User login
Delirium: Apply the ‘4 Ps’ for comprehensive treatment
Four principles of treating delirium can help protect medical/surgical patients at risk for morbidity and functional decline. These principals—which I call the “four Ps”—are prompt identification, protection, pragmatic intervention, and pharmacotherapy.
This article describes an up-to-date, “four-Ps” approach to treating delirium—including use of antipsychotics and supportive care—and offers evidence and case reports to address these clinical questions:
- What causes delirium?
- Does delirium worsen prognosis?
- Can delirium be prevented?
FOUR ‘Ps’ FOR TREATING DELIRIUM
When a patient’s mental status changes dramatically (Box 1),1 identifying potential delirium causes requires careful medical, psychiatric, and neurologic assessment. Assimilating this information is as essential to positive outcomes as are intensive nursing care and appropriate interventions.
- Disturbance of consciousness (i.e. reduced clarity of awareness of the environment) with reduced ability to focus, sustain, or shift attention
- A change in cognition (such as memory deficit, disorientation, language disturbance) or the development of a perceptual disturbance that is not better accounted for by a preexisting, established, or evolving dementia
- The disturbance develops over a short period of time (usually hours to days) and tends to fluctuate during the course of a 24-hour period
- There is evidence from the history, physical examination, or laboratory findings that the disturbance is caused by the direct physiologic consequences of a general medical condition
Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders (4th ed., text rev). Copyright 2000. American Psychiatric Publishing.
Prompt identification. Delirium often goes unrecognized, delaying treatment. Easily administered rating scales—such as the Delirium Rating Scale (DRS)2 and the Confusion Assessment Method (CAM)3 —can help detect emerging symptoms.
Patient protection. Provide intensive nursing care—often one-to-one observation and containment—and, where possible, enlist the family in reassuring and calming the patient. Restraints may be needed to safeguard against injury and to prevent the patient from removing or dislocating monitoring equipment and IV access.
Pragmatic intervention. With medical colleagues, begin treating biochemical and physiologic abnormalities that are the most likely and most remediable contributors (Box 2).2,4-6 Review the patient’s medications and discontinue or replace any that may be causing delirium.
Pharmacotherapy. Based on clinical studies, antipsychotics appear to possess antidelirium properties and may be considered as one part of a patient’s treatment plan. Interpreting these studies is complicated, however, by delirium’s complexity, numerous causes, and presumed mechanisms, as well as the transience of some forms. For ethical reasons, no placebo-controlled studies of delirium treatment have been done.
EVIDENCE ON ANTIPSYCHOTICS
Haloperidol has been the drug of choice for managing delirium because it is less likely to cause hypotension and sedation than other neuroleptics. Optimum haloperidol dosing in delirium has not been established, but the usual range is 2 to 6 mg every 4 to 6 hours, depending on the patient’s age and delirium severity.
Instances of QTc interval prolongation have been reported with high-dose IV haloperidol (> 100 mg). This life-threatening effect—which can induce torsades de pointes dysrhythmia, ventricular tachycardias, and fibrillation—is very rare, quite variable, and unpredictable. It probably is a function of total dose and neuroleptic administration rate.
Atypical antipsychotics share haloperidol’s advantages over first-generation neuroleptics, with lower potential for dystonic reactions, parkinsonian side effects, and tardive dyskinesia. Preliminary evidence suggests that atypicals may be safe and effective in treating delirium, although no randomized controlled trials have been done and accurate dose-response curves have not been established. Low to modest dosages have been used in case series.
Risperidone. Two prospective, open-label trials—each with 10 patients—suggest that low-dose risperidone is effective for treating delirium:
- In one trial, risperidone given at an average dosage of 1.7 mg/d was effective in 80% of patients with delirium, and one patient responded to 0.5 mg/d. Some patients experienced sleepiness or mild drug-induced parkinsonism.7
- In the other trial, risperidone was started at 0.5 mg twice daily, with additional doses allowed on day 1 for cognitive and behavioral symptoms. This dosage was maintained until DRS scores declined to ≤12, then was reduced by 50% and continued until day 6. Mean maintenance dosage was 0.75 mg/d. Two patients discontinued risperidone because of sedation or hypotension.8
At least 10% to 30% of hospitalized medically ill patients develop delirium, and rates approach 40% after age 65.4 Especially in older patients, delirium is a risk factor for:
- prolonged hospital stays
- increased morbidity and mortality
- increased functional decline and need for custodial care after hospital discharge.2
Risk factors. Prospectively identified risk factors for delirium include pre-existing dementia; age >65 years; serious medical illness; alcohol/sedative withdrawal; abnormal serum sodium, potassium, or blood glucose levels; vision or hearing impairment; hypoxia; malnutrition; and fever. Medication—particularly anticholinergic drugs—is one of the most common delirium triggers in susceptible patients.5
The most common underlying disorders that increase delirium risk in older patients are hip fracture, dementia, infections, and cerebrovascular events.6
In a larger prospective study, 64 patients (mean age 67) with delirium were treated with risperidone, given at a mean dose of 2.6 +/- 1.7 mg/d at day 3. This dosage was effective in 90% of patients and significantly improved all symptoms, as measured with scales including the DRS. Two patients (3%) experienced adverse effects.9
No significant differences in response frequency were seen in a 7-day, double-blind comparison of flexibly-dosed risperidone (starting at 0.5 mg bid) and haloperidol (starting at 0.75 mg bid) in 28 patients with delirium. Symptom severity decreased for each group, as measured with the Memorial Delirium Assessment Scale. One patient receiving haloperidol experienced mild akathisia, but no others reported clinically significant side effects.10
Quetiapine. In a retrospective review, the charts of 11 patients who received quetiapine for delirium were compared with those of 11 similar patients treated with haloperidol. DRS scores improved by >50% in 10 of 11 patients in both groups, with similar onset of effect, treatment duration, and overall clinical improvement.11 Small prospective trials with flexible dosing schedules have reported similar results.12,13
In a study of 12 older hospitalized patients with delirium, quetiapine at a mean dosage of 93.75 +/-23.31 mg/d was associated with significant DRS score improvements. Interestingly, patients’ Mini-Mental State Examination and Clock-Drawing Test scores continued to improve 3 months after their delirium symptoms stabilized.14
Olanzapine. In a prospective trial, hospitalized patients with delirium were randomly assigned to receive enteral olanzapine or haloperidol. Delirium symptoms decreased across 5 days in both groups, and clinical improvement was similar. Some patients receiving haloperidol reported extrapyramidal symptoms, whereas those receiving olanzapine reported no adverse effects.15
Parenteral forms of some atypicals (aripiprazole, olanzapine, and ziprasidone) have become available and may increase this class’ usefulness in treating delirium.
Other drugs. Benzodiazepines appear ineffective and generally play only an adjunctive role in treating delirium. An exception may be delirium induced by acute alcohol or benzodiazepine withdrawal. Sedating antidepressants have been used as hypnotics in patients with delirium, but supporting evidence is lacking.
Other drug classes—general anesthetics, narcotics, cholinomimetics—may help manage the dangerously hyperactive delirious patient, but the literature contains no systematic analyses.
WHAT CAUSES DELIRIUM?
Delirium’s pathophysiology is not completely understood, although most authors believe several mechanisms are involved.
The brain’s exclusively oxidative metabolism and its systems’ hierarchical vulnerability to substrate deficiency—as might occur in even transient hypoxia or hypotension—appear to play important roles. Factors such as fever and stress that increase metabolic demand on the brain intensify the effects of oxygen deficiency or circulatory compromise.
At least three molecular mechanisms have been proposed for delirium, including cholinergic transmission disruption, monoaminergic dysfunction, and cytokine release ( Box 3).16-19 These mechanisms may interact, cascading into a common final pathway that results in delirium.
Features not considered essential to delirium’s diagnosis—such as visual hallucinations or aggressive behaviors—indicate that additional cortical and subcortical systems are involved.
CASE REPORT: DRUG-DRUG INTERACTION
Three days after hip replacement surgery, Mr. S, age 64, becomes confused, distractible, and combative. He is alert one minute and somnolent the next. His arms and legs jerk involuntarily, and his muscle tone is diffusely increased. He talks with absent friends and family as though they are present in his hospital room. His body temperature and blood pressure fluctuate widely, despite no evidence of infection.
Cholinergic transmission disruption
The greater a medication’s anticholinergic activity, the greater its risk of causing delirium. Combining drugs with anticholinergic effects—such as theophylline, warfarin, or codeine (Table19)—compounds the delirium risk.
Acetylcholine-secreting neurons—widely if sparsely distributed throughout the brain—affect arousal, attention, memory, and sleep regulation. Acetylcholine is produced by oxidative metabolism and thus is vulnerable to physiologic disturbances that increase oxygen demand or disrupt oxygen supply.
Anticholinergic poisoning and abuse of anticholinergic substances are known to cause acute delirium—a finding that supports the key role of acetylcholine in maintaining alertness and concentration. Agents that enhance cholinergic transmission—such as the cholinesterase inhibitor physostigmine—can effectively treat drug-induced delirium.
Monoaminergic dysfunction
The principal monoamines of dopamine, serotonin, and norepinephrine help sustain attention, regulate the sleep-wake cycle, inhibit affective responses, and modulate aggressive and impulsive behaviors. Treating patients with dopamine and serotonin agonists can cause psychotic symptoms.
Glutamate—a monoamine neurotransmitter with excitatory properties—is released during metabolic stress and likely contributes to the psychotic features sometimes seen in delirium.
Cytokine release
Infection in a distant organ, such as gallbladder or kidney, is known to cause delirium. Cytokines such as interleukins and interferon-alpha are polypeptides secreted by macrophagesin response to tissue injury. They easily cross the blood-brain barrier and stimulate glial cells to release more cytokines, which interfere with neurotransmitter synthesis and transmission.
Table
Drugs whose anticholinergic effects may increase the risk of delirium
| Drug | Anticholinergic level* |
|---|---|
| Cimetidine | 0.86 |
| Prednisolone | 0.55 |
| Theophylline | 0.44 |
| Digoxin | 0.25 |
| Lanoxin | 0.25 |
| Nifedipine | 0.22 |
| Ranitidine | 0.22 |
| Furosemide | 0.22 |
| Isosorbide | 0.15 |
| Warfarin | 0.12 |
| Dipyridamole | 0.11 |
| Codeine | 0.11 |
| * ng/mL in atropine equivalents | |
| Source: Adapted from reference 19. | |
For several years, Mr. S has been taking the monoamine oxidase inhibitor (MAOI) phenelzine, 30 mg/d, for depression maintenance treatment. On admission, he insisted that the MAOI be continued during hospitalization because it had relieved his severe depressions.
Within 24 hours of surgery, he was given the skeletal muscle relaxant cyclobenzaprine, 5 mg tid, for painful muscle spasms in the operated hip. When this brought little relief, the dosage was increased to 10 mg tid. Delirium and autonomic instability developed approximately 4 hours after the first 10-mg dose and gradually worsened.
The two drugs are discontinued, and Mr S. gradually recovers after several days of physiologic support, protection, and sedation in the intensive-care unit.
Discussion. Mr. S developed serotonin syndrome from a drug-drug interaction. Phenelzine inhibited serotonin metabolism, and cyclobenzaprine—a drug chemically similar to tricyclic antidepressants—inhibited serotonin reuptake, resulting in substantially increased CNS serotonergic activity.20 Serotonin syndrome symptoms include delirium, autonomic dysfunction, and neurologic signs such as myoclonus and rigidity when patients are taking drugs that enhance serotonergic transmission.
DOES DELIRIUM WORSEN PROGNOSIS?
In the largest study of delirium in older patients, Inouye et al21 examined outcomes of 727 consecutive patients age 65 and older with various medical diagnoses who were admitted to three teaching hospitals. Delirium was diagnosed in 88 patients (12%) at admission.
Within 3 months of hospital discharge, 165 (25%) of 663 patients had died or been newly admitted to a nursing home. After the authors controlled the data for age, gender, dementia, illness severity, and functional status, they found that delirium:
- tripled the likelihood of nursing home placement at hospital discharge and after 3 months (adjusted odds ratio [OR] for delirium 3.0)
- more than doubled the likelihood of death or new nursing home placement at discharge (OR for delirium 2.1) and after 3 months (OR for delirium 2.6).
They concluded that delirium was a significant predictor of functional decline at hospital discharge and also at follow-up in older patients.
Interestingly, although these authors did not find a statistically significant association between delirium and death alone, the risk of death was particularly strong for patients who were not demented (OR for delirium, 3.77). Similarly, Rabins and Folstein22 found higher mortality rates in medically ill patients diagnosed with delirium on hospital admission than in demented, cognitively intact, or depressed patients. After 1 year, the death rate remained higher in those who had been delirious than in those with dementia.
In a 12-month observational study comparing 243 older medical inpatients with delirium and 118 controls without delirium, McCusker et al23 found that:
- patients with delirium were twice as likely to die within 12 months as those without delirium
- the greater severity of delirium symptoms, the higher the risk of death in patients with delirium but without dementia.
In a recent study, some of the same investigators found that delirium symptoms—especially inattention, disorientation, and impaired memory—persisted for 12 months after hospital discharge in medical inpatients age 65 and older with or without dementia. Mean numbers of delirium symptoms at diagnosis and 12-month follow-up, respectively, were:
- 4.5 and 3.5 in patients with dementia
- 3.4 and 2.2 in patients without dementia.24
CASE REPORT: DELIRIUM AS PROGNOSTIC SIGN
Mrs. W, age 70, is hospitalized for treatment of anemia and dehydration after falling at home. She has metastatic adenocarcinoma of the colon and is hypernatremic and hypotensive on admission.
Within 24 hours, she becomes floridly delirious, despite transfusion of two units of packed red cells and IV fluid replacement. She receives IM haloperidol to reduce the agitation and counteract delirium. Head CT reveals mild, diffuse cerebral atrophy but no metastasis or subdural hematoma.
Although aggressive treatment corrects her electrolyte disturbance and dehydration and restores normal vital signs, the delirium does not resolve. She is discharged to a nursing home, where she is discovered dead in bed 1 week later.
Discussion. Delirium independently increases the risk of death during hospitalization and thereafter, particularly in older patients. As in the case of Mrs. W, delirium is a common preterminal event in cancer patients.25
Evidence suggests that delirium is a marker for declining functional status and of relatively poor outcomes in older patients. In patients who are hospitalized, however, the relative effects of comorbid medical and neurologic conditions on prognosis are difficult to differentiate from the effects of delirium.
CAN DELIRIUM BE PREVENTED?
Researchers at Yale University examined whether a multicomponent, nonpharmacologic intervention could reduce delirium incidence and episode duration in 852 at-risk hospitalized medical patients age 70 and older.26 Patients were randomly assigned to intervention or usual care and then observed daily until discharge. Interventions included protocols for orientation, mobilization, sleep hygiene, and sensory enhancement, as well as prompt treatment of dehydration.
Delirium occurred in 10% of the intervention group and in 15% of the usual-care group (matched odds ratio 0.6). Total days with delirium (105 vs. 161; P = 0.02) and total episodes (62 vs. 90; P = 0.03) were significantly lower in the intervention group. A potential source of bias in this study was a lack of randomization in assigning patients to intervention or usual care. Follow-up studies found that:
- The intervention increased health care costs for patients at high risk for delirium but had no significant effect on overall costs for patients at intermediate risk.27
- Delirium risk decreased the most (89%) in older patients who were most adherent to the intervention protocols during hospitalization.28
- Among the 705 patients who survived at least 6 months after discharge, those who had been in the intervention and usual-care groups showed similar functional and cognitive status and rates of depression, delirium, nursing home placement, and rehospitalization.29
CASE REPORT: A SUCCESSFUL INTERVENTION
Mr. A, age 66, who has moderate-to-severe chronic obstructive pulmonary disease, is hospitalized for surgery to remove a suspicious lung nodule. Two years ago, he experienced delirium following a transurethral prostatectomy. His hemoglobin is 9.1 g/dL (normal, 11.5 to 14 g/dL), defined as anemia related to chronic disease.
Because of his history of postoperative delirium, the hospital staff initiates preventive measures. Before surgery, he is given two units of blood for anemia. To assist with orientation, he and his family receive information about delirium, and his hearing aid—which has been malfunctioning—is readjusted to improve his auditory acuity. During surgery, his oxygen saturation and blood pressure are monitored scrupulously.
Afterward, no mental status changes are observed, and Mr. A recovers uneventfully. The surgery revealed a benign granuloma.
Discussion. Surgical patients such as Mr. A—particularly those with hemoglobin <10 g/dL—face a higher risk for delirium than medical patients do. The reason, although undetermined, may be related to unavoidable tissue injury and hemorrhage associated with surgery.30
Nonpharmacologic intervention shows promise in preventing delirium, but more evidence is needed to develop simpler, less-costly strategies for at-risk hospitalized patients and to preserve their functional status after discharge.
Related resources
- Cook IA. Guideline Watch. Practice guideline for the treatment of patients with delirium. American Psychiatric Association, August 2004. www.psych.org/psych_pract/treatg/pg/prac_guide.cfm (scroll down to “Delirium” under topic list). Accessed Dec. 14, 2004.
Drug brand names
- Aripiprazole • Abilify
- Cyclobenzapine • Flexeril
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Phenylzine • Nardil
- Physostigmine • Antilirium
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Warfarin • Coumadin
- Ziprasidone • Geodon
Disclosures
Dr. O’Connor reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Diagnostic and statistical manual of mental disorders, 4th edition, text rev. Washington, DC: American Psychiatric Association, 2000.
2. Trzepacz PT, Mulsant BH, Amanda Dew M, et al. Is delirium different when it occurs with dementia? A study using the delirium rating scale. J Neuropsychiatry Clin Neurosci 1998;10:199-204.
3. Inouye SK, Charpentier PA. Precipitating factors for delirium in hospitalized elderly persons. Predictive model and interrelationship with baseline vulnerability. JAMA 1996;275:852-7.
4. Liptzin B. Clinical diagnosis and management of delirium. In: Stoudemire A, Fogel BS, Greenberg DB (eds). Psychiatric care of the medical patient (2nd ed). New York: Oxford University Press, 2000;581-96.
5. Bourgeois JA, Seaman JS, Servis M. Delirium, dementia, and amnestic disorders. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry (4th ed). Washington, DC: American Psychiatric Publishing, 2003;270.-
6. Rahkonen T, Makela H, Paanila S, et al. Delirium in elderly people without severe predisposing disorders: etiology and 1-year prognosis after discharge. Int Psychogeriatr 2000;12(4):473-81.
7. Horikawa N, Yamazaki T, Miyamoto K, et al. Treatment of delirium with risperidone: results of a prospective open trial with 10 patients. Gen Hosp Psychiatry 2003;25(4):289-92.
8. Mittal D, Jimerson NA, Neely EP, et al. Risperidone in the treatment of delirium: results from a prospective open-label trial. J Clin Psychiatry 2004;65(5):662-7.
9. Parellada E, Baeza I, de Pablo J, Martinez G. Risperidone in the treatment of patients with delirium. J Clin Psychiatry 2004;65(3):348-53.
10. Han CS, Kim YK. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics 2004;45:297-301.
11. Schwartz TL, Masand PS. Treatment of delirium with quetiapine. Prim Care Companion J Clin Psychiatry 2000;2(1):10-12.
12. Sasaki Y, Matsuyama T, Inoue S, et al. A prospective, open-label, flexible-dose study of quetiapine in the treatment of delirium. J Clin Psychiatry 2003;64(11):1316-21.
13. Pae CU, Lee SJ, Lee CU, et al. A pilot trial of quetiapine for the treatment of patients with delirium. Hum Psychopharmacol 2004;19(2):125-7.
14. Kim KY, Bader GM, Kotlyar V, Gropper D. Treatment of delirium in older adults with quetiapine. J Geriatr Psychiatry Neurol 2003;16(1):29-31.
15. Skrobik YK, Bergeron N, Dumont M, Gottfried SB. Olanzapine vs haloperidol: treating delirium in a critical care setting. Intensive Care Med 2004;30(3):444-9.
16. Van der Mast RC. Pathophysiology of delirium. J Geriatr Psychiatry Neurol 1998;11:138-45.
17. Trzepacz PT. Update on the neuropathogenesis of delirium. Dement Geriatr Cogn Disord 1999;10:330-4.
18. Mussi C, Ferrari R, Ascari S, et al. Importance of serum anticholinergic activity in the assessment of elderly patients with delirium. J Geriatr Psychiatry Neurol 1999;12:82-6.
19. Tune L, Carr S, Hoag E, Cooper T. Anticholinergic effects of drugs commonly prescribed for the elderly: potential means for assessing risk of delirium.[see comment]. Am J Psychiatry 1992;149:1393-4.
20. Keck PE, Jr, Arnold LM. The serotonin syndrome. Psychiatr Ann 2000;30:333-43.
21. Inouye SK, Rushing JT, Foreman MD, et al. Does delirium contribute to poor hospital outcomes? A three-site epidemiologic study. J Gen Intern Med 1998;13:234-42.
22. Rabins PV, Folstein MF. Delirium and dementia: diagnostic criteria and fatality rates. Br J Psychiatry 1982;140:149-53.
23. McCusker J, Cole M, Abrahamowicz M, et al. Delirium predicts 12-month mortality. Arch Intern Med 2002;162(4):457-63.
24. McCusker J, Cole M, Dendukuri N, et al. The course of delirium in older medical inpatients: a prospective study. J Gen Intern Med 2003;18(9):696-704.
25. Greenberg DB. Preventing delirium at the end of life: lessons from recent research. Primary Care Companion J Clin Psychiatry 2003;5:62-7.
26. Inouye SK, Bogardus ST, Jr, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med 1999;340:669-76.
27. Rizzo JA, Bogardus ST, Jr, Leo-Summers L, et al. Multicomponent targeted intervention to prevent delirium in hospitalized older patients: what is the economic value? Med Care 2001;39(7):740-52.
28. Inouye SK, Bogardus ST, Jr, Williams CS, et al. The role of adherence on the effectiveness of nonpharmacologic interventions: evidence from the delirium prevention trial. Arch Intern Med 2003;163(8):958-64.
29. Bogardus ST, Jr, Desai MM, Williams CS, et al. The effects of a targeted multicomponent delirium intervention on postdischarge outcomes for hospitalized older adults. Am J Med 2003;114(5):383-90.
30. Marcantonio ER, Goldman L, Orav EJ, et al. The association of intraoperative factors with the development of postoperative delirium. Am J Med 1998;105(5):380-4.
Four principles of treating delirium can help protect medical/surgical patients at risk for morbidity and functional decline. These principals—which I call the “four Ps”—are prompt identification, protection, pragmatic intervention, and pharmacotherapy.
This article describes an up-to-date, “four-Ps” approach to treating delirium—including use of antipsychotics and supportive care—and offers evidence and case reports to address these clinical questions:
- What causes delirium?
- Does delirium worsen prognosis?
- Can delirium be prevented?
FOUR ‘Ps’ FOR TREATING DELIRIUM
When a patient’s mental status changes dramatically (Box 1),1 identifying potential delirium causes requires careful medical, psychiatric, and neurologic assessment. Assimilating this information is as essential to positive outcomes as are intensive nursing care and appropriate interventions.
- Disturbance of consciousness (i.e. reduced clarity of awareness of the environment) with reduced ability to focus, sustain, or shift attention
- A change in cognition (such as memory deficit, disorientation, language disturbance) or the development of a perceptual disturbance that is not better accounted for by a preexisting, established, or evolving dementia
- The disturbance develops over a short period of time (usually hours to days) and tends to fluctuate during the course of a 24-hour period
- There is evidence from the history, physical examination, or laboratory findings that the disturbance is caused by the direct physiologic consequences of a general medical condition
Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders (4th ed., text rev). Copyright 2000. American Psychiatric Publishing.
Prompt identification. Delirium often goes unrecognized, delaying treatment. Easily administered rating scales—such as the Delirium Rating Scale (DRS)2 and the Confusion Assessment Method (CAM)3 —can help detect emerging symptoms.
Patient protection. Provide intensive nursing care—often one-to-one observation and containment—and, where possible, enlist the family in reassuring and calming the patient. Restraints may be needed to safeguard against injury and to prevent the patient from removing or dislocating monitoring equipment and IV access.
Pragmatic intervention. With medical colleagues, begin treating biochemical and physiologic abnormalities that are the most likely and most remediable contributors (Box 2).2,4-6 Review the patient’s medications and discontinue or replace any that may be causing delirium.
Pharmacotherapy. Based on clinical studies, antipsychotics appear to possess antidelirium properties and may be considered as one part of a patient’s treatment plan. Interpreting these studies is complicated, however, by delirium’s complexity, numerous causes, and presumed mechanisms, as well as the transience of some forms. For ethical reasons, no placebo-controlled studies of delirium treatment have been done.
EVIDENCE ON ANTIPSYCHOTICS
Haloperidol has been the drug of choice for managing delirium because it is less likely to cause hypotension and sedation than other neuroleptics. Optimum haloperidol dosing in delirium has not been established, but the usual range is 2 to 6 mg every 4 to 6 hours, depending on the patient’s age and delirium severity.
Instances of QTc interval prolongation have been reported with high-dose IV haloperidol (> 100 mg). This life-threatening effect—which can induce torsades de pointes dysrhythmia, ventricular tachycardias, and fibrillation—is very rare, quite variable, and unpredictable. It probably is a function of total dose and neuroleptic administration rate.
Atypical antipsychotics share haloperidol’s advantages over first-generation neuroleptics, with lower potential for dystonic reactions, parkinsonian side effects, and tardive dyskinesia. Preliminary evidence suggests that atypicals may be safe and effective in treating delirium, although no randomized controlled trials have been done and accurate dose-response curves have not been established. Low to modest dosages have been used in case series.
Risperidone. Two prospective, open-label trials—each with 10 patients—suggest that low-dose risperidone is effective for treating delirium:
- In one trial, risperidone given at an average dosage of 1.7 mg/d was effective in 80% of patients with delirium, and one patient responded to 0.5 mg/d. Some patients experienced sleepiness or mild drug-induced parkinsonism.7
- In the other trial, risperidone was started at 0.5 mg twice daily, with additional doses allowed on day 1 for cognitive and behavioral symptoms. This dosage was maintained until DRS scores declined to ≤12, then was reduced by 50% and continued until day 6. Mean maintenance dosage was 0.75 mg/d. Two patients discontinued risperidone because of sedation or hypotension.8
At least 10% to 30% of hospitalized medically ill patients develop delirium, and rates approach 40% after age 65.4 Especially in older patients, delirium is a risk factor for:
- prolonged hospital stays
- increased morbidity and mortality
- increased functional decline and need for custodial care after hospital discharge.2
Risk factors. Prospectively identified risk factors for delirium include pre-existing dementia; age >65 years; serious medical illness; alcohol/sedative withdrawal; abnormal serum sodium, potassium, or blood glucose levels; vision or hearing impairment; hypoxia; malnutrition; and fever. Medication—particularly anticholinergic drugs—is one of the most common delirium triggers in susceptible patients.5
The most common underlying disorders that increase delirium risk in older patients are hip fracture, dementia, infections, and cerebrovascular events.6
In a larger prospective study, 64 patients (mean age 67) with delirium were treated with risperidone, given at a mean dose of 2.6 +/- 1.7 mg/d at day 3. This dosage was effective in 90% of patients and significantly improved all symptoms, as measured with scales including the DRS. Two patients (3%) experienced adverse effects.9
No significant differences in response frequency were seen in a 7-day, double-blind comparison of flexibly-dosed risperidone (starting at 0.5 mg bid) and haloperidol (starting at 0.75 mg bid) in 28 patients with delirium. Symptom severity decreased for each group, as measured with the Memorial Delirium Assessment Scale. One patient receiving haloperidol experienced mild akathisia, but no others reported clinically significant side effects.10
Quetiapine. In a retrospective review, the charts of 11 patients who received quetiapine for delirium were compared with those of 11 similar patients treated with haloperidol. DRS scores improved by >50% in 10 of 11 patients in both groups, with similar onset of effect, treatment duration, and overall clinical improvement.11 Small prospective trials with flexible dosing schedules have reported similar results.12,13
In a study of 12 older hospitalized patients with delirium, quetiapine at a mean dosage of 93.75 +/-23.31 mg/d was associated with significant DRS score improvements. Interestingly, patients’ Mini-Mental State Examination and Clock-Drawing Test scores continued to improve 3 months after their delirium symptoms stabilized.14
Olanzapine. In a prospective trial, hospitalized patients with delirium were randomly assigned to receive enteral olanzapine or haloperidol. Delirium symptoms decreased across 5 days in both groups, and clinical improvement was similar. Some patients receiving haloperidol reported extrapyramidal symptoms, whereas those receiving olanzapine reported no adverse effects.15
Parenteral forms of some atypicals (aripiprazole, olanzapine, and ziprasidone) have become available and may increase this class’ usefulness in treating delirium.
Other drugs. Benzodiazepines appear ineffective and generally play only an adjunctive role in treating delirium. An exception may be delirium induced by acute alcohol or benzodiazepine withdrawal. Sedating antidepressants have been used as hypnotics in patients with delirium, but supporting evidence is lacking.
Other drug classes—general anesthetics, narcotics, cholinomimetics—may help manage the dangerously hyperactive delirious patient, but the literature contains no systematic analyses.
WHAT CAUSES DELIRIUM?
Delirium’s pathophysiology is not completely understood, although most authors believe several mechanisms are involved.
The brain’s exclusively oxidative metabolism and its systems’ hierarchical vulnerability to substrate deficiency—as might occur in even transient hypoxia or hypotension—appear to play important roles. Factors such as fever and stress that increase metabolic demand on the brain intensify the effects of oxygen deficiency or circulatory compromise.
At least three molecular mechanisms have been proposed for delirium, including cholinergic transmission disruption, monoaminergic dysfunction, and cytokine release ( Box 3).16-19 These mechanisms may interact, cascading into a common final pathway that results in delirium.
Features not considered essential to delirium’s diagnosis—such as visual hallucinations or aggressive behaviors—indicate that additional cortical and subcortical systems are involved.
CASE REPORT: DRUG-DRUG INTERACTION
Three days after hip replacement surgery, Mr. S, age 64, becomes confused, distractible, and combative. He is alert one minute and somnolent the next. His arms and legs jerk involuntarily, and his muscle tone is diffusely increased. He talks with absent friends and family as though they are present in his hospital room. His body temperature and blood pressure fluctuate widely, despite no evidence of infection.
Cholinergic transmission disruption
The greater a medication’s anticholinergic activity, the greater its risk of causing delirium. Combining drugs with anticholinergic effects—such as theophylline, warfarin, or codeine (Table19)—compounds the delirium risk.
Acetylcholine-secreting neurons—widely if sparsely distributed throughout the brain—affect arousal, attention, memory, and sleep regulation. Acetylcholine is produced by oxidative metabolism and thus is vulnerable to physiologic disturbances that increase oxygen demand or disrupt oxygen supply.
Anticholinergic poisoning and abuse of anticholinergic substances are known to cause acute delirium—a finding that supports the key role of acetylcholine in maintaining alertness and concentration. Agents that enhance cholinergic transmission—such as the cholinesterase inhibitor physostigmine—can effectively treat drug-induced delirium.
Monoaminergic dysfunction
The principal monoamines of dopamine, serotonin, and norepinephrine help sustain attention, regulate the sleep-wake cycle, inhibit affective responses, and modulate aggressive and impulsive behaviors. Treating patients with dopamine and serotonin agonists can cause psychotic symptoms.
Glutamate—a monoamine neurotransmitter with excitatory properties—is released during metabolic stress and likely contributes to the psychotic features sometimes seen in delirium.
Cytokine release
Infection in a distant organ, such as gallbladder or kidney, is known to cause delirium. Cytokines such as interleukins and interferon-alpha are polypeptides secreted by macrophagesin response to tissue injury. They easily cross the blood-brain barrier and stimulate glial cells to release more cytokines, which interfere with neurotransmitter synthesis and transmission.
Table
Drugs whose anticholinergic effects may increase the risk of delirium
| Drug | Anticholinergic level* |
|---|---|
| Cimetidine | 0.86 |
| Prednisolone | 0.55 |
| Theophylline | 0.44 |
| Digoxin | 0.25 |
| Lanoxin | 0.25 |
| Nifedipine | 0.22 |
| Ranitidine | 0.22 |
| Furosemide | 0.22 |
| Isosorbide | 0.15 |
| Warfarin | 0.12 |
| Dipyridamole | 0.11 |
| Codeine | 0.11 |
| * ng/mL in atropine equivalents | |
| Source: Adapted from reference 19. | |
For several years, Mr. S has been taking the monoamine oxidase inhibitor (MAOI) phenelzine, 30 mg/d, for depression maintenance treatment. On admission, he insisted that the MAOI be continued during hospitalization because it had relieved his severe depressions.
Within 24 hours of surgery, he was given the skeletal muscle relaxant cyclobenzaprine, 5 mg tid, for painful muscle spasms in the operated hip. When this brought little relief, the dosage was increased to 10 mg tid. Delirium and autonomic instability developed approximately 4 hours after the first 10-mg dose and gradually worsened.
The two drugs are discontinued, and Mr S. gradually recovers after several days of physiologic support, protection, and sedation in the intensive-care unit.
Discussion. Mr. S developed serotonin syndrome from a drug-drug interaction. Phenelzine inhibited serotonin metabolism, and cyclobenzaprine—a drug chemically similar to tricyclic antidepressants—inhibited serotonin reuptake, resulting in substantially increased CNS serotonergic activity.20 Serotonin syndrome symptoms include delirium, autonomic dysfunction, and neurologic signs such as myoclonus and rigidity when patients are taking drugs that enhance serotonergic transmission.
DOES DELIRIUM WORSEN PROGNOSIS?
In the largest study of delirium in older patients, Inouye et al21 examined outcomes of 727 consecutive patients age 65 and older with various medical diagnoses who were admitted to three teaching hospitals. Delirium was diagnosed in 88 patients (12%) at admission.
Within 3 months of hospital discharge, 165 (25%) of 663 patients had died or been newly admitted to a nursing home. After the authors controlled the data for age, gender, dementia, illness severity, and functional status, they found that delirium:
- tripled the likelihood of nursing home placement at hospital discharge and after 3 months (adjusted odds ratio [OR] for delirium 3.0)
- more than doubled the likelihood of death or new nursing home placement at discharge (OR for delirium 2.1) and after 3 months (OR for delirium 2.6).
They concluded that delirium was a significant predictor of functional decline at hospital discharge and also at follow-up in older patients.
Interestingly, although these authors did not find a statistically significant association between delirium and death alone, the risk of death was particularly strong for patients who were not demented (OR for delirium, 3.77). Similarly, Rabins and Folstein22 found higher mortality rates in medically ill patients diagnosed with delirium on hospital admission than in demented, cognitively intact, or depressed patients. After 1 year, the death rate remained higher in those who had been delirious than in those with dementia.
In a 12-month observational study comparing 243 older medical inpatients with delirium and 118 controls without delirium, McCusker et al23 found that:
- patients with delirium were twice as likely to die within 12 months as those without delirium
- the greater severity of delirium symptoms, the higher the risk of death in patients with delirium but without dementia.
In a recent study, some of the same investigators found that delirium symptoms—especially inattention, disorientation, and impaired memory—persisted for 12 months after hospital discharge in medical inpatients age 65 and older with or without dementia. Mean numbers of delirium symptoms at diagnosis and 12-month follow-up, respectively, were:
- 4.5 and 3.5 in patients with dementia
- 3.4 and 2.2 in patients without dementia.24
CASE REPORT: DELIRIUM AS PROGNOSTIC SIGN
Mrs. W, age 70, is hospitalized for treatment of anemia and dehydration after falling at home. She has metastatic adenocarcinoma of the colon and is hypernatremic and hypotensive on admission.
Within 24 hours, she becomes floridly delirious, despite transfusion of two units of packed red cells and IV fluid replacement. She receives IM haloperidol to reduce the agitation and counteract delirium. Head CT reveals mild, diffuse cerebral atrophy but no metastasis or subdural hematoma.
Although aggressive treatment corrects her electrolyte disturbance and dehydration and restores normal vital signs, the delirium does not resolve. She is discharged to a nursing home, where she is discovered dead in bed 1 week later.
Discussion. Delirium independently increases the risk of death during hospitalization and thereafter, particularly in older patients. As in the case of Mrs. W, delirium is a common preterminal event in cancer patients.25
Evidence suggests that delirium is a marker for declining functional status and of relatively poor outcomes in older patients. In patients who are hospitalized, however, the relative effects of comorbid medical and neurologic conditions on prognosis are difficult to differentiate from the effects of delirium.
CAN DELIRIUM BE PREVENTED?
Researchers at Yale University examined whether a multicomponent, nonpharmacologic intervention could reduce delirium incidence and episode duration in 852 at-risk hospitalized medical patients age 70 and older.26 Patients were randomly assigned to intervention or usual care and then observed daily until discharge. Interventions included protocols for orientation, mobilization, sleep hygiene, and sensory enhancement, as well as prompt treatment of dehydration.
Delirium occurred in 10% of the intervention group and in 15% of the usual-care group (matched odds ratio 0.6). Total days with delirium (105 vs. 161; P = 0.02) and total episodes (62 vs. 90; P = 0.03) were significantly lower in the intervention group. A potential source of bias in this study was a lack of randomization in assigning patients to intervention or usual care. Follow-up studies found that:
- The intervention increased health care costs for patients at high risk for delirium but had no significant effect on overall costs for patients at intermediate risk.27
- Delirium risk decreased the most (89%) in older patients who were most adherent to the intervention protocols during hospitalization.28
- Among the 705 patients who survived at least 6 months after discharge, those who had been in the intervention and usual-care groups showed similar functional and cognitive status and rates of depression, delirium, nursing home placement, and rehospitalization.29
CASE REPORT: A SUCCESSFUL INTERVENTION
Mr. A, age 66, who has moderate-to-severe chronic obstructive pulmonary disease, is hospitalized for surgery to remove a suspicious lung nodule. Two years ago, he experienced delirium following a transurethral prostatectomy. His hemoglobin is 9.1 g/dL (normal, 11.5 to 14 g/dL), defined as anemia related to chronic disease.
Because of his history of postoperative delirium, the hospital staff initiates preventive measures. Before surgery, he is given two units of blood for anemia. To assist with orientation, he and his family receive information about delirium, and his hearing aid—which has been malfunctioning—is readjusted to improve his auditory acuity. During surgery, his oxygen saturation and blood pressure are monitored scrupulously.
Afterward, no mental status changes are observed, and Mr. A recovers uneventfully. The surgery revealed a benign granuloma.
Discussion. Surgical patients such as Mr. A—particularly those with hemoglobin <10 g/dL—face a higher risk for delirium than medical patients do. The reason, although undetermined, may be related to unavoidable tissue injury and hemorrhage associated with surgery.30
Nonpharmacologic intervention shows promise in preventing delirium, but more evidence is needed to develop simpler, less-costly strategies for at-risk hospitalized patients and to preserve their functional status after discharge.
Related resources
- Cook IA. Guideline Watch. Practice guideline for the treatment of patients with delirium. American Psychiatric Association, August 2004. www.psych.org/psych_pract/treatg/pg/prac_guide.cfm (scroll down to “Delirium” under topic list). Accessed Dec. 14, 2004.
Drug brand names
- Aripiprazole • Abilify
- Cyclobenzapine • Flexeril
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Phenylzine • Nardil
- Physostigmine • Antilirium
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Warfarin • Coumadin
- Ziprasidone • Geodon
Disclosures
Dr. O’Connor reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Four principles of treating delirium can help protect medical/surgical patients at risk for morbidity and functional decline. These principals—which I call the “four Ps”—are prompt identification, protection, pragmatic intervention, and pharmacotherapy.
This article describes an up-to-date, “four-Ps” approach to treating delirium—including use of antipsychotics and supportive care—and offers evidence and case reports to address these clinical questions:
- What causes delirium?
- Does delirium worsen prognosis?
- Can delirium be prevented?
FOUR ‘Ps’ FOR TREATING DELIRIUM
When a patient’s mental status changes dramatically (Box 1),1 identifying potential delirium causes requires careful medical, psychiatric, and neurologic assessment. Assimilating this information is as essential to positive outcomes as are intensive nursing care and appropriate interventions.
- Disturbance of consciousness (i.e. reduced clarity of awareness of the environment) with reduced ability to focus, sustain, or shift attention
- A change in cognition (such as memory deficit, disorientation, language disturbance) or the development of a perceptual disturbance that is not better accounted for by a preexisting, established, or evolving dementia
- The disturbance develops over a short period of time (usually hours to days) and tends to fluctuate during the course of a 24-hour period
- There is evidence from the history, physical examination, or laboratory findings that the disturbance is caused by the direct physiologic consequences of a general medical condition
Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders (4th ed., text rev). Copyright 2000. American Psychiatric Publishing.
Prompt identification. Delirium often goes unrecognized, delaying treatment. Easily administered rating scales—such as the Delirium Rating Scale (DRS)2 and the Confusion Assessment Method (CAM)3 —can help detect emerging symptoms.
Patient protection. Provide intensive nursing care—often one-to-one observation and containment—and, where possible, enlist the family in reassuring and calming the patient. Restraints may be needed to safeguard against injury and to prevent the patient from removing or dislocating monitoring equipment and IV access.
Pragmatic intervention. With medical colleagues, begin treating biochemical and physiologic abnormalities that are the most likely and most remediable contributors (Box 2).2,4-6 Review the patient’s medications and discontinue or replace any that may be causing delirium.
Pharmacotherapy. Based on clinical studies, antipsychotics appear to possess antidelirium properties and may be considered as one part of a patient’s treatment plan. Interpreting these studies is complicated, however, by delirium’s complexity, numerous causes, and presumed mechanisms, as well as the transience of some forms. For ethical reasons, no placebo-controlled studies of delirium treatment have been done.
EVIDENCE ON ANTIPSYCHOTICS
Haloperidol has been the drug of choice for managing delirium because it is less likely to cause hypotension and sedation than other neuroleptics. Optimum haloperidol dosing in delirium has not been established, but the usual range is 2 to 6 mg every 4 to 6 hours, depending on the patient’s age and delirium severity.
Instances of QTc interval prolongation have been reported with high-dose IV haloperidol (> 100 mg). This life-threatening effect—which can induce torsades de pointes dysrhythmia, ventricular tachycardias, and fibrillation—is very rare, quite variable, and unpredictable. It probably is a function of total dose and neuroleptic administration rate.
Atypical antipsychotics share haloperidol’s advantages over first-generation neuroleptics, with lower potential for dystonic reactions, parkinsonian side effects, and tardive dyskinesia. Preliminary evidence suggests that atypicals may be safe and effective in treating delirium, although no randomized controlled trials have been done and accurate dose-response curves have not been established. Low to modest dosages have been used in case series.
Risperidone. Two prospective, open-label trials—each with 10 patients—suggest that low-dose risperidone is effective for treating delirium:
- In one trial, risperidone given at an average dosage of 1.7 mg/d was effective in 80% of patients with delirium, and one patient responded to 0.5 mg/d. Some patients experienced sleepiness or mild drug-induced parkinsonism.7
- In the other trial, risperidone was started at 0.5 mg twice daily, with additional doses allowed on day 1 for cognitive and behavioral symptoms. This dosage was maintained until DRS scores declined to ≤12, then was reduced by 50% and continued until day 6. Mean maintenance dosage was 0.75 mg/d. Two patients discontinued risperidone because of sedation or hypotension.8
At least 10% to 30% of hospitalized medically ill patients develop delirium, and rates approach 40% after age 65.4 Especially in older patients, delirium is a risk factor for:
- prolonged hospital stays
- increased morbidity and mortality
- increased functional decline and need for custodial care after hospital discharge.2
Risk factors. Prospectively identified risk factors for delirium include pre-existing dementia; age >65 years; serious medical illness; alcohol/sedative withdrawal; abnormal serum sodium, potassium, or blood glucose levels; vision or hearing impairment; hypoxia; malnutrition; and fever. Medication—particularly anticholinergic drugs—is one of the most common delirium triggers in susceptible patients.5
The most common underlying disorders that increase delirium risk in older patients are hip fracture, dementia, infections, and cerebrovascular events.6
In a larger prospective study, 64 patients (mean age 67) with delirium were treated with risperidone, given at a mean dose of 2.6 +/- 1.7 mg/d at day 3. This dosage was effective in 90% of patients and significantly improved all symptoms, as measured with scales including the DRS. Two patients (3%) experienced adverse effects.9
No significant differences in response frequency were seen in a 7-day, double-blind comparison of flexibly-dosed risperidone (starting at 0.5 mg bid) and haloperidol (starting at 0.75 mg bid) in 28 patients with delirium. Symptom severity decreased for each group, as measured with the Memorial Delirium Assessment Scale. One patient receiving haloperidol experienced mild akathisia, but no others reported clinically significant side effects.10
Quetiapine. In a retrospective review, the charts of 11 patients who received quetiapine for delirium were compared with those of 11 similar patients treated with haloperidol. DRS scores improved by >50% in 10 of 11 patients in both groups, with similar onset of effect, treatment duration, and overall clinical improvement.11 Small prospective trials with flexible dosing schedules have reported similar results.12,13
In a study of 12 older hospitalized patients with delirium, quetiapine at a mean dosage of 93.75 +/-23.31 mg/d was associated with significant DRS score improvements. Interestingly, patients’ Mini-Mental State Examination and Clock-Drawing Test scores continued to improve 3 months after their delirium symptoms stabilized.14
Olanzapine. In a prospective trial, hospitalized patients with delirium were randomly assigned to receive enteral olanzapine or haloperidol. Delirium symptoms decreased across 5 days in both groups, and clinical improvement was similar. Some patients receiving haloperidol reported extrapyramidal symptoms, whereas those receiving olanzapine reported no adverse effects.15
Parenteral forms of some atypicals (aripiprazole, olanzapine, and ziprasidone) have become available and may increase this class’ usefulness in treating delirium.
Other drugs. Benzodiazepines appear ineffective and generally play only an adjunctive role in treating delirium. An exception may be delirium induced by acute alcohol or benzodiazepine withdrawal. Sedating antidepressants have been used as hypnotics in patients with delirium, but supporting evidence is lacking.
Other drug classes—general anesthetics, narcotics, cholinomimetics—may help manage the dangerously hyperactive delirious patient, but the literature contains no systematic analyses.
WHAT CAUSES DELIRIUM?
Delirium’s pathophysiology is not completely understood, although most authors believe several mechanisms are involved.
The brain’s exclusively oxidative metabolism and its systems’ hierarchical vulnerability to substrate deficiency—as might occur in even transient hypoxia or hypotension—appear to play important roles. Factors such as fever and stress that increase metabolic demand on the brain intensify the effects of oxygen deficiency or circulatory compromise.
At least three molecular mechanisms have been proposed for delirium, including cholinergic transmission disruption, monoaminergic dysfunction, and cytokine release ( Box 3).16-19 These mechanisms may interact, cascading into a common final pathway that results in delirium.
Features not considered essential to delirium’s diagnosis—such as visual hallucinations or aggressive behaviors—indicate that additional cortical and subcortical systems are involved.
CASE REPORT: DRUG-DRUG INTERACTION
Three days after hip replacement surgery, Mr. S, age 64, becomes confused, distractible, and combative. He is alert one minute and somnolent the next. His arms and legs jerk involuntarily, and his muscle tone is diffusely increased. He talks with absent friends and family as though they are present in his hospital room. His body temperature and blood pressure fluctuate widely, despite no evidence of infection.
Cholinergic transmission disruption
The greater a medication’s anticholinergic activity, the greater its risk of causing delirium. Combining drugs with anticholinergic effects—such as theophylline, warfarin, or codeine (Table19)—compounds the delirium risk.
Acetylcholine-secreting neurons—widely if sparsely distributed throughout the brain—affect arousal, attention, memory, and sleep regulation. Acetylcholine is produced by oxidative metabolism and thus is vulnerable to physiologic disturbances that increase oxygen demand or disrupt oxygen supply.
Anticholinergic poisoning and abuse of anticholinergic substances are known to cause acute delirium—a finding that supports the key role of acetylcholine in maintaining alertness and concentration. Agents that enhance cholinergic transmission—such as the cholinesterase inhibitor physostigmine—can effectively treat drug-induced delirium.
Monoaminergic dysfunction
The principal monoamines of dopamine, serotonin, and norepinephrine help sustain attention, regulate the sleep-wake cycle, inhibit affective responses, and modulate aggressive and impulsive behaviors. Treating patients with dopamine and serotonin agonists can cause psychotic symptoms.
Glutamate—a monoamine neurotransmitter with excitatory properties—is released during metabolic stress and likely contributes to the psychotic features sometimes seen in delirium.
Cytokine release
Infection in a distant organ, such as gallbladder or kidney, is known to cause delirium. Cytokines such as interleukins and interferon-alpha are polypeptides secreted by macrophagesin response to tissue injury. They easily cross the blood-brain barrier and stimulate glial cells to release more cytokines, which interfere with neurotransmitter synthesis and transmission.
Table
Drugs whose anticholinergic effects may increase the risk of delirium
| Drug | Anticholinergic level* |
|---|---|
| Cimetidine | 0.86 |
| Prednisolone | 0.55 |
| Theophylline | 0.44 |
| Digoxin | 0.25 |
| Lanoxin | 0.25 |
| Nifedipine | 0.22 |
| Ranitidine | 0.22 |
| Furosemide | 0.22 |
| Isosorbide | 0.15 |
| Warfarin | 0.12 |
| Dipyridamole | 0.11 |
| Codeine | 0.11 |
| * ng/mL in atropine equivalents | |
| Source: Adapted from reference 19. | |
For several years, Mr. S has been taking the monoamine oxidase inhibitor (MAOI) phenelzine, 30 mg/d, for depression maintenance treatment. On admission, he insisted that the MAOI be continued during hospitalization because it had relieved his severe depressions.
Within 24 hours of surgery, he was given the skeletal muscle relaxant cyclobenzaprine, 5 mg tid, for painful muscle spasms in the operated hip. When this brought little relief, the dosage was increased to 10 mg tid. Delirium and autonomic instability developed approximately 4 hours after the first 10-mg dose and gradually worsened.
The two drugs are discontinued, and Mr S. gradually recovers after several days of physiologic support, protection, and sedation in the intensive-care unit.
Discussion. Mr. S developed serotonin syndrome from a drug-drug interaction. Phenelzine inhibited serotonin metabolism, and cyclobenzaprine—a drug chemically similar to tricyclic antidepressants—inhibited serotonin reuptake, resulting in substantially increased CNS serotonergic activity.20 Serotonin syndrome symptoms include delirium, autonomic dysfunction, and neurologic signs such as myoclonus and rigidity when patients are taking drugs that enhance serotonergic transmission.
DOES DELIRIUM WORSEN PROGNOSIS?
In the largest study of delirium in older patients, Inouye et al21 examined outcomes of 727 consecutive patients age 65 and older with various medical diagnoses who were admitted to three teaching hospitals. Delirium was diagnosed in 88 patients (12%) at admission.
Within 3 months of hospital discharge, 165 (25%) of 663 patients had died or been newly admitted to a nursing home. After the authors controlled the data for age, gender, dementia, illness severity, and functional status, they found that delirium:
- tripled the likelihood of nursing home placement at hospital discharge and after 3 months (adjusted odds ratio [OR] for delirium 3.0)
- more than doubled the likelihood of death or new nursing home placement at discharge (OR for delirium 2.1) and after 3 months (OR for delirium 2.6).
They concluded that delirium was a significant predictor of functional decline at hospital discharge and also at follow-up in older patients.
Interestingly, although these authors did not find a statistically significant association between delirium and death alone, the risk of death was particularly strong for patients who were not demented (OR for delirium, 3.77). Similarly, Rabins and Folstein22 found higher mortality rates in medically ill patients diagnosed with delirium on hospital admission than in demented, cognitively intact, or depressed patients. After 1 year, the death rate remained higher in those who had been delirious than in those with dementia.
In a 12-month observational study comparing 243 older medical inpatients with delirium and 118 controls without delirium, McCusker et al23 found that:
- patients with delirium were twice as likely to die within 12 months as those without delirium
- the greater severity of delirium symptoms, the higher the risk of death in patients with delirium but without dementia.
In a recent study, some of the same investigators found that delirium symptoms—especially inattention, disorientation, and impaired memory—persisted for 12 months after hospital discharge in medical inpatients age 65 and older with or without dementia. Mean numbers of delirium symptoms at diagnosis and 12-month follow-up, respectively, were:
- 4.5 and 3.5 in patients with dementia
- 3.4 and 2.2 in patients without dementia.24
CASE REPORT: DELIRIUM AS PROGNOSTIC SIGN
Mrs. W, age 70, is hospitalized for treatment of anemia and dehydration after falling at home. She has metastatic adenocarcinoma of the colon and is hypernatremic and hypotensive on admission.
Within 24 hours, she becomes floridly delirious, despite transfusion of two units of packed red cells and IV fluid replacement. She receives IM haloperidol to reduce the agitation and counteract delirium. Head CT reveals mild, diffuse cerebral atrophy but no metastasis or subdural hematoma.
Although aggressive treatment corrects her electrolyte disturbance and dehydration and restores normal vital signs, the delirium does not resolve. She is discharged to a nursing home, where she is discovered dead in bed 1 week later.
Discussion. Delirium independently increases the risk of death during hospitalization and thereafter, particularly in older patients. As in the case of Mrs. W, delirium is a common preterminal event in cancer patients.25
Evidence suggests that delirium is a marker for declining functional status and of relatively poor outcomes in older patients. In patients who are hospitalized, however, the relative effects of comorbid medical and neurologic conditions on prognosis are difficult to differentiate from the effects of delirium.
CAN DELIRIUM BE PREVENTED?
Researchers at Yale University examined whether a multicomponent, nonpharmacologic intervention could reduce delirium incidence and episode duration in 852 at-risk hospitalized medical patients age 70 and older.26 Patients were randomly assigned to intervention or usual care and then observed daily until discharge. Interventions included protocols for orientation, mobilization, sleep hygiene, and sensory enhancement, as well as prompt treatment of dehydration.
Delirium occurred in 10% of the intervention group and in 15% of the usual-care group (matched odds ratio 0.6). Total days with delirium (105 vs. 161; P = 0.02) and total episodes (62 vs. 90; P = 0.03) were significantly lower in the intervention group. A potential source of bias in this study was a lack of randomization in assigning patients to intervention or usual care. Follow-up studies found that:
- The intervention increased health care costs for patients at high risk for delirium but had no significant effect on overall costs for patients at intermediate risk.27
- Delirium risk decreased the most (89%) in older patients who were most adherent to the intervention protocols during hospitalization.28
- Among the 705 patients who survived at least 6 months after discharge, those who had been in the intervention and usual-care groups showed similar functional and cognitive status and rates of depression, delirium, nursing home placement, and rehospitalization.29
CASE REPORT: A SUCCESSFUL INTERVENTION
Mr. A, age 66, who has moderate-to-severe chronic obstructive pulmonary disease, is hospitalized for surgery to remove a suspicious lung nodule. Two years ago, he experienced delirium following a transurethral prostatectomy. His hemoglobin is 9.1 g/dL (normal, 11.5 to 14 g/dL), defined as anemia related to chronic disease.
Because of his history of postoperative delirium, the hospital staff initiates preventive measures. Before surgery, he is given two units of blood for anemia. To assist with orientation, he and his family receive information about delirium, and his hearing aid—which has been malfunctioning—is readjusted to improve his auditory acuity. During surgery, his oxygen saturation and blood pressure are monitored scrupulously.
Afterward, no mental status changes are observed, and Mr. A recovers uneventfully. The surgery revealed a benign granuloma.
Discussion. Surgical patients such as Mr. A—particularly those with hemoglobin <10 g/dL—face a higher risk for delirium than medical patients do. The reason, although undetermined, may be related to unavoidable tissue injury and hemorrhage associated with surgery.30
Nonpharmacologic intervention shows promise in preventing delirium, but more evidence is needed to develop simpler, less-costly strategies for at-risk hospitalized patients and to preserve their functional status after discharge.
Related resources
- Cook IA. Guideline Watch. Practice guideline for the treatment of patients with delirium. American Psychiatric Association, August 2004. www.psych.org/psych_pract/treatg/pg/prac_guide.cfm (scroll down to “Delirium” under topic list). Accessed Dec. 14, 2004.
Drug brand names
- Aripiprazole • Abilify
- Cyclobenzapine • Flexeril
- Haloperidol • Haldol
- Olanzapine • Zyprexa
- Phenylzine • Nardil
- Physostigmine • Antilirium
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Warfarin • Coumadin
- Ziprasidone • Geodon
Disclosures
Dr. O’Connor reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Diagnostic and statistical manual of mental disorders, 4th edition, text rev. Washington, DC: American Psychiatric Association, 2000.
2. Trzepacz PT, Mulsant BH, Amanda Dew M, et al. Is delirium different when it occurs with dementia? A study using the delirium rating scale. J Neuropsychiatry Clin Neurosci 1998;10:199-204.
3. Inouye SK, Charpentier PA. Precipitating factors for delirium in hospitalized elderly persons. Predictive model and interrelationship with baseline vulnerability. JAMA 1996;275:852-7.
4. Liptzin B. Clinical diagnosis and management of delirium. In: Stoudemire A, Fogel BS, Greenberg DB (eds). Psychiatric care of the medical patient (2nd ed). New York: Oxford University Press, 2000;581-96.
5. Bourgeois JA, Seaman JS, Servis M. Delirium, dementia, and amnestic disorders. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry (4th ed). Washington, DC: American Psychiatric Publishing, 2003;270.-
6. Rahkonen T, Makela H, Paanila S, et al. Delirium in elderly people without severe predisposing disorders: etiology and 1-year prognosis after discharge. Int Psychogeriatr 2000;12(4):473-81.
7. Horikawa N, Yamazaki T, Miyamoto K, et al. Treatment of delirium with risperidone: results of a prospective open trial with 10 patients. Gen Hosp Psychiatry 2003;25(4):289-92.
8. Mittal D, Jimerson NA, Neely EP, et al. Risperidone in the treatment of delirium: results from a prospective open-label trial. J Clin Psychiatry 2004;65(5):662-7.
9. Parellada E, Baeza I, de Pablo J, Martinez G. Risperidone in the treatment of patients with delirium. J Clin Psychiatry 2004;65(3):348-53.
10. Han CS, Kim YK. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics 2004;45:297-301.
11. Schwartz TL, Masand PS. Treatment of delirium with quetiapine. Prim Care Companion J Clin Psychiatry 2000;2(1):10-12.
12. Sasaki Y, Matsuyama T, Inoue S, et al. A prospective, open-label, flexible-dose study of quetiapine in the treatment of delirium. J Clin Psychiatry 2003;64(11):1316-21.
13. Pae CU, Lee SJ, Lee CU, et al. A pilot trial of quetiapine for the treatment of patients with delirium. Hum Psychopharmacol 2004;19(2):125-7.
14. Kim KY, Bader GM, Kotlyar V, Gropper D. Treatment of delirium in older adults with quetiapine. J Geriatr Psychiatry Neurol 2003;16(1):29-31.
15. Skrobik YK, Bergeron N, Dumont M, Gottfried SB. Olanzapine vs haloperidol: treating delirium in a critical care setting. Intensive Care Med 2004;30(3):444-9.
16. Van der Mast RC. Pathophysiology of delirium. J Geriatr Psychiatry Neurol 1998;11:138-45.
17. Trzepacz PT. Update on the neuropathogenesis of delirium. Dement Geriatr Cogn Disord 1999;10:330-4.
18. Mussi C, Ferrari R, Ascari S, et al. Importance of serum anticholinergic activity in the assessment of elderly patients with delirium. J Geriatr Psychiatry Neurol 1999;12:82-6.
19. Tune L, Carr S, Hoag E, Cooper T. Anticholinergic effects of drugs commonly prescribed for the elderly: potential means for assessing risk of delirium.[see comment]. Am J Psychiatry 1992;149:1393-4.
20. Keck PE, Jr, Arnold LM. The serotonin syndrome. Psychiatr Ann 2000;30:333-43.
21. Inouye SK, Rushing JT, Foreman MD, et al. Does delirium contribute to poor hospital outcomes? A three-site epidemiologic study. J Gen Intern Med 1998;13:234-42.
22. Rabins PV, Folstein MF. Delirium and dementia: diagnostic criteria and fatality rates. Br J Psychiatry 1982;140:149-53.
23. McCusker J, Cole M, Abrahamowicz M, et al. Delirium predicts 12-month mortality. Arch Intern Med 2002;162(4):457-63.
24. McCusker J, Cole M, Dendukuri N, et al. The course of delirium in older medical inpatients: a prospective study. J Gen Intern Med 2003;18(9):696-704.
25. Greenberg DB. Preventing delirium at the end of life: lessons from recent research. Primary Care Companion J Clin Psychiatry 2003;5:62-7.
26. Inouye SK, Bogardus ST, Jr, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med 1999;340:669-76.
27. Rizzo JA, Bogardus ST, Jr, Leo-Summers L, et al. Multicomponent targeted intervention to prevent delirium in hospitalized older patients: what is the economic value? Med Care 2001;39(7):740-52.
28. Inouye SK, Bogardus ST, Jr, Williams CS, et al. The role of adherence on the effectiveness of nonpharmacologic interventions: evidence from the delirium prevention trial. Arch Intern Med 2003;163(8):958-64.
29. Bogardus ST, Jr, Desai MM, Williams CS, et al. The effects of a targeted multicomponent delirium intervention on postdischarge outcomes for hospitalized older adults. Am J Med 2003;114(5):383-90.
30. Marcantonio ER, Goldman L, Orav EJ, et al. The association of intraoperative factors with the development of postoperative delirium. Am J Med 1998;105(5):380-4.
1. Diagnostic and statistical manual of mental disorders, 4th edition, text rev. Washington, DC: American Psychiatric Association, 2000.
2. Trzepacz PT, Mulsant BH, Amanda Dew M, et al. Is delirium different when it occurs with dementia? A study using the delirium rating scale. J Neuropsychiatry Clin Neurosci 1998;10:199-204.
3. Inouye SK, Charpentier PA. Precipitating factors for delirium in hospitalized elderly persons. Predictive model and interrelationship with baseline vulnerability. JAMA 1996;275:852-7.
4. Liptzin B. Clinical diagnosis and management of delirium. In: Stoudemire A, Fogel BS, Greenberg DB (eds). Psychiatric care of the medical patient (2nd ed). New York: Oxford University Press, 2000;581-96.
5. Bourgeois JA, Seaman JS, Servis M. Delirium, dementia, and amnestic disorders. In: Hales RE, Yudofsky SC (eds). Textbook of clinical psychiatry (4th ed). Washington, DC: American Psychiatric Publishing, 2003;270.-
6. Rahkonen T, Makela H, Paanila S, et al. Delirium in elderly people without severe predisposing disorders: etiology and 1-year prognosis after discharge. Int Psychogeriatr 2000;12(4):473-81.
7. Horikawa N, Yamazaki T, Miyamoto K, et al. Treatment of delirium with risperidone: results of a prospective open trial with 10 patients. Gen Hosp Psychiatry 2003;25(4):289-92.
8. Mittal D, Jimerson NA, Neely EP, et al. Risperidone in the treatment of delirium: results from a prospective open-label trial. J Clin Psychiatry 2004;65(5):662-7.
9. Parellada E, Baeza I, de Pablo J, Martinez G. Risperidone in the treatment of patients with delirium. J Clin Psychiatry 2004;65(3):348-53.
10. Han CS, Kim YK. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics 2004;45:297-301.
11. Schwartz TL, Masand PS. Treatment of delirium with quetiapine. Prim Care Companion J Clin Psychiatry 2000;2(1):10-12.
12. Sasaki Y, Matsuyama T, Inoue S, et al. A prospective, open-label, flexible-dose study of quetiapine in the treatment of delirium. J Clin Psychiatry 2003;64(11):1316-21.
13. Pae CU, Lee SJ, Lee CU, et al. A pilot trial of quetiapine for the treatment of patients with delirium. Hum Psychopharmacol 2004;19(2):125-7.
14. Kim KY, Bader GM, Kotlyar V, Gropper D. Treatment of delirium in older adults with quetiapine. J Geriatr Psychiatry Neurol 2003;16(1):29-31.
15. Skrobik YK, Bergeron N, Dumont M, Gottfried SB. Olanzapine vs haloperidol: treating delirium in a critical care setting. Intensive Care Med 2004;30(3):444-9.
16. Van der Mast RC. Pathophysiology of delirium. J Geriatr Psychiatry Neurol 1998;11:138-45.
17. Trzepacz PT. Update on the neuropathogenesis of delirium. Dement Geriatr Cogn Disord 1999;10:330-4.
18. Mussi C, Ferrari R, Ascari S, et al. Importance of serum anticholinergic activity in the assessment of elderly patients with delirium. J Geriatr Psychiatry Neurol 1999;12:82-6.
19. Tune L, Carr S, Hoag E, Cooper T. Anticholinergic effects of drugs commonly prescribed for the elderly: potential means for assessing risk of delirium.[see comment]. Am J Psychiatry 1992;149:1393-4.
20. Keck PE, Jr, Arnold LM. The serotonin syndrome. Psychiatr Ann 2000;30:333-43.
21. Inouye SK, Rushing JT, Foreman MD, et al. Does delirium contribute to poor hospital outcomes? A three-site epidemiologic study. J Gen Intern Med 1998;13:234-42.
22. Rabins PV, Folstein MF. Delirium and dementia: diagnostic criteria and fatality rates. Br J Psychiatry 1982;140:149-53.
23. McCusker J, Cole M, Abrahamowicz M, et al. Delirium predicts 12-month mortality. Arch Intern Med 2002;162(4):457-63.
24. McCusker J, Cole M, Dendukuri N, et al. The course of delirium in older medical inpatients: a prospective study. J Gen Intern Med 2003;18(9):696-704.
25. Greenberg DB. Preventing delirium at the end of life: lessons from recent research. Primary Care Companion J Clin Psychiatry 2003;5:62-7.
26. Inouye SK, Bogardus ST, Jr, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med 1999;340:669-76.
27. Rizzo JA, Bogardus ST, Jr, Leo-Summers L, et al. Multicomponent targeted intervention to prevent delirium in hospitalized older patients: what is the economic value? Med Care 2001;39(7):740-52.
28. Inouye SK, Bogardus ST, Jr, Williams CS, et al. The role of adherence on the effectiveness of nonpharmacologic interventions: evidence from the delirium prevention trial. Arch Intern Med 2003;163(8):958-64.
29. Bogardus ST, Jr, Desai MM, Williams CS, et al. The effects of a targeted multicomponent delirium intervention on postdischarge outcomes for hospitalized older adults. Am J Med 2003;114(5):383-90.
30. Marcantonio ER, Goldman L, Orav EJ, et al. The association of intraoperative factors with the development of postoperative delirium. Am J Med 1998;105(5):380-4.
5-minute first aid for psychosis
Adding just 5 to 10 minutes of psychotherapy to medication monitoring visits can help patients overcome hallucinations, delusions, and other psychotic symptoms. Targeted cognitive-behavioral therapy (CBT) can:
- prevent crisis visits and hospitalizations
- improve long-term medication and treatment adherence
- enhance the therapeutic alliance.
Treatment goals for patients with chronic mental illness are changing as clinicians, patients, and families aspire for more than improved symptoms ( Box ).1-14 This article describes brief interventions to target medication nonadherence and positive and negative symptoms in patients with schizophrenia, schizoaffective disorder, bipolar disorder, major depressive disorder, and other chronic disorders.
CASE: VOICES FROM THE PAST
Ms. W, age 45, is seen every 6 to 8 weeks in an outpatient medication management clinic for symptoms of schizoaffective disorder, depressed type; posttraumatic stress disorder; and generalized anxiety disorder. She has a history of severe abuse by her father, self-mutilation in response to anxiety and stress, and repeated hospitalizations following visits to her mother.
She recently visited her mother again and saw her father as well. The trip led to increased symptoms of intrusive traumatic memories, thoughts of suicide with plans to overdose, visual hallucinations of her father, and increased auditory hallucinations with derogatory content.
Goals of the first therapy session after Ms. W’s trip home were to reduce her suicidal thoughts and prevent hospitalization. We encouraged her to list her positive qualities, accomplishments, important relationships, religious beliefs, goals, and dreams. She then wrote all these reasons to live on a cue card. Reading the card twice in the session stopped her suicidal thoughts, and she expressed some hope.
We encouraged her to read the card whenever suicidal ideas became strong. We scheduled her next visit 1 week later, and she contracted not to attempt suicide during that time.
DEVELOPING AN ALLIANCE
To develop an alliance with psychotic patients such as Ms. W, the first task is to help them leave each session feeling understood, validated, and enjoying the therapist’s company. This alone provides a powerful counterbalance to the isolation, demoralization, and hopelessness they bring to therapy.
Pharmacologic and psychosocial interventions are changing treatment goals for patients with serious mental illness from improved symptoms to functional recovery, improved quality of life, and reintegration into the community.1,2 Patients, families and clinicians increasingly view self-determination, independence, and recovery as realistic treatment goals.3,4
Medication limits. Drugs are crucial to managing psychotic symptoms but inadequate for achieving recovery:
- many patients with positive psychotic symptoms respond only partially or not at all5
- functional improvement does not always follow symptomatic improvement6
- medication nonadherence remains high, leading to repeated relapses.7
Dual-therapy benefits. A combination of antipsychotics and psychotherapy has been found to increase the chances of recovery in schizophrenia.8 Psychotherapy is also highly valued by patients and their families:
- In patient satisfaction studies, 72% to 90% of participants with psychotic disorders said individual psychotherapy improved their lives.9,10
- In a survey of 3,099 National Alliance for the Mentally Ill family members, 88% rated psychotherapy as having some (53%) or considerable (35%) value.11
Access problems. Despite psychotherapy’s benefits, access is extremely limited. In one survey, only 7.3% of patients with nonaffective psychosis received at least “minimally adequate” care (four or more medication visits that did not include psychotherapy).12 Incorporating therapeutic techniques into medication monitoring clinics is one way to improve access to therapy for patients with serious mental illnesses.
Keep it brief. Psychotherapy in medication clinics differs from traditional models’ 15- to 45-minute sessions.13 Patients with psychotic illness prefer brief interventions; a study of 212 patients found that 85% of those with schizophrenia preferred sessions:
- less often than once a week
- that focus on solving practical problems.14
5 steps in effective cognitive-behavioral interventions
|
In normalization, the stress vulnerability model is used to explain psychosis to the patient. Psychotic symptoms are emphasized as something normal people can experience in extreme situations, such as:
- hallucinations in states of sleep deprivation or medical and drug-induced states
- paranoia as error in thinking in states of heightened vigilance and perceived threat.15
Universality is the understanding that many people have experiences similar to the patient’s.
In a collaborative therapeutic alliance, the patient is not a passive recipient but an active collaborator in therapy. He or she contributes to decisions—such as the length of therapy and topics to be discussed—and gives feedback on interventions and therapist style.
Focusing on life goals makes therapy meaningful to the patient.
Set priorities. Because only one or two therapeutic interventions can be tried during a medication-monitoring visit, problems need to be prioritized. As with Ms. W, the first visit’s goal was crisis intervention: to reduce suicidal thoughts and prevent hospitalization. Table 1 offers a framework for effective therapeutic interventions.
Save time by giving patients out-of-session assignments, which:
- collect important information to review with patients during the next monitoring session
- help empower patients to manage their symptoms.
IMPROVING ADHERENCE
Medication nonadherence and partial adherence can result from:
- illness-related factors such as lack of insight
- patient-related factors such as attitudes and beliefs about medication
- treatment factors such as side effects
- physician-related factors such as showing an authoritarian attitude toward patients
- system-related factors such as treatment access problems.
Table 2
Interventions to improve patient medication adherence
| Issue | Intervention |
|---|---|
| Assessing medication adherence and beliefs |
|
| Dysfunctional beliefs about medication (“Taking it means I am weak.” “It can turn me into a zombie.” “I will be dependent on medication.”) |
|
| Lack of insight (“I do not need medication”) |
|
| Forgetting to take medication |
|
| Lack of a shared understanding of the illness between patient and physician |
|
CASE: NOT REALLY HER FATHER
By the second session 1 week later, Ms. W’s suicidal thoughts had become infrequent and mild, and she was using the coping card as needed. This visit focused on visual hallucinations associated with anxiety about facing her father. We encouraged her to describe the hallucinations in great detail, and she realized that she visualized her father as he had looked 20 years ago, not as he looks today. Her anxiety decreased as she considered that she might be seeing not him but an image. Her homework assignment was to closely observe the hallucinations. Because she was more stable, the next visit was scheduled in 2 weeks.
By the third session, she reported that the visual hallucinations had disappeared, and the focusing technique had helped her. She continued to hear voices, however, particularly in the evening when she was alone and anxious or depressed. With prompting, she identified activities she could engage in at night, such as calling her mother and praying with her mother on the phone. This reduced her loneliness and helped her relax.
Table 3
Interventions to manage auditory and visual hallucinations
| Problem | Intervention |
|---|---|
| Acting on hallucinations | Ask questions such as: |
| |
| Tell patient, “It is not the voices themselves but the thoughts in your mind in response to the voices that determine whether or not you follow them” | |
| List thoughts patient generates when choosing not to follow voice commands and encourage patient to read the list when hearing voices | |
| Triggers of negative emotions that cause voices | Ask questions such as: |
| |
| Identify techniques to deal with triggers and rate their effectiveness | |
| Dysfunctional beliefs that voices cannot be controlled or are prophetic | When voices are strong, coach patient to rate them on a scale of 0 to 10, try different distraction techniques, and rate them again |
| Encourage patient to write down what the voices say and whether their prophecies come true; reviewing the record in subsequent session shows voices are not prophetic | |
| Voices during the session | Hum a familiar tune with patient |
| Ask patient to read out loud | |
| Visual hallucinations | Encourage patient to examine details of what they see; this alone can make hallucinations disappear |
| Encourage patient to try to make hallucinations funny, such as making the image’s nose long (personal communication: e-mail Morton Sosland MD) |
One month later, the voices had diminished greatly, and Ms. W returned to her regular medication monitoring appointments of every 6 to 8 weeks.
MANAGING POSITIVE SYMPTOMS
In serious mental illnesses such as schizophrenia, the most common hallucinations are auditory ( Table 3 ),19 followed by visual and other types.20 Sometimes patients view hallucinations as helpful, providing reassurance, advice, or companionship. The content may be an expression of the patient’s own beliefs.
Table 4
Interventions to help patients examine common delusions
| Symptom | Questions to ask the patient |
|---|---|
| Behaviors of acting on delusions |
|
| Delusion with changing conviction |
|
| Delusion with complete conviction |
|
| Addressing underlying beliefs |
|
| Delusion associated with lack of real world knowledge | Provide real-world knowledge. For example, for delusion that people can read a patient’s mind, inform patient that scientific experiments have shown that no one can read complex thoughts of others |
| Delusion involving physician | For example, say, “It is normal for you to sometimes question my intentions and believe that I am part of the conspiracy. I can assure you that is not the case. Anytime you have those doubts I would like the opportunity to clarify those for you. Can I rely on you to bring those doubts to my attention?” |
| When patient’s body language or behavior changes, ask if patient is suspicious and paranoid about you | |
| Behavioral experiment for delusions | For example, a patient believed people parking cars on his street would break into his apartment. Homework was designed with two columns on a paper, one for him to check when someone parked and the other if they broke in. Next visit, patient returned with no checks in the break-ins column |
- Are the hallucinations distressing, and does the patient want them to stop?
- What triggers them (usually depressed mood, anxiety, anger, or boredom)?
- What coping mechanisms has the patient used, and how effective have they been?
- What is the source of the patient’s distress?
Table 5
Interventions for managing schizophrenia’s negative symptoms
| Symptom | Intervention |
|---|---|
| Anergia/anhedonia |
|
| Impaired attention |
|
| Alogia |
|
Never dispute a patient’s delusional beliefs. Maintain an attitude of benevolent curiosity to elicit the reasoning processes by which he or she came to believe the delusions. By encouraging the patient to become curious about the experience, you can create a chink of insight and help the him or her achieve important goals despite disturbing sensory experiences and beliefs.
Thought disorder can be addressed by gently pointing out that you are having trouble understanding the patient’s speech. Ask if other people whom the patient trusts have commented on his or her speech.
Because thought disorder worsens the longer a patient talks, suggest a 5-sentence rule during sessions. You and the patient try to speak no more than 5 sentences at a time before pausing to let the other person speak. Encourage the patient to monitor your speech and to indicate when you violate the rule. Monitoring your speech helps patients start monitoring their own.
Thought disorder worsens when patients experience negative emotions such as anxiety. When this occurs, move the discussion to a neutral topic or encourage deep regular breathing for 2 minutes to reduce anxiety.
MANAGING NEGATIVE SYMPTOMS
Negative symptoms of schizophrenia ( Table 5 ) overlap with depression and with medication side effects. Anhedonia and social withdrawal, for example, may reflect a patient’s depression and demoralization, rather than just schizophrenia’s biological core symptoms.
Similarly, limited facial expression may be caused by drug side effects, rather than absence of affect. Negative symptoms also can occur in the absence of depression or side effects, such as when a patient’s automatic thoughts related to expectations of failure lead to lack of motivation.
Negative symptoms usually bother patients much less than positive symptoms do. Thus, enlisting family members to help patients monitor and deal with negative symptoms can be very useful.
CASE SUMMARY
Ms. W’s stress-related psychotic symptoms resolved to baseline with cognitive therapy done in a regular medication management clinic. Throughout this episode, her medication dosages remained unchanged. The interventions added about 10 minutes to sessions, effectively dealt with her symptom exacerbation, and prevented hospitalization.
Psychotropics remain a critical component of treating psychotic disorders, and psychotherapy can also be very helpful. But in the many situations when psychotherapy is not available, brief psychotherapeutic techniques can:
- increase patient and family satisfaction
- enhance the therapeutic alliance
- improve medication adherence
- promote recovery.
1. American Psychiatric Association. Work group on Schizophrenia. Practice guidelines for the treatment of patients with schizophrenia. Am J Psychiatry 2004;161:29(suppl):26-7.
2. Kane JM. Long-term treatment of schizophrenia: moving from a relapse-prevention model to a recovery model. J Clin Psychiatry 2004;64(11):1384-5.
3. Coursey RD, Alford J, Safarjan B. Significant advances in understanding and treating serious mental lllness. Prof Psychol Res Pract 1997;28(3):205-16.
4. Cunningham R. In my own voice: how early intervention led to great success. NAMI Voice 2004;1:1-5.
5. Conley RR, Buchanan RW. Evaluation of treatment-resistant schizophrenia. Schizophr Bull 1997;23:663-74.
6. Harvey PD, Green M, Keefe RS, Velligan DI. Cognitive functioning in schizophrenia: a consensus statement on its role in the definition and evaluation of effective treatments for the illness. J Clin Psychiatry 2004;65(3):361-72.
7. Bridge JA, Barbe RP. Reducing hospital readmission in depression and schizophrenia: current evidence. Curr Opin Psychiatry 2004;17(6):505-11.
8. Lieberman RP, Kopelowicz A, Ventura J, et al. Operational criteria and factors related to recovery from schizophrenia. Int Rev Psychiatry 2002;14(4):256-72.
9. Leggatt M. Schizophrenia: the consumer’s viewpoint. In: Burrows GD, Norman TR, Rubinstein G (eds). Handbook of studies on schizophrenia, vol 2. New York: Elsevier Science Publishers, 1986;143-53.
10. Coursey RD, Keller AB, Farrell EW. Individual psychotherapy and persons with serious mental illness: the client’s perspective. Schizophr Bull 1995;21:283-301.
11. Hatfield A, Gearon J, Coursey R. Family members’ ratings of the use and value of mental health services: results of a national NAMI survey. Psychiatr Serv 1996;47:825-31.
12. Wang PS, Demler O, Kessler RC. Adequacy of treatment for serious mental illness in the United States. Am J Public Health 2002;92(1):92-8.
13. Rector N, Beck A. CBT for schizophrenia. Can J Psychiatry 2002;47(1):39-48.
14. Coursey RD, Keller A, Farrell EW. Individual psychotherapy and serious mental illness: the clients’ perspective. Schizophr Bull 1995;21:283-301.
15. Kingdon DG, Turkington D. Explanations of schizophrenia. In: Kingdon DG, Turkington D (eds). Cognitive-behavioral therapy of schizophrenia. New York: Guilford Press, 1994;9.-
16. Green MF. What are the functional consequences of neurocognitive deficits in schizophrenia? Am J Psychiatry. 1996;153:361-9.
17. Velligan DI, Bow-Thomas CC, Huntzinger C, et al. Randomized controlled trial of the use of compensatory strategies to enhance adaptive functioning in outpatients with schizophrenia. Am J Psychiatry 2000;157:1317-23.
18. Gilmer T, Dolder C, Lacro J, et al. Adherence to treatment with antipsychotic medication and health care costs among Medicaid beneficiaries with schizophrenia. Am J Psychiatry 2004;161(4):692-99.
19. Romme MAJ. Hearing voices. Schizophr Bull 1989;15:209-16.
20. Andreasen NC, Flaum M. Schizophrenia: the characteristic symptoms. Schizophr Bull 1991;17(1):27-49.
Adding just 5 to 10 minutes of psychotherapy to medication monitoring visits can help patients overcome hallucinations, delusions, and other psychotic symptoms. Targeted cognitive-behavioral therapy (CBT) can:
- prevent crisis visits and hospitalizations
- improve long-term medication and treatment adherence
- enhance the therapeutic alliance.
Treatment goals for patients with chronic mental illness are changing as clinicians, patients, and families aspire for more than improved symptoms ( Box ).1-14 This article describes brief interventions to target medication nonadherence and positive and negative symptoms in patients with schizophrenia, schizoaffective disorder, bipolar disorder, major depressive disorder, and other chronic disorders.
CASE: VOICES FROM THE PAST
Ms. W, age 45, is seen every 6 to 8 weeks in an outpatient medication management clinic for symptoms of schizoaffective disorder, depressed type; posttraumatic stress disorder; and generalized anxiety disorder. She has a history of severe abuse by her father, self-mutilation in response to anxiety and stress, and repeated hospitalizations following visits to her mother.
She recently visited her mother again and saw her father as well. The trip led to increased symptoms of intrusive traumatic memories, thoughts of suicide with plans to overdose, visual hallucinations of her father, and increased auditory hallucinations with derogatory content.
Goals of the first therapy session after Ms. W’s trip home were to reduce her suicidal thoughts and prevent hospitalization. We encouraged her to list her positive qualities, accomplishments, important relationships, religious beliefs, goals, and dreams. She then wrote all these reasons to live on a cue card. Reading the card twice in the session stopped her suicidal thoughts, and she expressed some hope.
We encouraged her to read the card whenever suicidal ideas became strong. We scheduled her next visit 1 week later, and she contracted not to attempt suicide during that time.
DEVELOPING AN ALLIANCE
To develop an alliance with psychotic patients such as Ms. W, the first task is to help them leave each session feeling understood, validated, and enjoying the therapist’s company. This alone provides a powerful counterbalance to the isolation, demoralization, and hopelessness they bring to therapy.
Pharmacologic and psychosocial interventions are changing treatment goals for patients with serious mental illness from improved symptoms to functional recovery, improved quality of life, and reintegration into the community.1,2 Patients, families and clinicians increasingly view self-determination, independence, and recovery as realistic treatment goals.3,4
Medication limits. Drugs are crucial to managing psychotic symptoms but inadequate for achieving recovery:
- many patients with positive psychotic symptoms respond only partially or not at all5
- functional improvement does not always follow symptomatic improvement6
- medication nonadherence remains high, leading to repeated relapses.7
Dual-therapy benefits. A combination of antipsychotics and psychotherapy has been found to increase the chances of recovery in schizophrenia.8 Psychotherapy is also highly valued by patients and their families:
- In patient satisfaction studies, 72% to 90% of participants with psychotic disorders said individual psychotherapy improved their lives.9,10
- In a survey of 3,099 National Alliance for the Mentally Ill family members, 88% rated psychotherapy as having some (53%) or considerable (35%) value.11
Access problems. Despite psychotherapy’s benefits, access is extremely limited. In one survey, only 7.3% of patients with nonaffective psychosis received at least “minimally adequate” care (four or more medication visits that did not include psychotherapy).12 Incorporating therapeutic techniques into medication monitoring clinics is one way to improve access to therapy for patients with serious mental illnesses.
Keep it brief. Psychotherapy in medication clinics differs from traditional models’ 15- to 45-minute sessions.13 Patients with psychotic illness prefer brief interventions; a study of 212 patients found that 85% of those with schizophrenia preferred sessions:
- less often than once a week
- that focus on solving practical problems.14
5 steps in effective cognitive-behavioral interventions
|
In normalization, the stress vulnerability model is used to explain psychosis to the patient. Psychotic symptoms are emphasized as something normal people can experience in extreme situations, such as:
- hallucinations in states of sleep deprivation or medical and drug-induced states
- paranoia as error in thinking in states of heightened vigilance and perceived threat.15
Universality is the understanding that many people have experiences similar to the patient’s.
In a collaborative therapeutic alliance, the patient is not a passive recipient but an active collaborator in therapy. He or she contributes to decisions—such as the length of therapy and topics to be discussed—and gives feedback on interventions and therapist style.
Focusing on life goals makes therapy meaningful to the patient.
Set priorities. Because only one or two therapeutic interventions can be tried during a medication-monitoring visit, problems need to be prioritized. As with Ms. W, the first visit’s goal was crisis intervention: to reduce suicidal thoughts and prevent hospitalization. Table 1 offers a framework for effective therapeutic interventions.
Save time by giving patients out-of-session assignments, which:
- collect important information to review with patients during the next monitoring session
- help empower patients to manage their symptoms.
IMPROVING ADHERENCE
Medication nonadherence and partial adherence can result from:
- illness-related factors such as lack of insight
- patient-related factors such as attitudes and beliefs about medication
- treatment factors such as side effects
- physician-related factors such as showing an authoritarian attitude toward patients
- system-related factors such as treatment access problems.
Table 2
Interventions to improve patient medication adherence
| Issue | Intervention |
|---|---|
| Assessing medication adherence and beliefs |
|
| Dysfunctional beliefs about medication (“Taking it means I am weak.” “It can turn me into a zombie.” “I will be dependent on medication.”) |
|
| Lack of insight (“I do not need medication”) |
|
| Forgetting to take medication |
|
| Lack of a shared understanding of the illness between patient and physician |
|
CASE: NOT REALLY HER FATHER
By the second session 1 week later, Ms. W’s suicidal thoughts had become infrequent and mild, and she was using the coping card as needed. This visit focused on visual hallucinations associated with anxiety about facing her father. We encouraged her to describe the hallucinations in great detail, and she realized that she visualized her father as he had looked 20 years ago, not as he looks today. Her anxiety decreased as she considered that she might be seeing not him but an image. Her homework assignment was to closely observe the hallucinations. Because she was more stable, the next visit was scheduled in 2 weeks.
By the third session, she reported that the visual hallucinations had disappeared, and the focusing technique had helped her. She continued to hear voices, however, particularly in the evening when she was alone and anxious or depressed. With prompting, she identified activities she could engage in at night, such as calling her mother and praying with her mother on the phone. This reduced her loneliness and helped her relax.
Table 3
Interventions to manage auditory and visual hallucinations
| Problem | Intervention |
|---|---|
| Acting on hallucinations | Ask questions such as: |
| |
| Tell patient, “It is not the voices themselves but the thoughts in your mind in response to the voices that determine whether or not you follow them” | |
| List thoughts patient generates when choosing not to follow voice commands and encourage patient to read the list when hearing voices | |
| Triggers of negative emotions that cause voices | Ask questions such as: |
| |
| Identify techniques to deal with triggers and rate their effectiveness | |
| Dysfunctional beliefs that voices cannot be controlled or are prophetic | When voices are strong, coach patient to rate them on a scale of 0 to 10, try different distraction techniques, and rate them again |
| Encourage patient to write down what the voices say and whether their prophecies come true; reviewing the record in subsequent session shows voices are not prophetic | |
| Voices during the session | Hum a familiar tune with patient |
| Ask patient to read out loud | |
| Visual hallucinations | Encourage patient to examine details of what they see; this alone can make hallucinations disappear |
| Encourage patient to try to make hallucinations funny, such as making the image’s nose long (personal communication: e-mail Morton Sosland MD) |
One month later, the voices had diminished greatly, and Ms. W returned to her regular medication monitoring appointments of every 6 to 8 weeks.
MANAGING POSITIVE SYMPTOMS
In serious mental illnesses such as schizophrenia, the most common hallucinations are auditory ( Table 3 ),19 followed by visual and other types.20 Sometimes patients view hallucinations as helpful, providing reassurance, advice, or companionship. The content may be an expression of the patient’s own beliefs.
Table 4
Interventions to help patients examine common delusions
| Symptom | Questions to ask the patient |
|---|---|
| Behaviors of acting on delusions |
|
| Delusion with changing conviction |
|
| Delusion with complete conviction |
|
| Addressing underlying beliefs |
|
| Delusion associated with lack of real world knowledge | Provide real-world knowledge. For example, for delusion that people can read a patient’s mind, inform patient that scientific experiments have shown that no one can read complex thoughts of others |
| Delusion involving physician | For example, say, “It is normal for you to sometimes question my intentions and believe that I am part of the conspiracy. I can assure you that is not the case. Anytime you have those doubts I would like the opportunity to clarify those for you. Can I rely on you to bring those doubts to my attention?” |
| When patient’s body language or behavior changes, ask if patient is suspicious and paranoid about you | |
| Behavioral experiment for delusions | For example, a patient believed people parking cars on his street would break into his apartment. Homework was designed with two columns on a paper, one for him to check when someone parked and the other if they broke in. Next visit, patient returned with no checks in the break-ins column |
- Are the hallucinations distressing, and does the patient want them to stop?
- What triggers them (usually depressed mood, anxiety, anger, or boredom)?
- What coping mechanisms has the patient used, and how effective have they been?
- What is the source of the patient’s distress?
Table 5
Interventions for managing schizophrenia’s negative symptoms
| Symptom | Intervention |
|---|---|
| Anergia/anhedonia |
|
| Impaired attention |
|
| Alogia |
|
Never dispute a patient’s delusional beliefs. Maintain an attitude of benevolent curiosity to elicit the reasoning processes by which he or she came to believe the delusions. By encouraging the patient to become curious about the experience, you can create a chink of insight and help the him or her achieve important goals despite disturbing sensory experiences and beliefs.
Thought disorder can be addressed by gently pointing out that you are having trouble understanding the patient’s speech. Ask if other people whom the patient trusts have commented on his or her speech.
Because thought disorder worsens the longer a patient talks, suggest a 5-sentence rule during sessions. You and the patient try to speak no more than 5 sentences at a time before pausing to let the other person speak. Encourage the patient to monitor your speech and to indicate when you violate the rule. Monitoring your speech helps patients start monitoring their own.
Thought disorder worsens when patients experience negative emotions such as anxiety. When this occurs, move the discussion to a neutral topic or encourage deep regular breathing for 2 minutes to reduce anxiety.
MANAGING NEGATIVE SYMPTOMS
Negative symptoms of schizophrenia ( Table 5 ) overlap with depression and with medication side effects. Anhedonia and social withdrawal, for example, may reflect a patient’s depression and demoralization, rather than just schizophrenia’s biological core symptoms.
Similarly, limited facial expression may be caused by drug side effects, rather than absence of affect. Negative symptoms also can occur in the absence of depression or side effects, such as when a patient’s automatic thoughts related to expectations of failure lead to lack of motivation.
Negative symptoms usually bother patients much less than positive symptoms do. Thus, enlisting family members to help patients monitor and deal with negative symptoms can be very useful.
CASE SUMMARY
Ms. W’s stress-related psychotic symptoms resolved to baseline with cognitive therapy done in a regular medication management clinic. Throughout this episode, her medication dosages remained unchanged. The interventions added about 10 minutes to sessions, effectively dealt with her symptom exacerbation, and prevented hospitalization.
Psychotropics remain a critical component of treating psychotic disorders, and psychotherapy can also be very helpful. But in the many situations when psychotherapy is not available, brief psychotherapeutic techniques can:
- increase patient and family satisfaction
- enhance the therapeutic alliance
- improve medication adherence
- promote recovery.
Adding just 5 to 10 minutes of psychotherapy to medication monitoring visits can help patients overcome hallucinations, delusions, and other psychotic symptoms. Targeted cognitive-behavioral therapy (CBT) can:
- prevent crisis visits and hospitalizations
- improve long-term medication and treatment adherence
- enhance the therapeutic alliance.
Treatment goals for patients with chronic mental illness are changing as clinicians, patients, and families aspire for more than improved symptoms ( Box ).1-14 This article describes brief interventions to target medication nonadherence and positive and negative symptoms in patients with schizophrenia, schizoaffective disorder, bipolar disorder, major depressive disorder, and other chronic disorders.
CASE: VOICES FROM THE PAST
Ms. W, age 45, is seen every 6 to 8 weeks in an outpatient medication management clinic for symptoms of schizoaffective disorder, depressed type; posttraumatic stress disorder; and generalized anxiety disorder. She has a history of severe abuse by her father, self-mutilation in response to anxiety and stress, and repeated hospitalizations following visits to her mother.
She recently visited her mother again and saw her father as well. The trip led to increased symptoms of intrusive traumatic memories, thoughts of suicide with plans to overdose, visual hallucinations of her father, and increased auditory hallucinations with derogatory content.
Goals of the first therapy session after Ms. W’s trip home were to reduce her suicidal thoughts and prevent hospitalization. We encouraged her to list her positive qualities, accomplishments, important relationships, religious beliefs, goals, and dreams. She then wrote all these reasons to live on a cue card. Reading the card twice in the session stopped her suicidal thoughts, and she expressed some hope.
We encouraged her to read the card whenever suicidal ideas became strong. We scheduled her next visit 1 week later, and she contracted not to attempt suicide during that time.
DEVELOPING AN ALLIANCE
To develop an alliance with psychotic patients such as Ms. W, the first task is to help them leave each session feeling understood, validated, and enjoying the therapist’s company. This alone provides a powerful counterbalance to the isolation, demoralization, and hopelessness they bring to therapy.
Pharmacologic and psychosocial interventions are changing treatment goals for patients with serious mental illness from improved symptoms to functional recovery, improved quality of life, and reintegration into the community.1,2 Patients, families and clinicians increasingly view self-determination, independence, and recovery as realistic treatment goals.3,4
Medication limits. Drugs are crucial to managing psychotic symptoms but inadequate for achieving recovery:
- many patients with positive psychotic symptoms respond only partially or not at all5
- functional improvement does not always follow symptomatic improvement6
- medication nonadherence remains high, leading to repeated relapses.7
Dual-therapy benefits. A combination of antipsychotics and psychotherapy has been found to increase the chances of recovery in schizophrenia.8 Psychotherapy is also highly valued by patients and their families:
- In patient satisfaction studies, 72% to 90% of participants with psychotic disorders said individual psychotherapy improved their lives.9,10
- In a survey of 3,099 National Alliance for the Mentally Ill family members, 88% rated psychotherapy as having some (53%) or considerable (35%) value.11
Access problems. Despite psychotherapy’s benefits, access is extremely limited. In one survey, only 7.3% of patients with nonaffective psychosis received at least “minimally adequate” care (four or more medication visits that did not include psychotherapy).12 Incorporating therapeutic techniques into medication monitoring clinics is one way to improve access to therapy for patients with serious mental illnesses.
Keep it brief. Psychotherapy in medication clinics differs from traditional models’ 15- to 45-minute sessions.13 Patients with psychotic illness prefer brief interventions; a study of 212 patients found that 85% of those with schizophrenia preferred sessions:
- less often than once a week
- that focus on solving practical problems.14
5 steps in effective cognitive-behavioral interventions
|
In normalization, the stress vulnerability model is used to explain psychosis to the patient. Psychotic symptoms are emphasized as something normal people can experience in extreme situations, such as:
- hallucinations in states of sleep deprivation or medical and drug-induced states
- paranoia as error in thinking in states of heightened vigilance and perceived threat.15
Universality is the understanding that many people have experiences similar to the patient’s.
In a collaborative therapeutic alliance, the patient is not a passive recipient but an active collaborator in therapy. He or she contributes to decisions—such as the length of therapy and topics to be discussed—and gives feedback on interventions and therapist style.
Focusing on life goals makes therapy meaningful to the patient.
Set priorities. Because only one or two therapeutic interventions can be tried during a medication-monitoring visit, problems need to be prioritized. As with Ms. W, the first visit’s goal was crisis intervention: to reduce suicidal thoughts and prevent hospitalization. Table 1 offers a framework for effective therapeutic interventions.
Save time by giving patients out-of-session assignments, which:
- collect important information to review with patients during the next monitoring session
- help empower patients to manage their symptoms.
IMPROVING ADHERENCE
Medication nonadherence and partial adherence can result from:
- illness-related factors such as lack of insight
- patient-related factors such as attitudes and beliefs about medication
- treatment factors such as side effects
- physician-related factors such as showing an authoritarian attitude toward patients
- system-related factors such as treatment access problems.
Table 2
Interventions to improve patient medication adherence
| Issue | Intervention |
|---|---|
| Assessing medication adherence and beliefs |
|
| Dysfunctional beliefs about medication (“Taking it means I am weak.” “It can turn me into a zombie.” “I will be dependent on medication.”) |
|
| Lack of insight (“I do not need medication”) |
|
| Forgetting to take medication |
|
| Lack of a shared understanding of the illness between patient and physician |
|
CASE: NOT REALLY HER FATHER
By the second session 1 week later, Ms. W’s suicidal thoughts had become infrequent and mild, and she was using the coping card as needed. This visit focused on visual hallucinations associated with anxiety about facing her father. We encouraged her to describe the hallucinations in great detail, and she realized that she visualized her father as he had looked 20 years ago, not as he looks today. Her anxiety decreased as she considered that she might be seeing not him but an image. Her homework assignment was to closely observe the hallucinations. Because she was more stable, the next visit was scheduled in 2 weeks.
By the third session, she reported that the visual hallucinations had disappeared, and the focusing technique had helped her. She continued to hear voices, however, particularly in the evening when she was alone and anxious or depressed. With prompting, she identified activities she could engage in at night, such as calling her mother and praying with her mother on the phone. This reduced her loneliness and helped her relax.
Table 3
Interventions to manage auditory and visual hallucinations
| Problem | Intervention |
|---|---|
| Acting on hallucinations | Ask questions such as: |
| |
| Tell patient, “It is not the voices themselves but the thoughts in your mind in response to the voices that determine whether or not you follow them” | |
| List thoughts patient generates when choosing not to follow voice commands and encourage patient to read the list when hearing voices | |
| Triggers of negative emotions that cause voices | Ask questions such as: |
| |
| Identify techniques to deal with triggers and rate their effectiveness | |
| Dysfunctional beliefs that voices cannot be controlled or are prophetic | When voices are strong, coach patient to rate them on a scale of 0 to 10, try different distraction techniques, and rate them again |
| Encourage patient to write down what the voices say and whether their prophecies come true; reviewing the record in subsequent session shows voices are not prophetic | |
| Voices during the session | Hum a familiar tune with patient |
| Ask patient to read out loud | |
| Visual hallucinations | Encourage patient to examine details of what they see; this alone can make hallucinations disappear |
| Encourage patient to try to make hallucinations funny, such as making the image’s nose long (personal communication: e-mail Morton Sosland MD) |
One month later, the voices had diminished greatly, and Ms. W returned to her regular medication monitoring appointments of every 6 to 8 weeks.
MANAGING POSITIVE SYMPTOMS
In serious mental illnesses such as schizophrenia, the most common hallucinations are auditory ( Table 3 ),19 followed by visual and other types.20 Sometimes patients view hallucinations as helpful, providing reassurance, advice, or companionship. The content may be an expression of the patient’s own beliefs.
Table 4
Interventions to help patients examine common delusions
| Symptom | Questions to ask the patient |
|---|---|
| Behaviors of acting on delusions |
|
| Delusion with changing conviction |
|
| Delusion with complete conviction |
|
| Addressing underlying beliefs |
|
| Delusion associated with lack of real world knowledge | Provide real-world knowledge. For example, for delusion that people can read a patient’s mind, inform patient that scientific experiments have shown that no one can read complex thoughts of others |
| Delusion involving physician | For example, say, “It is normal for you to sometimes question my intentions and believe that I am part of the conspiracy. I can assure you that is not the case. Anytime you have those doubts I would like the opportunity to clarify those for you. Can I rely on you to bring those doubts to my attention?” |
| When patient’s body language or behavior changes, ask if patient is suspicious and paranoid about you | |
| Behavioral experiment for delusions | For example, a patient believed people parking cars on his street would break into his apartment. Homework was designed with two columns on a paper, one for him to check when someone parked and the other if they broke in. Next visit, patient returned with no checks in the break-ins column |
- Are the hallucinations distressing, and does the patient want them to stop?
- What triggers them (usually depressed mood, anxiety, anger, or boredom)?
- What coping mechanisms has the patient used, and how effective have they been?
- What is the source of the patient’s distress?
Table 5
Interventions for managing schizophrenia’s negative symptoms
| Symptom | Intervention |
|---|---|
| Anergia/anhedonia |
|
| Impaired attention |
|
| Alogia |
|
Never dispute a patient’s delusional beliefs. Maintain an attitude of benevolent curiosity to elicit the reasoning processes by which he or she came to believe the delusions. By encouraging the patient to become curious about the experience, you can create a chink of insight and help the him or her achieve important goals despite disturbing sensory experiences and beliefs.
Thought disorder can be addressed by gently pointing out that you are having trouble understanding the patient’s speech. Ask if other people whom the patient trusts have commented on his or her speech.
Because thought disorder worsens the longer a patient talks, suggest a 5-sentence rule during sessions. You and the patient try to speak no more than 5 sentences at a time before pausing to let the other person speak. Encourage the patient to monitor your speech and to indicate when you violate the rule. Monitoring your speech helps patients start monitoring their own.
Thought disorder worsens when patients experience negative emotions such as anxiety. When this occurs, move the discussion to a neutral topic or encourage deep regular breathing for 2 minutes to reduce anxiety.
MANAGING NEGATIVE SYMPTOMS
Negative symptoms of schizophrenia ( Table 5 ) overlap with depression and with medication side effects. Anhedonia and social withdrawal, for example, may reflect a patient’s depression and demoralization, rather than just schizophrenia’s biological core symptoms.
Similarly, limited facial expression may be caused by drug side effects, rather than absence of affect. Negative symptoms also can occur in the absence of depression or side effects, such as when a patient’s automatic thoughts related to expectations of failure lead to lack of motivation.
Negative symptoms usually bother patients much less than positive symptoms do. Thus, enlisting family members to help patients monitor and deal with negative symptoms can be very useful.
CASE SUMMARY
Ms. W’s stress-related psychotic symptoms resolved to baseline with cognitive therapy done in a regular medication management clinic. Throughout this episode, her medication dosages remained unchanged. The interventions added about 10 minutes to sessions, effectively dealt with her symptom exacerbation, and prevented hospitalization.
Psychotropics remain a critical component of treating psychotic disorders, and psychotherapy can also be very helpful. But in the many situations when psychotherapy is not available, brief psychotherapeutic techniques can:
- increase patient and family satisfaction
- enhance the therapeutic alliance
- improve medication adherence
- promote recovery.
1. American Psychiatric Association. Work group on Schizophrenia. Practice guidelines for the treatment of patients with schizophrenia. Am J Psychiatry 2004;161:29(suppl):26-7.
2. Kane JM. Long-term treatment of schizophrenia: moving from a relapse-prevention model to a recovery model. J Clin Psychiatry 2004;64(11):1384-5.
3. Coursey RD, Alford J, Safarjan B. Significant advances in understanding and treating serious mental lllness. Prof Psychol Res Pract 1997;28(3):205-16.
4. Cunningham R. In my own voice: how early intervention led to great success. NAMI Voice 2004;1:1-5.
5. Conley RR, Buchanan RW. Evaluation of treatment-resistant schizophrenia. Schizophr Bull 1997;23:663-74.
6. Harvey PD, Green M, Keefe RS, Velligan DI. Cognitive functioning in schizophrenia: a consensus statement on its role in the definition and evaluation of effective treatments for the illness. J Clin Psychiatry 2004;65(3):361-72.
7. Bridge JA, Barbe RP. Reducing hospital readmission in depression and schizophrenia: current evidence. Curr Opin Psychiatry 2004;17(6):505-11.
8. Lieberman RP, Kopelowicz A, Ventura J, et al. Operational criteria and factors related to recovery from schizophrenia. Int Rev Psychiatry 2002;14(4):256-72.
9. Leggatt M. Schizophrenia: the consumer’s viewpoint. In: Burrows GD, Norman TR, Rubinstein G (eds). Handbook of studies on schizophrenia, vol 2. New York: Elsevier Science Publishers, 1986;143-53.
10. Coursey RD, Keller AB, Farrell EW. Individual psychotherapy and persons with serious mental illness: the client’s perspective. Schizophr Bull 1995;21:283-301.
11. Hatfield A, Gearon J, Coursey R. Family members’ ratings of the use and value of mental health services: results of a national NAMI survey. Psychiatr Serv 1996;47:825-31.
12. Wang PS, Demler O, Kessler RC. Adequacy of treatment for serious mental illness in the United States. Am J Public Health 2002;92(1):92-8.
13. Rector N, Beck A. CBT for schizophrenia. Can J Psychiatry 2002;47(1):39-48.
14. Coursey RD, Keller A, Farrell EW. Individual psychotherapy and serious mental illness: the clients’ perspective. Schizophr Bull 1995;21:283-301.
15. Kingdon DG, Turkington D. Explanations of schizophrenia. In: Kingdon DG, Turkington D (eds). Cognitive-behavioral therapy of schizophrenia. New York: Guilford Press, 1994;9.-
16. Green MF. What are the functional consequences of neurocognitive deficits in schizophrenia? Am J Psychiatry. 1996;153:361-9.
17. Velligan DI, Bow-Thomas CC, Huntzinger C, et al. Randomized controlled trial of the use of compensatory strategies to enhance adaptive functioning in outpatients with schizophrenia. Am J Psychiatry 2000;157:1317-23.
18. Gilmer T, Dolder C, Lacro J, et al. Adherence to treatment with antipsychotic medication and health care costs among Medicaid beneficiaries with schizophrenia. Am J Psychiatry 2004;161(4):692-99.
19. Romme MAJ. Hearing voices. Schizophr Bull 1989;15:209-16.
20. Andreasen NC, Flaum M. Schizophrenia: the characteristic symptoms. Schizophr Bull 1991;17(1):27-49.
1. American Psychiatric Association. Work group on Schizophrenia. Practice guidelines for the treatment of patients with schizophrenia. Am J Psychiatry 2004;161:29(suppl):26-7.
2. Kane JM. Long-term treatment of schizophrenia: moving from a relapse-prevention model to a recovery model. J Clin Psychiatry 2004;64(11):1384-5.
3. Coursey RD, Alford J, Safarjan B. Significant advances in understanding and treating serious mental lllness. Prof Psychol Res Pract 1997;28(3):205-16.
4. Cunningham R. In my own voice: how early intervention led to great success. NAMI Voice 2004;1:1-5.
5. Conley RR, Buchanan RW. Evaluation of treatment-resistant schizophrenia. Schizophr Bull 1997;23:663-74.
6. Harvey PD, Green M, Keefe RS, Velligan DI. Cognitive functioning in schizophrenia: a consensus statement on its role in the definition and evaluation of effective treatments for the illness. J Clin Psychiatry 2004;65(3):361-72.
7. Bridge JA, Barbe RP. Reducing hospital readmission in depression and schizophrenia: current evidence. Curr Opin Psychiatry 2004;17(6):505-11.
8. Lieberman RP, Kopelowicz A, Ventura J, et al. Operational criteria and factors related to recovery from schizophrenia. Int Rev Psychiatry 2002;14(4):256-72.
9. Leggatt M. Schizophrenia: the consumer’s viewpoint. In: Burrows GD, Norman TR, Rubinstein G (eds). Handbook of studies on schizophrenia, vol 2. New York: Elsevier Science Publishers, 1986;143-53.
10. Coursey RD, Keller AB, Farrell EW. Individual psychotherapy and persons with serious mental illness: the client’s perspective. Schizophr Bull 1995;21:283-301.
11. Hatfield A, Gearon J, Coursey R. Family members’ ratings of the use and value of mental health services: results of a national NAMI survey. Psychiatr Serv 1996;47:825-31.
12. Wang PS, Demler O, Kessler RC. Adequacy of treatment for serious mental illness in the United States. Am J Public Health 2002;92(1):92-8.
13. Rector N, Beck A. CBT for schizophrenia. Can J Psychiatry 2002;47(1):39-48.
14. Coursey RD, Keller A, Farrell EW. Individual psychotherapy and serious mental illness: the clients’ perspective. Schizophr Bull 1995;21:283-301.
15. Kingdon DG, Turkington D. Explanations of schizophrenia. In: Kingdon DG, Turkington D (eds). Cognitive-behavioral therapy of schizophrenia. New York: Guilford Press, 1994;9.-
16. Green MF. What are the functional consequences of neurocognitive deficits in schizophrenia? Am J Psychiatry. 1996;153:361-9.
17. Velligan DI, Bow-Thomas CC, Huntzinger C, et al. Randomized controlled trial of the use of compensatory strategies to enhance adaptive functioning in outpatients with schizophrenia. Am J Psychiatry 2000;157:1317-23.
18. Gilmer T, Dolder C, Lacro J, et al. Adherence to treatment with antipsychotic medication and health care costs among Medicaid beneficiaries with schizophrenia. Am J Psychiatry 2004;161(4):692-99.
19. Romme MAJ. Hearing voices. Schizophr Bull 1989;15:209-16.
20. Andreasen NC, Flaum M. Schizophrenia: the characteristic symptoms. Schizophr Bull 1991;17(1):27-49.
Help children and teens stop impulsive hair pulling
Trichotillomania (TTM) is distressing to pediatric patients who pull their hair and to their parents who feel helpless to stop the destructive behavior. Hair-pulling with psychiatric comorbidity requires comprehensive assessment and treatment, but we have found that cognitive-behavioral therapy (CBT) alone can help children and adolescents with uncomplicated TTM.
This article describes a typical patient with adolescent-onset mild-to-moderate TTM and the three-step CBT approach—awareness training, stimulus control, and habit reversal—that we find effective in reducing pediatric hair pulling.
Jane, age 12, was referred to our clinic by her primary doctor after an 8-week trial of fluoxetine, 80 mg/d, failed to stop her hair pulling. Jane, who is right-handed, has been pulling her hair for 2 years, mostly in the right front scalp. Her shame over the hair loss makes her reluctant to participate in social activities. A dermatologist found no medical cause for her behavior, such as alopecia or folliculitis.
Jane’s parents say she has no history of a major mood disorder or anxiety. Her hair pulling causes significant “tension and stress” for all family members.
WHY DO PATIENTS PULL HAIR?
Cognitive-behavioral theory suggests that chronic TTM originates as a normal response to stress that often escapes personal and social awareness but gradually increases in frequency and severity (Box).1-8 Thus, hair pulling becomes associated with internal and external cues through conditioning and is maintained primarily by positive reinforcement. Hair-pulling urges that are reinforced by pulling intensify the need to pull, perpetuating the behavioral cycle.
A genetic link? Familial research has associated TTM with increased rates of obsessive-compulsive disorder (OCD) or other excessive habits—such as nail biting or skin picking—among first-degree relatives.6,9,10 Neuroimaging of persons with TTM has shown hyperactivity in the left cerebellum and right superior parietal lobe11 as well as possible structural abnormalities in the left putamen,12 left inferior frontal gyrus, and right cluneal cortex.13
These findings do not necessarily indicate pre-existing brain pathology, however. Perhaps TTM leads to changes in brain structure or function, or both TTM and the brain abnormalities may be caused by another as-yet-unknown variable.
Decreased pain sensitivity. Patients with TTM often report that hair pulling is not painful,2 though we suspect that persons without TTM would disagree and derive no pleasure from it. Changes in pain sensitivity may influence the reinforcing quality of pulling behavior. One possible mechanism for such alterations is upregulation of the endogenous opioid system; some intriguing evidence suggests that opioid receptor antagonists such as naltrexone may reduce pulling.14
Trichotillomania (TTM) is an impulse control disorder characterized by repetitive hair pulling,1 which typically emerges during adolescence. In a large clinical sample of adult hair pullers, mean age of onset was 13.2 Very-early onset (before age 5) may be a more benign form of TTM that tends to abate spontaneously and requires little or no therapeutic intervention.3
Despite the absence of body hair in prepubertal children, their pulling patterns are consistent with those of adults. The scalp is the most common pulling site, followed by eyelashes and eyebrows.4
Psychiatric comorbidity. In two studies evaluating psychiatric comorbidity in pediatric clinical samples, 60% to 70% of children and teens with TTM had at least one comorbid axis I disorder.5,6 Disruptive behavior disorders were most common in one study,6 whereas overanxious disorder was most common in the other.5 In a large clinical sample of adults with TTM, 51% met criteria for comorbid depression.2
Early identification and treatment of TTM are recommended because of the disorder’s distressing nature and social stigma. Early interventions also may help prevent later adult psychiatric comorbidity and functional impairment, although no studies have been done to demonstrate this benefit.7,8
Pain tolerance at the preferred pulling site has not been studied, however. For patients who feel pain from hair pulling, the pain itself may reinforce the behavior by distracting the individual from negative emotional or physiologic states.15
CASE CONTINUED: COUNTING THE WAYS
Jane and her parents agree that she pulls her hair 5 to 8 times daily, one hair at a time with her right index finger and thumb while doing homework or watching TV. The trigger, she says, is “an itch” on her scalp; “sometimes pulling relieves the itch.” She fails to resist pulling her hair 9 out of 10 times.
Table 1
Defining hair pulling: What to ask the pediatric patient
| Response description | How many times do you pull your hair each day? |
| How many hairs do you pull each time? | |
| From what body areas do you pull hair? | |
| What are all the steps involved in pulling (Touching the head before pulling? Pulling one hair at a time with the thumb and index finger)? | |
| Response detection | Under what circumstances do you sense the urge to pull? |
| How strong is the urge on a scale of 1 to 10, with 10 being the greatest intensity you ever felt? | |
| How do you try to resist and overcome the urge to pull? | |
| Precursors | External cues (Do you pull when you look at yourself in a mirror?) |
| Internal cues (Do you pull when you are nervous?) | |
| High-risk situations | What are you usually doing when you get the urge to pull? (reading, talking on the telephone, watching TV, using a computer, etc.) |
| Consequences that reinforce the behavior | Do you pull to reduce physical sensations (such as itching) at the site of pulling? |
| Does pulling relieve sadness or worry about problems at home or in school? | |
| Do you pull to create a more even hairline? |
Psychiatric comorbidity is common—if not the norm—in adults with TTM. Although axis I comorbidity is also seen in children and adolescents, their hair pulling is frequently uncomplicated. Jane meets criteria for TTM, as determined by the Trichotillomania Diagnostic Interview,16 but her history does not support a comorbid disorder. After discussing the diagnosis with Jane and her parents, the psychiatrist begins treatment with CBT alone.
MEDICATION OR CBT?
SSRIs. Literature on TTM pharmacotherapy is very limited and equivocal. Medications that have helped adults with TTM have been described,17 but the lack of a single, randomized, controlled trial in pediatric TTM severely limits treatment recommendations for children.
Selective serotonin reuptake inhibitors (SSRIs) have shown efficacy for treating anger and other impulse control problems but not for TTM. Some practitioners use SSRIs for TTM because of the belief that TTM is a variant of OCD. However, TTM may be maintained by positive reinforcement rather than compulsive tendencies and thus may not respond to SSRIs.
CBT. Evidence on CBT justifies cautious recommendations for pediatric TTM. In randomized trials, CBT reduced hair pulling in adults and was more effective than SSRIs or placebo.18,19
REDUCING THE URGE
Obtain detailed information about a child or adolescent’s hair-pulling episodes (Table 1), as recognizing triggers and reactions is vital to effective CBT. Explain to the patient that:
- the pleasure or satisfaction she derives from pulling reinforces the urge to pull
- she can reduce the urge by learning and using awareness training, stimulus control, and habit reversal (Table 2).
Awareness training involves patient self-monitoring to gain awareness of urges to pull and of pulling behavior. The child must become alert to every hair pulled and to response precursors, such as placing her hand on her head. For a patient such as Jane, a useful technique is to post reminders on the TV and school notebook and in the bedroom and bathroom—wherever pulling typically occurs.
A “PULLING CALENDAR”
Jane begins a daily “pulling calendar” in which she records each time she pulls a hair while watching TV or doing homework. She is asked to include the total number of hairs pulled and the intensity of the “itch to pull” on a scale of 1 to 10.
Stimulus control. Most patients can identify high-risk situations, such as time in the bathroom, talking on the phone, watching TV, driving, reading, or while falling asleep. Boredom, frustration, anxiety, and sadness may serve as pulling cues.
With stimulus control, the patient tries to reduce her ability to freely engage in pulling behavior in high-risk situations. For instance, you might encourage a child who pulls hairs while doing homework to stick Band-Aid®-type adhesive strips on her thumb and index finger tips before she starts studying as an impediment to gripping hairs. Such “speed bumps” may allow her to delay pulling and reach for tools that assist in habit reversal.
TREATMENT THAT APPEALS
Jane agrees to apply adhesive strips to her fingers and understands why. Because she is a fan of Peter Pan, we place Peter Pan stickers on her books and notebooks and on the TV remote control as reminders not to pull.
Table 2
CBT strategies to reduce the hair-pulling urge
| Awareness training | Increases patient’s awareness of pulling |
| Stimulus control | Establishes an environment less conducive to pulling |
| Habit reversal/ response | Patient develops alternate activities that provide competing positive reinforcement comparable to that gained from pulling |
Habit reversal and competing response procedures provide pleasurable physical stimulation as an alternative to pulling. The most effective methods engage the same motions as used in hair pulling. Examples include sculpting with clay, hulling sunflower seeds, and playing with Koosh® balls—small rubbery balls filled with a jellylike plasma and covered with hundreds of soft “tentacles.”
‘CALMER, HAPPIER’
We explain habit reversal to Jane and instruct her to use the Koosh ball a few times a day. She enjoys pulling its rubber strands, an action that uses the same muscles as hair pulling. Because she will need Koosh balls during all identified high-risk situations, we instruct her to buy one for her book bag and to leave one near the couch where she watches TV.
Over time, Jane reports a gradual decrease of hair pulling with the use of awareness training and stimulus control techniques. Using the Koosh ball (habit reversal) helps her improve. By the 10th week, Jane and her parents report a 70% decrease in hair pulling, based on the pulling calendar entries and other objective evidence of treatment response. All report feeling “calmer and happier.”
CONCLUSION
Cognitive and behavioral strategies are useful and safe for treating pediatric TTM. Enlisting the parents and patient in identifying problem situations and applying creative solutions may increase the chances of success.
Follow-up is important for maintaining new cognitive and behavioral patterns. We recommend that you see patients monthly for at least 3 months, depending on how the patient feels about additional sessions. We encourage families to call and report on progress or relapses. Booster CBT sessions can help deal with setbacks.
Related resources
- Trichotillomania Learning Center, Inc.; devoted to improving TTM understanding and providing access to treatments and support groups. www.trich.org. Accessed Sept. 17, 2004.
- Golomb RG, Vavrichek SM. The hair pulling “habit” and you: how to solve the trichotillomania puzzle (rev ed). Silver Spring, MD: Writer’s Cooperative of Greater Washington; 2000. Book for children and teenagers.
Drug brand names
- Fluoxetine • Prozac
- Naltrexone • Depade, ReVia
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
Preparation of this article was supported in part by a grant from the National Institute of Mental Health (MH61457).
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th ed., text rev. Washington, DC: American Psychiatric Association Press; 2000;674-7.
2. Christenson GA, Mackenzie TB, Mitchell JE. Characteristics of 60 adult chronic hairpullers. Am J Psychiatry 1991;148:365-70.
3. Swedo SE, Leonard HL. Trichotillomania: an obsessive compulsive spectrum disorder? Psychiatr Clin North Am 1992;15:777-90.
4. Reeve E. Hair pulling in children and adolescents. In: Stein DJ, Christenson GA, Hollander E, eds. Trichotillomania. Washington, DC: American Psychiatric Association Press, 1999;201-24.
5. Reeve EA, Bernstein GA, Christenson GA. Clinical characteristics and psychiatric comorbidity in children with trichotillomania. J Am Acad Child Adolesc Psychiatry 1992;31:132-8.
6. King RA, Scahill L, Vitulano LA, et al. Childhood trichotillomania: clinical phenomenology, comorbidity, and family genetics. J Am Acad Child Adolesc Psychiatry 1995;34:1451-9.
7. Franklin ME, Bux DA, Foa EB. Pediatric trichotillomania: conceptualization and treatment implications. In: Orvashel H, Faust J, Hersen M, eds. Handbook of conceptualization and treatment of child psychopathology. Oxford, UK: Elsevier Science; 2001;379-98.
8. Keuthen NJ, Franklin ME. Trichotillomania: psychopathology and treatment development [presentation]. Reno, NV: Association for the Advancement of Behavior Therapy annual meeting, 2002.
9. Bienvenu OJ, Samuels JF, Riddle MA, et al. The relationship of obsessive-compulsive disorder to possible spectrum disorders: results from a family study. Biol Psychiatry 2000;48:287-93.
10. Lenane MC, Swedo SE, Rapoport JL, et al. Rates of obsessive compulsive disorder in first degree relatives of patients with trichotillomania: a research note. J Child Psychol Psychiatry 1992;33:925-33.
11. Swedo SE, Rapoport JL, Leonard HL, et al. Regional cerebral glucose metabolism of women in trichotillomania. Arch Gen Psychiatry 1991;48:828-33.
12. O’Sullivan RL, Rauch SL, Breiter HC, et al. Reduced basal ganglia volumes in trichotillomania measured via morphometric magnetic resonance imaging. Biol Psychiatry 1997;42:39-45.
13. Grachev ID. MRI-based morphometric topographic parcellation of human neocortex in trichotillomania. Psychiatry Clin Neurosci 1997;51:315-21.
14. Carrion VG. Naltrexone for the treatment of trichotillomania: a case report. J Clin Psychopharmacol 1995;15:444-5.
15. Christenson GA, Mansueto CS. Trichotillomania: descriptive characteristics and phenomenology. In: Stein DJ, Christenson GA, Hollander E, eds. Trichotillomania. Washington, DC: American Psychiatric Press, 1999;1-41.
16. Rothbaum BO, Ninan PT. The assessment of trichotillomania. Behav Res Ther 1994;32(6):651-62.
17. Lundt LP. Trichotillomania: a heads-up on severe cases. Current Psychiatry 2004;3(5):89-105.
18. Ninan PT, Rothbaum BO, Marsteller FA, et al. A placebo-controlled trial of cognitive-behavioral therapy and clomipramine in trichotillomania. J Clin Psychiatry. 2000;61:47-50.
19. Azrin NH, Nunn RG, Frantz SE. Treatment of hairpulling (trichotillomania): a comparative study of habit reversal and negative practice training. J Behav Ther Exp Psychiatry 1980;11:13-20.
Trichotillomania (TTM) is distressing to pediatric patients who pull their hair and to their parents who feel helpless to stop the destructive behavior. Hair-pulling with psychiatric comorbidity requires comprehensive assessment and treatment, but we have found that cognitive-behavioral therapy (CBT) alone can help children and adolescents with uncomplicated TTM.
This article describes a typical patient with adolescent-onset mild-to-moderate TTM and the three-step CBT approach—awareness training, stimulus control, and habit reversal—that we find effective in reducing pediatric hair pulling.
Jane, age 12, was referred to our clinic by her primary doctor after an 8-week trial of fluoxetine, 80 mg/d, failed to stop her hair pulling. Jane, who is right-handed, has been pulling her hair for 2 years, mostly in the right front scalp. Her shame over the hair loss makes her reluctant to participate in social activities. A dermatologist found no medical cause for her behavior, such as alopecia or folliculitis.
Jane’s parents say she has no history of a major mood disorder or anxiety. Her hair pulling causes significant “tension and stress” for all family members.
WHY DO PATIENTS PULL HAIR?
Cognitive-behavioral theory suggests that chronic TTM originates as a normal response to stress that often escapes personal and social awareness but gradually increases in frequency and severity (Box).1-8 Thus, hair pulling becomes associated with internal and external cues through conditioning and is maintained primarily by positive reinforcement. Hair-pulling urges that are reinforced by pulling intensify the need to pull, perpetuating the behavioral cycle.
A genetic link? Familial research has associated TTM with increased rates of obsessive-compulsive disorder (OCD) or other excessive habits—such as nail biting or skin picking—among first-degree relatives.6,9,10 Neuroimaging of persons with TTM has shown hyperactivity in the left cerebellum and right superior parietal lobe11 as well as possible structural abnormalities in the left putamen,12 left inferior frontal gyrus, and right cluneal cortex.13
These findings do not necessarily indicate pre-existing brain pathology, however. Perhaps TTM leads to changes in brain structure or function, or both TTM and the brain abnormalities may be caused by another as-yet-unknown variable.
Decreased pain sensitivity. Patients with TTM often report that hair pulling is not painful,2 though we suspect that persons without TTM would disagree and derive no pleasure from it. Changes in pain sensitivity may influence the reinforcing quality of pulling behavior. One possible mechanism for such alterations is upregulation of the endogenous opioid system; some intriguing evidence suggests that opioid receptor antagonists such as naltrexone may reduce pulling.14
Trichotillomania (TTM) is an impulse control disorder characterized by repetitive hair pulling,1 which typically emerges during adolescence. In a large clinical sample of adult hair pullers, mean age of onset was 13.2 Very-early onset (before age 5) may be a more benign form of TTM that tends to abate spontaneously and requires little or no therapeutic intervention.3
Despite the absence of body hair in prepubertal children, their pulling patterns are consistent with those of adults. The scalp is the most common pulling site, followed by eyelashes and eyebrows.4
Psychiatric comorbidity. In two studies evaluating psychiatric comorbidity in pediatric clinical samples, 60% to 70% of children and teens with TTM had at least one comorbid axis I disorder.5,6 Disruptive behavior disorders were most common in one study,6 whereas overanxious disorder was most common in the other.5 In a large clinical sample of adults with TTM, 51% met criteria for comorbid depression.2
Early identification and treatment of TTM are recommended because of the disorder’s distressing nature and social stigma. Early interventions also may help prevent later adult psychiatric comorbidity and functional impairment, although no studies have been done to demonstrate this benefit.7,8
Pain tolerance at the preferred pulling site has not been studied, however. For patients who feel pain from hair pulling, the pain itself may reinforce the behavior by distracting the individual from negative emotional or physiologic states.15
CASE CONTINUED: COUNTING THE WAYS
Jane and her parents agree that she pulls her hair 5 to 8 times daily, one hair at a time with her right index finger and thumb while doing homework or watching TV. The trigger, she says, is “an itch” on her scalp; “sometimes pulling relieves the itch.” She fails to resist pulling her hair 9 out of 10 times.
Table 1
Defining hair pulling: What to ask the pediatric patient
| Response description | How many times do you pull your hair each day? |
| How many hairs do you pull each time? | |
| From what body areas do you pull hair? | |
| What are all the steps involved in pulling (Touching the head before pulling? Pulling one hair at a time with the thumb and index finger)? | |
| Response detection | Under what circumstances do you sense the urge to pull? |
| How strong is the urge on a scale of 1 to 10, with 10 being the greatest intensity you ever felt? | |
| How do you try to resist and overcome the urge to pull? | |
| Precursors | External cues (Do you pull when you look at yourself in a mirror?) |
| Internal cues (Do you pull when you are nervous?) | |
| High-risk situations | What are you usually doing when you get the urge to pull? (reading, talking on the telephone, watching TV, using a computer, etc.) |
| Consequences that reinforce the behavior | Do you pull to reduce physical sensations (such as itching) at the site of pulling? |
| Does pulling relieve sadness or worry about problems at home or in school? | |
| Do you pull to create a more even hairline? |
Psychiatric comorbidity is common—if not the norm—in adults with TTM. Although axis I comorbidity is also seen in children and adolescents, their hair pulling is frequently uncomplicated. Jane meets criteria for TTM, as determined by the Trichotillomania Diagnostic Interview,16 but her history does not support a comorbid disorder. After discussing the diagnosis with Jane and her parents, the psychiatrist begins treatment with CBT alone.
MEDICATION OR CBT?
SSRIs. Literature on TTM pharmacotherapy is very limited and equivocal. Medications that have helped adults with TTM have been described,17 but the lack of a single, randomized, controlled trial in pediatric TTM severely limits treatment recommendations for children.
Selective serotonin reuptake inhibitors (SSRIs) have shown efficacy for treating anger and other impulse control problems but not for TTM. Some practitioners use SSRIs for TTM because of the belief that TTM is a variant of OCD. However, TTM may be maintained by positive reinforcement rather than compulsive tendencies and thus may not respond to SSRIs.
CBT. Evidence on CBT justifies cautious recommendations for pediatric TTM. In randomized trials, CBT reduced hair pulling in adults and was more effective than SSRIs or placebo.18,19
REDUCING THE URGE
Obtain detailed information about a child or adolescent’s hair-pulling episodes (Table 1), as recognizing triggers and reactions is vital to effective CBT. Explain to the patient that:
- the pleasure or satisfaction she derives from pulling reinforces the urge to pull
- she can reduce the urge by learning and using awareness training, stimulus control, and habit reversal (Table 2).
Awareness training involves patient self-monitoring to gain awareness of urges to pull and of pulling behavior. The child must become alert to every hair pulled and to response precursors, such as placing her hand on her head. For a patient such as Jane, a useful technique is to post reminders on the TV and school notebook and in the bedroom and bathroom—wherever pulling typically occurs.
A “PULLING CALENDAR”
Jane begins a daily “pulling calendar” in which she records each time she pulls a hair while watching TV or doing homework. She is asked to include the total number of hairs pulled and the intensity of the “itch to pull” on a scale of 1 to 10.
Stimulus control. Most patients can identify high-risk situations, such as time in the bathroom, talking on the phone, watching TV, driving, reading, or while falling asleep. Boredom, frustration, anxiety, and sadness may serve as pulling cues.
With stimulus control, the patient tries to reduce her ability to freely engage in pulling behavior in high-risk situations. For instance, you might encourage a child who pulls hairs while doing homework to stick Band-Aid®-type adhesive strips on her thumb and index finger tips before she starts studying as an impediment to gripping hairs. Such “speed bumps” may allow her to delay pulling and reach for tools that assist in habit reversal.
TREATMENT THAT APPEALS
Jane agrees to apply adhesive strips to her fingers and understands why. Because she is a fan of Peter Pan, we place Peter Pan stickers on her books and notebooks and on the TV remote control as reminders not to pull.
Table 2
CBT strategies to reduce the hair-pulling urge
| Awareness training | Increases patient’s awareness of pulling |
| Stimulus control | Establishes an environment less conducive to pulling |
| Habit reversal/ response | Patient develops alternate activities that provide competing positive reinforcement comparable to that gained from pulling |
Habit reversal and competing response procedures provide pleasurable physical stimulation as an alternative to pulling. The most effective methods engage the same motions as used in hair pulling. Examples include sculpting with clay, hulling sunflower seeds, and playing with Koosh® balls—small rubbery balls filled with a jellylike plasma and covered with hundreds of soft “tentacles.”
‘CALMER, HAPPIER’
We explain habit reversal to Jane and instruct her to use the Koosh ball a few times a day. She enjoys pulling its rubber strands, an action that uses the same muscles as hair pulling. Because she will need Koosh balls during all identified high-risk situations, we instruct her to buy one for her book bag and to leave one near the couch where she watches TV.
Over time, Jane reports a gradual decrease of hair pulling with the use of awareness training and stimulus control techniques. Using the Koosh ball (habit reversal) helps her improve. By the 10th week, Jane and her parents report a 70% decrease in hair pulling, based on the pulling calendar entries and other objective evidence of treatment response. All report feeling “calmer and happier.”
CONCLUSION
Cognitive and behavioral strategies are useful and safe for treating pediatric TTM. Enlisting the parents and patient in identifying problem situations and applying creative solutions may increase the chances of success.
Follow-up is important for maintaining new cognitive and behavioral patterns. We recommend that you see patients monthly for at least 3 months, depending on how the patient feels about additional sessions. We encourage families to call and report on progress or relapses. Booster CBT sessions can help deal with setbacks.
Related resources
- Trichotillomania Learning Center, Inc.; devoted to improving TTM understanding and providing access to treatments and support groups. www.trich.org. Accessed Sept. 17, 2004.
- Golomb RG, Vavrichek SM. The hair pulling “habit” and you: how to solve the trichotillomania puzzle (rev ed). Silver Spring, MD: Writer’s Cooperative of Greater Washington; 2000. Book for children and teenagers.
Drug brand names
- Fluoxetine • Prozac
- Naltrexone • Depade, ReVia
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
Preparation of this article was supported in part by a grant from the National Institute of Mental Health (MH61457).
Trichotillomania (TTM) is distressing to pediatric patients who pull their hair and to their parents who feel helpless to stop the destructive behavior. Hair-pulling with psychiatric comorbidity requires comprehensive assessment and treatment, but we have found that cognitive-behavioral therapy (CBT) alone can help children and adolescents with uncomplicated TTM.
This article describes a typical patient with adolescent-onset mild-to-moderate TTM and the three-step CBT approach—awareness training, stimulus control, and habit reversal—that we find effective in reducing pediatric hair pulling.
Jane, age 12, was referred to our clinic by her primary doctor after an 8-week trial of fluoxetine, 80 mg/d, failed to stop her hair pulling. Jane, who is right-handed, has been pulling her hair for 2 years, mostly in the right front scalp. Her shame over the hair loss makes her reluctant to participate in social activities. A dermatologist found no medical cause for her behavior, such as alopecia or folliculitis.
Jane’s parents say she has no history of a major mood disorder or anxiety. Her hair pulling causes significant “tension and stress” for all family members.
WHY DO PATIENTS PULL HAIR?
Cognitive-behavioral theory suggests that chronic TTM originates as a normal response to stress that often escapes personal and social awareness but gradually increases in frequency and severity (Box).1-8 Thus, hair pulling becomes associated with internal and external cues through conditioning and is maintained primarily by positive reinforcement. Hair-pulling urges that are reinforced by pulling intensify the need to pull, perpetuating the behavioral cycle.
A genetic link? Familial research has associated TTM with increased rates of obsessive-compulsive disorder (OCD) or other excessive habits—such as nail biting or skin picking—among first-degree relatives.6,9,10 Neuroimaging of persons with TTM has shown hyperactivity in the left cerebellum and right superior parietal lobe11 as well as possible structural abnormalities in the left putamen,12 left inferior frontal gyrus, and right cluneal cortex.13
These findings do not necessarily indicate pre-existing brain pathology, however. Perhaps TTM leads to changes in brain structure or function, or both TTM and the brain abnormalities may be caused by another as-yet-unknown variable.
Decreased pain sensitivity. Patients with TTM often report that hair pulling is not painful,2 though we suspect that persons without TTM would disagree and derive no pleasure from it. Changes in pain sensitivity may influence the reinforcing quality of pulling behavior. One possible mechanism for such alterations is upregulation of the endogenous opioid system; some intriguing evidence suggests that opioid receptor antagonists such as naltrexone may reduce pulling.14
Trichotillomania (TTM) is an impulse control disorder characterized by repetitive hair pulling,1 which typically emerges during adolescence. In a large clinical sample of adult hair pullers, mean age of onset was 13.2 Very-early onset (before age 5) may be a more benign form of TTM that tends to abate spontaneously and requires little or no therapeutic intervention.3
Despite the absence of body hair in prepubertal children, their pulling patterns are consistent with those of adults. The scalp is the most common pulling site, followed by eyelashes and eyebrows.4
Psychiatric comorbidity. In two studies evaluating psychiatric comorbidity in pediatric clinical samples, 60% to 70% of children and teens with TTM had at least one comorbid axis I disorder.5,6 Disruptive behavior disorders were most common in one study,6 whereas overanxious disorder was most common in the other.5 In a large clinical sample of adults with TTM, 51% met criteria for comorbid depression.2
Early identification and treatment of TTM are recommended because of the disorder’s distressing nature and social stigma. Early interventions also may help prevent later adult psychiatric comorbidity and functional impairment, although no studies have been done to demonstrate this benefit.7,8
Pain tolerance at the preferred pulling site has not been studied, however. For patients who feel pain from hair pulling, the pain itself may reinforce the behavior by distracting the individual from negative emotional or physiologic states.15
CASE CONTINUED: COUNTING THE WAYS
Jane and her parents agree that she pulls her hair 5 to 8 times daily, one hair at a time with her right index finger and thumb while doing homework or watching TV. The trigger, she says, is “an itch” on her scalp; “sometimes pulling relieves the itch.” She fails to resist pulling her hair 9 out of 10 times.
Table 1
Defining hair pulling: What to ask the pediatric patient
| Response description | How many times do you pull your hair each day? |
| How many hairs do you pull each time? | |
| From what body areas do you pull hair? | |
| What are all the steps involved in pulling (Touching the head before pulling? Pulling one hair at a time with the thumb and index finger)? | |
| Response detection | Under what circumstances do you sense the urge to pull? |
| How strong is the urge on a scale of 1 to 10, with 10 being the greatest intensity you ever felt? | |
| How do you try to resist and overcome the urge to pull? | |
| Precursors | External cues (Do you pull when you look at yourself in a mirror?) |
| Internal cues (Do you pull when you are nervous?) | |
| High-risk situations | What are you usually doing when you get the urge to pull? (reading, talking on the telephone, watching TV, using a computer, etc.) |
| Consequences that reinforce the behavior | Do you pull to reduce physical sensations (such as itching) at the site of pulling? |
| Does pulling relieve sadness or worry about problems at home or in school? | |
| Do you pull to create a more even hairline? |
Psychiatric comorbidity is common—if not the norm—in adults with TTM. Although axis I comorbidity is also seen in children and adolescents, their hair pulling is frequently uncomplicated. Jane meets criteria for TTM, as determined by the Trichotillomania Diagnostic Interview,16 but her history does not support a comorbid disorder. After discussing the diagnosis with Jane and her parents, the psychiatrist begins treatment with CBT alone.
MEDICATION OR CBT?
SSRIs. Literature on TTM pharmacotherapy is very limited and equivocal. Medications that have helped adults with TTM have been described,17 but the lack of a single, randomized, controlled trial in pediatric TTM severely limits treatment recommendations for children.
Selective serotonin reuptake inhibitors (SSRIs) have shown efficacy for treating anger and other impulse control problems but not for TTM. Some practitioners use SSRIs for TTM because of the belief that TTM is a variant of OCD. However, TTM may be maintained by positive reinforcement rather than compulsive tendencies and thus may not respond to SSRIs.
CBT. Evidence on CBT justifies cautious recommendations for pediatric TTM. In randomized trials, CBT reduced hair pulling in adults and was more effective than SSRIs or placebo.18,19
REDUCING THE URGE
Obtain detailed information about a child or adolescent’s hair-pulling episodes (Table 1), as recognizing triggers and reactions is vital to effective CBT. Explain to the patient that:
- the pleasure or satisfaction she derives from pulling reinforces the urge to pull
- she can reduce the urge by learning and using awareness training, stimulus control, and habit reversal (Table 2).
Awareness training involves patient self-monitoring to gain awareness of urges to pull and of pulling behavior. The child must become alert to every hair pulled and to response precursors, such as placing her hand on her head. For a patient such as Jane, a useful technique is to post reminders on the TV and school notebook and in the bedroom and bathroom—wherever pulling typically occurs.
A “PULLING CALENDAR”
Jane begins a daily “pulling calendar” in which she records each time she pulls a hair while watching TV or doing homework. She is asked to include the total number of hairs pulled and the intensity of the “itch to pull” on a scale of 1 to 10.
Stimulus control. Most patients can identify high-risk situations, such as time in the bathroom, talking on the phone, watching TV, driving, reading, or while falling asleep. Boredom, frustration, anxiety, and sadness may serve as pulling cues.
With stimulus control, the patient tries to reduce her ability to freely engage in pulling behavior in high-risk situations. For instance, you might encourage a child who pulls hairs while doing homework to stick Band-Aid®-type adhesive strips on her thumb and index finger tips before she starts studying as an impediment to gripping hairs. Such “speed bumps” may allow her to delay pulling and reach for tools that assist in habit reversal.
TREATMENT THAT APPEALS
Jane agrees to apply adhesive strips to her fingers and understands why. Because she is a fan of Peter Pan, we place Peter Pan stickers on her books and notebooks and on the TV remote control as reminders not to pull.
Table 2
CBT strategies to reduce the hair-pulling urge
| Awareness training | Increases patient’s awareness of pulling |
| Stimulus control | Establishes an environment less conducive to pulling |
| Habit reversal/ response | Patient develops alternate activities that provide competing positive reinforcement comparable to that gained from pulling |
Habit reversal and competing response procedures provide pleasurable physical stimulation as an alternative to pulling. The most effective methods engage the same motions as used in hair pulling. Examples include sculpting with clay, hulling sunflower seeds, and playing with Koosh® balls—small rubbery balls filled with a jellylike plasma and covered with hundreds of soft “tentacles.”
‘CALMER, HAPPIER’
We explain habit reversal to Jane and instruct her to use the Koosh ball a few times a day. She enjoys pulling its rubber strands, an action that uses the same muscles as hair pulling. Because she will need Koosh balls during all identified high-risk situations, we instruct her to buy one for her book bag and to leave one near the couch where she watches TV.
Over time, Jane reports a gradual decrease of hair pulling with the use of awareness training and stimulus control techniques. Using the Koosh ball (habit reversal) helps her improve. By the 10th week, Jane and her parents report a 70% decrease in hair pulling, based on the pulling calendar entries and other objective evidence of treatment response. All report feeling “calmer and happier.”
CONCLUSION
Cognitive and behavioral strategies are useful and safe for treating pediatric TTM. Enlisting the parents and patient in identifying problem situations and applying creative solutions may increase the chances of success.
Follow-up is important for maintaining new cognitive and behavioral patterns. We recommend that you see patients monthly for at least 3 months, depending on how the patient feels about additional sessions. We encourage families to call and report on progress or relapses. Booster CBT sessions can help deal with setbacks.
Related resources
- Trichotillomania Learning Center, Inc.; devoted to improving TTM understanding and providing access to treatments and support groups. www.trich.org. Accessed Sept. 17, 2004.
- Golomb RG, Vavrichek SM. The hair pulling “habit” and you: how to solve the trichotillomania puzzle (rev ed). Silver Spring, MD: Writer’s Cooperative of Greater Washington; 2000. Book for children and teenagers.
Drug brand names
- Fluoxetine • Prozac
- Naltrexone • Depade, ReVia
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
Preparation of this article was supported in part by a grant from the National Institute of Mental Health (MH61457).
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th ed., text rev. Washington, DC: American Psychiatric Association Press; 2000;674-7.
2. Christenson GA, Mackenzie TB, Mitchell JE. Characteristics of 60 adult chronic hairpullers. Am J Psychiatry 1991;148:365-70.
3. Swedo SE, Leonard HL. Trichotillomania: an obsessive compulsive spectrum disorder? Psychiatr Clin North Am 1992;15:777-90.
4. Reeve E. Hair pulling in children and adolescents. In: Stein DJ, Christenson GA, Hollander E, eds. Trichotillomania. Washington, DC: American Psychiatric Association Press, 1999;201-24.
5. Reeve EA, Bernstein GA, Christenson GA. Clinical characteristics and psychiatric comorbidity in children with trichotillomania. J Am Acad Child Adolesc Psychiatry 1992;31:132-8.
6. King RA, Scahill L, Vitulano LA, et al. Childhood trichotillomania: clinical phenomenology, comorbidity, and family genetics. J Am Acad Child Adolesc Psychiatry 1995;34:1451-9.
7. Franklin ME, Bux DA, Foa EB. Pediatric trichotillomania: conceptualization and treatment implications. In: Orvashel H, Faust J, Hersen M, eds. Handbook of conceptualization and treatment of child psychopathology. Oxford, UK: Elsevier Science; 2001;379-98.
8. Keuthen NJ, Franklin ME. Trichotillomania: psychopathology and treatment development [presentation]. Reno, NV: Association for the Advancement of Behavior Therapy annual meeting, 2002.
9. Bienvenu OJ, Samuels JF, Riddle MA, et al. The relationship of obsessive-compulsive disorder to possible spectrum disorders: results from a family study. Biol Psychiatry 2000;48:287-93.
10. Lenane MC, Swedo SE, Rapoport JL, et al. Rates of obsessive compulsive disorder in first degree relatives of patients with trichotillomania: a research note. J Child Psychol Psychiatry 1992;33:925-33.
11. Swedo SE, Rapoport JL, Leonard HL, et al. Regional cerebral glucose metabolism of women in trichotillomania. Arch Gen Psychiatry 1991;48:828-33.
12. O’Sullivan RL, Rauch SL, Breiter HC, et al. Reduced basal ganglia volumes in trichotillomania measured via morphometric magnetic resonance imaging. Biol Psychiatry 1997;42:39-45.
13. Grachev ID. MRI-based morphometric topographic parcellation of human neocortex in trichotillomania. Psychiatry Clin Neurosci 1997;51:315-21.
14. Carrion VG. Naltrexone for the treatment of trichotillomania: a case report. J Clin Psychopharmacol 1995;15:444-5.
15. Christenson GA, Mansueto CS. Trichotillomania: descriptive characteristics and phenomenology. In: Stein DJ, Christenson GA, Hollander E, eds. Trichotillomania. Washington, DC: American Psychiatric Press, 1999;1-41.
16. Rothbaum BO, Ninan PT. The assessment of trichotillomania. Behav Res Ther 1994;32(6):651-62.
17. Lundt LP. Trichotillomania: a heads-up on severe cases. Current Psychiatry 2004;3(5):89-105.
18. Ninan PT, Rothbaum BO, Marsteller FA, et al. A placebo-controlled trial of cognitive-behavioral therapy and clomipramine in trichotillomania. J Clin Psychiatry. 2000;61:47-50.
19. Azrin NH, Nunn RG, Frantz SE. Treatment of hairpulling (trichotillomania): a comparative study of habit reversal and negative practice training. J Behav Ther Exp Psychiatry 1980;11:13-20.
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th ed., text rev. Washington, DC: American Psychiatric Association Press; 2000;674-7.
2. Christenson GA, Mackenzie TB, Mitchell JE. Characteristics of 60 adult chronic hairpullers. Am J Psychiatry 1991;148:365-70.
3. Swedo SE, Leonard HL. Trichotillomania: an obsessive compulsive spectrum disorder? Psychiatr Clin North Am 1992;15:777-90.
4. Reeve E. Hair pulling in children and adolescents. In: Stein DJ, Christenson GA, Hollander E, eds. Trichotillomania. Washington, DC: American Psychiatric Association Press, 1999;201-24.
5. Reeve EA, Bernstein GA, Christenson GA. Clinical characteristics and psychiatric comorbidity in children with trichotillomania. J Am Acad Child Adolesc Psychiatry 1992;31:132-8.
6. King RA, Scahill L, Vitulano LA, et al. Childhood trichotillomania: clinical phenomenology, comorbidity, and family genetics. J Am Acad Child Adolesc Psychiatry 1995;34:1451-9.
7. Franklin ME, Bux DA, Foa EB. Pediatric trichotillomania: conceptualization and treatment implications. In: Orvashel H, Faust J, Hersen M, eds. Handbook of conceptualization and treatment of child psychopathology. Oxford, UK: Elsevier Science; 2001;379-98.
8. Keuthen NJ, Franklin ME. Trichotillomania: psychopathology and treatment development [presentation]. Reno, NV: Association for the Advancement of Behavior Therapy annual meeting, 2002.
9. Bienvenu OJ, Samuels JF, Riddle MA, et al. The relationship of obsessive-compulsive disorder to possible spectrum disorders: results from a family study. Biol Psychiatry 2000;48:287-93.
10. Lenane MC, Swedo SE, Rapoport JL, et al. Rates of obsessive compulsive disorder in first degree relatives of patients with trichotillomania: a research note. J Child Psychol Psychiatry 1992;33:925-33.
11. Swedo SE, Rapoport JL, Leonard HL, et al. Regional cerebral glucose metabolism of women in trichotillomania. Arch Gen Psychiatry 1991;48:828-33.
12. O’Sullivan RL, Rauch SL, Breiter HC, et al. Reduced basal ganglia volumes in trichotillomania measured via morphometric magnetic resonance imaging. Biol Psychiatry 1997;42:39-45.
13. Grachev ID. MRI-based morphometric topographic parcellation of human neocortex in trichotillomania. Psychiatry Clin Neurosci 1997;51:315-21.
14. Carrion VG. Naltrexone for the treatment of trichotillomania: a case report. J Clin Psychopharmacol 1995;15:444-5.
15. Christenson GA, Mansueto CS. Trichotillomania: descriptive characteristics and phenomenology. In: Stein DJ, Christenson GA, Hollander E, eds. Trichotillomania. Washington, DC: American Psychiatric Press, 1999;1-41.
16. Rothbaum BO, Ninan PT. The assessment of trichotillomania. Behav Res Ther 1994;32(6):651-62.
17. Lundt LP. Trichotillomania: a heads-up on severe cases. Current Psychiatry 2004;3(5):89-105.
18. Ninan PT, Rothbaum BO, Marsteller FA, et al. A placebo-controlled trial of cognitive-behavioral therapy and clomipramine in trichotillomania. J Clin Psychiatry. 2000;61:47-50.
19. Azrin NH, Nunn RG, Frantz SE. Treatment of hairpulling (trichotillomania): a comparative study of habit reversal and negative practice training. J Behav Ther Exp Psychiatry 1980;11:13-20.
Identify and manage 2 common non-Alzheimer’s dementias
Primary care doctors refer patients with dementia to psychiatrists when the diagnosis or disease course is unclear. Psychiatrists thus must often discern non-Alzheimer’s dementias— particularly the vascular and Lewy body types— from Alzheimer’s dementia. This article describes:
- features that distinguish vascular, Lewy body, and Alzheimer’s dementias
- cognitive and medical tests to help determine dementia type and facilitate treatment
- risk factors that promote cognitive and functional decline
- strategies for using medication while minimizing side-effect risks.
CASE REPORT: DISRUPTIVE IN DAY CARE
Ms. Z, age 82, is referred to a psychiatrist after numerous failed attempts by her primary care physician to stop her medical and psychiatric deterioration.
Table 1
Estimated dementia type prevalence among patients with dementia
| Dementia type | Prevalence |
|---|---|
| Alzheimer's | 65% |
| Lewy body | 0-15% |
| Vascular | 10-15% |
| Mixed | 10-15% |
| Source: reference 1 | |
The patient was functioning well at home until 6 months ago, when her husband’s death triggered a dramatic functional decline. She has Parkinson’s disease and has had dementia symptoms for 3 years, but family members do not recall a dementia diagnosis.
Ms. Z has become increasingly disruptive in day care; she yelled at and slapped a staff member during one episode. Her son is concerned that additional outbursts will prompt her dismissal. Her Mini-Mental State Examination (MMSE) score is 19, indicating moderate dementia.
Donepezil, 10 mg/d across 2 years, has not slowed Ms. Z’s memory decline. Carbidopa/levadopa, 25/250 mg tid over 1 year, has not improved her Parkinson’s symptoms. Risperidone, 0.5 mg bid, caused marked sedation and unsteady gait and was stopped after 4 weeks. She also is taking hydrocodone/acetaminophen, 5/500 mg/d for osteoarthritis, and lisinopril/hydrochlorothiazide, 10/12.5 mg/d for hypertension.
Discussion. As with Ms. Z, a significant other can mask a dementia patient’s cognitive deficits, but these deficits become apparent after the partner dies. Family members then discover that a parent or sibling cannot function independently.
Treatment should target Ms. Z’s aggression to allow her to stay in day care and her son to care for her at home. Determining the dementia type is crucial to planning treatment and preserving function.
WHICH DEMENTIA IS WHICH?
Non-Alzheimer’s dementias account for up to 35% of dementia cases (Table 1).1 The pathologic correlations separating Alzheimer’s, vascular, and Lewy body dementias are often confusing:
- Beta-amyloid plaques are common in Alzheimer’s and Lewy body dementias, although neurofibrillary tangles are much less common in the Lewy body type.
- Synaptic cholinergic deficiencies are seen in Alzheimer’s and vascular dementias.
- Hypertension and hyperlipidemia—both traditional vascular risk factors—also appear to contribute to Alzheimer’s dementia.
Vascular dementia. Large, single-vessel hemispheric infarcts cause substantial damage, whereas multiple small vascular lesions (such as lacunae or mini-infarcts) can have more-subtle effects when strategically located, such as in the basal ganglia, hippocampus, or thalamus. These smaller lesions can disrupt frontal cortical-subcortical neural pathways and contribute to difficulties with executive functions (judgment, insight), emotional control, and behavior.
Lesions from a cerebrovascular accident, however, do not necessarily cause dementia, and the mechanism by which lesions cause dementia is not fully understood. Post-stroke dementia sometimes is progressive, suggesting a degenerative rather than vascular cause.
Lewy body dementia is associated with Parkinson’s disease, as Lewy body inclusion deposits are common to both disorders. The deposits typically appear in the cerebral cortex in Lewy body dementia but not in Parkinson’s.
Amyloid protein deposits alter the clinical presentation. Patients with these lesions have fewer visual hallucinations and motor problems, making diagnosis more difficult.
Lewy body dementia, like all major dementias, usually surfaces after age 75. Its clinical course generally is considered worse than that of Alzheimer’s dementia, but these two dementia types do not differ substantially in age of onset, age of death, or survival rates.
Table 2
Clinical features that characterize Lewy body dementia
| Central | Progressive cognitive decline that interferes with normal social and occupational function; deficits on tests of attention, frontal-subcortical skills, and visuospatial ability can be especially prominent |
| Core | Two of three needed for probable diagnosis:
|
| Supportive | Repeated falls Syncope Transient loss of consciousness REM sleep behavior disorder Systematized delusions Hallucinations in other modalities Neuroleptic sensitivity Depression |
| Features less likely to be present | History of stroke Another physical illness or brain disorder that interferes with cognitive performance |
| Source: reference 6 | |
FEATURES OF VASCULAR DEMENTIA
Onset can be gradual but is more often sudden— usually occurring shortly after an ischemic stroke. Disease progression can be gradual or dramatic, depending on the vascular event type. Cognitive and physical decline in vascular dementia usually is stepwise over time, whereas decline in Alzheimer’s dementia is more gradual with progressive severity.
Patients with vascular dementia classically present with memory loss temporally associated with other typical stroke stigmata. Brain imaging often uncovers evidence of stroke that is otherwise not clinically evident.
CNS manifestations of vascular dementia often include memory loss, emotional lability (including depression), and executive-task dysfunction. Patients usually have atrial fibrillation or vascular risk factors, including diabetes mellitus, hypertension, hyperlipidemia, obesity, or tobacco use. Patients with previous stroke, coronary artery disease, or peripheral vascular disease are at increased risk.
Vascular dementia is categorized by stroke type:
Embolic infarct. Emboli, typically cardiac in origin, can occlude small or large cerebral arteries, resulting in correspondingly sized infarcts. Atrial fibrillation can promote areas in the atria with relatively low flow turbulence. Blood clots can form that eventually embolize via the carotid arteries. Multiple emboli can occur, causing progressive dementia.
Cerebral hemorrhage —small or large—can be devastating. Hypertension is the major risk factor for this form of stroke.
Multi-infarct dementia. Multiple cerebral blood vessel infarcts classically lead to stepwise functional decline after each event. Multiple small infarcts can occur in various brain regions, including the cortex and basal ganglia. Binswanger’s disease, a variant of vascular dementia in which incomplete ischemia is limited to the hemispheric white matter, tends to be fairly progressive.2
Small-vessel disease. Reduced blood flow and tissue perfusion can cause small-vessel disease. Often the ischemia is “silent,” detectable only on MRI or CT. The infarcts typically cause lacunar lesions, nerve demyelination, and gliosis.3 These can occur to some extent in nondemented patients but become significant with more-extensive disease.
FEATURES OF LEWY BODY DEMENTIA
As with all dementias, permanent memory loss must be present to diagnose this dementia sub-type. Overall cognitive deficits may be more prominent than memory loss, however. The patient may have trouble performing cognitive tasks that employ visuospatial abilities, executive functions, and attention. Neuropsychiatric symptoms that overlap with Alzheimer’s dementia include apathy, anxiety, agitation, depression, anhedonia, and paranoia.
The presence of visual hallucinations, fluctuating cognition, or extrapyramidal symptoms (EPS) distinguish Lewy body from Alzheimer’s dementia.
Visual hallucinations are prominent in Lewy body dementia and often prompt psychiatric referral (Table 2). They usually surface early in the disease course and tend to persist. Other sensory hallucinations also can occur.
The hallucinations often are detailed and vivid and the patient may be aware they are occurring, especially if the dementia is not advanced. Treatment might not be necessary for mild hallucinations, which can concern the caregiver more than the patient.
Antipsychotics paradoxically worsen hallucinations in Lewy body dementia, and many patients present to psychiatrists after failing an empiric trial. A failed antipsychotic course in a patient diagnosed with Alzheimer’s dementia could indicate that the diagnosis is incorrect.
Fluctuating cognition occurs in 50% to 75% of Lewy body cases. Alertness, attention, and concentration are variable and can cycle within hours to weeks. The patient often is fairly interactive and social for a time, then has periods of diminished function and being “out of it.” Some patients have recurrent delirium and undergo multiple workups in search of a cause.
EPS. As many as 75% of Lewy body patients have parkinsonian motor features.4 Because these features are not essential to the diagnosis, their absence is the most common reason Lewy body dementia goes unrecognized.1
Motor involvement varies and can be worsened by antipsychotics. Overuse of antipsychotics in Alzheimer’s or vascular dementia also can cause motor symptoms that mimic Lewy body features.
EPS orientation tends to be axial, showing less facial expressivity and more postural imbalance. Peripheral signs such as tremor and extremity rigidity tend to be less dominant.
MAKING THE DIAGNOSIS
Vascular and Lewy body dementia diagnoses are primarily based on clinical features and findings. Memory loss is necessary for either diagnosis.
Vascular dementia. Most consensus criteria require presence of dementia, physical or radiologic signs of a stroke, and a temporal relationship between the stroke and the dementia for a vascular dementia diagnosis.
Hachinski’s “ischemia scale” can help differentiate multi-infarct from Alzheimer’s dementia.5 Cases are scored on a 0-to-9 scale, with point values for abrupt onset; stepwise course; history of stroke; and presence of somatic complaints, emotional lability, hypertension, and focal neurologic signs. A score ≥4 suggests vascular dementia.
The scale, however, does not account for imaging studies, vascular risk factors other than hypertension, or repeated silent strokes that can cause symptoms. Also, some patients who score below the cutoff have strategic infarct dementias.
Lewy body dementia. Clinical consensus guidelines developed by McKeith et al6 can help clinicians recognize and categorize this dementia type (Table 2). Several studies of diagnostic criteria have shown very good specificity but variable sensitivity.7 Because no standard imaging modalities or serum markers exist, presence of progressive memory loss, fluctuating cognition, visual hallucinations, and EPS should drive the diagnosis.
Lewy body dementia is commonly misdiagnosed as Parkinson’s dementia. The two types are readily differentiated by onset of memory loss, which emerges late in Parkinson’s dementia but is early and prominent in Lewy body dementia.
CASE CONTINUED: HISTORY LEADS TO DIAGNOSIS
Ms. Z was diagnosed as having Lewy body dementia, as her cognitive decline clearly preceded her motor deficits. Further questioning revealed fluctuating attention levels and a history of visual hallucinations.
TESTING PATIENT FUNCTION
Neuropsychiatric tests. DSM-IV recommends testing memory, orientation, language, praxis, constructional ability, and executive control function in patients with dementia. Numerous tests can aid in diagnosis, but they generally are too lengthy to be practical. The MMSE takes 5 to 10 minutes, but it might miss mild memory loss or executive dysfunction.
Giving a quick clock-drawing test in tandem with the MMSE can help measure basic executive control and constructional ability. Also, patients with Lewy body or vascular dementia often are more proficient than patients with Alzheimer’s dementia on verbal memory tests but less proficient on visuospatial performance. Consider referring clinically challenging patients for more-extensive neuropsychiatric testing.
Lab tests. Blood tests including TSH and B12/folate screens are usually performed but rarely positive. Rapid plasma reagin testing for syphilis is no longer recommended unless syphilis is suspected.
Table 3
Potential cognitive side effects associated with psychotropic classes*
| Drug class | Potential cognitive side effects |
|---|---|
| Antidepressants Tricyclics, SSRIs, SNRIs | Confusion, sedation, falls |
| Antihistamines | Confusion, sedation, dizziness |
| Antipsychotics | Sedation, fatigue, anxiety |
| Antispasmodics | Confusion, sedation |
| Benzodiazepines | Sedation, confusion, ataxia, depression |
| Opioids | Sedation, confusion, dizziness |
| Sleep-promoting agents | Amnesia, confusion, ataxia |
| * Not all agents in each class are associated with listed side effects | |
| SSRIs: Selective serotonin reuptake inhibitors | |
| SNRIs: Serotonin-norepinephrine reuptake inhibitors | |
Radiologic imaging. Radiologic imaging (MRI or CT) can show infarcts in vascular dementia and can rule out:
- a brain tumor
- a subdural hemorrhage after recent head trauma
- or normal-pressure hydrocephalus in patients with dementia, gait instability, and/or urinary incontinence.
Brain imaging in Lewy body dementia can show hippocampal preservation8 but is not specific and does not significantly support the diagnosis. Specialized tests such as single-photon emission computed tomography or positron-emission tomography show occipital hypoperfusion9 but are expensive, not sufficiently specific, and do not add substantial value over clinical criteria.
MANAGING SYMPTOMS
Medication may be necessary if the patient is frequently and significantly agitated. Consider prescribing a selective serotonin reuptake inhibitor, an anticonvulsant such as divalproex or carbamazepine as a mood stabilizer, or a short-acting benzodiazepine. Start low and titrate slowly if needed.
Find out if the patient is taking medications that may be causing bothersome side effects. Avoid agents with potential cognitive or anticholinergic effects (Table 3); the latter can cause confusion, sedation, and falls in the elderly.
Cholinesterase inhibitors, FDA-approved for use in Alzheimer’s dementia, have been shown to reduce cognitive and global functioning decline in vascular dementia.10 A cholinergic deficit present in vascular dementia may explain the drugs’ effectiveness. Donepezil, galantamine, and rivastigmine have all shown positive effects on cognition.
Because patients with Lewy body hallucinations have greater synaptic acetylcholine deficits, cholinesterase inhibitors tend to be more effective in Lewy body dementia than in other dementia subtypes. In small open-label studies, patients taking cholinesterase inhibitors for Lewy body dementia have shown sustained improvements (up to 96 months) in cognition and behavior. Wild et al,11 however, concluded that the evidence supporting use of these agents—specifically rivastigmine—is weak.
Also, cholinesterase inhibitors offer fairly modest effectiveness, do not work for all patients, and do not prevent cognitive decline even when taken regularly. Because cholinesterase inhibitors are costly and most Medicare patients lack prescription medication coverage, an initial short (6-month) trial is recommended. Re-evaluate the patient periodically by using caregiver reports, caregiver assessment scales, and basic cognitive testing.
Cholinesterase inhibitor dosing is the same for vascular and Lewy body dementia as it is for Alzheimer’s disease. Tell patients to take the agents with food to minimize potential intestinal side effects.
Memantine. In European studies, memantine has shown positive effects on cognition and function in vascular dementia. Memantine, a N-methyl-D-aspartate receptor antagonist, is FDA-approved for moderate to severe Alzheimer’s dementia.12
DELAYING DECLINE
Controlling risk factors. Controlling vascular risk factors—especially high blood pressure—is the most effective way to prevent or treat vascular dementia. In primary prevention studies, patients with good hypertension and hyperlipidemia control developed dementia more slowly than did nontreated cohorts.
In patients with coronary artery disease, statins have been shown to lower cholesterol and stabilize pre-existing plaques in the arterial wall, reducing the risk of plaque rupture. Low-density lipoproteincholesterol goals vary according to vascular risk factors but should be <100 mg/dL for patients with vascular dementia, who are at highest risk. Blood pressure goals are ≤140 mm Hg (systolic) and ≤90 mm Hg (diastolic).
Glycemic control (fasting blood glucose <110 mg/dL) and smoking cessation can also reduce the risk of further vascular events. Most patients should be taking an antiplatelet medication, preferably aspirin, to reduce clotting risk.
Although Lewy body dementia has no known risk factors other than age, research will determine whether vascular or other factors contribute to its development.
CASE CONTINUED: TARGETING AGGRESSION
Ms. Z was given divalproex, 250 mg bid, to reduce her frequent aggression. Her visual hallucinations were considered mild and not problematic and therefore were not treated. She responded well to the medication, allowing her to remain in day care and avoid nursing home placement.
Related resources
- Alzheimer’s Association. http://www.alz.org
- American Geriatrics Society. http://www.americangeriatrics.org
Drug brand names
- Carbamazepine • Tegretol, others
- Carbidopa/Levodopa • Various
- Divalproex • Depakote
- Donepezil • Aricept
- Galantamine • Reminyl
- Hydrocodone/acetaminophen • Vicodin, others
- Lisinopril/hydrochlorothiazide • Prinzide, Zestoretic
- Memantine • Namenda
- Risperdone • Risperdal
- Rivastigmine • Exelon
Disclosure
Dr. Bartz is a speaker for Forest Pharmaceuticals and Novartis Pharmaceuticals Corp.
1. McKeith JG, Ballard CG, Perry RH, et al. Prospective validation of consensus criteria for the diagnosis of dementia with Lewy bodies. Neurology 2000;54:1050-8.
2. Roman GC, Erkinjuntti T, Wallin A, et al. Subcortical ischemic vascular dementia. Lancet Neurol 2002;17:426-36.
3. Pohjasraara T, Mantyla R, Ylikoski MA, et al. Comparison of different clinical criteria (DSM-III, ADDTC, ICD-10, NINDS-AIREN, DSM-IV) for the diagnosis of vascular dementia. Stroke 2000;31:2952-7.
4. Del Ser T, McKeith I, Anand R, et al. Dementia with Lewy bodies: findings from an international multicenter study. Int J Geriatr Psychiatry 2000;15:1034-45.
5. Hachinski VC, Iliff LD, Zilhka E, et al. Cerebral blood flow in dementia. Arch Neurol 1975;32:632-7.
6. McKeith IG, Galasko D, Kosaka K, et al. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the consortium on DLB international workshop. Neurology 1996;47:1113-24.
7. Luis CA, Barker WW, Gajaraj K, et al. Sensitivity and specificity of three clinical criteria for dementia with Lewy bodies in an autopsy-verified sample. Int J Geriatr Psychiatry 1999;14:526-33.
8. Barber R, Ballard C, McKeith IG, et al. MRI volumetric study of dementia with Lewy bodies: a comparison with AD and vascular dementia. Neurology 2000;54:1304-9.
9. Lobotesis K, Fenwick JD, Phipps A, et al. Occipital hypoperfusion on SPECT in dementia with Lewy bodies but not AD. Neurology 2001;56:643-9.
10. Pratt RD, Perdomo CA. Results of clinical studies with donepezil in vascular dementia. Am J Geriatr Psychiatry 2002;10(suppl 1):88-9.
11. Wild R, Pettit T, Burns A. Cholinesterase inhibitors for dementia with Lewy bodies. Cochrane Database Syst Rev 2003;3:CD003672.-
12. Tariot PN, Farlow MR, Grossberg GT, et al. Memantine treatment in patients with moderate to severe Alzheimer disease already receiving donepezil: a randomized controlled trial. JAMA 2004;291:317-24.
Primary care doctors refer patients with dementia to psychiatrists when the diagnosis or disease course is unclear. Psychiatrists thus must often discern non-Alzheimer’s dementias— particularly the vascular and Lewy body types— from Alzheimer’s dementia. This article describes:
- features that distinguish vascular, Lewy body, and Alzheimer’s dementias
- cognitive and medical tests to help determine dementia type and facilitate treatment
- risk factors that promote cognitive and functional decline
- strategies for using medication while minimizing side-effect risks.
CASE REPORT: DISRUPTIVE IN DAY CARE
Ms. Z, age 82, is referred to a psychiatrist after numerous failed attempts by her primary care physician to stop her medical and psychiatric deterioration.
Table 1
Estimated dementia type prevalence among patients with dementia
| Dementia type | Prevalence |
|---|---|
| Alzheimer's | 65% |
| Lewy body | 0-15% |
| Vascular | 10-15% |
| Mixed | 10-15% |
| Source: reference 1 | |
The patient was functioning well at home until 6 months ago, when her husband’s death triggered a dramatic functional decline. She has Parkinson’s disease and has had dementia symptoms for 3 years, but family members do not recall a dementia diagnosis.
Ms. Z has become increasingly disruptive in day care; she yelled at and slapped a staff member during one episode. Her son is concerned that additional outbursts will prompt her dismissal. Her Mini-Mental State Examination (MMSE) score is 19, indicating moderate dementia.
Donepezil, 10 mg/d across 2 years, has not slowed Ms. Z’s memory decline. Carbidopa/levadopa, 25/250 mg tid over 1 year, has not improved her Parkinson’s symptoms. Risperidone, 0.5 mg bid, caused marked sedation and unsteady gait and was stopped after 4 weeks. She also is taking hydrocodone/acetaminophen, 5/500 mg/d for osteoarthritis, and lisinopril/hydrochlorothiazide, 10/12.5 mg/d for hypertension.
Discussion. As with Ms. Z, a significant other can mask a dementia patient’s cognitive deficits, but these deficits become apparent after the partner dies. Family members then discover that a parent or sibling cannot function independently.
Treatment should target Ms. Z’s aggression to allow her to stay in day care and her son to care for her at home. Determining the dementia type is crucial to planning treatment and preserving function.
WHICH DEMENTIA IS WHICH?
Non-Alzheimer’s dementias account for up to 35% of dementia cases (Table 1).1 The pathologic correlations separating Alzheimer’s, vascular, and Lewy body dementias are often confusing:
- Beta-amyloid plaques are common in Alzheimer’s and Lewy body dementias, although neurofibrillary tangles are much less common in the Lewy body type.
- Synaptic cholinergic deficiencies are seen in Alzheimer’s and vascular dementias.
- Hypertension and hyperlipidemia—both traditional vascular risk factors—also appear to contribute to Alzheimer’s dementia.
Vascular dementia. Large, single-vessel hemispheric infarcts cause substantial damage, whereas multiple small vascular lesions (such as lacunae or mini-infarcts) can have more-subtle effects when strategically located, such as in the basal ganglia, hippocampus, or thalamus. These smaller lesions can disrupt frontal cortical-subcortical neural pathways and contribute to difficulties with executive functions (judgment, insight), emotional control, and behavior.
Lesions from a cerebrovascular accident, however, do not necessarily cause dementia, and the mechanism by which lesions cause dementia is not fully understood. Post-stroke dementia sometimes is progressive, suggesting a degenerative rather than vascular cause.
Lewy body dementia is associated with Parkinson’s disease, as Lewy body inclusion deposits are common to both disorders. The deposits typically appear in the cerebral cortex in Lewy body dementia but not in Parkinson’s.
Amyloid protein deposits alter the clinical presentation. Patients with these lesions have fewer visual hallucinations and motor problems, making diagnosis more difficult.
Lewy body dementia, like all major dementias, usually surfaces after age 75. Its clinical course generally is considered worse than that of Alzheimer’s dementia, but these two dementia types do not differ substantially in age of onset, age of death, or survival rates.
Table 2
Clinical features that characterize Lewy body dementia
| Central | Progressive cognitive decline that interferes with normal social and occupational function; deficits on tests of attention, frontal-subcortical skills, and visuospatial ability can be especially prominent |
| Core | Two of three needed for probable diagnosis:
|
| Supportive | Repeated falls Syncope Transient loss of consciousness REM sleep behavior disorder Systematized delusions Hallucinations in other modalities Neuroleptic sensitivity Depression |
| Features less likely to be present | History of stroke Another physical illness or brain disorder that interferes with cognitive performance |
| Source: reference 6 | |
FEATURES OF VASCULAR DEMENTIA
Onset can be gradual but is more often sudden— usually occurring shortly after an ischemic stroke. Disease progression can be gradual or dramatic, depending on the vascular event type. Cognitive and physical decline in vascular dementia usually is stepwise over time, whereas decline in Alzheimer’s dementia is more gradual with progressive severity.
Patients with vascular dementia classically present with memory loss temporally associated with other typical stroke stigmata. Brain imaging often uncovers evidence of stroke that is otherwise not clinically evident.
CNS manifestations of vascular dementia often include memory loss, emotional lability (including depression), and executive-task dysfunction. Patients usually have atrial fibrillation or vascular risk factors, including diabetes mellitus, hypertension, hyperlipidemia, obesity, or tobacco use. Patients with previous stroke, coronary artery disease, or peripheral vascular disease are at increased risk.
Vascular dementia is categorized by stroke type:
Embolic infarct. Emboli, typically cardiac in origin, can occlude small or large cerebral arteries, resulting in correspondingly sized infarcts. Atrial fibrillation can promote areas in the atria with relatively low flow turbulence. Blood clots can form that eventually embolize via the carotid arteries. Multiple emboli can occur, causing progressive dementia.
Cerebral hemorrhage —small or large—can be devastating. Hypertension is the major risk factor for this form of stroke.
Multi-infarct dementia. Multiple cerebral blood vessel infarcts classically lead to stepwise functional decline after each event. Multiple small infarcts can occur in various brain regions, including the cortex and basal ganglia. Binswanger’s disease, a variant of vascular dementia in which incomplete ischemia is limited to the hemispheric white matter, tends to be fairly progressive.2
Small-vessel disease. Reduced blood flow and tissue perfusion can cause small-vessel disease. Often the ischemia is “silent,” detectable only on MRI or CT. The infarcts typically cause lacunar lesions, nerve demyelination, and gliosis.3 These can occur to some extent in nondemented patients but become significant with more-extensive disease.
FEATURES OF LEWY BODY DEMENTIA
As with all dementias, permanent memory loss must be present to diagnose this dementia sub-type. Overall cognitive deficits may be more prominent than memory loss, however. The patient may have trouble performing cognitive tasks that employ visuospatial abilities, executive functions, and attention. Neuropsychiatric symptoms that overlap with Alzheimer’s dementia include apathy, anxiety, agitation, depression, anhedonia, and paranoia.
The presence of visual hallucinations, fluctuating cognition, or extrapyramidal symptoms (EPS) distinguish Lewy body from Alzheimer’s dementia.
Visual hallucinations are prominent in Lewy body dementia and often prompt psychiatric referral (Table 2). They usually surface early in the disease course and tend to persist. Other sensory hallucinations also can occur.
The hallucinations often are detailed and vivid and the patient may be aware they are occurring, especially if the dementia is not advanced. Treatment might not be necessary for mild hallucinations, which can concern the caregiver more than the patient.
Antipsychotics paradoxically worsen hallucinations in Lewy body dementia, and many patients present to psychiatrists after failing an empiric trial. A failed antipsychotic course in a patient diagnosed with Alzheimer’s dementia could indicate that the diagnosis is incorrect.
Fluctuating cognition occurs in 50% to 75% of Lewy body cases. Alertness, attention, and concentration are variable and can cycle within hours to weeks. The patient often is fairly interactive and social for a time, then has periods of diminished function and being “out of it.” Some patients have recurrent delirium and undergo multiple workups in search of a cause.
EPS. As many as 75% of Lewy body patients have parkinsonian motor features.4 Because these features are not essential to the diagnosis, their absence is the most common reason Lewy body dementia goes unrecognized.1
Motor involvement varies and can be worsened by antipsychotics. Overuse of antipsychotics in Alzheimer’s or vascular dementia also can cause motor symptoms that mimic Lewy body features.
EPS orientation tends to be axial, showing less facial expressivity and more postural imbalance. Peripheral signs such as tremor and extremity rigidity tend to be less dominant.
MAKING THE DIAGNOSIS
Vascular and Lewy body dementia diagnoses are primarily based on clinical features and findings. Memory loss is necessary for either diagnosis.
Vascular dementia. Most consensus criteria require presence of dementia, physical or radiologic signs of a stroke, and a temporal relationship between the stroke and the dementia for a vascular dementia diagnosis.
Hachinski’s “ischemia scale” can help differentiate multi-infarct from Alzheimer’s dementia.5 Cases are scored on a 0-to-9 scale, with point values for abrupt onset; stepwise course; history of stroke; and presence of somatic complaints, emotional lability, hypertension, and focal neurologic signs. A score ≥4 suggests vascular dementia.
The scale, however, does not account for imaging studies, vascular risk factors other than hypertension, or repeated silent strokes that can cause symptoms. Also, some patients who score below the cutoff have strategic infarct dementias.
Lewy body dementia. Clinical consensus guidelines developed by McKeith et al6 can help clinicians recognize and categorize this dementia type (Table 2). Several studies of diagnostic criteria have shown very good specificity but variable sensitivity.7 Because no standard imaging modalities or serum markers exist, presence of progressive memory loss, fluctuating cognition, visual hallucinations, and EPS should drive the diagnosis.
Lewy body dementia is commonly misdiagnosed as Parkinson’s dementia. The two types are readily differentiated by onset of memory loss, which emerges late in Parkinson’s dementia but is early and prominent in Lewy body dementia.
CASE CONTINUED: HISTORY LEADS TO DIAGNOSIS
Ms. Z was diagnosed as having Lewy body dementia, as her cognitive decline clearly preceded her motor deficits. Further questioning revealed fluctuating attention levels and a history of visual hallucinations.
TESTING PATIENT FUNCTION
Neuropsychiatric tests. DSM-IV recommends testing memory, orientation, language, praxis, constructional ability, and executive control function in patients with dementia. Numerous tests can aid in diagnosis, but they generally are too lengthy to be practical. The MMSE takes 5 to 10 minutes, but it might miss mild memory loss or executive dysfunction.
Giving a quick clock-drawing test in tandem with the MMSE can help measure basic executive control and constructional ability. Also, patients with Lewy body or vascular dementia often are more proficient than patients with Alzheimer’s dementia on verbal memory tests but less proficient on visuospatial performance. Consider referring clinically challenging patients for more-extensive neuropsychiatric testing.
Lab tests. Blood tests including TSH and B12/folate screens are usually performed but rarely positive. Rapid plasma reagin testing for syphilis is no longer recommended unless syphilis is suspected.
Table 3
Potential cognitive side effects associated with psychotropic classes*
| Drug class | Potential cognitive side effects |
|---|---|
| Antidepressants Tricyclics, SSRIs, SNRIs | Confusion, sedation, falls |
| Antihistamines | Confusion, sedation, dizziness |
| Antipsychotics | Sedation, fatigue, anxiety |
| Antispasmodics | Confusion, sedation |
| Benzodiazepines | Sedation, confusion, ataxia, depression |
| Opioids | Sedation, confusion, dizziness |
| Sleep-promoting agents | Amnesia, confusion, ataxia |
| * Not all agents in each class are associated with listed side effects | |
| SSRIs: Selective serotonin reuptake inhibitors | |
| SNRIs: Serotonin-norepinephrine reuptake inhibitors | |
Radiologic imaging. Radiologic imaging (MRI or CT) can show infarcts in vascular dementia and can rule out:
- a brain tumor
- a subdural hemorrhage after recent head trauma
- or normal-pressure hydrocephalus in patients with dementia, gait instability, and/or urinary incontinence.
Brain imaging in Lewy body dementia can show hippocampal preservation8 but is not specific and does not significantly support the diagnosis. Specialized tests such as single-photon emission computed tomography or positron-emission tomography show occipital hypoperfusion9 but are expensive, not sufficiently specific, and do not add substantial value over clinical criteria.
MANAGING SYMPTOMS
Medication may be necessary if the patient is frequently and significantly agitated. Consider prescribing a selective serotonin reuptake inhibitor, an anticonvulsant such as divalproex or carbamazepine as a mood stabilizer, or a short-acting benzodiazepine. Start low and titrate slowly if needed.
Find out if the patient is taking medications that may be causing bothersome side effects. Avoid agents with potential cognitive or anticholinergic effects (Table 3); the latter can cause confusion, sedation, and falls in the elderly.
Cholinesterase inhibitors, FDA-approved for use in Alzheimer’s dementia, have been shown to reduce cognitive and global functioning decline in vascular dementia.10 A cholinergic deficit present in vascular dementia may explain the drugs’ effectiveness. Donepezil, galantamine, and rivastigmine have all shown positive effects on cognition.
Because patients with Lewy body hallucinations have greater synaptic acetylcholine deficits, cholinesterase inhibitors tend to be more effective in Lewy body dementia than in other dementia subtypes. In small open-label studies, patients taking cholinesterase inhibitors for Lewy body dementia have shown sustained improvements (up to 96 months) in cognition and behavior. Wild et al,11 however, concluded that the evidence supporting use of these agents—specifically rivastigmine—is weak.
Also, cholinesterase inhibitors offer fairly modest effectiveness, do not work for all patients, and do not prevent cognitive decline even when taken regularly. Because cholinesterase inhibitors are costly and most Medicare patients lack prescription medication coverage, an initial short (6-month) trial is recommended. Re-evaluate the patient periodically by using caregiver reports, caregiver assessment scales, and basic cognitive testing.
Cholinesterase inhibitor dosing is the same for vascular and Lewy body dementia as it is for Alzheimer’s disease. Tell patients to take the agents with food to minimize potential intestinal side effects.
Memantine. In European studies, memantine has shown positive effects on cognition and function in vascular dementia. Memantine, a N-methyl-D-aspartate receptor antagonist, is FDA-approved for moderate to severe Alzheimer’s dementia.12
DELAYING DECLINE
Controlling risk factors. Controlling vascular risk factors—especially high blood pressure—is the most effective way to prevent or treat vascular dementia. In primary prevention studies, patients with good hypertension and hyperlipidemia control developed dementia more slowly than did nontreated cohorts.
In patients with coronary artery disease, statins have been shown to lower cholesterol and stabilize pre-existing plaques in the arterial wall, reducing the risk of plaque rupture. Low-density lipoproteincholesterol goals vary according to vascular risk factors but should be <100 mg/dL for patients with vascular dementia, who are at highest risk. Blood pressure goals are ≤140 mm Hg (systolic) and ≤90 mm Hg (diastolic).
Glycemic control (fasting blood glucose <110 mg/dL) and smoking cessation can also reduce the risk of further vascular events. Most patients should be taking an antiplatelet medication, preferably aspirin, to reduce clotting risk.
Although Lewy body dementia has no known risk factors other than age, research will determine whether vascular or other factors contribute to its development.
CASE CONTINUED: TARGETING AGGRESSION
Ms. Z was given divalproex, 250 mg bid, to reduce her frequent aggression. Her visual hallucinations were considered mild and not problematic and therefore were not treated. She responded well to the medication, allowing her to remain in day care and avoid nursing home placement.
Related resources
- Alzheimer’s Association. http://www.alz.org
- American Geriatrics Society. http://www.americangeriatrics.org
Drug brand names
- Carbamazepine • Tegretol, others
- Carbidopa/Levodopa • Various
- Divalproex • Depakote
- Donepezil • Aricept
- Galantamine • Reminyl
- Hydrocodone/acetaminophen • Vicodin, others
- Lisinopril/hydrochlorothiazide • Prinzide, Zestoretic
- Memantine • Namenda
- Risperdone • Risperdal
- Rivastigmine • Exelon
Disclosure
Dr. Bartz is a speaker for Forest Pharmaceuticals and Novartis Pharmaceuticals Corp.
Primary care doctors refer patients with dementia to psychiatrists when the diagnosis or disease course is unclear. Psychiatrists thus must often discern non-Alzheimer’s dementias— particularly the vascular and Lewy body types— from Alzheimer’s dementia. This article describes:
- features that distinguish vascular, Lewy body, and Alzheimer’s dementias
- cognitive and medical tests to help determine dementia type and facilitate treatment
- risk factors that promote cognitive and functional decline
- strategies for using medication while minimizing side-effect risks.
CASE REPORT: DISRUPTIVE IN DAY CARE
Ms. Z, age 82, is referred to a psychiatrist after numerous failed attempts by her primary care physician to stop her medical and psychiatric deterioration.
Table 1
Estimated dementia type prevalence among patients with dementia
| Dementia type | Prevalence |
|---|---|
| Alzheimer's | 65% |
| Lewy body | 0-15% |
| Vascular | 10-15% |
| Mixed | 10-15% |
| Source: reference 1 | |
The patient was functioning well at home until 6 months ago, when her husband’s death triggered a dramatic functional decline. She has Parkinson’s disease and has had dementia symptoms for 3 years, but family members do not recall a dementia diagnosis.
Ms. Z has become increasingly disruptive in day care; she yelled at and slapped a staff member during one episode. Her son is concerned that additional outbursts will prompt her dismissal. Her Mini-Mental State Examination (MMSE) score is 19, indicating moderate dementia.
Donepezil, 10 mg/d across 2 years, has not slowed Ms. Z’s memory decline. Carbidopa/levadopa, 25/250 mg tid over 1 year, has not improved her Parkinson’s symptoms. Risperidone, 0.5 mg bid, caused marked sedation and unsteady gait and was stopped after 4 weeks. She also is taking hydrocodone/acetaminophen, 5/500 mg/d for osteoarthritis, and lisinopril/hydrochlorothiazide, 10/12.5 mg/d for hypertension.
Discussion. As with Ms. Z, a significant other can mask a dementia patient’s cognitive deficits, but these deficits become apparent after the partner dies. Family members then discover that a parent or sibling cannot function independently.
Treatment should target Ms. Z’s aggression to allow her to stay in day care and her son to care for her at home. Determining the dementia type is crucial to planning treatment and preserving function.
WHICH DEMENTIA IS WHICH?
Non-Alzheimer’s dementias account for up to 35% of dementia cases (Table 1).1 The pathologic correlations separating Alzheimer’s, vascular, and Lewy body dementias are often confusing:
- Beta-amyloid plaques are common in Alzheimer’s and Lewy body dementias, although neurofibrillary tangles are much less common in the Lewy body type.
- Synaptic cholinergic deficiencies are seen in Alzheimer’s and vascular dementias.
- Hypertension and hyperlipidemia—both traditional vascular risk factors—also appear to contribute to Alzheimer’s dementia.
Vascular dementia. Large, single-vessel hemispheric infarcts cause substantial damage, whereas multiple small vascular lesions (such as lacunae or mini-infarcts) can have more-subtle effects when strategically located, such as in the basal ganglia, hippocampus, or thalamus. These smaller lesions can disrupt frontal cortical-subcortical neural pathways and contribute to difficulties with executive functions (judgment, insight), emotional control, and behavior.
Lesions from a cerebrovascular accident, however, do not necessarily cause dementia, and the mechanism by which lesions cause dementia is not fully understood. Post-stroke dementia sometimes is progressive, suggesting a degenerative rather than vascular cause.
Lewy body dementia is associated with Parkinson’s disease, as Lewy body inclusion deposits are common to both disorders. The deposits typically appear in the cerebral cortex in Lewy body dementia but not in Parkinson’s.
Amyloid protein deposits alter the clinical presentation. Patients with these lesions have fewer visual hallucinations and motor problems, making diagnosis more difficult.
Lewy body dementia, like all major dementias, usually surfaces after age 75. Its clinical course generally is considered worse than that of Alzheimer’s dementia, but these two dementia types do not differ substantially in age of onset, age of death, or survival rates.
Table 2
Clinical features that characterize Lewy body dementia
| Central | Progressive cognitive decline that interferes with normal social and occupational function; deficits on tests of attention, frontal-subcortical skills, and visuospatial ability can be especially prominent |
| Core | Two of three needed for probable diagnosis:
|
| Supportive | Repeated falls Syncope Transient loss of consciousness REM sleep behavior disorder Systematized delusions Hallucinations in other modalities Neuroleptic sensitivity Depression |
| Features less likely to be present | History of stroke Another physical illness or brain disorder that interferes with cognitive performance |
| Source: reference 6 | |
FEATURES OF VASCULAR DEMENTIA
Onset can be gradual but is more often sudden— usually occurring shortly after an ischemic stroke. Disease progression can be gradual or dramatic, depending on the vascular event type. Cognitive and physical decline in vascular dementia usually is stepwise over time, whereas decline in Alzheimer’s dementia is more gradual with progressive severity.
Patients with vascular dementia classically present with memory loss temporally associated with other typical stroke stigmata. Brain imaging often uncovers evidence of stroke that is otherwise not clinically evident.
CNS manifestations of vascular dementia often include memory loss, emotional lability (including depression), and executive-task dysfunction. Patients usually have atrial fibrillation or vascular risk factors, including diabetes mellitus, hypertension, hyperlipidemia, obesity, or tobacco use. Patients with previous stroke, coronary artery disease, or peripheral vascular disease are at increased risk.
Vascular dementia is categorized by stroke type:
Embolic infarct. Emboli, typically cardiac in origin, can occlude small or large cerebral arteries, resulting in correspondingly sized infarcts. Atrial fibrillation can promote areas in the atria with relatively low flow turbulence. Blood clots can form that eventually embolize via the carotid arteries. Multiple emboli can occur, causing progressive dementia.
Cerebral hemorrhage —small or large—can be devastating. Hypertension is the major risk factor for this form of stroke.
Multi-infarct dementia. Multiple cerebral blood vessel infarcts classically lead to stepwise functional decline after each event. Multiple small infarcts can occur in various brain regions, including the cortex and basal ganglia. Binswanger’s disease, a variant of vascular dementia in which incomplete ischemia is limited to the hemispheric white matter, tends to be fairly progressive.2
Small-vessel disease. Reduced blood flow and tissue perfusion can cause small-vessel disease. Often the ischemia is “silent,” detectable only on MRI or CT. The infarcts typically cause lacunar lesions, nerve demyelination, and gliosis.3 These can occur to some extent in nondemented patients but become significant with more-extensive disease.
FEATURES OF LEWY BODY DEMENTIA
As with all dementias, permanent memory loss must be present to diagnose this dementia sub-type. Overall cognitive deficits may be more prominent than memory loss, however. The patient may have trouble performing cognitive tasks that employ visuospatial abilities, executive functions, and attention. Neuropsychiatric symptoms that overlap with Alzheimer’s dementia include apathy, anxiety, agitation, depression, anhedonia, and paranoia.
The presence of visual hallucinations, fluctuating cognition, or extrapyramidal symptoms (EPS) distinguish Lewy body from Alzheimer’s dementia.
Visual hallucinations are prominent in Lewy body dementia and often prompt psychiatric referral (Table 2). They usually surface early in the disease course and tend to persist. Other sensory hallucinations also can occur.
The hallucinations often are detailed and vivid and the patient may be aware they are occurring, especially if the dementia is not advanced. Treatment might not be necessary for mild hallucinations, which can concern the caregiver more than the patient.
Antipsychotics paradoxically worsen hallucinations in Lewy body dementia, and many patients present to psychiatrists after failing an empiric trial. A failed antipsychotic course in a patient diagnosed with Alzheimer’s dementia could indicate that the diagnosis is incorrect.
Fluctuating cognition occurs in 50% to 75% of Lewy body cases. Alertness, attention, and concentration are variable and can cycle within hours to weeks. The patient often is fairly interactive and social for a time, then has periods of diminished function and being “out of it.” Some patients have recurrent delirium and undergo multiple workups in search of a cause.
EPS. As many as 75% of Lewy body patients have parkinsonian motor features.4 Because these features are not essential to the diagnosis, their absence is the most common reason Lewy body dementia goes unrecognized.1
Motor involvement varies and can be worsened by antipsychotics. Overuse of antipsychotics in Alzheimer’s or vascular dementia also can cause motor symptoms that mimic Lewy body features.
EPS orientation tends to be axial, showing less facial expressivity and more postural imbalance. Peripheral signs such as tremor and extremity rigidity tend to be less dominant.
MAKING THE DIAGNOSIS
Vascular and Lewy body dementia diagnoses are primarily based on clinical features and findings. Memory loss is necessary for either diagnosis.
Vascular dementia. Most consensus criteria require presence of dementia, physical or radiologic signs of a stroke, and a temporal relationship between the stroke and the dementia for a vascular dementia diagnosis.
Hachinski’s “ischemia scale” can help differentiate multi-infarct from Alzheimer’s dementia.5 Cases are scored on a 0-to-9 scale, with point values for abrupt onset; stepwise course; history of stroke; and presence of somatic complaints, emotional lability, hypertension, and focal neurologic signs. A score ≥4 suggests vascular dementia.
The scale, however, does not account for imaging studies, vascular risk factors other than hypertension, or repeated silent strokes that can cause symptoms. Also, some patients who score below the cutoff have strategic infarct dementias.
Lewy body dementia. Clinical consensus guidelines developed by McKeith et al6 can help clinicians recognize and categorize this dementia type (Table 2). Several studies of diagnostic criteria have shown very good specificity but variable sensitivity.7 Because no standard imaging modalities or serum markers exist, presence of progressive memory loss, fluctuating cognition, visual hallucinations, and EPS should drive the diagnosis.
Lewy body dementia is commonly misdiagnosed as Parkinson’s dementia. The two types are readily differentiated by onset of memory loss, which emerges late in Parkinson’s dementia but is early and prominent in Lewy body dementia.
CASE CONTINUED: HISTORY LEADS TO DIAGNOSIS
Ms. Z was diagnosed as having Lewy body dementia, as her cognitive decline clearly preceded her motor deficits. Further questioning revealed fluctuating attention levels and a history of visual hallucinations.
TESTING PATIENT FUNCTION
Neuropsychiatric tests. DSM-IV recommends testing memory, orientation, language, praxis, constructional ability, and executive control function in patients with dementia. Numerous tests can aid in diagnosis, but they generally are too lengthy to be practical. The MMSE takes 5 to 10 minutes, but it might miss mild memory loss or executive dysfunction.
Giving a quick clock-drawing test in tandem with the MMSE can help measure basic executive control and constructional ability. Also, patients with Lewy body or vascular dementia often are more proficient than patients with Alzheimer’s dementia on verbal memory tests but less proficient on visuospatial performance. Consider referring clinically challenging patients for more-extensive neuropsychiatric testing.
Lab tests. Blood tests including TSH and B12/folate screens are usually performed but rarely positive. Rapid plasma reagin testing for syphilis is no longer recommended unless syphilis is suspected.
Table 3
Potential cognitive side effects associated with psychotropic classes*
| Drug class | Potential cognitive side effects |
|---|---|
| Antidepressants Tricyclics, SSRIs, SNRIs | Confusion, sedation, falls |
| Antihistamines | Confusion, sedation, dizziness |
| Antipsychotics | Sedation, fatigue, anxiety |
| Antispasmodics | Confusion, sedation |
| Benzodiazepines | Sedation, confusion, ataxia, depression |
| Opioids | Sedation, confusion, dizziness |
| Sleep-promoting agents | Amnesia, confusion, ataxia |
| * Not all agents in each class are associated with listed side effects | |
| SSRIs: Selective serotonin reuptake inhibitors | |
| SNRIs: Serotonin-norepinephrine reuptake inhibitors | |
Radiologic imaging. Radiologic imaging (MRI or CT) can show infarcts in vascular dementia and can rule out:
- a brain tumor
- a subdural hemorrhage after recent head trauma
- or normal-pressure hydrocephalus in patients with dementia, gait instability, and/or urinary incontinence.
Brain imaging in Lewy body dementia can show hippocampal preservation8 but is not specific and does not significantly support the diagnosis. Specialized tests such as single-photon emission computed tomography or positron-emission tomography show occipital hypoperfusion9 but are expensive, not sufficiently specific, and do not add substantial value over clinical criteria.
MANAGING SYMPTOMS
Medication may be necessary if the patient is frequently and significantly agitated. Consider prescribing a selective serotonin reuptake inhibitor, an anticonvulsant such as divalproex or carbamazepine as a mood stabilizer, or a short-acting benzodiazepine. Start low and titrate slowly if needed.
Find out if the patient is taking medications that may be causing bothersome side effects. Avoid agents with potential cognitive or anticholinergic effects (Table 3); the latter can cause confusion, sedation, and falls in the elderly.
Cholinesterase inhibitors, FDA-approved for use in Alzheimer’s dementia, have been shown to reduce cognitive and global functioning decline in vascular dementia.10 A cholinergic deficit present in vascular dementia may explain the drugs’ effectiveness. Donepezil, galantamine, and rivastigmine have all shown positive effects on cognition.
Because patients with Lewy body hallucinations have greater synaptic acetylcholine deficits, cholinesterase inhibitors tend to be more effective in Lewy body dementia than in other dementia subtypes. In small open-label studies, patients taking cholinesterase inhibitors for Lewy body dementia have shown sustained improvements (up to 96 months) in cognition and behavior. Wild et al,11 however, concluded that the evidence supporting use of these agents—specifically rivastigmine—is weak.
Also, cholinesterase inhibitors offer fairly modest effectiveness, do not work for all patients, and do not prevent cognitive decline even when taken regularly. Because cholinesterase inhibitors are costly and most Medicare patients lack prescription medication coverage, an initial short (6-month) trial is recommended. Re-evaluate the patient periodically by using caregiver reports, caregiver assessment scales, and basic cognitive testing.
Cholinesterase inhibitor dosing is the same for vascular and Lewy body dementia as it is for Alzheimer’s disease. Tell patients to take the agents with food to minimize potential intestinal side effects.
Memantine. In European studies, memantine has shown positive effects on cognition and function in vascular dementia. Memantine, a N-methyl-D-aspartate receptor antagonist, is FDA-approved for moderate to severe Alzheimer’s dementia.12
DELAYING DECLINE
Controlling risk factors. Controlling vascular risk factors—especially high blood pressure—is the most effective way to prevent or treat vascular dementia. In primary prevention studies, patients with good hypertension and hyperlipidemia control developed dementia more slowly than did nontreated cohorts.
In patients with coronary artery disease, statins have been shown to lower cholesterol and stabilize pre-existing plaques in the arterial wall, reducing the risk of plaque rupture. Low-density lipoproteincholesterol goals vary according to vascular risk factors but should be <100 mg/dL for patients with vascular dementia, who are at highest risk. Blood pressure goals are ≤140 mm Hg (systolic) and ≤90 mm Hg (diastolic).
Glycemic control (fasting blood glucose <110 mg/dL) and smoking cessation can also reduce the risk of further vascular events. Most patients should be taking an antiplatelet medication, preferably aspirin, to reduce clotting risk.
Although Lewy body dementia has no known risk factors other than age, research will determine whether vascular or other factors contribute to its development.
CASE CONTINUED: TARGETING AGGRESSION
Ms. Z was given divalproex, 250 mg bid, to reduce her frequent aggression. Her visual hallucinations were considered mild and not problematic and therefore were not treated. She responded well to the medication, allowing her to remain in day care and avoid nursing home placement.
Related resources
- Alzheimer’s Association. http://www.alz.org
- American Geriatrics Society. http://www.americangeriatrics.org
Drug brand names
- Carbamazepine • Tegretol, others
- Carbidopa/Levodopa • Various
- Divalproex • Depakote
- Donepezil • Aricept
- Galantamine • Reminyl
- Hydrocodone/acetaminophen • Vicodin, others
- Lisinopril/hydrochlorothiazide • Prinzide, Zestoretic
- Memantine • Namenda
- Risperdone • Risperdal
- Rivastigmine • Exelon
Disclosure
Dr. Bartz is a speaker for Forest Pharmaceuticals and Novartis Pharmaceuticals Corp.
1. McKeith JG, Ballard CG, Perry RH, et al. Prospective validation of consensus criteria for the diagnosis of dementia with Lewy bodies. Neurology 2000;54:1050-8.
2. Roman GC, Erkinjuntti T, Wallin A, et al. Subcortical ischemic vascular dementia. Lancet Neurol 2002;17:426-36.
3. Pohjasraara T, Mantyla R, Ylikoski MA, et al. Comparison of different clinical criteria (DSM-III, ADDTC, ICD-10, NINDS-AIREN, DSM-IV) for the diagnosis of vascular dementia. Stroke 2000;31:2952-7.
4. Del Ser T, McKeith I, Anand R, et al. Dementia with Lewy bodies: findings from an international multicenter study. Int J Geriatr Psychiatry 2000;15:1034-45.
5. Hachinski VC, Iliff LD, Zilhka E, et al. Cerebral blood flow in dementia. Arch Neurol 1975;32:632-7.
6. McKeith IG, Galasko D, Kosaka K, et al. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the consortium on DLB international workshop. Neurology 1996;47:1113-24.
7. Luis CA, Barker WW, Gajaraj K, et al. Sensitivity and specificity of three clinical criteria for dementia with Lewy bodies in an autopsy-verified sample. Int J Geriatr Psychiatry 1999;14:526-33.
8. Barber R, Ballard C, McKeith IG, et al. MRI volumetric study of dementia with Lewy bodies: a comparison with AD and vascular dementia. Neurology 2000;54:1304-9.
9. Lobotesis K, Fenwick JD, Phipps A, et al. Occipital hypoperfusion on SPECT in dementia with Lewy bodies but not AD. Neurology 2001;56:643-9.
10. Pratt RD, Perdomo CA. Results of clinical studies with donepezil in vascular dementia. Am J Geriatr Psychiatry 2002;10(suppl 1):88-9.
11. Wild R, Pettit T, Burns A. Cholinesterase inhibitors for dementia with Lewy bodies. Cochrane Database Syst Rev 2003;3:CD003672.-
12. Tariot PN, Farlow MR, Grossberg GT, et al. Memantine treatment in patients with moderate to severe Alzheimer disease already receiving donepezil: a randomized controlled trial. JAMA 2004;291:317-24.
1. McKeith JG, Ballard CG, Perry RH, et al. Prospective validation of consensus criteria for the diagnosis of dementia with Lewy bodies. Neurology 2000;54:1050-8.
2. Roman GC, Erkinjuntti T, Wallin A, et al. Subcortical ischemic vascular dementia. Lancet Neurol 2002;17:426-36.
3. Pohjasraara T, Mantyla R, Ylikoski MA, et al. Comparison of different clinical criteria (DSM-III, ADDTC, ICD-10, NINDS-AIREN, DSM-IV) for the diagnosis of vascular dementia. Stroke 2000;31:2952-7.
4. Del Ser T, McKeith I, Anand R, et al. Dementia with Lewy bodies: findings from an international multicenter study. Int J Geriatr Psychiatry 2000;15:1034-45.
5. Hachinski VC, Iliff LD, Zilhka E, et al. Cerebral blood flow in dementia. Arch Neurol 1975;32:632-7.
6. McKeith IG, Galasko D, Kosaka K, et al. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the consortium on DLB international workshop. Neurology 1996;47:1113-24.
7. Luis CA, Barker WW, Gajaraj K, et al. Sensitivity and specificity of three clinical criteria for dementia with Lewy bodies in an autopsy-verified sample. Int J Geriatr Psychiatry 1999;14:526-33.
8. Barber R, Ballard C, McKeith IG, et al. MRI volumetric study of dementia with Lewy bodies: a comparison with AD and vascular dementia. Neurology 2000;54:1304-9.
9. Lobotesis K, Fenwick JD, Phipps A, et al. Occipital hypoperfusion on SPECT in dementia with Lewy bodies but not AD. Neurology 2001;56:643-9.
10. Pratt RD, Perdomo CA. Results of clinical studies with donepezil in vascular dementia. Am J Geriatr Psychiatry 2002;10(suppl 1):88-9.
11. Wild R, Pettit T, Burns A. Cholinesterase inhibitors for dementia with Lewy bodies. Cochrane Database Syst Rev 2003;3:CD003672.-
12. Tariot PN, Farlow MR, Grossberg GT, et al. Memantine treatment in patients with moderate to severe Alzheimer disease already receiving donepezil: a randomized controlled trial. JAMA 2004;291:317-24.
Treatment-resistant schizophrenia: What role for mood stabilizers?
In patients with treatment-resistant schizophrenia, lithium and anticonvulsants have become such common adjuncts to antipsychotics that 50% of inpatients may be receiving them.1 Evidence supporting this practice is mixed:
- Initial case reports and open-label studies that showed benefit have not always been followed by randomized clinical trials.
- Lack of clear benefit also has been described (Table 1).
This article examines the extent of this prescribing pattern, its evidence base, and mechanisms of action that may help explain why some adjunctive mood stabilizers are more effective than others for treatment-resistant schizophrenia.
EXTENT OF USE
For 5 years, the rate at which inpatients with schizophrenia received adjunctive mood stabilizers has held steady at approximately 50% in New York State Office of Mental Health (NYSOMH) facilities (Figure1). These facilities provide intermediate and long-term care for the seriously, persistently mentally ill. Adjunctive mood stabilizers might not be used as often for outpatients or for inpatients treated in short-stay facilities.
Table 1
Evidence for adjunctive use of lithium or anticonvulsants for treating schizophrenia
| Agent | Case reports and open studies | Randomized, double-blind trials | Benefit? |
|---|---|---|---|
| Lithium | Yes (many) | Yes (several, +/-) | Probably not |
| Carbamazepine | Yes (many) | Yes (several; small total sample) | Limited |
| Valproate | Yes (many) | Yes | Yes |
| Gabapentin | Yes (very few, +/-) | None | Probably not |
| Lamotrigine | Yes (few, +/-) | Yes (2, +) | Yes |
| Topiramate | Yes (very few, +/-) | Yes (1, +/-) | Probably not |
| Oxcarbazepine | Yes (very few, +/-) | None | Probably not |
| + = positive results | |||
| - = negative results | |||
| +/- = both positive and negative results | |||
Valproate is the most commonly used anticonvulsant, with one out of three patients with schizophrenia receiving it. Adjunctive gabapentin use is declining, probably because of inadequate efficacy—as will be discussed later. Use of adjunctive lamotrigine is expected to increase as more data become available on its usefulness in treatment-resistant schizophrenia.
Clinicians are using substantial dosages of adjunctive mood stabilizers. During first-quarter 2004, average daily dosages for 4,788 NYSOMH patients (80% with schizophrenia or schizoaffective disorder) receiving antipsychotics were:
- valproate, 1639 mg (n = 1921)
- gabapentin, 1524 mg (n = 303)
- oxcarbazepine, 1226 mg (n = 201)
- carbamazepine, 908 mg (n = 112)
- lithium, 894 mg (n = 715)
- topiramate, 234 mg (n = 269)
- lamotrigine, 204 mg (n = 231).2
Mood-stabilizer combinations were also used. Approximately one-half of patients receiving adjunctive mood stabilizers—with the exception of valproate—were receiving more than one. In patients receiving valproate, the rate of mood-stabilizer co-prescribing was about 25%.2
WHAT IS THE EVIDENCE?
Evidence supporting the use of adjunctive lithium or anticonvulsants to treat schizophrenia varies in quality and quantity (Table 1). Case reports and open studies offer the weakest evidence but can spur double-blind, randomized clinical trials (RCTs). Unfortunately, RCTs are not often done, and the published studies usually suffer from methodologic flaws such as:
- inadequate number of subjects (insufficient statistical power to detect differences)
- lack of control of confounds such as mood symptoms (seen when studies include patients with schizoaffective disorder)
- inadequate duration
- inappropriate target populations (patients with acute exacerbations of schizophrenia instead of persistent symptoms in treatment-resistant schizophrenia).
Because controlled trials of the use of adjunctive mood stabilizers are relatively scarce, clinical practice has transcended clinical research. Clinicians need effective regimens for treatment-resistant schizophrenia, and mood-stabilizer augmentation helps some patients.
Lithium is perhaps the best-known mood stabilizer. Although early studies showed adjunctive lithium useful in treating schizophrenia, later and better-designed trials did not. The authors of a recent meta-analysis of randomized clinical trials (n = 611 in 20 studies) concluded that despite some evidence supporting the efficacy of lithium augmentation, overall results were inconclusive. A large trial would be required to detect a small benefit in patients with schizophrenia who lack affective symptoms.3
Carbamazepine use among patients with schizophrenia is declining, primarily because this drug induces its own metabolism and can require frequent dose adjustments. Adjunctive carbamazepine has been used to manage persistent aggressive behavior in patients with schizophrenia and schizoaffective disorder. Evidence comes primarily from small trials or case reports (Table 2),4-8 but results of a larger clinical trial (n = 162) by Okuma et al6 are also available
In the Okuma report—a double-blind, placebo-controlled trial of carbamazepine in patients with DSM-III schizophrenia or schizoaffective disorder—carbamazepine did not significantly improve patients’ total Brief Psychiatric Rating Scale (BPRS) scores. Compared with placebo, however, some benefit with carbamazepine did emerge in measures of suspiciousness, uncooperativeness, and excitement.
A systematic review and meta-analysis (n = 283 in 10 studies) detected a trend toward reduced psychopathology with carbamazepine augmentation for schizophrenia. BPRS scores declined by 20% and 35% in the six trials (n = 147) for which data were available (P = 0.08 and 0.09, respectively).9 Because the double-blind trial by Okuma et al6 was not randomized, it was not included in this meta-analysis.9
Figure 1 10-year trend in use of adjunctive mood stabilizers for schizophrenia

Valproate. Among the anticonvulsants, the greatest body of evidence supports the use of valproate in patients with schizophrenia,10 although a recent meta-analysis (n = 378 in 5 studies) indicates inconsistent beneficial effects.11
Initial double-blind, RCTs of adjunctive valproate in patients with schizophrenia were limited in size and failed to show benefit with adjunctive valproate12-15 (Table 2). A more recent study16 showed that adjunctive valproate affects acute psychotic symptoms rather than mood. This study, however, did not answer whether adjunctive valproate would help patients with persistent symptoms of schizophrenia.
Table 2
Double-blind studies of adjunctive carbamazepine in schizophrenia
| Author (yr) | n | Duration (days) | Design | Diagnosis | Outcome |
|---|---|---|---|---|---|
| Neppe (1983) | 11 | 42 | Crossover | Mixed, 8 with schizophrenia | “Overall clinical rating” improved |
| Dose et al (1987) | 22 | 28 | HAL + CBZ vs HAL + placebo | Schizophrenia or schizoaffective disorder | No difference on BPRS |
| Okuma et al (1989) | 162 | 28 | NL + CBZ vs NL + placebo | Schizophrenia or schizoaffective disorder | No difference on BPRS; possible improvement in suspiciousness, uncooperativeness, and excitement |
| Nachshoni et al (1994) | 28 | 49 | NL + CBZ vs NL + placebo | “Residual schizophrenia with negative symptoms” | No difference on BPRS or SANS |
| Simhandl et al (1996) | 42 | 42 | NL + CBZ vs NL + lithium vs NL + placebo | Schizophrenia(treatment- nonresponsive) | No difference on BPRS; CGI improved from baseline in groups receiving CBZ and lithium |
| n = number of subjects | |||||
| BPRS = Brief Psychiatric Rating Scale | |||||
| CGI = Clinical Global Impression scale | |||||
| CBZ = carbamazepine | |||||
| HAL = haloperidol | |||||
| NL = neuroleptic (first-generation antipsychotic) | |||||
| SANS = Scale for the Assessment of Negative Symptoms | |||||
In this large (n = 249), multicenter, randomized, double-blind trial, hospitalized patients with an acute exacerbation of schizophrenia received olanzapine or risperidone plus divalproex or placebo for 28 days. Patients with schizoaffective disorder and treatment-resistant schizophrenia were excluded.
By day 6, dosages reached 6 mg/d for risperidone and 15 mg/d for olanzapine. Divalproex was started at 15 mg/kg and titrated to a maximum of 30 mg/kg by day 14. Mean divalproex dosage was approximately 2300 mg/d (mean plasma level approximately 100 mg/mL).
Positive and Negative Syndrome Scale (PANSS) total scores improved significantly in patients receiving adjunctive divalproex compared with those receiving antipsychotic monotherapy, and significant differences occurred as early as day 3. The major effect was seen on schizophrenia’s positive symptoms. A post-hoc analysis17 also showed greater reductions in hostility (as measured by the hostility item in the PANSS Positive Subscale) in patients receiving adjunctive divalproex compared with antipsychotic monotherapy. This effect was independent of the effect on positive symptoms or sedation.
A large, multi-site, 84-day acute schizophrenia RCT similar to the 28-day trial—but using extended-release divalproex—is being conducted. An extended-release preparation may be particularly helpful in encouraging medication adherence for patients taking complicated medication regimens.
Table 3
Double-blind studies of adjunctive valproate in schizophrenia
| Author (yr) | n | Duration (days) | Design | Diagnosis | Outcome |
|---|---|---|---|---|---|
| Ko et al (1985) | 6 | 28 | Crossover | Neurolepticresistant patients with chronic schizophrenia, not exacerbation | No valproate effect noted |
| Fisk and York (1987) | 62 | 42 | Antipsychotic + valproate vs antipsychotic + placebo | Chronic psychosis and tardive dyskinesia | No differences in mental state and behavior, as measured by“ Krawiecka scale”* |
| Dose et al (1998) | 42 | 28 | HAL + valproate vs HAL + placebo | Acute, nonmanic schizophrenic or schizoaffective psychosis | No difference on BPRS; possible effect on “hostile belligerence” |
| Wassef et al (2000) | 12 | 21 | HAL + valproate vs HAL + placebo | Acute exacerbation of chronic schizophrenia | CGI and SANS scores improved significantly, but BPRS scores did not |
| Casey et al (2003) | 249 | 28 | RIS + valproate vs OLZ + valproate vs RIS + placebo vs OLZ + placebo | Acute exacerbation of schizophrenia | PANSS scores improved |
| * Krawiecka M, Goldberg D, Vaughan M. A standardized psychiatric assessment scale for rating chronic psychotic patients. Acta Psychiatr Scand 1977;55(4):299-308. | |||||
| n = number of subjects | |||||
| BPRS = Brief Psychiatric Rating Scale | |||||
| CGI = Clinical Global Impression scale | |||||
| HAL = haloperidol | |||||
| OLZ = olanzapine | |||||
| PANSS = Positive and Negative Syndrome Scale | |||||
| RIS = risperidone | |||||
| SANS = Scale for the Assessment of Negative Symptoms | |||||
In a recent large (n = 10,262), retrospective, pharmacoepidemiologic analysis,18 valproate augmentation led to longer persistence of treatment than did the strategy of switching antipsychotics. Average valproate dosages were small, however (<425 mg/d), as were antipsychotic dosages (risperidone <1.7 mg/d, quetiapine <120 mg/d, and olanzapine <7.5 mg/d). Patients’ diagnostic categories were not available. One interpretation of this study is that valproate augmentation would be more successful than switching antipsychotics, assuming that treatment persistence can be viewed as a positive outcome.
Table 4
Double-blind studies of adjunctive lamotrigine in schizophrenia
| Author (yr) | n | Duration (days) | Design | Diagnosis | Outcome |
|---|---|---|---|---|---|
| Tiihonen et al (2003) | 34 | 84 | Crossover; clozapine with or without lamotrigine | Clozapine-resistant male inpatients with chronic schizophrenia, not exacerbation | BPRS, PANSS positive, and PANSS general psychopathology symptom scores improved Negative symptoms did not improve |
| Kremer et al (2004) | 38 | 70 | Antipsychotic* + lamotrigine vs antipsychotic* + placebo | Treatment- resistant inpatients with schizophrenia | Completers’ PANSS positive, general psychopathology and total symptom scores improved No difference in negative symptoms or total BPRS scores No difference with intent-to-treat analyses |
| n = number of patients | |||||
| * First- or second-generation antipsychotic | |||||
| BPRS = Brief Psychiatric Rating Scale | |||||
| PANSS = Positive and Negative Syndrome Scale | |||||
Lamotrigine is the only other anticonvulsant for which published, double-blind, randomized evidence of use in patients with schizophrenia is available (Table 4).19,20 Adjunctive lamotrigine may be effective in managing treatment-resistant schizophrenia, as was shown in a small (n = 34), double-blind, placebo-controlled, crossover trial.19 Hospitalized patients whose symptoms were inadequately controlled with clozapine monotherapy received lamotrigine, 200 mg/d, for up to 12 weeks. Adjunctive lamotrigine improved positive but not negative symptoms.
Similar results were seen in treatment-resistant inpatients with schizophrenia (n = 38) in a 10-week, double-blind, parallel group trial by Kremer et al.20 Adjunctive lamotrigine improved PANSS positive, general psychopathology, and total symptom scores in the 31 patients who completed the trial. No differences were seen, however, in negative symptoms, total BPRS scores, or in the intent-to-treat analysis. These results have spurred the launch of a large, multi-site, RCT of adjunctive lamotrigine in patients with schizophrenia who have responded inadequately to antipsychotics alone.
Topiramate, one of the few psychotropics associated with weight loss, has attracted interest as an adjunct to second-generation antipsychotics to address weight gain. Although case reports have shown benefit,21 one showed deterioration in both positive and negative symptoms when topiramate was added to second-generation antipsychotics.22
Table 5
Double-blind study of adjunctive topiramate in schizophrenia
| Author (yr) | n | Duration (days) | Design | Diagnosis | Outcome |
|---|---|---|---|---|---|
| Tiihonen (2004)* | 26 | 84 | Crossover; SGA plus topiramate or placebo | Treatment- resistant male inpatients with chronic schizophrenia | PANSS general scores improved No difference in total PANSS, PANSS positive, or PANSS negative scores |
| * 2004 Collegium Internationale Neuro-Psychopharmacologicum (CINP) presentation, and personal communication (6/22/04) | |||||
| n = number of patients | |||||
| PANSS = Positive and Negative Syndrome Scale | |||||
| SGA = Second-generation antipsychotic (patients were taking clozapine, olanzapine, or quetiapine) | |||||
An unpublished, randomized, crossover trial compared second-generation antipsychotics plus topiramate or placebo in 26 male inpatients with chronic schizophrenia. With adjunctive topiramate, the authors found a statistically significant improvement in the PANSS general psychopathology subscale but not in PANSS total, positive subscale, or negative subscale scores (Table 5) (Tiihonen J, personal communication 6/22/04).
Other agents. Very little information—all uncontrolled—supports adjunctive use of gabapentin or oxcarbazepine for patients with schizophrenia.23-28 Of concern are reports of patients suffering worsening of psychosis with gabapentin25 or of dysphoria and irritability with oxcarbazepine (attributed to a pharmacokinetic interaction).26
Conclusion. More trials are needed to examine the use of adjunctive mood stabilizers in patients with schizophrenia—particularly in those with chronic symptoms. Although mood stabilizers are widely used in this population, important questions remain unanswered, including:
- characteristics of patients likely to require adjunctive treatment
- how long treatment should continue.
MECHANISMS OF ACTION
Unlike antipsychotics, mood stabilizers do not exert their therapeutic effects by acting directly on dopamine (D2) receptors. Differences in mechanism of action among the anticonvulsants may help explain why some—such as valproate and lamotrigine—have been useful for bipolar disorder or schizophrenia and others—such as gabapentin—have not.29
One possibility is that anticonvulsants that affect voltage-gated sodium channels—such as valproate, lamotrigine, carbamazepine and oxcarbazepine—may be most useful for patients with bipolar disorder or schizophrenia. On the other hand, agents that affect voltage-gated calcium channels—such as gabapentin—may be efficacious as anticonvulsants but not as efficacious for bipolar disorder or schizophrenia.
Ketter et al30 proposed an anticonvulsant classification system based on predominant psychotropic profiles:
- the “GABA-ergic” group predominantly potentiates the inhibitory neurotransmitter GABA, resulting in sedation, fatigue, cognitive slowing, and weight gain, as well as possible anxiolytic and antimanic effects
- the “anti-glutamate” group predominantly attenuates glutamate excitatory neurotransmission and is associated with activation, weight loss, and possibly anxiogenic and antidepressant effects.
In the GABA-ergic group are anticonvulsants such as barbiturates, benzodiazepines, valproate, gabapentin, tiagabine, and vigabatrin. The antiglutamate group includes agents such as felbamate and lamotrigine. A “mixed” category includes anticonvulsants with GABA-ergic and anti-glutaminergic actions such as topiramate, which has sedating and weight-loss properties.
Because GABA appears to modulate dopamine neurotransmission,31 this may explain valproate’s role as an adjunctive agent for schizophrenia. Similarly, mechanisms related to Nmethyl-D-aspartate (NMDA) and non-NMDA glutamate receptor function may explain lamotrigine’s usefulness in this setting.19,20
SUMMARY
Clinicians resort to combination therapies when monotherapies fail to adequately control symptoms or maintain response. Co-prescribing of anticonvulsants with antipsychotics for inpatients with schizophrenia is common practice in New York State and most likely elsewhere. In general, antipsychotics’ and mood stabilizers’ different—and perhaps complementary—mechanisms of action explain the synergism between them. Mechanisms of action also may explain why some anticonvulsants help in schizophrenia (or bipolar disorder) whereas others do not.
Evidence for using adjunctive anticonvulsants is variable. The strongest data support using valproate (and perhaps lamotrigine), followed by carbamazepine and then topiramate. Gabapentin and oxcarbazepine have only anecdotal evidence, some of it negative. Well-designed, randomized clinical trials with the appropriate populations are needed.
Related resources
- Stahl SM. Essential psychopharmacology of antipsychotics and mood stabilizers. New York: Cambridge University Press, 2002.
- Harvard Medical School Department of Psychiatry’s psychopharmacology algorithm project. Osser DN, Patterson RD. Consultant for the pharmacotherapy of schizophrenia. Available at http://mhc.com/Algorithms/. Accessed Nov. 5, 2004.
Drug brand names
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Lithium • Lithobid, Eskalith
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Topiramate • Topamax
- Valproate (valproic acid, divalproex sodium) • Depakene, Depakote
Disclosure
Dr. Citrome receives research grants/contracts from Abbott Laboratories, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb Co., Eli Lilly & Co., Janssen Pharmaceutica, and Pfizer Inc. He is a consultant to and/or speaker for Bristol-Myers Squibb Co., Eli Lilly & Co., Pfizer Inc., Abbott Laboratories, AstraZeneca Pharmaceuticals, and Novartis Pharmaceuticals Corp.
Acknowledgment
Adapted from Citrome L. “Antipsychotic polypharmacy versus augmentation with anticonvulsants: the U.S. perspective” (presentation). Paris: Collegium Internationale Neuro-Psychopharmacologicum (CINP), June 2004 [abstract in Int J Neuropsychopharmacol. 2004; 7(suppl 1):S69], and from Citrome L. “Mood-stabilizer use in schizophrenia: 1994-2002” (NR350) (poster). New York: American Psychiatric Association annual meeting, May 2004.
1. Citrome L, Jaffe A, Levine J. Datapoints - mood stabilizers: utilization trends in patients diagnosed with schizophrenia 1994-2001. Psychiatr Serv 2002;53(10):1212.-
2. Citrome L. Antipsychotic polypharmacy versus augmentation with anticonvulsants: the U.S.perspective (presentation). Paris: Collegium Internationale Neuro-Psychopharmacologicum(CINP), June 2004 [abstract in Int J Neuropsychopharmacol 2004;7(suppl 1):S69].
3. Leucht S, Kissling W, McGrath J. Lithium for schizophrenia revisited: a systematic review and meta-analysis of randomized clinical trials. J Clin Psychiatry 2004;65(2):177-86.
4. Neppe VM. Carbamazepine as adjunctive treatment in nonepileptic chronic inpatients with EEG temporal lobe abnormalities. J Clin Psychiatry 1983;44:326-31.
5. Dose M, Apelt S, Emrich HM. Carbamazepine as an adjunct of antipsychotic therapy. Psychiatry Res 1987;22:303-10.
6. Okuma T, Yamashita I, Takahashi R, et al. A double-blind study of adjunctive carbamazepine versus placebo on excited states of schizophrenic and schizoaffective disorders. Acta Psychiatr Scand 1989;80:250-9.
7. Nachshoni T, Levin Y, Levy A, et al. A double-blind trial of carbamazepine in negative symptom schizophrenia. Biol Psychiatry 1994;35(1):22-26.
8. Simhandl C, Meszaros K, Denk E, et al. Adjunctive carbamazepine or lithium carbonate in therapy-resistant chronic schizophrenia. Can J Psychiatry 1996;41(5):317.-
9. Leucht S, McGrath J, White P, et al. Carbamazepine augmentation for schizophrenia: how good is the evidence? J Clin Psychiatry 2002;63(3):218-24.
10. Citrome L. Schizophrenia and valproate. Psychopharmacol Bull 2003;37(suppl 2):74-88.
11. Basan A, Kissling W, Leucht S. Valproate as an adjunct to antipsychotics for schizophrenia: a systematic review of randomized trials. Schizophr Res 2004;70(1):33-7.
12. Ko GN, Korpi ER, Freed WJ, et al. Effect of valproic acid on behavior and plasma amino acid concentrations in chronic schizophrenia patients. Biol Psychiatry 1985;20:209-15.
13. Dose M, Hellweg R, Yassouridis A, et al. Combined treatment of schizophrenic psychoses with haloperidol and valproate. Pharmacopsychiatry 1998;31(4):122-5.
14. Fisk GG, York SM. The effect of sodium valproate on tardive dyskinesia—revisited. Br J Psychiatry 1987;150:542-6.
15. Wassef AA, Dott SG, Harris A, et al. Randomized, placebo-controlled pilot study of divalproex sodium in the treatment of acute exacerbations of chronic schizophrenia. J Clin Psychopharmacol 2000;20(3):357-361.
16. Casey DE, Daniel DG, Wassef AA, et al. Effect of divalproex combined with olanzapine or risperidone in patients with an acute exacerbation of schizophrenia. Neuropsychopharmacol 2003;28(1):182-92.
17. Citrome L, Casey DE, Daniel DG, et al. Effects of adjunctive valproate on hostility in patients with schizophrenia receiving olanzapine or risperidone: a double-blind multi-center study. Psychiatr Serv 2004;55(3):290-4.
18. Cramer JA, Sernyak M. Results of a naturalistic study of treatment options: switching atypical antipsychotic drugs or augmenting with valproate. Clin Ther 2004;26(6):905-14.
19. Tiihonen J, Hallikainen T, Ryynanen OP, et al. Lamotrigine in treatment-resistant schizophrenia: a randomized placebo-controlled trial. Biol Psychiatry 2003;54(11):1241-8.
20. Kremer I, Vass A, Gurelik I, et al. Placebo-controlled trial of lamotrigine added to conventional and atypical antipsychotics in schizophrenia. Biol Psychiatry 2004;56(6):441-6.
21. Drapalski AL, Rosse RB, Peebles RR, et al. Topiramate improves deficit symptoms in a patient with schizophrenia when added to a stable regimen of antipsychotic medication. Clin Neuropharmacol 2001;24:290-4.
22. Millson RC, Owen JA, Lorberg GW, Tackaberry L. Topiramate for refractory schizophrenia. Am J Psychiatry 2002;159(4):675.-
23. Chouinard G, Beauclair L, Belanger MC. Gabapentin: long term antianxiety and hypnotic effects in psychiatric patients with comorbid anxiety-related disorders. Can J Psychiatry 1998;43:305.-
24. Megna JL, Devitt PJ, Sauro MD, Dewan MJ. Gabapentin’s effect on agitation in severely and persistently mentally ill patients. Ann Pharmacother 2002;35:12-16.
25. Jablonowski K, Margolese HC, Chouinard G. Gabapentin-induced paradoxical exacerbation of psychosis in a patient with schizophrenia. Can J Psychiatry 2002;47(10):975-6.
26. Baird P. The interactive metabolism effect of oxcarbazepine coadministered with tricyclic antidepressant therapy for OCD symptoms. J Clin Psychopharmacol 2003;23(4):419.-
27. Centorrino F, Albert MJ, Berry JM, et al. Oxcarbazepine: clinical experience with hospitalized psychiatric patients. Bipolar Disord 2003;5(5):370-4.
28. Leweke FM, Gerth CW, Koethe D, et al. Oxcarbazepine as an adjunct for schizophrenia. Am J Psychiatry 2004;161(6):1130-1.
29. Stahl SM. Psychopharmacology of anticonvulsants: do all anticonvulsants have the same mechanism of action? J Clin Psychiatry 2004;65(2):149-50.
30. Ketter TA, Wong PW. The emerging differential roles of GABAergic and antiglutaminergic agents in bipolar disorders. J Clin Psychiatry 2003;64(suppl 3):15-20.
31. Wassef A, Baker J, Kochan LD. GABA and schizophrenia: a review of basic science and clinical studies. J Clin Psychopharmacol 2003;23(6):601-40.
In patients with treatment-resistant schizophrenia, lithium and anticonvulsants have become such common adjuncts to antipsychotics that 50% of inpatients may be receiving them.1 Evidence supporting this practice is mixed:
- Initial case reports and open-label studies that showed benefit have not always been followed by randomized clinical trials.
- Lack of clear benefit also has been described (Table 1).
This article examines the extent of this prescribing pattern, its evidence base, and mechanisms of action that may help explain why some adjunctive mood stabilizers are more effective than others for treatment-resistant schizophrenia.
EXTENT OF USE
For 5 years, the rate at which inpatients with schizophrenia received adjunctive mood stabilizers has held steady at approximately 50% in New York State Office of Mental Health (NYSOMH) facilities (Figure1). These facilities provide intermediate and long-term care for the seriously, persistently mentally ill. Adjunctive mood stabilizers might not be used as often for outpatients or for inpatients treated in short-stay facilities.
Table 1
Evidence for adjunctive use of lithium or anticonvulsants for treating schizophrenia
| Agent | Case reports and open studies | Randomized, double-blind trials | Benefit? |
|---|---|---|---|
| Lithium | Yes (many) | Yes (several, +/-) | Probably not |
| Carbamazepine | Yes (many) | Yes (several; small total sample) | Limited |
| Valproate | Yes (many) | Yes | Yes |
| Gabapentin | Yes (very few, +/-) | None | Probably not |
| Lamotrigine | Yes (few, +/-) | Yes (2, +) | Yes |
| Topiramate | Yes (very few, +/-) | Yes (1, +/-) | Probably not |
| Oxcarbazepine | Yes (very few, +/-) | None | Probably not |
| + = positive results | |||
| - = negative results | |||
| +/- = both positive and negative results | |||
Valproate is the most commonly used anticonvulsant, with one out of three patients with schizophrenia receiving it. Adjunctive gabapentin use is declining, probably because of inadequate efficacy—as will be discussed later. Use of adjunctive lamotrigine is expected to increase as more data become available on its usefulness in treatment-resistant schizophrenia.
Clinicians are using substantial dosages of adjunctive mood stabilizers. During first-quarter 2004, average daily dosages for 4,788 NYSOMH patients (80% with schizophrenia or schizoaffective disorder) receiving antipsychotics were:
- valproate, 1639 mg (n = 1921)
- gabapentin, 1524 mg (n = 303)
- oxcarbazepine, 1226 mg (n = 201)
- carbamazepine, 908 mg (n = 112)
- lithium, 894 mg (n = 715)
- topiramate, 234 mg (n = 269)
- lamotrigine, 204 mg (n = 231).2
Mood-stabilizer combinations were also used. Approximately one-half of patients receiving adjunctive mood stabilizers—with the exception of valproate—were receiving more than one. In patients receiving valproate, the rate of mood-stabilizer co-prescribing was about 25%.2
WHAT IS THE EVIDENCE?
Evidence supporting the use of adjunctive lithium or anticonvulsants to treat schizophrenia varies in quality and quantity (Table 1). Case reports and open studies offer the weakest evidence but can spur double-blind, randomized clinical trials (RCTs). Unfortunately, RCTs are not often done, and the published studies usually suffer from methodologic flaws such as:
- inadequate number of subjects (insufficient statistical power to detect differences)
- lack of control of confounds such as mood symptoms (seen when studies include patients with schizoaffective disorder)
- inadequate duration
- inappropriate target populations (patients with acute exacerbations of schizophrenia instead of persistent symptoms in treatment-resistant schizophrenia).
Because controlled trials of the use of adjunctive mood stabilizers are relatively scarce, clinical practice has transcended clinical research. Clinicians need effective regimens for treatment-resistant schizophrenia, and mood-stabilizer augmentation helps some patients.
Lithium is perhaps the best-known mood stabilizer. Although early studies showed adjunctive lithium useful in treating schizophrenia, later and better-designed trials did not. The authors of a recent meta-analysis of randomized clinical trials (n = 611 in 20 studies) concluded that despite some evidence supporting the efficacy of lithium augmentation, overall results were inconclusive. A large trial would be required to detect a small benefit in patients with schizophrenia who lack affective symptoms.3
Carbamazepine use among patients with schizophrenia is declining, primarily because this drug induces its own metabolism and can require frequent dose adjustments. Adjunctive carbamazepine has been used to manage persistent aggressive behavior in patients with schizophrenia and schizoaffective disorder. Evidence comes primarily from small trials or case reports (Table 2),4-8 but results of a larger clinical trial (n = 162) by Okuma et al6 are also available
In the Okuma report—a double-blind, placebo-controlled trial of carbamazepine in patients with DSM-III schizophrenia or schizoaffective disorder—carbamazepine did not significantly improve patients’ total Brief Psychiatric Rating Scale (BPRS) scores. Compared with placebo, however, some benefit with carbamazepine did emerge in measures of suspiciousness, uncooperativeness, and excitement.
A systematic review and meta-analysis (n = 283 in 10 studies) detected a trend toward reduced psychopathology with carbamazepine augmentation for schizophrenia. BPRS scores declined by 20% and 35% in the six trials (n = 147) for which data were available (P = 0.08 and 0.09, respectively).9 Because the double-blind trial by Okuma et al6 was not randomized, it was not included in this meta-analysis.9
Figure 1 10-year trend in use of adjunctive mood stabilizers for schizophrenia
Valproate. Among the anticonvulsants, the greatest body of evidence supports the use of valproate in patients with schizophrenia,10 although a recent meta-analysis (n = 378 in 5 studies) indicates inconsistent beneficial effects.11
Initial double-blind, RCTs of adjunctive valproate in patients with schizophrenia were limited in size and failed to show benefit with adjunctive valproate12-15 (Table 2). A more recent study16 showed that adjunctive valproate affects acute psychotic symptoms rather than mood. This study, however, did not answer whether adjunctive valproate would help patients with persistent symptoms of schizophrenia.
Table 2
Double-blind studies of adjunctive carbamazepine in schizophrenia
| Author (yr) | n | Duration (days) | Design | Diagnosis | Outcome |
|---|---|---|---|---|---|
| Neppe (1983) | 11 | 42 | Crossover | Mixed, 8 with schizophrenia | “Overall clinical rating” improved |
| Dose et al (1987) | 22 | 28 | HAL + CBZ vs HAL + placebo | Schizophrenia or schizoaffective disorder | No difference on BPRS |
| Okuma et al (1989) | 162 | 28 | NL + CBZ vs NL + placebo | Schizophrenia or schizoaffective disorder | No difference on BPRS; possible improvement in suspiciousness, uncooperativeness, and excitement |
| Nachshoni et al (1994) | 28 | 49 | NL + CBZ vs NL + placebo | “Residual schizophrenia with negative symptoms” | No difference on BPRS or SANS |
| Simhandl et al (1996) | 42 | 42 | NL + CBZ vs NL + lithium vs NL + placebo | Schizophrenia(treatment- nonresponsive) | No difference on BPRS; CGI improved from baseline in groups receiving CBZ and lithium |
| n = number of subjects | |||||
| BPRS = Brief Psychiatric Rating Scale | |||||
| CGI = Clinical Global Impression scale | |||||
| CBZ = carbamazepine | |||||
| HAL = haloperidol | |||||
| NL = neuroleptic (first-generation antipsychotic) | |||||
| SANS = Scale for the Assessment of Negative Symptoms | |||||
In this large (n = 249), multicenter, randomized, double-blind trial, hospitalized patients with an acute exacerbation of schizophrenia received olanzapine or risperidone plus divalproex or placebo for 28 days. Patients with schizoaffective disorder and treatment-resistant schizophrenia were excluded.
By day 6, dosages reached 6 mg/d for risperidone and 15 mg/d for olanzapine. Divalproex was started at 15 mg/kg and titrated to a maximum of 30 mg/kg by day 14. Mean divalproex dosage was approximately 2300 mg/d (mean plasma level approximately 100 mg/mL).
Positive and Negative Syndrome Scale (PANSS) total scores improved significantly in patients receiving adjunctive divalproex compared with those receiving antipsychotic monotherapy, and significant differences occurred as early as day 3. The major effect was seen on schizophrenia’s positive symptoms. A post-hoc analysis17 also showed greater reductions in hostility (as measured by the hostility item in the PANSS Positive Subscale) in patients receiving adjunctive divalproex compared with antipsychotic monotherapy. This effect was independent of the effect on positive symptoms or sedation.
A large, multi-site, 84-day acute schizophrenia RCT similar to the 28-day trial—but using extended-release divalproex—is being conducted. An extended-release preparation may be particularly helpful in encouraging medication adherence for patients taking complicated medication regimens.
Table 3
Double-blind studies of adjunctive valproate in schizophrenia
| Author (yr) | n | Duration (days) | Design | Diagnosis | Outcome |
|---|---|---|---|---|---|
| Ko et al (1985) | 6 | 28 | Crossover | Neurolepticresistant patients with chronic schizophrenia, not exacerbation | No valproate effect noted |
| Fisk and York (1987) | 62 | 42 | Antipsychotic + valproate vs antipsychotic + placebo | Chronic psychosis and tardive dyskinesia | No differences in mental state and behavior, as measured by“ Krawiecka scale”* |
| Dose et al (1998) | 42 | 28 | HAL + valproate vs HAL + placebo | Acute, nonmanic schizophrenic or schizoaffective psychosis | No difference on BPRS; possible effect on “hostile belligerence” |
| Wassef et al (2000) | 12 | 21 | HAL + valproate vs HAL + placebo | Acute exacerbation of chronic schizophrenia | CGI and SANS scores improved significantly, but BPRS scores did not |
| Casey et al (2003) | 249 | 28 | RIS + valproate vs OLZ + valproate vs RIS + placebo vs OLZ + placebo | Acute exacerbation of schizophrenia | PANSS scores improved |
| * Krawiecka M, Goldberg D, Vaughan M. A standardized psychiatric assessment scale for rating chronic psychotic patients. Acta Psychiatr Scand 1977;55(4):299-308. | |||||
| n = number of subjects | |||||
| BPRS = Brief Psychiatric Rating Scale | |||||
| CGI = Clinical Global Impression scale | |||||
| HAL = haloperidol | |||||
| OLZ = olanzapine | |||||
| PANSS = Positive and Negative Syndrome Scale | |||||
| RIS = risperidone | |||||
| SANS = Scale for the Assessment of Negative Symptoms | |||||
In a recent large (n = 10,262), retrospective, pharmacoepidemiologic analysis,18 valproate augmentation led to longer persistence of treatment than did the strategy of switching antipsychotics. Average valproate dosages were small, however (<425 mg/d), as were antipsychotic dosages (risperidone <1.7 mg/d, quetiapine <120 mg/d, and olanzapine <7.5 mg/d). Patients’ diagnostic categories were not available. One interpretation of this study is that valproate augmentation would be more successful than switching antipsychotics, assuming that treatment persistence can be viewed as a positive outcome.
Table 4
Double-blind studies of adjunctive lamotrigine in schizophrenia
| Author (yr) | n | Duration (days) | Design | Diagnosis | Outcome |
|---|---|---|---|---|---|
| Tiihonen et al (2003) | 34 | 84 | Crossover; clozapine with or without lamotrigine | Clozapine-resistant male inpatients with chronic schizophrenia, not exacerbation | BPRS, PANSS positive, and PANSS general psychopathology symptom scores improved Negative symptoms did not improve |
| Kremer et al (2004) | 38 | 70 | Antipsychotic* + lamotrigine vs antipsychotic* + placebo | Treatment- resistant inpatients with schizophrenia | Completers’ PANSS positive, general psychopathology and total symptom scores improved No difference in negative symptoms or total BPRS scores No difference with intent-to-treat analyses |
| n = number of patients | |||||
| * First- or second-generation antipsychotic | |||||
| BPRS = Brief Psychiatric Rating Scale | |||||
| PANSS = Positive and Negative Syndrome Scale | |||||
Lamotrigine is the only other anticonvulsant for which published, double-blind, randomized evidence of use in patients with schizophrenia is available (Table 4).19,20 Adjunctive lamotrigine may be effective in managing treatment-resistant schizophrenia, as was shown in a small (n = 34), double-blind, placebo-controlled, crossover trial.19 Hospitalized patients whose symptoms were inadequately controlled with clozapine monotherapy received lamotrigine, 200 mg/d, for up to 12 weeks. Adjunctive lamotrigine improved positive but not negative symptoms.
Similar results were seen in treatment-resistant inpatients with schizophrenia (n = 38) in a 10-week, double-blind, parallel group trial by Kremer et al.20 Adjunctive lamotrigine improved PANSS positive, general psychopathology, and total symptom scores in the 31 patients who completed the trial. No differences were seen, however, in negative symptoms, total BPRS scores, or in the intent-to-treat analysis. These results have spurred the launch of a large, multi-site, RCT of adjunctive lamotrigine in patients with schizophrenia who have responded inadequately to antipsychotics alone.
Topiramate, one of the few psychotropics associated with weight loss, has attracted interest as an adjunct to second-generation antipsychotics to address weight gain. Although case reports have shown benefit,21 one showed deterioration in both positive and negative symptoms when topiramate was added to second-generation antipsychotics.22
Table 5
Double-blind study of adjunctive topiramate in schizophrenia
| Author (yr) | n | Duration (days) | Design | Diagnosis | Outcome |
|---|---|---|---|---|---|
| Tiihonen (2004)* | 26 | 84 | Crossover; SGA plus topiramate or placebo | Treatment- resistant male inpatients with chronic schizophrenia | PANSS general scores improved No difference in total PANSS, PANSS positive, or PANSS negative scores |
| * 2004 Collegium Internationale Neuro-Psychopharmacologicum (CINP) presentation, and personal communication (6/22/04) | |||||
| n = number of patients | |||||
| PANSS = Positive and Negative Syndrome Scale | |||||
| SGA = Second-generation antipsychotic (patients were taking clozapine, olanzapine, or quetiapine) | |||||
An unpublished, randomized, crossover trial compared second-generation antipsychotics plus topiramate or placebo in 26 male inpatients with chronic schizophrenia. With adjunctive topiramate, the authors found a statistically significant improvement in the PANSS general psychopathology subscale but not in PANSS total, positive subscale, or negative subscale scores (Table 5) (Tiihonen J, personal communication 6/22/04).
Other agents. Very little information—all uncontrolled—supports adjunctive use of gabapentin or oxcarbazepine for patients with schizophrenia.23-28 Of concern are reports of patients suffering worsening of psychosis with gabapentin25 or of dysphoria and irritability with oxcarbazepine (attributed to a pharmacokinetic interaction).26
Conclusion. More trials are needed to examine the use of adjunctive mood stabilizers in patients with schizophrenia—particularly in those with chronic symptoms. Although mood stabilizers are widely used in this population, important questions remain unanswered, including:
- characteristics of patients likely to require adjunctive treatment
- how long treatment should continue.
MECHANISMS OF ACTION
Unlike antipsychotics, mood stabilizers do not exert their therapeutic effects by acting directly on dopamine (D2) receptors. Differences in mechanism of action among the anticonvulsants may help explain why some—such as valproate and lamotrigine—have been useful for bipolar disorder or schizophrenia and others—such as gabapentin—have not.29
One possibility is that anticonvulsants that affect voltage-gated sodium channels—such as valproate, lamotrigine, carbamazepine and oxcarbazepine—may be most useful for patients with bipolar disorder or schizophrenia. On the other hand, agents that affect voltage-gated calcium channels—such as gabapentin—may be efficacious as anticonvulsants but not as efficacious for bipolar disorder or schizophrenia.
Ketter et al30 proposed an anticonvulsant classification system based on predominant psychotropic profiles:
- the “GABA-ergic” group predominantly potentiates the inhibitory neurotransmitter GABA, resulting in sedation, fatigue, cognitive slowing, and weight gain, as well as possible anxiolytic and antimanic effects
- the “anti-glutamate” group predominantly attenuates glutamate excitatory neurotransmission and is associated with activation, weight loss, and possibly anxiogenic and antidepressant effects.
In the GABA-ergic group are anticonvulsants such as barbiturates, benzodiazepines, valproate, gabapentin, tiagabine, and vigabatrin. The antiglutamate group includes agents such as felbamate and lamotrigine. A “mixed” category includes anticonvulsants with GABA-ergic and anti-glutaminergic actions such as topiramate, which has sedating and weight-loss properties.
Because GABA appears to modulate dopamine neurotransmission,31 this may explain valproate’s role as an adjunctive agent for schizophrenia. Similarly, mechanisms related to Nmethyl-D-aspartate (NMDA) and non-NMDA glutamate receptor function may explain lamotrigine’s usefulness in this setting.19,20
SUMMARY
Clinicians resort to combination therapies when monotherapies fail to adequately control symptoms or maintain response. Co-prescribing of anticonvulsants with antipsychotics for inpatients with schizophrenia is common practice in New York State and most likely elsewhere. In general, antipsychotics’ and mood stabilizers’ different—and perhaps complementary—mechanisms of action explain the synergism between them. Mechanisms of action also may explain why some anticonvulsants help in schizophrenia (or bipolar disorder) whereas others do not.
Evidence for using adjunctive anticonvulsants is variable. The strongest data support using valproate (and perhaps lamotrigine), followed by carbamazepine and then topiramate. Gabapentin and oxcarbazepine have only anecdotal evidence, some of it negative. Well-designed, randomized clinical trials with the appropriate populations are needed.
Related resources
- Stahl SM. Essential psychopharmacology of antipsychotics and mood stabilizers. New York: Cambridge University Press, 2002.
- Harvard Medical School Department of Psychiatry’s psychopharmacology algorithm project. Osser DN, Patterson RD. Consultant for the pharmacotherapy of schizophrenia. Available at http://mhc.com/Algorithms/. Accessed Nov. 5, 2004.
Drug brand names
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Lithium • Lithobid, Eskalith
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Topiramate • Topamax
- Valproate (valproic acid, divalproex sodium) • Depakene, Depakote
Disclosure
Dr. Citrome receives research grants/contracts from Abbott Laboratories, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb Co., Eli Lilly & Co., Janssen Pharmaceutica, and Pfizer Inc. He is a consultant to and/or speaker for Bristol-Myers Squibb Co., Eli Lilly & Co., Pfizer Inc., Abbott Laboratories, AstraZeneca Pharmaceuticals, and Novartis Pharmaceuticals Corp.
Acknowledgment
Adapted from Citrome L. “Antipsychotic polypharmacy versus augmentation with anticonvulsants: the U.S. perspective” (presentation). Paris: Collegium Internationale Neuro-Psychopharmacologicum (CINP), June 2004 [abstract in Int J Neuropsychopharmacol. 2004; 7(suppl 1):S69], and from Citrome L. “Mood-stabilizer use in schizophrenia: 1994-2002” (NR350) (poster). New York: American Psychiatric Association annual meeting, May 2004.
In patients with treatment-resistant schizophrenia, lithium and anticonvulsants have become such common adjuncts to antipsychotics that 50% of inpatients may be receiving them.1 Evidence supporting this practice is mixed:
- Initial case reports and open-label studies that showed benefit have not always been followed by randomized clinical trials.
- Lack of clear benefit also has been described (Table 1).
This article examines the extent of this prescribing pattern, its evidence base, and mechanisms of action that may help explain why some adjunctive mood stabilizers are more effective than others for treatment-resistant schizophrenia.
EXTENT OF USE
For 5 years, the rate at which inpatients with schizophrenia received adjunctive mood stabilizers has held steady at approximately 50% in New York State Office of Mental Health (NYSOMH) facilities (Figure1). These facilities provide intermediate and long-term care for the seriously, persistently mentally ill. Adjunctive mood stabilizers might not be used as often for outpatients or for inpatients treated in short-stay facilities.
Table 1
Evidence for adjunctive use of lithium or anticonvulsants for treating schizophrenia
| Agent | Case reports and open studies | Randomized, double-blind trials | Benefit? |
|---|---|---|---|
| Lithium | Yes (many) | Yes (several, +/-) | Probably not |
| Carbamazepine | Yes (many) | Yes (several; small total sample) | Limited |
| Valproate | Yes (many) | Yes | Yes |
| Gabapentin | Yes (very few, +/-) | None | Probably not |
| Lamotrigine | Yes (few, +/-) | Yes (2, +) | Yes |
| Topiramate | Yes (very few, +/-) | Yes (1, +/-) | Probably not |
| Oxcarbazepine | Yes (very few, +/-) | None | Probably not |
| + = positive results | |||
| - = negative results | |||
| +/- = both positive and negative results | |||
Valproate is the most commonly used anticonvulsant, with one out of three patients with schizophrenia receiving it. Adjunctive gabapentin use is declining, probably because of inadequate efficacy—as will be discussed later. Use of adjunctive lamotrigine is expected to increase as more data become available on its usefulness in treatment-resistant schizophrenia.
Clinicians are using substantial dosages of adjunctive mood stabilizers. During first-quarter 2004, average daily dosages for 4,788 NYSOMH patients (80% with schizophrenia or schizoaffective disorder) receiving antipsychotics were:
- valproate, 1639 mg (n = 1921)
- gabapentin, 1524 mg (n = 303)
- oxcarbazepine, 1226 mg (n = 201)
- carbamazepine, 908 mg (n = 112)
- lithium, 894 mg (n = 715)
- topiramate, 234 mg (n = 269)
- lamotrigine, 204 mg (n = 231).2
Mood-stabilizer combinations were also used. Approximately one-half of patients receiving adjunctive mood stabilizers—with the exception of valproate—were receiving more than one. In patients receiving valproate, the rate of mood-stabilizer co-prescribing was about 25%.2
WHAT IS THE EVIDENCE?
Evidence supporting the use of adjunctive lithium or anticonvulsants to treat schizophrenia varies in quality and quantity (Table 1). Case reports and open studies offer the weakest evidence but can spur double-blind, randomized clinical trials (RCTs). Unfortunately, RCTs are not often done, and the published studies usually suffer from methodologic flaws such as:
- inadequate number of subjects (insufficient statistical power to detect differences)
- lack of control of confounds such as mood symptoms (seen when studies include patients with schizoaffective disorder)
- inadequate duration
- inappropriate target populations (patients with acute exacerbations of schizophrenia instead of persistent symptoms in treatment-resistant schizophrenia).
Because controlled trials of the use of adjunctive mood stabilizers are relatively scarce, clinical practice has transcended clinical research. Clinicians need effective regimens for treatment-resistant schizophrenia, and mood-stabilizer augmentation helps some patients.
Lithium is perhaps the best-known mood stabilizer. Although early studies showed adjunctive lithium useful in treating schizophrenia, later and better-designed trials did not. The authors of a recent meta-analysis of randomized clinical trials (n = 611 in 20 studies) concluded that despite some evidence supporting the efficacy of lithium augmentation, overall results were inconclusive. A large trial would be required to detect a small benefit in patients with schizophrenia who lack affective symptoms.3
Carbamazepine use among patients with schizophrenia is declining, primarily because this drug induces its own metabolism and can require frequent dose adjustments. Adjunctive carbamazepine has been used to manage persistent aggressive behavior in patients with schizophrenia and schizoaffective disorder. Evidence comes primarily from small trials or case reports (Table 2),4-8 but results of a larger clinical trial (n = 162) by Okuma et al6 are also available
In the Okuma report—a double-blind, placebo-controlled trial of carbamazepine in patients with DSM-III schizophrenia or schizoaffective disorder—carbamazepine did not significantly improve patients’ total Brief Psychiatric Rating Scale (BPRS) scores. Compared with placebo, however, some benefit with carbamazepine did emerge in measures of suspiciousness, uncooperativeness, and excitement.
A systematic review and meta-analysis (n = 283 in 10 studies) detected a trend toward reduced psychopathology with carbamazepine augmentation for schizophrenia. BPRS scores declined by 20% and 35% in the six trials (n = 147) for which data were available (P = 0.08 and 0.09, respectively).9 Because the double-blind trial by Okuma et al6 was not randomized, it was not included in this meta-analysis.9
Figure 1 10-year trend in use of adjunctive mood stabilizers for schizophrenia
Valproate. Among the anticonvulsants, the greatest body of evidence supports the use of valproate in patients with schizophrenia,10 although a recent meta-analysis (n = 378 in 5 studies) indicates inconsistent beneficial effects.11
Initial double-blind, RCTs of adjunctive valproate in patients with schizophrenia were limited in size and failed to show benefit with adjunctive valproate12-15 (Table 2). A more recent study16 showed that adjunctive valproate affects acute psychotic symptoms rather than mood. This study, however, did not answer whether adjunctive valproate would help patients with persistent symptoms of schizophrenia.
Table 2
Double-blind studies of adjunctive carbamazepine in schizophrenia
| Author (yr) | n | Duration (days) | Design | Diagnosis | Outcome |
|---|---|---|---|---|---|
| Neppe (1983) | 11 | 42 | Crossover | Mixed, 8 with schizophrenia | “Overall clinical rating” improved |
| Dose et al (1987) | 22 | 28 | HAL + CBZ vs HAL + placebo | Schizophrenia or schizoaffective disorder | No difference on BPRS |
| Okuma et al (1989) | 162 | 28 | NL + CBZ vs NL + placebo | Schizophrenia or schizoaffective disorder | No difference on BPRS; possible improvement in suspiciousness, uncooperativeness, and excitement |
| Nachshoni et al (1994) | 28 | 49 | NL + CBZ vs NL + placebo | “Residual schizophrenia with negative symptoms” | No difference on BPRS or SANS |
| Simhandl et al (1996) | 42 | 42 | NL + CBZ vs NL + lithium vs NL + placebo | Schizophrenia(treatment- nonresponsive) | No difference on BPRS; CGI improved from baseline in groups receiving CBZ and lithium |
| n = number of subjects | |||||
| BPRS = Brief Psychiatric Rating Scale | |||||
| CGI = Clinical Global Impression scale | |||||
| CBZ = carbamazepine | |||||
| HAL = haloperidol | |||||
| NL = neuroleptic (first-generation antipsychotic) | |||||
| SANS = Scale for the Assessment of Negative Symptoms | |||||
In this large (n = 249), multicenter, randomized, double-blind trial, hospitalized patients with an acute exacerbation of schizophrenia received olanzapine or risperidone plus divalproex or placebo for 28 days. Patients with schizoaffective disorder and treatment-resistant schizophrenia were excluded.
By day 6, dosages reached 6 mg/d for risperidone and 15 mg/d for olanzapine. Divalproex was started at 15 mg/kg and titrated to a maximum of 30 mg/kg by day 14. Mean divalproex dosage was approximately 2300 mg/d (mean plasma level approximately 100 mg/mL).
Positive and Negative Syndrome Scale (PANSS) total scores improved significantly in patients receiving adjunctive divalproex compared with those receiving antipsychotic monotherapy, and significant differences occurred as early as day 3. The major effect was seen on schizophrenia’s positive symptoms. A post-hoc analysis17 also showed greater reductions in hostility (as measured by the hostility item in the PANSS Positive Subscale) in patients receiving adjunctive divalproex compared with antipsychotic monotherapy. This effect was independent of the effect on positive symptoms or sedation.
A large, multi-site, 84-day acute schizophrenia RCT similar to the 28-day trial—but using extended-release divalproex—is being conducted. An extended-release preparation may be particularly helpful in encouraging medication adherence for patients taking complicated medication regimens.
Table 3
Double-blind studies of adjunctive valproate in schizophrenia
| Author (yr) | n | Duration (days) | Design | Diagnosis | Outcome |
|---|---|---|---|---|---|
| Ko et al (1985) | 6 | 28 | Crossover | Neurolepticresistant patients with chronic schizophrenia, not exacerbation | No valproate effect noted |
| Fisk and York (1987) | 62 | 42 | Antipsychotic + valproate vs antipsychotic + placebo | Chronic psychosis and tardive dyskinesia | No differences in mental state and behavior, as measured by“ Krawiecka scale”* |
| Dose et al (1998) | 42 | 28 | HAL + valproate vs HAL + placebo | Acute, nonmanic schizophrenic or schizoaffective psychosis | No difference on BPRS; possible effect on “hostile belligerence” |
| Wassef et al (2000) | 12 | 21 | HAL + valproate vs HAL + placebo | Acute exacerbation of chronic schizophrenia | CGI and SANS scores improved significantly, but BPRS scores did not |
| Casey et al (2003) | 249 | 28 | RIS + valproate vs OLZ + valproate vs RIS + placebo vs OLZ + placebo | Acute exacerbation of schizophrenia | PANSS scores improved |
| * Krawiecka M, Goldberg D, Vaughan M. A standardized psychiatric assessment scale for rating chronic psychotic patients. Acta Psychiatr Scand 1977;55(4):299-308. | |||||
| n = number of subjects | |||||
| BPRS = Brief Psychiatric Rating Scale | |||||
| CGI = Clinical Global Impression scale | |||||
| HAL = haloperidol | |||||
| OLZ = olanzapine | |||||
| PANSS = Positive and Negative Syndrome Scale | |||||
| RIS = risperidone | |||||
| SANS = Scale for the Assessment of Negative Symptoms | |||||
In a recent large (n = 10,262), retrospective, pharmacoepidemiologic analysis,18 valproate augmentation led to longer persistence of treatment than did the strategy of switching antipsychotics. Average valproate dosages were small, however (<425 mg/d), as were antipsychotic dosages (risperidone <1.7 mg/d, quetiapine <120 mg/d, and olanzapine <7.5 mg/d). Patients’ diagnostic categories were not available. One interpretation of this study is that valproate augmentation would be more successful than switching antipsychotics, assuming that treatment persistence can be viewed as a positive outcome.
Table 4
Double-blind studies of adjunctive lamotrigine in schizophrenia
| Author (yr) | n | Duration (days) | Design | Diagnosis | Outcome |
|---|---|---|---|---|---|
| Tiihonen et al (2003) | 34 | 84 | Crossover; clozapine with or without lamotrigine | Clozapine-resistant male inpatients with chronic schizophrenia, not exacerbation | BPRS, PANSS positive, and PANSS general psychopathology symptom scores improved Negative symptoms did not improve |
| Kremer et al (2004) | 38 | 70 | Antipsychotic* + lamotrigine vs antipsychotic* + placebo | Treatment- resistant inpatients with schizophrenia | Completers’ PANSS positive, general psychopathology and total symptom scores improved No difference in negative symptoms or total BPRS scores No difference with intent-to-treat analyses |
| n = number of patients | |||||
| * First- or second-generation antipsychotic | |||||
| BPRS = Brief Psychiatric Rating Scale | |||||
| PANSS = Positive and Negative Syndrome Scale | |||||
Lamotrigine is the only other anticonvulsant for which published, double-blind, randomized evidence of use in patients with schizophrenia is available (Table 4).19,20 Adjunctive lamotrigine may be effective in managing treatment-resistant schizophrenia, as was shown in a small (n = 34), double-blind, placebo-controlled, crossover trial.19 Hospitalized patients whose symptoms were inadequately controlled with clozapine monotherapy received lamotrigine, 200 mg/d, for up to 12 weeks. Adjunctive lamotrigine improved positive but not negative symptoms.
Similar results were seen in treatment-resistant inpatients with schizophrenia (n = 38) in a 10-week, double-blind, parallel group trial by Kremer et al.20 Adjunctive lamotrigine improved PANSS positive, general psychopathology, and total symptom scores in the 31 patients who completed the trial. No differences were seen, however, in negative symptoms, total BPRS scores, or in the intent-to-treat analysis. These results have spurred the launch of a large, multi-site, RCT of adjunctive lamotrigine in patients with schizophrenia who have responded inadequately to antipsychotics alone.
Topiramate, one of the few psychotropics associated with weight loss, has attracted interest as an adjunct to second-generation antipsychotics to address weight gain. Although case reports have shown benefit,21 one showed deterioration in both positive and negative symptoms when topiramate was added to second-generation antipsychotics.22
Table 5
Double-blind study of adjunctive topiramate in schizophrenia
| Author (yr) | n | Duration (days) | Design | Diagnosis | Outcome |
|---|---|---|---|---|---|
| Tiihonen (2004)* | 26 | 84 | Crossover; SGA plus topiramate or placebo | Treatment- resistant male inpatients with chronic schizophrenia | PANSS general scores improved No difference in total PANSS, PANSS positive, or PANSS negative scores |
| * 2004 Collegium Internationale Neuro-Psychopharmacologicum (CINP) presentation, and personal communication (6/22/04) | |||||
| n = number of patients | |||||
| PANSS = Positive and Negative Syndrome Scale | |||||
| SGA = Second-generation antipsychotic (patients were taking clozapine, olanzapine, or quetiapine) | |||||
An unpublished, randomized, crossover trial compared second-generation antipsychotics plus topiramate or placebo in 26 male inpatients with chronic schizophrenia. With adjunctive topiramate, the authors found a statistically significant improvement in the PANSS general psychopathology subscale but not in PANSS total, positive subscale, or negative subscale scores (Table 5) (Tiihonen J, personal communication 6/22/04).
Other agents. Very little information—all uncontrolled—supports adjunctive use of gabapentin or oxcarbazepine for patients with schizophrenia.23-28 Of concern are reports of patients suffering worsening of psychosis with gabapentin25 or of dysphoria and irritability with oxcarbazepine (attributed to a pharmacokinetic interaction).26
Conclusion. More trials are needed to examine the use of adjunctive mood stabilizers in patients with schizophrenia—particularly in those with chronic symptoms. Although mood stabilizers are widely used in this population, important questions remain unanswered, including:
- characteristics of patients likely to require adjunctive treatment
- how long treatment should continue.
MECHANISMS OF ACTION
Unlike antipsychotics, mood stabilizers do not exert their therapeutic effects by acting directly on dopamine (D2) receptors. Differences in mechanism of action among the anticonvulsants may help explain why some—such as valproate and lamotrigine—have been useful for bipolar disorder or schizophrenia and others—such as gabapentin—have not.29
One possibility is that anticonvulsants that affect voltage-gated sodium channels—such as valproate, lamotrigine, carbamazepine and oxcarbazepine—may be most useful for patients with bipolar disorder or schizophrenia. On the other hand, agents that affect voltage-gated calcium channels—such as gabapentin—may be efficacious as anticonvulsants but not as efficacious for bipolar disorder or schizophrenia.
Ketter et al30 proposed an anticonvulsant classification system based on predominant psychotropic profiles:
- the “GABA-ergic” group predominantly potentiates the inhibitory neurotransmitter GABA, resulting in sedation, fatigue, cognitive slowing, and weight gain, as well as possible anxiolytic and antimanic effects
- the “anti-glutamate” group predominantly attenuates glutamate excitatory neurotransmission and is associated with activation, weight loss, and possibly anxiogenic and antidepressant effects.
In the GABA-ergic group are anticonvulsants such as barbiturates, benzodiazepines, valproate, gabapentin, tiagabine, and vigabatrin. The antiglutamate group includes agents such as felbamate and lamotrigine. A “mixed” category includes anticonvulsants with GABA-ergic and anti-glutaminergic actions such as topiramate, which has sedating and weight-loss properties.
Because GABA appears to modulate dopamine neurotransmission,31 this may explain valproate’s role as an adjunctive agent for schizophrenia. Similarly, mechanisms related to Nmethyl-D-aspartate (NMDA) and non-NMDA glutamate receptor function may explain lamotrigine’s usefulness in this setting.19,20
SUMMARY
Clinicians resort to combination therapies when monotherapies fail to adequately control symptoms or maintain response. Co-prescribing of anticonvulsants with antipsychotics for inpatients with schizophrenia is common practice in New York State and most likely elsewhere. In general, antipsychotics’ and mood stabilizers’ different—and perhaps complementary—mechanisms of action explain the synergism between them. Mechanisms of action also may explain why some anticonvulsants help in schizophrenia (or bipolar disorder) whereas others do not.
Evidence for using adjunctive anticonvulsants is variable. The strongest data support using valproate (and perhaps lamotrigine), followed by carbamazepine and then topiramate. Gabapentin and oxcarbazepine have only anecdotal evidence, some of it negative. Well-designed, randomized clinical trials with the appropriate populations are needed.
Related resources
- Stahl SM. Essential psychopharmacology of antipsychotics and mood stabilizers. New York: Cambridge University Press, 2002.
- Harvard Medical School Department of Psychiatry’s psychopharmacology algorithm project. Osser DN, Patterson RD. Consultant for the pharmacotherapy of schizophrenia. Available at http://mhc.com/Algorithms/. Accessed Nov. 5, 2004.
Drug brand names
- Carbamazepine • Tegretol
- Clozapine • Clozaril
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Lithium • Lithobid, Eskalith
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Topiramate • Topamax
- Valproate (valproic acid, divalproex sodium) • Depakene, Depakote
Disclosure
Dr. Citrome receives research grants/contracts from Abbott Laboratories, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb Co., Eli Lilly & Co., Janssen Pharmaceutica, and Pfizer Inc. He is a consultant to and/or speaker for Bristol-Myers Squibb Co., Eli Lilly & Co., Pfizer Inc., Abbott Laboratories, AstraZeneca Pharmaceuticals, and Novartis Pharmaceuticals Corp.
Acknowledgment
Adapted from Citrome L. “Antipsychotic polypharmacy versus augmentation with anticonvulsants: the U.S. perspective” (presentation). Paris: Collegium Internationale Neuro-Psychopharmacologicum (CINP), June 2004 [abstract in Int J Neuropsychopharmacol. 2004; 7(suppl 1):S69], and from Citrome L. “Mood-stabilizer use in schizophrenia: 1994-2002” (NR350) (poster). New York: American Psychiatric Association annual meeting, May 2004.
1. Citrome L, Jaffe A, Levine J. Datapoints - mood stabilizers: utilization trends in patients diagnosed with schizophrenia 1994-2001. Psychiatr Serv 2002;53(10):1212.-
2. Citrome L. Antipsychotic polypharmacy versus augmentation with anticonvulsants: the U.S.perspective (presentation). Paris: Collegium Internationale Neuro-Psychopharmacologicum(CINP), June 2004 [abstract in Int J Neuropsychopharmacol 2004;7(suppl 1):S69].
3. Leucht S, Kissling W, McGrath J. Lithium for schizophrenia revisited: a systematic review and meta-analysis of randomized clinical trials. J Clin Psychiatry 2004;65(2):177-86.
4. Neppe VM. Carbamazepine as adjunctive treatment in nonepileptic chronic inpatients with EEG temporal lobe abnormalities. J Clin Psychiatry 1983;44:326-31.
5. Dose M, Apelt S, Emrich HM. Carbamazepine as an adjunct of antipsychotic therapy. Psychiatry Res 1987;22:303-10.
6. Okuma T, Yamashita I, Takahashi R, et al. A double-blind study of adjunctive carbamazepine versus placebo on excited states of schizophrenic and schizoaffective disorders. Acta Psychiatr Scand 1989;80:250-9.
7. Nachshoni T, Levin Y, Levy A, et al. A double-blind trial of carbamazepine in negative symptom schizophrenia. Biol Psychiatry 1994;35(1):22-26.
8. Simhandl C, Meszaros K, Denk E, et al. Adjunctive carbamazepine or lithium carbonate in therapy-resistant chronic schizophrenia. Can J Psychiatry 1996;41(5):317.-
9. Leucht S, McGrath J, White P, et al. Carbamazepine augmentation for schizophrenia: how good is the evidence? J Clin Psychiatry 2002;63(3):218-24.
10. Citrome L. Schizophrenia and valproate. Psychopharmacol Bull 2003;37(suppl 2):74-88.
11. Basan A, Kissling W, Leucht S. Valproate as an adjunct to antipsychotics for schizophrenia: a systematic review of randomized trials. Schizophr Res 2004;70(1):33-7.
12. Ko GN, Korpi ER, Freed WJ, et al. Effect of valproic acid on behavior and plasma amino acid concentrations in chronic schizophrenia patients. Biol Psychiatry 1985;20:209-15.
13. Dose M, Hellweg R, Yassouridis A, et al. Combined treatment of schizophrenic psychoses with haloperidol and valproate. Pharmacopsychiatry 1998;31(4):122-5.
14. Fisk GG, York SM. The effect of sodium valproate on tardive dyskinesia—revisited. Br J Psychiatry 1987;150:542-6.
15. Wassef AA, Dott SG, Harris A, et al. Randomized, placebo-controlled pilot study of divalproex sodium in the treatment of acute exacerbations of chronic schizophrenia. J Clin Psychopharmacol 2000;20(3):357-361.
16. Casey DE, Daniel DG, Wassef AA, et al. Effect of divalproex combined with olanzapine or risperidone in patients with an acute exacerbation of schizophrenia. Neuropsychopharmacol 2003;28(1):182-92.
17. Citrome L, Casey DE, Daniel DG, et al. Effects of adjunctive valproate on hostility in patients with schizophrenia receiving olanzapine or risperidone: a double-blind multi-center study. Psychiatr Serv 2004;55(3):290-4.
18. Cramer JA, Sernyak M. Results of a naturalistic study of treatment options: switching atypical antipsychotic drugs or augmenting with valproate. Clin Ther 2004;26(6):905-14.
19. Tiihonen J, Hallikainen T, Ryynanen OP, et al. Lamotrigine in treatment-resistant schizophrenia: a randomized placebo-controlled trial. Biol Psychiatry 2003;54(11):1241-8.
20. Kremer I, Vass A, Gurelik I, et al. Placebo-controlled trial of lamotrigine added to conventional and atypical antipsychotics in schizophrenia. Biol Psychiatry 2004;56(6):441-6.
21. Drapalski AL, Rosse RB, Peebles RR, et al. Topiramate improves deficit symptoms in a patient with schizophrenia when added to a stable regimen of antipsychotic medication. Clin Neuropharmacol 2001;24:290-4.
22. Millson RC, Owen JA, Lorberg GW, Tackaberry L. Topiramate for refractory schizophrenia. Am J Psychiatry 2002;159(4):675.-
23. Chouinard G, Beauclair L, Belanger MC. Gabapentin: long term antianxiety and hypnotic effects in psychiatric patients with comorbid anxiety-related disorders. Can J Psychiatry 1998;43:305.-
24. Megna JL, Devitt PJ, Sauro MD, Dewan MJ. Gabapentin’s effect on agitation in severely and persistently mentally ill patients. Ann Pharmacother 2002;35:12-16.
25. Jablonowski K, Margolese HC, Chouinard G. Gabapentin-induced paradoxical exacerbation of psychosis in a patient with schizophrenia. Can J Psychiatry 2002;47(10):975-6.
26. Baird P. The interactive metabolism effect of oxcarbazepine coadministered with tricyclic antidepressant therapy for OCD symptoms. J Clin Psychopharmacol 2003;23(4):419.-
27. Centorrino F, Albert MJ, Berry JM, et al. Oxcarbazepine: clinical experience with hospitalized psychiatric patients. Bipolar Disord 2003;5(5):370-4.
28. Leweke FM, Gerth CW, Koethe D, et al. Oxcarbazepine as an adjunct for schizophrenia. Am J Psychiatry 2004;161(6):1130-1.
29. Stahl SM. Psychopharmacology of anticonvulsants: do all anticonvulsants have the same mechanism of action? J Clin Psychiatry 2004;65(2):149-50.
30. Ketter TA, Wong PW. The emerging differential roles of GABAergic and antiglutaminergic agents in bipolar disorders. J Clin Psychiatry 2003;64(suppl 3):15-20.
31. Wassef A, Baker J, Kochan LD. GABA and schizophrenia: a review of basic science and clinical studies. J Clin Psychopharmacol 2003;23(6):601-40.
1. Citrome L, Jaffe A, Levine J. Datapoints - mood stabilizers: utilization trends in patients diagnosed with schizophrenia 1994-2001. Psychiatr Serv 2002;53(10):1212.-
2. Citrome L. Antipsychotic polypharmacy versus augmentation with anticonvulsants: the U.S.perspective (presentation). Paris: Collegium Internationale Neuro-Psychopharmacologicum(CINP), June 2004 [abstract in Int J Neuropsychopharmacol 2004;7(suppl 1):S69].
3. Leucht S, Kissling W, McGrath J. Lithium for schizophrenia revisited: a systematic review and meta-analysis of randomized clinical trials. J Clin Psychiatry 2004;65(2):177-86.
4. Neppe VM. Carbamazepine as adjunctive treatment in nonepileptic chronic inpatients with EEG temporal lobe abnormalities. J Clin Psychiatry 1983;44:326-31.
5. Dose M, Apelt S, Emrich HM. Carbamazepine as an adjunct of antipsychotic therapy. Psychiatry Res 1987;22:303-10.
6. Okuma T, Yamashita I, Takahashi R, et al. A double-blind study of adjunctive carbamazepine versus placebo on excited states of schizophrenic and schizoaffective disorders. Acta Psychiatr Scand 1989;80:250-9.
7. Nachshoni T, Levin Y, Levy A, et al. A double-blind trial of carbamazepine in negative symptom schizophrenia. Biol Psychiatry 1994;35(1):22-26.
8. Simhandl C, Meszaros K, Denk E, et al. Adjunctive carbamazepine or lithium carbonate in therapy-resistant chronic schizophrenia. Can J Psychiatry 1996;41(5):317.-
9. Leucht S, McGrath J, White P, et al. Carbamazepine augmentation for schizophrenia: how good is the evidence? J Clin Psychiatry 2002;63(3):218-24.
10. Citrome L. Schizophrenia and valproate. Psychopharmacol Bull 2003;37(suppl 2):74-88.
11. Basan A, Kissling W, Leucht S. Valproate as an adjunct to antipsychotics for schizophrenia: a systematic review of randomized trials. Schizophr Res 2004;70(1):33-7.
12. Ko GN, Korpi ER, Freed WJ, et al. Effect of valproic acid on behavior and plasma amino acid concentrations in chronic schizophrenia patients. Biol Psychiatry 1985;20:209-15.
13. Dose M, Hellweg R, Yassouridis A, et al. Combined treatment of schizophrenic psychoses with haloperidol and valproate. Pharmacopsychiatry 1998;31(4):122-5.
14. Fisk GG, York SM. The effect of sodium valproate on tardive dyskinesia—revisited. Br J Psychiatry 1987;150:542-6.
15. Wassef AA, Dott SG, Harris A, et al. Randomized, placebo-controlled pilot study of divalproex sodium in the treatment of acute exacerbations of chronic schizophrenia. J Clin Psychopharmacol 2000;20(3):357-361.
16. Casey DE, Daniel DG, Wassef AA, et al. Effect of divalproex combined with olanzapine or risperidone in patients with an acute exacerbation of schizophrenia. Neuropsychopharmacol 2003;28(1):182-92.
17. Citrome L, Casey DE, Daniel DG, et al. Effects of adjunctive valproate on hostility in patients with schizophrenia receiving olanzapine or risperidone: a double-blind multi-center study. Psychiatr Serv 2004;55(3):290-4.
18. Cramer JA, Sernyak M. Results of a naturalistic study of treatment options: switching atypical antipsychotic drugs or augmenting with valproate. Clin Ther 2004;26(6):905-14.
19. Tiihonen J, Hallikainen T, Ryynanen OP, et al. Lamotrigine in treatment-resistant schizophrenia: a randomized placebo-controlled trial. Biol Psychiatry 2003;54(11):1241-8.
20. Kremer I, Vass A, Gurelik I, et al. Placebo-controlled trial of lamotrigine added to conventional and atypical antipsychotics in schizophrenia. Biol Psychiatry 2004;56(6):441-6.
21. Drapalski AL, Rosse RB, Peebles RR, et al. Topiramate improves deficit symptoms in a patient with schizophrenia when added to a stable regimen of antipsychotic medication. Clin Neuropharmacol 2001;24:290-4.
22. Millson RC, Owen JA, Lorberg GW, Tackaberry L. Topiramate for refractory schizophrenia. Am J Psychiatry 2002;159(4):675.-
23. Chouinard G, Beauclair L, Belanger MC. Gabapentin: long term antianxiety and hypnotic effects in psychiatric patients with comorbid anxiety-related disorders. Can J Psychiatry 1998;43:305.-
24. Megna JL, Devitt PJ, Sauro MD, Dewan MJ. Gabapentin’s effect on agitation in severely and persistently mentally ill patients. Ann Pharmacother 2002;35:12-16.
25. Jablonowski K, Margolese HC, Chouinard G. Gabapentin-induced paradoxical exacerbation of psychosis in a patient with schizophrenia. Can J Psychiatry 2002;47(10):975-6.
26. Baird P. The interactive metabolism effect of oxcarbazepine coadministered with tricyclic antidepressant therapy for OCD symptoms. J Clin Psychopharmacol 2003;23(4):419.-
27. Centorrino F, Albert MJ, Berry JM, et al. Oxcarbazepine: clinical experience with hospitalized psychiatric patients. Bipolar Disord 2003;5(5):370-4.
28. Leweke FM, Gerth CW, Koethe D, et al. Oxcarbazepine as an adjunct for schizophrenia. Am J Psychiatry 2004;161(6):1130-1.
29. Stahl SM. Psychopharmacology of anticonvulsants: do all anticonvulsants have the same mechanism of action? J Clin Psychiatry 2004;65(2):149-50.
30. Ketter TA, Wong PW. The emerging differential roles of GABAergic and antiglutaminergic agents in bipolar disorders. J Clin Psychiatry 2003;64(suppl 3):15-20.
31. Wassef A, Baker J, Kochan LD. GABA and schizophrenia: a review of basic science and clinical studies. J Clin Psychopharmacol 2003;23(6):601-40.
Bodybuilding’s dark side: Clues to anabolic steroid use
Anabolic steroid use by athletes and body-builders has captured public attention but remains poorly understood by most physicians. This is not surprising because users of anabolic-androgenic steroids (AAS):
- rarely seek treatment or disclose their drug use
- frequently distrust professionals.
If you are a clinician who regularly sees male adolescents and young men, you need to become familiar with—and watch for—this often-secret form of substance abuse. This article provides the groundwork for that understanding, starting with the story of “Aaron”—a composite patient whose case represents experiences and verbatim quotes from AAS users known to the authors.
CASE REPORT: ‘I FEEL INVINCIBLE’
At his first visit, Aaron, age 18, told the psychiatrist he had no complaints but was coming to please his parents. “I have a lot of arguments with my Dad,” he said, “and they keep thinking something’s wrong with me.”
The patient was very muscular and dressed in baggy sweats that masked his body proportions. He was appropriately groomed and darkly tanned but displayed some acne. The clinician guessed he weighed about 175 lbs and stood at about 65 inches, with very low body fat. Although superficially confident, he seemed restless, somewhat anxious, and guarded as the interview progressed.
Aaron admitted he experienced prominent mood swings. During rage outbursts, he had damaged objects and put his fist through the wall. “There’s holes all over the wall of my room,” he joked.
He also had assaulted a motorist in a traffic altercation, then left the scene. “Did you hurt him?” the clinician asked. Somewhat sheepishly, Aaron responded, “Well, I bought the newspaper and kept checking the obituaries for about 2 weeks afterwards.”
He spoke with pride about his weightlifting, which was the focus of his life. He revealed that he was preparing for a body-building contest in 2 months. The psychiatrist asked him about use of supplements—protein shakes, creatine, and “andro” (androstenedione)—all of which Aaron acknowledged. The psychiatrist then gently asked about anabolic steroid use (Box 1).
Initially, Aaron strongly denied using AAS. The psychiatrist persisted, pointing out that no information would be disclosed to his parents, and asked again using colloquial terms from the AAS subculture: “Anybody who is prepping for an untested contest in a couple of months is going to be on a cycle. Come on, what are you taking?”
Anabolic-androgenic steroids (AAS) are hormones that include testosterone—nature’s own AAS—and more than 100 synthetically developed testosterone relatives. All AAS possess anabolic (muscle-building) and androgenic (masculinizing) properties; no known compound can produce one of these effects without the other.
Because of their masculinizing effects, AAS are rarely used by women—and even then in much lower doses than those used by men. Thus, this article focuses on evaluating and treating male adolescents and men.
AAS are not:
- Corticosteroids (such as cortisol) are often called “steroids” but possess no muscle-building properties. Corticosteroids’ prominent but idiosyncratic psychiatric effects are usually seen in consultation-liaison settings where patients have been prescribed these drugs, rather than among substance abusers.
- Androstenedione (“andro”) and its relatives are adrenal steroids that are weakly metabolized into testosterone or other AAS. These substances were sold legally without prescription in the United States for many years but were banned by federal law in October 2004. Their anabolic and psychiatric effects are much weaker than those of AAS.
- Athletic “supplements” with names designed to sound like AAS (such as beginning with “Ana…”) or supplements claimed to be “testosterone-releasers” or the like. If sold legally in supplement stores, an athletic supplement is not an AAS. Psychiatric effects are extremely unlikely.
Eventually it emerged that Aaron had taken five 8- to 20-week AAS “cycles” (courses), during which he had “stacked” (combined) various “injectables” such as IM testosterone and “orals” such as methyltestosterone (Table 1). His current cycle included:
- a blend of testosterone esters (Sustanon), 500 mg IM once a week
- boldenone (Equipoise), a veterinary AAS normally used for horses, 200 mg IM per week
- oxymetholone (Anadrol), 50 mg orally per day.
Table 1
Commonly used anabolic-androgenic steroids
| ‘Injectables’ (usually administered only by injection) | |
| Boldenone (Equipoise)* | |
| Methenolone (Primobolan depot) | |
| Nandrolone (Deca-Durabolin, Durabolin, Laurabolin, others) | |
| Stanozolol (Winstrol-V)* | |
| Testosterone esters (Depo-testosterone, Sten, Sustanon, others) | |
| Trenbolone (Finajet, Parabolan) | |
| ‘Orals’ | |
| Methandienone (formerly called methandrostenolone) (Dianabol, others) | |
| Methenolone (Primobolan) | |
| Methyltestosterone (Android, others) | |
| Mibolerone (Checque Drops)* | |
| Oxandrolone (Anavar, Lipidex) | |
| Oxmetholone (Anadrol, Anapolon) | |
| Stanoxolol (Stromba, Winstrol) | |
| Other anabolic substances sold on the ‘black market’ | |
| Human growth hormone (HGH) | Possesses anabolic properties |
| Extremely expensive | |
| Almost impossible to detect by testing | |
| Lacks androgenic effects | |
| Psychiatric effects appear negligible | |
| Large doses can cause acromegaly | |
| Clenbuterol | Beta-adrenergic agonist with stimulant and anabolic properties |
| Used less commonly than AAS | |
| Lacks androgenic effects and assists fat loss | |
| Can produce psychiatric effects similar to those of amphetamine abuse (rare, in the authors’ experience) | |
| Human chorionic gonadotropin (HCG) | Stimulates testes to produce more testosterone, creating an AAS effect |
| Most commonly used near the end of an AAS “cycle” to “jump-start” the hypothalamic-pituitary-testicular axis and minimize AAS withdrawal | |
| * Veterinary preparation | |
| AAS: anabolic-androgenic steroid | |
His friends had taught him to self-inject AAS at age 15; he admitted that he was also occasionally self-injecting the opioid analgesic nalbuphine intravenously because of “pain in my ‘delts’ from military presses.”
During his cycles, Aaron experienced hypomanic symptoms, including euphoria, prominent irritability, increased libido, decreased need for sleep, and grandiosity. “I feel invincible,” he said. His aggressive outbursts had worsened with increasing AAS doses; in addition to attacking the motorist, he also had been physically violent with his girlfriend. “She’s scared of me when I’m on juice,” he conceded.
During the withdrawal phase after stopping each cycle, Aaron described prominent depression with anhedonia, hypersomnia, loss of libido, and suicidal ideation. “I once almost jumped off a bridge after my fourth cycle,” he admitted. “I couldn’t wait to get on my next cycle to feel good again.” His depressions were also characterized by body-image obsessions; he would regularly spend at least 1 hour a day examining his musculature in a mirror, and sometimes refused to go out in public because he “was getting too small.”
Perhaps most disturbing was his increasing use of opioids. In addition to self-injecting nalbuphine, he also ingested oral opioids such as oxycodone almost daily. He mentioned that several of his friends in the gym had progressed from injecting nalbuphine to injecting morphine or heroin, and he knew two bodybuilders who had died from apparently unintentional opioid overdoses.
Aaron said his parents, teachers, and non-bodybuilding friends were unaware of this history. He claimed his parents were proud that their son had apparently eschewed drugs and alcohol to pursue a healthy athletic lifestyle.
RECOGNIZING AAS USE
In our experience with treating substance abusers, we find that AAS users may be the least likely to disclose their drug use to clinicians. In a recent study,1 20 of 36 AAS users (56%) reported they had never revealed their AAS use to any physician. When asked to rate their trust in sources of information about AAS, 17 of 42 AAS users (40%) said they trusted information from their drug dealers at least as much as information from any physician they had seen.
Some expressed contempt for physicians as “geeks” or “pencil-necks” who could not comprehend the body-building lifestyle. They gave doctors high marks on knowledge of tobacco, alcohol, and ordinary “street drugs” but much lower ratings on AAS knowledge. Other investigators have shown that many clinicians are unfamiliar with AAS.2,3
AAS users embrace these beliefs for two other reasons. First, to admit to AAS use is to admit that one’s muscularity and physical prowess is the result of taking a drug; there is no comparable motivation to withhold information about, say, one’s use of marijuana or cocaine.
Second, AAS users are much less likely than other substance abusers to view their behavior as pathologic. We have argued that our culture is partially to blame.4 Americans pay to watch 300-lb football linemen and AAS-using movie stars. Makers of cars, computers, and electronics do not hesitate to advertise their products as “on steroids,” but they would never claim their products were “on cocaine.” In this climate, it is easy to forget that AAS use is an illicit substance abuse.
Formula: FFMI = (W x (100 - BF)/100)H2 + 6.1 x (1.8 - H)
W = weight in kilograms
BF = body fat percentage
H = height in meters
Obtain height in meters and weight in kilograms. Ideally, measure body fat using calipers, electrical impedance, or some other method. Alternately, estimate body fat by visual inspection:
- 20% = average 30-year-old American man
- 10% = quite lean
- 5% = approaching lowest body fat normally attainable
FFMI values for American men:
20 = average
22 = visibly muscular
25 = approximate maximum attainable by a lean individual without using drugs
Example 1
Young male weightlifter is 69 inches tall, weighs 175 lbs, and is moderately lean, with body fat of 10%; he denies AAS use
H = 69 inches x .0254 meters/inch = 1.75 m
H2= 1.75 x 1.75 = 3.06 m2
W = 175 pounds x 0.454 kilograms/lb = 79.5 kg
Therefore, FFMI = (79.5 x (100-10)/100)/3.06 + 6.1 x (1.8 - 1.75) = 23.7
This degree of muscularity can be attained without using AAS
Example 2
Young male weightlifter is 66 inches tall, weighs 175 lbs, and is very lean, with body fat of 6%; he also denies AAS use
H = 66 inches x .0254 meters/inch = 1.68 m
H2= 1.68 x 1.68 = 2.82 m2
W = 175 pounds x 0.454 kilograms/lb = 79.5 kg
Therefore, FFMI = (79.5 x (100-6)/100)2.82 + 6.1 x (1.8 - 1.68) = 27.2
This level of muscularity is extremely unlikely without drugs. Patient is almost certainly lying and should be gently confronted, especially if other symptoms (Table 2) suggest AAS use
Table 2
Clues to possible AAS use in men
| Muscularity |
| Estimated fat-free mass index (FFMI) >26 (see Box 2) |
| Recent rapid muscle gains (>8 lb/month) |
| Striae over pectoralis muscles caused by rapid hypertrophy of underlying muscle |
| Other physical signs |
| Acne |
| Gynecomastia |
| Testicular atrophy |
| Psychiatric signs |
| Uncharacteristically aggressive behavior |
Uncharacteristic hypomanic symptoms
|
Uncharacteristic depressive symptoms
|
To overcome these treatment obstacles, we recommend that you:
- Become as knowledgeable about AAS use as you are about other forms of substance abuse (see Related resources).
- Approach AAS users as you would any other substance abusers—as individuals at risk for potentially serious medical and psychiatric consequences.
- Maintain a high index of suspicion when evaluating any muscular young male patient, even if he initially denies AAS use.
AAS use can often be suspected by looking at the patient as he walks in the door. Using what we call the “fat-free mass index” (FFMI) to calculate muscularity (Box 2), we have shown that a lean man can achieve only a certain amount of muscularity without using drugs.5 Although this finding needs to be replicated elsewhere, in our experience a man is almost certainly lying if he:
- is relatively lean (with approximately 10% body fat)
- displays an FFMI >26
- and claims he has not used drugs.
If a patient has an elevated FFMI and other cues suggesting AAS use (Table 2), gently but persistently question him if he denies using these drugs.
TREATING AAS-ASSOCIATED SYNDROMES
When you have established a history of AAS use, you will be far better prepared to anticipate and possibly treat its associated syndromes. Discussion of these effects is beyond the scope of this paper; for details, see reviews of AAS-associated medical effects,3,6 psychiatric effects,6,7 and general treatment principles.8 We focus here on the four scenarios clinicians encounter most often in practice and offer some pragmatic suggestions.
Forensic cases. AAS users almost never voluntarily seek help to stop their drug use. Such a request would be somewhat analogous to a girl with anorexia nervosa voluntarily asking for help to gain weight. We are unaware of any rehabilitation centers, clinics, 12-step programs, or the like for AAS users—there is no demand for them.
Thus, an AAS user may first come to clinical attention through legal channels. For example, if an AAS user committed a violent crime while experiencing hypomanic effects from these drugs, he might be required to undergo random urine testing as a condition of probation. This may be reasonable, provided that the tests are unannounced and urine is always collected under direct observation.
Monitoring clinicians may serve as little better than policemen, although sometimes it is possible to forge an alliance with the patient.
Depression. Exogenous AAS administration suppresses endogenous testosterone production through feedback mechanisms involving the hypothalamic-pituitary-testicular axis.3,6 Thus, during a long cycle, the user’s testes may shrink to half their normal size and stop producing testosterone and spermatozoa.
If the user then stops AAS rapidly, he may plunge into a profoundly hypogonadal state associated with symptoms of major depression. In a field study of 77 steroid users (71 male and 6 female), 6 (7.8%) reported they attempted suicide during AAS withdrawal.9 Depression associated with AAS withdrawal may prompt users to resume AAS quickly, triggering a syndrome of AAS dependence.6,10,11
Fortunately, AAS-withdrawal depression is usually self-limited and responds—in our experience and that of others12—to standard antidepressants. We recommend aggressively treating such depressions, as doing so may prevent resumption of AAS use and eventual AAS dependence.
Body-image disorders. AAS users often report body-image disorders, especially muscle dysmorphia—a form of body dysmorphic disorder where individuals become preoccupied with the belief that they are not adequately muscular.13,14 Anxieties about muscularity are a risk factor for subsequent AAS use15 and a major contributor to AAS dependence.8,11
Body dysmorphic disorder responds to pharmacologic and cognitive-behavioral interventions.3,16 Young men showing pathologic concerns about their muscularity or displaying related body-image pathology may benefit from prompt treatment before they are tempted to use AAS.
Progression to opioid dependence. An ominous development among American17 and British18 AAS users is a growing tendency to use opioids. In two studies of individuals with opioid dependence,19,20 7% to 9% reported beginning as AAS users, then learning about opioids from fellow bodybuilders and often buying their first illicit opioids from the person who had sold them AAS. Most learned as teenagers to use needles to inject AAS intramuscularly, so beginning to using opioids intravenously was only a small step.
In the last 5 years, we have become anecdotally aware of numerous AAS users who developed heroin addiction requiring repeated inpatient detoxification or who died of unintentional opioid overdoses. We suspect this phenomenon is under-recognized and urge clinicians to watch for it.
- Pope HG Jr, Brower KJ. Anabolic-androgenic steroid abuse. In: Sadock BJ, Sadock VA (eds). Comprehensive textbook of psychiatry (8th ed). Philadelphia: Lippincott Williams & Wilkins (in press).
- Yesalis CE (ed). Anabolic steroids in sport and exercise (2nd ed). Champaign, IL: Human Kinetics, 2000.
- The Taylor Hooton Foundation. Started by the father of a high school athlete who committed suicide during a depressive episode apparently precipitated by AAS withdrawal. Includes links to related Web sites. http://www.taylorhooton.org/about.asp. Accessed Nov. 10, 2004.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Pope HG, Jr, Kanayama G, Ionescu-Pioggia M, Hudson JI. Anabolic steroid users’ attitudes towards physicians. Addiction 2004;99:1189-94.
2. Dawson RT. Drugs in sport—the role of the physician. J Endocrinol 2001;170:55-61.
3. Kutscher EC, Lund BC, Perry PJ. Anabolic steroids: a review for the clinician. Sports Med 2002;32:285-96.
4. Pope HG, Jr, Phillips KA, Olivardia R. The Adonis complex: the secret crisis of male body obsession. New York: Free Press, 2000.
5. Kouri EM, Pope HG, Jr, Katz DL, Oliva PS. Fat-free mass index in users and non-users of anabolic-androgenic steroids. Clin J Sport Med 1995;5:223-8.
6. Brower KJ. Anabolic steroid abuse and dependence. Curr Psychiatry Rep 2002;4:377-83.
7. Pope HG, Jr, Katz DL. Psychiatric effects of exogenous anabolic-androgenic steroids. In: Wolkowitz OM, Rothschild AJ (eds). Psychoneuroendocrinology: the scientific basis of clinical practice. Washington. DC: American Psychiatric Publishing, 2003;331-58.
8. Pope HG, Jr, Brower KJ. Anabolic-androgenic steroids. In: Galanter M, Kleber HD (eds). American Psychiatric Publishing textbook of substance abuse treatment (3rd ed). Washington DC: American Psychiatric Publishing, 2004;257-64.
9. Malone DA, Jr, Dimeff R, Lombardo JA, Sample BRH. Psychiatric effects and psychoactive substance use in anabolic-androgenic steroid users. Clin J Sports Med 1995;5:25-31
10. Kashkin KB, Kleber HD. Hooked on hormones? An anabolic steroid addiction hypothesis. JAMA 1989;262:3166-70.
11. Brower KJ, Eliopulos GA, Blow FC, et al. Evidence for physical and psychological dependence on anabolic androgenic steroids in eight weight lifters. Am J Psychiatry. 1990;147(4):510-2.
12. Malone DA, Jr, Dimeff RJ. The use of fluoxetine in depression associated with anabolic steroid withdrawal: a case series. J Clin Psychiatry. 1992;53:130-2.
13. Pope HG, Jr, Gruber AJ, Choi PY. Muscle dysmorphia: an underrecognized form of body dysmorphic disorder. Psychosomatics 1997;38:548-57.
14. Olivardia R, Pope HG, Jr, Hudson JI. ‘Muscle dysmorphia’ in male weightlifters: a case-control study. Am J Psychiatry 2000;157:1291-6.
15. Kanayama G, Pope HG, Jr, Cohane G, Hudson JI. Risk factors for anabolic-androgenic steroid use among weightlifters: a case-control study. Drug Alcohol Depend 2003;71:77-86.
16. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: a review of empirical data and a proposed treatment algorithm. Psychiatr Clin North Am 2000;7:59-82.
17. Wines JD, Jr, Gruber AJ, Pope HG, Jr, Lukas SE. Nalbuphine hydrochloride dependence in anabolic steroid users. Am J Addictions 1999;8:161-4.
18. McBride AJ, Williamson K, Petersen T. Three cases of nalbuphine hydrochloride dependence associated with anabolic steroid abuse. Br J Sports Med 1996;30:69-70.
19. Kanayama G, Cohane G, Weiss RD, Pope HG, Jr. Past anabolic-androgenic steroid use among men admitted for substance abuse treatment: an underrecognized problem? J Clin Psychiatry. 2003;64:156-60.
20. Arvary D, Pope HG, Jr. Anabolic steroids: a possible gateway to opioid dependence. N Engl J Med 2000;342:1532.-
Anabolic steroid use by athletes and body-builders has captured public attention but remains poorly understood by most physicians. This is not surprising because users of anabolic-androgenic steroids (AAS):
- rarely seek treatment or disclose their drug use
- frequently distrust professionals.
If you are a clinician who regularly sees male adolescents and young men, you need to become familiar with—and watch for—this often-secret form of substance abuse. This article provides the groundwork for that understanding, starting with the story of “Aaron”—a composite patient whose case represents experiences and verbatim quotes from AAS users known to the authors.
CASE REPORT: ‘I FEEL INVINCIBLE’
At his first visit, Aaron, age 18, told the psychiatrist he had no complaints but was coming to please his parents. “I have a lot of arguments with my Dad,” he said, “and they keep thinking something’s wrong with me.”
The patient was very muscular and dressed in baggy sweats that masked his body proportions. He was appropriately groomed and darkly tanned but displayed some acne. The clinician guessed he weighed about 175 lbs and stood at about 65 inches, with very low body fat. Although superficially confident, he seemed restless, somewhat anxious, and guarded as the interview progressed.
Aaron admitted he experienced prominent mood swings. During rage outbursts, he had damaged objects and put his fist through the wall. “There’s holes all over the wall of my room,” he joked.
He also had assaulted a motorist in a traffic altercation, then left the scene. “Did you hurt him?” the clinician asked. Somewhat sheepishly, Aaron responded, “Well, I bought the newspaper and kept checking the obituaries for about 2 weeks afterwards.”
He spoke with pride about his weightlifting, which was the focus of his life. He revealed that he was preparing for a body-building contest in 2 months. The psychiatrist asked him about use of supplements—protein shakes, creatine, and “andro” (androstenedione)—all of which Aaron acknowledged. The psychiatrist then gently asked about anabolic steroid use (Box 1).
Initially, Aaron strongly denied using AAS. The psychiatrist persisted, pointing out that no information would be disclosed to his parents, and asked again using colloquial terms from the AAS subculture: “Anybody who is prepping for an untested contest in a couple of months is going to be on a cycle. Come on, what are you taking?”
Anabolic-androgenic steroids (AAS) are hormones that include testosterone—nature’s own AAS—and more than 100 synthetically developed testosterone relatives. All AAS possess anabolic (muscle-building) and androgenic (masculinizing) properties; no known compound can produce one of these effects without the other.
Because of their masculinizing effects, AAS are rarely used by women—and even then in much lower doses than those used by men. Thus, this article focuses on evaluating and treating male adolescents and men.
AAS are not:
- Corticosteroids (such as cortisol) are often called “steroids” but possess no muscle-building properties. Corticosteroids’ prominent but idiosyncratic psychiatric effects are usually seen in consultation-liaison settings where patients have been prescribed these drugs, rather than among substance abusers.
- Androstenedione (“andro”) and its relatives are adrenal steroids that are weakly metabolized into testosterone or other AAS. These substances were sold legally without prescription in the United States for many years but were banned by federal law in October 2004. Their anabolic and psychiatric effects are much weaker than those of AAS.
- Athletic “supplements” with names designed to sound like AAS (such as beginning with “Ana…”) or supplements claimed to be “testosterone-releasers” or the like. If sold legally in supplement stores, an athletic supplement is not an AAS. Psychiatric effects are extremely unlikely.
Eventually it emerged that Aaron had taken five 8- to 20-week AAS “cycles” (courses), during which he had “stacked” (combined) various “injectables” such as IM testosterone and “orals” such as methyltestosterone (Table 1). His current cycle included:
- a blend of testosterone esters (Sustanon), 500 mg IM once a week
- boldenone (Equipoise), a veterinary AAS normally used for horses, 200 mg IM per week
- oxymetholone (Anadrol), 50 mg orally per day.
Table 1
Commonly used anabolic-androgenic steroids
| ‘Injectables’ (usually administered only by injection) | |
| Boldenone (Equipoise)* | |
| Methenolone (Primobolan depot) | |
| Nandrolone (Deca-Durabolin, Durabolin, Laurabolin, others) | |
| Stanozolol (Winstrol-V)* | |
| Testosterone esters (Depo-testosterone, Sten, Sustanon, others) | |
| Trenbolone (Finajet, Parabolan) | |
| ‘Orals’ | |
| Methandienone (formerly called methandrostenolone) (Dianabol, others) | |
| Methenolone (Primobolan) | |
| Methyltestosterone (Android, others) | |
| Mibolerone (Checque Drops)* | |
| Oxandrolone (Anavar, Lipidex) | |
| Oxmetholone (Anadrol, Anapolon) | |
| Stanoxolol (Stromba, Winstrol) | |
| Other anabolic substances sold on the ‘black market’ | |
| Human growth hormone (HGH) | Possesses anabolic properties |
| Extremely expensive | |
| Almost impossible to detect by testing | |
| Lacks androgenic effects | |
| Psychiatric effects appear negligible | |
| Large doses can cause acromegaly | |
| Clenbuterol | Beta-adrenergic agonist with stimulant and anabolic properties |
| Used less commonly than AAS | |
| Lacks androgenic effects and assists fat loss | |
| Can produce psychiatric effects similar to those of amphetamine abuse (rare, in the authors’ experience) | |
| Human chorionic gonadotropin (HCG) | Stimulates testes to produce more testosterone, creating an AAS effect |
| Most commonly used near the end of an AAS “cycle” to “jump-start” the hypothalamic-pituitary-testicular axis and minimize AAS withdrawal | |
| * Veterinary preparation | |
| AAS: anabolic-androgenic steroid | |
His friends had taught him to self-inject AAS at age 15; he admitted that he was also occasionally self-injecting the opioid analgesic nalbuphine intravenously because of “pain in my ‘delts’ from military presses.”
During his cycles, Aaron experienced hypomanic symptoms, including euphoria, prominent irritability, increased libido, decreased need for sleep, and grandiosity. “I feel invincible,” he said. His aggressive outbursts had worsened with increasing AAS doses; in addition to attacking the motorist, he also had been physically violent with his girlfriend. “She’s scared of me when I’m on juice,” he conceded.
During the withdrawal phase after stopping each cycle, Aaron described prominent depression with anhedonia, hypersomnia, loss of libido, and suicidal ideation. “I once almost jumped off a bridge after my fourth cycle,” he admitted. “I couldn’t wait to get on my next cycle to feel good again.” His depressions were also characterized by body-image obsessions; he would regularly spend at least 1 hour a day examining his musculature in a mirror, and sometimes refused to go out in public because he “was getting too small.”
Perhaps most disturbing was his increasing use of opioids. In addition to self-injecting nalbuphine, he also ingested oral opioids such as oxycodone almost daily. He mentioned that several of his friends in the gym had progressed from injecting nalbuphine to injecting morphine or heroin, and he knew two bodybuilders who had died from apparently unintentional opioid overdoses.
Aaron said his parents, teachers, and non-bodybuilding friends were unaware of this history. He claimed his parents were proud that their son had apparently eschewed drugs and alcohol to pursue a healthy athletic lifestyle.
RECOGNIZING AAS USE
In our experience with treating substance abusers, we find that AAS users may be the least likely to disclose their drug use to clinicians. In a recent study,1 20 of 36 AAS users (56%) reported they had never revealed their AAS use to any physician. When asked to rate their trust in sources of information about AAS, 17 of 42 AAS users (40%) said they trusted information from their drug dealers at least as much as information from any physician they had seen.
Some expressed contempt for physicians as “geeks” or “pencil-necks” who could not comprehend the body-building lifestyle. They gave doctors high marks on knowledge of tobacco, alcohol, and ordinary “street drugs” but much lower ratings on AAS knowledge. Other investigators have shown that many clinicians are unfamiliar with AAS.2,3
AAS users embrace these beliefs for two other reasons. First, to admit to AAS use is to admit that one’s muscularity and physical prowess is the result of taking a drug; there is no comparable motivation to withhold information about, say, one’s use of marijuana or cocaine.
Second, AAS users are much less likely than other substance abusers to view their behavior as pathologic. We have argued that our culture is partially to blame.4 Americans pay to watch 300-lb football linemen and AAS-using movie stars. Makers of cars, computers, and electronics do not hesitate to advertise their products as “on steroids,” but they would never claim their products were “on cocaine.” In this climate, it is easy to forget that AAS use is an illicit substance abuse.
Formula: FFMI = (W x (100 - BF)/100)H2 + 6.1 x (1.8 - H)
W = weight in kilograms
BF = body fat percentage
H = height in meters
Obtain height in meters and weight in kilograms. Ideally, measure body fat using calipers, electrical impedance, or some other method. Alternately, estimate body fat by visual inspection:
- 20% = average 30-year-old American man
- 10% = quite lean
- 5% = approaching lowest body fat normally attainable
FFMI values for American men:
20 = average
22 = visibly muscular
25 = approximate maximum attainable by a lean individual without using drugs
Example 1
Young male weightlifter is 69 inches tall, weighs 175 lbs, and is moderately lean, with body fat of 10%; he denies AAS use
H = 69 inches x .0254 meters/inch = 1.75 m
H2= 1.75 x 1.75 = 3.06 m2
W = 175 pounds x 0.454 kilograms/lb = 79.5 kg
Therefore, FFMI = (79.5 x (100-10)/100)/3.06 + 6.1 x (1.8 - 1.75) = 23.7
This degree of muscularity can be attained without using AAS
Example 2
Young male weightlifter is 66 inches tall, weighs 175 lbs, and is very lean, with body fat of 6%; he also denies AAS use
H = 66 inches x .0254 meters/inch = 1.68 m
H2= 1.68 x 1.68 = 2.82 m2
W = 175 pounds x 0.454 kilograms/lb = 79.5 kg
Therefore, FFMI = (79.5 x (100-6)/100)2.82 + 6.1 x (1.8 - 1.68) = 27.2
This level of muscularity is extremely unlikely without drugs. Patient is almost certainly lying and should be gently confronted, especially if other symptoms (Table 2) suggest AAS use
Table 2
Clues to possible AAS use in men
| Muscularity |
| Estimated fat-free mass index (FFMI) >26 (see Box 2) |
| Recent rapid muscle gains (>8 lb/month) |
| Striae over pectoralis muscles caused by rapid hypertrophy of underlying muscle |
| Other physical signs |
| Acne |
| Gynecomastia |
| Testicular atrophy |
| Psychiatric signs |
| Uncharacteristically aggressive behavior |
Uncharacteristic hypomanic symptoms
|
Uncharacteristic depressive symptoms
|
To overcome these treatment obstacles, we recommend that you:
- Become as knowledgeable about AAS use as you are about other forms of substance abuse (see Related resources).
- Approach AAS users as you would any other substance abusers—as individuals at risk for potentially serious medical and psychiatric consequences.
- Maintain a high index of suspicion when evaluating any muscular young male patient, even if he initially denies AAS use.
AAS use can often be suspected by looking at the patient as he walks in the door. Using what we call the “fat-free mass index” (FFMI) to calculate muscularity (Box 2), we have shown that a lean man can achieve only a certain amount of muscularity without using drugs.5 Although this finding needs to be replicated elsewhere, in our experience a man is almost certainly lying if he:
- is relatively lean (with approximately 10% body fat)
- displays an FFMI >26
- and claims he has not used drugs.
If a patient has an elevated FFMI and other cues suggesting AAS use (Table 2), gently but persistently question him if he denies using these drugs.
TREATING AAS-ASSOCIATED SYNDROMES
When you have established a history of AAS use, you will be far better prepared to anticipate and possibly treat its associated syndromes. Discussion of these effects is beyond the scope of this paper; for details, see reviews of AAS-associated medical effects,3,6 psychiatric effects,6,7 and general treatment principles.8 We focus here on the four scenarios clinicians encounter most often in practice and offer some pragmatic suggestions.
Forensic cases. AAS users almost never voluntarily seek help to stop their drug use. Such a request would be somewhat analogous to a girl with anorexia nervosa voluntarily asking for help to gain weight. We are unaware of any rehabilitation centers, clinics, 12-step programs, or the like for AAS users—there is no demand for them.
Thus, an AAS user may first come to clinical attention through legal channels. For example, if an AAS user committed a violent crime while experiencing hypomanic effects from these drugs, he might be required to undergo random urine testing as a condition of probation. This may be reasonable, provided that the tests are unannounced and urine is always collected under direct observation.
Monitoring clinicians may serve as little better than policemen, although sometimes it is possible to forge an alliance with the patient.
Depression. Exogenous AAS administration suppresses endogenous testosterone production through feedback mechanisms involving the hypothalamic-pituitary-testicular axis.3,6 Thus, during a long cycle, the user’s testes may shrink to half their normal size and stop producing testosterone and spermatozoa.
If the user then stops AAS rapidly, he may plunge into a profoundly hypogonadal state associated with symptoms of major depression. In a field study of 77 steroid users (71 male and 6 female), 6 (7.8%) reported they attempted suicide during AAS withdrawal.9 Depression associated with AAS withdrawal may prompt users to resume AAS quickly, triggering a syndrome of AAS dependence.6,10,11
Fortunately, AAS-withdrawal depression is usually self-limited and responds—in our experience and that of others12—to standard antidepressants. We recommend aggressively treating such depressions, as doing so may prevent resumption of AAS use and eventual AAS dependence.
Body-image disorders. AAS users often report body-image disorders, especially muscle dysmorphia—a form of body dysmorphic disorder where individuals become preoccupied with the belief that they are not adequately muscular.13,14 Anxieties about muscularity are a risk factor for subsequent AAS use15 and a major contributor to AAS dependence.8,11
Body dysmorphic disorder responds to pharmacologic and cognitive-behavioral interventions.3,16 Young men showing pathologic concerns about their muscularity or displaying related body-image pathology may benefit from prompt treatment before they are tempted to use AAS.
Progression to opioid dependence. An ominous development among American17 and British18 AAS users is a growing tendency to use opioids. In two studies of individuals with opioid dependence,19,20 7% to 9% reported beginning as AAS users, then learning about opioids from fellow bodybuilders and often buying their first illicit opioids from the person who had sold them AAS. Most learned as teenagers to use needles to inject AAS intramuscularly, so beginning to using opioids intravenously was only a small step.
In the last 5 years, we have become anecdotally aware of numerous AAS users who developed heroin addiction requiring repeated inpatient detoxification or who died of unintentional opioid overdoses. We suspect this phenomenon is under-recognized and urge clinicians to watch for it.
- Pope HG Jr, Brower KJ. Anabolic-androgenic steroid abuse. In: Sadock BJ, Sadock VA (eds). Comprehensive textbook of psychiatry (8th ed). Philadelphia: Lippincott Williams & Wilkins (in press).
- Yesalis CE (ed). Anabolic steroids in sport and exercise (2nd ed). Champaign, IL: Human Kinetics, 2000.
- The Taylor Hooton Foundation. Started by the father of a high school athlete who committed suicide during a depressive episode apparently precipitated by AAS withdrawal. Includes links to related Web sites. http://www.taylorhooton.org/about.asp. Accessed Nov. 10, 2004.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Anabolic steroid use by athletes and body-builders has captured public attention but remains poorly understood by most physicians. This is not surprising because users of anabolic-androgenic steroids (AAS):
- rarely seek treatment or disclose their drug use
- frequently distrust professionals.
If you are a clinician who regularly sees male adolescents and young men, you need to become familiar with—and watch for—this often-secret form of substance abuse. This article provides the groundwork for that understanding, starting with the story of “Aaron”—a composite patient whose case represents experiences and verbatim quotes from AAS users known to the authors.
CASE REPORT: ‘I FEEL INVINCIBLE’
At his first visit, Aaron, age 18, told the psychiatrist he had no complaints but was coming to please his parents. “I have a lot of arguments with my Dad,” he said, “and they keep thinking something’s wrong with me.”
The patient was very muscular and dressed in baggy sweats that masked his body proportions. He was appropriately groomed and darkly tanned but displayed some acne. The clinician guessed he weighed about 175 lbs and stood at about 65 inches, with very low body fat. Although superficially confident, he seemed restless, somewhat anxious, and guarded as the interview progressed.
Aaron admitted he experienced prominent mood swings. During rage outbursts, he had damaged objects and put his fist through the wall. “There’s holes all over the wall of my room,” he joked.
He also had assaulted a motorist in a traffic altercation, then left the scene. “Did you hurt him?” the clinician asked. Somewhat sheepishly, Aaron responded, “Well, I bought the newspaper and kept checking the obituaries for about 2 weeks afterwards.”
He spoke with pride about his weightlifting, which was the focus of his life. He revealed that he was preparing for a body-building contest in 2 months. The psychiatrist asked him about use of supplements—protein shakes, creatine, and “andro” (androstenedione)—all of which Aaron acknowledged. The psychiatrist then gently asked about anabolic steroid use (Box 1).
Initially, Aaron strongly denied using AAS. The psychiatrist persisted, pointing out that no information would be disclosed to his parents, and asked again using colloquial terms from the AAS subculture: “Anybody who is prepping for an untested contest in a couple of months is going to be on a cycle. Come on, what are you taking?”
Anabolic-androgenic steroids (AAS) are hormones that include testosterone—nature’s own AAS—and more than 100 synthetically developed testosterone relatives. All AAS possess anabolic (muscle-building) and androgenic (masculinizing) properties; no known compound can produce one of these effects without the other.
Because of their masculinizing effects, AAS are rarely used by women—and even then in much lower doses than those used by men. Thus, this article focuses on evaluating and treating male adolescents and men.
AAS are not:
- Corticosteroids (such as cortisol) are often called “steroids” but possess no muscle-building properties. Corticosteroids’ prominent but idiosyncratic psychiatric effects are usually seen in consultation-liaison settings where patients have been prescribed these drugs, rather than among substance abusers.
- Androstenedione (“andro”) and its relatives are adrenal steroids that are weakly metabolized into testosterone or other AAS. These substances were sold legally without prescription in the United States for many years but were banned by federal law in October 2004. Their anabolic and psychiatric effects are much weaker than those of AAS.
- Athletic “supplements” with names designed to sound like AAS (such as beginning with “Ana…”) or supplements claimed to be “testosterone-releasers” or the like. If sold legally in supplement stores, an athletic supplement is not an AAS. Psychiatric effects are extremely unlikely.
Eventually it emerged that Aaron had taken five 8- to 20-week AAS “cycles” (courses), during which he had “stacked” (combined) various “injectables” such as IM testosterone and “orals” such as methyltestosterone (Table 1). His current cycle included:
- a blend of testosterone esters (Sustanon), 500 mg IM once a week
- boldenone (Equipoise), a veterinary AAS normally used for horses, 200 mg IM per week
- oxymetholone (Anadrol), 50 mg orally per day.
Table 1
Commonly used anabolic-androgenic steroids
| ‘Injectables’ (usually administered only by injection) | |
| Boldenone (Equipoise)* | |
| Methenolone (Primobolan depot) | |
| Nandrolone (Deca-Durabolin, Durabolin, Laurabolin, others) | |
| Stanozolol (Winstrol-V)* | |
| Testosterone esters (Depo-testosterone, Sten, Sustanon, others) | |
| Trenbolone (Finajet, Parabolan) | |
| ‘Orals’ | |
| Methandienone (formerly called methandrostenolone) (Dianabol, others) | |
| Methenolone (Primobolan) | |
| Methyltestosterone (Android, others) | |
| Mibolerone (Checque Drops)* | |
| Oxandrolone (Anavar, Lipidex) | |
| Oxmetholone (Anadrol, Anapolon) | |
| Stanoxolol (Stromba, Winstrol) | |
| Other anabolic substances sold on the ‘black market’ | |
| Human growth hormone (HGH) | Possesses anabolic properties |
| Extremely expensive | |
| Almost impossible to detect by testing | |
| Lacks androgenic effects | |
| Psychiatric effects appear negligible | |
| Large doses can cause acromegaly | |
| Clenbuterol | Beta-adrenergic agonist with stimulant and anabolic properties |
| Used less commonly than AAS | |
| Lacks androgenic effects and assists fat loss | |
| Can produce psychiatric effects similar to those of amphetamine abuse (rare, in the authors’ experience) | |
| Human chorionic gonadotropin (HCG) | Stimulates testes to produce more testosterone, creating an AAS effect |
| Most commonly used near the end of an AAS “cycle” to “jump-start” the hypothalamic-pituitary-testicular axis and minimize AAS withdrawal | |
| * Veterinary preparation | |
| AAS: anabolic-androgenic steroid | |
His friends had taught him to self-inject AAS at age 15; he admitted that he was also occasionally self-injecting the opioid analgesic nalbuphine intravenously because of “pain in my ‘delts’ from military presses.”
During his cycles, Aaron experienced hypomanic symptoms, including euphoria, prominent irritability, increased libido, decreased need for sleep, and grandiosity. “I feel invincible,” he said. His aggressive outbursts had worsened with increasing AAS doses; in addition to attacking the motorist, he also had been physically violent with his girlfriend. “She’s scared of me when I’m on juice,” he conceded.
During the withdrawal phase after stopping each cycle, Aaron described prominent depression with anhedonia, hypersomnia, loss of libido, and suicidal ideation. “I once almost jumped off a bridge after my fourth cycle,” he admitted. “I couldn’t wait to get on my next cycle to feel good again.” His depressions were also characterized by body-image obsessions; he would regularly spend at least 1 hour a day examining his musculature in a mirror, and sometimes refused to go out in public because he “was getting too small.”
Perhaps most disturbing was his increasing use of opioids. In addition to self-injecting nalbuphine, he also ingested oral opioids such as oxycodone almost daily. He mentioned that several of his friends in the gym had progressed from injecting nalbuphine to injecting morphine or heroin, and he knew two bodybuilders who had died from apparently unintentional opioid overdoses.
Aaron said his parents, teachers, and non-bodybuilding friends were unaware of this history. He claimed his parents were proud that their son had apparently eschewed drugs and alcohol to pursue a healthy athletic lifestyle.
RECOGNIZING AAS USE
In our experience with treating substance abusers, we find that AAS users may be the least likely to disclose their drug use to clinicians. In a recent study,1 20 of 36 AAS users (56%) reported they had never revealed their AAS use to any physician. When asked to rate their trust in sources of information about AAS, 17 of 42 AAS users (40%) said they trusted information from their drug dealers at least as much as information from any physician they had seen.
Some expressed contempt for physicians as “geeks” or “pencil-necks” who could not comprehend the body-building lifestyle. They gave doctors high marks on knowledge of tobacco, alcohol, and ordinary “street drugs” but much lower ratings on AAS knowledge. Other investigators have shown that many clinicians are unfamiliar with AAS.2,3
AAS users embrace these beliefs for two other reasons. First, to admit to AAS use is to admit that one’s muscularity and physical prowess is the result of taking a drug; there is no comparable motivation to withhold information about, say, one’s use of marijuana or cocaine.
Second, AAS users are much less likely than other substance abusers to view their behavior as pathologic. We have argued that our culture is partially to blame.4 Americans pay to watch 300-lb football linemen and AAS-using movie stars. Makers of cars, computers, and electronics do not hesitate to advertise their products as “on steroids,” but they would never claim their products were “on cocaine.” In this climate, it is easy to forget that AAS use is an illicit substance abuse.
Formula: FFMI = (W x (100 - BF)/100)H2 + 6.1 x (1.8 - H)
W = weight in kilograms
BF = body fat percentage
H = height in meters
Obtain height in meters and weight in kilograms. Ideally, measure body fat using calipers, electrical impedance, or some other method. Alternately, estimate body fat by visual inspection:
- 20% = average 30-year-old American man
- 10% = quite lean
- 5% = approaching lowest body fat normally attainable
FFMI values for American men:
20 = average
22 = visibly muscular
25 = approximate maximum attainable by a lean individual without using drugs
Example 1
Young male weightlifter is 69 inches tall, weighs 175 lbs, and is moderately lean, with body fat of 10%; he denies AAS use
H = 69 inches x .0254 meters/inch = 1.75 m
H2= 1.75 x 1.75 = 3.06 m2
W = 175 pounds x 0.454 kilograms/lb = 79.5 kg
Therefore, FFMI = (79.5 x (100-10)/100)/3.06 + 6.1 x (1.8 - 1.75) = 23.7
This degree of muscularity can be attained without using AAS
Example 2
Young male weightlifter is 66 inches tall, weighs 175 lbs, and is very lean, with body fat of 6%; he also denies AAS use
H = 66 inches x .0254 meters/inch = 1.68 m
H2= 1.68 x 1.68 = 2.82 m2
W = 175 pounds x 0.454 kilograms/lb = 79.5 kg
Therefore, FFMI = (79.5 x (100-6)/100)2.82 + 6.1 x (1.8 - 1.68) = 27.2
This level of muscularity is extremely unlikely without drugs. Patient is almost certainly lying and should be gently confronted, especially if other symptoms (Table 2) suggest AAS use
Table 2
Clues to possible AAS use in men
| Muscularity |
| Estimated fat-free mass index (FFMI) >26 (see Box 2) |
| Recent rapid muscle gains (>8 lb/month) |
| Striae over pectoralis muscles caused by rapid hypertrophy of underlying muscle |
| Other physical signs |
| Acne |
| Gynecomastia |
| Testicular atrophy |
| Psychiatric signs |
| Uncharacteristically aggressive behavior |
Uncharacteristic hypomanic symptoms
|
Uncharacteristic depressive symptoms
|
To overcome these treatment obstacles, we recommend that you:
- Become as knowledgeable about AAS use as you are about other forms of substance abuse (see Related resources).
- Approach AAS users as you would any other substance abusers—as individuals at risk for potentially serious medical and psychiatric consequences.
- Maintain a high index of suspicion when evaluating any muscular young male patient, even if he initially denies AAS use.
AAS use can often be suspected by looking at the patient as he walks in the door. Using what we call the “fat-free mass index” (FFMI) to calculate muscularity (Box 2), we have shown that a lean man can achieve only a certain amount of muscularity without using drugs.5 Although this finding needs to be replicated elsewhere, in our experience a man is almost certainly lying if he:
- is relatively lean (with approximately 10% body fat)
- displays an FFMI >26
- and claims he has not used drugs.
If a patient has an elevated FFMI and other cues suggesting AAS use (Table 2), gently but persistently question him if he denies using these drugs.
TREATING AAS-ASSOCIATED SYNDROMES
When you have established a history of AAS use, you will be far better prepared to anticipate and possibly treat its associated syndromes. Discussion of these effects is beyond the scope of this paper; for details, see reviews of AAS-associated medical effects,3,6 psychiatric effects,6,7 and general treatment principles.8 We focus here on the four scenarios clinicians encounter most often in practice and offer some pragmatic suggestions.
Forensic cases. AAS users almost never voluntarily seek help to stop their drug use. Such a request would be somewhat analogous to a girl with anorexia nervosa voluntarily asking for help to gain weight. We are unaware of any rehabilitation centers, clinics, 12-step programs, or the like for AAS users—there is no demand for them.
Thus, an AAS user may first come to clinical attention through legal channels. For example, if an AAS user committed a violent crime while experiencing hypomanic effects from these drugs, he might be required to undergo random urine testing as a condition of probation. This may be reasonable, provided that the tests are unannounced and urine is always collected under direct observation.
Monitoring clinicians may serve as little better than policemen, although sometimes it is possible to forge an alliance with the patient.
Depression. Exogenous AAS administration suppresses endogenous testosterone production through feedback mechanisms involving the hypothalamic-pituitary-testicular axis.3,6 Thus, during a long cycle, the user’s testes may shrink to half their normal size and stop producing testosterone and spermatozoa.
If the user then stops AAS rapidly, he may plunge into a profoundly hypogonadal state associated with symptoms of major depression. In a field study of 77 steroid users (71 male and 6 female), 6 (7.8%) reported they attempted suicide during AAS withdrawal.9 Depression associated with AAS withdrawal may prompt users to resume AAS quickly, triggering a syndrome of AAS dependence.6,10,11
Fortunately, AAS-withdrawal depression is usually self-limited and responds—in our experience and that of others12—to standard antidepressants. We recommend aggressively treating such depressions, as doing so may prevent resumption of AAS use and eventual AAS dependence.
Body-image disorders. AAS users often report body-image disorders, especially muscle dysmorphia—a form of body dysmorphic disorder where individuals become preoccupied with the belief that they are not adequately muscular.13,14 Anxieties about muscularity are a risk factor for subsequent AAS use15 and a major contributor to AAS dependence.8,11
Body dysmorphic disorder responds to pharmacologic and cognitive-behavioral interventions.3,16 Young men showing pathologic concerns about their muscularity or displaying related body-image pathology may benefit from prompt treatment before they are tempted to use AAS.
Progression to opioid dependence. An ominous development among American17 and British18 AAS users is a growing tendency to use opioids. In two studies of individuals with opioid dependence,19,20 7% to 9% reported beginning as AAS users, then learning about opioids from fellow bodybuilders and often buying their first illicit opioids from the person who had sold them AAS. Most learned as teenagers to use needles to inject AAS intramuscularly, so beginning to using opioids intravenously was only a small step.
In the last 5 years, we have become anecdotally aware of numerous AAS users who developed heroin addiction requiring repeated inpatient detoxification or who died of unintentional opioid overdoses. We suspect this phenomenon is under-recognized and urge clinicians to watch for it.
- Pope HG Jr, Brower KJ. Anabolic-androgenic steroid abuse. In: Sadock BJ, Sadock VA (eds). Comprehensive textbook of psychiatry (8th ed). Philadelphia: Lippincott Williams & Wilkins (in press).
- Yesalis CE (ed). Anabolic steroids in sport and exercise (2nd ed). Champaign, IL: Human Kinetics, 2000.
- The Taylor Hooton Foundation. Started by the father of a high school athlete who committed suicide during a depressive episode apparently precipitated by AAS withdrawal. Includes links to related Web sites. http://www.taylorhooton.org/about.asp. Accessed Nov. 10, 2004.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Pope HG, Jr, Kanayama G, Ionescu-Pioggia M, Hudson JI. Anabolic steroid users’ attitudes towards physicians. Addiction 2004;99:1189-94.
2. Dawson RT. Drugs in sport—the role of the physician. J Endocrinol 2001;170:55-61.
3. Kutscher EC, Lund BC, Perry PJ. Anabolic steroids: a review for the clinician. Sports Med 2002;32:285-96.
4. Pope HG, Jr, Phillips KA, Olivardia R. The Adonis complex: the secret crisis of male body obsession. New York: Free Press, 2000.
5. Kouri EM, Pope HG, Jr, Katz DL, Oliva PS. Fat-free mass index in users and non-users of anabolic-androgenic steroids. Clin J Sport Med 1995;5:223-8.
6. Brower KJ. Anabolic steroid abuse and dependence. Curr Psychiatry Rep 2002;4:377-83.
7. Pope HG, Jr, Katz DL. Psychiatric effects of exogenous anabolic-androgenic steroids. In: Wolkowitz OM, Rothschild AJ (eds). Psychoneuroendocrinology: the scientific basis of clinical practice. Washington. DC: American Psychiatric Publishing, 2003;331-58.
8. Pope HG, Jr, Brower KJ. Anabolic-androgenic steroids. In: Galanter M, Kleber HD (eds). American Psychiatric Publishing textbook of substance abuse treatment (3rd ed). Washington DC: American Psychiatric Publishing, 2004;257-64.
9. Malone DA, Jr, Dimeff R, Lombardo JA, Sample BRH. Psychiatric effects and psychoactive substance use in anabolic-androgenic steroid users. Clin J Sports Med 1995;5:25-31
10. Kashkin KB, Kleber HD. Hooked on hormones? An anabolic steroid addiction hypothesis. JAMA 1989;262:3166-70.
11. Brower KJ, Eliopulos GA, Blow FC, et al. Evidence for physical and psychological dependence on anabolic androgenic steroids in eight weight lifters. Am J Psychiatry. 1990;147(4):510-2.
12. Malone DA, Jr, Dimeff RJ. The use of fluoxetine in depression associated with anabolic steroid withdrawal: a case series. J Clin Psychiatry. 1992;53:130-2.
13. Pope HG, Jr, Gruber AJ, Choi PY. Muscle dysmorphia: an underrecognized form of body dysmorphic disorder. Psychosomatics 1997;38:548-57.
14. Olivardia R, Pope HG, Jr, Hudson JI. ‘Muscle dysmorphia’ in male weightlifters: a case-control study. Am J Psychiatry 2000;157:1291-6.
15. Kanayama G, Pope HG, Jr, Cohane G, Hudson JI. Risk factors for anabolic-androgenic steroid use among weightlifters: a case-control study. Drug Alcohol Depend 2003;71:77-86.
16. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: a review of empirical data and a proposed treatment algorithm. Psychiatr Clin North Am 2000;7:59-82.
17. Wines JD, Jr, Gruber AJ, Pope HG, Jr, Lukas SE. Nalbuphine hydrochloride dependence in anabolic steroid users. Am J Addictions 1999;8:161-4.
18. McBride AJ, Williamson K, Petersen T. Three cases of nalbuphine hydrochloride dependence associated with anabolic steroid abuse. Br J Sports Med 1996;30:69-70.
19. Kanayama G, Cohane G, Weiss RD, Pope HG, Jr. Past anabolic-androgenic steroid use among men admitted for substance abuse treatment: an underrecognized problem? J Clin Psychiatry. 2003;64:156-60.
20. Arvary D, Pope HG, Jr. Anabolic steroids: a possible gateway to opioid dependence. N Engl J Med 2000;342:1532.-
1. Pope HG, Jr, Kanayama G, Ionescu-Pioggia M, Hudson JI. Anabolic steroid users’ attitudes towards physicians. Addiction 2004;99:1189-94.
2. Dawson RT. Drugs in sport—the role of the physician. J Endocrinol 2001;170:55-61.
3. Kutscher EC, Lund BC, Perry PJ. Anabolic steroids: a review for the clinician. Sports Med 2002;32:285-96.
4. Pope HG, Jr, Phillips KA, Olivardia R. The Adonis complex: the secret crisis of male body obsession. New York: Free Press, 2000.
5. Kouri EM, Pope HG, Jr, Katz DL, Oliva PS. Fat-free mass index in users and non-users of anabolic-androgenic steroids. Clin J Sport Med 1995;5:223-8.
6. Brower KJ. Anabolic steroid abuse and dependence. Curr Psychiatry Rep 2002;4:377-83.
7. Pope HG, Jr, Katz DL. Psychiatric effects of exogenous anabolic-androgenic steroids. In: Wolkowitz OM, Rothschild AJ (eds). Psychoneuroendocrinology: the scientific basis of clinical practice. Washington. DC: American Psychiatric Publishing, 2003;331-58.
8. Pope HG, Jr, Brower KJ. Anabolic-androgenic steroids. In: Galanter M, Kleber HD (eds). American Psychiatric Publishing textbook of substance abuse treatment (3rd ed). Washington DC: American Psychiatric Publishing, 2004;257-64.
9. Malone DA, Jr, Dimeff R, Lombardo JA, Sample BRH. Psychiatric effects and psychoactive substance use in anabolic-androgenic steroid users. Clin J Sports Med 1995;5:25-31
10. Kashkin KB, Kleber HD. Hooked on hormones? An anabolic steroid addiction hypothesis. JAMA 1989;262:3166-70.
11. Brower KJ, Eliopulos GA, Blow FC, et al. Evidence for physical and psychological dependence on anabolic androgenic steroids in eight weight lifters. Am J Psychiatry. 1990;147(4):510-2.
12. Malone DA, Jr, Dimeff RJ. The use of fluoxetine in depression associated with anabolic steroid withdrawal: a case series. J Clin Psychiatry. 1992;53:130-2.
13. Pope HG, Jr, Gruber AJ, Choi PY. Muscle dysmorphia: an underrecognized form of body dysmorphic disorder. Psychosomatics 1997;38:548-57.
14. Olivardia R, Pope HG, Jr, Hudson JI. ‘Muscle dysmorphia’ in male weightlifters: a case-control study. Am J Psychiatry 2000;157:1291-6.
15. Kanayama G, Pope HG, Jr, Cohane G, Hudson JI. Risk factors for anabolic-androgenic steroid use among weightlifters: a case-control study. Drug Alcohol Depend 2003;71:77-86.
16. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: a review of empirical data and a proposed treatment algorithm. Psychiatr Clin North Am 2000;7:59-82.
17. Wines JD, Jr, Gruber AJ, Pope HG, Jr, Lukas SE. Nalbuphine hydrochloride dependence in anabolic steroid users. Am J Addictions 1999;8:161-4.
18. McBride AJ, Williamson K, Petersen T. Three cases of nalbuphine hydrochloride dependence associated with anabolic steroid abuse. Br J Sports Med 1996;30:69-70.
19. Kanayama G, Cohane G, Weiss RD, Pope HG, Jr. Past anabolic-androgenic steroid use among men admitted for substance abuse treatment: an underrecognized problem? J Clin Psychiatry. 2003;64:156-60.
20. Arvary D, Pope HG, Jr. Anabolic steroids: a possible gateway to opioid dependence. N Engl J Med 2000;342:1532.-
Sex and antidepressants: When to switch drugs or try an antidote
Antidepressants’ sexual side effects can often be managed—while preserving the antidepressant effect—by altering dosages, switching to another drug class, or adding an “antidote.” Understanding the benefits and risks of each strategy can help you:
- base treatment choices on your patient’s history and side-effect experience
- improve long-term compliance with antidepressant regimens.
EFFECTS VARY BY ANTIDEPRESSANT CLASS
Antidepressants may affect one or more phases of sexual functioning:
- desire (libido)
- arousal (erection or vaginal lubrication)
- orgasm/ejaculation.
Sexual symptoms linked to antidepressants range from diminished interest/arousal and delayed orgasm to heightened sexual functioning (Table 1). Resulting sexual dysfunction can impair quality of life and intimate relationships and discourage patients from taking antidepressants (Box) 1,2
Table 1
Sexual side effects linked to antidepressants
| Most common effects | Shown by these drugs |
|---|---|
| Decreased desire | TCAs, MAOIs, SSRIs |
| Delayed or absent ejaculation/orgasm | TCAs, MAOIs, SSRIs |
| Impaired erection | TCAs, MAOIs, SSRIs |
| Less common effects | |
| Increased desire | Bupropion |
| Spontaneous/prolonged erections | SSRIs, CMI,bupropion, trazodone, nefazodone |
| Premature/retrograde/painful ejaculations | TCAs, trazodone, nefazodone |
| Priapism | SSRIs, CMI, bupropion, trazodone, nefazodone |
| Spontaneous orgasms (associated with yawning) | SSRIs, CMI, bupropion |
| Altered sexual sensation and sensitivity | SSRIs, CMI, bupropion |
| TCAs: tricyclics | |
| MAOIs: monoamine oxidase inhibitors | |
| SSRIs: selective serotonin reuptake inhibitors | |
| CMI: clomipramine | |
Although most reports have focused on SSRIs, all antidepressant classes have been associated with sexual dysfunction, with prevalence likely influenced by differences in neurotransmitter modulation (Table 2).1,3,4 The highest rates of sexual side effects have been reported with SSRIs, certain tricyclic antidepressants (TCAs), and monoamine oxidase inhibitors (MAOIs).
A recent study reported similarly high rates with mirtazapine, but its small sample size limits conclusions about side effect prevalence with this drug.1 Other studies have found significantly lower rates with bupropion and nefazodone.
TCAs’ sexual side-effect rates and types depend on how much each drug inhibits serotonin reuptake. Clomipramine appears to have the highest rates of sexual dysfunction—particularly anorgasmia—probably because it inhibits the serotonin transporter more than do other TCAs.5 In TCAs with lesser effects on serotonergic neurotransmission, alpha-adrenergic and cholinergic receptor blockade may cause sexual side effects—particularly erectile dysfunction (ED).
Cholinergic agonists such as bethanechol, 10 to 50 mg/d, may reverse sexual dysfunction caused by anticholinergic effects.6 Cyproheptadine—a nonselective serotonin receptor antagonist—has also shown benefit at 4 to 12 mg/d in treating TCA-related sexual side effects.7
MAOIs. Sexual side effects appear to be more prevalent with MAOIs than with TCAs,4 perhaps similar to the rate seen with SSRIs. MAOIs directly increase serotonergic neurotransmission, and their substantial alpha-adrenergic antagonist effects may also produce sexual side effects.
Waiting for symptoms to subside may be appropriate, as anorgasmia caused by MAOIs may remit spontaneously. Sildenafil8 and cyproheptadine9 may reverse MAOI sexual side effects, although serious toxicity has been reported in a patient taking cyproheptadine and an MAOI.10
SSRIs. Increased serotonergic neurotransmission is widely believed to cause SSRI sexual side effects. Resulting secondary effects—such as inhibited central dopamine release, increased prolactin secretion, and inhibited nitric oxide synthesis—may also play important roles.
In general, SSRIs appear to alter sexual functioning in 40% to 60% of patients—both men and women. Anorgasmia is the most commonly reported sexual symptom.
Although all SSRIs are associated with sexual dysfunction, some studies have found higher rates with paroxetine. One study associated paroxetine with significantly higher rates of ED compared with other SSRIs. The authors attributed this finding to paroxetine’s greater anticholinergic effects or to its directly decreasing nitric oxide synthesis.3
SSRI MANAGEMENT STRATEGIES
Waiting. The simplest, safest way to manage SSRI-related sexual dysfunction is to wait and see if side effects resolve spontaneously. Sexual side effects improve without treatment in approximately 20% of cases,3 although improvement is often incomplete. Moreover, several months may pass before symptoms diminish adequately, making this strategy impractical for patients with substantial sexual dysfunction.
Dosing changes. Because SSRIs’ sexual side effects appear to be dose-related,11 carefully reducing the dosage may reduce sexual dysfunction without compromising antidepressant efficacy. This strategy is most likely to sustain remission when you avoid dosages that have proven ineffective. For example, consider a patient who achieves remission of depressive symptoms when fluoxetine is increased from 20 to 40 mg/d. If sexual side effects emerge at 40 mg/d, relapse may be less likely at 30 mg/d than at 20 mg/d.
Sexual side effects are common in patients taking selective serotonin reuptake inhibitors.1 Sexual side effects diminish patients’ quality of life and significantly decrease adherence to antidepressant regimens,2 which in turn diminishes depression treatment efficacy.
Hidden problem. Drug-related sexual side effects often go undetected because:
- patients are too embarrassed to discuss sexual problems with their physicians
- onset is often later and more insidious than that of other antidepressant side effects
- they may be difficult to distinguish from pre-existing sexual dysfunction caused by depression, other medical reasons, or psychosocial factors
- physicians often fail to educate patients about them.
Clinical tips. These problems point out the importance of obtaining a sexual history before starting antidepressant therapy, educating patients about the potential for sexual side effects with antidepressants (including when they occur and what may be done to manage them), and directly asking patients about specific sexual side effects at follow-up visits.
Other strategies that lessen sexual side effects for some patients include:
- dividing the dosage
- delaying dosing until after sexual activity
- allowing 2- to 3-day “drug holidays” over weekends, when sexual activity is more likely to occur.12
Drug holidays probably would not help patients taking fluoxetine, as plasma concentrations would not drop sufficiently in 2 to 3 days to alleviate sexual side effects. Also, drug holidays are presumably safest for patients who are in maintenance treatment, are asymptomatic, and have no history of rapid symptom recurrence or withdrawal effects when discontinuing SSRIs.12
Switching medications. When sexual side effects do not resolve spontaneously or with dose reduction, consider switching to an antidepressant with a lower incidence of sexual dysfunction.
Table 2
Prevalence of antidepressant sexual side effects
| SSRIs | % of patients affected |
|---|---|
| Citalopram | 38 to 731,3 |
| Fluoxetine | 36 to 581,3 |
| Fluvoxamine | 623 |
| Paroxetine | 42 to 711,3 |
| Sertraline | 40 to 631,3 |
| Other antidepressants | |
| Bupropion | 20 to 241 |
| Mirtazapine | 24 to 401,3 |
| MAO inhibitors | 404 |
| Nefazodone | 8 to 291,3 |
| Tricyclics (excluding clomipramine) | 30 4 |
| Venlafaxine | 40 to 671,3 |
| SSRI: selective serotonin reuptake inhibitor | |
Bupropion has been shown to improve sexual functioning in patients treated for depression. One study reported improved sexual functioning in patients with SSRI-induced sexual side effects who were switched to bupropion.13 Similar studies have shown benefits with substituting nefazodone or mirtazapine for an SSRI.
These uncontrolled studies suggest that switching some patients to a non-SSRI antidepressant may diminish sexual side effects while continuing antidepressant efficacy. Bupropion or nefazodone may be more effective for this purpose, as mirtazapine showed a high rate of sexual side effects in a large observational study.1
Use caution when switching from an SSRI to nefazodone, as cytochrome P-450 2D6 isoenzyme inhibition may increase levels of mCPP—a nefazodone metabolite with anxiogenic properties. To avoid this interaction, taper the SSRI before starting nefazodone.
Switching medications may not be ideal for patients with an unacceptable depression relapse risk, characterized by severe dysfunction, suicidal ideation, or past treatment resistance.
USING AN ANTIDOTE
Adding a second medication to antidepressant therapy is another strategy to consider. An antidote seems most practical when:
- a patient clearly benefits from an antidepressant regimen
- the risk of losing efficacy with a new medication is high
- reducing the dosage or waiting for sexual dysfunction to resolve spontaneously are impractical or have failed.
Most reports of sexual side effect antidotes have been open-label trials of drugs thought to:
- improve some aspect of sexual functioning as with dopamine or noradrenergic agonists)
- or block antidepressant mechanisms suspected of contributing to sexual side effects (as with serotonin receptor antagonists or cholinergic agonists).
Unfortunately, controlled trials with many of these strategies have been less than promising (Table 3).5,14-28 Several trials reported high placebo-response rates—which may complicate assessment of any sexual side effect treatment—and most produced negative results. Two notable exceptions have been sildenafil and bupropion.
Sildenafil, a phosphodiesterase-5 inhibitor, showed greater benefit than placebo in a prospective trial of 90 depressed men (mean age 45) diagnosed with sexual dysfunction caused by an SSRI.28 The men took sildenafil, 50 to 100 mg, 1 hour before sexual activity.
After 6 weeks, 55% of sildenafil-treated patients were rated as much/very much improved on the Clinical Global Impression Scale adapted for Sexual Function, compared with 4% of those taking placebo, a statistically significant difference. Measures used to assess sexual function showed that arousal, erectile function, and orgasm improved significantly, with a lesser effect on desire. This suggests that adjunctive sildenafil reduces SSRIs’ sexual side effects, and this benefit may extend beyond improving ED.
Table 3
Evidence for antidotes used to treat antidepressant sexual side effects
| Drug/dosage Dopaminergic agents | Study designs and outcomes |
|---|---|
| Amantadine, 100 to 400 mg/d14 | Open-label (+) |
| Placebo-controlled (−) | |
| Bupropion SR, 75 to 300 mg/d15 | Open-label (+) |
| Placebo-controlled (+) | |
| Ephedrine16 | Placebo-controlled (−) |
| Methylphenidate, 10 to 30 mg/d14 | Open-label (+) |
| Pramipexole, 0.125 to 2.0 mg/d18 | Open-label (+) |
| Ropinirole, 1 to 4 mg/d19 | Open-label (+) |
| 5-HT antagonists | |
| Cyproheptadine, 2 to 16 mg/d20 | Open-label (+) |
| Granisetron, 1 to 1.5 mg/d21 | Open-label (+) |
| Placebo-controlled (−) | |
| Mianserin, 30 mg/d22 | Open-label (+) |
| Mirtazapine, 15 to 45 mg/d23 | Open-label (+) |
| Placebo-controlled (−) | |
| Nefazodone, 50 to 150 mg/d24 | Open-label (+) |
| Noradrenergic agent | |
| Yohimbine, 5.4 mg/d25 | Open-label (+) |
| Placebo-controlled (−) | |
| Others | |
| Bethanechol, 10 to 50 mg/d6 | Open-label (+) |
| Buspirone, 15 to 60 mg/d26 | Placebo-controlled (+)(−) |
| Ginkgo biloba, 60 to 240 mg/d27 | Open-label (+) |
| Placebo-controlled (−) | |
| Sildenafil, 25 to 200 mg28 | Open-label (+) |
| Placebo-controlled: (+) | |
| (+) = evidence supports effectiveness | |
| (−) = evidence does not support effectiveness | |
| Source: Prepared from references 6 and 14-28. | |
Sildenafil improves peripheral vasodilatation due to smooth muscle relaxation caused by enhanced nitric oxide release. Other sexual side effects—such as delayed orgasm/ejaculation—may improve because of indirect effects of increased penile and clitoral blood flow caused by vasodilatation.29
Sildenafil treatment was well-tolerated; the most common side effects were headache (40.5%), flushing (16.7%), dyspepsia (7.1%), nasal congestion (11.9%), and transient visual disturbances (11.9%).
Bupropion has also shown therapeutic efficacy for SSRI-related sexual dysfunction in a 4-week, placebo-controlled trial of 55 patients (mean age 39) diagnosed with SSRI-induced sexual dysfunction.15 Compared with the placebo group, those receiving add-on bupropion SR, 150 mg bid, improved significantly more in sexual desire and frequency of sexual activity, as measured by the Changes in Sexual Functioning Questionnaire.
Measures of arousal, orgasm, and global sexual functioning did not differ significantly between the two groups. Bupropion added to SSRI treatment was well-tolerated; most-commonly reported side effects were irritability (12%), dry mouth (12%), and headache (15%).
Other ED treatments. Two additional phosphodiesterase-5 inhibitors have become available in the past year. Like sildenafil, tadalafil and vardenafil are indicated for treating ED. They may be useful as alternatives for patients who do not respond to or tolerate sildenafil, although no published studies have examined their use in antidepressant-induced sexual dysfunction.
Recommendation. Based on the evidence, it seems reasonable to start with bupropion or sildenafil when considering an antidote for sexual side effects caused by SSRIs or other medications with strong serotonergic effects. Determining which agent would be “first-line” depends on patient factors, as summarized in Table 130,31For example:
- Bupropion has been reported to augment SSRIs’ antidepressant effects32 and thus may provide added benefit in patients with residual depressive symptoms.
- Bupropion is more effective than sildenafil for improving sexual desire and thus would be preferred for patients in whom this sexual dysfunction symptom is prominent.
- Sildenafil appears to be more effective than bupropion for improving overall sexual satisfaction for men experiencing substantial erectile dysfunction.
Table 4
Bupropion vs. sildenafil as antidote therapy for antidepressant sexual side effects
| Bupropion |
| Possible advantages |
| May reduce residual depressive symptoms, if present32 |
| Appears to improve sexual desire15 |
| Possible disadvantages |
| Daily dosing may increase side-effect risk, but less effective when taken as needed30 |
| Less-clear benefits for arousal and orgasm-related symptoms |
| Sildenafil |
| Possible advantages |
| Can be taken as needed as opposed to daily31 |
| Benefits for arousal and orgasm-related symptoms demonstrated in men31 |
| Possible disadvantages |
| Benefit less-proven for women than for men |
| Reduced sexual spontaneity |
| Unclear benefits for sexual desire31 |
Contraindicated in patients taking organic nitrates because of potentiation of hypotensive effects. Caution advised in patients with:
|
| Source: Prepared from references 15 and 30-32. |
Related resources
- Worthington JJ 3rd, Peters PM. Treatment of antidepressant-induced sexual dysfunction. Drugs Today (Barc) 2003;39(11):887-96.
- Montgomery SA, Baldwin DS, Riley A. Antidepressant medications: a review of the evidence for drug-induced sexual dysfunction. J Affect Disord 2002;69(1-3):119-40.
Drug brand names
- Amantadine • Symmetrel
- Bethanechol • Duvoid, Urecholine, Urabeth
- Bupropion SR • Wellbutrin SR
- Buspirone • Buspar
- Citalopram • Celexa
- Clomipramine • Anafranil
- Cyproheptadine • Periactin
- Fluoxetine • Prozac
- Granisetron • Kytril
- Methyphenidate • Ritalin
- Mianserin • Bolvidon, Norval
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Pramipexole • Mirapex
- Ropinirole • Requip
- Sertraline • Zoloft
- Sildenafil • Viagra
- Tadalafil • Cialis
- Vardenafil • Levitra
- Venlafaxine • Effexor
Disclosure
Dr. Nelson receives research support from Eli Lilly and Co. and Forest Laboratories and is a speaker for Pfizer Inc. and Wyeth Pharmaceuticals.
1. Clayton AH, Pradko JF, Croft HA, et al. Prevalence of sexual dysfunction among newer antidepressants. J Clin Psychiatry 2002;63(4):357-66.
2. Worthington JJ, 3rd, Peters PM. Treatment of antidepressant-induced sexual dysfunction. Drugs Today (Barc) 2003;39(11):887-96.
3. Montejo AL, Llorca G, Izquierdo JA, Rico-Villademoros F. Incidence of sexual dysfunction associated with antidepressant agents: a prospective multicenter study of 1022 outpatients.Spanish Working Group for the Study of Psychotropic-Related Sexual Dysfunction. J Clin Psychiatry 2001;62(suppl 3):10-21.
4. Harrison WM, Rabkin JG, Ehrhardt AA, et al. Effects of antidepressant medication on sexual function: a controlled study. J Clin Psychopharmacol 1986;6(3):144-9.
5. Monteiro WO, Noshirvani HF, Marks IM, Lelliott PT. Anorgasmia from clomipramine in obsessive-compulsive disorder. A controlled trial. Br J Psychiatry 1987;151:107-12.
6. Gross MD. Reversal by bethanechol of sexual dysfunction caused by anticholinergic antidepressants. Am J Psychiatry 1982;139(9):1193-4.
7. Sovner R. Treatment of tricyclic antidepressant-induced orgasmic inhibition with cyproheptadine. J Clin Psychopharmacol 1984;4(3):169.-
8. Gupta S, Masand P, Ashton AK, Berry SL. Phenelzine-induced sexual dysfunction treated with sildenafil. J Sex Marital Ther 1999;25(2):131-5.
9. Decastro RM. Reversal of MAOI-induced anorgasmia with cyproheptadine. Am J Psychiatry 1985;142(6):783.-
10. Kahn DA. Possible toxic interaction between cyproheptadine and phenelzine. Am J Psychiatry 1987;144(9):1242-3.
11. Montejo-Gonzalez AL, Llorca G, Izquierdo JA, et al. SSRI-induced sexual dysfunction: fluoxetine, paroxetine, sertraline, and fluvoxamine in a prospective, multicenter, and descriptive clinical study of 344 patients. J Sex Marital Ther 1997;23:176-94.
12. Rothschild AJ. Selective serotonin reuptake inhibitor-induced sexual dysfunction: efficacy of a drug holiday. Am J Psychiatry 1995;152(10):1514-16.
13. Clayton AH, McGarvey EL, Abouesh AI, Pinkerton RC. Substitution of an SSRI with bupropion sustained release following SSRI-induced sexual dysfunction. J Clin Psychiatry 2001;62(3):185-90.
14. Shrivastava RK. Amantadine in the treatment of sexual dysfunction associated with selective serotonin reuptake inhibitors. J Clin Psychopharmacol 1995;15:83-84.
15. Clayton AH, Warnock JK, Kornstein SG, et al. A placebo-controlled trial of bupropion SR as an antidote for selective serotonin reuptake inhibitor-induced sexual dysfunction. J Clin Psychiatry, 2004;65(1):62-7.
16. Meston CM. A randomized, placebo-controlled, crossover study of ephedrine for SSRI-induced female sexual dysfunction. J Sex Marital Ther 2004;30(2):57-68.
17. Roeloffs C, Bartlik B, Kaplan PM, Kocsis JH. Methylphenidate and SSRI-induced sexual side effects. J Clin Psychiatry 1996;57(11):548.-
18. DeBattista C, Solvason HB, Breen JA, Schatzberg AF. Pramipexole augmentation of a selective serotonin reuptake inhibitor in the treatment of depression. J Clin Psychopharmacol 2000;20(2):274-5.
19. Worthington JJ, 3rd, Simon NM, Korbly NB, et al. Ropinirole for antidepressant-induced sexual dysfunction. Int Clin Psychopharmacol 2002;17(6):307-10.
20. Aizenberg D, Zemishlany Z, Weizman A. Cyproheptadine treatment of sexual dysfunction induced by serotonin reuptake inhibitors. Clin Neuropharmacol 1995;18:320-4.
21. Nelson EB, Keck PE, Jr, McElroy SL. Resolution of fluoxetine-induced sexual dysfunction with the 5-HT 3 antagonist granisetron (letter). J Clin Psychiatry 1997;58:496-7.
22. Aizenberg D, Naor S, Zemishlany Z, Weizman A. The serotonin antagonist mianserin for treatment of serotonin reuptake inhibitor-induced sexual dysfunction in women: an open-label add-on study. Clin Neuropharmacol 1999;22:347-50.
23. Farah A. Relief of SSRI-induced sexual dysfunction with mirtazapine treatment. J Clin Psychiatry 1999;60:260-1.
24. Reynolds RD. Sertraline-induced anorgasmia treated with intermittent nefazodone. J Clin Psychiatry 1997;58:89.-
25. Jacobsen F. Fluoxetine-induced sexual dysfunction and an open trial of yohimbine. J Clin Psychiatry 1992;53:119-22.
26. Michelson D, Bancroft J, Targum S, et al. Female sexual dysfunction associated with antidepressant administration: a randomized, placebo-controlled study of pharmacologic intervention. Am J Psychiatry 2000;157(2):239-43.
27. Kang BJ, Lee SJ, Kim MD, Cho MJ. A placebo-controlled, double-blind trial of Ginkgo biloba for antidepressant-induced sexual dysfunction. Hum Psychopharmacol 2002;17(6):279-84.
28. Nurnberg HG, Hensley PL. Sildenafil citrate for the management of antidepressant-associated erectile dysfunction. J Clin Psychiatry 2003;64(suppl 10):20-5.
29. Zajecka J. Strategies for the treatment of antidepressant-related sexual dysfunction. J Clin Psychiatry 2001;62(suppl 3):35-43.
30. DeBattista C, Solvason HB, Poirier J, et al. A prospective trial of bupropion SR augmentation of partial and non-responders to serotonergic antidepressants. J Clin Psychopharmacol 2003;23:27-30.
31. Ashton AK, Rosen RC. Bupropion as an antidote for serotonin reuptake inhibitor-induced sexual dysfunction. J Clin Psychiatry 1998;59:112-15.
32. Nurnberg HG, Gelenberg A, Hargreave TB, et al. Efficacy of sildenafil citrate for the treatment of erectile dysfunction in men taking serotonin reuptake inhibitors. Am J Psychiatry 2001;158:1926-8.
Antidepressants’ sexual side effects can often be managed—while preserving the antidepressant effect—by altering dosages, switching to another drug class, or adding an “antidote.” Understanding the benefits and risks of each strategy can help you:
- base treatment choices on your patient’s history and side-effect experience
- improve long-term compliance with antidepressant regimens.
EFFECTS VARY BY ANTIDEPRESSANT CLASS
Antidepressants may affect one or more phases of sexual functioning:
- desire (libido)
- arousal (erection or vaginal lubrication)
- orgasm/ejaculation.
Sexual symptoms linked to antidepressants range from diminished interest/arousal and delayed orgasm to heightened sexual functioning (Table 1). Resulting sexual dysfunction can impair quality of life and intimate relationships and discourage patients from taking antidepressants (Box) 1,2
Table 1
Sexual side effects linked to antidepressants
| Most common effects | Shown by these drugs |
|---|---|
| Decreased desire | TCAs, MAOIs, SSRIs |
| Delayed or absent ejaculation/orgasm | TCAs, MAOIs, SSRIs |
| Impaired erection | TCAs, MAOIs, SSRIs |
| Less common effects | |
| Increased desire | Bupropion |
| Spontaneous/prolonged erections | SSRIs, CMI,bupropion, trazodone, nefazodone |
| Premature/retrograde/painful ejaculations | TCAs, trazodone, nefazodone |
| Priapism | SSRIs, CMI, bupropion, trazodone, nefazodone |
| Spontaneous orgasms (associated with yawning) | SSRIs, CMI, bupropion |
| Altered sexual sensation and sensitivity | SSRIs, CMI, bupropion |
| TCAs: tricyclics | |
| MAOIs: monoamine oxidase inhibitors | |
| SSRIs: selective serotonin reuptake inhibitors | |
| CMI: clomipramine | |
Although most reports have focused on SSRIs, all antidepressant classes have been associated with sexual dysfunction, with prevalence likely influenced by differences in neurotransmitter modulation (Table 2).1,3,4 The highest rates of sexual side effects have been reported with SSRIs, certain tricyclic antidepressants (TCAs), and monoamine oxidase inhibitors (MAOIs).
A recent study reported similarly high rates with mirtazapine, but its small sample size limits conclusions about side effect prevalence with this drug.1 Other studies have found significantly lower rates with bupropion and nefazodone.
TCAs’ sexual side-effect rates and types depend on how much each drug inhibits serotonin reuptake. Clomipramine appears to have the highest rates of sexual dysfunction—particularly anorgasmia—probably because it inhibits the serotonin transporter more than do other TCAs.5 In TCAs with lesser effects on serotonergic neurotransmission, alpha-adrenergic and cholinergic receptor blockade may cause sexual side effects—particularly erectile dysfunction (ED).
Cholinergic agonists such as bethanechol, 10 to 50 mg/d, may reverse sexual dysfunction caused by anticholinergic effects.6 Cyproheptadine—a nonselective serotonin receptor antagonist—has also shown benefit at 4 to 12 mg/d in treating TCA-related sexual side effects.7
MAOIs. Sexual side effects appear to be more prevalent with MAOIs than with TCAs,4 perhaps similar to the rate seen with SSRIs. MAOIs directly increase serotonergic neurotransmission, and their substantial alpha-adrenergic antagonist effects may also produce sexual side effects.
Waiting for symptoms to subside may be appropriate, as anorgasmia caused by MAOIs may remit spontaneously. Sildenafil8 and cyproheptadine9 may reverse MAOI sexual side effects, although serious toxicity has been reported in a patient taking cyproheptadine and an MAOI.10
SSRIs. Increased serotonergic neurotransmission is widely believed to cause SSRI sexual side effects. Resulting secondary effects—such as inhibited central dopamine release, increased prolactin secretion, and inhibited nitric oxide synthesis—may also play important roles.
In general, SSRIs appear to alter sexual functioning in 40% to 60% of patients—both men and women. Anorgasmia is the most commonly reported sexual symptom.
Although all SSRIs are associated with sexual dysfunction, some studies have found higher rates with paroxetine. One study associated paroxetine with significantly higher rates of ED compared with other SSRIs. The authors attributed this finding to paroxetine’s greater anticholinergic effects or to its directly decreasing nitric oxide synthesis.3
SSRI MANAGEMENT STRATEGIES
Waiting. The simplest, safest way to manage SSRI-related sexual dysfunction is to wait and see if side effects resolve spontaneously. Sexual side effects improve without treatment in approximately 20% of cases,3 although improvement is often incomplete. Moreover, several months may pass before symptoms diminish adequately, making this strategy impractical for patients with substantial sexual dysfunction.
Dosing changes. Because SSRIs’ sexual side effects appear to be dose-related,11 carefully reducing the dosage may reduce sexual dysfunction without compromising antidepressant efficacy. This strategy is most likely to sustain remission when you avoid dosages that have proven ineffective. For example, consider a patient who achieves remission of depressive symptoms when fluoxetine is increased from 20 to 40 mg/d. If sexual side effects emerge at 40 mg/d, relapse may be less likely at 30 mg/d than at 20 mg/d.
Sexual side effects are common in patients taking selective serotonin reuptake inhibitors.1 Sexual side effects diminish patients’ quality of life and significantly decrease adherence to antidepressant regimens,2 which in turn diminishes depression treatment efficacy.
Hidden problem. Drug-related sexual side effects often go undetected because:
- patients are too embarrassed to discuss sexual problems with their physicians
- onset is often later and more insidious than that of other antidepressant side effects
- they may be difficult to distinguish from pre-existing sexual dysfunction caused by depression, other medical reasons, or psychosocial factors
- physicians often fail to educate patients about them.
Clinical tips. These problems point out the importance of obtaining a sexual history before starting antidepressant therapy, educating patients about the potential for sexual side effects with antidepressants (including when they occur and what may be done to manage them), and directly asking patients about specific sexual side effects at follow-up visits.
Other strategies that lessen sexual side effects for some patients include:
- dividing the dosage
- delaying dosing until after sexual activity
- allowing 2- to 3-day “drug holidays” over weekends, when sexual activity is more likely to occur.12
Drug holidays probably would not help patients taking fluoxetine, as plasma concentrations would not drop sufficiently in 2 to 3 days to alleviate sexual side effects. Also, drug holidays are presumably safest for patients who are in maintenance treatment, are asymptomatic, and have no history of rapid symptom recurrence or withdrawal effects when discontinuing SSRIs.12
Switching medications. When sexual side effects do not resolve spontaneously or with dose reduction, consider switching to an antidepressant with a lower incidence of sexual dysfunction.
Table 2
Prevalence of antidepressant sexual side effects
| SSRIs | % of patients affected |
|---|---|
| Citalopram | 38 to 731,3 |
| Fluoxetine | 36 to 581,3 |
| Fluvoxamine | 623 |
| Paroxetine | 42 to 711,3 |
| Sertraline | 40 to 631,3 |
| Other antidepressants | |
| Bupropion | 20 to 241 |
| Mirtazapine | 24 to 401,3 |
| MAO inhibitors | 404 |
| Nefazodone | 8 to 291,3 |
| Tricyclics (excluding clomipramine) | 30 4 |
| Venlafaxine | 40 to 671,3 |
| SSRI: selective serotonin reuptake inhibitor | |
Bupropion has been shown to improve sexual functioning in patients treated for depression. One study reported improved sexual functioning in patients with SSRI-induced sexual side effects who were switched to bupropion.13 Similar studies have shown benefits with substituting nefazodone or mirtazapine for an SSRI.
These uncontrolled studies suggest that switching some patients to a non-SSRI antidepressant may diminish sexual side effects while continuing antidepressant efficacy. Bupropion or nefazodone may be more effective for this purpose, as mirtazapine showed a high rate of sexual side effects in a large observational study.1
Use caution when switching from an SSRI to nefazodone, as cytochrome P-450 2D6 isoenzyme inhibition may increase levels of mCPP—a nefazodone metabolite with anxiogenic properties. To avoid this interaction, taper the SSRI before starting nefazodone.
Switching medications may not be ideal for patients with an unacceptable depression relapse risk, characterized by severe dysfunction, suicidal ideation, or past treatment resistance.
USING AN ANTIDOTE
Adding a second medication to antidepressant therapy is another strategy to consider. An antidote seems most practical when:
- a patient clearly benefits from an antidepressant regimen
- the risk of losing efficacy with a new medication is high
- reducing the dosage or waiting for sexual dysfunction to resolve spontaneously are impractical or have failed.
Most reports of sexual side effect antidotes have been open-label trials of drugs thought to:
- improve some aspect of sexual functioning as with dopamine or noradrenergic agonists)
- or block antidepressant mechanisms suspected of contributing to sexual side effects (as with serotonin receptor antagonists or cholinergic agonists).
Unfortunately, controlled trials with many of these strategies have been less than promising (Table 3).5,14-28 Several trials reported high placebo-response rates—which may complicate assessment of any sexual side effect treatment—and most produced negative results. Two notable exceptions have been sildenafil and bupropion.
Sildenafil, a phosphodiesterase-5 inhibitor, showed greater benefit than placebo in a prospective trial of 90 depressed men (mean age 45) diagnosed with sexual dysfunction caused by an SSRI.28 The men took sildenafil, 50 to 100 mg, 1 hour before sexual activity.
After 6 weeks, 55% of sildenafil-treated patients were rated as much/very much improved on the Clinical Global Impression Scale adapted for Sexual Function, compared with 4% of those taking placebo, a statistically significant difference. Measures used to assess sexual function showed that arousal, erectile function, and orgasm improved significantly, with a lesser effect on desire. This suggests that adjunctive sildenafil reduces SSRIs’ sexual side effects, and this benefit may extend beyond improving ED.
Table 3
Evidence for antidotes used to treat antidepressant sexual side effects
| Drug/dosage Dopaminergic agents | Study designs and outcomes |
|---|---|
| Amantadine, 100 to 400 mg/d14 | Open-label (+) |
| Placebo-controlled (−) | |
| Bupropion SR, 75 to 300 mg/d15 | Open-label (+) |
| Placebo-controlled (+) | |
| Ephedrine16 | Placebo-controlled (−) |
| Methylphenidate, 10 to 30 mg/d14 | Open-label (+) |
| Pramipexole, 0.125 to 2.0 mg/d18 | Open-label (+) |
| Ropinirole, 1 to 4 mg/d19 | Open-label (+) |
| 5-HT antagonists | |
| Cyproheptadine, 2 to 16 mg/d20 | Open-label (+) |
| Granisetron, 1 to 1.5 mg/d21 | Open-label (+) |
| Placebo-controlled (−) | |
| Mianserin, 30 mg/d22 | Open-label (+) |
| Mirtazapine, 15 to 45 mg/d23 | Open-label (+) |
| Placebo-controlled (−) | |
| Nefazodone, 50 to 150 mg/d24 | Open-label (+) |
| Noradrenergic agent | |
| Yohimbine, 5.4 mg/d25 | Open-label (+) |
| Placebo-controlled (−) | |
| Others | |
| Bethanechol, 10 to 50 mg/d6 | Open-label (+) |
| Buspirone, 15 to 60 mg/d26 | Placebo-controlled (+)(−) |
| Ginkgo biloba, 60 to 240 mg/d27 | Open-label (+) |
| Placebo-controlled (−) | |
| Sildenafil, 25 to 200 mg28 | Open-label (+) |
| Placebo-controlled: (+) | |
| (+) = evidence supports effectiveness | |
| (−) = evidence does not support effectiveness | |
| Source: Prepared from references 6 and 14-28. | |
Sildenafil improves peripheral vasodilatation due to smooth muscle relaxation caused by enhanced nitric oxide release. Other sexual side effects—such as delayed orgasm/ejaculation—may improve because of indirect effects of increased penile and clitoral blood flow caused by vasodilatation.29
Sildenafil treatment was well-tolerated; the most common side effects were headache (40.5%), flushing (16.7%), dyspepsia (7.1%), nasal congestion (11.9%), and transient visual disturbances (11.9%).
Bupropion has also shown therapeutic efficacy for SSRI-related sexual dysfunction in a 4-week, placebo-controlled trial of 55 patients (mean age 39) diagnosed with SSRI-induced sexual dysfunction.15 Compared with the placebo group, those receiving add-on bupropion SR, 150 mg bid, improved significantly more in sexual desire and frequency of sexual activity, as measured by the Changes in Sexual Functioning Questionnaire.
Measures of arousal, orgasm, and global sexual functioning did not differ significantly between the two groups. Bupropion added to SSRI treatment was well-tolerated; most-commonly reported side effects were irritability (12%), dry mouth (12%), and headache (15%).
Other ED treatments. Two additional phosphodiesterase-5 inhibitors have become available in the past year. Like sildenafil, tadalafil and vardenafil are indicated for treating ED. They may be useful as alternatives for patients who do not respond to or tolerate sildenafil, although no published studies have examined their use in antidepressant-induced sexual dysfunction.
Recommendation. Based on the evidence, it seems reasonable to start with bupropion or sildenafil when considering an antidote for sexual side effects caused by SSRIs or other medications with strong serotonergic effects. Determining which agent would be “first-line” depends on patient factors, as summarized in Table 130,31For example:
- Bupropion has been reported to augment SSRIs’ antidepressant effects32 and thus may provide added benefit in patients with residual depressive symptoms.
- Bupropion is more effective than sildenafil for improving sexual desire and thus would be preferred for patients in whom this sexual dysfunction symptom is prominent.
- Sildenafil appears to be more effective than bupropion for improving overall sexual satisfaction for men experiencing substantial erectile dysfunction.
Table 4
Bupropion vs. sildenafil as antidote therapy for antidepressant sexual side effects
| Bupropion |
| Possible advantages |
| May reduce residual depressive symptoms, if present32 |
| Appears to improve sexual desire15 |
| Possible disadvantages |
| Daily dosing may increase side-effect risk, but less effective when taken as needed30 |
| Less-clear benefits for arousal and orgasm-related symptoms |
| Sildenafil |
| Possible advantages |
| Can be taken as needed as opposed to daily31 |
| Benefits for arousal and orgasm-related symptoms demonstrated in men31 |
| Possible disadvantages |
| Benefit less-proven for women than for men |
| Reduced sexual spontaneity |
| Unclear benefits for sexual desire31 |
Contraindicated in patients taking organic nitrates because of potentiation of hypotensive effects. Caution advised in patients with:
|
| Source: Prepared from references 15 and 30-32. |
Related resources
- Worthington JJ 3rd, Peters PM. Treatment of antidepressant-induced sexual dysfunction. Drugs Today (Barc) 2003;39(11):887-96.
- Montgomery SA, Baldwin DS, Riley A. Antidepressant medications: a review of the evidence for drug-induced sexual dysfunction. J Affect Disord 2002;69(1-3):119-40.
Drug brand names
- Amantadine • Symmetrel
- Bethanechol • Duvoid, Urecholine, Urabeth
- Bupropion SR • Wellbutrin SR
- Buspirone • Buspar
- Citalopram • Celexa
- Clomipramine • Anafranil
- Cyproheptadine • Periactin
- Fluoxetine • Prozac
- Granisetron • Kytril
- Methyphenidate • Ritalin
- Mianserin • Bolvidon, Norval
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Pramipexole • Mirapex
- Ropinirole • Requip
- Sertraline • Zoloft
- Sildenafil • Viagra
- Tadalafil • Cialis
- Vardenafil • Levitra
- Venlafaxine • Effexor
Disclosure
Dr. Nelson receives research support from Eli Lilly and Co. and Forest Laboratories and is a speaker for Pfizer Inc. and Wyeth Pharmaceuticals.
Antidepressants’ sexual side effects can often be managed—while preserving the antidepressant effect—by altering dosages, switching to another drug class, or adding an “antidote.” Understanding the benefits and risks of each strategy can help you:
- base treatment choices on your patient’s history and side-effect experience
- improve long-term compliance with antidepressant regimens.
EFFECTS VARY BY ANTIDEPRESSANT CLASS
Antidepressants may affect one or more phases of sexual functioning:
- desire (libido)
- arousal (erection or vaginal lubrication)
- orgasm/ejaculation.
Sexual symptoms linked to antidepressants range from diminished interest/arousal and delayed orgasm to heightened sexual functioning (Table 1). Resulting sexual dysfunction can impair quality of life and intimate relationships and discourage patients from taking antidepressants (Box) 1,2
Table 1
Sexual side effects linked to antidepressants
| Most common effects | Shown by these drugs |
|---|---|
| Decreased desire | TCAs, MAOIs, SSRIs |
| Delayed or absent ejaculation/orgasm | TCAs, MAOIs, SSRIs |
| Impaired erection | TCAs, MAOIs, SSRIs |
| Less common effects | |
| Increased desire | Bupropion |
| Spontaneous/prolonged erections | SSRIs, CMI,bupropion, trazodone, nefazodone |
| Premature/retrograde/painful ejaculations | TCAs, trazodone, nefazodone |
| Priapism | SSRIs, CMI, bupropion, trazodone, nefazodone |
| Spontaneous orgasms (associated with yawning) | SSRIs, CMI, bupropion |
| Altered sexual sensation and sensitivity | SSRIs, CMI, bupropion |
| TCAs: tricyclics | |
| MAOIs: monoamine oxidase inhibitors | |
| SSRIs: selective serotonin reuptake inhibitors | |
| CMI: clomipramine | |
Although most reports have focused on SSRIs, all antidepressant classes have been associated with sexual dysfunction, with prevalence likely influenced by differences in neurotransmitter modulation (Table 2).1,3,4 The highest rates of sexual side effects have been reported with SSRIs, certain tricyclic antidepressants (TCAs), and monoamine oxidase inhibitors (MAOIs).
A recent study reported similarly high rates with mirtazapine, but its small sample size limits conclusions about side effect prevalence with this drug.1 Other studies have found significantly lower rates with bupropion and nefazodone.
TCAs’ sexual side-effect rates and types depend on how much each drug inhibits serotonin reuptake. Clomipramine appears to have the highest rates of sexual dysfunction—particularly anorgasmia—probably because it inhibits the serotonin transporter more than do other TCAs.5 In TCAs with lesser effects on serotonergic neurotransmission, alpha-adrenergic and cholinergic receptor blockade may cause sexual side effects—particularly erectile dysfunction (ED).
Cholinergic agonists such as bethanechol, 10 to 50 mg/d, may reverse sexual dysfunction caused by anticholinergic effects.6 Cyproheptadine—a nonselective serotonin receptor antagonist—has also shown benefit at 4 to 12 mg/d in treating TCA-related sexual side effects.7
MAOIs. Sexual side effects appear to be more prevalent with MAOIs than with TCAs,4 perhaps similar to the rate seen with SSRIs. MAOIs directly increase serotonergic neurotransmission, and their substantial alpha-adrenergic antagonist effects may also produce sexual side effects.
Waiting for symptoms to subside may be appropriate, as anorgasmia caused by MAOIs may remit spontaneously. Sildenafil8 and cyproheptadine9 may reverse MAOI sexual side effects, although serious toxicity has been reported in a patient taking cyproheptadine and an MAOI.10
SSRIs. Increased serotonergic neurotransmission is widely believed to cause SSRI sexual side effects. Resulting secondary effects—such as inhibited central dopamine release, increased prolactin secretion, and inhibited nitric oxide synthesis—may also play important roles.
In general, SSRIs appear to alter sexual functioning in 40% to 60% of patients—both men and women. Anorgasmia is the most commonly reported sexual symptom.
Although all SSRIs are associated with sexual dysfunction, some studies have found higher rates with paroxetine. One study associated paroxetine with significantly higher rates of ED compared with other SSRIs. The authors attributed this finding to paroxetine’s greater anticholinergic effects or to its directly decreasing nitric oxide synthesis.3
SSRI MANAGEMENT STRATEGIES
Waiting. The simplest, safest way to manage SSRI-related sexual dysfunction is to wait and see if side effects resolve spontaneously. Sexual side effects improve without treatment in approximately 20% of cases,3 although improvement is often incomplete. Moreover, several months may pass before symptoms diminish adequately, making this strategy impractical for patients with substantial sexual dysfunction.
Dosing changes. Because SSRIs’ sexual side effects appear to be dose-related,11 carefully reducing the dosage may reduce sexual dysfunction without compromising antidepressant efficacy. This strategy is most likely to sustain remission when you avoid dosages that have proven ineffective. For example, consider a patient who achieves remission of depressive symptoms when fluoxetine is increased from 20 to 40 mg/d. If sexual side effects emerge at 40 mg/d, relapse may be less likely at 30 mg/d than at 20 mg/d.
Sexual side effects are common in patients taking selective serotonin reuptake inhibitors.1 Sexual side effects diminish patients’ quality of life and significantly decrease adherence to antidepressant regimens,2 which in turn diminishes depression treatment efficacy.
Hidden problem. Drug-related sexual side effects often go undetected because:
- patients are too embarrassed to discuss sexual problems with their physicians
- onset is often later and more insidious than that of other antidepressant side effects
- they may be difficult to distinguish from pre-existing sexual dysfunction caused by depression, other medical reasons, or psychosocial factors
- physicians often fail to educate patients about them.
Clinical tips. These problems point out the importance of obtaining a sexual history before starting antidepressant therapy, educating patients about the potential for sexual side effects with antidepressants (including when they occur and what may be done to manage them), and directly asking patients about specific sexual side effects at follow-up visits.
Other strategies that lessen sexual side effects for some patients include:
- dividing the dosage
- delaying dosing until after sexual activity
- allowing 2- to 3-day “drug holidays” over weekends, when sexual activity is more likely to occur.12
Drug holidays probably would not help patients taking fluoxetine, as plasma concentrations would not drop sufficiently in 2 to 3 days to alleviate sexual side effects. Also, drug holidays are presumably safest for patients who are in maintenance treatment, are asymptomatic, and have no history of rapid symptom recurrence or withdrawal effects when discontinuing SSRIs.12
Switching medications. When sexual side effects do not resolve spontaneously or with dose reduction, consider switching to an antidepressant with a lower incidence of sexual dysfunction.
Table 2
Prevalence of antidepressant sexual side effects
| SSRIs | % of patients affected |
|---|---|
| Citalopram | 38 to 731,3 |
| Fluoxetine | 36 to 581,3 |
| Fluvoxamine | 623 |
| Paroxetine | 42 to 711,3 |
| Sertraline | 40 to 631,3 |
| Other antidepressants | |
| Bupropion | 20 to 241 |
| Mirtazapine | 24 to 401,3 |
| MAO inhibitors | 404 |
| Nefazodone | 8 to 291,3 |
| Tricyclics (excluding clomipramine) | 30 4 |
| Venlafaxine | 40 to 671,3 |
| SSRI: selective serotonin reuptake inhibitor | |
Bupropion has been shown to improve sexual functioning in patients treated for depression. One study reported improved sexual functioning in patients with SSRI-induced sexual side effects who were switched to bupropion.13 Similar studies have shown benefits with substituting nefazodone or mirtazapine for an SSRI.
These uncontrolled studies suggest that switching some patients to a non-SSRI antidepressant may diminish sexual side effects while continuing antidepressant efficacy. Bupropion or nefazodone may be more effective for this purpose, as mirtazapine showed a high rate of sexual side effects in a large observational study.1
Use caution when switching from an SSRI to nefazodone, as cytochrome P-450 2D6 isoenzyme inhibition may increase levels of mCPP—a nefazodone metabolite with anxiogenic properties. To avoid this interaction, taper the SSRI before starting nefazodone.
Switching medications may not be ideal for patients with an unacceptable depression relapse risk, characterized by severe dysfunction, suicidal ideation, or past treatment resistance.
USING AN ANTIDOTE
Adding a second medication to antidepressant therapy is another strategy to consider. An antidote seems most practical when:
- a patient clearly benefits from an antidepressant regimen
- the risk of losing efficacy with a new medication is high
- reducing the dosage or waiting for sexual dysfunction to resolve spontaneously are impractical or have failed.
Most reports of sexual side effect antidotes have been open-label trials of drugs thought to:
- improve some aspect of sexual functioning as with dopamine or noradrenergic agonists)
- or block antidepressant mechanisms suspected of contributing to sexual side effects (as with serotonin receptor antagonists or cholinergic agonists).
Unfortunately, controlled trials with many of these strategies have been less than promising (Table 3).5,14-28 Several trials reported high placebo-response rates—which may complicate assessment of any sexual side effect treatment—and most produced negative results. Two notable exceptions have been sildenafil and bupropion.
Sildenafil, a phosphodiesterase-5 inhibitor, showed greater benefit than placebo in a prospective trial of 90 depressed men (mean age 45) diagnosed with sexual dysfunction caused by an SSRI.28 The men took sildenafil, 50 to 100 mg, 1 hour before sexual activity.
After 6 weeks, 55% of sildenafil-treated patients were rated as much/very much improved on the Clinical Global Impression Scale adapted for Sexual Function, compared with 4% of those taking placebo, a statistically significant difference. Measures used to assess sexual function showed that arousal, erectile function, and orgasm improved significantly, with a lesser effect on desire. This suggests that adjunctive sildenafil reduces SSRIs’ sexual side effects, and this benefit may extend beyond improving ED.
Table 3
Evidence for antidotes used to treat antidepressant sexual side effects
| Drug/dosage Dopaminergic agents | Study designs and outcomes |
|---|---|
| Amantadine, 100 to 400 mg/d14 | Open-label (+) |
| Placebo-controlled (−) | |
| Bupropion SR, 75 to 300 mg/d15 | Open-label (+) |
| Placebo-controlled (+) | |
| Ephedrine16 | Placebo-controlled (−) |
| Methylphenidate, 10 to 30 mg/d14 | Open-label (+) |
| Pramipexole, 0.125 to 2.0 mg/d18 | Open-label (+) |
| Ropinirole, 1 to 4 mg/d19 | Open-label (+) |
| 5-HT antagonists | |
| Cyproheptadine, 2 to 16 mg/d20 | Open-label (+) |
| Granisetron, 1 to 1.5 mg/d21 | Open-label (+) |
| Placebo-controlled (−) | |
| Mianserin, 30 mg/d22 | Open-label (+) |
| Mirtazapine, 15 to 45 mg/d23 | Open-label (+) |
| Placebo-controlled (−) | |
| Nefazodone, 50 to 150 mg/d24 | Open-label (+) |
| Noradrenergic agent | |
| Yohimbine, 5.4 mg/d25 | Open-label (+) |
| Placebo-controlled (−) | |
| Others | |
| Bethanechol, 10 to 50 mg/d6 | Open-label (+) |
| Buspirone, 15 to 60 mg/d26 | Placebo-controlled (+)(−) |
| Ginkgo biloba, 60 to 240 mg/d27 | Open-label (+) |
| Placebo-controlled (−) | |
| Sildenafil, 25 to 200 mg28 | Open-label (+) |
| Placebo-controlled: (+) | |
| (+) = evidence supports effectiveness | |
| (−) = evidence does not support effectiveness | |
| Source: Prepared from references 6 and 14-28. | |
Sildenafil improves peripheral vasodilatation due to smooth muscle relaxation caused by enhanced nitric oxide release. Other sexual side effects—such as delayed orgasm/ejaculation—may improve because of indirect effects of increased penile and clitoral blood flow caused by vasodilatation.29
Sildenafil treatment was well-tolerated; the most common side effects were headache (40.5%), flushing (16.7%), dyspepsia (7.1%), nasal congestion (11.9%), and transient visual disturbances (11.9%).
Bupropion has also shown therapeutic efficacy for SSRI-related sexual dysfunction in a 4-week, placebo-controlled trial of 55 patients (mean age 39) diagnosed with SSRI-induced sexual dysfunction.15 Compared with the placebo group, those receiving add-on bupropion SR, 150 mg bid, improved significantly more in sexual desire and frequency of sexual activity, as measured by the Changes in Sexual Functioning Questionnaire.
Measures of arousal, orgasm, and global sexual functioning did not differ significantly between the two groups. Bupropion added to SSRI treatment was well-tolerated; most-commonly reported side effects were irritability (12%), dry mouth (12%), and headache (15%).
Other ED treatments. Two additional phosphodiesterase-5 inhibitors have become available in the past year. Like sildenafil, tadalafil and vardenafil are indicated for treating ED. They may be useful as alternatives for patients who do not respond to or tolerate sildenafil, although no published studies have examined their use in antidepressant-induced sexual dysfunction.
Recommendation. Based on the evidence, it seems reasonable to start with bupropion or sildenafil when considering an antidote for sexual side effects caused by SSRIs or other medications with strong serotonergic effects. Determining which agent would be “first-line” depends on patient factors, as summarized in Table 130,31For example:
- Bupropion has been reported to augment SSRIs’ antidepressant effects32 and thus may provide added benefit in patients with residual depressive symptoms.
- Bupropion is more effective than sildenafil for improving sexual desire and thus would be preferred for patients in whom this sexual dysfunction symptom is prominent.
- Sildenafil appears to be more effective than bupropion for improving overall sexual satisfaction for men experiencing substantial erectile dysfunction.
Table 4
Bupropion vs. sildenafil as antidote therapy for antidepressant sexual side effects
| Bupropion |
| Possible advantages |
| May reduce residual depressive symptoms, if present32 |
| Appears to improve sexual desire15 |
| Possible disadvantages |
| Daily dosing may increase side-effect risk, but less effective when taken as needed30 |
| Less-clear benefits for arousal and orgasm-related symptoms |
| Sildenafil |
| Possible advantages |
| Can be taken as needed as opposed to daily31 |
| Benefits for arousal and orgasm-related symptoms demonstrated in men31 |
| Possible disadvantages |
| Benefit less-proven for women than for men |
| Reduced sexual spontaneity |
| Unclear benefits for sexual desire31 |
Contraindicated in patients taking organic nitrates because of potentiation of hypotensive effects. Caution advised in patients with:
|
| Source: Prepared from references 15 and 30-32. |
Related resources
- Worthington JJ 3rd, Peters PM. Treatment of antidepressant-induced sexual dysfunction. Drugs Today (Barc) 2003;39(11):887-96.
- Montgomery SA, Baldwin DS, Riley A. Antidepressant medications: a review of the evidence for drug-induced sexual dysfunction. J Affect Disord 2002;69(1-3):119-40.
Drug brand names
- Amantadine • Symmetrel
- Bethanechol • Duvoid, Urecholine, Urabeth
- Bupropion SR • Wellbutrin SR
- Buspirone • Buspar
- Citalopram • Celexa
- Clomipramine • Anafranil
- Cyproheptadine • Periactin
- Fluoxetine • Prozac
- Granisetron • Kytril
- Methyphenidate • Ritalin
- Mianserin • Bolvidon, Norval
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Pramipexole • Mirapex
- Ropinirole • Requip
- Sertraline • Zoloft
- Sildenafil • Viagra
- Tadalafil • Cialis
- Vardenafil • Levitra
- Venlafaxine • Effexor
Disclosure
Dr. Nelson receives research support from Eli Lilly and Co. and Forest Laboratories and is a speaker for Pfizer Inc. and Wyeth Pharmaceuticals.
1. Clayton AH, Pradko JF, Croft HA, et al. Prevalence of sexual dysfunction among newer antidepressants. J Clin Psychiatry 2002;63(4):357-66.
2. Worthington JJ, 3rd, Peters PM. Treatment of antidepressant-induced sexual dysfunction. Drugs Today (Barc) 2003;39(11):887-96.
3. Montejo AL, Llorca G, Izquierdo JA, Rico-Villademoros F. Incidence of sexual dysfunction associated with antidepressant agents: a prospective multicenter study of 1022 outpatients.Spanish Working Group for the Study of Psychotropic-Related Sexual Dysfunction. J Clin Psychiatry 2001;62(suppl 3):10-21.
4. Harrison WM, Rabkin JG, Ehrhardt AA, et al. Effects of antidepressant medication on sexual function: a controlled study. J Clin Psychopharmacol 1986;6(3):144-9.
5. Monteiro WO, Noshirvani HF, Marks IM, Lelliott PT. Anorgasmia from clomipramine in obsessive-compulsive disorder. A controlled trial. Br J Psychiatry 1987;151:107-12.
6. Gross MD. Reversal by bethanechol of sexual dysfunction caused by anticholinergic antidepressants. Am J Psychiatry 1982;139(9):1193-4.
7. Sovner R. Treatment of tricyclic antidepressant-induced orgasmic inhibition with cyproheptadine. J Clin Psychopharmacol 1984;4(3):169.-
8. Gupta S, Masand P, Ashton AK, Berry SL. Phenelzine-induced sexual dysfunction treated with sildenafil. J Sex Marital Ther 1999;25(2):131-5.
9. Decastro RM. Reversal of MAOI-induced anorgasmia with cyproheptadine. Am J Psychiatry 1985;142(6):783.-
10. Kahn DA. Possible toxic interaction between cyproheptadine and phenelzine. Am J Psychiatry 1987;144(9):1242-3.
11. Montejo-Gonzalez AL, Llorca G, Izquierdo JA, et al. SSRI-induced sexual dysfunction: fluoxetine, paroxetine, sertraline, and fluvoxamine in a prospective, multicenter, and descriptive clinical study of 344 patients. J Sex Marital Ther 1997;23:176-94.
12. Rothschild AJ. Selective serotonin reuptake inhibitor-induced sexual dysfunction: efficacy of a drug holiday. Am J Psychiatry 1995;152(10):1514-16.
13. Clayton AH, McGarvey EL, Abouesh AI, Pinkerton RC. Substitution of an SSRI with bupropion sustained release following SSRI-induced sexual dysfunction. J Clin Psychiatry 2001;62(3):185-90.
14. Shrivastava RK. Amantadine in the treatment of sexual dysfunction associated with selective serotonin reuptake inhibitors. J Clin Psychopharmacol 1995;15:83-84.
15. Clayton AH, Warnock JK, Kornstein SG, et al. A placebo-controlled trial of bupropion SR as an antidote for selective serotonin reuptake inhibitor-induced sexual dysfunction. J Clin Psychiatry, 2004;65(1):62-7.
16. Meston CM. A randomized, placebo-controlled, crossover study of ephedrine for SSRI-induced female sexual dysfunction. J Sex Marital Ther 2004;30(2):57-68.
17. Roeloffs C, Bartlik B, Kaplan PM, Kocsis JH. Methylphenidate and SSRI-induced sexual side effects. J Clin Psychiatry 1996;57(11):548.-
18. DeBattista C, Solvason HB, Breen JA, Schatzberg AF. Pramipexole augmentation of a selective serotonin reuptake inhibitor in the treatment of depression. J Clin Psychopharmacol 2000;20(2):274-5.
19. Worthington JJ, 3rd, Simon NM, Korbly NB, et al. Ropinirole for antidepressant-induced sexual dysfunction. Int Clin Psychopharmacol 2002;17(6):307-10.
20. Aizenberg D, Zemishlany Z, Weizman A. Cyproheptadine treatment of sexual dysfunction induced by serotonin reuptake inhibitors. Clin Neuropharmacol 1995;18:320-4.
21. Nelson EB, Keck PE, Jr, McElroy SL. Resolution of fluoxetine-induced sexual dysfunction with the 5-HT 3 antagonist granisetron (letter). J Clin Psychiatry 1997;58:496-7.
22. Aizenberg D, Naor S, Zemishlany Z, Weizman A. The serotonin antagonist mianserin for treatment of serotonin reuptake inhibitor-induced sexual dysfunction in women: an open-label add-on study. Clin Neuropharmacol 1999;22:347-50.
23. Farah A. Relief of SSRI-induced sexual dysfunction with mirtazapine treatment. J Clin Psychiatry 1999;60:260-1.
24. Reynolds RD. Sertraline-induced anorgasmia treated with intermittent nefazodone. J Clin Psychiatry 1997;58:89.-
25. Jacobsen F. Fluoxetine-induced sexual dysfunction and an open trial of yohimbine. J Clin Psychiatry 1992;53:119-22.
26. Michelson D, Bancroft J, Targum S, et al. Female sexual dysfunction associated with antidepressant administration: a randomized, placebo-controlled study of pharmacologic intervention. Am J Psychiatry 2000;157(2):239-43.
27. Kang BJ, Lee SJ, Kim MD, Cho MJ. A placebo-controlled, double-blind trial of Ginkgo biloba for antidepressant-induced sexual dysfunction. Hum Psychopharmacol 2002;17(6):279-84.
28. Nurnberg HG, Hensley PL. Sildenafil citrate for the management of antidepressant-associated erectile dysfunction. J Clin Psychiatry 2003;64(suppl 10):20-5.
29. Zajecka J. Strategies for the treatment of antidepressant-related sexual dysfunction. J Clin Psychiatry 2001;62(suppl 3):35-43.
30. DeBattista C, Solvason HB, Poirier J, et al. A prospective trial of bupropion SR augmentation of partial and non-responders to serotonergic antidepressants. J Clin Psychopharmacol 2003;23:27-30.
31. Ashton AK, Rosen RC. Bupropion as an antidote for serotonin reuptake inhibitor-induced sexual dysfunction. J Clin Psychiatry 1998;59:112-15.
32. Nurnberg HG, Gelenberg A, Hargreave TB, et al. Efficacy of sildenafil citrate for the treatment of erectile dysfunction in men taking serotonin reuptake inhibitors. Am J Psychiatry 2001;158:1926-8.
1. Clayton AH, Pradko JF, Croft HA, et al. Prevalence of sexual dysfunction among newer antidepressants. J Clin Psychiatry 2002;63(4):357-66.
2. Worthington JJ, 3rd, Peters PM. Treatment of antidepressant-induced sexual dysfunction. Drugs Today (Barc) 2003;39(11):887-96.
3. Montejo AL, Llorca G, Izquierdo JA, Rico-Villademoros F. Incidence of sexual dysfunction associated with antidepressant agents: a prospective multicenter study of 1022 outpatients.Spanish Working Group for the Study of Psychotropic-Related Sexual Dysfunction. J Clin Psychiatry 2001;62(suppl 3):10-21.
4. Harrison WM, Rabkin JG, Ehrhardt AA, et al. Effects of antidepressant medication on sexual function: a controlled study. J Clin Psychopharmacol 1986;6(3):144-9.
5. Monteiro WO, Noshirvani HF, Marks IM, Lelliott PT. Anorgasmia from clomipramine in obsessive-compulsive disorder. A controlled trial. Br J Psychiatry 1987;151:107-12.
6. Gross MD. Reversal by bethanechol of sexual dysfunction caused by anticholinergic antidepressants. Am J Psychiatry 1982;139(9):1193-4.
7. Sovner R. Treatment of tricyclic antidepressant-induced orgasmic inhibition with cyproheptadine. J Clin Psychopharmacol 1984;4(3):169.-
8. Gupta S, Masand P, Ashton AK, Berry SL. Phenelzine-induced sexual dysfunction treated with sildenafil. J Sex Marital Ther 1999;25(2):131-5.
9. Decastro RM. Reversal of MAOI-induced anorgasmia with cyproheptadine. Am J Psychiatry 1985;142(6):783.-
10. Kahn DA. Possible toxic interaction between cyproheptadine and phenelzine. Am J Psychiatry 1987;144(9):1242-3.
11. Montejo-Gonzalez AL, Llorca G, Izquierdo JA, et al. SSRI-induced sexual dysfunction: fluoxetine, paroxetine, sertraline, and fluvoxamine in a prospective, multicenter, and descriptive clinical study of 344 patients. J Sex Marital Ther 1997;23:176-94.
12. Rothschild AJ. Selective serotonin reuptake inhibitor-induced sexual dysfunction: efficacy of a drug holiday. Am J Psychiatry 1995;152(10):1514-16.
13. Clayton AH, McGarvey EL, Abouesh AI, Pinkerton RC. Substitution of an SSRI with bupropion sustained release following SSRI-induced sexual dysfunction. J Clin Psychiatry 2001;62(3):185-90.
14. Shrivastava RK. Amantadine in the treatment of sexual dysfunction associated with selective serotonin reuptake inhibitors. J Clin Psychopharmacol 1995;15:83-84.
15. Clayton AH, Warnock JK, Kornstein SG, et al. A placebo-controlled trial of bupropion SR as an antidote for selective serotonin reuptake inhibitor-induced sexual dysfunction. J Clin Psychiatry, 2004;65(1):62-7.
16. Meston CM. A randomized, placebo-controlled, crossover study of ephedrine for SSRI-induced female sexual dysfunction. J Sex Marital Ther 2004;30(2):57-68.
17. Roeloffs C, Bartlik B, Kaplan PM, Kocsis JH. Methylphenidate and SSRI-induced sexual side effects. J Clin Psychiatry 1996;57(11):548.-
18. DeBattista C, Solvason HB, Breen JA, Schatzberg AF. Pramipexole augmentation of a selective serotonin reuptake inhibitor in the treatment of depression. J Clin Psychopharmacol 2000;20(2):274-5.
19. Worthington JJ, 3rd, Simon NM, Korbly NB, et al. Ropinirole for antidepressant-induced sexual dysfunction. Int Clin Psychopharmacol 2002;17(6):307-10.
20. Aizenberg D, Zemishlany Z, Weizman A. Cyproheptadine treatment of sexual dysfunction induced by serotonin reuptake inhibitors. Clin Neuropharmacol 1995;18:320-4.
21. Nelson EB, Keck PE, Jr, McElroy SL. Resolution of fluoxetine-induced sexual dysfunction with the 5-HT 3 antagonist granisetron (letter). J Clin Psychiatry 1997;58:496-7.
22. Aizenberg D, Naor S, Zemishlany Z, Weizman A. The serotonin antagonist mianserin for treatment of serotonin reuptake inhibitor-induced sexual dysfunction in women: an open-label add-on study. Clin Neuropharmacol 1999;22:347-50.
23. Farah A. Relief of SSRI-induced sexual dysfunction with mirtazapine treatment. J Clin Psychiatry 1999;60:260-1.
24. Reynolds RD. Sertraline-induced anorgasmia treated with intermittent nefazodone. J Clin Psychiatry 1997;58:89.-
25. Jacobsen F. Fluoxetine-induced sexual dysfunction and an open trial of yohimbine. J Clin Psychiatry 1992;53:119-22.
26. Michelson D, Bancroft J, Targum S, et al. Female sexual dysfunction associated with antidepressant administration: a randomized, placebo-controlled study of pharmacologic intervention. Am J Psychiatry 2000;157(2):239-43.
27. Kang BJ, Lee SJ, Kim MD, Cho MJ. A placebo-controlled, double-blind trial of Ginkgo biloba for antidepressant-induced sexual dysfunction. Hum Psychopharmacol 2002;17(6):279-84.
28. Nurnberg HG, Hensley PL. Sildenafil citrate for the management of antidepressant-associated erectile dysfunction. J Clin Psychiatry 2003;64(suppl 10):20-5.
29. Zajecka J. Strategies for the treatment of antidepressant-related sexual dysfunction. J Clin Psychiatry 2001;62(suppl 3):35-43.
30. DeBattista C, Solvason HB, Poirier J, et al. A prospective trial of bupropion SR augmentation of partial and non-responders to serotonergic antidepressants. J Clin Psychopharmacol 2003;23:27-30.
31. Ashton AK, Rosen RC. Bupropion as an antidote for serotonin reuptake inhibitor-induced sexual dysfunction. J Clin Psychiatry 1998;59:112-15.
32. Nurnberg HG, Gelenberg A, Hargreave TB, et al. Efficacy of sildenafil citrate for the treatment of erectile dysfunction in men taking serotonin reuptake inhibitors. Am J Psychiatry 2001;158:1926-8.
Blocking the ‘munchies’ receptor: A novel approach to obesity
Marijuana has long been known to stimulate appetite, particularly for sweet foods.1 The naughty boys in my fraternity called it “the munchies;” the professionals call it hyperphagia. Cannabinoid receptor (CB1) stimulation by marijuana’s main active component—9-THC—is believed to induce this behavior. Clinicians have successfully used this effect to treat AIDS-related wasting syndrome and other anorexic conditions.2
CB1 is widely expressed throughout the brain and seems to inhibit release of various neurotransmitters.3 How this effect leads to increased appetite is unclear, but it may result from a decrease in the appetite-suppressing effects of hormones such as leptin. In other words, tweaking the CB1 receptor may take the “brakes” off appetite.
Some researchers have speculated that if stimulating CB1 triggers appetite, blocking the receptor might inhibit it (Figure 1).
THE ‘MUNCHIES’ IN MICE
Rimonabant (SR141716), an experimental agent, is a potent and selective CB1 antagonist.
Ravinet Trillou et al fed mice a high-fat diet known to induce obesity.4 The mice were randomized to receive rimonabant or placebo while maintained on the highly palatable diet. The authors asked: Would rimonabant help the mice lose weight even when they could eat as much delicious fatty food as they wanted?
Figure 1 Blocking CB1 may prevent weight gain
Δ9-THC activates the cannabinoid receptor (CB1), stimulating appetite and leading to weight gain in mice (left). When the same receptor is blocked, appetite is controlled (right).
Source: Illustration for CURRENT PSYCHIATRY by Marcia HartsockRimonabant induced a sustained body weight reduction of approximately 20% in the treatment group compared with the placebo group across 5 weeks (Figure 2). Estimated fat stores among the treatment group were depleted by slightly more than 50%.
The authors noted that the mice in the treatment group had decreased their food intake, but the decrease was not sufficient to explain the weight loss. They speculate that rimonabant could activate metabolic processes and decrease intake.
RIMONABANT’S ROLE IN PSYCHIATRY
Phase III human trials of rimonabant are under way for obesity as well as smoking cessation.5 In uncontrolled studies, rimonabant has been shown to help people avoid weight gain while quitting smoking.5
If rimonabant shows effectiveness in controlled trials and is safe in humans, it could be most valuable. Obesity in industrial countries is epidemic and causes serious secondary morbidity, including diabetes, arthritis, and hypertension. Rimonabant, if approved by the FDA, could reach the market by early 2006.6
It is unknown whether rimonabant’s metabolic effects could offset those of many psychotropics. As psychiatrists, we often must stop an effective antipsychotic or antidepressant because it is causing significant weight gain. A treatment that would prevent medication-induced weight gain could improve patient compliance and, ultimately, outcomes.
MANAGING SCHIZOPHRENIA
Some evidence also suggests that rimonabant may offer additional benefits for patients with schizophrenia beyond weight reduction or smoking cessation.
Figure 2 Rimonabant’s effects on weight in mice on a high-fat diet
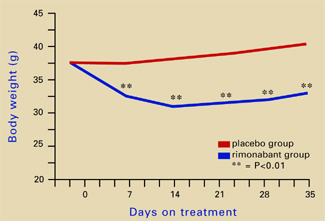
Source: Adapted from reference 4.Leweke et al found increased endogenous cannabinoids in the CSF of patients with schizophrenia, suggesting that a cannabinoid signaling imbalance may contribute to the disorder’s pathogenesis.7 However, 72 patients with schizophrenia or schizoaffective disorder who took rimonabant for 6 weeks showed no improvement compared with a placebo group.8
1. Abel EL. Cannabis: effects on hunger and thirst. Behav Biol 1975;15:255-81.
2. Beal JE, Olson R, Laubenstein L, et al. Dronabinol as a treatment for anorexia associated with weight loss in patients with AIDS. J Pain Symptom Manage 1995;10:89-97.
3. Iversen L. Cannabis and the brain. Brain 2003;126:1252-70.
4. Ravinet Trillou C, Arnone M, Delgorge C, et al. Anti-obesity effect of SR141716, a CB1 receptor antagonist, in diet-induced obese mice. Am J Physiol Regul Integr Comp Physiol 2003;284:R345-53.
5. Fernandez JR, Allison DB. Rimonabant Sanofi-Synthelabo. Curr Opin Investig Drugs 2004;5:430-5.
6. The Website for the Drug Development Industry. Acomplia (rimonabant)—investigational agent for the management of obesity. London: SPGMedia. Available at: http://www. drugdevelopment-technology.com/projects/rimonabant/. Accessed Oct. 14, 2004.
7. Leweke FM, Giuffrida A, Wurster U, et al. Elevated endogenous cannabinoids in schizophrenia. Neuroreport 1999;10:1665-9.
8. Meltzer HY, Arvanitis L, Bauer D, et al. Placebo-controlled evaluation of four novel compounds for the treatment of schizophrenia and schizoaffective disorder. Am J Psychiatry 2004;161:975-84.
Marijuana has long been known to stimulate appetite, particularly for sweet foods.1 The naughty boys in my fraternity called it “the munchies;” the professionals call it hyperphagia. Cannabinoid receptor (CB1) stimulation by marijuana’s main active component—9-THC—is believed to induce this behavior. Clinicians have successfully used this effect to treat AIDS-related wasting syndrome and other anorexic conditions.2
CB1 is widely expressed throughout the brain and seems to inhibit release of various neurotransmitters.3 How this effect leads to increased appetite is unclear, but it may result from a decrease in the appetite-suppressing effects of hormones such as leptin. In other words, tweaking the CB1 receptor may take the “brakes” off appetite.
Some researchers have speculated that if stimulating CB1 triggers appetite, blocking the receptor might inhibit it (Figure 1).
THE ‘MUNCHIES’ IN MICE
Rimonabant (SR141716), an experimental agent, is a potent and selective CB1 antagonist.
Ravinet Trillou et al fed mice a high-fat diet known to induce obesity.4 The mice were randomized to receive rimonabant or placebo while maintained on the highly palatable diet. The authors asked: Would rimonabant help the mice lose weight even when they could eat as much delicious fatty food as they wanted?
Figure 1 Blocking CB1 may prevent weight gain
Δ9-THC activates the cannabinoid receptor (CB1), stimulating appetite and leading to weight gain in mice (left). When the same receptor is blocked, appetite is controlled (right).
Source: Illustration for CURRENT PSYCHIATRY by Marcia HartsockRimonabant induced a sustained body weight reduction of approximately 20% in the treatment group compared with the placebo group across 5 weeks (Figure 2). Estimated fat stores among the treatment group were depleted by slightly more than 50%.
The authors noted that the mice in the treatment group had decreased their food intake, but the decrease was not sufficient to explain the weight loss. They speculate that rimonabant could activate metabolic processes and decrease intake.
RIMONABANT’S ROLE IN PSYCHIATRY
Phase III human trials of rimonabant are under way for obesity as well as smoking cessation.5 In uncontrolled studies, rimonabant has been shown to help people avoid weight gain while quitting smoking.5
If rimonabant shows effectiveness in controlled trials and is safe in humans, it could be most valuable. Obesity in industrial countries is epidemic and causes serious secondary morbidity, including diabetes, arthritis, and hypertension. Rimonabant, if approved by the FDA, could reach the market by early 2006.6
It is unknown whether rimonabant’s metabolic effects could offset those of many psychotropics. As psychiatrists, we often must stop an effective antipsychotic or antidepressant because it is causing significant weight gain. A treatment that would prevent medication-induced weight gain could improve patient compliance and, ultimately, outcomes.
MANAGING SCHIZOPHRENIA
Some evidence also suggests that rimonabant may offer additional benefits for patients with schizophrenia beyond weight reduction or smoking cessation.
Figure 2 Rimonabant’s effects on weight in mice on a high-fat diet
Source: Adapted from reference 4.Leweke et al found increased endogenous cannabinoids in the CSF of patients with schizophrenia, suggesting that a cannabinoid signaling imbalance may contribute to the disorder’s pathogenesis.7 However, 72 patients with schizophrenia or schizoaffective disorder who took rimonabant for 6 weeks showed no improvement compared with a placebo group.8
Marijuana has long been known to stimulate appetite, particularly for sweet foods.1 The naughty boys in my fraternity called it “the munchies;” the professionals call it hyperphagia. Cannabinoid receptor (CB1) stimulation by marijuana’s main active component—9-THC—is believed to induce this behavior. Clinicians have successfully used this effect to treat AIDS-related wasting syndrome and other anorexic conditions.2
CB1 is widely expressed throughout the brain and seems to inhibit release of various neurotransmitters.3 How this effect leads to increased appetite is unclear, but it may result from a decrease in the appetite-suppressing effects of hormones such as leptin. In other words, tweaking the CB1 receptor may take the “brakes” off appetite.
Some researchers have speculated that if stimulating CB1 triggers appetite, blocking the receptor might inhibit it (Figure 1).
THE ‘MUNCHIES’ IN MICE
Rimonabant (SR141716), an experimental agent, is a potent and selective CB1 antagonist.
Ravinet Trillou et al fed mice a high-fat diet known to induce obesity.4 The mice were randomized to receive rimonabant or placebo while maintained on the highly palatable diet. The authors asked: Would rimonabant help the mice lose weight even when they could eat as much delicious fatty food as they wanted?
Figure 1 Blocking CB1 may prevent weight gain
Δ9-THC activates the cannabinoid receptor (CB1), stimulating appetite and leading to weight gain in mice (left). When the same receptor is blocked, appetite is controlled (right).
Source: Illustration for CURRENT PSYCHIATRY by Marcia HartsockRimonabant induced a sustained body weight reduction of approximately 20% in the treatment group compared with the placebo group across 5 weeks (Figure 2). Estimated fat stores among the treatment group were depleted by slightly more than 50%.
The authors noted that the mice in the treatment group had decreased their food intake, but the decrease was not sufficient to explain the weight loss. They speculate that rimonabant could activate metabolic processes and decrease intake.
RIMONABANT’S ROLE IN PSYCHIATRY
Phase III human trials of rimonabant are under way for obesity as well as smoking cessation.5 In uncontrolled studies, rimonabant has been shown to help people avoid weight gain while quitting smoking.5
If rimonabant shows effectiveness in controlled trials and is safe in humans, it could be most valuable. Obesity in industrial countries is epidemic and causes serious secondary morbidity, including diabetes, arthritis, and hypertension. Rimonabant, if approved by the FDA, could reach the market by early 2006.6
It is unknown whether rimonabant’s metabolic effects could offset those of many psychotropics. As psychiatrists, we often must stop an effective antipsychotic or antidepressant because it is causing significant weight gain. A treatment that would prevent medication-induced weight gain could improve patient compliance and, ultimately, outcomes.
MANAGING SCHIZOPHRENIA
Some evidence also suggests that rimonabant may offer additional benefits for patients with schizophrenia beyond weight reduction or smoking cessation.
Figure 2 Rimonabant’s effects on weight in mice on a high-fat diet
Source: Adapted from reference 4.Leweke et al found increased endogenous cannabinoids in the CSF of patients with schizophrenia, suggesting that a cannabinoid signaling imbalance may contribute to the disorder’s pathogenesis.7 However, 72 patients with schizophrenia or schizoaffective disorder who took rimonabant for 6 weeks showed no improvement compared with a placebo group.8
1. Abel EL. Cannabis: effects on hunger and thirst. Behav Biol 1975;15:255-81.
2. Beal JE, Olson R, Laubenstein L, et al. Dronabinol as a treatment for anorexia associated with weight loss in patients with AIDS. J Pain Symptom Manage 1995;10:89-97.
3. Iversen L. Cannabis and the brain. Brain 2003;126:1252-70.
4. Ravinet Trillou C, Arnone M, Delgorge C, et al. Anti-obesity effect of SR141716, a CB1 receptor antagonist, in diet-induced obese mice. Am J Physiol Regul Integr Comp Physiol 2003;284:R345-53.
5. Fernandez JR, Allison DB. Rimonabant Sanofi-Synthelabo. Curr Opin Investig Drugs 2004;5:430-5.
6. The Website for the Drug Development Industry. Acomplia (rimonabant)—investigational agent for the management of obesity. London: SPGMedia. Available at: http://www. drugdevelopment-technology.com/projects/rimonabant/. Accessed Oct. 14, 2004.
7. Leweke FM, Giuffrida A, Wurster U, et al. Elevated endogenous cannabinoids in schizophrenia. Neuroreport 1999;10:1665-9.
8. Meltzer HY, Arvanitis L, Bauer D, et al. Placebo-controlled evaluation of four novel compounds for the treatment of schizophrenia and schizoaffective disorder. Am J Psychiatry 2004;161:975-84.
1. Abel EL. Cannabis: effects on hunger and thirst. Behav Biol 1975;15:255-81.
2. Beal JE, Olson R, Laubenstein L, et al. Dronabinol as a treatment for anorexia associated with weight loss in patients with AIDS. J Pain Symptom Manage 1995;10:89-97.
3. Iversen L. Cannabis and the brain. Brain 2003;126:1252-70.
4. Ravinet Trillou C, Arnone M, Delgorge C, et al. Anti-obesity effect of SR141716, a CB1 receptor antagonist, in diet-induced obese mice. Am J Physiol Regul Integr Comp Physiol 2003;284:R345-53.
5. Fernandez JR, Allison DB. Rimonabant Sanofi-Synthelabo. Curr Opin Investig Drugs 2004;5:430-5.
6. The Website for the Drug Development Industry. Acomplia (rimonabant)—investigational agent for the management of obesity. London: SPGMedia. Available at: http://www. drugdevelopment-technology.com/projects/rimonabant/. Accessed Oct. 14, 2004.
7. Leweke FM, Giuffrida A, Wurster U, et al. Elevated endogenous cannabinoids in schizophrenia. Neuroreport 1999;10:1665-9.
8. Meltzer HY, Arvanitis L, Bauer D, et al. Placebo-controlled evaluation of four novel compounds for the treatment of schizophrenia and schizoaffective disorder. Am J Psychiatry 2004;161:975-84.
Stumped? 5 steps to find the latest evidence
When grappling with difficult cases, clinicians often wonder, “What does the evidence say, and how can I find it?” Thanks to evidence-based medicine (EBM), study results are easier to track down and apply to patient care.
From our experience, we tell how to use EBM’s 5 steps and offer tips and shortcuts to help you quickly find the evidence you need.
SPEEDING RESEARCH TO PRACTICE
Health care is rich in evidence-based innovations, but successful innovations are often disseminated slowly—if at all—to practitioners.1 Studies that demonstrate effective treatments for mental disorders may take considerable time to find their way into clinical practice.2 Similar delays have been noted in other specialties, depriving patients of the most up-to-date medical treatments. Academic medical center surveys show that up to 40% of clinical decisions are not supported by the literature.3,4
Faculty at McMaster University in Canada developed evidence-based medicine as a medical education model by which physicians would rely on the literature—rather than textbooks or tradition—to solve patient problems.7 EBM’s influence on psychiatry has been greatest in the United Kingdom through efforts of its National Health Service, the Centre for Evidence-Based Mental Health at the University of Oxford, and the journal, Evidence-Based Mental Health.5
The U.S. experience. Given managed care’s influence on American medicine, one might expect EBM to have had a similar effect in the United States. This has not been the case, however, perhaps because for-profit HMOs have focused more on controlling costs rather than improving quality.
The U.S. Agency for Healthcare Research and Quality has funded evidence-based practice centers that produce systematic reviews but has done relatively little to promote EBM teaching and practice. Instead, professional organizations such as the American College of Physicians and journals such as JAMA have taken the lead in teaching physicians about EBM.
Residents learning EBM. Most EBM instruction occurs in medical school primary care departments. This is changing, however, now that the Accreditation Council for Graduate Medical Education (ACGME) requires all residents to show competence in EBM methods.8 ACGME requires residency programs in all specialties—including psychiatry—to ensure that graduates achieve EBM core competencies, including being able to use the process described in this article.
Two problems that daunt psychiatrists and other physicians—information overload and uncritical acceptance of information—contribute to less-than-optimal care.5
Information overload. With thousands of medical journals and millions of articles being published, no clinician can keep up with all developments in his or her field. Furthermore, study results often appear contradictory.
Review articles summarize the literature, but most are “journalistic” or “narrative”—not systematic reviews—and thus are subject to author bias in the studies cited and methods used to summarize conflicting results.4 Textbook chapters have the added problem of being almost immediately out-of-date.6
Uncritical acceptance of information occurs when clinicians rely too heavily on personal experiences, noncritiqued study results, expert opinion, and pharmaceutical industry influence.4,6
Two approaches could narrow the gap between research and practice:
- clinical practice guidelines and pathways, a “top-down” approach favored by administrators
- evidence-based medicine, a “bottom-up” approach favored—and developed by—medical educators (Box 1).5,7,8
EBM and patient care. EBM has been described as “partly a philosophy, partly a skill, and partly…a set of tools.”9 David Sackett—often considered the father of EBM—has defined it as “the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients.”10
Although some critics disagree, clinical expertise plays an important role in EBM, as the clinician must integrate research evidence, patient preferences, and the patient’s clinical condition when making decisions.11
EBM’S 5 ACTION STEPS
With EBM, evidence from the medical literature is applied to patient care through 5 action steps:
- Formulate the question.
- Search for answers.
- Appraise the evidence.
- Apply the evidence to the patient.
- Assess the outcome.5,6,12
Step 1: Formulate the question. EBM begins with a clinical question related to the diagnosis, treatment, prognosis, or cause of a patient’s illness. The question is formatted to include the patient’s problem or diagnosis, the intervention of interest and any comparison intervention, and the outcome of interest.
Take, for example, this question: “In patients with bipolar disorder, is lamotrigine as effective as lithium in preventing relapse?” In this format:
- bipolar disorder is the diagnosis
- lamotrigine is the intervention of interest
- lithium is the comparison intervention
- relapse is the outcome of interest.
Step 2: Search for answers. Because answering different types of questions requires different types of evidence, this step involves determining the most appropriate type of evidence and searching for it.13
Evidence hierarchies (Table 1) 5,6,12,14 indicate that certain types of evidence are considered more credible than others. The higher the level of evidence, the more likely it is to provide valid, unbiased estimates of an intervention’s effect.
Table 1
Hierarchy for studies of therapy or harm
| Quality* | Type of evidence |
|---|---|
| 1a | Systematic review of randomized controlled trials (RCTs) |
| 1b | Individual RCT with narrow confidence interval |
| 2a | Systematic review of cohort studies |
| 2b | Individual cohort study RCT with <80% follow-up |
| 2c | Outcomes research Ecological study |
| 3a | Systematic review of case-control studies |
| 3b | Individual case-control study |
| 4 | Case series |
| 5 | Expert opinion |
| * Highest- to lowest-quality evidence | |
| Source: Adapted from references 5,6,12, and 14 | |
For example, observational studies may give misleading results, compared with randomized, controlled, clinical trials.15 Expert opinion—which does not necessarily reflect the best evidence in the literature—is considered the lowest evidence level.16
Beginning the literature search with Medline—as many clinicians do—is relatively inefficient. Searching the massive National Library of Medicine database often identifies a large number of articles, which you then must appraise for validity.
More efficient is Haynes’ “4S” strategy of:
It gives priority to sources of high-quality, pre-appraised information ( Table 2), so that you may omit Step 3—appraisal—in the EBM process.
Table 2
“4S” approach to answering clinical questions
| Category | Examples | Web site |
|---|---|---|
| Systems (comprehensive sources) | Clinical Evidence | http://www.clinicalevidence.com |
| National electronic Library for Mental Health | http://www.nelmh.org | |
| APA Practice Guidelines | http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm | |
| National Guideline Clearinghouse | http://www.guideline.gov | |
| Synopses (structured abstracts) | Evidence-Based Mental Health | http://ebmh.bmjjournals.com |
| ACP Journal Club | http://www.acpjc.org/ | |
| Syntheses (systematic reviews) | Cochrane Database of Systematic Reviews | http://www.update-software.com/abstracts/mainindex.htm |
| Database of Abstracts of Reviews of Effectiveness (DARE) | http://www.york.ac.uk/inst/crd/darehp.htm | |
| Health Technology Assessment (HTA) database | http://www.york.ac.uk/inst/crd/htahp.htm | |
| Studies (original articles) | Medline (PubMed) | http://www.ncbi.nlm.nih.gov/entrez/query/static/clinical.html |
| Source: Adapted from references 12 and 17. | ||
Systems. A system is an information source that covers a variety of diagnoses, summarizes the results of high-quality systematic reviews, is frequently updated, and is linked to the original studies. Three examples are:
- Clinical Evidence, a journal published semi-annually in the United Kingdom that is also available online (www.clinicalevidence.com). Its ease of use, frequent updates, and clear links to the best evidence make it a good starting point.
- National electronic Library for Mental Health (NeLMH) (www.nelmh.org), created by the U.K.’s Centre for Evidence-Based Mental Health.18 It provides information only about depression, schizophrenia, and suicide but may become the model for evidence-based psychiatry.
- Evidence-based clinical practice guidelines developed by the American Psychiatric Association9 and other organizations. Many of these are included in the National Guideline Clearinghouse (www.guideline.gov), produced by the U.S. Department of Health and Human Service’s Agency for Healthcare Research and Quality.
Synopses. If a system does not answer a clinical question, look for synopses—structured abstracts of high-quality systematic reviews or original articles. Synopses are brief and pre-appraised for quality, allowing you to quickly get the point without reading a lengthy article. For psychiatry, Evidence-Based Mental Health and ACP Journal Club are the best synopses sources.
Syntheses. If you don’t find a synopsis to answer your question, then search for a synthesis—a high-quality systematic review. The best source is the Cochrane Database of Systematic Reviews;20 others include:
- Database of Abstracts of Reviews of Effectiveness (DARE)
- Health Technology Assessment (HTA) database.
Table 3
Web sites for learning more about EBM
| Organization | Web site |
|---|---|
| Centre for Evidence-Based Medicine (Oxford) | http://www.cebm.net |
| Centre for Evidence-Based Medicine (Toronto) | http://www.cebm.utoronto.ca |
| Centre for Evidence-Based Mental Health | http://www.cebmh.com |
| EBM Education Center of Excellence | http://www.hsl.unc.edu/ahec/ebmcoe/pages/teaching.htm |
| Evidence-based Medicine Resource Center | http://www.ebmny.org |
| Netting the Evidence | http://www.nettingtheevidence.org.uk |
| University of Sheffield Health Informatics | http://www.shef.ac.uk/~scharr/ir/mschi/ |
| Users’ Guides to the Medical Literature | http://ugi.usersguides.org |
Studies. Only if the first three “S’s” fail to yield an answer would you then search Medline or similar databases for applicable studies.
The PubMed Clinical Queries interface lets you specify the type of question (therapy, diagnosis, etiology, or prognosis) and whether the search is to be sensitive or specific. You can also use filters built into this interface when searching for systematic reviews.
Step 3: Appraise the evidence. After you find an article, appraise its validity and importance. Checklists for appraising studies may be found in EBM texts4,6,12 or downloaded from Web sites (Table 3). Specific appraisal questions to ask depend on the study design and your clinical question.
Step 4: Apply the results to your patient. Assuming the evidence is valid, important, and feasible in your setting, consider your patient’s preferences21 and apply the results.
Step 5: Assess the outcome. Evaluate your performance in searching the literature, and assess the patient’s response.
STREAMLINING THE EBM PROCESS
Studies in academic settings have shown that the full 5-step model can be incorporated into daily practice.6,12 In nonacademic settings, however, practitioners complain about lack of time and information resources, as well as inadequate EBM skills.11,12 Two shortcuts can streamline the process:
Use the 5-step process selectively; it is not required for every patient encounter.6,12 After you research a question for one patient with a particular diagnosis, you can apply the answer to similar patients. Because most psychiatrists’ patients fall into relatively few diagnostic categories, only the exceptional patient would trigger the full 5-step process.
Use pre-appraised information sources. With online databases such as Clinical Evidence and Evidence-Based Mental Health, you can find information quickly, often in the time it takes to use textbooks.5,12,17
Excellent EBM texts4,6,12 and online resources may be useful (Table 3). Courses are listed on the EBM Education Center of Excellence Web site, and the Centre for Evidence-Based Mental Health at Oxford University offers an outstanding course for psychiatrists.
Related resources
- Gray GE. Concise guide to evidence-based psychiatry. Washington, DC: American Psychiatric Publishing, 2004.
- Greenhalgh T. How to read a paper: the basics of evidence-based medicine (2nd ed). London, BMJ Books, 2001.
- Guyatt G, Rennie D (eds). Users’ guides to the medical literature: a manual for evidence-based clinical care. Chicago: AMA Press, 2002.
- Sackett DL, Straus SE, Richardson WS, et al. Evidence-based medicine: how to practice and teach EBM (2nd ed). New York: Churchill Livingstone, 2000.
Acknowledgment
Supported in part by a grant from the National Institute of Mental Health (5-R24-MH61456-03).
1. Berwick DM. Disseminating innovations in health care. JAMA 2003;289:1969-75
2. Drake RE, Goldman HH, Leff HS, et al. Implementing evidence-based practices in routine mental health settings. Psychiatr Serv 2001;52:179-82
3. Geddes JR, Game D, Jenkins NE, et al. What proportion of primary psychiatric interventions are based on evidence from randomised controlled trials? Qual Health Care 1996;5:215-17.
4. Greenhalgh T. How to read a paper: the basics of evidence based medicine (2nd ed). London: BMJ Books, 2001.
5. Gray GE. Evidence-based medicine: an introduction for psychiatrists. J Psychiatr Pract 2002;8:5-13.
6. Sackett DL, Straus SE, Richardson WS, et al. Evidence-based medicine: How to practice and teach EBM (2nd ed). New York: Churchill Livingstone, 2000.
7. Evidence-Based Medicine Working Group. Evidence-based medicine: a new approach to the teaching of medicine. JAMA 1992;268:2420-5.
8. Accreditation Council for Graduate Medical Education General competencies [ACGME Outcome Project Web site], 2001. Available at: http://www.acgme.org/outcome/. Accessed May 5, 2004.
9. Dawes M. Preface. In: Dawes M, Davies P, Gray A, et al (eds). Evidence-based practice: a primer for health professionals New York: Churchill Livingstone, 1999.
10. Sackett DL, Rosenberg WMC, Gray JAM, et al. Evidence-based medicine: what it is and what it isn’t. BMJ 1996;312:71-2.
11. Straus SE, McAlister FA. Evidence-based medicine: a commentary on common criticisms. Can Med Assoc J 2000;163:837-41.
12. Gray GE. Concise guide to evidence-based psychiatry Washington, DC: American Psychiatric Publishing, 2004.
13. Glasziou P, Vandenbroucke J, Chalmers I. Assessing the quality of research. BMJ 2004;328:39-41.
14. Phillips B, Ball C, Sackett D, et al. Centre for Evidence-Based Medicine: Levels of evidence and grades of recommendations, May 2001. Available at: http://www.cebm.net/levels_of_evidence.asp. Accessed Sept. 18, 2004.
15. Lacchetti C, Guyatt G. Therapy and validity: surprising results of randomized controlled trials. In: Guyatt G, Rennie D (eds). Users’ guides to the medical literature: a manual for evidence-based clinical care. Chicago: AMA Press, 2002.
16. Antman EM, Lau J, Kupelnick B, et al. A comparison of results of meta-analyses of randomized control trials and recommendations of clinical experts: treatments for myocardial infarction. JAMA 1992;268:240-8.
17. Haynes RB. Of studies, summaries, synopses, and systems: the “4S” evolution of services for finding current best evidence. Evid Based Ment Health 2001;4:37-9.
18. Dearness KL, Tomlin A. Development of the National Electronic Library for Mental Health: providing evidence-based information for all. Health Info Libr J 2001;18:167-74.
19. American Psychiatric Association. Practice guidelines for the treatment of psychiatric disorders: compendium 2002. Washington, DC: American Psychiatric Publishing, 2002.
20. Antes G. Oxman AD for the Cochrane Collaboration. The Cochrane Collaboration in the 20th Century. In: Egger M, Smith GD, Altman DG (eds). Systematic reviews in health care: meta-analysis in context London: BMJBooks, 2001.
21. Say RE, Thomson R. The importance of patient p in treatment decisions—challenges for doctors. BMJ 2003;327:542-5.
When grappling with difficult cases, clinicians often wonder, “What does the evidence say, and how can I find it?” Thanks to evidence-based medicine (EBM), study results are easier to track down and apply to patient care.
From our experience, we tell how to use EBM’s 5 steps and offer tips and shortcuts to help you quickly find the evidence you need.
SPEEDING RESEARCH TO PRACTICE
Health care is rich in evidence-based innovations, but successful innovations are often disseminated slowly—if at all—to practitioners.1 Studies that demonstrate effective treatments for mental disorders may take considerable time to find their way into clinical practice.2 Similar delays have been noted in other specialties, depriving patients of the most up-to-date medical treatments. Academic medical center surveys show that up to 40% of clinical decisions are not supported by the literature.3,4
Faculty at McMaster University in Canada developed evidence-based medicine as a medical education model by which physicians would rely on the literature—rather than textbooks or tradition—to solve patient problems.7 EBM’s influence on psychiatry has been greatest in the United Kingdom through efforts of its National Health Service, the Centre for Evidence-Based Mental Health at the University of Oxford, and the journal, Evidence-Based Mental Health.5
The U.S. experience. Given managed care’s influence on American medicine, one might expect EBM to have had a similar effect in the United States. This has not been the case, however, perhaps because for-profit HMOs have focused more on controlling costs rather than improving quality.
The U.S. Agency for Healthcare Research and Quality has funded evidence-based practice centers that produce systematic reviews but has done relatively little to promote EBM teaching and practice. Instead, professional organizations such as the American College of Physicians and journals such as JAMA have taken the lead in teaching physicians about EBM.
Residents learning EBM. Most EBM instruction occurs in medical school primary care departments. This is changing, however, now that the Accreditation Council for Graduate Medical Education (ACGME) requires all residents to show competence in EBM methods.8 ACGME requires residency programs in all specialties—including psychiatry—to ensure that graduates achieve EBM core competencies, including being able to use the process described in this article.
Two problems that daunt psychiatrists and other physicians—information overload and uncritical acceptance of information—contribute to less-than-optimal care.5
Information overload. With thousands of medical journals and millions of articles being published, no clinician can keep up with all developments in his or her field. Furthermore, study results often appear contradictory.
Review articles summarize the literature, but most are “journalistic” or “narrative”—not systematic reviews—and thus are subject to author bias in the studies cited and methods used to summarize conflicting results.4 Textbook chapters have the added problem of being almost immediately out-of-date.6
Uncritical acceptance of information occurs when clinicians rely too heavily on personal experiences, noncritiqued study results, expert opinion, and pharmaceutical industry influence.4,6
Two approaches could narrow the gap between research and practice:
- clinical practice guidelines and pathways, a “top-down” approach favored by administrators
- evidence-based medicine, a “bottom-up” approach favored—and developed by—medical educators (Box 1).5,7,8
EBM and patient care. EBM has been described as “partly a philosophy, partly a skill, and partly…a set of tools.”9 David Sackett—often considered the father of EBM—has defined it as “the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients.”10
Although some critics disagree, clinical expertise plays an important role in EBM, as the clinician must integrate research evidence, patient preferences, and the patient’s clinical condition when making decisions.11
EBM’S 5 ACTION STEPS
With EBM, evidence from the medical literature is applied to patient care through 5 action steps:
- Formulate the question.
- Search for answers.
- Appraise the evidence.
- Apply the evidence to the patient.
- Assess the outcome.5,6,12
Step 1: Formulate the question. EBM begins with a clinical question related to the diagnosis, treatment, prognosis, or cause of a patient’s illness. The question is formatted to include the patient’s problem or diagnosis, the intervention of interest and any comparison intervention, and the outcome of interest.
Take, for example, this question: “In patients with bipolar disorder, is lamotrigine as effective as lithium in preventing relapse?” In this format:
- bipolar disorder is the diagnosis
- lamotrigine is the intervention of interest
- lithium is the comparison intervention
- relapse is the outcome of interest.
Step 2: Search for answers. Because answering different types of questions requires different types of evidence, this step involves determining the most appropriate type of evidence and searching for it.13
Evidence hierarchies (Table 1) 5,6,12,14 indicate that certain types of evidence are considered more credible than others. The higher the level of evidence, the more likely it is to provide valid, unbiased estimates of an intervention’s effect.
Table 1
Hierarchy for studies of therapy or harm
| Quality* | Type of evidence |
|---|---|
| 1a | Systematic review of randomized controlled trials (RCTs) |
| 1b | Individual RCT with narrow confidence interval |
| 2a | Systematic review of cohort studies |
| 2b | Individual cohort study RCT with <80% follow-up |
| 2c | Outcomes research Ecological study |
| 3a | Systematic review of case-control studies |
| 3b | Individual case-control study |
| 4 | Case series |
| 5 | Expert opinion |
| * Highest- to lowest-quality evidence | |
| Source: Adapted from references 5,6,12, and 14 | |
For example, observational studies may give misleading results, compared with randomized, controlled, clinical trials.15 Expert opinion—which does not necessarily reflect the best evidence in the literature—is considered the lowest evidence level.16
Beginning the literature search with Medline—as many clinicians do—is relatively inefficient. Searching the massive National Library of Medicine database often identifies a large number of articles, which you then must appraise for validity.
More efficient is Haynes’ “4S” strategy of:
It gives priority to sources of high-quality, pre-appraised information ( Table 2), so that you may omit Step 3—appraisal—in the EBM process.
Table 2
“4S” approach to answering clinical questions
| Category | Examples | Web site |
|---|---|---|
| Systems (comprehensive sources) | Clinical Evidence | http://www.clinicalevidence.com |
| National electronic Library for Mental Health | http://www.nelmh.org | |
| APA Practice Guidelines | http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm | |
| National Guideline Clearinghouse | http://www.guideline.gov | |
| Synopses (structured abstracts) | Evidence-Based Mental Health | http://ebmh.bmjjournals.com |
| ACP Journal Club | http://www.acpjc.org/ | |
| Syntheses (systematic reviews) | Cochrane Database of Systematic Reviews | http://www.update-software.com/abstracts/mainindex.htm |
| Database of Abstracts of Reviews of Effectiveness (DARE) | http://www.york.ac.uk/inst/crd/darehp.htm | |
| Health Technology Assessment (HTA) database | http://www.york.ac.uk/inst/crd/htahp.htm | |
| Studies (original articles) | Medline (PubMed) | http://www.ncbi.nlm.nih.gov/entrez/query/static/clinical.html |
| Source: Adapted from references 12 and 17. | ||
Systems. A system is an information source that covers a variety of diagnoses, summarizes the results of high-quality systematic reviews, is frequently updated, and is linked to the original studies. Three examples are:
- Clinical Evidence, a journal published semi-annually in the United Kingdom that is also available online (www.clinicalevidence.com). Its ease of use, frequent updates, and clear links to the best evidence make it a good starting point.
- National electronic Library for Mental Health (NeLMH) (www.nelmh.org), created by the U.K.’s Centre for Evidence-Based Mental Health.18 It provides information only about depression, schizophrenia, and suicide but may become the model for evidence-based psychiatry.
- Evidence-based clinical practice guidelines developed by the American Psychiatric Association9 and other organizations. Many of these are included in the National Guideline Clearinghouse (www.guideline.gov), produced by the U.S. Department of Health and Human Service’s Agency for Healthcare Research and Quality.
Synopses. If a system does not answer a clinical question, look for synopses—structured abstracts of high-quality systematic reviews or original articles. Synopses are brief and pre-appraised for quality, allowing you to quickly get the point without reading a lengthy article. For psychiatry, Evidence-Based Mental Health and ACP Journal Club are the best synopses sources.
Syntheses. If you don’t find a synopsis to answer your question, then search for a synthesis—a high-quality systematic review. The best source is the Cochrane Database of Systematic Reviews;20 others include:
- Database of Abstracts of Reviews of Effectiveness (DARE)
- Health Technology Assessment (HTA) database.
Table 3
Web sites for learning more about EBM
| Organization | Web site |
|---|---|
| Centre for Evidence-Based Medicine (Oxford) | http://www.cebm.net |
| Centre for Evidence-Based Medicine (Toronto) | http://www.cebm.utoronto.ca |
| Centre for Evidence-Based Mental Health | http://www.cebmh.com |
| EBM Education Center of Excellence | http://www.hsl.unc.edu/ahec/ebmcoe/pages/teaching.htm |
| Evidence-based Medicine Resource Center | http://www.ebmny.org |
| Netting the Evidence | http://www.nettingtheevidence.org.uk |
| University of Sheffield Health Informatics | http://www.shef.ac.uk/~scharr/ir/mschi/ |
| Users’ Guides to the Medical Literature | http://ugi.usersguides.org |
Studies. Only if the first three “S’s” fail to yield an answer would you then search Medline or similar databases for applicable studies.
The PubMed Clinical Queries interface lets you specify the type of question (therapy, diagnosis, etiology, or prognosis) and whether the search is to be sensitive or specific. You can also use filters built into this interface when searching for systematic reviews.
Step 3: Appraise the evidence. After you find an article, appraise its validity and importance. Checklists for appraising studies may be found in EBM texts4,6,12 or downloaded from Web sites (Table 3). Specific appraisal questions to ask depend on the study design and your clinical question.
Step 4: Apply the results to your patient. Assuming the evidence is valid, important, and feasible in your setting, consider your patient’s preferences21 and apply the results.
Step 5: Assess the outcome. Evaluate your performance in searching the literature, and assess the patient’s response.
STREAMLINING THE EBM PROCESS
Studies in academic settings have shown that the full 5-step model can be incorporated into daily practice.6,12 In nonacademic settings, however, practitioners complain about lack of time and information resources, as well as inadequate EBM skills.11,12 Two shortcuts can streamline the process:
Use the 5-step process selectively; it is not required for every patient encounter.6,12 After you research a question for one patient with a particular diagnosis, you can apply the answer to similar patients. Because most psychiatrists’ patients fall into relatively few diagnostic categories, only the exceptional patient would trigger the full 5-step process.
Use pre-appraised information sources. With online databases such as Clinical Evidence and Evidence-Based Mental Health, you can find information quickly, often in the time it takes to use textbooks.5,12,17
Excellent EBM texts4,6,12 and online resources may be useful (Table 3). Courses are listed on the EBM Education Center of Excellence Web site, and the Centre for Evidence-Based Mental Health at Oxford University offers an outstanding course for psychiatrists.
Related resources
- Gray GE. Concise guide to evidence-based psychiatry. Washington, DC: American Psychiatric Publishing, 2004.
- Greenhalgh T. How to read a paper: the basics of evidence-based medicine (2nd ed). London, BMJ Books, 2001.
- Guyatt G, Rennie D (eds). Users’ guides to the medical literature: a manual for evidence-based clinical care. Chicago: AMA Press, 2002.
- Sackett DL, Straus SE, Richardson WS, et al. Evidence-based medicine: how to practice and teach EBM (2nd ed). New York: Churchill Livingstone, 2000.
Acknowledgment
Supported in part by a grant from the National Institute of Mental Health (5-R24-MH61456-03).
When grappling with difficult cases, clinicians often wonder, “What does the evidence say, and how can I find it?” Thanks to evidence-based medicine (EBM), study results are easier to track down and apply to patient care.
From our experience, we tell how to use EBM’s 5 steps and offer tips and shortcuts to help you quickly find the evidence you need.
SPEEDING RESEARCH TO PRACTICE
Health care is rich in evidence-based innovations, but successful innovations are often disseminated slowly—if at all—to practitioners.1 Studies that demonstrate effective treatments for mental disorders may take considerable time to find their way into clinical practice.2 Similar delays have been noted in other specialties, depriving patients of the most up-to-date medical treatments. Academic medical center surveys show that up to 40% of clinical decisions are not supported by the literature.3,4
Faculty at McMaster University in Canada developed evidence-based medicine as a medical education model by which physicians would rely on the literature—rather than textbooks or tradition—to solve patient problems.7 EBM’s influence on psychiatry has been greatest in the United Kingdom through efforts of its National Health Service, the Centre for Evidence-Based Mental Health at the University of Oxford, and the journal, Evidence-Based Mental Health.5
The U.S. experience. Given managed care’s influence on American medicine, one might expect EBM to have had a similar effect in the United States. This has not been the case, however, perhaps because for-profit HMOs have focused more on controlling costs rather than improving quality.
The U.S. Agency for Healthcare Research and Quality has funded evidence-based practice centers that produce systematic reviews but has done relatively little to promote EBM teaching and practice. Instead, professional organizations such as the American College of Physicians and journals such as JAMA have taken the lead in teaching physicians about EBM.
Residents learning EBM. Most EBM instruction occurs in medical school primary care departments. This is changing, however, now that the Accreditation Council for Graduate Medical Education (ACGME) requires all residents to show competence in EBM methods.8 ACGME requires residency programs in all specialties—including psychiatry—to ensure that graduates achieve EBM core competencies, including being able to use the process described in this article.
Two problems that daunt psychiatrists and other physicians—information overload and uncritical acceptance of information—contribute to less-than-optimal care.5
Information overload. With thousands of medical journals and millions of articles being published, no clinician can keep up with all developments in his or her field. Furthermore, study results often appear contradictory.
Review articles summarize the literature, but most are “journalistic” or “narrative”—not systematic reviews—and thus are subject to author bias in the studies cited and methods used to summarize conflicting results.4 Textbook chapters have the added problem of being almost immediately out-of-date.6
Uncritical acceptance of information occurs when clinicians rely too heavily on personal experiences, noncritiqued study results, expert opinion, and pharmaceutical industry influence.4,6
Two approaches could narrow the gap between research and practice:
- clinical practice guidelines and pathways, a “top-down” approach favored by administrators
- evidence-based medicine, a “bottom-up” approach favored—and developed by—medical educators (Box 1).5,7,8
EBM and patient care. EBM has been described as “partly a philosophy, partly a skill, and partly…a set of tools.”9 David Sackett—often considered the father of EBM—has defined it as “the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients.”10
Although some critics disagree, clinical expertise plays an important role in EBM, as the clinician must integrate research evidence, patient preferences, and the patient’s clinical condition when making decisions.11
EBM’S 5 ACTION STEPS
With EBM, evidence from the medical literature is applied to patient care through 5 action steps:
- Formulate the question.
- Search for answers.
- Appraise the evidence.
- Apply the evidence to the patient.
- Assess the outcome.5,6,12
Step 1: Formulate the question. EBM begins with a clinical question related to the diagnosis, treatment, prognosis, or cause of a patient’s illness. The question is formatted to include the patient’s problem or diagnosis, the intervention of interest and any comparison intervention, and the outcome of interest.
Take, for example, this question: “In patients with bipolar disorder, is lamotrigine as effective as lithium in preventing relapse?” In this format:
- bipolar disorder is the diagnosis
- lamotrigine is the intervention of interest
- lithium is the comparison intervention
- relapse is the outcome of interest.
Step 2: Search for answers. Because answering different types of questions requires different types of evidence, this step involves determining the most appropriate type of evidence and searching for it.13
Evidence hierarchies (Table 1) 5,6,12,14 indicate that certain types of evidence are considered more credible than others. The higher the level of evidence, the more likely it is to provide valid, unbiased estimates of an intervention’s effect.
Table 1
Hierarchy for studies of therapy or harm
| Quality* | Type of evidence |
|---|---|
| 1a | Systematic review of randomized controlled trials (RCTs) |
| 1b | Individual RCT with narrow confidence interval |
| 2a | Systematic review of cohort studies |
| 2b | Individual cohort study RCT with <80% follow-up |
| 2c | Outcomes research Ecological study |
| 3a | Systematic review of case-control studies |
| 3b | Individual case-control study |
| 4 | Case series |
| 5 | Expert opinion |
| * Highest- to lowest-quality evidence | |
| Source: Adapted from references 5,6,12, and 14 | |
For example, observational studies may give misleading results, compared with randomized, controlled, clinical trials.15 Expert opinion—which does not necessarily reflect the best evidence in the literature—is considered the lowest evidence level.16
Beginning the literature search with Medline—as many clinicians do—is relatively inefficient. Searching the massive National Library of Medicine database often identifies a large number of articles, which you then must appraise for validity.
More efficient is Haynes’ “4S” strategy of:
It gives priority to sources of high-quality, pre-appraised information ( Table 2), so that you may omit Step 3—appraisal—in the EBM process.
Table 2
“4S” approach to answering clinical questions
| Category | Examples | Web site |
|---|---|---|
| Systems (comprehensive sources) | Clinical Evidence | http://www.clinicalevidence.com |
| National electronic Library for Mental Health | http://www.nelmh.org | |
| APA Practice Guidelines | http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm | |
| National Guideline Clearinghouse | http://www.guideline.gov | |
| Synopses (structured abstracts) | Evidence-Based Mental Health | http://ebmh.bmjjournals.com |
| ACP Journal Club | http://www.acpjc.org/ | |
| Syntheses (systematic reviews) | Cochrane Database of Systematic Reviews | http://www.update-software.com/abstracts/mainindex.htm |
| Database of Abstracts of Reviews of Effectiveness (DARE) | http://www.york.ac.uk/inst/crd/darehp.htm | |
| Health Technology Assessment (HTA) database | http://www.york.ac.uk/inst/crd/htahp.htm | |
| Studies (original articles) | Medline (PubMed) | http://www.ncbi.nlm.nih.gov/entrez/query/static/clinical.html |
| Source: Adapted from references 12 and 17. | ||
Systems. A system is an information source that covers a variety of diagnoses, summarizes the results of high-quality systematic reviews, is frequently updated, and is linked to the original studies. Three examples are:
- Clinical Evidence, a journal published semi-annually in the United Kingdom that is also available online (www.clinicalevidence.com). Its ease of use, frequent updates, and clear links to the best evidence make it a good starting point.
- National electronic Library for Mental Health (NeLMH) (www.nelmh.org), created by the U.K.’s Centre for Evidence-Based Mental Health.18 It provides information only about depression, schizophrenia, and suicide but may become the model for evidence-based psychiatry.
- Evidence-based clinical practice guidelines developed by the American Psychiatric Association9 and other organizations. Many of these are included in the National Guideline Clearinghouse (www.guideline.gov), produced by the U.S. Department of Health and Human Service’s Agency for Healthcare Research and Quality.
Synopses. If a system does not answer a clinical question, look for synopses—structured abstracts of high-quality systematic reviews or original articles. Synopses are brief and pre-appraised for quality, allowing you to quickly get the point without reading a lengthy article. For psychiatry, Evidence-Based Mental Health and ACP Journal Club are the best synopses sources.
Syntheses. If you don’t find a synopsis to answer your question, then search for a synthesis—a high-quality systematic review. The best source is the Cochrane Database of Systematic Reviews;20 others include:
- Database of Abstracts of Reviews of Effectiveness (DARE)
- Health Technology Assessment (HTA) database.
Table 3
Web sites for learning more about EBM
| Organization | Web site |
|---|---|
| Centre for Evidence-Based Medicine (Oxford) | http://www.cebm.net |
| Centre for Evidence-Based Medicine (Toronto) | http://www.cebm.utoronto.ca |
| Centre for Evidence-Based Mental Health | http://www.cebmh.com |
| EBM Education Center of Excellence | http://www.hsl.unc.edu/ahec/ebmcoe/pages/teaching.htm |
| Evidence-based Medicine Resource Center | http://www.ebmny.org |
| Netting the Evidence | http://www.nettingtheevidence.org.uk |
| University of Sheffield Health Informatics | http://www.shef.ac.uk/~scharr/ir/mschi/ |
| Users’ Guides to the Medical Literature | http://ugi.usersguides.org |
Studies. Only if the first three “S’s” fail to yield an answer would you then search Medline or similar databases for applicable studies.
The PubMed Clinical Queries interface lets you specify the type of question (therapy, diagnosis, etiology, or prognosis) and whether the search is to be sensitive or specific. You can also use filters built into this interface when searching for systematic reviews.
Step 3: Appraise the evidence. After you find an article, appraise its validity and importance. Checklists for appraising studies may be found in EBM texts4,6,12 or downloaded from Web sites (Table 3). Specific appraisal questions to ask depend on the study design and your clinical question.
Step 4: Apply the results to your patient. Assuming the evidence is valid, important, and feasible in your setting, consider your patient’s preferences21 and apply the results.
Step 5: Assess the outcome. Evaluate your performance in searching the literature, and assess the patient’s response.
STREAMLINING THE EBM PROCESS
Studies in academic settings have shown that the full 5-step model can be incorporated into daily practice.6,12 In nonacademic settings, however, practitioners complain about lack of time and information resources, as well as inadequate EBM skills.11,12 Two shortcuts can streamline the process:
Use the 5-step process selectively; it is not required for every patient encounter.6,12 After you research a question for one patient with a particular diagnosis, you can apply the answer to similar patients. Because most psychiatrists’ patients fall into relatively few diagnostic categories, only the exceptional patient would trigger the full 5-step process.
Use pre-appraised information sources. With online databases such as Clinical Evidence and Evidence-Based Mental Health, you can find information quickly, often in the time it takes to use textbooks.5,12,17
Excellent EBM texts4,6,12 and online resources may be useful (Table 3). Courses are listed on the EBM Education Center of Excellence Web site, and the Centre for Evidence-Based Mental Health at Oxford University offers an outstanding course for psychiatrists.
Related resources
- Gray GE. Concise guide to evidence-based psychiatry. Washington, DC: American Psychiatric Publishing, 2004.
- Greenhalgh T. How to read a paper: the basics of evidence-based medicine (2nd ed). London, BMJ Books, 2001.
- Guyatt G, Rennie D (eds). Users’ guides to the medical literature: a manual for evidence-based clinical care. Chicago: AMA Press, 2002.
- Sackett DL, Straus SE, Richardson WS, et al. Evidence-based medicine: how to practice and teach EBM (2nd ed). New York: Churchill Livingstone, 2000.
Acknowledgment
Supported in part by a grant from the National Institute of Mental Health (5-R24-MH61456-03).
1. Berwick DM. Disseminating innovations in health care. JAMA 2003;289:1969-75
2. Drake RE, Goldman HH, Leff HS, et al. Implementing evidence-based practices in routine mental health settings. Psychiatr Serv 2001;52:179-82
3. Geddes JR, Game D, Jenkins NE, et al. What proportion of primary psychiatric interventions are based on evidence from randomised controlled trials? Qual Health Care 1996;5:215-17.
4. Greenhalgh T. How to read a paper: the basics of evidence based medicine (2nd ed). London: BMJ Books, 2001.
5. Gray GE. Evidence-based medicine: an introduction for psychiatrists. J Psychiatr Pract 2002;8:5-13.
6. Sackett DL, Straus SE, Richardson WS, et al. Evidence-based medicine: How to practice and teach EBM (2nd ed). New York: Churchill Livingstone, 2000.
7. Evidence-Based Medicine Working Group. Evidence-based medicine: a new approach to the teaching of medicine. JAMA 1992;268:2420-5.
8. Accreditation Council for Graduate Medical Education General competencies [ACGME Outcome Project Web site], 2001. Available at: http://www.acgme.org/outcome/. Accessed May 5, 2004.
9. Dawes M. Preface. In: Dawes M, Davies P, Gray A, et al (eds). Evidence-based practice: a primer for health professionals New York: Churchill Livingstone, 1999.
10. Sackett DL, Rosenberg WMC, Gray JAM, et al. Evidence-based medicine: what it is and what it isn’t. BMJ 1996;312:71-2.
11. Straus SE, McAlister FA. Evidence-based medicine: a commentary on common criticisms. Can Med Assoc J 2000;163:837-41.
12. Gray GE. Concise guide to evidence-based psychiatry Washington, DC: American Psychiatric Publishing, 2004.
13. Glasziou P, Vandenbroucke J, Chalmers I. Assessing the quality of research. BMJ 2004;328:39-41.
14. Phillips B, Ball C, Sackett D, et al. Centre for Evidence-Based Medicine: Levels of evidence and grades of recommendations, May 2001. Available at: http://www.cebm.net/levels_of_evidence.asp. Accessed Sept. 18, 2004.
15. Lacchetti C, Guyatt G. Therapy and validity: surprising results of randomized controlled trials. In: Guyatt G, Rennie D (eds). Users’ guides to the medical literature: a manual for evidence-based clinical care. Chicago: AMA Press, 2002.
16. Antman EM, Lau J, Kupelnick B, et al. A comparison of results of meta-analyses of randomized control trials and recommendations of clinical experts: treatments for myocardial infarction. JAMA 1992;268:240-8.
17. Haynes RB. Of studies, summaries, synopses, and systems: the “4S” evolution of services for finding current best evidence. Evid Based Ment Health 2001;4:37-9.
18. Dearness KL, Tomlin A. Development of the National Electronic Library for Mental Health: providing evidence-based information for all. Health Info Libr J 2001;18:167-74.
19. American Psychiatric Association. Practice guidelines for the treatment of psychiatric disorders: compendium 2002. Washington, DC: American Psychiatric Publishing, 2002.
20. Antes G. Oxman AD for the Cochrane Collaboration. The Cochrane Collaboration in the 20th Century. In: Egger M, Smith GD, Altman DG (eds). Systematic reviews in health care: meta-analysis in context London: BMJBooks, 2001.
21. Say RE, Thomson R. The importance of patient p in treatment decisions—challenges for doctors. BMJ 2003;327:542-5.
1. Berwick DM. Disseminating innovations in health care. JAMA 2003;289:1969-75
2. Drake RE, Goldman HH, Leff HS, et al. Implementing evidence-based practices in routine mental health settings. Psychiatr Serv 2001;52:179-82
3. Geddes JR, Game D, Jenkins NE, et al. What proportion of primary psychiatric interventions are based on evidence from randomised controlled trials? Qual Health Care 1996;5:215-17.
4. Greenhalgh T. How to read a paper: the basics of evidence based medicine (2nd ed). London: BMJ Books, 2001.
5. Gray GE. Evidence-based medicine: an introduction for psychiatrists. J Psychiatr Pract 2002;8:5-13.
6. Sackett DL, Straus SE, Richardson WS, et al. Evidence-based medicine: How to practice and teach EBM (2nd ed). New York: Churchill Livingstone, 2000.
7. Evidence-Based Medicine Working Group. Evidence-based medicine: a new approach to the teaching of medicine. JAMA 1992;268:2420-5.
8. Accreditation Council for Graduate Medical Education General competencies [ACGME Outcome Project Web site], 2001. Available at: http://www.acgme.org/outcome/. Accessed May 5, 2004.
9. Dawes M. Preface. In: Dawes M, Davies P, Gray A, et al (eds). Evidence-based practice: a primer for health professionals New York: Churchill Livingstone, 1999.
10. Sackett DL, Rosenberg WMC, Gray JAM, et al. Evidence-based medicine: what it is and what it isn’t. BMJ 1996;312:71-2.
11. Straus SE, McAlister FA. Evidence-based medicine: a commentary on common criticisms. Can Med Assoc J 2000;163:837-41.
12. Gray GE. Concise guide to evidence-based psychiatry Washington, DC: American Psychiatric Publishing, 2004.
13. Glasziou P, Vandenbroucke J, Chalmers I. Assessing the quality of research. BMJ 2004;328:39-41.
14. Phillips B, Ball C, Sackett D, et al. Centre for Evidence-Based Medicine: Levels of evidence and grades of recommendations, May 2001. Available at: http://www.cebm.net/levels_of_evidence.asp. Accessed Sept. 18, 2004.
15. Lacchetti C, Guyatt G. Therapy and validity: surprising results of randomized controlled trials. In: Guyatt G, Rennie D (eds). Users’ guides to the medical literature: a manual for evidence-based clinical care. Chicago: AMA Press, 2002.
16. Antman EM, Lau J, Kupelnick B, et al. A comparison of results of meta-analyses of randomized control trials and recommendations of clinical experts: treatments for myocardial infarction. JAMA 1992;268:240-8.
17. Haynes RB. Of studies, summaries, synopses, and systems: the “4S” evolution of services for finding current best evidence. Evid Based Ment Health 2001;4:37-9.
18. Dearness KL, Tomlin A. Development of the National Electronic Library for Mental Health: providing evidence-based information for all. Health Info Libr J 2001;18:167-74.
19. American Psychiatric Association. Practice guidelines for the treatment of psychiatric disorders: compendium 2002. Washington, DC: American Psychiatric Publishing, 2002.
20. Antes G. Oxman AD for the Cochrane Collaboration. The Cochrane Collaboration in the 20th Century. In: Egger M, Smith GD, Altman DG (eds). Systematic reviews in health care: meta-analysis in context London: BMJBooks, 2001.
21. Say RE, Thomson R. The importance of patient p in treatment decisions—challenges for doctors. BMJ 2003;327:542-5.
Psychogenic or epileptic seizures? How to clinch the diagnosis
When you evaluate patients whose seizures could be epileptic or psychogenic, the evidence points to three useful diagnostic steps:
- Step 1: Characterize the seizure by its triggers and presentation.
- Step 2: Identify psychiatric comorbidity that might be precipitating psychogenic nonepileptic seizures (PNES).1
- Step 3: Obtain video EEG and blood tests for physiologic confirmation of epilepsy.
Using a case illustration, this article describes how to accomplish these steps by seeking clues in the patient’s seizure and psychiatric histories and choosing high-yield laboratory tests. When a PNES diagnosis becomes clear, we suggest an empathic approach that can help patients develop healthier responses to stress.
Patients with psychogenic nonepileptic seizure (PNES)have high rates of repressed anger and life stressors. Psychodynamic interpretations postulate PNES as an unconscious conversion of emotional distress into physical symptoms, unlike factitious disorder’s intentionality. Repressed traumatic childhood sexual experience may be significant.2
Family dynamics. PNES may be a maladaptive communication method by which an individual uses behavior to manipulate the environment to meet emotional needs or to compensate for an environment intolerant of direct verbal expression.3
Characteristics. PNES patients are a heterogeneous group. They average a full-scale IQ of 92 in the lower quartile of intellectual capacity and neuropsychological functioning. PNES usually presents in the 20s but may occur at any age. PNES is more common in women than men (ratio 4:1).4,5
Comorbidities. Up to 40% of patients treated at epilepsy centers are reported to have both epilepsy and PNES.4,5 In a 1-year study at an EEG-video monitoring unit, however, only 9.4% of PNES patients had interictal epileptiform discharges to support a coexisting diagnosis of epilepsy.4
PNES may be highly associated with somatoform disorder, mood disorder, anxiety disorder, brief reactive psychosis, or schizophreniform disorder.6
CASE: A DIFFERENT KIND OF SEIZURE
Ms. X’s husband brought her to the emergency room after her third tonic-clonic convulsion within 1 week. He reported that her eyes suddenly rolled up and she became limp and fell down after they argued about money. She suffered a minor temple laceration, but this seizure—unlike past episodes—was not associated with mouth foaming or fecal or urinary incontinence.
Ms. X, age 35, has a history of seizure disorder and 5 years of unemployment when seizures were uncontrolled. Her seizures have been stabilized for 18 months with phenytoin, 300 mg bid. She has been hospitalized twice for major depressive disorder, most recently 2 years ago. Since then, her depression has been in remission with paroxetine, 20 mg once daily. She does not abuse drugs or alcohol. She has been married 8 years, has no children, and receives disability income.
Ms. X was stabilized and admitted for neurologic evaluation. CT and MRI were normal, EEG recordings were unremarkable, and blood workup revealed slightly elevated creatine kinase but normal prolactin. Her phenytoin serum level was 12 mcg/mL (therapeutic range, 5 to 20 mcg/mL). When video-EEG recording during one seizure revealed no abnormality, the neurologist requested psychiatric consultation.
PNES: NOT A ‘PSEUDO’ SEIZURE
Patients with PNES are a heterogeneous population (Box)2-6 that appears repeatedly at emergency rooms, resulting in multiple investigations and treatment with antiepileptic medications. Those with both PNES and epileptic seizure disorders, such as Ms. X, present a particularly difficult clinical dilemma as:
- discontinuing anticonvulsants may exacerbate epileptic seizures
- increasing the medication in the mistaken belief that a seizure breakthrough has occurred could result in toxic serum levels.
Psychological stressors may precipitate PNES in a person who has never had a seizure or in someone with co-existing epilepsy. Patients with PNES frequently deny a correlation between emotional stress and their seizures, whereas the opposite usually holds for patients who have experienced an epileptic seizure.7,8
PNES has been called “pseudoseizure” a term we believe is unfair to patients because the etiologic determinants are mostly subconscious.9 Although one author has defended the term,10 we agree with others that “pseudoseizure” can give a misleading impression that patients feign their symptoms.9
Psychiatric comorbidity. When PNES is suspected, a careful history is essential to identify precipitating psychiatric comorbidity, such as somatoform, somatization, conversion, or dissociative disorder. PNES may also be precipitated by or coexist with mood and anxiety disorders, schizophrenia, malingering and factitious disorders, diffuse organic brain disease, and developmental disorders (Table 1).11,12
CASE CONTINUED: AN IMPORTANT CLUE
Ms. X was admitted to the psychiatric unit. Her psychiatric history showed recurrent depressive disorder and excluded head injury. She was mildly depressed but expressed minimal cognitive and biological depressive symptoms in the mental status examination. She denied suicidal or homicidal thoughts. Perception, thought process, and cognition were normal.
With her consent, the psychiatrist obtained collateral information from her brother. He reported that his sister had received a diagnosis of “pseudoseizures” about 5 years before this presentation. The brother was unsure of any emotional precipitants.
Table 1
Psychiatric disorders that may precipitate or coexist with PNES
| Psychopathology | Differentiation |
|---|---|
| Somatoform disorders | Physical symptoms suggest a medical condition but are not the result of a medical condition, substance, or another mental disorder such as panic disorder or schizophrenia |
| Conversion disorder | Psychological symptoms expressed as neurologic symptoms—such as paralysis, blindness, or paresthesia—in the absence of a known medical or neurologic disorder |
| Dissociative disorder | Disruption in consciousness, memory, identity, or perception that may be sudden or gradual, transient or chronic |
| Depressive disorders | Mood or anxiety symptoms related to depressive, bipolar, panic, posttraumatic stress, or acute stress disorders may coexist with PNES |
| Psychotic disorders | Schizophrenia may be associated with seizure-like events in some patients12 |
| Factitious disorder | Seizure-like symptoms may be produced intentionally for secondary gain (as in malingering) or feigned to assume a sick role (as in factitious disorder) |
| Developmental disorders | In a patient with mental retardation, PNES may result from reinforced operant behavior patterns |
| Source: Diagnostic and statistical manual of mental disorders (4th ed., text rev).11 | |
PNES OR EPILEPSY?
Initial assessment of suspected PNES includes a medical, psychiatric, social, psychological, and substance abuse history, as well as a thorough physical examination.
In patients with suspected PNES, obtain collateral histories of seizure precipitants, abortants, childhood events, and family history. Ms. X, for example, has a history of depression and at least one past episode of probable PNES, as described by her brother. An argument with her husband apparently precipitated the most recent seizure episode.
Table 2
Psychogenic seizures PNES vs. epileptic seizures: Differences in presentation*
| Clinical features | Psychogenic nonepileptic seizures (PNES) | Epileptic seizures |
|---|---|---|
| Duration | Variable | Short (20 to 70 seconds) |
| Pattern | Variable | Stereotyped |
| Frequency | Variable | Paroxysmal, cluster |
| Cause | Emotional | Organic |
| Occurs in presence of others | Yes | Variable |
| Occurs during sleep | Rare | Yes |
| Incontinence | Rare | Frequent |
| Biting pattern | Tip of tongue, lips | Side of tongue, cheek |
| Convulsion | Bizarre, trashing, sexual movements | Tonic-clonic |
| Injury | Infrequent, mild | Infrequent, severe |
| Pupillary reflex | Normal | Slow, nonreactive |
| Babinski’s reflex | No | Yes, if convulsion |
| Orientation afterwards | Clear | Confused |
| Postictal stupor | Rare | Frequent |
| Serum prolactin | Normal | Elevated (>18 ng/mL in men; >30 ng/mL in nonpregnant women) |
| EEG | Normal | Abnormal or variable |
| * Apply loosely, as the spectrum of seizure types within epilepsy is very large. | ||
| Source: Adapted from reference 13. | ||
PNES features. Clinical features (Table 2)13—although not definitive—can help differentiate PNES from epileptic seizure.1 PNES features to look for include:
- prolonged and bizarre prodrome
- prominent out-of-phase ictal or postictal activity
- clear-cut precipitants, especially in an emotionally charged atmosphere
- lack of falls or injuries
- fluctuating consciousness or vivid recall of details during ictal moments.
PNES’ physical symptoms are not voluntary. Patients often have out-of-phase upper- and lower-extremity movements and vocalization as the event starts, as opposed to about 20 seconds into the event when true tonic-clonic seizure makes the tonic-clonic transformation. Other common features are high-amplitude, forward pelvic thrusting, and lack of rigidity. Weeping during an apparent seizure strongly suggests a nonepileptic event.14
Ictal duration can be useful in assessment. Events that resemble tonic-clonic seizure but continue for >70 seconds or <20 seconds raise suspicion of nonepileptic seizures, although status epilepticus is possible.
Prolactin elevation. Epileptic tonic-clonic and partial complex seizures increase serum prolactin and are most reliable approximately 20 minutes after event onset. Nipple manipulation can spuriously increase serum prolactin, so observe female patients for this behavior if a seizure occurs in your presence. Psychotropics such as chlorpromazine and haloperidol may also elevate serum prolactin.
INVESTIGATIONS
Video EEG recording is available in most neurologic centers and is the investigation of choice. Epileptic seizure is characterized by recruitment of seizure activity in a physiologic distribution and postictal slowing, which would be difficult for a patient to imitate.
Unlike traditional EEG, video EEG shows evidence of electrographic paroxysmal changes immediately before, during, or after an epileptic seizure.15 Seizure presentations without paroxysmal electrographic changes would be considered PNES.
Traditional EEG is not recommended for a PNES workup because seizure activity is not recorded and myogenic infarcts may obscure readings. Moreover, because interictal EEG changes may occur even in patients with PNES, these changes in isolation cannot be interpreted as evidence of epilepsy.16
Laboratory testing includes full blood count, electrolytes, urea and creatinine, urine drug screen, and thyroid and liver function tests, as well as serum levels in patients taking anticonvulsants. These tests may exclude some seizure causes (such as hypokalemia or hypocalcemia with electrolyte disturbances) and provide baseline values for monitoring drug toxicity. Thyroid function testing will rule out hypo- or hyperthyroidism in patients with comorbid depressive or anxiety disorders. Urine drug screen reveals evidence of drug abuse—a possible organic seizure disorder precipitant.
Normal serum prolactin (men: 2 to 18 ng/mL; nonpregnant women: 3 to 30 ng/mL), cortisol (5 to 22 mcg/dL, morning blood specimen), and creatine kinase (50 to 200 U/L) rise substantially after an epileptic—but not psychogenic—seizure.17 Note, however, that creatine kinase and prolactin may be as elevated in PNES as in an epileptic seizure if PNES presents with vigorous muscular activity.18
Psychological testing may help distinguish PNES from epileptic seizure:
- Minnesota Multiphasic Personality Inventory (MMPI) is fairly sensitive and shows statistically significant differences between PNES and epileptic seizures in hypochondriasis, depression, hysteria, and schizophrenia.19
- Washington Psychosocial Seizure Inventory helps identify etiologic subgroups among PNES patients.9
Others. As in Ms. X’s case, CT and MRI for cerebral pathology may not help.20 Provocative techniques21 based on suggestibility also may have little value because PNES can be provoked in patients with documented epileptic seizures. Hypnosis has been used in attempts to demonstrate the psychogenic component of nonepileptic seizures by reversing ictal and postictal amnesia. Patients with PNES seem to be more responsive to hypnosis than those with epileptic seizures.22
CASE CONTINUED: EXPLAINING THE DIAGNOSIS
The psychiatric team concluded that even though Ms. X has a seizure disorder, this particular episode was psychogenic. This conclusion was based on the emotional precipitant, her brother’s collateral history, video EEG recordings, and her history of depression.
The psychiatrist explained to Ms. X that PNES and seizure disorders can coexist and that a PNES diagnosis does not imply that a patient is lying. It simply means that some seizures are precipitated by psychoemotional events.
Unlike some patients with PNES, Ms. X accepted the diagnosis without anger. Because her epilepsy and depression were stable, the psychiatrist did not change her phenytoin or paroxetine dosages. She was discharged, with follow-up care by a psychiatrist and neurologist.
TELLING AND TREATING THE PATIENT
It is important to present a PNES diagnosis with care because some patients react with aggressive denial and suicidal behavior. A patient who believes he or she has been perceived as a liar or “fake” may feel humiliated,9 which is why we prefer the term “PNES” rather than “pseudoseizure.”
PNES treatment calls for collaboration among the neurologist, psychiatrist, psychologist, therapists, support workers, and family. When PNES is clearly the only cause of seizures, avoid treating with anticonvulsants. If PNES coexists with a treated seizure disorder, no change in anticonvulsant dosage is necessary, especially if blood levels are normal.
Target the underlying psychiatric disorder, using medication and cognitive-behavioral therapy as appropriate. Advise patients and families that the seizure-like events may continue for some time but will disappear as the patient develops more-effective and appropriate coping strategies.
Prognosis. Favorable prognostic factors include being female, effective early intervention, normal premorbid psychological make-up, and good family support. Studies have shown that:
- up to 40% of treated PNES patients remained event-free for a median of 5 years.23
- prognosis may depend on spell type (catatonic is more favorable than “thrashing”) and illness duration (<1 year is more favorable than >1 year).24
Related resources
- Riley LT, Roy A. Pseudoseizures. Baltimore: Lippincott, Williams and Wilkins, 1982.
- Epilepsy.com. Psychogenic seizures. Resource for patients. www.epilepsy.com/epilepsy/seizure_psychogenic.html Accessed Oct. 14, 2004.
- Epilepsy Foundation. Information for patients and families. www.epilepsyfoundation.org. Search for nonepileptic seizures. Accessed Oct. 14, 2004.
Drug brand names
- Chlorpromazine • Thorazine
- Haloperidol • Haldol
- Phenytoin • Dilantin
- Paroxetine • Paxil
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Riley TL, Brannon WL, Jr. Recognition of pseudoseizures. Acta Neurol Scand 1991;83(2):129-32.
2. Goodwin J, Simms M, Bergman R. Hysterical seizures: a sequel to incest. Am J Orthopsychiatry 1979;49:698-703.
3. Krawetz P, Fleisher W, Pillay N, et al. Family functioning in subjects with pseudoseizures and epilepsy. J Nerv Ment Dis 2001;189(1):38-43.
4. Gates JR, Luciano D, Devinsky O. The classification and treatment of nonepileptic events. In: Devinsky O, Theodore WH (eds). Epilepsy and behavior. New York: Wiley-Liss, 1991;251-63.
5. Vossler DG. Nonepileptic seizures of physiologic origin. J Epilepsy 1995;8:1-10.
6. Wyllie E, Glazer JP, Benbadis S, et al. Psychiatric features of children and adolescents with pseudoseizures. Arch Pediatr Adolesc Med 1999;153(3):244-8.
7. Luciano D, Perrine K, Clayton B, Devinsky O. Stress as a seizure precipitant and its relationship to ictal focus [abstract]. Epilepsia 1992;33(suppl 3):130.-
8. Betts T. Epilepsy and stress [editorial]. BMJ 1992;305:378-9.
9. Chabolla DR, Krahn LE, So EL, Rummans TA. Psychogenic nonepileptic seizures. Mayo Foundation for Medical Education and Research (symposium, part Ii, vol. 71[5]). May 1996;493-500.
10. Slavney PR. In defense of pseudoseizure (comment). Gen Hosp Psychiatry 1994;16(4):243-5.
11. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association, 2000.
12. Matsuura M, Oana Y, Kato M, et al. A multicenter study on the prevalence of psychiatric disorders among new referrals for epilepsy in Japan. Epilepsia 2003;44(1):107-14.
13. Oommen KJ. Pseudoseizures: Diagnostic guidelines. Comprehensive Oklahoma Program for Epilepsy (COPE), 2000. Available at w3.ouhsc.edu/neuro/division/cope/pseudosz.htm. Accessed Oct. 14, 2004.
14. Walczak TS, Bogolioubov A. Weeping during psychogenic non-epileptic seizures. Epilepsia 1996;37(2):208-10.
15. Mohan KK, Markand ON, Salanova V. Diagnostic utility of video EEG monitoring in paroxysmal events. Acta Neurol Scand 1996;94(5):320-5.
16. Reuber M, Fernandez G, Bauer J, et al. Interictal EEG abnormalities in patients with psychogenic nonepileptic seizures. Epilepsia 2002;43(9):1013-20.
17. Laxer KD, Mullooly JP, Howell B. Prolactin changes after seizures classified by EEG monitoring. Neurology 1985;35:31-5.
18. Alving J. Serum prolactin levels are elevated also after pseudoepileptic seizures. Seizure 1998;7(2):85-9.
19. Henrichs TF, Tucker DM, Farha J, Novelly RA. MMPI indices in the identification of patients evidencing pseudoseizures. Epilepsia 1988;29:184-7.
20. Lelliott PT, Fenwick P. Cerebral pathology in pseudoseizures. Acta Neurol Scand 1992;85(3):177-80.
21. Guberman A. Psychogenic pseudoseizures in non-epileptic patients. Can J Psychiatry 1982;27:401-4.
22. Kuyk J, Jacobs LD, Aldenkamp AP, et al. Pseudoepileptic seizures: hypnosis as a diagnostic tool. Seizure 1995;4(2):123-8.
23. Holmes GL, Sackellares JC, McKiernan J, et al. Evaluation of childhood pseudoseizures using EEG telemetry and video tape monitoring. J Pediatr 1980;97(4):554-8.
24. Selwa LM, Geyer J, Nikakhtar N, et al. Nonepileptic seizure outcome varies by type of spell and duration of illness. Epilepsia 2000;41(10):1330-4.
When you evaluate patients whose seizures could be epileptic or psychogenic, the evidence points to three useful diagnostic steps:
- Step 1: Characterize the seizure by its triggers and presentation.
- Step 2: Identify psychiatric comorbidity that might be precipitating psychogenic nonepileptic seizures (PNES).1
- Step 3: Obtain video EEG and blood tests for physiologic confirmation of epilepsy.
Using a case illustration, this article describes how to accomplish these steps by seeking clues in the patient’s seizure and psychiatric histories and choosing high-yield laboratory tests. When a PNES diagnosis becomes clear, we suggest an empathic approach that can help patients develop healthier responses to stress.
Patients with psychogenic nonepileptic seizure (PNES)have high rates of repressed anger and life stressors. Psychodynamic interpretations postulate PNES as an unconscious conversion of emotional distress into physical symptoms, unlike factitious disorder’s intentionality. Repressed traumatic childhood sexual experience may be significant.2
Family dynamics. PNES may be a maladaptive communication method by which an individual uses behavior to manipulate the environment to meet emotional needs or to compensate for an environment intolerant of direct verbal expression.3
Characteristics. PNES patients are a heterogeneous group. They average a full-scale IQ of 92 in the lower quartile of intellectual capacity and neuropsychological functioning. PNES usually presents in the 20s but may occur at any age. PNES is more common in women than men (ratio 4:1).4,5
Comorbidities. Up to 40% of patients treated at epilepsy centers are reported to have both epilepsy and PNES.4,5 In a 1-year study at an EEG-video monitoring unit, however, only 9.4% of PNES patients had interictal epileptiform discharges to support a coexisting diagnosis of epilepsy.4
PNES may be highly associated with somatoform disorder, mood disorder, anxiety disorder, brief reactive psychosis, or schizophreniform disorder.6
CASE: A DIFFERENT KIND OF SEIZURE
Ms. X’s husband brought her to the emergency room after her third tonic-clonic convulsion within 1 week. He reported that her eyes suddenly rolled up and she became limp and fell down after they argued about money. She suffered a minor temple laceration, but this seizure—unlike past episodes—was not associated with mouth foaming or fecal or urinary incontinence.
Ms. X, age 35, has a history of seizure disorder and 5 years of unemployment when seizures were uncontrolled. Her seizures have been stabilized for 18 months with phenytoin, 300 mg bid. She has been hospitalized twice for major depressive disorder, most recently 2 years ago. Since then, her depression has been in remission with paroxetine, 20 mg once daily. She does not abuse drugs or alcohol. She has been married 8 years, has no children, and receives disability income.
Ms. X was stabilized and admitted for neurologic evaluation. CT and MRI were normal, EEG recordings were unremarkable, and blood workup revealed slightly elevated creatine kinase but normal prolactin. Her phenytoin serum level was 12 mcg/mL (therapeutic range, 5 to 20 mcg/mL). When video-EEG recording during one seizure revealed no abnormality, the neurologist requested psychiatric consultation.
PNES: NOT A ‘PSEUDO’ SEIZURE
Patients with PNES are a heterogeneous population (Box)2-6 that appears repeatedly at emergency rooms, resulting in multiple investigations and treatment with antiepileptic medications. Those with both PNES and epileptic seizure disorders, such as Ms. X, present a particularly difficult clinical dilemma as:
- discontinuing anticonvulsants may exacerbate epileptic seizures
- increasing the medication in the mistaken belief that a seizure breakthrough has occurred could result in toxic serum levels.
Psychological stressors may precipitate PNES in a person who has never had a seizure or in someone with co-existing epilepsy. Patients with PNES frequently deny a correlation between emotional stress and their seizures, whereas the opposite usually holds for patients who have experienced an epileptic seizure.7,8
PNES has been called “pseudoseizure” a term we believe is unfair to patients because the etiologic determinants are mostly subconscious.9 Although one author has defended the term,10 we agree with others that “pseudoseizure” can give a misleading impression that patients feign their symptoms.9
Psychiatric comorbidity. When PNES is suspected, a careful history is essential to identify precipitating psychiatric comorbidity, such as somatoform, somatization, conversion, or dissociative disorder. PNES may also be precipitated by or coexist with mood and anxiety disorders, schizophrenia, malingering and factitious disorders, diffuse organic brain disease, and developmental disorders (Table 1).11,12
CASE CONTINUED: AN IMPORTANT CLUE
Ms. X was admitted to the psychiatric unit. Her psychiatric history showed recurrent depressive disorder and excluded head injury. She was mildly depressed but expressed minimal cognitive and biological depressive symptoms in the mental status examination. She denied suicidal or homicidal thoughts. Perception, thought process, and cognition were normal.
With her consent, the psychiatrist obtained collateral information from her brother. He reported that his sister had received a diagnosis of “pseudoseizures” about 5 years before this presentation. The brother was unsure of any emotional precipitants.
Table 1
Psychiatric disorders that may precipitate or coexist with PNES
| Psychopathology | Differentiation |
|---|---|
| Somatoform disorders | Physical symptoms suggest a medical condition but are not the result of a medical condition, substance, or another mental disorder such as panic disorder or schizophrenia |
| Conversion disorder | Psychological symptoms expressed as neurologic symptoms—such as paralysis, blindness, or paresthesia—in the absence of a known medical or neurologic disorder |
| Dissociative disorder | Disruption in consciousness, memory, identity, or perception that may be sudden or gradual, transient or chronic |
| Depressive disorders | Mood or anxiety symptoms related to depressive, bipolar, panic, posttraumatic stress, or acute stress disorders may coexist with PNES |
| Psychotic disorders | Schizophrenia may be associated with seizure-like events in some patients12 |
| Factitious disorder | Seizure-like symptoms may be produced intentionally for secondary gain (as in malingering) or feigned to assume a sick role (as in factitious disorder) |
| Developmental disorders | In a patient with mental retardation, PNES may result from reinforced operant behavior patterns |
| Source: Diagnostic and statistical manual of mental disorders (4th ed., text rev).11 | |
PNES OR EPILEPSY?
Initial assessment of suspected PNES includes a medical, psychiatric, social, psychological, and substance abuse history, as well as a thorough physical examination.
In patients with suspected PNES, obtain collateral histories of seizure precipitants, abortants, childhood events, and family history. Ms. X, for example, has a history of depression and at least one past episode of probable PNES, as described by her brother. An argument with her husband apparently precipitated the most recent seizure episode.
Table 2
Psychogenic seizures PNES vs. epileptic seizures: Differences in presentation*
| Clinical features | Psychogenic nonepileptic seizures (PNES) | Epileptic seizures |
|---|---|---|
| Duration | Variable | Short (20 to 70 seconds) |
| Pattern | Variable | Stereotyped |
| Frequency | Variable | Paroxysmal, cluster |
| Cause | Emotional | Organic |
| Occurs in presence of others | Yes | Variable |
| Occurs during sleep | Rare | Yes |
| Incontinence | Rare | Frequent |
| Biting pattern | Tip of tongue, lips | Side of tongue, cheek |
| Convulsion | Bizarre, trashing, sexual movements | Tonic-clonic |
| Injury | Infrequent, mild | Infrequent, severe |
| Pupillary reflex | Normal | Slow, nonreactive |
| Babinski’s reflex | No | Yes, if convulsion |
| Orientation afterwards | Clear | Confused |
| Postictal stupor | Rare | Frequent |
| Serum prolactin | Normal | Elevated (>18 ng/mL in men; >30 ng/mL in nonpregnant women) |
| EEG | Normal | Abnormal or variable |
| * Apply loosely, as the spectrum of seizure types within epilepsy is very large. | ||
| Source: Adapted from reference 13. | ||
PNES features. Clinical features (Table 2)13—although not definitive—can help differentiate PNES from epileptic seizure.1 PNES features to look for include:
- prolonged and bizarre prodrome
- prominent out-of-phase ictal or postictal activity
- clear-cut precipitants, especially in an emotionally charged atmosphere
- lack of falls or injuries
- fluctuating consciousness or vivid recall of details during ictal moments.
PNES’ physical symptoms are not voluntary. Patients often have out-of-phase upper- and lower-extremity movements and vocalization as the event starts, as opposed to about 20 seconds into the event when true tonic-clonic seizure makes the tonic-clonic transformation. Other common features are high-amplitude, forward pelvic thrusting, and lack of rigidity. Weeping during an apparent seizure strongly suggests a nonepileptic event.14
Ictal duration can be useful in assessment. Events that resemble tonic-clonic seizure but continue for >70 seconds or <20 seconds raise suspicion of nonepileptic seizures, although status epilepticus is possible.
Prolactin elevation. Epileptic tonic-clonic and partial complex seizures increase serum prolactin and are most reliable approximately 20 minutes after event onset. Nipple manipulation can spuriously increase serum prolactin, so observe female patients for this behavior if a seizure occurs in your presence. Psychotropics such as chlorpromazine and haloperidol may also elevate serum prolactin.
INVESTIGATIONS
Video EEG recording is available in most neurologic centers and is the investigation of choice. Epileptic seizure is characterized by recruitment of seizure activity in a physiologic distribution and postictal slowing, which would be difficult for a patient to imitate.
Unlike traditional EEG, video EEG shows evidence of electrographic paroxysmal changes immediately before, during, or after an epileptic seizure.15 Seizure presentations without paroxysmal electrographic changes would be considered PNES.
Traditional EEG is not recommended for a PNES workup because seizure activity is not recorded and myogenic infarcts may obscure readings. Moreover, because interictal EEG changes may occur even in patients with PNES, these changes in isolation cannot be interpreted as evidence of epilepsy.16
Laboratory testing includes full blood count, electrolytes, urea and creatinine, urine drug screen, and thyroid and liver function tests, as well as serum levels in patients taking anticonvulsants. These tests may exclude some seizure causes (such as hypokalemia or hypocalcemia with electrolyte disturbances) and provide baseline values for monitoring drug toxicity. Thyroid function testing will rule out hypo- or hyperthyroidism in patients with comorbid depressive or anxiety disorders. Urine drug screen reveals evidence of drug abuse—a possible organic seizure disorder precipitant.
Normal serum prolactin (men: 2 to 18 ng/mL; nonpregnant women: 3 to 30 ng/mL), cortisol (5 to 22 mcg/dL, morning blood specimen), and creatine kinase (50 to 200 U/L) rise substantially after an epileptic—but not psychogenic—seizure.17 Note, however, that creatine kinase and prolactin may be as elevated in PNES as in an epileptic seizure if PNES presents with vigorous muscular activity.18
Psychological testing may help distinguish PNES from epileptic seizure:
- Minnesota Multiphasic Personality Inventory (MMPI) is fairly sensitive and shows statistically significant differences between PNES and epileptic seizures in hypochondriasis, depression, hysteria, and schizophrenia.19
- Washington Psychosocial Seizure Inventory helps identify etiologic subgroups among PNES patients.9
Others. As in Ms. X’s case, CT and MRI for cerebral pathology may not help.20 Provocative techniques21 based on suggestibility also may have little value because PNES can be provoked in patients with documented epileptic seizures. Hypnosis has been used in attempts to demonstrate the psychogenic component of nonepileptic seizures by reversing ictal and postictal amnesia. Patients with PNES seem to be more responsive to hypnosis than those with epileptic seizures.22
CASE CONTINUED: EXPLAINING THE DIAGNOSIS
The psychiatric team concluded that even though Ms. X has a seizure disorder, this particular episode was psychogenic. This conclusion was based on the emotional precipitant, her brother’s collateral history, video EEG recordings, and her history of depression.
The psychiatrist explained to Ms. X that PNES and seizure disorders can coexist and that a PNES diagnosis does not imply that a patient is lying. It simply means that some seizures are precipitated by psychoemotional events.
Unlike some patients with PNES, Ms. X accepted the diagnosis without anger. Because her epilepsy and depression were stable, the psychiatrist did not change her phenytoin or paroxetine dosages. She was discharged, with follow-up care by a psychiatrist and neurologist.
TELLING AND TREATING THE PATIENT
It is important to present a PNES diagnosis with care because some patients react with aggressive denial and suicidal behavior. A patient who believes he or she has been perceived as a liar or “fake” may feel humiliated,9 which is why we prefer the term “PNES” rather than “pseudoseizure.”
PNES treatment calls for collaboration among the neurologist, psychiatrist, psychologist, therapists, support workers, and family. When PNES is clearly the only cause of seizures, avoid treating with anticonvulsants. If PNES coexists with a treated seizure disorder, no change in anticonvulsant dosage is necessary, especially if blood levels are normal.
Target the underlying psychiatric disorder, using medication and cognitive-behavioral therapy as appropriate. Advise patients and families that the seizure-like events may continue for some time but will disappear as the patient develops more-effective and appropriate coping strategies.
Prognosis. Favorable prognostic factors include being female, effective early intervention, normal premorbid psychological make-up, and good family support. Studies have shown that:
- up to 40% of treated PNES patients remained event-free for a median of 5 years.23
- prognosis may depend on spell type (catatonic is more favorable than “thrashing”) and illness duration (<1 year is more favorable than >1 year).24
Related resources
- Riley LT, Roy A. Pseudoseizures. Baltimore: Lippincott, Williams and Wilkins, 1982.
- Epilepsy.com. Psychogenic seizures. Resource for patients. www.epilepsy.com/epilepsy/seizure_psychogenic.html Accessed Oct. 14, 2004.
- Epilepsy Foundation. Information for patients and families. www.epilepsyfoundation.org. Search for nonepileptic seizures. Accessed Oct. 14, 2004.
Drug brand names
- Chlorpromazine • Thorazine
- Haloperidol • Haldol
- Phenytoin • Dilantin
- Paroxetine • Paxil
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
When you evaluate patients whose seizures could be epileptic or psychogenic, the evidence points to three useful diagnostic steps:
- Step 1: Characterize the seizure by its triggers and presentation.
- Step 2: Identify psychiatric comorbidity that might be precipitating psychogenic nonepileptic seizures (PNES).1
- Step 3: Obtain video EEG and blood tests for physiologic confirmation of epilepsy.
Using a case illustration, this article describes how to accomplish these steps by seeking clues in the patient’s seizure and psychiatric histories and choosing high-yield laboratory tests. When a PNES diagnosis becomes clear, we suggest an empathic approach that can help patients develop healthier responses to stress.
Patients with psychogenic nonepileptic seizure (PNES)have high rates of repressed anger and life stressors. Psychodynamic interpretations postulate PNES as an unconscious conversion of emotional distress into physical symptoms, unlike factitious disorder’s intentionality. Repressed traumatic childhood sexual experience may be significant.2
Family dynamics. PNES may be a maladaptive communication method by which an individual uses behavior to manipulate the environment to meet emotional needs or to compensate for an environment intolerant of direct verbal expression.3
Characteristics. PNES patients are a heterogeneous group. They average a full-scale IQ of 92 in the lower quartile of intellectual capacity and neuropsychological functioning. PNES usually presents in the 20s but may occur at any age. PNES is more common in women than men (ratio 4:1).4,5
Comorbidities. Up to 40% of patients treated at epilepsy centers are reported to have both epilepsy and PNES.4,5 In a 1-year study at an EEG-video monitoring unit, however, only 9.4% of PNES patients had interictal epileptiform discharges to support a coexisting diagnosis of epilepsy.4
PNES may be highly associated with somatoform disorder, mood disorder, anxiety disorder, brief reactive psychosis, or schizophreniform disorder.6
CASE: A DIFFERENT KIND OF SEIZURE
Ms. X’s husband brought her to the emergency room after her third tonic-clonic convulsion within 1 week. He reported that her eyes suddenly rolled up and she became limp and fell down after they argued about money. She suffered a minor temple laceration, but this seizure—unlike past episodes—was not associated with mouth foaming or fecal or urinary incontinence.
Ms. X, age 35, has a history of seizure disorder and 5 years of unemployment when seizures were uncontrolled. Her seizures have been stabilized for 18 months with phenytoin, 300 mg bid. She has been hospitalized twice for major depressive disorder, most recently 2 years ago. Since then, her depression has been in remission with paroxetine, 20 mg once daily. She does not abuse drugs or alcohol. She has been married 8 years, has no children, and receives disability income.
Ms. X was stabilized and admitted for neurologic evaluation. CT and MRI were normal, EEG recordings were unremarkable, and blood workup revealed slightly elevated creatine kinase but normal prolactin. Her phenytoin serum level was 12 mcg/mL (therapeutic range, 5 to 20 mcg/mL). When video-EEG recording during one seizure revealed no abnormality, the neurologist requested psychiatric consultation.
PNES: NOT A ‘PSEUDO’ SEIZURE
Patients with PNES are a heterogeneous population (Box)2-6 that appears repeatedly at emergency rooms, resulting in multiple investigations and treatment with antiepileptic medications. Those with both PNES and epileptic seizure disorders, such as Ms. X, present a particularly difficult clinical dilemma as:
- discontinuing anticonvulsants may exacerbate epileptic seizures
- increasing the medication in the mistaken belief that a seizure breakthrough has occurred could result in toxic serum levels.
Psychological stressors may precipitate PNES in a person who has never had a seizure or in someone with co-existing epilepsy. Patients with PNES frequently deny a correlation between emotional stress and their seizures, whereas the opposite usually holds for patients who have experienced an epileptic seizure.7,8
PNES has been called “pseudoseizure” a term we believe is unfair to patients because the etiologic determinants are mostly subconscious.9 Although one author has defended the term,10 we agree with others that “pseudoseizure” can give a misleading impression that patients feign their symptoms.9
Psychiatric comorbidity. When PNES is suspected, a careful history is essential to identify precipitating psychiatric comorbidity, such as somatoform, somatization, conversion, or dissociative disorder. PNES may also be precipitated by or coexist with mood and anxiety disorders, schizophrenia, malingering and factitious disorders, diffuse organic brain disease, and developmental disorders (Table 1).11,12
CASE CONTINUED: AN IMPORTANT CLUE
Ms. X was admitted to the psychiatric unit. Her psychiatric history showed recurrent depressive disorder and excluded head injury. She was mildly depressed but expressed minimal cognitive and biological depressive symptoms in the mental status examination. She denied suicidal or homicidal thoughts. Perception, thought process, and cognition were normal.
With her consent, the psychiatrist obtained collateral information from her brother. He reported that his sister had received a diagnosis of “pseudoseizures” about 5 years before this presentation. The brother was unsure of any emotional precipitants.
Table 1
Psychiatric disorders that may precipitate or coexist with PNES
| Psychopathology | Differentiation |
|---|---|
| Somatoform disorders | Physical symptoms suggest a medical condition but are not the result of a medical condition, substance, or another mental disorder such as panic disorder or schizophrenia |
| Conversion disorder | Psychological symptoms expressed as neurologic symptoms—such as paralysis, blindness, or paresthesia—in the absence of a known medical or neurologic disorder |
| Dissociative disorder | Disruption in consciousness, memory, identity, or perception that may be sudden or gradual, transient or chronic |
| Depressive disorders | Mood or anxiety symptoms related to depressive, bipolar, panic, posttraumatic stress, or acute stress disorders may coexist with PNES |
| Psychotic disorders | Schizophrenia may be associated with seizure-like events in some patients12 |
| Factitious disorder | Seizure-like symptoms may be produced intentionally for secondary gain (as in malingering) or feigned to assume a sick role (as in factitious disorder) |
| Developmental disorders | In a patient with mental retardation, PNES may result from reinforced operant behavior patterns |
| Source: Diagnostic and statistical manual of mental disorders (4th ed., text rev).11 | |
PNES OR EPILEPSY?
Initial assessment of suspected PNES includes a medical, psychiatric, social, psychological, and substance abuse history, as well as a thorough physical examination.
In patients with suspected PNES, obtain collateral histories of seizure precipitants, abortants, childhood events, and family history. Ms. X, for example, has a history of depression and at least one past episode of probable PNES, as described by her brother. An argument with her husband apparently precipitated the most recent seizure episode.
Table 2
Psychogenic seizures PNES vs. epileptic seizures: Differences in presentation*
| Clinical features | Psychogenic nonepileptic seizures (PNES) | Epileptic seizures |
|---|---|---|
| Duration | Variable | Short (20 to 70 seconds) |
| Pattern | Variable | Stereotyped |
| Frequency | Variable | Paroxysmal, cluster |
| Cause | Emotional | Organic |
| Occurs in presence of others | Yes | Variable |
| Occurs during sleep | Rare | Yes |
| Incontinence | Rare | Frequent |
| Biting pattern | Tip of tongue, lips | Side of tongue, cheek |
| Convulsion | Bizarre, trashing, sexual movements | Tonic-clonic |
| Injury | Infrequent, mild | Infrequent, severe |
| Pupillary reflex | Normal | Slow, nonreactive |
| Babinski’s reflex | No | Yes, if convulsion |
| Orientation afterwards | Clear | Confused |
| Postictal stupor | Rare | Frequent |
| Serum prolactin | Normal | Elevated (>18 ng/mL in men; >30 ng/mL in nonpregnant women) |
| EEG | Normal | Abnormal or variable |
| * Apply loosely, as the spectrum of seizure types within epilepsy is very large. | ||
| Source: Adapted from reference 13. | ||
PNES features. Clinical features (Table 2)13—although not definitive—can help differentiate PNES from epileptic seizure.1 PNES features to look for include:
- prolonged and bizarre prodrome
- prominent out-of-phase ictal or postictal activity
- clear-cut precipitants, especially in an emotionally charged atmosphere
- lack of falls or injuries
- fluctuating consciousness or vivid recall of details during ictal moments.
PNES’ physical symptoms are not voluntary. Patients often have out-of-phase upper- and lower-extremity movements and vocalization as the event starts, as opposed to about 20 seconds into the event when true tonic-clonic seizure makes the tonic-clonic transformation. Other common features are high-amplitude, forward pelvic thrusting, and lack of rigidity. Weeping during an apparent seizure strongly suggests a nonepileptic event.14
Ictal duration can be useful in assessment. Events that resemble tonic-clonic seizure but continue for >70 seconds or <20 seconds raise suspicion of nonepileptic seizures, although status epilepticus is possible.
Prolactin elevation. Epileptic tonic-clonic and partial complex seizures increase serum prolactin and are most reliable approximately 20 minutes after event onset. Nipple manipulation can spuriously increase serum prolactin, so observe female patients for this behavior if a seizure occurs in your presence. Psychotropics such as chlorpromazine and haloperidol may also elevate serum prolactin.
INVESTIGATIONS
Video EEG recording is available in most neurologic centers and is the investigation of choice. Epileptic seizure is characterized by recruitment of seizure activity in a physiologic distribution and postictal slowing, which would be difficult for a patient to imitate.
Unlike traditional EEG, video EEG shows evidence of electrographic paroxysmal changes immediately before, during, or after an epileptic seizure.15 Seizure presentations without paroxysmal electrographic changes would be considered PNES.
Traditional EEG is not recommended for a PNES workup because seizure activity is not recorded and myogenic infarcts may obscure readings. Moreover, because interictal EEG changes may occur even in patients with PNES, these changes in isolation cannot be interpreted as evidence of epilepsy.16
Laboratory testing includes full blood count, electrolytes, urea and creatinine, urine drug screen, and thyroid and liver function tests, as well as serum levels in patients taking anticonvulsants. These tests may exclude some seizure causes (such as hypokalemia or hypocalcemia with electrolyte disturbances) and provide baseline values for monitoring drug toxicity. Thyroid function testing will rule out hypo- or hyperthyroidism in patients with comorbid depressive or anxiety disorders. Urine drug screen reveals evidence of drug abuse—a possible organic seizure disorder precipitant.
Normal serum prolactin (men: 2 to 18 ng/mL; nonpregnant women: 3 to 30 ng/mL), cortisol (5 to 22 mcg/dL, morning blood specimen), and creatine kinase (50 to 200 U/L) rise substantially after an epileptic—but not psychogenic—seizure.17 Note, however, that creatine kinase and prolactin may be as elevated in PNES as in an epileptic seizure if PNES presents with vigorous muscular activity.18
Psychological testing may help distinguish PNES from epileptic seizure:
- Minnesota Multiphasic Personality Inventory (MMPI) is fairly sensitive and shows statistically significant differences between PNES and epileptic seizures in hypochondriasis, depression, hysteria, and schizophrenia.19
- Washington Psychosocial Seizure Inventory helps identify etiologic subgroups among PNES patients.9
Others. As in Ms. X’s case, CT and MRI for cerebral pathology may not help.20 Provocative techniques21 based on suggestibility also may have little value because PNES can be provoked in patients with documented epileptic seizures. Hypnosis has been used in attempts to demonstrate the psychogenic component of nonepileptic seizures by reversing ictal and postictal amnesia. Patients with PNES seem to be more responsive to hypnosis than those with epileptic seizures.22
CASE CONTINUED: EXPLAINING THE DIAGNOSIS
The psychiatric team concluded that even though Ms. X has a seizure disorder, this particular episode was psychogenic. This conclusion was based on the emotional precipitant, her brother’s collateral history, video EEG recordings, and her history of depression.
The psychiatrist explained to Ms. X that PNES and seizure disorders can coexist and that a PNES diagnosis does not imply that a patient is lying. It simply means that some seizures are precipitated by psychoemotional events.
Unlike some patients with PNES, Ms. X accepted the diagnosis without anger. Because her epilepsy and depression were stable, the psychiatrist did not change her phenytoin or paroxetine dosages. She was discharged, with follow-up care by a psychiatrist and neurologist.
TELLING AND TREATING THE PATIENT
It is important to present a PNES diagnosis with care because some patients react with aggressive denial and suicidal behavior. A patient who believes he or she has been perceived as a liar or “fake” may feel humiliated,9 which is why we prefer the term “PNES” rather than “pseudoseizure.”
PNES treatment calls for collaboration among the neurologist, psychiatrist, psychologist, therapists, support workers, and family. When PNES is clearly the only cause of seizures, avoid treating with anticonvulsants. If PNES coexists with a treated seizure disorder, no change in anticonvulsant dosage is necessary, especially if blood levels are normal.
Target the underlying psychiatric disorder, using medication and cognitive-behavioral therapy as appropriate. Advise patients and families that the seizure-like events may continue for some time but will disappear as the patient develops more-effective and appropriate coping strategies.
Prognosis. Favorable prognostic factors include being female, effective early intervention, normal premorbid psychological make-up, and good family support. Studies have shown that:
- up to 40% of treated PNES patients remained event-free for a median of 5 years.23
- prognosis may depend on spell type (catatonic is more favorable than “thrashing”) and illness duration (<1 year is more favorable than >1 year).24
Related resources
- Riley LT, Roy A. Pseudoseizures. Baltimore: Lippincott, Williams and Wilkins, 1982.
- Epilepsy.com. Psychogenic seizures. Resource for patients. www.epilepsy.com/epilepsy/seizure_psychogenic.html Accessed Oct. 14, 2004.
- Epilepsy Foundation. Information for patients and families. www.epilepsyfoundation.org. Search for nonepileptic seizures. Accessed Oct. 14, 2004.
Drug brand names
- Chlorpromazine • Thorazine
- Haloperidol • Haldol
- Phenytoin • Dilantin
- Paroxetine • Paxil
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Riley TL, Brannon WL, Jr. Recognition of pseudoseizures. Acta Neurol Scand 1991;83(2):129-32.
2. Goodwin J, Simms M, Bergman R. Hysterical seizures: a sequel to incest. Am J Orthopsychiatry 1979;49:698-703.
3. Krawetz P, Fleisher W, Pillay N, et al. Family functioning in subjects with pseudoseizures and epilepsy. J Nerv Ment Dis 2001;189(1):38-43.
4. Gates JR, Luciano D, Devinsky O. The classification and treatment of nonepileptic events. In: Devinsky O, Theodore WH (eds). Epilepsy and behavior. New York: Wiley-Liss, 1991;251-63.
5. Vossler DG. Nonepileptic seizures of physiologic origin. J Epilepsy 1995;8:1-10.
6. Wyllie E, Glazer JP, Benbadis S, et al. Psychiatric features of children and adolescents with pseudoseizures. Arch Pediatr Adolesc Med 1999;153(3):244-8.
7. Luciano D, Perrine K, Clayton B, Devinsky O. Stress as a seizure precipitant and its relationship to ictal focus [abstract]. Epilepsia 1992;33(suppl 3):130.-
8. Betts T. Epilepsy and stress [editorial]. BMJ 1992;305:378-9.
9. Chabolla DR, Krahn LE, So EL, Rummans TA. Psychogenic nonepileptic seizures. Mayo Foundation for Medical Education and Research (symposium, part Ii, vol. 71[5]). May 1996;493-500.
10. Slavney PR. In defense of pseudoseizure (comment). Gen Hosp Psychiatry 1994;16(4):243-5.
11. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association, 2000.
12. Matsuura M, Oana Y, Kato M, et al. A multicenter study on the prevalence of psychiatric disorders among new referrals for epilepsy in Japan. Epilepsia 2003;44(1):107-14.
13. Oommen KJ. Pseudoseizures: Diagnostic guidelines. Comprehensive Oklahoma Program for Epilepsy (COPE), 2000. Available at w3.ouhsc.edu/neuro/division/cope/pseudosz.htm. Accessed Oct. 14, 2004.
14. Walczak TS, Bogolioubov A. Weeping during psychogenic non-epileptic seizures. Epilepsia 1996;37(2):208-10.
15. Mohan KK, Markand ON, Salanova V. Diagnostic utility of video EEG monitoring in paroxysmal events. Acta Neurol Scand 1996;94(5):320-5.
16. Reuber M, Fernandez G, Bauer J, et al. Interictal EEG abnormalities in patients with psychogenic nonepileptic seizures. Epilepsia 2002;43(9):1013-20.
17. Laxer KD, Mullooly JP, Howell B. Prolactin changes after seizures classified by EEG monitoring. Neurology 1985;35:31-5.
18. Alving J. Serum prolactin levels are elevated also after pseudoepileptic seizures. Seizure 1998;7(2):85-9.
19. Henrichs TF, Tucker DM, Farha J, Novelly RA. MMPI indices in the identification of patients evidencing pseudoseizures. Epilepsia 1988;29:184-7.
20. Lelliott PT, Fenwick P. Cerebral pathology in pseudoseizures. Acta Neurol Scand 1992;85(3):177-80.
21. Guberman A. Psychogenic pseudoseizures in non-epileptic patients. Can J Psychiatry 1982;27:401-4.
22. Kuyk J, Jacobs LD, Aldenkamp AP, et al. Pseudoepileptic seizures: hypnosis as a diagnostic tool. Seizure 1995;4(2):123-8.
23. Holmes GL, Sackellares JC, McKiernan J, et al. Evaluation of childhood pseudoseizures using EEG telemetry and video tape monitoring. J Pediatr 1980;97(4):554-8.
24. Selwa LM, Geyer J, Nikakhtar N, et al. Nonepileptic seizure outcome varies by type of spell and duration of illness. Epilepsia 2000;41(10):1330-4.
1. Riley TL, Brannon WL, Jr. Recognition of pseudoseizures. Acta Neurol Scand 1991;83(2):129-32.
2. Goodwin J, Simms M, Bergman R. Hysterical seizures: a sequel to incest. Am J Orthopsychiatry 1979;49:698-703.
3. Krawetz P, Fleisher W, Pillay N, et al. Family functioning in subjects with pseudoseizures and epilepsy. J Nerv Ment Dis 2001;189(1):38-43.
4. Gates JR, Luciano D, Devinsky O. The classification and treatment of nonepileptic events. In: Devinsky O, Theodore WH (eds). Epilepsy and behavior. New York: Wiley-Liss, 1991;251-63.
5. Vossler DG. Nonepileptic seizures of physiologic origin. J Epilepsy 1995;8:1-10.
6. Wyllie E, Glazer JP, Benbadis S, et al. Psychiatric features of children and adolescents with pseudoseizures. Arch Pediatr Adolesc Med 1999;153(3):244-8.
7. Luciano D, Perrine K, Clayton B, Devinsky O. Stress as a seizure precipitant and its relationship to ictal focus [abstract]. Epilepsia 1992;33(suppl 3):130.-
8. Betts T. Epilepsy and stress [editorial]. BMJ 1992;305:378-9.
9. Chabolla DR, Krahn LE, So EL, Rummans TA. Psychogenic nonepileptic seizures. Mayo Foundation for Medical Education and Research (symposium, part Ii, vol. 71[5]). May 1996;493-500.
10. Slavney PR. In defense of pseudoseizure (comment). Gen Hosp Psychiatry 1994;16(4):243-5.
11. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed, text rev). Washington, DC: American Psychiatric Association, 2000.
12. Matsuura M, Oana Y, Kato M, et al. A multicenter study on the prevalence of psychiatric disorders among new referrals for epilepsy in Japan. Epilepsia 2003;44(1):107-14.
13. Oommen KJ. Pseudoseizures: Diagnostic guidelines. Comprehensive Oklahoma Program for Epilepsy (COPE), 2000. Available at w3.ouhsc.edu/neuro/division/cope/pseudosz.htm. Accessed Oct. 14, 2004.
14. Walczak TS, Bogolioubov A. Weeping during psychogenic non-epileptic seizures. Epilepsia 1996;37(2):208-10.
15. Mohan KK, Markand ON, Salanova V. Diagnostic utility of video EEG monitoring in paroxysmal events. Acta Neurol Scand 1996;94(5):320-5.
16. Reuber M, Fernandez G, Bauer J, et al. Interictal EEG abnormalities in patients with psychogenic nonepileptic seizures. Epilepsia 2002;43(9):1013-20.
17. Laxer KD, Mullooly JP, Howell B. Prolactin changes after seizures classified by EEG monitoring. Neurology 1985;35:31-5.
18. Alving J. Serum prolactin levels are elevated also after pseudoepileptic seizures. Seizure 1998;7(2):85-9.
19. Henrichs TF, Tucker DM, Farha J, Novelly RA. MMPI indices in the identification of patients evidencing pseudoseizures. Epilepsia 1988;29:184-7.
20. Lelliott PT, Fenwick P. Cerebral pathology in pseudoseizures. Acta Neurol Scand 1992;85(3):177-80.
21. Guberman A. Psychogenic pseudoseizures in non-epileptic patients. Can J Psychiatry 1982;27:401-4.
22. Kuyk J, Jacobs LD, Aldenkamp AP, et al. Pseudoepileptic seizures: hypnosis as a diagnostic tool. Seizure 1995;4(2):123-8.
23. Holmes GL, Sackellares JC, McKiernan J, et al. Evaluation of childhood pseudoseizures using EEG telemetry and video tape monitoring. J Pediatr 1980;97(4):554-8.
24. Selwa LM, Geyer J, Nikakhtar N, et al. Nonepileptic seizure outcome varies by type of spell and duration of illness. Epilepsia 2000;41(10):1330-4.