User login
How to Handle Medicare Documentation Audits

The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
PIAA Director of Research and Loss Prevention Discusses Hospitalist Insurance Premiums
Click here to listen to more of our interview with Divya Parikh
Click here to listen to more of our interview with Divya Parikh
Click here to listen to more of our interview with Divya Parikh
Why Hospitalists Remain Outside Malpractice Insurers' High-Risk Categories, For Now

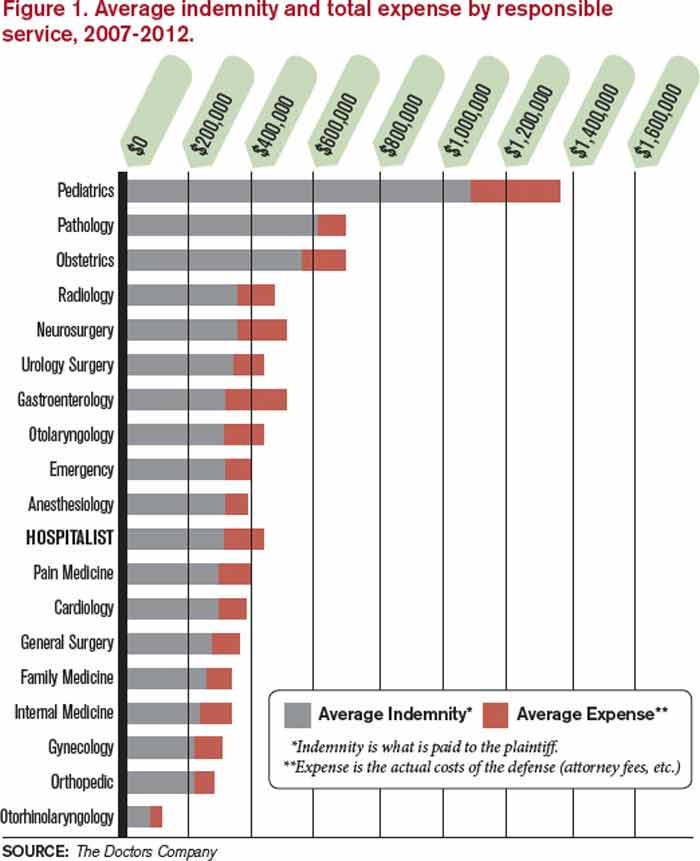
Source: The Doctors Company
Ten years ago, the national headlines on malpractice insurance were staggering. Media reports catalogued OB-GYNs who proclaimed they were shutting down their private practices in the face of runaway premiums. Surgeons and other proceduralists decried payments tied to lawsuits they’d argue were arbitrary and capricious. And the American Medical Association (AMA) made announcement after announcement about states being in a “malpractice crisis.”
In recent years, premiums have actually dropped and stabilized at levels that most physicians agree are manageable for bottom lines. But, in that time, there has been scant discussion about hospital medicine’s relationship with malpractice. It’s not because the issue isn’t omnipresent for all healthcare practitioners, including the relatively nascent specialty that is HM.
Practice management experts say anecdotally that delayed diagnosis of, or treatment for, a spinal epidural abscess (SEA) is likely to get more than a few hospitalists sued. And, the proliferation of co-management of other specialties—particularly those with higher risk of incidence and higher premiums than internal medicine—open up hospitalists to further liability.
The issue is that at less than 20 years as a specialty, HM is in its infancy when it comes to its interaction with malpractice premiums. Health insurance companies and trade groups that track the insurance industry are just beginning to have enough data on claims, premiums, and payouts to make recommendations on risk factors, risk mitigation, and potential trends.
Still, even in a landscape of limited information, there are a few rules of thumb hospitalist group leaders should live by when it comes to managing exposure to malpractice cases, according to interviews with a half dozen healthcare professionals:
- Know how your coverage works. Is there “tail coverage” that ensures you have protection for incidents that happened at an institution where you no longer practice? Even though hospital-employed physicians rarely have rate discussions directly (the hospital typically covers premiums as part of the compensation package), take the time to learn the basic details.
- Be diligent in documentation. Note concerns in charts when appropriate, and stand up for your point of view. There’s a fine line between picking fights with other physicians involved in a patient’s care and making your concerns known, but don’t be afraid to put your clinical view on the record.
- Avoid the practice of “defensive medicine.” Ordering tests and procedures that aren’t clinically necessary might seem like it can serve as a protection from later lawsuits, but it adds to healthcare costs and is just not the right thing to do, says hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, who has studied the phenomenon (see “Culture Shift Necessary to Defeat “Defensive” Medicine,” on p. 38).
- Recognize the risks associated with co-management. Caring for neurology, cardiology, and other subspecialty patients is a revenue boost for HM groups, but when some of those complex cases have adverse events, the hospitalist who interacted with the patient daily could be included in a lawsuit.
- Focus on communication skills. An analysis of claims data by The Doctors Company (TDC) (www.thedoctors.com), a medical malpractice insurance company exclusively endorsed by SHM, reports that the second most common factor contributing to patient injury by hospitalists is “communication breakdown among healthcare professionals.”
- Manage workloads to avoid burnout. Don’t take on too many patients at the expense of being involved in hospital committees or quality initiatives.
To be sure, many of the same tenets of being a productive hospitalist with high patient satisfaction scores—maintain manageable censuses; focus on patient centeredness; and use checklists, technology, and regimented protocols to reduce adverse events—translate very well to being a lower-risk hospitalist in relation to malpractice cases.
When you’re “thinking of patient satisfaction strategies, also think of them as risk mitigation strategies,” says John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., an SHM co-founder and practice management columnist for The Hospitalist. “They overlap tremendously.”
A History Lesson
Medical malpractice has been around for centuries and has two prevailing goals: 1) to provide monetary remuneration to patients who have been injured via substandard care and 2) to deter that poor treatment through fiscal punishment.
Malpractice lawsuits were not prevalent enough to be a major medical concern until the early 1800s. By the middle of the 19th century, the country hit its first periods of crisis.1 Cycles ebbed and flowed from there, with malpractice premiums causing crises in the 1980s and again in the early 2000s.
continued below...
Now, rates for medical professional liability insurance have been dropping for seven years, and an eighth straight annual decline is expected this year, according to Mike Matray, the editor of trade publication Medical Liability Monitor and the chief content officer of its associated website, www.mymedicalmalpracticeinsurance.com.
“We are in the longest, deepest soft market that the malpractice insurance industry has ever been in,” he says. “Right now, things are really good for the doctors, as far as rates coming down.”
Matray says he understands that declining rates may seem immaterial to a physician who receives an insurance bill that eats into the bottom line. For some specialties, that premium can be as high as $200,000 per physician, per year—or more.
“I’m not saying it isn’t expensive,” he adds. “It’s expensive to run a medical practice. At the same time, medical malpractice insurance is less expensive in today’s dollars than it was in 2005.”
The reduction in rates is multi-faceted. Prominently, state-level tort reforms like non-economic damage caps, health courts, and arbitration hearings are making it harder to bring cases to trial, particularly for lawyers who take cases on contingency. Second, frivolous lawsuits “are making an impression on jury pools,” Matray says, which means fewer filed claims and fewer cases that make it to trial. Third, this soft cycle has outlasted the typical pattern of rates falling for three to four years before rebounding.
“A lot of smart actuaries keep saying this has to change soon, because in a soft market there is a lot of competition,” he says, noting that in order to compete for low rates, insurance companies offer credits to clients and use their own reserve cash piles. “So things are really going to change in the next couple of years.”

—Robin Diamond, senior vice president and chief patient safety officer, The Doctors Company
In Need of Data, Patience
So what does it all mean for hospitalists and HM group leaders looking to be proactive about medical malpractice liability insurance? Patience is required.
For starters, there is no designated premium category for hospitalists. Much like the situation that exists for coding issues, the closest proxy for HM is internal medicine. According to Medical Liability Monitor, the premium paid by internal medicine physicians as of July 1, 2012, varied widely across the country. In South Florida, internal medicine insurance premiums in Miami, Dade, and Broward counties were between $42,000 and $46,000 per year. In South Dakota, one insurer reported rates of just under $4,000 per year. There is no average or median figure available, and Matray notes that actual rates paid can vary from county to county.
Moreover, it is difficult for group leaders or hospital executives to use past history to negotiate rates with insurers because of a shortage of reliable data. In its spring 2013 newsletter, the PIAA (formerly known as the Physician Insurers Association of America) published its first report on hospitalist claims reported to its Data Sharing Project. Of the 92,868 closed claims reported from 2002-2011, just 312, or 0.3%, named hospitalists as the defendant.
The data also showed that, of those claims, 20% were settled through insurance company payments. Those payments totaled $17.1 million, with an average payout to a claimant (known as the indemnity) of $272,553 per claim. Overall, hospitalists had a 20% paid-to-closed ratio, totaling more than $17.1 million. By comparison, the percent of paid-to-closed claims for all physicians was 29.3%, according to PIAA.
In a separate data set compiled this year by TDC, 34% of allegations against hospitalists were related to missed or failed diagnoses, with 28% tied to “improper management of treatment.” Twelve percent of allegations were the result of either improper medication management or ordering errors.
Robin Diamond, TDC’s senior vice president and chief patient safety officer, says that teasing out trends from the initial data can be challenging. Hospitalists, she says, can deal with so many different patients, diseases, and severity levels that it is difficult to draw conclusions.
“Hospital medicine is different than other specialties, because the hospitalist treats a broad range of patients in an acute care setting—from a pediatric patient to an adult patient with many chronic illnesses,” she says.
Divya Parikh, PIAA’s director of research and loss prevention, says HM group leaders should avoid reading too much into the first batch of data, because it’s a small sample size.
“A big part of that is we feel that a lot of hospitalists are intermingled into the other medical specialties,” she says. “So this becomes a very small subset where they are distinctly identified as hospitalists. And that’s the challenge.”
In particular, Parikh is curious to see whether HM’s rate of claims paid through insurance payments drops from 20% (already below the overall healthcare industry average). “It will be interesting as we proceed...to see if they begin to mitigate areas of risk where we used to see a lot of claims,” she adds. “If you look at a hospital setting, there has been some shift change in what the errors are. And, what you’d hope with hospitalists within these environments who are really owning this specialty, is that you’d see a decrease in that. There would be that connective care. There would be the patient that felt that they had an individual who was their go-to individual throughout their care at a hospital.”
A Peek at the Future
Insurers have begun compiling claims data on hospitalists and are taking a longer-term view of the specialty. TDC, for example, has analyzed its data and identified characteristics it says make a low-risk hospitalist, an analysis the company says is the first of its kind (see Figure 1). The insurer adds that it sees its responsibility as making sure everyone understands the hospitalist’s role within the acute care setting so that its pricing is commensurate with the liability risk.
Source: The Doctors Company
“We’re looking at the systems within the hospitalist group, as well as how well that group is integrating with the hospital where they’re practicing,” Diamond says. “What kind of patient mix is this particular hospitalist group seeing in that particular hospital, because it can be different in a large healthcare corporation in Manhattan, New York, from a community hospital in rural Texas.”
The growing popularity of hospitalists taking on co-management responsibilities for other specialties is another trend to keep an eye on, as it creates what insurers call “vicarious liability.” Working together in teams with other specialties can improve communication, reduce errors during transitions of care, and create better outcomes. However, in instances where there are problems, being on a care team means hospitalists can open themselves to liability. To mitigate that risk, hospitalists can look to other groups that have dealt with shared liability issues in the past, Parikh says.
“Historically, you would have seen it with anesthesiology,” she explains. “And one huge improvement anesthesiologists have made when a patient comes in for a surgery now is they come out, introduce themselves, say hello, and tell you what’s going on. They put a face to the name, so that it’s not just a no-name anesthesiologist who gets included in the lawsuit as well because they’re naming everybody in the group.”
But, holistically, the best long-term mitigation strategy appears to be tort reform and new ways of looking at the way in which healthcare liability issues are handled in the U.S., says Anupam Jena, MD, PhD, assistant professor of healthcare policy and medicine at Harvard Medical School, and an internist at Massachusetts General Hospital, both in Boston. Dr. Jena says that there is limited evidence that enacted malpractice reforms have produced more than a 2% to 5% reduction in healthcare spending compared to states that have not.2 Instead, healthcare leaders should push for the elimination of defensive medicine, which he says contributes the lion’s share of the estimated $50 billion annual cost of malpractice liability across the country.
“Do I think the country is in a malpractice crisis? No,” he says. “Do I think that defensive medicine is larger than we think it is? Yes.
“If physicians practice as they felt they should practice without ordering extra tests and procedures, my guess would be you could reduce healthcare spending by substantially more than $50 billion.”
Richard Quinn is a freelance writer in New Jersey.
References
- Spiegel AD, Kavaler F. America’s first medical malpractice crisis, 1835-1865. J Community Health. 1997;22:283-308.
- Chandra A, Jena A, Seabury, S. Defensive medicine may be costlier than it seems. The Wall Street Journal website. http://online.wsj.com/article/SB10001424127887323701904578280112638373302.html. Accessed September 21, 2013.
Source: The Doctors Company
Ten years ago, the national headlines on malpractice insurance were staggering. Media reports catalogued OB-GYNs who proclaimed they were shutting down their private practices in the face of runaway premiums. Surgeons and other proceduralists decried payments tied to lawsuits they’d argue were arbitrary and capricious. And the American Medical Association (AMA) made announcement after announcement about states being in a “malpractice crisis.”
In recent years, premiums have actually dropped and stabilized at levels that most physicians agree are manageable for bottom lines. But, in that time, there has been scant discussion about hospital medicine’s relationship with malpractice. It’s not because the issue isn’t omnipresent for all healthcare practitioners, including the relatively nascent specialty that is HM.
Practice management experts say anecdotally that delayed diagnosis of, or treatment for, a spinal epidural abscess (SEA) is likely to get more than a few hospitalists sued. And, the proliferation of co-management of other specialties—particularly those with higher risk of incidence and higher premiums than internal medicine—open up hospitalists to further liability.
The issue is that at less than 20 years as a specialty, HM is in its infancy when it comes to its interaction with malpractice premiums. Health insurance companies and trade groups that track the insurance industry are just beginning to have enough data on claims, premiums, and payouts to make recommendations on risk factors, risk mitigation, and potential trends.
Still, even in a landscape of limited information, there are a few rules of thumb hospitalist group leaders should live by when it comes to managing exposure to malpractice cases, according to interviews with a half dozen healthcare professionals:
- Know how your coverage works. Is there “tail coverage” that ensures you have protection for incidents that happened at an institution where you no longer practice? Even though hospital-employed physicians rarely have rate discussions directly (the hospital typically covers premiums as part of the compensation package), take the time to learn the basic details.
- Be diligent in documentation. Note concerns in charts when appropriate, and stand up for your point of view. There’s a fine line between picking fights with other physicians involved in a patient’s care and making your concerns known, but don’t be afraid to put your clinical view on the record.
- Avoid the practice of “defensive medicine.” Ordering tests and procedures that aren’t clinically necessary might seem like it can serve as a protection from later lawsuits, but it adds to healthcare costs and is just not the right thing to do, says hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, who has studied the phenomenon (see “Culture Shift Necessary to Defeat “Defensive” Medicine,” on p. 38).
- Recognize the risks associated with co-management. Caring for neurology, cardiology, and other subspecialty patients is a revenue boost for HM groups, but when some of those complex cases have adverse events, the hospitalist who interacted with the patient daily could be included in a lawsuit.
- Focus on communication skills. An analysis of claims data by The Doctors Company (TDC) (www.thedoctors.com), a medical malpractice insurance company exclusively endorsed by SHM, reports that the second most common factor contributing to patient injury by hospitalists is “communication breakdown among healthcare professionals.”
- Manage workloads to avoid burnout. Don’t take on too many patients at the expense of being involved in hospital committees or quality initiatives.
To be sure, many of the same tenets of being a productive hospitalist with high patient satisfaction scores—maintain manageable censuses; focus on patient centeredness; and use checklists, technology, and regimented protocols to reduce adverse events—translate very well to being a lower-risk hospitalist in relation to malpractice cases.
When you’re “thinking of patient satisfaction strategies, also think of them as risk mitigation strategies,” says John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., an SHM co-founder and practice management columnist for The Hospitalist. “They overlap tremendously.”
A History Lesson
Medical malpractice has been around for centuries and has two prevailing goals: 1) to provide monetary remuneration to patients who have been injured via substandard care and 2) to deter that poor treatment through fiscal punishment.
Malpractice lawsuits were not prevalent enough to be a major medical concern until the early 1800s. By the middle of the 19th century, the country hit its first periods of crisis.1 Cycles ebbed and flowed from there, with malpractice premiums causing crises in the 1980s and again in the early 2000s.
continued below...
Now, rates for medical professional liability insurance have been dropping for seven years, and an eighth straight annual decline is expected this year, according to Mike Matray, the editor of trade publication Medical Liability Monitor and the chief content officer of its associated website, www.mymedicalmalpracticeinsurance.com.
“We are in the longest, deepest soft market that the malpractice insurance industry has ever been in,” he says. “Right now, things are really good for the doctors, as far as rates coming down.”
Matray says he understands that declining rates may seem immaterial to a physician who receives an insurance bill that eats into the bottom line. For some specialties, that premium can be as high as $200,000 per physician, per year—or more.
“I’m not saying it isn’t expensive,” he adds. “It’s expensive to run a medical practice. At the same time, medical malpractice insurance is less expensive in today’s dollars than it was in 2005.”
The reduction in rates is multi-faceted. Prominently, state-level tort reforms like non-economic damage caps, health courts, and arbitration hearings are making it harder to bring cases to trial, particularly for lawyers who take cases on contingency. Second, frivolous lawsuits “are making an impression on jury pools,” Matray says, which means fewer filed claims and fewer cases that make it to trial. Third, this soft cycle has outlasted the typical pattern of rates falling for three to four years before rebounding.
“A lot of smart actuaries keep saying this has to change soon, because in a soft market there is a lot of competition,” he says, noting that in order to compete for low rates, insurance companies offer credits to clients and use their own reserve cash piles. “So things are really going to change in the next couple of years.”
—Robin Diamond, senior vice president and chief patient safety officer, The Doctors Company
In Need of Data, Patience
So what does it all mean for hospitalists and HM group leaders looking to be proactive about medical malpractice liability insurance? Patience is required.
For starters, there is no designated premium category for hospitalists. Much like the situation that exists for coding issues, the closest proxy for HM is internal medicine. According to Medical Liability Monitor, the premium paid by internal medicine physicians as of July 1, 2012, varied widely across the country. In South Florida, internal medicine insurance premiums in Miami, Dade, and Broward counties were between $42,000 and $46,000 per year. In South Dakota, one insurer reported rates of just under $4,000 per year. There is no average or median figure available, and Matray notes that actual rates paid can vary from county to county.
Moreover, it is difficult for group leaders or hospital executives to use past history to negotiate rates with insurers because of a shortage of reliable data. In its spring 2013 newsletter, the PIAA (formerly known as the Physician Insurers Association of America) published its first report on hospitalist claims reported to its Data Sharing Project. Of the 92,868 closed claims reported from 2002-2011, just 312, or 0.3%, named hospitalists as the defendant.
The data also showed that, of those claims, 20% were settled through insurance company payments. Those payments totaled $17.1 million, with an average payout to a claimant (known as the indemnity) of $272,553 per claim. Overall, hospitalists had a 20% paid-to-closed ratio, totaling more than $17.1 million. By comparison, the percent of paid-to-closed claims for all physicians was 29.3%, according to PIAA.
In a separate data set compiled this year by TDC, 34% of allegations against hospitalists were related to missed or failed diagnoses, with 28% tied to “improper management of treatment.” Twelve percent of allegations were the result of either improper medication management or ordering errors.
Robin Diamond, TDC’s senior vice president and chief patient safety officer, says that teasing out trends from the initial data can be challenging. Hospitalists, she says, can deal with so many different patients, diseases, and severity levels that it is difficult to draw conclusions.
“Hospital medicine is different than other specialties, because the hospitalist treats a broad range of patients in an acute care setting—from a pediatric patient to an adult patient with many chronic illnesses,” she says.
Divya Parikh, PIAA’s director of research and loss prevention, says HM group leaders should avoid reading too much into the first batch of data, because it’s a small sample size.
“A big part of that is we feel that a lot of hospitalists are intermingled into the other medical specialties,” she says. “So this becomes a very small subset where they are distinctly identified as hospitalists. And that’s the challenge.”
In particular, Parikh is curious to see whether HM’s rate of claims paid through insurance payments drops from 20% (already below the overall healthcare industry average). “It will be interesting as we proceed...to see if they begin to mitigate areas of risk where we used to see a lot of claims,” she adds. “If you look at a hospital setting, there has been some shift change in what the errors are. And, what you’d hope with hospitalists within these environments who are really owning this specialty, is that you’d see a decrease in that. There would be that connective care. There would be the patient that felt that they had an individual who was their go-to individual throughout their care at a hospital.”
A Peek at the Future
Insurers have begun compiling claims data on hospitalists and are taking a longer-term view of the specialty. TDC, for example, has analyzed its data and identified characteristics it says make a low-risk hospitalist, an analysis the company says is the first of its kind (see Figure 1). The insurer adds that it sees its responsibility as making sure everyone understands the hospitalist’s role within the acute care setting so that its pricing is commensurate with the liability risk.
Source: The Doctors Company
“We’re looking at the systems within the hospitalist group, as well as how well that group is integrating with the hospital where they’re practicing,” Diamond says. “What kind of patient mix is this particular hospitalist group seeing in that particular hospital, because it can be different in a large healthcare corporation in Manhattan, New York, from a community hospital in rural Texas.”
The growing popularity of hospitalists taking on co-management responsibilities for other specialties is another trend to keep an eye on, as it creates what insurers call “vicarious liability.” Working together in teams with other specialties can improve communication, reduce errors during transitions of care, and create better outcomes. However, in instances where there are problems, being on a care team means hospitalists can open themselves to liability. To mitigate that risk, hospitalists can look to other groups that have dealt with shared liability issues in the past, Parikh says.
“Historically, you would have seen it with anesthesiology,” she explains. “And one huge improvement anesthesiologists have made when a patient comes in for a surgery now is they come out, introduce themselves, say hello, and tell you what’s going on. They put a face to the name, so that it’s not just a no-name anesthesiologist who gets included in the lawsuit as well because they’re naming everybody in the group.”
But, holistically, the best long-term mitigation strategy appears to be tort reform and new ways of looking at the way in which healthcare liability issues are handled in the U.S., says Anupam Jena, MD, PhD, assistant professor of healthcare policy and medicine at Harvard Medical School, and an internist at Massachusetts General Hospital, both in Boston. Dr. Jena says that there is limited evidence that enacted malpractice reforms have produced more than a 2% to 5% reduction in healthcare spending compared to states that have not.2 Instead, healthcare leaders should push for the elimination of defensive medicine, which he says contributes the lion’s share of the estimated $50 billion annual cost of malpractice liability across the country.
“Do I think the country is in a malpractice crisis? No,” he says. “Do I think that defensive medicine is larger than we think it is? Yes.
“If physicians practice as they felt they should practice without ordering extra tests and procedures, my guess would be you could reduce healthcare spending by substantially more than $50 billion.”
Richard Quinn is a freelance writer in New Jersey.
References
- Spiegel AD, Kavaler F. America’s first medical malpractice crisis, 1835-1865. J Community Health. 1997;22:283-308.
- Chandra A, Jena A, Seabury, S. Defensive medicine may be costlier than it seems. The Wall Street Journal website. http://online.wsj.com/article/SB10001424127887323701904578280112638373302.html. Accessed September 21, 2013.
Source: The Doctors Company
Ten years ago, the national headlines on malpractice insurance were staggering. Media reports catalogued OB-GYNs who proclaimed they were shutting down their private practices in the face of runaway premiums. Surgeons and other proceduralists decried payments tied to lawsuits they’d argue were arbitrary and capricious. And the American Medical Association (AMA) made announcement after announcement about states being in a “malpractice crisis.”
In recent years, premiums have actually dropped and stabilized at levels that most physicians agree are manageable for bottom lines. But, in that time, there has been scant discussion about hospital medicine’s relationship with malpractice. It’s not because the issue isn’t omnipresent for all healthcare practitioners, including the relatively nascent specialty that is HM.
Practice management experts say anecdotally that delayed diagnosis of, or treatment for, a spinal epidural abscess (SEA) is likely to get more than a few hospitalists sued. And, the proliferation of co-management of other specialties—particularly those with higher risk of incidence and higher premiums than internal medicine—open up hospitalists to further liability.
The issue is that at less than 20 years as a specialty, HM is in its infancy when it comes to its interaction with malpractice premiums. Health insurance companies and trade groups that track the insurance industry are just beginning to have enough data on claims, premiums, and payouts to make recommendations on risk factors, risk mitigation, and potential trends.
Still, even in a landscape of limited information, there are a few rules of thumb hospitalist group leaders should live by when it comes to managing exposure to malpractice cases, according to interviews with a half dozen healthcare professionals:
- Know how your coverage works. Is there “tail coverage” that ensures you have protection for incidents that happened at an institution where you no longer practice? Even though hospital-employed physicians rarely have rate discussions directly (the hospital typically covers premiums as part of the compensation package), take the time to learn the basic details.
- Be diligent in documentation. Note concerns in charts when appropriate, and stand up for your point of view. There’s a fine line between picking fights with other physicians involved in a patient’s care and making your concerns known, but don’t be afraid to put your clinical view on the record.
- Avoid the practice of “defensive medicine.” Ordering tests and procedures that aren’t clinically necessary might seem like it can serve as a protection from later lawsuits, but it adds to healthcare costs and is just not the right thing to do, says hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, who has studied the phenomenon (see “Culture Shift Necessary to Defeat “Defensive” Medicine,” on p. 38).
- Recognize the risks associated with co-management. Caring for neurology, cardiology, and other subspecialty patients is a revenue boost for HM groups, but when some of those complex cases have adverse events, the hospitalist who interacted with the patient daily could be included in a lawsuit.
- Focus on communication skills. An analysis of claims data by The Doctors Company (TDC) (www.thedoctors.com), a medical malpractice insurance company exclusively endorsed by SHM, reports that the second most common factor contributing to patient injury by hospitalists is “communication breakdown among healthcare professionals.”
- Manage workloads to avoid burnout. Don’t take on too many patients at the expense of being involved in hospital committees or quality initiatives.
To be sure, many of the same tenets of being a productive hospitalist with high patient satisfaction scores—maintain manageable censuses; focus on patient centeredness; and use checklists, technology, and regimented protocols to reduce adverse events—translate very well to being a lower-risk hospitalist in relation to malpractice cases.
When you’re “thinking of patient satisfaction strategies, also think of them as risk mitigation strategies,” says John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., an SHM co-founder and practice management columnist for The Hospitalist. “They overlap tremendously.”
A History Lesson
Medical malpractice has been around for centuries and has two prevailing goals: 1) to provide monetary remuneration to patients who have been injured via substandard care and 2) to deter that poor treatment through fiscal punishment.
Malpractice lawsuits were not prevalent enough to be a major medical concern until the early 1800s. By the middle of the 19th century, the country hit its first periods of crisis.1 Cycles ebbed and flowed from there, with malpractice premiums causing crises in the 1980s and again in the early 2000s.
continued below...
Now, rates for medical professional liability insurance have been dropping for seven years, and an eighth straight annual decline is expected this year, according to Mike Matray, the editor of trade publication Medical Liability Monitor and the chief content officer of its associated website, www.mymedicalmalpracticeinsurance.com.
“We are in the longest, deepest soft market that the malpractice insurance industry has ever been in,” he says. “Right now, things are really good for the doctors, as far as rates coming down.”
Matray says he understands that declining rates may seem immaterial to a physician who receives an insurance bill that eats into the bottom line. For some specialties, that premium can be as high as $200,000 per physician, per year—or more.
“I’m not saying it isn’t expensive,” he adds. “It’s expensive to run a medical practice. At the same time, medical malpractice insurance is less expensive in today’s dollars than it was in 2005.”
The reduction in rates is multi-faceted. Prominently, state-level tort reforms like non-economic damage caps, health courts, and arbitration hearings are making it harder to bring cases to trial, particularly for lawyers who take cases on contingency. Second, frivolous lawsuits “are making an impression on jury pools,” Matray says, which means fewer filed claims and fewer cases that make it to trial. Third, this soft cycle has outlasted the typical pattern of rates falling for three to four years before rebounding.
“A lot of smart actuaries keep saying this has to change soon, because in a soft market there is a lot of competition,” he says, noting that in order to compete for low rates, insurance companies offer credits to clients and use their own reserve cash piles. “So things are really going to change in the next couple of years.”
—Robin Diamond, senior vice president and chief patient safety officer, The Doctors Company
In Need of Data, Patience
So what does it all mean for hospitalists and HM group leaders looking to be proactive about medical malpractice liability insurance? Patience is required.
For starters, there is no designated premium category for hospitalists. Much like the situation that exists for coding issues, the closest proxy for HM is internal medicine. According to Medical Liability Monitor, the premium paid by internal medicine physicians as of July 1, 2012, varied widely across the country. In South Florida, internal medicine insurance premiums in Miami, Dade, and Broward counties were between $42,000 and $46,000 per year. In South Dakota, one insurer reported rates of just under $4,000 per year. There is no average or median figure available, and Matray notes that actual rates paid can vary from county to county.
Moreover, it is difficult for group leaders or hospital executives to use past history to negotiate rates with insurers because of a shortage of reliable data. In its spring 2013 newsletter, the PIAA (formerly known as the Physician Insurers Association of America) published its first report on hospitalist claims reported to its Data Sharing Project. Of the 92,868 closed claims reported from 2002-2011, just 312, or 0.3%, named hospitalists as the defendant.
The data also showed that, of those claims, 20% were settled through insurance company payments. Those payments totaled $17.1 million, with an average payout to a claimant (known as the indemnity) of $272,553 per claim. Overall, hospitalists had a 20% paid-to-closed ratio, totaling more than $17.1 million. By comparison, the percent of paid-to-closed claims for all physicians was 29.3%, according to PIAA.
In a separate data set compiled this year by TDC, 34% of allegations against hospitalists were related to missed or failed diagnoses, with 28% tied to “improper management of treatment.” Twelve percent of allegations were the result of either improper medication management or ordering errors.
Robin Diamond, TDC’s senior vice president and chief patient safety officer, says that teasing out trends from the initial data can be challenging. Hospitalists, she says, can deal with so many different patients, diseases, and severity levels that it is difficult to draw conclusions.
“Hospital medicine is different than other specialties, because the hospitalist treats a broad range of patients in an acute care setting—from a pediatric patient to an adult patient with many chronic illnesses,” she says.
Divya Parikh, PIAA’s director of research and loss prevention, says HM group leaders should avoid reading too much into the first batch of data, because it’s a small sample size.
“A big part of that is we feel that a lot of hospitalists are intermingled into the other medical specialties,” she says. “So this becomes a very small subset where they are distinctly identified as hospitalists. And that’s the challenge.”
In particular, Parikh is curious to see whether HM’s rate of claims paid through insurance payments drops from 20% (already below the overall healthcare industry average). “It will be interesting as we proceed...to see if they begin to mitigate areas of risk where we used to see a lot of claims,” she adds. “If you look at a hospital setting, there has been some shift change in what the errors are. And, what you’d hope with hospitalists within these environments who are really owning this specialty, is that you’d see a decrease in that. There would be that connective care. There would be the patient that felt that they had an individual who was their go-to individual throughout their care at a hospital.”
A Peek at the Future
Insurers have begun compiling claims data on hospitalists and are taking a longer-term view of the specialty. TDC, for example, has analyzed its data and identified characteristics it says make a low-risk hospitalist, an analysis the company says is the first of its kind (see Figure 1). The insurer adds that it sees its responsibility as making sure everyone understands the hospitalist’s role within the acute care setting so that its pricing is commensurate with the liability risk.
Source: The Doctors Company
“We’re looking at the systems within the hospitalist group, as well as how well that group is integrating with the hospital where they’re practicing,” Diamond says. “What kind of patient mix is this particular hospitalist group seeing in that particular hospital, because it can be different in a large healthcare corporation in Manhattan, New York, from a community hospital in rural Texas.”
The growing popularity of hospitalists taking on co-management responsibilities for other specialties is another trend to keep an eye on, as it creates what insurers call “vicarious liability.” Working together in teams with other specialties can improve communication, reduce errors during transitions of care, and create better outcomes. However, in instances where there are problems, being on a care team means hospitalists can open themselves to liability. To mitigate that risk, hospitalists can look to other groups that have dealt with shared liability issues in the past, Parikh says.
“Historically, you would have seen it with anesthesiology,” she explains. “And one huge improvement anesthesiologists have made when a patient comes in for a surgery now is they come out, introduce themselves, say hello, and tell you what’s going on. They put a face to the name, so that it’s not just a no-name anesthesiologist who gets included in the lawsuit as well because they’re naming everybody in the group.”
But, holistically, the best long-term mitigation strategy appears to be tort reform and new ways of looking at the way in which healthcare liability issues are handled in the U.S., says Anupam Jena, MD, PhD, assistant professor of healthcare policy and medicine at Harvard Medical School, and an internist at Massachusetts General Hospital, both in Boston. Dr. Jena says that there is limited evidence that enacted malpractice reforms have produced more than a 2% to 5% reduction in healthcare spending compared to states that have not.2 Instead, healthcare leaders should push for the elimination of defensive medicine, which he says contributes the lion’s share of the estimated $50 billion annual cost of malpractice liability across the country.
“Do I think the country is in a malpractice crisis? No,” he says. “Do I think that defensive medicine is larger than we think it is? Yes.
“If physicians practice as they felt they should practice without ordering extra tests and procedures, my guess would be you could reduce healthcare spending by substantially more than $50 billion.”
Richard Quinn is a freelance writer in New Jersey.
References
- Spiegel AD, Kavaler F. America’s first medical malpractice crisis, 1835-1865. J Community Health. 1997;22:283-308.
- Chandra A, Jena A, Seabury, S. Defensive medicine may be costlier than it seems. The Wall Street Journal website. http://online.wsj.com/article/SB10001424127887323701904578280112638373302.html. Accessed September 21, 2013.
Addendum to MRI Report Not Communicated to Providers
In September 2006, a 42-year-old woman was transported to a medical center in New York City with symptoms of a manic bipolar episode. She was admitted and stabilized, and she remained in the hospital for 11 days.
During her hospitalization, an MRI of the brain was performed. The radiologist initially noted no significant findings. However, several hours later, he prepared an addendum to his report, indicating the presence of a mass suggestive of a meningioma. The addendum was never transmitted to the patient’s attending physician, and she was discharged.
In December 2007, the patient had a seizure and was transported to the same medical center. The physician who reviewed the patient’s records discovered the addendum to the MRI report. It was determined that the seizure was caused by the meningioma.
The tumor was surgically removed but recurred, necessitating a second procedure. The patient continues to experience periodic seizures. She claimed that the defendants failed to timely treat her meningioma.
The matter ultimately proceeded against only the radiologist and the hospital. The plaintiff specifically claimed that the radiologist should have ensured that the addendum was transmitted to her physicians.
The defendant claimed that any failure to immediately address the meningioma did not change the patient’s outcome and that the treatment at that time would have entailed monitoring the tumor for signs of growth.
Outcome
According to a published account, a $4 million settlement was reached.
Comment
This case is frustrating: Frustrating because the radiologist made the correct interpretation, but that information never made it to the patient’s primary provider. He made the right diagnostic call—how can he be on the hook for a hospital-related “systems error”?
A frustrated patient injured by a systems error will attempt to blame everyone, including the clinician. Will the jury be persuaded to blame the clinician too? It depends on the interrelationship between the clinician’s practice and the system that failed.
For example, if an ambulatory patient in a large HMO complex slips and falls on a recently mopped bathroom floor, there will be no case against a clinician because the arguable negligence was the failure to notify the patient that the floor was wet. The system that failed and the clinician’s services are distinct.
By contrast, if an unsteady ambulatory patient is examined by a clinician and then sent to walk down the hallway for x-rays, and the patient slips and falls, there is likely a case against the clinician. The clinician discovered that the patient was unsteady during the examination, and it was a foreseeable risk that an unsteady patient could fall and suffer injury. The plaintiff will claim that a reasonably prudent clinician, recognizing the risk, would arrange for wheelchair transport.
In the present case, the radiologist and hospital settled for $4 million. We can rationally infer that the plaintiff’s legal team was able to produce an expert to testify (during deposition) that the standard of care required that the radiologist not just interpret the MRI correctly, but also ensure that the test’s findings were communicated to the patient’s attending physician.
Would a jury agree and fault the radiologist for the “systems error”? We don’t know. We do know the plaintiff’s attorney felt this argument was strong enough to keep the radiologist in the case and force a settlement against him—which usually results in an adverse National Practitioner Data Bank recording.
What risks exist in your practice? Once a clinician-patient relationship is established, risks that seem out of your control could land you with liability if a jury believes that the elimination of that risk was in your control—and therefore your responsibility.
Once a clinician-patient relationship is established, take reasonable steps to protect patients. Between the extremes of omniscience at one end of the spectrum and willful blindness on the other, we are left with the clinician’s duty to avert reasonably foreseeable harms.
Here, if the radiologist had any reason to believe that the addendum may not have been forwarded, he had an obligation to take affirmative steps to ensure it was communicated. Yet, if his system had functioned previously without flaw, faulting him would be unfair. Apparently, the plaintiff’s attorney had some evidence suggesting that the radiologist had knowledge that the existing system was flawed—and under those circumstances, simply entering an addendum with the hope that it would be communicated was risky.
In sum, if you see potential harm looming for a patient, take action before “mere risk” materializes into actual harm. —DML
In September 2006, a 42-year-old woman was transported to a medical center in New York City with symptoms of a manic bipolar episode. She was admitted and stabilized, and she remained in the hospital for 11 days.
During her hospitalization, an MRI of the brain was performed. The radiologist initially noted no significant findings. However, several hours later, he prepared an addendum to his report, indicating the presence of a mass suggestive of a meningioma. The addendum was never transmitted to the patient’s attending physician, and she was discharged.
In December 2007, the patient had a seizure and was transported to the same medical center. The physician who reviewed the patient’s records discovered the addendum to the MRI report. It was determined that the seizure was caused by the meningioma.
The tumor was surgically removed but recurred, necessitating a second procedure. The patient continues to experience periodic seizures. She claimed that the defendants failed to timely treat her meningioma.
The matter ultimately proceeded against only the radiologist and the hospital. The plaintiff specifically claimed that the radiologist should have ensured that the addendum was transmitted to her physicians.
The defendant claimed that any failure to immediately address the meningioma did not change the patient’s outcome and that the treatment at that time would have entailed monitoring the tumor for signs of growth.
Outcome
According to a published account, a $4 million settlement was reached.
Comment
This case is frustrating: Frustrating because the radiologist made the correct interpretation, but that information never made it to the patient’s primary provider. He made the right diagnostic call—how can he be on the hook for a hospital-related “systems error”?
A frustrated patient injured by a systems error will attempt to blame everyone, including the clinician. Will the jury be persuaded to blame the clinician too? It depends on the interrelationship between the clinician’s practice and the system that failed.
For example, if an ambulatory patient in a large HMO complex slips and falls on a recently mopped bathroom floor, there will be no case against a clinician because the arguable negligence was the failure to notify the patient that the floor was wet. The system that failed and the clinician’s services are distinct.
By contrast, if an unsteady ambulatory patient is examined by a clinician and then sent to walk down the hallway for x-rays, and the patient slips and falls, there is likely a case against the clinician. The clinician discovered that the patient was unsteady during the examination, and it was a foreseeable risk that an unsteady patient could fall and suffer injury. The plaintiff will claim that a reasonably prudent clinician, recognizing the risk, would arrange for wheelchair transport.
In the present case, the radiologist and hospital settled for $4 million. We can rationally infer that the plaintiff’s legal team was able to produce an expert to testify (during deposition) that the standard of care required that the radiologist not just interpret the MRI correctly, but also ensure that the test’s findings were communicated to the patient’s attending physician.
Would a jury agree and fault the radiologist for the “systems error”? We don’t know. We do know the plaintiff’s attorney felt this argument was strong enough to keep the radiologist in the case and force a settlement against him—which usually results in an adverse National Practitioner Data Bank recording.
What risks exist in your practice? Once a clinician-patient relationship is established, risks that seem out of your control could land you with liability if a jury believes that the elimination of that risk was in your control—and therefore your responsibility.
Once a clinician-patient relationship is established, take reasonable steps to protect patients. Between the extremes of omniscience at one end of the spectrum and willful blindness on the other, we are left with the clinician’s duty to avert reasonably foreseeable harms.
Here, if the radiologist had any reason to believe that the addendum may not have been forwarded, he had an obligation to take affirmative steps to ensure it was communicated. Yet, if his system had functioned previously without flaw, faulting him would be unfair. Apparently, the plaintiff’s attorney had some evidence suggesting that the radiologist had knowledge that the existing system was flawed—and under those circumstances, simply entering an addendum with the hope that it would be communicated was risky.
In sum, if you see potential harm looming for a patient, take action before “mere risk” materializes into actual harm. —DML
In September 2006, a 42-year-old woman was transported to a medical center in New York City with symptoms of a manic bipolar episode. She was admitted and stabilized, and she remained in the hospital for 11 days.
During her hospitalization, an MRI of the brain was performed. The radiologist initially noted no significant findings. However, several hours later, he prepared an addendum to his report, indicating the presence of a mass suggestive of a meningioma. The addendum was never transmitted to the patient’s attending physician, and she was discharged.
In December 2007, the patient had a seizure and was transported to the same medical center. The physician who reviewed the patient’s records discovered the addendum to the MRI report. It was determined that the seizure was caused by the meningioma.
The tumor was surgically removed but recurred, necessitating a second procedure. The patient continues to experience periodic seizures. She claimed that the defendants failed to timely treat her meningioma.
The matter ultimately proceeded against only the radiologist and the hospital. The plaintiff specifically claimed that the radiologist should have ensured that the addendum was transmitted to her physicians.
The defendant claimed that any failure to immediately address the meningioma did not change the patient’s outcome and that the treatment at that time would have entailed monitoring the tumor for signs of growth.
Outcome
According to a published account, a $4 million settlement was reached.
Comment
This case is frustrating: Frustrating because the radiologist made the correct interpretation, but that information never made it to the patient’s primary provider. He made the right diagnostic call—how can he be on the hook for a hospital-related “systems error”?
A frustrated patient injured by a systems error will attempt to blame everyone, including the clinician. Will the jury be persuaded to blame the clinician too? It depends on the interrelationship between the clinician’s practice and the system that failed.
For example, if an ambulatory patient in a large HMO complex slips and falls on a recently mopped bathroom floor, there will be no case against a clinician because the arguable negligence was the failure to notify the patient that the floor was wet. The system that failed and the clinician’s services are distinct.
By contrast, if an unsteady ambulatory patient is examined by a clinician and then sent to walk down the hallway for x-rays, and the patient slips and falls, there is likely a case against the clinician. The clinician discovered that the patient was unsteady during the examination, and it was a foreseeable risk that an unsteady patient could fall and suffer injury. The plaintiff will claim that a reasonably prudent clinician, recognizing the risk, would arrange for wheelchair transport.
In the present case, the radiologist and hospital settled for $4 million. We can rationally infer that the plaintiff’s legal team was able to produce an expert to testify (during deposition) that the standard of care required that the radiologist not just interpret the MRI correctly, but also ensure that the test’s findings were communicated to the patient’s attending physician.
Would a jury agree and fault the radiologist for the “systems error”? We don’t know. We do know the plaintiff’s attorney felt this argument was strong enough to keep the radiologist in the case and force a settlement against him—which usually results in an adverse National Practitioner Data Bank recording.
What risks exist in your practice? Once a clinician-patient relationship is established, risks that seem out of your control could land you with liability if a jury believes that the elimination of that risk was in your control—and therefore your responsibility.
Once a clinician-patient relationship is established, take reasonable steps to protect patients. Between the extremes of omniscience at one end of the spectrum and willful blindness on the other, we are left with the clinician’s duty to avert reasonably foreseeable harms.
Here, if the radiologist had any reason to believe that the addendum may not have been forwarded, he had an obligation to take affirmative steps to ensure it was communicated. Yet, if his system had functioned previously without flaw, faulting him would be unfair. Apparently, the plaintiff’s attorney had some evidence suggesting that the radiologist had knowledge that the existing system was flawed—and under those circumstances, simply entering an addendum with the hope that it would be communicated was risky.
In sum, if you see potential harm looming for a patient, take action before “mere risk” materializes into actual harm. —DML
Did poor communication lead to her death?

A woman in her 50s underwent hysterectomy performed by a surgeon, who then assigned an ObGyn to her follow-up care. The day after surgery, the patient had severe abdominal pain with decreased blood pressure and increased heart and respiration rates. The ObGyn admitted the patient to the intensive care unit (ICU), and then designated Dr. A, the patient’s family practitioner to continue her care. Dr. A was not available, so his associate, Dr. B, took over. Over the phone, Dr. B requested pulmonary, cardiology, and infectious disease consults. In the ICU the next day, the patient suffered respiratory arrest and was intubated. When her abdomen became rigid and swollen, emergency surgery revealed that a colon perforation had allowed fecal matter to reach the abdominal cavity. The woman died the next day from complications of sepsis, peritonitis, and multiple organ failure.
ESTATE’S CLAIM None of the physicians assigned to her care ever saw the patient in the ICU. Earlier surgery could have prevented her death. The physicians involved in her care failed to communicate with each other properly.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $3.2 million Illinois settlement was reached with the hospital.
BOTH PARENTS HAD PLATELET ANTIBODIES
When a 32-year-old woman became pregnant with her third child, she sought treatment at a clinic. The mother informed the nurse practi-tioner that her two other children had been diagnosed with low platelets at birth, but they were now healthy and had no further problems.
The woman gave birth vaginally to her third child at term. The newborn had Apgar scores of 8 and 8, at 1 and 5 minutes, respectively. However, the child’s platelet level was 26 x 103/µL. The baby was transferred to another hospital the next day, where he was diagnosed with hydrocephalus and neonatal alloimmune thrombocytopenia. He suffered a massive intracranial hemorrhage, which caused severe neurologic injuries and brain damage. A shunt was placed. The child has significant cognitive deficits as well as cerebral palsy with mild developmental delays. Testing showed that each parent had a different genotype for platelet antibodies.
PARENTS’ CLAIM The parents should have been tested for platelet antibodies prior to this birth due to the family’s history. A prenatal diagnosis of neonatal alloimmune thrombocytopenia would have allowed for treatment with gamma globulin, which could have avoided the intracranial hemorrhage.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $4.8 million California settlement was reached.
CORD PROLAPSE NOT CARED FOR IN AMBULANCE
At 36 weeks’ gestation, a mother called an ambulance when her membranes ruptured and she noticed an umbilical cord prolapse.
The child was in a breech presentation, experienced oxygen deprivation, and sustained severe neurologic damage.
PARENTS’ CLAIM The ambulance service was negligent in its care. The ambulance service dispatcher advised the mother to stand, squat, and push before the ambulance arrived. The ambulance attendants failed to take basic actions to relieve pressure on the prolapsed umbilical cord. The ambulance did not stop at two closer hospitals, which delayed arrival for an additional 20 minutes.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $2.7 million settlement was reached, but before it was submitted to the court for approval, the child died. The defendants then sought to revoke the settlement, but the parents claimed breach of contract. The defendants claimed that the agreement was orally negotiated independent of defense counsel and was unenforceable due to the child’s death and lack of court approval. A Texas judge issued summary judgment on breach of contract and awarded $2.7 million plus $40,000 in attorney fees to the parents.

SECOND- AND THIRD-DEGREE BURNS TO PERINEUM
A mother received an epidural injection during vaginal delivery. Six hours later, the patient asked a nurse for a warm compress to place on her perineum. The nurse heated the compress in a microwave and then applied it to the perineal area. The compress caused second- and third-degree burns to the patient’s labia and inner left thigh. She underwent surgical repair of the burned area, and, a year later, had plastic surgery.
PATIENT’S CLAIM The nurse was negligent in overheating the compress.
DEFENDANTS’ DEFENSE The hospital agreed that the nurse who heated and applied the compress had been negligent. The hospital paid all medical expenses relating to the burns, including follow-up surgeries.
VERDICT A $190,000 Utah verdict was returned for noneconomic damages.
DOCUMENTATION MAKES A DIFFERENCE FOR OBGYN AFTER CHILD DIES
A 30-year-old physician was pregnant with her first child. Due to a low amniotic fluid index and lagging fetal growth, she saw a maternal-fetal medicine specialist, who suggested labor induction at 39 weeks.
Labor progressed slowly. After three attempts at vacuum-assisted delivery, the ObGyn recommended cesarean delivery. The parents eventually consented to cesarean delivery after another failed vacuum-assisted attempt. Although the ObGyn had recommended cesarean 2 hours earlier, surgery was not ordered on an emergent basis.
At birth, the baby’s resuscitation took more than 20 minutes. The child lost nearly one-third of her blood volume; she had a subgaleal hemorrhage. Both parties agreed that the vacuum device probably caused the bleeding.
The child had hypoxic ischemic encephalopathy and disseminated intravascular coagulation. She suffered a myocardial infarction at 3 days of age. Without electrical brain activity, life support was removed, and the child died at 5 days of age. An autopsy found possible hypereosinophilic syndrome as the concurrent cause of death.
PARENTS’ CLAIM The mother claimed she was not informed of the risks, benefits, and alternatives to vacuum extraction; she would not have consented had she known the risks. The mother, her husband, and two family members maintained that the ObGyn offered the possibility of cesarean delivery as a question, but did not insist on it. The mother claimed she wanted what was best for the baby, and never refused a cesarean. The resuscitation efforts caused eosinophilic infiltration into several organs.
PHYSICIAN’S DEFENSE The ObGyn charted that the parents were “adamant about having a vaginal delivery,” and said she told the parents what she charted. The obstetric nurse testified that the mother delayed consent because she felt vaginal delivery was imminent. The ObGyn acted properly; eosinophilia caused the baby’s death.
VERDICT An Illinois defense verdict was returned.
HIGH BP TO BLAME FOR DEATHS OF BOTH MOTHER AND CHILD
A 23-year-old woman’s pregnancy was at high risk because of very high blood pressure (BP). At 34 weeks’ gestation, she went to a county hospital with symptoms of high BP; she was treated and discharged 3 days later. She returned to the hospital to be checked twice more within a month. The day after the third visit, she suffered a seizure and was taken to a university hospital, where emergency cesarean delivery was performed. The mother died from an aortic rupture during delivery.
The child was born with brain injuries and died at age 4 years due to neurologic complications.
ESTATE’S CLAIM The mother was not properly treated at the county hospital, resulting in both deaths; she should not have been discharged. Under monitoring, she would have undergone delivery before the aortic rupture occurred, avoiding the baby’s brain injury.
DEFENDANTS’ DEFENSE The mother was stable when released; aortic rupture is unpredictable and unpreventable, and would have occurred under any circumstances. It is highly unusual that a woman of her age would have an aortic rupture.
VERDICT A $3,062,803 California verdict was returned. The parties then settled for $1,782,000 (with the county assuming the medical lien).
NECROTIZING FASCIITIS FROM PERFORATED COLON
A woman underwent laparoscopic-assisted vaginal hysterectomy performed by her ObGyn, and was discharged after 3 days. The next day, she went to another hospital’s emergency department (ED) with abdominal distention and rigidity, severe abdominal pain, and vomiting. She had a toxic appearance, rapid pulse rate, and hypotension. In emergency surgery, several liters of dark brown, foul-smelling fluid were found in her abdomen, and feculent peritonitis and necrotizing fasciitis were diagnosed due to a perforated sigmoid colon. She required multiple hospitalizations and operations.
PATIENT’S CLAIM Perforation occurred during hysterectomy. The ObGyn failed to recognize the injury prior to discharge. The hospital staff did not properly assess her or communicate her symptoms to the ObGyn.
DEFENDANTS’ DEFENSE There was no negligence; proper care was given.
VERDICT A $2,922,503 Florida verdict was returned, with the jury finding the ObGyn 30% at fault and the hospital 70% at fault.
FAILURE TO REACT TO FETAL DISTRESS: $15.6M
After delivery at full term, a child suffered convulsions and seizures on her second day of life. A CT scan showed brain injuries. At age 11 years, she has severe learning and developmental delays, and requires 24-hour care.
PARENTS’ CLAIM Severe decelerations with slow return to baseline occurred several times during labor and delivery. The nurse midwife failed to recognize and react to fetal distress. A cesarean delivery should have been performed instead of a vaginal delivery. The delay in delivery caused the child’s injuries.
DEFENDANTS’ DEFENSE A prenatal neurogenetic disorder caused the child’s injuries.
VERDICT A $15.6 million Maryland verdict was returned. It will not be automatically reduced; the awarded noneconomic damages do not exceed the state cap.
LATE DELIVERY; SEVERE INJURY TO CHILD
At 40 weeks’ gestation, a woman was admitted to the hospital in labor. When the mother’s membranes were ruptured, a small amount of meconium was noted, but the fetal monitor strips were reassuring. Two hours later, the nurse and midwife noted a pattern of decelerations, but they felt the pattern was nonrepetitive and reactive. Thirty minutes later, the nurse and midwife noted decelerations to 90 bpm with pushing, but did not call a physician.
Another midwife arrived to assist the first midwife who was new to practice. The mother was given oxygen, her position was changed, and an IV fluid bolus was administered. Thirty minutes later, the nurses recognized late decelerations and called a Code White twice while the fetal heart rate continued to decelerate. After the attending physician unsuccessfully attempted vacuum extraction, an emergency cesarean delivery was performed.
The child’s Apgar scores were 2, 3, and 3, at 1, 5, and 10 minutes, respectively. The cord blood pH was 6.66, indicating severe metabolic acidosis. She developed seizures within the first few minutes of life. Imaging studies showed global hypoxic ischemic encephalopathy. The child cannot walk, talk, or sit up unsupported at age 8, and requires a G-tube. She is cortically blind and requires antiseizure medication.
PARENTS’ CLAIM The nurse, two midwives, and physician were negligent in their care of the mother and child.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $5 million Massachusetts settlement was reached.
WHAT CAUSED INFECTION AFTER ABORTION?
A 20-year-old woman underwent a surgical termination of pregnancy performed by an ObGyn. After discharge, the patient developed pain and other complications requiring rehospitalization and additional surgery for a pelvic infection.
PATIENT’S CLAIM Complications were due to a uterine perforation that spontaneously sealed before it could be detected. The ObGyn was negligent in the performance of the elective abortion. The patient has a large scar on her abdomen because of the additional operation.
PHYSICIAN’S DEFENSE Perforation of the uterus is a known complication of the procedure. However, no perforation occurred; it was not found on imaging, and spontaneous sealing of a perforation cannot occur. The patient’s complications were due to a subclinical infection that was activated by the surgery.
VERDICT A New York defense verdict was returned.
We want to hear from you. Tell us what you think!
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
A woman in her 50s underwent hysterectomy performed by a surgeon, who then assigned an ObGyn to her follow-up care. The day after surgery, the patient had severe abdominal pain with decreased blood pressure and increased heart and respiration rates. The ObGyn admitted the patient to the intensive care unit (ICU), and then designated Dr. A, the patient’s family practitioner to continue her care. Dr. A was not available, so his associate, Dr. B, took over. Over the phone, Dr. B requested pulmonary, cardiology, and infectious disease consults. In the ICU the next day, the patient suffered respiratory arrest and was intubated. When her abdomen became rigid and swollen, emergency surgery revealed that a colon perforation had allowed fecal matter to reach the abdominal cavity. The woman died the next day from complications of sepsis, peritonitis, and multiple organ failure.
ESTATE’S CLAIM None of the physicians assigned to her care ever saw the patient in the ICU. Earlier surgery could have prevented her death. The physicians involved in her care failed to communicate with each other properly.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $3.2 million Illinois settlement was reached with the hospital.
BOTH PARENTS HAD PLATELET ANTIBODIES
When a 32-year-old woman became pregnant with her third child, she sought treatment at a clinic. The mother informed the nurse practi-tioner that her two other children had been diagnosed with low platelets at birth, but they were now healthy and had no further problems.
The woman gave birth vaginally to her third child at term. The newborn had Apgar scores of 8 and 8, at 1 and 5 minutes, respectively. However, the child’s platelet level was 26 x 103/µL. The baby was transferred to another hospital the next day, where he was diagnosed with hydrocephalus and neonatal alloimmune thrombocytopenia. He suffered a massive intracranial hemorrhage, which caused severe neurologic injuries and brain damage. A shunt was placed. The child has significant cognitive deficits as well as cerebral palsy with mild developmental delays. Testing showed that each parent had a different genotype for platelet antibodies.
PARENTS’ CLAIM The parents should have been tested for platelet antibodies prior to this birth due to the family’s history. A prenatal diagnosis of neonatal alloimmune thrombocytopenia would have allowed for treatment with gamma globulin, which could have avoided the intracranial hemorrhage.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $4.8 million California settlement was reached.
CORD PROLAPSE NOT CARED FOR IN AMBULANCE
At 36 weeks’ gestation, a mother called an ambulance when her membranes ruptured and she noticed an umbilical cord prolapse.
The child was in a breech presentation, experienced oxygen deprivation, and sustained severe neurologic damage.
PARENTS’ CLAIM The ambulance service was negligent in its care. The ambulance service dispatcher advised the mother to stand, squat, and push before the ambulance arrived. The ambulance attendants failed to take basic actions to relieve pressure on the prolapsed umbilical cord. The ambulance did not stop at two closer hospitals, which delayed arrival for an additional 20 minutes.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $2.7 million settlement was reached, but before it was submitted to the court for approval, the child died. The defendants then sought to revoke the settlement, but the parents claimed breach of contract. The defendants claimed that the agreement was orally negotiated independent of defense counsel and was unenforceable due to the child’s death and lack of court approval. A Texas judge issued summary judgment on breach of contract and awarded $2.7 million plus $40,000 in attorney fees to the parents.
SECOND- AND THIRD-DEGREE BURNS TO PERINEUM
A mother received an epidural injection during vaginal delivery. Six hours later, the patient asked a nurse for a warm compress to place on her perineum. The nurse heated the compress in a microwave and then applied it to the perineal area. The compress caused second- and third-degree burns to the patient’s labia and inner left thigh. She underwent surgical repair of the burned area, and, a year later, had plastic surgery.
PATIENT’S CLAIM The nurse was negligent in overheating the compress.
DEFENDANTS’ DEFENSE The hospital agreed that the nurse who heated and applied the compress had been negligent. The hospital paid all medical expenses relating to the burns, including follow-up surgeries.
VERDICT A $190,000 Utah verdict was returned for noneconomic damages.
DOCUMENTATION MAKES A DIFFERENCE FOR OBGYN AFTER CHILD DIES
A 30-year-old physician was pregnant with her first child. Due to a low amniotic fluid index and lagging fetal growth, she saw a maternal-fetal medicine specialist, who suggested labor induction at 39 weeks.
Labor progressed slowly. After three attempts at vacuum-assisted delivery, the ObGyn recommended cesarean delivery. The parents eventually consented to cesarean delivery after another failed vacuum-assisted attempt. Although the ObGyn had recommended cesarean 2 hours earlier, surgery was not ordered on an emergent basis.
At birth, the baby’s resuscitation took more than 20 minutes. The child lost nearly one-third of her blood volume; she had a subgaleal hemorrhage. Both parties agreed that the vacuum device probably caused the bleeding.
The child had hypoxic ischemic encephalopathy and disseminated intravascular coagulation. She suffered a myocardial infarction at 3 days of age. Without electrical brain activity, life support was removed, and the child died at 5 days of age. An autopsy found possible hypereosinophilic syndrome as the concurrent cause of death.
PARENTS’ CLAIM The mother claimed she was not informed of the risks, benefits, and alternatives to vacuum extraction; she would not have consented had she known the risks. The mother, her husband, and two family members maintained that the ObGyn offered the possibility of cesarean delivery as a question, but did not insist on it. The mother claimed she wanted what was best for the baby, and never refused a cesarean. The resuscitation efforts caused eosinophilic infiltration into several organs.
PHYSICIAN’S DEFENSE The ObGyn charted that the parents were “adamant about having a vaginal delivery,” and said she told the parents what she charted. The obstetric nurse testified that the mother delayed consent because she felt vaginal delivery was imminent. The ObGyn acted properly; eosinophilia caused the baby’s death.
VERDICT An Illinois defense verdict was returned.
HIGH BP TO BLAME FOR DEATHS OF BOTH MOTHER AND CHILD
A 23-year-old woman’s pregnancy was at high risk because of very high blood pressure (BP). At 34 weeks’ gestation, she went to a county hospital with symptoms of high BP; she was treated and discharged 3 days later. She returned to the hospital to be checked twice more within a month. The day after the third visit, she suffered a seizure and was taken to a university hospital, where emergency cesarean delivery was performed. The mother died from an aortic rupture during delivery.
The child was born with brain injuries and died at age 4 years due to neurologic complications.
ESTATE’S CLAIM The mother was not properly treated at the county hospital, resulting in both deaths; she should not have been discharged. Under monitoring, she would have undergone delivery before the aortic rupture occurred, avoiding the baby’s brain injury.
DEFENDANTS’ DEFENSE The mother was stable when released; aortic rupture is unpredictable and unpreventable, and would have occurred under any circumstances. It is highly unusual that a woman of her age would have an aortic rupture.
VERDICT A $3,062,803 California verdict was returned. The parties then settled for $1,782,000 (with the county assuming the medical lien).
NECROTIZING FASCIITIS FROM PERFORATED COLON
A woman underwent laparoscopic-assisted vaginal hysterectomy performed by her ObGyn, and was discharged after 3 days. The next day, she went to another hospital’s emergency department (ED) with abdominal distention and rigidity, severe abdominal pain, and vomiting. She had a toxic appearance, rapid pulse rate, and hypotension. In emergency surgery, several liters of dark brown, foul-smelling fluid were found in her abdomen, and feculent peritonitis and necrotizing fasciitis were diagnosed due to a perforated sigmoid colon. She required multiple hospitalizations and operations.
PATIENT’S CLAIM Perforation occurred during hysterectomy. The ObGyn failed to recognize the injury prior to discharge. The hospital staff did not properly assess her or communicate her symptoms to the ObGyn.
DEFENDANTS’ DEFENSE There was no negligence; proper care was given.
VERDICT A $2,922,503 Florida verdict was returned, with the jury finding the ObGyn 30% at fault and the hospital 70% at fault.
FAILURE TO REACT TO FETAL DISTRESS: $15.6M
After delivery at full term, a child suffered convulsions and seizures on her second day of life. A CT scan showed brain injuries. At age 11 years, she has severe learning and developmental delays, and requires 24-hour care.
PARENTS’ CLAIM Severe decelerations with slow return to baseline occurred several times during labor and delivery. The nurse midwife failed to recognize and react to fetal distress. A cesarean delivery should have been performed instead of a vaginal delivery. The delay in delivery caused the child’s injuries.
DEFENDANTS’ DEFENSE A prenatal neurogenetic disorder caused the child’s injuries.
VERDICT A $15.6 million Maryland verdict was returned. It will not be automatically reduced; the awarded noneconomic damages do not exceed the state cap.
LATE DELIVERY; SEVERE INJURY TO CHILD
At 40 weeks’ gestation, a woman was admitted to the hospital in labor. When the mother’s membranes were ruptured, a small amount of meconium was noted, but the fetal monitor strips were reassuring. Two hours later, the nurse and midwife noted a pattern of decelerations, but they felt the pattern was nonrepetitive and reactive. Thirty minutes later, the nurse and midwife noted decelerations to 90 bpm with pushing, but did not call a physician.
Another midwife arrived to assist the first midwife who was new to practice. The mother was given oxygen, her position was changed, and an IV fluid bolus was administered. Thirty minutes later, the nurses recognized late decelerations and called a Code White twice while the fetal heart rate continued to decelerate. After the attending physician unsuccessfully attempted vacuum extraction, an emergency cesarean delivery was performed.
The child’s Apgar scores were 2, 3, and 3, at 1, 5, and 10 minutes, respectively. The cord blood pH was 6.66, indicating severe metabolic acidosis. She developed seizures within the first few minutes of life. Imaging studies showed global hypoxic ischemic encephalopathy. The child cannot walk, talk, or sit up unsupported at age 8, and requires a G-tube. She is cortically blind and requires antiseizure medication.
PARENTS’ CLAIM The nurse, two midwives, and physician were negligent in their care of the mother and child.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $5 million Massachusetts settlement was reached.
WHAT CAUSED INFECTION AFTER ABORTION?
A 20-year-old woman underwent a surgical termination of pregnancy performed by an ObGyn. After discharge, the patient developed pain and other complications requiring rehospitalization and additional surgery for a pelvic infection.
PATIENT’S CLAIM Complications were due to a uterine perforation that spontaneously sealed before it could be detected. The ObGyn was negligent in the performance of the elective abortion. The patient has a large scar on her abdomen because of the additional operation.
PHYSICIAN’S DEFENSE Perforation of the uterus is a known complication of the procedure. However, no perforation occurred; it was not found on imaging, and spontaneous sealing of a perforation cannot occur. The patient’s complications were due to a subclinical infection that was activated by the surgery.
VERDICT A New York defense verdict was returned.
We want to hear from you. Tell us what you think!
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
A woman in her 50s underwent hysterectomy performed by a surgeon, who then assigned an ObGyn to her follow-up care. The day after surgery, the patient had severe abdominal pain with decreased blood pressure and increased heart and respiration rates. The ObGyn admitted the patient to the intensive care unit (ICU), and then designated Dr. A, the patient’s family practitioner to continue her care. Dr. A was not available, so his associate, Dr. B, took over. Over the phone, Dr. B requested pulmonary, cardiology, and infectious disease consults. In the ICU the next day, the patient suffered respiratory arrest and was intubated. When her abdomen became rigid and swollen, emergency surgery revealed that a colon perforation had allowed fecal matter to reach the abdominal cavity. The woman died the next day from complications of sepsis, peritonitis, and multiple organ failure.
ESTATE’S CLAIM None of the physicians assigned to her care ever saw the patient in the ICU. Earlier surgery could have prevented her death. The physicians involved in her care failed to communicate with each other properly.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $3.2 million Illinois settlement was reached with the hospital.
BOTH PARENTS HAD PLATELET ANTIBODIES
When a 32-year-old woman became pregnant with her third child, she sought treatment at a clinic. The mother informed the nurse practi-tioner that her two other children had been diagnosed with low platelets at birth, but they were now healthy and had no further problems.
The woman gave birth vaginally to her third child at term. The newborn had Apgar scores of 8 and 8, at 1 and 5 minutes, respectively. However, the child’s platelet level was 26 x 103/µL. The baby was transferred to another hospital the next day, where he was diagnosed with hydrocephalus and neonatal alloimmune thrombocytopenia. He suffered a massive intracranial hemorrhage, which caused severe neurologic injuries and brain damage. A shunt was placed. The child has significant cognitive deficits as well as cerebral palsy with mild developmental delays. Testing showed that each parent had a different genotype for platelet antibodies.
PARENTS’ CLAIM The parents should have been tested for platelet antibodies prior to this birth due to the family’s history. A prenatal diagnosis of neonatal alloimmune thrombocytopenia would have allowed for treatment with gamma globulin, which could have avoided the intracranial hemorrhage.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $4.8 million California settlement was reached.
CORD PROLAPSE NOT CARED FOR IN AMBULANCE
At 36 weeks’ gestation, a mother called an ambulance when her membranes ruptured and she noticed an umbilical cord prolapse.
The child was in a breech presentation, experienced oxygen deprivation, and sustained severe neurologic damage.
PARENTS’ CLAIM The ambulance service was negligent in its care. The ambulance service dispatcher advised the mother to stand, squat, and push before the ambulance arrived. The ambulance attendants failed to take basic actions to relieve pressure on the prolapsed umbilical cord. The ambulance did not stop at two closer hospitals, which delayed arrival for an additional 20 minutes.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $2.7 million settlement was reached, but before it was submitted to the court for approval, the child died. The defendants then sought to revoke the settlement, but the parents claimed breach of contract. The defendants claimed that the agreement was orally negotiated independent of defense counsel and was unenforceable due to the child’s death and lack of court approval. A Texas judge issued summary judgment on breach of contract and awarded $2.7 million plus $40,000 in attorney fees to the parents.
SECOND- AND THIRD-DEGREE BURNS TO PERINEUM
A mother received an epidural injection during vaginal delivery. Six hours later, the patient asked a nurse for a warm compress to place on her perineum. The nurse heated the compress in a microwave and then applied it to the perineal area. The compress caused second- and third-degree burns to the patient’s labia and inner left thigh. She underwent surgical repair of the burned area, and, a year later, had plastic surgery.
PATIENT’S CLAIM The nurse was negligent in overheating the compress.
DEFENDANTS’ DEFENSE The hospital agreed that the nurse who heated and applied the compress had been negligent. The hospital paid all medical expenses relating to the burns, including follow-up surgeries.
VERDICT A $190,000 Utah verdict was returned for noneconomic damages.
DOCUMENTATION MAKES A DIFFERENCE FOR OBGYN AFTER CHILD DIES
A 30-year-old physician was pregnant with her first child. Due to a low amniotic fluid index and lagging fetal growth, she saw a maternal-fetal medicine specialist, who suggested labor induction at 39 weeks.
Labor progressed slowly. After three attempts at vacuum-assisted delivery, the ObGyn recommended cesarean delivery. The parents eventually consented to cesarean delivery after another failed vacuum-assisted attempt. Although the ObGyn had recommended cesarean 2 hours earlier, surgery was not ordered on an emergent basis.
At birth, the baby’s resuscitation took more than 20 minutes. The child lost nearly one-third of her blood volume; she had a subgaleal hemorrhage. Both parties agreed that the vacuum device probably caused the bleeding.
The child had hypoxic ischemic encephalopathy and disseminated intravascular coagulation. She suffered a myocardial infarction at 3 days of age. Without electrical brain activity, life support was removed, and the child died at 5 days of age. An autopsy found possible hypereosinophilic syndrome as the concurrent cause of death.
PARENTS’ CLAIM The mother claimed she was not informed of the risks, benefits, and alternatives to vacuum extraction; she would not have consented had she known the risks. The mother, her husband, and two family members maintained that the ObGyn offered the possibility of cesarean delivery as a question, but did not insist on it. The mother claimed she wanted what was best for the baby, and never refused a cesarean. The resuscitation efforts caused eosinophilic infiltration into several organs.
PHYSICIAN’S DEFENSE The ObGyn charted that the parents were “adamant about having a vaginal delivery,” and said she told the parents what she charted. The obstetric nurse testified that the mother delayed consent because she felt vaginal delivery was imminent. The ObGyn acted properly; eosinophilia caused the baby’s death.
VERDICT An Illinois defense verdict was returned.
HIGH BP TO BLAME FOR DEATHS OF BOTH MOTHER AND CHILD
A 23-year-old woman’s pregnancy was at high risk because of very high blood pressure (BP). At 34 weeks’ gestation, she went to a county hospital with symptoms of high BP; she was treated and discharged 3 days later. She returned to the hospital to be checked twice more within a month. The day after the third visit, she suffered a seizure and was taken to a university hospital, where emergency cesarean delivery was performed. The mother died from an aortic rupture during delivery.
The child was born with brain injuries and died at age 4 years due to neurologic complications.
ESTATE’S CLAIM The mother was not properly treated at the county hospital, resulting in both deaths; she should not have been discharged. Under monitoring, she would have undergone delivery before the aortic rupture occurred, avoiding the baby’s brain injury.
DEFENDANTS’ DEFENSE The mother was stable when released; aortic rupture is unpredictable and unpreventable, and would have occurred under any circumstances. It is highly unusual that a woman of her age would have an aortic rupture.
VERDICT A $3,062,803 California verdict was returned. The parties then settled for $1,782,000 (with the county assuming the medical lien).
NECROTIZING FASCIITIS FROM PERFORATED COLON
A woman underwent laparoscopic-assisted vaginal hysterectomy performed by her ObGyn, and was discharged after 3 days. The next day, she went to another hospital’s emergency department (ED) with abdominal distention and rigidity, severe abdominal pain, and vomiting. She had a toxic appearance, rapid pulse rate, and hypotension. In emergency surgery, several liters of dark brown, foul-smelling fluid were found in her abdomen, and feculent peritonitis and necrotizing fasciitis were diagnosed due to a perforated sigmoid colon. She required multiple hospitalizations and operations.
PATIENT’S CLAIM Perforation occurred during hysterectomy. The ObGyn failed to recognize the injury prior to discharge. The hospital staff did not properly assess her or communicate her symptoms to the ObGyn.
DEFENDANTS’ DEFENSE There was no negligence; proper care was given.
VERDICT A $2,922,503 Florida verdict was returned, with the jury finding the ObGyn 30% at fault and the hospital 70% at fault.
FAILURE TO REACT TO FETAL DISTRESS: $15.6M
After delivery at full term, a child suffered convulsions and seizures on her second day of life. A CT scan showed brain injuries. At age 11 years, she has severe learning and developmental delays, and requires 24-hour care.
PARENTS’ CLAIM Severe decelerations with slow return to baseline occurred several times during labor and delivery. The nurse midwife failed to recognize and react to fetal distress. A cesarean delivery should have been performed instead of a vaginal delivery. The delay in delivery caused the child’s injuries.
DEFENDANTS’ DEFENSE A prenatal neurogenetic disorder caused the child’s injuries.
VERDICT A $15.6 million Maryland verdict was returned. It will not be automatically reduced; the awarded noneconomic damages do not exceed the state cap.
LATE DELIVERY; SEVERE INJURY TO CHILD
At 40 weeks’ gestation, a woman was admitted to the hospital in labor. When the mother’s membranes were ruptured, a small amount of meconium was noted, but the fetal monitor strips were reassuring. Two hours later, the nurse and midwife noted a pattern of decelerations, but they felt the pattern was nonrepetitive and reactive. Thirty minutes later, the nurse and midwife noted decelerations to 90 bpm with pushing, but did not call a physician.
Another midwife arrived to assist the first midwife who was new to practice. The mother was given oxygen, her position was changed, and an IV fluid bolus was administered. Thirty minutes later, the nurses recognized late decelerations and called a Code White twice while the fetal heart rate continued to decelerate. After the attending physician unsuccessfully attempted vacuum extraction, an emergency cesarean delivery was performed.
The child’s Apgar scores were 2, 3, and 3, at 1, 5, and 10 minutes, respectively. The cord blood pH was 6.66, indicating severe metabolic acidosis. She developed seizures within the first few minutes of life. Imaging studies showed global hypoxic ischemic encephalopathy. The child cannot walk, talk, or sit up unsupported at age 8, and requires a G-tube. She is cortically blind and requires antiseizure medication.
PARENTS’ CLAIM The nurse, two midwives, and physician were negligent in their care of the mother and child.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $5 million Massachusetts settlement was reached.
WHAT CAUSED INFECTION AFTER ABORTION?
A 20-year-old woman underwent a surgical termination of pregnancy performed by an ObGyn. After discharge, the patient developed pain and other complications requiring rehospitalization and additional surgery for a pelvic infection.
PATIENT’S CLAIM Complications were due to a uterine perforation that spontaneously sealed before it could be detected. The ObGyn was negligent in the performance of the elective abortion. The patient has a large scar on her abdomen because of the additional operation.
PHYSICIAN’S DEFENSE Perforation of the uterus is a known complication of the procedure. However, no perforation occurred; it was not found on imaging, and spontaneous sealing of a perforation cannot occur. The patient’s complications were due to a subclinical infection that was activated by the surgery.
VERDICT A New York defense verdict was returned.
We want to hear from you. Tell us what you think!
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Data Mining Expert Explains Role Performance Tools Will Play in Future
Click here to listen to more of our interview with Paul Roscoe, CEO of the Washington, D.C.-based Advisory Board Company
Click here to listen to more of our interview with Paul Roscoe, CEO of the Washington, D.C.-based Advisory Board Company
Click here to listen to more of our interview with Paul Roscoe, CEO of the Washington, D.C.-based Advisory Board Company
The Why and How Data Mining Is Applicable to Hospital Medicine
Click here to listen to excerpts of our interview with Dr. Deitelzweig, chair of SHM’s Practice Analysis Committee.
Click here to listen to excerpts of our interview with Dr. Deitelzweig, chair of SHM’s Practice Analysis Committee.
Click here to listen to excerpts of our interview with Dr. Deitelzweig, chair of SHM’s Practice Analysis Committee.
Hospitalist James O’Callaghan Finds Career Satisfaction in Pediatric Medicine


It took a while for James J. O’Callaghan, MD, FAAP, FHM, to settle on a career path. First, he pursued the life of a chemical engineer. Then, in his third year at Rensselaer Polytechnic Institute in Troy, N.Y., he realized the kind of job he would be getting into was not quite for him. His then-girlfriend was a pre-med student, and it wasn’t long until he switched majors.
Hospital medicine drew his interest during residency, when he spent a monthlong rotation with a small group of physicians at a community hospital in Cleveland.
“Their days consisted of rounding on pediatric inpatients, examining normal newborns, completing pediatric consults in the ED, and performing minor procedures on the floor,” he says. “To me, it seemed the perfect job.”
Dr. O’Callaghan married an adult-medicine hospitalist and moved to Seattle, but he could not find a good fit in a hospitalist practice. He did private practice for two years, and in 2004, he landed a position in pediatric hospital medicine.
“I quickly changed career paths,” he says.
Dr. O’Callaghan is now a regional pediatric hospitalist at Evergreen Hospital in Kirkland, Wash., and a medical hospitalist at Seattle Children’s Hospital. He is a clinical assistant professor at the University of Washington and one of nine new Team Hospitalist members, The Hospitalist’s volunteer editorial advisory group.
As the section head for pediatrics at Evergreen, Dr. O’Callaghan spends most of his time seeing patients. However, he has in recent years developed a keen interest in quality improvement (QI). He’s the lead pediatric hospitalist on two clinical pathways at Seattle Children’s and has been an active member of SHM’s Hospital Quality and Patient Safety Committee since 2012.
“I want to continue to expand on this QI work,” he says, “with the goal of developing into a formal QI role at either, or both, hospitals.”
Question: What do you like most about working as a hospitalist?
Answer: I like the fact that the work I am doing as a hospitalist can have both an immediate impact on a single patient and a prolonged impact on multiple patients. I can admit a child with community-acquired pneumonia and, through my treatment, prevent serious sequelae from developing. However, I can also develop an evidenced-based, community-acquired pneumonia pathway and, potentially, affect the care of hundreds of children. There is immediate gratification in treating today’s patient and delayed gratification knowing that you are helping many of tomorrow’s patients.
Q: What do you dislike?
A: One of the hardest parts of a career in HM is trying to effect culture change. Hospital systems are typically large, complex organizations with their own culture. In order to successfully produce sustainable, long-term improvement, you must change this culture. You can perform a robust search of the literature to produce a brilliant clinical-care path, but unless you can affect behavior, your work and effort may not last. It can be frustrating to think you have the answer to a clinical problem only to see your effort fail because you could not change culture.
Q: What’s the biggest change you’ve seen in HM in your career?
A: In the early years, much of the conversation in HM was centered on the viability of a career in HM. Could one make a sustainable career in HM? Would hospitals and health systems continue to support physicians in HM? The biggest change I have seen is that we are no longer having those conversations. Now, the conversations are focused on determining which areas of medicine will be owned by HM: First it was QI work, then patient safety, and now resource utilization and cost containment. We are no longer spending time and energy worrying about the future of HM, but rather now our efforts are focused on the present work of HM. As a sustainable career, HM is here to stay.
Q: For group leaders, why is it important for you to continue seeing patients?
A: In my QI work, I have studied Lean thinking and methodology. Lean thinking teaches you that change and improvement do not come down from leadership, but rather develop up from front-line workers. Group leaders need to continue seeing patients to truly understand the processes and problems inherent in clinical work. Effective solutions must come from those actually doing the work, rather than from those managing the work from above.
Q: What does it mean to you to be elected a Fellow in Hospital Medicine?
A: It meant that I had committed fully to a career in hospital medicine. I use the FHM designation proudly in all my communications, as a signal to others of my commitment and dedication to hospital medicine. Someday, I hope to earn the designation of SFHM, as a validation and recognition of my contributions to the field of pediatric hospital medicine.
Q: When you aren’t working, what is important to you?
A: After family, it is important for me to maintain a healthy lifestyle and stay in shape. I am able to commute to Seattle Children’s Hospital by bicycle and I try to run two to three times a week. I squeeze in half-marathons and marathons, along with century [100 miles] and double-century bicycle rides each year.
Q: If you weren’t a doctor, what would you be doing right now?
A: I would love to be a stay-at-home father for my boys and also devote the time and energy into pursuing a career in trail running.
Q: What’s the best book you’ve read recently?
A: I recently read Jim Collins’ “Good to Great” as part of a management training course at Seattle Children’s Hospital. This easy-to-read, highly entertaining book clearly demonstrates the culture changes that need to occur for companies to move from good to great. As a field, hospital medicine, with its focus on QI work and patient safety, is now in the midst of trying to become “great.”
Q: How many Apple products (phones, iPods, tablets, iTunes, etc.) do you interface with in a given week?
A: As many as possible. My wife and I own two iPhones, two iPads, and a MacBook Air, which she thinks we share but, in actuality, is mine. We are hoping to purchase a Mac desktop, and then we will have fully given over to the dark side.
Richard Quinn is a freelance writer in New Jersey.
It took a while for James J. O’Callaghan, MD, FAAP, FHM, to settle on a career path. First, he pursued the life of a chemical engineer. Then, in his third year at Rensselaer Polytechnic Institute in Troy, N.Y., he realized the kind of job he would be getting into was not quite for him. His then-girlfriend was a pre-med student, and it wasn’t long until he switched majors.
Hospital medicine drew his interest during residency, when he spent a monthlong rotation with a small group of physicians at a community hospital in Cleveland.
“Their days consisted of rounding on pediatric inpatients, examining normal newborns, completing pediatric consults in the ED, and performing minor procedures on the floor,” he says. “To me, it seemed the perfect job.”
Dr. O’Callaghan married an adult-medicine hospitalist and moved to Seattle, but he could not find a good fit in a hospitalist practice. He did private practice for two years, and in 2004, he landed a position in pediatric hospital medicine.
“I quickly changed career paths,” he says.
Dr. O’Callaghan is now a regional pediatric hospitalist at Evergreen Hospital in Kirkland, Wash., and a medical hospitalist at Seattle Children’s Hospital. He is a clinical assistant professor at the University of Washington and one of nine new Team Hospitalist members, The Hospitalist’s volunteer editorial advisory group.
As the section head for pediatrics at Evergreen, Dr. O’Callaghan spends most of his time seeing patients. However, he has in recent years developed a keen interest in quality improvement (QI). He’s the lead pediatric hospitalist on two clinical pathways at Seattle Children’s and has been an active member of SHM’s Hospital Quality and Patient Safety Committee since 2012.
“I want to continue to expand on this QI work,” he says, “with the goal of developing into a formal QI role at either, or both, hospitals.”
Question: What do you like most about working as a hospitalist?
Answer: I like the fact that the work I am doing as a hospitalist can have both an immediate impact on a single patient and a prolonged impact on multiple patients. I can admit a child with community-acquired pneumonia and, through my treatment, prevent serious sequelae from developing. However, I can also develop an evidenced-based, community-acquired pneumonia pathway and, potentially, affect the care of hundreds of children. There is immediate gratification in treating today’s patient and delayed gratification knowing that you are helping many of tomorrow’s patients.
Q: What do you dislike?
A: One of the hardest parts of a career in HM is trying to effect culture change. Hospital systems are typically large, complex organizations with their own culture. In order to successfully produce sustainable, long-term improvement, you must change this culture. You can perform a robust search of the literature to produce a brilliant clinical-care path, but unless you can affect behavior, your work and effort may not last. It can be frustrating to think you have the answer to a clinical problem only to see your effort fail because you could not change culture.
Q: What’s the biggest change you’ve seen in HM in your career?
A: In the early years, much of the conversation in HM was centered on the viability of a career in HM. Could one make a sustainable career in HM? Would hospitals and health systems continue to support physicians in HM? The biggest change I have seen is that we are no longer having those conversations. Now, the conversations are focused on determining which areas of medicine will be owned by HM: First it was QI work, then patient safety, and now resource utilization and cost containment. We are no longer spending time and energy worrying about the future of HM, but rather now our efforts are focused on the present work of HM. As a sustainable career, HM is here to stay.
Q: For group leaders, why is it important for you to continue seeing patients?
A: In my QI work, I have studied Lean thinking and methodology. Lean thinking teaches you that change and improvement do not come down from leadership, but rather develop up from front-line workers. Group leaders need to continue seeing patients to truly understand the processes and problems inherent in clinical work. Effective solutions must come from those actually doing the work, rather than from those managing the work from above.
Q: What does it mean to you to be elected a Fellow in Hospital Medicine?
A: It meant that I had committed fully to a career in hospital medicine. I use the FHM designation proudly in all my communications, as a signal to others of my commitment and dedication to hospital medicine. Someday, I hope to earn the designation of SFHM, as a validation and recognition of my contributions to the field of pediatric hospital medicine.
Q: When you aren’t working, what is important to you?
A: After family, it is important for me to maintain a healthy lifestyle and stay in shape. I am able to commute to Seattle Children’s Hospital by bicycle and I try to run two to three times a week. I squeeze in half-marathons and marathons, along with century [100 miles] and double-century bicycle rides each year.
Q: If you weren’t a doctor, what would you be doing right now?
A: I would love to be a stay-at-home father for my boys and also devote the time and energy into pursuing a career in trail running.
Q: What’s the best book you’ve read recently?
A: I recently read Jim Collins’ “Good to Great” as part of a management training course at Seattle Children’s Hospital. This easy-to-read, highly entertaining book clearly demonstrates the culture changes that need to occur for companies to move from good to great. As a field, hospital medicine, with its focus on QI work and patient safety, is now in the midst of trying to become “great.”
Q: How many Apple products (phones, iPods, tablets, iTunes, etc.) do you interface with in a given week?
A: As many as possible. My wife and I own two iPhones, two iPads, and a MacBook Air, which she thinks we share but, in actuality, is mine. We are hoping to purchase a Mac desktop, and then we will have fully given over to the dark side.
Richard Quinn is a freelance writer in New Jersey.
It took a while for James J. O’Callaghan, MD, FAAP, FHM, to settle on a career path. First, he pursued the life of a chemical engineer. Then, in his third year at Rensselaer Polytechnic Institute in Troy, N.Y., he realized the kind of job he would be getting into was not quite for him. His then-girlfriend was a pre-med student, and it wasn’t long until he switched majors.
Hospital medicine drew his interest during residency, when he spent a monthlong rotation with a small group of physicians at a community hospital in Cleveland.
“Their days consisted of rounding on pediatric inpatients, examining normal newborns, completing pediatric consults in the ED, and performing minor procedures on the floor,” he says. “To me, it seemed the perfect job.”
Dr. O’Callaghan married an adult-medicine hospitalist and moved to Seattle, but he could not find a good fit in a hospitalist practice. He did private practice for two years, and in 2004, he landed a position in pediatric hospital medicine.
“I quickly changed career paths,” he says.
Dr. O’Callaghan is now a regional pediatric hospitalist at Evergreen Hospital in Kirkland, Wash., and a medical hospitalist at Seattle Children’s Hospital. He is a clinical assistant professor at the University of Washington and one of nine new Team Hospitalist members, The Hospitalist’s volunteer editorial advisory group.
As the section head for pediatrics at Evergreen, Dr. O’Callaghan spends most of his time seeing patients. However, he has in recent years developed a keen interest in quality improvement (QI). He’s the lead pediatric hospitalist on two clinical pathways at Seattle Children’s and has been an active member of SHM’s Hospital Quality and Patient Safety Committee since 2012.
“I want to continue to expand on this QI work,” he says, “with the goal of developing into a formal QI role at either, or both, hospitals.”
Question: What do you like most about working as a hospitalist?
Answer: I like the fact that the work I am doing as a hospitalist can have both an immediate impact on a single patient and a prolonged impact on multiple patients. I can admit a child with community-acquired pneumonia and, through my treatment, prevent serious sequelae from developing. However, I can also develop an evidenced-based, community-acquired pneumonia pathway and, potentially, affect the care of hundreds of children. There is immediate gratification in treating today’s patient and delayed gratification knowing that you are helping many of tomorrow’s patients.
Q: What do you dislike?
A: One of the hardest parts of a career in HM is trying to effect culture change. Hospital systems are typically large, complex organizations with their own culture. In order to successfully produce sustainable, long-term improvement, you must change this culture. You can perform a robust search of the literature to produce a brilliant clinical-care path, but unless you can affect behavior, your work and effort may not last. It can be frustrating to think you have the answer to a clinical problem only to see your effort fail because you could not change culture.
Q: What’s the biggest change you’ve seen in HM in your career?
A: In the early years, much of the conversation in HM was centered on the viability of a career in HM. Could one make a sustainable career in HM? Would hospitals and health systems continue to support physicians in HM? The biggest change I have seen is that we are no longer having those conversations. Now, the conversations are focused on determining which areas of medicine will be owned by HM: First it was QI work, then patient safety, and now resource utilization and cost containment. We are no longer spending time and energy worrying about the future of HM, but rather now our efforts are focused on the present work of HM. As a sustainable career, HM is here to stay.
Q: For group leaders, why is it important for you to continue seeing patients?
A: In my QI work, I have studied Lean thinking and methodology. Lean thinking teaches you that change and improvement do not come down from leadership, but rather develop up from front-line workers. Group leaders need to continue seeing patients to truly understand the processes and problems inherent in clinical work. Effective solutions must come from those actually doing the work, rather than from those managing the work from above.
Q: What does it mean to you to be elected a Fellow in Hospital Medicine?
A: It meant that I had committed fully to a career in hospital medicine. I use the FHM designation proudly in all my communications, as a signal to others of my commitment and dedication to hospital medicine. Someday, I hope to earn the designation of SFHM, as a validation and recognition of my contributions to the field of pediatric hospital medicine.
Q: When you aren’t working, what is important to you?
A: After family, it is important for me to maintain a healthy lifestyle and stay in shape. I am able to commute to Seattle Children’s Hospital by bicycle and I try to run two to three times a week. I squeeze in half-marathons and marathons, along with century [100 miles] and double-century bicycle rides each year.
Q: If you weren’t a doctor, what would you be doing right now?
A: I would love to be a stay-at-home father for my boys and also devote the time and energy into pursuing a career in trail running.
Q: What’s the best book you’ve read recently?
A: I recently read Jim Collins’ “Good to Great” as part of a management training course at Seattle Children’s Hospital. This easy-to-read, highly entertaining book clearly demonstrates the culture changes that need to occur for companies to move from good to great. As a field, hospital medicine, with its focus on QI work and patient safety, is now in the midst of trying to become “great.”
Q: How many Apple products (phones, iPods, tablets, iTunes, etc.) do you interface with in a given week?
A: As many as possible. My wife and I own two iPhones, two iPads, and a MacBook Air, which she thinks we share but, in actuality, is mine. We are hoping to purchase a Mac desktop, and then we will have fully given over to the dark side.
Richard Quinn is a freelance writer in New Jersey.
Feds Extend HIPAA Obligations, Violation Penalties
Key Takeaways for Hospitalist Groups

- Covered entities and business associates should review their business associate agreements and determine whether the agreements qualify for grandfathered status and, if needed, enter into new business-associate agreements.
- Covered entities and business associates will need to review their policies and procedures so that they can implement all necessary changes in a timely manner.
- Notices of Privacy Practices will need to be revised, and appropriate training should be provided to personnel of covered entities and business associates.
- Any vendor or business that performs functions for a covered entity or another business associate involving the use or disclosure of PHI should determine whether it is a “business associate” and, if so, what needs to be done in order to comply with the Final Rule.
On Jan. 17, 2013, the Office for Civil Rights (OCR) of the U.S. Department of Health and Human Services (HHS) issued an omnibus Final Rule implementing various provisions of the Health Information Technology for Economic and Clinical Health, or HITECH, Act. The Final Rule revises the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the interim final Breach Notification Rule.
The HITECH Act, which took effect as part of the American Recovery and Reinvestment Act of 2009, expanded the obligations of covered entities and business associates to protect the confidentiality and security of protected health information (PHI).
Under HIPAA, “covered entities” may disclose PHI to “business associates,” and permit business associates to create and receive PHI on behalf of the covered entity, subject to the terms of a business-associate agreement between the parties. A “covered entity” is defined as a health plan, healthcare clearinghouse, or healthcare provider (e.g. physician practice or hospital) that transmits health information electronically. In general, the HIPAA regulations have traditionally defined a “business associate” as a person (other than a member of the covered entity’s workforce) or entity who, on behalf of a covered entity, performs a function or activity involving the use or disclosure of PHI, such as the performance of financial, legal, actuarial, accounting, consulting, data aggregation, management, administrative, or accreditation services to or for a covered entity.
Prior to the HITECH Act, business associates were contractually obligated to maintain the privacy and security of PHI but could not be sanctioned for failing to comply with HIPAA. The HITECH Act expands those obligations and exposure of business associates by:
- Applying many of the privacy and security standards to business associates;
- Subjecting business associates to the breach-notification requirements; and
- Imposing civil and criminal penalties on business associates for HIPAA violations.
In addition, the HITECH Act strengthened the penalties and enforcement mechanisms under HIPAA and required periodic audits to ensure that covered entities and business associates are compliant.
Expansion of Breach-Notification Requirements
The Final Rule expands the breach-notification obligations of covered entities and business associates by revising the definition of “breach” and the risk-assessment process for determining whether notification is required. A use or disclosure of unsecured PHI that is not permitted under the Privacy Rule is presumed to be a breach (and therefore requires notification to the individual, OCR, and possibly the media) unless the incident satisfies an exception, or the covered entity or business associate demonstrates a low probability that PHI has been compromised.1 This risk analysis is based on at least the following four factors:
- The nature and extent of the PHI, including the types of identifiers and the likelihood of re-identification;
- The unauthorized person who used or accessed the PHI;
- Whether the PHI was actually acquired or viewed; and
- The extent to which the risk is mitigated (e.g. by obtaining reliable assurances by a recipient of PHI that the information will be destroyed or will not be used or disclosed).
Expansion of Business-Associate Obligations
The Final Rule implements the HITECH Act’s expansion of business associates’ HIPAA obligations by applying the Privacy and Security Rules directly to business associates and by imposing civil and criminal penalties on business associates for HIPAA violations. It also extends obligations and potential penalties to subcontractors of business associates if a business associate delegates a function, activity, or service to the subcontractor, and the subcontractor creates, receives, maintains, or transmits PHI on behalf of the business associate. Any business associate that delegates a function involving the use or disclosure of PHI to a subcontractor will be required to enter into a business-associate agreement with the subcontractor.
Additional Provisions
The Final Rule addresses the following additional issues by:
- Requiring covered entities to modify their Notices of Privacy Practices;
- Allowing individuals to obtain a copy of PHI in an electronic format if the covered entity uses an electronic health record;
- Restricting marketing activities;
- Allowing covered entities to disclose relevant PHI of a deceased person to a family member, close friend, or other person designated by the deceased, unless the disclosure is inconsistent with the deceased person’s known prior expressed preference;
- Requiring covered entities to agree to an individual’s request to restrict disclosure of PHI to a health plan when the individual (or someone other than the health plan) pays for the healthcare item or service in full;
- Revising the definition of PHI to exclude information about a person who has been deceased for more than 50 years;
- Prohibiting the sale of PHI without authorization from the individual, and adding a requirement of authorization in order for a covered entity to receive remuneration for disclosing PHI;
- Clarifying OCR’s view that covered entities are allowed to send electronic PHI to individuals in unencrypted e-mails only after notifying the individual of the risk;
- Prohibiting health plans from using or disclosing genetic information for underwriting, as required by the Genetic Information Nondiscrimination Act of 2008 (GINA);
- Allowing disclosure of proof of immunization to schools if agreed by the parent, guardian, or individual;
- Permitting compound authorizations for clinical-research studies; and
- Revising the Enforcement Rule (which was previously revised in 2009 as an interim Final Rule), which:
- Requires the secretary of HHS to investigate a HIPAA complaint if a preliminary investigation indicates a possible violation due to willful neglect;
- Permits HHS to disclose PHI to other government agencies (including state attorneys general) for civil or criminal law-enforcement purposes; and
- Revises standards for determining the levels of civil money penalties.
Effective Date, Compliance Date
Although most provisions of the Final Rule became effective on March 26, many provisions impacting covered entities and business associates (including subcontractors) required compliance by Sept. 23. However, if certain conditions are met, the Final Rule allows additional time to revise business associate agreements to make them compliant. In particular, transition provisions will allow covered entities and business associates to continue to operate under existing business-associate agreements for up to one year beyond the compliance date (until Sept. 22, 2014) if the business-associate agreement:
- Is in writing;
- Is in place prior to Jan. 25, 2013 (the publication date of the Final Rule);
- Is compliant with the Privacy and Security Rules, in effect immediately prior to Jan. 25, 2013; and
- Is not modified or renewed.
This additional time for grandfathered business-associate agreements applies only to the written-documentation requirement. Covered entities, business associates and subcontractors will be required to comply with all other HIPAA requirements beginning on the compliance date, even if the business-associate agreement qualifies for grandfathered status
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Footnote
The exceptions relate to (i) unintentional, good-faith access, acquisition or use by members of the covered entity’s or business associate’s workforce, (ii) inadvertent disclosure limited to persons with authorized access and not resulting in further unpermitted use or disclosure, and (iii) good-faith belief that the unauthorized recipient would be unable to retain the PHI.
Key Takeaways for Hospitalist Groups
- Covered entities and business associates should review their business associate agreements and determine whether the agreements qualify for grandfathered status and, if needed, enter into new business-associate agreements.
- Covered entities and business associates will need to review their policies and procedures so that they can implement all necessary changes in a timely manner.
- Notices of Privacy Practices will need to be revised, and appropriate training should be provided to personnel of covered entities and business associates.
- Any vendor or business that performs functions for a covered entity or another business associate involving the use or disclosure of PHI should determine whether it is a “business associate” and, if so, what needs to be done in order to comply with the Final Rule.
On Jan. 17, 2013, the Office for Civil Rights (OCR) of the U.S. Department of Health and Human Services (HHS) issued an omnibus Final Rule implementing various provisions of the Health Information Technology for Economic and Clinical Health, or HITECH, Act. The Final Rule revises the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the interim final Breach Notification Rule.
The HITECH Act, which took effect as part of the American Recovery and Reinvestment Act of 2009, expanded the obligations of covered entities and business associates to protect the confidentiality and security of protected health information (PHI).
Under HIPAA, “covered entities” may disclose PHI to “business associates,” and permit business associates to create and receive PHI on behalf of the covered entity, subject to the terms of a business-associate agreement between the parties. A “covered entity” is defined as a health plan, healthcare clearinghouse, or healthcare provider (e.g. physician practice or hospital) that transmits health information electronically. In general, the HIPAA regulations have traditionally defined a “business associate” as a person (other than a member of the covered entity’s workforce) or entity who, on behalf of a covered entity, performs a function or activity involving the use or disclosure of PHI, such as the performance of financial, legal, actuarial, accounting, consulting, data aggregation, management, administrative, or accreditation services to or for a covered entity.
Prior to the HITECH Act, business associates were contractually obligated to maintain the privacy and security of PHI but could not be sanctioned for failing to comply with HIPAA. The HITECH Act expands those obligations and exposure of business associates by:
- Applying many of the privacy and security standards to business associates;
- Subjecting business associates to the breach-notification requirements; and
- Imposing civil and criminal penalties on business associates for HIPAA violations.
In addition, the HITECH Act strengthened the penalties and enforcement mechanisms under HIPAA and required periodic audits to ensure that covered entities and business associates are compliant.
Expansion of Breach-Notification Requirements
The Final Rule expands the breach-notification obligations of covered entities and business associates by revising the definition of “breach” and the risk-assessment process for determining whether notification is required. A use or disclosure of unsecured PHI that is not permitted under the Privacy Rule is presumed to be a breach (and therefore requires notification to the individual, OCR, and possibly the media) unless the incident satisfies an exception, or the covered entity or business associate demonstrates a low probability that PHI has been compromised.1 This risk analysis is based on at least the following four factors:
- The nature and extent of the PHI, including the types of identifiers and the likelihood of re-identification;
- The unauthorized person who used or accessed the PHI;
- Whether the PHI was actually acquired or viewed; and
- The extent to which the risk is mitigated (e.g. by obtaining reliable assurances by a recipient of PHI that the information will be destroyed or will not be used or disclosed).
Expansion of Business-Associate Obligations
The Final Rule implements the HITECH Act’s expansion of business associates’ HIPAA obligations by applying the Privacy and Security Rules directly to business associates and by imposing civil and criminal penalties on business associates for HIPAA violations. It also extends obligations and potential penalties to subcontractors of business associates if a business associate delegates a function, activity, or service to the subcontractor, and the subcontractor creates, receives, maintains, or transmits PHI on behalf of the business associate. Any business associate that delegates a function involving the use or disclosure of PHI to a subcontractor will be required to enter into a business-associate agreement with the subcontractor.
Additional Provisions
The Final Rule addresses the following additional issues by:
- Requiring covered entities to modify their Notices of Privacy Practices;
- Allowing individuals to obtain a copy of PHI in an electronic format if the covered entity uses an electronic health record;
- Restricting marketing activities;
- Allowing covered entities to disclose relevant PHI of a deceased person to a family member, close friend, or other person designated by the deceased, unless the disclosure is inconsistent with the deceased person’s known prior expressed preference;
- Requiring covered entities to agree to an individual’s request to restrict disclosure of PHI to a health plan when the individual (or someone other than the health plan) pays for the healthcare item or service in full;
- Revising the definition of PHI to exclude information about a person who has been deceased for more than 50 years;
- Prohibiting the sale of PHI without authorization from the individual, and adding a requirement of authorization in order for a covered entity to receive remuneration for disclosing PHI;
- Clarifying OCR’s view that covered entities are allowed to send electronic PHI to individuals in unencrypted e-mails only after notifying the individual of the risk;
- Prohibiting health plans from using or disclosing genetic information for underwriting, as required by the Genetic Information Nondiscrimination Act of 2008 (GINA);
- Allowing disclosure of proof of immunization to schools if agreed by the parent, guardian, or individual;
- Permitting compound authorizations for clinical-research studies; and
- Revising the Enforcement Rule (which was previously revised in 2009 as an interim Final Rule), which:
- Requires the secretary of HHS to investigate a HIPAA complaint if a preliminary investigation indicates a possible violation due to willful neglect;
- Permits HHS to disclose PHI to other government agencies (including state attorneys general) for civil or criminal law-enforcement purposes; and
- Revises standards for determining the levels of civil money penalties.
Effective Date, Compliance Date
Although most provisions of the Final Rule became effective on March 26, many provisions impacting covered entities and business associates (including subcontractors) required compliance by Sept. 23. However, if certain conditions are met, the Final Rule allows additional time to revise business associate agreements to make them compliant. In particular, transition provisions will allow covered entities and business associates to continue to operate under existing business-associate agreements for up to one year beyond the compliance date (until Sept. 22, 2014) if the business-associate agreement:
- Is in writing;
- Is in place prior to Jan. 25, 2013 (the publication date of the Final Rule);
- Is compliant with the Privacy and Security Rules, in effect immediately prior to Jan. 25, 2013; and
- Is not modified or renewed.
This additional time for grandfathered business-associate agreements applies only to the written-documentation requirement. Covered entities, business associates and subcontractors will be required to comply with all other HIPAA requirements beginning on the compliance date, even if the business-associate agreement qualifies for grandfathered status
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Footnote
The exceptions relate to (i) unintentional, good-faith access, acquisition or use by members of the covered entity’s or business associate’s workforce, (ii) inadvertent disclosure limited to persons with authorized access and not resulting in further unpermitted use or disclosure, and (iii) good-faith belief that the unauthorized recipient would be unable to retain the PHI.
Key Takeaways for Hospitalist Groups
- Covered entities and business associates should review their business associate agreements and determine whether the agreements qualify for grandfathered status and, if needed, enter into new business-associate agreements.
- Covered entities and business associates will need to review their policies and procedures so that they can implement all necessary changes in a timely manner.
- Notices of Privacy Practices will need to be revised, and appropriate training should be provided to personnel of covered entities and business associates.
- Any vendor or business that performs functions for a covered entity or another business associate involving the use or disclosure of PHI should determine whether it is a “business associate” and, if so, what needs to be done in order to comply with the Final Rule.
On Jan. 17, 2013, the Office for Civil Rights (OCR) of the U.S. Department of Health and Human Services (HHS) issued an omnibus Final Rule implementing various provisions of the Health Information Technology for Economic and Clinical Health, or HITECH, Act. The Final Rule revises the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the interim final Breach Notification Rule.
The HITECH Act, which took effect as part of the American Recovery and Reinvestment Act of 2009, expanded the obligations of covered entities and business associates to protect the confidentiality and security of protected health information (PHI).
Under HIPAA, “covered entities” may disclose PHI to “business associates,” and permit business associates to create and receive PHI on behalf of the covered entity, subject to the terms of a business-associate agreement between the parties. A “covered entity” is defined as a health plan, healthcare clearinghouse, or healthcare provider (e.g. physician practice or hospital) that transmits health information electronically. In general, the HIPAA regulations have traditionally defined a “business associate” as a person (other than a member of the covered entity’s workforce) or entity who, on behalf of a covered entity, performs a function or activity involving the use or disclosure of PHI, such as the performance of financial, legal, actuarial, accounting, consulting, data aggregation, management, administrative, or accreditation services to or for a covered entity.
Prior to the HITECH Act, business associates were contractually obligated to maintain the privacy and security of PHI but could not be sanctioned for failing to comply with HIPAA. The HITECH Act expands those obligations and exposure of business associates by:
- Applying many of the privacy and security standards to business associates;
- Subjecting business associates to the breach-notification requirements; and
- Imposing civil and criminal penalties on business associates for HIPAA violations.
In addition, the HITECH Act strengthened the penalties and enforcement mechanisms under HIPAA and required periodic audits to ensure that covered entities and business associates are compliant.
Expansion of Breach-Notification Requirements
The Final Rule expands the breach-notification obligations of covered entities and business associates by revising the definition of “breach” and the risk-assessment process for determining whether notification is required. A use or disclosure of unsecured PHI that is not permitted under the Privacy Rule is presumed to be a breach (and therefore requires notification to the individual, OCR, and possibly the media) unless the incident satisfies an exception, or the covered entity or business associate demonstrates a low probability that PHI has been compromised.1 This risk analysis is based on at least the following four factors:
- The nature and extent of the PHI, including the types of identifiers and the likelihood of re-identification;
- The unauthorized person who used or accessed the PHI;
- Whether the PHI was actually acquired or viewed; and
- The extent to which the risk is mitigated (e.g. by obtaining reliable assurances by a recipient of PHI that the information will be destroyed or will not be used or disclosed).
Expansion of Business-Associate Obligations
The Final Rule implements the HITECH Act’s expansion of business associates’ HIPAA obligations by applying the Privacy and Security Rules directly to business associates and by imposing civil and criminal penalties on business associates for HIPAA violations. It also extends obligations and potential penalties to subcontractors of business associates if a business associate delegates a function, activity, or service to the subcontractor, and the subcontractor creates, receives, maintains, or transmits PHI on behalf of the business associate. Any business associate that delegates a function involving the use or disclosure of PHI to a subcontractor will be required to enter into a business-associate agreement with the subcontractor.
Additional Provisions
The Final Rule addresses the following additional issues by:
- Requiring covered entities to modify their Notices of Privacy Practices;
- Allowing individuals to obtain a copy of PHI in an electronic format if the covered entity uses an electronic health record;
- Restricting marketing activities;
- Allowing covered entities to disclose relevant PHI of a deceased person to a family member, close friend, or other person designated by the deceased, unless the disclosure is inconsistent with the deceased person’s known prior expressed preference;
- Requiring covered entities to agree to an individual’s request to restrict disclosure of PHI to a health plan when the individual (or someone other than the health plan) pays for the healthcare item or service in full;
- Revising the definition of PHI to exclude information about a person who has been deceased for more than 50 years;
- Prohibiting the sale of PHI without authorization from the individual, and adding a requirement of authorization in order for a covered entity to receive remuneration for disclosing PHI;
- Clarifying OCR’s view that covered entities are allowed to send electronic PHI to individuals in unencrypted e-mails only after notifying the individual of the risk;
- Prohibiting health plans from using or disclosing genetic information for underwriting, as required by the Genetic Information Nondiscrimination Act of 2008 (GINA);
- Allowing disclosure of proof of immunization to schools if agreed by the parent, guardian, or individual;
- Permitting compound authorizations for clinical-research studies; and
- Revising the Enforcement Rule (which was previously revised in 2009 as an interim Final Rule), which:
- Requires the secretary of HHS to investigate a HIPAA complaint if a preliminary investigation indicates a possible violation due to willful neglect;
- Permits HHS to disclose PHI to other government agencies (including state attorneys general) for civil or criminal law-enforcement purposes; and
- Revises standards for determining the levels of civil money penalties.
Effective Date, Compliance Date
Although most provisions of the Final Rule became effective on March 26, many provisions impacting covered entities and business associates (including subcontractors) required compliance by Sept. 23. However, if certain conditions are met, the Final Rule allows additional time to revise business associate agreements to make them compliant. In particular, transition provisions will allow covered entities and business associates to continue to operate under existing business-associate agreements for up to one year beyond the compliance date (until Sept. 22, 2014) if the business-associate agreement:
- Is in writing;
- Is in place prior to Jan. 25, 2013 (the publication date of the Final Rule);
- Is compliant with the Privacy and Security Rules, in effect immediately prior to Jan. 25, 2013; and
- Is not modified or renewed.
This additional time for grandfathered business-associate agreements applies only to the written-documentation requirement. Covered entities, business associates and subcontractors will be required to comply with all other HIPAA requirements beginning on the compliance date, even if the business-associate agreement qualifies for grandfathered status
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Footnote
The exceptions relate to (i) unintentional, good-faith access, acquisition or use by members of the covered entity’s or business associate’s workforce, (ii) inadvertent disclosure limited to persons with authorized access and not resulting in further unpermitted use or disclosure, and (iii) good-faith belief that the unauthorized recipient would be unable to retain the PHI.
When in Doubt, Blame the Drug
A 54-year-old woman with chronic renal disease was diagnosed with gout and prescribed allopurinol. Two days later, she was evaluated by her nephrologist, whom she informed about her new medication.
Subsequently, the patient developed fever and rash. Laboratory analysis indicated elevated transaminase levels and eosinophilia. She was admitted to the hospital.
During her stay, an infectious disease consultation was obtained, and the allopurinol was discontinued. When the patient’s condition improved, she was discharged.
Following discharge, the patient resumed taking allopurinol, and her rash returned. Eleven days later, she returned to the hospital, where she was diagnosed with toxic epidermal necrolysis. She was found to have a desquamating rash covering 62% of her body. The patient was transferred to a burn center but eventually succumbed to multi-organ failure.
The patient’s estate filed a medical malpractice lawsuit against the nephrologist alleging negligence—specifically, failure to diagnose toxic epidermal necrolysis and failure to review her medications more carefully.
Outcome
A $5.1 million verdict was returned against the nephrologist.
Comment
Many medications cause rash and are subsequently withdrawn; in a few cases, the effects are life threatening. Toxic epidermal necrolysis (TEN) and Stevens-Johnson syndrome (SJS) are relatively uncommon but potentially fatal examples.
From the limited facts presented, we know that a 54-year-old woman with established renal disease of unknown magnitude was prescribed allopurinol for gout and consulted the nephrologist two days later. It is unclear if the patient had the rash during the first visit with her nephrologist. But we do know that she was eventually admitted and maintained on allopurinol while she had the rash, pending infectious disease consultation. At some point, the allopurinol was apparently stopped and the rash improved. After discharge, the patient resumed taking allopurinol. The rash not only returned but also worsened, necessitating her readmission to a burn center.
TEN, like SJS, is often induced by certain medications, including sulfonamides, macrolides, penicillins, and quinolones. Allopurinol, phenobarbital, phenytoin, carbamazepine, valproic acid, and lamotrigine are frequently implicated as well.
TEN is rare but serious. The initial presentation may be subtle, with influenza-like symptoms such as malaise, fever, cough, rhinitis, headache, and arthralgia—and the most discriminating sign: rash.
The rash begins as a poorly defined, erythematous macular rash with purpuric centers. The lesions predominate on the torso and face, sparing the scalp. Mucosal membranes are involved in more than 90% of cases.1 Pain at the site of the skin lesions is often the predominate symptom and is often out of proportion to physical findings. Over a period of hours to days, the rash coalesces to form flaccid blisters and sheetlike epidermal detachment.2 In established cases, patients will nearly universally demonstrate Nikolsky’s sign: Mild frictional contact with the skin results in epithelial desquamation and immediate blistering.
Management involves immediate withdrawal of the offending agent and hospitalization for aggressive management. The mortality rate is high (30% to 60%3) and generally attributed to sepsis or multi-organ failure.
As clinicians, we are sometimes hesitant to label a rash allergic—thereby forever disqualifying an entire class of useful agents from that patient. However, in this case, the fact that the rash occurred simultaneously with a constellation of signs and symptoms perhaps made the rash appear to be part of an infectious process and not a drug-induced reaction. That is the challenge with TEN and SJS: The symptoms are subtle, flu-like, and confounding.
Here, the nephrologist apparently did not take action to stop the allopurinol after the patient first developed the rash. The jury was persuaded that a reasonably prudent clinician would have recognized the clinical presentation and stopped the allopurinol—and certainly not restarted it following discharge (especially after the allopurinol was stopped in the hospital and the rash began to improve).
This case brings to mind two physicians from my training who made an impression. The first was a second-year internal medicine resident. I remember quietly remarking to another student during rounds, “He is really good.” Overhearing, an attending physician answered, “He is really good because in his workup he always considers a presentation as a function of an underlying process, and walks through each of those processes in formulating his differential.” “Walking through” various disease categories forces the clinician to consider them all: infectious, autoimmune, neoplastic, environmental/toxic, vascular, traumatic, metabolic, inflammatory. In challenging cases, I’ve found it helpful to step backward into those broad basic categories of disease and reconsider the clinical picture. Here, doing so may have allowed the clinician to reconsider inflammatory and autoimmune processes and revisit the possibility of iatrogenic toxic/environmental causes (ie, the allopurinol).
The second physician was a nephrology fellow, who left me with this: “When in doubt, blame the drug.” Since nephrologists are expert drug-blamers, I suspect the early stages of this unfortunate case presented a clinical challenge. In sum, before you “missile lock” onto a diagnosis, consider taking a mental step back to consider broad categories of disease. —DML
References
1. Letko E, Papaliodis DN, Papaliodis GN, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: a review of the literature. Ann Allergy Asthma Immunol. 2005;94(4):419-436.
2. Cohen V, Jellinek SP, Schwartz RA, et al. Toxic epidermal necrolysis. Medscape; 2013. http://emedicine.medscape.com/article/229698-overview. Accessed September 9, 2013.
3. Schulz JT, Sheridan RL, Ryan CM, et al. A 10-year experience with toxic epidermal necrolysis.
J Burn Care Rehabil. 2000;21(3):199-204.
A 54-year-old woman with chronic renal disease was diagnosed with gout and prescribed allopurinol. Two days later, she was evaluated by her nephrologist, whom she informed about her new medication.
Subsequently, the patient developed fever and rash. Laboratory analysis indicated elevated transaminase levels and eosinophilia. She was admitted to the hospital.
During her stay, an infectious disease consultation was obtained, and the allopurinol was discontinued. When the patient’s condition improved, she was discharged.
Following discharge, the patient resumed taking allopurinol, and her rash returned. Eleven days later, she returned to the hospital, where she was diagnosed with toxic epidermal necrolysis. She was found to have a desquamating rash covering 62% of her body. The patient was transferred to a burn center but eventually succumbed to multi-organ failure.
The patient’s estate filed a medical malpractice lawsuit against the nephrologist alleging negligence—specifically, failure to diagnose toxic epidermal necrolysis and failure to review her medications more carefully.
Outcome
A $5.1 million verdict was returned against the nephrologist.
Comment
Many medications cause rash and are subsequently withdrawn; in a few cases, the effects are life threatening. Toxic epidermal necrolysis (TEN) and Stevens-Johnson syndrome (SJS) are relatively uncommon but potentially fatal examples.
From the limited facts presented, we know that a 54-year-old woman with established renal disease of unknown magnitude was prescribed allopurinol for gout and consulted the nephrologist two days later. It is unclear if the patient had the rash during the first visit with her nephrologist. But we do know that she was eventually admitted and maintained on allopurinol while she had the rash, pending infectious disease consultation. At some point, the allopurinol was apparently stopped and the rash improved. After discharge, the patient resumed taking allopurinol. The rash not only returned but also worsened, necessitating her readmission to a burn center.
TEN, like SJS, is often induced by certain medications, including sulfonamides, macrolides, penicillins, and quinolones. Allopurinol, phenobarbital, phenytoin, carbamazepine, valproic acid, and lamotrigine are frequently implicated as well.
TEN is rare but serious. The initial presentation may be subtle, with influenza-like symptoms such as malaise, fever, cough, rhinitis, headache, and arthralgia—and the most discriminating sign: rash.
The rash begins as a poorly defined, erythematous macular rash with purpuric centers. The lesions predominate on the torso and face, sparing the scalp. Mucosal membranes are involved in more than 90% of cases.1 Pain at the site of the skin lesions is often the predominate symptom and is often out of proportion to physical findings. Over a period of hours to days, the rash coalesces to form flaccid blisters and sheetlike epidermal detachment.2 In established cases, patients will nearly universally demonstrate Nikolsky’s sign: Mild frictional contact with the skin results in epithelial desquamation and immediate blistering.
Management involves immediate withdrawal of the offending agent and hospitalization for aggressive management. The mortality rate is high (30% to 60%3) and generally attributed to sepsis or multi-organ failure.
As clinicians, we are sometimes hesitant to label a rash allergic—thereby forever disqualifying an entire class of useful agents from that patient. However, in this case, the fact that the rash occurred simultaneously with a constellation of signs and symptoms perhaps made the rash appear to be part of an infectious process and not a drug-induced reaction. That is the challenge with TEN and SJS: The symptoms are subtle, flu-like, and confounding.
Here, the nephrologist apparently did not take action to stop the allopurinol after the patient first developed the rash. The jury was persuaded that a reasonably prudent clinician would have recognized the clinical presentation and stopped the allopurinol—and certainly not restarted it following discharge (especially after the allopurinol was stopped in the hospital and the rash began to improve).
This case brings to mind two physicians from my training who made an impression. The first was a second-year internal medicine resident. I remember quietly remarking to another student during rounds, “He is really good.” Overhearing, an attending physician answered, “He is really good because in his workup he always considers a presentation as a function of an underlying process, and walks through each of those processes in formulating his differential.” “Walking through” various disease categories forces the clinician to consider them all: infectious, autoimmune, neoplastic, environmental/toxic, vascular, traumatic, metabolic, inflammatory. In challenging cases, I’ve found it helpful to step backward into those broad basic categories of disease and reconsider the clinical picture. Here, doing so may have allowed the clinician to reconsider inflammatory and autoimmune processes and revisit the possibility of iatrogenic toxic/environmental causes (ie, the allopurinol).
The second physician was a nephrology fellow, who left me with this: “When in doubt, blame the drug.” Since nephrologists are expert drug-blamers, I suspect the early stages of this unfortunate case presented a clinical challenge. In sum, before you “missile lock” onto a diagnosis, consider taking a mental step back to consider broad categories of disease. —DML
References
1. Letko E, Papaliodis DN, Papaliodis GN, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: a review of the literature. Ann Allergy Asthma Immunol. 2005;94(4):419-436.
2. Cohen V, Jellinek SP, Schwartz RA, et al. Toxic epidermal necrolysis. Medscape; 2013. http://emedicine.medscape.com/article/229698-overview. Accessed September 9, 2013.
3. Schulz JT, Sheridan RL, Ryan CM, et al. A 10-year experience with toxic epidermal necrolysis.
J Burn Care Rehabil. 2000;21(3):199-204.
A 54-year-old woman with chronic renal disease was diagnosed with gout and prescribed allopurinol. Two days later, she was evaluated by her nephrologist, whom she informed about her new medication.
Subsequently, the patient developed fever and rash. Laboratory analysis indicated elevated transaminase levels and eosinophilia. She was admitted to the hospital.
During her stay, an infectious disease consultation was obtained, and the allopurinol was discontinued. When the patient’s condition improved, she was discharged.
Following discharge, the patient resumed taking allopurinol, and her rash returned. Eleven days later, she returned to the hospital, where she was diagnosed with toxic epidermal necrolysis. She was found to have a desquamating rash covering 62% of her body. The patient was transferred to a burn center but eventually succumbed to multi-organ failure.
The patient’s estate filed a medical malpractice lawsuit against the nephrologist alleging negligence—specifically, failure to diagnose toxic epidermal necrolysis and failure to review her medications more carefully.
Outcome
A $5.1 million verdict was returned against the nephrologist.
Comment
Many medications cause rash and are subsequently withdrawn; in a few cases, the effects are life threatening. Toxic epidermal necrolysis (TEN) and Stevens-Johnson syndrome (SJS) are relatively uncommon but potentially fatal examples.
From the limited facts presented, we know that a 54-year-old woman with established renal disease of unknown magnitude was prescribed allopurinol for gout and consulted the nephrologist two days later. It is unclear if the patient had the rash during the first visit with her nephrologist. But we do know that she was eventually admitted and maintained on allopurinol while she had the rash, pending infectious disease consultation. At some point, the allopurinol was apparently stopped and the rash improved. After discharge, the patient resumed taking allopurinol. The rash not only returned but also worsened, necessitating her readmission to a burn center.
TEN, like SJS, is often induced by certain medications, including sulfonamides, macrolides, penicillins, and quinolones. Allopurinol, phenobarbital, phenytoin, carbamazepine, valproic acid, and lamotrigine are frequently implicated as well.
TEN is rare but serious. The initial presentation may be subtle, with influenza-like symptoms such as malaise, fever, cough, rhinitis, headache, and arthralgia—and the most discriminating sign: rash.
The rash begins as a poorly defined, erythematous macular rash with purpuric centers. The lesions predominate on the torso and face, sparing the scalp. Mucosal membranes are involved in more than 90% of cases.1 Pain at the site of the skin lesions is often the predominate symptom and is often out of proportion to physical findings. Over a period of hours to days, the rash coalesces to form flaccid blisters and sheetlike epidermal detachment.2 In established cases, patients will nearly universally demonstrate Nikolsky’s sign: Mild frictional contact with the skin results in epithelial desquamation and immediate blistering.
Management involves immediate withdrawal of the offending agent and hospitalization for aggressive management. The mortality rate is high (30% to 60%3) and generally attributed to sepsis or multi-organ failure.
As clinicians, we are sometimes hesitant to label a rash allergic—thereby forever disqualifying an entire class of useful agents from that patient. However, in this case, the fact that the rash occurred simultaneously with a constellation of signs and symptoms perhaps made the rash appear to be part of an infectious process and not a drug-induced reaction. That is the challenge with TEN and SJS: The symptoms are subtle, flu-like, and confounding.
Here, the nephrologist apparently did not take action to stop the allopurinol after the patient first developed the rash. The jury was persuaded that a reasonably prudent clinician would have recognized the clinical presentation and stopped the allopurinol—and certainly not restarted it following discharge (especially after the allopurinol was stopped in the hospital and the rash began to improve).
This case brings to mind two physicians from my training who made an impression. The first was a second-year internal medicine resident. I remember quietly remarking to another student during rounds, “He is really good.” Overhearing, an attending physician answered, “He is really good because in his workup he always considers a presentation as a function of an underlying process, and walks through each of those processes in formulating his differential.” “Walking through” various disease categories forces the clinician to consider them all: infectious, autoimmune, neoplastic, environmental/toxic, vascular, traumatic, metabolic, inflammatory. In challenging cases, I’ve found it helpful to step backward into those broad basic categories of disease and reconsider the clinical picture. Here, doing so may have allowed the clinician to reconsider inflammatory and autoimmune processes and revisit the possibility of iatrogenic toxic/environmental causes (ie, the allopurinol).
The second physician was a nephrology fellow, who left me with this: “When in doubt, blame the drug.” Since nephrologists are expert drug-blamers, I suspect the early stages of this unfortunate case presented a clinical challenge. In sum, before you “missile lock” onto a diagnosis, consider taking a mental step back to consider broad categories of disease. —DML
References
1. Letko E, Papaliodis DN, Papaliodis GN, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: a review of the literature. Ann Allergy Asthma Immunol. 2005;94(4):419-436.
2. Cohen V, Jellinek SP, Schwartz RA, et al. Toxic epidermal necrolysis. Medscape; 2013. http://emedicine.medscape.com/article/229698-overview. Accessed September 9, 2013.
3. Schulz JT, Sheridan RL, Ryan CM, et al. A 10-year experience with toxic epidermal necrolysis.
J Burn Care Rehabil. 2000;21(3):199-204.