User login
Measles: More than the rash
To the Editor: I read the excellent overview article on measles by Drs. Kumar and Sabella.1 However, there are additional important clinical points regarding measles diagnosis that deserve further comment. Prior to definitive diagnosis, measles is a clinical diagnosis. Properly, much attention is given to the rash, but there are important clinical clues besides the rash that are helpful diagnostically.
Some clinical findings are more characteristic of a disease than others, eg, eye findings in measles, and clinicians should specifically look for them. Other findings not characteristic but consistent with the diagnosis are less helpful, eg, measles with diarrhea.2 Measles is a systemic infection with several extradermatologic manifestations. Characteristically, measles involves the respiratory tract, manifested by runny nose, dry cough, or shortness of breath, ie, measles pneumonia.2
Gastrointestinal involvement may be manifested as nausea, vomiting, diarrhea, or abdominal pain. Abdominal pain, when located in the right lower quadrant, may mimic acute appendicitis, ie, pseudoappendicitis. In patients undergoing appendectomy, pathologically the appendix is normal but contains multinucleated giant cells (Warthin-Finkeldey cells). Measles pseudoappendicitis can be perplexing because it presents before the rash. Even without appendiceal involvement (pseudoappendicitis), Warthin-Finkeldey cells are also present in the nasal mucosa. If nasal swab cytology shows Warthin-Finkeldey cells, an early diagnosis of measles may be made days before IgM measles antibodies are reported.3
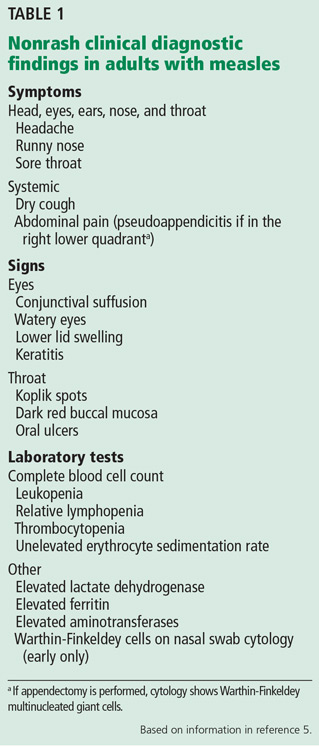
Other often-overlooked important clues are eye findings, eg, watery eyes, lower lid edema, conjunctival suffusion, and keratitis. No other disease in the differential diagnosis of measles presents with watery eyes with bilateral lower lid edema and conjunctival suffusion. Headache, mental confusion or oral ulcers may suggest alternate diagnoses. Typically, nonspecific laboratory abnormalities include leukopenia and thrombocytopenia, and importantly, the erythrocyte sedimentation rate is not elevated (Table 1).4,5
In measles, much is made of Koplik spots, which are found early on dark red buccal mucosa (vs Fordyce spots).1 However, if these are missed or not present, clinicians can use other characteristic findings to make a presumptive diagnosis of measles.
- Kumar D, Sabella C. Measles: back again. Cleve Clin J Med 2016; 83:340–344.
- Leibovici L, Sharir T, Kalter-Leibovici O, Alpert G, Epstein LM. An outbreak of measles among young adults. Clinical and laboratory features in 461 patients. J Adolesc Health Care 1988; 9:203–207.
- Cunha BA, Hage JE, Turi GK. A 45-year-old male with rash, fever and diarrhea. J Clin Microbiol 2012; 50:1835,2184.
- Cunha BA, Mickail N. Fever and rash in an adult traveler: the many masquerades of measles. Travel Med Inf Dis 2011; 9:255–257.
- Cunha CB, Cunha BA. Rash and fever in the intensive care unit. In: Fink MP, Abraham E, Vincent JL, Kochanek P, editors. Textbook of Critical Care Medicine (7th Ed). Elsevier, Philadelphia, 2016:97–115.
To the Editor: I read the excellent overview article on measles by Drs. Kumar and Sabella.1 However, there are additional important clinical points regarding measles diagnosis that deserve further comment. Prior to definitive diagnosis, measles is a clinical diagnosis. Properly, much attention is given to the rash, but there are important clinical clues besides the rash that are helpful diagnostically.
Some clinical findings are more characteristic of a disease than others, eg, eye findings in measles, and clinicians should specifically look for them. Other findings not characteristic but consistent with the diagnosis are less helpful, eg, measles with diarrhea.2 Measles is a systemic infection with several extradermatologic manifestations. Characteristically, measles involves the respiratory tract, manifested by runny nose, dry cough, or shortness of breath, ie, measles pneumonia.2
Gastrointestinal involvement may be manifested as nausea, vomiting, diarrhea, or abdominal pain. Abdominal pain, when located in the right lower quadrant, may mimic acute appendicitis, ie, pseudoappendicitis. In patients undergoing appendectomy, pathologically the appendix is normal but contains multinucleated giant cells (Warthin-Finkeldey cells). Measles pseudoappendicitis can be perplexing because it presents before the rash. Even without appendiceal involvement (pseudoappendicitis), Warthin-Finkeldey cells are also present in the nasal mucosa. If nasal swab cytology shows Warthin-Finkeldey cells, an early diagnosis of measles may be made days before IgM measles antibodies are reported.3
Other often-overlooked important clues are eye findings, eg, watery eyes, lower lid edema, conjunctival suffusion, and keratitis. No other disease in the differential diagnosis of measles presents with watery eyes with bilateral lower lid edema and conjunctival suffusion. Headache, mental confusion or oral ulcers may suggest alternate diagnoses. Typically, nonspecific laboratory abnormalities include leukopenia and thrombocytopenia, and importantly, the erythrocyte sedimentation rate is not elevated (Table 1).4,5
In measles, much is made of Koplik spots, which are found early on dark red buccal mucosa (vs Fordyce spots).1 However, if these are missed or not present, clinicians can use other characteristic findings to make a presumptive diagnosis of measles.
To the Editor: I read the excellent overview article on measles by Drs. Kumar and Sabella.1 However, there are additional important clinical points regarding measles diagnosis that deserve further comment. Prior to definitive diagnosis, measles is a clinical diagnosis. Properly, much attention is given to the rash, but there are important clinical clues besides the rash that are helpful diagnostically.
Some clinical findings are more characteristic of a disease than others, eg, eye findings in measles, and clinicians should specifically look for them. Other findings not characteristic but consistent with the diagnosis are less helpful, eg, measles with diarrhea.2 Measles is a systemic infection with several extradermatologic manifestations. Characteristically, measles involves the respiratory tract, manifested by runny nose, dry cough, or shortness of breath, ie, measles pneumonia.2
Gastrointestinal involvement may be manifested as nausea, vomiting, diarrhea, or abdominal pain. Abdominal pain, when located in the right lower quadrant, may mimic acute appendicitis, ie, pseudoappendicitis. In patients undergoing appendectomy, pathologically the appendix is normal but contains multinucleated giant cells (Warthin-Finkeldey cells). Measles pseudoappendicitis can be perplexing because it presents before the rash. Even without appendiceal involvement (pseudoappendicitis), Warthin-Finkeldey cells are also present in the nasal mucosa. If nasal swab cytology shows Warthin-Finkeldey cells, an early diagnosis of measles may be made days before IgM measles antibodies are reported.3
Other often-overlooked important clues are eye findings, eg, watery eyes, lower lid edema, conjunctival suffusion, and keratitis. No other disease in the differential diagnosis of measles presents with watery eyes with bilateral lower lid edema and conjunctival suffusion. Headache, mental confusion or oral ulcers may suggest alternate diagnoses. Typically, nonspecific laboratory abnormalities include leukopenia and thrombocytopenia, and importantly, the erythrocyte sedimentation rate is not elevated (Table 1).4,5
In measles, much is made of Koplik spots, which are found early on dark red buccal mucosa (vs Fordyce spots).1 However, if these are missed or not present, clinicians can use other characteristic findings to make a presumptive diagnosis of measles.
- Kumar D, Sabella C. Measles: back again. Cleve Clin J Med 2016; 83:340–344.
- Leibovici L, Sharir T, Kalter-Leibovici O, Alpert G, Epstein LM. An outbreak of measles among young adults. Clinical and laboratory features in 461 patients. J Adolesc Health Care 1988; 9:203–207.
- Cunha BA, Hage JE, Turi GK. A 45-year-old male with rash, fever and diarrhea. J Clin Microbiol 2012; 50:1835,2184.
- Cunha BA, Mickail N. Fever and rash in an adult traveler: the many masquerades of measles. Travel Med Inf Dis 2011; 9:255–257.
- Cunha CB, Cunha BA. Rash and fever in the intensive care unit. In: Fink MP, Abraham E, Vincent JL, Kochanek P, editors. Textbook of Critical Care Medicine (7th Ed). Elsevier, Philadelphia, 2016:97–115.
- Kumar D, Sabella C. Measles: back again. Cleve Clin J Med 2016; 83:340–344.
- Leibovici L, Sharir T, Kalter-Leibovici O, Alpert G, Epstein LM. An outbreak of measles among young adults. Clinical and laboratory features in 461 patients. J Adolesc Health Care 1988; 9:203–207.
- Cunha BA, Hage JE, Turi GK. A 45-year-old male with rash, fever and diarrhea. J Clin Microbiol 2012; 50:1835,2184.
- Cunha BA, Mickail N. Fever and rash in an adult traveler: the many masquerades of measles. Travel Med Inf Dis 2011; 9:255–257.
- Cunha CB, Cunha BA. Rash and fever in the intensive care unit. In: Fink MP, Abraham E, Vincent JL, Kochanek P, editors. Textbook of Critical Care Medicine (7th Ed). Elsevier, Philadelphia, 2016:97–115.
In reply: Measles: More than the rash
In Reply: We thank Dr. Cunha for his comments and appreciate the opportunity to emphasize important points that he highlights.
We agree that measles is a systemic illness with important extradermatologic manifestations that are critical to the diagnosis, and that the nondermatologic manifestations often precede the rash and serve to distinguish measles from other systemic illnesses. As discussed in our review, the respiratory prodrome of cough, coryza, and conjunctivitis is very distinctive and serves as an important clue to the diagnosis. Likewise, we acknowledge the importance of gastrointestinal findings in measles and note appendicitis as an important complication that is well described. Although Koplik spots are pathognomonic, we do stress that these often are not present at the time of presentation.
Finally, we agree that measles is a clinical diagnosis, and that the clinical manifestations beyond the dermatologic manifestations noted in our review and highlighted by Dr. Cunha are extremely helpful to the clinician in considering the diagnosis.
In Reply: We thank Dr. Cunha for his comments and appreciate the opportunity to emphasize important points that he highlights.
We agree that measles is a systemic illness with important extradermatologic manifestations that are critical to the diagnosis, and that the nondermatologic manifestations often precede the rash and serve to distinguish measles from other systemic illnesses. As discussed in our review, the respiratory prodrome of cough, coryza, and conjunctivitis is very distinctive and serves as an important clue to the diagnosis. Likewise, we acknowledge the importance of gastrointestinal findings in measles and note appendicitis as an important complication that is well described. Although Koplik spots are pathognomonic, we do stress that these often are not present at the time of presentation.
Finally, we agree that measles is a clinical diagnosis, and that the clinical manifestations beyond the dermatologic manifestations noted in our review and highlighted by Dr. Cunha are extremely helpful to the clinician in considering the diagnosis.
In Reply: We thank Dr. Cunha for his comments and appreciate the opportunity to emphasize important points that he highlights.
We agree that measles is a systemic illness with important extradermatologic manifestations that are critical to the diagnosis, and that the nondermatologic manifestations often precede the rash and serve to distinguish measles from other systemic illnesses. As discussed in our review, the respiratory prodrome of cough, coryza, and conjunctivitis is very distinctive and serves as an important clue to the diagnosis. Likewise, we acknowledge the importance of gastrointestinal findings in measles and note appendicitis as an important complication that is well described. Although Koplik spots are pathognomonic, we do stress that these often are not present at the time of presentation.
Finally, we agree that measles is a clinical diagnosis, and that the clinical manifestations beyond the dermatologic manifestations noted in our review and highlighted by Dr. Cunha are extremely helpful to the clinician in considering the diagnosis.
Prescribing opioids
To the Editor: As a primary care physician who has practiced for 31 years, I have a few concerns about the article “Prescribing opioids in primary care: Safely starting, monitoring, and stopping” by Drs. Daniel Tobin, Rebecca Andrews, and William Becker in your March 2016 issue.
Prescribing narcotics and other controlled medications has become a hot topic with legal implications. Many physicians have lost their license, and some have lost their freedom as well.
The article notes that primary care physicians provide most of the care for chronic pain but implies that we don’t know what we are doing. Although we might not have completed a residency in the management of chronic pain, we were required to attend a graduate medical school and to complete residency programs. We are also required to read the medical literature and keep up with our CME requirements. We too strive to keep up with and practice the latest cutting-edge medicine. And we have experience. After seeing thousands of patients and writing millions of prescriptions, I think I do know something about whether or not a medicine is safe, effective, and cost-effective. I have encountered quite a few patients with pain, and not one of them has overdosed by taking the medications as prescribed.
Most of what is being said and published about pain medication focuses on the epidemic of young people who are getting pain medications (prescription narcotics) and street narcotics (heroin) illegally. Directly, it has nothing to do with conscientious physicians prescribing narcotics for pain, but indirectly, it has to do with all adults in society. We are allowing our young people to be destroyed by drugs and by a lack of proper discipline in our homes that spills over into society. Where are our children getting these drugs, and who is bringing them into our neighborhoods? The practice of medicine is not the primary problem. I am for scientific, conscientious regulations concerning controlled substances. Medicine needs to inform all doctors about the changing laws surrounding the prescribing of controlled substances.
Cigarettes and alcohol are sold on every corner, and places selling marijuana are popping up everywhere. The former two drugs are harming and killing more young people than all the illegal drugs combined, and marijuana is fast approaching number three. I feel we need to stop picking on the medical profession and stop trying to blame it for all the woes that our young people are encountering every day. The reality is that legal and illegal drugs are not going to go away. We need to love our children more and better prepare them while in our homes to deal with the evils in our society.
To the Editor: As a primary care physician who has practiced for 31 years, I have a few concerns about the article “Prescribing opioids in primary care: Safely starting, monitoring, and stopping” by Drs. Daniel Tobin, Rebecca Andrews, and William Becker in your March 2016 issue.
Prescribing narcotics and other controlled medications has become a hot topic with legal implications. Many physicians have lost their license, and some have lost their freedom as well.
The article notes that primary care physicians provide most of the care for chronic pain but implies that we don’t know what we are doing. Although we might not have completed a residency in the management of chronic pain, we were required to attend a graduate medical school and to complete residency programs. We are also required to read the medical literature and keep up with our CME requirements. We too strive to keep up with and practice the latest cutting-edge medicine. And we have experience. After seeing thousands of patients and writing millions of prescriptions, I think I do know something about whether or not a medicine is safe, effective, and cost-effective. I have encountered quite a few patients with pain, and not one of them has overdosed by taking the medications as prescribed.
Most of what is being said and published about pain medication focuses on the epidemic of young people who are getting pain medications (prescription narcotics) and street narcotics (heroin) illegally. Directly, it has nothing to do with conscientious physicians prescribing narcotics for pain, but indirectly, it has to do with all adults in society. We are allowing our young people to be destroyed by drugs and by a lack of proper discipline in our homes that spills over into society. Where are our children getting these drugs, and who is bringing them into our neighborhoods? The practice of medicine is not the primary problem. I am for scientific, conscientious regulations concerning controlled substances. Medicine needs to inform all doctors about the changing laws surrounding the prescribing of controlled substances.
Cigarettes and alcohol are sold on every corner, and places selling marijuana are popping up everywhere. The former two drugs are harming and killing more young people than all the illegal drugs combined, and marijuana is fast approaching number three. I feel we need to stop picking on the medical profession and stop trying to blame it for all the woes that our young people are encountering every day. The reality is that legal and illegal drugs are not going to go away. We need to love our children more and better prepare them while in our homes to deal with the evils in our society.
To the Editor: As a primary care physician who has practiced for 31 years, I have a few concerns about the article “Prescribing opioids in primary care: Safely starting, monitoring, and stopping” by Drs. Daniel Tobin, Rebecca Andrews, and William Becker in your March 2016 issue.
Prescribing narcotics and other controlled medications has become a hot topic with legal implications. Many physicians have lost their license, and some have lost their freedom as well.
The article notes that primary care physicians provide most of the care for chronic pain but implies that we don’t know what we are doing. Although we might not have completed a residency in the management of chronic pain, we were required to attend a graduate medical school and to complete residency programs. We are also required to read the medical literature and keep up with our CME requirements. We too strive to keep up with and practice the latest cutting-edge medicine. And we have experience. After seeing thousands of patients and writing millions of prescriptions, I think I do know something about whether or not a medicine is safe, effective, and cost-effective. I have encountered quite a few patients with pain, and not one of them has overdosed by taking the medications as prescribed.
Most of what is being said and published about pain medication focuses on the epidemic of young people who are getting pain medications (prescription narcotics) and street narcotics (heroin) illegally. Directly, it has nothing to do with conscientious physicians prescribing narcotics for pain, but indirectly, it has to do with all adults in society. We are allowing our young people to be destroyed by drugs and by a lack of proper discipline in our homes that spills over into society. Where are our children getting these drugs, and who is bringing them into our neighborhoods? The practice of medicine is not the primary problem. I am for scientific, conscientious regulations concerning controlled substances. Medicine needs to inform all doctors about the changing laws surrounding the prescribing of controlled substances.
Cigarettes and alcohol are sold on every corner, and places selling marijuana are popping up everywhere. The former two drugs are harming and killing more young people than all the illegal drugs combined, and marijuana is fast approaching number three. I feel we need to stop picking on the medical profession and stop trying to blame it for all the woes that our young people are encountering every day. The reality is that legal and illegal drugs are not going to go away. We need to love our children more and better prepare them while in our homes to deal with the evils in our society.
In reply: Prescribing opioids
In Reply: We thank Dr. Pettiway for his remarks. The intent of our article was to identify common challenges when prescribing opioids for chronic pain and offer tips to the provider struggling with how to do so safely. We hope these comments will offer additional clarity.
First, as general internists who are essentially “self-trained” in the management of chronic pain, we fully acknowledge the importance of practical experience in learning how to prescribe opioids safely and effectively. Dr. Pettiway is correct that a dedicated physician who keeps up with the medical literature, attends relevant continuing medical education courses, and strives to provide deliberate, rational, and evidence-based care to his or her patients can do so effectively. However, the medical literature suggests that medical school training in the management of chronic pain is sparse; one review found that in 2011 only 5 out of 133 US medical schools required coursework on pain management, and only 13 offered it as an elective.1 Many primary care providers do feel unprepared to handle this challenge.
Additionally, Dr. Pettiway raises a good question about where misused prescription opioids originate and whether prescribers are responsible. The data show that the majority of misused prescription opioids are obtained from a family member or friend and not directly from a physician.2,3 However, this supply does generally originate from a prescription. Providers need to educate their patients about the risk for diversion, the need to keep pills safely hidden and locked away, and the importance of safely discarding unused supplies. Responsible prescribers need to anticipate these concerns and educate patients about them.
In summary, we firmly believe that primary care providers are capable of safe, effective, and responsible opioid prescribing and hope that our paper provides additional guidance on how to do so.
- Roehr B. US needs new strategy to help 116 million patients in chronic pain. BMJ 2011; 343:d4206.
- Becker WC, Tobin DG, Fiellin DA. Nonmedical use of opioid analgesics obtained directly from physicians: prevalence and correlates. Arch Intern Med 2011; 171:1034–1036.
- Substance Abuse and Mental health Services Administration. Results from the 2013 National Survey on Drug Use and Health: summary of national findings. HHS Publication No. (SMA) 14-4863. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2014. www.samhsa.gov/data/sites/default/files/NSDUHresultsPDFWHTML2013/Web/NSDUHresults2013.htm. Accessed June 29, 2016.
In Reply: We thank Dr. Pettiway for his remarks. The intent of our article was to identify common challenges when prescribing opioids for chronic pain and offer tips to the provider struggling with how to do so safely. We hope these comments will offer additional clarity.
First, as general internists who are essentially “self-trained” in the management of chronic pain, we fully acknowledge the importance of practical experience in learning how to prescribe opioids safely and effectively. Dr. Pettiway is correct that a dedicated physician who keeps up with the medical literature, attends relevant continuing medical education courses, and strives to provide deliberate, rational, and evidence-based care to his or her patients can do so effectively. However, the medical literature suggests that medical school training in the management of chronic pain is sparse; one review found that in 2011 only 5 out of 133 US medical schools required coursework on pain management, and only 13 offered it as an elective.1 Many primary care providers do feel unprepared to handle this challenge.
Additionally, Dr. Pettiway raises a good question about where misused prescription opioids originate and whether prescribers are responsible. The data show that the majority of misused prescription opioids are obtained from a family member or friend and not directly from a physician.2,3 However, this supply does generally originate from a prescription. Providers need to educate their patients about the risk for diversion, the need to keep pills safely hidden and locked away, and the importance of safely discarding unused supplies. Responsible prescribers need to anticipate these concerns and educate patients about them.
In summary, we firmly believe that primary care providers are capable of safe, effective, and responsible opioid prescribing and hope that our paper provides additional guidance on how to do so.
In Reply: We thank Dr. Pettiway for his remarks. The intent of our article was to identify common challenges when prescribing opioids for chronic pain and offer tips to the provider struggling with how to do so safely. We hope these comments will offer additional clarity.
First, as general internists who are essentially “self-trained” in the management of chronic pain, we fully acknowledge the importance of practical experience in learning how to prescribe opioids safely and effectively. Dr. Pettiway is correct that a dedicated physician who keeps up with the medical literature, attends relevant continuing medical education courses, and strives to provide deliberate, rational, and evidence-based care to his or her patients can do so effectively. However, the medical literature suggests that medical school training in the management of chronic pain is sparse; one review found that in 2011 only 5 out of 133 US medical schools required coursework on pain management, and only 13 offered it as an elective.1 Many primary care providers do feel unprepared to handle this challenge.
Additionally, Dr. Pettiway raises a good question about where misused prescription opioids originate and whether prescribers are responsible. The data show that the majority of misused prescription opioids are obtained from a family member or friend and not directly from a physician.2,3 However, this supply does generally originate from a prescription. Providers need to educate their patients about the risk for diversion, the need to keep pills safely hidden and locked away, and the importance of safely discarding unused supplies. Responsible prescribers need to anticipate these concerns and educate patients about them.
In summary, we firmly believe that primary care providers are capable of safe, effective, and responsible opioid prescribing and hope that our paper provides additional guidance on how to do so.
- Roehr B. US needs new strategy to help 116 million patients in chronic pain. BMJ 2011; 343:d4206.
- Becker WC, Tobin DG, Fiellin DA. Nonmedical use of opioid analgesics obtained directly from physicians: prevalence and correlates. Arch Intern Med 2011; 171:1034–1036.
- Substance Abuse and Mental health Services Administration. Results from the 2013 National Survey on Drug Use and Health: summary of national findings. HHS Publication No. (SMA) 14-4863. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2014. www.samhsa.gov/data/sites/default/files/NSDUHresultsPDFWHTML2013/Web/NSDUHresults2013.htm. Accessed June 29, 2016.
- Roehr B. US needs new strategy to help 116 million patients in chronic pain. BMJ 2011; 343:d4206.
- Becker WC, Tobin DG, Fiellin DA. Nonmedical use of opioid analgesics obtained directly from physicians: prevalence and correlates. Arch Intern Med 2011; 171:1034–1036.
- Substance Abuse and Mental health Services Administration. Results from the 2013 National Survey on Drug Use and Health: summary of national findings. HHS Publication No. (SMA) 14-4863. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2014. www.samhsa.gov/data/sites/default/files/NSDUHresultsPDFWHTML2013/Web/NSDUHresults2013.htm. Accessed June 29, 2016.