User login
Troubling trend as both diabetes types rise among U.S. youth
The incidence of type 1 and type 2 diabetes continues to rise among children and adolescents in the United States, new data from the SEARCH for Diabetes in Youth study show.
The SEARCH data demonstrate an increase in the youth population aged 0-19 diagnosed with type 1 or type 2 diabetes in five representative U.S. centers. Between 2002 and 2018, the annual incidence rose by about 2% per year for type 1 diabetes and 5% per year for type 2 diabetes. The rates of increase for both types were greater among non-White than White youth.
These increases “will result in an expanding population of young adults at risk of developing early complications of diabetes whose health care needs will exceed those of their peers,” write Lynne E. Wagenknecht, DrPH, of Wake Forest University School of Medicine, Winston-Salem, N.C., and colleagues in their article, recently published in The Lancet Diabetes & Endocrinology.
In an accompanying editorial, Jonathan E. Shaw, MD, and Dianna J. Magliano, PhD, both at the Baker Heart and Diabetes Institute, Melbourne, write that one of the most “concerning findings” was a 7%-9% annual increase in the incidence of type 2 diabetes among Hispanic, Asian, and Pacific Islander populations.
“This is a health care crisis in the making. ...Youth and young-adult-onset type 2 diabetes are growing problems leading to poor outcomes and to widening social inequality, adversely affecting a population that might already be disadvantaged. Better information about its natural history, prevention, and management is urgently needed,” they write.
Upward trends in both diabetes types
Overall, 18,169 children and adolescents with type 1 diabetes and 5,293 with type 2 diabetes were identified over the 17-year study period in SEARCH. After adjustment for age, sex, and race/ethnicity, there was a significant increase in type 1 diabetes incidence from 19.5 cases/100,000 population in 2002-2003 to 22.2/100,000 in 2017-2018, a 2.02% annual increase.
The upward trend was even greater for type 2 diabetes, from 9.0/100,000 in 2002-2003 to 17.9/100,000 in 2017-2018, a 5.31% annual increase.
The annual rate of increase in type 1 diabetes was highest among Asian/Pacific Islander youth (4.84%), followed by Hispanic (4.14%) and Black youth (2.93%): All significantly rose over the 17 years.
For type 2 diabetes, significant annual rates of increase were also highest for Asian/Pacific Islanders (8.92%), followed by Hispanic (7.17%) and Black youth (5.99%).
Among youth aged 15-19 years, the overall incidence of type 2 diabetes exceeded that of type 1 diabetes (19.7 vs. 14.6/100,000).
The incidence of type 2 diabetes may be rising because of increased rates of obesity, as well as increased screening of at-risk youth, the authors say.
And, the editorialists note, obesity is also a risk factor for type 1 diabetes.
Peak incidence of type 1 diabetes occurred at age 10 years, while for type 2 diabetes, the peak was at 16 years. There were also seasonal peaks, occurring in January for type 1 diabetes and in August for type 2 diabetes. Those seasonal patterns have been previously reported; they are possibly because of increased viral infections and decreased sun exposure for the former, and increased physical exams in preparation for school in the latter, the authors speculate.
Dr. Shaw and Dr. Magliano note that the reduced incidence after age 16 years “might simply reflect a failure to diagnose,” suggesting that there will likely be an upturn in incidence in the subsequent decade.
The editorialists also point out: “Not only does the long duration of diabetes that youth-onset leads to cause a large burden of fatal and nonfatal complications, but it magnifies intergenerational effects.”
“When type 2 diabetes is already present before pregnancy, birth outcomes are worse, and the long-term metabolic health of the offspring is adversely affected. This does not bode well for the epidemic of diabetes and its complications.”
The study was funded by the Centers for Disease Control and Prevention and National Institutes of Health. The authors and Dr. Magliano have reported no relevant financial relationships. Dr. Shaw has reported receiving honoraria for lectures and for advisory boards and grants from AstraZeneca, Boehringer Ingelheim, Pfizer, Eli Lilly, Sanofi, Roche, Mylan, and Zuellig Pharma.
A version of this article originally appeared on Medscape.com.
The incidence of type 1 and type 2 diabetes continues to rise among children and adolescents in the United States, new data from the SEARCH for Diabetes in Youth study show.
The SEARCH data demonstrate an increase in the youth population aged 0-19 diagnosed with type 1 or type 2 diabetes in five representative U.S. centers. Between 2002 and 2018, the annual incidence rose by about 2% per year for type 1 diabetes and 5% per year for type 2 diabetes. The rates of increase for both types were greater among non-White than White youth.
These increases “will result in an expanding population of young adults at risk of developing early complications of diabetes whose health care needs will exceed those of their peers,” write Lynne E. Wagenknecht, DrPH, of Wake Forest University School of Medicine, Winston-Salem, N.C., and colleagues in their article, recently published in The Lancet Diabetes & Endocrinology.
In an accompanying editorial, Jonathan E. Shaw, MD, and Dianna J. Magliano, PhD, both at the Baker Heart and Diabetes Institute, Melbourne, write that one of the most “concerning findings” was a 7%-9% annual increase in the incidence of type 2 diabetes among Hispanic, Asian, and Pacific Islander populations.
“This is a health care crisis in the making. ...Youth and young-adult-onset type 2 diabetes are growing problems leading to poor outcomes and to widening social inequality, adversely affecting a population that might already be disadvantaged. Better information about its natural history, prevention, and management is urgently needed,” they write.
Upward trends in both diabetes types
Overall, 18,169 children and adolescents with type 1 diabetes and 5,293 with type 2 diabetes were identified over the 17-year study period in SEARCH. After adjustment for age, sex, and race/ethnicity, there was a significant increase in type 1 diabetes incidence from 19.5 cases/100,000 population in 2002-2003 to 22.2/100,000 in 2017-2018, a 2.02% annual increase.
The upward trend was even greater for type 2 diabetes, from 9.0/100,000 in 2002-2003 to 17.9/100,000 in 2017-2018, a 5.31% annual increase.
The annual rate of increase in type 1 diabetes was highest among Asian/Pacific Islander youth (4.84%), followed by Hispanic (4.14%) and Black youth (2.93%): All significantly rose over the 17 years.
For type 2 diabetes, significant annual rates of increase were also highest for Asian/Pacific Islanders (8.92%), followed by Hispanic (7.17%) and Black youth (5.99%).
Among youth aged 15-19 years, the overall incidence of type 2 diabetes exceeded that of type 1 diabetes (19.7 vs. 14.6/100,000).
The incidence of type 2 diabetes may be rising because of increased rates of obesity, as well as increased screening of at-risk youth, the authors say.
And, the editorialists note, obesity is also a risk factor for type 1 diabetes.
Peak incidence of type 1 diabetes occurred at age 10 years, while for type 2 diabetes, the peak was at 16 years. There were also seasonal peaks, occurring in January for type 1 diabetes and in August for type 2 diabetes. Those seasonal patterns have been previously reported; they are possibly because of increased viral infections and decreased sun exposure for the former, and increased physical exams in preparation for school in the latter, the authors speculate.
Dr. Shaw and Dr. Magliano note that the reduced incidence after age 16 years “might simply reflect a failure to diagnose,” suggesting that there will likely be an upturn in incidence in the subsequent decade.
The editorialists also point out: “Not only does the long duration of diabetes that youth-onset leads to cause a large burden of fatal and nonfatal complications, but it magnifies intergenerational effects.”
“When type 2 diabetes is already present before pregnancy, birth outcomes are worse, and the long-term metabolic health of the offspring is adversely affected. This does not bode well for the epidemic of diabetes and its complications.”
The study was funded by the Centers for Disease Control and Prevention and National Institutes of Health. The authors and Dr. Magliano have reported no relevant financial relationships. Dr. Shaw has reported receiving honoraria for lectures and for advisory boards and grants from AstraZeneca, Boehringer Ingelheim, Pfizer, Eli Lilly, Sanofi, Roche, Mylan, and Zuellig Pharma.
A version of this article originally appeared on Medscape.com.
The incidence of type 1 and type 2 diabetes continues to rise among children and adolescents in the United States, new data from the SEARCH for Diabetes in Youth study show.
The SEARCH data demonstrate an increase in the youth population aged 0-19 diagnosed with type 1 or type 2 diabetes in five representative U.S. centers. Between 2002 and 2018, the annual incidence rose by about 2% per year for type 1 diabetes and 5% per year for type 2 diabetes. The rates of increase for both types were greater among non-White than White youth.
These increases “will result in an expanding population of young adults at risk of developing early complications of diabetes whose health care needs will exceed those of their peers,” write Lynne E. Wagenknecht, DrPH, of Wake Forest University School of Medicine, Winston-Salem, N.C., and colleagues in their article, recently published in The Lancet Diabetes & Endocrinology.
In an accompanying editorial, Jonathan E. Shaw, MD, and Dianna J. Magliano, PhD, both at the Baker Heart and Diabetes Institute, Melbourne, write that one of the most “concerning findings” was a 7%-9% annual increase in the incidence of type 2 diabetes among Hispanic, Asian, and Pacific Islander populations.
“This is a health care crisis in the making. ...Youth and young-adult-onset type 2 diabetes are growing problems leading to poor outcomes and to widening social inequality, adversely affecting a population that might already be disadvantaged. Better information about its natural history, prevention, and management is urgently needed,” they write.
Upward trends in both diabetes types
Overall, 18,169 children and adolescents with type 1 diabetes and 5,293 with type 2 diabetes were identified over the 17-year study period in SEARCH. After adjustment for age, sex, and race/ethnicity, there was a significant increase in type 1 diabetes incidence from 19.5 cases/100,000 population in 2002-2003 to 22.2/100,000 in 2017-2018, a 2.02% annual increase.
The upward trend was even greater for type 2 diabetes, from 9.0/100,000 in 2002-2003 to 17.9/100,000 in 2017-2018, a 5.31% annual increase.
The annual rate of increase in type 1 diabetes was highest among Asian/Pacific Islander youth (4.84%), followed by Hispanic (4.14%) and Black youth (2.93%): All significantly rose over the 17 years.
For type 2 diabetes, significant annual rates of increase were also highest for Asian/Pacific Islanders (8.92%), followed by Hispanic (7.17%) and Black youth (5.99%).
Among youth aged 15-19 years, the overall incidence of type 2 diabetes exceeded that of type 1 diabetes (19.7 vs. 14.6/100,000).
The incidence of type 2 diabetes may be rising because of increased rates of obesity, as well as increased screening of at-risk youth, the authors say.
And, the editorialists note, obesity is also a risk factor for type 1 diabetes.
Peak incidence of type 1 diabetes occurred at age 10 years, while for type 2 diabetes, the peak was at 16 years. There were also seasonal peaks, occurring in January for type 1 diabetes and in August for type 2 diabetes. Those seasonal patterns have been previously reported; they are possibly because of increased viral infections and decreased sun exposure for the former, and increased physical exams in preparation for school in the latter, the authors speculate.
Dr. Shaw and Dr. Magliano note that the reduced incidence after age 16 years “might simply reflect a failure to diagnose,” suggesting that there will likely be an upturn in incidence in the subsequent decade.
The editorialists also point out: “Not only does the long duration of diabetes that youth-onset leads to cause a large burden of fatal and nonfatal complications, but it magnifies intergenerational effects.”
“When type 2 diabetes is already present before pregnancy, birth outcomes are worse, and the long-term metabolic health of the offspring is adversely affected. This does not bode well for the epidemic of diabetes and its complications.”
The study was funded by the Centers for Disease Control and Prevention and National Institutes of Health. The authors and Dr. Magliano have reported no relevant financial relationships. Dr. Shaw has reported receiving honoraria for lectures and for advisory boards and grants from AstraZeneca, Boehringer Ingelheim, Pfizer, Eli Lilly, Sanofi, Roche, Mylan, and Zuellig Pharma.
A version of this article originally appeared on Medscape.com.
FROM THE LANCET DIABETES & ENDOCRINOLOGY
Two FDA clearances add diabetes technology options
Two diabetes management devices that aid in the precision of insulin delivery have been recently cleared by the Food and Drug Administration.
On March 2, the FDA cleared the Android version of Bigfoot Biomedical’s Unity Mobile App for use with its system of smart pen caps that are compatible with different disposable insulin pens for administering both long-acting and rapid-acting insulin.
The system, which has been compatible with iOS devices since May 2021, is “the first and only FDA-cleared smart injection system that turns CGM [continuous glucose monitoring] data into dosing recommendations displayed right on the pen cap for people using multiple daily [insulin] injection therapy,” according to a company statement.
The Bigfoot app allows users to input and review provider treatment recommendations, displays current glucose ranges, and delivers real-time alerts.
Once it is commercially launched, the Android phone application will be available via the Google Play Store. “Given that 41% of U.S. smartphone users choose Android devices, this clearance enables expanded access to a large group of people with diabetes,” the company said.
On March 6, the FDA cleared the Abbott FreeStyle Libre 2 and FreeStyle Libre 3 devices as “integrated” CGM sensors. This means that they can now be used as components in automated insulin delivery systems, along with insulin pumps and connectivity software.
Abbott is working with insulin pump manufacturers Insulet and Tandem in the United States for integration with the FreeStyle Libre versions 2 and 3. Outside the United States, the Libre 3 is already authorized to work with mylife Loop from Ypsomed and CamDiab in Germany. Further launches are expected in the United Kingdom, Switzerland, and the Netherlands later this year.
The modified FreeStyle Libre 2 and FreeStyle Libre 3 sensors have been cleared for use by patients as young as age 2 years and for up to 15 days, in contrast to the previous versions, which were available for patients as young as 4 years for use up to 14 days. The FDA has cleared all Libre sensors – 2 and 3, current and future versions – for use by pregnant women with any type of diabetes.
The modified sensors will be available in the United States later this year and will eventually replace the Libre sensors in current use, the company said in a statement.
“The FreeStyle Libre portfolio is still the most affordable CGM on the market,” an Abbott representative said in an interview.
A version of this article first appeared on Medscape.com.
Two diabetes management devices that aid in the precision of insulin delivery have been recently cleared by the Food and Drug Administration.
On March 2, the FDA cleared the Android version of Bigfoot Biomedical’s Unity Mobile App for use with its system of smart pen caps that are compatible with different disposable insulin pens for administering both long-acting and rapid-acting insulin.
The system, which has been compatible with iOS devices since May 2021, is “the first and only FDA-cleared smart injection system that turns CGM [continuous glucose monitoring] data into dosing recommendations displayed right on the pen cap for people using multiple daily [insulin] injection therapy,” according to a company statement.
The Bigfoot app allows users to input and review provider treatment recommendations, displays current glucose ranges, and delivers real-time alerts.
Once it is commercially launched, the Android phone application will be available via the Google Play Store. “Given that 41% of U.S. smartphone users choose Android devices, this clearance enables expanded access to a large group of people with diabetes,” the company said.
On March 6, the FDA cleared the Abbott FreeStyle Libre 2 and FreeStyle Libre 3 devices as “integrated” CGM sensors. This means that they can now be used as components in automated insulin delivery systems, along with insulin pumps and connectivity software.
Abbott is working with insulin pump manufacturers Insulet and Tandem in the United States for integration with the FreeStyle Libre versions 2 and 3. Outside the United States, the Libre 3 is already authorized to work with mylife Loop from Ypsomed and CamDiab in Germany. Further launches are expected in the United Kingdom, Switzerland, and the Netherlands later this year.
The modified FreeStyle Libre 2 and FreeStyle Libre 3 sensors have been cleared for use by patients as young as age 2 years and for up to 15 days, in contrast to the previous versions, which were available for patients as young as 4 years for use up to 14 days. The FDA has cleared all Libre sensors – 2 and 3, current and future versions – for use by pregnant women with any type of diabetes.
The modified sensors will be available in the United States later this year and will eventually replace the Libre sensors in current use, the company said in a statement.
“The FreeStyle Libre portfolio is still the most affordable CGM on the market,” an Abbott representative said in an interview.
A version of this article first appeared on Medscape.com.
Two diabetes management devices that aid in the precision of insulin delivery have been recently cleared by the Food and Drug Administration.
On March 2, the FDA cleared the Android version of Bigfoot Biomedical’s Unity Mobile App for use with its system of smart pen caps that are compatible with different disposable insulin pens for administering both long-acting and rapid-acting insulin.
The system, which has been compatible with iOS devices since May 2021, is “the first and only FDA-cleared smart injection system that turns CGM [continuous glucose monitoring] data into dosing recommendations displayed right on the pen cap for people using multiple daily [insulin] injection therapy,” according to a company statement.
The Bigfoot app allows users to input and review provider treatment recommendations, displays current glucose ranges, and delivers real-time alerts.
Once it is commercially launched, the Android phone application will be available via the Google Play Store. “Given that 41% of U.S. smartphone users choose Android devices, this clearance enables expanded access to a large group of people with diabetes,” the company said.
On March 6, the FDA cleared the Abbott FreeStyle Libre 2 and FreeStyle Libre 3 devices as “integrated” CGM sensors. This means that they can now be used as components in automated insulin delivery systems, along with insulin pumps and connectivity software.
Abbott is working with insulin pump manufacturers Insulet and Tandem in the United States for integration with the FreeStyle Libre versions 2 and 3. Outside the United States, the Libre 3 is already authorized to work with mylife Loop from Ypsomed and CamDiab in Germany. Further launches are expected in the United Kingdom, Switzerland, and the Netherlands later this year.
The modified FreeStyle Libre 2 and FreeStyle Libre 3 sensors have been cleared for use by patients as young as age 2 years and for up to 15 days, in contrast to the previous versions, which were available for patients as young as 4 years for use up to 14 days. The FDA has cleared all Libre sensors – 2 and 3, current and future versions – for use by pregnant women with any type of diabetes.
The modified sensors will be available in the United States later this year and will eventually replace the Libre sensors in current use, the company said in a statement.
“The FreeStyle Libre portfolio is still the most affordable CGM on the market,” an Abbott representative said in an interview.
A version of this article first appeared on Medscape.com.
Heart-healthy actions promote longer, disease-free life
Adults who follow a heart-healthy lifestyle are more likely to live longer and to be free of chronic health conditions, based on data from a pair of related studies from the United States and United Kingdom involving nearly 200,000 individuals.

The studies, presented at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting in Boston, assessed the impact of cardiovascular health on life expectancy and freedom from chronic diseases. Cardiovascular health (CVH) was based on the Life’s Essential 8 (LE8) score, a composite of health metrics released by the American Heart Association in 2022. The LE8 was developed to guide research and assessment of cardiovascular health, and includes diet, physical activity, tobacco/nicotine exposure, sleep, body mass index, non-HDL cholesterol, blood glucose, and blood pressure.
In one study, Xuan Wang, MD, a postdoctoral fellow and biostatistician in the department of epidemiology at Tulane University, New Orleans, and colleagues reviewed data from 136,599 adults in the United Kingdom Biobank who were free of cardiovascular disease, diabetes, cancer, and dementia at baseline, and for whom complete LE8 data were available.
CVH was classified as poor, intermediate, and ideal, defined as LE8 scores of less than 50, 50 to 80, and 80 or higher, respectively.
The goal of the study was to examine the role of CVH based on LE8 scores on the percentage of life expectancy free of chronic diseases.
Men and women with ideal CVH averaged 5.2 years and 6.3 years more of total life expectancy at age 50 years, compared with those with poor CVH. Out of total life expectancy, the percentage of life expectancy free of chronic diseases was 75.9% and 83.4% for men and women, respectively, compared with 64.9% and 69.4%, respectively, for men and women with poor CVH.
The researchers also found that disparities in the percentage of disease-free years for both men and women were reduced in the high CVH groups.
The findings were limited by several factors including the use of only CVD, diabetes, cancer, and dementia in the definition of “disease-free life expectancy,” the researchers noted in a press release accompanying the study. Other limitations include the lack of data on e-cigarettes, and the homogeneous White study population. More research is needed in diverse populations who experience a stronger impact from negative social determinants of health, they said.
In a second study, Hao Ma, MD, and colleagues reviewed data from 23,003 adults who participated in the National Health and Nutrition Examination Survey (NHANES) between 2005 and 2018 with mortality linked to the National Death Index through Dec. 31, 2019. The goal of the second study was to examine the association between CVH based on LE8 scores and life expectancy.
Over a median follow-up of 7.8 years, deaths occurred in 772 men and 587 women, said Dr. Ma, a postdoctoral fellow and biostatistician in epidemiology at Tulane University and coauthor on Dr. Wang’s study.
The estimated life expectancies at age 50 years for men with poor, intermediate, and ideal cardiovascular health based on the LE8 were 25.5 years, 31.2 years, and 33.1 years, respectively.
For women, the corresponding life expectancies for women at age 50 with poor, intermediate, and ideal CVH were 29.5 years, 34.2 years, and 38.4 years, respectively.
Men and women had similar gains in life expectancy from adhering to a heart-healthy lifestyle as defined by the LE8 score that reduced their risk of death from cardiovascular disease (41.8% and 44.1%, respectively).
Associations of cardiovascular health and life expectancy were similar for non-Hispanic Whites and non-Hispanic Blacks, but not among people of Mexican heritage, and more research is needed in diverse populations, the researchers wrote.
The study was limited by several factors including potential changes in cardiovascular health during the follow-up period, and by the limited analysis of racial and ethnic groups to non-Hispanic white, non-Hispanic Black, and people of Mexican heritage because of small sample sizes for other racial/ethnic groups, the researchers noted in a press release accompanying the study.
The message for clinicians and their patients is that adherence to cardiovascular health as defined by the LE8 will help not only extend life, but enhance quality of life, Dr. Xang and Dr. Ma said in an interview. “If your overall CVH score is low, we might be able to focus on one element first and improve them one by one,” they said. Sedentary lifestyle and an unhealthy diet are barriers to improving LE8 metrics that can be addressed, they added.
More research is needed to examine the effects of LE8 on high-risk patients, the researchers told this news organization. “No studies have yet focused on these patients with chronic diseases. We suspect that LE8 will play a role even in these high-risk groups,” they said. Further studies should include diverse populations and evaluations of the association between CVH change and health outcomes, they added.
“Overall, we see this 7.5-year difference [in life expectancy] going from poor to high cardiovascular health,” said Donald M. Lloyd-Jones, MD, of Northwestern University, Chicago, in a video accompanying the presentation of the study findings. The impact on life expectancy is yet another reason to motivate people to improve their cardiovascular health, said Dr. Lloyd-Jones, immediate past president of the American Heart Association and lead author on the writing group for Life’s Essential 8. “The earlier we do this, the better, and the greater the gains in life expectancy we’re likely to see in the U.S. population,” he said.
People maintaining high cardiovascular health into midlife are avoiding not only cardiovascular disease, but other chronic diseases of aging, Dr. Lloyd-Jones added. These conditions are delayed until much later in the lifespan, which allows people to enjoy better quality of life for more of their remaining years, he said.
The meeting was sponsored by the American Heart Association.
Both studies were supported by the National Heart, Lung, and Blood Institute and the National Institute of Diabetes and Digestive and Kidney Diseases, part of the National Institutes of Health; the Fogarty International Center; and the Tulane Research Centers of Excellence Awards. The researchers had no financial conflicts to disclose.
Adults who follow a heart-healthy lifestyle are more likely to live longer and to be free of chronic health conditions, based on data from a pair of related studies from the United States and United Kingdom involving nearly 200,000 individuals.
The studies, presented at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting in Boston, assessed the impact of cardiovascular health on life expectancy and freedom from chronic diseases. Cardiovascular health (CVH) was based on the Life’s Essential 8 (LE8) score, a composite of health metrics released by the American Heart Association in 2022. The LE8 was developed to guide research and assessment of cardiovascular health, and includes diet, physical activity, tobacco/nicotine exposure, sleep, body mass index, non-HDL cholesterol, blood glucose, and blood pressure.
In one study, Xuan Wang, MD, a postdoctoral fellow and biostatistician in the department of epidemiology at Tulane University, New Orleans, and colleagues reviewed data from 136,599 adults in the United Kingdom Biobank who were free of cardiovascular disease, diabetes, cancer, and dementia at baseline, and for whom complete LE8 data were available.
CVH was classified as poor, intermediate, and ideal, defined as LE8 scores of less than 50, 50 to 80, and 80 or higher, respectively.
The goal of the study was to examine the role of CVH based on LE8 scores on the percentage of life expectancy free of chronic diseases.
Men and women with ideal CVH averaged 5.2 years and 6.3 years more of total life expectancy at age 50 years, compared with those with poor CVH. Out of total life expectancy, the percentage of life expectancy free of chronic diseases was 75.9% and 83.4% for men and women, respectively, compared with 64.9% and 69.4%, respectively, for men and women with poor CVH.
The researchers also found that disparities in the percentage of disease-free years for both men and women were reduced in the high CVH groups.
The findings were limited by several factors including the use of only CVD, diabetes, cancer, and dementia in the definition of “disease-free life expectancy,” the researchers noted in a press release accompanying the study. Other limitations include the lack of data on e-cigarettes, and the homogeneous White study population. More research is needed in diverse populations who experience a stronger impact from negative social determinants of health, they said.
In a second study, Hao Ma, MD, and colleagues reviewed data from 23,003 adults who participated in the National Health and Nutrition Examination Survey (NHANES) between 2005 and 2018 with mortality linked to the National Death Index through Dec. 31, 2019. The goal of the second study was to examine the association between CVH based on LE8 scores and life expectancy.
Over a median follow-up of 7.8 years, deaths occurred in 772 men and 587 women, said Dr. Ma, a postdoctoral fellow and biostatistician in epidemiology at Tulane University and coauthor on Dr. Wang’s study.
The estimated life expectancies at age 50 years for men with poor, intermediate, and ideal cardiovascular health based on the LE8 were 25.5 years, 31.2 years, and 33.1 years, respectively.
For women, the corresponding life expectancies for women at age 50 with poor, intermediate, and ideal CVH were 29.5 years, 34.2 years, and 38.4 years, respectively.
Men and women had similar gains in life expectancy from adhering to a heart-healthy lifestyle as defined by the LE8 score that reduced their risk of death from cardiovascular disease (41.8% and 44.1%, respectively).
Associations of cardiovascular health and life expectancy were similar for non-Hispanic Whites and non-Hispanic Blacks, but not among people of Mexican heritage, and more research is needed in diverse populations, the researchers wrote.
The study was limited by several factors including potential changes in cardiovascular health during the follow-up period, and by the limited analysis of racial and ethnic groups to non-Hispanic white, non-Hispanic Black, and people of Mexican heritage because of small sample sizes for other racial/ethnic groups, the researchers noted in a press release accompanying the study.
The message for clinicians and their patients is that adherence to cardiovascular health as defined by the LE8 will help not only extend life, but enhance quality of life, Dr. Xang and Dr. Ma said in an interview. “If your overall CVH score is low, we might be able to focus on one element first and improve them one by one,” they said. Sedentary lifestyle and an unhealthy diet are barriers to improving LE8 metrics that can be addressed, they added.
More research is needed to examine the effects of LE8 on high-risk patients, the researchers told this news organization. “No studies have yet focused on these patients with chronic diseases. We suspect that LE8 will play a role even in these high-risk groups,” they said. Further studies should include diverse populations and evaluations of the association between CVH change and health outcomes, they added.
“Overall, we see this 7.5-year difference [in life expectancy] going from poor to high cardiovascular health,” said Donald M. Lloyd-Jones, MD, of Northwestern University, Chicago, in a video accompanying the presentation of the study findings. The impact on life expectancy is yet another reason to motivate people to improve their cardiovascular health, said Dr. Lloyd-Jones, immediate past president of the American Heart Association and lead author on the writing group for Life’s Essential 8. “The earlier we do this, the better, and the greater the gains in life expectancy we’re likely to see in the U.S. population,” he said.
People maintaining high cardiovascular health into midlife are avoiding not only cardiovascular disease, but other chronic diseases of aging, Dr. Lloyd-Jones added. These conditions are delayed until much later in the lifespan, which allows people to enjoy better quality of life for more of their remaining years, he said.
The meeting was sponsored by the American Heart Association.
Both studies were supported by the National Heart, Lung, and Blood Institute and the National Institute of Diabetes and Digestive and Kidney Diseases, part of the National Institutes of Health; the Fogarty International Center; and the Tulane Research Centers of Excellence Awards. The researchers had no financial conflicts to disclose.
Adults who follow a heart-healthy lifestyle are more likely to live longer and to be free of chronic health conditions, based on data from a pair of related studies from the United States and United Kingdom involving nearly 200,000 individuals.
The studies, presented at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting in Boston, assessed the impact of cardiovascular health on life expectancy and freedom from chronic diseases. Cardiovascular health (CVH) was based on the Life’s Essential 8 (LE8) score, a composite of health metrics released by the American Heart Association in 2022. The LE8 was developed to guide research and assessment of cardiovascular health, and includes diet, physical activity, tobacco/nicotine exposure, sleep, body mass index, non-HDL cholesterol, blood glucose, and blood pressure.
In one study, Xuan Wang, MD, a postdoctoral fellow and biostatistician in the department of epidemiology at Tulane University, New Orleans, and colleagues reviewed data from 136,599 adults in the United Kingdom Biobank who were free of cardiovascular disease, diabetes, cancer, and dementia at baseline, and for whom complete LE8 data were available.
CVH was classified as poor, intermediate, and ideal, defined as LE8 scores of less than 50, 50 to 80, and 80 or higher, respectively.
The goal of the study was to examine the role of CVH based on LE8 scores on the percentage of life expectancy free of chronic diseases.
Men and women with ideal CVH averaged 5.2 years and 6.3 years more of total life expectancy at age 50 years, compared with those with poor CVH. Out of total life expectancy, the percentage of life expectancy free of chronic diseases was 75.9% and 83.4% for men and women, respectively, compared with 64.9% and 69.4%, respectively, for men and women with poor CVH.
The researchers also found that disparities in the percentage of disease-free years for both men and women were reduced in the high CVH groups.
The findings were limited by several factors including the use of only CVD, diabetes, cancer, and dementia in the definition of “disease-free life expectancy,” the researchers noted in a press release accompanying the study. Other limitations include the lack of data on e-cigarettes, and the homogeneous White study population. More research is needed in diverse populations who experience a stronger impact from negative social determinants of health, they said.
In a second study, Hao Ma, MD, and colleagues reviewed data from 23,003 adults who participated in the National Health and Nutrition Examination Survey (NHANES) between 2005 and 2018 with mortality linked to the National Death Index through Dec. 31, 2019. The goal of the second study was to examine the association between CVH based on LE8 scores and life expectancy.
Over a median follow-up of 7.8 years, deaths occurred in 772 men and 587 women, said Dr. Ma, a postdoctoral fellow and biostatistician in epidemiology at Tulane University and coauthor on Dr. Wang’s study.
The estimated life expectancies at age 50 years for men with poor, intermediate, and ideal cardiovascular health based on the LE8 were 25.5 years, 31.2 years, and 33.1 years, respectively.
For women, the corresponding life expectancies for women at age 50 with poor, intermediate, and ideal CVH were 29.5 years, 34.2 years, and 38.4 years, respectively.
Men and women had similar gains in life expectancy from adhering to a heart-healthy lifestyle as defined by the LE8 score that reduced their risk of death from cardiovascular disease (41.8% and 44.1%, respectively).
Associations of cardiovascular health and life expectancy were similar for non-Hispanic Whites and non-Hispanic Blacks, but not among people of Mexican heritage, and more research is needed in diverse populations, the researchers wrote.
The study was limited by several factors including potential changes in cardiovascular health during the follow-up period, and by the limited analysis of racial and ethnic groups to non-Hispanic white, non-Hispanic Black, and people of Mexican heritage because of small sample sizes for other racial/ethnic groups, the researchers noted in a press release accompanying the study.
The message for clinicians and their patients is that adherence to cardiovascular health as defined by the LE8 will help not only extend life, but enhance quality of life, Dr. Xang and Dr. Ma said in an interview. “If your overall CVH score is low, we might be able to focus on one element first and improve them one by one,” they said. Sedentary lifestyle and an unhealthy diet are barriers to improving LE8 metrics that can be addressed, they added.
More research is needed to examine the effects of LE8 on high-risk patients, the researchers told this news organization. “No studies have yet focused on these patients with chronic diseases. We suspect that LE8 will play a role even in these high-risk groups,” they said. Further studies should include diverse populations and evaluations of the association between CVH change and health outcomes, they added.
“Overall, we see this 7.5-year difference [in life expectancy] going from poor to high cardiovascular health,” said Donald M. Lloyd-Jones, MD, of Northwestern University, Chicago, in a video accompanying the presentation of the study findings. The impact on life expectancy is yet another reason to motivate people to improve their cardiovascular health, said Dr. Lloyd-Jones, immediate past president of the American Heart Association and lead author on the writing group for Life’s Essential 8. “The earlier we do this, the better, and the greater the gains in life expectancy we’re likely to see in the U.S. population,” he said.
People maintaining high cardiovascular health into midlife are avoiding not only cardiovascular disease, but other chronic diseases of aging, Dr. Lloyd-Jones added. These conditions are delayed until much later in the lifespan, which allows people to enjoy better quality of life for more of their remaining years, he said.
The meeting was sponsored by the American Heart Association.
Both studies were supported by the National Heart, Lung, and Blood Institute and the National Institute of Diabetes and Digestive and Kidney Diseases, part of the National Institutes of Health; the Fogarty International Center; and the Tulane Research Centers of Excellence Awards. The researchers had no financial conflicts to disclose.
FROM EPI/LIFESTYLE 2023
High CV risk factor burden in young adults a ‘smoldering’ crisis
New data show a high and rising burden of most cardiovascular (CV) risk factors among young adults aged 20-44 years in the United States.
In this age group, over the past 10 years, there has been an increase in the prevalence of diabetes and obesity, no improvement in the prevalence of hypertension, and a decrease in the prevalence of hyperlipidemia.
Yet medical treatment rates for CV risk factors are “surprisingly” low among young adults, study investigator Rishi Wadhera, MD, with Beth Israel Deaconess Medical Center and Harvard Medical School, both in Boston, told this news organization.

The findings are “extremely concerning. We’re witnessing a smoldering public health crisis. The onset of these risk factors earlier in life is associated with a higher lifetime risk of heart disease and potentially life-threatening,” Dr. Wadhera added.
The study was presented March 5 at the joint scientific sessions of the American College of Cardiology and the World Heart Federation and was simultaneously published in JAMA.
The burden of CV risk factors among young adults is “unacceptably high and increasing,” write the co-authors of a JAMA editorial.
“The time is now for aggressive preventive measures in young adults. Without immediate action there will continue to be a rise in heart disease and the burden it places on patients, families, and communities,” say Norrina Allen, PhD, and John Wilkins, MD, with Northwestern University, Chicago.
Preventing a tsunami of heart disease
The findings stem from a cross-sectional study of 12,294 U.S. adults aged 20-44 years (mean age, 32; 51% women) who participated in National Health and Nutrition Examination Survey (NHANES) cycles for 2009-2010 to 2017-2020.
Overall, the prevalence of hypertension was 9.3% in 2009-2010 and increased to 11.5% in 2017-2020. The prevalence of diabetes rose from 3.0% to 4.1%, and the prevalence of obesity rose from 32.7% to 40.9%. The prevalence of hyperlipidemia decreased from 40.5% to 36.1%.
Black adults consistently had high rates of hypertension during the study period – 16.2% in 2009-2010 and 20.1% in 2017-2020 – and significant increases in hypertension occurred among Mexican American adults (from 6.5% to 9.5%) and other Hispanic adults (from 4.4% to 10.5%), while Mexican American adults had a significant uptick in diabetes (from 4.3% to 7.5%).
Equally concerning, said Dr. Wadhera, is the fact that only about 55% of young adults with hypertension were receiving antihypertensive medication, and just 1 in 2 young adults with diabetes were receiving treatment. “These low rates were driven, in part, by many young adults not being aware of their diagnosis,” he noted.
The NHANES data also show that the percentage of young adults who were treated for hypertension and who achieved blood pressure control did not change significantly over the study period (65.0% in 2009-2010 and 74.8% in 2017-2020). Blood sugar control among young adults being treated for diabetes remained suboptimal throughout the study period (45.5% in 2009-2010 and 56.6% in 2017-2020).
“The fact that blood pressure control and glycemic control are so poor is really worrisome,” Jeffrey Berger, MD, director of the Center for the Prevention of Cardiovascular Disease at NYU Langone Heart, who wasn’t involved in the study, told this news organization.

“Even in the lipid control, while it did get a little bit better, it’s still only around 30%-40%. So, I think we have ways to go as a society,” Dr. Berger noted.
Double down on screening
Dr. Wadhera said “we need to double down on efforts to screen for and treat cardiovascular risk factors like high blood pressure and diabetes in young adults. We need to intensify clinical and public health interventions focused on primordial and primary prevention in young adults now so that we can avoid a tsunami of cardiovascular disease in the long term.”
“It’s critically important that young adults speak with their health care provider about whether – and when – they should undergo screening for high blood pressure, diabetes, and high cholesterol,” Dr. Wadhera added.
Dr. Berger said one problem is that younger people often have a “superman or superwoman” view and don’t comprehend that they are at risk for some of these conditions. Studies such as this “reinforce the idea that it’s never too young to be checked out.”
As a cardiologist who specializes in cardiovascular prevention, Dr. Berger said he sometimes hears patients say things like, “I don’t ever want to need a cardiologist,” or “I hope I never need a cardiologist.”
“My response is, ‘There are many different types of cardiologists,’ and I think it would really be helpful for many people to see a prevention-focused cardiologist way before they have problems,” he said in an interview.
“As a system, medicine has become very good at treating patients with different diseases. I think we need to get better in terms of preventing some of these problems,” Dr. Berger added.
In their editorial, Dr. Allen and Dr. Wilkins say the “foundation of cardiovascular health begins early in life. These worsening trends in risk factors highlight the importance of focusing on prevention in adolescence and young adulthood in order to promote cardiovascular health across the lifetime.”
The study was funded by a grant from the National Heart, Lung, and Blood Institute. Dr. Wadhera has served as a consultant for Abbott and CVS Health. Dr. Wilkins has received personal fees from 3M. Dr. Berger has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
New data show a high and rising burden of most cardiovascular (CV) risk factors among young adults aged 20-44 years in the United States.
In this age group, over the past 10 years, there has been an increase in the prevalence of diabetes and obesity, no improvement in the prevalence of hypertension, and a decrease in the prevalence of hyperlipidemia.
Yet medical treatment rates for CV risk factors are “surprisingly” low among young adults, study investigator Rishi Wadhera, MD, with Beth Israel Deaconess Medical Center and Harvard Medical School, both in Boston, told this news organization.
The findings are “extremely concerning. We’re witnessing a smoldering public health crisis. The onset of these risk factors earlier in life is associated with a higher lifetime risk of heart disease and potentially life-threatening,” Dr. Wadhera added.
The study was presented March 5 at the joint scientific sessions of the American College of Cardiology and the World Heart Federation and was simultaneously published in JAMA.
The burden of CV risk factors among young adults is “unacceptably high and increasing,” write the co-authors of a JAMA editorial.
“The time is now for aggressive preventive measures in young adults. Without immediate action there will continue to be a rise in heart disease and the burden it places on patients, families, and communities,” say Norrina Allen, PhD, and John Wilkins, MD, with Northwestern University, Chicago.
Preventing a tsunami of heart disease
The findings stem from a cross-sectional study of 12,294 U.S. adults aged 20-44 years (mean age, 32; 51% women) who participated in National Health and Nutrition Examination Survey (NHANES) cycles for 2009-2010 to 2017-2020.
Overall, the prevalence of hypertension was 9.3% in 2009-2010 and increased to 11.5% in 2017-2020. The prevalence of diabetes rose from 3.0% to 4.1%, and the prevalence of obesity rose from 32.7% to 40.9%. The prevalence of hyperlipidemia decreased from 40.5% to 36.1%.
Black adults consistently had high rates of hypertension during the study period – 16.2% in 2009-2010 and 20.1% in 2017-2020 – and significant increases in hypertension occurred among Mexican American adults (from 6.5% to 9.5%) and other Hispanic adults (from 4.4% to 10.5%), while Mexican American adults had a significant uptick in diabetes (from 4.3% to 7.5%).
Equally concerning, said Dr. Wadhera, is the fact that only about 55% of young adults with hypertension were receiving antihypertensive medication, and just 1 in 2 young adults with diabetes were receiving treatment. “These low rates were driven, in part, by many young adults not being aware of their diagnosis,” he noted.
The NHANES data also show that the percentage of young adults who were treated for hypertension and who achieved blood pressure control did not change significantly over the study period (65.0% in 2009-2010 and 74.8% in 2017-2020). Blood sugar control among young adults being treated for diabetes remained suboptimal throughout the study period (45.5% in 2009-2010 and 56.6% in 2017-2020).
“The fact that blood pressure control and glycemic control are so poor is really worrisome,” Jeffrey Berger, MD, director of the Center for the Prevention of Cardiovascular Disease at NYU Langone Heart, who wasn’t involved in the study, told this news organization.
“Even in the lipid control, while it did get a little bit better, it’s still only around 30%-40%. So, I think we have ways to go as a society,” Dr. Berger noted.
Double down on screening
Dr. Wadhera said “we need to double down on efforts to screen for and treat cardiovascular risk factors like high blood pressure and diabetes in young adults. We need to intensify clinical and public health interventions focused on primordial and primary prevention in young adults now so that we can avoid a tsunami of cardiovascular disease in the long term.”
“It’s critically important that young adults speak with their health care provider about whether – and when – they should undergo screening for high blood pressure, diabetes, and high cholesterol,” Dr. Wadhera added.
Dr. Berger said one problem is that younger people often have a “superman or superwoman” view and don’t comprehend that they are at risk for some of these conditions. Studies such as this “reinforce the idea that it’s never too young to be checked out.”
As a cardiologist who specializes in cardiovascular prevention, Dr. Berger said he sometimes hears patients say things like, “I don’t ever want to need a cardiologist,” or “I hope I never need a cardiologist.”
“My response is, ‘There are many different types of cardiologists,’ and I think it would really be helpful for many people to see a prevention-focused cardiologist way before they have problems,” he said in an interview.
“As a system, medicine has become very good at treating patients with different diseases. I think we need to get better in terms of preventing some of these problems,” Dr. Berger added.
In their editorial, Dr. Allen and Dr. Wilkins say the “foundation of cardiovascular health begins early in life. These worsening trends in risk factors highlight the importance of focusing on prevention in adolescence and young adulthood in order to promote cardiovascular health across the lifetime.”
The study was funded by a grant from the National Heart, Lung, and Blood Institute. Dr. Wadhera has served as a consultant for Abbott and CVS Health. Dr. Wilkins has received personal fees from 3M. Dr. Berger has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
New data show a high and rising burden of most cardiovascular (CV) risk factors among young adults aged 20-44 years in the United States.
In this age group, over the past 10 years, there has been an increase in the prevalence of diabetes and obesity, no improvement in the prevalence of hypertension, and a decrease in the prevalence of hyperlipidemia.
Yet medical treatment rates for CV risk factors are “surprisingly” low among young adults, study investigator Rishi Wadhera, MD, with Beth Israel Deaconess Medical Center and Harvard Medical School, both in Boston, told this news organization.
The findings are “extremely concerning. We’re witnessing a smoldering public health crisis. The onset of these risk factors earlier in life is associated with a higher lifetime risk of heart disease and potentially life-threatening,” Dr. Wadhera added.
The study was presented March 5 at the joint scientific sessions of the American College of Cardiology and the World Heart Federation and was simultaneously published in JAMA.
The burden of CV risk factors among young adults is “unacceptably high and increasing,” write the co-authors of a JAMA editorial.
“The time is now for aggressive preventive measures in young adults. Without immediate action there will continue to be a rise in heart disease and the burden it places on patients, families, and communities,” say Norrina Allen, PhD, and John Wilkins, MD, with Northwestern University, Chicago.
Preventing a tsunami of heart disease
The findings stem from a cross-sectional study of 12,294 U.S. adults aged 20-44 years (mean age, 32; 51% women) who participated in National Health and Nutrition Examination Survey (NHANES) cycles for 2009-2010 to 2017-2020.
Overall, the prevalence of hypertension was 9.3% in 2009-2010 and increased to 11.5% in 2017-2020. The prevalence of diabetes rose from 3.0% to 4.1%, and the prevalence of obesity rose from 32.7% to 40.9%. The prevalence of hyperlipidemia decreased from 40.5% to 36.1%.
Black adults consistently had high rates of hypertension during the study period – 16.2% in 2009-2010 and 20.1% in 2017-2020 – and significant increases in hypertension occurred among Mexican American adults (from 6.5% to 9.5%) and other Hispanic adults (from 4.4% to 10.5%), while Mexican American adults had a significant uptick in diabetes (from 4.3% to 7.5%).
Equally concerning, said Dr. Wadhera, is the fact that only about 55% of young adults with hypertension were receiving antihypertensive medication, and just 1 in 2 young adults with diabetes were receiving treatment. “These low rates were driven, in part, by many young adults not being aware of their diagnosis,” he noted.
The NHANES data also show that the percentage of young adults who were treated for hypertension and who achieved blood pressure control did not change significantly over the study period (65.0% in 2009-2010 and 74.8% in 2017-2020). Blood sugar control among young adults being treated for diabetes remained suboptimal throughout the study period (45.5% in 2009-2010 and 56.6% in 2017-2020).
“The fact that blood pressure control and glycemic control are so poor is really worrisome,” Jeffrey Berger, MD, director of the Center for the Prevention of Cardiovascular Disease at NYU Langone Heart, who wasn’t involved in the study, told this news organization.
“Even in the lipid control, while it did get a little bit better, it’s still only around 30%-40%. So, I think we have ways to go as a society,” Dr. Berger noted.
Double down on screening
Dr. Wadhera said “we need to double down on efforts to screen for and treat cardiovascular risk factors like high blood pressure and diabetes in young adults. We need to intensify clinical and public health interventions focused on primordial and primary prevention in young adults now so that we can avoid a tsunami of cardiovascular disease in the long term.”
“It’s critically important that young adults speak with their health care provider about whether – and when – they should undergo screening for high blood pressure, diabetes, and high cholesterol,” Dr. Wadhera added.
Dr. Berger said one problem is that younger people often have a “superman or superwoman” view and don’t comprehend that they are at risk for some of these conditions. Studies such as this “reinforce the idea that it’s never too young to be checked out.”
As a cardiologist who specializes in cardiovascular prevention, Dr. Berger said he sometimes hears patients say things like, “I don’t ever want to need a cardiologist,” or “I hope I never need a cardiologist.”
“My response is, ‘There are many different types of cardiologists,’ and I think it would really be helpful for many people to see a prevention-focused cardiologist way before they have problems,” he said in an interview.
“As a system, medicine has become very good at treating patients with different diseases. I think we need to get better in terms of preventing some of these problems,” Dr. Berger added.
In their editorial, Dr. Allen and Dr. Wilkins say the “foundation of cardiovascular health begins early in life. These worsening trends in risk factors highlight the importance of focusing on prevention in adolescence and young adulthood in order to promote cardiovascular health across the lifetime.”
The study was funded by a grant from the National Heart, Lung, and Blood Institute. Dr. Wadhera has served as a consultant for Abbott and CVS Health. Dr. Wilkins has received personal fees from 3M. Dr. Berger has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACC 2023
COORDINATEd effort boosts optimal therapy in patients with T2D and ASCVD
NEW ORLEANS – Twenty cardiology clinics successfully intensified the medical care they gave patients with type 2 diabetes (T2D) and atherosclerotic cardiovascular disease (ASCVD) after receiving a simple and scalable investigational intervention that gave the clinics’ staffs guidance on best prescribing practices and implementation and also provided quality-improvement feedback.
Within a year, these clinics quadrupled optimal medical management of these patients, compared with control clinics, in a randomized trial involving a total of 43 clinics and 1,049 patients.
“This multifaceted intervention is effective in increasing the prescription of evidence-based therapies in adults with T2D and ASCVD,” Neha J. Pagidipati, MD, said at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
“The next step is to scale this intervention across cardiology practices” interested in improving the quality of care they deliver to these patients, added Dr. Pagidipati, a cardiologist specializing in cardiometabolic disease prevention at Duke University in Durham, N.C.
The goal is getting patients on triple therapy
The primary outcome of the COORDINATE-Diabetes trial was the change in the number of patients with T2D and ASCVD who received prescriptions for agents from three recommended medication classes and at recommended dosages: a high-intensity statin, a renin-angiotensin system inhibitor (RASi), and at least one agent from either of two classes that have both cardiovascular-protective and antihyperglycemic effects: the sodium-glucose cotransporter 2 (SGLT2) inhibitors, or the glucagonlike peptide 1 (GLP-1)–receptor agonists.
Among the 457 patients treated at the 20 cardiology clinics who received the quality-improvement intervention, 37.9% were on the promoted triple therapy after 12 months, compared with 14.5% of the 588 patients treated at the 23 clinics that continued with their usual care approach. This 23.4–percentage point increase in triple-class prescribing at recommended dosages represented a significant 4.4-fold increase in the goal prescribing endpoint after adjustment for possible confounders, Dr. Pagidipati reported.
Simultaneously with her report, the findings also appeared online in JAMA.
At baseline, 41%-50% of the patients were on both a high-intensity statin and a RASi, with a total of about 58%-67% on a high-intensity statin and about 70%-75% on a RASi. Fewer than 1% of patients were on SGLT2 inhibitors or GLP-1–receptor agonists at baseline. By design, no patient could be on all three categories of medication at baseline.
At their last follow-up visit (after 12 months for 97% of patients, or after 6 months for the remainder) 71% of the patients at practices that received the intervention were on a high-intensity statin, 81% were taking a RASi, and 60% were on an SGLT2 inhibitor or GLP-1–receptor agonist. Among the control patients, 58% were on a high-intensity statin, 68% on a RASi, and 36% were on one of the antihyperglycemic agents.
Effective interventions and the need for a champion
The clinics randomized to the active arm received instruction from a three-member team, either from an in-person or virtual one-time visit, on an intervention comprising several initiatives:
- Analysis of the barriers to evidence-based care at each clinic.
- Development of local interdisciplinary care pathways to address the identified barriers.
- Facilitation of care coordination among clinicians – particularly among cardiology, endocrinology, and primary care clinicians.
- Education of the clinic staff, including provision of educational materials.
- Auditing of clinic performance using specified metrics and feedback on the findings.
Clinics in the usual care group were given current clinical practice guidelines.
The investigational intervention was, by design, “low-tech and designed to be scalable,” explained Dr. Pagidipati, and once the COVID pandemic started the intervention team shifted to a virtual consultation with participating practices that was mostly front-loaded, followed by monthly phone calls to give clinics feedback on their progress.
Among the most helpful aspects of the intervention was involving the entire clinic staff, including pharmacists, nurses, and advanced care practitioners; boosting familiarity with the relevant medications and their appropriate use; and advice on navigating insurance-coverage barriers such as prior authorizations.
“What was most critical was having a local champion who took on making this effort an important part” of what the clinic was trying to do, she explained. “All it takes is passion, and the tenacity of a bulldog,” Dr. Pagidipati said.
Research advances often don’t translate into management changes
“We don’t do a great job of translating findings from trials to patient care, so any method we can use to improve that will improve practice,” commented Kristen B. Campbell, PharmD, a clinical pharmacist at Duke who was not involved in the study.
“Although the trial was not powered to look at patient outcomes, we think that patients will benefit” because all the recommended medication uses have been proven to help patients in prior trials, Dr. Campbell noted.

“A particular strength of this study was its simple design. All the interventions are low-tech and scalable.”
The low level of use of guideline-directed medical therapy in American adults with type 2 diabetes and atherosclerotic cardiovascular disease is “incredible,” said Christopher B. Granger, MD, a senior investigator on the study and a cardiologist and professor at Duke.
The researchers who ran the study are now focused on evaluating which cardiology clinics and patients had the most success from the intervention and are using that information to further refine implementation. They are also planning to encourage cardiology practices as well as other relevant medical groups to incorporate the intervention and implementation model used in the trial. The intervention program is detailed and available at no charge on the COORDINATE-Diabetes website.
COORDINATE-Diabetes received funding from Boehringer Ingelheim and Eli Lilly. Dr. Pagidipati has received personal fees from Boehringer Ingelheim, Lilly, AstraZeneca, Novartis, Novo Nordisk, Merck, and CRISPR Therapeutics, and she has received research grants from Amgen, Novartis, Novo Nordisk, and Eggland’s Best. Dr. Campbell had no disclosures. Dr. Granger has received personal fees and research funding from numerous companies.
NEW ORLEANS – Twenty cardiology clinics successfully intensified the medical care they gave patients with type 2 diabetes (T2D) and atherosclerotic cardiovascular disease (ASCVD) after receiving a simple and scalable investigational intervention that gave the clinics’ staffs guidance on best prescribing practices and implementation and also provided quality-improvement feedback.
Within a year, these clinics quadrupled optimal medical management of these patients, compared with control clinics, in a randomized trial involving a total of 43 clinics and 1,049 patients.
“This multifaceted intervention is effective in increasing the prescription of evidence-based therapies in adults with T2D and ASCVD,” Neha J. Pagidipati, MD, said at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
“The next step is to scale this intervention across cardiology practices” interested in improving the quality of care they deliver to these patients, added Dr. Pagidipati, a cardiologist specializing in cardiometabolic disease prevention at Duke University in Durham, N.C.
The goal is getting patients on triple therapy
The primary outcome of the COORDINATE-Diabetes trial was the change in the number of patients with T2D and ASCVD who received prescriptions for agents from three recommended medication classes and at recommended dosages: a high-intensity statin, a renin-angiotensin system inhibitor (RASi), and at least one agent from either of two classes that have both cardiovascular-protective and antihyperglycemic effects: the sodium-glucose cotransporter 2 (SGLT2) inhibitors, or the glucagonlike peptide 1 (GLP-1)–receptor agonists.
Among the 457 patients treated at the 20 cardiology clinics who received the quality-improvement intervention, 37.9% were on the promoted triple therapy after 12 months, compared with 14.5% of the 588 patients treated at the 23 clinics that continued with their usual care approach. This 23.4–percentage point increase in triple-class prescribing at recommended dosages represented a significant 4.4-fold increase in the goal prescribing endpoint after adjustment for possible confounders, Dr. Pagidipati reported.
Simultaneously with her report, the findings also appeared online in JAMA.
At baseline, 41%-50% of the patients were on both a high-intensity statin and a RASi, with a total of about 58%-67% on a high-intensity statin and about 70%-75% on a RASi. Fewer than 1% of patients were on SGLT2 inhibitors or GLP-1–receptor agonists at baseline. By design, no patient could be on all three categories of medication at baseline.
At their last follow-up visit (after 12 months for 97% of patients, or after 6 months for the remainder) 71% of the patients at practices that received the intervention were on a high-intensity statin, 81% were taking a RASi, and 60% were on an SGLT2 inhibitor or GLP-1–receptor agonist. Among the control patients, 58% were on a high-intensity statin, 68% on a RASi, and 36% were on one of the antihyperglycemic agents.
Effective interventions and the need for a champion
The clinics randomized to the active arm received instruction from a three-member team, either from an in-person or virtual one-time visit, on an intervention comprising several initiatives:
- Analysis of the barriers to evidence-based care at each clinic.
- Development of local interdisciplinary care pathways to address the identified barriers.
- Facilitation of care coordination among clinicians – particularly among cardiology, endocrinology, and primary care clinicians.
- Education of the clinic staff, including provision of educational materials.
- Auditing of clinic performance using specified metrics and feedback on the findings.
Clinics in the usual care group were given current clinical practice guidelines.
The investigational intervention was, by design, “low-tech and designed to be scalable,” explained Dr. Pagidipati, and once the COVID pandemic started the intervention team shifted to a virtual consultation with participating practices that was mostly front-loaded, followed by monthly phone calls to give clinics feedback on their progress.
Among the most helpful aspects of the intervention was involving the entire clinic staff, including pharmacists, nurses, and advanced care practitioners; boosting familiarity with the relevant medications and their appropriate use; and advice on navigating insurance-coverage barriers such as prior authorizations.
“What was most critical was having a local champion who took on making this effort an important part” of what the clinic was trying to do, she explained. “All it takes is passion, and the tenacity of a bulldog,” Dr. Pagidipati said.
Research advances often don’t translate into management changes
“We don’t do a great job of translating findings from trials to patient care, so any method we can use to improve that will improve practice,” commented Kristen B. Campbell, PharmD, a clinical pharmacist at Duke who was not involved in the study.
“Although the trial was not powered to look at patient outcomes, we think that patients will benefit” because all the recommended medication uses have been proven to help patients in prior trials, Dr. Campbell noted.
“A particular strength of this study was its simple design. All the interventions are low-tech and scalable.”
The low level of use of guideline-directed medical therapy in American adults with type 2 diabetes and atherosclerotic cardiovascular disease is “incredible,” said Christopher B. Granger, MD, a senior investigator on the study and a cardiologist and professor at Duke.
The researchers who ran the study are now focused on evaluating which cardiology clinics and patients had the most success from the intervention and are using that information to further refine implementation. They are also planning to encourage cardiology practices as well as other relevant medical groups to incorporate the intervention and implementation model used in the trial. The intervention program is detailed and available at no charge on the COORDINATE-Diabetes website.
COORDINATE-Diabetes received funding from Boehringer Ingelheim and Eli Lilly. Dr. Pagidipati has received personal fees from Boehringer Ingelheim, Lilly, AstraZeneca, Novartis, Novo Nordisk, Merck, and CRISPR Therapeutics, and she has received research grants from Amgen, Novartis, Novo Nordisk, and Eggland’s Best. Dr. Campbell had no disclosures. Dr. Granger has received personal fees and research funding from numerous companies.
NEW ORLEANS – Twenty cardiology clinics successfully intensified the medical care they gave patients with type 2 diabetes (T2D) and atherosclerotic cardiovascular disease (ASCVD) after receiving a simple and scalable investigational intervention that gave the clinics’ staffs guidance on best prescribing practices and implementation and also provided quality-improvement feedback.
Within a year, these clinics quadrupled optimal medical management of these patients, compared with control clinics, in a randomized trial involving a total of 43 clinics and 1,049 patients.
“This multifaceted intervention is effective in increasing the prescription of evidence-based therapies in adults with T2D and ASCVD,” Neha J. Pagidipati, MD, said at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
“The next step is to scale this intervention across cardiology practices” interested in improving the quality of care they deliver to these patients, added Dr. Pagidipati, a cardiologist specializing in cardiometabolic disease prevention at Duke University in Durham, N.C.
The goal is getting patients on triple therapy
The primary outcome of the COORDINATE-Diabetes trial was the change in the number of patients with T2D and ASCVD who received prescriptions for agents from three recommended medication classes and at recommended dosages: a high-intensity statin, a renin-angiotensin system inhibitor (RASi), and at least one agent from either of two classes that have both cardiovascular-protective and antihyperglycemic effects: the sodium-glucose cotransporter 2 (SGLT2) inhibitors, or the glucagonlike peptide 1 (GLP-1)–receptor agonists.
Among the 457 patients treated at the 20 cardiology clinics who received the quality-improvement intervention, 37.9% were on the promoted triple therapy after 12 months, compared with 14.5% of the 588 patients treated at the 23 clinics that continued with their usual care approach. This 23.4–percentage point increase in triple-class prescribing at recommended dosages represented a significant 4.4-fold increase in the goal prescribing endpoint after adjustment for possible confounders, Dr. Pagidipati reported.
Simultaneously with her report, the findings also appeared online in JAMA.
At baseline, 41%-50% of the patients were on both a high-intensity statin and a RASi, with a total of about 58%-67% on a high-intensity statin and about 70%-75% on a RASi. Fewer than 1% of patients were on SGLT2 inhibitors or GLP-1–receptor agonists at baseline. By design, no patient could be on all three categories of medication at baseline.
At their last follow-up visit (after 12 months for 97% of patients, or after 6 months for the remainder) 71% of the patients at practices that received the intervention were on a high-intensity statin, 81% were taking a RASi, and 60% were on an SGLT2 inhibitor or GLP-1–receptor agonist. Among the control patients, 58% were on a high-intensity statin, 68% on a RASi, and 36% were on one of the antihyperglycemic agents.
Effective interventions and the need for a champion
The clinics randomized to the active arm received instruction from a three-member team, either from an in-person or virtual one-time visit, on an intervention comprising several initiatives:
- Analysis of the barriers to evidence-based care at each clinic.
- Development of local interdisciplinary care pathways to address the identified barriers.
- Facilitation of care coordination among clinicians – particularly among cardiology, endocrinology, and primary care clinicians.
- Education of the clinic staff, including provision of educational materials.
- Auditing of clinic performance using specified metrics and feedback on the findings.
Clinics in the usual care group were given current clinical practice guidelines.
The investigational intervention was, by design, “low-tech and designed to be scalable,” explained Dr. Pagidipati, and once the COVID pandemic started the intervention team shifted to a virtual consultation with participating practices that was mostly front-loaded, followed by monthly phone calls to give clinics feedback on their progress.
Among the most helpful aspects of the intervention was involving the entire clinic staff, including pharmacists, nurses, and advanced care practitioners; boosting familiarity with the relevant medications and their appropriate use; and advice on navigating insurance-coverage barriers such as prior authorizations.
“What was most critical was having a local champion who took on making this effort an important part” of what the clinic was trying to do, she explained. “All it takes is passion, and the tenacity of a bulldog,” Dr. Pagidipati said.
Research advances often don’t translate into management changes
“We don’t do a great job of translating findings from trials to patient care, so any method we can use to improve that will improve practice,” commented Kristen B. Campbell, PharmD, a clinical pharmacist at Duke who was not involved in the study.
“Although the trial was not powered to look at patient outcomes, we think that patients will benefit” because all the recommended medication uses have been proven to help patients in prior trials, Dr. Campbell noted.
“A particular strength of this study was its simple design. All the interventions are low-tech and scalable.”
The low level of use of guideline-directed medical therapy in American adults with type 2 diabetes and atherosclerotic cardiovascular disease is “incredible,” said Christopher B. Granger, MD, a senior investigator on the study and a cardiologist and professor at Duke.
The researchers who ran the study are now focused on evaluating which cardiology clinics and patients had the most success from the intervention and are using that information to further refine implementation. They are also planning to encourage cardiology practices as well as other relevant medical groups to incorporate the intervention and implementation model used in the trial. The intervention program is detailed and available at no charge on the COORDINATE-Diabetes website.
COORDINATE-Diabetes received funding from Boehringer Ingelheim and Eli Lilly. Dr. Pagidipati has received personal fees from Boehringer Ingelheim, Lilly, AstraZeneca, Novartis, Novo Nordisk, Merck, and CRISPR Therapeutics, and she has received research grants from Amgen, Novartis, Novo Nordisk, and Eggland’s Best. Dr. Campbell had no disclosures. Dr. Granger has received personal fees and research funding from numerous companies.
AT ACC 2023
Biomarkers linked to elevated T2D MACE risk in DECLARE-TIMI 58

The researchers found that N-terminal pro-B-type natriuretic peptide (NT-proBNP) and high-sensitivity cardiac troponin T (hsTnT) levels helped identify a subset of T2D patients at higher risk of major adverse cardiovascular events who would benefit most from dapagliflozin.
“We’ve shown previously that these two biomarkers are very robust risk indicators for cardiovascular death and heart failure events,” senior study author David A. Morrow, MD, of Harvard University, Boston, said in an interview. “In this study, we now show that the two biomarkers also yield important prognostic information for MACE [major adverse cardiovascular events].”
Although NT-proBNP is typically measured to diagnose heart failure, and hsTnT to diagnose acute MI, Dr. Morrow pointed out that this analysis demonstrated the potential for using the two tests to evaluate risks in T2D patients.
Study results
The secondary analysis included 14,565 patients in the DECLARE-TIMI 58 trial. The patients had T2D and multiple risk factors for atherosclerotic cardiovascular disease (about 60%) or established ASCVD (about 40%). All patients had available blood samples and the data were collected from May 2013 to September 2018. The primary outcome was MACE, a composite of MI, ischemic stroke, and cardiovascular death. The results were reported online in JAMA Cardiology.
The analysis found that higher baseline concentrations of NT-proBNP increased MACE risks by 62% (95% confidence interval, 1.49-1.76) and hsTnT elevated those risks by 59% (95% CI, 1.46-1.74).
Among placebo patients, when divided into risk quartiles, those in the highest quartile had significantly higher risk with both elevated NT-proBNP and hsTnT, compared with those with low concentrations. For example, patients with established ASCVD had a 22.9% risk vs. 9.5% with elevated NT-proBNP (P < .001) and a 24.2% vs. 7.2% risk with elevated hsTnT (P < .001). The gap was similar for patients with multiple risk factors.
Dr. Morrow noted that the main DECLARE-TIMI 58 trial showed that dapagliflozin reduced the rates of cardiovascular death or hospitalization for heart failure in patients with T2D, when compared to placebo, but didn’t reach statistical significance for MACE (N Engl J Med. 2019;380:347-57).
“We have previously shown that among patients with T2D who have high risk indicators, such as prior MI or long-standing diabetes, dapagliflozin also appeared to reduce MACE,” Dr. Morrow said. “In this study, we find that these two widely available biomarkers also identify a high-risk group who may have even more potential benefits from treatment with an SGLT2i.”
Dr. Morrow noted that the study design – a nested prospective biomarker study within a randomized, double-blind, placebo-controlled clinical trial – “is a particular strength.”
Results clarify which patients will benefit
This secondary analysis of DECLARE-TIMI 58 brings more clarity to the types of T2D patients who will get the most cardiovascular benefits from dapagliflozin, said Matthew J. Budoff, MD, professor of medicine at University of California, Los Angeles, and Endowed Chair of Preventive Cardiology at the Lundquist Institute in Torrance, Calif.

“The big picture is, we’ve known for some time from epidemiologic studies that these biomarkers, when they’re elevated, mean that the patient is at higher risk of having a cardiovascular event,” he said, “but I think what it helps us with is in knowing in whom to use dapagliflozin for prevention of ASCVD. The effect in the DECLARE-TIMI 58 trial was quite modest, but if you can subgroup it, in these high-risk people there’s a more profound effect. It helps in risk stratification because the absolute benefit is larger.”
The specific biomarkers, NT-proBNP and hsTnT, “haven’t been explored very much in clinical trials,” Dr. Budoff said, “so I do think that it’s nice that in a randomized trial it plays out the way we might expect.”
He added that “for many clinicians this is novel, because I don’t think they were aware of the biomarker data, so I think that this does add some clinical benefit in that context.” The findings also strengthen the case to get T2D patients with higher ASCVD risk onto SGLT2 inhibitors if they’re not already, he said.
Dr. Morrow disclosed relationships with AstraZeneca, Roche Diagnostics, Abbott Laboratories, Anthos Therapeutics, ARCA Biopharma, Merck, Novartis, Pfizer, Regeneron, Siemens, and InCarda outside the reported work.
Dr. Budoff has no relevant disclosures.
The researchers found that N-terminal pro-B-type natriuretic peptide (NT-proBNP) and high-sensitivity cardiac troponin T (hsTnT) levels helped identify a subset of T2D patients at higher risk of major adverse cardiovascular events who would benefit most from dapagliflozin.
“We’ve shown previously that these two biomarkers are very robust risk indicators for cardiovascular death and heart failure events,” senior study author David A. Morrow, MD, of Harvard University, Boston, said in an interview. “In this study, we now show that the two biomarkers also yield important prognostic information for MACE [major adverse cardiovascular events].”
Although NT-proBNP is typically measured to diagnose heart failure, and hsTnT to diagnose acute MI, Dr. Morrow pointed out that this analysis demonstrated the potential for using the two tests to evaluate risks in T2D patients.
Study results
The secondary analysis included 14,565 patients in the DECLARE-TIMI 58 trial. The patients had T2D and multiple risk factors for atherosclerotic cardiovascular disease (about 60%) or established ASCVD (about 40%). All patients had available blood samples and the data were collected from May 2013 to September 2018. The primary outcome was MACE, a composite of MI, ischemic stroke, and cardiovascular death. The results were reported online in JAMA Cardiology.
The analysis found that higher baseline concentrations of NT-proBNP increased MACE risks by 62% (95% confidence interval, 1.49-1.76) and hsTnT elevated those risks by 59% (95% CI, 1.46-1.74).
Among placebo patients, when divided into risk quartiles, those in the highest quartile had significantly higher risk with both elevated NT-proBNP and hsTnT, compared with those with low concentrations. For example, patients with established ASCVD had a 22.9% risk vs. 9.5% with elevated NT-proBNP (P < .001) and a 24.2% vs. 7.2% risk with elevated hsTnT (P < .001). The gap was similar for patients with multiple risk factors.
Dr. Morrow noted that the main DECLARE-TIMI 58 trial showed that dapagliflozin reduced the rates of cardiovascular death or hospitalization for heart failure in patients with T2D, when compared to placebo, but didn’t reach statistical significance for MACE (N Engl J Med. 2019;380:347-57).
“We have previously shown that among patients with T2D who have high risk indicators, such as prior MI or long-standing diabetes, dapagliflozin also appeared to reduce MACE,” Dr. Morrow said. “In this study, we find that these two widely available biomarkers also identify a high-risk group who may have even more potential benefits from treatment with an SGLT2i.”
Dr. Morrow noted that the study design – a nested prospective biomarker study within a randomized, double-blind, placebo-controlled clinical trial – “is a particular strength.”
Results clarify which patients will benefit
This secondary analysis of DECLARE-TIMI 58 brings more clarity to the types of T2D patients who will get the most cardiovascular benefits from dapagliflozin, said Matthew J. Budoff, MD, professor of medicine at University of California, Los Angeles, and Endowed Chair of Preventive Cardiology at the Lundquist Institute in Torrance, Calif.
“The big picture is, we’ve known for some time from epidemiologic studies that these biomarkers, when they’re elevated, mean that the patient is at higher risk of having a cardiovascular event,” he said, “but I think what it helps us with is in knowing in whom to use dapagliflozin for prevention of ASCVD. The effect in the DECLARE-TIMI 58 trial was quite modest, but if you can subgroup it, in these high-risk people there’s a more profound effect. It helps in risk stratification because the absolute benefit is larger.”
The specific biomarkers, NT-proBNP and hsTnT, “haven’t been explored very much in clinical trials,” Dr. Budoff said, “so I do think that it’s nice that in a randomized trial it plays out the way we might expect.”
He added that “for many clinicians this is novel, because I don’t think they were aware of the biomarker data, so I think that this does add some clinical benefit in that context.” The findings also strengthen the case to get T2D patients with higher ASCVD risk onto SGLT2 inhibitors if they’re not already, he said.
Dr. Morrow disclosed relationships with AstraZeneca, Roche Diagnostics, Abbott Laboratories, Anthos Therapeutics, ARCA Biopharma, Merck, Novartis, Pfizer, Regeneron, Siemens, and InCarda outside the reported work.
Dr. Budoff has no relevant disclosures.
The researchers found that N-terminal pro-B-type natriuretic peptide (NT-proBNP) and high-sensitivity cardiac troponin T (hsTnT) levels helped identify a subset of T2D patients at higher risk of major adverse cardiovascular events who would benefit most from dapagliflozin.
“We’ve shown previously that these two biomarkers are very robust risk indicators for cardiovascular death and heart failure events,” senior study author David A. Morrow, MD, of Harvard University, Boston, said in an interview. “In this study, we now show that the two biomarkers also yield important prognostic information for MACE [major adverse cardiovascular events].”
Although NT-proBNP is typically measured to diagnose heart failure, and hsTnT to diagnose acute MI, Dr. Morrow pointed out that this analysis demonstrated the potential for using the two tests to evaluate risks in T2D patients.
Study results
The secondary analysis included 14,565 patients in the DECLARE-TIMI 58 trial. The patients had T2D and multiple risk factors for atherosclerotic cardiovascular disease (about 60%) or established ASCVD (about 40%). All patients had available blood samples and the data were collected from May 2013 to September 2018. The primary outcome was MACE, a composite of MI, ischemic stroke, and cardiovascular death. The results were reported online in JAMA Cardiology.
The analysis found that higher baseline concentrations of NT-proBNP increased MACE risks by 62% (95% confidence interval, 1.49-1.76) and hsTnT elevated those risks by 59% (95% CI, 1.46-1.74).
Among placebo patients, when divided into risk quartiles, those in the highest quartile had significantly higher risk with both elevated NT-proBNP and hsTnT, compared with those with low concentrations. For example, patients with established ASCVD had a 22.9% risk vs. 9.5% with elevated NT-proBNP (P < .001) and a 24.2% vs. 7.2% risk with elevated hsTnT (P < .001). The gap was similar for patients with multiple risk factors.
Dr. Morrow noted that the main DECLARE-TIMI 58 trial showed that dapagliflozin reduced the rates of cardiovascular death or hospitalization for heart failure in patients with T2D, when compared to placebo, but didn’t reach statistical significance for MACE (N Engl J Med. 2019;380:347-57).
“We have previously shown that among patients with T2D who have high risk indicators, such as prior MI or long-standing diabetes, dapagliflozin also appeared to reduce MACE,” Dr. Morrow said. “In this study, we find that these two widely available biomarkers also identify a high-risk group who may have even more potential benefits from treatment with an SGLT2i.”
Dr. Morrow noted that the study design – a nested prospective biomarker study within a randomized, double-blind, placebo-controlled clinical trial – “is a particular strength.”
Results clarify which patients will benefit
This secondary analysis of DECLARE-TIMI 58 brings more clarity to the types of T2D patients who will get the most cardiovascular benefits from dapagliflozin, said Matthew J. Budoff, MD, professor of medicine at University of California, Los Angeles, and Endowed Chair of Preventive Cardiology at the Lundquist Institute in Torrance, Calif.
“The big picture is, we’ve known for some time from epidemiologic studies that these biomarkers, when they’re elevated, mean that the patient is at higher risk of having a cardiovascular event,” he said, “but I think what it helps us with is in knowing in whom to use dapagliflozin for prevention of ASCVD. The effect in the DECLARE-TIMI 58 trial was quite modest, but if you can subgroup it, in these high-risk people there’s a more profound effect. It helps in risk stratification because the absolute benefit is larger.”
The specific biomarkers, NT-proBNP and hsTnT, “haven’t been explored very much in clinical trials,” Dr. Budoff said, “so I do think that it’s nice that in a randomized trial it plays out the way we might expect.”
He added that “for many clinicians this is novel, because I don’t think they were aware of the biomarker data, so I think that this does add some clinical benefit in that context.” The findings also strengthen the case to get T2D patients with higher ASCVD risk onto SGLT2 inhibitors if they’re not already, he said.
Dr. Morrow disclosed relationships with AstraZeneca, Roche Diagnostics, Abbott Laboratories, Anthos Therapeutics, ARCA Biopharma, Merck, Novartis, Pfizer, Regeneron, Siemens, and InCarda outside the reported work.
Dr. Budoff has no relevant disclosures.
FROM JAMA CARDIOLOGY
Can skin care aid use of diabetes devices?
Technologies that allow people to monitor blood sugar and automate the administration of insulin have radically transformed the lives of patients – and children in particular – with type 1 diabetes. But the devices often come with a cost: Insulin pumps and continuous glucose monitors can irritate the skin at the points of contact, causing some people to stop using their pumps or monitors altogether.
Regular use of lipid-rich skin creams can reduce eczema in children who use insulin pumps and continuous glucose monitors to manage type 1 diabetes, Danish researchers reported last month. The article is currently undergoing peer review at The Lancet Diabetes and Endocrinology, and the authors said they hope their approach will deter more children from abandoning diabetes technology.
“A simple thing can actually change a lot,” said Anna Korsgaard Berg, MD, a pediatrician who specializes in diabetes care at Copenhagen University Hospital’s Steno Diabetes Center in Herlev, Denmark, and a coauthor of the new study. “Not all skin reactions can be solved by the skin care program, but it can help improve the issue.”
More than 1.5 million children and adolescents worldwide live with type 1 diabetes, a condition that requires continuous insulin infusion. Insulin pumps meet this need in many wealthier countries, and are often used in combination with sensors that measure a child’s glucose level. Both the American Diabetes Association and the International Society for Adolescent and Pediatric Diabetes recommend insulin pumps and continuous glucose monitors as core treatment tools.
Dr. Berg and colleagues, who have previously shown that as many as 90% of children who use these devices experience some kind of skin reaction, want to minimize the rate of such discomfort in hopes that fewer children stop using the devices. According to a 2014 study, 18% of people with type 1 diabetes who stopped using continuous glucose monitors did so because of skin irritation.
Lather on that lipid-rich lotion
Dr. Berg and colleagues studied 170 children and adolescents with type 1 diabetes (average age, 11 years) who use insulin pumps, continuous glucose monitors, or both. From March 2020 to July 2021, 112 children (55 girls) employed a skin care program developed for the study, while the other 58 (34 girls) did not receive any skin care advice.
The skin care group received instructions about how to gently insert and remove their insulin pumps or glucose monitors, to minimize skin damage. They also were told to avoid disinfectants such as alcohol, which can irritate skin. The children in this group used a cream containing 70% lipids to help rehydrate their skin, applying the salve each day a device was not inserted into their skin.
Eczema can be a real problem for kids who use insulin pumps and continuous glucose monitors to manage type 1 diabetes. Researchers found that regular use of lipid-rich skin creams can reduce its incidence.
Although insulin pumps and glucose monitors are kept in place for longer periods of time than they once were, Dr. Berg and colleagues noted, users do periodically remove them when bathing or when undergoing medical tests that involve x-rays. On days when the devices were not in place for a period of time, children in the skin care group were encouraged to follow the protocol.
Study results
One-third of children in the skin care group developed eczema or experienced a wound, compared with almost half of the children in the control group, according to the researchers. The absolute difference in developing eczema or wounds between the two groups was 12.9 % (95% confidence interval, –28.7% to 2.9%).
Children in the skin care group were much less likely to develop wounds, the researchers found, when they focused only on wounds and not eczema (odds ratio, 0.29, 95% CI, 0.12-0.68).
Dr. Berg said she would like to explore whether other techniques, such as a combination of patches, adhesives, or other lotions, yield even better results.
“Anything that can help people use technology more consistently is better for both quality of life and diabetes outcomes,” said Priya Prahalad, MD, a specialist in pediatric endocrinology and diabetes at Stanford Medicine Children’s Health in Palo Alto and Sunnyvale, Calif.
Dr. Prahalad, who was not involved in the Danish study, said that although the sample sizes in the trial were relatively small, the data are “headed in the right direction.”
Pediatricians already recommend using moisturizing creams at the sites where pumps or glucose monitors are inserted into the skin, she noted. But the new study simply employed an especially moisturizing cream to mitigate skin damage.
Although one reason for skin irritation may be the repeated insertion and removal of devices, Dr. Berg and Dr. Prahalad stressed that the medical devices themselves may contain allergy-causing components. Device makers are not required to disclose what’s inside the boxes.
“I do not understand why the full content of a device is not by law mandatory to declare, when declaration by law is mandatory for many other products and drugs but not for medical devices,” Dr. Berg said.
Dr. Berg reports receiving lipid cream from Teva Pharmaceuticals and research support from Medtronic. Dr. Prahalad reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Technologies that allow people to monitor blood sugar and automate the administration of insulin have radically transformed the lives of patients – and children in particular – with type 1 diabetes. But the devices often come with a cost: Insulin pumps and continuous glucose monitors can irritate the skin at the points of contact, causing some people to stop using their pumps or monitors altogether.
Regular use of lipid-rich skin creams can reduce eczema in children who use insulin pumps and continuous glucose monitors to manage type 1 diabetes, Danish researchers reported last month. The article is currently undergoing peer review at The Lancet Diabetes and Endocrinology, and the authors said they hope their approach will deter more children from abandoning diabetes technology.
“A simple thing can actually change a lot,” said Anna Korsgaard Berg, MD, a pediatrician who specializes in diabetes care at Copenhagen University Hospital’s Steno Diabetes Center in Herlev, Denmark, and a coauthor of the new study. “Not all skin reactions can be solved by the skin care program, but it can help improve the issue.”
More than 1.5 million children and adolescents worldwide live with type 1 diabetes, a condition that requires continuous insulin infusion. Insulin pumps meet this need in many wealthier countries, and are often used in combination with sensors that measure a child’s glucose level. Both the American Diabetes Association and the International Society for Adolescent and Pediatric Diabetes recommend insulin pumps and continuous glucose monitors as core treatment tools.
Dr. Berg and colleagues, who have previously shown that as many as 90% of children who use these devices experience some kind of skin reaction, want to minimize the rate of such discomfort in hopes that fewer children stop using the devices. According to a 2014 study, 18% of people with type 1 diabetes who stopped using continuous glucose monitors did so because of skin irritation.
Lather on that lipid-rich lotion
Dr. Berg and colleagues studied 170 children and adolescents with type 1 diabetes (average age, 11 years) who use insulin pumps, continuous glucose monitors, or both. From March 2020 to July 2021, 112 children (55 girls) employed a skin care program developed for the study, while the other 58 (34 girls) did not receive any skin care advice.
The skin care group received instructions about how to gently insert and remove their insulin pumps or glucose monitors, to minimize skin damage. They also were told to avoid disinfectants such as alcohol, which can irritate skin. The children in this group used a cream containing 70% lipids to help rehydrate their skin, applying the salve each day a device was not inserted into their skin.
Eczema can be a real problem for kids who use insulin pumps and continuous glucose monitors to manage type 1 diabetes. Researchers found that regular use of lipid-rich skin creams can reduce its incidence.
Although insulin pumps and glucose monitors are kept in place for longer periods of time than they once were, Dr. Berg and colleagues noted, users do periodically remove them when bathing or when undergoing medical tests that involve x-rays. On days when the devices were not in place for a period of time, children in the skin care group were encouraged to follow the protocol.
Study results
One-third of children in the skin care group developed eczema or experienced a wound, compared with almost half of the children in the control group, according to the researchers. The absolute difference in developing eczema or wounds between the two groups was 12.9 % (95% confidence interval, –28.7% to 2.9%).
Children in the skin care group were much less likely to develop wounds, the researchers found, when they focused only on wounds and not eczema (odds ratio, 0.29, 95% CI, 0.12-0.68).
Dr. Berg said she would like to explore whether other techniques, such as a combination of patches, adhesives, or other lotions, yield even better results.
“Anything that can help people use technology more consistently is better for both quality of life and diabetes outcomes,” said Priya Prahalad, MD, a specialist in pediatric endocrinology and diabetes at Stanford Medicine Children’s Health in Palo Alto and Sunnyvale, Calif.
Dr. Prahalad, who was not involved in the Danish study, said that although the sample sizes in the trial were relatively small, the data are “headed in the right direction.”
Pediatricians already recommend using moisturizing creams at the sites where pumps or glucose monitors are inserted into the skin, she noted. But the new study simply employed an especially moisturizing cream to mitigate skin damage.
Although one reason for skin irritation may be the repeated insertion and removal of devices, Dr. Berg and Dr. Prahalad stressed that the medical devices themselves may contain allergy-causing components. Device makers are not required to disclose what’s inside the boxes.
“I do not understand why the full content of a device is not by law mandatory to declare, when declaration by law is mandatory for many other products and drugs but not for medical devices,” Dr. Berg said.
Dr. Berg reports receiving lipid cream from Teva Pharmaceuticals and research support from Medtronic. Dr. Prahalad reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Technologies that allow people to monitor blood sugar and automate the administration of insulin have radically transformed the lives of patients – and children in particular – with type 1 diabetes. But the devices often come with a cost: Insulin pumps and continuous glucose monitors can irritate the skin at the points of contact, causing some people to stop using their pumps or monitors altogether.
Regular use of lipid-rich skin creams can reduce eczema in children who use insulin pumps and continuous glucose monitors to manage type 1 diabetes, Danish researchers reported last month. The article is currently undergoing peer review at The Lancet Diabetes and Endocrinology, and the authors said they hope their approach will deter more children from abandoning diabetes technology.
“A simple thing can actually change a lot,” said Anna Korsgaard Berg, MD, a pediatrician who specializes in diabetes care at Copenhagen University Hospital’s Steno Diabetes Center in Herlev, Denmark, and a coauthor of the new study. “Not all skin reactions can be solved by the skin care program, but it can help improve the issue.”
More than 1.5 million children and adolescents worldwide live with type 1 diabetes, a condition that requires continuous insulin infusion. Insulin pumps meet this need in many wealthier countries, and are often used in combination with sensors that measure a child’s glucose level. Both the American Diabetes Association and the International Society for Adolescent and Pediatric Diabetes recommend insulin pumps and continuous glucose monitors as core treatment tools.
Dr. Berg and colleagues, who have previously shown that as many as 90% of children who use these devices experience some kind of skin reaction, want to minimize the rate of such discomfort in hopes that fewer children stop using the devices. According to a 2014 study, 18% of people with type 1 diabetes who stopped using continuous glucose monitors did so because of skin irritation.
Lather on that lipid-rich lotion
Dr. Berg and colleagues studied 170 children and adolescents with type 1 diabetes (average age, 11 years) who use insulin pumps, continuous glucose monitors, or both. From March 2020 to July 2021, 112 children (55 girls) employed a skin care program developed for the study, while the other 58 (34 girls) did not receive any skin care advice.
The skin care group received instructions about how to gently insert and remove their insulin pumps or glucose monitors, to minimize skin damage. They also were told to avoid disinfectants such as alcohol, which can irritate skin. The children in this group used a cream containing 70% lipids to help rehydrate their skin, applying the salve each day a device was not inserted into their skin.
Eczema can be a real problem for kids who use insulin pumps and continuous glucose monitors to manage type 1 diabetes. Researchers found that regular use of lipid-rich skin creams can reduce its incidence.
Although insulin pumps and glucose monitors are kept in place for longer periods of time than they once were, Dr. Berg and colleagues noted, users do periodically remove them when bathing or when undergoing medical tests that involve x-rays. On days when the devices were not in place for a period of time, children in the skin care group were encouraged to follow the protocol.
Study results
One-third of children in the skin care group developed eczema or experienced a wound, compared with almost half of the children in the control group, according to the researchers. The absolute difference in developing eczema or wounds between the two groups was 12.9 % (95% confidence interval, –28.7% to 2.9%).
Children in the skin care group were much less likely to develop wounds, the researchers found, when they focused only on wounds and not eczema (odds ratio, 0.29, 95% CI, 0.12-0.68).
Dr. Berg said she would like to explore whether other techniques, such as a combination of patches, adhesives, or other lotions, yield even better results.
“Anything that can help people use technology more consistently is better for both quality of life and diabetes outcomes,” said Priya Prahalad, MD, a specialist in pediatric endocrinology and diabetes at Stanford Medicine Children’s Health in Palo Alto and Sunnyvale, Calif.
Dr. Prahalad, who was not involved in the Danish study, said that although the sample sizes in the trial were relatively small, the data are “headed in the right direction.”
Pediatricians already recommend using moisturizing creams at the sites where pumps or glucose monitors are inserted into the skin, she noted. But the new study simply employed an especially moisturizing cream to mitigate skin damage.
Although one reason for skin irritation may be the repeated insertion and removal of devices, Dr. Berg and Dr. Prahalad stressed that the medical devices themselves may contain allergy-causing components. Device makers are not required to disclose what’s inside the boxes.
“I do not understand why the full content of a device is not by law mandatory to declare, when declaration by law is mandatory for many other products and drugs but not for medical devices,” Dr. Berg said.
Dr. Berg reports receiving lipid cream from Teva Pharmaceuticals and research support from Medtronic. Dr. Prahalad reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Lilly cuts insulin price by 70%, caps out-of-pocket cost
Eli Lilly will cut prices for most of its insulins in the United States by 70% and cap out-of-pocket costs for insulin at $35 per month, the company announced on March 1.
“Lilly is taking these actions to make it easier to access Lilly insulin and help Americans who may have difficulty navigating a complex healthcare system that may keep them from getting affordable insulin,” the company said in a statement.
The $35 price cap is effective immediately at participating retail pharmacies for people with commercial insurance. Those without insurance can go to InsulinAffordability.com and download the Lilly Insulin Value Program savings card to receive Lilly insulins for $35 per month.
The company says it will cut the list price of its nonbranded Insulin Lispro Injection 100 units/mL to $25 a vial, effective May 1, 2023. The list price of the branded Humalog (insulin lispro injection) 100 units/mL will be cut by 70%, effective in the fourth quarter of 2023.
Lilly is among the three main companies that manufacture insulin, along with Novo Nordisk and Sanofi, that have come under fire over the cost of insulin in the US. Studies have shown that up to 25% of people with type 1 diabetes ration insulin because of costs, putting their health and often their lives in jeopardy.
Prices in the United States are around 10 times higher than in other countries. California is the latest state to say it plans to sue these big three companies over the high price of insulin and has announced plans to make its own cheaper versions.
Asked at a telephone press briefing if the lawsuit prompted the company’s move, Lilly chair and CEO David A. Ricks said: “Of course there are complaints against the industry and the company. We see those as completely unfounded. However, we can probably all agree that patients should have a consistent and lower-cost experience at the pharmacy counter, and that’s what today’s announcement is about. We’re doing this completely voluntarily because it’s time and it’s the right thing to do.”
On hearing the company announcement, Laura Nally, MD, a pediatric endocrinologist living with type 1 diabetes, @drnallypants, tweeted: “YES. After years of advocacy, the list price of Lispro/Humalog is now similar to what it was in the late 1990s. Cheers to all the #pwd [people with diabetes] who have advocated through #insulin4all! But we still have work to do to improve access to other diabetes medications & supplies.”
#insulin4all is a worldwide campaign to ensure that people with type 1 diabetes have access to affordable insulin and other supplies needed to manage the condition, such as glucose strips. It is supported, among others, by the advocacy group T1International.
Also giving his reaction to the Lilly announcement, Chuck Henderson, CEO of the American Diabetes Association, said: “We applaud Eli Lilly for taking the important step to limit cost-sharing for its insulin, and we encourage other insulin manufacturers to do the same.
“While we have been able to help achieve significant progress on the issue of insulin affordability, including Medicare’s new out-of-pocket cost cap on insulin, state copay caps, and patient assistance developments from insulin manufacturers, we know that our work is not done,” he added.
“ADA will work to ensure that Eli Lilly’s patient assistance program is benefiting patients as intended and continue the fight so that everyone who needs insulin has access.”
And Endocrine Society chief medical officer Robert Lash, MD, said: “Lilly’s move to apply a $35/month cap for people with private insurance will be a significant improvement for adults and children with diabetes who use Lilly’s products.
“We encourage all insulin manufacturers to join in the effort to reduce out-of-pocket costs for people who need insulin.”
Lilly will also launch a new insulin biosimilar, Rezvoglar (insulin glargine-aglr) injection, which is similar to and interchangeable with insulin glargine (Lantus). The cost will by $92 for a five pack of KwikPens, a 78% discount, compared with the cost of Lantus, beginning April 1, 2023.
A version of this article first appeared on Medscape.com.
Eli Lilly will cut prices for most of its insulins in the United States by 70% and cap out-of-pocket costs for insulin at $35 per month, the company announced on March 1.
“Lilly is taking these actions to make it easier to access Lilly insulin and help Americans who may have difficulty navigating a complex healthcare system that may keep them from getting affordable insulin,” the company said in a statement.
The $35 price cap is effective immediately at participating retail pharmacies for people with commercial insurance. Those without insurance can go to InsulinAffordability.com and download the Lilly Insulin Value Program savings card to receive Lilly insulins for $35 per month.
The company says it will cut the list price of its nonbranded Insulin Lispro Injection 100 units/mL to $25 a vial, effective May 1, 2023. The list price of the branded Humalog (insulin lispro injection) 100 units/mL will be cut by 70%, effective in the fourth quarter of 2023.
Lilly is among the three main companies that manufacture insulin, along with Novo Nordisk and Sanofi, that have come under fire over the cost of insulin in the US. Studies have shown that up to 25% of people with type 1 diabetes ration insulin because of costs, putting their health and often their lives in jeopardy.
Prices in the United States are around 10 times higher than in other countries. California is the latest state to say it plans to sue these big three companies over the high price of insulin and has announced plans to make its own cheaper versions.
Asked at a telephone press briefing if the lawsuit prompted the company’s move, Lilly chair and CEO David A. Ricks said: “Of course there are complaints against the industry and the company. We see those as completely unfounded. However, we can probably all agree that patients should have a consistent and lower-cost experience at the pharmacy counter, and that’s what today’s announcement is about. We’re doing this completely voluntarily because it’s time and it’s the right thing to do.”
On hearing the company announcement, Laura Nally, MD, a pediatric endocrinologist living with type 1 diabetes, @drnallypants, tweeted: “YES. After years of advocacy, the list price of Lispro/Humalog is now similar to what it was in the late 1990s. Cheers to all the #pwd [people with diabetes] who have advocated through #insulin4all! But we still have work to do to improve access to other diabetes medications & supplies.”
#insulin4all is a worldwide campaign to ensure that people with type 1 diabetes have access to affordable insulin and other supplies needed to manage the condition, such as glucose strips. It is supported, among others, by the advocacy group T1International.
Also giving his reaction to the Lilly announcement, Chuck Henderson, CEO of the American Diabetes Association, said: “We applaud Eli Lilly for taking the important step to limit cost-sharing for its insulin, and we encourage other insulin manufacturers to do the same.
“While we have been able to help achieve significant progress on the issue of insulin affordability, including Medicare’s new out-of-pocket cost cap on insulin, state copay caps, and patient assistance developments from insulin manufacturers, we know that our work is not done,” he added.
“ADA will work to ensure that Eli Lilly’s patient assistance program is benefiting patients as intended and continue the fight so that everyone who needs insulin has access.”
And Endocrine Society chief medical officer Robert Lash, MD, said: “Lilly’s move to apply a $35/month cap for people with private insurance will be a significant improvement for adults and children with diabetes who use Lilly’s products.
“We encourage all insulin manufacturers to join in the effort to reduce out-of-pocket costs for people who need insulin.”
Lilly will also launch a new insulin biosimilar, Rezvoglar (insulin glargine-aglr) injection, which is similar to and interchangeable with insulin glargine (Lantus). The cost will by $92 for a five pack of KwikPens, a 78% discount, compared with the cost of Lantus, beginning April 1, 2023.
A version of this article first appeared on Medscape.com.
Eli Lilly will cut prices for most of its insulins in the United States by 70% and cap out-of-pocket costs for insulin at $35 per month, the company announced on March 1.
“Lilly is taking these actions to make it easier to access Lilly insulin and help Americans who may have difficulty navigating a complex healthcare system that may keep them from getting affordable insulin,” the company said in a statement.
The $35 price cap is effective immediately at participating retail pharmacies for people with commercial insurance. Those without insurance can go to InsulinAffordability.com and download the Lilly Insulin Value Program savings card to receive Lilly insulins for $35 per month.
The company says it will cut the list price of its nonbranded Insulin Lispro Injection 100 units/mL to $25 a vial, effective May 1, 2023. The list price of the branded Humalog (insulin lispro injection) 100 units/mL will be cut by 70%, effective in the fourth quarter of 2023.
Lilly is among the three main companies that manufacture insulin, along with Novo Nordisk and Sanofi, that have come under fire over the cost of insulin in the US. Studies have shown that up to 25% of people with type 1 diabetes ration insulin because of costs, putting their health and often their lives in jeopardy.
Prices in the United States are around 10 times higher than in other countries. California is the latest state to say it plans to sue these big three companies over the high price of insulin and has announced plans to make its own cheaper versions.
Asked at a telephone press briefing if the lawsuit prompted the company’s move, Lilly chair and CEO David A. Ricks said: “Of course there are complaints against the industry and the company. We see those as completely unfounded. However, we can probably all agree that patients should have a consistent and lower-cost experience at the pharmacy counter, and that’s what today’s announcement is about. We’re doing this completely voluntarily because it’s time and it’s the right thing to do.”
On hearing the company announcement, Laura Nally, MD, a pediatric endocrinologist living with type 1 diabetes, @drnallypants, tweeted: “YES. After years of advocacy, the list price of Lispro/Humalog is now similar to what it was in the late 1990s. Cheers to all the #pwd [people with diabetes] who have advocated through #insulin4all! But we still have work to do to improve access to other diabetes medications & supplies.”
#insulin4all is a worldwide campaign to ensure that people with type 1 diabetes have access to affordable insulin and other supplies needed to manage the condition, such as glucose strips. It is supported, among others, by the advocacy group T1International.
Also giving his reaction to the Lilly announcement, Chuck Henderson, CEO of the American Diabetes Association, said: “We applaud Eli Lilly for taking the important step to limit cost-sharing for its insulin, and we encourage other insulin manufacturers to do the same.
“While we have been able to help achieve significant progress on the issue of insulin affordability, including Medicare’s new out-of-pocket cost cap on insulin, state copay caps, and patient assistance developments from insulin manufacturers, we know that our work is not done,” he added.
“ADA will work to ensure that Eli Lilly’s patient assistance program is benefiting patients as intended and continue the fight so that everyone who needs insulin has access.”
And Endocrine Society chief medical officer Robert Lash, MD, said: “Lilly’s move to apply a $35/month cap for people with private insurance will be a significant improvement for adults and children with diabetes who use Lilly’s products.
“We encourage all insulin manufacturers to join in the effort to reduce out-of-pocket costs for people who need insulin.”
Lilly will also launch a new insulin biosimilar, Rezvoglar (insulin glargine-aglr) injection, which is similar to and interchangeable with insulin glargine (Lantus). The cost will by $92 for a five pack of KwikPens, a 78% discount, compared with the cost of Lantus, beginning April 1, 2023.
A version of this article first appeared on Medscape.com.
Old drug verapamil may have new use in type 1 diabetes
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
Insomnia, short sleep linked to greater risk for MI
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.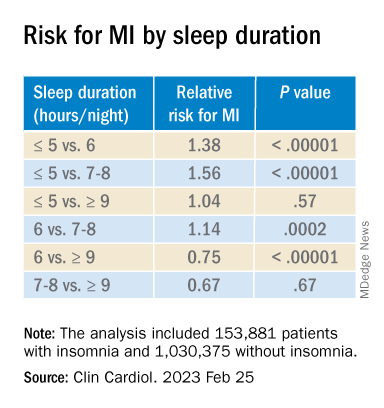
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACC 2023