl (two points), elevated troponin levels, ECG ischemic changes, estimated glomerular filtration rate (eGFR) less than 45, previous vascular event (one point each two). The calculator predicted probabilities of death in one year ranging from 2% (score of zero) to 75% (score of six). The calculator allowed stratification into low (score: zero to one), intermediate (score: two), or high (score: three or greater) risk. High-risk patients appeared to benefit from intervention with significantly reduced risk for mortality (odds ratio 0.44).
Bottom line: A simple risk calculator stratifies elderly patients into low, intermediate, or high risk to predict mortality from NSTEMI. High-risk patients appear to achieve a mortality benefit from intervention.
Citation: Angeli F, Cavallini C, Verdecchia P, et al. A risk score for predicting 1-year mortality in patients ≥75 years of age presenting with non-ST-elevation acute coronary syndrome. Am J Cardiol. 2015;116(2):208-213.
Family Physicians Propose Payment for PCPs’ Hospital Consult Visits
The American Academy of Family Physicians (AAFP) has appealed to some of the nation's largest insurers, asking for coverage of hospital consults conducted by PCPs on behalf of hospitalists for their patients who are in the hospital.
"We believe that there is value in paying primary care physicians to see their patients in a hospital setting and that there is some evidence to suggest that doing so has benefits in terms of both improved outcomes and cost savings to the health system," says AAFP's commercial insurance strategist Brennan Cantrell. Cantrell's letter to the insurers asks them to review their coverage and payment policies.
Some insurers have downplayed the value of a hospital consultation by the outpatient physician, but advocates have emphasized its value in improving communication and enhancing care transitions.
"Payors' responses to our letter have been positive,” Cantrell tells The Hospitalist. The seven companies indicate that they have policies to permit separate payment for consults done by hospitalists and by PCPs brought in for hospital consults.
Hospitalist Claudia K. Geyer, MD, SFHM, chair of SHM's Family Medicine Committee, says AAFP's consultation initiative could help to formalize the social consult visit for primary care physicians, turning it into a true multidisciplinary approach to managing transitions. However, which patients are most appropriate for this type of consult, how it is initiated, and how many PCPs would be willing and able to provide the service—even if it were billable—require further clarification.
"The key would be for the hospitalist and PCP to work together as a team," Dr. Geyer says.
Visit our website for more information on inpatient visits by PCPs.
The American Academy of Family Physicians (AAFP) has appealed to some of the nation's largest insurers, asking for coverage of hospital consults conducted by PCPs on behalf of hospitalists for their patients who are in the hospital.
"We believe that there is value in paying primary care physicians to see their patients in a hospital setting and that there is some evidence to suggest that doing so has benefits in terms of both improved outcomes and cost savings to the health system," says AAFP's commercial insurance strategist Brennan Cantrell. Cantrell's letter to the insurers asks them to review their coverage and payment policies.
Some insurers have downplayed the value of a hospital consultation by the outpatient physician, but advocates have emphasized its value in improving communication and enhancing care transitions.
"Payors' responses to our letter have been positive,” Cantrell tells The Hospitalist. The seven companies indicate that they have policies to permit separate payment for consults done by hospitalists and by PCPs brought in for hospital consults.
Hospitalist Claudia K. Geyer, MD, SFHM, chair of SHM's Family Medicine Committee, says AAFP's consultation initiative could help to formalize the social consult visit for primary care physicians, turning it into a true multidisciplinary approach to managing transitions. However, which patients are most appropriate for this type of consult, how it is initiated, and how many PCPs would be willing and able to provide the service—even if it were billable—require further clarification.
"The key would be for the hospitalist and PCP to work together as a team," Dr. Geyer says.
Visit our website for more information on inpatient visits by PCPs.
The American Academy of Family Physicians (AAFP) has appealed to some of the nation's largest insurers, asking for coverage of hospital consults conducted by PCPs on behalf of hospitalists for their patients who are in the hospital.
"We believe that there is value in paying primary care physicians to see their patients in a hospital setting and that there is some evidence to suggest that doing so has benefits in terms of both improved outcomes and cost savings to the health system," says AAFP's commercial insurance strategist Brennan Cantrell. Cantrell's letter to the insurers asks them to review their coverage and payment policies.
Some insurers have downplayed the value of a hospital consultation by the outpatient physician, but advocates have emphasized its value in improving communication and enhancing care transitions.
"Payors' responses to our letter have been positive,” Cantrell tells The Hospitalist. The seven companies indicate that they have policies to permit separate payment for consults done by hospitalists and by PCPs brought in for hospital consults.
Hospitalist Claudia K. Geyer, MD, SFHM, chair of SHM's Family Medicine Committee, says AAFP's consultation initiative could help to formalize the social consult visit for primary care physicians, turning it into a true multidisciplinary approach to managing transitions. However, which patients are most appropriate for this type of consult, how it is initiated, and how many PCPs would be willing and able to provide the service—even if it were billable—require further clarification.
"The key would be for the hospitalist and PCP to work together as a team," Dr. Geyer says.
Visit our website for more information on inpatient visits by PCPs.
App Helps Hospitalists Prevent Inpatient Falls
Every year, hundreds of thousands of hospitalized patients fall. Now, hospitalists can get help in dramatically reducing those numbers. According to Erin DuPree, MD, FACOG, vice president and chief medical officer at The Joint Commission's Center for Transforming Healthcare, 30% to 50% of inpatients sustain an injury in a fall, incurring hospital costs of roughly $14,000 and adding, on average, 6.3 days to a hospital stay. It's an ongoing challenge.
"Hospitals have been working on preventing falls forever," Dr. DuPree says. "It's complex, and we needed to look at this in a data-driven way."
The center has done just that, and the result is a new web application called the Preventing Falls Targeted Solutions Tool. Anyone at a Joint Commission–accredited organization can gain complimentary access to the app, which guides users through a systematic, data-driven, Lean Six Sigma approach to reducing falls.
"It guides them through data collection and analyzes the data," Dr. DuPree adds. "Then the tool identifies your top contributing factors to falls and the solutions for those factors. We know every hospital has different contributing factors that matter; this is very local and dependent on the data that's entered."
Seven healthcare institutions in Missouri, Texas, Minnesota, California, North Carolina, and New Hampshire assisted the Joint Commission in developing the tool. Altogether, the pilot institutions reduced their rate of falls by an average of 35% and decreased their rate of patients injured in a fall by an average of 62%.
Hospitalists have a crucial role to play in bringing this process to their own workplace. "It's an opportunity for them to assert their leadership in their clinical role by collaborating with other disciplines on a big patient-safety issue," Dr. DuPree says.
It's also an opportunity for hospitalists to learn about quality improvement, she adds. "If they want to learn something about Lean Six Sigma," she says, "they can do a pilot project on their unit. I hope hospitalists gain access to the tool and start a falls project or work with their team to see what things in the tool could be of value to them."
Visit our website for more information on hospitalists and preventing inpatient falls.
Every year, hundreds of thousands of hospitalized patients fall. Now, hospitalists can get help in dramatically reducing those numbers. According to Erin DuPree, MD, FACOG, vice president and chief medical officer at The Joint Commission's Center for Transforming Healthcare, 30% to 50% of inpatients sustain an injury in a fall, incurring hospital costs of roughly $14,000 and adding, on average, 6.3 days to a hospital stay. It's an ongoing challenge.
"Hospitals have been working on preventing falls forever," Dr. DuPree says. "It's complex, and we needed to look at this in a data-driven way."
The center has done just that, and the result is a new web application called the Preventing Falls Targeted Solutions Tool. Anyone at a Joint Commission–accredited organization can gain complimentary access to the app, which guides users through a systematic, data-driven, Lean Six Sigma approach to reducing falls.
"It guides them through data collection and analyzes the data," Dr. DuPree adds. "Then the tool identifies your top contributing factors to falls and the solutions for those factors. We know every hospital has different contributing factors that matter; this is very local and dependent on the data that's entered."
Seven healthcare institutions in Missouri, Texas, Minnesota, California, North Carolina, and New Hampshire assisted the Joint Commission in developing the tool. Altogether, the pilot institutions reduced their rate of falls by an average of 35% and decreased their rate of patients injured in a fall by an average of 62%.
Hospitalists have a crucial role to play in bringing this process to their own workplace. "It's an opportunity for them to assert their leadership in their clinical role by collaborating with other disciplines on a big patient-safety issue," Dr. DuPree says.
It's also an opportunity for hospitalists to learn about quality improvement, she adds. "If they want to learn something about Lean Six Sigma," she says, "they can do a pilot project on their unit. I hope hospitalists gain access to the tool and start a falls project or work with their team to see what things in the tool could be of value to them."
Visit our website for more information on hospitalists and preventing inpatient falls.
Every year, hundreds of thousands of hospitalized patients fall. Now, hospitalists can get help in dramatically reducing those numbers. According to Erin DuPree, MD, FACOG, vice president and chief medical officer at The Joint Commission's Center for Transforming Healthcare, 30% to 50% of inpatients sustain an injury in a fall, incurring hospital costs of roughly $14,000 and adding, on average, 6.3 days to a hospital stay. It's an ongoing challenge.
"Hospitals have been working on preventing falls forever," Dr. DuPree says. "It's complex, and we needed to look at this in a data-driven way."
The center has done just that, and the result is a new web application called the Preventing Falls Targeted Solutions Tool. Anyone at a Joint Commission–accredited organization can gain complimentary access to the app, which guides users through a systematic, data-driven, Lean Six Sigma approach to reducing falls.
"It guides them through data collection and analyzes the data," Dr. DuPree adds. "Then the tool identifies your top contributing factors to falls and the solutions for those factors. We know every hospital has different contributing factors that matter; this is very local and dependent on the data that's entered."
Seven healthcare institutions in Missouri, Texas, Minnesota, California, North Carolina, and New Hampshire assisted the Joint Commission in developing the tool. Altogether, the pilot institutions reduced their rate of falls by an average of 35% and decreased their rate of patients injured in a fall by an average of 62%.
Hospitalists have a crucial role to play in bringing this process to their own workplace. "It's an opportunity for them to assert their leadership in their clinical role by collaborating with other disciplines on a big patient-safety issue," Dr. DuPree says.
It's also an opportunity for hospitalists to learn about quality improvement, she adds. "If they want to learn something about Lean Six Sigma," she says, "they can do a pilot project on their unit. I hope hospitalists gain access to the tool and start a falls project or work with their team to see what things in the tool could be of value to them."
Visit our website for more information on hospitalists and preventing inpatient falls.
Rise of the Chief Patient Experience Officer
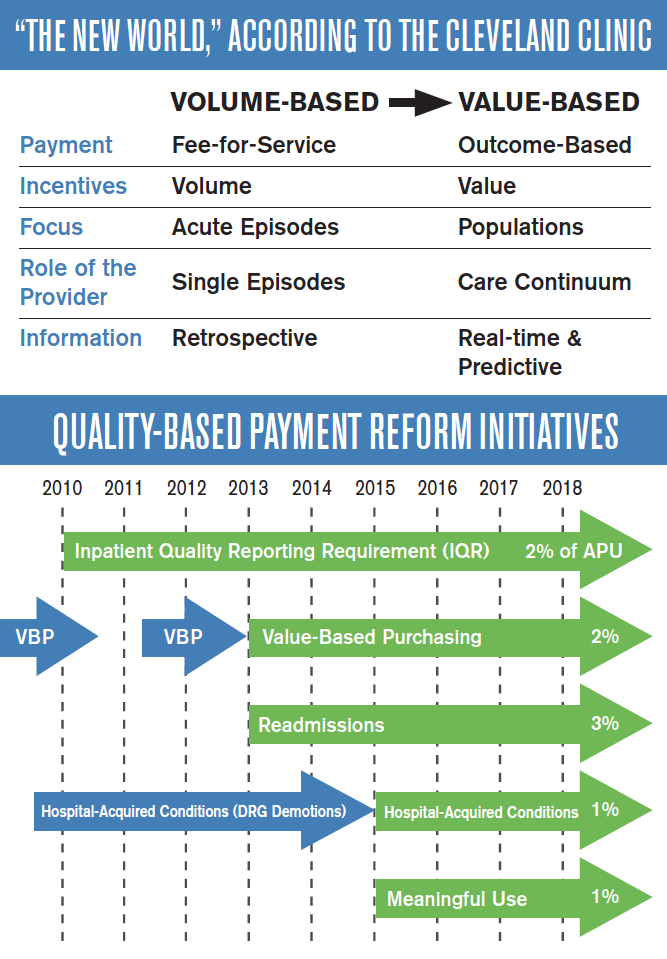
The Cleveland Clinic was the first major academic medical center to make improving patient experience a strategic goal. In 2007, the medical institution hired its first chief patient experience officer (CXO) and established the Office of Patient Experience. These were also firsts.
“When we took a step back to evaluate why we come to work every day, we realized it’s for one reason—the patients,” says Adrienne Boissy, MD, MA, the clinic’s CXO. “Toby [Cosgrove, MD, president and CEO of Cleveland Clinic] had some key early experiences, which prompted us to think about patient experience as an organizational priority. These experiences led him to recognize the importance of caring for the soul of the patient, not just the body.
“The CXO was embedded into our executive team, which effectively wove it into our fabric.”
Since then, more than 60 other medical institutions across the country have followed suit.
But improving patient experience isn’t just “nice to do,” Dr. Boissy says. “The great part of these shifts in healthcare is that the government has created the burning platform for us. Organizations won’t survive in the current market if they don’t make it a strategic priority.”
So what are the key drivers of a positive patient experience?
“You cannot deliver an exceptional patient experience without safe care, high quality, or high value,” says Dr. Boissy, who adds that hospitalists shouldn’t underestimate their role in the patient’s experience.
“Hospitalists are leaders whether they have an official title or not,” she adds. “People watch how they behave and interact with patients and colleagues. Raising your own awareness about your ability to influence is key. Model the skills you hope to embed.”
The Cleveland Clinic was the first major academic medical center to make improving patient experience a strategic goal. In 2007, the medical institution hired its first chief patient experience officer (CXO) and established the Office of Patient Experience. These were also firsts.
“When we took a step back to evaluate why we come to work every day, we realized it’s for one reason—the patients,” says Adrienne Boissy, MD, MA, the clinic’s CXO. “Toby [Cosgrove, MD, president and CEO of Cleveland Clinic] had some key early experiences, which prompted us to think about patient experience as an organizational priority. These experiences led him to recognize the importance of caring for the soul of the patient, not just the body.
“The CXO was embedded into our executive team, which effectively wove it into our fabric.”
Since then, more than 60 other medical institutions across the country have followed suit.
But improving patient experience isn’t just “nice to do,” Dr. Boissy says. “The great part of these shifts in healthcare is that the government has created the burning platform for us. Organizations won’t survive in the current market if they don’t make it a strategic priority.”
So what are the key drivers of a positive patient experience?
“You cannot deliver an exceptional patient experience without safe care, high quality, or high value,” says Dr. Boissy, who adds that hospitalists shouldn’t underestimate their role in the patient’s experience.
“Hospitalists are leaders whether they have an official title or not,” she adds. “People watch how they behave and interact with patients and colleagues. Raising your own awareness about your ability to influence is key. Model the skills you hope to embed.”
The Cleveland Clinic was the first major academic medical center to make improving patient experience a strategic goal. In 2007, the medical institution hired its first chief patient experience officer (CXO) and established the Office of Patient Experience. These were also firsts.
“When we took a step back to evaluate why we come to work every day, we realized it’s for one reason—the patients,” says Adrienne Boissy, MD, MA, the clinic’s CXO. “Toby [Cosgrove, MD, president and CEO of Cleveland Clinic] had some key early experiences, which prompted us to think about patient experience as an organizational priority. These experiences led him to recognize the importance of caring for the soul of the patient, not just the body.
“The CXO was embedded into our executive team, which effectively wove it into our fabric.”
Since then, more than 60 other medical institutions across the country have followed suit.
But improving patient experience isn’t just “nice to do,” Dr. Boissy says. “The great part of these shifts in healthcare is that the government has created the burning platform for us. Organizations won’t survive in the current market if they don’t make it a strategic priority.”
So what are the key drivers of a positive patient experience?
“You cannot deliver an exceptional patient experience without safe care, high quality, or high value,” says Dr. Boissy, who adds that hospitalists shouldn’t underestimate their role in the patient’s experience.
“Hospitalists are leaders whether they have an official title or not,” she adds. “People watch how they behave and interact with patients and colleagues. Raising your own awareness about your ability to influence is key. Model the skills you hope to embed.”
Cognitive, Emotional Memory Disconnect Impacts Patient Satisfaction
There are two types of memory, the cognitive and the emotional, and the latter is more enduring. Maya Angelou characterized the distinction between these two types of memory most eloquently and succinctly when she said, “I’ve learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel.” She was ahead of her time, because neurocognitive research has objectified with science what Ms. Angelou captured so elegantly in her prose. Emotional events are processed in the sensory systems and then transmitted to the medial-temporal lobe and the amygdale for the formation of an emotional memory. When the memory is cued and retrieved from the amygdale, it triggers an emotional response. Emotional experiences leave strong traces in the brain. Memories about emotional situations are stored in both the conscious and unconscious memory, which is part of the reason emotional memories are so enduring.1 Studies of patients with severe anterograde amnesia following circumscribed bilateral hippocampal brain damage showed enduring memories of emotion despite the absence of conscious memories.2 This has a demonstrably practical application in patients with dementia, who we now know have feelings of happiness and sadness long after they have forgotten what caused the emotion.3
The distinction is important because patients judge the quality of their medical care based on emotions. The patient satisfaction disconnect arises from the fact that physicians live in their cognitive memory, while patients live in their emotional memory. Being cognitive and objective is a critical skill a physician must bring to the bedside every day; the reason we don’t allow physicians to treat family members is that their ability to remain objective will be impaired. I realized that my emotion, my passion, and my empathy for the dying would impair my judgment when I started medical school, and I launched myself on a conscious and systematic discipline to keep those feelings out of my mind during patient care. The effort worked and, for the most part, I have been able to remain objective and unemotional as I care for my patients. Recently, however, I realized that my focus on objectivity negatively impacts patient experience. As a result, I have expanded my view: While I must stay objective and detached with my thinking, I must be emotionally engaged to provide a great patient experience.
I can remain objective and detached in my clinical judgment as I engage and connect emotionally during my patient encounters. This delicate balancing act has taken years of trial and error, however. I recently cared for a woman in her 60s who had fallen and broke her hip. Everyone was pleased that a top orthopedic surgeon was on call and able to give her the first-rate care she needed to begin walking again. The surgery went smoothly, and she was transferred to the medical/surgical ward, where things took a turn for the worse. She had a lot of anxiety in addition to her osteoporosis. Objectively, she was doing great, and we had a big success on our hands; however, she remained anxious, and she peppered the surgeon with fears that, while unfounded, were very real in her mind. The surgeon brushed them off, saying that her fears were not real and that he didn’t need to address them; his response made her emotional state spiral out of control. Her nurse notified me of the situation, and I came to her bedside. She was very agitated. I sat down at a low level and just started listening. She got all of her anxieties out in words. I held her hand, looked her in the eye, and assured her that I would be there for her and that things were going to be alright. Subsequently, she wrote letters of gratitude and proclaimed to any medical staff who would listen what a talented and great doctor I was. I did not have the skill to fix her broken hip; if it had been left to me alone, she would still be bed-bound. But I did have the human skills to connect with her and fix her agitated mind. If we remember the enduring power of the emotional memory, we can create great patient experiences.
The importance of these experiences was illustrated to me at the 2014 Dignity Health Patient Experience Summit, a powerful event featuring motivational speakers and leaders from across the country. The most powerful speakers, however, were patients. These patients had received terrible diagnoses that committed them to a prolonged interaction with the healthcare system. They were scared of what their diagnoses would mean for their future, they were subjected to uncomfortable procedures in which they struggled to maintain their dignity, and they repeatedly met the indifference of healthcare providers and clerical people who were only there to do a job. They related how the lack of caring and empathy made fears and anxiety much worse. But each of them had a story about that one person, that one care provider, who took the time to reassure them, to show that they cared, and to ensure that the patient did not feel alone. In most of these stories, the stand-out care providers took the time to hold their hands and reassure the patients. They took the time to connect with the patient’s emotional memory in a positive way, and that simple gesture of empathy had a powerful and lasting impact on the patient.
Invariably, the care provider at the heart of the patients’ stories was a nurse. Nurses have the reputation for being angels of mercy because they do the simple, empathetic gestures that let a patient know they are being cared for. These feelings endure in the patients’ memories long after the treatment is over. Doctors can, and should, be that type of care provider. It requires us to recognize that patients are scared and anxious, even though they may do their best not to show it. We, as physicians, often don’t see their anxiety, and we are so focused on the cognitive memory that we don’t address the anxiety and fear that is just under the surface. But taking just a few minutes to acknowledge their emotions, to explore them, and to reassure the patient that we are there for them has a lasting impact. In my group, we talk about the “human-business-human” encounter with patients. We begin all interactions with a human interaction (“Hello, I am Dr. McIlraith…”), conduct the business we came to provide (“Now I am going to examine you…”), and end with a human interaction (“What else can I do for you today?”). Patients expect physical contact with us during the “business” part of that interaction. I find that respectful, reassuring, and appropriate physical contact during the final “human” portion of that interaction helps solidify my patients’ experience. It helps make them feel that they have been cared for, particularly if the visit includes bad news.
Much of the recent focus on patient satisfaction has been driven by financial incentives. In 2013, CMS began penalizing hospitals 1.25% for poor HCAHPS scores as a part of the Affordable Care Act. In 2014, the maximum penalty increased to 2%, and to 3% in 2015. Hospitals have notoriously high overhead costs and slim profit margins, so these penalties can have a profound impact on the financial viability of an institution. But, while hospitals across the country have taken notice (see related article in this edition of The Hospitalist), I find doctors are more motivated by the well-being of their patients than are their hospital administrators. Satisfied patients are more compliant with treatment plans and have better outcomes.4,5 Hospitalists spend a lot of effort making sure their heart failure patients are on an ACE inhibitor, and their heart attack patients are discharged on aspirin, beta blockers, and statins so that they will have a good outcome following treatment for their acute illness. The same outcome-driven, evidence-based practice of medicine relates to patient satisfaction, however. Success in HCAHPS is as important as core measures when it comes to patient outcomes. And if I can’t convince you patient satisfaction is important because of the good it does for hospitals and patients, think about yourself for a minute. Satisfied patients are much less likely to sue their physicians.6 Practicing quality, evidence-based medicine will keep you out of peer review; however, satisfied patients will keep you out of the courtroom.
I frequently hear the comment that “we can do great on patient satisfaction, but then it gets busy, and patient satisfaction goes out the window.” My own experience contradicts this maxim, however. It is not how much time you spend with your patient but, rather, what you do with the time you have. One of the most powerful things we can do is listen. I used to make the mistake that I only wanted to hear the information I needed to figure out my patients’ problems so I could start treating them; however, I have come to learn that being heard is, in itself, therapy for my patients. It is often quoted that physicians interrupt their patients within 18 seconds of starting the interview.7 A lot of physicians dispense with attentive listening when they are under time pressure, when they should instead dispense with lengthy discourses on the patient treatment plan. It is important to educate our patients on their illness and treatment, I admit. I find a lot of hospitalists want to impart their knowledge and their treatment rationale to their patients; however, they frequently give patients and families much more information than they can hold in their cognitive memory. And time pressures are not the only anxieties hospitalists carry with them to the bedside. Our increasingly metric-driven profession means that we not only have to worry about morning discharges, interdisciplinary rounds, length of stay, and so on, but we also have to consider patient experience. It is not easy to hide all the stress we are under when we come to the bedside of a patient, but we have to. The easiest way to do that is to take a deep breath, sit next to the patient, ask an open-ended question, and then say nothing until the patient is done speaking. Active listening with good eye contact and encouragement to continue solidifies the patient’s experience of being heard. There are extreme cases when a patient is in a manic phase and won’t ever stop speaking; bend the rules a bit in those circumstances. However, the above rule works very effectively in the majority of physician-patient interactions. Being heard leaves an enduring emotional memory with our patients.
Hospital medicine often looks to other industries for inspiration on how we can improve. The airline industry is often held up as an example of how we can model patient safety, for instance, but these comparisons oversimplify the challenges we face. The same is true with patient satisfaction. In the business world, adages like “The customer is always right” are central to customer satisfaction, yet completely irrelevant to HM practice. Patients and families frequently have inappropriate and unrealistic expectations of their hospitalist physicians. We cannot, and should not, tell the patient addicted to narcotics that they can have as much IV Dilaudid as they would like. We cannot fix the patient with end-stage cancer, heart failure, or dementia. This is where we have to part ways with comparisons to principles that guide other industries if we are going to find a way forward with patient experience in hospital medicine. Because we have to set limits for patients, we often have to give our patients and families bad news, and because we have to tell them things they don’t like to hear, like “You can’t have any salt in your diet,” or “You must quit drinking alcohol,” we must develop our own principles on patient experience and satisfaction. Otherwise our options are either delivering inappropriate medical care or abandoning the pursuit of patient satisfaction all together. This is when we must remember that emotional memories are more enduring. We can’t always give our patients what they want, and we can’t always tell them what they want to hear, but we can always show them that we care. When we show our patients that we care in a palpable way, we leave them with the feeling that they have been cared for regardless of their condition, and the positive memory will endure despite the negative information we may have to convey. Maybe they won’t cut down on their salt or quit drinking alcohol, but they will never forget that their hospitalist physician cared.
And if they remember that the physician cared, it is much more likely that they will cut down on the salt or quit drinking alcohol when they go home. To paraphrase Maya Angelou, “I can’t always tell my patients what they want to hear, I can’t always tell them that their lifestyle is appropriate, but I can always show them that I care.”
Dr. McIlraith is chairman of the department of hospital medicine of Mercy Medical Group in Sacramento, Calif.
References
- LeDoux JE. Emotional memory. Scholarpedia. Accessed August 2, 2015.
- Feinstein JS, Duff MC, D Tranel D. Sustained experience of emotion after loss of memory in patients with amnesia. Proc Natl Acad Sci. 2010:107(17):7674-7679.
- Guzmán-Vélez E, Feinstein JS, Tranel D. Feelings without memory in Alzheimer disease. Cogn Behav Neurol. 2014;27(3):117-129.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. March 2001. Accessed August 2, 2015.
- Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med. 2011;24(3):229-239.
- Stelfox HT, Gandhi TK, Orav EJ, Gustafson ML. The relation of patient statisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005;118(10):1126-1133.
- Beckman HB, Frankel RM. The effect of physician behavior on the collection of data. Ann Intern Med. 1984;101(5):692-696.
There are two types of memory, the cognitive and the emotional, and the latter is more enduring. Maya Angelou characterized the distinction between these two types of memory most eloquently and succinctly when she said, “I’ve learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel.” She was ahead of her time, because neurocognitive research has objectified with science what Ms. Angelou captured so elegantly in her prose. Emotional events are processed in the sensory systems and then transmitted to the medial-temporal lobe and the amygdale for the formation of an emotional memory. When the memory is cued and retrieved from the amygdale, it triggers an emotional response. Emotional experiences leave strong traces in the brain. Memories about emotional situations are stored in both the conscious and unconscious memory, which is part of the reason emotional memories are so enduring.1 Studies of patients with severe anterograde amnesia following circumscribed bilateral hippocampal brain damage showed enduring memories of emotion despite the absence of conscious memories.2 This has a demonstrably practical application in patients with dementia, who we now know have feelings of happiness and sadness long after they have forgotten what caused the emotion.3
The distinction is important because patients judge the quality of their medical care based on emotions. The patient satisfaction disconnect arises from the fact that physicians live in their cognitive memory, while patients live in their emotional memory. Being cognitive and objective is a critical skill a physician must bring to the bedside every day; the reason we don’t allow physicians to treat family members is that their ability to remain objective will be impaired. I realized that my emotion, my passion, and my empathy for the dying would impair my judgment when I started medical school, and I launched myself on a conscious and systematic discipline to keep those feelings out of my mind during patient care. The effort worked and, for the most part, I have been able to remain objective and unemotional as I care for my patients. Recently, however, I realized that my focus on objectivity negatively impacts patient experience. As a result, I have expanded my view: While I must stay objective and detached with my thinking, I must be emotionally engaged to provide a great patient experience.
I can remain objective and detached in my clinical judgment as I engage and connect emotionally during my patient encounters. This delicate balancing act has taken years of trial and error, however. I recently cared for a woman in her 60s who had fallen and broke her hip. Everyone was pleased that a top orthopedic surgeon was on call and able to give her the first-rate care she needed to begin walking again. The surgery went smoothly, and she was transferred to the medical/surgical ward, where things took a turn for the worse. She had a lot of anxiety in addition to her osteoporosis. Objectively, she was doing great, and we had a big success on our hands; however, she remained anxious, and she peppered the surgeon with fears that, while unfounded, were very real in her mind. The surgeon brushed them off, saying that her fears were not real and that he didn’t need to address them; his response made her emotional state spiral out of control. Her nurse notified me of the situation, and I came to her bedside. She was very agitated. I sat down at a low level and just started listening. She got all of her anxieties out in words. I held her hand, looked her in the eye, and assured her that I would be there for her and that things were going to be alright. Subsequently, she wrote letters of gratitude and proclaimed to any medical staff who would listen what a talented and great doctor I was. I did not have the skill to fix her broken hip; if it had been left to me alone, she would still be bed-bound. But I did have the human skills to connect with her and fix her agitated mind. If we remember the enduring power of the emotional memory, we can create great patient experiences.
The importance of these experiences was illustrated to me at the 2014 Dignity Health Patient Experience Summit, a powerful event featuring motivational speakers and leaders from across the country. The most powerful speakers, however, were patients. These patients had received terrible diagnoses that committed them to a prolonged interaction with the healthcare system. They were scared of what their diagnoses would mean for their future, they were subjected to uncomfortable procedures in which they struggled to maintain their dignity, and they repeatedly met the indifference of healthcare providers and clerical people who were only there to do a job. They related how the lack of caring and empathy made fears and anxiety much worse. But each of them had a story about that one person, that one care provider, who took the time to reassure them, to show that they cared, and to ensure that the patient did not feel alone. In most of these stories, the stand-out care providers took the time to hold their hands and reassure the patients. They took the time to connect with the patient’s emotional memory in a positive way, and that simple gesture of empathy had a powerful and lasting impact on the patient.
Invariably, the care provider at the heart of the patients’ stories was a nurse. Nurses have the reputation for being angels of mercy because they do the simple, empathetic gestures that let a patient know they are being cared for. These feelings endure in the patients’ memories long after the treatment is over. Doctors can, and should, be that type of care provider. It requires us to recognize that patients are scared and anxious, even though they may do their best not to show it. We, as physicians, often don’t see their anxiety, and we are so focused on the cognitive memory that we don’t address the anxiety and fear that is just under the surface. But taking just a few minutes to acknowledge their emotions, to explore them, and to reassure the patient that we are there for them has a lasting impact. In my group, we talk about the “human-business-human” encounter with patients. We begin all interactions with a human interaction (“Hello, I am Dr. McIlraith…”), conduct the business we came to provide (“Now I am going to examine you…”), and end with a human interaction (“What else can I do for you today?”). Patients expect physical contact with us during the “business” part of that interaction. I find that respectful, reassuring, and appropriate physical contact during the final “human” portion of that interaction helps solidify my patients’ experience. It helps make them feel that they have been cared for, particularly if the visit includes bad news.
Much of the recent focus on patient satisfaction has been driven by financial incentives. In 2013, CMS began penalizing hospitals 1.25% for poor HCAHPS scores as a part of the Affordable Care Act. In 2014, the maximum penalty increased to 2%, and to 3% in 2015. Hospitals have notoriously high overhead costs and slim profit margins, so these penalties can have a profound impact on the financial viability of an institution. But, while hospitals across the country have taken notice (see related article in this edition of The Hospitalist), I find doctors are more motivated by the well-being of their patients than are their hospital administrators. Satisfied patients are more compliant with treatment plans and have better outcomes.4,5 Hospitalists spend a lot of effort making sure their heart failure patients are on an ACE inhibitor, and their heart attack patients are discharged on aspirin, beta blockers, and statins so that they will have a good outcome following treatment for their acute illness. The same outcome-driven, evidence-based practice of medicine relates to patient satisfaction, however. Success in HCAHPS is as important as core measures when it comes to patient outcomes. And if I can’t convince you patient satisfaction is important because of the good it does for hospitals and patients, think about yourself for a minute. Satisfied patients are much less likely to sue their physicians.6 Practicing quality, evidence-based medicine will keep you out of peer review; however, satisfied patients will keep you out of the courtroom.
I frequently hear the comment that “we can do great on patient satisfaction, but then it gets busy, and patient satisfaction goes out the window.” My own experience contradicts this maxim, however. It is not how much time you spend with your patient but, rather, what you do with the time you have. One of the most powerful things we can do is listen. I used to make the mistake that I only wanted to hear the information I needed to figure out my patients’ problems so I could start treating them; however, I have come to learn that being heard is, in itself, therapy for my patients. It is often quoted that physicians interrupt their patients within 18 seconds of starting the interview.7 A lot of physicians dispense with attentive listening when they are under time pressure, when they should instead dispense with lengthy discourses on the patient treatment plan. It is important to educate our patients on their illness and treatment, I admit. I find a lot of hospitalists want to impart their knowledge and their treatment rationale to their patients; however, they frequently give patients and families much more information than they can hold in their cognitive memory. And time pressures are not the only anxieties hospitalists carry with them to the bedside. Our increasingly metric-driven profession means that we not only have to worry about morning discharges, interdisciplinary rounds, length of stay, and so on, but we also have to consider patient experience. It is not easy to hide all the stress we are under when we come to the bedside of a patient, but we have to. The easiest way to do that is to take a deep breath, sit next to the patient, ask an open-ended question, and then say nothing until the patient is done speaking. Active listening with good eye contact and encouragement to continue solidifies the patient’s experience of being heard. There are extreme cases when a patient is in a manic phase and won’t ever stop speaking; bend the rules a bit in those circumstances. However, the above rule works very effectively in the majority of physician-patient interactions. Being heard leaves an enduring emotional memory with our patients.
Hospital medicine often looks to other industries for inspiration on how we can improve. The airline industry is often held up as an example of how we can model patient safety, for instance, but these comparisons oversimplify the challenges we face. The same is true with patient satisfaction. In the business world, adages like “The customer is always right” are central to customer satisfaction, yet completely irrelevant to HM practice. Patients and families frequently have inappropriate and unrealistic expectations of their hospitalist physicians. We cannot, and should not, tell the patient addicted to narcotics that they can have as much IV Dilaudid as they would like. We cannot fix the patient with end-stage cancer, heart failure, or dementia. This is where we have to part ways with comparisons to principles that guide other industries if we are going to find a way forward with patient experience in hospital medicine. Because we have to set limits for patients, we often have to give our patients and families bad news, and because we have to tell them things they don’t like to hear, like “You can’t have any salt in your diet,” or “You must quit drinking alcohol,” we must develop our own principles on patient experience and satisfaction. Otherwise our options are either delivering inappropriate medical care or abandoning the pursuit of patient satisfaction all together. This is when we must remember that emotional memories are more enduring. We can’t always give our patients what they want, and we can’t always tell them what they want to hear, but we can always show them that we care. When we show our patients that we care in a palpable way, we leave them with the feeling that they have been cared for regardless of their condition, and the positive memory will endure despite the negative information we may have to convey. Maybe they won’t cut down on their salt or quit drinking alcohol, but they will never forget that their hospitalist physician cared.
And if they remember that the physician cared, it is much more likely that they will cut down on the salt or quit drinking alcohol when they go home. To paraphrase Maya Angelou, “I can’t always tell my patients what they want to hear, I can’t always tell them that their lifestyle is appropriate, but I can always show them that I care.”
Dr. McIlraith is chairman of the department of hospital medicine of Mercy Medical Group in Sacramento, Calif.
References
- LeDoux JE. Emotional memory. Scholarpedia. Accessed August 2, 2015.
- Feinstein JS, Duff MC, D Tranel D. Sustained experience of emotion after loss of memory in patients with amnesia. Proc Natl Acad Sci. 2010:107(17):7674-7679.
- Guzmán-Vélez E, Feinstein JS, Tranel D. Feelings without memory in Alzheimer disease. Cogn Behav Neurol. 2014;27(3):117-129.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. March 2001. Accessed August 2, 2015.
- Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med. 2011;24(3):229-239.
- Stelfox HT, Gandhi TK, Orav EJ, Gustafson ML. The relation of patient statisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005;118(10):1126-1133.
- Beckman HB, Frankel RM. The effect of physician behavior on the collection of data. Ann Intern Med. 1984;101(5):692-696.
There are two types of memory, the cognitive and the emotional, and the latter is more enduring. Maya Angelou characterized the distinction between these two types of memory most eloquently and succinctly when she said, “I’ve learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel.” She was ahead of her time, because neurocognitive research has objectified with science what Ms. Angelou captured so elegantly in her prose. Emotional events are processed in the sensory systems and then transmitted to the medial-temporal lobe and the amygdale for the formation of an emotional memory. When the memory is cued and retrieved from the amygdale, it triggers an emotional response. Emotional experiences leave strong traces in the brain. Memories about emotional situations are stored in both the conscious and unconscious memory, which is part of the reason emotional memories are so enduring.1 Studies of patients with severe anterograde amnesia following circumscribed bilateral hippocampal brain damage showed enduring memories of emotion despite the absence of conscious memories.2 This has a demonstrably practical application in patients with dementia, who we now know have feelings of happiness and sadness long after they have forgotten what caused the emotion.3
The distinction is important because patients judge the quality of their medical care based on emotions. The patient satisfaction disconnect arises from the fact that physicians live in their cognitive memory, while patients live in their emotional memory. Being cognitive and objective is a critical skill a physician must bring to the bedside every day; the reason we don’t allow physicians to treat family members is that their ability to remain objective will be impaired. I realized that my emotion, my passion, and my empathy for the dying would impair my judgment when I started medical school, and I launched myself on a conscious and systematic discipline to keep those feelings out of my mind during patient care. The effort worked and, for the most part, I have been able to remain objective and unemotional as I care for my patients. Recently, however, I realized that my focus on objectivity negatively impacts patient experience. As a result, I have expanded my view: While I must stay objective and detached with my thinking, I must be emotionally engaged to provide a great patient experience.
I can remain objective and detached in my clinical judgment as I engage and connect emotionally during my patient encounters. This delicate balancing act has taken years of trial and error, however. I recently cared for a woman in her 60s who had fallen and broke her hip. Everyone was pleased that a top orthopedic surgeon was on call and able to give her the first-rate care she needed to begin walking again. The surgery went smoothly, and she was transferred to the medical/surgical ward, where things took a turn for the worse. She had a lot of anxiety in addition to her osteoporosis. Objectively, she was doing great, and we had a big success on our hands; however, she remained anxious, and she peppered the surgeon with fears that, while unfounded, were very real in her mind. The surgeon brushed them off, saying that her fears were not real and that he didn’t need to address them; his response made her emotional state spiral out of control. Her nurse notified me of the situation, and I came to her bedside. She was very agitated. I sat down at a low level and just started listening. She got all of her anxieties out in words. I held her hand, looked her in the eye, and assured her that I would be there for her and that things were going to be alright. Subsequently, she wrote letters of gratitude and proclaimed to any medical staff who would listen what a talented and great doctor I was. I did not have the skill to fix her broken hip; if it had been left to me alone, she would still be bed-bound. But I did have the human skills to connect with her and fix her agitated mind. If we remember the enduring power of the emotional memory, we can create great patient experiences.
The importance of these experiences was illustrated to me at the 2014 Dignity Health Patient Experience Summit, a powerful event featuring motivational speakers and leaders from across the country. The most powerful speakers, however, were patients. These patients had received terrible diagnoses that committed them to a prolonged interaction with the healthcare system. They were scared of what their diagnoses would mean for their future, they were subjected to uncomfortable procedures in which they struggled to maintain their dignity, and they repeatedly met the indifference of healthcare providers and clerical people who were only there to do a job. They related how the lack of caring and empathy made fears and anxiety much worse. But each of them had a story about that one person, that one care provider, who took the time to reassure them, to show that they cared, and to ensure that the patient did not feel alone. In most of these stories, the stand-out care providers took the time to hold their hands and reassure the patients. They took the time to connect with the patient’s emotional memory in a positive way, and that simple gesture of empathy had a powerful and lasting impact on the patient.
Invariably, the care provider at the heart of the patients’ stories was a nurse. Nurses have the reputation for being angels of mercy because they do the simple, empathetic gestures that let a patient know they are being cared for. These feelings endure in the patients’ memories long after the treatment is over. Doctors can, and should, be that type of care provider. It requires us to recognize that patients are scared and anxious, even though they may do their best not to show it. We, as physicians, often don’t see their anxiety, and we are so focused on the cognitive memory that we don’t address the anxiety and fear that is just under the surface. But taking just a few minutes to acknowledge their emotions, to explore them, and to reassure the patient that we are there for them has a lasting impact. In my group, we talk about the “human-business-human” encounter with patients. We begin all interactions with a human interaction (“Hello, I am Dr. McIlraith…”), conduct the business we came to provide (“Now I am going to examine you…”), and end with a human interaction (“What else can I do for you today?”). Patients expect physical contact with us during the “business” part of that interaction. I find that respectful, reassuring, and appropriate physical contact during the final “human” portion of that interaction helps solidify my patients’ experience. It helps make them feel that they have been cared for, particularly if the visit includes bad news.
Much of the recent focus on patient satisfaction has been driven by financial incentives. In 2013, CMS began penalizing hospitals 1.25% for poor HCAHPS scores as a part of the Affordable Care Act. In 2014, the maximum penalty increased to 2%, and to 3% in 2015. Hospitals have notoriously high overhead costs and slim profit margins, so these penalties can have a profound impact on the financial viability of an institution. But, while hospitals across the country have taken notice (see related article in this edition of The Hospitalist), I find doctors are more motivated by the well-being of their patients than are their hospital administrators. Satisfied patients are more compliant with treatment plans and have better outcomes.4,5 Hospitalists spend a lot of effort making sure their heart failure patients are on an ACE inhibitor, and their heart attack patients are discharged on aspirin, beta blockers, and statins so that they will have a good outcome following treatment for their acute illness. The same outcome-driven, evidence-based practice of medicine relates to patient satisfaction, however. Success in HCAHPS is as important as core measures when it comes to patient outcomes. And if I can’t convince you patient satisfaction is important because of the good it does for hospitals and patients, think about yourself for a minute. Satisfied patients are much less likely to sue their physicians.6 Practicing quality, evidence-based medicine will keep you out of peer review; however, satisfied patients will keep you out of the courtroom.
I frequently hear the comment that “we can do great on patient satisfaction, but then it gets busy, and patient satisfaction goes out the window.” My own experience contradicts this maxim, however. It is not how much time you spend with your patient but, rather, what you do with the time you have. One of the most powerful things we can do is listen. I used to make the mistake that I only wanted to hear the information I needed to figure out my patients’ problems so I could start treating them; however, I have come to learn that being heard is, in itself, therapy for my patients. It is often quoted that physicians interrupt their patients within 18 seconds of starting the interview.7 A lot of physicians dispense with attentive listening when they are under time pressure, when they should instead dispense with lengthy discourses on the patient treatment plan. It is important to educate our patients on their illness and treatment, I admit. I find a lot of hospitalists want to impart their knowledge and their treatment rationale to their patients; however, they frequently give patients and families much more information than they can hold in their cognitive memory. And time pressures are not the only anxieties hospitalists carry with them to the bedside. Our increasingly metric-driven profession means that we not only have to worry about morning discharges, interdisciplinary rounds, length of stay, and so on, but we also have to consider patient experience. It is not easy to hide all the stress we are under when we come to the bedside of a patient, but we have to. The easiest way to do that is to take a deep breath, sit next to the patient, ask an open-ended question, and then say nothing until the patient is done speaking. Active listening with good eye contact and encouragement to continue solidifies the patient’s experience of being heard. There are extreme cases when a patient is in a manic phase and won’t ever stop speaking; bend the rules a bit in those circumstances. However, the above rule works very effectively in the majority of physician-patient interactions. Being heard leaves an enduring emotional memory with our patients.
Hospital medicine often looks to other industries for inspiration on how we can improve. The airline industry is often held up as an example of how we can model patient safety, for instance, but these comparisons oversimplify the challenges we face. The same is true with patient satisfaction. In the business world, adages like “The customer is always right” are central to customer satisfaction, yet completely irrelevant to HM practice. Patients and families frequently have inappropriate and unrealistic expectations of their hospitalist physicians. We cannot, and should not, tell the patient addicted to narcotics that they can have as much IV Dilaudid as they would like. We cannot fix the patient with end-stage cancer, heart failure, or dementia. This is where we have to part ways with comparisons to principles that guide other industries if we are going to find a way forward with patient experience in hospital medicine. Because we have to set limits for patients, we often have to give our patients and families bad news, and because we have to tell them things they don’t like to hear, like “You can’t have any salt in your diet,” or “You must quit drinking alcohol,” we must develop our own principles on patient experience and satisfaction. Otherwise our options are either delivering inappropriate medical care or abandoning the pursuit of patient satisfaction all together. This is when we must remember that emotional memories are more enduring. We can’t always give our patients what they want, and we can’t always tell them what they want to hear, but we can always show them that we care. When we show our patients that we care in a palpable way, we leave them with the feeling that they have been cared for regardless of their condition, and the positive memory will endure despite the negative information we may have to convey. Maybe they won’t cut down on their salt or quit drinking alcohol, but they will never forget that their hospitalist physician cared.
And if they remember that the physician cared, it is much more likely that they will cut down on the salt or quit drinking alcohol when they go home. To paraphrase Maya Angelou, “I can’t always tell my patients what they want to hear, I can’t always tell them that their lifestyle is appropriate, but I can always show them that I care.”
Dr. McIlraith is chairman of the department of hospital medicine of Mercy Medical Group in Sacramento, Calif.
References
- LeDoux JE. Emotional memory. Scholarpedia. Accessed August 2, 2015.
- Feinstein JS, Duff MC, D Tranel D. Sustained experience of emotion after loss of memory in patients with amnesia. Proc Natl Acad Sci. 2010:107(17):7674-7679.
- Guzmán-Vélez E, Feinstein JS, Tranel D. Feelings without memory in Alzheimer disease. Cogn Behav Neurol. 2014;27(3):117-129.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. March 2001. Accessed August 2, 2015.
- Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med. 2011;24(3):229-239.
- Stelfox HT, Gandhi TK, Orav EJ, Gustafson ML. The relation of patient statisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005;118(10):1126-1133.
- Beckman HB, Frankel RM. The effect of physician behavior on the collection of data. Ann Intern Med. 1984;101(5):692-696.
Increased Mortality With Perioperative Beta-Blockade in Low-Risk Patients Undergoing Noncardiac Surgery
Clinical question: Does the use of perioperative beta-blockers affect the outcomes in patients undergoing noncardiac surgery?
Bottom line: Determining the presence or absence of cardiac risk factors is important when deciding whether to use beta-blockers during the perioperative period for patients undergoing noncardiac surgery. This study shows that although perioperative beta-blockade may benefit patients with high cardiac risk, it increases short-term mortality in those with no cardiac risk factors. (LOE = 2b)
Reference: Friedell ML, Van Way CW, Freyberg RW, Almenoff PL. Beta-blockade and operative mortality in noncardiac surgery: harmful or helpful. JAMA Surg. 2015;150(7):658-663.
Study design: Cohort (retrospective)
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (any location) with outpatient follow-up
Synopsis: Using data collected from the Veterans Health Administration, these investigators identified more than 325,000 patients hospitalized for surgery. The use of perioperative beta-blockers in this cohort was determined by using pharmacy data. It was unclear whether the beta-blocker was a new medication or a continuation of a home medication and the study did not measure if the beta-blocker was given preoperatively or postoperatively.
Each patient was assigned a cardiac risk score (1 point each for the presence of renal failure, coronary artery disease, diabetes, and abdominal/thoracic surgery) and grouped into 1 of 3 categories: 0 risk factors, 1 to 2 risk factors, and 3 to 4 risk factors. The results showed that the effect of the beta-blockers on mortality varied according to the presence of cardiac risk factors in patients undergoing noncardiac surgery (n = 314,114). In an adjusted analysis, patients with no cardiac risk factors who received beta-blockers had increased 30-day mortality compared with those who did not receive beta-blockers (odds ratio [OR] 1.19, 95% CI 1.06-1.35).
The opposite was true for patients with 3 to 4 cardiac risk factors: Those who received beta-blockers were less likely to die than those who did not receive them (OR 0.63, 95% CI 0.43-0.93). For patients with 1 to 2 risk factors, there was a nonsignificant reduction in mortality with the use of beta-blockers. For the minority of the cohort who actually underwent cardiac surgery (n = 12,375), there was no significant interaction seen between the number of cardiac risk factors and the use of beta-blockers on mortality. Of note, more than 90% of patients in this study population were men, thus these findings may not be generalizable to women.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Does the use of perioperative beta-blockers affect the outcomes in patients undergoing noncardiac surgery?
Bottom line: Determining the presence or absence of cardiac risk factors is important when deciding whether to use beta-blockers during the perioperative period for patients undergoing noncardiac surgery. This study shows that although perioperative beta-blockade may benefit patients with high cardiac risk, it increases short-term mortality in those with no cardiac risk factors. (LOE = 2b)
Reference: Friedell ML, Van Way CW, Freyberg RW, Almenoff PL. Beta-blockade and operative mortality in noncardiac surgery: harmful or helpful. JAMA Surg. 2015;150(7):658-663.
Study design: Cohort (retrospective)
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (any location) with outpatient follow-up
Synopsis: Using data collected from the Veterans Health Administration, these investigators identified more than 325,000 patients hospitalized for surgery. The use of perioperative beta-blockers in this cohort was determined by using pharmacy data. It was unclear whether the beta-blocker was a new medication or a continuation of a home medication and the study did not measure if the beta-blocker was given preoperatively or postoperatively.
Each patient was assigned a cardiac risk score (1 point each for the presence of renal failure, coronary artery disease, diabetes, and abdominal/thoracic surgery) and grouped into 1 of 3 categories: 0 risk factors, 1 to 2 risk factors, and 3 to 4 risk factors. The results showed that the effect of the beta-blockers on mortality varied according to the presence of cardiac risk factors in patients undergoing noncardiac surgery (n = 314,114). In an adjusted analysis, patients with no cardiac risk factors who received beta-blockers had increased 30-day mortality compared with those who did not receive beta-blockers (odds ratio [OR] 1.19, 95% CI 1.06-1.35).
The opposite was true for patients with 3 to 4 cardiac risk factors: Those who received beta-blockers were less likely to die than those who did not receive them (OR 0.63, 95% CI 0.43-0.93). For patients with 1 to 2 risk factors, there was a nonsignificant reduction in mortality with the use of beta-blockers. For the minority of the cohort who actually underwent cardiac surgery (n = 12,375), there was no significant interaction seen between the number of cardiac risk factors and the use of beta-blockers on mortality. Of note, more than 90% of patients in this study population were men, thus these findings may not be generalizable to women.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Does the use of perioperative beta-blockers affect the outcomes in patients undergoing noncardiac surgery?
Bottom line: Determining the presence or absence of cardiac risk factors is important when deciding whether to use beta-blockers during the perioperative period for patients undergoing noncardiac surgery. This study shows that although perioperative beta-blockade may benefit patients with high cardiac risk, it increases short-term mortality in those with no cardiac risk factors. (LOE = 2b)
Reference: Friedell ML, Van Way CW, Freyberg RW, Almenoff PL. Beta-blockade and operative mortality in noncardiac surgery: harmful or helpful. JAMA Surg. 2015;150(7):658-663.
Study design: Cohort (retrospective)
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (any location) with outpatient follow-up
Synopsis: Using data collected from the Veterans Health Administration, these investigators identified more than 325,000 patients hospitalized for surgery. The use of perioperative beta-blockers in this cohort was determined by using pharmacy data. It was unclear whether the beta-blocker was a new medication or a continuation of a home medication and the study did not measure if the beta-blocker was given preoperatively or postoperatively.
Each patient was assigned a cardiac risk score (1 point each for the presence of renal failure, coronary artery disease, diabetes, and abdominal/thoracic surgery) and grouped into 1 of 3 categories: 0 risk factors, 1 to 2 risk factors, and 3 to 4 risk factors. The results showed that the effect of the beta-blockers on mortality varied according to the presence of cardiac risk factors in patients undergoing noncardiac surgery (n = 314,114). In an adjusted analysis, patients with no cardiac risk factors who received beta-blockers had increased 30-day mortality compared with those who did not receive beta-blockers (odds ratio [OR] 1.19, 95% CI 1.06-1.35).
The opposite was true for patients with 3 to 4 cardiac risk factors: Those who received beta-blockers were less likely to die than those who did not receive them (OR 0.63, 95% CI 0.43-0.93). For patients with 1 to 2 risk factors, there was a nonsignificant reduction in mortality with the use of beta-blockers. For the minority of the cohort who actually underwent cardiac surgery (n = 12,375), there was no significant interaction seen between the number of cardiac risk factors and the use of beta-blockers on mortality. Of note, more than 90% of patients in this study population were men, thus these findings may not be generalizable to women.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Wells Score Not Helpful in Hospitalized Patients With Suspected DVT
Clinical question: How useful is the Wells score for risk-stratifying hospitalized patients with suspected deep vein thrombosis?
Bottom line: The Wells score is not helpful in the inpatient setting to predict the presence or absence of deep vein thrombosis (DVT). Based on this study, if a hospitalized patient has a low Wells score, the risk of having DVT is still relatively high (6%). If a patient has a moderate or high score, however, the risk of having DVT is fairly low (10% to 16%). In all 3 categories, a patient would need further testing with ultrasound to evaluate for DVT. (LOE = 2b)
Reference: Silveira PC, Ip IK, Goldhaber SZ, Piazza G, Benson CB, Khorasani R. Performance of Wells score for deep vein thrombosis in the inpatient setting. JAMA Intern Med. 2015;175(7):1112-1117.
Study design: Diagnostic test evaluation
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (any location)
Synopsis: The Wells score has been previously validated to risk-stratify outpatients with suspected DVT but its utility in the inpatient setting is unknown. These investigators evaluated 1135 hospitalized patients with suspected DVT who underwent a lower extremity ultrasound study in the hospital. When ordering these studies, clinicians were required to enter information regarding clinical predictors in order to calculate an individual patient's Wells score. The patients were divided into 3 Wells score categories that determined their pre-test probability for DVT (low risk = 0 or lower, moderate risk = 1 or 2, high risk = 3 or higher). Baseline characteristics for the patients in the study showed that 71% were recently bedridden or had recent major surgery and almost 40% had active cancer.
Overall, 12% of patients in the study had proximal DVT confirmed by a lower extremity ultrasound study. When classified by Wells score categories, the incidence of proximal DVT was 5.9%, 9.5%, and 16.4% in low, moderate, and high pre-test probability groups, respectively. The area under the receiving operating characteristics curve for the Wells score as a diagnostic test was 0.60.
This indicates that the ability of the Wells score to discriminate between the presence and absence of DVT in hospitalized patients was only slightly better than chance. The authors postulate that the reason for this is that hospitalized patients are inherently different from outpatients: they have a higher prevalence of immobilization and/or have active cancer; they receive routine DVT prophylaxis; and they are more likely to have other comorbidities that increase DVT risk, such as heart failure and chronic obstructive pulmonary disease — risk factors that are not accounted for in the Wells score calculation. As such, the Wells score is less meaningful in this population.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: How useful is the Wells score for risk-stratifying hospitalized patients with suspected deep vein thrombosis?
Bottom line: The Wells score is not helpful in the inpatient setting to predict the presence or absence of deep vein thrombosis (DVT). Based on this study, if a hospitalized patient has a low Wells score, the risk of having DVT is still relatively high (6%). If a patient has a moderate or high score, however, the risk of having DVT is fairly low (10% to 16%). In all 3 categories, a patient would need further testing with ultrasound to evaluate for DVT. (LOE = 2b)
Reference: Silveira PC, Ip IK, Goldhaber SZ, Piazza G, Benson CB, Khorasani R. Performance of Wells score for deep vein thrombosis in the inpatient setting. JAMA Intern Med. 2015;175(7):1112-1117.
Study design: Diagnostic test evaluation
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (any location)
Synopsis: The Wells score has been previously validated to risk-stratify outpatients with suspected DVT but its utility in the inpatient setting is unknown. These investigators evaluated 1135 hospitalized patients with suspected DVT who underwent a lower extremity ultrasound study in the hospital. When ordering these studies, clinicians were required to enter information regarding clinical predictors in order to calculate an individual patient's Wells score. The patients were divided into 3 Wells score categories that determined their pre-test probability for DVT (low risk = 0 or lower, moderate risk = 1 or 2, high risk = 3 or higher). Baseline characteristics for the patients in the study showed that 71% were recently bedridden or had recent major surgery and almost 40% had active cancer.
Overall, 12% of patients in the study had proximal DVT confirmed by a lower extremity ultrasound study. When classified by Wells score categories, the incidence of proximal DVT was 5.9%, 9.5%, and 16.4% in low, moderate, and high pre-test probability groups, respectively. The area under the receiving operating characteristics curve for the Wells score as a diagnostic test was 0.60.
This indicates that the ability of the Wells score to discriminate between the presence and absence of DVT in hospitalized patients was only slightly better than chance. The authors postulate that the reason for this is that hospitalized patients are inherently different from outpatients: they have a higher prevalence of immobilization and/or have active cancer; they receive routine DVT prophylaxis; and they are more likely to have other comorbidities that increase DVT risk, such as heart failure and chronic obstructive pulmonary disease — risk factors that are not accounted for in the Wells score calculation. As such, the Wells score is less meaningful in this population.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: How useful is the Wells score for risk-stratifying hospitalized patients with suspected deep vein thrombosis?
Bottom line: The Wells score is not helpful in the inpatient setting to predict the presence or absence of deep vein thrombosis (DVT). Based on this study, if a hospitalized patient has a low Wells score, the risk of having DVT is still relatively high (6%). If a patient has a moderate or high score, however, the risk of having DVT is fairly low (10% to 16%). In all 3 categories, a patient would need further testing with ultrasound to evaluate for DVT. (LOE = 2b)
Reference: Silveira PC, Ip IK, Goldhaber SZ, Piazza G, Benson CB, Khorasani R. Performance of Wells score for deep vein thrombosis in the inpatient setting. JAMA Intern Med. 2015;175(7):1112-1117.
Study design: Diagnostic test evaluation
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (any location)
Synopsis: The Wells score has been previously validated to risk-stratify outpatients with suspected DVT but its utility in the inpatient setting is unknown. These investigators evaluated 1135 hospitalized patients with suspected DVT who underwent a lower extremity ultrasound study in the hospital. When ordering these studies, clinicians were required to enter information regarding clinical predictors in order to calculate an individual patient's Wells score. The patients were divided into 3 Wells score categories that determined their pre-test probability for DVT (low risk = 0 or lower, moderate risk = 1 or 2, high risk = 3 or higher). Baseline characteristics for the patients in the study showed that 71% were recently bedridden or had recent major surgery and almost 40% had active cancer.
Overall, 12% of patients in the study had proximal DVT confirmed by a lower extremity ultrasound study. When classified by Wells score categories, the incidence of proximal DVT was 5.9%, 9.5%, and 16.4% in low, moderate, and high pre-test probability groups, respectively. The area under the receiving operating characteristics curve for the Wells score as a diagnostic test was 0.60.
This indicates that the ability of the Wells score to discriminate between the presence and absence of DVT in hospitalized patients was only slightly better than chance. The authors postulate that the reason for this is that hospitalized patients are inherently different from outpatients: they have a higher prevalence of immobilization and/or have active cancer; they receive routine DVT prophylaxis; and they are more likely to have other comorbidities that increase DVT risk, such as heart failure and chronic obstructive pulmonary disease — risk factors that are not accounted for in the Wells score calculation. As such, the Wells score is less meaningful in this population.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.