User login
ACOG’s push for medical liability reform: What’s the latest?
It’s a conundrum. There seems to be no doubt about the need for medical liability reform—in fact, there is wide-spread support for it. And yet....
Four years after Captain Chesley “Sully” Sullenberger saved a planeload of passengers during an emergency landing—the “miracle on the Hudson”—he’s become a national champion of medical liability reform. In a recent interview with Politico, Sullenberger equated the 200,000 lives estimated to be lost each year due to medical errors to “20 jetliners crashing per week,” a situation he insists would close airports and ground flights until the problem was solved. But these 200,000 deaths cause little more than a ripple of concern, he claims.1
Among the solutions he proposes is “a whole different approach to reviewing medical errors, figuring out what’s behind them, not just blaming doctors and nurses.”1
Captain Sullenberger is discovering the difficult reality we’ve experienced for too many years: Solutions just don’t come very fast to medical liability reform, despite wide-spread support for it.
At the American Congress of Obstetricians and Gynecologists (ACOG), our campaign for medical liability reform has focused, as always, on patients, using the campaign line: “Who will delivery my baby?” ACOG supports caps on noneconomic damages and other reforms, such as those contained in the California Medical Injury Compensation Reform Act (MICRA), the gold standard for medical liability reform. We will continue to push for national MICRA reform until we’ve won that important protection for all ObGyns and their patients.
Until we reach that goal, we’re working to accomplish meaningful steps to liability reform where we can, including testing state alternatives. And our colleague organizations? Many of them, once insisting on federal adoption of MICRA or nothing at all, now actively support meaningful alternatives, too.
What do we want?
Proposals for tort reform, based on California’s MICRA statute, include:
- mandatory periodic payments of all future damages exceeding $100,000
- a $250,000 ceiling on noneconomic damage awards
- a requirement that claims must be filed within 2 years of the date by which the alleged injury reasonably should have been discovered but in no event more than 4 years from the time of the alleged injury. In the case of alleged injury to children under 4 years of age, claims must be filed by the child’s 8th birthday.
- limits on punitive damages, with 50% of punitive damage awards going to a state disciplinary fund
- limits on attorney contingency fees
- reductions in awards based on the amount paid from another source, such as health or disability insurance
- a requirement for “clear and convincing evidence” rather than the usual “preponderance of evidence” when a health-care professional who provided delivery services but not prenatal care is sued
- alternative systems for dispute resolution.
10 alternative reforms
Good ideas include:
1. Require a certificate of merit from the plaintiff
This proposal would require the plaintiff to file an affidavit with the court to demonstrate that the case has merit before the complaint can move forward. Certificates would necessitate the written opinion of a legally qualified health-care provider affirming that the defendant failed to meet the care standards that would be followed by a reasonably prudent health-care provider—and that this failure caused or directly contributed to the damages claimed.
2. Facilitate early settlement offers
Under this idea, a physician or hospital would be allowed to offer economic damages to an injured party without involving the courts. This offer would not constitute an admission of liability and would be inadmissible if a lawsuit were later filed in the case. Physicians would have an incentive to make a good-faith offer as early as possible after the injury is discovered, and patients would have an incentive to accept legitimate offers of compensation. Early-offer programs would require the injured party to meet a higher burden of proof for alleged negligence if that party chooses to reject the offer and file a lawsuit.
3. Create health-care courts
Health-care courts would allow for a bench or jury trial presided over by a specially trained judge to exclusively hear medical liability cases. Such courts have the potential to correct severe deficiencies in the current medical justice system and to reduce health-system errors and improve patient safety.
4. Allow a physician to say, “I’m sorry”
This proposal would encourage physicians to directly discuss errors and injuries with patients, to apologize and outline corrective action. Such discussions would be inadmissible if a patient later files a lawsuit.
5. Establish medical review panels
Any claim against a physician would be reviewed by a panel of experts who would provide an opinion on whether the physician failed to act within the relevant standards of care.
6. Require a claim to be screened and mediated
A plaintiff ’s claim would have to be evaluated by a screening panel before it could proceed to litigation. The panel would identify claims hat merit compensation and encourage early resolution of those claims. It also would encourage withdrawal or dismissal of non-meritorious claims.
7. Protect physicians who follow evidence-based guidelines
Health-care providers who follow guidelines based on solid evidence, and those who have legitimate justifications for departing from guidelines, would be protected from liability claims.
8. Allow the voluntary resolution of disputes
This proposal would motivate states to encourage the creation of other innovative systems to compensate individuals who are injured in the course of receiving health-care services.
9. Require expert witnesses to meet certain standards
This alternative would limit expert-witness standing to individuals who:
- are licensed and trained in the same specialty as the defendant
- have particular expertise in the disease process or procedure performed in the case
- have been in active medical practice in the same specialty as the defendant within 5 years of the claim or who have been taught at an accredited medical school on the care and type of treatment at issue.
10. Create catastrophic injury systems
These systems would establish a fund for individuals who have experienced bad outcomes. Birth injury funds are an example of this model.
Who’s on our side?
Congressional policy wonks give liability reform a thumbs up
In early 2010, the Medicare Payment Advisory Commission (MedPAC), a nonpartisan advisory counsel to the US Congress, identified three important ways that our current malpractice system harms the Medicare program and Medicare beneficiaries, the aged, and disabled:
- Medicare payments to providers include some liability costs (folded into hospital diagnosis-related group [DRG] payments; factored into physician fee schedule calculation)
- Defensive medicine drives up costs for Medicare
- Malpractice impairs the quality and safety of care to beneficiaries. That is, the current system does not improve patient safety.
MedPAC staff recommended that the commissioners urge Congress to pass government-subsidized malpractice reinsurance for providers who meet certain safety criteria or create a federal administrative adjudication process. The commissioners expressed an interest in alternatives to address the costs of medical malpractice, including ways to encourage states and providers to address medical malpractice in a manner most appropriate for them. However, when MedPAC returned to this topic at its next meeting later the same year, the commissioners mentioned medical liability only to dismiss it as an incidental issue in opening remarks.
The Congressional Budget Office (CBO) estimates that medical malpractice costs our health-care system $35 billion in direct costs, with billions more as a result of defensive medicine.
CBO has scored these medical liability reform proposals as providing significant savings to our federal budget:
- a $250,000 cap on subjective, noneconomic damages (with no limit on economic damages)
- collateral source rule allowing evidence of outside payments to be submitted in court
- a ban on subrogation by certain collateral sources
- caps on attorney contingency fees
- periodic payments of future damages
- a reasonable statute of limitations.
In addition, in 2011, CBO scored comprehensive medical liability reform as saving the federal government $62.4 billion over 10 years. As longtime Illinois Senator Everett Dirksen was known to say, “A billion here, a billion there, and pretty soon you’re talking real money.”
Many Republican congressional leaders “walk the walk”
Republicans have long claimed medical liability reform as their issue. And they walk the walk.
Representative Phil Gingrey, MD, of Georgia, an ACOG Fellow, has led the medical liability reform fight on Capitol Hill for a number of years. His bill, the Protecting Access to Healthcare Act (HR 5), which would have brought MICRA to the national level, was repeatedly passed by the Republican majority of the House of Representatives, only to be ignored by the Democrats controlling the Senate.
Again this year, Dr. Gingrey introduced legislation to protect physicians from unexpected liability. His Standard of Care Protection Act (HR 1473) would ensure that provisions of the Affordable Care Act (ACA) cannot be used to create new causes of action against medical professionals. HR 1473 would ensure that Medicare, Medicaid, and other federal programs that establish government standards and guidelines for health-care providers cannot be used to create new causes of action.
Federal health-care programs are changing to ensure that payment reflects quality of care. As a result, new payment rules, guidelines, and standards are being written into federal laws and regulations. HR 1473 would make clear that these cannot be used to define the applicable standard of care or duty of care in a medical liability lawsuit.
ACOG supports Dr. Gingrey’s bill, as well as a second, companion approach that would ensure that ObGyns who follow guidelines and standards of care developed by their medical society are protected from liability, with sensible exceptions for egregious harm and negligence.
Representative Charlie Dent, Republican of Pennsylvania, also has introduced ACOG-supported medical liability legislation. The Health Care Safety Net Enhancement Act (HR 36) would provide federal liability protection for physicians providing care under the Emergency Medical Treatment and Active Labor Act (EMTALA). HR 36 is commonly referred to as Good Samaritan legislation, intended to protect doctors who rush to the aid of a sick individual. The likelihood of any of these bills getting enacted into law is slim. Even some conservative Republicans oppose federal liability reform as an intrusion into states’ rights.
Some Democrats have said good things
In his proposed budget for fiscal year 2012, President Barack Obama asked Congress for funding to address medical liability issues.
He proposed “to restrain health-care costs” through “a more aggressive effort to reform our medical malpractice system to reduce defensive medicine, promote patient safety, and improve patient outcomes.” He encouraged Republicans to work constructively with him on medical malpractice as part of an overall effort to restrain health-care costs.2
The President asked Congress for “$250 million in grants to states to reform the way they resolve medical malpractice disputes,” including health courts, safe harbors, early disclosure and offer, and other legal reforms such as joint and several liability and collateral source rules.2
Congress never funded the President’s request.
President Obama repeated his request in his fiscal year 2013 budget proposal. Congress didn’t fund it then, either.
Earlier, in March 2009, in remarks to the Business Roundtable, President Obama noted that “the cost issue is the thing that we actually think is the big driver in this whole debate...things like comparative effectiveness, health IT, prevention, figuring out how our reimbursement structures are designed under Medicare and Medicaid. Medical liability issues—I think all those things have to be on the table.”3
In an interview the same month, Senator Ron Wyden, Democrat of Oregon, said, “I think [medical liability reform is] an essential piece for there to be enduring reform, reform that will stick and will get a significant bipar-tisan vote in the United States Senate.”4
Senator Wyden’s Healthy Americans Act (S 391) included incentives to get states to enact malpractice reforms as a key to overhauling the health-care system.
Also in March 2009, Representative Rob Andrews, Democrat of New Jersey, Chairman of the House Education and Labor, Health Subcommittee, pointed to the need for medical liability reform.
“It’s hard for me to imagine a [health-care reform] result that gets to the president’s desk that doesn’t deal with the medical mal-practice issue in some way.”4
And Senator Max Baucus, Democrat of Montana, Chairman of the Senate Finance Committee, proposed providing states grant money to develop alternative litigation models, such as encouraging disclosure and compensation in the case of error, and establishing health courts whose judges have health-care expertise.
As early as May 2006, President Obama (then a Senator from Illinois) and Senator Hillary Rodham Clinton, Democrat of New York, urged a focus on patient safety.
“Instead of focusing on the few areas of intense disagreement,” they wrote in the New England Journal of Medicine, “such as the possibility of mandating caps on the financial damages awarded to patients, we believe that the discussion should center on a more fundamental issue: the need to improve patient safety....”
“To improve both patient safety and the medical liability climate, the tort system must achieve four goals: reduce the rates of preventable patient injuries, promote open communication between physicians and patients, ensure patients access to fair compensation for legitimate medical injuries, and reduce liability insurance premiums for health-care providers. Addressing just one of these issues is not sufficient.”5
And then there are the trial lawyers
Readers of OBG Management know all too well that the role of trial lawyers in medical liability reform has been to block meaningful reforms from passing and to repeal reforms currently in place. The Association of Trial Lawyers of America, now known as the American Association for Justice, tries to portray itself as defending vulnerable patients against a few bad apples. Its Web site (www.justice.org) points to recent National Practitioner Data Bank (NPDB) figures indicating that “just 6% of doctors are responsible for 58% of all negligence incidents. The civil justice system seeks to weed out those few doctors whose actions have such devastating impact on patients.”
The Web site includes these bullet points:
- 6% of doctors have been responsible for 58% of all malpractice payments since 1991
- 2% of doctors having three or more mal-practice payments were responsible for 33% of all payments
- 1% of doctors having four or more malprac-tice payments were responsible for 20% of all payments
- 82% of doctors have never had a medical malpractice payment.
Tell that to ObGyns, who, in 2012, paid an average of 12.4% of their gross income for liability insurance premiums in 2012, and nearly 60% of whom changed their practices based on the risk or fear of professional liability claims or litigation. And this despite the fact that 43.9% of claims were dropped or settled without any payment on behalf of the ObGyn.
Action at the state level
We need a federal solution, but since that isn’t within reach, we’re looking to the states for action. And there’s a lot of action in some states, including Connecticut, Florida, Georgia, Hawaii, Illinois, Iowa, Missouri, Oregon, Rhode Island, Tennessee, and Utah.
Advocates in these states are trying a number of different approaches, hoping that some type of meaningful reform will be signed into law. Here’s a sampling of what’s under way.
Connecticut
HB 6687, amend certificates of merit in medical liability actions. Status: April 1, 2013: Joint Committee on Judiciary hearing. The bill would eliminate the need for a detailed basis for the formation of an opinion and replace it with a lower threshold stating the appearance of one or more specific breaches of the prevailing professional standard of care.
In addition, HB 6687 would allow any expert who may testify in court to satisfy the certificate of merit requirement, but at trial the “expert,” in order to testify, needs to have the court determine him or her to be qualified to testify based on discovery and evidentiary issues that are decided at trial. This expert then could sign a certificate of merit but have the court determine that he or she is indeed not an expert for that case. HB 6687 delays the challenging of qualifications of an expert only after the completion of discovery, adding substantial time and cost to defending meritless suits. Finally, the bill allows for a second bite of the apple for cases that did not meet this watered down standard for certificate of merit and would eliminate the automatic dismissal of cases filed with inadequate certificates that did not meet the rules of the court.
SB 1154, amend Connecticut’s failure of suit statute to allow a plaintiff whose lawsuit was dismissed due to a failure to file a certificate of good faith as required by statute, to commence a new action.
HB 5229, limit noneconomic damages in medical liability cases to $250,000 for each health-care provider and institution per event, and $750,000 overall for each event.
HB 5270, establish peer-review panels in medical liability actions. The panels would consist of physicians, medical professionals, and individuals outside the medical profession who would review claims of alleged negligence and determine whether there is probable cause that the medical liability claims have been made in good faith prior to the action being referred to mandatory mediation.
SB 97, extend the statute of limitations in medical liability cases, allowing for an action to be brought no more than 10 years from the date of the act or omission that serves as the basis for the claim.
Florida
The Birth-Related Neurological Injury Compensation Association (NICA). NICA is a statutory organization that manages the compensation plan used to pay for the care of infants born with certain neurological injuries. This plan is available to eligible families statewide without litigation. By eliminating costly legal proceedings, and through professional management of its disbursements, NICA ensures that birth-injured infants receive the care they need while reducing the financial burden on medical providers and families. Defensive work continues on the NICA Board and trial bar.
HB 7015, expert witness. Status: March 28, 2013, the House Justice Appropriations Subcommittee reported favorably. This bill would adopt the Daubert standard for expert witness testimony. It provides that a witness qualified as an expert by knowledge, skill, experience, training, or education may testify in the form of an opinion as to the facts at issue in a case.
Georgia
HB 499, Provider Shield Act. Georgia is the first state to introduce legislation based on the American Medical Association’s model bill, “The Provider Shield Act,” which clarifies language in the Affordable Care Act by providing that a physician’s failure to comply with, or a breach of, any federal statute, regulation, program, guideline, or other provision shall not: (1) be admissible; (2) be used to determine the standard of care; or (3) be the legal basis for a presumption of negligence.
Status: Enacted May 6, 2013. The law prohibits the use of payer guidelines and quality criteria outlined in federal law as a legal basis for negligence or standard of care in determining medical liability. Physicians are concerned that without such protections, the medical profession could be exposed to charges of negligence that aren’t based on clinical standards or the patient’s unique medical needs. Implementation of any guideline by any public or private payor, or the establishment of any payment standard or reimbursement criteria under any federal laws or regulations related to health care, shall not be construed, without competent expert testimony establishing the appropriate standard of care, to establish a legal basis for negligence or the standard of care or duty of care owed by a health-care provider to a patient in any civil action for medical malpractice or product liability.
This first-of-its-kind legislation reinforces the concept that medical decisions should be based on a patient’s unique medical needs. HB 499 makes it clear that federal standards or guidelines designed to enhance access to high-quality health care cannot be used to invent new legal actions against physicians.
Hawaii
SB 1308, health-care provider benevolent gesture legislation.
Illinois
On March 22, 2013, several pieces of tort-reform legislation were re-referred to the House Committee on Rules, effectively killing the bills for the session. The House Speaker would have to choose to “release” any of the bills in order for them to move again; this is highly unlikely.
HB 138 would have deleted existing-venue language providing that an action may commence in any county if all defendants are nonresidents of the state, and replaced it with language providing that, if no defendants that are joined in good faith and with probable cause for the purpose of obtaining a judgment against them are residents of the state, an action may be commenced only in the county in which the transaction or some part thereof occurred out of which the cause of action arose.
HB 2220 and HB 2222 provided that, with respect to certain types of actions, for any defendant whose fault is less than 25% of the total fault attributable to the plaintiff, the defendants sued by the plaintiff, and any third-party defendant who could have been sued by the plaintiff (instead of any third-party defendant except the plaintiff’s employer), shall be severally liable for all other damages. In addition, these bills provided that, for any defendant whose fault is 25% or greater of the total fault attributable to the plaintiff, the defendants sued by the plaintiff, and any third-party defendants who could have been sued by the plaintiff (instead of any third-party defendants except the plaintiff’s employer), shall be jointly and severally liable for all other damages.
HB 2221 created requirements regarding qualifications, testimony, disclosure and compensation of expert testimony and standards for reviewing courts to follow in ruling on the admissibility of expert testimony.
Iowa
SSB 1054 and HSB 36, expert’s certificate of merit affidavit and noneconomic cap. These bills provide that in any medical liability action, the plaintiff is required, within 180 days of the defendant’s answer, to serve the defendant with an expert’s certificate of merit affidavit for each expert scheduled to testify. They also would limit noneconomic damage awards in medical liability cases to $1 million.
Missouri
HJR 6 proposes a constitutional amendment allowing the legislature to cap noneconomic damages in medical liability cases.
SJR 1 grants the legislature the power to limit, by statute, jury awards for noneconomic damages.
SB 64 changes the evidentiary standard in medical liability cases to “clear and convincing” for noneconomic damages.
Oregon
SB 483, early discussion and resolution. Status: Passed by the legislature. This bill establishes an early discussion and resolution (EDC) process within the Oregon Patient Safety Commission. This voluntary process is intended to facilitate open communication about all outcomes of care, including serious events, between the provider, health-care facility, and the patient. When an adverse health-care incident occurs, the patient, health-care provider or health-care facility where the incident occurred may file a notice of adverse health-care incident with the Commission. This notice triggers discussion of the health-care incident and, if appropriate, an offer of compensation. If discussion does not result in the resolution of the claim, the bill gives the parties the option of participating in Commission-facilitated mediation. The entire process is voluntary.
SJR 30, proposed amendment to constitution, $1 million limit on noneconomic awards in medical liability cases. Slated for next general election.
Rhode Island
HB 5380, apology bill. Status: Heard in House Judiciary Committee on March 27, 2013; no action was taken. This bill provides that statements by a health-care provider to a patient or to the patient’s family regarding the outcome of such patient’s medical care and treatment, such as an apology or expression of sympathy, shall be inadmissible as evidence or an admission of liability in any claim or action against the provider.
Tennessee
Joint and several liability. Status: On March 26, 2013, the House Civil Justice Subcommittee reported favorably. This bill would codify current state law by providing that if multiple defendants are found liable in a civil action governed by comparative fault, a defendant shall only be severally liable for the percentage of damages for which fault is attributed to such defendant by the trier of fact, and no defendant shall be held jointly liable for any damages.
SB 274, medical liability expert witness reform.
Utah
HB 135, rules, arbitration. Status: March 21, 2013, sent to Governor Gary Herbert for his approval. HB 135 provides that a party in a medical liability action or arbitration may not attempt to allocate fault to any health-care provider unless a certificate of compliance has been issued. HB 135 also requires that evidence from a medical review panel remain unreportable to a health-care facility or health insurance plan.
Summing up
Medical liability reform—the obvious need for it, the good reasons to do it, and the fact that it remains beyond reach—is a constant source of frustration among many ObGyns. Maybe Captain Sully can save the day.
How medical liability affects the ObGyn specialty
ACOG’s 2012 Survey on Professional Liability, our 11th survey since 1983, assessed the effects of professional liability litigation and insurance issues on the practice of obstetrics and gynecology.6 The survey, conducted under the direction of ACOG’s Vice President for Fellowship and Deputy Executive Vice President Albert Strunk, MD, JD, included segments on demographics, patient care, liability claims experience, and practice changes associated with the cost of liability insurance and the fear of litigation. The survey went to 32,238 Fellows and Junior Fellows. Of these, 9,006 completed the questionnaire. Here are major findings.
Provider profiles
A total of 72.5% of respondents provided both obstetric and gynecologic care, slightly lower than the percentage identified in the 2009 survey, which was 74.3%. Fewer than 7% of respondents provided obstetric care only; 19.8% provided gynecologic care only. Of those restricting their services to gynecology, 88.9% had previously offered obstetric care. The average age at which these physicians stopped practicing obstetrics was 49 years.
Cost of liability insurance
ObGyns spent an average of 12.4% of their gross income on liability insurance premiums in 2012, down from 18% in 2009.
How liability issues affected practice
Since the previous survey in 2009, 57.9% of respondents made one or more changes to their practice to mitigate the risk or fear of professional liability claims or litigation.
Obstetric practice. Among respondents who made changes to their obstetric practice, 27.4% decreased the number of high-risk patients they see, 23.8% increased the number of cesarean deliveries they perform, 18.9% stopped offering and performing vaginal birth after cesarean (VBAC), 11.5% reduced the total number of deliveries, and 6.2% stopped practicing obstetrics altogether.
Gynecologic practice. Respondents who changed their gynecologic practice cut back on surgical procedures (18.9%), stopped performing major gynecologic surgery (6.7%), and stopped performing all surgery (1.8%).
Other changes. Medical liability issues contributed to the decisions of 12.3% of respondents to choose salaried employment with a hospital, government, or other institution.
Claims experience
Obstetric claims were likely to involve a neurologically impaired infant (28.8%) as the primary allegation, followed by stillbirth or neonatal death (14.4%).
Other variables involved in obstetric claims included electronic fetal monitoring (20.9%), shoulder dystocia and/or brachial plexus injury (15.5%), and actions of ObGyn residents (11.4%).
Gynecologic claims. Survey respondents reported a total of 1,496 gynecologic claims. Major injury to the patient was the primary allegation of 29.1% of these claims. A delay in diagnosis or failure to diagnose was the second most common primary allegation (22.1%), followed by minor injury to the patient (20.7%).Of the claims involving a delayed or missed diagnosis, 41.8% involved cancer. Of these, breast cancer was the most frequent type of cancer (39.1%), followed by uterine cancer (20.3%), ovarian cancer (14.5%), and cervical cancer (10.9%).
Many gynecologic claims (44.4%) involved surgical complications arising from hysterectomy (28.7%) and laparoscopic procedures (14.6%).
Claims outcomes. A total of 43.9% of claims were dropped or settled without any payment on behalf of the ObGyn. Of these, 29.0% were dropped by the plaintiff, 11.2% were dismissed by the court, and 3.7% were settled without payment on behalf of the ObGyn.The average for all paid claims was $510,473.
The average payment for claims involving a neurologically impaired infant was $982,051. Other average payments for obstetric claims include $364,794 for “other infant injury–major” and $271,149 for stillbirth or neonatal death.
Average payments for gynecologic claims include $407,500 for a failure to diagnose breast cancer and $315,633 for “patient injury–major.”
Most challenging locales. It will come as no surprise to many readers that average medical liability payouts are especially high in six states:
New York - $677,866,050
Pennsylvania - $319,710,250
Illinois - $242,108,800
New Jersey - $221,170,750
Florida - $218,123,050
California - $215,519,200.
Fifty-eight percent of payouts nationwide were for female patients.7
Tell us what you think, at [email protected]. Please include your name and city and state.
1.Cheney K. ‘Miracle’ pilot on mission against medical errors. Politico.com. August 1, 2013. http://www.politico.com/story/2013/08/sully-sullenberger-mission-medical-erros-95009.html. Accessed August 6, 2013.
2.Office of Management and Budget. Fiscal Year 2012 Budget of the US Government. http://www.whitehouse.gov/files/documents/budget_2012.pdf. Accessed August 8, 2013.
3.Obama’s remarks to the Business Roundtable, March 12, 2009. Wall Street Journal: Washington Wire. http://blogs.wsj.com/washwire/2009/03/12/obamas-remarks-to-the-business-roundtable/. Accessed August 8, 2013.
4.Werner E. Health debate could spur malpractice changes. Salt Lake Tribune. March 17, 2009. http://www.sltrib.com/ci_11933162. Accessed August 8, 2013.
5.Clinton HR, Obama B. Perspective: Making patient safety the centerpiece of medical liability reform. N Engl J Med. 2006;354(21):2205–2208.
6.American Congress of Obstetricians and Gynecologists. Survey on Professional Liability. 2012 Survey Results. http://www.acog.org/About_ACOG/ACOG_Departments/Professional_Liability/2012_Survey_Results. Accessed August 7, 2013.
7. Latner AW. Six states account for 50% of malpractice payouts. Clinical Advisor. April 17, 2012. http://www.clinicaladvisor.com/six-states-account-for-50-of-malpractice-payouts/article/236931. Accessed August 7, 2013.
It’s a conundrum. There seems to be no doubt about the need for medical liability reform—in fact, there is wide-spread support for it. And yet....
Four years after Captain Chesley “Sully” Sullenberger saved a planeload of passengers during an emergency landing—the “miracle on the Hudson”—he’s become a national champion of medical liability reform. In a recent interview with Politico, Sullenberger equated the 200,000 lives estimated to be lost each year due to medical errors to “20 jetliners crashing per week,” a situation he insists would close airports and ground flights until the problem was solved. But these 200,000 deaths cause little more than a ripple of concern, he claims.1
Among the solutions he proposes is “a whole different approach to reviewing medical errors, figuring out what’s behind them, not just blaming doctors and nurses.”1
Captain Sullenberger is discovering the difficult reality we’ve experienced for too many years: Solutions just don’t come very fast to medical liability reform, despite wide-spread support for it.
At the American Congress of Obstetricians and Gynecologists (ACOG), our campaign for medical liability reform has focused, as always, on patients, using the campaign line: “Who will delivery my baby?” ACOG supports caps on noneconomic damages and other reforms, such as those contained in the California Medical Injury Compensation Reform Act (MICRA), the gold standard for medical liability reform. We will continue to push for national MICRA reform until we’ve won that important protection for all ObGyns and their patients.
Until we reach that goal, we’re working to accomplish meaningful steps to liability reform where we can, including testing state alternatives. And our colleague organizations? Many of them, once insisting on federal adoption of MICRA or nothing at all, now actively support meaningful alternatives, too.
What do we want?
Proposals for tort reform, based on California’s MICRA statute, include:
- mandatory periodic payments of all future damages exceeding $100,000
- a $250,000 ceiling on noneconomic damage awards
- a requirement that claims must be filed within 2 years of the date by which the alleged injury reasonably should have been discovered but in no event more than 4 years from the time of the alleged injury. In the case of alleged injury to children under 4 years of age, claims must be filed by the child’s 8th birthday.
- limits on punitive damages, with 50% of punitive damage awards going to a state disciplinary fund
- limits on attorney contingency fees
- reductions in awards based on the amount paid from another source, such as health or disability insurance
- a requirement for “clear and convincing evidence” rather than the usual “preponderance of evidence” when a health-care professional who provided delivery services but not prenatal care is sued
- alternative systems for dispute resolution.
10 alternative reforms
Good ideas include:
1. Require a certificate of merit from the plaintiff
This proposal would require the plaintiff to file an affidavit with the court to demonstrate that the case has merit before the complaint can move forward. Certificates would necessitate the written opinion of a legally qualified health-care provider affirming that the defendant failed to meet the care standards that would be followed by a reasonably prudent health-care provider—and that this failure caused or directly contributed to the damages claimed.
2. Facilitate early settlement offers
Under this idea, a physician or hospital would be allowed to offer economic damages to an injured party without involving the courts. This offer would not constitute an admission of liability and would be inadmissible if a lawsuit were later filed in the case. Physicians would have an incentive to make a good-faith offer as early as possible after the injury is discovered, and patients would have an incentive to accept legitimate offers of compensation. Early-offer programs would require the injured party to meet a higher burden of proof for alleged negligence if that party chooses to reject the offer and file a lawsuit.
3. Create health-care courts
Health-care courts would allow for a bench or jury trial presided over by a specially trained judge to exclusively hear medical liability cases. Such courts have the potential to correct severe deficiencies in the current medical justice system and to reduce health-system errors and improve patient safety.
4. Allow a physician to say, “I’m sorry”
This proposal would encourage physicians to directly discuss errors and injuries with patients, to apologize and outline corrective action. Such discussions would be inadmissible if a patient later files a lawsuit.
5. Establish medical review panels
Any claim against a physician would be reviewed by a panel of experts who would provide an opinion on whether the physician failed to act within the relevant standards of care.
6. Require a claim to be screened and mediated
A plaintiff ’s claim would have to be evaluated by a screening panel before it could proceed to litigation. The panel would identify claims hat merit compensation and encourage early resolution of those claims. It also would encourage withdrawal or dismissal of non-meritorious claims.
7. Protect physicians who follow evidence-based guidelines
Health-care providers who follow guidelines based on solid evidence, and those who have legitimate justifications for departing from guidelines, would be protected from liability claims.
8. Allow the voluntary resolution of disputes
This proposal would motivate states to encourage the creation of other innovative systems to compensate individuals who are injured in the course of receiving health-care services.
9. Require expert witnesses to meet certain standards
This alternative would limit expert-witness standing to individuals who:
- are licensed and trained in the same specialty as the defendant
- have particular expertise in the disease process or procedure performed in the case
- have been in active medical practice in the same specialty as the defendant within 5 years of the claim or who have been taught at an accredited medical school on the care and type of treatment at issue.
10. Create catastrophic injury systems
These systems would establish a fund for individuals who have experienced bad outcomes. Birth injury funds are an example of this model.
Who’s on our side?
Congressional policy wonks give liability reform a thumbs up
In early 2010, the Medicare Payment Advisory Commission (MedPAC), a nonpartisan advisory counsel to the US Congress, identified three important ways that our current malpractice system harms the Medicare program and Medicare beneficiaries, the aged, and disabled:
- Medicare payments to providers include some liability costs (folded into hospital diagnosis-related group [DRG] payments; factored into physician fee schedule calculation)
- Defensive medicine drives up costs for Medicare
- Malpractice impairs the quality and safety of care to beneficiaries. That is, the current system does not improve patient safety.
MedPAC staff recommended that the commissioners urge Congress to pass government-subsidized malpractice reinsurance for providers who meet certain safety criteria or create a federal administrative adjudication process. The commissioners expressed an interest in alternatives to address the costs of medical malpractice, including ways to encourage states and providers to address medical malpractice in a manner most appropriate for them. However, when MedPAC returned to this topic at its next meeting later the same year, the commissioners mentioned medical liability only to dismiss it as an incidental issue in opening remarks.
The Congressional Budget Office (CBO) estimates that medical malpractice costs our health-care system $35 billion in direct costs, with billions more as a result of defensive medicine.
CBO has scored these medical liability reform proposals as providing significant savings to our federal budget:
- a $250,000 cap on subjective, noneconomic damages (with no limit on economic damages)
- collateral source rule allowing evidence of outside payments to be submitted in court
- a ban on subrogation by certain collateral sources
- caps on attorney contingency fees
- periodic payments of future damages
- a reasonable statute of limitations.
In addition, in 2011, CBO scored comprehensive medical liability reform as saving the federal government $62.4 billion over 10 years. As longtime Illinois Senator Everett Dirksen was known to say, “A billion here, a billion there, and pretty soon you’re talking real money.”
Many Republican congressional leaders “walk the walk”
Republicans have long claimed medical liability reform as their issue. And they walk the walk.
Representative Phil Gingrey, MD, of Georgia, an ACOG Fellow, has led the medical liability reform fight on Capitol Hill for a number of years. His bill, the Protecting Access to Healthcare Act (HR 5), which would have brought MICRA to the national level, was repeatedly passed by the Republican majority of the House of Representatives, only to be ignored by the Democrats controlling the Senate.
Again this year, Dr. Gingrey introduced legislation to protect physicians from unexpected liability. His Standard of Care Protection Act (HR 1473) would ensure that provisions of the Affordable Care Act (ACA) cannot be used to create new causes of action against medical professionals. HR 1473 would ensure that Medicare, Medicaid, and other federal programs that establish government standards and guidelines for health-care providers cannot be used to create new causes of action.
Federal health-care programs are changing to ensure that payment reflects quality of care. As a result, new payment rules, guidelines, and standards are being written into federal laws and regulations. HR 1473 would make clear that these cannot be used to define the applicable standard of care or duty of care in a medical liability lawsuit.
ACOG supports Dr. Gingrey’s bill, as well as a second, companion approach that would ensure that ObGyns who follow guidelines and standards of care developed by their medical society are protected from liability, with sensible exceptions for egregious harm and negligence.
Representative Charlie Dent, Republican of Pennsylvania, also has introduced ACOG-supported medical liability legislation. The Health Care Safety Net Enhancement Act (HR 36) would provide federal liability protection for physicians providing care under the Emergency Medical Treatment and Active Labor Act (EMTALA). HR 36 is commonly referred to as Good Samaritan legislation, intended to protect doctors who rush to the aid of a sick individual. The likelihood of any of these bills getting enacted into law is slim. Even some conservative Republicans oppose federal liability reform as an intrusion into states’ rights.
Some Democrats have said good things
In his proposed budget for fiscal year 2012, President Barack Obama asked Congress for funding to address medical liability issues.
He proposed “to restrain health-care costs” through “a more aggressive effort to reform our medical malpractice system to reduce defensive medicine, promote patient safety, and improve patient outcomes.” He encouraged Republicans to work constructively with him on medical malpractice as part of an overall effort to restrain health-care costs.2
The President asked Congress for “$250 million in grants to states to reform the way they resolve medical malpractice disputes,” including health courts, safe harbors, early disclosure and offer, and other legal reforms such as joint and several liability and collateral source rules.2
Congress never funded the President’s request.
President Obama repeated his request in his fiscal year 2013 budget proposal. Congress didn’t fund it then, either.
Earlier, in March 2009, in remarks to the Business Roundtable, President Obama noted that “the cost issue is the thing that we actually think is the big driver in this whole debate...things like comparative effectiveness, health IT, prevention, figuring out how our reimbursement structures are designed under Medicare and Medicaid. Medical liability issues—I think all those things have to be on the table.”3
In an interview the same month, Senator Ron Wyden, Democrat of Oregon, said, “I think [medical liability reform is] an essential piece for there to be enduring reform, reform that will stick and will get a significant bipar-tisan vote in the United States Senate.”4
Senator Wyden’s Healthy Americans Act (S 391) included incentives to get states to enact malpractice reforms as a key to overhauling the health-care system.
Also in March 2009, Representative Rob Andrews, Democrat of New Jersey, Chairman of the House Education and Labor, Health Subcommittee, pointed to the need for medical liability reform.
“It’s hard for me to imagine a [health-care reform] result that gets to the president’s desk that doesn’t deal with the medical mal-practice issue in some way.”4
And Senator Max Baucus, Democrat of Montana, Chairman of the Senate Finance Committee, proposed providing states grant money to develop alternative litigation models, such as encouraging disclosure and compensation in the case of error, and establishing health courts whose judges have health-care expertise.
As early as May 2006, President Obama (then a Senator from Illinois) and Senator Hillary Rodham Clinton, Democrat of New York, urged a focus on patient safety.
“Instead of focusing on the few areas of intense disagreement,” they wrote in the New England Journal of Medicine, “such as the possibility of mandating caps on the financial damages awarded to patients, we believe that the discussion should center on a more fundamental issue: the need to improve patient safety....”
“To improve both patient safety and the medical liability climate, the tort system must achieve four goals: reduce the rates of preventable patient injuries, promote open communication between physicians and patients, ensure patients access to fair compensation for legitimate medical injuries, and reduce liability insurance premiums for health-care providers. Addressing just one of these issues is not sufficient.”5
And then there are the trial lawyers
Readers of OBG Management know all too well that the role of trial lawyers in medical liability reform has been to block meaningful reforms from passing and to repeal reforms currently in place. The Association of Trial Lawyers of America, now known as the American Association for Justice, tries to portray itself as defending vulnerable patients against a few bad apples. Its Web site (www.justice.org) points to recent National Practitioner Data Bank (NPDB) figures indicating that “just 6% of doctors are responsible for 58% of all negligence incidents. The civil justice system seeks to weed out those few doctors whose actions have such devastating impact on patients.”
The Web site includes these bullet points:
- 6% of doctors have been responsible for 58% of all malpractice payments since 1991
- 2% of doctors having three or more mal-practice payments were responsible for 33% of all payments
- 1% of doctors having four or more malprac-tice payments were responsible for 20% of all payments
- 82% of doctors have never had a medical malpractice payment.
Tell that to ObGyns, who, in 2012, paid an average of 12.4% of their gross income for liability insurance premiums in 2012, and nearly 60% of whom changed their practices based on the risk or fear of professional liability claims or litigation. And this despite the fact that 43.9% of claims were dropped or settled without any payment on behalf of the ObGyn.
Action at the state level
We need a federal solution, but since that isn’t within reach, we’re looking to the states for action. And there’s a lot of action in some states, including Connecticut, Florida, Georgia, Hawaii, Illinois, Iowa, Missouri, Oregon, Rhode Island, Tennessee, and Utah.
Advocates in these states are trying a number of different approaches, hoping that some type of meaningful reform will be signed into law. Here’s a sampling of what’s under way.
Connecticut
HB 6687, amend certificates of merit in medical liability actions. Status: April 1, 2013: Joint Committee on Judiciary hearing. The bill would eliminate the need for a detailed basis for the formation of an opinion and replace it with a lower threshold stating the appearance of one or more specific breaches of the prevailing professional standard of care.
In addition, HB 6687 would allow any expert who may testify in court to satisfy the certificate of merit requirement, but at trial the “expert,” in order to testify, needs to have the court determine him or her to be qualified to testify based on discovery and evidentiary issues that are decided at trial. This expert then could sign a certificate of merit but have the court determine that he or she is indeed not an expert for that case. HB 6687 delays the challenging of qualifications of an expert only after the completion of discovery, adding substantial time and cost to defending meritless suits. Finally, the bill allows for a second bite of the apple for cases that did not meet this watered down standard for certificate of merit and would eliminate the automatic dismissal of cases filed with inadequate certificates that did not meet the rules of the court.
SB 1154, amend Connecticut’s failure of suit statute to allow a plaintiff whose lawsuit was dismissed due to a failure to file a certificate of good faith as required by statute, to commence a new action.
HB 5229, limit noneconomic damages in medical liability cases to $250,000 for each health-care provider and institution per event, and $750,000 overall for each event.
HB 5270, establish peer-review panels in medical liability actions. The panels would consist of physicians, medical professionals, and individuals outside the medical profession who would review claims of alleged negligence and determine whether there is probable cause that the medical liability claims have been made in good faith prior to the action being referred to mandatory mediation.
SB 97, extend the statute of limitations in medical liability cases, allowing for an action to be brought no more than 10 years from the date of the act or omission that serves as the basis for the claim.
Florida
The Birth-Related Neurological Injury Compensation Association (NICA). NICA is a statutory organization that manages the compensation plan used to pay for the care of infants born with certain neurological injuries. This plan is available to eligible families statewide without litigation. By eliminating costly legal proceedings, and through professional management of its disbursements, NICA ensures that birth-injured infants receive the care they need while reducing the financial burden on medical providers and families. Defensive work continues on the NICA Board and trial bar.
HB 7015, expert witness. Status: March 28, 2013, the House Justice Appropriations Subcommittee reported favorably. This bill would adopt the Daubert standard for expert witness testimony. It provides that a witness qualified as an expert by knowledge, skill, experience, training, or education may testify in the form of an opinion as to the facts at issue in a case.
Georgia
HB 499, Provider Shield Act. Georgia is the first state to introduce legislation based on the American Medical Association’s model bill, “The Provider Shield Act,” which clarifies language in the Affordable Care Act by providing that a physician’s failure to comply with, or a breach of, any federal statute, regulation, program, guideline, or other provision shall not: (1) be admissible; (2) be used to determine the standard of care; or (3) be the legal basis for a presumption of negligence.
Status: Enacted May 6, 2013. The law prohibits the use of payer guidelines and quality criteria outlined in federal law as a legal basis for negligence or standard of care in determining medical liability. Physicians are concerned that without such protections, the medical profession could be exposed to charges of negligence that aren’t based on clinical standards or the patient’s unique medical needs. Implementation of any guideline by any public or private payor, or the establishment of any payment standard or reimbursement criteria under any federal laws or regulations related to health care, shall not be construed, without competent expert testimony establishing the appropriate standard of care, to establish a legal basis for negligence or the standard of care or duty of care owed by a health-care provider to a patient in any civil action for medical malpractice or product liability.
This first-of-its-kind legislation reinforces the concept that medical decisions should be based on a patient’s unique medical needs. HB 499 makes it clear that federal standards or guidelines designed to enhance access to high-quality health care cannot be used to invent new legal actions against physicians.
Hawaii
SB 1308, health-care provider benevolent gesture legislation.
Illinois
On March 22, 2013, several pieces of tort-reform legislation were re-referred to the House Committee on Rules, effectively killing the bills for the session. The House Speaker would have to choose to “release” any of the bills in order for them to move again; this is highly unlikely.
HB 138 would have deleted existing-venue language providing that an action may commence in any county if all defendants are nonresidents of the state, and replaced it with language providing that, if no defendants that are joined in good faith and with probable cause for the purpose of obtaining a judgment against them are residents of the state, an action may be commenced only in the county in which the transaction or some part thereof occurred out of which the cause of action arose.
HB 2220 and HB 2222 provided that, with respect to certain types of actions, for any defendant whose fault is less than 25% of the total fault attributable to the plaintiff, the defendants sued by the plaintiff, and any third-party defendant who could have been sued by the plaintiff (instead of any third-party defendant except the plaintiff’s employer), shall be severally liable for all other damages. In addition, these bills provided that, for any defendant whose fault is 25% or greater of the total fault attributable to the plaintiff, the defendants sued by the plaintiff, and any third-party defendants who could have been sued by the plaintiff (instead of any third-party defendants except the plaintiff’s employer), shall be jointly and severally liable for all other damages.
HB 2221 created requirements regarding qualifications, testimony, disclosure and compensation of expert testimony and standards for reviewing courts to follow in ruling on the admissibility of expert testimony.
Iowa
SSB 1054 and HSB 36, expert’s certificate of merit affidavit and noneconomic cap. These bills provide that in any medical liability action, the plaintiff is required, within 180 days of the defendant’s answer, to serve the defendant with an expert’s certificate of merit affidavit for each expert scheduled to testify. They also would limit noneconomic damage awards in medical liability cases to $1 million.
Missouri
HJR 6 proposes a constitutional amendment allowing the legislature to cap noneconomic damages in medical liability cases.
SJR 1 grants the legislature the power to limit, by statute, jury awards for noneconomic damages.
SB 64 changes the evidentiary standard in medical liability cases to “clear and convincing” for noneconomic damages.
Oregon
SB 483, early discussion and resolution. Status: Passed by the legislature. This bill establishes an early discussion and resolution (EDC) process within the Oregon Patient Safety Commission. This voluntary process is intended to facilitate open communication about all outcomes of care, including serious events, between the provider, health-care facility, and the patient. When an adverse health-care incident occurs, the patient, health-care provider or health-care facility where the incident occurred may file a notice of adverse health-care incident with the Commission. This notice triggers discussion of the health-care incident and, if appropriate, an offer of compensation. If discussion does not result in the resolution of the claim, the bill gives the parties the option of participating in Commission-facilitated mediation. The entire process is voluntary.
SJR 30, proposed amendment to constitution, $1 million limit on noneconomic awards in medical liability cases. Slated for next general election.
Rhode Island
HB 5380, apology bill. Status: Heard in House Judiciary Committee on March 27, 2013; no action was taken. This bill provides that statements by a health-care provider to a patient or to the patient’s family regarding the outcome of such patient’s medical care and treatment, such as an apology or expression of sympathy, shall be inadmissible as evidence or an admission of liability in any claim or action against the provider.
Tennessee
Joint and several liability. Status: On March 26, 2013, the House Civil Justice Subcommittee reported favorably. This bill would codify current state law by providing that if multiple defendants are found liable in a civil action governed by comparative fault, a defendant shall only be severally liable for the percentage of damages for which fault is attributed to such defendant by the trier of fact, and no defendant shall be held jointly liable for any damages.
SB 274, medical liability expert witness reform.
Utah
HB 135, rules, arbitration. Status: March 21, 2013, sent to Governor Gary Herbert for his approval. HB 135 provides that a party in a medical liability action or arbitration may not attempt to allocate fault to any health-care provider unless a certificate of compliance has been issued. HB 135 also requires that evidence from a medical review panel remain unreportable to a health-care facility or health insurance plan.
Summing up
Medical liability reform—the obvious need for it, the good reasons to do it, and the fact that it remains beyond reach—is a constant source of frustration among many ObGyns. Maybe Captain Sully can save the day.
How medical liability affects the ObGyn specialty
ACOG’s 2012 Survey on Professional Liability, our 11th survey since 1983, assessed the effects of professional liability litigation and insurance issues on the practice of obstetrics and gynecology.6 The survey, conducted under the direction of ACOG’s Vice President for Fellowship and Deputy Executive Vice President Albert Strunk, MD, JD, included segments on demographics, patient care, liability claims experience, and practice changes associated with the cost of liability insurance and the fear of litigation. The survey went to 32,238 Fellows and Junior Fellows. Of these, 9,006 completed the questionnaire. Here are major findings.
Provider profiles
A total of 72.5% of respondents provided both obstetric and gynecologic care, slightly lower than the percentage identified in the 2009 survey, which was 74.3%. Fewer than 7% of respondents provided obstetric care only; 19.8% provided gynecologic care only. Of those restricting their services to gynecology, 88.9% had previously offered obstetric care. The average age at which these physicians stopped practicing obstetrics was 49 years.
Cost of liability insurance
ObGyns spent an average of 12.4% of their gross income on liability insurance premiums in 2012, down from 18% in 2009.
How liability issues affected practice
Since the previous survey in 2009, 57.9% of respondents made one or more changes to their practice to mitigate the risk or fear of professional liability claims or litigation.
Obstetric practice. Among respondents who made changes to their obstetric practice, 27.4% decreased the number of high-risk patients they see, 23.8% increased the number of cesarean deliveries they perform, 18.9% stopped offering and performing vaginal birth after cesarean (VBAC), 11.5% reduced the total number of deliveries, and 6.2% stopped practicing obstetrics altogether.
Gynecologic practice. Respondents who changed their gynecologic practice cut back on surgical procedures (18.9%), stopped performing major gynecologic surgery (6.7%), and stopped performing all surgery (1.8%).
Other changes. Medical liability issues contributed to the decisions of 12.3% of respondents to choose salaried employment with a hospital, government, or other institution.
Claims experience
Obstetric claims were likely to involve a neurologically impaired infant (28.8%) as the primary allegation, followed by stillbirth or neonatal death (14.4%).
Other variables involved in obstetric claims included electronic fetal monitoring (20.9%), shoulder dystocia and/or brachial plexus injury (15.5%), and actions of ObGyn residents (11.4%).
Gynecologic claims. Survey respondents reported a total of 1,496 gynecologic claims. Major injury to the patient was the primary allegation of 29.1% of these claims. A delay in diagnosis or failure to diagnose was the second most common primary allegation (22.1%), followed by minor injury to the patient (20.7%).Of the claims involving a delayed or missed diagnosis, 41.8% involved cancer. Of these, breast cancer was the most frequent type of cancer (39.1%), followed by uterine cancer (20.3%), ovarian cancer (14.5%), and cervical cancer (10.9%).
Many gynecologic claims (44.4%) involved surgical complications arising from hysterectomy (28.7%) and laparoscopic procedures (14.6%).
Claims outcomes. A total of 43.9% of claims were dropped or settled without any payment on behalf of the ObGyn. Of these, 29.0% were dropped by the plaintiff, 11.2% were dismissed by the court, and 3.7% were settled without payment on behalf of the ObGyn.The average for all paid claims was $510,473.
The average payment for claims involving a neurologically impaired infant was $982,051. Other average payments for obstetric claims include $364,794 for “other infant injury–major” and $271,149 for stillbirth or neonatal death.
Average payments for gynecologic claims include $407,500 for a failure to diagnose breast cancer and $315,633 for “patient injury–major.”
Most challenging locales. It will come as no surprise to many readers that average medical liability payouts are especially high in six states:
New York - $677,866,050
Pennsylvania - $319,710,250
Illinois - $242,108,800
New Jersey - $221,170,750
Florida - $218,123,050
California - $215,519,200.
Fifty-eight percent of payouts nationwide were for female patients.7
Tell us what you think, at [email protected]. Please include your name and city and state.
It’s a conundrum. There seems to be no doubt about the need for medical liability reform—in fact, there is wide-spread support for it. And yet....
Four years after Captain Chesley “Sully” Sullenberger saved a planeload of passengers during an emergency landing—the “miracle on the Hudson”—he’s become a national champion of medical liability reform. In a recent interview with Politico, Sullenberger equated the 200,000 lives estimated to be lost each year due to medical errors to “20 jetliners crashing per week,” a situation he insists would close airports and ground flights until the problem was solved. But these 200,000 deaths cause little more than a ripple of concern, he claims.1
Among the solutions he proposes is “a whole different approach to reviewing medical errors, figuring out what’s behind them, not just blaming doctors and nurses.”1
Captain Sullenberger is discovering the difficult reality we’ve experienced for too many years: Solutions just don’t come very fast to medical liability reform, despite wide-spread support for it.
At the American Congress of Obstetricians and Gynecologists (ACOG), our campaign for medical liability reform has focused, as always, on patients, using the campaign line: “Who will delivery my baby?” ACOG supports caps on noneconomic damages and other reforms, such as those contained in the California Medical Injury Compensation Reform Act (MICRA), the gold standard for medical liability reform. We will continue to push for national MICRA reform until we’ve won that important protection for all ObGyns and their patients.
Until we reach that goal, we’re working to accomplish meaningful steps to liability reform where we can, including testing state alternatives. And our colleague organizations? Many of them, once insisting on federal adoption of MICRA or nothing at all, now actively support meaningful alternatives, too.
What do we want?
Proposals for tort reform, based on California’s MICRA statute, include:
- mandatory periodic payments of all future damages exceeding $100,000
- a $250,000 ceiling on noneconomic damage awards
- a requirement that claims must be filed within 2 years of the date by which the alleged injury reasonably should have been discovered but in no event more than 4 years from the time of the alleged injury. In the case of alleged injury to children under 4 years of age, claims must be filed by the child’s 8th birthday.
- limits on punitive damages, with 50% of punitive damage awards going to a state disciplinary fund
- limits on attorney contingency fees
- reductions in awards based on the amount paid from another source, such as health or disability insurance
- a requirement for “clear and convincing evidence” rather than the usual “preponderance of evidence” when a health-care professional who provided delivery services but not prenatal care is sued
- alternative systems for dispute resolution.
10 alternative reforms
Good ideas include:
1. Require a certificate of merit from the plaintiff
This proposal would require the plaintiff to file an affidavit with the court to demonstrate that the case has merit before the complaint can move forward. Certificates would necessitate the written opinion of a legally qualified health-care provider affirming that the defendant failed to meet the care standards that would be followed by a reasonably prudent health-care provider—and that this failure caused or directly contributed to the damages claimed.
2. Facilitate early settlement offers
Under this idea, a physician or hospital would be allowed to offer economic damages to an injured party without involving the courts. This offer would not constitute an admission of liability and would be inadmissible if a lawsuit were later filed in the case. Physicians would have an incentive to make a good-faith offer as early as possible after the injury is discovered, and patients would have an incentive to accept legitimate offers of compensation. Early-offer programs would require the injured party to meet a higher burden of proof for alleged negligence if that party chooses to reject the offer and file a lawsuit.
3. Create health-care courts
Health-care courts would allow for a bench or jury trial presided over by a specially trained judge to exclusively hear medical liability cases. Such courts have the potential to correct severe deficiencies in the current medical justice system and to reduce health-system errors and improve patient safety.
4. Allow a physician to say, “I’m sorry”
This proposal would encourage physicians to directly discuss errors and injuries with patients, to apologize and outline corrective action. Such discussions would be inadmissible if a patient later files a lawsuit.
5. Establish medical review panels
Any claim against a physician would be reviewed by a panel of experts who would provide an opinion on whether the physician failed to act within the relevant standards of care.
6. Require a claim to be screened and mediated
A plaintiff ’s claim would have to be evaluated by a screening panel before it could proceed to litigation. The panel would identify claims hat merit compensation and encourage early resolution of those claims. It also would encourage withdrawal or dismissal of non-meritorious claims.
7. Protect physicians who follow evidence-based guidelines
Health-care providers who follow guidelines based on solid evidence, and those who have legitimate justifications for departing from guidelines, would be protected from liability claims.
8. Allow the voluntary resolution of disputes
This proposal would motivate states to encourage the creation of other innovative systems to compensate individuals who are injured in the course of receiving health-care services.
9. Require expert witnesses to meet certain standards
This alternative would limit expert-witness standing to individuals who:
- are licensed and trained in the same specialty as the defendant
- have particular expertise in the disease process or procedure performed in the case
- have been in active medical practice in the same specialty as the defendant within 5 years of the claim or who have been taught at an accredited medical school on the care and type of treatment at issue.
10. Create catastrophic injury systems
These systems would establish a fund for individuals who have experienced bad outcomes. Birth injury funds are an example of this model.
Who’s on our side?
Congressional policy wonks give liability reform a thumbs up
In early 2010, the Medicare Payment Advisory Commission (MedPAC), a nonpartisan advisory counsel to the US Congress, identified three important ways that our current malpractice system harms the Medicare program and Medicare beneficiaries, the aged, and disabled:
- Medicare payments to providers include some liability costs (folded into hospital diagnosis-related group [DRG] payments; factored into physician fee schedule calculation)
- Defensive medicine drives up costs for Medicare
- Malpractice impairs the quality and safety of care to beneficiaries. That is, the current system does not improve patient safety.
MedPAC staff recommended that the commissioners urge Congress to pass government-subsidized malpractice reinsurance for providers who meet certain safety criteria or create a federal administrative adjudication process. The commissioners expressed an interest in alternatives to address the costs of medical malpractice, including ways to encourage states and providers to address medical malpractice in a manner most appropriate for them. However, when MedPAC returned to this topic at its next meeting later the same year, the commissioners mentioned medical liability only to dismiss it as an incidental issue in opening remarks.
The Congressional Budget Office (CBO) estimates that medical malpractice costs our health-care system $35 billion in direct costs, with billions more as a result of defensive medicine.
CBO has scored these medical liability reform proposals as providing significant savings to our federal budget:
- a $250,000 cap on subjective, noneconomic damages (with no limit on economic damages)
- collateral source rule allowing evidence of outside payments to be submitted in court
- a ban on subrogation by certain collateral sources
- caps on attorney contingency fees
- periodic payments of future damages
- a reasonable statute of limitations.
In addition, in 2011, CBO scored comprehensive medical liability reform as saving the federal government $62.4 billion over 10 years. As longtime Illinois Senator Everett Dirksen was known to say, “A billion here, a billion there, and pretty soon you’re talking real money.”
Many Republican congressional leaders “walk the walk”
Republicans have long claimed medical liability reform as their issue. And they walk the walk.
Representative Phil Gingrey, MD, of Georgia, an ACOG Fellow, has led the medical liability reform fight on Capitol Hill for a number of years. His bill, the Protecting Access to Healthcare Act (HR 5), which would have brought MICRA to the national level, was repeatedly passed by the Republican majority of the House of Representatives, only to be ignored by the Democrats controlling the Senate.
Again this year, Dr. Gingrey introduced legislation to protect physicians from unexpected liability. His Standard of Care Protection Act (HR 1473) would ensure that provisions of the Affordable Care Act (ACA) cannot be used to create new causes of action against medical professionals. HR 1473 would ensure that Medicare, Medicaid, and other federal programs that establish government standards and guidelines for health-care providers cannot be used to create new causes of action.
Federal health-care programs are changing to ensure that payment reflects quality of care. As a result, new payment rules, guidelines, and standards are being written into federal laws and regulations. HR 1473 would make clear that these cannot be used to define the applicable standard of care or duty of care in a medical liability lawsuit.
ACOG supports Dr. Gingrey’s bill, as well as a second, companion approach that would ensure that ObGyns who follow guidelines and standards of care developed by their medical society are protected from liability, with sensible exceptions for egregious harm and negligence.
Representative Charlie Dent, Republican of Pennsylvania, also has introduced ACOG-supported medical liability legislation. The Health Care Safety Net Enhancement Act (HR 36) would provide federal liability protection for physicians providing care under the Emergency Medical Treatment and Active Labor Act (EMTALA). HR 36 is commonly referred to as Good Samaritan legislation, intended to protect doctors who rush to the aid of a sick individual. The likelihood of any of these bills getting enacted into law is slim. Even some conservative Republicans oppose federal liability reform as an intrusion into states’ rights.
Some Democrats have said good things
In his proposed budget for fiscal year 2012, President Barack Obama asked Congress for funding to address medical liability issues.
He proposed “to restrain health-care costs” through “a more aggressive effort to reform our medical malpractice system to reduce defensive medicine, promote patient safety, and improve patient outcomes.” He encouraged Republicans to work constructively with him on medical malpractice as part of an overall effort to restrain health-care costs.2
The President asked Congress for “$250 million in grants to states to reform the way they resolve medical malpractice disputes,” including health courts, safe harbors, early disclosure and offer, and other legal reforms such as joint and several liability and collateral source rules.2
Congress never funded the President’s request.
President Obama repeated his request in his fiscal year 2013 budget proposal. Congress didn’t fund it then, either.
Earlier, in March 2009, in remarks to the Business Roundtable, President Obama noted that “the cost issue is the thing that we actually think is the big driver in this whole debate...things like comparative effectiveness, health IT, prevention, figuring out how our reimbursement structures are designed under Medicare and Medicaid. Medical liability issues—I think all those things have to be on the table.”3
In an interview the same month, Senator Ron Wyden, Democrat of Oregon, said, “I think [medical liability reform is] an essential piece for there to be enduring reform, reform that will stick and will get a significant bipar-tisan vote in the United States Senate.”4
Senator Wyden’s Healthy Americans Act (S 391) included incentives to get states to enact malpractice reforms as a key to overhauling the health-care system.
Also in March 2009, Representative Rob Andrews, Democrat of New Jersey, Chairman of the House Education and Labor, Health Subcommittee, pointed to the need for medical liability reform.
“It’s hard for me to imagine a [health-care reform] result that gets to the president’s desk that doesn’t deal with the medical mal-practice issue in some way.”4
And Senator Max Baucus, Democrat of Montana, Chairman of the Senate Finance Committee, proposed providing states grant money to develop alternative litigation models, such as encouraging disclosure and compensation in the case of error, and establishing health courts whose judges have health-care expertise.
As early as May 2006, President Obama (then a Senator from Illinois) and Senator Hillary Rodham Clinton, Democrat of New York, urged a focus on patient safety.
“Instead of focusing on the few areas of intense disagreement,” they wrote in the New England Journal of Medicine, “such as the possibility of mandating caps on the financial damages awarded to patients, we believe that the discussion should center on a more fundamental issue: the need to improve patient safety....”
“To improve both patient safety and the medical liability climate, the tort system must achieve four goals: reduce the rates of preventable patient injuries, promote open communication between physicians and patients, ensure patients access to fair compensation for legitimate medical injuries, and reduce liability insurance premiums for health-care providers. Addressing just one of these issues is not sufficient.”5
And then there are the trial lawyers
Readers of OBG Management know all too well that the role of trial lawyers in medical liability reform has been to block meaningful reforms from passing and to repeal reforms currently in place. The Association of Trial Lawyers of America, now known as the American Association for Justice, tries to portray itself as defending vulnerable patients against a few bad apples. Its Web site (www.justice.org) points to recent National Practitioner Data Bank (NPDB) figures indicating that “just 6% of doctors are responsible for 58% of all negligence incidents. The civil justice system seeks to weed out those few doctors whose actions have such devastating impact on patients.”
The Web site includes these bullet points:
- 6% of doctors have been responsible for 58% of all malpractice payments since 1991
- 2% of doctors having three or more mal-practice payments were responsible for 33% of all payments
- 1% of doctors having four or more malprac-tice payments were responsible for 20% of all payments
- 82% of doctors have never had a medical malpractice payment.
Tell that to ObGyns, who, in 2012, paid an average of 12.4% of their gross income for liability insurance premiums in 2012, and nearly 60% of whom changed their practices based on the risk or fear of professional liability claims or litigation. And this despite the fact that 43.9% of claims were dropped or settled without any payment on behalf of the ObGyn.
Action at the state level
We need a federal solution, but since that isn’t within reach, we’re looking to the states for action. And there’s a lot of action in some states, including Connecticut, Florida, Georgia, Hawaii, Illinois, Iowa, Missouri, Oregon, Rhode Island, Tennessee, and Utah.
Advocates in these states are trying a number of different approaches, hoping that some type of meaningful reform will be signed into law. Here’s a sampling of what’s under way.
Connecticut
HB 6687, amend certificates of merit in medical liability actions. Status: April 1, 2013: Joint Committee on Judiciary hearing. The bill would eliminate the need for a detailed basis for the formation of an opinion and replace it with a lower threshold stating the appearance of one or more specific breaches of the prevailing professional standard of care.
In addition, HB 6687 would allow any expert who may testify in court to satisfy the certificate of merit requirement, but at trial the “expert,” in order to testify, needs to have the court determine him or her to be qualified to testify based on discovery and evidentiary issues that are decided at trial. This expert then could sign a certificate of merit but have the court determine that he or she is indeed not an expert for that case. HB 6687 delays the challenging of qualifications of an expert only after the completion of discovery, adding substantial time and cost to defending meritless suits. Finally, the bill allows for a second bite of the apple for cases that did not meet this watered down standard for certificate of merit and would eliminate the automatic dismissal of cases filed with inadequate certificates that did not meet the rules of the court.
SB 1154, amend Connecticut’s failure of suit statute to allow a plaintiff whose lawsuit was dismissed due to a failure to file a certificate of good faith as required by statute, to commence a new action.
HB 5229, limit noneconomic damages in medical liability cases to $250,000 for each health-care provider and institution per event, and $750,000 overall for each event.
HB 5270, establish peer-review panels in medical liability actions. The panels would consist of physicians, medical professionals, and individuals outside the medical profession who would review claims of alleged negligence and determine whether there is probable cause that the medical liability claims have been made in good faith prior to the action being referred to mandatory mediation.
SB 97, extend the statute of limitations in medical liability cases, allowing for an action to be brought no more than 10 years from the date of the act or omission that serves as the basis for the claim.
Florida
The Birth-Related Neurological Injury Compensation Association (NICA). NICA is a statutory organization that manages the compensation plan used to pay for the care of infants born with certain neurological injuries. This plan is available to eligible families statewide without litigation. By eliminating costly legal proceedings, and through professional management of its disbursements, NICA ensures that birth-injured infants receive the care they need while reducing the financial burden on medical providers and families. Defensive work continues on the NICA Board and trial bar.
HB 7015, expert witness. Status: March 28, 2013, the House Justice Appropriations Subcommittee reported favorably. This bill would adopt the Daubert standard for expert witness testimony. It provides that a witness qualified as an expert by knowledge, skill, experience, training, or education may testify in the form of an opinion as to the facts at issue in a case.
Georgia
HB 499, Provider Shield Act. Georgia is the first state to introduce legislation based on the American Medical Association’s model bill, “The Provider Shield Act,” which clarifies language in the Affordable Care Act by providing that a physician’s failure to comply with, or a breach of, any federal statute, regulation, program, guideline, or other provision shall not: (1) be admissible; (2) be used to determine the standard of care; or (3) be the legal basis for a presumption of negligence.
Status: Enacted May 6, 2013. The law prohibits the use of payer guidelines and quality criteria outlined in federal law as a legal basis for negligence or standard of care in determining medical liability. Physicians are concerned that without such protections, the medical profession could be exposed to charges of negligence that aren’t based on clinical standards or the patient’s unique medical needs. Implementation of any guideline by any public or private payor, or the establishment of any payment standard or reimbursement criteria under any federal laws or regulations related to health care, shall not be construed, without competent expert testimony establishing the appropriate standard of care, to establish a legal basis for negligence or the standard of care or duty of care owed by a health-care provider to a patient in any civil action for medical malpractice or product liability.
This first-of-its-kind legislation reinforces the concept that medical decisions should be based on a patient’s unique medical needs. HB 499 makes it clear that federal standards or guidelines designed to enhance access to high-quality health care cannot be used to invent new legal actions against physicians.
Hawaii
SB 1308, health-care provider benevolent gesture legislation.
Illinois
On March 22, 2013, several pieces of tort-reform legislation were re-referred to the House Committee on Rules, effectively killing the bills for the session. The House Speaker would have to choose to “release” any of the bills in order for them to move again; this is highly unlikely.
HB 138 would have deleted existing-venue language providing that an action may commence in any county if all defendants are nonresidents of the state, and replaced it with language providing that, if no defendants that are joined in good faith and with probable cause for the purpose of obtaining a judgment against them are residents of the state, an action may be commenced only in the county in which the transaction or some part thereof occurred out of which the cause of action arose.
HB 2220 and HB 2222 provided that, with respect to certain types of actions, for any defendant whose fault is less than 25% of the total fault attributable to the plaintiff, the defendants sued by the plaintiff, and any third-party defendant who could have been sued by the plaintiff (instead of any third-party defendant except the plaintiff’s employer), shall be severally liable for all other damages. In addition, these bills provided that, for any defendant whose fault is 25% or greater of the total fault attributable to the plaintiff, the defendants sued by the plaintiff, and any third-party defendants who could have been sued by the plaintiff (instead of any third-party defendants except the plaintiff’s employer), shall be jointly and severally liable for all other damages.
HB 2221 created requirements regarding qualifications, testimony, disclosure and compensation of expert testimony and standards for reviewing courts to follow in ruling on the admissibility of expert testimony.
Iowa
SSB 1054 and HSB 36, expert’s certificate of merit affidavit and noneconomic cap. These bills provide that in any medical liability action, the plaintiff is required, within 180 days of the defendant’s answer, to serve the defendant with an expert’s certificate of merit affidavit for each expert scheduled to testify. They also would limit noneconomic damage awards in medical liability cases to $1 million.
Missouri
HJR 6 proposes a constitutional amendment allowing the legislature to cap noneconomic damages in medical liability cases.
SJR 1 grants the legislature the power to limit, by statute, jury awards for noneconomic damages.
SB 64 changes the evidentiary standard in medical liability cases to “clear and convincing” for noneconomic damages.
Oregon
SB 483, early discussion and resolution. Status: Passed by the legislature. This bill establishes an early discussion and resolution (EDC) process within the Oregon Patient Safety Commission. This voluntary process is intended to facilitate open communication about all outcomes of care, including serious events, between the provider, health-care facility, and the patient. When an adverse health-care incident occurs, the patient, health-care provider or health-care facility where the incident occurred may file a notice of adverse health-care incident with the Commission. This notice triggers discussion of the health-care incident and, if appropriate, an offer of compensation. If discussion does not result in the resolution of the claim, the bill gives the parties the option of participating in Commission-facilitated mediation. The entire process is voluntary.
SJR 30, proposed amendment to constitution, $1 million limit on noneconomic awards in medical liability cases. Slated for next general election.
Rhode Island
HB 5380, apology bill. Status: Heard in House Judiciary Committee on March 27, 2013; no action was taken. This bill provides that statements by a health-care provider to a patient or to the patient’s family regarding the outcome of such patient’s medical care and treatment, such as an apology or expression of sympathy, shall be inadmissible as evidence or an admission of liability in any claim or action against the provider.
Tennessee
Joint and several liability. Status: On March 26, 2013, the House Civil Justice Subcommittee reported favorably. This bill would codify current state law by providing that if multiple defendants are found liable in a civil action governed by comparative fault, a defendant shall only be severally liable for the percentage of damages for which fault is attributed to such defendant by the trier of fact, and no defendant shall be held jointly liable for any damages.
SB 274, medical liability expert witness reform.
Utah
HB 135, rules, arbitration. Status: March 21, 2013, sent to Governor Gary Herbert for his approval. HB 135 provides that a party in a medical liability action or arbitration may not attempt to allocate fault to any health-care provider unless a certificate of compliance has been issued. HB 135 also requires that evidence from a medical review panel remain unreportable to a health-care facility or health insurance plan.
Summing up
Medical liability reform—the obvious need for it, the good reasons to do it, and the fact that it remains beyond reach—is a constant source of frustration among many ObGyns. Maybe Captain Sully can save the day.
How medical liability affects the ObGyn specialty
ACOG’s 2012 Survey on Professional Liability, our 11th survey since 1983, assessed the effects of professional liability litigation and insurance issues on the practice of obstetrics and gynecology.6 The survey, conducted under the direction of ACOG’s Vice President for Fellowship and Deputy Executive Vice President Albert Strunk, MD, JD, included segments on demographics, patient care, liability claims experience, and practice changes associated with the cost of liability insurance and the fear of litigation. The survey went to 32,238 Fellows and Junior Fellows. Of these, 9,006 completed the questionnaire. Here are major findings.
Provider profiles
A total of 72.5% of respondents provided both obstetric and gynecologic care, slightly lower than the percentage identified in the 2009 survey, which was 74.3%. Fewer than 7% of respondents provided obstetric care only; 19.8% provided gynecologic care only. Of those restricting their services to gynecology, 88.9% had previously offered obstetric care. The average age at which these physicians stopped practicing obstetrics was 49 years.
Cost of liability insurance
ObGyns spent an average of 12.4% of their gross income on liability insurance premiums in 2012, down from 18% in 2009.
How liability issues affected practice
Since the previous survey in 2009, 57.9% of respondents made one or more changes to their practice to mitigate the risk or fear of professional liability claims or litigation.
Obstetric practice. Among respondents who made changes to their obstetric practice, 27.4% decreased the number of high-risk patients they see, 23.8% increased the number of cesarean deliveries they perform, 18.9% stopped offering and performing vaginal birth after cesarean (VBAC), 11.5% reduced the total number of deliveries, and 6.2% stopped practicing obstetrics altogether.
Gynecologic practice. Respondents who changed their gynecologic practice cut back on surgical procedures (18.9%), stopped performing major gynecologic surgery (6.7%), and stopped performing all surgery (1.8%).
Other changes. Medical liability issues contributed to the decisions of 12.3% of respondents to choose salaried employment with a hospital, government, or other institution.
Claims experience
Obstetric claims were likely to involve a neurologically impaired infant (28.8%) as the primary allegation, followed by stillbirth or neonatal death (14.4%).
Other variables involved in obstetric claims included electronic fetal monitoring (20.9%), shoulder dystocia and/or brachial plexus injury (15.5%), and actions of ObGyn residents (11.4%).
Gynecologic claims. Survey respondents reported a total of 1,496 gynecologic claims. Major injury to the patient was the primary allegation of 29.1% of these claims. A delay in diagnosis or failure to diagnose was the second most common primary allegation (22.1%), followed by minor injury to the patient (20.7%).Of the claims involving a delayed or missed diagnosis, 41.8% involved cancer. Of these, breast cancer was the most frequent type of cancer (39.1%), followed by uterine cancer (20.3%), ovarian cancer (14.5%), and cervical cancer (10.9%).
Many gynecologic claims (44.4%) involved surgical complications arising from hysterectomy (28.7%) and laparoscopic procedures (14.6%).
Claims outcomes. A total of 43.9% of claims were dropped or settled without any payment on behalf of the ObGyn. Of these, 29.0% were dropped by the plaintiff, 11.2% were dismissed by the court, and 3.7% were settled without payment on behalf of the ObGyn.The average for all paid claims was $510,473.
The average payment for claims involving a neurologically impaired infant was $982,051. Other average payments for obstetric claims include $364,794 for “other infant injury–major” and $271,149 for stillbirth or neonatal death.
Average payments for gynecologic claims include $407,500 for a failure to diagnose breast cancer and $315,633 for “patient injury–major.”
Most challenging locales. It will come as no surprise to many readers that average medical liability payouts are especially high in six states:
New York - $677,866,050
Pennsylvania - $319,710,250
Illinois - $242,108,800
New Jersey - $221,170,750
Florida - $218,123,050
California - $215,519,200.
Fifty-eight percent of payouts nationwide were for female patients.7
Tell us what you think, at [email protected]. Please include your name and city and state.
1.Cheney K. ‘Miracle’ pilot on mission against medical errors. Politico.com. August 1, 2013. http://www.politico.com/story/2013/08/sully-sullenberger-mission-medical-erros-95009.html. Accessed August 6, 2013.
2.Office of Management and Budget. Fiscal Year 2012 Budget of the US Government. http://www.whitehouse.gov/files/documents/budget_2012.pdf. Accessed August 8, 2013.
3.Obama’s remarks to the Business Roundtable, March 12, 2009. Wall Street Journal: Washington Wire. http://blogs.wsj.com/washwire/2009/03/12/obamas-remarks-to-the-business-roundtable/. Accessed August 8, 2013.
4.Werner E. Health debate could spur malpractice changes. Salt Lake Tribune. March 17, 2009. http://www.sltrib.com/ci_11933162. Accessed August 8, 2013.
5.Clinton HR, Obama B. Perspective: Making patient safety the centerpiece of medical liability reform. N Engl J Med. 2006;354(21):2205–2208.
6.American Congress of Obstetricians and Gynecologists. Survey on Professional Liability. 2012 Survey Results. http://www.acog.org/About_ACOG/ACOG_Departments/Professional_Liability/2012_Survey_Results. Accessed August 7, 2013.
7. Latner AW. Six states account for 50% of malpractice payouts. Clinical Advisor. April 17, 2012. http://www.clinicaladvisor.com/six-states-account-for-50-of-malpractice-payouts/article/236931. Accessed August 7, 2013.
1.Cheney K. ‘Miracle’ pilot on mission against medical errors. Politico.com. August 1, 2013. http://www.politico.com/story/2013/08/sully-sullenberger-mission-medical-erros-95009.html. Accessed August 6, 2013.
2.Office of Management and Budget. Fiscal Year 2012 Budget of the US Government. http://www.whitehouse.gov/files/documents/budget_2012.pdf. Accessed August 8, 2013.
3.Obama’s remarks to the Business Roundtable, March 12, 2009. Wall Street Journal: Washington Wire. http://blogs.wsj.com/washwire/2009/03/12/obamas-remarks-to-the-business-roundtable/. Accessed August 8, 2013.
4.Werner E. Health debate could spur malpractice changes. Salt Lake Tribune. March 17, 2009. http://www.sltrib.com/ci_11933162. Accessed August 8, 2013.
5.Clinton HR, Obama B. Perspective: Making patient safety the centerpiece of medical liability reform. N Engl J Med. 2006;354(21):2205–2208.
6.American Congress of Obstetricians and Gynecologists. Survey on Professional Liability. 2012 Survey Results. http://www.acog.org/About_ACOG/ACOG_Departments/Professional_Liability/2012_Survey_Results. Accessed August 7, 2013.
7. Latner AW. Six states account for 50% of malpractice payouts. Clinical Advisor. April 17, 2012. http://www.clinicaladvisor.com/six-states-account-for-50-of-malpractice-payouts/article/236931. Accessed August 7, 2013.
- ACOG proposals for reform
- Action at the state level
- How medical liability affects the ObGyn specialty

Altering Record Compounds Fatal Mistake
A 17-year-old girl underwent a routine tonsillectomy without complications at a surgical center. Following the procedure, the patient was returned to the recovery room and administered fentanyl for pain.
The recovery room nurse assigned to monitor the patient spent 20 minutes treating another patient and then went on break, signing out to a second recovery room nurse. On receiving the signout, the second recovery room nurse discovered that the patient was in respiratory distress and began resuscitation efforts. The patient was resuscitated but died 15 days later.
The plaintiff claimed that the girl was left unmonitored by nurses assigned to the unit and that the monitoring equipment was not used, not set properly, or muted.
During her deposition, the second recovery room nurse admitted under oath that the first recovery room nurse falsified the patient’s chart; the first nurse claimed that she had assessed the patient during an important time period when she had not.
OUTCOME
The case was settled for $6 million: $1 million against the surgical center’s primary policy and $5 million against its excess policy.
COMMENT
Cases such as this one are unfortunate and avoidable—and tragically, too common. On any medical malpractice lawyer’s desk is a teetering stack of potential cases; much of that stack involves narcotics. This case raises two important areas to discuss: the dangers of parenteral narcotics and the perils of falsifying medical records.
First, when parenteral narcotics are given, proper monitoring safeguards must be in place. Malpractice cases frequently involve a scenario in which patients are given parenteral narcotics and left alone, out of sight, and unmonitored. This simply can’t be done. Close supervision and monitoring—with both equipment and eyes—are required to safeguard your patients and avoid malpractice risk.
Other malpractice scenarios involve the ambulatory patient who is given parenteral narcotics in a clinic setting and discharged after a 10-minute “observation” period—a period during which peak drug effect is probably not realized. The patient is unsafely discharged before that peak is reached and suffers potentially fatal side effects. Even when direct fatal effects are not realized, the patient is discharged with impaired motor coordination and cognitive judgment, placing the patient at risk in his/her surroundings.
If a clinician commits to giving parenteral narcotics, he or she commits to providing “real-time” monitoring until the narcotic effects have safely diminished and the patient’s condition is thoroughly documented in the record. Generally speaking, the patient must be reasonably clear of the effects of narcotics before discharge. (Remember the special case of naloxone, administered for opiate excesses, in which narcan is metabolized before the opiate; the patient can relapse into a coma/apnea if the naloxone fully metabolizes before the opiate.)
Here, this young woman was probably opiate naïve. While the amount she was given was certain, her response to the drug was not. She was left alone for at least 20 minutes and did not have a functioning SaO2 monitor. Close monitoring of this patient was required but not provided.
As a result of this case, the surgical center changed several policies: Nurses must be on a one-to-one ratio with patients who have received narcotics during anesthesia. Furthermore, nurses must have line-of-sight to see patients at all times, and importantly, may not mute monitors (eg, oximetry monitors).
The second salient point of this case is never, ever alter or falsify patient records! It will be discovered, and your credibility will be irretrievably damaged. Plaintiff lawyers live for this, and yet clinicians continue to do it. Don’t.
When altered medical records are discovered, the plaintiff’s theory of the case will be “cover up,” and jurors will be invited to punish the clinician for it. The jurors will do so.
Also problematic is a case that is otherwise defensible, but which becomes much more difficult to defend because a clinician has altered the records. Remember, the plaintiff must prove all aspects of negligence, including causation and damages. In some cases, the clinician knows an obvious mistake was made, but does not know that the eventual damages may be minimal or attributable to another cause. By altering the medical record, the clinician may enhance the damages value of a case by introducing a punitive element. Altering records may result in a lawsuit being filed when it otherwise wouldn’t have, or maintained when it would have been dropped before trial. In sum, don’t create a case against yourself by altering the medical records.
Here, the falsification of records came to light during the deposition of the second nurse—who, being under oath, probably had little choice but to testify that the first nurse falsified the records. No doubt, this falsification made a bad case worse and gave the plaintiff leverage in securing more favorable settlement terms.
You can’t make it right by rewriting history, but you can make it right by showing concern for the patient in your actions following a problem. You can also make it right by troubleshooting problems in a closed-door, formal peer review conference. Peer review conferences are designed for full and frank communication between clinicians and staff to solve problems, and as such they are protected from plaintiff disclosure.
This is an unfortunate case and a tragic loss of a young woman’s life. As clinicians, we must respect the potential life-ending power of parenteral narcotics. —DML
A 17-year-old girl underwent a routine tonsillectomy without complications at a surgical center. Following the procedure, the patient was returned to the recovery room and administered fentanyl for pain.
The recovery room nurse assigned to monitor the patient spent 20 minutes treating another patient and then went on break, signing out to a second recovery room nurse. On receiving the signout, the second recovery room nurse discovered that the patient was in respiratory distress and began resuscitation efforts. The patient was resuscitated but died 15 days later.
The plaintiff claimed that the girl was left unmonitored by nurses assigned to the unit and that the monitoring equipment was not used, not set properly, or muted.
During her deposition, the second recovery room nurse admitted under oath that the first recovery room nurse falsified the patient’s chart; the first nurse claimed that she had assessed the patient during an important time period when she had not.
OUTCOME
The case was settled for $6 million: $1 million against the surgical center’s primary policy and $5 million against its excess policy.
COMMENT
Cases such as this one are unfortunate and avoidable—and tragically, too common. On any medical malpractice lawyer’s desk is a teetering stack of potential cases; much of that stack involves narcotics. This case raises two important areas to discuss: the dangers of parenteral narcotics and the perils of falsifying medical records.
First, when parenteral narcotics are given, proper monitoring safeguards must be in place. Malpractice cases frequently involve a scenario in which patients are given parenteral narcotics and left alone, out of sight, and unmonitored. This simply can’t be done. Close supervision and monitoring—with both equipment and eyes—are required to safeguard your patients and avoid malpractice risk.
Other malpractice scenarios involve the ambulatory patient who is given parenteral narcotics in a clinic setting and discharged after a 10-minute “observation” period—a period during which peak drug effect is probably not realized. The patient is unsafely discharged before that peak is reached and suffers potentially fatal side effects. Even when direct fatal effects are not realized, the patient is discharged with impaired motor coordination and cognitive judgment, placing the patient at risk in his/her surroundings.
If a clinician commits to giving parenteral narcotics, he or she commits to providing “real-time” monitoring until the narcotic effects have safely diminished and the patient’s condition is thoroughly documented in the record. Generally speaking, the patient must be reasonably clear of the effects of narcotics before discharge. (Remember the special case of naloxone, administered for opiate excesses, in which narcan is metabolized before the opiate; the patient can relapse into a coma/apnea if the naloxone fully metabolizes before the opiate.)
Here, this young woman was probably opiate naïve. While the amount she was given was certain, her response to the drug was not. She was left alone for at least 20 minutes and did not have a functioning SaO2 monitor. Close monitoring of this patient was required but not provided.
As a result of this case, the surgical center changed several policies: Nurses must be on a one-to-one ratio with patients who have received narcotics during anesthesia. Furthermore, nurses must have line-of-sight to see patients at all times, and importantly, may not mute monitors (eg, oximetry monitors).
The second salient point of this case is never, ever alter or falsify patient records! It will be discovered, and your credibility will be irretrievably damaged. Plaintiff lawyers live for this, and yet clinicians continue to do it. Don’t.
When altered medical records are discovered, the plaintiff’s theory of the case will be “cover up,” and jurors will be invited to punish the clinician for it. The jurors will do so.
Also problematic is a case that is otherwise defensible, but which becomes much more difficult to defend because a clinician has altered the records. Remember, the plaintiff must prove all aspects of negligence, including causation and damages. In some cases, the clinician knows an obvious mistake was made, but does not know that the eventual damages may be minimal or attributable to another cause. By altering the medical record, the clinician may enhance the damages value of a case by introducing a punitive element. Altering records may result in a lawsuit being filed when it otherwise wouldn’t have, or maintained when it would have been dropped before trial. In sum, don’t create a case against yourself by altering the medical records.
Here, the falsification of records came to light during the deposition of the second nurse—who, being under oath, probably had little choice but to testify that the first nurse falsified the records. No doubt, this falsification made a bad case worse and gave the plaintiff leverage in securing more favorable settlement terms.
You can’t make it right by rewriting history, but you can make it right by showing concern for the patient in your actions following a problem. You can also make it right by troubleshooting problems in a closed-door, formal peer review conference. Peer review conferences are designed for full and frank communication between clinicians and staff to solve problems, and as such they are protected from plaintiff disclosure.
This is an unfortunate case and a tragic loss of a young woman’s life. As clinicians, we must respect the potential life-ending power of parenteral narcotics. —DML
A 17-year-old girl underwent a routine tonsillectomy without complications at a surgical center. Following the procedure, the patient was returned to the recovery room and administered fentanyl for pain.
The recovery room nurse assigned to monitor the patient spent 20 minutes treating another patient and then went on break, signing out to a second recovery room nurse. On receiving the signout, the second recovery room nurse discovered that the patient was in respiratory distress and began resuscitation efforts. The patient was resuscitated but died 15 days later.
The plaintiff claimed that the girl was left unmonitored by nurses assigned to the unit and that the monitoring equipment was not used, not set properly, or muted.
During her deposition, the second recovery room nurse admitted under oath that the first recovery room nurse falsified the patient’s chart; the first nurse claimed that she had assessed the patient during an important time period when she had not.
OUTCOME
The case was settled for $6 million: $1 million against the surgical center’s primary policy and $5 million against its excess policy.
COMMENT
Cases such as this one are unfortunate and avoidable—and tragically, too common. On any medical malpractice lawyer’s desk is a teetering stack of potential cases; much of that stack involves narcotics. This case raises two important areas to discuss: the dangers of parenteral narcotics and the perils of falsifying medical records.
First, when parenteral narcotics are given, proper monitoring safeguards must be in place. Malpractice cases frequently involve a scenario in which patients are given parenteral narcotics and left alone, out of sight, and unmonitored. This simply can’t be done. Close supervision and monitoring—with both equipment and eyes—are required to safeguard your patients and avoid malpractice risk.
Other malpractice scenarios involve the ambulatory patient who is given parenteral narcotics in a clinic setting and discharged after a 10-minute “observation” period—a period during which peak drug effect is probably not realized. The patient is unsafely discharged before that peak is reached and suffers potentially fatal side effects. Even when direct fatal effects are not realized, the patient is discharged with impaired motor coordination and cognitive judgment, placing the patient at risk in his/her surroundings.
If a clinician commits to giving parenteral narcotics, he or she commits to providing “real-time” monitoring until the narcotic effects have safely diminished and the patient’s condition is thoroughly documented in the record. Generally speaking, the patient must be reasonably clear of the effects of narcotics before discharge. (Remember the special case of naloxone, administered for opiate excesses, in which narcan is metabolized before the opiate; the patient can relapse into a coma/apnea if the naloxone fully metabolizes before the opiate.)
Here, this young woman was probably opiate naïve. While the amount she was given was certain, her response to the drug was not. She was left alone for at least 20 minutes and did not have a functioning SaO2 monitor. Close monitoring of this patient was required but not provided.
As a result of this case, the surgical center changed several policies: Nurses must be on a one-to-one ratio with patients who have received narcotics during anesthesia. Furthermore, nurses must have line-of-sight to see patients at all times, and importantly, may not mute monitors (eg, oximetry monitors).
The second salient point of this case is never, ever alter or falsify patient records! It will be discovered, and your credibility will be irretrievably damaged. Plaintiff lawyers live for this, and yet clinicians continue to do it. Don’t.
When altered medical records are discovered, the plaintiff’s theory of the case will be “cover up,” and jurors will be invited to punish the clinician for it. The jurors will do so.
Also problematic is a case that is otherwise defensible, but which becomes much more difficult to defend because a clinician has altered the records. Remember, the plaintiff must prove all aspects of negligence, including causation and damages. In some cases, the clinician knows an obvious mistake was made, but does not know that the eventual damages may be minimal or attributable to another cause. By altering the medical record, the clinician may enhance the damages value of a case by introducing a punitive element. Altering records may result in a lawsuit being filed when it otherwise wouldn’t have, or maintained when it would have been dropped before trial. In sum, don’t create a case against yourself by altering the medical records.
Here, the falsification of records came to light during the deposition of the second nurse—who, being under oath, probably had little choice but to testify that the first nurse falsified the records. No doubt, this falsification made a bad case worse and gave the plaintiff leverage in securing more favorable settlement terms.
You can’t make it right by rewriting history, but you can make it right by showing concern for the patient in your actions following a problem. You can also make it right by troubleshooting problems in a closed-door, formal peer review conference. Peer review conferences are designed for full and frank communication between clinicians and staff to solve problems, and as such they are protected from plaintiff disclosure.
This is an unfortunate case and a tragic loss of a young woman’s life. As clinicians, we must respect the potential life-ending power of parenteral narcotics. —DML
Study Investigator Explains Why Copper Surfaces Can Help Prevent Infections
Click here to listen to more of our interview with Dr. Schmidt
Click here to listen to more of our interview with Dr. Schmidt
Click here to listen to more of our interview with Dr. Schmidt
Goals, Patient-Centered Decisions Drive Hospitalist Julianna Lindsey


Growing up on a farm in rural Kentucky could have led to a career in the family business for Julianna Lindsey, MD, MBA, FHM. Except she knew at an early age that she wanted to be a doctor.
“My family physician was very influential on my decision to become a physician,” she says. “[He] mentored and encouraged me from a young age; it was very powerful for me.”
Dr. Lindsey earned bachelor’s degrees in biomedical science from the University of South Alabama and biochemistry from Western Kentucky University. She graduated from the University of Kentucky College of Medicine and completed her internal-medicine residency at the University of Kentucky. In 2011, she earned her master’s in business administration from the University of Tennessee.
Immediately following residency, she worked for the Veterans Affairs Medical Center in Lexington, Ky., as an ED physician. In 2002, she latched on to a career in HM when she and her husband, a gastroenterologist, relocated to Knoxville, Tenn. She recently launched a startup company, Synergy Surgicalists, with two orthopedic surgeons, and also provides process-improvement and leadership-development consulting.
She says she was told early in her career to know your goals and stay focused.
“That has been the guiding light for me throughout my career,” says Dr. Lindsey, one of nine new Team Hospitalist members, The Hospitalist’s volunteer editorial advisory group. “My goal is to make medical care better and safer for hospitalized patients. We increasingly need to figure out how to do that with fewer and fewer resources. Regardless, we can never move backward on delivering better and safer care to patients.”
Question: How did you decide to become a hospitalist?
Answer: I have always been drawn to the practice of acute-care medicine. I enjoy taking care of patients and their families in their times of need. From the purely diagnostic standpoint, I very much enjoy the critical decision-making required in the diagnosis and treatment of the acutely ill patient.
Q: What do you like most about working as a hospitalist?
A: I enjoy the opportunity to “dig in” and positively affect processes and patient outcomes throughout hospitals.
Q: What do you dislike most?
A: Fighting the “scope creep” that is continually pushing on us as hospitalists. Hospitalists are constantly being asked to admit patients whose problems are outside the scope of our practice as medically trained physicians. A few examples of this include acute surgical abdomens, intracranial hemorrhages, and blunt-trauma cases.
Q: What’s the biggest change you’ve seen in HM in your career?
A: The explosion of hospitalist programs throughout the country. Hospitalists programs are now even being built by payors and long-term-care facilities.
Q: For group leaders, why is it important for you to continue seeing patients?
A: In order to improve upon a process, you must know the process; to truly know the process, you must live the process. If you are not at the bedside delivering care to patients, there will be a disconnect between you, as a leader, and your physicians, who are at the bedside delivering care.
Q: What are your interests outside of patient care?
A: I believe the success—or failure—of a hospital, physician group, corporation, etc. is directly related to leadership. I enjoy leadership development because I see that as “mission critical” to the success of delivering better and safer patient care in any health-care system. As physicians, most of us never receive meaningful leadership training, yet are expected to come out of residency ready to lead. I enjoy providing physicians the tools to lead effectively. It makes the careers of physician leaders more fulfilling, as well as the careers of those physicians who are “following.”
Q: What is your biggest professional challenge?
A: Continuing to provide better and safer patient care with diminishing resources.
Q: What is your biggest professional reward?
A: Making a difference in the lives of patients. It is very rewarding to me to be able to come into a hospital and put processes in place, then actually see the risk-adjusted mortality rates improve. One of my teams’ biggest wins was taking over an HM program in a hospital with a mortality rate of 4, and seeing that mortality rate cut literally in half within six months.
Q: When you aren’t working, what is important to you?
A: My husband and children are the most important aspect of my life. My husband is a gastroenterologist; we have been married for 13 years. We have two healthy, happy kiddos ages 8 and 10.
Q: What’s next professionally? Where do you see yourself in 10 years?
A: I am partnering with two orthopedic surgeons in a startup company, Synergy Surgicalists. Our company mirrors the hospitalist model utilizing general and orthopedic surgeons. It’s very exciting to have the opportunity to bring value to hospitals and patients on a larger scale. Also, for the immediate future, I have accepted the role of interim executive medical director for hospital medicine for University of Texas Southwestern and Parkland hospitals. We are completely restructuring those programs in preparation for moving into two beautiful new (and very large) hospitals. I’m very excited about working with a truly excellent group of physicians and leaders while we are recruiting a permanent executive director and expanding our ranks.
Q: If you weren’t a doctor, what would you be doing right now?
A: I cannot imagine not being a physician. I suppose if pressed, I imagine I would have landed somewhere in the financial industry. I am also a musician, but have a hard time seeing myself employed in that industry.
Q: What’s the best book you’ve read recently?
A: “Widow Walk” by Gerard LaSalle. He is a physician author who pens a beautiful story. It’s just an enjoyable read of American historical fiction set in the Pacific Northwest.
Q: How many Apple products do you interface with in a given week?
A: Sadly, I interface with 11 (11!) different Apple products in any given week. (Even sadder: I just came into an iPod Shuffle, so I’m up to 12 … )
Q: What’s next in your Netflix queue?
A: “Fringe,” Season 2, Episode 19.
Richard Quinn is a freelance writer in New Jersey.
Growing up on a farm in rural Kentucky could have led to a career in the family business for Julianna Lindsey, MD, MBA, FHM. Except she knew at an early age that she wanted to be a doctor.
“My family physician was very influential on my decision to become a physician,” she says. “[He] mentored and encouraged me from a young age; it was very powerful for me.”
Dr. Lindsey earned bachelor’s degrees in biomedical science from the University of South Alabama and biochemistry from Western Kentucky University. She graduated from the University of Kentucky College of Medicine and completed her internal-medicine residency at the University of Kentucky. In 2011, she earned her master’s in business administration from the University of Tennessee.
Immediately following residency, she worked for the Veterans Affairs Medical Center in Lexington, Ky., as an ED physician. In 2002, she latched on to a career in HM when she and her husband, a gastroenterologist, relocated to Knoxville, Tenn. She recently launched a startup company, Synergy Surgicalists, with two orthopedic surgeons, and also provides process-improvement and leadership-development consulting.
She says she was told early in her career to know your goals and stay focused.
“That has been the guiding light for me throughout my career,” says Dr. Lindsey, one of nine new Team Hospitalist members, The Hospitalist’s volunteer editorial advisory group. “My goal is to make medical care better and safer for hospitalized patients. We increasingly need to figure out how to do that with fewer and fewer resources. Regardless, we can never move backward on delivering better and safer care to patients.”
Question: How did you decide to become a hospitalist?
Answer: I have always been drawn to the practice of acute-care medicine. I enjoy taking care of patients and their families in their times of need. From the purely diagnostic standpoint, I very much enjoy the critical decision-making required in the diagnosis and treatment of the acutely ill patient.
Q: What do you like most about working as a hospitalist?
A: I enjoy the opportunity to “dig in” and positively affect processes and patient outcomes throughout hospitals.
Q: What do you dislike most?
A: Fighting the “scope creep” that is continually pushing on us as hospitalists. Hospitalists are constantly being asked to admit patients whose problems are outside the scope of our practice as medically trained physicians. A few examples of this include acute surgical abdomens, intracranial hemorrhages, and blunt-trauma cases.
Q: What’s the biggest change you’ve seen in HM in your career?
A: The explosion of hospitalist programs throughout the country. Hospitalists programs are now even being built by payors and long-term-care facilities.
Q: For group leaders, why is it important for you to continue seeing patients?
A: In order to improve upon a process, you must know the process; to truly know the process, you must live the process. If you are not at the bedside delivering care to patients, there will be a disconnect between you, as a leader, and your physicians, who are at the bedside delivering care.
Q: What are your interests outside of patient care?
A: I believe the success—or failure—of a hospital, physician group, corporation, etc. is directly related to leadership. I enjoy leadership development because I see that as “mission critical” to the success of delivering better and safer patient care in any health-care system. As physicians, most of us never receive meaningful leadership training, yet are expected to come out of residency ready to lead. I enjoy providing physicians the tools to lead effectively. It makes the careers of physician leaders more fulfilling, as well as the careers of those physicians who are “following.”
Q: What is your biggest professional challenge?
A: Continuing to provide better and safer patient care with diminishing resources.
Q: What is your biggest professional reward?
A: Making a difference in the lives of patients. It is very rewarding to me to be able to come into a hospital and put processes in place, then actually see the risk-adjusted mortality rates improve. One of my teams’ biggest wins was taking over an HM program in a hospital with a mortality rate of 4, and seeing that mortality rate cut literally in half within six months.
Q: When you aren’t working, what is important to you?
A: My husband and children are the most important aspect of my life. My husband is a gastroenterologist; we have been married for 13 years. We have two healthy, happy kiddos ages 8 and 10.
Q: What’s next professionally? Where do you see yourself in 10 years?
A: I am partnering with two orthopedic surgeons in a startup company, Synergy Surgicalists. Our company mirrors the hospitalist model utilizing general and orthopedic surgeons. It’s very exciting to have the opportunity to bring value to hospitals and patients on a larger scale. Also, for the immediate future, I have accepted the role of interim executive medical director for hospital medicine for University of Texas Southwestern and Parkland hospitals. We are completely restructuring those programs in preparation for moving into two beautiful new (and very large) hospitals. I’m very excited about working with a truly excellent group of physicians and leaders while we are recruiting a permanent executive director and expanding our ranks.
Q: If you weren’t a doctor, what would you be doing right now?
A: I cannot imagine not being a physician. I suppose if pressed, I imagine I would have landed somewhere in the financial industry. I am also a musician, but have a hard time seeing myself employed in that industry.
Q: What’s the best book you’ve read recently?
A: “Widow Walk” by Gerard LaSalle. He is a physician author who pens a beautiful story. It’s just an enjoyable read of American historical fiction set in the Pacific Northwest.
Q: How many Apple products do you interface with in a given week?
A: Sadly, I interface with 11 (11!) different Apple products in any given week. (Even sadder: I just came into an iPod Shuffle, so I’m up to 12 … )
Q: What’s next in your Netflix queue?
A: “Fringe,” Season 2, Episode 19.
Richard Quinn is a freelance writer in New Jersey.
Growing up on a farm in rural Kentucky could have led to a career in the family business for Julianna Lindsey, MD, MBA, FHM. Except she knew at an early age that she wanted to be a doctor.
“My family physician was very influential on my decision to become a physician,” she says. “[He] mentored and encouraged me from a young age; it was very powerful for me.”
Dr. Lindsey earned bachelor’s degrees in biomedical science from the University of South Alabama and biochemistry from Western Kentucky University. She graduated from the University of Kentucky College of Medicine and completed her internal-medicine residency at the University of Kentucky. In 2011, she earned her master’s in business administration from the University of Tennessee.
Immediately following residency, she worked for the Veterans Affairs Medical Center in Lexington, Ky., as an ED physician. In 2002, she latched on to a career in HM when she and her husband, a gastroenterologist, relocated to Knoxville, Tenn. She recently launched a startup company, Synergy Surgicalists, with two orthopedic surgeons, and also provides process-improvement and leadership-development consulting.
She says she was told early in her career to know your goals and stay focused.
“That has been the guiding light for me throughout my career,” says Dr. Lindsey, one of nine new Team Hospitalist members, The Hospitalist’s volunteer editorial advisory group. “My goal is to make medical care better and safer for hospitalized patients. We increasingly need to figure out how to do that with fewer and fewer resources. Regardless, we can never move backward on delivering better and safer care to patients.”
Question: How did you decide to become a hospitalist?
Answer: I have always been drawn to the practice of acute-care medicine. I enjoy taking care of patients and their families in their times of need. From the purely diagnostic standpoint, I very much enjoy the critical decision-making required in the diagnosis and treatment of the acutely ill patient.
Q: What do you like most about working as a hospitalist?
A: I enjoy the opportunity to “dig in” and positively affect processes and patient outcomes throughout hospitals.
Q: What do you dislike most?
A: Fighting the “scope creep” that is continually pushing on us as hospitalists. Hospitalists are constantly being asked to admit patients whose problems are outside the scope of our practice as medically trained physicians. A few examples of this include acute surgical abdomens, intracranial hemorrhages, and blunt-trauma cases.
Q: What’s the biggest change you’ve seen in HM in your career?
A: The explosion of hospitalist programs throughout the country. Hospitalists programs are now even being built by payors and long-term-care facilities.
Q: For group leaders, why is it important for you to continue seeing patients?
A: In order to improve upon a process, you must know the process; to truly know the process, you must live the process. If you are not at the bedside delivering care to patients, there will be a disconnect between you, as a leader, and your physicians, who are at the bedside delivering care.
Q: What are your interests outside of patient care?
A: I believe the success—or failure—of a hospital, physician group, corporation, etc. is directly related to leadership. I enjoy leadership development because I see that as “mission critical” to the success of delivering better and safer patient care in any health-care system. As physicians, most of us never receive meaningful leadership training, yet are expected to come out of residency ready to lead. I enjoy providing physicians the tools to lead effectively. It makes the careers of physician leaders more fulfilling, as well as the careers of those physicians who are “following.”
Q: What is your biggest professional challenge?
A: Continuing to provide better and safer patient care with diminishing resources.
Q: What is your biggest professional reward?
A: Making a difference in the lives of patients. It is very rewarding to me to be able to come into a hospital and put processes in place, then actually see the risk-adjusted mortality rates improve. One of my teams’ biggest wins was taking over an HM program in a hospital with a mortality rate of 4, and seeing that mortality rate cut literally in half within six months.
Q: When you aren’t working, what is important to you?
A: My husband and children are the most important aspect of my life. My husband is a gastroenterologist; we have been married for 13 years. We have two healthy, happy kiddos ages 8 and 10.
Q: What’s next professionally? Where do you see yourself in 10 years?
A: I am partnering with two orthopedic surgeons in a startup company, Synergy Surgicalists. Our company mirrors the hospitalist model utilizing general and orthopedic surgeons. It’s very exciting to have the opportunity to bring value to hospitals and patients on a larger scale. Also, for the immediate future, I have accepted the role of interim executive medical director for hospital medicine for University of Texas Southwestern and Parkland hospitals. We are completely restructuring those programs in preparation for moving into two beautiful new (and very large) hospitals. I’m very excited about working with a truly excellent group of physicians and leaders while we are recruiting a permanent executive director and expanding our ranks.
Q: If you weren’t a doctor, what would you be doing right now?
A: I cannot imagine not being a physician. I suppose if pressed, I imagine I would have landed somewhere in the financial industry. I am also a musician, but have a hard time seeing myself employed in that industry.
Q: What’s the best book you’ve read recently?
A: “Widow Walk” by Gerard LaSalle. He is a physician author who pens a beautiful story. It’s just an enjoyable read of American historical fiction set in the Pacific Northwest.
Q: How many Apple products do you interface with in a given week?
A: Sadly, I interface with 11 (11!) different Apple products in any given week. (Even sadder: I just came into an iPod Shuffle, so I’m up to 12 … )
Q: What’s next in your Netflix queue?
A: “Fringe,” Season 2, Episode 19.
Richard Quinn is a freelance writer in New Jersey.
Academic Hospitalist Academy Provides Resources for Success

SHM asked Academic Hospitalist Academy course co-directors Jeffrey Glasheen, MD, SFHM, and Bradley Sharpe, MD, SFHM, why academic hospitalists should attend this year’s academy.
Question: What has you personally excited about this year’s Academic Hospitalist Academy?
Dr. Sharpe: I’ll be honest—it is one of my favorite weeks of the year. It is a tremendous opportunity to engage with academic hospitalists and help them develop the core skills they need to be successful.
Dr. Glasheen: For me, it’s about the energy, the talent, and the excitement that the attendees bring to the course. It ends up being a tremendously energizing week for me personally. To see the talent in the room begin to find outlets for success is truly invigorating.
Q: If you were talking one on one with an academic hospitalist, what would you say to encourage them to attend?
Dr. Sharpe: Based on previous attendees, these four days could truly change your life. We are confident you will leave with newfound energy and enthusiasm and key building blocks to help you be successful when you go back home. Don’t miss it.
Dr. Glasheen: There is a magical transformation that happens every year. Very talented individuals enter the program. Nearly uniformly, they are struggling with the same issues around mentorship, sense of purpose, direction, and resources for success. They all want to be successful but sense there is something that is missing, and within the course of four days, they find it.
Q: What have you heard from previous AHA attendees?
Dr. Sharpe: Here are a couple of emails I received: “I can’t say enough about the AHA. It was possibly the most important 3 days of my young career. Thank you both for the knowledge and guidance.” “I have fond memories of the whole AHA conference. The great Jeff Wiese!!! But most of all, the small group sessions were extremely helpful.”
Dr. Glasheen: To a person, they all say the meeting is “transformational.” They gain skills in teaching, confidence in evaluating learners, methods for scholarly success, and a roadmap for navigating the tricky world on academic medicine. But beyond that, they gain a peer network. They leave tied in with 80 other national colleagues that are struggling with the same issues. This network becomes their home away from home—people they can turn to with a question, catch up with at a national meeting, and look to as exemplars in the field.
SHM asked Academic Hospitalist Academy course co-directors Jeffrey Glasheen, MD, SFHM, and Bradley Sharpe, MD, SFHM, why academic hospitalists should attend this year’s academy.
Question: What has you personally excited about this year’s Academic Hospitalist Academy?
Dr. Sharpe: I’ll be honest—it is one of my favorite weeks of the year. It is a tremendous opportunity to engage with academic hospitalists and help them develop the core skills they need to be successful.
Dr. Glasheen: For me, it’s about the energy, the talent, and the excitement that the attendees bring to the course. It ends up being a tremendously energizing week for me personally. To see the talent in the room begin to find outlets for success is truly invigorating.
Q: If you were talking one on one with an academic hospitalist, what would you say to encourage them to attend?
Dr. Sharpe: Based on previous attendees, these four days could truly change your life. We are confident you will leave with newfound energy and enthusiasm and key building blocks to help you be successful when you go back home. Don’t miss it.
Dr. Glasheen: There is a magical transformation that happens every year. Very talented individuals enter the program. Nearly uniformly, they are struggling with the same issues around mentorship, sense of purpose, direction, and resources for success. They all want to be successful but sense there is something that is missing, and within the course of four days, they find it.
Q: What have you heard from previous AHA attendees?
Dr. Sharpe: Here are a couple of emails I received: “I can’t say enough about the AHA. It was possibly the most important 3 days of my young career. Thank you both for the knowledge and guidance.” “I have fond memories of the whole AHA conference. The great Jeff Wiese!!! But most of all, the small group sessions were extremely helpful.”
Dr. Glasheen: To a person, they all say the meeting is “transformational.” They gain skills in teaching, confidence in evaluating learners, methods for scholarly success, and a roadmap for navigating the tricky world on academic medicine. But beyond that, they gain a peer network. They leave tied in with 80 other national colleagues that are struggling with the same issues. This network becomes their home away from home—people they can turn to with a question, catch up with at a national meeting, and look to as exemplars in the field.
SHM asked Academic Hospitalist Academy course co-directors Jeffrey Glasheen, MD, SFHM, and Bradley Sharpe, MD, SFHM, why academic hospitalists should attend this year’s academy.
Question: What has you personally excited about this year’s Academic Hospitalist Academy?
Dr. Sharpe: I’ll be honest—it is one of my favorite weeks of the year. It is a tremendous opportunity to engage with academic hospitalists and help them develop the core skills they need to be successful.
Dr. Glasheen: For me, it’s about the energy, the talent, and the excitement that the attendees bring to the course. It ends up being a tremendously energizing week for me personally. To see the talent in the room begin to find outlets for success is truly invigorating.
Q: If you were talking one on one with an academic hospitalist, what would you say to encourage them to attend?
Dr. Sharpe: Based on previous attendees, these four days could truly change your life. We are confident you will leave with newfound energy and enthusiasm and key building blocks to help you be successful when you go back home. Don’t miss it.
Dr. Glasheen: There is a magical transformation that happens every year. Very talented individuals enter the program. Nearly uniformly, they are struggling with the same issues around mentorship, sense of purpose, direction, and resources for success. They all want to be successful but sense there is something that is missing, and within the course of four days, they find it.
Q: What have you heard from previous AHA attendees?
Dr. Sharpe: Here are a couple of emails I received: “I can’t say enough about the AHA. It was possibly the most important 3 days of my young career. Thank you both for the knowledge and guidance.” “I have fond memories of the whole AHA conference. The great Jeff Wiese!!! But most of all, the small group sessions were extremely helpful.”
Dr. Glasheen: To a person, they all say the meeting is “transformational.” They gain skills in teaching, confidence in evaluating learners, methods for scholarly success, and a roadmap for navigating the tricky world on academic medicine. But beyond that, they gain a peer network. They leave tied in with 80 other national colleagues that are struggling with the same issues. This network becomes their home away from home—people they can turn to with a question, catch up with at a national meeting, and look to as exemplars in the field.
Should you report a patient who misuses a prescription?
Dear Dr. Mossman:
My patient, Ms. X, returned to see me after she had spent 3 months in jail. When I accessed her medication history in our state’s prescription registry, I discovered that, during her incarceration, a local pharmacy continued to fill her prescription for clonazepam. After anxiously explaining that her roommate had filled the prescriptions, Ms. X pleaded with me not to tell anyone. Do I have to report this to legal authorities? If I do, will I be breaching confidentiality?
Submitted by Dr. L
Preserving the confidentiality of patient encounters is an ethical responsibility as old as the Hippocratic Oath,1 but protecting privacy is not an absolute duty. As psychiatrists familiar with the Tarasoff case2 know, clinical events sometimes create moral and legal obligations that outweigh our confidentiality obligations.
What Dr. L should do may hinge on specific details of Ms. X’s previous and current treatment, but in this article, we’ll examine some general issues that affect Dr. L’s choices. These include:
• reporting a past crime
• liability risks associated with violating confidentiality.
Monitoring controlled substances
Dr. L’s clinical situation probably would not have arisen 10 years ago because until recently, she would have had no easy way to learn that Ms. X’s prescription had been filled. In 2002, Congress responded to increasing concern about “epidemic” abuse of controlled substances—especially opioids—by authorizing state grants for prescription drug monitoring programs (PDMPs).3
PDMPs are internet-based registries that let physicians quickly find out when and where their patients have filled prescriptions for controlled substances (defined in the Table).4,5 As the rate of opioid-related deaths has risen,6 at least 43 states have initiated PDMPs; soon, all U.S. jurisdictions likely will have such programs.7 Data about the impact of PDMPs, although limited, suggest that PDMPs reduce “doctor shopping” and prescription drug abuse.8
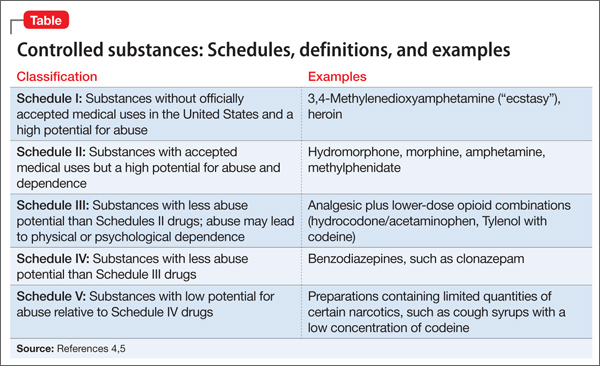
The U.S. Department of Health and Human Services is promoting the development of electronic architecture standards to facilitate information exchange across jurisdictions,9 but states currently run their own PDMPs independently and have varying regulations about how physicians should use PDMPs.10 Excerpts from the rules used in Ohio’s prescription reporting system appear in the Box.11
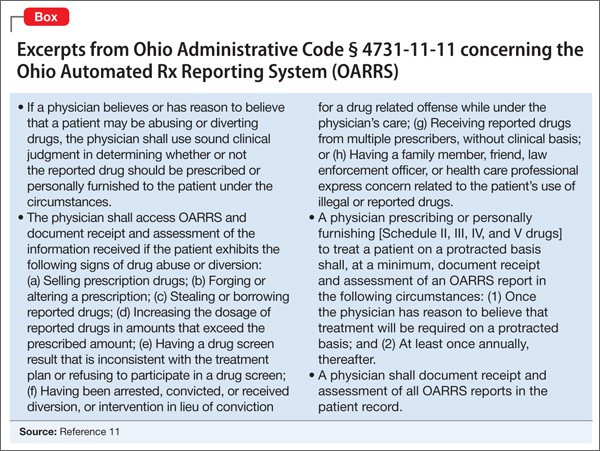
Reporting past crimes
What Ms. X told Dr. L implies that someone—the patient, her roommate, or both—misused a prescription to obtain a controlled substance. Simple improper possession of a scheduled drug is a federal misdemeanor offense,12 and deception and conspiracy to obtain a scheduled drug are federal-level felonies.13 Such actions also violate state laws. Dr. L therefore knows that a crime has occurred.
Are doctors obligated or legally required to breach confidentiality and tell authorities about a patient’s past criminal acts? Writing several years ago, Appelbaum and Meisel14 and Goldman and Gutheil15 said the answer, in general, is “no.”
In recent years, state legislatures have modified criminal codes to encourage people to disclose their knowledge of certain crimes to police. For example, failures to report environmental offenses and financial misdealings have become criminal acts.16 A minority of states now punish failure to report other kinds of illegal behavior, but these laws focus mainly on violent crimes (often involving harm to vulnerable persons).17 Although Ohio has a law that obligates everyone to report knowledge of any felony, it makes exceptions when the information is learned during a customarily confidential relationship—including a physician’s treatment of a patient.18 Unless Dr. L herself has aided or concealed a crime (both illegal acts19), concerns about possible prosecution should not affect her decision to report what she has learned thus far.14
Deciding how to proceed
If Dr. L still feels inclined to do something about the misused prescription, what are her options? What clinical, legal, and moral obligations to act should she consider?
Obtain the facts. First, Dr. L should try to learn more about what happened. Jails are reluctant to give inmates benzodiazepines20; did Ms. X receive clonazepam while in jail? When and how did Ms. X learn about her roommate’s actions? Did Ms. X obtain previous prescriptions from Dr. L with the intention of letting her roommate use them? Answers to these questions can help Dr. L determine whether her patient participated in prescription misuse, an important factor in deciding what clinical or legal actions to take.
Should the patient take the lead? Learning more about the situation might suggest that Ms. X should report what has happened herself. If, for example, the roommate has coerced Ms. X to engage in illegal conduct, Dr. L might help Ms. X figure out how to tell police what has happened—preferably after Ms. X has obtained legal advice.14
Consider implications for treatment. Last, what Ms. X reveals might significantly alter her future interactions with Dr. L. This is particularly true if Dr. L concluded that Ms. X would likely divert drugs in the future, or that the patient had established her relationship with Dr. L for purposes of improperly obtaining drugs. Federal regulations require that doctors prescribe drugs only for “legitimate medical purposes,” and issuing prescriptions to a patient who is known to be delivering the drugs to others violates this law.22
Bottom Line
Growing concern about prescription drug misuse has led to nationwide implementation of systems for monitoring patients’ access to, and receipt of, controlled substances. Psychiatrists are expected to be more vigilant about patients’ use of scheduled drugs and, when they believe that a prescription has been misused, to take appropriate clinical or legal action.
Related Resources
- Office of National Drug Control Policy. Epidemic: responding to America’s prescription drug abuse crisis. www.whitehouse.gov/sites/default/files/ondcp/issues-content/ prescription-drugs/rx_abuse_plan.pdf.
- California Department of Alcohol and Drug Misuse. Preventing prescription drug misuse. www.prescriptiondrugmisuse.org.
- U.S. Food and Drug Administration. Combating misuse and abuse of prescription drugs: Q&A with Michael Klein, PhD. www.fda.gov/ForConsumers/ConsumerUpdates/ ucm220112.htm.
Drug Brand Names
Clonazepam • Klonopin Hydrocodone/acetaminophen • Vicodin
Methylphenidate • Ritalin Hydromorphone • Dilaudid
Disclosure
Dr. Mossman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. von Staden H. “In a pure and holy way”: personal and professional conduct in the Hippocratic Oath? J Hist Med Allied Sci. 1996;51(4):404-437.
2. Tarasoff v Regents of the University of California, 17 Cal.3d 425, 551 P.2d 334, 131 Cal Rptr 14 (Cal 1976).
3. PubLNo.107-177,115Stat748.
4. ControlledSubstancesAct,21USC§812(b)(2007).
5. Schedules of Controlled Substances, 21 CFR. § 1308.11– 1308.15 (2013).
6. Dowell D, Kunins HV, Farley TA. Opioid analgesics— risky drugs, not risky patients. JAMA. 2013;309: 2219-2220.
7. US Department of Justice. Harold Rogers Prescription Drug Monitoring Program FY 2013 Competitive Grant Announcement. Washington, DC: Bureau of Justice Assistance, Office of Justice Programs; 2013. OMB No. 1121-0329.
8. Worley J. Prescription drug monitoring programs, a response to doctor shopping: purpose, effectiveness, and directions for future research. Issues Ment Health Nurs. 2012;33:319-328.
9. PubLNo.112-144,126Stat993.
10. Finklea KM, Bagalman E, Sacco L. Prescription Drug Monitoring Programs. Washington, DC: Library of Congress, Congressional Research Service; 2013. Report No. R42593.
11. Ohio State Medical Association. 4731-11-11 Standards and procedures for review of Ohio Automated Rx Reporting System (OARRS). http://www.osma.org/files/pdf/sept- 2011-draft-4731-11-11-ph-of-n-ru-20110520-1541.pdf. Accessed August 5, 2013.
12. Prohibited Acts C, 21 USC §843(a)(3) (2007).
13. PenaltyforSimplePossession,21USC§844(a)(2007).
14. Appelbaum PS, Meisel A. Therapists’ obligations to report their patients’ criminal acts. Bull Am Acad Psychiatry Law. 1986;14(3):221-230.
15. Goldman MJ, Gutheil TG. The misperceived duty to report patients’ past crimes. Bull Am Acad Psychiatry Law. 1994; 22(3):407-410.
16. Thompson SG. The white-collar police force: “duty to report” statutes in criminal law theory. William Mary Bill Rights J. 2002;11(1):3-65.
17. Trombley B. No stitches for snitches: the need for a duty-to-report law in Arkansas. Univ Ark Little Rock Law J. 2012; 34:813-832.
18. OhioRevisedCode§2921.22.
19. Section2:Principals,18USC§2(a).
20. Reeves R. Guideline, education, and peer comparison to reduce prescriptions of benzodiazepines and low-dose quetiapine in prison. J Correct Health Care. 2012;18(1): 45-52.
21. Appelbaum PS. Suits against clinicians for warning of patients’ violence. Psychiatr Serv. 1996;47(7):683-684.
22. UnitedStatesvRosen,582F2d1032(5thCir1978).
23. State Medical Board of Ohio. Regarding the duty of a physician to report criminal behavior to law enforcement. http://www.med.ohio.gov/pdf/NEWS/Duty%20to%20Report_March%202013.pdf. Adopted March 2013. Accessed July 1, 2013.
24. Missouri Department of Health & Senior Services. Preventing Prescription Fraud. http://health.mo.gov/ safety/bndd/publications.php. Accessed July 1, 2013.
Dear Dr. Mossman:
My patient, Ms. X, returned to see me after she had spent 3 months in jail. When I accessed her medication history in our state’s prescription registry, I discovered that, during her incarceration, a local pharmacy continued to fill her prescription for clonazepam. After anxiously explaining that her roommate had filled the prescriptions, Ms. X pleaded with me not to tell anyone. Do I have to report this to legal authorities? If I do, will I be breaching confidentiality?
Submitted by Dr. L
Preserving the confidentiality of patient encounters is an ethical responsibility as old as the Hippocratic Oath,1 but protecting privacy is not an absolute duty. As psychiatrists familiar with the Tarasoff case2 know, clinical events sometimes create moral and legal obligations that outweigh our confidentiality obligations.
What Dr. L should do may hinge on specific details of Ms. X’s previous and current treatment, but in this article, we’ll examine some general issues that affect Dr. L’s choices. These include:
• reporting a past crime
• liability risks associated with violating confidentiality.
Monitoring controlled substances
Dr. L’s clinical situation probably would not have arisen 10 years ago because until recently, she would have had no easy way to learn that Ms. X’s prescription had been filled. In 2002, Congress responded to increasing concern about “epidemic” abuse of controlled substances—especially opioids—by authorizing state grants for prescription drug monitoring programs (PDMPs).3
PDMPs are internet-based registries that let physicians quickly find out when and where their patients have filled prescriptions for controlled substances (defined in the Table).4,5 As the rate of opioid-related deaths has risen,6 at least 43 states have initiated PDMPs; soon, all U.S. jurisdictions likely will have such programs.7 Data about the impact of PDMPs, although limited, suggest that PDMPs reduce “doctor shopping” and prescription drug abuse.8
The U.S. Department of Health and Human Services is promoting the development of electronic architecture standards to facilitate information exchange across jurisdictions,9 but states currently run their own PDMPs independently and have varying regulations about how physicians should use PDMPs.10 Excerpts from the rules used in Ohio’s prescription reporting system appear in the Box.11
Reporting past crimes
What Ms. X told Dr. L implies that someone—the patient, her roommate, or both—misused a prescription to obtain a controlled substance. Simple improper possession of a scheduled drug is a federal misdemeanor offense,12 and deception and conspiracy to obtain a scheduled drug are federal-level felonies.13 Such actions also violate state laws. Dr. L therefore knows that a crime has occurred.
Are doctors obligated or legally required to breach confidentiality and tell authorities about a patient’s past criminal acts? Writing several years ago, Appelbaum and Meisel14 and Goldman and Gutheil15 said the answer, in general, is “no.”
In recent years, state legislatures have modified criminal codes to encourage people to disclose their knowledge of certain crimes to police. For example, failures to report environmental offenses and financial misdealings have become criminal acts.16 A minority of states now punish failure to report other kinds of illegal behavior, but these laws focus mainly on violent crimes (often involving harm to vulnerable persons).17 Although Ohio has a law that obligates everyone to report knowledge of any felony, it makes exceptions when the information is learned during a customarily confidential relationship—including a physician’s treatment of a patient.18 Unless Dr. L herself has aided or concealed a crime (both illegal acts19), concerns about possible prosecution should not affect her decision to report what she has learned thus far.14
Deciding how to proceed
If Dr. L still feels inclined to do something about the misused prescription, what are her options? What clinical, legal, and moral obligations to act should she consider?
Obtain the facts. First, Dr. L should try to learn more about what happened. Jails are reluctant to give inmates benzodiazepines20; did Ms. X receive clonazepam while in jail? When and how did Ms. X learn about her roommate’s actions? Did Ms. X obtain previous prescriptions from Dr. L with the intention of letting her roommate use them? Answers to these questions can help Dr. L determine whether her patient participated in prescription misuse, an important factor in deciding what clinical or legal actions to take.
Should the patient take the lead? Learning more about the situation might suggest that Ms. X should report what has happened herself. If, for example, the roommate has coerced Ms. X to engage in illegal conduct, Dr. L might help Ms. X figure out how to tell police what has happened—preferably after Ms. X has obtained legal advice.14
Consider implications for treatment. Last, what Ms. X reveals might significantly alter her future interactions with Dr. L. This is particularly true if Dr. L concluded that Ms. X would likely divert drugs in the future, or that the patient had established her relationship with Dr. L for purposes of improperly obtaining drugs. Federal regulations require that doctors prescribe drugs only for “legitimate medical purposes,” and issuing prescriptions to a patient who is known to be delivering the drugs to others violates this law.22
Bottom Line
Growing concern about prescription drug misuse has led to nationwide implementation of systems for monitoring patients’ access to, and receipt of, controlled substances. Psychiatrists are expected to be more vigilant about patients’ use of scheduled drugs and, when they believe that a prescription has been misused, to take appropriate clinical or legal action.
Related Resources
- Office of National Drug Control Policy. Epidemic: responding to America’s prescription drug abuse crisis. www.whitehouse.gov/sites/default/files/ondcp/issues-content/ prescription-drugs/rx_abuse_plan.pdf.
- California Department of Alcohol and Drug Misuse. Preventing prescription drug misuse. www.prescriptiondrugmisuse.org.
- U.S. Food and Drug Administration. Combating misuse and abuse of prescription drugs: Q&A with Michael Klein, PhD. www.fda.gov/ForConsumers/ConsumerUpdates/ ucm220112.htm.
Drug Brand Names
Clonazepam • Klonopin Hydrocodone/acetaminophen • Vicodin
Methylphenidate • Ritalin Hydromorphone • Dilaudid
Disclosure
Dr. Mossman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dear Dr. Mossman:
My patient, Ms. X, returned to see me after she had spent 3 months in jail. When I accessed her medication history in our state’s prescription registry, I discovered that, during her incarceration, a local pharmacy continued to fill her prescription for clonazepam. After anxiously explaining that her roommate had filled the prescriptions, Ms. X pleaded with me not to tell anyone. Do I have to report this to legal authorities? If I do, will I be breaching confidentiality?
Submitted by Dr. L
Preserving the confidentiality of patient encounters is an ethical responsibility as old as the Hippocratic Oath,1 but protecting privacy is not an absolute duty. As psychiatrists familiar with the Tarasoff case2 know, clinical events sometimes create moral and legal obligations that outweigh our confidentiality obligations.
What Dr. L should do may hinge on specific details of Ms. X’s previous and current treatment, but in this article, we’ll examine some general issues that affect Dr. L’s choices. These include:
• reporting a past crime
• liability risks associated with violating confidentiality.
Monitoring controlled substances
Dr. L’s clinical situation probably would not have arisen 10 years ago because until recently, she would have had no easy way to learn that Ms. X’s prescription had been filled. In 2002, Congress responded to increasing concern about “epidemic” abuse of controlled substances—especially opioids—by authorizing state grants for prescription drug monitoring programs (PDMPs).3
PDMPs are internet-based registries that let physicians quickly find out when and where their patients have filled prescriptions for controlled substances (defined in the Table).4,5 As the rate of opioid-related deaths has risen,6 at least 43 states have initiated PDMPs; soon, all U.S. jurisdictions likely will have such programs.7 Data about the impact of PDMPs, although limited, suggest that PDMPs reduce “doctor shopping” and prescription drug abuse.8
The U.S. Department of Health and Human Services is promoting the development of electronic architecture standards to facilitate information exchange across jurisdictions,9 but states currently run their own PDMPs independently and have varying regulations about how physicians should use PDMPs.10 Excerpts from the rules used in Ohio’s prescription reporting system appear in the Box.11
Reporting past crimes
What Ms. X told Dr. L implies that someone—the patient, her roommate, or both—misused a prescription to obtain a controlled substance. Simple improper possession of a scheduled drug is a federal misdemeanor offense,12 and deception and conspiracy to obtain a scheduled drug are federal-level felonies.13 Such actions also violate state laws. Dr. L therefore knows that a crime has occurred.
Are doctors obligated or legally required to breach confidentiality and tell authorities about a patient’s past criminal acts? Writing several years ago, Appelbaum and Meisel14 and Goldman and Gutheil15 said the answer, in general, is “no.”
In recent years, state legislatures have modified criminal codes to encourage people to disclose their knowledge of certain crimes to police. For example, failures to report environmental offenses and financial misdealings have become criminal acts.16 A minority of states now punish failure to report other kinds of illegal behavior, but these laws focus mainly on violent crimes (often involving harm to vulnerable persons).17 Although Ohio has a law that obligates everyone to report knowledge of any felony, it makes exceptions when the information is learned during a customarily confidential relationship—including a physician’s treatment of a patient.18 Unless Dr. L herself has aided or concealed a crime (both illegal acts19), concerns about possible prosecution should not affect her decision to report what she has learned thus far.14
Deciding how to proceed
If Dr. L still feels inclined to do something about the misused prescription, what are her options? What clinical, legal, and moral obligations to act should she consider?
Obtain the facts. First, Dr. L should try to learn more about what happened. Jails are reluctant to give inmates benzodiazepines20; did Ms. X receive clonazepam while in jail? When and how did Ms. X learn about her roommate’s actions? Did Ms. X obtain previous prescriptions from Dr. L with the intention of letting her roommate use them? Answers to these questions can help Dr. L determine whether her patient participated in prescription misuse, an important factor in deciding what clinical or legal actions to take.
Should the patient take the lead? Learning more about the situation might suggest that Ms. X should report what has happened herself. If, for example, the roommate has coerced Ms. X to engage in illegal conduct, Dr. L might help Ms. X figure out how to tell police what has happened—preferably after Ms. X has obtained legal advice.14
Consider implications for treatment. Last, what Ms. X reveals might significantly alter her future interactions with Dr. L. This is particularly true if Dr. L concluded that Ms. X would likely divert drugs in the future, or that the patient had established her relationship with Dr. L for purposes of improperly obtaining drugs. Federal regulations require that doctors prescribe drugs only for “legitimate medical purposes,” and issuing prescriptions to a patient who is known to be delivering the drugs to others violates this law.22
Bottom Line
Growing concern about prescription drug misuse has led to nationwide implementation of systems for monitoring patients’ access to, and receipt of, controlled substances. Psychiatrists are expected to be more vigilant about patients’ use of scheduled drugs and, when they believe that a prescription has been misused, to take appropriate clinical or legal action.
Related Resources
- Office of National Drug Control Policy. Epidemic: responding to America’s prescription drug abuse crisis. www.whitehouse.gov/sites/default/files/ondcp/issues-content/ prescription-drugs/rx_abuse_plan.pdf.
- California Department of Alcohol and Drug Misuse. Preventing prescription drug misuse. www.prescriptiondrugmisuse.org.
- U.S. Food and Drug Administration. Combating misuse and abuse of prescription drugs: Q&A with Michael Klein, PhD. www.fda.gov/ForConsumers/ConsumerUpdates/ ucm220112.htm.
Drug Brand Names
Clonazepam • Klonopin Hydrocodone/acetaminophen • Vicodin
Methylphenidate • Ritalin Hydromorphone • Dilaudid
Disclosure
Dr. Mossman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. von Staden H. “In a pure and holy way”: personal and professional conduct in the Hippocratic Oath? J Hist Med Allied Sci. 1996;51(4):404-437.
2. Tarasoff v Regents of the University of California, 17 Cal.3d 425, 551 P.2d 334, 131 Cal Rptr 14 (Cal 1976).
3. PubLNo.107-177,115Stat748.
4. ControlledSubstancesAct,21USC§812(b)(2007).
5. Schedules of Controlled Substances, 21 CFR. § 1308.11– 1308.15 (2013).
6. Dowell D, Kunins HV, Farley TA. Opioid analgesics— risky drugs, not risky patients. JAMA. 2013;309: 2219-2220.
7. US Department of Justice. Harold Rogers Prescription Drug Monitoring Program FY 2013 Competitive Grant Announcement. Washington, DC: Bureau of Justice Assistance, Office of Justice Programs; 2013. OMB No. 1121-0329.
8. Worley J. Prescription drug monitoring programs, a response to doctor shopping: purpose, effectiveness, and directions for future research. Issues Ment Health Nurs. 2012;33:319-328.
9. PubLNo.112-144,126Stat993.
10. Finklea KM, Bagalman E, Sacco L. Prescription Drug Monitoring Programs. Washington, DC: Library of Congress, Congressional Research Service; 2013. Report No. R42593.
11. Ohio State Medical Association. 4731-11-11 Standards and procedures for review of Ohio Automated Rx Reporting System (OARRS). http://www.osma.org/files/pdf/sept- 2011-draft-4731-11-11-ph-of-n-ru-20110520-1541.pdf. Accessed August 5, 2013.
12. Prohibited Acts C, 21 USC §843(a)(3) (2007).
13. PenaltyforSimplePossession,21USC§844(a)(2007).
14. Appelbaum PS, Meisel A. Therapists’ obligations to report their patients’ criminal acts. Bull Am Acad Psychiatry Law. 1986;14(3):221-230.
15. Goldman MJ, Gutheil TG. The misperceived duty to report patients’ past crimes. Bull Am Acad Psychiatry Law. 1994; 22(3):407-410.
16. Thompson SG. The white-collar police force: “duty to report” statutes in criminal law theory. William Mary Bill Rights J. 2002;11(1):3-65.
17. Trombley B. No stitches for snitches: the need for a duty-to-report law in Arkansas. Univ Ark Little Rock Law J. 2012; 34:813-832.
18. OhioRevisedCode§2921.22.
19. Section2:Principals,18USC§2(a).
20. Reeves R. Guideline, education, and peer comparison to reduce prescriptions of benzodiazepines and low-dose quetiapine in prison. J Correct Health Care. 2012;18(1): 45-52.
21. Appelbaum PS. Suits against clinicians for warning of patients’ violence. Psychiatr Serv. 1996;47(7):683-684.
22. UnitedStatesvRosen,582F2d1032(5thCir1978).
23. State Medical Board of Ohio. Regarding the duty of a physician to report criminal behavior to law enforcement. http://www.med.ohio.gov/pdf/NEWS/Duty%20to%20Report_March%202013.pdf. Adopted March 2013. Accessed July 1, 2013.
24. Missouri Department of Health & Senior Services. Preventing Prescription Fraud. http://health.mo.gov/ safety/bndd/publications.php. Accessed July 1, 2013.
1. von Staden H. “In a pure and holy way”: personal and professional conduct in the Hippocratic Oath? J Hist Med Allied Sci. 1996;51(4):404-437.
2. Tarasoff v Regents of the University of California, 17 Cal.3d 425, 551 P.2d 334, 131 Cal Rptr 14 (Cal 1976).
3. PubLNo.107-177,115Stat748.
4. ControlledSubstancesAct,21USC§812(b)(2007).
5. Schedules of Controlled Substances, 21 CFR. § 1308.11– 1308.15 (2013).
6. Dowell D, Kunins HV, Farley TA. Opioid analgesics— risky drugs, not risky patients. JAMA. 2013;309: 2219-2220.
7. US Department of Justice. Harold Rogers Prescription Drug Monitoring Program FY 2013 Competitive Grant Announcement. Washington, DC: Bureau of Justice Assistance, Office of Justice Programs; 2013. OMB No. 1121-0329.
8. Worley J. Prescription drug monitoring programs, a response to doctor shopping: purpose, effectiveness, and directions for future research. Issues Ment Health Nurs. 2012;33:319-328.
9. PubLNo.112-144,126Stat993.
10. Finklea KM, Bagalman E, Sacco L. Prescription Drug Monitoring Programs. Washington, DC: Library of Congress, Congressional Research Service; 2013. Report No. R42593.
11. Ohio State Medical Association. 4731-11-11 Standards and procedures for review of Ohio Automated Rx Reporting System (OARRS). http://www.osma.org/files/pdf/sept- 2011-draft-4731-11-11-ph-of-n-ru-20110520-1541.pdf. Accessed August 5, 2013.
12. Prohibited Acts C, 21 USC §843(a)(3) (2007).
13. PenaltyforSimplePossession,21USC§844(a)(2007).
14. Appelbaum PS, Meisel A. Therapists’ obligations to report their patients’ criminal acts. Bull Am Acad Psychiatry Law. 1986;14(3):221-230.
15. Goldman MJ, Gutheil TG. The misperceived duty to report patients’ past crimes. Bull Am Acad Psychiatry Law. 1994; 22(3):407-410.
16. Thompson SG. The white-collar police force: “duty to report” statutes in criminal law theory. William Mary Bill Rights J. 2002;11(1):3-65.
17. Trombley B. No stitches for snitches: the need for a duty-to-report law in Arkansas. Univ Ark Little Rock Law J. 2012; 34:813-832.
18. OhioRevisedCode§2921.22.
19. Section2:Principals,18USC§2(a).
20. Reeves R. Guideline, education, and peer comparison to reduce prescriptions of benzodiazepines and low-dose quetiapine in prison. J Correct Health Care. 2012;18(1): 45-52.
21. Appelbaum PS. Suits against clinicians for warning of patients’ violence. Psychiatr Serv. 1996;47(7):683-684.
22. UnitedStatesvRosen,582F2d1032(5thCir1978).
23. State Medical Board of Ohio. Regarding the duty of a physician to report criminal behavior to law enforcement. http://www.med.ohio.gov/pdf/NEWS/Duty%20to%20Report_March%202013.pdf. Adopted March 2013. Accessed July 1, 2013.
24. Missouri Department of Health & Senior Services. Preventing Prescription Fraud. http://health.mo.gov/ safety/bndd/publications.php. Accessed July 1, 2013.
Ill-advised genetic counseling: $1M verdict

A mother had given birth to two children with thalamic abnormalities that resulted in seizures, developmental delays, and death. Before getting pregnant again, the parents sought genetic counseling and were told that identifying the specific defective gene would be impossible. The geneticist advised them that a child conceived with a donor egg and father’s sperm would have essentially the same risk as the general population. The parents asked in writing if it would be safer to
use both donor egg and donor sperm; the geneticist responded that the difference in risk was negligible.
The mother gave birth in June 2007 to a child conceived with a donated egg and the father’s sperm. After the child began to show the same symptoms as the others, an MRI of the child’s brain revealed a thalamic abnormality, and testing revealed Alpers syndrome caused by POLG gene mutations. The third child died in September 2008.
PARENTS’ CLAIM The chances of having a child with Alpers syndrome are
about 1:200,000 in the general population; if one parent is a known carrier, the chance is 1:1,000. If the parents had known this risk, they would have used donor egg and donor sperm to conceive or adopted. They were not told about Alpers syndrome and its relationship to the POLG gene until after their third child was born. The geneticist was negligent in failing to provide this information.
PHYSICIAN’S DEFENSE The parents received appropriate and accurate genetic counseling.
VERDICT A $1 million Florida verdict was returned.
What caused a delay in breast cancer diagnosis?
A 39-year-old woman underwent mammography in October 2004. After recommending a spotcompression film of a left-breast lesion, and then ultrasonography, the radiologist concluded that the lesion was benign, and suggested a 1-year follow-up. Reports were sent to the patient and her primary care physician.
In August 2006, when mammography was suspicious for breast cancer, a biopsy diagnosed infiltrating ductal carcinoma of the left breast. After undergoing a mastectomy, radiation therapy, and chemotherapy, the patient was cancer-free at the time of the trial.
patient’s CLAIM The radiologist failed to properly interpret the 2004 mammography.
physician’s DEFENSE The radiologist’s interpretations of the 2004 tests were correct. The patient failed to follow up in 1 year, as recommended, and this delayed the cancer diagnosis. The patient’s survival indicated that she had been cured of her breast cancer.
VERDICT A confidential settlement was reached with the hospital before the trial. An Illinois defense verdict was returned for the radiologist.
Heparin overdose for preemie
At 27 weeks' gestation, a woman went to a clinic with preeclampsia. After she was stabilized, the baby was born by emergency cesarean delivery.
At birth, the baby was thrombocytopenic (platelet count, 37,000/mL) with a heart rate of 60 bpm. The child’s cord blood pH was 7.27, indicating no significant hypoxia. At 1 minute of life, the child’s heart rate had not improved. After trying three times to place an endotracheal tube, chest compressions were begun at 10 minutes of life. An umbilical vein catheter (UVC) was placed at 22 minutes. Heparin was used to flush the UVC. After 40 minutes, the baby’s pH was 6.88, indicating severe acidosis. The infant was transferred to another hospital 3 hours after birth.
Head ultrasonography at 5 days of life revealed hemorrhagic and ischemic changes in the baby’s brain. The child suffered massive brain damage, is ventilator-dependent, and has a G-tube for feeding. She cannot sit up, walk, or speak, and will require specialized care for life.
Parent's claim Emergency resuscitation was not performed at birth: the low heart rate and thrombocytopenia were not treated; the UVC was not immediately placed. Twice, adult doses of heparin were used instead of normal saline to flush the UVC; heparin caused bleeding in the baby’s brain.
Defendant's Defense The case was settled during trial.
Verdict A $3 million Maryland settlement was reached.

Uterine rupture: $130M verdict
After a woman's first child was born by cesarean delivery, vaginal birth after cesarean (VBAC) was planned for her second pregnancy. When a nurse recognized a ruptured uterus, the ObGyn ordered a cesarean delivery. The newborn suffered severe brain damage, with seizures. She has cerebral palsy with near-normal intelligence, but cannot talk or walk and continues to have seizures.
Parents' claim The baby’s injuries occurred due to a failure to respond to fetal distress. When the intrauterine pressure catheter (IUPC) stopped working for 27 minutes, the nurse did not notify the ObGyn or apply an external monitor. Fetal heart decelerations occurred, including a prolonged deceleration for 3 minutes; the nurse did not notify the ObGyn, reposition the mother, provide oxygen and extra fluids, or discontinue oxytocin. A cesarean delivery should have occurred 30 to 60 minutes earlier.
Defendants' defense The fetal heart rates were what typically occur during the second stage of labor. The hospital’s accepted practices were followed. When the IUPC failed, the nurse measured contractions by hand and analyzed the fetal heartbeat from audible sounds; therefore, it was not necessary to notify the ObGyn. The physician was promptly called when uterine rupture was suspected. Uterine rupture and placental abruption caused the child’s injury. Uterine rupture cannot be predicted or prevented and is a known complication of VBAC.
Verdict After the parents declined an $8 million settlement, the matter was tried to a defense verdict. That decision was overturned on appeal, and, at a second trial, a $130 million New York verdict was returned against the hospital that employed the ObGyn and nurse.
Uterus, small bowel injured during D&C
A 65-year-old woman underwent dilation and curettage (D&C) to screen for uterine cancer performed by an ObGyn and a general surgeon. Her uterus and small intestine were perforated during the procedure, and a second operation was required to repair the damage.
Patient's claim Both physicians were negligent in performing D&C.
Physician's defense The ObGyn denied negligence and countered that the injuries are known complications of the procedure.
Verdict The surgeon settled for a confidential amount before trial. A New Jersey defense verdict was returned for the ObGyn.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
A mother had given birth to two children with thalamic abnormalities that resulted in seizures, developmental delays, and death. Before getting pregnant again, the parents sought genetic counseling and were told that identifying the specific defective gene would be impossible. The geneticist advised them that a child conceived with a donor egg and father’s sperm would have essentially the same risk as the general population. The parents asked in writing if it would be safer to
use both donor egg and donor sperm; the geneticist responded that the difference in risk was negligible.
The mother gave birth in June 2007 to a child conceived with a donated egg and the father’s sperm. After the child began to show the same symptoms as the others, an MRI of the child’s brain revealed a thalamic abnormality, and testing revealed Alpers syndrome caused by POLG gene mutations. The third child died in September 2008.
PARENTS’ CLAIM The chances of having a child with Alpers syndrome are
about 1:200,000 in the general population; if one parent is a known carrier, the chance is 1:1,000. If the parents had known this risk, they would have used donor egg and donor sperm to conceive or adopted. They were not told about Alpers syndrome and its relationship to the POLG gene until after their third child was born. The geneticist was negligent in failing to provide this information.
PHYSICIAN’S DEFENSE The parents received appropriate and accurate genetic counseling.
VERDICT A $1 million Florida verdict was returned.
What caused a delay in breast cancer diagnosis?
A 39-year-old woman underwent mammography in October 2004. After recommending a spotcompression film of a left-breast lesion, and then ultrasonography, the radiologist concluded that the lesion was benign, and suggested a 1-year follow-up. Reports were sent to the patient and her primary care physician.
In August 2006, when mammography was suspicious for breast cancer, a biopsy diagnosed infiltrating ductal carcinoma of the left breast. After undergoing a mastectomy, radiation therapy, and chemotherapy, the patient was cancer-free at the time of the trial.
patient’s CLAIM The radiologist failed to properly interpret the 2004 mammography.
physician’s DEFENSE The radiologist’s interpretations of the 2004 tests were correct. The patient failed to follow up in 1 year, as recommended, and this delayed the cancer diagnosis. The patient’s survival indicated that she had been cured of her breast cancer.
VERDICT A confidential settlement was reached with the hospital before the trial. An Illinois defense verdict was returned for the radiologist.
Heparin overdose for preemie
At 27 weeks' gestation, a woman went to a clinic with preeclampsia. After she was stabilized, the baby was born by emergency cesarean delivery.
At birth, the baby was thrombocytopenic (platelet count, 37,000/mL) with a heart rate of 60 bpm. The child’s cord blood pH was 7.27, indicating no significant hypoxia. At 1 minute of life, the child’s heart rate had not improved. After trying three times to place an endotracheal tube, chest compressions were begun at 10 minutes of life. An umbilical vein catheter (UVC) was placed at 22 minutes. Heparin was used to flush the UVC. After 40 minutes, the baby’s pH was 6.88, indicating severe acidosis. The infant was transferred to another hospital 3 hours after birth.
Head ultrasonography at 5 days of life revealed hemorrhagic and ischemic changes in the baby’s brain. The child suffered massive brain damage, is ventilator-dependent, and has a G-tube for feeding. She cannot sit up, walk, or speak, and will require specialized care for life.
Parent's claim Emergency resuscitation was not performed at birth: the low heart rate and thrombocytopenia were not treated; the UVC was not immediately placed. Twice, adult doses of heparin were used instead of normal saline to flush the UVC; heparin caused bleeding in the baby’s brain.
Defendant's Defense The case was settled during trial.
Verdict A $3 million Maryland settlement was reached.
Uterine rupture: $130M verdict
After a woman's first child was born by cesarean delivery, vaginal birth after cesarean (VBAC) was planned for her second pregnancy. When a nurse recognized a ruptured uterus, the ObGyn ordered a cesarean delivery. The newborn suffered severe brain damage, with seizures. She has cerebral palsy with near-normal intelligence, but cannot talk or walk and continues to have seizures.
Parents' claim The baby’s injuries occurred due to a failure to respond to fetal distress. When the intrauterine pressure catheter (IUPC) stopped working for 27 minutes, the nurse did not notify the ObGyn or apply an external monitor. Fetal heart decelerations occurred, including a prolonged deceleration for 3 minutes; the nurse did not notify the ObGyn, reposition the mother, provide oxygen and extra fluids, or discontinue oxytocin. A cesarean delivery should have occurred 30 to 60 minutes earlier.
Defendants' defense The fetal heart rates were what typically occur during the second stage of labor. The hospital’s accepted practices were followed. When the IUPC failed, the nurse measured contractions by hand and analyzed the fetal heartbeat from audible sounds; therefore, it was not necessary to notify the ObGyn. The physician was promptly called when uterine rupture was suspected. Uterine rupture and placental abruption caused the child’s injury. Uterine rupture cannot be predicted or prevented and is a known complication of VBAC.
Verdict After the parents declined an $8 million settlement, the matter was tried to a defense verdict. That decision was overturned on appeal, and, at a second trial, a $130 million New York verdict was returned against the hospital that employed the ObGyn and nurse.
Uterus, small bowel injured during D&C
A 65-year-old woman underwent dilation and curettage (D&C) to screen for uterine cancer performed by an ObGyn and a general surgeon. Her uterus and small intestine were perforated during the procedure, and a second operation was required to repair the damage.
Patient's claim Both physicians were negligent in performing D&C.
Physician's defense The ObGyn denied negligence and countered that the injuries are known complications of the procedure.
Verdict The surgeon settled for a confidential amount before trial. A New Jersey defense verdict was returned for the ObGyn.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
A mother had given birth to two children with thalamic abnormalities that resulted in seizures, developmental delays, and death. Before getting pregnant again, the parents sought genetic counseling and were told that identifying the specific defective gene would be impossible. The geneticist advised them that a child conceived with a donor egg and father’s sperm would have essentially the same risk as the general population. The parents asked in writing if it would be safer to
use both donor egg and donor sperm; the geneticist responded that the difference in risk was negligible.
The mother gave birth in June 2007 to a child conceived with a donated egg and the father’s sperm. After the child began to show the same symptoms as the others, an MRI of the child’s brain revealed a thalamic abnormality, and testing revealed Alpers syndrome caused by POLG gene mutations. The third child died in September 2008.
PARENTS’ CLAIM The chances of having a child with Alpers syndrome are
about 1:200,000 in the general population; if one parent is a known carrier, the chance is 1:1,000. If the parents had known this risk, they would have used donor egg and donor sperm to conceive or adopted. They were not told about Alpers syndrome and its relationship to the POLG gene until after their third child was born. The geneticist was negligent in failing to provide this information.
PHYSICIAN’S DEFENSE The parents received appropriate and accurate genetic counseling.
VERDICT A $1 million Florida verdict was returned.
What caused a delay in breast cancer diagnosis?
A 39-year-old woman underwent mammography in October 2004. After recommending a spotcompression film of a left-breast lesion, and then ultrasonography, the radiologist concluded that the lesion was benign, and suggested a 1-year follow-up. Reports were sent to the patient and her primary care physician.
In August 2006, when mammography was suspicious for breast cancer, a biopsy diagnosed infiltrating ductal carcinoma of the left breast. After undergoing a mastectomy, radiation therapy, and chemotherapy, the patient was cancer-free at the time of the trial.
patient’s CLAIM The radiologist failed to properly interpret the 2004 mammography.
physician’s DEFENSE The radiologist’s interpretations of the 2004 tests were correct. The patient failed to follow up in 1 year, as recommended, and this delayed the cancer diagnosis. The patient’s survival indicated that she had been cured of her breast cancer.
VERDICT A confidential settlement was reached with the hospital before the trial. An Illinois defense verdict was returned for the radiologist.
Heparin overdose for preemie
At 27 weeks' gestation, a woman went to a clinic with preeclampsia. After she was stabilized, the baby was born by emergency cesarean delivery.
At birth, the baby was thrombocytopenic (platelet count, 37,000/mL) with a heart rate of 60 bpm. The child’s cord blood pH was 7.27, indicating no significant hypoxia. At 1 minute of life, the child’s heart rate had not improved. After trying three times to place an endotracheal tube, chest compressions were begun at 10 minutes of life. An umbilical vein catheter (UVC) was placed at 22 minutes. Heparin was used to flush the UVC. After 40 minutes, the baby’s pH was 6.88, indicating severe acidosis. The infant was transferred to another hospital 3 hours after birth.
Head ultrasonography at 5 days of life revealed hemorrhagic and ischemic changes in the baby’s brain. The child suffered massive brain damage, is ventilator-dependent, and has a G-tube for feeding. She cannot sit up, walk, or speak, and will require specialized care for life.
Parent's claim Emergency resuscitation was not performed at birth: the low heart rate and thrombocytopenia were not treated; the UVC was not immediately placed. Twice, adult doses of heparin were used instead of normal saline to flush the UVC; heparin caused bleeding in the baby’s brain.
Defendant's Defense The case was settled during trial.
Verdict A $3 million Maryland settlement was reached.
Uterine rupture: $130M verdict
After a woman's first child was born by cesarean delivery, vaginal birth after cesarean (VBAC) was planned for her second pregnancy. When a nurse recognized a ruptured uterus, the ObGyn ordered a cesarean delivery. The newborn suffered severe brain damage, with seizures. She has cerebral palsy with near-normal intelligence, but cannot talk or walk and continues to have seizures.
Parents' claim The baby’s injuries occurred due to a failure to respond to fetal distress. When the intrauterine pressure catheter (IUPC) stopped working for 27 minutes, the nurse did not notify the ObGyn or apply an external monitor. Fetal heart decelerations occurred, including a prolonged deceleration for 3 minutes; the nurse did not notify the ObGyn, reposition the mother, provide oxygen and extra fluids, or discontinue oxytocin. A cesarean delivery should have occurred 30 to 60 minutes earlier.
Defendants' defense The fetal heart rates were what typically occur during the second stage of labor. The hospital’s accepted practices were followed. When the IUPC failed, the nurse measured contractions by hand and analyzed the fetal heartbeat from audible sounds; therefore, it was not necessary to notify the ObGyn. The physician was promptly called when uterine rupture was suspected. Uterine rupture and placental abruption caused the child’s injury. Uterine rupture cannot be predicted or prevented and is a known complication of VBAC.
Verdict After the parents declined an $8 million settlement, the matter was tried to a defense verdict. That decision was overturned on appeal, and, at a second trial, a $130 million New York verdict was returned against the hospital that employed the ObGyn and nurse.
Uterus, small bowel injured during D&C
A 65-year-old woman underwent dilation and curettage (D&C) to screen for uterine cancer performed by an ObGyn and a general surgeon. Her uterus and small intestine were perforated during the procedure, and a second operation was required to repair the damage.
Patient's claim Both physicians were negligent in performing D&C.
Physician's defense The ObGyn denied negligence and countered that the injuries are known complications of the procedure.
Verdict The surgeon settled for a confidential amount before trial. A New Jersey defense verdict was returned for the ObGyn.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.

Who’s Responsible for Oral Lesions?
Cases reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
A 47-year-old man in Michigan went to his internist with complaints of oral discomfort and white patches on his tongue. He was subsequently diagnosed with oral leukoplakia, which is considered precancerous. The patient’s symptoms were treated, but no further follow-up testing was recommended or scheduled.
Subsequently, a second internist evaluated the patient in the emergency department of a major medical center and provided symptomatic treatment without arranging follow-up. The patient was later diagnosed with stage IV oral cancer and required radiation therapy, chemotherapy, and surgery to remove the lesion. In addition, he underwent a second procedure to reconstruct his jaw using bone grafting.
The plaintiff alleged negligence in the failure to refer him for a biopsy, maintaining that earlier diagnosis and treatment would have prevented the need for extensive surgery and treatment. The defendants claimed that the treatment given was appropriate and that the plaintiff’s drug use, to which he admitted, had caused or contributed to his disease.
Outcome
According to a published account, a $367,500 verdict was returned against the medical center, with 60% comparative negligence being found against the medical center and 40% attributed to the patient. (Explanation follows.)
Comment
Persistent oral lesions require a definitive diagnosis and should be considered cancerous until proven otherwise. Oral cancer can present as an obvious mass but can be as subtle as a mucosal change.1 Oral leukoplakia is the most common premalignant lesion and is defined by the World Health Organization as “a white patch or plaque that cannot be characterized clinically or pathologically as any other disease.”
In the United States, cancers of the oral cavity and oropharynx are the ninth most common cancer.2 Approximately 90% of oral cancers are squamous cell carcinoma, occurring most commonly on the tongue, floor of the mouth, and vermilion border of the lower lip. A full 60% of oral carcinomas are advanced by the time they are detected, and about 15% of patients have another cancer in a nearby area, such as the larynx, esophagus, or lungs. Tobacco use and heavy alcohol use are the two main risk factors, accounting for 75% of oral carcinomas.3
When primary care providers casually address oral lesions, there is potential for a missed diagnosis. This potential is greater when a clinician may erroneously believe that a dentist will evaluate the lesion at a routine follow-up—but that follow-up never happens.
Oral care presents an overlap between dentistry and medicine, with both clinicians sharing responsibility but sometimes finding ways of excusing themselves from it. Problematically, dentists and oromaxillofacial surgeons may not be part of the usual referral network for primary care providers. This presents barriers to referring patients and receiving feedback after the evaluation takes place.
When a decision is made to refer the patient for a suspicious oral lesion, do so formally with a referral to otolaryngology or an oromaxillofacial surgeon. Should the patient wish instead to follow up with his or her dentist, make sure that a specific date is chosen (not “at the next six-month routine visit”). Ensure the referral is part of your formal plan and recorded and documented. Follow up with referral documentation to the dentist, and schedule your own follow-up to be sure the evaluation occurred and the dentist’s feedback is received. Both dentists and primary care clinicians should work together to ensure that a suspicious lesion receives a biopsy.
In this case, a decision to biopsy the lesion may have resulted in the need for less extensive surgery and treatment and a better prognosis. Here, we have a legally interesting situation in which the jury found comparative negligence and reduced the plaintiff’s award based on the jury’s perception that he contributed to his condition (ostensibly because of his drug use).
As clinicians, we are duty-bound to take optimal care of every one of our patients—no matter how we find them. Blaming a patient for a bad outcome can be risky. Even as a defense strategy in a medical malpractice case, alleging plaintiff contribution is tricky: It can backfire badly if the jury is angered by clinician attempts to assign a share of the blame to the patient.
Comparative negligence provides an offset for the patient’s contribution to his situation. Many jurisdictions follow a “50% rule” and bar plaintiff recovery if he/she is deemed half responsible (50%) or more, and others follow a modified “51% rule” in which the plaintiff can recover if he/she was half responsible, but not more (ie, 51% at fault). Thirteen states follow a pure comparative negligence rule that permits recovery if the plaintiff is more than 51% responsible (in theory, even 99%).
This case was tried in Michigan, which follows the modified comparative negligence (“51%”) rule. Here, the jury found the defendant 60% at fault and the plaintiff 40% percent at fault and reduced the award accordingly. Because the jury found the plaintiff less than 51% responsible, he was able to maintain his claim and recover 60% of the damages.
Contributory negligence is an older defense that operates as a complete bar to recovery if the plaintiff contributed to the incident in any way. Only a handful of states still follow strict contributory negligence law.
In summary, take oral lesions seriously. If you encounter a patient with such a lesion, establish a clear plan to refer the patient or to monitor the lesion carefully. A definitive diagnosis is required for any persistent lesion. Explain to the patient that the lesion must be properly evaluated to be sure it is not serious. As primary care providers, we are responsible for oral lesions. —DML
References
1. Gonsalves WC, Chi AC, Neville BW. Common oral lesions: part II—masses and neoplasia. Am Fam Phys. 2007;75(4):509-512.
2. Jemal A, Murray T, Ward E, et al. Cancer statistics, 2005 [published correction appears in CA Cancer J Clin. 2005;55:259]. CA Cancer J Clin. 2005;55:10-30.
3. Weinberg MA, Estefan DJ. Assessing oral malignancies. Am Fam Phys. 2002;65:1379-84.
Cases reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
A 47-year-old man in Michigan went to his internist with complaints of oral discomfort and white patches on his tongue. He was subsequently diagnosed with oral leukoplakia, which is considered precancerous. The patient’s symptoms were treated, but no further follow-up testing was recommended or scheduled.
Subsequently, a second internist evaluated the patient in the emergency department of a major medical center and provided symptomatic treatment without arranging follow-up. The patient was later diagnosed with stage IV oral cancer and required radiation therapy, chemotherapy, and surgery to remove the lesion. In addition, he underwent a second procedure to reconstruct his jaw using bone grafting.
The plaintiff alleged negligence in the failure to refer him for a biopsy, maintaining that earlier diagnosis and treatment would have prevented the need for extensive surgery and treatment. The defendants claimed that the treatment given was appropriate and that the plaintiff’s drug use, to which he admitted, had caused or contributed to his disease.
Outcome
According to a published account, a $367,500 verdict was returned against the medical center, with 60% comparative negligence being found against the medical center and 40% attributed to the patient. (Explanation follows.)
Comment
Persistent oral lesions require a definitive diagnosis and should be considered cancerous until proven otherwise. Oral cancer can present as an obvious mass but can be as subtle as a mucosal change.1 Oral leukoplakia is the most common premalignant lesion and is defined by the World Health Organization as “a white patch or plaque that cannot be characterized clinically or pathologically as any other disease.”
In the United States, cancers of the oral cavity and oropharynx are the ninth most common cancer.2 Approximately 90% of oral cancers are squamous cell carcinoma, occurring most commonly on the tongue, floor of the mouth, and vermilion border of the lower lip. A full 60% of oral carcinomas are advanced by the time they are detected, and about 15% of patients have another cancer in a nearby area, such as the larynx, esophagus, or lungs. Tobacco use and heavy alcohol use are the two main risk factors, accounting for 75% of oral carcinomas.3
When primary care providers casually address oral lesions, there is potential for a missed diagnosis. This potential is greater when a clinician may erroneously believe that a dentist will evaluate the lesion at a routine follow-up—but that follow-up never happens.
Oral care presents an overlap between dentistry and medicine, with both clinicians sharing responsibility but sometimes finding ways of excusing themselves from it. Problematically, dentists and oromaxillofacial surgeons may not be part of the usual referral network for primary care providers. This presents barriers to referring patients and receiving feedback after the evaluation takes place.
When a decision is made to refer the patient for a suspicious oral lesion, do so formally with a referral to otolaryngology or an oromaxillofacial surgeon. Should the patient wish instead to follow up with his or her dentist, make sure that a specific date is chosen (not “at the next six-month routine visit”). Ensure the referral is part of your formal plan and recorded and documented. Follow up with referral documentation to the dentist, and schedule your own follow-up to be sure the evaluation occurred and the dentist’s feedback is received. Both dentists and primary care clinicians should work together to ensure that a suspicious lesion receives a biopsy.
In this case, a decision to biopsy the lesion may have resulted in the need for less extensive surgery and treatment and a better prognosis. Here, we have a legally interesting situation in which the jury found comparative negligence and reduced the plaintiff’s award based on the jury’s perception that he contributed to his condition (ostensibly because of his drug use).
As clinicians, we are duty-bound to take optimal care of every one of our patients—no matter how we find them. Blaming a patient for a bad outcome can be risky. Even as a defense strategy in a medical malpractice case, alleging plaintiff contribution is tricky: It can backfire badly if the jury is angered by clinician attempts to assign a share of the blame to the patient.
Comparative negligence provides an offset for the patient’s contribution to his situation. Many jurisdictions follow a “50% rule” and bar plaintiff recovery if he/she is deemed half responsible (50%) or more, and others follow a modified “51% rule” in which the plaintiff can recover if he/she was half responsible, but not more (ie, 51% at fault). Thirteen states follow a pure comparative negligence rule that permits recovery if the plaintiff is more than 51% responsible (in theory, even 99%).
This case was tried in Michigan, which follows the modified comparative negligence (“51%”) rule. Here, the jury found the defendant 60% at fault and the plaintiff 40% percent at fault and reduced the award accordingly. Because the jury found the plaintiff less than 51% responsible, he was able to maintain his claim and recover 60% of the damages.
Contributory negligence is an older defense that operates as a complete bar to recovery if the plaintiff contributed to the incident in any way. Only a handful of states still follow strict contributory negligence law.
In summary, take oral lesions seriously. If you encounter a patient with such a lesion, establish a clear plan to refer the patient or to monitor the lesion carefully. A definitive diagnosis is required for any persistent lesion. Explain to the patient that the lesion must be properly evaluated to be sure it is not serious. As primary care providers, we are responsible for oral lesions. —DML
References
1. Gonsalves WC, Chi AC, Neville BW. Common oral lesions: part II—masses and neoplasia. Am Fam Phys. 2007;75(4):509-512.
2. Jemal A, Murray T, Ward E, et al. Cancer statistics, 2005 [published correction appears in CA Cancer J Clin. 2005;55:259]. CA Cancer J Clin. 2005;55:10-30.
3. Weinberg MA, Estefan DJ. Assessing oral malignancies. Am Fam Phys. 2002;65:1379-84.
Cases reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
A 47-year-old man in Michigan went to his internist with complaints of oral discomfort and white patches on his tongue. He was subsequently diagnosed with oral leukoplakia, which is considered precancerous. The patient’s symptoms were treated, but no further follow-up testing was recommended or scheduled.
Subsequently, a second internist evaluated the patient in the emergency department of a major medical center and provided symptomatic treatment without arranging follow-up. The patient was later diagnosed with stage IV oral cancer and required radiation therapy, chemotherapy, and surgery to remove the lesion. In addition, he underwent a second procedure to reconstruct his jaw using bone grafting.
The plaintiff alleged negligence in the failure to refer him for a biopsy, maintaining that earlier diagnosis and treatment would have prevented the need for extensive surgery and treatment. The defendants claimed that the treatment given was appropriate and that the plaintiff’s drug use, to which he admitted, had caused or contributed to his disease.
Outcome
According to a published account, a $367,500 verdict was returned against the medical center, with 60% comparative negligence being found against the medical center and 40% attributed to the patient. (Explanation follows.)
Comment
Persistent oral lesions require a definitive diagnosis and should be considered cancerous until proven otherwise. Oral cancer can present as an obvious mass but can be as subtle as a mucosal change.1 Oral leukoplakia is the most common premalignant lesion and is defined by the World Health Organization as “a white patch or plaque that cannot be characterized clinically or pathologically as any other disease.”
In the United States, cancers of the oral cavity and oropharynx are the ninth most common cancer.2 Approximately 90% of oral cancers are squamous cell carcinoma, occurring most commonly on the tongue, floor of the mouth, and vermilion border of the lower lip. A full 60% of oral carcinomas are advanced by the time they are detected, and about 15% of patients have another cancer in a nearby area, such as the larynx, esophagus, or lungs. Tobacco use and heavy alcohol use are the two main risk factors, accounting for 75% of oral carcinomas.3
When primary care providers casually address oral lesions, there is potential for a missed diagnosis. This potential is greater when a clinician may erroneously believe that a dentist will evaluate the lesion at a routine follow-up—but that follow-up never happens.
Oral care presents an overlap between dentistry and medicine, with both clinicians sharing responsibility but sometimes finding ways of excusing themselves from it. Problematically, dentists and oromaxillofacial surgeons may not be part of the usual referral network for primary care providers. This presents barriers to referring patients and receiving feedback after the evaluation takes place.
When a decision is made to refer the patient for a suspicious oral lesion, do so formally with a referral to otolaryngology or an oromaxillofacial surgeon. Should the patient wish instead to follow up with his or her dentist, make sure that a specific date is chosen (not “at the next six-month routine visit”). Ensure the referral is part of your formal plan and recorded and documented. Follow up with referral documentation to the dentist, and schedule your own follow-up to be sure the evaluation occurred and the dentist’s feedback is received. Both dentists and primary care clinicians should work together to ensure that a suspicious lesion receives a biopsy.
In this case, a decision to biopsy the lesion may have resulted in the need for less extensive surgery and treatment and a better prognosis. Here, we have a legally interesting situation in which the jury found comparative negligence and reduced the plaintiff’s award based on the jury’s perception that he contributed to his condition (ostensibly because of his drug use).
As clinicians, we are duty-bound to take optimal care of every one of our patients—no matter how we find them. Blaming a patient for a bad outcome can be risky. Even as a defense strategy in a medical malpractice case, alleging plaintiff contribution is tricky: It can backfire badly if the jury is angered by clinician attempts to assign a share of the blame to the patient.
Comparative negligence provides an offset for the patient’s contribution to his situation. Many jurisdictions follow a “50% rule” and bar plaintiff recovery if he/she is deemed half responsible (50%) or more, and others follow a modified “51% rule” in which the plaintiff can recover if he/she was half responsible, but not more (ie, 51% at fault). Thirteen states follow a pure comparative negligence rule that permits recovery if the plaintiff is more than 51% responsible (in theory, even 99%).
This case was tried in Michigan, which follows the modified comparative negligence (“51%”) rule. Here, the jury found the defendant 60% at fault and the plaintiff 40% percent at fault and reduced the award accordingly. Because the jury found the plaintiff less than 51% responsible, he was able to maintain his claim and recover 60% of the damages.
Contributory negligence is an older defense that operates as a complete bar to recovery if the plaintiff contributed to the incident in any way. Only a handful of states still follow strict contributory negligence law.
In summary, take oral lesions seriously. If you encounter a patient with such a lesion, establish a clear plan to refer the patient or to monitor the lesion carefully. A definitive diagnosis is required for any persistent lesion. Explain to the patient that the lesion must be properly evaluated to be sure it is not serious. As primary care providers, we are responsible for oral lesions. —DML
References
1. Gonsalves WC, Chi AC, Neville BW. Common oral lesions: part II—masses and neoplasia. Am Fam Phys. 2007;75(4):509-512.
2. Jemal A, Murray T, Ward E, et al. Cancer statistics, 2005 [published correction appears in CA Cancer J Clin. 2005;55:259]. CA Cancer J Clin. 2005;55:10-30.
3. Weinberg MA, Estefan DJ. Assessing oral malignancies. Am Fam Phys. 2002;65:1379-84.
In Appendicitis Case, Patient Sues Clinic, Clinic Sues NP
A 17-year-old girl with diminished appetite, abdominal pain, and vomiting presented to a pediatrics clinic in New York, where she was examined by a nurse practitioner. She was found to have hematuria as well, and the NP diagnosed viral gastroenteritis.
Eight days later, the patient returned to the clinic with worsening pain. The pediatrician who examined her had her transported to a hospital, where a ruptured appendix was diagnosed. The patient underwent immediate surgery, which included resection of portions of her colon and intestines.
Despite a good recovery, the patient claimed that she suffers residual gastrointestinal dysfunction. She further claimed that the NP should have diagnosed appendicitis during her initial visit, which would have allowed for less invasive treatment.
Initially, the plaintiff brought suit against the clinic and several employees, but not the NP. She later moved to add the NP, but that motion was denied due to the statute of limitations. The clinic then impleaded the NP, arguing that it was her negligence in failing to diagnose the appendicitis.
The matter proceeded to trial against the NP and the clinic. The defendants claimed that the plaintiff’s symptoms did not suggest appendicitis at the time of the NP’s examination.
Outcome
According to a published account, a defense verdict was returned.
Comment
I used to tell students, “There are only two things in medicine that you need to know well: the common and the dangerous. For everything else, there is time.” I realize now that I sound like that guy from the Dos Equis commercial.
Consider this, however: If we don’t remember the difference between polymyositis and polymyalgia rheumatic, who cares? In such cases, we have time for review—and the patient will be better served by a clinician who has the intellectual curiosity to review conditions that he or she hasn’t seen in a while.
But the diseases that are both common and dangerous require our full proficiency. Basic competence requires us to be well versed in common diseases. And dangerous conditions, even if relatively rare, must be recognized and managed immediately. Entities that are common and dangerous—such as appendicitis—should enter our thoughts often.
In this case, we have a 17-year-old girl presenting to an outpatient clinic setting with abdominal pain, vomiting, and anorexia. Unfortunately, we are not given some important historical information, including duration and location of the pain and the presence or absence of pain migration. Physical exam findings are not described.
The trouble with appendicitis is that there is no single sign or symptom that can effectively diagnose it or exclude it from the differential. When evaluating a patient in a setting in which real-time laboratory testing is not generally ordered, clinicians must distinguish between self-limiting and dangerous abdominal pain. Where does that leave us in this case? Abdominal pain and vomiting are common, and ill patients frequently report anorexia.
Other clinical features associated with appendicitis may be more helpful. For example, pain migration has been described as “the most discriminating feature of the patient’s history,”1 with a sensitivity and specificity of approximately 80%.2 When present, psoas sign is fairly specific (0.95), but not sensitive (0.16).3
When evaluating patients in an outpatient setting, we have a snapshot of a disease process—a still frame of a movie. We are told what happened up to that point (with varying degrees of accuracy). But like the patient, we don’t know what will happen after the patient leaves the office: The still frame is gone, but the movie continues.
It can be helpful to inform patients of the concerning diagnoses in your differential and alert them to patterns of clinical progression that warrant return or immediate emergency department evaluation. Calling the patient to see how he or she is doing can be very useful for clinicians, and generally highly valued and appreciated by patients. Here, if gastroenteritis were suspected, a phone call after a few hours of antiemetic and rehydration therapy may have been helpful to determine if the patient’s symptoms had improved. This, of course, would not be conclusive—but at least it would give the clinician additional information and the patient additional comfort.
In this case, the jury was persuaded that the NP provided good treatment and acted within the standard of care. Diagnosing appendicitis can be tricky, even under the best circumstances. The NP’s defense was probably aided by good documentation showing that appendicitis seemed less likely at the time of her evaluation. Ultimately, she performed well enough that her care withstood scrutiny from the plaintiff, the plaintiff’s expert witness, and eventually, her own practice.
This case was interesting from a legal perspective in that the plaintiff originally failed to file suit against the NP—probably resorting to liability under the theory of respondeat superior (generally, employer liability for employee actions). While the plaintiff was unsuccessful in adding the NP later, due to the statue of limitations, the NP was brought into the case by her own practice, through a procedure known as “impleader.” An impleader action is brought by a co-defendant. Under typical impleader rules, the defendant becomes a “third-party plaintiff” and brings suit against a “third-party defendant” (in this case, the practice and the NP, respectively).
In sum, always keep important diagnoses in mind, and document well. Anticipate a changing clinical course, and instruct patients on how to respond to those changes. In certain cases, we are well served to pick up the phone, check on the patient, and make the presentation less of a static picture and more of a dynamic movie. —DML
References
1. Craig S, Brenner BE. Appendicitis (updated October 26, 2012). Medscape Reference. http://emedicine.medscape.com/article/773895-overview. Accessed August 14, 2013.
2. Yeh B. Evidence-based emergency medicine/rational clinical examination abstract: does this adult patient have appendicitis?.Ann Emerg Med. 2008;52(3):301-303.
3. Wagner J, McKinney WP, Carpenter JL. Does this patient have appendicitis? JAMA. 1996;276(19):1589-1594.
A 17-year-old girl with diminished appetite, abdominal pain, and vomiting presented to a pediatrics clinic in New York, where she was examined by a nurse practitioner. She was found to have hematuria as well, and the NP diagnosed viral gastroenteritis.
Eight days later, the patient returned to the clinic with worsening pain. The pediatrician who examined her had her transported to a hospital, where a ruptured appendix was diagnosed. The patient underwent immediate surgery, which included resection of portions of her colon and intestines.
Despite a good recovery, the patient claimed that she suffers residual gastrointestinal dysfunction. She further claimed that the NP should have diagnosed appendicitis during her initial visit, which would have allowed for less invasive treatment.
Initially, the plaintiff brought suit against the clinic and several employees, but not the NP. She later moved to add the NP, but that motion was denied due to the statute of limitations. The clinic then impleaded the NP, arguing that it was her negligence in failing to diagnose the appendicitis.
The matter proceeded to trial against the NP and the clinic. The defendants claimed that the plaintiff’s symptoms did not suggest appendicitis at the time of the NP’s examination.
Outcome
According to a published account, a defense verdict was returned.
Comment
I used to tell students, “There are only two things in medicine that you need to know well: the common and the dangerous. For everything else, there is time.” I realize now that I sound like that guy from the Dos Equis commercial.
Consider this, however: If we don’t remember the difference between polymyositis and polymyalgia rheumatic, who cares? In such cases, we have time for review—and the patient will be better served by a clinician who has the intellectual curiosity to review conditions that he or she hasn’t seen in a while.
But the diseases that are both common and dangerous require our full proficiency. Basic competence requires us to be well versed in common diseases. And dangerous conditions, even if relatively rare, must be recognized and managed immediately. Entities that are common and dangerous—such as appendicitis—should enter our thoughts often.
In this case, we have a 17-year-old girl presenting to an outpatient clinic setting with abdominal pain, vomiting, and anorexia. Unfortunately, we are not given some important historical information, including duration and location of the pain and the presence or absence of pain migration. Physical exam findings are not described.
The trouble with appendicitis is that there is no single sign or symptom that can effectively diagnose it or exclude it from the differential. When evaluating a patient in a setting in which real-time laboratory testing is not generally ordered, clinicians must distinguish between self-limiting and dangerous abdominal pain. Where does that leave us in this case? Abdominal pain and vomiting are common, and ill patients frequently report anorexia.
Other clinical features associated with appendicitis may be more helpful. For example, pain migration has been described as “the most discriminating feature of the patient’s history,”1 with a sensitivity and specificity of approximately 80%.2 When present, psoas sign is fairly specific (0.95), but not sensitive (0.16).3
When evaluating patients in an outpatient setting, we have a snapshot of a disease process—a still frame of a movie. We are told what happened up to that point (with varying degrees of accuracy). But like the patient, we don’t know what will happen after the patient leaves the office: The still frame is gone, but the movie continues.
It can be helpful to inform patients of the concerning diagnoses in your differential and alert them to patterns of clinical progression that warrant return or immediate emergency department evaluation. Calling the patient to see how he or she is doing can be very useful for clinicians, and generally highly valued and appreciated by patients. Here, if gastroenteritis were suspected, a phone call after a few hours of antiemetic and rehydration therapy may have been helpful to determine if the patient’s symptoms had improved. This, of course, would not be conclusive—but at least it would give the clinician additional information and the patient additional comfort.
In this case, the jury was persuaded that the NP provided good treatment and acted within the standard of care. Diagnosing appendicitis can be tricky, even under the best circumstances. The NP’s defense was probably aided by good documentation showing that appendicitis seemed less likely at the time of her evaluation. Ultimately, she performed well enough that her care withstood scrutiny from the plaintiff, the plaintiff’s expert witness, and eventually, her own practice.
This case was interesting from a legal perspective in that the plaintiff originally failed to file suit against the NP—probably resorting to liability under the theory of respondeat superior (generally, employer liability for employee actions). While the plaintiff was unsuccessful in adding the NP later, due to the statue of limitations, the NP was brought into the case by her own practice, through a procedure known as “impleader.” An impleader action is brought by a co-defendant. Under typical impleader rules, the defendant becomes a “third-party plaintiff” and brings suit against a “third-party defendant” (in this case, the practice and the NP, respectively).
In sum, always keep important diagnoses in mind, and document well. Anticipate a changing clinical course, and instruct patients on how to respond to those changes. In certain cases, we are well served to pick up the phone, check on the patient, and make the presentation less of a static picture and more of a dynamic movie. —DML
References
1. Craig S, Brenner BE. Appendicitis (updated October 26, 2012). Medscape Reference. http://emedicine.medscape.com/article/773895-overview. Accessed August 14, 2013.
2. Yeh B. Evidence-based emergency medicine/rational clinical examination abstract: does this adult patient have appendicitis?.Ann Emerg Med. 2008;52(3):301-303.
3. Wagner J, McKinney WP, Carpenter JL. Does this patient have appendicitis? JAMA. 1996;276(19):1589-1594.
A 17-year-old girl with diminished appetite, abdominal pain, and vomiting presented to a pediatrics clinic in New York, where she was examined by a nurse practitioner. She was found to have hematuria as well, and the NP diagnosed viral gastroenteritis.
Eight days later, the patient returned to the clinic with worsening pain. The pediatrician who examined her had her transported to a hospital, where a ruptured appendix was diagnosed. The patient underwent immediate surgery, which included resection of portions of her colon and intestines.
Despite a good recovery, the patient claimed that she suffers residual gastrointestinal dysfunction. She further claimed that the NP should have diagnosed appendicitis during her initial visit, which would have allowed for less invasive treatment.
Initially, the plaintiff brought suit against the clinic and several employees, but not the NP. She later moved to add the NP, but that motion was denied due to the statute of limitations. The clinic then impleaded the NP, arguing that it was her negligence in failing to diagnose the appendicitis.
The matter proceeded to trial against the NP and the clinic. The defendants claimed that the plaintiff’s symptoms did not suggest appendicitis at the time of the NP’s examination.
Outcome
According to a published account, a defense verdict was returned.
Comment
I used to tell students, “There are only two things in medicine that you need to know well: the common and the dangerous. For everything else, there is time.” I realize now that I sound like that guy from the Dos Equis commercial.
Consider this, however: If we don’t remember the difference between polymyositis and polymyalgia rheumatic, who cares? In such cases, we have time for review—and the patient will be better served by a clinician who has the intellectual curiosity to review conditions that he or she hasn’t seen in a while.
But the diseases that are both common and dangerous require our full proficiency. Basic competence requires us to be well versed in common diseases. And dangerous conditions, even if relatively rare, must be recognized and managed immediately. Entities that are common and dangerous—such as appendicitis—should enter our thoughts often.
In this case, we have a 17-year-old girl presenting to an outpatient clinic setting with abdominal pain, vomiting, and anorexia. Unfortunately, we are not given some important historical information, including duration and location of the pain and the presence or absence of pain migration. Physical exam findings are not described.
The trouble with appendicitis is that there is no single sign or symptom that can effectively diagnose it or exclude it from the differential. When evaluating a patient in a setting in which real-time laboratory testing is not generally ordered, clinicians must distinguish between self-limiting and dangerous abdominal pain. Where does that leave us in this case? Abdominal pain and vomiting are common, and ill patients frequently report anorexia.
Other clinical features associated with appendicitis may be more helpful. For example, pain migration has been described as “the most discriminating feature of the patient’s history,”1 with a sensitivity and specificity of approximately 80%.2 When present, psoas sign is fairly specific (0.95), but not sensitive (0.16).3
When evaluating patients in an outpatient setting, we have a snapshot of a disease process—a still frame of a movie. We are told what happened up to that point (with varying degrees of accuracy). But like the patient, we don’t know what will happen after the patient leaves the office: The still frame is gone, but the movie continues.
It can be helpful to inform patients of the concerning diagnoses in your differential and alert them to patterns of clinical progression that warrant return or immediate emergency department evaluation. Calling the patient to see how he or she is doing can be very useful for clinicians, and generally highly valued and appreciated by patients. Here, if gastroenteritis were suspected, a phone call after a few hours of antiemetic and rehydration therapy may have been helpful to determine if the patient’s symptoms had improved. This, of course, would not be conclusive—but at least it would give the clinician additional information and the patient additional comfort.
In this case, the jury was persuaded that the NP provided good treatment and acted within the standard of care. Diagnosing appendicitis can be tricky, even under the best circumstances. The NP’s defense was probably aided by good documentation showing that appendicitis seemed less likely at the time of her evaluation. Ultimately, she performed well enough that her care withstood scrutiny from the plaintiff, the plaintiff’s expert witness, and eventually, her own practice.
This case was interesting from a legal perspective in that the plaintiff originally failed to file suit against the NP—probably resorting to liability under the theory of respondeat superior (generally, employer liability for employee actions). While the plaintiff was unsuccessful in adding the NP later, due to the statue of limitations, the NP was brought into the case by her own practice, through a procedure known as “impleader.” An impleader action is brought by a co-defendant. Under typical impleader rules, the defendant becomes a “third-party plaintiff” and brings suit against a “third-party defendant” (in this case, the practice and the NP, respectively).
In sum, always keep important diagnoses in mind, and document well. Anticipate a changing clinical course, and instruct patients on how to respond to those changes. In certain cases, we are well served to pick up the phone, check on the patient, and make the presentation less of a static picture and more of a dynamic movie. —DML
References
1. Craig S, Brenner BE. Appendicitis (updated October 26, 2012). Medscape Reference. http://emedicine.medscape.com/article/773895-overview. Accessed August 14, 2013.
2. Yeh B. Evidence-based emergency medicine/rational clinical examination abstract: does this adult patient have appendicitis?.Ann Emerg Med. 2008;52(3):301-303.
3. Wagner J, McKinney WP, Carpenter JL. Does this patient have appendicitis? JAMA. 1996;276(19):1589-1594.
C difficile Infection Misdiagnosed
A 42-year-old woman underwent a hysterectomy performed by the defendant gynecologist at a New York City medical center. During the patient’s postsurgical hospitalization, she had a persistent fever, and it was noted that her leukocyte count had doubled. The gynecologist made a diagnosis of urinary tract infection (UTI) and prescribed ciprofloxacin. The woman was discharged four days after her surgery.
Four days later, she returned to the gynecologist’s office complaining of severe abdominal pain and vomiting. The gynecologist prescribed antacids and advised her to continue taking ciprofloxacin.
Three days after the office visit, the patient was hospitalized and diagnosed with Clostridium difficile colitis, which had caused colon perforation and subsequent peritonitis. The patient’s condition required a partial resection of the colon and creation of a colostomy, which was reversed six months later. The patient now has abdominal scarring and has developed an incisional hernia.
The plaintiff claimed that her C difficile infection developed shortly after her hysterectomy and that the defendant should have diagnosed and treated it, thus avoiding the resulting damage to her colon. The plaintiff claimed that she was given prophylactic antibiotics prior to surgery and that the defendant should have considered that the antibiotics and/or the procedure placed her at risk for C difficile colitis. The plaintiff also contended that ciprofloxacin should not have been prescribed and that its use likely worsened her infection.
The defendant claimed that the plaintiff’s symptoms did not suggest a C difficile infection and that no testing was warranted. The defendant acknowledged that ciprofloxacin may have allowed the proliferation of the plaintiff’s infection but that it was not negligent for him to prescribe the drug. Finally, the defendant claimed that the plaintiff’s infection was not preventable and could not have been diagnosed earlier.
Outcome
According to a published account, a $776,000 verdict was returned.
Comment
Complications arising from the use of antibiotics are well known but occur with relative infrequency. Although clindamycin is known for causing pseudomembranous colitis, virtually any antibiotic may be implicated.
It is possible for pseudomembranous colitis to occur after a single dose, and symptoms can develop several weeks after antibiotics have been stopped. Other lesser-known risk factors for this condition include use of proton pump inhibitors or antineoplastic agents; any condition that slows gut motility; age older than 65; use of enteral tube feeding; chronic debilitation; and critical illness.
In this case, the patient presented with abdominal pain and vomiting (not unusual symptoms following general surgery), but apparently without diarrhea; this complicates the early diagnostic picture for colitis. The symptoms were unfortunate for the patient, but it would have been a difficult diagnosis for the clinician to make.
The jury was likely impressed by testimony describing the patient’s colonic perforation and would have been shocked by the need to perform a colostomy (even though it was reversed six months later). Some jurors automatically equate an unfortunate result with malpractice and will quickly reach that conclusion when presented with a compelling story—skipping the issue of whether the clinician actually made a mistake.
It is the defense attorney’s job to make sure that jurors selected for malpractice cases will actually decide that malpractice exists before concluding negligence and awarding damages. I used to ask potential jurors if they agreed with this statement: “In this day and age, if a patient has a bad outcome, someone probably made a mistake.” A surprising number of potential jurors would answer “Yes,” indicating a predisposition to hold clinicians accountable for a bad outcome, even clinicians who performed well and acted in conformity with the standard of care.
Sometimes all we, as clinicians, can do is show patients the concern and attention they deserve, do our best, and make sure an adequate professional liability policy is in place. —DML
Cases reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
A 42-year-old woman underwent a hysterectomy performed by the defendant gynecologist at a New York City medical center. During the patient’s postsurgical hospitalization, she had a persistent fever, and it was noted that her leukocyte count had doubled. The gynecologist made a diagnosis of urinary tract infection (UTI) and prescribed ciprofloxacin. The woman was discharged four days after her surgery.
Four days later, she returned to the gynecologist’s office complaining of severe abdominal pain and vomiting. The gynecologist prescribed antacids and advised her to continue taking ciprofloxacin.
Three days after the office visit, the patient was hospitalized and diagnosed with Clostridium difficile colitis, which had caused colon perforation and subsequent peritonitis. The patient’s condition required a partial resection of the colon and creation of a colostomy, which was reversed six months later. The patient now has abdominal scarring and has developed an incisional hernia.
The plaintiff claimed that her C difficile infection developed shortly after her hysterectomy and that the defendant should have diagnosed and treated it, thus avoiding the resulting damage to her colon. The plaintiff claimed that she was given prophylactic antibiotics prior to surgery and that the defendant should have considered that the antibiotics and/or the procedure placed her at risk for C difficile colitis. The plaintiff also contended that ciprofloxacin should not have been prescribed and that its use likely worsened her infection.
The defendant claimed that the plaintiff’s symptoms did not suggest a C difficile infection and that no testing was warranted. The defendant acknowledged that ciprofloxacin may have allowed the proliferation of the plaintiff’s infection but that it was not negligent for him to prescribe the drug. Finally, the defendant claimed that the plaintiff’s infection was not preventable and could not have been diagnosed earlier.
Outcome
According to a published account, a $776,000 verdict was returned.
Comment
Complications arising from the use of antibiotics are well known but occur with relative infrequency. Although clindamycin is known for causing pseudomembranous colitis, virtually any antibiotic may be implicated.
It is possible for pseudomembranous colitis to occur after a single dose, and symptoms can develop several weeks after antibiotics have been stopped. Other lesser-known risk factors for this condition include use of proton pump inhibitors or antineoplastic agents; any condition that slows gut motility; age older than 65; use of enteral tube feeding; chronic debilitation; and critical illness.
In this case, the patient presented with abdominal pain and vomiting (not unusual symptoms following general surgery), but apparently without diarrhea; this complicates the early diagnostic picture for colitis. The symptoms were unfortunate for the patient, but it would have been a difficult diagnosis for the clinician to make.
The jury was likely impressed by testimony describing the patient’s colonic perforation and would have been shocked by the need to perform a colostomy (even though it was reversed six months later). Some jurors automatically equate an unfortunate result with malpractice and will quickly reach that conclusion when presented with a compelling story—skipping the issue of whether the clinician actually made a mistake.
It is the defense attorney’s job to make sure that jurors selected for malpractice cases will actually decide that malpractice exists before concluding negligence and awarding damages. I used to ask potential jurors if they agreed with this statement: “In this day and age, if a patient has a bad outcome, someone probably made a mistake.” A surprising number of potential jurors would answer “Yes,” indicating a predisposition to hold clinicians accountable for a bad outcome, even clinicians who performed well and acted in conformity with the standard of care.
Sometimes all we, as clinicians, can do is show patients the concern and attention they deserve, do our best, and make sure an adequate professional liability policy is in place. —DML
Cases reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.
A 42-year-old woman underwent a hysterectomy performed by the defendant gynecologist at a New York City medical center. During the patient’s postsurgical hospitalization, she had a persistent fever, and it was noted that her leukocyte count had doubled. The gynecologist made a diagnosis of urinary tract infection (UTI) and prescribed ciprofloxacin. The woman was discharged four days after her surgery.
Four days later, she returned to the gynecologist’s office complaining of severe abdominal pain and vomiting. The gynecologist prescribed antacids and advised her to continue taking ciprofloxacin.
Three days after the office visit, the patient was hospitalized and diagnosed with Clostridium difficile colitis, which had caused colon perforation and subsequent peritonitis. The patient’s condition required a partial resection of the colon and creation of a colostomy, which was reversed six months later. The patient now has abdominal scarring and has developed an incisional hernia.
The plaintiff claimed that her C difficile infection developed shortly after her hysterectomy and that the defendant should have diagnosed and treated it, thus avoiding the resulting damage to her colon. The plaintiff claimed that she was given prophylactic antibiotics prior to surgery and that the defendant should have considered that the antibiotics and/or the procedure placed her at risk for C difficile colitis. The plaintiff also contended that ciprofloxacin should not have been prescribed and that its use likely worsened her infection.
The defendant claimed that the plaintiff’s symptoms did not suggest a C difficile infection and that no testing was warranted. The defendant acknowledged that ciprofloxacin may have allowed the proliferation of the plaintiff’s infection but that it was not negligent for him to prescribe the drug. Finally, the defendant claimed that the plaintiff’s infection was not preventable and could not have been diagnosed earlier.
Outcome
According to a published account, a $776,000 verdict was returned.
Comment
Complications arising from the use of antibiotics are well known but occur with relative infrequency. Although clindamycin is known for causing pseudomembranous colitis, virtually any antibiotic may be implicated.
It is possible for pseudomembranous colitis to occur after a single dose, and symptoms can develop several weeks after antibiotics have been stopped. Other lesser-known risk factors for this condition include use of proton pump inhibitors or antineoplastic agents; any condition that slows gut motility; age older than 65; use of enteral tube feeding; chronic debilitation; and critical illness.
In this case, the patient presented with abdominal pain and vomiting (not unusual symptoms following general surgery), but apparently without diarrhea; this complicates the early diagnostic picture for colitis. The symptoms were unfortunate for the patient, but it would have been a difficult diagnosis for the clinician to make.
The jury was likely impressed by testimony describing the patient’s colonic perforation and would have been shocked by the need to perform a colostomy (even though it was reversed six months later). Some jurors automatically equate an unfortunate result with malpractice and will quickly reach that conclusion when presented with a compelling story—skipping the issue of whether the clinician actually made a mistake.
It is the defense attorney’s job to make sure that jurors selected for malpractice cases will actually decide that malpractice exists before concluding negligence and awarding damages. I used to ask potential jurors if they agreed with this statement: “In this day and age, if a patient has a bad outcome, someone probably made a mistake.” A surprising number of potential jurors would answer “Yes,” indicating a predisposition to hold clinicians accountable for a bad outcome, even clinicians who performed well and acted in conformity with the standard of care.
Sometimes all we, as clinicians, can do is show patients the concern and attention they deserve, do our best, and make sure an adequate professional liability policy is in place. —DML
Cases reprinted with permission from Medical Malpractice Verdicts, Settlements and Experts, Lewis Laska, Editor, (800) 298-6288.