User login
VIDEO: Meta-analysis lead author Dr. Richard Gray on dose intensity benefit
SAN ANTONIO – Increasing the dose intensity of adjuvant chemotherapy reduced risks of breast cancer recurrence and death by about 15% in an Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) meta-analysis of individual patient data from 25 randomized trials among 34,122 women. Lead author Richard Gray, MSc, professor of medical statistics in the Nuffield Department of Population Health at University of Oxford, England, discussed the findings for various dose-intensification approaches and likely impact on clinical practice in an interview at the San Antonio Breast Cancer Symposium.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – Increasing the dose intensity of adjuvant chemotherapy reduced risks of breast cancer recurrence and death by about 15% in an Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) meta-analysis of individual patient data from 25 randomized trials among 34,122 women. Lead author Richard Gray, MSc, professor of medical statistics in the Nuffield Department of Population Health at University of Oxford, England, discussed the findings for various dose-intensification approaches and likely impact on clinical practice in an interview at the San Antonio Breast Cancer Symposium.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – Increasing the dose intensity of adjuvant chemotherapy reduced risks of breast cancer recurrence and death by about 15% in an Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) meta-analysis of individual patient data from 25 randomized trials among 34,122 women. Lead author Richard Gray, MSc, professor of medical statistics in the Nuffield Department of Population Health at University of Oxford, England, discussed the findings for various dose-intensification approaches and likely impact on clinical practice in an interview at the San Antonio Breast Cancer Symposium.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
REPORTING FROM SABCS 2017

Half of all breast cancer survivors conceived naturally within 3 months of trying
SAN ANTONIO – Half of premenopausal breast cancer patients who had completed chemotherapy conceived by intercourse alone within 3 months of beginning to attempt conception, a study showed.
This single-center study provides some guidance for women and the physicians caring for them that an attempt at natural conception is worthwhile if ovarian function has returned after chemotherapy, said Nikita Sinha.
Speaking at the annual meeting of the American Society for Reproductive Medicine, Ms. Sinha, a medical student at the University of California, San Francisco, said that this is a worthwhile strategy, “even for patients with limited ovarian reserve, prior to using cryopreserved tissue.” Cytotoxicity of chemotherapy was not associated with decreased chances for conception, she said.
Ms. Sinha and her colleagues designed a prospective cohort study to follow women aged 18-44 years who had been diagnosed with breast cancer and had received a fertility preservation consult. A total of 297 women who had completed cancer treatment were contacted and asked to complete a survey that asked questions about their oncologic and reproductive history. Of these, 200 (67%) completed the survey, but 43 more patients were excluded because they had not received chemotherapy.
Of the remaining 157 women, 40 (25%) attempted to conceive. Return of ovarian function occurred in 36 of the 40 women (90%). Of these 36 women, 4 also began their attempts to conceive with assisted reproductive technology (ART) because of age, previous history of infertility, or a preimplantation genetic diagnosis of the BRCA mutation. Thus, a total of eight patients (20%) first attempted to conceive with ART.
Three-fourths of women in both groups had eggs or embryos cryopreserved before their chemotherapy. In the ART group, a total of five women (62.5%) became pregnant: One first attempted intrauterine insemination and became pregnant; two first attempted pregnancy by egg donation, and one became pregnant; and three of five women who attempted embryo transfer from cryopreserved eggs or embryos became pregnant.
Of the 32 women who first attempted to conceive by intercourse, 18 became pregnant after 3 months, and 16 women had a live birth, for a 50% live birth rate for this group. Of the remaining 14 women who did not become pregnant by intercourse, 8 went on to attempt conception by ART.
Of these eight women, intrauterine insemination was attempted by three, with two resulting pregnancies. The single patient who used letrozole became pregnant. Of the four patients who attempted frozen embryo transfer, two became pregnant, for a total of five pregnancies (62.5%).
Comparing the 18 women who became pregnant with the 14 women who did not, Ms. Sinha and her colleagues found no significant differences in age, parity, hormone receptor status, pre- or postchemotherapy antral follicle count, type of chemotherapy, or time since chemotherapy. Receiving leuprolide acetate during therapy was not a significant factor.
Of the patients who became pregnant, 2 of 28 (7%) have had a recurrence of their breast cancer; both of these patients are estrogen receptor positive, said Ms. Sinha. One of the 12 patients who didn’t become pregnant also has had a recurrence; she is estrogen receptor negative.
In this study, the winnowing process of patient selection resulted in a limited sample size, with the potential for selection bias, said Ms. Sinha. Data collection is ongoing for breast cancer patients who receive fertility preservation consultations at her facility, she said.
The women trying to conceive were, on average, 37 years old at their initial attempt at conception, and had completed chemotherapy about 4 years ago. Most patients received cytotoxic chemotherapy, and 25 (63%) had estrogen receptor–positive cancer.
Previous work had shown that up to 80% of women of reproductive age will have some ovarian function resume after treatment with gonadotoxic chemotherapy agents, said Ms. Sinha.
However, the fertility risk for cancer survivors is twofold, said Ms. Sinha. “While acute ovarian failure is a well-known risk, there remains an increased risk of early menopause despite resumption of menses, especially in younger aged women” who are cancer survivors, she said.
Ms. Sinha reported that her work was supported by the University of California, San Francisco Clinical and Translational Science Institute.
[email protected]
On Twitter @karioakes
SAN ANTONIO – Half of premenopausal breast cancer patients who had completed chemotherapy conceived by intercourse alone within 3 months of beginning to attempt conception, a study showed.
This single-center study provides some guidance for women and the physicians caring for them that an attempt at natural conception is worthwhile if ovarian function has returned after chemotherapy, said Nikita Sinha.
Speaking at the annual meeting of the American Society for Reproductive Medicine, Ms. Sinha, a medical student at the University of California, San Francisco, said that this is a worthwhile strategy, “even for patients with limited ovarian reserve, prior to using cryopreserved tissue.” Cytotoxicity of chemotherapy was not associated with decreased chances for conception, she said.
Ms. Sinha and her colleagues designed a prospective cohort study to follow women aged 18-44 years who had been diagnosed with breast cancer and had received a fertility preservation consult. A total of 297 women who had completed cancer treatment were contacted and asked to complete a survey that asked questions about their oncologic and reproductive history. Of these, 200 (67%) completed the survey, but 43 more patients were excluded because they had not received chemotherapy.
Of the remaining 157 women, 40 (25%) attempted to conceive. Return of ovarian function occurred in 36 of the 40 women (90%). Of these 36 women, 4 also began their attempts to conceive with assisted reproductive technology (ART) because of age, previous history of infertility, or a preimplantation genetic diagnosis of the BRCA mutation. Thus, a total of eight patients (20%) first attempted to conceive with ART.
Three-fourths of women in both groups had eggs or embryos cryopreserved before their chemotherapy. In the ART group, a total of five women (62.5%) became pregnant: One first attempted intrauterine insemination and became pregnant; two first attempted pregnancy by egg donation, and one became pregnant; and three of five women who attempted embryo transfer from cryopreserved eggs or embryos became pregnant.
Of the 32 women who first attempted to conceive by intercourse, 18 became pregnant after 3 months, and 16 women had a live birth, for a 50% live birth rate for this group. Of the remaining 14 women who did not become pregnant by intercourse, 8 went on to attempt conception by ART.
Of these eight women, intrauterine insemination was attempted by three, with two resulting pregnancies. The single patient who used letrozole became pregnant. Of the four patients who attempted frozen embryo transfer, two became pregnant, for a total of five pregnancies (62.5%).
Comparing the 18 women who became pregnant with the 14 women who did not, Ms. Sinha and her colleagues found no significant differences in age, parity, hormone receptor status, pre- or postchemotherapy antral follicle count, type of chemotherapy, or time since chemotherapy. Receiving leuprolide acetate during therapy was not a significant factor.
Of the patients who became pregnant, 2 of 28 (7%) have had a recurrence of their breast cancer; both of these patients are estrogen receptor positive, said Ms. Sinha. One of the 12 patients who didn’t become pregnant also has had a recurrence; she is estrogen receptor negative.
In this study, the winnowing process of patient selection resulted in a limited sample size, with the potential for selection bias, said Ms. Sinha. Data collection is ongoing for breast cancer patients who receive fertility preservation consultations at her facility, she said.
The women trying to conceive were, on average, 37 years old at their initial attempt at conception, and had completed chemotherapy about 4 years ago. Most patients received cytotoxic chemotherapy, and 25 (63%) had estrogen receptor–positive cancer.
Previous work had shown that up to 80% of women of reproductive age will have some ovarian function resume after treatment with gonadotoxic chemotherapy agents, said Ms. Sinha.
However, the fertility risk for cancer survivors is twofold, said Ms. Sinha. “While acute ovarian failure is a well-known risk, there remains an increased risk of early menopause despite resumption of menses, especially in younger aged women” who are cancer survivors, she said.
Ms. Sinha reported that her work was supported by the University of California, San Francisco Clinical and Translational Science Institute.
[email protected]
On Twitter @karioakes
SAN ANTONIO – Half of premenopausal breast cancer patients who had completed chemotherapy conceived by intercourse alone within 3 months of beginning to attempt conception, a study showed.
This single-center study provides some guidance for women and the physicians caring for them that an attempt at natural conception is worthwhile if ovarian function has returned after chemotherapy, said Nikita Sinha.
Speaking at the annual meeting of the American Society for Reproductive Medicine, Ms. Sinha, a medical student at the University of California, San Francisco, said that this is a worthwhile strategy, “even for patients with limited ovarian reserve, prior to using cryopreserved tissue.” Cytotoxicity of chemotherapy was not associated with decreased chances for conception, she said.
Ms. Sinha and her colleagues designed a prospective cohort study to follow women aged 18-44 years who had been diagnosed with breast cancer and had received a fertility preservation consult. A total of 297 women who had completed cancer treatment were contacted and asked to complete a survey that asked questions about their oncologic and reproductive history. Of these, 200 (67%) completed the survey, but 43 more patients were excluded because they had not received chemotherapy.
Of the remaining 157 women, 40 (25%) attempted to conceive. Return of ovarian function occurred in 36 of the 40 women (90%). Of these 36 women, 4 also began their attempts to conceive with assisted reproductive technology (ART) because of age, previous history of infertility, or a preimplantation genetic diagnosis of the BRCA mutation. Thus, a total of eight patients (20%) first attempted to conceive with ART.
Three-fourths of women in both groups had eggs or embryos cryopreserved before their chemotherapy. In the ART group, a total of five women (62.5%) became pregnant: One first attempted intrauterine insemination and became pregnant; two first attempted pregnancy by egg donation, and one became pregnant; and three of five women who attempted embryo transfer from cryopreserved eggs or embryos became pregnant.
Of the 32 women who first attempted to conceive by intercourse, 18 became pregnant after 3 months, and 16 women had a live birth, for a 50% live birth rate for this group. Of the remaining 14 women who did not become pregnant by intercourse, 8 went on to attempt conception by ART.
Of these eight women, intrauterine insemination was attempted by three, with two resulting pregnancies. The single patient who used letrozole became pregnant. Of the four patients who attempted frozen embryo transfer, two became pregnant, for a total of five pregnancies (62.5%).
Comparing the 18 women who became pregnant with the 14 women who did not, Ms. Sinha and her colleagues found no significant differences in age, parity, hormone receptor status, pre- or postchemotherapy antral follicle count, type of chemotherapy, or time since chemotherapy. Receiving leuprolide acetate during therapy was not a significant factor.
Of the patients who became pregnant, 2 of 28 (7%) have had a recurrence of their breast cancer; both of these patients are estrogen receptor positive, said Ms. Sinha. One of the 12 patients who didn’t become pregnant also has had a recurrence; she is estrogen receptor negative.
In this study, the winnowing process of patient selection resulted in a limited sample size, with the potential for selection bias, said Ms. Sinha. Data collection is ongoing for breast cancer patients who receive fertility preservation consultations at her facility, she said.
The women trying to conceive were, on average, 37 years old at their initial attempt at conception, and had completed chemotherapy about 4 years ago. Most patients received cytotoxic chemotherapy, and 25 (63%) had estrogen receptor–positive cancer.
Previous work had shown that up to 80% of women of reproductive age will have some ovarian function resume after treatment with gonadotoxic chemotherapy agents, said Ms. Sinha.
However, the fertility risk for cancer survivors is twofold, said Ms. Sinha. “While acute ovarian failure is a well-known risk, there remains an increased risk of early menopause despite resumption of menses, especially in younger aged women” who are cancer survivors, she said.
Ms. Sinha reported that her work was supported by the University of California, San Francisco Clinical and Translational Science Institute.
[email protected]
On Twitter @karioakes
AT ASRM 2017
Key clinical point:
Major finding: Of 36 women whose ovarian function resumed after chemotherapy, 18 (50%) conceived within 3 months of attempting conception.
Data source: A single-center prospective cohort study of women diagnosed with breast cancer who received fertility preservation consultation.
Disclosures: The study was funded by the University of California, San Francisco Clinical and Translational Science Institute.
No benefit to trastuzumab in low HER2 breast cancer
SAN ANTONIO – Adding trastuzumab to the standard regimen for patients with early-stage breast cancer and low levels of HER2 does not improve outcomes, according to new findings presented at the San Antonio Breast Cancer Symposium.
In a randomized trial of more than 3,000 patients, the
Patients in both arms did well, explained lead study author Louis Fehrenbacher, MD, medical director of Kaiser Permanente Oncology Clinical Trials and an oncologist with the Kaiser Permanente Vallejo (Calif.) Medical Center. “But the primary endpoint of IDFS was not met and none of the secondary endpoints were met. No trends of efficacy were seen.”
Current guidelines classify a breast cancer as HER2 positive if immunohistochemistry testing shows high levels of HER2 protein, defined as IHC 3+, or increased copies of the HER2 gene in situ hybridization. Adding 1 year of treatment with trastuzumab to standard adjuvant chemotherapy has been found to significantly reduce cancer recurrence and to improve survival for patients with early-stage HER2-positive breast cancer.
However, data from some of the early trastuzumab clinical trials suggested that patients with HER2-low breast cancer may benefit from the HER2-targeted treatment as well.
In 2005, the “stunning” results from the NSABP B-31 trial, of trastuzumab used in HER2+ breast cancer, were presented at the annual meeting of the American Society of Clinical Oncology. The study criteria included having a FISH+ test greater than 2.0 or IHC 3+, and testing was initially performed at a local laboratory site. When testing was conducted by the NSABP, submitted tissue samples showed that 9.7% of patients were not HER2 IHC 3+ or FISH+ greater than 2.0.
There were 174 patients defined as HER2 low, and not HER2 +.
“When the analysis was performed looking at the benefit of using trastuzumab in these patients considered low, it was found that the result was essentially identical, the benefit was equal, and statistically there was no interaction between FISH testing of IHC testing,” said Dr. Fehrenbacher. “These results were bewildering as the hypothesis was that only the HER2 amplified patients would benefit.
Because of these results, the NCI [National Cancer Institute] and the NSABP [National Surgical Adjuvant Breast and Bowel Project] initiated another trial, the N9831, which also found the same benefit in patients who were HER2 low.
About 15% of breast cancers are HER2 positive and another 45% have low levels of HER2, but these patients are not currently treated with adjuvant trastuzumab. Therefore, the current study, the NSABP-B-47, was designed and conducted to see if these early results could be validated in a large, prospective, randomized trial.
The study included 3,270 patients with early-stage breast cancer that was either IHC 1+, IHC 2+, and/or ISH negative in the trial. The patients were randomized 1:1 to standard adjuvant chemotherapy with or without a year of trastuzumab.
The standard regimen consisted of either one of the two chemotherapy regimens, per physician choice: The non-anthracycline regimen is TC (docetaxel 75 mg/m2, cyclophosphamide 600 mg/m2) administered intravenously every 3 weeks for six cycles; the anthracycline regimen is AC followed by weekly paclitaxel (doxorubicin 60 mg/m2 and cyclophosphamide 600 mg/m2 administered intravenously either every 3 weeks or every 2 weeks. The same regimen applied to the group that received additional trastuzumab.
The primary endpoint was to determine whether the addition of trastuzumab to chemotherapy improved invasive disease-free survival.
At a median follow-up of 46.1 months, 264 patients had IDFS events. The 5-year estimates for recurrence-free interval, distant recurrence–free interval, and overall survival were not statistically different for patients receiving trastuzumab compared with those not receiving trastuzumab.
There was no difference in outcomes for IHC 1+ (HR for IDFS 0.88, 95% CI, 0.63-1.22) or IHC 2+ (HR for IDFS 1.14 95% CI, 0.79-1.65).
“The retrospective outcome difference between local tested HER2 + and center tested HER2-low patients identified in two major adjuvant trials are not readily explained,” said Dr. Fehrenbacher. “There is no benefit with trastuzumab therapy in patients with a FISH ratio of less than 2 and IHC staining intensity of 1+ or 2+.
SOURCE: Fehrenbacher et al. GS1-02
SAN ANTONIO – Adding trastuzumab to the standard regimen for patients with early-stage breast cancer and low levels of HER2 does not improve outcomes, according to new findings presented at the San Antonio Breast Cancer Symposium.
In a randomized trial of more than 3,000 patients, the
Patients in both arms did well, explained lead study author Louis Fehrenbacher, MD, medical director of Kaiser Permanente Oncology Clinical Trials and an oncologist with the Kaiser Permanente Vallejo (Calif.) Medical Center. “But the primary endpoint of IDFS was not met and none of the secondary endpoints were met. No trends of efficacy were seen.”
Current guidelines classify a breast cancer as HER2 positive if immunohistochemistry testing shows high levels of HER2 protein, defined as IHC 3+, or increased copies of the HER2 gene in situ hybridization. Adding 1 year of treatment with trastuzumab to standard adjuvant chemotherapy has been found to significantly reduce cancer recurrence and to improve survival for patients with early-stage HER2-positive breast cancer.
However, data from some of the early trastuzumab clinical trials suggested that patients with HER2-low breast cancer may benefit from the HER2-targeted treatment as well.
In 2005, the “stunning” results from the NSABP B-31 trial, of trastuzumab used in HER2+ breast cancer, were presented at the annual meeting of the American Society of Clinical Oncology. The study criteria included having a FISH+ test greater than 2.0 or IHC 3+, and testing was initially performed at a local laboratory site. When testing was conducted by the NSABP, submitted tissue samples showed that 9.7% of patients were not HER2 IHC 3+ or FISH+ greater than 2.0.
There were 174 patients defined as HER2 low, and not HER2 +.
“When the analysis was performed looking at the benefit of using trastuzumab in these patients considered low, it was found that the result was essentially identical, the benefit was equal, and statistically there was no interaction between FISH testing of IHC testing,” said Dr. Fehrenbacher. “These results were bewildering as the hypothesis was that only the HER2 amplified patients would benefit.
Because of these results, the NCI [National Cancer Institute] and the NSABP [National Surgical Adjuvant Breast and Bowel Project] initiated another trial, the N9831, which also found the same benefit in patients who were HER2 low.
About 15% of breast cancers are HER2 positive and another 45% have low levels of HER2, but these patients are not currently treated with adjuvant trastuzumab. Therefore, the current study, the NSABP-B-47, was designed and conducted to see if these early results could be validated in a large, prospective, randomized trial.
The study included 3,270 patients with early-stage breast cancer that was either IHC 1+, IHC 2+, and/or ISH negative in the trial. The patients were randomized 1:1 to standard adjuvant chemotherapy with or without a year of trastuzumab.
The standard regimen consisted of either one of the two chemotherapy regimens, per physician choice: The non-anthracycline regimen is TC (docetaxel 75 mg/m2, cyclophosphamide 600 mg/m2) administered intravenously every 3 weeks for six cycles; the anthracycline regimen is AC followed by weekly paclitaxel (doxorubicin 60 mg/m2 and cyclophosphamide 600 mg/m2 administered intravenously either every 3 weeks or every 2 weeks. The same regimen applied to the group that received additional trastuzumab.
The primary endpoint was to determine whether the addition of trastuzumab to chemotherapy improved invasive disease-free survival.
At a median follow-up of 46.1 months, 264 patients had IDFS events. The 5-year estimates for recurrence-free interval, distant recurrence–free interval, and overall survival were not statistically different for patients receiving trastuzumab compared with those not receiving trastuzumab.
There was no difference in outcomes for IHC 1+ (HR for IDFS 0.88, 95% CI, 0.63-1.22) or IHC 2+ (HR for IDFS 1.14 95% CI, 0.79-1.65).
“The retrospective outcome difference between local tested HER2 + and center tested HER2-low patients identified in two major adjuvant trials are not readily explained,” said Dr. Fehrenbacher. “There is no benefit with trastuzumab therapy in patients with a FISH ratio of less than 2 and IHC staining intensity of 1+ or 2+.
SOURCE: Fehrenbacher et al. GS1-02
SAN ANTONIO – Adding trastuzumab to the standard regimen for patients with early-stage breast cancer and low levels of HER2 does not improve outcomes, according to new findings presented at the San Antonio Breast Cancer Symposium.
In a randomized trial of more than 3,000 patients, the
Patients in both arms did well, explained lead study author Louis Fehrenbacher, MD, medical director of Kaiser Permanente Oncology Clinical Trials and an oncologist with the Kaiser Permanente Vallejo (Calif.) Medical Center. “But the primary endpoint of IDFS was not met and none of the secondary endpoints were met. No trends of efficacy were seen.”
Current guidelines classify a breast cancer as HER2 positive if immunohistochemistry testing shows high levels of HER2 protein, defined as IHC 3+, or increased copies of the HER2 gene in situ hybridization. Adding 1 year of treatment with trastuzumab to standard adjuvant chemotherapy has been found to significantly reduce cancer recurrence and to improve survival for patients with early-stage HER2-positive breast cancer.
However, data from some of the early trastuzumab clinical trials suggested that patients with HER2-low breast cancer may benefit from the HER2-targeted treatment as well.
In 2005, the “stunning” results from the NSABP B-31 trial, of trastuzumab used in HER2+ breast cancer, were presented at the annual meeting of the American Society of Clinical Oncology. The study criteria included having a FISH+ test greater than 2.0 or IHC 3+, and testing was initially performed at a local laboratory site. When testing was conducted by the NSABP, submitted tissue samples showed that 9.7% of patients were not HER2 IHC 3+ or FISH+ greater than 2.0.
There were 174 patients defined as HER2 low, and not HER2 +.
“When the analysis was performed looking at the benefit of using trastuzumab in these patients considered low, it was found that the result was essentially identical, the benefit was equal, and statistically there was no interaction between FISH testing of IHC testing,” said Dr. Fehrenbacher. “These results were bewildering as the hypothesis was that only the HER2 amplified patients would benefit.
Because of these results, the NCI [National Cancer Institute] and the NSABP [National Surgical Adjuvant Breast and Bowel Project] initiated another trial, the N9831, which also found the same benefit in patients who were HER2 low.
About 15% of breast cancers are HER2 positive and another 45% have low levels of HER2, but these patients are not currently treated with adjuvant trastuzumab. Therefore, the current study, the NSABP-B-47, was designed and conducted to see if these early results could be validated in a large, prospective, randomized trial.
The study included 3,270 patients with early-stage breast cancer that was either IHC 1+, IHC 2+, and/or ISH negative in the trial. The patients were randomized 1:1 to standard adjuvant chemotherapy with or without a year of trastuzumab.
The standard regimen consisted of either one of the two chemotherapy regimens, per physician choice: The non-anthracycline regimen is TC (docetaxel 75 mg/m2, cyclophosphamide 600 mg/m2) administered intravenously every 3 weeks for six cycles; the anthracycline regimen is AC followed by weekly paclitaxel (doxorubicin 60 mg/m2 and cyclophosphamide 600 mg/m2 administered intravenously either every 3 weeks or every 2 weeks. The same regimen applied to the group that received additional trastuzumab.
The primary endpoint was to determine whether the addition of trastuzumab to chemotherapy improved invasive disease-free survival.
At a median follow-up of 46.1 months, 264 patients had IDFS events. The 5-year estimates for recurrence-free interval, distant recurrence–free interval, and overall survival were not statistically different for patients receiving trastuzumab compared with those not receiving trastuzumab.
There was no difference in outcomes for IHC 1+ (HR for IDFS 0.88, 95% CI, 0.63-1.22) or IHC 2+ (HR for IDFS 1.14 95% CI, 0.79-1.65).
“The retrospective outcome difference between local tested HER2 + and center tested HER2-low patients identified in two major adjuvant trials are not readily explained,” said Dr. Fehrenbacher. “There is no benefit with trastuzumab therapy in patients with a FISH ratio of less than 2 and IHC staining intensity of 1+ or 2+.
SOURCE: Fehrenbacher et al. GS1-02
REPORTING FROM SABCS 2017
Key clinical point: In contrast to earlier reports, trastuzumab does not improve outcomes in breast cancer patients with low HER2 levels.
Major finding: The 5-year invasive disease–free survival was 89.6% for those who received trastuzumab, compared with 89.2% for those who did not (HR 0.98 95% CI 0.77-1.26, P = .90).
Data source: Phase 3 randomized, prospective clinical trial of 3,720 heavily pretreated breast cancer patients with low HER2 levels.
Disclosures: The National Cancer Institute and Genentech supported the study. Dr. Fehrenbacher declared no conflicts of interest.
Source: Fehrenbacher et al. GS1-02.
Newer hormonal contraception formulations linked to breast cancer risk*
The risk of developing breast cancer is about 20% higher among women who are current or recent users of hormonal contraceptives, compared with women who never used them, according to a prospective cohort study that included current contraception formulations.

Lina S. Mørch, PhD, of the University of Copenhagen, and colleagues conducted a nationwide, prospective cohort study of 1,797,932 women in Denmark who were aged 15-49 years between 1995 and 2012. The risk of developing breast cancer among all women currently using or who had recently used hormonal contraception correlated to a relative risk (RR) of 1.20 (95% confidence interval [CI], 1.14-1.26). The report was published in the New England Journal of Medicine.
The risk of breast cancer was heavily associated with the length of time during which the women had taken hormonal contraceptives. Women with less than a year of exposure had the lowest risk elevation (RR 1.09, 95% CI, 0.96-1.23), while women with more than 10 years of exposure faced the greatest increase in risk (RR 1.38, 95% CI, 1.26-1.51, P = .002).
The increased risk persisted even after women had stopped taking contraceptives. Researchers found that contraception use of less than a year (RR 1.01, 95% CI, 0.88-1.15), between 1 year and 5 years (RR 1.07, 95% CI, 0.94-1.20), and between 5 years and 10 years (RR 1.30, 95% CI, 1.06-1.58) correlated to increased risks of breast cancer 5-10 years after cessation of use. The number of events in women who had used hormonal contraceptive for more than 10 years was too small to accurately determine risks and was not reported in the study.
The combinations and formulations of oral contraceptives had little effect on breast cancer risk elevation, the researchers found. Triphasic and monophasic formulations containing levonorgestrel had similar relative risk levels of 1.21 (95% CI, 1.04-1.41) and 1.45 (95% CI, 1.26-1.67), respectively (P = .07). The relative risk was similar for intrauterine devices containing levonorgestrel (RR 1.21, 95% CI, 1.11-1.33).
The difference in risk between current and recent users of hormonal contraception and women who never took it was 13 (CI, 10-16) per 100,000 person-years, which translates into an one extra breast cancer diagnosis for every 7,690 women using hormonal contraception for 1 year.
“The estimated number of additional breast cancers that were associated with hormonal contraception did not include extra cases diagnosed after the discontinuation of long-term use. Even so, the estimated number of additional breast cancers among premenopausal women that were attributable to hormonal contraception is likely to be low,” the researchers wrote. “This risk should be weighed against important benefits of hormonal contraceptives such as good contraceptive efficacy and reduced risks of ovarian, endometrial, and perhaps colorectal cancer (at least for combined oral contraceptives that were commonly used in the 1970s and 1980s).
”Dr. Mørch and a coauthor received grant support from the Novo Nordisk Foundation and became employed by Novo Nordisk Foundation after the study was accepted for publication. No other relevant disclosures were reported.
Source: Mørch L. et al. N Engl J Med 2017;377(23):2228-39.
*12/7/2017: The headline for this story has been corrected to reflect an association between contraception and breast cancer risk.
The association between increased breast cancer risk and hormonal contraceptives is well documented but the research by Mørch et al. offers several factors for physicians to consider when prescribing hormonal contraceptives.
Mørch et al. found a 20% total increase in breast cancer in women but that finding is not consistent across age groups. As seen in the study, breast cancer risk was more than five times higher in women in their 40s than in women in their 30s, with an overall increase in breast cancer risk of 13 women per 100,000 women. The increased risk of breast cancer was much less pronounced in women under 35, at only 2 women per 100,000 women. For women in their 40s, hormonal contraceptives not only increase their cancer risk, but they can suffer uncommon adverse side effects such as myocardial infarction and stroke as well. Older women should consider using alternative methods of contraception, such as nonhormonal long-acting, reversible contraceptives.
But the breast cancer risk needs to be balanced against the benefits, including the association between oral contraceptives and substantial reductions in the risk of ovarian, endometrial, and colorectal cancers later in life.
Ultimately, the need for contraceptives that do not increase breast cancer risk is evident.
David J. Hunter , MBBS, ScD, is from the University of Oxford, England. He reported having no relevant financial disclosures. These comments are adapted from an editorial (N Engl J Med. 2017;377[23]:2276-7).
The association between increased breast cancer risk and hormonal contraceptives is well documented but the research by Mørch et al. offers several factors for physicians to consider when prescribing hormonal contraceptives.
Mørch et al. found a 20% total increase in breast cancer in women but that finding is not consistent across age groups. As seen in the study, breast cancer risk was more than five times higher in women in their 40s than in women in their 30s, with an overall increase in breast cancer risk of 13 women per 100,000 women. The increased risk of breast cancer was much less pronounced in women under 35, at only 2 women per 100,000 women. For women in their 40s, hormonal contraceptives not only increase their cancer risk, but they can suffer uncommon adverse side effects such as myocardial infarction and stroke as well. Older women should consider using alternative methods of contraception, such as nonhormonal long-acting, reversible contraceptives.
But the breast cancer risk needs to be balanced against the benefits, including the association between oral contraceptives and substantial reductions in the risk of ovarian, endometrial, and colorectal cancers later in life.
Ultimately, the need for contraceptives that do not increase breast cancer risk is evident.
David J. Hunter , MBBS, ScD, is from the University of Oxford, England. He reported having no relevant financial disclosures. These comments are adapted from an editorial (N Engl J Med. 2017;377[23]:2276-7).
The association between increased breast cancer risk and hormonal contraceptives is well documented but the research by Mørch et al. offers several factors for physicians to consider when prescribing hormonal contraceptives.
Mørch et al. found a 20% total increase in breast cancer in women but that finding is not consistent across age groups. As seen in the study, breast cancer risk was more than five times higher in women in their 40s than in women in their 30s, with an overall increase in breast cancer risk of 13 women per 100,000 women. The increased risk of breast cancer was much less pronounced in women under 35, at only 2 women per 100,000 women. For women in their 40s, hormonal contraceptives not only increase their cancer risk, but they can suffer uncommon adverse side effects such as myocardial infarction and stroke as well. Older women should consider using alternative methods of contraception, such as nonhormonal long-acting, reversible contraceptives.
But the breast cancer risk needs to be balanced against the benefits, including the association between oral contraceptives and substantial reductions in the risk of ovarian, endometrial, and colorectal cancers later in life.
Ultimately, the need for contraceptives that do not increase breast cancer risk is evident.
David J. Hunter , MBBS, ScD, is from the University of Oxford, England. He reported having no relevant financial disclosures. These comments are adapted from an editorial (N Engl J Med. 2017;377[23]:2276-7).
The risk of developing breast cancer is about 20% higher among women who are current or recent users of hormonal contraceptives, compared with women who never used them, according to a prospective cohort study that included current contraception formulations.
Lina S. Mørch, PhD, of the University of Copenhagen, and colleagues conducted a nationwide, prospective cohort study of 1,797,932 women in Denmark who were aged 15-49 years between 1995 and 2012. The risk of developing breast cancer among all women currently using or who had recently used hormonal contraception correlated to a relative risk (RR) of 1.20 (95% confidence interval [CI], 1.14-1.26). The report was published in the New England Journal of Medicine.
The risk of breast cancer was heavily associated with the length of time during which the women had taken hormonal contraceptives. Women with less than a year of exposure had the lowest risk elevation (RR 1.09, 95% CI, 0.96-1.23), while women with more than 10 years of exposure faced the greatest increase in risk (RR 1.38, 95% CI, 1.26-1.51, P = .002).
The increased risk persisted even after women had stopped taking contraceptives. Researchers found that contraception use of less than a year (RR 1.01, 95% CI, 0.88-1.15), between 1 year and 5 years (RR 1.07, 95% CI, 0.94-1.20), and between 5 years and 10 years (RR 1.30, 95% CI, 1.06-1.58) correlated to increased risks of breast cancer 5-10 years after cessation of use. The number of events in women who had used hormonal contraceptive for more than 10 years was too small to accurately determine risks and was not reported in the study.
The combinations and formulations of oral contraceptives had little effect on breast cancer risk elevation, the researchers found. Triphasic and monophasic formulations containing levonorgestrel had similar relative risk levels of 1.21 (95% CI, 1.04-1.41) and 1.45 (95% CI, 1.26-1.67), respectively (P = .07). The relative risk was similar for intrauterine devices containing levonorgestrel (RR 1.21, 95% CI, 1.11-1.33).
The difference in risk between current and recent users of hormonal contraception and women who never took it was 13 (CI, 10-16) per 100,000 person-years, which translates into an one extra breast cancer diagnosis for every 7,690 women using hormonal contraception for 1 year.
“The estimated number of additional breast cancers that were associated with hormonal contraception did not include extra cases diagnosed after the discontinuation of long-term use. Even so, the estimated number of additional breast cancers among premenopausal women that were attributable to hormonal contraception is likely to be low,” the researchers wrote. “This risk should be weighed against important benefits of hormonal contraceptives such as good contraceptive efficacy and reduced risks of ovarian, endometrial, and perhaps colorectal cancer (at least for combined oral contraceptives that were commonly used in the 1970s and 1980s).
”Dr. Mørch and a coauthor received grant support from the Novo Nordisk Foundation and became employed by Novo Nordisk Foundation after the study was accepted for publication. No other relevant disclosures were reported.
Source: Mørch L. et al. N Engl J Med 2017;377(23):2228-39.
*12/7/2017: The headline for this story has been corrected to reflect an association between contraception and breast cancer risk.
The risk of developing breast cancer is about 20% higher among women who are current or recent users of hormonal contraceptives, compared with women who never used them, according to a prospective cohort study that included current contraception formulations.
Lina S. Mørch, PhD, of the University of Copenhagen, and colleagues conducted a nationwide, prospective cohort study of 1,797,932 women in Denmark who were aged 15-49 years between 1995 and 2012. The risk of developing breast cancer among all women currently using or who had recently used hormonal contraception correlated to a relative risk (RR) of 1.20 (95% confidence interval [CI], 1.14-1.26). The report was published in the New England Journal of Medicine.
The risk of breast cancer was heavily associated with the length of time during which the women had taken hormonal contraceptives. Women with less than a year of exposure had the lowest risk elevation (RR 1.09, 95% CI, 0.96-1.23), while women with more than 10 years of exposure faced the greatest increase in risk (RR 1.38, 95% CI, 1.26-1.51, P = .002).
The increased risk persisted even after women had stopped taking contraceptives. Researchers found that contraception use of less than a year (RR 1.01, 95% CI, 0.88-1.15), between 1 year and 5 years (RR 1.07, 95% CI, 0.94-1.20), and between 5 years and 10 years (RR 1.30, 95% CI, 1.06-1.58) correlated to increased risks of breast cancer 5-10 years after cessation of use. The number of events in women who had used hormonal contraceptive for more than 10 years was too small to accurately determine risks and was not reported in the study.
The combinations and formulations of oral contraceptives had little effect on breast cancer risk elevation, the researchers found. Triphasic and monophasic formulations containing levonorgestrel had similar relative risk levels of 1.21 (95% CI, 1.04-1.41) and 1.45 (95% CI, 1.26-1.67), respectively (P = .07). The relative risk was similar for intrauterine devices containing levonorgestrel (RR 1.21, 95% CI, 1.11-1.33).
The difference in risk between current and recent users of hormonal contraception and women who never took it was 13 (CI, 10-16) per 100,000 person-years, which translates into an one extra breast cancer diagnosis for every 7,690 women using hormonal contraception for 1 year.
“The estimated number of additional breast cancers that were associated with hormonal contraception did not include extra cases diagnosed after the discontinuation of long-term use. Even so, the estimated number of additional breast cancers among premenopausal women that were attributable to hormonal contraception is likely to be low,” the researchers wrote. “This risk should be weighed against important benefits of hormonal contraceptives such as good contraceptive efficacy and reduced risks of ovarian, endometrial, and perhaps colorectal cancer (at least for combined oral contraceptives that were commonly used in the 1970s and 1980s).
”Dr. Mørch and a coauthor received grant support from the Novo Nordisk Foundation and became employed by Novo Nordisk Foundation after the study was accepted for publication. No other relevant disclosures were reported.
Source: Mørch L. et al. N Engl J Med 2017;377(23):2228-39.
*12/7/2017: The headline for this story has been corrected to reflect an association between contraception and breast cancer risk.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: The relative risk of breast cancer was 1.20 for current and recent users of hormonal contraception, compared with women who never used hormonal contraception (95% CI 1.14-1.26).
Data source: Nationwide, prospective cohort study of 1,797,932 women in Denmark aged 15-49 years between 1995 and 2012.
Disclosures: Dr. Mørch and a coauthor received grant support from the Novo Nordisk Foundation and became employed by Novo Nordisk Foundation after the study was accepted for publication. No other relevant disclosures were reported.
Source: Mørch L et al. N Engl J Med 2017;377(23):2228-39.
Mammography screening’s benefits for breast cancer mortality questioned
Twenty-four years’ worth of data from the Netherlands’ mammography screening program suggest that it has achieved only a marginal impact on breast cancer mortality, according to a paper published online Dec. 5 in the British Medical Journal.
Researchers used data on the stage-specific incidence of breast cancer in the Netherlands during 1989-2012 and estimated the mortality effect of a nationwide, population-based mammography breast cancer screening program, which was introduced in 1988 and targeted women aged 50-75 years.
While there were considerable increases in the incidence of in situ tumors and stage 1 cancers during 1989-2012, the incidence of stages 2-4 cancers was relatively stable over this period. In women aged more than 50 years, who would have been eligible to participate in the screening program, the incidence of stages 2-4 cancers decreased by a nonsignificant 0.16%; from 168/100,000 women in 1989 to 166/100,000 in 2012.
Even when researchers limited their analysis to the period from 1995 to 2012, when the screening program was fully operational and participation rates were around 80%, the incidence of stages 2-4 cancers remained steady. It was also stable in women younger than 50 years, who would not have been eligible for screening.
To estimate the effects of mammography screening on mortality, researchers assumed a scenario without efficient treatment of breast cancer, in which the mortality increase of 0.09% per year seen from 1967 to 1995 would persist until 2012. Under this scenario, they calculated that screening would have at least prevented the predicted 2% increase in breast cancer mortality over that period. Combined with the 0.16% nonsignificant reduction in stages 2-4 cancers over the 23 years of screening, this equated to a total mortality decrease of around 3%.
This reduction paled in comparison to the contributions made by improved treatment and patient management, which the authors suggested would be associated with a 28% reduction in mortality.
“The data on advanced breast cancer in the Netherlands indicate that the Dutch national mammography screening programme would have had little influence on the decreases in breast cancer mortality observed over the past 24 years,” wrote Philippe Autier, MD, and his colleagues from the International Prevention Research Institute in Lyon, France. “This conclusion accords with the mounting evidence that randomised trials have overestimated the ability of mammography screening to reduce the risk of deaths from breast cancer in the entire life period after first exposure to mammography screening.”
However, mammography screening also was associated with a sixfold increase in the incidence of in situ cancers among women aged 50-74 years, over the 23-year study period.
The incidence of stage 1 cancers tripled in woman aged 50-69 years, and increased 3.5-fold in those aged 70-74 years. In comparison, over the same period the rates of stage 1 cancers in women younger than 50 years or older than 75 years increased 1.3-fold.
This amounted to a 50% increase in in situ and stage 1 cancers diagnosed among women who were invited to screening, compared with those younger than 50 years. Even in a best-case scenario, the advent of digital mammography would mean 10,038 overdiagnosed cancers for 640 breast cancer deaths prevented by screening.
“Thus for 1 woman who would not die from breast cancer because of screening, about 16 women would be overdiagnosed with an in situ or a stage 1 cancer,” the authors wrote. “Hence, the advent of digital technologies has probably worsened the overdiagnosis problem without clear evidence for improvements in the ability of screening to curb the risk of breast cancer death.”
The study was partly supported by the International Prevention Research Institute. No conflicts of interest were declared.
SOURCE: Autier P et al. BMJ. 2017 Dec 5;359:j5224.
Twenty-four years’ worth of data from the Netherlands’ mammography screening program suggest that it has achieved only a marginal impact on breast cancer mortality, according to a paper published online Dec. 5 in the British Medical Journal.
Researchers used data on the stage-specific incidence of breast cancer in the Netherlands during 1989-2012 and estimated the mortality effect of a nationwide, population-based mammography breast cancer screening program, which was introduced in 1988 and targeted women aged 50-75 years.
While there were considerable increases in the incidence of in situ tumors and stage 1 cancers during 1989-2012, the incidence of stages 2-4 cancers was relatively stable over this period. In women aged more than 50 years, who would have been eligible to participate in the screening program, the incidence of stages 2-4 cancers decreased by a nonsignificant 0.16%; from 168/100,000 women in 1989 to 166/100,000 in 2012.
Even when researchers limited their analysis to the period from 1995 to 2012, when the screening program was fully operational and participation rates were around 80%, the incidence of stages 2-4 cancers remained steady. It was also stable in women younger than 50 years, who would not have been eligible for screening.
To estimate the effects of mammography screening on mortality, researchers assumed a scenario without efficient treatment of breast cancer, in which the mortality increase of 0.09% per year seen from 1967 to 1995 would persist until 2012. Under this scenario, they calculated that screening would have at least prevented the predicted 2% increase in breast cancer mortality over that period. Combined with the 0.16% nonsignificant reduction in stages 2-4 cancers over the 23 years of screening, this equated to a total mortality decrease of around 3%.
This reduction paled in comparison to the contributions made by improved treatment and patient management, which the authors suggested would be associated with a 28% reduction in mortality.
“The data on advanced breast cancer in the Netherlands indicate that the Dutch national mammography screening programme would have had little influence on the decreases in breast cancer mortality observed over the past 24 years,” wrote Philippe Autier, MD, and his colleagues from the International Prevention Research Institute in Lyon, France. “This conclusion accords with the mounting evidence that randomised trials have overestimated the ability of mammography screening to reduce the risk of deaths from breast cancer in the entire life period after first exposure to mammography screening.”
However, mammography screening also was associated with a sixfold increase in the incidence of in situ cancers among women aged 50-74 years, over the 23-year study period.
The incidence of stage 1 cancers tripled in woman aged 50-69 years, and increased 3.5-fold in those aged 70-74 years. In comparison, over the same period the rates of stage 1 cancers in women younger than 50 years or older than 75 years increased 1.3-fold.
This amounted to a 50% increase in in situ and stage 1 cancers diagnosed among women who were invited to screening, compared with those younger than 50 years. Even in a best-case scenario, the advent of digital mammography would mean 10,038 overdiagnosed cancers for 640 breast cancer deaths prevented by screening.
“Thus for 1 woman who would not die from breast cancer because of screening, about 16 women would be overdiagnosed with an in situ or a stage 1 cancer,” the authors wrote. “Hence, the advent of digital technologies has probably worsened the overdiagnosis problem without clear evidence for improvements in the ability of screening to curb the risk of breast cancer death.”
The study was partly supported by the International Prevention Research Institute. No conflicts of interest were declared.
SOURCE: Autier P et al. BMJ. 2017 Dec 5;359:j5224.
Twenty-four years’ worth of data from the Netherlands’ mammography screening program suggest that it has achieved only a marginal impact on breast cancer mortality, according to a paper published online Dec. 5 in the British Medical Journal.
Researchers used data on the stage-specific incidence of breast cancer in the Netherlands during 1989-2012 and estimated the mortality effect of a nationwide, population-based mammography breast cancer screening program, which was introduced in 1988 and targeted women aged 50-75 years.
While there were considerable increases in the incidence of in situ tumors and stage 1 cancers during 1989-2012, the incidence of stages 2-4 cancers was relatively stable over this period. In women aged more than 50 years, who would have been eligible to participate in the screening program, the incidence of stages 2-4 cancers decreased by a nonsignificant 0.16%; from 168/100,000 women in 1989 to 166/100,000 in 2012.
Even when researchers limited their analysis to the period from 1995 to 2012, when the screening program was fully operational and participation rates were around 80%, the incidence of stages 2-4 cancers remained steady. It was also stable in women younger than 50 years, who would not have been eligible for screening.
To estimate the effects of mammography screening on mortality, researchers assumed a scenario without efficient treatment of breast cancer, in which the mortality increase of 0.09% per year seen from 1967 to 1995 would persist until 2012. Under this scenario, they calculated that screening would have at least prevented the predicted 2% increase in breast cancer mortality over that period. Combined with the 0.16% nonsignificant reduction in stages 2-4 cancers over the 23 years of screening, this equated to a total mortality decrease of around 3%.
This reduction paled in comparison to the contributions made by improved treatment and patient management, which the authors suggested would be associated with a 28% reduction in mortality.
“The data on advanced breast cancer in the Netherlands indicate that the Dutch national mammography screening programme would have had little influence on the decreases in breast cancer mortality observed over the past 24 years,” wrote Philippe Autier, MD, and his colleagues from the International Prevention Research Institute in Lyon, France. “This conclusion accords with the mounting evidence that randomised trials have overestimated the ability of mammography screening to reduce the risk of deaths from breast cancer in the entire life period after first exposure to mammography screening.”
However, mammography screening also was associated with a sixfold increase in the incidence of in situ cancers among women aged 50-74 years, over the 23-year study period.
The incidence of stage 1 cancers tripled in woman aged 50-69 years, and increased 3.5-fold in those aged 70-74 years. In comparison, over the same period the rates of stage 1 cancers in women younger than 50 years or older than 75 years increased 1.3-fold.
This amounted to a 50% increase in in situ and stage 1 cancers diagnosed among women who were invited to screening, compared with those younger than 50 years. Even in a best-case scenario, the advent of digital mammography would mean 10,038 overdiagnosed cancers for 640 breast cancer deaths prevented by screening.
“Thus for 1 woman who would not die from breast cancer because of screening, about 16 women would be overdiagnosed with an in situ or a stage 1 cancer,” the authors wrote. “Hence, the advent of digital technologies has probably worsened the overdiagnosis problem without clear evidence for improvements in the ability of screening to curb the risk of breast cancer death.”
The study was partly supported by the International Prevention Research Institute. No conflicts of interest were declared.
SOURCE: Autier P et al. BMJ. 2017 Dec 5;359:j5224.
FROM BMJ
Key clinical point: Data from the Netherlands’ mammography screening program suggests it has only achieved a small, nonsignificant reduction in breast cancer mortality at a cost of a significant increase in overdiagnosis of stage 1 and in situ breast cancers.
Major finding: The incidence of stages 2-4 cancers decreased only by a nonsignificant 0.16% over the 23 years of mammography screening in the Netherlands.
Data source: Population-based study using 23 years worth of data from the Netherlands.
Disclosures: The study was partly supported by the International Prevention Research Institute. No conflicts of interest were declared.
Source: Autier P et al. BMJ. 2017 Dec 5;359:j5224.
E-health app helps weight loss, QOL for African American breast cancer survivors
MONTREAL – African American breast cancer survivors who participated in fitness tracking and an online support program saw small but significant reductions in weight and improvement in quality of life, according to a new study.
Further, patients who reported a low baseline quality of life (QOL) achieved as much or more weight loss as did those whose QOL was initially high, said Jeanne Ferrante, MD, MPH, professor of family medicine and community health at Robert Wood Johnson Medical School, New Brunswick, N.J.
Overall, but not cancer-related, QOL improved during the 6 months of the study as well.
“Low quality of life at baseline was not a barrier to weight loss, and there’s the potential for weight loss to improve quality of life” in this group of cancer survivors, Dr. Ferrante said at the annual meeting of the North American Primary Care Research Group.
Although weight loss is known to improve functional status and QOL, few studies have examined these issues in African American breast cancer survivors, who may have more comorbidities and a greater risk for obesity compared with the general population, said Dr. Ferrante.
Dr. Ferrante and her coinvestigators hypothesized that QOL would be a predictor of weight loss, and that weight loss, in turn, would have a positive impact on QOL. They conducted a secondary data analysis of a trial of participants using a physical activity monitor alone (in this study, a Fitbit), compared with using the wrist-worn activity monitor together with an Internet program, SparkPeople, designed to provide information and support for increased activity and weight loss.
Eligible participants (n = 61) were African American women who had completed treatment for early stage (0-III) breast cancer, were aged 21-75 (mean 62) years, and had a body mass index of at least 25 kg/m2 (mean, 37; range 26-52). They had to be English speaking, and have Internet and smartphone access. Half the number of participants were retired, half were college graduates, and about a third were married.
One-third of the women reported that they had five or more chronic conditions at enrollment. The mean waist circumference at baseline was 45 inches, and the mean weight was 216 pounds. Patients who had bariatric surgery, had recently lost at least 5% of their body weight, or had limitations to exercise participation or other serious medical or psychiatric conditions were excluded.
To assess QOL, the investigators used the Quality of Life in Adult Cancer Survivors (Q-LACS) scale, which measures both generic and cancer-specific quality of life.
The women in the study also reported how many days out of the past 30 days their mental and their physical health was “not good.”
At baseline, the mean QOL was 108, generic quality of life was 70, and cancer-specific quality of life was 39; lower numbers are better on the scale. Patients reported that their mental health had not been good for 9 of the past 30 days, on average, and that their physical health had not been good for a mean of 6 of the past 30 days.
After 6 months (but not at 3 months), the mean improvement for overall QOL on the Q-LACS scale was –7 (P = .054). Generic QOL improved significantly at both 3 and 6 months (P = .051 and P = .017, respectively), but cancer-specific QOL did not change significantly.
The women saw no significant change over the 6 months in the number of “not good” mental and physical health days.
Waist circumference reduction was about a half inch at 3 months (–0.45 inches, not significant), with a drop at 6 months of 0.91 inches from baseline that met criteria for statistical significance. (P = .013).
The study’s limitations included its small sample size and relatively short duration, said Dr. Ferrante; however, the study continued for 12 months and those data are being analyzed now. Some bias may have been introduced by the need for Internet connection and a smartphone as well, she said.
The investigators are now piloting use of a premium version of the SparkPeople app that offers more customization and interaction with participants.
Dr. Ferrante reported no conflicts of interest.
[email protected]
On Twitter @karioakes
MONTREAL – African American breast cancer survivors who participated in fitness tracking and an online support program saw small but significant reductions in weight and improvement in quality of life, according to a new study.
Further, patients who reported a low baseline quality of life (QOL) achieved as much or more weight loss as did those whose QOL was initially high, said Jeanne Ferrante, MD, MPH, professor of family medicine and community health at Robert Wood Johnson Medical School, New Brunswick, N.J.
Overall, but not cancer-related, QOL improved during the 6 months of the study as well.
“Low quality of life at baseline was not a barrier to weight loss, and there’s the potential for weight loss to improve quality of life” in this group of cancer survivors, Dr. Ferrante said at the annual meeting of the North American Primary Care Research Group.
Although weight loss is known to improve functional status and QOL, few studies have examined these issues in African American breast cancer survivors, who may have more comorbidities and a greater risk for obesity compared with the general population, said Dr. Ferrante.
Dr. Ferrante and her coinvestigators hypothesized that QOL would be a predictor of weight loss, and that weight loss, in turn, would have a positive impact on QOL. They conducted a secondary data analysis of a trial of participants using a physical activity monitor alone (in this study, a Fitbit), compared with using the wrist-worn activity monitor together with an Internet program, SparkPeople, designed to provide information and support for increased activity and weight loss.
Eligible participants (n = 61) were African American women who had completed treatment for early stage (0-III) breast cancer, were aged 21-75 (mean 62) years, and had a body mass index of at least 25 kg/m2 (mean, 37; range 26-52). They had to be English speaking, and have Internet and smartphone access. Half the number of participants were retired, half were college graduates, and about a third were married.
One-third of the women reported that they had five or more chronic conditions at enrollment. The mean waist circumference at baseline was 45 inches, and the mean weight was 216 pounds. Patients who had bariatric surgery, had recently lost at least 5% of their body weight, or had limitations to exercise participation or other serious medical or psychiatric conditions were excluded.
To assess QOL, the investigators used the Quality of Life in Adult Cancer Survivors (Q-LACS) scale, which measures both generic and cancer-specific quality of life.
The women in the study also reported how many days out of the past 30 days their mental and their physical health was “not good.”
At baseline, the mean QOL was 108, generic quality of life was 70, and cancer-specific quality of life was 39; lower numbers are better on the scale. Patients reported that their mental health had not been good for 9 of the past 30 days, on average, and that their physical health had not been good for a mean of 6 of the past 30 days.
After 6 months (but not at 3 months), the mean improvement for overall QOL on the Q-LACS scale was –7 (P = .054). Generic QOL improved significantly at both 3 and 6 months (P = .051 and P = .017, respectively), but cancer-specific QOL did not change significantly.
The women saw no significant change over the 6 months in the number of “not good” mental and physical health days.
Waist circumference reduction was about a half inch at 3 months (–0.45 inches, not significant), with a drop at 6 months of 0.91 inches from baseline that met criteria for statistical significance. (P = .013).
The study’s limitations included its small sample size and relatively short duration, said Dr. Ferrante; however, the study continued for 12 months and those data are being analyzed now. Some bias may have been introduced by the need for Internet connection and a smartphone as well, she said.
The investigators are now piloting use of a premium version of the SparkPeople app that offers more customization and interaction with participants.
Dr. Ferrante reported no conflicts of interest.
[email protected]
On Twitter @karioakes
MONTREAL – African American breast cancer survivors who participated in fitness tracking and an online support program saw small but significant reductions in weight and improvement in quality of life, according to a new study.
Further, patients who reported a low baseline quality of life (QOL) achieved as much or more weight loss as did those whose QOL was initially high, said Jeanne Ferrante, MD, MPH, professor of family medicine and community health at Robert Wood Johnson Medical School, New Brunswick, N.J.
Overall, but not cancer-related, QOL improved during the 6 months of the study as well.
“Low quality of life at baseline was not a barrier to weight loss, and there’s the potential for weight loss to improve quality of life” in this group of cancer survivors, Dr. Ferrante said at the annual meeting of the North American Primary Care Research Group.
Although weight loss is known to improve functional status and QOL, few studies have examined these issues in African American breast cancer survivors, who may have more comorbidities and a greater risk for obesity compared with the general population, said Dr. Ferrante.
Dr. Ferrante and her coinvestigators hypothesized that QOL would be a predictor of weight loss, and that weight loss, in turn, would have a positive impact on QOL. They conducted a secondary data analysis of a trial of participants using a physical activity monitor alone (in this study, a Fitbit), compared with using the wrist-worn activity monitor together with an Internet program, SparkPeople, designed to provide information and support for increased activity and weight loss.
Eligible participants (n = 61) were African American women who had completed treatment for early stage (0-III) breast cancer, were aged 21-75 (mean 62) years, and had a body mass index of at least 25 kg/m2 (mean, 37; range 26-52). They had to be English speaking, and have Internet and smartphone access. Half the number of participants were retired, half were college graduates, and about a third were married.
One-third of the women reported that they had five or more chronic conditions at enrollment. The mean waist circumference at baseline was 45 inches, and the mean weight was 216 pounds. Patients who had bariatric surgery, had recently lost at least 5% of their body weight, or had limitations to exercise participation or other serious medical or psychiatric conditions were excluded.
To assess QOL, the investigators used the Quality of Life in Adult Cancer Survivors (Q-LACS) scale, which measures both generic and cancer-specific quality of life.
The women in the study also reported how many days out of the past 30 days their mental and their physical health was “not good.”
At baseline, the mean QOL was 108, generic quality of life was 70, and cancer-specific quality of life was 39; lower numbers are better on the scale. Patients reported that their mental health had not been good for 9 of the past 30 days, on average, and that their physical health had not been good for a mean of 6 of the past 30 days.
After 6 months (but not at 3 months), the mean improvement for overall QOL on the Q-LACS scale was –7 (P = .054). Generic QOL improved significantly at both 3 and 6 months (P = .051 and P = .017, respectively), but cancer-specific QOL did not change significantly.
The women saw no significant change over the 6 months in the number of “not good” mental and physical health days.
Waist circumference reduction was about a half inch at 3 months (–0.45 inches, not significant), with a drop at 6 months of 0.91 inches from baseline that met criteria for statistical significance. (P = .013).
The study’s limitations included its small sample size and relatively short duration, said Dr. Ferrante; however, the study continued for 12 months and those data are being analyzed now. Some bias may have been introduced by the need for Internet connection and a smartphone as well, she said.
The investigators are now piloting use of a premium version of the SparkPeople app that offers more customization and interaction with participants.
Dr. Ferrante reported no conflicts of interest.
[email protected]
On Twitter @karioakes
AT NAPCRG 2017
Key clinical point:
Major finding: Participants lost a mean 4.79 pounds from baseline (mean 2.14%, P less than .001).
Data source: Subanalysis from study of 61 African American survivors of early stage breast cancer, with BMI of 25 or higher.
Disclosures: Dr. Ferrante reported no conflicts of interest.
FDA approves first trastuzumab biosimilar
The Food and Drug Administration has approved trastuzumab-dkst (Ogivri) as a biosimilar to trastuzumab (Herceptin) for the treatment of patients with HER2+ breast or metastatic gastric or gastroesophageal junction adenocarcinoma.
This is the first biosimilar approved in the United States for the treatment of breast cancer or gastric cancer and the second biosimilar approved for the treatment of cancer, the FDA said in a statement.
The approval of trastuzumab-dkst is based on structural and functional characterization, animal study data, human pharmacokinetic and pharmacodynamic data, clinical immunogenicity data, and other clinical safety and effectiveness data.
Common expected side effects of trastuzumab-dkst for the treatment of HER2+ breast cancer include headache, diarrhea, nausea, chills, fever, infection, congestive heart failure, insomnia, cough, and rash. Common expected side effects for the treatment of HER2+ metastatic gastric cancer include neutropenia, diarrhea, fatigue, anemia, stomatitis, weight loss, upper respiratory tract infections, fever, thrombocytopenia, mucosal inflammation, nasopharyngitis, and dysgeusia.
The biosimilar label contains a Boxed Warning – as trastuzumab does – about increased risks of cardiomyopathy, infusion reactions, pulmonary toxicity, and fetal toxicity.
The FDA’s Oncologic Drugs Advisory Committee voted unanimously in July to recommend approval of the biosimilar, made by Mylan and Biocon.
The Food and Drug Administration has approved trastuzumab-dkst (Ogivri) as a biosimilar to trastuzumab (Herceptin) for the treatment of patients with HER2+ breast or metastatic gastric or gastroesophageal junction adenocarcinoma.
This is the first biosimilar approved in the United States for the treatment of breast cancer or gastric cancer and the second biosimilar approved for the treatment of cancer, the FDA said in a statement.
The approval of trastuzumab-dkst is based on structural and functional characterization, animal study data, human pharmacokinetic and pharmacodynamic data, clinical immunogenicity data, and other clinical safety and effectiveness data.
Common expected side effects of trastuzumab-dkst for the treatment of HER2+ breast cancer include headache, diarrhea, nausea, chills, fever, infection, congestive heart failure, insomnia, cough, and rash. Common expected side effects for the treatment of HER2+ metastatic gastric cancer include neutropenia, diarrhea, fatigue, anemia, stomatitis, weight loss, upper respiratory tract infections, fever, thrombocytopenia, mucosal inflammation, nasopharyngitis, and dysgeusia.
The biosimilar label contains a Boxed Warning – as trastuzumab does – about increased risks of cardiomyopathy, infusion reactions, pulmonary toxicity, and fetal toxicity.
The FDA’s Oncologic Drugs Advisory Committee voted unanimously in July to recommend approval of the biosimilar, made by Mylan and Biocon.
The Food and Drug Administration has approved trastuzumab-dkst (Ogivri) as a biosimilar to trastuzumab (Herceptin) for the treatment of patients with HER2+ breast or metastatic gastric or gastroesophageal junction adenocarcinoma.
This is the first biosimilar approved in the United States for the treatment of breast cancer or gastric cancer and the second biosimilar approved for the treatment of cancer, the FDA said in a statement.
The approval of trastuzumab-dkst is based on structural and functional characterization, animal study data, human pharmacokinetic and pharmacodynamic data, clinical immunogenicity data, and other clinical safety and effectiveness data.
Common expected side effects of trastuzumab-dkst for the treatment of HER2+ breast cancer include headache, diarrhea, nausea, chills, fever, infection, congestive heart failure, insomnia, cough, and rash. Common expected side effects for the treatment of HER2+ metastatic gastric cancer include neutropenia, diarrhea, fatigue, anemia, stomatitis, weight loss, upper respiratory tract infections, fever, thrombocytopenia, mucosal inflammation, nasopharyngitis, and dysgeusia.
The biosimilar label contains a Boxed Warning – as trastuzumab does – about increased risks of cardiomyopathy, infusion reactions, pulmonary toxicity, and fetal toxicity.
The FDA’s Oncologic Drugs Advisory Committee voted unanimously in July to recommend approval of the biosimilar, made by Mylan and Biocon.
SABCS 2017: Top picks from Dr. William J. Gradishar
Oncology Practice Associate Editor William J. Gradishar, MD, reveals several anticipated studies from the 40th annual San Antonio Breast Cancer Symposium, set to begin on Wednesday, Dec. 6:

• GS1-01. Increasing the dose density of adjuvant chemotherapy by shortening intervals between courses or by sequential drug administration significantly reduces both disease recurrence and breast cancer mortality: an EBCTCG meta-analysis of 21,000 women in 16 randomized trials.
• GS4-02. Randomized comparison of adjuvant aromatase inhibitor exemestane plus ovarian function suppression vs. tamoxifen plus OFS in premenopausal women with hormone receptor–positive early breast cancer: Update of the combined TEXT and SOFT trials.
• GS1-03. Perioperative aromatase inhibitor treatment in determining or predicting long-term outcome in early breast cancer–the POETIC Trial.
• GS1-06. Extended adjuvant bisphosphonate treatment over 5 years in early breast cancer does not improve disease-free and overall survival, compared with 2 years of treatment: Phase III data from the SUCCESS A study.
• GS2-05. First-line ribociclib vs. placebo with goserelin and tamoxifen or a nonsteroidal aromatase inhibitor in premenopausal women with hormone receptor–positive, HER2-negative advanced breast cancer: Results from the randomized phase III MONALEESA-7 trial.
• GS2-06. Phase Ib/II study evaluating safety and efficacy of pembrolizumab and trastuzumab in patients with trastuzumab-resistant HER2-positive metastatic breast cancer: Results from the PANACEA (IBCSG 45-13/KEYNOTE-014) study.
• GS2-07. MANTA – A randomized phase 2 study of fulvestrant in combination with the dual mTOR inhibitor AZD2014 or everolimus or fulvestrant alone in estrogen receptor–positive advanced or metastatic breast cancer.
• GS3-01. A prospective, randomized, multicenter phase 3 trial of additional 2 versus additional 5 years of anastrozole after initial 5 years of adjuvant endocrine therapy – results from 3,484 postmenopausal women in the ABCSG-16 trial.
• GS3-02. Invasive disease-free survival and gene-expression signatures in CALGB (Alliance) 40601, a randomized phase III neoadjuvant trial of dual HER2 targeting with lapatinib added to chemotherapy plus trastuzumab.
• GS3-03. A phase III, multicenter, double-blind randomized trial of celecoxib versus placebo in primary breast cancer patients (REACT – Randomized European Celecoxib Trial).
• GS3-04. A randomized phase III study of adjuvant trastuzumab for a duration of 9 weeks versus 1 year, combined with adjuvant taxane-anthracycline chemotherapy, for early HER2-positive breast cancer (the SOLD study).
• GS3-06. Long-term follow-up of CALGB 40502/NCCTG N063H (Alliance): A randomized phase III trial of weekly paclitaxel, compared with weekly nanoparticle albumin-bound (nab)–paclitaxel or ixabepilone +/– bevacizumab as first-line therapy for locally recurrent or metastatic breast cancer.
• GS3-08. Pathological complete response predicts event-free and distant disease-free survival in the I-SPY2 TRIAL.
• GS4-01. Pooled analysis of five randomized trials investigating temporary ovarian suppression with gonadotropin-releasing hormone analogues during chemotherapy as a strategy to preserve ovarian function and fertility in premenopausal early breast cancer patients.
• GS4-02. Randomized comparison of adjuvant aromatase inhibitor exemestane plus ovarian function suppression vs. tamoxifen plus OFS in premenopausal women with hormone receptor–positive early breast cancer: Update of the combined TEXT and SOFT trials.
• GS4-03. Randomized comparison of adjuvant tamoxifen plus ovarian function suppression versus tamoxifen in premenopausal women with hormone receptor–positive early breast cancer: Update of the SOFT trial.
• GS4-04. Randomized blinded sham- and waitlist-controlled trial of acupuncture for joint symptoms related to aromatase inhibitors in women with early-stage breast cancer.
• GS5-03. Risk of arm morbidity after local therapy in young breast cancer survivors.
• GS5-05. Primary endocrine therapy for ER-positive ductal carcinoma in situ: CALGB 40903 (Alliance).
• GS6-01. Integration of clinical variables for the prediction of late distant recurrence in patients with estrogen receptor–positive breast cancer treated with 5 years of endocrine therapy.
• GS6-02. The benefit of abemaciclib in prognostic subgroups: An exploratory analysis of combined data from the MONARCH 2 and 3 studies.
• GS6-07. EMBRACA: A phase 3 trial comparing talazoparib, an oral PARP inhibitor, to physician’s choice of therapy in patients with advanced breast cancer and a germline BRCA mutation.
Dr. Gradishar is the Betsy Bramsen Professor of Breast Oncology, professor of medicine, and interim chief of the division of hematology/oncology, Northwestern University Feinberg School of Medicine, Chicago, and deputy director for the Clinical Network and director of the Maggie Daley Center for Women’s Cancer Care, Robert H. Lurie Comprehensive Cancer Center Network of Northwestern University, Chicago.
Oncology Practice Associate Editor William J. Gradishar, MD, reveals several anticipated studies from the 40th annual San Antonio Breast Cancer Symposium, set to begin on Wednesday, Dec. 6:
• GS1-01. Increasing the dose density of adjuvant chemotherapy by shortening intervals between courses or by sequential drug administration significantly reduces both disease recurrence and breast cancer mortality: an EBCTCG meta-analysis of 21,000 women in 16 randomized trials.
• GS4-02. Randomized comparison of adjuvant aromatase inhibitor exemestane plus ovarian function suppression vs. tamoxifen plus OFS in premenopausal women with hormone receptor–positive early breast cancer: Update of the combined TEXT and SOFT trials.
• GS1-03. Perioperative aromatase inhibitor treatment in determining or predicting long-term outcome in early breast cancer–the POETIC Trial.
• GS1-06. Extended adjuvant bisphosphonate treatment over 5 years in early breast cancer does not improve disease-free and overall survival, compared with 2 years of treatment: Phase III data from the SUCCESS A study.
• GS2-05. First-line ribociclib vs. placebo with goserelin and tamoxifen or a nonsteroidal aromatase inhibitor in premenopausal women with hormone receptor–positive, HER2-negative advanced breast cancer: Results from the randomized phase III MONALEESA-7 trial.
• GS2-06. Phase Ib/II study evaluating safety and efficacy of pembrolizumab and trastuzumab in patients with trastuzumab-resistant HER2-positive metastatic breast cancer: Results from the PANACEA (IBCSG 45-13/KEYNOTE-014) study.
• GS2-07. MANTA – A randomized phase 2 study of fulvestrant in combination with the dual mTOR inhibitor AZD2014 or everolimus or fulvestrant alone in estrogen receptor–positive advanced or metastatic breast cancer.
• GS3-01. A prospective, randomized, multicenter phase 3 trial of additional 2 versus additional 5 years of anastrozole after initial 5 years of adjuvant endocrine therapy – results from 3,484 postmenopausal women in the ABCSG-16 trial.
• GS3-02. Invasive disease-free survival and gene-expression signatures in CALGB (Alliance) 40601, a randomized phase III neoadjuvant trial of dual HER2 targeting with lapatinib added to chemotherapy plus trastuzumab.
• GS3-03. A phase III, multicenter, double-blind randomized trial of celecoxib versus placebo in primary breast cancer patients (REACT – Randomized European Celecoxib Trial).
• GS3-04. A randomized phase III study of adjuvant trastuzumab for a duration of 9 weeks versus 1 year, combined with adjuvant taxane-anthracycline chemotherapy, for early HER2-positive breast cancer (the SOLD study).
• GS3-06. Long-term follow-up of CALGB 40502/NCCTG N063H (Alliance): A randomized phase III trial of weekly paclitaxel, compared with weekly nanoparticle albumin-bound (nab)–paclitaxel or ixabepilone +/– bevacizumab as first-line therapy for locally recurrent or metastatic breast cancer.
• GS3-08. Pathological complete response predicts event-free and distant disease-free survival in the I-SPY2 TRIAL.
• GS4-01. Pooled analysis of five randomized trials investigating temporary ovarian suppression with gonadotropin-releasing hormone analogues during chemotherapy as a strategy to preserve ovarian function and fertility in premenopausal early breast cancer patients.
• GS4-02. Randomized comparison of adjuvant aromatase inhibitor exemestane plus ovarian function suppression vs. tamoxifen plus OFS in premenopausal women with hormone receptor–positive early breast cancer: Update of the combined TEXT and SOFT trials.
• GS4-03. Randomized comparison of adjuvant tamoxifen plus ovarian function suppression versus tamoxifen in premenopausal women with hormone receptor–positive early breast cancer: Update of the SOFT trial.
• GS4-04. Randomized blinded sham- and waitlist-controlled trial of acupuncture for joint symptoms related to aromatase inhibitors in women with early-stage breast cancer.
• GS5-03. Risk of arm morbidity after local therapy in young breast cancer survivors.
• GS5-05. Primary endocrine therapy for ER-positive ductal carcinoma in situ: CALGB 40903 (Alliance).
• GS6-01. Integration of clinical variables for the prediction of late distant recurrence in patients with estrogen receptor–positive breast cancer treated with 5 years of endocrine therapy.
• GS6-02. The benefit of abemaciclib in prognostic subgroups: An exploratory analysis of combined data from the MONARCH 2 and 3 studies.
• GS6-07. EMBRACA: A phase 3 trial comparing talazoparib, an oral PARP inhibitor, to physician’s choice of therapy in patients with advanced breast cancer and a germline BRCA mutation.
Dr. Gradishar is the Betsy Bramsen Professor of Breast Oncology, professor of medicine, and interim chief of the division of hematology/oncology, Northwestern University Feinberg School of Medicine, Chicago, and deputy director for the Clinical Network and director of the Maggie Daley Center for Women’s Cancer Care, Robert H. Lurie Comprehensive Cancer Center Network of Northwestern University, Chicago.
Oncology Practice Associate Editor William J. Gradishar, MD, reveals several anticipated studies from the 40th annual San Antonio Breast Cancer Symposium, set to begin on Wednesday, Dec. 6:
• GS1-01. Increasing the dose density of adjuvant chemotherapy by shortening intervals between courses or by sequential drug administration significantly reduces both disease recurrence and breast cancer mortality: an EBCTCG meta-analysis of 21,000 women in 16 randomized trials.
• GS4-02. Randomized comparison of adjuvant aromatase inhibitor exemestane plus ovarian function suppression vs. tamoxifen plus OFS in premenopausal women with hormone receptor–positive early breast cancer: Update of the combined TEXT and SOFT trials.
• GS1-03. Perioperative aromatase inhibitor treatment in determining or predicting long-term outcome in early breast cancer–the POETIC Trial.
• GS1-06. Extended adjuvant bisphosphonate treatment over 5 years in early breast cancer does not improve disease-free and overall survival, compared with 2 years of treatment: Phase III data from the SUCCESS A study.
• GS2-05. First-line ribociclib vs. placebo with goserelin and tamoxifen or a nonsteroidal aromatase inhibitor in premenopausal women with hormone receptor–positive, HER2-negative advanced breast cancer: Results from the randomized phase III MONALEESA-7 trial.
• GS2-06. Phase Ib/II study evaluating safety and efficacy of pembrolizumab and trastuzumab in patients with trastuzumab-resistant HER2-positive metastatic breast cancer: Results from the PANACEA (IBCSG 45-13/KEYNOTE-014) study.
• GS2-07. MANTA – A randomized phase 2 study of fulvestrant in combination with the dual mTOR inhibitor AZD2014 or everolimus or fulvestrant alone in estrogen receptor–positive advanced or metastatic breast cancer.
• GS3-01. A prospective, randomized, multicenter phase 3 trial of additional 2 versus additional 5 years of anastrozole after initial 5 years of adjuvant endocrine therapy – results from 3,484 postmenopausal women in the ABCSG-16 trial.
• GS3-02. Invasive disease-free survival and gene-expression signatures in CALGB (Alliance) 40601, a randomized phase III neoadjuvant trial of dual HER2 targeting with lapatinib added to chemotherapy plus trastuzumab.
• GS3-03. A phase III, multicenter, double-blind randomized trial of celecoxib versus placebo in primary breast cancer patients (REACT – Randomized European Celecoxib Trial).
• GS3-04. A randomized phase III study of adjuvant trastuzumab for a duration of 9 weeks versus 1 year, combined with adjuvant taxane-anthracycline chemotherapy, for early HER2-positive breast cancer (the SOLD study).
• GS3-06. Long-term follow-up of CALGB 40502/NCCTG N063H (Alliance): A randomized phase III trial of weekly paclitaxel, compared with weekly nanoparticle albumin-bound (nab)–paclitaxel or ixabepilone +/– bevacizumab as first-line therapy for locally recurrent or metastatic breast cancer.
• GS3-08. Pathological complete response predicts event-free and distant disease-free survival in the I-SPY2 TRIAL.
• GS4-01. Pooled analysis of five randomized trials investigating temporary ovarian suppression with gonadotropin-releasing hormone analogues during chemotherapy as a strategy to preserve ovarian function and fertility in premenopausal early breast cancer patients.
• GS4-02. Randomized comparison of adjuvant aromatase inhibitor exemestane plus ovarian function suppression vs. tamoxifen plus OFS in premenopausal women with hormone receptor–positive early breast cancer: Update of the combined TEXT and SOFT trials.
• GS4-03. Randomized comparison of adjuvant tamoxifen plus ovarian function suppression versus tamoxifen in premenopausal women with hormone receptor–positive early breast cancer: Update of the SOFT trial.
• GS4-04. Randomized blinded sham- and waitlist-controlled trial of acupuncture for joint symptoms related to aromatase inhibitors in women with early-stage breast cancer.
• GS5-03. Risk of arm morbidity after local therapy in young breast cancer survivors.
• GS5-05. Primary endocrine therapy for ER-positive ductal carcinoma in situ: CALGB 40903 (Alliance).
• GS6-01. Integration of clinical variables for the prediction of late distant recurrence in patients with estrogen receptor–positive breast cancer treated with 5 years of endocrine therapy.
• GS6-02. The benefit of abemaciclib in prognostic subgroups: An exploratory analysis of combined data from the MONARCH 2 and 3 studies.
• GS6-07. EMBRACA: A phase 3 trial comparing talazoparib, an oral PARP inhibitor, to physician’s choice of therapy in patients with advanced breast cancer and a germline BRCA mutation.
Dr. Gradishar is the Betsy Bramsen Professor of Breast Oncology, professor of medicine, and interim chief of the division of hematology/oncology, Northwestern University Feinberg School of Medicine, Chicago, and deputy director for the Clinical Network and director of the Maggie Daley Center for Women’s Cancer Care, Robert H. Lurie Comprehensive Cancer Center Network of Northwestern University, Chicago.
FROM SABCS 2017
Breakthrough cancer gene assay approved, CMS proposes coverage
The Food and Drug Administration approved a new genetic sequencing test that detects mutations across 324 genes in tumor biopsy specimens with an accuracy of 94.6%.
The FoundationOne CDx (F1CDx) test from Foundation Medicine “can identify which patients with any of five tumor types” – non–small-cell lung cancer, melanoma, breast cancer, colorectal cancer, or ovarian cancer – “may benefit from 15 different FDA-approved targeted treatment options,” as well as clinical trial eligibility, “with one test report, avoiding duplicative biopsies,” the agency said in a statement.
On the same day as the approval, the Centers for Medicare & Medicaid Services proposed nationwide coverage for Medicare beneficiaries with recurrent or metastatic disease. CMS is accepting public comments on the proposal for 30 days. The cost of the test is $5,800.
F1CDx went through the FDA and CMS Parallel Review Program, in which the agencies review medical devices concurrently to help reduce the time between approval and Medicare coverage.
F1CDx reads the order of nucleotides on DNA isolated from biopsy specimens to detect a range of genetic anomalies, including base substitutions, insertion and deletion alterations, copy number alterations, and select gene rearrangements, as well as genomic signatures including microsatellite instability and tumor mutational burden. Clinical performance was established by comparing the F1CDx to previously approved tests.
The Food and Drug Administration approved a new genetic sequencing test that detects mutations across 324 genes in tumor biopsy specimens with an accuracy of 94.6%.
The FoundationOne CDx (F1CDx) test from Foundation Medicine “can identify which patients with any of five tumor types” – non–small-cell lung cancer, melanoma, breast cancer, colorectal cancer, or ovarian cancer – “may benefit from 15 different FDA-approved targeted treatment options,” as well as clinical trial eligibility, “with one test report, avoiding duplicative biopsies,” the agency said in a statement.
On the same day as the approval, the Centers for Medicare & Medicaid Services proposed nationwide coverage for Medicare beneficiaries with recurrent or metastatic disease. CMS is accepting public comments on the proposal for 30 days. The cost of the test is $5,800.
F1CDx went through the FDA and CMS Parallel Review Program, in which the agencies review medical devices concurrently to help reduce the time between approval and Medicare coverage.
F1CDx reads the order of nucleotides on DNA isolated from biopsy specimens to detect a range of genetic anomalies, including base substitutions, insertion and deletion alterations, copy number alterations, and select gene rearrangements, as well as genomic signatures including microsatellite instability and tumor mutational burden. Clinical performance was established by comparing the F1CDx to previously approved tests.
The Food and Drug Administration approved a new genetic sequencing test that detects mutations across 324 genes in tumor biopsy specimens with an accuracy of 94.6%.
The FoundationOne CDx (F1CDx) test from Foundation Medicine “can identify which patients with any of five tumor types” – non–small-cell lung cancer, melanoma, breast cancer, colorectal cancer, or ovarian cancer – “may benefit from 15 different FDA-approved targeted treatment options,” as well as clinical trial eligibility, “with one test report, avoiding duplicative biopsies,” the agency said in a statement.
On the same day as the approval, the Centers for Medicare & Medicaid Services proposed nationwide coverage for Medicare beneficiaries with recurrent or metastatic disease. CMS is accepting public comments on the proposal for 30 days. The cost of the test is $5,800.
F1CDx went through the FDA and CMS Parallel Review Program, in which the agencies review medical devices concurrently to help reduce the time between approval and Medicare coverage.
F1CDx reads the order of nucleotides on DNA isolated from biopsy specimens to detect a range of genetic anomalies, including base substitutions, insertion and deletion alterations, copy number alterations, and select gene rearrangements, as well as genomic signatures including microsatellite instability and tumor mutational burden. Clinical performance was established by comparing the F1CDx to previously approved tests.
Targeted therapies forge ahead in multiple breast cancer subtypes
As our understanding of the biology of breast cancer has improved, treatment has become increasingly personalized. Targeted therapies continue to significantly improve patient outcomes in multiple subtypes, with several recent drug approvals. Here, we discuss some of these latest developments.
A disease of many faces
Clinically speaking, breast cancers can be divided into at least 5 subtypes on the basis of the genes they express (Figure 1). The luminal subtypes make up the largest proportion and are characterized by the expression of hormone receptor (HR) genes. Luminal A tumors are negative for human epidermal growth factor receptor 2 (HER2; HER2-negative), whereas luminal B tumors often co-express the HER2 genes.1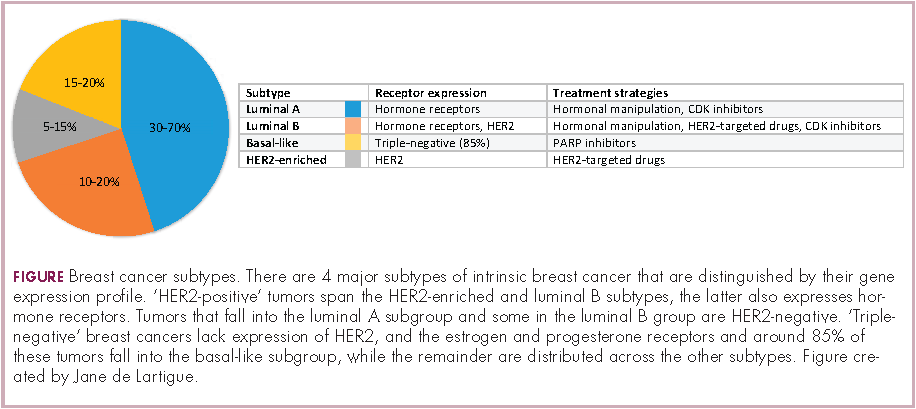
The remainder of HER2-positive patients fall into the HER2-enriched category, in which HER2 expression is the defining characteristic. Basal-like tumors, meanwhile, represent the most heterogeneous subtype, overlapping to a large extent with tumors dubbed “triple-negative” because of their lack of either HER2 or ESR1 and PGR gene expression. The fifth subtype is known as normal breast-like and remains poorly characterized.
In recent years, there have been significant advancements in the genomic characterization of breast cancer that have begun to provide a more comprehensive understanding of the driver molecular mechanisms, which has helped to explain some of the limitations of current targeted approaches and to reveal new possible treatments, with a shift toward increasingly personalized strategies.2
HER2: what’s neu?
An estimated 18%-20% of breast tumors are HER2 positive, displaying amplification of the HER2/neu gene or overexpression of its protein product.3 Historically, HER2 positivity correlated with a highly aggressive and metastatic form of disease, conferring poor prognosis.4,5 The HER2-targeted monoclonal antibody (mAb), trastuzumab serves as a prime example of the power of personalized medicine. Evidence suggests that trastuzumab has altered the natural history of HER2-positive breast cancer, such that trastuzumab-treated patients with HER2-positive breast cancer now have a better prognosis than do patients with HER2-negative disease.6,7
Several additional HER2-targeted drugs have joined trastuzumab on the market, including other mAbs, small molecule tyrosine kinase inhibitors (TKIs), and an antibody–drug conjugate that combines the specificity of a mAb with the anti-tumor potency of a cytotoxic drug. These drugs have further improved patient outcomes in both early and advanced disease settings (Table 1).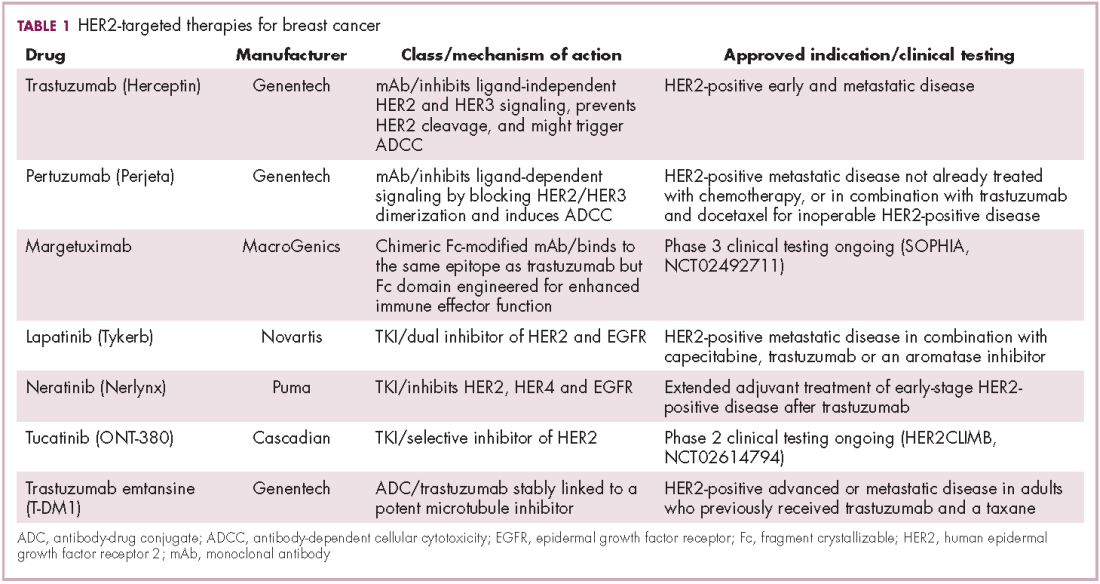
The most recent regulatory approval was for neratinib, a potent TKI inhibiting all members of the HER protein family. On the basis of the phase 3 ExteNET study, neratinib was granted approval by the US Food and Drug Administration (FDA) for extended adjuvant treatment of patients with HER2-positive, early-stage breast cancer previously treated with trastuzumab. In a 5-year analysis of the study, invasive disease-free survival (DFS) was 90.4% with neratinib, compared with 87.9% with placebo (hazard ratio [HR], 0.74; P = .017).8,9
The tide of advancements in HER2-targeted therapy looks set to continue in the coming years as potentially practice-changing data emerges from ongoing clinical trials and, as the patent on trastuzumab has expired, a number of biosimilars, such as MYL-1401O have the potential to help patients who may not have access to trastuzumab.10
One of the biggest remaining challenges is identifying drugs that can effectively treat patients with brain metastases because the blood–brain barrier presents an impediment to the delivery of effective concentrations of anticancer drugs. Initially, it was hoped that the small molecule inhibitors lapatinib and neratinib could cross the blood–brain barrier and may be more effective in patients with brain metastases, but that hypothesis has not borne out in randomized clinical trials.11
Tucatinib (ONT-380) has shown significant promise in this respect. In a phase 1 trial, ONT-380 had significant efficacy in patients with and without central nervous system metastases; the overall response rate (ORR) in the CNS was 36%. ONT-380 is also notable for its specificity for HER2, without significant inhibition of HER1 and EGFR, which could translate into a better toxicity profile.12
Doubling down on resistant tumors
Since the success of HER2-targeted therapy is limited by the development of resistance, there has been significant interest in assessing the potential of dual HER2 blockade, exploiting the unique mechanisms of action of different drugs in combination therapy, and ensuring more complete inhibition of the HER2 pathway. Although numerous different combinations have been tested, a double antibody combination has proved most effective.
In fact, dual HER2 targeting with trastuzumab and pertuzumab in combination with chemotherapy has replaced a trastuzumab-chemotherapy regimen as the new standard of care in the metastatic setting. A 6-month improvement in progression-free survival (PFS) sealed FDA approval for the combination and in a recently published final analysis of the trial overall survival (OS) was also improved to a level unprecedented in the first-line setting.13,14The double antibody combination has also been successful in the neoadjuvant setting. Approval followed the results of the phase 2 NeoSphere trial, in which the combination was associated with a significant improvement in pathologic complete response (pCR) rate, a measure that acts as a surrogate for improved survival in the neoadjuvant setting. In a 5-year analysis of the NeoSphere trial, improved pCR did indeed translate into improved PFS and DFS.15,16
The results of the phase 3 APHINITY trial evaluating this combination in the adjuvant setting have been hotly anticipated. In a presentation at the 2017 American Society of Clinical Oncology (ASCO) meeting in June, the study authors reported that in 4,085 patients with operable HER2-positive disease, it significantly reduced the risk of disease recurrence or death compared with trastuzumab and chemotherapy alone.17
There is an ongoing effort to determine if it is possible to de-escalate treatment by removing the chemotherapy component. At least in the neoadjuvant setting, pCR rates in the chemotherapy-free arms of several studies suggest that a proportion of patients might benefit from this strategy15,18,19 and the challenge now is to identify them. To that end, the phase 2 PAMELA trial identified the HER2-enriched subtype as a strong predictor of response to neoadjuvant dual blockade (lapatinib and trastuzumab) without chemotherapy. The pCR rate was 40.6% for the combination in patients with the HER2-enriched subtype of breast cancer and only 10% in patients with non–HER2-enriched tumors.20
Targeting resistance to endocrine therapy
Another coup for personalized medicine in breast cancer is the treatment of hormone receptor–positive cases with endocrine therapy, which has become the cornerstone of treatment in the metastatic and adjuvant settings. Those drugs are designed to block the growth-stimulating effects of the estrogen and progesterone hormones on tumor cells. They include the selective estrogen receptor (ER) modulator tamoxifen, aromatase inhibitors (AIs) such as letrozole, anastrozole, and exemestane, which work by blocking the activity of the aromatase enzyme that converts androgens into estrogens, and the selective estrogen-receptor down-regulator fulvestrant.
As with HER2-targeted therapy, patients treated with endocrine therapy often develop resistance. Activation of alternate signaling cascades, such as the P13K–Akt–mTOR (phosphatidylinositol-3-kinase–Akt–mammalian target of rapamycin) pathway, or downstream targets of ER signaling, including the cyclin-dependent kinases, CDK4 and CDK6, have emerged as important mechanisms of resistance.21,22
Drugs directed against these secondary targets, aimed to enhance the efficacy of endocrine therapies, have shown significant promise (Table 2). The mTOR inhibitor everolimus received FDA approval in 2012 in combination with exemestane for the treatment of advanced HR-positive, HER2-negative breast cancer.23 More recently, everolimus has also proven effective in combination with either fulvestrant or letrozole, according to the phase 2 PrECOG 0102 and BOLERO-4 studies, both doubling PFS compared with endocrine therapy alone.24,25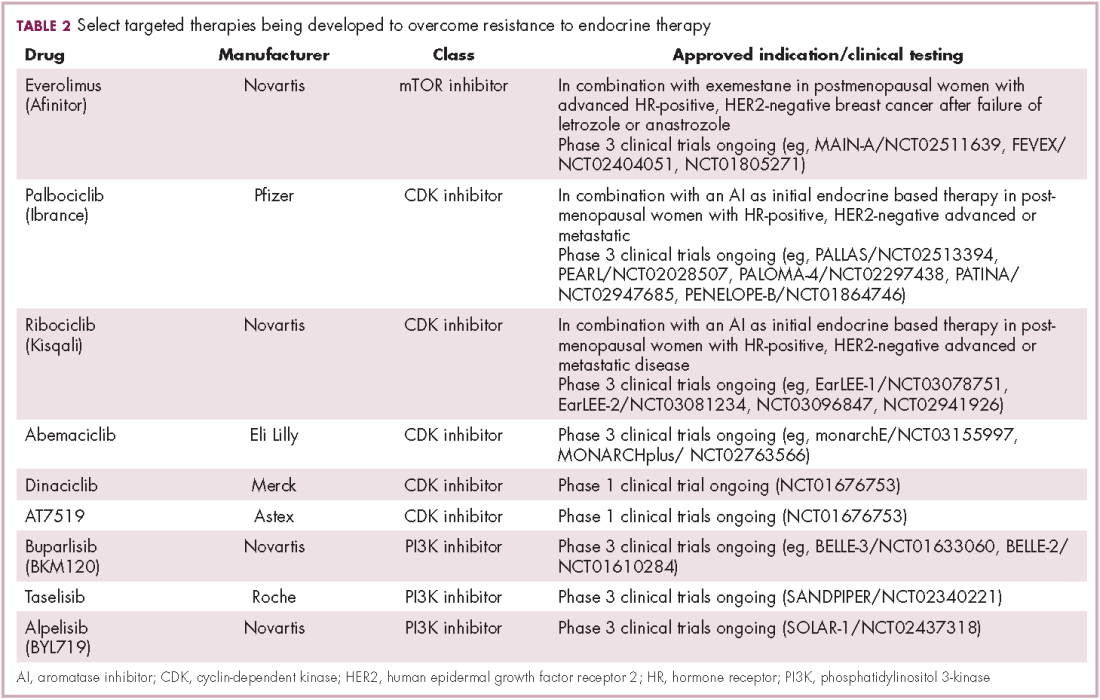
Buparlisib is an oral reversible pan-PI3K inhibitor, and the results of the first phase 3 trial of this drug in metastatic breast cancer (MBC) were recently reported. Among 1,147 postmenopausal women with HR-positive, HER2-negative MBC that progressed on or after AI therapy, the combination of buparlisib and fulvestrant prolonged PFS compared with fulvestrant alone (median PFS, 6.9 vs 5 months; HR,0.78; P < .001). However, Novartis, which was developing buparlisib, reported that the combination will not be pursued further due to increased toxicity.26
Two other PI3K inhibitors are currently in phase 3 clinical trials; taselisib and alpelisib, both selective PI3K-alpha inhibitors. The results of a phase 1 dose-escalation study of taselisib were recently published and the ORR among patients with PIK3CA-mutant solid tumors was 36%, including responses in 4 patients with breast cancer.27 Meanwhile, alpelisib has also demonstrated early promise in combination with both letrozole and fulvestrant in patients with ER-positive MBC refractory to endocrine therapy. In combination with letrozole, the clinical benefit rate was 35% overall (44% in patients with PIK3CA mutations, compared with 20% in patients with wild-type PIK3CA status). The combination of alpesilib and fulvestrant produced an ORR of 27%, and both combinations were well tolerated.28,29
Another exciting therapeutic avenue is CDK4 and CDK6 inhibitors. These proteins are critical regulators of cell cycle progression, ensuring transition from G1 to S phase occurs at the appropriate time. The CDK pathway is also a downstream target of ER activation and, unsurprisingly, aberrant expression of the proteins involved in this pathway is commonly observed in breast tumors.
Palbociclib became the first FDA-approved member of this drug class, receiving accelerated approval in patients with HR-positive, HER2-negative metastatic breast cancer, in combination with letrozole in 2015. This became full regulatory approval in combination with any AI earlier this year, following the phase 3 PALOMA-3 study, in which the combination of palbociclib and fulvestrant (accelerated approval was based upon a trial testing palbociclib and letrozole) improved PFS by 5 months (HR, 0.46; P < .0001).30
In addition, a second CDK4/6 inhibitor hit the market this year. Ribociclib demonstrated a significant PFS benefit in combination with letrozole; median PFS was 25.3 months, compared with 16 months for letrozole alone, translating to a 44% reduction in the risk of disease progression or death.31
Abemaciclib, which has greater selectivity for CDK4 than its predecessors, also appears to be heading towards approval. It was granted priority review by the FDA based on data from the MONARCH-2 trial, showing a significant improvement in PFS for the combination of abemaciclib and fulvestrant (median PFS, 16.4 vs 9.3 months for fulvestrant alone; HR, 0.553; P < .001).32
Teasing out ‘HER2-positive’ subtypes
Until recently, “HER2-positive” and “HR-positive” tumors have been treated as separate subtypes, despite the fact that about half of HER2-positive tumors fall into the luminal A subtype and are also HR-positive. Patients were typically treated with HER2-targeted therapy regardless of their endocrine status because of the aggressive nature of HER2-positive disease.
Increasingly, researchers are reconsidering this view, especially as several studies have shown differential response rates to HER2-targeted therapy in HR-positive compared with HR-negative patients and accumulating evidence suggests that there is significant crosstalk between the HER2 and HR pathways, which may be responsible for the development of resistance with both treatment paradigms.
Findings from several studies have shown a benefit to combining HER2-targeted and hormonal therapies in patients with luminal (HR-positive), HER2-positive disease. In the metastatic setting, the results of the phase 2 PERTAIN study, presented at the 2017 ASCO annual meeting suggest that dual HER2 blockade could prove even more effective. The addition of pertuzumab to a combination of trastuzumab and an AI improved PFS by more than 3 months (median PFS, 19.89 vs 15.8 months; HR, 0.65; P = .007).33
The clinical application of these combinations may be limited by the additional cost – several studies have suggested that they are not cost effective – and toxicity, but have served to drive the development of new clinical trial designs as the importance of considering luminal and nonluminal HER2-positive tumors has become increasingly apparent.
PARP inhibitors make a dent in BRCA1/2-mutated cancers
The most renowned breast cancer genes, BRCA1 and BRCA2 are present in about 5%-10% of all breast cancers. They play a central role in the homologous recombination pathway that fixes double-strand breaks in the DNA. Genome sequencing studies have revealed that the presence of the BRCA1/2 genes and other DNA repair defects is highest among patients with the basal-like subtype of breast cancer, in particular those who have triple-negative disease.34,35
This type of breast cancer has proved stubbornly resistant to efforts to improve patient outcomes with targeted therapies. BRCA1/2 mutations and other DNA repair defects that confer a so-called BRCAness phenotype, render tumor cells dependent on other pathways for DNA repair and there has been considerable interest in therapeutically exploiting this through the development of inhibitors of the poly(ADP-ribose) polymerase (PARP) enzyme, which is involved in the repair of single-strand breaks in the DNA. The double damage to DNA repair mechanisms through PARP inhibition in patients with BRCA1/2-mutant tumors proves overwhelming to cancerous cells.
Despite more than a decade of investigation in breast cancer, PARP inhibitors have yet to yield any FDA-approved treatment options. That may be set to change imminently, following the success of olaparib (Table 3). In the first randomized phase 3 trial of a PARP inhibitor in breast cancer (OlympiAD), olaparib was compared with standard chemotherapy in patients with BRCA1/2-mutated MBC who had received up to 2 previous lines of chemotherapy. Olaparib reduced the risk of disease progression by 42% compared with standard chemotherapy and was well tolerated.36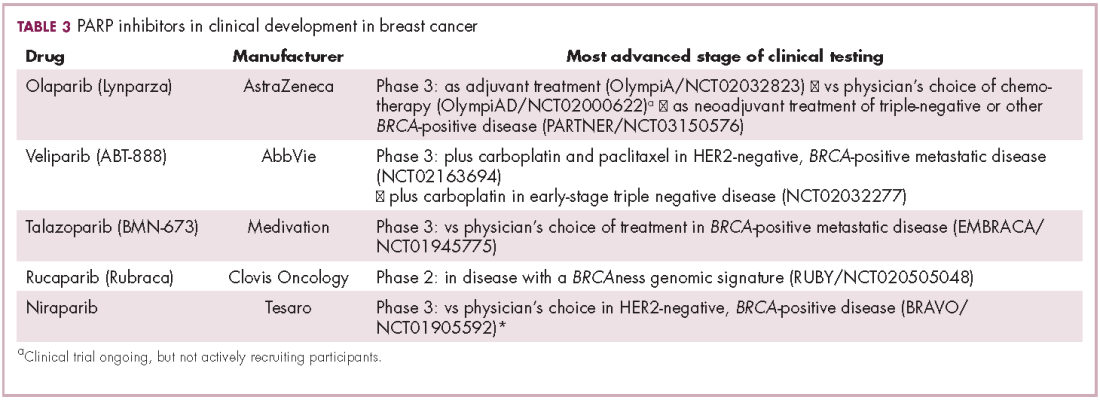
The novel PARP inhibitor talazoparib, which is the most potent to date, is also demonstrating significant efficacy in clinical trials. The results of the phase 2 ABRAZO trial were presented at the ASCO annual meeting. Two cohorts were treated; the first included 49 patients who had responded to their last platinum-containing regimen for metastatic disease and progressed more than 8 weeks after last platinum dose and the other included 35 patients previously treated with 3 or more nonplatinum regimens for metastatic disease. ORR was 28% across the 2 cohorts; 23% and 33% in BRCA1- and BRCA2-mutant carriers, respectively; and 26% in patients with triple-negative breast cancer.37 PARP inhibition is not faring so well in early-stage triple-negative disease; a phase 3 trial of veliparib in combination with chemotherapy did not meet its primary endpoint.38
As our understanding of the biology of breast cancer has improved, treatment has become increasingly personalized. Targeted therapies continue to significantly improve patient outcomes in multiple subtypes, with several recent drug approvals. Here, we discuss some of these latest developments.
A disease of many faces
Clinically speaking, breast cancers can be divided into at least 5 subtypes on the basis of the genes they express (Figure 1). The luminal subtypes make up the largest proportion and are characterized by the expression of hormone receptor (HR) genes. Luminal A tumors are negative for human epidermal growth factor receptor 2 (HER2; HER2-negative), whereas luminal B tumors often co-express the HER2 genes.1
The remainder of HER2-positive patients fall into the HER2-enriched category, in which HER2 expression is the defining characteristic. Basal-like tumors, meanwhile, represent the most heterogeneous subtype, overlapping to a large extent with tumors dubbed “triple-negative” because of their lack of either HER2 or ESR1 and PGR gene expression. The fifth subtype is known as normal breast-like and remains poorly characterized.
In recent years, there have been significant advancements in the genomic characterization of breast cancer that have begun to provide a more comprehensive understanding of the driver molecular mechanisms, which has helped to explain some of the limitations of current targeted approaches and to reveal new possible treatments, with a shift toward increasingly personalized strategies.2
HER2: what’s neu?
An estimated 18%-20% of breast tumors are HER2 positive, displaying amplification of the HER2/neu gene or overexpression of its protein product.3 Historically, HER2 positivity correlated with a highly aggressive and metastatic form of disease, conferring poor prognosis.4,5 The HER2-targeted monoclonal antibody (mAb), trastuzumab serves as a prime example of the power of personalized medicine. Evidence suggests that trastuzumab has altered the natural history of HER2-positive breast cancer, such that trastuzumab-treated patients with HER2-positive breast cancer now have a better prognosis than do patients with HER2-negative disease.6,7
Several additional HER2-targeted drugs have joined trastuzumab on the market, including other mAbs, small molecule tyrosine kinase inhibitors (TKIs), and an antibody–drug conjugate that combines the specificity of a mAb with the anti-tumor potency of a cytotoxic drug. These drugs have further improved patient outcomes in both early and advanced disease settings (Table 1).
The most recent regulatory approval was for neratinib, a potent TKI inhibiting all members of the HER protein family. On the basis of the phase 3 ExteNET study, neratinib was granted approval by the US Food and Drug Administration (FDA) for extended adjuvant treatment of patients with HER2-positive, early-stage breast cancer previously treated with trastuzumab. In a 5-year analysis of the study, invasive disease-free survival (DFS) was 90.4% with neratinib, compared with 87.9% with placebo (hazard ratio [HR], 0.74; P = .017).8,9
The tide of advancements in HER2-targeted therapy looks set to continue in the coming years as potentially practice-changing data emerges from ongoing clinical trials and, as the patent on trastuzumab has expired, a number of biosimilars, such as MYL-1401O have the potential to help patients who may not have access to trastuzumab.10
One of the biggest remaining challenges is identifying drugs that can effectively treat patients with brain metastases because the blood–brain barrier presents an impediment to the delivery of effective concentrations of anticancer drugs. Initially, it was hoped that the small molecule inhibitors lapatinib and neratinib could cross the blood–brain barrier and may be more effective in patients with brain metastases, but that hypothesis has not borne out in randomized clinical trials.11
Tucatinib (ONT-380) has shown significant promise in this respect. In a phase 1 trial, ONT-380 had significant efficacy in patients with and without central nervous system metastases; the overall response rate (ORR) in the CNS was 36%. ONT-380 is also notable for its specificity for HER2, without significant inhibition of HER1 and EGFR, which could translate into a better toxicity profile.12
Doubling down on resistant tumors
Since the success of HER2-targeted therapy is limited by the development of resistance, there has been significant interest in assessing the potential of dual HER2 blockade, exploiting the unique mechanisms of action of different drugs in combination therapy, and ensuring more complete inhibition of the HER2 pathway. Although numerous different combinations have been tested, a double antibody combination has proved most effective.
In fact, dual HER2 targeting with trastuzumab and pertuzumab in combination with chemotherapy has replaced a trastuzumab-chemotherapy regimen as the new standard of care in the metastatic setting. A 6-month improvement in progression-free survival (PFS) sealed FDA approval for the combination and in a recently published final analysis of the trial overall survival (OS) was also improved to a level unprecedented in the first-line setting.13,14The double antibody combination has also been successful in the neoadjuvant setting. Approval followed the results of the phase 2 NeoSphere trial, in which the combination was associated with a significant improvement in pathologic complete response (pCR) rate, a measure that acts as a surrogate for improved survival in the neoadjuvant setting. In a 5-year analysis of the NeoSphere trial, improved pCR did indeed translate into improved PFS and DFS.15,16
The results of the phase 3 APHINITY trial evaluating this combination in the adjuvant setting have been hotly anticipated. In a presentation at the 2017 American Society of Clinical Oncology (ASCO) meeting in June, the study authors reported that in 4,085 patients with operable HER2-positive disease, it significantly reduced the risk of disease recurrence or death compared with trastuzumab and chemotherapy alone.17
There is an ongoing effort to determine if it is possible to de-escalate treatment by removing the chemotherapy component. At least in the neoadjuvant setting, pCR rates in the chemotherapy-free arms of several studies suggest that a proportion of patients might benefit from this strategy15,18,19 and the challenge now is to identify them. To that end, the phase 2 PAMELA trial identified the HER2-enriched subtype as a strong predictor of response to neoadjuvant dual blockade (lapatinib and trastuzumab) without chemotherapy. The pCR rate was 40.6% for the combination in patients with the HER2-enriched subtype of breast cancer and only 10% in patients with non–HER2-enriched tumors.20
Targeting resistance to endocrine therapy
Another coup for personalized medicine in breast cancer is the treatment of hormone receptor–positive cases with endocrine therapy, which has become the cornerstone of treatment in the metastatic and adjuvant settings. Those drugs are designed to block the growth-stimulating effects of the estrogen and progesterone hormones on tumor cells. They include the selective estrogen receptor (ER) modulator tamoxifen, aromatase inhibitors (AIs) such as letrozole, anastrozole, and exemestane, which work by blocking the activity of the aromatase enzyme that converts androgens into estrogens, and the selective estrogen-receptor down-regulator fulvestrant.
As with HER2-targeted therapy, patients treated with endocrine therapy often develop resistance. Activation of alternate signaling cascades, such as the P13K–Akt–mTOR (phosphatidylinositol-3-kinase–Akt–mammalian target of rapamycin) pathway, or downstream targets of ER signaling, including the cyclin-dependent kinases, CDK4 and CDK6, have emerged as important mechanisms of resistance.21,22
Drugs directed against these secondary targets, aimed to enhance the efficacy of endocrine therapies, have shown significant promise (Table 2). The mTOR inhibitor everolimus received FDA approval in 2012 in combination with exemestane for the treatment of advanced HR-positive, HER2-negative breast cancer.23 More recently, everolimus has also proven effective in combination with either fulvestrant or letrozole, according to the phase 2 PrECOG 0102 and BOLERO-4 studies, both doubling PFS compared with endocrine therapy alone.24,25
Buparlisib is an oral reversible pan-PI3K inhibitor, and the results of the first phase 3 trial of this drug in metastatic breast cancer (MBC) were recently reported. Among 1,147 postmenopausal women with HR-positive, HER2-negative MBC that progressed on or after AI therapy, the combination of buparlisib and fulvestrant prolonged PFS compared with fulvestrant alone (median PFS, 6.9 vs 5 months; HR,0.78; P < .001). However, Novartis, which was developing buparlisib, reported that the combination will not be pursued further due to increased toxicity.26
Two other PI3K inhibitors are currently in phase 3 clinical trials; taselisib and alpelisib, both selective PI3K-alpha inhibitors. The results of a phase 1 dose-escalation study of taselisib were recently published and the ORR among patients with PIK3CA-mutant solid tumors was 36%, including responses in 4 patients with breast cancer.27 Meanwhile, alpelisib has also demonstrated early promise in combination with both letrozole and fulvestrant in patients with ER-positive MBC refractory to endocrine therapy. In combination with letrozole, the clinical benefit rate was 35% overall (44% in patients with PIK3CA mutations, compared with 20% in patients with wild-type PIK3CA status). The combination of alpesilib and fulvestrant produced an ORR of 27%, and both combinations were well tolerated.28,29
Another exciting therapeutic avenue is CDK4 and CDK6 inhibitors. These proteins are critical regulators of cell cycle progression, ensuring transition from G1 to S phase occurs at the appropriate time. The CDK pathway is also a downstream target of ER activation and, unsurprisingly, aberrant expression of the proteins involved in this pathway is commonly observed in breast tumors.
Palbociclib became the first FDA-approved member of this drug class, receiving accelerated approval in patients with HR-positive, HER2-negative metastatic breast cancer, in combination with letrozole in 2015. This became full regulatory approval in combination with any AI earlier this year, following the phase 3 PALOMA-3 study, in which the combination of palbociclib and fulvestrant (accelerated approval was based upon a trial testing palbociclib and letrozole) improved PFS by 5 months (HR, 0.46; P < .0001).30
In addition, a second CDK4/6 inhibitor hit the market this year. Ribociclib demonstrated a significant PFS benefit in combination with letrozole; median PFS was 25.3 months, compared with 16 months for letrozole alone, translating to a 44% reduction in the risk of disease progression or death.31
Abemaciclib, which has greater selectivity for CDK4 than its predecessors, also appears to be heading towards approval. It was granted priority review by the FDA based on data from the MONARCH-2 trial, showing a significant improvement in PFS for the combination of abemaciclib and fulvestrant (median PFS, 16.4 vs 9.3 months for fulvestrant alone; HR, 0.553; P < .001).32
Teasing out ‘HER2-positive’ subtypes
Until recently, “HER2-positive” and “HR-positive” tumors have been treated as separate subtypes, despite the fact that about half of HER2-positive tumors fall into the luminal A subtype and are also HR-positive. Patients were typically treated with HER2-targeted therapy regardless of their endocrine status because of the aggressive nature of HER2-positive disease.
Increasingly, researchers are reconsidering this view, especially as several studies have shown differential response rates to HER2-targeted therapy in HR-positive compared with HR-negative patients and accumulating evidence suggests that there is significant crosstalk between the HER2 and HR pathways, which may be responsible for the development of resistance with both treatment paradigms.
Findings from several studies have shown a benefit to combining HER2-targeted and hormonal therapies in patients with luminal (HR-positive), HER2-positive disease. In the metastatic setting, the results of the phase 2 PERTAIN study, presented at the 2017 ASCO annual meeting suggest that dual HER2 blockade could prove even more effective. The addition of pertuzumab to a combination of trastuzumab and an AI improved PFS by more than 3 months (median PFS, 19.89 vs 15.8 months; HR, 0.65; P = .007).33
The clinical application of these combinations may be limited by the additional cost – several studies have suggested that they are not cost effective – and toxicity, but have served to drive the development of new clinical trial designs as the importance of considering luminal and nonluminal HER2-positive tumors has become increasingly apparent.
PARP inhibitors make a dent in BRCA1/2-mutated cancers
The most renowned breast cancer genes, BRCA1 and BRCA2 are present in about 5%-10% of all breast cancers. They play a central role in the homologous recombination pathway that fixes double-strand breaks in the DNA. Genome sequencing studies have revealed that the presence of the BRCA1/2 genes and other DNA repair defects is highest among patients with the basal-like subtype of breast cancer, in particular those who have triple-negative disease.34,35
This type of breast cancer has proved stubbornly resistant to efforts to improve patient outcomes with targeted therapies. BRCA1/2 mutations and other DNA repair defects that confer a so-called BRCAness phenotype, render tumor cells dependent on other pathways for DNA repair and there has been considerable interest in therapeutically exploiting this through the development of inhibitors of the poly(ADP-ribose) polymerase (PARP) enzyme, which is involved in the repair of single-strand breaks in the DNA. The double damage to DNA repair mechanisms through PARP inhibition in patients with BRCA1/2-mutant tumors proves overwhelming to cancerous cells.
Despite more than a decade of investigation in breast cancer, PARP inhibitors have yet to yield any FDA-approved treatment options. That may be set to change imminently, following the success of olaparib (Table 3). In the first randomized phase 3 trial of a PARP inhibitor in breast cancer (OlympiAD), olaparib was compared with standard chemotherapy in patients with BRCA1/2-mutated MBC who had received up to 2 previous lines of chemotherapy. Olaparib reduced the risk of disease progression by 42% compared with standard chemotherapy and was well tolerated.36
The novel PARP inhibitor talazoparib, which is the most potent to date, is also demonstrating significant efficacy in clinical trials. The results of the phase 2 ABRAZO trial were presented at the ASCO annual meeting. Two cohorts were treated; the first included 49 patients who had responded to their last platinum-containing regimen for metastatic disease and progressed more than 8 weeks after last platinum dose and the other included 35 patients previously treated with 3 or more nonplatinum regimens for metastatic disease. ORR was 28% across the 2 cohorts; 23% and 33% in BRCA1- and BRCA2-mutant carriers, respectively; and 26% in patients with triple-negative breast cancer.37 PARP inhibition is not faring so well in early-stage triple-negative disease; a phase 3 trial of veliparib in combination with chemotherapy did not meet its primary endpoint.38
As our understanding of the biology of breast cancer has improved, treatment has become increasingly personalized. Targeted therapies continue to significantly improve patient outcomes in multiple subtypes, with several recent drug approvals. Here, we discuss some of these latest developments.
A disease of many faces
Clinically speaking, breast cancers can be divided into at least 5 subtypes on the basis of the genes they express (Figure 1). The luminal subtypes make up the largest proportion and are characterized by the expression of hormone receptor (HR) genes. Luminal A tumors are negative for human epidermal growth factor receptor 2 (HER2; HER2-negative), whereas luminal B tumors often co-express the HER2 genes.1
The remainder of HER2-positive patients fall into the HER2-enriched category, in which HER2 expression is the defining characteristic. Basal-like tumors, meanwhile, represent the most heterogeneous subtype, overlapping to a large extent with tumors dubbed “triple-negative” because of their lack of either HER2 or ESR1 and PGR gene expression. The fifth subtype is known as normal breast-like and remains poorly characterized.
In recent years, there have been significant advancements in the genomic characterization of breast cancer that have begun to provide a more comprehensive understanding of the driver molecular mechanisms, which has helped to explain some of the limitations of current targeted approaches and to reveal new possible treatments, with a shift toward increasingly personalized strategies.2
HER2: what’s neu?
An estimated 18%-20% of breast tumors are HER2 positive, displaying amplification of the HER2/neu gene or overexpression of its protein product.3 Historically, HER2 positivity correlated with a highly aggressive and metastatic form of disease, conferring poor prognosis.4,5 The HER2-targeted monoclonal antibody (mAb), trastuzumab serves as a prime example of the power of personalized medicine. Evidence suggests that trastuzumab has altered the natural history of HER2-positive breast cancer, such that trastuzumab-treated patients with HER2-positive breast cancer now have a better prognosis than do patients with HER2-negative disease.6,7
Several additional HER2-targeted drugs have joined trastuzumab on the market, including other mAbs, small molecule tyrosine kinase inhibitors (TKIs), and an antibody–drug conjugate that combines the specificity of a mAb with the anti-tumor potency of a cytotoxic drug. These drugs have further improved patient outcomes in both early and advanced disease settings (Table 1).
The most recent regulatory approval was for neratinib, a potent TKI inhibiting all members of the HER protein family. On the basis of the phase 3 ExteNET study, neratinib was granted approval by the US Food and Drug Administration (FDA) for extended adjuvant treatment of patients with HER2-positive, early-stage breast cancer previously treated with trastuzumab. In a 5-year analysis of the study, invasive disease-free survival (DFS) was 90.4% with neratinib, compared with 87.9% with placebo (hazard ratio [HR], 0.74; P = .017).8,9
The tide of advancements in HER2-targeted therapy looks set to continue in the coming years as potentially practice-changing data emerges from ongoing clinical trials and, as the patent on trastuzumab has expired, a number of biosimilars, such as MYL-1401O have the potential to help patients who may not have access to trastuzumab.10
One of the biggest remaining challenges is identifying drugs that can effectively treat patients with brain metastases because the blood–brain barrier presents an impediment to the delivery of effective concentrations of anticancer drugs. Initially, it was hoped that the small molecule inhibitors lapatinib and neratinib could cross the blood–brain barrier and may be more effective in patients with brain metastases, but that hypothesis has not borne out in randomized clinical trials.11
Tucatinib (ONT-380) has shown significant promise in this respect. In a phase 1 trial, ONT-380 had significant efficacy in patients with and without central nervous system metastases; the overall response rate (ORR) in the CNS was 36%. ONT-380 is also notable for its specificity for HER2, without significant inhibition of HER1 and EGFR, which could translate into a better toxicity profile.12
Doubling down on resistant tumors
Since the success of HER2-targeted therapy is limited by the development of resistance, there has been significant interest in assessing the potential of dual HER2 blockade, exploiting the unique mechanisms of action of different drugs in combination therapy, and ensuring more complete inhibition of the HER2 pathway. Although numerous different combinations have been tested, a double antibody combination has proved most effective.
In fact, dual HER2 targeting with trastuzumab and pertuzumab in combination with chemotherapy has replaced a trastuzumab-chemotherapy regimen as the new standard of care in the metastatic setting. A 6-month improvement in progression-free survival (PFS) sealed FDA approval for the combination and in a recently published final analysis of the trial overall survival (OS) was also improved to a level unprecedented in the first-line setting.13,14The double antibody combination has also been successful in the neoadjuvant setting. Approval followed the results of the phase 2 NeoSphere trial, in which the combination was associated with a significant improvement in pathologic complete response (pCR) rate, a measure that acts as a surrogate for improved survival in the neoadjuvant setting. In a 5-year analysis of the NeoSphere trial, improved pCR did indeed translate into improved PFS and DFS.15,16
The results of the phase 3 APHINITY trial evaluating this combination in the adjuvant setting have been hotly anticipated. In a presentation at the 2017 American Society of Clinical Oncology (ASCO) meeting in June, the study authors reported that in 4,085 patients with operable HER2-positive disease, it significantly reduced the risk of disease recurrence or death compared with trastuzumab and chemotherapy alone.17
There is an ongoing effort to determine if it is possible to de-escalate treatment by removing the chemotherapy component. At least in the neoadjuvant setting, pCR rates in the chemotherapy-free arms of several studies suggest that a proportion of patients might benefit from this strategy15,18,19 and the challenge now is to identify them. To that end, the phase 2 PAMELA trial identified the HER2-enriched subtype as a strong predictor of response to neoadjuvant dual blockade (lapatinib and trastuzumab) without chemotherapy. The pCR rate was 40.6% for the combination in patients with the HER2-enriched subtype of breast cancer and only 10% in patients with non–HER2-enriched tumors.20
Targeting resistance to endocrine therapy
Another coup for personalized medicine in breast cancer is the treatment of hormone receptor–positive cases with endocrine therapy, which has become the cornerstone of treatment in the metastatic and adjuvant settings. Those drugs are designed to block the growth-stimulating effects of the estrogen and progesterone hormones on tumor cells. They include the selective estrogen receptor (ER) modulator tamoxifen, aromatase inhibitors (AIs) such as letrozole, anastrozole, and exemestane, which work by blocking the activity of the aromatase enzyme that converts androgens into estrogens, and the selective estrogen-receptor down-regulator fulvestrant.
As with HER2-targeted therapy, patients treated with endocrine therapy often develop resistance. Activation of alternate signaling cascades, such as the P13K–Akt–mTOR (phosphatidylinositol-3-kinase–Akt–mammalian target of rapamycin) pathway, or downstream targets of ER signaling, including the cyclin-dependent kinases, CDK4 and CDK6, have emerged as important mechanisms of resistance.21,22
Drugs directed against these secondary targets, aimed to enhance the efficacy of endocrine therapies, have shown significant promise (Table 2). The mTOR inhibitor everolimus received FDA approval in 2012 in combination with exemestane for the treatment of advanced HR-positive, HER2-negative breast cancer.23 More recently, everolimus has also proven effective in combination with either fulvestrant or letrozole, according to the phase 2 PrECOG 0102 and BOLERO-4 studies, both doubling PFS compared with endocrine therapy alone.24,25
Buparlisib is an oral reversible pan-PI3K inhibitor, and the results of the first phase 3 trial of this drug in metastatic breast cancer (MBC) were recently reported. Among 1,147 postmenopausal women with HR-positive, HER2-negative MBC that progressed on or after AI therapy, the combination of buparlisib and fulvestrant prolonged PFS compared with fulvestrant alone (median PFS, 6.9 vs 5 months; HR,0.78; P < .001). However, Novartis, which was developing buparlisib, reported that the combination will not be pursued further due to increased toxicity.26
Two other PI3K inhibitors are currently in phase 3 clinical trials; taselisib and alpelisib, both selective PI3K-alpha inhibitors. The results of a phase 1 dose-escalation study of taselisib were recently published and the ORR among patients with PIK3CA-mutant solid tumors was 36%, including responses in 4 patients with breast cancer.27 Meanwhile, alpelisib has also demonstrated early promise in combination with both letrozole and fulvestrant in patients with ER-positive MBC refractory to endocrine therapy. In combination with letrozole, the clinical benefit rate was 35% overall (44% in patients with PIK3CA mutations, compared with 20% in patients with wild-type PIK3CA status). The combination of alpesilib and fulvestrant produced an ORR of 27%, and both combinations were well tolerated.28,29
Another exciting therapeutic avenue is CDK4 and CDK6 inhibitors. These proteins are critical regulators of cell cycle progression, ensuring transition from G1 to S phase occurs at the appropriate time. The CDK pathway is also a downstream target of ER activation and, unsurprisingly, aberrant expression of the proteins involved in this pathway is commonly observed in breast tumors.
Palbociclib became the first FDA-approved member of this drug class, receiving accelerated approval in patients with HR-positive, HER2-negative metastatic breast cancer, in combination with letrozole in 2015. This became full regulatory approval in combination with any AI earlier this year, following the phase 3 PALOMA-3 study, in which the combination of palbociclib and fulvestrant (accelerated approval was based upon a trial testing palbociclib and letrozole) improved PFS by 5 months (HR, 0.46; P < .0001).30
In addition, a second CDK4/6 inhibitor hit the market this year. Ribociclib demonstrated a significant PFS benefit in combination with letrozole; median PFS was 25.3 months, compared with 16 months for letrozole alone, translating to a 44% reduction in the risk of disease progression or death.31
Abemaciclib, which has greater selectivity for CDK4 than its predecessors, also appears to be heading towards approval. It was granted priority review by the FDA based on data from the MONARCH-2 trial, showing a significant improvement in PFS for the combination of abemaciclib and fulvestrant (median PFS, 16.4 vs 9.3 months for fulvestrant alone; HR, 0.553; P < .001).32
Teasing out ‘HER2-positive’ subtypes
Until recently, “HER2-positive” and “HR-positive” tumors have been treated as separate subtypes, despite the fact that about half of HER2-positive tumors fall into the luminal A subtype and are also HR-positive. Patients were typically treated with HER2-targeted therapy regardless of their endocrine status because of the aggressive nature of HER2-positive disease.
Increasingly, researchers are reconsidering this view, especially as several studies have shown differential response rates to HER2-targeted therapy in HR-positive compared with HR-negative patients and accumulating evidence suggests that there is significant crosstalk between the HER2 and HR pathways, which may be responsible for the development of resistance with both treatment paradigms.
Findings from several studies have shown a benefit to combining HER2-targeted and hormonal therapies in patients with luminal (HR-positive), HER2-positive disease. In the metastatic setting, the results of the phase 2 PERTAIN study, presented at the 2017 ASCO annual meeting suggest that dual HER2 blockade could prove even more effective. The addition of pertuzumab to a combination of trastuzumab and an AI improved PFS by more than 3 months (median PFS, 19.89 vs 15.8 months; HR, 0.65; P = .007).33
The clinical application of these combinations may be limited by the additional cost – several studies have suggested that they are not cost effective – and toxicity, but have served to drive the development of new clinical trial designs as the importance of considering luminal and nonluminal HER2-positive tumors has become increasingly apparent.
PARP inhibitors make a dent in BRCA1/2-mutated cancers
The most renowned breast cancer genes, BRCA1 and BRCA2 are present in about 5%-10% of all breast cancers. They play a central role in the homologous recombination pathway that fixes double-strand breaks in the DNA. Genome sequencing studies have revealed that the presence of the BRCA1/2 genes and other DNA repair defects is highest among patients with the basal-like subtype of breast cancer, in particular those who have triple-negative disease.34,35
This type of breast cancer has proved stubbornly resistant to efforts to improve patient outcomes with targeted therapies. BRCA1/2 mutations and other DNA repair defects that confer a so-called BRCAness phenotype, render tumor cells dependent on other pathways for DNA repair and there has been considerable interest in therapeutically exploiting this through the development of inhibitors of the poly(ADP-ribose) polymerase (PARP) enzyme, which is involved in the repair of single-strand breaks in the DNA. The double damage to DNA repair mechanisms through PARP inhibition in patients with BRCA1/2-mutant tumors proves overwhelming to cancerous cells.
Despite more than a decade of investigation in breast cancer, PARP inhibitors have yet to yield any FDA-approved treatment options. That may be set to change imminently, following the success of olaparib (Table 3). In the first randomized phase 3 trial of a PARP inhibitor in breast cancer (OlympiAD), olaparib was compared with standard chemotherapy in patients with BRCA1/2-mutated MBC who had received up to 2 previous lines of chemotherapy. Olaparib reduced the risk of disease progression by 42% compared with standard chemotherapy and was well tolerated.36
The novel PARP inhibitor talazoparib, which is the most potent to date, is also demonstrating significant efficacy in clinical trials. The results of the phase 2 ABRAZO trial were presented at the ASCO annual meeting. Two cohorts were treated; the first included 49 patients who had responded to their last platinum-containing regimen for metastatic disease and progressed more than 8 weeks after last platinum dose and the other included 35 patients previously treated with 3 or more nonplatinum regimens for metastatic disease. ORR was 28% across the 2 cohorts; 23% and 33% in BRCA1- and BRCA2-mutant carriers, respectively; and 26% in patients with triple-negative breast cancer.37 PARP inhibition is not faring so well in early-stage triple-negative disease; a phase 3 trial of veliparib in combination with chemotherapy did not meet its primary endpoint.38