User login
The Billing & Coding Bandwagon

It’s no secret that documenting and coding one’s work is not the average hospitalist’s favorite thing to do. It’s probably not even in the top 10 or 20. In fact, many consider the whole documentation process a “thorn in the side.”
“When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’ ” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
Like it or not, healthcare providers live in a highly regulated world, says Richard D. Pinson, MD, FACP, CCS, who became a certified coding specialist and formed his own consulting company, Houston-based HCQ Consulting, to help hospitals and physicians achieve diagnostic accuracy for inpatient care. Documentation and coding have become a serious, high-stakes word game, he says. “Perfectly good clinical documentation, especially with some important diagnoses, may not correspond at all to what is required by the strict coding rules that govern code assignments,” he says.
A hospitalist’s documentation is at the heart of accurate coding, whether it’s for the hospital’s DRG reimbursement, quality and performance scores, or for assigning current procedural terminology (CPT) and evaluation and management (E/M) codes for billing for their own professional services. And if hospitalists don’t buy into the coding mindset, they risk decreased reimbursement for their services, monetary losses for the hospital, Medicare audits, compromised quality scores for both the hospital and themselves, and noncompliance.
“If your documentation is not up to par, then the hospital may get fined and lose money, and you can’t prove your worth as a hospitalist,” Dr. Nweke says.
What’s at Stake?

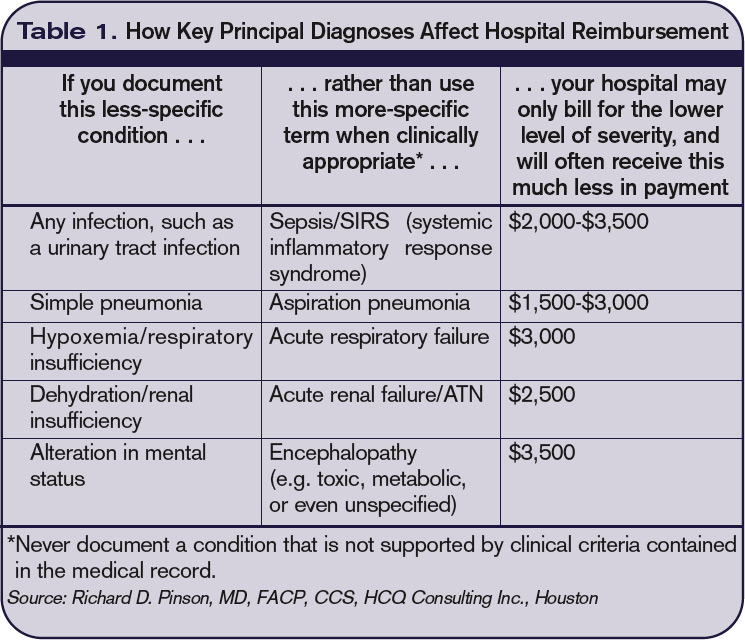
Inadequate documentation results in “undercoding” a patient’s condition and underpayment to your hospital (see Table 1, right). Undercoding also can result in inadequate representation of the severity of a patient’s illness, complexity, and cost of care. If a patient gets worse in the hospital, then that initial lower severity of illness might show up in poor performance scores on outcome measures. If a patient’s severity of illness is miscoded, Medicare might question the medical necessity for inpatient admission and deny payment.
On the other hand, if overcoding occurs because the clinical criteria for a specific diagnosis have not been met, Medicare will take action to recover the overpayment, leveling penalties and sanctions. (For more information on Medicare’s Recovery Audit Contractor program, dubbed “Medicare’s repo men” by Dr. Pinson, see “Take Proactive Approach to Recovery Audit Contractors,” p. 28.)
Lack of specificity also hampers reimbursement for professional fees, says Barb Pierce, CCS-P, ACS-EM, president of Barb Pierce Coding and Consulting Inc. of West Des Moines, Iowa. “Unfortunately,” she observes, “the code isn’t just based on decision-making, which is why physicians went to school for all those years. The guidelines [Documentation Guidelines for Evaluation and Management Services] mandate that if you forget one little bullet in history or examination, even if you’ve got the riskiest, highest-level, decision-making patient in front of you, that could pull down the whole code selection.”1
How costly might such small mistakes be for an HM group? According to the State of Hospital Medicine: 2010 Report Based on 2009 Data survey, internal-medicine hospitalists generate a median of 1.86 work relative value units (wRVUs) per encounter, and collect $45.57 per wRVU.2 If a hospitalist has 2,200 encounters per year and averages only 1.65 wRVUs per encounter, improving documentation and coding performance could add an additional 0.21 wRVUs, meeting the national average. Multiplying those 2,200 encounters by the national average of 1.86, the hospitalist could potentially add an additional 462 wRVUs for the year. Such documentation improvement—up to the national average—would equate to $21,053 in additional billed revenue without increasing the physician’s overall workload.
Dr. Pinson explains that physicians often perceive their time constraints as so severe that they’d be hard pressed to find the time to learn about documentation and coding. But he maintains that even short seminars yield “a huge amount of information that would astound [hospitalists], in terms of usefulness for their own clinical practices.”
Barriers to the Coding Mindset

Most hospitalists receive little or no training in documentation and coding during medical school or residency. The lack of education is further complicated because there are several coding sets healthcare providers must master, each with different rules governing assignment of diagnoses and levels of care (see “Coding Sets: Separate but Overlapping,” above).
Inexperience with coding guidelines can lead to mismatches. Nelly Leon-Chisen, RHIA, director of coding and classification for the American Hospital Association (AHA), gives one example: The ICD-9-CM Official Coding Guideline stipulates that coders cannot assign diagnosis codes based on lab results.3 So although it might appear intuitive to a physician that repeated blood sugars and monitoring of insulin levels indicate a patient has diabetes, the coder cannot assign the diagnosis unless it’s explicitly stated in the record.
Some physicians could simply be using outmoded terminology, such as “renal insufficiency” instead of “acute renal failure,” Dr. Pinson notes. If hospitalists learn to focus on evidence-based clinical criteria to support the codes, it leads to more effective care, he says.
The nature of hospitalist programs might not lend itself to efficient revenue-cycle processes for their own professional billing, says Jeri Leong, RN, CPC, CPC-H, president and CEO of Honolulu-based Healthcare Coding Consultants of Hawaii. If the HM group contracts with several hospitals, the hospitalists will be together rarely as a group, “so they don’t have the luxury of sitting down together with their billers to get important feedback and coding updates,” she says.
Leong’s company identifies missed charges, for instance, when charge tags from different shifts do not get married together (Hospitalist A might round on the patient in the morning and turn in a charge tag; Hospitalist B might do a procedure in the afternoon, but the two tags do not get combined). Examples such as these, she says, “can be an issue from a compliance perspective, and can leave money on the table.”
One of the problems Kathy DeVault, RHIA, CCS, CCS-P, manager of professional practice resources for the American Health Information Management Association (AHIMA), sees is a lack of continuity between initial admitting diagnosis and discharge summaries. For example, a hospitalist might admit a patient for acute renal failure—the correct diagnosis—and be able to reverse the condition fairly quickly, especially if the failure is due to dehydration.
The patient, whose issue is resolved, could be discharged by an attending physician who does not note the acute diagnosis in the summary. “That acute condition disappears, and the RAC auditor may then challenge the claim for payment,” DeVault says.
The Remedies
While physicians might think that they don’t have the time to acquire coding education, there could be other incentives coming down the pike. Dr. Pinson has noticed that hospitals are beginning to incorporate documentation accuracy into their contractual reimbursement formulas.
Documentation fixes vary according to domain. A hospital’s clinical documentation specialists can query physicians for clarity and detail in their notes; for instance, a diagnosis of congestive heart failure (CHF) must be accompanied by additional documentation stating whether the CHF is acute or chronic, and whether it is systolic or diastolic.
Many hospitals have instituted clinical documentation improvement (CDI) programs, sometimes called clinical documentation integrity programs, to address documentation discrepancies. CDI programs are essential to hospitals’ financial survival, Dr. Pinson says, and hospitalists are ideally positioned to join those efforts.
“[The hospitalists] are the most important people to the hospital in all of this,” he says. “They’re at the center of this whirlpool. If you have these skills, your value to the hospital and to your group is greatly enhanced.” (Visit the-hospitalist.org to listen to Dr. Pinson discuss HM’s role in documentation improvement.)
Leon-Chisen also says that the relationship between coders and physicians should be collaborative. “If it’s adversarial, nobody wins,” she points out, adding that CDI programs present an opportunity for mutual education.
Conducting audits of the practice’s documentation and coding can identify coding strengths and weaknesses, says Pierce, who is faculty for SHM’s billing and coding pre-course and regularly consults with hospitalist groups. Audits are helpful, she says, not just for increasing group revenue, but for compliance reasons as well. “You need to know what you’re doing well, and what you’re not doing quite so well, and get it fixed internally before an entity like Medicare discovers it,” she says.
It’s no doubt difficult for a busy HM group to stay on top of annual coding updates and changes to guidelines for reporting their services, Leong notes. Her company has worked with many hospitalist groups over the years, offering coding workshops, “back end” audits, and real-time feedback of E/M and CPT coding choices. If all of the hospitalists in a group cannot convene simultaneously, Leong provides the feedback (in the form of a scorecard) to the group’s physician champion, who becomes the lead contact to help those physicians who struggle more with their coding. (Leong talks more about real-time feedback and capturing CPT and E/M codes at the-hospitalist.org.)
In lieu of hiring professional coders, some HM groups use electronic coding devices. The software could be a standalone product, or it could interface with other products, such as electronic medical records (EMRs). These programs assist with a variety of coding-related activities, such as CPT or ICD-9 lookups, or calculation of E/M key components with assignment of an appropriate level of billing. Leong, however, cautions too much reliance on technology.
“While these devices can be accurate, compact, and convenient, it’s important to maintain a current [software] subscription to keep abreast of updates to the code sets, which occur sometimes as often as quarterly,” she says.
Pierce adds that coding tools should be double-checked against an audit tool. She has sometimes found discrepancies when auditing against an EMR product that assigns the E/M level.

Attitude Adjustment
Coding experts emphasize that physicians need not worry about mastering coding manuals, but they should forge relationships with both their hospital’s billers and the coders for their practice.
Dr. Nweke took advantage of coding and billing workshops offered by her group, HMG, and through the seminars began to understand what a DRG meant not just for her hospital but for her own evaluations and the expansion of her HM group, too. “Now, when I get questions from billers and coders, I try to answer them quickly,” she says. “I don’t look upon them as the enemy, but rather as people who are helping me document appropriately, so I don’t get audited by Medicare. I think the way you view the coders and billers definitely affects your willingness to learn.”
Dr. Nweke also takes a broader view of her role as a hospitalist. “You are there to take care of patients and assist with transitioning them in and out of the hospital, but you’re also there to ensure that the hospital remains afloat financially,” she says. “Your documentation plays a huge role in that. We have a huge contribution to make.”
The patient gains, too, says Leon-Chisen, who explains that documentation should be as accurate as possible “because someone else—the patient’s primary physician—will be taking over care of that patient and needs to understand what happened in the hospital.”
“The bottom line,” Dr. Pinson says, “is that we need accurate documentation that can be correctly coded to reflect the true complexity of care and severity of illness. If we do that, good things will follow.” TH
Gretchen Henkel is a freelance writer based in California.
References
- 1997 Documentation Guidelines for Evaluation and Management Services. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed April 11, 2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Society of Hospital Medicine and Medical Group Management Association; Philadelphia and Englewood, Colo.; 2010.
- ICD-9-CM Official Coding Guidelines. CMS and National Center for Health Statistics; Washington, D.C.; 2008. Available at: www.ama-assn.org/resources/doc/cpt/icd9cm_coding_guidelines_08_09_full.pdf. Accessed April 10, 2011.
Take Proactive Approach to Recovery Audit Contractors
The congressionally authorized Medicare Recovery Audit Contractor (RAC) program began with a three-year demonstration pilot project in 2005. In August 2010, the program expanded to the entire country. The RAC’s main objective is to identify improper Medicare payments, both overpayments and underpayments, to providers. CMS, which administrates Medicare and the RAC program, has agreements with contractors who are authorized to audit and review claims that are up to three years old.
According to Elizabeth Baskett, senior associate director of policy at the AHA, medical necessity review was a big focus of the RAC demonstration project and now is “under way in the permanent RAC program. We are bracing ourselves for a significant amount of denials.”
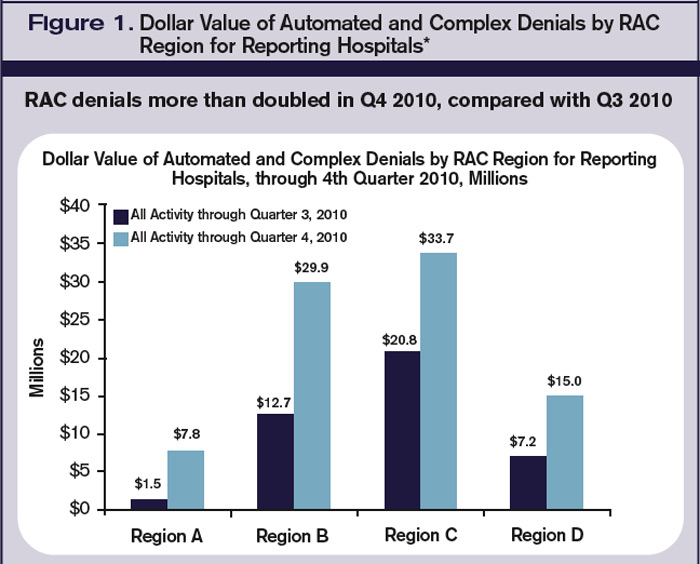
The AHA has created a free, Web-based survey called RAC Trac (www.aha.org/aha/issues/RAC/ractrac.html) to assess the nationwide impact the RAC program has on U.S. hospitals. In a report released Feb. 24, the RAC Trac survey shows that $82 million in denials were reported, more than double the dollar amount of denials reported in the third quarter of 2010 (see Figure 1, below). It also shows 57% of the more than 1,850 participating hospitals cited “medically unnecessary” as a reason for a denial of a claim.
Nearly 80% of the participating hospitals reported RAC activity in 2010, with general medical and surgical hospitals reporting the most activity. Fifty percent of reporting hospitals noted that their administrative burden—in the form of hiring consultants, copying medical records, hiring legal counsel, and the like—had increased as a result of RAC activity.
Most importantly, the report shows the average dollar value of automated denials was $399. But when a complex review—one involving a human review of requested records—was conducted, the average value of the denial was $5,281. Additionally, inpatient facilities were most likely to experience complex denials, which account for 90% of the value of denied claims.
Leong says RAC audits are just one area of “exposure to review for hospitals and providers. Other third-party payers, including individual commercial insurance companies,” she says, “also do routine post-payment review and recoupment, several years after payment.”—GH
It’s no secret that documenting and coding one’s work is not the average hospitalist’s favorite thing to do. It’s probably not even in the top 10 or 20. In fact, many consider the whole documentation process a “thorn in the side.”
“When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’ ” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
Like it or not, healthcare providers live in a highly regulated world, says Richard D. Pinson, MD, FACP, CCS, who became a certified coding specialist and formed his own consulting company, Houston-based HCQ Consulting, to help hospitals and physicians achieve diagnostic accuracy for inpatient care. Documentation and coding have become a serious, high-stakes word game, he says. “Perfectly good clinical documentation, especially with some important diagnoses, may not correspond at all to what is required by the strict coding rules that govern code assignments,” he says.
A hospitalist’s documentation is at the heart of accurate coding, whether it’s for the hospital’s DRG reimbursement, quality and performance scores, or for assigning current procedural terminology (CPT) and evaluation and management (E/M) codes for billing for their own professional services. And if hospitalists don’t buy into the coding mindset, they risk decreased reimbursement for their services, monetary losses for the hospital, Medicare audits, compromised quality scores for both the hospital and themselves, and noncompliance.
“If your documentation is not up to par, then the hospital may get fined and lose money, and you can’t prove your worth as a hospitalist,” Dr. Nweke says.
What’s at Stake?
Inadequate documentation results in “undercoding” a patient’s condition and underpayment to your hospital (see Table 1, right). Undercoding also can result in inadequate representation of the severity of a patient’s illness, complexity, and cost of care. If a patient gets worse in the hospital, then that initial lower severity of illness might show up in poor performance scores on outcome measures. If a patient’s severity of illness is miscoded, Medicare might question the medical necessity for inpatient admission and deny payment.
On the other hand, if overcoding occurs because the clinical criteria for a specific diagnosis have not been met, Medicare will take action to recover the overpayment, leveling penalties and sanctions. (For more information on Medicare’s Recovery Audit Contractor program, dubbed “Medicare’s repo men” by Dr. Pinson, see “Take Proactive Approach to Recovery Audit Contractors,” p. 28.)
Lack of specificity also hampers reimbursement for professional fees, says Barb Pierce, CCS-P, ACS-EM, president of Barb Pierce Coding and Consulting Inc. of West Des Moines, Iowa. “Unfortunately,” she observes, “the code isn’t just based on decision-making, which is why physicians went to school for all those years. The guidelines [Documentation Guidelines for Evaluation and Management Services] mandate that if you forget one little bullet in history or examination, even if you’ve got the riskiest, highest-level, decision-making patient in front of you, that could pull down the whole code selection.”1
How costly might such small mistakes be for an HM group? According to the State of Hospital Medicine: 2010 Report Based on 2009 Data survey, internal-medicine hospitalists generate a median of 1.86 work relative value units (wRVUs) per encounter, and collect $45.57 per wRVU.2 If a hospitalist has 2,200 encounters per year and averages only 1.65 wRVUs per encounter, improving documentation and coding performance could add an additional 0.21 wRVUs, meeting the national average. Multiplying those 2,200 encounters by the national average of 1.86, the hospitalist could potentially add an additional 462 wRVUs for the year. Such documentation improvement—up to the national average—would equate to $21,053 in additional billed revenue without increasing the physician’s overall workload.
Dr. Pinson explains that physicians often perceive their time constraints as so severe that they’d be hard pressed to find the time to learn about documentation and coding. But he maintains that even short seminars yield “a huge amount of information that would astound [hospitalists], in terms of usefulness for their own clinical practices.”
Barriers to the Coding Mindset
Most hospitalists receive little or no training in documentation and coding during medical school or residency. The lack of education is further complicated because there are several coding sets healthcare providers must master, each with different rules governing assignment of diagnoses and levels of care (see “Coding Sets: Separate but Overlapping,” above).
Inexperience with coding guidelines can lead to mismatches. Nelly Leon-Chisen, RHIA, director of coding and classification for the American Hospital Association (AHA), gives one example: The ICD-9-CM Official Coding Guideline stipulates that coders cannot assign diagnosis codes based on lab results.3 So although it might appear intuitive to a physician that repeated blood sugars and monitoring of insulin levels indicate a patient has diabetes, the coder cannot assign the diagnosis unless it’s explicitly stated in the record.
Some physicians could simply be using outmoded terminology, such as “renal insufficiency” instead of “acute renal failure,” Dr. Pinson notes. If hospitalists learn to focus on evidence-based clinical criteria to support the codes, it leads to more effective care, he says.
The nature of hospitalist programs might not lend itself to efficient revenue-cycle processes for their own professional billing, says Jeri Leong, RN, CPC, CPC-H, president and CEO of Honolulu-based Healthcare Coding Consultants of Hawaii. If the HM group contracts with several hospitals, the hospitalists will be together rarely as a group, “so they don’t have the luxury of sitting down together with their billers to get important feedback and coding updates,” she says.
Leong’s company identifies missed charges, for instance, when charge tags from different shifts do not get married together (Hospitalist A might round on the patient in the morning and turn in a charge tag; Hospitalist B might do a procedure in the afternoon, but the two tags do not get combined). Examples such as these, she says, “can be an issue from a compliance perspective, and can leave money on the table.”
One of the problems Kathy DeVault, RHIA, CCS, CCS-P, manager of professional practice resources for the American Health Information Management Association (AHIMA), sees is a lack of continuity between initial admitting diagnosis and discharge summaries. For example, a hospitalist might admit a patient for acute renal failure—the correct diagnosis—and be able to reverse the condition fairly quickly, especially if the failure is due to dehydration.
The patient, whose issue is resolved, could be discharged by an attending physician who does not note the acute diagnosis in the summary. “That acute condition disappears, and the RAC auditor may then challenge the claim for payment,” DeVault says.
The Remedies
While physicians might think that they don’t have the time to acquire coding education, there could be other incentives coming down the pike. Dr. Pinson has noticed that hospitals are beginning to incorporate documentation accuracy into their contractual reimbursement formulas.
Documentation fixes vary according to domain. A hospital’s clinical documentation specialists can query physicians for clarity and detail in their notes; for instance, a diagnosis of congestive heart failure (CHF) must be accompanied by additional documentation stating whether the CHF is acute or chronic, and whether it is systolic or diastolic.
Many hospitals have instituted clinical documentation improvement (CDI) programs, sometimes called clinical documentation integrity programs, to address documentation discrepancies. CDI programs are essential to hospitals’ financial survival, Dr. Pinson says, and hospitalists are ideally positioned to join those efforts.
“[The hospitalists] are the most important people to the hospital in all of this,” he says. “They’re at the center of this whirlpool. If you have these skills, your value to the hospital and to your group is greatly enhanced.” (Visit the-hospitalist.org to listen to Dr. Pinson discuss HM’s role in documentation improvement.)
Leon-Chisen also says that the relationship between coders and physicians should be collaborative. “If it’s adversarial, nobody wins,” she points out, adding that CDI programs present an opportunity for mutual education.
Conducting audits of the practice’s documentation and coding can identify coding strengths and weaknesses, says Pierce, who is faculty for SHM’s billing and coding pre-course and regularly consults with hospitalist groups. Audits are helpful, she says, not just for increasing group revenue, but for compliance reasons as well. “You need to know what you’re doing well, and what you’re not doing quite so well, and get it fixed internally before an entity like Medicare discovers it,” she says.
It’s no doubt difficult for a busy HM group to stay on top of annual coding updates and changes to guidelines for reporting their services, Leong notes. Her company has worked with many hospitalist groups over the years, offering coding workshops, “back end” audits, and real-time feedback of E/M and CPT coding choices. If all of the hospitalists in a group cannot convene simultaneously, Leong provides the feedback (in the form of a scorecard) to the group’s physician champion, who becomes the lead contact to help those physicians who struggle more with their coding. (Leong talks more about real-time feedback and capturing CPT and E/M codes at the-hospitalist.org.)
In lieu of hiring professional coders, some HM groups use electronic coding devices. The software could be a standalone product, or it could interface with other products, such as electronic medical records (EMRs). These programs assist with a variety of coding-related activities, such as CPT or ICD-9 lookups, or calculation of E/M key components with assignment of an appropriate level of billing. Leong, however, cautions too much reliance on technology.
“While these devices can be accurate, compact, and convenient, it’s important to maintain a current [software] subscription to keep abreast of updates to the code sets, which occur sometimes as often as quarterly,” she says.
Pierce adds that coding tools should be double-checked against an audit tool. She has sometimes found discrepancies when auditing against an EMR product that assigns the E/M level.
Attitude Adjustment
Coding experts emphasize that physicians need not worry about mastering coding manuals, but they should forge relationships with both their hospital’s billers and the coders for their practice.
Dr. Nweke took advantage of coding and billing workshops offered by her group, HMG, and through the seminars began to understand what a DRG meant not just for her hospital but for her own evaluations and the expansion of her HM group, too. “Now, when I get questions from billers and coders, I try to answer them quickly,” she says. “I don’t look upon them as the enemy, but rather as people who are helping me document appropriately, so I don’t get audited by Medicare. I think the way you view the coders and billers definitely affects your willingness to learn.”
Dr. Nweke also takes a broader view of her role as a hospitalist. “You are there to take care of patients and assist with transitioning them in and out of the hospital, but you’re also there to ensure that the hospital remains afloat financially,” she says. “Your documentation plays a huge role in that. We have a huge contribution to make.”
The patient gains, too, says Leon-Chisen, who explains that documentation should be as accurate as possible “because someone else—the patient’s primary physician—will be taking over care of that patient and needs to understand what happened in the hospital.”
“The bottom line,” Dr. Pinson says, “is that we need accurate documentation that can be correctly coded to reflect the true complexity of care and severity of illness. If we do that, good things will follow.” TH
Gretchen Henkel is a freelance writer based in California.
References
- 1997 Documentation Guidelines for Evaluation and Management Services. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed April 11, 2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Society of Hospital Medicine and Medical Group Management Association; Philadelphia and Englewood, Colo.; 2010.
- ICD-9-CM Official Coding Guidelines. CMS and National Center for Health Statistics; Washington, D.C.; 2008. Available at: www.ama-assn.org/resources/doc/cpt/icd9cm_coding_guidelines_08_09_full.pdf. Accessed April 10, 2011.
Take Proactive Approach to Recovery Audit Contractors
The congressionally authorized Medicare Recovery Audit Contractor (RAC) program began with a three-year demonstration pilot project in 2005. In August 2010, the program expanded to the entire country. The RAC’s main objective is to identify improper Medicare payments, both overpayments and underpayments, to providers. CMS, which administrates Medicare and the RAC program, has agreements with contractors who are authorized to audit and review claims that are up to three years old.
According to Elizabeth Baskett, senior associate director of policy at the AHA, medical necessity review was a big focus of the RAC demonstration project and now is “under way in the permanent RAC program. We are bracing ourselves for a significant amount of denials.”
The AHA has created a free, Web-based survey called RAC Trac (www.aha.org/aha/issues/RAC/ractrac.html) to assess the nationwide impact the RAC program has on U.S. hospitals. In a report released Feb. 24, the RAC Trac survey shows that $82 million in denials were reported, more than double the dollar amount of denials reported in the third quarter of 2010 (see Figure 1, below). It also shows 57% of the more than 1,850 participating hospitals cited “medically unnecessary” as a reason for a denial of a claim.
Nearly 80% of the participating hospitals reported RAC activity in 2010, with general medical and surgical hospitals reporting the most activity. Fifty percent of reporting hospitals noted that their administrative burden—in the form of hiring consultants, copying medical records, hiring legal counsel, and the like—had increased as a result of RAC activity.
Most importantly, the report shows the average dollar value of automated denials was $399. But when a complex review—one involving a human review of requested records—was conducted, the average value of the denial was $5,281. Additionally, inpatient facilities were most likely to experience complex denials, which account for 90% of the value of denied claims.
Leong says RAC audits are just one area of “exposure to review for hospitals and providers. Other third-party payers, including individual commercial insurance companies,” she says, “also do routine post-payment review and recoupment, several years after payment.”—GH
It’s no secret that documenting and coding one’s work is not the average hospitalist’s favorite thing to do. It’s probably not even in the top 10 or 20. In fact, many consider the whole documentation process a “thorn in the side.”
“When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’ ” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
Like it or not, healthcare providers live in a highly regulated world, says Richard D. Pinson, MD, FACP, CCS, who became a certified coding specialist and formed his own consulting company, Houston-based HCQ Consulting, to help hospitals and physicians achieve diagnostic accuracy for inpatient care. Documentation and coding have become a serious, high-stakes word game, he says. “Perfectly good clinical documentation, especially with some important diagnoses, may not correspond at all to what is required by the strict coding rules that govern code assignments,” he says.
A hospitalist’s documentation is at the heart of accurate coding, whether it’s for the hospital’s DRG reimbursement, quality and performance scores, or for assigning current procedural terminology (CPT) and evaluation and management (E/M) codes for billing for their own professional services. And if hospitalists don’t buy into the coding mindset, they risk decreased reimbursement for their services, monetary losses for the hospital, Medicare audits, compromised quality scores for both the hospital and themselves, and noncompliance.
“If your documentation is not up to par, then the hospital may get fined and lose money, and you can’t prove your worth as a hospitalist,” Dr. Nweke says.
What’s at Stake?
Inadequate documentation results in “undercoding” a patient’s condition and underpayment to your hospital (see Table 1, right). Undercoding also can result in inadequate representation of the severity of a patient’s illness, complexity, and cost of care. If a patient gets worse in the hospital, then that initial lower severity of illness might show up in poor performance scores on outcome measures. If a patient’s severity of illness is miscoded, Medicare might question the medical necessity for inpatient admission and deny payment.
On the other hand, if overcoding occurs because the clinical criteria for a specific diagnosis have not been met, Medicare will take action to recover the overpayment, leveling penalties and sanctions. (For more information on Medicare’s Recovery Audit Contractor program, dubbed “Medicare’s repo men” by Dr. Pinson, see “Take Proactive Approach to Recovery Audit Contractors,” p. 28.)
Lack of specificity also hampers reimbursement for professional fees, says Barb Pierce, CCS-P, ACS-EM, president of Barb Pierce Coding and Consulting Inc. of West Des Moines, Iowa. “Unfortunately,” she observes, “the code isn’t just based on decision-making, which is why physicians went to school for all those years. The guidelines [Documentation Guidelines for Evaluation and Management Services] mandate that if you forget one little bullet in history or examination, even if you’ve got the riskiest, highest-level, decision-making patient in front of you, that could pull down the whole code selection.”1
How costly might such small mistakes be for an HM group? According to the State of Hospital Medicine: 2010 Report Based on 2009 Data survey, internal-medicine hospitalists generate a median of 1.86 work relative value units (wRVUs) per encounter, and collect $45.57 per wRVU.2 If a hospitalist has 2,200 encounters per year and averages only 1.65 wRVUs per encounter, improving documentation and coding performance could add an additional 0.21 wRVUs, meeting the national average. Multiplying those 2,200 encounters by the national average of 1.86, the hospitalist could potentially add an additional 462 wRVUs for the year. Such documentation improvement—up to the national average—would equate to $21,053 in additional billed revenue without increasing the physician’s overall workload.
Dr. Pinson explains that physicians often perceive their time constraints as so severe that they’d be hard pressed to find the time to learn about documentation and coding. But he maintains that even short seminars yield “a huge amount of information that would astound [hospitalists], in terms of usefulness for their own clinical practices.”
Barriers to the Coding Mindset
Most hospitalists receive little or no training in documentation and coding during medical school or residency. The lack of education is further complicated because there are several coding sets healthcare providers must master, each with different rules governing assignment of diagnoses and levels of care (see “Coding Sets: Separate but Overlapping,” above).
Inexperience with coding guidelines can lead to mismatches. Nelly Leon-Chisen, RHIA, director of coding and classification for the American Hospital Association (AHA), gives one example: The ICD-9-CM Official Coding Guideline stipulates that coders cannot assign diagnosis codes based on lab results.3 So although it might appear intuitive to a physician that repeated blood sugars and monitoring of insulin levels indicate a patient has diabetes, the coder cannot assign the diagnosis unless it’s explicitly stated in the record.
Some physicians could simply be using outmoded terminology, such as “renal insufficiency” instead of “acute renal failure,” Dr. Pinson notes. If hospitalists learn to focus on evidence-based clinical criteria to support the codes, it leads to more effective care, he says.
The nature of hospitalist programs might not lend itself to efficient revenue-cycle processes for their own professional billing, says Jeri Leong, RN, CPC, CPC-H, president and CEO of Honolulu-based Healthcare Coding Consultants of Hawaii. If the HM group contracts with several hospitals, the hospitalists will be together rarely as a group, “so they don’t have the luxury of sitting down together with their billers to get important feedback and coding updates,” she says.
Leong’s company identifies missed charges, for instance, when charge tags from different shifts do not get married together (Hospitalist A might round on the patient in the morning and turn in a charge tag; Hospitalist B might do a procedure in the afternoon, but the two tags do not get combined). Examples such as these, she says, “can be an issue from a compliance perspective, and can leave money on the table.”
One of the problems Kathy DeVault, RHIA, CCS, CCS-P, manager of professional practice resources for the American Health Information Management Association (AHIMA), sees is a lack of continuity between initial admitting diagnosis and discharge summaries. For example, a hospitalist might admit a patient for acute renal failure—the correct diagnosis—and be able to reverse the condition fairly quickly, especially if the failure is due to dehydration.
The patient, whose issue is resolved, could be discharged by an attending physician who does not note the acute diagnosis in the summary. “That acute condition disappears, and the RAC auditor may then challenge the claim for payment,” DeVault says.
The Remedies
While physicians might think that they don’t have the time to acquire coding education, there could be other incentives coming down the pike. Dr. Pinson has noticed that hospitals are beginning to incorporate documentation accuracy into their contractual reimbursement formulas.
Documentation fixes vary according to domain. A hospital’s clinical documentation specialists can query physicians for clarity and detail in their notes; for instance, a diagnosis of congestive heart failure (CHF) must be accompanied by additional documentation stating whether the CHF is acute or chronic, and whether it is systolic or diastolic.
Many hospitals have instituted clinical documentation improvement (CDI) programs, sometimes called clinical documentation integrity programs, to address documentation discrepancies. CDI programs are essential to hospitals’ financial survival, Dr. Pinson says, and hospitalists are ideally positioned to join those efforts.
“[The hospitalists] are the most important people to the hospital in all of this,” he says. “They’re at the center of this whirlpool. If you have these skills, your value to the hospital and to your group is greatly enhanced.” (Visit the-hospitalist.org to listen to Dr. Pinson discuss HM’s role in documentation improvement.)
Leon-Chisen also says that the relationship between coders and physicians should be collaborative. “If it’s adversarial, nobody wins,” she points out, adding that CDI programs present an opportunity for mutual education.
Conducting audits of the practice’s documentation and coding can identify coding strengths and weaknesses, says Pierce, who is faculty for SHM’s billing and coding pre-course and regularly consults with hospitalist groups. Audits are helpful, she says, not just for increasing group revenue, but for compliance reasons as well. “You need to know what you’re doing well, and what you’re not doing quite so well, and get it fixed internally before an entity like Medicare discovers it,” she says.
It’s no doubt difficult for a busy HM group to stay on top of annual coding updates and changes to guidelines for reporting their services, Leong notes. Her company has worked with many hospitalist groups over the years, offering coding workshops, “back end” audits, and real-time feedback of E/M and CPT coding choices. If all of the hospitalists in a group cannot convene simultaneously, Leong provides the feedback (in the form of a scorecard) to the group’s physician champion, who becomes the lead contact to help those physicians who struggle more with their coding. (Leong talks more about real-time feedback and capturing CPT and E/M codes at the-hospitalist.org.)
In lieu of hiring professional coders, some HM groups use electronic coding devices. The software could be a standalone product, or it could interface with other products, such as electronic medical records (EMRs). These programs assist with a variety of coding-related activities, such as CPT or ICD-9 lookups, or calculation of E/M key components with assignment of an appropriate level of billing. Leong, however, cautions too much reliance on technology.
“While these devices can be accurate, compact, and convenient, it’s important to maintain a current [software] subscription to keep abreast of updates to the code sets, which occur sometimes as often as quarterly,” she says.
Pierce adds that coding tools should be double-checked against an audit tool. She has sometimes found discrepancies when auditing against an EMR product that assigns the E/M level.
Attitude Adjustment
Coding experts emphasize that physicians need not worry about mastering coding manuals, but they should forge relationships with both their hospital’s billers and the coders for their practice.
Dr. Nweke took advantage of coding and billing workshops offered by her group, HMG, and through the seminars began to understand what a DRG meant not just for her hospital but for her own evaluations and the expansion of her HM group, too. “Now, when I get questions from billers and coders, I try to answer them quickly,” she says. “I don’t look upon them as the enemy, but rather as people who are helping me document appropriately, so I don’t get audited by Medicare. I think the way you view the coders and billers definitely affects your willingness to learn.”
Dr. Nweke also takes a broader view of her role as a hospitalist. “You are there to take care of patients and assist with transitioning them in and out of the hospital, but you’re also there to ensure that the hospital remains afloat financially,” she says. “Your documentation plays a huge role in that. We have a huge contribution to make.”
The patient gains, too, says Leon-Chisen, who explains that documentation should be as accurate as possible “because someone else—the patient’s primary physician—will be taking over care of that patient and needs to understand what happened in the hospital.”
“The bottom line,” Dr. Pinson says, “is that we need accurate documentation that can be correctly coded to reflect the true complexity of care and severity of illness. If we do that, good things will follow.” TH
Gretchen Henkel is a freelance writer based in California.
References
- 1997 Documentation Guidelines for Evaluation and Management Services. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed April 11, 2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Society of Hospital Medicine and Medical Group Management Association; Philadelphia and Englewood, Colo.; 2010.
- ICD-9-CM Official Coding Guidelines. CMS and National Center for Health Statistics; Washington, D.C.; 2008. Available at: www.ama-assn.org/resources/doc/cpt/icd9cm_coding_guidelines_08_09_full.pdf. Accessed April 10, 2011.
Take Proactive Approach to Recovery Audit Contractors
The congressionally authorized Medicare Recovery Audit Contractor (RAC) program began with a three-year demonstration pilot project in 2005. In August 2010, the program expanded to the entire country. The RAC’s main objective is to identify improper Medicare payments, both overpayments and underpayments, to providers. CMS, which administrates Medicare and the RAC program, has agreements with contractors who are authorized to audit and review claims that are up to three years old.
According to Elizabeth Baskett, senior associate director of policy at the AHA, medical necessity review was a big focus of the RAC demonstration project and now is “under way in the permanent RAC program. We are bracing ourselves for a significant amount of denials.”
The AHA has created a free, Web-based survey called RAC Trac (www.aha.org/aha/issues/RAC/ractrac.html) to assess the nationwide impact the RAC program has on U.S. hospitals. In a report released Feb. 24, the RAC Trac survey shows that $82 million in denials were reported, more than double the dollar amount of denials reported in the third quarter of 2010 (see Figure 1, below). It also shows 57% of the more than 1,850 participating hospitals cited “medically unnecessary” as a reason for a denial of a claim.
Nearly 80% of the participating hospitals reported RAC activity in 2010, with general medical and surgical hospitals reporting the most activity. Fifty percent of reporting hospitals noted that their administrative burden—in the form of hiring consultants, copying medical records, hiring legal counsel, and the like—had increased as a result of RAC activity.
Most importantly, the report shows the average dollar value of automated denials was $399. But when a complex review—one involving a human review of requested records—was conducted, the average value of the denial was $5,281. Additionally, inpatient facilities were most likely to experience complex denials, which account for 90% of the value of denied claims.
Leong says RAC audits are just one area of “exposure to review for hospitals and providers. Other third-party payers, including individual commercial insurance companies,” she says, “also do routine post-payment review and recoupment, several years after payment.”—GH
Due Diligence: Denials
Before submitting a claim, hospitalists should ensure that the service is rendered, that it is completely and accurately documented in the medical record, that the correct information is entered on the claim form, and that it is a covered benefit and eligible for payment.
Although the latter two elements typically are delegated to the billing team, hospitalists should encourage or request feedback regarding payment and denials. The ensuing open dialogue between physicians and billers might prove helpful in understanding and resolving future billing issues. Less-experienced billers first respond to claim denials by submitting documentation (i.e. “appeal with paper”) despite the inappropriateness of this action. If the denial is upheld, this attempt is viewed as unsuccessful and, without further consideration, “written off.” However, careful examination of the payor’s initial claim determination could elicit a more suitable response.
Service Provider
Provider enrollment issues can sidetrack claim submissions. Physicians must register their NPI (national provider identifier) with the correct practice location and group assignment, particularly when previously practicing physicians join a new group practice. Failure to do so is an infrequent, yet valid, cause for denial.
Alternatively, enrollment issues play a greater role when services involve nurse practitioners (NPs) and physician assistants (PAs) who are enrolled with Medicare but might be prohibited from enrolling with other payors. For example, an NP independently provides subsequent hospital care (e.g. 99232) to a Medicare beneficiary. The claim is submitted in the NP’s name and reimbursed at the correct amount by Medicare as the primary insurer. The remaining balance is submitted to the secondary insurer, who does not enroll NPPs. The claim is rejected. If the physician group has a contractual agreement to recognize NPP services by reporting them under the collaborating physician’s name, the claim can be resubmitted in the physician’s name. In absence of such an agreement, the claim should be written off.
Location
The place of service (POS) must match the reported service/procedure code. For example, a hospitalist is asked to see a patient in the ED. The patient requires further testing but does not meet the criterion for an inpatient stay. The hospitalist admits the patient to observation, treats him, and discharges him to home.
Hospitalists need to avoid the common mistake of mismatching the service code with the location/POS. Observation services performed by the “physician of record” should be reported with the corresponding codes: initial observation care (99218-99220), subsequent observation care (99224-99226), or observation discharge (99217), as appropriate.1 The correct POS should be reported as outpatient hospital (POS 22), not inpatient hospital (POS 21). Trying to report outpatient codes with an inpatient POS will result in claim denial.
A similar denial occurs when trying to report inpatient codes (99231-99233) in an outpatient location (e.g. 23-ED). These denials require claim resubmission with the correct POS and/or service/procedure code. A complete list of POS codes and corresponding definitions can be obtained from Chapter 26, Section 10.5 of the Medicare Claims Processing Manual, available at www.cms.hhs.gov/manuals/downloads/clm104c26.pdf.
Diagnosis
Denials involving diagnoses produce issues of “medical necessity.”1 Examine these denials carefully. Consider the service/procedure code when trying to formulate a response to the denial. The diagnosis code represents the reason for the service or procedure and might be a sign, symptom, or condition with which the patient presents. Medicare reimburses for procedures and services that are deemed “reasonable and necessary.”
In an effort to unify standards, Medicare has developed national coverage determinations (NCDs) to identify coverage requirements for frequent or problematic procedures or services. These coverage requirements can identify specific conditions (i.e. ICD-9-CM codes) for which the services or procedures are considered medically necessary. In the absence of a national coverage policy, an item or service could be covered at the discretion of Medicare contractors based on a local coverage determination (LCD), which varies by contractor.
Medical necessity denials often involve a mismatched or missing diagnosis. For example, a payor might deny a claim for cardiopulmonary resuscitation (92950) that is associated with a diagnosis code of congestive heart failure (428.0), despite this being the underlying condition that prompted the decline in the patient’s condition. The payor might only accept “cardiac arrest” (427.5) as the “medically necessary” diagnosis for cardiopulmonary resuscitation, as this is the direct reason necessitating the procedure. After reviewing the documentation to ensure that the documentation supports the diagnosis, the claim can be resubmitted with a confirmed and corrected diagnosis code.
Initial-Request Response
While diagnoses can lead to medical necessity issues, not all medical necessity denials are due to incorrect diagnoses. Some “medical necessity” denials result from a failure to respond to a payor request. More specifically, if the “medical necessity” denial involves a covered evaluation and management visit, the denial is more likely the result of a failure to respond to a prepayment request for documentation.
Medicare typically issues prepayment requests for documentation for the following inpatient CPT codes: 99223, 99233, 99232, 99239, and 99292.1 If the documentation is not provided to the Medicare review department within a designated time frame (e.g. 30-45 days), the claim is automatically denied. The reason for denial is cited as being “not deemed a medical necessity.” These claims do not require electronic resubmission, and instead require submission of documentation to the Medicare appeals department. Once the supporting documentation is reviewed, reimbursement is issued.
Supportive Documentation
There are times when payor requests for additional information or documentation is handled in a timely fashion. However, the paper submission might have been incomplete, as the encounter note itself might not contain the cumulative information representing the reported service.
For example, other pieces of pertinent information may be obtained from the data or order section of the chart. If the individual responsible for gathering the requested documentation does not review it before submission, important or referenced entries may be missed, and the complexity of the billed service might be sacrificed. The provider should submit any entry with the same date as the requested documentation in support: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility of the encounter note is crucial when the documentation is sent for review. Most reviewers will seek another reviewer’s assistance in translating, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied, resulting in a nonpayment or a refund. Electronic medical records (EMRs) are assisting physicians and other providers with legibility issues and improving review findings. If a physician is still writing notes by hand, a transcription might be sent along with the documentation to prevent unnecessary denials. Only consider this for requests involving providers with problematic handwriting. A legible signature is required. If a denial ensues in absence of a signature, the provider can submit an appeal with an acceptable attestation.
Modifier Considerations
Some services are denied for being “incidental/integral” to another reimbursed service (i.e. bundled). Payors implement electronic payment edits that disallow separate payment for “related” services. The industry standard, known as the National Correct Coding Initiative (NCCI), identifies code pairs that should not be reported together on the same date by either a single physician or physicians of the same specialty within a provider group.
When a claim is denied for this reason, billers tend to automatically and erroneously resubmit the claim with a modifier appended to the disallowed or “bundled” procedure code. Documentation should be reviewed to determine if the denied service is separately reportable from the paid service. The biller might append the appropriate modifier and resubmit the claim only when well supported by documentation.
For example, the hospitalist evaluated a patient with congestive heart failure and pleural effusions. The hospitalist determined that the patient requires placement of a central venous catheter (36556). Because the patient’s underlying condition was evaluated, and resulted in the decision to place a catheter, both the visit (99233) and the procedure (36556) can be reported. If submitted without modifiers, some payors will deny payment for the visit for being integral to the catheter placement. In this case, the claim should be resubmitted with modifier 25 appended to the visit. Payors might still require documentation review to ensure legitimacy of this modifier before the claim is paid. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Reference
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: AMA Press; 2011.
Before submitting a claim, hospitalists should ensure that the service is rendered, that it is completely and accurately documented in the medical record, that the correct information is entered on the claim form, and that it is a covered benefit and eligible for payment.
Although the latter two elements typically are delegated to the billing team, hospitalists should encourage or request feedback regarding payment and denials. The ensuing open dialogue between physicians and billers might prove helpful in understanding and resolving future billing issues. Less-experienced billers first respond to claim denials by submitting documentation (i.e. “appeal with paper”) despite the inappropriateness of this action. If the denial is upheld, this attempt is viewed as unsuccessful and, without further consideration, “written off.” However, careful examination of the payor’s initial claim determination could elicit a more suitable response.
Service Provider
Provider enrollment issues can sidetrack claim submissions. Physicians must register their NPI (national provider identifier) with the correct practice location and group assignment, particularly when previously practicing physicians join a new group practice. Failure to do so is an infrequent, yet valid, cause for denial.
Alternatively, enrollment issues play a greater role when services involve nurse practitioners (NPs) and physician assistants (PAs) who are enrolled with Medicare but might be prohibited from enrolling with other payors. For example, an NP independently provides subsequent hospital care (e.g. 99232) to a Medicare beneficiary. The claim is submitted in the NP’s name and reimbursed at the correct amount by Medicare as the primary insurer. The remaining balance is submitted to the secondary insurer, who does not enroll NPPs. The claim is rejected. If the physician group has a contractual agreement to recognize NPP services by reporting them under the collaborating physician’s name, the claim can be resubmitted in the physician’s name. In absence of such an agreement, the claim should be written off.
Location
The place of service (POS) must match the reported service/procedure code. For example, a hospitalist is asked to see a patient in the ED. The patient requires further testing but does not meet the criterion for an inpatient stay. The hospitalist admits the patient to observation, treats him, and discharges him to home.
Hospitalists need to avoid the common mistake of mismatching the service code with the location/POS. Observation services performed by the “physician of record” should be reported with the corresponding codes: initial observation care (99218-99220), subsequent observation care (99224-99226), or observation discharge (99217), as appropriate.1 The correct POS should be reported as outpatient hospital (POS 22), not inpatient hospital (POS 21). Trying to report outpatient codes with an inpatient POS will result in claim denial.
A similar denial occurs when trying to report inpatient codes (99231-99233) in an outpatient location (e.g. 23-ED). These denials require claim resubmission with the correct POS and/or service/procedure code. A complete list of POS codes and corresponding definitions can be obtained from Chapter 26, Section 10.5 of the Medicare Claims Processing Manual, available at www.cms.hhs.gov/manuals/downloads/clm104c26.pdf.
Diagnosis
Denials involving diagnoses produce issues of “medical necessity.”1 Examine these denials carefully. Consider the service/procedure code when trying to formulate a response to the denial. The diagnosis code represents the reason for the service or procedure and might be a sign, symptom, or condition with which the patient presents. Medicare reimburses for procedures and services that are deemed “reasonable and necessary.”
In an effort to unify standards, Medicare has developed national coverage determinations (NCDs) to identify coverage requirements for frequent or problematic procedures or services. These coverage requirements can identify specific conditions (i.e. ICD-9-CM codes) for which the services or procedures are considered medically necessary. In the absence of a national coverage policy, an item or service could be covered at the discretion of Medicare contractors based on a local coverage determination (LCD), which varies by contractor.
Medical necessity denials often involve a mismatched or missing diagnosis. For example, a payor might deny a claim for cardiopulmonary resuscitation (92950) that is associated with a diagnosis code of congestive heart failure (428.0), despite this being the underlying condition that prompted the decline in the patient’s condition. The payor might only accept “cardiac arrest” (427.5) as the “medically necessary” diagnosis for cardiopulmonary resuscitation, as this is the direct reason necessitating the procedure. After reviewing the documentation to ensure that the documentation supports the diagnosis, the claim can be resubmitted with a confirmed and corrected diagnosis code.
Initial-Request Response
While diagnoses can lead to medical necessity issues, not all medical necessity denials are due to incorrect diagnoses. Some “medical necessity” denials result from a failure to respond to a payor request. More specifically, if the “medical necessity” denial involves a covered evaluation and management visit, the denial is more likely the result of a failure to respond to a prepayment request for documentation.
Medicare typically issues prepayment requests for documentation for the following inpatient CPT codes: 99223, 99233, 99232, 99239, and 99292.1 If the documentation is not provided to the Medicare review department within a designated time frame (e.g. 30-45 days), the claim is automatically denied. The reason for denial is cited as being “not deemed a medical necessity.” These claims do not require electronic resubmission, and instead require submission of documentation to the Medicare appeals department. Once the supporting documentation is reviewed, reimbursement is issued.
Supportive Documentation
There are times when payor requests for additional information or documentation is handled in a timely fashion. However, the paper submission might have been incomplete, as the encounter note itself might not contain the cumulative information representing the reported service.
For example, other pieces of pertinent information may be obtained from the data or order section of the chart. If the individual responsible for gathering the requested documentation does not review it before submission, important or referenced entries may be missed, and the complexity of the billed service might be sacrificed. The provider should submit any entry with the same date as the requested documentation in support: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility of the encounter note is crucial when the documentation is sent for review. Most reviewers will seek another reviewer’s assistance in translating, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied, resulting in a nonpayment or a refund. Electronic medical records (EMRs) are assisting physicians and other providers with legibility issues and improving review findings. If a physician is still writing notes by hand, a transcription might be sent along with the documentation to prevent unnecessary denials. Only consider this for requests involving providers with problematic handwriting. A legible signature is required. If a denial ensues in absence of a signature, the provider can submit an appeal with an acceptable attestation.
Modifier Considerations
Some services are denied for being “incidental/integral” to another reimbursed service (i.e. bundled). Payors implement electronic payment edits that disallow separate payment for “related” services. The industry standard, known as the National Correct Coding Initiative (NCCI), identifies code pairs that should not be reported together on the same date by either a single physician or physicians of the same specialty within a provider group.
When a claim is denied for this reason, billers tend to automatically and erroneously resubmit the claim with a modifier appended to the disallowed or “bundled” procedure code. Documentation should be reviewed to determine if the denied service is separately reportable from the paid service. The biller might append the appropriate modifier and resubmit the claim only when well supported by documentation.
For example, the hospitalist evaluated a patient with congestive heart failure and pleural effusions. The hospitalist determined that the patient requires placement of a central venous catheter (36556). Because the patient’s underlying condition was evaluated, and resulted in the decision to place a catheter, both the visit (99233) and the procedure (36556) can be reported. If submitted without modifiers, some payors will deny payment for the visit for being integral to the catheter placement. In this case, the claim should be resubmitted with modifier 25 appended to the visit. Payors might still require documentation review to ensure legitimacy of this modifier before the claim is paid. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Reference
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: AMA Press; 2011.
Before submitting a claim, hospitalists should ensure that the service is rendered, that it is completely and accurately documented in the medical record, that the correct information is entered on the claim form, and that it is a covered benefit and eligible for payment.
Although the latter two elements typically are delegated to the billing team, hospitalists should encourage or request feedback regarding payment and denials. The ensuing open dialogue between physicians and billers might prove helpful in understanding and resolving future billing issues. Less-experienced billers first respond to claim denials by submitting documentation (i.e. “appeal with paper”) despite the inappropriateness of this action. If the denial is upheld, this attempt is viewed as unsuccessful and, without further consideration, “written off.” However, careful examination of the payor’s initial claim determination could elicit a more suitable response.
Service Provider
Provider enrollment issues can sidetrack claim submissions. Physicians must register their NPI (national provider identifier) with the correct practice location and group assignment, particularly when previously practicing physicians join a new group practice. Failure to do so is an infrequent, yet valid, cause for denial.
Alternatively, enrollment issues play a greater role when services involve nurse practitioners (NPs) and physician assistants (PAs) who are enrolled with Medicare but might be prohibited from enrolling with other payors. For example, an NP independently provides subsequent hospital care (e.g. 99232) to a Medicare beneficiary. The claim is submitted in the NP’s name and reimbursed at the correct amount by Medicare as the primary insurer. The remaining balance is submitted to the secondary insurer, who does not enroll NPPs. The claim is rejected. If the physician group has a contractual agreement to recognize NPP services by reporting them under the collaborating physician’s name, the claim can be resubmitted in the physician’s name. In absence of such an agreement, the claim should be written off.
Location
The place of service (POS) must match the reported service/procedure code. For example, a hospitalist is asked to see a patient in the ED. The patient requires further testing but does not meet the criterion for an inpatient stay. The hospitalist admits the patient to observation, treats him, and discharges him to home.
Hospitalists need to avoid the common mistake of mismatching the service code with the location/POS. Observation services performed by the “physician of record” should be reported with the corresponding codes: initial observation care (99218-99220), subsequent observation care (99224-99226), or observation discharge (99217), as appropriate.1 The correct POS should be reported as outpatient hospital (POS 22), not inpatient hospital (POS 21). Trying to report outpatient codes with an inpatient POS will result in claim denial.
A similar denial occurs when trying to report inpatient codes (99231-99233) in an outpatient location (e.g. 23-ED). These denials require claim resubmission with the correct POS and/or service/procedure code. A complete list of POS codes and corresponding definitions can be obtained from Chapter 26, Section 10.5 of the Medicare Claims Processing Manual, available at www.cms.hhs.gov/manuals/downloads/clm104c26.pdf.
Diagnosis
Denials involving diagnoses produce issues of “medical necessity.”1 Examine these denials carefully. Consider the service/procedure code when trying to formulate a response to the denial. The diagnosis code represents the reason for the service or procedure and might be a sign, symptom, or condition with which the patient presents. Medicare reimburses for procedures and services that are deemed “reasonable and necessary.”
In an effort to unify standards, Medicare has developed national coverage determinations (NCDs) to identify coverage requirements for frequent or problematic procedures or services. These coverage requirements can identify specific conditions (i.e. ICD-9-CM codes) for which the services or procedures are considered medically necessary. In the absence of a national coverage policy, an item or service could be covered at the discretion of Medicare contractors based on a local coverage determination (LCD), which varies by contractor.
Medical necessity denials often involve a mismatched or missing diagnosis. For example, a payor might deny a claim for cardiopulmonary resuscitation (92950) that is associated with a diagnosis code of congestive heart failure (428.0), despite this being the underlying condition that prompted the decline in the patient’s condition. The payor might only accept “cardiac arrest” (427.5) as the “medically necessary” diagnosis for cardiopulmonary resuscitation, as this is the direct reason necessitating the procedure. After reviewing the documentation to ensure that the documentation supports the diagnosis, the claim can be resubmitted with a confirmed and corrected diagnosis code.
Initial-Request Response
While diagnoses can lead to medical necessity issues, not all medical necessity denials are due to incorrect diagnoses. Some “medical necessity” denials result from a failure to respond to a payor request. More specifically, if the “medical necessity” denial involves a covered evaluation and management visit, the denial is more likely the result of a failure to respond to a prepayment request for documentation.
Medicare typically issues prepayment requests for documentation for the following inpatient CPT codes: 99223, 99233, 99232, 99239, and 99292.1 If the documentation is not provided to the Medicare review department within a designated time frame (e.g. 30-45 days), the claim is automatically denied. The reason for denial is cited as being “not deemed a medical necessity.” These claims do not require electronic resubmission, and instead require submission of documentation to the Medicare appeals department. Once the supporting documentation is reviewed, reimbursement is issued.
Supportive Documentation
There are times when payor requests for additional information or documentation is handled in a timely fashion. However, the paper submission might have been incomplete, as the encounter note itself might not contain the cumulative information representing the reported service.
For example, other pieces of pertinent information may be obtained from the data or order section of the chart. If the individual responsible for gathering the requested documentation does not review it before submission, important or referenced entries may be missed, and the complexity of the billed service might be sacrificed. The provider should submit any entry with the same date as the requested documentation in support: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility of the encounter note is crucial when the documentation is sent for review. Most reviewers will seek another reviewer’s assistance in translating, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied, resulting in a nonpayment or a refund. Electronic medical records (EMRs) are assisting physicians and other providers with legibility issues and improving review findings. If a physician is still writing notes by hand, a transcription might be sent along with the documentation to prevent unnecessary denials. Only consider this for requests involving providers with problematic handwriting. A legible signature is required. If a denial ensues in absence of a signature, the provider can submit an appeal with an acceptable attestation.
Modifier Considerations
Some services are denied for being “incidental/integral” to another reimbursed service (i.e. bundled). Payors implement electronic payment edits that disallow separate payment for “related” services. The industry standard, known as the National Correct Coding Initiative (NCCI), identifies code pairs that should not be reported together on the same date by either a single physician or physicians of the same specialty within a provider group.
When a claim is denied for this reason, billers tend to automatically and erroneously resubmit the claim with a modifier appended to the disallowed or “bundled” procedure code. Documentation should be reviewed to determine if the denied service is separately reportable from the paid service. The biller might append the appropriate modifier and resubmit the claim only when well supported by documentation.
For example, the hospitalist evaluated a patient with congestive heart failure and pleural effusions. The hospitalist determined that the patient requires placement of a central venous catheter (36556). Because the patient’s underlying condition was evaluated, and resulted in the decision to place a catheter, both the visit (99233) and the procedure (36556) can be reported. If submitted without modifiers, some payors will deny payment for the visit for being integral to the catheter placement. In this case, the claim should be resubmitted with modifier 25 appended to the visit. Payors might still require documentation review to ensure legitimacy of this modifier before the claim is paid. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Reference
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: AMA Press; 2011.
The To-Don’t List, Part 2


A couple of additions to the list that I started last month, in which I mentioned the problems associated with fixed-duration day shifts, a contractual vacation provision, tenure-based salary increases, poor roles for NPs and PAs, and blinded performance reporting. I think most practices would be better off without those things, and this month I’ll add a few more to the list.
I readily admit that there are some relatively rare situations in which the following things might be a good idea. But most hospitalist practices should think about alternatives.
Extra shifts. I think every hospitalist should have, within reason, a chance to work more or less than others in an HM group. And, of course, compensation should match the amount of work. So those who want to work more than the normal, or contractually required, number of shifts should have at it. But I think it is best to avoid categorizing the work into “normal” shifts and “extra” shifts. Essentially, all shifts should be thought of as “normal.”
What is the problem with having an “extra” shift category? It pretty reliably leads to confusion.
This confusion is easiest to illustrate with an example. Consider Dr. Krause, a hospitalist working in a practice with a seven-on/seven-off schedule. However, the first week in July, she works only six days, but she plans to “pay that back” and more when she works a 10-day stretch two months hence. So far, this sounds easy. By the end of September, Dr. Krause will have worked two extra shifts.
But when another hospitalist in Dr. Krause’s group is out sick in August, several hospitalists in the group rearrange their schedules to fill in. In September, Dr. Krause works the two days that she originally was scheduled to be off and trades away three of the consecutive days she was to work in September.
While it will be clear to Dr. Krause that she will be “even” in the number of shifts worked at the end of September, it probably isn’t clear to anyone else. The person who determines payroll will probably have a really hard time figuring out whether Dr. Krause is to be paid extra for “extra” shifts during any two-week pay period.
The most reliable way to figure out if a doctor worked extra shifts is to add up all worked shifts at the end of the year. But that would mean waiting until the end of the year to compensate the doctor for any extra shifts worked. And most docs would find that really unattractive.
It would be easy enough to just add up the shifts worked every pay period (usually two weeks) and compensate for any above the number expected, but that would then require lowering the salary for any pay period in which the doctor works fewer than the expected number. Although it might not be popular, I see this as the best arrangement. That is, just pay per shift so that there is no need to keep track of whether any particular shift is “normal” or “extra.”
Even if this illustration doesn’t convince you how messy it can be to keep track of extra vs. normal shifts, trust me on this one. It causes lots of problems for lots of physician practices. If your practice is among the few that has a clear-cut system that doesn’t confuse those in payroll, then stick with it.
Shift duration symmetry. Rarely is there a reason to keep every shift the same duration.
Let’s consider a common scenario. A small hospitalist group has a schedule that consists of a 12-hour day shift followed by a 12-hour night shift. As patient volume grows, the day-shift doctor(s) often have to stay after their shift to finish the initial care of new referrals, or the night doctor typically starts their shift with several patients in the ED awaiting admission. So the practice makes a good decision and creates an evening shift, which often is referred to as a “swing shift.” And because all existing shifts are 12 hours, the evening shift will be 12 hours, right?
Not so fast.
Why should the evening shift be the same duration as the day shift? Shouldn’t it be however long is necessary? Practices of no more than about 15 FTEs typically require an evening shift of only about four to six hours. It should start an hour or so before the last day doctor should be finishing work; it should continue until the night doctor has resolved the backlog of patients. As the practice volume grows, it will probably be necessary to lengthen the evening shift until it eventually reaches the same length as other shifts. But there is almost never a real workload or patient-care reason that the shift length needs to be the same duration as other shifts when it is first put into place.
While an evening shift should have a clearly defined start time, it will work best if the end of shift time is left loose and is based on just how busy that night it. For example, it might be reasonable to have the evening doctor accept their last new referral no later than a specified time (10 p.m. is the deadline in my hospitalist group). The swing shift can leave after completing the care of that patient and addressing any other issues that came up during the shift. Some nights, that will mean the evening doctor can leave at 10 p.m.; other nights, it might be 11 p.m. or midnight.
While we’re talking about it, there is no clear reason day and night shifts need to be the same length, either. It is fine to make both 12 hours long, but that isn’t the only reasonable option.
Of course, your compensation formula might influence what can be reasonably done with shift lengths. But if a practice compensates the doctors in a way that requires that all shifts be identical in duration, then the compensation method needs another look. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
A couple of additions to the list that I started last month, in which I mentioned the problems associated with fixed-duration day shifts, a contractual vacation provision, tenure-based salary increases, poor roles for NPs and PAs, and blinded performance reporting. I think most practices would be better off without those things, and this month I’ll add a few more to the list.
I readily admit that there are some relatively rare situations in which the following things might be a good idea. But most hospitalist practices should think about alternatives.
Extra shifts. I think every hospitalist should have, within reason, a chance to work more or less than others in an HM group. And, of course, compensation should match the amount of work. So those who want to work more than the normal, or contractually required, number of shifts should have at it. But I think it is best to avoid categorizing the work into “normal” shifts and “extra” shifts. Essentially, all shifts should be thought of as “normal.”
What is the problem with having an “extra” shift category? It pretty reliably leads to confusion.
This confusion is easiest to illustrate with an example. Consider Dr. Krause, a hospitalist working in a practice with a seven-on/seven-off schedule. However, the first week in July, she works only six days, but she plans to “pay that back” and more when she works a 10-day stretch two months hence. So far, this sounds easy. By the end of September, Dr. Krause will have worked two extra shifts.
But when another hospitalist in Dr. Krause’s group is out sick in August, several hospitalists in the group rearrange their schedules to fill in. In September, Dr. Krause works the two days that she originally was scheduled to be off and trades away three of the consecutive days she was to work in September.
While it will be clear to Dr. Krause that she will be “even” in the number of shifts worked at the end of September, it probably isn’t clear to anyone else. The person who determines payroll will probably have a really hard time figuring out whether Dr. Krause is to be paid extra for “extra” shifts during any two-week pay period.
The most reliable way to figure out if a doctor worked extra shifts is to add up all worked shifts at the end of the year. But that would mean waiting until the end of the year to compensate the doctor for any extra shifts worked. And most docs would find that really unattractive.
It would be easy enough to just add up the shifts worked every pay period (usually two weeks) and compensate for any above the number expected, but that would then require lowering the salary for any pay period in which the doctor works fewer than the expected number. Although it might not be popular, I see this as the best arrangement. That is, just pay per shift so that there is no need to keep track of whether any particular shift is “normal” or “extra.”
Even if this illustration doesn’t convince you how messy it can be to keep track of extra vs. normal shifts, trust me on this one. It causes lots of problems for lots of physician practices. If your practice is among the few that has a clear-cut system that doesn’t confuse those in payroll, then stick with it.
Shift duration symmetry. Rarely is there a reason to keep every shift the same duration.
Let’s consider a common scenario. A small hospitalist group has a schedule that consists of a 12-hour day shift followed by a 12-hour night shift. As patient volume grows, the day-shift doctor(s) often have to stay after their shift to finish the initial care of new referrals, or the night doctor typically starts their shift with several patients in the ED awaiting admission. So the practice makes a good decision and creates an evening shift, which often is referred to as a “swing shift.” And because all existing shifts are 12 hours, the evening shift will be 12 hours, right?
Not so fast.
Why should the evening shift be the same duration as the day shift? Shouldn’t it be however long is necessary? Practices of no more than about 15 FTEs typically require an evening shift of only about four to six hours. It should start an hour or so before the last day doctor should be finishing work; it should continue until the night doctor has resolved the backlog of patients. As the practice volume grows, it will probably be necessary to lengthen the evening shift until it eventually reaches the same length as other shifts. But there is almost never a real workload or patient-care reason that the shift length needs to be the same duration as other shifts when it is first put into place.
While an evening shift should have a clearly defined start time, it will work best if the end of shift time is left loose and is based on just how busy that night it. For example, it might be reasonable to have the evening doctor accept their last new referral no later than a specified time (10 p.m. is the deadline in my hospitalist group). The swing shift can leave after completing the care of that patient and addressing any other issues that came up during the shift. Some nights, that will mean the evening doctor can leave at 10 p.m.; other nights, it might be 11 p.m. or midnight.
While we’re talking about it, there is no clear reason day and night shifts need to be the same length, either. It is fine to make both 12 hours long, but that isn’t the only reasonable option.
Of course, your compensation formula might influence what can be reasonably done with shift lengths. But if a practice compensates the doctors in a way that requires that all shifts be identical in duration, then the compensation method needs another look. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
A couple of additions to the list that I started last month, in which I mentioned the problems associated with fixed-duration day shifts, a contractual vacation provision, tenure-based salary increases, poor roles for NPs and PAs, and blinded performance reporting. I think most practices would be better off without those things, and this month I’ll add a few more to the list.
I readily admit that there are some relatively rare situations in which the following things might be a good idea. But most hospitalist practices should think about alternatives.
Extra shifts. I think every hospitalist should have, within reason, a chance to work more or less than others in an HM group. And, of course, compensation should match the amount of work. So those who want to work more than the normal, or contractually required, number of shifts should have at it. But I think it is best to avoid categorizing the work into “normal” shifts and “extra” shifts. Essentially, all shifts should be thought of as “normal.”
What is the problem with having an “extra” shift category? It pretty reliably leads to confusion.
This confusion is easiest to illustrate with an example. Consider Dr. Krause, a hospitalist working in a practice with a seven-on/seven-off schedule. However, the first week in July, she works only six days, but she plans to “pay that back” and more when she works a 10-day stretch two months hence. So far, this sounds easy. By the end of September, Dr. Krause will have worked two extra shifts.
But when another hospitalist in Dr. Krause’s group is out sick in August, several hospitalists in the group rearrange their schedules to fill in. In September, Dr. Krause works the two days that she originally was scheduled to be off and trades away three of the consecutive days she was to work in September.
While it will be clear to Dr. Krause that she will be “even” in the number of shifts worked at the end of September, it probably isn’t clear to anyone else. The person who determines payroll will probably have a really hard time figuring out whether Dr. Krause is to be paid extra for “extra” shifts during any two-week pay period.
The most reliable way to figure out if a doctor worked extra shifts is to add up all worked shifts at the end of the year. But that would mean waiting until the end of the year to compensate the doctor for any extra shifts worked. And most docs would find that really unattractive.
It would be easy enough to just add up the shifts worked every pay period (usually two weeks) and compensate for any above the number expected, but that would then require lowering the salary for any pay period in which the doctor works fewer than the expected number. Although it might not be popular, I see this as the best arrangement. That is, just pay per shift so that there is no need to keep track of whether any particular shift is “normal” or “extra.”
Even if this illustration doesn’t convince you how messy it can be to keep track of extra vs. normal shifts, trust me on this one. It causes lots of problems for lots of physician practices. If your practice is among the few that has a clear-cut system that doesn’t confuse those in payroll, then stick with it.
Shift duration symmetry. Rarely is there a reason to keep every shift the same duration.
Let’s consider a common scenario. A small hospitalist group has a schedule that consists of a 12-hour day shift followed by a 12-hour night shift. As patient volume grows, the day-shift doctor(s) often have to stay after their shift to finish the initial care of new referrals, or the night doctor typically starts their shift with several patients in the ED awaiting admission. So the practice makes a good decision and creates an evening shift, which often is referred to as a “swing shift.” And because all existing shifts are 12 hours, the evening shift will be 12 hours, right?
Not so fast.
Why should the evening shift be the same duration as the day shift? Shouldn’t it be however long is necessary? Practices of no more than about 15 FTEs typically require an evening shift of only about four to six hours. It should start an hour or so before the last day doctor should be finishing work; it should continue until the night doctor has resolved the backlog of patients. As the practice volume grows, it will probably be necessary to lengthen the evening shift until it eventually reaches the same length as other shifts. But there is almost never a real workload or patient-care reason that the shift length needs to be the same duration as other shifts when it is first put into place.
While an evening shift should have a clearly defined start time, it will work best if the end of shift time is left loose and is based on just how busy that night it. For example, it might be reasonable to have the evening doctor accept their last new referral no later than a specified time (10 p.m. is the deadline in my hospitalist group). The swing shift can leave after completing the care of that patient and addressing any other issues that came up during the shift. Some nights, that will mean the evening doctor can leave at 10 p.m.; other nights, it might be 11 p.m. or midnight.
While we’re talking about it, there is no clear reason day and night shifts need to be the same length, either. It is fine to make both 12 hours long, but that isn’t the only reasonable option.
Of course, your compensation formula might influence what can be reasonably done with shift lengths. But if a practice compensates the doctors in a way that requires that all shifts be identical in duration, then the compensation method needs another look. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Blocked intestine after cesarean—a nonsurgical cause?…and more
a nonsurgical cause?

A 34-YEAR-OLD WOMAN GAVE BIRTH to a healthy baby by cesarean delivery. Several weeks later, the mother reported abdominal pain, distention, and nausea. Her ObGyn suspected it was related to a somatic disorder.
Two months after delivery, the mother came to the emergency department with increasingly severe symptoms. One month later, at another hospital, physicians diagnosed a bowel obstruction. During emergency surgery, a lap sponge was found within the lumen of the patient’s small intestine.
PATIENT’S CLAIM The ObGyn left the lap sponge in her abdomen during cesarean delivery.
PHYSICIAN’S DEFENSE The sponge count from the cesarean delivery was correct. The ObGyn suggested that the patient had swallowed the sponge, because it was found within the lumen of the intestine, not in free space. The surgeon who removed the sponge agreed with the ObGyn, and recommended a psychiatric consult.
VERDICT A Louisiana defense verdict was returned.
Did vacuum extraction cause developmental delays?
SUCCESSFUL DELIVERY was performed using vacuum extraction. Later, mild balance and coordination issues, cognitive deficits, and speech delay were diagnosed in the child.
PATIENT’S CLAIM Use of the vacuum extractor was unnecessary; the instrument caused a subdural bleed that resulted in the child’s developmental delays.
PHYSICIAN’S DEFENSE Vacuum extraction was necessary because the baby was not progressing down the birth canal and was beginning to show signs of distress. Vacuum extraction did not cause the child’s injuries.
VERDICT A confidential South Carolina settlement was reached during jury deliberations.
Suture fails to dissolve; fistula develops
A WOMAN UNDERWENT SURGERY for uterine fibroids, during which injury to the bladder was repaired with a single suture.
A few weeks later, she developed abdominal pain, blood in her urine, and urinary incontinence. It was determined that the suture had not dissolved, and caused obstruction of the right ureter and kidney. A vesicovaginal fistula developed when the stitch migrated through the anterior wall of the vagina.
PATIENT’S CLAIM The gynecologist was at fault for injuring the bladder during surgery, and repairing it with a nondissolving suture.
PHYSICIAN’S DEFENSE Injury to the bladder and ureters is a known risk of the procedure. The correct type of suture was used; it was supposed to dissolve. The gynecologist tested the bladder and ureters using Indigo carmine-based dye before closing.
Over time, as the suture failed to dissolve, scar tissue occluded the ureter. Subsequent surgery returned the patient to baseline health.
VERDICT A Pennsylvania defense verdict was returned.
Baby stillborn. Vasa previa missed?
ULTRASONOGRAPHY REVEALED that the patient probably had a vasa previa. Her ObGyn referred her to an OB specialist, who ordered a second scan, which ruled out vasa previa. A month later, the patient was taken to the hospital with vaginal bleeding. It was determined that she was in labor, and her ObGyn performed a cesarean delivery. The baby was stillborn.
PATIENT’S CLAIM Both ObGyns failed to diagnose a vasa previa, which caused the stillbirth. Proper diagnosis would have allowed for cesarean delivery before labor began, resulting in a successful birth.
PHYSICIANS’ DEFENSE The pregnancy was properly managed. Vasa previa had been ruled out by ultrasonography. Placental abruption or a fetal-maternal hemorrhage was responsible for the stillbirth.
VERDICT A Kentucky defense verdict was returned.
Delay in delivery, then uterine infection, then hysterectomy
A 29-YEAR-OLD WOMAN was 34 weeks’ pregnant with her third child when she suspected that her water broke, and went to the hospital. Testing revealed the membranes had ruptured, but the ObGyn elected to delay delivery.
Amniotic fluid continued to leak for 5 days when suddenly the woman’s temperature spiked. A healthy baby was delivered by cesarean section 24 hours later.
After delivery, an intrauterine infection was diagnosed in the mother. She was transferred to another hospital, where she underwent a hysterectomy.
PATIENT’S CLAIM The ObGyn was negligent in failing to deliver the child when membranes initially broke. Leaking amniotic fluid contributed to the uterine infection.
PHYSICIAN’S DEFENSE It was appropriate to allow the pregnancy to continue because the fetus was premature. Infection could have occurred regardless of when delivery was performed.
VERDICT A $25,000 Mississippi verdict was returned.
What caused this child’s brain damage?
DURING PROLONGED DELIVERY, the physician assistant and residents in charge of labor and delivery noted meconiumstained amniotic fluid discharge. When advised, the mother’s ObGyn directed the hospital staff to perform amnioinfusion. The child was born vaginally several hours later and determined to have suffered brain damage.
The child cannot swallow and receives nutrition through a feeding tube. She cannot speak, is confined to a wheelchair, and has the cognitive function of an 18-month old.
PATIENT’S CLAIM The child suffered a hypoxic event caused by meconium aspiration, resulting in encephalopathy and cerebral palsy. The finding of stained amniotic fluid should have prompted the ObGyn to perform an emergency cesarean delivery.
PHYSICIAN’S DEFENSE Electronic fetal monitoring never indicated fetal distress. Amnioinfusion cleared the amniotic fluid, making a cesarean delivery unnecessary. The child’s condition resulted from preexisting neurological problems and/or a genetic condition that also caused microcephaly, a heart defect, and polydactylism.
VERDICT A New York defense verdict was returned.
Bowel is perforated: “Now I can’t conceive”
A WOMAN WAS GIVEN A DIAGNOSIS of endometriosis. During laparoscopic surgery to treat the condition, the gynecologist used a unipolar laparoscopic coagulator wand.
Eighteen days later, the patient went to the emergency department with severe lower abdominal pain. Peritonitis, caused by bowel perforation, was diagnosed, and she underwent surgery. A portion of bowel was removed. A colostomy was created, which was later reversed.
She developed adhesions from the peritonitis and required additional surgeries that, she alleged, caused subsequent fertility treatments to be unsuccessful.
PATIENT’S CLAIM The coagulator wand perforated the bowel. The gynecologist was negligent in his use of the wand; the wand manufacturer and the electrosurgical generator manufacturer were negligent in the equipment’s design; and the hospital was negligent in its maintenance of the equipment.
DEFENDANTS’ DEFENSE The instrument manufacturer denied any design defect and argued that the injury was not a burn but was caused by the coagulator wand making contact with another surgical instrument. The physician, generator manufacturer, and hospital denied negligence.
VERDICT The claim against the gynecologist was dismissed by summary judgment. The hospital and the generator manufacturer settled for an undisclosed amount. A $2.2 million California verdict was reached against the wand manufacturer.
Child has spina bifida despite evaluation
ULTRASONOGRAPHY RESULTS indicated normal fetal growth during a woman’s pregnancy. However, the child was born with spina bifida and required back and brain surgery shortly after birth. She wears ankle and foot orthotics and is incontinent.
PATIENT’S CLAIM The ObGyn failed to perform a prenatal alpha-fetoprotein test. The radiologist misinterpreted the sonogram.
PHYSICIANS’ DEFENSE The ObGyn believes that most spina bifida conditions are detectable by ultrasonography, and the radiologist’s report did not indicate spina bifida.
VERDICT The radiologist settled for $1 million before the trial. A $2.5 million New Jersey verdict was returned against the ObGyn.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
a nonsurgical cause?
A 34-YEAR-OLD WOMAN GAVE BIRTH to a healthy baby by cesarean delivery. Several weeks later, the mother reported abdominal pain, distention, and nausea. Her ObGyn suspected it was related to a somatic disorder.
Two months after delivery, the mother came to the emergency department with increasingly severe symptoms. One month later, at another hospital, physicians diagnosed a bowel obstruction. During emergency surgery, a lap sponge was found within the lumen of the patient’s small intestine.
PATIENT’S CLAIM The ObGyn left the lap sponge in her abdomen during cesarean delivery.
PHYSICIAN’S DEFENSE The sponge count from the cesarean delivery was correct. The ObGyn suggested that the patient had swallowed the sponge, because it was found within the lumen of the intestine, not in free space. The surgeon who removed the sponge agreed with the ObGyn, and recommended a psychiatric consult.
VERDICT A Louisiana defense verdict was returned.
Did vacuum extraction cause developmental delays?
SUCCESSFUL DELIVERY was performed using vacuum extraction. Later, mild balance and coordination issues, cognitive deficits, and speech delay were diagnosed in the child.
PATIENT’S CLAIM Use of the vacuum extractor was unnecessary; the instrument caused a subdural bleed that resulted in the child’s developmental delays.
PHYSICIAN’S DEFENSE Vacuum extraction was necessary because the baby was not progressing down the birth canal and was beginning to show signs of distress. Vacuum extraction did not cause the child’s injuries.
VERDICT A confidential South Carolina settlement was reached during jury deliberations.
Suture fails to dissolve; fistula develops
A WOMAN UNDERWENT SURGERY for uterine fibroids, during which injury to the bladder was repaired with a single suture.
A few weeks later, she developed abdominal pain, blood in her urine, and urinary incontinence. It was determined that the suture had not dissolved, and caused obstruction of the right ureter and kidney. A vesicovaginal fistula developed when the stitch migrated through the anterior wall of the vagina.
PATIENT’S CLAIM The gynecologist was at fault for injuring the bladder during surgery, and repairing it with a nondissolving suture.
PHYSICIAN’S DEFENSE Injury to the bladder and ureters is a known risk of the procedure. The correct type of suture was used; it was supposed to dissolve. The gynecologist tested the bladder and ureters using Indigo carmine-based dye before closing.
Over time, as the suture failed to dissolve, scar tissue occluded the ureter. Subsequent surgery returned the patient to baseline health.
VERDICT A Pennsylvania defense verdict was returned.
Baby stillborn. Vasa previa missed?
ULTRASONOGRAPHY REVEALED that the patient probably had a vasa previa. Her ObGyn referred her to an OB specialist, who ordered a second scan, which ruled out vasa previa. A month later, the patient was taken to the hospital with vaginal bleeding. It was determined that she was in labor, and her ObGyn performed a cesarean delivery. The baby was stillborn.
PATIENT’S CLAIM Both ObGyns failed to diagnose a vasa previa, which caused the stillbirth. Proper diagnosis would have allowed for cesarean delivery before labor began, resulting in a successful birth.
PHYSICIANS’ DEFENSE The pregnancy was properly managed. Vasa previa had been ruled out by ultrasonography. Placental abruption or a fetal-maternal hemorrhage was responsible for the stillbirth.
VERDICT A Kentucky defense verdict was returned.
Delay in delivery, then uterine infection, then hysterectomy
A 29-YEAR-OLD WOMAN was 34 weeks’ pregnant with her third child when she suspected that her water broke, and went to the hospital. Testing revealed the membranes had ruptured, but the ObGyn elected to delay delivery.
Amniotic fluid continued to leak for 5 days when suddenly the woman’s temperature spiked. A healthy baby was delivered by cesarean section 24 hours later.
After delivery, an intrauterine infection was diagnosed in the mother. She was transferred to another hospital, where she underwent a hysterectomy.
PATIENT’S CLAIM The ObGyn was negligent in failing to deliver the child when membranes initially broke. Leaking amniotic fluid contributed to the uterine infection.
PHYSICIAN’S DEFENSE It was appropriate to allow the pregnancy to continue because the fetus was premature. Infection could have occurred regardless of when delivery was performed.
VERDICT A $25,000 Mississippi verdict was returned.
What caused this child’s brain damage?
DURING PROLONGED DELIVERY, the physician assistant and residents in charge of labor and delivery noted meconiumstained amniotic fluid discharge. When advised, the mother’s ObGyn directed the hospital staff to perform amnioinfusion. The child was born vaginally several hours later and determined to have suffered brain damage.
The child cannot swallow and receives nutrition through a feeding tube. She cannot speak, is confined to a wheelchair, and has the cognitive function of an 18-month old.
PATIENT’S CLAIM The child suffered a hypoxic event caused by meconium aspiration, resulting in encephalopathy and cerebral palsy. The finding of stained amniotic fluid should have prompted the ObGyn to perform an emergency cesarean delivery.
PHYSICIAN’S DEFENSE Electronic fetal monitoring never indicated fetal distress. Amnioinfusion cleared the amniotic fluid, making a cesarean delivery unnecessary. The child’s condition resulted from preexisting neurological problems and/or a genetic condition that also caused microcephaly, a heart defect, and polydactylism.
VERDICT A New York defense verdict was returned.
Bowel is perforated: “Now I can’t conceive”
A WOMAN WAS GIVEN A DIAGNOSIS of endometriosis. During laparoscopic surgery to treat the condition, the gynecologist used a unipolar laparoscopic coagulator wand.
Eighteen days later, the patient went to the emergency department with severe lower abdominal pain. Peritonitis, caused by bowel perforation, was diagnosed, and she underwent surgery. A portion of bowel was removed. A colostomy was created, which was later reversed.
She developed adhesions from the peritonitis and required additional surgeries that, she alleged, caused subsequent fertility treatments to be unsuccessful.
PATIENT’S CLAIM The coagulator wand perforated the bowel. The gynecologist was negligent in his use of the wand; the wand manufacturer and the electrosurgical generator manufacturer were negligent in the equipment’s design; and the hospital was negligent in its maintenance of the equipment.
DEFENDANTS’ DEFENSE The instrument manufacturer denied any design defect and argued that the injury was not a burn but was caused by the coagulator wand making contact with another surgical instrument. The physician, generator manufacturer, and hospital denied negligence.
VERDICT The claim against the gynecologist was dismissed by summary judgment. The hospital and the generator manufacturer settled for an undisclosed amount. A $2.2 million California verdict was reached against the wand manufacturer.
Child has spina bifida despite evaluation
ULTRASONOGRAPHY RESULTS indicated normal fetal growth during a woman’s pregnancy. However, the child was born with spina bifida and required back and brain surgery shortly after birth. She wears ankle and foot orthotics and is incontinent.
PATIENT’S CLAIM The ObGyn failed to perform a prenatal alpha-fetoprotein test. The radiologist misinterpreted the sonogram.
PHYSICIANS’ DEFENSE The ObGyn believes that most spina bifida conditions are detectable by ultrasonography, and the radiologist’s report did not indicate spina bifida.
VERDICT The radiologist settled for $1 million before the trial. A $2.5 million New Jersey verdict was returned against the ObGyn.
a nonsurgical cause?
A 34-YEAR-OLD WOMAN GAVE BIRTH to a healthy baby by cesarean delivery. Several weeks later, the mother reported abdominal pain, distention, and nausea. Her ObGyn suspected it was related to a somatic disorder.
Two months after delivery, the mother came to the emergency department with increasingly severe symptoms. One month later, at another hospital, physicians diagnosed a bowel obstruction. During emergency surgery, a lap sponge was found within the lumen of the patient’s small intestine.
PATIENT’S CLAIM The ObGyn left the lap sponge in her abdomen during cesarean delivery.
PHYSICIAN’S DEFENSE The sponge count from the cesarean delivery was correct. The ObGyn suggested that the patient had swallowed the sponge, because it was found within the lumen of the intestine, not in free space. The surgeon who removed the sponge agreed with the ObGyn, and recommended a psychiatric consult.
VERDICT A Louisiana defense verdict was returned.
Did vacuum extraction cause developmental delays?
SUCCESSFUL DELIVERY was performed using vacuum extraction. Later, mild balance and coordination issues, cognitive deficits, and speech delay were diagnosed in the child.
PATIENT’S CLAIM Use of the vacuum extractor was unnecessary; the instrument caused a subdural bleed that resulted in the child’s developmental delays.
PHYSICIAN’S DEFENSE Vacuum extraction was necessary because the baby was not progressing down the birth canal and was beginning to show signs of distress. Vacuum extraction did not cause the child’s injuries.
VERDICT A confidential South Carolina settlement was reached during jury deliberations.
Suture fails to dissolve; fistula develops
A WOMAN UNDERWENT SURGERY for uterine fibroids, during which injury to the bladder was repaired with a single suture.
A few weeks later, she developed abdominal pain, blood in her urine, and urinary incontinence. It was determined that the suture had not dissolved, and caused obstruction of the right ureter and kidney. A vesicovaginal fistula developed when the stitch migrated through the anterior wall of the vagina.
PATIENT’S CLAIM The gynecologist was at fault for injuring the bladder during surgery, and repairing it with a nondissolving suture.
PHYSICIAN’S DEFENSE Injury to the bladder and ureters is a known risk of the procedure. The correct type of suture was used; it was supposed to dissolve. The gynecologist tested the bladder and ureters using Indigo carmine-based dye before closing.
Over time, as the suture failed to dissolve, scar tissue occluded the ureter. Subsequent surgery returned the patient to baseline health.
VERDICT A Pennsylvania defense verdict was returned.
Baby stillborn. Vasa previa missed?
ULTRASONOGRAPHY REVEALED that the patient probably had a vasa previa. Her ObGyn referred her to an OB specialist, who ordered a second scan, which ruled out vasa previa. A month later, the patient was taken to the hospital with vaginal bleeding. It was determined that she was in labor, and her ObGyn performed a cesarean delivery. The baby was stillborn.
PATIENT’S CLAIM Both ObGyns failed to diagnose a vasa previa, which caused the stillbirth. Proper diagnosis would have allowed for cesarean delivery before labor began, resulting in a successful birth.
PHYSICIANS’ DEFENSE The pregnancy was properly managed. Vasa previa had been ruled out by ultrasonography. Placental abruption or a fetal-maternal hemorrhage was responsible for the stillbirth.
VERDICT A Kentucky defense verdict was returned.
Delay in delivery, then uterine infection, then hysterectomy
A 29-YEAR-OLD WOMAN was 34 weeks’ pregnant with her third child when she suspected that her water broke, and went to the hospital. Testing revealed the membranes had ruptured, but the ObGyn elected to delay delivery.
Amniotic fluid continued to leak for 5 days when suddenly the woman’s temperature spiked. A healthy baby was delivered by cesarean section 24 hours later.
After delivery, an intrauterine infection was diagnosed in the mother. She was transferred to another hospital, where she underwent a hysterectomy.
PATIENT’S CLAIM The ObGyn was negligent in failing to deliver the child when membranes initially broke. Leaking amniotic fluid contributed to the uterine infection.
PHYSICIAN’S DEFENSE It was appropriate to allow the pregnancy to continue because the fetus was premature. Infection could have occurred regardless of when delivery was performed.
VERDICT A $25,000 Mississippi verdict was returned.
What caused this child’s brain damage?
DURING PROLONGED DELIVERY, the physician assistant and residents in charge of labor and delivery noted meconiumstained amniotic fluid discharge. When advised, the mother’s ObGyn directed the hospital staff to perform amnioinfusion. The child was born vaginally several hours later and determined to have suffered brain damage.
The child cannot swallow and receives nutrition through a feeding tube. She cannot speak, is confined to a wheelchair, and has the cognitive function of an 18-month old.
PATIENT’S CLAIM The child suffered a hypoxic event caused by meconium aspiration, resulting in encephalopathy and cerebral palsy. The finding of stained amniotic fluid should have prompted the ObGyn to perform an emergency cesarean delivery.
PHYSICIAN’S DEFENSE Electronic fetal monitoring never indicated fetal distress. Amnioinfusion cleared the amniotic fluid, making a cesarean delivery unnecessary. The child’s condition resulted from preexisting neurological problems and/or a genetic condition that also caused microcephaly, a heart defect, and polydactylism.
VERDICT A New York defense verdict was returned.
Bowel is perforated: “Now I can’t conceive”
A WOMAN WAS GIVEN A DIAGNOSIS of endometriosis. During laparoscopic surgery to treat the condition, the gynecologist used a unipolar laparoscopic coagulator wand.
Eighteen days later, the patient went to the emergency department with severe lower abdominal pain. Peritonitis, caused by bowel perforation, was diagnosed, and she underwent surgery. A portion of bowel was removed. A colostomy was created, which was later reversed.
She developed adhesions from the peritonitis and required additional surgeries that, she alleged, caused subsequent fertility treatments to be unsuccessful.
PATIENT’S CLAIM The coagulator wand perforated the bowel. The gynecologist was negligent in his use of the wand; the wand manufacturer and the electrosurgical generator manufacturer were negligent in the equipment’s design; and the hospital was negligent in its maintenance of the equipment.
DEFENDANTS’ DEFENSE The instrument manufacturer denied any design defect and argued that the injury was not a burn but was caused by the coagulator wand making contact with another surgical instrument. The physician, generator manufacturer, and hospital denied negligence.
VERDICT The claim against the gynecologist was dismissed by summary judgment. The hospital and the generator manufacturer settled for an undisclosed amount. A $2.2 million California verdict was reached against the wand manufacturer.
Child has spina bifida despite evaluation
ULTRASONOGRAPHY RESULTS indicated normal fetal growth during a woman’s pregnancy. However, the child was born with spina bifida and required back and brain surgery shortly after birth. She wears ankle and foot orthotics and is incontinent.
PATIENT’S CLAIM The ObGyn failed to perform a prenatal alpha-fetoprotein test. The radiologist misinterpreted the sonogram.
PHYSICIANS’ DEFENSE The ObGyn believes that most spina bifida conditions are detectable by ultrasonography, and the radiologist’s report did not indicate spina bifida.
VERDICT The radiologist settled for $1 million before the trial. A $2.5 million New Jersey verdict was returned against the ObGyn.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
Managing Your Dermatology Practice: E-Prescribing Update
About this time last year, I wrote about electronic prescribing and the incentives that had been put in place to encourage adoption. Apparently, most of you were unimpressed; a year later e-prescribing use has increased only marginally.
The Centers for Medicare and Medicaid Services thought it could turn the tide in 2009 by adding a financial incentive: a 2% bonus on Medicare Part B payments. That didn't do the trick either; accessibility and cost issues remained, and the various "G" codes that had to be added to Medicare claims to document e-prescribing were confusing and annoying.
In 2010, CMS made it much easier to collect the incentive with minimum e-prescribing effort: If you could show that you were using a qualified e-prescribing program on only 25 Medicare claims over the course of the entire year, you got a 2% bonus on every Medicare Part B claim you filed over the entire year. They also replaced myriad confusing "G" codes with a single one, G8553.
If none of these incentives have swayed you, 2011 might be the year you are finally persuaded: CMS has not sweetened the deal.
In fact, the bonus is reduced to 1% this year. But 2011 is the last year you can avoid going electronic without generating a penalty.
In 2012, physicians filing at least the minimum 25 Medicare claims will receive a 1% bonus, but those not doing so will incur a 1% penalty.
In 2013, the incentive drops to 0.5%, and the penalty increases to 1.5%. In 2014, and beyond, there will be no incentive, but the penalty will rise to 2% and remain there.
To be clear (and I have been asked about this more than once), faxing a prescription to a pharmacy is not e-prescribing, which, by definition, is computer-to-computer (paperless) communication of prescriptions.
Many electronic medical record users are under the erroneous impression that they are e-prescribing via their EMR, when the EMR is simply generating faxes that arrive, on paper, in the pharmacy's fax machine. That is not considered e-prescribing by CMS, and it does not qualify for the financial incentive program.
A coalition of insurance and technology companies called the National ePrescribing Patient Safety Initiative (NEPSI) has provided $100 million in funding to offer free e-prescribing technology that qualifies for the program to physicians nationwide.
NEPSI members include Allscripts, Surescripts, and NaviMedix, as well as Google, Dell, Cisco Systems, Fujitsu, Microsoft, Sprint Nextel, Aetna, Horizon Blue Cross Blue Shield, WellPoint, and Wolters Kluwer Health. (I have no financial interest in any company or product mentioned in this column.)
Thanks to the efforts of NEPSI and others, e-prescribing is now easy for most practices to set up and use. Pharmacies have already done most of the work to make themselves compatible; about 70% of U.S. pharmacies can now handle electronic prescriptions.
Setup methods vary, but the concepts and requirements for each company are generally similar. You can incorporate bona fide e-prescribing into many electronic health record systems, or set it up as a separate, stand-alone system. In most cases, all you need to get started is an Internet-enabled computer with a high-speed connection and a database of patients.
Keep in mind that this will not be a complete transition; once you're set up, you cannot throw away your paper prescription pads. Besides the 30% of pharmacies not yet equipped for e-prescribing, the Drug Enforcement Administration strongly discourages sending controlled substance prescriptions electronically. (The DEA has, however, relaxed its rules somewhat on this issue in the past year.)
A nonprofit foundation called eHealth Initiative has released an excellent guide for physicians on e-prescribing.
A list of other companies currently offering e-prescribing software, along with links to their respective Web sites, can be found at www.ehealthinitiative.org/is sues/meaningful-use.html.
Whether or not a mere 1% incentive impresses you, you'll need to sign up this year or next to avoid a penalty; and with the free NEPSI program and only 25 e-prescriptions required to qualify, you will expend a minimum of cost and inconvenience in giving it a try.
About this time last year, I wrote about electronic prescribing and the incentives that had been put in place to encourage adoption. Apparently, most of you were unimpressed; a year later e-prescribing use has increased only marginally.
The Centers for Medicare and Medicaid Services thought it could turn the tide in 2009 by adding a financial incentive: a 2% bonus on Medicare Part B payments. That didn't do the trick either; accessibility and cost issues remained, and the various "G" codes that had to be added to Medicare claims to document e-prescribing were confusing and annoying.
In 2010, CMS made it much easier to collect the incentive with minimum e-prescribing effort: If you could show that you were using a qualified e-prescribing program on only 25 Medicare claims over the course of the entire year, you got a 2% bonus on every Medicare Part B claim you filed over the entire year. They also replaced myriad confusing "G" codes with a single one, G8553.
If none of these incentives have swayed you, 2011 might be the year you are finally persuaded: CMS has not sweetened the deal.
In fact, the bonus is reduced to 1% this year. But 2011 is the last year you can avoid going electronic without generating a penalty.
In 2012, physicians filing at least the minimum 25 Medicare claims will receive a 1% bonus, but those not doing so will incur a 1% penalty.
In 2013, the incentive drops to 0.5%, and the penalty increases to 1.5%. In 2014, and beyond, there will be no incentive, but the penalty will rise to 2% and remain there.
To be clear (and I have been asked about this more than once), faxing a prescription to a pharmacy is not e-prescribing, which, by definition, is computer-to-computer (paperless) communication of prescriptions.
Many electronic medical record users are under the erroneous impression that they are e-prescribing via their EMR, when the EMR is simply generating faxes that arrive, on paper, in the pharmacy's fax machine. That is not considered e-prescribing by CMS, and it does not qualify for the financial incentive program.
A coalition of insurance and technology companies called the National ePrescribing Patient Safety Initiative (NEPSI) has provided $100 million in funding to offer free e-prescribing technology that qualifies for the program to physicians nationwide.
NEPSI members include Allscripts, Surescripts, and NaviMedix, as well as Google, Dell, Cisco Systems, Fujitsu, Microsoft, Sprint Nextel, Aetna, Horizon Blue Cross Blue Shield, WellPoint, and Wolters Kluwer Health. (I have no financial interest in any company or product mentioned in this column.)
Thanks to the efforts of NEPSI and others, e-prescribing is now easy for most practices to set up and use. Pharmacies have already done most of the work to make themselves compatible; about 70% of U.S. pharmacies can now handle electronic prescriptions.
Setup methods vary, but the concepts and requirements for each company are generally similar. You can incorporate bona fide e-prescribing into many electronic health record systems, or set it up as a separate, stand-alone system. In most cases, all you need to get started is an Internet-enabled computer with a high-speed connection and a database of patients.
Keep in mind that this will not be a complete transition; once you're set up, you cannot throw away your paper prescription pads. Besides the 30% of pharmacies not yet equipped for e-prescribing, the Drug Enforcement Administration strongly discourages sending controlled substance prescriptions electronically. (The DEA has, however, relaxed its rules somewhat on this issue in the past year.)
A nonprofit foundation called eHealth Initiative has released an excellent guide for physicians on e-prescribing.
A list of other companies currently offering e-prescribing software, along with links to their respective Web sites, can be found at www.ehealthinitiative.org/is sues/meaningful-use.html.
Whether or not a mere 1% incentive impresses you, you'll need to sign up this year or next to avoid a penalty; and with the free NEPSI program and only 25 e-prescriptions required to qualify, you will expend a minimum of cost and inconvenience in giving it a try.
About this time last year, I wrote about electronic prescribing and the incentives that had been put in place to encourage adoption. Apparently, most of you were unimpressed; a year later e-prescribing use has increased only marginally.
The Centers for Medicare and Medicaid Services thought it could turn the tide in 2009 by adding a financial incentive: a 2% bonus on Medicare Part B payments. That didn't do the trick either; accessibility and cost issues remained, and the various "G" codes that had to be added to Medicare claims to document e-prescribing were confusing and annoying.
In 2010, CMS made it much easier to collect the incentive with minimum e-prescribing effort: If you could show that you were using a qualified e-prescribing program on only 25 Medicare claims over the course of the entire year, you got a 2% bonus on every Medicare Part B claim you filed over the entire year. They also replaced myriad confusing "G" codes with a single one, G8553.
If none of these incentives have swayed you, 2011 might be the year you are finally persuaded: CMS has not sweetened the deal.
In fact, the bonus is reduced to 1% this year. But 2011 is the last year you can avoid going electronic without generating a penalty.
In 2012, physicians filing at least the minimum 25 Medicare claims will receive a 1% bonus, but those not doing so will incur a 1% penalty.
In 2013, the incentive drops to 0.5%, and the penalty increases to 1.5%. In 2014, and beyond, there will be no incentive, but the penalty will rise to 2% and remain there.
To be clear (and I have been asked about this more than once), faxing a prescription to a pharmacy is not e-prescribing, which, by definition, is computer-to-computer (paperless) communication of prescriptions.
Many electronic medical record users are under the erroneous impression that they are e-prescribing via their EMR, when the EMR is simply generating faxes that arrive, on paper, in the pharmacy's fax machine. That is not considered e-prescribing by CMS, and it does not qualify for the financial incentive program.
A coalition of insurance and technology companies called the National ePrescribing Patient Safety Initiative (NEPSI) has provided $100 million in funding to offer free e-prescribing technology that qualifies for the program to physicians nationwide.
NEPSI members include Allscripts, Surescripts, and NaviMedix, as well as Google, Dell, Cisco Systems, Fujitsu, Microsoft, Sprint Nextel, Aetna, Horizon Blue Cross Blue Shield, WellPoint, and Wolters Kluwer Health. (I have no financial interest in any company or product mentioned in this column.)
Thanks to the efforts of NEPSI and others, e-prescribing is now easy for most practices to set up and use. Pharmacies have already done most of the work to make themselves compatible; about 70% of U.S. pharmacies can now handle electronic prescriptions.
Setup methods vary, but the concepts and requirements for each company are generally similar. You can incorporate bona fide e-prescribing into many electronic health record systems, or set it up as a separate, stand-alone system. In most cases, all you need to get started is an Internet-enabled computer with a high-speed connection and a database of patients.
Keep in mind that this will not be a complete transition; once you're set up, you cannot throw away your paper prescription pads. Besides the 30% of pharmacies not yet equipped for e-prescribing, the Drug Enforcement Administration strongly discourages sending controlled substance prescriptions electronically. (The DEA has, however, relaxed its rules somewhat on this issue in the past year.)
A nonprofit foundation called eHealth Initiative has released an excellent guide for physicians on e-prescribing.
A list of other companies currently offering e-prescribing software, along with links to their respective Web sites, can be found at www.ehealthinitiative.org/is sues/meaningful-use.html.
Whether or not a mere 1% incentive impresses you, you'll need to sign up this year or next to avoid a penalty; and with the free NEPSI program and only 25 e-prescriptions required to qualify, you will expend a minimum of cost and inconvenience in giving it a try.
Letters to the Editor
Pennsylvania group director sounds the call for hospitalist emancipation
Terms such as partners, associates, and K-1 are much less common in HM than other specialties. Instead, we are more familiar with such terms as medical director, employee, corporation-owned, hospital-owned, W-2. In most HM practices, there tends to be more of a hierarchal structure with unequal distribution of say and authority; 100% of the decision-making authority lies with two or three people in the group or organization.
I look around at my friends’ practices in other fields, the majority being privately owned with partnership track and equitable standing in the group, and I contrast that with what I see in nearly every HM group in my area. In HM, our fellow hospitalist must answer to his or her medical director, who then answers to the hospital administration. In many of the large, multistate corporations, the medical director answers to hospital administration as well as to a regional director, who then answers to the CMO of the corporation, who then answers to the CEO.
Rarely do you see a field of medicine that has such little autonomy. I believe it is time for hospitalists to step up to the plate and create practices in which we answer to ourselves and determine our own destinies.
Another phenomenon in HM demonstrates how everyone wants a piece of the HM action. In a 20-mile radius of where I practice, there are HM groups that have been started by specialists in other fields, including infectious disease, pulmonary, emergency medicine, and anesthesia. A cardiology acquaintance of mine recently started three hospitalist practices—single-handedly. These new additions are in addition to the HM groups started by hospital administrations and large multistate corporations.
The majority, but certainly not all, of these people or entities have very little understanding of what running a hospitalist practice entails. They might understand an HM practice to the extent that I understand how a hip replacement is done, procedurally, from my reading of a textbook or an operative note. Unless one currently practices or has recently practiced as a hospitalist, then it is difficult to fully grasp all the nuances of running an HM practice. Never have I seen a GI physician start up a cardiology group, nor have I seen an ER group start up an endocrine practice. Yet the majority of HM practices nationwide are started and controlled by entities other than the hospitalists themselves.
This recent epiphany has prompted me to sound the call for hospitalist emancipation. With a new generation of HM leaders, who now have both clinical and administrative experience in HM, it is time for hospitalists, not other specialists nor hospital administrators, to pave the course of our future in light of emerging healthcare reforms. Of course, we still need to work intimately with our parent hospitals, align our goals and vision, and be mindful of the construct in which HM is practiced. But I believe it is time for us to take control of our practices, because only we know what’s best for our patients and our fellow hospitalists.
Edward Ma, MD, hospitalist,
managing partner, Medical Inpatient Care Associates,
West Chester, Pa.,
president, The Hospitalist Consulting Group, LLC
ACGME not the only game in town for graduate medical education
I enjoy reading your column, but feel I must correct you regarding graduate medical education. You stated in your January 2011 column (“Turn to ACGME for Transfer, Resident Supervision Rules,” p. 39) that all U.S. postgraduate physician-training programs are governed by rules of the ACGME. Please note that there are hundreds of osteopathic postgraduate training programs throughout the country that are governed by the rules of the American Osteopathic Association and the osteopathic specialty colleges that sponsor these residencies and fellowships. If you need more information regarding this segment of postgraduate training, I would be more than happy to share more information with you.
Joanne Kaiser-Smith, DO,
FACOI, FACP, assistant dean,
Graduate Medical Education,
University of Medicine and Dentistry New Jersey,
School of Osteopathic Medicine, Stratford, N.J.
Dr. Hospitalist responds:
Dr. Kaiser-Smith: Thank you for your letter to the editor. You are absolutely correct. My intention was not to overlook the postgraduate training of osteopathic physicians, which, as you pointed out, is governed differently from the postgraduate allopathic training programs.
Thank you for sharing this information with our readers.
New Zealanders have pharmaceutical choice, but most choose subsidized meds
Dr. Williams’ excellent article (see “Hospitalist Down Under,” Feb-ruary 2011, p. 1) about his experiences at a country hospital in New Zealand and comparisons with the U.S. system has had a warm reception in this country. However, one statement he makes needs correction.
Dr. Williams states that if a drug was not available on the New Zealand “formulary” (the Pharmaceutical Schedule), then it is not available. The New Zealand government has separate drug evaluation (Medsafe) and funding (PHARMAC) agencies, each of which has different remits. Medsafe decides which medicines are safe and effective to use in New Zealand. PHARMAC decides which medicines will be funded by the government, and publishes this list in the Pharmaceutical Schedule.
Any Medsafe-approved drug can be prescribed for New Zealand patients, even those not on the schedule. About 20% of medicines used in New Zealand are purchased privately.
Our experience is that when faced with a choice, New Zealanders usually opt for government-funded medicines (those subsidized by PHARMAC). For this reason, the majority of medicines prescribed for New Zealand patients are funded by the government.
Thanks again for the excellent article.
Simon England,
communications manager,
PHARMAC, Wellington,
New Zealand
Pennsylvania group director sounds the call for hospitalist emancipation
Terms such as partners, associates, and K-1 are much less common in HM than other specialties. Instead, we are more familiar with such terms as medical director, employee, corporation-owned, hospital-owned, W-2. In most HM practices, there tends to be more of a hierarchal structure with unequal distribution of say and authority; 100% of the decision-making authority lies with two or three people in the group or organization.
I look around at my friends’ practices in other fields, the majority being privately owned with partnership track and equitable standing in the group, and I contrast that with what I see in nearly every HM group in my area. In HM, our fellow hospitalist must answer to his or her medical director, who then answers to the hospital administration. In many of the large, multistate corporations, the medical director answers to hospital administration as well as to a regional director, who then answers to the CMO of the corporation, who then answers to the CEO.
Rarely do you see a field of medicine that has such little autonomy. I believe it is time for hospitalists to step up to the plate and create practices in which we answer to ourselves and determine our own destinies.
Another phenomenon in HM demonstrates how everyone wants a piece of the HM action. In a 20-mile radius of where I practice, there are HM groups that have been started by specialists in other fields, including infectious disease, pulmonary, emergency medicine, and anesthesia. A cardiology acquaintance of mine recently started three hospitalist practices—single-handedly. These new additions are in addition to the HM groups started by hospital administrations and large multistate corporations.
The majority, but certainly not all, of these people or entities have very little understanding of what running a hospitalist practice entails. They might understand an HM practice to the extent that I understand how a hip replacement is done, procedurally, from my reading of a textbook or an operative note. Unless one currently practices or has recently practiced as a hospitalist, then it is difficult to fully grasp all the nuances of running an HM practice. Never have I seen a GI physician start up a cardiology group, nor have I seen an ER group start up an endocrine practice. Yet the majority of HM practices nationwide are started and controlled by entities other than the hospitalists themselves.
This recent epiphany has prompted me to sound the call for hospitalist emancipation. With a new generation of HM leaders, who now have both clinical and administrative experience in HM, it is time for hospitalists, not other specialists nor hospital administrators, to pave the course of our future in light of emerging healthcare reforms. Of course, we still need to work intimately with our parent hospitals, align our goals and vision, and be mindful of the construct in which HM is practiced. But I believe it is time for us to take control of our practices, because only we know what’s best for our patients and our fellow hospitalists.
Edward Ma, MD, hospitalist,
managing partner, Medical Inpatient Care Associates,
West Chester, Pa.,
president, The Hospitalist Consulting Group, LLC
ACGME not the only game in town for graduate medical education
I enjoy reading your column, but feel I must correct you regarding graduate medical education. You stated in your January 2011 column (“Turn to ACGME for Transfer, Resident Supervision Rules,” p. 39) that all U.S. postgraduate physician-training programs are governed by rules of the ACGME. Please note that there are hundreds of osteopathic postgraduate training programs throughout the country that are governed by the rules of the American Osteopathic Association and the osteopathic specialty colleges that sponsor these residencies and fellowships. If you need more information regarding this segment of postgraduate training, I would be more than happy to share more information with you.
Joanne Kaiser-Smith, DO,
FACOI, FACP, assistant dean,
Graduate Medical Education,
University of Medicine and Dentistry New Jersey,
School of Osteopathic Medicine, Stratford, N.J.
Dr. Hospitalist responds:
Dr. Kaiser-Smith: Thank you for your letter to the editor. You are absolutely correct. My intention was not to overlook the postgraduate training of osteopathic physicians, which, as you pointed out, is governed differently from the postgraduate allopathic training programs.
Thank you for sharing this information with our readers.
New Zealanders have pharmaceutical choice, but most choose subsidized meds
Dr. Williams’ excellent article (see “Hospitalist Down Under,” Feb-ruary 2011, p. 1) about his experiences at a country hospital in New Zealand and comparisons with the U.S. system has had a warm reception in this country. However, one statement he makes needs correction.
Dr. Williams states that if a drug was not available on the New Zealand “formulary” (the Pharmaceutical Schedule), then it is not available. The New Zealand government has separate drug evaluation (Medsafe) and funding (PHARMAC) agencies, each of which has different remits. Medsafe decides which medicines are safe and effective to use in New Zealand. PHARMAC decides which medicines will be funded by the government, and publishes this list in the Pharmaceutical Schedule.
Any Medsafe-approved drug can be prescribed for New Zealand patients, even those not on the schedule. About 20% of medicines used in New Zealand are purchased privately.
Our experience is that when faced with a choice, New Zealanders usually opt for government-funded medicines (those subsidized by PHARMAC). For this reason, the majority of medicines prescribed for New Zealand patients are funded by the government.
Thanks again for the excellent article.
Simon England,
communications manager,
PHARMAC, Wellington,
New Zealand
Pennsylvania group director sounds the call for hospitalist emancipation
Terms such as partners, associates, and K-1 are much less common in HM than other specialties. Instead, we are more familiar with such terms as medical director, employee, corporation-owned, hospital-owned, W-2. In most HM practices, there tends to be more of a hierarchal structure with unequal distribution of say and authority; 100% of the decision-making authority lies with two or three people in the group or organization.
I look around at my friends’ practices in other fields, the majority being privately owned with partnership track and equitable standing in the group, and I contrast that with what I see in nearly every HM group in my area. In HM, our fellow hospitalist must answer to his or her medical director, who then answers to the hospital administration. In many of the large, multistate corporations, the medical director answers to hospital administration as well as to a regional director, who then answers to the CMO of the corporation, who then answers to the CEO.
Rarely do you see a field of medicine that has such little autonomy. I believe it is time for hospitalists to step up to the plate and create practices in which we answer to ourselves and determine our own destinies.
Another phenomenon in HM demonstrates how everyone wants a piece of the HM action. In a 20-mile radius of where I practice, there are HM groups that have been started by specialists in other fields, including infectious disease, pulmonary, emergency medicine, and anesthesia. A cardiology acquaintance of mine recently started three hospitalist practices—single-handedly. These new additions are in addition to the HM groups started by hospital administrations and large multistate corporations.
The majority, but certainly not all, of these people or entities have very little understanding of what running a hospitalist practice entails. They might understand an HM practice to the extent that I understand how a hip replacement is done, procedurally, from my reading of a textbook or an operative note. Unless one currently practices or has recently practiced as a hospitalist, then it is difficult to fully grasp all the nuances of running an HM practice. Never have I seen a GI physician start up a cardiology group, nor have I seen an ER group start up an endocrine practice. Yet the majority of HM practices nationwide are started and controlled by entities other than the hospitalists themselves.
This recent epiphany has prompted me to sound the call for hospitalist emancipation. With a new generation of HM leaders, who now have both clinical and administrative experience in HM, it is time for hospitalists, not other specialists nor hospital administrators, to pave the course of our future in light of emerging healthcare reforms. Of course, we still need to work intimately with our parent hospitals, align our goals and vision, and be mindful of the construct in which HM is practiced. But I believe it is time for us to take control of our practices, because only we know what’s best for our patients and our fellow hospitalists.
Edward Ma, MD, hospitalist,
managing partner, Medical Inpatient Care Associates,
West Chester, Pa.,
president, The Hospitalist Consulting Group, LLC
ACGME not the only game in town for graduate medical education
I enjoy reading your column, but feel I must correct you regarding graduate medical education. You stated in your January 2011 column (“Turn to ACGME for Transfer, Resident Supervision Rules,” p. 39) that all U.S. postgraduate physician-training programs are governed by rules of the ACGME. Please note that there are hundreds of osteopathic postgraduate training programs throughout the country that are governed by the rules of the American Osteopathic Association and the osteopathic specialty colleges that sponsor these residencies and fellowships. If you need more information regarding this segment of postgraduate training, I would be more than happy to share more information with you.
Joanne Kaiser-Smith, DO,
FACOI, FACP, assistant dean,
Graduate Medical Education,
University of Medicine and Dentistry New Jersey,
School of Osteopathic Medicine, Stratford, N.J.
Dr. Hospitalist responds:
Dr. Kaiser-Smith: Thank you for your letter to the editor. You are absolutely correct. My intention was not to overlook the postgraduate training of osteopathic physicians, which, as you pointed out, is governed differently from the postgraduate allopathic training programs.
Thank you for sharing this information with our readers.
New Zealanders have pharmaceutical choice, but most choose subsidized meds
Dr. Williams’ excellent article (see “Hospitalist Down Under,” Feb-ruary 2011, p. 1) about his experiences at a country hospital in New Zealand and comparisons with the U.S. system has had a warm reception in this country. However, one statement he makes needs correction.
Dr. Williams states that if a drug was not available on the New Zealand “formulary” (the Pharmaceutical Schedule), then it is not available. The New Zealand government has separate drug evaluation (Medsafe) and funding (PHARMAC) agencies, each of which has different remits. Medsafe decides which medicines are safe and effective to use in New Zealand. PHARMAC decides which medicines will be funded by the government, and publishes this list in the Pharmaceutical Schedule.
Any Medsafe-approved drug can be prescribed for New Zealand patients, even those not on the schedule. About 20% of medicines used in New Zealand are purchased privately.
Our experience is that when faced with a choice, New Zealanders usually opt for government-funded medicines (those subsidized by PHARMAC). For this reason, the majority of medicines prescribed for New Zealand patients are funded by the government.
Thanks again for the excellent article.
Simon England,
communications manager,
PHARMAC, Wellington,
New Zealand
ONLINE EXCLUSIVE: Listen to HM experts discuss comanagement opportunities
Click here to listen to Dr. McKean
Click here to listen to Dr. Wachter
Click here to listen to Dr. Siegal
Click here to listen to Dr. Cheng
Click here to listen to Dr. Auerbach
Click here to listen to Dr. McKean
Click here to listen to Dr. Wachter
Click here to listen to Dr. Siegal
Click here to listen to Dr. Cheng
Click here to listen to Dr. Auerbach
Click here to listen to Dr. McKean
Click here to listen to Dr. Wachter
Click here to listen to Dr. Siegal
Click here to listen to Dr. Cheng
Click here to listen to Dr. Auerbach
ONLINE EXCLUSIVE: Comanagement Business Models
One of the emerging trends in comanagement by hospitalists (see “The Comanagement Conundrum,” p. 1, April 2011) is an expanded role in the perioperative care of surgical patients—extending from before the operation into rehabilitation. To be successful, hospitalists should think more broadly than the usual focus on medical needs immediately post-surgery, says Burke Kealey, MD, director of perioperative comanagement at Regions Hospital in St. Paul, Minn.
The perioperative service at Regions includes staffing of a pre-operative clinic, a partnership with the hospital’s anesthesia department, and use of a pre-operative patient checklist. Many primary-care physicians (PCPs) want to retain a role in the pre-operative assessments of their patients, so the Regions service has tried to partner with physicians in the community to work on standardizing the process.
Dr. Kealey, an SHM board member, was hired by Regions’ orthopedic department right out of residency in 1995 to do medical comanagement of its patients. His service later was absorbed into an emerging HM department. It has experimented with models including the use of nurse practitioners and physician assistants.
—Burke Kealey, MD, director of perioperative comanagement, Regions Hospital, St. Paul, Minn., SHM board member
Today, Regions dedicates three of its 16 full-time hospitalist teams to comanagement services, largely on the orthopedics floor, but also for cardiovascular surgery and urology. “As hospitalists, we can help to facilitate using the best, up-to-date medical knowledge” both before and after surgery, he says.
At the University of Rochester School of Medicine in New York, a group of fellowship-trained geriatric hospitalists has taken on comanagement of hip fracture patients at the Geriatric Fracture Center, leading to improved processes and patient outcomes.1 According to hospitalist Susan M. Friedman, MD, MPH, the program began as a collaboration between a geriatrician and an orthopedic surgeon. They found that their patients’ outcomes seemed to be better when they worked together on a case, so they sat down to talk about what they were doing and how to standardize it.
“From the start, they set the tone for how this is supposed work, and when it doesn’t, they find out why and address it,” Dr. Friedman says. The program does not use a formal service agreement, but there is a strong emphasis on co-ownership, mutual respect, and communication. “One thing that has helped us a lot is data-gathering,” she adds. The hip fracture comanagement has cut lengths of stay and readmissions by half and complications by one-third for the mostly elderly patients.
Larry Beresford is a freelance writer based in Oakland, Calif.
Reference
- Friedman SM, Mendelson DA, Bingham KW, Kates SL. Impact of co-managed geriatric fracture center on short-term hip fracture outcomes. Arch Intern Med. 2009;169(18):1712-1717.
One of the emerging trends in comanagement by hospitalists (see “The Comanagement Conundrum,” p. 1, April 2011) is an expanded role in the perioperative care of surgical patients—extending from before the operation into rehabilitation. To be successful, hospitalists should think more broadly than the usual focus on medical needs immediately post-surgery, says Burke Kealey, MD, director of perioperative comanagement at Regions Hospital in St. Paul, Minn.
The perioperative service at Regions includes staffing of a pre-operative clinic, a partnership with the hospital’s anesthesia department, and use of a pre-operative patient checklist. Many primary-care physicians (PCPs) want to retain a role in the pre-operative assessments of their patients, so the Regions service has tried to partner with physicians in the community to work on standardizing the process.
Dr. Kealey, an SHM board member, was hired by Regions’ orthopedic department right out of residency in 1995 to do medical comanagement of its patients. His service later was absorbed into an emerging HM department. It has experimented with models including the use of nurse practitioners and physician assistants.
—Burke Kealey, MD, director of perioperative comanagement, Regions Hospital, St. Paul, Minn., SHM board member
Today, Regions dedicates three of its 16 full-time hospitalist teams to comanagement services, largely on the orthopedics floor, but also for cardiovascular surgery and urology. “As hospitalists, we can help to facilitate using the best, up-to-date medical knowledge” both before and after surgery, he says.
At the University of Rochester School of Medicine in New York, a group of fellowship-trained geriatric hospitalists has taken on comanagement of hip fracture patients at the Geriatric Fracture Center, leading to improved processes and patient outcomes.1 According to hospitalist Susan M. Friedman, MD, MPH, the program began as a collaboration between a geriatrician and an orthopedic surgeon. They found that their patients’ outcomes seemed to be better when they worked together on a case, so they sat down to talk about what they were doing and how to standardize it.
“From the start, they set the tone for how this is supposed work, and when it doesn’t, they find out why and address it,” Dr. Friedman says. The program does not use a formal service agreement, but there is a strong emphasis on co-ownership, mutual respect, and communication. “One thing that has helped us a lot is data-gathering,” she adds. The hip fracture comanagement has cut lengths of stay and readmissions by half and complications by one-third for the mostly elderly patients.
Larry Beresford is a freelance writer based in Oakland, Calif.
Reference
- Friedman SM, Mendelson DA, Bingham KW, Kates SL. Impact of co-managed geriatric fracture center on short-term hip fracture outcomes. Arch Intern Med. 2009;169(18):1712-1717.
One of the emerging trends in comanagement by hospitalists (see “The Comanagement Conundrum,” p. 1, April 2011) is an expanded role in the perioperative care of surgical patients—extending from before the operation into rehabilitation. To be successful, hospitalists should think more broadly than the usual focus on medical needs immediately post-surgery, says Burke Kealey, MD, director of perioperative comanagement at Regions Hospital in St. Paul, Minn.
The perioperative service at Regions includes staffing of a pre-operative clinic, a partnership with the hospital’s anesthesia department, and use of a pre-operative patient checklist. Many primary-care physicians (PCPs) want to retain a role in the pre-operative assessments of their patients, so the Regions service has tried to partner with physicians in the community to work on standardizing the process.
Dr. Kealey, an SHM board member, was hired by Regions’ orthopedic department right out of residency in 1995 to do medical comanagement of its patients. His service later was absorbed into an emerging HM department. It has experimented with models including the use of nurse practitioners and physician assistants.
—Burke Kealey, MD, director of perioperative comanagement, Regions Hospital, St. Paul, Minn., SHM board member
Today, Regions dedicates three of its 16 full-time hospitalist teams to comanagement services, largely on the orthopedics floor, but also for cardiovascular surgery and urology. “As hospitalists, we can help to facilitate using the best, up-to-date medical knowledge” both before and after surgery, he says.
At the University of Rochester School of Medicine in New York, a group of fellowship-trained geriatric hospitalists has taken on comanagement of hip fracture patients at the Geriatric Fracture Center, leading to improved processes and patient outcomes.1 According to hospitalist Susan M. Friedman, MD, MPH, the program began as a collaboration between a geriatrician and an orthopedic surgeon. They found that their patients’ outcomes seemed to be better when they worked together on a case, so they sat down to talk about what they were doing and how to standardize it.
“From the start, they set the tone for how this is supposed work, and when it doesn’t, they find out why and address it,” Dr. Friedman says. The program does not use a formal service agreement, but there is a strong emphasis on co-ownership, mutual respect, and communication. “One thing that has helped us a lot is data-gathering,” she adds. The hip fracture comanagement has cut lengths of stay and readmissions by half and complications by one-third for the mostly elderly patients.
Larry Beresford is a freelance writer based in Oakland, Calif.
Reference
- Friedman SM, Mendelson DA, Bingham KW, Kates SL. Impact of co-managed geriatric fracture center on short-term hip fracture outcomes. Arch Intern Med. 2009;169(18):1712-1717.
Q&A with Hospitalist Administrator Amit Prachand

Amit Prachand, MEng
Division Administrator, Hospital Medicine
Northwestern Memorial Hospital and Feinberg School of Medicine,
Northwestern University, Chicago
Question: What motivated you to join SHM’s Administrators Task Force (ATF)?
A: I wanted to be able to directly interface with the community of leaders in similar administrator roles in order to obtain a stronger perspective of the role, its rewards and challenges, and of the creative solutions different practices have implemented to address issues relevant to hospital medicine and the overall healthcare delivery model. I was also relatively new to hospital medicine practice management, and even healthcare, so I wanted to put myself in the best position to soak in as much as possible as well as help facilitate the sharing of ideas amongst my new group of peers.
Q: How is the Administrators Task Force moving HM forward?
A: One of our main thrusts in the task force is to help expand the administrative membership in SHM. As hospitalist programs mature and the environment in which hospital medicine is practiced evolves, it is imperative that we develop the community, the infrastructure, and the tools required to partner with our stakeholders—both internal and external—to help lead hospital medicine forward.
Q: Has your participation in the Administrators Task Force helped your group?
A: The ATF has helped develop direct lines of communication with peers. This helps when it come to issues for which we are finding the best solutions for; areas such as on-boarding of new physicians, negotiations with hospitals, coding and billing improvement, and meaningful performance reporting.
Q: How is the task force helping hospitals improve patient care?
A: By having a peer group on the administrative side, I believe we are now able to more readily share ideas that support the ideas around patient-care improvement that are being shared amongst the physician membership.
One of the key roles we play as an administrator is to help develop the systems and structures that help improve patient care. That may range from advocating for physician representation on certain hospital committees to facilitating a process/QI project that involves hospitalists and other members of the extended patient-care team, such as physicians from other medical specialties, nursing, pharmacists, case management, bed management, environmental services, and information technology.
Q: How is the task force helping hospitals improve healthcare overall?
A: We are continually improving the infrastructure for administrators to share ideas and solutions to address overall healthcare issues (payment reform, readmissions, compliance, cost). It is through this infrastructure that we can identify best implementation practices of ideas. The webinar series (www.hospitalmedicine.org/roundtables) that we’ve developed addresses many of the issues that healthcare in general is facing. This series has exceeded expectations for participation and interest.
Q: What do you like most about your job as an administrator?
A: It is never dull, always exciting. From the firefighting to the long-term planning, the role keeps me on my toes. I enjoy being in a position that is so tightly intertwined with so many critical functions and disciplines across the medical center in a profession—hospital medicine—that is continuing to lead advances in healthcare delivery.
—Brendon Shank
Amit Prachand, MEng
Division Administrator, Hospital Medicine
Northwestern Memorial Hospital and Feinberg School of Medicine,
Northwestern University, Chicago
Question: What motivated you to join SHM’s Administrators Task Force (ATF)?
A: I wanted to be able to directly interface with the community of leaders in similar administrator roles in order to obtain a stronger perspective of the role, its rewards and challenges, and of the creative solutions different practices have implemented to address issues relevant to hospital medicine and the overall healthcare delivery model. I was also relatively new to hospital medicine practice management, and even healthcare, so I wanted to put myself in the best position to soak in as much as possible as well as help facilitate the sharing of ideas amongst my new group of peers.
Q: How is the Administrators Task Force moving HM forward?
A: One of our main thrusts in the task force is to help expand the administrative membership in SHM. As hospitalist programs mature and the environment in which hospital medicine is practiced evolves, it is imperative that we develop the community, the infrastructure, and the tools required to partner with our stakeholders—both internal and external—to help lead hospital medicine forward.
Q: Has your participation in the Administrators Task Force helped your group?
A: The ATF has helped develop direct lines of communication with peers. This helps when it come to issues for which we are finding the best solutions for; areas such as on-boarding of new physicians, negotiations with hospitals, coding and billing improvement, and meaningful performance reporting.
Q: How is the task force helping hospitals improve patient care?
A: By having a peer group on the administrative side, I believe we are now able to more readily share ideas that support the ideas around patient-care improvement that are being shared amongst the physician membership.
One of the key roles we play as an administrator is to help develop the systems and structures that help improve patient care. That may range from advocating for physician representation on certain hospital committees to facilitating a process/QI project that involves hospitalists and other members of the extended patient-care team, such as physicians from other medical specialties, nursing, pharmacists, case management, bed management, environmental services, and information technology.
Q: How is the task force helping hospitals improve healthcare overall?
A: We are continually improving the infrastructure for administrators to share ideas and solutions to address overall healthcare issues (payment reform, readmissions, compliance, cost). It is through this infrastructure that we can identify best implementation practices of ideas. The webinar series (www.hospitalmedicine.org/roundtables) that we’ve developed addresses many of the issues that healthcare in general is facing. This series has exceeded expectations for participation and interest.
Q: What do you like most about your job as an administrator?
A: It is never dull, always exciting. From the firefighting to the long-term planning, the role keeps me on my toes. I enjoy being in a position that is so tightly intertwined with so many critical functions and disciplines across the medical center in a profession—hospital medicine—that is continuing to lead advances in healthcare delivery.
—Brendon Shank
Amit Prachand, MEng
Division Administrator, Hospital Medicine
Northwestern Memorial Hospital and Feinberg School of Medicine,
Northwestern University, Chicago
Question: What motivated you to join SHM’s Administrators Task Force (ATF)?
A: I wanted to be able to directly interface with the community of leaders in similar administrator roles in order to obtain a stronger perspective of the role, its rewards and challenges, and of the creative solutions different practices have implemented to address issues relevant to hospital medicine and the overall healthcare delivery model. I was also relatively new to hospital medicine practice management, and even healthcare, so I wanted to put myself in the best position to soak in as much as possible as well as help facilitate the sharing of ideas amongst my new group of peers.
Q: How is the Administrators Task Force moving HM forward?
A: One of our main thrusts in the task force is to help expand the administrative membership in SHM. As hospitalist programs mature and the environment in which hospital medicine is practiced evolves, it is imperative that we develop the community, the infrastructure, and the tools required to partner with our stakeholders—both internal and external—to help lead hospital medicine forward.
Q: Has your participation in the Administrators Task Force helped your group?
A: The ATF has helped develop direct lines of communication with peers. This helps when it come to issues for which we are finding the best solutions for; areas such as on-boarding of new physicians, negotiations with hospitals, coding and billing improvement, and meaningful performance reporting.
Q: How is the task force helping hospitals improve patient care?
A: By having a peer group on the administrative side, I believe we are now able to more readily share ideas that support the ideas around patient-care improvement that are being shared amongst the physician membership.
One of the key roles we play as an administrator is to help develop the systems and structures that help improve patient care. That may range from advocating for physician representation on certain hospital committees to facilitating a process/QI project that involves hospitalists and other members of the extended patient-care team, such as physicians from other medical specialties, nursing, pharmacists, case management, bed management, environmental services, and information technology.
Q: How is the task force helping hospitals improve healthcare overall?
A: We are continually improving the infrastructure for administrators to share ideas and solutions to address overall healthcare issues (payment reform, readmissions, compliance, cost). It is through this infrastructure that we can identify best implementation practices of ideas. The webinar series (www.hospitalmedicine.org/roundtables) that we’ve developed addresses many of the issues that healthcare in general is facing. This series has exceeded expectations for participation and interest.
Q: What do you like most about your job as an administrator?
A: It is never dull, always exciting. From the firefighting to the long-term planning, the role keeps me on my toes. I enjoy being in a position that is so tightly intertwined with so many critical functions and disciplines across the medical center in a profession—hospital medicine—that is continuing to lead advances in healthcare delivery.
—Brendon Shank
Q&A with Hospitalist Administrator Kristi Gylten

Kristi Gylten, MBA
Director, Hospitalist Service,
Rapid City (S.D.) Regional Hospital
Question: What motivated you to join the Administrators Task Force (ATF)?
Answer: I wanted to have the opportunity to meet and network with my peers, and to be a part of developing resources and a place “on the map” for hospitalist administrators. The Administrators Task Force is bringing awareness to the administrative and business side of hospital medicine through the eyes of the hospitalist administrators.
Q: Has your participation on the task force helped out your group?
A: My group has benefited through the access and utilization of the available tools and resources to evaluate my own program, including tools like dashboards, job descriptions, patient communication, and marketing materials. The ATF has increased my awareness of the resources available, clinical and operational, to hospitalist groups, including my own.
Q: How is the ATF helping hospitals improve healthcare overall?
A: I believe the task force has its pulse on how healthcare could ideally be provided in the future. And, to me, it is extremely exciting to be part of the team that will help design the future of inpatient medicine and, in part, the continuum of care.
As hospitalist administrators, you have a close and collaborative relationship with the inpatient providers. And I think that because of that relationship and the fact that they live and breathe inpatient medicine, you are able to engage your team in improving many aspects of healthcare.
Q: What do you like most about your job as an administrator?
A: I like the wide variety of opportunities and challenges the role presents: human resources, contracting, recruitment, marketing and public relations, customer satisfaction, quality, and financials. The list goes on. No one day is like the previous, and it’s never dull. And most of all, I enjoy the challenge of strategizing and planning for the future of providing healthcare.
—Brendon Shank
Kristi Gylten, MBA
Director, Hospitalist Service,
Rapid City (S.D.) Regional Hospital
Question: What motivated you to join the Administrators Task Force (ATF)?
Answer: I wanted to have the opportunity to meet and network with my peers, and to be a part of developing resources and a place “on the map” for hospitalist administrators. The Administrators Task Force is bringing awareness to the administrative and business side of hospital medicine through the eyes of the hospitalist administrators.
Q: Has your participation on the task force helped out your group?
A: My group has benefited through the access and utilization of the available tools and resources to evaluate my own program, including tools like dashboards, job descriptions, patient communication, and marketing materials. The ATF has increased my awareness of the resources available, clinical and operational, to hospitalist groups, including my own.
Q: How is the ATF helping hospitals improve healthcare overall?
A: I believe the task force has its pulse on how healthcare could ideally be provided in the future. And, to me, it is extremely exciting to be part of the team that will help design the future of inpatient medicine and, in part, the continuum of care.
As hospitalist administrators, you have a close and collaborative relationship with the inpatient providers. And I think that because of that relationship and the fact that they live and breathe inpatient medicine, you are able to engage your team in improving many aspects of healthcare.
Q: What do you like most about your job as an administrator?
A: I like the wide variety of opportunities and challenges the role presents: human resources, contracting, recruitment, marketing and public relations, customer satisfaction, quality, and financials. The list goes on. No one day is like the previous, and it’s never dull. And most of all, I enjoy the challenge of strategizing and planning for the future of providing healthcare.
—Brendon Shank
Kristi Gylten, MBA
Director, Hospitalist Service,
Rapid City (S.D.) Regional Hospital
Question: What motivated you to join the Administrators Task Force (ATF)?
Answer: I wanted to have the opportunity to meet and network with my peers, and to be a part of developing resources and a place “on the map” for hospitalist administrators. The Administrators Task Force is bringing awareness to the administrative and business side of hospital medicine through the eyes of the hospitalist administrators.
Q: Has your participation on the task force helped out your group?
A: My group has benefited through the access and utilization of the available tools and resources to evaluate my own program, including tools like dashboards, job descriptions, patient communication, and marketing materials. The ATF has increased my awareness of the resources available, clinical and operational, to hospitalist groups, including my own.
Q: How is the ATF helping hospitals improve healthcare overall?
A: I believe the task force has its pulse on how healthcare could ideally be provided in the future. And, to me, it is extremely exciting to be part of the team that will help design the future of inpatient medicine and, in part, the continuum of care.
As hospitalist administrators, you have a close and collaborative relationship with the inpatient providers. And I think that because of that relationship and the fact that they live and breathe inpatient medicine, you are able to engage your team in improving many aspects of healthcare.
Q: What do you like most about your job as an administrator?
A: I like the wide variety of opportunities and challenges the role presents: human resources, contracting, recruitment, marketing and public relations, customer satisfaction, quality, and financials. The list goes on. No one day is like the previous, and it’s never dull. And most of all, I enjoy the challenge of strategizing and planning for the future of providing healthcare.
—Brendon Shank