User login
Racial, age disparities confirmed in triple-negative breast cancer
Odds of triple-negative breast cancer (TNBC) are elevated for minority women and younger women, results of a nationwide cross-sectional cohort study of more than a million breast cancer cases confirm.
Previous studies have suggested certain sociodemographic groups are disproportionately affected by TNBC, but have been limited by the population studied, size, and characteristics assessed, note the investigators, who were led by Lia C. Scott, PhD, MPH, of the division of epidemiology and biostatistics at the School of Public Health, Georgia State University, Atlanta. “It is imperative that cancer research identify factors that drive disparities and focus on prevention,” they wrote in Cancer.
Dr. Scott and coinvestigators used the United States Cancer Statistics database to identify 1,151,724 cases of breast cancer diagnosed during 2010-2014 in 39 states having the necessary data. TNBC accounted for roughly 8.4% of all cases.
In unadjusted analyses using non-Hispanic white women as the comparator, odds of TNBC were significantly higher for non-Hispanic black women (odds ratio, 2.27), Hispanic women (OR, 1.22), and American Indian/Alaska Native women (OR, 1.26). On the other hand, odds were lower for Asian women (OR, 0.92).
By age group, compared with women 50-64 years old, women younger than 40 years were most likely to have the TNBC phenotype (OR, 1.95), while women aged 75 or older were least likely (OR, 0.75). Odds of TNBC were also significantly elevated for women whose cancer was diagnosed at stage III or higher (OR, 1.69) or at stage IV (OR, 1.47).
Findings were essentially the same in analyses simultaneously adjusted for age, race, and stage.
“The results of the current study demonstrated that there is a significant burden of disease in TNBC diagnosed among women of color, specifically non-Hispanic black women, and younger women,” Dr. Scott and coinvestigators write. “Given the large sample size and geospatial coverage of the data, these results are somewhat different from and also more generalizable, compared with data from previous studies.”
“With the advent and availability of more comprehensive cancer data, such as the United States Cancer Statistics database, it is important that we continue to explore disparities in order to better inform practice and policy around screenable cancers like breast cancer,” she further commented in a statement. “We hope that this update on the epidemiology of triple-negative breast cancer can provide a basis to further explore contributing factors in future research.”
Dr. Scott disclosed that she received a Dissertation Training Grant (F31-Diversity) from the National Institutes of Health. The study was funded by the National Institute on Minority Health and Health Disparities of the National Institutes of Health; the Centers for Disease Control and Prevention’s National Program of Cancer Registries contributed funds to cover the standard research data center fees for researchers conducting analyses under approved research projects.
SOURCE: Scott LC et al. Cancer. 2019 Jul 8. doi: 10.1002/cncr.32207.
Odds of triple-negative breast cancer (TNBC) are elevated for minority women and younger women, results of a nationwide cross-sectional cohort study of more than a million breast cancer cases confirm.
Previous studies have suggested certain sociodemographic groups are disproportionately affected by TNBC, but have been limited by the population studied, size, and characteristics assessed, note the investigators, who were led by Lia C. Scott, PhD, MPH, of the division of epidemiology and biostatistics at the School of Public Health, Georgia State University, Atlanta. “It is imperative that cancer research identify factors that drive disparities and focus on prevention,” they wrote in Cancer.
Dr. Scott and coinvestigators used the United States Cancer Statistics database to identify 1,151,724 cases of breast cancer diagnosed during 2010-2014 in 39 states having the necessary data. TNBC accounted for roughly 8.4% of all cases.
In unadjusted analyses using non-Hispanic white women as the comparator, odds of TNBC were significantly higher for non-Hispanic black women (odds ratio, 2.27), Hispanic women (OR, 1.22), and American Indian/Alaska Native women (OR, 1.26). On the other hand, odds were lower for Asian women (OR, 0.92).
By age group, compared with women 50-64 years old, women younger than 40 years were most likely to have the TNBC phenotype (OR, 1.95), while women aged 75 or older were least likely (OR, 0.75). Odds of TNBC were also significantly elevated for women whose cancer was diagnosed at stage III or higher (OR, 1.69) or at stage IV (OR, 1.47).
Findings were essentially the same in analyses simultaneously adjusted for age, race, and stage.
“The results of the current study demonstrated that there is a significant burden of disease in TNBC diagnosed among women of color, specifically non-Hispanic black women, and younger women,” Dr. Scott and coinvestigators write. “Given the large sample size and geospatial coverage of the data, these results are somewhat different from and also more generalizable, compared with data from previous studies.”
“With the advent and availability of more comprehensive cancer data, such as the United States Cancer Statistics database, it is important that we continue to explore disparities in order to better inform practice and policy around screenable cancers like breast cancer,” she further commented in a statement. “We hope that this update on the epidemiology of triple-negative breast cancer can provide a basis to further explore contributing factors in future research.”
Dr. Scott disclosed that she received a Dissertation Training Grant (F31-Diversity) from the National Institutes of Health. The study was funded by the National Institute on Minority Health and Health Disparities of the National Institutes of Health; the Centers for Disease Control and Prevention’s National Program of Cancer Registries contributed funds to cover the standard research data center fees for researchers conducting analyses under approved research projects.
SOURCE: Scott LC et al. Cancer. 2019 Jul 8. doi: 10.1002/cncr.32207.
Odds of triple-negative breast cancer (TNBC) are elevated for minority women and younger women, results of a nationwide cross-sectional cohort study of more than a million breast cancer cases confirm.
Previous studies have suggested certain sociodemographic groups are disproportionately affected by TNBC, but have been limited by the population studied, size, and characteristics assessed, note the investigators, who were led by Lia C. Scott, PhD, MPH, of the division of epidemiology and biostatistics at the School of Public Health, Georgia State University, Atlanta. “It is imperative that cancer research identify factors that drive disparities and focus on prevention,” they wrote in Cancer.
Dr. Scott and coinvestigators used the United States Cancer Statistics database to identify 1,151,724 cases of breast cancer diagnosed during 2010-2014 in 39 states having the necessary data. TNBC accounted for roughly 8.4% of all cases.
In unadjusted analyses using non-Hispanic white women as the comparator, odds of TNBC were significantly higher for non-Hispanic black women (odds ratio, 2.27), Hispanic women (OR, 1.22), and American Indian/Alaska Native women (OR, 1.26). On the other hand, odds were lower for Asian women (OR, 0.92).
By age group, compared with women 50-64 years old, women younger than 40 years were most likely to have the TNBC phenotype (OR, 1.95), while women aged 75 or older were least likely (OR, 0.75). Odds of TNBC were also significantly elevated for women whose cancer was diagnosed at stage III or higher (OR, 1.69) or at stage IV (OR, 1.47).
Findings were essentially the same in analyses simultaneously adjusted for age, race, and stage.
“The results of the current study demonstrated that there is a significant burden of disease in TNBC diagnosed among women of color, specifically non-Hispanic black women, and younger women,” Dr. Scott and coinvestigators write. “Given the large sample size and geospatial coverage of the data, these results are somewhat different from and also more generalizable, compared with data from previous studies.”
“With the advent and availability of more comprehensive cancer data, such as the United States Cancer Statistics database, it is important that we continue to explore disparities in order to better inform practice and policy around screenable cancers like breast cancer,” she further commented in a statement. “We hope that this update on the epidemiology of triple-negative breast cancer can provide a basis to further explore contributing factors in future research.”
Dr. Scott disclosed that she received a Dissertation Training Grant (F31-Diversity) from the National Institutes of Health. The study was funded by the National Institute on Minority Health and Health Disparities of the National Institutes of Health; the Centers for Disease Control and Prevention’s National Program of Cancer Registries contributed funds to cover the standard research data center fees for researchers conducting analyses under approved research projects.
SOURCE: Scott LC et al. Cancer. 2019 Jul 8. doi: 10.1002/cncr.32207.
FROM CANCER
Increased cancer death linked to radioactive iodine therapy
Radioactive iodine therapy for hyperthyroidism may be associated with an increased risk of death from cancer, according to a longitudinal cohort study published in the July 1 issue of JAMA Internal Medicine.

The study followed 18,805 individuals whose hyperthyroidism was treated with radioactive iodine in the United States and United Kingdom between 1946 and 1964.
Researchers found positive dose-response relationships between radioactive iodine therapy and most of the solid cancers that were evaluated. However these only attained statistical significance in the case of female breast cancer – where there was a 12% increase in the risk of death from breast cancer from a 100-mGy tissue- or organ-absorbed dose – or for all solid cancers combined, where a 100-mGy dose to the stomach was associated with a 6% increase in death from all solid cancers.
Based on this, the authors estimated that 8% of solid cancer deaths, including 14% of breast cancer deaths, could be attributed to the radiation. When combined with current US mortality rates, that translated to around 13 excess solid cancer deaths, including three deaths from breast cancer, for every 1000 patients receiving a 100 mGy absorbed dose to the stomach or breast at age 40 years.
However they noted that patients with Graves disease are now recommended to receive higher doses, and calculated that for 150-mGy, 200-mGy and 250-mGy dosages there would be 19-32 excess solid cancer deaths per 1000 patients treated at age 40 years.
“To our knowledge, this is the first study to characterize the dose-response relationship between RAI treatment and site-specific cancer mortality in patients with hyperthyroidism using reliable estimates of absorbed dose to exposed organs or tissues,” wrote Cari M. Kitahara, PhD, from the Division of Cancer Epidemiology and Genetics at the National Cancer Institute, and co-authors.
Radioactive iodine therapy did not appear to be associated with an increased risk of death from leukemia, non-Hodgkin lymphoma or multiple myeloma.
The authors noted that this was unexpected given previous findings of an elevated risk of leukemia in patients with thyroid cancer who received higher levels of radiation. They suggested that the greater uncertainty in calculation of red bone marrow exposure compared to that of other organs and tissue, as well as the relatively small number of leukemia deaths, may have limited their ability to detect a dose-response relationship.
The study was funded by the National Cancer Institute. One author declared membership of a consortium supported by the pharmaceutical sector.
SOURCE: Kitahara C et al. JAMA Internal Medicine 2019, July 1. DOI:10.1001/jamainternmed.2019.0981.
Radioactive iodine therapy for hyperthyroidism may be associated with an increased risk of death from cancer, according to a longitudinal cohort study published in the July 1 issue of JAMA Internal Medicine.
The study followed 18,805 individuals whose hyperthyroidism was treated with radioactive iodine in the United States and United Kingdom between 1946 and 1964.
Researchers found positive dose-response relationships between radioactive iodine therapy and most of the solid cancers that were evaluated. However these only attained statistical significance in the case of female breast cancer – where there was a 12% increase in the risk of death from breast cancer from a 100-mGy tissue- or organ-absorbed dose – or for all solid cancers combined, where a 100-mGy dose to the stomach was associated with a 6% increase in death from all solid cancers.
Based on this, the authors estimated that 8% of solid cancer deaths, including 14% of breast cancer deaths, could be attributed to the radiation. When combined with current US mortality rates, that translated to around 13 excess solid cancer deaths, including three deaths from breast cancer, for every 1000 patients receiving a 100 mGy absorbed dose to the stomach or breast at age 40 years.
However they noted that patients with Graves disease are now recommended to receive higher doses, and calculated that for 150-mGy, 200-mGy and 250-mGy dosages there would be 19-32 excess solid cancer deaths per 1000 patients treated at age 40 years.
“To our knowledge, this is the first study to characterize the dose-response relationship between RAI treatment and site-specific cancer mortality in patients with hyperthyroidism using reliable estimates of absorbed dose to exposed organs or tissues,” wrote Cari M. Kitahara, PhD, from the Division of Cancer Epidemiology and Genetics at the National Cancer Institute, and co-authors.
Radioactive iodine therapy did not appear to be associated with an increased risk of death from leukemia, non-Hodgkin lymphoma or multiple myeloma.
The authors noted that this was unexpected given previous findings of an elevated risk of leukemia in patients with thyroid cancer who received higher levels of radiation. They suggested that the greater uncertainty in calculation of red bone marrow exposure compared to that of other organs and tissue, as well as the relatively small number of leukemia deaths, may have limited their ability to detect a dose-response relationship.
The study was funded by the National Cancer Institute. One author declared membership of a consortium supported by the pharmaceutical sector.
SOURCE: Kitahara C et al. JAMA Internal Medicine 2019, July 1. DOI:10.1001/jamainternmed.2019.0981.
Radioactive iodine therapy for hyperthyroidism may be associated with an increased risk of death from cancer, according to a longitudinal cohort study published in the July 1 issue of JAMA Internal Medicine.
The study followed 18,805 individuals whose hyperthyroidism was treated with radioactive iodine in the United States and United Kingdom between 1946 and 1964.
Researchers found positive dose-response relationships between radioactive iodine therapy and most of the solid cancers that were evaluated. However these only attained statistical significance in the case of female breast cancer – where there was a 12% increase in the risk of death from breast cancer from a 100-mGy tissue- or organ-absorbed dose – or for all solid cancers combined, where a 100-mGy dose to the stomach was associated with a 6% increase in death from all solid cancers.
Based on this, the authors estimated that 8% of solid cancer deaths, including 14% of breast cancer deaths, could be attributed to the radiation. When combined with current US mortality rates, that translated to around 13 excess solid cancer deaths, including three deaths from breast cancer, for every 1000 patients receiving a 100 mGy absorbed dose to the stomach or breast at age 40 years.
However they noted that patients with Graves disease are now recommended to receive higher doses, and calculated that for 150-mGy, 200-mGy and 250-mGy dosages there would be 19-32 excess solid cancer deaths per 1000 patients treated at age 40 years.
“To our knowledge, this is the first study to characterize the dose-response relationship between RAI treatment and site-specific cancer mortality in patients with hyperthyroidism using reliable estimates of absorbed dose to exposed organs or tissues,” wrote Cari M. Kitahara, PhD, from the Division of Cancer Epidemiology and Genetics at the National Cancer Institute, and co-authors.
Radioactive iodine therapy did not appear to be associated with an increased risk of death from leukemia, non-Hodgkin lymphoma or multiple myeloma.
The authors noted that this was unexpected given previous findings of an elevated risk of leukemia in patients with thyroid cancer who received higher levels of radiation. They suggested that the greater uncertainty in calculation of red bone marrow exposure compared to that of other organs and tissue, as well as the relatively small number of leukemia deaths, may have limited their ability to detect a dose-response relationship.
The study was funded by the National Cancer Institute. One author declared membership of a consortium supported by the pharmaceutical sector.
SOURCE: Kitahara C et al. JAMA Internal Medicine 2019, July 1. DOI:10.1001/jamainternmed.2019.0981.
FROM JAMA INTERNAL MEDICINE
Breast density alone should not prompt supplemental imaging discussions
Breast density should be a factor in assessing breast cancer risk and recommending supplemental imaging, but not the primary factor, according to a study of women who were screened for the disease.
“Counseling strategies that identified women for supplemental imaging based on breast density and BCSC 5-year risk were more efficient compared with strategies based on age and density or density alone,” wrote Karla Kerlikowske, MD, of the Department of Veterans Affairs, and her coauthors. The study was published in JAMA Internal Medicine.
To assess breast cancer risk and strategies for recommending supplemental screening, the researchers assembled a cohort of 638,856 women aged 40 to 74 years who received mammograms at Breast Cancer Surveillance Consortium (BCSC) facilities from Jan. 3, 2005, to Dec. 31, 2014. Participants were identified as high risk via combinations of Breast Imaging Reporting and Data System (BI-RADS) breast density, BCSC 5-year breast cancer risk, and age.
Women with dense breasts made up 47% of those screened, and 60% of those with advanced cancers. Low advanced cancer rates (less than .61 per 1,000 mammograms) occurred in 34.5% of women with dense breasts, while high advanced cancer rates (greater than or equal to .61 cases per 1,000 mammograms) occurred in women with heterogeneously dense breasts and a 5-year risk of 2.5% or higher (6.0% of screened women) and those with extremely dense breasts and a 5-year risk of 1.0% or higher (6.5% of screened women).
In a hypothetical cohort of 100,000 women, supplemental imaging for all 47,012 women with dense breasts would mean a ratio of 1,866 supplemental imaging discussions per potential advanced breast cancer prevented. If imaging was considered based on a combination of density plus BCSC 5-year risk, the number of women screened would be reduced to 12,506 and the ratio would become 1,097 supplemental imaging discussions per potential advanced cancer prevented.
The coauthors acknowledged their study’s limitations, including their lack of ability to determine if women at high risk of advanced cancer would benefit from supplemental screening. In addition, they were unable to evaluate digital breast tomosynthesis outcomes, though they noted that, to their knowledge, “no published evidence indicates that advanced cancer rates differ for digital mammography vs. tomosynthesis according to breast density.”
The study was funded by the Patient-Centered Outcomes Research Institute, the Breast Cancer Surveillance Consortium, the National Cancer Institute, the Agency for Health Research and Quality, and the Lake Champlain Cancer Research Organization. The authors reported several potential conflicts of interest, including being members of various working groups, advisory boards, committees, task forces, and panels.
SOURCE: Kerlikowske K et al. JAMA Intern Med. 2019 Jul 1. doi:10.1001/jamainternmed.2019.1758 .
Identifying women at risk of breast cancer is key, but physicians and policymakers should pause and reassess how exactly to go about it, according to Ilana B. Richman, MD, and Susan H. Busch, PhD of the Yale School of Medicine.
The latest proposal from the U.S. Food and Drug Administration focuses on recommending additional screening for women with dense breasts, but that can be too broad of a stroke. “Breast density is only one aspect of breast cancer risk,” the coauthors noted, and limiting supplemental screening recommendations to women with dense breasts may leave out many others at legitimate risk.
So how should supplemental screening be handled moving forward? In their accompanying study, Kerlikowske et al. rejected 2 strategies while embracing elements of 3 others, but none of them were recognized as the proper path to take.
At the same time, the coauthors asked, “Why legislate this particular area of medicine?” And what is the exact opportunity cost of supplemental screening? There is no simple answer, which highlights “both the overall inefficiency of supplemental screening and the insensitivity of a targeted approach.” In short, more work is needed.
These comments are adapted from an accompanying editorial (JAMA Intern Med. 2019 Jul 1. doi:10.1001/jamainternmed.2019.1737 ). Dr. Richman reported receiving funding from the Centers for Medicare and Medicaid Services to develop quality measures, along with funding from the National Center for Advancing Translational Sciences.
Identifying women at risk of breast cancer is key, but physicians and policymakers should pause and reassess how exactly to go about it, according to Ilana B. Richman, MD, and Susan H. Busch, PhD of the Yale School of Medicine.
The latest proposal from the U.S. Food and Drug Administration focuses on recommending additional screening for women with dense breasts, but that can be too broad of a stroke. “Breast density is only one aspect of breast cancer risk,” the coauthors noted, and limiting supplemental screening recommendations to women with dense breasts may leave out many others at legitimate risk.
So how should supplemental screening be handled moving forward? In their accompanying study, Kerlikowske et al. rejected 2 strategies while embracing elements of 3 others, but none of them were recognized as the proper path to take.
At the same time, the coauthors asked, “Why legislate this particular area of medicine?” And what is the exact opportunity cost of supplemental screening? There is no simple answer, which highlights “both the overall inefficiency of supplemental screening and the insensitivity of a targeted approach.” In short, more work is needed.
These comments are adapted from an accompanying editorial (JAMA Intern Med. 2019 Jul 1. doi:10.1001/jamainternmed.2019.1737 ). Dr. Richman reported receiving funding from the Centers for Medicare and Medicaid Services to develop quality measures, along with funding from the National Center for Advancing Translational Sciences.
Identifying women at risk of breast cancer is key, but physicians and policymakers should pause and reassess how exactly to go about it, according to Ilana B. Richman, MD, and Susan H. Busch, PhD of the Yale School of Medicine.
The latest proposal from the U.S. Food and Drug Administration focuses on recommending additional screening for women with dense breasts, but that can be too broad of a stroke. “Breast density is only one aspect of breast cancer risk,” the coauthors noted, and limiting supplemental screening recommendations to women with dense breasts may leave out many others at legitimate risk.
So how should supplemental screening be handled moving forward? In their accompanying study, Kerlikowske et al. rejected 2 strategies while embracing elements of 3 others, but none of them were recognized as the proper path to take.
At the same time, the coauthors asked, “Why legislate this particular area of medicine?” And what is the exact opportunity cost of supplemental screening? There is no simple answer, which highlights “both the overall inefficiency of supplemental screening and the insensitivity of a targeted approach.” In short, more work is needed.
These comments are adapted from an accompanying editorial (JAMA Intern Med. 2019 Jul 1. doi:10.1001/jamainternmed.2019.1737 ). Dr. Richman reported receiving funding from the Centers for Medicare and Medicaid Services to develop quality measures, along with funding from the National Center for Advancing Translational Sciences.
Breast density should be a factor in assessing breast cancer risk and recommending supplemental imaging, but not the primary factor, according to a study of women who were screened for the disease.
“Counseling strategies that identified women for supplemental imaging based on breast density and BCSC 5-year risk were more efficient compared with strategies based on age and density or density alone,” wrote Karla Kerlikowske, MD, of the Department of Veterans Affairs, and her coauthors. The study was published in JAMA Internal Medicine.
To assess breast cancer risk and strategies for recommending supplemental screening, the researchers assembled a cohort of 638,856 women aged 40 to 74 years who received mammograms at Breast Cancer Surveillance Consortium (BCSC) facilities from Jan. 3, 2005, to Dec. 31, 2014. Participants were identified as high risk via combinations of Breast Imaging Reporting and Data System (BI-RADS) breast density, BCSC 5-year breast cancer risk, and age.
Women with dense breasts made up 47% of those screened, and 60% of those with advanced cancers. Low advanced cancer rates (less than .61 per 1,000 mammograms) occurred in 34.5% of women with dense breasts, while high advanced cancer rates (greater than or equal to .61 cases per 1,000 mammograms) occurred in women with heterogeneously dense breasts and a 5-year risk of 2.5% or higher (6.0% of screened women) and those with extremely dense breasts and a 5-year risk of 1.0% or higher (6.5% of screened women).
In a hypothetical cohort of 100,000 women, supplemental imaging for all 47,012 women with dense breasts would mean a ratio of 1,866 supplemental imaging discussions per potential advanced breast cancer prevented. If imaging was considered based on a combination of density plus BCSC 5-year risk, the number of women screened would be reduced to 12,506 and the ratio would become 1,097 supplemental imaging discussions per potential advanced cancer prevented.
The coauthors acknowledged their study’s limitations, including their lack of ability to determine if women at high risk of advanced cancer would benefit from supplemental screening. In addition, they were unable to evaluate digital breast tomosynthesis outcomes, though they noted that, to their knowledge, “no published evidence indicates that advanced cancer rates differ for digital mammography vs. tomosynthesis according to breast density.”
The study was funded by the Patient-Centered Outcomes Research Institute, the Breast Cancer Surveillance Consortium, the National Cancer Institute, the Agency for Health Research and Quality, and the Lake Champlain Cancer Research Organization. The authors reported several potential conflicts of interest, including being members of various working groups, advisory boards, committees, task forces, and panels.
SOURCE: Kerlikowske K et al. JAMA Intern Med. 2019 Jul 1. doi:10.1001/jamainternmed.2019.1758 .
Breast density should be a factor in assessing breast cancer risk and recommending supplemental imaging, but not the primary factor, according to a study of women who were screened for the disease.
“Counseling strategies that identified women for supplemental imaging based on breast density and BCSC 5-year risk were more efficient compared with strategies based on age and density or density alone,” wrote Karla Kerlikowske, MD, of the Department of Veterans Affairs, and her coauthors. The study was published in JAMA Internal Medicine.
To assess breast cancer risk and strategies for recommending supplemental screening, the researchers assembled a cohort of 638,856 women aged 40 to 74 years who received mammograms at Breast Cancer Surveillance Consortium (BCSC) facilities from Jan. 3, 2005, to Dec. 31, 2014. Participants were identified as high risk via combinations of Breast Imaging Reporting and Data System (BI-RADS) breast density, BCSC 5-year breast cancer risk, and age.
Women with dense breasts made up 47% of those screened, and 60% of those with advanced cancers. Low advanced cancer rates (less than .61 per 1,000 mammograms) occurred in 34.5% of women with dense breasts, while high advanced cancer rates (greater than or equal to .61 cases per 1,000 mammograms) occurred in women with heterogeneously dense breasts and a 5-year risk of 2.5% or higher (6.0% of screened women) and those with extremely dense breasts and a 5-year risk of 1.0% or higher (6.5% of screened women).
In a hypothetical cohort of 100,000 women, supplemental imaging for all 47,012 women with dense breasts would mean a ratio of 1,866 supplemental imaging discussions per potential advanced breast cancer prevented. If imaging was considered based on a combination of density plus BCSC 5-year risk, the number of women screened would be reduced to 12,506 and the ratio would become 1,097 supplemental imaging discussions per potential advanced cancer prevented.
The coauthors acknowledged their study’s limitations, including their lack of ability to determine if women at high risk of advanced cancer would benefit from supplemental screening. In addition, they were unable to evaluate digital breast tomosynthesis outcomes, though they noted that, to their knowledge, “no published evidence indicates that advanced cancer rates differ for digital mammography vs. tomosynthesis according to breast density.”
The study was funded by the Patient-Centered Outcomes Research Institute, the Breast Cancer Surveillance Consortium, the National Cancer Institute, the Agency for Health Research and Quality, and the Lake Champlain Cancer Research Organization. The authors reported several potential conflicts of interest, including being members of various working groups, advisory boards, committees, task forces, and panels.
SOURCE: Kerlikowske K et al. JAMA Intern Med. 2019 Jul 1. doi:10.1001/jamainternmed.2019.1758 .
FROM JAMA INTERNAL MEDICINE
CVD risk upped in postmenopausal breast cancer survivors
according to a new study of nearly 300 women.
Previous studies have shown that cardiovascular risk is greater among postmenopausal women treated for breast cancer compared with those without cancer, but specific risk factors have not been well studied, wrote Daniel de Araujo Brito Buttros, MD, of Paulista State University, Sao Paulo, Brazil, and colleagues.
In a study published in Menopause, the researchers evaluated several CVD risk factors in 96 postmenopausal women with breast cancer and 192 women without breast cancer, including metabolic syndrome, subclinical atherosclerosis, and heat shock proteins (HSP) 60 and 70.
Overall, breast cancer patients had significantly higher HSP60 levels and lower HSP70 levels than those of their cancer-free peers. These two proteins have an antagonistic relationship in cardiovascular disease, with HSP60 considered a risk factor for CVD, and HSP70 considered a protective factor. Average HSP60 levels for the breast cancer and control groups were 35 ng/mL and 10.8 ng/mL, respectively; average HSP70 levels were 0.5 ng/mL and 1.3 ng/mL, respectively.
Both diabetes and metabolic syndrome were significantly more common among breast cancer patients vs. controls (19.8% vs. 6.8% and 54.2% vs. 30.7%, respectively). Carotid artery plaque also was more common in breast cancer patients vs. controls (19.8% vs. 9.4%, respectively, P = 0.013).
In addition, systolic and diastolic blood pressure levels were significantly higher among the breast cancer patients, as were triglycerides and glucose.
The findings were limited by several factors including the cross-sectional design that could not prove a causal relationship between CVD risk and breast cancer, the researchers noted.
However, the results demonstrate the increased CVD risk for breast cancer patients, and “[therefore], women diagnosed with breast cancer might receive multidisciplinary care, including cardiology consultation at the time of breast cancer diagnosis and also during oncologic follow-up visits,” they said.
“Heart disease appears more commonly in women treated for breast cancer because of the toxicities of chemotherapy, radiation therapy, and use of aromatase inhibitors, which lower estrogen. Heart-healthy lifestyle modifications will decrease both the risk of recurrent breast cancer and the risk of developing heart disease,” JoAnn Pinkerton, MD, executive director of the North American Menopause Society, said in a statement. “Women should schedule a cardiology consultation when breast cancer is diagnosed and continue with ongoing follow-up after cancer treatments are completed,” she emphasized.
The researchers had no financial conflicts to disclose.
SOURCE: Buttros DAB et al. Menopause. 2019. doi: 10.1097/GME.0000000000001348.
according to a new study of nearly 300 women.
Previous studies have shown that cardiovascular risk is greater among postmenopausal women treated for breast cancer compared with those without cancer, but specific risk factors have not been well studied, wrote Daniel de Araujo Brito Buttros, MD, of Paulista State University, Sao Paulo, Brazil, and colleagues.
In a study published in Menopause, the researchers evaluated several CVD risk factors in 96 postmenopausal women with breast cancer and 192 women without breast cancer, including metabolic syndrome, subclinical atherosclerosis, and heat shock proteins (HSP) 60 and 70.
Overall, breast cancer patients had significantly higher HSP60 levels and lower HSP70 levels than those of their cancer-free peers. These two proteins have an antagonistic relationship in cardiovascular disease, with HSP60 considered a risk factor for CVD, and HSP70 considered a protective factor. Average HSP60 levels for the breast cancer and control groups were 35 ng/mL and 10.8 ng/mL, respectively; average HSP70 levels were 0.5 ng/mL and 1.3 ng/mL, respectively.
Both diabetes and metabolic syndrome were significantly more common among breast cancer patients vs. controls (19.8% vs. 6.8% and 54.2% vs. 30.7%, respectively). Carotid artery plaque also was more common in breast cancer patients vs. controls (19.8% vs. 9.4%, respectively, P = 0.013).
In addition, systolic and diastolic blood pressure levels were significantly higher among the breast cancer patients, as were triglycerides and glucose.
The findings were limited by several factors including the cross-sectional design that could not prove a causal relationship between CVD risk and breast cancer, the researchers noted.
However, the results demonstrate the increased CVD risk for breast cancer patients, and “[therefore], women diagnosed with breast cancer might receive multidisciplinary care, including cardiology consultation at the time of breast cancer diagnosis and also during oncologic follow-up visits,” they said.
“Heart disease appears more commonly in women treated for breast cancer because of the toxicities of chemotherapy, radiation therapy, and use of aromatase inhibitors, which lower estrogen. Heart-healthy lifestyle modifications will decrease both the risk of recurrent breast cancer and the risk of developing heart disease,” JoAnn Pinkerton, MD, executive director of the North American Menopause Society, said in a statement. “Women should schedule a cardiology consultation when breast cancer is diagnosed and continue with ongoing follow-up after cancer treatments are completed,” she emphasized.
The researchers had no financial conflicts to disclose.
SOURCE: Buttros DAB et al. Menopause. 2019. doi: 10.1097/GME.0000000000001348.
according to a new study of nearly 300 women.
Previous studies have shown that cardiovascular risk is greater among postmenopausal women treated for breast cancer compared with those without cancer, but specific risk factors have not been well studied, wrote Daniel de Araujo Brito Buttros, MD, of Paulista State University, Sao Paulo, Brazil, and colleagues.
In a study published in Menopause, the researchers evaluated several CVD risk factors in 96 postmenopausal women with breast cancer and 192 women without breast cancer, including metabolic syndrome, subclinical atherosclerosis, and heat shock proteins (HSP) 60 and 70.
Overall, breast cancer patients had significantly higher HSP60 levels and lower HSP70 levels than those of their cancer-free peers. These two proteins have an antagonistic relationship in cardiovascular disease, with HSP60 considered a risk factor for CVD, and HSP70 considered a protective factor. Average HSP60 levels for the breast cancer and control groups were 35 ng/mL and 10.8 ng/mL, respectively; average HSP70 levels were 0.5 ng/mL and 1.3 ng/mL, respectively.
Both diabetes and metabolic syndrome were significantly more common among breast cancer patients vs. controls (19.8% vs. 6.8% and 54.2% vs. 30.7%, respectively). Carotid artery plaque also was more common in breast cancer patients vs. controls (19.8% vs. 9.4%, respectively, P = 0.013).
In addition, systolic and diastolic blood pressure levels were significantly higher among the breast cancer patients, as were triglycerides and glucose.
The findings were limited by several factors including the cross-sectional design that could not prove a causal relationship between CVD risk and breast cancer, the researchers noted.
However, the results demonstrate the increased CVD risk for breast cancer patients, and “[therefore], women diagnosed with breast cancer might receive multidisciplinary care, including cardiology consultation at the time of breast cancer diagnosis and also during oncologic follow-up visits,” they said.
“Heart disease appears more commonly in women treated for breast cancer because of the toxicities of chemotherapy, radiation therapy, and use of aromatase inhibitors, which lower estrogen. Heart-healthy lifestyle modifications will decrease both the risk of recurrent breast cancer and the risk of developing heart disease,” JoAnn Pinkerton, MD, executive director of the North American Menopause Society, said in a statement. “Women should schedule a cardiology consultation when breast cancer is diagnosed and continue with ongoing follow-up after cancer treatments are completed,” she emphasized.
The researchers had no financial conflicts to disclose.
SOURCE: Buttros DAB et al. Menopause. 2019. doi: 10.1097/GME.0000000000001348.
FROM MENOPAUSE
APHINITY trial: Biomarker analysis IDs predictive, prognostic factors
CHICAGO – Higher levels of several immune markers confer better response and outcomes in patients with HER2-positive breast cancer treated with trastuzumab and pertuzumab, according to a comprehensive biomarker analysis of data from the randomized, phase 3 APHINITY trial.

APHINITY randomized 4,805 patients with HER2-positive breast cancer to adjuvant chemotherapy with trastuzumab plus either pertuzumab or placebo and demonstrated a small improvement of just 1.7% in invasive disease–free survival at 4 years with the addition of adjuvant pertuzumab. The current analysis involved a nested case-control assessment of 1,023 patient samples from the trial to identify “biomarkers beyond clinical parameters” that could identify subgroups of patients who might benefit more from the addition of pertuzumab, Ian E. Krop, MD, PhD, reported at the annual meeting of the American Society of Clinical Oncology.
The genomic and immune marker-based analysis included DNA, whole transcriptome, tumor-infiltrating lymphocytes (TILs), and HER2 analyses, and after adjustment for treatment, hormone receptor status, nodal status, age, and chemotherapy type. Topoisomerase II-alpha amplification and higher messenger RNA expression of an immune signature consisting of interferon-gamma (IFNG), programmed death-ligand 1 (PD-L1), and chemokine (C-X-C motif) ligand 9 (CXCL9) were associated with better prognosis (hazard ratios, 0.68 and 0.91, respectively), said Dr. Krop, associate chief of the division of breast oncology at the Susan F. Smith Center for Women’s Cancers and clinical research director of the breast oncology center at Dana-Farber Cancer Institute, both in Boston.
TILs also suggested better outcomes (HR, 0.91), and HER2 copy number of six or greater versus lower levels of HER2 copy number was also associated with better prognosis (HR, 0.68), he noted.
Conversely, PI3K/PTEN/AKT gene alterations and MYC and ZNF703 amplification each were associated with worse outcomes (HRs, 1.35, 1.61, and 1.62, respectively).
As for predictive value, no significant association was seen between any of the amplification events and benefit of pertuzumab, nor was an interaction seen between the three-gene signature and pertuzumab benefit, Dr. Krop said.
“But if you look at the individual genes and ... the highest quartiles of expression of these genes – particularly interferon gamma and CXCL9 – it did appear that there was a statistically significant improvement in the benefit of pertuzumab if you had the highest levels of these genes, compared to lower levels of these genes,” he added.
The hazard ratios for CXCL9 of 0%-75% and greater than 75%, for example, were 0.95 and 0.49, respectively.
The interaction P values for IFNG and CXCL9 were statistically significant, but a trend toward benefit with PD-L1 did not reach statistical significance, Dr. Krop noted.
As with IFNG and CXCL9, the highest quartiles of TILs also predicted greater pertuzumab benefit (HRs for TILs at 0-75% and greater than 75%, 0.95 and 0.35, respectively), and the association was highly significant (P = .003).
HER2 copy number of six or greater was also associated with significantly greater benefit with pertuzumab (HRs for copy number of six or greater vs. less than six, 0.75 and 1.41, respectively).
A trend was seen toward decreased benefit of pertuzumab in patients with P13K/PTEN/AKT alteration, but this was not statistically significant, he noted.
However, the trend, coupled with the poor prognosis found to be associated with P13K-altered cancers, “would suggest that we need to identify new therapies – alternative approaches – to maximize treatment benefit in this cancer subtype,” he said.
“This biomarker analysis is possibly the largest and most comprehensive to date in HER2-positive breast cancer,” Dr. Krop said, noting that the findings provide support for an immune-mediated mechanism of action for pertuzumab, and suggest a need for alternative therapies for patients with low levels of TILs or immune gene markers in order to maximize their outcomes.
“We hope these data will be useful to refine future trials of early-stage HER2-positive breast cancer,” he said.
Dr. Krop reported relationships – including employment, leadership, and stock ownership – with AMAG, as well as honoraria from Genentech/Roche; consulting or advisory roles with Context Therapeutics, Daiichi Sankyo, Genentech/Roche, MacroGenics, Seattle Genetics, and Taiho Pharmaceutical; and research funding from Genentech and Pfizer to his institution.
SOURCE: Krop IE et al. ASCO 2019, Abstract 1012 .
CHICAGO – Higher levels of several immune markers confer better response and outcomes in patients with HER2-positive breast cancer treated with trastuzumab and pertuzumab, according to a comprehensive biomarker analysis of data from the randomized, phase 3 APHINITY trial.
APHINITY randomized 4,805 patients with HER2-positive breast cancer to adjuvant chemotherapy with trastuzumab plus either pertuzumab or placebo and demonstrated a small improvement of just 1.7% in invasive disease–free survival at 4 years with the addition of adjuvant pertuzumab. The current analysis involved a nested case-control assessment of 1,023 patient samples from the trial to identify “biomarkers beyond clinical parameters” that could identify subgroups of patients who might benefit more from the addition of pertuzumab, Ian E. Krop, MD, PhD, reported at the annual meeting of the American Society of Clinical Oncology.
The genomic and immune marker-based analysis included DNA, whole transcriptome, tumor-infiltrating lymphocytes (TILs), and HER2 analyses, and after adjustment for treatment, hormone receptor status, nodal status, age, and chemotherapy type. Topoisomerase II-alpha amplification and higher messenger RNA expression of an immune signature consisting of interferon-gamma (IFNG), programmed death-ligand 1 (PD-L1), and chemokine (C-X-C motif) ligand 9 (CXCL9) were associated with better prognosis (hazard ratios, 0.68 and 0.91, respectively), said Dr. Krop, associate chief of the division of breast oncology at the Susan F. Smith Center for Women’s Cancers and clinical research director of the breast oncology center at Dana-Farber Cancer Institute, both in Boston.
TILs also suggested better outcomes (HR, 0.91), and HER2 copy number of six or greater versus lower levels of HER2 copy number was also associated with better prognosis (HR, 0.68), he noted.
Conversely, PI3K/PTEN/AKT gene alterations and MYC and ZNF703 amplification each were associated with worse outcomes (HRs, 1.35, 1.61, and 1.62, respectively).
As for predictive value, no significant association was seen between any of the amplification events and benefit of pertuzumab, nor was an interaction seen between the three-gene signature and pertuzumab benefit, Dr. Krop said.
“But if you look at the individual genes and ... the highest quartiles of expression of these genes – particularly interferon gamma and CXCL9 – it did appear that there was a statistically significant improvement in the benefit of pertuzumab if you had the highest levels of these genes, compared to lower levels of these genes,” he added.
The hazard ratios for CXCL9 of 0%-75% and greater than 75%, for example, were 0.95 and 0.49, respectively.
The interaction P values for IFNG and CXCL9 were statistically significant, but a trend toward benefit with PD-L1 did not reach statistical significance, Dr. Krop noted.
As with IFNG and CXCL9, the highest quartiles of TILs also predicted greater pertuzumab benefit (HRs for TILs at 0-75% and greater than 75%, 0.95 and 0.35, respectively), and the association was highly significant (P = .003).
HER2 copy number of six or greater was also associated with significantly greater benefit with pertuzumab (HRs for copy number of six or greater vs. less than six, 0.75 and 1.41, respectively).
A trend was seen toward decreased benefit of pertuzumab in patients with P13K/PTEN/AKT alteration, but this was not statistically significant, he noted.
However, the trend, coupled with the poor prognosis found to be associated with P13K-altered cancers, “would suggest that we need to identify new therapies – alternative approaches – to maximize treatment benefit in this cancer subtype,” he said.
“This biomarker analysis is possibly the largest and most comprehensive to date in HER2-positive breast cancer,” Dr. Krop said, noting that the findings provide support for an immune-mediated mechanism of action for pertuzumab, and suggest a need for alternative therapies for patients with low levels of TILs or immune gene markers in order to maximize their outcomes.
“We hope these data will be useful to refine future trials of early-stage HER2-positive breast cancer,” he said.
Dr. Krop reported relationships – including employment, leadership, and stock ownership – with AMAG, as well as honoraria from Genentech/Roche; consulting or advisory roles with Context Therapeutics, Daiichi Sankyo, Genentech/Roche, MacroGenics, Seattle Genetics, and Taiho Pharmaceutical; and research funding from Genentech and Pfizer to his institution.
SOURCE: Krop IE et al. ASCO 2019, Abstract 1012 .
CHICAGO – Higher levels of several immune markers confer better response and outcomes in patients with HER2-positive breast cancer treated with trastuzumab and pertuzumab, according to a comprehensive biomarker analysis of data from the randomized, phase 3 APHINITY trial.
APHINITY randomized 4,805 patients with HER2-positive breast cancer to adjuvant chemotherapy with trastuzumab plus either pertuzumab or placebo and demonstrated a small improvement of just 1.7% in invasive disease–free survival at 4 years with the addition of adjuvant pertuzumab. The current analysis involved a nested case-control assessment of 1,023 patient samples from the trial to identify “biomarkers beyond clinical parameters” that could identify subgroups of patients who might benefit more from the addition of pertuzumab, Ian E. Krop, MD, PhD, reported at the annual meeting of the American Society of Clinical Oncology.
The genomic and immune marker-based analysis included DNA, whole transcriptome, tumor-infiltrating lymphocytes (TILs), and HER2 analyses, and after adjustment for treatment, hormone receptor status, nodal status, age, and chemotherapy type. Topoisomerase II-alpha amplification and higher messenger RNA expression of an immune signature consisting of interferon-gamma (IFNG), programmed death-ligand 1 (PD-L1), and chemokine (C-X-C motif) ligand 9 (CXCL9) were associated with better prognosis (hazard ratios, 0.68 and 0.91, respectively), said Dr. Krop, associate chief of the division of breast oncology at the Susan F. Smith Center for Women’s Cancers and clinical research director of the breast oncology center at Dana-Farber Cancer Institute, both in Boston.
TILs also suggested better outcomes (HR, 0.91), and HER2 copy number of six or greater versus lower levels of HER2 copy number was also associated with better prognosis (HR, 0.68), he noted.
Conversely, PI3K/PTEN/AKT gene alterations and MYC and ZNF703 amplification each were associated with worse outcomes (HRs, 1.35, 1.61, and 1.62, respectively).
As for predictive value, no significant association was seen between any of the amplification events and benefit of pertuzumab, nor was an interaction seen between the three-gene signature and pertuzumab benefit, Dr. Krop said.
“But if you look at the individual genes and ... the highest quartiles of expression of these genes – particularly interferon gamma and CXCL9 – it did appear that there was a statistically significant improvement in the benefit of pertuzumab if you had the highest levels of these genes, compared to lower levels of these genes,” he added.
The hazard ratios for CXCL9 of 0%-75% and greater than 75%, for example, were 0.95 and 0.49, respectively.
The interaction P values for IFNG and CXCL9 were statistically significant, but a trend toward benefit with PD-L1 did not reach statistical significance, Dr. Krop noted.
As with IFNG and CXCL9, the highest quartiles of TILs also predicted greater pertuzumab benefit (HRs for TILs at 0-75% and greater than 75%, 0.95 and 0.35, respectively), and the association was highly significant (P = .003).
HER2 copy number of six or greater was also associated with significantly greater benefit with pertuzumab (HRs for copy number of six or greater vs. less than six, 0.75 and 1.41, respectively).
A trend was seen toward decreased benefit of pertuzumab in patients with P13K/PTEN/AKT alteration, but this was not statistically significant, he noted.
However, the trend, coupled with the poor prognosis found to be associated with P13K-altered cancers, “would suggest that we need to identify new therapies – alternative approaches – to maximize treatment benefit in this cancer subtype,” he said.
“This biomarker analysis is possibly the largest and most comprehensive to date in HER2-positive breast cancer,” Dr. Krop said, noting that the findings provide support for an immune-mediated mechanism of action for pertuzumab, and suggest a need for alternative therapies for patients with low levels of TILs or immune gene markers in order to maximize their outcomes.
“We hope these data will be useful to refine future trials of early-stage HER2-positive breast cancer,” he said.
Dr. Krop reported relationships – including employment, leadership, and stock ownership – with AMAG, as well as honoraria from Genentech/Roche; consulting or advisory roles with Context Therapeutics, Daiichi Sankyo, Genentech/Roche, MacroGenics, Seattle Genetics, and Taiho Pharmaceutical; and research funding from Genentech and Pfizer to his institution.
SOURCE: Krop IE et al. ASCO 2019, Abstract 1012 .
REPORTING FROM ASCO 2019
Chemo-free neoadjuvant approaches emerge in NSCLC and breast cancer
In this edition of “How I will treat my next patient,” I take a look at two “chemo-free” neoadjuvant studies reported at the annual meeting of the American Society of Clinical Oncology. One summarizes the potential utility of immune checkpoint inhibitors (ICIs) in non–small cell lung cancer (NSCLC) patients who are – or can become – candidates for curative resection and the other highlights the potential utility of neoadjuvant trastuzumab emtansine (T-DM1) for HER2-positive breast cancer patients.
NEOSTAR in NSCLC

With the accumulation of comorbid conditions in an aging population, we all see NSCLC patients who are potential candidates for curative surgery, but for whom we have concerns about standard preoperative chemotherapy plus or minus radiation. At ASCO 2019, abstracts 8503 (atezolizumab, the LCMC3 trial) and 8504 (nivolumab plus or minus ipilimumab, NEOSTAR) addressed the neoadjuvant use of ICIs. I will focus on NEOSTAR, because the major pathologic response (mPR) rate – reduction in viable tumor cells to 10% or less – was higher with the combination of nivolumab plus ipilimumab in NEOSTAR than with single agent nivolumab or atezolizumab in the NEOSTAR or LCMC3 trials, respectively.
Briefly, 44 patients with stage I-IIIA NSCLC were randomized to nivolumab plus or minus ipilimumab. In total, 93% completed 6 weeks of neoadjuvant therapy and 89% were resected. The mPR rate was 33% with nivolumab plus ipilimumab (about twice as high as with nivolumab alone in NEOSTAR or atezolizumab in LCMC3).
Among resected patients, nivolumab plus ipilimumab had a 44% mPR rate and a pathologic complete response rate of 38%. Although RECIST (Response Evaluation Criteria in Solid Tumors) responses were more likely in patients who had an mPR, 11% of patients had radiographic “nodal immune flare” because of noncaseating granulomas in regional (or nonregional) nodes. Elevated baseline programmed death-ligand 1 was associated with a higher rate of mPR. Surgical complications seemed similar to expectations – 1 bronchopleural fistula and 8 air leaks among the 39 resected patients.
What this means in practice
Although the mPR endpoint has no validated association with survival and the studies were relatively small, neoadjuvant use of ICIs in patients for whom tolerance to standard chemotherapy plus or minus radiation might be problematic is attractive – especially in view of the reality of an approximately 50% relapse rate after surgical resection with standard therapy.
If I had a potential candidate for neoadjuvant ICI therapy – especially one with a high proportion of cells with PD-L1 or someone with an equivocal distant metastasis on a preoperative PET-CT – I would consider using an ICI as given in LCMC3 or NEOSTAR.
PREDIX in HER2-positive breast cancer
As Mark Pegram, MD, of Stanford (Calif.) University suggested in his discussion at the local/regional/adjuvant breast cancer session at ASCO 2019, the goal of HER2-targeted therapy was originally that it could replace – not supplement – the use of cytotoxic chemotherapy.
Abstracts 500 (the KRISTINE trial: neoadjuvant T-DM1 plus pertuzumab vs. docetaxel, carboplatin, and trastuzumab plus pertuzumab); 501 (the PREDIX study: T-DM1 vs. docetaxel plus trastuzumab plus pertuzumab [DTP] for six cycles); and 502 (HER2 heterogeneity as a predictor of response) addressed the potential for the antibody-drug conjugate to replace standard preoperative cytotoxic chemotherapy plus HER2-targeting.
In PREDIX, it was anticipated that toxicity would be lower with T-DM1 than with DTP – and it was, with better quality of life scores. The authors found a pathologic complete response rate of 45% among 98 participants with stage IIA-IIIA HER2-positive breast cancer, with higher rates among hormone receptor–negative than hormone receptor–positive patients, as expected.
PREDIX patients were allowed to switch from T-DM1 to DTP for progression, lack of clinical/radiographic response, or toxicity. More than twice as many patients switched from DTP to T-DM1 than vice versa for progression or lack of response.
What this means in practice
Although neither DTP nor T-DM1 are National Comprehensive Cancer Network guideline-endorsed neoadjuvant regimens at present, the KRISTINE and PREDIX trials and Abstract 502 advance the discussion about further personalizing therapy for HER2-amplified breast cancer with high HER2 copy number and lack of intratumor heterogeneity for HER2. They also raise questions about de-escalating therapy for patients with good prognosis and HER2-positive cancers, and the creative use of T-DM1 in the neoadjuvant setting.
Neoadjuvant T-DM1 may not be standard of care yet, but watch this space.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I will treat my next patient,” I take a look at two “chemo-free” neoadjuvant studies reported at the annual meeting of the American Society of Clinical Oncology. One summarizes the potential utility of immune checkpoint inhibitors (ICIs) in non–small cell lung cancer (NSCLC) patients who are – or can become – candidates for curative resection and the other highlights the potential utility of neoadjuvant trastuzumab emtansine (T-DM1) for HER2-positive breast cancer patients.
NEOSTAR in NSCLC
With the accumulation of comorbid conditions in an aging population, we all see NSCLC patients who are potential candidates for curative surgery, but for whom we have concerns about standard preoperative chemotherapy plus or minus radiation. At ASCO 2019, abstracts 8503 (atezolizumab, the LCMC3 trial) and 8504 (nivolumab plus or minus ipilimumab, NEOSTAR) addressed the neoadjuvant use of ICIs. I will focus on NEOSTAR, because the major pathologic response (mPR) rate – reduction in viable tumor cells to 10% or less – was higher with the combination of nivolumab plus ipilimumab in NEOSTAR than with single agent nivolumab or atezolizumab in the NEOSTAR or LCMC3 trials, respectively.
Briefly, 44 patients with stage I-IIIA NSCLC were randomized to nivolumab plus or minus ipilimumab. In total, 93% completed 6 weeks of neoadjuvant therapy and 89% were resected. The mPR rate was 33% with nivolumab plus ipilimumab (about twice as high as with nivolumab alone in NEOSTAR or atezolizumab in LCMC3).
Among resected patients, nivolumab plus ipilimumab had a 44% mPR rate and a pathologic complete response rate of 38%. Although RECIST (Response Evaluation Criteria in Solid Tumors) responses were more likely in patients who had an mPR, 11% of patients had radiographic “nodal immune flare” because of noncaseating granulomas in regional (or nonregional) nodes. Elevated baseline programmed death-ligand 1 was associated with a higher rate of mPR. Surgical complications seemed similar to expectations – 1 bronchopleural fistula and 8 air leaks among the 39 resected patients.
What this means in practice
Although the mPR endpoint has no validated association with survival and the studies were relatively small, neoadjuvant use of ICIs in patients for whom tolerance to standard chemotherapy plus or minus radiation might be problematic is attractive – especially in view of the reality of an approximately 50% relapse rate after surgical resection with standard therapy.
If I had a potential candidate for neoadjuvant ICI therapy – especially one with a high proportion of cells with PD-L1 or someone with an equivocal distant metastasis on a preoperative PET-CT – I would consider using an ICI as given in LCMC3 or NEOSTAR.
PREDIX in HER2-positive breast cancer
As Mark Pegram, MD, of Stanford (Calif.) University suggested in his discussion at the local/regional/adjuvant breast cancer session at ASCO 2019, the goal of HER2-targeted therapy was originally that it could replace – not supplement – the use of cytotoxic chemotherapy.
Abstracts 500 (the KRISTINE trial: neoadjuvant T-DM1 plus pertuzumab vs. docetaxel, carboplatin, and trastuzumab plus pertuzumab); 501 (the PREDIX study: T-DM1 vs. docetaxel plus trastuzumab plus pertuzumab [DTP] for six cycles); and 502 (HER2 heterogeneity as a predictor of response) addressed the potential for the antibody-drug conjugate to replace standard preoperative cytotoxic chemotherapy plus HER2-targeting.
In PREDIX, it was anticipated that toxicity would be lower with T-DM1 than with DTP – and it was, with better quality of life scores. The authors found a pathologic complete response rate of 45% among 98 participants with stage IIA-IIIA HER2-positive breast cancer, with higher rates among hormone receptor–negative than hormone receptor–positive patients, as expected.
PREDIX patients were allowed to switch from T-DM1 to DTP for progression, lack of clinical/radiographic response, or toxicity. More than twice as many patients switched from DTP to T-DM1 than vice versa for progression or lack of response.
What this means in practice
Although neither DTP nor T-DM1 are National Comprehensive Cancer Network guideline-endorsed neoadjuvant regimens at present, the KRISTINE and PREDIX trials and Abstract 502 advance the discussion about further personalizing therapy for HER2-amplified breast cancer with high HER2 copy number and lack of intratumor heterogeneity for HER2. They also raise questions about de-escalating therapy for patients with good prognosis and HER2-positive cancers, and the creative use of T-DM1 in the neoadjuvant setting.
Neoadjuvant T-DM1 may not be standard of care yet, but watch this space.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I will treat my next patient,” I take a look at two “chemo-free” neoadjuvant studies reported at the annual meeting of the American Society of Clinical Oncology. One summarizes the potential utility of immune checkpoint inhibitors (ICIs) in non–small cell lung cancer (NSCLC) patients who are – or can become – candidates for curative resection and the other highlights the potential utility of neoadjuvant trastuzumab emtansine (T-DM1) for HER2-positive breast cancer patients.
NEOSTAR in NSCLC
With the accumulation of comorbid conditions in an aging population, we all see NSCLC patients who are potential candidates for curative surgery, but for whom we have concerns about standard preoperative chemotherapy plus or minus radiation. At ASCO 2019, abstracts 8503 (atezolizumab, the LCMC3 trial) and 8504 (nivolumab plus or minus ipilimumab, NEOSTAR) addressed the neoadjuvant use of ICIs. I will focus on NEOSTAR, because the major pathologic response (mPR) rate – reduction in viable tumor cells to 10% or less – was higher with the combination of nivolumab plus ipilimumab in NEOSTAR than with single agent nivolumab or atezolizumab in the NEOSTAR or LCMC3 trials, respectively.
Briefly, 44 patients with stage I-IIIA NSCLC were randomized to nivolumab plus or minus ipilimumab. In total, 93% completed 6 weeks of neoadjuvant therapy and 89% were resected. The mPR rate was 33% with nivolumab plus ipilimumab (about twice as high as with nivolumab alone in NEOSTAR or atezolizumab in LCMC3).
Among resected patients, nivolumab plus ipilimumab had a 44% mPR rate and a pathologic complete response rate of 38%. Although RECIST (Response Evaluation Criteria in Solid Tumors) responses were more likely in patients who had an mPR, 11% of patients had radiographic “nodal immune flare” because of noncaseating granulomas in regional (or nonregional) nodes. Elevated baseline programmed death-ligand 1 was associated with a higher rate of mPR. Surgical complications seemed similar to expectations – 1 bronchopleural fistula and 8 air leaks among the 39 resected patients.
What this means in practice
Although the mPR endpoint has no validated association with survival and the studies were relatively small, neoadjuvant use of ICIs in patients for whom tolerance to standard chemotherapy plus or minus radiation might be problematic is attractive – especially in view of the reality of an approximately 50% relapse rate after surgical resection with standard therapy.
If I had a potential candidate for neoadjuvant ICI therapy – especially one with a high proportion of cells with PD-L1 or someone with an equivocal distant metastasis on a preoperative PET-CT – I would consider using an ICI as given in LCMC3 or NEOSTAR.
PREDIX in HER2-positive breast cancer
As Mark Pegram, MD, of Stanford (Calif.) University suggested in his discussion at the local/regional/adjuvant breast cancer session at ASCO 2019, the goal of HER2-targeted therapy was originally that it could replace – not supplement – the use of cytotoxic chemotherapy.
Abstracts 500 (the KRISTINE trial: neoadjuvant T-DM1 plus pertuzumab vs. docetaxel, carboplatin, and trastuzumab plus pertuzumab); 501 (the PREDIX study: T-DM1 vs. docetaxel plus trastuzumab plus pertuzumab [DTP] for six cycles); and 502 (HER2 heterogeneity as a predictor of response) addressed the potential for the antibody-drug conjugate to replace standard preoperative cytotoxic chemotherapy plus HER2-targeting.
In PREDIX, it was anticipated that toxicity would be lower with T-DM1 than with DTP – and it was, with better quality of life scores. The authors found a pathologic complete response rate of 45% among 98 participants with stage IIA-IIIA HER2-positive breast cancer, with higher rates among hormone receptor–negative than hormone receptor–positive patients, as expected.
PREDIX patients were allowed to switch from T-DM1 to DTP for progression, lack of clinical/radiographic response, or toxicity. More than twice as many patients switched from DTP to T-DM1 than vice versa for progression or lack of response.
What this means in practice
Although neither DTP nor T-DM1 are National Comprehensive Cancer Network guideline-endorsed neoadjuvant regimens at present, the KRISTINE and PREDIX trials and Abstract 502 advance the discussion about further personalizing therapy for HER2-amplified breast cancer with high HER2 copy number and lack of intratumor heterogeneity for HER2. They also raise questions about de-escalating therapy for patients with good prognosis and HER2-positive cancers, and the creative use of T-DM1 in the neoadjuvant setting.
Neoadjuvant T-DM1 may not be standard of care yet, but watch this space.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
Novel chip system could improve preclinical drug studies
A novel multiorgan body-on-a-chip system shows promise to improve the preclinical evaluation of various anticancer therapies, investigators report.
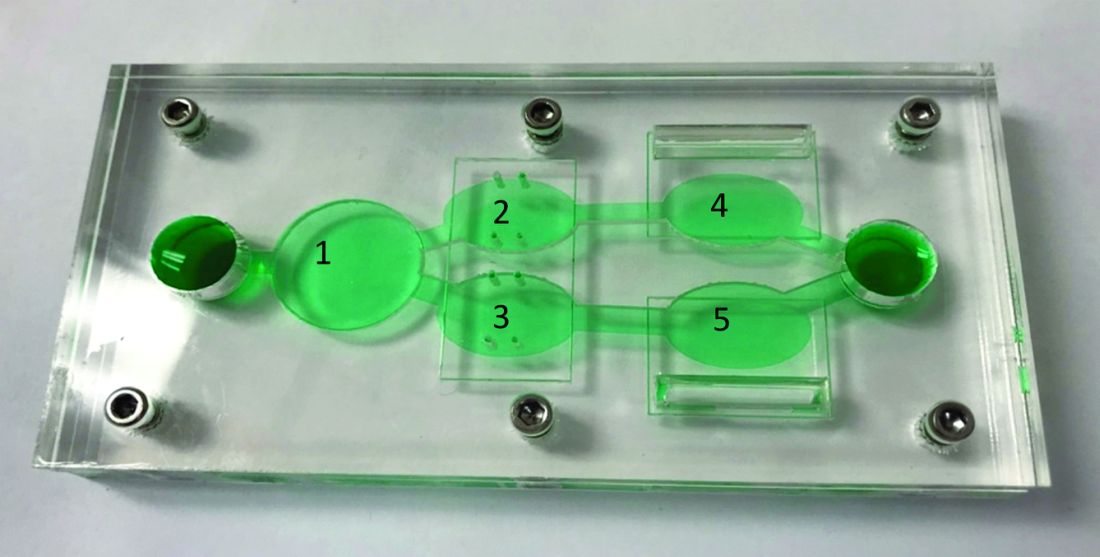
“Initially, organ-on-a-chip systems were designed for specific applications with limited ability for reconfiguration and typically with cells from a single organ,” wrote Christopher W. McAleer, PhD, of Hesperos Inc., Orlando, and colleagues. Their report is in Science Translational Medicine.
“To address these issues, a reconfigurable body-on-a-chip system was developed with the capacity to house multiple organ-like tissue constructs,” the authors explained.
The researchers used two different system configurations to evaluate the off-target organ toxicities, metabolism, and efficacy of diclofenac and imatinib (system 1), in addition to tamoxifen (system 2). Both therapies were combined with verapamil in the study.
In system 1, cancer-derived bone marrow cells were cultured with primary hepatocytes, and were analyzed for anti-leukemic activity. In this configuration, both imatinib and diclofenac showed cytostatic activity on cancer progression in the bone marrow cells.
“Liver viability was not affected by imatinib; however, diclofenac reduced liver viability by 30%,” the researchers wrote.
System 2 included a wide variety of cell-lines, including primary hepatocytes, induced pluripotent stem cell-derived cardiomyocytes, a multidrug-resistant vulva cancer line, and a non-multidrug-resistant breast cancer line.
In this configuration, tamoxifen monotherapy and tamoxifen coadministered with verapamil resulted in off-target cardiac toxicities, but did not alter cell viability.
“These systems demonstrate the utility of a human cell–based in vitro culture system to evaluate both on-target efficacy and off-target toxicity for parent drugs and their metabolites,” Dr. McAleer and colleagues wrote.
The researchers acknowledged that the dosing parameters used in the model were acute. As a result, chronic, low-dose treatment strategies may reflect clinical conditions more accurately.
“These systems can augment and reduce the use of animals and increase the efficiency of drug evaluations in preclinical studies,” they concluded.
The study was supported by Hesperos Internal Development funds, the NIH, and Roche. The authors reported financial affiliations with Hesperos and Roche.
SOURCE: McAleer CW et al. Sci Transl Med. 2019 Jun 19. doi: 10.1126/scitranslmed.aav1386.
A novel multiorgan body-on-a-chip system shows promise to improve the preclinical evaluation of various anticancer therapies, investigators report.
“Initially, organ-on-a-chip systems were designed for specific applications with limited ability for reconfiguration and typically with cells from a single organ,” wrote Christopher W. McAleer, PhD, of Hesperos Inc., Orlando, and colleagues. Their report is in Science Translational Medicine.
“To address these issues, a reconfigurable body-on-a-chip system was developed with the capacity to house multiple organ-like tissue constructs,” the authors explained.
The researchers used two different system configurations to evaluate the off-target organ toxicities, metabolism, and efficacy of diclofenac and imatinib (system 1), in addition to tamoxifen (system 2). Both therapies were combined with verapamil in the study.
In system 1, cancer-derived bone marrow cells were cultured with primary hepatocytes, and were analyzed for anti-leukemic activity. In this configuration, both imatinib and diclofenac showed cytostatic activity on cancer progression in the bone marrow cells.
“Liver viability was not affected by imatinib; however, diclofenac reduced liver viability by 30%,” the researchers wrote.
System 2 included a wide variety of cell-lines, including primary hepatocytes, induced pluripotent stem cell-derived cardiomyocytes, a multidrug-resistant vulva cancer line, and a non-multidrug-resistant breast cancer line.
In this configuration, tamoxifen monotherapy and tamoxifen coadministered with verapamil resulted in off-target cardiac toxicities, but did not alter cell viability.
“These systems demonstrate the utility of a human cell–based in vitro culture system to evaluate both on-target efficacy and off-target toxicity for parent drugs and their metabolites,” Dr. McAleer and colleagues wrote.
The researchers acknowledged that the dosing parameters used in the model were acute. As a result, chronic, low-dose treatment strategies may reflect clinical conditions more accurately.
“These systems can augment and reduce the use of animals and increase the efficiency of drug evaluations in preclinical studies,” they concluded.
The study was supported by Hesperos Internal Development funds, the NIH, and Roche. The authors reported financial affiliations with Hesperos and Roche.
SOURCE: McAleer CW et al. Sci Transl Med. 2019 Jun 19. doi: 10.1126/scitranslmed.aav1386.
A novel multiorgan body-on-a-chip system shows promise to improve the preclinical evaluation of various anticancer therapies, investigators report.
“Initially, organ-on-a-chip systems were designed for specific applications with limited ability for reconfiguration and typically with cells from a single organ,” wrote Christopher W. McAleer, PhD, of Hesperos Inc., Orlando, and colleagues. Their report is in Science Translational Medicine.
“To address these issues, a reconfigurable body-on-a-chip system was developed with the capacity to house multiple organ-like tissue constructs,” the authors explained.
The researchers used two different system configurations to evaluate the off-target organ toxicities, metabolism, and efficacy of diclofenac and imatinib (system 1), in addition to tamoxifen (system 2). Both therapies were combined with verapamil in the study.
In system 1, cancer-derived bone marrow cells were cultured with primary hepatocytes, and were analyzed for anti-leukemic activity. In this configuration, both imatinib and diclofenac showed cytostatic activity on cancer progression in the bone marrow cells.
“Liver viability was not affected by imatinib; however, diclofenac reduced liver viability by 30%,” the researchers wrote.
System 2 included a wide variety of cell-lines, including primary hepatocytes, induced pluripotent stem cell-derived cardiomyocytes, a multidrug-resistant vulva cancer line, and a non-multidrug-resistant breast cancer line.
In this configuration, tamoxifen monotherapy and tamoxifen coadministered with verapamil resulted in off-target cardiac toxicities, but did not alter cell viability.
“These systems demonstrate the utility of a human cell–based in vitro culture system to evaluate both on-target efficacy and off-target toxicity for parent drugs and their metabolites,” Dr. McAleer and colleagues wrote.
The researchers acknowledged that the dosing parameters used in the model were acute. As a result, chronic, low-dose treatment strategies may reflect clinical conditions more accurately.
“These systems can augment and reduce the use of animals and increase the efficiency of drug evaluations in preclinical studies,” they concluded.
The study was supported by Hesperos Internal Development funds, the NIH, and Roche. The authors reported financial affiliations with Hesperos and Roche.
SOURCE: McAleer CW et al. Sci Transl Med. 2019 Jun 19. doi: 10.1126/scitranslmed.aav1386.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point: A novel multiorgan body-on-a-chip system shows promise to improve the preclinical evaluation of anticancer therapies.
Major finding: Overall, results support the utility of the system to assess both off-target toxicity and on-target efficacy for various anticancer drugs.
Study details: A study exploring the utility of a multi-organ-on-a-chip system to assess safety and effectiveness of anticancer therapies in the preclinical setting.
Disclosures: The study was supported by Hesperos Internal Development funds, the NIH, and Roche. The authors reported financial affiliations with Hesperos and Roche.
Source: McAleer CW et al. Sci Transl Med. 2019 Jun 19. doi: 10.1126/scitranslmed.aav1386.
PALOMA-3 biomarker analysis: Liquid biopsy could ID progression risk
CHICAGO – Tumor protein 53 (TP53) mutation, fibroblast growth factor receptor 1 (FGFR1) amplification, and tumor purity in plasma each predict early progression on palbociclib and/or fulvestrant in patients with advanced estrogen receptor–positive (ER+) breast cancer, according to genomic analyses of PALOMA-3 trial data.

Overall, the presence of one or more of these genomic changes identified 131 out of 310 patients from the phase 3 trial who had baseline samples available, Ben O’Leary, MBBS, said at the annual meeting of the American Society of Clinical Oncology.
“So, a significant minority of patients – 42.3% – potentially who fall into a more poor-prognosis group,” said Dr. O’Leary of the Institute of Cancer Research at the Royal Marsden Hospital in London.
The findings suggest that a “liquid biopsy” at the start of treatment could identify patients at risk for progression.
The PALOMA-3 trial randomized 521 patients with ER+, human epidermal growth factor receptor 2 (HER2)–negative advanced breast cancer who had previously progressed on endocrine therapy 2:1 to CDK4/CDK6 inhibition with palbociclib plus fulvestrant (P+F) or placebo plus fulvestrant (F), and it showed that adding palbociclib significantly improved progression-free survival (PFS) (N Engl J Med. Jul 16 2015;373:209-19).
For the current analysis, the investigators assessed circulating tumor DNA (ctDNA) in baseline plasma samples from 459 study participants in an effort to identify genomic biomarkers for progression, to examine the association between baseline tumor fraction and clinical outcome, and to explore differences in predictive markers by treatment arm. A custom amplicon-sequencing analysis was performed to look for mutations in 17 different relevant genes, and another was used to estimate tumor fraction by looking at about 800 common germline single-nucleotide polymorphisms and to assess copy-number gain in the amplification status in 11 different genes, Dr. O’Leary said.
Results for mutations and circulating nucleic acids were available in 203 and 107 patients from the P+F and F groups, respectively, and on multivariable analysis of all 310 patients (including palbociclib as a variable in the model and with ctDNA fraction as a continuous variable), higher baseline tumor purity in plasma was associated with highly significantly worse PFS (HR 1.2 per 10% increase in purity), and baseline TP53 mutation and FGFR1 amplification each were associated with significantly shorter PFS (HRs, 1.8 and 2.9, respectively).
“[It is] very important to note ... that we did look specifically for interaction between our genomic changes and treatment, and we didn’t find any evidence of a significant interaction, so these genomic markers [are] prognostic rather than predictive in terms of the two treatment arms of the trial,” he said.
A survival analysis showed a median PFS of 3.7 vs. 12.7 months in patients with vs. without TP53 mutation in the P+F arm, and 1.8 vs. 5.4 months, respectively, in the F arm, with similar HRs of 2.0 and 2.3 in the arms, respectively.
“Even in the [P+F] arm, you see almost half of the patients with a TP53 mutation ... have relapsed by 2 months, the earliest clinical assessment in the trial,” he noted.
For FGFR1, the PFS was 3.9 vs. 12 months with vs. without amplification in the P+F arms, and 1.8 vs. 5.8 months, respectively in th F arm, with HRs of 3.4 and 3.6, respectively.
These findings are notable because markers of early progression on endocrine therapy in combination with CDK4/6 inhibitors remain limited – despite the key role of these combinations in treating ER+ advanced breast cancer, Dr. O’Leary explained.
“Although many patients derive a great deal of benefit from these combinations, there are a subset of patients who will relapse relatively early, and ... we don’t have an established means of identifying those patients at the present,” he said. “From the technical perspective, liquid biopsies have emerged in recent years as a promising means of genotyping patients’ cancers from circulating tumor DNA, and in addition, the overall level of circulating tumor DNA – the fractional purity – has been associated with poor prognosis, specifically in the triple-negative breast cancer setting.”
The results, which require independent validation, could potentially inform future clinical trials of CDK4/6 inhibitor combinations in advanced ER+ breast cancer to identify a high-risk group of patients who require escalation of therapy, he concluded.
Dr. O’Leary reported receiving research funding from Pfizer to his institution.
SOURCE: O’Leary B et al. ASCO 2019, Abstract 1010.
CHICAGO – Tumor protein 53 (TP53) mutation, fibroblast growth factor receptor 1 (FGFR1) amplification, and tumor purity in plasma each predict early progression on palbociclib and/or fulvestrant in patients with advanced estrogen receptor–positive (ER+) breast cancer, according to genomic analyses of PALOMA-3 trial data.
Overall, the presence of one or more of these genomic changes identified 131 out of 310 patients from the phase 3 trial who had baseline samples available, Ben O’Leary, MBBS, said at the annual meeting of the American Society of Clinical Oncology.
“So, a significant minority of patients – 42.3% – potentially who fall into a more poor-prognosis group,” said Dr. O’Leary of the Institute of Cancer Research at the Royal Marsden Hospital in London.
The findings suggest that a “liquid biopsy” at the start of treatment could identify patients at risk for progression.
The PALOMA-3 trial randomized 521 patients with ER+, human epidermal growth factor receptor 2 (HER2)–negative advanced breast cancer who had previously progressed on endocrine therapy 2:1 to CDK4/CDK6 inhibition with palbociclib plus fulvestrant (P+F) or placebo plus fulvestrant (F), and it showed that adding palbociclib significantly improved progression-free survival (PFS) (N Engl J Med. Jul 16 2015;373:209-19).
For the current analysis, the investigators assessed circulating tumor DNA (ctDNA) in baseline plasma samples from 459 study participants in an effort to identify genomic biomarkers for progression, to examine the association between baseline tumor fraction and clinical outcome, and to explore differences in predictive markers by treatment arm. A custom amplicon-sequencing analysis was performed to look for mutations in 17 different relevant genes, and another was used to estimate tumor fraction by looking at about 800 common germline single-nucleotide polymorphisms and to assess copy-number gain in the amplification status in 11 different genes, Dr. O’Leary said.
Results for mutations and circulating nucleic acids were available in 203 and 107 patients from the P+F and F groups, respectively, and on multivariable analysis of all 310 patients (including palbociclib as a variable in the model and with ctDNA fraction as a continuous variable), higher baseline tumor purity in plasma was associated with highly significantly worse PFS (HR 1.2 per 10% increase in purity), and baseline TP53 mutation and FGFR1 amplification each were associated with significantly shorter PFS (HRs, 1.8 and 2.9, respectively).
“[It is] very important to note ... that we did look specifically for interaction between our genomic changes and treatment, and we didn’t find any evidence of a significant interaction, so these genomic markers [are] prognostic rather than predictive in terms of the two treatment arms of the trial,” he said.
A survival analysis showed a median PFS of 3.7 vs. 12.7 months in patients with vs. without TP53 mutation in the P+F arm, and 1.8 vs. 5.4 months, respectively, in the F arm, with similar HRs of 2.0 and 2.3 in the arms, respectively.
“Even in the [P+F] arm, you see almost half of the patients with a TP53 mutation ... have relapsed by 2 months, the earliest clinical assessment in the trial,” he noted.
For FGFR1, the PFS was 3.9 vs. 12 months with vs. without amplification in the P+F arms, and 1.8 vs. 5.8 months, respectively in th F arm, with HRs of 3.4 and 3.6, respectively.
These findings are notable because markers of early progression on endocrine therapy in combination with CDK4/6 inhibitors remain limited – despite the key role of these combinations in treating ER+ advanced breast cancer, Dr. O’Leary explained.
“Although many patients derive a great deal of benefit from these combinations, there are a subset of patients who will relapse relatively early, and ... we don’t have an established means of identifying those patients at the present,” he said. “From the technical perspective, liquid biopsies have emerged in recent years as a promising means of genotyping patients’ cancers from circulating tumor DNA, and in addition, the overall level of circulating tumor DNA – the fractional purity – has been associated with poor prognosis, specifically in the triple-negative breast cancer setting.”
The results, which require independent validation, could potentially inform future clinical trials of CDK4/6 inhibitor combinations in advanced ER+ breast cancer to identify a high-risk group of patients who require escalation of therapy, he concluded.
Dr. O’Leary reported receiving research funding from Pfizer to his institution.
SOURCE: O’Leary B et al. ASCO 2019, Abstract 1010.
CHICAGO – Tumor protein 53 (TP53) mutation, fibroblast growth factor receptor 1 (FGFR1) amplification, and tumor purity in plasma each predict early progression on palbociclib and/or fulvestrant in patients with advanced estrogen receptor–positive (ER+) breast cancer, according to genomic analyses of PALOMA-3 trial data.
Overall, the presence of one or more of these genomic changes identified 131 out of 310 patients from the phase 3 trial who had baseline samples available, Ben O’Leary, MBBS, said at the annual meeting of the American Society of Clinical Oncology.
“So, a significant minority of patients – 42.3% – potentially who fall into a more poor-prognosis group,” said Dr. O’Leary of the Institute of Cancer Research at the Royal Marsden Hospital in London.
The findings suggest that a “liquid biopsy” at the start of treatment could identify patients at risk for progression.
The PALOMA-3 trial randomized 521 patients with ER+, human epidermal growth factor receptor 2 (HER2)–negative advanced breast cancer who had previously progressed on endocrine therapy 2:1 to CDK4/CDK6 inhibition with palbociclib plus fulvestrant (P+F) or placebo plus fulvestrant (F), and it showed that adding palbociclib significantly improved progression-free survival (PFS) (N Engl J Med. Jul 16 2015;373:209-19).
For the current analysis, the investigators assessed circulating tumor DNA (ctDNA) in baseline plasma samples from 459 study participants in an effort to identify genomic biomarkers for progression, to examine the association between baseline tumor fraction and clinical outcome, and to explore differences in predictive markers by treatment arm. A custom amplicon-sequencing analysis was performed to look for mutations in 17 different relevant genes, and another was used to estimate tumor fraction by looking at about 800 common germline single-nucleotide polymorphisms and to assess copy-number gain in the amplification status in 11 different genes, Dr. O’Leary said.
Results for mutations and circulating nucleic acids were available in 203 and 107 patients from the P+F and F groups, respectively, and on multivariable analysis of all 310 patients (including palbociclib as a variable in the model and with ctDNA fraction as a continuous variable), higher baseline tumor purity in plasma was associated with highly significantly worse PFS (HR 1.2 per 10% increase in purity), and baseline TP53 mutation and FGFR1 amplification each were associated with significantly shorter PFS (HRs, 1.8 and 2.9, respectively).
“[It is] very important to note ... that we did look specifically for interaction between our genomic changes and treatment, and we didn’t find any evidence of a significant interaction, so these genomic markers [are] prognostic rather than predictive in terms of the two treatment arms of the trial,” he said.
A survival analysis showed a median PFS of 3.7 vs. 12.7 months in patients with vs. without TP53 mutation in the P+F arm, and 1.8 vs. 5.4 months, respectively, in the F arm, with similar HRs of 2.0 and 2.3 in the arms, respectively.
“Even in the [P+F] arm, you see almost half of the patients with a TP53 mutation ... have relapsed by 2 months, the earliest clinical assessment in the trial,” he noted.
For FGFR1, the PFS was 3.9 vs. 12 months with vs. without amplification in the P+F arms, and 1.8 vs. 5.8 months, respectively in th F arm, with HRs of 3.4 and 3.6, respectively.
These findings are notable because markers of early progression on endocrine therapy in combination with CDK4/6 inhibitors remain limited – despite the key role of these combinations in treating ER+ advanced breast cancer, Dr. O’Leary explained.
“Although many patients derive a great deal of benefit from these combinations, there are a subset of patients who will relapse relatively early, and ... we don’t have an established means of identifying those patients at the present,” he said. “From the technical perspective, liquid biopsies have emerged in recent years as a promising means of genotyping patients’ cancers from circulating tumor DNA, and in addition, the overall level of circulating tumor DNA – the fractional purity – has been associated with poor prognosis, specifically in the triple-negative breast cancer setting.”
The results, which require independent validation, could potentially inform future clinical trials of CDK4/6 inhibitor combinations in advanced ER+ breast cancer to identify a high-risk group of patients who require escalation of therapy, he concluded.
Dr. O’Leary reported receiving research funding from Pfizer to his institution.
SOURCE: O’Leary B et al. ASCO 2019, Abstract 1010.
REPORTING FROM ASCO 2019
Niraparib-pembrolizumab combo finds niche in breast, ovarian cancers
The strategy of simultaneously exploiting deficient DNA damage repair and unleashing the immune response could expand treatment options for hard-to-treat breast and ovarian cancers, findings of the TOPACIO/KEYNOTE-162 trial suggest.
Triple-negative breast cancer (TNBC) and high-grade serous ovarian carcinoma share a number of genomic features, including a high frequency of BRCA1 and BRCA2 inactivation (Nature. 2012;490:61-70), as well as potential immunoreactivity (Lancet Oncol. 2018;19:40-50).
The open-label, single-arm phase 1/2 trial therefore tested the combination of niraparib (Zejula), an oral poly (ADP-ribose) polymerase (PARP) inhibitor, and pembrolizumab (Keytruda), an antibody to programmed death 1 (PD-1), among more than 100 patients with advanced or metastatic TNBC or recurrent platinum-resistant ovarian carcinoma. Patients were enrolled irrespective of BRCA mutation status or programmed death-ligand 1 (PD-L1) expression.
Main results, reported in JAMA Oncology, showed that the combination was safe, and about a fifth of patients with each type of cancer had an objective response. Median progression-free survival (PFS) was about 2 months in those with TNBC overall (although it exceeded 8 months in the subset with a tumor BRCA mutation) and about 3 months in those with ovarian cancer.
TNBC cohort
Investigators led by Shaveta Vinayak, MD, of the division of oncology at Fred Hutchinson Cancer Research Center, and University of Washington School of Medicine, Seattle Cancer Care Alliance, Seattle, studied 55 patients with TNBC treated with niraparib-pembrolizumab in the trial.
In the efficacy-evaluable population of 47 patients, the objective response rate (ORR) was 21%, and the disease control rate (DCR) was 49%. With a median duration of follow-up of 14.8 months, the median duration of response was not reached.
Activity of the combination varied by tumor BRCA mutation status. Compared with counterparts having BRCA wild-type tumors, patients having tumors with BRCA mutations had a numerically higher ORR (47% vs. 11%), DCR (80% vs. 33%), and PFS (8.3 vs. 2.1 months).
Some 18% of patients had treatment-related anemia, 15% thrombocytopenia, and 7% fatigue. In addition, 15% of patients had immune-related adverse events, with 4% having grade 3 immune-related adverse events.
“Combination niraparib plus pembrolizumab provides promising antitumor activity in patients with advanced or metastatic TNBC, with numerically higher response rates in those with tumor BRCA mutations,” Dr. Vinayak and colleagues conclude. “The combination therapy was safe with a tolerable safety profile, warranting further investigation.”
Ovarian cancer cohort
Investigators led by Panagiotis A. Konstantinopoulos, MD, PhD, of the division of gynecologic oncology, department of medical oncology at Dana-Farber Cancer Institute, Harvard Medical School, Boston, studied 62 patients with ovarian carcinoma treated with niraparib-pembrolizumab in the trial.
In the efficacy-evaluable population of 60 patients, the ORR was 18% and the DCR was 65%. The ORRs were similar regardless of patients’ platinum-based chemotherapy sensitivity, previous bevacizumab treatment, or tumor BRCA or homologous recombination deficiency (HRD) biomarker status.
With a median duration of follow-up of 12.4 months, the median duration of response was not reached, ranging from 4.2 to roughly 14.5 months. Median progression-free survival was 3.4 months.
The leading treatment-related adverse events of grade 3 or higher in this cohort were anemia (21%) and thrombocytopenia (9%). In addition, 19% of patients had immune-related adverse events, with 9% having grade 3 or higher immune-related adverse events.
“Niraparib in combination with pembrolizumab is tolerable, with promising antitumor activity for patients with ovarian carcinoma who have limited treatment options regardless of platinum status, biomarker status, or prior treatment with bevacizumab,” Dr. Konstantinopoulos and colleagues conclude. “Responses in patients without tumor BRCA mutations or non-HRD cancers were higher than expected with either agent as monotherapy.”
Dr. Vinayak disclosed receiving clinical trial funding from TESARO; serving on an advisory board for TESARO; and serving on an advisory board for OncoSec Medical (uncompensated). Dr. Konstantinopoulos disclosed serving on advisory boards for AstraZeneca, Pfizer, and Merck. The trial was supported by TESARO: a GSK company and Merck, and in part by Stand Up to Cancer (a program of the Entertainment Industry Foundation); the Ovarian Cancer Research Fund Alliance; and National Ovarian Cancer Coalition Dream Team Translational Research.
SOURCE: Vinayak A et al. JAMA Oncol. 2019 Jun 13. doi: 10.1001/jamaoncol.2019.1029. Konstantinopoulos PA et al. JAMA Oncol. 2019 Jun 13. doi: 10.1001/jamaoncol.2019.1048.
“Targeting DNA repair and immune checkpoint pathways has emerged as an important concept in cancer therapy, well supported by preclinical and clinical data in ovarian cancer and TNBC. However, there are some limitations to the two studies presented herein,” maintain editorialists Kunle Odunsi, MD, PhD, and Tanja Pejovic, MD, PhD.
Patients varied considerably with respect to number of prior chemotherapy regimens, they elaborate. Also, there may have been some misclassification of patients into DNA damage repair (DDR) groups, and small sample sizes precluded rigorous subgroup analyses.
“Because DDR and, by extension, tumor mutational burden and PD-L1 status do not fully explain the effects of the combination of PARP inhibitors and anti–PD-1 therapy, additional predictive biomarkers based on tumor intrinsic or adaptive mechanisms of resistance are needed for both cancer types,” the editorialists contend. In particular, knowledge of the tumor microenvironment could be used to tailor therapy for individual patients.
“The TOPACIO clinical studies are clearly steps in the right direction for patients with [platinum-resistant ovarian carcinoma] and TNBC,” they conclude. “However, larger confirmatory randomized clinical trials are needed that use panels of integrated biomarkers that would allow identification of patients most likely to respond.”
Dr. Odunsi is the deputy director and chair of the department of gynecologic oncology, executive director of the Center for Immunotherapy, and co-leader of the Tumor Immunology and Immunotherapy Research Program–Roswell Park Comprehensive Cancer Center, Buffalo, N.Y. Dr. Pejovic is associate professor, division of gynecologic oncology, department of obstetrics & gynecology, Knight Cancer Institute, Oregon Health & Science University, Portland, Ore. These remarks are adapted from a related editorial (JAMA Oncol. 2019 Jun 13. doi: 10.1001/jamaoncol.2019.1009 ).
“Targeting DNA repair and immune checkpoint pathways has emerged as an important concept in cancer therapy, well supported by preclinical and clinical data in ovarian cancer and TNBC. However, there are some limitations to the two studies presented herein,” maintain editorialists Kunle Odunsi, MD, PhD, and Tanja Pejovic, MD, PhD.
Patients varied considerably with respect to number of prior chemotherapy regimens, they elaborate. Also, there may have been some misclassification of patients into DNA damage repair (DDR) groups, and small sample sizes precluded rigorous subgroup analyses.
“Because DDR and, by extension, tumor mutational burden and PD-L1 status do not fully explain the effects of the combination of PARP inhibitors and anti–PD-1 therapy, additional predictive biomarkers based on tumor intrinsic or adaptive mechanisms of resistance are needed for both cancer types,” the editorialists contend. In particular, knowledge of the tumor microenvironment could be used to tailor therapy for individual patients.
“The TOPACIO clinical studies are clearly steps in the right direction for patients with [platinum-resistant ovarian carcinoma] and TNBC,” they conclude. “However, larger confirmatory randomized clinical trials are needed that use panels of integrated biomarkers that would allow identification of patients most likely to respond.”
Dr. Odunsi is the deputy director and chair of the department of gynecologic oncology, executive director of the Center for Immunotherapy, and co-leader of the Tumor Immunology and Immunotherapy Research Program–Roswell Park Comprehensive Cancer Center, Buffalo, N.Y. Dr. Pejovic is associate professor, division of gynecologic oncology, department of obstetrics & gynecology, Knight Cancer Institute, Oregon Health & Science University, Portland, Ore. These remarks are adapted from a related editorial (JAMA Oncol. 2019 Jun 13. doi: 10.1001/jamaoncol.2019.1009 ).
“Targeting DNA repair and immune checkpoint pathways has emerged as an important concept in cancer therapy, well supported by preclinical and clinical data in ovarian cancer and TNBC. However, there are some limitations to the two studies presented herein,” maintain editorialists Kunle Odunsi, MD, PhD, and Tanja Pejovic, MD, PhD.
Patients varied considerably with respect to number of prior chemotherapy regimens, they elaborate. Also, there may have been some misclassification of patients into DNA damage repair (DDR) groups, and small sample sizes precluded rigorous subgroup analyses.
“Because DDR and, by extension, tumor mutational burden and PD-L1 status do not fully explain the effects of the combination of PARP inhibitors and anti–PD-1 therapy, additional predictive biomarkers based on tumor intrinsic or adaptive mechanisms of resistance are needed for both cancer types,” the editorialists contend. In particular, knowledge of the tumor microenvironment could be used to tailor therapy for individual patients.
“The TOPACIO clinical studies are clearly steps in the right direction for patients with [platinum-resistant ovarian carcinoma] and TNBC,” they conclude. “However, larger confirmatory randomized clinical trials are needed that use panels of integrated biomarkers that would allow identification of patients most likely to respond.”
Dr. Odunsi is the deputy director and chair of the department of gynecologic oncology, executive director of the Center for Immunotherapy, and co-leader of the Tumor Immunology and Immunotherapy Research Program–Roswell Park Comprehensive Cancer Center, Buffalo, N.Y. Dr. Pejovic is associate professor, division of gynecologic oncology, department of obstetrics & gynecology, Knight Cancer Institute, Oregon Health & Science University, Portland, Ore. These remarks are adapted from a related editorial (JAMA Oncol. 2019 Jun 13. doi: 10.1001/jamaoncol.2019.1009 ).
The strategy of simultaneously exploiting deficient DNA damage repair and unleashing the immune response could expand treatment options for hard-to-treat breast and ovarian cancers, findings of the TOPACIO/KEYNOTE-162 trial suggest.
Triple-negative breast cancer (TNBC) and high-grade serous ovarian carcinoma share a number of genomic features, including a high frequency of BRCA1 and BRCA2 inactivation (Nature. 2012;490:61-70), as well as potential immunoreactivity (Lancet Oncol. 2018;19:40-50).
The open-label, single-arm phase 1/2 trial therefore tested the combination of niraparib (Zejula), an oral poly (ADP-ribose) polymerase (PARP) inhibitor, and pembrolizumab (Keytruda), an antibody to programmed death 1 (PD-1), among more than 100 patients with advanced or metastatic TNBC or recurrent platinum-resistant ovarian carcinoma. Patients were enrolled irrespective of BRCA mutation status or programmed death-ligand 1 (PD-L1) expression.
Main results, reported in JAMA Oncology, showed that the combination was safe, and about a fifth of patients with each type of cancer had an objective response. Median progression-free survival (PFS) was about 2 months in those with TNBC overall (although it exceeded 8 months in the subset with a tumor BRCA mutation) and about 3 months in those with ovarian cancer.
TNBC cohort
Investigators led by Shaveta Vinayak, MD, of the division of oncology at Fred Hutchinson Cancer Research Center, and University of Washington School of Medicine, Seattle Cancer Care Alliance, Seattle, studied 55 patients with TNBC treated with niraparib-pembrolizumab in the trial.
In the efficacy-evaluable population of 47 patients, the objective response rate (ORR) was 21%, and the disease control rate (DCR) was 49%. With a median duration of follow-up of 14.8 months, the median duration of response was not reached.
Activity of the combination varied by tumor BRCA mutation status. Compared with counterparts having BRCA wild-type tumors, patients having tumors with BRCA mutations had a numerically higher ORR (47% vs. 11%), DCR (80% vs. 33%), and PFS (8.3 vs. 2.1 months).
Some 18% of patients had treatment-related anemia, 15% thrombocytopenia, and 7% fatigue. In addition, 15% of patients had immune-related adverse events, with 4% having grade 3 immune-related adverse events.
“Combination niraparib plus pembrolizumab provides promising antitumor activity in patients with advanced or metastatic TNBC, with numerically higher response rates in those with tumor BRCA mutations,” Dr. Vinayak and colleagues conclude. “The combination therapy was safe with a tolerable safety profile, warranting further investigation.”
Ovarian cancer cohort
Investigators led by Panagiotis A. Konstantinopoulos, MD, PhD, of the division of gynecologic oncology, department of medical oncology at Dana-Farber Cancer Institute, Harvard Medical School, Boston, studied 62 patients with ovarian carcinoma treated with niraparib-pembrolizumab in the trial.
In the efficacy-evaluable population of 60 patients, the ORR was 18% and the DCR was 65%. The ORRs were similar regardless of patients’ platinum-based chemotherapy sensitivity, previous bevacizumab treatment, or tumor BRCA or homologous recombination deficiency (HRD) biomarker status.
With a median duration of follow-up of 12.4 months, the median duration of response was not reached, ranging from 4.2 to roughly 14.5 months. Median progression-free survival was 3.4 months.
The leading treatment-related adverse events of grade 3 or higher in this cohort were anemia (21%) and thrombocytopenia (9%). In addition, 19% of patients had immune-related adverse events, with 9% having grade 3 or higher immune-related adverse events.
“Niraparib in combination with pembrolizumab is tolerable, with promising antitumor activity for patients with ovarian carcinoma who have limited treatment options regardless of platinum status, biomarker status, or prior treatment with bevacizumab,” Dr. Konstantinopoulos and colleagues conclude. “Responses in patients without tumor BRCA mutations or non-HRD cancers were higher than expected with either agent as monotherapy.”
Dr. Vinayak disclosed receiving clinical trial funding from TESARO; serving on an advisory board for TESARO; and serving on an advisory board for OncoSec Medical (uncompensated). Dr. Konstantinopoulos disclosed serving on advisory boards for AstraZeneca, Pfizer, and Merck. The trial was supported by TESARO: a GSK company and Merck, and in part by Stand Up to Cancer (a program of the Entertainment Industry Foundation); the Ovarian Cancer Research Fund Alliance; and National Ovarian Cancer Coalition Dream Team Translational Research.
SOURCE: Vinayak A et al. JAMA Oncol. 2019 Jun 13. doi: 10.1001/jamaoncol.2019.1029. Konstantinopoulos PA et al. JAMA Oncol. 2019 Jun 13. doi: 10.1001/jamaoncol.2019.1048.
The strategy of simultaneously exploiting deficient DNA damage repair and unleashing the immune response could expand treatment options for hard-to-treat breast and ovarian cancers, findings of the TOPACIO/KEYNOTE-162 trial suggest.
Triple-negative breast cancer (TNBC) and high-grade serous ovarian carcinoma share a number of genomic features, including a high frequency of BRCA1 and BRCA2 inactivation (Nature. 2012;490:61-70), as well as potential immunoreactivity (Lancet Oncol. 2018;19:40-50).
The open-label, single-arm phase 1/2 trial therefore tested the combination of niraparib (Zejula), an oral poly (ADP-ribose) polymerase (PARP) inhibitor, and pembrolizumab (Keytruda), an antibody to programmed death 1 (PD-1), among more than 100 patients with advanced or metastatic TNBC or recurrent platinum-resistant ovarian carcinoma. Patients were enrolled irrespective of BRCA mutation status or programmed death-ligand 1 (PD-L1) expression.
Main results, reported in JAMA Oncology, showed that the combination was safe, and about a fifth of patients with each type of cancer had an objective response. Median progression-free survival (PFS) was about 2 months in those with TNBC overall (although it exceeded 8 months in the subset with a tumor BRCA mutation) and about 3 months in those with ovarian cancer.
TNBC cohort
Investigators led by Shaveta Vinayak, MD, of the division of oncology at Fred Hutchinson Cancer Research Center, and University of Washington School of Medicine, Seattle Cancer Care Alliance, Seattle, studied 55 patients with TNBC treated with niraparib-pembrolizumab in the trial.
In the efficacy-evaluable population of 47 patients, the objective response rate (ORR) was 21%, and the disease control rate (DCR) was 49%. With a median duration of follow-up of 14.8 months, the median duration of response was not reached.
Activity of the combination varied by tumor BRCA mutation status. Compared with counterparts having BRCA wild-type tumors, patients having tumors with BRCA mutations had a numerically higher ORR (47% vs. 11%), DCR (80% vs. 33%), and PFS (8.3 vs. 2.1 months).
Some 18% of patients had treatment-related anemia, 15% thrombocytopenia, and 7% fatigue. In addition, 15% of patients had immune-related adverse events, with 4% having grade 3 immune-related adverse events.
“Combination niraparib plus pembrolizumab provides promising antitumor activity in patients with advanced or metastatic TNBC, with numerically higher response rates in those with tumor BRCA mutations,” Dr. Vinayak and colleagues conclude. “The combination therapy was safe with a tolerable safety profile, warranting further investigation.”
Ovarian cancer cohort
Investigators led by Panagiotis A. Konstantinopoulos, MD, PhD, of the division of gynecologic oncology, department of medical oncology at Dana-Farber Cancer Institute, Harvard Medical School, Boston, studied 62 patients with ovarian carcinoma treated with niraparib-pembrolizumab in the trial.
In the efficacy-evaluable population of 60 patients, the ORR was 18% and the DCR was 65%. The ORRs were similar regardless of patients’ platinum-based chemotherapy sensitivity, previous bevacizumab treatment, or tumor BRCA or homologous recombination deficiency (HRD) biomarker status.
With a median duration of follow-up of 12.4 months, the median duration of response was not reached, ranging from 4.2 to roughly 14.5 months. Median progression-free survival was 3.4 months.
The leading treatment-related adverse events of grade 3 or higher in this cohort were anemia (21%) and thrombocytopenia (9%). In addition, 19% of patients had immune-related adverse events, with 9% having grade 3 or higher immune-related adverse events.
“Niraparib in combination with pembrolizumab is tolerable, with promising antitumor activity for patients with ovarian carcinoma who have limited treatment options regardless of platinum status, biomarker status, or prior treatment with bevacizumab,” Dr. Konstantinopoulos and colleagues conclude. “Responses in patients without tumor BRCA mutations or non-HRD cancers were higher than expected with either agent as monotherapy.”
Dr. Vinayak disclosed receiving clinical trial funding from TESARO; serving on an advisory board for TESARO; and serving on an advisory board for OncoSec Medical (uncompensated). Dr. Konstantinopoulos disclosed serving on advisory boards for AstraZeneca, Pfizer, and Merck. The trial was supported by TESARO: a GSK company and Merck, and in part by Stand Up to Cancer (a program of the Entertainment Industry Foundation); the Ovarian Cancer Research Fund Alliance; and National Ovarian Cancer Coalition Dream Team Translational Research.
SOURCE: Vinayak A et al. JAMA Oncol. 2019 Jun 13. doi: 10.1001/jamaoncol.2019.1029. Konstantinopoulos PA et al. JAMA Oncol. 2019 Jun 13. doi: 10.1001/jamaoncol.2019.1048.
FROM JAMA ONCOLOGY
TAILORx: Clinical data add value to recurrence score
CHICAGO – , according to a secondary analysis of data from the practice-changing TAILORx study.

Specifically, tumor size and histology-based risk stratification improves the prediction of disease-free survival and distant recurrence, and – for some patient groups – chemotherapy benefit, Joseph A. Sparano, MD, reported at the annual meeting of the American Society of Clinical Oncology.
Combining these tools could help determine whether endocrine therapy (ET) alone or ET with adjuvant chemotherapy is the best treatment approach for a given patient, said Dr. Sparano, professor of medicine and obstetrics, gynecology, and women’s health at Albert Einstein College of Medicine, New York.
The phase 3 TAILORx study established that ET alone is noninferior to adjuvant chemotherapy (CT) plus ET in patients with early breast cancer and RS of 11-25, and that ET alone has some benefit over ET+CT in women aged 50 years and younger with RS of 16-25, he explained.
Those findings were presented at the 2018 ASCO annual meeting and subsequently published in the New England Journal of Medicine.
The current analysis focused on the integration of clinical and genomic features for prognosis, and the results were published online June 3 in a corresponding article in the New England Journal of Medicine.
“The totality of the data, including TAILORx and the prior prospective validation studies, indicate that assessment of genomic risk with the 21-gene recurrence score provides complementary prognostic information to pathologic features, and is also predictive of a large chemotherapy benefit if the recurrence score is greater than 25, or lack thereof if 25 or lower,” he said.
However, there is a three-way interaction between age, RS, and CT use, which results in an absolute CT benefit in women aged 50 or younger of about 2% for RS of 16-20, and about 7% for RS of 21-25, he added.
“Assessment of clinical risk using pathological features also provides prognostic information that doesn’t correlate well with the recurrence score, therefore it stands to reason that integration of clinical and genomic risk offers the potential for greater precision in prognosis and, ultimately, guiding the use of adjuvant therapy,” he said.
Clinical risk for this analysis was assessed using a binary clinical risk categorization employed in the MINDACT trial and calibrated to greater than 92% 10-year breast cancer-specific survival for ET alone based on Adjuvant! version 8.0. Low-grade tumors up to 3 cm, intermediate-grade tumors up to 2 cm, and high-grade tumors up to 1 cm were categorized as low clinical risk (LCR), and all others not meeting these criteria were categorized as high clinical risk (HCR), he explained.
Of 9,427 patients included in the analysis, 70% had LCR and 30% had HCR.
“For distant recurrence, high clinical risk was associated with a 2.5- to 3-fold higher recurrence rate for those with a recurrence score of 11 or higher, and in a multivariate model for distant recurrence in the [group with a] recurrence score of 11-25, high clinical risk was independently associated with a 2.4-fold higher recurrence risk,” he said. “Continuous recurrence score also provided significant prognostic information, with each 1-unit increase associated with an 8% higher distant recurrence risk.”
For the overall population, clinical risk added significant prognostic information to the RS for both distant recurrence and disease-free survival, and stratification by age showed that among women over age 50 years, the hazard ratios for distant recurrence ranged from 2.20 to 2.36, and did not substantially vary by age or RS, he said.
However, for the overall population, adding clinical risk to the RS did not improve prediction of chemotherapy benefit.
“This was also true for the two-thirds of women who were over 50 years of age. For the remaining women 50 or younger, there was a trend favoring chemo, irrespective of clinical risk, though not significant – a finding consistent with the treatment interaction previously described,” he said.
Finally, the absolute differences in 9-year distant recurrence rates by clinical risk stratified by age, RS, and CT use showed an absolute 4%-6% higher distant recurrence risk for HCR vs. LCR among those over age 50 with RS of 0-25 irrespective of CT use, and a 13% difference for those with RS of 26-100 who were treated with CT.
“For those 50 or younger, clinical risk had no impact on recurrence if the RS was 0-10. For RS of 11-25, the difference was about 9% with endocrine therapy alone, and 2% with chemo plus ET, reflecting absolute chemo benefit in younger women who had high clinical risk,” he said, adding that for those with RS of 26-100, there was a 9% higher absolute recurrence rate in the HCR vs. LCR population.
“We therefore further evaluated absolute differences in distance recurrence rates associated with chemotherapy use in women 50 and younger with RS of 16-25, further stratified by RS and clinical risk,” he said, noting that when not stratified by clinical risk, as reported in the primary analysis, the absolute CT benefit was 1.6% for RS of 16-20, and 6.5% for RS of 21-25.
When stratified by clinical risk, the absolute CT benefit ranged from 6% to 9% in those with RS of 21-25, irrespective of clinical risk, and in those with RS of 16-20 and HCR.
“This accounted for 51% of patients with RS of 16-25,” he said. “However, there was no demonstrable chemo benefit for those with LCR and RS of 16-20, who accounted for the remaining 49%.”
Additional analysis looking at age at diagnosis and CT benefit showed a benefit in premenopausal women aged 46-50 years (but not postmenopausal women), a trend toward benefit in those aged 41-45 years, and no benefit in those aged 40 years and younger, who are less likely to develop premature menopause as a consequence of cytotoxic CT.
“In addition, we saw no consistent effect favoring chemotherapy in older women. Taken together, these findings suggest the chemo benefit observed for the RS 16-25 group may, in fact, be due to a castration effect associated with cytotoxic therapy rather than an effect in eradicating micrometastatic disease,” Dr. Sparano said.
Applying this framework to the TAILORx study population categorized 68% of those aged 50 years and younger into a low integrated risk group with less than 5% risk of distant recurrence. This included all patients with RS of 0-10 irrespective of clinical risk (14% of the patient population; distant recurrence rate 1.8% or less), and all with RS of 11-25 and LCR (54% of the patient population, 4.7% distant recurrence rate).
In contrast, 25% fell into the high integrated risk group (greater than 10% distant recurrence risk), including those with RS of 11-25 and HCR (17% of the patient population; distant recurrence rate 12.3%), and RS of 26-100 and HCR (8% of the patient population; distant recurrence rate 15.2%).
“This framework encompasses 93% of all TAILORx subjects, with the remaining 7% having a distant recurrence risk of between 5% and 10%,” he said.
Overall, the primary results of TAILORx remain unchanged based on this secondary analysis as the addition of clinical risk did not predict CT benefit in the RS 11-25 group, he noted.
“However, for women 50 and under and RS 16-25, integrated risk distinguished 50% who derived no chemo benefit from the 50% who derived an absolute benefit of approximately 6%-9% – a level that is higher than an unselected population,” he said, reiterating that the absolute CT benefit was greater in premenopausal women aged 45-50 with RS 16-25, suggesting that the absolute CR benefit seen in younger women in TAILORx may be due to an endocrine effect.
“Integrated risk clearly provides greater prognostic precision and may have clinical utility; the prognostic precision afforded by the integrated risk model is superior to that by the use of clinical or genomic features alone, and in addition, the genomic assay also provides predictive information for chemo benefit that is not captured by clinical features alone,” he concluded.
As an example of the potential clinical utility of this integrated approach for guiding treatment in women aged 50 years or younger, he presented “a highly stratified integrated risk assessment model” separating TAILORx patients into low integrated risk (58% of the study population) and high integrated risk (31% of the study population).
In the low integrated risk patients with RS of 0-10 and any clinical risk level, or with RS of 11-25 and LCR, tamoxifen alone appears adequate, he said.
In those with high integrated risk and RS of 16-25 with HCR, ovarian function suppression plus an aromatase inhibitor (OFS/AI) could be considered as an alternative to chemo, and in those with high integrated risk, RS of 26-100, and HCR who have not developed chemotherapy-induced menopause, ovarian function suppression and an AI could be added to chemotherapy.
“Indeed, data from the SOFT and TEXT trials indicate that patients with a high RS risk experienced an absolute improvement of up to 10%-15% in 5-year breast cancer–free interval with an OFS/AI, compared with tamoxifen, whereas improvement was minimal in those at lowest risk, supporting the strategy of using integrated clinical and genomic risk to select for ovarian function suppression plus an AI,” he said.
During a discussion of the findings and how they might impact practice, Vered Stearns, MD, an oncology professor and codirector of the Breast Cancer Program at Johns Hopkins University, Baltimore, noted that in her practice she will “carefully select women for whom genomic assay [use] is appropriate.
“I will also assess clinical risk and RS to inform recommendations for chemotherapy use, and possibly appropriate endocrine agents in select populations,” she said.

Dr. Stearns further noted that the interaction between RS and age as reported by Dr. Sparano is exploratory and should be interpreted with caution as the majority of those aged 50 and younger received tamoxifen alone and the question remains as to whether they would have received similar benefits from ovarian suppression and tamoxifen/AI instead of chemo-endocrine therapy.
“Indeed, indirect hypotheses from other studies suggest that may be the case,” she said, adding that these women may be offered ovarian suppression and tamoxifen or AI based on the SOFT and TEXT results.
“TAILORx remains a rich resource for new explorations, new biomarkers, new models, and new machine learning opportunities,” she said.
TAILORx was funded by the National Institutes of Health. Dr. Sparano reported stock ownership, a consulting role, and research funding from several pharmaceutical companies. Dr. Stearns reported consulting or advisory roles with Iridium Therapeutics; research funding from Abbvie, Biocept, MedImmune, Novartis, Pfizer, and Puma Biotechnology; and an “other relationship” with Immunomedics.
SOURCE: Sparano JA et al. ASCO 2019. Abstract 503.
CHICAGO – , according to a secondary analysis of data from the practice-changing TAILORx study.
Specifically, tumor size and histology-based risk stratification improves the prediction of disease-free survival and distant recurrence, and – for some patient groups – chemotherapy benefit, Joseph A. Sparano, MD, reported at the annual meeting of the American Society of Clinical Oncology.
Combining these tools could help determine whether endocrine therapy (ET) alone or ET with adjuvant chemotherapy is the best treatment approach for a given patient, said Dr. Sparano, professor of medicine and obstetrics, gynecology, and women’s health at Albert Einstein College of Medicine, New York.
The phase 3 TAILORx study established that ET alone is noninferior to adjuvant chemotherapy (CT) plus ET in patients with early breast cancer and RS of 11-25, and that ET alone has some benefit over ET+CT in women aged 50 years and younger with RS of 16-25, he explained.
Those findings were presented at the 2018 ASCO annual meeting and subsequently published in the New England Journal of Medicine.
The current analysis focused on the integration of clinical and genomic features for prognosis, and the results were published online June 3 in a corresponding article in the New England Journal of Medicine.
“The totality of the data, including TAILORx and the prior prospective validation studies, indicate that assessment of genomic risk with the 21-gene recurrence score provides complementary prognostic information to pathologic features, and is also predictive of a large chemotherapy benefit if the recurrence score is greater than 25, or lack thereof if 25 or lower,” he said.
However, there is a three-way interaction between age, RS, and CT use, which results in an absolute CT benefit in women aged 50 or younger of about 2% for RS of 16-20, and about 7% for RS of 21-25, he added.
“Assessment of clinical risk using pathological features also provides prognostic information that doesn’t correlate well with the recurrence score, therefore it stands to reason that integration of clinical and genomic risk offers the potential for greater precision in prognosis and, ultimately, guiding the use of adjuvant therapy,” he said.
Clinical risk for this analysis was assessed using a binary clinical risk categorization employed in the MINDACT trial and calibrated to greater than 92% 10-year breast cancer-specific survival for ET alone based on Adjuvant! version 8.0. Low-grade tumors up to 3 cm, intermediate-grade tumors up to 2 cm, and high-grade tumors up to 1 cm were categorized as low clinical risk (LCR), and all others not meeting these criteria were categorized as high clinical risk (HCR), he explained.
Of 9,427 patients included in the analysis, 70% had LCR and 30% had HCR.
“For distant recurrence, high clinical risk was associated with a 2.5- to 3-fold higher recurrence rate for those with a recurrence score of 11 or higher, and in a multivariate model for distant recurrence in the [group with a] recurrence score of 11-25, high clinical risk was independently associated with a 2.4-fold higher recurrence risk,” he said. “Continuous recurrence score also provided significant prognostic information, with each 1-unit increase associated with an 8% higher distant recurrence risk.”
For the overall population, clinical risk added significant prognostic information to the RS for both distant recurrence and disease-free survival, and stratification by age showed that among women over age 50 years, the hazard ratios for distant recurrence ranged from 2.20 to 2.36, and did not substantially vary by age or RS, he said.
However, for the overall population, adding clinical risk to the RS did not improve prediction of chemotherapy benefit.
“This was also true for the two-thirds of women who were over 50 years of age. For the remaining women 50 or younger, there was a trend favoring chemo, irrespective of clinical risk, though not significant – a finding consistent with the treatment interaction previously described,” he said.
Finally, the absolute differences in 9-year distant recurrence rates by clinical risk stratified by age, RS, and CT use showed an absolute 4%-6% higher distant recurrence risk for HCR vs. LCR among those over age 50 with RS of 0-25 irrespective of CT use, and a 13% difference for those with RS of 26-100 who were treated with CT.
“For those 50 or younger, clinical risk had no impact on recurrence if the RS was 0-10. For RS of 11-25, the difference was about 9% with endocrine therapy alone, and 2% with chemo plus ET, reflecting absolute chemo benefit in younger women who had high clinical risk,” he said, adding that for those with RS of 26-100, there was a 9% higher absolute recurrence rate in the HCR vs. LCR population.
“We therefore further evaluated absolute differences in distance recurrence rates associated with chemotherapy use in women 50 and younger with RS of 16-25, further stratified by RS and clinical risk,” he said, noting that when not stratified by clinical risk, as reported in the primary analysis, the absolute CT benefit was 1.6% for RS of 16-20, and 6.5% for RS of 21-25.
When stratified by clinical risk, the absolute CT benefit ranged from 6% to 9% in those with RS of 21-25, irrespective of clinical risk, and in those with RS of 16-20 and HCR.
“This accounted for 51% of patients with RS of 16-25,” he said. “However, there was no demonstrable chemo benefit for those with LCR and RS of 16-20, who accounted for the remaining 49%.”
Additional analysis looking at age at diagnosis and CT benefit showed a benefit in premenopausal women aged 46-50 years (but not postmenopausal women), a trend toward benefit in those aged 41-45 years, and no benefit in those aged 40 years and younger, who are less likely to develop premature menopause as a consequence of cytotoxic CT.
“In addition, we saw no consistent effect favoring chemotherapy in older women. Taken together, these findings suggest the chemo benefit observed for the RS 16-25 group may, in fact, be due to a castration effect associated with cytotoxic therapy rather than an effect in eradicating micrometastatic disease,” Dr. Sparano said.
Applying this framework to the TAILORx study population categorized 68% of those aged 50 years and younger into a low integrated risk group with less than 5% risk of distant recurrence. This included all patients with RS of 0-10 irrespective of clinical risk (14% of the patient population; distant recurrence rate 1.8% or less), and all with RS of 11-25 and LCR (54% of the patient population, 4.7% distant recurrence rate).
In contrast, 25% fell into the high integrated risk group (greater than 10% distant recurrence risk), including those with RS of 11-25 and HCR (17% of the patient population; distant recurrence rate 12.3%), and RS of 26-100 and HCR (8% of the patient population; distant recurrence rate 15.2%).
“This framework encompasses 93% of all TAILORx subjects, with the remaining 7% having a distant recurrence risk of between 5% and 10%,” he said.
Overall, the primary results of TAILORx remain unchanged based on this secondary analysis as the addition of clinical risk did not predict CT benefit in the RS 11-25 group, he noted.
“However, for women 50 and under and RS 16-25, integrated risk distinguished 50% who derived no chemo benefit from the 50% who derived an absolute benefit of approximately 6%-9% – a level that is higher than an unselected population,” he said, reiterating that the absolute CT benefit was greater in premenopausal women aged 45-50 with RS 16-25, suggesting that the absolute CR benefit seen in younger women in TAILORx may be due to an endocrine effect.
“Integrated risk clearly provides greater prognostic precision and may have clinical utility; the prognostic precision afforded by the integrated risk model is superior to that by the use of clinical or genomic features alone, and in addition, the genomic assay also provides predictive information for chemo benefit that is not captured by clinical features alone,” he concluded.
As an example of the potential clinical utility of this integrated approach for guiding treatment in women aged 50 years or younger, he presented “a highly stratified integrated risk assessment model” separating TAILORx patients into low integrated risk (58% of the study population) and high integrated risk (31% of the study population).
In the low integrated risk patients with RS of 0-10 and any clinical risk level, or with RS of 11-25 and LCR, tamoxifen alone appears adequate, he said.
In those with high integrated risk and RS of 16-25 with HCR, ovarian function suppression plus an aromatase inhibitor (OFS/AI) could be considered as an alternative to chemo, and in those with high integrated risk, RS of 26-100, and HCR who have not developed chemotherapy-induced menopause, ovarian function suppression and an AI could be added to chemotherapy.
“Indeed, data from the SOFT and TEXT trials indicate that patients with a high RS risk experienced an absolute improvement of up to 10%-15% in 5-year breast cancer–free interval with an OFS/AI, compared with tamoxifen, whereas improvement was minimal in those at lowest risk, supporting the strategy of using integrated clinical and genomic risk to select for ovarian function suppression plus an AI,” he said.
During a discussion of the findings and how they might impact practice, Vered Stearns, MD, an oncology professor and codirector of the Breast Cancer Program at Johns Hopkins University, Baltimore, noted that in her practice she will “carefully select women for whom genomic assay [use] is appropriate.
“I will also assess clinical risk and RS to inform recommendations for chemotherapy use, and possibly appropriate endocrine agents in select populations,” she said.
Dr. Stearns further noted that the interaction between RS and age as reported by Dr. Sparano is exploratory and should be interpreted with caution as the majority of those aged 50 and younger received tamoxifen alone and the question remains as to whether they would have received similar benefits from ovarian suppression and tamoxifen/AI instead of chemo-endocrine therapy.
“Indeed, indirect hypotheses from other studies suggest that may be the case,” she said, adding that these women may be offered ovarian suppression and tamoxifen or AI based on the SOFT and TEXT results.
“TAILORx remains a rich resource for new explorations, new biomarkers, new models, and new machine learning opportunities,” she said.
TAILORx was funded by the National Institutes of Health. Dr. Sparano reported stock ownership, a consulting role, and research funding from several pharmaceutical companies. Dr. Stearns reported consulting or advisory roles with Iridium Therapeutics; research funding from Abbvie, Biocept, MedImmune, Novartis, Pfizer, and Puma Biotechnology; and an “other relationship” with Immunomedics.
SOURCE: Sparano JA et al. ASCO 2019. Abstract 503.
CHICAGO – , according to a secondary analysis of data from the practice-changing TAILORx study.
Specifically, tumor size and histology-based risk stratification improves the prediction of disease-free survival and distant recurrence, and – for some patient groups – chemotherapy benefit, Joseph A. Sparano, MD, reported at the annual meeting of the American Society of Clinical Oncology.
Combining these tools could help determine whether endocrine therapy (ET) alone or ET with adjuvant chemotherapy is the best treatment approach for a given patient, said Dr. Sparano, professor of medicine and obstetrics, gynecology, and women’s health at Albert Einstein College of Medicine, New York.
The phase 3 TAILORx study established that ET alone is noninferior to adjuvant chemotherapy (CT) plus ET in patients with early breast cancer and RS of 11-25, and that ET alone has some benefit over ET+CT in women aged 50 years and younger with RS of 16-25, he explained.
Those findings were presented at the 2018 ASCO annual meeting and subsequently published in the New England Journal of Medicine.
The current analysis focused on the integration of clinical and genomic features for prognosis, and the results were published online June 3 in a corresponding article in the New England Journal of Medicine.
“The totality of the data, including TAILORx and the prior prospective validation studies, indicate that assessment of genomic risk with the 21-gene recurrence score provides complementary prognostic information to pathologic features, and is also predictive of a large chemotherapy benefit if the recurrence score is greater than 25, or lack thereof if 25 or lower,” he said.
However, there is a three-way interaction between age, RS, and CT use, which results in an absolute CT benefit in women aged 50 or younger of about 2% for RS of 16-20, and about 7% for RS of 21-25, he added.
“Assessment of clinical risk using pathological features also provides prognostic information that doesn’t correlate well with the recurrence score, therefore it stands to reason that integration of clinical and genomic risk offers the potential for greater precision in prognosis and, ultimately, guiding the use of adjuvant therapy,” he said.
Clinical risk for this analysis was assessed using a binary clinical risk categorization employed in the MINDACT trial and calibrated to greater than 92% 10-year breast cancer-specific survival for ET alone based on Adjuvant! version 8.0. Low-grade tumors up to 3 cm, intermediate-grade tumors up to 2 cm, and high-grade tumors up to 1 cm were categorized as low clinical risk (LCR), and all others not meeting these criteria were categorized as high clinical risk (HCR), he explained.
Of 9,427 patients included in the analysis, 70% had LCR and 30% had HCR.
“For distant recurrence, high clinical risk was associated with a 2.5- to 3-fold higher recurrence rate for those with a recurrence score of 11 or higher, and in a multivariate model for distant recurrence in the [group with a] recurrence score of 11-25, high clinical risk was independently associated with a 2.4-fold higher recurrence risk,” he said. “Continuous recurrence score also provided significant prognostic information, with each 1-unit increase associated with an 8% higher distant recurrence risk.”
For the overall population, clinical risk added significant prognostic information to the RS for both distant recurrence and disease-free survival, and stratification by age showed that among women over age 50 years, the hazard ratios for distant recurrence ranged from 2.20 to 2.36, and did not substantially vary by age or RS, he said.
However, for the overall population, adding clinical risk to the RS did not improve prediction of chemotherapy benefit.
“This was also true for the two-thirds of women who were over 50 years of age. For the remaining women 50 or younger, there was a trend favoring chemo, irrespective of clinical risk, though not significant – a finding consistent with the treatment interaction previously described,” he said.
Finally, the absolute differences in 9-year distant recurrence rates by clinical risk stratified by age, RS, and CT use showed an absolute 4%-6% higher distant recurrence risk for HCR vs. LCR among those over age 50 with RS of 0-25 irrespective of CT use, and a 13% difference for those with RS of 26-100 who were treated with CT.
“For those 50 or younger, clinical risk had no impact on recurrence if the RS was 0-10. For RS of 11-25, the difference was about 9% with endocrine therapy alone, and 2% with chemo plus ET, reflecting absolute chemo benefit in younger women who had high clinical risk,” he said, adding that for those with RS of 26-100, there was a 9% higher absolute recurrence rate in the HCR vs. LCR population.
“We therefore further evaluated absolute differences in distance recurrence rates associated with chemotherapy use in women 50 and younger with RS of 16-25, further stratified by RS and clinical risk,” he said, noting that when not stratified by clinical risk, as reported in the primary analysis, the absolute CT benefit was 1.6% for RS of 16-20, and 6.5% for RS of 21-25.
When stratified by clinical risk, the absolute CT benefit ranged from 6% to 9% in those with RS of 21-25, irrespective of clinical risk, and in those with RS of 16-20 and HCR.
“This accounted for 51% of patients with RS of 16-25,” he said. “However, there was no demonstrable chemo benefit for those with LCR and RS of 16-20, who accounted for the remaining 49%.”
Additional analysis looking at age at diagnosis and CT benefit showed a benefit in premenopausal women aged 46-50 years (but not postmenopausal women), a trend toward benefit in those aged 41-45 years, and no benefit in those aged 40 years and younger, who are less likely to develop premature menopause as a consequence of cytotoxic CT.
“In addition, we saw no consistent effect favoring chemotherapy in older women. Taken together, these findings suggest the chemo benefit observed for the RS 16-25 group may, in fact, be due to a castration effect associated with cytotoxic therapy rather than an effect in eradicating micrometastatic disease,” Dr. Sparano said.
Applying this framework to the TAILORx study population categorized 68% of those aged 50 years and younger into a low integrated risk group with less than 5% risk of distant recurrence. This included all patients with RS of 0-10 irrespective of clinical risk (14% of the patient population; distant recurrence rate 1.8% or less), and all with RS of 11-25 and LCR (54% of the patient population, 4.7% distant recurrence rate).
In contrast, 25% fell into the high integrated risk group (greater than 10% distant recurrence risk), including those with RS of 11-25 and HCR (17% of the patient population; distant recurrence rate 12.3%), and RS of 26-100 and HCR (8% of the patient population; distant recurrence rate 15.2%).
“This framework encompasses 93% of all TAILORx subjects, with the remaining 7% having a distant recurrence risk of between 5% and 10%,” he said.
Overall, the primary results of TAILORx remain unchanged based on this secondary analysis as the addition of clinical risk did not predict CT benefit in the RS 11-25 group, he noted.
“However, for women 50 and under and RS 16-25, integrated risk distinguished 50% who derived no chemo benefit from the 50% who derived an absolute benefit of approximately 6%-9% – a level that is higher than an unselected population,” he said, reiterating that the absolute CT benefit was greater in premenopausal women aged 45-50 with RS 16-25, suggesting that the absolute CR benefit seen in younger women in TAILORx may be due to an endocrine effect.
“Integrated risk clearly provides greater prognostic precision and may have clinical utility; the prognostic precision afforded by the integrated risk model is superior to that by the use of clinical or genomic features alone, and in addition, the genomic assay also provides predictive information for chemo benefit that is not captured by clinical features alone,” he concluded.
As an example of the potential clinical utility of this integrated approach for guiding treatment in women aged 50 years or younger, he presented “a highly stratified integrated risk assessment model” separating TAILORx patients into low integrated risk (58% of the study population) and high integrated risk (31% of the study population).
In the low integrated risk patients with RS of 0-10 and any clinical risk level, or with RS of 11-25 and LCR, tamoxifen alone appears adequate, he said.
In those with high integrated risk and RS of 16-25 with HCR, ovarian function suppression plus an aromatase inhibitor (OFS/AI) could be considered as an alternative to chemo, and in those with high integrated risk, RS of 26-100, and HCR who have not developed chemotherapy-induced menopause, ovarian function suppression and an AI could be added to chemotherapy.
“Indeed, data from the SOFT and TEXT trials indicate that patients with a high RS risk experienced an absolute improvement of up to 10%-15% in 5-year breast cancer–free interval with an OFS/AI, compared with tamoxifen, whereas improvement was minimal in those at lowest risk, supporting the strategy of using integrated clinical and genomic risk to select for ovarian function suppression plus an AI,” he said.
During a discussion of the findings and how they might impact practice, Vered Stearns, MD, an oncology professor and codirector of the Breast Cancer Program at Johns Hopkins University, Baltimore, noted that in her practice she will “carefully select women for whom genomic assay [use] is appropriate.
“I will also assess clinical risk and RS to inform recommendations for chemotherapy use, and possibly appropriate endocrine agents in select populations,” she said.
Dr. Stearns further noted that the interaction between RS and age as reported by Dr. Sparano is exploratory and should be interpreted with caution as the majority of those aged 50 and younger received tamoxifen alone and the question remains as to whether they would have received similar benefits from ovarian suppression and tamoxifen/AI instead of chemo-endocrine therapy.
“Indeed, indirect hypotheses from other studies suggest that may be the case,” she said, adding that these women may be offered ovarian suppression and tamoxifen or AI based on the SOFT and TEXT results.
“TAILORx remains a rich resource for new explorations, new biomarkers, new models, and new machine learning opportunities,” she said.
TAILORx was funded by the National Institutes of Health. Dr. Sparano reported stock ownership, a consulting role, and research funding from several pharmaceutical companies. Dr. Stearns reported consulting or advisory roles with Iridium Therapeutics; research funding from Abbvie, Biocept, MedImmune, Novartis, Pfizer, and Puma Biotechnology; and an “other relationship” with Immunomedics.
SOURCE: Sparano JA et al. ASCO 2019. Abstract 503.
REPORTING FROM ASCO 2019