User login
Speakers at HM13 Stress Overarching Reform, Day-to-Day Implementation

To some HM13 attendees, the keynote speakers might have seemed to be talking about different things.
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Center for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services (CMS), hinted at promising results from the first accountable-care organizations (ACOs) and noted a meaningful reduction in 30-day readmission rates for the first time in years.
David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, told hospitalists that unless they’re getting patient care right every time, they’re not getting it right enough. And nothing would make him happier than seeing fewer hospitalists at SHM’s annual meeting—because that would mean fewer hospitalized patients.
HM pioneer Bob Wachter, MD, MHM, said it’s time for hospitalists to link their quality-improvement (QI) efforts and safety acumen to projects focused on cutting costs and reducing waste in the health-care system.
So while each made their points in a different way, each plenary speaker left many meeting-goers with a similar thought: Hospitalists are positioned at the nexus of big-picture reform and day-to-day implementation. So if hospitalists as a specialty continue to embrace teamwork, evidence-based practice, quality, safety, and a sense that the patient comes first, they will cement themselves as leaders in the next iteration of health-care delivery.
“There is enormous change going on in the healthcare system,” says SHM CEO Larry Wellikson. “And we are right in the middle of this. We are essential. If we are bad, we are going to sink it. And if we’re great, we are going to take it to another level.”
Needle Movement
Dr. Conway said some of that progress already is evident. He disclosed that initial findings from the first data sets coming from the first ACOs are showing promising results, though he can’t go into detail until the information is publicly released. However, he did boast that after decades of Medicare readmission rates hovering around 19%, data from late 2012 and early 2013 show that figure has dropped to below 18%.
“That is a 1.5% to 2% shift in readmissions nationally,” he said. “It is a credit to the work you and others are doing in the field. That’s hundreds of thousands of Medicare beneficiaries that are not readmitted every year, that stay home healthy. … It’s a tremendous example of moving a national needle.”
He dismissed those who attribute the initial readmission progress solely to penalties instituted on readmissions, though he acknowledged that CMS is using both carrots and sticks to push change.

“It’s a combination of interventions,” he said.
And all of those initiatives must be aimed jointly at improving the patient experience, said Dr. Feinberg, a child psychiatrist by training whose mantra is “patient-centeredness.” Dr. Feinberg’s reputation is that of a physician-administrator who puts patients first. For example, even though his health system (www.uclahealth.org) is in the 99th percentile for patient satisfaction, he is unhappy. That’s because the top ranking means roughly 85 out of every 100 patients served are pretty happy with their experience.
“It means that we’re the cream of the crap,” he said. “Of the last 100 people we took care of, 15 of them—and, by definition, those 15 people are someone’s mom, someone’s brother, someone’s coworker—would not refer us to a friend, or rate us a 9 or 10. So, I think, while we’ve really moved the needle, we’re really not done until we get it right with every patient, every time.”
He added that those who argue against difficult or time-consuming innovations and improvements that better patient care are arguing against the moral high ground of how they would want a family member to be treated in the hospital.
“The pushback I hear is, ‘Some of this stuff is unpreventable,’” Dr. Feinberg said. “Well, maybe it’s unpreventable the way we’re doing it now. But maybe we need to think differently. Maybe it is unpreventable, but if this decreases the prevalence, or makes it better, then to me, it’s important to do.”
Dr. Feinberg, who took over as UCLA Health System’s president in 2011, says he still spends several hours every day talking to patients. For those who say there’s not enough time to stay connected to patients and that all the time spent making sure patients are happy takes away from other activities, he says they’re forgetting what brought them into medicine in the first place: healing. He blames the delivery system for stifling what he believes is a provider’s desire to help people.
“We haven’t allowed the culture to come out,” he said. “I think it’s there.”

Dr. Wachter has a similar faith in the hospitalist culture—although his is based in the pluripotent nature of the specialty. Hospitalists have worked hard to be viewed as “generalists, able to solve all kinds of problems,” and that means the specialty is poised to adapt and thrive.
“We will morph into what is needed,” said Dr. Wachter, a past president of SHM whose titles include chief of the division of hospital medicine at the University of California at San Francisco and chair of the American Board of Internal Medicine. “That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists.
“We will fill new niches,” he said.

What Dr. Wachter does not want to see is that the field grows “fat and happy,” as it is now firmly entrenched in the U.S. health-care delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs and waste, and, ultimately, improve the patient experience.
But he cautioned against conceptually separating QI and cost reduction. Instead, they should be viewed as equally meaningful parts of his oft-quoted value equation, which, viewed from the health-care consumer’s point of view, is quality divided by cost.
“You can’t survive and thrive in a world with the kinds of pressures that we have to improve performance if you do business the same old way,” he added. “It’s no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care.”
Richard Quinn is a freelance writer in New Jersey.
To some HM13 attendees, the keynote speakers might have seemed to be talking about different things.
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Center for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services (CMS), hinted at promising results from the first accountable-care organizations (ACOs) and noted a meaningful reduction in 30-day readmission rates for the first time in years.
David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, told hospitalists that unless they’re getting patient care right every time, they’re not getting it right enough. And nothing would make him happier than seeing fewer hospitalists at SHM’s annual meeting—because that would mean fewer hospitalized patients.
HM pioneer Bob Wachter, MD, MHM, said it’s time for hospitalists to link their quality-improvement (QI) efforts and safety acumen to projects focused on cutting costs and reducing waste in the health-care system.
So while each made their points in a different way, each plenary speaker left many meeting-goers with a similar thought: Hospitalists are positioned at the nexus of big-picture reform and day-to-day implementation. So if hospitalists as a specialty continue to embrace teamwork, evidence-based practice, quality, safety, and a sense that the patient comes first, they will cement themselves as leaders in the next iteration of health-care delivery.
“There is enormous change going on in the healthcare system,” says SHM CEO Larry Wellikson. “And we are right in the middle of this. We are essential. If we are bad, we are going to sink it. And if we’re great, we are going to take it to another level.”
Needle Movement
Dr. Conway said some of that progress already is evident. He disclosed that initial findings from the first data sets coming from the first ACOs are showing promising results, though he can’t go into detail until the information is publicly released. However, he did boast that after decades of Medicare readmission rates hovering around 19%, data from late 2012 and early 2013 show that figure has dropped to below 18%.
“That is a 1.5% to 2% shift in readmissions nationally,” he said. “It is a credit to the work you and others are doing in the field. That’s hundreds of thousands of Medicare beneficiaries that are not readmitted every year, that stay home healthy. … It’s a tremendous example of moving a national needle.”
He dismissed those who attribute the initial readmission progress solely to penalties instituted on readmissions, though he acknowledged that CMS is using both carrots and sticks to push change.
“It’s a combination of interventions,” he said.
And all of those initiatives must be aimed jointly at improving the patient experience, said Dr. Feinberg, a child psychiatrist by training whose mantra is “patient-centeredness.” Dr. Feinberg’s reputation is that of a physician-administrator who puts patients first. For example, even though his health system (www.uclahealth.org) is in the 99th percentile for patient satisfaction, he is unhappy. That’s because the top ranking means roughly 85 out of every 100 patients served are pretty happy with their experience.
“It means that we’re the cream of the crap,” he said. “Of the last 100 people we took care of, 15 of them—and, by definition, those 15 people are someone’s mom, someone’s brother, someone’s coworker—would not refer us to a friend, or rate us a 9 or 10. So, I think, while we’ve really moved the needle, we’re really not done until we get it right with every patient, every time.”
He added that those who argue against difficult or time-consuming innovations and improvements that better patient care are arguing against the moral high ground of how they would want a family member to be treated in the hospital.
“The pushback I hear is, ‘Some of this stuff is unpreventable,’” Dr. Feinberg said. “Well, maybe it’s unpreventable the way we’re doing it now. But maybe we need to think differently. Maybe it is unpreventable, but if this decreases the prevalence, or makes it better, then to me, it’s important to do.”
Dr. Feinberg, who took over as UCLA Health System’s president in 2011, says he still spends several hours every day talking to patients. For those who say there’s not enough time to stay connected to patients and that all the time spent making sure patients are happy takes away from other activities, he says they’re forgetting what brought them into medicine in the first place: healing. He blames the delivery system for stifling what he believes is a provider’s desire to help people.
“We haven’t allowed the culture to come out,” he said. “I think it’s there.”
Dr. Wachter has a similar faith in the hospitalist culture—although his is based in the pluripotent nature of the specialty. Hospitalists have worked hard to be viewed as “generalists, able to solve all kinds of problems,” and that means the specialty is poised to adapt and thrive.
“We will morph into what is needed,” said Dr. Wachter, a past president of SHM whose titles include chief of the division of hospital medicine at the University of California at San Francisco and chair of the American Board of Internal Medicine. “That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists.
“We will fill new niches,” he said.
What Dr. Wachter does not want to see is that the field grows “fat and happy,” as it is now firmly entrenched in the U.S. health-care delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs and waste, and, ultimately, improve the patient experience.
But he cautioned against conceptually separating QI and cost reduction. Instead, they should be viewed as equally meaningful parts of his oft-quoted value equation, which, viewed from the health-care consumer’s point of view, is quality divided by cost.
“You can’t survive and thrive in a world with the kinds of pressures that we have to improve performance if you do business the same old way,” he added. “It’s no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care.”
Richard Quinn is a freelance writer in New Jersey.
To some HM13 attendees, the keynote speakers might have seemed to be talking about different things.
Patrick Conway, MD, MSc, FAAP, SFHM, chief medical officer and director of the Center for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services (CMS), hinted at promising results from the first accountable-care organizations (ACOs) and noted a meaningful reduction in 30-day readmission rates for the first time in years.
David Feinberg, MD, MBA, president of UCLA Health System in Los Angeles, told hospitalists that unless they’re getting patient care right every time, they’re not getting it right enough. And nothing would make him happier than seeing fewer hospitalists at SHM’s annual meeting—because that would mean fewer hospitalized patients.
HM pioneer Bob Wachter, MD, MHM, said it’s time for hospitalists to link their quality-improvement (QI) efforts and safety acumen to projects focused on cutting costs and reducing waste in the health-care system.
So while each made their points in a different way, each plenary speaker left many meeting-goers with a similar thought: Hospitalists are positioned at the nexus of big-picture reform and day-to-day implementation. So if hospitalists as a specialty continue to embrace teamwork, evidence-based practice, quality, safety, and a sense that the patient comes first, they will cement themselves as leaders in the next iteration of health-care delivery.
“There is enormous change going on in the healthcare system,” says SHM CEO Larry Wellikson. “And we are right in the middle of this. We are essential. If we are bad, we are going to sink it. And if we’re great, we are going to take it to another level.”
Needle Movement
Dr. Conway said some of that progress already is evident. He disclosed that initial findings from the first data sets coming from the first ACOs are showing promising results, though he can’t go into detail until the information is publicly released. However, he did boast that after decades of Medicare readmission rates hovering around 19%, data from late 2012 and early 2013 show that figure has dropped to below 18%.
“That is a 1.5% to 2% shift in readmissions nationally,” he said. “It is a credit to the work you and others are doing in the field. That’s hundreds of thousands of Medicare beneficiaries that are not readmitted every year, that stay home healthy. … It’s a tremendous example of moving a national needle.”
He dismissed those who attribute the initial readmission progress solely to penalties instituted on readmissions, though he acknowledged that CMS is using both carrots and sticks to push change.
“It’s a combination of interventions,” he said.
And all of those initiatives must be aimed jointly at improving the patient experience, said Dr. Feinberg, a child psychiatrist by training whose mantra is “patient-centeredness.” Dr. Feinberg’s reputation is that of a physician-administrator who puts patients first. For example, even though his health system (www.uclahealth.org) is in the 99th percentile for patient satisfaction, he is unhappy. That’s because the top ranking means roughly 85 out of every 100 patients served are pretty happy with their experience.
“It means that we’re the cream of the crap,” he said. “Of the last 100 people we took care of, 15 of them—and, by definition, those 15 people are someone’s mom, someone’s brother, someone’s coworker—would not refer us to a friend, or rate us a 9 or 10. So, I think, while we’ve really moved the needle, we’re really not done until we get it right with every patient, every time.”
He added that those who argue against difficult or time-consuming innovations and improvements that better patient care are arguing against the moral high ground of how they would want a family member to be treated in the hospital.
“The pushback I hear is, ‘Some of this stuff is unpreventable,’” Dr. Feinberg said. “Well, maybe it’s unpreventable the way we’re doing it now. But maybe we need to think differently. Maybe it is unpreventable, but if this decreases the prevalence, or makes it better, then to me, it’s important to do.”
Dr. Feinberg, who took over as UCLA Health System’s president in 2011, says he still spends several hours every day talking to patients. For those who say there’s not enough time to stay connected to patients and that all the time spent making sure patients are happy takes away from other activities, he says they’re forgetting what brought them into medicine in the first place: healing. He blames the delivery system for stifling what he believes is a provider’s desire to help people.
“We haven’t allowed the culture to come out,” he said. “I think it’s there.”
Dr. Wachter has a similar faith in the hospitalist culture—although his is based in the pluripotent nature of the specialty. Hospitalists have worked hard to be viewed as “generalists, able to solve all kinds of problems,” and that means the specialty is poised to adapt and thrive.
“We will morph into what is needed,” said Dr. Wachter, a past president of SHM whose titles include chief of the division of hospital medicine at the University of California at San Francisco and chair of the American Board of Internal Medicine. “That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists.
“We will fill new niches,” he said.
What Dr. Wachter does not want to see is that the field grows “fat and happy,” as it is now firmly entrenched in the U.S. health-care delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs and waste, and, ultimately, improve the patient experience.
But he cautioned against conceptually separating QI and cost reduction. Instead, they should be viewed as equally meaningful parts of his oft-quoted value equation, which, viewed from the health-care consumer’s point of view, is quality divided by cost.
“You can’t survive and thrive in a world with the kinds of pressures that we have to improve performance if you do business the same old way,” he added. “It’s no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care.”
Richard Quinn is a freelance writer in New Jersey.
Most Health-Care Professionals Use Personal Smartphones for Work
Proportion of U.S. health-care workers who used their personal smartphones for work in the past year.5 The survey, conducted by Cisco Systems Inc., found that 36% of workers believe their employers are ready for “bring your own device” policies, while 41% say their devices are not password-protected and 53% access unsecure wi-fi networks at work. Additionally, 9 out of 10 workers receive no financial support from employers for using their smartphones at work.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
Proportion of U.S. health-care workers who used their personal smartphones for work in the past year.5 The survey, conducted by Cisco Systems Inc., found that 36% of workers believe their employers are ready for “bring your own device” policies, while 41% say their devices are not password-protected and 53% access unsecure wi-fi networks at work. Additionally, 9 out of 10 workers receive no financial support from employers for using their smartphones at work.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
Proportion of U.S. health-care workers who used their personal smartphones for work in the past year.5 The survey, conducted by Cisco Systems Inc., found that 36% of workers believe their employers are ready for “bring your own device” policies, while 41% say their devices are not password-protected and 53% access unsecure wi-fi networks at work. Additionally, 9 out of 10 workers receive no financial support from employers for using their smartphones at work.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
Health-Care Journalists Tackle Barriers to Hospital Safety Records

The Association of Health Care Journalists, a professional association that includes 1,400 journalists, is tackling some of the barriers consumers and advocates face when trying to access such information as hospital safety records. AHCJ’s www.HospitalInfections.org is a free, searchable news application that went live in March with detailed reports of deficiencies cited in federal inspection visits for acute- and critical-access hospitals nationwide.
Through years of advocacy, AHCJ has filed Freedom of Information Act requests and negotiated with the Centers for Medicare & Medicaid Services (CMS) to get access to hospital safety information in electronic form.
CMS’ Hospital Compare website (www.medicare.gov/hospitalcompare) and the Joint Commission’s Quality Check (www.qualitycheck.org) program both publicly report hospital quality data, but they have significant time lags and data that are difficult for the average consumer to understand, according to AHCJ. The association touts its new site as an “early attempt by an advocacy group to make hospital safety information easier to access and more consumer-driven.”
“Being able to easily review the performance of your local hospital is vital for health-care journalists and for the public,” AHCJ president Charles Ornstein, a senior reporter at ProPublica in New York, said in a statement.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
The Association of Health Care Journalists, a professional association that includes 1,400 journalists, is tackling some of the barriers consumers and advocates face when trying to access such information as hospital safety records. AHCJ’s www.HospitalInfections.org is a free, searchable news application that went live in March with detailed reports of deficiencies cited in federal inspection visits for acute- and critical-access hospitals nationwide.
Through years of advocacy, AHCJ has filed Freedom of Information Act requests and negotiated with the Centers for Medicare & Medicaid Services (CMS) to get access to hospital safety information in electronic form.
CMS’ Hospital Compare website (www.medicare.gov/hospitalcompare) and the Joint Commission’s Quality Check (www.qualitycheck.org) program both publicly report hospital quality data, but they have significant time lags and data that are difficult for the average consumer to understand, according to AHCJ. The association touts its new site as an “early attempt by an advocacy group to make hospital safety information easier to access and more consumer-driven.”
“Being able to easily review the performance of your local hospital is vital for health-care journalists and for the public,” AHCJ president Charles Ornstein, a senior reporter at ProPublica in New York, said in a statement.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
The Association of Health Care Journalists, a professional association that includes 1,400 journalists, is tackling some of the barriers consumers and advocates face when trying to access such information as hospital safety records. AHCJ’s www.HospitalInfections.org is a free, searchable news application that went live in March with detailed reports of deficiencies cited in federal inspection visits for acute- and critical-access hospitals nationwide.
Through years of advocacy, AHCJ has filed Freedom of Information Act requests and negotiated with the Centers for Medicare & Medicaid Services (CMS) to get access to hospital safety information in electronic form.
CMS’ Hospital Compare website (www.medicare.gov/hospitalcompare) and the Joint Commission’s Quality Check (www.qualitycheck.org) program both publicly report hospital quality data, but they have significant time lags and data that are difficult for the average consumer to understand, according to AHCJ. The association touts its new site as an “early attempt by an advocacy group to make hospital safety information easier to access and more consumer-driven.”
“Being able to easily review the performance of your local hospital is vital for health-care journalists and for the public,” AHCJ president Charles Ornstein, a senior reporter at ProPublica in New York, said in a statement.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
Medical Centers Take Tips from Other Industries
Curriculums using Lean quality-improvement (QI) principles and techniques are becoming entrenched in medical teaching programs across the country.
A curriculum based on Lean QI is teaching medical residents at Boston Medical Center techniques based on successes in manufacturing and service industries, according to Charlene Weigel, MD, who now works as a hospitalist at Mount Auburn Hospital in Cambridge, Mass. Residents also are learning about implementation of Lean principles at the medical center, Dr. Weigel and co-authors report in a study published in the American Journal of Medical Quality.1
“In Week One, we gave an introduction to QI and explained what Lean means,” Dr. Weigel says. Three other interactive sessions explored such techniques as how to create process maps and root-cause analysis, and identifying steps that aren’t helpful. The 90 residents and eight Boston University School of Public Health students also created 17 group QI project plans. “The goal was for the QI classwork and ideas to become implemented in hospital QI projects, but logistically, we had to scale back expectations for that initial go-round,” Dr. Weigel says.
The medical center recently started a second cycle of the QI course, with students from the first cycle encouraged to continue their QI projects on their own. One group submitted its project as an Institute for Healthcare Improvement storyboard at a national meeting.
“The experience also exposed the residents to our interprofessional team structure, which reflects their future working relationships and professional roles in QI,” Dr. Weigel says.
Lean concepts also are the basis for the Perfecting Patient Care University (PPCU, www.prhi.org/perfecting-patient-care/what-is-ppc), a QI training program for health-care leaders and clinicians offered in a variety of formats by the Pittsburgh Regional Health Initiative, a regional health collaborative. An evaluation of outcomes at PPCU was published online in the American Journal of Medical Quality in April.2 The same journal also describes the curriculum, program evaluation, and lessons learned by SHM’s Quality and Safety Educators Academy (http://sites.hospitalmedicine.org/qsea), which provides training in QI and patient safety for teaching faculty.3 The academy, a 2.5-day course, is co-sponsored by the Alliance for Academic Internal Medicine.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
Curriculums using Lean quality-improvement (QI) principles and techniques are becoming entrenched in medical teaching programs across the country.
A curriculum based on Lean QI is teaching medical residents at Boston Medical Center techniques based on successes in manufacturing and service industries, according to Charlene Weigel, MD, who now works as a hospitalist at Mount Auburn Hospital in Cambridge, Mass. Residents also are learning about implementation of Lean principles at the medical center, Dr. Weigel and co-authors report in a study published in the American Journal of Medical Quality.1
“In Week One, we gave an introduction to QI and explained what Lean means,” Dr. Weigel says. Three other interactive sessions explored such techniques as how to create process maps and root-cause analysis, and identifying steps that aren’t helpful. The 90 residents and eight Boston University School of Public Health students also created 17 group QI project plans. “The goal was for the QI classwork and ideas to become implemented in hospital QI projects, but logistically, we had to scale back expectations for that initial go-round,” Dr. Weigel says.
The medical center recently started a second cycle of the QI course, with students from the first cycle encouraged to continue their QI projects on their own. One group submitted its project as an Institute for Healthcare Improvement storyboard at a national meeting.
“The experience also exposed the residents to our interprofessional team structure, which reflects their future working relationships and professional roles in QI,” Dr. Weigel says.
Lean concepts also are the basis for the Perfecting Patient Care University (PPCU, www.prhi.org/perfecting-patient-care/what-is-ppc), a QI training program for health-care leaders and clinicians offered in a variety of formats by the Pittsburgh Regional Health Initiative, a regional health collaborative. An evaluation of outcomes at PPCU was published online in the American Journal of Medical Quality in April.2 The same journal also describes the curriculum, program evaluation, and lessons learned by SHM’s Quality and Safety Educators Academy (http://sites.hospitalmedicine.org/qsea), which provides training in QI and patient safety for teaching faculty.3 The academy, a 2.5-day course, is co-sponsored by the Alliance for Academic Internal Medicine.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
Curriculums using Lean quality-improvement (QI) principles and techniques are becoming entrenched in medical teaching programs across the country.
A curriculum based on Lean QI is teaching medical residents at Boston Medical Center techniques based on successes in manufacturing and service industries, according to Charlene Weigel, MD, who now works as a hospitalist at Mount Auburn Hospital in Cambridge, Mass. Residents also are learning about implementation of Lean principles at the medical center, Dr. Weigel and co-authors report in a study published in the American Journal of Medical Quality.1
“In Week One, we gave an introduction to QI and explained what Lean means,” Dr. Weigel says. Three other interactive sessions explored such techniques as how to create process maps and root-cause analysis, and identifying steps that aren’t helpful. The 90 residents and eight Boston University School of Public Health students also created 17 group QI project plans. “The goal was for the QI classwork and ideas to become implemented in hospital QI projects, but logistically, we had to scale back expectations for that initial go-round,” Dr. Weigel says.
The medical center recently started a second cycle of the QI course, with students from the first cycle encouraged to continue their QI projects on their own. One group submitted its project as an Institute for Healthcare Improvement storyboard at a national meeting.
“The experience also exposed the residents to our interprofessional team structure, which reflects their future working relationships and professional roles in QI,” Dr. Weigel says.
Lean concepts also are the basis for the Perfecting Patient Care University (PPCU, www.prhi.org/perfecting-patient-care/what-is-ppc), a QI training program for health-care leaders and clinicians offered in a variety of formats by the Pittsburgh Regional Health Initiative, a regional health collaborative. An evaluation of outcomes at PPCU was published online in the American Journal of Medical Quality in April.2 The same journal also describes the curriculum, program evaluation, and lessons learned by SHM’s Quality and Safety Educators Academy (http://sites.hospitalmedicine.org/qsea), which provides training in QI and patient safety for teaching faculty.3 The academy, a 2.5-day course, is co-sponsored by the Alliance for Academic Internal Medicine.
Larry Beresford is a freelance writer in San Francisco
References
- Weigel C, Suen W, Gupta G. Using Lean methodology to teach quality improvement to internal medicine residents at a safety net hospital. Am J Med Qual. 2013 Feb 4 [Epub ahead of print].
- Morganti KG, Lovejoy S, Beckjord EB, Haviland AM, Haas AC, Farley DO. A retrospective evaluation of the Perfecting Patient Care University training program for health care organizations. Am J Med Qual. 2013 Apr 9 [Epub ahead of print].
- Myers JS, Tess A, Glasheen JJ, et al. The Quality and Safety Educators’ Academy: fulfilling an unmet need for faculty development. Am J Med Qual. 2013 Apr 11 [Epub ahead of print].
- Dong XQ, Simon MA. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern Med. 2013 Apr 8:1-7. doi: 10.1001/jamainternmed.2013.238 [Epub ahead of print].
- Cisco mConcierge. 90% American workers use their own smartphones for work. Cisco mConcierge website. Available at: http://www.ciscomcon.com/sw/swchannel/registration/internet/registrationcfm?SWAPPID=91&RegPageID=350200&SWTHEMEID=12949. Accessed
‘Hill Trip’ Connects Legislators to Hospitalists, Health Care Issues

A veritable perfect storm of relationships brought hospitalist Jairy Hunter, MD, MBA, SFHM, to “Hospitalists on the Hill 2013,” a daylong advocacy affair that preceded HM13 last month.
First, Dr. Hunter was born and bred—and now lives—in South Carolina, a close-knit state where leaders across industries tend to run in the same circles, or at least have relatives who do. Second, Dr. Hunter’s father, Jairy Hunter Jr., is the longtime president of Charleston Southern University, where Sen. Tim Scott (R-S.C.) earned his undergraduate degree when it was still called Baptist College at Charleston. And three, Dr. Hunter is associate executive medical director of one of the state’s flagship health-care institutions, Medical University of South Carolina in Charleston.
So it was that SHM set Dr. Hunter up in meetings with the offices of Scott, Sen. Lindsey Graham (R-S.C.), and Rep. Jim Clyburn (D-S.C.), and—for the day at least—made Dr. Hunter the voice of hospital medicine.
“It was a little bit demystifying of an experience to be able to know there’s actually people you can talk to and you can develop a relationship with,” says Dr. Hunter, who also serves on Team Hospitalist. “I thought that was very rewarding.”
The connections made by Dr. Hunter are the point of the annual trek made by SHM leaders and members to lobby legislators and federal staffers “on the way policies affect your practice and your patients,” SHM says on its website (www.hospitalmedicine.org/advocacy). This year’s volunteer effort was by far the largest ever, says Public Policy Committee chair Ron Greeno, MD, FCCP, MHM. More than 150 hospitalists participated in training, 113 hospitalists visited Capitol Hill, and scores more had to be turned away. All told, hospitalists held 409 individual meetings with legislators and staff members.
“Quite frankly, if we’d have had the budget, we could have had another 100 to 150 people come,” Dr. Greeno says. “That’s how many people wanted to go.”
Dr. Greeno attributes the interest to two factors. One, having the annual meeting at the Gaylord National Resort & Convention Center, just outside Washington, D.C, makes the Hill trip a natural extension. Two, the current landscape of health-care reform has motivated many physicians to become more involved than they might otherwise be. One challenge of having so many first-timers making this year’s trip was making sure they were properly prepared. To hone the message, SHM gave the group a few hours of education by former legislative staffer Stephanie Vance of Advocacy Associates, a communications firm that helps organizations, such as medical societies, tailor their message to policymakers. Vance told hospitalists a personal visit with a constituent often becomes the most influential type of advocacy.
“That’s why it was easy to make an initial connection, because these staffers are from where I’m from, friends with people that I’m friends with,” Dr. Hunter says.

Unique Approach
SHM CEO Larry Wellikson, MD, SFHM, says the society tries to differentiate itself from other organizations through its grassroots approach to advocacy. More important, the society refrains from giving a long list of legislative requests that are self-serving.
“We’re someone they want to talk to because we’re not coming there to just say, ‘Here’s a power play for hospitalists,’” Dr. Wellikson says. “We come and try to provide solutions.”
To that end, this year’s lobbying effort was targeted to topics important both to HM and the health-care system:
- Repealing the sustainable growth rate (SGR) formula for Medicare payments, specifically via the proposed Medicare Physician Payment Innovation Act of 2013 (H.R. 574);
- Solving the quagmire of observation status time not counting toward the required three consecutive overnights as an inpatient needed to qualify for Medicare benefits at a skilled nursing facility, by supporting the Improving Access to Medicare Coverage Act of 2013 (H.R. 1179, S. 569); and
- Getting the federal government to commit to providing $434 million in funding for the Agency for Healthcare Research and Quality (AHRQ) in fiscal 2014.
“The message that we’re sending resonated with the people we met with on both sides of the aisle,” Dr. Greeno says. “The SGR, for instance, they know there needs to be a fix. We want to serve as a resource for them as they start to figure out the answer to the question: What are we going to replace it with?
“What we want to do is make everybody on the Hill understand that we can be relied upon as a resource when they’re looking for solutions,” he says.
Focused on Follow-Up
And that’s where rank-and-filers, such as Dr. Hunter, have to take charge. So for his Hill Day visits, he tried to stand out. Everyone he met with got a lapel pin in the shape of a South Carolina state flag, which has become a popular fashion statement in recent years. And Scott also got a pin from Charleston Southern University, his alma mater. The gestures were small, but they served as icebreakers and reminders that Dr. Hunter and the people he met are bound by service to the residents of the Palmetto State.
Dr. Hunter also hopes the small token will be that little extra that makes him memorable enough that the next time a Congressional staffer has an SGR question, they’ll ask him and not a doctor from another specialty.
“I’m interested to see how much feedback I get back from them,” he says. “I can feed them all day long, but I don’t want to be that crazy guy bugging them. If they respond back to me, I can hopefully make more inroads.”
He certainly would if Dr. Greeno gets his way. Moving forward, SHM hopes to be able to rely more on local advocates pushing for reform than just a once-a-year major event and formal positions drafted by SHM’s staffers or the Public Policy Committee. Dr. Greeno says the physicians who participated in this year’s Hill trip are likely to find they will be asked to be the first cohort of a grassroots initiative meant to deliver the society’s message more routinely.
“These are not easy things to change because there are not easy solutions,” Dr. Greeno adds. “If you have just one meeting on the Hill, you’ll have no impact at all. You have to follow up. You have to do it consistently. And you have to have a consistent message. And we will.”
Richard Quinn is a freelance writer in New Jersey.
A veritable perfect storm of relationships brought hospitalist Jairy Hunter, MD, MBA, SFHM, to “Hospitalists on the Hill 2013,” a daylong advocacy affair that preceded HM13 last month.
First, Dr. Hunter was born and bred—and now lives—in South Carolina, a close-knit state where leaders across industries tend to run in the same circles, or at least have relatives who do. Second, Dr. Hunter’s father, Jairy Hunter Jr., is the longtime president of Charleston Southern University, where Sen. Tim Scott (R-S.C.) earned his undergraduate degree when it was still called Baptist College at Charleston. And three, Dr. Hunter is associate executive medical director of one of the state’s flagship health-care institutions, Medical University of South Carolina in Charleston.
So it was that SHM set Dr. Hunter up in meetings with the offices of Scott, Sen. Lindsey Graham (R-S.C.), and Rep. Jim Clyburn (D-S.C.), and—for the day at least—made Dr. Hunter the voice of hospital medicine.
“It was a little bit demystifying of an experience to be able to know there’s actually people you can talk to and you can develop a relationship with,” says Dr. Hunter, who also serves on Team Hospitalist. “I thought that was very rewarding.”
The connections made by Dr. Hunter are the point of the annual trek made by SHM leaders and members to lobby legislators and federal staffers “on the way policies affect your practice and your patients,” SHM says on its website (www.hospitalmedicine.org/advocacy). This year’s volunteer effort was by far the largest ever, says Public Policy Committee chair Ron Greeno, MD, FCCP, MHM. More than 150 hospitalists participated in training, 113 hospitalists visited Capitol Hill, and scores more had to be turned away. All told, hospitalists held 409 individual meetings with legislators and staff members.
“Quite frankly, if we’d have had the budget, we could have had another 100 to 150 people come,” Dr. Greeno says. “That’s how many people wanted to go.”
Dr. Greeno attributes the interest to two factors. One, having the annual meeting at the Gaylord National Resort & Convention Center, just outside Washington, D.C, makes the Hill trip a natural extension. Two, the current landscape of health-care reform has motivated many physicians to become more involved than they might otherwise be. One challenge of having so many first-timers making this year’s trip was making sure they were properly prepared. To hone the message, SHM gave the group a few hours of education by former legislative staffer Stephanie Vance of Advocacy Associates, a communications firm that helps organizations, such as medical societies, tailor their message to policymakers. Vance told hospitalists a personal visit with a constituent often becomes the most influential type of advocacy.
“That’s why it was easy to make an initial connection, because these staffers are from where I’m from, friends with people that I’m friends with,” Dr. Hunter says.
Unique Approach
SHM CEO Larry Wellikson, MD, SFHM, says the society tries to differentiate itself from other organizations through its grassroots approach to advocacy. More important, the society refrains from giving a long list of legislative requests that are self-serving.
“We’re someone they want to talk to because we’re not coming there to just say, ‘Here’s a power play for hospitalists,’” Dr. Wellikson says. “We come and try to provide solutions.”
To that end, this year’s lobbying effort was targeted to topics important both to HM and the health-care system:
- Repealing the sustainable growth rate (SGR) formula for Medicare payments, specifically via the proposed Medicare Physician Payment Innovation Act of 2013 (H.R. 574);
- Solving the quagmire of observation status time not counting toward the required three consecutive overnights as an inpatient needed to qualify for Medicare benefits at a skilled nursing facility, by supporting the Improving Access to Medicare Coverage Act of 2013 (H.R. 1179, S. 569); and
- Getting the federal government to commit to providing $434 million in funding for the Agency for Healthcare Research and Quality (AHRQ) in fiscal 2014.
“The message that we’re sending resonated with the people we met with on both sides of the aisle,” Dr. Greeno says. “The SGR, for instance, they know there needs to be a fix. We want to serve as a resource for them as they start to figure out the answer to the question: What are we going to replace it with?
“What we want to do is make everybody on the Hill understand that we can be relied upon as a resource when they’re looking for solutions,” he says.
Focused on Follow-Up
And that’s where rank-and-filers, such as Dr. Hunter, have to take charge. So for his Hill Day visits, he tried to stand out. Everyone he met with got a lapel pin in the shape of a South Carolina state flag, which has become a popular fashion statement in recent years. And Scott also got a pin from Charleston Southern University, his alma mater. The gestures were small, but they served as icebreakers and reminders that Dr. Hunter and the people he met are bound by service to the residents of the Palmetto State.
Dr. Hunter also hopes the small token will be that little extra that makes him memorable enough that the next time a Congressional staffer has an SGR question, they’ll ask him and not a doctor from another specialty.
“I’m interested to see how much feedback I get back from them,” he says. “I can feed them all day long, but I don’t want to be that crazy guy bugging them. If they respond back to me, I can hopefully make more inroads.”
He certainly would if Dr. Greeno gets his way. Moving forward, SHM hopes to be able to rely more on local advocates pushing for reform than just a once-a-year major event and formal positions drafted by SHM’s staffers or the Public Policy Committee. Dr. Greeno says the physicians who participated in this year’s Hill trip are likely to find they will be asked to be the first cohort of a grassroots initiative meant to deliver the society’s message more routinely.
“These are not easy things to change because there are not easy solutions,” Dr. Greeno adds. “If you have just one meeting on the Hill, you’ll have no impact at all. You have to follow up. You have to do it consistently. And you have to have a consistent message. And we will.”
Richard Quinn is a freelance writer in New Jersey.
A veritable perfect storm of relationships brought hospitalist Jairy Hunter, MD, MBA, SFHM, to “Hospitalists on the Hill 2013,” a daylong advocacy affair that preceded HM13 last month.
First, Dr. Hunter was born and bred—and now lives—in South Carolina, a close-knit state where leaders across industries tend to run in the same circles, or at least have relatives who do. Second, Dr. Hunter’s father, Jairy Hunter Jr., is the longtime president of Charleston Southern University, where Sen. Tim Scott (R-S.C.) earned his undergraduate degree when it was still called Baptist College at Charleston. And three, Dr. Hunter is associate executive medical director of one of the state’s flagship health-care institutions, Medical University of South Carolina in Charleston.
So it was that SHM set Dr. Hunter up in meetings with the offices of Scott, Sen. Lindsey Graham (R-S.C.), and Rep. Jim Clyburn (D-S.C.), and—for the day at least—made Dr. Hunter the voice of hospital medicine.
“It was a little bit demystifying of an experience to be able to know there’s actually people you can talk to and you can develop a relationship with,” says Dr. Hunter, who also serves on Team Hospitalist. “I thought that was very rewarding.”
The connections made by Dr. Hunter are the point of the annual trek made by SHM leaders and members to lobby legislators and federal staffers “on the way policies affect your practice and your patients,” SHM says on its website (www.hospitalmedicine.org/advocacy). This year’s volunteer effort was by far the largest ever, says Public Policy Committee chair Ron Greeno, MD, FCCP, MHM. More than 150 hospitalists participated in training, 113 hospitalists visited Capitol Hill, and scores more had to be turned away. All told, hospitalists held 409 individual meetings with legislators and staff members.
“Quite frankly, if we’d have had the budget, we could have had another 100 to 150 people come,” Dr. Greeno says. “That’s how many people wanted to go.”
Dr. Greeno attributes the interest to two factors. One, having the annual meeting at the Gaylord National Resort & Convention Center, just outside Washington, D.C, makes the Hill trip a natural extension. Two, the current landscape of health-care reform has motivated many physicians to become more involved than they might otherwise be. One challenge of having so many first-timers making this year’s trip was making sure they were properly prepared. To hone the message, SHM gave the group a few hours of education by former legislative staffer Stephanie Vance of Advocacy Associates, a communications firm that helps organizations, such as medical societies, tailor their message to policymakers. Vance told hospitalists a personal visit with a constituent often becomes the most influential type of advocacy.
“That’s why it was easy to make an initial connection, because these staffers are from where I’m from, friends with people that I’m friends with,” Dr. Hunter says.
Unique Approach
SHM CEO Larry Wellikson, MD, SFHM, says the society tries to differentiate itself from other organizations through its grassroots approach to advocacy. More important, the society refrains from giving a long list of legislative requests that are self-serving.
“We’re someone they want to talk to because we’re not coming there to just say, ‘Here’s a power play for hospitalists,’” Dr. Wellikson says. “We come and try to provide solutions.”
To that end, this year’s lobbying effort was targeted to topics important both to HM and the health-care system:
- Repealing the sustainable growth rate (SGR) formula for Medicare payments, specifically via the proposed Medicare Physician Payment Innovation Act of 2013 (H.R. 574);
- Solving the quagmire of observation status time not counting toward the required three consecutive overnights as an inpatient needed to qualify for Medicare benefits at a skilled nursing facility, by supporting the Improving Access to Medicare Coverage Act of 2013 (H.R. 1179, S. 569); and
- Getting the federal government to commit to providing $434 million in funding for the Agency for Healthcare Research and Quality (AHRQ) in fiscal 2014.
“The message that we’re sending resonated with the people we met with on both sides of the aisle,” Dr. Greeno says. “The SGR, for instance, they know there needs to be a fix. We want to serve as a resource for them as they start to figure out the answer to the question: What are we going to replace it with?
“What we want to do is make everybody on the Hill understand that we can be relied upon as a resource when they’re looking for solutions,” he says.
Focused on Follow-Up
And that’s where rank-and-filers, such as Dr. Hunter, have to take charge. So for his Hill Day visits, he tried to stand out. Everyone he met with got a lapel pin in the shape of a South Carolina state flag, which has become a popular fashion statement in recent years. And Scott also got a pin from Charleston Southern University, his alma mater. The gestures were small, but they served as icebreakers and reminders that Dr. Hunter and the people he met are bound by service to the residents of the Palmetto State.
Dr. Hunter also hopes the small token will be that little extra that makes him memorable enough that the next time a Congressional staffer has an SGR question, they’ll ask him and not a doctor from another specialty.
“I’m interested to see how much feedback I get back from them,” he says. “I can feed them all day long, but I don’t want to be that crazy guy bugging them. If they respond back to me, I can hopefully make more inroads.”
He certainly would if Dr. Greeno gets his way. Moving forward, SHM hopes to be able to rely more on local advocates pushing for reform than just a once-a-year major event and formal positions drafted by SHM’s staffers or the Public Policy Committee. Dr. Greeno says the physicians who participated in this year’s Hill trip are likely to find they will be asked to be the first cohort of a grassroots initiative meant to deliver the society’s message more routinely.
“These are not easy things to change because there are not easy solutions,” Dr. Greeno adds. “If you have just one meeting on the Hill, you’ll have no impact at all. You have to follow up. You have to do it consistently. And you have to have a consistent message. And we will.”
Richard Quinn is a freelance writer in New Jersey.
Hospitalists Applaud Stress-Free CME Sessions, MOC Training at HM13




Hospitalist Roman Cortez, MD, who helps run Inpatient Medical Service in Kailua, Hawaii, is up for recertification of his internal-medicine boards in 2015. So after attending—and loving—his first SHM annual meeting last year in San Diego, he couldn’t think of a better place to earn credits for the American Board of Internal Medicine (ABIM) Maintenance of Certification (MOC) than HM13 in National Harbor, Md.
“It’s more motivational to sit through a seminar than to do it on your own, obviously,” Dr. Cortez says. “It’s like going to the gym. Nobody wants to work out at home, but if you go to the gym, you’re more motivated because you look around and your peers are working out. It’s the same thing with your mind.”
Working on one’s mind and career development is a major aim of SHMa’s annual meeting. From credit-worthy CME pre-courses to the daylong MOC class to the newest class of Fellows, Senior Fellows, and Masters of Hospital Medicine, clinicians like Dr. Cortez can use the yearly gathering as a chance to benchmark their professional progress.
Dr. Cortez, one of three partners who launched their HM group about five years ago, says having tutors, a regimented curricula via the pre-course, and a packed room of like-minded physicians helps hospitalists who are looking for one-stop shopping rather than working on Practice Improvement Modules (PIMs) in a room at their hospital or at home while balancing domestic duties.
“It seems like SHM has streamlined it for us,” Dr. Cortez says.
Ethan Cumbler, MD, FACP, of the University of Colorado at Denver believes the MOC courses are working. Dr. Cumbler is faculty for the pre-course and says there has been a noticeable uptick in how comfortable physicians at the meeting are with quality-improvement (QI) terminology and concepts.
“I think that over the years, the audiences that we’re seeing are savvier as to the process,” he adds. “I remember the first year that the quality-improvement module went out, people were shocked.
“I see clear differences between now and where we were three, four years ago,” he says.
Moving forward, Dr. Cumbler believes that ABIM and the people who help compile PIMs and test questions have to continue to evolve with physicians.
“What we have to figure out how to do as teachers of the Maintenance of Certification modules is how to make this engaging, interesting, and relevant,” he says. And “the people who are writing these questions have to take those same considerations into account. If you are teaching things which are relevant and important, then smart people will learn them.”
New Recruits, New Paths
Larry Spratling, MD, chief medical officer at Banner Baywood Medical Center in Mesa, Ariz., expects to see even more changes to the career trajectory of hospitalists. A pulmonary-disease specialist by training, he believes that as the payment systems are reformed to reward the quality of treatment, many more hospitalists will find their careers outside the walls of institutions.
Theoretically, improved outcomes that reduce readmissions would equate to fewer overall patients, potentially requiring fewer hospitalists in the future. The recent proliferation of hospitalists in long-term acute-care hospitals (LTACs), rehabilitation centers, skilled-nursing facilities (SNFs), and other facilities likely will continue that trend, as HM practitioners adapt to the needs of what Dr. Spratling calls “hospital space in a new system.” Dr. Spratling goes as far as to wonder if the specialty’s skill set might even presage a new name, perhaps something like acute-care medical specialists.
“The acute-care management skills that they have in the hospital, we can use them in these other sites of care,” he adds. “They aren’t just limited to the hospital anymore.”
Another angle of career development is career inception, so newly minted by SHM president Eric Howell, MD, SFHM. In fact, Dr. Howell made recruitment of the next generation of hospitalists and HM leaders a major plank of his one-year term. Of the society’s 12,000 members, just 500 are medical students and house staff members. He’d like to triple that figure by HM14.
He believes that the same professional and personal factors that have swelled the specialty’s ranks to some 40,000 practitioners will appeal to younger physicians. On the clinical side, that includes a focus on QI at a time when health care is being pushed to be better and a chance to be a leader in the hospital of the future. On a positive note, Dr. Howell, chief of hospital medicine at Johns Hopkins Bayview Medical Center in Baltimore, says hospitalists continue to see their compensation rise along with good work-life balance.
“For our specialty to be just as powerful, and just as important, and thrive just as much in the next 16 years as it has in the past 16 years, we are going to need high-quality recruits—and a lot of them,” Dr. Howell says.
Richard Quinn is a freelance writer in New Jersey.
Hospitalist Roman Cortez, MD, who helps run Inpatient Medical Service in Kailua, Hawaii, is up for recertification of his internal-medicine boards in 2015. So after attending—and loving—his first SHM annual meeting last year in San Diego, he couldn’t think of a better place to earn credits for the American Board of Internal Medicine (ABIM) Maintenance of Certification (MOC) than HM13 in National Harbor, Md.
“It’s more motivational to sit through a seminar than to do it on your own, obviously,” Dr. Cortez says. “It’s like going to the gym. Nobody wants to work out at home, but if you go to the gym, you’re more motivated because you look around and your peers are working out. It’s the same thing with your mind.”
Working on one’s mind and career development is a major aim of SHMa’s annual meeting. From credit-worthy CME pre-courses to the daylong MOC class to the newest class of Fellows, Senior Fellows, and Masters of Hospital Medicine, clinicians like Dr. Cortez can use the yearly gathering as a chance to benchmark their professional progress.
Dr. Cortez, one of three partners who launched their HM group about five years ago, says having tutors, a regimented curricula via the pre-course, and a packed room of like-minded physicians helps hospitalists who are looking for one-stop shopping rather than working on Practice Improvement Modules (PIMs) in a room at their hospital or at home while balancing domestic duties.
“It seems like SHM has streamlined it for us,” Dr. Cortez says.
Ethan Cumbler, MD, FACP, of the University of Colorado at Denver believes the MOC courses are working. Dr. Cumbler is faculty for the pre-course and says there has been a noticeable uptick in how comfortable physicians at the meeting are with quality-improvement (QI) terminology and concepts.
“I think that over the years, the audiences that we’re seeing are savvier as to the process,” he adds. “I remember the first year that the quality-improvement module went out, people were shocked.
“I see clear differences between now and where we were three, four years ago,” he says.
Moving forward, Dr. Cumbler believes that ABIM and the people who help compile PIMs and test questions have to continue to evolve with physicians.
“What we have to figure out how to do as teachers of the Maintenance of Certification modules is how to make this engaging, interesting, and relevant,” he says. And “the people who are writing these questions have to take those same considerations into account. If you are teaching things which are relevant and important, then smart people will learn them.”
New Recruits, New Paths
Larry Spratling, MD, chief medical officer at Banner Baywood Medical Center in Mesa, Ariz., expects to see even more changes to the career trajectory of hospitalists. A pulmonary-disease specialist by training, he believes that as the payment systems are reformed to reward the quality of treatment, many more hospitalists will find their careers outside the walls of institutions.
Theoretically, improved outcomes that reduce readmissions would equate to fewer overall patients, potentially requiring fewer hospitalists in the future. The recent proliferation of hospitalists in long-term acute-care hospitals (LTACs), rehabilitation centers, skilled-nursing facilities (SNFs), and other facilities likely will continue that trend, as HM practitioners adapt to the needs of what Dr. Spratling calls “hospital space in a new system.” Dr. Spratling goes as far as to wonder if the specialty’s skill set might even presage a new name, perhaps something like acute-care medical specialists.
“The acute-care management skills that they have in the hospital, we can use them in these other sites of care,” he adds. “They aren’t just limited to the hospital anymore.”
Another angle of career development is career inception, so newly minted by SHM president Eric Howell, MD, SFHM. In fact, Dr. Howell made recruitment of the next generation of hospitalists and HM leaders a major plank of his one-year term. Of the society’s 12,000 members, just 500 are medical students and house staff members. He’d like to triple that figure by HM14.
He believes that the same professional and personal factors that have swelled the specialty’s ranks to some 40,000 practitioners will appeal to younger physicians. On the clinical side, that includes a focus on QI at a time when health care is being pushed to be better and a chance to be a leader in the hospital of the future. On a positive note, Dr. Howell, chief of hospital medicine at Johns Hopkins Bayview Medical Center in Baltimore, says hospitalists continue to see their compensation rise along with good work-life balance.
“For our specialty to be just as powerful, and just as important, and thrive just as much in the next 16 years as it has in the past 16 years, we are going to need high-quality recruits—and a lot of them,” Dr. Howell says.
Richard Quinn is a freelance writer in New Jersey.
Hospitalist Roman Cortez, MD, who helps run Inpatient Medical Service in Kailua, Hawaii, is up for recertification of his internal-medicine boards in 2015. So after attending—and loving—his first SHM annual meeting last year in San Diego, he couldn’t think of a better place to earn credits for the American Board of Internal Medicine (ABIM) Maintenance of Certification (MOC) than HM13 in National Harbor, Md.
“It’s more motivational to sit through a seminar than to do it on your own, obviously,” Dr. Cortez says. “It’s like going to the gym. Nobody wants to work out at home, but if you go to the gym, you’re more motivated because you look around and your peers are working out. It’s the same thing with your mind.”
Working on one’s mind and career development is a major aim of SHMa’s annual meeting. From credit-worthy CME pre-courses to the daylong MOC class to the newest class of Fellows, Senior Fellows, and Masters of Hospital Medicine, clinicians like Dr. Cortez can use the yearly gathering as a chance to benchmark their professional progress.
Dr. Cortez, one of three partners who launched their HM group about five years ago, says having tutors, a regimented curricula via the pre-course, and a packed room of like-minded physicians helps hospitalists who are looking for one-stop shopping rather than working on Practice Improvement Modules (PIMs) in a room at their hospital or at home while balancing domestic duties.
“It seems like SHM has streamlined it for us,” Dr. Cortez says.
Ethan Cumbler, MD, FACP, of the University of Colorado at Denver believes the MOC courses are working. Dr. Cumbler is faculty for the pre-course and says there has been a noticeable uptick in how comfortable physicians at the meeting are with quality-improvement (QI) terminology and concepts.
“I think that over the years, the audiences that we’re seeing are savvier as to the process,” he adds. “I remember the first year that the quality-improvement module went out, people were shocked.
“I see clear differences between now and where we were three, four years ago,” he says.
Moving forward, Dr. Cumbler believes that ABIM and the people who help compile PIMs and test questions have to continue to evolve with physicians.
“What we have to figure out how to do as teachers of the Maintenance of Certification modules is how to make this engaging, interesting, and relevant,” he says. And “the people who are writing these questions have to take those same considerations into account. If you are teaching things which are relevant and important, then smart people will learn them.”
New Recruits, New Paths
Larry Spratling, MD, chief medical officer at Banner Baywood Medical Center in Mesa, Ariz., expects to see even more changes to the career trajectory of hospitalists. A pulmonary-disease specialist by training, he believes that as the payment systems are reformed to reward the quality of treatment, many more hospitalists will find their careers outside the walls of institutions.
Theoretically, improved outcomes that reduce readmissions would equate to fewer overall patients, potentially requiring fewer hospitalists in the future. The recent proliferation of hospitalists in long-term acute-care hospitals (LTACs), rehabilitation centers, skilled-nursing facilities (SNFs), and other facilities likely will continue that trend, as HM practitioners adapt to the needs of what Dr. Spratling calls “hospital space in a new system.” Dr. Spratling goes as far as to wonder if the specialty’s skill set might even presage a new name, perhaps something like acute-care medical specialists.
“The acute-care management skills that they have in the hospital, we can use them in these other sites of care,” he adds. “They aren’t just limited to the hospital anymore.”
Another angle of career development is career inception, so newly minted by SHM president Eric Howell, MD, SFHM. In fact, Dr. Howell made recruitment of the next generation of hospitalists and HM leaders a major plank of his one-year term. Of the society’s 12,000 members, just 500 are medical students and house staff members. He’d like to triple that figure by HM14.
He believes that the same professional and personal factors that have swelled the specialty’s ranks to some 40,000 practitioners will appeal to younger physicians. On the clinical side, that includes a focus on QI at a time when health care is being pushed to be better and a chance to be a leader in the hospital of the future. On a positive note, Dr. Howell, chief of hospital medicine at Johns Hopkins Bayview Medical Center in Baltimore, says hospitalists continue to see their compensation rise along with good work-life balance.
“For our specialty to be just as powerful, and just as important, and thrive just as much in the next 16 years as it has in the past 16 years, we are going to need high-quality recruits—and a lot of them,” Dr. Howell says.
Richard Quinn is a freelance writer in New Jersey.
Behavioral Economics Can Accelerate Adoption of Choosing Wisely Campaign

SHM has gotten behind the Choosing Wisely campaign in a big way. Earlier this year, SHM announced lists of suggested practices for adult and pediatric hospital medicine (see Table 1). To keep it on the front burner, hospitalists John Bulger and Ian Jenkins held a pre-course at HM13 devoted entirely to quality-improvement (QI) approaches to implementing and sustaining the practices outlined in the campaign. During the main meeting, they did an encore presentation, with Doug Carlson and Ricardo Quinonez presenting the elements of Choosing Wisely for pediatric hospital medicine.
The widely publicized campaign arose from an American Board of Internal Medicine (ABIM) Foundation grant program to “facilitate the development of innovative, emerging strategies to advance appropriate health-care decision-making and stewardship of health-care resources.” (For more information, visit www.abimfoundation.org.)
Adoption of many of the suggested Choosing Wisely practices will require a change in deeply ingrained, habitual behaviors. We assert that rational, reflective, cognitive processes might not be enough to overturn these behaviors, and that we must look to other mental systems to achieve the consistent adoption of the campaign’s suggested practices. An analogy exists in economics, where theories behind classical economics are challenged by behavioral economics.
What is behavioral economics? Classical economics asserts the individual as “homo economicus”: a person making rational, predictable decisions to advance their interests. However, due to social or professional influence, behavior often does not comport to expected ends. We succumb, sympathize, or follow the pack, diverging from the rulebook. Behavioral economics attempts to understand and compensate for these deviations.
In medicine, we often yield to cognitive biases. To simplify decision-making, we generalize our observations to arrive at decisions quickly. Daniel Kahneman, winner of the Nobel Memorial Prize in Economic Sciences, describes Type I thinking as fast and automatic, and Type II thinking as slow and effortful. Using Kahneman’s framework, we attempt to understand where reasoning may stray and, in turn, introduce environmental changes to achieve better outcomes.
How does this relate to Choosing Wisely? Embracing and embedding the practices of the Choosing Wisely campaign in day-to-day practice will require change in how we approach the clinical decisions we make each day. How can we create the conditions so as not to yield to the status quo?
The MINDSPACE framework
King et al in a recent Health Affairs article describe the MINDSPACE framework (see Table 2), which captures nine effects on behavior—messenger, incentives, norms, defaults, salience, priming, affect, commitments, and ego—that mostly involve automatic systems (Kahneman’s Type I), and how we can leverage them to minimize ineffective health care.1 Below, we describe Choosing Wisely’s HM components and how MINDSPACE can help promote better practice.
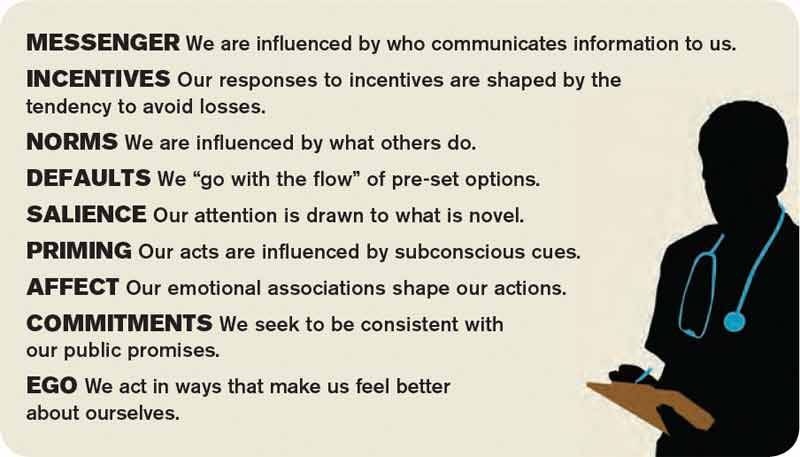
Messenger refers to the importance we place on the source of information conveyed to us. In the campaign, the ABIM Foundation engaged professional societies to come up with a list of specialty-specific practices. We know physicians pay more attention to messages from professional societies than, for example, insurance companies. Having the chair of medicine, the chief of hospital medicine, or the vice president of quality officially sanction the campaign’s practices at your organization leverages messengers.
Incentives, while widely used in health care, have had mixed results in terms of their utility in improving outcomes. People are loss-averse, and behavioral economics leverages that finding, which means incentives structured as penalties seem to have more powerful effects than bonuses. While the familiar pay-for-performance programs might not yield desired results, the evidence base continues to grow, and we have lots to learn. Does a 2% bonus change culture? What would really facilitate modifications in your test ordering patterns?
Norms, or what we perceive as the views of the majority, shape our behavior. How do we establish new ones? We all know the axiom “culture eats strategy for breakfast,” and, like patterned antibiotic administration, redirecting behavior requires examination of why we order items. Often, we order not because the drug combination conforms to standards, but because our training programs imbue us with less-than-ideal habits. These habits become standards, and their root causes require layered examination.
Defaults suggest that we are more likely to embrace a certain behavior if we otherwise need to “opt out” to avoid the behavior. We know that, for example, automatic enrollment in retirement savings plans has dramatically increased participation in such programs. For the Choosing Wisely campaign, the suggested practices should be set up as the default option. Examples include appropriate auto-stop orders for urinary catheters, telemetry, oximetry, or the requirement for added clicks to order daily CBCs. Think about ED orders and how they become substitute defaults once patients arrive on the wards. How do you disrupt the inertia?
Salience is when an individual makes a decision based on what is novel or what their attention is drawn to. Anticipating what subspecialists might expect, what your CMO demands, or what trainees envisage in their supervising attendings all may subconsciously override best judgment and deter best practice.
Priming describes how simple cues—often detected by our subconscious—influence decisions we make. When a physician, perhaps out of concern but often due to poorly reasoned or cavalier messaging, scribes “consider test X,” we involuntarily complete the act. We assume, because of the prime, that we need to act accordingly.
Affect is when we rely on gut feelings to make decisions. Emotions guide our ordering a urinary catheter for incontinence or transfusing to a HGB of 10, even when evidence contradicts what we might know as correct. Countering these actions requires credible stops to convert our emotions to reason (think clinical decision support with teeth).
Commitments are made in advance of an undertaking, behavioral economics suggests, as a way to combat the moment when willpower fails and desired behaviors go by the wayside. By publically signing a contract, in front of your group, chair, or medical director, and going on record as having pledged something, chances of success increase.
Ego, which underpins the need for a positive self-image, can drive the kind of automatic behavior that enables one to compare favorably to others. This effect has driven much of the motivation to perform well on public reporting of hospital quality measures. But ideal reporting of results must be valid; otherwise, attribution of subpar outcomes justifies the usual refrains of “not my responsibility” or the “system needs fixing, not me.”
Conclusions
Choosing Wisely is an ambitious undertaking made up of more than 90 suggested best practices put forth by 25 medical societies. In their book “Nudge,” authors Richard Thaler and Cass Sunstein describe how automatic behaviors arise from the environment or context in which choices to engage in such behaviors are presented.2 For the Choosing Wisely campaign to have staying power, we submit that institutional leaders and front-line clinicians will need to create a context where the safest, most cost-effective choices are the automatic, or nearly automatic, ones.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected]. Dr. Flansbaum is director of hospitalist services at Lenox Hill Hospital in New York City and an SHM Public Policy Committee member.
References
- King D, Greaves F, Vlaev I, Darzi A. Approaches based on behavioral economics could help nudge patients and providers toward lower health spending growth. Health Aff (Millwood). 2013;32(4):661-668.
- Thaler RH, Sunstein CR. Nudge: improving decisions about health, wealth and happiness. New Haven, Conn: Yale University Press; 2008.
SHM has gotten behind the Choosing Wisely campaign in a big way. Earlier this year, SHM announced lists of suggested practices for adult and pediatric hospital medicine (see Table 1). To keep it on the front burner, hospitalists John Bulger and Ian Jenkins held a pre-course at HM13 devoted entirely to quality-improvement (QI) approaches to implementing and sustaining the practices outlined in the campaign. During the main meeting, they did an encore presentation, with Doug Carlson and Ricardo Quinonez presenting the elements of Choosing Wisely for pediatric hospital medicine.
The widely publicized campaign arose from an American Board of Internal Medicine (ABIM) Foundation grant program to “facilitate the development of innovative, emerging strategies to advance appropriate health-care decision-making and stewardship of health-care resources.” (For more information, visit www.abimfoundation.org.)
Adoption of many of the suggested Choosing Wisely practices will require a change in deeply ingrained, habitual behaviors. We assert that rational, reflective, cognitive processes might not be enough to overturn these behaviors, and that we must look to other mental systems to achieve the consistent adoption of the campaign’s suggested practices. An analogy exists in economics, where theories behind classical economics are challenged by behavioral economics.
What is behavioral economics? Classical economics asserts the individual as “homo economicus”: a person making rational, predictable decisions to advance their interests. However, due to social or professional influence, behavior often does not comport to expected ends. We succumb, sympathize, or follow the pack, diverging from the rulebook. Behavioral economics attempts to understand and compensate for these deviations.
In medicine, we often yield to cognitive biases. To simplify decision-making, we generalize our observations to arrive at decisions quickly. Daniel Kahneman, winner of the Nobel Memorial Prize in Economic Sciences, describes Type I thinking as fast and automatic, and Type II thinking as slow and effortful. Using Kahneman’s framework, we attempt to understand where reasoning may stray and, in turn, introduce environmental changes to achieve better outcomes.
How does this relate to Choosing Wisely? Embracing and embedding the practices of the Choosing Wisely campaign in day-to-day practice will require change in how we approach the clinical decisions we make each day. How can we create the conditions so as not to yield to the status quo?
The MINDSPACE framework
King et al in a recent Health Affairs article describe the MINDSPACE framework (see Table 2), which captures nine effects on behavior—messenger, incentives, norms, defaults, salience, priming, affect, commitments, and ego—that mostly involve automatic systems (Kahneman’s Type I), and how we can leverage them to minimize ineffective health care.1 Below, we describe Choosing Wisely’s HM components and how MINDSPACE can help promote better practice.
Messenger refers to the importance we place on the source of information conveyed to us. In the campaign, the ABIM Foundation engaged professional societies to come up with a list of specialty-specific practices. We know physicians pay more attention to messages from professional societies than, for example, insurance companies. Having the chair of medicine, the chief of hospital medicine, or the vice president of quality officially sanction the campaign’s practices at your organization leverages messengers.
Incentives, while widely used in health care, have had mixed results in terms of their utility in improving outcomes. People are loss-averse, and behavioral economics leverages that finding, which means incentives structured as penalties seem to have more powerful effects than bonuses. While the familiar pay-for-performance programs might not yield desired results, the evidence base continues to grow, and we have lots to learn. Does a 2% bonus change culture? What would really facilitate modifications in your test ordering patterns?
Norms, or what we perceive as the views of the majority, shape our behavior. How do we establish new ones? We all know the axiom “culture eats strategy for breakfast,” and, like patterned antibiotic administration, redirecting behavior requires examination of why we order items. Often, we order not because the drug combination conforms to standards, but because our training programs imbue us with less-than-ideal habits. These habits become standards, and their root causes require layered examination.
Defaults suggest that we are more likely to embrace a certain behavior if we otherwise need to “opt out” to avoid the behavior. We know that, for example, automatic enrollment in retirement savings plans has dramatically increased participation in such programs. For the Choosing Wisely campaign, the suggested practices should be set up as the default option. Examples include appropriate auto-stop orders for urinary catheters, telemetry, oximetry, or the requirement for added clicks to order daily CBCs. Think about ED orders and how they become substitute defaults once patients arrive on the wards. How do you disrupt the inertia?
Salience is when an individual makes a decision based on what is novel or what their attention is drawn to. Anticipating what subspecialists might expect, what your CMO demands, or what trainees envisage in their supervising attendings all may subconsciously override best judgment and deter best practice.
Priming describes how simple cues—often detected by our subconscious—influence decisions we make. When a physician, perhaps out of concern but often due to poorly reasoned or cavalier messaging, scribes “consider test X,” we involuntarily complete the act. We assume, because of the prime, that we need to act accordingly.
Affect is when we rely on gut feelings to make decisions. Emotions guide our ordering a urinary catheter for incontinence or transfusing to a HGB of 10, even when evidence contradicts what we might know as correct. Countering these actions requires credible stops to convert our emotions to reason (think clinical decision support with teeth).
Commitments are made in advance of an undertaking, behavioral economics suggests, as a way to combat the moment when willpower fails and desired behaviors go by the wayside. By publically signing a contract, in front of your group, chair, or medical director, and going on record as having pledged something, chances of success increase.
Ego, which underpins the need for a positive self-image, can drive the kind of automatic behavior that enables one to compare favorably to others. This effect has driven much of the motivation to perform well on public reporting of hospital quality measures. But ideal reporting of results must be valid; otherwise, attribution of subpar outcomes justifies the usual refrains of “not my responsibility” or the “system needs fixing, not me.”
Conclusions
Choosing Wisely is an ambitious undertaking made up of more than 90 suggested best practices put forth by 25 medical societies. In their book “Nudge,” authors Richard Thaler and Cass Sunstein describe how automatic behaviors arise from the environment or context in which choices to engage in such behaviors are presented.2 For the Choosing Wisely campaign to have staying power, we submit that institutional leaders and front-line clinicians will need to create a context where the safest, most cost-effective choices are the automatic, or nearly automatic, ones.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected]. Dr. Flansbaum is director of hospitalist services at Lenox Hill Hospital in New York City and an SHM Public Policy Committee member.
References
- King D, Greaves F, Vlaev I, Darzi A. Approaches based on behavioral economics could help nudge patients and providers toward lower health spending growth. Health Aff (Millwood). 2013;32(4):661-668.
- Thaler RH, Sunstein CR. Nudge: improving decisions about health, wealth and happiness. New Haven, Conn: Yale University Press; 2008.
SHM has gotten behind the Choosing Wisely campaign in a big way. Earlier this year, SHM announced lists of suggested practices for adult and pediatric hospital medicine (see Table 1). To keep it on the front burner, hospitalists John Bulger and Ian Jenkins held a pre-course at HM13 devoted entirely to quality-improvement (QI) approaches to implementing and sustaining the practices outlined in the campaign. During the main meeting, they did an encore presentation, with Doug Carlson and Ricardo Quinonez presenting the elements of Choosing Wisely for pediatric hospital medicine.
The widely publicized campaign arose from an American Board of Internal Medicine (ABIM) Foundation grant program to “facilitate the development of innovative, emerging strategies to advance appropriate health-care decision-making and stewardship of health-care resources.” (For more information, visit www.abimfoundation.org.)
Adoption of many of the suggested Choosing Wisely practices will require a change in deeply ingrained, habitual behaviors. We assert that rational, reflective, cognitive processes might not be enough to overturn these behaviors, and that we must look to other mental systems to achieve the consistent adoption of the campaign’s suggested practices. An analogy exists in economics, where theories behind classical economics are challenged by behavioral economics.
What is behavioral economics? Classical economics asserts the individual as “homo economicus”: a person making rational, predictable decisions to advance their interests. However, due to social or professional influence, behavior often does not comport to expected ends. We succumb, sympathize, or follow the pack, diverging from the rulebook. Behavioral economics attempts to understand and compensate for these deviations.
In medicine, we often yield to cognitive biases. To simplify decision-making, we generalize our observations to arrive at decisions quickly. Daniel Kahneman, winner of the Nobel Memorial Prize in Economic Sciences, describes Type I thinking as fast and automatic, and Type II thinking as slow and effortful. Using Kahneman’s framework, we attempt to understand where reasoning may stray and, in turn, introduce environmental changes to achieve better outcomes.
How does this relate to Choosing Wisely? Embracing and embedding the practices of the Choosing Wisely campaign in day-to-day practice will require change in how we approach the clinical decisions we make each day. How can we create the conditions so as not to yield to the status quo?
The MINDSPACE framework
King et al in a recent Health Affairs article describe the MINDSPACE framework (see Table 2), which captures nine effects on behavior—messenger, incentives, norms, defaults, salience, priming, affect, commitments, and ego—that mostly involve automatic systems (Kahneman’s Type I), and how we can leverage them to minimize ineffective health care.1 Below, we describe Choosing Wisely’s HM components and how MINDSPACE can help promote better practice.
Messenger refers to the importance we place on the source of information conveyed to us. In the campaign, the ABIM Foundation engaged professional societies to come up with a list of specialty-specific practices. We know physicians pay more attention to messages from professional societies than, for example, insurance companies. Having the chair of medicine, the chief of hospital medicine, or the vice president of quality officially sanction the campaign’s practices at your organization leverages messengers.
Incentives, while widely used in health care, have had mixed results in terms of their utility in improving outcomes. People are loss-averse, and behavioral economics leverages that finding, which means incentives structured as penalties seem to have more powerful effects than bonuses. While the familiar pay-for-performance programs might not yield desired results, the evidence base continues to grow, and we have lots to learn. Does a 2% bonus change culture? What would really facilitate modifications in your test ordering patterns?
Norms, or what we perceive as the views of the majority, shape our behavior. How do we establish new ones? We all know the axiom “culture eats strategy for breakfast,” and, like patterned antibiotic administration, redirecting behavior requires examination of why we order items. Often, we order not because the drug combination conforms to standards, but because our training programs imbue us with less-than-ideal habits. These habits become standards, and their root causes require layered examination.
Defaults suggest that we are more likely to embrace a certain behavior if we otherwise need to “opt out” to avoid the behavior. We know that, for example, automatic enrollment in retirement savings plans has dramatically increased participation in such programs. For the Choosing Wisely campaign, the suggested practices should be set up as the default option. Examples include appropriate auto-stop orders for urinary catheters, telemetry, oximetry, or the requirement for added clicks to order daily CBCs. Think about ED orders and how they become substitute defaults once patients arrive on the wards. How do you disrupt the inertia?
Salience is when an individual makes a decision based on what is novel or what their attention is drawn to. Anticipating what subspecialists might expect, what your CMO demands, or what trainees envisage in their supervising attendings all may subconsciously override best judgment and deter best practice.
Priming describes how simple cues—often detected by our subconscious—influence decisions we make. When a physician, perhaps out of concern but often due to poorly reasoned or cavalier messaging, scribes “consider test X,” we involuntarily complete the act. We assume, because of the prime, that we need to act accordingly.
Affect is when we rely on gut feelings to make decisions. Emotions guide our ordering a urinary catheter for incontinence or transfusing to a HGB of 10, even when evidence contradicts what we might know as correct. Countering these actions requires credible stops to convert our emotions to reason (think clinical decision support with teeth).
Commitments are made in advance of an undertaking, behavioral economics suggests, as a way to combat the moment when willpower fails and desired behaviors go by the wayside. By publically signing a contract, in front of your group, chair, or medical director, and going on record as having pledged something, chances of success increase.
Ego, which underpins the need for a positive self-image, can drive the kind of automatic behavior that enables one to compare favorably to others. This effect has driven much of the motivation to perform well on public reporting of hospital quality measures. But ideal reporting of results must be valid; otherwise, attribution of subpar outcomes justifies the usual refrains of “not my responsibility” or the “system needs fixing, not me.”
Conclusions
Choosing Wisely is an ambitious undertaking made up of more than 90 suggested best practices put forth by 25 medical societies. In their book “Nudge,” authors Richard Thaler and Cass Sunstein describe how automatic behaviors arise from the environment or context in which choices to engage in such behaviors are presented.2 For the Choosing Wisely campaign to have staying power, we submit that institutional leaders and front-line clinicians will need to create a context where the safest, most cost-effective choices are the automatic, or nearly automatic, ones.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected]. Dr. Flansbaum is director of hospitalist services at Lenox Hill Hospital in New York City and an SHM Public Policy Committee member.
References
- King D, Greaves F, Vlaev I, Darzi A. Approaches based on behavioral economics could help nudge patients and providers toward lower health spending growth. Health Aff (Millwood). 2013;32(4):661-668.
- Thaler RH, Sunstein CR. Nudge: improving decisions about health, wealth and happiness. New Haven, Conn: Yale University Press; 2008.
When Staying Up Late Should Pay Off
Most people believe that nocturnists should get paid 20% to 33% more than their day-shift counterparts, according to a recent survey at www.the-hospitalist.org. Results of the survey, however, do not necessarily reflect the realities of supply and demand in local markets, according to members of SHM’s Practice Analysis Committee.
Practice size, volume of work, and the inconvenience of working at night contribute to the amount nocturnists get paid, says Leslie Flores, MHA, a committee member and partner in Nelson Flores Hospital Medicine Consultants. “We usually see a range between [a] 15% to 20% premium for nocturnist work,” she adds.
Survey respondents were asked to choose how much of a premium nocturnists should get paid, with the answers ranging from 20% to 60% to the same as everyone else. Two-thirds of the 212 respondents chose 20% or 33% bonus pay for nocturnists; 17% chose “the same as everyone else”; and another 17% chose 50% or 66%.
Committee member Troy Ahlstrom, MD, SFHM, senior chief information officer at Hospitals of Northern Michigan, says the survey does not reflect the reality of important factors that influence the market, such as supply and demand for nocturnists, local and regional factors that impact the level of supply and demand, and economic influence nationally.
“If you ask a practice manager or a hospital administrator that question, they would say nocturnists should make whatever is necessary to meet the demands for filling that job,” Dr. Ahlstrom says. “It’s a market-driven phenomenon.”
Hospitals don’t want to pay more, he notes, but they do want “to pay the right amount for the right job.”
Check out our website for more information about hospitalist compensation.
Most people believe that nocturnists should get paid 20% to 33% more than their day-shift counterparts, according to a recent survey at www.the-hospitalist.org. Results of the survey, however, do not necessarily reflect the realities of supply and demand in local markets, according to members of SHM’s Practice Analysis Committee.
Practice size, volume of work, and the inconvenience of working at night contribute to the amount nocturnists get paid, says Leslie Flores, MHA, a committee member and partner in Nelson Flores Hospital Medicine Consultants. “We usually see a range between [a] 15% to 20% premium for nocturnist work,” she adds.
Survey respondents were asked to choose how much of a premium nocturnists should get paid, with the answers ranging from 20% to 60% to the same as everyone else. Two-thirds of the 212 respondents chose 20% or 33% bonus pay for nocturnists; 17% chose “the same as everyone else”; and another 17% chose 50% or 66%.
Committee member Troy Ahlstrom, MD, SFHM, senior chief information officer at Hospitals of Northern Michigan, says the survey does not reflect the reality of important factors that influence the market, such as supply and demand for nocturnists, local and regional factors that impact the level of supply and demand, and economic influence nationally.
“If you ask a practice manager or a hospital administrator that question, they would say nocturnists should make whatever is necessary to meet the demands for filling that job,” Dr. Ahlstrom says. “It’s a market-driven phenomenon.”
Hospitals don’t want to pay more, he notes, but they do want “to pay the right amount for the right job.”
Check out our website for more information about hospitalist compensation.
Most people believe that nocturnists should get paid 20% to 33% more than their day-shift counterparts, according to a recent survey at www.the-hospitalist.org. Results of the survey, however, do not necessarily reflect the realities of supply and demand in local markets, according to members of SHM’s Practice Analysis Committee.
Practice size, volume of work, and the inconvenience of working at night contribute to the amount nocturnists get paid, says Leslie Flores, MHA, a committee member and partner in Nelson Flores Hospital Medicine Consultants. “We usually see a range between [a] 15% to 20% premium for nocturnist work,” she adds.
Survey respondents were asked to choose how much of a premium nocturnists should get paid, with the answers ranging from 20% to 60% to the same as everyone else. Two-thirds of the 212 respondents chose 20% or 33% bonus pay for nocturnists; 17% chose “the same as everyone else”; and another 17% chose 50% or 66%.
Committee member Troy Ahlstrom, MD, SFHM, senior chief information officer at Hospitals of Northern Michigan, says the survey does not reflect the reality of important factors that influence the market, such as supply and demand for nocturnists, local and regional factors that impact the level of supply and demand, and economic influence nationally.
“If you ask a practice manager or a hospital administrator that question, they would say nocturnists should make whatever is necessary to meet the demands for filling that job,” Dr. Ahlstrom says. “It’s a market-driven phenomenon.”
Hospitals don’t want to pay more, he notes, but they do want “to pay the right amount for the right job.”
Check out our website for more information about hospitalist compensation.
Physician Reviews of HM-Related Research
Clinical question: Does fluid management guided by daily plasma natriuretic peptide-driven (BNP) levels in mechanically ventilated patients improve weaning outcomes compared with usual therapy dictated by clinical acumen?
Background: Ventilator weaning contributes at least 40% of the total duration of mechanical ventilation; strategies aimed at optimizing this process could provide substantial benefit. Previous studies have demonstrated that BNP levels prior to ventilator weaning independently predict weaning failure. No current objective practical guide to fluid management during ventilator weaning exists.
Study design: Randomized controlled trial.
Setting: Multiple international centers.
Synopsis: Three hundred four patients who met specific inclusion and exclusion criteria were randomized to either a BNP-driven or physician-guided strategy for fluid management during ventilator weaning. Patients with renal failure were excluded because of the influence of renal function on BNP levels.
All patients in both groups were ventilated with an automatic computer-driven weaning system to standardize the weaning process. In the BNP-driven group, diuretic use was higher, resulting in a more negative fluid balance and significantly shorter time to successful extubation (58.6 hours vs. 42.2 hours, P=0.03). The effect on weaning time was strongest in patients with left ventricular systolic dysfunction, whereas those with COPD seemed less likely to benefit. The two groups did not differ in baseline characteristics, length of stay, mortality, or development of adverse outcomes of renal failure, shock, or electrolyte disturbances.
Bottom line: Compared with physician-guided fluid management, a BNP-driven fluid management protocol decreased duration of ventilator weaning without significant differences in adverse events, mortality rate, or length of stay between the two groups.
Citation: Dessap AM, Roche-Campo F, Kouatchet A, et al. Natriuretic peptide-driven fluid management during ventilator weaning. Am J Respir Crit Care Med. 2012;186(12):1256-1263.
Visit our website for more physician reviews of recent HM-relevant literature.
Clinical question: Does fluid management guided by daily plasma natriuretic peptide-driven (BNP) levels in mechanically ventilated patients improve weaning outcomes compared with usual therapy dictated by clinical acumen?
Background: Ventilator weaning contributes at least 40% of the total duration of mechanical ventilation; strategies aimed at optimizing this process could provide substantial benefit. Previous studies have demonstrated that BNP levels prior to ventilator weaning independently predict weaning failure. No current objective practical guide to fluid management during ventilator weaning exists.
Study design: Randomized controlled trial.
Setting: Multiple international centers.
Synopsis: Three hundred four patients who met specific inclusion and exclusion criteria were randomized to either a BNP-driven or physician-guided strategy for fluid management during ventilator weaning. Patients with renal failure were excluded because of the influence of renal function on BNP levels.
All patients in both groups were ventilated with an automatic computer-driven weaning system to standardize the weaning process. In the BNP-driven group, diuretic use was higher, resulting in a more negative fluid balance and significantly shorter time to successful extubation (58.6 hours vs. 42.2 hours, P=0.03). The effect on weaning time was strongest in patients with left ventricular systolic dysfunction, whereas those with COPD seemed less likely to benefit. The two groups did not differ in baseline characteristics, length of stay, mortality, or development of adverse outcomes of renal failure, shock, or electrolyte disturbances.
Bottom line: Compared with physician-guided fluid management, a BNP-driven fluid management protocol decreased duration of ventilator weaning without significant differences in adverse events, mortality rate, or length of stay between the two groups.
Citation: Dessap AM, Roche-Campo F, Kouatchet A, et al. Natriuretic peptide-driven fluid management during ventilator weaning. Am J Respir Crit Care Med. 2012;186(12):1256-1263.
Visit our website for more physician reviews of recent HM-relevant literature.
Clinical question: Does fluid management guided by daily plasma natriuretic peptide-driven (BNP) levels in mechanically ventilated patients improve weaning outcomes compared with usual therapy dictated by clinical acumen?
Background: Ventilator weaning contributes at least 40% of the total duration of mechanical ventilation; strategies aimed at optimizing this process could provide substantial benefit. Previous studies have demonstrated that BNP levels prior to ventilator weaning independently predict weaning failure. No current objective practical guide to fluid management during ventilator weaning exists.
Study design: Randomized controlled trial.
Setting: Multiple international centers.
Synopsis: Three hundred four patients who met specific inclusion and exclusion criteria were randomized to either a BNP-driven or physician-guided strategy for fluid management during ventilator weaning. Patients with renal failure were excluded because of the influence of renal function on BNP levels.
All patients in both groups were ventilated with an automatic computer-driven weaning system to standardize the weaning process. In the BNP-driven group, diuretic use was higher, resulting in a more negative fluid balance and significantly shorter time to successful extubation (58.6 hours vs. 42.2 hours, P=0.03). The effect on weaning time was strongest in patients with left ventricular systolic dysfunction, whereas those with COPD seemed less likely to benefit. The two groups did not differ in baseline characteristics, length of stay, mortality, or development of adverse outcomes of renal failure, shock, or electrolyte disturbances.
Bottom line: Compared with physician-guided fluid management, a BNP-driven fluid management protocol decreased duration of ventilator weaning without significant differences in adverse events, mortality rate, or length of stay between the two groups.
Citation: Dessap AM, Roche-Campo F, Kouatchet A, et al. Natriuretic peptide-driven fluid management during ventilator weaning. Am J Respir Crit Care Med. 2012;186(12):1256-1263.
Visit our website for more physician reviews of recent HM-relevant literature.
Wachter Sees Bright Future for Hospital Medicine

He believes HM's reputation as "generalists able to solve all kinds of problems" means the specialty is poised to adapt and thrive, he told a crowded ballroom at HM13's final keynote address yesterday at the Gaylord National Resort & Convention Center.
The annual plenary session was the effective wrap-up of SHM's four-day annual meeting, which drew some 2,700 attendees.
"We will morph into what is needed," he said. "That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists…we will fill new niches."
Watch a 2-minute video excerpt from Dr. Wachter's HM13 keynote address
What Dr. Wachter does not want to see is that the field grows "fat and happy" as it is now firmly entrenched in the U.S. healthcare delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs, and, ultimately, improve the patient experience.
"You can't survive and thrive in a world with the kinds of pressures that we have to improve performance, if you do business the same old way," he added. "It's no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care."
He believes HM's reputation as "generalists able to solve all kinds of problems" means the specialty is poised to adapt and thrive, he told a crowded ballroom at HM13's final keynote address yesterday at the Gaylord National Resort & Convention Center.
The annual plenary session was the effective wrap-up of SHM's four-day annual meeting, which drew some 2,700 attendees.
"We will morph into what is needed," he said. "That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists…we will fill new niches."
Watch a 2-minute video excerpt from Dr. Wachter's HM13 keynote address
What Dr. Wachter does not want to see is that the field grows "fat and happy" as it is now firmly entrenched in the U.S. healthcare delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs, and, ultimately, improve the patient experience.
"You can't survive and thrive in a world with the kinds of pressures that we have to improve performance, if you do business the same old way," he added. "It's no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care."
He believes HM's reputation as "generalists able to solve all kinds of problems" means the specialty is poised to adapt and thrive, he told a crowded ballroom at HM13's final keynote address yesterday at the Gaylord National Resort & Convention Center.
The annual plenary session was the effective wrap-up of SHM's four-day annual meeting, which drew some 2,700 attendees.
"We will morph into what is needed," he said. "That will be all sorts of things: comanagement, dealing with the residency limits in teaching hospitals, systems improvement, cost reductions, transitions, working in skilled nursing facilities, all the specialty hospitalists…we will fill new niches."
Watch a 2-minute video excerpt from Dr. Wachter's HM13 keynote address
What Dr. Wachter does not want to see is that the field grows "fat and happy" as it is now firmly entrenched in the U.S. healthcare delivery system. In fact, he urged hospitalists to welcome change, particularly initiatives that improve quality and safety, reduce costs, and, ultimately, improve the patient experience.
"You can't survive and thrive in a world with the kinds of pressures that we have to improve performance, if you do business the same old way," he added. "It's no longer possible to achieve the things you need to achieve handling these as single projects. You need to transform the way you think about care."