User login
ObGyn leaving for vacation urges induction — and more

AN OBGYN OFFERED TO INDUCE LABOR at 39 weeks’ gestation for a couple’s first child because she was anticipating a vacation. In counseling, the ObGyn revealed no significant risks. The parents agreed and went to the hospital that afternoon.
Induction included cervical ripening with misoprostol followed by oxytocin, resulting in uterine tachysystole and an abnormal fetal heart-rate pattern. The child was born by cesarean delivery 25 hours after labor began.
The child suffered hypoxia, which caused hypoxic-ischemic encephalopathy, cerebral palsy, and spastic quadriparesis. He will always require 24-hour care.
PATIENT’S CLAIM Induction of labor was medically unnecessary. Informed consent was incomplete: induced labor increases the risks of hyperstimulation of labor, failure to progress, and cesarean delivery. The ObGyn was negligent: She had admitted several patients to labor and delivery that day, and delivered five babies in 19 hours, including three “unscheduled” cesarean deliveries. Because of the patient load, she was busy with other patients when a cesarean delivery became urgently needed for this baby. Hyperstimulation and fetal heart-rate abnormalities continued for several hours.
DEFENDANTS’ DEFENSE The suit was settled before trial.
VERDICT A $5.5 million Missouri settlement was reached against the ObGyn and hospital. The hospital was also required to implement new policies on induction, augmentation of labor, and informed consent.
Insulin wasn’t given to diabetic mother during labor
A PREGNANT WOMAN had pregestational insulin-dependent diabetes. She was not given insulin despite having an elevated blood glucose level at admission and during 26 hours of labor. The mother developed diabetic ketoacidosis. The fetus suffered severe ketoacidosis-induced hypoxic ischemic encephalopathy. At delivery, the infant was resuscitated, but was severely brain damaged. Life-support was withdrawn after 6 days, and the child died.
PATIENT’S CLAIM The mother alleged emotional distress for injury to the fetus in the womb, and wrongful death of the infant.
PHYSICIAN’S DEFENSE Settlements were reached during pretrial mediation.
VERDICT Virginia settlements included $1,000,000 for the wrongful death claim and $200,000 for the mother.
Bowel was perforated during hysterectomy
AFTER CONSERVATIVE MANAGEMENT of menorrhagia and dysmenorrhea, a 49-year-old woman underwent total abdominal hysterectomy. Her ObGyn performed the surgery, and his partner monitored the woman’s 2-day hospital stay. A return of bowel function was noted before her discharge.
Six days postoperatively, the patient contacted the ObGyn’s office, complaining of passing fecal matter through her vagina. Readmitted to the hospital, she was found to have a bowel perforation and vaginal fistula. The next day, the bowel was surgically repaired, and a colostomy was performed. The colostomy was reversed, successfully, 6 months later.
PATIENT’S CLAIM The ObGyn was negligent in failing to diagnose and repair the bowel perforation during surgery. A 2-cm perforation would have been visible, and subsequent surgeries and colostomy could have been avoided. She suffered another surgical scar, and could have lifelong problems with motility and bowel function. She has permanent abdominal pain.
PHYSICIAN’S DEFENSE Bowel injury is a known risk of the procedure. The woman had pre-existing abdominal adhesions from prior surgeries, which made a bowel injury more likely. The injury was undetectable during the initial surgery because it was a partial cut or tear that progressed to full perforation after normal bowel function returned. The perforation was diagnosed and repaired as quickly as possible.
VERDICT An Illinois defense verdict was returned.
Genetic defect missed on prenatal US
A PREGNANT WOMAN SAW a maternal-fetal medicine specialist, and a sonogram showed a jaw abnormality. The child was born with Treacher Collins syndrome, a genetic defect that leads to craniofacial deformities. The child has a misaligned jaw and trachea, is deaf and disfigured. She has undergone several surgeries and is expected to require more.
PATIENT’S CLAIM The mother would have chosen to terminate the pregnancy had she been given an accurate diagnosis after ultrasonography.
PHYSICIAN’S DEFENSE The case was settled before trial.
VERDICT A $2.25 million New Jersey settlement was reached.
Did inept response to fetal distress cause brain damage?
DURING LABOR, the fetus showed signs of absent or minimal heart-rate variability that lasted until delivery. The child was born with brain damage, does not have use of his limbs, is blind, and requires 24-hour care.
PATIENT’S CLAIM Neither the resident nor nurses responded to signs of fetal distress. The resident also failed to respond to tachysystole. The ObGyn did not properly supervise the resident, did not review fetal monitoring strips, and did not examine the mother until 8 hours after she arrived. Labor was allowed to continue despite fetal distress; reduced oxygen flow to the fetus caused the injury.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A $14 million New Jersey settlement was reached against the hospital and ObGyn.
Excessive traction blamed for nerve injury
AN INFANT’S LEFT ARM WAS FLACCID after vaginal delivery. The child has limited range of motion and loss of strength in the left arm. Shoulder surgery has been recommended.
PATIENT’S CLAIM Excessive force and traction were exerted on the baby’s head after encountering shoulder dystocia. This caused a stretch injury to the brachial plexus nerves at C5–6.
PHYSICIAN’S DEFENSE The McRobert’s maneuver was properly used to resolve shoulder dystocia. Only gentle downward traction was used.
VERDICT An Illinois defense verdict was returned.
Drug error leads to nipple necrosis
AT RIGHT BREAST EXCISIONAL BIOPSY, a woman was given four localized injections in the same tissue space: methylene blue dye; bupivacaine, 0.25 mg with epinephrine; sodium phosphate, 2 cc; and sodium bicarbonate, 2 cc. After surgery, the patient’s right nipple began to turn black and became necrotic. A wound specialist advised her to have the nipple removed and the area debrided. She received wound treatment for several months.
PATIENT’S CLAIM Medical center staff was negligent, including OR nurses and physician who injected the sodium phosphate.
DEFENDANTS’ DEFENSE The physician who administered the sodium phosphate testified that she injected less than 1 cc before realizing the mistake. An OR nurse contacted the pharmacy; the pharmacist did not believe that there would be any damage. After surgery, the defendants admitted their error to the woman.
VERDICT Suits against the physician who injected the sodium phosphate and OR nurses were dismissed prior to trial. A $23,363 Idaho verdict was returned against the medical center.
Death postop from bowel injury
A WOMAN UNDERWENT SURGERY for blocked fallopian tubes and adhesions—procedures recommended by her ObGyn to improve her chance of successful in vitro fertilization. A surgeon performed the procedures, noting that a superficial bowel injury had occurred, and she was discharged.
The next morning, she called the ObGyn’s office to report abdominal pain; he did not ask her to come to the office. She died 2 days later.
ESTATE’S CLAIM The ObGyn should not have agreed to discharge her, particularly because the surgeon had noticed the bowel injury. The ObGyn should have examined her when she called to report abdominal pain the morning after surgery.
PHYSICIAN’S DEFENSE It was proper to rely on the surgeon’s judgment, particularly because abdominal surgery and evaluation of bowel injury were not within the ObGyn’s expertise. Abdominal pain 1 or 2 days after abdominal surgery is insufficient reason to suspect bowel perforation or evaluation. The ObGyn called the woman two times later that day, and, based on her description, believed that she was improving.
VERDICT A Virginia defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The Editors acknowledge the assistance of Victor Bergman, Esq, of Shamberg, Johnson & Bergman, in preparing this installment of Medical Verdicts.
We want to hear from you! Tell us what you think.
AN OBGYN OFFERED TO INDUCE LABOR at 39 weeks’ gestation for a couple’s first child because she was anticipating a vacation. In counseling, the ObGyn revealed no significant risks. The parents agreed and went to the hospital that afternoon.
Induction included cervical ripening with misoprostol followed by oxytocin, resulting in uterine tachysystole and an abnormal fetal heart-rate pattern. The child was born by cesarean delivery 25 hours after labor began.
The child suffered hypoxia, which caused hypoxic-ischemic encephalopathy, cerebral palsy, and spastic quadriparesis. He will always require 24-hour care.
PATIENT’S CLAIM Induction of labor was medically unnecessary. Informed consent was incomplete: induced labor increases the risks of hyperstimulation of labor, failure to progress, and cesarean delivery. The ObGyn was negligent: She had admitted several patients to labor and delivery that day, and delivered five babies in 19 hours, including three “unscheduled” cesarean deliveries. Because of the patient load, she was busy with other patients when a cesarean delivery became urgently needed for this baby. Hyperstimulation and fetal heart-rate abnormalities continued for several hours.
DEFENDANTS’ DEFENSE The suit was settled before trial.
VERDICT A $5.5 million Missouri settlement was reached against the ObGyn and hospital. The hospital was also required to implement new policies on induction, augmentation of labor, and informed consent.
Insulin wasn’t given to diabetic mother during labor
A PREGNANT WOMAN had pregestational insulin-dependent diabetes. She was not given insulin despite having an elevated blood glucose level at admission and during 26 hours of labor. The mother developed diabetic ketoacidosis. The fetus suffered severe ketoacidosis-induced hypoxic ischemic encephalopathy. At delivery, the infant was resuscitated, but was severely brain damaged. Life-support was withdrawn after 6 days, and the child died.
PATIENT’S CLAIM The mother alleged emotional distress for injury to the fetus in the womb, and wrongful death of the infant.
PHYSICIAN’S DEFENSE Settlements were reached during pretrial mediation.
VERDICT Virginia settlements included $1,000,000 for the wrongful death claim and $200,000 for the mother.
Bowel was perforated during hysterectomy
AFTER CONSERVATIVE MANAGEMENT of menorrhagia and dysmenorrhea, a 49-year-old woman underwent total abdominal hysterectomy. Her ObGyn performed the surgery, and his partner monitored the woman’s 2-day hospital stay. A return of bowel function was noted before her discharge.
Six days postoperatively, the patient contacted the ObGyn’s office, complaining of passing fecal matter through her vagina. Readmitted to the hospital, she was found to have a bowel perforation and vaginal fistula. The next day, the bowel was surgically repaired, and a colostomy was performed. The colostomy was reversed, successfully, 6 months later.
PATIENT’S CLAIM The ObGyn was negligent in failing to diagnose and repair the bowel perforation during surgery. A 2-cm perforation would have been visible, and subsequent surgeries and colostomy could have been avoided. She suffered another surgical scar, and could have lifelong problems with motility and bowel function. She has permanent abdominal pain.
PHYSICIAN’S DEFENSE Bowel injury is a known risk of the procedure. The woman had pre-existing abdominal adhesions from prior surgeries, which made a bowel injury more likely. The injury was undetectable during the initial surgery because it was a partial cut or tear that progressed to full perforation after normal bowel function returned. The perforation was diagnosed and repaired as quickly as possible.
VERDICT An Illinois defense verdict was returned.
Genetic defect missed on prenatal US
A PREGNANT WOMAN SAW a maternal-fetal medicine specialist, and a sonogram showed a jaw abnormality. The child was born with Treacher Collins syndrome, a genetic defect that leads to craniofacial deformities. The child has a misaligned jaw and trachea, is deaf and disfigured. She has undergone several surgeries and is expected to require more.
PATIENT’S CLAIM The mother would have chosen to terminate the pregnancy had she been given an accurate diagnosis after ultrasonography.
PHYSICIAN’S DEFENSE The case was settled before trial.
VERDICT A $2.25 million New Jersey settlement was reached.
Did inept response to fetal distress cause brain damage?
DURING LABOR, the fetus showed signs of absent or minimal heart-rate variability that lasted until delivery. The child was born with brain damage, does not have use of his limbs, is blind, and requires 24-hour care.
PATIENT’S CLAIM Neither the resident nor nurses responded to signs of fetal distress. The resident also failed to respond to tachysystole. The ObGyn did not properly supervise the resident, did not review fetal monitoring strips, and did not examine the mother until 8 hours after she arrived. Labor was allowed to continue despite fetal distress; reduced oxygen flow to the fetus caused the injury.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A $14 million New Jersey settlement was reached against the hospital and ObGyn.
Excessive traction blamed for nerve injury
AN INFANT’S LEFT ARM WAS FLACCID after vaginal delivery. The child has limited range of motion and loss of strength in the left arm. Shoulder surgery has been recommended.
PATIENT’S CLAIM Excessive force and traction were exerted on the baby’s head after encountering shoulder dystocia. This caused a stretch injury to the brachial plexus nerves at C5–6.
PHYSICIAN’S DEFENSE The McRobert’s maneuver was properly used to resolve shoulder dystocia. Only gentle downward traction was used.
VERDICT An Illinois defense verdict was returned.
Drug error leads to nipple necrosis
AT RIGHT BREAST EXCISIONAL BIOPSY, a woman was given four localized injections in the same tissue space: methylene blue dye; bupivacaine, 0.25 mg with epinephrine; sodium phosphate, 2 cc; and sodium bicarbonate, 2 cc. After surgery, the patient’s right nipple began to turn black and became necrotic. A wound specialist advised her to have the nipple removed and the area debrided. She received wound treatment for several months.
PATIENT’S CLAIM Medical center staff was negligent, including OR nurses and physician who injected the sodium phosphate.
DEFENDANTS’ DEFENSE The physician who administered the sodium phosphate testified that she injected less than 1 cc before realizing the mistake. An OR nurse contacted the pharmacy; the pharmacist did not believe that there would be any damage. After surgery, the defendants admitted their error to the woman.
VERDICT Suits against the physician who injected the sodium phosphate and OR nurses were dismissed prior to trial. A $23,363 Idaho verdict was returned against the medical center.
Death postop from bowel injury
A WOMAN UNDERWENT SURGERY for blocked fallopian tubes and adhesions—procedures recommended by her ObGyn to improve her chance of successful in vitro fertilization. A surgeon performed the procedures, noting that a superficial bowel injury had occurred, and she was discharged.
The next morning, she called the ObGyn’s office to report abdominal pain; he did not ask her to come to the office. She died 2 days later.
ESTATE’S CLAIM The ObGyn should not have agreed to discharge her, particularly because the surgeon had noticed the bowel injury. The ObGyn should have examined her when she called to report abdominal pain the morning after surgery.
PHYSICIAN’S DEFENSE It was proper to rely on the surgeon’s judgment, particularly because abdominal surgery and evaluation of bowel injury were not within the ObGyn’s expertise. Abdominal pain 1 or 2 days after abdominal surgery is insufficient reason to suspect bowel perforation or evaluation. The ObGyn called the woman two times later that day, and, based on her description, believed that she was improving.
VERDICT A Virginia defense verdict was returned.
AN OBGYN OFFERED TO INDUCE LABOR at 39 weeks’ gestation for a couple’s first child because she was anticipating a vacation. In counseling, the ObGyn revealed no significant risks. The parents agreed and went to the hospital that afternoon.
Induction included cervical ripening with misoprostol followed by oxytocin, resulting in uterine tachysystole and an abnormal fetal heart-rate pattern. The child was born by cesarean delivery 25 hours after labor began.
The child suffered hypoxia, which caused hypoxic-ischemic encephalopathy, cerebral palsy, and spastic quadriparesis. He will always require 24-hour care.
PATIENT’S CLAIM Induction of labor was medically unnecessary. Informed consent was incomplete: induced labor increases the risks of hyperstimulation of labor, failure to progress, and cesarean delivery. The ObGyn was negligent: She had admitted several patients to labor and delivery that day, and delivered five babies in 19 hours, including three “unscheduled” cesarean deliveries. Because of the patient load, she was busy with other patients when a cesarean delivery became urgently needed for this baby. Hyperstimulation and fetal heart-rate abnormalities continued for several hours.
DEFENDANTS’ DEFENSE The suit was settled before trial.
VERDICT A $5.5 million Missouri settlement was reached against the ObGyn and hospital. The hospital was also required to implement new policies on induction, augmentation of labor, and informed consent.
Insulin wasn’t given to diabetic mother during labor
A PREGNANT WOMAN had pregestational insulin-dependent diabetes. She was not given insulin despite having an elevated blood glucose level at admission and during 26 hours of labor. The mother developed diabetic ketoacidosis. The fetus suffered severe ketoacidosis-induced hypoxic ischemic encephalopathy. At delivery, the infant was resuscitated, but was severely brain damaged. Life-support was withdrawn after 6 days, and the child died.
PATIENT’S CLAIM The mother alleged emotional distress for injury to the fetus in the womb, and wrongful death of the infant.
PHYSICIAN’S DEFENSE Settlements were reached during pretrial mediation.
VERDICT Virginia settlements included $1,000,000 for the wrongful death claim and $200,000 for the mother.
Bowel was perforated during hysterectomy
AFTER CONSERVATIVE MANAGEMENT of menorrhagia and dysmenorrhea, a 49-year-old woman underwent total abdominal hysterectomy. Her ObGyn performed the surgery, and his partner monitored the woman’s 2-day hospital stay. A return of bowel function was noted before her discharge.
Six days postoperatively, the patient contacted the ObGyn’s office, complaining of passing fecal matter through her vagina. Readmitted to the hospital, she was found to have a bowel perforation and vaginal fistula. The next day, the bowel was surgically repaired, and a colostomy was performed. The colostomy was reversed, successfully, 6 months later.
PATIENT’S CLAIM The ObGyn was negligent in failing to diagnose and repair the bowel perforation during surgery. A 2-cm perforation would have been visible, and subsequent surgeries and colostomy could have been avoided. She suffered another surgical scar, and could have lifelong problems with motility and bowel function. She has permanent abdominal pain.
PHYSICIAN’S DEFENSE Bowel injury is a known risk of the procedure. The woman had pre-existing abdominal adhesions from prior surgeries, which made a bowel injury more likely. The injury was undetectable during the initial surgery because it was a partial cut or tear that progressed to full perforation after normal bowel function returned. The perforation was diagnosed and repaired as quickly as possible.
VERDICT An Illinois defense verdict was returned.
Genetic defect missed on prenatal US
A PREGNANT WOMAN SAW a maternal-fetal medicine specialist, and a sonogram showed a jaw abnormality. The child was born with Treacher Collins syndrome, a genetic defect that leads to craniofacial deformities. The child has a misaligned jaw and trachea, is deaf and disfigured. She has undergone several surgeries and is expected to require more.
PATIENT’S CLAIM The mother would have chosen to terminate the pregnancy had she been given an accurate diagnosis after ultrasonography.
PHYSICIAN’S DEFENSE The case was settled before trial.
VERDICT A $2.25 million New Jersey settlement was reached.
Did inept response to fetal distress cause brain damage?
DURING LABOR, the fetus showed signs of absent or minimal heart-rate variability that lasted until delivery. The child was born with brain damage, does not have use of his limbs, is blind, and requires 24-hour care.
PATIENT’S CLAIM Neither the resident nor nurses responded to signs of fetal distress. The resident also failed to respond to tachysystole. The ObGyn did not properly supervise the resident, did not review fetal monitoring strips, and did not examine the mother until 8 hours after she arrived. Labor was allowed to continue despite fetal distress; reduced oxygen flow to the fetus caused the injury.
DEFENDANTS’ DEFENSE The case was settled before trial.
VERDICT A $14 million New Jersey settlement was reached against the hospital and ObGyn.
Excessive traction blamed for nerve injury
AN INFANT’S LEFT ARM WAS FLACCID after vaginal delivery. The child has limited range of motion and loss of strength in the left arm. Shoulder surgery has been recommended.
PATIENT’S CLAIM Excessive force and traction were exerted on the baby’s head after encountering shoulder dystocia. This caused a stretch injury to the brachial plexus nerves at C5–6.
PHYSICIAN’S DEFENSE The McRobert’s maneuver was properly used to resolve shoulder dystocia. Only gentle downward traction was used.
VERDICT An Illinois defense verdict was returned.
Drug error leads to nipple necrosis
AT RIGHT BREAST EXCISIONAL BIOPSY, a woman was given four localized injections in the same tissue space: methylene blue dye; bupivacaine, 0.25 mg with epinephrine; sodium phosphate, 2 cc; and sodium bicarbonate, 2 cc. After surgery, the patient’s right nipple began to turn black and became necrotic. A wound specialist advised her to have the nipple removed and the area debrided. She received wound treatment for several months.
PATIENT’S CLAIM Medical center staff was negligent, including OR nurses and physician who injected the sodium phosphate.
DEFENDANTS’ DEFENSE The physician who administered the sodium phosphate testified that she injected less than 1 cc before realizing the mistake. An OR nurse contacted the pharmacy; the pharmacist did not believe that there would be any damage. After surgery, the defendants admitted their error to the woman.
VERDICT Suits against the physician who injected the sodium phosphate and OR nurses were dismissed prior to trial. A $23,363 Idaho verdict was returned against the medical center.
Death postop from bowel injury
A WOMAN UNDERWENT SURGERY for blocked fallopian tubes and adhesions—procedures recommended by her ObGyn to improve her chance of successful in vitro fertilization. A surgeon performed the procedures, noting that a superficial bowel injury had occurred, and she was discharged.
The next morning, she called the ObGyn’s office to report abdominal pain; he did not ask her to come to the office. She died 2 days later.
ESTATE’S CLAIM The ObGyn should not have agreed to discharge her, particularly because the surgeon had noticed the bowel injury. The ObGyn should have examined her when she called to report abdominal pain the morning after surgery.
PHYSICIAN’S DEFENSE It was proper to rely on the surgeon’s judgment, particularly because abdominal surgery and evaluation of bowel injury were not within the ObGyn’s expertise. Abdominal pain 1 or 2 days after abdominal surgery is insufficient reason to suspect bowel perforation or evaluation. The ObGyn called the woman two times later that day, and, based on her description, believed that she was improving.
VERDICT A Virginia defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The Editors acknowledge the assistance of Victor Bergman, Esq, of Shamberg, Johnson & Bergman, in preparing this installment of Medical Verdicts.
We want to hear from you! Tell us what you think.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The Editors acknowledge the assistance of Victor Bergman, Esq, of Shamberg, Johnson & Bergman, in preparing this installment of Medical Verdicts.
We want to hear from you! Tell us what you think.
How state budget crises are putting the squeeze on Medicaid (and you)
Is private ObGyn practice on its way out?
Lucia DiVenere (October 2011)
Medicare and Medicaid are on the brink of insolvency, and you’re not just a bystander
Robert L. Barbieri, MD (Editorial, October 2011)
14 questions (and answers) about health reform and you
Janelle Yates, Senior Editor, with Lucia DiVenere (July 2010)
Is the patient-centered medical home a win-all or lose-all proposition for ObGyns?
Janelle Yates (October 2010)
Ms. DiVenere reports no financial relationships relevant to this article.
Tough economic times have pushed 2.8 million more people onto Medicaid rolls, now crowded with more than 60 million low-income individuals and families—nearly 20% of the US population.
Because Medicaid is a means-tested entitlement program, states and the federal government must fund as much health care as beneficiaries use, an expense that increases substantially each year.
Through the Medicaid program, more than 30 million adult women have access to an annual gynecologic exam, family planning services, and prenatal care. Without such coverage, many of them would go without care, potentially driving our nation’s health-care costs even higher. Two thirds of ObGyns treat Medicaid patients, and Medicaid accounts for 18%, on average, of an ObGyn practice’s revenue.1
In this article, I describe how the burgeoning ranks of Medicaid beneficiaries are straining state budgets and prompting legislators to cut provider payments to make up the shortfall. The federal government also plays a role in shrinking reimbursements for physicians and other providers.

Medicaid costs are outpacing economic growth
In fiscal 2011, Medicaid enrollment grew an average of 5.5%, and states are anticipating a growth rate of 4.1% in 2012.2 Total Medicaid spending is also increasing rapidly. In fiscal 2010, it was $361.8 billion (excluding administrative costs)—a 6% increase over fiscal 2009. By the end of fiscal 2011, it was expected to hit $398.6 billion—a 10.1% increase over 2010.3
Medicaid costs are also absorbing a greater share of state budgets. In fiscal 2009, they accounted for 21.9% of total state expenditures, 22.3% in fiscal 2010, and 23.6% in fiscal 2011.3 Many states have had to reduce spending in other important areas as a result (TABLE 1).
Medicaid costs are shared by federal and state governments. The federal government pays, on average, 57% of state program costs. In fiscal 2010, the federal government covered 64.6% of all Medicaid costs.
State general funds at the end of 2011 were well below their pre-recession levels, due to lower revenues and increased expenditures, including continued obligations for state workers’ pensions and retiree health care. At the same time, 49 state governments are required to balance their budgets. As a result, states are likely to face austere budgets for at least the next several years, and will continue to make difficult spending decisions.
As state and federal budgets face pressure to reduce overall spending, Medicaid lies in nearly all budget crosshairs.
TABLE 1
Medicaid absorbs an ever-greater percentage of state expenditures
| State | Percentage | ||
|---|---|---|---|
| Fiscal 2009 | Fiscal 2010 | Fiscal 2011 | |
| New England | |||
| Connecticut | 27.9 | 25.4 | 27.2 |
| Maine | 29.9 | 28.6 | 28.6 |
| Massachusetts | 17.8 | 18.8 | 20.2 |
| New Hampshire | 26.5 | 24.9 | 25.2 |
| Rhode Island | 24.9 | 25.0 | 24.7 |
| Vermont | 25.5 | 25.9 | 26.6 |
| Mid-Atlantic | |||
| Delaware | 12.3 | 14.4 | 16.2 |
| Maryland | 19.3 | 20.4 | 21.6 |
| New Jersey | 19.8 | 21.3 | 21.9 |
| New york | 26.7 | 28.7 | 29.1 |
| Pennsylvania | 30.2 | 29.6 | 31.1 |
| Great Lakes | |||
| Illinois | 24.8 | 23.6 | 28.9 |
| Indiana | 21.8 | 23.1 | 24.4 |
| Michigan | 23.0 | 24.2 | 24.0 |
| Ohio | 20.6 | 21.3 | 23.2 |
| Wisconsin | 15.7 | 17.1 | 17.0 |
| Plains | |||
| Iowa | 17.9 | 18.6 | 19.3 |
| Kansas | 17.4 | 18.8 | 18.6 |
| Minnesota | 24.0 | 25.1 | 25.1 |
| Missouri | 35.6 | 34.4 | 36.3 |
| Nebraska | 17.6 | 17.2 | 16.5 |
| North Dakota | 14.1 | 13.7 | 14.6 |
| South Dakota | 21.6 | 21.7 | 23.2 |
| Southeast | |||
| Alabama | 25.6 | 25.8 | 25.3 |
| Arkansas | 19.7 | 20.0 | 20.5 |
| Florida | 26.7 | 30.0 | 28.0 |
| Georgia | 19.0 | 19.5 | 20.5 |
| Kentucky | 22.5 | 21.9 | 22.8 |
| Louisiana | 22.0 | 23.7 | 23.5 |
| Mississippi | 24.8 | 22.9 | 22.6 |
| North Carolina | 25.0 | 24.2 | 22.1 |
| South Carolina | 22.0 | 22.6 | 19.9 |
| Tennessee | 25.4 | 28.8 | 28.1 |
| Virginia | 16.4 | 16.1 | 16.9 |
| West Virginia | 11.9 | 12.6 | 13.0 |
| Southwest | |||
| Arizona | 29.3 | 27.7 | 28.0 |
| New Mexico | 20.7 | 22.1 | 20.2 |
| Oklahoma | 17.7 | 17.1 | 18.5 |
| Texas | 22.8 | 24.6 | 26.3 |
| Rocky Mountain | |||
| Colorado | 14.1 | 15.3 | 19.4 |
| Idaho | 22.8 | 23.0 | 25.6 |
| Montana | 15.2 | 15.4 | 15.7 |
| Utah | 14.9 | 11.9 | 14.3 |
| Wyoming | 8.1 | 7.3 | 7.0 |
| Far West | |||
| Alaska | 8.1 | 12.0 | 9.0 |
| California | 20.6 | 18.9 | 24.2 |
| Hawaii | 11.3 | 13.3 | 15.9 |
| Nevada | 16.0 | 18.3 | 18.7 |
| Oregon | 14.3 | 13.1 | 14.6 |
| Washington | 21.4 | 23.0 | 24.4 |
| Average | 21.9 | 22.3 | 23.6 |
The fiscal health of Medicaid matters—here’s why
Twelve percent of women 18 to 64 years old rely on Medicaid for health-care coverage, and three quarters of all adult Medicaid beneficiaries are women. Sixty-nine percent of women in the 18- to 64-year-old age group are in their reproductive years. Medicaid pays for 42% of all births in the United States—as many as 64% of all births in Arkansas and Oklahoma.4
Medicaid covers essential well-woman care, including maternity care, breast and cervical cancer screening and treatment, care for disabled women, and family planning.
Medicaid is the largest source of public funding for contraception and sterilization services, covering 71% of these costs. States clearly find it in their best interest and the best interest of public health to encourage use of family planning, which can improve women’s health and reduce the number of unintended pregnancies and abortions. In 2010, 27 states extended family planning coverage to women whose incomes, while still low, were higher than the standard Medicaid eligibility requirements.
Many states cover nutrition and substance abuse counseling, health education, psychosocial counseling, breastfeeding, and case management. TABLE 2 on page 16a lists mandatory and optional Medicaid services.
TABLE 2
Benefits of the Medicaid program
| Mandatory | Optional |
|---|---|
| Physician services Laboratory and radiographic services Hospitalization Outpatient services Early and periodic screening, diagnostic, and treatment services for people younger than 21 years Family planning Rural and federally qualified health center services Nurse midwife services Nursing facility services for people older than 21 years Home health care for people entitled to nursing facility care Smoking cessation for pregnant women* Free-standing birth center services* | Prescription drugs Clinic services Dental services, dentures Physical therapy and rehabilitation Prosthetic devices, eyeglasses Primary-care case management Intermediate-care facilities for the mentally retarded Inpatient psychiatric care for people younger than 21 years Home health care and other services provided under home- and community-based waivers Personal care services Hospice care Health home services for people with chronic conditions* Home- and community-based attendant services and supports* |
| * Benefits added under the Patient Protection and Affordable Care Act | |
Coming: Another 4.5 million women on Medicaid rolls
Under the Patient Protection and Affordable Care Act, Medicaid will expand to cover another 4.5 million women in 2014. Beginning January 1, 2014, state Medicaid programs are required to cover nonpregnant, non-elderly individuals who have incomes as high as 133% of the federal poverty level ($10,890 for an individual in 2011). The federal government will cover the full expense of insuring these newly eligible individuals for calendar years 2014, 2015, and 2016. Federal financing will phase down to 90% by 2020, and will likely decrease further after that.
States that participate in Medicaid must cover pregnant women who have an income at or below 133% of the federal poverty level. States are required to disregard 5% of an individual’s income when determining Medicaid eligibility, a rule that effectively brings the maximum eligibility level to 138% of the federal poverty level, opening the Medicaid doors to additional low-income individuals.
Today, coverage lasts throughout pregnancy and 2 months beyond. States may choose to extend eligibility to pregnant women who have incomes that exceed 133% of the poverty level; at present, 45 states do so, with the District of Columbia topping the list by covering pregnant women who have incomes at or below 300% of the poverty level.
Many measures show that Medicaid has improved access to health care for low- income women, saving lives and dollars. Your experience—wherever you practice— undoubtedly echoes that observation.
Prenatal care. You also know that prenatal care helps ensure healthy babies. Obstetric services often go beyond traditional medical needs to include a full spectrum of care that helps ensure a healthy pregnancy, delivery, and postpartum period.
Of course, inadequate use of prenatal care is associated with increased risks of low birth weight, preterm birth, neonatal mortality, infant mortality, and maternal mortality. Preterm births alone increase US health-care costs by $26 billion each year.5 Pregnancy-related maternal mortality is three to four times higher, and infant mortality is more than six times higher, among women who receive no prenatal care, compared with those who receive prenatal care.
Gynecologic services covered through Medicaid also help preserve health and reduce health-care costs. Eighty-four percent of women on Medicaid have had a Pap test in the past 2 years, compared with 80% of women who have private insurance and 59% of women who lack insurance.6 Routine gynecologic care is vital to prevent cervical cancer and other diseases. Women without a regular doctor don’t get regular Pap tests and mammography; nor do they get screened for other serious health risks, including high cholesterol and diabetes.
Despite the proven benefits of access to regular care, 23% of women on Medicaid report problems finding a new doctor who will accept their insurance, compared with 7% of Medicare beneficiaries and 13% of women who have private insurance.
Why the difficulty in finding a doctor? A leading reason is the inadequacy of Medicaid payment rates.
Cutting payments to physicians
Medicaid provider payments are often the first item cut in a state budget crisis. States are required to cover many health services and are restricted from charging patients significant co-pays, so they often trim budgets at the expense of physicians. Thirty-nine states reduced physician and provider payments in 2011, and 46 states plan to do so in fiscal 2012. In addition, in fiscal 2011, 47 states put in place at least one new policy to control Medicaid costs; most states implemented several of these policies. All 50 states plan to do so in fiscal 2012.
Under federal rules, states must ensure that payment rates are consistent with efficiency, economy, and quality of care. They also must ensure that payment is sufficient to enlist enough providers to render care and services to the same extent that care and services are available to the general population in the same geographic area. States must request and receive permission from the federal government before reducing provider payment rates. However, even with this safeguard in place, physician payments—and patient access to care—are in jeopardy.
For example, in 2008, the California legislature issued several rounds of cuts, including a 10% cut in physician and provider payments, to make up for budget shortfalls. Physicians, hospitals, pharmacists, and other health professionals sued in response, and the 9th US Circuit Court of Appeals blocked the payment cut.
In 2011, California Governor Jerry Brown again put the 10% cut in place, this time with approval from the federal Center for Medicare and Medicaid Services (CMS).
In response, California physicians, led by the state medical association, sued California again. They argued that payment cuts reduce access to care among Medicaid beneficiaries by prompting physicians to stop accepting these patients. The California Department of Health Care Services countered that the cuts are necessary to offset a critical budget shortfall and will not affect access to care. The situation in California highlights the conflicts between physicians and many states over Medicaid payment rates.
The US Supreme Court agreed to review the case on only one question—whether individuals and private parties, including doctors and Medicaid recipients, can sue the state for failing to pay rates that meet the federal adequacy requirement. On October 3, 2011, the Supreme Court heard oral arguments in this group of cases, known as Douglas v. Independent Living Center of Southern California. ACOG joined the case in support of physicians.
Medicaid versus Medicare
It’s easy to see how important Medicaid is to women’s health, and how important physician payment rates are to women’s access to care. You might expect, then, that states would recognize the value of adequate physician payment—but they don’t, always.
At present, Medicaid pays for obstetric care at 93% of the Medicare rate. Still, obstetric care fares slightly better than many physician services. In many states, it costs physicians much more than Medicaid pays to provide non-obstetric care to Mediaid patients. Although 23 states pay for obstetric care at a rate lower than that offered by Medicare, 27 states offer greater support, and 16 states offer reimbursement well above the Medicare rate.
A federal target, too
The states aren’t the only entities with an eye on Medicaid cuts. The US Congress, too, is considering proposals to dramatically change the program. The options include issuing block grants for Medicaid; reducing the federal match; and including Medicaid in global or health spending caps. ACOG has an extensive campaign under way to ensure that any changes to Medicaid do not come at the expense of women’s health.
The Congressional Joint Special Committee on Deficit Reduction—more commonly known as the Supercommittee— represents the latest effort at deficit reduction. When its work imploded in December 2011, federal programs came online for a 2% across-the-board cut (“sequester”) that will take effect on January 1, 2013. The Medicaid program is exempt from this cut, no doubt in recognition of the already-precarious nature of this program, which has become a safety net for millions of American families struggling through the recession.
Because so many American women rely on Medicaid for obstetric and gynecologic care, it is critical that we protect funding levels and maintain eligibility for this program.
ACOG plays a prominent role in advocating for preservation of women’s access to care and adequate physician reimbursement levels. you can help by contacting your state legislators and representatives in the uS Congress to emphasize the importance of these efforts.
We want to hear from you! Tell us what you think.
1. American Congress of Obstetricians and Gynecologists. 2008 Socioeconomic Survey of ACOG Fellows. Washington DC: ACOG; 2008.
2. Holahan J, Headen I. Kaiser Commission on Medicaid and the Uninsured. Medicaid Coverage and Spending in Health Reform: National and State-by-State Results for Adults at or Below 133% FPL. Washington DC: Kaiser Family Foundation; 2010.
3. National Association of State Budget Officers. State Expenditure Report 2010. Washington DC: NASBO; December 2011.
4. National Governors Association Center for Best Practices. 2010 Maternal and Child Health Update. Issue Brief. Washington DC: National Governors Association; 2011. http://www.nga.org/files/live/sites/NGA/files/pdf/MCHUPDATE2010.PDF. Accessed January 12, 2011.
5. Behrman RE, Butler AS. eds Committee on Understanding Premature Birth and Assuring Healthy Outcomes. Preterm Birth: Causes, Consequences, and Prevention. Washington, DC: Institute of Medicine; 2007.
6. Kaiser Family Foundation. Kaiser Women’s Health Survey 2004. Washington DC: KFF; 2005.

Lucia DiVenere,
Ms. DiVenere is Senior Director of Government Affairs at the American Congress of Obstetricians and Gynecologists.
Lucia DiVenere,
Ms. DiVenere is Senior Director of Government Affairs at the American Congress of Obstetricians and Gynecologists.
Lucia DiVenere,
Ms. DiVenere is Senior Director of Government Affairs at the American Congress of Obstetricians and Gynecologists.
Is private ObGyn practice on its way out?
Lucia DiVenere (October 2011)
Medicare and Medicaid are on the brink of insolvency, and you’re not just a bystander
Robert L. Barbieri, MD (Editorial, October 2011)
14 questions (and answers) about health reform and you
Janelle Yates, Senior Editor, with Lucia DiVenere (July 2010)
Is the patient-centered medical home a win-all or lose-all proposition for ObGyns?
Janelle Yates (October 2010)
Ms. DiVenere reports no financial relationships relevant to this article.
Tough economic times have pushed 2.8 million more people onto Medicaid rolls, now crowded with more than 60 million low-income individuals and families—nearly 20% of the US population.
Because Medicaid is a means-tested entitlement program, states and the federal government must fund as much health care as beneficiaries use, an expense that increases substantially each year.
Through the Medicaid program, more than 30 million adult women have access to an annual gynecologic exam, family planning services, and prenatal care. Without such coverage, many of them would go without care, potentially driving our nation’s health-care costs even higher. Two thirds of ObGyns treat Medicaid patients, and Medicaid accounts for 18%, on average, of an ObGyn practice’s revenue.1
In this article, I describe how the burgeoning ranks of Medicaid beneficiaries are straining state budgets and prompting legislators to cut provider payments to make up the shortfall. The federal government also plays a role in shrinking reimbursements for physicians and other providers.
Medicaid costs are outpacing economic growth
In fiscal 2011, Medicaid enrollment grew an average of 5.5%, and states are anticipating a growth rate of 4.1% in 2012.2 Total Medicaid spending is also increasing rapidly. In fiscal 2010, it was $361.8 billion (excluding administrative costs)—a 6% increase over fiscal 2009. By the end of fiscal 2011, it was expected to hit $398.6 billion—a 10.1% increase over 2010.3
Medicaid costs are also absorbing a greater share of state budgets. In fiscal 2009, they accounted for 21.9% of total state expenditures, 22.3% in fiscal 2010, and 23.6% in fiscal 2011.3 Many states have had to reduce spending in other important areas as a result (TABLE 1).
Medicaid costs are shared by federal and state governments. The federal government pays, on average, 57% of state program costs. In fiscal 2010, the federal government covered 64.6% of all Medicaid costs.
State general funds at the end of 2011 were well below their pre-recession levels, due to lower revenues and increased expenditures, including continued obligations for state workers’ pensions and retiree health care. At the same time, 49 state governments are required to balance their budgets. As a result, states are likely to face austere budgets for at least the next several years, and will continue to make difficult spending decisions.
As state and federal budgets face pressure to reduce overall spending, Medicaid lies in nearly all budget crosshairs.
TABLE 1
Medicaid absorbs an ever-greater percentage of state expenditures
| State | Percentage | ||
|---|---|---|---|
| Fiscal 2009 | Fiscal 2010 | Fiscal 2011 | |
| New England | |||
| Connecticut | 27.9 | 25.4 | 27.2 |
| Maine | 29.9 | 28.6 | 28.6 |
| Massachusetts | 17.8 | 18.8 | 20.2 |
| New Hampshire | 26.5 | 24.9 | 25.2 |
| Rhode Island | 24.9 | 25.0 | 24.7 |
| Vermont | 25.5 | 25.9 | 26.6 |
| Mid-Atlantic | |||
| Delaware | 12.3 | 14.4 | 16.2 |
| Maryland | 19.3 | 20.4 | 21.6 |
| New Jersey | 19.8 | 21.3 | 21.9 |
| New york | 26.7 | 28.7 | 29.1 |
| Pennsylvania | 30.2 | 29.6 | 31.1 |
| Great Lakes | |||
| Illinois | 24.8 | 23.6 | 28.9 |
| Indiana | 21.8 | 23.1 | 24.4 |
| Michigan | 23.0 | 24.2 | 24.0 |
| Ohio | 20.6 | 21.3 | 23.2 |
| Wisconsin | 15.7 | 17.1 | 17.0 |
| Plains | |||
| Iowa | 17.9 | 18.6 | 19.3 |
| Kansas | 17.4 | 18.8 | 18.6 |
| Minnesota | 24.0 | 25.1 | 25.1 |
| Missouri | 35.6 | 34.4 | 36.3 |
| Nebraska | 17.6 | 17.2 | 16.5 |
| North Dakota | 14.1 | 13.7 | 14.6 |
| South Dakota | 21.6 | 21.7 | 23.2 |
| Southeast | |||
| Alabama | 25.6 | 25.8 | 25.3 |
| Arkansas | 19.7 | 20.0 | 20.5 |
| Florida | 26.7 | 30.0 | 28.0 |
| Georgia | 19.0 | 19.5 | 20.5 |
| Kentucky | 22.5 | 21.9 | 22.8 |
| Louisiana | 22.0 | 23.7 | 23.5 |
| Mississippi | 24.8 | 22.9 | 22.6 |
| North Carolina | 25.0 | 24.2 | 22.1 |
| South Carolina | 22.0 | 22.6 | 19.9 |
| Tennessee | 25.4 | 28.8 | 28.1 |
| Virginia | 16.4 | 16.1 | 16.9 |
| West Virginia | 11.9 | 12.6 | 13.0 |
| Southwest | |||
| Arizona | 29.3 | 27.7 | 28.0 |
| New Mexico | 20.7 | 22.1 | 20.2 |
| Oklahoma | 17.7 | 17.1 | 18.5 |
| Texas | 22.8 | 24.6 | 26.3 |
| Rocky Mountain | |||
| Colorado | 14.1 | 15.3 | 19.4 |
| Idaho | 22.8 | 23.0 | 25.6 |
| Montana | 15.2 | 15.4 | 15.7 |
| Utah | 14.9 | 11.9 | 14.3 |
| Wyoming | 8.1 | 7.3 | 7.0 |
| Far West | |||
| Alaska | 8.1 | 12.0 | 9.0 |
| California | 20.6 | 18.9 | 24.2 |
| Hawaii | 11.3 | 13.3 | 15.9 |
| Nevada | 16.0 | 18.3 | 18.7 |
| Oregon | 14.3 | 13.1 | 14.6 |
| Washington | 21.4 | 23.0 | 24.4 |
| Average | 21.9 | 22.3 | 23.6 |
The fiscal health of Medicaid matters—here’s why
Twelve percent of women 18 to 64 years old rely on Medicaid for health-care coverage, and three quarters of all adult Medicaid beneficiaries are women. Sixty-nine percent of women in the 18- to 64-year-old age group are in their reproductive years. Medicaid pays for 42% of all births in the United States—as many as 64% of all births in Arkansas and Oklahoma.4
Medicaid covers essential well-woman care, including maternity care, breast and cervical cancer screening and treatment, care for disabled women, and family planning.
Medicaid is the largest source of public funding for contraception and sterilization services, covering 71% of these costs. States clearly find it in their best interest and the best interest of public health to encourage use of family planning, which can improve women’s health and reduce the number of unintended pregnancies and abortions. In 2010, 27 states extended family planning coverage to women whose incomes, while still low, were higher than the standard Medicaid eligibility requirements.
Many states cover nutrition and substance abuse counseling, health education, psychosocial counseling, breastfeeding, and case management. TABLE 2 on page 16a lists mandatory and optional Medicaid services.
TABLE 2
Benefits of the Medicaid program
| Mandatory | Optional |
|---|---|
| Physician services Laboratory and radiographic services Hospitalization Outpatient services Early and periodic screening, diagnostic, and treatment services for people younger than 21 years Family planning Rural and federally qualified health center services Nurse midwife services Nursing facility services for people older than 21 years Home health care for people entitled to nursing facility care Smoking cessation for pregnant women* Free-standing birth center services* | Prescription drugs Clinic services Dental services, dentures Physical therapy and rehabilitation Prosthetic devices, eyeglasses Primary-care case management Intermediate-care facilities for the mentally retarded Inpatient psychiatric care for people younger than 21 years Home health care and other services provided under home- and community-based waivers Personal care services Hospice care Health home services for people with chronic conditions* Home- and community-based attendant services and supports* |
| * Benefits added under the Patient Protection and Affordable Care Act | |
Coming: Another 4.5 million women on Medicaid rolls
Under the Patient Protection and Affordable Care Act, Medicaid will expand to cover another 4.5 million women in 2014. Beginning January 1, 2014, state Medicaid programs are required to cover nonpregnant, non-elderly individuals who have incomes as high as 133% of the federal poverty level ($10,890 for an individual in 2011). The federal government will cover the full expense of insuring these newly eligible individuals for calendar years 2014, 2015, and 2016. Federal financing will phase down to 90% by 2020, and will likely decrease further after that.
States that participate in Medicaid must cover pregnant women who have an income at or below 133% of the federal poverty level. States are required to disregard 5% of an individual’s income when determining Medicaid eligibility, a rule that effectively brings the maximum eligibility level to 138% of the federal poverty level, opening the Medicaid doors to additional low-income individuals.
Today, coverage lasts throughout pregnancy and 2 months beyond. States may choose to extend eligibility to pregnant women who have incomes that exceed 133% of the poverty level; at present, 45 states do so, with the District of Columbia topping the list by covering pregnant women who have incomes at or below 300% of the poverty level.
Many measures show that Medicaid has improved access to health care for low- income women, saving lives and dollars. Your experience—wherever you practice— undoubtedly echoes that observation.
Prenatal care. You also know that prenatal care helps ensure healthy babies. Obstetric services often go beyond traditional medical needs to include a full spectrum of care that helps ensure a healthy pregnancy, delivery, and postpartum period.
Of course, inadequate use of prenatal care is associated with increased risks of low birth weight, preterm birth, neonatal mortality, infant mortality, and maternal mortality. Preterm births alone increase US health-care costs by $26 billion each year.5 Pregnancy-related maternal mortality is three to four times higher, and infant mortality is more than six times higher, among women who receive no prenatal care, compared with those who receive prenatal care.
Gynecologic services covered through Medicaid also help preserve health and reduce health-care costs. Eighty-four percent of women on Medicaid have had a Pap test in the past 2 years, compared with 80% of women who have private insurance and 59% of women who lack insurance.6 Routine gynecologic care is vital to prevent cervical cancer and other diseases. Women without a regular doctor don’t get regular Pap tests and mammography; nor do they get screened for other serious health risks, including high cholesterol and diabetes.
Despite the proven benefits of access to regular care, 23% of women on Medicaid report problems finding a new doctor who will accept their insurance, compared with 7% of Medicare beneficiaries and 13% of women who have private insurance.
Why the difficulty in finding a doctor? A leading reason is the inadequacy of Medicaid payment rates.
Cutting payments to physicians
Medicaid provider payments are often the first item cut in a state budget crisis. States are required to cover many health services and are restricted from charging patients significant co-pays, so they often trim budgets at the expense of physicians. Thirty-nine states reduced physician and provider payments in 2011, and 46 states plan to do so in fiscal 2012. In addition, in fiscal 2011, 47 states put in place at least one new policy to control Medicaid costs; most states implemented several of these policies. All 50 states plan to do so in fiscal 2012.
Under federal rules, states must ensure that payment rates are consistent with efficiency, economy, and quality of care. They also must ensure that payment is sufficient to enlist enough providers to render care and services to the same extent that care and services are available to the general population in the same geographic area. States must request and receive permission from the federal government before reducing provider payment rates. However, even with this safeguard in place, physician payments—and patient access to care—are in jeopardy.
For example, in 2008, the California legislature issued several rounds of cuts, including a 10% cut in physician and provider payments, to make up for budget shortfalls. Physicians, hospitals, pharmacists, and other health professionals sued in response, and the 9th US Circuit Court of Appeals blocked the payment cut.
In 2011, California Governor Jerry Brown again put the 10% cut in place, this time with approval from the federal Center for Medicare and Medicaid Services (CMS).
In response, California physicians, led by the state medical association, sued California again. They argued that payment cuts reduce access to care among Medicaid beneficiaries by prompting physicians to stop accepting these patients. The California Department of Health Care Services countered that the cuts are necessary to offset a critical budget shortfall and will not affect access to care. The situation in California highlights the conflicts between physicians and many states over Medicaid payment rates.
The US Supreme Court agreed to review the case on only one question—whether individuals and private parties, including doctors and Medicaid recipients, can sue the state for failing to pay rates that meet the federal adequacy requirement. On October 3, 2011, the Supreme Court heard oral arguments in this group of cases, known as Douglas v. Independent Living Center of Southern California. ACOG joined the case in support of physicians.
Medicaid versus Medicare
It’s easy to see how important Medicaid is to women’s health, and how important physician payment rates are to women’s access to care. You might expect, then, that states would recognize the value of adequate physician payment—but they don’t, always.
At present, Medicaid pays for obstetric care at 93% of the Medicare rate. Still, obstetric care fares slightly better than many physician services. In many states, it costs physicians much more than Medicaid pays to provide non-obstetric care to Mediaid patients. Although 23 states pay for obstetric care at a rate lower than that offered by Medicare, 27 states offer greater support, and 16 states offer reimbursement well above the Medicare rate.
A federal target, too
The states aren’t the only entities with an eye on Medicaid cuts. The US Congress, too, is considering proposals to dramatically change the program. The options include issuing block grants for Medicaid; reducing the federal match; and including Medicaid in global or health spending caps. ACOG has an extensive campaign under way to ensure that any changes to Medicaid do not come at the expense of women’s health.
The Congressional Joint Special Committee on Deficit Reduction—more commonly known as the Supercommittee— represents the latest effort at deficit reduction. When its work imploded in December 2011, federal programs came online for a 2% across-the-board cut (“sequester”) that will take effect on January 1, 2013. The Medicaid program is exempt from this cut, no doubt in recognition of the already-precarious nature of this program, which has become a safety net for millions of American families struggling through the recession.
Because so many American women rely on Medicaid for obstetric and gynecologic care, it is critical that we protect funding levels and maintain eligibility for this program.
ACOG plays a prominent role in advocating for preservation of women’s access to care and adequate physician reimbursement levels. you can help by contacting your state legislators and representatives in the uS Congress to emphasize the importance of these efforts.
We want to hear from you! Tell us what you think.
Is private ObGyn practice on its way out?
Lucia DiVenere (October 2011)
Medicare and Medicaid are on the brink of insolvency, and you’re not just a bystander
Robert L. Barbieri, MD (Editorial, October 2011)
14 questions (and answers) about health reform and you
Janelle Yates, Senior Editor, with Lucia DiVenere (July 2010)
Is the patient-centered medical home a win-all or lose-all proposition for ObGyns?
Janelle Yates (October 2010)
Ms. DiVenere reports no financial relationships relevant to this article.
Tough economic times have pushed 2.8 million more people onto Medicaid rolls, now crowded with more than 60 million low-income individuals and families—nearly 20% of the US population.
Because Medicaid is a means-tested entitlement program, states and the federal government must fund as much health care as beneficiaries use, an expense that increases substantially each year.
Through the Medicaid program, more than 30 million adult women have access to an annual gynecologic exam, family planning services, and prenatal care. Without such coverage, many of them would go without care, potentially driving our nation’s health-care costs even higher. Two thirds of ObGyns treat Medicaid patients, and Medicaid accounts for 18%, on average, of an ObGyn practice’s revenue.1
In this article, I describe how the burgeoning ranks of Medicaid beneficiaries are straining state budgets and prompting legislators to cut provider payments to make up the shortfall. The federal government also plays a role in shrinking reimbursements for physicians and other providers.
Medicaid costs are outpacing economic growth
In fiscal 2011, Medicaid enrollment grew an average of 5.5%, and states are anticipating a growth rate of 4.1% in 2012.2 Total Medicaid spending is also increasing rapidly. In fiscal 2010, it was $361.8 billion (excluding administrative costs)—a 6% increase over fiscal 2009. By the end of fiscal 2011, it was expected to hit $398.6 billion—a 10.1% increase over 2010.3
Medicaid costs are also absorbing a greater share of state budgets. In fiscal 2009, they accounted for 21.9% of total state expenditures, 22.3% in fiscal 2010, and 23.6% in fiscal 2011.3 Many states have had to reduce spending in other important areas as a result (TABLE 1).
Medicaid costs are shared by federal and state governments. The federal government pays, on average, 57% of state program costs. In fiscal 2010, the federal government covered 64.6% of all Medicaid costs.
State general funds at the end of 2011 were well below their pre-recession levels, due to lower revenues and increased expenditures, including continued obligations for state workers’ pensions and retiree health care. At the same time, 49 state governments are required to balance their budgets. As a result, states are likely to face austere budgets for at least the next several years, and will continue to make difficult spending decisions.
As state and federal budgets face pressure to reduce overall spending, Medicaid lies in nearly all budget crosshairs.
TABLE 1
Medicaid absorbs an ever-greater percentage of state expenditures
| State | Percentage | ||
|---|---|---|---|
| Fiscal 2009 | Fiscal 2010 | Fiscal 2011 | |
| New England | |||
| Connecticut | 27.9 | 25.4 | 27.2 |
| Maine | 29.9 | 28.6 | 28.6 |
| Massachusetts | 17.8 | 18.8 | 20.2 |
| New Hampshire | 26.5 | 24.9 | 25.2 |
| Rhode Island | 24.9 | 25.0 | 24.7 |
| Vermont | 25.5 | 25.9 | 26.6 |
| Mid-Atlantic | |||
| Delaware | 12.3 | 14.4 | 16.2 |
| Maryland | 19.3 | 20.4 | 21.6 |
| New Jersey | 19.8 | 21.3 | 21.9 |
| New york | 26.7 | 28.7 | 29.1 |
| Pennsylvania | 30.2 | 29.6 | 31.1 |
| Great Lakes | |||
| Illinois | 24.8 | 23.6 | 28.9 |
| Indiana | 21.8 | 23.1 | 24.4 |
| Michigan | 23.0 | 24.2 | 24.0 |
| Ohio | 20.6 | 21.3 | 23.2 |
| Wisconsin | 15.7 | 17.1 | 17.0 |
| Plains | |||
| Iowa | 17.9 | 18.6 | 19.3 |
| Kansas | 17.4 | 18.8 | 18.6 |
| Minnesota | 24.0 | 25.1 | 25.1 |
| Missouri | 35.6 | 34.4 | 36.3 |
| Nebraska | 17.6 | 17.2 | 16.5 |
| North Dakota | 14.1 | 13.7 | 14.6 |
| South Dakota | 21.6 | 21.7 | 23.2 |
| Southeast | |||
| Alabama | 25.6 | 25.8 | 25.3 |
| Arkansas | 19.7 | 20.0 | 20.5 |
| Florida | 26.7 | 30.0 | 28.0 |
| Georgia | 19.0 | 19.5 | 20.5 |
| Kentucky | 22.5 | 21.9 | 22.8 |
| Louisiana | 22.0 | 23.7 | 23.5 |
| Mississippi | 24.8 | 22.9 | 22.6 |
| North Carolina | 25.0 | 24.2 | 22.1 |
| South Carolina | 22.0 | 22.6 | 19.9 |
| Tennessee | 25.4 | 28.8 | 28.1 |
| Virginia | 16.4 | 16.1 | 16.9 |
| West Virginia | 11.9 | 12.6 | 13.0 |
| Southwest | |||
| Arizona | 29.3 | 27.7 | 28.0 |
| New Mexico | 20.7 | 22.1 | 20.2 |
| Oklahoma | 17.7 | 17.1 | 18.5 |
| Texas | 22.8 | 24.6 | 26.3 |
| Rocky Mountain | |||
| Colorado | 14.1 | 15.3 | 19.4 |
| Idaho | 22.8 | 23.0 | 25.6 |
| Montana | 15.2 | 15.4 | 15.7 |
| Utah | 14.9 | 11.9 | 14.3 |
| Wyoming | 8.1 | 7.3 | 7.0 |
| Far West | |||
| Alaska | 8.1 | 12.0 | 9.0 |
| California | 20.6 | 18.9 | 24.2 |
| Hawaii | 11.3 | 13.3 | 15.9 |
| Nevada | 16.0 | 18.3 | 18.7 |
| Oregon | 14.3 | 13.1 | 14.6 |
| Washington | 21.4 | 23.0 | 24.4 |
| Average | 21.9 | 22.3 | 23.6 |
The fiscal health of Medicaid matters—here’s why
Twelve percent of women 18 to 64 years old rely on Medicaid for health-care coverage, and three quarters of all adult Medicaid beneficiaries are women. Sixty-nine percent of women in the 18- to 64-year-old age group are in their reproductive years. Medicaid pays for 42% of all births in the United States—as many as 64% of all births in Arkansas and Oklahoma.4
Medicaid covers essential well-woman care, including maternity care, breast and cervical cancer screening and treatment, care for disabled women, and family planning.
Medicaid is the largest source of public funding for contraception and sterilization services, covering 71% of these costs. States clearly find it in their best interest and the best interest of public health to encourage use of family planning, which can improve women’s health and reduce the number of unintended pregnancies and abortions. In 2010, 27 states extended family planning coverage to women whose incomes, while still low, were higher than the standard Medicaid eligibility requirements.
Many states cover nutrition and substance abuse counseling, health education, psychosocial counseling, breastfeeding, and case management. TABLE 2 on page 16a lists mandatory and optional Medicaid services.
TABLE 2
Benefits of the Medicaid program
| Mandatory | Optional |
|---|---|
| Physician services Laboratory and radiographic services Hospitalization Outpatient services Early and periodic screening, diagnostic, and treatment services for people younger than 21 years Family planning Rural and federally qualified health center services Nurse midwife services Nursing facility services for people older than 21 years Home health care for people entitled to nursing facility care Smoking cessation for pregnant women* Free-standing birth center services* | Prescription drugs Clinic services Dental services, dentures Physical therapy and rehabilitation Prosthetic devices, eyeglasses Primary-care case management Intermediate-care facilities for the mentally retarded Inpatient psychiatric care for people younger than 21 years Home health care and other services provided under home- and community-based waivers Personal care services Hospice care Health home services for people with chronic conditions* Home- and community-based attendant services and supports* |
| * Benefits added under the Patient Protection and Affordable Care Act | |
Coming: Another 4.5 million women on Medicaid rolls
Under the Patient Protection and Affordable Care Act, Medicaid will expand to cover another 4.5 million women in 2014. Beginning January 1, 2014, state Medicaid programs are required to cover nonpregnant, non-elderly individuals who have incomes as high as 133% of the federal poverty level ($10,890 for an individual in 2011). The federal government will cover the full expense of insuring these newly eligible individuals for calendar years 2014, 2015, and 2016. Federal financing will phase down to 90% by 2020, and will likely decrease further after that.
States that participate in Medicaid must cover pregnant women who have an income at or below 133% of the federal poverty level. States are required to disregard 5% of an individual’s income when determining Medicaid eligibility, a rule that effectively brings the maximum eligibility level to 138% of the federal poverty level, opening the Medicaid doors to additional low-income individuals.
Today, coverage lasts throughout pregnancy and 2 months beyond. States may choose to extend eligibility to pregnant women who have incomes that exceed 133% of the poverty level; at present, 45 states do so, with the District of Columbia topping the list by covering pregnant women who have incomes at or below 300% of the poverty level.
Many measures show that Medicaid has improved access to health care for low- income women, saving lives and dollars. Your experience—wherever you practice— undoubtedly echoes that observation.
Prenatal care. You also know that prenatal care helps ensure healthy babies. Obstetric services often go beyond traditional medical needs to include a full spectrum of care that helps ensure a healthy pregnancy, delivery, and postpartum period.
Of course, inadequate use of prenatal care is associated with increased risks of low birth weight, preterm birth, neonatal mortality, infant mortality, and maternal mortality. Preterm births alone increase US health-care costs by $26 billion each year.5 Pregnancy-related maternal mortality is three to four times higher, and infant mortality is more than six times higher, among women who receive no prenatal care, compared with those who receive prenatal care.
Gynecologic services covered through Medicaid also help preserve health and reduce health-care costs. Eighty-four percent of women on Medicaid have had a Pap test in the past 2 years, compared with 80% of women who have private insurance and 59% of women who lack insurance.6 Routine gynecologic care is vital to prevent cervical cancer and other diseases. Women without a regular doctor don’t get regular Pap tests and mammography; nor do they get screened for other serious health risks, including high cholesterol and diabetes.
Despite the proven benefits of access to regular care, 23% of women on Medicaid report problems finding a new doctor who will accept their insurance, compared with 7% of Medicare beneficiaries and 13% of women who have private insurance.
Why the difficulty in finding a doctor? A leading reason is the inadequacy of Medicaid payment rates.
Cutting payments to physicians
Medicaid provider payments are often the first item cut in a state budget crisis. States are required to cover many health services and are restricted from charging patients significant co-pays, so they often trim budgets at the expense of physicians. Thirty-nine states reduced physician and provider payments in 2011, and 46 states plan to do so in fiscal 2012. In addition, in fiscal 2011, 47 states put in place at least one new policy to control Medicaid costs; most states implemented several of these policies. All 50 states plan to do so in fiscal 2012.
Under federal rules, states must ensure that payment rates are consistent with efficiency, economy, and quality of care. They also must ensure that payment is sufficient to enlist enough providers to render care and services to the same extent that care and services are available to the general population in the same geographic area. States must request and receive permission from the federal government before reducing provider payment rates. However, even with this safeguard in place, physician payments—and patient access to care—are in jeopardy.
For example, in 2008, the California legislature issued several rounds of cuts, including a 10% cut in physician and provider payments, to make up for budget shortfalls. Physicians, hospitals, pharmacists, and other health professionals sued in response, and the 9th US Circuit Court of Appeals blocked the payment cut.
In 2011, California Governor Jerry Brown again put the 10% cut in place, this time with approval from the federal Center for Medicare and Medicaid Services (CMS).
In response, California physicians, led by the state medical association, sued California again. They argued that payment cuts reduce access to care among Medicaid beneficiaries by prompting physicians to stop accepting these patients. The California Department of Health Care Services countered that the cuts are necessary to offset a critical budget shortfall and will not affect access to care. The situation in California highlights the conflicts between physicians and many states over Medicaid payment rates.
The US Supreme Court agreed to review the case on only one question—whether individuals and private parties, including doctors and Medicaid recipients, can sue the state for failing to pay rates that meet the federal adequacy requirement. On October 3, 2011, the Supreme Court heard oral arguments in this group of cases, known as Douglas v. Independent Living Center of Southern California. ACOG joined the case in support of physicians.
Medicaid versus Medicare
It’s easy to see how important Medicaid is to women’s health, and how important physician payment rates are to women’s access to care. You might expect, then, that states would recognize the value of adequate physician payment—but they don’t, always.
At present, Medicaid pays for obstetric care at 93% of the Medicare rate. Still, obstetric care fares slightly better than many physician services. In many states, it costs physicians much more than Medicaid pays to provide non-obstetric care to Mediaid patients. Although 23 states pay for obstetric care at a rate lower than that offered by Medicare, 27 states offer greater support, and 16 states offer reimbursement well above the Medicare rate.
A federal target, too
The states aren’t the only entities with an eye on Medicaid cuts. The US Congress, too, is considering proposals to dramatically change the program. The options include issuing block grants for Medicaid; reducing the federal match; and including Medicaid in global or health spending caps. ACOG has an extensive campaign under way to ensure that any changes to Medicaid do not come at the expense of women’s health.
The Congressional Joint Special Committee on Deficit Reduction—more commonly known as the Supercommittee— represents the latest effort at deficit reduction. When its work imploded in December 2011, federal programs came online for a 2% across-the-board cut (“sequester”) that will take effect on January 1, 2013. The Medicaid program is exempt from this cut, no doubt in recognition of the already-precarious nature of this program, which has become a safety net for millions of American families struggling through the recession.
Because so many American women rely on Medicaid for obstetric and gynecologic care, it is critical that we protect funding levels and maintain eligibility for this program.
ACOG plays a prominent role in advocating for preservation of women’s access to care and adequate physician reimbursement levels. you can help by contacting your state legislators and representatives in the uS Congress to emphasize the importance of these efforts.
We want to hear from you! Tell us what you think.
1. American Congress of Obstetricians and Gynecologists. 2008 Socioeconomic Survey of ACOG Fellows. Washington DC: ACOG; 2008.
2. Holahan J, Headen I. Kaiser Commission on Medicaid and the Uninsured. Medicaid Coverage and Spending in Health Reform: National and State-by-State Results for Adults at or Below 133% FPL. Washington DC: Kaiser Family Foundation; 2010.
3. National Association of State Budget Officers. State Expenditure Report 2010. Washington DC: NASBO; December 2011.
4. National Governors Association Center for Best Practices. 2010 Maternal and Child Health Update. Issue Brief. Washington DC: National Governors Association; 2011. http://www.nga.org/files/live/sites/NGA/files/pdf/MCHUPDATE2010.PDF. Accessed January 12, 2011.
5. Behrman RE, Butler AS. eds Committee on Understanding Premature Birth and Assuring Healthy Outcomes. Preterm Birth: Causes, Consequences, and Prevention. Washington, DC: Institute of Medicine; 2007.
6. Kaiser Family Foundation. Kaiser Women’s Health Survey 2004. Washington DC: KFF; 2005.
1. American Congress of Obstetricians and Gynecologists. 2008 Socioeconomic Survey of ACOG Fellows. Washington DC: ACOG; 2008.
2. Holahan J, Headen I. Kaiser Commission on Medicaid and the Uninsured. Medicaid Coverage and Spending in Health Reform: National and State-by-State Results for Adults at or Below 133% FPL. Washington DC: Kaiser Family Foundation; 2010.
3. National Association of State Budget Officers. State Expenditure Report 2010. Washington DC: NASBO; December 2011.
4. National Governors Association Center for Best Practices. 2010 Maternal and Child Health Update. Issue Brief. Washington DC: National Governors Association; 2011. http://www.nga.org/files/live/sites/NGA/files/pdf/MCHUPDATE2010.PDF. Accessed January 12, 2011.
5. Behrman RE, Butler AS. eds Committee on Understanding Premature Birth and Assuring Healthy Outcomes. Preterm Birth: Causes, Consequences, and Prevention. Washington, DC: Institute of Medicine; 2007.
6. Kaiser Family Foundation. Kaiser Women’s Health Survey 2004. Washington DC: KFF; 2005.
Medical Decision-Making Factors Include Quantity of Information, Complexity
Physicians should formulate a complete and accurate description of a patient’s condition with an equivalent plan of care for each encounter. While acuity and severity can be inferred by healthcare professionals without excessive detail or repetitive documentation of previously entered information, adequate documentation for every service date assists in conveying patient complexity during medical record review.
Regardless of how complex a patient’s condition might be, physicians tend to undervalue their services. This is due, in part, to the routine nature of patient care for seasoned physicians; it is also due in part to a general lack of understanding with respect to the documentation guidelines.
Consider the following scenario: A 68-year-old male with diabetes and a history of chronic obstructive bronchitis was hospitalized after a five-day history of progressive cough with increasing purulent sputum, shortness of breath, and fever. He was treated for an exacerbation of chronic bronchitis within the past six weeks. Upon admission, the patient had an increased temperature (102°F), increased heart rate (96 beats per minute), and increased respiratory rate (28 shallow breaths per minute). His breath sounds included in the right lower lobe rhonchi, and his pulse oximetry was 89% on room air. Chest X-ray confirmed right lower lobe infiltrates along with chronic changes.
Although some physicians would consider this “low complexity” due to the frequency in which they encounter this type of case, others will more appropriately identify this as moderately complex.
MDM Categories
Medical decision-making (MDM) remains consistent in both the 1995 and 1997 guidelines.1,2 Complexity is categorized as straightforward, low, moderate, or high, based on the content of physician documentation. Each visit level is associated with a particular level of complexity. Only the care plan for a given date of service is considered when assigning MDM complexity. For each encounter, the physician receives credit for the number of diagnoses and/or treatment options, the amount and/or complexity of data ordered/reviewed, and the risk of complications/morbidity/mortality (see Table 1).
Number of diagnoses or treatment options. Physicians should document problems addressed and managed daily despite any changes to the treatment plan. Credit is provided for each problem with an associated plan, even if the plan states “continue treatment.” Credit also depends upon the quantity of problems addressed, as well as the problem type. An established problem in which the care plan has been established by the physician or group practice member during the current hospitalization is less complex than a new problem for which a diagnosis, prognosis, or plan has not been determined. Severity of the problem affects the weight of complexity. A worsening problem is more complex than an improving problem. Physician documentation should:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- When documentation indicates a continuation of current management options (e.g. “continue meds”), be sure that the management options to be continued are noted somewhere in the progress note for that encounter (e.g. medication list).
The plan of care outlines problems that the physician personally manages and those that impact management options, even if another physician directly oversees the problem. For example, the hospitalist might primarily manage diabetes, while the pulmonologist manages pneumonia. Since the pneumonia may impact the hospitalist’s plan for diabetic management, the hospitalist can receive credit for the pneumonia diagnosis if there is a non-overlapping, hospitalist-related care plan or comment about the pneumonia.
Amount and/or complexity of data ordered/reviewed. “Data” is classified as pathology/laboratory testing, radiology, and medicine-based diagnostics. Pertinent orders or results could be noted in the visit record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note or make an entry that refers to another auditor-accessible location for ordered tests and studies;
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”);
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary;
- Indicate when images, tracings, or specimens are “personally reviewed”; and
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Risks of complication and/or morbidity or mortality. Risk involves the patient’s presenting problem, diagnostic procedures ordered, and management options selected. It is measured as minimal, low, moderate, or high when compared with corresponding items assigned to each risk level (see Table 2). The highest individual item detected on the table determines the overall patient risk for that encounter.
Chronic conditions and invasive procedures pose more risk than acute, uncomplicated illnesses or non-invasive procedures. Stable or improving problems are not as menacing as progressing problems; minor exacerbations are less hazardous than severe exacerbations; and medication risk varies with the type and potential for adverse effects. A patient maintains the same level of risk for a given medication whether the dosage is increased, decreased, or continued without change. Physicians should:
- Status all problems in the plan of care; identify them as stable, worsening, exacerbating (mild or severe), when applicable;
- Document all diagnostic or therapeutic procedures considered;
- Identify surgical risk factors involving comorbid conditions, when appropriate; and
- Associate the labs ordered to monitor for toxicity with the corresponding medication (e.g. “Continue Coumadin, monitor PT/INR”).
Determining complexity of medical decision-making. The final complexity of MDM depends upon the second-highest MDM category. The physician does not have to meet the requirements for all three MDM categories. For example, if a physician satisfies the requirements for a “multiple” number of diagnoses/treatment options, “limited” data, and “high” risk, the physician achieves moderate complexity decision-making (see Table 3). Remember that decision-making is just one of three components in evaluation and management services, along with history and exam.
Beware of payor variation, as it could have a significant impact on visit-level selection.3 Become acquainted with rules applicable to the geographical area. Review insurer websites for guidelines, policies, and “frequently asked questions” that can help improve documentation skills and support billing practices.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf. Accessed Nov. 14, 2011.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed Nov. 14, 2011.
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2010. Northbrook, IL: American College of Chest Physicians, 2009; 87-118.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011:1-20.
Physicians should formulate a complete and accurate description of a patient’s condition with an equivalent plan of care for each encounter. While acuity and severity can be inferred by healthcare professionals without excessive detail or repetitive documentation of previously entered information, adequate documentation for every service date assists in conveying patient complexity during medical record review.
Regardless of how complex a patient’s condition might be, physicians tend to undervalue their services. This is due, in part, to the routine nature of patient care for seasoned physicians; it is also due in part to a general lack of understanding with respect to the documentation guidelines.
Consider the following scenario: A 68-year-old male with diabetes and a history of chronic obstructive bronchitis was hospitalized after a five-day history of progressive cough with increasing purulent sputum, shortness of breath, and fever. He was treated for an exacerbation of chronic bronchitis within the past six weeks. Upon admission, the patient had an increased temperature (102°F), increased heart rate (96 beats per minute), and increased respiratory rate (28 shallow breaths per minute). His breath sounds included in the right lower lobe rhonchi, and his pulse oximetry was 89% on room air. Chest X-ray confirmed right lower lobe infiltrates along with chronic changes.
Although some physicians would consider this “low complexity” due to the frequency in which they encounter this type of case, others will more appropriately identify this as moderately complex.
MDM Categories
Medical decision-making (MDM) remains consistent in both the 1995 and 1997 guidelines.1,2 Complexity is categorized as straightforward, low, moderate, or high, based on the content of physician documentation. Each visit level is associated with a particular level of complexity. Only the care plan for a given date of service is considered when assigning MDM complexity. For each encounter, the physician receives credit for the number of diagnoses and/or treatment options, the amount and/or complexity of data ordered/reviewed, and the risk of complications/morbidity/mortality (see Table 1).
Number of diagnoses or treatment options. Physicians should document problems addressed and managed daily despite any changes to the treatment plan. Credit is provided for each problem with an associated plan, even if the plan states “continue treatment.” Credit also depends upon the quantity of problems addressed, as well as the problem type. An established problem in which the care plan has been established by the physician or group practice member during the current hospitalization is less complex than a new problem for which a diagnosis, prognosis, or plan has not been determined. Severity of the problem affects the weight of complexity. A worsening problem is more complex than an improving problem. Physician documentation should:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- When documentation indicates a continuation of current management options (e.g. “continue meds”), be sure that the management options to be continued are noted somewhere in the progress note for that encounter (e.g. medication list).
The plan of care outlines problems that the physician personally manages and those that impact management options, even if another physician directly oversees the problem. For example, the hospitalist might primarily manage diabetes, while the pulmonologist manages pneumonia. Since the pneumonia may impact the hospitalist’s plan for diabetic management, the hospitalist can receive credit for the pneumonia diagnosis if there is a non-overlapping, hospitalist-related care plan or comment about the pneumonia.
Amount and/or complexity of data ordered/reviewed. “Data” is classified as pathology/laboratory testing, radiology, and medicine-based diagnostics. Pertinent orders or results could be noted in the visit record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note or make an entry that refers to another auditor-accessible location for ordered tests and studies;
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”);
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary;
- Indicate when images, tracings, or specimens are “personally reviewed”; and
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Risks of complication and/or morbidity or mortality. Risk involves the patient’s presenting problem, diagnostic procedures ordered, and management options selected. It is measured as minimal, low, moderate, or high when compared with corresponding items assigned to each risk level (see Table 2). The highest individual item detected on the table determines the overall patient risk for that encounter.
Chronic conditions and invasive procedures pose more risk than acute, uncomplicated illnesses or non-invasive procedures. Stable or improving problems are not as menacing as progressing problems; minor exacerbations are less hazardous than severe exacerbations; and medication risk varies with the type and potential for adverse effects. A patient maintains the same level of risk for a given medication whether the dosage is increased, decreased, or continued without change. Physicians should:
- Status all problems in the plan of care; identify them as stable, worsening, exacerbating (mild or severe), when applicable;
- Document all diagnostic or therapeutic procedures considered;
- Identify surgical risk factors involving comorbid conditions, when appropriate; and
- Associate the labs ordered to monitor for toxicity with the corresponding medication (e.g. “Continue Coumadin, monitor PT/INR”).
Determining complexity of medical decision-making. The final complexity of MDM depends upon the second-highest MDM category. The physician does not have to meet the requirements for all three MDM categories. For example, if a physician satisfies the requirements for a “multiple” number of diagnoses/treatment options, “limited” data, and “high” risk, the physician achieves moderate complexity decision-making (see Table 3). Remember that decision-making is just one of three components in evaluation and management services, along with history and exam.
Beware of payor variation, as it could have a significant impact on visit-level selection.3 Become acquainted with rules applicable to the geographical area. Review insurer websites for guidelines, policies, and “frequently asked questions” that can help improve documentation skills and support billing practices.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf. Accessed Nov. 14, 2011.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed Nov. 14, 2011.
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2010. Northbrook, IL: American College of Chest Physicians, 2009; 87-118.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011:1-20.
Physicians should formulate a complete and accurate description of a patient’s condition with an equivalent plan of care for each encounter. While acuity and severity can be inferred by healthcare professionals without excessive detail or repetitive documentation of previously entered information, adequate documentation for every service date assists in conveying patient complexity during medical record review.
Regardless of how complex a patient’s condition might be, physicians tend to undervalue their services. This is due, in part, to the routine nature of patient care for seasoned physicians; it is also due in part to a general lack of understanding with respect to the documentation guidelines.
Consider the following scenario: A 68-year-old male with diabetes and a history of chronic obstructive bronchitis was hospitalized after a five-day history of progressive cough with increasing purulent sputum, shortness of breath, and fever. He was treated for an exacerbation of chronic bronchitis within the past six weeks. Upon admission, the patient had an increased temperature (102°F), increased heart rate (96 beats per minute), and increased respiratory rate (28 shallow breaths per minute). His breath sounds included in the right lower lobe rhonchi, and his pulse oximetry was 89% on room air. Chest X-ray confirmed right lower lobe infiltrates along with chronic changes.
Although some physicians would consider this “low complexity” due to the frequency in which they encounter this type of case, others will more appropriately identify this as moderately complex.
MDM Categories
Medical decision-making (MDM) remains consistent in both the 1995 and 1997 guidelines.1,2 Complexity is categorized as straightforward, low, moderate, or high, based on the content of physician documentation. Each visit level is associated with a particular level of complexity. Only the care plan for a given date of service is considered when assigning MDM complexity. For each encounter, the physician receives credit for the number of diagnoses and/or treatment options, the amount and/or complexity of data ordered/reviewed, and the risk of complications/morbidity/mortality (see Table 1).
Number of diagnoses or treatment options. Physicians should document problems addressed and managed daily despite any changes to the treatment plan. Credit is provided for each problem with an associated plan, even if the plan states “continue treatment.” Credit also depends upon the quantity of problems addressed, as well as the problem type. An established problem in which the care plan has been established by the physician or group practice member during the current hospitalization is less complex than a new problem for which a diagnosis, prognosis, or plan has not been determined. Severity of the problem affects the weight of complexity. A worsening problem is more complex than an improving problem. Physician documentation should:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- When documentation indicates a continuation of current management options (e.g. “continue meds”), be sure that the management options to be continued are noted somewhere in the progress note for that encounter (e.g. medication list).
The plan of care outlines problems that the physician personally manages and those that impact management options, even if another physician directly oversees the problem. For example, the hospitalist might primarily manage diabetes, while the pulmonologist manages pneumonia. Since the pneumonia may impact the hospitalist’s plan for diabetic management, the hospitalist can receive credit for the pneumonia diagnosis if there is a non-overlapping, hospitalist-related care plan or comment about the pneumonia.
Amount and/or complexity of data ordered/reviewed. “Data” is classified as pathology/laboratory testing, radiology, and medicine-based diagnostics. Pertinent orders or results could be noted in the visit record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note or make an entry that refers to another auditor-accessible location for ordered tests and studies;
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”);
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary;
- Indicate when images, tracings, or specimens are “personally reviewed”; and
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Risks of complication and/or morbidity or mortality. Risk involves the patient’s presenting problem, diagnostic procedures ordered, and management options selected. It is measured as minimal, low, moderate, or high when compared with corresponding items assigned to each risk level (see Table 2). The highest individual item detected on the table determines the overall patient risk for that encounter.
Chronic conditions and invasive procedures pose more risk than acute, uncomplicated illnesses or non-invasive procedures. Stable or improving problems are not as menacing as progressing problems; minor exacerbations are less hazardous than severe exacerbations; and medication risk varies with the type and potential for adverse effects. A patient maintains the same level of risk for a given medication whether the dosage is increased, decreased, or continued without change. Physicians should:
- Status all problems in the plan of care; identify them as stable, worsening, exacerbating (mild or severe), when applicable;
- Document all diagnostic or therapeutic procedures considered;
- Identify surgical risk factors involving comorbid conditions, when appropriate; and
- Associate the labs ordered to monitor for toxicity with the corresponding medication (e.g. “Continue Coumadin, monitor PT/INR”).
Determining complexity of medical decision-making. The final complexity of MDM depends upon the second-highest MDM category. The physician does not have to meet the requirements for all three MDM categories. For example, if a physician satisfies the requirements for a “multiple” number of diagnoses/treatment options, “limited” data, and “high” risk, the physician achieves moderate complexity decision-making (see Table 3). Remember that decision-making is just one of three components in evaluation and management services, along with history and exam.
Beware of payor variation, as it could have a significant impact on visit-level selection.3 Become acquainted with rules applicable to the geographical area. Review insurer websites for guidelines, policies, and “frequently asked questions” that can help improve documentation skills and support billing practices.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf. Accessed Nov. 14, 2011.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed Nov. 14, 2011.
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2010. Northbrook, IL: American College of Chest Physicians, 2009; 87-118.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011:1-20.
Managing Your Dermatology Practice: Sample Credit Card Policy Letter for Patients
Thanks for all of the emails and requests to receive a copy of Dr. Joseph S. Eastern's credit card policy letter based on his blog post, "Your 2012 Resolution- Stop Extending Credit!"
The following is a copy of the letter Dr. Joseph S. Eastern gives to all new patients on their first visit explaining his office's credit card policy.
His office staff keeps the patient's credit card number on file, and uses it to bill any outstanding balances.
PLEASE NOTE:
This generic letter is intended to be used as an example for a letter you might draft for a similar purpose. However, we take no responsibility for your use of its content, either verbatim or altered, or any inappropriate usage.
To Our Patients:
As you know if you have ever checked into a hotel or rented a car, the first thing you are asked for is a credit card, which is imprinted and later used to pay your bill. This is an advantage for both you and the hotel or rental company, since it makes checkout easier, faster, and more efficient.
We have implemented a similar policy. You will be asked for a credit card number at the time you check in and the information will be held securely until your insurances have paid their portion and notified us of the amount of your share. At that time, any remaining balance owed by you will be charged to your credit card, and a copy of the charge will be mailed to you.
This will be an advantage to you, since you will no longer have to write out and mail us checks. It will be an advantage to us as well, since it will greatly decrease the number of statements that we have to generate and send out. The combination will benefit everybody in helping to keep the cost of health care down.
This in no way will compromise your ability to dispute a charge or question your insurance company’s determination of payment.
Co-pays due at the time of the visit will, of course, still be due at the time of the visit.
If you have any questions about this payment method, do not hesitate to ask.
Sincerely yours,
I authorize ********************, PA to charge outstanding balances on my account to the following credit card:
Visa Mastercard American Express Other: ____________________________
Account number ________________________________ Expiration Date ____________
Thanks for all of the emails and requests to receive a copy of Dr. Joseph S. Eastern's credit card policy letter based on his blog post, "Your 2012 Resolution- Stop Extending Credit!"
The following is a copy of the letter Dr. Joseph S. Eastern gives to all new patients on their first visit explaining his office's credit card policy.
His office staff keeps the patient's credit card number on file, and uses it to bill any outstanding balances.
PLEASE NOTE:
This generic letter is intended to be used as an example for a letter you might draft for a similar purpose. However, we take no responsibility for your use of its content, either verbatim or altered, or any inappropriate usage.
To Our Patients:
As you know if you have ever checked into a hotel or rented a car, the first thing you are asked for is a credit card, which is imprinted and later used to pay your bill. This is an advantage for both you and the hotel or rental company, since it makes checkout easier, faster, and more efficient.
We have implemented a similar policy. You will be asked for a credit card number at the time you check in and the information will be held securely until your insurances have paid their portion and notified us of the amount of your share. At that time, any remaining balance owed by you will be charged to your credit card, and a copy of the charge will be mailed to you.
This will be an advantage to you, since you will no longer have to write out and mail us checks. It will be an advantage to us as well, since it will greatly decrease the number of statements that we have to generate and send out. The combination will benefit everybody in helping to keep the cost of health care down.
This in no way will compromise your ability to dispute a charge or question your insurance company’s determination of payment.
Co-pays due at the time of the visit will, of course, still be due at the time of the visit.
If you have any questions about this payment method, do not hesitate to ask.
Sincerely yours,
I authorize ********************, PA to charge outstanding balances on my account to the following credit card:
Visa Mastercard American Express Other: ____________________________
Account number ________________________________ Expiration Date ____________
Thanks for all of the emails and requests to receive a copy of Dr. Joseph S. Eastern's credit card policy letter based on his blog post, "Your 2012 Resolution- Stop Extending Credit!"
The following is a copy of the letter Dr. Joseph S. Eastern gives to all new patients on their first visit explaining his office's credit card policy.
His office staff keeps the patient's credit card number on file, and uses it to bill any outstanding balances.
PLEASE NOTE:
This generic letter is intended to be used as an example for a letter you might draft for a similar purpose. However, we take no responsibility for your use of its content, either verbatim or altered, or any inappropriate usage.
To Our Patients:
As you know if you have ever checked into a hotel or rented a car, the first thing you are asked for is a credit card, which is imprinted and later used to pay your bill. This is an advantage for both you and the hotel or rental company, since it makes checkout easier, faster, and more efficient.
We have implemented a similar policy. You will be asked for a credit card number at the time you check in and the information will be held securely until your insurances have paid their portion and notified us of the amount of your share. At that time, any remaining balance owed by you will be charged to your credit card, and a copy of the charge will be mailed to you.
This will be an advantage to you, since you will no longer have to write out and mail us checks. It will be an advantage to us as well, since it will greatly decrease the number of statements that we have to generate and send out. The combination will benefit everybody in helping to keep the cost of health care down.
This in no way will compromise your ability to dispute a charge or question your insurance company’s determination of payment.
Co-pays due at the time of the visit will, of course, still be due at the time of the visit.
If you have any questions about this payment method, do not hesitate to ask.
Sincerely yours,
I authorize ********************, PA to charge outstanding balances on my account to the following credit card:
Visa Mastercard American Express Other: ____________________________
Account number ________________________________ Expiration Date ____________
Managing Your Dermatology Practice: Defending Your Online Reputation
Have you ever run across a negative or even malicious comment about you or your office on the Web, in full view of the world? You’re certainly not alone.
Chances are the comment was on a doctor-rating site, whose supposedly "objective" evaluations are anything but fair or accurate; one curmudgeon, angry about something that has nothing to do with your clinical skills, can trash your reputation, as thousands of satisfied patients remain silent.
What to do? You could hire one of the many companies in the rapidly burgeoning field of online reputation management; but that can cost hundreds to thousands of dollars per month for monitoring and intervention, and there are no guarantees of success.
A better solution is to generate your own search results – positive ones – that will overwhelm any negative comments that search engines might find. Start with social networking sites.
However you feel about networking, there’s no getting around the fact that personal pages on Facebook, LinkedIn, and Twitter rank high on major search engines. (Some consultants say a favorable LinkedIn profile is particularly helpful because of that site’s reputation as a "professional" network.) Your community activities, charitable work, interesting hobbies – anything that casts you in a favorable light – need to be mentioned prominently in your network profiles.
You can also use Google’s profiling tool (google.com/profiles) to create a sterling bio, complete with links to URLs, photos, and anything else that shows you in the best possible light. And your Google profile will be at or near the top of any Google search.
Wikipedia articles also go to the top of most searches, so if you’re notable enough to merit mention in one – or to have one of your own – see that it is done and updated regularly. You can’t do that yourself, however; Wikipedia’s conflict of interest rules forbid writing or editing content about yourself. Someone with a theoretical "neutral point of view" will have to do it.
If you don’t yet have a website, now would be a good time to have one built for you. A professionally designed site will be far more attractive and polished than anything you could build yourself. Furthermore, an experienced designer will employ "search engine optimization" (SEO), meaning content will be created in a way that is readily visible to search engine users.
Leave design and SEO to the pros, but don’t delegate the content itself. As captain of the ship, you are responsible for all the facts and opinions on your site. And remember that once it’s online, it’s online forever; consider the ramifications of anything you post on any site (yours or others) before hitting the "send" button. "The most damaging item about you," one consultant told me, "could well be something you posted yourself." Just ask former Congressman Anthony Weiner.
That said, don’t be shy about creating content. Make your (noncontroversial) opinions known on Facebook and Twitter. If social networks are not your thing, add a blog to your website and write about what you know, and what interests you. If you have expertise in a particular field, write about that.
Incidentally, if the URL for your website is not your name, you should also register your name as a separate domain – if only to be sure that a trickster, or someone with the same name and a bad reputation, doesn’t get it.
Set up an RSS news feed for yourself, so you’ll know immediately when your name pops up on news gossip, or blog sites If something untrue is posted, take action. Reputable news sites and blogs have their own reputations to protect, and so can usually be persuaded to correct anything that is demonstrably false. Try to get the error removed entirely, or corrected within the original article. An erratum on the last page of the next edition will be ignored, and will leave the false information intact.
Unfair comments on doctor-rating sites are unlikely to be removed unless they are blatantly libelous, but there is nothing wrong with asking pleased patients to write favorable reviews. Turnabout is fair play.
Have you ever run across a negative or even malicious comment about you or your office on the Web, in full view of the world? You’re certainly not alone.
Chances are the comment was on a doctor-rating site, whose supposedly "objective" evaluations are anything but fair or accurate; one curmudgeon, angry about something that has nothing to do with your clinical skills, can trash your reputation, as thousands of satisfied patients remain silent.
What to do? You could hire one of the many companies in the rapidly burgeoning field of online reputation management; but that can cost hundreds to thousands of dollars per month for monitoring and intervention, and there are no guarantees of success.
A better solution is to generate your own search results – positive ones – that will overwhelm any negative comments that search engines might find. Start with social networking sites.
However you feel about networking, there’s no getting around the fact that personal pages on Facebook, LinkedIn, and Twitter rank high on major search engines. (Some consultants say a favorable LinkedIn profile is particularly helpful because of that site’s reputation as a "professional" network.) Your community activities, charitable work, interesting hobbies – anything that casts you in a favorable light – need to be mentioned prominently in your network profiles.
You can also use Google’s profiling tool (google.com/profiles) to create a sterling bio, complete with links to URLs, photos, and anything else that shows you in the best possible light. And your Google profile will be at or near the top of any Google search.
Wikipedia articles also go to the top of most searches, so if you’re notable enough to merit mention in one – or to have one of your own – see that it is done and updated regularly. You can’t do that yourself, however; Wikipedia’s conflict of interest rules forbid writing or editing content about yourself. Someone with a theoretical "neutral point of view" will have to do it.
If you don’t yet have a website, now would be a good time to have one built for you. A professionally designed site will be far more attractive and polished than anything you could build yourself. Furthermore, an experienced designer will employ "search engine optimization" (SEO), meaning content will be created in a way that is readily visible to search engine users.
Leave design and SEO to the pros, but don’t delegate the content itself. As captain of the ship, you are responsible for all the facts and opinions on your site. And remember that once it’s online, it’s online forever; consider the ramifications of anything you post on any site (yours or others) before hitting the "send" button. "The most damaging item about you," one consultant told me, "could well be something you posted yourself." Just ask former Congressman Anthony Weiner.
That said, don’t be shy about creating content. Make your (noncontroversial) opinions known on Facebook and Twitter. If social networks are not your thing, add a blog to your website and write about what you know, and what interests you. If you have expertise in a particular field, write about that.
Incidentally, if the URL for your website is not your name, you should also register your name as a separate domain – if only to be sure that a trickster, or someone with the same name and a bad reputation, doesn’t get it.
Set up an RSS news feed for yourself, so you’ll know immediately when your name pops up on news gossip, or blog sites If something untrue is posted, take action. Reputable news sites and blogs have their own reputations to protect, and so can usually be persuaded to correct anything that is demonstrably false. Try to get the error removed entirely, or corrected within the original article. An erratum on the last page of the next edition will be ignored, and will leave the false information intact.
Unfair comments on doctor-rating sites are unlikely to be removed unless they are blatantly libelous, but there is nothing wrong with asking pleased patients to write favorable reviews. Turnabout is fair play.
Have you ever run across a negative or even malicious comment about you or your office on the Web, in full view of the world? You’re certainly not alone.
Chances are the comment was on a doctor-rating site, whose supposedly "objective" evaluations are anything but fair or accurate; one curmudgeon, angry about something that has nothing to do with your clinical skills, can trash your reputation, as thousands of satisfied patients remain silent.
What to do? You could hire one of the many companies in the rapidly burgeoning field of online reputation management; but that can cost hundreds to thousands of dollars per month for monitoring and intervention, and there are no guarantees of success.
A better solution is to generate your own search results – positive ones – that will overwhelm any negative comments that search engines might find. Start with social networking sites.
However you feel about networking, there’s no getting around the fact that personal pages on Facebook, LinkedIn, and Twitter rank high on major search engines. (Some consultants say a favorable LinkedIn profile is particularly helpful because of that site’s reputation as a "professional" network.) Your community activities, charitable work, interesting hobbies – anything that casts you in a favorable light – need to be mentioned prominently in your network profiles.
You can also use Google’s profiling tool (google.com/profiles) to create a sterling bio, complete with links to URLs, photos, and anything else that shows you in the best possible light. And your Google profile will be at or near the top of any Google search.
Wikipedia articles also go to the top of most searches, so if you’re notable enough to merit mention in one – or to have one of your own – see that it is done and updated regularly. You can’t do that yourself, however; Wikipedia’s conflict of interest rules forbid writing or editing content about yourself. Someone with a theoretical "neutral point of view" will have to do it.
If you don’t yet have a website, now would be a good time to have one built for you. A professionally designed site will be far more attractive and polished than anything you could build yourself. Furthermore, an experienced designer will employ "search engine optimization" (SEO), meaning content will be created in a way that is readily visible to search engine users.
Leave design and SEO to the pros, but don’t delegate the content itself. As captain of the ship, you are responsible for all the facts and opinions on your site. And remember that once it’s online, it’s online forever; consider the ramifications of anything you post on any site (yours or others) before hitting the "send" button. "The most damaging item about you," one consultant told me, "could well be something you posted yourself." Just ask former Congressman Anthony Weiner.
That said, don’t be shy about creating content. Make your (noncontroversial) opinions known on Facebook and Twitter. If social networks are not your thing, add a blog to your website and write about what you know, and what interests you. If you have expertise in a particular field, write about that.
Incidentally, if the URL for your website is not your name, you should also register your name as a separate domain – if only to be sure that a trickster, or someone with the same name and a bad reputation, doesn’t get it.
Set up an RSS news feed for yourself, so you’ll know immediately when your name pops up on news gossip, or blog sites If something untrue is posted, take action. Reputable news sites and blogs have their own reputations to protect, and so can usually be persuaded to correct anything that is demonstrably false. Try to get the error removed entirely, or corrected within the original article. An erratum on the last page of the next edition will be ignored, and will leave the false information intact.
Unfair comments on doctor-rating sites are unlikely to be removed unless they are blatantly libelous, but there is nothing wrong with asking pleased patients to write favorable reviews. Turnabout is fair play.
IT Security—What All Orthopedic Surgeons Must Know
Data on liability claims offer bright spots for ObGyns— and sobering statistics
Good news on the medical liability front, Doctor!
Yes, that’s right, good news.
According to data from the Physician Insurers Association of America (PIAA), the number of claims that were paid in the ObGyn category between 2006 and 2011 was 44% lower than the number of claims paid between 1986 and 1991.
The percentage of claims that were paid also decreased over the same quarter century. During 1986–1990, 37.25% of all claims were paid in the ObGyn category, compared with 31.73% during 2006–2010.1
And when claims for both periods are calculated in 2010 dollars, the amount paid also declined—by more than $138 million!
These are three of the findings that reflect “significant improvement” in obstetrics and gynecology in medical liability, says John B. Stanchfield, MD, an endocrinologist who, for 25 years, was medical director of the Utah Medical Insurance Association (UMIA)—a member company of PIAA. PIAA is the insurance industry trade association.
PIAA member companies in the United States “include large national insurance companies, mid-size regional writers, single-state insurers, and specialty companies that serve specific health care–provider niche markets. Collectively, these companies provide insurance protection to more than 60% of America’s private practice physicians and write approximately 46%, or $5.2 billion, of the total industry premium.”2
The improvement in ObGyn comes as no surprise to Dr. Stanchfield because the specialty was “the first group that got ‘risk-managed’ almost universally across the country,” he says. “In our little company out here in Utah, in 1985, we were told that if we didn’t do something [about lawsuits in obstetrics and gynecology], we weren’t going to be able to insure that class anymore because we wouldn’t be able to collect enough money. That’s what the actuaries told us, but it wasn’t unique to us—it was a nationwide problem.”
Why was the ObGyn specialty, in particular, in need of aggressive risk management? What made ObGyn claims unique?
“It’s infant injury,” says Dr. Stanchfield. “It’s injury to the baby. Those claims, you start talking at a million dollars.”
Another reason may be that some claims in this specialty category involve doctors other than ObGyns who provide obstetric care—for example, family practice physicians.

A risk manager’s perspective
After receiving the warning about ObGyn claims, UMIA got busy. First, it formed a committee comprising perinatologists, ObGyns, family practice physicians, claims specialists, and attorneys. “We analyzed all claims that were paid, looking for common denominators,” says Dr. Stanchfield. Improvement was clearly needed in about 10 areas, so “we basically created a risk-management program and then mandated it.” In the process, the organization published a booklet entitled Insurance Recommendations for Obstetrical Practice, of which Dr. Stanchfield was the editor.3
The booklet offers guidance on 10 potential “problem” areas:
- antepartum testing
- hypertension and pregnancy
- operative vaginal delivery
- breech delivery
- oxytocin administration
- vaginal birth after cesarean
- use of misoprostol
- shoulder dystocia
- preterm labor
- hospital standards.
Fewer claims and more physicians
The declining number and percentage of paid claims in obstetrics and gynecology over 25 years may be even more impressive than the figures suggest, says Dr. Stanchfield.
“Gestalt tells me that through the years there are more practicing physicians rather than fewer,” so the denominator is increasing even as these claims are declining—making the decrease “even more powerful.”
The numbers haven’t improved to the same degree in other specialties, Dr. Stanchfield says. “If you look at global data, the decrease in paid claims might have been 10% to 15%. In ObGyn, if you compare the last 5-year block of data with the first 5-year block, the number of paid claims is almost cut in half.”
What brought about this improvement?
“There weren’t any groundbreaking medical or surgical technological advances during this period. It was just doing it better. And the main push to doing it better in this country, in my opinion, is risk management.”
Slicing the data
Now for the not-so-great news: In 2010 alone, more than $55 million was paid out in the ObGyn category for 10 patient conditions. Topping the list were “pregnancy” and “brain-damaged infant.” The $55 million figure represents the money paid for the top 10 most commonly cited conditions in cases closed during 2010 (TABLE 1).
TABLE 1
Claims categorized under the rather broad category of pregnancy usually were placed there because a more appropriate category was lacking, says Dr. Stanchfield. These claims typically involve “things that happen—usually to the baby—that result in a lawsuit other than brain damage per se.” For example, a claim that involved skull fracture without brain damage might fall into this zone, he says.
Problematic procedures
Slicing the data a different way, problems related to the 10 most commonly cited ObGyn procedures cost PIAA companies more than $120 million dollars in 2010—and that figure is only for the top 10.1 The top three procedures, in terms of number of claims closed in 2010, were operative procedures on the uterus, manually assisted delivery, and cesarean delivery (TABLE 2).
TABLE 2
Manually assisted delivery does not include vacuum extraction or forceps delivery, notes Dr. Stanchfield. “Manually assisted delivery is basically standing there like a quarterback and catching the baby.”
Top 10 “medical misadventures”
And another slice of data reveals the 10 most prevalent medical misadventures in the ObGyn specialty in 2010 (TABLE 3):
- improper performance of a procedure
- no medical misadventure (i.e., no misadventure was identifiable)
- errors in diagnosis
- failure to supervise or monitor a case
- delay in performance of a procedure
- failure to recognize a complication
- surgical foreign body left in a patient after a procedure
- necessary treatment or management was “not performed”
- failure to instruct or communicate with a patient
- medication errors.
The total indemnity paid for these so-called misadventures was more than $136 million.1
TABLE 3
Putting the dollars in perspective
PIAA also collects data on the number of claims reported, and indemnity dollars paid, for other specialties.
“Of the 28 specialty groups included in the database, ObGyn ranks second”—behind internal medicine—“in the number of claims closed between 1985 and 2010,” a PIAA report notes. The ObGyn specialty also ranks second—behind dentists—in the percentage (35%) of those claims that were paid (for dentists, the figure was 46%). Obstetrics and gynecology was also responsible for the single largest indemnity payment—$13,000,000.1
Medical liability: A national disaster?
According to figures from the PIAA Data Sharing Project, an ongoing claim study that includes 22 PIAA member companies, $19.7 billion in losses (total indemnity plus expenses) were reported during the period from 1985 through 2008. Those losses represented approximately 25% of the physicians who were practicing during that time.
“So if you multiply that $19.7 billion figure by four”—to extrapolate it to the full spectrum of physicians practicing between 1985 and 2008—“you’ve got almost $80 billion coming out of the pockets of the doctors in this country,” says Dr. Stanchfield. If you compare that $80 billion figure to the World Trade Center disaster, which involved approximately $42 billion in losses, the need for federal tort reform is highlighted, he says. In 24 years, the physicians “in this country have paid for almost two World Trade Center disasters. That’s an incredible dollar cost.”
From Dr. Stanchfield’s perspective as a risk manager, the best thing physicians can do to protect themselves is to practice medicine wisely.
“One of our speakers used to say, ‘Look, just practice good, middle-of-the-road medicine. Don’t get yourself out on the fringes where you’re doing something questionable. Just practice rock-solid, conservative, safe medicine.’”
We want to hear from you! Tell us what you think.
1. Physician Insurers Association of America. 2011 Risk Management Review. Rockville, Md: PIAA; 2011.
2. Physician Insurers Association of America. PIAA Backgrounder. Rockville, Md: PIAA; 2011.
3. Stanchfied JB, ed. Insurance Recommendations for Obstetrical Practice. Revised ed. Salt Lake City, Utah: Utah Medical Insurance Association; 2009.
Good news on the medical liability front, Doctor!
Yes, that’s right, good news.
According to data from the Physician Insurers Association of America (PIAA), the number of claims that were paid in the ObGyn category between 2006 and 2011 was 44% lower than the number of claims paid between 1986 and 1991.
The percentage of claims that were paid also decreased over the same quarter century. During 1986–1990, 37.25% of all claims were paid in the ObGyn category, compared with 31.73% during 2006–2010.1
And when claims for both periods are calculated in 2010 dollars, the amount paid also declined—by more than $138 million!
These are three of the findings that reflect “significant improvement” in obstetrics and gynecology in medical liability, says John B. Stanchfield, MD, an endocrinologist who, for 25 years, was medical director of the Utah Medical Insurance Association (UMIA)—a member company of PIAA. PIAA is the insurance industry trade association.
PIAA member companies in the United States “include large national insurance companies, mid-size regional writers, single-state insurers, and specialty companies that serve specific health care–provider niche markets. Collectively, these companies provide insurance protection to more than 60% of America’s private practice physicians and write approximately 46%, or $5.2 billion, of the total industry premium.”2
The improvement in ObGyn comes as no surprise to Dr. Stanchfield because the specialty was “the first group that got ‘risk-managed’ almost universally across the country,” he says. “In our little company out here in Utah, in 1985, we were told that if we didn’t do something [about lawsuits in obstetrics and gynecology], we weren’t going to be able to insure that class anymore because we wouldn’t be able to collect enough money. That’s what the actuaries told us, but it wasn’t unique to us—it was a nationwide problem.”
Why was the ObGyn specialty, in particular, in need of aggressive risk management? What made ObGyn claims unique?
“It’s infant injury,” says Dr. Stanchfield. “It’s injury to the baby. Those claims, you start talking at a million dollars.”
Another reason may be that some claims in this specialty category involve doctors other than ObGyns who provide obstetric care—for example, family practice physicians.
A risk manager’s perspective
After receiving the warning about ObGyn claims, UMIA got busy. First, it formed a committee comprising perinatologists, ObGyns, family practice physicians, claims specialists, and attorneys. “We analyzed all claims that were paid, looking for common denominators,” says Dr. Stanchfield. Improvement was clearly needed in about 10 areas, so “we basically created a risk-management program and then mandated it.” In the process, the organization published a booklet entitled Insurance Recommendations for Obstetrical Practice, of which Dr. Stanchfield was the editor.3
The booklet offers guidance on 10 potential “problem” areas:
- antepartum testing
- hypertension and pregnancy
- operative vaginal delivery
- breech delivery
- oxytocin administration
- vaginal birth after cesarean
- use of misoprostol
- shoulder dystocia
- preterm labor
- hospital standards.
Fewer claims and more physicians
The declining number and percentage of paid claims in obstetrics and gynecology over 25 years may be even more impressive than the figures suggest, says Dr. Stanchfield.
“Gestalt tells me that through the years there are more practicing physicians rather than fewer,” so the denominator is increasing even as these claims are declining—making the decrease “even more powerful.”
The numbers haven’t improved to the same degree in other specialties, Dr. Stanchfield says. “If you look at global data, the decrease in paid claims might have been 10% to 15%. In ObGyn, if you compare the last 5-year block of data with the first 5-year block, the number of paid claims is almost cut in half.”
What brought about this improvement?
“There weren’t any groundbreaking medical or surgical technological advances during this period. It was just doing it better. And the main push to doing it better in this country, in my opinion, is risk management.”
Slicing the data
Now for the not-so-great news: In 2010 alone, more than $55 million was paid out in the ObGyn category for 10 patient conditions. Topping the list were “pregnancy” and “brain-damaged infant.” The $55 million figure represents the money paid for the top 10 most commonly cited conditions in cases closed during 2010 (TABLE 1).
TABLE 1
Claims categorized under the rather broad category of pregnancy usually were placed there because a more appropriate category was lacking, says Dr. Stanchfield. These claims typically involve “things that happen—usually to the baby—that result in a lawsuit other than brain damage per se.” For example, a claim that involved skull fracture without brain damage might fall into this zone, he says.
Problematic procedures
Slicing the data a different way, problems related to the 10 most commonly cited ObGyn procedures cost PIAA companies more than $120 million dollars in 2010—and that figure is only for the top 10.1 The top three procedures, in terms of number of claims closed in 2010, were operative procedures on the uterus, manually assisted delivery, and cesarean delivery (TABLE 2).
TABLE 2
Manually assisted delivery does not include vacuum extraction or forceps delivery, notes Dr. Stanchfield. “Manually assisted delivery is basically standing there like a quarterback and catching the baby.”
Top 10 “medical misadventures”
And another slice of data reveals the 10 most prevalent medical misadventures in the ObGyn specialty in 2010 (TABLE 3):
- improper performance of a procedure
- no medical misadventure (i.e., no misadventure was identifiable)
- errors in diagnosis
- failure to supervise or monitor a case
- delay in performance of a procedure
- failure to recognize a complication
- surgical foreign body left in a patient after a procedure
- necessary treatment or management was “not performed”
- failure to instruct or communicate with a patient
- medication errors.
The total indemnity paid for these so-called misadventures was more than $136 million.1
TABLE 3
Putting the dollars in perspective
PIAA also collects data on the number of claims reported, and indemnity dollars paid, for other specialties.
“Of the 28 specialty groups included in the database, ObGyn ranks second”—behind internal medicine—“in the number of claims closed between 1985 and 2010,” a PIAA report notes. The ObGyn specialty also ranks second—behind dentists—in the percentage (35%) of those claims that were paid (for dentists, the figure was 46%). Obstetrics and gynecology was also responsible for the single largest indemnity payment—$13,000,000.1
Medical liability: A national disaster?
According to figures from the PIAA Data Sharing Project, an ongoing claim study that includes 22 PIAA member companies, $19.7 billion in losses (total indemnity plus expenses) were reported during the period from 1985 through 2008. Those losses represented approximately 25% of the physicians who were practicing during that time.
“So if you multiply that $19.7 billion figure by four”—to extrapolate it to the full spectrum of physicians practicing between 1985 and 2008—“you’ve got almost $80 billion coming out of the pockets of the doctors in this country,” says Dr. Stanchfield. If you compare that $80 billion figure to the World Trade Center disaster, which involved approximately $42 billion in losses, the need for federal tort reform is highlighted, he says. In 24 years, the physicians “in this country have paid for almost two World Trade Center disasters. That’s an incredible dollar cost.”
From Dr. Stanchfield’s perspective as a risk manager, the best thing physicians can do to protect themselves is to practice medicine wisely.
“One of our speakers used to say, ‘Look, just practice good, middle-of-the-road medicine. Don’t get yourself out on the fringes where you’re doing something questionable. Just practice rock-solid, conservative, safe medicine.’”
We want to hear from you! Tell us what you think.
Good news on the medical liability front, Doctor!
Yes, that’s right, good news.
According to data from the Physician Insurers Association of America (PIAA), the number of claims that were paid in the ObGyn category between 2006 and 2011 was 44% lower than the number of claims paid between 1986 and 1991.
The percentage of claims that were paid also decreased over the same quarter century. During 1986–1990, 37.25% of all claims were paid in the ObGyn category, compared with 31.73% during 2006–2010.1
And when claims for both periods are calculated in 2010 dollars, the amount paid also declined—by more than $138 million!
These are three of the findings that reflect “significant improvement” in obstetrics and gynecology in medical liability, says John B. Stanchfield, MD, an endocrinologist who, for 25 years, was medical director of the Utah Medical Insurance Association (UMIA)—a member company of PIAA. PIAA is the insurance industry trade association.
PIAA member companies in the United States “include large national insurance companies, mid-size regional writers, single-state insurers, and specialty companies that serve specific health care–provider niche markets. Collectively, these companies provide insurance protection to more than 60% of America’s private practice physicians and write approximately 46%, or $5.2 billion, of the total industry premium.”2
The improvement in ObGyn comes as no surprise to Dr. Stanchfield because the specialty was “the first group that got ‘risk-managed’ almost universally across the country,” he says. “In our little company out here in Utah, in 1985, we were told that if we didn’t do something [about lawsuits in obstetrics and gynecology], we weren’t going to be able to insure that class anymore because we wouldn’t be able to collect enough money. That’s what the actuaries told us, but it wasn’t unique to us—it was a nationwide problem.”
Why was the ObGyn specialty, in particular, in need of aggressive risk management? What made ObGyn claims unique?
“It’s infant injury,” says Dr. Stanchfield. “It’s injury to the baby. Those claims, you start talking at a million dollars.”
Another reason may be that some claims in this specialty category involve doctors other than ObGyns who provide obstetric care—for example, family practice physicians.
A risk manager’s perspective
After receiving the warning about ObGyn claims, UMIA got busy. First, it formed a committee comprising perinatologists, ObGyns, family practice physicians, claims specialists, and attorneys. “We analyzed all claims that were paid, looking for common denominators,” says Dr. Stanchfield. Improvement was clearly needed in about 10 areas, so “we basically created a risk-management program and then mandated it.” In the process, the organization published a booklet entitled Insurance Recommendations for Obstetrical Practice, of which Dr. Stanchfield was the editor.3
The booklet offers guidance on 10 potential “problem” areas:
- antepartum testing
- hypertension and pregnancy
- operative vaginal delivery
- breech delivery
- oxytocin administration
- vaginal birth after cesarean
- use of misoprostol
- shoulder dystocia
- preterm labor
- hospital standards.
Fewer claims and more physicians
The declining number and percentage of paid claims in obstetrics and gynecology over 25 years may be even more impressive than the figures suggest, says Dr. Stanchfield.
“Gestalt tells me that through the years there are more practicing physicians rather than fewer,” so the denominator is increasing even as these claims are declining—making the decrease “even more powerful.”
The numbers haven’t improved to the same degree in other specialties, Dr. Stanchfield says. “If you look at global data, the decrease in paid claims might have been 10% to 15%. In ObGyn, if you compare the last 5-year block of data with the first 5-year block, the number of paid claims is almost cut in half.”
What brought about this improvement?
“There weren’t any groundbreaking medical or surgical technological advances during this period. It was just doing it better. And the main push to doing it better in this country, in my opinion, is risk management.”
Slicing the data
Now for the not-so-great news: In 2010 alone, more than $55 million was paid out in the ObGyn category for 10 patient conditions. Topping the list were “pregnancy” and “brain-damaged infant.” The $55 million figure represents the money paid for the top 10 most commonly cited conditions in cases closed during 2010 (TABLE 1).
TABLE 1
Claims categorized under the rather broad category of pregnancy usually were placed there because a more appropriate category was lacking, says Dr. Stanchfield. These claims typically involve “things that happen—usually to the baby—that result in a lawsuit other than brain damage per se.” For example, a claim that involved skull fracture without brain damage might fall into this zone, he says.
Problematic procedures
Slicing the data a different way, problems related to the 10 most commonly cited ObGyn procedures cost PIAA companies more than $120 million dollars in 2010—and that figure is only for the top 10.1 The top three procedures, in terms of number of claims closed in 2010, were operative procedures on the uterus, manually assisted delivery, and cesarean delivery (TABLE 2).
TABLE 2
Manually assisted delivery does not include vacuum extraction or forceps delivery, notes Dr. Stanchfield. “Manually assisted delivery is basically standing there like a quarterback and catching the baby.”
Top 10 “medical misadventures”
And another slice of data reveals the 10 most prevalent medical misadventures in the ObGyn specialty in 2010 (TABLE 3):
- improper performance of a procedure
- no medical misadventure (i.e., no misadventure was identifiable)
- errors in diagnosis
- failure to supervise or monitor a case
- delay in performance of a procedure
- failure to recognize a complication
- surgical foreign body left in a patient after a procedure
- necessary treatment or management was “not performed”
- failure to instruct or communicate with a patient
- medication errors.
The total indemnity paid for these so-called misadventures was more than $136 million.1
TABLE 3
Putting the dollars in perspective
PIAA also collects data on the number of claims reported, and indemnity dollars paid, for other specialties.
“Of the 28 specialty groups included in the database, ObGyn ranks second”—behind internal medicine—“in the number of claims closed between 1985 and 2010,” a PIAA report notes. The ObGyn specialty also ranks second—behind dentists—in the percentage (35%) of those claims that were paid (for dentists, the figure was 46%). Obstetrics and gynecology was also responsible for the single largest indemnity payment—$13,000,000.1
Medical liability: A national disaster?
According to figures from the PIAA Data Sharing Project, an ongoing claim study that includes 22 PIAA member companies, $19.7 billion in losses (total indemnity plus expenses) were reported during the period from 1985 through 2008. Those losses represented approximately 25% of the physicians who were practicing during that time.
“So if you multiply that $19.7 billion figure by four”—to extrapolate it to the full spectrum of physicians practicing between 1985 and 2008—“you’ve got almost $80 billion coming out of the pockets of the doctors in this country,” says Dr. Stanchfield. If you compare that $80 billion figure to the World Trade Center disaster, which involved approximately $42 billion in losses, the need for federal tort reform is highlighted, he says. In 24 years, the physicians “in this country have paid for almost two World Trade Center disasters. That’s an incredible dollar cost.”
From Dr. Stanchfield’s perspective as a risk manager, the best thing physicians can do to protect themselves is to practice medicine wisely.
“One of our speakers used to say, ‘Look, just practice good, middle-of-the-road medicine. Don’t get yourself out on the fringes where you’re doing something questionable. Just practice rock-solid, conservative, safe medicine.’”
We want to hear from you! Tell us what you think.
1. Physician Insurers Association of America. 2011 Risk Management Review. Rockville, Md: PIAA; 2011.
2. Physician Insurers Association of America. PIAA Backgrounder. Rockville, Md: PIAA; 2011.
3. Stanchfied JB, ed. Insurance Recommendations for Obstetrical Practice. Revised ed. Salt Lake City, Utah: Utah Medical Insurance Association; 2009.
1. Physician Insurers Association of America. 2011 Risk Management Review. Rockville, Md: PIAA; 2011.
2. Physician Insurers Association of America. PIAA Backgrounder. Rockville, Md: PIAA; 2011.
3. Stanchfied JB, ed. Insurance Recommendations for Obstetrical Practice. Revised ed. Salt Lake City, Utah: Utah Medical Insurance Association; 2009.
Head entrapment in premature baby ... more

DURING BREECH VAGINAL DELIVERY of a premature infant, the child’s head became entrapped. A maternal-fetal medicine specialist was called in. Delivery took 22 minutes. The child has cerebral palsy, with severe developmental delays, and requires a gastrostomy tube and tracheotomy.
PATIENT’S CLAIM Lack of oxygen for 22 minutes before delivery caused brain damage. Inappropriate maneuvers used by the physicians and nurses to relieve head entrapment also contributed to the injury. An emergency cesarean delivery should have been performed when vaginal delivery was delayed.
DEFENDANTS’ DEFENSE The appropriate maneuvers were performed to release the entrapped head. The child’s problems were due to her prematurity and fetal inflammatory response syndrome.
VERDICT In Illinois, a summary judgment was granted for the maternal-fetal medicine physician. A directed verdict was given for one nurse. A jury returned a defense verdict for the hospital, a labor and delivery nurse, and one of the ObGyns. The jury deadlocked on the claims against a second ObGyn.
Stenotic os thwarts two biopsies
AT HER ANNUAL VISIT in June 2006, a 48-year-old woman reported heavy bleeding. Her ObGyn asked the woman to return for re-examination. Twelve days later, ultrasonography revealed an enlarged uterus. The ObGyn attempted to perform a biopsy, but failed because of a stenotic os.
In September 2006, after a course of hormones, the ObGyn again tried to obtain a biopsy, but once more encountered the stenotic os. A hysterectomy was discussed, but the patient declined. In October 2007, the woman agreed to a hysterectomy. During surgery, the ObGyn identified cancer, and a gynecologic oncologist was called in. The woman was found to have stage-IV endometrial cancer. She underwent chemotherapy; at trial, the cancer was in remission.
PATIENT’S CLAIM Cancer should have been diagnosed earlier.
PHYSICIAN’S DEFENSE There was no negligence; the patient had rejected hysterectomy in September 2006. In addition, the cancer initially was not endometrial, but had started in an area of adenomyosis deep in the uterine wall.
VERDICT A Kentucky defense verdict was returned.
Brachial plexus injury after shoulder dystocia
AN OBESE WOMAN had gestational diabetes; the fetus was estimated to be macrosomic. When shoulder dystocia was encountered at delivery, the ObGyn delivered the child using several maneuvers. The child was born with a brachial plexus injury.
PATIENT’S CLAIM The physician was negligent in not scheduling a cesarean delivery because the fetus was large. When dystocia occurred, the ObGyn continued to apply traction to the infant’s head and neck, causing injury.
PHYSICIAN’S DEFENSE The proper maneuvers were undertaken to deliver the child as quickly and safely as possible.
VERDICT A $72,500 Texas settlement was reached.
Was informed consent neglected?
A 35-YEAR-OLD WOMAN underwent diagnostic laparoscopy in March 2005 because of severe pelvic pain. During surgery, the ObGyn observed adhesions and scarring that obstructed visualization of the pelvic area. He converted to an open procedure and discovered advanced-stage endometriosis. Because of his concern that endometriosis might perforate the patient’s colon, he performed supracervical hysterectomy.
PATIENT’S CLAIM The ObGyn was negligent in converting to an open procedure and performing the hysterectomy without obtaining informed consent. She suffered post-traumatic stress disorder because of the surgery.
PHYSICIAN’S DEFENSE The only option for treating the conditions he found was a hysterectomy. The patient had a history of anxiety prior to surgery.
VERDICT A Tennessee defense verdict was returned.
Nipples “too high” after breast reduction surgery
A 25-YEAR-OLD WOMAN underwent breast reduction surgery.
PATIENT’S CLAIM The plastic surgeon placed her nipples too high on her chest, making it impossible to find a bra that covered them, and making it difficult to find clothing to wear.
PHYSICIAN’S DEFENSE Unforeseeable postoperative changes caused the woman’s breasts to drop, giving the appearance of the nipples being too high. The nipples were properly located during surgery.
VERDICT A $170,000 Georgia verdict was returned.
Placental abruption; stillbirth follows
A 24-YEAR-OLD WOMAN AWOKE one day during the 39th week of pregnancy with abrupt onset of vaginal bleeding. She arrived at the emergency department (ED) at 12:30 am, and was transferred to labor and delivery at 1:12 am. A sonogram at 1:24 am revealed a fetal heart rate of 2 beats in 40 seconds, and a fetal scalp electrode did not register a heartbeat.
The mother was immediately prepped for emergency cesarean delivery, but a second sonogram performed in the OR showed no fetal heartbeat. Cesarean delivery was cancelled and labor was induced. The stillborn fetus was delivered vaginally several hours later, when a >60% placental abruption was found.
PATIENT’S CLAIM She was not treated in a timely manner in the ED or on labor and delivery. An emergency cesarean delivery should have been performed earlier.
DEFENDANTS’ DEFENSE All treatment had been timely. Placental abruption was the cause of fetal demise; the child was not viable shortly after the mother’s arrival. The time allowed for transfer from the ED to labor and delivery, evaluation, and emergency cesarean preparation was appropriate. The child could not possibly have been born alive.
VERDICT An Illinois defense verdict was returned.
Child’s enlarged heart unnoticed; lethal result
A WOMAN UNDERWENT four prenatal sonograms because she was found to have a single umbilical artery. Delivery was uneventful.
At 26 days, the infant became ill and was vomiting. The pediatrician sent the parents and baby to the emergency department, where Dr. A undertook his care. A radiologist read a three-view plain radiograph remotely and reported nothing abnormal. The infant was discharged.
When the parents returned the child to the ED the next morning, he was in cardiac failure related to an enlarged heart. He died before he could be transported to another hospital.
PATIENT’S CLAIM The ObGyn failed to diagnose the child’s defective heart in utero. Dr. A relied on the radiologist’s report; he should have personally viewed the radiograph, as it clearly showed the defective and enlarged heart. The defect could have been surgically repaired. The hospital nurses and radiologist were also negligent.
DEFENDANTS’ DEFENSE The hospital and radiologist settled for undisclosed amounts, and the trial proceeded against the ObGyn and Dr. A.
The ObGyn maintained that none of the prenatal sonograms was troubling; she had complied with the standard of care. Dr. A claimed that it was reasonable to rely on the radiologist’s report. Both physicians claimed they could not have done anything to avoid the child’s death; the hospital, radiologist, and pediatrician were at fault.
VERDICT A Kentucky defense verdict was returned.
Death from occult uterine Ca
A WOMAN SAW HER GYNECOLOGIST in January 1999 with postmenopausal bleeding and severe pelvic pain, but the physician could not determine a source of the problems.
Several months later, another gynecologist found that she had uterine sarcoma. She died of metastatic leiomyosarcoma at age 52 in July 2000.
ESTATE’S CLAIM The first gynecologist was negligent in failing to diagnose and treat the cancer, failing to consult or refer her to a specialist, and in prescribing hormones, which are contraindicated and caused the cancer to grow more rapidly.
PHYSICIAN’S DEFENSE The cancer had metastasized before the woman’s first visit, but was too small to be detected at that time. The decedent was already taking hormones when he saw her in January 1999; he only changed the type and brand. Hormones would not cause this type of cancer to grow more rapidly.
VERDICT A Texas defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
DURING BREECH VAGINAL DELIVERY of a premature infant, the child’s head became entrapped. A maternal-fetal medicine specialist was called in. Delivery took 22 minutes. The child has cerebral palsy, with severe developmental delays, and requires a gastrostomy tube and tracheotomy.
PATIENT’S CLAIM Lack of oxygen for 22 minutes before delivery caused brain damage. Inappropriate maneuvers used by the physicians and nurses to relieve head entrapment also contributed to the injury. An emergency cesarean delivery should have been performed when vaginal delivery was delayed.
DEFENDANTS’ DEFENSE The appropriate maneuvers were performed to release the entrapped head. The child’s problems were due to her prematurity and fetal inflammatory response syndrome.
VERDICT In Illinois, a summary judgment was granted for the maternal-fetal medicine physician. A directed verdict was given for one nurse. A jury returned a defense verdict for the hospital, a labor and delivery nurse, and one of the ObGyns. The jury deadlocked on the claims against a second ObGyn.
Stenotic os thwarts two biopsies
AT HER ANNUAL VISIT in June 2006, a 48-year-old woman reported heavy bleeding. Her ObGyn asked the woman to return for re-examination. Twelve days later, ultrasonography revealed an enlarged uterus. The ObGyn attempted to perform a biopsy, but failed because of a stenotic os.
In September 2006, after a course of hormones, the ObGyn again tried to obtain a biopsy, but once more encountered the stenotic os. A hysterectomy was discussed, but the patient declined. In October 2007, the woman agreed to a hysterectomy. During surgery, the ObGyn identified cancer, and a gynecologic oncologist was called in. The woman was found to have stage-IV endometrial cancer. She underwent chemotherapy; at trial, the cancer was in remission.
PATIENT’S CLAIM Cancer should have been diagnosed earlier.
PHYSICIAN’S DEFENSE There was no negligence; the patient had rejected hysterectomy in September 2006. In addition, the cancer initially was not endometrial, but had started in an area of adenomyosis deep in the uterine wall.
VERDICT A Kentucky defense verdict was returned.
Brachial plexus injury after shoulder dystocia
AN OBESE WOMAN had gestational diabetes; the fetus was estimated to be macrosomic. When shoulder dystocia was encountered at delivery, the ObGyn delivered the child using several maneuvers. The child was born with a brachial plexus injury.
PATIENT’S CLAIM The physician was negligent in not scheduling a cesarean delivery because the fetus was large. When dystocia occurred, the ObGyn continued to apply traction to the infant’s head and neck, causing injury.
PHYSICIAN’S DEFENSE The proper maneuvers were undertaken to deliver the child as quickly and safely as possible.
VERDICT A $72,500 Texas settlement was reached.
Was informed consent neglected?
A 35-YEAR-OLD WOMAN underwent diagnostic laparoscopy in March 2005 because of severe pelvic pain. During surgery, the ObGyn observed adhesions and scarring that obstructed visualization of the pelvic area. He converted to an open procedure and discovered advanced-stage endometriosis. Because of his concern that endometriosis might perforate the patient’s colon, he performed supracervical hysterectomy.
PATIENT’S CLAIM The ObGyn was negligent in converting to an open procedure and performing the hysterectomy without obtaining informed consent. She suffered post-traumatic stress disorder because of the surgery.
PHYSICIAN’S DEFENSE The only option for treating the conditions he found was a hysterectomy. The patient had a history of anxiety prior to surgery.
VERDICT A Tennessee defense verdict was returned.
Nipples “too high” after breast reduction surgery
A 25-YEAR-OLD WOMAN underwent breast reduction surgery.
PATIENT’S CLAIM The plastic surgeon placed her nipples too high on her chest, making it impossible to find a bra that covered them, and making it difficult to find clothing to wear.
PHYSICIAN’S DEFENSE Unforeseeable postoperative changes caused the woman’s breasts to drop, giving the appearance of the nipples being too high. The nipples were properly located during surgery.
VERDICT A $170,000 Georgia verdict was returned.
Placental abruption; stillbirth follows
A 24-YEAR-OLD WOMAN AWOKE one day during the 39th week of pregnancy with abrupt onset of vaginal bleeding. She arrived at the emergency department (ED) at 12:30 am, and was transferred to labor and delivery at 1:12 am. A sonogram at 1:24 am revealed a fetal heart rate of 2 beats in 40 seconds, and a fetal scalp electrode did not register a heartbeat.
The mother was immediately prepped for emergency cesarean delivery, but a second sonogram performed in the OR showed no fetal heartbeat. Cesarean delivery was cancelled and labor was induced. The stillborn fetus was delivered vaginally several hours later, when a >60% placental abruption was found.
PATIENT’S CLAIM She was not treated in a timely manner in the ED or on labor and delivery. An emergency cesarean delivery should have been performed earlier.
DEFENDANTS’ DEFENSE All treatment had been timely. Placental abruption was the cause of fetal demise; the child was not viable shortly after the mother’s arrival. The time allowed for transfer from the ED to labor and delivery, evaluation, and emergency cesarean preparation was appropriate. The child could not possibly have been born alive.
VERDICT An Illinois defense verdict was returned.
Child’s enlarged heart unnoticed; lethal result
A WOMAN UNDERWENT four prenatal sonograms because she was found to have a single umbilical artery. Delivery was uneventful.
At 26 days, the infant became ill and was vomiting. The pediatrician sent the parents and baby to the emergency department, where Dr. A undertook his care. A radiologist read a three-view plain radiograph remotely and reported nothing abnormal. The infant was discharged.
When the parents returned the child to the ED the next morning, he was in cardiac failure related to an enlarged heart. He died before he could be transported to another hospital.
PATIENT’S CLAIM The ObGyn failed to diagnose the child’s defective heart in utero. Dr. A relied on the radiologist’s report; he should have personally viewed the radiograph, as it clearly showed the defective and enlarged heart. The defect could have been surgically repaired. The hospital nurses and radiologist were also negligent.
DEFENDANTS’ DEFENSE The hospital and radiologist settled for undisclosed amounts, and the trial proceeded against the ObGyn and Dr. A.
The ObGyn maintained that none of the prenatal sonograms was troubling; she had complied with the standard of care. Dr. A claimed that it was reasonable to rely on the radiologist’s report. Both physicians claimed they could not have done anything to avoid the child’s death; the hospital, radiologist, and pediatrician were at fault.
VERDICT A Kentucky defense verdict was returned.
Death from occult uterine Ca
A WOMAN SAW HER GYNECOLOGIST in January 1999 with postmenopausal bleeding and severe pelvic pain, but the physician could not determine a source of the problems.
Several months later, another gynecologist found that she had uterine sarcoma. She died of metastatic leiomyosarcoma at age 52 in July 2000.
ESTATE’S CLAIM The first gynecologist was negligent in failing to diagnose and treat the cancer, failing to consult or refer her to a specialist, and in prescribing hormones, which are contraindicated and caused the cancer to grow more rapidly.
PHYSICIAN’S DEFENSE The cancer had metastasized before the woman’s first visit, but was too small to be detected at that time. The decedent was already taking hormones when he saw her in January 1999; he only changed the type and brand. Hormones would not cause this type of cancer to grow more rapidly.
VERDICT A Texas defense verdict was returned.
DURING BREECH VAGINAL DELIVERY of a premature infant, the child’s head became entrapped. A maternal-fetal medicine specialist was called in. Delivery took 22 minutes. The child has cerebral palsy, with severe developmental delays, and requires a gastrostomy tube and tracheotomy.
PATIENT’S CLAIM Lack of oxygen for 22 minutes before delivery caused brain damage. Inappropriate maneuvers used by the physicians and nurses to relieve head entrapment also contributed to the injury. An emergency cesarean delivery should have been performed when vaginal delivery was delayed.
DEFENDANTS’ DEFENSE The appropriate maneuvers were performed to release the entrapped head. The child’s problems were due to her prematurity and fetal inflammatory response syndrome.
VERDICT In Illinois, a summary judgment was granted for the maternal-fetal medicine physician. A directed verdict was given for one nurse. A jury returned a defense verdict for the hospital, a labor and delivery nurse, and one of the ObGyns. The jury deadlocked on the claims against a second ObGyn.
Stenotic os thwarts two biopsies
AT HER ANNUAL VISIT in June 2006, a 48-year-old woman reported heavy bleeding. Her ObGyn asked the woman to return for re-examination. Twelve days later, ultrasonography revealed an enlarged uterus. The ObGyn attempted to perform a biopsy, but failed because of a stenotic os.
In September 2006, after a course of hormones, the ObGyn again tried to obtain a biopsy, but once more encountered the stenotic os. A hysterectomy was discussed, but the patient declined. In October 2007, the woman agreed to a hysterectomy. During surgery, the ObGyn identified cancer, and a gynecologic oncologist was called in. The woman was found to have stage-IV endometrial cancer. She underwent chemotherapy; at trial, the cancer was in remission.
PATIENT’S CLAIM Cancer should have been diagnosed earlier.
PHYSICIAN’S DEFENSE There was no negligence; the patient had rejected hysterectomy in September 2006. In addition, the cancer initially was not endometrial, but had started in an area of adenomyosis deep in the uterine wall.
VERDICT A Kentucky defense verdict was returned.
Brachial plexus injury after shoulder dystocia
AN OBESE WOMAN had gestational diabetes; the fetus was estimated to be macrosomic. When shoulder dystocia was encountered at delivery, the ObGyn delivered the child using several maneuvers. The child was born with a brachial plexus injury.
PATIENT’S CLAIM The physician was negligent in not scheduling a cesarean delivery because the fetus was large. When dystocia occurred, the ObGyn continued to apply traction to the infant’s head and neck, causing injury.
PHYSICIAN’S DEFENSE The proper maneuvers were undertaken to deliver the child as quickly and safely as possible.
VERDICT A $72,500 Texas settlement was reached.
Was informed consent neglected?
A 35-YEAR-OLD WOMAN underwent diagnostic laparoscopy in March 2005 because of severe pelvic pain. During surgery, the ObGyn observed adhesions and scarring that obstructed visualization of the pelvic area. He converted to an open procedure and discovered advanced-stage endometriosis. Because of his concern that endometriosis might perforate the patient’s colon, he performed supracervical hysterectomy.
PATIENT’S CLAIM The ObGyn was negligent in converting to an open procedure and performing the hysterectomy without obtaining informed consent. She suffered post-traumatic stress disorder because of the surgery.
PHYSICIAN’S DEFENSE The only option for treating the conditions he found was a hysterectomy. The patient had a history of anxiety prior to surgery.
VERDICT A Tennessee defense verdict was returned.
Nipples “too high” after breast reduction surgery
A 25-YEAR-OLD WOMAN underwent breast reduction surgery.
PATIENT’S CLAIM The plastic surgeon placed her nipples too high on her chest, making it impossible to find a bra that covered them, and making it difficult to find clothing to wear.
PHYSICIAN’S DEFENSE Unforeseeable postoperative changes caused the woman’s breasts to drop, giving the appearance of the nipples being too high. The nipples were properly located during surgery.
VERDICT A $170,000 Georgia verdict was returned.
Placental abruption; stillbirth follows
A 24-YEAR-OLD WOMAN AWOKE one day during the 39th week of pregnancy with abrupt onset of vaginal bleeding. She arrived at the emergency department (ED) at 12:30 am, and was transferred to labor and delivery at 1:12 am. A sonogram at 1:24 am revealed a fetal heart rate of 2 beats in 40 seconds, and a fetal scalp electrode did not register a heartbeat.
The mother was immediately prepped for emergency cesarean delivery, but a second sonogram performed in the OR showed no fetal heartbeat. Cesarean delivery was cancelled and labor was induced. The stillborn fetus was delivered vaginally several hours later, when a >60% placental abruption was found.
PATIENT’S CLAIM She was not treated in a timely manner in the ED or on labor and delivery. An emergency cesarean delivery should have been performed earlier.
DEFENDANTS’ DEFENSE All treatment had been timely. Placental abruption was the cause of fetal demise; the child was not viable shortly after the mother’s arrival. The time allowed for transfer from the ED to labor and delivery, evaluation, and emergency cesarean preparation was appropriate. The child could not possibly have been born alive.
VERDICT An Illinois defense verdict was returned.
Child’s enlarged heart unnoticed; lethal result
A WOMAN UNDERWENT four prenatal sonograms because she was found to have a single umbilical artery. Delivery was uneventful.
At 26 days, the infant became ill and was vomiting. The pediatrician sent the parents and baby to the emergency department, where Dr. A undertook his care. A radiologist read a three-view plain radiograph remotely and reported nothing abnormal. The infant was discharged.
When the parents returned the child to the ED the next morning, he was in cardiac failure related to an enlarged heart. He died before he could be transported to another hospital.
PATIENT’S CLAIM The ObGyn failed to diagnose the child’s defective heart in utero. Dr. A relied on the radiologist’s report; he should have personally viewed the radiograph, as it clearly showed the defective and enlarged heart. The defect could have been surgically repaired. The hospital nurses and radiologist were also negligent.
DEFENDANTS’ DEFENSE The hospital and radiologist settled for undisclosed amounts, and the trial proceeded against the ObGyn and Dr. A.
The ObGyn maintained that none of the prenatal sonograms was troubling; she had complied with the standard of care. Dr. A claimed that it was reasonable to rely on the radiologist’s report. Both physicians claimed they could not have done anything to avoid the child’s death; the hospital, radiologist, and pediatrician were at fault.
VERDICT A Kentucky defense verdict was returned.
Death from occult uterine Ca
A WOMAN SAW HER GYNECOLOGIST in January 1999 with postmenopausal bleeding and severe pelvic pain, but the physician could not determine a source of the problems.
Several months later, another gynecologist found that she had uterine sarcoma. She died of metastatic leiomyosarcoma at age 52 in July 2000.
ESTATE’S CLAIM The first gynecologist was negligent in failing to diagnose and treat the cancer, failing to consult or refer her to a specialist, and in prescribing hormones, which are contraindicated and caused the cancer to grow more rapidly.
PHYSICIAN’S DEFENSE The cancer had metastasized before the woman’s first visit, but was too small to be detected at that time. The decedent was already taking hormones when he saw her in January 1999; he only changed the type and brand. Hormones would not cause this type of cancer to grow more rapidly.
VERDICT A Texas defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
Survey Insights: Peeking under the Hood of Academic HM
The 2011 State of Hospital Medicine report offers some tantalizing insights into the operation of academic hospital medicine practices and how they compare with their nonacademic peers. Some results are not surprising, such as the fact that academic hospital medicine groups tend to be larger than nonacademic groups, and that compensation and clinical-FTE-adjusted productivity both tend to be lower for academic hospitalists. Interestingly, turnover rates were about the same in academic and nonacademic practices.
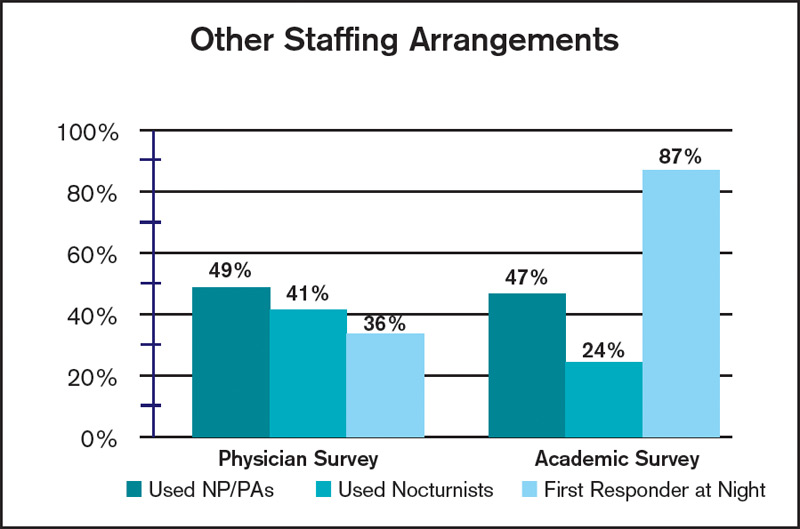
Among the more unexpected findings, however, is that academic HM practices tend to employ a higher proportion of women (44%) than nonacademic practices (35%). In addition, academic practices employed a wider range of staffing models, with only 43% of practices using shift-based staffing, compared with 78% of nonacademic respondents. Similarly, only 47% of academic groups provided on-site coverage at night, compared with 81% of nonacademic groups.
Additional differences between the way academic and nonacademic HM groups staff their programs are shown in the table, “Other Staffing Arrangements.” While the use of nurse practitioners and physician assistants (PA) was similar for academic and nonacademic practices, academic groups were much less likely to utilize nocturnists, and far more likely to have a nonphysician first responder at night (resident, nonphysician provider/PA, or other) than nonacademic groups.
It will be interesting to follow these trends over time. Because of new resident work-hour limits that went into effect in July, SHM Practice Analysis Committee (PAC) member Andrew White, MD, expects that there will be very few places that continue to use residents to cross-cover at night. “I suspect most academic centers have or will hire nocturnists,” he says, “but we’ll see.”
On the other hand, PAC member Scarlett Blue, RN, believes that continued growth in HM, coupled with a competitive job market, could result in increased use of nonphysician first responders at night—and in general. “Hospital medicine group leaders who are looking for alternative ways to meet the supply-demand conundrum may find a blended physician-NP/PA team to be one such answer,” she says.
Finally, the clinical services provided by academic HM groups vary from their nonacademic counterparts in some other important ways. Only 25% of academic practices provide care for ICU patients, compared with 78% of nonacademic practices, while 75% of academic groups perform procedures, compared with only 52% of nonacademic groups. And while the overwhelming majority of both academic and nonacademic practices provide surgical comanagement, academic practices were more than twice as likely to provide comanagement for medical subspecialty patients (45%, compared with 20% for nonacademic practices).
PAC member Troy Ahlstrom, MD, explains, tongue-in-cheek, that “academic hospitalists don’t do procedures because they have oodles of residents, fellows, and interventional radiologists to do them instead, and academics do more medical comanagement because the subspecialist who only does Waldenstrom’s macroglobulinemia probably doesn’t do diabetes.”
Whatever the reason, there are meaningful differences between academic and nonacademic HM practices that bear watching over time. You can help us identify and track these differences by ensuring that your group participates in SHM’s annual State of Hospital Medicine survey, launching this month.
The 2011 State of Hospital Medicine report offers some tantalizing insights into the operation of academic hospital medicine practices and how they compare with their nonacademic peers. Some results are not surprising, such as the fact that academic hospital medicine groups tend to be larger than nonacademic groups, and that compensation and clinical-FTE-adjusted productivity both tend to be lower for academic hospitalists. Interestingly, turnover rates were about the same in academic and nonacademic practices.
Among the more unexpected findings, however, is that academic HM practices tend to employ a higher proportion of women (44%) than nonacademic practices (35%). In addition, academic practices employed a wider range of staffing models, with only 43% of practices using shift-based staffing, compared with 78% of nonacademic respondents. Similarly, only 47% of academic groups provided on-site coverage at night, compared with 81% of nonacademic groups.
Additional differences between the way academic and nonacademic HM groups staff their programs are shown in the table, “Other Staffing Arrangements.” While the use of nurse practitioners and physician assistants (PA) was similar for academic and nonacademic practices, academic groups were much less likely to utilize nocturnists, and far more likely to have a nonphysician first responder at night (resident, nonphysician provider/PA, or other) than nonacademic groups.
It will be interesting to follow these trends over time. Because of new resident work-hour limits that went into effect in July, SHM Practice Analysis Committee (PAC) member Andrew White, MD, expects that there will be very few places that continue to use residents to cross-cover at night. “I suspect most academic centers have or will hire nocturnists,” he says, “but we’ll see.”
On the other hand, PAC member Scarlett Blue, RN, believes that continued growth in HM, coupled with a competitive job market, could result in increased use of nonphysician first responders at night—and in general. “Hospital medicine group leaders who are looking for alternative ways to meet the supply-demand conundrum may find a blended physician-NP/PA team to be one such answer,” she says.
Finally, the clinical services provided by academic HM groups vary from their nonacademic counterparts in some other important ways. Only 25% of academic practices provide care for ICU patients, compared with 78% of nonacademic practices, while 75% of academic groups perform procedures, compared with only 52% of nonacademic groups. And while the overwhelming majority of both academic and nonacademic practices provide surgical comanagement, academic practices were more than twice as likely to provide comanagement for medical subspecialty patients (45%, compared with 20% for nonacademic practices).
PAC member Troy Ahlstrom, MD, explains, tongue-in-cheek, that “academic hospitalists don’t do procedures because they have oodles of residents, fellows, and interventional radiologists to do them instead, and academics do more medical comanagement because the subspecialist who only does Waldenstrom’s macroglobulinemia probably doesn’t do diabetes.”
Whatever the reason, there are meaningful differences between academic and nonacademic HM practices that bear watching over time. You can help us identify and track these differences by ensuring that your group participates in SHM’s annual State of Hospital Medicine survey, launching this month.
The 2011 State of Hospital Medicine report offers some tantalizing insights into the operation of academic hospital medicine practices and how they compare with their nonacademic peers. Some results are not surprising, such as the fact that academic hospital medicine groups tend to be larger than nonacademic groups, and that compensation and clinical-FTE-adjusted productivity both tend to be lower for academic hospitalists. Interestingly, turnover rates were about the same in academic and nonacademic practices.
Among the more unexpected findings, however, is that academic HM practices tend to employ a higher proportion of women (44%) than nonacademic practices (35%). In addition, academic practices employed a wider range of staffing models, with only 43% of practices using shift-based staffing, compared with 78% of nonacademic respondents. Similarly, only 47% of academic groups provided on-site coverage at night, compared with 81% of nonacademic groups.
Additional differences between the way academic and nonacademic HM groups staff their programs are shown in the table, “Other Staffing Arrangements.” While the use of nurse practitioners and physician assistants (PA) was similar for academic and nonacademic practices, academic groups were much less likely to utilize nocturnists, and far more likely to have a nonphysician first responder at night (resident, nonphysician provider/PA, or other) than nonacademic groups.
It will be interesting to follow these trends over time. Because of new resident work-hour limits that went into effect in July, SHM Practice Analysis Committee (PAC) member Andrew White, MD, expects that there will be very few places that continue to use residents to cross-cover at night. “I suspect most academic centers have or will hire nocturnists,” he says, “but we’ll see.”
On the other hand, PAC member Scarlett Blue, RN, believes that continued growth in HM, coupled with a competitive job market, could result in increased use of nonphysician first responders at night—and in general. “Hospital medicine group leaders who are looking for alternative ways to meet the supply-demand conundrum may find a blended physician-NP/PA team to be one such answer,” she says.
Finally, the clinical services provided by academic HM groups vary from their nonacademic counterparts in some other important ways. Only 25% of academic practices provide care for ICU patients, compared with 78% of nonacademic practices, while 75% of academic groups perform procedures, compared with only 52% of nonacademic groups. And while the overwhelming majority of both academic and nonacademic practices provide surgical comanagement, academic practices were more than twice as likely to provide comanagement for medical subspecialty patients (45%, compared with 20% for nonacademic practices).
PAC member Troy Ahlstrom, MD, explains, tongue-in-cheek, that “academic hospitalists don’t do procedures because they have oodles of residents, fellows, and interventional radiologists to do them instead, and academics do more medical comanagement because the subspecialist who only does Waldenstrom’s macroglobulinemia probably doesn’t do diabetes.”
Whatever the reason, there are meaningful differences between academic and nonacademic HM practices that bear watching over time. You can help us identify and track these differences by ensuring that your group participates in SHM’s annual State of Hospital Medicine survey, launching this month.
HM’s Role in Helping Hospitals Profit
A new report shows that 1 in 5 community hospitals operates in the red, but the chief strategy officer of the firm that conducted the survey thinks hospitals can help change that.
The second annual survey from healthcare information technology (HIT) provider Anthelio and leadership group Community Hospital 100 found that 22% of community hospitals operate with margins below 2%; another 38% operate below 1%. Rick Kneipper, Anthelio’s cofounder and chief strategy officer, says that hospitalists can be at the forefront “of the creative changes needed” to reduce costs and improve profitability.
“Hospital medicine groups and hospitals could free up significant funds to devote to improved patient-care services if they focus on their core competency of patient care and farm out their non-core, back-office services to experts who can use leverage to provide more efficient services at significantly reduced costs,” Kneipper wrote in an email to The Hospitalist. “Financial pressures have historically forced most industries to stop trying to be vertically integrated [trying to be ‘all things to all people’] and instead to focus on their core competencies—it’s time for healthcare to do the same.”
—Rick Kneipper, cofounder, chief strategy officer, Anthelio
HM’s foothold at the intersection of clinical care and safety and QI positions the specialty to “respond to the new challenges of readmission penalties, evidenced-based medicine requirements, EMR implementation, and operation challenges,” Kneipper wrote.
For the full survey, please visit www.antheliohealth.com and search “survey.”
A new report shows that 1 in 5 community hospitals operates in the red, but the chief strategy officer of the firm that conducted the survey thinks hospitals can help change that.
The second annual survey from healthcare information technology (HIT) provider Anthelio and leadership group Community Hospital 100 found that 22% of community hospitals operate with margins below 2%; another 38% operate below 1%. Rick Kneipper, Anthelio’s cofounder and chief strategy officer, says that hospitalists can be at the forefront “of the creative changes needed” to reduce costs and improve profitability.
“Hospital medicine groups and hospitals could free up significant funds to devote to improved patient-care services if they focus on their core competency of patient care and farm out their non-core, back-office services to experts who can use leverage to provide more efficient services at significantly reduced costs,” Kneipper wrote in an email to The Hospitalist. “Financial pressures have historically forced most industries to stop trying to be vertically integrated [trying to be ‘all things to all people’] and instead to focus on their core competencies—it’s time for healthcare to do the same.”
—Rick Kneipper, cofounder, chief strategy officer, Anthelio
HM’s foothold at the intersection of clinical care and safety and QI positions the specialty to “respond to the new challenges of readmission penalties, evidenced-based medicine requirements, EMR implementation, and operation challenges,” Kneipper wrote.
For the full survey, please visit www.antheliohealth.com and search “survey.”
A new report shows that 1 in 5 community hospitals operates in the red, but the chief strategy officer of the firm that conducted the survey thinks hospitals can help change that.
The second annual survey from healthcare information technology (HIT) provider Anthelio and leadership group Community Hospital 100 found that 22% of community hospitals operate with margins below 2%; another 38% operate below 1%. Rick Kneipper, Anthelio’s cofounder and chief strategy officer, says that hospitalists can be at the forefront “of the creative changes needed” to reduce costs and improve profitability.
“Hospital medicine groups and hospitals could free up significant funds to devote to improved patient-care services if they focus on their core competency of patient care and farm out their non-core, back-office services to experts who can use leverage to provide more efficient services at significantly reduced costs,” Kneipper wrote in an email to The Hospitalist. “Financial pressures have historically forced most industries to stop trying to be vertically integrated [trying to be ‘all things to all people’] and instead to focus on their core competencies—it’s time for healthcare to do the same.”
—Rick Kneipper, cofounder, chief strategy officer, Anthelio
HM’s foothold at the intersection of clinical care and safety and QI positions the specialty to “respond to the new challenges of readmission penalties, evidenced-based medicine requirements, EMR implementation, and operation challenges,” Kneipper wrote.
For the full survey, please visit www.antheliohealth.com and search “survey.”