User login
Movers and Shakers in Hospital Medicine

Hospitalist Robert McNab, DO, has been named the new medical education director of Freeman Health System in Joplin, Mo. He will continue as a hospitalist and director of the internal-medicine residency program. Dr. McNab brings more than 10 years of teaching experience to the Freeman Graduate Medical Education Program.
Brian Harte, MD, SFHM, Cleveland Clinic hospitalist and president of South Pointe Hospital in Warrensville Heights, Ohio, is now president of Hillcrest Hospital in Mayfield Heights, Ohio. Dr. Harte is an SHM board member and serves as the board treasurer. In addition to his new role, Dr. Harte will continue to practice as a hospitalist at Hillcrest Hospital.
Anita Dhople, MD, is the new hospitalist medical director for the Rockledge, Fla.-based Health First health system. Dr. Dhople will oversee all hospitalist services at four affiliated hospitals. Dr. Dhople comes to Health First from the Piedmont Physicians Group in Atlanta.
Matthew Heinz, MD, has been appointed director of provider outreach in the U.S. Department of Health and Human Services’ Office of Intergovernmental and External Affairs (IEA). Dr. Heinz is a practicing hospitalist at Tucson (Ariz.) Medical Center and a former representative in the Arizona state legislature.
Business Moves


IPC: The Hospitalist Company, based in North Hollywood, Calif., has announced the acquisition of two private hospitalist practices: Sound Senior Geriatrics LLC (SSG) in Mystic, Conn., and Cape Coral Hospitalists Inc. (CCH) based in Fort Meyers, Fla. IPC contracts hospitalist services in 28 states.
Bayhealth hospital network in Dover, Del., has partnered with Apogee Physicians to provide 24-hour hospitalist services at Kent General Hospital in Dover and Milford Memorial Hospital in Milford. Bayhealth has been serving communities in central and southern Delaware for more than 75 years. Phoenix-based Apogee Physicians has been providing contracted hospitalist services since 2002.
Cogent Healthcare is partnering with South Georgia Medical Center (SGMC) to provide hospitalist services at the 285-bed acute-care nonprofit main campus and the 55-bed Smith Northview Campus in Valdosta, Ga. SGMC currently serves 15 counties in south-central Georgia and north Florida. Cogent provides contracted hospitalist services at more than 100 hospitals throughout the United States.
Cogent Healthcare Inc., based in Brentwood, Tenn., recently announced Dean Weiland as the private hospitalist staffing company’s new president and CEO. Weiland served as an executive during a merger between Renal Advantage and Liberty Dialysis in 2010. Before that, he served as CEO of The Work Institute.
Hill Country Memorial Hospital (HCM) in Fredericksburg, Texas, has announced plans to expand its 24-hour hospitalist service from only weekends to seven days a week. The decision comes as a reaction to the positive benefits HCM has experienced since it began its weekend hospitalist service in 2011.
Hospitalist Robert McNab, DO, has been named the new medical education director of Freeman Health System in Joplin, Mo. He will continue as a hospitalist and director of the internal-medicine residency program. Dr. McNab brings more than 10 years of teaching experience to the Freeman Graduate Medical Education Program.
Brian Harte, MD, SFHM, Cleveland Clinic hospitalist and president of South Pointe Hospital in Warrensville Heights, Ohio, is now president of Hillcrest Hospital in Mayfield Heights, Ohio. Dr. Harte is an SHM board member and serves as the board treasurer. In addition to his new role, Dr. Harte will continue to practice as a hospitalist at Hillcrest Hospital.
Anita Dhople, MD, is the new hospitalist medical director for the Rockledge, Fla.-based Health First health system. Dr. Dhople will oversee all hospitalist services at four affiliated hospitals. Dr. Dhople comes to Health First from the Piedmont Physicians Group in Atlanta.
Matthew Heinz, MD, has been appointed director of provider outreach in the U.S. Department of Health and Human Services’ Office of Intergovernmental and External Affairs (IEA). Dr. Heinz is a practicing hospitalist at Tucson (Ariz.) Medical Center and a former representative in the Arizona state legislature.
Business Moves
IPC: The Hospitalist Company, based in North Hollywood, Calif., has announced the acquisition of two private hospitalist practices: Sound Senior Geriatrics LLC (SSG) in Mystic, Conn., and Cape Coral Hospitalists Inc. (CCH) based in Fort Meyers, Fla. IPC contracts hospitalist services in 28 states.
Bayhealth hospital network in Dover, Del., has partnered with Apogee Physicians to provide 24-hour hospitalist services at Kent General Hospital in Dover and Milford Memorial Hospital in Milford. Bayhealth has been serving communities in central and southern Delaware for more than 75 years. Phoenix-based Apogee Physicians has been providing contracted hospitalist services since 2002.
Cogent Healthcare is partnering with South Georgia Medical Center (SGMC) to provide hospitalist services at the 285-bed acute-care nonprofit main campus and the 55-bed Smith Northview Campus in Valdosta, Ga. SGMC currently serves 15 counties in south-central Georgia and north Florida. Cogent provides contracted hospitalist services at more than 100 hospitals throughout the United States.
Cogent Healthcare Inc., based in Brentwood, Tenn., recently announced Dean Weiland as the private hospitalist staffing company’s new president and CEO. Weiland served as an executive during a merger between Renal Advantage and Liberty Dialysis in 2010. Before that, he served as CEO of The Work Institute.
Hill Country Memorial Hospital (HCM) in Fredericksburg, Texas, has announced plans to expand its 24-hour hospitalist service from only weekends to seven days a week. The decision comes as a reaction to the positive benefits HCM has experienced since it began its weekend hospitalist service in 2011.
Hospitalist Robert McNab, DO, has been named the new medical education director of Freeman Health System in Joplin, Mo. He will continue as a hospitalist and director of the internal-medicine residency program. Dr. McNab brings more than 10 years of teaching experience to the Freeman Graduate Medical Education Program.
Brian Harte, MD, SFHM, Cleveland Clinic hospitalist and president of South Pointe Hospital in Warrensville Heights, Ohio, is now president of Hillcrest Hospital in Mayfield Heights, Ohio. Dr. Harte is an SHM board member and serves as the board treasurer. In addition to his new role, Dr. Harte will continue to practice as a hospitalist at Hillcrest Hospital.
Anita Dhople, MD, is the new hospitalist medical director for the Rockledge, Fla.-based Health First health system. Dr. Dhople will oversee all hospitalist services at four affiliated hospitals. Dr. Dhople comes to Health First from the Piedmont Physicians Group in Atlanta.
Matthew Heinz, MD, has been appointed director of provider outreach in the U.S. Department of Health and Human Services’ Office of Intergovernmental and External Affairs (IEA). Dr. Heinz is a practicing hospitalist at Tucson (Ariz.) Medical Center and a former representative in the Arizona state legislature.
Business Moves
IPC: The Hospitalist Company, based in North Hollywood, Calif., has announced the acquisition of two private hospitalist practices: Sound Senior Geriatrics LLC (SSG) in Mystic, Conn., and Cape Coral Hospitalists Inc. (CCH) based in Fort Meyers, Fla. IPC contracts hospitalist services in 28 states.
Bayhealth hospital network in Dover, Del., has partnered with Apogee Physicians to provide 24-hour hospitalist services at Kent General Hospital in Dover and Milford Memorial Hospital in Milford. Bayhealth has been serving communities in central and southern Delaware for more than 75 years. Phoenix-based Apogee Physicians has been providing contracted hospitalist services since 2002.
Cogent Healthcare is partnering with South Georgia Medical Center (SGMC) to provide hospitalist services at the 285-bed acute-care nonprofit main campus and the 55-bed Smith Northview Campus in Valdosta, Ga. SGMC currently serves 15 counties in south-central Georgia and north Florida. Cogent provides contracted hospitalist services at more than 100 hospitals throughout the United States.
Cogent Healthcare Inc., based in Brentwood, Tenn., recently announced Dean Weiland as the private hospitalist staffing company’s new president and CEO. Weiland served as an executive during a merger between Renal Advantage and Liberty Dialysis in 2010. Before that, he served as CEO of The Work Institute.
Hill Country Memorial Hospital (HCM) in Fredericksburg, Texas, has announced plans to expand its 24-hour hospitalist service from only weekends to seven days a week. The decision comes as a reaction to the positive benefits HCM has experienced since it began its weekend hospitalist service in 2011.
Pediatric Hospital Medicine Marks 10th Anniversary

With a record number of attendees, Pediatric Hospital Medicine 2013 (PHM) swept into New Orleans last month, carrying with it unbridled enthusiasm about the past, present, and future.
Virginia Moyer, MD, MPH, vice president for maintenance of certification and quality for the American Board of Pediatrics (ABP) and professor of pediatrics and chief of academic general pediatrics at Texas Children’s Hospital, delivered a keynote address to 700 attendees that focused on the challenges and opportunities of providing evidence-based, high-quality care in the hospital, as well as ABP’s role in meeting these challenges.
“If evidence-based medicine is an individual sport,” Dr. Moyer said, “then quality improvement is a team sport.”
Barriers to quality improvement (QI)— such as lack of will, lack of data, and lack of training—can be surmounted in a team environment, she said. ABP is continuing in its efforts to support QI education through its Maintenance of Certification (MOC) Part 4 modules, as well as other educational activities.
Other highlights of the 10th annual Pediatric Hospital Medicine meeting:
- The addition of a new “Community Hospitalists” track was given high marks by those in attendance. It covered such topics as perioperative management of medically complex pediatric patients, community-acquired pneumonia, and osteomyelitis.
- A 10-year retrospective of pediatric hospital medicine was given by a panel of notable pediatric hospitalists, including Erin Stucky Fisher, MD, FAAP, MHM, chief of hospital medicine at Rady Children’s Hospital in San Diego; Mary Ottolini, MD, MPH, chief of hospital medicine at Children’s National Medical Center in Washington; Jack Percelay, MD, MPH, FAAP, associate clinical professor at Pace University; and Daniel Rauch, MD, FAAP, pediatric hospitalist program director at the NYU School of Medicine in New York City. A host of new programs has been established by the PHM community, including the Quality Improvement Innovation Networks (QuIIN); the Value in Pediatrics (VIP) network; the International Network for Simulation-Based Pediatric Innovation, Research, and Education (INSPIRE); patient- and family-centered rounds; and the I-PASS Handoff Program. The panel also discussed future challenges, including reduction of unnecessary treatments, interfacing, and perhaps incorporating “hyphen hospitalists,” and learning from advances made by the adult HM community.
- The ever-popular “Top Articles in Pediatric Hospital Medicine” session was presented by H. Barrett Fromme, MD, associate professor of pediatrics at the University of Chicago, and Ben Bauer, MD, director of pediatric hospital medicine at Riley Hospital for Children at Indiana University Health in Indianapolis, which was met with raucous approval by the audience. The presentation not only educated those in attendance about the most cutting-edge pediatric literature, but it also included dance moves most likely to attract the opposite sex and clothing appropriate for the Australian pediatric hospitalist.
- The three presidents of the sponsoring societies—Thomas McInerney, MD, FAAP, of the American Academy of Pediatrics, David Keller, MD, of the Academic Pediatric Association, and Eric Howell, MD, SFHM, of SHM—presented each society’s contributions to the growth of PHM, as well as future areas for cooperative sponsorship. These include the development of the AAP Section of Hospital Medicine Library website (sohmlibrary.org), the APA Quality Scholars program, and SHM’s efforts to increase interest in hospital medicine in medical students and trainees. “Ask not what hospital medicine can do for you,” Dr. Howell implored, “ask what you can do for hospital medicine!”
- Members of the Joint Council of Pediatric Hospital Medicine (JCPHM) presented the recent recommendations of the council arising from an April 2013 meeting with the ABP in Chapel Hill, N.C. Despite acknowledgements that no decision will be met with uniform satisfaction by all the stakeholders, the JCPHM concluded that the path that would best advance the field of PHM, provide for high-quality care of hospitalized children, and ensure the public trust would be a two-year fellowship sponsored by ABP. This would ultimately lead to approved certification eligibility for fellowship graduates by the American Board of Medical Specialties (ABMS); it would also make provisions for “grandfathering” in current pediatric hospitalists. Concerns from med-peds, community hospitalists, and recent residency graduate communities were addressed by the panel.
- A recurrent theme of reducing unnecessary treatments, interventions, and, perhaps, hospitalizations was summarized eloquently by Alan Schroeder, MD, director of the pediatric ICU and chief of pediatric inpatient care at Santa Clara (Calif.) Valley Health. Barriers to reducing unnecessary care can be substantial, including pressure from families, pressure from colleagues, profit motive, and the “n’s of 1,” according to Dr. Schroeder. Ultimately, however, avoiding testing and treatments that have no benefit to children will improve care. “Ask, ‘How will this test benefit my patient?’ not ‘How will this test change management?’” Dr. Schroeder advised.
Dr. Chang is The Hospitalist’s pediatric editor and a med-peds-trained hospitalist working at the University of California San Diego and Rady Children’s Hospital.
With a record number of attendees, Pediatric Hospital Medicine 2013 (PHM) swept into New Orleans last month, carrying with it unbridled enthusiasm about the past, present, and future.
Virginia Moyer, MD, MPH, vice president for maintenance of certification and quality for the American Board of Pediatrics (ABP) and professor of pediatrics and chief of academic general pediatrics at Texas Children’s Hospital, delivered a keynote address to 700 attendees that focused on the challenges and opportunities of providing evidence-based, high-quality care in the hospital, as well as ABP’s role in meeting these challenges.
“If evidence-based medicine is an individual sport,” Dr. Moyer said, “then quality improvement is a team sport.”
Barriers to quality improvement (QI)— such as lack of will, lack of data, and lack of training—can be surmounted in a team environment, she said. ABP is continuing in its efforts to support QI education through its Maintenance of Certification (MOC) Part 4 modules, as well as other educational activities.
Other highlights of the 10th annual Pediatric Hospital Medicine meeting:
- The addition of a new “Community Hospitalists” track was given high marks by those in attendance. It covered such topics as perioperative management of medically complex pediatric patients, community-acquired pneumonia, and osteomyelitis.
- A 10-year retrospective of pediatric hospital medicine was given by a panel of notable pediatric hospitalists, including Erin Stucky Fisher, MD, FAAP, MHM, chief of hospital medicine at Rady Children’s Hospital in San Diego; Mary Ottolini, MD, MPH, chief of hospital medicine at Children’s National Medical Center in Washington; Jack Percelay, MD, MPH, FAAP, associate clinical professor at Pace University; and Daniel Rauch, MD, FAAP, pediatric hospitalist program director at the NYU School of Medicine in New York City. A host of new programs has been established by the PHM community, including the Quality Improvement Innovation Networks (QuIIN); the Value in Pediatrics (VIP) network; the International Network for Simulation-Based Pediatric Innovation, Research, and Education (INSPIRE); patient- and family-centered rounds; and the I-PASS Handoff Program. The panel also discussed future challenges, including reduction of unnecessary treatments, interfacing, and perhaps incorporating “hyphen hospitalists,” and learning from advances made by the adult HM community.
- The ever-popular “Top Articles in Pediatric Hospital Medicine” session was presented by H. Barrett Fromme, MD, associate professor of pediatrics at the University of Chicago, and Ben Bauer, MD, director of pediatric hospital medicine at Riley Hospital for Children at Indiana University Health in Indianapolis, which was met with raucous approval by the audience. The presentation not only educated those in attendance about the most cutting-edge pediatric literature, but it also included dance moves most likely to attract the opposite sex and clothing appropriate for the Australian pediatric hospitalist.
- The three presidents of the sponsoring societies—Thomas McInerney, MD, FAAP, of the American Academy of Pediatrics, David Keller, MD, of the Academic Pediatric Association, and Eric Howell, MD, SFHM, of SHM—presented each society’s contributions to the growth of PHM, as well as future areas for cooperative sponsorship. These include the development of the AAP Section of Hospital Medicine Library website (sohmlibrary.org), the APA Quality Scholars program, and SHM’s efforts to increase interest in hospital medicine in medical students and trainees. “Ask not what hospital medicine can do for you,” Dr. Howell implored, “ask what you can do for hospital medicine!”
- Members of the Joint Council of Pediatric Hospital Medicine (JCPHM) presented the recent recommendations of the council arising from an April 2013 meeting with the ABP in Chapel Hill, N.C. Despite acknowledgements that no decision will be met with uniform satisfaction by all the stakeholders, the JCPHM concluded that the path that would best advance the field of PHM, provide for high-quality care of hospitalized children, and ensure the public trust would be a two-year fellowship sponsored by ABP. This would ultimately lead to approved certification eligibility for fellowship graduates by the American Board of Medical Specialties (ABMS); it would also make provisions for “grandfathering” in current pediatric hospitalists. Concerns from med-peds, community hospitalists, and recent residency graduate communities were addressed by the panel.
- A recurrent theme of reducing unnecessary treatments, interventions, and, perhaps, hospitalizations was summarized eloquently by Alan Schroeder, MD, director of the pediatric ICU and chief of pediatric inpatient care at Santa Clara (Calif.) Valley Health. Barriers to reducing unnecessary care can be substantial, including pressure from families, pressure from colleagues, profit motive, and the “n’s of 1,” according to Dr. Schroeder. Ultimately, however, avoiding testing and treatments that have no benefit to children will improve care. “Ask, ‘How will this test benefit my patient?’ not ‘How will this test change management?’” Dr. Schroeder advised.
Dr. Chang is The Hospitalist’s pediatric editor and a med-peds-trained hospitalist working at the University of California San Diego and Rady Children’s Hospital.
With a record number of attendees, Pediatric Hospital Medicine 2013 (PHM) swept into New Orleans last month, carrying with it unbridled enthusiasm about the past, present, and future.
Virginia Moyer, MD, MPH, vice president for maintenance of certification and quality for the American Board of Pediatrics (ABP) and professor of pediatrics and chief of academic general pediatrics at Texas Children’s Hospital, delivered a keynote address to 700 attendees that focused on the challenges and opportunities of providing evidence-based, high-quality care in the hospital, as well as ABP’s role in meeting these challenges.
“If evidence-based medicine is an individual sport,” Dr. Moyer said, “then quality improvement is a team sport.”
Barriers to quality improvement (QI)— such as lack of will, lack of data, and lack of training—can be surmounted in a team environment, she said. ABP is continuing in its efforts to support QI education through its Maintenance of Certification (MOC) Part 4 modules, as well as other educational activities.
Other highlights of the 10th annual Pediatric Hospital Medicine meeting:
- The addition of a new “Community Hospitalists” track was given high marks by those in attendance. It covered such topics as perioperative management of medically complex pediatric patients, community-acquired pneumonia, and osteomyelitis.
- A 10-year retrospective of pediatric hospital medicine was given by a panel of notable pediatric hospitalists, including Erin Stucky Fisher, MD, FAAP, MHM, chief of hospital medicine at Rady Children’s Hospital in San Diego; Mary Ottolini, MD, MPH, chief of hospital medicine at Children’s National Medical Center in Washington; Jack Percelay, MD, MPH, FAAP, associate clinical professor at Pace University; and Daniel Rauch, MD, FAAP, pediatric hospitalist program director at the NYU School of Medicine in New York City. A host of new programs has been established by the PHM community, including the Quality Improvement Innovation Networks (QuIIN); the Value in Pediatrics (VIP) network; the International Network for Simulation-Based Pediatric Innovation, Research, and Education (INSPIRE); patient- and family-centered rounds; and the I-PASS Handoff Program. The panel also discussed future challenges, including reduction of unnecessary treatments, interfacing, and perhaps incorporating “hyphen hospitalists,” and learning from advances made by the adult HM community.
- The ever-popular “Top Articles in Pediatric Hospital Medicine” session was presented by H. Barrett Fromme, MD, associate professor of pediatrics at the University of Chicago, and Ben Bauer, MD, director of pediatric hospital medicine at Riley Hospital for Children at Indiana University Health in Indianapolis, which was met with raucous approval by the audience. The presentation not only educated those in attendance about the most cutting-edge pediatric literature, but it also included dance moves most likely to attract the opposite sex and clothing appropriate for the Australian pediatric hospitalist.
- The three presidents of the sponsoring societies—Thomas McInerney, MD, FAAP, of the American Academy of Pediatrics, David Keller, MD, of the Academic Pediatric Association, and Eric Howell, MD, SFHM, of SHM—presented each society’s contributions to the growth of PHM, as well as future areas for cooperative sponsorship. These include the development of the AAP Section of Hospital Medicine Library website (sohmlibrary.org), the APA Quality Scholars program, and SHM’s efforts to increase interest in hospital medicine in medical students and trainees. “Ask not what hospital medicine can do for you,” Dr. Howell implored, “ask what you can do for hospital medicine!”
- Members of the Joint Council of Pediatric Hospital Medicine (JCPHM) presented the recent recommendations of the council arising from an April 2013 meeting with the ABP in Chapel Hill, N.C. Despite acknowledgements that no decision will be met with uniform satisfaction by all the stakeholders, the JCPHM concluded that the path that would best advance the field of PHM, provide for high-quality care of hospitalized children, and ensure the public trust would be a two-year fellowship sponsored by ABP. This would ultimately lead to approved certification eligibility for fellowship graduates by the American Board of Medical Specialties (ABMS); it would also make provisions for “grandfathering” in current pediatric hospitalists. Concerns from med-peds, community hospitalists, and recent residency graduate communities were addressed by the panel.
- A recurrent theme of reducing unnecessary treatments, interventions, and, perhaps, hospitalizations was summarized eloquently by Alan Schroeder, MD, director of the pediatric ICU and chief of pediatric inpatient care at Santa Clara (Calif.) Valley Health. Barriers to reducing unnecessary care can be substantial, including pressure from families, pressure from colleagues, profit motive, and the “n’s of 1,” according to Dr. Schroeder. Ultimately, however, avoiding testing and treatments that have no benefit to children will improve care. “Ask, ‘How will this test benefit my patient?’ not ‘How will this test change management?’” Dr. Schroeder advised.
Dr. Chang is The Hospitalist’s pediatric editor and a med-peds-trained hospitalist working at the University of California San Diego and Rady Children’s Hospital.
Career Boost a Benefit of Winning SHM’s Research, Innovations, and Clinical Vignettes Poster Competition
Back to the Furture Past RIV winners talk about what the recognition meant for their careers By Larry Beresford

After winning SHM’s annual Research, Innovations, and Clinical Vignettes (RIV) scientific abstract and poster competition for an abstract illustrating a program that promoted flu vaccinations for families of neonatal patients, Shetal Shah, MD, FAAP, became a leading advocate for two laws mandating that New York hospitals offer vaccinations to families.
A poster that described a VTE prevention program led Gregory Maynard, MD, MSc, SFHM, to join SHM’s VTE Prevention Collaborative and, eventually, to become senior vice president of the society’s Center for Hospital Innovation and Improvement.
A prize-winning innovations poster for improving team communication by Vineet Chopra, MD, MS, FACP, FHM, and colleagues later took off as a new technology company.
Leonard Feldman, MD, FAAP, SFHM, won for a poster that explained online CME curriculum for hospitalists as consultants; the curriculum now resides on SHM’s website.
The evidence is clear: RIV abstracts are a vital part of hospital medicine.
Nearly 800 abstracts were submitted for HM13.
Awards are given in three categories:
- Research posters report clinical or basic science data, systematically review a clinical problem, or address efficiency, cost, or method of health-care delivery or medical decision-making;
- Innovations posters describe an existing innovative program in hospital medicine, often with preliminary data; and
- Clinical vignettes, either adult or pediatric, report on one or more cases illustrating a new disease entity, a prominent or unusual feature of an established disease, or an area of clinical controversy.
The Hospitalist asked 11 past RIV winners what the poster contest meant to their careers. Some added more data and analysis and went on to be published in such medical journals as the Journal of Hospital Medicine. Some used the recognition to launch or boost research-oriented careers; others saw their careers go in different directions.
“Winning a national poster competition gives you the confidence to continue to pursue your interest and take it to a higher level, like successfully competing for funding and publishing your line of inquiry,” says hospitalist and researcher Vineet Arora, MD, MPP, FHM, of the University of Chicago, who won the 2006 RIV research competition. “Sometimes, presenting posters can be lonely, but at SHM, you get a lot of traffic. You get a chance to practice your spiel, communicating science and research in a very concise way, which is an important skill to have.”
David Metzger, MD, PhD, also from the University of Chicago, who won the RIV research award in 2005, says recognition is a big deal, but “one of the biggest values of the RIV competition is just getting information out to colleagues, with the opportunity to talk with your peers. That’s the real prize.
“I’ve been involved in presenting posters at SHM every year that the society has been in existence,” he says. “I’ve met so many people and talked about what they’re doing. That’s what a medical society should do—bring people together like this.”

Title: Administrator, academic consult service; teaching staff physician
Institution: Saint Joseph Mercy Hospital, Ypsilanti, Mich.
Year: 2008
RIV: “A Case of Salty Voluminous Urine” (clinical vignette)
Dr. Tassava was honored two years in a row for topics drawn from her experience as a hospitalist working in the surgical ICU. Her HM08 entry won top poster, and her HM09 poster, “Permissive Hypernatremia: Co-Management of Intracranial Pressure in a Patient with Diabetes Insipidus,” was selected for an oral presentation.
The HM09 vignette described how the hypernatremia that occurs with diabetes insipidus could be used in a novel way to control intracranial pressure in a 17-year-old patient who had a traumatic brain injury from an auto accident.
“She had a beautiful outcome,” Dr. Tassava says. “She started college and she came back to our unit for a visit after her recovery.”
Dr. Tassava enjoyed the opportunity to explain to her peers how diabetes insipidus presented and how she managed the case. “I was a little surprised at how much discussion was generated by my case,” she says, “even though I knew this was an important and novel approach.”
When her hospital added intensivists, her work and research in the ICU ended and her career moved more toward hospitalist administration. She now runs the academic consult service at St. Joseph, serves as lead physician for the orthopedic surgery floor, instructs and mentors medical residents, and chairs the hospital’s Coagulation Collaborative Practice Team (Coagulation CPT). She credits the RIV honors with helping her to gain recognition as an academic hospitalist who was nominated for leadership roles. She has moved out of research for now but plans to pursue anticoagulation research in the future.
“I really appreciated the recognition for my curiosity and scientific approach, which was acknowledged by my surgical colleagues,” Dr. Tassava says. “I absolutely love the CPT. I am the hospital’s principal educator with regard to anticoagulation. Over the past year, I have given medicine and cardiology grand rounds, and have presented on the newest anticoagulants.”
Dr. Tassava still collaborates with her residents on abstracts, several of which have been submitted to SHM, the American College of Physicians, and other medical societies.
“I still love research,” she says. “I have a million ideas.”

Title: Chief of the division of hospital medicine; senior vice president, SHM’s Center for Innovation and Improvement
Institution: University of California at San Diego (UCSD)
Year: 2008
RIV: “Prevention of Hospital-Acquired Venous Thromboembolism: Prospective Validation of a VTE Risk Assessment Model and Protocol” (research)
Citations: Maynard G, Stein J. Designing and implementing effective VTE prevention protocols: lessons from collaboratives. J Thromb Thrombolysis. 2010;29(2):159-166. Maynard G, Morris T, Jenkins I, et al. Optimizing prevention of hospital acquired venous thromboembolism: prospective validation of a VTE risk assessment model. J Hosp Med. 2010;5(1):10-18.
Dr. Maynard’s abstract described a project funded by the federal Agency for Healthcare Research and Quality to design and implement an organized, comprehensive protocol for VTE prevention within the hospital setting. The project also included a toolkit to help other hospitals do the same thing. The same group received SHM’s Award of Excellence for Teamwork.
This work, combined with similar efforts by Jason Stein, MD, and colleagues at Emory University in Atlanta and others, provided the foundation for SHM’s VTE resource room and the mentored implementation program of SHM’s VTE Prevention Collaborative, which had been launched in 2007 as one of the society’s first large-scale quality-improvement (QI) initiatives.
“SHM wanted to do something about VTE prevention, and when we got our AHRQ grant, I was interested in doing the same,” Dr. Maynard says. “We published our implementation guides on the AHRQ and SHM websites, along with a lot of valuable supporting materials.”
Dr. Maynard later took on leadership roles with SHM’s quality initiatives on glycemic control and care transitions, which made him the logical choice to become senior vice president of SHM’s Center for Hospital Innovation and Improvement.
He says the RIV honor lifted his profile not only within SHM, but also throughout the field, and it was instrumental in obtaining continued funding to advance the VTE initiative. “We did this tremendous work—with great results,” he says. “But I don’t think our local administrators appreciated it quite as much until we started to get external, national recognition.”
Dr. Maynard earned his master’s degree in biostatistics and clinical research design from the University of Michigan—skills he later brought to the academic setting at UCSD.
“It was a nice way for a hospitalist, who’s really a medical generalist, to become an expert in something,” he says. “I could never be more of an expert in cardiology than a cardiologist, or more of an expert in DVT than a hematologist or critical-care specialist. But I could help both of them do what they couldn’t do as effectively, which was to implement protocols reliably using a QI framework.”

Title: Assistant professor of general internal medicine, hospital medicine, and public health
Institution: Vanderbilt University, Nashville, Tenn.
Year: 2009
RIV: “Predictors of Early Post-Discharge Mortality in Critically Ill Patients: Lessons for Quality Performance and Quality Assessment” (research)
Citation: Vasilevskis EE, Kuzniewicz MW, Cason BA, et al. Predictors of early post-discharge mortality in critically ill patients: a retrospective cohort study from the California Intensive Care Outcomes project. J Crit Care. 2011;26(1):65-75.
Dr. Vasilevskis has submitted abstracts to the RIV competition almost every year since 2007, when he was completing a fellowship at the University of California at San Francisco’s Institute for Health Policy Studies. He was honored in 2009 for a project based on the California Intensive Care Outcomes Project, which drew data from 35 hospitals to demonstrate that shortening ICU length of stay was predictive of early post-discharge mortality in the most severely ill patients.
He has continued to research quality and safety in the ICU, and he has published dozens of journal articles.
“My initial focus was on traditional mortality and length-of-stay outcomes,” he says. “I am now pursuing additional outcomes, most notably delirium in the ICU patient. I work with an amazing group of researchers that are trying to better measure, define, and treat delirium in the ICU—an outcome associated with a number of poor patient outcomes.”
Dr. Vasilevskis also is researching the causes of hospital readmissions and the development of novel ways to improve care transitions for elderly patients. He is pursuing a master’s of public health at Vanderbilt, and is co-principal investigator of an investigation of the Hospital Medicine Reengineering Network to improve transitions of care, supported by the Association of American Medical Colleges.
In addition to his 2009 win, he captured the HM10 and HM12 research categories. His HM12 poster, “Veterans Administration Acute Care 30-Day Mortality Model: Development, Validation and Performance Variation,” was singled out by the judging committee for its impressive sample size (1,114,327 patients in a retrospective cohort study of 131 VA hospitals), as well as for how it combined administrative and clinical risk models.
Dr. Vasilevskis says the opportunity to present his research at SHM and the recognition he received encouraged him to continue as a hospitalist engaged in medical research. He has been a member of SHM’s Research Committee since 2009, an RIV judge at HM11, and chaired the HM13 RIV competition subcommittee.

Title: Assistant professor of medicine
Institution: University of Michigan Health System, Ann Arbor
Year: 2009
RIV: “MComm: Redefining Medical Communications in the 21st Century” (innovations)
Early in his career, Dr. Chopra was curious about how to improve the way patient care is delivered in the hospital setting. He was particularly interested in the inordinate amount of time hospitalists spend every day on communication.
“I saw one-way paging systems as a problem for communication between members of the medical team,” he says. “Doctors get paged and break off from what they’re doing to return the page—to someone who often isn’t there to take the call back. Sometimes the system gives us the wrong number or a cryptic message that makes no sense.”
A technological solution to this problem, which he and hospitalist Prasanth Gogineni, MD, conceived, designed, and created, then tested at the University of Michigan, is called MComm. Dr. Chopra describes it as a novel, uniform way of messaging for the entire medical team using wireless servers, PUSH technology, and iPhones. MComm was built around existing hospital workflow and patient-specific task lists, assigning priority to each message and documenting that it was delivered. The junior faculty members submitted an abstract about their innovative application, not really expecting it to get accepted. But when it won the poster competition and was selected for a plenary presentation, things got busy in a hurry. Specifically, the university hospital’s Office of Technology Transfer took a keen interest.
“We met with a number of people who had business experience in the health-care-technology space and found a CEO for the company we formed to develop MComm,” Dr. Chopra says. “I found myself getting pulled into it very quickly, with a lot of conversations about commercialization, revenue-sharing models, intellectual property, and the like.”
But running a company was not something Dr. Chopra wanted to do. Two years ago, that company, Synaptin, went one way and he went another—he stayed at Michigan as a medical researcher. He remains deeply interested in how care is delivered to hospitalized patients, but with a focus on such patient-safety questions as how to prevent negative outcomes from indwelling venous catheters.
“Winning the poster competition opened doors for me—there’s no doubt in my mind,” he says. “We demonstrated the ability to deliver a project of significance, from concept to prototype, without formal training in this area. If we didn’t have that recognition, I’m not sure I would have been ready to step into a research career as quickly. It helped me realize that medical research was what I wanted to do.”
Title: Associate program director, internal-medicine residency; assistant dean of scholarship and discovery
Institution: Pritzker School of Medicine, University of Chicago
Year: 2006
RIV: “Measuring Quality of Hospital Care for Vulnerable Elders: Use of ACOVE Quality Indicators” (research)
Citation: Arora VM, Fish M, Basu A, et al. Relationship between quality of care of hospitalized vulnerable elders and postdischarge mortality. J Am Geriatrics. 2010;58:1642-1648.

Title: Associate professor, department of medicine; associate faculty member, Harris School and the Department of Economics
Institution: University of Chicago
Year: 2005
RIV: “Effects of Hospitalists on Outcomes and Costs in a Multicenter Trial of Academic Hospitalists” (research)
Dr. Meltzer was the lead author, with 11 other prominent hospitalists, of an abstract based on a multisite study of the cost and outcome implications of the hospitalist model—still a relatively new concept in 2001, when the research began. Although the study did not uncover large cost savings realized from the hospitalist model of care, as some advocates had hoped, important findings and implications for the emerging field were teased out of the data.
At the time, only a few randomly controlled, multisite studies of costs and outcomes for the hospitalist model had been performed. The study, Dr. Meltzer says, required a complicated analysis to discover that hospitalists, in fact, saved their facilities money, with their most important impact realized post-hospitalization, such as on nursing-home costs. It was important to control for spillover effect and the fact that hospitalists do a better job of teaching house staff, while a physician’s years of experience was another important variable, he says.
Dr. Meltzer was a medical researcher interested in medical specialization when the term “hospitalist” was first coined in 1996. “I thought, here was a chance to study a medical specialty in its formative stages,” he says.
He still works as a hospitalist, although with limited clinical time. In addition to his administrative work as division chief, he directs the Center for Health and the Social Sciences at the University of Chicago. His research interests include cost-effectiveness, technology assessment, and information research.
In 2010, his poster “Effects of Hospitalists on 1-Year Post-Discharge Resource Utilization by Medicare Beneficiaries” took the top prize in the HM10 research competition. In 2011, he was appointed to the methodology committee of the federal Patient-Centered Outcomes Research Institute (PCORI), which was created by the Affordable Care Act to advise the government on clinical-effectiveness research. He also sits on the Advisory Council to the National Institute of General Medical Sciences at the Institute of Medicine, and on the Congressional Budget Office’s panel of health advisors.
In a career full of recognition, Dr. Meltzer says it’s hard to pinpoint the impact of winning the poster contest. But he has continued to submit abstracts to SHM every year and appreciates the opportunities for interaction with peers at the poster exhibits.

Title: Director of perioperative and consultative medicine
Institution: University of Michigan, Ann Arbor
Year: 2006
RIV: “Disseminated Histoplasmosis Presenting As Painful Oral Ulcers” (clinical vignettes)
Dr. Grant’s winning vignette presented a patient with a complex medical history, including heart disease and four months of painful oral ulcers, for which prior evaluations had been inconclusive, despite conducting biopsies. Following administration of high-dose corticosteroids, the patient’s condition worsened on multiple fronts. The vignette showed how the medical team was able to diagnose an unusual presentation of a fungal infection called histoplasmosis, which is prevalent in parts of the Midwest surrounding the Ohio and Mississippi river valleys.
“We see a lot of cases in the hospital where there are different angles you could take to turn it into a clinical vignette or a nice poster with good teaching points,” Dr. Grant says. “In this case, just digging deeper into the actual diagnosis was important because the empiric use of steroids can be fatal for some patients. Steroids are given for a lot of good reasons, but in this patient they caused immune suppression, allowing a smoldering infection to become very active.”
Dr. Grant did not submit the vignette for publication. “That was probably a mistake on my part,” he says, acknowledging the common complaint of too little time and too many competing priorities. But his interest in research has continued.
“I became involved at a national level with issues of perioperative medicine and last August published a textbook on the subject,” he reports.1 “VTE is another area of interest I have developed since my hospital medicine fellowship.”
He serves as the VTE resource expert on the Michigan Hospital Medicine Safety Consortium, a quality collaborative of more than 40 hospitals with Blue Cross/Blue Shield of Michigan. “It’s exciting to be able to look at the risk factors, what kinds of patients get VTEs, and whether they were appropriately prophylaxed in the hospital,” he says.
VTE is a national quality priority, and Dr. Grant expects abstracts to emerge from the consortium’s work.
He says he appreciates the opportunities that arise from participating in poster sessions at SHM, where medical students, residents, and working hospitalists talk to the presenters of interesting cases.
“It gives you a real back-and-forth, which is good for the person asking the question and for the presenter,” he says, noting hospitalists from other parts of the country were not as familiar with histoplasmosis.
He says winning the HM06 poster contest helped him “get his feet wet” and feel more prepared for a career in academic hospital medicine. “I’m sure the award solidified my employers’ satisfaction in hiring me—and in giving me more desirable academic roles and responsibilities,” he adds.

Title: Assistant professor of medicine pediatrics; director of the general internal-medicine comprehensive consultation service
Institution: Johns Hopkins Hospital, Baltimore
Year: 2009
RIV: “An Internet-Based Consult Curriculum for Hospitalists” (innovations)
Dr. Feldman’s poster described an online CME curriculum for hospitalists acting as medical consultants. The concept grew out of a perceived deficiency in his own medical education when, in 2004, he was asked to lead the consultation service at Johns Hopkins—just six months after finishing his residency.
“I had no idea what I was doing as a general-internal-medicine consultant,” he says. “I maybe received two weeks of experience as a consultant during my residency. I was willing to take it on, learning on the job and asking for help. But it occurred to me that I’m probably not alone in feeling unprepared.”
In his quest for self-education, Dr. Feldman wondered whether he should write a textbook on the subject. “But the information changes so quickly, I thought I’d have a better chance to reach people online,” he notes.
After talking to publishers and CME companies, he came up with the concept of learning modules on perioperative and consultative medicine topics, which could be taken online while earning CME credits. Johns Hopkins served as the CME certifier, and medical-education company Advanced Studies in Medicine joined as a partner. Once the project got off the ground, a medical advisory committee was convened.
“Winning the SHM poster competition is a great honor to have on a CV. It really helps to legitimize your name in the world of hospital medicine,” Dr. Feldman says. “It also provided confirmation that we were on the right track with the curriculum project. People valued what we were doing.”
Dr. Feldman and SHM have since become affiliated, and the “Consultative and Perioperative Medicine Essentials for Hospitalists” modules are available on SHM’s website (www.shmconsults.com). The site has 12,000 registered members completing 500 CME modules every month.
“I do a lot of the editing still,” Dr. Feldman says. “We update the modules every two years and are still creating new ones.”
Dr. Feldman also pursues a number of clinical-research interests, including resident education and costs of care.

Title: Assistant professor of medicine
Institution: Medical University of South Carolina, Charleston
Year: 2009
RIV: “Intensivists versus Hospitalists in the ICU: A Prospective Cohort Study Comparing Mortality and Length of Stay Between Two Staffing Models” (research) Citation: Wise KR, Akopov VA, Williams BR, Ido MS, Leeper KV, Dressler DD. Hospitalists and intensivists in the medical ICU: a prospective and observational study comparing mortality and length of stay between two staffing models. J Hosp Med. 2012;7(3):183-189.
Dr. Wise was recognized for research that began while she worked at Emory University in Atlanta, comparing hospitalists and intensivists in such outcomes as length of stay and mortality rates for patients in the ICU. The study was one of the first statistically rigorous examinations of this critical quality question. With an eye toward improving patient safety, national quality advocates such as the Leapfrog Group have called for hospitals to employ intensivists (critical-care specialists) to manage the care of ICU patients. In reality, Dr. Wise says, there aren’t enough intensivists to meet the need.
“Hospitalists are in the ICU anyway,” she says. “We just don’t have enough data to answer how well they do [in comparison to intensivists].”
Through a prospective cohort study of more than 1,000 patients, Dr. Wise’s group found that there was essentially no statistical difference in mortality rates between patients treated by intensivist teams or hospitalist ICU teams.
“We were also able to look at some of the intermediate-acuity patients—fairly complicated but not requiring ventilators,” she explains. “Our study wasn’t sufficiently powered for this subgroup, but it was an interesting piece of data to raise the question: Where should we deploy this scarce resource of intensivists? Which pockets of patients?”
Presenting her abstract at SHM’s annual meeting was a “good experience.”
“I’d done public speaking before, but never with an audience of about 500 people,” she says. “To go out there and field their questions was a real professional growing experience. Several people interested in the topic sought me out at the conference, introduced themselves, and we have subsequently stayed in touch.”
The manuscript published in JHM has been cited four times, including in a position paper from SHM and the Society of Critical Care Medicine.3 Another outgrowth of the research was being asked to contribute a chapter on hospitalists’ role in the ICU to a textbook on hospital medicine. Based on her still-fresh HM presentation, Dr. Wise was one of the few publicly identified experts on the subject. The chapter, co-authored by fellow Emory hospitalist Michael Heisler, MD, MPH, “The Role of the Hospitalist in Critical Care” was included in Principles and Practices of Hospital Medicine.4

Title: Neonatal intensivist
Institution: Stony Brook University Hospital, Great Neck, N.Y.
Year: 2006
RIV: “Administration of Inactivated Trivalent Influenza Vaccine (TIV) to Parents of Infants in the Neonatal Intensive Care Unit (NICU): A Novel Strategy to Increase Vaccination Rates” (innovations)
Citation: Shah SI, Caprio M, Hendricks-Munoz K. Administration of inactivated trivalent influenza vaccine to parents of high-risk infants in the neonatal intensive care unit. Pediatrics. 2007;120;e617-e621.
Dr. Shah was in his final year of a fellowship in neonatology at New York University when he took on the challenge of improving immunization access to protect premature, highly vulnerable patients in the NICU from influenza infections. Because these children are too young to be vaccinated directly, the concept of cocooning them from infection involves extending protection to everyone around them.
“We came up with the idea of offering flu vaccinations 24/7 in the NICU to the children’s parents,” he says. “It worked well for us as a way to define an indicated therapy for a defined population, even if it was a little outside the box. By the end of the flu season, 95% of the parents were vaccinated.”
SHM recognized the project as the top RIV innovations poster at HM06, but that was just the beginning.
“When I moved to SUNY Stony Brook, I continued to study and advocate for these vaccinations,” Dr. Shah says. “We were giving 500 to 700 vaccinations a year. Then I wrote a national resolution for the American Academy of Pediatrics, which was significant because it meant AAP was behind the project.”
Dr. Shah later became chair of AAP’s Long Island Chapter Legislative Committee and joined a statewide pediatric advocacy group. In 2009, the New York legislature enacted the Neonatal Influenza Protection Act, which required hospitals in the state to offer parents the vaccine, with Dr. Shah’s research and advocacy providing an essential basis for its passage. He’s even been recognized for his research in congressional citations.
Based on that success with influenza vaccinations, Dr. Shah and his colleagues looked at other diseases, starting with pertussis, and then tetanus, diphtheria, and whooping cough.5 All the while, they continued tracking immunization rates. A second state law, passed in 2011, added pertussis to the vaccinations. Next on his advocacy agenda is a project to promote smoking-cessation interventions in the NICU.6
“These parents come to see us every day,” he says. “What can we do, through the parents, to promote the health and well-being of their high-risk newborns?”

Title: Assistant professor of medicine; medical director of inpatient palliative-care consultation
Institution: University of Texas Health Sciences Center, San Antonio
Year: 2009
RIV: “When to Depend on the Kinins of Strangers: An Unusual Case of Abdominal Pain” (clinical vignettes)
Publication: An article on the ethics of determining code status for patients with advanced cancer and a book chapter on the “last hours of life” for a forthcoming book on palliative care and hospital medicine.
As a medical resident, Dr. Morrow met a 27-year-old woman who had chronic abdominal pain and had made multiple visits to the ED for this complaint. The patient had a history of substance abuse and requested dilaudid for her pain—making it easy for staff to consign her to the stereotype of the difficult patient.
“I met her after an interesting finding,” he says. “It turns out that on the previous emergency room visit, she received a CAT scan, which showed duodenal and small-bowel thickening consistent with hereditary angioedema, although with an unusual presentation. As it happened, we had onsite a world expert in angioedema.”
The expert was able to confirm the diagnosis, Dr. Morrow says.
“By giving her this ‘legitimate,’ organic diagnosis, it just changed the whole dynamic of her relationship with her doctors,” he says. “She knew that they knew something was really wrong. The residents were empowered to have something to hang their hats on. And we were able to get better control of her pain.”
Dr. Morrow says he came on the scene late in the discovery process, but he helped to solve the puzzle, and then put together the abstract and poster that told the story of making the diagnosis.
“In my previous job, I was hired as a hospitalist but helped to build the palliative-care program within the hospital-medicine service,” he says. “In my current job, I was brought in to build the inpatient palliative-care-consultation service, although I still moonlight as a hospitalist to stay sharp.”
Dr. Morrow says he enjoys sharing stories of difficult cases and submitting case studies about them to medical conferences, often with clever titles incorporating puns (e.g. the 2009 SHM poster citing kinins, polypeptides in the blood that cause inflammation). Another example is “The Angina Monologues,” a story of an 82-year-old patient with chronic angina pectoris and complex pain syndromes that were difficult to bring under control. Palliative care also emphasizes patients’ stories, he says, in order to understand the person behind the diagnosis.
Larry Beresford is a freelance writer in San Francisco. References available at www.the-hospitalist.org.
References
2. Yoder J. Association between hospital noise levels and inpatient sleep among middle-aged and older adults: Far from a quiet night. Abstract, Society of Hospital Medicine, 2011.
3. McKean SC, Ross JJ, Dressler DD, Brotman DJ, Ginsberg JS. Principles and Practice of Hospital Medicine. McGraw-Hill Medical; New York City: 2012.
4. Siegal EM, Dressler DD, Dichter JR, Gorman MJ, Lipsett PA. Training a hospitalist workforce to address the intensivist shortage in American hospitals: a position paper from the Society of Hospital Medicine and the Society of Critical Care Medicine. J Hosp Med. 2012;7:359-364.
5. Dylag A, Shah SI. Administration of tetanus, diphtheria, and acellular pertussis vaccine to parents of high-risk infants in the neonatal intensive care unit. Pediatrics. 2008;122:e550-e555.
6. Shah S. Smoking cessation counseling and PPSV 23-valent pneumococcal polysaccharide vaccine administration parents of neonatal intensive care unit (NICU)-admitted infants: A life-changing opportunity. J Neonatal-Perinatal Med. 2011;4:263-267.
Back to the Furture Past RIV winners talk about what the recognition meant for their careers By Larry Beresford
After winning SHM’s annual Research, Innovations, and Clinical Vignettes (RIV) scientific abstract and poster competition for an abstract illustrating a program that promoted flu vaccinations for families of neonatal patients, Shetal Shah, MD, FAAP, became a leading advocate for two laws mandating that New York hospitals offer vaccinations to families.
A poster that described a VTE prevention program led Gregory Maynard, MD, MSc, SFHM, to join SHM’s VTE Prevention Collaborative and, eventually, to become senior vice president of the society’s Center for Hospital Innovation and Improvement.
A prize-winning innovations poster for improving team communication by Vineet Chopra, MD, MS, FACP, FHM, and colleagues later took off as a new technology company.
Leonard Feldman, MD, FAAP, SFHM, won for a poster that explained online CME curriculum for hospitalists as consultants; the curriculum now resides on SHM’s website.
The evidence is clear: RIV abstracts are a vital part of hospital medicine.
Nearly 800 abstracts were submitted for HM13.
Awards are given in three categories:
- Research posters report clinical or basic science data, systematically review a clinical problem, or address efficiency, cost, or method of health-care delivery or medical decision-making;
- Innovations posters describe an existing innovative program in hospital medicine, often with preliminary data; and
- Clinical vignettes, either adult or pediatric, report on one or more cases illustrating a new disease entity, a prominent or unusual feature of an established disease, or an area of clinical controversy.
The Hospitalist asked 11 past RIV winners what the poster contest meant to their careers. Some added more data and analysis and went on to be published in such medical journals as the Journal of Hospital Medicine. Some used the recognition to launch or boost research-oriented careers; others saw their careers go in different directions.
“Winning a national poster competition gives you the confidence to continue to pursue your interest and take it to a higher level, like successfully competing for funding and publishing your line of inquiry,” says hospitalist and researcher Vineet Arora, MD, MPP, FHM, of the University of Chicago, who won the 2006 RIV research competition. “Sometimes, presenting posters can be lonely, but at SHM, you get a lot of traffic. You get a chance to practice your spiel, communicating science and research in a very concise way, which is an important skill to have.”
David Metzger, MD, PhD, also from the University of Chicago, who won the RIV research award in 2005, says recognition is a big deal, but “one of the biggest values of the RIV competition is just getting information out to colleagues, with the opportunity to talk with your peers. That’s the real prize.
“I’ve been involved in presenting posters at SHM every year that the society has been in existence,” he says. “I’ve met so many people and talked about what they’re doing. That’s what a medical society should do—bring people together like this.”
Title: Administrator, academic consult service; teaching staff physician
Institution: Saint Joseph Mercy Hospital, Ypsilanti, Mich.
Year: 2008
RIV: “A Case of Salty Voluminous Urine” (clinical vignette)
Dr. Tassava was honored two years in a row for topics drawn from her experience as a hospitalist working in the surgical ICU. Her HM08 entry won top poster, and her HM09 poster, “Permissive Hypernatremia: Co-Management of Intracranial Pressure in a Patient with Diabetes Insipidus,” was selected for an oral presentation.
The HM09 vignette described how the hypernatremia that occurs with diabetes insipidus could be used in a novel way to control intracranial pressure in a 17-year-old patient who had a traumatic brain injury from an auto accident.
“She had a beautiful outcome,” Dr. Tassava says. “She started college and she came back to our unit for a visit after her recovery.”
Dr. Tassava enjoyed the opportunity to explain to her peers how diabetes insipidus presented and how she managed the case. “I was a little surprised at how much discussion was generated by my case,” she says, “even though I knew this was an important and novel approach.”
When her hospital added intensivists, her work and research in the ICU ended and her career moved more toward hospitalist administration. She now runs the academic consult service at St. Joseph, serves as lead physician for the orthopedic surgery floor, instructs and mentors medical residents, and chairs the hospital’s Coagulation Collaborative Practice Team (Coagulation CPT). She credits the RIV honors with helping her to gain recognition as an academic hospitalist who was nominated for leadership roles. She has moved out of research for now but plans to pursue anticoagulation research in the future.
“I really appreciated the recognition for my curiosity and scientific approach, which was acknowledged by my surgical colleagues,” Dr. Tassava says. “I absolutely love the CPT. I am the hospital’s principal educator with regard to anticoagulation. Over the past year, I have given medicine and cardiology grand rounds, and have presented on the newest anticoagulants.”
Dr. Tassava still collaborates with her residents on abstracts, several of which have been submitted to SHM, the American College of Physicians, and other medical societies.
“I still love research,” she says. “I have a million ideas.”
Title: Chief of the division of hospital medicine; senior vice president, SHM’s Center for Innovation and Improvement
Institution: University of California at San Diego (UCSD)
Year: 2008
RIV: “Prevention of Hospital-Acquired Venous Thromboembolism: Prospective Validation of a VTE Risk Assessment Model and Protocol” (research)
Citations: Maynard G, Stein J. Designing and implementing effective VTE prevention protocols: lessons from collaboratives. J Thromb Thrombolysis. 2010;29(2):159-166. Maynard G, Morris T, Jenkins I, et al. Optimizing prevention of hospital acquired venous thromboembolism: prospective validation of a VTE risk assessment model. J Hosp Med. 2010;5(1):10-18.
Dr. Maynard’s abstract described a project funded by the federal Agency for Healthcare Research and Quality to design and implement an organized, comprehensive protocol for VTE prevention within the hospital setting. The project also included a toolkit to help other hospitals do the same thing. The same group received SHM’s Award of Excellence for Teamwork.
This work, combined with similar efforts by Jason Stein, MD, and colleagues at Emory University in Atlanta and others, provided the foundation for SHM’s VTE resource room and the mentored implementation program of SHM’s VTE Prevention Collaborative, which had been launched in 2007 as one of the society’s first large-scale quality-improvement (QI) initiatives.
“SHM wanted to do something about VTE prevention, and when we got our AHRQ grant, I was interested in doing the same,” Dr. Maynard says. “We published our implementation guides on the AHRQ and SHM websites, along with a lot of valuable supporting materials.”
Dr. Maynard later took on leadership roles with SHM’s quality initiatives on glycemic control and care transitions, which made him the logical choice to become senior vice president of SHM’s Center for Hospital Innovation and Improvement.
He says the RIV honor lifted his profile not only within SHM, but also throughout the field, and it was instrumental in obtaining continued funding to advance the VTE initiative. “We did this tremendous work—with great results,” he says. “But I don’t think our local administrators appreciated it quite as much until we started to get external, national recognition.”
Dr. Maynard earned his master’s degree in biostatistics and clinical research design from the University of Michigan—skills he later brought to the academic setting at UCSD.
“It was a nice way for a hospitalist, who’s really a medical generalist, to become an expert in something,” he says. “I could never be more of an expert in cardiology than a cardiologist, or more of an expert in DVT than a hematologist or critical-care specialist. But I could help both of them do what they couldn’t do as effectively, which was to implement protocols reliably using a QI framework.”
Title: Assistant professor of general internal medicine, hospital medicine, and public health
Institution: Vanderbilt University, Nashville, Tenn.
Year: 2009
RIV: “Predictors of Early Post-Discharge Mortality in Critically Ill Patients: Lessons for Quality Performance and Quality Assessment” (research)
Citation: Vasilevskis EE, Kuzniewicz MW, Cason BA, et al. Predictors of early post-discharge mortality in critically ill patients: a retrospective cohort study from the California Intensive Care Outcomes project. J Crit Care. 2011;26(1):65-75.
Dr. Vasilevskis has submitted abstracts to the RIV competition almost every year since 2007, when he was completing a fellowship at the University of California at San Francisco’s Institute for Health Policy Studies. He was honored in 2009 for a project based on the California Intensive Care Outcomes Project, which drew data from 35 hospitals to demonstrate that shortening ICU length of stay was predictive of early post-discharge mortality in the most severely ill patients.
He has continued to research quality and safety in the ICU, and he has published dozens of journal articles.
“My initial focus was on traditional mortality and length-of-stay outcomes,” he says. “I am now pursuing additional outcomes, most notably delirium in the ICU patient. I work with an amazing group of researchers that are trying to better measure, define, and treat delirium in the ICU—an outcome associated with a number of poor patient outcomes.”
Dr. Vasilevskis also is researching the causes of hospital readmissions and the development of novel ways to improve care transitions for elderly patients. He is pursuing a master’s of public health at Vanderbilt, and is co-principal investigator of an investigation of the Hospital Medicine Reengineering Network to improve transitions of care, supported by the Association of American Medical Colleges.
In addition to his 2009 win, he captured the HM10 and HM12 research categories. His HM12 poster, “Veterans Administration Acute Care 30-Day Mortality Model: Development, Validation and Performance Variation,” was singled out by the judging committee for its impressive sample size (1,114,327 patients in a retrospective cohort study of 131 VA hospitals), as well as for how it combined administrative and clinical risk models.
Dr. Vasilevskis says the opportunity to present his research at SHM and the recognition he received encouraged him to continue as a hospitalist engaged in medical research. He has been a member of SHM’s Research Committee since 2009, an RIV judge at HM11, and chaired the HM13 RIV competition subcommittee.
Title: Assistant professor of medicine
Institution: University of Michigan Health System, Ann Arbor
Year: 2009
RIV: “MComm: Redefining Medical Communications in the 21st Century” (innovations)
Early in his career, Dr. Chopra was curious about how to improve the way patient care is delivered in the hospital setting. He was particularly interested in the inordinate amount of time hospitalists spend every day on communication.
“I saw one-way paging systems as a problem for communication between members of the medical team,” he says. “Doctors get paged and break off from what they’re doing to return the page—to someone who often isn’t there to take the call back. Sometimes the system gives us the wrong number or a cryptic message that makes no sense.”
A technological solution to this problem, which he and hospitalist Prasanth Gogineni, MD, conceived, designed, and created, then tested at the University of Michigan, is called MComm. Dr. Chopra describes it as a novel, uniform way of messaging for the entire medical team using wireless servers, PUSH technology, and iPhones. MComm was built around existing hospital workflow and patient-specific task lists, assigning priority to each message and documenting that it was delivered. The junior faculty members submitted an abstract about their innovative application, not really expecting it to get accepted. But when it won the poster competition and was selected for a plenary presentation, things got busy in a hurry. Specifically, the university hospital’s Office of Technology Transfer took a keen interest.
“We met with a number of people who had business experience in the health-care-technology space and found a CEO for the company we formed to develop MComm,” Dr. Chopra says. “I found myself getting pulled into it very quickly, with a lot of conversations about commercialization, revenue-sharing models, intellectual property, and the like.”
But running a company was not something Dr. Chopra wanted to do. Two years ago, that company, Synaptin, went one way and he went another—he stayed at Michigan as a medical researcher. He remains deeply interested in how care is delivered to hospitalized patients, but with a focus on such patient-safety questions as how to prevent negative outcomes from indwelling venous catheters.
“Winning the poster competition opened doors for me—there’s no doubt in my mind,” he says. “We demonstrated the ability to deliver a project of significance, from concept to prototype, without formal training in this area. If we didn’t have that recognition, I’m not sure I would have been ready to step into a research career as quickly. It helped me realize that medical research was what I wanted to do.”
Title: Associate program director, internal-medicine residency; assistant dean of scholarship and discovery
Institution: Pritzker School of Medicine, University of Chicago
Year: 2006
RIV: “Measuring Quality of Hospital Care for Vulnerable Elders: Use of ACOVE Quality Indicators” (research)
Citation: Arora VM, Fish M, Basu A, et al. Relationship between quality of care of hospitalized vulnerable elders and postdischarge mortality. J Am Geriatrics. 2010;58:1642-1648.
Title: Associate professor, department of medicine; associate faculty member, Harris School and the Department of Economics
Institution: University of Chicago
Year: 2005
RIV: “Effects of Hospitalists on Outcomes and Costs in a Multicenter Trial of Academic Hospitalists” (research)
Dr. Meltzer was the lead author, with 11 other prominent hospitalists, of an abstract based on a multisite study of the cost and outcome implications of the hospitalist model—still a relatively new concept in 2001, when the research began. Although the study did not uncover large cost savings realized from the hospitalist model of care, as some advocates had hoped, important findings and implications for the emerging field were teased out of the data.
At the time, only a few randomly controlled, multisite studies of costs and outcomes for the hospitalist model had been performed. The study, Dr. Meltzer says, required a complicated analysis to discover that hospitalists, in fact, saved their facilities money, with their most important impact realized post-hospitalization, such as on nursing-home costs. It was important to control for spillover effect and the fact that hospitalists do a better job of teaching house staff, while a physician’s years of experience was another important variable, he says.
Dr. Meltzer was a medical researcher interested in medical specialization when the term “hospitalist” was first coined in 1996. “I thought, here was a chance to study a medical specialty in its formative stages,” he says.
He still works as a hospitalist, although with limited clinical time. In addition to his administrative work as division chief, he directs the Center for Health and the Social Sciences at the University of Chicago. His research interests include cost-effectiveness, technology assessment, and information research.
In 2010, his poster “Effects of Hospitalists on 1-Year Post-Discharge Resource Utilization by Medicare Beneficiaries” took the top prize in the HM10 research competition. In 2011, he was appointed to the methodology committee of the federal Patient-Centered Outcomes Research Institute (PCORI), which was created by the Affordable Care Act to advise the government on clinical-effectiveness research. He also sits on the Advisory Council to the National Institute of General Medical Sciences at the Institute of Medicine, and on the Congressional Budget Office’s panel of health advisors.
In a career full of recognition, Dr. Meltzer says it’s hard to pinpoint the impact of winning the poster contest. But he has continued to submit abstracts to SHM every year and appreciates the opportunities for interaction with peers at the poster exhibits.
Title: Director of perioperative and consultative medicine
Institution: University of Michigan, Ann Arbor
Year: 2006
RIV: “Disseminated Histoplasmosis Presenting As Painful Oral Ulcers” (clinical vignettes)
Dr. Grant’s winning vignette presented a patient with a complex medical history, including heart disease and four months of painful oral ulcers, for which prior evaluations had been inconclusive, despite conducting biopsies. Following administration of high-dose corticosteroids, the patient’s condition worsened on multiple fronts. The vignette showed how the medical team was able to diagnose an unusual presentation of a fungal infection called histoplasmosis, which is prevalent in parts of the Midwest surrounding the Ohio and Mississippi river valleys.
“We see a lot of cases in the hospital where there are different angles you could take to turn it into a clinical vignette or a nice poster with good teaching points,” Dr. Grant says. “In this case, just digging deeper into the actual diagnosis was important because the empiric use of steroids can be fatal for some patients. Steroids are given for a lot of good reasons, but in this patient they caused immune suppression, allowing a smoldering infection to become very active.”
Dr. Grant did not submit the vignette for publication. “That was probably a mistake on my part,” he says, acknowledging the common complaint of too little time and too many competing priorities. But his interest in research has continued.
“I became involved at a national level with issues of perioperative medicine and last August published a textbook on the subject,” he reports.1 “VTE is another area of interest I have developed since my hospital medicine fellowship.”
He serves as the VTE resource expert on the Michigan Hospital Medicine Safety Consortium, a quality collaborative of more than 40 hospitals with Blue Cross/Blue Shield of Michigan. “It’s exciting to be able to look at the risk factors, what kinds of patients get VTEs, and whether they were appropriately prophylaxed in the hospital,” he says.
VTE is a national quality priority, and Dr. Grant expects abstracts to emerge from the consortium’s work.
He says he appreciates the opportunities that arise from participating in poster sessions at SHM, where medical students, residents, and working hospitalists talk to the presenters of interesting cases.
“It gives you a real back-and-forth, which is good for the person asking the question and for the presenter,” he says, noting hospitalists from other parts of the country were not as familiar with histoplasmosis.
He says winning the HM06 poster contest helped him “get his feet wet” and feel more prepared for a career in academic hospital medicine. “I’m sure the award solidified my employers’ satisfaction in hiring me—and in giving me more desirable academic roles and responsibilities,” he adds.
Title: Assistant professor of medicine pediatrics; director of the general internal-medicine comprehensive consultation service
Institution: Johns Hopkins Hospital, Baltimore
Year: 2009
RIV: “An Internet-Based Consult Curriculum for Hospitalists” (innovations)
Dr. Feldman’s poster described an online CME curriculum for hospitalists acting as medical consultants. The concept grew out of a perceived deficiency in his own medical education when, in 2004, he was asked to lead the consultation service at Johns Hopkins—just six months after finishing his residency.
“I had no idea what I was doing as a general-internal-medicine consultant,” he says. “I maybe received two weeks of experience as a consultant during my residency. I was willing to take it on, learning on the job and asking for help. But it occurred to me that I’m probably not alone in feeling unprepared.”
In his quest for self-education, Dr. Feldman wondered whether he should write a textbook on the subject. “But the information changes so quickly, I thought I’d have a better chance to reach people online,” he notes.
After talking to publishers and CME companies, he came up with the concept of learning modules on perioperative and consultative medicine topics, which could be taken online while earning CME credits. Johns Hopkins served as the CME certifier, and medical-education company Advanced Studies in Medicine joined as a partner. Once the project got off the ground, a medical advisory committee was convened.
“Winning the SHM poster competition is a great honor to have on a CV. It really helps to legitimize your name in the world of hospital medicine,” Dr. Feldman says. “It also provided confirmation that we were on the right track with the curriculum project. People valued what we were doing.”
Dr. Feldman and SHM have since become affiliated, and the “Consultative and Perioperative Medicine Essentials for Hospitalists” modules are available on SHM’s website (www.shmconsults.com). The site has 12,000 registered members completing 500 CME modules every month.
“I do a lot of the editing still,” Dr. Feldman says. “We update the modules every two years and are still creating new ones.”
Dr. Feldman also pursues a number of clinical-research interests, including resident education and costs of care.
Title: Assistant professor of medicine
Institution: Medical University of South Carolina, Charleston
Year: 2009
RIV: “Intensivists versus Hospitalists in the ICU: A Prospective Cohort Study Comparing Mortality and Length of Stay Between Two Staffing Models” (research) Citation: Wise KR, Akopov VA, Williams BR, Ido MS, Leeper KV, Dressler DD. Hospitalists and intensivists in the medical ICU: a prospective and observational study comparing mortality and length of stay between two staffing models. J Hosp Med. 2012;7(3):183-189.
Dr. Wise was recognized for research that began while she worked at Emory University in Atlanta, comparing hospitalists and intensivists in such outcomes as length of stay and mortality rates for patients in the ICU. The study was one of the first statistically rigorous examinations of this critical quality question. With an eye toward improving patient safety, national quality advocates such as the Leapfrog Group have called for hospitals to employ intensivists (critical-care specialists) to manage the care of ICU patients. In reality, Dr. Wise says, there aren’t enough intensivists to meet the need.
“Hospitalists are in the ICU anyway,” she says. “We just don’t have enough data to answer how well they do [in comparison to intensivists].”
Through a prospective cohort study of more than 1,000 patients, Dr. Wise’s group found that there was essentially no statistical difference in mortality rates between patients treated by intensivist teams or hospitalist ICU teams.
“We were also able to look at some of the intermediate-acuity patients—fairly complicated but not requiring ventilators,” she explains. “Our study wasn’t sufficiently powered for this subgroup, but it was an interesting piece of data to raise the question: Where should we deploy this scarce resource of intensivists? Which pockets of patients?”
Presenting her abstract at SHM’s annual meeting was a “good experience.”
“I’d done public speaking before, but never with an audience of about 500 people,” she says. “To go out there and field their questions was a real professional growing experience. Several people interested in the topic sought me out at the conference, introduced themselves, and we have subsequently stayed in touch.”
The manuscript published in JHM has been cited four times, including in a position paper from SHM and the Society of Critical Care Medicine.3 Another outgrowth of the research was being asked to contribute a chapter on hospitalists’ role in the ICU to a textbook on hospital medicine. Based on her still-fresh HM presentation, Dr. Wise was one of the few publicly identified experts on the subject. The chapter, co-authored by fellow Emory hospitalist Michael Heisler, MD, MPH, “The Role of the Hospitalist in Critical Care” was included in Principles and Practices of Hospital Medicine.4
Title: Neonatal intensivist
Institution: Stony Brook University Hospital, Great Neck, N.Y.
Year: 2006
RIV: “Administration of Inactivated Trivalent Influenza Vaccine (TIV) to Parents of Infants in the Neonatal Intensive Care Unit (NICU): A Novel Strategy to Increase Vaccination Rates” (innovations)
Citation: Shah SI, Caprio M, Hendricks-Munoz K. Administration of inactivated trivalent influenza vaccine to parents of high-risk infants in the neonatal intensive care unit. Pediatrics. 2007;120;e617-e621.
Dr. Shah was in his final year of a fellowship in neonatology at New York University when he took on the challenge of improving immunization access to protect premature, highly vulnerable patients in the NICU from influenza infections. Because these children are too young to be vaccinated directly, the concept of cocooning them from infection involves extending protection to everyone around them.
“We came up with the idea of offering flu vaccinations 24/7 in the NICU to the children’s parents,” he says. “It worked well for us as a way to define an indicated therapy for a defined population, even if it was a little outside the box. By the end of the flu season, 95% of the parents were vaccinated.”
SHM recognized the project as the top RIV innovations poster at HM06, but that was just the beginning.
“When I moved to SUNY Stony Brook, I continued to study and advocate for these vaccinations,” Dr. Shah says. “We were giving 500 to 700 vaccinations a year. Then I wrote a national resolution for the American Academy of Pediatrics, which was significant because it meant AAP was behind the project.”
Dr. Shah later became chair of AAP’s Long Island Chapter Legislative Committee and joined a statewide pediatric advocacy group. In 2009, the New York legislature enacted the Neonatal Influenza Protection Act, which required hospitals in the state to offer parents the vaccine, with Dr. Shah’s research and advocacy providing an essential basis for its passage. He’s even been recognized for his research in congressional citations.
Based on that success with influenza vaccinations, Dr. Shah and his colleagues looked at other diseases, starting with pertussis, and then tetanus, diphtheria, and whooping cough.5 All the while, they continued tracking immunization rates. A second state law, passed in 2011, added pertussis to the vaccinations. Next on his advocacy agenda is a project to promote smoking-cessation interventions in the NICU.6
“These parents come to see us every day,” he says. “What can we do, through the parents, to promote the health and well-being of their high-risk newborns?”
Title: Assistant professor of medicine; medical director of inpatient palliative-care consultation
Institution: University of Texas Health Sciences Center, San Antonio
Year: 2009
RIV: “When to Depend on the Kinins of Strangers: An Unusual Case of Abdominal Pain” (clinical vignettes)
Publication: An article on the ethics of determining code status for patients with advanced cancer and a book chapter on the “last hours of life” for a forthcoming book on palliative care and hospital medicine.
As a medical resident, Dr. Morrow met a 27-year-old woman who had chronic abdominal pain and had made multiple visits to the ED for this complaint. The patient had a history of substance abuse and requested dilaudid for her pain—making it easy for staff to consign her to the stereotype of the difficult patient.
“I met her after an interesting finding,” he says. “It turns out that on the previous emergency room visit, she received a CAT scan, which showed duodenal and small-bowel thickening consistent with hereditary angioedema, although with an unusual presentation. As it happened, we had onsite a world expert in angioedema.”
The expert was able to confirm the diagnosis, Dr. Morrow says.
“By giving her this ‘legitimate,’ organic diagnosis, it just changed the whole dynamic of her relationship with her doctors,” he says. “She knew that they knew something was really wrong. The residents were empowered to have something to hang their hats on. And we were able to get better control of her pain.”
Dr. Morrow says he came on the scene late in the discovery process, but he helped to solve the puzzle, and then put together the abstract and poster that told the story of making the diagnosis.
“In my previous job, I was hired as a hospitalist but helped to build the palliative-care program within the hospital-medicine service,” he says. “In my current job, I was brought in to build the inpatient palliative-care-consultation service, although I still moonlight as a hospitalist to stay sharp.”
Dr. Morrow says he enjoys sharing stories of difficult cases and submitting case studies about them to medical conferences, often with clever titles incorporating puns (e.g. the 2009 SHM poster citing kinins, polypeptides in the blood that cause inflammation). Another example is “The Angina Monologues,” a story of an 82-year-old patient with chronic angina pectoris and complex pain syndromes that were difficult to bring under control. Palliative care also emphasizes patients’ stories, he says, in order to understand the person behind the diagnosis.
Larry Beresford is a freelance writer in San Francisco. References available at www.the-hospitalist.org.
References
2. Yoder J. Association between hospital noise levels and inpatient sleep among middle-aged and older adults: Far from a quiet night. Abstract, Society of Hospital Medicine, 2011.
3. McKean SC, Ross JJ, Dressler DD, Brotman DJ, Ginsberg JS. Principles and Practice of Hospital Medicine. McGraw-Hill Medical; New York City: 2012.
4. Siegal EM, Dressler DD, Dichter JR, Gorman MJ, Lipsett PA. Training a hospitalist workforce to address the intensivist shortage in American hospitals: a position paper from the Society of Hospital Medicine and the Society of Critical Care Medicine. J Hosp Med. 2012;7:359-364.
5. Dylag A, Shah SI. Administration of tetanus, diphtheria, and acellular pertussis vaccine to parents of high-risk infants in the neonatal intensive care unit. Pediatrics. 2008;122:e550-e555.
6. Shah S. Smoking cessation counseling and PPSV 23-valent pneumococcal polysaccharide vaccine administration parents of neonatal intensive care unit (NICU)-admitted infants: A life-changing opportunity. J Neonatal-Perinatal Med. 2011;4:263-267.
Back to the Furture Past RIV winners talk about what the recognition meant for their careers By Larry Beresford
After winning SHM’s annual Research, Innovations, and Clinical Vignettes (RIV) scientific abstract and poster competition for an abstract illustrating a program that promoted flu vaccinations for families of neonatal patients, Shetal Shah, MD, FAAP, became a leading advocate for two laws mandating that New York hospitals offer vaccinations to families.
A poster that described a VTE prevention program led Gregory Maynard, MD, MSc, SFHM, to join SHM’s VTE Prevention Collaborative and, eventually, to become senior vice president of the society’s Center for Hospital Innovation and Improvement.
A prize-winning innovations poster for improving team communication by Vineet Chopra, MD, MS, FACP, FHM, and colleagues later took off as a new technology company.
Leonard Feldman, MD, FAAP, SFHM, won for a poster that explained online CME curriculum for hospitalists as consultants; the curriculum now resides on SHM’s website.
The evidence is clear: RIV abstracts are a vital part of hospital medicine.
Nearly 800 abstracts were submitted for HM13.
Awards are given in three categories:
- Research posters report clinical or basic science data, systematically review a clinical problem, or address efficiency, cost, or method of health-care delivery or medical decision-making;
- Innovations posters describe an existing innovative program in hospital medicine, often with preliminary data; and
- Clinical vignettes, either adult or pediatric, report on one or more cases illustrating a new disease entity, a prominent or unusual feature of an established disease, or an area of clinical controversy.
The Hospitalist asked 11 past RIV winners what the poster contest meant to their careers. Some added more data and analysis and went on to be published in such medical journals as the Journal of Hospital Medicine. Some used the recognition to launch or boost research-oriented careers; others saw their careers go in different directions.
“Winning a national poster competition gives you the confidence to continue to pursue your interest and take it to a higher level, like successfully competing for funding and publishing your line of inquiry,” says hospitalist and researcher Vineet Arora, MD, MPP, FHM, of the University of Chicago, who won the 2006 RIV research competition. “Sometimes, presenting posters can be lonely, but at SHM, you get a lot of traffic. You get a chance to practice your spiel, communicating science and research in a very concise way, which is an important skill to have.”
David Metzger, MD, PhD, also from the University of Chicago, who won the RIV research award in 2005, says recognition is a big deal, but “one of the biggest values of the RIV competition is just getting information out to colleagues, with the opportunity to talk with your peers. That’s the real prize.
“I’ve been involved in presenting posters at SHM every year that the society has been in existence,” he says. “I’ve met so many people and talked about what they’re doing. That’s what a medical society should do—bring people together like this.”
Title: Administrator, academic consult service; teaching staff physician
Institution: Saint Joseph Mercy Hospital, Ypsilanti, Mich.
Year: 2008
RIV: “A Case of Salty Voluminous Urine” (clinical vignette)
Dr. Tassava was honored two years in a row for topics drawn from her experience as a hospitalist working in the surgical ICU. Her HM08 entry won top poster, and her HM09 poster, “Permissive Hypernatremia: Co-Management of Intracranial Pressure in a Patient with Diabetes Insipidus,” was selected for an oral presentation.
The HM09 vignette described how the hypernatremia that occurs with diabetes insipidus could be used in a novel way to control intracranial pressure in a 17-year-old patient who had a traumatic brain injury from an auto accident.
“She had a beautiful outcome,” Dr. Tassava says. “She started college and she came back to our unit for a visit after her recovery.”
Dr. Tassava enjoyed the opportunity to explain to her peers how diabetes insipidus presented and how she managed the case. “I was a little surprised at how much discussion was generated by my case,” she says, “even though I knew this was an important and novel approach.”
When her hospital added intensivists, her work and research in the ICU ended and her career moved more toward hospitalist administration. She now runs the academic consult service at St. Joseph, serves as lead physician for the orthopedic surgery floor, instructs and mentors medical residents, and chairs the hospital’s Coagulation Collaborative Practice Team (Coagulation CPT). She credits the RIV honors with helping her to gain recognition as an academic hospitalist who was nominated for leadership roles. She has moved out of research for now but plans to pursue anticoagulation research in the future.
“I really appreciated the recognition for my curiosity and scientific approach, which was acknowledged by my surgical colleagues,” Dr. Tassava says. “I absolutely love the CPT. I am the hospital’s principal educator with regard to anticoagulation. Over the past year, I have given medicine and cardiology grand rounds, and have presented on the newest anticoagulants.”
Dr. Tassava still collaborates with her residents on abstracts, several of which have been submitted to SHM, the American College of Physicians, and other medical societies.
“I still love research,” she says. “I have a million ideas.”
Title: Chief of the division of hospital medicine; senior vice president, SHM’s Center for Innovation and Improvement
Institution: University of California at San Diego (UCSD)
Year: 2008
RIV: “Prevention of Hospital-Acquired Venous Thromboembolism: Prospective Validation of a VTE Risk Assessment Model and Protocol” (research)
Citations: Maynard G, Stein J. Designing and implementing effective VTE prevention protocols: lessons from collaboratives. J Thromb Thrombolysis. 2010;29(2):159-166. Maynard G, Morris T, Jenkins I, et al. Optimizing prevention of hospital acquired venous thromboembolism: prospective validation of a VTE risk assessment model. J Hosp Med. 2010;5(1):10-18.
Dr. Maynard’s abstract described a project funded by the federal Agency for Healthcare Research and Quality to design and implement an organized, comprehensive protocol for VTE prevention within the hospital setting. The project also included a toolkit to help other hospitals do the same thing. The same group received SHM’s Award of Excellence for Teamwork.
This work, combined with similar efforts by Jason Stein, MD, and colleagues at Emory University in Atlanta and others, provided the foundation for SHM’s VTE resource room and the mentored implementation program of SHM’s VTE Prevention Collaborative, which had been launched in 2007 as one of the society’s first large-scale quality-improvement (QI) initiatives.
“SHM wanted to do something about VTE prevention, and when we got our AHRQ grant, I was interested in doing the same,” Dr. Maynard says. “We published our implementation guides on the AHRQ and SHM websites, along with a lot of valuable supporting materials.”
Dr. Maynard later took on leadership roles with SHM’s quality initiatives on glycemic control and care transitions, which made him the logical choice to become senior vice president of SHM’s Center for Hospital Innovation and Improvement.
He says the RIV honor lifted his profile not only within SHM, but also throughout the field, and it was instrumental in obtaining continued funding to advance the VTE initiative. “We did this tremendous work—with great results,” he says. “But I don’t think our local administrators appreciated it quite as much until we started to get external, national recognition.”
Dr. Maynard earned his master’s degree in biostatistics and clinical research design from the University of Michigan—skills he later brought to the academic setting at UCSD.
“It was a nice way for a hospitalist, who’s really a medical generalist, to become an expert in something,” he says. “I could never be more of an expert in cardiology than a cardiologist, or more of an expert in DVT than a hematologist or critical-care specialist. But I could help both of them do what they couldn’t do as effectively, which was to implement protocols reliably using a QI framework.”
Title: Assistant professor of general internal medicine, hospital medicine, and public health
Institution: Vanderbilt University, Nashville, Tenn.
Year: 2009
RIV: “Predictors of Early Post-Discharge Mortality in Critically Ill Patients: Lessons for Quality Performance and Quality Assessment” (research)
Citation: Vasilevskis EE, Kuzniewicz MW, Cason BA, et al. Predictors of early post-discharge mortality in critically ill patients: a retrospective cohort study from the California Intensive Care Outcomes project. J Crit Care. 2011;26(1):65-75.
Dr. Vasilevskis has submitted abstracts to the RIV competition almost every year since 2007, when he was completing a fellowship at the University of California at San Francisco’s Institute for Health Policy Studies. He was honored in 2009 for a project based on the California Intensive Care Outcomes Project, which drew data from 35 hospitals to demonstrate that shortening ICU length of stay was predictive of early post-discharge mortality in the most severely ill patients.
He has continued to research quality and safety in the ICU, and he has published dozens of journal articles.
“My initial focus was on traditional mortality and length-of-stay outcomes,” he says. “I am now pursuing additional outcomes, most notably delirium in the ICU patient. I work with an amazing group of researchers that are trying to better measure, define, and treat delirium in the ICU—an outcome associated with a number of poor patient outcomes.”
Dr. Vasilevskis also is researching the causes of hospital readmissions and the development of novel ways to improve care transitions for elderly patients. He is pursuing a master’s of public health at Vanderbilt, and is co-principal investigator of an investigation of the Hospital Medicine Reengineering Network to improve transitions of care, supported by the Association of American Medical Colleges.
In addition to his 2009 win, he captured the HM10 and HM12 research categories. His HM12 poster, “Veterans Administration Acute Care 30-Day Mortality Model: Development, Validation and Performance Variation,” was singled out by the judging committee for its impressive sample size (1,114,327 patients in a retrospective cohort study of 131 VA hospitals), as well as for how it combined administrative and clinical risk models.
Dr. Vasilevskis says the opportunity to present his research at SHM and the recognition he received encouraged him to continue as a hospitalist engaged in medical research. He has been a member of SHM’s Research Committee since 2009, an RIV judge at HM11, and chaired the HM13 RIV competition subcommittee.
Title: Assistant professor of medicine
Institution: University of Michigan Health System, Ann Arbor
Year: 2009
RIV: “MComm: Redefining Medical Communications in the 21st Century” (innovations)
Early in his career, Dr. Chopra was curious about how to improve the way patient care is delivered in the hospital setting. He was particularly interested in the inordinate amount of time hospitalists spend every day on communication.
“I saw one-way paging systems as a problem for communication between members of the medical team,” he says. “Doctors get paged and break off from what they’re doing to return the page—to someone who often isn’t there to take the call back. Sometimes the system gives us the wrong number or a cryptic message that makes no sense.”
A technological solution to this problem, which he and hospitalist Prasanth Gogineni, MD, conceived, designed, and created, then tested at the University of Michigan, is called MComm. Dr. Chopra describes it as a novel, uniform way of messaging for the entire medical team using wireless servers, PUSH technology, and iPhones. MComm was built around existing hospital workflow and patient-specific task lists, assigning priority to each message and documenting that it was delivered. The junior faculty members submitted an abstract about their innovative application, not really expecting it to get accepted. But when it won the poster competition and was selected for a plenary presentation, things got busy in a hurry. Specifically, the university hospital’s Office of Technology Transfer took a keen interest.
“We met with a number of people who had business experience in the health-care-technology space and found a CEO for the company we formed to develop MComm,” Dr. Chopra says. “I found myself getting pulled into it very quickly, with a lot of conversations about commercialization, revenue-sharing models, intellectual property, and the like.”
But running a company was not something Dr. Chopra wanted to do. Two years ago, that company, Synaptin, went one way and he went another—he stayed at Michigan as a medical researcher. He remains deeply interested in how care is delivered to hospitalized patients, but with a focus on such patient-safety questions as how to prevent negative outcomes from indwelling venous catheters.
“Winning the poster competition opened doors for me—there’s no doubt in my mind,” he says. “We demonstrated the ability to deliver a project of significance, from concept to prototype, without formal training in this area. If we didn’t have that recognition, I’m not sure I would have been ready to step into a research career as quickly. It helped me realize that medical research was what I wanted to do.”
Title: Associate program director, internal-medicine residency; assistant dean of scholarship and discovery
Institution: Pritzker School of Medicine, University of Chicago
Year: 2006
RIV: “Measuring Quality of Hospital Care for Vulnerable Elders: Use of ACOVE Quality Indicators” (research)
Citation: Arora VM, Fish M, Basu A, et al. Relationship between quality of care of hospitalized vulnerable elders and postdischarge mortality. J Am Geriatrics. 2010;58:1642-1648.
Title: Associate professor, department of medicine; associate faculty member, Harris School and the Department of Economics
Institution: University of Chicago
Year: 2005
RIV: “Effects of Hospitalists on Outcomes and Costs in a Multicenter Trial of Academic Hospitalists” (research)
Dr. Meltzer was the lead author, with 11 other prominent hospitalists, of an abstract based on a multisite study of the cost and outcome implications of the hospitalist model—still a relatively new concept in 2001, when the research began. Although the study did not uncover large cost savings realized from the hospitalist model of care, as some advocates had hoped, important findings and implications for the emerging field were teased out of the data.
At the time, only a few randomly controlled, multisite studies of costs and outcomes for the hospitalist model had been performed. The study, Dr. Meltzer says, required a complicated analysis to discover that hospitalists, in fact, saved their facilities money, with their most important impact realized post-hospitalization, such as on nursing-home costs. It was important to control for spillover effect and the fact that hospitalists do a better job of teaching house staff, while a physician’s years of experience was another important variable, he says.
Dr. Meltzer was a medical researcher interested in medical specialization when the term “hospitalist” was first coined in 1996. “I thought, here was a chance to study a medical specialty in its formative stages,” he says.
He still works as a hospitalist, although with limited clinical time. In addition to his administrative work as division chief, he directs the Center for Health and the Social Sciences at the University of Chicago. His research interests include cost-effectiveness, technology assessment, and information research.
In 2010, his poster “Effects of Hospitalists on 1-Year Post-Discharge Resource Utilization by Medicare Beneficiaries” took the top prize in the HM10 research competition. In 2011, he was appointed to the methodology committee of the federal Patient-Centered Outcomes Research Institute (PCORI), which was created by the Affordable Care Act to advise the government on clinical-effectiveness research. He also sits on the Advisory Council to the National Institute of General Medical Sciences at the Institute of Medicine, and on the Congressional Budget Office’s panel of health advisors.
In a career full of recognition, Dr. Meltzer says it’s hard to pinpoint the impact of winning the poster contest. But he has continued to submit abstracts to SHM every year and appreciates the opportunities for interaction with peers at the poster exhibits.
Title: Director of perioperative and consultative medicine
Institution: University of Michigan, Ann Arbor
Year: 2006
RIV: “Disseminated Histoplasmosis Presenting As Painful Oral Ulcers” (clinical vignettes)
Dr. Grant’s winning vignette presented a patient with a complex medical history, including heart disease and four months of painful oral ulcers, for which prior evaluations had been inconclusive, despite conducting biopsies. Following administration of high-dose corticosteroids, the patient’s condition worsened on multiple fronts. The vignette showed how the medical team was able to diagnose an unusual presentation of a fungal infection called histoplasmosis, which is prevalent in parts of the Midwest surrounding the Ohio and Mississippi river valleys.
“We see a lot of cases in the hospital where there are different angles you could take to turn it into a clinical vignette or a nice poster with good teaching points,” Dr. Grant says. “In this case, just digging deeper into the actual diagnosis was important because the empiric use of steroids can be fatal for some patients. Steroids are given for a lot of good reasons, but in this patient they caused immune suppression, allowing a smoldering infection to become very active.”
Dr. Grant did not submit the vignette for publication. “That was probably a mistake on my part,” he says, acknowledging the common complaint of too little time and too many competing priorities. But his interest in research has continued.
“I became involved at a national level with issues of perioperative medicine and last August published a textbook on the subject,” he reports.1 “VTE is another area of interest I have developed since my hospital medicine fellowship.”
He serves as the VTE resource expert on the Michigan Hospital Medicine Safety Consortium, a quality collaborative of more than 40 hospitals with Blue Cross/Blue Shield of Michigan. “It’s exciting to be able to look at the risk factors, what kinds of patients get VTEs, and whether they were appropriately prophylaxed in the hospital,” he says.
VTE is a national quality priority, and Dr. Grant expects abstracts to emerge from the consortium’s work.
He says he appreciates the opportunities that arise from participating in poster sessions at SHM, where medical students, residents, and working hospitalists talk to the presenters of interesting cases.
“It gives you a real back-and-forth, which is good for the person asking the question and for the presenter,” he says, noting hospitalists from other parts of the country were not as familiar with histoplasmosis.
He says winning the HM06 poster contest helped him “get his feet wet” and feel more prepared for a career in academic hospital medicine. “I’m sure the award solidified my employers’ satisfaction in hiring me—and in giving me more desirable academic roles and responsibilities,” he adds.
Title: Assistant professor of medicine pediatrics; director of the general internal-medicine comprehensive consultation service
Institution: Johns Hopkins Hospital, Baltimore
Year: 2009
RIV: “An Internet-Based Consult Curriculum for Hospitalists” (innovations)
Dr. Feldman’s poster described an online CME curriculum for hospitalists acting as medical consultants. The concept grew out of a perceived deficiency in his own medical education when, in 2004, he was asked to lead the consultation service at Johns Hopkins—just six months after finishing his residency.
“I had no idea what I was doing as a general-internal-medicine consultant,” he says. “I maybe received two weeks of experience as a consultant during my residency. I was willing to take it on, learning on the job and asking for help. But it occurred to me that I’m probably not alone in feeling unprepared.”
In his quest for self-education, Dr. Feldman wondered whether he should write a textbook on the subject. “But the information changes so quickly, I thought I’d have a better chance to reach people online,” he notes.
After talking to publishers and CME companies, he came up with the concept of learning modules on perioperative and consultative medicine topics, which could be taken online while earning CME credits. Johns Hopkins served as the CME certifier, and medical-education company Advanced Studies in Medicine joined as a partner. Once the project got off the ground, a medical advisory committee was convened.
“Winning the SHM poster competition is a great honor to have on a CV. It really helps to legitimize your name in the world of hospital medicine,” Dr. Feldman says. “It also provided confirmation that we were on the right track with the curriculum project. People valued what we were doing.”
Dr. Feldman and SHM have since become affiliated, and the “Consultative and Perioperative Medicine Essentials for Hospitalists” modules are available on SHM’s website (www.shmconsults.com). The site has 12,000 registered members completing 500 CME modules every month.
“I do a lot of the editing still,” Dr. Feldman says. “We update the modules every two years and are still creating new ones.”
Dr. Feldman also pursues a number of clinical-research interests, including resident education and costs of care.
Title: Assistant professor of medicine
Institution: Medical University of South Carolina, Charleston
Year: 2009
RIV: “Intensivists versus Hospitalists in the ICU: A Prospective Cohort Study Comparing Mortality and Length of Stay Between Two Staffing Models” (research) Citation: Wise KR, Akopov VA, Williams BR, Ido MS, Leeper KV, Dressler DD. Hospitalists and intensivists in the medical ICU: a prospective and observational study comparing mortality and length of stay between two staffing models. J Hosp Med. 2012;7(3):183-189.
Dr. Wise was recognized for research that began while she worked at Emory University in Atlanta, comparing hospitalists and intensivists in such outcomes as length of stay and mortality rates for patients in the ICU. The study was one of the first statistically rigorous examinations of this critical quality question. With an eye toward improving patient safety, national quality advocates such as the Leapfrog Group have called for hospitals to employ intensivists (critical-care specialists) to manage the care of ICU patients. In reality, Dr. Wise says, there aren’t enough intensivists to meet the need.
“Hospitalists are in the ICU anyway,” she says. “We just don’t have enough data to answer how well they do [in comparison to intensivists].”
Through a prospective cohort study of more than 1,000 patients, Dr. Wise’s group found that there was essentially no statistical difference in mortality rates between patients treated by intensivist teams or hospitalist ICU teams.
“We were also able to look at some of the intermediate-acuity patients—fairly complicated but not requiring ventilators,” she explains. “Our study wasn’t sufficiently powered for this subgroup, but it was an interesting piece of data to raise the question: Where should we deploy this scarce resource of intensivists? Which pockets of patients?”
Presenting her abstract at SHM’s annual meeting was a “good experience.”
“I’d done public speaking before, but never with an audience of about 500 people,” she says. “To go out there and field their questions was a real professional growing experience. Several people interested in the topic sought me out at the conference, introduced themselves, and we have subsequently stayed in touch.”
The manuscript published in JHM has been cited four times, including in a position paper from SHM and the Society of Critical Care Medicine.3 Another outgrowth of the research was being asked to contribute a chapter on hospitalists’ role in the ICU to a textbook on hospital medicine. Based on her still-fresh HM presentation, Dr. Wise was one of the few publicly identified experts on the subject. The chapter, co-authored by fellow Emory hospitalist Michael Heisler, MD, MPH, “The Role of the Hospitalist in Critical Care” was included in Principles and Practices of Hospital Medicine.4
Title: Neonatal intensivist
Institution: Stony Brook University Hospital, Great Neck, N.Y.
Year: 2006
RIV: “Administration of Inactivated Trivalent Influenza Vaccine (TIV) to Parents of Infants in the Neonatal Intensive Care Unit (NICU): A Novel Strategy to Increase Vaccination Rates” (innovations)
Citation: Shah SI, Caprio M, Hendricks-Munoz K. Administration of inactivated trivalent influenza vaccine to parents of high-risk infants in the neonatal intensive care unit. Pediatrics. 2007;120;e617-e621.
Dr. Shah was in his final year of a fellowship in neonatology at New York University when he took on the challenge of improving immunization access to protect premature, highly vulnerable patients in the NICU from influenza infections. Because these children are too young to be vaccinated directly, the concept of cocooning them from infection involves extending protection to everyone around them.
“We came up with the idea of offering flu vaccinations 24/7 in the NICU to the children’s parents,” he says. “It worked well for us as a way to define an indicated therapy for a defined population, even if it was a little outside the box. By the end of the flu season, 95% of the parents were vaccinated.”
SHM recognized the project as the top RIV innovations poster at HM06, but that was just the beginning.
“When I moved to SUNY Stony Brook, I continued to study and advocate for these vaccinations,” Dr. Shah says. “We were giving 500 to 700 vaccinations a year. Then I wrote a national resolution for the American Academy of Pediatrics, which was significant because it meant AAP was behind the project.”
Dr. Shah later became chair of AAP’s Long Island Chapter Legislative Committee and joined a statewide pediatric advocacy group. In 2009, the New York legislature enacted the Neonatal Influenza Protection Act, which required hospitals in the state to offer parents the vaccine, with Dr. Shah’s research and advocacy providing an essential basis for its passage. He’s even been recognized for his research in congressional citations.
Based on that success with influenza vaccinations, Dr. Shah and his colleagues looked at other diseases, starting with pertussis, and then tetanus, diphtheria, and whooping cough.5 All the while, they continued tracking immunization rates. A second state law, passed in 2011, added pertussis to the vaccinations. Next on his advocacy agenda is a project to promote smoking-cessation interventions in the NICU.6
“These parents come to see us every day,” he says. “What can we do, through the parents, to promote the health and well-being of their high-risk newborns?”
Title: Assistant professor of medicine; medical director of inpatient palliative-care consultation
Institution: University of Texas Health Sciences Center, San Antonio
Year: 2009
RIV: “When to Depend on the Kinins of Strangers: An Unusual Case of Abdominal Pain” (clinical vignettes)
Publication: An article on the ethics of determining code status for patients with advanced cancer and a book chapter on the “last hours of life” for a forthcoming book on palliative care and hospital medicine.
As a medical resident, Dr. Morrow met a 27-year-old woman who had chronic abdominal pain and had made multiple visits to the ED for this complaint. The patient had a history of substance abuse and requested dilaudid for her pain—making it easy for staff to consign her to the stereotype of the difficult patient.
“I met her after an interesting finding,” he says. “It turns out that on the previous emergency room visit, she received a CAT scan, which showed duodenal and small-bowel thickening consistent with hereditary angioedema, although with an unusual presentation. As it happened, we had onsite a world expert in angioedema.”
The expert was able to confirm the diagnosis, Dr. Morrow says.
“By giving her this ‘legitimate,’ organic diagnosis, it just changed the whole dynamic of her relationship with her doctors,” he says. “She knew that they knew something was really wrong. The residents were empowered to have something to hang their hats on. And we were able to get better control of her pain.”
Dr. Morrow says he came on the scene late in the discovery process, but he helped to solve the puzzle, and then put together the abstract and poster that told the story of making the diagnosis.
“In my previous job, I was hired as a hospitalist but helped to build the palliative-care program within the hospital-medicine service,” he says. “In my current job, I was brought in to build the inpatient palliative-care-consultation service, although I still moonlight as a hospitalist to stay sharp.”
Dr. Morrow says he enjoys sharing stories of difficult cases and submitting case studies about them to medical conferences, often with clever titles incorporating puns (e.g. the 2009 SHM poster citing kinins, polypeptides in the blood that cause inflammation). Another example is “The Angina Monologues,” a story of an 82-year-old patient with chronic angina pectoris and complex pain syndromes that were difficult to bring under control. Palliative care also emphasizes patients’ stories, he says, in order to understand the person behind the diagnosis.
Larry Beresford is a freelance writer in San Francisco. References available at www.the-hospitalist.org.
References
2. Yoder J. Association between hospital noise levels and inpatient sleep among middle-aged and older adults: Far from a quiet night. Abstract, Society of Hospital Medicine, 2011.
3. McKean SC, Ross JJ, Dressler DD, Brotman DJ, Ginsberg JS. Principles and Practice of Hospital Medicine. McGraw-Hill Medical; New York City: 2012.
4. Siegal EM, Dressler DD, Dichter JR, Gorman MJ, Lipsett PA. Training a hospitalist workforce to address the intensivist shortage in American hospitals: a position paper from the Society of Hospital Medicine and the Society of Critical Care Medicine. J Hosp Med. 2012;7:359-364.
5. Dylag A, Shah SI. Administration of tetanus, diphtheria, and acellular pertussis vaccine to parents of high-risk infants in the neonatal intensive care unit. Pediatrics. 2008;122:e550-e555.
6. Shah S. Smoking cessation counseling and PPSV 23-valent pneumococcal polysaccharide vaccine administration parents of neonatal intensive care unit (NICU)-admitted infants: A life-changing opportunity. J Neonatal-Perinatal Med. 2011;4:263-267.
Medicare Penalties Make Hospital-Acquired-Infection Solutions a Priority
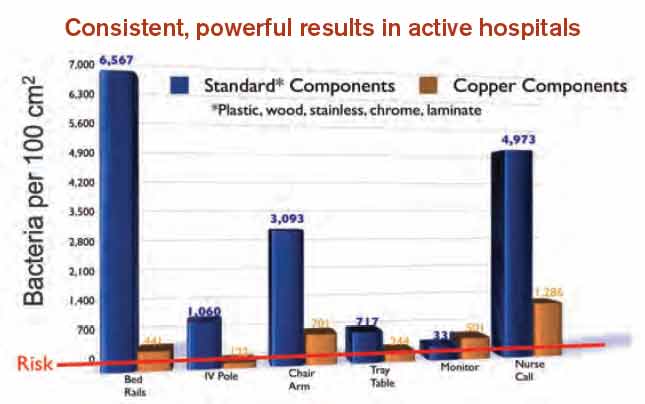
A shift in governmental regulations regarding reimbursement for hospital-acquired infections (HAIs) is forcing hospitals to take a closer look at how to reduce them. A recent study in Infection Control and Hospital Epidemiology shows that copper-alloy surfaces may be one such solution.3 According to the study, although only 9% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases.1
“Before these regulations, hospitals didn’t necessarily want technology to decrease HAI rates, because the more infections and complications, the longer the length of patient stay, the greater the reimbursement, and the better the bottom line,” says Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association.
Three regulations that have resulted in reimbursements to hospitals getting cut include:
- The Deficit Reduction Act of 2005, which was implemented on Oct. 1, 2008, which states that Medicare will not reimburse for certain types of HAIs;
- Section 3025 of the Affordable Care Act (signed into law in 2010), which incentivizes hospitals to decrease their readmission rates, which frequently are caused by HAIs. Beginning this fall, hospitals are getting reduced reimbursement when their readmission rates exceed a certain threshold. The maximum penalty in 2013 is 1% and will increase to 3% by 2015; and
- Section 1886 of the Affordable Care Act, which describes value-based purchasing and makes hospitals eligible to receive incentive payments for achieving better care on certain quality metrics. Funding for the program comes from withholding payment from poor-performing hospitals. The financial impact to hospitals started this year. In 2014, urinary tract infections and vascular-catheter-associated infections will be among the targeted conditions measured by CMS to calculate incentives and penalties.
“Hospitals are now feeling a direct impact from all of this,” Dr. Georgiou says. “Back in 2008, hospitals were noticing, but it was hard to get their attention since only one program was impacting their bottom line. But, pretty soon, hospitals risk losing upwards of 5% of their Medicare reimbursement for decreased quality.
“Reducing HAIs is clearly on the priority list of chief operating officers. They are very aware of the impact to their bottom line. They are looking to their vendors and suppliers to develop strategies to work with their hospitals to improve performance around these metrics.”
Karen Appold is a freelance writer in Pennsylvania.
A shift in governmental regulations regarding reimbursement for hospital-acquired infections (HAIs) is forcing hospitals to take a closer look at how to reduce them. A recent study in Infection Control and Hospital Epidemiology shows that copper-alloy surfaces may be one such solution.3 According to the study, although only 9% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases.1
“Before these regulations, hospitals didn’t necessarily want technology to decrease HAI rates, because the more infections and complications, the longer the length of patient stay, the greater the reimbursement, and the better the bottom line,” says Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association.
Three regulations that have resulted in reimbursements to hospitals getting cut include:
- The Deficit Reduction Act of 2005, which was implemented on Oct. 1, 2008, which states that Medicare will not reimburse for certain types of HAIs;
- Section 3025 of the Affordable Care Act (signed into law in 2010), which incentivizes hospitals to decrease their readmission rates, which frequently are caused by HAIs. Beginning this fall, hospitals are getting reduced reimbursement when their readmission rates exceed a certain threshold. The maximum penalty in 2013 is 1% and will increase to 3% by 2015; and
- Section 1886 of the Affordable Care Act, which describes value-based purchasing and makes hospitals eligible to receive incentive payments for achieving better care on certain quality metrics. Funding for the program comes from withholding payment from poor-performing hospitals. The financial impact to hospitals started this year. In 2014, urinary tract infections and vascular-catheter-associated infections will be among the targeted conditions measured by CMS to calculate incentives and penalties.
“Hospitals are now feeling a direct impact from all of this,” Dr. Georgiou says. “Back in 2008, hospitals were noticing, but it was hard to get their attention since only one program was impacting their bottom line. But, pretty soon, hospitals risk losing upwards of 5% of their Medicare reimbursement for decreased quality.
“Reducing HAIs is clearly on the priority list of chief operating officers. They are very aware of the impact to their bottom line. They are looking to their vendors and suppliers to develop strategies to work with their hospitals to improve performance around these metrics.”
Karen Appold is a freelance writer in Pennsylvania.
A shift in governmental regulations regarding reimbursement for hospital-acquired infections (HAIs) is forcing hospitals to take a closer look at how to reduce them. A recent study in Infection Control and Hospital Epidemiology shows that copper-alloy surfaces may be one such solution.3 According to the study, although only 9% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases.1
“Before these regulations, hospitals didn’t necessarily want technology to decrease HAI rates, because the more infections and complications, the longer the length of patient stay, the greater the reimbursement, and the better the bottom line,” says Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association.
Three regulations that have resulted in reimbursements to hospitals getting cut include:
- The Deficit Reduction Act of 2005, which was implemented on Oct. 1, 2008, which states that Medicare will not reimburse for certain types of HAIs;
- Section 3025 of the Affordable Care Act (signed into law in 2010), which incentivizes hospitals to decrease their readmission rates, which frequently are caused by HAIs. Beginning this fall, hospitals are getting reduced reimbursement when their readmission rates exceed a certain threshold. The maximum penalty in 2013 is 1% and will increase to 3% by 2015; and
- Section 1886 of the Affordable Care Act, which describes value-based purchasing and makes hospitals eligible to receive incentive payments for achieving better care on certain quality metrics. Funding for the program comes from withholding payment from poor-performing hospitals. The financial impact to hospitals started this year. In 2014, urinary tract infections and vascular-catheter-associated infections will be among the targeted conditions measured by CMS to calculate incentives and penalties.
“Hospitals are now feeling a direct impact from all of this,” Dr. Georgiou says. “Back in 2008, hospitals were noticing, but it was hard to get their attention since only one program was impacting their bottom line. But, pretty soon, hospitals risk losing upwards of 5% of their Medicare reimbursement for decreased quality.
“Reducing HAIs is clearly on the priority list of chief operating officers. They are very aware of the impact to their bottom line. They are looking to their vendors and suppliers to develop strategies to work with their hospitals to improve performance around these metrics.”
Karen Appold is a freelance writer in Pennsylvania.
Medical Training Programs Adapt to Duty-Hour Changes
A new study that showed no long-term decrease in patient outcomes after landmark 2003 reforms could portend good news for the latest duty-hour regulations implemented in 2011.
The Journal of General Internal Medicine report, “Teaching Hospital Five-Year Mortality Trends in the Wake of Duty Hour Reforms,” found that the 2003 changes were associated with “no significant change in mortality in the early years after implementation, and with a trend toward improved mortality among medical patients in the fourth and fifth years.” One of the authors says it’s not evident whether the improved outcomes are because of the reforms.
“We don’t think it’s an effect of work-hour reforms itself, but more likely a marker that teaching hospitals are staying ahead of the curve in general,” says Patrick Romano, MD, MPH, FACP, FAAP, a professor of medicine and pediatrics at the University of California at Davis School of Medicine in Sacramento.
Dr. Romano, who along with colleagues has been studying duty-hour reforms for years, says the new research shows that teaching hospitals were able to adapt over the long term to staffing rules. Researchers are now curious how health care will adapt to the more restrictive 2011 changes promulgated by the Accreditation Council for Graduate Medical Education (ACGME), which mostly limits first-year residents to a maximum 16-hour shift and older residents to 24 hours.
“Even though there were more handoffs [caused by the 2003 reforms], even though there were more opportunities for error due to handoffs, teaching hospitals were able to update,” Dr. Romano says. “Maybe that’s optimistic for 2011.
“Is the glass half full or half empty?”
Visit our website for more information on duty hours.
A new study that showed no long-term decrease in patient outcomes after landmark 2003 reforms could portend good news for the latest duty-hour regulations implemented in 2011.
The Journal of General Internal Medicine report, “Teaching Hospital Five-Year Mortality Trends in the Wake of Duty Hour Reforms,” found that the 2003 changes were associated with “no significant change in mortality in the early years after implementation, and with a trend toward improved mortality among medical patients in the fourth and fifth years.” One of the authors says it’s not evident whether the improved outcomes are because of the reforms.
“We don’t think it’s an effect of work-hour reforms itself, but more likely a marker that teaching hospitals are staying ahead of the curve in general,” says Patrick Romano, MD, MPH, FACP, FAAP, a professor of medicine and pediatrics at the University of California at Davis School of Medicine in Sacramento.
Dr. Romano, who along with colleagues has been studying duty-hour reforms for years, says the new research shows that teaching hospitals were able to adapt over the long term to staffing rules. Researchers are now curious how health care will adapt to the more restrictive 2011 changes promulgated by the Accreditation Council for Graduate Medical Education (ACGME), which mostly limits first-year residents to a maximum 16-hour shift and older residents to 24 hours.
“Even though there were more handoffs [caused by the 2003 reforms], even though there were more opportunities for error due to handoffs, teaching hospitals were able to update,” Dr. Romano says. “Maybe that’s optimistic for 2011.
“Is the glass half full or half empty?”
Visit our website for more information on duty hours.
A new study that showed no long-term decrease in patient outcomes after landmark 2003 reforms could portend good news for the latest duty-hour regulations implemented in 2011.
The Journal of General Internal Medicine report, “Teaching Hospital Five-Year Mortality Trends in the Wake of Duty Hour Reforms,” found that the 2003 changes were associated with “no significant change in mortality in the early years after implementation, and with a trend toward improved mortality among medical patients in the fourth and fifth years.” One of the authors says it’s not evident whether the improved outcomes are because of the reforms.
“We don’t think it’s an effect of work-hour reforms itself, but more likely a marker that teaching hospitals are staying ahead of the curve in general,” says Patrick Romano, MD, MPH, FACP, FAAP, a professor of medicine and pediatrics at the University of California at Davis School of Medicine in Sacramento.
Dr. Romano, who along with colleagues has been studying duty-hour reforms for years, says the new research shows that teaching hospitals were able to adapt over the long term to staffing rules. Researchers are now curious how health care will adapt to the more restrictive 2011 changes promulgated by the Accreditation Council for Graduate Medical Education (ACGME), which mostly limits first-year residents to a maximum 16-hour shift and older residents to 24 hours.
“Even though there were more handoffs [caused by the 2003 reforms], even though there were more opportunities for error due to handoffs, teaching hospitals were able to update,” Dr. Romano says. “Maybe that’s optimistic for 2011.
“Is the glass half full or half empty?”
Visit our website for more information on duty hours.
Steroids May Increase Venous Thromboembolism Risk
Clinical question: Is exogenous glucocorticoid administration associated with an increased risk of VTE?
Background: Endogenous hypercortisolism is linked to increased VTE rates, and pathophysiologic data exist to suggest glucocorticoids increase clotting, but few studies have measured the clinical link between glucocorticoid administration and VTE events.
Study design: Case-control study.
Setting: Denmark.
Synopsis: The authors analyzed Danish national registries, which include information on diagnoses and prescriptions. The study selection period was Jan. 1, 2005, to Dec. 31, 2011. During this period, 38,675 cases of VTE (both DVT and pulmonary embolism) were identified in the population of Denmark. These cases were matched with 387,650 controls. Three routes of glucocorticoid use were studied: systemic (oral and intravenous), inhaled, and intestinal-acting. Cases were classified as present (within 90 days of VTE event), recent (within 91 to 365 days), or former (more than 365 days prior) users of glucocorticoids. Categories were also created for new versus continuous users.
Glucocorticoid use was associated with a significant increase in VTE occurrence. The strongest link was in new and recent users, and the effect diminished over time. Key limitations of the study included its reliance on registry data, as well as the fact that cases had more comorbid conditions than controls (e.g. recent infection, chronic illnesses).
Bottom line: Recipients of glucocorticoids had an increased risk of VTE; the effect was strongest in new and recent users.
Citation: Johannesdottir SA, Horvath-Puho E, Dekkers OM, et al. Use of glucocorticoids and risk of venous thromboembolism. JAMA Intern Med. 2013;173(9):743-752.
Visit our website for more physician reviews of recent HM-relevant literature.
Clinical question: Is exogenous glucocorticoid administration associated with an increased risk of VTE?
Background: Endogenous hypercortisolism is linked to increased VTE rates, and pathophysiologic data exist to suggest glucocorticoids increase clotting, but few studies have measured the clinical link between glucocorticoid administration and VTE events.
Study design: Case-control study.
Setting: Denmark.
Synopsis: The authors analyzed Danish national registries, which include information on diagnoses and prescriptions. The study selection period was Jan. 1, 2005, to Dec. 31, 2011. During this period, 38,675 cases of VTE (both DVT and pulmonary embolism) were identified in the population of Denmark. These cases were matched with 387,650 controls. Three routes of glucocorticoid use were studied: systemic (oral and intravenous), inhaled, and intestinal-acting. Cases were classified as present (within 90 days of VTE event), recent (within 91 to 365 days), or former (more than 365 days prior) users of glucocorticoids. Categories were also created for new versus continuous users.
Glucocorticoid use was associated with a significant increase in VTE occurrence. The strongest link was in new and recent users, and the effect diminished over time. Key limitations of the study included its reliance on registry data, as well as the fact that cases had more comorbid conditions than controls (e.g. recent infection, chronic illnesses).
Bottom line: Recipients of glucocorticoids had an increased risk of VTE; the effect was strongest in new and recent users.
Citation: Johannesdottir SA, Horvath-Puho E, Dekkers OM, et al. Use of glucocorticoids and risk of venous thromboembolism. JAMA Intern Med. 2013;173(9):743-752.
Visit our website for more physician reviews of recent HM-relevant literature.
Clinical question: Is exogenous glucocorticoid administration associated with an increased risk of VTE?
Background: Endogenous hypercortisolism is linked to increased VTE rates, and pathophysiologic data exist to suggest glucocorticoids increase clotting, but few studies have measured the clinical link between glucocorticoid administration and VTE events.
Study design: Case-control study.
Setting: Denmark.
Synopsis: The authors analyzed Danish national registries, which include information on diagnoses and prescriptions. The study selection period was Jan. 1, 2005, to Dec. 31, 2011. During this period, 38,675 cases of VTE (both DVT and pulmonary embolism) were identified in the population of Denmark. These cases were matched with 387,650 controls. Three routes of glucocorticoid use were studied: systemic (oral and intravenous), inhaled, and intestinal-acting. Cases were classified as present (within 90 days of VTE event), recent (within 91 to 365 days), or former (more than 365 days prior) users of glucocorticoids. Categories were also created for new versus continuous users.
Glucocorticoid use was associated with a significant increase in VTE occurrence. The strongest link was in new and recent users, and the effect diminished over time. Key limitations of the study included its reliance on registry data, as well as the fact that cases had more comorbid conditions than controls (e.g. recent infection, chronic illnesses).
Bottom line: Recipients of glucocorticoids had an increased risk of VTE; the effect was strongest in new and recent users.
Citation: Johannesdottir SA, Horvath-Puho E, Dekkers OM, et al. Use of glucocorticoids and risk of venous thromboembolism. JAMA Intern Med. 2013;173(9):743-752.
Visit our website for more physician reviews of recent HM-relevant literature.
Team Approach Vital to Treating Patients with Mental Illness
A recent report about medication management for hospitalized patients with psychiatric comorbidities shows that collaboration between hospitalists and specialists is key to improving the care of these patients.
The paper, "Challenges in Pharmacologic Management of the Hospitalized Patient with Psychiatric Comorbidity," suggests that "when making complex psychopharmacologic decisions," hospitalists should collaborate with pharmacists and psychiatrists. The study aims to help hospitalists make informed decisions when considering whether to continue home psychotropic medication in medically ill patients.
Martha Ward, MD, assistant professor in the department of psychiatry and behavioral sciences at Emory University School of Medicine in Atlanta and lead author of the study, says hospitalists are rightly focused on the acute problem in front of them, and they sometimes do not have time to address chronic, nonemergent issues, such as a psychiatric comorbidity.
"It's a mindset," Dr. Ward says. "At times when you're focused minute to minute on an emergent issue, it can be difficult to look at the chronic issues that don't come to the forefront."
Dr. Ward says it's important for hospitalists to never "reflexively discontinue" medications for patients with mental illness. Instead, she suggests weighing the risks and benefits of how existing medications would interact with new treatments.
Working with pharmacists, psychiatrists, or even tapping online resources that provide information about drug interactions is a good first step, she adds. Otherwise, physicians risk introducing complicating factors, such as potential adverse events related to psychiatric decompensation or psychotropic drug withdrawal.
Over the long term, Dr. Ward says, hospitalists should be educated in psychiatry, starting in medical school and in residency. "I'm somewhat biased," adds Dr. Ward, who is trained in both internal medicine and psychiatry. "I think internal-medicine doctors could benefit greatly from additional training. I think that's one of the biggest deficiencies in our curriculum."
Visit our website for more information about hospital medicine and psychiatry.
A recent report about medication management for hospitalized patients with psychiatric comorbidities shows that collaboration between hospitalists and specialists is key to improving the care of these patients.
The paper, "Challenges in Pharmacologic Management of the Hospitalized Patient with Psychiatric Comorbidity," suggests that "when making complex psychopharmacologic decisions," hospitalists should collaborate with pharmacists and psychiatrists. The study aims to help hospitalists make informed decisions when considering whether to continue home psychotropic medication in medically ill patients.
Martha Ward, MD, assistant professor in the department of psychiatry and behavioral sciences at Emory University School of Medicine in Atlanta and lead author of the study, says hospitalists are rightly focused on the acute problem in front of them, and they sometimes do not have time to address chronic, nonemergent issues, such as a psychiatric comorbidity.
"It's a mindset," Dr. Ward says. "At times when you're focused minute to minute on an emergent issue, it can be difficult to look at the chronic issues that don't come to the forefront."
Dr. Ward says it's important for hospitalists to never "reflexively discontinue" medications for patients with mental illness. Instead, she suggests weighing the risks and benefits of how existing medications would interact with new treatments.
Working with pharmacists, psychiatrists, or even tapping online resources that provide information about drug interactions is a good first step, she adds. Otherwise, physicians risk introducing complicating factors, such as potential adverse events related to psychiatric decompensation or psychotropic drug withdrawal.
Over the long term, Dr. Ward says, hospitalists should be educated in psychiatry, starting in medical school and in residency. "I'm somewhat biased," adds Dr. Ward, who is trained in both internal medicine and psychiatry. "I think internal-medicine doctors could benefit greatly from additional training. I think that's one of the biggest deficiencies in our curriculum."
Visit our website for more information about hospital medicine and psychiatry.
A recent report about medication management for hospitalized patients with psychiatric comorbidities shows that collaboration between hospitalists and specialists is key to improving the care of these patients.
The paper, "Challenges in Pharmacologic Management of the Hospitalized Patient with Psychiatric Comorbidity," suggests that "when making complex psychopharmacologic decisions," hospitalists should collaborate with pharmacists and psychiatrists. The study aims to help hospitalists make informed decisions when considering whether to continue home psychotropic medication in medically ill patients.
Martha Ward, MD, assistant professor in the department of psychiatry and behavioral sciences at Emory University School of Medicine in Atlanta and lead author of the study, says hospitalists are rightly focused on the acute problem in front of them, and they sometimes do not have time to address chronic, nonemergent issues, such as a psychiatric comorbidity.
"It's a mindset," Dr. Ward says. "At times when you're focused minute to minute on an emergent issue, it can be difficult to look at the chronic issues that don't come to the forefront."
Dr. Ward says it's important for hospitalists to never "reflexively discontinue" medications for patients with mental illness. Instead, she suggests weighing the risks and benefits of how existing medications would interact with new treatments.
Working with pharmacists, psychiatrists, or even tapping online resources that provide information about drug interactions is a good first step, she adds. Otherwise, physicians risk introducing complicating factors, such as potential adverse events related to psychiatric decompensation or psychotropic drug withdrawal.
Over the long term, Dr. Ward says, hospitalists should be educated in psychiatry, starting in medical school and in residency. "I'm somewhat biased," adds Dr. Ward, who is trained in both internal medicine and psychiatry. "I think internal-medicine doctors could benefit greatly from additional training. I think that's one of the biggest deficiencies in our curriculum."
Visit our website for more information about hospital medicine and psychiatry.
Hospital to Gauge Health Benefits of Therapeutic Garden
A hospital in Portland, Ore., has received a $560,000 grant from the TKF Foundation to design and build a therapeutic 6,800-square-foot, four-seasons garden onsite, then measure stress levels among patients, family, visitors, and staff members who go to it.
Legacy Emanuel Medical Center was awarded one of six National Open Spaces Sacred Places grants last June. The center is part of the six-hospital Legacy Health system, which serves the greater Portland region and Vancouver, Wash., and has a history of innovative green spaces connected with its hospital and hospice facilities, explains Teresia Hazen, MEd, HTR, QMHP, a registered horticultural therapist, Legacy’s director of therapeutic gardens, and the grant’s project manager.
The garden will be built in an open-air terrace between the hospital's family birth center and cardiovascular ICU. Grant funding will support incorporating such design elements as portals and pathways, public spaces, and areas where visitors can have some privacy, reflecting therapeutic garden characteristics defined by the American Horticultural Therapy Association, Hazen says. Researchers will then monitor the stress levels and heart rates of expectant mothers and their babies in utero, family members visiting ICU patients, and hospital staff members who spend time in the hospital garden.
Isadora Roth, MD, a hospitalist at two Legacy Health hospitals, appreciates the availability of hospital gardens for her patients and herself. "I often see patients out there, and they seem happier, more relaxed, and less anxious," Dr. Roth says. "I really think it has therapeutic benefits."
The new garden is scheduled to be completed in December; data will start to be gathered next April, Hazen says. Legacy also is planning a Therapeutic Landscapes Symposium on April 4, 2014, in Portland.
Visit our website for more information on stress and hospitalists.
A hospital in Portland, Ore., has received a $560,000 grant from the TKF Foundation to design and build a therapeutic 6,800-square-foot, four-seasons garden onsite, then measure stress levels among patients, family, visitors, and staff members who go to it.
Legacy Emanuel Medical Center was awarded one of six National Open Spaces Sacred Places grants last June. The center is part of the six-hospital Legacy Health system, which serves the greater Portland region and Vancouver, Wash., and has a history of innovative green spaces connected with its hospital and hospice facilities, explains Teresia Hazen, MEd, HTR, QMHP, a registered horticultural therapist, Legacy’s director of therapeutic gardens, and the grant’s project manager.
The garden will be built in an open-air terrace between the hospital's family birth center and cardiovascular ICU. Grant funding will support incorporating such design elements as portals and pathways, public spaces, and areas where visitors can have some privacy, reflecting therapeutic garden characteristics defined by the American Horticultural Therapy Association, Hazen says. Researchers will then monitor the stress levels and heart rates of expectant mothers and their babies in utero, family members visiting ICU patients, and hospital staff members who spend time in the hospital garden.
Isadora Roth, MD, a hospitalist at two Legacy Health hospitals, appreciates the availability of hospital gardens for her patients and herself. "I often see patients out there, and they seem happier, more relaxed, and less anxious," Dr. Roth says. "I really think it has therapeutic benefits."
The new garden is scheduled to be completed in December; data will start to be gathered next April, Hazen says. Legacy also is planning a Therapeutic Landscapes Symposium on April 4, 2014, in Portland.
Visit our website for more information on stress and hospitalists.
A hospital in Portland, Ore., has received a $560,000 grant from the TKF Foundation to design and build a therapeutic 6,800-square-foot, four-seasons garden onsite, then measure stress levels among patients, family, visitors, and staff members who go to it.
Legacy Emanuel Medical Center was awarded one of six National Open Spaces Sacred Places grants last June. The center is part of the six-hospital Legacy Health system, which serves the greater Portland region and Vancouver, Wash., and has a history of innovative green spaces connected with its hospital and hospice facilities, explains Teresia Hazen, MEd, HTR, QMHP, a registered horticultural therapist, Legacy’s director of therapeutic gardens, and the grant’s project manager.
The garden will be built in an open-air terrace between the hospital's family birth center and cardiovascular ICU. Grant funding will support incorporating such design elements as portals and pathways, public spaces, and areas where visitors can have some privacy, reflecting therapeutic garden characteristics defined by the American Horticultural Therapy Association, Hazen says. Researchers will then monitor the stress levels and heart rates of expectant mothers and their babies in utero, family members visiting ICU patients, and hospital staff members who spend time in the hospital garden.
Isadora Roth, MD, a hospitalist at two Legacy Health hospitals, appreciates the availability of hospital gardens for her patients and herself. "I often see patients out there, and they seem happier, more relaxed, and less anxious," Dr. Roth says. "I really think it has therapeutic benefits."
The new garden is scheduled to be completed in December; data will start to be gathered next April, Hazen says. Legacy also is planning a Therapeutic Landscapes Symposium on April 4, 2014, in Portland.
Visit our website for more information on stress and hospitalists.
Listen to John Vazquez, MD, discuss neurophobia and tips for adjusting to discomfort in treating neuro patients
Click here to listen to more of our interview with Dr. Vazquez
Click here to listen to more of our interview with Dr. Vazquez
Click here to listen to more of our interview with Dr. Vazquez
“Telestroke” care and “teleneurology” give hospitalists additional resources
To deal with the demand for neurologists, hospitals are increasingly turning to a new idea: patching a neurologist into the exam room from afar, Skype-style. This approach to caring for patients with strokes and other neurologic conditions—“telestroke” care or “teleneurology”—is an emerging valuable resource, says Edgar Kenton, MD, who is in the process of expanding such a system at Geisinger Health System in Danville, Pa.
It’s a hub-and-spoke system, with a central hospital as the “hub” and other hospitals as the “spokes” that connect with the hub, using computers and real-time video. Geisinger has six spokes, with plans for about another half-dozen.
“We’re able to talk to the physician, we can see the patient, we can see the families if they’re there, and get a lot of information,” says Dr. Kenton, director of the stroke program at Geisinger.
It’s crucial to see patients when they’re suspected of having stroke symptoms, he says, so that the neurologist can get crucial insight they can’t get over the phone. With a laptop, tablet, or smartphone, the neurologist can do a consult regardless of location.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says he expects that one paradoxical effect of telestroke care is that more patients with neurological conditions ultimately will end up under the care of hospitalists. That’s because centers will be more likely to take on a patient, consult with a neurologist using telestroke care or teleneurology, then admit the patient—after the neurologist has logged off.
“I do think that we are going to see an increase in the number of neurologic-type patients that are cared for primarily by hospitalists,” he says. “I’m there for the acute consultation. But often those patients are then subsequently admitted to a hospitalist service for the very reason that I was called. They don’t have local resources for neurology or a neurohospitalist.
“I actually think there’s going to be more involvement on the hospitalist front for neurologic patients, even patients with neurologic emergencies, because of telemedicine,” Dr. Barrett says. TH
Tom Collins is a freelance writer in South Florida.
To deal with the demand for neurologists, hospitals are increasingly turning to a new idea: patching a neurologist into the exam room from afar, Skype-style. This approach to caring for patients with strokes and other neurologic conditions—“telestroke” care or “teleneurology”—is an emerging valuable resource, says Edgar Kenton, MD, who is in the process of expanding such a system at Geisinger Health System in Danville, Pa.
It’s a hub-and-spoke system, with a central hospital as the “hub” and other hospitals as the “spokes” that connect with the hub, using computers and real-time video. Geisinger has six spokes, with plans for about another half-dozen.
“We’re able to talk to the physician, we can see the patient, we can see the families if they’re there, and get a lot of information,” says Dr. Kenton, director of the stroke program at Geisinger.
It’s crucial to see patients when they’re suspected of having stroke symptoms, he says, so that the neurologist can get crucial insight they can’t get over the phone. With a laptop, tablet, or smartphone, the neurologist can do a consult regardless of location.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says he expects that one paradoxical effect of telestroke care is that more patients with neurological conditions ultimately will end up under the care of hospitalists. That’s because centers will be more likely to take on a patient, consult with a neurologist using telestroke care or teleneurology, then admit the patient—after the neurologist has logged off.
“I do think that we are going to see an increase in the number of neurologic-type patients that are cared for primarily by hospitalists,” he says. “I’m there for the acute consultation. But often those patients are then subsequently admitted to a hospitalist service for the very reason that I was called. They don’t have local resources for neurology or a neurohospitalist.
“I actually think there’s going to be more involvement on the hospitalist front for neurologic patients, even patients with neurologic emergencies, because of telemedicine,” Dr. Barrett says. TH
Tom Collins is a freelance writer in South Florida.
To deal with the demand for neurologists, hospitals are increasingly turning to a new idea: patching a neurologist into the exam room from afar, Skype-style. This approach to caring for patients with strokes and other neurologic conditions—“telestroke” care or “teleneurology”—is an emerging valuable resource, says Edgar Kenton, MD, who is in the process of expanding such a system at Geisinger Health System in Danville, Pa.
It’s a hub-and-spoke system, with a central hospital as the “hub” and other hospitals as the “spokes” that connect with the hub, using computers and real-time video. Geisinger has six spokes, with plans for about another half-dozen.
“We’re able to talk to the physician, we can see the patient, we can see the families if they’re there, and get a lot of information,” says Dr. Kenton, director of the stroke program at Geisinger.
It’s crucial to see patients when they’re suspected of having stroke symptoms, he says, so that the neurologist can get crucial insight they can’t get over the phone. With a laptop, tablet, or smartphone, the neurologist can do a consult regardless of location.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says he expects that one paradoxical effect of telestroke care is that more patients with neurological conditions ultimately will end up under the care of hospitalists. That’s because centers will be more likely to take on a patient, consult with a neurologist using telestroke care or teleneurology, then admit the patient—after the neurologist has logged off.
“I do think that we are going to see an increase in the number of neurologic-type patients that are cared for primarily by hospitalists,” he says. “I’m there for the acute consultation. But often those patients are then subsequently admitted to a hospitalist service for the very reason that I was called. They don’t have local resources for neurology or a neurohospitalist.
“I actually think there’s going to be more involvement on the hospitalist front for neurologic patients, even patients with neurologic emergencies, because of telemedicine,” Dr. Barrett says. TH
Tom Collins is a freelance writer in South Florida.