User login
Moore Medical Center a Casualty of Tornado’s Fury
After a monstrous tornado roared through Moore, Okla., chewing up and spitting out everything in its path, hospitalist Joe R. Womble, MD, who was off that day, wondered what had become of his colleagues, his patients, and his hospital, Moore Medical Center.
The initial news was encouraging: Everyone who had been inside the hospital—roughly 200 to 300 people, including a few dozen patients—had survived. He thought that boded well for the hospital as well.
“When I was getting information back from people who were there and I was hearing that everyone was fine, all the patients and staff, and no one got injured, I was thinking that either the hospital was missed by the storm, or that it must not have really damaged it very significantly,” says Dr. Womble. “And then they started showing aerial shots [on TV] and I was just shocked. My jaw was just dropped. The main entrance that I would go in every day was literally stacked three or four cars deep with … about 30 cars.” Likewise, the storm ripped through patient rooms on the second floor, obliterating some and reducing others to their steel innards.
About a week after the storm, word came back that Moore Medical Center will have to be demolished.
“Nobody knows what will happen next, but a lot of us speculate that they will not rebuild an inpatient facility,” says Dr. Womble. “It’s the only hospital in that city of Moore, and it’s just me and my partner to take care of virtually everyone that comes in with any kind of medical problem.
“And so I definitely feel a tie to the community. … Now that it’s gone, it’s just hard to put into words,” he says. “I would just say devastating, I guess.”
After a monstrous tornado roared through Moore, Okla., chewing up and spitting out everything in its path, hospitalist Joe R. Womble, MD, who was off that day, wondered what had become of his colleagues, his patients, and his hospital, Moore Medical Center.
The initial news was encouraging: Everyone who had been inside the hospital—roughly 200 to 300 people, including a few dozen patients—had survived. He thought that boded well for the hospital as well.
“When I was getting information back from people who were there and I was hearing that everyone was fine, all the patients and staff, and no one got injured, I was thinking that either the hospital was missed by the storm, or that it must not have really damaged it very significantly,” says Dr. Womble. “And then they started showing aerial shots [on TV] and I was just shocked. My jaw was just dropped. The main entrance that I would go in every day was literally stacked three or four cars deep with … about 30 cars.” Likewise, the storm ripped through patient rooms on the second floor, obliterating some and reducing others to their steel innards.
About a week after the storm, word came back that Moore Medical Center will have to be demolished.
“Nobody knows what will happen next, but a lot of us speculate that they will not rebuild an inpatient facility,” says Dr. Womble. “It’s the only hospital in that city of Moore, and it’s just me and my partner to take care of virtually everyone that comes in with any kind of medical problem.
“And so I definitely feel a tie to the community. … Now that it’s gone, it’s just hard to put into words,” he says. “I would just say devastating, I guess.”
After a monstrous tornado roared through Moore, Okla., chewing up and spitting out everything in its path, hospitalist Joe R. Womble, MD, who was off that day, wondered what had become of his colleagues, his patients, and his hospital, Moore Medical Center.
The initial news was encouraging: Everyone who had been inside the hospital—roughly 200 to 300 people, including a few dozen patients—had survived. He thought that boded well for the hospital as well.
“When I was getting information back from people who were there and I was hearing that everyone was fine, all the patients and staff, and no one got injured, I was thinking that either the hospital was missed by the storm, or that it must not have really damaged it very significantly,” says Dr. Womble. “And then they started showing aerial shots [on TV] and I was just shocked. My jaw was just dropped. The main entrance that I would go in every day was literally stacked three or four cars deep with … about 30 cars.” Likewise, the storm ripped through patient rooms on the second floor, obliterating some and reducing others to their steel innards.
About a week after the storm, word came back that Moore Medical Center will have to be demolished.
“Nobody knows what will happen next, but a lot of us speculate that they will not rebuild an inpatient facility,” says Dr. Womble. “It’s the only hospital in that city of Moore, and it’s just me and my partner to take care of virtually everyone that comes in with any kind of medical problem.
“And so I definitely feel a tie to the community. … Now that it’s gone, it’s just hard to put into words,” he says. “I would just say devastating, I guess.”
Should Skyrocketing Health Care Costs Concern Hospitalists?
Median hospitalist compensation has grown steadily over the past decade, but physicians aren’t immune to the sting of accelerated premiums, copays, and contributions imposed by health insurers.
According to the Hay Group’s 2011 Physician Compensation Survey, the number of physicians who contributing to health insurance premiums increased to 68% in 2011 from 58% in 2010. The survey showed only 9% of physicians did not pay anything for medical coverage, down from 19% in 2010.
Moreover, the expected physician contribution was between 1% and 25% of the premium.
Dan Fuller, president and cofounder of Alpharetta, Ga.-based IN Compass Health, has noticed an uptick in candidates’ interest in their health-care benefits. “Especially for physicians who have families, health benefits have become one of the top issues in recruiting,” the SHM Practice Analysis Committee (PAC) member says.
Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America in Nashville, Tenn., reports that he is seeing an upward trend in employees’ contributions to premiums and out-of-pocket costs. He’s also observed colleagues becoming more selective when choosing their own health-care plans and how they use those plans.
Gretchen Henkel is a freelance writer in California.
Median hospitalist compensation has grown steadily over the past decade, but physicians aren’t immune to the sting of accelerated premiums, copays, and contributions imposed by health insurers.
According to the Hay Group’s 2011 Physician Compensation Survey, the number of physicians who contributing to health insurance premiums increased to 68% in 2011 from 58% in 2010. The survey showed only 9% of physicians did not pay anything for medical coverage, down from 19% in 2010.
Moreover, the expected physician contribution was between 1% and 25% of the premium.
Dan Fuller, president and cofounder of Alpharetta, Ga.-based IN Compass Health, has noticed an uptick in candidates’ interest in their health-care benefits. “Especially for physicians who have families, health benefits have become one of the top issues in recruiting,” the SHM Practice Analysis Committee (PAC) member says.
Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America in Nashville, Tenn., reports that he is seeing an upward trend in employees’ contributions to premiums and out-of-pocket costs. He’s also observed colleagues becoming more selective when choosing their own health-care plans and how they use those plans.
Gretchen Henkel is a freelance writer in California.
Median hospitalist compensation has grown steadily over the past decade, but physicians aren’t immune to the sting of accelerated premiums, copays, and contributions imposed by health insurers.
According to the Hay Group’s 2011 Physician Compensation Survey, the number of physicians who contributing to health insurance premiums increased to 68% in 2011 from 58% in 2010. The survey showed only 9% of physicians did not pay anything for medical coverage, down from 19% in 2010.
Moreover, the expected physician contribution was between 1% and 25% of the premium.
Dan Fuller, president and cofounder of Alpharetta, Ga.-based IN Compass Health, has noticed an uptick in candidates’ interest in their health-care benefits. “Especially for physicians who have families, health benefits have become one of the top issues in recruiting,” the SHM Practice Analysis Committee (PAC) member says.
Christopher Frost, MD, FHM, medical director of hospital medicine at the Hospital Corporation of America in Nashville, Tenn., reports that he is seeing an upward trend in employees’ contributions to premiums and out-of-pocket costs. He’s also observed colleagues becoming more selective when choosing their own health-care plans and how they use those plans.
Gretchen Henkel is a freelance writer in California.
Pediatric Hospital Medicine Conference Marks 10th Year
This year marks an exciting milestone for pediatric hospitalists: the 10th anniversary of the only national conference dedicated to pediatric hospital medicine (PHM). Although the first meeting might have been just a handful of pediatric hospitalists gathering to better understand an emerging specialty, Pediatric Hospital Medicine 2013 will be a bustling gathering of leaders in the now-established field.
New this year are three conundrum sessions and a Sunday plenary session focusing on pediatric overuse in the hospital setting. And in response to participant demand, the concurrent workshop sessions have been expanded to include nine educational tracks, including the debut of the early-career and community hospitalist tracks.
PHM 2013 is sponsored by the American Academy of Pediatrics (AAP), the AAP Section on Hospital Medicine (SOHM), the Academic Pediatric Association, and SHM.
This year marks an exciting milestone for pediatric hospitalists: the 10th anniversary of the only national conference dedicated to pediatric hospital medicine (PHM). Although the first meeting might have been just a handful of pediatric hospitalists gathering to better understand an emerging specialty, Pediatric Hospital Medicine 2013 will be a bustling gathering of leaders in the now-established field.
New this year are three conundrum sessions and a Sunday plenary session focusing on pediatric overuse in the hospital setting. And in response to participant demand, the concurrent workshop sessions have been expanded to include nine educational tracks, including the debut of the early-career and community hospitalist tracks.
PHM 2013 is sponsored by the American Academy of Pediatrics (AAP), the AAP Section on Hospital Medicine (SOHM), the Academic Pediatric Association, and SHM.
This year marks an exciting milestone for pediatric hospitalists: the 10th anniversary of the only national conference dedicated to pediatric hospital medicine (PHM). Although the first meeting might have been just a handful of pediatric hospitalists gathering to better understand an emerging specialty, Pediatric Hospital Medicine 2013 will be a bustling gathering of leaders in the now-established field.
New this year are three conundrum sessions and a Sunday plenary session focusing on pediatric overuse in the hospital setting. And in response to participant demand, the concurrent workshop sessions have been expanded to include nine educational tracks, including the debut of the early-career and community hospitalist tracks.
PHM 2013 is sponsored by the American Academy of Pediatrics (AAP), the AAP Section on Hospital Medicine (SOHM), the Academic Pediatric Association, and SHM.
Advanced-Practice Providers Have More to Offer Hospital Medicine Groups

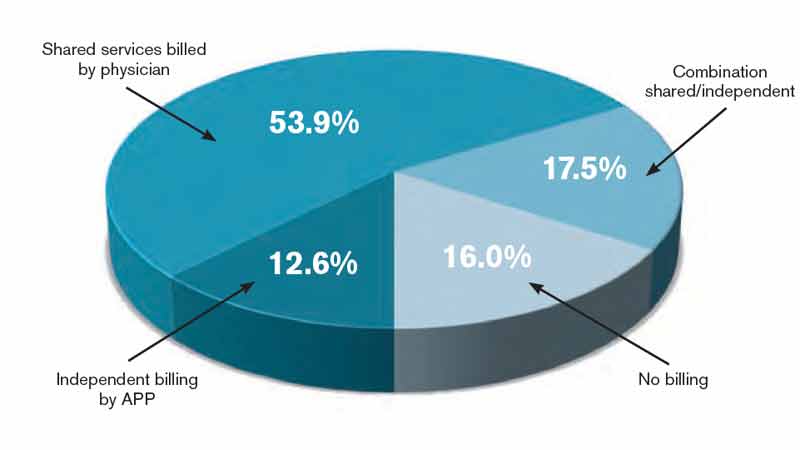
Advanced-practice providers (APPs) continue to make their presence felt in the world of hospital medicine. According to survey data from the 2012 State of Hospital Medicine report, more than half (53.9%) of respondent groups serving adults have nurse practitioners (NP) and/or physician assistants (PA) integrated into their practices. The median ratio of APPs to hospitalist physicians in these groups has remained about the same as in previous surveys, with respondents reporting 0.2 FTE NPs per FTE physician, and 0.1 FTE PAs per FTE physician. We’ve also learned that APPs tend to be stable members of most hospitalist practices, with more than 70% of groups reporting no turnover among their APPs during the survey period.
Unfortunately, we don’t yet have much information on the specific roles APPs are filling in HM practices; hopefully, this will be a subject for the next State of Hospital Medicine survey, scheduled to launch in January 2014.
The 2012 survey did provide new information about how APP work is billed by HM groups. More than half the time, APP work is billed as a shared service under a physician’s provider number (see Table 1). Only on rare occasions is APP work billed separately under the APP’s provider number.
Perhaps most surprising of all, 16% of adult HM groups with APPs reported that their APPs don’t generally provide billable services, or no charges were submitted to payors for their services. This figure rose to 23% for hospital-employed groups.
Almost everywhere I go in my consulting work, we are asked about the value APPs can provide to hospitalist practice, and what their optimal roles are. I am extremely supportive of integrating APPs into hospitalist practice and believe they can play valuable roles supporting both excellent patient care and overall group efficiency.
But in my experience, many HM groups fail to execute well on this promise. As the survey results suggest, sometimes APPs are relegated to nonbillable tasks that could be performed by individuals at a lower skill level. Sometimes the hospitalists tend to think of the APPs as “free” help, and no real attempt is made to account for their contribution or capture their billable work. And some groups are so focused on ensuring they capture the 100% reimbursement available by billing under the physician’s name (rather than the 85% reimbursement typically available to APPs) that they lose sight of the fact that the extra physician time and effort involved might cost more than the incremental additional reimbursement received.
As a specialty, we still have a lot to learn about the optimal ways to deploy APPs to support high-quality, effective hospitalist practice. In the meantime, it can be valuable for HM groups to ensure that APPs are functioning in roles that take advantage of their advanced skills and licensure scope, and that efforts are being made to ensure the capture of all billable services provided.
I hope you will plan to participate in the 2014 State of Hospital Medicine survey and share your own practice’s experience with APPs.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
Advanced-practice providers (APPs) continue to make their presence felt in the world of hospital medicine. According to survey data from the 2012 State of Hospital Medicine report, more than half (53.9%) of respondent groups serving adults have nurse practitioners (NP) and/or physician assistants (PA) integrated into their practices. The median ratio of APPs to hospitalist physicians in these groups has remained about the same as in previous surveys, with respondents reporting 0.2 FTE NPs per FTE physician, and 0.1 FTE PAs per FTE physician. We’ve also learned that APPs tend to be stable members of most hospitalist practices, with more than 70% of groups reporting no turnover among their APPs during the survey period.
Unfortunately, we don’t yet have much information on the specific roles APPs are filling in HM practices; hopefully, this will be a subject for the next State of Hospital Medicine survey, scheduled to launch in January 2014.
The 2012 survey did provide new information about how APP work is billed by HM groups. More than half the time, APP work is billed as a shared service under a physician’s provider number (see Table 1). Only on rare occasions is APP work billed separately under the APP’s provider number.
Perhaps most surprising of all, 16% of adult HM groups with APPs reported that their APPs don’t generally provide billable services, or no charges were submitted to payors for their services. This figure rose to 23% for hospital-employed groups.
Almost everywhere I go in my consulting work, we are asked about the value APPs can provide to hospitalist practice, and what their optimal roles are. I am extremely supportive of integrating APPs into hospitalist practice and believe they can play valuable roles supporting both excellent patient care and overall group efficiency.
But in my experience, many HM groups fail to execute well on this promise. As the survey results suggest, sometimes APPs are relegated to nonbillable tasks that could be performed by individuals at a lower skill level. Sometimes the hospitalists tend to think of the APPs as “free” help, and no real attempt is made to account for their contribution or capture their billable work. And some groups are so focused on ensuring they capture the 100% reimbursement available by billing under the physician’s name (rather than the 85% reimbursement typically available to APPs) that they lose sight of the fact that the extra physician time and effort involved might cost more than the incremental additional reimbursement received.
As a specialty, we still have a lot to learn about the optimal ways to deploy APPs to support high-quality, effective hospitalist practice. In the meantime, it can be valuable for HM groups to ensure that APPs are functioning in roles that take advantage of their advanced skills and licensure scope, and that efforts are being made to ensure the capture of all billable services provided.
I hope you will plan to participate in the 2014 State of Hospital Medicine survey and share your own practice’s experience with APPs.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
Advanced-practice providers (APPs) continue to make their presence felt in the world of hospital medicine. According to survey data from the 2012 State of Hospital Medicine report, more than half (53.9%) of respondent groups serving adults have nurse practitioners (NP) and/or physician assistants (PA) integrated into their practices. The median ratio of APPs to hospitalist physicians in these groups has remained about the same as in previous surveys, with respondents reporting 0.2 FTE NPs per FTE physician, and 0.1 FTE PAs per FTE physician. We’ve also learned that APPs tend to be stable members of most hospitalist practices, with more than 70% of groups reporting no turnover among their APPs during the survey period.
Unfortunately, we don’t yet have much information on the specific roles APPs are filling in HM practices; hopefully, this will be a subject for the next State of Hospital Medicine survey, scheduled to launch in January 2014.
The 2012 survey did provide new information about how APP work is billed by HM groups. More than half the time, APP work is billed as a shared service under a physician’s provider number (see Table 1). Only on rare occasions is APP work billed separately under the APP’s provider number.
Perhaps most surprising of all, 16% of adult HM groups with APPs reported that their APPs don’t generally provide billable services, or no charges were submitted to payors for their services. This figure rose to 23% for hospital-employed groups.
Almost everywhere I go in my consulting work, we are asked about the value APPs can provide to hospitalist practice, and what their optimal roles are. I am extremely supportive of integrating APPs into hospitalist practice and believe they can play valuable roles supporting both excellent patient care and overall group efficiency.
But in my experience, many HM groups fail to execute well on this promise. As the survey results suggest, sometimes APPs are relegated to nonbillable tasks that could be performed by individuals at a lower skill level. Sometimes the hospitalists tend to think of the APPs as “free” help, and no real attempt is made to account for their contribution or capture their billable work. And some groups are so focused on ensuring they capture the 100% reimbursement available by billing under the physician’s name (rather than the 85% reimbursement typically available to APPs) that they lose sight of the fact that the extra physician time and effort involved might cost more than the incremental additional reimbursement received.
As a specialty, we still have a lot to learn about the optimal ways to deploy APPs to support high-quality, effective hospitalist practice. In the meantime, it can be valuable for HM groups to ensure that APPs are functioning in roles that take advantage of their advanced skills and licensure scope, and that efforts are being made to ensure the capture of all billable services provided.
I hope you will plan to participate in the 2014 State of Hospital Medicine survey and share your own practice’s experience with APPs.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
Start Planning Now for HM14

Whether you couldn’t make it to HM13 or you’re bringing back all the energy from the conference back to your hospital, now is the time to start planning for the next national conference exclusively designed for the nation’s 40,000 hospitalists.
For newcomers, HM14 will offer unprecedented access, networking, and CME-accredited educational sessions for hospitalists in all career stages. And for veterans of SHM’s annual meeting, 2014 will introduce two new pre-courses: “Cardiology and Evidence-Based Medicine” and “Bending the Cost Curve,” one of the hottest topics in public health, which will have its own dedicated track as well.
In addition to offering the best CME-accredited educational experience, HM14 will also give hospitalists the chance to enjoy an all-new official headquarters for the meeting: Mandalay Bay Hotel & Casino in Las Vegas.
Pre-Courses
Enhance the HM14 educational experience, broaden your skills, and earn additional CME credits. Choose from one of the following HM-focused topics:
- Medical Procedures for the Hospitalist;
- Portable Ultrasound for the Hospitalist;
- Perioperative Medicine;
- ABIM Maintenance of Certification;
- Practice Management;
- Neurology;
- Cardiology (new); and
- Evidence-Based Medicine (new).
Content Areas
The educational tracks offered at HM14 enable attendees to take courses in various designated tracks designed to better focus and enrich the annual meeting for attendees.
Tracks focus on the following cutting-edge content areas:
- Clinical;
- Rapid Fire;
- Practice Management;
- Academic/Research;
- Quality;
- Bending the Cost Curve (new);
- Pediatric;
- Potpourri;
- Comanagement; and
- Workshops.
Brendon Shank is SHM’s associate vice president of communications.
HM14 HEADQUARTERS: THE MANDALAY BAY HOTEL & CASINO

Enjoy casual elegance and comfort in the main tower’s rooms and suites, or relax in unparalleled sophistication and style at The Hotel at Mandalay Bay. At HM14 in March, hospitalists will:
- Bask in ultimate aquatic relaxation at the unforgettable, 11-acre Mandalay Bay Beach;
- Explore the Shark Reef Aquarium, featuring more than 2,000 exotic animals in a breathtaking 1.6-million-gallon habitat; and
- Taste the variety of foods at the 20-plus restaurants Mandalay Bay has to offer, including beach dining.
Whether you couldn’t make it to HM13 or you’re bringing back all the energy from the conference back to your hospital, now is the time to start planning for the next national conference exclusively designed for the nation’s 40,000 hospitalists.
For newcomers, HM14 will offer unprecedented access, networking, and CME-accredited educational sessions for hospitalists in all career stages. And for veterans of SHM’s annual meeting, 2014 will introduce two new pre-courses: “Cardiology and Evidence-Based Medicine” and “Bending the Cost Curve,” one of the hottest topics in public health, which will have its own dedicated track as well.
In addition to offering the best CME-accredited educational experience, HM14 will also give hospitalists the chance to enjoy an all-new official headquarters for the meeting: Mandalay Bay Hotel & Casino in Las Vegas.
Pre-Courses
Enhance the HM14 educational experience, broaden your skills, and earn additional CME credits. Choose from one of the following HM-focused topics:
- Medical Procedures for the Hospitalist;
- Portable Ultrasound for the Hospitalist;
- Perioperative Medicine;
- ABIM Maintenance of Certification;
- Practice Management;
- Neurology;
- Cardiology (new); and
- Evidence-Based Medicine (new).
Content Areas
The educational tracks offered at HM14 enable attendees to take courses in various designated tracks designed to better focus and enrich the annual meeting for attendees.
Tracks focus on the following cutting-edge content areas:
- Clinical;
- Rapid Fire;
- Practice Management;
- Academic/Research;
- Quality;
- Bending the Cost Curve (new);
- Pediatric;
- Potpourri;
- Comanagement; and
- Workshops.
Brendon Shank is SHM’s associate vice president of communications.
HM14 HEADQUARTERS: THE MANDALAY BAY HOTEL & CASINO
Enjoy casual elegance and comfort in the main tower’s rooms and suites, or relax in unparalleled sophistication and style at The Hotel at Mandalay Bay. At HM14 in March, hospitalists will:
- Bask in ultimate aquatic relaxation at the unforgettable, 11-acre Mandalay Bay Beach;
- Explore the Shark Reef Aquarium, featuring more than 2,000 exotic animals in a breathtaking 1.6-million-gallon habitat; and
- Taste the variety of foods at the 20-plus restaurants Mandalay Bay has to offer, including beach dining.
Whether you couldn’t make it to HM13 or you’re bringing back all the energy from the conference back to your hospital, now is the time to start planning for the next national conference exclusively designed for the nation’s 40,000 hospitalists.
For newcomers, HM14 will offer unprecedented access, networking, and CME-accredited educational sessions for hospitalists in all career stages. And for veterans of SHM’s annual meeting, 2014 will introduce two new pre-courses: “Cardiology and Evidence-Based Medicine” and “Bending the Cost Curve,” one of the hottest topics in public health, which will have its own dedicated track as well.
In addition to offering the best CME-accredited educational experience, HM14 will also give hospitalists the chance to enjoy an all-new official headquarters for the meeting: Mandalay Bay Hotel & Casino in Las Vegas.
Pre-Courses
Enhance the HM14 educational experience, broaden your skills, and earn additional CME credits. Choose from one of the following HM-focused topics:
- Medical Procedures for the Hospitalist;
- Portable Ultrasound for the Hospitalist;
- Perioperative Medicine;
- ABIM Maintenance of Certification;
- Practice Management;
- Neurology;
- Cardiology (new); and
- Evidence-Based Medicine (new).
Content Areas
The educational tracks offered at HM14 enable attendees to take courses in various designated tracks designed to better focus and enrich the annual meeting for attendees.
Tracks focus on the following cutting-edge content areas:
- Clinical;
- Rapid Fire;
- Practice Management;
- Academic/Research;
- Quality;
- Bending the Cost Curve (new);
- Pediatric;
- Potpourri;
- Comanagement; and
- Workshops.
Brendon Shank is SHM’s associate vice president of communications.
HM14 HEADQUARTERS: THE MANDALAY BAY HOTEL & CASINO
Enjoy casual elegance and comfort in the main tower’s rooms and suites, or relax in unparalleled sophistication and style at The Hotel at Mandalay Bay. At HM14 in March, hospitalists will:
- Bask in ultimate aquatic relaxation at the unforgettable, 11-acre Mandalay Bay Beach;
- Explore the Shark Reef Aquarium, featuring more than 2,000 exotic animals in a breathtaking 1.6-million-gallon habitat; and
- Taste the variety of foods at the 20-plus restaurants Mandalay Bay has to offer, including beach dining.
RIV Presenters at HM13 Explore Common Hospitalist Concerns
Two oral research poster presentations at HM13 explored malpractice concerns of hospitalists and the issue of defensive-medicine-related overutilization—popular topics considering how policymakers are attempting to bend the cost curve in the direction of greater efficiency and value.
Hospitalist Alan Kachalia, MD, JD, and colleagues at Brigham and Women’s Hospital in Boston conducted a randomized national survey of 1,020 hospitalists and analyzed their responses to common clinical scenarios. They found evidence of inappropriate overutilization and deviance from scientific evidence or recognized treatment guidelines, which the research team pegged to the practice of defensive medicine.
Dr. Kachalia’s presentation, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists,” was named best of the oral presentations in the research category.
“Our survey found substantial overutilization, frequently caused by defensive medicine,” in response to questions about practice patterns for two common clinical scenarios: preoperative evaluation and syncope, Dr. Kachalia said. Physicians who practiced at Veterans Affairs medical centers had less association with defensive medicine, while those who paid for their own liability insurance reported more. Overall, defensive medicine was reported for 37% of preoperative evaluations and 58% of the syncope scenarios.
More than 800 abstracts were submitted for HM13’s Research, Innovations, and Clinical Vignettes (RIV) competition. Nearly 600 were accepted, put on display at the annual meeting, and published online (www.shmabstracts.com). More than 100 abstracts were judged, with 15 of the Research and Innovations entries invited to make oral presentations of their projects. Three others gave “Best of RIV” plenary presentations at the conference.
The diversity and richness of HM13’s oral and poster presentations also will be highlighted in the Innovations department of The Hospitalist over the next year.
Asked to suggest policy responses to these findings, Dr. Kachalia said reform of the malpractice system is needed. “What a lot of us argue is that to get physicians to follow treatment guidelines, make them more clear and practical,” he said. “We’d also like to see safe harbors [from lawsuits] for following recognized guidelines.”
Adam Schaffer, MD, also a hospitalist at Brigham and Women’s Hospital in Boston, and colleagues reviewed a medical liability insurance carrier’s database of more than 30,000 closed claims for those in which a hospitalist was the attending of record. Dr. Schaffer’s retrospective, observational analysis, “Medical Malpractice: Causes and Outcomes of Claims Against Hospitalists,” of the claims database from 1997 to 2011 found 272 claims—almost 1%—for which the attending was a hospitalist.
“The claims rate was almost four times lower for hospitalists than for nonhospitalist internal-medicine physicians,” he said.
The average payment for claims against hospitalists also was smaller. He noted that the types of claims were similar and tended to fall in three general categories: errors in medical treatment, missed or delayed diagnoses, and medication-related errors (although claims also tended to have multiple contributing factors).
Research like Dr. Schaffer’s could help to inform patient-safety efforts and reduce legal malpractice risk, he said. If hospitalists have fewer malpractice claims, that information might also be used to argue for lower malpractice premium rates.
Larry Beresford is a freelance writer in Oakland, Calif.
Two oral research poster presentations at HM13 explored malpractice concerns of hospitalists and the issue of defensive-medicine-related overutilization—popular topics considering how policymakers are attempting to bend the cost curve in the direction of greater efficiency and value.
Hospitalist Alan Kachalia, MD, JD, and colleagues at Brigham and Women’s Hospital in Boston conducted a randomized national survey of 1,020 hospitalists and analyzed their responses to common clinical scenarios. They found evidence of inappropriate overutilization and deviance from scientific evidence or recognized treatment guidelines, which the research team pegged to the practice of defensive medicine.
Dr. Kachalia’s presentation, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists,” was named best of the oral presentations in the research category.
“Our survey found substantial overutilization, frequently caused by defensive medicine,” in response to questions about practice patterns for two common clinical scenarios: preoperative evaluation and syncope, Dr. Kachalia said. Physicians who practiced at Veterans Affairs medical centers had less association with defensive medicine, while those who paid for their own liability insurance reported more. Overall, defensive medicine was reported for 37% of preoperative evaluations and 58% of the syncope scenarios.
More than 800 abstracts were submitted for HM13’s Research, Innovations, and Clinical Vignettes (RIV) competition. Nearly 600 were accepted, put on display at the annual meeting, and published online (www.shmabstracts.com). More than 100 abstracts were judged, with 15 of the Research and Innovations entries invited to make oral presentations of their projects. Three others gave “Best of RIV” plenary presentations at the conference.
The diversity and richness of HM13’s oral and poster presentations also will be highlighted in the Innovations department of The Hospitalist over the next year.
Asked to suggest policy responses to these findings, Dr. Kachalia said reform of the malpractice system is needed. “What a lot of us argue is that to get physicians to follow treatment guidelines, make them more clear and practical,” he said. “We’d also like to see safe harbors [from lawsuits] for following recognized guidelines.”
Adam Schaffer, MD, also a hospitalist at Brigham and Women’s Hospital in Boston, and colleagues reviewed a medical liability insurance carrier’s database of more than 30,000 closed claims for those in which a hospitalist was the attending of record. Dr. Schaffer’s retrospective, observational analysis, “Medical Malpractice: Causes and Outcomes of Claims Against Hospitalists,” of the claims database from 1997 to 2011 found 272 claims—almost 1%—for which the attending was a hospitalist.
“The claims rate was almost four times lower for hospitalists than for nonhospitalist internal-medicine physicians,” he said.
The average payment for claims against hospitalists also was smaller. He noted that the types of claims were similar and tended to fall in three general categories: errors in medical treatment, missed or delayed diagnoses, and medication-related errors (although claims also tended to have multiple contributing factors).
Research like Dr. Schaffer’s could help to inform patient-safety efforts and reduce legal malpractice risk, he said. If hospitalists have fewer malpractice claims, that information might also be used to argue for lower malpractice premium rates.
Larry Beresford is a freelance writer in Oakland, Calif.
Two oral research poster presentations at HM13 explored malpractice concerns of hospitalists and the issue of defensive-medicine-related overutilization—popular topics considering how policymakers are attempting to bend the cost curve in the direction of greater efficiency and value.
Hospitalist Alan Kachalia, MD, JD, and colleagues at Brigham and Women’s Hospital in Boston conducted a randomized national survey of 1,020 hospitalists and analyzed their responses to common clinical scenarios. They found evidence of inappropriate overutilization and deviance from scientific evidence or recognized treatment guidelines, which the research team pegged to the practice of defensive medicine.
Dr. Kachalia’s presentation, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists,” was named best of the oral presentations in the research category.
“Our survey found substantial overutilization, frequently caused by defensive medicine,” in response to questions about practice patterns for two common clinical scenarios: preoperative evaluation and syncope, Dr. Kachalia said. Physicians who practiced at Veterans Affairs medical centers had less association with defensive medicine, while those who paid for their own liability insurance reported more. Overall, defensive medicine was reported for 37% of preoperative evaluations and 58% of the syncope scenarios.
More than 800 abstracts were submitted for HM13’s Research, Innovations, and Clinical Vignettes (RIV) competition. Nearly 600 were accepted, put on display at the annual meeting, and published online (www.shmabstracts.com). More than 100 abstracts were judged, with 15 of the Research and Innovations entries invited to make oral presentations of their projects. Three others gave “Best of RIV” plenary presentations at the conference.
The diversity and richness of HM13’s oral and poster presentations also will be highlighted in the Innovations department of The Hospitalist over the next year.
Asked to suggest policy responses to these findings, Dr. Kachalia said reform of the malpractice system is needed. “What a lot of us argue is that to get physicians to follow treatment guidelines, make them more clear and practical,” he said. “We’d also like to see safe harbors [from lawsuits] for following recognized guidelines.”
Adam Schaffer, MD, also a hospitalist at Brigham and Women’s Hospital in Boston, and colleagues reviewed a medical liability insurance carrier’s database of more than 30,000 closed claims for those in which a hospitalist was the attending of record. Dr. Schaffer’s retrospective, observational analysis, “Medical Malpractice: Causes and Outcomes of Claims Against Hospitalists,” of the claims database from 1997 to 2011 found 272 claims—almost 1%—for which the attending was a hospitalist.
“The claims rate was almost four times lower for hospitalists than for nonhospitalist internal-medicine physicians,” he said.
The average payment for claims against hospitalists also was smaller. He noted that the types of claims were similar and tended to fall in three general categories: errors in medical treatment, missed or delayed diagnoses, and medication-related errors (although claims also tended to have multiple contributing factors).
Research like Dr. Schaffer’s could help to inform patient-safety efforts and reduce legal malpractice risk, he said. If hospitalists have fewer malpractice claims, that information might also be used to argue for lower malpractice premium rates.
Larry Beresford is a freelance writer in Oakland, Calif.
Hospitalists Share Information, Insights Through RIV Posters at HM13
One of the busiest times of HM13—and, come to think of it, every recent annual meeting—is the poster session for the Research, Innovations, and Clinical Vignettes (RIV) competition. This year, more than 800 abstracts were submitted and reviewed, with nearly 600 being accepted for presentation at HM13. That meant thousands of hospitalists thumbtacking posters to rows and rows of portable bulletin boards in the Gaylord National Resort & Convention Center’s massive exhibit hall.
With all those posters and accompanying oral presentations, it’s impossible for RIV judges to chat with everybody, so they choose finalists based on the abstracts, then listen to quick-hit summaries before choosing a winner on site. And meeting attendees are just as strapped for time, so they do the best they can to see as many posters as they can, taking time to network with old connections and make new ones.
So with all the limitations on how many people will interact with your poster, the small chance of winning Best in Show, and the hundreds of work hours that go into a poster presentation, why do it?
“To share is what I think is really important,” says Todd Hecht, MD, FACP, SFHM, associate professor of clinical medicine at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia. “If you don’t let other people know what you’re doing, they can’t bring it to their institutions, nor can you learn from others and bring their innovations to your own hospital.”
Dr. Hecht, director of the Anticoagulation Management Center and Anticoagulation Management Program at the Hospital of the University of Pennsylvania, takes the poster sessions very seriously. This year, he entered a poster in both the Innovations and Vignette categories. His Innovations poster, “Impact of a Multidisciplinary Safety Checklist on the Rate of Preventable Hospital Complications and Standardization of Care,” was a finalist.
That meant that, at the very least, he’d be able to explain to at least two judges what motivated his research team’s project. And what was the inspiration? A 90-year-old male patient with metastatic melanoma who, in the fall of 2011, refused to take medication for VTE prophylaxis, as lesions on his skin made the process rather painful. After refusing the doses for a bit, though, the high-risk patient unsurprisingly developed a pulmonary embolism (PE).
The man survived the PE, but Dr. Hecht and his colleagues began to wonder how many patients refuse VTE prophylaxis. So they investigated, and it turned out that from December 2010 to February 2011, 26.4% of the prescribed doses of prophylaxis on the medicine floors they studied were missed. Moreover, nearly 80% of all missed doses on the medicine floors were due to patient refusal.
“It was astonishing to me that it was that high,” Dr. Hecht says. “If there were 1,000 doses in a month, 260 of them were not being given—and 205 of them were not given because they were refused.”
Checklist Integration
So Dr. Hecht and colleagues set out to create a checklist that could be used daily on multidisciplinary rounds to help reduce the risk of VTE. First question on the list: Has prophylaxis been ordered, and if so, is the patient refusing it? Knowing that patients are “refusing” medication can lead to discussions about why that is happening, which in turn can lead to ways to convince the patient that the preventative measure is a good idea.
Dr. Hecht says the team also realized a checklist creates the opportunity to improve other quality metrics, such as hospital-associated infections (HAIs). Two questions on the checklist ask whether indwelling urinary catheters (IUCs) and central venous catheters (CVCs) can be removed. Two questions ask if telemetry can be stopped and whether there are any pain-management concerns. A final query asks whether there are any nursing, social work, or discharge-related questions—a step that, according to Dr. Hecht, loops the entire multidisciplinary team into the care-plan discussion.
“An ongoing challenge is making sure it’s not just questions being asked and being answered by rote,” Dr. Hecht says. “Just pause and think for just a second for each question. You can get through the checklist in 10 seconds, but you can’t go through the checklist in two seconds.”
The project’s results are what made it a finalist. After the checklist intervention, the number of missed doses of VTE prophylaxis plummeted 59% to just 10.9% (P<0.001) from September to November 2012; the number of “patient refused” doses dropped to 6.3% (P<0.001).
Not only was Dr. Hecht caught off guard by his findings, but so were the judges who visited his poster—Mangla Gulati, MD, FHM, of the University of Maryland School of Medicine and Rachel George, MD, MBA, FHM, of Cogent HMG.
“I wonder if it’s like that in every hospital,” Dr. George says. “I’d like to know.”
The positive reaction and feedback to Dr. Hecht’s poster, however, was not enough to win the Innovations category. That honor went to “SEPTRIS: Improving Sepsis Recognition and Management Through a Mobile Educational Game,” which was developed by a team of researchers at Stanford University in Palo Alto, Calif. The video game
(http://med.stanford.edu/septris/)—a mashup of sepsis and the once-popular Tetris puzzle game—already has been played 17,000 times and is on its way to being shared in other languages.
“Win or lose, it doesn’t matter,” Dr. Hecht says. “The goal is to share your information with other people and learn from them.”
Peter Watson, MD, FACP, FHM, sees it the same way. That’s why this year he was both judge and judged. The division head of hospital medicine for Henry Ford Medical Group in Detroit was part of a group presenting “Feasibility and Efficacy of a Specialized Pilot Training Program to Enhance Inpatient Communication Skills of Hospitalists.” He was a judge for the Research portion of the contest. He says he’s hard-pressed to say which process he enjoyed more, but one trick of the poster trade he passes along is that “judging actually makes you a better presenter on the back end,” especially when it comes to describing in less than five minutes a poster whose work may date back 12 to 18 months.
“In your brain,” he says, “you have a Tolstoy novel of information, but you have to break that down into a paragraph of CliffsNotes, and actually convince the people that are judging you that you have a really cool project that either is going to have a big impact in the field or may lead to other big studies or is going to impress somebody so much that they’re going to go back to their institution and say, ‘Hey, I’m going to do that.’”
Dr. Watson also urges people not to be discouraged by not winning the poster contest. First, all of the accepted abstracts get published online (www.shmabstracts.com) by the Journal of Hospital Medicine, a high point for medical students, residents, and early-career physicians looking to make a mark. Second, presenting information of value to one’s peers is the definition of a specialty that prides itself on collaboration.
“To see a second-year medical student presenting all the way up to a very senior division chief and everything in between is a really good example for our profession,” he says. “That’s really the magic of this meeting.”
Richard Quinn is a freelance writer in New Jersey.
One of the busiest times of HM13—and, come to think of it, every recent annual meeting—is the poster session for the Research, Innovations, and Clinical Vignettes (RIV) competition. This year, more than 800 abstracts were submitted and reviewed, with nearly 600 being accepted for presentation at HM13. That meant thousands of hospitalists thumbtacking posters to rows and rows of portable bulletin boards in the Gaylord National Resort & Convention Center’s massive exhibit hall.
With all those posters and accompanying oral presentations, it’s impossible for RIV judges to chat with everybody, so they choose finalists based on the abstracts, then listen to quick-hit summaries before choosing a winner on site. And meeting attendees are just as strapped for time, so they do the best they can to see as many posters as they can, taking time to network with old connections and make new ones.
So with all the limitations on how many people will interact with your poster, the small chance of winning Best in Show, and the hundreds of work hours that go into a poster presentation, why do it?
“To share is what I think is really important,” says Todd Hecht, MD, FACP, SFHM, associate professor of clinical medicine at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia. “If you don’t let other people know what you’re doing, they can’t bring it to their institutions, nor can you learn from others and bring their innovations to your own hospital.”
Dr. Hecht, director of the Anticoagulation Management Center and Anticoagulation Management Program at the Hospital of the University of Pennsylvania, takes the poster sessions very seriously. This year, he entered a poster in both the Innovations and Vignette categories. His Innovations poster, “Impact of a Multidisciplinary Safety Checklist on the Rate of Preventable Hospital Complications and Standardization of Care,” was a finalist.
That meant that, at the very least, he’d be able to explain to at least two judges what motivated his research team’s project. And what was the inspiration? A 90-year-old male patient with metastatic melanoma who, in the fall of 2011, refused to take medication for VTE prophylaxis, as lesions on his skin made the process rather painful. After refusing the doses for a bit, though, the high-risk patient unsurprisingly developed a pulmonary embolism (PE).
The man survived the PE, but Dr. Hecht and his colleagues began to wonder how many patients refuse VTE prophylaxis. So they investigated, and it turned out that from December 2010 to February 2011, 26.4% of the prescribed doses of prophylaxis on the medicine floors they studied were missed. Moreover, nearly 80% of all missed doses on the medicine floors were due to patient refusal.
“It was astonishing to me that it was that high,” Dr. Hecht says. “If there were 1,000 doses in a month, 260 of them were not being given—and 205 of them were not given because they were refused.”
Checklist Integration
So Dr. Hecht and colleagues set out to create a checklist that could be used daily on multidisciplinary rounds to help reduce the risk of VTE. First question on the list: Has prophylaxis been ordered, and if so, is the patient refusing it? Knowing that patients are “refusing” medication can lead to discussions about why that is happening, which in turn can lead to ways to convince the patient that the preventative measure is a good idea.
Dr. Hecht says the team also realized a checklist creates the opportunity to improve other quality metrics, such as hospital-associated infections (HAIs). Two questions on the checklist ask whether indwelling urinary catheters (IUCs) and central venous catheters (CVCs) can be removed. Two questions ask if telemetry can be stopped and whether there are any pain-management concerns. A final query asks whether there are any nursing, social work, or discharge-related questions—a step that, according to Dr. Hecht, loops the entire multidisciplinary team into the care-plan discussion.
“An ongoing challenge is making sure it’s not just questions being asked and being answered by rote,” Dr. Hecht says. “Just pause and think for just a second for each question. You can get through the checklist in 10 seconds, but you can’t go through the checklist in two seconds.”
The project’s results are what made it a finalist. After the checklist intervention, the number of missed doses of VTE prophylaxis plummeted 59% to just 10.9% (P<0.001) from September to November 2012; the number of “patient refused” doses dropped to 6.3% (P<0.001).
Not only was Dr. Hecht caught off guard by his findings, but so were the judges who visited his poster—Mangla Gulati, MD, FHM, of the University of Maryland School of Medicine and Rachel George, MD, MBA, FHM, of Cogent HMG.
“I wonder if it’s like that in every hospital,” Dr. George says. “I’d like to know.”
The positive reaction and feedback to Dr. Hecht’s poster, however, was not enough to win the Innovations category. That honor went to “SEPTRIS: Improving Sepsis Recognition and Management Through a Mobile Educational Game,” which was developed by a team of researchers at Stanford University in Palo Alto, Calif. The video game
(http://med.stanford.edu/septris/)—a mashup of sepsis and the once-popular Tetris puzzle game—already has been played 17,000 times and is on its way to being shared in other languages.
“Win or lose, it doesn’t matter,” Dr. Hecht says. “The goal is to share your information with other people and learn from them.”
Peter Watson, MD, FACP, FHM, sees it the same way. That’s why this year he was both judge and judged. The division head of hospital medicine for Henry Ford Medical Group in Detroit was part of a group presenting “Feasibility and Efficacy of a Specialized Pilot Training Program to Enhance Inpatient Communication Skills of Hospitalists.” He was a judge for the Research portion of the contest. He says he’s hard-pressed to say which process he enjoyed more, but one trick of the poster trade he passes along is that “judging actually makes you a better presenter on the back end,” especially when it comes to describing in less than five minutes a poster whose work may date back 12 to 18 months.
“In your brain,” he says, “you have a Tolstoy novel of information, but you have to break that down into a paragraph of CliffsNotes, and actually convince the people that are judging you that you have a really cool project that either is going to have a big impact in the field or may lead to other big studies or is going to impress somebody so much that they’re going to go back to their institution and say, ‘Hey, I’m going to do that.’”
Dr. Watson also urges people not to be discouraged by not winning the poster contest. First, all of the accepted abstracts get published online (www.shmabstracts.com) by the Journal of Hospital Medicine, a high point for medical students, residents, and early-career physicians looking to make a mark. Second, presenting information of value to one’s peers is the definition of a specialty that prides itself on collaboration.
“To see a second-year medical student presenting all the way up to a very senior division chief and everything in between is a really good example for our profession,” he says. “That’s really the magic of this meeting.”
Richard Quinn is a freelance writer in New Jersey.
One of the busiest times of HM13—and, come to think of it, every recent annual meeting—is the poster session for the Research, Innovations, and Clinical Vignettes (RIV) competition. This year, more than 800 abstracts were submitted and reviewed, with nearly 600 being accepted for presentation at HM13. That meant thousands of hospitalists thumbtacking posters to rows and rows of portable bulletin boards in the Gaylord National Resort & Convention Center’s massive exhibit hall.
With all those posters and accompanying oral presentations, it’s impossible for RIV judges to chat with everybody, so they choose finalists based on the abstracts, then listen to quick-hit summaries before choosing a winner on site. And meeting attendees are just as strapped for time, so they do the best they can to see as many posters as they can, taking time to network with old connections and make new ones.
So with all the limitations on how many people will interact with your poster, the small chance of winning Best in Show, and the hundreds of work hours that go into a poster presentation, why do it?
“To share is what I think is really important,” says Todd Hecht, MD, FACP, SFHM, associate professor of clinical medicine at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia. “If you don’t let other people know what you’re doing, they can’t bring it to their institutions, nor can you learn from others and bring their innovations to your own hospital.”
Dr. Hecht, director of the Anticoagulation Management Center and Anticoagulation Management Program at the Hospital of the University of Pennsylvania, takes the poster sessions very seriously. This year, he entered a poster in both the Innovations and Vignette categories. His Innovations poster, “Impact of a Multidisciplinary Safety Checklist on the Rate of Preventable Hospital Complications and Standardization of Care,” was a finalist.
That meant that, at the very least, he’d be able to explain to at least two judges what motivated his research team’s project. And what was the inspiration? A 90-year-old male patient with metastatic melanoma who, in the fall of 2011, refused to take medication for VTE prophylaxis, as lesions on his skin made the process rather painful. After refusing the doses for a bit, though, the high-risk patient unsurprisingly developed a pulmonary embolism (PE).
The man survived the PE, but Dr. Hecht and his colleagues began to wonder how many patients refuse VTE prophylaxis. So they investigated, and it turned out that from December 2010 to February 2011, 26.4% of the prescribed doses of prophylaxis on the medicine floors they studied were missed. Moreover, nearly 80% of all missed doses on the medicine floors were due to patient refusal.
“It was astonishing to me that it was that high,” Dr. Hecht says. “If there were 1,000 doses in a month, 260 of them were not being given—and 205 of them were not given because they were refused.”
Checklist Integration
So Dr. Hecht and colleagues set out to create a checklist that could be used daily on multidisciplinary rounds to help reduce the risk of VTE. First question on the list: Has prophylaxis been ordered, and if so, is the patient refusing it? Knowing that patients are “refusing” medication can lead to discussions about why that is happening, which in turn can lead to ways to convince the patient that the preventative measure is a good idea.
Dr. Hecht says the team also realized a checklist creates the opportunity to improve other quality metrics, such as hospital-associated infections (HAIs). Two questions on the checklist ask whether indwelling urinary catheters (IUCs) and central venous catheters (CVCs) can be removed. Two questions ask if telemetry can be stopped and whether there are any pain-management concerns. A final query asks whether there are any nursing, social work, or discharge-related questions—a step that, according to Dr. Hecht, loops the entire multidisciplinary team into the care-plan discussion.
“An ongoing challenge is making sure it’s not just questions being asked and being answered by rote,” Dr. Hecht says. “Just pause and think for just a second for each question. You can get through the checklist in 10 seconds, but you can’t go through the checklist in two seconds.”
The project’s results are what made it a finalist. After the checklist intervention, the number of missed doses of VTE prophylaxis plummeted 59% to just 10.9% (P<0.001) from September to November 2012; the number of “patient refused” doses dropped to 6.3% (P<0.001).
Not only was Dr. Hecht caught off guard by his findings, but so were the judges who visited his poster—Mangla Gulati, MD, FHM, of the University of Maryland School of Medicine and Rachel George, MD, MBA, FHM, of Cogent HMG.
“I wonder if it’s like that in every hospital,” Dr. George says. “I’d like to know.”
The positive reaction and feedback to Dr. Hecht’s poster, however, was not enough to win the Innovations category. That honor went to “SEPTRIS: Improving Sepsis Recognition and Management Through a Mobile Educational Game,” which was developed by a team of researchers at Stanford University in Palo Alto, Calif. The video game
(http://med.stanford.edu/septris/)—a mashup of sepsis and the once-popular Tetris puzzle game—already has been played 17,000 times and is on its way to being shared in other languages.
“Win or lose, it doesn’t matter,” Dr. Hecht says. “The goal is to share your information with other people and learn from them.”
Peter Watson, MD, FACP, FHM, sees it the same way. That’s why this year he was both judge and judged. The division head of hospital medicine for Henry Ford Medical Group in Detroit was part of a group presenting “Feasibility and Efficacy of a Specialized Pilot Training Program to Enhance Inpatient Communication Skills of Hospitalists.” He was a judge for the Research portion of the contest. He says he’s hard-pressed to say which process he enjoyed more, but one trick of the poster trade he passes along is that “judging actually makes you a better presenter on the back end,” especially when it comes to describing in less than five minutes a poster whose work may date back 12 to 18 months.
“In your brain,” he says, “you have a Tolstoy novel of information, but you have to break that down into a paragraph of CliffsNotes, and actually convince the people that are judging you that you have a really cool project that either is going to have a big impact in the field or may lead to other big studies or is going to impress somebody so much that they’re going to go back to their institution and say, ‘Hey, I’m going to do that.’”
Dr. Watson also urges people not to be discouraged by not winning the poster contest. First, all of the accepted abstracts get published online (www.shmabstracts.com) by the Journal of Hospital Medicine, a high point for medical students, residents, and early-career physicians looking to make a mark. Second, presenting information of value to one’s peers is the definition of a specialty that prides itself on collaboration.
“To see a second-year medical student presenting all the way up to a very senior division chief and everything in between is a really good example for our profession,” he says. “That’s really the magic of this meeting.”
Richard Quinn is a freelance writer in New Jersey.
Quality Improvement (QI) Remains a Central Theme at HM13


Like a grinning child at a carnival, Iqbal M. Binoj, MD, steps right up and gives it a try—except instead of tossing rings, he’s gripping an intraosseous infusion drill.
A tutor shows him how the device, which looks remarkably like a glue gun, inserts into the bones of the shoulder or knee and drills down until it hits the marrow. He is guided on using a steady speed to maintain the integrity of the cavity. He’s also taught about the maneuver’s low complication rates and ability to expedite workups.
“I’ve seen it used before, but I never did it,” says Dr. Binoj, a hospitalist with Cogent HMG at Genesis Medical Center in Davenport, Iowa.
Well, he never did it before a hands-on pre-course at HM13 that focused on improving hospitalists’ proficiency at such procedures as lumbar punctures and ultrasound-guided vascular access. Quality improvement (QI) is always a focus of SHM’s annual meeting, but sometimes the science of improving care is viewed from up on high.
Not everything needs to be a national imitative, an institution-wide project, or even a unit-based intervention. Sometimes, it’s as simple as teaching a room full of hospitalists how to use an intraosseous infusion drill, says Michelle Fox, RN, BSN, senior director of clinical affairs with Vidacare, which manufactures the drill used in the demonstration.
“Hospitalists have an increasing role in doing these procedures, not only in the environment they predominantly support but in other areas of the hospital,” Fox says, adding that “the primary goal of this course is to give them the opportunity to perfect those skills.”
Hospitalist Bradley Rosen, MD, MBA, FHM, medical of the inpatient specialty program at Cedars-Sinai in Los Angeles, says the point of hands-on demonstrations is to translate QI to the bedside. Take ultrasound devices, he says. In the past few years, the technology has become less expensive, better in resolution, more common, and more portable. Hospitalists must ensure hands-on training that keeps pace with that technology.
“We actually want people to get gloves on, hands on, learn where they may have challenges in terms of their own dexterity or workflow, which hand is dominant, and how to visualize on the ultrasound machine a three-dimensional structure in 2D,” he says. “We don’t want people watching from the sidelines. ... We try to get people in it and engaged.”
And once hospitalists master procedures or diagnostic maneuvers, they invariably are sought out by other physicians to pass that knowledge on to others, Dr. Rosen says.
“In so doing, we get involved in larger quality initiatives and systemwide changes that can go top-down,” he adds, “but from our perspective, it starts with the individual practitioner. And I think SHM has always advocated and preached the importance of the individual hospitalist doing the best possible job for your patient, and the group, and the institution.”
Shared Excellence
What’s best for individual institutions moving forward is what worries SHM immediate past president Shaun Frost, MD, SFHM. He fears CMS’ Value-Based Payment Modifier (VBPM) program could have the unintended consequence of spurring some hospitals to hang on to innovative ideas in order to keep a competitive business advantage.
In health care, where quality and affordability have long been viewed as valuable for nonmonetary reasons, “the medical profession willingly shares new information” to improve patient care, Dr. Frost said in his farewell speech. But he is concerned that commodification—imbuing monetary value into something that previously had none—could change that dynamic, a situation he says is “ethically not acceptable.”
“When somebody builds a better mousetrap, it should be freely shared so that all patients have the opportunity to benefit,” Dr. Frost said. “The pursuit of economic competitive advantage should not prevent us from collaborating and sharing new ideas that hopefully make the health system better.”
Kendall Rogers, MD, FACP, SFHM, chief of the division of hospital medicine at the University of New Mexico Health Sciences Center in Albuquerque, N.M., says part of that improvement in quality and patient safety will come via hospitalists pushing for improvements to health information technology (HIT), particularly to maximize computerized physician order entry (CPOE) and order sets. He empathizes with those who complain about the operability of existing systems but urges physicians to stop complaining and take action.
“We need to stop accepting what our existing limitations are, and we need to be the innovators,” he says. “Many of us aren’t even thinking about, ‘What are the products we need?’ We’re just reacting to the products we currently have and stating how they don’t meet our needs.”
He suggests people communally report safety or troubleshooting issues, in part via Hospital Medicine Exchange (HMX), an online community SHM launched last year to discuss HM issues (www.hmxchange.org). He also wants hospitalists to push HIT vendors to provide improved functionality, and for institutions to provide necessary training.
“We just need to be vocal,” says Dr. Rogers, chair of SHM’s IT Executive Committee. “I do believe this is all leading us to a good place, but there’s a dip down before we have a swing up.”
Frustration Surge
In the long run, hospitalist Anuj Mehta, MD, medical director of the adult hospitalist program at Nyack Hospital in New York, agrees with Dr. Rogers. But as a provider seeing patients day after day, he says it’s often easier to not engage HIT than it is to slog through it.
“We try to work around the system, and sometimes it’s a much longer workaround,” he says. “So what happens is loss of productivity, greater length of stay, poor patient satisfaction, more screen time, and less bedside time.”
Dr. Mehta says frustration is building as society—outside of medicine—moves rapidly through such technology as smartphones, tablets, and other intuitive devices that make actions easier. He notes that his toddler daughter could learn how to navigate an iPad in a fraction of the time it takes him to complete an HIT training course.
“You cannot have physicians going through learning for four hours, learning a system to do step one before step two before step three,” he laments. “It should flow naturally. I don’t think the IT people have realized that as of yet.”
Richard Quinn is a freelance writer in New Jersey.
Like a grinning child at a carnival, Iqbal M. Binoj, MD, steps right up and gives it a try—except instead of tossing rings, he’s gripping an intraosseous infusion drill.
A tutor shows him how the device, which looks remarkably like a glue gun, inserts into the bones of the shoulder or knee and drills down until it hits the marrow. He is guided on using a steady speed to maintain the integrity of the cavity. He’s also taught about the maneuver’s low complication rates and ability to expedite workups.
“I’ve seen it used before, but I never did it,” says Dr. Binoj, a hospitalist with Cogent HMG at Genesis Medical Center in Davenport, Iowa.
Well, he never did it before a hands-on pre-course at HM13 that focused on improving hospitalists’ proficiency at such procedures as lumbar punctures and ultrasound-guided vascular access. Quality improvement (QI) is always a focus of SHM’s annual meeting, but sometimes the science of improving care is viewed from up on high.
Not everything needs to be a national imitative, an institution-wide project, or even a unit-based intervention. Sometimes, it’s as simple as teaching a room full of hospitalists how to use an intraosseous infusion drill, says Michelle Fox, RN, BSN, senior director of clinical affairs with Vidacare, which manufactures the drill used in the demonstration.
“Hospitalists have an increasing role in doing these procedures, not only in the environment they predominantly support but in other areas of the hospital,” Fox says, adding that “the primary goal of this course is to give them the opportunity to perfect those skills.”
Hospitalist Bradley Rosen, MD, MBA, FHM, medical of the inpatient specialty program at Cedars-Sinai in Los Angeles, says the point of hands-on demonstrations is to translate QI to the bedside. Take ultrasound devices, he says. In the past few years, the technology has become less expensive, better in resolution, more common, and more portable. Hospitalists must ensure hands-on training that keeps pace with that technology.
“We actually want people to get gloves on, hands on, learn where they may have challenges in terms of their own dexterity or workflow, which hand is dominant, and how to visualize on the ultrasound machine a three-dimensional structure in 2D,” he says. “We don’t want people watching from the sidelines. ... We try to get people in it and engaged.”
And once hospitalists master procedures or diagnostic maneuvers, they invariably are sought out by other physicians to pass that knowledge on to others, Dr. Rosen says.
“In so doing, we get involved in larger quality initiatives and systemwide changes that can go top-down,” he adds, “but from our perspective, it starts with the individual practitioner. And I think SHM has always advocated and preached the importance of the individual hospitalist doing the best possible job for your patient, and the group, and the institution.”
Shared Excellence
What’s best for individual institutions moving forward is what worries SHM immediate past president Shaun Frost, MD, SFHM. He fears CMS’ Value-Based Payment Modifier (VBPM) program could have the unintended consequence of spurring some hospitals to hang on to innovative ideas in order to keep a competitive business advantage.
In health care, where quality and affordability have long been viewed as valuable for nonmonetary reasons, “the medical profession willingly shares new information” to improve patient care, Dr. Frost said in his farewell speech. But he is concerned that commodification—imbuing monetary value into something that previously had none—could change that dynamic, a situation he says is “ethically not acceptable.”
“When somebody builds a better mousetrap, it should be freely shared so that all patients have the opportunity to benefit,” Dr. Frost said. “The pursuit of economic competitive advantage should not prevent us from collaborating and sharing new ideas that hopefully make the health system better.”
Kendall Rogers, MD, FACP, SFHM, chief of the division of hospital medicine at the University of New Mexico Health Sciences Center in Albuquerque, N.M., says part of that improvement in quality and patient safety will come via hospitalists pushing for improvements to health information technology (HIT), particularly to maximize computerized physician order entry (CPOE) and order sets. He empathizes with those who complain about the operability of existing systems but urges physicians to stop complaining and take action.
“We need to stop accepting what our existing limitations are, and we need to be the innovators,” he says. “Many of us aren’t even thinking about, ‘What are the products we need?’ We’re just reacting to the products we currently have and stating how they don’t meet our needs.”
He suggests people communally report safety or troubleshooting issues, in part via Hospital Medicine Exchange (HMX), an online community SHM launched last year to discuss HM issues (www.hmxchange.org). He also wants hospitalists to push HIT vendors to provide improved functionality, and for institutions to provide necessary training.
“We just need to be vocal,” says Dr. Rogers, chair of SHM’s IT Executive Committee. “I do believe this is all leading us to a good place, but there’s a dip down before we have a swing up.”
Frustration Surge
In the long run, hospitalist Anuj Mehta, MD, medical director of the adult hospitalist program at Nyack Hospital in New York, agrees with Dr. Rogers. But as a provider seeing patients day after day, he says it’s often easier to not engage HIT than it is to slog through it.
“We try to work around the system, and sometimes it’s a much longer workaround,” he says. “So what happens is loss of productivity, greater length of stay, poor patient satisfaction, more screen time, and less bedside time.”
Dr. Mehta says frustration is building as society—outside of medicine—moves rapidly through such technology as smartphones, tablets, and other intuitive devices that make actions easier. He notes that his toddler daughter could learn how to navigate an iPad in a fraction of the time it takes him to complete an HIT training course.
“You cannot have physicians going through learning for four hours, learning a system to do step one before step two before step three,” he laments. “It should flow naturally. I don’t think the IT people have realized that as of yet.”
Richard Quinn is a freelance writer in New Jersey.
Like a grinning child at a carnival, Iqbal M. Binoj, MD, steps right up and gives it a try—except instead of tossing rings, he’s gripping an intraosseous infusion drill.
A tutor shows him how the device, which looks remarkably like a glue gun, inserts into the bones of the shoulder or knee and drills down until it hits the marrow. He is guided on using a steady speed to maintain the integrity of the cavity. He’s also taught about the maneuver’s low complication rates and ability to expedite workups.
“I’ve seen it used before, but I never did it,” says Dr. Binoj, a hospitalist with Cogent HMG at Genesis Medical Center in Davenport, Iowa.
Well, he never did it before a hands-on pre-course at HM13 that focused on improving hospitalists’ proficiency at such procedures as lumbar punctures and ultrasound-guided vascular access. Quality improvement (QI) is always a focus of SHM’s annual meeting, but sometimes the science of improving care is viewed from up on high.
Not everything needs to be a national imitative, an institution-wide project, or even a unit-based intervention. Sometimes, it’s as simple as teaching a room full of hospitalists how to use an intraosseous infusion drill, says Michelle Fox, RN, BSN, senior director of clinical affairs with Vidacare, which manufactures the drill used in the demonstration.
“Hospitalists have an increasing role in doing these procedures, not only in the environment they predominantly support but in other areas of the hospital,” Fox says, adding that “the primary goal of this course is to give them the opportunity to perfect those skills.”
Hospitalist Bradley Rosen, MD, MBA, FHM, medical of the inpatient specialty program at Cedars-Sinai in Los Angeles, says the point of hands-on demonstrations is to translate QI to the bedside. Take ultrasound devices, he says. In the past few years, the technology has become less expensive, better in resolution, more common, and more portable. Hospitalists must ensure hands-on training that keeps pace with that technology.
“We actually want people to get gloves on, hands on, learn where they may have challenges in terms of their own dexterity or workflow, which hand is dominant, and how to visualize on the ultrasound machine a three-dimensional structure in 2D,” he says. “We don’t want people watching from the sidelines. ... We try to get people in it and engaged.”
And once hospitalists master procedures or diagnostic maneuvers, they invariably are sought out by other physicians to pass that knowledge on to others, Dr. Rosen says.
“In so doing, we get involved in larger quality initiatives and systemwide changes that can go top-down,” he adds, “but from our perspective, it starts with the individual practitioner. And I think SHM has always advocated and preached the importance of the individual hospitalist doing the best possible job for your patient, and the group, and the institution.”
Shared Excellence
What’s best for individual institutions moving forward is what worries SHM immediate past president Shaun Frost, MD, SFHM. He fears CMS’ Value-Based Payment Modifier (VBPM) program could have the unintended consequence of spurring some hospitals to hang on to innovative ideas in order to keep a competitive business advantage.
In health care, where quality and affordability have long been viewed as valuable for nonmonetary reasons, “the medical profession willingly shares new information” to improve patient care, Dr. Frost said in his farewell speech. But he is concerned that commodification—imbuing monetary value into something that previously had none—could change that dynamic, a situation he says is “ethically not acceptable.”
“When somebody builds a better mousetrap, it should be freely shared so that all patients have the opportunity to benefit,” Dr. Frost said. “The pursuit of economic competitive advantage should not prevent us from collaborating and sharing new ideas that hopefully make the health system better.”
Kendall Rogers, MD, FACP, SFHM, chief of the division of hospital medicine at the University of New Mexico Health Sciences Center in Albuquerque, N.M., says part of that improvement in quality and patient safety will come via hospitalists pushing for improvements to health information technology (HIT), particularly to maximize computerized physician order entry (CPOE) and order sets. He empathizes with those who complain about the operability of existing systems but urges physicians to stop complaining and take action.
“We need to stop accepting what our existing limitations are, and we need to be the innovators,” he says. “Many of us aren’t even thinking about, ‘What are the products we need?’ We’re just reacting to the products we currently have and stating how they don’t meet our needs.”
He suggests people communally report safety or troubleshooting issues, in part via Hospital Medicine Exchange (HMX), an online community SHM launched last year to discuss HM issues (www.hmxchange.org). He also wants hospitalists to push HIT vendors to provide improved functionality, and for institutions to provide necessary training.
“We just need to be vocal,” says Dr. Rogers, chair of SHM’s IT Executive Committee. “I do believe this is all leading us to a good place, but there’s a dip down before we have a swing up.”
Frustration Surge
In the long run, hospitalist Anuj Mehta, MD, medical director of the adult hospitalist program at Nyack Hospital in New York, agrees with Dr. Rogers. But as a provider seeing patients day after day, he says it’s often easier to not engage HIT than it is to slog through it.
“We try to work around the system, and sometimes it’s a much longer workaround,” he says. “So what happens is loss of productivity, greater length of stay, poor patient satisfaction, more screen time, and less bedside time.”
Dr. Mehta says frustration is building as society—outside of medicine—moves rapidly through such technology as smartphones, tablets, and other intuitive devices that make actions easier. He notes that his toddler daughter could learn how to navigate an iPad in a fraction of the time it takes him to complete an HIT training course.
“You cannot have physicians going through learning for four hours, learning a system to do step one before step two before step three,” he laments. “It should flow naturally. I don’t think the IT people have realized that as of yet.”
Richard Quinn is a freelance writer in New Jersey.
Pediatric Hospitalist Charts Decade-Long Journey in Health Care

Dear Mark,
I am pleased and excited that you are willing to abandon your plan for being a vagabond and will give serious consideration to joining the faculty of the Department of Pediatrics to become a core member of a new [general pediatric inpatient] program that I believe has exciting potential.
So reads the first line of my very first job offer letter. Obviously, my chairman had a sense of humor. But he also was not off target, as before May 21 of my third year of residency, I had no meaningful work lined up. Dreams of locum tenens work in Hawaii or a California coastal town quickly disappeared as I received only offers for work in small-town Mississippi and Oklahoma. Eleven years later, I don’t think I could have planned a more fulfilling early career, particularly when the alternative might have been surfing on the Mississippi River.
I would like this opportunity, in my final column as The Hospitalist’s pediatric editor, to reflect on this odyssey from vagabond to hospitalist.
The Early Years
As a new attending, I was appropriately terrified of how much I didn’t know. I also had ambitious goals at first, wanting to emulate my two favorite role models from residency, Charles Ginsburg and Heinz Eichenwald. We might call them hospitalists now, but back then they were old-fashioned, generalist inpatient clinician-educators, even while chairing the department of pediatrics over their separate tenures. They were the smartest and wisest teachers that I have ever met. These early years were a pseudo-fellowship of sorts; under their tutelage, I soaked up more than I ever had during residency.
Despite all of this learning, I remained sheltered in my clinician-educator bubble. The path to excellence for me was defined through frequent trips to the library (where journals used to be stored) and trying to teach as well as my mentors did. I largely was ignorant of the national hospitalist movement, until the 2007 SHM annual meeting was held in my backyard in Dallas. Listening to Bob Wachter that year, and then Don Berwick the following year, I suddenly realized the tremendous and intertwined importance of the quality movement and hospitalists. We were going to fix medicine. OK, maybe not all of medicine, but it happened to be the perfect time for me to learn about our health-care crisis, quality, and the role of hospital medicine.
If my first five years were about clinical medicine, the next five years were all about lessons in leadership. I had a new role, directing 8 15 20 25 hospitalists—and now was accountable for the group’s results. I’ve often said that an explicit leadership role is like stepping behind a curtain, where your own previous n=1 perspective is now the challenge of herding a group of n=25. And let’s be clear that it’s one thing to manage the group and keep the ship afloat, but it’s entirely another thing to lead the group toward success.
A Path for Me
Although the cacophony of managing that many voices was deafening early on, I found solace in the lessons of quality improvement (QI), where no project lives without a team that is all going the same direction. Between the national opportunities for collaborative improvement and the day-to-day experiences within my group, I found two simple principles worked well: 1) engage the team and 2) deliver objective results.
And just as I had craved a clinical learning environment early on, I now found myself learning from local and national peers putting their leadership skills in action to produce quality outcomes. The beauty of collaborative teamwork is that it creates self-sustaining capacity for more positive results.
Looking forward, the opportunities seem limitless for pediatric hospital medicine. From the inherent fulfillment of our day-to-day bedside work to the explicit leadership that we offer the complex hospital system, our family of pediatric hospitalists has blazed career paths in all directions. We are program directors. We are directors of quality and safety. We are division directors and section chiefs. We are professors. We are fellowship-trained. We are CEOs, of entire hospitals and the CMO of CMS. There has never been a better time to be a pediatric hospitalist.
This rapid ascent has to be the fastest in the history of medicine and might surprise the unsuspecting, but these career paths really should have been expected. Residents and students still identify the most with their ward months—we always will be leaders in education. Hospitals and health-care systems recognize the value of hospitalists as systems improvers and will forever need enlightened physicians to guide safer, better care. But we also remain generalists, perched over the exact intersection of acute illness and health. From this vantage point, we have the perfect perspective from which to lead the transformation of our health-care system. I’m not sure there is a leadership position in health care that a hospitalist will not fill in the near future.
A New Frontier
With all of this opportunity before us, there exists an imperative for true leadership. And unlike all of our past requirements for achievement, relying on our quantitative abilities will no longer be enough. Rather, we will need to focus on the qualitative “soft” skills, whether you call this emotional intelligence, interpersonal communication, or behavioral economics. The creation of value-based, care-delivery systems requires high-functioning units. We will need to design and lead teams from the bedside to the boardroom.
In the coming years, this leadership imperative will only intensify, as we all will be pressured to do more with less. We will be asked to improve quality and decrease costs. We will need to broaden our focus to health in addition to acute illness. Doing more with less will require courage and leadership. If you look at our growth curve to date, we have an abundance of both.
Dr. Shen is medical director of hospital medicine at Dell Children's Medical Center in Austin, Texas. He served as The Hospitalist's pediatric editor since 2010 and this marks his last column in his role as editor. In his newfound spare time, he looks forward to defining value in health care.
Dear Mark,
I am pleased and excited that you are willing to abandon your plan for being a vagabond and will give serious consideration to joining the faculty of the Department of Pediatrics to become a core member of a new [general pediatric inpatient] program that I believe has exciting potential.
So reads the first line of my very first job offer letter. Obviously, my chairman had a sense of humor. But he also was not off target, as before May 21 of my third year of residency, I had no meaningful work lined up. Dreams of locum tenens work in Hawaii or a California coastal town quickly disappeared as I received only offers for work in small-town Mississippi and Oklahoma. Eleven years later, I don’t think I could have planned a more fulfilling early career, particularly when the alternative might have been surfing on the Mississippi River.
I would like this opportunity, in my final column as The Hospitalist’s pediatric editor, to reflect on this odyssey from vagabond to hospitalist.
The Early Years
As a new attending, I was appropriately terrified of how much I didn’t know. I also had ambitious goals at first, wanting to emulate my two favorite role models from residency, Charles Ginsburg and Heinz Eichenwald. We might call them hospitalists now, but back then they were old-fashioned, generalist inpatient clinician-educators, even while chairing the department of pediatrics over their separate tenures. They were the smartest and wisest teachers that I have ever met. These early years were a pseudo-fellowship of sorts; under their tutelage, I soaked up more than I ever had during residency.
Despite all of this learning, I remained sheltered in my clinician-educator bubble. The path to excellence for me was defined through frequent trips to the library (where journals used to be stored) and trying to teach as well as my mentors did. I largely was ignorant of the national hospitalist movement, until the 2007 SHM annual meeting was held in my backyard in Dallas. Listening to Bob Wachter that year, and then Don Berwick the following year, I suddenly realized the tremendous and intertwined importance of the quality movement and hospitalists. We were going to fix medicine. OK, maybe not all of medicine, but it happened to be the perfect time for me to learn about our health-care crisis, quality, and the role of hospital medicine.
If my first five years were about clinical medicine, the next five years were all about lessons in leadership. I had a new role, directing 8 15 20 25 hospitalists—and now was accountable for the group’s results. I’ve often said that an explicit leadership role is like stepping behind a curtain, where your own previous n=1 perspective is now the challenge of herding a group of n=25. And let’s be clear that it’s one thing to manage the group and keep the ship afloat, but it’s entirely another thing to lead the group toward success.
A Path for Me
Although the cacophony of managing that many voices was deafening early on, I found solace in the lessons of quality improvement (QI), where no project lives without a team that is all going the same direction. Between the national opportunities for collaborative improvement and the day-to-day experiences within my group, I found two simple principles worked well: 1) engage the team and 2) deliver objective results.
And just as I had craved a clinical learning environment early on, I now found myself learning from local and national peers putting their leadership skills in action to produce quality outcomes. The beauty of collaborative teamwork is that it creates self-sustaining capacity for more positive results.
Looking forward, the opportunities seem limitless for pediatric hospital medicine. From the inherent fulfillment of our day-to-day bedside work to the explicit leadership that we offer the complex hospital system, our family of pediatric hospitalists has blazed career paths in all directions. We are program directors. We are directors of quality and safety. We are division directors and section chiefs. We are professors. We are fellowship-trained. We are CEOs, of entire hospitals and the CMO of CMS. There has never been a better time to be a pediatric hospitalist.
This rapid ascent has to be the fastest in the history of medicine and might surprise the unsuspecting, but these career paths really should have been expected. Residents and students still identify the most with their ward months—we always will be leaders in education. Hospitals and health-care systems recognize the value of hospitalists as systems improvers and will forever need enlightened physicians to guide safer, better care. But we also remain generalists, perched over the exact intersection of acute illness and health. From this vantage point, we have the perfect perspective from which to lead the transformation of our health-care system. I’m not sure there is a leadership position in health care that a hospitalist will not fill in the near future.
A New Frontier
With all of this opportunity before us, there exists an imperative for true leadership. And unlike all of our past requirements for achievement, relying on our quantitative abilities will no longer be enough. Rather, we will need to focus on the qualitative “soft” skills, whether you call this emotional intelligence, interpersonal communication, or behavioral economics. The creation of value-based, care-delivery systems requires high-functioning units. We will need to design and lead teams from the bedside to the boardroom.
In the coming years, this leadership imperative will only intensify, as we all will be pressured to do more with less. We will be asked to improve quality and decrease costs. We will need to broaden our focus to health in addition to acute illness. Doing more with less will require courage and leadership. If you look at our growth curve to date, we have an abundance of both.
Dr. Shen is medical director of hospital medicine at Dell Children's Medical Center in Austin, Texas. He served as The Hospitalist's pediatric editor since 2010 and this marks his last column in his role as editor. In his newfound spare time, he looks forward to defining value in health care.
Dear Mark,
I am pleased and excited that you are willing to abandon your plan for being a vagabond and will give serious consideration to joining the faculty of the Department of Pediatrics to become a core member of a new [general pediatric inpatient] program that I believe has exciting potential.
So reads the first line of my very first job offer letter. Obviously, my chairman had a sense of humor. But he also was not off target, as before May 21 of my third year of residency, I had no meaningful work lined up. Dreams of locum tenens work in Hawaii or a California coastal town quickly disappeared as I received only offers for work in small-town Mississippi and Oklahoma. Eleven years later, I don’t think I could have planned a more fulfilling early career, particularly when the alternative might have been surfing on the Mississippi River.
I would like this opportunity, in my final column as The Hospitalist’s pediatric editor, to reflect on this odyssey from vagabond to hospitalist.
The Early Years
As a new attending, I was appropriately terrified of how much I didn’t know. I also had ambitious goals at first, wanting to emulate my two favorite role models from residency, Charles Ginsburg and Heinz Eichenwald. We might call them hospitalists now, but back then they were old-fashioned, generalist inpatient clinician-educators, even while chairing the department of pediatrics over their separate tenures. They were the smartest and wisest teachers that I have ever met. These early years were a pseudo-fellowship of sorts; under their tutelage, I soaked up more than I ever had during residency.
Despite all of this learning, I remained sheltered in my clinician-educator bubble. The path to excellence for me was defined through frequent trips to the library (where journals used to be stored) and trying to teach as well as my mentors did. I largely was ignorant of the national hospitalist movement, until the 2007 SHM annual meeting was held in my backyard in Dallas. Listening to Bob Wachter that year, and then Don Berwick the following year, I suddenly realized the tremendous and intertwined importance of the quality movement and hospitalists. We were going to fix medicine. OK, maybe not all of medicine, but it happened to be the perfect time for me to learn about our health-care crisis, quality, and the role of hospital medicine.
If my first five years were about clinical medicine, the next five years were all about lessons in leadership. I had a new role, directing 8 15 20 25 hospitalists—and now was accountable for the group’s results. I’ve often said that an explicit leadership role is like stepping behind a curtain, where your own previous n=1 perspective is now the challenge of herding a group of n=25. And let’s be clear that it’s one thing to manage the group and keep the ship afloat, but it’s entirely another thing to lead the group toward success.
A Path for Me
Although the cacophony of managing that many voices was deafening early on, I found solace in the lessons of quality improvement (QI), where no project lives without a team that is all going the same direction. Between the national opportunities for collaborative improvement and the day-to-day experiences within my group, I found two simple principles worked well: 1) engage the team and 2) deliver objective results.
And just as I had craved a clinical learning environment early on, I now found myself learning from local and national peers putting their leadership skills in action to produce quality outcomes. The beauty of collaborative teamwork is that it creates self-sustaining capacity for more positive results.
Looking forward, the opportunities seem limitless for pediatric hospital medicine. From the inherent fulfillment of our day-to-day bedside work to the explicit leadership that we offer the complex hospital system, our family of pediatric hospitalists has blazed career paths in all directions. We are program directors. We are directors of quality and safety. We are division directors and section chiefs. We are professors. We are fellowship-trained. We are CEOs, of entire hospitals and the CMO of CMS. There has never been a better time to be a pediatric hospitalist.
This rapid ascent has to be the fastest in the history of medicine and might surprise the unsuspecting, but these career paths really should have been expected. Residents and students still identify the most with their ward months—we always will be leaders in education. Hospitals and health-care systems recognize the value of hospitalists as systems improvers and will forever need enlightened physicians to guide safer, better care. But we also remain generalists, perched over the exact intersection of acute illness and health. From this vantage point, we have the perfect perspective from which to lead the transformation of our health-care system. I’m not sure there is a leadership position in health care that a hospitalist will not fill in the near future.
A New Frontier
With all of this opportunity before us, there exists an imperative for true leadership. And unlike all of our past requirements for achievement, relying on our quantitative abilities will no longer be enough. Rather, we will need to focus on the qualitative “soft” skills, whether you call this emotional intelligence, interpersonal communication, or behavioral economics. The creation of value-based, care-delivery systems requires high-functioning units. We will need to design and lead teams from the bedside to the boardroom.
In the coming years, this leadership imperative will only intensify, as we all will be pressured to do more with less. We will be asked to improve quality and decrease costs. We will need to broaden our focus to health in addition to acute illness. Doing more with less will require courage and leadership. If you look at our growth curve to date, we have an abundance of both.
Dr. Shen is medical director of hospital medicine at Dell Children's Medical Center in Austin, Texas. He served as The Hospitalist's pediatric editor since 2010 and this marks his last column in his role as editor. In his newfound spare time, he looks forward to defining value in health care.
Hospital Medicine Leaders Flock to HM13 for Answers, Encouragement

Ibe Mbanu, MD, MBA, MPH, became medical director of the adult hospitalist department at Bon Secours St. Mary’s Hospital in Richmond, Va., about six months ago. Since then, he’s been besieged by a torrent of reform-based challenges he says make his job exponentially more difficult than that of medical directors just a few years ago.
Accountable-care organizations (ACOs), value-based purchasing, and discussions about bundled payments for episodic care are changing rapidly, and as a new administrator in a group with 24 hospitalists and three nonphysician providers (NPPs), he felt he needed to attend his first SHM annual meeting to keep up.
“The landscape in health care is rapidly evolving, at a frantic pace,” Dr. Mbanu says. “I essentially came here to just try to get a condensed source of information on how to manage the changes that are coming through the pipeline, and how to effectively run my department.”
Managing a practice is a challenge, and many of the more than 2,700 attendees at HM13 said the four-day confab’s focus on the topic was a major draw. From a rebooted continuing medical education (CME) pre-course appropriately named “What Keeps You Awake at Night? Hot Topics in Hospitalist Practice Management” to dozens of breakout sessions on the topic, it’s clear that successful practice management is a concern for many hospitalists.
“Before, the drivers were pretty clear,” Dr. Mbanu says. “Volume, productivity. Now we’re switching more toward a business model that’s changing from volume to value. Trying to adapt to that change is pretty challenging.
“Now it’s critical to really understand the environment.”
Comanagement Conundrum
One particularly hot topic this year was the trend of hospitalists taking on more comanagement responsibilities for patients previously managed by other specialties, including neurology, surgery, and others. Frank Volpicelli, MD, a first-year hospitalist and instructor at New York University (NYU) Langone Medical Center in New York, was one of three members of his HM group that attended the “Perioperative Medicine: Medical Consultation and Co-Management” pre-course. This summer, his group is going to establish a presence in the preoperative clinic.
“We hope very strongly that we can prevent some complications, identify patients that we should be following when they come into the hospital, and help the surgeons out,” he says. “No. 1, keep them in the [operating room] more, and No. 2, get in front of some of the complications that they are less comfortable managing.”
Ralph Velazquez, MD, senior vice president of care management for OSF Healthcare System in Peoria, Ill., isn’t so sure comanagement of more and more patients is the best practice-management model moving forward. For example, as physician compensation is tied more to how much their care costs to deliver, a hospitalist comanaging a surgical patient’s elective knee replacement could be financially penalized for the cost of that person’s stay, despite having nothing to do with the most expensive portion of the bill.
“You have a financial model that says do more billings, but as you start developing analytics … you may see there is no difference between the model that’s doing more billing, in terms of improving quality, and the one that is doing less,” Dr. Velazquez says. “So if you’re getting the same amount of quality, and the only thing you’re doing is generating more cost by doing more billing, you need to reevaluate your strategy.”
He believes some patients benefit from comanagement, but HM groups have to be diligent in seeking them out.
“We look for simple solutions and one-size-fits-all,” he adds. “Comanagement in complex patients—definitely there’s a need for that. Comanagement in noncomplex patients, elective patients—there’s no need for that. It’s just additional cost. I don’t think it’s going to produce any value.”
Startup Academy
John Colombo, MD, FACP, a 30-year veteran of internal medicine who moved to HM a few years ago when one of the hospitals he worked at asked him to launch a hospitalist group, thinks bundled payments might alleviate that value conundrum. Then again, he’s not quite sure. That’s why attended his first annual meeting.
“I found it difficult starting a new program from scratch,” says Dr. Colombo, of Crozer Keystone Health System in Drexel Hill, Pa. “Even with the materials available, there’s not a lot of ‘how to do it’ out there. There’s no ‘Starting Hospitals for Dummies’ book.”
Dr. Colombo spent much of his meeting focused on recruiting, compensation, bonus structures, and scheduling concerns. He said all are important in the hospital-heavy metropolitan Philadelphia region where he works. Plus, with departures and retirements at other programs in his health system, Dr. Colombo went from no HM experience three years ago to being in charge of four HM programs.
“The biggest thing is, I wanted to make sure I hadn’t stepped in something that I shouldn’t have already,” he adds. “There’s many different ways to do things. So I’ve learned a few different ways. I found value.”
Demonstrate Value
Another way to discover value in running a practice is looking at the business side of the house, says Denice Cora-Bramble, MD, MBA, chief medical officer and executive vice president of Ambulatory & Community Health Services at the Children’s National Medical Center in Washington, D.C.
Dr. Bramble says many hospitalists need to understand that while clinical care is what brought them to medicine, their future paychecks depend on recognizing how to provide that care in a way that demonstrates business value.
“When you finish residency, if you have not intentionally sought out those courses or those seminars, you need to recognize that as a blind spot,” she says. “You need to fill that toolkit as it relates to the business side of medicine.
“You don’t necessarily have to know all the answers, but you need to know the right questions to ask,” she says.
Dr. Bramble adds that hospitalist leaders should take advantage of certificate programs, leadership courses, basic budgeting classes, or anything that gives them added education about the economics of healthcare.
“It all comes down to demonstrating your outcomes, demonstrating the value that you bring to that institution,” she says. “And with health-care reform, I think hospitalists are uniquely positioned to be able to partner with other areas of the hospital to look at this value-based approach.”
Gary Gammon, MD, FHM, the newly named medical director of the Hospitalist Service at FirstHealth Moore Regional Hospital in Pinehurst, N.C., is doing his part to demonstrate value to his administrators. While his group does multidisciplinary rounds on patients, one of his questions for the pre-course faculty was to make sure that system of rounding is an evidence-based practice. He’s also looking for ways to establish more hegemony to his practice to ensure the rounds are effective, regardless of which physicians and others are participating.
The feedback he received was that most people view multidisciplinary rounds as a best practice. Now, Dr. Gammon can feel more authoritative that he and his 32 hospitalists and 12 extenders are practicing HM the way it should be practiced.
“I wanted to hear just what I heard, which is the leaders in the community feel that it’s helping, feel that it’s the right thing to do, feel that there’s objective data,” he says. “This is the stuff that makes me say, ‘OK, I’ve got the same problems everybody else has.’”
Richard Quinn is a freelance writer in New Jersey.
Ibe Mbanu, MD, MBA, MPH, became medical director of the adult hospitalist department at Bon Secours St. Mary’s Hospital in Richmond, Va., about six months ago. Since then, he’s been besieged by a torrent of reform-based challenges he says make his job exponentially more difficult than that of medical directors just a few years ago.
Accountable-care organizations (ACOs), value-based purchasing, and discussions about bundled payments for episodic care are changing rapidly, and as a new administrator in a group with 24 hospitalists and three nonphysician providers (NPPs), he felt he needed to attend his first SHM annual meeting to keep up.
“The landscape in health care is rapidly evolving, at a frantic pace,” Dr. Mbanu says. “I essentially came here to just try to get a condensed source of information on how to manage the changes that are coming through the pipeline, and how to effectively run my department.”
Managing a practice is a challenge, and many of the more than 2,700 attendees at HM13 said the four-day confab’s focus on the topic was a major draw. From a rebooted continuing medical education (CME) pre-course appropriately named “What Keeps You Awake at Night? Hot Topics in Hospitalist Practice Management” to dozens of breakout sessions on the topic, it’s clear that successful practice management is a concern for many hospitalists.
“Before, the drivers were pretty clear,” Dr. Mbanu says. “Volume, productivity. Now we’re switching more toward a business model that’s changing from volume to value. Trying to adapt to that change is pretty challenging.
“Now it’s critical to really understand the environment.”
Comanagement Conundrum
One particularly hot topic this year was the trend of hospitalists taking on more comanagement responsibilities for patients previously managed by other specialties, including neurology, surgery, and others. Frank Volpicelli, MD, a first-year hospitalist and instructor at New York University (NYU) Langone Medical Center in New York, was one of three members of his HM group that attended the “Perioperative Medicine: Medical Consultation and Co-Management” pre-course. This summer, his group is going to establish a presence in the preoperative clinic.
“We hope very strongly that we can prevent some complications, identify patients that we should be following when they come into the hospital, and help the surgeons out,” he says. “No. 1, keep them in the [operating room] more, and No. 2, get in front of some of the complications that they are less comfortable managing.”
Ralph Velazquez, MD, senior vice president of care management for OSF Healthcare System in Peoria, Ill., isn’t so sure comanagement of more and more patients is the best practice-management model moving forward. For example, as physician compensation is tied more to how much their care costs to deliver, a hospitalist comanaging a surgical patient’s elective knee replacement could be financially penalized for the cost of that person’s stay, despite having nothing to do with the most expensive portion of the bill.
“You have a financial model that says do more billings, but as you start developing analytics … you may see there is no difference between the model that’s doing more billing, in terms of improving quality, and the one that is doing less,” Dr. Velazquez says. “So if you’re getting the same amount of quality, and the only thing you’re doing is generating more cost by doing more billing, you need to reevaluate your strategy.”
He believes some patients benefit from comanagement, but HM groups have to be diligent in seeking them out.
“We look for simple solutions and one-size-fits-all,” he adds. “Comanagement in complex patients—definitely there’s a need for that. Comanagement in noncomplex patients, elective patients—there’s no need for that. It’s just additional cost. I don’t think it’s going to produce any value.”
Startup Academy
John Colombo, MD, FACP, a 30-year veteran of internal medicine who moved to HM a few years ago when one of the hospitals he worked at asked him to launch a hospitalist group, thinks bundled payments might alleviate that value conundrum. Then again, he’s not quite sure. That’s why attended his first annual meeting.
“I found it difficult starting a new program from scratch,” says Dr. Colombo, of Crozer Keystone Health System in Drexel Hill, Pa. “Even with the materials available, there’s not a lot of ‘how to do it’ out there. There’s no ‘Starting Hospitals for Dummies’ book.”
Dr. Colombo spent much of his meeting focused on recruiting, compensation, bonus structures, and scheduling concerns. He said all are important in the hospital-heavy metropolitan Philadelphia region where he works. Plus, with departures and retirements at other programs in his health system, Dr. Colombo went from no HM experience three years ago to being in charge of four HM programs.
“The biggest thing is, I wanted to make sure I hadn’t stepped in something that I shouldn’t have already,” he adds. “There’s many different ways to do things. So I’ve learned a few different ways. I found value.”
Demonstrate Value
Another way to discover value in running a practice is looking at the business side of the house, says Denice Cora-Bramble, MD, MBA, chief medical officer and executive vice president of Ambulatory & Community Health Services at the Children’s National Medical Center in Washington, D.C.
Dr. Bramble says many hospitalists need to understand that while clinical care is what brought them to medicine, their future paychecks depend on recognizing how to provide that care in a way that demonstrates business value.
“When you finish residency, if you have not intentionally sought out those courses or those seminars, you need to recognize that as a blind spot,” she says. “You need to fill that toolkit as it relates to the business side of medicine.
“You don’t necessarily have to know all the answers, but you need to know the right questions to ask,” she says.
Dr. Bramble adds that hospitalist leaders should take advantage of certificate programs, leadership courses, basic budgeting classes, or anything that gives them added education about the economics of healthcare.
“It all comes down to demonstrating your outcomes, demonstrating the value that you bring to that institution,” she says. “And with health-care reform, I think hospitalists are uniquely positioned to be able to partner with other areas of the hospital to look at this value-based approach.”
Gary Gammon, MD, FHM, the newly named medical director of the Hospitalist Service at FirstHealth Moore Regional Hospital in Pinehurst, N.C., is doing his part to demonstrate value to his administrators. While his group does multidisciplinary rounds on patients, one of his questions for the pre-course faculty was to make sure that system of rounding is an evidence-based practice. He’s also looking for ways to establish more hegemony to his practice to ensure the rounds are effective, regardless of which physicians and others are participating.
The feedback he received was that most people view multidisciplinary rounds as a best practice. Now, Dr. Gammon can feel more authoritative that he and his 32 hospitalists and 12 extenders are practicing HM the way it should be practiced.
“I wanted to hear just what I heard, which is the leaders in the community feel that it’s helping, feel that it’s the right thing to do, feel that there’s objective data,” he says. “This is the stuff that makes me say, ‘OK, I’ve got the same problems everybody else has.’”
Richard Quinn is a freelance writer in New Jersey.
Ibe Mbanu, MD, MBA, MPH, became medical director of the adult hospitalist department at Bon Secours St. Mary’s Hospital in Richmond, Va., about six months ago. Since then, he’s been besieged by a torrent of reform-based challenges he says make his job exponentially more difficult than that of medical directors just a few years ago.
Accountable-care organizations (ACOs), value-based purchasing, and discussions about bundled payments for episodic care are changing rapidly, and as a new administrator in a group with 24 hospitalists and three nonphysician providers (NPPs), he felt he needed to attend his first SHM annual meeting to keep up.
“The landscape in health care is rapidly evolving, at a frantic pace,” Dr. Mbanu says. “I essentially came here to just try to get a condensed source of information on how to manage the changes that are coming through the pipeline, and how to effectively run my department.”
Managing a practice is a challenge, and many of the more than 2,700 attendees at HM13 said the four-day confab’s focus on the topic was a major draw. From a rebooted continuing medical education (CME) pre-course appropriately named “What Keeps You Awake at Night? Hot Topics in Hospitalist Practice Management” to dozens of breakout sessions on the topic, it’s clear that successful practice management is a concern for many hospitalists.
“Before, the drivers were pretty clear,” Dr. Mbanu says. “Volume, productivity. Now we’re switching more toward a business model that’s changing from volume to value. Trying to adapt to that change is pretty challenging.
“Now it’s critical to really understand the environment.”
Comanagement Conundrum
One particularly hot topic this year was the trend of hospitalists taking on more comanagement responsibilities for patients previously managed by other specialties, including neurology, surgery, and others. Frank Volpicelli, MD, a first-year hospitalist and instructor at New York University (NYU) Langone Medical Center in New York, was one of three members of his HM group that attended the “Perioperative Medicine: Medical Consultation and Co-Management” pre-course. This summer, his group is going to establish a presence in the preoperative clinic.
“We hope very strongly that we can prevent some complications, identify patients that we should be following when they come into the hospital, and help the surgeons out,” he says. “No. 1, keep them in the [operating room] more, and No. 2, get in front of some of the complications that they are less comfortable managing.”
Ralph Velazquez, MD, senior vice president of care management for OSF Healthcare System in Peoria, Ill., isn’t so sure comanagement of more and more patients is the best practice-management model moving forward. For example, as physician compensation is tied more to how much their care costs to deliver, a hospitalist comanaging a surgical patient’s elective knee replacement could be financially penalized for the cost of that person’s stay, despite having nothing to do with the most expensive portion of the bill.
“You have a financial model that says do more billings, but as you start developing analytics … you may see there is no difference between the model that’s doing more billing, in terms of improving quality, and the one that is doing less,” Dr. Velazquez says. “So if you’re getting the same amount of quality, and the only thing you’re doing is generating more cost by doing more billing, you need to reevaluate your strategy.”
He believes some patients benefit from comanagement, but HM groups have to be diligent in seeking them out.
“We look for simple solutions and one-size-fits-all,” he adds. “Comanagement in complex patients—definitely there’s a need for that. Comanagement in noncomplex patients, elective patients—there’s no need for that. It’s just additional cost. I don’t think it’s going to produce any value.”
Startup Academy
John Colombo, MD, FACP, a 30-year veteran of internal medicine who moved to HM a few years ago when one of the hospitals he worked at asked him to launch a hospitalist group, thinks bundled payments might alleviate that value conundrum. Then again, he’s not quite sure. That’s why attended his first annual meeting.
“I found it difficult starting a new program from scratch,” says Dr. Colombo, of Crozer Keystone Health System in Drexel Hill, Pa. “Even with the materials available, there’s not a lot of ‘how to do it’ out there. There’s no ‘Starting Hospitals for Dummies’ book.”
Dr. Colombo spent much of his meeting focused on recruiting, compensation, bonus structures, and scheduling concerns. He said all are important in the hospital-heavy metropolitan Philadelphia region where he works. Plus, with departures and retirements at other programs in his health system, Dr. Colombo went from no HM experience three years ago to being in charge of four HM programs.
“The biggest thing is, I wanted to make sure I hadn’t stepped in something that I shouldn’t have already,” he adds. “There’s many different ways to do things. So I’ve learned a few different ways. I found value.”
Demonstrate Value
Another way to discover value in running a practice is looking at the business side of the house, says Denice Cora-Bramble, MD, MBA, chief medical officer and executive vice president of Ambulatory & Community Health Services at the Children’s National Medical Center in Washington, D.C.
Dr. Bramble says many hospitalists need to understand that while clinical care is what brought them to medicine, their future paychecks depend on recognizing how to provide that care in a way that demonstrates business value.
“When you finish residency, if you have not intentionally sought out those courses or those seminars, you need to recognize that as a blind spot,” she says. “You need to fill that toolkit as it relates to the business side of medicine.
“You don’t necessarily have to know all the answers, but you need to know the right questions to ask,” she says.
Dr. Bramble adds that hospitalist leaders should take advantage of certificate programs, leadership courses, basic budgeting classes, or anything that gives them added education about the economics of healthcare.
“It all comes down to demonstrating your outcomes, demonstrating the value that you bring to that institution,” she says. “And with health-care reform, I think hospitalists are uniquely positioned to be able to partner with other areas of the hospital to look at this value-based approach.”
Gary Gammon, MD, FHM, the newly named medical director of the Hospitalist Service at FirstHealth Moore Regional Hospital in Pinehurst, N.C., is doing his part to demonstrate value to his administrators. While his group does multidisciplinary rounds on patients, one of his questions for the pre-course faculty was to make sure that system of rounding is an evidence-based practice. He’s also looking for ways to establish more hegemony to his practice to ensure the rounds are effective, regardless of which physicians and others are participating.
The feedback he received was that most people view multidisciplinary rounds as a best practice. Now, Dr. Gammon can feel more authoritative that he and his 32 hospitalists and 12 extenders are practicing HM the way it should be practiced.
“I wanted to hear just what I heard, which is the leaders in the community feel that it’s helping, feel that it’s the right thing to do, feel that there’s objective data,” he says. “This is the stuff that makes me say, ‘OK, I’ve got the same problems everybody else has.’”
Richard Quinn is a freelance writer in New Jersey.