User login
The To-Don’t List

Last month, I wrote about the attributes of hospitalist practices that I associate with success. This month, I’ll do the opposite. That is, I’ll write about strategies your practice could, or even should, do without. Of course, all of these things are open to debate, and some thoughtful people might (and in my experience, probably will) arrive at different conclusions.
So I offer my list as food for thought, and if your practice relies on some of these strategies, you shouldn’t feel threatened by my opinion. But you might want to think about whether they’ve been made part of your practice by design, or if things just evolved this way without careful consideration of alternatives. I’ve listed them in no particular order.
Fixed-duration day shifts. My sense is that the majority of practices have a day shift with a predetermined start and end. That is, the hospitalist is expected to arrive and depart at the same time each day.
This seems to make a lot of sense, but it ignores the dramatic variations in workload a practice will have. For example, a practice that is appropriately staffed with four daytime hospitalists, and schedules each of them to work a 12-hour shift, provides 48 hours of daytime hospitalist manpower each day. But that will turn out to be precisely the right level of staffing only a few days a year. On all other days, daytime staffing will be optimal with a different number of hours. So it would make sense for the doctors to work more or less on those days.
Telling doctors that their shift always starts at the same time has significant lifestyle advantages. But it can inhibit the doctors who would be happy to start earlier to address more discharges early in the day and potentially go home earlier. So, just like most other doctors at your hospital have, why not let the doctors have significant latitude in when they start and stop working each day? In most cases, it might be necessary to have a time by which every doctor must be available to respond to pages (and one who must be on-site before the night doctor leaves), but they should feel free to actually arrive and start working when they choose. Most will make good choices and will likely feel a little more empowered and happy with their work.
And, at the end of the day, it might be reasonable to allow some of the day-shift doctors to leave when their work is done, and allow the others to stay to handle admissions until the night shift takes over. Those who leave early might still be required to respond to pages until a specified time.
Shifts that don’t involve rounding on “continuity” patients, such as night and evening (“swing”) shifts, usually should be arranged with predetermined start. I wrote in more detail on this topic in January 2007 and October 2010.
Contractual vacation provisions. Hospitalists should have significant amounts of time off. We work a lot of evenings, nights, and weekends, and we must have liberal amounts of time away from work. But for many practices, there is no advantage in classifying this time as vacation (or CME, etc.) time. In most cases, it makes the most sense to simply specify how much work (e.g. number of shifts) a doctor is to do each year and not specify a number of days or hours of vacation time. For more detail, read “The Vacation Conundrum” from March 2007.
If your practice has a vacation system that works well, then stick with it. But if you or your administrators are going nuts trying to categorize nonworking days between vacation and days the doctor simply wasn’t scheduled, then it might be best to stop trying. Just settle on the number of shifts (or some other metric) that a doctor is to work each year.
Tenure-based salary increases. It makes a lot of sense to pay doctors in most specialties an increasing salary based on his or her tenure with the practice. As they build a patient population and a referral stream, they generate more revenue and should benefit accordingly. But a new hospitalist who joins an existing group almost never has to build the referrals. In most cases, the group hired the doctor because the referrals are already coming and the practice needs more help, or the new doctor is replacing a departing one. So paying a new hospitalist a lower salary that increases automatically every few years isn’t really a raise earned by the doctor’s improved financial performance. Usually it’s just a system of withholding money that could be available for compensation for the doctor’s first few years in the practice. This lower starting salary might adversely impact recruiting. For more, see “Compensation Conundrum” from December 2009.
Poor roles for nonphysician providers (NPPs). I’ve worked with a lot of practices that have NPs and PAs (and, in some cases, RNs) who are doing what amounts to clerical work. They’re faxing discharge summaries, making calls to schedule patient appointments, dividing up the overnight admissions for the day rounders, etc.
Don’t make this mistake. Hire a secretary for that sort of work. And be sure that the roles occupied by trained clinicians (PAs, NPs, RNs, etc.) are professionally satisfying and will position them to make an effective contribution to the practice.
For more on this topic, see “The 411 on NPPs” from September 2008 and “Role Refinement” from September 2009; the latter features the perspective of Ryan Genzink, a thoughtful PA-C from Michigan.
Blinded performance reporting. First, make sure your practice provides regular, meaningful reports on each doctor’s performance and the group as a whole. This usually takes the form of a dashboard or report card. In my experience, too few practices do this. Make sure your group isn’t in that category.
Groups that do provide performance data often allow each doctor to see only his or her data. If data about other individuals in the group are provided, the names have often been removed. With exception of certain human resources issues (e.g. counseling a doctor to prevent termination), I think all performance data in the group should be shared by name with the whole group. In most practices, everyone should know by name which doctors are the high and low producers, each doctor’s compensation, and CPT coding practices (e.g. the portion of discharges coded at the high level).
When clinical performance can be attributed to individual providers, report those metrics openly, too. This usually creates greater cohesion within the group and helps foster a mentality of practice ownership. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Last month, I wrote about the attributes of hospitalist practices that I associate with success. This month, I’ll do the opposite. That is, I’ll write about strategies your practice could, or even should, do without. Of course, all of these things are open to debate, and some thoughtful people might (and in my experience, probably will) arrive at different conclusions.
So I offer my list as food for thought, and if your practice relies on some of these strategies, you shouldn’t feel threatened by my opinion. But you might want to think about whether they’ve been made part of your practice by design, or if things just evolved this way without careful consideration of alternatives. I’ve listed them in no particular order.
Fixed-duration day shifts. My sense is that the majority of practices have a day shift with a predetermined start and end. That is, the hospitalist is expected to arrive and depart at the same time each day.
This seems to make a lot of sense, but it ignores the dramatic variations in workload a practice will have. For example, a practice that is appropriately staffed with four daytime hospitalists, and schedules each of them to work a 12-hour shift, provides 48 hours of daytime hospitalist manpower each day. But that will turn out to be precisely the right level of staffing only a few days a year. On all other days, daytime staffing will be optimal with a different number of hours. So it would make sense for the doctors to work more or less on those days.
Telling doctors that their shift always starts at the same time has significant lifestyle advantages. But it can inhibit the doctors who would be happy to start earlier to address more discharges early in the day and potentially go home earlier. So, just like most other doctors at your hospital have, why not let the doctors have significant latitude in when they start and stop working each day? In most cases, it might be necessary to have a time by which every doctor must be available to respond to pages (and one who must be on-site before the night doctor leaves), but they should feel free to actually arrive and start working when they choose. Most will make good choices and will likely feel a little more empowered and happy with their work.
And, at the end of the day, it might be reasonable to allow some of the day-shift doctors to leave when their work is done, and allow the others to stay to handle admissions until the night shift takes over. Those who leave early might still be required to respond to pages until a specified time.
Shifts that don’t involve rounding on “continuity” patients, such as night and evening (“swing”) shifts, usually should be arranged with predetermined start. I wrote in more detail on this topic in January 2007 and October 2010.
Contractual vacation provisions. Hospitalists should have significant amounts of time off. We work a lot of evenings, nights, and weekends, and we must have liberal amounts of time away from work. But for many practices, there is no advantage in classifying this time as vacation (or CME, etc.) time. In most cases, it makes the most sense to simply specify how much work (e.g. number of shifts) a doctor is to do each year and not specify a number of days or hours of vacation time. For more detail, read “The Vacation Conundrum” from March 2007.
If your practice has a vacation system that works well, then stick with it. But if you or your administrators are going nuts trying to categorize nonworking days between vacation and days the doctor simply wasn’t scheduled, then it might be best to stop trying. Just settle on the number of shifts (or some other metric) that a doctor is to work each year.
Tenure-based salary increases. It makes a lot of sense to pay doctors in most specialties an increasing salary based on his or her tenure with the practice. As they build a patient population and a referral stream, they generate more revenue and should benefit accordingly. But a new hospitalist who joins an existing group almost never has to build the referrals. In most cases, the group hired the doctor because the referrals are already coming and the practice needs more help, or the new doctor is replacing a departing one. So paying a new hospitalist a lower salary that increases automatically every few years isn’t really a raise earned by the doctor’s improved financial performance. Usually it’s just a system of withholding money that could be available for compensation for the doctor’s first few years in the practice. This lower starting salary might adversely impact recruiting. For more, see “Compensation Conundrum” from December 2009.
Poor roles for nonphysician providers (NPPs). I’ve worked with a lot of practices that have NPs and PAs (and, in some cases, RNs) who are doing what amounts to clerical work. They’re faxing discharge summaries, making calls to schedule patient appointments, dividing up the overnight admissions for the day rounders, etc.
Don’t make this mistake. Hire a secretary for that sort of work. And be sure that the roles occupied by trained clinicians (PAs, NPs, RNs, etc.) are professionally satisfying and will position them to make an effective contribution to the practice.
For more on this topic, see “The 411 on NPPs” from September 2008 and “Role Refinement” from September 2009; the latter features the perspective of Ryan Genzink, a thoughtful PA-C from Michigan.
Blinded performance reporting. First, make sure your practice provides regular, meaningful reports on each doctor’s performance and the group as a whole. This usually takes the form of a dashboard or report card. In my experience, too few practices do this. Make sure your group isn’t in that category.
Groups that do provide performance data often allow each doctor to see only his or her data. If data about other individuals in the group are provided, the names have often been removed. With exception of certain human resources issues (e.g. counseling a doctor to prevent termination), I think all performance data in the group should be shared by name with the whole group. In most practices, everyone should know by name which doctors are the high and low producers, each doctor’s compensation, and CPT coding practices (e.g. the portion of discharges coded at the high level).
When clinical performance can be attributed to individual providers, report those metrics openly, too. This usually creates greater cohesion within the group and helps foster a mentality of practice ownership. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Last month, I wrote about the attributes of hospitalist practices that I associate with success. This month, I’ll do the opposite. That is, I’ll write about strategies your practice could, or even should, do without. Of course, all of these things are open to debate, and some thoughtful people might (and in my experience, probably will) arrive at different conclusions.
So I offer my list as food for thought, and if your practice relies on some of these strategies, you shouldn’t feel threatened by my opinion. But you might want to think about whether they’ve been made part of your practice by design, or if things just evolved this way without careful consideration of alternatives. I’ve listed them in no particular order.
Fixed-duration day shifts. My sense is that the majority of practices have a day shift with a predetermined start and end. That is, the hospitalist is expected to arrive and depart at the same time each day.
This seems to make a lot of sense, but it ignores the dramatic variations in workload a practice will have. For example, a practice that is appropriately staffed with four daytime hospitalists, and schedules each of them to work a 12-hour shift, provides 48 hours of daytime hospitalist manpower each day. But that will turn out to be precisely the right level of staffing only a few days a year. On all other days, daytime staffing will be optimal with a different number of hours. So it would make sense for the doctors to work more or less on those days.
Telling doctors that their shift always starts at the same time has significant lifestyle advantages. But it can inhibit the doctors who would be happy to start earlier to address more discharges early in the day and potentially go home earlier. So, just like most other doctors at your hospital have, why not let the doctors have significant latitude in when they start and stop working each day? In most cases, it might be necessary to have a time by which every doctor must be available to respond to pages (and one who must be on-site before the night doctor leaves), but they should feel free to actually arrive and start working when they choose. Most will make good choices and will likely feel a little more empowered and happy with their work.
And, at the end of the day, it might be reasonable to allow some of the day-shift doctors to leave when their work is done, and allow the others to stay to handle admissions until the night shift takes over. Those who leave early might still be required to respond to pages until a specified time.
Shifts that don’t involve rounding on “continuity” patients, such as night and evening (“swing”) shifts, usually should be arranged with predetermined start. I wrote in more detail on this topic in January 2007 and October 2010.
Contractual vacation provisions. Hospitalists should have significant amounts of time off. We work a lot of evenings, nights, and weekends, and we must have liberal amounts of time away from work. But for many practices, there is no advantage in classifying this time as vacation (or CME, etc.) time. In most cases, it makes the most sense to simply specify how much work (e.g. number of shifts) a doctor is to do each year and not specify a number of days or hours of vacation time. For more detail, read “The Vacation Conundrum” from March 2007.
If your practice has a vacation system that works well, then stick with it. But if you or your administrators are going nuts trying to categorize nonworking days between vacation and days the doctor simply wasn’t scheduled, then it might be best to stop trying. Just settle on the number of shifts (or some other metric) that a doctor is to work each year.
Tenure-based salary increases. It makes a lot of sense to pay doctors in most specialties an increasing salary based on his or her tenure with the practice. As they build a patient population and a referral stream, they generate more revenue and should benefit accordingly. But a new hospitalist who joins an existing group almost never has to build the referrals. In most cases, the group hired the doctor because the referrals are already coming and the practice needs more help, or the new doctor is replacing a departing one. So paying a new hospitalist a lower salary that increases automatically every few years isn’t really a raise earned by the doctor’s improved financial performance. Usually it’s just a system of withholding money that could be available for compensation for the doctor’s first few years in the practice. This lower starting salary might adversely impact recruiting. For more, see “Compensation Conundrum” from December 2009.
Poor roles for nonphysician providers (NPPs). I’ve worked with a lot of practices that have NPs and PAs (and, in some cases, RNs) who are doing what amounts to clerical work. They’re faxing discharge summaries, making calls to schedule patient appointments, dividing up the overnight admissions for the day rounders, etc.
Don’t make this mistake. Hire a secretary for that sort of work. And be sure that the roles occupied by trained clinicians (PAs, NPs, RNs, etc.) are professionally satisfying and will position them to make an effective contribution to the practice.
For more on this topic, see “The 411 on NPPs” from September 2008 and “Role Refinement” from September 2009; the latter features the perspective of Ryan Genzink, a thoughtful PA-C from Michigan.
Blinded performance reporting. First, make sure your practice provides regular, meaningful reports on each doctor’s performance and the group as a whole. This usually takes the form of a dashboard or report card. In my experience, too few practices do this. Make sure your group isn’t in that category.
Groups that do provide performance data often allow each doctor to see only his or her data. If data about other individuals in the group are provided, the names have often been removed. With exception of certain human resources issues (e.g. counseling a doctor to prevent termination), I think all performance data in the group should be shared by name with the whole group. In most practices, everyone should know by name which doctors are the high and low producers, each doctor’s compensation, and CPT coding practices (e.g. the portion of discharges coded at the high level).
When clinical performance can be attributed to individual providers, report those metrics openly, too. This usually creates greater cohesion within the group and helps foster a mentality of practice ownership. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Hiring Technologically Advanced Staff
Misplaced intubation results in brain damage
PATIENT’S CLAIM The ED physician should have remained with the patient until she was in the ICU; promethazine was contraindicated and led to cardiopulmonary arrest; the ED physician failed to intubate the patient in a timely manner.
DEFENDANTS’ DEFENSE The physician’s return to the ED was proper because he handed over care to the critical care physician; promethazine was not contraindicated; appropriate care was provided, including attempts at resuscitation. The nursing staff never informed the ED physician of the patient’s history of congestive heart failure with a previous pregnancy.
VERDICT A Florida defense verdict was returned.
Heated solution burns genital area
A WOMAN UNDERWENT endometrial ablation for menorrhagia. A few days later, she discovered infected and painful blisters in her genital area.
PATIENT’S CLAIM The gynecologist was negligent in how he performed endometrial ablation. He ignored several warning beeps from the machine while the wand was filling the woman’s uterus with heated solution, and he removed the wand while it was still releasing hot liquid. The heated solution leaked from the uterus and damaged the vagina, rectal area, and other genital areas. The patient was not informed that the liquid had escaped, nor did she receive treatment for her second- and third-degree burns before she was discharged.
DEFENDANTS’ DEFENSE The gynecologist admitted that he never reviewed the operator’s manual for the procedure but denied negligence. He claimed two nurses assisting him failed to respond to his instructions to turn off the machine in time to avoid the incident. The nurses denied hearing any such instructions.
VERDICT The hospital was given a directed verdict and dismissed from the case. A $32,000 verdict was returned against the gynecologist.
Surgical towel found 6 years later
AFTER SUFFERING ABDOMINAL PAIN, a woman underwent a hysterectomy. She continued to report abdominal pain to her gynecologist for several years. Six years after the initial surgery, she sought care from another physician. During an exploratory laparotomy, a blue surgical towel was found adhered to the patient’s abdominal wall and bowel.
PATIENT’S CLAIM The gynecologist was negligent in leaving the surgical towel in the abdomen, and in failing to appropriately respond to her complaints of postoperative pain.
DEFENDANTS’ DEFENSE The hospital provides white radiopaque sponges for internal use during surgery, and those sponges were carefully counted. The blue towels were not counted because they are not intended for internal use; they are provided for medical personnel to wipe hands and medical equipment. The gynecologist claimed the hospital had not informed him that it was not counting blue towels, and that it was reasonable to expect that the blue towels had been counted.
VERDICT A $564,000 Indiana verdict was reached against the gynecologist; the hospital was vindicated.
Biopsy showed dysplasia; woman dies
AFTER AN ABNORMAL PAP SMEAR, a 27-year-old woman underwent colposcopy and cervical biopsy. When he received the test results, the gynecologist told her to return in 6 months. Three months later, she began having suspicious symptoms. When further testing yielded abnormal findings, she was referred to a gynecologic oncologist, who diagnosed cervical cancer. The woman underwent radical hysterectomy, radiotherapy, and chemotherapy, but the cancer had metastasized, and she died.
ESTATE’S CLAIM The gynecologist should have ordered additional testing when the original biopsy report was inconclusive. Advising 6-month follow-up was negligent.
PHYSICIAN’S DEFENSE The report indicated cervical dysplasia, making the 6-month time-frame proper.
VERDICT A South Carolina defense verdict was returned.
Premature baby succumbs
A PREGNANT WOMAN WAS REFERRED to a perinatal evaluation center for a full cervical examination because prior pregnancies had required cerclage. She was treated by Dr. A, a first-year intern, under the supervision of Dr. B, a fourth-year resident, and Dr. C, the attending ObGyn. Cerclage was not performed. Ten days later, the child was born at 19 weeks’ gestation, and died shortly after birth.
PATIENT’S CLAIM The hospital should have had a policy mandating that an attending physician evaluate obstetric patients whose cervical exam is abnormal. Cerclage should have been performed; cervical weakness had been treated in her second and third pregnancies, resulting in successful deliveries at 29 weeks and 34 weeks, respectively. The attending ObGyn never examined the patient.
DEFENDANTS’ DEFENSE The hospital claimed that a cervical examination showed that cerclage was unnecessary. Dr. C indicated that the correct decision and treatment were rendered; the intern and resident had reported their findings to him.
VERDICT A $3 million Pennsylvania verdict was returned.
Breast discharge during pregnancy
AT 7 MONTHS’ GESTATION, a 29-year-old woman reported burning pain and clear discharge from her right breast. The ObGyn told her he believed the complaints were related to her pregnancy; he did not examine her breasts.
The ObGyn’s partner palpated a lump in the woman’s right breast at her 6-week postpartum visit. Triple negative breast cancer was diagnosed. She underwent chemotherapy, mastectomy, and radiotherapy, but died of metastatic breast cancer.
ESTATE’S CLAIM The ObGyn failed to conduct a breast examination when the woman first complained of symptoms. This caused a delay in diagnosis, which reduced her chance of survival.
PHYSICIAN’S DEFENSE The ObGyn first denied the patient reported breast symptoms at her 7-month visit, as his records did not indicate a complaint. However, in a documented telephone call 4 days before the visit, the patient complained of burning pain and clear fluid leaking from her right breast. The ObGyn admitted that he would have followed up on the phone call, and that she must have told him complaints had subsided, or he would have noted continuing symptoms and performed a breast exam. He claimed a 3-month delay in diagnosis did not change the outcome because hers was a highly aggressive type of tumor that 1) is unresponsive to treatment and 2) carries an extremely poor survival rate compared with other types of breast cancer.
VERDICT A $1.5 million Illinois verdict was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.

PATIENT’S CLAIM The ED physician should have remained with the patient until she was in the ICU; promethazine was contraindicated and led to cardiopulmonary arrest; the ED physician failed to intubate the patient in a timely manner.
DEFENDANTS’ DEFENSE The physician’s return to the ED was proper because he handed over care to the critical care physician; promethazine was not contraindicated; appropriate care was provided, including attempts at resuscitation. The nursing staff never informed the ED physician of the patient’s history of congestive heart failure with a previous pregnancy.
VERDICT A Florida defense verdict was returned.
Heated solution burns genital area
A WOMAN UNDERWENT endometrial ablation for menorrhagia. A few days later, she discovered infected and painful blisters in her genital area.
PATIENT’S CLAIM The gynecologist was negligent in how he performed endometrial ablation. He ignored several warning beeps from the machine while the wand was filling the woman’s uterus with heated solution, and he removed the wand while it was still releasing hot liquid. The heated solution leaked from the uterus and damaged the vagina, rectal area, and other genital areas. The patient was not informed that the liquid had escaped, nor did she receive treatment for her second- and third-degree burns before she was discharged.
DEFENDANTS’ DEFENSE The gynecologist admitted that he never reviewed the operator’s manual for the procedure but denied negligence. He claimed two nurses assisting him failed to respond to his instructions to turn off the machine in time to avoid the incident. The nurses denied hearing any such instructions.
VERDICT The hospital was given a directed verdict and dismissed from the case. A $32,000 verdict was returned against the gynecologist.
Surgical towel found 6 years later
AFTER SUFFERING ABDOMINAL PAIN, a woman underwent a hysterectomy. She continued to report abdominal pain to her gynecologist for several years. Six years after the initial surgery, she sought care from another physician. During an exploratory laparotomy, a blue surgical towel was found adhered to the patient’s abdominal wall and bowel.
PATIENT’S CLAIM The gynecologist was negligent in leaving the surgical towel in the abdomen, and in failing to appropriately respond to her complaints of postoperative pain.
DEFENDANTS’ DEFENSE The hospital provides white radiopaque sponges for internal use during surgery, and those sponges were carefully counted. The blue towels were not counted because they are not intended for internal use; they are provided for medical personnel to wipe hands and medical equipment. The gynecologist claimed the hospital had not informed him that it was not counting blue towels, and that it was reasonable to expect that the blue towels had been counted.
VERDICT A $564,000 Indiana verdict was reached against the gynecologist; the hospital was vindicated.
Biopsy showed dysplasia; woman dies
AFTER AN ABNORMAL PAP SMEAR, a 27-year-old woman underwent colposcopy and cervical biopsy. When he received the test results, the gynecologist told her to return in 6 months. Three months later, she began having suspicious symptoms. When further testing yielded abnormal findings, she was referred to a gynecologic oncologist, who diagnosed cervical cancer. The woman underwent radical hysterectomy, radiotherapy, and chemotherapy, but the cancer had metastasized, and she died.
ESTATE’S CLAIM The gynecologist should have ordered additional testing when the original biopsy report was inconclusive. Advising 6-month follow-up was negligent.
PHYSICIAN’S DEFENSE The report indicated cervical dysplasia, making the 6-month time-frame proper.
VERDICT A South Carolina defense verdict was returned.
Premature baby succumbs
A PREGNANT WOMAN WAS REFERRED to a perinatal evaluation center for a full cervical examination because prior pregnancies had required cerclage. She was treated by Dr. A, a first-year intern, under the supervision of Dr. B, a fourth-year resident, and Dr. C, the attending ObGyn. Cerclage was not performed. Ten days later, the child was born at 19 weeks’ gestation, and died shortly after birth.
PATIENT’S CLAIM The hospital should have had a policy mandating that an attending physician evaluate obstetric patients whose cervical exam is abnormal. Cerclage should have been performed; cervical weakness had been treated in her second and third pregnancies, resulting in successful deliveries at 29 weeks and 34 weeks, respectively. The attending ObGyn never examined the patient.
DEFENDANTS’ DEFENSE The hospital claimed that a cervical examination showed that cerclage was unnecessary. Dr. C indicated that the correct decision and treatment were rendered; the intern and resident had reported their findings to him.
VERDICT A $3 million Pennsylvania verdict was returned.
Breast discharge during pregnancy
AT 7 MONTHS’ GESTATION, a 29-year-old woman reported burning pain and clear discharge from her right breast. The ObGyn told her he believed the complaints were related to her pregnancy; he did not examine her breasts.
The ObGyn’s partner palpated a lump in the woman’s right breast at her 6-week postpartum visit. Triple negative breast cancer was diagnosed. She underwent chemotherapy, mastectomy, and radiotherapy, but died of metastatic breast cancer.
ESTATE’S CLAIM The ObGyn failed to conduct a breast examination when the woman first complained of symptoms. This caused a delay in diagnosis, which reduced her chance of survival.
PHYSICIAN’S DEFENSE The ObGyn first denied the patient reported breast symptoms at her 7-month visit, as his records did not indicate a complaint. However, in a documented telephone call 4 days before the visit, the patient complained of burning pain and clear fluid leaking from her right breast. The ObGyn admitted that he would have followed up on the phone call, and that she must have told him complaints had subsided, or he would have noted continuing symptoms and performed a breast exam. He claimed a 3-month delay in diagnosis did not change the outcome because hers was a highly aggressive type of tumor that 1) is unresponsive to treatment and 2) carries an extremely poor survival rate compared with other types of breast cancer.
VERDICT A $1.5 million Illinois verdict was reached.
PATIENT’S CLAIM The ED physician should have remained with the patient until she was in the ICU; promethazine was contraindicated and led to cardiopulmonary arrest; the ED physician failed to intubate the patient in a timely manner.
DEFENDANTS’ DEFENSE The physician’s return to the ED was proper because he handed over care to the critical care physician; promethazine was not contraindicated; appropriate care was provided, including attempts at resuscitation. The nursing staff never informed the ED physician of the patient’s history of congestive heart failure with a previous pregnancy.
VERDICT A Florida defense verdict was returned.
Heated solution burns genital area
A WOMAN UNDERWENT endometrial ablation for menorrhagia. A few days later, she discovered infected and painful blisters in her genital area.
PATIENT’S CLAIM The gynecologist was negligent in how he performed endometrial ablation. He ignored several warning beeps from the machine while the wand was filling the woman’s uterus with heated solution, and he removed the wand while it was still releasing hot liquid. The heated solution leaked from the uterus and damaged the vagina, rectal area, and other genital areas. The patient was not informed that the liquid had escaped, nor did she receive treatment for her second- and third-degree burns before she was discharged.
DEFENDANTS’ DEFENSE The gynecologist admitted that he never reviewed the operator’s manual for the procedure but denied negligence. He claimed two nurses assisting him failed to respond to his instructions to turn off the machine in time to avoid the incident. The nurses denied hearing any such instructions.
VERDICT The hospital was given a directed verdict and dismissed from the case. A $32,000 verdict was returned against the gynecologist.
Surgical towel found 6 years later
AFTER SUFFERING ABDOMINAL PAIN, a woman underwent a hysterectomy. She continued to report abdominal pain to her gynecologist for several years. Six years after the initial surgery, she sought care from another physician. During an exploratory laparotomy, a blue surgical towel was found adhered to the patient’s abdominal wall and bowel.
PATIENT’S CLAIM The gynecologist was negligent in leaving the surgical towel in the abdomen, and in failing to appropriately respond to her complaints of postoperative pain.
DEFENDANTS’ DEFENSE The hospital provides white radiopaque sponges for internal use during surgery, and those sponges were carefully counted. The blue towels were not counted because they are not intended for internal use; they are provided for medical personnel to wipe hands and medical equipment. The gynecologist claimed the hospital had not informed him that it was not counting blue towels, and that it was reasonable to expect that the blue towels had been counted.
VERDICT A $564,000 Indiana verdict was reached against the gynecologist; the hospital was vindicated.
Biopsy showed dysplasia; woman dies
AFTER AN ABNORMAL PAP SMEAR, a 27-year-old woman underwent colposcopy and cervical biopsy. When he received the test results, the gynecologist told her to return in 6 months. Three months later, she began having suspicious symptoms. When further testing yielded abnormal findings, she was referred to a gynecologic oncologist, who diagnosed cervical cancer. The woman underwent radical hysterectomy, radiotherapy, and chemotherapy, but the cancer had metastasized, and she died.
ESTATE’S CLAIM The gynecologist should have ordered additional testing when the original biopsy report was inconclusive. Advising 6-month follow-up was negligent.
PHYSICIAN’S DEFENSE The report indicated cervical dysplasia, making the 6-month time-frame proper.
VERDICT A South Carolina defense verdict was returned.
Premature baby succumbs
A PREGNANT WOMAN WAS REFERRED to a perinatal evaluation center for a full cervical examination because prior pregnancies had required cerclage. She was treated by Dr. A, a first-year intern, under the supervision of Dr. B, a fourth-year resident, and Dr. C, the attending ObGyn. Cerclage was not performed. Ten days later, the child was born at 19 weeks’ gestation, and died shortly after birth.
PATIENT’S CLAIM The hospital should have had a policy mandating that an attending physician evaluate obstetric patients whose cervical exam is abnormal. Cerclage should have been performed; cervical weakness had been treated in her second and third pregnancies, resulting in successful deliveries at 29 weeks and 34 weeks, respectively. The attending ObGyn never examined the patient.
DEFENDANTS’ DEFENSE The hospital claimed that a cervical examination showed that cerclage was unnecessary. Dr. C indicated that the correct decision and treatment were rendered; the intern and resident had reported their findings to him.
VERDICT A $3 million Pennsylvania verdict was returned.
Breast discharge during pregnancy
AT 7 MONTHS’ GESTATION, a 29-year-old woman reported burning pain and clear discharge from her right breast. The ObGyn told her he believed the complaints were related to her pregnancy; he did not examine her breasts.
The ObGyn’s partner palpated a lump in the woman’s right breast at her 6-week postpartum visit. Triple negative breast cancer was diagnosed. She underwent chemotherapy, mastectomy, and radiotherapy, but died of metastatic breast cancer.
ESTATE’S CLAIM The ObGyn failed to conduct a breast examination when the woman first complained of symptoms. This caused a delay in diagnosis, which reduced her chance of survival.
PHYSICIAN’S DEFENSE The ObGyn first denied the patient reported breast symptoms at her 7-month visit, as his records did not indicate a complaint. However, in a documented telephone call 4 days before the visit, the patient complained of burning pain and clear fluid leaking from her right breast. The ObGyn admitted that he would have followed up on the phone call, and that she must have told him complaints had subsided, or he would have noted continuing symptoms and performed a breast exam. He claimed a 3-month delay in diagnosis did not change the outcome because hers was a highly aggressive type of tumor that 1) is unresponsive to treatment and 2) carries an extremely poor survival rate compared with other types of breast cancer.
VERDICT A $1.5 million Illinois verdict was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
Managing Your Dermatology Practice: "What's This" Rounds
How often does this happen to you? You're in a social situation, minding your own business. Someone walks up to you, hikes up his or her shirt, pants, or dress to reveal a lump, bump, or rash, and without a second thought, asks, "What's this?"
I call it "What's This Rounds." My wife and I joke about it. Each time we enter a gathering, one of us invariably will say, "I wonder what we'll see at 'What's This Rounds' tonight!"
It can happen anywhere: at a party, a ball game, or while we're strolling down the street. A man once stopped me in front of the T. Rex skeleton at the American Museum of Natural History in New York to inquire about a dermatofibroma on his leg. (To this day I have no clue who he was.)
Incredibly, I've had "what's this" phone calls as well. (Why anyone thinks I'll know what "this" is, without seeing it, is completely beyond me.) These days, I'm getting "what's this" e-mails, too - from patients and physicians!
It happens to all of us, and we joke about it. But what do you do? You don't want to appear rude or aloof; but there are obvious legal and ethical issues to consider, especially when the individuals are not under your care (as they almost never are).
Does a casual "what's this" question create a physician-patient relationship? Do you owe a "duty of care" to such people, just because they've asked you to identify a bump or rash?
As so often happens, the law in this situation is inconsistent, and unreliable; few if any written statutes directly address the issue, and courts have gone both ways.
Some judges have ruled that "informal consultations" are analogous to "Good Samaritan" encounters (although Good Samaritan laws seldom specifically cover such situations) and in the same way, cannot create a liability. Other courts have found that existence of a doctor-patient relationship has to be decided on a case-by-case basis.
Obviously, a lot depends on where you practice; legal precedents vary state by state, and it may be wise to review the situation in your state (or ask your attorney or malpractice carrier to do it for you).
Nevertheless, some basic guidelines are in order, no matter where you live.
When a relative or acquaintance asks my advice, whenever possible, I answer that this isn't the time or place. They need to come to my office (or see their own doctor) where they can be examined with the proper equipment and lighting, in proper privacy.
When I must give an answer, I always preface it with a disclaimer: We are talking informally, as opposed to professionally, and the person asking should not be relying on my advice, because I am not legally his or her doctor (as those are the two essential requirements for legal liability).
It goes without saying that I never discuss other patients, or matters outside my field of expertise, and I never prescribe medications informally.
When a colleague grabs me in the hall and asks about treating a patient I haven't seen, I preface it with a similar disclaimer. I emphasize that my advice is necessarily general and abstract because individual situations vary, and I can't really be more specific without examining the patient myself.
When the request is via e-mail (as it is, more and more often), I have a prepared, template response suggesting that a comprehensive evaluation is necessary, so that any specific diagnosis and treatment recommendations will be based on a full understanding of the patient's specific medical history, and not on secondhand or incomplete information.
If the patient already has a specific, well established diagnosis, I may suggest some potential treatment options in general, abstract terms. At the end of the template, my lawyer added a sentence emphasizing that my response does not imply a formal consulting relationship, nor am I advocating a particular course of action.
Some lawyers suggest keeping a record of informal consults in an office folder designated specifically for that purpose. You can't create a chart for a patient you have never seen, of course, but the doctor soliciting your advice may well have made a note in the patient's chart about it.
In the absence of any documentation by you, that will be the only written record. To protect yourself, you may wish to write your own note in a "miscellaneous" file that does not imply a doctor-patient relationship, but allows you to document your side of the conversation, emphasizing the informal, nonspecific, and inconclusive nature of the advice.
How often does this happen to you? You're in a social situation, minding your own business. Someone walks up to you, hikes up his or her shirt, pants, or dress to reveal a lump, bump, or rash, and without a second thought, asks, "What's this?"
I call it "What's This Rounds." My wife and I joke about it. Each time we enter a gathering, one of us invariably will say, "I wonder what we'll see at 'What's This Rounds' tonight!"
It can happen anywhere: at a party, a ball game, or while we're strolling down the street. A man once stopped me in front of the T. Rex skeleton at the American Museum of Natural History in New York to inquire about a dermatofibroma on his leg. (To this day I have no clue who he was.)
Incredibly, I've had "what's this" phone calls as well. (Why anyone thinks I'll know what "this" is, without seeing it, is completely beyond me.) These days, I'm getting "what's this" e-mails, too - from patients and physicians!
It happens to all of us, and we joke about it. But what do you do? You don't want to appear rude or aloof; but there are obvious legal and ethical issues to consider, especially when the individuals are not under your care (as they almost never are).
Does a casual "what's this" question create a physician-patient relationship? Do you owe a "duty of care" to such people, just because they've asked you to identify a bump or rash?
As so often happens, the law in this situation is inconsistent, and unreliable; few if any written statutes directly address the issue, and courts have gone both ways.
Some judges have ruled that "informal consultations" are analogous to "Good Samaritan" encounters (although Good Samaritan laws seldom specifically cover such situations) and in the same way, cannot create a liability. Other courts have found that existence of a doctor-patient relationship has to be decided on a case-by-case basis.
Obviously, a lot depends on where you practice; legal precedents vary state by state, and it may be wise to review the situation in your state (or ask your attorney or malpractice carrier to do it for you).
Nevertheless, some basic guidelines are in order, no matter where you live.
When a relative or acquaintance asks my advice, whenever possible, I answer that this isn't the time or place. They need to come to my office (or see their own doctor) where they can be examined with the proper equipment and lighting, in proper privacy.
When I must give an answer, I always preface it with a disclaimer: We are talking informally, as opposed to professionally, and the person asking should not be relying on my advice, because I am not legally his or her doctor (as those are the two essential requirements for legal liability).
It goes without saying that I never discuss other patients, or matters outside my field of expertise, and I never prescribe medications informally.
When a colleague grabs me in the hall and asks about treating a patient I haven't seen, I preface it with a similar disclaimer. I emphasize that my advice is necessarily general and abstract because individual situations vary, and I can't really be more specific without examining the patient myself.
When the request is via e-mail (as it is, more and more often), I have a prepared, template response suggesting that a comprehensive evaluation is necessary, so that any specific diagnosis and treatment recommendations will be based on a full understanding of the patient's specific medical history, and not on secondhand or incomplete information.
If the patient already has a specific, well established diagnosis, I may suggest some potential treatment options in general, abstract terms. At the end of the template, my lawyer added a sentence emphasizing that my response does not imply a formal consulting relationship, nor am I advocating a particular course of action.
Some lawyers suggest keeping a record of informal consults in an office folder designated specifically for that purpose. You can't create a chart for a patient you have never seen, of course, but the doctor soliciting your advice may well have made a note in the patient's chart about it.
In the absence of any documentation by you, that will be the only written record. To protect yourself, you may wish to write your own note in a "miscellaneous" file that does not imply a doctor-patient relationship, but allows you to document your side of the conversation, emphasizing the informal, nonspecific, and inconclusive nature of the advice.
How often does this happen to you? You're in a social situation, minding your own business. Someone walks up to you, hikes up his or her shirt, pants, or dress to reveal a lump, bump, or rash, and without a second thought, asks, "What's this?"
I call it "What's This Rounds." My wife and I joke about it. Each time we enter a gathering, one of us invariably will say, "I wonder what we'll see at 'What's This Rounds' tonight!"
It can happen anywhere: at a party, a ball game, or while we're strolling down the street. A man once stopped me in front of the T. Rex skeleton at the American Museum of Natural History in New York to inquire about a dermatofibroma on his leg. (To this day I have no clue who he was.)
Incredibly, I've had "what's this" phone calls as well. (Why anyone thinks I'll know what "this" is, without seeing it, is completely beyond me.) These days, I'm getting "what's this" e-mails, too - from patients and physicians!
It happens to all of us, and we joke about it. But what do you do? You don't want to appear rude or aloof; but there are obvious legal and ethical issues to consider, especially when the individuals are not under your care (as they almost never are).
Does a casual "what's this" question create a physician-patient relationship? Do you owe a "duty of care" to such people, just because they've asked you to identify a bump or rash?
As so often happens, the law in this situation is inconsistent, and unreliable; few if any written statutes directly address the issue, and courts have gone both ways.
Some judges have ruled that "informal consultations" are analogous to "Good Samaritan" encounters (although Good Samaritan laws seldom specifically cover such situations) and in the same way, cannot create a liability. Other courts have found that existence of a doctor-patient relationship has to be decided on a case-by-case basis.
Obviously, a lot depends on where you practice; legal precedents vary state by state, and it may be wise to review the situation in your state (or ask your attorney or malpractice carrier to do it for you).
Nevertheless, some basic guidelines are in order, no matter where you live.
When a relative or acquaintance asks my advice, whenever possible, I answer that this isn't the time or place. They need to come to my office (or see their own doctor) where they can be examined with the proper equipment and lighting, in proper privacy.
When I must give an answer, I always preface it with a disclaimer: We are talking informally, as opposed to professionally, and the person asking should not be relying on my advice, because I am not legally his or her doctor (as those are the two essential requirements for legal liability).
It goes without saying that I never discuss other patients, or matters outside my field of expertise, and I never prescribe medications informally.
When a colleague grabs me in the hall and asks about treating a patient I haven't seen, I preface it with a similar disclaimer. I emphasize that my advice is necessarily general and abstract because individual situations vary, and I can't really be more specific without examining the patient myself.
When the request is via e-mail (as it is, more and more often), I have a prepared, template response suggesting that a comprehensive evaluation is necessary, so that any specific diagnosis and treatment recommendations will be based on a full understanding of the patient's specific medical history, and not on secondhand or incomplete information.
If the patient already has a specific, well established diagnosis, I may suggest some potential treatment options in general, abstract terms. At the end of the template, my lawyer added a sentence emphasizing that my response does not imply a formal consulting relationship, nor am I advocating a particular course of action.
Some lawyers suggest keeping a record of informal consults in an office folder designated specifically for that purpose. You can't create a chart for a patient you have never seen, of course, but the doctor soliciting your advice may well have made a note in the patient's chart about it.
In the absence of any documentation by you, that will be the only written record. To protect yourself, you may wish to write your own note in a "miscellaneous" file that does not imply a doctor-patient relationship, but allows you to document your side of the conversation, emphasizing the informal, nonspecific, and inconclusive nature of the advice.
Managerial Muscle
Ajay Kharbanda, MBA, CMPE, is regional director of Arlington-based Texas Health Resources, a nonprofit healthcare system that serves 16 counties in North and Central Texas with 4,100 beds at 24 acute-care and short-stay hospitals. Kharbanda, chair of SHM’s Administrators Task Force, chatted with The Hospitalist about his work, his involvement in SHM leadership, and how administrators can work with HM to improve the healthcare delivery.
Question: How would you characterize your role?
Answer: I work closely with the medical director of the hospitalist group to support physician practice operations for employed hospitalist physicians.
Q: What do you like most about your job as an administrator?
A: I serve professionals who make a difference in people’s lives, and I work with a specialty that is making a difference in how healthcare is being delivered in the country. Additionally, I work for a health system that has the mission to improve the health of the people in the communities we serve.

Q: What motivated you to join—and lead—SHM’s Administrators Task Force?
A: I have been a member of both MGMA (Medical Group Management Association) and SHM for many years, and I have seen SHM mature in the sense of meeting needs of nonclinicians who are looking for an avenue to network and seek answers to our common issues. I remember going to annual meetings, looking for familiar faces, and seeking out peers among the stream of physicians attending the event. Several of us saw the need for an avenue, especially at the annual meetings, for administrators to huddle and brainstorm.
As nonphysician administrators, we send a powerful message about our commitment to the specialty of hospital medicine by becoming a member of the society, and we do need to remember that this is a community unique to our needs as hospital medicine practice administrators.
Q: How is the task force moving HM forward?
A: The Administrators Task Force (ATF) is helping to develop initiatives and programs that promote and define the role of nonphysician practice administrators in hospital medicine. The ATF is charged with facilitating and enhancing the integration of administrators into the society. We strive to strengthen the society’s ability to fulfill its mission by developing and using the talents of current and future administrative leaders.
Q: How is the ATF helping hospitals improve patient care?
A: I believe it is by strengthening the role of the society. ATF has reached out to administrators nationwide to build awareness of the value of SHM resources, and we advised on the practice management [curriculum] for HM10. Plus, we have created the Web-based Practice Administrators’ Roundtable Series. These quarterly events provide an opportunity to discuss issues of common concern and share best practices around various topics. Following a brief formal presentation, participants are encouraged to take part in the discussion.
We all know that SHM offers a remarkable avenue for clinical knowledge, and we are helping to build an avenue for nonclinicians.
Q: Are there ways for other hospitalists and administrators to get involved with SHM?
A: First, visit the Practice Management Institute Web page at www.hospitalmedicine.org. It has information about the Practice Administrators’ Roundtable Series and resources on staffing and scheduling, career satisfaction, and coding and documentation.
Second, come to HM11, SHM’s annual meeting. We will be hosting a special-interest forum specifically designed for administrators. TH
Brendon Shank is vice president of communications for SHM.
Ajay Kharbanda, MBA, CMPE, is regional director of Arlington-based Texas Health Resources, a nonprofit healthcare system that serves 16 counties in North and Central Texas with 4,100 beds at 24 acute-care and short-stay hospitals. Kharbanda, chair of SHM’s Administrators Task Force, chatted with The Hospitalist about his work, his involvement in SHM leadership, and how administrators can work with HM to improve the healthcare delivery.
Question: How would you characterize your role?
Answer: I work closely with the medical director of the hospitalist group to support physician practice operations for employed hospitalist physicians.
Q: What do you like most about your job as an administrator?
A: I serve professionals who make a difference in people’s lives, and I work with a specialty that is making a difference in how healthcare is being delivered in the country. Additionally, I work for a health system that has the mission to improve the health of the people in the communities we serve.
Q: What motivated you to join—and lead—SHM’s Administrators Task Force?
A: I have been a member of both MGMA (Medical Group Management Association) and SHM for many years, and I have seen SHM mature in the sense of meeting needs of nonclinicians who are looking for an avenue to network and seek answers to our common issues. I remember going to annual meetings, looking for familiar faces, and seeking out peers among the stream of physicians attending the event. Several of us saw the need for an avenue, especially at the annual meetings, for administrators to huddle and brainstorm.
As nonphysician administrators, we send a powerful message about our commitment to the specialty of hospital medicine by becoming a member of the society, and we do need to remember that this is a community unique to our needs as hospital medicine practice administrators.
Q: How is the task force moving HM forward?
A: The Administrators Task Force (ATF) is helping to develop initiatives and programs that promote and define the role of nonphysician practice administrators in hospital medicine. The ATF is charged with facilitating and enhancing the integration of administrators into the society. We strive to strengthen the society’s ability to fulfill its mission by developing and using the talents of current and future administrative leaders.
Q: How is the ATF helping hospitals improve patient care?
A: I believe it is by strengthening the role of the society. ATF has reached out to administrators nationwide to build awareness of the value of SHM resources, and we advised on the practice management [curriculum] for HM10. Plus, we have created the Web-based Practice Administrators’ Roundtable Series. These quarterly events provide an opportunity to discuss issues of common concern and share best practices around various topics. Following a brief formal presentation, participants are encouraged to take part in the discussion.
We all know that SHM offers a remarkable avenue for clinical knowledge, and we are helping to build an avenue for nonclinicians.
Q: Are there ways for other hospitalists and administrators to get involved with SHM?
A: First, visit the Practice Management Institute Web page at www.hospitalmedicine.org. It has information about the Practice Administrators’ Roundtable Series and resources on staffing and scheduling, career satisfaction, and coding and documentation.
Second, come to HM11, SHM’s annual meeting. We will be hosting a special-interest forum specifically designed for administrators. TH
Brendon Shank is vice president of communications for SHM.
Ajay Kharbanda, MBA, CMPE, is regional director of Arlington-based Texas Health Resources, a nonprofit healthcare system that serves 16 counties in North and Central Texas with 4,100 beds at 24 acute-care and short-stay hospitals. Kharbanda, chair of SHM’s Administrators Task Force, chatted with The Hospitalist about his work, his involvement in SHM leadership, and how administrators can work with HM to improve the healthcare delivery.
Question: How would you characterize your role?
Answer: I work closely with the medical director of the hospitalist group to support physician practice operations for employed hospitalist physicians.
Q: What do you like most about your job as an administrator?
A: I serve professionals who make a difference in people’s lives, and I work with a specialty that is making a difference in how healthcare is being delivered in the country. Additionally, I work for a health system that has the mission to improve the health of the people in the communities we serve.
Q: What motivated you to join—and lead—SHM’s Administrators Task Force?
A: I have been a member of both MGMA (Medical Group Management Association) and SHM for many years, and I have seen SHM mature in the sense of meeting needs of nonclinicians who are looking for an avenue to network and seek answers to our common issues. I remember going to annual meetings, looking for familiar faces, and seeking out peers among the stream of physicians attending the event. Several of us saw the need for an avenue, especially at the annual meetings, for administrators to huddle and brainstorm.
As nonphysician administrators, we send a powerful message about our commitment to the specialty of hospital medicine by becoming a member of the society, and we do need to remember that this is a community unique to our needs as hospital medicine practice administrators.
Q: How is the task force moving HM forward?
A: The Administrators Task Force (ATF) is helping to develop initiatives and programs that promote and define the role of nonphysician practice administrators in hospital medicine. The ATF is charged with facilitating and enhancing the integration of administrators into the society. We strive to strengthen the society’s ability to fulfill its mission by developing and using the talents of current and future administrative leaders.
Q: How is the ATF helping hospitals improve patient care?
A: I believe it is by strengthening the role of the society. ATF has reached out to administrators nationwide to build awareness of the value of SHM resources, and we advised on the practice management [curriculum] for HM10. Plus, we have created the Web-based Practice Administrators’ Roundtable Series. These quarterly events provide an opportunity to discuss issues of common concern and share best practices around various topics. Following a brief formal presentation, participants are encouraged to take part in the discussion.
We all know that SHM offers a remarkable avenue for clinical knowledge, and we are helping to build an avenue for nonclinicians.
Q: Are there ways for other hospitalists and administrators to get involved with SHM?
A: First, visit the Practice Management Institute Web page at www.hospitalmedicine.org. It has information about the Practice Administrators’ Roundtable Series and resources on staffing and scheduling, career satisfaction, and coding and documentation.
Second, come to HM11, SHM’s annual meeting. We will be hosting a special-interest forum specifically designed for administrators. TH
Brendon Shank is vice president of communications for SHM.
CPT 2011 Update
In the past, observation services typically did not exceed 24 hours or two calendar days. However, changes in healthcare policy coupled with the impetus to reduce wasteful spending have spurred an atmosphere of scrutiny over hospital admissions. Sometimes there are discrepancies between a hospital’s utilization review committee and a payor’s utilization review committee in determining the appropriateness of healthcare services and supplies, in accordance with each party’s definition of medical necessity. This situation has caused an increase in both the number and cost of observation stays.
In response, subsequent observation-care codes (99224-99226) were developed and published in the 2011 edition of Current Procedural Terminology (CPT).1

Codes and Their Uses
CPT outlines three subsequent observation care codes:
- 99224: Subsequent observation care, per day, for the evaluation and management (E/M) of a patient, which requires at least two of these three key components: problem-focused interval history; problem-focused examination; and medical decision-making that is straightforward or of low complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is stable, recovering, or improving. Physicians typically spend 15 minutes at the bedside and on the patient’s hospital floor or unit.
- 99225: Subsequent observation care, per day, for the E/M of a patient, which requires at least two of these three key components: expanded problem focused interval history; expanded problem focused examination; and medical decision-making of moderate complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is responding inadequately to therapy or has developed a minor complication. Physicians typically spend 25 minutes at the bedside and on the patient’s hospital floor or unit.
- 99226: Subsequent observation care, per day, for the E/M of a patient, which requires at least two of these three key components: detailed interval history; detailed examination; and medical decision-making of high complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is unstable or has developed a significant complication or a significant new problem. Physicians typically spend 35 minutes at the bedside and on the patient’s hospital floor or unit.
Subsequent observation-care codes replicate the key components and time requirements established for subsequent hospital care services (99231-99233). However, the relative value units (RVUs) of physician work associated with subsequent observation care are not weighted equally (see Table 1, below). Subsequent observation care is a less-intense service, and therefore is valued at a lesser rate.
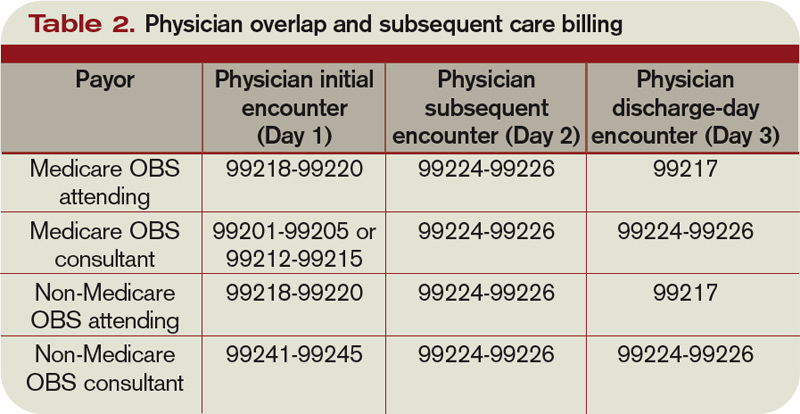
The attending of record writes the orders to admit the patient to observation (OBS); indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. Specialists typically are called onto an OBS case for their opinion/advice (i.e. consultants) but do not function as the attending of record.
According to CPT 2011, subsequent OBS care codes can be reported by both the attending physician of record and specialists who provide medically necessary, nonoverlapping care to patients on any day other than the admission or discharge day (see Table 2, above). At press time, CMS and private payors had not provided written clarification on the use of subsequent observation-care codes. Therefore, it is imperative to monitor payments, denials, and policy clarifications providing further billing instruction.
On the Horizon
Prior reporting guidelines required the reporting of subsequent observation-care days with established outpatient codes (99212-99215). Some member plans insisted on referrals for all outpatient visits regardless nature of the service. Without the mandated referral for established patient visits performed in the observation setting, physician services were denied for coverage.
The creation of subsequent observation codes might play a role in decreasing these denials. Be sure to review the private payors’ fee schedules for inclusion of 99224-99226 codes. If missing, contact the payor or include it as an agenda item during your contract negotiations.
For more information on observation care services, check out “Observation Care” in the July 2010 issue of The Hospitalist. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology: Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.8. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 16, 2011.
In the past, observation services typically did not exceed 24 hours or two calendar days. However, changes in healthcare policy coupled with the impetus to reduce wasteful spending have spurred an atmosphere of scrutiny over hospital admissions. Sometimes there are discrepancies between a hospital’s utilization review committee and a payor’s utilization review committee in determining the appropriateness of healthcare services and supplies, in accordance with each party’s definition of medical necessity. This situation has caused an increase in both the number and cost of observation stays.
In response, subsequent observation-care codes (99224-99226) were developed and published in the 2011 edition of Current Procedural Terminology (CPT).1
Codes and Their Uses
CPT outlines three subsequent observation care codes:
- 99224: Subsequent observation care, per day, for the evaluation and management (E/M) of a patient, which requires at least two of these three key components: problem-focused interval history; problem-focused examination; and medical decision-making that is straightforward or of low complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is stable, recovering, or improving. Physicians typically spend 15 minutes at the bedside and on the patient’s hospital floor or unit.
- 99225: Subsequent observation care, per day, for the E/M of a patient, which requires at least two of these three key components: expanded problem focused interval history; expanded problem focused examination; and medical decision-making of moderate complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is responding inadequately to therapy or has developed a minor complication. Physicians typically spend 25 minutes at the bedside and on the patient’s hospital floor or unit.
- 99226: Subsequent observation care, per day, for the E/M of a patient, which requires at least two of these three key components: detailed interval history; detailed examination; and medical decision-making of high complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is unstable or has developed a significant complication or a significant new problem. Physicians typically spend 35 minutes at the bedside and on the patient’s hospital floor or unit.
Subsequent observation-care codes replicate the key components and time requirements established for subsequent hospital care services (99231-99233). However, the relative value units (RVUs) of physician work associated with subsequent observation care are not weighted equally (see Table 1, below). Subsequent observation care is a less-intense service, and therefore is valued at a lesser rate.
The attending of record writes the orders to admit the patient to observation (OBS); indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. Specialists typically are called onto an OBS case for their opinion/advice (i.e. consultants) but do not function as the attending of record.
According to CPT 2011, subsequent OBS care codes can be reported by both the attending physician of record and specialists who provide medically necessary, nonoverlapping care to patients on any day other than the admission or discharge day (see Table 2, above). At press time, CMS and private payors had not provided written clarification on the use of subsequent observation-care codes. Therefore, it is imperative to monitor payments, denials, and policy clarifications providing further billing instruction.
On the Horizon
Prior reporting guidelines required the reporting of subsequent observation-care days with established outpatient codes (99212-99215). Some member plans insisted on referrals for all outpatient visits regardless nature of the service. Without the mandated referral for established patient visits performed in the observation setting, physician services were denied for coverage.
The creation of subsequent observation codes might play a role in decreasing these denials. Be sure to review the private payors’ fee schedules for inclusion of 99224-99226 codes. If missing, contact the payor or include it as an agenda item during your contract negotiations.
For more information on observation care services, check out “Observation Care” in the July 2010 issue of The Hospitalist. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology: Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.8. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 16, 2011.
In the past, observation services typically did not exceed 24 hours or two calendar days. However, changes in healthcare policy coupled with the impetus to reduce wasteful spending have spurred an atmosphere of scrutiny over hospital admissions. Sometimes there are discrepancies between a hospital’s utilization review committee and a payor’s utilization review committee in determining the appropriateness of healthcare services and supplies, in accordance with each party’s definition of medical necessity. This situation has caused an increase in both the number and cost of observation stays.
In response, subsequent observation-care codes (99224-99226) were developed and published in the 2011 edition of Current Procedural Terminology (CPT).1
Codes and Their Uses
CPT outlines three subsequent observation care codes:
- 99224: Subsequent observation care, per day, for the evaluation and management (E/M) of a patient, which requires at least two of these three key components: problem-focused interval history; problem-focused examination; and medical decision-making that is straightforward or of low complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is stable, recovering, or improving. Physicians typically spend 15 minutes at the bedside and on the patient’s hospital floor or unit.
- 99225: Subsequent observation care, per day, for the E/M of a patient, which requires at least two of these three key components: expanded problem focused interval history; expanded problem focused examination; and medical decision-making of moderate complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is responding inadequately to therapy or has developed a minor complication. Physicians typically spend 25 minutes at the bedside and on the patient’s hospital floor or unit.
- 99226: Subsequent observation care, per day, for the E/M of a patient, which requires at least two of these three key components: detailed interval history; detailed examination; and medical decision-making of high complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is unstable or has developed a significant complication or a significant new problem. Physicians typically spend 35 minutes at the bedside and on the patient’s hospital floor or unit.
Subsequent observation-care codes replicate the key components and time requirements established for subsequent hospital care services (99231-99233). However, the relative value units (RVUs) of physician work associated with subsequent observation care are not weighted equally (see Table 1, below). Subsequent observation care is a less-intense service, and therefore is valued at a lesser rate.
The attending of record writes the orders to admit the patient to observation (OBS); indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. Specialists typically are called onto an OBS case for their opinion/advice (i.e. consultants) but do not function as the attending of record.
According to CPT 2011, subsequent OBS care codes can be reported by both the attending physician of record and specialists who provide medically necessary, nonoverlapping care to patients on any day other than the admission or discharge day (see Table 2, above). At press time, CMS and private payors had not provided written clarification on the use of subsequent observation-care codes. Therefore, it is imperative to monitor payments, denials, and policy clarifications providing further billing instruction.
On the Horizon
Prior reporting guidelines required the reporting of subsequent observation-care days with established outpatient codes (99212-99215). Some member plans insisted on referrals for all outpatient visits regardless nature of the service. Without the mandated referral for established patient visits performed in the observation setting, physician services were denied for coverage.
The creation of subsequent observation codes might play a role in decreasing these denials. Be sure to review the private payors’ fee schedules for inclusion of 99224-99226 codes. If missing, contact the payor or include it as an agenda item during your contract negotiations.
For more information on observation care services, check out “Observation Care” in the July 2010 issue of The Hospitalist. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology: Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.8. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 16, 2011.
Flexibility Is King
Michael Radzienda, MD, FHM, once worked in a hospitalist program in which physicians were scheduled 30 days straight on clinical duty and 30 days off clinical duty. Although it sounds harsh by today’s standards, that job was so satisfying, he says, the schedule never felt like a burden. Conversely, he’s seen hospitalists work five days on and five days off, and the job was treacherous.
His point: Work schedules are just one influential piece of the job satisfaction pie.
“Satisfaction has more to do with work relationships and opportunities for growth,” says Dr. Radzienda, chief of hospital medicine and director of hospital medicine service at Medical College of Wisconsin/Froedtert Memorial Lutheran General Hospital in Milwaukee.
Shift-based staffing has become the norm, as more than 70% of hospitalist groups use a shift-based staffing model, according to the State of Hospital Medicine: 2010 Report Based on 2009 Data.1 That figure is up 40% from SHM’s 2005-2006 survey. Conversely, the number of HM groups employing call-based and hybrid (some shift, some call) coverage is declining—2.8% of groups employ call-based schedules, and 26.9% use a hybrid schedule. Those figures have dropped significantly from the 2005-2006 report, from 25% and 35%, respectively.
If you are going to make HM a career, you’ll need time to be with your family and pursue other interests, Dr. Radzienda says. As HM groups turn to more shift-based models, in which hospitalists work a set number of predetermined shifts and have no call responsibility, the challenge is setting a schedule that balances productivity and quality time off.
Fixed = Inflexible
The most popular way to schedule is through blocks of five days on/five days off (5/5) or seven days on/seven days off (7/7), in which hospitalists work 12 or 14 hours at a time, says Troy Ahlstrom, MD, FHM, a member of SHM’s Practice Analysis Committee and CFO of Hospitalists of Northern Michigan, a hospitalist-owned and -managed group based in Traverse City, Mich. Many HM groups employ this model because it’s easy to schedule and is attractive to residents who want a fixed schedule. But from a career satisfaction standpoint, the 5/5 and 7/7 schedule models present their own issues.
Fairness is the first potential pitfall. If all of the physicians in a group work the same schedule, they all have to log the same number of shifts and receive the same compensation. This leaves little to no wiggle room for hospitalists who want to make more money by picking up more shifts or those who want to work fewer shifts, Dr. Ahlstrom says. “People have different income goals,” he adds.
Second, physicians have to see the same number of patients throughout the day. This doesn’t take into consideration the reality that some hospitalists naturally work faster than others, thereby forcing the slower-paced doctors to keep up with an imposed patient load. “Invariably, no matter what you do, people are different,” Dr. Ahlstrom says.
Another consideration is that when physicians are working 12 to 14 hours a day, essentially they have no time for activities other than work and sleep, which doesn’t match the realities of life. Inevitably, things in personal lives crop up, which leads to swapping shifts that the group scheduler doesn’t know about or overloading the scheduler with shift-change requests, Dr. Ahlstrom explains.
Additionally, 7/7 schedules and their ilk squeeze a year’s worth of work into a compressed time frame, which can lead to intense stress and burnout, says John Nelson, MD, FACP, MHM, director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., SHM co-founder, and practice management columnist for The Hospitalist. “Maximizing the number of days off is not the holy grail,” he says. “If you choose to shut your life down on days that you work, that is going to be toxic.”
Flexibility Equates to Fairness
Dr. Nelson has long advocated a flexible shift schedule that accommodates individual preferences by giving physicians in the group autonomy in deciding how much or how little they want to work. While the group as a whole has to get all the work done, the flexibility comes from one physician taking more shifts as another takes less.
Dr. Radzienda tries to create teams within his group by pairing hospitalists with similar scheduling preferences. For example, he might have a pair working 5/5 and another working 14/14. “Up front, it takes a lot of work, but once you template it out, it becomes a good strategy,” he says.
He also strives to build robust backup plans and jeopardy models (see “Surge Protection,” September 2010, p. 43) into the schedule for short-notice callouts, as you never know when a hospitalist will need to miss a day or two because of illness or a family emergency. “Psychologically, it helps to know that you don’t have to be a hero if you’re ill or emotionally strained,” Dr. Radzienda says.
Dr. Ahlstrom agrees that a flex-schedule strategy has a positive impact on hospitalists’ career satisfaction and longevity. He suggests hospitalists be allowed to specify how many patients they want to see and be compensated according to their workload through built-in bonuses for physicians who work more. Dr. Nelson suggests paying hospitalists per relative value unit (RVU) of work. “I think hospitalists would like it and find it liberating to be paid on production,” he says.
An added bonus to flexible work hours and patient load, according to Dr. Ahlstrom, is that pay difference “will lead to a far more collegial atmosphere, because physicians know they are getting compensated fairly for the amount of work done.”
Another advantage of a flexible schedule is hospitalists knowing they have the option of ramping up or scaling back the number of shifts they work, Dr. Ahlstrom says—for example, a physician who wants to reduce shifts in order to coach his daughter’s softball team or have Friday nights off to watch her son play high school football.
“You prevent burnout by allowing people to change their work schedule depending on what’s going on in their life,” Dr. Ahlstrom says. TH
Lisa Ryan is a freelance writer based in New Jersey.
Michael Radzienda, MD, FHM, once worked in a hospitalist program in which physicians were scheduled 30 days straight on clinical duty and 30 days off clinical duty. Although it sounds harsh by today’s standards, that job was so satisfying, he says, the schedule never felt like a burden. Conversely, he’s seen hospitalists work five days on and five days off, and the job was treacherous.
His point: Work schedules are just one influential piece of the job satisfaction pie.
“Satisfaction has more to do with work relationships and opportunities for growth,” says Dr. Radzienda, chief of hospital medicine and director of hospital medicine service at Medical College of Wisconsin/Froedtert Memorial Lutheran General Hospital in Milwaukee.
Shift-based staffing has become the norm, as more than 70% of hospitalist groups use a shift-based staffing model, according to the State of Hospital Medicine: 2010 Report Based on 2009 Data.1 That figure is up 40% from SHM’s 2005-2006 survey. Conversely, the number of HM groups employing call-based and hybrid (some shift, some call) coverage is declining—2.8% of groups employ call-based schedules, and 26.9% use a hybrid schedule. Those figures have dropped significantly from the 2005-2006 report, from 25% and 35%, respectively.
If you are going to make HM a career, you’ll need time to be with your family and pursue other interests, Dr. Radzienda says. As HM groups turn to more shift-based models, in which hospitalists work a set number of predetermined shifts and have no call responsibility, the challenge is setting a schedule that balances productivity and quality time off.
Fixed = Inflexible
The most popular way to schedule is through blocks of five days on/five days off (5/5) or seven days on/seven days off (7/7), in which hospitalists work 12 or 14 hours at a time, says Troy Ahlstrom, MD, FHM, a member of SHM’s Practice Analysis Committee and CFO of Hospitalists of Northern Michigan, a hospitalist-owned and -managed group based in Traverse City, Mich. Many HM groups employ this model because it’s easy to schedule and is attractive to residents who want a fixed schedule. But from a career satisfaction standpoint, the 5/5 and 7/7 schedule models present their own issues.
Fairness is the first potential pitfall. If all of the physicians in a group work the same schedule, they all have to log the same number of shifts and receive the same compensation. This leaves little to no wiggle room for hospitalists who want to make more money by picking up more shifts or those who want to work fewer shifts, Dr. Ahlstrom says. “People have different income goals,” he adds.
Second, physicians have to see the same number of patients throughout the day. This doesn’t take into consideration the reality that some hospitalists naturally work faster than others, thereby forcing the slower-paced doctors to keep up with an imposed patient load. “Invariably, no matter what you do, people are different,” Dr. Ahlstrom says.
Another consideration is that when physicians are working 12 to 14 hours a day, essentially they have no time for activities other than work and sleep, which doesn’t match the realities of life. Inevitably, things in personal lives crop up, which leads to swapping shifts that the group scheduler doesn’t know about or overloading the scheduler with shift-change requests, Dr. Ahlstrom explains.
Additionally, 7/7 schedules and their ilk squeeze a year’s worth of work into a compressed time frame, which can lead to intense stress and burnout, says John Nelson, MD, FACP, MHM, director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., SHM co-founder, and practice management columnist for The Hospitalist. “Maximizing the number of days off is not the holy grail,” he says. “If you choose to shut your life down on days that you work, that is going to be toxic.”
Flexibility Equates to Fairness
Dr. Nelson has long advocated a flexible shift schedule that accommodates individual preferences by giving physicians in the group autonomy in deciding how much or how little they want to work. While the group as a whole has to get all the work done, the flexibility comes from one physician taking more shifts as another takes less.
Dr. Radzienda tries to create teams within his group by pairing hospitalists with similar scheduling preferences. For example, he might have a pair working 5/5 and another working 14/14. “Up front, it takes a lot of work, but once you template it out, it becomes a good strategy,” he says.
He also strives to build robust backup plans and jeopardy models (see “Surge Protection,” September 2010, p. 43) into the schedule for short-notice callouts, as you never know when a hospitalist will need to miss a day or two because of illness or a family emergency. “Psychologically, it helps to know that you don’t have to be a hero if you’re ill or emotionally strained,” Dr. Radzienda says.
Dr. Ahlstrom agrees that a flex-schedule strategy has a positive impact on hospitalists’ career satisfaction and longevity. He suggests hospitalists be allowed to specify how many patients they want to see and be compensated according to their workload through built-in bonuses for physicians who work more. Dr. Nelson suggests paying hospitalists per relative value unit (RVU) of work. “I think hospitalists would like it and find it liberating to be paid on production,” he says.
An added bonus to flexible work hours and patient load, according to Dr. Ahlstrom, is that pay difference “will lead to a far more collegial atmosphere, because physicians know they are getting compensated fairly for the amount of work done.”
Another advantage of a flexible schedule is hospitalists knowing they have the option of ramping up or scaling back the number of shifts they work, Dr. Ahlstrom says—for example, a physician who wants to reduce shifts in order to coach his daughter’s softball team or have Friday nights off to watch her son play high school football.
“You prevent burnout by allowing people to change their work schedule depending on what’s going on in their life,” Dr. Ahlstrom says. TH
Lisa Ryan is a freelance writer based in New Jersey.
Michael Radzienda, MD, FHM, once worked in a hospitalist program in which physicians were scheduled 30 days straight on clinical duty and 30 days off clinical duty. Although it sounds harsh by today’s standards, that job was so satisfying, he says, the schedule never felt like a burden. Conversely, he’s seen hospitalists work five days on and five days off, and the job was treacherous.
His point: Work schedules are just one influential piece of the job satisfaction pie.
“Satisfaction has more to do with work relationships and opportunities for growth,” says Dr. Radzienda, chief of hospital medicine and director of hospital medicine service at Medical College of Wisconsin/Froedtert Memorial Lutheran General Hospital in Milwaukee.
Shift-based staffing has become the norm, as more than 70% of hospitalist groups use a shift-based staffing model, according to the State of Hospital Medicine: 2010 Report Based on 2009 Data.1 That figure is up 40% from SHM’s 2005-2006 survey. Conversely, the number of HM groups employing call-based and hybrid (some shift, some call) coverage is declining—2.8% of groups employ call-based schedules, and 26.9% use a hybrid schedule. Those figures have dropped significantly from the 2005-2006 report, from 25% and 35%, respectively.
If you are going to make HM a career, you’ll need time to be with your family and pursue other interests, Dr. Radzienda says. As HM groups turn to more shift-based models, in which hospitalists work a set number of predetermined shifts and have no call responsibility, the challenge is setting a schedule that balances productivity and quality time off.
Fixed = Inflexible
The most popular way to schedule is through blocks of five days on/five days off (5/5) or seven days on/seven days off (7/7), in which hospitalists work 12 or 14 hours at a time, says Troy Ahlstrom, MD, FHM, a member of SHM’s Practice Analysis Committee and CFO of Hospitalists of Northern Michigan, a hospitalist-owned and -managed group based in Traverse City, Mich. Many HM groups employ this model because it’s easy to schedule and is attractive to residents who want a fixed schedule. But from a career satisfaction standpoint, the 5/5 and 7/7 schedule models present their own issues.
Fairness is the first potential pitfall. If all of the physicians in a group work the same schedule, they all have to log the same number of shifts and receive the same compensation. This leaves little to no wiggle room for hospitalists who want to make more money by picking up more shifts or those who want to work fewer shifts, Dr. Ahlstrom says. “People have different income goals,” he adds.
Second, physicians have to see the same number of patients throughout the day. This doesn’t take into consideration the reality that some hospitalists naturally work faster than others, thereby forcing the slower-paced doctors to keep up with an imposed patient load. “Invariably, no matter what you do, people are different,” Dr. Ahlstrom says.
Another consideration is that when physicians are working 12 to 14 hours a day, essentially they have no time for activities other than work and sleep, which doesn’t match the realities of life. Inevitably, things in personal lives crop up, which leads to swapping shifts that the group scheduler doesn’t know about or overloading the scheduler with shift-change requests, Dr. Ahlstrom explains.
Additionally, 7/7 schedules and their ilk squeeze a year’s worth of work into a compressed time frame, which can lead to intense stress and burnout, says John Nelson, MD, FACP, MHM, director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., SHM co-founder, and practice management columnist for The Hospitalist. “Maximizing the number of days off is not the holy grail,” he says. “If you choose to shut your life down on days that you work, that is going to be toxic.”
Flexibility Equates to Fairness
Dr. Nelson has long advocated a flexible shift schedule that accommodates individual preferences by giving physicians in the group autonomy in deciding how much or how little they want to work. While the group as a whole has to get all the work done, the flexibility comes from one physician taking more shifts as another takes less.
Dr. Radzienda tries to create teams within his group by pairing hospitalists with similar scheduling preferences. For example, he might have a pair working 5/5 and another working 14/14. “Up front, it takes a lot of work, but once you template it out, it becomes a good strategy,” he says.
He also strives to build robust backup plans and jeopardy models (see “Surge Protection,” September 2010, p. 43) into the schedule for short-notice callouts, as you never know when a hospitalist will need to miss a day or two because of illness or a family emergency. “Psychologically, it helps to know that you don’t have to be a hero if you’re ill or emotionally strained,” Dr. Radzienda says.
Dr. Ahlstrom agrees that a flex-schedule strategy has a positive impact on hospitalists’ career satisfaction and longevity. He suggests hospitalists be allowed to specify how many patients they want to see and be compensated according to their workload through built-in bonuses for physicians who work more. Dr. Nelson suggests paying hospitalists per relative value unit (RVU) of work. “I think hospitalists would like it and find it liberating to be paid on production,” he says.
An added bonus to flexible work hours and patient load, according to Dr. Ahlstrom, is that pay difference “will lead to a far more collegial atmosphere, because physicians know they are getting compensated fairly for the amount of work done.”
Another advantage of a flexible schedule is hospitalists knowing they have the option of ramping up or scaling back the number of shifts they work, Dr. Ahlstrom says—for example, a physician who wants to reduce shifts in order to coach his daughter’s softball team or have Friday nights off to watch her son play high school football.
“You prevent burnout by allowing people to change their work schedule depending on what’s going on in their life,” Dr. Ahlstrom says. TH
Lisa Ryan is a freelance writer based in New Jersey.
Woman refuses hysterectomy, dies of invasive cancer
dies of invasive cancer

A 37-YEAR-OLD WOMAN VISITED HER GYNECOLOGIST for an annual physical exam. A Pap smear revealed human papillomavirus (HPV) infection and abnormal cells. The pathology report after cone biopsy indicated adenoid cystic carcinoma. The physician told the patient that she needed a hysterectomy, which she refused.
The patient visited her primary care physician 9 months later because of abdominal bloating. He palpated a pelvic mass and sent her for a CT scan, which showed a mass within the pelvis as well as liver metastases. Surgery was not an option because of the metastases. Chemotherapy was started but the woman died in less than a month.
ESTATE’S CLAIM Although the gynecologist told the patient she needed a hysterectomy, he did not 1) correctly report the results of the biopsy or 2) explain the reasons why he was recommending hysterectomy.
PHYSICIAN’S DEFENSE The patient was properly treated when advised to have a hysterectomy. She refused treatment
VERDICT A $1.4 million Virginia settlement was reached.
NEONATAL DEATH FROM GROUP B STREP
AN INMATE AT A STATE PRISON gave birth to a healthy baby at 39 weeks’ gestation. The baby died the next day from a perinatal group B Streptococcal (GBS) infection.
ESTATE’S CLAIM The two ObGyns who treated the mother were negligent: the mother’s GBS status was unknown; she was never informed that she needed GBS testing; testing was not administered.
PHYSICIANS’ DEFENSE The primary ObGyn (Dr. A) denied negligence. The other (Dr. B) claimed that he had no duty to administer GBS testing because he was not the primary ObGyn. Prophylactic antibiotics in the absence of certain risk factors—none were present—were inappropriate.
VERDICT A $150,000 California settlement was reached with Dr. A. A defense verdict was returned for Dr. B.
>> READ New group B strep guidelines clarify management of key groups.
DIFFICULT DELIVERY, INJURED BABY
FETAL HEART RATE TRACING was not reassuring, and the fetus did not descend during prolonged labor and delivery. After more than 15 minutes of bradycardia, the hospital staff contacted the ObGyn, who then ordered cesarean delivery. At the initiation of surgery, the anesthetic was insufficient and the mother was unable to tolerate the abdominal incision.
The child has cerebral palsy and suffers motor delays and moderate cognitive deficits.
PATIENTS’ CLAIM The ObGyn failed to recognize cephalopelvic dispro-portion. The hospital staff misread fetal monitoring strips, delaying response to fetal distress because the umbilical cord was compressed between the baby’s cheekbone and maternal pelvis. A cesarean delivery should have been performed earlier, immediately after the baby showed signs of distress. The staff administered the wrong type of anesthetic to the mother before surgery.
DEFENDANTS’ DEFENSE Proper care was provided. An occult prolapsed cord was unpredictable, unpreventable, and unforeseeable.
VERDICT A $6.5 million Illinois settlement was reached, including $300,000 for the mother.
FISTULA CAUSES INCONTINENCE, PROMPTS MULTIPLE SURGERIES
SEVERAL WEEKS AFTER a vaginal hysterectomy, a woman presented with urinary incontinence; vesicovaginal fistula was diagnosed. She underwent 9 surgeries to repair the bladder injury and fistula.
PATIENT’S CLAIM The injury occurred because the gynecologist used improper technique when retracting the bladder. He should have inspected the bladder for injury before finishing the operation.
PHYSICIAN’S DEFENSE Bladder injury is a known risk of laparoscopic transvaginal hysterectomy.
VERDICT A $796,617 Michigan verdict was returned.
URETER KINKS DURING DIFFICULT HYSTERECTOMY
A 36-YEAR-OLD WOMAN PRESENTED to her gynecologist complaining of heavy menses and abdominal and pelvic pain, especially in the lower left quadrant. Total abdominal hysterectomy was scheduled. During surgery, the gynecologist found that the bladder was densely adhered to the uterus. Brisk bleeding followed attempts to separate the bladder from the uterus. The physician placed a single suture to stop the bleeding, and the procedure was completed.
Three days later, she had pain in the right kidney area; testing determined her right ureter was kinked. She was sent to another hospital for placement of a stent and nephrostomy tube, which were removed 4 months later.
PATIENT’S CLAIM The gynecologist was negligent in failing to provide the patient with alternatives to hysterectomy, and in injuring the ureter during hysterectomy.
PHYSICIAN’S DEFENSE Four treatment options were provided to the patient. The injury is a known complication of the surgery. The patient has completely recovered.
VERDICT A Pennsylvania defense verdict was returned.
WOMAN DELIVERS AT HOME AFTER FETUS DIES
AT 16 WEEKS’ GESTATION, a woman went to the hospital complaining of vaginal discharge. Ultrasonography revealed that the fetus had died. The woman’s cervix was not dilated; when the hospital staff attempted to discharge her, she resisted. Hospital officials threatened to call the police if she did not leave. She left, and later delivered the dead fetus at home. She then called her ObGyn, who promptly admitted her for emergency dilation and curettage to remove the remaining placental tissue.
PATIENT’S CLAIM She alleged a violation of the Emergency Medical Treatment and Active Labor Act (EMTALA), arguing that instead of stabilizing her, she was sent home under the threat of police intervention.
DEFENDANT’S DEFENSE The hospital claimed it had done all it could for the patient; she was not ready to deliver the fetus. She was given instructions to see her ObGyn or return if her condition changed. She never returned.
VERDICT A Maine verdict of $50,000 compensatory damages was returned against the hospital. The jury added $150,000 for punitive damages.
A SECOND ECTOPIC PREGNANCY?
FOUR YEARS AFTER SUFFERING a ruptured tubal ectopic pregnancy that necessitated salpingectomy, a 30-year-old woman became pregnant again. At her first prenatal visit to a hospital clinic, she saw a certified nurse midwife. The patient reported the prior ectopic pregnancy and complained of spotting with left-sided pain, nausea, and vomiting. Six days later, she went to the emergency department and was given a diagnosis of a ruptured fallopian tube from an ectopic pregnancy. Surgery was performed to remove the fallopian tube, thus making her unable to naturally conceive a child.
PATIENT’S CLAIM The midwife should have responded immediately to the patient’s symptoms, ordered a sonogram, and sent her to the hospital. Any of several available options would have saved the fallopian tube if the ectopic pregnancy had been diagnosed before rupture. The patient has spiritual and moral objections to in vitro fertilization.
MIDWIFE’S DEFENSE The midwife ordered a Stat sonogram at the first prenatal visit, but the prescription form was never removed from the chart, and the sonogram never scheduled. It was the hospital’s responsibility to get the form to the plaintiff and have the procedure scheduled. The midwife was therefore not at fault.
VERDICT A $2.5 million Maryland verdict was returned; it was reduced under the state cap to $650,000.
OBGYN UNDERESTIMATES BIRTH WEIGHT—BY APPROXIMATELY 50%
A PREGNANT WOMAN WITH BACK PAIN went to the emergency department. She was discharged but returned the next day with the same complaint, and, shortly, went into labor. The ObGyn, who estimated fetal weight at 7 or 8 lbs, delivered the baby using a vacuum extractor. Shoulder dystocia was encountered, and four maneuvers were used to deliver the baby, who weighed more than 11 lbs at birth. The baby suffered global brachial plexus injury.
PATIENT’S CLAIM The ObGyn was negligent: in underestimating fetal weight; in failing to offer cesarean delivery after 2 hours of second-stage labor; and in applying excessive force to deliver the baby.
PHYSICIAN’S DEFENSE Fetal weight is almost impossible to accurately estimate. A cesarean delivery was unnecessary. Only gentle traction was used to deliver the child.
VERDICT An Illinois defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
dies of invasive cancer
A 37-YEAR-OLD WOMAN VISITED HER GYNECOLOGIST for an annual physical exam. A Pap smear revealed human papillomavirus (HPV) infection and abnormal cells. The pathology report after cone biopsy indicated adenoid cystic carcinoma. The physician told the patient that she needed a hysterectomy, which she refused.
The patient visited her primary care physician 9 months later because of abdominal bloating. He palpated a pelvic mass and sent her for a CT scan, which showed a mass within the pelvis as well as liver metastases. Surgery was not an option because of the metastases. Chemotherapy was started but the woman died in less than a month.
ESTATE’S CLAIM Although the gynecologist told the patient she needed a hysterectomy, he did not 1) correctly report the results of the biopsy or 2) explain the reasons why he was recommending hysterectomy.
PHYSICIAN’S DEFENSE The patient was properly treated when advised to have a hysterectomy. She refused treatment
VERDICT A $1.4 million Virginia settlement was reached.
NEONATAL DEATH FROM GROUP B STREP
AN INMATE AT A STATE PRISON gave birth to a healthy baby at 39 weeks’ gestation. The baby died the next day from a perinatal group B Streptococcal (GBS) infection.
ESTATE’S CLAIM The two ObGyns who treated the mother were negligent: the mother’s GBS status was unknown; she was never informed that she needed GBS testing; testing was not administered.
PHYSICIANS’ DEFENSE The primary ObGyn (Dr. A) denied negligence. The other (Dr. B) claimed that he had no duty to administer GBS testing because he was not the primary ObGyn. Prophylactic antibiotics in the absence of certain risk factors—none were present—were inappropriate.
VERDICT A $150,000 California settlement was reached with Dr. A. A defense verdict was returned for Dr. B.
>> READ New group B strep guidelines clarify management of key groups.
DIFFICULT DELIVERY, INJURED BABY
FETAL HEART RATE TRACING was not reassuring, and the fetus did not descend during prolonged labor and delivery. After more than 15 minutes of bradycardia, the hospital staff contacted the ObGyn, who then ordered cesarean delivery. At the initiation of surgery, the anesthetic was insufficient and the mother was unable to tolerate the abdominal incision.
The child has cerebral palsy and suffers motor delays and moderate cognitive deficits.
PATIENTS’ CLAIM The ObGyn failed to recognize cephalopelvic dispro-portion. The hospital staff misread fetal monitoring strips, delaying response to fetal distress because the umbilical cord was compressed between the baby’s cheekbone and maternal pelvis. A cesarean delivery should have been performed earlier, immediately after the baby showed signs of distress. The staff administered the wrong type of anesthetic to the mother before surgery.
DEFENDANTS’ DEFENSE Proper care was provided. An occult prolapsed cord was unpredictable, unpreventable, and unforeseeable.
VERDICT A $6.5 million Illinois settlement was reached, including $300,000 for the mother.
FISTULA CAUSES INCONTINENCE, PROMPTS MULTIPLE SURGERIES
SEVERAL WEEKS AFTER a vaginal hysterectomy, a woman presented with urinary incontinence; vesicovaginal fistula was diagnosed. She underwent 9 surgeries to repair the bladder injury and fistula.
PATIENT’S CLAIM The injury occurred because the gynecologist used improper technique when retracting the bladder. He should have inspected the bladder for injury before finishing the operation.
PHYSICIAN’S DEFENSE Bladder injury is a known risk of laparoscopic transvaginal hysterectomy.
VERDICT A $796,617 Michigan verdict was returned.
URETER KINKS DURING DIFFICULT HYSTERECTOMY
A 36-YEAR-OLD WOMAN PRESENTED to her gynecologist complaining of heavy menses and abdominal and pelvic pain, especially in the lower left quadrant. Total abdominal hysterectomy was scheduled. During surgery, the gynecologist found that the bladder was densely adhered to the uterus. Brisk bleeding followed attempts to separate the bladder from the uterus. The physician placed a single suture to stop the bleeding, and the procedure was completed.
Three days later, she had pain in the right kidney area; testing determined her right ureter was kinked. She was sent to another hospital for placement of a stent and nephrostomy tube, which were removed 4 months later.
PATIENT’S CLAIM The gynecologist was negligent in failing to provide the patient with alternatives to hysterectomy, and in injuring the ureter during hysterectomy.
PHYSICIAN’S DEFENSE Four treatment options were provided to the patient. The injury is a known complication of the surgery. The patient has completely recovered.
VERDICT A Pennsylvania defense verdict was returned.
WOMAN DELIVERS AT HOME AFTER FETUS DIES
AT 16 WEEKS’ GESTATION, a woman went to the hospital complaining of vaginal discharge. Ultrasonography revealed that the fetus had died. The woman’s cervix was not dilated; when the hospital staff attempted to discharge her, she resisted. Hospital officials threatened to call the police if she did not leave. She left, and later delivered the dead fetus at home. She then called her ObGyn, who promptly admitted her for emergency dilation and curettage to remove the remaining placental tissue.
PATIENT’S CLAIM She alleged a violation of the Emergency Medical Treatment and Active Labor Act (EMTALA), arguing that instead of stabilizing her, she was sent home under the threat of police intervention.
DEFENDANT’S DEFENSE The hospital claimed it had done all it could for the patient; she was not ready to deliver the fetus. She was given instructions to see her ObGyn or return if her condition changed. She never returned.
VERDICT A Maine verdict of $50,000 compensatory damages was returned against the hospital. The jury added $150,000 for punitive damages.
A SECOND ECTOPIC PREGNANCY?
FOUR YEARS AFTER SUFFERING a ruptured tubal ectopic pregnancy that necessitated salpingectomy, a 30-year-old woman became pregnant again. At her first prenatal visit to a hospital clinic, she saw a certified nurse midwife. The patient reported the prior ectopic pregnancy and complained of spotting with left-sided pain, nausea, and vomiting. Six days later, she went to the emergency department and was given a diagnosis of a ruptured fallopian tube from an ectopic pregnancy. Surgery was performed to remove the fallopian tube, thus making her unable to naturally conceive a child.
PATIENT’S CLAIM The midwife should have responded immediately to the patient’s symptoms, ordered a sonogram, and sent her to the hospital. Any of several available options would have saved the fallopian tube if the ectopic pregnancy had been diagnosed before rupture. The patient has spiritual and moral objections to in vitro fertilization.
MIDWIFE’S DEFENSE The midwife ordered a Stat sonogram at the first prenatal visit, but the prescription form was never removed from the chart, and the sonogram never scheduled. It was the hospital’s responsibility to get the form to the plaintiff and have the procedure scheduled. The midwife was therefore not at fault.
VERDICT A $2.5 million Maryland verdict was returned; it was reduced under the state cap to $650,000.
OBGYN UNDERESTIMATES BIRTH WEIGHT—BY APPROXIMATELY 50%
A PREGNANT WOMAN WITH BACK PAIN went to the emergency department. She was discharged but returned the next day with the same complaint, and, shortly, went into labor. The ObGyn, who estimated fetal weight at 7 or 8 lbs, delivered the baby using a vacuum extractor. Shoulder dystocia was encountered, and four maneuvers were used to deliver the baby, who weighed more than 11 lbs at birth. The baby suffered global brachial plexus injury.
PATIENT’S CLAIM The ObGyn was negligent: in underestimating fetal weight; in failing to offer cesarean delivery after 2 hours of second-stage labor; and in applying excessive force to deliver the baby.
PHYSICIAN’S DEFENSE Fetal weight is almost impossible to accurately estimate. A cesarean delivery was unnecessary. Only gentle traction was used to deliver the child.
VERDICT An Illinois defense verdict was returned.
dies of invasive cancer
A 37-YEAR-OLD WOMAN VISITED HER GYNECOLOGIST for an annual physical exam. A Pap smear revealed human papillomavirus (HPV) infection and abnormal cells. The pathology report after cone biopsy indicated adenoid cystic carcinoma. The physician told the patient that she needed a hysterectomy, which she refused.
The patient visited her primary care physician 9 months later because of abdominal bloating. He palpated a pelvic mass and sent her for a CT scan, which showed a mass within the pelvis as well as liver metastases. Surgery was not an option because of the metastases. Chemotherapy was started but the woman died in less than a month.
ESTATE’S CLAIM Although the gynecologist told the patient she needed a hysterectomy, he did not 1) correctly report the results of the biopsy or 2) explain the reasons why he was recommending hysterectomy.
PHYSICIAN’S DEFENSE The patient was properly treated when advised to have a hysterectomy. She refused treatment
VERDICT A $1.4 million Virginia settlement was reached.
NEONATAL DEATH FROM GROUP B STREP
AN INMATE AT A STATE PRISON gave birth to a healthy baby at 39 weeks’ gestation. The baby died the next day from a perinatal group B Streptococcal (GBS) infection.
ESTATE’S CLAIM The two ObGyns who treated the mother were negligent: the mother’s GBS status was unknown; she was never informed that she needed GBS testing; testing was not administered.
PHYSICIANS’ DEFENSE The primary ObGyn (Dr. A) denied negligence. The other (Dr. B) claimed that he had no duty to administer GBS testing because he was not the primary ObGyn. Prophylactic antibiotics in the absence of certain risk factors—none were present—were inappropriate.
VERDICT A $150,000 California settlement was reached with Dr. A. A defense verdict was returned for Dr. B.
>> READ New group B strep guidelines clarify management of key groups.
DIFFICULT DELIVERY, INJURED BABY
FETAL HEART RATE TRACING was not reassuring, and the fetus did not descend during prolonged labor and delivery. After more than 15 minutes of bradycardia, the hospital staff contacted the ObGyn, who then ordered cesarean delivery. At the initiation of surgery, the anesthetic was insufficient and the mother was unable to tolerate the abdominal incision.
The child has cerebral palsy and suffers motor delays and moderate cognitive deficits.
PATIENTS’ CLAIM The ObGyn failed to recognize cephalopelvic dispro-portion. The hospital staff misread fetal monitoring strips, delaying response to fetal distress because the umbilical cord was compressed between the baby’s cheekbone and maternal pelvis. A cesarean delivery should have been performed earlier, immediately after the baby showed signs of distress. The staff administered the wrong type of anesthetic to the mother before surgery.
DEFENDANTS’ DEFENSE Proper care was provided. An occult prolapsed cord was unpredictable, unpreventable, and unforeseeable.
VERDICT A $6.5 million Illinois settlement was reached, including $300,000 for the mother.
FISTULA CAUSES INCONTINENCE, PROMPTS MULTIPLE SURGERIES
SEVERAL WEEKS AFTER a vaginal hysterectomy, a woman presented with urinary incontinence; vesicovaginal fistula was diagnosed. She underwent 9 surgeries to repair the bladder injury and fistula.
PATIENT’S CLAIM The injury occurred because the gynecologist used improper technique when retracting the bladder. He should have inspected the bladder for injury before finishing the operation.
PHYSICIAN’S DEFENSE Bladder injury is a known risk of laparoscopic transvaginal hysterectomy.
VERDICT A $796,617 Michigan verdict was returned.
URETER KINKS DURING DIFFICULT HYSTERECTOMY
A 36-YEAR-OLD WOMAN PRESENTED to her gynecologist complaining of heavy menses and abdominal and pelvic pain, especially in the lower left quadrant. Total abdominal hysterectomy was scheduled. During surgery, the gynecologist found that the bladder was densely adhered to the uterus. Brisk bleeding followed attempts to separate the bladder from the uterus. The physician placed a single suture to stop the bleeding, and the procedure was completed.
Three days later, she had pain in the right kidney area; testing determined her right ureter was kinked. She was sent to another hospital for placement of a stent and nephrostomy tube, which were removed 4 months later.
PATIENT’S CLAIM The gynecologist was negligent in failing to provide the patient with alternatives to hysterectomy, and in injuring the ureter during hysterectomy.
PHYSICIAN’S DEFENSE Four treatment options were provided to the patient. The injury is a known complication of the surgery. The patient has completely recovered.
VERDICT A Pennsylvania defense verdict was returned.
WOMAN DELIVERS AT HOME AFTER FETUS DIES
AT 16 WEEKS’ GESTATION, a woman went to the hospital complaining of vaginal discharge. Ultrasonography revealed that the fetus had died. The woman’s cervix was not dilated; when the hospital staff attempted to discharge her, she resisted. Hospital officials threatened to call the police if she did not leave. She left, and later delivered the dead fetus at home. She then called her ObGyn, who promptly admitted her for emergency dilation and curettage to remove the remaining placental tissue.
PATIENT’S CLAIM She alleged a violation of the Emergency Medical Treatment and Active Labor Act (EMTALA), arguing that instead of stabilizing her, she was sent home under the threat of police intervention.
DEFENDANT’S DEFENSE The hospital claimed it had done all it could for the patient; she was not ready to deliver the fetus. She was given instructions to see her ObGyn or return if her condition changed. She never returned.
VERDICT A Maine verdict of $50,000 compensatory damages was returned against the hospital. The jury added $150,000 for punitive damages.
A SECOND ECTOPIC PREGNANCY?
FOUR YEARS AFTER SUFFERING a ruptured tubal ectopic pregnancy that necessitated salpingectomy, a 30-year-old woman became pregnant again. At her first prenatal visit to a hospital clinic, she saw a certified nurse midwife. The patient reported the prior ectopic pregnancy and complained of spotting with left-sided pain, nausea, and vomiting. Six days later, she went to the emergency department and was given a diagnosis of a ruptured fallopian tube from an ectopic pregnancy. Surgery was performed to remove the fallopian tube, thus making her unable to naturally conceive a child.
PATIENT’S CLAIM The midwife should have responded immediately to the patient’s symptoms, ordered a sonogram, and sent her to the hospital. Any of several available options would have saved the fallopian tube if the ectopic pregnancy had been diagnosed before rupture. The patient has spiritual and moral objections to in vitro fertilization.
MIDWIFE’S DEFENSE The midwife ordered a Stat sonogram at the first prenatal visit, but the prescription form was never removed from the chart, and the sonogram never scheduled. It was the hospital’s responsibility to get the form to the plaintiff and have the procedure scheduled. The midwife was therefore not at fault.
VERDICT A $2.5 million Maryland verdict was returned; it was reduced under the state cap to $650,000.
OBGYN UNDERESTIMATES BIRTH WEIGHT—BY APPROXIMATELY 50%
A PREGNANT WOMAN WITH BACK PAIN went to the emergency department. She was discharged but returned the next day with the same complaint, and, shortly, went into labor. The ObGyn, who estimated fetal weight at 7 or 8 lbs, delivered the baby using a vacuum extractor. Shoulder dystocia was encountered, and four maneuvers were used to deliver the baby, who weighed more than 11 lbs at birth. The baby suffered global brachial plexus injury.
PATIENT’S CLAIM The ObGyn was negligent: in underestimating fetal weight; in failing to offer cesarean delivery after 2 hours of second-stage labor; and in applying excessive force to deliver the baby.
PHYSICIAN’S DEFENSE Fetal weight is almost impossible to accurately estimate. A cesarean delivery was unnecessary. Only gentle traction was used to deliver the child.
VERDICT An Illinois defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
For better or, maybe, worse, patients are judging your care online
- Twitter 101 for ObGyns: Pearls, pitfalls, and potential
(September 2011)
CASE: Unfairly labeled and now unnerved
Dr. Y, your colleague, calls you; she’s distraught. She performed a Google search of her name and found what she describes as a hateful review on a physician-rating Web site from someone claiming to be her patient. The reviewer declared that Dr. Y. was “rude” and interested only in “pushing one drug.”
“She must be a shill for a drug company….”
You’ve referred many patients to Dr. Y, and you’ve always heard wonderful things about her care. You know that she has never accepted pharma money for lectures or research.
“What should I do?” Dr. Y pleads with you.
We physicians probably don’t think twice about looking up reviews and ratings of hotels and restaurants. But many of us balk at the thought of our professional services being reviewed in such a manner. We’re aware that patients discuss their care, of course, but the Internet— well, that provides a megaphone of global reach for what was once mere water-cooler chat.
And reading angry words in print hurts more than hearing them secondhand.
With the Internet hosting more than 30 sites that rate health-care providers and hospitals, most of us can expect to be reviewed at some point. Only about 15% of people report consulting online physician reviews, however, and fewer than 5% have posted an online review themselves.1,2
What do you need to know about these sites and their potential to have an impact on your practice? Here are some important observations and pearls from the literature and from my experience at the receiving end of ratings.
Types of physician online rating
The first step in navigating the morass of Internet review and rating sites is to understand the types of sites that you’ll encounter.
Angie’s List. This site rates all kinds of services, including physicians. Membership requires registration and a fee. A member can post a review of a given physician every 6 months. Although the names of reviewers are not posted, they are available to the physicians being reviewed—if they ask.
Free Web sites that require registration of some kind. These are general review sites, such as www.yelp.com or specific sites for physicians, such as www.DoctorScorecard.com, which states that a reviewer is allowed to rate a given physician only once.
Free Web sites that don’t require registration. One simply finds the physician’s name and either clicks on the number of stars or writes a review, or both. Two examples: www.vitals.com and www.drscore.com. These sites claim to limit the number of reviews: vitals.com, one review a month; drscore.com, one a quarter. A spokesperson for drscore.com, claiming that such information is proprietary, declined to tell me how, without the controls offered by registration, the site prevents a physician or an angry patient from stuffing the ballot box.

How valid are online reviews?
You might think that the patients most likely to rate a physician or post a comment about her (or his) care are ones who are unhappy with their medical care. You would be wrong: 70% to 90% of online ratings of physicians are positive.3,4 It’s unclear if the positive-negative division of ratings varies between Web sites that require registration (and therefore have a greater degree of accountability) and those that do not. A recent informal sampling of sites reveals that most physicians have five or fewer reviews on any one site—a sample far too small for the rating to be considered valid or to offer meaningful feedback to a physician.
What can I do to protect my reputation?”
Good question. The answer is multifaceted.
- Give your patients an opportunity to provide feedback after an appointment. If they can off-load to you at, or immediately after, their visit, they may be less inclined to post damaging comments elsewhere. And you might actually learn valuable information about your practice and your staff— and how convenient parking is.
- Consider an anonymous survey for the patient to complete before leaving the office or to mail back in a stamped envelope.
- Does the idea of a third-party Internet ranking site appeal to you? Find one that allows you to create a profile and have your staff direct patients to that site.
- Develop a robust Internet presence. Web content that is under your control is more likely to appear at the top of the first search-engine response page (SERP)—thereby pushing potentially negative reviews out of this prime real estate (links that appear on the bottom half of the first page of search results, and beyond, are far less likely to be viewed or clicked). If your Web site isn’t listed first, consult with a search engine optimization specialist about trying to change that. Other ways to generate positive hits on the first SERP? Use Twitter (as long as you are using a version of your name as the username); start a blog; and write guest posts on other Web sites.
- It’s possible to register with all the physician rating sites and receive alerts when you are mentioned, but that could be time-consuming. This strategy is also unlikely to be productive: First, not all sites allow rebuttal or other feedback from physicians. Second, even if you were able to respond, what you can say is limited by HIPAA. Last, although you can flag malicious content for removal, what you consider malicious and what the site administrator considers malicious could differ.
For the fictional Dr. Y., whose story was told at the beginning of this article, this is the best possible answer to her dilemma: Leave the review alone. It’s an opinion, and while hurtful, it isn’t slander and is unlikely to meet the requirements for removal. However, it might be wise to follow up with the bullet-point recommendations I’ve made, above.
Can you muzzle your patient population? One company, Medical Justice, Greensboro, N.C., provides practices with a patient contract that allows the physician to retain copyright to patients’ online comments. The contract doesn’t preclude posting, but the physician is free to remove negative comments. The company’s product was described by its founder and chief executive officer in an article in the December 2009 issue of OBG Management (“Should you worry that patients will use the Web to grade you?,” at www.obgmanagement.com).
Even if—and that’s a big “if”—patients are willing to sign on the dotted line, it’s unclear how such a contract could stop anonymous posting. And, by analogy, would you eat at a restaurant where you were required to turn over copyright to your online comments before you saw the menu?
I’m a believer in physician ratings: If I’m doing a good job for my patients, I like to know that. And, if there’s room for improvement, I can change or fix something I do only if I know about it.
My physician group has had a patient survey in place for several years. It’s similar to the CHECKBOOK/CSS program, although it is accomplished by mail.
I’m proud that I receive high scores from my patients. Whenever I find that some facet of my ratings is slipping, I redouble my efforts. Online, 70% to 90% of my reviews are positive, which is in line with physicians’ experiences reported in the literature that I cited for this article.
Most negative opinions in medicine stem from communication difficulties
As a parent of two medically fragile children who has spent a greater part of 7 years at the other end of the stethoscope, I understand this only too well. So I strive to provide the kind of service that I would want from my providers. I ask my patients if:
- they understand my recommendations
- they agree with the management plan
- there is anything else I have not addressed (and not while I have my hand on the doorknob!).
If I sense that my patient is unhappy, I ask her what’s wrong, and I do my best to allay her fears or mitigate her problems that are under my control. last, I’m not afraid of online reviews—although my preference is for a scientifically valid questionnaire with a focus on achieving adequate numbers.
I believe that, when patients search for health information, they deserve accurate content not only about their health condition but about their physician, too.—Jennifer Gunter, MD
Other models that are worth considering
The United Kingdom’s National Health Service (NHS) operates a health-care rating site (NHS Choices; http://www.nhs.uk), where, among many other services, patients can provide feedback about both physicians and hospitals (anonymous if desired, although an e-mail address is required for validation).1 What’s unique about NHS Choices is that it is moderated; there are specific ground rules for providing ratings; and physicians are encouraged to respond to individual ratings.
In several geographic markets in the United States, Consumer’s CHECKBOOK/ Center for the Study of Services (CHECKBOOK/CSS), a not-for-profit consumer education organization, has piloted an online survey of physicians. Patients are sampled randomly from the enrollment of a list of insurers and invited to participate. The system verifies that the patient being surveyed has made a visit to the physician in question during the past year.
CHECKBOOK/CSS uses questions developed by the US Agency for Healthcare Research and Quality. The reports generated by the system are based on a statistically valid number of surveys (on average, 49 completed surveys for one physician). They are available without charge to the public at the organization’s Web site (http://www.checkbook.org/patientcentral).
A recent perusal of CHECKBOOK/CSS in one market easily found an “above average” rating for a member of the OBG Management Board of Editors….
Let’s make this a useful thing
Here is what we can say with reasonable certainty, based on observation:
- Most online reviews are positive
- Most physicians have far too few ratings on any one Web site to approach a meaningful degree of scientific validity
- Lack of accountability on many ratings Web sites raises the specter of sham negative or positive reviews. The CHECKBOOK/CSS model that I described appears to address many of these concerns.
Most patients have valuable comments and opinions about their medical care; we should remember that listening is our most important clinical skill. Finding a way to make online feedback valid and productive for both patients and physicians should be a goal for our professional societies.
We want to hear from you! Tell us what you think.
1. Lagu T, Lindenauer PK. Putting the public back in public reporting of health care quality. JAMA. 2010;304(15):1711-1712.
2. Fox S, Jones S. The social life of health information. Pew Internet and American Life Project Web site. http://www.pewinternet.org/Reports/2009/8-The-Social-Life-of-Health-Information. aspx. Published June 11, 2009. Accessed January 12, 2011.
3. Lagu T, Hannon NS, Rothberg MB, Lindenauer PK. Patients’ evaluations of health care providers in the era of social networking: an analysis of physician rating websites. J Gen Intern Med. 2010;25(9):942-946.
4. Lopez A, Detz A, Ratanawongsa N, Schillinger D, Sarkar U. What do your patients say about you on the internet? A thematic analysis of online reviews of primary care physicians [abstract]. Presented at: 33rd Annual Society of General Internal Medicine Meeting; May 1, 2010; Minneapolis, MN.

Jennifer Gunter, MD
Dr. Gunter is in ObGyn practice in San Francisco, Calif. She is the author of The Preemie Primer: A Complete Guide for Parents of Premature Babies—from Birth through the Toddler Years and Beyond (Da Capo Press, 2010). Dr. Gunter writes a blog at www.preemieprimer.com/blog/.
Dr. Gunter reports no financial relationships relevant to this article.
Jennifer Gunter, MD
Dr. Gunter is in ObGyn practice in San Francisco, Calif. She is the author of The Preemie Primer: A Complete Guide for Parents of Premature Babies—from Birth through the Toddler Years and Beyond (Da Capo Press, 2010). Dr. Gunter writes a blog at www.preemieprimer.com/blog/.
Dr. Gunter reports no financial relationships relevant to this article.
Jennifer Gunter, MD
Dr. Gunter is in ObGyn practice in San Francisco, Calif. She is the author of The Preemie Primer: A Complete Guide for Parents of Premature Babies—from Birth through the Toddler Years and Beyond (Da Capo Press, 2010). Dr. Gunter writes a blog at www.preemieprimer.com/blog/.
Dr. Gunter reports no financial relationships relevant to this article.
- Twitter 101 for ObGyns: Pearls, pitfalls, and potential
(September 2011)
CASE: Unfairly labeled and now unnerved
Dr. Y, your colleague, calls you; she’s distraught. She performed a Google search of her name and found what she describes as a hateful review on a physician-rating Web site from someone claiming to be her patient. The reviewer declared that Dr. Y. was “rude” and interested only in “pushing one drug.”
“She must be a shill for a drug company….”
You’ve referred many patients to Dr. Y, and you’ve always heard wonderful things about her care. You know that she has never accepted pharma money for lectures or research.
“What should I do?” Dr. Y pleads with you.
We physicians probably don’t think twice about looking up reviews and ratings of hotels and restaurants. But many of us balk at the thought of our professional services being reviewed in such a manner. We’re aware that patients discuss their care, of course, but the Internet— well, that provides a megaphone of global reach for what was once mere water-cooler chat.
And reading angry words in print hurts more than hearing them secondhand.
With the Internet hosting more than 30 sites that rate health-care providers and hospitals, most of us can expect to be reviewed at some point. Only about 15% of people report consulting online physician reviews, however, and fewer than 5% have posted an online review themselves.1,2
What do you need to know about these sites and their potential to have an impact on your practice? Here are some important observations and pearls from the literature and from my experience at the receiving end of ratings.
Types of physician online rating
The first step in navigating the morass of Internet review and rating sites is to understand the types of sites that you’ll encounter.
Angie’s List. This site rates all kinds of services, including physicians. Membership requires registration and a fee. A member can post a review of a given physician every 6 months. Although the names of reviewers are not posted, they are available to the physicians being reviewed—if they ask.
Free Web sites that require registration of some kind. These are general review sites, such as www.yelp.com or specific sites for physicians, such as www.DoctorScorecard.com, which states that a reviewer is allowed to rate a given physician only once.
Free Web sites that don’t require registration. One simply finds the physician’s name and either clicks on the number of stars or writes a review, or both. Two examples: www.vitals.com and www.drscore.com. These sites claim to limit the number of reviews: vitals.com, one review a month; drscore.com, one a quarter. A spokesperson for drscore.com, claiming that such information is proprietary, declined to tell me how, without the controls offered by registration, the site prevents a physician or an angry patient from stuffing the ballot box.
How valid are online reviews?
You might think that the patients most likely to rate a physician or post a comment about her (or his) care are ones who are unhappy with their medical care. You would be wrong: 70% to 90% of online ratings of physicians are positive.3,4 It’s unclear if the positive-negative division of ratings varies between Web sites that require registration (and therefore have a greater degree of accountability) and those that do not. A recent informal sampling of sites reveals that most physicians have five or fewer reviews on any one site—a sample far too small for the rating to be considered valid or to offer meaningful feedback to a physician.
What can I do to protect my reputation?”
Good question. The answer is multifaceted.
- Give your patients an opportunity to provide feedback after an appointment. If they can off-load to you at, or immediately after, their visit, they may be less inclined to post damaging comments elsewhere. And you might actually learn valuable information about your practice and your staff— and how convenient parking is.
- Consider an anonymous survey for the patient to complete before leaving the office or to mail back in a stamped envelope.
- Does the idea of a third-party Internet ranking site appeal to you? Find one that allows you to create a profile and have your staff direct patients to that site.
- Develop a robust Internet presence. Web content that is under your control is more likely to appear at the top of the first search-engine response page (SERP)—thereby pushing potentially negative reviews out of this prime real estate (links that appear on the bottom half of the first page of search results, and beyond, are far less likely to be viewed or clicked). If your Web site isn’t listed first, consult with a search engine optimization specialist about trying to change that. Other ways to generate positive hits on the first SERP? Use Twitter (as long as you are using a version of your name as the username); start a blog; and write guest posts on other Web sites.
- It’s possible to register with all the physician rating sites and receive alerts when you are mentioned, but that could be time-consuming. This strategy is also unlikely to be productive: First, not all sites allow rebuttal or other feedback from physicians. Second, even if you were able to respond, what you can say is limited by HIPAA. Last, although you can flag malicious content for removal, what you consider malicious and what the site administrator considers malicious could differ.
For the fictional Dr. Y., whose story was told at the beginning of this article, this is the best possible answer to her dilemma: Leave the review alone. It’s an opinion, and while hurtful, it isn’t slander and is unlikely to meet the requirements for removal. However, it might be wise to follow up with the bullet-point recommendations I’ve made, above.
Can you muzzle your patient population? One company, Medical Justice, Greensboro, N.C., provides practices with a patient contract that allows the physician to retain copyright to patients’ online comments. The contract doesn’t preclude posting, but the physician is free to remove negative comments. The company’s product was described by its founder and chief executive officer in an article in the December 2009 issue of OBG Management (“Should you worry that patients will use the Web to grade you?,” at www.obgmanagement.com).
Even if—and that’s a big “if”—patients are willing to sign on the dotted line, it’s unclear how such a contract could stop anonymous posting. And, by analogy, would you eat at a restaurant where you were required to turn over copyright to your online comments before you saw the menu?
I’m a believer in physician ratings: If I’m doing a good job for my patients, I like to know that. And, if there’s room for improvement, I can change or fix something I do only if I know about it.
My physician group has had a patient survey in place for several years. It’s similar to the CHECKBOOK/CSS program, although it is accomplished by mail.
I’m proud that I receive high scores from my patients. Whenever I find that some facet of my ratings is slipping, I redouble my efforts. Online, 70% to 90% of my reviews are positive, which is in line with physicians’ experiences reported in the literature that I cited for this article.
Most negative opinions in medicine stem from communication difficulties
As a parent of two medically fragile children who has spent a greater part of 7 years at the other end of the stethoscope, I understand this only too well. So I strive to provide the kind of service that I would want from my providers. I ask my patients if:
- they understand my recommendations
- they agree with the management plan
- there is anything else I have not addressed (and not while I have my hand on the doorknob!).
If I sense that my patient is unhappy, I ask her what’s wrong, and I do my best to allay her fears or mitigate her problems that are under my control. last, I’m not afraid of online reviews—although my preference is for a scientifically valid questionnaire with a focus on achieving adequate numbers.
I believe that, when patients search for health information, they deserve accurate content not only about their health condition but about their physician, too.—Jennifer Gunter, MD
Other models that are worth considering
The United Kingdom’s National Health Service (NHS) operates a health-care rating site (NHS Choices; http://www.nhs.uk), where, among many other services, patients can provide feedback about both physicians and hospitals (anonymous if desired, although an e-mail address is required for validation).1 What’s unique about NHS Choices is that it is moderated; there are specific ground rules for providing ratings; and physicians are encouraged to respond to individual ratings.
In several geographic markets in the United States, Consumer’s CHECKBOOK/ Center for the Study of Services (CHECKBOOK/CSS), a not-for-profit consumer education organization, has piloted an online survey of physicians. Patients are sampled randomly from the enrollment of a list of insurers and invited to participate. The system verifies that the patient being surveyed has made a visit to the physician in question during the past year.
CHECKBOOK/CSS uses questions developed by the US Agency for Healthcare Research and Quality. The reports generated by the system are based on a statistically valid number of surveys (on average, 49 completed surveys for one physician). They are available without charge to the public at the organization’s Web site (http://www.checkbook.org/patientcentral).
A recent perusal of CHECKBOOK/CSS in one market easily found an “above average” rating for a member of the OBG Management Board of Editors….
Let’s make this a useful thing
Here is what we can say with reasonable certainty, based on observation:
- Most online reviews are positive
- Most physicians have far too few ratings on any one Web site to approach a meaningful degree of scientific validity
- Lack of accountability on many ratings Web sites raises the specter of sham negative or positive reviews. The CHECKBOOK/CSS model that I described appears to address many of these concerns.
Most patients have valuable comments and opinions about their medical care; we should remember that listening is our most important clinical skill. Finding a way to make online feedback valid and productive for both patients and physicians should be a goal for our professional societies.
We want to hear from you! Tell us what you think.
- Twitter 101 for ObGyns: Pearls, pitfalls, and potential
(September 2011)
CASE: Unfairly labeled and now unnerved
Dr. Y, your colleague, calls you; she’s distraught. She performed a Google search of her name and found what she describes as a hateful review on a physician-rating Web site from someone claiming to be her patient. The reviewer declared that Dr. Y. was “rude” and interested only in “pushing one drug.”
“She must be a shill for a drug company….”
You’ve referred many patients to Dr. Y, and you’ve always heard wonderful things about her care. You know that she has never accepted pharma money for lectures or research.
“What should I do?” Dr. Y pleads with you.
We physicians probably don’t think twice about looking up reviews and ratings of hotels and restaurants. But many of us balk at the thought of our professional services being reviewed in such a manner. We’re aware that patients discuss their care, of course, but the Internet— well, that provides a megaphone of global reach for what was once mere water-cooler chat.
And reading angry words in print hurts more than hearing them secondhand.
With the Internet hosting more than 30 sites that rate health-care providers and hospitals, most of us can expect to be reviewed at some point. Only about 15% of people report consulting online physician reviews, however, and fewer than 5% have posted an online review themselves.1,2
What do you need to know about these sites and their potential to have an impact on your practice? Here are some important observations and pearls from the literature and from my experience at the receiving end of ratings.
Types of physician online rating
The first step in navigating the morass of Internet review and rating sites is to understand the types of sites that you’ll encounter.
Angie’s List. This site rates all kinds of services, including physicians. Membership requires registration and a fee. A member can post a review of a given physician every 6 months. Although the names of reviewers are not posted, they are available to the physicians being reviewed—if they ask.
Free Web sites that require registration of some kind. These are general review sites, such as www.yelp.com or specific sites for physicians, such as www.DoctorScorecard.com, which states that a reviewer is allowed to rate a given physician only once.
Free Web sites that don’t require registration. One simply finds the physician’s name and either clicks on the number of stars or writes a review, or both. Two examples: www.vitals.com and www.drscore.com. These sites claim to limit the number of reviews: vitals.com, one review a month; drscore.com, one a quarter. A spokesperson for drscore.com, claiming that such information is proprietary, declined to tell me how, without the controls offered by registration, the site prevents a physician or an angry patient from stuffing the ballot box.
How valid are online reviews?
You might think that the patients most likely to rate a physician or post a comment about her (or his) care are ones who are unhappy with their medical care. You would be wrong: 70% to 90% of online ratings of physicians are positive.3,4 It’s unclear if the positive-negative division of ratings varies between Web sites that require registration (and therefore have a greater degree of accountability) and those that do not. A recent informal sampling of sites reveals that most physicians have five or fewer reviews on any one site—a sample far too small for the rating to be considered valid or to offer meaningful feedback to a physician.
What can I do to protect my reputation?”
Good question. The answer is multifaceted.
- Give your patients an opportunity to provide feedback after an appointment. If they can off-load to you at, or immediately after, their visit, they may be less inclined to post damaging comments elsewhere. And you might actually learn valuable information about your practice and your staff— and how convenient parking is.
- Consider an anonymous survey for the patient to complete before leaving the office or to mail back in a stamped envelope.
- Does the idea of a third-party Internet ranking site appeal to you? Find one that allows you to create a profile and have your staff direct patients to that site.
- Develop a robust Internet presence. Web content that is under your control is more likely to appear at the top of the first search-engine response page (SERP)—thereby pushing potentially negative reviews out of this prime real estate (links that appear on the bottom half of the first page of search results, and beyond, are far less likely to be viewed or clicked). If your Web site isn’t listed first, consult with a search engine optimization specialist about trying to change that. Other ways to generate positive hits on the first SERP? Use Twitter (as long as you are using a version of your name as the username); start a blog; and write guest posts on other Web sites.
- It’s possible to register with all the physician rating sites and receive alerts when you are mentioned, but that could be time-consuming. This strategy is also unlikely to be productive: First, not all sites allow rebuttal or other feedback from physicians. Second, even if you were able to respond, what you can say is limited by HIPAA. Last, although you can flag malicious content for removal, what you consider malicious and what the site administrator considers malicious could differ.
For the fictional Dr. Y., whose story was told at the beginning of this article, this is the best possible answer to her dilemma: Leave the review alone. It’s an opinion, and while hurtful, it isn’t slander and is unlikely to meet the requirements for removal. However, it might be wise to follow up with the bullet-point recommendations I’ve made, above.
Can you muzzle your patient population? One company, Medical Justice, Greensboro, N.C., provides practices with a patient contract that allows the physician to retain copyright to patients’ online comments. The contract doesn’t preclude posting, but the physician is free to remove negative comments. The company’s product was described by its founder and chief executive officer in an article in the December 2009 issue of OBG Management (“Should you worry that patients will use the Web to grade you?,” at www.obgmanagement.com).
Even if—and that’s a big “if”—patients are willing to sign on the dotted line, it’s unclear how such a contract could stop anonymous posting. And, by analogy, would you eat at a restaurant where you were required to turn over copyright to your online comments before you saw the menu?
I’m a believer in physician ratings: If I’m doing a good job for my patients, I like to know that. And, if there’s room for improvement, I can change or fix something I do only if I know about it.
My physician group has had a patient survey in place for several years. It’s similar to the CHECKBOOK/CSS program, although it is accomplished by mail.
I’m proud that I receive high scores from my patients. Whenever I find that some facet of my ratings is slipping, I redouble my efforts. Online, 70% to 90% of my reviews are positive, which is in line with physicians’ experiences reported in the literature that I cited for this article.
Most negative opinions in medicine stem from communication difficulties
As a parent of two medically fragile children who has spent a greater part of 7 years at the other end of the stethoscope, I understand this only too well. So I strive to provide the kind of service that I would want from my providers. I ask my patients if:
- they understand my recommendations
- they agree with the management plan
- there is anything else I have not addressed (and not while I have my hand on the doorknob!).
If I sense that my patient is unhappy, I ask her what’s wrong, and I do my best to allay her fears or mitigate her problems that are under my control. last, I’m not afraid of online reviews—although my preference is for a scientifically valid questionnaire with a focus on achieving adequate numbers.
I believe that, when patients search for health information, they deserve accurate content not only about their health condition but about their physician, too.—Jennifer Gunter, MD
Other models that are worth considering
The United Kingdom’s National Health Service (NHS) operates a health-care rating site (NHS Choices; http://www.nhs.uk), where, among many other services, patients can provide feedback about both physicians and hospitals (anonymous if desired, although an e-mail address is required for validation).1 What’s unique about NHS Choices is that it is moderated; there are specific ground rules for providing ratings; and physicians are encouraged to respond to individual ratings.
In several geographic markets in the United States, Consumer’s CHECKBOOK/ Center for the Study of Services (CHECKBOOK/CSS), a not-for-profit consumer education organization, has piloted an online survey of physicians. Patients are sampled randomly from the enrollment of a list of insurers and invited to participate. The system verifies that the patient being surveyed has made a visit to the physician in question during the past year.
CHECKBOOK/CSS uses questions developed by the US Agency for Healthcare Research and Quality. The reports generated by the system are based on a statistically valid number of surveys (on average, 49 completed surveys for one physician). They are available without charge to the public at the organization’s Web site (http://www.checkbook.org/patientcentral).
A recent perusal of CHECKBOOK/CSS in one market easily found an “above average” rating for a member of the OBG Management Board of Editors….
Let’s make this a useful thing
Here is what we can say with reasonable certainty, based on observation:
- Most online reviews are positive
- Most physicians have far too few ratings on any one Web site to approach a meaningful degree of scientific validity
- Lack of accountability on many ratings Web sites raises the specter of sham negative or positive reviews. The CHECKBOOK/CSS model that I described appears to address many of these concerns.
Most patients have valuable comments and opinions about their medical care; we should remember that listening is our most important clinical skill. Finding a way to make online feedback valid and productive for both patients and physicians should be a goal for our professional societies.
We want to hear from you! Tell us what you think.
1. Lagu T, Lindenauer PK. Putting the public back in public reporting of health care quality. JAMA. 2010;304(15):1711-1712.
2. Fox S, Jones S. The social life of health information. Pew Internet and American Life Project Web site. http://www.pewinternet.org/Reports/2009/8-The-Social-Life-of-Health-Information. aspx. Published June 11, 2009. Accessed January 12, 2011.
3. Lagu T, Hannon NS, Rothberg MB, Lindenauer PK. Patients’ evaluations of health care providers in the era of social networking: an analysis of physician rating websites. J Gen Intern Med. 2010;25(9):942-946.
4. Lopez A, Detz A, Ratanawongsa N, Schillinger D, Sarkar U. What do your patients say about you on the internet? A thematic analysis of online reviews of primary care physicians [abstract]. Presented at: 33rd Annual Society of General Internal Medicine Meeting; May 1, 2010; Minneapolis, MN.
1. Lagu T, Lindenauer PK. Putting the public back in public reporting of health care quality. JAMA. 2010;304(15):1711-1712.
2. Fox S, Jones S. The social life of health information. Pew Internet and American Life Project Web site. http://www.pewinternet.org/Reports/2009/8-The-Social-Life-of-Health-Information. aspx. Published June 11, 2009. Accessed January 12, 2011.
3. Lagu T, Hannon NS, Rothberg MB, Lindenauer PK. Patients’ evaluations of health care providers in the era of social networking: an analysis of physician rating websites. J Gen Intern Med. 2010;25(9):942-946.
4. Lopez A, Detz A, Ratanawongsa N, Schillinger D, Sarkar U. What do your patients say about you on the internet? A thematic analysis of online reviews of primary care physicians [abstract]. Presented at: 33rd Annual Society of General Internal Medicine Meeting; May 1, 2010; Minneapolis, MN.
Websites
Is a website essential to the success of your practice? No, not really, despite everything those spammers tell you.
About 20% of private medical practices have a website, and the rest seem to be doing fine without one. The reality is that most users of medical care are older folk; and most older folk still find their doctors the old-fashioned ways: through referrals from primary practitioners, and by word-of-mouth from family and friends.
By the time the youngsters who use the Internet to find everything reach the age where medical care is a priority, almost every private practice will certainly have a Web presence. (But by then, of course, something way cooler will have come along to replace the Web!)
That said, aggressive cosmetic practices in highly competitive areas clearly seem to benefit from Web exposure; and for the rest of us, although a well-designed website is not a necessity, it can certainly make life easier for doctors, staff, and patients.
The key phrase, of course, is "well-designed." A badly designed site will do far more harm than good, so this is one project to leave to the professionals.
Doing it yourself might sound like fun, but good site design is a lot harder than it looks. And if you resort to a standard template, as most amateurs do, you won't like the result.
Almost every generic, template-based website I've seen looks shabby and amateurish. Broken links, misspelled text, stock snapshot-quality photos - exactly the opposite of the professional image you want to project.
In addition, template-based sites tend to be overlooked by search engines. What's the point of having a website if patients can't find it?
A buzz phrase among professional Web designers is "search engine optimization" (SEO). A pro will give you a professional look and a Web presence that is readily visible to search engine users.
On the other hand, don't let your designer get carried away with fancy gimmicks and expensive effects. A big turnoff for me, on any website, is anything blocking fast, easy navigation.
Anytime I find myself waiting for a fancy flash introduction to load, for example, I'm gone. Tell your designer to stick with simple, interactive, user-friendly Java scripts.
Once patients have found your site, they had better find it easy to navigate, or they will be gone, too. Make clear immediately what you want visitors to do. Advertising professionals call this the "call to action." If potential patients don't know what to do within seconds of landing on your site, they will usually click the back button and go to the next hit on the search engine.
Communication links ("Contact Us," "Make an Appointment," "Call for Consultation") should be readily available. Don't expect patients to sift through the site to find them.
Don't let your patients get lost, either. Well-organized websites have hyperlinked paths on each page that allow users to determine immediately where they are. For example, "Home > Services > Fillers" means a patient is on the Fillers page of the Services section, with an easy path back to the Home page. (Designers call this "breadcrumbing.")
Leave design and navigation to the pros, but don't delegate content. Only you know what you want to say on your site and as the captain of the ship, you are responsible for all the facts and opinions on it.
Decide what you want your site to say before any design begins, and write it out, in plain English. Once the designer has your content to work with, he or she can create a unique framework to complement it.
Good photo- graphs are vital to a good practice site. Patients should be able to see that your office is an attractive place, staffed with compassionate and cheerful professionals. A professional photographer can convey that message and make your site distinctive.
Photos are often the most prominent elements of a website. They should send a warm and professional first impression.
Contact information must be front and center, and on every page. Patients don't want to hunt for a way to contact you. Post contact information prominently, in large, easy-to-read fonts.
Contact forms should be simple, with a few basic fields. If you make patients work too hard to contact you by having them complete a complex form and a string of scary questions, you will lose them.
And don't just rely on online contact; give them other options as well. Some people - particularly the elderly - still prefer to pick up the phone!
Is a website essential to the success of your practice? No, not really, despite everything those spammers tell you.
About 20% of private medical practices have a website, and the rest seem to be doing fine without one. The reality is that most users of medical care are older folk; and most older folk still find their doctors the old-fashioned ways: through referrals from primary practitioners, and by word-of-mouth from family and friends.
By the time the youngsters who use the Internet to find everything reach the age where medical care is a priority, almost every private practice will certainly have a Web presence. (But by then, of course, something way cooler will have come along to replace the Web!)
That said, aggressive cosmetic practices in highly competitive areas clearly seem to benefit from Web exposure; and for the rest of us, although a well-designed website is not a necessity, it can certainly make life easier for doctors, staff, and patients.
The key phrase, of course, is "well-designed." A badly designed site will do far more harm than good, so this is one project to leave to the professionals.
Doing it yourself might sound like fun, but good site design is a lot harder than it looks. And if you resort to a standard template, as most amateurs do, you won't like the result.
Almost every generic, template-based website I've seen looks shabby and amateurish. Broken links, misspelled text, stock snapshot-quality photos - exactly the opposite of the professional image you want to project.
In addition, template-based sites tend to be overlooked by search engines. What's the point of having a website if patients can't find it?
A buzz phrase among professional Web designers is "search engine optimization" (SEO). A pro will give you a professional look and a Web presence that is readily visible to search engine users.
On the other hand, don't let your designer get carried away with fancy gimmicks and expensive effects. A big turnoff for me, on any website, is anything blocking fast, easy navigation.
Anytime I find myself waiting for a fancy flash introduction to load, for example, I'm gone. Tell your designer to stick with simple, interactive, user-friendly Java scripts.
Once patients have found your site, they had better find it easy to navigate, or they will be gone, too. Make clear immediately what you want visitors to do. Advertising professionals call this the "call to action." If potential patients don't know what to do within seconds of landing on your site, they will usually click the back button and go to the next hit on the search engine.
Communication links ("Contact Us," "Make an Appointment," "Call for Consultation") should be readily available. Don't expect patients to sift through the site to find them.
Don't let your patients get lost, either. Well-organized websites have hyperlinked paths on each page that allow users to determine immediately where they are. For example, "Home > Services > Fillers" means a patient is on the Fillers page of the Services section, with an easy path back to the Home page. (Designers call this "breadcrumbing.")
Leave design and navigation to the pros, but don't delegate content. Only you know what you want to say on your site and as the captain of the ship, you are responsible for all the facts and opinions on it.
Decide what you want your site to say before any design begins, and write it out, in plain English. Once the designer has your content to work with, he or she can create a unique framework to complement it.
Good photo- graphs are vital to a good practice site. Patients should be able to see that your office is an attractive place, staffed with compassionate and cheerful professionals. A professional photographer can convey that message and make your site distinctive.
Photos are often the most prominent elements of a website. They should send a warm and professional first impression.
Contact information must be front and center, and on every page. Patients don't want to hunt for a way to contact you. Post contact information prominently, in large, easy-to-read fonts.
Contact forms should be simple, with a few basic fields. If you make patients work too hard to contact you by having them complete a complex form and a string of scary questions, you will lose them.
And don't just rely on online contact; give them other options as well. Some people - particularly the elderly - still prefer to pick up the phone!
Is a website essential to the success of your practice? No, not really, despite everything those spammers tell you.
About 20% of private medical practices have a website, and the rest seem to be doing fine without one. The reality is that most users of medical care are older folk; and most older folk still find their doctors the old-fashioned ways: through referrals from primary practitioners, and by word-of-mouth from family and friends.
By the time the youngsters who use the Internet to find everything reach the age where medical care is a priority, almost every private practice will certainly have a Web presence. (But by then, of course, something way cooler will have come along to replace the Web!)
That said, aggressive cosmetic practices in highly competitive areas clearly seem to benefit from Web exposure; and for the rest of us, although a well-designed website is not a necessity, it can certainly make life easier for doctors, staff, and patients.
The key phrase, of course, is "well-designed." A badly designed site will do far more harm than good, so this is one project to leave to the professionals.
Doing it yourself might sound like fun, but good site design is a lot harder than it looks. And if you resort to a standard template, as most amateurs do, you won't like the result.
Almost every generic, template-based website I've seen looks shabby and amateurish. Broken links, misspelled text, stock snapshot-quality photos - exactly the opposite of the professional image you want to project.
In addition, template-based sites tend to be overlooked by search engines. What's the point of having a website if patients can't find it?
A buzz phrase among professional Web designers is "search engine optimization" (SEO). A pro will give you a professional look and a Web presence that is readily visible to search engine users.
On the other hand, don't let your designer get carried away with fancy gimmicks and expensive effects. A big turnoff for me, on any website, is anything blocking fast, easy navigation.
Anytime I find myself waiting for a fancy flash introduction to load, for example, I'm gone. Tell your designer to stick with simple, interactive, user-friendly Java scripts.
Once patients have found your site, they had better find it easy to navigate, or they will be gone, too. Make clear immediately what you want visitors to do. Advertising professionals call this the "call to action." If potential patients don't know what to do within seconds of landing on your site, they will usually click the back button and go to the next hit on the search engine.
Communication links ("Contact Us," "Make an Appointment," "Call for Consultation") should be readily available. Don't expect patients to sift through the site to find them.
Don't let your patients get lost, either. Well-organized websites have hyperlinked paths on each page that allow users to determine immediately where they are. For example, "Home > Services > Fillers" means a patient is on the Fillers page of the Services section, with an easy path back to the Home page. (Designers call this "breadcrumbing.")
Leave design and navigation to the pros, but don't delegate content. Only you know what you want to say on your site and as the captain of the ship, you are responsible for all the facts and opinions on it.
Decide what you want your site to say before any design begins, and write it out, in plain English. Once the designer has your content to work with, he or she can create a unique framework to complement it.
Good photo- graphs are vital to a good practice site. Patients should be able to see that your office is an attractive place, staffed with compassionate and cheerful professionals. A professional photographer can convey that message and make your site distinctive.
Photos are often the most prominent elements of a website. They should send a warm and professional first impression.
Contact information must be front and center, and on every page. Patients don't want to hunt for a way to contact you. Post contact information prominently, in large, easy-to-read fonts.
Contact forms should be simple, with a few basic fields. If you make patients work too hard to contact you by having them complete a complex form and a string of scary questions, you will lose them.
And don't just rely on online contact; give them other options as well. Some people - particularly the elderly - still prefer to pick up the phone!