User login
HHS proposes auto-enrollment for 2015 ACA plans
Federal health officials propose to automatically reenroll consumers in Affordable Care Act health plans for 2015 if they purchased coverage through the federally run marketplace earlier this year.
The auto-enrollment feature is part of an effort by the Health & Human Services department to make the ACA’s second open enrollment period run more smoothly than the first.

The auto-enrollment feature puts the federal marketplace in line with the Federal Employee Health Benefits Program (FEHBP) and many employer-sponsored plans. Close to 90% of federal employees who use the FEHBP system don’t switch plans each year, but instead auto-enroll in their current plan with updated premiums and benefits, according to HHS.
Under the proposed rule, released on June 26, the agency will automatically reenroll consumers in the same plan they had in 2014. If that plan is unavailable, the marketplace will select a similar plan.
During the open enrollment period this fall, consumers who are happy with the selected plan won’t have to make new selections. But they have the option to select a different plan.
The proposed rule notes, however, that even if consumers are auto-enrolled, they may need to provide updated income information to continue to receive a tax credit to subsidize their insurance premiums.
State-run marketplaces can follow the federal government’s lead or propose an alternative, according to HHS.
On Twitter @maryellenny
Federal health officials propose to automatically reenroll consumers in Affordable Care Act health plans for 2015 if they purchased coverage through the federally run marketplace earlier this year.
The auto-enrollment feature is part of an effort by the Health & Human Services department to make the ACA’s second open enrollment period run more smoothly than the first.
The auto-enrollment feature puts the federal marketplace in line with the Federal Employee Health Benefits Program (FEHBP) and many employer-sponsored plans. Close to 90% of federal employees who use the FEHBP system don’t switch plans each year, but instead auto-enroll in their current plan with updated premiums and benefits, according to HHS.
Under the proposed rule, released on June 26, the agency will automatically reenroll consumers in the same plan they had in 2014. If that plan is unavailable, the marketplace will select a similar plan.
During the open enrollment period this fall, consumers who are happy with the selected plan won’t have to make new selections. But they have the option to select a different plan.
The proposed rule notes, however, that even if consumers are auto-enrolled, they may need to provide updated income information to continue to receive a tax credit to subsidize their insurance premiums.
State-run marketplaces can follow the federal government’s lead or propose an alternative, according to HHS.
On Twitter @maryellenny
Federal health officials propose to automatically reenroll consumers in Affordable Care Act health plans for 2015 if they purchased coverage through the federally run marketplace earlier this year.
The auto-enrollment feature is part of an effort by the Health & Human Services department to make the ACA’s second open enrollment period run more smoothly than the first.
The auto-enrollment feature puts the federal marketplace in line with the Federal Employee Health Benefits Program (FEHBP) and many employer-sponsored plans. Close to 90% of federal employees who use the FEHBP system don’t switch plans each year, but instead auto-enroll in their current plan with updated premiums and benefits, according to HHS.
Under the proposed rule, released on June 26, the agency will automatically reenroll consumers in the same plan they had in 2014. If that plan is unavailable, the marketplace will select a similar plan.
During the open enrollment period this fall, consumers who are happy with the selected plan won’t have to make new selections. But they have the option to select a different plan.
The proposed rule notes, however, that even if consumers are auto-enrolled, they may need to provide updated income information to continue to receive a tax credit to subsidize their insurance premiums.
State-run marketplaces can follow the federal government’s lead or propose an alternative, according to HHS.
On Twitter @maryellenny

Health insurance gap widens between large and small companies
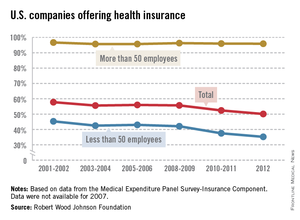
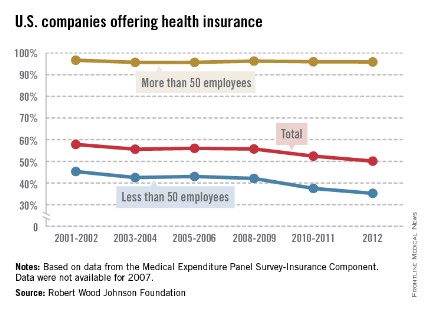
Almost 96% of larger companies still offer health insurance to their employees, but the trend toward smaller companies not providing coverage has accelerated in the last few years, according to the Robert Wood Johnson Foundation.
In 2012, 50.1% of all U.S. firms offered health insurance to their employees, down from 57.8% in 2001-2002. (All estimates represent 2-year averages, except for 2012.) That decline occurred almost entirely among smaller companies – those with fewer than 50 employees – as the percentage offering coverage fell from 45.3% in 2001-2002 to 35.2% in 2012, with two-thirds of the decline occurring after 2008-2009, the RWJF analysis showed.
Among larger companies, the decline was much smaller: from 96.7% in 2001-2002 to 95.9% in 2012.
The data for the analysis came from the Agency for Healthcare Research and Quality’s Medical Expenditure Panel Survey-Insurance Component.
Almost 96% of larger companies still offer health insurance to their employees, but the trend toward smaller companies not providing coverage has accelerated in the last few years, according to the Robert Wood Johnson Foundation.
In 2012, 50.1% of all U.S. firms offered health insurance to their employees, down from 57.8% in 2001-2002. (All estimates represent 2-year averages, except for 2012.) That decline occurred almost entirely among smaller companies – those with fewer than 50 employees – as the percentage offering coverage fell from 45.3% in 2001-2002 to 35.2% in 2012, with two-thirds of the decline occurring after 2008-2009, the RWJF analysis showed.
Among larger companies, the decline was much smaller: from 96.7% in 2001-2002 to 95.9% in 2012.
The data for the analysis came from the Agency for Healthcare Research and Quality’s Medical Expenditure Panel Survey-Insurance Component.
Almost 96% of larger companies still offer health insurance to their employees, but the trend toward smaller companies not providing coverage has accelerated in the last few years, according to the Robert Wood Johnson Foundation.
In 2012, 50.1% of all U.S. firms offered health insurance to their employees, down from 57.8% in 2001-2002. (All estimates represent 2-year averages, except for 2012.) That decline occurred almost entirely among smaller companies – those with fewer than 50 employees – as the percentage offering coverage fell from 45.3% in 2001-2002 to 35.2% in 2012, with two-thirds of the decline occurring after 2008-2009, the RWJF analysis showed.
Among larger companies, the decline was much smaller: from 96.7% in 2001-2002 to 95.9% in 2012.
The data for the analysis came from the Agency for Healthcare Research and Quality’s Medical Expenditure Panel Survey-Insurance Component.
Maintenance of certification took center stage at AMA Congress of Delegates
CHICAGO – The American Medical Association should continue to work with the American Board of Medical Specialties to address physicians’ concerns about Maintenance of Certification – that was the consensus at the annual meeting of the AMA House of Delegates.
The AMA’s delegates defeated a resolution that asked the organization to put a moratorium on MOC until it was proven to improve the quality of care and patient outcomes. However, they did agree to a new policy that directs the AMA to:

• Explore with independent entities the feasibility of conducting a study to evaluate the effect MOC requirements and Maintenance of Licensure principles have on workforce, practice costs, patient outcomes, patient safety, and patient access.
• Work with the American Board of Medical Specialties and its 24 member boards to collect data on why physicians choose to maintain or discontinue their board certification.
• Work with the ABMS and the Federation of State Medical Boards to study whether MOC and the principles of Maintenance of Licensure are important factors to physicians when deciding whether to retire and whether they have a direct effect on workforce.
• Oppose making MOC mandatory as a condition of medical licensure, and encourage physicians to strive constantly to improve their care of patients by the means they find most effective.
The new policy applies to both the ABMS MOC process and the Osteopathic Continuous Certification (OCC) process.
Physicians have increasingly voiced their concerns about MOC. Dr. Paul Teirstein, chief of cardiology and director of interventional cardiology for Scripps Clinic in La Jolla, Calif., launched a petition drive to overhaul the American Board of Internal Medicine’s MOC process. The petition has more than 17,000 signatures.
The ABIM says that it is listening to physicians and is making changes in the process, but also recently said that more than 150,000 physicians had participated in its MOC process – making the May 1 deadline to be listed on the ABIM website as having met the MOC criteria.
But anger is still bubbling up, and was expressed at the AMA’s meeting.
"Practicing physicians on the front lines are increasingly burdened, hassled, and confused by the onerous and expensive process of Maintenance of Certification and Maintenance of Licensure," said Dr. James A. Goodyear, a delegate from Pennsylvania.
Dr. Goodyear introduced the resolution to seek a moratorium on the MOC.
But Dr. Darlyne Menscer, a member of the AMA Council on Medical Education, told the delegates that such a moratorium would put a wedge in the close working relationship the AMA has had with the ABMS. "This is more prescriptive than we can commit to as a council, although we definitely do hear the concerns of the House," added Dr. Menscer.
The AMA has been discussing the concerns about MOC with the ABMS, most recently holding a meeting in Chicago in early June.
Dr. Joshua Cohen, a delegate from the American Academy of Neurology, and a member of the AMA Foundation’s Board of Directors, who attended that meeting, also argued against a moratorium. "It would make it impossible for the AMA to improve the process going forward," said Dr. Cohen.
Dr. Chuck Wilson, a pediatrician and delegate from the North Carolina delegation, also opposed any major change in direction for the AMA. He noted that if the AMA was seen as opposed to MOC, it might not be viewed well. "We all want it to be less onerous," said Dr. Wilson. But, he noted, "the Council on Medical Education is working in that direction. Let’s give them a chance to be successful."
In a statement after the HOD meeting, the AMA said that it "continues to ensure the MOC process does not disrupt physician practice or reduce the capacity of the overall physician workforce." Concerns about MOC "center around the need for relevance to the daily practice of physicians and the better integration into physician practices to optimally support learning and improvement."
On Twitter @aliciaault
CHICAGO – The American Medical Association should continue to work with the American Board of Medical Specialties to address physicians’ concerns about Maintenance of Certification – that was the consensus at the annual meeting of the AMA House of Delegates.
The AMA’s delegates defeated a resolution that asked the organization to put a moratorium on MOC until it was proven to improve the quality of care and patient outcomes. However, they did agree to a new policy that directs the AMA to:
• Explore with independent entities the feasibility of conducting a study to evaluate the effect MOC requirements and Maintenance of Licensure principles have on workforce, practice costs, patient outcomes, patient safety, and patient access.
• Work with the American Board of Medical Specialties and its 24 member boards to collect data on why physicians choose to maintain or discontinue their board certification.
• Work with the ABMS and the Federation of State Medical Boards to study whether MOC and the principles of Maintenance of Licensure are important factors to physicians when deciding whether to retire and whether they have a direct effect on workforce.
• Oppose making MOC mandatory as a condition of medical licensure, and encourage physicians to strive constantly to improve their care of patients by the means they find most effective.
The new policy applies to both the ABMS MOC process and the Osteopathic Continuous Certification (OCC) process.
Physicians have increasingly voiced their concerns about MOC. Dr. Paul Teirstein, chief of cardiology and director of interventional cardiology for Scripps Clinic in La Jolla, Calif., launched a petition drive to overhaul the American Board of Internal Medicine’s MOC process. The petition has more than 17,000 signatures.
The ABIM says that it is listening to physicians and is making changes in the process, but also recently said that more than 150,000 physicians had participated in its MOC process – making the May 1 deadline to be listed on the ABIM website as having met the MOC criteria.
But anger is still bubbling up, and was expressed at the AMA’s meeting.
"Practicing physicians on the front lines are increasingly burdened, hassled, and confused by the onerous and expensive process of Maintenance of Certification and Maintenance of Licensure," said Dr. James A. Goodyear, a delegate from Pennsylvania.
Dr. Goodyear introduced the resolution to seek a moratorium on the MOC.
But Dr. Darlyne Menscer, a member of the AMA Council on Medical Education, told the delegates that such a moratorium would put a wedge in the close working relationship the AMA has had with the ABMS. "This is more prescriptive than we can commit to as a council, although we definitely do hear the concerns of the House," added Dr. Menscer.
The AMA has been discussing the concerns about MOC with the ABMS, most recently holding a meeting in Chicago in early June.
Dr. Joshua Cohen, a delegate from the American Academy of Neurology, and a member of the AMA Foundation’s Board of Directors, who attended that meeting, also argued against a moratorium. "It would make it impossible for the AMA to improve the process going forward," said Dr. Cohen.
Dr. Chuck Wilson, a pediatrician and delegate from the North Carolina delegation, also opposed any major change in direction for the AMA. He noted that if the AMA was seen as opposed to MOC, it might not be viewed well. "We all want it to be less onerous," said Dr. Wilson. But, he noted, "the Council on Medical Education is working in that direction. Let’s give them a chance to be successful."
In a statement after the HOD meeting, the AMA said that it "continues to ensure the MOC process does not disrupt physician practice or reduce the capacity of the overall physician workforce." Concerns about MOC "center around the need for relevance to the daily practice of physicians and the better integration into physician practices to optimally support learning and improvement."
On Twitter @aliciaault
CHICAGO – The American Medical Association should continue to work with the American Board of Medical Specialties to address physicians’ concerns about Maintenance of Certification – that was the consensus at the annual meeting of the AMA House of Delegates.
The AMA’s delegates defeated a resolution that asked the organization to put a moratorium on MOC until it was proven to improve the quality of care and patient outcomes. However, they did agree to a new policy that directs the AMA to:
• Explore with independent entities the feasibility of conducting a study to evaluate the effect MOC requirements and Maintenance of Licensure principles have on workforce, practice costs, patient outcomes, patient safety, and patient access.
• Work with the American Board of Medical Specialties and its 24 member boards to collect data on why physicians choose to maintain or discontinue their board certification.
• Work with the ABMS and the Federation of State Medical Boards to study whether MOC and the principles of Maintenance of Licensure are important factors to physicians when deciding whether to retire and whether they have a direct effect on workforce.
• Oppose making MOC mandatory as a condition of medical licensure, and encourage physicians to strive constantly to improve their care of patients by the means they find most effective.
The new policy applies to both the ABMS MOC process and the Osteopathic Continuous Certification (OCC) process.
Physicians have increasingly voiced their concerns about MOC. Dr. Paul Teirstein, chief of cardiology and director of interventional cardiology for Scripps Clinic in La Jolla, Calif., launched a petition drive to overhaul the American Board of Internal Medicine’s MOC process. The petition has more than 17,000 signatures.
The ABIM says that it is listening to physicians and is making changes in the process, but also recently said that more than 150,000 physicians had participated in its MOC process – making the May 1 deadline to be listed on the ABIM website as having met the MOC criteria.
But anger is still bubbling up, and was expressed at the AMA’s meeting.
"Practicing physicians on the front lines are increasingly burdened, hassled, and confused by the onerous and expensive process of Maintenance of Certification and Maintenance of Licensure," said Dr. James A. Goodyear, a delegate from Pennsylvania.
Dr. Goodyear introduced the resolution to seek a moratorium on the MOC.
But Dr. Darlyne Menscer, a member of the AMA Council on Medical Education, told the delegates that such a moratorium would put a wedge in the close working relationship the AMA has had with the ABMS. "This is more prescriptive than we can commit to as a council, although we definitely do hear the concerns of the House," added Dr. Menscer.
The AMA has been discussing the concerns about MOC with the ABMS, most recently holding a meeting in Chicago in early June.
Dr. Joshua Cohen, a delegate from the American Academy of Neurology, and a member of the AMA Foundation’s Board of Directors, who attended that meeting, also argued against a moratorium. "It would make it impossible for the AMA to improve the process going forward," said Dr. Cohen.
Dr. Chuck Wilson, a pediatrician and delegate from the North Carolina delegation, also opposed any major change in direction for the AMA. He noted that if the AMA was seen as opposed to MOC, it might not be viewed well. "We all want it to be less onerous," said Dr. Wilson. But, he noted, "the Council on Medical Education is working in that direction. Let’s give them a chance to be successful."
In a statement after the HOD meeting, the AMA said that it "continues to ensure the MOC process does not disrupt physician practice or reduce the capacity of the overall physician workforce." Concerns about MOC "center around the need for relevance to the daily practice of physicians and the better integration into physician practices to optimally support learning and improvement."
On Twitter @aliciaault
AT THE AMA HOD MEETING

Survey: Insurance companies, government blamed for cost of health care
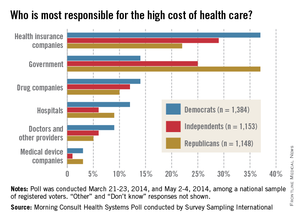
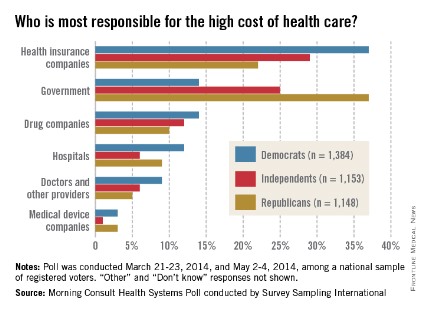
When it comes to the increasingly high cost of health care, Americans are most likely to put the blame on health insurance companies and the government, according to a survey from digital media company Morning Consult.
Among all responders, 30% said that insurance companies were most responsible for the high costs of health care, while 25% put the blame on the government and another 12% named the drug companies, Morning Consult reported.
Things change a bit, though, when viewed through a political lens. Among Democrats, 37% said that insurance companies bore the most responsibility, compared with 14% for the government and 14% for drug companies. Republicans saw the situation a bit differently, with government leading the way at 37%, insurance companies at 22%, and drug companies at 10%. Among Independents, 29% put primary responsibility on insurance companies, 25% on the government, and 10% on drug companies, the survey showed.
Among other entities included in the survey, 9% of all respondents said that hospitals were most responsible for the high cost of health care, 7% blamed physicians, and 2% blamed medical device companies.
The survey was conducted online during March 21-23, 2014, and May 2-4, 2014, among a national sample of 3,687 registered voters. It was performed by Survey Sampling International.
When it comes to the increasingly high cost of health care, Americans are most likely to put the blame on health insurance companies and the government, according to a survey from digital media company Morning Consult.
Among all responders, 30% said that insurance companies were most responsible for the high costs of health care, while 25% put the blame on the government and another 12% named the drug companies, Morning Consult reported.
Things change a bit, though, when viewed through a political lens. Among Democrats, 37% said that insurance companies bore the most responsibility, compared with 14% for the government and 14% for drug companies. Republicans saw the situation a bit differently, with government leading the way at 37%, insurance companies at 22%, and drug companies at 10%. Among Independents, 29% put primary responsibility on insurance companies, 25% on the government, and 10% on drug companies, the survey showed.
Among other entities included in the survey, 9% of all respondents said that hospitals were most responsible for the high cost of health care, 7% blamed physicians, and 2% blamed medical device companies.
The survey was conducted online during March 21-23, 2014, and May 2-4, 2014, among a national sample of 3,687 registered voters. It was performed by Survey Sampling International.
When it comes to the increasingly high cost of health care, Americans are most likely to put the blame on health insurance companies and the government, according to a survey from digital media company Morning Consult.
Among all responders, 30% said that insurance companies were most responsible for the high costs of health care, while 25% put the blame on the government and another 12% named the drug companies, Morning Consult reported.
Things change a bit, though, when viewed through a political lens. Among Democrats, 37% said that insurance companies bore the most responsibility, compared with 14% for the government and 14% for drug companies. Republicans saw the situation a bit differently, with government leading the way at 37%, insurance companies at 22%, and drug companies at 10%. Among Independents, 29% put primary responsibility on insurance companies, 25% on the government, and 10% on drug companies, the survey showed.
Among other entities included in the survey, 9% of all respondents said that hospitals were most responsible for the high cost of health care, 7% blamed physicians, and 2% blamed medical device companies.
The survey was conducted online during March 21-23, 2014, and May 2-4, 2014, among a national sample of 3,687 registered voters. It was performed by Survey Sampling International.
Variation in admission rates from EDs raising eyebrows
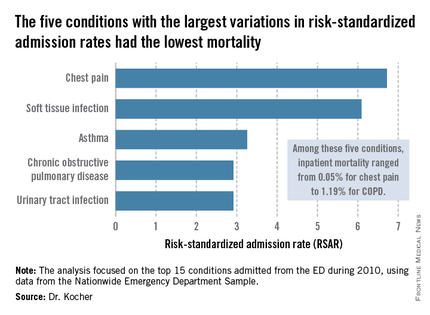
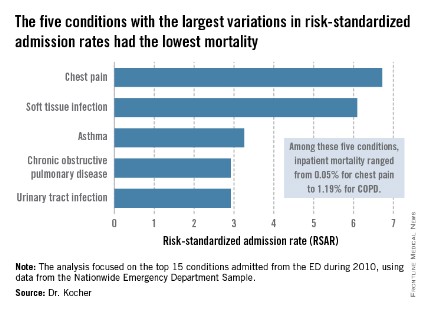
DALLAS – Emergency departments across the United States vary widely in their admission rates for the 15 most common medical and surgical conditions resulting in hospitalization.
The variability is important from a cost perspective because ED admission is increasingly the dominant route by which patients enter the hospital, Dr. Keith E. Kocher observed at the annual meeting of the Society for Academic Emergency Medicine. "We’re talking about potentially billions of dollars that may be in play if we narrow these differences." The 15 conditions collectively account for more than $266 billion/year in hospital charges to payers.
Dr. Kocher, an emergency medicine physician at the University of Michigan, Ann Arbor, and his colleagues conducted a retrospective analysis of the Nationwide Emergency Department Sample for 2010. This database, maintained by the Agency for Healthcare Research and Quality, contains extensive records on the millions of ED visits at nearly 1,000 hospitals in 28 states.
Their analysis adjusted for the severity of case mix by incorporating demographics, comorbid conditions, primary payer, median income, and patient zip code. The researchers then determined risk-standardized admission rates – the number of predicted admissions for each ED given the institutional case mix, divided by the number of expected admissions had those patients been treated at the average ED, multiplied by the mean admission rate for the sample.
The five disorders with the least variation in admission rates among the 15 most commonly admitted conditions were heart failure, stroke, acute renal failure, acute MI, and sepsis. All are characterized by relatively high inpatient mortality.

The five with the greatest variation in admission rates were chest pain, soft tissue infection, asthma, chronic obstructive pulmonary disease, and urinary tract infection. Importantly, these conditions were among those with the lowest inpatient mortality, ranging from 0.05% for patients admitted from the ED for chest pain to a high of 1.19% for those admitted for COPD.
"High-mortality/low-variation diagnoses like sepsis and MI provide little opportunity to realize meaningful spending reductions. Instead, the Big-5 high-variation/low-mortality conditions represent the greatest source of potential savings," Dr. Kocher said.
The ED could become "a workshop for developing innovative strategies for care coordination and alternatives to acute hospitalization, particularly around a select group of high-variation/low-mortality conditions" with the goal of reducing health costs, he said.

If EDs with high-risk–standardized admission rates above the median reduced admissions for the five high-variation/low-mortality conditions to the median rate, it would save an estimated $16.9 billion in charges and $5.1 billion in costs per year. Another option might be to set incentives to induce EDs with high-risk–standardized admission rates in the top quartile to reduce admissions to the 75th percentile; the resulting saving would be $7 billion less in charges and $2.1 billion less in costs per year.
Incentivizing top quartile and bottom quartile EDs to meet the median rate would yield an estimated $2.8 billion reduction in charges and a $0.8 billion decrease in costs per year.
The in-hospital mortality implications of moving admission rates toward the median are not known, Dr. Kocher acknowledged. "We’re not implying that we know the optimal rate of admission. In fact, it probably varies from condition to condition."
Further, a formal economic analysis of net expenditures would need to incorporate the increased outpatient expenditures of shifting care to ambulatory settings, he said.
The study was supported by the Agency for Healthcare Research and Quality. Dr. Kocher reported having no financial conflicts.
DALLAS – Emergency departments across the United States vary widely in their admission rates for the 15 most common medical and surgical conditions resulting in hospitalization.
The variability is important from a cost perspective because ED admission is increasingly the dominant route by which patients enter the hospital, Dr. Keith E. Kocher observed at the annual meeting of the Society for Academic Emergency Medicine. "We’re talking about potentially billions of dollars that may be in play if we narrow these differences." The 15 conditions collectively account for more than $266 billion/year in hospital charges to payers.
Dr. Kocher, an emergency medicine physician at the University of Michigan, Ann Arbor, and his colleagues conducted a retrospective analysis of the Nationwide Emergency Department Sample for 2010. This database, maintained by the Agency for Healthcare Research and Quality, contains extensive records on the millions of ED visits at nearly 1,000 hospitals in 28 states.
Their analysis adjusted for the severity of case mix by incorporating demographics, comorbid conditions, primary payer, median income, and patient zip code. The researchers then determined risk-standardized admission rates – the number of predicted admissions for each ED given the institutional case mix, divided by the number of expected admissions had those patients been treated at the average ED, multiplied by the mean admission rate for the sample.
The five disorders with the least variation in admission rates among the 15 most commonly admitted conditions were heart failure, stroke, acute renal failure, acute MI, and sepsis. All are characterized by relatively high inpatient mortality.
The five with the greatest variation in admission rates were chest pain, soft tissue infection, asthma, chronic obstructive pulmonary disease, and urinary tract infection. Importantly, these conditions were among those with the lowest inpatient mortality, ranging from 0.05% for patients admitted from the ED for chest pain to a high of 1.19% for those admitted for COPD.
"High-mortality/low-variation diagnoses like sepsis and MI provide little opportunity to realize meaningful spending reductions. Instead, the Big-5 high-variation/low-mortality conditions represent the greatest source of potential savings," Dr. Kocher said.
The ED could become "a workshop for developing innovative strategies for care coordination and alternatives to acute hospitalization, particularly around a select group of high-variation/low-mortality conditions" with the goal of reducing health costs, he said.
If EDs with high-risk–standardized admission rates above the median reduced admissions for the five high-variation/low-mortality conditions to the median rate, it would save an estimated $16.9 billion in charges and $5.1 billion in costs per year. Another option might be to set incentives to induce EDs with high-risk–standardized admission rates in the top quartile to reduce admissions to the 75th percentile; the resulting saving would be $7 billion less in charges and $2.1 billion less in costs per year.
Incentivizing top quartile and bottom quartile EDs to meet the median rate would yield an estimated $2.8 billion reduction in charges and a $0.8 billion decrease in costs per year.
The in-hospital mortality implications of moving admission rates toward the median are not known, Dr. Kocher acknowledged. "We’re not implying that we know the optimal rate of admission. In fact, it probably varies from condition to condition."
Further, a formal economic analysis of net expenditures would need to incorporate the increased outpatient expenditures of shifting care to ambulatory settings, he said.
The study was supported by the Agency for Healthcare Research and Quality. Dr. Kocher reported having no financial conflicts.
DALLAS – Emergency departments across the United States vary widely in their admission rates for the 15 most common medical and surgical conditions resulting in hospitalization.
The variability is important from a cost perspective because ED admission is increasingly the dominant route by which patients enter the hospital, Dr. Keith E. Kocher observed at the annual meeting of the Society for Academic Emergency Medicine. "We’re talking about potentially billions of dollars that may be in play if we narrow these differences." The 15 conditions collectively account for more than $266 billion/year in hospital charges to payers.
Dr. Kocher, an emergency medicine physician at the University of Michigan, Ann Arbor, and his colleagues conducted a retrospective analysis of the Nationwide Emergency Department Sample for 2010. This database, maintained by the Agency for Healthcare Research and Quality, contains extensive records on the millions of ED visits at nearly 1,000 hospitals in 28 states.
Their analysis adjusted for the severity of case mix by incorporating demographics, comorbid conditions, primary payer, median income, and patient zip code. The researchers then determined risk-standardized admission rates – the number of predicted admissions for each ED given the institutional case mix, divided by the number of expected admissions had those patients been treated at the average ED, multiplied by the mean admission rate for the sample.
The five disorders with the least variation in admission rates among the 15 most commonly admitted conditions were heart failure, stroke, acute renal failure, acute MI, and sepsis. All are characterized by relatively high inpatient mortality.
The five with the greatest variation in admission rates were chest pain, soft tissue infection, asthma, chronic obstructive pulmonary disease, and urinary tract infection. Importantly, these conditions were among those with the lowest inpatient mortality, ranging from 0.05% for patients admitted from the ED for chest pain to a high of 1.19% for those admitted for COPD.
"High-mortality/low-variation diagnoses like sepsis and MI provide little opportunity to realize meaningful spending reductions. Instead, the Big-5 high-variation/low-mortality conditions represent the greatest source of potential savings," Dr. Kocher said.
The ED could become "a workshop for developing innovative strategies for care coordination and alternatives to acute hospitalization, particularly around a select group of high-variation/low-mortality conditions" with the goal of reducing health costs, he said.
If EDs with high-risk–standardized admission rates above the median reduced admissions for the five high-variation/low-mortality conditions to the median rate, it would save an estimated $16.9 billion in charges and $5.1 billion in costs per year. Another option might be to set incentives to induce EDs with high-risk–standardized admission rates in the top quartile to reduce admissions to the 75th percentile; the resulting saving would be $7 billion less in charges and $2.1 billion less in costs per year.
Incentivizing top quartile and bottom quartile EDs to meet the median rate would yield an estimated $2.8 billion reduction in charges and a $0.8 billion decrease in costs per year.
The in-hospital mortality implications of moving admission rates toward the median are not known, Dr. Kocher acknowledged. "We’re not implying that we know the optimal rate of admission. In fact, it probably varies from condition to condition."
Further, a formal economic analysis of net expenditures would need to incorporate the increased outpatient expenditures of shifting care to ambulatory settings, he said.
The study was supported by the Agency for Healthcare Research and Quality. Dr. Kocher reported having no financial conflicts.
AT SAEM 2014
Key clinical point: Reducing variation in admission rates from EDs for selected common conditions with low inpatient mortality rates could save billions of dollars in health care expenditures annually.
Major finding: If EDs with hospital admission rates above the national median for five target conditions were to reduce those rates to the median, payers would save an estimated $16.9 billion in charges annually.
Data source: This was a retrospective analysis of the 2010 Nationwide Emergency Department Sample, which contains detailed records on millions of ED visits at nearly 1,000 hospitals in 28 states.
Disclosures: This study was supported by the AHRQ. The presenter reported having no financial conflicts.
'Code Black' offers insider look at ED challenges
"Code Black," the award-winning documentary about working in the emergency department at Los Angeles County Hospital, opens in theaters in 40 U.S. cities this summer.
It’s the film debut for young emergency physician Ryan McGarry, who both stars in and directs the feature-length documentary. It highlights the thrills and challenges of working in a busy emergency department through the eyes of senior residents, including Dr. McGarry, who completed his training while working on the film. The young doctors start the film as fresh-faced idealists in the "C-Booth" trauma bay at L.A. County Hospital, the famed birthplace of emergency medicine. Later they move to the county’s newly built hospital, which, though state-of-the-art, lacks some of the camaraderie of the original ED.

"Code Black" was the Best Documentary winner at the Los Angeles Film Festival and the Hamptons International Film Festival. And it was the Audience Award winner at both the Starz Denver Film Festival and the Aspen Filmfest.
Dr. McGarry, who is now an attending physician at New York-Presbyterian Hospital in New York City, discussed why he made the film and how it is likely to impact the health care debate.
Question: What inspired you to make this film?
Dr. McGarry: As documentaries go, this one was kind of an accident in the sense of its narrative development. I set out to capture what I thought was a phenomenally intense, and in some ways, dated and brutal trauma bay. At this point, most people associate modern health care with a lot of sterility and technology and white and blue spaces that are kind of contained. And this shows the opposite. This looks like battlefield medicine. To my surprise, it was working very well. Of course, at the time I was a young medical student, so my basis for evaluating that matured along with the film. As time went on, we migrated from the old L.A. County Hospital to a newer space. So in the course of filming, they closed down an 80-year-old structure in favor of a brand new, billion-dollar, shining, technology-laden palace. What we found was that as we were brought up to speed on modern health care, and of course regulation, the care became much more complicated.
Question: What do you want the audience to take away from the film?
Dr. McGarry: It’s hopefully a primer for health care discussion that has not yet existed. There are plenty of films that ride the political undertones of health care very well and, I think, if anything, they seem to keep people in their camps. They don’t really bring people to the middle. They may make discussion more satisfying for people who are politically charged, but from the provider’s point of view, I’m not sure if they get us anywhere. "Code Black" does not have a call to action, as they call it in the documentary world. That’s on purpose. What we’re hoping for is for people to watch it and be a bit more primed when we talk about health care. My prediction – this could be wrong – is that the real discussion for the next quarter-century, as we improve access with the [Affordable Care Act], is going to be the patient-doctor connection and some deregulation. There are just too many barriers right now. The equation is too complicated. The healing and listening that people want are not happening.

Question: So would you like to see policy makers ease up on some of the health care regulations?
Dr. McGarry: We all want safety. But as a scientist would say, these regulations ought to be evidence based. What we know as physicians is that any evidence-based truth is a hard thing to prove, period. I think a lot of these regulations are well intentioned. Nobody doubts that. But yesterday, the Joint Commission visited our hospital. Everybody was working hard on a shift trying to move patients through, trying to provide both quick and safe care, and one of the things that they were watching out for was keeping the employee bags and coffee off the computer desks. Meanwhile, I have patients with chest pain, patients with stroke, patients with fractures, who are not getting the attention they need because we’re totally focused on pleasing the federal regulators that our bags and coffee aren’t out.
Question: The film is from the perspective of young doctors and talks a lot about their initial idealism. Do you think the messages in the film will also resonate with older doctors?
Dr. McGarry: One of the more surprising aspects of "Code Black" is the nostalgia factor, that fact that both physicians that have been working for awhile and those that have become administrators watched this film. We thought it would be offensive to them, especially people from private hospitals, whom we are sort of tough on in the movie. We thought that they would find us a little unrealistic and idealistic. Interestingly, they all watched it and they said, "I long for the day in my residency when all I had to worry about was just getting the science right, getting that patient connection right."
Question: Working in C-Booth was a great experience for ED physicians in training. Can you ever recapture that feeling in the new, heavily regulated environment?
Dr. McGarry: One thing we wouldn’t want to return to would be the lack of privacy. The biggest aspect of C-Booth that probably we wouldn’t be proud of would be the lack of privacy. I’m definitely for privacy and for a dignified experience. After that, I feel like things are quite undefined. I think we have expectations that technology, in particular, is a huge answer to medicine. But we know it can be expensive and it can be dangerous. And in the case of electronic medical records, it certainly doesn’t make things faster. We know that every institution that has gone from paper charts to an EMR has found not just an immediate slowing of care, but a permanent slowing. And yet there are benefits with being able to quickly look up old medical information. But what about when my patient is waiting 20 minutes for pain medicine because it takes almost that long to get them in the computer, pull up the order, select the medicine, and go through all these stupid hard stops that are built in. Before, I could just write it down on a piece of paper, communicate it to the nurse, and get it done. If you’re the one in pain, is that worth it? I don’t know.
Question: How did you find the time to make this movie?
Dr. McGarry: There were a lot of consequences there. I probably pushed it from a health perspective. I really found myself in a unique position as both a filmmaker and subject. For almost 3 years, I would do every ounce of my residency and then would race from the hospital to the edit room and would live and breathe it for 3 years. You would imagine there’s a cost to that. Lost a girlfriend. Didn’t sleep. Happily, I came through without any major damage, but that’s a heck of a lot of emergency medicine.
Question: What are you doing next? Are you working on another film and how are balancing that with your day job in medicine?
Dr. McGarry: This is a different game than it was in residency. I have an option for a scripted series, so basically it means that producers have identified it as a viable project for a fiction series like you would see on HBO. That’s in active development. We just shot a 3-minute spot with the New York and L.A. ballets, which involves these dancers in the old abandoned general hospital. As far as balancing all this, I’m so lucky in that. Cornell/New York Presbyterian and Dr. Neal Flomenbaum have been incredibly supportive of me and allowing me to be full time there, but with the work flexibility to jump on these projects as they come.
On Twitter @maryellenny
"Code Black," the award-winning documentary about working in the emergency department at Los Angeles County Hospital, opens in theaters in 40 U.S. cities this summer.
It’s the film debut for young emergency physician Ryan McGarry, who both stars in and directs the feature-length documentary. It highlights the thrills and challenges of working in a busy emergency department through the eyes of senior residents, including Dr. McGarry, who completed his training while working on the film. The young doctors start the film as fresh-faced idealists in the "C-Booth" trauma bay at L.A. County Hospital, the famed birthplace of emergency medicine. Later they move to the county’s newly built hospital, which, though state-of-the-art, lacks some of the camaraderie of the original ED.
"Code Black" was the Best Documentary winner at the Los Angeles Film Festival and the Hamptons International Film Festival. And it was the Audience Award winner at both the Starz Denver Film Festival and the Aspen Filmfest.
Dr. McGarry, who is now an attending physician at New York-Presbyterian Hospital in New York City, discussed why he made the film and how it is likely to impact the health care debate.
Question: What inspired you to make this film?
Dr. McGarry: As documentaries go, this one was kind of an accident in the sense of its narrative development. I set out to capture what I thought was a phenomenally intense, and in some ways, dated and brutal trauma bay. At this point, most people associate modern health care with a lot of sterility and technology and white and blue spaces that are kind of contained. And this shows the opposite. This looks like battlefield medicine. To my surprise, it was working very well. Of course, at the time I was a young medical student, so my basis for evaluating that matured along with the film. As time went on, we migrated from the old L.A. County Hospital to a newer space. So in the course of filming, they closed down an 80-year-old structure in favor of a brand new, billion-dollar, shining, technology-laden palace. What we found was that as we were brought up to speed on modern health care, and of course regulation, the care became much more complicated.
Question: What do you want the audience to take away from the film?
Dr. McGarry: It’s hopefully a primer for health care discussion that has not yet existed. There are plenty of films that ride the political undertones of health care very well and, I think, if anything, they seem to keep people in their camps. They don’t really bring people to the middle. They may make discussion more satisfying for people who are politically charged, but from the provider’s point of view, I’m not sure if they get us anywhere. "Code Black" does not have a call to action, as they call it in the documentary world. That’s on purpose. What we’re hoping for is for people to watch it and be a bit more primed when we talk about health care. My prediction – this could be wrong – is that the real discussion for the next quarter-century, as we improve access with the [Affordable Care Act], is going to be the patient-doctor connection and some deregulation. There are just too many barriers right now. The equation is too complicated. The healing and listening that people want are not happening.
Question: So would you like to see policy makers ease up on some of the health care regulations?
Dr. McGarry: We all want safety. But as a scientist would say, these regulations ought to be evidence based. What we know as physicians is that any evidence-based truth is a hard thing to prove, period. I think a lot of these regulations are well intentioned. Nobody doubts that. But yesterday, the Joint Commission visited our hospital. Everybody was working hard on a shift trying to move patients through, trying to provide both quick and safe care, and one of the things that they were watching out for was keeping the employee bags and coffee off the computer desks. Meanwhile, I have patients with chest pain, patients with stroke, patients with fractures, who are not getting the attention they need because we’re totally focused on pleasing the federal regulators that our bags and coffee aren’t out.
Question: The film is from the perspective of young doctors and talks a lot about their initial idealism. Do you think the messages in the film will also resonate with older doctors?
Dr. McGarry: One of the more surprising aspects of "Code Black" is the nostalgia factor, that fact that both physicians that have been working for awhile and those that have become administrators watched this film. We thought it would be offensive to them, especially people from private hospitals, whom we are sort of tough on in the movie. We thought that they would find us a little unrealistic and idealistic. Interestingly, they all watched it and they said, "I long for the day in my residency when all I had to worry about was just getting the science right, getting that patient connection right."
Question: Working in C-Booth was a great experience for ED physicians in training. Can you ever recapture that feeling in the new, heavily regulated environment?
Dr. McGarry: One thing we wouldn’t want to return to would be the lack of privacy. The biggest aspect of C-Booth that probably we wouldn’t be proud of would be the lack of privacy. I’m definitely for privacy and for a dignified experience. After that, I feel like things are quite undefined. I think we have expectations that technology, in particular, is a huge answer to medicine. But we know it can be expensive and it can be dangerous. And in the case of electronic medical records, it certainly doesn’t make things faster. We know that every institution that has gone from paper charts to an EMR has found not just an immediate slowing of care, but a permanent slowing. And yet there are benefits with being able to quickly look up old medical information. But what about when my patient is waiting 20 minutes for pain medicine because it takes almost that long to get them in the computer, pull up the order, select the medicine, and go through all these stupid hard stops that are built in. Before, I could just write it down on a piece of paper, communicate it to the nurse, and get it done. If you’re the one in pain, is that worth it? I don’t know.
Question: How did you find the time to make this movie?
Dr. McGarry: There were a lot of consequences there. I probably pushed it from a health perspective. I really found myself in a unique position as both a filmmaker and subject. For almost 3 years, I would do every ounce of my residency and then would race from the hospital to the edit room and would live and breathe it for 3 years. You would imagine there’s a cost to that. Lost a girlfriend. Didn’t sleep. Happily, I came through without any major damage, but that’s a heck of a lot of emergency medicine.
Question: What are you doing next? Are you working on another film and how are balancing that with your day job in medicine?
Dr. McGarry: This is a different game than it was in residency. I have an option for a scripted series, so basically it means that producers have identified it as a viable project for a fiction series like you would see on HBO. That’s in active development. We just shot a 3-minute spot with the New York and L.A. ballets, which involves these dancers in the old abandoned general hospital. As far as balancing all this, I’m so lucky in that. Cornell/New York Presbyterian and Dr. Neal Flomenbaum have been incredibly supportive of me and allowing me to be full time there, but with the work flexibility to jump on these projects as they come.
On Twitter @maryellenny
"Code Black," the award-winning documentary about working in the emergency department at Los Angeles County Hospital, opens in theaters in 40 U.S. cities this summer.
It’s the film debut for young emergency physician Ryan McGarry, who both stars in and directs the feature-length documentary. It highlights the thrills and challenges of working in a busy emergency department through the eyes of senior residents, including Dr. McGarry, who completed his training while working on the film. The young doctors start the film as fresh-faced idealists in the "C-Booth" trauma bay at L.A. County Hospital, the famed birthplace of emergency medicine. Later they move to the county’s newly built hospital, which, though state-of-the-art, lacks some of the camaraderie of the original ED.
"Code Black" was the Best Documentary winner at the Los Angeles Film Festival and the Hamptons International Film Festival. And it was the Audience Award winner at both the Starz Denver Film Festival and the Aspen Filmfest.
Dr. McGarry, who is now an attending physician at New York-Presbyterian Hospital in New York City, discussed why he made the film and how it is likely to impact the health care debate.
Question: What inspired you to make this film?
Dr. McGarry: As documentaries go, this one was kind of an accident in the sense of its narrative development. I set out to capture what I thought was a phenomenally intense, and in some ways, dated and brutal trauma bay. At this point, most people associate modern health care with a lot of sterility and technology and white and blue spaces that are kind of contained. And this shows the opposite. This looks like battlefield medicine. To my surprise, it was working very well. Of course, at the time I was a young medical student, so my basis for evaluating that matured along with the film. As time went on, we migrated from the old L.A. County Hospital to a newer space. So in the course of filming, they closed down an 80-year-old structure in favor of a brand new, billion-dollar, shining, technology-laden palace. What we found was that as we were brought up to speed on modern health care, and of course regulation, the care became much more complicated.
Question: What do you want the audience to take away from the film?
Dr. McGarry: It’s hopefully a primer for health care discussion that has not yet existed. There are plenty of films that ride the political undertones of health care very well and, I think, if anything, they seem to keep people in their camps. They don’t really bring people to the middle. They may make discussion more satisfying for people who are politically charged, but from the provider’s point of view, I’m not sure if they get us anywhere. "Code Black" does not have a call to action, as they call it in the documentary world. That’s on purpose. What we’re hoping for is for people to watch it and be a bit more primed when we talk about health care. My prediction – this could be wrong – is that the real discussion for the next quarter-century, as we improve access with the [Affordable Care Act], is going to be the patient-doctor connection and some deregulation. There are just too many barriers right now. The equation is too complicated. The healing and listening that people want are not happening.
Question: So would you like to see policy makers ease up on some of the health care regulations?
Dr. McGarry: We all want safety. But as a scientist would say, these regulations ought to be evidence based. What we know as physicians is that any evidence-based truth is a hard thing to prove, period. I think a lot of these regulations are well intentioned. Nobody doubts that. But yesterday, the Joint Commission visited our hospital. Everybody was working hard on a shift trying to move patients through, trying to provide both quick and safe care, and one of the things that they were watching out for was keeping the employee bags and coffee off the computer desks. Meanwhile, I have patients with chest pain, patients with stroke, patients with fractures, who are not getting the attention they need because we’re totally focused on pleasing the federal regulators that our bags and coffee aren’t out.
Question: The film is from the perspective of young doctors and talks a lot about their initial idealism. Do you think the messages in the film will also resonate with older doctors?
Dr. McGarry: One of the more surprising aspects of "Code Black" is the nostalgia factor, that fact that both physicians that have been working for awhile and those that have become administrators watched this film. We thought it would be offensive to them, especially people from private hospitals, whom we are sort of tough on in the movie. We thought that they would find us a little unrealistic and idealistic. Interestingly, they all watched it and they said, "I long for the day in my residency when all I had to worry about was just getting the science right, getting that patient connection right."
Question: Working in C-Booth was a great experience for ED physicians in training. Can you ever recapture that feeling in the new, heavily regulated environment?
Dr. McGarry: One thing we wouldn’t want to return to would be the lack of privacy. The biggest aspect of C-Booth that probably we wouldn’t be proud of would be the lack of privacy. I’m definitely for privacy and for a dignified experience. After that, I feel like things are quite undefined. I think we have expectations that technology, in particular, is a huge answer to medicine. But we know it can be expensive and it can be dangerous. And in the case of electronic medical records, it certainly doesn’t make things faster. We know that every institution that has gone from paper charts to an EMR has found not just an immediate slowing of care, but a permanent slowing. And yet there are benefits with being able to quickly look up old medical information. But what about when my patient is waiting 20 minutes for pain medicine because it takes almost that long to get them in the computer, pull up the order, select the medicine, and go through all these stupid hard stops that are built in. Before, I could just write it down on a piece of paper, communicate it to the nurse, and get it done. If you’re the one in pain, is that worth it? I don’t know.
Question: How did you find the time to make this movie?
Dr. McGarry: There were a lot of consequences there. I probably pushed it from a health perspective. I really found myself in a unique position as both a filmmaker and subject. For almost 3 years, I would do every ounce of my residency and then would race from the hospital to the edit room and would live and breathe it for 3 years. You would imagine there’s a cost to that. Lost a girlfriend. Didn’t sleep. Happily, I came through without any major damage, but that’s a heck of a lot of emergency medicine.
Question: What are you doing next? Are you working on another film and how are balancing that with your day job in medicine?
Dr. McGarry: This is a different game than it was in residency. I have an option for a scripted series, so basically it means that producers have identified it as a viable project for a fiction series like you would see on HBO. That’s in active development. We just shot a 3-minute spot with the New York and L.A. ballets, which involves these dancers in the old abandoned general hospital. As far as balancing all this, I’m so lucky in that. Cornell/New York Presbyterian and Dr. Neal Flomenbaum have been incredibly supportive of me and allowing me to be full time there, but with the work flexibility to jump on these projects as they come.
On Twitter @maryellenny

ED doc survey: 22% of advanced imaging is ‘medically unnecessary’
DALLAS – On average, 22% of the CTs and MRIs ordered by emergency physicians are "medically unnecessary," based on responses by 435 emergency physicians participating in a national survey.
"The overwhelming majority of physicians in our sample recognized the issue of overimaging in the ED, and it’s not just something they felt was going on among others in their group. It’s something they personally acknowledged participating in," Dr. Hemal K. Kanzaria said at the annual meeting of the Society for Academic Emergency Medicine.

The two most common reasons for ordering "medically unnecessary" advanced diagnostic imaging studies were fear of missing a diagnosis despite low pretest probability, cited by 69% of respondents, and fear of litigation, cited by 64%, noted Dr. Kanzaria, a Robert Woods Johnson Foundation Clinical Scholar and emergency medicine fellow at the University of California, Los Angeles.
Patient and family expectations were identified as a driving force in ordering medically unnecessary imaging, 40% of respondents said. A mere 1% of respondents cited administrative pressure to increase group reimbursement as a main contributor, he added.
Advanced diagnostic imaging in EDs has increased appreciably in recent years, with little evidence of a resultant improvement in patient outcomes. The trend has drawn scrutiny from health policy experts in light of estimates that the U.S. annually spends $210 billion on unnecessary medical tests, procedures, and services. Yet there are little data on emergency physicians’ perceptions regarding overordering of CTs and MRIs, the causes, and the potential solutions.
"Basically, we need to know what physicians are thinking (about the issue), and that’s why we did this study," Dr. Kanzaria explained.
Two focus groups of multispecialty physicians and expert opinion from physicians who have researched overordering of diagnostic imaging were used to create the questions, which were then revised in response to a pilot study conducted among 16 emergency physicians.
The resulting 19-item survey took about 10 minutes to complete. The survey defined a "medically unnecessary" imaging study as "one you wouldn’t order if you had no external pressure and were only concerned about providing optimal medical care."
The nonrandom sample for the survey included 478 academic and community practice emergency physicians in 29 states; the completion rate was a whopping 91% (435 respondents). Respondents’ average age was 42 years with a mean 14 years in clinical practice; 68% were board-certified in emergency medicine. The pattern of survey responses did not differ based upon physician age, years in practice, or board certification status.
More than 85% of the emergency physicians said they believe too many diagnostic tests are ordered in their own ED. More specifically, a similarly lofty percentage believe medically unnecessary CTs and MRIs are ordered in their ED under common clinical scenarios described in the survey, such as head CTs for nontraumatic headaches and pan scans for trauma patients. Fully 97% of EPs acknowledged ordering medically unnecessary CTs and MRIs.
More than 50% of respondents identified as "extremely or very helpful" proposed solutions to "medically unnecessary" advanced imaging in the ED.
Topping the options was tort reform, which 79% of emergency physicians thought would make a major difference. However, Dr. Kanzaria called malpractice reform necessary but not sufficient to change practice. "Recent studies on tort reform efforts have not actually shown subsequent significant effects on cost reduction or a change in test-ordering behavior."
A more promising option may be shared decision making with patients regarding diagnostic testing for low-probability outcomes, he said. "The literature on shared decision making is still in its infancy, but what’s out there [indicates this option] is really promising as an avenue to improve communication and potentially to reduce overuse. So, I think we should consider ways to incorporate shared decision making into emergency care," Dr. Kanzaria said.
Another popular suggestion was to provide feedback to emergency physicians regarding their own test ordering behavior compared to that of their peers, something Dr. Kanzaria called "incredibly simple to do."
Education aimed at steering patients, families, and referring physicians away from the prevailing "no miss" attitude in favor of greater understanding of the probabilistic limits of diagnostic testing was also widely endorsed by the survey respondents.
Dr. Kanzaria’s research is funded by the Robert Wood Johnson Foundation Clinical Scholars Program. He reported having no financial conflicts.
DALLAS – On average, 22% of the CTs and MRIs ordered by emergency physicians are "medically unnecessary," based on responses by 435 emergency physicians participating in a national survey.
"The overwhelming majority of physicians in our sample recognized the issue of overimaging in the ED, and it’s not just something they felt was going on among others in their group. It’s something they personally acknowledged participating in," Dr. Hemal K. Kanzaria said at the annual meeting of the Society for Academic Emergency Medicine.
The two most common reasons for ordering "medically unnecessary" advanced diagnostic imaging studies were fear of missing a diagnosis despite low pretest probability, cited by 69% of respondents, and fear of litigation, cited by 64%, noted Dr. Kanzaria, a Robert Woods Johnson Foundation Clinical Scholar and emergency medicine fellow at the University of California, Los Angeles.
Patient and family expectations were identified as a driving force in ordering medically unnecessary imaging, 40% of respondents said. A mere 1% of respondents cited administrative pressure to increase group reimbursement as a main contributor, he added.
Advanced diagnostic imaging in EDs has increased appreciably in recent years, with little evidence of a resultant improvement in patient outcomes. The trend has drawn scrutiny from health policy experts in light of estimates that the U.S. annually spends $210 billion on unnecessary medical tests, procedures, and services. Yet there are little data on emergency physicians’ perceptions regarding overordering of CTs and MRIs, the causes, and the potential solutions.
"Basically, we need to know what physicians are thinking (about the issue), and that’s why we did this study," Dr. Kanzaria explained.
Two focus groups of multispecialty physicians and expert opinion from physicians who have researched overordering of diagnostic imaging were used to create the questions, which were then revised in response to a pilot study conducted among 16 emergency physicians.
The resulting 19-item survey took about 10 minutes to complete. The survey defined a "medically unnecessary" imaging study as "one you wouldn’t order if you had no external pressure and were only concerned about providing optimal medical care."
The nonrandom sample for the survey included 478 academic and community practice emergency physicians in 29 states; the completion rate was a whopping 91% (435 respondents). Respondents’ average age was 42 years with a mean 14 years in clinical practice; 68% were board-certified in emergency medicine. The pattern of survey responses did not differ based upon physician age, years in practice, or board certification status.
More than 85% of the emergency physicians said they believe too many diagnostic tests are ordered in their own ED. More specifically, a similarly lofty percentage believe medically unnecessary CTs and MRIs are ordered in their ED under common clinical scenarios described in the survey, such as head CTs for nontraumatic headaches and pan scans for trauma patients. Fully 97% of EPs acknowledged ordering medically unnecessary CTs and MRIs.
More than 50% of respondents identified as "extremely or very helpful" proposed solutions to "medically unnecessary" advanced imaging in the ED.
Topping the options was tort reform, which 79% of emergency physicians thought would make a major difference. However, Dr. Kanzaria called malpractice reform necessary but not sufficient to change practice. "Recent studies on tort reform efforts have not actually shown subsequent significant effects on cost reduction or a change in test-ordering behavior."
A more promising option may be shared decision making with patients regarding diagnostic testing for low-probability outcomes, he said. "The literature on shared decision making is still in its infancy, but what’s out there [indicates this option] is really promising as an avenue to improve communication and potentially to reduce overuse. So, I think we should consider ways to incorporate shared decision making into emergency care," Dr. Kanzaria said.
Another popular suggestion was to provide feedback to emergency physicians regarding their own test ordering behavior compared to that of their peers, something Dr. Kanzaria called "incredibly simple to do."
Education aimed at steering patients, families, and referring physicians away from the prevailing "no miss" attitude in favor of greater understanding of the probabilistic limits of diagnostic testing was also widely endorsed by the survey respondents.
Dr. Kanzaria’s research is funded by the Robert Wood Johnson Foundation Clinical Scholars Program. He reported having no financial conflicts.
DALLAS – On average, 22% of the CTs and MRIs ordered by emergency physicians are "medically unnecessary," based on responses by 435 emergency physicians participating in a national survey.
"The overwhelming majority of physicians in our sample recognized the issue of overimaging in the ED, and it’s not just something they felt was going on among others in their group. It’s something they personally acknowledged participating in," Dr. Hemal K. Kanzaria said at the annual meeting of the Society for Academic Emergency Medicine.
The two most common reasons for ordering "medically unnecessary" advanced diagnostic imaging studies were fear of missing a diagnosis despite low pretest probability, cited by 69% of respondents, and fear of litigation, cited by 64%, noted Dr. Kanzaria, a Robert Woods Johnson Foundation Clinical Scholar and emergency medicine fellow at the University of California, Los Angeles.
Patient and family expectations were identified as a driving force in ordering medically unnecessary imaging, 40% of respondents said. A mere 1% of respondents cited administrative pressure to increase group reimbursement as a main contributor, he added.
Advanced diagnostic imaging in EDs has increased appreciably in recent years, with little evidence of a resultant improvement in patient outcomes. The trend has drawn scrutiny from health policy experts in light of estimates that the U.S. annually spends $210 billion on unnecessary medical tests, procedures, and services. Yet there are little data on emergency physicians’ perceptions regarding overordering of CTs and MRIs, the causes, and the potential solutions.
"Basically, we need to know what physicians are thinking (about the issue), and that’s why we did this study," Dr. Kanzaria explained.
Two focus groups of multispecialty physicians and expert opinion from physicians who have researched overordering of diagnostic imaging were used to create the questions, which were then revised in response to a pilot study conducted among 16 emergency physicians.
The resulting 19-item survey took about 10 minutes to complete. The survey defined a "medically unnecessary" imaging study as "one you wouldn’t order if you had no external pressure and were only concerned about providing optimal medical care."
The nonrandom sample for the survey included 478 academic and community practice emergency physicians in 29 states; the completion rate was a whopping 91% (435 respondents). Respondents’ average age was 42 years with a mean 14 years in clinical practice; 68% were board-certified in emergency medicine. The pattern of survey responses did not differ based upon physician age, years in practice, or board certification status.
More than 85% of the emergency physicians said they believe too many diagnostic tests are ordered in their own ED. More specifically, a similarly lofty percentage believe medically unnecessary CTs and MRIs are ordered in their ED under common clinical scenarios described in the survey, such as head CTs for nontraumatic headaches and pan scans for trauma patients. Fully 97% of EPs acknowledged ordering medically unnecessary CTs and MRIs.
More than 50% of respondents identified as "extremely or very helpful" proposed solutions to "medically unnecessary" advanced imaging in the ED.
Topping the options was tort reform, which 79% of emergency physicians thought would make a major difference. However, Dr. Kanzaria called malpractice reform necessary but not sufficient to change practice. "Recent studies on tort reform efforts have not actually shown subsequent significant effects on cost reduction or a change in test-ordering behavior."
A more promising option may be shared decision making with patients regarding diagnostic testing for low-probability outcomes, he said. "The literature on shared decision making is still in its infancy, but what’s out there [indicates this option] is really promising as an avenue to improve communication and potentially to reduce overuse. So, I think we should consider ways to incorporate shared decision making into emergency care," Dr. Kanzaria said.
Another popular suggestion was to provide feedback to emergency physicians regarding their own test ordering behavior compared to that of their peers, something Dr. Kanzaria called "incredibly simple to do."
Education aimed at steering patients, families, and referring physicians away from the prevailing "no miss" attitude in favor of greater understanding of the probabilistic limits of diagnostic testing was also widely endorsed by the survey respondents.
Dr. Kanzaria’s research is funded by the Robert Wood Johnson Foundation Clinical Scholars Program. He reported having no financial conflicts.
AT SAEM 2014

Ensure business associate agreements comply with HIPAA rule, attorneys advise
CHICAGO – A new HIPAA rule means physicians face broader liability for protected health information breaches by their business associates.
The final omnibus rule on the Health Insurance Portability and Accountability Act broadens the definition of who and what is considered a business associate and places more responsibility on doctors for protected health information (PHI) acts or omissions by such associates.

About "28%-49% of breaches in the health care industry are associated with business associates and how they’re using data," health law attorney Clinton R. Mikel said at a physicians’ legal issues conference held by the American Bar Association.
"It’s important to know who your business associates are, how you’re [interacting] with them and what they’re doing with your data."
The final HIPAA omnibus rule went into effect in September 2013, but allowed covered entities and businesses to continue operating under some existing contracts for up to 1 year. Grandfathered business agreements must be revised to meet the new HIPAA requirements by Sept. 22, 2014.
Under the omnibus rule, a business associate is defined as any person or entity that creates, receives, maintains, or transmits PHI on behalf of a covered entity. The regulation means that business associates now include patient safety organizations, data transmission organizations, personal health record vendors, entities that transmit and need routine access to PHI, and data storage vendors – paper based and cloud based.
On physicians’ immediate checklist of things to be reviewed and updated is their existing business-associate agreement template, said Mr. Mikel, a partner at The Health Law Partners, PC, in Southfield, Mich. The revised agreement should ensure that associates comply with all measures of the Security Rule for electronic PHI and that business associates report any breach of unsecured PHI.
In addition, business associates should enter into contracts only with subcontractors that comply with such agreements and restrict subcontractors from disclosing PHI in an inappropriate manner.
Distribute the new template as soon as possible for all new contracts and evaluate outstanding business associate relationships, Mr. Mikel advised.
Proper data security from cloud-based vendors is especially important in light of the new HIPAA rule, said Hemant Pathak, assistant general counsel for Microsoft. Make certain they are told where and how their data is stored in "the cloud" and have clear data maps and geographic boundary information.
Vendors should be "transparent about what their operations are, have a breach procedure, and be willing to share" their policies, Mr. Pathak added. "It should not be something that is obtuse. It should be something that is clear and transparent."
Under the omnibus rule, both the doctor and vendor are on the hook if PHI is exposed.
"It’s important for both of us in protecting our reputations and understanding what the needs are from a compliance" standpoint, Mr. Pathak said.
CHICAGO – A new HIPAA rule means physicians face broader liability for protected health information breaches by their business associates.
The final omnibus rule on the Health Insurance Portability and Accountability Act broadens the definition of who and what is considered a business associate and places more responsibility on doctors for protected health information (PHI) acts or omissions by such associates.
About "28%-49% of breaches in the health care industry are associated with business associates and how they’re using data," health law attorney Clinton R. Mikel said at a physicians’ legal issues conference held by the American Bar Association.
"It’s important to know who your business associates are, how you’re [interacting] with them and what they’re doing with your data."
The final HIPAA omnibus rule went into effect in September 2013, but allowed covered entities and businesses to continue operating under some existing contracts for up to 1 year. Grandfathered business agreements must be revised to meet the new HIPAA requirements by Sept. 22, 2014.
Under the omnibus rule, a business associate is defined as any person or entity that creates, receives, maintains, or transmits PHI on behalf of a covered entity. The regulation means that business associates now include patient safety organizations, data transmission organizations, personal health record vendors, entities that transmit and need routine access to PHI, and data storage vendors – paper based and cloud based.
On physicians’ immediate checklist of things to be reviewed and updated is their existing business-associate agreement template, said Mr. Mikel, a partner at The Health Law Partners, PC, in Southfield, Mich. The revised agreement should ensure that associates comply with all measures of the Security Rule for electronic PHI and that business associates report any breach of unsecured PHI.
In addition, business associates should enter into contracts only with subcontractors that comply with such agreements and restrict subcontractors from disclosing PHI in an inappropriate manner.
Distribute the new template as soon as possible for all new contracts and evaluate outstanding business associate relationships, Mr. Mikel advised.
Proper data security from cloud-based vendors is especially important in light of the new HIPAA rule, said Hemant Pathak, assistant general counsel for Microsoft. Make certain they are told where and how their data is stored in "the cloud" and have clear data maps and geographic boundary information.
Vendors should be "transparent about what their operations are, have a breach procedure, and be willing to share" their policies, Mr. Pathak added. "It should not be something that is obtuse. It should be something that is clear and transparent."
Under the omnibus rule, both the doctor and vendor are on the hook if PHI is exposed.
"It’s important for both of us in protecting our reputations and understanding what the needs are from a compliance" standpoint, Mr. Pathak said.
CHICAGO – A new HIPAA rule means physicians face broader liability for protected health information breaches by their business associates.
The final omnibus rule on the Health Insurance Portability and Accountability Act broadens the definition of who and what is considered a business associate and places more responsibility on doctors for protected health information (PHI) acts or omissions by such associates.
About "28%-49% of breaches in the health care industry are associated with business associates and how they’re using data," health law attorney Clinton R. Mikel said at a physicians’ legal issues conference held by the American Bar Association.
"It’s important to know who your business associates are, how you’re [interacting] with them and what they’re doing with your data."
The final HIPAA omnibus rule went into effect in September 2013, but allowed covered entities and businesses to continue operating under some existing contracts for up to 1 year. Grandfathered business agreements must be revised to meet the new HIPAA requirements by Sept. 22, 2014.
Under the omnibus rule, a business associate is defined as any person or entity that creates, receives, maintains, or transmits PHI on behalf of a covered entity. The regulation means that business associates now include patient safety organizations, data transmission organizations, personal health record vendors, entities that transmit and need routine access to PHI, and data storage vendors – paper based and cloud based.
On physicians’ immediate checklist of things to be reviewed and updated is their existing business-associate agreement template, said Mr. Mikel, a partner at The Health Law Partners, PC, in Southfield, Mich. The revised agreement should ensure that associates comply with all measures of the Security Rule for electronic PHI and that business associates report any breach of unsecured PHI.
In addition, business associates should enter into contracts only with subcontractors that comply with such agreements and restrict subcontractors from disclosing PHI in an inappropriate manner.
Distribute the new template as soon as possible for all new contracts and evaluate outstanding business associate relationships, Mr. Mikel advised.
Proper data security from cloud-based vendors is especially important in light of the new HIPAA rule, said Hemant Pathak, assistant general counsel for Microsoft. Make certain they are told where and how their data is stored in "the cloud" and have clear data maps and geographic boundary information.
Vendors should be "transparent about what their operations are, have a breach procedure, and be willing to share" their policies, Mr. Pathak added. "It should not be something that is obtuse. It should be something that is clear and transparent."
Under the omnibus rule, both the doctor and vendor are on the hook if PHI is exposed.
"It’s important for both of us in protecting our reputations and understanding what the needs are from a compliance" standpoint, Mr. Pathak said.
AT AN ABA CONFERENCE

Republicans more likely to report being hurt by health reform
Six out of 10 Americans say that they have not been affected by the Affordable Care Act, with an unsurprising political split among those who say it has either helped or hurt them, according to a report from the Kaiser Family Foundation.
Among Republicans, 37% say that they have been hurt by the health reform law and 5% say that they have been helped. The numbers were basically reversed for Democrats, with 26% saying that they have been helped and 8% reporting that they been hurt. Independents lean more toward the Republicans, with 27% saying that they have been hurt and 11% saying that they have been helped, Kaiser reported in its latest Health Tracking Poll.
Those who report being hurt by the law were most likely to cite their increased health care costs (14% of the public overall), while those who say they have been helped most often say that someone in their family was able to get or keep coverage (5% of the public overall), Kaiser said.
The survey involved a nationally representative sample of 1,505 adults and was conducted May 13-19.

Six out of 10 Americans say that they have not been affected by the Affordable Care Act, with an unsurprising political split among those who say it has either helped or hurt them, according to a report from the Kaiser Family Foundation.
Among Republicans, 37% say that they have been hurt by the health reform law and 5% say that they have been helped. The numbers were basically reversed for Democrats, with 26% saying that they have been helped and 8% reporting that they been hurt. Independents lean more toward the Republicans, with 27% saying that they have been hurt and 11% saying that they have been helped, Kaiser reported in its latest Health Tracking Poll.
Those who report being hurt by the law were most likely to cite their increased health care costs (14% of the public overall), while those who say they have been helped most often say that someone in their family was able to get or keep coverage (5% of the public overall), Kaiser said.
The survey involved a nationally representative sample of 1,505 adults and was conducted May 13-19.
Six out of 10 Americans say that they have not been affected by the Affordable Care Act, with an unsurprising political split among those who say it has either helped or hurt them, according to a report from the Kaiser Family Foundation.
Among Republicans, 37% say that they have been hurt by the health reform law and 5% say that they have been helped. The numbers were basically reversed for Democrats, with 26% saying that they have been helped and 8% reporting that they been hurt. Independents lean more toward the Republicans, with 27% saying that they have been hurt and 11% saying that they have been helped, Kaiser reported in its latest Health Tracking Poll.
Those who report being hurt by the law were most likely to cite their increased health care costs (14% of the public overall), while those who say they have been helped most often say that someone in their family was able to get or keep coverage (5% of the public overall), Kaiser said.
The survey involved a nationally representative sample of 1,505 adults and was conducted May 13-19.
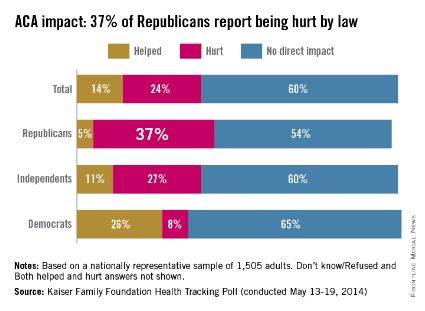
AMA: Obama needs to take immediate action on VA health care
CHICAGO – The American Medical Association’s policy-making body called on President Obama to take immediate action to increase access to care for the nation’s veterans by encouraging them to use physicians outside the Veterans Affairs system.
The House of Delegates also urged state medical societies to create registries of physicians willing and able to take veterans as patients.
The action comes as Congress moves to pass legislation to help alleviate delays in the VA system that have led to long wait times for appointments. The revelation that phony wait lists were created in an attempt to cover up the delays led to the resignation of VA Secretary Eric Shinseki on May 30.

The U.S. House of Representatives on June 10 unanimously passed a bill sponsored by Rep. Jeff Miller (R-Fla.) that would allow veterans to seek care outside the VA system. A similar bipartisan bill in the U.S. Senate that is sponsored by Sen. Bernie Sanders (I-Vt.) and Sen. John McCain (R-Ariz.) may be voted on this week.
The proposal adopted by the AMA House of Delegates at its annual meeting was sponsored by delegations from Florida, Texas, New York, and California. In addition to asking President Obama to provide timely access to health care for veterans by allowing for, and paying for, care outside the VA system, it also calls on Congress to act rapidly on a long-term solution that will provide timely access to care. And, the resolution requested that the AMA issue a press release by June 12 that calls attention to its new policy on care for veterans.
Most of the delegates were in favor of the new policy.
Dr. David McKalip, a Florida neurosurgeon, said his delegation sought the policy because a solution was needed now. He said that he was already providing care to veterans, and that there was "an abundance of care" available outside the VA.
Others said they, too, were already treating veterans, either in emergency departments or in their offices. Dr. Mario Motta, a cardiologist and delegate from Massachusetts, said that he often treated veterans for acute problems and then would send them back to the VA for follow-up. But, they often end up back in his office when they can’t get in to see a cardiologist in the VA system, he said. "We need to fix this issue," said Dr. Motta.
Some delegates said that the AMA should not be trying to fix what is essentially a VA problem.
Dr. Richard Evans, a general surgeon from Dover-Foxcroft, Maine, and a veteran, said that he, too, treated many veterans. But he said that it seemed like the AMA was merely trying to take advantage of a hot topic. "I’m certain everyone in this room is supportive of veterans’ care," said Dr. Evans. But, he added, "I see no need for this resolution."
Another physician-veteran, Dr. Thomas G. Peters, an alternate delegate from Florida, said that all physicians should be willing to see veterans. But, said the Jacksonville-based transplant surgeon, "the responsibility to fix the VA should be with the VA."
The American Academy of Family Physicians also recently urged the President to enlist physicians in the community to help alleviate the backlog at the VA.
In a June 4 letter, Dr. Jeff Cain, AAFP board chair, also said the group was recommending that civilian physicians be allowed to order diagnostic tests at VA facilities, and refer to specialists at those facilities, and to allow prescriptions written by civilian physicians to be filled at VA pharmacies.
"While these policy recommendations are not a solution to all the challenges facing the VA health system, they do represent an opportunity to alleviate the current backlog and facilitate access to primary care services for thousands of veterans," Dr. Cain said in the letter.
On Twitter @aliciaault
CHICAGO – The American Medical Association’s policy-making body called on President Obama to take immediate action to increase access to care for the nation’s veterans by encouraging them to use physicians outside the Veterans Affairs system.
The House of Delegates also urged state medical societies to create registries of physicians willing and able to take veterans as patients.
The action comes as Congress moves to pass legislation to help alleviate delays in the VA system that have led to long wait times for appointments. The revelation that phony wait lists were created in an attempt to cover up the delays led to the resignation of VA Secretary Eric Shinseki on May 30.
The U.S. House of Representatives on June 10 unanimously passed a bill sponsored by Rep. Jeff Miller (R-Fla.) that would allow veterans to seek care outside the VA system. A similar bipartisan bill in the U.S. Senate that is sponsored by Sen. Bernie Sanders (I-Vt.) and Sen. John McCain (R-Ariz.) may be voted on this week.
The proposal adopted by the AMA House of Delegates at its annual meeting was sponsored by delegations from Florida, Texas, New York, and California. In addition to asking President Obama to provide timely access to health care for veterans by allowing for, and paying for, care outside the VA system, it also calls on Congress to act rapidly on a long-term solution that will provide timely access to care. And, the resolution requested that the AMA issue a press release by June 12 that calls attention to its new policy on care for veterans.
Most of the delegates were in favor of the new policy.
Dr. David McKalip, a Florida neurosurgeon, said his delegation sought the policy because a solution was needed now. He said that he was already providing care to veterans, and that there was "an abundance of care" available outside the VA.
Others said they, too, were already treating veterans, either in emergency departments or in their offices. Dr. Mario Motta, a cardiologist and delegate from Massachusetts, said that he often treated veterans for acute problems and then would send them back to the VA for follow-up. But, they often end up back in his office when they can’t get in to see a cardiologist in the VA system, he said. "We need to fix this issue," said Dr. Motta.
Some delegates said that the AMA should not be trying to fix what is essentially a VA problem.
Dr. Richard Evans, a general surgeon from Dover-Foxcroft, Maine, and a veteran, said that he, too, treated many veterans. But he said that it seemed like the AMA was merely trying to take advantage of a hot topic. "I’m certain everyone in this room is supportive of veterans’ care," said Dr. Evans. But, he added, "I see no need for this resolution."
Another physician-veteran, Dr. Thomas G. Peters, an alternate delegate from Florida, said that all physicians should be willing to see veterans. But, said the Jacksonville-based transplant surgeon, "the responsibility to fix the VA should be with the VA."
The American Academy of Family Physicians also recently urged the President to enlist physicians in the community to help alleviate the backlog at the VA.
In a June 4 letter, Dr. Jeff Cain, AAFP board chair, also said the group was recommending that civilian physicians be allowed to order diagnostic tests at VA facilities, and refer to specialists at those facilities, and to allow prescriptions written by civilian physicians to be filled at VA pharmacies.
"While these policy recommendations are not a solution to all the challenges facing the VA health system, they do represent an opportunity to alleviate the current backlog and facilitate access to primary care services for thousands of veterans," Dr. Cain said in the letter.
On Twitter @aliciaault
CHICAGO – The American Medical Association’s policy-making body called on President Obama to take immediate action to increase access to care for the nation’s veterans by encouraging them to use physicians outside the Veterans Affairs system.
The House of Delegates also urged state medical societies to create registries of physicians willing and able to take veterans as patients.
The action comes as Congress moves to pass legislation to help alleviate delays in the VA system that have led to long wait times for appointments. The revelation that phony wait lists were created in an attempt to cover up the delays led to the resignation of VA Secretary Eric Shinseki on May 30.
The U.S. House of Representatives on June 10 unanimously passed a bill sponsored by Rep. Jeff Miller (R-Fla.) that would allow veterans to seek care outside the VA system. A similar bipartisan bill in the U.S. Senate that is sponsored by Sen. Bernie Sanders (I-Vt.) and Sen. John McCain (R-Ariz.) may be voted on this week.
The proposal adopted by the AMA House of Delegates at its annual meeting was sponsored by delegations from Florida, Texas, New York, and California. In addition to asking President Obama to provide timely access to health care for veterans by allowing for, and paying for, care outside the VA system, it also calls on Congress to act rapidly on a long-term solution that will provide timely access to care. And, the resolution requested that the AMA issue a press release by June 12 that calls attention to its new policy on care for veterans.
Most of the delegates were in favor of the new policy.
Dr. David McKalip, a Florida neurosurgeon, said his delegation sought the policy because a solution was needed now. He said that he was already providing care to veterans, and that there was "an abundance of care" available outside the VA.
Others said they, too, were already treating veterans, either in emergency departments or in their offices. Dr. Mario Motta, a cardiologist and delegate from Massachusetts, said that he often treated veterans for acute problems and then would send them back to the VA for follow-up. But, they often end up back in his office when they can’t get in to see a cardiologist in the VA system, he said. "We need to fix this issue," said Dr. Motta.
Some delegates said that the AMA should not be trying to fix what is essentially a VA problem.
Dr. Richard Evans, a general surgeon from Dover-Foxcroft, Maine, and a veteran, said that he, too, treated many veterans. But he said that it seemed like the AMA was merely trying to take advantage of a hot topic. "I’m certain everyone in this room is supportive of veterans’ care," said Dr. Evans. But, he added, "I see no need for this resolution."
Another physician-veteran, Dr. Thomas G. Peters, an alternate delegate from Florida, said that all physicians should be willing to see veterans. But, said the Jacksonville-based transplant surgeon, "the responsibility to fix the VA should be with the VA."
The American Academy of Family Physicians also recently urged the President to enlist physicians in the community to help alleviate the backlog at the VA.
In a June 4 letter, Dr. Jeff Cain, AAFP board chair, also said the group was recommending that civilian physicians be allowed to order diagnostic tests at VA facilities, and refer to specialists at those facilities, and to allow prescriptions written by civilian physicians to be filled at VA pharmacies.
"While these policy recommendations are not a solution to all the challenges facing the VA health system, they do represent an opportunity to alleviate the current backlog and facilitate access to primary care services for thousands of veterans," Dr. Cain said in the letter.
On Twitter @aliciaault
AT THE AMA HOD MEETING
