User login
Immunostaining boosts pathologists’ accuracy in Barrett’s esophagus
SAN DIEGO – Years of experience and an academic medical center affiliation predicted the accuracy of pathologists reviewing biopsies from patients with Barrett’s esophagus, according to the results of a multinational study.
Those with 5 or more years of experience were less likely to make major diagnostic errors in reviewing Barrett’s esophagus biopsies (odds ratio [OR], 0.48, 95% confidence interval, 0.31-0.74). Pathologists who worked in nonacademic settings were more likely to make a major diagnostic error (OR, 1.76; 95% CI, 1.15-2.69) when reviewing hematoxylin and eosin-stained slides alone, but the addition of p53 immunostaining greatly improved accuracy.
Current guidelines recommend expert evaluation of Barrett’s esophagus biopsies that show dysplasia, but exact determination of expert review status had been lacking, according to Marnix Jansen, MD, a pathologist at University College London.
“The guidelines say that biopsies with dysplasia need to be reviewed by an expert pathologist, but don’t define what makes an expert pathologist,” Dr. Jansen said in an interview at the annual Digestive Disease Week.
“We wanted to advance the field by for the first time creating objective and quantitative standards” to delineate the characteristics of an expert pathologist in reviewing Barrett’s esophagus tissue samples, said Dr. Jansen. The study’s first author is Myrtle J. van der Wel, MD, of Amsterdam University Medical Center, the Netherlands.
More than 6,000 individual case diagnoses were used in the study, which included pathologists from more than 20 countries. Before the pathologists began reviewing the case set, they answered a questionnaire about training, practice context, years of experience, case volume, and other demographic characteristics.
“We then sent those biopsies around the world to ... 55 pathologists in the U.S., in Europe, Japan, Australia, even some in South America – so really around the whole globe,” explained Dr. Jansen. Biopsies were assessed by each pathologist before and after p53 immunostaining.
“Once we had the final dataset – which is massive, because we had 6,000 case diagnoses within our dataset – we could then regress those variables back onto the consensus data,” providing a first-ever look at “clear predictors of what the pathologist looks like that will score on a par with where the experts are,” said Dr. Jansen.
The results? “You need at least 5 years of experience. On top of that, if you are a pathologist working in a [nonacademic center], you are at a slightly increased risk of making major diagnostic errors,” said Dr. Jansen. However, the analysis convincingly showed that the addition of p53 immunostaining neutralized the risk for these pathologists – a strength of having such a large dataset, he said.
The study also affirmed the safety of digital pathology for expert review, said Dr. Jansen: “One of the reassuring points of our study was that we found that the best concordance was for nondysplastic Barrett’s, and high-grade dysplasia, which really replicates known glass slide characteristics. So we can really say that digital pathology is safe for this application – which is very relevant for pathologists that are taking in cases from outside for expert review.”
Concordance rates for nondysplastic Barrett’s esophagus and high-grade dysplasia were over 70%; for low-grade dysplasia, rates were intermediate at 42%.
Going forward, the study can inform the next iteration of guidelines for pathologist review of Barrett’s dysplasia, said Dr. Jansen. Rather than just recommending expert review, the guidelines can include a quantitative assessment of what’s needed. “You need to have to have at least 5 years of experience, and if you work in a [community hospital], to use a p53, and that is collectively what amounts to expertise in Barrett’s pathology.”
A follow-up study with a similar design is planned within the United Kingdom, the Netherlands, and the United States. This study, which Dr. Jansen said would enroll hundreds of pathologists, will include an intervention arm that administers a tutorial with the aim of improving concordance scoring.
Dr. Jansen reported no relevant conflicts of interest.
SAN DIEGO – Years of experience and an academic medical center affiliation predicted the accuracy of pathologists reviewing biopsies from patients with Barrett’s esophagus, according to the results of a multinational study.
Those with 5 or more years of experience were less likely to make major diagnostic errors in reviewing Barrett’s esophagus biopsies (odds ratio [OR], 0.48, 95% confidence interval, 0.31-0.74). Pathologists who worked in nonacademic settings were more likely to make a major diagnostic error (OR, 1.76; 95% CI, 1.15-2.69) when reviewing hematoxylin and eosin-stained slides alone, but the addition of p53 immunostaining greatly improved accuracy.
Current guidelines recommend expert evaluation of Barrett’s esophagus biopsies that show dysplasia, but exact determination of expert review status had been lacking, according to Marnix Jansen, MD, a pathologist at University College London.
“The guidelines say that biopsies with dysplasia need to be reviewed by an expert pathologist, but don’t define what makes an expert pathologist,” Dr. Jansen said in an interview at the annual Digestive Disease Week.
“We wanted to advance the field by for the first time creating objective and quantitative standards” to delineate the characteristics of an expert pathologist in reviewing Barrett’s esophagus tissue samples, said Dr. Jansen. The study’s first author is Myrtle J. van der Wel, MD, of Amsterdam University Medical Center, the Netherlands.
More than 6,000 individual case diagnoses were used in the study, which included pathologists from more than 20 countries. Before the pathologists began reviewing the case set, they answered a questionnaire about training, practice context, years of experience, case volume, and other demographic characteristics.
“We then sent those biopsies around the world to ... 55 pathologists in the U.S., in Europe, Japan, Australia, even some in South America – so really around the whole globe,” explained Dr. Jansen. Biopsies were assessed by each pathologist before and after p53 immunostaining.
“Once we had the final dataset – which is massive, because we had 6,000 case diagnoses within our dataset – we could then regress those variables back onto the consensus data,” providing a first-ever look at “clear predictors of what the pathologist looks like that will score on a par with where the experts are,” said Dr. Jansen.
The results? “You need at least 5 years of experience. On top of that, if you are a pathologist working in a [nonacademic center], you are at a slightly increased risk of making major diagnostic errors,” said Dr. Jansen. However, the analysis convincingly showed that the addition of p53 immunostaining neutralized the risk for these pathologists – a strength of having such a large dataset, he said.
The study also affirmed the safety of digital pathology for expert review, said Dr. Jansen: “One of the reassuring points of our study was that we found that the best concordance was for nondysplastic Barrett’s, and high-grade dysplasia, which really replicates known glass slide characteristics. So we can really say that digital pathology is safe for this application – which is very relevant for pathologists that are taking in cases from outside for expert review.”
Concordance rates for nondysplastic Barrett’s esophagus and high-grade dysplasia were over 70%; for low-grade dysplasia, rates were intermediate at 42%.
Going forward, the study can inform the next iteration of guidelines for pathologist review of Barrett’s dysplasia, said Dr. Jansen. Rather than just recommending expert review, the guidelines can include a quantitative assessment of what’s needed. “You need to have to have at least 5 years of experience, and if you work in a [community hospital], to use a p53, and that is collectively what amounts to expertise in Barrett’s pathology.”
A follow-up study with a similar design is planned within the United Kingdom, the Netherlands, and the United States. This study, which Dr. Jansen said would enroll hundreds of pathologists, will include an intervention arm that administers a tutorial with the aim of improving concordance scoring.
Dr. Jansen reported no relevant conflicts of interest.
SAN DIEGO – Years of experience and an academic medical center affiliation predicted the accuracy of pathologists reviewing biopsies from patients with Barrett’s esophagus, according to the results of a multinational study.
Those with 5 or more years of experience were less likely to make major diagnostic errors in reviewing Barrett’s esophagus biopsies (odds ratio [OR], 0.48, 95% confidence interval, 0.31-0.74). Pathologists who worked in nonacademic settings were more likely to make a major diagnostic error (OR, 1.76; 95% CI, 1.15-2.69) when reviewing hematoxylin and eosin-stained slides alone, but the addition of p53 immunostaining greatly improved accuracy.
Current guidelines recommend expert evaluation of Barrett’s esophagus biopsies that show dysplasia, but exact determination of expert review status had been lacking, according to Marnix Jansen, MD, a pathologist at University College London.
“The guidelines say that biopsies with dysplasia need to be reviewed by an expert pathologist, but don’t define what makes an expert pathologist,” Dr. Jansen said in an interview at the annual Digestive Disease Week.
“We wanted to advance the field by for the first time creating objective and quantitative standards” to delineate the characteristics of an expert pathologist in reviewing Barrett’s esophagus tissue samples, said Dr. Jansen. The study’s first author is Myrtle J. van der Wel, MD, of Amsterdam University Medical Center, the Netherlands.
More than 6,000 individual case diagnoses were used in the study, which included pathologists from more than 20 countries. Before the pathologists began reviewing the case set, they answered a questionnaire about training, practice context, years of experience, case volume, and other demographic characteristics.
“We then sent those biopsies around the world to ... 55 pathologists in the U.S., in Europe, Japan, Australia, even some in South America – so really around the whole globe,” explained Dr. Jansen. Biopsies were assessed by each pathologist before and after p53 immunostaining.
“Once we had the final dataset – which is massive, because we had 6,000 case diagnoses within our dataset – we could then regress those variables back onto the consensus data,” providing a first-ever look at “clear predictors of what the pathologist looks like that will score on a par with where the experts are,” said Dr. Jansen.
The results? “You need at least 5 years of experience. On top of that, if you are a pathologist working in a [nonacademic center], you are at a slightly increased risk of making major diagnostic errors,” said Dr. Jansen. However, the analysis convincingly showed that the addition of p53 immunostaining neutralized the risk for these pathologists – a strength of having such a large dataset, he said.
The study also affirmed the safety of digital pathology for expert review, said Dr. Jansen: “One of the reassuring points of our study was that we found that the best concordance was for nondysplastic Barrett’s, and high-grade dysplasia, which really replicates known glass slide characteristics. So we can really say that digital pathology is safe for this application – which is very relevant for pathologists that are taking in cases from outside for expert review.”
Concordance rates for nondysplastic Barrett’s esophagus and high-grade dysplasia were over 70%; for low-grade dysplasia, rates were intermediate at 42%.
Going forward, the study can inform the next iteration of guidelines for pathologist review of Barrett’s dysplasia, said Dr. Jansen. Rather than just recommending expert review, the guidelines can include a quantitative assessment of what’s needed. “You need to have to have at least 5 years of experience, and if you work in a [community hospital], to use a p53, and that is collectively what amounts to expertise in Barrett’s pathology.”
A follow-up study with a similar design is planned within the United Kingdom, the Netherlands, and the United States. This study, which Dr. Jansen said would enroll hundreds of pathologists, will include an intervention arm that administers a tutorial with the aim of improving concordance scoring.
Dr. Jansen reported no relevant conflicts of interest.
REPORTING FROM DDW 2019
When the parent is a psychiatrist: How are children affected?
SAN FRANCISCO – Research into how the children of psychiatrists fare psychologically is sparse. But anecdotally, children report that having a psychiatrist parent is a gift – not only for them – but for their friends’ families, Michelle B. Riba, MD, said at the annual meeting of the American Psychiatric Association.

In this video, Dr. Riba is interviewed by Carol A. Bernstein, MD, about what she expected when she helped start the Children of Psychiatrists workshop at the APA meeting with Leah J. Dickstein, MD, and how it draws a standing room–only crowd each year.
“In general ... people feel very appreciative of having an empathic, knowledgeable parent to help guide them – and not overguide them,” Dr. Riba said. Psychiatrists also can provide insight into the causes of societal challenges such as homelessness. One audience member in this year’s workshop discussed the value of having a psychiatrist parent put a school suicide into perspective. Dr. Bernstein said she is viewed by her daughter’s friends as “the psychiatrist in residence.”
The children of psychiatrists who spoke on the panel this year said they liked being able to facilitate care for their friends. “They didn’t feel burdened by [having a psychiatrist parent],” Dr. Riba said. “We asked about that very question today.”
Dr. Riba, a past president of the APA, is professor of psychiatry at the University of Michigan, Ann Arbor. She also serves as director of the consultation-liaison fellowship, and director of the PsychOncology program at the university’s Rogel Cancer Center. She had no disclosures.
Dr. Bernstein, also an APA past president, is professor of psychiatry and obstetrics and gynecology, and vice chair for faculty development in psychiatry at the Albert Einstein College of Medicine, New York. She previously served as vice chair for education in psychiatry and director of residency training in psychiatry at the NYU School of Medicine. Dr. Bernstein had no disclosures.
SAN FRANCISCO – Research into how the children of psychiatrists fare psychologically is sparse. But anecdotally, children report that having a psychiatrist parent is a gift – not only for them – but for their friends’ families, Michelle B. Riba, MD, said at the annual meeting of the American Psychiatric Association.
In this video, Dr. Riba is interviewed by Carol A. Bernstein, MD, about what she expected when she helped start the Children of Psychiatrists workshop at the APA meeting with Leah J. Dickstein, MD, and how it draws a standing room–only crowd each year.
“In general ... people feel very appreciative of having an empathic, knowledgeable parent to help guide them – and not overguide them,” Dr. Riba said. Psychiatrists also can provide insight into the causes of societal challenges such as homelessness. One audience member in this year’s workshop discussed the value of having a psychiatrist parent put a school suicide into perspective. Dr. Bernstein said she is viewed by her daughter’s friends as “the psychiatrist in residence.”
The children of psychiatrists who spoke on the panel this year said they liked being able to facilitate care for their friends. “They didn’t feel burdened by [having a psychiatrist parent],” Dr. Riba said. “We asked about that very question today.”
Dr. Riba, a past president of the APA, is professor of psychiatry at the University of Michigan, Ann Arbor. She also serves as director of the consultation-liaison fellowship, and director of the PsychOncology program at the university’s Rogel Cancer Center. She had no disclosures.
Dr. Bernstein, also an APA past president, is professor of psychiatry and obstetrics and gynecology, and vice chair for faculty development in psychiatry at the Albert Einstein College of Medicine, New York. She previously served as vice chair for education in psychiatry and director of residency training in psychiatry at the NYU School of Medicine. Dr. Bernstein had no disclosures.
SAN FRANCISCO – Research into how the children of psychiatrists fare psychologically is sparse. But anecdotally, children report that having a psychiatrist parent is a gift – not only for them – but for their friends’ families, Michelle B. Riba, MD, said at the annual meeting of the American Psychiatric Association.
In this video, Dr. Riba is interviewed by Carol A. Bernstein, MD, about what she expected when she helped start the Children of Psychiatrists workshop at the APA meeting with Leah J. Dickstein, MD, and how it draws a standing room–only crowd each year.
“In general ... people feel very appreciative of having an empathic, knowledgeable parent to help guide them – and not overguide them,” Dr. Riba said. Psychiatrists also can provide insight into the causes of societal challenges such as homelessness. One audience member in this year’s workshop discussed the value of having a psychiatrist parent put a school suicide into perspective. Dr. Bernstein said she is viewed by her daughter’s friends as “the psychiatrist in residence.”
The children of psychiatrists who spoke on the panel this year said they liked being able to facilitate care for their friends. “They didn’t feel burdened by [having a psychiatrist parent],” Dr. Riba said. “We asked about that very question today.”
Dr. Riba, a past president of the APA, is professor of psychiatry at the University of Michigan, Ann Arbor. She also serves as director of the consultation-liaison fellowship, and director of the PsychOncology program at the university’s Rogel Cancer Center. She had no disclosures.
Dr. Bernstein, also an APA past president, is professor of psychiatry and obstetrics and gynecology, and vice chair for faculty development in psychiatry at the Albert Einstein College of Medicine, New York. She previously served as vice chair for education in psychiatry and director of residency training in psychiatry at the NYU School of Medicine. Dr. Bernstein had no disclosures.
REPORTING FROM APA 2019

Button batteries that pass to the stomach may warrant rapid endoscopic removal
SAN DIEGO – A button battery lodged in a child’s esophagus is an acknowledged emergency, but there is less evidence about retrieval of button batteries that have passed to the stomach. Observation alone has been recommended when an x-ray determines that the button battery has passed to the stomach within 2 hours of ingestion, when the battery is less than 20 mm, and the child is aged at least 5 years.
At the annual Digestive Disease Week, Racha Khalaf, MD, and Thomas Walker, MD, both of Children’s Hospital Colorado, Aurora, presented data that call this approach into question. Their retrospective cohort study of 4 years’ worth of records from four pediatric centers in the United States identified 68 cases in which a pediatric gastroenterologist had endoscopically removed the button battery. In 60% of those cases, the battery had already caused mucosal damage varying from minor to deep necrosis and perforation.
Further, the degree of injury was not correlated with symptoms, strengthening the recommendation for retrieving the button battery from the stomach.
In our exclusive video interview, Dr. Khalaf and Dr. Walker discussed the impact of their findings for guidelines for pediatric gastroenterologists and Poison Control Center advice to parents about ingestion of button batteries.
Their study was partly supported by a Cystic Fibrosis Foundational Grant Award and by National Institutes of Health Training Grants.
SAN DIEGO – A button battery lodged in a child’s esophagus is an acknowledged emergency, but there is less evidence about retrieval of button batteries that have passed to the stomach. Observation alone has been recommended when an x-ray determines that the button battery has passed to the stomach within 2 hours of ingestion, when the battery is less than 20 mm, and the child is aged at least 5 years.
At the annual Digestive Disease Week, Racha Khalaf, MD, and Thomas Walker, MD, both of Children’s Hospital Colorado, Aurora, presented data that call this approach into question. Their retrospective cohort study of 4 years’ worth of records from four pediatric centers in the United States identified 68 cases in which a pediatric gastroenterologist had endoscopically removed the button battery. In 60% of those cases, the battery had already caused mucosal damage varying from minor to deep necrosis and perforation.
Further, the degree of injury was not correlated with symptoms, strengthening the recommendation for retrieving the button battery from the stomach.
In our exclusive video interview, Dr. Khalaf and Dr. Walker discussed the impact of their findings for guidelines for pediatric gastroenterologists and Poison Control Center advice to parents about ingestion of button batteries.
Their study was partly supported by a Cystic Fibrosis Foundational Grant Award and by National Institutes of Health Training Grants.
SAN DIEGO – A button battery lodged in a child’s esophagus is an acknowledged emergency, but there is less evidence about retrieval of button batteries that have passed to the stomach. Observation alone has been recommended when an x-ray determines that the button battery has passed to the stomach within 2 hours of ingestion, when the battery is less than 20 mm, and the child is aged at least 5 years.
At the annual Digestive Disease Week, Racha Khalaf, MD, and Thomas Walker, MD, both of Children’s Hospital Colorado, Aurora, presented data that call this approach into question. Their retrospective cohort study of 4 years’ worth of records from four pediatric centers in the United States identified 68 cases in which a pediatric gastroenterologist had endoscopically removed the button battery. In 60% of those cases, the battery had already caused mucosal damage varying from minor to deep necrosis and perforation.
Further, the degree of injury was not correlated with symptoms, strengthening the recommendation for retrieving the button battery from the stomach.
In our exclusive video interview, Dr. Khalaf and Dr. Walker discussed the impact of their findings for guidelines for pediatric gastroenterologists and Poison Control Center advice to parents about ingestion of button batteries.
Their study was partly supported by a Cystic Fibrosis Foundational Grant Award and by National Institutes of Health Training Grants.
REPORTING FROM DDW 2019
Toolkit for providing mental health care to Muslim patients launched
SAN FRANCISCO – A toolkit that seeks to help clinicians provide culturally and religiously informed mental health care for Muslim patients was officially launched at the annual meeting of the American Psychiatric Association.
Rania Awaad, MD, and Belinda S. Bandstra, MD, sat down at the annual meeting of the American Psychiatric Association to discuss how to use the toolkit and why it – and other resources on providing nuanced mental health care – are needed.

In this video, Dr. Awaad explores some of the origins of Islamophobia in the United States and how she came to do this work while in medical school. The travel ban affecting mostly Muslim countries has had a ripple effect on community members, she said. “The feeling is ‘My country isn’t named in the travel ban, but will I be next?’ ”
In addition to the fear and distrust fostered by the political climate are the challenges of abiding by the Islamic faith’s precepts.
“Patients will just do things on their own – and not consult their clinician,” Dr. Awaad said, referring to those might change the times in which they take medication during the sacred month of Ramadan because of fasting that is expected of observant Muslims. “It’s important for the patients to know that anyone acutely ill is exempt from fasting.” Medical- and faith-based consultation are important for these patients, Dr. Awaad said, pointing to a recent article that outlines best practices for treating patients with psychiatric disorders during Ramadan (Lancet Psychiatry. 2019 May 2. doi: 10.1016/S2215-0366[19]30161-0).
She also discussed “Islamophobia and Psychiatry” (Springer, 2019), a book she coedited that she said provides evidence of the detrimental effect that Islamophobia has on the mental health of Muslims.
Dr. Awaad is director of the Muslim Mental Health Lab and Wellness Program and codirector of the Diversity Clinic at Stanford (Calif.) University. Dr. Bandstra is assistant director of residency training in Stanford’s department of psychiatry and behavioral sciences. Dr. Awaad and Dr. Bandstra had no relevant disclosures.
SAN FRANCISCO – A toolkit that seeks to help clinicians provide culturally and religiously informed mental health care for Muslim patients was officially launched at the annual meeting of the American Psychiatric Association.
Rania Awaad, MD, and Belinda S. Bandstra, MD, sat down at the annual meeting of the American Psychiatric Association to discuss how to use the toolkit and why it – and other resources on providing nuanced mental health care – are needed.
In this video, Dr. Awaad explores some of the origins of Islamophobia in the United States and how she came to do this work while in medical school. The travel ban affecting mostly Muslim countries has had a ripple effect on community members, she said. “The feeling is ‘My country isn’t named in the travel ban, but will I be next?’ ”
In addition to the fear and distrust fostered by the political climate are the challenges of abiding by the Islamic faith’s precepts.
“Patients will just do things on their own – and not consult their clinician,” Dr. Awaad said, referring to those might change the times in which they take medication during the sacred month of Ramadan because of fasting that is expected of observant Muslims. “It’s important for the patients to know that anyone acutely ill is exempt from fasting.” Medical- and faith-based consultation are important for these patients, Dr. Awaad said, pointing to a recent article that outlines best practices for treating patients with psychiatric disorders during Ramadan (Lancet Psychiatry. 2019 May 2. doi: 10.1016/S2215-0366[19]30161-0).
She also discussed “Islamophobia and Psychiatry” (Springer, 2019), a book she coedited that she said provides evidence of the detrimental effect that Islamophobia has on the mental health of Muslims.
Dr. Awaad is director of the Muslim Mental Health Lab and Wellness Program and codirector of the Diversity Clinic at Stanford (Calif.) University. Dr. Bandstra is assistant director of residency training in Stanford’s department of psychiatry and behavioral sciences. Dr. Awaad and Dr. Bandstra had no relevant disclosures.
SAN FRANCISCO – A toolkit that seeks to help clinicians provide culturally and religiously informed mental health care for Muslim patients was officially launched at the annual meeting of the American Psychiatric Association.
Rania Awaad, MD, and Belinda S. Bandstra, MD, sat down at the annual meeting of the American Psychiatric Association to discuss how to use the toolkit and why it – and other resources on providing nuanced mental health care – are needed.
In this video, Dr. Awaad explores some of the origins of Islamophobia in the United States and how she came to do this work while in medical school. The travel ban affecting mostly Muslim countries has had a ripple effect on community members, she said. “The feeling is ‘My country isn’t named in the travel ban, but will I be next?’ ”
In addition to the fear and distrust fostered by the political climate are the challenges of abiding by the Islamic faith’s precepts.
“Patients will just do things on their own – and not consult their clinician,” Dr. Awaad said, referring to those might change the times in which they take medication during the sacred month of Ramadan because of fasting that is expected of observant Muslims. “It’s important for the patients to know that anyone acutely ill is exempt from fasting.” Medical- and faith-based consultation are important for these patients, Dr. Awaad said, pointing to a recent article that outlines best practices for treating patients with psychiatric disorders during Ramadan (Lancet Psychiatry. 2019 May 2. doi: 10.1016/S2215-0366[19]30161-0).
She also discussed “Islamophobia and Psychiatry” (Springer, 2019), a book she coedited that she said provides evidence of the detrimental effect that Islamophobia has on the mental health of Muslims.
Dr. Awaad is director of the Muslim Mental Health Lab and Wellness Program and codirector of the Diversity Clinic at Stanford (Calif.) University. Dr. Bandstra is assistant director of residency training in Stanford’s department of psychiatry and behavioral sciences. Dr. Awaad and Dr. Bandstra had no relevant disclosures.
REPORTING FROM APA 2019

Hip-hop offers lens into psyche of black boys, men
SAN FRANCISCO – The lyrics found in hip-hop can help mental health professionals understand the triumphs and trauma experienced by African American boys and men, Sarah Y. Vinson, MD, said at the annual meeting of the American Psychiatric Association. This understanding can enable clinicians to recognize hopelessness and pain in those patients that they otherwise might have missed.
In this video, Dr. Vinson said her session at the APA meeting looked at the history of hip-hop and focused on the perspectives embedded in the work of several artists/groups, including N.W.A, Tupac Shakur, Childish Gambino (aka Donald Glover), J. Cole, and Kendrick Lamar.
One of the take-home points for clinicians, Dr. Vinson said, is that hip-hop, an art form that has spread across the world, came out of resilience. Another is that suicidality in black men might not look the same as it does in other patients. “It doesn’t necessarily look like cutting your own wrists or having thoughts of killing yourself – it may look like reckless behaviors that put you at risk of being killed by somebody else.”
Dr. Vinson, who is triple boarded in child and adolescent, adult, and forensic psychiatry, is in private practice in Atlanta. She had no financial disclosures.
SAN FRANCISCO – The lyrics found in hip-hop can help mental health professionals understand the triumphs and trauma experienced by African American boys and men, Sarah Y. Vinson, MD, said at the annual meeting of the American Psychiatric Association. This understanding can enable clinicians to recognize hopelessness and pain in those patients that they otherwise might have missed.
In this video, Dr. Vinson said her session at the APA meeting looked at the history of hip-hop and focused on the perspectives embedded in the work of several artists/groups, including N.W.A, Tupac Shakur, Childish Gambino (aka Donald Glover), J. Cole, and Kendrick Lamar.
One of the take-home points for clinicians, Dr. Vinson said, is that hip-hop, an art form that has spread across the world, came out of resilience. Another is that suicidality in black men might not look the same as it does in other patients. “It doesn’t necessarily look like cutting your own wrists or having thoughts of killing yourself – it may look like reckless behaviors that put you at risk of being killed by somebody else.”
Dr. Vinson, who is triple boarded in child and adolescent, adult, and forensic psychiatry, is in private practice in Atlanta. She had no financial disclosures.
SAN FRANCISCO – The lyrics found in hip-hop can help mental health professionals understand the triumphs and trauma experienced by African American boys and men, Sarah Y. Vinson, MD, said at the annual meeting of the American Psychiatric Association. This understanding can enable clinicians to recognize hopelessness and pain in those patients that they otherwise might have missed.
In this video, Dr. Vinson said her session at the APA meeting looked at the history of hip-hop and focused on the perspectives embedded in the work of several artists/groups, including N.W.A, Tupac Shakur, Childish Gambino (aka Donald Glover), J. Cole, and Kendrick Lamar.
One of the take-home points for clinicians, Dr. Vinson said, is that hip-hop, an art form that has spread across the world, came out of resilience. Another is that suicidality in black men might not look the same as it does in other patients. “It doesn’t necessarily look like cutting your own wrists or having thoughts of killing yourself – it may look like reckless behaviors that put you at risk of being killed by somebody else.”
Dr. Vinson, who is triple boarded in child and adolescent, adult, and forensic psychiatry, is in private practice in Atlanta. She had no financial disclosures.
REPORTING FROM APA 2019

Ultrasound’s arrhythmia localization surpassed ECG’s accuracy
SAN FRANCISCO – A new type of echocardiography that uses a high frame rate to track tissue motion allowed researchers to noninvasively map the source of cardiac arrhythmias in patients with significantly more precision than did standard 12-lead ECG recordings in a pilot, single-center study with 55 patients.
Electromechanical wave imaging (EWI) correctly identified the arrhythmia source in 53 of 55 (96%) patients scheduled to undergo arrhythmia ablation, whereas only 39 of the same 55 patients (71%) were correctly mapped using recordings from a standard 12-lead ECG read by several trained electrophysiologists. The findings from this pilot study suggested that EWI performed with noninvasive ultrasound can provide useful, added information to 12-lead ECG tracings to localize cardiac arrhythmias of various types prior to invasive procedures, Elaine Y. Wan, MD, said at the annual scientific sessions of the Heart Rhythm Society.
She cautioned, however, that future studies must still establish that adding EWI to standard preprocedural assessment can benefit patients by, for example, reducing their radiation dosages or shortening their procedure times.
Patients at Columbia University Medical Center in New York scheduled to undergo ablation for a cardiac arrhythmia first had noninvasive assessment with EWI and 12-lead ECG. Patients averaged 56 years old; 45% had an atrial flutter, 22% had Wolff-Parkinson-White syndrome accessory pathways, 20% had premature ventricular complexes, and 13% had an atrial tachycardia. The researchers used 3D electroanatomic arrhythmia mapping performed during ablation as the arrhythmia-localization standard against which they compared both the EWI and ECG results.
EWI can map cardiac electromechanical activity in all four heart chambers by tracking, with high temporal and spatial resolution, transient tissue deformations that occur in response to local electrical activation of cardiac myocytes, the depolarizations in cardiac muscle that produce tissue movement. The technique captures 2,000 image frames per second, creating a “video of tissue movement that lets us see where the movement started,” explained Dr. Wan, a cardiac electrophysiologist at Columbia.
Dr. Wan and associates previously reported use of EWI to successfully map accessory pathways in all 14 children with Wolff-Parkinson-White syndrome they tested versus success in 11 of these 14 patients (79%) when using expert interpretation of 12-lead ECG recordings (JACC Clin Electrophysiol. 2019 Apr;5[4]:427-37).
The new study is the first report on using EWI in adults, Dr. Wan noted. Advantages of EWI over 12-lead ECG include its lack of dependence on correct lead placement, and EWI does not share the inherent limitation of 12-lead ECG for localizing arrhythmias on the heart’s posterior wall, she said in a video interview.
SOURCE: Wan EY et al. Heart Rhythm 2019, Abstract S-LCT04-03.
SAN FRANCISCO – A new type of echocardiography that uses a high frame rate to track tissue motion allowed researchers to noninvasively map the source of cardiac arrhythmias in patients with significantly more precision than did standard 12-lead ECG recordings in a pilot, single-center study with 55 patients.
Electromechanical wave imaging (EWI) correctly identified the arrhythmia source in 53 of 55 (96%) patients scheduled to undergo arrhythmia ablation, whereas only 39 of the same 55 patients (71%) were correctly mapped using recordings from a standard 12-lead ECG read by several trained electrophysiologists. The findings from this pilot study suggested that EWI performed with noninvasive ultrasound can provide useful, added information to 12-lead ECG tracings to localize cardiac arrhythmias of various types prior to invasive procedures, Elaine Y. Wan, MD, said at the annual scientific sessions of the Heart Rhythm Society.
She cautioned, however, that future studies must still establish that adding EWI to standard preprocedural assessment can benefit patients by, for example, reducing their radiation dosages or shortening their procedure times.
Patients at Columbia University Medical Center in New York scheduled to undergo ablation for a cardiac arrhythmia first had noninvasive assessment with EWI and 12-lead ECG. Patients averaged 56 years old; 45% had an atrial flutter, 22% had Wolff-Parkinson-White syndrome accessory pathways, 20% had premature ventricular complexes, and 13% had an atrial tachycardia. The researchers used 3D electroanatomic arrhythmia mapping performed during ablation as the arrhythmia-localization standard against which they compared both the EWI and ECG results.
EWI can map cardiac electromechanical activity in all four heart chambers by tracking, with high temporal and spatial resolution, transient tissue deformations that occur in response to local electrical activation of cardiac myocytes, the depolarizations in cardiac muscle that produce tissue movement. The technique captures 2,000 image frames per second, creating a “video of tissue movement that lets us see where the movement started,” explained Dr. Wan, a cardiac electrophysiologist at Columbia.
Dr. Wan and associates previously reported use of EWI to successfully map accessory pathways in all 14 children with Wolff-Parkinson-White syndrome they tested versus success in 11 of these 14 patients (79%) when using expert interpretation of 12-lead ECG recordings (JACC Clin Electrophysiol. 2019 Apr;5[4]:427-37).
The new study is the first report on using EWI in adults, Dr. Wan noted. Advantages of EWI over 12-lead ECG include its lack of dependence on correct lead placement, and EWI does not share the inherent limitation of 12-lead ECG for localizing arrhythmias on the heart’s posterior wall, she said in a video interview.
SOURCE: Wan EY et al. Heart Rhythm 2019, Abstract S-LCT04-03.
SAN FRANCISCO – A new type of echocardiography that uses a high frame rate to track tissue motion allowed researchers to noninvasively map the source of cardiac arrhythmias in patients with significantly more precision than did standard 12-lead ECG recordings in a pilot, single-center study with 55 patients.
Electromechanical wave imaging (EWI) correctly identified the arrhythmia source in 53 of 55 (96%) patients scheduled to undergo arrhythmia ablation, whereas only 39 of the same 55 patients (71%) were correctly mapped using recordings from a standard 12-lead ECG read by several trained electrophysiologists. The findings from this pilot study suggested that EWI performed with noninvasive ultrasound can provide useful, added information to 12-lead ECG tracings to localize cardiac arrhythmias of various types prior to invasive procedures, Elaine Y. Wan, MD, said at the annual scientific sessions of the Heart Rhythm Society.
She cautioned, however, that future studies must still establish that adding EWI to standard preprocedural assessment can benefit patients by, for example, reducing their radiation dosages or shortening their procedure times.
Patients at Columbia University Medical Center in New York scheduled to undergo ablation for a cardiac arrhythmia first had noninvasive assessment with EWI and 12-lead ECG. Patients averaged 56 years old; 45% had an atrial flutter, 22% had Wolff-Parkinson-White syndrome accessory pathways, 20% had premature ventricular complexes, and 13% had an atrial tachycardia. The researchers used 3D electroanatomic arrhythmia mapping performed during ablation as the arrhythmia-localization standard against which they compared both the EWI and ECG results.
EWI can map cardiac electromechanical activity in all four heart chambers by tracking, with high temporal and spatial resolution, transient tissue deformations that occur in response to local electrical activation of cardiac myocytes, the depolarizations in cardiac muscle that produce tissue movement. The technique captures 2,000 image frames per second, creating a “video of tissue movement that lets us see where the movement started,” explained Dr. Wan, a cardiac electrophysiologist at Columbia.
Dr. Wan and associates previously reported use of EWI to successfully map accessory pathways in all 14 children with Wolff-Parkinson-White syndrome they tested versus success in 11 of these 14 patients (79%) when using expert interpretation of 12-lead ECG recordings (JACC Clin Electrophysiol. 2019 Apr;5[4]:427-37).
The new study is the first report on using EWI in adults, Dr. Wan noted. Advantages of EWI over 12-lead ECG include its lack of dependence on correct lead placement, and EWI does not share the inherent limitation of 12-lead ECG for localizing arrhythmias on the heart’s posterior wall, she said in a video interview.
SOURCE: Wan EY et al. Heart Rhythm 2019, Abstract S-LCT04-03.
REPORTING FROM HEART RHYTHM 2019

Ultrasound or biopsy for evaluation of endometrium? It depends
NASHVILLE, TENN. – Biopsy isn’t usually the first step in evaluating the endometrium of a reproductive-age woman who presents with abnormal uterine bleeding, but that’s not always the case, according to James M. Shwayder, MD.

“If we have young women come in, generally speaking, we don’t think much about doing biopsies, but there are those patients who really require a biopsy very early on: If they are obese and if they have long histories of oligomenorrhea ... they are at significantly greater risk for either endometrial hyperplasia or cancer, so in those patients I recommend biopsy very early on,” Dr. Shwayder said in this video interview about his presentation entitled “Modern Evaluation of the Endometrium: When to Use Ultrasound, When to Biopsy,” as presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Conversely, in some cases when biopsy is typically considered the first-line step in evaluation, ultrasound may actually be better, he argued.
“[ACOG] recommends that women over 45 ... should have a biopsy done as their first-line evaluation. I kind of take issue with that a little bit,” said Dr. Shwayder, a professor at the University of Mississippi Medical Center, Jackson, and president and chief executive officer of Shwayder Consulting in Venice, Fla.
Data suggest that a “blind biopsy” could miss up to 18% of cases involving either a submucous myoma or a polyp and that one-third to one-fourth of patients have a structural defect such as a polyp or fibroid that can’t be diagnosed with a biopsy, he explained, noting that sonohysterography is best for preoperative evaluation in such case.
Ultrasound also has utility for evaluating other abnormalities, and it can be a very simple way to evaluate the patient and decide whether they need further evaluation or further treatment, he said.
Dr. Shwayder also discussed evidence for making a choice between biopsy and ultrasound for initial evaluation in postmenopausal women and for assessing women with asymptomatic thickened endometrium.
Dr. Shwayder is a consultant for GE Ultrasound.
NASHVILLE, TENN. – Biopsy isn’t usually the first step in evaluating the endometrium of a reproductive-age woman who presents with abnormal uterine bleeding, but that’s not always the case, according to James M. Shwayder, MD.
“If we have young women come in, generally speaking, we don’t think much about doing biopsies, but there are those patients who really require a biopsy very early on: If they are obese and if they have long histories of oligomenorrhea ... they are at significantly greater risk for either endometrial hyperplasia or cancer, so in those patients I recommend biopsy very early on,” Dr. Shwayder said in this video interview about his presentation entitled “Modern Evaluation of the Endometrium: When to Use Ultrasound, When to Biopsy,” as presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Conversely, in some cases when biopsy is typically considered the first-line step in evaluation, ultrasound may actually be better, he argued.
“[ACOG] recommends that women over 45 ... should have a biopsy done as their first-line evaluation. I kind of take issue with that a little bit,” said Dr. Shwayder, a professor at the University of Mississippi Medical Center, Jackson, and president and chief executive officer of Shwayder Consulting in Venice, Fla.
Data suggest that a “blind biopsy” could miss up to 18% of cases involving either a submucous myoma or a polyp and that one-third to one-fourth of patients have a structural defect such as a polyp or fibroid that can’t be diagnosed with a biopsy, he explained, noting that sonohysterography is best for preoperative evaluation in such case.
Ultrasound also has utility for evaluating other abnormalities, and it can be a very simple way to evaluate the patient and decide whether they need further evaluation or further treatment, he said.
Dr. Shwayder also discussed evidence for making a choice between biopsy and ultrasound for initial evaluation in postmenopausal women and for assessing women with asymptomatic thickened endometrium.
Dr. Shwayder is a consultant for GE Ultrasound.
NASHVILLE, TENN. – Biopsy isn’t usually the first step in evaluating the endometrium of a reproductive-age woman who presents with abnormal uterine bleeding, but that’s not always the case, according to James M. Shwayder, MD.
“If we have young women come in, generally speaking, we don’t think much about doing biopsies, but there are those patients who really require a biopsy very early on: If they are obese and if they have long histories of oligomenorrhea ... they are at significantly greater risk for either endometrial hyperplasia or cancer, so in those patients I recommend biopsy very early on,” Dr. Shwayder said in this video interview about his presentation entitled “Modern Evaluation of the Endometrium: When to Use Ultrasound, When to Biopsy,” as presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Conversely, in some cases when biopsy is typically considered the first-line step in evaluation, ultrasound may actually be better, he argued.
“[ACOG] recommends that women over 45 ... should have a biopsy done as their first-line evaluation. I kind of take issue with that a little bit,” said Dr. Shwayder, a professor at the University of Mississippi Medical Center, Jackson, and president and chief executive officer of Shwayder Consulting in Venice, Fla.
Data suggest that a “blind biopsy” could miss up to 18% of cases involving either a submucous myoma or a polyp and that one-third to one-fourth of patients have a structural defect such as a polyp or fibroid that can’t be diagnosed with a biopsy, he explained, noting that sonohysterography is best for preoperative evaluation in such case.
Ultrasound also has utility for evaluating other abnormalities, and it can be a very simple way to evaluate the patient and decide whether they need further evaluation or further treatment, he said.
Dr. Shwayder also discussed evidence for making a choice between biopsy and ultrasound for initial evaluation in postmenopausal women and for assessing women with asymptomatic thickened endometrium.
Dr. Shwayder is a consultant for GE Ultrasound.
EXPERT ANALYSIS FROM ACOG 2019

Immediate postpartum LARC: ‘Agony and ecstasy’
NASHVILLE, TENN. – according to Eve Espey, MD.
“I think [the rate] is going to settle out at around 15%-20%, but good cost-effectiveness studies show that, even if it were that high, it is still highly cost effective,” she said during an update on contraceptives at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Immediate postpartum long-acting reversible contraception (LARC), including an IUD or implant, may reduce rapid-repeat pregnancy, she added, noting, however, that while Medicaid is covering it in many states, “it turns out that payment models are very cumbersome; they actually don’t work very well.”
At the University of New Mexico (UNM) in Albuquerque, where Dr .Espey is a professor and chair of the department of obstetrics and gynecology and director of the family planning fellowship, immediate postpartum LARC is offered to women with Medicaid coverage, and payment is received in about 97% of cases.
It took about 4 years of persistent effort to make that happen, she said, adding that the UNM Hospital still is the only one in the state offering the service, although efforts are underway to help other hospitals “troubleshoot the issues.”
Another challenge is the lack of private insurance coverage for immediate postpartum LARC, she said.
“I was super enthusiastic about this a few years ago, and I remain super enthusiastic about it, but I think it’s going to take another 5 years or so [for better coverage], and honestly I think what we really need is an inpatient LARC CPT code to make this happen.”
In this video interview, Dr. Espey discusses the “agony and ecstasy” of immediate postpartum LARC, summarizing the main points regarding its benefits and challenges as presented during an “EdTalk” she gave at the meeting.
Dr. Espey reported having no relevant financial disclosures.
NASHVILLE, TENN. – according to Eve Espey, MD.
“I think [the rate] is going to settle out at around 15%-20%, but good cost-effectiveness studies show that, even if it were that high, it is still highly cost effective,” she said during an update on contraceptives at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Immediate postpartum long-acting reversible contraception (LARC), including an IUD or implant, may reduce rapid-repeat pregnancy, she added, noting, however, that while Medicaid is covering it in many states, “it turns out that payment models are very cumbersome; they actually don’t work very well.”
At the University of New Mexico (UNM) in Albuquerque, where Dr .Espey is a professor and chair of the department of obstetrics and gynecology and director of the family planning fellowship, immediate postpartum LARC is offered to women with Medicaid coverage, and payment is received in about 97% of cases.
It took about 4 years of persistent effort to make that happen, she said, adding that the UNM Hospital still is the only one in the state offering the service, although efforts are underway to help other hospitals “troubleshoot the issues.”
Another challenge is the lack of private insurance coverage for immediate postpartum LARC, she said.
“I was super enthusiastic about this a few years ago, and I remain super enthusiastic about it, but I think it’s going to take another 5 years or so [for better coverage], and honestly I think what we really need is an inpatient LARC CPT code to make this happen.”
In this video interview, Dr. Espey discusses the “agony and ecstasy” of immediate postpartum LARC, summarizing the main points regarding its benefits and challenges as presented during an “EdTalk” she gave at the meeting.
Dr. Espey reported having no relevant financial disclosures.
NASHVILLE, TENN. – according to Eve Espey, MD.
“I think [the rate] is going to settle out at around 15%-20%, but good cost-effectiveness studies show that, even if it were that high, it is still highly cost effective,” she said during an update on contraceptives at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Immediate postpartum long-acting reversible contraception (LARC), including an IUD or implant, may reduce rapid-repeat pregnancy, she added, noting, however, that while Medicaid is covering it in many states, “it turns out that payment models are very cumbersome; they actually don’t work very well.”
At the University of New Mexico (UNM) in Albuquerque, where Dr .Espey is a professor and chair of the department of obstetrics and gynecology and director of the family planning fellowship, immediate postpartum LARC is offered to women with Medicaid coverage, and payment is received in about 97% of cases.
It took about 4 years of persistent effort to make that happen, she said, adding that the UNM Hospital still is the only one in the state offering the service, although efforts are underway to help other hospitals “troubleshoot the issues.”
Another challenge is the lack of private insurance coverage for immediate postpartum LARC, she said.
“I was super enthusiastic about this a few years ago, and I remain super enthusiastic about it, but I think it’s going to take another 5 years or so [for better coverage], and honestly I think what we really need is an inpatient LARC CPT code to make this happen.”
In this video interview, Dr. Espey discusses the “agony and ecstasy” of immediate postpartum LARC, summarizing the main points regarding its benefits and challenges as presented during an “EdTalk” she gave at the meeting.
Dr. Espey reported having no relevant financial disclosures.
EXPERT ANALYSIS FROM ACOG 2019

Sustainable weight loss seen 5 years after endoscopic sleeve gastroplasty

The finding comes from the first long-term analysis of outcomes following endoscopic sleeve gastroplasty, a relatively new, minimally invasive weight-loss procedure that offers patients an alternative to bariatric surgery.
“Endoscopic sleeve gastrectomy is a 1-day outpatient procedure that uses a suturing device attached to an endoscope to create a series of sutures that cinch the stomach like an accordion down to roughly the size of a banana, and leaves no scars,” lead study author Reem Z. Sharaiha, MD, MSc, said during a media briefing in advance of the annual Digestive Disease Week®. “The procedure causes patients to eat less because they feel full faster. This results in weight loss.”
Digestive Disease Week is jointly sponsored by the American Association for the Study of Liver Diseases (AASLD), the American Gastroenterological Association (AGA) Institute, the American Society for Gastrointestinal Endoscopy (ASGE), and the Society for Surgery of the Alimentary Tract (SSAT).
While previous studies have tracked ESG results for 1-2 years, her research team followed 203 patients who underwent the procedure between August 2013 and October 2018. “We felt that a longer-term study was needed to make sure weight loss was sustainable with this method of treatment, because research shows that if you keep weight loss for an extended period of time, you’re more likely to keep it off permanently, which is ultimately what we want for these patients,” said Dr. Sharaiha, who is an attending physician at New York–Presbyterian/Weill Cornell Medicine, New York.
At baseline, the mean age of the 203 patients was 46 years, 67% were female, and their mean body mass index was 39 kg/m2. Dr. Sharaiha and colleagues observed that maximum weight loss was generally achieved by 24 months after the procedure, after which patients tended to regain a small amount of their lost weight. For example, at 1 year, the mean weight loss was 18.1 kg, with a total body weight loss of 15.2% (P less than .0001 for both associations). At 2 years, the mean weight loss was 17.3 kg, with a total body weight loss of 14.5% (P less than .0001 for both associations). At 3 years, the mean weight loss was 20.8 kg, with a total body weight loss of 14.5% (P less than .0001 for both associations). At 5 years, the mean weight loss was 18.7 kg (P = .0003) and the total body weight loss was 14.5% (P = .0002).
Overall, patients gained an average 2.4 kg of weight after achieving their minimum weight after ESG until the end of follow-up. The researchers also found that failure to lose at least 10% of total body weight within the first 3 months after ESG decreased the chance of subsequent significant weight loss by 80%. Fewer than 1% of patients experienced complications, an improvement over surgical procedures.
“Our study showed very sustainable, significant weight loss for our patients between the 1 and 5 year mark,” Dr. Sharaiha said. “Out to 5 years, there was an average 15% total body weight loss. This is significant, because studies have shown that when people lose at least 10% of their body weight, they see improvement in blood pressure, diabetes, and heart outcomes, which are the comorbidities associated with obesity. We hope these findings will help persuade insurance companies that ESG is not experimental, but has value over patients’ lifespans.”
Dr. Sharaiha and colleagues plan to follow the current cohort for the next 10-20 years. “It’s important to show the value of these endoscopic procedures, so we’ll be looking at improvement in comorbidities such as diabetes, high blood pressure, and cholesterol,” she said. “We’re also part of a randomized study that’s currently under way looking at ESG in combination with diet and exercise.”
She reported having no financial disclosures.
The finding comes from the first long-term analysis of outcomes following endoscopic sleeve gastroplasty, a relatively new, minimally invasive weight-loss procedure that offers patients an alternative to bariatric surgery.
“Endoscopic sleeve gastrectomy is a 1-day outpatient procedure that uses a suturing device attached to an endoscope to create a series of sutures that cinch the stomach like an accordion down to roughly the size of a banana, and leaves no scars,” lead study author Reem Z. Sharaiha, MD, MSc, said during a media briefing in advance of the annual Digestive Disease Week®. “The procedure causes patients to eat less because they feel full faster. This results in weight loss.”
Digestive Disease Week is jointly sponsored by the American Association for the Study of Liver Diseases (AASLD), the American Gastroenterological Association (AGA) Institute, the American Society for Gastrointestinal Endoscopy (ASGE), and the Society for Surgery of the Alimentary Tract (SSAT).
While previous studies have tracked ESG results for 1-2 years, her research team followed 203 patients who underwent the procedure between August 2013 and October 2018. “We felt that a longer-term study was needed to make sure weight loss was sustainable with this method of treatment, because research shows that if you keep weight loss for an extended period of time, you’re more likely to keep it off permanently, which is ultimately what we want for these patients,” said Dr. Sharaiha, who is an attending physician at New York–Presbyterian/Weill Cornell Medicine, New York.
At baseline, the mean age of the 203 patients was 46 years, 67% were female, and their mean body mass index was 39 kg/m2. Dr. Sharaiha and colleagues observed that maximum weight loss was generally achieved by 24 months after the procedure, after which patients tended to regain a small amount of their lost weight. For example, at 1 year, the mean weight loss was 18.1 kg, with a total body weight loss of 15.2% (P less than .0001 for both associations). At 2 years, the mean weight loss was 17.3 kg, with a total body weight loss of 14.5% (P less than .0001 for both associations). At 3 years, the mean weight loss was 20.8 kg, with a total body weight loss of 14.5% (P less than .0001 for both associations). At 5 years, the mean weight loss was 18.7 kg (P = .0003) and the total body weight loss was 14.5% (P = .0002).
Overall, patients gained an average 2.4 kg of weight after achieving their minimum weight after ESG until the end of follow-up. The researchers also found that failure to lose at least 10% of total body weight within the first 3 months after ESG decreased the chance of subsequent significant weight loss by 80%. Fewer than 1% of patients experienced complications, an improvement over surgical procedures.
“Our study showed very sustainable, significant weight loss for our patients between the 1 and 5 year mark,” Dr. Sharaiha said. “Out to 5 years, there was an average 15% total body weight loss. This is significant, because studies have shown that when people lose at least 10% of their body weight, they see improvement in blood pressure, diabetes, and heart outcomes, which are the comorbidities associated with obesity. We hope these findings will help persuade insurance companies that ESG is not experimental, but has value over patients’ lifespans.”
Dr. Sharaiha and colleagues plan to follow the current cohort for the next 10-20 years. “It’s important to show the value of these endoscopic procedures, so we’ll be looking at improvement in comorbidities such as diabetes, high blood pressure, and cholesterol,” she said. “We’re also part of a randomized study that’s currently under way looking at ESG in combination with diet and exercise.”
She reported having no financial disclosures.
The finding comes from the first long-term analysis of outcomes following endoscopic sleeve gastroplasty, a relatively new, minimally invasive weight-loss procedure that offers patients an alternative to bariatric surgery.
“Endoscopic sleeve gastrectomy is a 1-day outpatient procedure that uses a suturing device attached to an endoscope to create a series of sutures that cinch the stomach like an accordion down to roughly the size of a banana, and leaves no scars,” lead study author Reem Z. Sharaiha, MD, MSc, said during a media briefing in advance of the annual Digestive Disease Week®. “The procedure causes patients to eat less because they feel full faster. This results in weight loss.”
Digestive Disease Week is jointly sponsored by the American Association for the Study of Liver Diseases (AASLD), the American Gastroenterological Association (AGA) Institute, the American Society for Gastrointestinal Endoscopy (ASGE), and the Society for Surgery of the Alimentary Tract (SSAT).
While previous studies have tracked ESG results for 1-2 years, her research team followed 203 patients who underwent the procedure between August 2013 and October 2018. “We felt that a longer-term study was needed to make sure weight loss was sustainable with this method of treatment, because research shows that if you keep weight loss for an extended period of time, you’re more likely to keep it off permanently, which is ultimately what we want for these patients,” said Dr. Sharaiha, who is an attending physician at New York–Presbyterian/Weill Cornell Medicine, New York.
At baseline, the mean age of the 203 patients was 46 years, 67% were female, and their mean body mass index was 39 kg/m2. Dr. Sharaiha and colleagues observed that maximum weight loss was generally achieved by 24 months after the procedure, after which patients tended to regain a small amount of their lost weight. For example, at 1 year, the mean weight loss was 18.1 kg, with a total body weight loss of 15.2% (P less than .0001 for both associations). At 2 years, the mean weight loss was 17.3 kg, with a total body weight loss of 14.5% (P less than .0001 for both associations). At 3 years, the mean weight loss was 20.8 kg, with a total body weight loss of 14.5% (P less than .0001 for both associations). At 5 years, the mean weight loss was 18.7 kg (P = .0003) and the total body weight loss was 14.5% (P = .0002).
Overall, patients gained an average 2.4 kg of weight after achieving their minimum weight after ESG until the end of follow-up. The researchers also found that failure to lose at least 10% of total body weight within the first 3 months after ESG decreased the chance of subsequent significant weight loss by 80%. Fewer than 1% of patients experienced complications, an improvement over surgical procedures.
“Our study showed very sustainable, significant weight loss for our patients between the 1 and 5 year mark,” Dr. Sharaiha said. “Out to 5 years, there was an average 15% total body weight loss. This is significant, because studies have shown that when people lose at least 10% of their body weight, they see improvement in blood pressure, diabetes, and heart outcomes, which are the comorbidities associated with obesity. We hope these findings will help persuade insurance companies that ESG is not experimental, but has value over patients’ lifespans.”
Dr. Sharaiha and colleagues plan to follow the current cohort for the next 10-20 years. “It’s important to show the value of these endoscopic procedures, so we’ll be looking at improvement in comorbidities such as diabetes, high blood pressure, and cholesterol,” she said. “We’re also part of a randomized study that’s currently under way looking at ESG in combination with diet and exercise.”
She reported having no financial disclosures.
FROM DDW 2019
Key clinical point: Endoscopic sleeve gastroplasty is an effective, minimally invasive weight-loss procedure that results in significant total body weight loss.
Major finding: Between 1 and 5 years after endoscopic sleeve gastroplasty, patients lost 15%-20% of their total body weight.
Study details: A retrospective study of prospectively collected data on 203 patients.
Disclosures: Dr. Sharaiha reported having no financial disclosures.

New risk score predicts cardiac-device infection
SAN FRANCISCO – Researchers have devised a five-item scoring formula to quantify the risk for infection in patients undergoing placement, revision, or removal of a cardiac-rhythm device based on data from nearly 20,000 patients enrolled in a recent infection-prophylaxis trial.
The risk score can help identify patients who might benefit from intensified antibiotic prophylaxis, and it can also help during shared decision making with patients to better understand the risk a patient faces from infection, compared with their predicted device benefit, David H. Birnie, MD, said at the annual scientific sessions of the Heart Rhythm Society.
The new risk score produced a concordance statistic, the area under the receiver-operator characteristic curve, of 0.704. It showed that, although it could use further validation, the score as it currently stands has substantial predictive value, said Dr. Birnie, professor of medicine at the University of Ottawa and deputy chief of cardiology at the University of Ottawa Heart Institute. “It’s certainly better than anything we have now,” he said in a video interview.
Dr. Birnie and his associates used data they collected on baseline characteristics and infection outcomes of the 19,603 patients enrolled in PADIT (Prevention of Arrhythmia Device Infection Trial) who underwent a rhythm-device procedure at 1 of 28 participating Canadian centers. The primary aim of PADIT was to assess the safety and efficacy of an intensified antibiotic-prophylaxis regimen, compared with a standard regimen of a cefazolin infusion just before the procedure. The study’s primary endpoint was the incidence of hospitalization for device infection during 1-year follow-up, and while the intensified prophylactic regimen linked with a 23% relative reduction in the hospitalization rate, compared with standard treatment, the difference was not statistically significant (J Am Coll Cardiol. 2018 Dec 18;72[24]:3098-109).
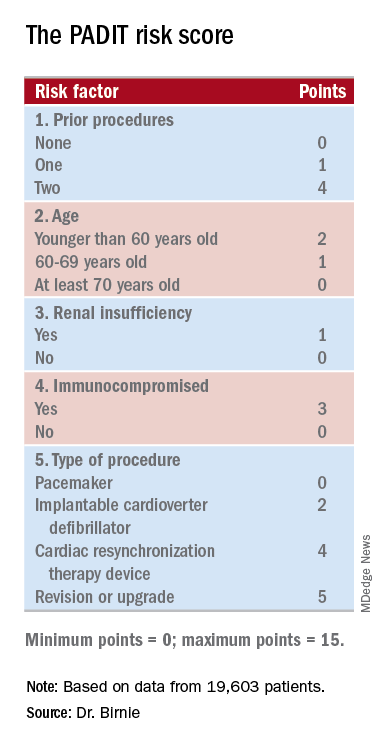
The researchers analyzed the baseline patient data and the blindly adjudicated infection outcomes and identified five factors that were independently associated with an increased infection rate. They organized the five factors and produced a formula they call the PADIT score (see chart). Those five factors are: prior procedures (the greater the number the greater the risk), age (which unexpectedly had an inverse relationship with infection incidence), depressed renal function, immuno-compromised status, and type of procedure. A patient can potentially score 0-15 points.
Among the PADIT patients a score of 0 correlated with about a 0.3% rate of hospitalization for a device-related infection during 1 year of follow-up, a score of 5 with about a 1.1% rate, a score of 6 with about a 1.8% rate, and a score of seven or more with a 3.4% infection rate over the following year. About 5% of patients had a score of 7 or more, and roughly another 5% had a score of 5 or 6, Dr. Birnie said. At his center, clinicians have begun routinely calculating scores for patients scheduled for an arrhythmia-device procedure, and they are considering routinely administering added antibiotic prophylaxis to patients with a preprocedural score of 6 or higher. They may also use the score to determine whether to use the antibacterial envelope recently reported to prevent cardiac-device infections (N Engl J Med. 2019 May 16;380[20]:1895-905).
“It’s very easy for patients to get to a PADIT score of 7 or higher,” Dr. Birnie noted. As an example, he cited a common patient, an 85-year-old with renal dysfunction who is under consideration for a second replacement of an implantable cardioverter defibrillator. The patient would score 1 point for renal insufficiency, 2 points for the type of device, and 4 points for having a prior history of two devices, and the consequent 3.4% risk for infection might counterbalance the potential benefit this elderly patient could expect from the new device. The score will be very important for targeting treatment, shared decision making, and selection of patients for future intervention trials, he concluded.

“I think this risk score will change practice by giving clinicians a better idea of a patient’s risk for infection,” commented Fred M. Kusumoto, MD, professor of medicine at the Mayo Medical School, Rochester, Minn., and director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla. The PADIT score will help identify patients for whom leaving a device in place is a better option than taking it out because of their infection risk. The risk score could also help improve the cost effectiveness of preventive treatments, such as antibiotic-eluting envelopes, by targeting treatment to higher-risk patients, Dr. Kusumoto said during a press briefing.
SOURCE: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.
I like this new infection risk score. It addresses a very clinically relevant issue. It’s important for the electrophysiology community to better understand how to best manage infections related to cardiac rhythm devices and ideally prevent them from happening.
I’m not a big fan of risk scores in general because they can sometimes detract from independent thinking about how to manage a patient. However, it is also helpful to have this type of risk-assessment information when discussing management options with a patient.
The PADIT risk score may also help identify which patients could potentially benefit the most from an antibiotic-eluting envelope when receiving an implanted cardiac-rhythm device. Recently reported results from WRAP-IT showed that routinely using envelopes cut the incidence of major infections by a relative 40%, but in absolute terms, the number needed to treat with the envelop to prevent one major infection was about 200 patients, a big number given the high cost of the envelope (N Engl J Med. 2019 May 16;380[20]:1895-905). It is therefore very interesting to think about using the PADIT risk score to better target an effective but expensive preventive measure like an antibiotic-eluting envelop to patients at the highest risk for infection.
Ulrika Birgersdotter-Green, MD , professor of medicine and director of pacemaker and ICD services at the University of California, San Diego, made these comments as a designated discussant for the report. She has been a consultant to and received honoraria from Abbott, Boston Scientific, and Medtronic.
I like this new infection risk score. It addresses a very clinically relevant issue. It’s important for the electrophysiology community to better understand how to best manage infections related to cardiac rhythm devices and ideally prevent them from happening.
I’m not a big fan of risk scores in general because they can sometimes detract from independent thinking about how to manage a patient. However, it is also helpful to have this type of risk-assessment information when discussing management options with a patient.
The PADIT risk score may also help identify which patients could potentially benefit the most from an antibiotic-eluting envelope when receiving an implanted cardiac-rhythm device. Recently reported results from WRAP-IT showed that routinely using envelopes cut the incidence of major infections by a relative 40%, but in absolute terms, the number needed to treat with the envelop to prevent one major infection was about 200 patients, a big number given the high cost of the envelope (N Engl J Med. 2019 May 16;380[20]:1895-905). It is therefore very interesting to think about using the PADIT risk score to better target an effective but expensive preventive measure like an antibiotic-eluting envelop to patients at the highest risk for infection.
Ulrika Birgersdotter-Green, MD , professor of medicine and director of pacemaker and ICD services at the University of California, San Diego, made these comments as a designated discussant for the report. She has been a consultant to and received honoraria from Abbott, Boston Scientific, and Medtronic.
I like this new infection risk score. It addresses a very clinically relevant issue. It’s important for the electrophysiology community to better understand how to best manage infections related to cardiac rhythm devices and ideally prevent them from happening.
I’m not a big fan of risk scores in general because they can sometimes detract from independent thinking about how to manage a patient. However, it is also helpful to have this type of risk-assessment information when discussing management options with a patient.
The PADIT risk score may also help identify which patients could potentially benefit the most from an antibiotic-eluting envelope when receiving an implanted cardiac-rhythm device. Recently reported results from WRAP-IT showed that routinely using envelopes cut the incidence of major infections by a relative 40%, but in absolute terms, the number needed to treat with the envelop to prevent one major infection was about 200 patients, a big number given the high cost of the envelope (N Engl J Med. 2019 May 16;380[20]:1895-905). It is therefore very interesting to think about using the PADIT risk score to better target an effective but expensive preventive measure like an antibiotic-eluting envelop to patients at the highest risk for infection.
Ulrika Birgersdotter-Green, MD , professor of medicine and director of pacemaker and ICD services at the University of California, San Diego, made these comments as a designated discussant for the report. She has been a consultant to and received honoraria from Abbott, Boston Scientific, and Medtronic.
SAN FRANCISCO – Researchers have devised a five-item scoring formula to quantify the risk for infection in patients undergoing placement, revision, or removal of a cardiac-rhythm device based on data from nearly 20,000 patients enrolled in a recent infection-prophylaxis trial.
The risk score can help identify patients who might benefit from intensified antibiotic prophylaxis, and it can also help during shared decision making with patients to better understand the risk a patient faces from infection, compared with their predicted device benefit, David H. Birnie, MD, said at the annual scientific sessions of the Heart Rhythm Society.
The new risk score produced a concordance statistic, the area under the receiver-operator characteristic curve, of 0.704. It showed that, although it could use further validation, the score as it currently stands has substantial predictive value, said Dr. Birnie, professor of medicine at the University of Ottawa and deputy chief of cardiology at the University of Ottawa Heart Institute. “It’s certainly better than anything we have now,” he said in a video interview.
Dr. Birnie and his associates used data they collected on baseline characteristics and infection outcomes of the 19,603 patients enrolled in PADIT (Prevention of Arrhythmia Device Infection Trial) who underwent a rhythm-device procedure at 1 of 28 participating Canadian centers. The primary aim of PADIT was to assess the safety and efficacy of an intensified antibiotic-prophylaxis regimen, compared with a standard regimen of a cefazolin infusion just before the procedure. The study’s primary endpoint was the incidence of hospitalization for device infection during 1-year follow-up, and while the intensified prophylactic regimen linked with a 23% relative reduction in the hospitalization rate, compared with standard treatment, the difference was not statistically significant (J Am Coll Cardiol. 2018 Dec 18;72[24]:3098-109).
The researchers analyzed the baseline patient data and the blindly adjudicated infection outcomes and identified five factors that were independently associated with an increased infection rate. They organized the five factors and produced a formula they call the PADIT score (see chart). Those five factors are: prior procedures (the greater the number the greater the risk), age (which unexpectedly had an inverse relationship with infection incidence), depressed renal function, immuno-compromised status, and type of procedure. A patient can potentially score 0-15 points.
Among the PADIT patients a score of 0 correlated with about a 0.3% rate of hospitalization for a device-related infection during 1 year of follow-up, a score of 5 with about a 1.1% rate, a score of 6 with about a 1.8% rate, and a score of seven or more with a 3.4% infection rate over the following year. About 5% of patients had a score of 7 or more, and roughly another 5% had a score of 5 or 6, Dr. Birnie said. At his center, clinicians have begun routinely calculating scores for patients scheduled for an arrhythmia-device procedure, and they are considering routinely administering added antibiotic prophylaxis to patients with a preprocedural score of 6 or higher. They may also use the score to determine whether to use the antibacterial envelope recently reported to prevent cardiac-device infections (N Engl J Med. 2019 May 16;380[20]:1895-905).
“It’s very easy for patients to get to a PADIT score of 7 or higher,” Dr. Birnie noted. As an example, he cited a common patient, an 85-year-old with renal dysfunction who is under consideration for a second replacement of an implantable cardioverter defibrillator. The patient would score 1 point for renal insufficiency, 2 points for the type of device, and 4 points for having a prior history of two devices, and the consequent 3.4% risk for infection might counterbalance the potential benefit this elderly patient could expect from the new device. The score will be very important for targeting treatment, shared decision making, and selection of patients for future intervention trials, he concluded.
“I think this risk score will change practice by giving clinicians a better idea of a patient’s risk for infection,” commented Fred M. Kusumoto, MD, professor of medicine at the Mayo Medical School, Rochester, Minn., and director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla. The PADIT score will help identify patients for whom leaving a device in place is a better option than taking it out because of their infection risk. The risk score could also help improve the cost effectiveness of preventive treatments, such as antibiotic-eluting envelopes, by targeting treatment to higher-risk patients, Dr. Kusumoto said during a press briefing.
SOURCE: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.
SAN FRANCISCO – Researchers have devised a five-item scoring formula to quantify the risk for infection in patients undergoing placement, revision, or removal of a cardiac-rhythm device based on data from nearly 20,000 patients enrolled in a recent infection-prophylaxis trial.
The risk score can help identify patients who might benefit from intensified antibiotic prophylaxis, and it can also help during shared decision making with patients to better understand the risk a patient faces from infection, compared with their predicted device benefit, David H. Birnie, MD, said at the annual scientific sessions of the Heart Rhythm Society.
The new risk score produced a concordance statistic, the area under the receiver-operator characteristic curve, of 0.704. It showed that, although it could use further validation, the score as it currently stands has substantial predictive value, said Dr. Birnie, professor of medicine at the University of Ottawa and deputy chief of cardiology at the University of Ottawa Heart Institute. “It’s certainly better than anything we have now,” he said in a video interview.
Dr. Birnie and his associates used data they collected on baseline characteristics and infection outcomes of the 19,603 patients enrolled in PADIT (Prevention of Arrhythmia Device Infection Trial) who underwent a rhythm-device procedure at 1 of 28 participating Canadian centers. The primary aim of PADIT was to assess the safety and efficacy of an intensified antibiotic-prophylaxis regimen, compared with a standard regimen of a cefazolin infusion just before the procedure. The study’s primary endpoint was the incidence of hospitalization for device infection during 1-year follow-up, and while the intensified prophylactic regimen linked with a 23% relative reduction in the hospitalization rate, compared with standard treatment, the difference was not statistically significant (J Am Coll Cardiol. 2018 Dec 18;72[24]:3098-109).
The researchers analyzed the baseline patient data and the blindly adjudicated infection outcomes and identified five factors that were independently associated with an increased infection rate. They organized the five factors and produced a formula they call the PADIT score (see chart). Those five factors are: prior procedures (the greater the number the greater the risk), age (which unexpectedly had an inverse relationship with infection incidence), depressed renal function, immuno-compromised status, and type of procedure. A patient can potentially score 0-15 points.
Among the PADIT patients a score of 0 correlated with about a 0.3% rate of hospitalization for a device-related infection during 1 year of follow-up, a score of 5 with about a 1.1% rate, a score of 6 with about a 1.8% rate, and a score of seven or more with a 3.4% infection rate over the following year. About 5% of patients had a score of 7 or more, and roughly another 5% had a score of 5 or 6, Dr. Birnie said. At his center, clinicians have begun routinely calculating scores for patients scheduled for an arrhythmia-device procedure, and they are considering routinely administering added antibiotic prophylaxis to patients with a preprocedural score of 6 or higher. They may also use the score to determine whether to use the antibacterial envelope recently reported to prevent cardiac-device infections (N Engl J Med. 2019 May 16;380[20]:1895-905).
“It’s very easy for patients to get to a PADIT score of 7 or higher,” Dr. Birnie noted. As an example, he cited a common patient, an 85-year-old with renal dysfunction who is under consideration for a second replacement of an implantable cardioverter defibrillator. The patient would score 1 point for renal insufficiency, 2 points for the type of device, and 4 points for having a prior history of two devices, and the consequent 3.4% risk for infection might counterbalance the potential benefit this elderly patient could expect from the new device. The score will be very important for targeting treatment, shared decision making, and selection of patients for future intervention trials, he concluded.
“I think this risk score will change practice by giving clinicians a better idea of a patient’s risk for infection,” commented Fred M. Kusumoto, MD, professor of medicine at the Mayo Medical School, Rochester, Minn., and director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla. The PADIT score will help identify patients for whom leaving a device in place is a better option than taking it out because of their infection risk. The risk score could also help improve the cost effectiveness of preventive treatments, such as antibiotic-eluting envelopes, by targeting treatment to higher-risk patients, Dr. Kusumoto said during a press briefing.
SOURCE: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.
REPORTING FROM HEART RHYTHM 2019
Key clinical point: Researchers have devised a five-item scoring formula to predict a patient’s risk for infection from an cardiac rhythm–device procedure.
Major finding: The risk score had an optimism-corrected concordance statistic of 0.704.
Study details: Investigators developed the risk score using data from PADIT, a multicenter, randomized trial with 19,603 patients.
Disclosures: PADIT received no commercial funding. Dr. Birnie had no relevant disclosures.
Source: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.
