User login
My experience of a COVID-19 vaccine breakthrough infection
Friday, July 16, 2021, marked the end of a week on duty in the hospital, and it was time to celebrate with a nice dinner out with my wife, since COVID-19 masking requirements had been lifted in our part of California for people like us who were fully vaccinated.
We always loved a nice dinner out and missed it so much during the pandemic. Unlike 6 months earlier, when I was administering dexamethasone, remdesivir, and high-flow oxygen to half of the patients on my panel, not a single patient was diagnosed with COVID-19, much less treated for it, during the previous week. We were doing so well in Sacramento that the hospital visitation rules had been relaxed and vaccinated patients were not required to have a negative COVID-19 test prior to hospital admission.
Saturday was game 5 of the NBA finals, so we had two couples join us for the game at our house; no masks because we were all vaccinated. On Sunday, we visited our neighbors who had just had a new baby boy and made them the gift of some baby books. The new mom had struggled with the decision of whether to get vaccinated during her pregnancy, but eventually decided to complete the vaccination cycle prior to delivery. She was fully immune at the time of the baby’s birth, wisely wanting the baby to have passive immunity through her. We kept an appropriate distance, and never touched baby or mom, but since masking guidelines had been lifted for the vaccinated,we didn’t bother with them.
On Monday, I felt a little something in my nose but still pursued my usual workout. Interestingly, my performance wasn’t up to my usual standards. There was a meeting that evening that I had to prepare for, when all of a sudden I felt very fatigued. I lay down and slept for a good hour, which disrupted my preparation. I warned the participants that I was feeling a little under the weather, but they wanted to proceed. At this point, I decided it was time to start wearing a mask again.
More meetings on Tuesday morning, but I made sure that I was fully masked. That little thing in my nose had blown up into a full-scale rhinitis, requiring Kleenex and decongestants. Plus, the fatigue was hitting me very hard. “Dang!” I thought. “I haven’t had a cold since 2019. All those COVID-19 precautions not only worked against COVID-19 (which I never got) but also worked against the common cold, which I had now.”
I finished up my meetings and laid down for a good hour and a half. As the father of two, I had plenty of experience with the common cold, and I knew that plenty of rest and hydration was the key to kicking this thing. Besides, my 55th birthday was coming up, and I wanted to make sure I was fully recovered for the festivities my wife was planning for me. Nonetheless, I scheduled myself for a COVID-19 test. I knew this couldn’t be COVID-19 because I was fully vaccinated, but it was hitting me so hard. It had to be a virus that my body had never seen before; maybe the human metapneumovirus. That was my line of reasoning, anyway.
Wednesday was another day on the couch because of continued severe fatigue and myalgias. I figured another good day of rest would help me kick this cold in time for my birthday celebration. Then the COVID-19 results came back positive. “How could this be? I was vaccinated?!” Admittedly I had been more relaxed with masking, per the CDC and county guidelines, but I always wore a mask when I was seeing patients in the hospital. Yeah, I wasn’t wearing an N95 anymore, and I had given up my goggles months ago, but we just weren’t seeing much COVID-19 anymore, so a plain surgical mask was all that was required and seemed sufficient. I had been reading articles about the new Delta variant that was becoming dominant across the country, and reports were that the vaccine was still effective against the Delta variant. However, I was experiencing the COVID-19 vaccine breakthrough infection because of the remarkable talent the Delta variant has for replicating and producing high levels of viremia.
My first thoughts were for my family, of course. As my illness unfolded, I had kept checking in with them to see if they had any of these “cold” symptoms I had; none of them did. When my test came back positive, we all went into quarantine immediately and they went to get tested; all of them were negative. Next, I contacted the people I had been meeting with that week and warned them that I had tested positive. Despite my mask, and their fully vaccinated status, they needed to get tested. They did, and they were negative. I realized that I was probably contagious, though asymptomatic, on Saturday night when we had friends over to watch the NBA finals. Yeah, everyone was vaccinated, but if I could get sick from this new Delta variant, they could too. The public health department sent me a survey when they found out about my positive test, and they pinpointed Saturday as the day I started to be contagious. I told my friends that I was probably contagious when they were over for the game, and that they should get tested. They did, and everyone came back negative for COVID-19.
Wait a minute; what about Sunday night? The newborn baby and the sleep-deprived mom. Oh no! I was contagious then as well. We kept our distance, and were only there for about 10 minutes, but if I felt bad from COVID-19, I felt worse for exposing them to the virus.
I am no Anthony Fauci, and I am grateful that we have had levelheaded scientists like him to lead us through this terrible experience. I am sure there will be many papers written about COVID-19 breakthrough infections in the future, but I have many thoughts from this experience. First, my practice of wearing an N95 and goggles for all patients, not just COVID-19 patients, during the height of the pandemic was effective. Prior to getting vaccinated, my antibody tests were negative, so I never contracted the illness when I stuck to this regimen. Second, we all want to get back to something that looks like “normal,” but because there are large unvaccinated populations in the community the virus will continue to propagate and evolve, and hence everyone is at risk. While the guidelines said it was okay to ease up on our restrictions, because so many people are not vaccinated, we all must continue to keep our guard up. Third, would a booster shot have saved me from this fate? Because I was on the front lines of the pandemic as a hospitalist, I was also among the first members of my community to get vaccinated, receiving my second shot on Jan. 14, 2021. My wife was not in any risk group, was not on any vaccine priority list, and didn’t complete the series until early April. If I was going to give the infection to anyone, it would have been her. Not only did she never develop symptoms, but she also repeatedly tested negative, as did everyone else that I was in contact with when I was most contagious. The thing that was different about me from everyone else was that I had gotten the vaccine well ahead of them. Had my immunity waned over the months?
The good news is that, while I wouldn’t characterize what I had as “mild,” it certainly wasn’t protracted. Yes, I was a good boy, and did the basics: stay hydrated and get plenty of sleep. I was really bad off for about 3 days, and I hate to think what it would have been like if I had coexisting conditions such as asthma or diabetes. We all know what a bad case of COVID-19 looks like in the unvaccinated, with months in the hospital, intravenous infusions, and high-flow oxygen for the lucky ones. I had nothing remotely like that. The dominant symptom I had was incapacitating fatigue and significant body aches. The second night I had some major chills, sweats, and wild dreams. From a respiratory standpoint, I had bad rhinitis and a wicked cough for a while that tapered off. My oxygen saturations dropped into the mid 90’s, but never below 94%. But if I had been ten times sicker, I doubt I would have survived. I was on quarantine for 10 days but I highly doubt I was at all contagious by day 5, based on my symptoms and the fact that nobody around me turned COVID positive with repeat testing.
I was so relieved that none of my contacts when I was most contagious turned positive for COVID-19. Though not scientific, I find that illustrative. While I should have canceled my meetings on Monday and Tuesday, everybody knew I had a “cold” and nobody wanted to cancel. Nobody thought it possible that I had COVID-19, especially me. The Delta variant is notorious for generating high levels of viremia, yet I didn’t get anybody sick, not even my wife. That suggests to me that, while the vaccine doesn’t eliminate the risk of infection – which we already knew – it probably significantly reduced my infectivity. For that I am very grateful. Now that I can say that I had the COVID-19 experience, I can tell you it feels terrible. But I would have felt much worse if I had gotten others ill. My personal belief is that while the vaccine didn’t save me from disease, it dramatically truncated my illness, and significantly reduced my risk of passing the virus on to my friends and family.
So where did I contract the virus? We were unmasked at dinner on Friday night, which was acceptable in Yolo County at that time. By the way, I actually live in Yolo County, not YOLO (you only live once) county. You can imagine the latter would be a bit more loosey-goosey with the masking requirements. That notwithstanding, I don’t think the dinner was where I picked it up because it was too short of an incubation period. My wife and I obviously reacted differently, as I discussed, but we were both at the restaurant. She didn’t get COVID-19 and I did. I think that I probably picked it up at the hospital, because, while I was wearing a mask there, I was only wearing a surgical mask, not an N95. And I wasn’t wearing goggles anymore. While none of my patients were officially diagnosed with COVID-19, I was encountering a lot of people, getting in relatively close contact, and guidelines were being relaxed, including preadmission COVID-19 testing.
I was an outlier, as I have pointed out; none of my other close contacts contracted COVID-19. A lot of politics and public opinion is driven by outlier cases, and even pure fabrications these days; we certainly can’t create public health policy based on an outlier. I am not suggesting that my experience is any basis for rewriting the rules of COVID-19. The experience has given me pause to think through many facets of this horrible illness we have had to deal with in so many ways, however. And I have also reexamined my own practice for protecting myself in the hospital. Clearly what I was doing in the height of the pandemic was effective, and my more relaxed recent practices were not. Now that I am fully recovered after a relatively unique encounter with the condition, I look forward to seeing what the scientists and public policy makers do with COVID-19 vaccine breakthrough cases. So, between us hospitalist friends and colleagues, regardless of the policy guidelines, I say we keep on masking.
Dr. McIlraith is the founding chairman of the hospital medicine department at Mercy Medical Group in Sacramento. He received the SHM Award for Outstanding Service in Hospital Medicine in 2016.
Friday, July 16, 2021, marked the end of a week on duty in the hospital, and it was time to celebrate with a nice dinner out with my wife, since COVID-19 masking requirements had been lifted in our part of California for people like us who were fully vaccinated.
We always loved a nice dinner out and missed it so much during the pandemic. Unlike 6 months earlier, when I was administering dexamethasone, remdesivir, and high-flow oxygen to half of the patients on my panel, not a single patient was diagnosed with COVID-19, much less treated for it, during the previous week. We were doing so well in Sacramento that the hospital visitation rules had been relaxed and vaccinated patients were not required to have a negative COVID-19 test prior to hospital admission.
Saturday was game 5 of the NBA finals, so we had two couples join us for the game at our house; no masks because we were all vaccinated. On Sunday, we visited our neighbors who had just had a new baby boy and made them the gift of some baby books. The new mom had struggled with the decision of whether to get vaccinated during her pregnancy, but eventually decided to complete the vaccination cycle prior to delivery. She was fully immune at the time of the baby’s birth, wisely wanting the baby to have passive immunity through her. We kept an appropriate distance, and never touched baby or mom, but since masking guidelines had been lifted for the vaccinated,we didn’t bother with them.
On Monday, I felt a little something in my nose but still pursued my usual workout. Interestingly, my performance wasn’t up to my usual standards. There was a meeting that evening that I had to prepare for, when all of a sudden I felt very fatigued. I lay down and slept for a good hour, which disrupted my preparation. I warned the participants that I was feeling a little under the weather, but they wanted to proceed. At this point, I decided it was time to start wearing a mask again.
More meetings on Tuesday morning, but I made sure that I was fully masked. That little thing in my nose had blown up into a full-scale rhinitis, requiring Kleenex and decongestants. Plus, the fatigue was hitting me very hard. “Dang!” I thought. “I haven’t had a cold since 2019. All those COVID-19 precautions not only worked against COVID-19 (which I never got) but also worked against the common cold, which I had now.”
I finished up my meetings and laid down for a good hour and a half. As the father of two, I had plenty of experience with the common cold, and I knew that plenty of rest and hydration was the key to kicking this thing. Besides, my 55th birthday was coming up, and I wanted to make sure I was fully recovered for the festivities my wife was planning for me. Nonetheless, I scheduled myself for a COVID-19 test. I knew this couldn’t be COVID-19 because I was fully vaccinated, but it was hitting me so hard. It had to be a virus that my body had never seen before; maybe the human metapneumovirus. That was my line of reasoning, anyway.
Wednesday was another day on the couch because of continued severe fatigue and myalgias. I figured another good day of rest would help me kick this cold in time for my birthday celebration. Then the COVID-19 results came back positive. “How could this be? I was vaccinated?!” Admittedly I had been more relaxed with masking, per the CDC and county guidelines, but I always wore a mask when I was seeing patients in the hospital. Yeah, I wasn’t wearing an N95 anymore, and I had given up my goggles months ago, but we just weren’t seeing much COVID-19 anymore, so a plain surgical mask was all that was required and seemed sufficient. I had been reading articles about the new Delta variant that was becoming dominant across the country, and reports were that the vaccine was still effective against the Delta variant. However, I was experiencing the COVID-19 vaccine breakthrough infection because of the remarkable talent the Delta variant has for replicating and producing high levels of viremia.
My first thoughts were for my family, of course. As my illness unfolded, I had kept checking in with them to see if they had any of these “cold” symptoms I had; none of them did. When my test came back positive, we all went into quarantine immediately and they went to get tested; all of them were negative. Next, I contacted the people I had been meeting with that week and warned them that I had tested positive. Despite my mask, and their fully vaccinated status, they needed to get tested. They did, and they were negative. I realized that I was probably contagious, though asymptomatic, on Saturday night when we had friends over to watch the NBA finals. Yeah, everyone was vaccinated, but if I could get sick from this new Delta variant, they could too. The public health department sent me a survey when they found out about my positive test, and they pinpointed Saturday as the day I started to be contagious. I told my friends that I was probably contagious when they were over for the game, and that they should get tested. They did, and everyone came back negative for COVID-19.
Wait a minute; what about Sunday night? The newborn baby and the sleep-deprived mom. Oh no! I was contagious then as well. We kept our distance, and were only there for about 10 minutes, but if I felt bad from COVID-19, I felt worse for exposing them to the virus.
I am no Anthony Fauci, and I am grateful that we have had levelheaded scientists like him to lead us through this terrible experience. I am sure there will be many papers written about COVID-19 breakthrough infections in the future, but I have many thoughts from this experience. First, my practice of wearing an N95 and goggles for all patients, not just COVID-19 patients, during the height of the pandemic was effective. Prior to getting vaccinated, my antibody tests were negative, so I never contracted the illness when I stuck to this regimen. Second, we all want to get back to something that looks like “normal,” but because there are large unvaccinated populations in the community the virus will continue to propagate and evolve, and hence everyone is at risk. While the guidelines said it was okay to ease up on our restrictions, because so many people are not vaccinated, we all must continue to keep our guard up. Third, would a booster shot have saved me from this fate? Because I was on the front lines of the pandemic as a hospitalist, I was also among the first members of my community to get vaccinated, receiving my second shot on Jan. 14, 2021. My wife was not in any risk group, was not on any vaccine priority list, and didn’t complete the series until early April. If I was going to give the infection to anyone, it would have been her. Not only did she never develop symptoms, but she also repeatedly tested negative, as did everyone else that I was in contact with when I was most contagious. The thing that was different about me from everyone else was that I had gotten the vaccine well ahead of them. Had my immunity waned over the months?
The good news is that, while I wouldn’t characterize what I had as “mild,” it certainly wasn’t protracted. Yes, I was a good boy, and did the basics: stay hydrated and get plenty of sleep. I was really bad off for about 3 days, and I hate to think what it would have been like if I had coexisting conditions such as asthma or diabetes. We all know what a bad case of COVID-19 looks like in the unvaccinated, with months in the hospital, intravenous infusions, and high-flow oxygen for the lucky ones. I had nothing remotely like that. The dominant symptom I had was incapacitating fatigue and significant body aches. The second night I had some major chills, sweats, and wild dreams. From a respiratory standpoint, I had bad rhinitis and a wicked cough for a while that tapered off. My oxygen saturations dropped into the mid 90’s, but never below 94%. But if I had been ten times sicker, I doubt I would have survived. I was on quarantine for 10 days but I highly doubt I was at all contagious by day 5, based on my symptoms and the fact that nobody around me turned COVID positive with repeat testing.
I was so relieved that none of my contacts when I was most contagious turned positive for COVID-19. Though not scientific, I find that illustrative. While I should have canceled my meetings on Monday and Tuesday, everybody knew I had a “cold” and nobody wanted to cancel. Nobody thought it possible that I had COVID-19, especially me. The Delta variant is notorious for generating high levels of viremia, yet I didn’t get anybody sick, not even my wife. That suggests to me that, while the vaccine doesn’t eliminate the risk of infection – which we already knew – it probably significantly reduced my infectivity. For that I am very grateful. Now that I can say that I had the COVID-19 experience, I can tell you it feels terrible. But I would have felt much worse if I had gotten others ill. My personal belief is that while the vaccine didn’t save me from disease, it dramatically truncated my illness, and significantly reduced my risk of passing the virus on to my friends and family.
So where did I contract the virus? We were unmasked at dinner on Friday night, which was acceptable in Yolo County at that time. By the way, I actually live in Yolo County, not YOLO (you only live once) county. You can imagine the latter would be a bit more loosey-goosey with the masking requirements. That notwithstanding, I don’t think the dinner was where I picked it up because it was too short of an incubation period. My wife and I obviously reacted differently, as I discussed, but we were both at the restaurant. She didn’t get COVID-19 and I did. I think that I probably picked it up at the hospital, because, while I was wearing a mask there, I was only wearing a surgical mask, not an N95. And I wasn’t wearing goggles anymore. While none of my patients were officially diagnosed with COVID-19, I was encountering a lot of people, getting in relatively close contact, and guidelines were being relaxed, including preadmission COVID-19 testing.
I was an outlier, as I have pointed out; none of my other close contacts contracted COVID-19. A lot of politics and public opinion is driven by outlier cases, and even pure fabrications these days; we certainly can’t create public health policy based on an outlier. I am not suggesting that my experience is any basis for rewriting the rules of COVID-19. The experience has given me pause to think through many facets of this horrible illness we have had to deal with in so many ways, however. And I have also reexamined my own practice for protecting myself in the hospital. Clearly what I was doing in the height of the pandemic was effective, and my more relaxed recent practices were not. Now that I am fully recovered after a relatively unique encounter with the condition, I look forward to seeing what the scientists and public policy makers do with COVID-19 vaccine breakthrough cases. So, between us hospitalist friends and colleagues, regardless of the policy guidelines, I say we keep on masking.
Dr. McIlraith is the founding chairman of the hospital medicine department at Mercy Medical Group in Sacramento. He received the SHM Award for Outstanding Service in Hospital Medicine in 2016.
Friday, July 16, 2021, marked the end of a week on duty in the hospital, and it was time to celebrate with a nice dinner out with my wife, since COVID-19 masking requirements had been lifted in our part of California for people like us who were fully vaccinated.
We always loved a nice dinner out and missed it so much during the pandemic. Unlike 6 months earlier, when I was administering dexamethasone, remdesivir, and high-flow oxygen to half of the patients on my panel, not a single patient was diagnosed with COVID-19, much less treated for it, during the previous week. We were doing so well in Sacramento that the hospital visitation rules had been relaxed and vaccinated patients were not required to have a negative COVID-19 test prior to hospital admission.
Saturday was game 5 of the NBA finals, so we had two couples join us for the game at our house; no masks because we were all vaccinated. On Sunday, we visited our neighbors who had just had a new baby boy and made them the gift of some baby books. The new mom had struggled with the decision of whether to get vaccinated during her pregnancy, but eventually decided to complete the vaccination cycle prior to delivery. She was fully immune at the time of the baby’s birth, wisely wanting the baby to have passive immunity through her. We kept an appropriate distance, and never touched baby or mom, but since masking guidelines had been lifted for the vaccinated,we didn’t bother with them.
On Monday, I felt a little something in my nose but still pursued my usual workout. Interestingly, my performance wasn’t up to my usual standards. There was a meeting that evening that I had to prepare for, when all of a sudden I felt very fatigued. I lay down and slept for a good hour, which disrupted my preparation. I warned the participants that I was feeling a little under the weather, but they wanted to proceed. At this point, I decided it was time to start wearing a mask again.
More meetings on Tuesday morning, but I made sure that I was fully masked. That little thing in my nose had blown up into a full-scale rhinitis, requiring Kleenex and decongestants. Plus, the fatigue was hitting me very hard. “Dang!” I thought. “I haven’t had a cold since 2019. All those COVID-19 precautions not only worked against COVID-19 (which I never got) but also worked against the common cold, which I had now.”
I finished up my meetings and laid down for a good hour and a half. As the father of two, I had plenty of experience with the common cold, and I knew that plenty of rest and hydration was the key to kicking this thing. Besides, my 55th birthday was coming up, and I wanted to make sure I was fully recovered for the festivities my wife was planning for me. Nonetheless, I scheduled myself for a COVID-19 test. I knew this couldn’t be COVID-19 because I was fully vaccinated, but it was hitting me so hard. It had to be a virus that my body had never seen before; maybe the human metapneumovirus. That was my line of reasoning, anyway.
Wednesday was another day on the couch because of continued severe fatigue and myalgias. I figured another good day of rest would help me kick this cold in time for my birthday celebration. Then the COVID-19 results came back positive. “How could this be? I was vaccinated?!” Admittedly I had been more relaxed with masking, per the CDC and county guidelines, but I always wore a mask when I was seeing patients in the hospital. Yeah, I wasn’t wearing an N95 anymore, and I had given up my goggles months ago, but we just weren’t seeing much COVID-19 anymore, so a plain surgical mask was all that was required and seemed sufficient. I had been reading articles about the new Delta variant that was becoming dominant across the country, and reports were that the vaccine was still effective against the Delta variant. However, I was experiencing the COVID-19 vaccine breakthrough infection because of the remarkable talent the Delta variant has for replicating and producing high levels of viremia.
My first thoughts were for my family, of course. As my illness unfolded, I had kept checking in with them to see if they had any of these “cold” symptoms I had; none of them did. When my test came back positive, we all went into quarantine immediately and they went to get tested; all of them were negative. Next, I contacted the people I had been meeting with that week and warned them that I had tested positive. Despite my mask, and their fully vaccinated status, they needed to get tested. They did, and they were negative. I realized that I was probably contagious, though asymptomatic, on Saturday night when we had friends over to watch the NBA finals. Yeah, everyone was vaccinated, but if I could get sick from this new Delta variant, they could too. The public health department sent me a survey when they found out about my positive test, and they pinpointed Saturday as the day I started to be contagious. I told my friends that I was probably contagious when they were over for the game, and that they should get tested. They did, and everyone came back negative for COVID-19.
Wait a minute; what about Sunday night? The newborn baby and the sleep-deprived mom. Oh no! I was contagious then as well. We kept our distance, and were only there for about 10 minutes, but if I felt bad from COVID-19, I felt worse for exposing them to the virus.
I am no Anthony Fauci, and I am grateful that we have had levelheaded scientists like him to lead us through this terrible experience. I am sure there will be many papers written about COVID-19 breakthrough infections in the future, but I have many thoughts from this experience. First, my practice of wearing an N95 and goggles for all patients, not just COVID-19 patients, during the height of the pandemic was effective. Prior to getting vaccinated, my antibody tests were negative, so I never contracted the illness when I stuck to this regimen. Second, we all want to get back to something that looks like “normal,” but because there are large unvaccinated populations in the community the virus will continue to propagate and evolve, and hence everyone is at risk. While the guidelines said it was okay to ease up on our restrictions, because so many people are not vaccinated, we all must continue to keep our guard up. Third, would a booster shot have saved me from this fate? Because I was on the front lines of the pandemic as a hospitalist, I was also among the first members of my community to get vaccinated, receiving my second shot on Jan. 14, 2021. My wife was not in any risk group, was not on any vaccine priority list, and didn’t complete the series until early April. If I was going to give the infection to anyone, it would have been her. Not only did she never develop symptoms, but she also repeatedly tested negative, as did everyone else that I was in contact with when I was most contagious. The thing that was different about me from everyone else was that I had gotten the vaccine well ahead of them. Had my immunity waned over the months?
The good news is that, while I wouldn’t characterize what I had as “mild,” it certainly wasn’t protracted. Yes, I was a good boy, and did the basics: stay hydrated and get plenty of sleep. I was really bad off for about 3 days, and I hate to think what it would have been like if I had coexisting conditions such as asthma or diabetes. We all know what a bad case of COVID-19 looks like in the unvaccinated, with months in the hospital, intravenous infusions, and high-flow oxygen for the lucky ones. I had nothing remotely like that. The dominant symptom I had was incapacitating fatigue and significant body aches. The second night I had some major chills, sweats, and wild dreams. From a respiratory standpoint, I had bad rhinitis and a wicked cough for a while that tapered off. My oxygen saturations dropped into the mid 90’s, but never below 94%. But if I had been ten times sicker, I doubt I would have survived. I was on quarantine for 10 days but I highly doubt I was at all contagious by day 5, based on my symptoms and the fact that nobody around me turned COVID positive with repeat testing.
I was so relieved that none of my contacts when I was most contagious turned positive for COVID-19. Though not scientific, I find that illustrative. While I should have canceled my meetings on Monday and Tuesday, everybody knew I had a “cold” and nobody wanted to cancel. Nobody thought it possible that I had COVID-19, especially me. The Delta variant is notorious for generating high levels of viremia, yet I didn’t get anybody sick, not even my wife. That suggests to me that, while the vaccine doesn’t eliminate the risk of infection – which we already knew – it probably significantly reduced my infectivity. For that I am very grateful. Now that I can say that I had the COVID-19 experience, I can tell you it feels terrible. But I would have felt much worse if I had gotten others ill. My personal belief is that while the vaccine didn’t save me from disease, it dramatically truncated my illness, and significantly reduced my risk of passing the virus on to my friends and family.
So where did I contract the virus? We were unmasked at dinner on Friday night, which was acceptable in Yolo County at that time. By the way, I actually live in Yolo County, not YOLO (you only live once) county. You can imagine the latter would be a bit more loosey-goosey with the masking requirements. That notwithstanding, I don’t think the dinner was where I picked it up because it was too short of an incubation period. My wife and I obviously reacted differently, as I discussed, but we were both at the restaurant. She didn’t get COVID-19 and I did. I think that I probably picked it up at the hospital, because, while I was wearing a mask there, I was only wearing a surgical mask, not an N95. And I wasn’t wearing goggles anymore. While none of my patients were officially diagnosed with COVID-19, I was encountering a lot of people, getting in relatively close contact, and guidelines were being relaxed, including preadmission COVID-19 testing.
I was an outlier, as I have pointed out; none of my other close contacts contracted COVID-19. A lot of politics and public opinion is driven by outlier cases, and even pure fabrications these days; we certainly can’t create public health policy based on an outlier. I am not suggesting that my experience is any basis for rewriting the rules of COVID-19. The experience has given me pause to think through many facets of this horrible illness we have had to deal with in so many ways, however. And I have also reexamined my own practice for protecting myself in the hospital. Clearly what I was doing in the height of the pandemic was effective, and my more relaxed recent practices were not. Now that I am fully recovered after a relatively unique encounter with the condition, I look forward to seeing what the scientists and public policy makers do with COVID-19 vaccine breakthrough cases. So, between us hospitalist friends and colleagues, regardless of the policy guidelines, I say we keep on masking.
Dr. McIlraith is the founding chairman of the hospital medicine department at Mercy Medical Group in Sacramento. He received the SHM Award for Outstanding Service in Hospital Medicine in 2016.
The authority/accountability balance
Evaluating your career trajectory
I have had the pleasure of working on the Society of Hospital Medicine’s signature Leadership Academies since 2010, and I enjoy working with hospital medicine leaders from around the country every year. I started as a hospital medicine leader in 2000 and served during the unprecedented growth of the field when it was “the most rapidly growing specialty in the history of medicine.”
Most businesses dream of having a year of double-digit growth; my department grew an average of 15% annually for more than 10 years. These unique experiences have taught me many lessons and afforded me the opportunity to watch many stars of hospital medicine rise, as well as to learn from several less-scrupulous leaders about the darker side of hospital politics.
One of the lessons I learned the hard way about hospital politics is striking the “Authority/Accountability balance” in your career. I shared this perspective at the SHM annual conference in 2018, at speaking engagements on the West Coast, and with my leadership group at the academies. I am sharing it with you because the feedback I have received has been very positive.
The Authority/Accountability balance is a tool for evaluating your current career trajectory and measuring if it is set up for success or failure. The essence is that your Authority and Accountability need to be balanced for you to be successful in your career, regardless of your station. Everybody from the hospitalist fresh out of residency to the CEO needs to have Authority and Accountability in balance to be successful. And as you use the tool to measure your own potential for success or failure, learn to apply it to those who report to you.
I believe the rising tide lifts all boats and the success of your subordinates, through mentoring and support, will add to your success. There is another, more cynical view of subordinates that can be identified using the Authority/Accountability balance, which I will address.
Authority
In this construct, “Authority” has a much broader meaning than just the ability to tell people what to do. The ability to tell people what to do is important but not sufficient for success in hospital politics.
Financial resources are essential for a successful Authority/Accountability balance – not only the hardware such as computers, telephones, pagers, and so on, but also clerical support, technical support, and analytic support so that you are getting high-quality data on the performance of the members of your hospital medicine group (HMG). These “soft” resources (clerical, technical, and analytical) are often overlooked as needs that HMG leaders must advocate for; I speak with many HMG leaders who remain under-resourced with “soft” assets. However, being appropriately resourced in these areas can be transformational for a group. Hospitalists don’t like doing clerical work, and if you don’t like a menial job assigned to you, you probably won’t do it very well. Having an unlicensed person dedicated to these clerical activities not only will cost less, but will ensure the job is done better.
Reporting structure is critically important, often overlooked, and historically misaligned in HMGs. When hospital medicine was starting in the late 1990s and early 2000s, rapidly growing hospitalist groups were typically led by young, early-career physicians who had chosen hospital medicine as a career. The problem was that they often lacked the seniority and connections at the executive level to advocate for their HMG. All too often the hospitalist group was tucked in under another department or division which, in turn, reported HMG updates and issues to the board of directors and the CEO.
A common reporting structure in the early days was that a senior member of the medical staff, or group, had once worked in the hospital and therefore “understood” the issues and challenges that the hospitalists were facing. It was up to this physician with seniority and connections to advocate for the hospitalists as they saw fit. The problem was that the hospital landscape was, and is, constantly evolving in innumerable ways. These “once removed” reporting structures for HMGs failed to get the required information on the rapidly changing, and evolving, hospitalist landscape to the desks of executives who had the financial and structural control to address the challenges that the hospitalists in the trenches were facing.
Numerous HMGs failed in the early days of hospital medicine because of this type of misaligned reporting structure. This is a lesson that should not be forgotten: Make sure your HMG leader has a seat at the table where executive decisions are made, including but not limited to the board of directors. To be in balance, you have to be “in the room where it happens.”
Accountability
The outcomes that you are responsible for need to be explicit, appropriately resourced with Authority, and clearly spelled out in your job description. Your job description is a document you should know, own, and revisit regularly with whomever you report to, in order to ensure success.
Once you have the Authority side of the equation appropriately resourced, setting outcomes that are a stretch, but still realistic and achievable within the scope of your position, is critical to your success. It is good to think about short-, medium-, and long-term goals, especially if you are in a leadership role. For example, one expectation you will have, regardless of your station, is that you keep up on your email and answer your phone. These are short-term goals that will often be included in your job description. However, taking on a new hospital contract and making sure that it has 24/7 hospitalist coverage, that all the hospitalists are meeting the geometric mean length of stay, and that all the physicians are having 15 encounters per day doesn’t happen immediately. Long-term goals, such as taking on a new hospital contract, are the big-picture stuff that can make or break the career of an HMG leader. Long-term goals also need to be delineated in the job description, along with specific time stamps and the resources you need to accomplish big ticket items – which are spelled out in the Authority side (that is, physician recruiter, secretary, background checks, and so on).
One of the classic misuses of Accountability is the “Fall Guy” scenario. The Fall Guy scenario is often used by cynical hospital and medical group executives to expand their influence while limiting their liability. In the Fall Guy scenario, the executive is surrounded with junior partners who are underpowered with Authority, and then the executive makes decisions for which the junior partners are Accountable. This allows the senior executive to make risky decisions on behalf of the hospital or medical group without the liability of being held accountable when the decision-making process fails. When the risky, and often ill-informed, decision fails, the junior partner who lacked the Authority to make the decision – but held the Accountability for it – becomes the Fall Guy for the failed endeavor. This is a critical outcome that the Authority/Accountability balance can help you avoid, if you use it wisely and properly.
If you find yourself in the Fall Guy position, it is time for a change. The Authority, the Accountability, or both need to change so that they are in better balance. Or your employer needs to change. Changing employers is an outcome worth avoiding, if at all possible. I have scrutinized thousands of resumes in my career, and frequent job changes always wave a red flag to prospective employers. However, changing jobs remains a crucial option if you are being set up for failure when Authority and Accountability are out of balance.
If you are unable to negotiate for the balance that will allow you to be successful with your current group, remember that HMG leaders are a prized commodity and in short supply. Leaving a group that has been your career is hard, but it is better to leave than stay in a position where you are set up for failure as the Fall Guy. Further, the most effective time to expand your Authority is when you are negotiating the terms of a new position. Changing positions is the nuclear option. However, it is better than becoming the Fall Guy, and a change can create opportunities that will accelerate your career and influence, if done right.
When I talk about Authority/Accountability balance, I always counter the Fall Guy with an ignominious historical figure: General George B. McClellan. General McClellan was the commander of the Army of the Potomac during the early years of the American Civil War. General McClellan had the industrial might of the Union north at his beck and call, as well as extraordinary resources for recruiting and retaining soldiers for his army. At every encounter with General Robert E. Lee’s Army of Northern Virginia, General McClellan outnumbered them, sometimes by more than two to one. Yet General McClellan was outfoxed repeatedly for the same reason: He failed to take decisive action.
Every time that McClellan failed, he blamed insufficient resources and told President Lincoln that he needed more troops and more equipment to be successful. In summary, while the Fall Guy scenario needs to be avoided, once you are adequately resourced, success requires taking decisive and strategic action, or you will suffer as did General McClellan. Failing to act when you are appropriately resourced can be just as damaging to your career and credibility as allowing yourself to become the Fall Guy.
Job description
Everybody has somebody that they report to, no matter how high up on the executive ladder they have climbed. Even the CEO must report to the board of directors. And that reporting structure usually involves periodic formal reviews. Your formal review is a good time to go over your job description, note what is relevant, remove what is irrelevant, and add new elements that have evolved in importance since your last review.
Job descriptions take many forms, but they always include a list of qualifications. If you have the job, you have the qualifications, so that is not likely to change. You may become more qualified for a higher-level position, but that is an entirely different discussion. I like to think of a well-written job description as including short-term and long-term goals. Short-term goals are usually the daily stuff that keeps operations running smoothly but garners little attention. Examples would include staying current on your emails, answering your phone, organizing meetings, and regularly attending various committees. Even some of these short-term goals can and will change over time. I always enjoyed quality oversight in my department, but as the department and my responsibilities grew, I realized I couldn’t do everything that I wanted to do. I needed to focus on the things only I could do and delegate those things that could be done by someone else, even though I wanted to continue doing them myself. I created a position for a clinical quality officer, and quality oversight moved off of my job description.
Long-term goals are the aspirational items, such as increasing market share, decreasing readmissions, improving patient satisfaction, and the like. Effective leaders are often focused on these aspirational, long-term goals, but they still must effectively execute their short-term goals. Stephen Covey outlines the dilemma with the “time management matrix” in his seminal work “The 7 Habits of Highly Effective People.” An in-depth discussion is beyond the scope of this article, but the time management matrix places tasks into one of four categories based on urgency and importance, and provides strategies for staying up on short-term goals while continually moving long-term goals forward.If you show up at your review with a list of accomplishments as well as an understanding of how the “time management matrix” affects your responsibilities, your boss will be impressed. It is also worth mentioning that Covey’s first habit is “Proactivity.” He uses the term Proactivity in a much more nuanced form than we typically think of, however. Simply put, Proactivity is the opposite of Reactivity, and it is another invaluable tool for success with those long-term goals that will help you make a name for yourself.
When you show up for your review, be it annual, biannual, or other, be prepared. Not only should you bring your job description and recommendations for how it should be adapted in the changing environment, but also bring examples of your accomplishments since the last review.
I talk with leaders frequently who are hardworking and diligent and hate bragging about their achievements; I get that. At the same time, if you don’t inform your superiors about your successes, there is no guarantee that they will hear about them or understand them in the appropriate context. Bragging about how great you are in the physician’s lounge is annoying; telling your boss about your accomplishments since the last review is critical to maintaining the momentum of past accomplishments. If you are not willing to toot your own horn, there is a very good chance that your horn will remain silent. I don’t think self-promotion comes easily to anyone, and it has to be done with a degree of humility and sensitivity; but it has to be done, so prepare for it.
Look out for yourself and others
We talk about teamwork and collaboration as hospitalists, and SHM is always underscoring the importance of teamwork and highlighting examples of successful teamwork in its many conferences and publications. Most hospital executives are focused on their own careers, however, and many have no reservations about damaging your career (your brand) if they think it will promote theirs. You have to look out for yourself and size up every leadership position you get into.
Physicians can expect their careers to last decades. The average hospital CEO has a tenure of less than 3.5 years, however, and when a new CEO is hired, almost half of chief financial, chief operating, and chief information officers are fired within 9 months. You may be focused on the long-term success of your organization as you plan your career, but many hospital administrators are interested only in short-term gains. It is similar to some members of Congress who are interested only in what they need to do now to win the next election and not in the long-term needs of the country. You should understand this disconnect when dealing with hospital executives, and how you and your credibility can become cannon fodder in their quest for short-term self-preservation.
You have to look out for and take care of yourself as you promote your group. With a better understanding of the Authority/Accountability balance, you have new tools to assess your chances of success and to advocate for yourself so that you and your group can be successful.
Despite my cynicism toward executives in the medical field, I personally advocate for supporting the career development of those around you and advise against furthering your career at the expense of others. Many unscrupulous executives will use this approach, surrounding themselves with Fall Guys, but my experience shows that this is not a sustainable strategy for success. It can lead to short-term gains, but eventually the piper must be paid. Moreover, the most successful medical executives and leaders that I have encountered have been those who genuinely cared about their subordinates, looked out for them, and selflessly promoted their careers.
In the age of social media, tearing others down seems to be the fastest way to get more “likes.” However, I strongly believe that you can’t build up your group, and our profession, just by tearing people down. Lending a helping hand may bring you less attention in the short term, but such action raises your stature, creates loyalty, and leads to sustainable success for the long run.
Dr. McIlraith is the founding chairman of the Hospital Medicine Department at Mercy Medical Group in Sacramento, Calif. He received the SHM Award for Outstanding Service in Hospital Medicine in 2016 and is currently a member of the SHM Practice Management and Awards Committees, as well as the SHM Critical Care Task Force.
Sources
Quinn R. HM Turns 20: A look at the evolution of hospital medicine. The Hospitalist. 2016 August. https://www.the-hospitalist.org/hospitalist/article/121525/hm-turns-20-look-evolution-hospital-medicine
Stephen R. Covey. The 7 Habits of Highly Effective People: Powerful Lessons in Personal Change. Simon & Schuster. 1989.
10 Statistics on CEO Turnover, Recruitment. Becker’s Hospital Review. 2020. https://www.beckershospitalreview.com/hospital-management-administration/10-statistics-on-ceo-turnover-recruitment.html
Evaluating your career trajectory
Evaluating your career trajectory
I have had the pleasure of working on the Society of Hospital Medicine’s signature Leadership Academies since 2010, and I enjoy working with hospital medicine leaders from around the country every year. I started as a hospital medicine leader in 2000 and served during the unprecedented growth of the field when it was “the most rapidly growing specialty in the history of medicine.”
Most businesses dream of having a year of double-digit growth; my department grew an average of 15% annually for more than 10 years. These unique experiences have taught me many lessons and afforded me the opportunity to watch many stars of hospital medicine rise, as well as to learn from several less-scrupulous leaders about the darker side of hospital politics.
One of the lessons I learned the hard way about hospital politics is striking the “Authority/Accountability balance” in your career. I shared this perspective at the SHM annual conference in 2018, at speaking engagements on the West Coast, and with my leadership group at the academies. I am sharing it with you because the feedback I have received has been very positive.
The Authority/Accountability balance is a tool for evaluating your current career trajectory and measuring if it is set up for success or failure. The essence is that your Authority and Accountability need to be balanced for you to be successful in your career, regardless of your station. Everybody from the hospitalist fresh out of residency to the CEO needs to have Authority and Accountability in balance to be successful. And as you use the tool to measure your own potential for success or failure, learn to apply it to those who report to you.
I believe the rising tide lifts all boats and the success of your subordinates, through mentoring and support, will add to your success. There is another, more cynical view of subordinates that can be identified using the Authority/Accountability balance, which I will address.
Authority
In this construct, “Authority” has a much broader meaning than just the ability to tell people what to do. The ability to tell people what to do is important but not sufficient for success in hospital politics.
Financial resources are essential for a successful Authority/Accountability balance – not only the hardware such as computers, telephones, pagers, and so on, but also clerical support, technical support, and analytic support so that you are getting high-quality data on the performance of the members of your hospital medicine group (HMG). These “soft” resources (clerical, technical, and analytical) are often overlooked as needs that HMG leaders must advocate for; I speak with many HMG leaders who remain under-resourced with “soft” assets. However, being appropriately resourced in these areas can be transformational for a group. Hospitalists don’t like doing clerical work, and if you don’t like a menial job assigned to you, you probably won’t do it very well. Having an unlicensed person dedicated to these clerical activities not only will cost less, but will ensure the job is done better.
Reporting structure is critically important, often overlooked, and historically misaligned in HMGs. When hospital medicine was starting in the late 1990s and early 2000s, rapidly growing hospitalist groups were typically led by young, early-career physicians who had chosen hospital medicine as a career. The problem was that they often lacked the seniority and connections at the executive level to advocate for their HMG. All too often the hospitalist group was tucked in under another department or division which, in turn, reported HMG updates and issues to the board of directors and the CEO.
A common reporting structure in the early days was that a senior member of the medical staff, or group, had once worked in the hospital and therefore “understood” the issues and challenges that the hospitalists were facing. It was up to this physician with seniority and connections to advocate for the hospitalists as they saw fit. The problem was that the hospital landscape was, and is, constantly evolving in innumerable ways. These “once removed” reporting structures for HMGs failed to get the required information on the rapidly changing, and evolving, hospitalist landscape to the desks of executives who had the financial and structural control to address the challenges that the hospitalists in the trenches were facing.
Numerous HMGs failed in the early days of hospital medicine because of this type of misaligned reporting structure. This is a lesson that should not be forgotten: Make sure your HMG leader has a seat at the table where executive decisions are made, including but not limited to the board of directors. To be in balance, you have to be “in the room where it happens.”
Accountability
The outcomes that you are responsible for need to be explicit, appropriately resourced with Authority, and clearly spelled out in your job description. Your job description is a document you should know, own, and revisit regularly with whomever you report to, in order to ensure success.
Once you have the Authority side of the equation appropriately resourced, setting outcomes that are a stretch, but still realistic and achievable within the scope of your position, is critical to your success. It is good to think about short-, medium-, and long-term goals, especially if you are in a leadership role. For example, one expectation you will have, regardless of your station, is that you keep up on your email and answer your phone. These are short-term goals that will often be included in your job description. However, taking on a new hospital contract and making sure that it has 24/7 hospitalist coverage, that all the hospitalists are meeting the geometric mean length of stay, and that all the physicians are having 15 encounters per day doesn’t happen immediately. Long-term goals, such as taking on a new hospital contract, are the big-picture stuff that can make or break the career of an HMG leader. Long-term goals also need to be delineated in the job description, along with specific time stamps and the resources you need to accomplish big ticket items – which are spelled out in the Authority side (that is, physician recruiter, secretary, background checks, and so on).
One of the classic misuses of Accountability is the “Fall Guy” scenario. The Fall Guy scenario is often used by cynical hospital and medical group executives to expand their influence while limiting their liability. In the Fall Guy scenario, the executive is surrounded with junior partners who are underpowered with Authority, and then the executive makes decisions for which the junior partners are Accountable. This allows the senior executive to make risky decisions on behalf of the hospital or medical group without the liability of being held accountable when the decision-making process fails. When the risky, and often ill-informed, decision fails, the junior partner who lacked the Authority to make the decision – but held the Accountability for it – becomes the Fall Guy for the failed endeavor. This is a critical outcome that the Authority/Accountability balance can help you avoid, if you use it wisely and properly.
If you find yourself in the Fall Guy position, it is time for a change. The Authority, the Accountability, or both need to change so that they are in better balance. Or your employer needs to change. Changing employers is an outcome worth avoiding, if at all possible. I have scrutinized thousands of resumes in my career, and frequent job changes always wave a red flag to prospective employers. However, changing jobs remains a crucial option if you are being set up for failure when Authority and Accountability are out of balance.
If you are unable to negotiate for the balance that will allow you to be successful with your current group, remember that HMG leaders are a prized commodity and in short supply. Leaving a group that has been your career is hard, but it is better to leave than stay in a position where you are set up for failure as the Fall Guy. Further, the most effective time to expand your Authority is when you are negotiating the terms of a new position. Changing positions is the nuclear option. However, it is better than becoming the Fall Guy, and a change can create opportunities that will accelerate your career and influence, if done right.
When I talk about Authority/Accountability balance, I always counter the Fall Guy with an ignominious historical figure: General George B. McClellan. General McClellan was the commander of the Army of the Potomac during the early years of the American Civil War. General McClellan had the industrial might of the Union north at his beck and call, as well as extraordinary resources for recruiting and retaining soldiers for his army. At every encounter with General Robert E. Lee’s Army of Northern Virginia, General McClellan outnumbered them, sometimes by more than two to one. Yet General McClellan was outfoxed repeatedly for the same reason: He failed to take decisive action.
Every time that McClellan failed, he blamed insufficient resources and told President Lincoln that he needed more troops and more equipment to be successful. In summary, while the Fall Guy scenario needs to be avoided, once you are adequately resourced, success requires taking decisive and strategic action, or you will suffer as did General McClellan. Failing to act when you are appropriately resourced can be just as damaging to your career and credibility as allowing yourself to become the Fall Guy.
Job description
Everybody has somebody that they report to, no matter how high up on the executive ladder they have climbed. Even the CEO must report to the board of directors. And that reporting structure usually involves periodic formal reviews. Your formal review is a good time to go over your job description, note what is relevant, remove what is irrelevant, and add new elements that have evolved in importance since your last review.
Job descriptions take many forms, but they always include a list of qualifications. If you have the job, you have the qualifications, so that is not likely to change. You may become more qualified for a higher-level position, but that is an entirely different discussion. I like to think of a well-written job description as including short-term and long-term goals. Short-term goals are usually the daily stuff that keeps operations running smoothly but garners little attention. Examples would include staying current on your emails, answering your phone, organizing meetings, and regularly attending various committees. Even some of these short-term goals can and will change over time. I always enjoyed quality oversight in my department, but as the department and my responsibilities grew, I realized I couldn’t do everything that I wanted to do. I needed to focus on the things only I could do and delegate those things that could be done by someone else, even though I wanted to continue doing them myself. I created a position for a clinical quality officer, and quality oversight moved off of my job description.
Long-term goals are the aspirational items, such as increasing market share, decreasing readmissions, improving patient satisfaction, and the like. Effective leaders are often focused on these aspirational, long-term goals, but they still must effectively execute their short-term goals. Stephen Covey outlines the dilemma with the “time management matrix” in his seminal work “The 7 Habits of Highly Effective People.” An in-depth discussion is beyond the scope of this article, but the time management matrix places tasks into one of four categories based on urgency and importance, and provides strategies for staying up on short-term goals while continually moving long-term goals forward.If you show up at your review with a list of accomplishments as well as an understanding of how the “time management matrix” affects your responsibilities, your boss will be impressed. It is also worth mentioning that Covey’s first habit is “Proactivity.” He uses the term Proactivity in a much more nuanced form than we typically think of, however. Simply put, Proactivity is the opposite of Reactivity, and it is another invaluable tool for success with those long-term goals that will help you make a name for yourself.
When you show up for your review, be it annual, biannual, or other, be prepared. Not only should you bring your job description and recommendations for how it should be adapted in the changing environment, but also bring examples of your accomplishments since the last review.
I talk with leaders frequently who are hardworking and diligent and hate bragging about their achievements; I get that. At the same time, if you don’t inform your superiors about your successes, there is no guarantee that they will hear about them or understand them in the appropriate context. Bragging about how great you are in the physician’s lounge is annoying; telling your boss about your accomplishments since the last review is critical to maintaining the momentum of past accomplishments. If you are not willing to toot your own horn, there is a very good chance that your horn will remain silent. I don’t think self-promotion comes easily to anyone, and it has to be done with a degree of humility and sensitivity; but it has to be done, so prepare for it.
Look out for yourself and others
We talk about teamwork and collaboration as hospitalists, and SHM is always underscoring the importance of teamwork and highlighting examples of successful teamwork in its many conferences and publications. Most hospital executives are focused on their own careers, however, and many have no reservations about damaging your career (your brand) if they think it will promote theirs. You have to look out for yourself and size up every leadership position you get into.
Physicians can expect their careers to last decades. The average hospital CEO has a tenure of less than 3.5 years, however, and when a new CEO is hired, almost half of chief financial, chief operating, and chief information officers are fired within 9 months. You may be focused on the long-term success of your organization as you plan your career, but many hospital administrators are interested only in short-term gains. It is similar to some members of Congress who are interested only in what they need to do now to win the next election and not in the long-term needs of the country. You should understand this disconnect when dealing with hospital executives, and how you and your credibility can become cannon fodder in their quest for short-term self-preservation.
You have to look out for and take care of yourself as you promote your group. With a better understanding of the Authority/Accountability balance, you have new tools to assess your chances of success and to advocate for yourself so that you and your group can be successful.
Despite my cynicism toward executives in the medical field, I personally advocate for supporting the career development of those around you and advise against furthering your career at the expense of others. Many unscrupulous executives will use this approach, surrounding themselves with Fall Guys, but my experience shows that this is not a sustainable strategy for success. It can lead to short-term gains, but eventually the piper must be paid. Moreover, the most successful medical executives and leaders that I have encountered have been those who genuinely cared about their subordinates, looked out for them, and selflessly promoted their careers.
In the age of social media, tearing others down seems to be the fastest way to get more “likes.” However, I strongly believe that you can’t build up your group, and our profession, just by tearing people down. Lending a helping hand may bring you less attention in the short term, but such action raises your stature, creates loyalty, and leads to sustainable success for the long run.
Dr. McIlraith is the founding chairman of the Hospital Medicine Department at Mercy Medical Group in Sacramento, Calif. He received the SHM Award for Outstanding Service in Hospital Medicine in 2016 and is currently a member of the SHM Practice Management and Awards Committees, as well as the SHM Critical Care Task Force.
Sources
Quinn R. HM Turns 20: A look at the evolution of hospital medicine. The Hospitalist. 2016 August. https://www.the-hospitalist.org/hospitalist/article/121525/hm-turns-20-look-evolution-hospital-medicine
Stephen R. Covey. The 7 Habits of Highly Effective People: Powerful Lessons in Personal Change. Simon & Schuster. 1989.
10 Statistics on CEO Turnover, Recruitment. Becker’s Hospital Review. 2020. https://www.beckershospitalreview.com/hospital-management-administration/10-statistics-on-ceo-turnover-recruitment.html
I have had the pleasure of working on the Society of Hospital Medicine’s signature Leadership Academies since 2010, and I enjoy working with hospital medicine leaders from around the country every year. I started as a hospital medicine leader in 2000 and served during the unprecedented growth of the field when it was “the most rapidly growing specialty in the history of medicine.”
Most businesses dream of having a year of double-digit growth; my department grew an average of 15% annually for more than 10 years. These unique experiences have taught me many lessons and afforded me the opportunity to watch many stars of hospital medicine rise, as well as to learn from several less-scrupulous leaders about the darker side of hospital politics.
One of the lessons I learned the hard way about hospital politics is striking the “Authority/Accountability balance” in your career. I shared this perspective at the SHM annual conference in 2018, at speaking engagements on the West Coast, and with my leadership group at the academies. I am sharing it with you because the feedback I have received has been very positive.
The Authority/Accountability balance is a tool for evaluating your current career trajectory and measuring if it is set up for success or failure. The essence is that your Authority and Accountability need to be balanced for you to be successful in your career, regardless of your station. Everybody from the hospitalist fresh out of residency to the CEO needs to have Authority and Accountability in balance to be successful. And as you use the tool to measure your own potential for success or failure, learn to apply it to those who report to you.
I believe the rising tide lifts all boats and the success of your subordinates, through mentoring and support, will add to your success. There is another, more cynical view of subordinates that can be identified using the Authority/Accountability balance, which I will address.
Authority
In this construct, “Authority” has a much broader meaning than just the ability to tell people what to do. The ability to tell people what to do is important but not sufficient for success in hospital politics.
Financial resources are essential for a successful Authority/Accountability balance – not only the hardware such as computers, telephones, pagers, and so on, but also clerical support, technical support, and analytic support so that you are getting high-quality data on the performance of the members of your hospital medicine group (HMG). These “soft” resources (clerical, technical, and analytical) are often overlooked as needs that HMG leaders must advocate for; I speak with many HMG leaders who remain under-resourced with “soft” assets. However, being appropriately resourced in these areas can be transformational for a group. Hospitalists don’t like doing clerical work, and if you don’t like a menial job assigned to you, you probably won’t do it very well. Having an unlicensed person dedicated to these clerical activities not only will cost less, but will ensure the job is done better.
Reporting structure is critically important, often overlooked, and historically misaligned in HMGs. When hospital medicine was starting in the late 1990s and early 2000s, rapidly growing hospitalist groups were typically led by young, early-career physicians who had chosen hospital medicine as a career. The problem was that they often lacked the seniority and connections at the executive level to advocate for their HMG. All too often the hospitalist group was tucked in under another department or division which, in turn, reported HMG updates and issues to the board of directors and the CEO.
A common reporting structure in the early days was that a senior member of the medical staff, or group, had once worked in the hospital and therefore “understood” the issues and challenges that the hospitalists were facing. It was up to this physician with seniority and connections to advocate for the hospitalists as they saw fit. The problem was that the hospital landscape was, and is, constantly evolving in innumerable ways. These “once removed” reporting structures for HMGs failed to get the required information on the rapidly changing, and evolving, hospitalist landscape to the desks of executives who had the financial and structural control to address the challenges that the hospitalists in the trenches were facing.
Numerous HMGs failed in the early days of hospital medicine because of this type of misaligned reporting structure. This is a lesson that should not be forgotten: Make sure your HMG leader has a seat at the table where executive decisions are made, including but not limited to the board of directors. To be in balance, you have to be “in the room where it happens.”
Accountability
The outcomes that you are responsible for need to be explicit, appropriately resourced with Authority, and clearly spelled out in your job description. Your job description is a document you should know, own, and revisit regularly with whomever you report to, in order to ensure success.
Once you have the Authority side of the equation appropriately resourced, setting outcomes that are a stretch, but still realistic and achievable within the scope of your position, is critical to your success. It is good to think about short-, medium-, and long-term goals, especially if you are in a leadership role. For example, one expectation you will have, regardless of your station, is that you keep up on your email and answer your phone. These are short-term goals that will often be included in your job description. However, taking on a new hospital contract and making sure that it has 24/7 hospitalist coverage, that all the hospitalists are meeting the geometric mean length of stay, and that all the physicians are having 15 encounters per day doesn’t happen immediately. Long-term goals, such as taking on a new hospital contract, are the big-picture stuff that can make or break the career of an HMG leader. Long-term goals also need to be delineated in the job description, along with specific time stamps and the resources you need to accomplish big ticket items – which are spelled out in the Authority side (that is, physician recruiter, secretary, background checks, and so on).
One of the classic misuses of Accountability is the “Fall Guy” scenario. The Fall Guy scenario is often used by cynical hospital and medical group executives to expand their influence while limiting their liability. In the Fall Guy scenario, the executive is surrounded with junior partners who are underpowered with Authority, and then the executive makes decisions for which the junior partners are Accountable. This allows the senior executive to make risky decisions on behalf of the hospital or medical group without the liability of being held accountable when the decision-making process fails. When the risky, and often ill-informed, decision fails, the junior partner who lacked the Authority to make the decision – but held the Accountability for it – becomes the Fall Guy for the failed endeavor. This is a critical outcome that the Authority/Accountability balance can help you avoid, if you use it wisely and properly.
If you find yourself in the Fall Guy position, it is time for a change. The Authority, the Accountability, or both need to change so that they are in better balance. Or your employer needs to change. Changing employers is an outcome worth avoiding, if at all possible. I have scrutinized thousands of resumes in my career, and frequent job changes always wave a red flag to prospective employers. However, changing jobs remains a crucial option if you are being set up for failure when Authority and Accountability are out of balance.
If you are unable to negotiate for the balance that will allow you to be successful with your current group, remember that HMG leaders are a prized commodity and in short supply. Leaving a group that has been your career is hard, but it is better to leave than stay in a position where you are set up for failure as the Fall Guy. Further, the most effective time to expand your Authority is when you are negotiating the terms of a new position. Changing positions is the nuclear option. However, it is better than becoming the Fall Guy, and a change can create opportunities that will accelerate your career and influence, if done right.
When I talk about Authority/Accountability balance, I always counter the Fall Guy with an ignominious historical figure: General George B. McClellan. General McClellan was the commander of the Army of the Potomac during the early years of the American Civil War. General McClellan had the industrial might of the Union north at his beck and call, as well as extraordinary resources for recruiting and retaining soldiers for his army. At every encounter with General Robert E. Lee’s Army of Northern Virginia, General McClellan outnumbered them, sometimes by more than two to one. Yet General McClellan was outfoxed repeatedly for the same reason: He failed to take decisive action.
Every time that McClellan failed, he blamed insufficient resources and told President Lincoln that he needed more troops and more equipment to be successful. In summary, while the Fall Guy scenario needs to be avoided, once you are adequately resourced, success requires taking decisive and strategic action, or you will suffer as did General McClellan. Failing to act when you are appropriately resourced can be just as damaging to your career and credibility as allowing yourself to become the Fall Guy.
Job description
Everybody has somebody that they report to, no matter how high up on the executive ladder they have climbed. Even the CEO must report to the board of directors. And that reporting structure usually involves periodic formal reviews. Your formal review is a good time to go over your job description, note what is relevant, remove what is irrelevant, and add new elements that have evolved in importance since your last review.
Job descriptions take many forms, but they always include a list of qualifications. If you have the job, you have the qualifications, so that is not likely to change. You may become more qualified for a higher-level position, but that is an entirely different discussion. I like to think of a well-written job description as including short-term and long-term goals. Short-term goals are usually the daily stuff that keeps operations running smoothly but garners little attention. Examples would include staying current on your emails, answering your phone, organizing meetings, and regularly attending various committees. Even some of these short-term goals can and will change over time. I always enjoyed quality oversight in my department, but as the department and my responsibilities grew, I realized I couldn’t do everything that I wanted to do. I needed to focus on the things only I could do and delegate those things that could be done by someone else, even though I wanted to continue doing them myself. I created a position for a clinical quality officer, and quality oversight moved off of my job description.
Long-term goals are the aspirational items, such as increasing market share, decreasing readmissions, improving patient satisfaction, and the like. Effective leaders are often focused on these aspirational, long-term goals, but they still must effectively execute their short-term goals. Stephen Covey outlines the dilemma with the “time management matrix” in his seminal work “The 7 Habits of Highly Effective People.” An in-depth discussion is beyond the scope of this article, but the time management matrix places tasks into one of four categories based on urgency and importance, and provides strategies for staying up on short-term goals while continually moving long-term goals forward.If you show up at your review with a list of accomplishments as well as an understanding of how the “time management matrix” affects your responsibilities, your boss will be impressed. It is also worth mentioning that Covey’s first habit is “Proactivity.” He uses the term Proactivity in a much more nuanced form than we typically think of, however. Simply put, Proactivity is the opposite of Reactivity, and it is another invaluable tool for success with those long-term goals that will help you make a name for yourself.
When you show up for your review, be it annual, biannual, or other, be prepared. Not only should you bring your job description and recommendations for how it should be adapted in the changing environment, but also bring examples of your accomplishments since the last review.
I talk with leaders frequently who are hardworking and diligent and hate bragging about their achievements; I get that. At the same time, if you don’t inform your superiors about your successes, there is no guarantee that they will hear about them or understand them in the appropriate context. Bragging about how great you are in the physician’s lounge is annoying; telling your boss about your accomplishments since the last review is critical to maintaining the momentum of past accomplishments. If you are not willing to toot your own horn, there is a very good chance that your horn will remain silent. I don’t think self-promotion comes easily to anyone, and it has to be done with a degree of humility and sensitivity; but it has to be done, so prepare for it.
Look out for yourself and others
We talk about teamwork and collaboration as hospitalists, and SHM is always underscoring the importance of teamwork and highlighting examples of successful teamwork in its many conferences and publications. Most hospital executives are focused on their own careers, however, and many have no reservations about damaging your career (your brand) if they think it will promote theirs. You have to look out for yourself and size up every leadership position you get into.
Physicians can expect their careers to last decades. The average hospital CEO has a tenure of less than 3.5 years, however, and when a new CEO is hired, almost half of chief financial, chief operating, and chief information officers are fired within 9 months. You may be focused on the long-term success of your organization as you plan your career, but many hospital administrators are interested only in short-term gains. It is similar to some members of Congress who are interested only in what they need to do now to win the next election and not in the long-term needs of the country. You should understand this disconnect when dealing with hospital executives, and how you and your credibility can become cannon fodder in their quest for short-term self-preservation.
You have to look out for and take care of yourself as you promote your group. With a better understanding of the Authority/Accountability balance, you have new tools to assess your chances of success and to advocate for yourself so that you and your group can be successful.
Despite my cynicism toward executives in the medical field, I personally advocate for supporting the career development of those around you and advise against furthering your career at the expense of others. Many unscrupulous executives will use this approach, surrounding themselves with Fall Guys, but my experience shows that this is not a sustainable strategy for success. It can lead to short-term gains, but eventually the piper must be paid. Moreover, the most successful medical executives and leaders that I have encountered have been those who genuinely cared about their subordinates, looked out for them, and selflessly promoted their careers.
In the age of social media, tearing others down seems to be the fastest way to get more “likes.” However, I strongly believe that you can’t build up your group, and our profession, just by tearing people down. Lending a helping hand may bring you less attention in the short term, but such action raises your stature, creates loyalty, and leads to sustainable success for the long run.
Dr. McIlraith is the founding chairman of the Hospital Medicine Department at Mercy Medical Group in Sacramento, Calif. He received the SHM Award for Outstanding Service in Hospital Medicine in 2016 and is currently a member of the SHM Practice Management and Awards Committees, as well as the SHM Critical Care Task Force.
Sources
Quinn R. HM Turns 20: A look at the evolution of hospital medicine. The Hospitalist. 2016 August. https://www.the-hospitalist.org/hospitalist/article/121525/hm-turns-20-look-evolution-hospital-medicine
Stephen R. Covey. The 7 Habits of Highly Effective People: Powerful Lessons in Personal Change. Simon & Schuster. 1989.
10 Statistics on CEO Turnover, Recruitment. Becker’s Hospital Review. 2020. https://www.beckershospitalreview.com/hospital-management-administration/10-statistics-on-ceo-turnover-recruitment.html
Characterizing Hospitalist Practice and Perceptions of Critical Care Delivery
Despite calls for board-certified intensivist physicians to lead critical care delivery,1-3 the intensivist shortage in the United States continues to worsen,4 with projected shortfalls of 22% by 2020 and 35% by 2030.5 Many hospitals currently have inadequate or no board-certified intensivist support.6 The intensivist shortage has necessitated the development of alternative intensive care unit (ICU) staffing models, including engagement in telemedicine,7 the utilization of advanced practice providers,8 and dependence on hospitalists9 to deliver critical care services to ICU patients. Presently, research does not clearly show consistent differences in clinical outcomes based on the training of the clinical provider, although optimized teamwork and team rounds in the ICU do seem to be associated with improved outcomes.10-12
In its 2016 annual survey of hospital medicine (HM) leaders, the Society of Hospital Medicine (SHM) documented that most HM groups care for ICU patients, with up to 80% of hospitalist groups in some regions delivering critical care.13 In many United States hospitals, hospitalists serve as the primary if not lone physician providers of critical care.6,14 HM, with its team-based approach and on-site presence, shares many of the key attributes and values that define high-functioning critical care teams, and many hospitalists likely capably deliver some critical care services.9 However, hospitalists are also a highly heterogeneous work force with varied exposure to and comfort with critical care medicine, making it difficult to generalize hospitalists’ scope of practice in the ICU.
Because hospitalists render a significant amount of critical care in the United States, we surveyed practicing hospitalists to understand their demographics and practice roles in the ICU setting and to ascertain how they are supported when doing so. Additionally, we sought to identify mismatches between the ICU services that hospitalists provide and what they feel prepared and supported to deliver. Finally, we attempted to elucidate how hospitalists who practice in the ICU might respond to novel educational offerings targeted to mitigate cognitive or procedural gaps.
METHODS
We developed and deployed a survey to address the aforementioned questions. The survey content was developed iteratively by the Critical Care Task Force of SHM’s Education Committee and subsequently approved by SHM’s Education Committee and Board of Directors. Members of the Critical Care Task Force include critical care physicians and hospitalists. The survey included 25 items (supplemental Appendix A). Seventeen questions addressed the demographics and practice roles of hospitalists in the ICU, 5 addressed cognitive and procedural practice gaps, and 3 addressed how hospitalists would respond to educational opportunities in critical care. We used conditional formatting to ensure that only respondents who deliver ICU care could answer questions related to ICU practice. The survey was delivered by using an online survey platform (Survey Monkey, San Mateo, CA).
The survey was deployed in 3 phases from March to October of 2016. Initially, we distributed a pilot survey to professional contacts of the Critical Care Task Force to solicit feedback and refine the survey’s format and content. These contacts were largely academic hospitalists from our local institutions. We then distributed the survey to hospitalists via professional networks with instructions to forward the link to interested hospitalists. Finally, we distributed the survey to approximately 4000 hospitalists randomly selected from SHM’s national listserv of approximately 12,000 hospitalists. Respondents could enter a drawing for a monetary prize upon completion of the survey.
None of the survey questions changed during the 3 phases of survey deployment, and the data reported herein were compiled from all 3 phases of the survey deployment. Frequency tables were created using Tableau (version 10.0; Tableau Software, Seattle, WA). Comparisons between categorical questions were made by using χ2 and Fischer exact tests to calculate P values for associations by using SAS (version 9.3; SAS Institute, Cary, NC). Associations with P values below .05 were considered statistically significant.
RESULTS
Objective 1: Demographics and Practice Role
Four hundred and twenty-five hospitalists responded to the survey. The first 2 phases (pilot survey and distribution via professional networks) generated 101 responses, and the third phase (via SHM’s listserv) generated an additional 324 responses. As the survey was anonymous, we could not determine which hospitals or geographic regions were represented. Three hundred and twenty-five of the 425 hospitalists who completed the survey (77%) reported that they delivered care in the ICU. Of these 325 hospitalists, 45 served only as consultants, while the remaining 280 (66% of the total sample) served as the primary attending physician in the ICU. Among these primary providers of care in the ICU, 60 (21%) practiced in rural settings and 220 (79%) practiced in nonrural settings (Figure 1).
The demographics of our respondents were similar to those of the SHM annual survey,13 in which 66% of respondents delivered ICU care. Forty-one percent of our respondents worked in critical access or small community hospitals, 24% in academic medical centers, and 34% in large community centers with an academic affiliation. The SHM annual survey cohort included more physicians from nonteaching hospitals (58.7%) and fewer from academic medical centers (14.8%).13
Hospitalists’ presence in the ICU varied by practice setting (Table 1). 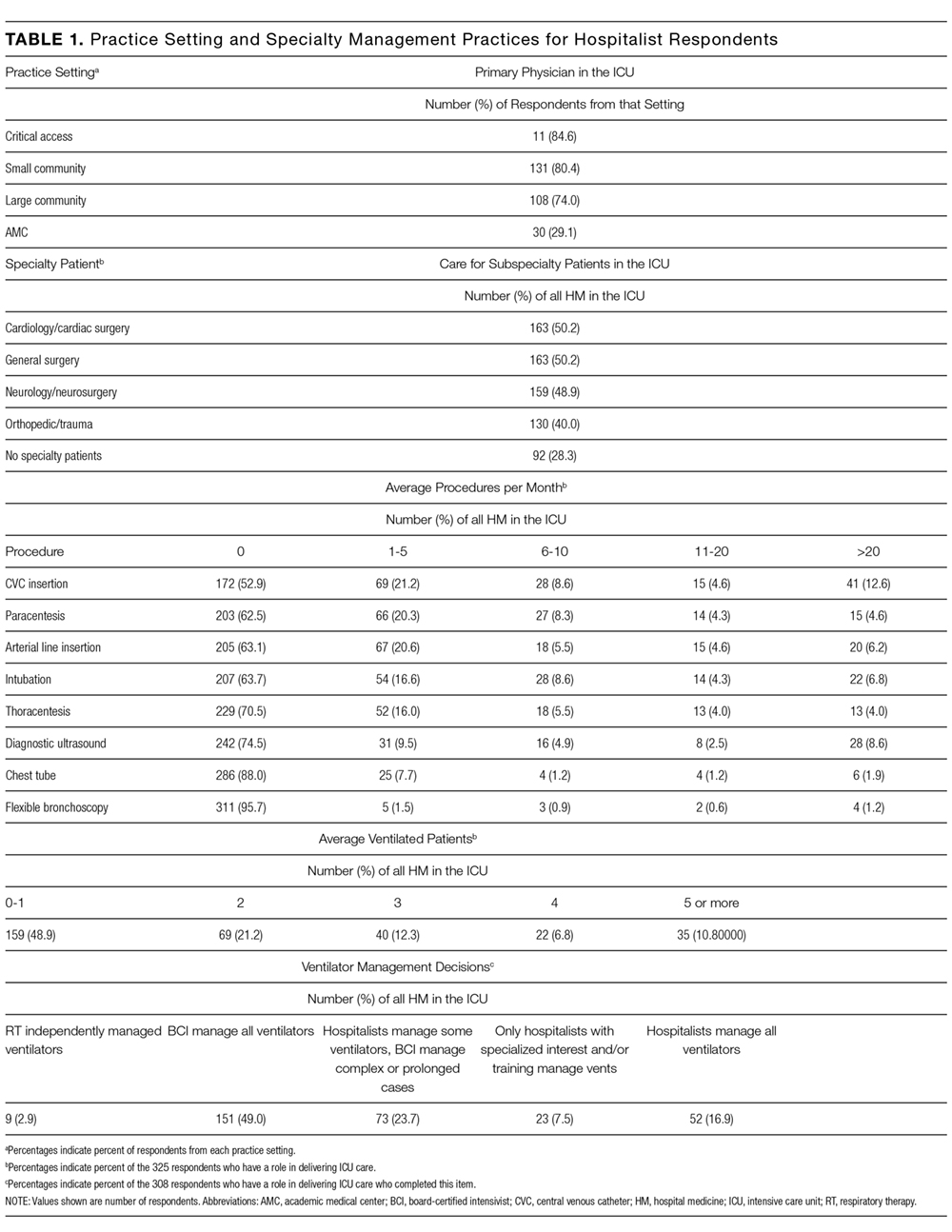
Hospitalists were significantly more prevalent in rural ICUs than in nonrural settings (96% vs 73%; Table 2). 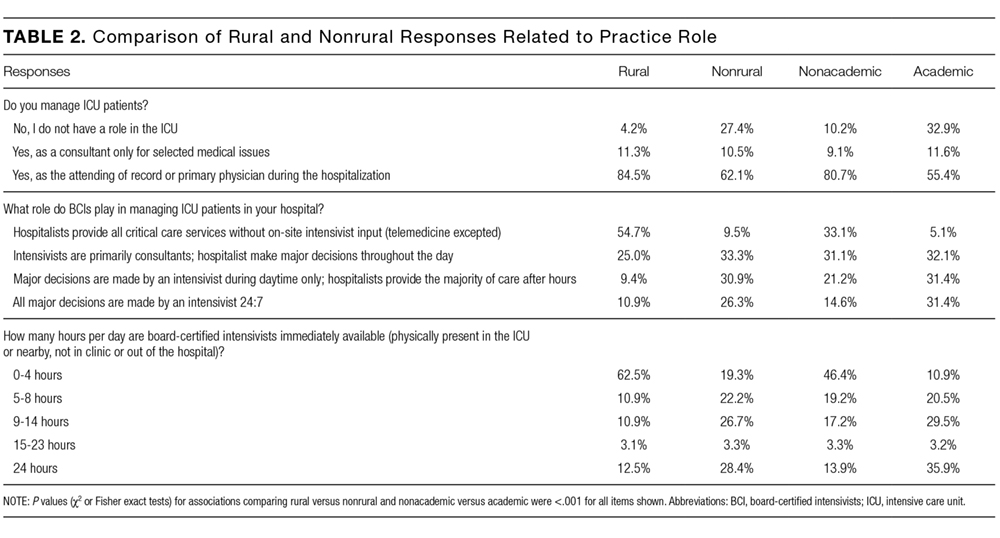
We found similar results when comparing academic hospitalists (those working in an academic medical center or academic-affiliated hospital) with nonacademic hospitalists (those working in critical access or small community centers). Specifically, hospitalists in nonacademic settings were significantly more prevalent in ICUs (90% vs 67%; Table 2), more likely to serve as the primary attending (81% vs 55%), and more likely to deliver all critical care services (64% vs 25%). Sixty-four percent of respondents from nonacademic settings reported that hospitalists manage all or most ICU patients in their hospital as opposed to 25% for academic respondents (χ2P value for association <.001). Intensivist availability was also significantly lower in nonacademic ICUs (Table 2).
We also sought to determine whether the ability to transfer critically ill patients to higher levels of care effectively mitigated shortfalls in intensivist staffing. When restricted to hospitalists who served as primary providers for ICU patients, 28% of all respondents and 51% of rural hospitalists reported transferring patients to a higher level of care.
Sixty-seven percent of hospitalists who served as primary physicians for ICU patients in any setting reported at least moderate difficulty arranging transfers to higher levels of care.
Objective 2: Identifying the Practice Gap
Hospitalists’ perceptions of practicing critical care beyond their skill level and without sufficient board-certified intensivist support varied by both practice location and practice type (Table 3). 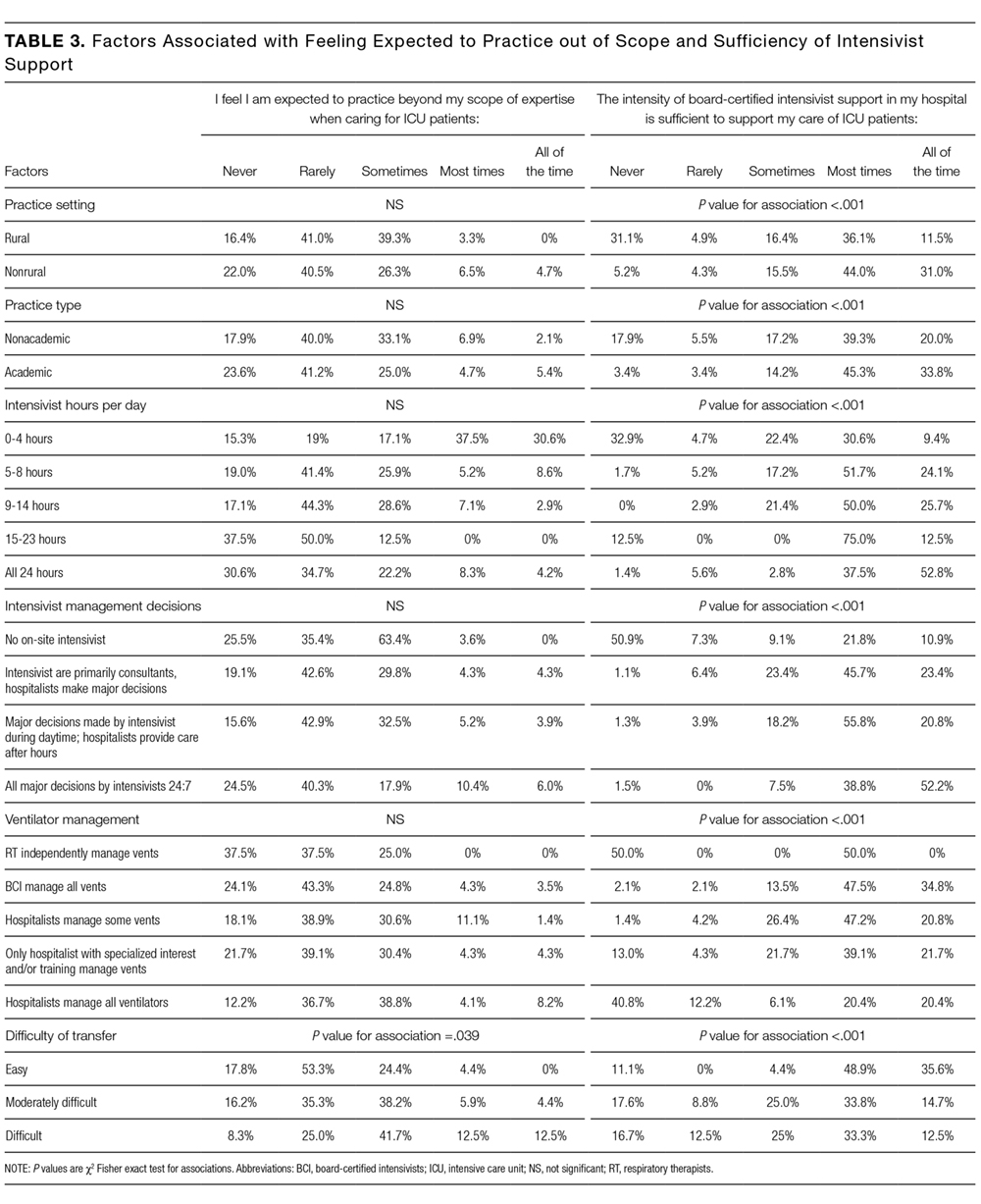
There were similar discrepancies between academic and nonacademic respondents. Forty-two percent of respondents practicing in nonacademic settings reported being expected to practice beyond their scope at least some of the time, and 18% reported that intensivist support was never sufficient. This contrasts with academic hospitalists, of whom 35% reported feeling expected to practice outside their scope, and less than 4% reported the available support from intensivists was never sufficient. For comparisons of academic and nonacademic respondents, only perceptions of sufficient board-certified intensivist support reached statistical significance (Table 3).
The role of intensivists in making management decisions and the strategy for ventilator management decisions correlated significantly with perception of intensivist support (P < .001) but not with the perception of practicing beyond one’s scope. The number of ventilated patients did not correlate significantly with either perception of intensivist support or of being expected to practice beyond scope.
Difficulty transferring patients to a higher level of care was the only attribute that significantly correlated with hospitalists’ perceptions of having to practice beyond their skill level (P < .05; Table 3). Difficulty of transfer was also significantly associated with perceived adequacy of board-certified intensivist support (P < .001). Total hours of intensivist coverage, intensivist role in decision making, and ventilator management arrangements also correlated significantly with the perceived adequacy of board-certified intensivist support (P < .001 for all; Table 3).
Objective 3: Assessing Interest in Critical Care Education
More than 85% of respondents indicated interest in obtaining additional critical care training and some form of certification short of fellowship training. Preferred modes of content delivery included courses or precourses at national meetings, academies, or online modules. Hospitalists in smaller communities indicated preference for online resources.
DISCUSSION
This survey of a large national cohort of hospitalists from diverse practice settings validates previous studies suggesting that hospitalists deliver critical care services, most notably in community and rural hospitals.13 A substantial subset of our respondents represented rural practice settings, which allowed us to compare rural and nonrural hospitalists as well as those practicing in academic and nonacademic settings. In assessing both the objective services that hospitalists provided as well as their subjective perceptions of how they practiced, we could correlate factors associated with the sense of practicing beyond one’s skill or feeling inadequately supported by board-certified intensivists.
More than a third of responding hospitalists who practiced in the ICU reported that they practiced beyond their self-perceived skill level, and almost three-fourths indicated that they practiced without consistent or adequate board-certified intensivist support. Rural and nonacademic hospitalists were far more likely to report delivering critical care beyond their comfort level and having insufficient board-certified intensivist support.
Calls for board-certified intensivists to deliver critical care to all critically ill patients do not reflect the reality in many American hospitals and, either by intent or by default, hospitalists have become the major and often sole providers of critical care services in many hospitals without robust intensivist support. We suspect that this phenomenon has been consistently underreported in the literature because academic hospitalists generally do not practice critical care.15
Many potential solutions to the intensivist shortage have been explored. Prior efforts in the United States have focused largely on care standardization and the recruitment of more trainees into existing critical care training pathways.16 Other countries have created multidisciplinary critical care training pathways that delink critical care from specific subspecialty training programs.17 Another potential solution to ensure that critically ill patients receive care from board-certified intensivists is to regionalize critical care such that the sickest patients are consistently transferred to referral centers with robust intensivist staffing.1,18 While such an approach has been effectively implemented for trauma patients7, it has yet to materialize on a systemic basis for other critically ill cohorts. Moreover, our data suggest that hospitalists who attempt to transfer patients to higher levels of critical care find doing so burdensome and difficult.
Our surveyed hospitalists overwhelmingly expressed interest in augmenting their critical care skills and knowledge. However, most existing critical care educational offerings are not optimized for hospitalists, either focusing on very specific skills or knowledge (eg, procedural techniques or point-of-care ultrasound) or providing entry-level or very foundational education. None of these offerings provide comprehensive, structured training schemas for hospitalists who need to evolve beyond basic critical care skills to manage critically ill patients competently and consistently for extended periods of time.
Our study has several limitations. First, we estimate that about 10% of invited participants responded to this survey, but as respondents could forward the survey via professional networks, this is only an estimate. It is possible but unlikely that some respondents could have completed the survey more than once. Second, because our analysis identified only associations, we cannot infer causality for any of our findings. Third, the questionnaire was not designed to capture the acuity threshold at which point each respondent would prefer to transfer their patients into an ICU setting or to another institution for assistance in critical care management. We recognize that definitions and perceptions of patient acuity vary markedly from one hospital to the next, and a patient who can be comfortably managed in a floor setting in one hospital may require ICU care in a smaller or less well-resourced hospital. Practice patterns relating to acuity thresholds could have a substantial impact both on critical care patient volumes and on provider perceptions and, as such, warrant further study.
Finally, as respondents participated voluntarily, our sample may have overrepresented hospitalists who practice or are interested in critical care, thereby overestimating the scope of the problem and hospitalists’ interest in nonfellowship critical care training and certification. However, this seems unlikely given that, relative to SHM’s annual survey, we overrepresented hospitalists from academic and large community medical centers who generally provide less critical care than other hospitalists.13 Provided that roughly 85% of the estimated 50,000 American hospitalists practice outside of academic medical centers,13 perhaps as many as 37,000 hospitalists regularly deliver care to critically ill patients in ICUs. In light of the evolving intensivist shortage,4,5 this number seems likely to continue to grow. Whatever biases may exist in our sample, it is evident that a substantial number of ICU patients are managed by hospitalists who feel unprepared and undersupported to perform the task.
Without a massive and sustained increase in the number of board-certified intensivists or a systemic national plan to regionalize critical care delivery, hospitalists will continue to practice critical care, frequently with inadequate knowledge, skills, or intensivist support. Fortunately, these same hospitalists appear to be highly interested in augmenting their skills to care for their critically ill patients. The HM and critical care communities must rise to this challenge and help these providers deliver safe, appropriate, and high-quality care to their critically ill patients.
Disclosure
Mark V. Williams, MD, FACP, MHM, receives funding from the Patient Centered Outcomes Research Institute, Agency for Healthcare Research and Quality, Centers for Medicare & Medicaid Services, and Society of Hospital Medicine honoraria.
Society of Hospital Medicine Resources
1. Barnato AE, Kahn JM, Rubenfeld GD, et al. Prioritizing the organization and management of intensive care services in the United States: the PrOMIS Conference. Crit Care Med. 2007;35(4):1003-1011. PubMed
2. The Leapfrog Group. Factsheet: ICU Physician Staffing. Leapfrog Hospital Survey. Washington, DC: The Leapfrog Group; 2016.
3. Baumann MH, Simpson SQ, Stahl M, Raoof S, Marciniuk DD, Gutterman DD. First, do no harm: less training not equal quality care. Am J Crit Care. Jul 2012;21(4):227-230. PubMed
4. Krell K. Critical care workforce. Crit Care Med. 2008;36(4):1350-1353. PubMed
5. Angus DC, Kelley MA, Schmitz RJ, White A, Popovich J, Jr. Caring for the critically ill patient. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: can we meet the requirements of an aging population? JAMA. 2000;284(21):2762-2770. PubMed
6. Hyzy RC, Flanders SA, Pronovost PJ, et al. Characteristics of intensive care units in Michigan: not an open and closed case. J Hosp Med. 2010;5(1):4-9. PubMed
7. Kahn JM, Cicero BD, Wallace DJ, Iwashyna TJ. Adoption of ICU telemedicine in the United States. Crit Care Med. 2014;42(2):362-368. PubMed
8. Kleinpell RM, Ely EW, Grabenkort R. Nurse practitioners and physician assistants in the intensive care unit: an evidence-based review. Crit Care Med. 2008;36(10):2888-2897. PubMed
9. Heisler M. Hospitalists and intensivists: partners in caring for the critically ill--the time has come. J Hosp Med. 2010;5(1):1-3. PubMed
10. Checkley W, Martin GS, Brown SM, et al. Structure, process, and annual ICU mortality across 69 centers: United States Critical Illness and Injury Trials Group Critical Illness Outcomes Study. Crit Care Med. 2014;42(2):344-356. PubMed
11. Wise KR, Akopov VA, Williams BR, Jr., Ido MS, Leeper KV, Jr., Dressler DD. Hospitalists and intensivists in the medical ICU: a prospective observational study comparing mortality and length of stay between two staffing models. J Hosp Med. 2012;7(3):183-189. PubMed
12. Yoo EJ, Edwards JD, Dean ML, Dudley RA. Multidisciplinary Critical Care and Intensivist Staffing: Results of a Statewide Survey and Association With Mortality. J Intensive Care Med. 2016;31(5):325-332. PubMed
13. Society of Hospital Medicine. 2016 State of Hospital Medicine Report. Philadelphia: Society of Hospital Medicine; 2016.
14. Siegal EM, Dressler DD, Dichter JR, Gorman MJ, Lipsett PA. Training a hospitalist workforce to address the intensivist shortage in American hospitals: a position paper from the Society of Hospital Medicine and the Society of Critical Care Medicine. Crit Care Med. 2012;40(6):1952-1956. PubMed
15. Weled BJ, Adzhigirey LA, Hodgman TM, et al. Critical Care Delivery: The Importance of Process of Care and ICU Structure to Improved Outcomes: An Update From the American College of Critical Care Medicine Task Force on Models of Critical Care. Crit Care Med. 2015;43(7):1520-1525. PubMed
16. Kelley MA, Angus D, Chalfin DB, et al. The critical care crisis in the United States: a report from the profession. Chest. 2004;125(4):1514-1517. PubMed
17. Bion JF, Ramsay G, Roussos C, Burchardi H. Intensive care training and specialty status in Europe: international comparisons. Task Force on Educational issues of the European Society of Intensive Care Medicine. Intensive Care Med. 1998;24(4);372-377. PubMed
18. Kahn JM, Branas CC, Schwab CW, Asch DA. Regionalization of medical critical care: what can we learn from the trauma experience? Crit Care Med. 2008;36(11):3085-3088. PubMed
Despite calls for board-certified intensivist physicians to lead critical care delivery,1-3 the intensivist shortage in the United States continues to worsen,4 with projected shortfalls of 22% by 2020 and 35% by 2030.5 Many hospitals currently have inadequate or no board-certified intensivist support.6 The intensivist shortage has necessitated the development of alternative intensive care unit (ICU) staffing models, including engagement in telemedicine,7 the utilization of advanced practice providers,8 and dependence on hospitalists9 to deliver critical care services to ICU patients. Presently, research does not clearly show consistent differences in clinical outcomes based on the training of the clinical provider, although optimized teamwork and team rounds in the ICU do seem to be associated with improved outcomes.10-12
In its 2016 annual survey of hospital medicine (HM) leaders, the Society of Hospital Medicine (SHM) documented that most HM groups care for ICU patients, with up to 80% of hospitalist groups in some regions delivering critical care.13 In many United States hospitals, hospitalists serve as the primary if not lone physician providers of critical care.6,14 HM, with its team-based approach and on-site presence, shares many of the key attributes and values that define high-functioning critical care teams, and many hospitalists likely capably deliver some critical care services.9 However, hospitalists are also a highly heterogeneous work force with varied exposure to and comfort with critical care medicine, making it difficult to generalize hospitalists’ scope of practice in the ICU.
Because hospitalists render a significant amount of critical care in the United States, we surveyed practicing hospitalists to understand their demographics and practice roles in the ICU setting and to ascertain how they are supported when doing so. Additionally, we sought to identify mismatches between the ICU services that hospitalists provide and what they feel prepared and supported to deliver. Finally, we attempted to elucidate how hospitalists who practice in the ICU might respond to novel educational offerings targeted to mitigate cognitive or procedural gaps.
METHODS
We developed and deployed a survey to address the aforementioned questions. The survey content was developed iteratively by the Critical Care Task Force of SHM’s Education Committee and subsequently approved by SHM’s Education Committee and Board of Directors. Members of the Critical Care Task Force include critical care physicians and hospitalists. The survey included 25 items (supplemental Appendix A). Seventeen questions addressed the demographics and practice roles of hospitalists in the ICU, 5 addressed cognitive and procedural practice gaps, and 3 addressed how hospitalists would respond to educational opportunities in critical care. We used conditional formatting to ensure that only respondents who deliver ICU care could answer questions related to ICU practice. The survey was delivered by using an online survey platform (Survey Monkey, San Mateo, CA).
The survey was deployed in 3 phases from March to October of 2016. Initially, we distributed a pilot survey to professional contacts of the Critical Care Task Force to solicit feedback and refine the survey’s format and content. These contacts were largely academic hospitalists from our local institutions. We then distributed the survey to hospitalists via professional networks with instructions to forward the link to interested hospitalists. Finally, we distributed the survey to approximately 4000 hospitalists randomly selected from SHM’s national listserv of approximately 12,000 hospitalists. Respondents could enter a drawing for a monetary prize upon completion of the survey.
None of the survey questions changed during the 3 phases of survey deployment, and the data reported herein were compiled from all 3 phases of the survey deployment. Frequency tables were created using Tableau (version 10.0; Tableau Software, Seattle, WA). Comparisons between categorical questions were made by using χ2 and Fischer exact tests to calculate P values for associations by using SAS (version 9.3; SAS Institute, Cary, NC). Associations with P values below .05 were considered statistically significant.
RESULTS
Objective 1: Demographics and Practice Role
Four hundred and twenty-five hospitalists responded to the survey. The first 2 phases (pilot survey and distribution via professional networks) generated 101 responses, and the third phase (via SHM’s listserv) generated an additional 324 responses. As the survey was anonymous, we could not determine which hospitals or geographic regions were represented. Three hundred and twenty-five of the 425 hospitalists who completed the survey (77%) reported that they delivered care in the ICU. Of these 325 hospitalists, 45 served only as consultants, while the remaining 280 (66% of the total sample) served as the primary attending physician in the ICU. Among these primary providers of care in the ICU, 60 (21%) practiced in rural settings and 220 (79%) practiced in nonrural settings (Figure 1).
The demographics of our respondents were similar to those of the SHM annual survey,13 in which 66% of respondents delivered ICU care. Forty-one percent of our respondents worked in critical access or small community hospitals, 24% in academic medical centers, and 34% in large community centers with an academic affiliation. The SHM annual survey cohort included more physicians from nonteaching hospitals (58.7%) and fewer from academic medical centers (14.8%).13
Hospitalists’ presence in the ICU varied by practice setting (Table 1).
Hospitalists were significantly more prevalent in rural ICUs than in nonrural settings (96% vs 73%; Table 2).
We found similar results when comparing academic hospitalists (those working in an academic medical center or academic-affiliated hospital) with nonacademic hospitalists (those working in critical access or small community centers). Specifically, hospitalists in nonacademic settings were significantly more prevalent in ICUs (90% vs 67%; Table 2), more likely to serve as the primary attending (81% vs 55%), and more likely to deliver all critical care services (64% vs 25%). Sixty-four percent of respondents from nonacademic settings reported that hospitalists manage all or most ICU patients in their hospital as opposed to 25% for academic respondents (χ2P value for association <.001). Intensivist availability was also significantly lower in nonacademic ICUs (Table 2).
We also sought to determine whether the ability to transfer critically ill patients to higher levels of care effectively mitigated shortfalls in intensivist staffing. When restricted to hospitalists who served as primary providers for ICU patients, 28% of all respondents and 51% of rural hospitalists reported transferring patients to a higher level of care.
Sixty-seven percent of hospitalists who served as primary physicians for ICU patients in any setting reported at least moderate difficulty arranging transfers to higher levels of care.
Objective 2: Identifying the Practice Gap
Hospitalists’ perceptions of practicing critical care beyond their skill level and without sufficient board-certified intensivist support varied by both practice location and practice type (Table 3).
There were similar discrepancies between academic and nonacademic respondents. Forty-two percent of respondents practicing in nonacademic settings reported being expected to practice beyond their scope at least some of the time, and 18% reported that intensivist support was never sufficient. This contrasts with academic hospitalists, of whom 35% reported feeling expected to practice outside their scope, and less than 4% reported the available support from intensivists was never sufficient. For comparisons of academic and nonacademic respondents, only perceptions of sufficient board-certified intensivist support reached statistical significance (Table 3).
The role of intensivists in making management decisions and the strategy for ventilator management decisions correlated significantly with perception of intensivist support (P < .001) but not with the perception of practicing beyond one’s scope. The number of ventilated patients did not correlate significantly with either perception of intensivist support or of being expected to practice beyond scope.
Difficulty transferring patients to a higher level of care was the only attribute that significantly correlated with hospitalists’ perceptions of having to practice beyond their skill level (P < .05; Table 3). Difficulty of transfer was also significantly associated with perceived adequacy of board-certified intensivist support (P < .001). Total hours of intensivist coverage, intensivist role in decision making, and ventilator management arrangements also correlated significantly with the perceived adequacy of board-certified intensivist support (P < .001 for all; Table 3).
Objective 3: Assessing Interest in Critical Care Education
More than 85% of respondents indicated interest in obtaining additional critical care training and some form of certification short of fellowship training. Preferred modes of content delivery included courses or precourses at national meetings, academies, or online modules. Hospitalists in smaller communities indicated preference for online resources.
DISCUSSION
This survey of a large national cohort of hospitalists from diverse practice settings validates previous studies suggesting that hospitalists deliver critical care services, most notably in community and rural hospitals.13 A substantial subset of our respondents represented rural practice settings, which allowed us to compare rural and nonrural hospitalists as well as those practicing in academic and nonacademic settings. In assessing both the objective services that hospitalists provided as well as their subjective perceptions of how they practiced, we could correlate factors associated with the sense of practicing beyond one’s skill or feeling inadequately supported by board-certified intensivists.
More than a third of responding hospitalists who practiced in the ICU reported that they practiced beyond their self-perceived skill level, and almost three-fourths indicated that they practiced without consistent or adequate board-certified intensivist support. Rural and nonacademic hospitalists were far more likely to report delivering critical care beyond their comfort level and having insufficient board-certified intensivist support.
Calls for board-certified intensivists to deliver critical care to all critically ill patients do not reflect the reality in many American hospitals and, either by intent or by default, hospitalists have become the major and often sole providers of critical care services in many hospitals without robust intensivist support. We suspect that this phenomenon has been consistently underreported in the literature because academic hospitalists generally do not practice critical care.15
Many potential solutions to the intensivist shortage have been explored. Prior efforts in the United States have focused largely on care standardization and the recruitment of more trainees into existing critical care training pathways.16 Other countries have created multidisciplinary critical care training pathways that delink critical care from specific subspecialty training programs.17 Another potential solution to ensure that critically ill patients receive care from board-certified intensivists is to regionalize critical care such that the sickest patients are consistently transferred to referral centers with robust intensivist staffing.1,18 While such an approach has been effectively implemented for trauma patients7, it has yet to materialize on a systemic basis for other critically ill cohorts. Moreover, our data suggest that hospitalists who attempt to transfer patients to higher levels of critical care find doing so burdensome and difficult.
Our surveyed hospitalists overwhelmingly expressed interest in augmenting their critical care skills and knowledge. However, most existing critical care educational offerings are not optimized for hospitalists, either focusing on very specific skills or knowledge (eg, procedural techniques or point-of-care ultrasound) or providing entry-level or very foundational education. None of these offerings provide comprehensive, structured training schemas for hospitalists who need to evolve beyond basic critical care skills to manage critically ill patients competently and consistently for extended periods of time.
Our study has several limitations. First, we estimate that about 10% of invited participants responded to this survey, but as respondents could forward the survey via professional networks, this is only an estimate. It is possible but unlikely that some respondents could have completed the survey more than once. Second, because our analysis identified only associations, we cannot infer causality for any of our findings. Third, the questionnaire was not designed to capture the acuity threshold at which point each respondent would prefer to transfer their patients into an ICU setting or to another institution for assistance in critical care management. We recognize that definitions and perceptions of patient acuity vary markedly from one hospital to the next, and a patient who can be comfortably managed in a floor setting in one hospital may require ICU care in a smaller or less well-resourced hospital. Practice patterns relating to acuity thresholds could have a substantial impact both on critical care patient volumes and on provider perceptions and, as such, warrant further study.
Finally, as respondents participated voluntarily, our sample may have overrepresented hospitalists who practice or are interested in critical care, thereby overestimating the scope of the problem and hospitalists’ interest in nonfellowship critical care training and certification. However, this seems unlikely given that, relative to SHM’s annual survey, we overrepresented hospitalists from academic and large community medical centers who generally provide less critical care than other hospitalists.13 Provided that roughly 85% of the estimated 50,000 American hospitalists practice outside of academic medical centers,13 perhaps as many as 37,000 hospitalists regularly deliver care to critically ill patients in ICUs. In light of the evolving intensivist shortage,4,5 this number seems likely to continue to grow. Whatever biases may exist in our sample, it is evident that a substantial number of ICU patients are managed by hospitalists who feel unprepared and undersupported to perform the task.
Without a massive and sustained increase in the number of board-certified intensivists or a systemic national plan to regionalize critical care delivery, hospitalists will continue to practice critical care, frequently with inadequate knowledge, skills, or intensivist support. Fortunately, these same hospitalists appear to be highly interested in augmenting their skills to care for their critically ill patients. The HM and critical care communities must rise to this challenge and help these providers deliver safe, appropriate, and high-quality care to their critically ill patients.
Disclosure
Mark V. Williams, MD, FACP, MHM, receives funding from the Patient Centered Outcomes Research Institute, Agency for Healthcare Research and Quality, Centers for Medicare & Medicaid Services, and Society of Hospital Medicine honoraria.
Society of Hospital Medicine Resources
Despite calls for board-certified intensivist physicians to lead critical care delivery,1-3 the intensivist shortage in the United States continues to worsen,4 with projected shortfalls of 22% by 2020 and 35% by 2030.5 Many hospitals currently have inadequate or no board-certified intensivist support.6 The intensivist shortage has necessitated the development of alternative intensive care unit (ICU) staffing models, including engagement in telemedicine,7 the utilization of advanced practice providers,8 and dependence on hospitalists9 to deliver critical care services to ICU patients. Presently, research does not clearly show consistent differences in clinical outcomes based on the training of the clinical provider, although optimized teamwork and team rounds in the ICU do seem to be associated with improved outcomes.10-12
In its 2016 annual survey of hospital medicine (HM) leaders, the Society of Hospital Medicine (SHM) documented that most HM groups care for ICU patients, with up to 80% of hospitalist groups in some regions delivering critical care.13 In many United States hospitals, hospitalists serve as the primary if not lone physician providers of critical care.6,14 HM, with its team-based approach and on-site presence, shares many of the key attributes and values that define high-functioning critical care teams, and many hospitalists likely capably deliver some critical care services.9 However, hospitalists are also a highly heterogeneous work force with varied exposure to and comfort with critical care medicine, making it difficult to generalize hospitalists’ scope of practice in the ICU.
Because hospitalists render a significant amount of critical care in the United States, we surveyed practicing hospitalists to understand their demographics and practice roles in the ICU setting and to ascertain how they are supported when doing so. Additionally, we sought to identify mismatches between the ICU services that hospitalists provide and what they feel prepared and supported to deliver. Finally, we attempted to elucidate how hospitalists who practice in the ICU might respond to novel educational offerings targeted to mitigate cognitive or procedural gaps.
METHODS
We developed and deployed a survey to address the aforementioned questions. The survey content was developed iteratively by the Critical Care Task Force of SHM’s Education Committee and subsequently approved by SHM’s Education Committee and Board of Directors. Members of the Critical Care Task Force include critical care physicians and hospitalists. The survey included 25 items (supplemental Appendix A). Seventeen questions addressed the demographics and practice roles of hospitalists in the ICU, 5 addressed cognitive and procedural practice gaps, and 3 addressed how hospitalists would respond to educational opportunities in critical care. We used conditional formatting to ensure that only respondents who deliver ICU care could answer questions related to ICU practice. The survey was delivered by using an online survey platform (Survey Monkey, San Mateo, CA).
The survey was deployed in 3 phases from March to October of 2016. Initially, we distributed a pilot survey to professional contacts of the Critical Care Task Force to solicit feedback and refine the survey’s format and content. These contacts were largely academic hospitalists from our local institutions. We then distributed the survey to hospitalists via professional networks with instructions to forward the link to interested hospitalists. Finally, we distributed the survey to approximately 4000 hospitalists randomly selected from SHM’s national listserv of approximately 12,000 hospitalists. Respondents could enter a drawing for a monetary prize upon completion of the survey.
None of the survey questions changed during the 3 phases of survey deployment, and the data reported herein were compiled from all 3 phases of the survey deployment. Frequency tables were created using Tableau (version 10.0; Tableau Software, Seattle, WA). Comparisons between categorical questions were made by using χ2 and Fischer exact tests to calculate P values for associations by using SAS (version 9.3; SAS Institute, Cary, NC). Associations with P values below .05 were considered statistically significant.
RESULTS
Objective 1: Demographics and Practice Role
Four hundred and twenty-five hospitalists responded to the survey. The first 2 phases (pilot survey and distribution via professional networks) generated 101 responses, and the third phase (via SHM’s listserv) generated an additional 324 responses. As the survey was anonymous, we could not determine which hospitals or geographic regions were represented. Three hundred and twenty-five of the 425 hospitalists who completed the survey (77%) reported that they delivered care in the ICU. Of these 325 hospitalists, 45 served only as consultants, while the remaining 280 (66% of the total sample) served as the primary attending physician in the ICU. Among these primary providers of care in the ICU, 60 (21%) practiced in rural settings and 220 (79%) practiced in nonrural settings (Figure 1).
The demographics of our respondents were similar to those of the SHM annual survey,13 in which 66% of respondents delivered ICU care. Forty-one percent of our respondents worked in critical access or small community hospitals, 24% in academic medical centers, and 34% in large community centers with an academic affiliation. The SHM annual survey cohort included more physicians from nonteaching hospitals (58.7%) and fewer from academic medical centers (14.8%).13
Hospitalists’ presence in the ICU varied by practice setting (Table 1).
Hospitalists were significantly more prevalent in rural ICUs than in nonrural settings (96% vs 73%; Table 2).
We found similar results when comparing academic hospitalists (those working in an academic medical center or academic-affiliated hospital) with nonacademic hospitalists (those working in critical access or small community centers). Specifically, hospitalists in nonacademic settings were significantly more prevalent in ICUs (90% vs 67%; Table 2), more likely to serve as the primary attending (81% vs 55%), and more likely to deliver all critical care services (64% vs 25%). Sixty-four percent of respondents from nonacademic settings reported that hospitalists manage all or most ICU patients in their hospital as opposed to 25% for academic respondents (χ2P value for association <.001). Intensivist availability was also significantly lower in nonacademic ICUs (Table 2).
We also sought to determine whether the ability to transfer critically ill patients to higher levels of care effectively mitigated shortfalls in intensivist staffing. When restricted to hospitalists who served as primary providers for ICU patients, 28% of all respondents and 51% of rural hospitalists reported transferring patients to a higher level of care.
Sixty-seven percent of hospitalists who served as primary physicians for ICU patients in any setting reported at least moderate difficulty arranging transfers to higher levels of care.
Objective 2: Identifying the Practice Gap
Hospitalists’ perceptions of practicing critical care beyond their skill level and without sufficient board-certified intensivist support varied by both practice location and practice type (Table 3).
There were similar discrepancies between academic and nonacademic respondents. Forty-two percent of respondents practicing in nonacademic settings reported being expected to practice beyond their scope at least some of the time, and 18% reported that intensivist support was never sufficient. This contrasts with academic hospitalists, of whom 35% reported feeling expected to practice outside their scope, and less than 4% reported the available support from intensivists was never sufficient. For comparisons of academic and nonacademic respondents, only perceptions of sufficient board-certified intensivist support reached statistical significance (Table 3).
The role of intensivists in making management decisions and the strategy for ventilator management decisions correlated significantly with perception of intensivist support (P < .001) but not with the perception of practicing beyond one’s scope. The number of ventilated patients did not correlate significantly with either perception of intensivist support or of being expected to practice beyond scope.
Difficulty transferring patients to a higher level of care was the only attribute that significantly correlated with hospitalists’ perceptions of having to practice beyond their skill level (P < .05; Table 3). Difficulty of transfer was also significantly associated with perceived adequacy of board-certified intensivist support (P < .001). Total hours of intensivist coverage, intensivist role in decision making, and ventilator management arrangements also correlated significantly with the perceived adequacy of board-certified intensivist support (P < .001 for all; Table 3).
Objective 3: Assessing Interest in Critical Care Education
More than 85% of respondents indicated interest in obtaining additional critical care training and some form of certification short of fellowship training. Preferred modes of content delivery included courses or precourses at national meetings, academies, or online modules. Hospitalists in smaller communities indicated preference for online resources.
DISCUSSION
This survey of a large national cohort of hospitalists from diverse practice settings validates previous studies suggesting that hospitalists deliver critical care services, most notably in community and rural hospitals.13 A substantial subset of our respondents represented rural practice settings, which allowed us to compare rural and nonrural hospitalists as well as those practicing in academic and nonacademic settings. In assessing both the objective services that hospitalists provided as well as their subjective perceptions of how they practiced, we could correlate factors associated with the sense of practicing beyond one’s skill or feeling inadequately supported by board-certified intensivists.
More than a third of responding hospitalists who practiced in the ICU reported that they practiced beyond their self-perceived skill level, and almost three-fourths indicated that they practiced without consistent or adequate board-certified intensivist support. Rural and nonacademic hospitalists were far more likely to report delivering critical care beyond their comfort level and having insufficient board-certified intensivist support.
Calls for board-certified intensivists to deliver critical care to all critically ill patients do not reflect the reality in many American hospitals and, either by intent or by default, hospitalists have become the major and often sole providers of critical care services in many hospitals without robust intensivist support. We suspect that this phenomenon has been consistently underreported in the literature because academic hospitalists generally do not practice critical care.15
Many potential solutions to the intensivist shortage have been explored. Prior efforts in the United States have focused largely on care standardization and the recruitment of more trainees into existing critical care training pathways.16 Other countries have created multidisciplinary critical care training pathways that delink critical care from specific subspecialty training programs.17 Another potential solution to ensure that critically ill patients receive care from board-certified intensivists is to regionalize critical care such that the sickest patients are consistently transferred to referral centers with robust intensivist staffing.1,18 While such an approach has been effectively implemented for trauma patients7, it has yet to materialize on a systemic basis for other critically ill cohorts. Moreover, our data suggest that hospitalists who attempt to transfer patients to higher levels of critical care find doing so burdensome and difficult.
Our surveyed hospitalists overwhelmingly expressed interest in augmenting their critical care skills and knowledge. However, most existing critical care educational offerings are not optimized for hospitalists, either focusing on very specific skills or knowledge (eg, procedural techniques or point-of-care ultrasound) or providing entry-level or very foundational education. None of these offerings provide comprehensive, structured training schemas for hospitalists who need to evolve beyond basic critical care skills to manage critically ill patients competently and consistently for extended periods of time.
Our study has several limitations. First, we estimate that about 10% of invited participants responded to this survey, but as respondents could forward the survey via professional networks, this is only an estimate. It is possible but unlikely that some respondents could have completed the survey more than once. Second, because our analysis identified only associations, we cannot infer causality for any of our findings. Third, the questionnaire was not designed to capture the acuity threshold at which point each respondent would prefer to transfer their patients into an ICU setting or to another institution for assistance in critical care management. We recognize that definitions and perceptions of patient acuity vary markedly from one hospital to the next, and a patient who can be comfortably managed in a floor setting in one hospital may require ICU care in a smaller or less well-resourced hospital. Practice patterns relating to acuity thresholds could have a substantial impact both on critical care patient volumes and on provider perceptions and, as such, warrant further study.
Finally, as respondents participated voluntarily, our sample may have overrepresented hospitalists who practice or are interested in critical care, thereby overestimating the scope of the problem and hospitalists’ interest in nonfellowship critical care training and certification. However, this seems unlikely given that, relative to SHM’s annual survey, we overrepresented hospitalists from academic and large community medical centers who generally provide less critical care than other hospitalists.13 Provided that roughly 85% of the estimated 50,000 American hospitalists practice outside of academic medical centers,13 perhaps as many as 37,000 hospitalists regularly deliver care to critically ill patients in ICUs. In light of the evolving intensivist shortage,4,5 this number seems likely to continue to grow. Whatever biases may exist in our sample, it is evident that a substantial number of ICU patients are managed by hospitalists who feel unprepared and undersupported to perform the task.
Without a massive and sustained increase in the number of board-certified intensivists or a systemic national plan to regionalize critical care delivery, hospitalists will continue to practice critical care, frequently with inadequate knowledge, skills, or intensivist support. Fortunately, these same hospitalists appear to be highly interested in augmenting their skills to care for their critically ill patients. The HM and critical care communities must rise to this challenge and help these providers deliver safe, appropriate, and high-quality care to their critically ill patients.
Disclosure
Mark V. Williams, MD, FACP, MHM, receives funding from the Patient Centered Outcomes Research Institute, Agency for Healthcare Research and Quality, Centers for Medicare & Medicaid Services, and Society of Hospital Medicine honoraria.
Society of Hospital Medicine Resources
1. Barnato AE, Kahn JM, Rubenfeld GD, et al. Prioritizing the organization and management of intensive care services in the United States: the PrOMIS Conference. Crit Care Med. 2007;35(4):1003-1011. PubMed
2. The Leapfrog Group. Factsheet: ICU Physician Staffing. Leapfrog Hospital Survey. Washington, DC: The Leapfrog Group; 2016.
3. Baumann MH, Simpson SQ, Stahl M, Raoof S, Marciniuk DD, Gutterman DD. First, do no harm: less training not equal quality care. Am J Crit Care. Jul 2012;21(4):227-230. PubMed
4. Krell K. Critical care workforce. Crit Care Med. 2008;36(4):1350-1353. PubMed
5. Angus DC, Kelley MA, Schmitz RJ, White A, Popovich J, Jr. Caring for the critically ill patient. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: can we meet the requirements of an aging population? JAMA. 2000;284(21):2762-2770. PubMed
6. Hyzy RC, Flanders SA, Pronovost PJ, et al. Characteristics of intensive care units in Michigan: not an open and closed case. J Hosp Med. 2010;5(1):4-9. PubMed
7. Kahn JM, Cicero BD, Wallace DJ, Iwashyna TJ. Adoption of ICU telemedicine in the United States. Crit Care Med. 2014;42(2):362-368. PubMed
8. Kleinpell RM, Ely EW, Grabenkort R. Nurse practitioners and physician assistants in the intensive care unit: an evidence-based review. Crit Care Med. 2008;36(10):2888-2897. PubMed
9. Heisler M. Hospitalists and intensivists: partners in caring for the critically ill--the time has come. J Hosp Med. 2010;5(1):1-3. PubMed
10. Checkley W, Martin GS, Brown SM, et al. Structure, process, and annual ICU mortality across 69 centers: United States Critical Illness and Injury Trials Group Critical Illness Outcomes Study. Crit Care Med. 2014;42(2):344-356. PubMed
11. Wise KR, Akopov VA, Williams BR, Jr., Ido MS, Leeper KV, Jr., Dressler DD. Hospitalists and intensivists in the medical ICU: a prospective observational study comparing mortality and length of stay between two staffing models. J Hosp Med. 2012;7(3):183-189. PubMed
12. Yoo EJ, Edwards JD, Dean ML, Dudley RA. Multidisciplinary Critical Care and Intensivist Staffing: Results of a Statewide Survey and Association With Mortality. J Intensive Care Med. 2016;31(5):325-332. PubMed
13. Society of Hospital Medicine. 2016 State of Hospital Medicine Report. Philadelphia: Society of Hospital Medicine; 2016.
14. Siegal EM, Dressler DD, Dichter JR, Gorman MJ, Lipsett PA. Training a hospitalist workforce to address the intensivist shortage in American hospitals: a position paper from the Society of Hospital Medicine and the Society of Critical Care Medicine. Crit Care Med. 2012;40(6):1952-1956. PubMed
15. Weled BJ, Adzhigirey LA, Hodgman TM, et al. Critical Care Delivery: The Importance of Process of Care and ICU Structure to Improved Outcomes: An Update From the American College of Critical Care Medicine Task Force on Models of Critical Care. Crit Care Med. 2015;43(7):1520-1525. PubMed
16. Kelley MA, Angus D, Chalfin DB, et al. The critical care crisis in the United States: a report from the profession. Chest. 2004;125(4):1514-1517. PubMed
17. Bion JF, Ramsay G, Roussos C, Burchardi H. Intensive care training and specialty status in Europe: international comparisons. Task Force on Educational issues of the European Society of Intensive Care Medicine. Intensive Care Med. 1998;24(4);372-377. PubMed
18. Kahn JM, Branas CC, Schwab CW, Asch DA. Regionalization of medical critical care: what can we learn from the trauma experience? Crit Care Med. 2008;36(11):3085-3088. PubMed
1. Barnato AE, Kahn JM, Rubenfeld GD, et al. Prioritizing the organization and management of intensive care services in the United States: the PrOMIS Conference. Crit Care Med. 2007;35(4):1003-1011. PubMed
2. The Leapfrog Group. Factsheet: ICU Physician Staffing. Leapfrog Hospital Survey. Washington, DC: The Leapfrog Group; 2016.
3. Baumann MH, Simpson SQ, Stahl M, Raoof S, Marciniuk DD, Gutterman DD. First, do no harm: less training not equal quality care. Am J Crit Care. Jul 2012;21(4):227-230. PubMed
4. Krell K. Critical care workforce. Crit Care Med. 2008;36(4):1350-1353. PubMed
5. Angus DC, Kelley MA, Schmitz RJ, White A, Popovich J, Jr. Caring for the critically ill patient. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: can we meet the requirements of an aging population? JAMA. 2000;284(21):2762-2770. PubMed
6. Hyzy RC, Flanders SA, Pronovost PJ, et al. Characteristics of intensive care units in Michigan: not an open and closed case. J Hosp Med. 2010;5(1):4-9. PubMed
7. Kahn JM, Cicero BD, Wallace DJ, Iwashyna TJ. Adoption of ICU telemedicine in the United States. Crit Care Med. 2014;42(2):362-368. PubMed
8. Kleinpell RM, Ely EW, Grabenkort R. Nurse practitioners and physician assistants in the intensive care unit: an evidence-based review. Crit Care Med. 2008;36(10):2888-2897. PubMed
9. Heisler M. Hospitalists and intensivists: partners in caring for the critically ill--the time has come. J Hosp Med. 2010;5(1):1-3. PubMed
10. Checkley W, Martin GS, Brown SM, et al. Structure, process, and annual ICU mortality across 69 centers: United States Critical Illness and Injury Trials Group Critical Illness Outcomes Study. Crit Care Med. 2014;42(2):344-356. PubMed
11. Wise KR, Akopov VA, Williams BR, Jr., Ido MS, Leeper KV, Jr., Dressler DD. Hospitalists and intensivists in the medical ICU: a prospective observational study comparing mortality and length of stay between two staffing models. J Hosp Med. 2012;7(3):183-189. PubMed
12. Yoo EJ, Edwards JD, Dean ML, Dudley RA. Multidisciplinary Critical Care and Intensivist Staffing: Results of a Statewide Survey and Association With Mortality. J Intensive Care Med. 2016;31(5):325-332. PubMed
13. Society of Hospital Medicine. 2016 State of Hospital Medicine Report. Philadelphia: Society of Hospital Medicine; 2016.
14. Siegal EM, Dressler DD, Dichter JR, Gorman MJ, Lipsett PA. Training a hospitalist workforce to address the intensivist shortage in American hospitals: a position paper from the Society of Hospital Medicine and the Society of Critical Care Medicine. Crit Care Med. 2012;40(6):1952-1956. PubMed
15. Weled BJ, Adzhigirey LA, Hodgman TM, et al. Critical Care Delivery: The Importance of Process of Care and ICU Structure to Improved Outcomes: An Update From the American College of Critical Care Medicine Task Force on Models of Critical Care. Crit Care Med. 2015;43(7):1520-1525. PubMed
16. Kelley MA, Angus D, Chalfin DB, et al. The critical care crisis in the United States: a report from the profession. Chest. 2004;125(4):1514-1517. PubMed
17. Bion JF, Ramsay G, Roussos C, Burchardi H. Intensive care training and specialty status in Europe: international comparisons. Task Force on Educational issues of the European Society of Intensive Care Medicine. Intensive Care Med. 1998;24(4);372-377. PubMed
18. Kahn JM, Branas CC, Schwab CW, Asch DA. Regionalization of medical critical care: what can we learn from the trauma experience? Crit Care Med. 2008;36(11):3085-3088. PubMed
© 2018 Society of Hospital Medicine
Cognitive, Emotional Memory Disconnect Impacts Patient Satisfaction
There are two types of memory, the cognitive and the emotional, and the latter is more enduring. Maya Angelou characterized the distinction between these two types of memory most eloquently and succinctly when she said, “I’ve learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel.” She was ahead of her time, because neurocognitive research has objectified with science what Ms. Angelou captured so elegantly in her prose. Emotional events are processed in the sensory systems and then transmitted to the medial-temporal lobe and the amygdale for the formation of an emotional memory. When the memory is cued and retrieved from the amygdale, it triggers an emotional response. Emotional experiences leave strong traces in the brain. Memories about emotional situations are stored in both the conscious and unconscious memory, which is part of the reason emotional memories are so enduring.1 Studies of patients with severe anterograde amnesia following circumscribed bilateral hippocampal brain damage showed enduring memories of emotion despite the absence of conscious memories.2 This has a demonstrably practical application in patients with dementia, who we now know have feelings of happiness and sadness long after they have forgotten what caused the emotion.3
The distinction is important because patients judge the quality of their medical care based on emotions. The patient satisfaction disconnect arises from the fact that physicians live in their cognitive memory, while patients live in their emotional memory. Being cognitive and objective is a critical skill a physician must bring to the bedside every day; the reason we don’t allow physicians to treat family members is that their ability to remain objective will be impaired. I realized that my emotion, my passion, and my empathy for the dying would impair my judgment when I started medical school, and I launched myself on a conscious and systematic discipline to keep those feelings out of my mind during patient care. The effort worked and, for the most part, I have been able to remain objective and unemotional as I care for my patients. Recently, however, I realized that my focus on objectivity negatively impacts patient experience. As a result, I have expanded my view: While I must stay objective and detached with my thinking, I must be emotionally engaged to provide a great patient experience.
I can remain objective and detached in my clinical judgment as I engage and connect emotionally during my patient encounters. This delicate balancing act has taken years of trial and error, however. I recently cared for a woman in her 60s who had fallen and broke her hip. Everyone was pleased that a top orthopedic surgeon was on call and able to give her the first-rate care she needed to begin walking again. The surgery went smoothly, and she was transferred to the medical/surgical ward, where things took a turn for the worse. She had a lot of anxiety in addition to her osteoporosis. Objectively, she was doing great, and we had a big success on our hands; however, she remained anxious, and she peppered the surgeon with fears that, while unfounded, were very real in her mind. The surgeon brushed them off, saying that her fears were not real and that he didn’t need to address them; his response made her emotional state spiral out of control. Her nurse notified me of the situation, and I came to her bedside. She was very agitated. I sat down at a low level and just started listening. She got all of her anxieties out in words. I held her hand, looked her in the eye, and assured her that I would be there for her and that things were going to be alright. Subsequently, she wrote letters of gratitude and proclaimed to any medical staff who would listen what a talented and great doctor I was. I did not have the skill to fix her broken hip; if it had been left to me alone, she would still be bed-bound. But I did have the human skills to connect with her and fix her agitated mind. If we remember the enduring power of the emotional memory, we can create great patient experiences.
The importance of these experiences was illustrated to me at the 2014 Dignity Health Patient Experience Summit, a powerful event featuring motivational speakers and leaders from across the country. The most powerful speakers, however, were patients. These patients had received terrible diagnoses that committed them to a prolonged interaction with the healthcare system. They were scared of what their diagnoses would mean for their future, they were subjected to uncomfortable procedures in which they struggled to maintain their dignity, and they repeatedly met the indifference of healthcare providers and clerical people who were only there to do a job. They related how the lack of caring and empathy made fears and anxiety much worse. But each of them had a story about that one person, that one care provider, who took the time to reassure them, to show that they cared, and to ensure that the patient did not feel alone. In most of these stories, the stand-out care providers took the time to hold their hands and reassure the patients. They took the time to connect with the patient’s emotional memory in a positive way, and that simple gesture of empathy had a powerful and lasting impact on the patient.
Invariably, the care provider at the heart of the patients’ stories was a nurse. Nurses have the reputation for being angels of mercy because they do the simple, empathetic gestures that let a patient know they are being cared for. These feelings endure in the patients’ memories long after the treatment is over. Doctors can, and should, be that type of care provider. It requires us to recognize that patients are scared and anxious, even though they may do their best not to show it. We, as physicians, often don’t see their anxiety, and we are so focused on the cognitive memory that we don’t address the anxiety and fear that is just under the surface. But taking just a few minutes to acknowledge their emotions, to explore them, and to reassure the patient that we are there for them has a lasting impact. In my group, we talk about the “human-business-human” encounter with patients. We begin all interactions with a human interaction (“Hello, I am Dr. McIlraith…”), conduct the business we came to provide (“Now I am going to examine you…”), and end with a human interaction (“What else can I do for you today?”). Patients expect physical contact with us during the “business” part of that interaction. I find that respectful, reassuring, and appropriate physical contact during the final “human” portion of that interaction helps solidify my patients’ experience. It helps make them feel that they have been cared for, particularly if the visit includes bad news.
Much of the recent focus on patient satisfaction has been driven by financial incentives. In 2013, CMS began penalizing hospitals 1.25% for poor HCAHPS scores as a part of the Affordable Care Act. In 2014, the maximum penalty increased to 2%, and to 3% in 2015. Hospitals have notoriously high overhead costs and slim profit margins, so these penalties can have a profound impact on the financial viability of an institution. But, while hospitals across the country have taken notice (see related article in this edition of The Hospitalist), I find doctors are more motivated by the well-being of their patients than are their hospital administrators. Satisfied patients are more compliant with treatment plans and have better outcomes.4,5 Hospitalists spend a lot of effort making sure their heart failure patients are on an ACE inhibitor, and their heart attack patients are discharged on aspirin, beta blockers, and statins so that they will have a good outcome following treatment for their acute illness. The same outcome-driven, evidence-based practice of medicine relates to patient satisfaction, however. Success in HCAHPS is as important as core measures when it comes to patient outcomes. And if I can’t convince you patient satisfaction is important because of the good it does for hospitals and patients, think about yourself for a minute. Satisfied patients are much less likely to sue their physicians.6 Practicing quality, evidence-based medicine will keep you out of peer review; however, satisfied patients will keep you out of the courtroom.
I frequently hear the comment that “we can do great on patient satisfaction, but then it gets busy, and patient satisfaction goes out the window.” My own experience contradicts this maxim, however. It is not how much time you spend with your patient but, rather, what you do with the time you have. One of the most powerful things we can do is listen. I used to make the mistake that I only wanted to hear the information I needed to figure out my patients’ problems so I could start treating them; however, I have come to learn that being heard is, in itself, therapy for my patients. It is often quoted that physicians interrupt their patients within 18 seconds of starting the interview.7 A lot of physicians dispense with attentive listening when they are under time pressure, when they should instead dispense with lengthy discourses on the patient treatment plan. It is important to educate our patients on their illness and treatment, I admit. I find a lot of hospitalists want to impart their knowledge and their treatment rationale to their patients; however, they frequently give patients and families much more information than they can hold in their cognitive memory. And time pressures are not the only anxieties hospitalists carry with them to the bedside. Our increasingly metric-driven profession means that we not only have to worry about morning discharges, interdisciplinary rounds, length of stay, and so on, but we also have to consider patient experience. It is not easy to hide all the stress we are under when we come to the bedside of a patient, but we have to. The easiest way to do that is to take a deep breath, sit next to the patient, ask an open-ended question, and then say nothing until the patient is done speaking. Active listening with good eye contact and encouragement to continue solidifies the patient’s experience of being heard. There are extreme cases when a patient is in a manic phase and won’t ever stop speaking; bend the rules a bit in those circumstances. However, the above rule works very effectively in the majority of physician-patient interactions. Being heard leaves an enduring emotional memory with our patients.
Hospital medicine often looks to other industries for inspiration on how we can improve. The airline industry is often held up as an example of how we can model patient safety, for instance, but these comparisons oversimplify the challenges we face. The same is true with patient satisfaction. In the business world, adages like “The customer is always right” are central to customer satisfaction, yet completely irrelevant to HM practice. Patients and families frequently have inappropriate and unrealistic expectations of their hospitalist physicians. We cannot, and should not, tell the patient addicted to narcotics that they can have as much IV Dilaudid as they would like. We cannot fix the patient with end-stage cancer, heart failure, or dementia. This is where we have to part ways with comparisons to principles that guide other industries if we are going to find a way forward with patient experience in hospital medicine. Because we have to set limits for patients, we often have to give our patients and families bad news, and because we have to tell them things they don’t like to hear, like “You can’t have any salt in your diet,” or “You must quit drinking alcohol,” we must develop our own principles on patient experience and satisfaction. Otherwise our options are either delivering inappropriate medical care or abandoning the pursuit of patient satisfaction all together. This is when we must remember that emotional memories are more enduring. We can’t always give our patients what they want, and we can’t always tell them what they want to hear, but we can always show them that we care. When we show our patients that we care in a palpable way, we leave them with the feeling that they have been cared for regardless of their condition, and the positive memory will endure despite the negative information we may have to convey. Maybe they won’t cut down on their salt or quit drinking alcohol, but they will never forget that their hospitalist physician cared.
And if they remember that the physician cared, it is much more likely that they will cut down on the salt or quit drinking alcohol when they go home. To paraphrase Maya Angelou, “I can’t always tell my patients what they want to hear, I can’t always tell them that their lifestyle is appropriate, but I can always show them that I care.”
Dr. McIlraith is chairman of the department of hospital medicine of Mercy Medical Group in Sacramento, Calif.
References
- LeDoux JE. Emotional memory. Scholarpedia. Accessed August 2, 2015.
- Feinstein JS, Duff MC, D Tranel D. Sustained experience of emotion after loss of memory in patients with amnesia. Proc Natl Acad Sci. 2010:107(17):7674-7679.
- Guzmán-Vélez E, Feinstein JS, Tranel D. Feelings without memory in Alzheimer disease. Cogn Behav Neurol. 2014;27(3):117-129.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. March 2001. Accessed August 2, 2015.
- Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med. 2011;24(3):229-239.
- Stelfox HT, Gandhi TK, Orav EJ, Gustafson ML. The relation of patient statisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005;118(10):1126-1133.
- Beckman HB, Frankel RM. The effect of physician behavior on the collection of data. Ann Intern Med. 1984;101(5):692-696.
There are two types of memory, the cognitive and the emotional, and the latter is more enduring. Maya Angelou characterized the distinction between these two types of memory most eloquently and succinctly when she said, “I’ve learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel.” She was ahead of her time, because neurocognitive research has objectified with science what Ms. Angelou captured so elegantly in her prose. Emotional events are processed in the sensory systems and then transmitted to the medial-temporal lobe and the amygdale for the formation of an emotional memory. When the memory is cued and retrieved from the amygdale, it triggers an emotional response. Emotional experiences leave strong traces in the brain. Memories about emotional situations are stored in both the conscious and unconscious memory, which is part of the reason emotional memories are so enduring.1 Studies of patients with severe anterograde amnesia following circumscribed bilateral hippocampal brain damage showed enduring memories of emotion despite the absence of conscious memories.2 This has a demonstrably practical application in patients with dementia, who we now know have feelings of happiness and sadness long after they have forgotten what caused the emotion.3
The distinction is important because patients judge the quality of their medical care based on emotions. The patient satisfaction disconnect arises from the fact that physicians live in their cognitive memory, while patients live in their emotional memory. Being cognitive and objective is a critical skill a physician must bring to the bedside every day; the reason we don’t allow physicians to treat family members is that their ability to remain objective will be impaired. I realized that my emotion, my passion, and my empathy for the dying would impair my judgment when I started medical school, and I launched myself on a conscious and systematic discipline to keep those feelings out of my mind during patient care. The effort worked and, for the most part, I have been able to remain objective and unemotional as I care for my patients. Recently, however, I realized that my focus on objectivity negatively impacts patient experience. As a result, I have expanded my view: While I must stay objective and detached with my thinking, I must be emotionally engaged to provide a great patient experience.
I can remain objective and detached in my clinical judgment as I engage and connect emotionally during my patient encounters. This delicate balancing act has taken years of trial and error, however. I recently cared for a woman in her 60s who had fallen and broke her hip. Everyone was pleased that a top orthopedic surgeon was on call and able to give her the first-rate care she needed to begin walking again. The surgery went smoothly, and she was transferred to the medical/surgical ward, where things took a turn for the worse. She had a lot of anxiety in addition to her osteoporosis. Objectively, she was doing great, and we had a big success on our hands; however, she remained anxious, and she peppered the surgeon with fears that, while unfounded, were very real in her mind. The surgeon brushed them off, saying that her fears were not real and that he didn’t need to address them; his response made her emotional state spiral out of control. Her nurse notified me of the situation, and I came to her bedside. She was very agitated. I sat down at a low level and just started listening. She got all of her anxieties out in words. I held her hand, looked her in the eye, and assured her that I would be there for her and that things were going to be alright. Subsequently, she wrote letters of gratitude and proclaimed to any medical staff who would listen what a talented and great doctor I was. I did not have the skill to fix her broken hip; if it had been left to me alone, she would still be bed-bound. But I did have the human skills to connect with her and fix her agitated mind. If we remember the enduring power of the emotional memory, we can create great patient experiences.
The importance of these experiences was illustrated to me at the 2014 Dignity Health Patient Experience Summit, a powerful event featuring motivational speakers and leaders from across the country. The most powerful speakers, however, were patients. These patients had received terrible diagnoses that committed them to a prolonged interaction with the healthcare system. They were scared of what their diagnoses would mean for their future, they were subjected to uncomfortable procedures in which they struggled to maintain their dignity, and they repeatedly met the indifference of healthcare providers and clerical people who were only there to do a job. They related how the lack of caring and empathy made fears and anxiety much worse. But each of them had a story about that one person, that one care provider, who took the time to reassure them, to show that they cared, and to ensure that the patient did not feel alone. In most of these stories, the stand-out care providers took the time to hold their hands and reassure the patients. They took the time to connect with the patient’s emotional memory in a positive way, and that simple gesture of empathy had a powerful and lasting impact on the patient.
Invariably, the care provider at the heart of the patients’ stories was a nurse. Nurses have the reputation for being angels of mercy because they do the simple, empathetic gestures that let a patient know they are being cared for. These feelings endure in the patients’ memories long after the treatment is over. Doctors can, and should, be that type of care provider. It requires us to recognize that patients are scared and anxious, even though they may do their best not to show it. We, as physicians, often don’t see their anxiety, and we are so focused on the cognitive memory that we don’t address the anxiety and fear that is just under the surface. But taking just a few minutes to acknowledge their emotions, to explore them, and to reassure the patient that we are there for them has a lasting impact. In my group, we talk about the “human-business-human” encounter with patients. We begin all interactions with a human interaction (“Hello, I am Dr. McIlraith…”), conduct the business we came to provide (“Now I am going to examine you…”), and end with a human interaction (“What else can I do for you today?”). Patients expect physical contact with us during the “business” part of that interaction. I find that respectful, reassuring, and appropriate physical contact during the final “human” portion of that interaction helps solidify my patients’ experience. It helps make them feel that they have been cared for, particularly if the visit includes bad news.
Much of the recent focus on patient satisfaction has been driven by financial incentives. In 2013, CMS began penalizing hospitals 1.25% for poor HCAHPS scores as a part of the Affordable Care Act. In 2014, the maximum penalty increased to 2%, and to 3% in 2015. Hospitals have notoriously high overhead costs and slim profit margins, so these penalties can have a profound impact on the financial viability of an institution. But, while hospitals across the country have taken notice (see related article in this edition of The Hospitalist), I find doctors are more motivated by the well-being of their patients than are their hospital administrators. Satisfied patients are more compliant with treatment plans and have better outcomes.4,5 Hospitalists spend a lot of effort making sure their heart failure patients are on an ACE inhibitor, and their heart attack patients are discharged on aspirin, beta blockers, and statins so that they will have a good outcome following treatment for their acute illness. The same outcome-driven, evidence-based practice of medicine relates to patient satisfaction, however. Success in HCAHPS is as important as core measures when it comes to patient outcomes. And if I can’t convince you patient satisfaction is important because of the good it does for hospitals and patients, think about yourself for a minute. Satisfied patients are much less likely to sue their physicians.6 Practicing quality, evidence-based medicine will keep you out of peer review; however, satisfied patients will keep you out of the courtroom.
I frequently hear the comment that “we can do great on patient satisfaction, but then it gets busy, and patient satisfaction goes out the window.” My own experience contradicts this maxim, however. It is not how much time you spend with your patient but, rather, what you do with the time you have. One of the most powerful things we can do is listen. I used to make the mistake that I only wanted to hear the information I needed to figure out my patients’ problems so I could start treating them; however, I have come to learn that being heard is, in itself, therapy for my patients. It is often quoted that physicians interrupt their patients within 18 seconds of starting the interview.7 A lot of physicians dispense with attentive listening when they are under time pressure, when they should instead dispense with lengthy discourses on the patient treatment plan. It is important to educate our patients on their illness and treatment, I admit. I find a lot of hospitalists want to impart their knowledge and their treatment rationale to their patients; however, they frequently give patients and families much more information than they can hold in their cognitive memory. And time pressures are not the only anxieties hospitalists carry with them to the bedside. Our increasingly metric-driven profession means that we not only have to worry about morning discharges, interdisciplinary rounds, length of stay, and so on, but we also have to consider patient experience. It is not easy to hide all the stress we are under when we come to the bedside of a patient, but we have to. The easiest way to do that is to take a deep breath, sit next to the patient, ask an open-ended question, and then say nothing until the patient is done speaking. Active listening with good eye contact and encouragement to continue solidifies the patient’s experience of being heard. There are extreme cases when a patient is in a manic phase and won’t ever stop speaking; bend the rules a bit in those circumstances. However, the above rule works very effectively in the majority of physician-patient interactions. Being heard leaves an enduring emotional memory with our patients.
Hospital medicine often looks to other industries for inspiration on how we can improve. The airline industry is often held up as an example of how we can model patient safety, for instance, but these comparisons oversimplify the challenges we face. The same is true with patient satisfaction. In the business world, adages like “The customer is always right” are central to customer satisfaction, yet completely irrelevant to HM practice. Patients and families frequently have inappropriate and unrealistic expectations of their hospitalist physicians. We cannot, and should not, tell the patient addicted to narcotics that they can have as much IV Dilaudid as they would like. We cannot fix the patient with end-stage cancer, heart failure, or dementia. This is where we have to part ways with comparisons to principles that guide other industries if we are going to find a way forward with patient experience in hospital medicine. Because we have to set limits for patients, we often have to give our patients and families bad news, and because we have to tell them things they don’t like to hear, like “You can’t have any salt in your diet,” or “You must quit drinking alcohol,” we must develop our own principles on patient experience and satisfaction. Otherwise our options are either delivering inappropriate medical care or abandoning the pursuit of patient satisfaction all together. This is when we must remember that emotional memories are more enduring. We can’t always give our patients what they want, and we can’t always tell them what they want to hear, but we can always show them that we care. When we show our patients that we care in a palpable way, we leave them with the feeling that they have been cared for regardless of their condition, and the positive memory will endure despite the negative information we may have to convey. Maybe they won’t cut down on their salt or quit drinking alcohol, but they will never forget that their hospitalist physician cared.
And if they remember that the physician cared, it is much more likely that they will cut down on the salt or quit drinking alcohol when they go home. To paraphrase Maya Angelou, “I can’t always tell my patients what they want to hear, I can’t always tell them that their lifestyle is appropriate, but I can always show them that I care.”
Dr. McIlraith is chairman of the department of hospital medicine of Mercy Medical Group in Sacramento, Calif.
References
- LeDoux JE. Emotional memory. Scholarpedia. Accessed August 2, 2015.
- Feinstein JS, Duff MC, D Tranel D. Sustained experience of emotion after loss of memory in patients with amnesia. Proc Natl Acad Sci. 2010:107(17):7674-7679.
- Guzmán-Vélez E, Feinstein JS, Tranel D. Feelings without memory in Alzheimer disease. Cogn Behav Neurol. 2014;27(3):117-129.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. March 2001. Accessed August 2, 2015.
- Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med. 2011;24(3):229-239.
- Stelfox HT, Gandhi TK, Orav EJ, Gustafson ML. The relation of patient statisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005;118(10):1126-1133.
- Beckman HB, Frankel RM. The effect of physician behavior on the collection of data. Ann Intern Med. 1984;101(5):692-696.
There are two types of memory, the cognitive and the emotional, and the latter is more enduring. Maya Angelou characterized the distinction between these two types of memory most eloquently and succinctly when she said, “I’ve learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel.” She was ahead of her time, because neurocognitive research has objectified with science what Ms. Angelou captured so elegantly in her prose. Emotional events are processed in the sensory systems and then transmitted to the medial-temporal lobe and the amygdale for the formation of an emotional memory. When the memory is cued and retrieved from the amygdale, it triggers an emotional response. Emotional experiences leave strong traces in the brain. Memories about emotional situations are stored in both the conscious and unconscious memory, which is part of the reason emotional memories are so enduring.1 Studies of patients with severe anterograde amnesia following circumscribed bilateral hippocampal brain damage showed enduring memories of emotion despite the absence of conscious memories.2 This has a demonstrably practical application in patients with dementia, who we now know have feelings of happiness and sadness long after they have forgotten what caused the emotion.3
The distinction is important because patients judge the quality of their medical care based on emotions. The patient satisfaction disconnect arises from the fact that physicians live in their cognitive memory, while patients live in their emotional memory. Being cognitive and objective is a critical skill a physician must bring to the bedside every day; the reason we don’t allow physicians to treat family members is that their ability to remain objective will be impaired. I realized that my emotion, my passion, and my empathy for the dying would impair my judgment when I started medical school, and I launched myself on a conscious and systematic discipline to keep those feelings out of my mind during patient care. The effort worked and, for the most part, I have been able to remain objective and unemotional as I care for my patients. Recently, however, I realized that my focus on objectivity negatively impacts patient experience. As a result, I have expanded my view: While I must stay objective and detached with my thinking, I must be emotionally engaged to provide a great patient experience.
I can remain objective and detached in my clinical judgment as I engage and connect emotionally during my patient encounters. This delicate balancing act has taken years of trial and error, however. I recently cared for a woman in her 60s who had fallen and broke her hip. Everyone was pleased that a top orthopedic surgeon was on call and able to give her the first-rate care she needed to begin walking again. The surgery went smoothly, and she was transferred to the medical/surgical ward, where things took a turn for the worse. She had a lot of anxiety in addition to her osteoporosis. Objectively, she was doing great, and we had a big success on our hands; however, she remained anxious, and she peppered the surgeon with fears that, while unfounded, were very real in her mind. The surgeon brushed them off, saying that her fears were not real and that he didn’t need to address them; his response made her emotional state spiral out of control. Her nurse notified me of the situation, and I came to her bedside. She was very agitated. I sat down at a low level and just started listening. She got all of her anxieties out in words. I held her hand, looked her in the eye, and assured her that I would be there for her and that things were going to be alright. Subsequently, she wrote letters of gratitude and proclaimed to any medical staff who would listen what a talented and great doctor I was. I did not have the skill to fix her broken hip; if it had been left to me alone, she would still be bed-bound. But I did have the human skills to connect with her and fix her agitated mind. If we remember the enduring power of the emotional memory, we can create great patient experiences.
The importance of these experiences was illustrated to me at the 2014 Dignity Health Patient Experience Summit, a powerful event featuring motivational speakers and leaders from across the country. The most powerful speakers, however, were patients. These patients had received terrible diagnoses that committed them to a prolonged interaction with the healthcare system. They were scared of what their diagnoses would mean for their future, they were subjected to uncomfortable procedures in which they struggled to maintain their dignity, and they repeatedly met the indifference of healthcare providers and clerical people who were only there to do a job. They related how the lack of caring and empathy made fears and anxiety much worse. But each of them had a story about that one person, that one care provider, who took the time to reassure them, to show that they cared, and to ensure that the patient did not feel alone. In most of these stories, the stand-out care providers took the time to hold their hands and reassure the patients. They took the time to connect with the patient’s emotional memory in a positive way, and that simple gesture of empathy had a powerful and lasting impact on the patient.
Invariably, the care provider at the heart of the patients’ stories was a nurse. Nurses have the reputation for being angels of mercy because they do the simple, empathetic gestures that let a patient know they are being cared for. These feelings endure in the patients’ memories long after the treatment is over. Doctors can, and should, be that type of care provider. It requires us to recognize that patients are scared and anxious, even though they may do their best not to show it. We, as physicians, often don’t see their anxiety, and we are so focused on the cognitive memory that we don’t address the anxiety and fear that is just under the surface. But taking just a few minutes to acknowledge their emotions, to explore them, and to reassure the patient that we are there for them has a lasting impact. In my group, we talk about the “human-business-human” encounter with patients. We begin all interactions with a human interaction (“Hello, I am Dr. McIlraith…”), conduct the business we came to provide (“Now I am going to examine you…”), and end with a human interaction (“What else can I do for you today?”). Patients expect physical contact with us during the “business” part of that interaction. I find that respectful, reassuring, and appropriate physical contact during the final “human” portion of that interaction helps solidify my patients’ experience. It helps make them feel that they have been cared for, particularly if the visit includes bad news.
Much of the recent focus on patient satisfaction has been driven by financial incentives. In 2013, CMS began penalizing hospitals 1.25% for poor HCAHPS scores as a part of the Affordable Care Act. In 2014, the maximum penalty increased to 2%, and to 3% in 2015. Hospitals have notoriously high overhead costs and slim profit margins, so these penalties can have a profound impact on the financial viability of an institution. But, while hospitals across the country have taken notice (see related article in this edition of The Hospitalist), I find doctors are more motivated by the well-being of their patients than are their hospital administrators. Satisfied patients are more compliant with treatment plans and have better outcomes.4,5 Hospitalists spend a lot of effort making sure their heart failure patients are on an ACE inhibitor, and their heart attack patients are discharged on aspirin, beta blockers, and statins so that they will have a good outcome following treatment for their acute illness. The same outcome-driven, evidence-based practice of medicine relates to patient satisfaction, however. Success in HCAHPS is as important as core measures when it comes to patient outcomes. And if I can’t convince you patient satisfaction is important because of the good it does for hospitals and patients, think about yourself for a minute. Satisfied patients are much less likely to sue their physicians.6 Practicing quality, evidence-based medicine will keep you out of peer review; however, satisfied patients will keep you out of the courtroom.
I frequently hear the comment that “we can do great on patient satisfaction, but then it gets busy, and patient satisfaction goes out the window.” My own experience contradicts this maxim, however. It is not how much time you spend with your patient but, rather, what you do with the time you have. One of the most powerful things we can do is listen. I used to make the mistake that I only wanted to hear the information I needed to figure out my patients’ problems so I could start treating them; however, I have come to learn that being heard is, in itself, therapy for my patients. It is often quoted that physicians interrupt their patients within 18 seconds of starting the interview.7 A lot of physicians dispense with attentive listening when they are under time pressure, when they should instead dispense with lengthy discourses on the patient treatment plan. It is important to educate our patients on their illness and treatment, I admit. I find a lot of hospitalists want to impart their knowledge and their treatment rationale to their patients; however, they frequently give patients and families much more information than they can hold in their cognitive memory. And time pressures are not the only anxieties hospitalists carry with them to the bedside. Our increasingly metric-driven profession means that we not only have to worry about morning discharges, interdisciplinary rounds, length of stay, and so on, but we also have to consider patient experience. It is not easy to hide all the stress we are under when we come to the bedside of a patient, but we have to. The easiest way to do that is to take a deep breath, sit next to the patient, ask an open-ended question, and then say nothing until the patient is done speaking. Active listening with good eye contact and encouragement to continue solidifies the patient’s experience of being heard. There are extreme cases when a patient is in a manic phase and won’t ever stop speaking; bend the rules a bit in those circumstances. However, the above rule works very effectively in the majority of physician-patient interactions. Being heard leaves an enduring emotional memory with our patients.
Hospital medicine often looks to other industries for inspiration on how we can improve. The airline industry is often held up as an example of how we can model patient safety, for instance, but these comparisons oversimplify the challenges we face. The same is true with patient satisfaction. In the business world, adages like “The customer is always right” are central to customer satisfaction, yet completely irrelevant to HM practice. Patients and families frequently have inappropriate and unrealistic expectations of their hospitalist physicians. We cannot, and should not, tell the patient addicted to narcotics that they can have as much IV Dilaudid as they would like. We cannot fix the patient with end-stage cancer, heart failure, or dementia. This is where we have to part ways with comparisons to principles that guide other industries if we are going to find a way forward with patient experience in hospital medicine. Because we have to set limits for patients, we often have to give our patients and families bad news, and because we have to tell them things they don’t like to hear, like “You can’t have any salt in your diet,” or “You must quit drinking alcohol,” we must develop our own principles on patient experience and satisfaction. Otherwise our options are either delivering inappropriate medical care or abandoning the pursuit of patient satisfaction all together. This is when we must remember that emotional memories are more enduring. We can’t always give our patients what they want, and we can’t always tell them what they want to hear, but we can always show them that we care. When we show our patients that we care in a palpable way, we leave them with the feeling that they have been cared for regardless of their condition, and the positive memory will endure despite the negative information we may have to convey. Maybe they won’t cut down on their salt or quit drinking alcohol, but they will never forget that their hospitalist physician cared.
And if they remember that the physician cared, it is much more likely that they will cut down on the salt or quit drinking alcohol when they go home. To paraphrase Maya Angelou, “I can’t always tell my patients what they want to hear, I can’t always tell them that their lifestyle is appropriate, but I can always show them that I care.”
Dr. McIlraith is chairman of the department of hospital medicine of Mercy Medical Group in Sacramento, Calif.
References
- LeDoux JE. Emotional memory. Scholarpedia. Accessed August 2, 2015.
- Feinstein JS, Duff MC, D Tranel D. Sustained experience of emotion after loss of memory in patients with amnesia. Proc Natl Acad Sci. 2010:107(17):7674-7679.
- Guzmán-Vélez E, Feinstein JS, Tranel D. Feelings without memory in Alzheimer disease. Cogn Behav Neurol. 2014;27(3):117-129.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. March 2001. Accessed August 2, 2015.
- Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med. 2011;24(3):229-239.
- Stelfox HT, Gandhi TK, Orav EJ, Gustafson ML. The relation of patient statisfaction with complaints against physicians and malpractice lawsuits. Am J Med. 2005;118(10):1126-1133.
- Beckman HB, Frankel RM. The effect of physician behavior on the collection of data. Ann Intern Med. 1984;101(5):692-696.