User login
CDC: Policy changes could prevent 100,000 deaths a year
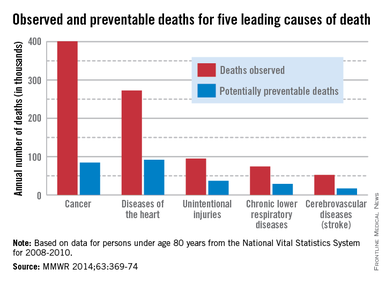
About one-third of heart disease deaths and one-fifth of cancer deaths could be prevented if overall U.S. death rates were the same as those in the states with the lowest rates, the Centers for Disease Control and Prevention reported May 1.
By using an average of the three states with the lowest death rates as a benchmark for each of the five causes, the analysis showed that 91,757 deaths from heart disease could be prevented each year. For cancer, 84,443 deaths could be prevented annually, according to the CDC report (MMWR 2014;63:369-74).
The total number of potentially preventable deaths is around 100,000, because the figures for each cause cannot be added together because someone who doesn’t die of heart disease may die of cancer or stroke, CDC Director Tom Frieden noted in a press briefing. For the rest of the top five causes of death, the numbers of avoidable deaths were 36,836 for unintentional injuries, 28,831 for chronic lower respiratory disease, and 16,973 for cerebrovascular disease.
The report highlights "the enormous variability among states" when it comes to public health policy, he said, with deaths for all five causes highest in the Southeast.
"In this country, your health and safety are determined more by your ZIP code than your genetic code," Dr. Frieden said. "We need to move the needle on policy change and programmatic change."
The analysis used mortality data from 2008 to 2010 for those younger than age 80 years from the National Vital Statistics System.
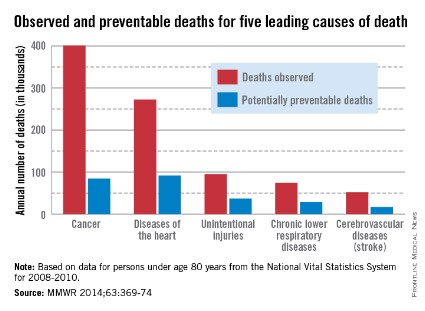
About one-third of heart disease deaths and one-fifth of cancer deaths could be prevented if overall U.S. death rates were the same as those in the states with the lowest rates, the Centers for Disease Control and Prevention reported May 1.
By using an average of the three states with the lowest death rates as a benchmark for each of the five causes, the analysis showed that 91,757 deaths from heart disease could be prevented each year. For cancer, 84,443 deaths could be prevented annually, according to the CDC report (MMWR 2014;63:369-74).
The total number of potentially preventable deaths is around 100,000, because the figures for each cause cannot be added together because someone who doesn’t die of heart disease may die of cancer or stroke, CDC Director Tom Frieden noted in a press briefing. For the rest of the top five causes of death, the numbers of avoidable deaths were 36,836 for unintentional injuries, 28,831 for chronic lower respiratory disease, and 16,973 for cerebrovascular disease.
The report highlights "the enormous variability among states" when it comes to public health policy, he said, with deaths for all five causes highest in the Southeast.
"In this country, your health and safety are determined more by your ZIP code than your genetic code," Dr. Frieden said. "We need to move the needle on policy change and programmatic change."
The analysis used mortality data from 2008 to 2010 for those younger than age 80 years from the National Vital Statistics System.
About one-third of heart disease deaths and one-fifth of cancer deaths could be prevented if overall U.S. death rates were the same as those in the states with the lowest rates, the Centers for Disease Control and Prevention reported May 1.
By using an average of the three states with the lowest death rates as a benchmark for each of the five causes, the analysis showed that 91,757 deaths from heart disease could be prevented each year. For cancer, 84,443 deaths could be prevented annually, according to the CDC report (MMWR 2014;63:369-74).
The total number of potentially preventable deaths is around 100,000, because the figures for each cause cannot be added together because someone who doesn’t die of heart disease may die of cancer or stroke, CDC Director Tom Frieden noted in a press briefing. For the rest of the top five causes of death, the numbers of avoidable deaths were 36,836 for unintentional injuries, 28,831 for chronic lower respiratory disease, and 16,973 for cerebrovascular disease.
The report highlights "the enormous variability among states" when it comes to public health policy, he said, with deaths for all five causes highest in the Southeast.
"In this country, your health and safety are determined more by your ZIP code than your genetic code," Dr. Frieden said. "We need to move the needle on policy change and programmatic change."
The analysis used mortality data from 2008 to 2010 for those younger than age 80 years from the National Vital Statistics System.
FROM MMWR
E&M codes could soon require more rigor
ORLANDO – With Medicare seeing a sharp spike in payments for evaluation and management services, a proposed overhaul of Current Procedural Terminology E&M codes could force physicians to provide substantially more documentation of their medical decision making.
The American Medical Association’s CPT editorial panel is scheduled to vote in mid-May on a recommendation to make such changes to E&M codes.

If the CPT panel’s changes are substantial enough, it’s even possible that the Centers for Medicare and Medicaid Services may embark on a revaluation of all the E&M codes, said Dr. Glenn Littenberg, a past member of the CPT editorial panel and a current CPT adviser to the American Society for Gastrointestinal Endoscopy.
If CMS decided to do so, revaluation potentially could be a good thing – if it results in a higher valuation for decision making, said Dr. Robert Wergin, president-elect of the American Academy of Family Physicians. But "if the motivation is to put up a barrier to code appropriately for the level of complexity of visits, it’s another step to undervalue the cognitive area," he said.
The federal government has been taking a closer look at coding, with the concern that electronic health records are making it easier to upcode.
A report in 2012 by the U.S. Department of Health & Human Services (HHS) inspector general found that between 2001 and 2010, physicians had increased their billing for higher-level E&M codes. Medicare payments for E&M services increased by 48% during the same period, from $22.7 billion to $33.5 billion. The Office of Inspector General labeled E&M services as "vulnerable to fraud and abuse."
Coding is a physician’s lifeblood, said Dr. Wergin. The AAFP is waiting to get more details on the CPT panel’s recommendations before it can say whether it supports the changes, he said.
The American College of Physicians said its officials could not comment, citing confidentiality agreements for ACP members who are on the CPT panel.
Detail your decision making
According to Dr. Littenberg, the CPT panel is proposing much more detailed documentation of decision making, including describing the number and complexity of problems. Medical decision making will be one of the two requirements to qualify for moderate to extensive E&M services for an office visit, an established patient, or follow-up hospital care.
The proposal is more prescriptive than current requirements, "and harder to grasp and keep in mind during an encounter," said Dr. Littenberg, who is also a gastroenterologist in Pasadena, Calif. He said he is "concerned about the impact of this," adding, "there are things about this proposal I don’t like, and I’ve said as much at CPT."
Decision making "is critical at arriving at a diagnosis and treatment plan," Dr. Wergin said, but the AAFP believes that it needs to be better defined by the CPT. "Let’s define medical decision making in a more meaningful way that makes sense to people like me," said Dr. Wergin, who added, "I have a lot of complicated patients."
If the focus is only on the presenting problem, it tends to undervalue the decision making that goes into evaluating a patient who may have multiple comorbidities and perhaps social issues as well, Dr. Wergin explained. To truly evaluate a patient, decision making should look at that individual as a whole, not as one issue, he said.
It appears that the panel is moving in that direction, Dr. Littenberg observed, but it will also require clear documentation that "reflects our thought process."
Note the basics
Physicians should be thinking more in terms of what would be required in documentation to defend an audit, he cautioned. The history, physical, and what led to decisions about diagnosis and treatment – the basic thinking behind what happened on that particular day – need to be within the notes.
That kind of documentation "is actually not that complicated, and yet we fail to do it a large percentage of the time," said Dr. Littenberg.
"It can’t just be a recap of a problem list and continue the same therapy and ‘See you next year,’ " he said. "That’s not ever going to pass a high-level audit."
On Twitter @aliciaault
ORLANDO – With Medicare seeing a sharp spike in payments for evaluation and management services, a proposed overhaul of Current Procedural Terminology E&M codes could force physicians to provide substantially more documentation of their medical decision making.
The American Medical Association’s CPT editorial panel is scheduled to vote in mid-May on a recommendation to make such changes to E&M codes.
If the CPT panel’s changes are substantial enough, it’s even possible that the Centers for Medicare and Medicaid Services may embark on a revaluation of all the E&M codes, said Dr. Glenn Littenberg, a past member of the CPT editorial panel and a current CPT adviser to the American Society for Gastrointestinal Endoscopy.
If CMS decided to do so, revaluation potentially could be a good thing – if it results in a higher valuation for decision making, said Dr. Robert Wergin, president-elect of the American Academy of Family Physicians. But "if the motivation is to put up a barrier to code appropriately for the level of complexity of visits, it’s another step to undervalue the cognitive area," he said.
The federal government has been taking a closer look at coding, with the concern that electronic health records are making it easier to upcode.
A report in 2012 by the U.S. Department of Health & Human Services (HHS) inspector general found that between 2001 and 2010, physicians had increased their billing for higher-level E&M codes. Medicare payments for E&M services increased by 48% during the same period, from $22.7 billion to $33.5 billion. The Office of Inspector General labeled E&M services as "vulnerable to fraud and abuse."
Coding is a physician’s lifeblood, said Dr. Wergin. The AAFP is waiting to get more details on the CPT panel’s recommendations before it can say whether it supports the changes, he said.
The American College of Physicians said its officials could not comment, citing confidentiality agreements for ACP members who are on the CPT panel.
Detail your decision making
According to Dr. Littenberg, the CPT panel is proposing much more detailed documentation of decision making, including describing the number and complexity of problems. Medical decision making will be one of the two requirements to qualify for moderate to extensive E&M services for an office visit, an established patient, or follow-up hospital care.
The proposal is more prescriptive than current requirements, "and harder to grasp and keep in mind during an encounter," said Dr. Littenberg, who is also a gastroenterologist in Pasadena, Calif. He said he is "concerned about the impact of this," adding, "there are things about this proposal I don’t like, and I’ve said as much at CPT."
Decision making "is critical at arriving at a diagnosis and treatment plan," Dr. Wergin said, but the AAFP believes that it needs to be better defined by the CPT. "Let’s define medical decision making in a more meaningful way that makes sense to people like me," said Dr. Wergin, who added, "I have a lot of complicated patients."
If the focus is only on the presenting problem, it tends to undervalue the decision making that goes into evaluating a patient who may have multiple comorbidities and perhaps social issues as well, Dr. Wergin explained. To truly evaluate a patient, decision making should look at that individual as a whole, not as one issue, he said.
It appears that the panel is moving in that direction, Dr. Littenberg observed, but it will also require clear documentation that "reflects our thought process."
Note the basics
Physicians should be thinking more in terms of what would be required in documentation to defend an audit, he cautioned. The history, physical, and what led to decisions about diagnosis and treatment – the basic thinking behind what happened on that particular day – need to be within the notes.
That kind of documentation "is actually not that complicated, and yet we fail to do it a large percentage of the time," said Dr. Littenberg.
"It can’t just be a recap of a problem list and continue the same therapy and ‘See you next year,’ " he said. "That’s not ever going to pass a high-level audit."
On Twitter @aliciaault
ORLANDO – With Medicare seeing a sharp spike in payments for evaluation and management services, a proposed overhaul of Current Procedural Terminology E&M codes could force physicians to provide substantially more documentation of their medical decision making.
The American Medical Association’s CPT editorial panel is scheduled to vote in mid-May on a recommendation to make such changes to E&M codes.
If the CPT panel’s changes are substantial enough, it’s even possible that the Centers for Medicare and Medicaid Services may embark on a revaluation of all the E&M codes, said Dr. Glenn Littenberg, a past member of the CPT editorial panel and a current CPT adviser to the American Society for Gastrointestinal Endoscopy.
If CMS decided to do so, revaluation potentially could be a good thing – if it results in a higher valuation for decision making, said Dr. Robert Wergin, president-elect of the American Academy of Family Physicians. But "if the motivation is to put up a barrier to code appropriately for the level of complexity of visits, it’s another step to undervalue the cognitive area," he said.
The federal government has been taking a closer look at coding, with the concern that electronic health records are making it easier to upcode.
A report in 2012 by the U.S. Department of Health & Human Services (HHS) inspector general found that between 2001 and 2010, physicians had increased their billing for higher-level E&M codes. Medicare payments for E&M services increased by 48% during the same period, from $22.7 billion to $33.5 billion. The Office of Inspector General labeled E&M services as "vulnerable to fraud and abuse."
Coding is a physician’s lifeblood, said Dr. Wergin. The AAFP is waiting to get more details on the CPT panel’s recommendations before it can say whether it supports the changes, he said.
The American College of Physicians said its officials could not comment, citing confidentiality agreements for ACP members who are on the CPT panel.
Detail your decision making
According to Dr. Littenberg, the CPT panel is proposing much more detailed documentation of decision making, including describing the number and complexity of problems. Medical decision making will be one of the two requirements to qualify for moderate to extensive E&M services for an office visit, an established patient, or follow-up hospital care.
The proposal is more prescriptive than current requirements, "and harder to grasp and keep in mind during an encounter," said Dr. Littenberg, who is also a gastroenterologist in Pasadena, Calif. He said he is "concerned about the impact of this," adding, "there are things about this proposal I don’t like, and I’ve said as much at CPT."
Decision making "is critical at arriving at a diagnosis and treatment plan," Dr. Wergin said, but the AAFP believes that it needs to be better defined by the CPT. "Let’s define medical decision making in a more meaningful way that makes sense to people like me," said Dr. Wergin, who added, "I have a lot of complicated patients."
If the focus is only on the presenting problem, it tends to undervalue the decision making that goes into evaluating a patient who may have multiple comorbidities and perhaps social issues as well, Dr. Wergin explained. To truly evaluate a patient, decision making should look at that individual as a whole, not as one issue, he said.
It appears that the panel is moving in that direction, Dr. Littenberg observed, but it will also require clear documentation that "reflects our thought process."
Note the basics
Physicians should be thinking more in terms of what would be required in documentation to defend an audit, he cautioned. The history, physical, and what led to decisions about diagnosis and treatment – the basic thinking behind what happened on that particular day – need to be within the notes.
That kind of documentation "is actually not that complicated, and yet we fail to do it a large percentage of the time," said Dr. Littenberg.
"It can’t just be a recap of a problem list and continue the same therapy and ‘See you next year,’ " he said. "That’s not ever going to pass a high-level audit."
On Twitter @aliciaault
AT ACP INTERNAL MEDICINE 2014

Affordable Care Act sign-ups hit 8 million
In the Affordable Care Act’s first open enrollment period, 8 million Americans signed up for private health insurance through the state and federal health marketplaces.
President Obama announced the latest figures on April 17, more than 2 weeks after the close of the first open enrollment period. Though March 31 was the deadline for signing up, individuals who had started the process by the deadline were given until April 15 to complete the process. During that time, nearly 1 million additional people signed up for health plans.

More young people have signed up for coverage as well. President Obama reported that in the federally run marketplaces, 35% of the sign-ups were from individuals under age 35, including children. About 28% of sign-ups were from young adults aged 18-34 years. That’s similar to the percentage of young adults who signed up for insurance in Massachusetts during the first year of its health reform effort, according to the White House.
"The Affordable Care Act is working," President Obama said during a White House press conference.
He once again called on the ACA’s opponents to stop trying to repeal it.
Rep. Fred Upton (R- Mich.), chairman of the House Energy and Commerce Committee, said the law has disrupted health care for millions of Americans, limited access to physicians, and caused insurance premiums to skyrocket.
"The administration still has not answered basic questions about enrollment and why it will not support fairness for all," Rep. Upton said in a statement.
On Twitter @maryellenny
In the Affordable Care Act’s first open enrollment period, 8 million Americans signed up for private health insurance through the state and federal health marketplaces.
President Obama announced the latest figures on April 17, more than 2 weeks after the close of the first open enrollment period. Though March 31 was the deadline for signing up, individuals who had started the process by the deadline were given until April 15 to complete the process. During that time, nearly 1 million additional people signed up for health plans.
More young people have signed up for coverage as well. President Obama reported that in the federally run marketplaces, 35% of the sign-ups were from individuals under age 35, including children. About 28% of sign-ups were from young adults aged 18-34 years. That’s similar to the percentage of young adults who signed up for insurance in Massachusetts during the first year of its health reform effort, according to the White House.
"The Affordable Care Act is working," President Obama said during a White House press conference.
He once again called on the ACA’s opponents to stop trying to repeal it.
Rep. Fred Upton (R- Mich.), chairman of the House Energy and Commerce Committee, said the law has disrupted health care for millions of Americans, limited access to physicians, and caused insurance premiums to skyrocket.
"The administration still has not answered basic questions about enrollment and why it will not support fairness for all," Rep. Upton said in a statement.
On Twitter @maryellenny
In the Affordable Care Act’s first open enrollment period, 8 million Americans signed up for private health insurance through the state and federal health marketplaces.
President Obama announced the latest figures on April 17, more than 2 weeks after the close of the first open enrollment period. Though March 31 was the deadline for signing up, individuals who had started the process by the deadline were given until April 15 to complete the process. During that time, nearly 1 million additional people signed up for health plans.
More young people have signed up for coverage as well. President Obama reported that in the federally run marketplaces, 35% of the sign-ups were from individuals under age 35, including children. About 28% of sign-ups were from young adults aged 18-34 years. That’s similar to the percentage of young adults who signed up for insurance in Massachusetts during the first year of its health reform effort, according to the White House.
"The Affordable Care Act is working," President Obama said during a White House press conference.
He once again called on the ACA’s opponents to stop trying to repeal it.
Rep. Fred Upton (R- Mich.), chairman of the House Energy and Commerce Committee, said the law has disrupted health care for millions of Americans, limited access to physicians, and caused insurance premiums to skyrocket.
"The administration still has not answered basic questions about enrollment and why it will not support fairness for all," Rep. Upton said in a statement.
On Twitter @maryellenny

Budget chief Burwell tapped for HHS
Sylvia Mathews Burwell, best known in Washington for managing last fall’s government shutdown, has been tapped to head the Department of Health & Human Services.
On April 11, President Obama announced that Kathleen Sebelius has resigned after 5 years as HHS secretary. The president will nominate Ms. Burwell, the current director of the White House Office of Management and Budget (OMB), to replace Ms. Sebelius.

Ms. Burwell faces confirmation by the Senate, but new rules mean that she will need only a majority of senators to vote in her favor.
Ms. Burwell, a Rhodes Scholar from Hinton, W.Va., was confirmed unanimously by the Senate last year to head the OMB. Before coming to the White House, she served as president of the Walmart Foundation and as president of the global development program at the Bill & Melinda Gates Foundation.
During the Clinton administration, Ms. Burwell worked as deputy director of OMB, as well as in other roles at the White House.
President Obama praised Ms. Burwell as "experienced" and "competent" and said she will bring common sense to the HHS job. "She knows how to deliver results," he said.
President Obama also commended the work done by Ms. Sebelius, saying that she turned around the struggling healthcare.gov website and helped to get 7.5 million Americans signed up for health insurance during the Affordable Care Act’s first open enrollment period.
"The final score speaks for itself," he said.
Ms. Sebelius will remain at the HHS helm until her successor is confirmed.
On Twitter @maryellenny
Sylvia Mathews Burwell, best known in Washington for managing last fall’s government shutdown, has been tapped to head the Department of Health & Human Services.
On April 11, President Obama announced that Kathleen Sebelius has resigned after 5 years as HHS secretary. The president will nominate Ms. Burwell, the current director of the White House Office of Management and Budget (OMB), to replace Ms. Sebelius.
Ms. Burwell faces confirmation by the Senate, but new rules mean that she will need only a majority of senators to vote in her favor.
Ms. Burwell, a Rhodes Scholar from Hinton, W.Va., was confirmed unanimously by the Senate last year to head the OMB. Before coming to the White House, she served as president of the Walmart Foundation and as president of the global development program at the Bill & Melinda Gates Foundation.
During the Clinton administration, Ms. Burwell worked as deputy director of OMB, as well as in other roles at the White House.
President Obama praised Ms. Burwell as "experienced" and "competent" and said she will bring common sense to the HHS job. "She knows how to deliver results," he said.
President Obama also commended the work done by Ms. Sebelius, saying that she turned around the struggling healthcare.gov website and helped to get 7.5 million Americans signed up for health insurance during the Affordable Care Act’s first open enrollment period.
"The final score speaks for itself," he said.
Ms. Sebelius will remain at the HHS helm until her successor is confirmed.
On Twitter @maryellenny
Sylvia Mathews Burwell, best known in Washington for managing last fall’s government shutdown, has been tapped to head the Department of Health & Human Services.
On April 11, President Obama announced that Kathleen Sebelius has resigned after 5 years as HHS secretary. The president will nominate Ms. Burwell, the current director of the White House Office of Management and Budget (OMB), to replace Ms. Sebelius.
Ms. Burwell faces confirmation by the Senate, but new rules mean that she will need only a majority of senators to vote in her favor.
Ms. Burwell, a Rhodes Scholar from Hinton, W.Va., was confirmed unanimously by the Senate last year to head the OMB. Before coming to the White House, she served as president of the Walmart Foundation and as president of the global development program at the Bill & Melinda Gates Foundation.
During the Clinton administration, Ms. Burwell worked as deputy director of OMB, as well as in other roles at the White House.
President Obama praised Ms. Burwell as "experienced" and "competent" and said she will bring common sense to the HHS job. "She knows how to deliver results," he said.
President Obama also commended the work done by Ms. Sebelius, saying that she turned around the struggling healthcare.gov website and helped to get 7.5 million Americans signed up for health insurance during the Affordable Care Act’s first open enrollment period.
"The final score speaks for itself," he said.
Ms. Sebelius will remain at the HHS helm until her successor is confirmed.
On Twitter @maryellenny

Medicare data dump frustrates doctors
For the first time, federal officials have publicly released data on how much Medicare pays individual physicians.
On April 9, the Centers for Medicare & Medicaid Services posted searchable files with information on more than 880,000 health care providers, including their specialty, the number of services they provided, what they charged, and what they were paid by Medicare.

Collectively, the data reveal $77 billion in Medicare Part B payments made in 2012.
The data set also allows the public to search for specific procedures and find out how often they were performed and the variation in payments.
For instance, in 2012, more than 91 million outpatient office visits were billed to Medicare with the CPT code 99213. The average Medicare-allowed amount was $69.59, with a range of $12.42 to $144.56. Chest x-rays were performed more than 17 million times in 2012; the average Medicare-allowed amount was $8.94, with a range of $6.52 to $28.56.
The Medicare-allowed amount for the more than 10 million emergency department visits billed to Medicare in 2012 ranged from $108.29 to $231.27, with an average allowed charge of $167.62.
In the short term, the large-scale data dump has yielded a slew of news stories about outlier physicians who raked in tens of millions from the Medicare program. Medicare officials said they expect that in the long term, the data will help root out fraud and highlight geographic payment variations.
"For too long, this information was not made public," Jonathan Blum, CMS principal deputy administrator, said during a press conference on April 9. "We believe the public has a right to know this information. The Medicare program is by and large funded with taxpayer dollars, and taxpayers have the right to understand what is being paid for and how it’s being paid for."
Aside from increased transparency, Mr. Blum said the agency is also counting on researchers, journalists, and the public to find patterns of waste or fraud that the agency may have missed.
But mostly, the data release has left physicians with unanswered questions – most notably how to address errors in the data. CMS officials did not provide physicians a chance to review their data before they were released, and so far, there is no formal mechanism for requesting corrections. The agency is working on setting up an appeals process, but it’s not ready yet, said Dr. Reid Blackwelder, president of the American Academy of Family Physicians. "It’s not an ideal situation at all."
For now, physicians can try e-mailing questions or complaints to CMS at [email protected].
Another lingering question is how to explain the information to patients.
"Payment data are particularly confusing since various complex factors contribute to their variability," said Dr. Norman E. Vinn, president of the American Osteopathic Association.
Physicians will be forced to explain to their patients that the CMS data are "raw" and don’t reflect the quality or competency of the physician or the treatment provided.

But Dr. Blackwelder said that if patients do bring up the data, it could be an opportunity to discuss why certain tests are frequently ordered or how Medicare actually pays physicians. For instance, Dr. Blackwelder said the Medicare charges reflect the cost of services, while the payments from the CMS are usually much lower.
"It’s a really important issue for patients to be aware of," he said.
While nearly all physician organizations voice their support of greater transparency on health care payments, they also object to the lack of context provided by the CMS.
The American Medical Association released a guide to the media highlighting the potential for errors in the data, as well as the lack of information about quality. The raw data could also be misleading in other ways, the AMA noted. For instance, since residents, physician assistants, and nurse practitioners sometimes file claims under a physician’s NPI (National Provider Identifier) number, the data listed for a particular physician may not accurately portray the services performed by that physician. Also, the data do not account for the patient mix, the demographics of the practice, or drug and supply costs.
"The AMA is disappointed that CMS did not include reasonable safeguards that would help the public understand the limitations of this data," Dr. Ardis Dee Hoven, AMA president, said in a statement.
The Medical Group Management Association raised similar concerns. "This release could result in patients making decisions about their care based on faulty assumptions about physicians," Dr. Susan Turney, president and CEO of MGMA, said in a statement. "Claims data are not a proxy for quality, especially when provided in isolation from a single payer."
The MGMA is also concerned that publishing individual provider information, including their address and NPI number, could leave them vulnerable to fraud.
For decades, the federal government was prohibited from releasing their type of individual payment data. However, in 2013, a federal court lifted the injunction that had barred the government from releasing its database of Medicare physician claims to the public. Since then, CMS has received numerous Freedom of Information Act requests seeking the data.
On Twitter @maryellenny
For the first time, federal officials have publicly released data on how much Medicare pays individual physicians.
On April 9, the Centers for Medicare & Medicaid Services posted searchable files with information on more than 880,000 health care providers, including their specialty, the number of services they provided, what they charged, and what they were paid by Medicare.
Collectively, the data reveal $77 billion in Medicare Part B payments made in 2012.
The data set also allows the public to search for specific procedures and find out how often they were performed and the variation in payments.
For instance, in 2012, more than 91 million outpatient office visits were billed to Medicare with the CPT code 99213. The average Medicare-allowed amount was $69.59, with a range of $12.42 to $144.56. Chest x-rays were performed more than 17 million times in 2012; the average Medicare-allowed amount was $8.94, with a range of $6.52 to $28.56.
The Medicare-allowed amount for the more than 10 million emergency department visits billed to Medicare in 2012 ranged from $108.29 to $231.27, with an average allowed charge of $167.62.
In the short term, the large-scale data dump has yielded a slew of news stories about outlier physicians who raked in tens of millions from the Medicare program. Medicare officials said they expect that in the long term, the data will help root out fraud and highlight geographic payment variations.
"For too long, this information was not made public," Jonathan Blum, CMS principal deputy administrator, said during a press conference on April 9. "We believe the public has a right to know this information. The Medicare program is by and large funded with taxpayer dollars, and taxpayers have the right to understand what is being paid for and how it’s being paid for."
Aside from increased transparency, Mr. Blum said the agency is also counting on researchers, journalists, and the public to find patterns of waste or fraud that the agency may have missed.
But mostly, the data release has left physicians with unanswered questions – most notably how to address errors in the data. CMS officials did not provide physicians a chance to review their data before they were released, and so far, there is no formal mechanism for requesting corrections. The agency is working on setting up an appeals process, but it’s not ready yet, said Dr. Reid Blackwelder, president of the American Academy of Family Physicians. "It’s not an ideal situation at all."
For now, physicians can try e-mailing questions or complaints to CMS at [email protected].
Another lingering question is how to explain the information to patients.
"Payment data are particularly confusing since various complex factors contribute to their variability," said Dr. Norman E. Vinn, president of the American Osteopathic Association.
Physicians will be forced to explain to their patients that the CMS data are "raw" and don’t reflect the quality or competency of the physician or the treatment provided.
But Dr. Blackwelder said that if patients do bring up the data, it could be an opportunity to discuss why certain tests are frequently ordered or how Medicare actually pays physicians. For instance, Dr. Blackwelder said the Medicare charges reflect the cost of services, while the payments from the CMS are usually much lower.
"It’s a really important issue for patients to be aware of," he said.
While nearly all physician organizations voice their support of greater transparency on health care payments, they also object to the lack of context provided by the CMS.
The American Medical Association released a guide to the media highlighting the potential for errors in the data, as well as the lack of information about quality. The raw data could also be misleading in other ways, the AMA noted. For instance, since residents, physician assistants, and nurse practitioners sometimes file claims under a physician’s NPI (National Provider Identifier) number, the data listed for a particular physician may not accurately portray the services performed by that physician. Also, the data do not account for the patient mix, the demographics of the practice, or drug and supply costs.
"The AMA is disappointed that CMS did not include reasonable safeguards that would help the public understand the limitations of this data," Dr. Ardis Dee Hoven, AMA president, said in a statement.
The Medical Group Management Association raised similar concerns. "This release could result in patients making decisions about their care based on faulty assumptions about physicians," Dr. Susan Turney, president and CEO of MGMA, said in a statement. "Claims data are not a proxy for quality, especially when provided in isolation from a single payer."
The MGMA is also concerned that publishing individual provider information, including their address and NPI number, could leave them vulnerable to fraud.
For decades, the federal government was prohibited from releasing their type of individual payment data. However, in 2013, a federal court lifted the injunction that had barred the government from releasing its database of Medicare physician claims to the public. Since then, CMS has received numerous Freedom of Information Act requests seeking the data.
On Twitter @maryellenny
For the first time, federal officials have publicly released data on how much Medicare pays individual physicians.
On April 9, the Centers for Medicare & Medicaid Services posted searchable files with information on more than 880,000 health care providers, including their specialty, the number of services they provided, what they charged, and what they were paid by Medicare.
Collectively, the data reveal $77 billion in Medicare Part B payments made in 2012.
The data set also allows the public to search for specific procedures and find out how often they were performed and the variation in payments.
For instance, in 2012, more than 91 million outpatient office visits were billed to Medicare with the CPT code 99213. The average Medicare-allowed amount was $69.59, with a range of $12.42 to $144.56. Chest x-rays were performed more than 17 million times in 2012; the average Medicare-allowed amount was $8.94, with a range of $6.52 to $28.56.
The Medicare-allowed amount for the more than 10 million emergency department visits billed to Medicare in 2012 ranged from $108.29 to $231.27, with an average allowed charge of $167.62.
In the short term, the large-scale data dump has yielded a slew of news stories about outlier physicians who raked in tens of millions from the Medicare program. Medicare officials said they expect that in the long term, the data will help root out fraud and highlight geographic payment variations.
"For too long, this information was not made public," Jonathan Blum, CMS principal deputy administrator, said during a press conference on April 9. "We believe the public has a right to know this information. The Medicare program is by and large funded with taxpayer dollars, and taxpayers have the right to understand what is being paid for and how it’s being paid for."
Aside from increased transparency, Mr. Blum said the agency is also counting on researchers, journalists, and the public to find patterns of waste or fraud that the agency may have missed.
But mostly, the data release has left physicians with unanswered questions – most notably how to address errors in the data. CMS officials did not provide physicians a chance to review their data before they were released, and so far, there is no formal mechanism for requesting corrections. The agency is working on setting up an appeals process, but it’s not ready yet, said Dr. Reid Blackwelder, president of the American Academy of Family Physicians. "It’s not an ideal situation at all."
For now, physicians can try e-mailing questions or complaints to CMS at [email protected].
Another lingering question is how to explain the information to patients.
"Payment data are particularly confusing since various complex factors contribute to their variability," said Dr. Norman E. Vinn, president of the American Osteopathic Association.
Physicians will be forced to explain to their patients that the CMS data are "raw" and don’t reflect the quality or competency of the physician or the treatment provided.
But Dr. Blackwelder said that if patients do bring up the data, it could be an opportunity to discuss why certain tests are frequently ordered or how Medicare actually pays physicians. For instance, Dr. Blackwelder said the Medicare charges reflect the cost of services, while the payments from the CMS are usually much lower.
"It’s a really important issue for patients to be aware of," he said.
While nearly all physician organizations voice their support of greater transparency on health care payments, they also object to the lack of context provided by the CMS.
The American Medical Association released a guide to the media highlighting the potential for errors in the data, as well as the lack of information about quality. The raw data could also be misleading in other ways, the AMA noted. For instance, since residents, physician assistants, and nurse practitioners sometimes file claims under a physician’s NPI (National Provider Identifier) number, the data listed for a particular physician may not accurately portray the services performed by that physician. Also, the data do not account for the patient mix, the demographics of the practice, or drug and supply costs.
"The AMA is disappointed that CMS did not include reasonable safeguards that would help the public understand the limitations of this data," Dr. Ardis Dee Hoven, AMA president, said in a statement.
The Medical Group Management Association raised similar concerns. "This release could result in patients making decisions about their care based on faulty assumptions about physicians," Dr. Susan Turney, president and CEO of MGMA, said in a statement. "Claims data are not a proxy for quality, especially when provided in isolation from a single payer."
The MGMA is also concerned that publishing individual provider information, including their address and NPI number, could leave them vulnerable to fraud.
For decades, the federal government was prohibited from releasing their type of individual payment data. However, in 2013, a federal court lifted the injunction that had barred the government from releasing its database of Medicare physician claims to the public. Since then, CMS has received numerous Freedom of Information Act requests seeking the data.
On Twitter @maryellenny

Physicians could get squeezed by Open Payments delay
Website delays may curtail physicians’ ability to review data on payments they received from drug and device makers before the federal government publishes it Sept. 30.
"There is a compelling need to ensure that physicians have an adequate amount of time to register with the Open Payments Program system, to review their consolidated reports, to dispute errors, and obtain corrections," Dr. James L. Madara, AMA executive vice president, wrote in a letter to the Centers for Medicare & Medicaid Services.
CMS got a late start in launching its online system for data collection, created as part of the Affordable Care Act.
The Open Payments Program – colloquially known as the Sunshine Act program – requires manufacturers of drugs, devices, biologicals, and medical supplies to report the honoraria, fees, and other payments that they make to doctors. The information will be published in a searchable database.

Manufacturers began tabulating data in August 2013 and were supposed to start reporting to the CMS through a website on Jan. 1. The program called for doctors to be able to register for the website at the same time so they could begin reviewing data.
CMS launched the website 6 weeks late on Feb. 18 and made it available only to manufacturers and group purchasing organizations. The first registration and reporting phase ended March 31. The agency has not begun the second phase yet.
Registration and review for physicians and teaching hospitals will begin no later than Aug. 1, according to CMS.
The AMA is urging the CMS "to adjust the public reporting date until the agency can ensure that physician due process rights are protected, and the agency has in place a process and system that will produce accurate reports."
The AMA said that it is concerned that the agency might not be able to ensure timeliness or accuracy because "the CMS is building a new system that reportedly has not been beta tested."
The ACA requires the CMS to give physicians 60 days to review data and settle any disputes, according to Neil Kirschner, senior associate for health policy and regulatory affairs at the American College of Physicians. He said that the ACP will continue to monitor the CMS’s progress and advocate for a minimum of a 60-day review period.
Officials at the American College of Cardiology also are wary of the situation.
"Given the difficulties that physicians have had in obtaining access to their Physician Quality Reporting System reports and other similar documents that require authentication of identity, the College is concerned that there will not be sufficient time to both communicate to them the need to register and for the registration and authentication to occur before the reports are available," said Lisa Goldstein, ACC associate director of regulatory affairs.
"Instead, many will likely be scrambling to register and authenticate their identities during the limited review period before the information is made public, reducing the amount of time the physicians have to review their reports and file disputes as appropriate," she said.
Dr. Brett Coldiron, president of the American Academy of Dermatology, said that the academy "wants to ensure that the information that is shared through Open Payments is as accurate as possible, and that implementation of the program is seamless and does not create undue administrative burdens on physicians."
On Twitter @aliciaault
Website delays may curtail physicians’ ability to review data on payments they received from drug and device makers before the federal government publishes it Sept. 30.
"There is a compelling need to ensure that physicians have an adequate amount of time to register with the Open Payments Program system, to review their consolidated reports, to dispute errors, and obtain corrections," Dr. James L. Madara, AMA executive vice president, wrote in a letter to the Centers for Medicare & Medicaid Services.
CMS got a late start in launching its online system for data collection, created as part of the Affordable Care Act.
The Open Payments Program – colloquially known as the Sunshine Act program – requires manufacturers of drugs, devices, biologicals, and medical supplies to report the honoraria, fees, and other payments that they make to doctors. The information will be published in a searchable database.
Manufacturers began tabulating data in August 2013 and were supposed to start reporting to the CMS through a website on Jan. 1. The program called for doctors to be able to register for the website at the same time so they could begin reviewing data.
CMS launched the website 6 weeks late on Feb. 18 and made it available only to manufacturers and group purchasing organizations. The first registration and reporting phase ended March 31. The agency has not begun the second phase yet.
Registration and review for physicians and teaching hospitals will begin no later than Aug. 1, according to CMS.
The AMA is urging the CMS "to adjust the public reporting date until the agency can ensure that physician due process rights are protected, and the agency has in place a process and system that will produce accurate reports."
The AMA said that it is concerned that the agency might not be able to ensure timeliness or accuracy because "the CMS is building a new system that reportedly has not been beta tested."
The ACA requires the CMS to give physicians 60 days to review data and settle any disputes, according to Neil Kirschner, senior associate for health policy and regulatory affairs at the American College of Physicians. He said that the ACP will continue to monitor the CMS’s progress and advocate for a minimum of a 60-day review period.
Officials at the American College of Cardiology also are wary of the situation.
"Given the difficulties that physicians have had in obtaining access to their Physician Quality Reporting System reports and other similar documents that require authentication of identity, the College is concerned that there will not be sufficient time to both communicate to them the need to register and for the registration and authentication to occur before the reports are available," said Lisa Goldstein, ACC associate director of regulatory affairs.
"Instead, many will likely be scrambling to register and authenticate their identities during the limited review period before the information is made public, reducing the amount of time the physicians have to review their reports and file disputes as appropriate," she said.
Dr. Brett Coldiron, president of the American Academy of Dermatology, said that the academy "wants to ensure that the information that is shared through Open Payments is as accurate as possible, and that implementation of the program is seamless and does not create undue administrative burdens on physicians."
On Twitter @aliciaault
Website delays may curtail physicians’ ability to review data on payments they received from drug and device makers before the federal government publishes it Sept. 30.
"There is a compelling need to ensure that physicians have an adequate amount of time to register with the Open Payments Program system, to review their consolidated reports, to dispute errors, and obtain corrections," Dr. James L. Madara, AMA executive vice president, wrote in a letter to the Centers for Medicare & Medicaid Services.
CMS got a late start in launching its online system for data collection, created as part of the Affordable Care Act.
The Open Payments Program – colloquially known as the Sunshine Act program – requires manufacturers of drugs, devices, biologicals, and medical supplies to report the honoraria, fees, and other payments that they make to doctors. The information will be published in a searchable database.
Manufacturers began tabulating data in August 2013 and were supposed to start reporting to the CMS through a website on Jan. 1. The program called for doctors to be able to register for the website at the same time so they could begin reviewing data.
CMS launched the website 6 weeks late on Feb. 18 and made it available only to manufacturers and group purchasing organizations. The first registration and reporting phase ended March 31. The agency has not begun the second phase yet.
Registration and review for physicians and teaching hospitals will begin no later than Aug. 1, according to CMS.
The AMA is urging the CMS "to adjust the public reporting date until the agency can ensure that physician due process rights are protected, and the agency has in place a process and system that will produce accurate reports."
The AMA said that it is concerned that the agency might not be able to ensure timeliness or accuracy because "the CMS is building a new system that reportedly has not been beta tested."
The ACA requires the CMS to give physicians 60 days to review data and settle any disputes, according to Neil Kirschner, senior associate for health policy and regulatory affairs at the American College of Physicians. He said that the ACP will continue to monitor the CMS’s progress and advocate for a minimum of a 60-day review period.
Officials at the American College of Cardiology also are wary of the situation.
"Given the difficulties that physicians have had in obtaining access to their Physician Quality Reporting System reports and other similar documents that require authentication of identity, the College is concerned that there will not be sufficient time to both communicate to them the need to register and for the registration and authentication to occur before the reports are available," said Lisa Goldstein, ACC associate director of regulatory affairs.
"Instead, many will likely be scrambling to register and authenticate their identities during the limited review period before the information is made public, reducing the amount of time the physicians have to review their reports and file disputes as appropriate," she said.
Dr. Brett Coldiron, president of the American Academy of Dermatology, said that the academy "wants to ensure that the information that is shared through Open Payments is as accurate as possible, and that implementation of the program is seamless and does not create undue administrative burdens on physicians."
On Twitter @aliciaault

Medicare releases physician payment data
On April 9, officials at the Centers for Medicare & Medicaid Services released an unprecedented amount of data detailing the payments made to more than 880,000 physicians and other health care providers.
The searchable files released by CMS include the provider name, address, specialty, and National Provider Identifier, as well as Medicare charges submitted and allowed and total Medicare payment for the year.
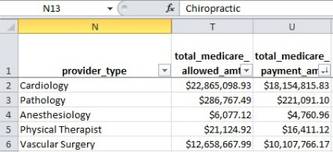
The data dump was harshly criticized by the American Medical Association, which said that the government had not given physicians a chance to review and correct their data. The data also lack context about quality of care, patient population, and site of service, the AMA said.
"Thoughtful observers concluded long ago that payments or costs were not the only metric to evaluate medical care," Dr. Ardis Dee Hoven, president of the AMA, said in a statement. "Quality, value, and outcomes are critical yardsticks for patients. The information released by CMS will not allow patients or payers to draw meaningful conclusions about the value or quality of care."
CMS will hold a press conference on the data dump on April 9. For more information on how to manage this new development in your practice, visit this website later this afternoon.
On Twitter @maryellenny
On April 9, officials at the Centers for Medicare & Medicaid Services released an unprecedented amount of data detailing the payments made to more than 880,000 physicians and other health care providers.
The searchable files released by CMS include the provider name, address, specialty, and National Provider Identifier, as well as Medicare charges submitted and allowed and total Medicare payment for the year.
The data dump was harshly criticized by the American Medical Association, which said that the government had not given physicians a chance to review and correct their data. The data also lack context about quality of care, patient population, and site of service, the AMA said.
"Thoughtful observers concluded long ago that payments or costs were not the only metric to evaluate medical care," Dr. Ardis Dee Hoven, president of the AMA, said in a statement. "Quality, value, and outcomes are critical yardsticks for patients. The information released by CMS will not allow patients or payers to draw meaningful conclusions about the value or quality of care."
CMS will hold a press conference on the data dump on April 9. For more information on how to manage this new development in your practice, visit this website later this afternoon.
On Twitter @maryellenny
On April 9, officials at the Centers for Medicare & Medicaid Services released an unprecedented amount of data detailing the payments made to more than 880,000 physicians and other health care providers.
The searchable files released by CMS include the provider name, address, specialty, and National Provider Identifier, as well as Medicare charges submitted and allowed and total Medicare payment for the year.
The data dump was harshly criticized by the American Medical Association, which said that the government had not given physicians a chance to review and correct their data. The data also lack context about quality of care, patient population, and site of service, the AMA said.
"Thoughtful observers concluded long ago that payments or costs were not the only metric to evaluate medical care," Dr. Ardis Dee Hoven, president of the AMA, said in a statement. "Quality, value, and outcomes are critical yardsticks for patients. The information released by CMS will not allow patients or payers to draw meaningful conclusions about the value or quality of care."
CMS will hold a press conference on the data dump on April 9. For more information on how to manage this new development in your practice, visit this website later this afternoon.
On Twitter @maryellenny

ACA coverage may lead to more malpractice claims
The volume of malpractice claims against physicians could increase by 5% as more Americans gain health care coverage and access health services under the Affordable Care Act, according to a study by the RAND Corporation released April 9.
That increase could translate into higher malpractice premiums for physicians, RAND researchers found in a study of the ACA’s impact on all liability insurances.

"The Affordable Care Act is unlikely to dramatically affect liability costs, but it may influence small and moderate changes in costs over the next several years," said lead author David Auerbach, a policy researcher at RAND. "For example, auto insurers may spend less for treating injuries, while it may cost a bit more to provide physicians with medical malpractice coverage."
RAND investigators theorized that a greater number of insured patients would escalate the rate of malpractice lawsuits because of more procedures, interactions, and visits with physicians. Previous analyses have found the uninsured currently use about half of the care that insured patients do, they said.
To test their theory, the researchers compared National Practitioner Data Bank (NPDB) data on liability claims from 2008 to 2010 to insurance coverage data from the Census Bureau’s American Community Survey (ACS). The results suggested that having insurance coverage is associated with a 2%-10% increase in malpractice activity. Thus, if 10% of a state’s population gains coverage, analysts estimated a 5% rise in malpractice claims.
"This study highlights the far-reaching impacts of the Affordable Care Act," said Jayne Plunkett, head of casualty reinsurance for Swiss Re, an international reinsurance company that sponsored the study. "Businesses and policymakers need to understand how and why their risk profiles might change as the Affordable Care Act is implemented."
But other insurers believe the study results are another uncertain forecast of the ACA’s future effects.
"You’re trying to look through a very cloudy crystal ball in making predictions about the Affordable Care Act," said Frank O’Neil, senior vice president and chief communications officer for ProAssurance, a national medical liability insurer. "There are a number of things that could cause a 5% change in medical liability rates that could happen at the same time as the implementation of the ACA, but be totally unrelated."
For example, if there is a sudden increase in either the frequency or the severity of malpractice claims in a particular state, that could impact the medical liability climate, Mr. O’Neil said. He added that other experts believe that new patients entering the health care system may be so appreciative of previously absent care that they would be reluctant to sue.
"There are a lot of unknowns yet, and I think it’s hard to agree or disagree with a prediction that doesn’t say over what time frame [an increase in claims] would occur," he said. The study "should be taken as just one other prediction."
The volume of malpractice claims against physicians could increase by 5% as more Americans gain health care coverage and access health services under the Affordable Care Act, according to a study by the RAND Corporation released April 9.
That increase could translate into higher malpractice premiums for physicians, RAND researchers found in a study of the ACA’s impact on all liability insurances.
"The Affordable Care Act is unlikely to dramatically affect liability costs, but it may influence small and moderate changes in costs over the next several years," said lead author David Auerbach, a policy researcher at RAND. "For example, auto insurers may spend less for treating injuries, while it may cost a bit more to provide physicians with medical malpractice coverage."
RAND investigators theorized that a greater number of insured patients would escalate the rate of malpractice lawsuits because of more procedures, interactions, and visits with physicians. Previous analyses have found the uninsured currently use about half of the care that insured patients do, they said.
To test their theory, the researchers compared National Practitioner Data Bank (NPDB) data on liability claims from 2008 to 2010 to insurance coverage data from the Census Bureau’s American Community Survey (ACS). The results suggested that having insurance coverage is associated with a 2%-10% increase in malpractice activity. Thus, if 10% of a state’s population gains coverage, analysts estimated a 5% rise in malpractice claims.
"This study highlights the far-reaching impacts of the Affordable Care Act," said Jayne Plunkett, head of casualty reinsurance for Swiss Re, an international reinsurance company that sponsored the study. "Businesses and policymakers need to understand how and why their risk profiles might change as the Affordable Care Act is implemented."
But other insurers believe the study results are another uncertain forecast of the ACA’s future effects.
"You’re trying to look through a very cloudy crystal ball in making predictions about the Affordable Care Act," said Frank O’Neil, senior vice president and chief communications officer for ProAssurance, a national medical liability insurer. "There are a number of things that could cause a 5% change in medical liability rates that could happen at the same time as the implementation of the ACA, but be totally unrelated."
For example, if there is a sudden increase in either the frequency or the severity of malpractice claims in a particular state, that could impact the medical liability climate, Mr. O’Neil said. He added that other experts believe that new patients entering the health care system may be so appreciative of previously absent care that they would be reluctant to sue.
"There are a lot of unknowns yet, and I think it’s hard to agree or disagree with a prediction that doesn’t say over what time frame [an increase in claims] would occur," he said. The study "should be taken as just one other prediction."
The volume of malpractice claims against physicians could increase by 5% as more Americans gain health care coverage and access health services under the Affordable Care Act, according to a study by the RAND Corporation released April 9.
That increase could translate into higher malpractice premiums for physicians, RAND researchers found in a study of the ACA’s impact on all liability insurances.
"The Affordable Care Act is unlikely to dramatically affect liability costs, but it may influence small and moderate changes in costs over the next several years," said lead author David Auerbach, a policy researcher at RAND. "For example, auto insurers may spend less for treating injuries, while it may cost a bit more to provide physicians with medical malpractice coverage."
RAND investigators theorized that a greater number of insured patients would escalate the rate of malpractice lawsuits because of more procedures, interactions, and visits with physicians. Previous analyses have found the uninsured currently use about half of the care that insured patients do, they said.
To test their theory, the researchers compared National Practitioner Data Bank (NPDB) data on liability claims from 2008 to 2010 to insurance coverage data from the Census Bureau’s American Community Survey (ACS). The results suggested that having insurance coverage is associated with a 2%-10% increase in malpractice activity. Thus, if 10% of a state’s population gains coverage, analysts estimated a 5% rise in malpractice claims.
"This study highlights the far-reaching impacts of the Affordable Care Act," said Jayne Plunkett, head of casualty reinsurance for Swiss Re, an international reinsurance company that sponsored the study. "Businesses and policymakers need to understand how and why their risk profiles might change as the Affordable Care Act is implemented."
But other insurers believe the study results are another uncertain forecast of the ACA’s future effects.
"You’re trying to look through a very cloudy crystal ball in making predictions about the Affordable Care Act," said Frank O’Neil, senior vice president and chief communications officer for ProAssurance, a national medical liability insurer. "There are a number of things that could cause a 5% change in medical liability rates that could happen at the same time as the implementation of the ACA, but be totally unrelated."
For example, if there is a sudden increase in either the frequency or the severity of malpractice claims in a particular state, that could impact the medical liability climate, Mr. O’Neil said. He added that other experts believe that new patients entering the health care system may be so appreciative of previously absent care that they would be reluctant to sue.
"There are a lot of unknowns yet, and I think it’s hard to agree or disagree with a prediction that doesn’t say over what time frame [an increase in claims] would occur," he said. The study "should be taken as just one other prediction."

Listen Now! Patrick Torcson, MD, MMM, SFHM, discusses how being a hospitalist prepared him for the C-suite
Click here to listen to more of our interview with Dr. Torcson
Click here to listen to more of our interview with Dr. Torcson
Click here to listen to more of our interview with Dr. Torcson
IOM identifies 17 social factors to collect in EHRs
The Institute of Medicine has identified the top 17 social and behavioral areas that should be addressed in all electronic health records to improve health outcomes and advance public health research efforts.
The IOM compiled the list as a guide for federal officials who are currently developing criteria for Stage 3 of the meaningful use program for EHRs, slated to begin in 2017.
A 13-member committee, which included physicians as well as experts in health information technology and social determinants of health, compiled a list of "candidate" domains that included sociodemographic, psychological, and behavioral factors. The committee also identified domains related to individual-level social relationships and the effect of neighborhoods and communities.

The candidate domains (in no particular order) are sexual orientation, race/ethnicity, country of origin, education, employment, financial resources strain (food and housing insecurity), health literacy, stress, negative mood and affect, psychological assets (patient engagement, conscientiousness, optimism, and self-efficacy), dietary patterns, physical activity, nicotine use and exposure, alcohol use, social connections and social isolation, exposure to violence, and area socioeconomic and racial/ethnic characteristics.
In selecting the domains, the IOM committee considered the evidence for whether the domains were associated with health outcomes, as well as whether collecting the information in an electronic health record would be useful for treatment and in public health research.
While some of the information, such as race, ethnicity, gender, language, and smoking status, is routinely collected in electronic health records now, the committee included them on the list to ensure they would remain a priority.
The IOM is planning a follow-up report to narrow down the current list and to recommend specific measures for each of the domains. The second report will also look closely at the barriers to collecting this type of social and behavioral information from patients.
On Twitter @maryellenny
The Institute of Medicine has identified the top 17 social and behavioral areas that should be addressed in all electronic health records to improve health outcomes and advance public health research efforts.
The IOM compiled the list as a guide for federal officials who are currently developing criteria for Stage 3 of the meaningful use program for EHRs, slated to begin in 2017.
A 13-member committee, which included physicians as well as experts in health information technology and social determinants of health, compiled a list of "candidate" domains that included sociodemographic, psychological, and behavioral factors. The committee also identified domains related to individual-level social relationships and the effect of neighborhoods and communities.
The candidate domains (in no particular order) are sexual orientation, race/ethnicity, country of origin, education, employment, financial resources strain (food and housing insecurity), health literacy, stress, negative mood and affect, psychological assets (patient engagement, conscientiousness, optimism, and self-efficacy), dietary patterns, physical activity, nicotine use and exposure, alcohol use, social connections and social isolation, exposure to violence, and area socioeconomic and racial/ethnic characteristics.
In selecting the domains, the IOM committee considered the evidence for whether the domains were associated with health outcomes, as well as whether collecting the information in an electronic health record would be useful for treatment and in public health research.
While some of the information, such as race, ethnicity, gender, language, and smoking status, is routinely collected in electronic health records now, the committee included them on the list to ensure they would remain a priority.
The IOM is planning a follow-up report to narrow down the current list and to recommend specific measures for each of the domains. The second report will also look closely at the barriers to collecting this type of social and behavioral information from patients.
On Twitter @maryellenny
The Institute of Medicine has identified the top 17 social and behavioral areas that should be addressed in all electronic health records to improve health outcomes and advance public health research efforts.
The IOM compiled the list as a guide for federal officials who are currently developing criteria for Stage 3 of the meaningful use program for EHRs, slated to begin in 2017.
A 13-member committee, which included physicians as well as experts in health information technology and social determinants of health, compiled a list of "candidate" domains that included sociodemographic, psychological, and behavioral factors. The committee also identified domains related to individual-level social relationships and the effect of neighborhoods and communities.
The candidate domains (in no particular order) are sexual orientation, race/ethnicity, country of origin, education, employment, financial resources strain (food and housing insecurity), health literacy, stress, negative mood and affect, psychological assets (patient engagement, conscientiousness, optimism, and self-efficacy), dietary patterns, physical activity, nicotine use and exposure, alcohol use, social connections and social isolation, exposure to violence, and area socioeconomic and racial/ethnic characteristics.
In selecting the domains, the IOM committee considered the evidence for whether the domains were associated with health outcomes, as well as whether collecting the information in an electronic health record would be useful for treatment and in public health research.
While some of the information, such as race, ethnicity, gender, language, and smoking status, is routinely collected in electronic health records now, the committee included them on the list to ensure they would remain a priority.
The IOM is planning a follow-up report to narrow down the current list and to recommend specific measures for each of the domains. The second report will also look closely at the barriers to collecting this type of social and behavioral information from patients.
On Twitter @maryellenny
