User login
Accountable care organizations may fuel new litigation theories
The aim of accountable care organizations is to improve health care quality, enhance care coordination, and reduce unnecessary costs. But the new health care delivery models are raising questions about possible hidden legal dangers for participating physicians.
"We’re talking about unchartered territory," said Christopher E. DiGiacinto, a medical liability defense attorney and partner in a New York law firm that focuses on the defense of professional liability claims including those brought against health care professionals and others. "There’s been a lot of uncertainty about how [ACOs] will affect the landscape of litigation. It could go any number of ways."

Mr. DiGiacinto cowrote an article in the 2013 summer issue of Risk Management Quarterly, the journal of the Association for Healthcare Risk Management of New York, detailing malpractice risks doctors may face within ACOs (RMQ Summer 2013). The liability dangers stem primarily from federal guidelines that outline how ACOs should operate and how doctors can enhance their practices.
For example, the Affordance Care Act requires that ACOs share medical information across multiple health care environments to improve knowledge among providers and to eliminate duplication of treatment across the care continuum. But such enhanced record maintenance could expose physicians to increased liability, Mr. DiGiacinto said. A plaintiff’s attorney could claim a doctor’s failure to access a patient’s prior medical records led to a subsequent poor medical outcome.
"There’s going to be a lot more data in this model, which is great for patients and allowing physicians to track patients," he said. "The downside for physicians is, where in the past, they might only be responsible for their own record and knowledge of the patient from their own perspective, now, they’re being responsible for knowing the [patient’s] history from other doctors. There’s going to be a wealth of information that could be used against them."
ACOs also create the potential for a heightened duty of informed consent for physicians, said Julian D. "Bo" Bobbitt Jr., senior partner and head of a health law group at a law firm in Raleigh, N.C. Federal guidelines call for ACOs to promote patient engagement during individualized treatment by involving patients and their families in making medical decisions.
"Under Medicare ACO regulations, there has to be a patient care plan and there has to be significant commitment to patient and family engagement and joint decision making," Mr. Bobbitt said. "What happens if you did a care plan, but you didn’t follow it? You were supposed to engage the family, but you didn’t?"
In such an instance, it’s possible a family member could sue, claiming he or she was not involved enough in the medical decision–making process, said Mr. Bobbitt.
Physicians who help create ACOs or hold administrative positions within the organizations may also be more at risk for being sued, say liability experts, whether or not they were directly involved in patient care.
In the past, entities such as HMOs were rarely sued for the actions of participants because such corporate structures are not generally responsible for the rendering of care, Mr. DiGiacinto said. However, federal guidelines recommend that medical professionals be involved in the corporate structure of ACOs, and that the organizations be accountable for the care they provide. This framework could fuel vicarious liability or corporate negligence claims in which the ACO itself is said to be liable for care provided to patients, according to the Accountable Care Legal Guide and RMQ article. In addition, physician leaders could potentially be sued for alleged negligent credentialing of other health professionals in the ACO, said legal experts.
But some, such as Christi J. Braun, believe suggested ACO litigation dangers are being overblown. Clinically integrated networks are designed to improve quality across all care providers, said Ms. Braun, a Washington-based health care antitrust attorney and cochair of the American Health Lawyers Association’s Accountable Care Organization Task Force.
"Even if you may not be following the protocols all the time, just the fact that you’re looking at best practices and trying to apply best practices makes it more likely that you’re going to provide better care on a more consistent basis," she said. "That actually reduces liability."
At the same time, physicians should not be so focused on following federal guidelines that they allow metrics and benchmarks to override quality medical judgment, said Brandy A. Boone, an Alabama-based senior risk management consultant for a national medical liability insurer.
"I think the biggest risk associated with ACOs or any other arrangement where physicians are incentivized to keep costs down by the prospect of making more money is the allegation that necessary tests or treatments were not offered or recommended because of the effect on reimbursement," Ms. Boone said. "We always caution our insured physicians that treatment recommendations should never be based on the patient’s ability to pay. While the majority of physicians would never actually let reimbursement sway their clinical decisions, avoiding that perception is also very important."
Only time will tell how ACO guidelines will affect malpractice cases. Often, it takes years for case law and legal precedents to develop around new issues and more clearly define boundaries, Mr. Bobbitt said.
In the meantime, litigation experts recommend that physicians joining ACOs protect themselves from lawsuits by thoroughly documenting patient interactions and clinical decision making. Mr. Bobbitt suggests also that physicians participating in ACOs become involved in developing best practice guidelines and ensuring those guidelines are clinically valid. Having a strong voice will empower physicians and assure ACO guidelines act as a lawsuit shield, rather than a sword.
"It can be a legal minefield, but it is navigable," Mr. Bobbitt said. "As an attorney and health care adviser, I try to convey that yes, there are legal issues – novel legal issues – but at the same time, this is such a positive improvement to health care, it is navigable if done right."
The aim of accountable care organizations is to improve health care quality, enhance care coordination, and reduce unnecessary costs. But the new health care delivery models are raising questions about possible hidden legal dangers for participating physicians.
"We’re talking about unchartered territory," said Christopher E. DiGiacinto, a medical liability defense attorney and partner in a New York law firm that focuses on the defense of professional liability claims including those brought against health care professionals and others. "There’s been a lot of uncertainty about how [ACOs] will affect the landscape of litigation. It could go any number of ways."
Mr. DiGiacinto cowrote an article in the 2013 summer issue of Risk Management Quarterly, the journal of the Association for Healthcare Risk Management of New York, detailing malpractice risks doctors may face within ACOs (RMQ Summer 2013). The liability dangers stem primarily from federal guidelines that outline how ACOs should operate and how doctors can enhance their practices.
For example, the Affordance Care Act requires that ACOs share medical information across multiple health care environments to improve knowledge among providers and to eliminate duplication of treatment across the care continuum. But such enhanced record maintenance could expose physicians to increased liability, Mr. DiGiacinto said. A plaintiff’s attorney could claim a doctor’s failure to access a patient’s prior medical records led to a subsequent poor medical outcome.
"There’s going to be a lot more data in this model, which is great for patients and allowing physicians to track patients," he said. "The downside for physicians is, where in the past, they might only be responsible for their own record and knowledge of the patient from their own perspective, now, they’re being responsible for knowing the [patient’s] history from other doctors. There’s going to be a wealth of information that could be used against them."
ACOs also create the potential for a heightened duty of informed consent for physicians, said Julian D. "Bo" Bobbitt Jr., senior partner and head of a health law group at a law firm in Raleigh, N.C. Federal guidelines call for ACOs to promote patient engagement during individualized treatment by involving patients and their families in making medical decisions.
"Under Medicare ACO regulations, there has to be a patient care plan and there has to be significant commitment to patient and family engagement and joint decision making," Mr. Bobbitt said. "What happens if you did a care plan, but you didn’t follow it? You were supposed to engage the family, but you didn’t?"
In such an instance, it’s possible a family member could sue, claiming he or she was not involved enough in the medical decision–making process, said Mr. Bobbitt.
Physicians who help create ACOs or hold administrative positions within the organizations may also be more at risk for being sued, say liability experts, whether or not they were directly involved in patient care.
In the past, entities such as HMOs were rarely sued for the actions of participants because such corporate structures are not generally responsible for the rendering of care, Mr. DiGiacinto said. However, federal guidelines recommend that medical professionals be involved in the corporate structure of ACOs, and that the organizations be accountable for the care they provide. This framework could fuel vicarious liability or corporate negligence claims in which the ACO itself is said to be liable for care provided to patients, according to the Accountable Care Legal Guide and RMQ article. In addition, physician leaders could potentially be sued for alleged negligent credentialing of other health professionals in the ACO, said legal experts.
But some, such as Christi J. Braun, believe suggested ACO litigation dangers are being overblown. Clinically integrated networks are designed to improve quality across all care providers, said Ms. Braun, a Washington-based health care antitrust attorney and cochair of the American Health Lawyers Association’s Accountable Care Organization Task Force.
"Even if you may not be following the protocols all the time, just the fact that you’re looking at best practices and trying to apply best practices makes it more likely that you’re going to provide better care on a more consistent basis," she said. "That actually reduces liability."
At the same time, physicians should not be so focused on following federal guidelines that they allow metrics and benchmarks to override quality medical judgment, said Brandy A. Boone, an Alabama-based senior risk management consultant for a national medical liability insurer.
"I think the biggest risk associated with ACOs or any other arrangement where physicians are incentivized to keep costs down by the prospect of making more money is the allegation that necessary tests or treatments were not offered or recommended because of the effect on reimbursement," Ms. Boone said. "We always caution our insured physicians that treatment recommendations should never be based on the patient’s ability to pay. While the majority of physicians would never actually let reimbursement sway their clinical decisions, avoiding that perception is also very important."
Only time will tell how ACO guidelines will affect malpractice cases. Often, it takes years for case law and legal precedents to develop around new issues and more clearly define boundaries, Mr. Bobbitt said.
In the meantime, litigation experts recommend that physicians joining ACOs protect themselves from lawsuits by thoroughly documenting patient interactions and clinical decision making. Mr. Bobbitt suggests also that physicians participating in ACOs become involved in developing best practice guidelines and ensuring those guidelines are clinically valid. Having a strong voice will empower physicians and assure ACO guidelines act as a lawsuit shield, rather than a sword.
"It can be a legal minefield, but it is navigable," Mr. Bobbitt said. "As an attorney and health care adviser, I try to convey that yes, there are legal issues – novel legal issues – but at the same time, this is such a positive improvement to health care, it is navigable if done right."
The aim of accountable care organizations is to improve health care quality, enhance care coordination, and reduce unnecessary costs. But the new health care delivery models are raising questions about possible hidden legal dangers for participating physicians.
"We’re talking about unchartered territory," said Christopher E. DiGiacinto, a medical liability defense attorney and partner in a New York law firm that focuses on the defense of professional liability claims including those brought against health care professionals and others. "There’s been a lot of uncertainty about how [ACOs] will affect the landscape of litigation. It could go any number of ways."
Mr. DiGiacinto cowrote an article in the 2013 summer issue of Risk Management Quarterly, the journal of the Association for Healthcare Risk Management of New York, detailing malpractice risks doctors may face within ACOs (RMQ Summer 2013). The liability dangers stem primarily from federal guidelines that outline how ACOs should operate and how doctors can enhance their practices.
For example, the Affordance Care Act requires that ACOs share medical information across multiple health care environments to improve knowledge among providers and to eliminate duplication of treatment across the care continuum. But such enhanced record maintenance could expose physicians to increased liability, Mr. DiGiacinto said. A plaintiff’s attorney could claim a doctor’s failure to access a patient’s prior medical records led to a subsequent poor medical outcome.
"There’s going to be a lot more data in this model, which is great for patients and allowing physicians to track patients," he said. "The downside for physicians is, where in the past, they might only be responsible for their own record and knowledge of the patient from their own perspective, now, they’re being responsible for knowing the [patient’s] history from other doctors. There’s going to be a wealth of information that could be used against them."
ACOs also create the potential for a heightened duty of informed consent for physicians, said Julian D. "Bo" Bobbitt Jr., senior partner and head of a health law group at a law firm in Raleigh, N.C. Federal guidelines call for ACOs to promote patient engagement during individualized treatment by involving patients and their families in making medical decisions.
"Under Medicare ACO regulations, there has to be a patient care plan and there has to be significant commitment to patient and family engagement and joint decision making," Mr. Bobbitt said. "What happens if you did a care plan, but you didn’t follow it? You were supposed to engage the family, but you didn’t?"
In such an instance, it’s possible a family member could sue, claiming he or she was not involved enough in the medical decision–making process, said Mr. Bobbitt.
Physicians who help create ACOs or hold administrative positions within the organizations may also be more at risk for being sued, say liability experts, whether or not they were directly involved in patient care.
In the past, entities such as HMOs were rarely sued for the actions of participants because such corporate structures are not generally responsible for the rendering of care, Mr. DiGiacinto said. However, federal guidelines recommend that medical professionals be involved in the corporate structure of ACOs, and that the organizations be accountable for the care they provide. This framework could fuel vicarious liability or corporate negligence claims in which the ACO itself is said to be liable for care provided to patients, according to the Accountable Care Legal Guide and RMQ article. In addition, physician leaders could potentially be sued for alleged negligent credentialing of other health professionals in the ACO, said legal experts.
But some, such as Christi J. Braun, believe suggested ACO litigation dangers are being overblown. Clinically integrated networks are designed to improve quality across all care providers, said Ms. Braun, a Washington-based health care antitrust attorney and cochair of the American Health Lawyers Association’s Accountable Care Organization Task Force.
"Even if you may not be following the protocols all the time, just the fact that you’re looking at best practices and trying to apply best practices makes it more likely that you’re going to provide better care on a more consistent basis," she said. "That actually reduces liability."
At the same time, physicians should not be so focused on following federal guidelines that they allow metrics and benchmarks to override quality medical judgment, said Brandy A. Boone, an Alabama-based senior risk management consultant for a national medical liability insurer.
"I think the biggest risk associated with ACOs or any other arrangement where physicians are incentivized to keep costs down by the prospect of making more money is the allegation that necessary tests or treatments were not offered or recommended because of the effect on reimbursement," Ms. Boone said. "We always caution our insured physicians that treatment recommendations should never be based on the patient’s ability to pay. While the majority of physicians would never actually let reimbursement sway their clinical decisions, avoiding that perception is also very important."
Only time will tell how ACO guidelines will affect malpractice cases. Often, it takes years for case law and legal precedents to develop around new issues and more clearly define boundaries, Mr. Bobbitt said.
In the meantime, litigation experts recommend that physicians joining ACOs protect themselves from lawsuits by thoroughly documenting patient interactions and clinical decision making. Mr. Bobbitt suggests also that physicians participating in ACOs become involved in developing best practice guidelines and ensuring those guidelines are clinically valid. Having a strong voice will empower physicians and assure ACO guidelines act as a lawsuit shield, rather than a sword.
"It can be a legal minefield, but it is navigable," Mr. Bobbitt said. "As an attorney and health care adviser, I try to convey that yes, there are legal issues – novel legal issues – but at the same time, this is such a positive improvement to health care, it is navigable if done right."

Proper Inpatient Documentation, Coding Essential to Avoid a Medicare Audit

Several years ago we sent a CPT coding auditor 15 chart notes generated by each doctor in our group. Among each doctors’ 15 notes were at least one or two billed as initial hospital care, follow up, discharge, critical care, and so on. This coding expert returned a report showing that, out of all the notes reviewed, a significant portion were not billed at the correct level. Most of the incorrectly billed notes were judged to reflect “up-coding,” and a few were seen as “down-coded.”
This was distressing and hard to believe.
So I took the same set of notes and paid a second coding expert for an independent review. She didn’t know about the first audit but returned a report that showed a nearly identical portion of incorrectly coded notes.
Two independent audits showing nearly the same portion of notes coded incorrectly was alarming. But it was difficult for my partners and me to address, because the auditors didn’t agree on the correct code for many of the notes. In some cases, both flagged a note as incorrectly coded but didn’t agree on the correct code. For a number of the notes, one auditor said the visit was “up-coded,” while the other said it was “down-coded.” There was so little agreement between the two of them that we had a hard time coming up with any firm conclusions about what we should do to improve our performance.
If experts who think about coding all the time can’t agree on the right code for a given note, how can hospitalists be expected to code nearly all of our visits accurately?
RAC: Recovery Audit Contractor
Despite what I believe is poor inter-rater reliability among coding auditors, we need to work diligently to comply with coding guidelines. A 2003 Federal law mandated a program of Recovery Audit Contractors, or RAC for short, to find cases of “up-coding” or other overbilling and require the provider to repay any resulting loss.
A number of companies are in the business of conducting RAC audits (one of them, CGI, is the Canadian company blamed for the failed “Obamacare” exchange websites), and there is a reasonable chance one of these companies has reviewed some of your charges—or those of your hospitalist colleagues.
The RAC auditors review information about your charges, and if they determine that you up-coded or overbilled, they send a “demand letter” summarizing their findings, along with the amount of money they have determined you should pay back. (Theoretically, they could notify you of “under-coding,” so that you can be paid more for past work, but I haven’t yet come across an example of that.)
It is common to appeal the RAC findings, but that can be a long process, and many organizations decide to pay back all the money requested by the RAC as quickly as possible to avoid paying interest on a delayed payment if the appeal is unsuccessful. In the case of a successful appeal, the money previously refunded by the doctor would be returned.
Page 338 of the CMS Fiscal Year 2015 “Justification of Estimates for Appropriations Committees” says that “…about 50 percent of the estimated 43,000 appeals [of adverse RAC audit findings] were fully or partially overturned…” This could mean the RACs are a sort of loose cannon, accusing many providers of overbilling while knowing that some won’t bother to appeal because they don’t understand the process or because the dollar amount involved for a single provider is too small to justify the time and expense of conducting the appeal. In this way, a RAC audit is like the $15 rebate on the last electronic gadget you bought. The seller knows that many people, including me, will fail to do the work required to claim the rebate.
Accuracy Strategies
There are a number of ways to help your group ensure appropriate CPT coding and reduce the chance a RAC will ask for money back.
Education. There are many ways to help providers in your practice understand the elements of documentation and coding. Periodic training classes (e.g. during orientation and annually thereafter) are useful but may not be enough. For me, this is a little like learning a foreign language by going to a couple of classes. Instead, I think “immersion training” is more effective. That might mean a doctor spends a few minutes with a certified coder on most working days for a few weeks. For example, they could meet for 15 minutes near lunchtime and review how the doctor plans to bill visits made that morning. Lastly, consider targeted education for each doctor, based on any problems found in an audit of his/her coding.
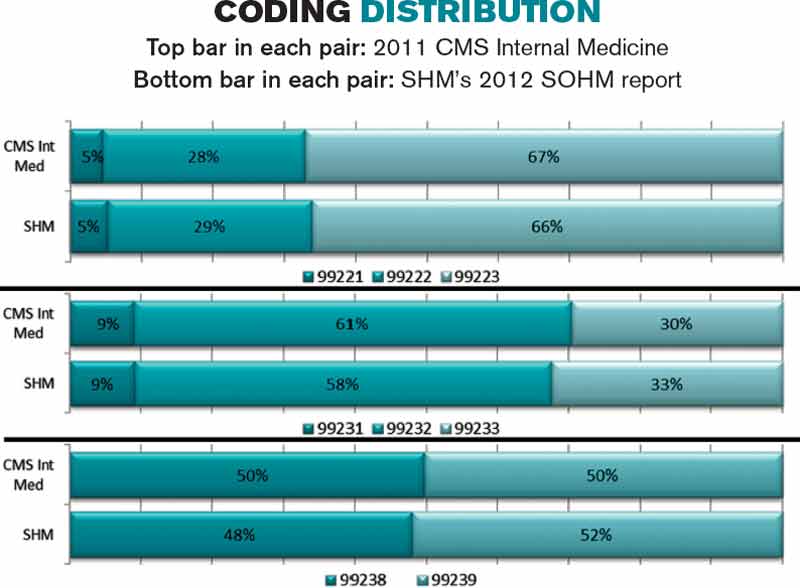
Review coding patterns. As I wrote in my August 2007 column, there is value in ensuring that each doctor in the group can see how her coding pattern differs from the group as a whole or any individual in the group. That is, what portion of follow-up visits was billed at the lowest, middle, and highest levels? What about admissions, discharges, and so on? I provided a sample report in that same column.
It also is worth taking the time to compare each doctor’s coding pattern to both the CMS Internal Medicine data and SHM’s State of Hospital Medicine report. The accompanying figure shows the most current data sets available.
Keep in mind that the goal is not to simply ensure that your coding pattern matches these external data sets; knowing where yours differs from these sets can suggest where you might want to investigate further or seek additional education.
Coding audits. Having a certified coder audit your performance at least annually is a good idea. It can help uncover areas in which you’d benefit from further review and training, and if, heaven forbid, questions are ever raised about whether you’re intentionally up-coding (fraud), showing that you’re audited regularly could help demonstrate your efforts to code correctly. In the latter case, it is probably more valuable if the audit is done independently of your employer.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Several years ago we sent a CPT coding auditor 15 chart notes generated by each doctor in our group. Among each doctors’ 15 notes were at least one or two billed as initial hospital care, follow up, discharge, critical care, and so on. This coding expert returned a report showing that, out of all the notes reviewed, a significant portion were not billed at the correct level. Most of the incorrectly billed notes were judged to reflect “up-coding,” and a few were seen as “down-coded.”
This was distressing and hard to believe.
So I took the same set of notes and paid a second coding expert for an independent review. She didn’t know about the first audit but returned a report that showed a nearly identical portion of incorrectly coded notes.
Two independent audits showing nearly the same portion of notes coded incorrectly was alarming. But it was difficult for my partners and me to address, because the auditors didn’t agree on the correct code for many of the notes. In some cases, both flagged a note as incorrectly coded but didn’t agree on the correct code. For a number of the notes, one auditor said the visit was “up-coded,” while the other said it was “down-coded.” There was so little agreement between the two of them that we had a hard time coming up with any firm conclusions about what we should do to improve our performance.
If experts who think about coding all the time can’t agree on the right code for a given note, how can hospitalists be expected to code nearly all of our visits accurately?
RAC: Recovery Audit Contractor
Despite what I believe is poor inter-rater reliability among coding auditors, we need to work diligently to comply with coding guidelines. A 2003 Federal law mandated a program of Recovery Audit Contractors, or RAC for short, to find cases of “up-coding” or other overbilling and require the provider to repay any resulting loss.
A number of companies are in the business of conducting RAC audits (one of them, CGI, is the Canadian company blamed for the failed “Obamacare” exchange websites), and there is a reasonable chance one of these companies has reviewed some of your charges—or those of your hospitalist colleagues.
The RAC auditors review information about your charges, and if they determine that you up-coded or overbilled, they send a “demand letter” summarizing their findings, along with the amount of money they have determined you should pay back. (Theoretically, they could notify you of “under-coding,” so that you can be paid more for past work, but I haven’t yet come across an example of that.)
It is common to appeal the RAC findings, but that can be a long process, and many organizations decide to pay back all the money requested by the RAC as quickly as possible to avoid paying interest on a delayed payment if the appeal is unsuccessful. In the case of a successful appeal, the money previously refunded by the doctor would be returned.
Page 338 of the CMS Fiscal Year 2015 “Justification of Estimates for Appropriations Committees” says that “…about 50 percent of the estimated 43,000 appeals [of adverse RAC audit findings] were fully or partially overturned…” This could mean the RACs are a sort of loose cannon, accusing many providers of overbilling while knowing that some won’t bother to appeal because they don’t understand the process or because the dollar amount involved for a single provider is too small to justify the time and expense of conducting the appeal. In this way, a RAC audit is like the $15 rebate on the last electronic gadget you bought. The seller knows that many people, including me, will fail to do the work required to claim the rebate.
Accuracy Strategies
There are a number of ways to help your group ensure appropriate CPT coding and reduce the chance a RAC will ask for money back.
Education. There are many ways to help providers in your practice understand the elements of documentation and coding. Periodic training classes (e.g. during orientation and annually thereafter) are useful but may not be enough. For me, this is a little like learning a foreign language by going to a couple of classes. Instead, I think “immersion training” is more effective. That might mean a doctor spends a few minutes with a certified coder on most working days for a few weeks. For example, they could meet for 15 minutes near lunchtime and review how the doctor plans to bill visits made that morning. Lastly, consider targeted education for each doctor, based on any problems found in an audit of his/her coding.
Review coding patterns. As I wrote in my August 2007 column, there is value in ensuring that each doctor in the group can see how her coding pattern differs from the group as a whole or any individual in the group. That is, what portion of follow-up visits was billed at the lowest, middle, and highest levels? What about admissions, discharges, and so on? I provided a sample report in that same column.
It also is worth taking the time to compare each doctor’s coding pattern to both the CMS Internal Medicine data and SHM’s State of Hospital Medicine report. The accompanying figure shows the most current data sets available.
Keep in mind that the goal is not to simply ensure that your coding pattern matches these external data sets; knowing where yours differs from these sets can suggest where you might want to investigate further or seek additional education.
Coding audits. Having a certified coder audit your performance at least annually is a good idea. It can help uncover areas in which you’d benefit from further review and training, and if, heaven forbid, questions are ever raised about whether you’re intentionally up-coding (fraud), showing that you’re audited regularly could help demonstrate your efforts to code correctly. In the latter case, it is probably more valuable if the audit is done independently of your employer.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Several years ago we sent a CPT coding auditor 15 chart notes generated by each doctor in our group. Among each doctors’ 15 notes were at least one or two billed as initial hospital care, follow up, discharge, critical care, and so on. This coding expert returned a report showing that, out of all the notes reviewed, a significant portion were not billed at the correct level. Most of the incorrectly billed notes were judged to reflect “up-coding,” and a few were seen as “down-coded.”
This was distressing and hard to believe.
So I took the same set of notes and paid a second coding expert for an independent review. She didn’t know about the first audit but returned a report that showed a nearly identical portion of incorrectly coded notes.
Two independent audits showing nearly the same portion of notes coded incorrectly was alarming. But it was difficult for my partners and me to address, because the auditors didn’t agree on the correct code for many of the notes. In some cases, both flagged a note as incorrectly coded but didn’t agree on the correct code. For a number of the notes, one auditor said the visit was “up-coded,” while the other said it was “down-coded.” There was so little agreement between the two of them that we had a hard time coming up with any firm conclusions about what we should do to improve our performance.
If experts who think about coding all the time can’t agree on the right code for a given note, how can hospitalists be expected to code nearly all of our visits accurately?
RAC: Recovery Audit Contractor
Despite what I believe is poor inter-rater reliability among coding auditors, we need to work diligently to comply with coding guidelines. A 2003 Federal law mandated a program of Recovery Audit Contractors, or RAC for short, to find cases of “up-coding” or other overbilling and require the provider to repay any resulting loss.
A number of companies are in the business of conducting RAC audits (one of them, CGI, is the Canadian company blamed for the failed “Obamacare” exchange websites), and there is a reasonable chance one of these companies has reviewed some of your charges—or those of your hospitalist colleagues.
The RAC auditors review information about your charges, and if they determine that you up-coded or overbilled, they send a “demand letter” summarizing their findings, along with the amount of money they have determined you should pay back. (Theoretically, they could notify you of “under-coding,” so that you can be paid more for past work, but I haven’t yet come across an example of that.)
It is common to appeal the RAC findings, but that can be a long process, and many organizations decide to pay back all the money requested by the RAC as quickly as possible to avoid paying interest on a delayed payment if the appeal is unsuccessful. In the case of a successful appeal, the money previously refunded by the doctor would be returned.
Page 338 of the CMS Fiscal Year 2015 “Justification of Estimates for Appropriations Committees” says that “…about 50 percent of the estimated 43,000 appeals [of adverse RAC audit findings] were fully or partially overturned…” This could mean the RACs are a sort of loose cannon, accusing many providers of overbilling while knowing that some won’t bother to appeal because they don’t understand the process or because the dollar amount involved for a single provider is too small to justify the time and expense of conducting the appeal. In this way, a RAC audit is like the $15 rebate on the last electronic gadget you bought. The seller knows that many people, including me, will fail to do the work required to claim the rebate.
Accuracy Strategies
There are a number of ways to help your group ensure appropriate CPT coding and reduce the chance a RAC will ask for money back.
Education. There are many ways to help providers in your practice understand the elements of documentation and coding. Periodic training classes (e.g. during orientation and annually thereafter) are useful but may not be enough. For me, this is a little like learning a foreign language by going to a couple of classes. Instead, I think “immersion training” is more effective. That might mean a doctor spends a few minutes with a certified coder on most working days for a few weeks. For example, they could meet for 15 minutes near lunchtime and review how the doctor plans to bill visits made that morning. Lastly, consider targeted education for each doctor, based on any problems found in an audit of his/her coding.
Review coding patterns. As I wrote in my August 2007 column, there is value in ensuring that each doctor in the group can see how her coding pattern differs from the group as a whole or any individual in the group. That is, what portion of follow-up visits was billed at the lowest, middle, and highest levels? What about admissions, discharges, and so on? I provided a sample report in that same column.
It also is worth taking the time to compare each doctor’s coding pattern to both the CMS Internal Medicine data and SHM’s State of Hospital Medicine report. The accompanying figure shows the most current data sets available.
Keep in mind that the goal is not to simply ensure that your coding pattern matches these external data sets; knowing where yours differs from these sets can suggest where you might want to investigate further or seek additional education.
Coding audits. Having a certified coder audit your performance at least annually is a good idea. It can help uncover areas in which you’d benefit from further review and training, and if, heaven forbid, questions are ever raised about whether you’re intentionally up-coding (fraud), showing that you’re audited regularly could help demonstrate your efforts to code correctly. In the latter case, it is probably more valuable if the audit is done independently of your employer.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Delay in ICD-10 Implementation to Impact Hospitalists, Physicians, Payers
On April 1, President Obama signed into law a bill that again delays a permanent fix of the sustainable growth rate formula, or SGR, the so-called “doc fix.” The bill also contained a surprise provision added by Congress to delay implementation of the switch from ICD-9 to ICD-10. The mandated conversion was supposed to take place by October 1 of this year; its delay will have a range of impacts on everyone from physicians to payers.
Hospitalists and others must weigh their options going forward, as many health systems and groups are already well on their way toward compliance with the 2014 deadline.
At this point, prevailing wisdom is that Congress added the delay as an appeasement to physician groups that would be unhappy about its failure to pass an SGR replacement, says Jeffrey Smith, senior director of federal affairs for CHIME, the College of Healthcare Information Management Executives.
“The appeasement, if in fact that was the motivation, was too little too late,” Smith says, adding Congress “caused a lot of unnecessary chaos.”
For instance, according to Modern Healthcare, executives at Catholic Health Initiatives had already invested millions of dollars updating software programs to handle the coding switch ahead of a new electronic health record system roll-out in 89 of its hospitals, which would not have been ready by the ICD-10 deadline.
“Anyone in the process has to circle the wagons again and reconsider their timelines,” Smith says. “The legislation has punished people trying to do the right thing.”
The transition to ICD-10 is a massive update to the 30-year-old ICD-9 codes, which no longer adequately reflect medical diagnoses, procedures, technology, and knowledge. There are five times more diagnosis codes and 21 times more procedural codes in ICD-10. It’s been on the table for at least a decade, and this was not the first delay.
In 2012, when fewer groups were on their way to compliance, CMS estimated that a one-year push-back of ICD-10 conversion could cost up to $306 million. With the latest delay, the American Health Information Management Association says CMS now estimates those costs between $1 billion and $6.6 billion.
However, according to the American Medical Association, which has actively lobbied to stop ICD-10 altogether, the costs of implementing ICD-10 range from $57,000 for small physician practices to as high as $8 million for large practices.
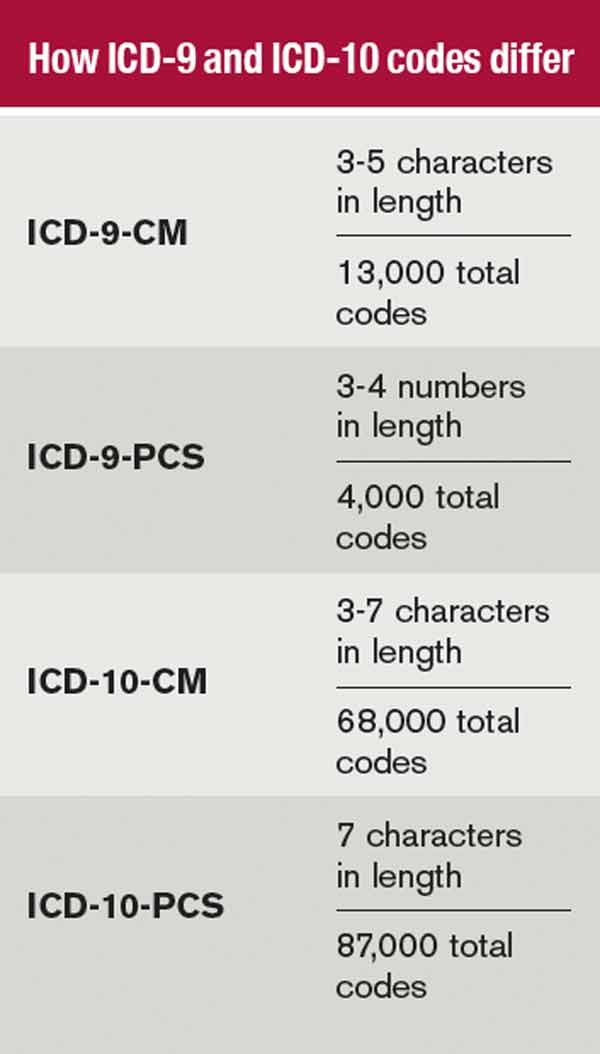
The increased number of codes, the increased number of characters per code, and the increased specificity require significant planning, training, software updates, and financial investments.
The Medical Group Management Association (MGMA) also pushed for ICD-10 delay, concerned that many groups would not be ready by Oct. 1. MGMA surveys showed as much, says Robert Tennant, senior policy advisor for MGMA.“We were concerned that if everyone has to flip the switch at the same time, there will be huge problems, as there were for healthcare.gov,” Tennant explains.
What MGMA would like to see is more thorough end-to-end testing and staggered roll-outs. Hospitals and health plans should be permitted to start using ICD-10 coding when they're ready, even if ahead of the next deadline, Tennant said. MGMA would also like to see a period of dual coding built in.
The ball is now in CMS' court.
“I think that CMS has within its power … the ability to embolden the industry to be more confident,” Smith says. “Even if it’s not going to require ICD-10 codes [by October 2014], hopefully they are still doing testing, still doing benchmarking, and by the time the deadline rolls around, it will touch every sector of the healthcare economy.”
Hospitalists, Smith says, should be more involved in the conversation going forward, to help maintain the momentum and preserve the investments made by their groups and institutions. Those not ready should push for compliance, rather than finding themselves in the same position a year from now.
Many of the hospital CIOs (chief information officers) he has talked to say that while they are stopping the car, they are keeping the engine running. Some will push for dual coding, even if only internally, because it’s proving to be a valuable tool in understanding their patient populations.
“It’s a frustrating time any time you have to kind of stop something with so much momentum, with hundreds of millions, if not billions, spent in advance of the conversion,” Smith says. “It does nothing to help care in this country to stay on ICD-9. Everybody understands those codes are completely exhausted, and the data we are getting out of it, while workable, is certainly not going to get us where we need to be in terms of transforming healthcare.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
On April 1, President Obama signed into law a bill that again delays a permanent fix of the sustainable growth rate formula, or SGR, the so-called “doc fix.” The bill also contained a surprise provision added by Congress to delay implementation of the switch from ICD-9 to ICD-10. The mandated conversion was supposed to take place by October 1 of this year; its delay will have a range of impacts on everyone from physicians to payers.
Hospitalists and others must weigh their options going forward, as many health systems and groups are already well on their way toward compliance with the 2014 deadline.
At this point, prevailing wisdom is that Congress added the delay as an appeasement to physician groups that would be unhappy about its failure to pass an SGR replacement, says Jeffrey Smith, senior director of federal affairs for CHIME, the College of Healthcare Information Management Executives.
“The appeasement, if in fact that was the motivation, was too little too late,” Smith says, adding Congress “caused a lot of unnecessary chaos.”
For instance, according to Modern Healthcare, executives at Catholic Health Initiatives had already invested millions of dollars updating software programs to handle the coding switch ahead of a new electronic health record system roll-out in 89 of its hospitals, which would not have been ready by the ICD-10 deadline.
“Anyone in the process has to circle the wagons again and reconsider their timelines,” Smith says. “The legislation has punished people trying to do the right thing.”
The transition to ICD-10 is a massive update to the 30-year-old ICD-9 codes, which no longer adequately reflect medical diagnoses, procedures, technology, and knowledge. There are five times more diagnosis codes and 21 times more procedural codes in ICD-10. It’s been on the table for at least a decade, and this was not the first delay.
In 2012, when fewer groups were on their way to compliance, CMS estimated that a one-year push-back of ICD-10 conversion could cost up to $306 million. With the latest delay, the American Health Information Management Association says CMS now estimates those costs between $1 billion and $6.6 billion.
However, according to the American Medical Association, which has actively lobbied to stop ICD-10 altogether, the costs of implementing ICD-10 range from $57,000 for small physician practices to as high as $8 million for large practices.
The increased number of codes, the increased number of characters per code, and the increased specificity require significant planning, training, software updates, and financial investments.
The Medical Group Management Association (MGMA) also pushed for ICD-10 delay, concerned that many groups would not be ready by Oct. 1. MGMA surveys showed as much, says Robert Tennant, senior policy advisor for MGMA.“We were concerned that if everyone has to flip the switch at the same time, there will be huge problems, as there were for healthcare.gov,” Tennant explains.
What MGMA would like to see is more thorough end-to-end testing and staggered roll-outs. Hospitals and health plans should be permitted to start using ICD-10 coding when they're ready, even if ahead of the next deadline, Tennant said. MGMA would also like to see a period of dual coding built in.
The ball is now in CMS' court.
“I think that CMS has within its power … the ability to embolden the industry to be more confident,” Smith says. “Even if it’s not going to require ICD-10 codes [by October 2014], hopefully they are still doing testing, still doing benchmarking, and by the time the deadline rolls around, it will touch every sector of the healthcare economy.”
Hospitalists, Smith says, should be more involved in the conversation going forward, to help maintain the momentum and preserve the investments made by their groups and institutions. Those not ready should push for compliance, rather than finding themselves in the same position a year from now.
Many of the hospital CIOs (chief information officers) he has talked to say that while they are stopping the car, they are keeping the engine running. Some will push for dual coding, even if only internally, because it’s proving to be a valuable tool in understanding their patient populations.
“It’s a frustrating time any time you have to kind of stop something with so much momentum, with hundreds of millions, if not billions, spent in advance of the conversion,” Smith says. “It does nothing to help care in this country to stay on ICD-9. Everybody understands those codes are completely exhausted, and the data we are getting out of it, while workable, is certainly not going to get us where we need to be in terms of transforming healthcare.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
On April 1, President Obama signed into law a bill that again delays a permanent fix of the sustainable growth rate formula, or SGR, the so-called “doc fix.” The bill also contained a surprise provision added by Congress to delay implementation of the switch from ICD-9 to ICD-10. The mandated conversion was supposed to take place by October 1 of this year; its delay will have a range of impacts on everyone from physicians to payers.
Hospitalists and others must weigh their options going forward, as many health systems and groups are already well on their way toward compliance with the 2014 deadline.
At this point, prevailing wisdom is that Congress added the delay as an appeasement to physician groups that would be unhappy about its failure to pass an SGR replacement, says Jeffrey Smith, senior director of federal affairs for CHIME, the College of Healthcare Information Management Executives.
“The appeasement, if in fact that was the motivation, was too little too late,” Smith says, adding Congress “caused a lot of unnecessary chaos.”
For instance, according to Modern Healthcare, executives at Catholic Health Initiatives had already invested millions of dollars updating software programs to handle the coding switch ahead of a new electronic health record system roll-out in 89 of its hospitals, which would not have been ready by the ICD-10 deadline.
“Anyone in the process has to circle the wagons again and reconsider their timelines,” Smith says. “The legislation has punished people trying to do the right thing.”
The transition to ICD-10 is a massive update to the 30-year-old ICD-9 codes, which no longer adequately reflect medical diagnoses, procedures, technology, and knowledge. There are five times more diagnosis codes and 21 times more procedural codes in ICD-10. It’s been on the table for at least a decade, and this was not the first delay.
In 2012, when fewer groups were on their way to compliance, CMS estimated that a one-year push-back of ICD-10 conversion could cost up to $306 million. With the latest delay, the American Health Information Management Association says CMS now estimates those costs between $1 billion and $6.6 billion.
However, according to the American Medical Association, which has actively lobbied to stop ICD-10 altogether, the costs of implementing ICD-10 range from $57,000 for small physician practices to as high as $8 million for large practices.
The increased number of codes, the increased number of characters per code, and the increased specificity require significant planning, training, software updates, and financial investments.
The Medical Group Management Association (MGMA) also pushed for ICD-10 delay, concerned that many groups would not be ready by Oct. 1. MGMA surveys showed as much, says Robert Tennant, senior policy advisor for MGMA.“We were concerned that if everyone has to flip the switch at the same time, there will be huge problems, as there were for healthcare.gov,” Tennant explains.
What MGMA would like to see is more thorough end-to-end testing and staggered roll-outs. Hospitals and health plans should be permitted to start using ICD-10 coding when they're ready, even if ahead of the next deadline, Tennant said. MGMA would also like to see a period of dual coding built in.
The ball is now in CMS' court.
“I think that CMS has within its power … the ability to embolden the industry to be more confident,” Smith says. “Even if it’s not going to require ICD-10 codes [by October 2014], hopefully they are still doing testing, still doing benchmarking, and by the time the deadline rolls around, it will touch every sector of the healthcare economy.”
Hospitalists, Smith says, should be more involved in the conversation going forward, to help maintain the momentum and preserve the investments made by their groups and institutions. Those not ready should push for compliance, rather than finding themselves in the same position a year from now.
Many of the hospital CIOs (chief information officers) he has talked to say that while they are stopping the car, they are keeping the engine running. Some will push for dual coding, even if only internally, because it’s proving to be a valuable tool in understanding their patient populations.
“It’s a frustrating time any time you have to kind of stop something with so much momentum, with hundreds of millions, if not billions, spent in advance of the conversion,” Smith says. “It does nothing to help care in this country to stay on ICD-9. Everybody understands those codes are completely exhausted, and the data we are getting out of it, while workable, is certainly not going to get us where we need to be in terms of transforming healthcare.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
Hospitals Lose $45.9 Billion in Uncompensated Care in 2012
Dollar value of uncompensated care provided by U.S. hospitals in 2012, expressed in terms of actual costs, according to data from the American Hospital Association’s Annual Survey of Hospitals.6 This figure represents 6.1% of total costs, an increase of 11.7% from 2011. The total includes both bad debt and charity care provided to patients unable to pay for their care, AHA says, but does not include underpayments by Medicare and Medicaid.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
Dollar value of uncompensated care provided by U.S. hospitals in 2012, expressed in terms of actual costs, according to data from the American Hospital Association’s Annual Survey of Hospitals.6 This figure represents 6.1% of total costs, an increase of 11.7% from 2011. The total includes both bad debt and charity care provided to patients unable to pay for their care, AHA says, but does not include underpayments by Medicare and Medicaid.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
Dollar value of uncompensated care provided by U.S. hospitals in 2012, expressed in terms of actual costs, according to data from the American Hospital Association’s Annual Survey of Hospitals.6 This figure represents 6.1% of total costs, an increase of 11.7% from 2011. The total includes both bad debt and charity care provided to patients unable to pay for their care, AHA says, but does not include underpayments by Medicare and Medicaid.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
Yogurt May Reduce Clostridium Difficile Infection Rate

The Philadelphia Inquirer recently reported that Holy Redeemer Hospital in Meadowbrook, Pa., cut its incidence of Clostridium difficile by two-thirds after its nutritionists began encouraging hospitalized patients with orders for antibiotics for more than one day to eat a widely available brand of yogurt.2 Seventy-five C. diff cases were reported in the hospital during 2011 and only 23 in 2012. The facility won an innovation award for the program from the Hospital and Healthsystem Association of Pennsylvania.
Other hospitals dispense probiotic dietary supplements, shown to have benefits against C. diff, in granular form. Medical experts have expressed skepticism that dispensing yogurt made the difference in cutting C. diff infections, arguing that there has not been enough research yet to support its widespread implementation in hospital settings.
Nationally, 337,000 cases of C. diff are reported in hospitals each year. A recent study reports that its spores are still commonly carried on the hands of healthcare workers who rubbed alcohol on their hands shortly after providing routine care to patients.3 Risk factors independently associated with hand contamination among healthcare workers in the exposed group included high-risk contacts and at least one contact without the use of gloves.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
The Philadelphia Inquirer recently reported that Holy Redeemer Hospital in Meadowbrook, Pa., cut its incidence of Clostridium difficile by two-thirds after its nutritionists began encouraging hospitalized patients with orders for antibiotics for more than one day to eat a widely available brand of yogurt.2 Seventy-five C. diff cases were reported in the hospital during 2011 and only 23 in 2012. The facility won an innovation award for the program from the Hospital and Healthsystem Association of Pennsylvania.
Other hospitals dispense probiotic dietary supplements, shown to have benefits against C. diff, in granular form. Medical experts have expressed skepticism that dispensing yogurt made the difference in cutting C. diff infections, arguing that there has not been enough research yet to support its widespread implementation in hospital settings.
Nationally, 337,000 cases of C. diff are reported in hospitals each year. A recent study reports that its spores are still commonly carried on the hands of healthcare workers who rubbed alcohol on their hands shortly after providing routine care to patients.3 Risk factors independently associated with hand contamination among healthcare workers in the exposed group included high-risk contacts and at least one contact without the use of gloves.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
The Philadelphia Inquirer recently reported that Holy Redeemer Hospital in Meadowbrook, Pa., cut its incidence of Clostridium difficile by two-thirds after its nutritionists began encouraging hospitalized patients with orders for antibiotics for more than one day to eat a widely available brand of yogurt.2 Seventy-five C. diff cases were reported in the hospital during 2011 and only 23 in 2012. The facility won an innovation award for the program from the Hospital and Healthsystem Association of Pennsylvania.
Other hospitals dispense probiotic dietary supplements, shown to have benefits against C. diff, in granular form. Medical experts have expressed skepticism that dispensing yogurt made the difference in cutting C. diff infections, arguing that there has not been enough research yet to support its widespread implementation in hospital settings.
Nationally, 337,000 cases of C. diff are reported in hospitals each year. A recent study reports that its spores are still commonly carried on the hands of healthcare workers who rubbed alcohol on their hands shortly after providing routine care to patients.3 Risk factors independently associated with hand contamination among healthcare workers in the exposed group included high-risk contacts and at least one contact without the use of gloves.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
Pre-Order Your State of Hospital Medicine Report Now
The State of Hospital Medicine Report is the authoritative source for hospitalists to compare and contrast their staffing, productivity, and compensation with other HM groups across the country. SHM publishes the State of Hospital Medicine every two years. SHM is accepting pre-orders now. For more information, visit www.hospitalmedicine.org/sohm.
The State of Hospital Medicine Report is the authoritative source for hospitalists to compare and contrast their staffing, productivity, and compensation with other HM groups across the country. SHM publishes the State of Hospital Medicine every two years. SHM is accepting pre-orders now. For more information, visit www.hospitalmedicine.org/sohm.
The State of Hospital Medicine Report is the authoritative source for hospitalists to compare and contrast their staffing, productivity, and compensation with other HM groups across the country. SHM publishes the State of Hospital Medicine every two years. SHM is accepting pre-orders now. For more information, visit www.hospitalmedicine.org/sohm.
Code-H Interactive Tool Helps Hospital Medicine Groups with Coding
Looking for ways to make your HM group run better? SHM is introducing new tools and information to keep you ahead of the curve.
CODE-H Interactive is an industry first: an interactive tool to help hospitalist groups code effectively and efficiently. CODE-H Interactive allows users to validate documentation against coding criteria and provides a guided tour through clinical documentation, allowing users to ensure they are choosing the correct billing code while providing a conceptual framework that enables the user to easily “connect the dots” between clinical documentation and the applicable CPT coding.
CODE-H Interactive includes two modules: one that reviews three admission notes and a second that reviews three daily notes. It also enables users to assess other E/M codes, such as consultations and ED visits. To get started, visit www.hospitalmedicine.org/CODEHI.
Looking for ways to make your HM group run better? SHM is introducing new tools and information to keep you ahead of the curve.
CODE-H Interactive is an industry first: an interactive tool to help hospitalist groups code effectively and efficiently. CODE-H Interactive allows users to validate documentation against coding criteria and provides a guided tour through clinical documentation, allowing users to ensure they are choosing the correct billing code while providing a conceptual framework that enables the user to easily “connect the dots” between clinical documentation and the applicable CPT coding.
CODE-H Interactive includes two modules: one that reviews three admission notes and a second that reviews three daily notes. It also enables users to assess other E/M codes, such as consultations and ED visits. To get started, visit www.hospitalmedicine.org/CODEHI.
Looking for ways to make your HM group run better? SHM is introducing new tools and information to keep you ahead of the curve.
CODE-H Interactive is an industry first: an interactive tool to help hospitalist groups code effectively and efficiently. CODE-H Interactive allows users to validate documentation against coding criteria and provides a guided tour through clinical documentation, allowing users to ensure they are choosing the correct billing code while providing a conceptual framework that enables the user to easily “connect the dots” between clinical documentation and the applicable CPT coding.
CODE-H Interactive includes two modules: one that reviews three admission notes and a second that reviews three daily notes. It also enables users to assess other E/M codes, such as consultations and ED visits. To get started, visit www.hospitalmedicine.org/CODEHI.
Medicare Rule Change Raises Stakes for Hospital Discharge Planning

When she presents information to hospitalists about the little-known revision to Medicare’s condition of participation for discharge planning by hospitals, most hospitalists have no idea what Amy Boutwell, MD, MPP, is talking about. Even hospitalists who are active in their institutions’ efforts to improve transitions of care out of the hospital setting are unaware of the change, which was published in the Centers for Medicare & Medicaid Services’ Transmittal 87 and became effective July 19, 2013.
“I just don’t hear hospital professionals talking about it,” says Dr. Boutwell, a hospitalist at Newton-Wellesley Hospital and president of Collaborative Healthcare Strategies in Lexington, Mass. “When I say, ‘There are new rules of the road for discharge planning and evaluation,’ many are not aware of it.”
The revised condition states that the hospital must have a discharge planning process that applies to all patients—not just Medicare beneficiaries. Not every patient needs to have a written discharge plan—although this is recommended—but all patients should be screened and, if indicated, evaluated at an early stage of their hospitalization for risk of adverse post-discharge outcomes. Observation patients are not included in this requirement.
The discharge plan is different from a discharge summary document, which must be completed by the inpatient attending physician, not the hospital, and is not directly addressed in the regulation. The regulation does address the need for transfer of essential information to the next provider of care and says the hospital should have a written policy and procedure in place for discharge planning. The policy and procedure should be developed with input from medical staff and approved by the hospital’s governing body.

Any hospitalist participating with a hospital QI team involved in Project BOOST is helping their hospital comply with this condition of participation.
—Mark Williams, MD, FACP, SFHM, principal investigator of SHM’s Project BOOST
Transmittal 87 represents the first major update of the discharge planning regulation (Standard 482.43) and accompanying interpretive guidelines in more than a decade, Dr. Boutwell says. It consolidates and reorganizes 24 “tags” of regulatory language down to 13 and contains blue advisory boxes recommending best practices in discharge planning, drawn from the suggestions of a technical expert panel convened by CMS.
That panel included many of the country’s recognized thought leaders on improving care transitions, such as Mark Williams, MD, FACP, SFHM, principal investigator of SHM’s Project BOOST; Eric Coleman, MD, MPH, head of the University of Colorado’s division of health care policy and research and creator of the widely-adopted Care Transitions Program (caretransitions.org), and Dr. Boutwell, co-founder of the STAAR initiative (www.ihi.org/engage/Initiatives/completed/STAAR).
The new condition raises baseline expectations for discharge planning and elevates care transitions efforts from a quality improvement issue to the realm of regulatory compliance, Dr. Boutwell says.
“This goes way beyond case review,” she adds. “It represents an evolution from discharge planning case by case to a system for improving transitions of care [for the hospital]. I’m impressed.”
The recommendations are consistent with best practices promoted by Project BOOST, STAAR, Project RED [Re-Engineered Discharge], and other national quality initiatives for improving care transitions.
“Any hospitalist participating with a hospital QI team involved in Project BOOST is helping their hospital comply with this condition of participation,” Dr. Williams says.
In the Byzantine structure of federal regulations, Medicare’s conditions of participation are the regulations providers must meet in order to participate in the Medicare program and bill for their services. Condition-level citations, if not resolved, can cause hospitals to be decertified from Medicare. The accompanying interpretive guidelines, with survey protocols, are the playbook to help state auditors and providers know how to interpret and apply the language of the regulations. The suggestions and examples of best practices contained in the new condition are not required of hospitals but, if followed, could increase their likelihood of achieving better patient outcomes and staying in compliance with the regulations on surveys.
“If hospitals were to actually implement all of the CMS advisory practice recommendations contained in this 35-page document, they’d be in really good shape for effectively managing transitions of care,” says Teresa L. Hamblin, RN, MS, a CMS consultant with Joint Commission Resources. “The government has provided robust practice recommendations that are a model for what hospitals can do. I’d advise doing your best to implement these recommendations. Check your current processes using this detailed document for reference.”
Discharge planning starts at admission, Hamblin says. If the hospitalist assumes that responsibility, it becomes easier to leave a paper trail in the patient’s chart. Other important lessons for hospitalists include participation in a multidisciplinary approach to discharge planning (i.e., interdisciplinary rounding) and development of policies and procedures in this area.
“If the hospital has not elected to do a discharge plan on every patient, request this for your own patients and recommend it as a policy,” Hamblin says. “Go the extra mile, making follow-up appointments for your patients, filling prescriptions in house, and calling the patient 24 to 72 hours after discharge.”
Weekend coverage, when case managers typically are not present, is a particular challenge in care transitions.
“Encourage your hospital to provide reliable weekend coverage for discharge planning. Involve the nurses,” Hamblin says. “Anything the hospitalist can do to help the hospital close this gap is important.”
Larry Beresford is a freelance writer in Alameda, Calif.
When she presents information to hospitalists about the little-known revision to Medicare’s condition of participation for discharge planning by hospitals, most hospitalists have no idea what Amy Boutwell, MD, MPP, is talking about. Even hospitalists who are active in their institutions’ efforts to improve transitions of care out of the hospital setting are unaware of the change, which was published in the Centers for Medicare & Medicaid Services’ Transmittal 87 and became effective July 19, 2013.
“I just don’t hear hospital professionals talking about it,” says Dr. Boutwell, a hospitalist at Newton-Wellesley Hospital and president of Collaborative Healthcare Strategies in Lexington, Mass. “When I say, ‘There are new rules of the road for discharge planning and evaluation,’ many are not aware of it.”
The revised condition states that the hospital must have a discharge planning process that applies to all patients—not just Medicare beneficiaries. Not every patient needs to have a written discharge plan—although this is recommended—but all patients should be screened and, if indicated, evaluated at an early stage of their hospitalization for risk of adverse post-discharge outcomes. Observation patients are not included in this requirement.
The discharge plan is different from a discharge summary document, which must be completed by the inpatient attending physician, not the hospital, and is not directly addressed in the regulation. The regulation does address the need for transfer of essential information to the next provider of care and says the hospital should have a written policy and procedure in place for discharge planning. The policy and procedure should be developed with input from medical staff and approved by the hospital’s governing body.
Any hospitalist participating with a hospital QI team involved in Project BOOST is helping their hospital comply with this condition of participation.
—Mark Williams, MD, FACP, SFHM, principal investigator of SHM’s Project BOOST
Transmittal 87 represents the first major update of the discharge planning regulation (Standard 482.43) and accompanying interpretive guidelines in more than a decade, Dr. Boutwell says. It consolidates and reorganizes 24 “tags” of regulatory language down to 13 and contains blue advisory boxes recommending best practices in discharge planning, drawn from the suggestions of a technical expert panel convened by CMS.
That panel included many of the country’s recognized thought leaders on improving care transitions, such as Mark Williams, MD, FACP, SFHM, principal investigator of SHM’s Project BOOST; Eric Coleman, MD, MPH, head of the University of Colorado’s division of health care policy and research and creator of the widely-adopted Care Transitions Program (caretransitions.org), and Dr. Boutwell, co-founder of the STAAR initiative (www.ihi.org/engage/Initiatives/completed/STAAR).
The new condition raises baseline expectations for discharge planning and elevates care transitions efforts from a quality improvement issue to the realm of regulatory compliance, Dr. Boutwell says.
“This goes way beyond case review,” she adds. “It represents an evolution from discharge planning case by case to a system for improving transitions of care [for the hospital]. I’m impressed.”
The recommendations are consistent with best practices promoted by Project BOOST, STAAR, Project RED [Re-Engineered Discharge], and other national quality initiatives for improving care transitions.
“Any hospitalist participating with a hospital QI team involved in Project BOOST is helping their hospital comply with this condition of participation,” Dr. Williams says.
In the Byzantine structure of federal regulations, Medicare’s conditions of participation are the regulations providers must meet in order to participate in the Medicare program and bill for their services. Condition-level citations, if not resolved, can cause hospitals to be decertified from Medicare. The accompanying interpretive guidelines, with survey protocols, are the playbook to help state auditors and providers know how to interpret and apply the language of the regulations. The suggestions and examples of best practices contained in the new condition are not required of hospitals but, if followed, could increase their likelihood of achieving better patient outcomes and staying in compliance with the regulations on surveys.
“If hospitals were to actually implement all of the CMS advisory practice recommendations contained in this 35-page document, they’d be in really good shape for effectively managing transitions of care,” says Teresa L. Hamblin, RN, MS, a CMS consultant with Joint Commission Resources. “The government has provided robust practice recommendations that are a model for what hospitals can do. I’d advise doing your best to implement these recommendations. Check your current processes using this detailed document for reference.”
Discharge planning starts at admission, Hamblin says. If the hospitalist assumes that responsibility, it becomes easier to leave a paper trail in the patient’s chart. Other important lessons for hospitalists include participation in a multidisciplinary approach to discharge planning (i.e., interdisciplinary rounding) and development of policies and procedures in this area.
“If the hospital has not elected to do a discharge plan on every patient, request this for your own patients and recommend it as a policy,” Hamblin says. “Go the extra mile, making follow-up appointments for your patients, filling prescriptions in house, and calling the patient 24 to 72 hours after discharge.”
Weekend coverage, when case managers typically are not present, is a particular challenge in care transitions.
“Encourage your hospital to provide reliable weekend coverage for discharge planning. Involve the nurses,” Hamblin says. “Anything the hospitalist can do to help the hospital close this gap is important.”
Larry Beresford is a freelance writer in Alameda, Calif.
When she presents information to hospitalists about the little-known revision to Medicare’s condition of participation for discharge planning by hospitals, most hospitalists have no idea what Amy Boutwell, MD, MPP, is talking about. Even hospitalists who are active in their institutions’ efforts to improve transitions of care out of the hospital setting are unaware of the change, which was published in the Centers for Medicare & Medicaid Services’ Transmittal 87 and became effective July 19, 2013.
“I just don’t hear hospital professionals talking about it,” says Dr. Boutwell, a hospitalist at Newton-Wellesley Hospital and president of Collaborative Healthcare Strategies in Lexington, Mass. “When I say, ‘There are new rules of the road for discharge planning and evaluation,’ many are not aware of it.”
The revised condition states that the hospital must have a discharge planning process that applies to all patients—not just Medicare beneficiaries. Not every patient needs to have a written discharge plan—although this is recommended—but all patients should be screened and, if indicated, evaluated at an early stage of their hospitalization for risk of adverse post-discharge outcomes. Observation patients are not included in this requirement.
The discharge plan is different from a discharge summary document, which must be completed by the inpatient attending physician, not the hospital, and is not directly addressed in the regulation. The regulation does address the need for transfer of essential information to the next provider of care and says the hospital should have a written policy and procedure in place for discharge planning. The policy and procedure should be developed with input from medical staff and approved by the hospital’s governing body.
Any hospitalist participating with a hospital QI team involved in Project BOOST is helping their hospital comply with this condition of participation.
—Mark Williams, MD, FACP, SFHM, principal investigator of SHM’s Project BOOST
Transmittal 87 represents the first major update of the discharge planning regulation (Standard 482.43) and accompanying interpretive guidelines in more than a decade, Dr. Boutwell says. It consolidates and reorganizes 24 “tags” of regulatory language down to 13 and contains blue advisory boxes recommending best practices in discharge planning, drawn from the suggestions of a technical expert panel convened by CMS.
That panel included many of the country’s recognized thought leaders on improving care transitions, such as Mark Williams, MD, FACP, SFHM, principal investigator of SHM’s Project BOOST; Eric Coleman, MD, MPH, head of the University of Colorado’s division of health care policy and research and creator of the widely-adopted Care Transitions Program (caretransitions.org), and Dr. Boutwell, co-founder of the STAAR initiative (www.ihi.org/engage/Initiatives/completed/STAAR).
The new condition raises baseline expectations for discharge planning and elevates care transitions efforts from a quality improvement issue to the realm of regulatory compliance, Dr. Boutwell says.
“This goes way beyond case review,” she adds. “It represents an evolution from discharge planning case by case to a system for improving transitions of care [for the hospital]. I’m impressed.”
The recommendations are consistent with best practices promoted by Project BOOST, STAAR, Project RED [Re-Engineered Discharge], and other national quality initiatives for improving care transitions.
“Any hospitalist participating with a hospital QI team involved in Project BOOST is helping their hospital comply with this condition of participation,” Dr. Williams says.
In the Byzantine structure of federal regulations, Medicare’s conditions of participation are the regulations providers must meet in order to participate in the Medicare program and bill for their services. Condition-level citations, if not resolved, can cause hospitals to be decertified from Medicare. The accompanying interpretive guidelines, with survey protocols, are the playbook to help state auditors and providers know how to interpret and apply the language of the regulations. The suggestions and examples of best practices contained in the new condition are not required of hospitals but, if followed, could increase their likelihood of achieving better patient outcomes and staying in compliance with the regulations on surveys.
“If hospitals were to actually implement all of the CMS advisory practice recommendations contained in this 35-page document, they’d be in really good shape for effectively managing transitions of care,” says Teresa L. Hamblin, RN, MS, a CMS consultant with Joint Commission Resources. “The government has provided robust practice recommendations that are a model for what hospitals can do. I’d advise doing your best to implement these recommendations. Check your current processes using this detailed document for reference.”
Discharge planning starts at admission, Hamblin says. If the hospitalist assumes that responsibility, it becomes easier to leave a paper trail in the patient’s chart. Other important lessons for hospitalists include participation in a multidisciplinary approach to discharge planning (i.e., interdisciplinary rounding) and development of policies and procedures in this area.
“If the hospital has not elected to do a discharge plan on every patient, request this for your own patients and recommend it as a policy,” Hamblin says. “Go the extra mile, making follow-up appointments for your patients, filling prescriptions in house, and calling the patient 24 to 72 hours after discharge.”
Weekend coverage, when case managers typically are not present, is a particular challenge in care transitions.
“Encourage your hospital to provide reliable weekend coverage for discharge planning. Involve the nurses,” Hamblin says. “Anything the hospitalist can do to help the hospital close this gap is important.”
Larry Beresford is a freelance writer in Alameda, Calif.
SGR Reform, ICD-10 Implementation Delays Frustrate Hospitalists, Physicians
Congress has once again delayed implementation of draconian Medicare cuts tied to the sustainable growth rate (SGR) formula. It was the 17th temporary patch applied to the ailing physician reimbursement program, so the decision caused little surprise.
But with the same legislation—the Protecting Access to Medicare Act of 2014—being used to delay the long-awaited debut of ICD-10, many hospitalists and physicians couldn’t help but wonder whether billing and coding would now be as much of a political football as the SGR fix.1
The upshot: It doesn’t seem that way.
“I think it’s two separate issues,” says Phyllis “PJ” Floyd, RN, BSN, MBA, NE-BC, CCA, director of health information services and clinical documentation improvement at Medical University of South Carolina (MUSC) in Charleston, S.C. “The fact that it was all in one bill, I don’t know that it was well thought out as much as it was, ‘Let’s put the ICD-10 in here at the same time.’
“It was just a few sentences, and then it wasn’t even brought up in the discussion on the floor.”
Four policy wonks interviewed by The Hospitalist concurred that while tying the ICD-10 delay to the SGR issue was an unexpected and frustrating development, the coding system likely will be implemented in the relative short term. Meanwhile, a long-term resolution of the SGR dilemma remains much more elusive.
“For about 12 hours, I felt relief about the ICD-10 [being delayed], and then I just realized, it’s still coming, presumably,” says John Nelson, MD, MHM, a co-founder and past president of SHM and medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. “[It’s] like a patient who needs surgery and finds out it’s canceled for the day and he’ll have it tomorrow. Well, that’s good for right now, but [he] still has to face this eventually.”
“Doc-Pay” Fix Near?
Congress’ recent decision to delay both an SGR fix and the ICD-10 are troubling to some hospitalists and others for different reasons.
The SGR extension through this year’s end means that physicians do not face a 24% cut to physician payments under Medicare. SHM has long lobbied against temporary patches to the SGR, repeatedly backing legislation that would once and for all scrap the formula and replace it with something sustainable.
The SGR formula was first crafted in 1997, but the now often-delayed cuts were a byproduct of the federal sequester that was included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. The cuts were implemented as a doomsday scenario that was never likely to actually happen, but despite negotiations over the past three years, no long-term compromise can be found. Paying for the reform remains the main stumbling block.
“I think, this year, Congress was as close as it’s been in a long time to enacting a serious fix, aided by the agreement of major professional societies like the American College of Physicians and American College of Surgeons,” says David Howard, PhD, an associate professor in the department of health policy and management at the Rollins School of Public Health at Emory University in Atlanta. “They were all on board with this solution. ... Who knows, maybe if the economic situation continues to improve [and] tax revenues continue to go up...that will create a more favorable environment for compromise.”
Dr. Howard adds that while Congress might be close to a solution in theory, agreement on how to offset the roughly $100 billion in costs “is just very difficult.” That is why the healthcare professor is pessimistic that a long-term fix is truly at hand.
“The places where Congress might have looked for savings to offset the cost of the doc fix, such as hospital reimbursement rates or payment rates to Medicare Advantage plans—those are exactly the areas that the Affordable Care Act is targeting to pay for insurance expansion,” Dr. Howard adds. “So those areas of savings are not going to be available to offset the cost of the doc fix.”
ICD-10 Delays “Unfair”

The medical coding conundrum presents a different set of issues. The delay in transitioning healthcare providers from the ICD-9 medical coding classification system to the more complicated ICD-10 means the upgraded system is now against an Oct. 1, 2015, deadline. This comes after the Centers for Medicare & Medicaid Services (CMS) already pushed back the original implementation date for ICD-10 by one year.
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, FACP, SFHM, says he thinks most doctors are content with the delay, particularly in light of some estimates that show that only about 20% of physicians “have actually initiated the ICD-10 transition.” But he also notes that it’s unfair to the health systems that have prepared for ICD-10.
“ICD-9 has a little more than 14,000 diagnostic codes and nearly 4,000 procedural codes. That is to be contrasted to ICD-10, which has more than 68,000 diagnostic codes ... and over 72,000 procedural codes,” Dr. Lenchus says. “So, it is not surprising that many take solace in the delay.”
–Dr. Lenchus
Dr. Nelson says the level of frustration for hospitalists is growing; however, the level of disruption for hospitals and health systems is reaching a boiling point.
“Of course, in some places, hospitalists may be the physician lead on ICD-10 efforts, so [they are] very much wrapped up in the problem of ‘What do we do now?’”
The answer, at least to the Coalition for ICD-10, a group of medical/technology trade groups, is to fight to ensure that the delays go no further. In an April letter to CMS Administrator Marilyn Tavenner, the coalition made that case, noting that in 2012, “CMS estimated the cost to the healthcare industry of a one-year delay to be as much as $6.6 billion, or approximately 30% of the $22 billion that CMS estimated had been invested or budgeted for ICD-10 implementation.”2
The letter went on to explain that the disruption and cost will grow each time the ICD-10 deadline is pushed.
“Furthermore, as CMS stated in 2012, implementation costs will continue to increase considerably with every year of a delay,” according to the letter. “The lost opportunity costs of failing to move to a more effective code set also continue to climb every year.”
Stay Engaged, Switch Gears
One of Floyd’s biggest concerns is that the ICD-10 implementation delays will affect physician engagement. The hospitalist groups at MUSC began training for ICD-10 in January 2013; however, the preparation and training were geared toward a 2014 implementation.
“You have to switch gears a little bit,” she says. “What we plan to do now is begin to do heavy auditing, and then from those audits we can give real-time feedback on what we’re doing well and what we’re not doing well. So I think that will be a method for engagement.”
She urges hospitalists, practice leaders, and informatics professionals to discuss ICD-10 not as a theoretical application, but as one tied to reimbursement that will have major impact in the years ahead. To that end, the American Health Information Management Association highlights the fact that the new coding system will result in higher-quality data that can improve performance measures, provide “increased sensitivity” to reimbursement methodologies, and help with stronger public health surveillance.3
“A lot of physicians see this as a hospital issue, and I think that’s why they shy away,” Floyd says. “Now there are some physicians who are interested in how well the hospital does, but the other piece is that it does affect things like [reduced] risk of mortality [and] comparison of data worldwide—those are things that we just have to continue to reiterate … and give them real examples.”
Richard Quinn is a freelance writer in New Jersey.
References
- Govtrack. H.R. 4302: Protecting Access to Medicare Act of 2014. https://www.govtrack.us/congress/bills/113/hr4302. Accessed June 5, 2014.
- Coalition for ICD. Letter to CMS Administrator Tavenner, April 11, 2014. http://coalitionforicd10.wordpress.com/2014/03/26/letter-from-the-coalition-for-icd-10. Accessed June 5, 2014.
- American Health Information Management Association. ICD-10-CM/PCS Transition: Planning and Preparation Checklist. http://journal.ahima.org/wp-content/uploads/ICD10-checklist.pdf. Accessed June 5, 2014.
Congress has once again delayed implementation of draconian Medicare cuts tied to the sustainable growth rate (SGR) formula. It was the 17th temporary patch applied to the ailing physician reimbursement program, so the decision caused little surprise.
But with the same legislation—the Protecting Access to Medicare Act of 2014—being used to delay the long-awaited debut of ICD-10, many hospitalists and physicians couldn’t help but wonder whether billing and coding would now be as much of a political football as the SGR fix.1
The upshot: It doesn’t seem that way.
“I think it’s two separate issues,” says Phyllis “PJ” Floyd, RN, BSN, MBA, NE-BC, CCA, director of health information services and clinical documentation improvement at Medical University of South Carolina (MUSC) in Charleston, S.C. “The fact that it was all in one bill, I don’t know that it was well thought out as much as it was, ‘Let’s put the ICD-10 in here at the same time.’
“It was just a few sentences, and then it wasn’t even brought up in the discussion on the floor.”
Four policy wonks interviewed by The Hospitalist concurred that while tying the ICD-10 delay to the SGR issue was an unexpected and frustrating development, the coding system likely will be implemented in the relative short term. Meanwhile, a long-term resolution of the SGR dilemma remains much more elusive.
“For about 12 hours, I felt relief about the ICD-10 [being delayed], and then I just realized, it’s still coming, presumably,” says John Nelson, MD, MHM, a co-founder and past president of SHM and medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. “[It’s] like a patient who needs surgery and finds out it’s canceled for the day and he’ll have it tomorrow. Well, that’s good for right now, but [he] still has to face this eventually.”
“Doc-Pay” Fix Near?
Congress’ recent decision to delay both an SGR fix and the ICD-10 are troubling to some hospitalists and others for different reasons.
The SGR extension through this year’s end means that physicians do not face a 24% cut to physician payments under Medicare. SHM has long lobbied against temporary patches to the SGR, repeatedly backing legislation that would once and for all scrap the formula and replace it with something sustainable.
The SGR formula was first crafted in 1997, but the now often-delayed cuts were a byproduct of the federal sequester that was included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. The cuts were implemented as a doomsday scenario that was never likely to actually happen, but despite negotiations over the past three years, no long-term compromise can be found. Paying for the reform remains the main stumbling block.
“I think, this year, Congress was as close as it’s been in a long time to enacting a serious fix, aided by the agreement of major professional societies like the American College of Physicians and American College of Surgeons,” says David Howard, PhD, an associate professor in the department of health policy and management at the Rollins School of Public Health at Emory University in Atlanta. “They were all on board with this solution. ... Who knows, maybe if the economic situation continues to improve [and] tax revenues continue to go up...that will create a more favorable environment for compromise.”
Dr. Howard adds that while Congress might be close to a solution in theory, agreement on how to offset the roughly $100 billion in costs “is just very difficult.” That is why the healthcare professor is pessimistic that a long-term fix is truly at hand.
“The places where Congress might have looked for savings to offset the cost of the doc fix, such as hospital reimbursement rates or payment rates to Medicare Advantage plans—those are exactly the areas that the Affordable Care Act is targeting to pay for insurance expansion,” Dr. Howard adds. “So those areas of savings are not going to be available to offset the cost of the doc fix.”
ICD-10 Delays “Unfair”
The medical coding conundrum presents a different set of issues. The delay in transitioning healthcare providers from the ICD-9 medical coding classification system to the more complicated ICD-10 means the upgraded system is now against an Oct. 1, 2015, deadline. This comes after the Centers for Medicare & Medicaid Services (CMS) already pushed back the original implementation date for ICD-10 by one year.
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, FACP, SFHM, says he thinks most doctors are content with the delay, particularly in light of some estimates that show that only about 20% of physicians “have actually initiated the ICD-10 transition.” But he also notes that it’s unfair to the health systems that have prepared for ICD-10.
“ICD-9 has a little more than 14,000 diagnostic codes and nearly 4,000 procedural codes. That is to be contrasted to ICD-10, which has more than 68,000 diagnostic codes ... and over 72,000 procedural codes,” Dr. Lenchus says. “So, it is not surprising that many take solace in the delay.”
–Dr. Lenchus
Dr. Nelson says the level of frustration for hospitalists is growing; however, the level of disruption for hospitals and health systems is reaching a boiling point.
“Of course, in some places, hospitalists may be the physician lead on ICD-10 efforts, so [they are] very much wrapped up in the problem of ‘What do we do now?’”
The answer, at least to the Coalition for ICD-10, a group of medical/technology trade groups, is to fight to ensure that the delays go no further. In an April letter to CMS Administrator Marilyn Tavenner, the coalition made that case, noting that in 2012, “CMS estimated the cost to the healthcare industry of a one-year delay to be as much as $6.6 billion, or approximately 30% of the $22 billion that CMS estimated had been invested or budgeted for ICD-10 implementation.”2
The letter went on to explain that the disruption and cost will grow each time the ICD-10 deadline is pushed.
“Furthermore, as CMS stated in 2012, implementation costs will continue to increase considerably with every year of a delay,” according to the letter. “The lost opportunity costs of failing to move to a more effective code set also continue to climb every year.”
Stay Engaged, Switch Gears
One of Floyd’s biggest concerns is that the ICD-10 implementation delays will affect physician engagement. The hospitalist groups at MUSC began training for ICD-10 in January 2013; however, the preparation and training were geared toward a 2014 implementation.
“You have to switch gears a little bit,” she says. “What we plan to do now is begin to do heavy auditing, and then from those audits we can give real-time feedback on what we’re doing well and what we’re not doing well. So I think that will be a method for engagement.”
She urges hospitalists, practice leaders, and informatics professionals to discuss ICD-10 not as a theoretical application, but as one tied to reimbursement that will have major impact in the years ahead. To that end, the American Health Information Management Association highlights the fact that the new coding system will result in higher-quality data that can improve performance measures, provide “increased sensitivity” to reimbursement methodologies, and help with stronger public health surveillance.3
“A lot of physicians see this as a hospital issue, and I think that’s why they shy away,” Floyd says. “Now there are some physicians who are interested in how well the hospital does, but the other piece is that it does affect things like [reduced] risk of mortality [and] comparison of data worldwide—those are things that we just have to continue to reiterate … and give them real examples.”
Richard Quinn is a freelance writer in New Jersey.
References
- Govtrack. H.R. 4302: Protecting Access to Medicare Act of 2014. https://www.govtrack.us/congress/bills/113/hr4302. Accessed June 5, 2014.
- Coalition for ICD. Letter to CMS Administrator Tavenner, April 11, 2014. http://coalitionforicd10.wordpress.com/2014/03/26/letter-from-the-coalition-for-icd-10. Accessed June 5, 2014.
- American Health Information Management Association. ICD-10-CM/PCS Transition: Planning and Preparation Checklist. http://journal.ahima.org/wp-content/uploads/ICD10-checklist.pdf. Accessed June 5, 2014.
Congress has once again delayed implementation of draconian Medicare cuts tied to the sustainable growth rate (SGR) formula. It was the 17th temporary patch applied to the ailing physician reimbursement program, so the decision caused little surprise.
But with the same legislation—the Protecting Access to Medicare Act of 2014—being used to delay the long-awaited debut of ICD-10, many hospitalists and physicians couldn’t help but wonder whether billing and coding would now be as much of a political football as the SGR fix.1
The upshot: It doesn’t seem that way.
“I think it’s two separate issues,” says Phyllis “PJ” Floyd, RN, BSN, MBA, NE-BC, CCA, director of health information services and clinical documentation improvement at Medical University of South Carolina (MUSC) in Charleston, S.C. “The fact that it was all in one bill, I don’t know that it was well thought out as much as it was, ‘Let’s put the ICD-10 in here at the same time.’
“It was just a few sentences, and then it wasn’t even brought up in the discussion on the floor.”
Four policy wonks interviewed by The Hospitalist concurred that while tying the ICD-10 delay to the SGR issue was an unexpected and frustrating development, the coding system likely will be implemented in the relative short term. Meanwhile, a long-term resolution of the SGR dilemma remains much more elusive.
“For about 12 hours, I felt relief about the ICD-10 [being delayed], and then I just realized, it’s still coming, presumably,” says John Nelson, MD, MHM, a co-founder and past president of SHM and medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. “[It’s] like a patient who needs surgery and finds out it’s canceled for the day and he’ll have it tomorrow. Well, that’s good for right now, but [he] still has to face this eventually.”
“Doc-Pay” Fix Near?
Congress’ recent decision to delay both an SGR fix and the ICD-10 are troubling to some hospitalists and others for different reasons.
The SGR extension through this year’s end means that physicians do not face a 24% cut to physician payments under Medicare. SHM has long lobbied against temporary patches to the SGR, repeatedly backing legislation that would once and for all scrap the formula and replace it with something sustainable.
The SGR formula was first crafted in 1997, but the now often-delayed cuts were a byproduct of the federal sequester that was included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. The cuts were implemented as a doomsday scenario that was never likely to actually happen, but despite negotiations over the past three years, no long-term compromise can be found. Paying for the reform remains the main stumbling block.
“I think, this year, Congress was as close as it’s been in a long time to enacting a serious fix, aided by the agreement of major professional societies like the American College of Physicians and American College of Surgeons,” says David Howard, PhD, an associate professor in the department of health policy and management at the Rollins School of Public Health at Emory University in Atlanta. “They were all on board with this solution. ... Who knows, maybe if the economic situation continues to improve [and] tax revenues continue to go up...that will create a more favorable environment for compromise.”
Dr. Howard adds that while Congress might be close to a solution in theory, agreement on how to offset the roughly $100 billion in costs “is just very difficult.” That is why the healthcare professor is pessimistic that a long-term fix is truly at hand.
“The places where Congress might have looked for savings to offset the cost of the doc fix, such as hospital reimbursement rates or payment rates to Medicare Advantage plans—those are exactly the areas that the Affordable Care Act is targeting to pay for insurance expansion,” Dr. Howard adds. “So those areas of savings are not going to be available to offset the cost of the doc fix.”
ICD-10 Delays “Unfair”
The medical coding conundrum presents a different set of issues. The delay in transitioning healthcare providers from the ICD-9 medical coding classification system to the more complicated ICD-10 means the upgraded system is now against an Oct. 1, 2015, deadline. This comes after the Centers for Medicare & Medicaid Services (CMS) already pushed back the original implementation date for ICD-10 by one year.
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, FACP, SFHM, says he thinks most doctors are content with the delay, particularly in light of some estimates that show that only about 20% of physicians “have actually initiated the ICD-10 transition.” But he also notes that it’s unfair to the health systems that have prepared for ICD-10.
“ICD-9 has a little more than 14,000 diagnostic codes and nearly 4,000 procedural codes. That is to be contrasted to ICD-10, which has more than 68,000 diagnostic codes ... and over 72,000 procedural codes,” Dr. Lenchus says. “So, it is not surprising that many take solace in the delay.”
–Dr. Lenchus
Dr. Nelson says the level of frustration for hospitalists is growing; however, the level of disruption for hospitals and health systems is reaching a boiling point.
“Of course, in some places, hospitalists may be the physician lead on ICD-10 efforts, so [they are] very much wrapped up in the problem of ‘What do we do now?’”
The answer, at least to the Coalition for ICD-10, a group of medical/technology trade groups, is to fight to ensure that the delays go no further. In an April letter to CMS Administrator Marilyn Tavenner, the coalition made that case, noting that in 2012, “CMS estimated the cost to the healthcare industry of a one-year delay to be as much as $6.6 billion, or approximately 30% of the $22 billion that CMS estimated had been invested or budgeted for ICD-10 implementation.”2
The letter went on to explain that the disruption and cost will grow each time the ICD-10 deadline is pushed.
“Furthermore, as CMS stated in 2012, implementation costs will continue to increase considerably with every year of a delay,” according to the letter. “The lost opportunity costs of failing to move to a more effective code set also continue to climb every year.”
Stay Engaged, Switch Gears
One of Floyd’s biggest concerns is that the ICD-10 implementation delays will affect physician engagement. The hospitalist groups at MUSC began training for ICD-10 in January 2013; however, the preparation and training were geared toward a 2014 implementation.
“You have to switch gears a little bit,” she says. “What we plan to do now is begin to do heavy auditing, and then from those audits we can give real-time feedback on what we’re doing well and what we’re not doing well. So I think that will be a method for engagement.”
She urges hospitalists, practice leaders, and informatics professionals to discuss ICD-10 not as a theoretical application, but as one tied to reimbursement that will have major impact in the years ahead. To that end, the American Health Information Management Association highlights the fact that the new coding system will result in higher-quality data that can improve performance measures, provide “increased sensitivity” to reimbursement methodologies, and help with stronger public health surveillance.3
“A lot of physicians see this as a hospital issue, and I think that’s why they shy away,” Floyd says. “Now there are some physicians who are interested in how well the hospital does, but the other piece is that it does affect things like [reduced] risk of mortality [and] comparison of data worldwide—those are things that we just have to continue to reiterate … and give them real examples.”
Richard Quinn is a freelance writer in New Jersey.
References
- Govtrack. H.R. 4302: Protecting Access to Medicare Act of 2014. https://www.govtrack.us/congress/bills/113/hr4302. Accessed June 5, 2014.
- Coalition for ICD. Letter to CMS Administrator Tavenner, April 11, 2014. http://coalitionforicd10.wordpress.com/2014/03/26/letter-from-the-coalition-for-icd-10. Accessed June 5, 2014.
- American Health Information Management Association. ICD-10-CM/PCS Transition: Planning and Preparation Checklist. http://journal.ahima.org/wp-content/uploads/ICD10-checklist.pdf. Accessed June 5, 2014.
Q&A: “Code Black” Offers Insider Look at ED Challenges
Interview by Mary Ellen Schneider
“Code Black,” the award-winning documentary about working in the ED at Los Angeles County Hospital, opened in theaters in 40 US cities this summer.
It’s the film debut for emergency physician Ryan McGarry, who both stars in and directs the feature-length documentary. It highlights the thrills and challenges of working in a busy ED through the eyes of senior residents, including Dr McGarry, who completed his training while working on the film. The young doctors start the film as fresh-faced idealists in the “C-Booth” trauma bay at LA County Hospital, the famed birthplace of emergency medicine. Later they move to the county’s newly built hospital, which, though state-of-the-art, lacks some of the camaraderie of the original ED.
“Code Black” was the Best Documentary winner at the Los Angeles Film Festival and the Hamptons International Film Festival. And it was the Audience Award winner at both the Starz Denver Film Festival and the Aspen Filmfest.

Dr McGarry, who is now an attending physician at New York-Presbyterian Hospital in New York City, discussed why he made the film and how it is likely to impact the health care debate.
Question: What inspired you to make this film?
Dr McGarry: As documentaries go, this one was kind of an accident in the sense of its narrative development. I set out to capture what I thought was a phenomenally intense, and in some ways, dated and brutal trauma bay. At this point, most people associate modern health care with a lot of sterility and technology and white and blue spaces that are kind of contained. And this shows the opposite. This looks like battlefield medicine. To my surprise, it was working very well. Of course, at the time I was a young medical student, so my basis for evaluating that matured along with the film. As time went on, we migrated from the old L.A. County Hospital to a newer space. So in the course of filming, they closed down an 80-year-old structure in favor of a brand new, billion-dollar, shining, technology-laden palace. What we found was that as we were brought up to speed on modern health care, and of course regulation, the care became much more complicated.
Question: What do you want the audience to take away from the film?
Dr McGarry: It’s hopefully a primer for health care discussion that has not yet existed. There are plenty of films that ride the political undertones of health care very well and, I think, if anything, they seem to keep people in their camps. They don’t really bring people to the middle. They may make discussion more satisfying for people who are politically charged, but from the provider’s point of view, I’m not sure if they get us anywhere. “Code Black” does not have a call to action, as they call it in the documentary world. That’s on purpose. What we’re hoping for is for people to watch it and be a bit more primed when we talk about health care. My prediction—this could be wrong—is that the real discussion for the next quarter-century, as we improve access with the [Affordable Care Act], is going to be the patient-doctor connection and some deregulation. There are just too many barriers right now. The equation is too complicated. The healing and listening that people want are not happening.
Question: So would you like to see policy makers ease up on some of the health care regulations?
Dr McGarry: We all want safety. But as a scientist would say, these regulations ought to be evidence based. What we know as physicians is that any evidence-based truth is a hard thing to prove, period. I think a lot of these regulations are well intentioned. Nobody doubts that. But yesterday, the Joint Commission visited our hospital. Everybody was working hard on a shift trying to move patients through, trying to provide both quick and safe care, and one of the things that [the regulators] were watching out for was keeping the employee bags and coffee off the computer desks. Meanwhile, I have patients with chest pain, patients with stroke, patients with fractures, who are not getting the attention they need because we’re totally focused on pleasing the federal regulators that our bags and coffee aren’t out.
Question: The film is from the perspective of young doctors and talks a lot about their initial idealism. Do you think the messages in the film will also resonate with older doctors?
Dr McGarry: One of the more surprising aspects of “Code Black” is the nostalgia factor, that fact that both physicians who have been working for a while and those who have become administrators watched this film. We thought it would be offensive to them—especially people from private hospitals, whom we are sort of tough on in the movie. We thought that they would find us a little unrealistic and idealistic. Interestingly, they all watched it and they said, “I long for the day in my residency when all I had to worry about was just getting the science right, getting that patient connection right.”
Question: Working in C-Booth was a great experience for ED physicians in training. Can you ever recapture that feeling in the new, heavily regulated environment?
Dr McGarry: One thing we wouldn’t want to return to would be the lack of privacy. The biggest aspect of C-Booth that probably we wouldn’t be proud of is the lack of privacy. I’m definitely for privacy and for a dignified experience. After that, I feel like things are quite undefined. I think we have expectations that technology, in particular, is a huge answer to medicine. But we know it can be expensive and it can be dangerous. And in the case of electronic medical records, it certainly doesn’t make things faster. We know that every institution that has gone from paper charts to an EMR has found not just an immediate slowing of care, but a permanent slowing. And yet there are benefits with being able to quickly look up old medical information. But what about when my patient is waiting 20 minutes for pain medicine because it takes almost that long to get them in the computer, pull up the order, select the medicine, and go through all these stupid hard stops that are built in? Before, I could just write it down on a piece of paper, communicate it to the nurse, and get it done. If you’re the one in pain, is [the EMR] worth it? I don’t know.

Question: How did you find the time to make this movie?
Dr McGarry: There were a lot of consequences. I probably pushed it from a health perspective. I really found myself in a unique position as both a filmmaker and subject. For almost 3 years, I would do every ounce of my residency and then would race from the hospital to the edit room and would live and breathe it for 3 years. You would imagine there’s a cost to that. Lost a girlfriend. Didn’t sleep. Happily, I came through without any major damage, but that’s a heck of a lot of emergency medicine.
Question: What are you doing next? Are you working on another film and how are you balancing your new project with your day job in medicine?
Dr McGarry: This is a different game than it was in residency. I have an option for a scripted series, so basically it means that producers have identified it as a viable project for a fiction series like you would see on HBO. That’s in active development. We just shot a 3-minute spot with the New York and L.A. ballets, which involves these dancers in the old abandoned general hospital. As far as balancing all this, I’m so lucky in that Cornell/New York-Presbyterian and Dr Neal Flomenbaum have been incredibly supportive of me, allowing me to be full time there but with the work flexibility to jump on these projects as they come.
On Twitter @maryellenny
Interview by Mary Ellen Schneider
“Code Black,” the award-winning documentary about working in the ED at Los Angeles County Hospital, opened in theaters in 40 US cities this summer.
It’s the film debut for emergency physician Ryan McGarry, who both stars in and directs the feature-length documentary. It highlights the thrills and challenges of working in a busy ED through the eyes of senior residents, including Dr McGarry, who completed his training while working on the film. The young doctors start the film as fresh-faced idealists in the “C-Booth” trauma bay at LA County Hospital, the famed birthplace of emergency medicine. Later they move to the county’s newly built hospital, which, though state-of-the-art, lacks some of the camaraderie of the original ED.
“Code Black” was the Best Documentary winner at the Los Angeles Film Festival and the Hamptons International Film Festival. And it was the Audience Award winner at both the Starz Denver Film Festival and the Aspen Filmfest.
Dr McGarry, who is now an attending physician at New York-Presbyterian Hospital in New York City, discussed why he made the film and how it is likely to impact the health care debate.
Question: What inspired you to make this film?
Dr McGarry: As documentaries go, this one was kind of an accident in the sense of its narrative development. I set out to capture what I thought was a phenomenally intense, and in some ways, dated and brutal trauma bay. At this point, most people associate modern health care with a lot of sterility and technology and white and blue spaces that are kind of contained. And this shows the opposite. This looks like battlefield medicine. To my surprise, it was working very well. Of course, at the time I was a young medical student, so my basis for evaluating that matured along with the film. As time went on, we migrated from the old L.A. County Hospital to a newer space. So in the course of filming, they closed down an 80-year-old structure in favor of a brand new, billion-dollar, shining, technology-laden palace. What we found was that as we were brought up to speed on modern health care, and of course regulation, the care became much more complicated.
Question: What do you want the audience to take away from the film?
Dr McGarry: It’s hopefully a primer for health care discussion that has not yet existed. There are plenty of films that ride the political undertones of health care very well and, I think, if anything, they seem to keep people in their camps. They don’t really bring people to the middle. They may make discussion more satisfying for people who are politically charged, but from the provider’s point of view, I’m not sure if they get us anywhere. “Code Black” does not have a call to action, as they call it in the documentary world. That’s on purpose. What we’re hoping for is for people to watch it and be a bit more primed when we talk about health care. My prediction—this could be wrong—is that the real discussion for the next quarter-century, as we improve access with the [Affordable Care Act], is going to be the patient-doctor connection and some deregulation. There are just too many barriers right now. The equation is too complicated. The healing and listening that people want are not happening.
Question: So would you like to see policy makers ease up on some of the health care regulations?
Dr McGarry: We all want safety. But as a scientist would say, these regulations ought to be evidence based. What we know as physicians is that any evidence-based truth is a hard thing to prove, period. I think a lot of these regulations are well intentioned. Nobody doubts that. But yesterday, the Joint Commission visited our hospital. Everybody was working hard on a shift trying to move patients through, trying to provide both quick and safe care, and one of the things that [the regulators] were watching out for was keeping the employee bags and coffee off the computer desks. Meanwhile, I have patients with chest pain, patients with stroke, patients with fractures, who are not getting the attention they need because we’re totally focused on pleasing the federal regulators that our bags and coffee aren’t out.
Question: The film is from the perspective of young doctors and talks a lot about their initial idealism. Do you think the messages in the film will also resonate with older doctors?
Dr McGarry: One of the more surprising aspects of “Code Black” is the nostalgia factor, that fact that both physicians who have been working for a while and those who have become administrators watched this film. We thought it would be offensive to them—especially people from private hospitals, whom we are sort of tough on in the movie. We thought that they would find us a little unrealistic and idealistic. Interestingly, they all watched it and they said, “I long for the day in my residency when all I had to worry about was just getting the science right, getting that patient connection right.”
Question: Working in C-Booth was a great experience for ED physicians in training. Can you ever recapture that feeling in the new, heavily regulated environment?
Dr McGarry: One thing we wouldn’t want to return to would be the lack of privacy. The biggest aspect of C-Booth that probably we wouldn’t be proud of is the lack of privacy. I’m definitely for privacy and for a dignified experience. After that, I feel like things are quite undefined. I think we have expectations that technology, in particular, is a huge answer to medicine. But we know it can be expensive and it can be dangerous. And in the case of electronic medical records, it certainly doesn’t make things faster. We know that every institution that has gone from paper charts to an EMR has found not just an immediate slowing of care, but a permanent slowing. And yet there are benefits with being able to quickly look up old medical information. But what about when my patient is waiting 20 minutes for pain medicine because it takes almost that long to get them in the computer, pull up the order, select the medicine, and go through all these stupid hard stops that are built in? Before, I could just write it down on a piece of paper, communicate it to the nurse, and get it done. If you’re the one in pain, is [the EMR] worth it? I don’t know.
Question: How did you find the time to make this movie?
Dr McGarry: There were a lot of consequences. I probably pushed it from a health perspective. I really found myself in a unique position as both a filmmaker and subject. For almost 3 years, I would do every ounce of my residency and then would race from the hospital to the edit room and would live and breathe it for 3 years. You would imagine there’s a cost to that. Lost a girlfriend. Didn’t sleep. Happily, I came through without any major damage, but that’s a heck of a lot of emergency medicine.
Question: What are you doing next? Are you working on another film and how are you balancing your new project with your day job in medicine?
Dr McGarry: This is a different game than it was in residency. I have an option for a scripted series, so basically it means that producers have identified it as a viable project for a fiction series like you would see on HBO. That’s in active development. We just shot a 3-minute spot with the New York and L.A. ballets, which involves these dancers in the old abandoned general hospital. As far as balancing all this, I’m so lucky in that Cornell/New York-Presbyterian and Dr Neal Flomenbaum have been incredibly supportive of me, allowing me to be full time there but with the work flexibility to jump on these projects as they come.
On Twitter @maryellenny
Interview by Mary Ellen Schneider
“Code Black,” the award-winning documentary about working in the ED at Los Angeles County Hospital, opened in theaters in 40 US cities this summer.
It’s the film debut for emergency physician Ryan McGarry, who both stars in and directs the feature-length documentary. It highlights the thrills and challenges of working in a busy ED through the eyes of senior residents, including Dr McGarry, who completed his training while working on the film. The young doctors start the film as fresh-faced idealists in the “C-Booth” trauma bay at LA County Hospital, the famed birthplace of emergency medicine. Later they move to the county’s newly built hospital, which, though state-of-the-art, lacks some of the camaraderie of the original ED.
“Code Black” was the Best Documentary winner at the Los Angeles Film Festival and the Hamptons International Film Festival. And it was the Audience Award winner at both the Starz Denver Film Festival and the Aspen Filmfest.
Dr McGarry, who is now an attending physician at New York-Presbyterian Hospital in New York City, discussed why he made the film and how it is likely to impact the health care debate.
Question: What inspired you to make this film?
Dr McGarry: As documentaries go, this one was kind of an accident in the sense of its narrative development. I set out to capture what I thought was a phenomenally intense, and in some ways, dated and brutal trauma bay. At this point, most people associate modern health care with a lot of sterility and technology and white and blue spaces that are kind of contained. And this shows the opposite. This looks like battlefield medicine. To my surprise, it was working very well. Of course, at the time I was a young medical student, so my basis for evaluating that matured along with the film. As time went on, we migrated from the old L.A. County Hospital to a newer space. So in the course of filming, they closed down an 80-year-old structure in favor of a brand new, billion-dollar, shining, technology-laden palace. What we found was that as we were brought up to speed on modern health care, and of course regulation, the care became much more complicated.
Question: What do you want the audience to take away from the film?
Dr McGarry: It’s hopefully a primer for health care discussion that has not yet existed. There are plenty of films that ride the political undertones of health care very well and, I think, if anything, they seem to keep people in their camps. They don’t really bring people to the middle. They may make discussion more satisfying for people who are politically charged, but from the provider’s point of view, I’m not sure if they get us anywhere. “Code Black” does not have a call to action, as they call it in the documentary world. That’s on purpose. What we’re hoping for is for people to watch it and be a bit more primed when we talk about health care. My prediction—this could be wrong—is that the real discussion for the next quarter-century, as we improve access with the [Affordable Care Act], is going to be the patient-doctor connection and some deregulation. There are just too many barriers right now. The equation is too complicated. The healing and listening that people want are not happening.
Question: So would you like to see policy makers ease up on some of the health care regulations?
Dr McGarry: We all want safety. But as a scientist would say, these regulations ought to be evidence based. What we know as physicians is that any evidence-based truth is a hard thing to prove, period. I think a lot of these regulations are well intentioned. Nobody doubts that. But yesterday, the Joint Commission visited our hospital. Everybody was working hard on a shift trying to move patients through, trying to provide both quick and safe care, and one of the things that [the regulators] were watching out for was keeping the employee bags and coffee off the computer desks. Meanwhile, I have patients with chest pain, patients with stroke, patients with fractures, who are not getting the attention they need because we’re totally focused on pleasing the federal regulators that our bags and coffee aren’t out.
Question: The film is from the perspective of young doctors and talks a lot about their initial idealism. Do you think the messages in the film will also resonate with older doctors?
Dr McGarry: One of the more surprising aspects of “Code Black” is the nostalgia factor, that fact that both physicians who have been working for a while and those who have become administrators watched this film. We thought it would be offensive to them—especially people from private hospitals, whom we are sort of tough on in the movie. We thought that they would find us a little unrealistic and idealistic. Interestingly, they all watched it and they said, “I long for the day in my residency when all I had to worry about was just getting the science right, getting that patient connection right.”
Question: Working in C-Booth was a great experience for ED physicians in training. Can you ever recapture that feeling in the new, heavily regulated environment?
Dr McGarry: One thing we wouldn’t want to return to would be the lack of privacy. The biggest aspect of C-Booth that probably we wouldn’t be proud of is the lack of privacy. I’m definitely for privacy and for a dignified experience. After that, I feel like things are quite undefined. I think we have expectations that technology, in particular, is a huge answer to medicine. But we know it can be expensive and it can be dangerous. And in the case of electronic medical records, it certainly doesn’t make things faster. We know that every institution that has gone from paper charts to an EMR has found not just an immediate slowing of care, but a permanent slowing. And yet there are benefits with being able to quickly look up old medical information. But what about when my patient is waiting 20 minutes for pain medicine because it takes almost that long to get them in the computer, pull up the order, select the medicine, and go through all these stupid hard stops that are built in? Before, I could just write it down on a piece of paper, communicate it to the nurse, and get it done. If you’re the one in pain, is [the EMR] worth it? I don’t know.
Question: How did you find the time to make this movie?
Dr McGarry: There were a lot of consequences. I probably pushed it from a health perspective. I really found myself in a unique position as both a filmmaker and subject. For almost 3 years, I would do every ounce of my residency and then would race from the hospital to the edit room and would live and breathe it for 3 years. You would imagine there’s a cost to that. Lost a girlfriend. Didn’t sleep. Happily, I came through without any major damage, but that’s a heck of a lot of emergency medicine.
Question: What are you doing next? Are you working on another film and how are you balancing your new project with your day job in medicine?
Dr McGarry: This is a different game than it was in residency. I have an option for a scripted series, so basically it means that producers have identified it as a viable project for a fiction series like you would see on HBO. That’s in active development. We just shot a 3-minute spot with the New York and L.A. ballets, which involves these dancers in the old abandoned general hospital. As far as balancing all this, I’m so lucky in that Cornell/New York-Presbyterian and Dr Neal Flomenbaum have been incredibly supportive of me, allowing me to be full time there but with the work flexibility to jump on these projects as they come.
On Twitter @maryellenny
