User login
The Hospitalist only
Medical Decision-Making Factors Include Quantity of Information, Complexity
Physicians should formulate a complete and accurate description of a patient’s condition with an equivalent plan of care for each encounter. While acuity and severity can be inferred by healthcare professionals without excessive detail or repetitive documentation of previously entered information, adequate documentation for every service date assists in conveying patient complexity during medical record review.
Regardless of how complex a patient’s condition might be, physicians tend to undervalue their services. This is due, in part, to the routine nature of patient care for seasoned physicians; it is also due in part to a general lack of understanding with respect to the documentation guidelines.
Consider the following scenario: A 68-year-old male with diabetes and a history of chronic obstructive bronchitis was hospitalized after a five-day history of progressive cough with increasing purulent sputum, shortness of breath, and fever. He was treated for an exacerbation of chronic bronchitis within the past six weeks. Upon admission, the patient had an increased temperature (102°F), increased heart rate (96 beats per minute), and increased respiratory rate (28 shallow breaths per minute). His breath sounds included in the right lower lobe rhonchi, and his pulse oximetry was 89% on room air. Chest X-ray confirmed right lower lobe infiltrates along with chronic changes.
Although some physicians would consider this “low complexity” due to the frequency in which they encounter this type of case, others will more appropriately identify this as moderately complex.
MDM Categories
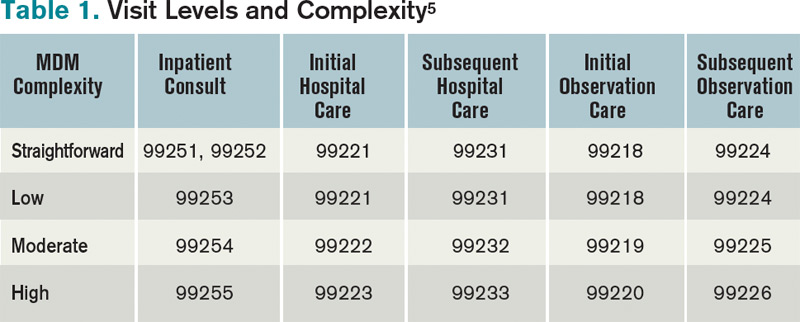
Medical decision-making (MDM) remains consistent in both the 1995 and 1997 guidelines.1,2 Complexity is categorized as straightforward, low, moderate, or high, based on the content of physician documentation. Each visit level is associated with a particular level of complexity. Only the care plan for a given date of service is considered when assigning MDM complexity. For each encounter, the physician receives credit for the number of diagnoses and/or treatment options, the amount and/or complexity of data ordered/reviewed, and the risk of complications/morbidity/mortality (see Table 1).
Number of diagnoses or treatment options. Physicians should document problems addressed and managed daily despite any changes to the treatment plan. Credit is provided for each problem with an associated plan, even if the plan states “continue treatment.” Credit also depends upon the quantity of problems addressed, as well as the problem type. An established problem in which the care plan has been established by the physician or group practice member during the current hospitalization is less complex than a new problem for which a diagnosis, prognosis, or plan has not been determined. Severity of the problem affects the weight of complexity. A worsening problem is more complex than an improving problem. Physician documentation should:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- When documentation indicates a continuation of current management options (e.g. “continue meds”), be sure that the management options to be continued are noted somewhere in the progress note for that encounter (e.g. medication list).
The plan of care outlines problems that the physician personally manages and those that impact management options, even if another physician directly oversees the problem. For example, the hospitalist might primarily manage diabetes, while the pulmonologist manages pneumonia. Since the pneumonia may impact the hospitalist’s plan for diabetic management, the hospitalist can receive credit for the pneumonia diagnosis if there is a non-overlapping, hospitalist-related care plan or comment about the pneumonia.
Amount and/or complexity of data ordered/reviewed. “Data” is classified as pathology/laboratory testing, radiology, and medicine-based diagnostics. Pertinent orders or results could be noted in the visit record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note or make an entry that refers to another auditor-accessible location for ordered tests and studies;
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”);
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary;
- Indicate when images, tracings, or specimens are “personally reviewed”; and
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
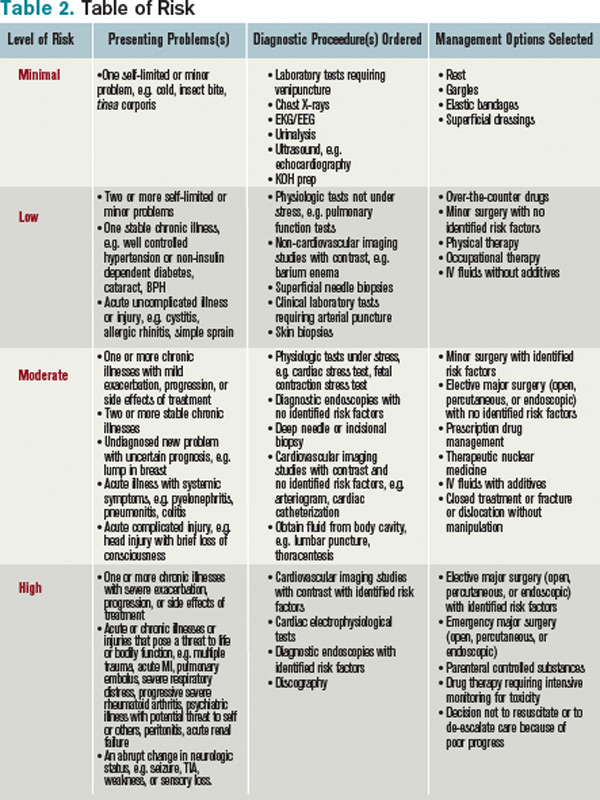
Risks of complication and/or morbidity or mortality. Risk involves the patient’s presenting problem, diagnostic procedures ordered, and management options selected. It is measured as minimal, low, moderate, or high when compared with corresponding items assigned to each risk level (see Table 2). The highest individual item detected on the table determines the overall patient risk for that encounter.
Chronic conditions and invasive procedures pose more risk than acute, uncomplicated illnesses or non-invasive procedures. Stable or improving problems are not as menacing as progressing problems; minor exacerbations are less hazardous than severe exacerbations; and medication risk varies with the type and potential for adverse effects. A patient maintains the same level of risk for a given medication whether the dosage is increased, decreased, or continued without change. Physicians should:
- Status all problems in the plan of care; identify them as stable, worsening, exacerbating (mild or severe), when applicable;
- Document all diagnostic or therapeutic procedures considered;
- Identify surgical risk factors involving comorbid conditions, when appropriate; and
- Associate the labs ordered to monitor for toxicity with the corresponding medication (e.g. “Continue Coumadin, monitor PT/INR”).
Determining complexity of medical decision-making. The final complexity of MDM depends upon the second-highest MDM category. The physician does not have to meet the requirements for all three MDM categories. For example, if a physician satisfies the requirements for a “multiple” number of diagnoses/treatment options, “limited” data, and “high” risk, the physician achieves moderate complexity decision-making (see Table 3). Remember that decision-making is just one of three components in evaluation and management services, along with history and exam.
Beware of payor variation, as it could have a significant impact on visit-level selection.3 Become acquainted with rules applicable to the geographical area. Review insurer websites for guidelines, policies, and “frequently asked questions” that can help improve documentation skills and support billing practices.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf. Accessed Nov. 14, 2011.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed Nov. 14, 2011.
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2010. Northbrook, IL: American College of Chest Physicians, 2009; 87-118.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011:1-20.
Physicians should formulate a complete and accurate description of a patient’s condition with an equivalent plan of care for each encounter. While acuity and severity can be inferred by healthcare professionals without excessive detail or repetitive documentation of previously entered information, adequate documentation for every service date assists in conveying patient complexity during medical record review.
Regardless of how complex a patient’s condition might be, physicians tend to undervalue their services. This is due, in part, to the routine nature of patient care for seasoned physicians; it is also due in part to a general lack of understanding with respect to the documentation guidelines.
Consider the following scenario: A 68-year-old male with diabetes and a history of chronic obstructive bronchitis was hospitalized after a five-day history of progressive cough with increasing purulent sputum, shortness of breath, and fever. He was treated for an exacerbation of chronic bronchitis within the past six weeks. Upon admission, the patient had an increased temperature (102°F), increased heart rate (96 beats per minute), and increased respiratory rate (28 shallow breaths per minute). His breath sounds included in the right lower lobe rhonchi, and his pulse oximetry was 89% on room air. Chest X-ray confirmed right lower lobe infiltrates along with chronic changes.
Although some physicians would consider this “low complexity” due to the frequency in which they encounter this type of case, others will more appropriately identify this as moderately complex.
MDM Categories
Medical decision-making (MDM) remains consistent in both the 1995 and 1997 guidelines.1,2 Complexity is categorized as straightforward, low, moderate, or high, based on the content of physician documentation. Each visit level is associated with a particular level of complexity. Only the care plan for a given date of service is considered when assigning MDM complexity. For each encounter, the physician receives credit for the number of diagnoses and/or treatment options, the amount and/or complexity of data ordered/reviewed, and the risk of complications/morbidity/mortality (see Table 1).
Number of diagnoses or treatment options. Physicians should document problems addressed and managed daily despite any changes to the treatment plan. Credit is provided for each problem with an associated plan, even if the plan states “continue treatment.” Credit also depends upon the quantity of problems addressed, as well as the problem type. An established problem in which the care plan has been established by the physician or group practice member during the current hospitalization is less complex than a new problem for which a diagnosis, prognosis, or plan has not been determined. Severity of the problem affects the weight of complexity. A worsening problem is more complex than an improving problem. Physician documentation should:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- When documentation indicates a continuation of current management options (e.g. “continue meds”), be sure that the management options to be continued are noted somewhere in the progress note for that encounter (e.g. medication list).
The plan of care outlines problems that the physician personally manages and those that impact management options, even if another physician directly oversees the problem. For example, the hospitalist might primarily manage diabetes, while the pulmonologist manages pneumonia. Since the pneumonia may impact the hospitalist’s plan for diabetic management, the hospitalist can receive credit for the pneumonia diagnosis if there is a non-overlapping, hospitalist-related care plan or comment about the pneumonia.
Amount and/or complexity of data ordered/reviewed. “Data” is classified as pathology/laboratory testing, radiology, and medicine-based diagnostics. Pertinent orders or results could be noted in the visit record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note or make an entry that refers to another auditor-accessible location for ordered tests and studies;
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”);
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary;
- Indicate when images, tracings, or specimens are “personally reviewed”; and
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Risks of complication and/or morbidity or mortality. Risk involves the patient’s presenting problem, diagnostic procedures ordered, and management options selected. It is measured as minimal, low, moderate, or high when compared with corresponding items assigned to each risk level (see Table 2). The highest individual item detected on the table determines the overall patient risk for that encounter.
Chronic conditions and invasive procedures pose more risk than acute, uncomplicated illnesses or non-invasive procedures. Stable or improving problems are not as menacing as progressing problems; minor exacerbations are less hazardous than severe exacerbations; and medication risk varies with the type and potential for adverse effects. A patient maintains the same level of risk for a given medication whether the dosage is increased, decreased, or continued without change. Physicians should:
- Status all problems in the plan of care; identify them as stable, worsening, exacerbating (mild or severe), when applicable;
- Document all diagnostic or therapeutic procedures considered;
- Identify surgical risk factors involving comorbid conditions, when appropriate; and
- Associate the labs ordered to monitor for toxicity with the corresponding medication (e.g. “Continue Coumadin, monitor PT/INR”).
Determining complexity of medical decision-making. The final complexity of MDM depends upon the second-highest MDM category. The physician does not have to meet the requirements for all three MDM categories. For example, if a physician satisfies the requirements for a “multiple” number of diagnoses/treatment options, “limited” data, and “high” risk, the physician achieves moderate complexity decision-making (see Table 3). Remember that decision-making is just one of three components in evaluation and management services, along with history and exam.
Beware of payor variation, as it could have a significant impact on visit-level selection.3 Become acquainted with rules applicable to the geographical area. Review insurer websites for guidelines, policies, and “frequently asked questions” that can help improve documentation skills and support billing practices.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf. Accessed Nov. 14, 2011.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed Nov. 14, 2011.
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2010. Northbrook, IL: American College of Chest Physicians, 2009; 87-118.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011:1-20.
Physicians should formulate a complete and accurate description of a patient’s condition with an equivalent plan of care for each encounter. While acuity and severity can be inferred by healthcare professionals without excessive detail or repetitive documentation of previously entered information, adequate documentation for every service date assists in conveying patient complexity during medical record review.
Regardless of how complex a patient’s condition might be, physicians tend to undervalue their services. This is due, in part, to the routine nature of patient care for seasoned physicians; it is also due in part to a general lack of understanding with respect to the documentation guidelines.
Consider the following scenario: A 68-year-old male with diabetes and a history of chronic obstructive bronchitis was hospitalized after a five-day history of progressive cough with increasing purulent sputum, shortness of breath, and fever. He was treated for an exacerbation of chronic bronchitis within the past six weeks. Upon admission, the patient had an increased temperature (102°F), increased heart rate (96 beats per minute), and increased respiratory rate (28 shallow breaths per minute). His breath sounds included in the right lower lobe rhonchi, and his pulse oximetry was 89% on room air. Chest X-ray confirmed right lower lobe infiltrates along with chronic changes.
Although some physicians would consider this “low complexity” due to the frequency in which they encounter this type of case, others will more appropriately identify this as moderately complex.
MDM Categories
Medical decision-making (MDM) remains consistent in both the 1995 and 1997 guidelines.1,2 Complexity is categorized as straightforward, low, moderate, or high, based on the content of physician documentation. Each visit level is associated with a particular level of complexity. Only the care plan for a given date of service is considered when assigning MDM complexity. For each encounter, the physician receives credit for the number of diagnoses and/or treatment options, the amount and/or complexity of data ordered/reviewed, and the risk of complications/morbidity/mortality (see Table 1).
Number of diagnoses or treatment options. Physicians should document problems addressed and managed daily despite any changes to the treatment plan. Credit is provided for each problem with an associated plan, even if the plan states “continue treatment.” Credit also depends upon the quantity of problems addressed, as well as the problem type. An established problem in which the care plan has been established by the physician or group practice member during the current hospitalization is less complex than a new problem for which a diagnosis, prognosis, or plan has not been determined. Severity of the problem affects the weight of complexity. A worsening problem is more complex than an improving problem. Physician documentation should:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- When documentation indicates a continuation of current management options (e.g. “continue meds”), be sure that the management options to be continued are noted somewhere in the progress note for that encounter (e.g. medication list).
The plan of care outlines problems that the physician personally manages and those that impact management options, even if another physician directly oversees the problem. For example, the hospitalist might primarily manage diabetes, while the pulmonologist manages pneumonia. Since the pneumonia may impact the hospitalist’s plan for diabetic management, the hospitalist can receive credit for the pneumonia diagnosis if there is a non-overlapping, hospitalist-related care plan or comment about the pneumonia.
Amount and/or complexity of data ordered/reviewed. “Data” is classified as pathology/laboratory testing, radiology, and medicine-based diagnostics. Pertinent orders or results could be noted in the visit record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note or make an entry that refers to another auditor-accessible location for ordered tests and studies;
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”);
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary;
- Indicate when images, tracings, or specimens are “personally reviewed”; and
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Risks of complication and/or morbidity or mortality. Risk involves the patient’s presenting problem, diagnostic procedures ordered, and management options selected. It is measured as minimal, low, moderate, or high when compared with corresponding items assigned to each risk level (see Table 2). The highest individual item detected on the table determines the overall patient risk for that encounter.
Chronic conditions and invasive procedures pose more risk than acute, uncomplicated illnesses or non-invasive procedures. Stable or improving problems are not as menacing as progressing problems; minor exacerbations are less hazardous than severe exacerbations; and medication risk varies with the type and potential for adverse effects. A patient maintains the same level of risk for a given medication whether the dosage is increased, decreased, or continued without change. Physicians should:
- Status all problems in the plan of care; identify them as stable, worsening, exacerbating (mild or severe), when applicable;
- Document all diagnostic or therapeutic procedures considered;
- Identify surgical risk factors involving comorbid conditions, when appropriate; and
- Associate the labs ordered to monitor for toxicity with the corresponding medication (e.g. “Continue Coumadin, monitor PT/INR”).
Determining complexity of medical decision-making. The final complexity of MDM depends upon the second-highest MDM category. The physician does not have to meet the requirements for all three MDM categories. For example, if a physician satisfies the requirements for a “multiple” number of diagnoses/treatment options, “limited” data, and “high” risk, the physician achieves moderate complexity decision-making (see Table 3). Remember that decision-making is just one of three components in evaluation and management services, along with history and exam.
Beware of payor variation, as it could have a significant impact on visit-level selection.3 Become acquainted with rules applicable to the geographical area. Review insurer websites for guidelines, policies, and “frequently asked questions” that can help improve documentation skills and support billing practices.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf. Accessed Nov. 14, 2011.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed Nov. 14, 2011.
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2010. Northbrook, IL: American College of Chest Physicians, 2009; 87-118.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011:1-20.
IPAB is Medicare's New Hammer for Spending Accountability
Now that the latest annual “doc fix” is in, physicians have been granted another reprieve from potentially crippling cuts to their Medicare reimbursement under the flawed sustainable growth rate (SGR) payment formula.
Beginning this year, there’s a new player in town that will have the authority to achieve what Congress has consistently failed to do—cut Medicare provider spending to keep it below a cap—and it can do so with unprecedented autonomy.
Say hello to the Independent Payment Advisory Board (IPAB), a creature of the Affordable Care Act (ACA) that will propose ways to reduce “overpayment” to Medicare providers if target-spending levels are exceeded.
What distinguishes the IPAB from the Medicare Payment Advisory Commission (MedPAC) is that its proposals will automatically become law, unless Congress enacts its own proposals that reduce Medicare provider spending by at least as much as IPAB’s, or the Senate musters a three-fifths majority vote to override IPAB’s proposals entirely. Further, the IPAB’s changes to Medicare cannot be overruled by the executive branch or a court of law.
MedPAC never wielded such authority; in fact, many of its cost-control recommendations were ignored.

—Judith Feder, PhD, professor of public policy, Georgetown University, Washington, D.C., former dean, Georgetown Public Policy Institute, fellow, the Urban Institute
The IPAB comes to life this year, with a $15 million appropriation from the ACA, and begins ramping up its operations (see “The IPAB Timetable,” p. 26). The board will be comprised of a 15-member, multi-stakeholder group—expected to include physicians, nurses, medical experts, economists, consumer advocates, and others—appointed by the President and subject to Senate confirmation.
Incendiary Reactions
Dubbed by its most vociferous and largely Republican critics as “dangerously powerful,” “the real death panel,” and “bureaucrats deciding whether you get care,” the IPAB even has some Democrats decrying its power grab. Rep. Pete Stark (D-Calif.) called the IPAB “an unprecedented abrogation of Congressional authority to an unelected, unaccountable body of so-called experts.”1
Even Allyson Schwartz (D-Pa.), who helped draft the ACA, has come out against the IPAB, joining a handful of Democrats and more than 200 Republicans in signing on to a bill (H.R. 452) to repeal the ACA’s IPAB provision. The Senate has a similar bill (S. 668).
Although the IPAB legally is barred from formally making recommendations to ration care, increase beneficiary premiums or cost sharing, and from restricting benefits or eligibility criteria, critics worry that its authority to control prices could hurt patients by driving Medicare payments so low that physicians cease to offer certain services to them.
Enforcement Power
IPAB will have unprecedented power to enforce Medicare’s provider spending benchmarks. Beginning in 2014, if Medicare’s projected spending growth rate per beneficiary rises above an inflation threshold of Gross Domestic Product per capita plus 1%, the IPAB would be triggered and would propose ways to trim provider payments. President Obama has since proposed a lower threshold of GDP per capita plus 0.5%, meaning that the IPAB would be triggered earlier and likely would have deeper cuts to make.
It is unclear how the spending growth benchmark will be affected by the $123 billion in Medicare payment cuts to hospitals and other providers over nine years, which were triggered when the so-called “super committee” failed to reach a budget-cutting consensus last fall.
U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius describes the IPAB as a “backstop to ensure that rising costs don’t accelerate out of control, threatening Medicare’s stability,” and she maintains that the board is a necessary fallback mechanism to enforce Medicare spending within budget while healthcare providers continue to prove the effectiveness of various value-based delivery and reimbursement reform projects the ACA is funding.2
Impact on Physicians
“The IPAB is a structural intervention to put pressure on Congress, the Executive, and CMS [Centers for Medicare & Medicaid Services] to guarantee the ACA’s investment in cost-containment, and it gives physicians the incentive to act on its principles,” says Judith Feder, PhD, professor of public policy at Georgetown University, former dean of the Georgetown Public Policy Institute, and a fellow at the Urban Institute.
Dr. Feder was a co-signer of a letter sent by 100 health policy experts and economists—including Congressional Budget Office founding director Alice Rivlin, now with the Brookings Institute—to congressional leaders last May urging them to abandon attempts to repeal the IPAB provision. Dr. Feder maintains that the IPAB will marshal “the expertise of professionals who can weigh evidence on how payment incentives affect care delivery and suggest sensible improvements, while forcing debate on difficult choices that Congress has thus far failed to address.”
Because of the changes the ACA has already made to provider reimbursement and Medicare Advantage plan funding, Feder says that Medicare’s average annual growth rate for the next decade is projected to be a full percentage point below per capita growth in GDP. On top of that, she says, “the ACA’s other payment reform experiments have the potential to improve quality and cut spending growth even further by reducing payment for overpriced or undesirable care–like unnecessary hospital readmissions–and rewarding efficiently provided, coordinated care.” By Feder’s analysis, the IPAB would not likely be triggered for a decade, but stands ready as a backup, if needed. Indeed, she favors extending IPAB’s authority beyond Medicare, to allow a system-wide spending target that creates an all-payer incentive to assure that providers really change their behavior to boost quality and efficiency.
Impact on Hospitalists
If the IPAB does come into play, Feder believes that hospitalists have less to worry about than other physician specialists, because the Board’s cost-reduction proposals would likely focus on services where overpayment is the most acute – like imaging and high-cost specialty procedures. “If hospitalists are promoting efficient, coordinated care, their position can only be enhanced by IPAB’s recommendations, to the extent that they can demonstrate value for the healthcare dollar spent,” she says.
Necessary quality and cost reforms that patients deserve, and physicians want to deliver, have been stymied for too long by a crippled Congress, and by powerful special interest agendas, says SHM Public Policy Committee member Bradley Flansbaum DO, MPH, FACP, SFHM, director of the HM program at Lenox Hill Hospital in New York City, and clinical assistant professor of medicine at NYU School of Medicine. Reform requires some real enforcement authority to put value-based quality above the fray, he adds.
“CMS just does not have the teeth to do that right now; they are in the cross-hairs, and an IPAB-like body is needed to insulate Congress from the politically-risky choices, bring evidence and expertise to the decisions, bust through the politics, and get the job done,” Dr. Flansbaum says.
Dr. Flansbaum illustrates the problem by pointing to recent clinical studies that show percutaneous vertebroplasty, which injects bone cement into the spine to treat fractures, to be no better than a placebo in relieving pain. Medicare and private health insurers have been covering vertebroplasty for many years, despite the absence of rigorous study of its effectiveness. The same likely holds true for scores of other expensive treatments and surgical procedures. “Who, exactly, is going to put the kibosh on this?” Dr. Flansbaum asks. “The free market, which includes surgeons, hospitals, and device companies, each with their agendas, or regulators?”
Dr. Flansbaum believes that, in order to effectively bring down costs, the IPAB should not be restricted to supply-side proposals (i.e. provider reimbursement), but also should be allowed to propose demand-side changes to Medicare’s benefit plans, such as tiered network pricing with higher premiums to cover the latest and most expensive technologies.
SHM supports the need for an independent entity to check the growth in Medicare spending, but it does not support the IPAB as it is currently established under the ACA because certain groups (including hospitals) are protected from its scrutiny during its first several years—a limitation that SHM says puts the board’s legitimacy into question and seriously weakens its potential cost-saving effectiveness. SHM supports replacing the IPAB with an independent board that (1) subjects all Medicare providers and suppliers to the same scrutiny without special interest carve-outs, (2) balances cost-saving with QI considerations, (3) protects delivery of quality services, and (4) ensures board membership that represents all potentially affected groups, including physicians. (Read the entire statement in the “Where We Stand” section of SHM’s Advocacy microsite at www.hospitalmedicine.org/advocacy.)
By removing the IPAB’s present handcuffs—opening its scope to all providers, as well as to demand-side changes in Medicare’s benefit structure—an IPAB-like entity with the proper staff and expertise can rationally think-out the choices that Congress will never make, according to Dr. Flansbaum.
“For the sake of our economy and our future generations, healthcare costs have to come down, even if that means some short-term pain,” he says. “Hospitals may take a hit. Some physician income might take a hit. Otherwise, there won’t be any hospitals or salaries to be hit.”
Christopher Guadagnino is a freelance writer in Philadelphia.
Reference
- Statement of Congressman Pete Stark Supporting Health Care Reform, March 21, 2010. Available at: http://www.stark.house.gov/index.php?option=com_content&view=article&id=1534:statement-of-congressman-pete-stark-supporting-health-care-reform&catid=67:floor-statements-2010-. Accessed Jan. 5, 2012.
- Kathleen Sebelius, “IPAB Will Protect Medicare.” Politico, June 23, 2011. Available at: http://dyn.politico.com/printstory.cfm?uuid=FDE594BA-87EE-4DA5-9841-33804926EF36. Accessed Jan. 5, 2012.
Now that the latest annual “doc fix” is in, physicians have been granted another reprieve from potentially crippling cuts to their Medicare reimbursement under the flawed sustainable growth rate (SGR) payment formula.
Beginning this year, there’s a new player in town that will have the authority to achieve what Congress has consistently failed to do—cut Medicare provider spending to keep it below a cap—and it can do so with unprecedented autonomy.
Say hello to the Independent Payment Advisory Board (IPAB), a creature of the Affordable Care Act (ACA) that will propose ways to reduce “overpayment” to Medicare providers if target-spending levels are exceeded.
What distinguishes the IPAB from the Medicare Payment Advisory Commission (MedPAC) is that its proposals will automatically become law, unless Congress enacts its own proposals that reduce Medicare provider spending by at least as much as IPAB’s, or the Senate musters a three-fifths majority vote to override IPAB’s proposals entirely. Further, the IPAB’s changes to Medicare cannot be overruled by the executive branch or a court of law.
MedPAC never wielded such authority; in fact, many of its cost-control recommendations were ignored.
—Judith Feder, PhD, professor of public policy, Georgetown University, Washington, D.C., former dean, Georgetown Public Policy Institute, fellow, the Urban Institute
The IPAB comes to life this year, with a $15 million appropriation from the ACA, and begins ramping up its operations (see “The IPAB Timetable,” p. 26). The board will be comprised of a 15-member, multi-stakeholder group—expected to include physicians, nurses, medical experts, economists, consumer advocates, and others—appointed by the President and subject to Senate confirmation.
Incendiary Reactions
Dubbed by its most vociferous and largely Republican critics as “dangerously powerful,” “the real death panel,” and “bureaucrats deciding whether you get care,” the IPAB even has some Democrats decrying its power grab. Rep. Pete Stark (D-Calif.) called the IPAB “an unprecedented abrogation of Congressional authority to an unelected, unaccountable body of so-called experts.”1
Even Allyson Schwartz (D-Pa.), who helped draft the ACA, has come out against the IPAB, joining a handful of Democrats and more than 200 Republicans in signing on to a bill (H.R. 452) to repeal the ACA’s IPAB provision. The Senate has a similar bill (S. 668).
Although the IPAB legally is barred from formally making recommendations to ration care, increase beneficiary premiums or cost sharing, and from restricting benefits or eligibility criteria, critics worry that its authority to control prices could hurt patients by driving Medicare payments so low that physicians cease to offer certain services to them.
Enforcement Power
IPAB will have unprecedented power to enforce Medicare’s provider spending benchmarks. Beginning in 2014, if Medicare’s projected spending growth rate per beneficiary rises above an inflation threshold of Gross Domestic Product per capita plus 1%, the IPAB would be triggered and would propose ways to trim provider payments. President Obama has since proposed a lower threshold of GDP per capita plus 0.5%, meaning that the IPAB would be triggered earlier and likely would have deeper cuts to make.
It is unclear how the spending growth benchmark will be affected by the $123 billion in Medicare payment cuts to hospitals and other providers over nine years, which were triggered when the so-called “super committee” failed to reach a budget-cutting consensus last fall.
U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius describes the IPAB as a “backstop to ensure that rising costs don’t accelerate out of control, threatening Medicare’s stability,” and she maintains that the board is a necessary fallback mechanism to enforce Medicare spending within budget while healthcare providers continue to prove the effectiveness of various value-based delivery and reimbursement reform projects the ACA is funding.2
Impact on Physicians
“The IPAB is a structural intervention to put pressure on Congress, the Executive, and CMS [Centers for Medicare & Medicaid Services] to guarantee the ACA’s investment in cost-containment, and it gives physicians the incentive to act on its principles,” says Judith Feder, PhD, professor of public policy at Georgetown University, former dean of the Georgetown Public Policy Institute, and a fellow at the Urban Institute.
Dr. Feder was a co-signer of a letter sent by 100 health policy experts and economists—including Congressional Budget Office founding director Alice Rivlin, now with the Brookings Institute—to congressional leaders last May urging them to abandon attempts to repeal the IPAB provision. Dr. Feder maintains that the IPAB will marshal “the expertise of professionals who can weigh evidence on how payment incentives affect care delivery and suggest sensible improvements, while forcing debate on difficult choices that Congress has thus far failed to address.”
Because of the changes the ACA has already made to provider reimbursement and Medicare Advantage plan funding, Feder says that Medicare’s average annual growth rate for the next decade is projected to be a full percentage point below per capita growth in GDP. On top of that, she says, “the ACA’s other payment reform experiments have the potential to improve quality and cut spending growth even further by reducing payment for overpriced or undesirable care–like unnecessary hospital readmissions–and rewarding efficiently provided, coordinated care.” By Feder’s analysis, the IPAB would not likely be triggered for a decade, but stands ready as a backup, if needed. Indeed, she favors extending IPAB’s authority beyond Medicare, to allow a system-wide spending target that creates an all-payer incentive to assure that providers really change their behavior to boost quality and efficiency.
Impact on Hospitalists
If the IPAB does come into play, Feder believes that hospitalists have less to worry about than other physician specialists, because the Board’s cost-reduction proposals would likely focus on services where overpayment is the most acute – like imaging and high-cost specialty procedures. “If hospitalists are promoting efficient, coordinated care, their position can only be enhanced by IPAB’s recommendations, to the extent that they can demonstrate value for the healthcare dollar spent,” she says.
Necessary quality and cost reforms that patients deserve, and physicians want to deliver, have been stymied for too long by a crippled Congress, and by powerful special interest agendas, says SHM Public Policy Committee member Bradley Flansbaum DO, MPH, FACP, SFHM, director of the HM program at Lenox Hill Hospital in New York City, and clinical assistant professor of medicine at NYU School of Medicine. Reform requires some real enforcement authority to put value-based quality above the fray, he adds.
“CMS just does not have the teeth to do that right now; they are in the cross-hairs, and an IPAB-like body is needed to insulate Congress from the politically-risky choices, bring evidence and expertise to the decisions, bust through the politics, and get the job done,” Dr. Flansbaum says.
Dr. Flansbaum illustrates the problem by pointing to recent clinical studies that show percutaneous vertebroplasty, which injects bone cement into the spine to treat fractures, to be no better than a placebo in relieving pain. Medicare and private health insurers have been covering vertebroplasty for many years, despite the absence of rigorous study of its effectiveness. The same likely holds true for scores of other expensive treatments and surgical procedures. “Who, exactly, is going to put the kibosh on this?” Dr. Flansbaum asks. “The free market, which includes surgeons, hospitals, and device companies, each with their agendas, or regulators?”
Dr. Flansbaum believes that, in order to effectively bring down costs, the IPAB should not be restricted to supply-side proposals (i.e. provider reimbursement), but also should be allowed to propose demand-side changes to Medicare’s benefit plans, such as tiered network pricing with higher premiums to cover the latest and most expensive technologies.
SHM supports the need for an independent entity to check the growth in Medicare spending, but it does not support the IPAB as it is currently established under the ACA because certain groups (including hospitals) are protected from its scrutiny during its first several years—a limitation that SHM says puts the board’s legitimacy into question and seriously weakens its potential cost-saving effectiveness. SHM supports replacing the IPAB with an independent board that (1) subjects all Medicare providers and suppliers to the same scrutiny without special interest carve-outs, (2) balances cost-saving with QI considerations, (3) protects delivery of quality services, and (4) ensures board membership that represents all potentially affected groups, including physicians. (Read the entire statement in the “Where We Stand” section of SHM’s Advocacy microsite at www.hospitalmedicine.org/advocacy.)
By removing the IPAB’s present handcuffs—opening its scope to all providers, as well as to demand-side changes in Medicare’s benefit structure—an IPAB-like entity with the proper staff and expertise can rationally think-out the choices that Congress will never make, according to Dr. Flansbaum.
“For the sake of our economy and our future generations, healthcare costs have to come down, even if that means some short-term pain,” he says. “Hospitals may take a hit. Some physician income might take a hit. Otherwise, there won’t be any hospitals or salaries to be hit.”
Christopher Guadagnino is a freelance writer in Philadelphia.
Reference
- Statement of Congressman Pete Stark Supporting Health Care Reform, March 21, 2010. Available at: http://www.stark.house.gov/index.php?option=com_content&view=article&id=1534:statement-of-congressman-pete-stark-supporting-health-care-reform&catid=67:floor-statements-2010-. Accessed Jan. 5, 2012.
- Kathleen Sebelius, “IPAB Will Protect Medicare.” Politico, June 23, 2011. Available at: http://dyn.politico.com/printstory.cfm?uuid=FDE594BA-87EE-4DA5-9841-33804926EF36. Accessed Jan. 5, 2012.
Now that the latest annual “doc fix” is in, physicians have been granted another reprieve from potentially crippling cuts to their Medicare reimbursement under the flawed sustainable growth rate (SGR) payment formula.
Beginning this year, there’s a new player in town that will have the authority to achieve what Congress has consistently failed to do—cut Medicare provider spending to keep it below a cap—and it can do so with unprecedented autonomy.
Say hello to the Independent Payment Advisory Board (IPAB), a creature of the Affordable Care Act (ACA) that will propose ways to reduce “overpayment” to Medicare providers if target-spending levels are exceeded.
What distinguishes the IPAB from the Medicare Payment Advisory Commission (MedPAC) is that its proposals will automatically become law, unless Congress enacts its own proposals that reduce Medicare provider spending by at least as much as IPAB’s, or the Senate musters a three-fifths majority vote to override IPAB’s proposals entirely. Further, the IPAB’s changes to Medicare cannot be overruled by the executive branch or a court of law.
MedPAC never wielded such authority; in fact, many of its cost-control recommendations were ignored.
—Judith Feder, PhD, professor of public policy, Georgetown University, Washington, D.C., former dean, Georgetown Public Policy Institute, fellow, the Urban Institute
The IPAB comes to life this year, with a $15 million appropriation from the ACA, and begins ramping up its operations (see “The IPAB Timetable,” p. 26). The board will be comprised of a 15-member, multi-stakeholder group—expected to include physicians, nurses, medical experts, economists, consumer advocates, and others—appointed by the President and subject to Senate confirmation.
Incendiary Reactions
Dubbed by its most vociferous and largely Republican critics as “dangerously powerful,” “the real death panel,” and “bureaucrats deciding whether you get care,” the IPAB even has some Democrats decrying its power grab. Rep. Pete Stark (D-Calif.) called the IPAB “an unprecedented abrogation of Congressional authority to an unelected, unaccountable body of so-called experts.”1
Even Allyson Schwartz (D-Pa.), who helped draft the ACA, has come out against the IPAB, joining a handful of Democrats and more than 200 Republicans in signing on to a bill (H.R. 452) to repeal the ACA’s IPAB provision. The Senate has a similar bill (S. 668).
Although the IPAB legally is barred from formally making recommendations to ration care, increase beneficiary premiums or cost sharing, and from restricting benefits or eligibility criteria, critics worry that its authority to control prices could hurt patients by driving Medicare payments so low that physicians cease to offer certain services to them.
Enforcement Power
IPAB will have unprecedented power to enforce Medicare’s provider spending benchmarks. Beginning in 2014, if Medicare’s projected spending growth rate per beneficiary rises above an inflation threshold of Gross Domestic Product per capita plus 1%, the IPAB would be triggered and would propose ways to trim provider payments. President Obama has since proposed a lower threshold of GDP per capita plus 0.5%, meaning that the IPAB would be triggered earlier and likely would have deeper cuts to make.
It is unclear how the spending growth benchmark will be affected by the $123 billion in Medicare payment cuts to hospitals and other providers over nine years, which were triggered when the so-called “super committee” failed to reach a budget-cutting consensus last fall.
U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius describes the IPAB as a “backstop to ensure that rising costs don’t accelerate out of control, threatening Medicare’s stability,” and she maintains that the board is a necessary fallback mechanism to enforce Medicare spending within budget while healthcare providers continue to prove the effectiveness of various value-based delivery and reimbursement reform projects the ACA is funding.2
Impact on Physicians
“The IPAB is a structural intervention to put pressure on Congress, the Executive, and CMS [Centers for Medicare & Medicaid Services] to guarantee the ACA’s investment in cost-containment, and it gives physicians the incentive to act on its principles,” says Judith Feder, PhD, professor of public policy at Georgetown University, former dean of the Georgetown Public Policy Institute, and a fellow at the Urban Institute.
Dr. Feder was a co-signer of a letter sent by 100 health policy experts and economists—including Congressional Budget Office founding director Alice Rivlin, now with the Brookings Institute—to congressional leaders last May urging them to abandon attempts to repeal the IPAB provision. Dr. Feder maintains that the IPAB will marshal “the expertise of professionals who can weigh evidence on how payment incentives affect care delivery and suggest sensible improvements, while forcing debate on difficult choices that Congress has thus far failed to address.”
Because of the changes the ACA has already made to provider reimbursement and Medicare Advantage plan funding, Feder says that Medicare’s average annual growth rate for the next decade is projected to be a full percentage point below per capita growth in GDP. On top of that, she says, “the ACA’s other payment reform experiments have the potential to improve quality and cut spending growth even further by reducing payment for overpriced or undesirable care–like unnecessary hospital readmissions–and rewarding efficiently provided, coordinated care.” By Feder’s analysis, the IPAB would not likely be triggered for a decade, but stands ready as a backup, if needed. Indeed, she favors extending IPAB’s authority beyond Medicare, to allow a system-wide spending target that creates an all-payer incentive to assure that providers really change their behavior to boost quality and efficiency.
Impact on Hospitalists
If the IPAB does come into play, Feder believes that hospitalists have less to worry about than other physician specialists, because the Board’s cost-reduction proposals would likely focus on services where overpayment is the most acute – like imaging and high-cost specialty procedures. “If hospitalists are promoting efficient, coordinated care, their position can only be enhanced by IPAB’s recommendations, to the extent that they can demonstrate value for the healthcare dollar spent,” she says.
Necessary quality and cost reforms that patients deserve, and physicians want to deliver, have been stymied for too long by a crippled Congress, and by powerful special interest agendas, says SHM Public Policy Committee member Bradley Flansbaum DO, MPH, FACP, SFHM, director of the HM program at Lenox Hill Hospital in New York City, and clinical assistant professor of medicine at NYU School of Medicine. Reform requires some real enforcement authority to put value-based quality above the fray, he adds.
“CMS just does not have the teeth to do that right now; they are in the cross-hairs, and an IPAB-like body is needed to insulate Congress from the politically-risky choices, bring evidence and expertise to the decisions, bust through the politics, and get the job done,” Dr. Flansbaum says.
Dr. Flansbaum illustrates the problem by pointing to recent clinical studies that show percutaneous vertebroplasty, which injects bone cement into the spine to treat fractures, to be no better than a placebo in relieving pain. Medicare and private health insurers have been covering vertebroplasty for many years, despite the absence of rigorous study of its effectiveness. The same likely holds true for scores of other expensive treatments and surgical procedures. “Who, exactly, is going to put the kibosh on this?” Dr. Flansbaum asks. “The free market, which includes surgeons, hospitals, and device companies, each with their agendas, or regulators?”
Dr. Flansbaum believes that, in order to effectively bring down costs, the IPAB should not be restricted to supply-side proposals (i.e. provider reimbursement), but also should be allowed to propose demand-side changes to Medicare’s benefit plans, such as tiered network pricing with higher premiums to cover the latest and most expensive technologies.
SHM supports the need for an independent entity to check the growth in Medicare spending, but it does not support the IPAB as it is currently established under the ACA because certain groups (including hospitals) are protected from its scrutiny during its first several years—a limitation that SHM says puts the board’s legitimacy into question and seriously weakens its potential cost-saving effectiveness. SHM supports replacing the IPAB with an independent board that (1) subjects all Medicare providers and suppliers to the same scrutiny without special interest carve-outs, (2) balances cost-saving with QI considerations, (3) protects delivery of quality services, and (4) ensures board membership that represents all potentially affected groups, including physicians. (Read the entire statement in the “Where We Stand” section of SHM’s Advocacy microsite at www.hospitalmedicine.org/advocacy.)
By removing the IPAB’s present handcuffs—opening its scope to all providers, as well as to demand-side changes in Medicare’s benefit structure—an IPAB-like entity with the proper staff and expertise can rationally think-out the choices that Congress will never make, according to Dr. Flansbaum.
“For the sake of our economy and our future generations, healthcare costs have to come down, even if that means some short-term pain,” he says. “Hospitals may take a hit. Some physician income might take a hit. Otherwise, there won’t be any hospitals or salaries to be hit.”
Christopher Guadagnino is a freelance writer in Philadelphia.
Reference
- Statement of Congressman Pete Stark Supporting Health Care Reform, March 21, 2010. Available at: http://www.stark.house.gov/index.php?option=com_content&view=article&id=1534:statement-of-congressman-pete-stark-supporting-health-care-reform&catid=67:floor-statements-2010-. Accessed Jan. 5, 2012.
- Kathleen Sebelius, “IPAB Will Protect Medicare.” Politico, June 23, 2011. Available at: http://dyn.politico.com/printstory.cfm?uuid=FDE594BA-87EE-4DA5-9841-33804926EF36. Accessed Jan. 5, 2012.
Seven-Day Schedule Could Improve Hospital Quality, Capacity
A new study evaluating outcomes for hospitals participating in the American Heart Association’s Get with the Guidelines program found no correlation between high performance on adhering to measures and care standards for acute myocardial infarction and for heart failure despite overlap between the sets of care processes (J Am Coll Cardio. 2011;58:637-644).
A total of 400,000 heart patients were studied, and 283 participating hospitals were stratified into thirds based on their adherence to core quality measures for each disease, with the upper third labeled superior in performance. Lead author Tracy Wang, MD, MHS, MSc, of the Duke Clinical Research Institute in Durham, N.C., and colleagues found that superior performance for only one of the two diseases led to such end-result outcomes as in-hospital mortality that were no better than for hospitals that were not high performers for either condition. But hospitals with superior performance for both conditions had lower in-hospital mortality rates.
“Perhaps quality is more than just following checklists,” Dr. Wang says. “There’s something special about these high-performing hospitals across the board, with better QI, perhaps a little more investment in infrastructure for quality.”
This result, Dr. Wang says, should give ammunition for hospitalists and other physicians to go to their hospital administrators to request more investment in quality improvement overall, not just for specific conditions.
A new study evaluating outcomes for hospitals participating in the American Heart Association’s Get with the Guidelines program found no correlation between high performance on adhering to measures and care standards for acute myocardial infarction and for heart failure despite overlap between the sets of care processes (J Am Coll Cardio. 2011;58:637-644).
A total of 400,000 heart patients were studied, and 283 participating hospitals were stratified into thirds based on their adherence to core quality measures for each disease, with the upper third labeled superior in performance. Lead author Tracy Wang, MD, MHS, MSc, of the Duke Clinical Research Institute in Durham, N.C., and colleagues found that superior performance for only one of the two diseases led to such end-result outcomes as in-hospital mortality that were no better than for hospitals that were not high performers for either condition. But hospitals with superior performance for both conditions had lower in-hospital mortality rates.
“Perhaps quality is more than just following checklists,” Dr. Wang says. “There’s something special about these high-performing hospitals across the board, with better QI, perhaps a little more investment in infrastructure for quality.”
This result, Dr. Wang says, should give ammunition for hospitalists and other physicians to go to their hospital administrators to request more investment in quality improvement overall, not just for specific conditions.
A new study evaluating outcomes for hospitals participating in the American Heart Association’s Get with the Guidelines program found no correlation between high performance on adhering to measures and care standards for acute myocardial infarction and for heart failure despite overlap between the sets of care processes (J Am Coll Cardio. 2011;58:637-644).
A total of 400,000 heart patients were studied, and 283 participating hospitals were stratified into thirds based on their adherence to core quality measures for each disease, with the upper third labeled superior in performance. Lead author Tracy Wang, MD, MHS, MSc, of the Duke Clinical Research Institute in Durham, N.C., and colleagues found that superior performance for only one of the two diseases led to such end-result outcomes as in-hospital mortality that were no better than for hospitals that were not high performers for either condition. But hospitals with superior performance for both conditions had lower in-hospital mortality rates.
“Perhaps quality is more than just following checklists,” Dr. Wang says. “There’s something special about these high-performing hospitals across the board, with better QI, perhaps a little more investment in infrastructure for quality.”
This result, Dr. Wang says, should give ammunition for hospitalists and other physicians to go to their hospital administrators to request more investment in quality improvement overall, not just for specific conditions.
Survey Insights: Peeking under the Hood of Academic HM
The 2011 State of Hospital Medicine report offers some tantalizing insights into the operation of academic hospital medicine practices and how they compare with their nonacademic peers. Some results are not surprising, such as the fact that academic hospital medicine groups tend to be larger than nonacademic groups, and that compensation and clinical-FTE-adjusted productivity both tend to be lower for academic hospitalists. Interestingly, turnover rates were about the same in academic and nonacademic practices.
Among the more unexpected findings, however, is that academic HM practices tend to employ a higher proportion of women (44%) than nonacademic practices (35%). In addition, academic practices employed a wider range of staffing models, with only 43% of practices using shift-based staffing, compared with 78% of nonacademic respondents. Similarly, only 47% of academic groups provided on-site coverage at night, compared with 81% of nonacademic groups.
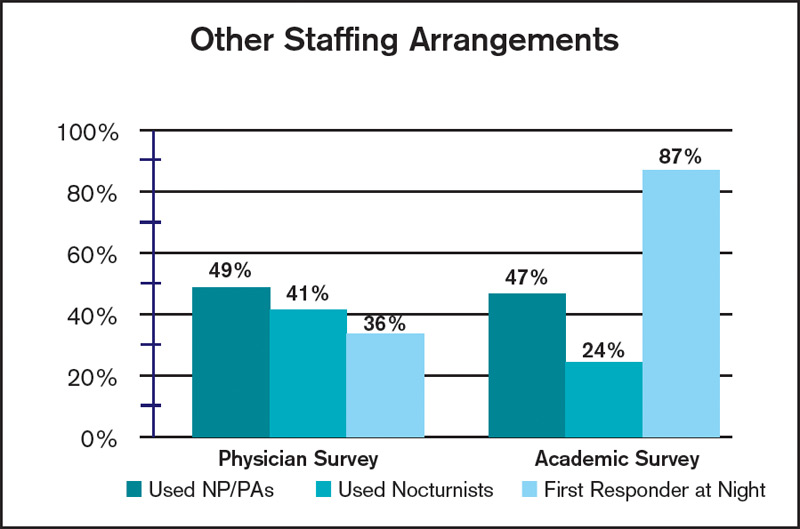
Additional differences between the way academic and nonacademic HM groups staff their programs are shown in the table, “Other Staffing Arrangements.” While the use of nurse practitioners and physician assistants (PA) was similar for academic and nonacademic practices, academic groups were much less likely to utilize nocturnists, and far more likely to have a nonphysician first responder at night (resident, nonphysician provider/PA, or other) than nonacademic groups.
It will be interesting to follow these trends over time. Because of new resident work-hour limits that went into effect in July, SHM Practice Analysis Committee (PAC) member Andrew White, MD, expects that there will be very few places that continue to use residents to cross-cover at night. “I suspect most academic centers have or will hire nocturnists,” he says, “but we’ll see.”
On the other hand, PAC member Scarlett Blue, RN, believes that continued growth in HM, coupled with a competitive job market, could result in increased use of nonphysician first responders at night—and in general. “Hospital medicine group leaders who are looking for alternative ways to meet the supply-demand conundrum may find a blended physician-NP/PA team to be one such answer,” she says.
Finally, the clinical services provided by academic HM groups vary from their nonacademic counterparts in some other important ways. Only 25% of academic practices provide care for ICU patients, compared with 78% of nonacademic practices, while 75% of academic groups perform procedures, compared with only 52% of nonacademic groups. And while the overwhelming majority of both academic and nonacademic practices provide surgical comanagement, academic practices were more than twice as likely to provide comanagement for medical subspecialty patients (45%, compared with 20% for nonacademic practices).
PAC member Troy Ahlstrom, MD, explains, tongue-in-cheek, that “academic hospitalists don’t do procedures because they have oodles of residents, fellows, and interventional radiologists to do them instead, and academics do more medical comanagement because the subspecialist who only does Waldenstrom’s macroglobulinemia probably doesn’t do diabetes.”
Whatever the reason, there are meaningful differences between academic and nonacademic HM practices that bear watching over time. You can help us identify and track these differences by ensuring that your group participates in SHM’s annual State of Hospital Medicine survey, launching this month.
The 2011 State of Hospital Medicine report offers some tantalizing insights into the operation of academic hospital medicine practices and how they compare with their nonacademic peers. Some results are not surprising, such as the fact that academic hospital medicine groups tend to be larger than nonacademic groups, and that compensation and clinical-FTE-adjusted productivity both tend to be lower for academic hospitalists. Interestingly, turnover rates were about the same in academic and nonacademic practices.
Among the more unexpected findings, however, is that academic HM practices tend to employ a higher proportion of women (44%) than nonacademic practices (35%). In addition, academic practices employed a wider range of staffing models, with only 43% of practices using shift-based staffing, compared with 78% of nonacademic respondents. Similarly, only 47% of academic groups provided on-site coverage at night, compared with 81% of nonacademic groups.
Additional differences between the way academic and nonacademic HM groups staff their programs are shown in the table, “Other Staffing Arrangements.” While the use of nurse practitioners and physician assistants (PA) was similar for academic and nonacademic practices, academic groups were much less likely to utilize nocturnists, and far more likely to have a nonphysician first responder at night (resident, nonphysician provider/PA, or other) than nonacademic groups.
It will be interesting to follow these trends over time. Because of new resident work-hour limits that went into effect in July, SHM Practice Analysis Committee (PAC) member Andrew White, MD, expects that there will be very few places that continue to use residents to cross-cover at night. “I suspect most academic centers have or will hire nocturnists,” he says, “but we’ll see.”
On the other hand, PAC member Scarlett Blue, RN, believes that continued growth in HM, coupled with a competitive job market, could result in increased use of nonphysician first responders at night—and in general. “Hospital medicine group leaders who are looking for alternative ways to meet the supply-demand conundrum may find a blended physician-NP/PA team to be one such answer,” she says.
Finally, the clinical services provided by academic HM groups vary from their nonacademic counterparts in some other important ways. Only 25% of academic practices provide care for ICU patients, compared with 78% of nonacademic practices, while 75% of academic groups perform procedures, compared with only 52% of nonacademic groups. And while the overwhelming majority of both academic and nonacademic practices provide surgical comanagement, academic practices were more than twice as likely to provide comanagement for medical subspecialty patients (45%, compared with 20% for nonacademic practices).
PAC member Troy Ahlstrom, MD, explains, tongue-in-cheek, that “academic hospitalists don’t do procedures because they have oodles of residents, fellows, and interventional radiologists to do them instead, and academics do more medical comanagement because the subspecialist who only does Waldenstrom’s macroglobulinemia probably doesn’t do diabetes.”
Whatever the reason, there are meaningful differences between academic and nonacademic HM practices that bear watching over time. You can help us identify and track these differences by ensuring that your group participates in SHM’s annual State of Hospital Medicine survey, launching this month.
The 2011 State of Hospital Medicine report offers some tantalizing insights into the operation of academic hospital medicine practices and how they compare with their nonacademic peers. Some results are not surprising, such as the fact that academic hospital medicine groups tend to be larger than nonacademic groups, and that compensation and clinical-FTE-adjusted productivity both tend to be lower for academic hospitalists. Interestingly, turnover rates were about the same in academic and nonacademic practices.
Among the more unexpected findings, however, is that academic HM practices tend to employ a higher proportion of women (44%) than nonacademic practices (35%). In addition, academic practices employed a wider range of staffing models, with only 43% of practices using shift-based staffing, compared with 78% of nonacademic respondents. Similarly, only 47% of academic groups provided on-site coverage at night, compared with 81% of nonacademic groups.
Additional differences between the way academic and nonacademic HM groups staff their programs are shown in the table, “Other Staffing Arrangements.” While the use of nurse practitioners and physician assistants (PA) was similar for academic and nonacademic practices, academic groups were much less likely to utilize nocturnists, and far more likely to have a nonphysician first responder at night (resident, nonphysician provider/PA, or other) than nonacademic groups.
It will be interesting to follow these trends over time. Because of new resident work-hour limits that went into effect in July, SHM Practice Analysis Committee (PAC) member Andrew White, MD, expects that there will be very few places that continue to use residents to cross-cover at night. “I suspect most academic centers have or will hire nocturnists,” he says, “but we’ll see.”
On the other hand, PAC member Scarlett Blue, RN, believes that continued growth in HM, coupled with a competitive job market, could result in increased use of nonphysician first responders at night—and in general. “Hospital medicine group leaders who are looking for alternative ways to meet the supply-demand conundrum may find a blended physician-NP/PA team to be one such answer,” she says.
Finally, the clinical services provided by academic HM groups vary from their nonacademic counterparts in some other important ways. Only 25% of academic practices provide care for ICU patients, compared with 78% of nonacademic practices, while 75% of academic groups perform procedures, compared with only 52% of nonacademic groups. And while the overwhelming majority of both academic and nonacademic practices provide surgical comanagement, academic practices were more than twice as likely to provide comanagement for medical subspecialty patients (45%, compared with 20% for nonacademic practices).
PAC member Troy Ahlstrom, MD, explains, tongue-in-cheek, that “academic hospitalists don’t do procedures because they have oodles of residents, fellows, and interventional radiologists to do them instead, and academics do more medical comanagement because the subspecialist who only does Waldenstrom’s macroglobulinemia probably doesn’t do diabetes.”
Whatever the reason, there are meaningful differences between academic and nonacademic HM practices that bear watching over time. You can help us identify and track these differences by ensuring that your group participates in SHM’s annual State of Hospital Medicine survey, launching this month.
HM’s Role in Helping Hospitals Profit
A new report shows that 1 in 5 community hospitals operates in the red, but the chief strategy officer of the firm that conducted the survey thinks hospitals can help change that.
The second annual survey from healthcare information technology (HIT) provider Anthelio and leadership group Community Hospital 100 found that 22% of community hospitals operate with margins below 2%; another 38% operate below 1%. Rick Kneipper, Anthelio’s cofounder and chief strategy officer, says that hospitalists can be at the forefront “of the creative changes needed” to reduce costs and improve profitability.
“Hospital medicine groups and hospitals could free up significant funds to devote to improved patient-care services if they focus on their core competency of patient care and farm out their non-core, back-office services to experts who can use leverage to provide more efficient services at significantly reduced costs,” Kneipper wrote in an email to The Hospitalist. “Financial pressures have historically forced most industries to stop trying to be vertically integrated [trying to be ‘all things to all people’] and instead to focus on their core competencies—it’s time for healthcare to do the same.”
—Rick Kneipper, cofounder, chief strategy officer, Anthelio
HM’s foothold at the intersection of clinical care and safety and QI positions the specialty to “respond to the new challenges of readmission penalties, evidenced-based medicine requirements, EMR implementation, and operation challenges,” Kneipper wrote.
For the full survey, please visit www.antheliohealth.com and search “survey.”
A new report shows that 1 in 5 community hospitals operates in the red, but the chief strategy officer of the firm that conducted the survey thinks hospitals can help change that.
The second annual survey from healthcare information technology (HIT) provider Anthelio and leadership group Community Hospital 100 found that 22% of community hospitals operate with margins below 2%; another 38% operate below 1%. Rick Kneipper, Anthelio’s cofounder and chief strategy officer, says that hospitalists can be at the forefront “of the creative changes needed” to reduce costs and improve profitability.
“Hospital medicine groups and hospitals could free up significant funds to devote to improved patient-care services if they focus on their core competency of patient care and farm out their non-core, back-office services to experts who can use leverage to provide more efficient services at significantly reduced costs,” Kneipper wrote in an email to The Hospitalist. “Financial pressures have historically forced most industries to stop trying to be vertically integrated [trying to be ‘all things to all people’] and instead to focus on their core competencies—it’s time for healthcare to do the same.”
—Rick Kneipper, cofounder, chief strategy officer, Anthelio
HM’s foothold at the intersection of clinical care and safety and QI positions the specialty to “respond to the new challenges of readmission penalties, evidenced-based medicine requirements, EMR implementation, and operation challenges,” Kneipper wrote.
For the full survey, please visit www.antheliohealth.com and search “survey.”
A new report shows that 1 in 5 community hospitals operates in the red, but the chief strategy officer of the firm that conducted the survey thinks hospitals can help change that.
The second annual survey from healthcare information technology (HIT) provider Anthelio and leadership group Community Hospital 100 found that 22% of community hospitals operate with margins below 2%; another 38% operate below 1%. Rick Kneipper, Anthelio’s cofounder and chief strategy officer, says that hospitalists can be at the forefront “of the creative changes needed” to reduce costs and improve profitability.
“Hospital medicine groups and hospitals could free up significant funds to devote to improved patient-care services if they focus on their core competency of patient care and farm out their non-core, back-office services to experts who can use leverage to provide more efficient services at significantly reduced costs,” Kneipper wrote in an email to The Hospitalist. “Financial pressures have historically forced most industries to stop trying to be vertically integrated [trying to be ‘all things to all people’] and instead to focus on their core competencies—it’s time for healthcare to do the same.”
—Rick Kneipper, cofounder, chief strategy officer, Anthelio
HM’s foothold at the intersection of clinical care and safety and QI positions the specialty to “respond to the new challenges of readmission penalties, evidenced-based medicine requirements, EMR implementation, and operation challenges,” Kneipper wrote.
For the full survey, please visit www.antheliohealth.com and search “survey.”
I Resolve…

It’s that time of year again. A new year is upon us. It’s resolution time.
I must admit, somewhat sheepishly, that I am a bit of “resolver.” What can I say? I like to resolve. I like to think about resolutions. I like to plan resolutions. I like to regale my uninterested wife with my resolutions. And I am, in fact, actually quite good at all phases of resolving, with one small exception—the follow-through.
You see, while I love to plan changes in my life, I’m horrible at making changes in my life. There’s nothing too shocking about that, I suppose. Most people fail when change is required. What is interesting, though, is that years of failure have yet to imbue me with the sense to stop resolving. I mean, how many times can a man fail at resolutions before he stumbles upon a resolution to stop resolving—a resolution I’d surely fail at?
But what are perhaps even more interesting are the things I’ve apparently resolved to do. I say “apparently” because not only do I typically not remember making the resolutions, but most often I also can’t even fathom why I’d resolve such things in the first place. But clearly I do. In fact, every year, I commit to about 10-20 resolutions. I actually write them down, threaten to make my wife read them, then stow them safely in my desk drawer, only to unearth them a year later to discover that I actually resolved to write a children’s book. True story; I just reviewed my resolutions from last year. I don’t remember why I put that on the list. But I did. And, of course, I failed—but I did, in fact, read a children’s book. Maybe that’s what I meant.
Over the years I’ve also resolved to make a hole-in-one, get better hair, and read War and Peace (on the toilet, during medical school). Fail, fail, and fail. The last one’s a great example of good intentions and no follow-through. Driven by the numerology (1,296 pages+1,296 days of medical school, excluding the last semester, of course, as most of us did=one page per day!) and the symbolism (medical school+grueling+war=challenging, long, grueling book about war) of the goal, I was ultimately undone by an inability to reliably differentiate a Bezukhov from a Bolkonsky, and constipation.
I bring this all up because it is time again for New Year’s resolutions. So here, in no particular order, are my 2012 resolutions.
Oh, That’s How Full Feels!
In 2012, I resolve to finally have a fully staffed HM group. From our group’s origins in 2003 to our current 30-member group, we have been intermittently understaffed to various degrees—a feeling I know most of you have experienced. For a couple of years we were fully staffed, but recent hospital expansions again place us at risk of being understaffed. As most of you know, it is exceedingly difficult to move the clinical, quality, and efficiency goals of a group forward without enough boots on the ground. So, if you’re in the market, the skiing in Colorado can’t be beat!
Appreciate VBP
I resolve to position our hospitalist group for the coming value-based purchasing world. We all know that the future belongs to those who can provide fundamental value—that is, higher-quality care at lower cost. This has been HM’s mantra the past decade. 2012 is the year I resolve to see our group fully realize this.
Leave the Cave
I resolve to (really) learn how to use Epic. We implemented our new Epic electronic health record in 2011. I’m a big proponent, but also a Luddite. I tinker around the edges of what is a truly powerful tool in advancing clinical care. I resolve to move past casual to highly functional user.
Make “10” Perfect
I resolve to figure out this new ICD-10 system. OK, technically it’s not “new.” It’s been complete since 1992 and in use in many countries for the better part of a decade. This is not a simple update of the ICD-9 system; rather, this is an entire overhaul that adds two more digits to the system. This takes the number of possible codes from 13,000 (ICD-9) to 68,000 (ICD-10). This allows for much more specificity and laterality—that is, you could have cellulitis of the right or left foot.
These changes are more than just job security for coders. The issue monetizes as payors decide not to pay for readmissions. Consider a patient who had a right-foot cellulitis, only to be admitted two weeks later with a left-foot cellulitis. ICD-9 does not have laterality, such that both stays would have the same code and the second admit could be denied as a 30-day readmission.
Twitter With Excitement
I resolve to figure out social media. I must admit that this is a red-alert, high-risk-of-failure resolution, partly because I don’t Facebook, tweet, or blog; heck, I’m not even LinkedIn! Additionally, I don’t have any friends. And finally, I just don’t get it. Then again, I didn’t get “The Simpsons” when they first came out. D’oh!
Get Hipper
And I resolve to re-enter the pop culture world in general. My social and cultural life came to a screeching halt near midnight on Sept. 29, 2007: One moment I was innocently watching the Colorado Rockies battle into their first playoffs in 12 years, and the next I was blasted onto a four-year hyper-blur of crying, spoon-feeding, and diaper-changing—for the non-parent readers, I’m describing child-rearing, not residency training, which is admittedly often marked by these same mileposts. Now 4 and 2 years old, my kiddos have finally reached the stages of self-care that allow for my gradual re-entry into the outside world.
As such, I resolve to go to a movie (in the theater) again. The last two movies we saw in the theatre in 2007 were chosen by my pregnant wife and contained an uncomfortable subliminal theme—Knocked Up (pregnant woman hates impregnating sloth of a man), Juno (pregnant woman has love-hate relationship with pasty, impregnating nerd in tight gym shorts).
I’m also interested to see what’s on TV and on the radio. When I last turned off the cathodes, “Lost” was big; ditto “The Sopranos.” And in a clearly ill-fated second season, “Dancing with the Stars” was well on its way to its undeniable cancellation. Musically, Britney was shaving her head and Jordin Sparks was edging out Sanjaya’s faux-hawk on “Idol.”
I’m also looking forward to learning what a Kardashian is (a sweater?), explaining the strange pull toward vampire romances, and discovering the difference between a Pippa and a Snooki. Should be fun. I just hope I don’t catch “Bieber Fever.”
Aspire To “Be The Cup”
Finally, in 2012, I resolve to live up to the coffee cup—you know, the Father’s Day 2011 gift emblazoned with “World’s Best Dad.” I’m sure you all feel this in your own way—that constant tension between work and life. In 2011, work won a few too many of the tug-o’-wars. Too many missed gymnastics lessons, soccer practices, parent events at daycare, and late dinners. 2012 will be different.
I resolve to teach my son the art of hitting a curveball (even if it’s off a tee) and my daughter her letters and numbers. The dogs will get more tennis balls, the wife fewer resolutions to review.
In fact, this year is going to be totally different. This is the year my to-do list doesn’t once again end as an “undid list.” This is the year I will accomplish my resolutions … not just one or two, but all of my resolutions.
And I might just write a children’s book for good measure.
Dr. Glasheen is The Hospitalist’s physician editor.
It’s that time of year again. A new year is upon us. It’s resolution time.
I must admit, somewhat sheepishly, that I am a bit of “resolver.” What can I say? I like to resolve. I like to think about resolutions. I like to plan resolutions. I like to regale my uninterested wife with my resolutions. And I am, in fact, actually quite good at all phases of resolving, with one small exception—the follow-through.
You see, while I love to plan changes in my life, I’m horrible at making changes in my life. There’s nothing too shocking about that, I suppose. Most people fail when change is required. What is interesting, though, is that years of failure have yet to imbue me with the sense to stop resolving. I mean, how many times can a man fail at resolutions before he stumbles upon a resolution to stop resolving—a resolution I’d surely fail at?
But what are perhaps even more interesting are the things I’ve apparently resolved to do. I say “apparently” because not only do I typically not remember making the resolutions, but most often I also can’t even fathom why I’d resolve such things in the first place. But clearly I do. In fact, every year, I commit to about 10-20 resolutions. I actually write them down, threaten to make my wife read them, then stow them safely in my desk drawer, only to unearth them a year later to discover that I actually resolved to write a children’s book. True story; I just reviewed my resolutions from last year. I don’t remember why I put that on the list. But I did. And, of course, I failed—but I did, in fact, read a children’s book. Maybe that’s what I meant.
Over the years I’ve also resolved to make a hole-in-one, get better hair, and read War and Peace (on the toilet, during medical school). Fail, fail, and fail. The last one’s a great example of good intentions and no follow-through. Driven by the numerology (1,296 pages+1,296 days of medical school, excluding the last semester, of course, as most of us did=one page per day!) and the symbolism (medical school+grueling+war=challenging, long, grueling book about war) of the goal, I was ultimately undone by an inability to reliably differentiate a Bezukhov from a Bolkonsky, and constipation.
I bring this all up because it is time again for New Year’s resolutions. So here, in no particular order, are my 2012 resolutions.
Oh, That’s How Full Feels!
In 2012, I resolve to finally have a fully staffed HM group. From our group’s origins in 2003 to our current 30-member group, we have been intermittently understaffed to various degrees—a feeling I know most of you have experienced. For a couple of years we were fully staffed, but recent hospital expansions again place us at risk of being understaffed. As most of you know, it is exceedingly difficult to move the clinical, quality, and efficiency goals of a group forward without enough boots on the ground. So, if you’re in the market, the skiing in Colorado can’t be beat!
Appreciate VBP
I resolve to position our hospitalist group for the coming value-based purchasing world. We all know that the future belongs to those who can provide fundamental value—that is, higher-quality care at lower cost. This has been HM’s mantra the past decade. 2012 is the year I resolve to see our group fully realize this.
Leave the Cave
I resolve to (really) learn how to use Epic. We implemented our new Epic electronic health record in 2011. I’m a big proponent, but also a Luddite. I tinker around the edges of what is a truly powerful tool in advancing clinical care. I resolve to move past casual to highly functional user.
Make “10” Perfect
I resolve to figure out this new ICD-10 system. OK, technically it’s not “new.” It’s been complete since 1992 and in use in many countries for the better part of a decade. This is not a simple update of the ICD-9 system; rather, this is an entire overhaul that adds two more digits to the system. This takes the number of possible codes from 13,000 (ICD-9) to 68,000 (ICD-10). This allows for much more specificity and laterality—that is, you could have cellulitis of the right or left foot.
These changes are more than just job security for coders. The issue monetizes as payors decide not to pay for readmissions. Consider a patient who had a right-foot cellulitis, only to be admitted two weeks later with a left-foot cellulitis. ICD-9 does not have laterality, such that both stays would have the same code and the second admit could be denied as a 30-day readmission.
Twitter With Excitement
I resolve to figure out social media. I must admit that this is a red-alert, high-risk-of-failure resolution, partly because I don’t Facebook, tweet, or blog; heck, I’m not even LinkedIn! Additionally, I don’t have any friends. And finally, I just don’t get it. Then again, I didn’t get “The Simpsons” when they first came out. D’oh!
Get Hipper
And I resolve to re-enter the pop culture world in general. My social and cultural life came to a screeching halt near midnight on Sept. 29, 2007: One moment I was innocently watching the Colorado Rockies battle into their first playoffs in 12 years, and the next I was blasted onto a four-year hyper-blur of crying, spoon-feeding, and diaper-changing—for the non-parent readers, I’m describing child-rearing, not residency training, which is admittedly often marked by these same mileposts. Now 4 and 2 years old, my kiddos have finally reached the stages of self-care that allow for my gradual re-entry into the outside world.
As such, I resolve to go to a movie (in the theater) again. The last two movies we saw in the theatre in 2007 were chosen by my pregnant wife and contained an uncomfortable subliminal theme—Knocked Up (pregnant woman hates impregnating sloth of a man), Juno (pregnant woman has love-hate relationship with pasty, impregnating nerd in tight gym shorts).
I’m also interested to see what’s on TV and on the radio. When I last turned off the cathodes, “Lost” was big; ditto “The Sopranos.” And in a clearly ill-fated second season, “Dancing with the Stars” was well on its way to its undeniable cancellation. Musically, Britney was shaving her head and Jordin Sparks was edging out Sanjaya’s faux-hawk on “Idol.”
I’m also looking forward to learning what a Kardashian is (a sweater?), explaining the strange pull toward vampire romances, and discovering the difference between a Pippa and a Snooki. Should be fun. I just hope I don’t catch “Bieber Fever.”
Aspire To “Be The Cup”
Finally, in 2012, I resolve to live up to the coffee cup—you know, the Father’s Day 2011 gift emblazoned with “World’s Best Dad.” I’m sure you all feel this in your own way—that constant tension between work and life. In 2011, work won a few too many of the tug-o’-wars. Too many missed gymnastics lessons, soccer practices, parent events at daycare, and late dinners. 2012 will be different.
I resolve to teach my son the art of hitting a curveball (even if it’s off a tee) and my daughter her letters and numbers. The dogs will get more tennis balls, the wife fewer resolutions to review.
In fact, this year is going to be totally different. This is the year my to-do list doesn’t once again end as an “undid list.” This is the year I will accomplish my resolutions … not just one or two, but all of my resolutions.
And I might just write a children’s book for good measure.
Dr. Glasheen is The Hospitalist’s physician editor.
It’s that time of year again. A new year is upon us. It’s resolution time.
I must admit, somewhat sheepishly, that I am a bit of “resolver.” What can I say? I like to resolve. I like to think about resolutions. I like to plan resolutions. I like to regale my uninterested wife with my resolutions. And I am, in fact, actually quite good at all phases of resolving, with one small exception—the follow-through.
You see, while I love to plan changes in my life, I’m horrible at making changes in my life. There’s nothing too shocking about that, I suppose. Most people fail when change is required. What is interesting, though, is that years of failure have yet to imbue me with the sense to stop resolving. I mean, how many times can a man fail at resolutions before he stumbles upon a resolution to stop resolving—a resolution I’d surely fail at?
But what are perhaps even more interesting are the things I’ve apparently resolved to do. I say “apparently” because not only do I typically not remember making the resolutions, but most often I also can’t even fathom why I’d resolve such things in the first place. But clearly I do. In fact, every year, I commit to about 10-20 resolutions. I actually write them down, threaten to make my wife read them, then stow them safely in my desk drawer, only to unearth them a year later to discover that I actually resolved to write a children’s book. True story; I just reviewed my resolutions from last year. I don’t remember why I put that on the list. But I did. And, of course, I failed—but I did, in fact, read a children’s book. Maybe that’s what I meant.
Over the years I’ve also resolved to make a hole-in-one, get better hair, and read War and Peace (on the toilet, during medical school). Fail, fail, and fail. The last one’s a great example of good intentions and no follow-through. Driven by the numerology (1,296 pages+1,296 days of medical school, excluding the last semester, of course, as most of us did=one page per day!) and the symbolism (medical school+grueling+war=challenging, long, grueling book about war) of the goal, I was ultimately undone by an inability to reliably differentiate a Bezukhov from a Bolkonsky, and constipation.
I bring this all up because it is time again for New Year’s resolutions. So here, in no particular order, are my 2012 resolutions.
Oh, That’s How Full Feels!
In 2012, I resolve to finally have a fully staffed HM group. From our group’s origins in 2003 to our current 30-member group, we have been intermittently understaffed to various degrees—a feeling I know most of you have experienced. For a couple of years we were fully staffed, but recent hospital expansions again place us at risk of being understaffed. As most of you know, it is exceedingly difficult to move the clinical, quality, and efficiency goals of a group forward without enough boots on the ground. So, if you’re in the market, the skiing in Colorado can’t be beat!
Appreciate VBP
I resolve to position our hospitalist group for the coming value-based purchasing world. We all know that the future belongs to those who can provide fundamental value—that is, higher-quality care at lower cost. This has been HM’s mantra the past decade. 2012 is the year I resolve to see our group fully realize this.
Leave the Cave
I resolve to (really) learn how to use Epic. We implemented our new Epic electronic health record in 2011. I’m a big proponent, but also a Luddite. I tinker around the edges of what is a truly powerful tool in advancing clinical care. I resolve to move past casual to highly functional user.
Make “10” Perfect
I resolve to figure out this new ICD-10 system. OK, technically it’s not “new.” It’s been complete since 1992 and in use in many countries for the better part of a decade. This is not a simple update of the ICD-9 system; rather, this is an entire overhaul that adds two more digits to the system. This takes the number of possible codes from 13,000 (ICD-9) to 68,000 (ICD-10). This allows for much more specificity and laterality—that is, you could have cellulitis of the right or left foot.
These changes are more than just job security for coders. The issue monetizes as payors decide not to pay for readmissions. Consider a patient who had a right-foot cellulitis, only to be admitted two weeks later with a left-foot cellulitis. ICD-9 does not have laterality, such that both stays would have the same code and the second admit could be denied as a 30-day readmission.
Twitter With Excitement
I resolve to figure out social media. I must admit that this is a red-alert, high-risk-of-failure resolution, partly because I don’t Facebook, tweet, or blog; heck, I’m not even LinkedIn! Additionally, I don’t have any friends. And finally, I just don’t get it. Then again, I didn’t get “The Simpsons” when they first came out. D’oh!
Get Hipper
And I resolve to re-enter the pop culture world in general. My social and cultural life came to a screeching halt near midnight on Sept. 29, 2007: One moment I was innocently watching the Colorado Rockies battle into their first playoffs in 12 years, and the next I was blasted onto a four-year hyper-blur of crying, spoon-feeding, and diaper-changing—for the non-parent readers, I’m describing child-rearing, not residency training, which is admittedly often marked by these same mileposts. Now 4 and 2 years old, my kiddos have finally reached the stages of self-care that allow for my gradual re-entry into the outside world.
As such, I resolve to go to a movie (in the theater) again. The last two movies we saw in the theatre in 2007 were chosen by my pregnant wife and contained an uncomfortable subliminal theme—Knocked Up (pregnant woman hates impregnating sloth of a man), Juno (pregnant woman has love-hate relationship with pasty, impregnating nerd in tight gym shorts).
I’m also interested to see what’s on TV and on the radio. When I last turned off the cathodes, “Lost” was big; ditto “The Sopranos.” And in a clearly ill-fated second season, “Dancing with the Stars” was well on its way to its undeniable cancellation. Musically, Britney was shaving her head and Jordin Sparks was edging out Sanjaya’s faux-hawk on “Idol.”
I’m also looking forward to learning what a Kardashian is (a sweater?), explaining the strange pull toward vampire romances, and discovering the difference between a Pippa and a Snooki. Should be fun. I just hope I don’t catch “Bieber Fever.”
Aspire To “Be The Cup”
Finally, in 2012, I resolve to live up to the coffee cup—you know, the Father’s Day 2011 gift emblazoned with “World’s Best Dad.” I’m sure you all feel this in your own way—that constant tension between work and life. In 2011, work won a few too many of the tug-o’-wars. Too many missed gymnastics lessons, soccer practices, parent events at daycare, and late dinners. 2012 will be different.
I resolve to teach my son the art of hitting a curveball (even if it’s off a tee) and my daughter her letters and numbers. The dogs will get more tennis balls, the wife fewer resolutions to review.
In fact, this year is going to be totally different. This is the year my to-do list doesn’t once again end as an “undid list.” This is the year I will accomplish my resolutions … not just one or two, but all of my resolutions.
And I might just write a children’s book for good measure.
Dr. Glasheen is The Hospitalist’s physician editor.
Reimbursement Readiness

Doctors shouldn’t have to worry about financial issues. The welfare of our patients should be our only concern.
We should be able to devote our full attention to studying how best to serve the needs of the people we care for. We shouldn’t need to spend time learning about healthcare reform or things like ICD-9 (or ICD-10!)—things that don’t help us provide better care to patients.
But these are pie-in-the-sky dreams. As far as I can tell, all healthcare systems require caregivers to attend to economics and data management that aren’t directly tied to clinical care. Our system depends on all caregivers devoting some time to learn how the system is organized, and keeping up with how it evolves. And the crisis in runaway costs in U.S. healthcare only increases the need for all who work in healthcare to devote significant time (too much) to the operational (nonclinical side) of healthcare.
Hospitalist practice is a much simpler business to manage and operate than most forms of clinical practice. There usually is no building to rent, few nonclinical employees to manage, and a comparatively simple financial model. And if employed by a hospital or other large entity, nonclinicians handle most of the “business management.” So when it comes to the number of brain cells diverted to business rather than clinical concerns, hospitalists start with an advantage over most other specialties.
Still, we have a lot of nonclinical stuff to keep up with. Consider the concept of “managing to Medicare reimbursement.” This means managing a practice or hospital in a way that minimizes the failure to capture all appropriate Medicare reimbursement dollars. Even if you’ve never heard of this concept before, there are probably a lot of people at your hospital who have this as their main responsibility, and clinicians should know something about it.
So in an effort to distract the fewest brain cells away from clinical matters, here is a very simple overview of some components of managing to Medicare reimbursement relevant to hospitalists. This isn’t a comprehensive list, only some hospitalist-relevant highlights.
Medicare Reimbursement Today
Accurate determination of inpatient vs. observation status. Wow, this can get complicated. Most hospitals have people who devote significant time to doing this for patients every day, and even those experts sometimes disagree on the appropriate status. But all hospitalists should have a basic understanding of how this works and a willingness to answer questions from the hospital’s experts, and, when appropriate, write additional information in the chart to clarify the appropriate status.
Optimal resource utilization, including length of stay. Because Medicare pays an essentially fixed amount based on the diagnoses for each inpatient admission, managing costs is critical to a hospital’s financial well-being. Hospitalists have a huge role in this. And regardless of how Medicare reimburses for services, there is clinical rationale for being careful about resources used and how long someone stays in a hospital. In many cases, more is not better—and it even could be worse—for the patient.
Optimal clinical documentation and accurate DRG assignment. Good documentation is important for clinical care, but beyond that, the precise way things are documented can have significant influence on Medicare reimbursement. Low potassium might in some cases lead to higher reimbursement, but a doctor must write “hypokalemia”; simply writing K+ means the hospital can’t include hypokalemia as a diagnosis. (A doctor, nurse practitioner, or physician assistant must write out “hypokalemia” only once for Medicare purposes; it would then be fine to use K+ in the chart every other time.)
Say you have a patient with a UTI and sepsis. Write only “urosepsis,” and the hospital must bill for cystitis—low reimbursement. Write “urinary tract infection with sepsis,” and the hospital can bill for higher reimbursement.
There should be people at your hospital who are experts at this, and all hospitalists should work with them to learn appropriate documentation language to describe illnesses correctly for billing purposes. Many hospitals use a system of “DRG queries,” which hospitalists should always respond to (though they should agree with the issue raised, such as “was the pneumonia likely due to aspiration?” only when clinically appropriate).
Change Is Coming
Don’t make the mistake of thinking Medicare reimbursement is a static phenomenon. It is undergoing rapid and significant evolution. For example, the Affordable Care Act, aka healthcare reform legislation, provides for a number of changes hospitalists need to understand.
I suggest that you make sure to understand your hospital’s or medical group’s position on accountable-care organizations (ACOs). It is a pretty complicated program that, in the first few years, has modest impact on reimbursement. If the ACO performs well, the additional reimbursement to an organization might pay for little more than the staff salaries of the staff that managed the considerable complexity of enrolling in and reporting for the program. And there is a risk the organization could lose money if it doesn’t perform well. So many organizations have decided not to pursue participation as an ACO, but they may decide to put in place most of the elements of an ACO without enrolling in the program. Some refer to this as an “aco” rather than an “ACO.”
Value-based purchasing (VBP) is set to influence hospital reimbursement rates starting in 2013 based on a hospital’s performance in 2012. SHM has a terrific VBP toolkit available online.
Bundled payments and financial penalties for readmissions also take effect in 2013. Now is the time ensure that you understand the implications of these programs; they are designed so that the financial impact to most organizations will be modest.
Reimbursement penalties for a specified list of hospital-acquired conditions (HACs) will begin in 2015. Conditions most relevant for hospitalists include vascular catheter-related bloodstream infections, catheter-related urinary infection, or manifestations of poor glycemic control (HONK, DKA, hypo-/hyperglycemia).
I plan to address some of these programs in greater detail in future practice management columns.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Doctors shouldn’t have to worry about financial issues. The welfare of our patients should be our only concern.
We should be able to devote our full attention to studying how best to serve the needs of the people we care for. We shouldn’t need to spend time learning about healthcare reform or things like ICD-9 (or ICD-10!)—things that don’t help us provide better care to patients.
But these are pie-in-the-sky dreams. As far as I can tell, all healthcare systems require caregivers to attend to economics and data management that aren’t directly tied to clinical care. Our system depends on all caregivers devoting some time to learn how the system is organized, and keeping up with how it evolves. And the crisis in runaway costs in U.S. healthcare only increases the need for all who work in healthcare to devote significant time (too much) to the operational (nonclinical side) of healthcare.
Hospitalist practice is a much simpler business to manage and operate than most forms of clinical practice. There usually is no building to rent, few nonclinical employees to manage, and a comparatively simple financial model. And if employed by a hospital or other large entity, nonclinicians handle most of the “business management.” So when it comes to the number of brain cells diverted to business rather than clinical concerns, hospitalists start with an advantage over most other specialties.
Still, we have a lot of nonclinical stuff to keep up with. Consider the concept of “managing to Medicare reimbursement.” This means managing a practice or hospital in a way that minimizes the failure to capture all appropriate Medicare reimbursement dollars. Even if you’ve never heard of this concept before, there are probably a lot of people at your hospital who have this as their main responsibility, and clinicians should know something about it.
So in an effort to distract the fewest brain cells away from clinical matters, here is a very simple overview of some components of managing to Medicare reimbursement relevant to hospitalists. This isn’t a comprehensive list, only some hospitalist-relevant highlights.
Medicare Reimbursement Today
Accurate determination of inpatient vs. observation status. Wow, this can get complicated. Most hospitals have people who devote significant time to doing this for patients every day, and even those experts sometimes disagree on the appropriate status. But all hospitalists should have a basic understanding of how this works and a willingness to answer questions from the hospital’s experts, and, when appropriate, write additional information in the chart to clarify the appropriate status.
Optimal resource utilization, including length of stay. Because Medicare pays an essentially fixed amount based on the diagnoses for each inpatient admission, managing costs is critical to a hospital’s financial well-being. Hospitalists have a huge role in this. And regardless of how Medicare reimburses for services, there is clinical rationale for being careful about resources used and how long someone stays in a hospital. In many cases, more is not better—and it even could be worse—for the patient.
Optimal clinical documentation and accurate DRG assignment. Good documentation is important for clinical care, but beyond that, the precise way things are documented can have significant influence on Medicare reimbursement. Low potassium might in some cases lead to higher reimbursement, but a doctor must write “hypokalemia”; simply writing K+ means the hospital can’t include hypokalemia as a diagnosis. (A doctor, nurse practitioner, or physician assistant must write out “hypokalemia” only once for Medicare purposes; it would then be fine to use K+ in the chart every other time.)
Say you have a patient with a UTI and sepsis. Write only “urosepsis,” and the hospital must bill for cystitis—low reimbursement. Write “urinary tract infection with sepsis,” and the hospital can bill for higher reimbursement.
There should be people at your hospital who are experts at this, and all hospitalists should work with them to learn appropriate documentation language to describe illnesses correctly for billing purposes. Many hospitals use a system of “DRG queries,” which hospitalists should always respond to (though they should agree with the issue raised, such as “was the pneumonia likely due to aspiration?” only when clinically appropriate).
Change Is Coming
Don’t make the mistake of thinking Medicare reimbursement is a static phenomenon. It is undergoing rapid and significant evolution. For example, the Affordable Care Act, aka healthcare reform legislation, provides for a number of changes hospitalists need to understand.
I suggest that you make sure to understand your hospital’s or medical group’s position on accountable-care organizations (ACOs). It is a pretty complicated program that, in the first few years, has modest impact on reimbursement. If the ACO performs well, the additional reimbursement to an organization might pay for little more than the staff salaries of the staff that managed the considerable complexity of enrolling in and reporting for the program. And there is a risk the organization could lose money if it doesn’t perform well. So many organizations have decided not to pursue participation as an ACO, but they may decide to put in place most of the elements of an ACO without enrolling in the program. Some refer to this as an “aco” rather than an “ACO.”
Value-based purchasing (VBP) is set to influence hospital reimbursement rates starting in 2013 based on a hospital’s performance in 2012. SHM has a terrific VBP toolkit available online.
Bundled payments and financial penalties for readmissions also take effect in 2013. Now is the time ensure that you understand the implications of these programs; they are designed so that the financial impact to most organizations will be modest.
Reimbursement penalties for a specified list of hospital-acquired conditions (HACs) will begin in 2015. Conditions most relevant for hospitalists include vascular catheter-related bloodstream infections, catheter-related urinary infection, or manifestations of poor glycemic control (HONK, DKA, hypo-/hyperglycemia).
I plan to address some of these programs in greater detail in future practice management columns.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Doctors shouldn’t have to worry about financial issues. The welfare of our patients should be our only concern.
We should be able to devote our full attention to studying how best to serve the needs of the people we care for. We shouldn’t need to spend time learning about healthcare reform or things like ICD-9 (or ICD-10!)—things that don’t help us provide better care to patients.
But these are pie-in-the-sky dreams. As far as I can tell, all healthcare systems require caregivers to attend to economics and data management that aren’t directly tied to clinical care. Our system depends on all caregivers devoting some time to learn how the system is organized, and keeping up with how it evolves. And the crisis in runaway costs in U.S. healthcare only increases the need for all who work in healthcare to devote significant time (too much) to the operational (nonclinical side) of healthcare.
Hospitalist practice is a much simpler business to manage and operate than most forms of clinical practice. There usually is no building to rent, few nonclinical employees to manage, and a comparatively simple financial model. And if employed by a hospital or other large entity, nonclinicians handle most of the “business management.” So when it comes to the number of brain cells diverted to business rather than clinical concerns, hospitalists start with an advantage over most other specialties.
Still, we have a lot of nonclinical stuff to keep up with. Consider the concept of “managing to Medicare reimbursement.” This means managing a practice or hospital in a way that minimizes the failure to capture all appropriate Medicare reimbursement dollars. Even if you’ve never heard of this concept before, there are probably a lot of people at your hospital who have this as their main responsibility, and clinicians should know something about it.
So in an effort to distract the fewest brain cells away from clinical matters, here is a very simple overview of some components of managing to Medicare reimbursement relevant to hospitalists. This isn’t a comprehensive list, only some hospitalist-relevant highlights.
Medicare Reimbursement Today
Accurate determination of inpatient vs. observation status. Wow, this can get complicated. Most hospitals have people who devote significant time to doing this for patients every day, and even those experts sometimes disagree on the appropriate status. But all hospitalists should have a basic understanding of how this works and a willingness to answer questions from the hospital’s experts, and, when appropriate, write additional information in the chart to clarify the appropriate status.
Optimal resource utilization, including length of stay. Because Medicare pays an essentially fixed amount based on the diagnoses for each inpatient admission, managing costs is critical to a hospital’s financial well-being. Hospitalists have a huge role in this. And regardless of how Medicare reimburses for services, there is clinical rationale for being careful about resources used and how long someone stays in a hospital. In many cases, more is not better—and it even could be worse—for the patient.
Optimal clinical documentation and accurate DRG assignment. Good documentation is important for clinical care, but beyond that, the precise way things are documented can have significant influence on Medicare reimbursement. Low potassium might in some cases lead to higher reimbursement, but a doctor must write “hypokalemia”; simply writing K+ means the hospital can’t include hypokalemia as a diagnosis. (A doctor, nurse practitioner, or physician assistant must write out “hypokalemia” only once for Medicare purposes; it would then be fine to use K+ in the chart every other time.)
Say you have a patient with a UTI and sepsis. Write only “urosepsis,” and the hospital must bill for cystitis—low reimbursement. Write “urinary tract infection with sepsis,” and the hospital can bill for higher reimbursement.
There should be people at your hospital who are experts at this, and all hospitalists should work with them to learn appropriate documentation language to describe illnesses correctly for billing purposes. Many hospitals use a system of “DRG queries,” which hospitalists should always respond to (though they should agree with the issue raised, such as “was the pneumonia likely due to aspiration?” only when clinically appropriate).
Change Is Coming
Don’t make the mistake of thinking Medicare reimbursement is a static phenomenon. It is undergoing rapid and significant evolution. For example, the Affordable Care Act, aka healthcare reform legislation, provides for a number of changes hospitalists need to understand.
I suggest that you make sure to understand your hospital’s or medical group’s position on accountable-care organizations (ACOs). It is a pretty complicated program that, in the first few years, has modest impact on reimbursement. If the ACO performs well, the additional reimbursement to an organization might pay for little more than the staff salaries of the staff that managed the considerable complexity of enrolling in and reporting for the program. And there is a risk the organization could lose money if it doesn’t perform well. So many organizations have decided not to pursue participation as an ACO, but they may decide to put in place most of the elements of an ACO without enrolling in the program. Some refer to this as an “aco” rather than an “ACO.”
Value-based purchasing (VBP) is set to influence hospital reimbursement rates starting in 2013 based on a hospital’s performance in 2012. SHM has a terrific VBP toolkit available online.
Bundled payments and financial penalties for readmissions also take effect in 2013. Now is the time ensure that you understand the implications of these programs; they are designed so that the financial impact to most organizations will be modest.
Reimbursement penalties for a specified list of hospital-acquired conditions (HACs) will begin in 2015. Conditions most relevant for hospitalists include vascular catheter-related bloodstream infections, catheter-related urinary infection, or manifestations of poor glycemic control (HONK, DKA, hypo-/hyperglycemia).
I plan to address some of these programs in greater detail in future practice management columns.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Leadership, Experience, Quality Factor into HM Compensation Formula

Last month, we looked at the three main factors affecting workload variability across different HM practices and its relationship to compensation. This month we will examine how physician pay varies within a single site.
For the purposes of this discussion, we will ignore volume of encounters by physician. It goes without saying that if two physicians are working and producing an equal amount at the same site, their compensation will be similar. Outside of volume variability, then, what causes differences in compensation?
Leadership: This is a hugely important piece of the puzzle, and one that merits some attention. There always should be differential pay attached to those physicians willing to shoulder the leadership burden. In my honest opinion, local HM group leaders are horrifically, grotesquely, and shockingly underpaid. They tend to be very hard-working, almost servants to the other members of the group, and usually are vastly underappreciated.
Money isn’t necessarily the answer here; maybe the reward is a lighter schedule or lighter rounding load, but the bottom line is that there should be a substantial differential for leaders. Unfortunately, I think that still tends to be the exception rather than the rule. Hospitalist group leaders have a heck of a hard job trying to lead other physicians, and they should be paid accordingly.
At the same time, the best leaders are the ones that are still working a clinical schedule and, because of that, still understand the day-to-day demands of the job. I am always a bit skeptical of the folks who are in positions of power but aren’t experiencing the daily workload.
Experience: This is a little bit tricky. In their simplest form, physician practices tend to have partners and non-partners. The timeline from employment to partnership is about two to three years. Upon becoming partner, additional benefits accrue, generally in the form of higher compensation or the ability to work a reduced schedule.
However, “experience” prima facie will not vault one into the partnership level upon joining a new group. That experience only counts for the group you are in. (And the partner collections from the insurance payor system? No change in reimbursement. We have a payor system that, at this point, does not adequately recognize experience or quality. I always have fun trying to explain this to my friends outside of healthcare. They tend to just shake their head and sigh. Hopefully we can get somewhere new with value-based purchasing and ACOs.) Anyway, enough digressing...
Nights: A fair number of groups use a night shift model. These shifts, due to their timing, will generate a lower volume of encounters and require a commensurately higher pay. As a result, the inclusion of nocturnist compensation in a pay model will skew the numbers. In a practice with a large number of hospitals and night shifts, nocturnists are a sought-after commodity.
Quality: Here is where things are going to get interesting in the very near future. A lot of hospitalist groups have quality measures that play a part in compensation, but it’s mostly small numbers, maybe 10% of total compensation. These measures tend to be internal quality metrics for things like chart completion, citizenship, or meeting attendance. Now, with the Centers for Medicare & Medicaid Services (CMS) getting into the game, hospitals are starting to sit up and pay attention. That means administrators want hospitalists to pay attention, too. Exactly how data for each physician will be extracted from the group, which typically is extracted from the hospital as a whole, is a valid question. However, expect quality measures to persistently factor into the compensation equation.
The response I’ve laid out is meant to foster discussion, not serve as a final determination, and represents only one hospitalist’s view on the subject.
Last month, we looked at the three main factors affecting workload variability across different HM practices and its relationship to compensation. This month we will examine how physician pay varies within a single site.
For the purposes of this discussion, we will ignore volume of encounters by physician. It goes without saying that if two physicians are working and producing an equal amount at the same site, their compensation will be similar. Outside of volume variability, then, what causes differences in compensation?
Leadership: This is a hugely important piece of the puzzle, and one that merits some attention. There always should be differential pay attached to those physicians willing to shoulder the leadership burden. In my honest opinion, local HM group leaders are horrifically, grotesquely, and shockingly underpaid. They tend to be very hard-working, almost servants to the other members of the group, and usually are vastly underappreciated.
Money isn’t necessarily the answer here; maybe the reward is a lighter schedule or lighter rounding load, but the bottom line is that there should be a substantial differential for leaders. Unfortunately, I think that still tends to be the exception rather than the rule. Hospitalist group leaders have a heck of a hard job trying to lead other physicians, and they should be paid accordingly.
At the same time, the best leaders are the ones that are still working a clinical schedule and, because of that, still understand the day-to-day demands of the job. I am always a bit skeptical of the folks who are in positions of power but aren’t experiencing the daily workload.
Experience: This is a little bit tricky. In their simplest form, physician practices tend to have partners and non-partners. The timeline from employment to partnership is about two to three years. Upon becoming partner, additional benefits accrue, generally in the form of higher compensation or the ability to work a reduced schedule.
However, “experience” prima facie will not vault one into the partnership level upon joining a new group. That experience only counts for the group you are in. (And the partner collections from the insurance payor system? No change in reimbursement. We have a payor system that, at this point, does not adequately recognize experience or quality. I always have fun trying to explain this to my friends outside of healthcare. They tend to just shake their head and sigh. Hopefully we can get somewhere new with value-based purchasing and ACOs.) Anyway, enough digressing...
Nights: A fair number of groups use a night shift model. These shifts, due to their timing, will generate a lower volume of encounters and require a commensurately higher pay. As a result, the inclusion of nocturnist compensation in a pay model will skew the numbers. In a practice with a large number of hospitals and night shifts, nocturnists are a sought-after commodity.
Quality: Here is where things are going to get interesting in the very near future. A lot of hospitalist groups have quality measures that play a part in compensation, but it’s mostly small numbers, maybe 10% of total compensation. These measures tend to be internal quality metrics for things like chart completion, citizenship, or meeting attendance. Now, with the Centers for Medicare & Medicaid Services (CMS) getting into the game, hospitals are starting to sit up and pay attention. That means administrators want hospitalists to pay attention, too. Exactly how data for each physician will be extracted from the group, which typically is extracted from the hospital as a whole, is a valid question. However, expect quality measures to persistently factor into the compensation equation.
The response I’ve laid out is meant to foster discussion, not serve as a final determination, and represents only one hospitalist’s view on the subject.
Last month, we looked at the three main factors affecting workload variability across different HM practices and its relationship to compensation. This month we will examine how physician pay varies within a single site.
For the purposes of this discussion, we will ignore volume of encounters by physician. It goes without saying that if two physicians are working and producing an equal amount at the same site, their compensation will be similar. Outside of volume variability, then, what causes differences in compensation?
Leadership: This is a hugely important piece of the puzzle, and one that merits some attention. There always should be differential pay attached to those physicians willing to shoulder the leadership burden. In my honest opinion, local HM group leaders are horrifically, grotesquely, and shockingly underpaid. They tend to be very hard-working, almost servants to the other members of the group, and usually are vastly underappreciated.
Money isn’t necessarily the answer here; maybe the reward is a lighter schedule or lighter rounding load, but the bottom line is that there should be a substantial differential for leaders. Unfortunately, I think that still tends to be the exception rather than the rule. Hospitalist group leaders have a heck of a hard job trying to lead other physicians, and they should be paid accordingly.
At the same time, the best leaders are the ones that are still working a clinical schedule and, because of that, still understand the day-to-day demands of the job. I am always a bit skeptical of the folks who are in positions of power but aren’t experiencing the daily workload.
Experience: This is a little bit tricky. In their simplest form, physician practices tend to have partners and non-partners. The timeline from employment to partnership is about two to three years. Upon becoming partner, additional benefits accrue, generally in the form of higher compensation or the ability to work a reduced schedule.
However, “experience” prima facie will not vault one into the partnership level upon joining a new group. That experience only counts for the group you are in. (And the partner collections from the insurance payor system? No change in reimbursement. We have a payor system that, at this point, does not adequately recognize experience or quality. I always have fun trying to explain this to my friends outside of healthcare. They tend to just shake their head and sigh. Hopefully we can get somewhere new with value-based purchasing and ACOs.) Anyway, enough digressing...
Nights: A fair number of groups use a night shift model. These shifts, due to their timing, will generate a lower volume of encounters and require a commensurately higher pay. As a result, the inclusion of nocturnist compensation in a pay model will skew the numbers. In a practice with a large number of hospitals and night shifts, nocturnists are a sought-after commodity.
Quality: Here is where things are going to get interesting in the very near future. A lot of hospitalist groups have quality measures that play a part in compensation, but it’s mostly small numbers, maybe 10% of total compensation. These measures tend to be internal quality metrics for things like chart completion, citizenship, or meeting attendance. Now, with the Centers for Medicare & Medicaid Services (CMS) getting into the game, hospitals are starting to sit up and pay attention. That means administrators want hospitalists to pay attention, too. Exactly how data for each physician will be extracted from the group, which typically is extracted from the hospital as a whole, is a valid question. However, expect quality measures to persistently factor into the compensation equation.
The response I’ve laid out is meant to foster discussion, not serve as a final determination, and represents only one hospitalist’s view on the subject.
Annals Study Might Not Cover All Situations
Just a quick comment regarding your editorial “Fiddling as HM Burns” (The Hospitalist, August 2011, p. 62) with regard to our hospital in the Florida Panhandle. The 60-plus patients we see daily are:
- Indigent (most) and uninsured working poor; and
- Unassigned (the local providers see their own patients).
Our length of stay is less than the providers’, but, of course, our follow-up expenses are high—we have a 15% 30-day readmission rate, and with no providers in the area that accept Medicaid, and almost no provision by the county to take care of indigent patients, the ER is the main de facto provider of healthcare. The majority of our discharges, therefore, have no follow-up plan.
I wonder if other hospitals in the Annals study (Ann Intern Med. 2011;155:152-159) had similar circumstances.
Stephen R. Gilmore, MD
Just a quick comment regarding your editorial “Fiddling as HM Burns” (The Hospitalist, August 2011, p. 62) with regard to our hospital in the Florida Panhandle. The 60-plus patients we see daily are:
- Indigent (most) and uninsured working poor; and
- Unassigned (the local providers see their own patients).
Our length of stay is less than the providers’, but, of course, our follow-up expenses are high—we have a 15% 30-day readmission rate, and with no providers in the area that accept Medicaid, and almost no provision by the county to take care of indigent patients, the ER is the main de facto provider of healthcare. The majority of our discharges, therefore, have no follow-up plan.
I wonder if other hospitals in the Annals study (Ann Intern Med. 2011;155:152-159) had similar circumstances.
Stephen R. Gilmore, MD
Just a quick comment regarding your editorial “Fiddling as HM Burns” (The Hospitalist, August 2011, p. 62) with regard to our hospital in the Florida Panhandle. The 60-plus patients we see daily are:
- Indigent (most) and uninsured working poor; and
- Unassigned (the local providers see their own patients).
Our length of stay is less than the providers’, but, of course, our follow-up expenses are high—we have a 15% 30-day readmission rate, and with no providers in the area that accept Medicaid, and almost no provision by the county to take care of indigent patients, the ER is the main de facto provider of healthcare. The majority of our discharges, therefore, have no follow-up plan.
I wonder if other hospitals in the Annals study (Ann Intern Med. 2011;155:152-159) had similar circumstances.
Stephen R. Gilmore, MD
Specialization Teams Offer Providers Opportunity, Strengthen HM Group Integrity
Of the 2.7 million visitors who visit Mount Rushmore each year, some unknowingly enlist in the Rushmore (elevation 5,725 feet) stress test. Having their acute coronary syndrome at the foot of the faces can be a memorable event, providing a subsequent introduction to Rapid City Regional Hospital’s (RCRH) ED, with an average door to balloon time of 70 minutes. Other tourists, including Harley Davidson riders at the annual motorcycle rally in nearby Sturgis, S.D., find their way to RCRH as one of 750 annual trauma admissions.
The ED is one of the busiest in the state, evaluating more than 50,000 patients a year. In many cases, it is the hospitalist team that provides care for visitors and the 375,000 people served by RCRH, which includes western South Dakota, the Black Hills, three Sioux Indian reservations, Ellsworth Air Force Base, and regions of North Dakota, Wyoming, and Nebraska.
The hospitalist program at RCRH originated in 2004 with three physicians: pulmonologist Stephen Calhoon and internists Gerald Hepnar and Greg Smith. They recognized the increasing demand for inpatient management of unassigned inpatients, together with diminishing community physician resources, as an opportunity to launch the program.
With exceptional support from our chief medical officer and infectious-disease specialist, the HM group has since grown to employ 20 physicians, six nocturnists, and five nurse practitioners. We care for an average of 140 patients daily in our 370-bed facility.
—Rita McGauvran, hospitalist, nurse practitioner, Rapid City (S.D.) Regional Hospital
The hospitalist group at RCRH is comanaged by Tony Blair and Robert Houser. During the day, eight physicians each care for approximately 16 patients, with an average seven-on/seven-off schedule that starts at 7 a.m. and ends at 5 p.m. One physician provides additional swing-shift coverage. The service is capped, to protect patients, and depending on the census. Three nocturnists and a nurse practitioner manage the night shift, 5 p.m. to 7 a.m. They work 10 shifts a month, with a monthly average of 390 admissions at night. Kristi Gylten provides administrative support, and we have a dedicated coding and billing staff to keep the entire program moving forward.
With growth came the need for restructuring. Initially, a two-team focus allowed close interdisciplinary communication with physicians, pharmacy, social work, and nurse practitioners as they met each morning to plan the day. As the group expanded, however, providing care on a team-based model was logistically less possible, due to the increasing numbers of patients and providers. The original team approach has since transitioned to each physician managing their own caseload and communicating, as needed, with support staff.
There are advantages in a larger group, and Dr. Houser believes that new areas of opportunity are now available. One such area is physician specialization. Interested hospitalists at RCRH are designing a consultative-based medicine delivery system, exploring an intensivist option, expanding the nocturnist program, and beginning a geographically based model for hospitalist patients offering continuity of location, staffing, and improved delivery of care. During the first six months of the pilot geographical model, nursing and patient satisfaction scores have skyrocketed, and cost savings already are apparent.
These interdisciplinary concentrations offer providers the options to pursue individual professional interests, while at the same time strengthening and preserving the groups’ integrity. Academically, medical students and family practice residents continue to be mentored by physicians with teaching interests as they rotate through the service.
One example of a hospitalist sub-group is our chronic inpatient service. This team was created within the last year to care for a subset of longer-term patients who are managed independently by two nurse practitioners in collaboration with Dr. Houser and Marc Aldrich, MD. The goal of the chronic team service is to provide continuity of care for patients and families, with a reduced length of stay. Many are difficult-to-place patients who have few family or material resources, live in rural locations, have dialysis needs, have wound-healing issues, are quadriplegic, etc. This team is supported by a dedicated pharmacist and social worker who meet with providers daily to analyze therapy, set goals, and measure progress.
Ongoing projects for the entire group include developing a comanagement model with the orthopedic and neurosurgery inpatient service, continuing to optimize computer order entry, exploring outreach to community physicians and facilities, and visiting other HM programs to learn more about geographical models.
In such a varied and rural location, the HM program at RCRH continues to grow and adapt to meet the challenges. Feel free to visit; you will be one of millions.
Rita McGauvran, hospitalist, nurse practitioner, Rapid City (S.D.) Regional Hospital
Of the 2.7 million visitors who visit Mount Rushmore each year, some unknowingly enlist in the Rushmore (elevation 5,725 feet) stress test. Having their acute coronary syndrome at the foot of the faces can be a memorable event, providing a subsequent introduction to Rapid City Regional Hospital’s (RCRH) ED, with an average door to balloon time of 70 minutes. Other tourists, including Harley Davidson riders at the annual motorcycle rally in nearby Sturgis, S.D., find their way to RCRH as one of 750 annual trauma admissions.
The ED is one of the busiest in the state, evaluating more than 50,000 patients a year. In many cases, it is the hospitalist team that provides care for visitors and the 375,000 people served by RCRH, which includes western South Dakota, the Black Hills, three Sioux Indian reservations, Ellsworth Air Force Base, and regions of North Dakota, Wyoming, and Nebraska.
The hospitalist program at RCRH originated in 2004 with three physicians: pulmonologist Stephen Calhoon and internists Gerald Hepnar and Greg Smith. They recognized the increasing demand for inpatient management of unassigned inpatients, together with diminishing community physician resources, as an opportunity to launch the program.
With exceptional support from our chief medical officer and infectious-disease specialist, the HM group has since grown to employ 20 physicians, six nocturnists, and five nurse practitioners. We care for an average of 140 patients daily in our 370-bed facility.
—Rita McGauvran, hospitalist, nurse practitioner, Rapid City (S.D.) Regional Hospital
The hospitalist group at RCRH is comanaged by Tony Blair and Robert Houser. During the day, eight physicians each care for approximately 16 patients, with an average seven-on/seven-off schedule that starts at 7 a.m. and ends at 5 p.m. One physician provides additional swing-shift coverage. The service is capped, to protect patients, and depending on the census. Three nocturnists and a nurse practitioner manage the night shift, 5 p.m. to 7 a.m. They work 10 shifts a month, with a monthly average of 390 admissions at night. Kristi Gylten provides administrative support, and we have a dedicated coding and billing staff to keep the entire program moving forward.
With growth came the need for restructuring. Initially, a two-team focus allowed close interdisciplinary communication with physicians, pharmacy, social work, and nurse practitioners as they met each morning to plan the day. As the group expanded, however, providing care on a team-based model was logistically less possible, due to the increasing numbers of patients and providers. The original team approach has since transitioned to each physician managing their own caseload and communicating, as needed, with support staff.
There are advantages in a larger group, and Dr. Houser believes that new areas of opportunity are now available. One such area is physician specialization. Interested hospitalists at RCRH are designing a consultative-based medicine delivery system, exploring an intensivist option, expanding the nocturnist program, and beginning a geographically based model for hospitalist patients offering continuity of location, staffing, and improved delivery of care. During the first six months of the pilot geographical model, nursing and patient satisfaction scores have skyrocketed, and cost savings already are apparent.
These interdisciplinary concentrations offer providers the options to pursue individual professional interests, while at the same time strengthening and preserving the groups’ integrity. Academically, medical students and family practice residents continue to be mentored by physicians with teaching interests as they rotate through the service.
One example of a hospitalist sub-group is our chronic inpatient service. This team was created within the last year to care for a subset of longer-term patients who are managed independently by two nurse practitioners in collaboration with Dr. Houser and Marc Aldrich, MD. The goal of the chronic team service is to provide continuity of care for patients and families, with a reduced length of stay. Many are difficult-to-place patients who have few family or material resources, live in rural locations, have dialysis needs, have wound-healing issues, are quadriplegic, etc. This team is supported by a dedicated pharmacist and social worker who meet with providers daily to analyze therapy, set goals, and measure progress.
Ongoing projects for the entire group include developing a comanagement model with the orthopedic and neurosurgery inpatient service, continuing to optimize computer order entry, exploring outreach to community physicians and facilities, and visiting other HM programs to learn more about geographical models.
In such a varied and rural location, the HM program at RCRH continues to grow and adapt to meet the challenges. Feel free to visit; you will be one of millions.
Rita McGauvran, hospitalist, nurse practitioner, Rapid City (S.D.) Regional Hospital
Of the 2.7 million visitors who visit Mount Rushmore each year, some unknowingly enlist in the Rushmore (elevation 5,725 feet) stress test. Having their acute coronary syndrome at the foot of the faces can be a memorable event, providing a subsequent introduction to Rapid City Regional Hospital’s (RCRH) ED, with an average door to balloon time of 70 minutes. Other tourists, including Harley Davidson riders at the annual motorcycle rally in nearby Sturgis, S.D., find their way to RCRH as one of 750 annual trauma admissions.
The ED is one of the busiest in the state, evaluating more than 50,000 patients a year. In many cases, it is the hospitalist team that provides care for visitors and the 375,000 people served by RCRH, which includes western South Dakota, the Black Hills, three Sioux Indian reservations, Ellsworth Air Force Base, and regions of North Dakota, Wyoming, and Nebraska.
The hospitalist program at RCRH originated in 2004 with three physicians: pulmonologist Stephen Calhoon and internists Gerald Hepnar and Greg Smith. They recognized the increasing demand for inpatient management of unassigned inpatients, together with diminishing community physician resources, as an opportunity to launch the program.
With exceptional support from our chief medical officer and infectious-disease specialist, the HM group has since grown to employ 20 physicians, six nocturnists, and five nurse practitioners. We care for an average of 140 patients daily in our 370-bed facility.
—Rita McGauvran, hospitalist, nurse practitioner, Rapid City (S.D.) Regional Hospital
The hospitalist group at RCRH is comanaged by Tony Blair and Robert Houser. During the day, eight physicians each care for approximately 16 patients, with an average seven-on/seven-off schedule that starts at 7 a.m. and ends at 5 p.m. One physician provides additional swing-shift coverage. The service is capped, to protect patients, and depending on the census. Three nocturnists and a nurse practitioner manage the night shift, 5 p.m. to 7 a.m. They work 10 shifts a month, with a monthly average of 390 admissions at night. Kristi Gylten provides administrative support, and we have a dedicated coding and billing staff to keep the entire program moving forward.
With growth came the need for restructuring. Initially, a two-team focus allowed close interdisciplinary communication with physicians, pharmacy, social work, and nurse practitioners as they met each morning to plan the day. As the group expanded, however, providing care on a team-based model was logistically less possible, due to the increasing numbers of patients and providers. The original team approach has since transitioned to each physician managing their own caseload and communicating, as needed, with support staff.
There are advantages in a larger group, and Dr. Houser believes that new areas of opportunity are now available. One such area is physician specialization. Interested hospitalists at RCRH are designing a consultative-based medicine delivery system, exploring an intensivist option, expanding the nocturnist program, and beginning a geographically based model for hospitalist patients offering continuity of location, staffing, and improved delivery of care. During the first six months of the pilot geographical model, nursing and patient satisfaction scores have skyrocketed, and cost savings already are apparent.
These interdisciplinary concentrations offer providers the options to pursue individual professional interests, while at the same time strengthening and preserving the groups’ integrity. Academically, medical students and family practice residents continue to be mentored by physicians with teaching interests as they rotate through the service.
One example of a hospitalist sub-group is our chronic inpatient service. This team was created within the last year to care for a subset of longer-term patients who are managed independently by two nurse practitioners in collaboration with Dr. Houser and Marc Aldrich, MD. The goal of the chronic team service is to provide continuity of care for patients and families, with a reduced length of stay. Many are difficult-to-place patients who have few family or material resources, live in rural locations, have dialysis needs, have wound-healing issues, are quadriplegic, etc. This team is supported by a dedicated pharmacist and social worker who meet with providers daily to analyze therapy, set goals, and measure progress.
Ongoing projects for the entire group include developing a comanagement model with the orthopedic and neurosurgery inpatient service, continuing to optimize computer order entry, exploring outreach to community physicians and facilities, and visiting other HM programs to learn more about geographical models.
In such a varied and rural location, the HM program at RCRH continues to grow and adapt to meet the challenges. Feel free to visit; you will be one of millions.
Rita McGauvran, hospitalist, nurse practitioner, Rapid City (S.D.) Regional Hospital