User login
Managing Your Dermatology Practice: Visit Your Office
Every year around now, as spring reawakens the outdoors, I like to take a tour of my office from the paradigm of a patient visiting for the first time, because more often than not, the indoors could use a bit of a revival as well.
We tend not to notice gradual deterioration in the environment we inhabit every day: Carpets fade and become dull with constant traffic and cleaning; wallpaper and paint accumulate dirt, stains, and damage; furniture gets dirty and dented; fabric rips; and hardware goes missing.
When did you last take a good look at your waiting room? Have your patients been snacking and spilling drinks, despite the signs begging them not to? Is the wallpaper smudged on the walls behind chairs where patients rest their heads? How is the carpeting and upholstery holding up?
Even if you don’t find anything obvious, it’s wise to check periodically for subtle evidence of age: Find some patches of protected carpeting and flooring – under desks, for example – and compare them to exposed floors.
And look at the décor itself – is it dated or just plain "old-looking?" Any interior designer will tell you they can determine quite accurately when a space was last decorated, simply by the color and style of the materials used. If your office is stuck in the ’90s, it’s probably time for a change.
Many patients assume that doctors who don’t keep up with technological innovations don’t keep up with anything else, either.
If you’re planning a vacation this summer (and I hope you are), that would be the perfect time for a redo. Your patients will be spared the dust and turmoil, tradespeople won’t have to work around your office hours, and you won’t have to cancel any hours that weren’t already canceled. Best of all, you’ll come back to a clean, fresh environment.
Start by reviewing your color scheme. If it’s hopelessly out of date and style, or if you are just tired of it, change it. Wallpaper and carpeting should be long-wearing industrial quality, paint should be high-quality "eggshell" finish to facilitate cleaning, and everything should be professionally applied. This is neither the time nor place for do-it-yourself experiments.
If your wall decorations have accumulated a few millimeters of dust, now would be a good time to replace at least some of them. This need not be an expensive proposition. If you or a family member is an artist or photographer, consider framing some of the best work. Or invite local artists or talented patients to display some of their creations on your walls.
Plants are great aesthetic accents and excellent stress reducers for apprehensive patients, yet many offices have little or no plant life. If you are hesitant to take on the extra work of plant upkeep, consider using one of the many corporate plant services that "rent" plants, keep them healthy, and replace them as necessary.
Furniture is another important consideration. You may be able to resurface and reupholster what you have now, but if not, shop carefully. Beware of non-medical products promoted specifically to physicians, as they tend to be overpriced. If you shop online, remember to factor in shipping costs, which can be considerable for furniture. Don’t be afraid to ask for discounts. You won’t get them if you don’t ask.
Consider joining your state or community business/industry association. Such organizations maintain a list of merchants willing to give discounts, and you may identify other member-businesses looking to acquire similar furniture or equipment, which could land all parties a significant quantity discount.
This is also a good time to clear out old textbooks, magazines, and files that you will never open again. And get your building maintenance crew to fix any nagging plumbing, electrical, or heating/air conditioning problems while pipes, ducts, and wires are more readily accessible.
Finally, spruce-up time is an excellent opportunity to inventory medical equipment. We’ve all seen "vintage" offices full of gadgets that were state-of-the-art decades ago. Nostalgia is nice, but would you want to be treated by a physician whose office could be moved straight to the Smithsonian, unaltered, as "Doctor’s Office Circa 1975?" Neither would your patients, for the most part. Many patients, particularly younger ones, assume that doctors who don’t keep up with technological innovations don’t keep up with anything else, either.
Every year around now, as spring reawakens the outdoors, I like to take a tour of my office from the paradigm of a patient visiting for the first time, because more often than not, the indoors could use a bit of a revival as well.
We tend not to notice gradual deterioration in the environment we inhabit every day: Carpets fade and become dull with constant traffic and cleaning; wallpaper and paint accumulate dirt, stains, and damage; furniture gets dirty and dented; fabric rips; and hardware goes missing.
When did you last take a good look at your waiting room? Have your patients been snacking and spilling drinks, despite the signs begging them not to? Is the wallpaper smudged on the walls behind chairs where patients rest their heads? How is the carpeting and upholstery holding up?
Even if you don’t find anything obvious, it’s wise to check periodically for subtle evidence of age: Find some patches of protected carpeting and flooring – under desks, for example – and compare them to exposed floors.
And look at the décor itself – is it dated or just plain "old-looking?" Any interior designer will tell you they can determine quite accurately when a space was last decorated, simply by the color and style of the materials used. If your office is stuck in the ’90s, it’s probably time for a change.
Many patients assume that doctors who don’t keep up with technological innovations don’t keep up with anything else, either.
If you’re planning a vacation this summer (and I hope you are), that would be the perfect time for a redo. Your patients will be spared the dust and turmoil, tradespeople won’t have to work around your office hours, and you won’t have to cancel any hours that weren’t already canceled. Best of all, you’ll come back to a clean, fresh environment.
Start by reviewing your color scheme. If it’s hopelessly out of date and style, or if you are just tired of it, change it. Wallpaper and carpeting should be long-wearing industrial quality, paint should be high-quality "eggshell" finish to facilitate cleaning, and everything should be professionally applied. This is neither the time nor place for do-it-yourself experiments.
If your wall decorations have accumulated a few millimeters of dust, now would be a good time to replace at least some of them. This need not be an expensive proposition. If you or a family member is an artist or photographer, consider framing some of the best work. Or invite local artists or talented patients to display some of their creations on your walls.
Plants are great aesthetic accents and excellent stress reducers for apprehensive patients, yet many offices have little or no plant life. If you are hesitant to take on the extra work of plant upkeep, consider using one of the many corporate plant services that "rent" plants, keep them healthy, and replace them as necessary.
Furniture is another important consideration. You may be able to resurface and reupholster what you have now, but if not, shop carefully. Beware of non-medical products promoted specifically to physicians, as they tend to be overpriced. If you shop online, remember to factor in shipping costs, which can be considerable for furniture. Don’t be afraid to ask for discounts. You won’t get them if you don’t ask.
Consider joining your state or community business/industry association. Such organizations maintain a list of merchants willing to give discounts, and you may identify other member-businesses looking to acquire similar furniture or equipment, which could land all parties a significant quantity discount.
This is also a good time to clear out old textbooks, magazines, and files that you will never open again. And get your building maintenance crew to fix any nagging plumbing, electrical, or heating/air conditioning problems while pipes, ducts, and wires are more readily accessible.
Finally, spruce-up time is an excellent opportunity to inventory medical equipment. We’ve all seen "vintage" offices full of gadgets that were state-of-the-art decades ago. Nostalgia is nice, but would you want to be treated by a physician whose office could be moved straight to the Smithsonian, unaltered, as "Doctor’s Office Circa 1975?" Neither would your patients, for the most part. Many patients, particularly younger ones, assume that doctors who don’t keep up with technological innovations don’t keep up with anything else, either.
Every year around now, as spring reawakens the outdoors, I like to take a tour of my office from the paradigm of a patient visiting for the first time, because more often than not, the indoors could use a bit of a revival as well.
We tend not to notice gradual deterioration in the environment we inhabit every day: Carpets fade and become dull with constant traffic and cleaning; wallpaper and paint accumulate dirt, stains, and damage; furniture gets dirty and dented; fabric rips; and hardware goes missing.
When did you last take a good look at your waiting room? Have your patients been snacking and spilling drinks, despite the signs begging them not to? Is the wallpaper smudged on the walls behind chairs where patients rest their heads? How is the carpeting and upholstery holding up?
Even if you don’t find anything obvious, it’s wise to check periodically for subtle evidence of age: Find some patches of protected carpeting and flooring – under desks, for example – and compare them to exposed floors.
And look at the décor itself – is it dated or just plain "old-looking?" Any interior designer will tell you they can determine quite accurately when a space was last decorated, simply by the color and style of the materials used. If your office is stuck in the ’90s, it’s probably time for a change.
Many patients assume that doctors who don’t keep up with technological innovations don’t keep up with anything else, either.
If you’re planning a vacation this summer (and I hope you are), that would be the perfect time for a redo. Your patients will be spared the dust and turmoil, tradespeople won’t have to work around your office hours, and you won’t have to cancel any hours that weren’t already canceled. Best of all, you’ll come back to a clean, fresh environment.
Start by reviewing your color scheme. If it’s hopelessly out of date and style, or if you are just tired of it, change it. Wallpaper and carpeting should be long-wearing industrial quality, paint should be high-quality "eggshell" finish to facilitate cleaning, and everything should be professionally applied. This is neither the time nor place for do-it-yourself experiments.
If your wall decorations have accumulated a few millimeters of dust, now would be a good time to replace at least some of them. This need not be an expensive proposition. If you or a family member is an artist or photographer, consider framing some of the best work. Or invite local artists or talented patients to display some of their creations on your walls.
Plants are great aesthetic accents and excellent stress reducers for apprehensive patients, yet many offices have little or no plant life. If you are hesitant to take on the extra work of plant upkeep, consider using one of the many corporate plant services that "rent" plants, keep them healthy, and replace them as necessary.
Furniture is another important consideration. You may be able to resurface and reupholster what you have now, but if not, shop carefully. Beware of non-medical products promoted specifically to physicians, as they tend to be overpriced. If you shop online, remember to factor in shipping costs, which can be considerable for furniture. Don’t be afraid to ask for discounts. You won’t get them if you don’t ask.
Consider joining your state or community business/industry association. Such organizations maintain a list of merchants willing to give discounts, and you may identify other member-businesses looking to acquire similar furniture or equipment, which could land all parties a significant quantity discount.
This is also a good time to clear out old textbooks, magazines, and files that you will never open again. And get your building maintenance crew to fix any nagging plumbing, electrical, or heating/air conditioning problems while pipes, ducts, and wires are more readily accessible.
Finally, spruce-up time is an excellent opportunity to inventory medical equipment. We’ve all seen "vintage" offices full of gadgets that were state-of-the-art decades ago. Nostalgia is nice, but would you want to be treated by a physician whose office could be moved straight to the Smithsonian, unaltered, as "Doctor’s Office Circa 1975?" Neither would your patients, for the most part. Many patients, particularly younger ones, assume that doctors who don’t keep up with technological innovations don’t keep up with anything else, either.
Child has congenital disorder after negative prenatal testing … and more

WHEN A POSSIBLE FETAL ABNORMALITY WAS SEEN on ultrasonography, the ObGyn suggested both parents have DNA testing for a hormonal disorder. Blood samples were taken in the hospital laboratory and sent to an outside lab. The parents were told that the results were negative.
The child was born with congenital adrenal hyperplasia, causing hormonal imbalance and development of ambiguous genitalia. She underwent genital reconstruction surgery at 4 months, and is expected to require additional surgery and lifelong hormone replacement therapy and monitoring.
PATIENTS’ CLAIM The hospital lab technician ordered the wrong test. The ObGyn was at fault for not confirming the test’s name. The parents would have terminated the pregnancy if they had been correctly informed of the child’s condition.
DEFENDANTS’ DEFENSE The test requested by the lab technician was similar in name to that ordered by the ObGyn. The ObGyn denied negligence; she relied on the lab to order the test she requested. The hospital claimed the error had been the fault of other entities involved in the handling and testing of the blood samples.
VERDICT A New Jersey jury found the hospital 75% and the lab technician 25% liable. The $1 million verdict included $625,000 for the child and $375,000 for her parents. A defense verdict was returned for the ObGyn.
Decision-to-delivery time challenged
A WOMAN WAS ADMITTED to the hospital for induction of labor for vaginal birth after cesarean delivery (VBAC). Because of fetal distress, the child was delivered by cesarean and later given a diagnosis of cerebral palsy. He has deficits involving grip, writing, and gait, and developmental delays.
PATIENT’S CLAIM Cesarean delivery should have been performed earlier because of a non-reassuring fetal heart rate.
PHYSICIAN’S DEFENSE The child’s heart rate was properly monitored in utero, and there were no contraindications to VBAC. As soon as the fetal tracings were disturbing, the physician converted to cesarean delivery. Only 18 minutes elapsed from the time of that decision until delivery. The child’s injury was mild and he has no cognitive impairment.
VERDICT A Mississippi defense verdict was returned.
Hematoma following vaginal hysterectomy
A 32-YEAR-OLD WOMAN underwent a vaginal hysterectomy. She developed a hematoma and was readmitted a week later for emergency surgery that included a bilateral salpingo-oophorectomy. She was scheduled for drainage of an abscess using interventional radiology, but the abscess ruptured during the preprocedure physical examination. The patient was discharged but returned the next day with serious pulmonary problems.
PATIENT’S CLAIM She chose vaginal hysterectomy to avoid scarring; now her abdomen was scarred from emergency surgery. The drainage procedure should have been performed despite the rupture. She was discharged prematurely after emergency surgery. A different antibiotic should have been prescribed.
PHYSICIAN’S DEFENSE A hematoma is a known complication of surgery. The drainage procedure was unnecessary after the rupture; the patient appeared to improve before she was discharged. Appropriate antibiotics were prescribed.
VERDICT A Ohio defense verdict was returned.
Oxygen deprivation blamed for fetal brain damage
LABOR WAS INDUCED after a mother reported a decrease in fetal movement. The child, age 9 at time of trial, has the developmental, motor, and language skills of a toddler.
PATIENT’S CLAIM The child’s grandparents, his legal guardians, claimed the doctors and nurses failed to properly monitor the oxytocin medication given to the mother, leading to oxygen deprivation that caused traumatic brain and neurological injuries.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT An Illinois settlement of $7.5 million was reached with the medical center before trial. Claims against the delivering ObGyn are still pending.

A 38-YEAR-OLD WOMAN underwent diagnostic hysteroscopy. During the procedure, visualization was poor and the gynecologist inadvertently perforated the uterus and rectum. Massive infection developed. Surgery to treat the infection and repair the injury included hysterectomy.
PATIENT’S CLAIM The gynecologist did not properly perform the hysteroscopy, and did not investigate for perforations at the end of the procedure. A small hole in the rectum allowed fecal contents to spill into the abdomen and pelvis, and caused the infection. The patient is now incapable of bearing children.
PHYSICIAN’S DEFENSE The infection that developed came solely from the perforation of the uterus, a known complication of hysteroscopy. The rectal perforation occurred during diagnostic laparoscopy and hysterectomy that was performed to treat the infection.
VERDICT A $650,000 Virginia settlement was reached.
12 lb, 7 oz baby, brachial plexus injury
A DIABETIC MOTHER GAINED 62 LBS during pregnancy. The baby, delivered vaginally, weighed 12 lbs, 7 oz. He suffered a brachial plexus injury, with avulsion injuries at C5, C6, and C7. The child’s right hand is in a pronated position; he cannot supinate without using his other hand to assist, despite three operations.
PATIENT’S CLAIM The ObGyn never discussed the risk of a large baby. Three weeks before delivery, ultrasonography estimated fetal weight at 9 lbs, 2 oz. The mother asked if cesarean delivery would be safer; the ObGyn responded that he believed the child weighed less than 10 lbs, and that a vaginal delivery would be appropriate.
PHYSICIAN’S DEFENSE The ObGyn did not offer cesarean delivery because he believed there was no medical necessity for that discussion.
VERDICT A $1,174,365 Ohio verdict was returned.
Despite gastroschisis, neonatal team called after birth
ULTRASONOGRAPHY showed fetal gastroschisis with a moderate amount of exposed bowel. The mother went into labor at 38 weeks. Electronic external fetal heart-rate tracing showed fetal bradycardia at 60–70 beats per minute (bpm). When the membranes were artificially ruptured, the amniotic fluid was full of thick meconium. A fetal scalp electrode showed a heart rate of 30–120 bpm; a second electrode confirmed the range.
The baby was delivered vaginally with Apgar scores of 2, 2, and 4 at 1, 5, and 10 minutes, respectively. The newborn was depressed, flaccid, blue, and unresponsive, with thick meconium below the vocal cords.
When the neonatal intensive care unit (NICU) team arrived, the baby was making no respiratory effort, and had a heart rate of 60 bpm. Meconium blocked the airway; he was intubated at 4 minutes of life. Arterial blood
sampling showed severe metabolic acidosis from hypoxia. Gastroschisis ruled out fetal cooling, which might have ameliorated the brain injury. The child suffered hypoxic ischemic encephalopathy from intrapartum asyphyxia that led to microcephaly. He requires a feeding tube and lifetime care.
PATIENT’S CLAIM Knowing that gastroschisis was present, the NICU team should have been called to the patient’s bedside before her membranes were ruptured. A cesarean delivery should have been performed when fetal distress was evident.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A $2.8 million Virginia settlement was reached: $1.8 million for the child; $1 million for the mother.
Twin-to-twin transfusion syndrome
A WOMAN EXPECTING TWINS had multiple ultrasonographic studies during pregnancy; all were read as normal. The babies were born prematurely and both died shortly after birth.
PATIENT’S CLAIM The radiologist and two ObGyns failed to correctly analyze the sonograms and diagnose and treat twin-to-twin transfusion syndrome.
PHYSICIANS’ DEFENSE The case was settled before trial.
VERDICT A $375,000 Virginia settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
WHEN A POSSIBLE FETAL ABNORMALITY WAS SEEN on ultrasonography, the ObGyn suggested both parents have DNA testing for a hormonal disorder. Blood samples were taken in the hospital laboratory and sent to an outside lab. The parents were told that the results were negative.
The child was born with congenital adrenal hyperplasia, causing hormonal imbalance and development of ambiguous genitalia. She underwent genital reconstruction surgery at 4 months, and is expected to require additional surgery and lifelong hormone replacement therapy and monitoring.
PATIENTS’ CLAIM The hospital lab technician ordered the wrong test. The ObGyn was at fault for not confirming the test’s name. The parents would have terminated the pregnancy if they had been correctly informed of the child’s condition.
DEFENDANTS’ DEFENSE The test requested by the lab technician was similar in name to that ordered by the ObGyn. The ObGyn denied negligence; she relied on the lab to order the test she requested. The hospital claimed the error had been the fault of other entities involved in the handling and testing of the blood samples.
VERDICT A New Jersey jury found the hospital 75% and the lab technician 25% liable. The $1 million verdict included $625,000 for the child and $375,000 for her parents. A defense verdict was returned for the ObGyn.
Decision-to-delivery time challenged
A WOMAN WAS ADMITTED to the hospital for induction of labor for vaginal birth after cesarean delivery (VBAC). Because of fetal distress, the child was delivered by cesarean and later given a diagnosis of cerebral palsy. He has deficits involving grip, writing, and gait, and developmental delays.
PATIENT’S CLAIM Cesarean delivery should have been performed earlier because of a non-reassuring fetal heart rate.
PHYSICIAN’S DEFENSE The child’s heart rate was properly monitored in utero, and there were no contraindications to VBAC. As soon as the fetal tracings were disturbing, the physician converted to cesarean delivery. Only 18 minutes elapsed from the time of that decision until delivery. The child’s injury was mild and he has no cognitive impairment.
VERDICT A Mississippi defense verdict was returned.
Hematoma following vaginal hysterectomy
A 32-YEAR-OLD WOMAN underwent a vaginal hysterectomy. She developed a hematoma and was readmitted a week later for emergency surgery that included a bilateral salpingo-oophorectomy. She was scheduled for drainage of an abscess using interventional radiology, but the abscess ruptured during the preprocedure physical examination. The patient was discharged but returned the next day with serious pulmonary problems.
PATIENT’S CLAIM She chose vaginal hysterectomy to avoid scarring; now her abdomen was scarred from emergency surgery. The drainage procedure should have been performed despite the rupture. She was discharged prematurely after emergency surgery. A different antibiotic should have been prescribed.
PHYSICIAN’S DEFENSE A hematoma is a known complication of surgery. The drainage procedure was unnecessary after the rupture; the patient appeared to improve before she was discharged. Appropriate antibiotics were prescribed.
VERDICT A Ohio defense verdict was returned.
Oxygen deprivation blamed for fetal brain damage
LABOR WAS INDUCED after a mother reported a decrease in fetal movement. The child, age 9 at time of trial, has the developmental, motor, and language skills of a toddler.
PATIENT’S CLAIM The child’s grandparents, his legal guardians, claimed the doctors and nurses failed to properly monitor the oxytocin medication given to the mother, leading to oxygen deprivation that caused traumatic brain and neurological injuries.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT An Illinois settlement of $7.5 million was reached with the medical center before trial. Claims against the delivering ObGyn are still pending.
A 38-YEAR-OLD WOMAN underwent diagnostic hysteroscopy. During the procedure, visualization was poor and the gynecologist inadvertently perforated the uterus and rectum. Massive infection developed. Surgery to treat the infection and repair the injury included hysterectomy.
PATIENT’S CLAIM The gynecologist did not properly perform the hysteroscopy, and did not investigate for perforations at the end of the procedure. A small hole in the rectum allowed fecal contents to spill into the abdomen and pelvis, and caused the infection. The patient is now incapable of bearing children.
PHYSICIAN’S DEFENSE The infection that developed came solely from the perforation of the uterus, a known complication of hysteroscopy. The rectal perforation occurred during diagnostic laparoscopy and hysterectomy that was performed to treat the infection.
VERDICT A $650,000 Virginia settlement was reached.
12 lb, 7 oz baby, brachial plexus injury
A DIABETIC MOTHER GAINED 62 LBS during pregnancy. The baby, delivered vaginally, weighed 12 lbs, 7 oz. He suffered a brachial plexus injury, with avulsion injuries at C5, C6, and C7. The child’s right hand is in a pronated position; he cannot supinate without using his other hand to assist, despite three operations.
PATIENT’S CLAIM The ObGyn never discussed the risk of a large baby. Three weeks before delivery, ultrasonography estimated fetal weight at 9 lbs, 2 oz. The mother asked if cesarean delivery would be safer; the ObGyn responded that he believed the child weighed less than 10 lbs, and that a vaginal delivery would be appropriate.
PHYSICIAN’S DEFENSE The ObGyn did not offer cesarean delivery because he believed there was no medical necessity for that discussion.
VERDICT A $1,174,365 Ohio verdict was returned.
Despite gastroschisis, neonatal team called after birth
ULTRASONOGRAPHY showed fetal gastroschisis with a moderate amount of exposed bowel. The mother went into labor at 38 weeks. Electronic external fetal heart-rate tracing showed fetal bradycardia at 60–70 beats per minute (bpm). When the membranes were artificially ruptured, the amniotic fluid was full of thick meconium. A fetal scalp electrode showed a heart rate of 30–120 bpm; a second electrode confirmed the range.
The baby was delivered vaginally with Apgar scores of 2, 2, and 4 at 1, 5, and 10 minutes, respectively. The newborn was depressed, flaccid, blue, and unresponsive, with thick meconium below the vocal cords.
When the neonatal intensive care unit (NICU) team arrived, the baby was making no respiratory effort, and had a heart rate of 60 bpm. Meconium blocked the airway; he was intubated at 4 minutes of life. Arterial blood
sampling showed severe metabolic acidosis from hypoxia. Gastroschisis ruled out fetal cooling, which might have ameliorated the brain injury. The child suffered hypoxic ischemic encephalopathy from intrapartum asyphyxia that led to microcephaly. He requires a feeding tube and lifetime care.
PATIENT’S CLAIM Knowing that gastroschisis was present, the NICU team should have been called to the patient’s bedside before her membranes were ruptured. A cesarean delivery should have been performed when fetal distress was evident.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A $2.8 million Virginia settlement was reached: $1.8 million for the child; $1 million for the mother.
Twin-to-twin transfusion syndrome
A WOMAN EXPECTING TWINS had multiple ultrasonographic studies during pregnancy; all were read as normal. The babies were born prematurely and both died shortly after birth.
PATIENT’S CLAIM The radiologist and two ObGyns failed to correctly analyze the sonograms and diagnose and treat twin-to-twin transfusion syndrome.
PHYSICIANS’ DEFENSE The case was settled before trial.
VERDICT A $375,000 Virginia settlement was reached.
WHEN A POSSIBLE FETAL ABNORMALITY WAS SEEN on ultrasonography, the ObGyn suggested both parents have DNA testing for a hormonal disorder. Blood samples were taken in the hospital laboratory and sent to an outside lab. The parents were told that the results were negative.
The child was born with congenital adrenal hyperplasia, causing hormonal imbalance and development of ambiguous genitalia. She underwent genital reconstruction surgery at 4 months, and is expected to require additional surgery and lifelong hormone replacement therapy and monitoring.
PATIENTS’ CLAIM The hospital lab technician ordered the wrong test. The ObGyn was at fault for not confirming the test’s name. The parents would have terminated the pregnancy if they had been correctly informed of the child’s condition.
DEFENDANTS’ DEFENSE The test requested by the lab technician was similar in name to that ordered by the ObGyn. The ObGyn denied negligence; she relied on the lab to order the test she requested. The hospital claimed the error had been the fault of other entities involved in the handling and testing of the blood samples.
VERDICT A New Jersey jury found the hospital 75% and the lab technician 25% liable. The $1 million verdict included $625,000 for the child and $375,000 for her parents. A defense verdict was returned for the ObGyn.
Decision-to-delivery time challenged
A WOMAN WAS ADMITTED to the hospital for induction of labor for vaginal birth after cesarean delivery (VBAC). Because of fetal distress, the child was delivered by cesarean and later given a diagnosis of cerebral palsy. He has deficits involving grip, writing, and gait, and developmental delays.
PATIENT’S CLAIM Cesarean delivery should have been performed earlier because of a non-reassuring fetal heart rate.
PHYSICIAN’S DEFENSE The child’s heart rate was properly monitored in utero, and there were no contraindications to VBAC. As soon as the fetal tracings were disturbing, the physician converted to cesarean delivery. Only 18 minutes elapsed from the time of that decision until delivery. The child’s injury was mild and he has no cognitive impairment.
VERDICT A Mississippi defense verdict was returned.
Hematoma following vaginal hysterectomy
A 32-YEAR-OLD WOMAN underwent a vaginal hysterectomy. She developed a hematoma and was readmitted a week later for emergency surgery that included a bilateral salpingo-oophorectomy. She was scheduled for drainage of an abscess using interventional radiology, but the abscess ruptured during the preprocedure physical examination. The patient was discharged but returned the next day with serious pulmonary problems.
PATIENT’S CLAIM She chose vaginal hysterectomy to avoid scarring; now her abdomen was scarred from emergency surgery. The drainage procedure should have been performed despite the rupture. She was discharged prematurely after emergency surgery. A different antibiotic should have been prescribed.
PHYSICIAN’S DEFENSE A hematoma is a known complication of surgery. The drainage procedure was unnecessary after the rupture; the patient appeared to improve before she was discharged. Appropriate antibiotics were prescribed.
VERDICT A Ohio defense verdict was returned.
Oxygen deprivation blamed for fetal brain damage
LABOR WAS INDUCED after a mother reported a decrease in fetal movement. The child, age 9 at time of trial, has the developmental, motor, and language skills of a toddler.
PATIENT’S CLAIM The child’s grandparents, his legal guardians, claimed the doctors and nurses failed to properly monitor the oxytocin medication given to the mother, leading to oxygen deprivation that caused traumatic brain and neurological injuries.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT An Illinois settlement of $7.5 million was reached with the medical center before trial. Claims against the delivering ObGyn are still pending.
A 38-YEAR-OLD WOMAN underwent diagnostic hysteroscopy. During the procedure, visualization was poor and the gynecologist inadvertently perforated the uterus and rectum. Massive infection developed. Surgery to treat the infection and repair the injury included hysterectomy.
PATIENT’S CLAIM The gynecologist did not properly perform the hysteroscopy, and did not investigate for perforations at the end of the procedure. A small hole in the rectum allowed fecal contents to spill into the abdomen and pelvis, and caused the infection. The patient is now incapable of bearing children.
PHYSICIAN’S DEFENSE The infection that developed came solely from the perforation of the uterus, a known complication of hysteroscopy. The rectal perforation occurred during diagnostic laparoscopy and hysterectomy that was performed to treat the infection.
VERDICT A $650,000 Virginia settlement was reached.
12 lb, 7 oz baby, brachial plexus injury
A DIABETIC MOTHER GAINED 62 LBS during pregnancy. The baby, delivered vaginally, weighed 12 lbs, 7 oz. He suffered a brachial plexus injury, with avulsion injuries at C5, C6, and C7. The child’s right hand is in a pronated position; he cannot supinate without using his other hand to assist, despite three operations.
PATIENT’S CLAIM The ObGyn never discussed the risk of a large baby. Three weeks before delivery, ultrasonography estimated fetal weight at 9 lbs, 2 oz. The mother asked if cesarean delivery would be safer; the ObGyn responded that he believed the child weighed less than 10 lbs, and that a vaginal delivery would be appropriate.
PHYSICIAN’S DEFENSE The ObGyn did not offer cesarean delivery because he believed there was no medical necessity for that discussion.
VERDICT A $1,174,365 Ohio verdict was returned.
Despite gastroschisis, neonatal team called after birth
ULTRASONOGRAPHY showed fetal gastroschisis with a moderate amount of exposed bowel. The mother went into labor at 38 weeks. Electronic external fetal heart-rate tracing showed fetal bradycardia at 60–70 beats per minute (bpm). When the membranes were artificially ruptured, the amniotic fluid was full of thick meconium. A fetal scalp electrode showed a heart rate of 30–120 bpm; a second electrode confirmed the range.
The baby was delivered vaginally with Apgar scores of 2, 2, and 4 at 1, 5, and 10 minutes, respectively. The newborn was depressed, flaccid, blue, and unresponsive, with thick meconium below the vocal cords.
When the neonatal intensive care unit (NICU) team arrived, the baby was making no respiratory effort, and had a heart rate of 60 bpm. Meconium blocked the airway; he was intubated at 4 minutes of life. Arterial blood
sampling showed severe metabolic acidosis from hypoxia. Gastroschisis ruled out fetal cooling, which might have ameliorated the brain injury. The child suffered hypoxic ischemic encephalopathy from intrapartum asyphyxia that led to microcephaly. He requires a feeding tube and lifetime care.
PATIENT’S CLAIM Knowing that gastroschisis was present, the NICU team should have been called to the patient’s bedside before her membranes were ruptured. A cesarean delivery should have been performed when fetal distress was evident.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A $2.8 million Virginia settlement was reached: $1.8 million for the child; $1 million for the mother.
Twin-to-twin transfusion syndrome
A WOMAN EXPECTING TWINS had multiple ultrasonographic studies during pregnancy; all were read as normal. The babies were born prematurely and both died shortly after birth.
PATIENT’S CLAIM The radiologist and two ObGyns failed to correctly analyze the sonograms and diagnose and treat twin-to-twin transfusion syndrome.
PHYSICIANS’ DEFENSE The case was settled before trial.
VERDICT A $375,000 Virginia settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
Time-based billing allows hospitalists to avoid
Providers typically rely on the “key components” (history, exam, medical decision-making) when documenting in the medical record. However, there are instances when the majority of the encounter constitutes counseling/coordination of care (C/CC). Physicians might only document a brief history and exam, or nothing at all. Utilizing time-based billing principles allows a physician to disregard the “key component” requirements and select a visit level reflective of this effort.
For example, a 64-year-old female is hospitalized with newly diagnosed diabetes and requires extensive counseling regarding disease management, lifestyle modification, and medication regime, as well as coordination of care for outpatient programs and services. The hospitalist reviews some of the pertinent information with the patient and leaves the room to coordinate the patient’s ongoing care (25 minutes). The hospitalist then asks a resident to assist with the remaining counseling efforts (20 minutes). Code 99232 (inpatient visit, 25 minutes total visit time) would be appropriate to report.
Counseling, Coordination of Care
Time may be used as the determining factor for the visit level, if more than 50% of the total visit time involves C/CC.1 Time is not used for visit-level selection if C/CC is minimal or absent from the patient encounter. Total visit time is acknowledged as the physician’s face-to-face (i.e. bedside) time combined with time spent on the unit/floor reviewing data, obtaining relevant patient information, and discussing the individual case with other involved healthcare providers.
Time associated with activities performed outside of the patient’s unit/floor is not considered when calculating total visit time. Time associated with teaching students/interns also is excluded; only the attending physician’s time counts.
When the requirements have been met, the physician selects the visit level that corresponds with the documented total visit time (see Table 1). In the scenario above, the visit level is chosen based on the attending physician’s documented time (25 minutes). The resident’s time cannot be included.

Documentation Requirements
Physicians must document the interaction during the patient encounter: history and exam, if updated or performed; discussion points; and patient response, if applicable. The medical record entry must contain both the C/CC time and the total visit time.2 “Total visit time=35 minutes; >50% spent counseling/coordinating care” or “20 of 35 minutes spent counseling/coordinating care.”
A payor may prefer one documentation style over another. It is always best to ask about the payor’s policy and review local documentation standards to ensure compliance.
Family Discussions
Physicians are always involved in family discussions. It is appropriate to count this as C/CC time. In the event that the family discussion takes place without the patient present, only count this as C/CC time if:
- The patient is unable or clinically incompetent to participate in discussions;
- The time is spent on the unit/floor with the family members or surrogate decision-makers obtaining a medical history, reviewing the patient’s condition or prognosis, or discussing treatment or limitation(s) of treatment; and
- The conversation bears directly on the management of the patient.4
The medical record should reflect these criteria. Do not consider the time if the discussion takes place in an area outside of the patient’s unit/floor, or if the time is spent counseling family members through their grieving process.
It is not uncommon for the family discussion to take place later in the day, after the physician has made earlier rounds. If the earlier encounter involved C/CC, the physician would report the cumulative time spent for that service date. If the earlier encounter was a typical patient evaluation (i.e. history update and physical) and management service (i.e. care plan review/revision), this second encounter might be regarded as a prolonged care service.
Prolonged Care
Prolonged care codes exist for both outpatient and inpatient services. A hospitalists’ focus involves the inpatient code series:
99356: Prolonged service in the inpatient or observation setting, requiring unit/floor time beyond the usual service, first hour; and
99357: Prolonged service in the inpatient or observation setting, requiring unit/floor time beyond the usual service, each additional 30 minutes.
Code 99356 is reported during the first hour of prolonged services, after the initial 30 minutes is reached; code 99357 is reported for each additional 30 minutes of prolonged care beyond the first hour, after the first 15 minutes of each additional segment. Both are “add on” codes and cannot be reported alone on a claim form; a “primary” code must be reported. Similarly, 99357 cannot be reported without 99356, and 99356 must be reported with one of the following inpatient service (primary) codes: 99218-99220, 99221-99223, 99231-99233, 99251-99255, 99304-99310. Only one unit of 99356 may be reported per patient per physician group per day, whereas multiple units of 99357 may be reported in a single day.
The CPT definition of prolonged care varies from that of the Centers for Medicare & Medicaid Services (CMS). Since 2009, CPT recognizes the total duration spent by a physician on a given date, even if the time spent by the physician on that date is not continuous; the time involves both face-to-face time and unit/floor time.5 CMS only attributes direct face-to-face time between the physician and the patient toward prolonged care billing. Time spent reviewing charts or discussion of a patient with house medical staff, waiting for test results, waiting for changes in the patient’s condition, waiting for end of a therapy session, or waiting for use of facilities cannot be billed as prolonged services.5 This is in direct opposition to its policy for C/CC services, and makes prolonged care services inefficient.
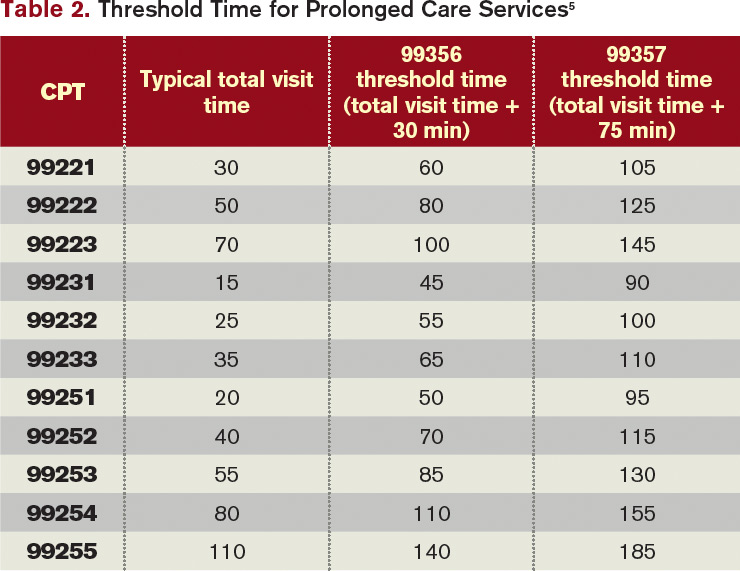
Medicare also identifies “threshold” time (see Table 2). The total physician visit time must exceed the time requirements associated with the “primary” codes by a 30-minute threshold (e.g. 99221+99356=30 minutes+30 minutes=60 minutes threshold time). The physician must document the total face-to-face time spent in separate notes throughout the day or, more realistically, in one cumulative note.
When two providers from the same group and same specialty perform services on the same date (e.g. physician A saw the patient during morning rounds, and physician B spoke with the patient/family in the afternoon), only one physician can report the cumulative service.6 As always, query payors for coverage, because some non-Medicare insurers do not recognize these codes.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare & Medicaid Services (CMS). Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2012.
- Centers for Medicare & Medicaid Services (CMS). Medicare Claims Processing Manual: Chapter 12, Section 30.6.1C. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2012.
- Centers for Medicare & Medicaid Services (CMS). Medicare National Coverage Determinations Manual: Chapter 1, Section 70.1. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/ncd103c1_Part1.pdf. Accessed Jan. 8, 2012.
- Centers for Medicare & Medicaid Services (CMS). Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1C. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011:7-21.
- Centers for Medicare & Medicaid Services (CMS). Medicare Claims Processing Manual: Chapter 12, Section 30.6.5. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2012.
Providers typically rely on the “key components” (history, exam, medical decision-making) when documenting in the medical record. However, there are instances when the majority of the encounter constitutes counseling/coordination of care (C/CC). Physicians might only document a brief history and exam, or nothing at all. Utilizing time-based billing principles allows a physician to disregard the “key component” requirements and select a visit level reflective of this effort.
For example, a 64-year-old female is hospitalized with newly diagnosed diabetes and requires extensive counseling regarding disease management, lifestyle modification, and medication regime, as well as coordination of care for outpatient programs and services. The hospitalist reviews some of the pertinent information with the patient and leaves the room to coordinate the patient’s ongoing care (25 minutes). The hospitalist then asks a resident to assist with the remaining counseling efforts (20 minutes). Code 99232 (inpatient visit, 25 minutes total visit time) would be appropriate to report.
Counseling, Coordination of Care
Time may be used as the determining factor for the visit level, if more than 50% of the total visit time involves C/CC.1 Time is not used for visit-level selection if C/CC is minimal or absent from the patient encounter. Total visit time is acknowledged as the physician’s face-to-face (i.e. bedside) time combined with time spent on the unit/floor reviewing data, obtaining relevant patient information, and discussing the individual case with other involved healthcare providers.
Time associated with activities performed outside of the patient’s unit/floor is not considered when calculating total visit time. Time associated with teaching students/interns also is excluded; only the attending physician’s time counts.
When the requirements have been met, the physician selects the visit level that corresponds with the documented total visit time (see Table 1). In the scenario above, the visit level is chosen based on the attending physician’s documented time (25 minutes). The resident’s time cannot be included.
Documentation Requirements
Physicians must document the interaction during the patient encounter: history and exam, if updated or performed; discussion points; and patient response, if applicable. The medical record entry must contain both the C/CC time and the total visit time.2 “Total visit time=35 minutes; >50% spent counseling/coordinating care” or “20 of 35 minutes spent counseling/coordinating care.”
A payor may prefer one documentation style over another. It is always best to ask about the payor’s policy and review local documentation standards to ensure compliance.
Family Discussions
Physicians are always involved in family discussions. It is appropriate to count this as C/CC time. In the event that the family discussion takes place without the patient present, only count this as C/CC time if:
- The patient is unable or clinically incompetent to participate in discussions;
- The time is spent on the unit/floor with the family members or surrogate decision-makers obtaining a medical history, reviewing the patient’s condition or prognosis, or discussing treatment or limitation(s) of treatment; and
- The conversation bears directly on the management of the patient.4
The medical record should reflect these criteria. Do not consider the time if the discussion takes place in an area outside of the patient’s unit/floor, or if the time is spent counseling family members through their grieving process.
It is not uncommon for the family discussion to take place later in the day, after the physician has made earlier rounds. If the earlier encounter involved C/CC, the physician would report the cumulative time spent for that service date. If the earlier encounter was a typical patient evaluation (i.e. history update and physical) and management service (i.e. care plan review/revision), this second encounter might be regarded as a prolonged care service.
Prolonged Care
Prolonged care codes exist for both outpatient and inpatient services. A hospitalists’ focus involves the inpatient code series:
99356: Prolonged service in the inpatient or observation setting, requiring unit/floor time beyond the usual service, first hour; and
99357: Prolonged service in the inpatient or observation setting, requiring unit/floor time beyond the usual service, each additional 30 minutes.
Code 99356 is reported during the first hour of prolonged services, after the initial 30 minutes is reached; code 99357 is reported for each additional 30 minutes of prolonged care beyond the first hour, after the first 15 minutes of each additional segment. Both are “add on” codes and cannot be reported alone on a claim form; a “primary” code must be reported. Similarly, 99357 cannot be reported without 99356, and 99356 must be reported with one of the following inpatient service (primary) codes: 99218-99220, 99221-99223, 99231-99233, 99251-99255, 99304-99310. Only one unit of 99356 may be reported per patient per physician group per day, whereas multiple units of 99357 may be reported in a single day.
The CPT definition of prolonged care varies from that of the Centers for Medicare & Medicaid Services (CMS). Since 2009, CPT recognizes the total duration spent by a physician on a given date, even if the time spent by the physician on that date is not continuous; the time involves both face-to-face time and unit/floor time.5 CMS only attributes direct face-to-face time between the physician and the patient toward prolonged care billing. Time spent reviewing charts or discussion of a patient with house medical staff, waiting for test results, waiting for changes in the patient’s condition, waiting for end of a therapy session, or waiting for use of facilities cannot be billed as prolonged services.5 This is in direct opposition to its policy for C/CC services, and makes prolonged care services inefficient.
Medicare also identifies “threshold” time (see Table 2). The total physician visit time must exceed the time requirements associated with the “primary” codes by a 30-minute threshold (e.g. 99221+99356=30 minutes+30 minutes=60 minutes threshold time). The physician must document the total face-to-face time spent in separate notes throughout the day or, more realistically, in one cumulative note.
When two providers from the same group and same specialty perform services on the same date (e.g. physician A saw the patient during morning rounds, and physician B spoke with the patient/family in the afternoon), only one physician can report the cumulative service.6 As always, query payors for coverage, because some non-Medicare insurers do not recognize these codes.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare & Medicaid Services (CMS). Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2012.
- Centers for Medicare & Medicaid Services (CMS). Medicare Claims Processing Manual: Chapter 12, Section 30.6.1C. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2012.
- Centers for Medicare & Medicaid Services (CMS). Medicare National Coverage Determinations Manual: Chapter 1, Section 70.1. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/ncd103c1_Part1.pdf. Accessed Jan. 8, 2012.
- Centers for Medicare & Medicaid Services (CMS). Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1C. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011:7-21.
- Centers for Medicare & Medicaid Services (CMS). Medicare Claims Processing Manual: Chapter 12, Section 30.6.5. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2012.
Providers typically rely on the “key components” (history, exam, medical decision-making) when documenting in the medical record. However, there are instances when the majority of the encounter constitutes counseling/coordination of care (C/CC). Physicians might only document a brief history and exam, or nothing at all. Utilizing time-based billing principles allows a physician to disregard the “key component” requirements and select a visit level reflective of this effort.
For example, a 64-year-old female is hospitalized with newly diagnosed diabetes and requires extensive counseling regarding disease management, lifestyle modification, and medication regime, as well as coordination of care for outpatient programs and services. The hospitalist reviews some of the pertinent information with the patient and leaves the room to coordinate the patient’s ongoing care (25 minutes). The hospitalist then asks a resident to assist with the remaining counseling efforts (20 minutes). Code 99232 (inpatient visit, 25 minutes total visit time) would be appropriate to report.
Counseling, Coordination of Care
Time may be used as the determining factor for the visit level, if more than 50% of the total visit time involves C/CC.1 Time is not used for visit-level selection if C/CC is minimal or absent from the patient encounter. Total visit time is acknowledged as the physician’s face-to-face (i.e. bedside) time combined with time spent on the unit/floor reviewing data, obtaining relevant patient information, and discussing the individual case with other involved healthcare providers.
Time associated with activities performed outside of the patient’s unit/floor is not considered when calculating total visit time. Time associated with teaching students/interns also is excluded; only the attending physician’s time counts.
When the requirements have been met, the physician selects the visit level that corresponds with the documented total visit time (see Table 1). In the scenario above, the visit level is chosen based on the attending physician’s documented time (25 minutes). The resident’s time cannot be included.
Documentation Requirements
Physicians must document the interaction during the patient encounter: history and exam, if updated or performed; discussion points; and patient response, if applicable. The medical record entry must contain both the C/CC time and the total visit time.2 “Total visit time=35 minutes; >50% spent counseling/coordinating care” or “20 of 35 minutes spent counseling/coordinating care.”
A payor may prefer one documentation style over another. It is always best to ask about the payor’s policy and review local documentation standards to ensure compliance.
Family Discussions
Physicians are always involved in family discussions. It is appropriate to count this as C/CC time. In the event that the family discussion takes place without the patient present, only count this as C/CC time if:
- The patient is unable or clinically incompetent to participate in discussions;
- The time is spent on the unit/floor with the family members or surrogate decision-makers obtaining a medical history, reviewing the patient’s condition or prognosis, or discussing treatment or limitation(s) of treatment; and
- The conversation bears directly on the management of the patient.4
The medical record should reflect these criteria. Do not consider the time if the discussion takes place in an area outside of the patient’s unit/floor, or if the time is spent counseling family members through their grieving process.
It is not uncommon for the family discussion to take place later in the day, after the physician has made earlier rounds. If the earlier encounter involved C/CC, the physician would report the cumulative time spent for that service date. If the earlier encounter was a typical patient evaluation (i.e. history update and physical) and management service (i.e. care plan review/revision), this second encounter might be regarded as a prolonged care service.
Prolonged Care
Prolonged care codes exist for both outpatient and inpatient services. A hospitalists’ focus involves the inpatient code series:
99356: Prolonged service in the inpatient or observation setting, requiring unit/floor time beyond the usual service, first hour; and
99357: Prolonged service in the inpatient or observation setting, requiring unit/floor time beyond the usual service, each additional 30 minutes.
Code 99356 is reported during the first hour of prolonged services, after the initial 30 minutes is reached; code 99357 is reported for each additional 30 minutes of prolonged care beyond the first hour, after the first 15 minutes of each additional segment. Both are “add on” codes and cannot be reported alone on a claim form; a “primary” code must be reported. Similarly, 99357 cannot be reported without 99356, and 99356 must be reported with one of the following inpatient service (primary) codes: 99218-99220, 99221-99223, 99231-99233, 99251-99255, 99304-99310. Only one unit of 99356 may be reported per patient per physician group per day, whereas multiple units of 99357 may be reported in a single day.
The CPT definition of prolonged care varies from that of the Centers for Medicare & Medicaid Services (CMS). Since 2009, CPT recognizes the total duration spent by a physician on a given date, even if the time spent by the physician on that date is not continuous; the time involves both face-to-face time and unit/floor time.5 CMS only attributes direct face-to-face time between the physician and the patient toward prolonged care billing. Time spent reviewing charts or discussion of a patient with house medical staff, waiting for test results, waiting for changes in the patient’s condition, waiting for end of a therapy session, or waiting for use of facilities cannot be billed as prolonged services.5 This is in direct opposition to its policy for C/CC services, and makes prolonged care services inefficient.
Medicare also identifies “threshold” time (see Table 2). The total physician visit time must exceed the time requirements associated with the “primary” codes by a 30-minute threshold (e.g. 99221+99356=30 minutes+30 minutes=60 minutes threshold time). The physician must document the total face-to-face time spent in separate notes throughout the day or, more realistically, in one cumulative note.
When two providers from the same group and same specialty perform services on the same date (e.g. physician A saw the patient during morning rounds, and physician B spoke with the patient/family in the afternoon), only one physician can report the cumulative service.6 As always, query payors for coverage, because some non-Medicare insurers do not recognize these codes.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare & Medicaid Services (CMS). Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2012.
- Centers for Medicare & Medicaid Services (CMS). Medicare Claims Processing Manual: Chapter 12, Section 30.6.1C. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2012.
- Centers for Medicare & Medicaid Services (CMS). Medicare National Coverage Determinations Manual: Chapter 1, Section 70.1. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/ncd103c1_Part1.pdf. Accessed Jan. 8, 2012.
- Centers for Medicare & Medicaid Services (CMS). Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1C. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011:7-21.
- Centers for Medicare & Medicaid Services (CMS). Medicare Claims Processing Manual: Chapter 12, Section 30.6.5. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2012.
Managing Your Dermatology Practice: Dealing With Deadbeats
My last few blogs have covered various techniques for assuring that you are paid for what you do. However, despite your best efforts, there will always be a few deadbeats whom you will need to pursue. For the record, I’m speaking not about patients who fall on hard times and are unable to pay, but those who are able to pay and do not.
The worst kinds of deadbeats are the ones who rob you twice; they accept payments from insurance companies and then spend the money themselves. Such crooks must be pursued aggressively, with all the means at your disposal; but to reiterate the point I’ve tried to drive home recently, the best cure is prevention.
You already know that you should collect as many fees as possible at the time of service. For cosmetic procedures you should require a substantial deposit in advance, with the balance due at the time of service. When that is impossible, maximize the chances you will be paid by making sure all available payment mechanisms are in place.
In the last several columns (click here to access them), I described my credit-card-on-file system; patients who fail to pay their credit card bill are the credit card company’s problem, not yours. In cases in which you suspect fees might exceed credit card limits, you can arrange a realistic payment schedule in advance and have the patient fill out a credit application. You can find forms for this online at allbusiness.com, lawdog.com, and other sites.
In some cases, it may be worth the trouble to run a background check. There are easy and affordable ways to do this. Dunn & Bradstreet, for example, will furnish a report containing payment records and details of any lawsuits, liens, and other legal actions for as little as $30. The more financial information you have on file, the more leverage you have if a patient later balks at paying the balance.

For cosmetic work, always take before and after photos and have all patients sign a written consent giving permission for the procedure, assuming full financial responsibility, and acknowledging that no guarantees have been given or implied. This defuses the common deadbeat tactics of professing ignorance of personal financial obligation and/or dissatisfaction with results.
Despite all your precautions, a deadbeat will inevitably slip through on occasion; but even then, you have options for extracting payment. Collection agencies are the traditional first line of attack for most medical practices. Ideally, your agency should specialize in handling medical accounts, so it will know exactly how much pressure to exert to avoid charges of harassment. Delinquent accounts should be submitted earlier rather than later to maximize the chances of success; my manager never allows an account to age more than 90 days, and if circumstances dictate, she refers them sooner than that.
When collection agencies fail, think about small claims court. You’ll need to learn the rules for filing in your state, but most charge a nominal fee and place a limit of $5,000 or so on claims. No attorneys are involved. If your paperwork is in order, the court will nearly always rule in your favor, but it will not provide the means for actual collection. In other words, you’ll still have to persuade the deadbeat to pay up. However, in many states, a court order will give you the authority to attach a lien to property or garnish wages, which often provides enough leverage to force payment.
What about those double deadbeats who steal the insurance checks? First, check your third-party contract; sometimes, the insurance company or HMO will be compelled to pay you directly and then will go after the patient itself to get back its money. (They won’t volunteer this service, however – you’ll have to ask for it.)
If that’s not an option, consider reporting the misdirected payment to the Internal Revenue Service as income to the patient, by submitting a 1099-Miscellaneous Income form. Be sure to notify the deadbeat that you will be doing this. Sometimes, the threat of such action will convince the crook to pay up; but if not, at least you’ll have the satisfaction of knowing he or she will have to pay taxes on the money.
My last few blogs have covered various techniques for assuring that you are paid for what you do. However, despite your best efforts, there will always be a few deadbeats whom you will need to pursue. For the record, I’m speaking not about patients who fall on hard times and are unable to pay, but those who are able to pay and do not.
The worst kinds of deadbeats are the ones who rob you twice; they accept payments from insurance companies and then spend the money themselves. Such crooks must be pursued aggressively, with all the means at your disposal; but to reiterate the point I’ve tried to drive home recently, the best cure is prevention.
You already know that you should collect as many fees as possible at the time of service. For cosmetic procedures you should require a substantial deposit in advance, with the balance due at the time of service. When that is impossible, maximize the chances you will be paid by making sure all available payment mechanisms are in place.
In the last several columns (click here to access them), I described my credit-card-on-file system; patients who fail to pay their credit card bill are the credit card company’s problem, not yours. In cases in which you suspect fees might exceed credit card limits, you can arrange a realistic payment schedule in advance and have the patient fill out a credit application. You can find forms for this online at allbusiness.com, lawdog.com, and other sites.
In some cases, it may be worth the trouble to run a background check. There are easy and affordable ways to do this. Dunn & Bradstreet, for example, will furnish a report containing payment records and details of any lawsuits, liens, and other legal actions for as little as $30. The more financial information you have on file, the more leverage you have if a patient later balks at paying the balance.
For cosmetic work, always take before and after photos and have all patients sign a written consent giving permission for the procedure, assuming full financial responsibility, and acknowledging that no guarantees have been given or implied. This defuses the common deadbeat tactics of professing ignorance of personal financial obligation and/or dissatisfaction with results.
Despite all your precautions, a deadbeat will inevitably slip through on occasion; but even then, you have options for extracting payment. Collection agencies are the traditional first line of attack for most medical practices. Ideally, your agency should specialize in handling medical accounts, so it will know exactly how much pressure to exert to avoid charges of harassment. Delinquent accounts should be submitted earlier rather than later to maximize the chances of success; my manager never allows an account to age more than 90 days, and if circumstances dictate, she refers them sooner than that.
When collection agencies fail, think about small claims court. You’ll need to learn the rules for filing in your state, but most charge a nominal fee and place a limit of $5,000 or so on claims. No attorneys are involved. If your paperwork is in order, the court will nearly always rule in your favor, but it will not provide the means for actual collection. In other words, you’ll still have to persuade the deadbeat to pay up. However, in many states, a court order will give you the authority to attach a lien to property or garnish wages, which often provides enough leverage to force payment.
What about those double deadbeats who steal the insurance checks? First, check your third-party contract; sometimes, the insurance company or HMO will be compelled to pay you directly and then will go after the patient itself to get back its money. (They won’t volunteer this service, however – you’ll have to ask for it.)
If that’s not an option, consider reporting the misdirected payment to the Internal Revenue Service as income to the patient, by submitting a 1099-Miscellaneous Income form. Be sure to notify the deadbeat that you will be doing this. Sometimes, the threat of such action will convince the crook to pay up; but if not, at least you’ll have the satisfaction of knowing he or she will have to pay taxes on the money.
My last few blogs have covered various techniques for assuring that you are paid for what you do. However, despite your best efforts, there will always be a few deadbeats whom you will need to pursue. For the record, I’m speaking not about patients who fall on hard times and are unable to pay, but those who are able to pay and do not.
The worst kinds of deadbeats are the ones who rob you twice; they accept payments from insurance companies and then spend the money themselves. Such crooks must be pursued aggressively, with all the means at your disposal; but to reiterate the point I’ve tried to drive home recently, the best cure is prevention.
You already know that you should collect as many fees as possible at the time of service. For cosmetic procedures you should require a substantial deposit in advance, with the balance due at the time of service. When that is impossible, maximize the chances you will be paid by making sure all available payment mechanisms are in place.
In the last several columns (click here to access them), I described my credit-card-on-file system; patients who fail to pay their credit card bill are the credit card company’s problem, not yours. In cases in which you suspect fees might exceed credit card limits, you can arrange a realistic payment schedule in advance and have the patient fill out a credit application. You can find forms for this online at allbusiness.com, lawdog.com, and other sites.
In some cases, it may be worth the trouble to run a background check. There are easy and affordable ways to do this. Dunn & Bradstreet, for example, will furnish a report containing payment records and details of any lawsuits, liens, and other legal actions for as little as $30. The more financial information you have on file, the more leverage you have if a patient later balks at paying the balance.
For cosmetic work, always take before and after photos and have all patients sign a written consent giving permission for the procedure, assuming full financial responsibility, and acknowledging that no guarantees have been given or implied. This defuses the common deadbeat tactics of professing ignorance of personal financial obligation and/or dissatisfaction with results.
Despite all your precautions, a deadbeat will inevitably slip through on occasion; but even then, you have options for extracting payment. Collection agencies are the traditional first line of attack for most medical practices. Ideally, your agency should specialize in handling medical accounts, so it will know exactly how much pressure to exert to avoid charges of harassment. Delinquent accounts should be submitted earlier rather than later to maximize the chances of success; my manager never allows an account to age more than 90 days, and if circumstances dictate, she refers them sooner than that.
When collection agencies fail, think about small claims court. You’ll need to learn the rules for filing in your state, but most charge a nominal fee and place a limit of $5,000 or so on claims. No attorneys are involved. If your paperwork is in order, the court will nearly always rule in your favor, but it will not provide the means for actual collection. In other words, you’ll still have to persuade the deadbeat to pay up. However, in many states, a court order will give you the authority to attach a lien to property or garnish wages, which often provides enough leverage to force payment.
What about those double deadbeats who steal the insurance checks? First, check your third-party contract; sometimes, the insurance company or HMO will be compelled to pay you directly and then will go after the patient itself to get back its money. (They won’t volunteer this service, however – you’ll have to ask for it.)
If that’s not an option, consider reporting the misdirected payment to the Internal Revenue Service as income to the patient, by submitting a 1099-Miscellaneous Income form. Be sure to notify the deadbeat that you will be doing this. Sometimes, the threat of such action will convince the crook to pay up; but if not, at least you’ll have the satisfaction of knowing he or she will have to pay taxes on the money.
Dealing With Deadbeats
My last few columns have covered various techniques for assuring that you are paid for what you do. However, despite your best efforts, there will always be a few deadbeats whom you will need to pursue. For the record, I’m speaking not about patients who fall on hard times and are unable to pay, but those who are able to pay and do not.
The worst kinds of deadbeats are the ones who rob you twice; they accept payments from insurance companies and then spend the money themselves. Such crooks must be pursued aggressively, with all the means at your disposal; but to reiterate the point I’ve tried to drive home recently, the best cure is prevention.
You already know that you should collect as many fees as possible at the time of service. For cosmetic procedures you should require a substantial deposit in advance, with the balance due at the time of service. When that is impossible, maximize the chances you will be paid by making sure all available payment mechanisms are in place.
In the last several columns (click here to access them), I described my credit-card-on-file system; patients who fail to pay their credit card bill are the credit card company’s problem, not yours. In cases in which you suspect fees might exceed credit card limits, you can arrange a realistic payment schedule in advance and have the patient fill out a credit application. You can find forms for this online at allbusiness.com, lawdog.com, and other sites.
In some cases, it may be worth the trouble to run a background check. There are easy and affordable ways to do this. Dunn & Bradstreet, for example, will furnish a report containing payment records and details of any lawsuits, liens, and other legal actions for as little as $30. The more financial information you have on file, the more leverage you have if a patient later balks at paying the balance.

For cosmetic work, always take before and after photos and have all patients sign a written consent giving permission for the procedure, assuming full financial responsibility, and acknowledging that no guarantees have been given or implied. This defuses the common deadbeat tactics of professing ignorance of personal financial obligation and/or dissatisfaction with results.
Despite all your precautions, a deadbeat will inevitably slip through on occasion; but even then, you have options for extracting payment. Collection agencies are the traditional first line of attack for most medical practices. Ideally, your agency should specialize in handling medical accounts, so it will know exactly how much pressure to exert to avoid charges of harassment. Delinquent accounts should be submitted earlier rather than later to maximize the chances of success; my manager never allows an account to age more than 90 days, and if circumstances dictate, she refers them sooner than that.
When collection agencies fail, think about small claims court. You’ll need to learn the rules for filing in your state, but most charge a nominal fee and place a limit of $5,000 or so on claims. No attorneys are involved. If your paperwork is in order, the court will nearly always rule in your favor, but it will not provide the means for actual collection. In other words, you’ll still have to persuade the deadbeat to pay up. However, in many states, a court order will give you the authority to attach a lien to property or garnish wages, which often provides enough leverage to force payment.
What about those double deadbeats who steal the insurance checks? First, check your third-party contract; sometimes, the insurance company or HMO will be compelled to pay you directly and then will go after the patient itself to get back its money. (They won’t volunteer this service, however – you’ll have to ask for it.)
If that’s not an option, consider reporting the misdirected payment to the Internal Revenue Service as income to the patient, by submitting a 1099-Miscellaneous Income form. Be sure to notify the deadbeat that you will be doing this. Sometimes, the threat of such action will convince the crook to pay up; but if not, at least you’ll have the satisfaction of knowing he or she will have to pay taxes on the money.
Dr. Eastern practices dermatology and dermatologic surgery in Bellevue, N.J.
My last few columns have covered various techniques for assuring that you are paid for what you do. However, despite your best efforts, there will always be a few deadbeats whom you will need to pursue. For the record, I’m speaking not about patients who fall on hard times and are unable to pay, but those who are able to pay and do not.
The worst kinds of deadbeats are the ones who rob you twice; they accept payments from insurance companies and then spend the money themselves. Such crooks must be pursued aggressively, with all the means at your disposal; but to reiterate the point I’ve tried to drive home recently, the best cure is prevention.
You already know that you should collect as many fees as possible at the time of service. For cosmetic procedures you should require a substantial deposit in advance, with the balance due at the time of service. When that is impossible, maximize the chances you will be paid by making sure all available payment mechanisms are in place.
In the last several columns (click here to access them), I described my credit-card-on-file system; patients who fail to pay their credit card bill are the credit card company’s problem, not yours. In cases in which you suspect fees might exceed credit card limits, you can arrange a realistic payment schedule in advance and have the patient fill out a credit application. You can find forms for this online at allbusiness.com, lawdog.com, and other sites.
In some cases, it may be worth the trouble to run a background check. There are easy and affordable ways to do this. Dunn & Bradstreet, for example, will furnish a report containing payment records and details of any lawsuits, liens, and other legal actions for as little as $30. The more financial information you have on file, the more leverage you have if a patient later balks at paying the balance.
For cosmetic work, always take before and after photos and have all patients sign a written consent giving permission for the procedure, assuming full financial responsibility, and acknowledging that no guarantees have been given or implied. This defuses the common deadbeat tactics of professing ignorance of personal financial obligation and/or dissatisfaction with results.
Despite all your precautions, a deadbeat will inevitably slip through on occasion; but even then, you have options for extracting payment. Collection agencies are the traditional first line of attack for most medical practices. Ideally, your agency should specialize in handling medical accounts, so it will know exactly how much pressure to exert to avoid charges of harassment. Delinquent accounts should be submitted earlier rather than later to maximize the chances of success; my manager never allows an account to age more than 90 days, and if circumstances dictate, she refers them sooner than that.
When collection agencies fail, think about small claims court. You’ll need to learn the rules for filing in your state, but most charge a nominal fee and place a limit of $5,000 or so on claims. No attorneys are involved. If your paperwork is in order, the court will nearly always rule in your favor, but it will not provide the means for actual collection. In other words, you’ll still have to persuade the deadbeat to pay up. However, in many states, a court order will give you the authority to attach a lien to property or garnish wages, which often provides enough leverage to force payment.
What about those double deadbeats who steal the insurance checks? First, check your third-party contract; sometimes, the insurance company or HMO will be compelled to pay you directly and then will go after the patient itself to get back its money. (They won’t volunteer this service, however – you’ll have to ask for it.)
If that’s not an option, consider reporting the misdirected payment to the Internal Revenue Service as income to the patient, by submitting a 1099-Miscellaneous Income form. Be sure to notify the deadbeat that you will be doing this. Sometimes, the threat of such action will convince the crook to pay up; but if not, at least you’ll have the satisfaction of knowing he or she will have to pay taxes on the money.
Dr. Eastern practices dermatology and dermatologic surgery in Bellevue, N.J.
My last few columns have covered various techniques for assuring that you are paid for what you do. However, despite your best efforts, there will always be a few deadbeats whom you will need to pursue. For the record, I’m speaking not about patients who fall on hard times and are unable to pay, but those who are able to pay and do not.
The worst kinds of deadbeats are the ones who rob you twice; they accept payments from insurance companies and then spend the money themselves. Such crooks must be pursued aggressively, with all the means at your disposal; but to reiterate the point I’ve tried to drive home recently, the best cure is prevention.
You already know that you should collect as many fees as possible at the time of service. For cosmetic procedures you should require a substantial deposit in advance, with the balance due at the time of service. When that is impossible, maximize the chances you will be paid by making sure all available payment mechanisms are in place.
In the last several columns (click here to access them), I described my credit-card-on-file system; patients who fail to pay their credit card bill are the credit card company’s problem, not yours. In cases in which you suspect fees might exceed credit card limits, you can arrange a realistic payment schedule in advance and have the patient fill out a credit application. You can find forms for this online at allbusiness.com, lawdog.com, and other sites.
In some cases, it may be worth the trouble to run a background check. There are easy and affordable ways to do this. Dunn & Bradstreet, for example, will furnish a report containing payment records and details of any lawsuits, liens, and other legal actions for as little as $30. The more financial information you have on file, the more leverage you have if a patient later balks at paying the balance.
For cosmetic work, always take before and after photos and have all patients sign a written consent giving permission for the procedure, assuming full financial responsibility, and acknowledging that no guarantees have been given or implied. This defuses the common deadbeat tactics of professing ignorance of personal financial obligation and/or dissatisfaction with results.
Despite all your precautions, a deadbeat will inevitably slip through on occasion; but even then, you have options for extracting payment. Collection agencies are the traditional first line of attack for most medical practices. Ideally, your agency should specialize in handling medical accounts, so it will know exactly how much pressure to exert to avoid charges of harassment. Delinquent accounts should be submitted earlier rather than later to maximize the chances of success; my manager never allows an account to age more than 90 days, and if circumstances dictate, she refers them sooner than that.
When collection agencies fail, think about small claims court. You’ll need to learn the rules for filing in your state, but most charge a nominal fee and place a limit of $5,000 or so on claims. No attorneys are involved. If your paperwork is in order, the court will nearly always rule in your favor, but it will not provide the means for actual collection. In other words, you’ll still have to persuade the deadbeat to pay up. However, in many states, a court order will give you the authority to attach a lien to property or garnish wages, which often provides enough leverage to force payment.
What about those double deadbeats who steal the insurance checks? First, check your third-party contract; sometimes, the insurance company or HMO will be compelled to pay you directly and then will go after the patient itself to get back its money. (They won’t volunteer this service, however – you’ll have to ask for it.)
If that’s not an option, consider reporting the misdirected payment to the Internal Revenue Service as income to the patient, by submitting a 1099-Miscellaneous Income form. Be sure to notify the deadbeat that you will be doing this. Sometimes, the threat of such action will convince the crook to pay up; but if not, at least you’ll have the satisfaction of knowing he or she will have to pay taxes on the money.
Dr. Eastern practices dermatology and dermatologic surgery in Bellevue, N.J.
Do you want to prevail at trial? Here are 10 keys to effective testimony
“10 strategies for the hot seat: Giving a successful deposition”
Andrew K. Worek, Esq (February 2012)
Mr. Worek reports no financial relationships relevant to this article.
You survived the deposition: Your attorney advised you that it went well and that nothing you said was catastrophically harmful to the defense of your case. Now it’s time to move on to trial.
A date has been set, and you’re anticipating it with a fair dose of trepidation. You may find yourself pacing nervously along the marble corridors of the courthouse or staring with foreboding at the witness stand, with its solitary chair and microphone. Rest assured: There is much to be done to navigate your way through the trial process.
In this article—a follow-up to “Strategies for the hot seat: Giving a successful deposition” (February 2012)—I offer 10 tips for getting through a medical malpractice trial.

1 Preparation is critical
How do you get to Carnegie Hall? You’ve heard the joke.
Preparation is absolutely critical. You are going to have six to 14 jurors, a judge, defense counsel, opposing counsel, the plaintiff, and a small audience watching your every move and hanging on every word, but there’s no need to be nervous if you have prepared.
That said, be informed that hours upon hours of discussion and review of the care rendered with your attorney may be necessary to ensure that you understand medical and legal issues and can address both with confidence.
Any hesitation or poorly chosen phrase can have a detrimental effect on your case. Review every aspect of your testimony, the exhibits you plan to use, and the questions likely to be asked by your own attorney and opposing counsel—and do so repeatedly. You should expect to spend several days immediately before trial in your lawyer’s office going over every detail, so clear your schedule.
Don’t stop until you are familiar with every aspect of your testimony and the facts. Anything less may cause you to appear un-prepared, confused, or, worse—incompetent.
2 Put on your educator’s cap
Now is the time to teach.
During your deposition, you concentrated on simply answering the question that was posed in the manner in which it was asked, and you tried to avoid educating opposing counsel. A trial is different—you have a panel of jurors who are eager to hear your side of the story. These are the people who will decide your fate. Now is the time to teach.
I was once told—and I truly believe—that most jurors understand science and medicine at the high school level. Of course, some jurors will have greater understanding, and some less. Teach the jury the reasons behind your medical decisions and explain why they were correct. A teaching approach—as opposed to monotone answers—will help hold the jury’s attention and address its inquisitiveness.
Work with your attorney to develop appropriate explanations of medical terms, diagnoses, and treatments at issue in the case.
3 Face the jury
We typically look at the person to whom we are speaking. In the courtroom, this tendency translates into a focus on the lawyer who is doing the questioning rather than the jury. In the big picture, however, you are testifying to the jury, not the attorney—so look at the jurors when you speak.
Your attorney may position himself (or herself) near the jury so that your gaze encompasses both him and the panel. However, even if the attorney asking questions is not near the jury, turn toward the jury when you answer.
It may help to turn your chair to angle slightly toward the jury when you take the witness stand to make yourself more comfortable and avoid appearing as though your head is on a swivel. Doing so will also help you face the jury more squarely and directly.
Look into the faces and eyes of the jury when you answer questions. Speak to them, not at them.
4 Be yourself
When you are preparing for trial with your attorney, review the answers you expect to give to various questions. Work on delivering those responses in your own words, the way you would present them to a patient or a peer. A jury can detect sincerity and its opposite—glibness.
You and your counsel may agree on the information or points to be disclosed in response to a certain question, but on the witness stand, you will have to respond with your own voice and vocabulary.
5 Prepare to be cross-examined
Most jurisdictions permit opposing counsel to call a defendant physician to the witness stand, “as if on cross-examination.” This means that the opposing attorney can ask you leading questions in an attempt to box you into “Yes” or “No” responses with little or no opportunity to explain. This is customary. You must be prepared to face heated examination.
A trial is an adversarial process, based on the general premise that, through heated exchanges and questioning, the truth will emerge. Opposing counsel will attempt to get you to answer questions based on the plaintiff’s view of the case. Most physicians find having their answers constrained in this manner to be very frustrating.
Work with your attorney until you are ready to answer even the toughest and narrowest of “Yes” or “No” questions. If a question cannot be answered reliably with a “Yes” or “No,” be prepared to point that fact out to the questioning attorney or the judge. Also be prepared to provide an explanation beyond “Yes” or “No” when it may be appropriate. The judge will ultimately decide whether an explanation is warranted; many judges permit elaboration.
Your own attorney will later have the opportunity to question you, as well. If you are not permitted to give an explanation during questioning by opposing counsel, your own attorney can afford you that opportunity. An opposing attorney who insists that a physician not explain runs the risk of diverting the jury’s focus to the unstated explanation rather than to the actual “Yes” or “No” response. Indicate when you would like to explain an answer, and retain your composure if refused.
When opposing counsel has finished questioning you, your own skillful defense attorney can rise from his chair and ask, “Doctor, what is it that you wanted to explain to the ladies and gentlemen of the jury?” Then, like the late radio commentator Paul Harvey, you can provide “the rest of the story.”
As you did during your deposition, you have the right to ask for clarification of a confusing or unintelligible question. The same is true for a question in which a medical principle or condition is improperly characterized or defined. If a question doesn’t make sense, ask for clarification. If the question is inaccurate, advise the opposing attorney of the improper characterization, and ask that he rephrase the question. On occasion, it may be best to respond to a mischaracterization of a medical principle by answering: “That’s not how it works.” By declining to offer more information, you can create a moment of uncomfortable silence while opposing counsel collects his thoughts and regroups.
6 Emulate a weather forecaster
Work with your attorney to find aspects of your testimony that will permit you to get off the witness stand and present a chart or graph or other evidence from a standing position before the jury. Think of how much more interesting a weather forecaster is than an anchor who sits behind a desk reading news. Lengthy testimony from the witness stand is boring for the jury and can be tiring for the witness. Get off the stand once or twice to illustrate a point or demonstrate, for example, how the McRoberts maneuver is accomplished. It will keep the jury focused and interested.
When you stand before the jury to illustrate a point, make sure every juror can see your presentation. Your attorney may also request that a photograph or other exhibit be “published” to the jury so that the panel members can pass it among themselves and examine it with their own hands.
7 Be on your best behavior
Jurors are curious. They are being asked to, quite literally, pass judgment on you, despite knowing next to nothing about you. Jurors typically take their duties very seriously and will naturally be motivated to analyze non-verbal as well as verbal cues in an effort to learn more about you. Be prepared: They will watch your every move and mannerism in the courtroom, so be conscious of your clothing, mannerisms, and behavior. This holds true in the hallways of the courthouse and any location within two or three blocks. It is not uncommon to encounter a juror a block or two away from a courthouse in a major city, or to see a juror in a nearby coffee shop.
8 Control your reactions to testimony
It may be difficult to sit and listen as opposing counsel presents his opening argument to the jury. It may be a challenge to listen to the plaintiff’s case during the first 2 or 3 days of the trial. The plaintiff goes first; you have to wait your turn.
Overt facial reactions to testimony are best avoided. Although it may be helpful for you to make notes during testimony, try not to pass or slide them across the table to your attorney, except for rare occasions. There will be periodic breaks in the testimony, during which you can discuss your notes with your attorney. Frantically jotting down notes and sliding them over to your attorney may cause the jury to conclude that you are overly emotional or lack confidence in your attorney.
9 Test the gadgets
If you are going to present an exhibit, such as a chart or graph, make absolutely certain that it is accurate. Any error will be noted by opposing counsel and may impair your credibility. Also consider whether the chart or diagram could be reinterpreted to support your opponent’s case. If it could, don’t use it.
High-tech gizmos were once frowned upon by old-school defense attorneys. Now, we’re well past the MTV generation, and high-tech illustrations and animations are common in courtrooms. Be careful to avoid any high-tech malfunctions, however, which can distract the jury during presentation of your evidence.
If you are planning to use a demonstrative exhibit such as a heart-rate monitor or portable pulse oximetry device, make sure the batteries are charged and that it works. Practice any maneuver you plan to perform using the device or machine. You don’t want to appear clumsy or unfamiliar with the device. If any demonstration involves a sharp or needle, use an abundance of caution! In a birth injury case, baby mannequins are sometimes used. Make sure they work as intended and don’t permit anyone to “play” with them in the courtroom during breaks in the case. Trial is a serious matter; any levity observed by a juror could leave a detrimental impression.
Over my career, I have seen 1) an orthopedic surgery expert drop several “easy to assemble” metal components, creating a cacophony of pings and clangs as they bounced across the marble floor; 2) a surgeon staple his own palm with an “empty” laparoscopic staple gun; and 3) a medical expert miss a step getting off the witness stand, causing him to tumble into the jury box, strike his head and render himself nearly unconscious. This last incident led to the cancellation of the afternoon court session.
10 Take your time— and a little water
It’s helpful to visit the courtroom with your attorney some time before the trial date to dispel the jitters that can arise in an unfamiliar place. Also take a moment to sit in the witness stand so that you can have some level of comfort when testifying and understand how well, or poorly, the jury will be able to see you (and vice versa).
During the trial, take your time when answering questions. You may want to speak slightly more slowly than normal so that all the jurors can hear and appreciate what you’re saying. The tempo and volume of your testimony may also need to be adjusted, depending on the acoustics of the courtroom, which can vary widely, particularly in some of the more majestic and ornate venues.
Most courtrooms offer water pitchers and cups. Take a half-cup of water with you to the stand. A full cup is easy to spill—and creates a mess when it does. Courtrooms are not known for having an ample supply of paper towels.
Your confident presence can humanize the courtroom
The trial of a medical malpractice case is a difficult and emotional experience for any physician. Preparing to testify with confidence and precision is an important step toward a successful defense. The courtroom is an unfamiliar, uncomfortable, and adversarial environment. With appropriate preparation, however, the daunting specter of the witness stand can be conquered.
They’re available in the archive at obgmanagement.com
- Data on liability claims offer bright spots for ObGyns—and sobering statistics
Janelle Yates (January 2012) - Sound strategies to avoid malpractice hazards on labor and delivery (Part 1)
Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (December 2010) - More strategies to avoid malpractice hazards on labor and delivery (Part 2)
Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (January 2011) - Afraid of getting sued? A plaintiff attorney offers counsel (but no sympathy)
Janelle Yates (October 2009) - 10 keys to defending (or, better, keeping clear of) a shoulder dystocia suit
Andrew K. Worek, Esq (March 2008)
We want to hear from you! Tell us what you think.

Andrew K. Worek, Esq
Mr. Worek is an attorney with the firm of Post & Post, LLC, in Berwyn, Pa. He has been an active trial attorney, specializing in medical malpractice defense, for 24 years.
Andrew K. Worek, Esq
Mr. Worek is an attorney with the firm of Post & Post, LLC, in Berwyn, Pa. He has been an active trial attorney, specializing in medical malpractice defense, for 24 years.
Andrew K. Worek, Esq
Mr. Worek is an attorney with the firm of Post & Post, LLC, in Berwyn, Pa. He has been an active trial attorney, specializing in medical malpractice defense, for 24 years.
“10 strategies for the hot seat: Giving a successful deposition”
Andrew K. Worek, Esq (February 2012)
Mr. Worek reports no financial relationships relevant to this article.
You survived the deposition: Your attorney advised you that it went well and that nothing you said was catastrophically harmful to the defense of your case. Now it’s time to move on to trial.
A date has been set, and you’re anticipating it with a fair dose of trepidation. You may find yourself pacing nervously along the marble corridors of the courthouse or staring with foreboding at the witness stand, with its solitary chair and microphone. Rest assured: There is much to be done to navigate your way through the trial process.
In this article—a follow-up to “Strategies for the hot seat: Giving a successful deposition” (February 2012)—I offer 10 tips for getting through a medical malpractice trial.
1 Preparation is critical
How do you get to Carnegie Hall? You’ve heard the joke.
Preparation is absolutely critical. You are going to have six to 14 jurors, a judge, defense counsel, opposing counsel, the plaintiff, and a small audience watching your every move and hanging on every word, but there’s no need to be nervous if you have prepared.
That said, be informed that hours upon hours of discussion and review of the care rendered with your attorney may be necessary to ensure that you understand medical and legal issues and can address both with confidence.
Any hesitation or poorly chosen phrase can have a detrimental effect on your case. Review every aspect of your testimony, the exhibits you plan to use, and the questions likely to be asked by your own attorney and opposing counsel—and do so repeatedly. You should expect to spend several days immediately before trial in your lawyer’s office going over every detail, so clear your schedule.
Don’t stop until you are familiar with every aspect of your testimony and the facts. Anything less may cause you to appear un-prepared, confused, or, worse—incompetent.
2 Put on your educator’s cap
Now is the time to teach.
During your deposition, you concentrated on simply answering the question that was posed in the manner in which it was asked, and you tried to avoid educating opposing counsel. A trial is different—you have a panel of jurors who are eager to hear your side of the story. These are the people who will decide your fate. Now is the time to teach.
I was once told—and I truly believe—that most jurors understand science and medicine at the high school level. Of course, some jurors will have greater understanding, and some less. Teach the jury the reasons behind your medical decisions and explain why they were correct. A teaching approach—as opposed to monotone answers—will help hold the jury’s attention and address its inquisitiveness.
Work with your attorney to develop appropriate explanations of medical terms, diagnoses, and treatments at issue in the case.
3 Face the jury
We typically look at the person to whom we are speaking. In the courtroom, this tendency translates into a focus on the lawyer who is doing the questioning rather than the jury. In the big picture, however, you are testifying to the jury, not the attorney—so look at the jurors when you speak.
Your attorney may position himself (or herself) near the jury so that your gaze encompasses both him and the panel. However, even if the attorney asking questions is not near the jury, turn toward the jury when you answer.
It may help to turn your chair to angle slightly toward the jury when you take the witness stand to make yourself more comfortable and avoid appearing as though your head is on a swivel. Doing so will also help you face the jury more squarely and directly.
Look into the faces and eyes of the jury when you answer questions. Speak to them, not at them.
4 Be yourself
When you are preparing for trial with your attorney, review the answers you expect to give to various questions. Work on delivering those responses in your own words, the way you would present them to a patient or a peer. A jury can detect sincerity and its opposite—glibness.
You and your counsel may agree on the information or points to be disclosed in response to a certain question, but on the witness stand, you will have to respond with your own voice and vocabulary.
5 Prepare to be cross-examined
Most jurisdictions permit opposing counsel to call a defendant physician to the witness stand, “as if on cross-examination.” This means that the opposing attorney can ask you leading questions in an attempt to box you into “Yes” or “No” responses with little or no opportunity to explain. This is customary. You must be prepared to face heated examination.
A trial is an adversarial process, based on the general premise that, through heated exchanges and questioning, the truth will emerge. Opposing counsel will attempt to get you to answer questions based on the plaintiff’s view of the case. Most physicians find having their answers constrained in this manner to be very frustrating.
Work with your attorney until you are ready to answer even the toughest and narrowest of “Yes” or “No” questions. If a question cannot be answered reliably with a “Yes” or “No,” be prepared to point that fact out to the questioning attorney or the judge. Also be prepared to provide an explanation beyond “Yes” or “No” when it may be appropriate. The judge will ultimately decide whether an explanation is warranted; many judges permit elaboration.
Your own attorney will later have the opportunity to question you, as well. If you are not permitted to give an explanation during questioning by opposing counsel, your own attorney can afford you that opportunity. An opposing attorney who insists that a physician not explain runs the risk of diverting the jury’s focus to the unstated explanation rather than to the actual “Yes” or “No” response. Indicate when you would like to explain an answer, and retain your composure if refused.
When opposing counsel has finished questioning you, your own skillful defense attorney can rise from his chair and ask, “Doctor, what is it that you wanted to explain to the ladies and gentlemen of the jury?” Then, like the late radio commentator Paul Harvey, you can provide “the rest of the story.”
As you did during your deposition, you have the right to ask for clarification of a confusing or unintelligible question. The same is true for a question in which a medical principle or condition is improperly characterized or defined. If a question doesn’t make sense, ask for clarification. If the question is inaccurate, advise the opposing attorney of the improper characterization, and ask that he rephrase the question. On occasion, it may be best to respond to a mischaracterization of a medical principle by answering: “That’s not how it works.” By declining to offer more information, you can create a moment of uncomfortable silence while opposing counsel collects his thoughts and regroups.
6 Emulate a weather forecaster
Work with your attorney to find aspects of your testimony that will permit you to get off the witness stand and present a chart or graph or other evidence from a standing position before the jury. Think of how much more interesting a weather forecaster is than an anchor who sits behind a desk reading news. Lengthy testimony from the witness stand is boring for the jury and can be tiring for the witness. Get off the stand once or twice to illustrate a point or demonstrate, for example, how the McRoberts maneuver is accomplished. It will keep the jury focused and interested.
When you stand before the jury to illustrate a point, make sure every juror can see your presentation. Your attorney may also request that a photograph or other exhibit be “published” to the jury so that the panel members can pass it among themselves and examine it with their own hands.
7 Be on your best behavior
Jurors are curious. They are being asked to, quite literally, pass judgment on you, despite knowing next to nothing about you. Jurors typically take their duties very seriously and will naturally be motivated to analyze non-verbal as well as verbal cues in an effort to learn more about you. Be prepared: They will watch your every move and mannerism in the courtroom, so be conscious of your clothing, mannerisms, and behavior. This holds true in the hallways of the courthouse and any location within two or three blocks. It is not uncommon to encounter a juror a block or two away from a courthouse in a major city, or to see a juror in a nearby coffee shop.
8 Control your reactions to testimony
It may be difficult to sit and listen as opposing counsel presents his opening argument to the jury. It may be a challenge to listen to the plaintiff’s case during the first 2 or 3 days of the trial. The plaintiff goes first; you have to wait your turn.
Overt facial reactions to testimony are best avoided. Although it may be helpful for you to make notes during testimony, try not to pass or slide them across the table to your attorney, except for rare occasions. There will be periodic breaks in the testimony, during which you can discuss your notes with your attorney. Frantically jotting down notes and sliding them over to your attorney may cause the jury to conclude that you are overly emotional or lack confidence in your attorney.
9 Test the gadgets
If you are going to present an exhibit, such as a chart or graph, make absolutely certain that it is accurate. Any error will be noted by opposing counsel and may impair your credibility. Also consider whether the chart or diagram could be reinterpreted to support your opponent’s case. If it could, don’t use it.
High-tech gizmos were once frowned upon by old-school defense attorneys. Now, we’re well past the MTV generation, and high-tech illustrations and animations are common in courtrooms. Be careful to avoid any high-tech malfunctions, however, which can distract the jury during presentation of your evidence.
If you are planning to use a demonstrative exhibit such as a heart-rate monitor or portable pulse oximetry device, make sure the batteries are charged and that it works. Practice any maneuver you plan to perform using the device or machine. You don’t want to appear clumsy or unfamiliar with the device. If any demonstration involves a sharp or needle, use an abundance of caution! In a birth injury case, baby mannequins are sometimes used. Make sure they work as intended and don’t permit anyone to “play” with them in the courtroom during breaks in the case. Trial is a serious matter; any levity observed by a juror could leave a detrimental impression.
Over my career, I have seen 1) an orthopedic surgery expert drop several “easy to assemble” metal components, creating a cacophony of pings and clangs as they bounced across the marble floor; 2) a surgeon staple his own palm with an “empty” laparoscopic staple gun; and 3) a medical expert miss a step getting off the witness stand, causing him to tumble into the jury box, strike his head and render himself nearly unconscious. This last incident led to the cancellation of the afternoon court session.
10 Take your time— and a little water
It’s helpful to visit the courtroom with your attorney some time before the trial date to dispel the jitters that can arise in an unfamiliar place. Also take a moment to sit in the witness stand so that you can have some level of comfort when testifying and understand how well, or poorly, the jury will be able to see you (and vice versa).
During the trial, take your time when answering questions. You may want to speak slightly more slowly than normal so that all the jurors can hear and appreciate what you’re saying. The tempo and volume of your testimony may also need to be adjusted, depending on the acoustics of the courtroom, which can vary widely, particularly in some of the more majestic and ornate venues.
Most courtrooms offer water pitchers and cups. Take a half-cup of water with you to the stand. A full cup is easy to spill—and creates a mess when it does. Courtrooms are not known for having an ample supply of paper towels.
Your confident presence can humanize the courtroom
The trial of a medical malpractice case is a difficult and emotional experience for any physician. Preparing to testify with confidence and precision is an important step toward a successful defense. The courtroom is an unfamiliar, uncomfortable, and adversarial environment. With appropriate preparation, however, the daunting specter of the witness stand can be conquered.
They’re available in the archive at obgmanagement.com
- Data on liability claims offer bright spots for ObGyns—and sobering statistics
Janelle Yates (January 2012) - Sound strategies to avoid malpractice hazards on labor and delivery (Part 1)
Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (December 2010) - More strategies to avoid malpractice hazards on labor and delivery (Part 2)
Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (January 2011) - Afraid of getting sued? A plaintiff attorney offers counsel (but no sympathy)
Janelle Yates (October 2009) - 10 keys to defending (or, better, keeping clear of) a shoulder dystocia suit
Andrew K. Worek, Esq (March 2008)
We want to hear from you! Tell us what you think.
“10 strategies for the hot seat: Giving a successful deposition”
Andrew K. Worek, Esq (February 2012)
Mr. Worek reports no financial relationships relevant to this article.
You survived the deposition: Your attorney advised you that it went well and that nothing you said was catastrophically harmful to the defense of your case. Now it’s time to move on to trial.
A date has been set, and you’re anticipating it with a fair dose of trepidation. You may find yourself pacing nervously along the marble corridors of the courthouse or staring with foreboding at the witness stand, with its solitary chair and microphone. Rest assured: There is much to be done to navigate your way through the trial process.
In this article—a follow-up to “Strategies for the hot seat: Giving a successful deposition” (February 2012)—I offer 10 tips for getting through a medical malpractice trial.
1 Preparation is critical
How do you get to Carnegie Hall? You’ve heard the joke.
Preparation is absolutely critical. You are going to have six to 14 jurors, a judge, defense counsel, opposing counsel, the plaintiff, and a small audience watching your every move and hanging on every word, but there’s no need to be nervous if you have prepared.
That said, be informed that hours upon hours of discussion and review of the care rendered with your attorney may be necessary to ensure that you understand medical and legal issues and can address both with confidence.
Any hesitation or poorly chosen phrase can have a detrimental effect on your case. Review every aspect of your testimony, the exhibits you plan to use, and the questions likely to be asked by your own attorney and opposing counsel—and do so repeatedly. You should expect to spend several days immediately before trial in your lawyer’s office going over every detail, so clear your schedule.
Don’t stop until you are familiar with every aspect of your testimony and the facts. Anything less may cause you to appear un-prepared, confused, or, worse—incompetent.
2 Put on your educator’s cap
Now is the time to teach.
During your deposition, you concentrated on simply answering the question that was posed in the manner in which it was asked, and you tried to avoid educating opposing counsel. A trial is different—you have a panel of jurors who are eager to hear your side of the story. These are the people who will decide your fate. Now is the time to teach.
I was once told—and I truly believe—that most jurors understand science and medicine at the high school level. Of course, some jurors will have greater understanding, and some less. Teach the jury the reasons behind your medical decisions and explain why they were correct. A teaching approach—as opposed to monotone answers—will help hold the jury’s attention and address its inquisitiveness.
Work with your attorney to develop appropriate explanations of medical terms, diagnoses, and treatments at issue in the case.
3 Face the jury
We typically look at the person to whom we are speaking. In the courtroom, this tendency translates into a focus on the lawyer who is doing the questioning rather than the jury. In the big picture, however, you are testifying to the jury, not the attorney—so look at the jurors when you speak.
Your attorney may position himself (or herself) near the jury so that your gaze encompasses both him and the panel. However, even if the attorney asking questions is not near the jury, turn toward the jury when you answer.
It may help to turn your chair to angle slightly toward the jury when you take the witness stand to make yourself more comfortable and avoid appearing as though your head is on a swivel. Doing so will also help you face the jury more squarely and directly.
Look into the faces and eyes of the jury when you answer questions. Speak to them, not at them.
4 Be yourself
When you are preparing for trial with your attorney, review the answers you expect to give to various questions. Work on delivering those responses in your own words, the way you would present them to a patient or a peer. A jury can detect sincerity and its opposite—glibness.
You and your counsel may agree on the information or points to be disclosed in response to a certain question, but on the witness stand, you will have to respond with your own voice and vocabulary.
5 Prepare to be cross-examined
Most jurisdictions permit opposing counsel to call a defendant physician to the witness stand, “as if on cross-examination.” This means that the opposing attorney can ask you leading questions in an attempt to box you into “Yes” or “No” responses with little or no opportunity to explain. This is customary. You must be prepared to face heated examination.
A trial is an adversarial process, based on the general premise that, through heated exchanges and questioning, the truth will emerge. Opposing counsel will attempt to get you to answer questions based on the plaintiff’s view of the case. Most physicians find having their answers constrained in this manner to be very frustrating.
Work with your attorney until you are ready to answer even the toughest and narrowest of “Yes” or “No” questions. If a question cannot be answered reliably with a “Yes” or “No,” be prepared to point that fact out to the questioning attorney or the judge. Also be prepared to provide an explanation beyond “Yes” or “No” when it may be appropriate. The judge will ultimately decide whether an explanation is warranted; many judges permit elaboration.
Your own attorney will later have the opportunity to question you, as well. If you are not permitted to give an explanation during questioning by opposing counsel, your own attorney can afford you that opportunity. An opposing attorney who insists that a physician not explain runs the risk of diverting the jury’s focus to the unstated explanation rather than to the actual “Yes” or “No” response. Indicate when you would like to explain an answer, and retain your composure if refused.
When opposing counsel has finished questioning you, your own skillful defense attorney can rise from his chair and ask, “Doctor, what is it that you wanted to explain to the ladies and gentlemen of the jury?” Then, like the late radio commentator Paul Harvey, you can provide “the rest of the story.”
As you did during your deposition, you have the right to ask for clarification of a confusing or unintelligible question. The same is true for a question in which a medical principle or condition is improperly characterized or defined. If a question doesn’t make sense, ask for clarification. If the question is inaccurate, advise the opposing attorney of the improper characterization, and ask that he rephrase the question. On occasion, it may be best to respond to a mischaracterization of a medical principle by answering: “That’s not how it works.” By declining to offer more information, you can create a moment of uncomfortable silence while opposing counsel collects his thoughts and regroups.
6 Emulate a weather forecaster
Work with your attorney to find aspects of your testimony that will permit you to get off the witness stand and present a chart or graph or other evidence from a standing position before the jury. Think of how much more interesting a weather forecaster is than an anchor who sits behind a desk reading news. Lengthy testimony from the witness stand is boring for the jury and can be tiring for the witness. Get off the stand once or twice to illustrate a point or demonstrate, for example, how the McRoberts maneuver is accomplished. It will keep the jury focused and interested.
When you stand before the jury to illustrate a point, make sure every juror can see your presentation. Your attorney may also request that a photograph or other exhibit be “published” to the jury so that the panel members can pass it among themselves and examine it with their own hands.
7 Be on your best behavior
Jurors are curious. They are being asked to, quite literally, pass judgment on you, despite knowing next to nothing about you. Jurors typically take their duties very seriously and will naturally be motivated to analyze non-verbal as well as verbal cues in an effort to learn more about you. Be prepared: They will watch your every move and mannerism in the courtroom, so be conscious of your clothing, mannerisms, and behavior. This holds true in the hallways of the courthouse and any location within two or three blocks. It is not uncommon to encounter a juror a block or two away from a courthouse in a major city, or to see a juror in a nearby coffee shop.
8 Control your reactions to testimony
It may be difficult to sit and listen as opposing counsel presents his opening argument to the jury. It may be a challenge to listen to the plaintiff’s case during the first 2 or 3 days of the trial. The plaintiff goes first; you have to wait your turn.
Overt facial reactions to testimony are best avoided. Although it may be helpful for you to make notes during testimony, try not to pass or slide them across the table to your attorney, except for rare occasions. There will be periodic breaks in the testimony, during which you can discuss your notes with your attorney. Frantically jotting down notes and sliding them over to your attorney may cause the jury to conclude that you are overly emotional or lack confidence in your attorney.
9 Test the gadgets
If you are going to present an exhibit, such as a chart or graph, make absolutely certain that it is accurate. Any error will be noted by opposing counsel and may impair your credibility. Also consider whether the chart or diagram could be reinterpreted to support your opponent’s case. If it could, don’t use it.
High-tech gizmos were once frowned upon by old-school defense attorneys. Now, we’re well past the MTV generation, and high-tech illustrations and animations are common in courtrooms. Be careful to avoid any high-tech malfunctions, however, which can distract the jury during presentation of your evidence.
If you are planning to use a demonstrative exhibit such as a heart-rate monitor or portable pulse oximetry device, make sure the batteries are charged and that it works. Practice any maneuver you plan to perform using the device or machine. You don’t want to appear clumsy or unfamiliar with the device. If any demonstration involves a sharp or needle, use an abundance of caution! In a birth injury case, baby mannequins are sometimes used. Make sure they work as intended and don’t permit anyone to “play” with them in the courtroom during breaks in the case. Trial is a serious matter; any levity observed by a juror could leave a detrimental impression.
Over my career, I have seen 1) an orthopedic surgery expert drop several “easy to assemble” metal components, creating a cacophony of pings and clangs as they bounced across the marble floor; 2) a surgeon staple his own palm with an “empty” laparoscopic staple gun; and 3) a medical expert miss a step getting off the witness stand, causing him to tumble into the jury box, strike his head and render himself nearly unconscious. This last incident led to the cancellation of the afternoon court session.
10 Take your time— and a little water
It’s helpful to visit the courtroom with your attorney some time before the trial date to dispel the jitters that can arise in an unfamiliar place. Also take a moment to sit in the witness stand so that you can have some level of comfort when testifying and understand how well, or poorly, the jury will be able to see you (and vice versa).
During the trial, take your time when answering questions. You may want to speak slightly more slowly than normal so that all the jurors can hear and appreciate what you’re saying. The tempo and volume of your testimony may also need to be adjusted, depending on the acoustics of the courtroom, which can vary widely, particularly in some of the more majestic and ornate venues.
Most courtrooms offer water pitchers and cups. Take a half-cup of water with you to the stand. A full cup is easy to spill—and creates a mess when it does. Courtrooms are not known for having an ample supply of paper towels.
Your confident presence can humanize the courtroom
The trial of a medical malpractice case is a difficult and emotional experience for any physician. Preparing to testify with confidence and precision is an important step toward a successful defense. The courtroom is an unfamiliar, uncomfortable, and adversarial environment. With appropriate preparation, however, the daunting specter of the witness stand can be conquered.
They’re available in the archive at obgmanagement.com
- Data on liability claims offer bright spots for ObGyns—and sobering statistics
Janelle Yates (January 2012) - Sound strategies to avoid malpractice hazards on labor and delivery (Part 1)
Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (December 2010) - More strategies to avoid malpractice hazards on labor and delivery (Part 2)
Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (January 2011) - Afraid of getting sued? A plaintiff attorney offers counsel (but no sympathy)
Janelle Yates (October 2009) - 10 keys to defending (or, better, keeping clear of) a shoulder dystocia suit
Andrew K. Worek, Esq (March 2008)
We want to hear from you! Tell us what you think.
Fetal decapitation at 21 weeks … and more

CERCLAGE WAS PERFORMED on a woman who had a short cervix. A week later, Dr. A, her ObGyn, found the cerclage weak, and placed her on bed rest. Three days later, she passed blood clots, and was admitted to the hospital, where Dr. B assumed her care. When membranes ruptured at 21 weeks’ gestation, the fetal feet extended out of the vagina. The baby’s head was amputated during delivery; the child weighed <1 lb. Nursing staff reattached the head with sutures and permitted the mother to hold the child.
PATIENT’S CLAIM Dr. A should have confirmed cerclage placement by ultrasonography. When he found the cerclage unstable, he should have hospitalized the patient. Dr. B used excessive force during delivery. The nurses failed to properly monitor the mother. She claimed psychological injury in having witnessed the infant’s decapitation and being allowed to hold the corpse. Unreasonable death was claimed on behalf of the child’s estate; with proper treatment, the child had a chance of survival.
DEFENDANTS’ DEFENSE Cerclage was performed properly; Dr. A’s care was appropriate. Dr. B did not use excessive force; the fetus had extremely thin skin that tore easily. The nurses’ treatment was appropriate. The hospital was required to allow the mother to hold her baby when requested. A fetus is not viable at 21 weeks.
VERDICT A $1,362,499 Kentucky verdict was returned against the ObGyns; a defense verdict was returned for the hospital. The jury refused to address the claim of wrongful death because a fetus is not viable at 21 weeks.
Which breast was it? 1 error cascades
A WOMAN UNDERWENT RIGHT-BREAST biopsy in the 1970s. In 2002, an architectural distortion appeared in the left breast on mammogram. The radiologist concluded that the abnormality was related to the biopsy—but failed to note that the biopsy had been performed on the right, not the left, breast. Mammography films made in 2003 and again in 2004 were incorrectly read as normal.
In December 2005, a radiologist found no change in the left breast. In June 2007, a radiologist reported a large area of parenchymal distortion but concluded that it was related to the previous biopsy.
In May 2008, another radiologist read the films and recommended follow-up to determine which breast underwent biopsy. The patient was found to have stage III breast cancer in the left breast with a positive lymph node. She underwent double mastectomy followed by breast reconstruction surgery.
PATIENT’S CLAIM Her ObGyns never read the radiographs themselves and did not detect the left-right error after reading the reports. Errors cascaded because radiologists relied only on a previous record, not reviewing the entire chart, and confusing right and left films, even though the films were clearly marked. Had the cancer been found in 2002, treatment would have been substantially less extensive.
DEFENDANTS’ DEFENSE The cancer was difficult to diagnose because it never changed in size. A double mastectomy was not required to treat the cancer.
VERDICT The statute of limitations restricted which radiologists were allowed to be included as defendants. A confidential settlement was reached with the ObGyn group and two of the radiologists.
OB’s priorities tested; child has cerebral palsy
WHEN A WOMAN WENT to the hospital for induction of labor, her ObGyn ruptured the membranes. Shortly thereafter, the fetal heart rate dropped and fetal distress was noted. Emergency cesarean delivery was ordered.
The ObGyn left to attend to another patient while nurses prepared the patient and contacted the anesthesiologist. After delivering another child, the ObGyn returned and delivered the baby, who has cerebral palsy.
PATIENT’S CLAIM The ObGyn should have stayed with this mother instead of delivering the other child. The delay caused the child’s brain damage.
PHYSICIAN’S DEFENSE Both patients’ deliveries were being carefully monitored; proper action was taken.
VERDICT A Georgia defense verdict was returned.
Post-hysterectomy vesicovaginal fistulae
WHEN A 46-YEAR-OLD WOMAN reported irregular bleeding, her gynecologist performed dilation and curettage in February. The pathology report was negative for malignancy; abnormal bleeding ceased.
In July, after symptoms returned, she underwent abdominal hysterectomy. In September, she reported leakage of urine from her vagina; cystoscopy revealed four vesicovaginal fistulae that were repaired by a urologic surgeon. Another fistula developed and was repaired subsequently.
PATIENT’S CLAIM The gynecologist failed to provide information about less invasive options, including endometrial ablation and hormone treatment. The fistulae developed because the gynecologist did not adequately identify the bladder before suturing the vaginal cuff.
PHYSICIAN’S DEFENSE The patient was given sufficient information and requested a hysterectomy; other treatments were offered. A fistula is a known complication of the procedure.
VERDICT A California defense verdict was returned.
Placental abruption: Child has brain damage
WHEN A LABOR AND DELIVERY NURSE called, Dr. A decided a cesarean delivery was needed. The on-call anesthesiologist was at another cesarean delivery, so the procedure was delayed for longer than an hour. Dr. B delivered the child, who was born severely depressed, was resuscitated, and transferred to the NICU. The child suffered hypoxic encephalopathy, is quadriplegic, and has hypotonia.
PATIENT’S CLAIM The cesarean delivery was not performed in a timely manner. Fetal distress occurred because of placental abruption. The child would not have been injured if 1) the nursing staff had summoned a back-up anesthesiologist and 2) the procedure had started within 30 minutes of the decision.
DEFENDANTS’ DEFENSE The hospital reported that Dr. A arrived at the hospital quickly, but decided to wait for Dr. B. Placental abruption occurred prior to the mother’s arrival at the hospital.
VERDICT The ObGyns settled for an undisclosed amount before trial. A California defense verdict was returned for the hospital.
Necrotizing infection in abdominal hematoma
DYSMENORRHEA and abnormal uterine bleeding developed in a 40-year-old woman. Her gynecologist recommended abdominal hysterectomy because she had undergone two cesarean deliveries. During surgery, bladder injury was recognized and repaired.
After several days, the patient suffered complications and was referred to a urogynecologist, who found a 2-mm vaginal fistula. Three days later, she was found unresponsive at home. During exploratory surgery, the gynecologist found necrotizing infection related to an abdominal hematoma. The patient died 2 weeks later.
ESTATE’S CLAIM The gynecologist was negligent in failing to identify signs of infection at two postoperative visits.
PHYSICIAN’S DEFENSE The patient was properly monitored and referred in a timely manner to the urogynecologist. Death was due to the aggressive nature of the infection, which did not develop until after the last office visit.
VERDICT A Tennessee defense verdict was returned.
C diff infection after antibiotics for cough
AT 34 WEEKS’ GESTATION, an ObGyn prescribed amoxicillin-clavulanate (Augmentin) for a woman’s cough. She developed diarrhea that did not respond to antidiarrheal medication and a change in diet. Another ObGyn prescribed empiric sulfamethoxazole and trimethoprim (Septra), and referred her to an infectious-disease specialist. The specialist prescribed empiric cefpodoxime proxetil (Vantin) and ordered stool cultures.
Before culture results were received, the patient went into labor and delivered by cesarean section. Her illness progressed to fulminant Clostridium difficile pseudomembranous colitis that required total colectomy. Re-anastomosis was accomplished a year later. She continues to have difficulty controlling bowel movements, and reports abdominal pain, frequent dehydration, and weight loss.
PATIENT’S CLAIM Antibiotics should not have been prescribed without a culture-proven bacterial illness. C. difficile should have been suspected and treated when diarrhea first developed. Empiric antibiotic treatment during pregnancy is contraindicated. The group’s practice model of having patients rotate among OBs impeded continuity of care.
PHYSICIANS’ DEFENSE C. difficile infection was difficult to diagnose because it is not known to arise in young, healthy women outside a hospital. Use of antibiotics was proper. The group’s practice model is appropriate; continuity of care was maintained.
VERDICT A Florida defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
CERCLAGE WAS PERFORMED on a woman who had a short cervix. A week later, Dr. A, her ObGyn, found the cerclage weak, and placed her on bed rest. Three days later, she passed blood clots, and was admitted to the hospital, where Dr. B assumed her care. When membranes ruptured at 21 weeks’ gestation, the fetal feet extended out of the vagina. The baby’s head was amputated during delivery; the child weighed <1 lb. Nursing staff reattached the head with sutures and permitted the mother to hold the child.
PATIENT’S CLAIM Dr. A should have confirmed cerclage placement by ultrasonography. When he found the cerclage unstable, he should have hospitalized the patient. Dr. B used excessive force during delivery. The nurses failed to properly monitor the mother. She claimed psychological injury in having witnessed the infant’s decapitation and being allowed to hold the corpse. Unreasonable death was claimed on behalf of the child’s estate; with proper treatment, the child had a chance of survival.
DEFENDANTS’ DEFENSE Cerclage was performed properly; Dr. A’s care was appropriate. Dr. B did not use excessive force; the fetus had extremely thin skin that tore easily. The nurses’ treatment was appropriate. The hospital was required to allow the mother to hold her baby when requested. A fetus is not viable at 21 weeks.
VERDICT A $1,362,499 Kentucky verdict was returned against the ObGyns; a defense verdict was returned for the hospital. The jury refused to address the claim of wrongful death because a fetus is not viable at 21 weeks.
Which breast was it? 1 error cascades
A WOMAN UNDERWENT RIGHT-BREAST biopsy in the 1970s. In 2002, an architectural distortion appeared in the left breast on mammogram. The radiologist concluded that the abnormality was related to the biopsy—but failed to note that the biopsy had been performed on the right, not the left, breast. Mammography films made in 2003 and again in 2004 were incorrectly read as normal.
In December 2005, a radiologist found no change in the left breast. In June 2007, a radiologist reported a large area of parenchymal distortion but concluded that it was related to the previous biopsy.
In May 2008, another radiologist read the films and recommended follow-up to determine which breast underwent biopsy. The patient was found to have stage III breast cancer in the left breast with a positive lymph node. She underwent double mastectomy followed by breast reconstruction surgery.
PATIENT’S CLAIM Her ObGyns never read the radiographs themselves and did not detect the left-right error after reading the reports. Errors cascaded because radiologists relied only on a previous record, not reviewing the entire chart, and confusing right and left films, even though the films were clearly marked. Had the cancer been found in 2002, treatment would have been substantially less extensive.
DEFENDANTS’ DEFENSE The cancer was difficult to diagnose because it never changed in size. A double mastectomy was not required to treat the cancer.
VERDICT The statute of limitations restricted which radiologists were allowed to be included as defendants. A confidential settlement was reached with the ObGyn group and two of the radiologists.
OB’s priorities tested; child has cerebral palsy
WHEN A WOMAN WENT to the hospital for induction of labor, her ObGyn ruptured the membranes. Shortly thereafter, the fetal heart rate dropped and fetal distress was noted. Emergency cesarean delivery was ordered.
The ObGyn left to attend to another patient while nurses prepared the patient and contacted the anesthesiologist. After delivering another child, the ObGyn returned and delivered the baby, who has cerebral palsy.
PATIENT’S CLAIM The ObGyn should have stayed with this mother instead of delivering the other child. The delay caused the child’s brain damage.
PHYSICIAN’S DEFENSE Both patients’ deliveries were being carefully monitored; proper action was taken.
VERDICT A Georgia defense verdict was returned.
Post-hysterectomy vesicovaginal fistulae
WHEN A 46-YEAR-OLD WOMAN reported irregular bleeding, her gynecologist performed dilation and curettage in February. The pathology report was negative for malignancy; abnormal bleeding ceased.
In July, after symptoms returned, she underwent abdominal hysterectomy. In September, she reported leakage of urine from her vagina; cystoscopy revealed four vesicovaginal fistulae that were repaired by a urologic surgeon. Another fistula developed and was repaired subsequently.
PATIENT’S CLAIM The gynecologist failed to provide information about less invasive options, including endometrial ablation and hormone treatment. The fistulae developed because the gynecologist did not adequately identify the bladder before suturing the vaginal cuff.
PHYSICIAN’S DEFENSE The patient was given sufficient information and requested a hysterectomy; other treatments were offered. A fistula is a known complication of the procedure.
VERDICT A California defense verdict was returned.
Placental abruption: Child has brain damage
WHEN A LABOR AND DELIVERY NURSE called, Dr. A decided a cesarean delivery was needed. The on-call anesthesiologist was at another cesarean delivery, so the procedure was delayed for longer than an hour. Dr. B delivered the child, who was born severely depressed, was resuscitated, and transferred to the NICU. The child suffered hypoxic encephalopathy, is quadriplegic, and has hypotonia.
PATIENT’S CLAIM The cesarean delivery was not performed in a timely manner. Fetal distress occurred because of placental abruption. The child would not have been injured if 1) the nursing staff had summoned a back-up anesthesiologist and 2) the procedure had started within 30 minutes of the decision.
DEFENDANTS’ DEFENSE The hospital reported that Dr. A arrived at the hospital quickly, but decided to wait for Dr. B. Placental abruption occurred prior to the mother’s arrival at the hospital.
VERDICT The ObGyns settled for an undisclosed amount before trial. A California defense verdict was returned for the hospital.
Necrotizing infection in abdominal hematoma
DYSMENORRHEA and abnormal uterine bleeding developed in a 40-year-old woman. Her gynecologist recommended abdominal hysterectomy because she had undergone two cesarean deliveries. During surgery, bladder injury was recognized and repaired.
After several days, the patient suffered complications and was referred to a urogynecologist, who found a 2-mm vaginal fistula. Three days later, she was found unresponsive at home. During exploratory surgery, the gynecologist found necrotizing infection related to an abdominal hematoma. The patient died 2 weeks later.
ESTATE’S CLAIM The gynecologist was negligent in failing to identify signs of infection at two postoperative visits.
PHYSICIAN’S DEFENSE The patient was properly monitored and referred in a timely manner to the urogynecologist. Death was due to the aggressive nature of the infection, which did not develop until after the last office visit.
VERDICT A Tennessee defense verdict was returned.
C diff infection after antibiotics for cough
AT 34 WEEKS’ GESTATION, an ObGyn prescribed amoxicillin-clavulanate (Augmentin) for a woman’s cough. She developed diarrhea that did not respond to antidiarrheal medication and a change in diet. Another ObGyn prescribed empiric sulfamethoxazole and trimethoprim (Septra), and referred her to an infectious-disease specialist. The specialist prescribed empiric cefpodoxime proxetil (Vantin) and ordered stool cultures.
Before culture results were received, the patient went into labor and delivered by cesarean section. Her illness progressed to fulminant Clostridium difficile pseudomembranous colitis that required total colectomy. Re-anastomosis was accomplished a year later. She continues to have difficulty controlling bowel movements, and reports abdominal pain, frequent dehydration, and weight loss.
PATIENT’S CLAIM Antibiotics should not have been prescribed without a culture-proven bacterial illness. C. difficile should have been suspected and treated when diarrhea first developed. Empiric antibiotic treatment during pregnancy is contraindicated. The group’s practice model of having patients rotate among OBs impeded continuity of care.
PHYSICIANS’ DEFENSE C. difficile infection was difficult to diagnose because it is not known to arise in young, healthy women outside a hospital. Use of antibiotics was proper. The group’s practice model is appropriate; continuity of care was maintained.
VERDICT A Florida defense verdict was returned.
CERCLAGE WAS PERFORMED on a woman who had a short cervix. A week later, Dr. A, her ObGyn, found the cerclage weak, and placed her on bed rest. Three days later, she passed blood clots, and was admitted to the hospital, where Dr. B assumed her care. When membranes ruptured at 21 weeks’ gestation, the fetal feet extended out of the vagina. The baby’s head was amputated during delivery; the child weighed <1 lb. Nursing staff reattached the head with sutures and permitted the mother to hold the child.
PATIENT’S CLAIM Dr. A should have confirmed cerclage placement by ultrasonography. When he found the cerclage unstable, he should have hospitalized the patient. Dr. B used excessive force during delivery. The nurses failed to properly monitor the mother. She claimed psychological injury in having witnessed the infant’s decapitation and being allowed to hold the corpse. Unreasonable death was claimed on behalf of the child’s estate; with proper treatment, the child had a chance of survival.
DEFENDANTS’ DEFENSE Cerclage was performed properly; Dr. A’s care was appropriate. Dr. B did not use excessive force; the fetus had extremely thin skin that tore easily. The nurses’ treatment was appropriate. The hospital was required to allow the mother to hold her baby when requested. A fetus is not viable at 21 weeks.
VERDICT A $1,362,499 Kentucky verdict was returned against the ObGyns; a defense verdict was returned for the hospital. The jury refused to address the claim of wrongful death because a fetus is not viable at 21 weeks.
Which breast was it? 1 error cascades
A WOMAN UNDERWENT RIGHT-BREAST biopsy in the 1970s. In 2002, an architectural distortion appeared in the left breast on mammogram. The radiologist concluded that the abnormality was related to the biopsy—but failed to note that the biopsy had been performed on the right, not the left, breast. Mammography films made in 2003 and again in 2004 were incorrectly read as normal.
In December 2005, a radiologist found no change in the left breast. In June 2007, a radiologist reported a large area of parenchymal distortion but concluded that it was related to the previous biopsy.
In May 2008, another radiologist read the films and recommended follow-up to determine which breast underwent biopsy. The patient was found to have stage III breast cancer in the left breast with a positive lymph node. She underwent double mastectomy followed by breast reconstruction surgery.
PATIENT’S CLAIM Her ObGyns never read the radiographs themselves and did not detect the left-right error after reading the reports. Errors cascaded because radiologists relied only on a previous record, not reviewing the entire chart, and confusing right and left films, even though the films were clearly marked. Had the cancer been found in 2002, treatment would have been substantially less extensive.
DEFENDANTS’ DEFENSE The cancer was difficult to diagnose because it never changed in size. A double mastectomy was not required to treat the cancer.
VERDICT The statute of limitations restricted which radiologists were allowed to be included as defendants. A confidential settlement was reached with the ObGyn group and two of the radiologists.
OB’s priorities tested; child has cerebral palsy
WHEN A WOMAN WENT to the hospital for induction of labor, her ObGyn ruptured the membranes. Shortly thereafter, the fetal heart rate dropped and fetal distress was noted. Emergency cesarean delivery was ordered.
The ObGyn left to attend to another patient while nurses prepared the patient and contacted the anesthesiologist. After delivering another child, the ObGyn returned and delivered the baby, who has cerebral palsy.
PATIENT’S CLAIM The ObGyn should have stayed with this mother instead of delivering the other child. The delay caused the child’s brain damage.
PHYSICIAN’S DEFENSE Both patients’ deliveries were being carefully monitored; proper action was taken.
VERDICT A Georgia defense verdict was returned.
Post-hysterectomy vesicovaginal fistulae
WHEN A 46-YEAR-OLD WOMAN reported irregular bleeding, her gynecologist performed dilation and curettage in February. The pathology report was negative for malignancy; abnormal bleeding ceased.
In July, after symptoms returned, she underwent abdominal hysterectomy. In September, she reported leakage of urine from her vagina; cystoscopy revealed four vesicovaginal fistulae that were repaired by a urologic surgeon. Another fistula developed and was repaired subsequently.
PATIENT’S CLAIM The gynecologist failed to provide information about less invasive options, including endometrial ablation and hormone treatment. The fistulae developed because the gynecologist did not adequately identify the bladder before suturing the vaginal cuff.
PHYSICIAN’S DEFENSE The patient was given sufficient information and requested a hysterectomy; other treatments were offered. A fistula is a known complication of the procedure.
VERDICT A California defense verdict was returned.
Placental abruption: Child has brain damage
WHEN A LABOR AND DELIVERY NURSE called, Dr. A decided a cesarean delivery was needed. The on-call anesthesiologist was at another cesarean delivery, so the procedure was delayed for longer than an hour. Dr. B delivered the child, who was born severely depressed, was resuscitated, and transferred to the NICU. The child suffered hypoxic encephalopathy, is quadriplegic, and has hypotonia.
PATIENT’S CLAIM The cesarean delivery was not performed in a timely manner. Fetal distress occurred because of placental abruption. The child would not have been injured if 1) the nursing staff had summoned a back-up anesthesiologist and 2) the procedure had started within 30 minutes of the decision.
DEFENDANTS’ DEFENSE The hospital reported that Dr. A arrived at the hospital quickly, but decided to wait for Dr. B. Placental abruption occurred prior to the mother’s arrival at the hospital.
VERDICT The ObGyns settled for an undisclosed amount before trial. A California defense verdict was returned for the hospital.
Necrotizing infection in abdominal hematoma
DYSMENORRHEA and abnormal uterine bleeding developed in a 40-year-old woman. Her gynecologist recommended abdominal hysterectomy because she had undergone two cesarean deliveries. During surgery, bladder injury was recognized and repaired.
After several days, the patient suffered complications and was referred to a urogynecologist, who found a 2-mm vaginal fistula. Three days later, she was found unresponsive at home. During exploratory surgery, the gynecologist found necrotizing infection related to an abdominal hematoma. The patient died 2 weeks later.
ESTATE’S CLAIM The gynecologist was negligent in failing to identify signs of infection at two postoperative visits.
PHYSICIAN’S DEFENSE The patient was properly monitored and referred in a timely manner to the urogynecologist. Death was due to the aggressive nature of the infection, which did not develop until after the last office visit.
VERDICT A Tennessee defense verdict was returned.
C diff infection after antibiotics for cough
AT 34 WEEKS’ GESTATION, an ObGyn prescribed amoxicillin-clavulanate (Augmentin) for a woman’s cough. She developed diarrhea that did not respond to antidiarrheal medication and a change in diet. Another ObGyn prescribed empiric sulfamethoxazole and trimethoprim (Septra), and referred her to an infectious-disease specialist. The specialist prescribed empiric cefpodoxime proxetil (Vantin) and ordered stool cultures.
Before culture results were received, the patient went into labor and delivered by cesarean section. Her illness progressed to fulminant Clostridium difficile pseudomembranous colitis that required total colectomy. Re-anastomosis was accomplished a year later. She continues to have difficulty controlling bowel movements, and reports abdominal pain, frequent dehydration, and weight loss.
PATIENT’S CLAIM Antibiotics should not have been prescribed without a culture-proven bacterial illness. C. difficile should have been suspected and treated when diarrhea first developed. Empiric antibiotic treatment during pregnancy is contraindicated. The group’s practice model of having patients rotate among OBs impeded continuity of care.
PHYSICIANS’ DEFENSE C. difficile infection was difficult to diagnose because it is not known to arise in young, healthy women outside a hospital. Use of antibiotics was proper. The group’s practice model is appropriate; continuity of care was maintained.
VERDICT A Florida defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
Keeping Credit Cards on File - FAQ
Each time the subject of credit cards on file comes up – as it did in my recent online column "Your 2012 Resolution - Stop Extending Credit." I am inundated with questions, comments, and requests for copies of the letter we give to patients explaining our credit card policy. The column was the most popular yet; as one of my editors put it, "Joe's goin' viral!"
I've put together an FAQ to answer the most common questions. However, if you have a question not addressed here, leave a comment below, or feel free to e-mail me at [email protected].
How do you safeguard the credit information you keep on file?
The same way we do medical information; it's all covered by the same HIPAA rules. If you have an EHR, it can go in the chart with everything else; if not, I suggest a separate portable file that can be locked up each night.

How do you keep the information current, as cards do expire?
The expiration date is right there next to the number; we check it at each visit, and ask for a new number or date if the card has expired.
Don’t your patients object to signing, in effect, a blank check?
Some did object initially – mostly older patients. Nowadays, a wide chasm seems to have formed in financial philosophies, right at about age 35 years. If you’re older than that, for example, when you receive your checking account statement each month you probably say, "Thank goodness they still include copies of my canceled checks." If you’re younger, you probably say, "Why do they send all this paper with each statement?"
But when we explain that we're doing nothing different than a hotel does at each check-in, and that it will work to their advantage by decreasing the bills they will receive and the checks they must write, most come around.
And they’re not "signing a blank check" – all credit card contracts give cardholders the right to challenge any charge against their account.
What’s the difference between this and "balance billing?"
"Balance billing" is asking patients to pay the difference between your normal fee and the insurance company's normal payment. That's a breach of your managed care contracts. What you want to charge to the patient's credit card is the portion of the insurance company–determined payment not covered by the company. For example, you charge $200, Medicare approves $100, and pays 80% of that. The other $20 is the patient’s responsibility, and that is what you charge to the credit card – instead of sending out a statement for that amount.
My office instituted this policy after you suggested it in your American Academy of Dermatology course. So far, one patient has called to ask if it is legal, and one insurance company has inquired about it. How do you respond to such queries?
Of course, it's legal. (See above.) Ask those patients if they question the legality every time they check into a hotel or rent a car. We have had no inquiries from insurers, but my response would be it's none of their business; you have every right to collect the patient-owed portion of your fees, and insurance companies have no say in how you do it.
How do you handle patients who refuse to hand over a number, particularly those who claim they have no credit cards?
We used to let refusers slide, but now we’ve made the policy mandatory. Patients who refuse without a good reason are asked, like any patient who refuses to cooperate with any standard office policy, to go elsewhere. Life’s too short. And "I don’t have any credit cards" does not count as a good reason.
Everybody has credit cards in this day and age. My office manager does have authority to make exceptions on a case-by-case basis, however.
One surgeon I know asks "no credit card" patients to pay a lawyer-style "retainer" which is held in escrow and used to pay receivable amounts as they come due. When presented with that alternative, most suddenly remember that they do have a credit card after all.
Each time the subject of credit cards on file comes up – as it did in my recent online column "Your 2012 Resolution - Stop Extending Credit." I am inundated with questions, comments, and requests for copies of the letter we give to patients explaining our credit card policy. The column was the most popular yet; as one of my editors put it, "Joe's goin' viral!"
I've put together an FAQ to answer the most common questions. However, if you have a question not addressed here, leave a comment below, or feel free to e-mail me at [email protected].
How do you safeguard the credit information you keep on file?
The same way we do medical information; it's all covered by the same HIPAA rules. If you have an EHR, it can go in the chart with everything else; if not, I suggest a separate portable file that can be locked up each night.
How do you keep the information current, as cards do expire?
The expiration date is right there next to the number; we check it at each visit, and ask for a new number or date if the card has expired.
Don’t your patients object to signing, in effect, a blank check?
Some did object initially – mostly older patients. Nowadays, a wide chasm seems to have formed in financial philosophies, right at about age 35 years. If you’re older than that, for example, when you receive your checking account statement each month you probably say, "Thank goodness they still include copies of my canceled checks." If you’re younger, you probably say, "Why do they send all this paper with each statement?"
But when we explain that we're doing nothing different than a hotel does at each check-in, and that it will work to their advantage by decreasing the bills they will receive and the checks they must write, most come around.
And they’re not "signing a blank check" – all credit card contracts give cardholders the right to challenge any charge against their account.
What’s the difference between this and "balance billing?"
"Balance billing" is asking patients to pay the difference between your normal fee and the insurance company's normal payment. That's a breach of your managed care contracts. What you want to charge to the patient's credit card is the portion of the insurance company–determined payment not covered by the company. For example, you charge $200, Medicare approves $100, and pays 80% of that. The other $20 is the patient’s responsibility, and that is what you charge to the credit card – instead of sending out a statement for that amount.
My office instituted this policy after you suggested it in your American Academy of Dermatology course. So far, one patient has called to ask if it is legal, and one insurance company has inquired about it. How do you respond to such queries?
Of course, it's legal. (See above.) Ask those patients if they question the legality every time they check into a hotel or rent a car. We have had no inquiries from insurers, but my response would be it's none of their business; you have every right to collect the patient-owed portion of your fees, and insurance companies have no say in how you do it.
How do you handle patients who refuse to hand over a number, particularly those who claim they have no credit cards?
We used to let refusers slide, but now we’ve made the policy mandatory. Patients who refuse without a good reason are asked, like any patient who refuses to cooperate with any standard office policy, to go elsewhere. Life’s too short. And "I don’t have any credit cards" does not count as a good reason.
Everybody has credit cards in this day and age. My office manager does have authority to make exceptions on a case-by-case basis, however.
One surgeon I know asks "no credit card" patients to pay a lawyer-style "retainer" which is held in escrow and used to pay receivable amounts as they come due. When presented with that alternative, most suddenly remember that they do have a credit card after all.
Each time the subject of credit cards on file comes up – as it did in my recent online column "Your 2012 Resolution - Stop Extending Credit." I am inundated with questions, comments, and requests for copies of the letter we give to patients explaining our credit card policy. The column was the most popular yet; as one of my editors put it, "Joe's goin' viral!"
I've put together an FAQ to answer the most common questions. However, if you have a question not addressed here, leave a comment below, or feel free to e-mail me at [email protected].
How do you safeguard the credit information you keep on file?
The same way we do medical information; it's all covered by the same HIPAA rules. If you have an EHR, it can go in the chart with everything else; if not, I suggest a separate portable file that can be locked up each night.
How do you keep the information current, as cards do expire?
The expiration date is right there next to the number; we check it at each visit, and ask for a new number or date if the card has expired.
Don’t your patients object to signing, in effect, a blank check?
Some did object initially – mostly older patients. Nowadays, a wide chasm seems to have formed in financial philosophies, right at about age 35 years. If you’re older than that, for example, when you receive your checking account statement each month you probably say, "Thank goodness they still include copies of my canceled checks." If you’re younger, you probably say, "Why do they send all this paper with each statement?"
But when we explain that we're doing nothing different than a hotel does at each check-in, and that it will work to their advantage by decreasing the bills they will receive and the checks they must write, most come around.
And they’re not "signing a blank check" – all credit card contracts give cardholders the right to challenge any charge against their account.
What’s the difference between this and "balance billing?"
"Balance billing" is asking patients to pay the difference between your normal fee and the insurance company's normal payment. That's a breach of your managed care contracts. What you want to charge to the patient's credit card is the portion of the insurance company–determined payment not covered by the company. For example, you charge $200, Medicare approves $100, and pays 80% of that. The other $20 is the patient’s responsibility, and that is what you charge to the credit card – instead of sending out a statement for that amount.
My office instituted this policy after you suggested it in your American Academy of Dermatology course. So far, one patient has called to ask if it is legal, and one insurance company has inquired about it. How do you respond to such queries?
Of course, it's legal. (See above.) Ask those patients if they question the legality every time they check into a hotel or rent a car. We have had no inquiries from insurers, but my response would be it's none of their business; you have every right to collect the patient-owed portion of your fees, and insurance companies have no say in how you do it.
How do you handle patients who refuse to hand over a number, particularly those who claim they have no credit cards?
We used to let refusers slide, but now we’ve made the policy mandatory. Patients who refuse without a good reason are asked, like any patient who refuses to cooperate with any standard office policy, to go elsewhere. Life’s too short. And "I don’t have any credit cards" does not count as a good reason.
Everybody has credit cards in this day and age. My office manager does have authority to make exceptions on a case-by-case basis, however.
One surgeon I know asks "no credit card" patients to pay a lawyer-style "retainer" which is held in escrow and used to pay receivable amounts as they come due. When presented with that alternative, most suddenly remember that they do have a credit card after all.
Managing Your Dermatology Practice: Keeping Credit Cards on File - FAQ
Each time the subject of credit cards on file comes up – as it did in my recent online column "Your 2012 Resolution - Stop Extending Credit." I am inundated with questions, comments, and requests for copies of the letter we give to patients explaining our credit card policy. The column was the most popular yet; as one of my editors put it, "Joe's goin' viral!"
I've put together an FAQ to answer the most common questions. However, if you have a question not addressed here, leave a comment below, or feel free to e-mail me at [email protected].
How do you safeguard the credit information you keep on file?
The same way we do medical information; it's all covered by the same HIPAA rules. If you have an EHR, it can go in the chart with everything else; if not, I suggest a separate portable file that can be locked up each night.

How do you keep the information current, as cards do expire?
The expiration date is right there next to the number; we check it at each visit, and ask for a new number or date if the card has expired.
Don’t your patients object to signing, in effect, a blank check?
Some did object initially – mostly older patients. Nowadays, a wide chasm seems to have formed in financial philosophies, right at about age 35 years. If you’re older than that, for example, when you receive your checking account statement each month you probably say, "Thank goodness they still include copies of my canceled checks." If you’re younger, you probably say, "Why do they send all this paper with each statement?"
But when we explain that we're doing nothing different than a hotel does at each check-in, and that it will work to their advantage by decreasing the bills they will receive and the checks they must write, most come around.
And they’re not "signing a blank check" – all credit card contracts give cardholders the right to challenge any charge against their account.
What’s the difference between this and "balance billing?"
"Balance billing" is asking patients to pay the difference between your normal fee and the insurance company's normal payment. That's a breach of your managed care contracts. What you want to charge to the patient's credit card is the portion of the insurance company–determined payment not covered by the company. For example, you charge $200, Medicare approves $100, and pays 80% of that. The other $20 is the patient’s responsibility, and that is what you charge to the credit card – instead of sending out a statement for that amount.
My office instituted this policy after you suggested it in your American Academy of Dermatology course. So far, one patient has called to ask if it is legal, and one insurance company has inquired about it. How do you respond to such queries?
Of course, it's legal. (See above.) Ask those patients if they question the legality every time they check into a hotel or rent a car. We have had no inquiries from insurers, but my response would be it's none of their business; you have every right to collect the patient-owed portion of your fees, and insurance companies have no say in how you do it.
How do you handle patients who refuse to hand over a number, particularly those who claim they have no credit cards?
We used to let refusers slide, but now we’ve made the policy mandatory. Patients who refuse without a good reason are asked, like any patient who refuses to cooperate with any standard office policy, to go elsewhere. Life’s too short. And "I don’t have any credit cards" does not count as a good reason.
Everybody has credit cards in this day and age. My office manager does have authority to make exceptions on a case-by-case basis, however.
One surgeon I know asks "no credit card" patients to pay a lawyer-style "retainer" which is held in escrow and used to pay receivable amounts as they come due. When presented with that alternative, most suddenly remember that they do have a credit card after all.
Each time the subject of credit cards on file comes up – as it did in my recent online column "Your 2012 Resolution - Stop Extending Credit." I am inundated with questions, comments, and requests for copies of the letter we give to patients explaining our credit card policy. The column was the most popular yet; as one of my editors put it, "Joe's goin' viral!"
I've put together an FAQ to answer the most common questions. However, if you have a question not addressed here, leave a comment below, or feel free to e-mail me at [email protected].
How do you safeguard the credit information you keep on file?
The same way we do medical information; it's all covered by the same HIPAA rules. If you have an EHR, it can go in the chart with everything else; if not, I suggest a separate portable file that can be locked up each night.
How do you keep the information current, as cards do expire?
The expiration date is right there next to the number; we check it at each visit, and ask for a new number or date if the card has expired.
Don’t your patients object to signing, in effect, a blank check?
Some did object initially – mostly older patients. Nowadays, a wide chasm seems to have formed in financial philosophies, right at about age 35 years. If you’re older than that, for example, when you receive your checking account statement each month you probably say, "Thank goodness they still include copies of my canceled checks." If you’re younger, you probably say, "Why do they send all this paper with each statement?"
But when we explain that we're doing nothing different than a hotel does at each check-in, and that it will work to their advantage by decreasing the bills they will receive and the checks they must write, most come around.
And they’re not "signing a blank check" – all credit card contracts give cardholders the right to challenge any charge against their account.
What’s the difference between this and "balance billing?"
"Balance billing" is asking patients to pay the difference between your normal fee and the insurance company's normal payment. That's a breach of your managed care contracts. What you want to charge to the patient's credit card is the portion of the insurance company–determined payment not covered by the company. For example, you charge $200, Medicare approves $100, and pays 80% of that. The other $20 is the patient’s responsibility, and that is what you charge to the credit card – instead of sending out a statement for that amount.
My office instituted this policy after you suggested it in your American Academy of Dermatology course. So far, one patient has called to ask if it is legal, and one insurance company has inquired about it. How do you respond to such queries?
Of course, it's legal. (See above.) Ask those patients if they question the legality every time they check into a hotel or rent a car. We have had no inquiries from insurers, but my response would be it's none of their business; you have every right to collect the patient-owed portion of your fees, and insurance companies have no say in how you do it.
How do you handle patients who refuse to hand over a number, particularly those who claim they have no credit cards?
We used to let refusers slide, but now we’ve made the policy mandatory. Patients who refuse without a good reason are asked, like any patient who refuses to cooperate with any standard office policy, to go elsewhere. Life’s too short. And "I don’t have any credit cards" does not count as a good reason.
Everybody has credit cards in this day and age. My office manager does have authority to make exceptions on a case-by-case basis, however.
One surgeon I know asks "no credit card" patients to pay a lawyer-style "retainer" which is held in escrow and used to pay receivable amounts as they come due. When presented with that alternative, most suddenly remember that they do have a credit card after all.
Each time the subject of credit cards on file comes up – as it did in my recent online column "Your 2012 Resolution - Stop Extending Credit." I am inundated with questions, comments, and requests for copies of the letter we give to patients explaining our credit card policy. The column was the most popular yet; as one of my editors put it, "Joe's goin' viral!"
I've put together an FAQ to answer the most common questions. However, if you have a question not addressed here, leave a comment below, or feel free to e-mail me at [email protected].
How do you safeguard the credit information you keep on file?
The same way we do medical information; it's all covered by the same HIPAA rules. If you have an EHR, it can go in the chart with everything else; if not, I suggest a separate portable file that can be locked up each night.
How do you keep the information current, as cards do expire?
The expiration date is right there next to the number; we check it at each visit, and ask for a new number or date if the card has expired.
Don’t your patients object to signing, in effect, a blank check?
Some did object initially – mostly older patients. Nowadays, a wide chasm seems to have formed in financial philosophies, right at about age 35 years. If you’re older than that, for example, when you receive your checking account statement each month you probably say, "Thank goodness they still include copies of my canceled checks." If you’re younger, you probably say, "Why do they send all this paper with each statement?"
But when we explain that we're doing nothing different than a hotel does at each check-in, and that it will work to their advantage by decreasing the bills they will receive and the checks they must write, most come around.
And they’re not "signing a blank check" – all credit card contracts give cardholders the right to challenge any charge against their account.
What’s the difference between this and "balance billing?"
"Balance billing" is asking patients to pay the difference between your normal fee and the insurance company's normal payment. That's a breach of your managed care contracts. What you want to charge to the patient's credit card is the portion of the insurance company–determined payment not covered by the company. For example, you charge $200, Medicare approves $100, and pays 80% of that. The other $20 is the patient’s responsibility, and that is what you charge to the credit card – instead of sending out a statement for that amount.
My office instituted this policy after you suggested it in your American Academy of Dermatology course. So far, one patient has called to ask if it is legal, and one insurance company has inquired about it. How do you respond to such queries?
Of course, it's legal. (See above.) Ask those patients if they question the legality every time they check into a hotel or rent a car. We have had no inquiries from insurers, but my response would be it's none of their business; you have every right to collect the patient-owed portion of your fees, and insurance companies have no say in how you do it.
How do you handle patients who refuse to hand over a number, particularly those who claim they have no credit cards?
We used to let refusers slide, but now we’ve made the policy mandatory. Patients who refuse without a good reason are asked, like any patient who refuses to cooperate with any standard office policy, to go elsewhere. Life’s too short. And "I don’t have any credit cards" does not count as a good reason.
Everybody has credit cards in this day and age. My office manager does have authority to make exceptions on a case-by-case basis, however.
One surgeon I know asks "no credit card" patients to pay a lawyer-style "retainer" which is held in escrow and used to pay receivable amounts as they come due. When presented with that alternative, most suddenly remember that they do have a credit card after all.
10 strategies for the hot seat: Giving a successful deposition
The unthinkable has happened: You’ve been sued.
You’ve spent the past several months explaining your care and treatment of the patient to your defense attorney. Now the plaintiff attorney wants to take your deposition.
Although a deposition is a routine part of a case (the defendant physician in a medical malpractice lawsuit is nearly always called on to give one), you’re anticipating the undertaking with understandable trepidation—maybe even fear.
There are significant differences between testifying in a deposition and testifying in a courtroom at trial. In this article, I offer 10 strategies for giving deposition testimony that strengthens your defense—or, at least, does not weaken it. In the next (March) issue of OBG Management, I will review tactics for giving testimony at trial.
“Do you want to prevail at trial? Here are 10 keys to effective testimony”
Andrew K. Worek, Esq (March 2012)
Out of the courtroom, still in the fire
A deposition is generally conducted in the conference room of the firm of one of the lawyers (defense or plaintiff attorney). It is an opportunity for the plaintiff lawyer to pose questions to the defendant physician. It is also an opportunity for the lawyer to challenge the physician’s answers, test his or her resolve, and collect sound bites that are unfavorable to the doctor’s defense. These sound bites can be read to the jury at trial.
On average, a physician deposition takes 3 or 4 hours to complete, although a duration of 6 to 8 hours is not uncommon. A deposition may begin in a relatively congenial atmosphere but devolve, at some point, to a highly contentious exchange.
Rather than leave the outcome of the deposition to chance, it is better to take a few considered preparatory steps and proceed judiciously during the deposition. Here are 10 strategies to help you come out on top.

1 Tell the truth
As a defendant, your credibility is the foundation upon which all of your past actions and forthcoming testimony—at deposition and at trial—will be judged. If you manage to protect and preserve that credibility, it will be a fortress of strength. If your credibility is compromised or breached, however, you will open yourself to attacks based on your decisions as a medical practitioner, and also upon your basic character as a human being.
Tell the truth, even when the truth may appear to cast you in an unfavorable light. On many occasions, I have seen a seemingly unfavorable issue become defensible as the evidence and case develop. The discovery of additional facts during the litigation may help strengthen the defense. Therefore, tell the truth, even if it appears to be unfavorable.
Many years ago, a mentor told me: “Honesty isn’t the best policy—it’s the only policy.”
As former Senator Alan Simpson once said: “If you have integrity, nothing else matters. If you don’t have integrity, nothing else matters.”
2 Prepare thoroughly with your defense attorney
Defending a lawsuit is a team effort. It requires cooperation between the physician, who brings medical knowledge and expertise to the table, and the defense attorney, who brings legal expertise. The more time you spend educating your attorney about the medicine, the better the result will be. And the more time the attorney spends raking you over the coals in preparation for the deposition, the better the outcome. If you view the education of your attorney and the overall defense of your case as a chore or inconvenience, you do yourself a great disservice.
Tell your defense attorney about any weaknesses that you perceive or suspect regarding the medical care rendered. It is better to develop a strategy to address a weakness rather than be surprised by or unprepared to answer a question on the issue during your deposition.
Provide your defense attorney with peer-reviewed literature and other reliable information about the medical care. Such information will help educate your attorney, may aid in defining the “standard of care,” and may be a source of potential differing views on the care rendered. Reliable literature will also alert you and your defense attorney to the potential alternative treatment theories that the plaintiff attorney is likely to raise during your deposition.
Make sure you clearly understand the meaning of “the standard of care” within the jurisdiction where your case is pending. Most jurisdictions permit a physician to be asked, point blank, “Doctor, did you meet the standard of care?” Responding that you don’t know what the definition of “standard of care” is or that you’re uncertain whether you met the standard of care would certainly be damaging to your defense.
Thorough preparation normally requires two or three meetings, each lasting 2 to 4 hours. Every potential question needs to be anticipated and evaluated. Keep in mind that every word of your testimony will be recorded by the court reporter, so concise and careful speech is a must. The ideal preparation is for your attorney to focus on your thought process and challenge your initial answers in role-playing sessions to expose any potential problems.
After the deposition, the best compliment you can pay your lawyer is to tell him or her that 1) there wasn’t a single question that surprised you and 2) the preparation was more grueling than the deposition.
As in other settings, half the battle is what you say, and the other half is how you say it. Both content and delivery are key.
3 Maintain your composure
A deposition is not the time to “get something off your chest.” Nor is it a license to tell the other guy “a thing or two.” A lawsuit can be emotionally devastating and exhausting—but if you need encouragement or feel an urge to vent frustrations, do it with your lawyer in private. The deposition room is not a place where weakness is rewarded.
There is no judge or jury at a deposition. Even if you give stellar and inspiring testimony, nobody is going to pronounce you the winner in the lawsuit. However, you can do serious damage to your case by making statements against your interest or becoming emotionally unwound.
The plaintiff attorney will probe your thinking, medical judgments, competence, and treatment decisions and performance. A good lawyer will spot any sign of inconsistency or weakness and dig deeper and deeper until you are caught between the horns of two seemingly inconsistent positions.
Composure is especially critical when a deposition is recorded on videotape. The Internet contains videos of a number of emotional deposition eruptions that, when replayed to a jury, undoubtedly produced catastrophic results.
Your dress and demeanor must remain professional whether or not the deposition is videotaped. A suit or sport coat and tie for men and similar professional attire for women are a must. Wearing a lab coat over a suit is generally only credible if the deposition is taking place in your clinical office or in a hospital.
4 Listen to the question
Each question is critical; listen closely. This may seem like a simple rule, but it is one that is frequently broken.
Listen to the question, and then take a breath before you answer. This pause will give your brain time to analyze the question and prepare a reasonable answer. It will also give your lawyer time to make a verbal objection, if one is warranted.
Make sure the question is intelligible before you begin to answer it. If you don’t understand it, say so and ask that it be rephrased.
If the question is medically inaccurate, point out the inaccuracy. For example, if the lawyer posits that preeclampsia is contagious, correct that statement and ask for the question to be rephrased. In cases involving birth trauma, the phrases “fetal stress” and “fetal distress” are often intermingled.
In the heat of a deposition, you will feel pressured. Don’t let that pressure cause you to blurt out an inaccurate or inappropriate answer to a poorly phrased question.
Listening to each question and taking a breath before responding will also keep you from becoming involved in a rapid-fire question-and-answer flurry with the opposing attorney. Such flurries rarely end favorably for the physician.
Listen to the question. Take it one question and one answer at a time.
5 Stop, look, listen
If your attorney makes an objection, stop talking. Don’t answer the question until your attorney gives you the go-ahead.
Sometimes a question is so inappropriate, you can rightfully refuse to answer. For example, an aggressive attorney might ask, “Doctor, am I correct that in medical school they taught you not to leave sponges in the patient’s belly?” Or, perhaps, “Doctor, did you think it might be a good idea to identify the ureter before you went slicing away at my poor client?” Such questions are, at times, merely designed to anger and impair the doctor’s focus.
In most instances, any objection from your lawyer will concern the technical phrasing of the question, and you will be instructed to answer.
Look at your attorney. Listen to the objection. The nature of the objection may give you valuable insight as to whether the phrasing of the question poses risks that are not readily apparent.
6 Answer only the question that is asked
This is another simple rule that is often broken. Many times, a physician will answer the question that is posed and then offer additional information that lies beyond the scope of the question. This approach creates three potential problems:
- It may lead the plaintiff attorney to ask about information that he or she hadn’t previously considered.
- It creates apparent inconsistency because the answer doesn’t match the question.
- It makes the deposition longer.
I once represented an anesthesiologist who was asked whether he evaluated the patient’s airway before intubation. He responded: “Yes, she was a red flag.”
From that point, the deposition became a downward spiral. Nobody had asked about “red flags”—or any other color of flag, for that matter—but that simple phrase changed the face of the litigation.
You can’t be penalized for not answering a question that was not asked. For example, if an attorney questions you for 4 hours but never touches on the patient’s history of a prior macrosomic delivery, you generally can’t be criticized at trial for failing to reveal the information in your deposition.
This is similar to strategy#6. As a general rule, you should refrain from volunteering information beyond the scope of the question.
The deposition is an adversarial process. Any information you volunteer has the potential to lead the opposing attorney into areas he or she hadn’t previously considered. When you volunteer information beyond the scope of the question, it may signal to opposing counsel that you are subliminally uncomfortable about some area of the case, and scores of additional questions may follow.
Opposing counsel is generally only able to obtain information from you via written questions (“interrogatories”) or directly during a deposition. If you engage in any informal pleasantries or discussions with opposing counsel in the deposition room, you could inadvertently provide information about yourself and your beliefs that the attorney would otherwise not be entitled to obtain. Therefore, anything beyond a simple handshake and “good afternoon” may be ill-advised.
This general rule of thumb isn’t hard and fast, however. Discuss this strategy with your attorney in advance of the deposition. In some instances, there may be information that should be volunteered during the process.
8 Know the medical chart
You will be questioned about your actions. If the answer is contained in the medical chart, it may be wise to refer to it to confirm the answer before you respond. If your handwriting or that of other parties is difficult to decipher, you must interpret the hieroglyphics before your deposition. It looks terrible when a physician stumbles and bumbles through his or her own handwriting or that of a trusted colleague. It’s even worse when the physician has to admit that he or she simply cannot decipher some or all of a critically important treatment note or order.
Similarly, if you are presented with a document, read it before you answer questions about it. Make sure that you receive all the pages and that the document is actually what the attorney represents it to be.
9 Resist the urge to educate
Physicians are highly intelligent people who, in addition to practicing medicine, educate their patients. A deposition room is not the place to be an educator, however. The opposing attorney may be unprepared, and by educating him or her, you may unwittingly assist them, ultimately leading to questions that produce unfavorable responses.
The opposing counsel in a medical malpractice action has very likely already consulted with an expert witness—quite possibly, with several. Those experts will have assisted the attorney in drafting questions to be put to you. Those questions will be intelligently designed to exploit potential weaknesses and conflicts in the defense.
Treat with great caution any statement by a lawyer to the effect of, “I’m just a lawyer. I don’t understand all this medical jargon.”
When a lawyer feigns ignorance, beware.
10 Take a break
A deposition can make you feel as though you are in a pressure cooker. If you need to take a break, ask your attorney to request one.
Also discuss with your attorney, ahead of time, how long the deposition is likely to take and whether scheduled or impromptu breaks are more appropriate.
Many attorneys can move from a congenial interrogation to heated questioning at the flip of a switch. You must be ready to answer questions under all conditions and stress levels. If you become emotional or combative, it may signal a weakness in your position or simply encourage opposing counsel to engage in similar tactics at the trial.
If you feel that you are losing your composure, it’s time to take a break.
You can make it through!
Although every situation and case are different, these 10 strategies should help you understand the deposition process and endure it. These strategies are guideposts that should be reviewed with your attorney. With careful preparation, you can both survive the process and bolster the defense of your case.
Has a deposition gone wrong?
Send us details of your worst deposition experience—and what you learned from it that can help your peers—and we will feature a selection in an upcoming issue of OBG Management. Simply email a short description to [email protected]. Include your name and city and state.
- Data on liability claims offer bright spots for ObGyns—and sobering statistics
Janelle Yates (January 2012) - Sound strategies to avoid malpractice hazards on labor and delivery (Part 1)
Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (December 2010) - More strategies to avoid malpractice hazards on labor and delivery (Part 2)
Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (January 2011) - Afraid of getting sued? A plaintiff attorney offers counsel (but no sympathy)
Janelle Yates (October 2009) - 10 keys to defending (or, better, keeping clear of) a shoulder dystocia suit
Andrew K. Worek, Esq (March 2008)
We want to hear from you! Tell us what you think.
| Mr. Worek offers tips on avoiding deposition pitfalls |

Andrew K. Worek, Esq
Mr. Worek is an attorney with the firm of Post & Post, LLC, in Berwyn, Pa. He has been an active trial attorney, specializing in medical malpractice defense, for 24 years.
Mr. Worek reports no financial relationships relevant to this article.
| Mr. Worek offers tips on avoiding deposition pitfalls |
Andrew K. Worek, Esq
Mr. Worek is an attorney with the firm of Post & Post, LLC, in Berwyn, Pa. He has been an active trial attorney, specializing in medical malpractice defense, for 24 years.
Mr. Worek reports no financial relationships relevant to this article.
| Mr. Worek offers tips on avoiding deposition pitfalls |
Andrew K. Worek, Esq
Mr. Worek is an attorney with the firm of Post & Post, LLC, in Berwyn, Pa. He has been an active trial attorney, specializing in medical malpractice defense, for 24 years.
Mr. Worek reports no financial relationships relevant to this article.
The unthinkable has happened: You’ve been sued.
You’ve spent the past several months explaining your care and treatment of the patient to your defense attorney. Now the plaintiff attorney wants to take your deposition.
Although a deposition is a routine part of a case (the defendant physician in a medical malpractice lawsuit is nearly always called on to give one), you’re anticipating the undertaking with understandable trepidation—maybe even fear.
There are significant differences between testifying in a deposition and testifying in a courtroom at trial. In this article, I offer 10 strategies for giving deposition testimony that strengthens your defense—or, at least, does not weaken it. In the next (March) issue of OBG Management, I will review tactics for giving testimony at trial.
“Do you want to prevail at trial? Here are 10 keys to effective testimony”
Andrew K. Worek, Esq (March 2012)
Out of the courtroom, still in the fire
A deposition is generally conducted in the conference room of the firm of one of the lawyers (defense or plaintiff attorney). It is an opportunity for the plaintiff lawyer to pose questions to the defendant physician. It is also an opportunity for the lawyer to challenge the physician’s answers, test his or her resolve, and collect sound bites that are unfavorable to the doctor’s defense. These sound bites can be read to the jury at trial.
On average, a physician deposition takes 3 or 4 hours to complete, although a duration of 6 to 8 hours is not uncommon. A deposition may begin in a relatively congenial atmosphere but devolve, at some point, to a highly contentious exchange.
Rather than leave the outcome of the deposition to chance, it is better to take a few considered preparatory steps and proceed judiciously during the deposition. Here are 10 strategies to help you come out on top.
1 Tell the truth
As a defendant, your credibility is the foundation upon which all of your past actions and forthcoming testimony—at deposition and at trial—will be judged. If you manage to protect and preserve that credibility, it will be a fortress of strength. If your credibility is compromised or breached, however, you will open yourself to attacks based on your decisions as a medical practitioner, and also upon your basic character as a human being.
Tell the truth, even when the truth may appear to cast you in an unfavorable light. On many occasions, I have seen a seemingly unfavorable issue become defensible as the evidence and case develop. The discovery of additional facts during the litigation may help strengthen the defense. Therefore, tell the truth, even if it appears to be unfavorable.
Many years ago, a mentor told me: “Honesty isn’t the best policy—it’s the only policy.”
As former Senator Alan Simpson once said: “If you have integrity, nothing else matters. If you don’t have integrity, nothing else matters.”
2 Prepare thoroughly with your defense attorney
Defending a lawsuit is a team effort. It requires cooperation between the physician, who brings medical knowledge and expertise to the table, and the defense attorney, who brings legal expertise. The more time you spend educating your attorney about the medicine, the better the result will be. And the more time the attorney spends raking you over the coals in preparation for the deposition, the better the outcome. If you view the education of your attorney and the overall defense of your case as a chore or inconvenience, you do yourself a great disservice.
Tell your defense attorney about any weaknesses that you perceive or suspect regarding the medical care rendered. It is better to develop a strategy to address a weakness rather than be surprised by or unprepared to answer a question on the issue during your deposition.
Provide your defense attorney with peer-reviewed literature and other reliable information about the medical care. Such information will help educate your attorney, may aid in defining the “standard of care,” and may be a source of potential differing views on the care rendered. Reliable literature will also alert you and your defense attorney to the potential alternative treatment theories that the plaintiff attorney is likely to raise during your deposition.
Make sure you clearly understand the meaning of “the standard of care” within the jurisdiction where your case is pending. Most jurisdictions permit a physician to be asked, point blank, “Doctor, did you meet the standard of care?” Responding that you don’t know what the definition of “standard of care” is or that you’re uncertain whether you met the standard of care would certainly be damaging to your defense.
Thorough preparation normally requires two or three meetings, each lasting 2 to 4 hours. Every potential question needs to be anticipated and evaluated. Keep in mind that every word of your testimony will be recorded by the court reporter, so concise and careful speech is a must. The ideal preparation is for your attorney to focus on your thought process and challenge your initial answers in role-playing sessions to expose any potential problems.
After the deposition, the best compliment you can pay your lawyer is to tell him or her that 1) there wasn’t a single question that surprised you and 2) the preparation was more grueling than the deposition.
As in other settings, half the battle is what you say, and the other half is how you say it. Both content and delivery are key.
3 Maintain your composure
A deposition is not the time to “get something off your chest.” Nor is it a license to tell the other guy “a thing or two.” A lawsuit can be emotionally devastating and exhausting—but if you need encouragement or feel an urge to vent frustrations, do it with your lawyer in private. The deposition room is not a place where weakness is rewarded.
There is no judge or jury at a deposition. Even if you give stellar and inspiring testimony, nobody is going to pronounce you the winner in the lawsuit. However, you can do serious damage to your case by making statements against your interest or becoming emotionally unwound.
The plaintiff attorney will probe your thinking, medical judgments, competence, and treatment decisions and performance. A good lawyer will spot any sign of inconsistency or weakness and dig deeper and deeper until you are caught between the horns of two seemingly inconsistent positions.
Composure is especially critical when a deposition is recorded on videotape. The Internet contains videos of a number of emotional deposition eruptions that, when replayed to a jury, undoubtedly produced catastrophic results.
Your dress and demeanor must remain professional whether or not the deposition is videotaped. A suit or sport coat and tie for men and similar professional attire for women are a must. Wearing a lab coat over a suit is generally only credible if the deposition is taking place in your clinical office or in a hospital.
4 Listen to the question
Each question is critical; listen closely. This may seem like a simple rule, but it is one that is frequently broken.
Listen to the question, and then take a breath before you answer. This pause will give your brain time to analyze the question and prepare a reasonable answer. It will also give your lawyer time to make a verbal objection, if one is warranted.
Make sure the question is intelligible before you begin to answer it. If you don’t understand it, say so and ask that it be rephrased.
If the question is medically inaccurate, point out the inaccuracy. For example, if the lawyer posits that preeclampsia is contagious, correct that statement and ask for the question to be rephrased. In cases involving birth trauma, the phrases “fetal stress” and “fetal distress” are often intermingled.
In the heat of a deposition, you will feel pressured. Don’t let that pressure cause you to blurt out an inaccurate or inappropriate answer to a poorly phrased question.
Listening to each question and taking a breath before responding will also keep you from becoming involved in a rapid-fire question-and-answer flurry with the opposing attorney. Such flurries rarely end favorably for the physician.
Listen to the question. Take it one question and one answer at a time.
5 Stop, look, listen
If your attorney makes an objection, stop talking. Don’t answer the question until your attorney gives you the go-ahead.
Sometimes a question is so inappropriate, you can rightfully refuse to answer. For example, an aggressive attorney might ask, “Doctor, am I correct that in medical school they taught you not to leave sponges in the patient’s belly?” Or, perhaps, “Doctor, did you think it might be a good idea to identify the ureter before you went slicing away at my poor client?” Such questions are, at times, merely designed to anger and impair the doctor’s focus.
In most instances, any objection from your lawyer will concern the technical phrasing of the question, and you will be instructed to answer.
Look at your attorney. Listen to the objection. The nature of the objection may give you valuable insight as to whether the phrasing of the question poses risks that are not readily apparent.
6 Answer only the question that is asked
This is another simple rule that is often broken. Many times, a physician will answer the question that is posed and then offer additional information that lies beyond the scope of the question. This approach creates three potential problems:
- It may lead the plaintiff attorney to ask about information that he or she hadn’t previously considered.
- It creates apparent inconsistency because the answer doesn’t match the question.
- It makes the deposition longer.
I once represented an anesthesiologist who was asked whether he evaluated the patient’s airway before intubation. He responded: “Yes, she was a red flag.”
From that point, the deposition became a downward spiral. Nobody had asked about “red flags”—or any other color of flag, for that matter—but that simple phrase changed the face of the litigation.
You can’t be penalized for not answering a question that was not asked. For example, if an attorney questions you for 4 hours but never touches on the patient’s history of a prior macrosomic delivery, you generally can’t be criticized at trial for failing to reveal the information in your deposition.
This is similar to strategy#6. As a general rule, you should refrain from volunteering information beyond the scope of the question.
The deposition is an adversarial process. Any information you volunteer has the potential to lead the opposing attorney into areas he or she hadn’t previously considered. When you volunteer information beyond the scope of the question, it may signal to opposing counsel that you are subliminally uncomfortable about some area of the case, and scores of additional questions may follow.
Opposing counsel is generally only able to obtain information from you via written questions (“interrogatories”) or directly during a deposition. If you engage in any informal pleasantries or discussions with opposing counsel in the deposition room, you could inadvertently provide information about yourself and your beliefs that the attorney would otherwise not be entitled to obtain. Therefore, anything beyond a simple handshake and “good afternoon” may be ill-advised.
This general rule of thumb isn’t hard and fast, however. Discuss this strategy with your attorney in advance of the deposition. In some instances, there may be information that should be volunteered during the process.
8 Know the medical chart
You will be questioned about your actions. If the answer is contained in the medical chart, it may be wise to refer to it to confirm the answer before you respond. If your handwriting or that of other parties is difficult to decipher, you must interpret the hieroglyphics before your deposition. It looks terrible when a physician stumbles and bumbles through his or her own handwriting or that of a trusted colleague. It’s even worse when the physician has to admit that he or she simply cannot decipher some or all of a critically important treatment note or order.
Similarly, if you are presented with a document, read it before you answer questions about it. Make sure that you receive all the pages and that the document is actually what the attorney represents it to be.
9 Resist the urge to educate
Physicians are highly intelligent people who, in addition to practicing medicine, educate their patients. A deposition room is not the place to be an educator, however. The opposing attorney may be unprepared, and by educating him or her, you may unwittingly assist them, ultimately leading to questions that produce unfavorable responses.
The opposing counsel in a medical malpractice action has very likely already consulted with an expert witness—quite possibly, with several. Those experts will have assisted the attorney in drafting questions to be put to you. Those questions will be intelligently designed to exploit potential weaknesses and conflicts in the defense.
Treat with great caution any statement by a lawyer to the effect of, “I’m just a lawyer. I don’t understand all this medical jargon.”
When a lawyer feigns ignorance, beware.
10 Take a break
A deposition can make you feel as though you are in a pressure cooker. If you need to take a break, ask your attorney to request one.
Also discuss with your attorney, ahead of time, how long the deposition is likely to take and whether scheduled or impromptu breaks are more appropriate.
Many attorneys can move from a congenial interrogation to heated questioning at the flip of a switch. You must be ready to answer questions under all conditions and stress levels. If you become emotional or combative, it may signal a weakness in your position or simply encourage opposing counsel to engage in similar tactics at the trial.
If you feel that you are losing your composure, it’s time to take a break.
You can make it through!
Although every situation and case are different, these 10 strategies should help you understand the deposition process and endure it. These strategies are guideposts that should be reviewed with your attorney. With careful preparation, you can both survive the process and bolster the defense of your case.
Has a deposition gone wrong?
Send us details of your worst deposition experience—and what you learned from it that can help your peers—and we will feature a selection in an upcoming issue of OBG Management. Simply email a short description to [email protected]. Include your name and city and state.
- Data on liability claims offer bright spots for ObGyns—and sobering statistics
Janelle Yates (January 2012) - Sound strategies to avoid malpractice hazards on labor and delivery (Part 1)
Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (December 2010) - More strategies to avoid malpractice hazards on labor and delivery (Part 2)
Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (January 2011) - Afraid of getting sued? A plaintiff attorney offers counsel (but no sympathy)
Janelle Yates (October 2009) - 10 keys to defending (or, better, keeping clear of) a shoulder dystocia suit
Andrew K. Worek, Esq (March 2008)
We want to hear from you! Tell us what you think.
The unthinkable has happened: You’ve been sued.
You’ve spent the past several months explaining your care and treatment of the patient to your defense attorney. Now the plaintiff attorney wants to take your deposition.
Although a deposition is a routine part of a case (the defendant physician in a medical malpractice lawsuit is nearly always called on to give one), you’re anticipating the undertaking with understandable trepidation—maybe even fear.
There are significant differences between testifying in a deposition and testifying in a courtroom at trial. In this article, I offer 10 strategies for giving deposition testimony that strengthens your defense—or, at least, does not weaken it. In the next (March) issue of OBG Management, I will review tactics for giving testimony at trial.
“Do you want to prevail at trial? Here are 10 keys to effective testimony”
Andrew K. Worek, Esq (March 2012)
Out of the courtroom, still in the fire
A deposition is generally conducted in the conference room of the firm of one of the lawyers (defense or plaintiff attorney). It is an opportunity for the plaintiff lawyer to pose questions to the defendant physician. It is also an opportunity for the lawyer to challenge the physician’s answers, test his or her resolve, and collect sound bites that are unfavorable to the doctor’s defense. These sound bites can be read to the jury at trial.
On average, a physician deposition takes 3 or 4 hours to complete, although a duration of 6 to 8 hours is not uncommon. A deposition may begin in a relatively congenial atmosphere but devolve, at some point, to a highly contentious exchange.
Rather than leave the outcome of the deposition to chance, it is better to take a few considered preparatory steps and proceed judiciously during the deposition. Here are 10 strategies to help you come out on top.
1 Tell the truth
As a defendant, your credibility is the foundation upon which all of your past actions and forthcoming testimony—at deposition and at trial—will be judged. If you manage to protect and preserve that credibility, it will be a fortress of strength. If your credibility is compromised or breached, however, you will open yourself to attacks based on your decisions as a medical practitioner, and also upon your basic character as a human being.
Tell the truth, even when the truth may appear to cast you in an unfavorable light. On many occasions, I have seen a seemingly unfavorable issue become defensible as the evidence and case develop. The discovery of additional facts during the litigation may help strengthen the defense. Therefore, tell the truth, even if it appears to be unfavorable.
Many years ago, a mentor told me: “Honesty isn’t the best policy—it’s the only policy.”
As former Senator Alan Simpson once said: “If you have integrity, nothing else matters. If you don’t have integrity, nothing else matters.”
2 Prepare thoroughly with your defense attorney
Defending a lawsuit is a team effort. It requires cooperation between the physician, who brings medical knowledge and expertise to the table, and the defense attorney, who brings legal expertise. The more time you spend educating your attorney about the medicine, the better the result will be. And the more time the attorney spends raking you over the coals in preparation for the deposition, the better the outcome. If you view the education of your attorney and the overall defense of your case as a chore or inconvenience, you do yourself a great disservice.
Tell your defense attorney about any weaknesses that you perceive or suspect regarding the medical care rendered. It is better to develop a strategy to address a weakness rather than be surprised by or unprepared to answer a question on the issue during your deposition.
Provide your defense attorney with peer-reviewed literature and other reliable information about the medical care. Such information will help educate your attorney, may aid in defining the “standard of care,” and may be a source of potential differing views on the care rendered. Reliable literature will also alert you and your defense attorney to the potential alternative treatment theories that the plaintiff attorney is likely to raise during your deposition.
Make sure you clearly understand the meaning of “the standard of care” within the jurisdiction where your case is pending. Most jurisdictions permit a physician to be asked, point blank, “Doctor, did you meet the standard of care?” Responding that you don’t know what the definition of “standard of care” is or that you’re uncertain whether you met the standard of care would certainly be damaging to your defense.
Thorough preparation normally requires two or three meetings, each lasting 2 to 4 hours. Every potential question needs to be anticipated and evaluated. Keep in mind that every word of your testimony will be recorded by the court reporter, so concise and careful speech is a must. The ideal preparation is for your attorney to focus on your thought process and challenge your initial answers in role-playing sessions to expose any potential problems.
After the deposition, the best compliment you can pay your lawyer is to tell him or her that 1) there wasn’t a single question that surprised you and 2) the preparation was more grueling than the deposition.
As in other settings, half the battle is what you say, and the other half is how you say it. Both content and delivery are key.
3 Maintain your composure
A deposition is not the time to “get something off your chest.” Nor is it a license to tell the other guy “a thing or two.” A lawsuit can be emotionally devastating and exhausting—but if you need encouragement or feel an urge to vent frustrations, do it with your lawyer in private. The deposition room is not a place where weakness is rewarded.
There is no judge or jury at a deposition. Even if you give stellar and inspiring testimony, nobody is going to pronounce you the winner in the lawsuit. However, you can do serious damage to your case by making statements against your interest or becoming emotionally unwound.
The plaintiff attorney will probe your thinking, medical judgments, competence, and treatment decisions and performance. A good lawyer will spot any sign of inconsistency or weakness and dig deeper and deeper until you are caught between the horns of two seemingly inconsistent positions.
Composure is especially critical when a deposition is recorded on videotape. The Internet contains videos of a number of emotional deposition eruptions that, when replayed to a jury, undoubtedly produced catastrophic results.
Your dress and demeanor must remain professional whether or not the deposition is videotaped. A suit or sport coat and tie for men and similar professional attire for women are a must. Wearing a lab coat over a suit is generally only credible if the deposition is taking place in your clinical office or in a hospital.
4 Listen to the question
Each question is critical; listen closely. This may seem like a simple rule, but it is one that is frequently broken.
Listen to the question, and then take a breath before you answer. This pause will give your brain time to analyze the question and prepare a reasonable answer. It will also give your lawyer time to make a verbal objection, if one is warranted.
Make sure the question is intelligible before you begin to answer it. If you don’t understand it, say so and ask that it be rephrased.
If the question is medically inaccurate, point out the inaccuracy. For example, if the lawyer posits that preeclampsia is contagious, correct that statement and ask for the question to be rephrased. In cases involving birth trauma, the phrases “fetal stress” and “fetal distress” are often intermingled.
In the heat of a deposition, you will feel pressured. Don’t let that pressure cause you to blurt out an inaccurate or inappropriate answer to a poorly phrased question.
Listening to each question and taking a breath before responding will also keep you from becoming involved in a rapid-fire question-and-answer flurry with the opposing attorney. Such flurries rarely end favorably for the physician.
Listen to the question. Take it one question and one answer at a time.
5 Stop, look, listen
If your attorney makes an objection, stop talking. Don’t answer the question until your attorney gives you the go-ahead.
Sometimes a question is so inappropriate, you can rightfully refuse to answer. For example, an aggressive attorney might ask, “Doctor, am I correct that in medical school they taught you not to leave sponges in the patient’s belly?” Or, perhaps, “Doctor, did you think it might be a good idea to identify the ureter before you went slicing away at my poor client?” Such questions are, at times, merely designed to anger and impair the doctor’s focus.
In most instances, any objection from your lawyer will concern the technical phrasing of the question, and you will be instructed to answer.
Look at your attorney. Listen to the objection. The nature of the objection may give you valuable insight as to whether the phrasing of the question poses risks that are not readily apparent.
6 Answer only the question that is asked
This is another simple rule that is often broken. Many times, a physician will answer the question that is posed and then offer additional information that lies beyond the scope of the question. This approach creates three potential problems:
- It may lead the plaintiff attorney to ask about information that he or she hadn’t previously considered.
- It creates apparent inconsistency because the answer doesn’t match the question.
- It makes the deposition longer.
I once represented an anesthesiologist who was asked whether he evaluated the patient’s airway before intubation. He responded: “Yes, she was a red flag.”
From that point, the deposition became a downward spiral. Nobody had asked about “red flags”—or any other color of flag, for that matter—but that simple phrase changed the face of the litigation.
You can’t be penalized for not answering a question that was not asked. For example, if an attorney questions you for 4 hours but never touches on the patient’s history of a prior macrosomic delivery, you generally can’t be criticized at trial for failing to reveal the information in your deposition.
This is similar to strategy#6. As a general rule, you should refrain from volunteering information beyond the scope of the question.
The deposition is an adversarial process. Any information you volunteer has the potential to lead the opposing attorney into areas he or she hadn’t previously considered. When you volunteer information beyond the scope of the question, it may signal to opposing counsel that you are subliminally uncomfortable about some area of the case, and scores of additional questions may follow.
Opposing counsel is generally only able to obtain information from you via written questions (“interrogatories”) or directly during a deposition. If you engage in any informal pleasantries or discussions with opposing counsel in the deposition room, you could inadvertently provide information about yourself and your beliefs that the attorney would otherwise not be entitled to obtain. Therefore, anything beyond a simple handshake and “good afternoon” may be ill-advised.
This general rule of thumb isn’t hard and fast, however. Discuss this strategy with your attorney in advance of the deposition. In some instances, there may be information that should be volunteered during the process.
8 Know the medical chart
You will be questioned about your actions. If the answer is contained in the medical chart, it may be wise to refer to it to confirm the answer before you respond. If your handwriting or that of other parties is difficult to decipher, you must interpret the hieroglyphics before your deposition. It looks terrible when a physician stumbles and bumbles through his or her own handwriting or that of a trusted colleague. It’s even worse when the physician has to admit that he or she simply cannot decipher some or all of a critically important treatment note or order.
Similarly, if you are presented with a document, read it before you answer questions about it. Make sure that you receive all the pages and that the document is actually what the attorney represents it to be.
9 Resist the urge to educate
Physicians are highly intelligent people who, in addition to practicing medicine, educate their patients. A deposition room is not the place to be an educator, however. The opposing attorney may be unprepared, and by educating him or her, you may unwittingly assist them, ultimately leading to questions that produce unfavorable responses.
The opposing counsel in a medical malpractice action has very likely already consulted with an expert witness—quite possibly, with several. Those experts will have assisted the attorney in drafting questions to be put to you. Those questions will be intelligently designed to exploit potential weaknesses and conflicts in the defense.
Treat with great caution any statement by a lawyer to the effect of, “I’m just a lawyer. I don’t understand all this medical jargon.”
When a lawyer feigns ignorance, beware.
10 Take a break
A deposition can make you feel as though you are in a pressure cooker. If you need to take a break, ask your attorney to request one.
Also discuss with your attorney, ahead of time, how long the deposition is likely to take and whether scheduled or impromptu breaks are more appropriate.
Many attorneys can move from a congenial interrogation to heated questioning at the flip of a switch. You must be ready to answer questions under all conditions and stress levels. If you become emotional or combative, it may signal a weakness in your position or simply encourage opposing counsel to engage in similar tactics at the trial.
If you feel that you are losing your composure, it’s time to take a break.
You can make it through!
Although every situation and case are different, these 10 strategies should help you understand the deposition process and endure it. These strategies are guideposts that should be reviewed with your attorney. With careful preparation, you can both survive the process and bolster the defense of your case.
Has a deposition gone wrong?
Send us details of your worst deposition experience—and what you learned from it that can help your peers—and we will feature a selection in an upcoming issue of OBG Management. Simply email a short description to [email protected]. Include your name and city and state.
- Data on liability claims offer bright spots for ObGyns—and sobering statistics
Janelle Yates (January 2012) - Sound strategies to avoid malpractice hazards on labor and delivery (Part 1)
Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (December 2010) - More strategies to avoid malpractice hazards on labor and delivery (Part 2)
Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (January 2011) - Afraid of getting sued? A plaintiff attorney offers counsel (but no sympathy)
Janelle Yates (October 2009) - 10 keys to defending (or, better, keeping clear of) a shoulder dystocia suit
Andrew K. Worek, Esq (March 2008)
We want to hear from you! Tell us what you think.