User login
High rate of arm morbidity in young breast cancer survivors
SAN ANTONIO – as compared with having a sentinel lymph node biopsy (SLNB), according to new findings.
In a large prospective cohort study that included 1,302 breast cancer patients aged 40 or younger, the incidence of arm swelling 1 year after diagnosis among women who underwent breast-conserving surgery was 6% for the SLNB group versus 24% for those who had ALND. Among patients who had a mastectomy, the rates were similar; 6% versus 23% for SLNB or ALND, respectively.
“Young breast cancer survivors report high rates of arm morbidity in the first year of follow-up,” said lead author Anne Kuijer, MD, of Dana-Farber Cancer Institute/Brigham and Women’s Hospital in Boston. “Axillary node dissection, increased BMI [body mass index] and socioeconomic status were all independently associated with an increased risk of arm swelling,” she said at the San Antonio Breast Cancer Symposium.
She noted that patients who received mastectomy with radiation therapy were twice as likely to have decreased range of motion at 1 year, compared with patients treated with breast-conserving treatment.
In this study, the authors evaluated the incidence of arm morbidity associated with both ALND and SLNB in patients who were enrolled in the Young Women’s Breast Cancer Study. This multicenter prospective cohort study was designed to explore biological, medical, and psychosocial issues experienced by young breast cancer patients.
Within this large cohort, 55% had undergone an SLNB only, and 41% an ALND. The remaining patients did not undergo either procedure.
The primary endpoint of this study was to examine the incidence of patient-reported arm swelling or decreased range of motion at 1 year after their breast cancer diagnosis. Patients used the Cancer Rehabilitation Evaluation System (CARES-SF) to measure their symptoms.
Overall, at 1 year, 13% of the cohort reported arm swelling, and 40% reported decreased range of motion in the ipsilateral arm.
Several factors were associated with a higher risk of arm morbidity. Patients with a BMI of greater than 25 were more likely to report arm swelling vs. those with lower BMI (odds ratio, 1.7; P = .03) as well as have less range of motion (OR, 1.5; P = .05). Women who reported feeling financially comfortable were 40% less likely to report swelling (P = .02) and 90% less likely to report decreased range of motion (P = .67).
In addition, those who underwent ALND were 3.4 times more likely to report swelling, compared with women who had SLNB, but it was not associated with a reduction in range of motion.
One limitation of the study is that the cohort included patients who had received treatment at large cancer centers in the Northeast, suggesting that they may have been of higher socioeconomic status and may have led more active lifestyles, compared with the general population. Another limitation is that arm morbidity was self-reported and not objectively measured.
“I think our findings highlight opportunities for preoperative counseling, early referral of patients to physical therapy, and identification of resources for support of those at increased risk,” said Dr. Kuijer.
SOURCE: Kuijer et al. SABCS Abstract GS5-03
SAN ANTONIO – as compared with having a sentinel lymph node biopsy (SLNB), according to new findings.
In a large prospective cohort study that included 1,302 breast cancer patients aged 40 or younger, the incidence of arm swelling 1 year after diagnosis among women who underwent breast-conserving surgery was 6% for the SLNB group versus 24% for those who had ALND. Among patients who had a mastectomy, the rates were similar; 6% versus 23% for SLNB or ALND, respectively.
“Young breast cancer survivors report high rates of arm morbidity in the first year of follow-up,” said lead author Anne Kuijer, MD, of Dana-Farber Cancer Institute/Brigham and Women’s Hospital in Boston. “Axillary node dissection, increased BMI [body mass index] and socioeconomic status were all independently associated with an increased risk of arm swelling,” she said at the San Antonio Breast Cancer Symposium.
She noted that patients who received mastectomy with radiation therapy were twice as likely to have decreased range of motion at 1 year, compared with patients treated with breast-conserving treatment.
In this study, the authors evaluated the incidence of arm morbidity associated with both ALND and SLNB in patients who were enrolled in the Young Women’s Breast Cancer Study. This multicenter prospective cohort study was designed to explore biological, medical, and psychosocial issues experienced by young breast cancer patients.
Within this large cohort, 55% had undergone an SLNB only, and 41% an ALND. The remaining patients did not undergo either procedure.
The primary endpoint of this study was to examine the incidence of patient-reported arm swelling or decreased range of motion at 1 year after their breast cancer diagnosis. Patients used the Cancer Rehabilitation Evaluation System (CARES-SF) to measure their symptoms.
Overall, at 1 year, 13% of the cohort reported arm swelling, and 40% reported decreased range of motion in the ipsilateral arm.
Several factors were associated with a higher risk of arm morbidity. Patients with a BMI of greater than 25 were more likely to report arm swelling vs. those with lower BMI (odds ratio, 1.7; P = .03) as well as have less range of motion (OR, 1.5; P = .05). Women who reported feeling financially comfortable were 40% less likely to report swelling (P = .02) and 90% less likely to report decreased range of motion (P = .67).
In addition, those who underwent ALND were 3.4 times more likely to report swelling, compared with women who had SLNB, but it was not associated with a reduction in range of motion.
One limitation of the study is that the cohort included patients who had received treatment at large cancer centers in the Northeast, suggesting that they may have been of higher socioeconomic status and may have led more active lifestyles, compared with the general population. Another limitation is that arm morbidity was self-reported and not objectively measured.
“I think our findings highlight opportunities for preoperative counseling, early referral of patients to physical therapy, and identification of resources for support of those at increased risk,” said Dr. Kuijer.
SOURCE: Kuijer et al. SABCS Abstract GS5-03
SAN ANTONIO – as compared with having a sentinel lymph node biopsy (SLNB), according to new findings.
In a large prospective cohort study that included 1,302 breast cancer patients aged 40 or younger, the incidence of arm swelling 1 year after diagnosis among women who underwent breast-conserving surgery was 6% for the SLNB group versus 24% for those who had ALND. Among patients who had a mastectomy, the rates were similar; 6% versus 23% for SLNB or ALND, respectively.
“Young breast cancer survivors report high rates of arm morbidity in the first year of follow-up,” said lead author Anne Kuijer, MD, of Dana-Farber Cancer Institute/Brigham and Women’s Hospital in Boston. “Axillary node dissection, increased BMI [body mass index] and socioeconomic status were all independently associated with an increased risk of arm swelling,” she said at the San Antonio Breast Cancer Symposium.
She noted that patients who received mastectomy with radiation therapy were twice as likely to have decreased range of motion at 1 year, compared with patients treated with breast-conserving treatment.
In this study, the authors evaluated the incidence of arm morbidity associated with both ALND and SLNB in patients who were enrolled in the Young Women’s Breast Cancer Study. This multicenter prospective cohort study was designed to explore biological, medical, and psychosocial issues experienced by young breast cancer patients.
Within this large cohort, 55% had undergone an SLNB only, and 41% an ALND. The remaining patients did not undergo either procedure.
The primary endpoint of this study was to examine the incidence of patient-reported arm swelling or decreased range of motion at 1 year after their breast cancer diagnosis. Patients used the Cancer Rehabilitation Evaluation System (CARES-SF) to measure their symptoms.
Overall, at 1 year, 13% of the cohort reported arm swelling, and 40% reported decreased range of motion in the ipsilateral arm.
Several factors were associated with a higher risk of arm morbidity. Patients with a BMI of greater than 25 were more likely to report arm swelling vs. those with lower BMI (odds ratio, 1.7; P = .03) as well as have less range of motion (OR, 1.5; P = .05). Women who reported feeling financially comfortable were 40% less likely to report swelling (P = .02) and 90% less likely to report decreased range of motion (P = .67).
In addition, those who underwent ALND were 3.4 times more likely to report swelling, compared with women who had SLNB, but it was not associated with a reduction in range of motion.
One limitation of the study is that the cohort included patients who had received treatment at large cancer centers in the Northeast, suggesting that they may have been of higher socioeconomic status and may have led more active lifestyles, compared with the general population. Another limitation is that arm morbidity was self-reported and not objectively measured.
“I think our findings highlight opportunities for preoperative counseling, early referral of patients to physical therapy, and identification of resources for support of those at increased risk,” said Dr. Kuijer.
SOURCE: Kuijer et al. SABCS Abstract GS5-03
REPORTING FROM SABCS 2017
Key clinical point: A significant rate of arm swelling and decreased range of motion was seen in young breast cancer patients 1 year after undergoing surgery.
Major finding: At 1 year, 13% of a large cohort of breast cancer patients aged 40 years or younger reported arm swelling, and 40% reported decreased range of motion in the ipsilateral arm.
Data source: Large prospective cohort study that included 1,302 breast cancer patients aged 40 or younger.
Disclosures:. This study was funded by the National Institutes of Health, the Susan G. Komen Foundation, The Pink Agenda, and the Breast Cancer Research Foundation. Dr. Kuijer and her colleagues declare no conflicts of interest.
Source: Kuijer et al. SABCS 2017 Abstract GS5-03.
VIDEO: SABCS 2017 roundtable with Dr. Hope S. Rugo and Dr. William J. Gradishar
SAN ANTONIO – Dr. William A. Gradishar and Dr. Hope S. Rugo reflect on some familiar questions at the conclusion of the San Antonio Breast Cancer Symposium: Should young, high-risk women receive ovarian suppression? What is the optimal duration for trastuzumab therapy? What about extended aromatase inhibitor therapy? But new questions were considered as well, based on results presented at the 40th annual symposium.
Will combining a checkpoint inhibitor with trastuzumab help overcome trastuzumab resistance?
Are CDK 4/6 inhibitors here to stay?
Does acupuncture relieve joint pain in women on adjuvant aromatase inhibitor treatment?
The potential approval of a few novel agents in 2018 – an antibody-drug conjugate and a new PARP inhibitor – were also discussed in the video roundtable.
Dr. William A. Gradishar is the Betsy Bramsen Professor of Breast Oncology at Northwestern University, Chicago. He had no disclosures to report. Dr. Hope S. Rugo is professor of medicine at the University of California, San Francisco. She disclosed that she receives research funding (institutional) from Plexxikon, Macrogenics, OBI Pharma, Eisai, Pfizer, Novartis, Lilly, Genentech, and Merck.
SAN ANTONIO – Dr. William A. Gradishar and Dr. Hope S. Rugo reflect on some familiar questions at the conclusion of the San Antonio Breast Cancer Symposium: Should young, high-risk women receive ovarian suppression? What is the optimal duration for trastuzumab therapy? What about extended aromatase inhibitor therapy? But new questions were considered as well, based on results presented at the 40th annual symposium.
Will combining a checkpoint inhibitor with trastuzumab help overcome trastuzumab resistance?
Are CDK 4/6 inhibitors here to stay?
Does acupuncture relieve joint pain in women on adjuvant aromatase inhibitor treatment?
The potential approval of a few novel agents in 2018 – an antibody-drug conjugate and a new PARP inhibitor – were also discussed in the video roundtable.
Dr. William A. Gradishar is the Betsy Bramsen Professor of Breast Oncology at Northwestern University, Chicago. He had no disclosures to report. Dr. Hope S. Rugo is professor of medicine at the University of California, San Francisco. She disclosed that she receives research funding (institutional) from Plexxikon, Macrogenics, OBI Pharma, Eisai, Pfizer, Novartis, Lilly, Genentech, and Merck.
SAN ANTONIO – Dr. William A. Gradishar and Dr. Hope S. Rugo reflect on some familiar questions at the conclusion of the San Antonio Breast Cancer Symposium: Should young, high-risk women receive ovarian suppression? What is the optimal duration for trastuzumab therapy? What about extended aromatase inhibitor therapy? But new questions were considered as well, based on results presented at the 40th annual symposium.
Will combining a checkpoint inhibitor with trastuzumab help overcome trastuzumab resistance?
Are CDK 4/6 inhibitors here to stay?
Does acupuncture relieve joint pain in women on adjuvant aromatase inhibitor treatment?
The potential approval of a few novel agents in 2018 – an antibody-drug conjugate and a new PARP inhibitor – were also discussed in the video roundtable.
Dr. William A. Gradishar is the Betsy Bramsen Professor of Breast Oncology at Northwestern University, Chicago. He had no disclosures to report. Dr. Hope S. Rugo is professor of medicine at the University of California, San Francisco. She disclosed that she receives research funding (institutional) from Plexxikon, Macrogenics, OBI Pharma, Eisai, Pfizer, Novartis, Lilly, Genentech, and Merck.
EXPERT ANALYSIS FROM SABCS 2017

CDK4/6 inhibitors have similar efficacy in older breast cancer patients
SAN ANTONIO – Treatment with cyclin-dependent kinase 4/6 inhibitors (CDK4/6) appears to have the same efficacy in older breast cancer patients, as compared to younger ones, according to new findings presented at the San Antonio Breast Cancer Symposium.
Women aged 65 years and older with hormone receptor (HR)–positive, HER2-negative metastatic breast cancer who received CDK4/6 inhibitors achieved a rate of progression-free survival (PFS) similar to that which has been reported in younger patients. Importantly, combining a CDK4/6 inhibitor with endocrine therapy led to superior PFS as compared to endocrine therapy alone.
However, older patients appeared to be less tolerant of associated adverse events and were more likely to discontinue treatment for that reason.
“Older patients with breast cancer benefit from treatment with CDK4/6 inhibitors ... for HR-positive, HER2-negative, metastatic breast cancer,” said the study’s lead author, Harpreet Singh, MD, scientific liaison for the FDA’s Cancer in Older Adults and a medical officer in the Office of Hematology and Oncology Products, Center for Drug Evaluation and Research, at the Food and Drug Administration.
“The severity of adverse events and rates of dose modifications and interruptions were higher in those 65 years of age and older and those 70 years and older,” Dr. Singh said. “Rates of selected adverse events were similar across pooled trials.”
Breast cancer is a disease of aging, and 72,000 breast cancers occur annually in women aged 70 years or older, she explained. “Most cancers in older women are lower risk tumors and most older patients will die of other causes, but approximately 40% of breast cancer related deaths are in women over the age of 70.
“But the accrual of older individuals in trials has been a persistent challenge,” said Dr. Singh. “Older patients traditionally have been underrepresented in oncology clinical trials, so pooling outcomes of older patients across clinical trials in the same drug class allows us to gain insight into how these patients may benefit.”
In the current study, which was an FDA-conducted review of FDA registration trials over a 10 year period, the authors found that fewer than 60% of new cases of breast cancer are diagnosed in women under the age of 65 years.
“But these women make up about 80% of the clinical trial populations even though they are only 57% of cases,” said Dr. Singh.
Only 17% of clinical trial populations comprised individuals aged 65-74 years – even though patients aged 75 years and older make up about 20% of new cases, they comprise only 4% of the clinical trial population.
The FDA has issued several guidances that encourage investigators to enroll older women into trials but does not require them to. Only 22% of patients over 70 received adjuvant or neoadjuvant therapy compared to close to 50% of younger patients, and as a result, very little is known about the safety and efficacy of these agents in older adults.
To assess the efficacy and safety of CDK4/6 inhibitors in an older population, Dr. Singh and her colleagues pooled and analyzed data from prospective, randomized, controlled trials that evaluated three different CDK4/6 inhibitors in combination with an aromatase inhibitor, as the first-line treatment for postmenopausal patients with HR-positive metastatic breast cancer. The cohort included 1,334 patients, (intention-to-treat population, 1,992), of whom 42% were aged 65 years or older, and 24% were 70 years or older.
The primary endpoint was PFS in patients aged 70 years and older, and in control groups.
For patients 70 years or older who received a CDK4/6 inhibitor in combination with an aromatase inhibitor, the estimated PFS was not reached (25.1 months, not reached), versus 16.8 months (13.7, 21.9) for those who received an aromatase inhibitor only.
For patients younger than 70 years of age, PFS also was superior among those who received a CDK4/6 inhibitor, compared with treatment with an aromatase inhibitor alone: 23.75(21.9, 25.4) months versus an estimated 13.8 months (12.9, 14.7).
There were no treatment differences across age subgroups and similar results with alternate age cut-offs (greater than 65 years, greater than 75 years, etc.).
When looking at safety, the authors found that older patients were more likely to stop treatment because of adverse events. Among those 70 years and older, 20% discontinued treatment as compared with 17% of those 65 years or older, and 8% of those under the age of 65 years. Virtually all patients in the three age groups experienced grade 1-2 events (younger than 65, 98%; greater than or equal to 65 years, 98%; greater than or equal to 70 years, 99%), and the majority experienced grade 3-4 events (76%, 83%, 85%, respectively), with the rate higher in the older age groups. More than three quarters of all patients experienced neutropenia (76%, 77%, 80%), and two-thirds or higher grade 3-4 neutropenia (65%, 69%, 72%). Adverse events leading to dose interruption and/or reduction were also higher in the older age groups (66%, 75%, 77%).
“But there are many signs of progress,” said Dr. Singh, referring to efforts in enrolling more older breast cancer patients in clinical trials. “There are ongoing efforts to modernize eligibility criteria which will include greater inclusion of older adults, and specifically, taking a rational approach to organ dysfunction and prior malignancies.”
The increased use of patient-reported outcomes will provide further information on the tolerability of therapy. “Also the acquisition of real-world data from more diverse oncology practices will help inform data on efficacy and safety of novel therapies in older adults,” concluded Dr. Singh.
SOURCE: Singh et al., SABCS 2017 Abstract GS5-06.
SAN ANTONIO – Treatment with cyclin-dependent kinase 4/6 inhibitors (CDK4/6) appears to have the same efficacy in older breast cancer patients, as compared to younger ones, according to new findings presented at the San Antonio Breast Cancer Symposium.
Women aged 65 years and older with hormone receptor (HR)–positive, HER2-negative metastatic breast cancer who received CDK4/6 inhibitors achieved a rate of progression-free survival (PFS) similar to that which has been reported in younger patients. Importantly, combining a CDK4/6 inhibitor with endocrine therapy led to superior PFS as compared to endocrine therapy alone.
However, older patients appeared to be less tolerant of associated adverse events and were more likely to discontinue treatment for that reason.
“Older patients with breast cancer benefit from treatment with CDK4/6 inhibitors ... for HR-positive, HER2-negative, metastatic breast cancer,” said the study’s lead author, Harpreet Singh, MD, scientific liaison for the FDA’s Cancer in Older Adults and a medical officer in the Office of Hematology and Oncology Products, Center for Drug Evaluation and Research, at the Food and Drug Administration.
“The severity of adverse events and rates of dose modifications and interruptions were higher in those 65 years of age and older and those 70 years and older,” Dr. Singh said. “Rates of selected adverse events were similar across pooled trials.”
Breast cancer is a disease of aging, and 72,000 breast cancers occur annually in women aged 70 years or older, she explained. “Most cancers in older women are lower risk tumors and most older patients will die of other causes, but approximately 40% of breast cancer related deaths are in women over the age of 70.
“But the accrual of older individuals in trials has been a persistent challenge,” said Dr. Singh. “Older patients traditionally have been underrepresented in oncology clinical trials, so pooling outcomes of older patients across clinical trials in the same drug class allows us to gain insight into how these patients may benefit.”
In the current study, which was an FDA-conducted review of FDA registration trials over a 10 year period, the authors found that fewer than 60% of new cases of breast cancer are diagnosed in women under the age of 65 years.
“But these women make up about 80% of the clinical trial populations even though they are only 57% of cases,” said Dr. Singh.
Only 17% of clinical trial populations comprised individuals aged 65-74 years – even though patients aged 75 years and older make up about 20% of new cases, they comprise only 4% of the clinical trial population.
The FDA has issued several guidances that encourage investigators to enroll older women into trials but does not require them to. Only 22% of patients over 70 received adjuvant or neoadjuvant therapy compared to close to 50% of younger patients, and as a result, very little is known about the safety and efficacy of these agents in older adults.
To assess the efficacy and safety of CDK4/6 inhibitors in an older population, Dr. Singh and her colleagues pooled and analyzed data from prospective, randomized, controlled trials that evaluated three different CDK4/6 inhibitors in combination with an aromatase inhibitor, as the first-line treatment for postmenopausal patients with HR-positive metastatic breast cancer. The cohort included 1,334 patients, (intention-to-treat population, 1,992), of whom 42% were aged 65 years or older, and 24% were 70 years or older.
The primary endpoint was PFS in patients aged 70 years and older, and in control groups.
For patients 70 years or older who received a CDK4/6 inhibitor in combination with an aromatase inhibitor, the estimated PFS was not reached (25.1 months, not reached), versus 16.8 months (13.7, 21.9) for those who received an aromatase inhibitor only.
For patients younger than 70 years of age, PFS also was superior among those who received a CDK4/6 inhibitor, compared with treatment with an aromatase inhibitor alone: 23.75(21.9, 25.4) months versus an estimated 13.8 months (12.9, 14.7).
There were no treatment differences across age subgroups and similar results with alternate age cut-offs (greater than 65 years, greater than 75 years, etc.).
When looking at safety, the authors found that older patients were more likely to stop treatment because of adverse events. Among those 70 years and older, 20% discontinued treatment as compared with 17% of those 65 years or older, and 8% of those under the age of 65 years. Virtually all patients in the three age groups experienced grade 1-2 events (younger than 65, 98%; greater than or equal to 65 years, 98%; greater than or equal to 70 years, 99%), and the majority experienced grade 3-4 events (76%, 83%, 85%, respectively), with the rate higher in the older age groups. More than three quarters of all patients experienced neutropenia (76%, 77%, 80%), and two-thirds or higher grade 3-4 neutropenia (65%, 69%, 72%). Adverse events leading to dose interruption and/or reduction were also higher in the older age groups (66%, 75%, 77%).
“But there are many signs of progress,” said Dr. Singh, referring to efforts in enrolling more older breast cancer patients in clinical trials. “There are ongoing efforts to modernize eligibility criteria which will include greater inclusion of older adults, and specifically, taking a rational approach to organ dysfunction and prior malignancies.”
The increased use of patient-reported outcomes will provide further information on the tolerability of therapy. “Also the acquisition of real-world data from more diverse oncology practices will help inform data on efficacy and safety of novel therapies in older adults,” concluded Dr. Singh.
SOURCE: Singh et al., SABCS 2017 Abstract GS5-06.
SAN ANTONIO – Treatment with cyclin-dependent kinase 4/6 inhibitors (CDK4/6) appears to have the same efficacy in older breast cancer patients, as compared to younger ones, according to new findings presented at the San Antonio Breast Cancer Symposium.
Women aged 65 years and older with hormone receptor (HR)–positive, HER2-negative metastatic breast cancer who received CDK4/6 inhibitors achieved a rate of progression-free survival (PFS) similar to that which has been reported in younger patients. Importantly, combining a CDK4/6 inhibitor with endocrine therapy led to superior PFS as compared to endocrine therapy alone.
However, older patients appeared to be less tolerant of associated adverse events and were more likely to discontinue treatment for that reason.
“Older patients with breast cancer benefit from treatment with CDK4/6 inhibitors ... for HR-positive, HER2-negative, metastatic breast cancer,” said the study’s lead author, Harpreet Singh, MD, scientific liaison for the FDA’s Cancer in Older Adults and a medical officer in the Office of Hematology and Oncology Products, Center for Drug Evaluation and Research, at the Food and Drug Administration.
“The severity of adverse events and rates of dose modifications and interruptions were higher in those 65 years of age and older and those 70 years and older,” Dr. Singh said. “Rates of selected adverse events were similar across pooled trials.”
Breast cancer is a disease of aging, and 72,000 breast cancers occur annually in women aged 70 years or older, she explained. “Most cancers in older women are lower risk tumors and most older patients will die of other causes, but approximately 40% of breast cancer related deaths are in women over the age of 70.
“But the accrual of older individuals in trials has been a persistent challenge,” said Dr. Singh. “Older patients traditionally have been underrepresented in oncology clinical trials, so pooling outcomes of older patients across clinical trials in the same drug class allows us to gain insight into how these patients may benefit.”
In the current study, which was an FDA-conducted review of FDA registration trials over a 10 year period, the authors found that fewer than 60% of new cases of breast cancer are diagnosed in women under the age of 65 years.
“But these women make up about 80% of the clinical trial populations even though they are only 57% of cases,” said Dr. Singh.
Only 17% of clinical trial populations comprised individuals aged 65-74 years – even though patients aged 75 years and older make up about 20% of new cases, they comprise only 4% of the clinical trial population.
The FDA has issued several guidances that encourage investigators to enroll older women into trials but does not require them to. Only 22% of patients over 70 received adjuvant or neoadjuvant therapy compared to close to 50% of younger patients, and as a result, very little is known about the safety and efficacy of these agents in older adults.
To assess the efficacy and safety of CDK4/6 inhibitors in an older population, Dr. Singh and her colleagues pooled and analyzed data from prospective, randomized, controlled trials that evaluated three different CDK4/6 inhibitors in combination with an aromatase inhibitor, as the first-line treatment for postmenopausal patients with HR-positive metastatic breast cancer. The cohort included 1,334 patients, (intention-to-treat population, 1,992), of whom 42% were aged 65 years or older, and 24% were 70 years or older.
The primary endpoint was PFS in patients aged 70 years and older, and in control groups.
For patients 70 years or older who received a CDK4/6 inhibitor in combination with an aromatase inhibitor, the estimated PFS was not reached (25.1 months, not reached), versus 16.8 months (13.7, 21.9) for those who received an aromatase inhibitor only.
For patients younger than 70 years of age, PFS also was superior among those who received a CDK4/6 inhibitor, compared with treatment with an aromatase inhibitor alone: 23.75(21.9, 25.4) months versus an estimated 13.8 months (12.9, 14.7).
There were no treatment differences across age subgroups and similar results with alternate age cut-offs (greater than 65 years, greater than 75 years, etc.).
When looking at safety, the authors found that older patients were more likely to stop treatment because of adverse events. Among those 70 years and older, 20% discontinued treatment as compared with 17% of those 65 years or older, and 8% of those under the age of 65 years. Virtually all patients in the three age groups experienced grade 1-2 events (younger than 65, 98%; greater than or equal to 65 years, 98%; greater than or equal to 70 years, 99%), and the majority experienced grade 3-4 events (76%, 83%, 85%, respectively), with the rate higher in the older age groups. More than three quarters of all patients experienced neutropenia (76%, 77%, 80%), and two-thirds or higher grade 3-4 neutropenia (65%, 69%, 72%). Adverse events leading to dose interruption and/or reduction were also higher in the older age groups (66%, 75%, 77%).
“But there are many signs of progress,” said Dr. Singh, referring to efforts in enrolling more older breast cancer patients in clinical trials. “There are ongoing efforts to modernize eligibility criteria which will include greater inclusion of older adults, and specifically, taking a rational approach to organ dysfunction and prior malignancies.”
The increased use of patient-reported outcomes will provide further information on the tolerability of therapy. “Also the acquisition of real-world data from more diverse oncology practices will help inform data on efficacy and safety of novel therapies in older adults,” concluded Dr. Singh.
SOURCE: Singh et al., SABCS 2017 Abstract GS5-06.
REPORTING FROM SABCS 2017
Key clinical point: Cyclin-dependent kinase 4 and 6 inhibitors are as effective in older breast cancer patients, as compared with younger ones.
Major finding: The PFS in patients aged 70 years or older treated with a CDK4/6 inhibitor plus an aromatase inhibitor was not reached vs. 16.8 months for those who received an aromatase inhibitor only.
Data source: Pooled retrospective subgroup analysis that included 1,334 breast cancer patients treated with CDK4/6 inhibitors and aromatase inhibitors.
Disclosures:. The study was run by the FDA. Dr. Singh and coauthors have no disclosures.
Source: Singh H et al., SABCS 2017 Abstract GS5-06.
PANACEA: pembrolizumab overcomes trastuzumab resistance for some
SAN ANTONIO – The immune checkpoint inhibitor pembrolizumab overcomes trastuzumab resistance in HER2-positive advanced breast cancer provided that the tumor expresses programmed death ligand 1 (PD-L1), a trial reported at the San Antonio Breast Cancer Symposium suggests. But presence of immune cells in the tumor is a major additional determinant of benefit.

The single-arm phase 1b/2 trial, called PANACEA (also KEYNOTE-014), enrolled 58 patients with HER2-positive advanced breast cancer that had progressed on trastuzumab (Herceptin) or trastuzumab emtansine (Kadcyla). All were given pembrolizumab (Keytruda), which unleashes antitumor immunity by targeting the programmed death-1 receptor on immune cells, in combination with trastuzumab.
With a median follow-up of 13.6 months, the cohort of patients having tumors positive for PD-L1 achieved an overall response rate of 15.2% and a disease control rate of 24%,” Dr. Loi reported in a press briefing and session, on behalf of the International Breast Cancer Study Group and Breast International Group. In contrast, there were no responses in the PD-L1–negative cohort.
Within the PD-L1–positive cohort, stromal levels of TILs in the metastatic lesion – which were low overall – influenced likelihood of benefit. The response rate was almost eight times higher in patients who had at least 5% of the stromal area densely infiltrated with TILs.
“The PANACEA study met its primary endpoint in the PD-L1–positive cohort. For responders, this combination offers durable control without chemotherapy,” Dr. Loi summarized.
“Metastatic HER2-positive breast cancer in this [heavily pretreated] setting is poorly immunogenic, as evidenced by the majority of patients having low TILs in their metastatic lesions. Saying that, however, we did observe a higher response rate in this study as compared to the equivalent triple-negative breast cancer studied in KEYNOTE-086,” she noted. “Future directions in this disease space should focus on combinations with effective anti-HER2 therapy, particularly in low-TIL patients.”
Predicting benefit
The trial is noteworthy for its efforts to identify the subset of patients most likely to benefit from immune checkpoint inhibition, according to press briefing moderator Virginia Kaklamani, MD, a professor of medicine in the division of hematology/oncology at the University of Texas Health Science Center, San Antonio, and a leader of the Breast Cancer Program at the UT Health San Antonio Cancer Center.

In similar studies among patients with HER2-negative breast cancer, PD-L1 did not pan out as a strong predictive biomarker. “What do you think the difference is between that subset and the HER2-positive subset?” Dr. Kaklamani asked.
“First off, I think that there are technical issues with the PD-L1 assay. And we find that patients with high TILs or immune infiltration usually have high levels of PD-L1 expression on their TILs,” Dr. Loi replied. “So I think that PD-L1 can be expressed on the tumor as well as the TIL, and it certainly seems to be the TIL infiltrate that probably enriches for responders to a PD-L1 checkpoint inhibitor on its own or in this case with trastuzumab.”
Study details
In the PANACEA trial (additionally known as IBCSG 45-13 and BIG 4-13), the most common adverse event of any grade and type with the pembrolizumab-trastuzumab combination was fatigue, seen in 21% of patients, Dr. Loi reported. For immune-related adverse events specifically, 19.0% of patients experienced an event, 10.3% experienced an event of grade 3 or worse, and 6.9% stopped treatment because of these events.
“These frequencies are consistent with what has been reported in other solid tumor types with pembrolizumab,” she commented. There were no cardiac events reported.
Efficacy analyses were restricted largely to the PD-L1–positive cohort, given the lack of any response in the negative cohort.
Median duration of response in the positive cohort was 3.5 months, and median duration of disease control was 11.1 months. Five patients (10.8%) remain on treatment with no progression; three of them have completed 2 years of pembrolizumab.
Median progression-free and overall survival were 2.7 and 16.1 months, respectively; corresponding 12-month rates were 13% and 65%. “There is a tantalizing suggestion of a tail on the curve. ... Obviously, this requires further follow-up, and the numbers are small,” Dr. Loi commented.
The median baseline stromal TIL level in metastatic lesions was just 1%. “This is 20 times less than what we observe in primary HER2-positive breast cancers,” she pointed out.
Compared with the PD-L1–negative cohort, the PD-L1–positive cohort had higher TIL levels. Additionally, within that latter cohort, TIL level was higher among patients achieving response versus not (P = .006) and patients achieving disease control versus not (P = .0006).
“We then went on to try to identify a TIL cutoff that could enrich the population for responders. This has been done in other solid tumor types,” Dr. Loi explained.
Analyses in the PD-L1-positive cohort showed that TIL levels down to 5% predicted benefit. The 41% of patients having 5% or more TILs were dramatically more likely to have a response (39% vs. 5%) and disease control (47% vs. 5%).
TIL levels varied widely according to site of the metastasis, with higher levels seen in metastases from lung and lymph nodes, and lower levels seen in those from liver and skin.
“At this stage, we are not sure which is the chicken and the egg: Patients could have disease in their lung and their lymph nodes because their immune system is better controlling their disease,” Dr. Loi commented. “How we treat these patients is still an open question. In patients with liver metastases, perhaps we need to be more aggressive with the primary or tumor-control anti-HER2 therapy.”
Improving efficacy
Going forward, one strategy for improving pembrolizumab efficacy in this patient population might be priming the immune response, according to Dr. Loi.
“In HER2 disease, it’s very clear that oncogenic signaling is the driver, so targeting HER2 potently also will help relieve tumor-mediated immune suppression,” she elaborated. “In this particular context, targeting HER2 well is the key. Whether you need the addition of a little bit of chemo or some radiation, all this needs to be studied.”
Another strategy for improving pembrolizumab efficacy might be moving the drug to earlier disease settings, Dr. Loi proposed.
“By the time you get to advanced stage and have had multiple treatments, you actually have low levels of T-cell infiltration in your metastatic lesion, for whatever reasons – tumor burden, immunosuppression, multiple lines of treatment. That all reduces your chance of responding to pembrolizumab, for example, as monotherapy,” she elaborated. “We don’t know yet if chemotherapy in addition to pembrolizumab could change that tumor microenvironment. But still, I think the earlier in lines you go, the more chance you are going to have of preexisting effective antitumor immunity that can be reactivated with the addition of pembrolizumab.”
Dr. Loi disclosed that her institution receives research funding from Novartis, Pfizer, Merck, Genentech/Roche, and Puma. Merck provided study drug and support for PANACEA.
SOURCE: Loi S et al. SABCS 2017 Abstract GS2-06.
SAN ANTONIO – The immune checkpoint inhibitor pembrolizumab overcomes trastuzumab resistance in HER2-positive advanced breast cancer provided that the tumor expresses programmed death ligand 1 (PD-L1), a trial reported at the San Antonio Breast Cancer Symposium suggests. But presence of immune cells in the tumor is a major additional determinant of benefit.
The single-arm phase 1b/2 trial, called PANACEA (also KEYNOTE-014), enrolled 58 patients with HER2-positive advanced breast cancer that had progressed on trastuzumab (Herceptin) or trastuzumab emtansine (Kadcyla). All were given pembrolizumab (Keytruda), which unleashes antitumor immunity by targeting the programmed death-1 receptor on immune cells, in combination with trastuzumab.
With a median follow-up of 13.6 months, the cohort of patients having tumors positive for PD-L1 achieved an overall response rate of 15.2% and a disease control rate of 24%,” Dr. Loi reported in a press briefing and session, on behalf of the International Breast Cancer Study Group and Breast International Group. In contrast, there were no responses in the PD-L1–negative cohort.
Within the PD-L1–positive cohort, stromal levels of TILs in the metastatic lesion – which were low overall – influenced likelihood of benefit. The response rate was almost eight times higher in patients who had at least 5% of the stromal area densely infiltrated with TILs.
“The PANACEA study met its primary endpoint in the PD-L1–positive cohort. For responders, this combination offers durable control without chemotherapy,” Dr. Loi summarized.
“Metastatic HER2-positive breast cancer in this [heavily pretreated] setting is poorly immunogenic, as evidenced by the majority of patients having low TILs in their metastatic lesions. Saying that, however, we did observe a higher response rate in this study as compared to the equivalent triple-negative breast cancer studied in KEYNOTE-086,” she noted. “Future directions in this disease space should focus on combinations with effective anti-HER2 therapy, particularly in low-TIL patients.”
Predicting benefit
The trial is noteworthy for its efforts to identify the subset of patients most likely to benefit from immune checkpoint inhibition, according to press briefing moderator Virginia Kaklamani, MD, a professor of medicine in the division of hematology/oncology at the University of Texas Health Science Center, San Antonio, and a leader of the Breast Cancer Program at the UT Health San Antonio Cancer Center.
In similar studies among patients with HER2-negative breast cancer, PD-L1 did not pan out as a strong predictive biomarker. “What do you think the difference is between that subset and the HER2-positive subset?” Dr. Kaklamani asked.
“First off, I think that there are technical issues with the PD-L1 assay. And we find that patients with high TILs or immune infiltration usually have high levels of PD-L1 expression on their TILs,” Dr. Loi replied. “So I think that PD-L1 can be expressed on the tumor as well as the TIL, and it certainly seems to be the TIL infiltrate that probably enriches for responders to a PD-L1 checkpoint inhibitor on its own or in this case with trastuzumab.”
Study details
In the PANACEA trial (additionally known as IBCSG 45-13 and BIG 4-13), the most common adverse event of any grade and type with the pembrolizumab-trastuzumab combination was fatigue, seen in 21% of patients, Dr. Loi reported. For immune-related adverse events specifically, 19.0% of patients experienced an event, 10.3% experienced an event of grade 3 or worse, and 6.9% stopped treatment because of these events.
“These frequencies are consistent with what has been reported in other solid tumor types with pembrolizumab,” she commented. There were no cardiac events reported.
Efficacy analyses were restricted largely to the PD-L1–positive cohort, given the lack of any response in the negative cohort.
Median duration of response in the positive cohort was 3.5 months, and median duration of disease control was 11.1 months. Five patients (10.8%) remain on treatment with no progression; three of them have completed 2 years of pembrolizumab.
Median progression-free and overall survival were 2.7 and 16.1 months, respectively; corresponding 12-month rates were 13% and 65%. “There is a tantalizing suggestion of a tail on the curve. ... Obviously, this requires further follow-up, and the numbers are small,” Dr. Loi commented.
The median baseline stromal TIL level in metastatic lesions was just 1%. “This is 20 times less than what we observe in primary HER2-positive breast cancers,” she pointed out.
Compared with the PD-L1–negative cohort, the PD-L1–positive cohort had higher TIL levels. Additionally, within that latter cohort, TIL level was higher among patients achieving response versus not (P = .006) and patients achieving disease control versus not (P = .0006).
“We then went on to try to identify a TIL cutoff that could enrich the population for responders. This has been done in other solid tumor types,” Dr. Loi explained.
Analyses in the PD-L1-positive cohort showed that TIL levels down to 5% predicted benefit. The 41% of patients having 5% or more TILs were dramatically more likely to have a response (39% vs. 5%) and disease control (47% vs. 5%).
TIL levels varied widely according to site of the metastasis, with higher levels seen in metastases from lung and lymph nodes, and lower levels seen in those from liver and skin.
“At this stage, we are not sure which is the chicken and the egg: Patients could have disease in their lung and their lymph nodes because their immune system is better controlling their disease,” Dr. Loi commented. “How we treat these patients is still an open question. In patients with liver metastases, perhaps we need to be more aggressive with the primary or tumor-control anti-HER2 therapy.”
Improving efficacy
Going forward, one strategy for improving pembrolizumab efficacy in this patient population might be priming the immune response, according to Dr. Loi.
“In HER2 disease, it’s very clear that oncogenic signaling is the driver, so targeting HER2 potently also will help relieve tumor-mediated immune suppression,” she elaborated. “In this particular context, targeting HER2 well is the key. Whether you need the addition of a little bit of chemo or some radiation, all this needs to be studied.”
Another strategy for improving pembrolizumab efficacy might be moving the drug to earlier disease settings, Dr. Loi proposed.
“By the time you get to advanced stage and have had multiple treatments, you actually have low levels of T-cell infiltration in your metastatic lesion, for whatever reasons – tumor burden, immunosuppression, multiple lines of treatment. That all reduces your chance of responding to pembrolizumab, for example, as monotherapy,” she elaborated. “We don’t know yet if chemotherapy in addition to pembrolizumab could change that tumor microenvironment. But still, I think the earlier in lines you go, the more chance you are going to have of preexisting effective antitumor immunity that can be reactivated with the addition of pembrolizumab.”
Dr. Loi disclosed that her institution receives research funding from Novartis, Pfizer, Merck, Genentech/Roche, and Puma. Merck provided study drug and support for PANACEA.
SOURCE: Loi S et al. SABCS 2017 Abstract GS2-06.
SAN ANTONIO – The immune checkpoint inhibitor pembrolizumab overcomes trastuzumab resistance in HER2-positive advanced breast cancer provided that the tumor expresses programmed death ligand 1 (PD-L1), a trial reported at the San Antonio Breast Cancer Symposium suggests. But presence of immune cells in the tumor is a major additional determinant of benefit.
The single-arm phase 1b/2 trial, called PANACEA (also KEYNOTE-014), enrolled 58 patients with HER2-positive advanced breast cancer that had progressed on trastuzumab (Herceptin) or trastuzumab emtansine (Kadcyla). All were given pembrolizumab (Keytruda), which unleashes antitumor immunity by targeting the programmed death-1 receptor on immune cells, in combination with trastuzumab.
With a median follow-up of 13.6 months, the cohort of patients having tumors positive for PD-L1 achieved an overall response rate of 15.2% and a disease control rate of 24%,” Dr. Loi reported in a press briefing and session, on behalf of the International Breast Cancer Study Group and Breast International Group. In contrast, there were no responses in the PD-L1–negative cohort.
Within the PD-L1–positive cohort, stromal levels of TILs in the metastatic lesion – which were low overall – influenced likelihood of benefit. The response rate was almost eight times higher in patients who had at least 5% of the stromal area densely infiltrated with TILs.
“The PANACEA study met its primary endpoint in the PD-L1–positive cohort. For responders, this combination offers durable control without chemotherapy,” Dr. Loi summarized.
“Metastatic HER2-positive breast cancer in this [heavily pretreated] setting is poorly immunogenic, as evidenced by the majority of patients having low TILs in their metastatic lesions. Saying that, however, we did observe a higher response rate in this study as compared to the equivalent triple-negative breast cancer studied in KEYNOTE-086,” she noted. “Future directions in this disease space should focus on combinations with effective anti-HER2 therapy, particularly in low-TIL patients.”
Predicting benefit
The trial is noteworthy for its efforts to identify the subset of patients most likely to benefit from immune checkpoint inhibition, according to press briefing moderator Virginia Kaklamani, MD, a professor of medicine in the division of hematology/oncology at the University of Texas Health Science Center, San Antonio, and a leader of the Breast Cancer Program at the UT Health San Antonio Cancer Center.
In similar studies among patients with HER2-negative breast cancer, PD-L1 did not pan out as a strong predictive biomarker. “What do you think the difference is between that subset and the HER2-positive subset?” Dr. Kaklamani asked.
“First off, I think that there are technical issues with the PD-L1 assay. And we find that patients with high TILs or immune infiltration usually have high levels of PD-L1 expression on their TILs,” Dr. Loi replied. “So I think that PD-L1 can be expressed on the tumor as well as the TIL, and it certainly seems to be the TIL infiltrate that probably enriches for responders to a PD-L1 checkpoint inhibitor on its own or in this case with trastuzumab.”
Study details
In the PANACEA trial (additionally known as IBCSG 45-13 and BIG 4-13), the most common adverse event of any grade and type with the pembrolizumab-trastuzumab combination was fatigue, seen in 21% of patients, Dr. Loi reported. For immune-related adverse events specifically, 19.0% of patients experienced an event, 10.3% experienced an event of grade 3 or worse, and 6.9% stopped treatment because of these events.
“These frequencies are consistent with what has been reported in other solid tumor types with pembrolizumab,” she commented. There were no cardiac events reported.
Efficacy analyses were restricted largely to the PD-L1–positive cohort, given the lack of any response in the negative cohort.
Median duration of response in the positive cohort was 3.5 months, and median duration of disease control was 11.1 months. Five patients (10.8%) remain on treatment with no progression; three of them have completed 2 years of pembrolizumab.
Median progression-free and overall survival were 2.7 and 16.1 months, respectively; corresponding 12-month rates were 13% and 65%. “There is a tantalizing suggestion of a tail on the curve. ... Obviously, this requires further follow-up, and the numbers are small,” Dr. Loi commented.
The median baseline stromal TIL level in metastatic lesions was just 1%. “This is 20 times less than what we observe in primary HER2-positive breast cancers,” she pointed out.
Compared with the PD-L1–negative cohort, the PD-L1–positive cohort had higher TIL levels. Additionally, within that latter cohort, TIL level was higher among patients achieving response versus not (P = .006) and patients achieving disease control versus not (P = .0006).
“We then went on to try to identify a TIL cutoff that could enrich the population for responders. This has been done in other solid tumor types,” Dr. Loi explained.
Analyses in the PD-L1-positive cohort showed that TIL levels down to 5% predicted benefit. The 41% of patients having 5% or more TILs were dramatically more likely to have a response (39% vs. 5%) and disease control (47% vs. 5%).
TIL levels varied widely according to site of the metastasis, with higher levels seen in metastases from lung and lymph nodes, and lower levels seen in those from liver and skin.
“At this stage, we are not sure which is the chicken and the egg: Patients could have disease in their lung and their lymph nodes because their immune system is better controlling their disease,” Dr. Loi commented. “How we treat these patients is still an open question. In patients with liver metastases, perhaps we need to be more aggressive with the primary or tumor-control anti-HER2 therapy.”
Improving efficacy
Going forward, one strategy for improving pembrolizumab efficacy in this patient population might be priming the immune response, according to Dr. Loi.
“In HER2 disease, it’s very clear that oncogenic signaling is the driver, so targeting HER2 potently also will help relieve tumor-mediated immune suppression,” she elaborated. “In this particular context, targeting HER2 well is the key. Whether you need the addition of a little bit of chemo or some radiation, all this needs to be studied.”
Another strategy for improving pembrolizumab efficacy might be moving the drug to earlier disease settings, Dr. Loi proposed.
“By the time you get to advanced stage and have had multiple treatments, you actually have low levels of T-cell infiltration in your metastatic lesion, for whatever reasons – tumor burden, immunosuppression, multiple lines of treatment. That all reduces your chance of responding to pembrolizumab, for example, as monotherapy,” she elaborated. “We don’t know yet if chemotherapy in addition to pembrolizumab could change that tumor microenvironment. But still, I think the earlier in lines you go, the more chance you are going to have of preexisting effective antitumor immunity that can be reactivated with the addition of pembrolizumab.”
Dr. Loi disclosed that her institution receives research funding from Novartis, Pfizer, Merck, Genentech/Roche, and Puma. Merck provided study drug and support for PANACEA.
SOURCE: Loi S et al. SABCS 2017 Abstract GS2-06.
REPORTING FROM SABCS 2017
Key clinical point:
Major finding: The PD-L1–positive cohort had an overall response rate of 15.2% and a disease control rate of 24%.
Data source: A single-arm phase 1b/2 trial among 58 women with trastuzumab-resistant HER2-positive advanced breast cancer (PANACEA study).
Disclosures: Dr. Loi disclosed that her institution receives research funding from Novartis, Pfizer, Merck, Genentech/Roche, and Puma. Merck provided study drug and support.
Source: Loi S et al. SABCS 2017 Abstract GS2-06.
Novel PARP inhibitor boosts PFS in HER2- breast cancer with BRCA mutations
SAN ANTONIO – In women with advanced HER2-negative breast cancer with germline BRCA mutations, an investigational oral PARP inhibitor talazoparib was associated with a near doubling in progression-free survival (PFS) when compared with single-agent chemotherapy, results of the phase 3 EMBRACA trial show.
After a median follow-up of 11.2 months, the median PFS by blinded central review – the primary endpoint – was 8.6 months for patients assigned to receive talazoparib, compared with 5.6 months for patients randomized to receive the physician’s choice of either capecitabine, eribulin, gemcitabine, or vinorelbine, reported Jennifer K. Litton, MD, from the University of Texas MD Anderson Cancer Center in Houston.

“Patients who were assigned to talazoparib had an improvement in their global health status versus patients who had deterioration when randomized.”
Talazoparib is an oral inhibitor of poly ADP-ribose polymerase (PARP) with a dual mechanism of action: It both inhibits the PARP enzyme directly and traps PARP on single-stranded DNA breaks, preventing repair of DNA damage and leading to the death of malignant cells.
In the phase 2 ABRAZO trial, the PARP inhibitor showed “encouraging” efficacy and safety in patients with germline BRCA1/BRCA2 mutations who had received platinum-based chemotherapy or at least three prior cytotoxic regimens.
Dr. Litton reported results of the EMBRACA trial, a phase 3 study in patients with locally advanced or metastatic HER2 negative breast cancer a germline BRCA1 or BRCA2 mutation. Patients were stratified by number of prior chemotherapy regimens, by having triple-negative breast cancer or hormone receptor-positive breast cancer, and by having a history of either central nervous system metastases or no CNS metastases; they were then randomized on a 2:1 basis to either oral talazoparib 1 mg daily (287 patients) or to the physician’s choice of therapy with one of the agents noted before.
The patient characteristics were generally well balanced, although there was a higher percentage of patients aged younger than 50 years in the talazoparib group than in the group treated with other agents (63.4% vs. 46.5%, respectively), slightly more CNS metastases (15% vs. 13.9%), and a higher percentage of patients with a disease-free interval (time from initial diagnosis to advanced breast cancer) shorter than 12 months (37.6% vs. 29.2%).
The primary endpoint of PFS by blinded central review showed the aforementioned significant benefit of talazoparib. A PFS by subgroup analysis showed that talazoparib was significantly better in all parameters except for patients who had previously received platinum-based therapy.
The trial was also powered to show overall survival as a secondary endpoint, but the data are not mature, Dr. Litton said. An interim OS analysis showed an apparent trend favoring the PARP inhibitor, with a median of 22.3 months, compared with 19.5 months with physician’s choice of treatment.
The 24- and 36-month probabilities of survival were 45% and 34% respectively for patients treated with talazoparib, compared with 37% and 0% for patients treated with other agents.
The objective response rate by investigator rating was 62.6% with talazoparib, compared with 27.2% for other drugs (odds ratio, 4.99; P less than .0001).
Anemia was the most common hematologic adverse event, with grade 3 or greater occurring in 39.2% of patients on the PARP inhibitor, compared with 4.8% of patients treated with other agents.
Talazoparib, unlike other PARP inhibitors, was also associated with grade 1 or 2 alopecia, which occurred in 25.2% of those patients, compared with 27.8% of those receiving the physician’s choice of treatment.
Grade 3 or 4 serious adverse events occurred in about 25.5% of patients in each study arm. Events leading to permanent drug discontinuation were more common with physician’s choice agents at 9.5%, compared with 7.7% of patients treated with talazoparib.

Kent Osborne, MD, the director of the Dan L. Duncan Cancer Center at Baylor College of Medicine, Houston, who moderated a briefing where Dr. Litton presented the data, commented that patients may not be as enthusiastic about the results as investigators seem to be.
“I’ve heard doctors like you and I say ‘This is really great, we’ve got some activity from a PARP inhibitor;’ patients look at it and say ‘Gee, a few more responses and a 3-month prolongation on average of my time to progression is not a very big advantage,’ ” he said to Dr. Litton.
“So what’s the next step in the development of these drugs? Are they going to be used in combinations? Are we going to come up with a mechanism of resistance that we can then overcome to extend the duration of their benefit?” he asked.
Dr. Litton replied that she was encouraged by fact that the tails of the survival curves appear to be separating and that some patients have complete responses and some have relatively durable responses.
“One of the things that we’re going to be looking at are the correlatives, trying to identify who these extraordinary responders are and the mechanisms of resistance as best we can,” she said.
This study was funded by Pfizer, which developed the inhibitor. Dr. Litton has disclosed research funding with EMD Serono, AstraZeneca, Pfizer, Genentech, and GlaxoSmithKline, and serves on advisory boards for Pfizer and AstraZeneca, all uncompensated.
SOURCE: Litton et al. SABCS 2017 Abstract GS6-07.
SAN ANTONIO – In women with advanced HER2-negative breast cancer with germline BRCA mutations, an investigational oral PARP inhibitor talazoparib was associated with a near doubling in progression-free survival (PFS) when compared with single-agent chemotherapy, results of the phase 3 EMBRACA trial show.
After a median follow-up of 11.2 months, the median PFS by blinded central review – the primary endpoint – was 8.6 months for patients assigned to receive talazoparib, compared with 5.6 months for patients randomized to receive the physician’s choice of either capecitabine, eribulin, gemcitabine, or vinorelbine, reported Jennifer K. Litton, MD, from the University of Texas MD Anderson Cancer Center in Houston.
“Patients who were assigned to talazoparib had an improvement in their global health status versus patients who had deterioration when randomized.”
Talazoparib is an oral inhibitor of poly ADP-ribose polymerase (PARP) with a dual mechanism of action: It both inhibits the PARP enzyme directly and traps PARP on single-stranded DNA breaks, preventing repair of DNA damage and leading to the death of malignant cells.
In the phase 2 ABRAZO trial, the PARP inhibitor showed “encouraging” efficacy and safety in patients with germline BRCA1/BRCA2 mutations who had received platinum-based chemotherapy or at least three prior cytotoxic regimens.
Dr. Litton reported results of the EMBRACA trial, a phase 3 study in patients with locally advanced or metastatic HER2 negative breast cancer a germline BRCA1 or BRCA2 mutation. Patients were stratified by number of prior chemotherapy regimens, by having triple-negative breast cancer or hormone receptor-positive breast cancer, and by having a history of either central nervous system metastases or no CNS metastases; they were then randomized on a 2:1 basis to either oral talazoparib 1 mg daily (287 patients) or to the physician’s choice of therapy with one of the agents noted before.
The patient characteristics were generally well balanced, although there was a higher percentage of patients aged younger than 50 years in the talazoparib group than in the group treated with other agents (63.4% vs. 46.5%, respectively), slightly more CNS metastases (15% vs. 13.9%), and a higher percentage of patients with a disease-free interval (time from initial diagnosis to advanced breast cancer) shorter than 12 months (37.6% vs. 29.2%).
The primary endpoint of PFS by blinded central review showed the aforementioned significant benefit of talazoparib. A PFS by subgroup analysis showed that talazoparib was significantly better in all parameters except for patients who had previously received platinum-based therapy.
The trial was also powered to show overall survival as a secondary endpoint, but the data are not mature, Dr. Litton said. An interim OS analysis showed an apparent trend favoring the PARP inhibitor, with a median of 22.3 months, compared with 19.5 months with physician’s choice of treatment.
The 24- and 36-month probabilities of survival were 45% and 34% respectively for patients treated with talazoparib, compared with 37% and 0% for patients treated with other agents.
The objective response rate by investigator rating was 62.6% with talazoparib, compared with 27.2% for other drugs (odds ratio, 4.99; P less than .0001).
Anemia was the most common hematologic adverse event, with grade 3 or greater occurring in 39.2% of patients on the PARP inhibitor, compared with 4.8% of patients treated with other agents.
Talazoparib, unlike other PARP inhibitors, was also associated with grade 1 or 2 alopecia, which occurred in 25.2% of those patients, compared with 27.8% of those receiving the physician’s choice of treatment.
Grade 3 or 4 serious adverse events occurred in about 25.5% of patients in each study arm. Events leading to permanent drug discontinuation were more common with physician’s choice agents at 9.5%, compared with 7.7% of patients treated with talazoparib.
Kent Osborne, MD, the director of the Dan L. Duncan Cancer Center at Baylor College of Medicine, Houston, who moderated a briefing where Dr. Litton presented the data, commented that patients may not be as enthusiastic about the results as investigators seem to be.
“I’ve heard doctors like you and I say ‘This is really great, we’ve got some activity from a PARP inhibitor;’ patients look at it and say ‘Gee, a few more responses and a 3-month prolongation on average of my time to progression is not a very big advantage,’ ” he said to Dr. Litton.
“So what’s the next step in the development of these drugs? Are they going to be used in combinations? Are we going to come up with a mechanism of resistance that we can then overcome to extend the duration of their benefit?” he asked.
Dr. Litton replied that she was encouraged by fact that the tails of the survival curves appear to be separating and that some patients have complete responses and some have relatively durable responses.
“One of the things that we’re going to be looking at are the correlatives, trying to identify who these extraordinary responders are and the mechanisms of resistance as best we can,” she said.
This study was funded by Pfizer, which developed the inhibitor. Dr. Litton has disclosed research funding with EMD Serono, AstraZeneca, Pfizer, Genentech, and GlaxoSmithKline, and serves on advisory boards for Pfizer and AstraZeneca, all uncompensated.
SOURCE: Litton et al. SABCS 2017 Abstract GS6-07.
SAN ANTONIO – In women with advanced HER2-negative breast cancer with germline BRCA mutations, an investigational oral PARP inhibitor talazoparib was associated with a near doubling in progression-free survival (PFS) when compared with single-agent chemotherapy, results of the phase 3 EMBRACA trial show.
After a median follow-up of 11.2 months, the median PFS by blinded central review – the primary endpoint – was 8.6 months for patients assigned to receive talazoparib, compared with 5.6 months for patients randomized to receive the physician’s choice of either capecitabine, eribulin, gemcitabine, or vinorelbine, reported Jennifer K. Litton, MD, from the University of Texas MD Anderson Cancer Center in Houston.
“Patients who were assigned to talazoparib had an improvement in their global health status versus patients who had deterioration when randomized.”
Talazoparib is an oral inhibitor of poly ADP-ribose polymerase (PARP) with a dual mechanism of action: It both inhibits the PARP enzyme directly and traps PARP on single-stranded DNA breaks, preventing repair of DNA damage and leading to the death of malignant cells.
In the phase 2 ABRAZO trial, the PARP inhibitor showed “encouraging” efficacy and safety in patients with germline BRCA1/BRCA2 mutations who had received platinum-based chemotherapy or at least three prior cytotoxic regimens.
Dr. Litton reported results of the EMBRACA trial, a phase 3 study in patients with locally advanced or metastatic HER2 negative breast cancer a germline BRCA1 or BRCA2 mutation. Patients were stratified by number of prior chemotherapy regimens, by having triple-negative breast cancer or hormone receptor-positive breast cancer, and by having a history of either central nervous system metastases or no CNS metastases; they were then randomized on a 2:1 basis to either oral talazoparib 1 mg daily (287 patients) or to the physician’s choice of therapy with one of the agents noted before.
The patient characteristics were generally well balanced, although there was a higher percentage of patients aged younger than 50 years in the talazoparib group than in the group treated with other agents (63.4% vs. 46.5%, respectively), slightly more CNS metastases (15% vs. 13.9%), and a higher percentage of patients with a disease-free interval (time from initial diagnosis to advanced breast cancer) shorter than 12 months (37.6% vs. 29.2%).
The primary endpoint of PFS by blinded central review showed the aforementioned significant benefit of talazoparib. A PFS by subgroup analysis showed that talazoparib was significantly better in all parameters except for patients who had previously received platinum-based therapy.
The trial was also powered to show overall survival as a secondary endpoint, but the data are not mature, Dr. Litton said. An interim OS analysis showed an apparent trend favoring the PARP inhibitor, with a median of 22.3 months, compared with 19.5 months with physician’s choice of treatment.
The 24- and 36-month probabilities of survival were 45% and 34% respectively for patients treated with talazoparib, compared with 37% and 0% for patients treated with other agents.
The objective response rate by investigator rating was 62.6% with talazoparib, compared with 27.2% for other drugs (odds ratio, 4.99; P less than .0001).
Anemia was the most common hematologic adverse event, with grade 3 or greater occurring in 39.2% of patients on the PARP inhibitor, compared with 4.8% of patients treated with other agents.
Talazoparib, unlike other PARP inhibitors, was also associated with grade 1 or 2 alopecia, which occurred in 25.2% of those patients, compared with 27.8% of those receiving the physician’s choice of treatment.
Grade 3 or 4 serious adverse events occurred in about 25.5% of patients in each study arm. Events leading to permanent drug discontinuation were more common with physician’s choice agents at 9.5%, compared with 7.7% of patients treated with talazoparib.
Kent Osborne, MD, the director of the Dan L. Duncan Cancer Center at Baylor College of Medicine, Houston, who moderated a briefing where Dr. Litton presented the data, commented that patients may not be as enthusiastic about the results as investigators seem to be.
“I’ve heard doctors like you and I say ‘This is really great, we’ve got some activity from a PARP inhibitor;’ patients look at it and say ‘Gee, a few more responses and a 3-month prolongation on average of my time to progression is not a very big advantage,’ ” he said to Dr. Litton.
“So what’s the next step in the development of these drugs? Are they going to be used in combinations? Are we going to come up with a mechanism of resistance that we can then overcome to extend the duration of their benefit?” he asked.
Dr. Litton replied that she was encouraged by fact that the tails of the survival curves appear to be separating and that some patients have complete responses and some have relatively durable responses.
“One of the things that we’re going to be looking at are the correlatives, trying to identify who these extraordinary responders are and the mechanisms of resistance as best we can,” she said.
This study was funded by Pfizer, which developed the inhibitor. Dr. Litton has disclosed research funding with EMD Serono, AstraZeneca, Pfizer, Genentech, and GlaxoSmithKline, and serves on advisory boards for Pfizer and AstraZeneca, all uncompensated.
SOURCE: Litton et al. SABCS 2017 Abstract GS6-07.
REPORTING FROM SABCS 2017
Key clinical point: The investigational PARP inhibitor talazoparib extended progression-free survival of advanced HER2-negative breast cancer with germline BRCA mutations.
Major finding: Talazoparib was associated with a 46% reduction in risk for progression when compared with standard single agent therapies.
Data source: Randomized clinical trial in 431 patients with advanced, previously treated breast cancer with germline BRCA1 and BRCA2 mutations.
Disclosures: This study was funded by Pfizer, which developed the inhibitor. Dr. Litton disclosed that she has received research funding from EMD Serono, AstraZeneca, Pfizer, Genentech, and GlaxoSmithKline and that she serves on advisory boards for Pfizer and AstraZeneca, all uncompensated.
Source: Litton J et al. SABCS 2017 Abstract GS6-07.
Extra years of adjuvant bisphosphonate not needed in early breast cancer
SAN ANTONIO – When it comes to adjuvant bisphosphonate therapy following adjuvant chemotherapy for high-risk early breast cancer, more is not better than less, phase 3 data from the randomized SUCCESS A study suggest.
Among 3,421 patients randomized to adjuvant bisphosphonate therapy following chemotherapy, there was barely a speck of difference in either disease-free survival (DFS) or overall survival (OS) between patients randomized to either 2 years or 5 years of adjuvant bisphosphonate therapy with zoledronate, reported Wolfgang Janni, MD, from University Hospital Ulm (Germany).
“We conclude 5 years of adjuvant zoledronate treatment should not be considered currently in these patients in the absence of decreased bone density,” he said at the San Antonio Breast Cancer Symposium.
Adjuvant bisphosphonate therapy in patients with early breast cancer is associated with improved breast cancer–specific survival and reduced rates of breast cancer recurrence in bone, especially for postmenopausal patients, as shown in a meta-analysis from the Early Breast Cancer Trialists’ Collaborative Group, Dr. Janni noted.
German breast cancer guidelines state that postmenopausal women should be offered bisphosphonates as part of their adjuvant systemic therapy, but the optimal duration of therapy is uncertain, prompting the investigators to examine the issue in a randomized trial.
SUCCESS A was a multicenter, phase 3, randomized trial with a multifactorial 2 x 2 design, in patients with high-risk node-negative and node-positive disease. Patients were randomized to FEC100 chemotherapy followed by docetaxel with or without gemcitabine. Chemotherapy was followed by endocrine therapy with 2 years of tamoxifen followed by 3 years of anastrozole (Arimidex). At the start of endocrine therapy, patients were further randomized to receive either 2 or 5 years of adjuvant zoledronate, 4 mg intravenously every 3 months for 2 years, or the same schedule over 2 years, followed by 4 mg every 6 months for 3 years.
A total of 2,987 of the 3,421 patients randomized to a zoledronate schedule were available for inclusion in the analysis.
As noted, adapted DFS and OS, measured starting from 2 years after the start of zoledronate with a maximum observation time of 48 months, were virtually identical between the two treatment groups, with respective P values of .827 and .713. Similarly, in a multivariate regression analysis model adjusted for age, body mass index, menopausal status, tumor size, nodal stage, histological grade and type, hormone receptor status, HER2 status, surgery type, and chemotherapy regimen, the hazard ratio for 5 vs. 2 years was 0.97 for DFS and 0.98 for OS. Neither endpoint was significantly different between the groups.
Similarly, there was no significant differences in the number of bone recurrences as first distant recurrences or in premenopausal vs. postmenopausal women.
Adverse events of any grade were significantly higher with 5 years of bisphosphonate therapy (46.2% vs. 27.2%, P less than .001), including significantly higher grade 3 or greater adverse events (7.6% vs. 5.1%, P = .006).
Following presentation of the data in an oral session, moderator Sibylle Loibl, MD, PhD, of the German Breast Group in Neu-Isenburg, Germany, questioned whether the follow-up was long enough to detect a clinically meaningful difference.
“The negative result of this study might be due to the small observation time,” Dr. Janni conceded.”We have a quite intensive drug regimen for the first 2 years, so this might also be a contributing factor [as to why] we did not see any difference.”
The SUCCESS A study was supported by AstraZeneca, Chugai, Janssen Diagnostics, Lilly, Novartis, and Sanofi-Aventis. Dr. Janni has reported financial relationships with AstraZeneca, Chugai, Janssen, Lilly, Novartis, and Sanofi.
SOURCE: Janni et al. SABCS 2017 Abstract GS1-06
SAN ANTONIO – When it comes to adjuvant bisphosphonate therapy following adjuvant chemotherapy for high-risk early breast cancer, more is not better than less, phase 3 data from the randomized SUCCESS A study suggest.
Among 3,421 patients randomized to adjuvant bisphosphonate therapy following chemotherapy, there was barely a speck of difference in either disease-free survival (DFS) or overall survival (OS) between patients randomized to either 2 years or 5 years of adjuvant bisphosphonate therapy with zoledronate, reported Wolfgang Janni, MD, from University Hospital Ulm (Germany).
“We conclude 5 years of adjuvant zoledronate treatment should not be considered currently in these patients in the absence of decreased bone density,” he said at the San Antonio Breast Cancer Symposium.
Adjuvant bisphosphonate therapy in patients with early breast cancer is associated with improved breast cancer–specific survival and reduced rates of breast cancer recurrence in bone, especially for postmenopausal patients, as shown in a meta-analysis from the Early Breast Cancer Trialists’ Collaborative Group, Dr. Janni noted.
German breast cancer guidelines state that postmenopausal women should be offered bisphosphonates as part of their adjuvant systemic therapy, but the optimal duration of therapy is uncertain, prompting the investigators to examine the issue in a randomized trial.
SUCCESS A was a multicenter, phase 3, randomized trial with a multifactorial 2 x 2 design, in patients with high-risk node-negative and node-positive disease. Patients were randomized to FEC100 chemotherapy followed by docetaxel with or without gemcitabine. Chemotherapy was followed by endocrine therapy with 2 years of tamoxifen followed by 3 years of anastrozole (Arimidex). At the start of endocrine therapy, patients were further randomized to receive either 2 or 5 years of adjuvant zoledronate, 4 mg intravenously every 3 months for 2 years, or the same schedule over 2 years, followed by 4 mg every 6 months for 3 years.
A total of 2,987 of the 3,421 patients randomized to a zoledronate schedule were available for inclusion in the analysis.
As noted, adapted DFS and OS, measured starting from 2 years after the start of zoledronate with a maximum observation time of 48 months, were virtually identical between the two treatment groups, with respective P values of .827 and .713. Similarly, in a multivariate regression analysis model adjusted for age, body mass index, menopausal status, tumor size, nodal stage, histological grade and type, hormone receptor status, HER2 status, surgery type, and chemotherapy regimen, the hazard ratio for 5 vs. 2 years was 0.97 for DFS and 0.98 for OS. Neither endpoint was significantly different between the groups.
Similarly, there was no significant differences in the number of bone recurrences as first distant recurrences or in premenopausal vs. postmenopausal women.
Adverse events of any grade were significantly higher with 5 years of bisphosphonate therapy (46.2% vs. 27.2%, P less than .001), including significantly higher grade 3 or greater adverse events (7.6% vs. 5.1%, P = .006).
Following presentation of the data in an oral session, moderator Sibylle Loibl, MD, PhD, of the German Breast Group in Neu-Isenburg, Germany, questioned whether the follow-up was long enough to detect a clinically meaningful difference.
“The negative result of this study might be due to the small observation time,” Dr. Janni conceded.”We have a quite intensive drug regimen for the first 2 years, so this might also be a contributing factor [as to why] we did not see any difference.”
The SUCCESS A study was supported by AstraZeneca, Chugai, Janssen Diagnostics, Lilly, Novartis, and Sanofi-Aventis. Dr. Janni has reported financial relationships with AstraZeneca, Chugai, Janssen, Lilly, Novartis, and Sanofi.
SOURCE: Janni et al. SABCS 2017 Abstract GS1-06
SAN ANTONIO – When it comes to adjuvant bisphosphonate therapy following adjuvant chemotherapy for high-risk early breast cancer, more is not better than less, phase 3 data from the randomized SUCCESS A study suggest.
Among 3,421 patients randomized to adjuvant bisphosphonate therapy following chemotherapy, there was barely a speck of difference in either disease-free survival (DFS) or overall survival (OS) between patients randomized to either 2 years or 5 years of adjuvant bisphosphonate therapy with zoledronate, reported Wolfgang Janni, MD, from University Hospital Ulm (Germany).
“We conclude 5 years of adjuvant zoledronate treatment should not be considered currently in these patients in the absence of decreased bone density,” he said at the San Antonio Breast Cancer Symposium.
Adjuvant bisphosphonate therapy in patients with early breast cancer is associated with improved breast cancer–specific survival and reduced rates of breast cancer recurrence in bone, especially for postmenopausal patients, as shown in a meta-analysis from the Early Breast Cancer Trialists’ Collaborative Group, Dr. Janni noted.
German breast cancer guidelines state that postmenopausal women should be offered bisphosphonates as part of their adjuvant systemic therapy, but the optimal duration of therapy is uncertain, prompting the investigators to examine the issue in a randomized trial.
SUCCESS A was a multicenter, phase 3, randomized trial with a multifactorial 2 x 2 design, in patients with high-risk node-negative and node-positive disease. Patients were randomized to FEC100 chemotherapy followed by docetaxel with or without gemcitabine. Chemotherapy was followed by endocrine therapy with 2 years of tamoxifen followed by 3 years of anastrozole (Arimidex). At the start of endocrine therapy, patients were further randomized to receive either 2 or 5 years of adjuvant zoledronate, 4 mg intravenously every 3 months for 2 years, or the same schedule over 2 years, followed by 4 mg every 6 months for 3 years.
A total of 2,987 of the 3,421 patients randomized to a zoledronate schedule were available for inclusion in the analysis.
As noted, adapted DFS and OS, measured starting from 2 years after the start of zoledronate with a maximum observation time of 48 months, were virtually identical between the two treatment groups, with respective P values of .827 and .713. Similarly, in a multivariate regression analysis model adjusted for age, body mass index, menopausal status, tumor size, nodal stage, histological grade and type, hormone receptor status, HER2 status, surgery type, and chemotherapy regimen, the hazard ratio for 5 vs. 2 years was 0.97 for DFS and 0.98 for OS. Neither endpoint was significantly different between the groups.
Similarly, there was no significant differences in the number of bone recurrences as first distant recurrences or in premenopausal vs. postmenopausal women.
Adverse events of any grade were significantly higher with 5 years of bisphosphonate therapy (46.2% vs. 27.2%, P less than .001), including significantly higher grade 3 or greater adverse events (7.6% vs. 5.1%, P = .006).
Following presentation of the data in an oral session, moderator Sibylle Loibl, MD, PhD, of the German Breast Group in Neu-Isenburg, Germany, questioned whether the follow-up was long enough to detect a clinically meaningful difference.
“The negative result of this study might be due to the small observation time,” Dr. Janni conceded.”We have a quite intensive drug regimen for the first 2 years, so this might also be a contributing factor [as to why] we did not see any difference.”
The SUCCESS A study was supported by AstraZeneca, Chugai, Janssen Diagnostics, Lilly, Novartis, and Sanofi-Aventis. Dr. Janni has reported financial relationships with AstraZeneca, Chugai, Janssen, Lilly, Novartis, and Sanofi.
SOURCE: Janni et al. SABCS 2017 Abstract GS1-06
REPORTING FROM SABCS 2017
Key clinical point: Five years of adjuvant bisphosphonate therapy offered no survival advantages over 2 years of therapy for women with early breast cancers.
Major finding: Neither adapted disease-free survival nor overall survival were significantly better with 3 extra years of zoledronate therapy.
Data source: Randomized phase 3 trial.
Disclosures: The SUCCESS A study was supported by AstraZeneca, Chugai, Janssen Diagnostics, Lilly, Novartis, and Sanofi-Aventis. Dr. Janni has reported financial relationships with AstraZeneca, Chugai, Janssen, Lilly, Novartis, and Sanofi.
Source: Janni et al., SABCS 2017 abstract GS1-06
VIDEO: CTCs may identify asymptomatic late breast cancer recurrences
SAN ANTONIO – Although the initial ardor over the use of circulating tumor cells (CTCs) in cancer diagnosis has cooled, new research suggests that they may play a role in identifying late breast cancer recurrences in otherwise asymptomatic patients, according to members of the ECOG-ACRIN cancer research group.
In this video interview from the the San Antonio Breast Cancer Symposium, Joseph A. Sparano, MD, of Montefiore Medical Center and Albert Einstein College of Medicine in New York, describes ECOG-ACRIN’s experiments showing that patients with hormone receptor–positive disease and HER2-negative breast cancer have a significantly elevated risk for recurrence, supporting CTCs as prognostic biomarkers for late recurrences.
If the findings can be replicated in prospective clinical trials, CTC assay results could help clinicians choose treatments for patients who are at risk for late recurrence.
ECOG-ACRIN received funding for this study from the Breast Cancer Research Foundation, Susan G. Komen, and the National Cancer Institute. Dr. Sparano declared no conflicts of interest.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – Although the initial ardor over the use of circulating tumor cells (CTCs) in cancer diagnosis has cooled, new research suggests that they may play a role in identifying late breast cancer recurrences in otherwise asymptomatic patients, according to members of the ECOG-ACRIN cancer research group.
In this video interview from the the San Antonio Breast Cancer Symposium, Joseph A. Sparano, MD, of Montefiore Medical Center and Albert Einstein College of Medicine in New York, describes ECOG-ACRIN’s experiments showing that patients with hormone receptor–positive disease and HER2-negative breast cancer have a significantly elevated risk for recurrence, supporting CTCs as prognostic biomarkers for late recurrences.
If the findings can be replicated in prospective clinical trials, CTC assay results could help clinicians choose treatments for patients who are at risk for late recurrence.
ECOG-ACRIN received funding for this study from the Breast Cancer Research Foundation, Susan G. Komen, and the National Cancer Institute. Dr. Sparano declared no conflicts of interest.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – Although the initial ardor over the use of circulating tumor cells (CTCs) in cancer diagnosis has cooled, new research suggests that they may play a role in identifying late breast cancer recurrences in otherwise asymptomatic patients, according to members of the ECOG-ACRIN cancer research group.
In this video interview from the the San Antonio Breast Cancer Symposium, Joseph A. Sparano, MD, of Montefiore Medical Center and Albert Einstein College of Medicine in New York, describes ECOG-ACRIN’s experiments showing that patients with hormone receptor–positive disease and HER2-negative breast cancer have a significantly elevated risk for recurrence, supporting CTCs as prognostic biomarkers for late recurrences.
If the findings can be replicated in prospective clinical trials, CTC assay results could help clinicians choose treatments for patients who are at risk for late recurrence.
ECOG-ACRIN received funding for this study from the Breast Cancer Research Foundation, Susan G. Komen, and the National Cancer Institute. Dr. Sparano declared no conflicts of interest.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
REPORTING FROM SABCS 2017

Hallmark tumor metabolism becomes a validated therapeutic target
Altered cell metabolism has long been recognized as a distinctive feature of malignant cells but, until recently, research efforts had focused on a single aspect. It has become increasingly evident that many metabolic pathways are altered in cancer cells. Improved understanding has yielded the first regulatory approval in this new class of drugs. Here, we discuss the latest developments in the therapeutic targeting of the cancer metabolism hallmark.
A cancer cell’s sweet tooth
The metabolism of cancer cells differs from that of normal cells, an observation that has spawned a dedicated field of research and new targeted drug development. The German physiologist Otto Warburg is credited as the father of the field with his observations about the way in which cancer cells derive energy from glucose.1
In normal cells, glucose is converted into pyruvate in the cytoplasm, which is then, most often, fed to the mitochondria that use oxidative phosphorylation to produce energy in the form of adenosine triphosphate (ATP). Cancer cells seem instead to favor using the pyruvate to produce lactate through glycolysis (Figure 1).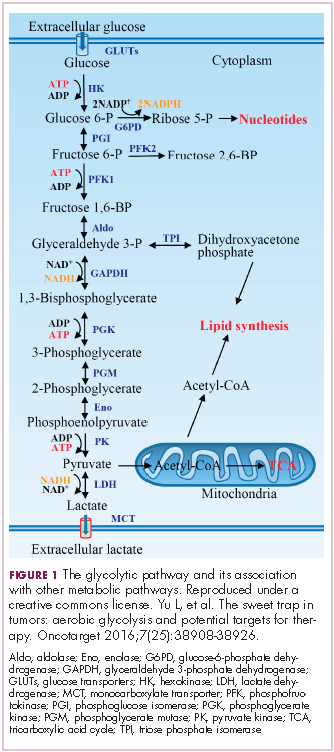
Glycolysis is usually reserved for conditions of poor oxygen availability, but although the tumor microenvironment is often hypoxic, cancer cells have been shown to use glycolysis even when oxygen is plentiful. As a result, the phenomenon is known as aerobic glycolysis, although it is most often referred to as the Warburg effect.2
Glycolysis is much less efficient than oxidative phosphorylation at producing energy, yielding only 2 ATP. In order to meet their energy demands in this way, cancer cells ramp up their glucose intake, an effect that has been exploited for the detection of cancer with positron-emission tomography.
Warburg postulated that this metabolic shift was a result of mitochondrial damage and defective oxidative phosphorylation, even going so far as to suggest that cancer was a mitochondrial disease. It has subsequently been shown that the mitochondria are mostly intact in cancer cells and that oxidative phosphorylation can still occur.3
The Warburg effect has been the subject of significant investigative efforts as researchers have attempted to better understand how this phenomenon comes about. Studies have shown that it is driven in large part by the transcription factors hypoxia inducible factor 1 alpha (HIF-1α) and c-Myc. In addition, numerous other signaling pathways, including the phosphatidylinositol 3-kinase (PI3K)-Akt-mammalian target of rapamycin (mTOR) pathway, and the activation of oncogenes and inactivation of tumor suppressors, are thought to play a central role.
HIF-1α is an oxygen-sensing transcription factor that coordinates cellular responses to reduced oxygen levels by binding to specific regions, known as hypoxia response elements, on target genes in the nucleus and regulating their subsequent expression. Oxygen levels and metabolism are tightly linked, and HIF-1α sits at the intersection of the 2 since many of its target genes are involved in metabolic pathways, including many glycolytic enzymes, but it also directly inhibits oxidative phosphorylation by suppressing key enzymes in this metabolic pathway.
The expression of HIF-1α and numerous glycolytic enzymes, including lactate dehydrogenase (LDH), phosphofructokinase (PFK), hexokinase II (HKII), and pyruvate dehydrogenase kinase (PDK) is increased in many tumor types. Other molecules that are associated with glucose uptake and metabolism are also dysregulated, such as the GLUT-1 glucose transporter.2,4-6
Targeting glycolysis and glucose uptake
According to one study, glucose transporters and glycolytic enzymes are overexpressed in 24 different types of cancer, representing more than 70% of all cancer cases.7 This enables cancer cells to respond metabolically as though they are experiencing hypoxia, even when oxygen is plentiful and, indeed, when hypoxia is a concern, to mount a faster response. It also provides a tempting avenue for anticancer drug design by exploiting the dependency of cancer cells on glycolysis to survive and thrive.
Inhibitors of HKII, LDH, PFK, PDK, and GLUT-1 have been and continue to be developed. For example, 2-deoxy-D-glucose is a glucose molecule in which the 2-hydroxyl group has been replaced by hydrogen, preventing further glycolysis; it acts as a competitive inhibitor of HKII. Dichloroacetate (DCA) activates the pyruvate dehydrogenase complex and inhibits the actions of the PDKs. Although development of DCA itself was unsuccessful, DCA derivatives continue to be pursued. WZB117 and STF-31 are novel small-molecule inhibitors of GLUT-1-mediated glucose transport. To date, where inhibitors of glycolysis have progressed into clinical trials, they have not proved successful, often limited by off-target effects and low potency.8-11
A variety of cell signaling pathways are implicated in metabolism by tightly regulating the ability of cells to gain access to and use nutrients. Through aberrations in these pathways, cancer cells can essentially go rogue, ignoring regulatory signals and taking up nutrients in an autonomous manner. One of the most frequently altered signaling pathways in human cancer, the PI3K-Akt-mTOR pathway, is also an important regulator of metabolism, coordinating the uptake of multiple nutrients, including glucose.
Akt in particular is thought to have a critical role in glucose metabolism and increased Akt pathway signaling has been shown to correlate with increased rates of glycolysis in cancer cells. Thus, Akt inhibitors could double as glycolytic or glucose transport inhibitors.12,13
A number of Akt inhibitors are being evaluated in clinical trials (Table) and results from the phase 2 LOTUS trial of ipatasertib (GDC-0068) were recently published.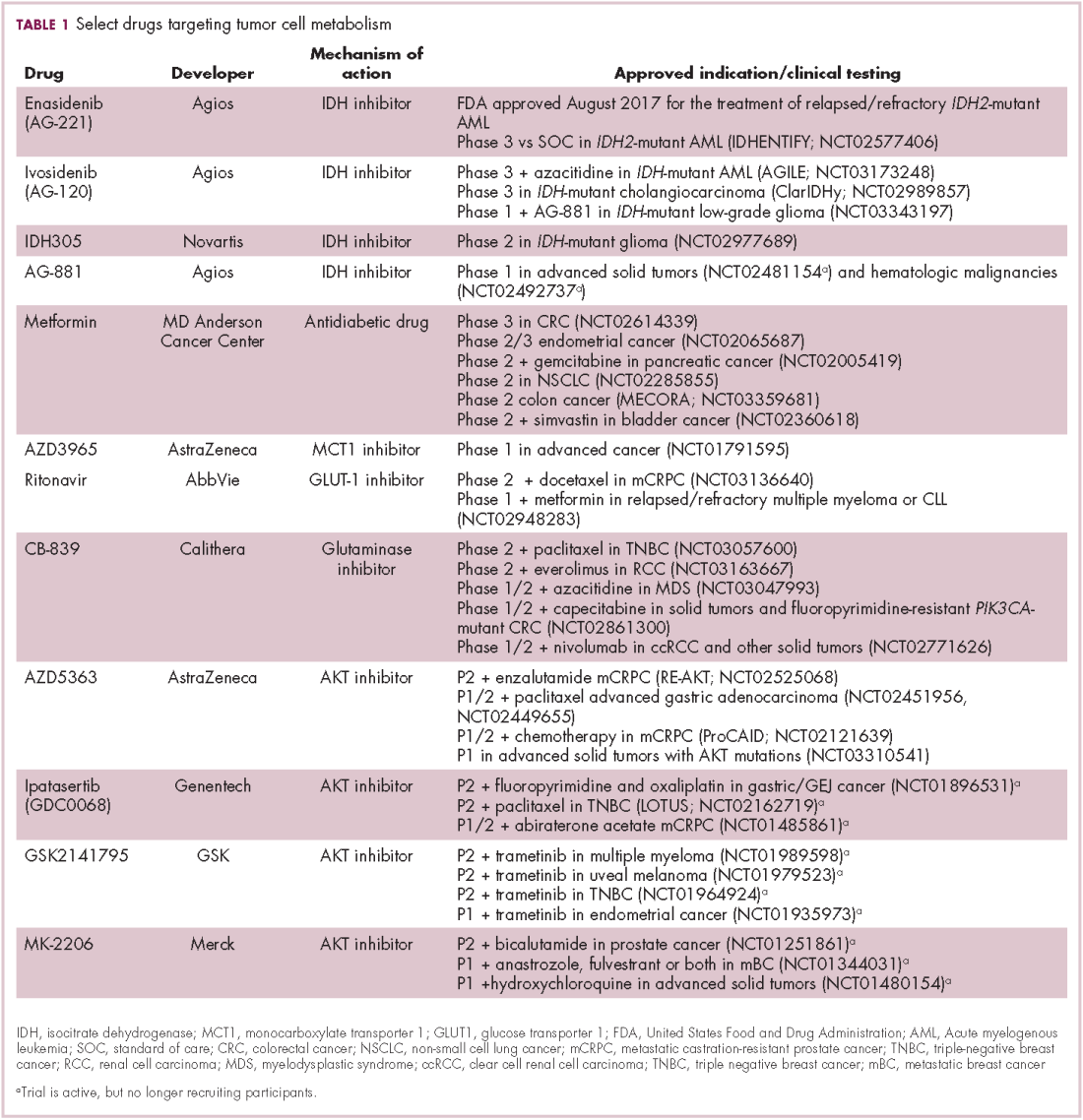
Among 124 patients randomly assigned to paclitaxel in combination with either ipatasertib or placebo, there was a modest improvement in progression-free survival (PFS) in the ipatasertib arm in patients with triple-negative breast cancer (TNBC; 6 months vs 4.2 months, respectively; hazard ratio [HR], 0.60; P = .037). The effect was more pronounced, though not statistically significant, in patients with phosphatase and tensin homolog (PTEN)-low tumors (6.2 months vs 3.7 months; HR, 0.59; P = .18). The most common grade 3 and higher adverse events (AEs) were diarrhea, reduced neutrophil count, and neutropenia.14
The Warburg paradox
Although the molecular mechanisms underlying the Warburg effect have been revealed to some extent, why cancer cells would choose to use such an energy-inefficient process when they have such high energy demands, remains something of a paradox. It’s still not entirely clear, but several explanations that are not necessarily mutually exclusive have been proposed and relate to the inherent benefits of glycolysis and might explain why cancer cells favor this pathway despite its poor energy yield. First, ATP is produced much more rapidly through glycolysis than oxidative phosphorylation, up to 100 times faster. Thus, using glycolysis is a trade-off, between making less energy and making it more quickly.
Second, cancer cells require more than just ATP to meet their metabolic demands. They need amino acids for protein synthesis; nucleotides for DNA replication; lipids for cell membrane synthesis; nicotinamide adenine dinucleotide phosphate (NADPH), which helps the cancer cell deal with oxidative stress; and various other metabolites. Glycolysis branches off into other metabolic pathways that generate many of these metabolites. Among these branched pathways is the pentose phosphate pathway (PPP), which is required for the generation of ribonucleotides and is a major source for NADPH. Cancer cells have been shown to upregulate the flux of glucose into the PPP to meet their anabolic demands and counter oxidative stress.
Third, the lactic acid produced through glycolysis is actively exported from tumor cells by monocarboxylate transporters (MCTs). This creates a highly acidic tumor microenvironment, which can promote several cancer-related processes and also plays a role in tumor-induced immunosuppression, by inhibiting the activity of tumor-infiltrating T cells, reducing dendritic cell maturation, and promoting the transformation of macrophages to a protumorigenic form.2,4,6
Beyond the Warburg effect
Although the focus has been on glucose metabolism and glycolysis, it has been increasingly recognized that many different metabolic pathways are altered. Fundamental changes to the metabolism of all 4 major classes of macromolecules – carbohydrates, lipids, proteins, and nucleic acids – have been observed, encompassing all aspects of cellular metabolism and enabling cancer cells to meet their complete metabolic requirements. There is also evidence that cancer cells are able to switch between different metabolic pathways depending on the availability of oxygen, their energetic needs, environmental stresses, and many other factors. Certainly, there is significant heterogeneity in the metabolic changes that occur in tumors, which vary from tumor to tumor and even within the same tumor and across the lifespan of a tumor as it progresses from an early stage to more advanced or metastatic disease.
The notion of the Warburg effect as a universal phenomenon in cancer cells is now being widely disregarded. Many tumors continue to use oxidative phosphorylation, particularly slower growing tumors, to meet their energy needs. More recently a “reverse” Warburg effect was described, whereby cancer cells are thought to influence the metabolism of the surrounding stromal fibroblasts and essentially outsource aerobic glycolysis to these cells, while performing energy-efficient oxidative phosphorylation themselves (Figure 2).5,15,16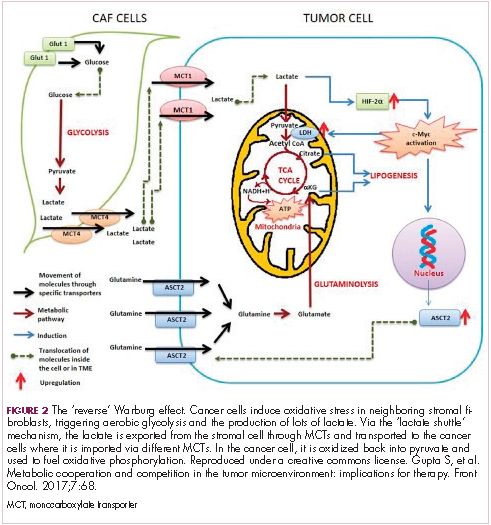
There is thought to be a “lactate shuttle” between the stromal and cancer cells. The stromal cells express high levels of efflux MCTs so that they can remove the subsequently high levels of lactate from the cytoplasm and avoid pickling themselves. The lactate is then shuttled to the cancer cells that have MCTs on their surface that are involved in lactate uptake. The cancer cells oxidize the lactate back into pyruvate, which can then be used in the tricarboxylic acid (TCA) cycle to feed oxidative phosphorylation for efficient ATP production. This hypothesis reflects a broader appreciation of the role of the microenvironment in contributing to cancer metabolism.17,18
An improved holistic understanding of cancer cell metabolism has led to the recognition of altered cancer metabolism as one of the hallmark abilities required for transformation of a normal cell into a cancerous one. It is categorized as “deregulation of bioenergetics” in the most up to date review of the cancer hallmarks.19 It has also begun to shape the therapeutic landscape as new drug targets have emerged.
IDH inhibitors first to market
A number of new metabolically-targeted treatment strategies are being developed. Most promising are small molecule inhibitors of the isocitrate dehydrogenase (IDH) enzymes. These enzymes play an essential role in the TCA cycle, catalyzing the conversion of isocitrate to alpha-ketoglutarate, generating carbon dioxide and NADPH. Recurrent mutations in the IDH1 and IDH2 genes have been observed in several different types of cancer, including glioma, acute myeloid leukemia (AML), and cholangiocarcinoma.
IDH mutations are known as neomorphic mutations because they confer a new function on the altered gene product. In this case, the mutant IDH enzyme converts alpha-ketoglutarate further into D-2-hydroxyglutarate (D-2HG). This molecule has a number of different effects that promote tumorigenesis, including fostering defective DNA repair (Figure 3).20,21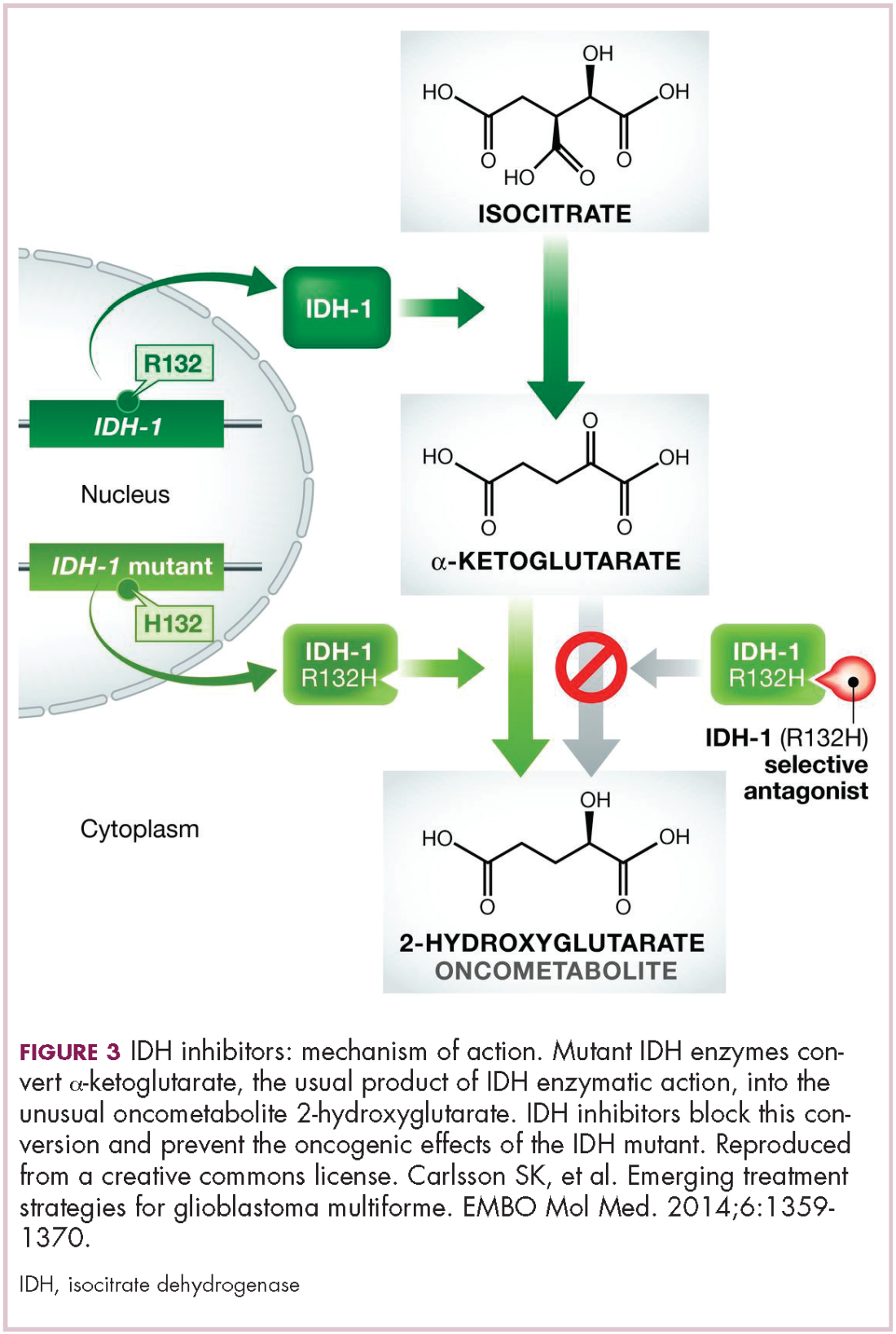
Intriguing research presented at the American Association of Cancer Research Annual Meeting revealed that IDH mutations may make cancer cells more vulnerable to poly (ADP-ribose) polymerase (PARP) inhibition, likely as a result of defects in homologous recombination pathways of DNA repair.22The pursuit of IDH as a potential therapeutic target has yielded the first regulatory approval for a metabolically targeted anticancer therapy. In August 2017, the United States Food and Drug Administration (FDA) approved enasidenib, an IDH2 inhibitor, for the treatment of relapsed or refractory AML with an IDH2 mutation. It was approved in combination with a companion diagnostic, the RealTime IDH2 Assay, which is used to detect IDH2 mutations.
The approval was based on a single-arm trial in which responses occurred in almost a quarter of the 199 patients treated with 100 mg oral enasidenib daily. After a median follow-up of 6.6 months, 23% of the patients experienced a complete response or a complete response with partial hematologic recovery lasting a median of 8.2 months. The most common AEs were nausea, vomiting, diarrhea, elevated bilirubin levels, and reduced appetite.23
Several other IDH inhibitors are also showing encouraging efficacy. Ivosidenib is an IDH1 inhibitor and the results of a phase 1 study in patients with cholangiocarcinoma were recently presented at a leading conference. Escalating doses of ivosidenib (100 mg twice daily to 1,200 mg once daily) were administered to 73 patients (as of December 2016). The confirmed partial response (PR) rate was 6%, the rate of stable disease was 56%, and PFS at 6 months was 40%. There were no dose-limiting toxicities (DLTs) and treatment-emergent AEs included fatigue, nausea, vomiting, diarrhea, decreased appetite, dysgeusia, and QT prolongation.24
Another study of ivosidenib was presented at the 2017 annual meeting of the Society for Neuro-Oncology. In that study, patients with glioma received daily doses of ivosidenib ranging from 300 mg to 900 mg. Two patients had a minor response, 83% had stable disease, and the median PFS was 13 months. There were no DLTs and most AEs were mild to moderate and included, most commonly, headache, nausea, diarrhea, and vomiting.25
Pursuing alternative targets and repurposing drugs
Other metabolic targets that are being pursued include glutaminase, given the observation of significantly enhanced glutamine uptake in cancer cells. CB-839 is a glutaminase inhibitor that is currently being evaluated in phase 1 and 2 clinical trials. Updated clinical trial data from a phase 1 trial of CB-839 in combination with paclitaxel in patients with advanced/metastatic TNBC were presented at the San Antonio Breast Cancer Symposium last year.26
As of October 2017, 49 patients had been treated with 400 mg, 600 mg, or 800 mg CB-839 twice daily in combination with 80 mg/m2 intravenous paclitaxel weekly. Among the 44 patients evaluable for response, the rate of PR was 22% and of disease control, 59%. The one DLT was grade 3 neutropenia at the 400 mg dose. Overall AEs were mostly low grade and reversible.
In recent years, lactate has emerged as more than just a by-product of altered cancer cell metabolism. It is responsible, at least in part, for the highly acidic tumor microenvironment that fosters many of the other hallmarks of cancer. In addition, lactate promotes angiogenesis by upregulating HIF-1α in endothelial cells. Depriving tumor cells of the ability to export lactate is a potentially promising therapeutic strategy. An MCT-1 inhibitor, AZD3965, is being evaluated in early stage clinical trials.
Finally, several drugs that are renowned for their use in other disease settings are being repurposed for cancer therapy because of their potential effects on cancer cell metabolism. Ritonavir, an antiretroviral drug used in the treatment of HIV, is an inhibitor of GLUT-1 and is being evaluated in phase 1 and 2 clinical trials. Meanwhile, long-term studies of metformin, a drug that has revolutionized the treatment of diabetes, have revealed a reduction in the emergence of new cancers in diabetic patients treated who are treated with it, and the drug has been shown to improve breast cancer survival rates. Its precise anticancer effects are somewhat unclear, but it is thought to act in part by inhibiting oxidative phosphorylation. Numerous clinical trials of metformin in different types of cancer are ongoing.27,2
1. Warburg O. On respiratory impairment in cancer cells. Science. 1956;124(3215):269-270.
2. Yu L, Chen X, Wang L, Chen S. The sweet trap in tumors: aerobic glycolysis and potential targets for therapy. Oncotarget. 2016;7(25):38908-38926.
3. Warburg O. On the origin of cancer cells. Science. 1956;123(3191):309-314.
4. Chen XS, Li LY, Guan YD, Yang JM, Cheng Y. Anticancer strategies based on the metabolic profile of tumor cells: therapeutic targeting of the Warburg effect. Acta Pharmacol Sin. 2016;37(8):1013-1019.
5. Gupta S, Roy A, Dwarakanath BS. Metabolic cooperation and competition in the tumor microenvironment: implications for therapy. Front Oncol. 2017;7:68.
6. Marchiq I, Pouyssegur J. Hypoxia, cancer metabolism and the therapeutic benefit of targeting lactate/H(+) symporters. J Mol Med (Berl). 2016;94(2):155-171.
7. Altenberg B, Greulich KO. Genes of glycolysis are ubiquitously overexpressed in 24 cancer classes. Genomics. 2004;84(6):1014-1020.
8. Yu L, Chen X, Sun X, Wang L, Chen S. The glycolytic switch in tumors: how many players are involved? J Cancer. 2017;8(17):3430-3440.
9. Zhang W, Zhang SL, Hu X, Tam KY. Targeting tumor metabolism for cancer treatment: is pyruvate dehydrogenase kinases (PDKs) a viable anticancer target? Int J Biol Sci. 2015;11(12):1390-1400.
10. Talekar M, Boreddy SR, Singh A, Amiji M. Tumor aerobic glycolysis: new insights into therapeutic strategies with targeted delivery. Expert Opin Biol Ther. 2014;14(8):1145-1159.
11. Ganapathy-Kanniappan S, Geschwind JF. Tumor glycolysis as a target for cancer therapy: progress and prospects. Mol Cancer. 2013;12:152.
12. Lien EC, Lyssiotis CA, Cantley LC. Metabolic reprogramming by the PI3K-Akt-mTOR pathway in cancer. In: Cramer T, Schmitt CA, eds. Metabolism in Cancer. Cham, Switzerland: Springer International Publishing; 2016:39-72.
13. Simons AL, Orcutt KP, Madsen JM, Scarbrough PM, Spitz DR. The role of Akt pathway signaling in glucose metabolism and metabolic oxidative stress. In: Spitz DR, Dornfeld KJ, Krishnan K, Gius D (eds). Oxidative stress in cancer biology and therapy. Humana Press (copyright holder, Springer Science+Business Media, LLC); 2012:21-46.
14. Kim S-B, Dent R, Im S-A, et al. Ipatasertib plus paclitaxel versus placebo plus paclitaxel as first-line therapy for metastatic triple-negative breast cancer (LOTUS): a multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol. 2017;18(10):1360-1372.
15. Fu Y, Liu S, Yin S, et al. The reverse Warburg effect is likely to be an Achilles’ heel of cancer that can be exploited for cancer therapy. Oncotarget. 2017;8(34):57813-57825.
16. Wilde L, Roche M, Domingo-Vidal M, et al. Metabolic coupling and the reverse Warburg effect in cancer: implications for novel biomarker and anticancer agent development. Semin Oncol. 2017;44(3):198-203.
17. Brooks GA. Cell–cell and intracellular lactate shuttles. Journal Physiol. 2009;587(23):5591-5600.
18. Chiarugi P, Cirri P. Metabolic exchanges within tumor microenvironment. Cancer Lett. 2016;380(1):272-280.
19. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646-674.
20. Fujii T, Khawaja MR, DiNardo CD, Atkins JT, Janku F. Targeting isocitrate dehydrogenase (IDH) in cancer. Discov Med. 2016;21(117):373-380.
21. Carlsson SK, Brothers SP, Wahlestedt C. Emerging treatment strategies for glioblastoma multiforme. EMBO Mol Med. 2014;6(11):1359-1370.
22. Lu Y, Kwintkiewicz J, Liu Y, et al. Chemosensitivity of IDH1-mutated gliomas due to an impairment in PARP1-mediated DNA repair. Cancer Res. 2017;77(7):1709-1718.
23. Stein EM, DiNardo CD, Pollyea DA, et al. Enasidenib in mutant IDH2 relapsed or refractory acute myeloid leukemia. Blood. 2017;130(6):722-731.
24. Lowery MA, Abou-Alfa GK, Burris HA, et al. Phase I study of AG-120, an IDH1 mutant enzyme inhibitor: results from the cholangiocarcinoma dose escalation and expansion cohorts. J Clin Oncol. 2017;35(15_suppl):4015-4015.
25. Mellinghoff IK, Touat M, Maher E, et al. ACTR-46. AG-120, a first-in-class mutant IDH1 inhibitor in patients with recurrent or progressive IDH1 mutant glioma: updated results from the phase 1 non-enhancing glioma population. Neuro Oncol. 2017;19(suppl_6):vi10-vi11.
26. Kalinsky K, Harding J, DeMichele A, et al. Phase 1 study of CB-839, a first-in-class oral inhibitor of glutaminase, in combination with paclitaxel in patients with advanced triple negative breast cancer. Paper presented at San Antonio Breast Cancer Symposium; December 5-9, 2017; San Antonio, Texas.
27. Hatoum D, McGowan EM. Recent advances in the use of metformin: can treating diabetes prevent breast cancer? Biomed Res Int. 2015;2015:548436.
28. Leone A, Di Gennaro E, Bruzzese F, Avallone A, Budillon A. New perspective for an old antidiabetic drug: metformin as anticancer agent. Cancer Treat Res. 2014;159:355-376.
Altered cell metabolism has long been recognized as a distinctive feature of malignant cells but, until recently, research efforts had focused on a single aspect. It has become increasingly evident that many metabolic pathways are altered in cancer cells. Improved understanding has yielded the first regulatory approval in this new class of drugs. Here, we discuss the latest developments in the therapeutic targeting of the cancer metabolism hallmark.
A cancer cell’s sweet tooth
The metabolism of cancer cells differs from that of normal cells, an observation that has spawned a dedicated field of research and new targeted drug development. The German physiologist Otto Warburg is credited as the father of the field with his observations about the way in which cancer cells derive energy from glucose.1
In normal cells, glucose is converted into pyruvate in the cytoplasm, which is then, most often, fed to the mitochondria that use oxidative phosphorylation to produce energy in the form of adenosine triphosphate (ATP). Cancer cells seem instead to favor using the pyruvate to produce lactate through glycolysis (Figure 1).
Glycolysis is usually reserved for conditions of poor oxygen availability, but although the tumor microenvironment is often hypoxic, cancer cells have been shown to use glycolysis even when oxygen is plentiful. As a result, the phenomenon is known as aerobic glycolysis, although it is most often referred to as the Warburg effect.2
Glycolysis is much less efficient than oxidative phosphorylation at producing energy, yielding only 2 ATP. In order to meet their energy demands in this way, cancer cells ramp up their glucose intake, an effect that has been exploited for the detection of cancer with positron-emission tomography.
Warburg postulated that this metabolic shift was a result of mitochondrial damage and defective oxidative phosphorylation, even going so far as to suggest that cancer was a mitochondrial disease. It has subsequently been shown that the mitochondria are mostly intact in cancer cells and that oxidative phosphorylation can still occur.3
The Warburg effect has been the subject of significant investigative efforts as researchers have attempted to better understand how this phenomenon comes about. Studies have shown that it is driven in large part by the transcription factors hypoxia inducible factor 1 alpha (HIF-1α) and c-Myc. In addition, numerous other signaling pathways, including the phosphatidylinositol 3-kinase (PI3K)-Akt-mammalian target of rapamycin (mTOR) pathway, and the activation of oncogenes and inactivation of tumor suppressors, are thought to play a central role.
HIF-1α is an oxygen-sensing transcription factor that coordinates cellular responses to reduced oxygen levels by binding to specific regions, known as hypoxia response elements, on target genes in the nucleus and regulating their subsequent expression. Oxygen levels and metabolism are tightly linked, and HIF-1α sits at the intersection of the 2 since many of its target genes are involved in metabolic pathways, including many glycolytic enzymes, but it also directly inhibits oxidative phosphorylation by suppressing key enzymes in this metabolic pathway.
The expression of HIF-1α and numerous glycolytic enzymes, including lactate dehydrogenase (LDH), phosphofructokinase (PFK), hexokinase II (HKII), and pyruvate dehydrogenase kinase (PDK) is increased in many tumor types. Other molecules that are associated with glucose uptake and metabolism are also dysregulated, such as the GLUT-1 glucose transporter.2,4-6
Targeting glycolysis and glucose uptake
According to one study, glucose transporters and glycolytic enzymes are overexpressed in 24 different types of cancer, representing more than 70% of all cancer cases.7 This enables cancer cells to respond metabolically as though they are experiencing hypoxia, even when oxygen is plentiful and, indeed, when hypoxia is a concern, to mount a faster response. It also provides a tempting avenue for anticancer drug design by exploiting the dependency of cancer cells on glycolysis to survive and thrive.
Inhibitors of HKII, LDH, PFK, PDK, and GLUT-1 have been and continue to be developed. For example, 2-deoxy-D-glucose is a glucose molecule in which the 2-hydroxyl group has been replaced by hydrogen, preventing further glycolysis; it acts as a competitive inhibitor of HKII. Dichloroacetate (DCA) activates the pyruvate dehydrogenase complex and inhibits the actions of the PDKs. Although development of DCA itself was unsuccessful, DCA derivatives continue to be pursued. WZB117 and STF-31 are novel small-molecule inhibitors of GLUT-1-mediated glucose transport. To date, where inhibitors of glycolysis have progressed into clinical trials, they have not proved successful, often limited by off-target effects and low potency.8-11
A variety of cell signaling pathways are implicated in metabolism by tightly regulating the ability of cells to gain access to and use nutrients. Through aberrations in these pathways, cancer cells can essentially go rogue, ignoring regulatory signals and taking up nutrients in an autonomous manner. One of the most frequently altered signaling pathways in human cancer, the PI3K-Akt-mTOR pathway, is also an important regulator of metabolism, coordinating the uptake of multiple nutrients, including glucose.
Akt in particular is thought to have a critical role in glucose metabolism and increased Akt pathway signaling has been shown to correlate with increased rates of glycolysis in cancer cells. Thus, Akt inhibitors could double as glycolytic or glucose transport inhibitors.12,13
A number of Akt inhibitors are being evaluated in clinical trials (Table) and results from the phase 2 LOTUS trial of ipatasertib (GDC-0068) were recently published.
Among 124 patients randomly assigned to paclitaxel in combination with either ipatasertib or placebo, there was a modest improvement in progression-free survival (PFS) in the ipatasertib arm in patients with triple-negative breast cancer (TNBC; 6 months vs 4.2 months, respectively; hazard ratio [HR], 0.60; P = .037). The effect was more pronounced, though not statistically significant, in patients with phosphatase and tensin homolog (PTEN)-low tumors (6.2 months vs 3.7 months; HR, 0.59; P = .18). The most common grade 3 and higher adverse events (AEs) were diarrhea, reduced neutrophil count, and neutropenia.14
The Warburg paradox
Although the molecular mechanisms underlying the Warburg effect have been revealed to some extent, why cancer cells would choose to use such an energy-inefficient process when they have such high energy demands, remains something of a paradox. It’s still not entirely clear, but several explanations that are not necessarily mutually exclusive have been proposed and relate to the inherent benefits of glycolysis and might explain why cancer cells favor this pathway despite its poor energy yield. First, ATP is produced much more rapidly through glycolysis than oxidative phosphorylation, up to 100 times faster. Thus, using glycolysis is a trade-off, between making less energy and making it more quickly.
Second, cancer cells require more than just ATP to meet their metabolic demands. They need amino acids for protein synthesis; nucleotides for DNA replication; lipids for cell membrane synthesis; nicotinamide adenine dinucleotide phosphate (NADPH), which helps the cancer cell deal with oxidative stress; and various other metabolites. Glycolysis branches off into other metabolic pathways that generate many of these metabolites. Among these branched pathways is the pentose phosphate pathway (PPP), which is required for the generation of ribonucleotides and is a major source for NADPH. Cancer cells have been shown to upregulate the flux of glucose into the PPP to meet their anabolic demands and counter oxidative stress.
Third, the lactic acid produced through glycolysis is actively exported from tumor cells by monocarboxylate transporters (MCTs). This creates a highly acidic tumor microenvironment, which can promote several cancer-related processes and also plays a role in tumor-induced immunosuppression, by inhibiting the activity of tumor-infiltrating T cells, reducing dendritic cell maturation, and promoting the transformation of macrophages to a protumorigenic form.2,4,6
Beyond the Warburg effect
Although the focus has been on glucose metabolism and glycolysis, it has been increasingly recognized that many different metabolic pathways are altered. Fundamental changes to the metabolism of all 4 major classes of macromolecules – carbohydrates, lipids, proteins, and nucleic acids – have been observed, encompassing all aspects of cellular metabolism and enabling cancer cells to meet their complete metabolic requirements. There is also evidence that cancer cells are able to switch between different metabolic pathways depending on the availability of oxygen, their energetic needs, environmental stresses, and many other factors. Certainly, there is significant heterogeneity in the metabolic changes that occur in tumors, which vary from tumor to tumor and even within the same tumor and across the lifespan of a tumor as it progresses from an early stage to more advanced or metastatic disease.
The notion of the Warburg effect as a universal phenomenon in cancer cells is now being widely disregarded. Many tumors continue to use oxidative phosphorylation, particularly slower growing tumors, to meet their energy needs. More recently a “reverse” Warburg effect was described, whereby cancer cells are thought to influence the metabolism of the surrounding stromal fibroblasts and essentially outsource aerobic glycolysis to these cells, while performing energy-efficient oxidative phosphorylation themselves (Figure 2).5,15,16
There is thought to be a “lactate shuttle” between the stromal and cancer cells. The stromal cells express high levels of efflux MCTs so that they can remove the subsequently high levels of lactate from the cytoplasm and avoid pickling themselves. The lactate is then shuttled to the cancer cells that have MCTs on their surface that are involved in lactate uptake. The cancer cells oxidize the lactate back into pyruvate, which can then be used in the tricarboxylic acid (TCA) cycle to feed oxidative phosphorylation for efficient ATP production. This hypothesis reflects a broader appreciation of the role of the microenvironment in contributing to cancer metabolism.17,18
An improved holistic understanding of cancer cell metabolism has led to the recognition of altered cancer metabolism as one of the hallmark abilities required for transformation of a normal cell into a cancerous one. It is categorized as “deregulation of bioenergetics” in the most up to date review of the cancer hallmarks.19 It has also begun to shape the therapeutic landscape as new drug targets have emerged.
IDH inhibitors first to market
A number of new metabolically-targeted treatment strategies are being developed. Most promising are small molecule inhibitors of the isocitrate dehydrogenase (IDH) enzymes. These enzymes play an essential role in the TCA cycle, catalyzing the conversion of isocitrate to alpha-ketoglutarate, generating carbon dioxide and NADPH. Recurrent mutations in the IDH1 and IDH2 genes have been observed in several different types of cancer, including glioma, acute myeloid leukemia (AML), and cholangiocarcinoma.
IDH mutations are known as neomorphic mutations because they confer a new function on the altered gene product. In this case, the mutant IDH enzyme converts alpha-ketoglutarate further into D-2-hydroxyglutarate (D-2HG). This molecule has a number of different effects that promote tumorigenesis, including fostering defective DNA repair (Figure 3).20,21
Intriguing research presented at the American Association of Cancer Research Annual Meeting revealed that IDH mutations may make cancer cells more vulnerable to poly (ADP-ribose) polymerase (PARP) inhibition, likely as a result of defects in homologous recombination pathways of DNA repair.22The pursuit of IDH as a potential therapeutic target has yielded the first regulatory approval for a metabolically targeted anticancer therapy. In August 2017, the United States Food and Drug Administration (FDA) approved enasidenib, an IDH2 inhibitor, for the treatment of relapsed or refractory AML with an IDH2 mutation. It was approved in combination with a companion diagnostic, the RealTime IDH2 Assay, which is used to detect IDH2 mutations.
The approval was based on a single-arm trial in which responses occurred in almost a quarter of the 199 patients treated with 100 mg oral enasidenib daily. After a median follow-up of 6.6 months, 23% of the patients experienced a complete response or a complete response with partial hematologic recovery lasting a median of 8.2 months. The most common AEs were nausea, vomiting, diarrhea, elevated bilirubin levels, and reduced appetite.23
Several other IDH inhibitors are also showing encouraging efficacy. Ivosidenib is an IDH1 inhibitor and the results of a phase 1 study in patients with cholangiocarcinoma were recently presented at a leading conference. Escalating doses of ivosidenib (100 mg twice daily to 1,200 mg once daily) were administered to 73 patients (as of December 2016). The confirmed partial response (PR) rate was 6%, the rate of stable disease was 56%, and PFS at 6 months was 40%. There were no dose-limiting toxicities (DLTs) and treatment-emergent AEs included fatigue, nausea, vomiting, diarrhea, decreased appetite, dysgeusia, and QT prolongation.24
Another study of ivosidenib was presented at the 2017 annual meeting of the Society for Neuro-Oncology. In that study, patients with glioma received daily doses of ivosidenib ranging from 300 mg to 900 mg. Two patients had a minor response, 83% had stable disease, and the median PFS was 13 months. There were no DLTs and most AEs were mild to moderate and included, most commonly, headache, nausea, diarrhea, and vomiting.25
Pursuing alternative targets and repurposing drugs
Other metabolic targets that are being pursued include glutaminase, given the observation of significantly enhanced glutamine uptake in cancer cells. CB-839 is a glutaminase inhibitor that is currently being evaluated in phase 1 and 2 clinical trials. Updated clinical trial data from a phase 1 trial of CB-839 in combination with paclitaxel in patients with advanced/metastatic TNBC were presented at the San Antonio Breast Cancer Symposium last year.26
As of October 2017, 49 patients had been treated with 400 mg, 600 mg, or 800 mg CB-839 twice daily in combination with 80 mg/m2 intravenous paclitaxel weekly. Among the 44 patients evaluable for response, the rate of PR was 22% and of disease control, 59%. The one DLT was grade 3 neutropenia at the 400 mg dose. Overall AEs were mostly low grade and reversible.
In recent years, lactate has emerged as more than just a by-product of altered cancer cell metabolism. It is responsible, at least in part, for the highly acidic tumor microenvironment that fosters many of the other hallmarks of cancer. In addition, lactate promotes angiogenesis by upregulating HIF-1α in endothelial cells. Depriving tumor cells of the ability to export lactate is a potentially promising therapeutic strategy. An MCT-1 inhibitor, AZD3965, is being evaluated in early stage clinical trials.
Finally, several drugs that are renowned for their use in other disease settings are being repurposed for cancer therapy because of their potential effects on cancer cell metabolism. Ritonavir, an antiretroviral drug used in the treatment of HIV, is an inhibitor of GLUT-1 and is being evaluated in phase 1 and 2 clinical trials. Meanwhile, long-term studies of metformin, a drug that has revolutionized the treatment of diabetes, have revealed a reduction in the emergence of new cancers in diabetic patients treated who are treated with it, and the drug has been shown to improve breast cancer survival rates. Its precise anticancer effects are somewhat unclear, but it is thought to act in part by inhibiting oxidative phosphorylation. Numerous clinical trials of metformin in different types of cancer are ongoing.27,2
Altered cell metabolism has long been recognized as a distinctive feature of malignant cells but, until recently, research efforts had focused on a single aspect. It has become increasingly evident that many metabolic pathways are altered in cancer cells. Improved understanding has yielded the first regulatory approval in this new class of drugs. Here, we discuss the latest developments in the therapeutic targeting of the cancer metabolism hallmark.
A cancer cell’s sweet tooth
The metabolism of cancer cells differs from that of normal cells, an observation that has spawned a dedicated field of research and new targeted drug development. The German physiologist Otto Warburg is credited as the father of the field with his observations about the way in which cancer cells derive energy from glucose.1
In normal cells, glucose is converted into pyruvate in the cytoplasm, which is then, most often, fed to the mitochondria that use oxidative phosphorylation to produce energy in the form of adenosine triphosphate (ATP). Cancer cells seem instead to favor using the pyruvate to produce lactate through glycolysis (Figure 1).
Glycolysis is usually reserved for conditions of poor oxygen availability, but although the tumor microenvironment is often hypoxic, cancer cells have been shown to use glycolysis even when oxygen is plentiful. As a result, the phenomenon is known as aerobic glycolysis, although it is most often referred to as the Warburg effect.2
Glycolysis is much less efficient than oxidative phosphorylation at producing energy, yielding only 2 ATP. In order to meet their energy demands in this way, cancer cells ramp up their glucose intake, an effect that has been exploited for the detection of cancer with positron-emission tomography.
Warburg postulated that this metabolic shift was a result of mitochondrial damage and defective oxidative phosphorylation, even going so far as to suggest that cancer was a mitochondrial disease. It has subsequently been shown that the mitochondria are mostly intact in cancer cells and that oxidative phosphorylation can still occur.3
The Warburg effect has been the subject of significant investigative efforts as researchers have attempted to better understand how this phenomenon comes about. Studies have shown that it is driven in large part by the transcription factors hypoxia inducible factor 1 alpha (HIF-1α) and c-Myc. In addition, numerous other signaling pathways, including the phosphatidylinositol 3-kinase (PI3K)-Akt-mammalian target of rapamycin (mTOR) pathway, and the activation of oncogenes and inactivation of tumor suppressors, are thought to play a central role.
HIF-1α is an oxygen-sensing transcription factor that coordinates cellular responses to reduced oxygen levels by binding to specific regions, known as hypoxia response elements, on target genes in the nucleus and regulating their subsequent expression. Oxygen levels and metabolism are tightly linked, and HIF-1α sits at the intersection of the 2 since many of its target genes are involved in metabolic pathways, including many glycolytic enzymes, but it also directly inhibits oxidative phosphorylation by suppressing key enzymes in this metabolic pathway.
The expression of HIF-1α and numerous glycolytic enzymes, including lactate dehydrogenase (LDH), phosphofructokinase (PFK), hexokinase II (HKII), and pyruvate dehydrogenase kinase (PDK) is increased in many tumor types. Other molecules that are associated with glucose uptake and metabolism are also dysregulated, such as the GLUT-1 glucose transporter.2,4-6
Targeting glycolysis and glucose uptake
According to one study, glucose transporters and glycolytic enzymes are overexpressed in 24 different types of cancer, representing more than 70% of all cancer cases.7 This enables cancer cells to respond metabolically as though they are experiencing hypoxia, even when oxygen is plentiful and, indeed, when hypoxia is a concern, to mount a faster response. It also provides a tempting avenue for anticancer drug design by exploiting the dependency of cancer cells on glycolysis to survive and thrive.
Inhibitors of HKII, LDH, PFK, PDK, and GLUT-1 have been and continue to be developed. For example, 2-deoxy-D-glucose is a glucose molecule in which the 2-hydroxyl group has been replaced by hydrogen, preventing further glycolysis; it acts as a competitive inhibitor of HKII. Dichloroacetate (DCA) activates the pyruvate dehydrogenase complex and inhibits the actions of the PDKs. Although development of DCA itself was unsuccessful, DCA derivatives continue to be pursued. WZB117 and STF-31 are novel small-molecule inhibitors of GLUT-1-mediated glucose transport. To date, where inhibitors of glycolysis have progressed into clinical trials, they have not proved successful, often limited by off-target effects and low potency.8-11
A variety of cell signaling pathways are implicated in metabolism by tightly regulating the ability of cells to gain access to and use nutrients. Through aberrations in these pathways, cancer cells can essentially go rogue, ignoring regulatory signals and taking up nutrients in an autonomous manner. One of the most frequently altered signaling pathways in human cancer, the PI3K-Akt-mTOR pathway, is also an important regulator of metabolism, coordinating the uptake of multiple nutrients, including glucose.
Akt in particular is thought to have a critical role in glucose metabolism and increased Akt pathway signaling has been shown to correlate with increased rates of glycolysis in cancer cells. Thus, Akt inhibitors could double as glycolytic or glucose transport inhibitors.12,13
A number of Akt inhibitors are being evaluated in clinical trials (Table) and results from the phase 2 LOTUS trial of ipatasertib (GDC-0068) were recently published.
Among 124 patients randomly assigned to paclitaxel in combination with either ipatasertib or placebo, there was a modest improvement in progression-free survival (PFS) in the ipatasertib arm in patients with triple-negative breast cancer (TNBC; 6 months vs 4.2 months, respectively; hazard ratio [HR], 0.60; P = .037). The effect was more pronounced, though not statistically significant, in patients with phosphatase and tensin homolog (PTEN)-low tumors (6.2 months vs 3.7 months; HR, 0.59; P = .18). The most common grade 3 and higher adverse events (AEs) were diarrhea, reduced neutrophil count, and neutropenia.14
The Warburg paradox
Although the molecular mechanisms underlying the Warburg effect have been revealed to some extent, why cancer cells would choose to use such an energy-inefficient process when they have such high energy demands, remains something of a paradox. It’s still not entirely clear, but several explanations that are not necessarily mutually exclusive have been proposed and relate to the inherent benefits of glycolysis and might explain why cancer cells favor this pathway despite its poor energy yield. First, ATP is produced much more rapidly through glycolysis than oxidative phosphorylation, up to 100 times faster. Thus, using glycolysis is a trade-off, between making less energy and making it more quickly.
Second, cancer cells require more than just ATP to meet their metabolic demands. They need amino acids for protein synthesis; nucleotides for DNA replication; lipids for cell membrane synthesis; nicotinamide adenine dinucleotide phosphate (NADPH), which helps the cancer cell deal with oxidative stress; and various other metabolites. Glycolysis branches off into other metabolic pathways that generate many of these metabolites. Among these branched pathways is the pentose phosphate pathway (PPP), which is required for the generation of ribonucleotides and is a major source for NADPH. Cancer cells have been shown to upregulate the flux of glucose into the PPP to meet their anabolic demands and counter oxidative stress.
Third, the lactic acid produced through glycolysis is actively exported from tumor cells by monocarboxylate transporters (MCTs). This creates a highly acidic tumor microenvironment, which can promote several cancer-related processes and also plays a role in tumor-induced immunosuppression, by inhibiting the activity of tumor-infiltrating T cells, reducing dendritic cell maturation, and promoting the transformation of macrophages to a protumorigenic form.2,4,6
Beyond the Warburg effect
Although the focus has been on glucose metabolism and glycolysis, it has been increasingly recognized that many different metabolic pathways are altered. Fundamental changes to the metabolism of all 4 major classes of macromolecules – carbohydrates, lipids, proteins, and nucleic acids – have been observed, encompassing all aspects of cellular metabolism and enabling cancer cells to meet their complete metabolic requirements. There is also evidence that cancer cells are able to switch between different metabolic pathways depending on the availability of oxygen, their energetic needs, environmental stresses, and many other factors. Certainly, there is significant heterogeneity in the metabolic changes that occur in tumors, which vary from tumor to tumor and even within the same tumor and across the lifespan of a tumor as it progresses from an early stage to more advanced or metastatic disease.
The notion of the Warburg effect as a universal phenomenon in cancer cells is now being widely disregarded. Many tumors continue to use oxidative phosphorylation, particularly slower growing tumors, to meet their energy needs. More recently a “reverse” Warburg effect was described, whereby cancer cells are thought to influence the metabolism of the surrounding stromal fibroblasts and essentially outsource aerobic glycolysis to these cells, while performing energy-efficient oxidative phosphorylation themselves (Figure 2).5,15,16
There is thought to be a “lactate shuttle” between the stromal and cancer cells. The stromal cells express high levels of efflux MCTs so that they can remove the subsequently high levels of lactate from the cytoplasm and avoid pickling themselves. The lactate is then shuttled to the cancer cells that have MCTs on their surface that are involved in lactate uptake. The cancer cells oxidize the lactate back into pyruvate, which can then be used in the tricarboxylic acid (TCA) cycle to feed oxidative phosphorylation for efficient ATP production. This hypothesis reflects a broader appreciation of the role of the microenvironment in contributing to cancer metabolism.17,18
An improved holistic understanding of cancer cell metabolism has led to the recognition of altered cancer metabolism as one of the hallmark abilities required for transformation of a normal cell into a cancerous one. It is categorized as “deregulation of bioenergetics” in the most up to date review of the cancer hallmarks.19 It has also begun to shape the therapeutic landscape as new drug targets have emerged.
IDH inhibitors first to market
A number of new metabolically-targeted treatment strategies are being developed. Most promising are small molecule inhibitors of the isocitrate dehydrogenase (IDH) enzymes. These enzymes play an essential role in the TCA cycle, catalyzing the conversion of isocitrate to alpha-ketoglutarate, generating carbon dioxide and NADPH. Recurrent mutations in the IDH1 and IDH2 genes have been observed in several different types of cancer, including glioma, acute myeloid leukemia (AML), and cholangiocarcinoma.
IDH mutations are known as neomorphic mutations because they confer a new function on the altered gene product. In this case, the mutant IDH enzyme converts alpha-ketoglutarate further into D-2-hydroxyglutarate (D-2HG). This molecule has a number of different effects that promote tumorigenesis, including fostering defective DNA repair (Figure 3).20,21
Intriguing research presented at the American Association of Cancer Research Annual Meeting revealed that IDH mutations may make cancer cells more vulnerable to poly (ADP-ribose) polymerase (PARP) inhibition, likely as a result of defects in homologous recombination pathways of DNA repair.22The pursuit of IDH as a potential therapeutic target has yielded the first regulatory approval for a metabolically targeted anticancer therapy. In August 2017, the United States Food and Drug Administration (FDA) approved enasidenib, an IDH2 inhibitor, for the treatment of relapsed or refractory AML with an IDH2 mutation. It was approved in combination with a companion diagnostic, the RealTime IDH2 Assay, which is used to detect IDH2 mutations.
The approval was based on a single-arm trial in which responses occurred in almost a quarter of the 199 patients treated with 100 mg oral enasidenib daily. After a median follow-up of 6.6 months, 23% of the patients experienced a complete response or a complete response with partial hematologic recovery lasting a median of 8.2 months. The most common AEs were nausea, vomiting, diarrhea, elevated bilirubin levels, and reduced appetite.23
Several other IDH inhibitors are also showing encouraging efficacy. Ivosidenib is an IDH1 inhibitor and the results of a phase 1 study in patients with cholangiocarcinoma were recently presented at a leading conference. Escalating doses of ivosidenib (100 mg twice daily to 1,200 mg once daily) were administered to 73 patients (as of December 2016). The confirmed partial response (PR) rate was 6%, the rate of stable disease was 56%, and PFS at 6 months was 40%. There were no dose-limiting toxicities (DLTs) and treatment-emergent AEs included fatigue, nausea, vomiting, diarrhea, decreased appetite, dysgeusia, and QT prolongation.24
Another study of ivosidenib was presented at the 2017 annual meeting of the Society for Neuro-Oncology. In that study, patients with glioma received daily doses of ivosidenib ranging from 300 mg to 900 mg. Two patients had a minor response, 83% had stable disease, and the median PFS was 13 months. There were no DLTs and most AEs were mild to moderate and included, most commonly, headache, nausea, diarrhea, and vomiting.25
Pursuing alternative targets and repurposing drugs
Other metabolic targets that are being pursued include glutaminase, given the observation of significantly enhanced glutamine uptake in cancer cells. CB-839 is a glutaminase inhibitor that is currently being evaluated in phase 1 and 2 clinical trials. Updated clinical trial data from a phase 1 trial of CB-839 in combination with paclitaxel in patients with advanced/metastatic TNBC were presented at the San Antonio Breast Cancer Symposium last year.26
As of October 2017, 49 patients had been treated with 400 mg, 600 mg, or 800 mg CB-839 twice daily in combination with 80 mg/m2 intravenous paclitaxel weekly. Among the 44 patients evaluable for response, the rate of PR was 22% and of disease control, 59%. The one DLT was grade 3 neutropenia at the 400 mg dose. Overall AEs were mostly low grade and reversible.
In recent years, lactate has emerged as more than just a by-product of altered cancer cell metabolism. It is responsible, at least in part, for the highly acidic tumor microenvironment that fosters many of the other hallmarks of cancer. In addition, lactate promotes angiogenesis by upregulating HIF-1α in endothelial cells. Depriving tumor cells of the ability to export lactate is a potentially promising therapeutic strategy. An MCT-1 inhibitor, AZD3965, is being evaluated in early stage clinical trials.
Finally, several drugs that are renowned for their use in other disease settings are being repurposed for cancer therapy because of their potential effects on cancer cell metabolism. Ritonavir, an antiretroviral drug used in the treatment of HIV, is an inhibitor of GLUT-1 and is being evaluated in phase 1 and 2 clinical trials. Meanwhile, long-term studies of metformin, a drug that has revolutionized the treatment of diabetes, have revealed a reduction in the emergence of new cancers in diabetic patients treated who are treated with it, and the drug has been shown to improve breast cancer survival rates. Its precise anticancer effects are somewhat unclear, but it is thought to act in part by inhibiting oxidative phosphorylation. Numerous clinical trials of metformin in different types of cancer are ongoing.27,2
1. Warburg O. On respiratory impairment in cancer cells. Science. 1956;124(3215):269-270.
2. Yu L, Chen X, Wang L, Chen S. The sweet trap in tumors: aerobic glycolysis and potential targets for therapy. Oncotarget. 2016;7(25):38908-38926.
3. Warburg O. On the origin of cancer cells. Science. 1956;123(3191):309-314.
4. Chen XS, Li LY, Guan YD, Yang JM, Cheng Y. Anticancer strategies based on the metabolic profile of tumor cells: therapeutic targeting of the Warburg effect. Acta Pharmacol Sin. 2016;37(8):1013-1019.
5. Gupta S, Roy A, Dwarakanath BS. Metabolic cooperation and competition in the tumor microenvironment: implications for therapy. Front Oncol. 2017;7:68.
6. Marchiq I, Pouyssegur J. Hypoxia, cancer metabolism and the therapeutic benefit of targeting lactate/H(+) symporters. J Mol Med (Berl). 2016;94(2):155-171.
7. Altenberg B, Greulich KO. Genes of glycolysis are ubiquitously overexpressed in 24 cancer classes. Genomics. 2004;84(6):1014-1020.
8. Yu L, Chen X, Sun X, Wang L, Chen S. The glycolytic switch in tumors: how many players are involved? J Cancer. 2017;8(17):3430-3440.
9. Zhang W, Zhang SL, Hu X, Tam KY. Targeting tumor metabolism for cancer treatment: is pyruvate dehydrogenase kinases (PDKs) a viable anticancer target? Int J Biol Sci. 2015;11(12):1390-1400.
10. Talekar M, Boreddy SR, Singh A, Amiji M. Tumor aerobic glycolysis: new insights into therapeutic strategies with targeted delivery. Expert Opin Biol Ther. 2014;14(8):1145-1159.
11. Ganapathy-Kanniappan S, Geschwind JF. Tumor glycolysis as a target for cancer therapy: progress and prospects. Mol Cancer. 2013;12:152.
12. Lien EC, Lyssiotis CA, Cantley LC. Metabolic reprogramming by the PI3K-Akt-mTOR pathway in cancer. In: Cramer T, Schmitt CA, eds. Metabolism in Cancer. Cham, Switzerland: Springer International Publishing; 2016:39-72.
13. Simons AL, Orcutt KP, Madsen JM, Scarbrough PM, Spitz DR. The role of Akt pathway signaling in glucose metabolism and metabolic oxidative stress. In: Spitz DR, Dornfeld KJ, Krishnan K, Gius D (eds). Oxidative stress in cancer biology and therapy. Humana Press (copyright holder, Springer Science+Business Media, LLC); 2012:21-46.
14. Kim S-B, Dent R, Im S-A, et al. Ipatasertib plus paclitaxel versus placebo plus paclitaxel as first-line therapy for metastatic triple-negative breast cancer (LOTUS): a multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol. 2017;18(10):1360-1372.
15. Fu Y, Liu S, Yin S, et al. The reverse Warburg effect is likely to be an Achilles’ heel of cancer that can be exploited for cancer therapy. Oncotarget. 2017;8(34):57813-57825.
16. Wilde L, Roche M, Domingo-Vidal M, et al. Metabolic coupling and the reverse Warburg effect in cancer: implications for novel biomarker and anticancer agent development. Semin Oncol. 2017;44(3):198-203.
17. Brooks GA. Cell–cell and intracellular lactate shuttles. Journal Physiol. 2009;587(23):5591-5600.
18. Chiarugi P, Cirri P. Metabolic exchanges within tumor microenvironment. Cancer Lett. 2016;380(1):272-280.
19. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646-674.
20. Fujii T, Khawaja MR, DiNardo CD, Atkins JT, Janku F. Targeting isocitrate dehydrogenase (IDH) in cancer. Discov Med. 2016;21(117):373-380.
21. Carlsson SK, Brothers SP, Wahlestedt C. Emerging treatment strategies for glioblastoma multiforme. EMBO Mol Med. 2014;6(11):1359-1370.
22. Lu Y, Kwintkiewicz J, Liu Y, et al. Chemosensitivity of IDH1-mutated gliomas due to an impairment in PARP1-mediated DNA repair. Cancer Res. 2017;77(7):1709-1718.
23. Stein EM, DiNardo CD, Pollyea DA, et al. Enasidenib in mutant IDH2 relapsed or refractory acute myeloid leukemia. Blood. 2017;130(6):722-731.
24. Lowery MA, Abou-Alfa GK, Burris HA, et al. Phase I study of AG-120, an IDH1 mutant enzyme inhibitor: results from the cholangiocarcinoma dose escalation and expansion cohorts. J Clin Oncol. 2017;35(15_suppl):4015-4015.
25. Mellinghoff IK, Touat M, Maher E, et al. ACTR-46. AG-120, a first-in-class mutant IDH1 inhibitor in patients with recurrent or progressive IDH1 mutant glioma: updated results from the phase 1 non-enhancing glioma population. Neuro Oncol. 2017;19(suppl_6):vi10-vi11.
26. Kalinsky K, Harding J, DeMichele A, et al. Phase 1 study of CB-839, a first-in-class oral inhibitor of glutaminase, in combination with paclitaxel in patients with advanced triple negative breast cancer. Paper presented at San Antonio Breast Cancer Symposium; December 5-9, 2017; San Antonio, Texas.
27. Hatoum D, McGowan EM. Recent advances in the use of metformin: can treating diabetes prevent breast cancer? Biomed Res Int. 2015;2015:548436.
28. Leone A, Di Gennaro E, Bruzzese F, Avallone A, Budillon A. New perspective for an old antidiabetic drug: metformin as anticancer agent. Cancer Treat Res. 2014;159:355-376.
1. Warburg O. On respiratory impairment in cancer cells. Science. 1956;124(3215):269-270.
2. Yu L, Chen X, Wang L, Chen S. The sweet trap in tumors: aerobic glycolysis and potential targets for therapy. Oncotarget. 2016;7(25):38908-38926.
3. Warburg O. On the origin of cancer cells. Science. 1956;123(3191):309-314.
4. Chen XS, Li LY, Guan YD, Yang JM, Cheng Y. Anticancer strategies based on the metabolic profile of tumor cells: therapeutic targeting of the Warburg effect. Acta Pharmacol Sin. 2016;37(8):1013-1019.
5. Gupta S, Roy A, Dwarakanath BS. Metabolic cooperation and competition in the tumor microenvironment: implications for therapy. Front Oncol. 2017;7:68.
6. Marchiq I, Pouyssegur J. Hypoxia, cancer metabolism and the therapeutic benefit of targeting lactate/H(+) symporters. J Mol Med (Berl). 2016;94(2):155-171.
7. Altenberg B, Greulich KO. Genes of glycolysis are ubiquitously overexpressed in 24 cancer classes. Genomics. 2004;84(6):1014-1020.
8. Yu L, Chen X, Sun X, Wang L, Chen S. The glycolytic switch in tumors: how many players are involved? J Cancer. 2017;8(17):3430-3440.
9. Zhang W, Zhang SL, Hu X, Tam KY. Targeting tumor metabolism for cancer treatment: is pyruvate dehydrogenase kinases (PDKs) a viable anticancer target? Int J Biol Sci. 2015;11(12):1390-1400.
10. Talekar M, Boreddy SR, Singh A, Amiji M. Tumor aerobic glycolysis: new insights into therapeutic strategies with targeted delivery. Expert Opin Biol Ther. 2014;14(8):1145-1159.
11. Ganapathy-Kanniappan S, Geschwind JF. Tumor glycolysis as a target for cancer therapy: progress and prospects. Mol Cancer. 2013;12:152.
12. Lien EC, Lyssiotis CA, Cantley LC. Metabolic reprogramming by the PI3K-Akt-mTOR pathway in cancer. In: Cramer T, Schmitt CA, eds. Metabolism in Cancer. Cham, Switzerland: Springer International Publishing; 2016:39-72.
13. Simons AL, Orcutt KP, Madsen JM, Scarbrough PM, Spitz DR. The role of Akt pathway signaling in glucose metabolism and metabolic oxidative stress. In: Spitz DR, Dornfeld KJ, Krishnan K, Gius D (eds). Oxidative stress in cancer biology and therapy. Humana Press (copyright holder, Springer Science+Business Media, LLC); 2012:21-46.
14. Kim S-B, Dent R, Im S-A, et al. Ipatasertib plus paclitaxel versus placebo plus paclitaxel as first-line therapy for metastatic triple-negative breast cancer (LOTUS): a multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol. 2017;18(10):1360-1372.
15. Fu Y, Liu S, Yin S, et al. The reverse Warburg effect is likely to be an Achilles’ heel of cancer that can be exploited for cancer therapy. Oncotarget. 2017;8(34):57813-57825.
16. Wilde L, Roche M, Domingo-Vidal M, et al. Metabolic coupling and the reverse Warburg effect in cancer: implications for novel biomarker and anticancer agent development. Semin Oncol. 2017;44(3):198-203.
17. Brooks GA. Cell–cell and intracellular lactate shuttles. Journal Physiol. 2009;587(23):5591-5600.
18. Chiarugi P, Cirri P. Metabolic exchanges within tumor microenvironment. Cancer Lett. 2016;380(1):272-280.
19. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646-674.
20. Fujii T, Khawaja MR, DiNardo CD, Atkins JT, Janku F. Targeting isocitrate dehydrogenase (IDH) in cancer. Discov Med. 2016;21(117):373-380.
21. Carlsson SK, Brothers SP, Wahlestedt C. Emerging treatment strategies for glioblastoma multiforme. EMBO Mol Med. 2014;6(11):1359-1370.
22. Lu Y, Kwintkiewicz J, Liu Y, et al. Chemosensitivity of IDH1-mutated gliomas due to an impairment in PARP1-mediated DNA repair. Cancer Res. 2017;77(7):1709-1718.
23. Stein EM, DiNardo CD, Pollyea DA, et al. Enasidenib in mutant IDH2 relapsed or refractory acute myeloid leukemia. Blood. 2017;130(6):722-731.
24. Lowery MA, Abou-Alfa GK, Burris HA, et al. Phase I study of AG-120, an IDH1 mutant enzyme inhibitor: results from the cholangiocarcinoma dose escalation and expansion cohorts. J Clin Oncol. 2017;35(15_suppl):4015-4015.
25. Mellinghoff IK, Touat M, Maher E, et al. ACTR-46. AG-120, a first-in-class mutant IDH1 inhibitor in patients with recurrent or progressive IDH1 mutant glioma: updated results from the phase 1 non-enhancing glioma population. Neuro Oncol. 2017;19(suppl_6):vi10-vi11.
26. Kalinsky K, Harding J, DeMichele A, et al. Phase 1 study of CB-839, a first-in-class oral inhibitor of glutaminase, in combination with paclitaxel in patients with advanced triple negative breast cancer. Paper presented at San Antonio Breast Cancer Symposium; December 5-9, 2017; San Antonio, Texas.
27. Hatoum D, McGowan EM. Recent advances in the use of metformin: can treating diabetes prevent breast cancer? Biomed Res Int. 2015;2015:548436.
28. Leone A, Di Gennaro E, Bruzzese F, Avallone A, Budillon A. New perspective for an old antidiabetic drug: metformin as anticancer agent. Cancer Treat Res. 2014;159:355-376.
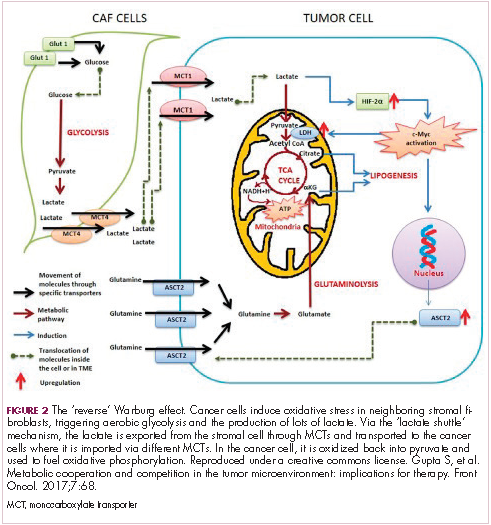
VIDEO: Novel PARP inhibitor boosts PFS in HER2– breast cancer with BRCA mutations
SAN ANTONIO – In women with advanced HER2-negative breast cancer with germline BRCA mutations, talazoparib, an investigational oral PARP inhibitor, was associated with a near doubling in progression-free survival, compared with single-agent chemotherapy in the phase 3 EMBRACA trial.
After a median follow-up of 11.2 months, median progression-free survival by blinded central review was 8.6 months for patients assigned to receive talazoparib, compared with 5.6 months for patients randomized to receive the physician’s choice of either capecitabine, eribulin, gemcitabine, or vinorelbine.
In this video interview from the San Antonio Breast Cancer Symposium, Jennifer K. Litton, MD, from the University of Texas MD Anderson Cancer Center in Houston discusses the comparative efficacy of the drug relative to standard chemotherapy agents in this population, and the association of the PARP inhibitor with improved patient-reported quality of life outcomes.
The EMBRACA study was funded by Pfizer. Dr. Litton has disclosed research funding with EMD Serono, AstraZeneca, Pfizer, Genentech, and GlaxoSmithKline, and serves on advisory boards for Pfizer and AstraZeneca, all uncompensated.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – In women with advanced HER2-negative breast cancer with germline BRCA mutations, talazoparib, an investigational oral PARP inhibitor, was associated with a near doubling in progression-free survival, compared with single-agent chemotherapy in the phase 3 EMBRACA trial.
After a median follow-up of 11.2 months, median progression-free survival by blinded central review was 8.6 months for patients assigned to receive talazoparib, compared with 5.6 months for patients randomized to receive the physician’s choice of either capecitabine, eribulin, gemcitabine, or vinorelbine.
In this video interview from the San Antonio Breast Cancer Symposium, Jennifer K. Litton, MD, from the University of Texas MD Anderson Cancer Center in Houston discusses the comparative efficacy of the drug relative to standard chemotherapy agents in this population, and the association of the PARP inhibitor with improved patient-reported quality of life outcomes.
The EMBRACA study was funded by Pfizer. Dr. Litton has disclosed research funding with EMD Serono, AstraZeneca, Pfizer, Genentech, and GlaxoSmithKline, and serves on advisory boards for Pfizer and AstraZeneca, all uncompensated.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – In women with advanced HER2-negative breast cancer with germline BRCA mutations, talazoparib, an investigational oral PARP inhibitor, was associated with a near doubling in progression-free survival, compared with single-agent chemotherapy in the phase 3 EMBRACA trial.
After a median follow-up of 11.2 months, median progression-free survival by blinded central review was 8.6 months for patients assigned to receive talazoparib, compared with 5.6 months for patients randomized to receive the physician’s choice of either capecitabine, eribulin, gemcitabine, or vinorelbine.
In this video interview from the San Antonio Breast Cancer Symposium, Jennifer K. Litton, MD, from the University of Texas MD Anderson Cancer Center in Houston discusses the comparative efficacy of the drug relative to standard chemotherapy agents in this population, and the association of the PARP inhibitor with improved patient-reported quality of life outcomes.
The EMBRACA study was funded by Pfizer. Dr. Litton has disclosed research funding with EMD Serono, AstraZeneca, Pfizer, Genentech, and GlaxoSmithKline, and serves on advisory boards for Pfizer and AstraZeneca, all uncompensated.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
REPORTING FROM SABCS 2017
Ovarian suppression during breast cancer chemo helps stave off early menopause, preserve fertility
SAN ANTONIO – Premenopausal women with early breast cancer should be offered temporary ovarian suppression during chemotherapy if they wish to remain fertile or avoid early menopause, suggests a meta-analysis of five randomized controlled trials among 873 women reported at the San Antonio Breast Cancer Symposium.

“Oocyte and embryo cryopreservation are standard strategies for fertility preservation in these patients, meaning increasing the chance of pregnancy after the end of treatment,” said lead author Matteo Lambertini, MD, medical oncologist and ESMO fellow at the Institut Jules Bordet in Brussels. “However, they do not prevent the risk of developing chemotherapy-induced premature ovarian insufficiency, and so patients are still at risk of developing early menopause.”
Data from individual trials of ovarian suppression have been mixed, and its use remains controversial, he further noted. As a result, guidelines from ASCO and ESMO for fertility preservation in cancer patients still consider ovarian suppression to be investigational.
Results of the new meta-analysis, reported in a press briefing and session, showed that, compared with control peers, premenopausal women given a gonadotropin-releasing hormone analog (GnRHa) to suppress ovarian function during breast cancer chemotherapy had a more than one-half reduction in odds of premature ovarian insufficiency and were almost twice as likely to become pregnant after completing their treatment.
“We believe that this strategy should now be considered a standard option to reduce the likelihood of chemotherapy-induced premature ovarian insufficiency and potentially improve future fertility in premenopausal early breast cancer patients who undergo adjuvant or neoadjuvant chemotherapy,” Dr. Lambertini maintained. The analysis and trial participants “remind us that there is a life after cancer and to cure the disease should not be considered enough any more.”
These new data are sufficient to put the controversy to rest, for several reasons, he contended. “First, this is an individual-patient meta-analysis of the five major randomized controlled trials in this setting, so it’s kind of the highest level of evidence that we can reach. Second, it’s very unlikely that we will have new randomized, controlled trials in this setting, and I would say also that, based on the results, it would probably be unethical to run randomized, controlled trials in this setting.”

Press briefing moderator Carlos L. Arteaga, MD, director of the Harold C. Simmons Comprehensive Cancer Center at UT Southwestern Medical Center, Dallas, wondered how trials were selected for inclusion in the meta-analysis.
Thirteen trials have been conducted on ovarian suppression in premenopausal patients with breast cancer, and the investigators included the five for which they were able to obtain patient-level data, a subset that contained both positive and negative trials, Dr. Lambertini replied. But findings would likely be the same had all trials been included, given that a 2015 analysis using trial-level data from the 12 trials completed at that time showed very similar results (Ann Oncol. 2015 Dec;26:2408-19).
“Societally, this is a hugely significant issue, but the difference you are showing I have to admit is rather modest,” commented Dr. Arteaga, who is also SABCS codirector and AACR past president. “So what kind of conversation do you have with the patient? Who are the ones who would be the best candidates for this approach?”
“The main message is that giving a GnRHa does not avoid the risk of early menopause in all patients, but still, it decreases significantly the number of patients who have this side effect,” Dr. Lambertini replied.
Two groups are optimal candidates for ovarian suppression, he proposed. “First, the patients who are concerned about developing early menopause and its related side effects, who are not interested per se in having a baby after the end of treatment, but may be preserving ovarian function. [Second], for patients interested in having a baby, so interested in fertility preservation, this strategy can be used after cryopreservation procedures or in patients who have no access, for different reasons, to cryopreservation strategies.”
Another point of view
In the session, attendee Kutluk Oktay, MD, PhD, professor of obstetrics & gynecology and reproductive sciences at Yale University, New Haven, and cochair of ASCO’s guideline committee on fertility preservation said, “I cannot agree with your conclusions based on what you presented to us.”
In particular, he took issue with the exclusion of additional trials in breast cancer as well as trials among patients with other types of cancers. “I’m wondering what the rationale is to limit this to breast cancer because chemotherapy is chemotherapy and ovary is ovary, so underlying disease should not matter. By limiting it to breast cancer, you are leaving out three important studies, all in hematological cancer, with better designs … three negative studies,” he commented.
From a clinical point of view, patients with lymphoma and patients with breast cancer differ greatly, Dr. Lambertini countered: The former are about 20 years younger, on average, and often receive less-granulotoxic chemotherapy. “For these reasons, I don’t believe that mixing these two populations would have been [appropriate] for analysis,” he said. “From a methodological point of view, the studies you have mentioned include overall [fewer] than 150 patients, so it’s a very small proportion in comparison to the data we have in breast cancer.”
Study details
For their meta-analysis, Dr. Lambertini and coinvestigators pooled individual patient data from five trials (PROMISE-GIM6, POEMS/SWOG S0230, Anglo-Celtic Group OPTION, GBG-37 ZORO, and a trial led by the Moffitt Cancer Center) that randomized premenopausal women with early breast cancer to adjuvant or neoadjuvant chemotherapy either with or without concurrent GnRHa therapy.
Two of the trials restricted enrollment to women with estrogen receptor (ER)-negative disease. The GnRHa agents used were triptorelin (Trelstar, Triptodur)and goserelin(Zoladex).
Main results showed that the rate of premature ovarian insufficiency, defined differently across trials, was 14.1% among women given a GnRHa and 30.9% among control women (adjusted odds ratio, 0.38; P less than .001), Dr. Lambertini reported. Findings were similar in subgroups stratified by age, ER status, and type and duration of chemotherapy.
The rate of amenorrhea, used as a standardized definition of premature ovarian insufficiency, was similar in the GnRHa and control groups at 1 year (36.8% and 40.4%) but sharply lower in the former at 2 years (18.2% vs. 30.0%; adjusted odds ratio, 0.51; P = .009).
Overall, 10.3% of women in the GnRHa group and 5.5% in the control group had at least one pregnancy after completing their breast cancer treatment (incidence rate ratio, 1.83; P = .030). “All of the randomized trials except for the POEMS study actually did not have fertility outcomes as a preplanned endpoint, and so the patients’ wish to have a pregnancy was not collected,” he noted; therefore, it was not possible to calculate pregnancy rates in the subset who actually wanted to conceive.
All pregnancies occurred among women aged 40 years or younger, and 86% occurred among women who had had ER-negative disease, likely reflecting use of adjuvant endocrine therapy in patients with ER-positive disease, he said. Of the 57 total pregnancies, 50 resulted in live births, and none of the infants had malformations; the other pregnancies ended in spontaneous or induced abortion.
With a median follow-up of 5 years, the groups did not differ significantly on rates of disease-free survival and overall survival, suggesting that ovarian suppression was safe, according to Dr. Lambertini. Findings were similar when patients were stratified by ER status.
“What I think researchers should do in the next year is to better understand how this strategy [of ovarian suppression] works because this is probably the main controversy right now, because it’s still not very clear how this strategy actually works,” he concluded.
SOURCE: Lambertini M et al., SABCS 2017 Abstract GS4-01.
SAN ANTONIO – Premenopausal women with early breast cancer should be offered temporary ovarian suppression during chemotherapy if they wish to remain fertile or avoid early menopause, suggests a meta-analysis of five randomized controlled trials among 873 women reported at the San Antonio Breast Cancer Symposium.
“Oocyte and embryo cryopreservation are standard strategies for fertility preservation in these patients, meaning increasing the chance of pregnancy after the end of treatment,” said lead author Matteo Lambertini, MD, medical oncologist and ESMO fellow at the Institut Jules Bordet in Brussels. “However, they do not prevent the risk of developing chemotherapy-induced premature ovarian insufficiency, and so patients are still at risk of developing early menopause.”
Data from individual trials of ovarian suppression have been mixed, and its use remains controversial, he further noted. As a result, guidelines from ASCO and ESMO for fertility preservation in cancer patients still consider ovarian suppression to be investigational.
Results of the new meta-analysis, reported in a press briefing and session, showed that, compared with control peers, premenopausal women given a gonadotropin-releasing hormone analog (GnRHa) to suppress ovarian function during breast cancer chemotherapy had a more than one-half reduction in odds of premature ovarian insufficiency and were almost twice as likely to become pregnant after completing their treatment.
“We believe that this strategy should now be considered a standard option to reduce the likelihood of chemotherapy-induced premature ovarian insufficiency and potentially improve future fertility in premenopausal early breast cancer patients who undergo adjuvant or neoadjuvant chemotherapy,” Dr. Lambertini maintained. The analysis and trial participants “remind us that there is a life after cancer and to cure the disease should not be considered enough any more.”
These new data are sufficient to put the controversy to rest, for several reasons, he contended. “First, this is an individual-patient meta-analysis of the five major randomized controlled trials in this setting, so it’s kind of the highest level of evidence that we can reach. Second, it’s very unlikely that we will have new randomized, controlled trials in this setting, and I would say also that, based on the results, it would probably be unethical to run randomized, controlled trials in this setting.”
Press briefing moderator Carlos L. Arteaga, MD, director of the Harold C. Simmons Comprehensive Cancer Center at UT Southwestern Medical Center, Dallas, wondered how trials were selected for inclusion in the meta-analysis.
Thirteen trials have been conducted on ovarian suppression in premenopausal patients with breast cancer, and the investigators included the five for which they were able to obtain patient-level data, a subset that contained both positive and negative trials, Dr. Lambertini replied. But findings would likely be the same had all trials been included, given that a 2015 analysis using trial-level data from the 12 trials completed at that time showed very similar results (Ann Oncol. 2015 Dec;26:2408-19).
“Societally, this is a hugely significant issue, but the difference you are showing I have to admit is rather modest,” commented Dr. Arteaga, who is also SABCS codirector and AACR past president. “So what kind of conversation do you have with the patient? Who are the ones who would be the best candidates for this approach?”
“The main message is that giving a GnRHa does not avoid the risk of early menopause in all patients, but still, it decreases significantly the number of patients who have this side effect,” Dr. Lambertini replied.
Two groups are optimal candidates for ovarian suppression, he proposed. “First, the patients who are concerned about developing early menopause and its related side effects, who are not interested per se in having a baby after the end of treatment, but may be preserving ovarian function. [Second], for patients interested in having a baby, so interested in fertility preservation, this strategy can be used after cryopreservation procedures or in patients who have no access, for different reasons, to cryopreservation strategies.”
Another point of view
In the session, attendee Kutluk Oktay, MD, PhD, professor of obstetrics & gynecology and reproductive sciences at Yale University, New Haven, and cochair of ASCO’s guideline committee on fertility preservation said, “I cannot agree with your conclusions based on what you presented to us.”
In particular, he took issue with the exclusion of additional trials in breast cancer as well as trials among patients with other types of cancers. “I’m wondering what the rationale is to limit this to breast cancer because chemotherapy is chemotherapy and ovary is ovary, so underlying disease should not matter. By limiting it to breast cancer, you are leaving out three important studies, all in hematological cancer, with better designs … three negative studies,” he commented.
From a clinical point of view, patients with lymphoma and patients with breast cancer differ greatly, Dr. Lambertini countered: The former are about 20 years younger, on average, and often receive less-granulotoxic chemotherapy. “For these reasons, I don’t believe that mixing these two populations would have been [appropriate] for analysis,” he said. “From a methodological point of view, the studies you have mentioned include overall [fewer] than 150 patients, so it’s a very small proportion in comparison to the data we have in breast cancer.”
Study details
For their meta-analysis, Dr. Lambertini and coinvestigators pooled individual patient data from five trials (PROMISE-GIM6, POEMS/SWOG S0230, Anglo-Celtic Group OPTION, GBG-37 ZORO, and a trial led by the Moffitt Cancer Center) that randomized premenopausal women with early breast cancer to adjuvant or neoadjuvant chemotherapy either with or without concurrent GnRHa therapy.
Two of the trials restricted enrollment to women with estrogen receptor (ER)-negative disease. The GnRHa agents used were triptorelin (Trelstar, Triptodur)and goserelin(Zoladex).
Main results showed that the rate of premature ovarian insufficiency, defined differently across trials, was 14.1% among women given a GnRHa and 30.9% among control women (adjusted odds ratio, 0.38; P less than .001), Dr. Lambertini reported. Findings were similar in subgroups stratified by age, ER status, and type and duration of chemotherapy.
The rate of amenorrhea, used as a standardized definition of premature ovarian insufficiency, was similar in the GnRHa and control groups at 1 year (36.8% and 40.4%) but sharply lower in the former at 2 years (18.2% vs. 30.0%; adjusted odds ratio, 0.51; P = .009).
Overall, 10.3% of women in the GnRHa group and 5.5% in the control group had at least one pregnancy after completing their breast cancer treatment (incidence rate ratio, 1.83; P = .030). “All of the randomized trials except for the POEMS study actually did not have fertility outcomes as a preplanned endpoint, and so the patients’ wish to have a pregnancy was not collected,” he noted; therefore, it was not possible to calculate pregnancy rates in the subset who actually wanted to conceive.
All pregnancies occurred among women aged 40 years or younger, and 86% occurred among women who had had ER-negative disease, likely reflecting use of adjuvant endocrine therapy in patients with ER-positive disease, he said. Of the 57 total pregnancies, 50 resulted in live births, and none of the infants had malformations; the other pregnancies ended in spontaneous or induced abortion.
With a median follow-up of 5 years, the groups did not differ significantly on rates of disease-free survival and overall survival, suggesting that ovarian suppression was safe, according to Dr. Lambertini. Findings were similar when patients were stratified by ER status.
“What I think researchers should do in the next year is to better understand how this strategy [of ovarian suppression] works because this is probably the main controversy right now, because it’s still not very clear how this strategy actually works,” he concluded.
SOURCE: Lambertini M et al., SABCS 2017 Abstract GS4-01.
SAN ANTONIO – Premenopausal women with early breast cancer should be offered temporary ovarian suppression during chemotherapy if they wish to remain fertile or avoid early menopause, suggests a meta-analysis of five randomized controlled trials among 873 women reported at the San Antonio Breast Cancer Symposium.
“Oocyte and embryo cryopreservation are standard strategies for fertility preservation in these patients, meaning increasing the chance of pregnancy after the end of treatment,” said lead author Matteo Lambertini, MD, medical oncologist and ESMO fellow at the Institut Jules Bordet in Brussels. “However, they do not prevent the risk of developing chemotherapy-induced premature ovarian insufficiency, and so patients are still at risk of developing early menopause.”
Data from individual trials of ovarian suppression have been mixed, and its use remains controversial, he further noted. As a result, guidelines from ASCO and ESMO for fertility preservation in cancer patients still consider ovarian suppression to be investigational.
Results of the new meta-analysis, reported in a press briefing and session, showed that, compared with control peers, premenopausal women given a gonadotropin-releasing hormone analog (GnRHa) to suppress ovarian function during breast cancer chemotherapy had a more than one-half reduction in odds of premature ovarian insufficiency and were almost twice as likely to become pregnant after completing their treatment.
“We believe that this strategy should now be considered a standard option to reduce the likelihood of chemotherapy-induced premature ovarian insufficiency and potentially improve future fertility in premenopausal early breast cancer patients who undergo adjuvant or neoadjuvant chemotherapy,” Dr. Lambertini maintained. The analysis and trial participants “remind us that there is a life after cancer and to cure the disease should not be considered enough any more.”
These new data are sufficient to put the controversy to rest, for several reasons, he contended. “First, this is an individual-patient meta-analysis of the five major randomized controlled trials in this setting, so it’s kind of the highest level of evidence that we can reach. Second, it’s very unlikely that we will have new randomized, controlled trials in this setting, and I would say also that, based on the results, it would probably be unethical to run randomized, controlled trials in this setting.”
Press briefing moderator Carlos L. Arteaga, MD, director of the Harold C. Simmons Comprehensive Cancer Center at UT Southwestern Medical Center, Dallas, wondered how trials were selected for inclusion in the meta-analysis.
Thirteen trials have been conducted on ovarian suppression in premenopausal patients with breast cancer, and the investigators included the five for which they were able to obtain patient-level data, a subset that contained both positive and negative trials, Dr. Lambertini replied. But findings would likely be the same had all trials been included, given that a 2015 analysis using trial-level data from the 12 trials completed at that time showed very similar results (Ann Oncol. 2015 Dec;26:2408-19).
“Societally, this is a hugely significant issue, but the difference you are showing I have to admit is rather modest,” commented Dr. Arteaga, who is also SABCS codirector and AACR past president. “So what kind of conversation do you have with the patient? Who are the ones who would be the best candidates for this approach?”
“The main message is that giving a GnRHa does not avoid the risk of early menopause in all patients, but still, it decreases significantly the number of patients who have this side effect,” Dr. Lambertini replied.
Two groups are optimal candidates for ovarian suppression, he proposed. “First, the patients who are concerned about developing early menopause and its related side effects, who are not interested per se in having a baby after the end of treatment, but may be preserving ovarian function. [Second], for patients interested in having a baby, so interested in fertility preservation, this strategy can be used after cryopreservation procedures or in patients who have no access, for different reasons, to cryopreservation strategies.”
Another point of view
In the session, attendee Kutluk Oktay, MD, PhD, professor of obstetrics & gynecology and reproductive sciences at Yale University, New Haven, and cochair of ASCO’s guideline committee on fertility preservation said, “I cannot agree with your conclusions based on what you presented to us.”
In particular, he took issue with the exclusion of additional trials in breast cancer as well as trials among patients with other types of cancers. “I’m wondering what the rationale is to limit this to breast cancer because chemotherapy is chemotherapy and ovary is ovary, so underlying disease should not matter. By limiting it to breast cancer, you are leaving out three important studies, all in hematological cancer, with better designs … three negative studies,” he commented.
From a clinical point of view, patients with lymphoma and patients with breast cancer differ greatly, Dr. Lambertini countered: The former are about 20 years younger, on average, and often receive less-granulotoxic chemotherapy. “For these reasons, I don’t believe that mixing these two populations would have been [appropriate] for analysis,” he said. “From a methodological point of view, the studies you have mentioned include overall [fewer] than 150 patients, so it’s a very small proportion in comparison to the data we have in breast cancer.”
Study details
For their meta-analysis, Dr. Lambertini and coinvestigators pooled individual patient data from five trials (PROMISE-GIM6, POEMS/SWOG S0230, Anglo-Celtic Group OPTION, GBG-37 ZORO, and a trial led by the Moffitt Cancer Center) that randomized premenopausal women with early breast cancer to adjuvant or neoadjuvant chemotherapy either with or without concurrent GnRHa therapy.
Two of the trials restricted enrollment to women with estrogen receptor (ER)-negative disease. The GnRHa agents used were triptorelin (Trelstar, Triptodur)and goserelin(Zoladex).
Main results showed that the rate of premature ovarian insufficiency, defined differently across trials, was 14.1% among women given a GnRHa and 30.9% among control women (adjusted odds ratio, 0.38; P less than .001), Dr. Lambertini reported. Findings were similar in subgroups stratified by age, ER status, and type and duration of chemotherapy.
The rate of amenorrhea, used as a standardized definition of premature ovarian insufficiency, was similar in the GnRHa and control groups at 1 year (36.8% and 40.4%) but sharply lower in the former at 2 years (18.2% vs. 30.0%; adjusted odds ratio, 0.51; P = .009).
Overall, 10.3% of women in the GnRHa group and 5.5% in the control group had at least one pregnancy after completing their breast cancer treatment (incidence rate ratio, 1.83; P = .030). “All of the randomized trials except for the POEMS study actually did not have fertility outcomes as a preplanned endpoint, and so the patients’ wish to have a pregnancy was not collected,” he noted; therefore, it was not possible to calculate pregnancy rates in the subset who actually wanted to conceive.
All pregnancies occurred among women aged 40 years or younger, and 86% occurred among women who had had ER-negative disease, likely reflecting use of adjuvant endocrine therapy in patients with ER-positive disease, he said. Of the 57 total pregnancies, 50 resulted in live births, and none of the infants had malformations; the other pregnancies ended in spontaneous or induced abortion.
With a median follow-up of 5 years, the groups did not differ significantly on rates of disease-free survival and overall survival, suggesting that ovarian suppression was safe, according to Dr. Lambertini. Findings were similar when patients were stratified by ER status.
“What I think researchers should do in the next year is to better understand how this strategy [of ovarian suppression] works because this is probably the main controversy right now, because it’s still not very clear how this strategy actually works,” he concluded.
SOURCE: Lambertini M et al., SABCS 2017 Abstract GS4-01.
REPORTING FROM SABCS 2017
Key clinical point:
Major finding: Compared with controls, women given a GnRHa during chemotherapy were less likely to develop premature ovarian insufficiency (adjusted OR, 0.38; P less than .001) and more likely to become pregnant after treatment (IRR, 1.83; P = .030).
Data source: A meta-analysis of individual patient data from five trials among 873 premenopausal women with early breast cancer.
Disclosures: Dr. Lambertini disclosed that he had no relevant conflicts of interest.
Source: Lambertini M et al., SABCS 2017 Abstract GS4-01.