User login
Dapagliflozin reduces hospitalizations in patients with CKD
These findings add to a growing body of evidence supporting a range of positive benefits from dapagliflozin, including reduced risks of mortality, cardiovascular events, and kidney events, lead author Meir Schechter, MD, PhD, of the Hebrew University of Jerusalem and colleagues wrote in Annals of Internal Medicine.“Although cardiovascular and kidney outcomes with SGLT2 inhibitors have been studied extensively, there is a paucity of data evaluating the effects of SGLT2 inhibitors on hospitalizations for any cause.”
The findings are based on a post hoc analysis of the DAPA-CKD trial, which involved 4,304 patients with CKD in 21 countries. Patients were randomized in a 1:1 ratio to receive dapagliflozin 10 mg orally once a day or matching placebo. The present analysis quantified first hospitalizations for any cause, all hospitalizations, cause-specific hospitalizations, and several related outcomes.
After a median follow-up of 2.4 years, 28% of the population had been hospitalized a total of 2,072 times.
Compared with placebo, dapagliflozin significantly reduced risk of first hospitalization by 16% (hazard ratio, 0.84; 95% confidence interval, 0.75-0.94) and rate of all hospitalizations by 21% (rate ratio, 0.79; 95% CI, 0.70-0.89). These findings remained significant regardless of type 2 diabetes status, with significant benefits seen across reasons for admission, including renal/urinary disorders, cardiac disorders, neoplasms, and metabolism/nutrition disorders. In addition, dapagliflozin was associated with shorter mean time in hospital (2.3 vs. 2.8 days; P = .027) and longer time alive and out of hospital (354.9 vs. 351.7; P = .023).
“These findings highlight additional benefits of dapagliflozin beyond those seen for cardiovascular and kidney events, all-cause and cause-specific mortality, eGFR [estimated glomerular filtration rate] slope, and albuminuria and should be considered when evaluating the totality of evidence favoring provision of dapagliflozin to patients with CKD,” the investigators concluded.
Positive data, positive experiences
Shree Mulay, MD, a nephrologist in private practice in western Tennessee, said this study is “one of several other articles that already exist” demonstrating the broad benefits of SGLT2 inhibitors.
“The evidence is pretty substantial,” Dr. Mulay said in an interview. “I think SGLT2 inhibitors are the new statin of this era. ... I won’t be surprised if in the next year or 2 or 3 they truly become the standard of care.”
Dr. Mulay also speaks from experience working in both the chronic and acute setting, where he’s observed “some magical stuff happening” in patients started on SGLT2 inhibitors, especially those in heart failure who are fluid overloaded.
“It’s phenomenal stuff,” Dr. Mulay said. “You can really stabilize patients’ hemodynamics.”
In the private health care setting, he described widespread enthusiasm among nephrologists, although others still appear skeptical.
“It’s really our cardiology colleagues that I feel are underprescribing it,” Dr. Mulay said. “So, I’m kind of taking it on myself, when I see a heart failure patient, to go ahead and put them on this.”
It’s unclear why some cardiologists seem apprehensive, Dr. Mulay continued, although he suggested that unclear guidelines and a lack of first-hand experience may be to blame.
Nephrologists and cardiologists sometimes agree
In the academic arena, Leslie Gewin, MD, associate professor at Washington University in St. Louis and the John Cochran VA Hospital, also in St. Louis, has seen similar support for SGLT2 inhibitors among both nephrologists and cardiologists.
“We had a joint nephrology-cardiology medicine grand rounds at Wash U in St. Louis maybe 2 weeks ago,” Dr. Gewin said in an interview. “The cardiologists and nephrologists tag-teamed to present data about SGLT2 inhibitors, and we kind of joked that this was the one thing we both could get behind and support.”
Still, she has seen some reluctance among non-nephrology clinicians lacking SGLT2 experience, specifically when managing patients who have poor kidney function.
“There can be some hesitancy among physicians if the GFR is low,” Dr. Gewin said. “That’s where I’ve had to sort of push the envelope with non-nephrologists, saying: ‘Look, we feel pretty comfortable starting down to a GFR of about 20.’ ”
Early rises in creatinine may also spook providers, she noted.
“Sometimes, when we start SGLT2 inhibitors, the creatinine increases slightly, and the [primary care provider] gets concerned,” Dr. Gewin said. “We say: ‘No, this is expected. Don’t worry, hold the course, this is a good drug.’ ”
Like Dr. Mulay, Dr. Gewin said the present study offers further encouragement for the efficacy of this drug class. She also said sufficient data have been published to allay earlier concerns about potential safety signals, such as bone fractures and amputations.
“SGLT2 inhibitors seem to be a lot safer than what we initially had thought,” Dr. Gewin said. “That’s very encouraging.”
The study was funded by AstraZeneca. The investigators disclosed additional relationships with Bayer, Janssen, Gilead, and others. Dr. Gewin and Dr. Mulay disclosed no relevant conflicts of interest.
These findings add to a growing body of evidence supporting a range of positive benefits from dapagliflozin, including reduced risks of mortality, cardiovascular events, and kidney events, lead author Meir Schechter, MD, PhD, of the Hebrew University of Jerusalem and colleagues wrote in Annals of Internal Medicine.“Although cardiovascular and kidney outcomes with SGLT2 inhibitors have been studied extensively, there is a paucity of data evaluating the effects of SGLT2 inhibitors on hospitalizations for any cause.”
The findings are based on a post hoc analysis of the DAPA-CKD trial, which involved 4,304 patients with CKD in 21 countries. Patients were randomized in a 1:1 ratio to receive dapagliflozin 10 mg orally once a day or matching placebo. The present analysis quantified first hospitalizations for any cause, all hospitalizations, cause-specific hospitalizations, and several related outcomes.
After a median follow-up of 2.4 years, 28% of the population had been hospitalized a total of 2,072 times.
Compared with placebo, dapagliflozin significantly reduced risk of first hospitalization by 16% (hazard ratio, 0.84; 95% confidence interval, 0.75-0.94) and rate of all hospitalizations by 21% (rate ratio, 0.79; 95% CI, 0.70-0.89). These findings remained significant regardless of type 2 diabetes status, with significant benefits seen across reasons for admission, including renal/urinary disorders, cardiac disorders, neoplasms, and metabolism/nutrition disorders. In addition, dapagliflozin was associated with shorter mean time in hospital (2.3 vs. 2.8 days; P = .027) and longer time alive and out of hospital (354.9 vs. 351.7; P = .023).
“These findings highlight additional benefits of dapagliflozin beyond those seen for cardiovascular and kidney events, all-cause and cause-specific mortality, eGFR [estimated glomerular filtration rate] slope, and albuminuria and should be considered when evaluating the totality of evidence favoring provision of dapagliflozin to patients with CKD,” the investigators concluded.
Positive data, positive experiences
Shree Mulay, MD, a nephrologist in private practice in western Tennessee, said this study is “one of several other articles that already exist” demonstrating the broad benefits of SGLT2 inhibitors.
“The evidence is pretty substantial,” Dr. Mulay said in an interview. “I think SGLT2 inhibitors are the new statin of this era. ... I won’t be surprised if in the next year or 2 or 3 they truly become the standard of care.”
Dr. Mulay also speaks from experience working in both the chronic and acute setting, where he’s observed “some magical stuff happening” in patients started on SGLT2 inhibitors, especially those in heart failure who are fluid overloaded.
“It’s phenomenal stuff,” Dr. Mulay said. “You can really stabilize patients’ hemodynamics.”
In the private health care setting, he described widespread enthusiasm among nephrologists, although others still appear skeptical.
“It’s really our cardiology colleagues that I feel are underprescribing it,” Dr. Mulay said. “So, I’m kind of taking it on myself, when I see a heart failure patient, to go ahead and put them on this.”
It’s unclear why some cardiologists seem apprehensive, Dr. Mulay continued, although he suggested that unclear guidelines and a lack of first-hand experience may be to blame.
Nephrologists and cardiologists sometimes agree
In the academic arena, Leslie Gewin, MD, associate professor at Washington University in St. Louis and the John Cochran VA Hospital, also in St. Louis, has seen similar support for SGLT2 inhibitors among both nephrologists and cardiologists.
“We had a joint nephrology-cardiology medicine grand rounds at Wash U in St. Louis maybe 2 weeks ago,” Dr. Gewin said in an interview. “The cardiologists and nephrologists tag-teamed to present data about SGLT2 inhibitors, and we kind of joked that this was the one thing we both could get behind and support.”
Still, she has seen some reluctance among non-nephrology clinicians lacking SGLT2 experience, specifically when managing patients who have poor kidney function.
“There can be some hesitancy among physicians if the GFR is low,” Dr. Gewin said. “That’s where I’ve had to sort of push the envelope with non-nephrologists, saying: ‘Look, we feel pretty comfortable starting down to a GFR of about 20.’ ”
Early rises in creatinine may also spook providers, she noted.
“Sometimes, when we start SGLT2 inhibitors, the creatinine increases slightly, and the [primary care provider] gets concerned,” Dr. Gewin said. “We say: ‘No, this is expected. Don’t worry, hold the course, this is a good drug.’ ”
Like Dr. Mulay, Dr. Gewin said the present study offers further encouragement for the efficacy of this drug class. She also said sufficient data have been published to allay earlier concerns about potential safety signals, such as bone fractures and amputations.
“SGLT2 inhibitors seem to be a lot safer than what we initially had thought,” Dr. Gewin said. “That’s very encouraging.”
The study was funded by AstraZeneca. The investigators disclosed additional relationships with Bayer, Janssen, Gilead, and others. Dr. Gewin and Dr. Mulay disclosed no relevant conflicts of interest.
These findings add to a growing body of evidence supporting a range of positive benefits from dapagliflozin, including reduced risks of mortality, cardiovascular events, and kidney events, lead author Meir Schechter, MD, PhD, of the Hebrew University of Jerusalem and colleagues wrote in Annals of Internal Medicine.“Although cardiovascular and kidney outcomes with SGLT2 inhibitors have been studied extensively, there is a paucity of data evaluating the effects of SGLT2 inhibitors on hospitalizations for any cause.”
The findings are based on a post hoc analysis of the DAPA-CKD trial, which involved 4,304 patients with CKD in 21 countries. Patients were randomized in a 1:1 ratio to receive dapagliflozin 10 mg orally once a day or matching placebo. The present analysis quantified first hospitalizations for any cause, all hospitalizations, cause-specific hospitalizations, and several related outcomes.
After a median follow-up of 2.4 years, 28% of the population had been hospitalized a total of 2,072 times.
Compared with placebo, dapagliflozin significantly reduced risk of first hospitalization by 16% (hazard ratio, 0.84; 95% confidence interval, 0.75-0.94) and rate of all hospitalizations by 21% (rate ratio, 0.79; 95% CI, 0.70-0.89). These findings remained significant regardless of type 2 diabetes status, with significant benefits seen across reasons for admission, including renal/urinary disorders, cardiac disorders, neoplasms, and metabolism/nutrition disorders. In addition, dapagliflozin was associated with shorter mean time in hospital (2.3 vs. 2.8 days; P = .027) and longer time alive and out of hospital (354.9 vs. 351.7; P = .023).
“These findings highlight additional benefits of dapagliflozin beyond those seen for cardiovascular and kidney events, all-cause and cause-specific mortality, eGFR [estimated glomerular filtration rate] slope, and albuminuria and should be considered when evaluating the totality of evidence favoring provision of dapagliflozin to patients with CKD,” the investigators concluded.
Positive data, positive experiences
Shree Mulay, MD, a nephrologist in private practice in western Tennessee, said this study is “one of several other articles that already exist” demonstrating the broad benefits of SGLT2 inhibitors.
“The evidence is pretty substantial,” Dr. Mulay said in an interview. “I think SGLT2 inhibitors are the new statin of this era. ... I won’t be surprised if in the next year or 2 or 3 they truly become the standard of care.”
Dr. Mulay also speaks from experience working in both the chronic and acute setting, where he’s observed “some magical stuff happening” in patients started on SGLT2 inhibitors, especially those in heart failure who are fluid overloaded.
“It’s phenomenal stuff,” Dr. Mulay said. “You can really stabilize patients’ hemodynamics.”
In the private health care setting, he described widespread enthusiasm among nephrologists, although others still appear skeptical.
“It’s really our cardiology colleagues that I feel are underprescribing it,” Dr. Mulay said. “So, I’m kind of taking it on myself, when I see a heart failure patient, to go ahead and put them on this.”
It’s unclear why some cardiologists seem apprehensive, Dr. Mulay continued, although he suggested that unclear guidelines and a lack of first-hand experience may be to blame.
Nephrologists and cardiologists sometimes agree
In the academic arena, Leslie Gewin, MD, associate professor at Washington University in St. Louis and the John Cochran VA Hospital, also in St. Louis, has seen similar support for SGLT2 inhibitors among both nephrologists and cardiologists.
“We had a joint nephrology-cardiology medicine grand rounds at Wash U in St. Louis maybe 2 weeks ago,” Dr. Gewin said in an interview. “The cardiologists and nephrologists tag-teamed to present data about SGLT2 inhibitors, and we kind of joked that this was the one thing we both could get behind and support.”
Still, she has seen some reluctance among non-nephrology clinicians lacking SGLT2 experience, specifically when managing patients who have poor kidney function.
“There can be some hesitancy among physicians if the GFR is low,” Dr. Gewin said. “That’s where I’ve had to sort of push the envelope with non-nephrologists, saying: ‘Look, we feel pretty comfortable starting down to a GFR of about 20.’ ”
Early rises in creatinine may also spook providers, she noted.
“Sometimes, when we start SGLT2 inhibitors, the creatinine increases slightly, and the [primary care provider] gets concerned,” Dr. Gewin said. “We say: ‘No, this is expected. Don’t worry, hold the course, this is a good drug.’ ”
Like Dr. Mulay, Dr. Gewin said the present study offers further encouragement for the efficacy of this drug class. She also said sufficient data have been published to allay earlier concerns about potential safety signals, such as bone fractures and amputations.
“SGLT2 inhibitors seem to be a lot safer than what we initially had thought,” Dr. Gewin said. “That’s very encouraging.”
The study was funded by AstraZeneca. The investigators disclosed additional relationships with Bayer, Janssen, Gilead, and others. Dr. Gewin and Dr. Mulay disclosed no relevant conflicts of interest.
FROM ANNALS OF INTERNAL MEDICINE
Shorter fever prevention duration effective after cardiac arrest
a randomized trial shows.
“Since 2005, active fever prevention in comatose patients has been advocated by the guidelines for 72 hours after an out-of-hospital cardiac arrest,” Christian Hassager, MD, of the University of Copenhagen, told this news organization. “Our study is the first randomized trial ever on this subject – and it challenges the guidelines.”
At 90 days, a primary endpoint – a composite of death from any cause or hospital discharge with a high Cerebral Performance Category score – occurred in 32.4% of those in the 36-hour group and 33.6% of those in the 72-hour group; mortality was 29.5% versus 30.3%, respectively.
The study was published online in The New England Journal of Medicine. The results were also presented at the Resuscitation Science Symposium during the American Heart Association scientific sessions.
No significant differences
Assessment of the two device-based fever-prevention strategies for the duration was a predefined, additional randomly assigned open-label intervention in the Blood Pressure and Oxygenation Targets in Post Resuscitation Care (BOX) trial, which involved comatose adult patients who had been resuscitated after out-of-hospital cardiac arrest at two Danish cardiac arrest centers.
The main BOX analysis compared different primary strategies in these patients in a two-by-two factorial design: higher versus lower blood pressure targets and higher versus lower oxygenation targets. They found no difference between the various strategies in terms of death and discharge from hospital in a poor neurologic state. Those results were presented at the European Society of Cardiology Congress on Aug. 27, and simultaneously published in separate articles in The New England Journal of Medicine.
For this current analysis, a total of 789 comatose patients (mean age, 62; 80% men) received device-based temperature control targeting 36° C for 24 hours followed by 37° C for either 12 or 48 hours (total intervention times, 36 and 72 hours, respectively) or until the patient regained consciousness.
Patients were kept sedated and were receiving mechanical ventilation during the temperature control at 36° C, the authors note. Target core body temperature was controlled using commercially available surface cooling at one of the sites in 286 patients (Criticool and Allon, Belmont Medical Technologies) and using intravenous cooling in 503 patients at the other site (Thermogard XP, and Cool Line Catheter, Zoll).
Body temperature was maintained at 37° C with the same type of device that had been used for 36° C during the initial 24 hours. If the patient awakened, cooling was terminated.
Physicians in both groups were permitted to use non–device-based fever treatment (that is, for a body temperature > 37.5° C) with drugs such as paracetamol, by uncovering the patient’s body, or both, at the discretion of the treating physician. Ice packs or pads were not used.
The primary outcome was a composite of death from any cause or hospital discharge with a Cerebral Performance Category of 3 or 4 (range, 1 to 5, with higher scores indicating more severe disability) within 90 days after randomization.
Secondary outcomes at 90 days included death from any cause and the Montreal Cognitive Assessment score (range, 0 to 30, with higher scores indicating better cognitive ability).
A primary endpoint event occurred in 32.3% of patients in the 36-hour group and in 33.6% of those in the 72-hour group (hazard ratio, 0.99). Mortality was 29.5% in the 36-hour group and 30.3% in the 72-hour group.
The median Montreal Cognitive Assessment scores were 26 and 27, respectively. No significant between-group differences in the incidence of adverse events were observed.
The authors concluded that “active device-based fever prevention for 36 or 72 hours after cardiac arrest did not result in significantly different percentages of patients dying or having severe disability or coma.”
Dr. Hassager added, “We will continue with a new trial where we will randomize to treatment as usual or immediate wakeup call and no temperature intervention at all.”
Findings ‘very persuasive’
Intensivist Ken Parhar, MD, clinical associate professor, Critical Care Medicine at the University of Calgary (Alta.) and Alberta Health Services, Edmonton, and medical director, Cardiovascular Intensive Care Unit, commented on the study.
“The findings are very clear and very persuasive,” he said. “I think this should be incorporated into future guidelines, though it would be nice to see the trial repeated in another center.”
Dr. Parhar has kept comatose patients under temperature control for less than 72 hours, but mainly because those patients started to wake up. “This study provides clarity on the safety of that process – that we don’t have to unnecessarily keep somebody sedated just for an arbitrary timeline,” he said. “Beyond 36 hours, we need to continue to use our judgment.”
The study was supported by a grant from the Novo Nordisk Foundation, as was the work of one of the coauthors. Dr. Hassager’s work was funded by a grant from the Lundbeck Foundation; he also received an individual research grant from the Novo Nordisk Foundation, as well as honoraria from ABIOMED. No other disclosures were declared.
A version of this article first appeared on Medscape.com.
a randomized trial shows.
“Since 2005, active fever prevention in comatose patients has been advocated by the guidelines for 72 hours after an out-of-hospital cardiac arrest,” Christian Hassager, MD, of the University of Copenhagen, told this news organization. “Our study is the first randomized trial ever on this subject – and it challenges the guidelines.”
At 90 days, a primary endpoint – a composite of death from any cause or hospital discharge with a high Cerebral Performance Category score – occurred in 32.4% of those in the 36-hour group and 33.6% of those in the 72-hour group; mortality was 29.5% versus 30.3%, respectively.
The study was published online in The New England Journal of Medicine. The results were also presented at the Resuscitation Science Symposium during the American Heart Association scientific sessions.
No significant differences
Assessment of the two device-based fever-prevention strategies for the duration was a predefined, additional randomly assigned open-label intervention in the Blood Pressure and Oxygenation Targets in Post Resuscitation Care (BOX) trial, which involved comatose adult patients who had been resuscitated after out-of-hospital cardiac arrest at two Danish cardiac arrest centers.
The main BOX analysis compared different primary strategies in these patients in a two-by-two factorial design: higher versus lower blood pressure targets and higher versus lower oxygenation targets. They found no difference between the various strategies in terms of death and discharge from hospital in a poor neurologic state. Those results were presented at the European Society of Cardiology Congress on Aug. 27, and simultaneously published in separate articles in The New England Journal of Medicine.
For this current analysis, a total of 789 comatose patients (mean age, 62; 80% men) received device-based temperature control targeting 36° C for 24 hours followed by 37° C for either 12 or 48 hours (total intervention times, 36 and 72 hours, respectively) or until the patient regained consciousness.
Patients were kept sedated and were receiving mechanical ventilation during the temperature control at 36° C, the authors note. Target core body temperature was controlled using commercially available surface cooling at one of the sites in 286 patients (Criticool and Allon, Belmont Medical Technologies) and using intravenous cooling in 503 patients at the other site (Thermogard XP, and Cool Line Catheter, Zoll).
Body temperature was maintained at 37° C with the same type of device that had been used for 36° C during the initial 24 hours. If the patient awakened, cooling was terminated.
Physicians in both groups were permitted to use non–device-based fever treatment (that is, for a body temperature > 37.5° C) with drugs such as paracetamol, by uncovering the patient’s body, or both, at the discretion of the treating physician. Ice packs or pads were not used.
The primary outcome was a composite of death from any cause or hospital discharge with a Cerebral Performance Category of 3 or 4 (range, 1 to 5, with higher scores indicating more severe disability) within 90 days after randomization.
Secondary outcomes at 90 days included death from any cause and the Montreal Cognitive Assessment score (range, 0 to 30, with higher scores indicating better cognitive ability).
A primary endpoint event occurred in 32.3% of patients in the 36-hour group and in 33.6% of those in the 72-hour group (hazard ratio, 0.99). Mortality was 29.5% in the 36-hour group and 30.3% in the 72-hour group.
The median Montreal Cognitive Assessment scores were 26 and 27, respectively. No significant between-group differences in the incidence of adverse events were observed.
The authors concluded that “active device-based fever prevention for 36 or 72 hours after cardiac arrest did not result in significantly different percentages of patients dying or having severe disability or coma.”
Dr. Hassager added, “We will continue with a new trial where we will randomize to treatment as usual or immediate wakeup call and no temperature intervention at all.”
Findings ‘very persuasive’
Intensivist Ken Parhar, MD, clinical associate professor, Critical Care Medicine at the University of Calgary (Alta.) and Alberta Health Services, Edmonton, and medical director, Cardiovascular Intensive Care Unit, commented on the study.
“The findings are very clear and very persuasive,” he said. “I think this should be incorporated into future guidelines, though it would be nice to see the trial repeated in another center.”
Dr. Parhar has kept comatose patients under temperature control for less than 72 hours, but mainly because those patients started to wake up. “This study provides clarity on the safety of that process – that we don’t have to unnecessarily keep somebody sedated just for an arbitrary timeline,” he said. “Beyond 36 hours, we need to continue to use our judgment.”
The study was supported by a grant from the Novo Nordisk Foundation, as was the work of one of the coauthors. Dr. Hassager’s work was funded by a grant from the Lundbeck Foundation; he also received an individual research grant from the Novo Nordisk Foundation, as well as honoraria from ABIOMED. No other disclosures were declared.
A version of this article first appeared on Medscape.com.
a randomized trial shows.
“Since 2005, active fever prevention in comatose patients has been advocated by the guidelines for 72 hours after an out-of-hospital cardiac arrest,” Christian Hassager, MD, of the University of Copenhagen, told this news organization. “Our study is the first randomized trial ever on this subject – and it challenges the guidelines.”
At 90 days, a primary endpoint – a composite of death from any cause or hospital discharge with a high Cerebral Performance Category score – occurred in 32.4% of those in the 36-hour group and 33.6% of those in the 72-hour group; mortality was 29.5% versus 30.3%, respectively.
The study was published online in The New England Journal of Medicine. The results were also presented at the Resuscitation Science Symposium during the American Heart Association scientific sessions.
No significant differences
Assessment of the two device-based fever-prevention strategies for the duration was a predefined, additional randomly assigned open-label intervention in the Blood Pressure and Oxygenation Targets in Post Resuscitation Care (BOX) trial, which involved comatose adult patients who had been resuscitated after out-of-hospital cardiac arrest at two Danish cardiac arrest centers.
The main BOX analysis compared different primary strategies in these patients in a two-by-two factorial design: higher versus lower blood pressure targets and higher versus lower oxygenation targets. They found no difference between the various strategies in terms of death and discharge from hospital in a poor neurologic state. Those results were presented at the European Society of Cardiology Congress on Aug. 27, and simultaneously published in separate articles in The New England Journal of Medicine.
For this current analysis, a total of 789 comatose patients (mean age, 62; 80% men) received device-based temperature control targeting 36° C for 24 hours followed by 37° C for either 12 or 48 hours (total intervention times, 36 and 72 hours, respectively) or until the patient regained consciousness.
Patients were kept sedated and were receiving mechanical ventilation during the temperature control at 36° C, the authors note. Target core body temperature was controlled using commercially available surface cooling at one of the sites in 286 patients (Criticool and Allon, Belmont Medical Technologies) and using intravenous cooling in 503 patients at the other site (Thermogard XP, and Cool Line Catheter, Zoll).
Body temperature was maintained at 37° C with the same type of device that had been used for 36° C during the initial 24 hours. If the patient awakened, cooling was terminated.
Physicians in both groups were permitted to use non–device-based fever treatment (that is, for a body temperature > 37.5° C) with drugs such as paracetamol, by uncovering the patient’s body, or both, at the discretion of the treating physician. Ice packs or pads were not used.
The primary outcome was a composite of death from any cause or hospital discharge with a Cerebral Performance Category of 3 or 4 (range, 1 to 5, with higher scores indicating more severe disability) within 90 days after randomization.
Secondary outcomes at 90 days included death from any cause and the Montreal Cognitive Assessment score (range, 0 to 30, with higher scores indicating better cognitive ability).
A primary endpoint event occurred in 32.3% of patients in the 36-hour group and in 33.6% of those in the 72-hour group (hazard ratio, 0.99). Mortality was 29.5% in the 36-hour group and 30.3% in the 72-hour group.
The median Montreal Cognitive Assessment scores were 26 and 27, respectively. No significant between-group differences in the incidence of adverse events were observed.
The authors concluded that “active device-based fever prevention for 36 or 72 hours after cardiac arrest did not result in significantly different percentages of patients dying or having severe disability or coma.”
Dr. Hassager added, “We will continue with a new trial where we will randomize to treatment as usual or immediate wakeup call and no temperature intervention at all.”
Findings ‘very persuasive’
Intensivist Ken Parhar, MD, clinical associate professor, Critical Care Medicine at the University of Calgary (Alta.) and Alberta Health Services, Edmonton, and medical director, Cardiovascular Intensive Care Unit, commented on the study.
“The findings are very clear and very persuasive,” he said. “I think this should be incorporated into future guidelines, though it would be nice to see the trial repeated in another center.”
Dr. Parhar has kept comatose patients under temperature control for less than 72 hours, but mainly because those patients started to wake up. “This study provides clarity on the safety of that process – that we don’t have to unnecessarily keep somebody sedated just for an arbitrary timeline,” he said. “Beyond 36 hours, we need to continue to use our judgment.”
The study was supported by a grant from the Novo Nordisk Foundation, as was the work of one of the coauthors. Dr. Hassager’s work was funded by a grant from the Lundbeck Foundation; he also received an individual research grant from the Novo Nordisk Foundation, as well as honoraria from ABIOMED. No other disclosures were declared.
A version of this article first appeared on Medscape.com.
FROM NEJM
IRONMAN galvanizes case for IV iron repletion in heart failure
CHICAGO – Another major study appears to back the use of intravenous iron repletion in patients with heart failure (HF) and iron deficiency, strengthening largely consistent evidence, researchers say, that the treatment may improve symptoms and prevent some HF-related hospital admissions.
To be sure, the IRONMAN trial, which compared intravenous iron versus usual care in such patients – most with reduced ejection fraction and not hospitalized – failed to show a benefit for its primary endpoint. The 18% reduction in risk for HF hospitalization or cardiovascular (CV) death seen in the trial, however encouraging, can only be called a trend (P = .07).
But the intervention showed signs of benefit for some secondary endpoints, including quality of life scores, and hinted at such an effect on HF hospitalization. Risk for the latter endpoint dropped 20% (P = .085) over a median follow-up of 2.7 years.
The findings “build upon the other data we have that correcting iron deficiency can help improve well-being, and particularly reduce the risk of hospitalization, in a broad range of [HF] patients,” said Paul Kalra, MD, of the University of Glasgow and Portsmouth (England) Hospitals University NHS Trust.
The tested regimen “was well tolerated with no safety concerns” and offers “reassurance about the long-term safety” of the intravenous iron it used, ferric derisomaltose (MonoFerric), in patients with HF, Dr. Kalra said at a media briefing on the trial.
The remarks preceded his formal presentation of IRONMAN at the American Heart Association scientific sessions. Dr. Kalra is also lead author on the trial’s publication in The Lancet.
IRONMAN strengthens the base of evidence supporting intravenous iron in HF with iron deficiency, especially chronic HF in outpatients, Dr. Kalra and others said. It also supports efficacy for a form of intravenous iron not previously tested in a major HF trial.
Still, “the totality of data are now supporting intravenous iron per se,” regardless of the iron agent used, said Dr. Kalra. But ferric derisomaltose may have dosing advantages, he observed, “and we’ve now got these long-term safety data.”
The strongest prior support for intravenous iron in HF came from hospitalized patients who received it as ferric carboxymaltose (Ferinject) and were followed only 12 months. That was in the AFFIRM-AHF trial, published 2 years ago, which also missed its primary endpoint – the same one used in IRONMAN. Some outcomes in the two trials were similar.
The risk for HF hospitalization or CV death for intravenous iron therapy, compared with usual care, in AFFIRM-AHF fell 21% (P = .059), missing significance but apparently driven by a 26% drop in risk for HF readmissions (P = .013). But neither that trial nor IRONMAN suggested a benefit for CV mortality on its own.
The COVID effect
In IRONMAN, Dr. Kalra said, usual care could include oral iron supplementation, which 17% of patients in the control group received. That could potentially have kept the intravenous iron group from making a better showing for the primary endpoint, he proposed.
And some iron doses and other treatments were missed by a substantial number of patients in both groups who entered the trial after the United Kingdom’s national lockdown in response to the COVID-19 pandemic, he observed. “Patients were not able to come into hospitals for research visits, or in fact when they were able, may not have wanted to.”
So, the group conducted a “prespecified” sensitivity analysis that excluded the 9% of patients enrolled by the end of March 2020, about the time of the first lockdown, and followed the remainder for another 6 months.
In that analysis, risk for HF hospitalization or CV death declined 24% in the intravenous iron group, a marginal but significant result (P = .047) that was dominated by an improvement in HF hospitalizations.
Effects on guidelines
The intravenous iron recommendations in the European HF guidelines refer only to ferric carboxymaltose without mentioning other forms, such as ferric derisomaltose, “but this is now a class effect given the similarities between AFFIRM-AHF and IRONMAN,” said Gregory D. Lewis, MD, Mass General Brigham, Boston, invited discussant for Dr. Kalra’s presentation at the AHA session.
“In the United States, we relegate IV iron to improvement in functional capacity as a comorbidity of heart failure. Perhaps this role will expand,” added Dr. Lewis, who is medical director of his center’s heart transplant program.
He also wondered aloud whether the purported clinical benefits of intravenous iron in HF patients with iron deficiency, not as yet supported by a significant primary-endpoint showing in one of the major trials, currently justify expansion of its use in practice.
“With the benefits of IV iron on exercise capacity and quality of life, and the safety of administering high doses of IV iron,” potentially reducing HF polypharmacy, he noted, “should we be considering IV iron more commonly for utilization in our patients even if we find that heart failure hospitalizations and mortality are only modestly improved?”
IRONMAN “asked whether there’s benefit to IV iron in the longer term,” Kiran Musunuru, MD, PhD, MPH, University of Pennsylvania,Philadelphia, observed at the media briefing. As the trial was reported, “that does in fact, seem to be the case,” said Dr. Musunuru, who was not involved in IRONMAN.
Therefore, he said, “this study reinforces the message that we should be routinely monitoring our heart failure patients for iron deficiency and supplementing them as needed.”
A commentary linked to the IRONMAN publication agreed. The trial “increases the evidence base for the treatment of iron deficiency with intravenous iron supplementation,” wrote the editorialists, led by Theresa A. McDonagh, MD, King’s College Hospital and School of Cardiovascular Sciences, London.
Patients with acute or chronic HF, iron deficiency, and reduced or mildly reduced ejection fractions “should be offered treatment with intravenous iron to reduce their risk of hospital admission for heart failure,” they concluded.
Mostly reduced-EF outpatients
The open-label, blinded-endpoint IRONMAN trial, conducted at 70 centers in the United Kingdom, entered adults with HF, ejection fractions 45% or lower within the previous 2 years, and iron deficiency defined as transferrin saturation less than 20% or serum ferritin levels below 100 mcg/L, the report states. They were either hospitalized for HF, had such a hospitalization within the past 6 months, or were outpatients with elevated natriuretic peptide levels; the third category accounted for two thirds of the trial population.
Of the 1,137 randomized patients, 569 were assigned to receive intravenous ferric derisomaltose at weight- and hemoglobin-adjusted dosages; 568 went to the usual-care group.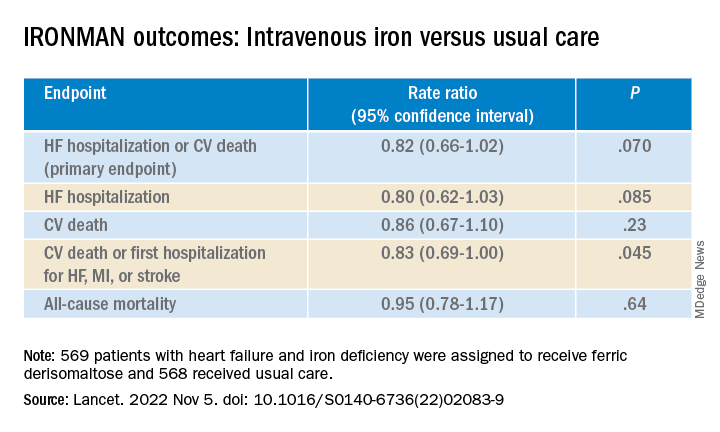
Those receiving intravenous iron visited the trial clinic 4 weeks later and then every 4 months. At those visits, they received a round of ferric derisomaltose if their ferritin levels were below 100 mcg/L, or 400 mcg/L or lower if transferrin saturation was below 25%, the published report states.
Mean scores on the Minnesota Living with Heart Failure Questionnaire improved by a marginally significant 3.33 points (P = .050) at 4 months in the intravenous iron group. The gain receded to a nonsignificant 2.57 points by 20 months (P = .23).
In COVID-related sensitivity analysis, the intravenous iron group showed a significant benefit for the primary endpoint and a trend for improved HF hospitalizations.
- HF hospitalization or CV death: RR, 0.76 (95% confidence interval, 0.58-1.00; P = .047)
- HF hospitalization: RR 0.76 (95% CI, 0.56-1.03; P = .077)
Fewer patients in the intravenous iron group experienced serious cardiac adverse events, 36% compared with 43% in for those on usual care, P = .016.
The recently updated European Society of Cardiology guidelines for HF made it a class 1 recommendation to assess iron status in every patient, Kalra observed. “It doesn›t specify how frequently, but I think we should be thinking about every 4-6 months.”
Dr. Kalra disclosed receiving research grants from Pharmacosmos; and consulting or lecturing for Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, Pfizer, Pharmacosmos, Servier, and Vifor Pharma. Dr. Musunuru disclosed significant ownership interest in Verve Therapeutics and Variant Bio. Dr. Lewis disclosed relationships with NXT, American Regent, and RIVUS; and receiving research grants from Cytokinetics and Amgen.
A version of this article first appeared on Medscape.com.
CHICAGO – Another major study appears to back the use of intravenous iron repletion in patients with heart failure (HF) and iron deficiency, strengthening largely consistent evidence, researchers say, that the treatment may improve symptoms and prevent some HF-related hospital admissions.
To be sure, the IRONMAN trial, which compared intravenous iron versus usual care in such patients – most with reduced ejection fraction and not hospitalized – failed to show a benefit for its primary endpoint. The 18% reduction in risk for HF hospitalization or cardiovascular (CV) death seen in the trial, however encouraging, can only be called a trend (P = .07).
But the intervention showed signs of benefit for some secondary endpoints, including quality of life scores, and hinted at such an effect on HF hospitalization. Risk for the latter endpoint dropped 20% (P = .085) over a median follow-up of 2.7 years.
The findings “build upon the other data we have that correcting iron deficiency can help improve well-being, and particularly reduce the risk of hospitalization, in a broad range of [HF] patients,” said Paul Kalra, MD, of the University of Glasgow and Portsmouth (England) Hospitals University NHS Trust.
The tested regimen “was well tolerated with no safety concerns” and offers “reassurance about the long-term safety” of the intravenous iron it used, ferric derisomaltose (MonoFerric), in patients with HF, Dr. Kalra said at a media briefing on the trial.
The remarks preceded his formal presentation of IRONMAN at the American Heart Association scientific sessions. Dr. Kalra is also lead author on the trial’s publication in The Lancet.
IRONMAN strengthens the base of evidence supporting intravenous iron in HF with iron deficiency, especially chronic HF in outpatients, Dr. Kalra and others said. It also supports efficacy for a form of intravenous iron not previously tested in a major HF trial.
Still, “the totality of data are now supporting intravenous iron per se,” regardless of the iron agent used, said Dr. Kalra. But ferric derisomaltose may have dosing advantages, he observed, “and we’ve now got these long-term safety data.”
The strongest prior support for intravenous iron in HF came from hospitalized patients who received it as ferric carboxymaltose (Ferinject) and were followed only 12 months. That was in the AFFIRM-AHF trial, published 2 years ago, which also missed its primary endpoint – the same one used in IRONMAN. Some outcomes in the two trials were similar.
The risk for HF hospitalization or CV death for intravenous iron therapy, compared with usual care, in AFFIRM-AHF fell 21% (P = .059), missing significance but apparently driven by a 26% drop in risk for HF readmissions (P = .013). But neither that trial nor IRONMAN suggested a benefit for CV mortality on its own.
The COVID effect
In IRONMAN, Dr. Kalra said, usual care could include oral iron supplementation, which 17% of patients in the control group received. That could potentially have kept the intravenous iron group from making a better showing for the primary endpoint, he proposed.
And some iron doses and other treatments were missed by a substantial number of patients in both groups who entered the trial after the United Kingdom’s national lockdown in response to the COVID-19 pandemic, he observed. “Patients were not able to come into hospitals for research visits, or in fact when they were able, may not have wanted to.”
So, the group conducted a “prespecified” sensitivity analysis that excluded the 9% of patients enrolled by the end of March 2020, about the time of the first lockdown, and followed the remainder for another 6 months.
In that analysis, risk for HF hospitalization or CV death declined 24% in the intravenous iron group, a marginal but significant result (P = .047) that was dominated by an improvement in HF hospitalizations.
Effects on guidelines
The intravenous iron recommendations in the European HF guidelines refer only to ferric carboxymaltose without mentioning other forms, such as ferric derisomaltose, “but this is now a class effect given the similarities between AFFIRM-AHF and IRONMAN,” said Gregory D. Lewis, MD, Mass General Brigham, Boston, invited discussant for Dr. Kalra’s presentation at the AHA session.
“In the United States, we relegate IV iron to improvement in functional capacity as a comorbidity of heart failure. Perhaps this role will expand,” added Dr. Lewis, who is medical director of his center’s heart transplant program.
He also wondered aloud whether the purported clinical benefits of intravenous iron in HF patients with iron deficiency, not as yet supported by a significant primary-endpoint showing in one of the major trials, currently justify expansion of its use in practice.
“With the benefits of IV iron on exercise capacity and quality of life, and the safety of administering high doses of IV iron,” potentially reducing HF polypharmacy, he noted, “should we be considering IV iron more commonly for utilization in our patients even if we find that heart failure hospitalizations and mortality are only modestly improved?”
IRONMAN “asked whether there’s benefit to IV iron in the longer term,” Kiran Musunuru, MD, PhD, MPH, University of Pennsylvania,Philadelphia, observed at the media briefing. As the trial was reported, “that does in fact, seem to be the case,” said Dr. Musunuru, who was not involved in IRONMAN.
Therefore, he said, “this study reinforces the message that we should be routinely monitoring our heart failure patients for iron deficiency and supplementing them as needed.”
A commentary linked to the IRONMAN publication agreed. The trial “increases the evidence base for the treatment of iron deficiency with intravenous iron supplementation,” wrote the editorialists, led by Theresa A. McDonagh, MD, King’s College Hospital and School of Cardiovascular Sciences, London.
Patients with acute or chronic HF, iron deficiency, and reduced or mildly reduced ejection fractions “should be offered treatment with intravenous iron to reduce their risk of hospital admission for heart failure,” they concluded.
Mostly reduced-EF outpatients
The open-label, blinded-endpoint IRONMAN trial, conducted at 70 centers in the United Kingdom, entered adults with HF, ejection fractions 45% or lower within the previous 2 years, and iron deficiency defined as transferrin saturation less than 20% or serum ferritin levels below 100 mcg/L, the report states. They were either hospitalized for HF, had such a hospitalization within the past 6 months, or were outpatients with elevated natriuretic peptide levels; the third category accounted for two thirds of the trial population.
Of the 1,137 randomized patients, 569 were assigned to receive intravenous ferric derisomaltose at weight- and hemoglobin-adjusted dosages; 568 went to the usual-care group.
Those receiving intravenous iron visited the trial clinic 4 weeks later and then every 4 months. At those visits, they received a round of ferric derisomaltose if their ferritin levels were below 100 mcg/L, or 400 mcg/L or lower if transferrin saturation was below 25%, the published report states.
Mean scores on the Minnesota Living with Heart Failure Questionnaire improved by a marginally significant 3.33 points (P = .050) at 4 months in the intravenous iron group. The gain receded to a nonsignificant 2.57 points by 20 months (P = .23).
In COVID-related sensitivity analysis, the intravenous iron group showed a significant benefit for the primary endpoint and a trend for improved HF hospitalizations.
- HF hospitalization or CV death: RR, 0.76 (95% confidence interval, 0.58-1.00; P = .047)
- HF hospitalization: RR 0.76 (95% CI, 0.56-1.03; P = .077)
Fewer patients in the intravenous iron group experienced serious cardiac adverse events, 36% compared with 43% in for those on usual care, P = .016.
The recently updated European Society of Cardiology guidelines for HF made it a class 1 recommendation to assess iron status in every patient, Kalra observed. “It doesn›t specify how frequently, but I think we should be thinking about every 4-6 months.”
Dr. Kalra disclosed receiving research grants from Pharmacosmos; and consulting or lecturing for Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, Pfizer, Pharmacosmos, Servier, and Vifor Pharma. Dr. Musunuru disclosed significant ownership interest in Verve Therapeutics and Variant Bio. Dr. Lewis disclosed relationships with NXT, American Regent, and RIVUS; and receiving research grants from Cytokinetics and Amgen.
A version of this article first appeared on Medscape.com.
CHICAGO – Another major study appears to back the use of intravenous iron repletion in patients with heart failure (HF) and iron deficiency, strengthening largely consistent evidence, researchers say, that the treatment may improve symptoms and prevent some HF-related hospital admissions.
To be sure, the IRONMAN trial, which compared intravenous iron versus usual care in such patients – most with reduced ejection fraction and not hospitalized – failed to show a benefit for its primary endpoint. The 18% reduction in risk for HF hospitalization or cardiovascular (CV) death seen in the trial, however encouraging, can only be called a trend (P = .07).
But the intervention showed signs of benefit for some secondary endpoints, including quality of life scores, and hinted at such an effect on HF hospitalization. Risk for the latter endpoint dropped 20% (P = .085) over a median follow-up of 2.7 years.
The findings “build upon the other data we have that correcting iron deficiency can help improve well-being, and particularly reduce the risk of hospitalization, in a broad range of [HF] patients,” said Paul Kalra, MD, of the University of Glasgow and Portsmouth (England) Hospitals University NHS Trust.
The tested regimen “was well tolerated with no safety concerns” and offers “reassurance about the long-term safety” of the intravenous iron it used, ferric derisomaltose (MonoFerric), in patients with HF, Dr. Kalra said at a media briefing on the trial.
The remarks preceded his formal presentation of IRONMAN at the American Heart Association scientific sessions. Dr. Kalra is also lead author on the trial’s publication in The Lancet.
IRONMAN strengthens the base of evidence supporting intravenous iron in HF with iron deficiency, especially chronic HF in outpatients, Dr. Kalra and others said. It also supports efficacy for a form of intravenous iron not previously tested in a major HF trial.
Still, “the totality of data are now supporting intravenous iron per se,” regardless of the iron agent used, said Dr. Kalra. But ferric derisomaltose may have dosing advantages, he observed, “and we’ve now got these long-term safety data.”
The strongest prior support for intravenous iron in HF came from hospitalized patients who received it as ferric carboxymaltose (Ferinject) and were followed only 12 months. That was in the AFFIRM-AHF trial, published 2 years ago, which also missed its primary endpoint – the same one used in IRONMAN. Some outcomes in the two trials were similar.
The risk for HF hospitalization or CV death for intravenous iron therapy, compared with usual care, in AFFIRM-AHF fell 21% (P = .059), missing significance but apparently driven by a 26% drop in risk for HF readmissions (P = .013). But neither that trial nor IRONMAN suggested a benefit for CV mortality on its own.
The COVID effect
In IRONMAN, Dr. Kalra said, usual care could include oral iron supplementation, which 17% of patients in the control group received. That could potentially have kept the intravenous iron group from making a better showing for the primary endpoint, he proposed.
And some iron doses and other treatments were missed by a substantial number of patients in both groups who entered the trial after the United Kingdom’s national lockdown in response to the COVID-19 pandemic, he observed. “Patients were not able to come into hospitals for research visits, or in fact when they were able, may not have wanted to.”
So, the group conducted a “prespecified” sensitivity analysis that excluded the 9% of patients enrolled by the end of March 2020, about the time of the first lockdown, and followed the remainder for another 6 months.
In that analysis, risk for HF hospitalization or CV death declined 24% in the intravenous iron group, a marginal but significant result (P = .047) that was dominated by an improvement in HF hospitalizations.
Effects on guidelines
The intravenous iron recommendations in the European HF guidelines refer only to ferric carboxymaltose without mentioning other forms, such as ferric derisomaltose, “but this is now a class effect given the similarities between AFFIRM-AHF and IRONMAN,” said Gregory D. Lewis, MD, Mass General Brigham, Boston, invited discussant for Dr. Kalra’s presentation at the AHA session.
“In the United States, we relegate IV iron to improvement in functional capacity as a comorbidity of heart failure. Perhaps this role will expand,” added Dr. Lewis, who is medical director of his center’s heart transplant program.
He also wondered aloud whether the purported clinical benefits of intravenous iron in HF patients with iron deficiency, not as yet supported by a significant primary-endpoint showing in one of the major trials, currently justify expansion of its use in practice.
“With the benefits of IV iron on exercise capacity and quality of life, and the safety of administering high doses of IV iron,” potentially reducing HF polypharmacy, he noted, “should we be considering IV iron more commonly for utilization in our patients even if we find that heart failure hospitalizations and mortality are only modestly improved?”
IRONMAN “asked whether there’s benefit to IV iron in the longer term,” Kiran Musunuru, MD, PhD, MPH, University of Pennsylvania,Philadelphia, observed at the media briefing. As the trial was reported, “that does in fact, seem to be the case,” said Dr. Musunuru, who was not involved in IRONMAN.
Therefore, he said, “this study reinforces the message that we should be routinely monitoring our heart failure patients for iron deficiency and supplementing them as needed.”
A commentary linked to the IRONMAN publication agreed. The trial “increases the evidence base for the treatment of iron deficiency with intravenous iron supplementation,” wrote the editorialists, led by Theresa A. McDonagh, MD, King’s College Hospital and School of Cardiovascular Sciences, London.
Patients with acute or chronic HF, iron deficiency, and reduced or mildly reduced ejection fractions “should be offered treatment with intravenous iron to reduce their risk of hospital admission for heart failure,” they concluded.
Mostly reduced-EF outpatients
The open-label, blinded-endpoint IRONMAN trial, conducted at 70 centers in the United Kingdom, entered adults with HF, ejection fractions 45% or lower within the previous 2 years, and iron deficiency defined as transferrin saturation less than 20% or serum ferritin levels below 100 mcg/L, the report states. They were either hospitalized for HF, had such a hospitalization within the past 6 months, or were outpatients with elevated natriuretic peptide levels; the third category accounted for two thirds of the trial population.
Of the 1,137 randomized patients, 569 were assigned to receive intravenous ferric derisomaltose at weight- and hemoglobin-adjusted dosages; 568 went to the usual-care group.
Those receiving intravenous iron visited the trial clinic 4 weeks later and then every 4 months. At those visits, they received a round of ferric derisomaltose if their ferritin levels were below 100 mcg/L, or 400 mcg/L or lower if transferrin saturation was below 25%, the published report states.
Mean scores on the Minnesota Living with Heart Failure Questionnaire improved by a marginally significant 3.33 points (P = .050) at 4 months in the intravenous iron group. The gain receded to a nonsignificant 2.57 points by 20 months (P = .23).
In COVID-related sensitivity analysis, the intravenous iron group showed a significant benefit for the primary endpoint and a trend for improved HF hospitalizations.
- HF hospitalization or CV death: RR, 0.76 (95% confidence interval, 0.58-1.00; P = .047)
- HF hospitalization: RR 0.76 (95% CI, 0.56-1.03; P = .077)
Fewer patients in the intravenous iron group experienced serious cardiac adverse events, 36% compared with 43% in for those on usual care, P = .016.
The recently updated European Society of Cardiology guidelines for HF made it a class 1 recommendation to assess iron status in every patient, Kalra observed. “It doesn›t specify how frequently, but I think we should be thinking about every 4-6 months.”
Dr. Kalra disclosed receiving research grants from Pharmacosmos; and consulting or lecturing for Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, Pfizer, Pharmacosmos, Servier, and Vifor Pharma. Dr. Musunuru disclosed significant ownership interest in Verve Therapeutics and Variant Bio. Dr. Lewis disclosed relationships with NXT, American Regent, and RIVUS; and receiving research grants from Cytokinetics and Amgen.
A version of this article first appeared on Medscape.com.
AT AHA 2022
Optimize HF meds rapidly and fully after hospital discharge: STRONG-HF
CHICAGO – Clinicians who prescribe heart failure meds are holding the best hand they’ve ever had, but with so much underuse and suboptimal dosing in actual practice, it seems many may not appreciate the value of their cards. But a major randomized trial that has captured the field’s attention may embolden them to go all in.
Results showed that a strategy of early, rapid up-titration of multiple guideline-directed meds in patients hospitalized with heart failure, compared with a usual-care approach, cut their 6-month risk for death or HF readmission by a steep 34% (P = .002).
The drugs had been started and partly up-titrated in the hospital with the goal of full up-titration within 2 weeks after discharge.
Patients well tolerated the high-intensity approach, researchers said. Their quality-of-life scores improved (P < .0001) compared with the usual-care group, and adverse events were considered few and manageable in the international trial with more than 1,000 patients.
Safety on the high-intensity strategy depended on close patient monitoring at frequently planned clinic visits along with guidance for the up-titrations from clinical signs and natriuretic peptide levels, observed Alexandre Mebazaa, MD, PhD, University of Paris and Public Hospitals of Paris.
Dr. Mebazaa is principal investigator on the trial, called STRONG-HF, which he presented at the American Heart Association scientific sessions, held in Chicago and virtually. He is also lead author on the study’s same-day publication in the Lancet.
The high-intensity strategy’s superiority emerged early in the trial, which was halted early on the data safety monitoring board’s recommendation, with about 90% of follow-ups completed. The board “felt it was unethical to keep patients in usual care,” Dr. Mebazaa said at a press conference.
A dramatic change
The next step, he said, will be to educate the heart failure community on the high-intensity care technique so it can swiftly enter clinical practice. Currently in acute heart failure, “very few patients are monitored after discharge and treated with full doses of heart failure therapies.”
Adoption of the strategy “would be a dramatic change from what’s currently being done,” said Martin B. Leon, MD, NewYork-Presbyterian/Columbia University Irving Medical Center, New York, who moderated the press conference.
Only an estimated 5% of patients with HF in the United States receive full guideline-directed medical therapy, Dr. Leon said, “so the generalizability of this strategy, with careful follow-up that has safety involved in it, is absolutely crucial.”
But the potential impact of this high-intensity approach on resource use is unknown, raising questions about how widely and consistently it could be implemented, said Dr. Leon, who is not connected with STRONG-HF.
The trial called for in-hospital initiation of the three distinct drug classes that, at the time, were the core of guideline-directed HF therapy, with up-titration to 50% of recommended dosage by hospital discharge, and then to 100% within 2 weeks later.
The meds included a beta-blocker, a mineralocorticoid receptor antagonist (MRA), and a renin-angiotensin system inhibitor (RASI). The latter could be an ACE inhibitor, angiotensin-receptor blocker (ARB), or angiotensin receptor-neprilysin inhibitor (ARNI).
How about a fourth drug?
Conspicuously absent from the list, for contemporary practice, was an SGLT2 inhibitor, a class that entered the HF guidelines well after STRONG-HF was designed. They would undoubtedly join the other three agents were the high-intensity strategy to enter practice, potentially changing its complexity and safety profile.
But Dr. Mebazaa and other experts don’t see that as a big challenge and would expect a smooth transition to a high-intensity approach that also includes the SGLT2 inhibitors.
STRONG-HF was necessary in part because many clinicians have been “reluctant” to take full advantage of three agents that had been the basis of guideline-directed therapy, he told this news organization.
That reluctance stemmed from concerns that beta-blockers might worsen the heart failure, ACE inhibitors could hurt the kidneys, or MRAs might cause hyperkalemia, Dr. Mebazaa said. The STRONG-HF high-intensity regimen, therefore, demanded multiple clinic visits for close follow-up.
But the SGLT2 inhibitors “are known to be rather safe drugs, at least much safer than the three others,” he said. So, it seems unlikely that their addition to a beta-blocker, RASI, and MRA in patients with HF would worsen the risk of adverse events.
John G.F. Cleland, MD, PhD, agrees. With addition of the fourth agent, “You may need to be a little bit more careful with renal function, just in that first couple of weeks,” he told this news organization. “But I think it would be easy to add an SGLT2 inhibitor into this regimen. And in general, there’s no titration with an SGLT2 inhibitor, so they’ll all be on full dose predischarge.”
Given the drugs’ diuretic-like action, moreover, some patients might be able to pull back on their loop diuretics, speculated Dr. Cleland, from the University of Glasgow’s School of Health and Wellbeing.
The prospect of a high-intensity strategy’s wide implementation in practice presents both “challenges and opportunities,” Amanda R. Vest, MBBS, MPH, Tufts University, Boston, told this news organization.
“There may be additional challenges in terms of ensuring we avoid hypotension or acute kidney injury in the up-titration phase,” said Dr. Vest, who is medical director of her center’s cardiac transplantation program but not connected with STRONG-HF.
“But it also gives us opportunities,” she added, “because there are some patients, especially in that vulnerable postdischarge phase, who are actually much more able to tolerate introduction of an SGLT2 inhibitor than, for example, an ACE inhibitor, ARB, or ARNI – or maybe a beta-blocker if they’ve been in a low cardiac-output state.” Effective dosing would depend on “the personalization and skill of the clinician in optimizing the medications in their correct sequence,” Dr. Vest said.
“It’s challenging to think that we would ever get to 100% up-titration,” she added, “and even in this excellent study, they didn’t get to 100%.” But as clinicians gain experience with the high-intensity strategy, especially as the SGLT2 inhibitors are included, “I think we can reasonably expect more progress to be made in these up-titration skills.”
No restrictions on LVEF
The researchers entered 1,078 patients hospitalized with acute HF in 14 countries across Africa, Europe, the Middle East, and South America, and randomly assigned them to the high-intensity management strategy or usual care.
About 60% of the patients were male and 77% were White. There were no entry restrictions based on left ventricular ejection fraction (LVEF), which exceeded 40% in almost a third of cases.
In the high-intensity care group’s 542 patients, the three agents were up-titrated to 50% of the maximum guideline-recommended dosage prior to hospital discharge, and to 100% within 2 weeks after discharge. Symptoms and laboratory biomarkers, including natriuretic peptides, were monitored closely at four planned clinical visits over the following 6 weeks.
The 536 patients assigned to usual care were discharged and managed according to local standards, with their meds handled by their own primary care doctors or cardiologists, the published report notes. They were reevaluated by STRONG-HF clinicians 90 days after discharge.
The number of clinic visits in the first 90 postdischarge days averaged 4.8 in the high-intensity care group and 1.0 for those receiving usual care. Full up-titration was far more likely in the high-intensity care group: 55% vs. 2% for RASI agents, 49% vs. 4% for beta-blockers, and 84% vs. 46% for MRAs.
They also fared significantly better on all measured parameters associated with decongestion, including weight, prevalence of peripheral edema, jugular venous pressure, NYHA functional class, and natriuretic peptide levels, the researchers said.
The primary endpoint of 180-day death from any cause or HF readmission was met by 15.2% of the high-intensity care group and 23.3% of usual-care patients, for an adjusted risk ratio (RR) of 0.66 (95% CI, 0.50-0.86; P = .0021).
Subgroup analyses saw no significant interactions by age, sex, race, geography, or baseline blood pressure, renal function, or LVEF. Patients with higher vs. lower baseline natriuretic peptide levels trend toward better responses to high-intensity care (P = .08)
The COVID effect
The group performed a sensitivity analysis that excluded deaths attributed to COVID-19 in STRONG-HF, which launched prior to the pandemic. The high-intensity strategy’s benefit for the primary endpoint grew, with an adjusted RR of 0.61 (95% CI, 0.46-0.82; P = .0005). There was no corresponding effect on death from any cause (P = .15).
Treatment-related adverse effects in the overall trial were seen in 41.1% of the high-intensity care group and in 29.5% of those assigned to usual care.
The higher rate in the high-intensity care arm “may be related to their higher number of [clinic] visits compared to usual care,” Dr. Mebazaa said. “However, serious adverse events and fatal adverse events were similar in both arms.”
Cardiac failure was the most common adverse event, developing in about 15% in both groups. It was followed by hypotension, hyperkalemia, and renal impairment, according to the published report.
Dr. Cleland cautioned that the risk of adverse events would potentially be higher should the high-intensity strategy become common clinical practice. The median age in STRONG-HF was 63, which is “10-15 years younger, on average, than the population with recently admitted heart failure that we see. There’s no doubt that older people have more multimorbidity.”
STRONG-HF was funded by Roche Diagnostics. Dr. Mebazaa discloses receiving grants from Roche Diagnostics, Abbott Laboratories, 4TEEN4, and Windtree Therapeutics; honoraria for lectures from Roche Diagnostics, Bayer, and Merck, Sharp & Dohme; and consulting for Corteria Pharmaceuticals, S-form Pharma, FIRE-1, Implicity, 4TEEN4, and Adrenomed; and to being a co-inventor on a patent involving combination therapy for patients having acute or persistent dyspnea.
Dr. Vest reports modest relationships with Boehringer Ingelheim, Corvia, and CareDx; and receiving research grants from the American Heart Association and the National Institutes of Health. Dr. Cleland discloses receiving honoraria from Idorsia; and research grants from Vifor Pharma, Medtronic, Bayer, and Bristol-Myers Squibb. Dr. Leon had no disclosures.
A version of this article first appeared on Medscape.com.
CHICAGO – Clinicians who prescribe heart failure meds are holding the best hand they’ve ever had, but with so much underuse and suboptimal dosing in actual practice, it seems many may not appreciate the value of their cards. But a major randomized trial that has captured the field’s attention may embolden them to go all in.
Results showed that a strategy of early, rapid up-titration of multiple guideline-directed meds in patients hospitalized with heart failure, compared with a usual-care approach, cut their 6-month risk for death or HF readmission by a steep 34% (P = .002).
The drugs had been started and partly up-titrated in the hospital with the goal of full up-titration within 2 weeks after discharge.
Patients well tolerated the high-intensity approach, researchers said. Their quality-of-life scores improved (P < .0001) compared with the usual-care group, and adverse events were considered few and manageable in the international trial with more than 1,000 patients.
Safety on the high-intensity strategy depended on close patient monitoring at frequently planned clinic visits along with guidance for the up-titrations from clinical signs and natriuretic peptide levels, observed Alexandre Mebazaa, MD, PhD, University of Paris and Public Hospitals of Paris.
Dr. Mebazaa is principal investigator on the trial, called STRONG-HF, which he presented at the American Heart Association scientific sessions, held in Chicago and virtually. He is also lead author on the study’s same-day publication in the Lancet.
The high-intensity strategy’s superiority emerged early in the trial, which was halted early on the data safety monitoring board’s recommendation, with about 90% of follow-ups completed. The board “felt it was unethical to keep patients in usual care,” Dr. Mebazaa said at a press conference.
A dramatic change
The next step, he said, will be to educate the heart failure community on the high-intensity care technique so it can swiftly enter clinical practice. Currently in acute heart failure, “very few patients are monitored after discharge and treated with full doses of heart failure therapies.”
Adoption of the strategy “would be a dramatic change from what’s currently being done,” said Martin B. Leon, MD, NewYork-Presbyterian/Columbia University Irving Medical Center, New York, who moderated the press conference.
Only an estimated 5% of patients with HF in the United States receive full guideline-directed medical therapy, Dr. Leon said, “so the generalizability of this strategy, with careful follow-up that has safety involved in it, is absolutely crucial.”
But the potential impact of this high-intensity approach on resource use is unknown, raising questions about how widely and consistently it could be implemented, said Dr. Leon, who is not connected with STRONG-HF.
The trial called for in-hospital initiation of the three distinct drug classes that, at the time, were the core of guideline-directed HF therapy, with up-titration to 50% of recommended dosage by hospital discharge, and then to 100% within 2 weeks later.
The meds included a beta-blocker, a mineralocorticoid receptor antagonist (MRA), and a renin-angiotensin system inhibitor (RASI). The latter could be an ACE inhibitor, angiotensin-receptor blocker (ARB), or angiotensin receptor-neprilysin inhibitor (ARNI).
How about a fourth drug?
Conspicuously absent from the list, for contemporary practice, was an SGLT2 inhibitor, a class that entered the HF guidelines well after STRONG-HF was designed. They would undoubtedly join the other three agents were the high-intensity strategy to enter practice, potentially changing its complexity and safety profile.
But Dr. Mebazaa and other experts don’t see that as a big challenge and would expect a smooth transition to a high-intensity approach that also includes the SGLT2 inhibitors.
STRONG-HF was necessary in part because many clinicians have been “reluctant” to take full advantage of three agents that had been the basis of guideline-directed therapy, he told this news organization.
That reluctance stemmed from concerns that beta-blockers might worsen the heart failure, ACE inhibitors could hurt the kidneys, or MRAs might cause hyperkalemia, Dr. Mebazaa said. The STRONG-HF high-intensity regimen, therefore, demanded multiple clinic visits for close follow-up.
But the SGLT2 inhibitors “are known to be rather safe drugs, at least much safer than the three others,” he said. So, it seems unlikely that their addition to a beta-blocker, RASI, and MRA in patients with HF would worsen the risk of adverse events.
John G.F. Cleland, MD, PhD, agrees. With addition of the fourth agent, “You may need to be a little bit more careful with renal function, just in that first couple of weeks,” he told this news organization. “But I think it would be easy to add an SGLT2 inhibitor into this regimen. And in general, there’s no titration with an SGLT2 inhibitor, so they’ll all be on full dose predischarge.”
Given the drugs’ diuretic-like action, moreover, some patients might be able to pull back on their loop diuretics, speculated Dr. Cleland, from the University of Glasgow’s School of Health and Wellbeing.
The prospect of a high-intensity strategy’s wide implementation in practice presents both “challenges and opportunities,” Amanda R. Vest, MBBS, MPH, Tufts University, Boston, told this news organization.
“There may be additional challenges in terms of ensuring we avoid hypotension or acute kidney injury in the up-titration phase,” said Dr. Vest, who is medical director of her center’s cardiac transplantation program but not connected with STRONG-HF.
“But it also gives us opportunities,” she added, “because there are some patients, especially in that vulnerable postdischarge phase, who are actually much more able to tolerate introduction of an SGLT2 inhibitor than, for example, an ACE inhibitor, ARB, or ARNI – or maybe a beta-blocker if they’ve been in a low cardiac-output state.” Effective dosing would depend on “the personalization and skill of the clinician in optimizing the medications in their correct sequence,” Dr. Vest said.
“It’s challenging to think that we would ever get to 100% up-titration,” she added, “and even in this excellent study, they didn’t get to 100%.” But as clinicians gain experience with the high-intensity strategy, especially as the SGLT2 inhibitors are included, “I think we can reasonably expect more progress to be made in these up-titration skills.”
No restrictions on LVEF
The researchers entered 1,078 patients hospitalized with acute HF in 14 countries across Africa, Europe, the Middle East, and South America, and randomly assigned them to the high-intensity management strategy or usual care.
About 60% of the patients were male and 77% were White. There were no entry restrictions based on left ventricular ejection fraction (LVEF), which exceeded 40% in almost a third of cases.
In the high-intensity care group’s 542 patients, the three agents were up-titrated to 50% of the maximum guideline-recommended dosage prior to hospital discharge, and to 100% within 2 weeks after discharge. Symptoms and laboratory biomarkers, including natriuretic peptides, were monitored closely at four planned clinical visits over the following 6 weeks.
The 536 patients assigned to usual care were discharged and managed according to local standards, with their meds handled by their own primary care doctors or cardiologists, the published report notes. They were reevaluated by STRONG-HF clinicians 90 days after discharge.
The number of clinic visits in the first 90 postdischarge days averaged 4.8 in the high-intensity care group and 1.0 for those receiving usual care. Full up-titration was far more likely in the high-intensity care group: 55% vs. 2% for RASI agents, 49% vs. 4% for beta-blockers, and 84% vs. 46% for MRAs.
They also fared significantly better on all measured parameters associated with decongestion, including weight, prevalence of peripheral edema, jugular venous pressure, NYHA functional class, and natriuretic peptide levels, the researchers said.
The primary endpoint of 180-day death from any cause or HF readmission was met by 15.2% of the high-intensity care group and 23.3% of usual-care patients, for an adjusted risk ratio (RR) of 0.66 (95% CI, 0.50-0.86; P = .0021).
Subgroup analyses saw no significant interactions by age, sex, race, geography, or baseline blood pressure, renal function, or LVEF. Patients with higher vs. lower baseline natriuretic peptide levels trend toward better responses to high-intensity care (P = .08)
The COVID effect
The group performed a sensitivity analysis that excluded deaths attributed to COVID-19 in STRONG-HF, which launched prior to the pandemic. The high-intensity strategy’s benefit for the primary endpoint grew, with an adjusted RR of 0.61 (95% CI, 0.46-0.82; P = .0005). There was no corresponding effect on death from any cause (P = .15).
Treatment-related adverse effects in the overall trial were seen in 41.1% of the high-intensity care group and in 29.5% of those assigned to usual care.
The higher rate in the high-intensity care arm “may be related to their higher number of [clinic] visits compared to usual care,” Dr. Mebazaa said. “However, serious adverse events and fatal adverse events were similar in both arms.”
Cardiac failure was the most common adverse event, developing in about 15% in both groups. It was followed by hypotension, hyperkalemia, and renal impairment, according to the published report.
Dr. Cleland cautioned that the risk of adverse events would potentially be higher should the high-intensity strategy become common clinical practice. The median age in STRONG-HF was 63, which is “10-15 years younger, on average, than the population with recently admitted heart failure that we see. There’s no doubt that older people have more multimorbidity.”
STRONG-HF was funded by Roche Diagnostics. Dr. Mebazaa discloses receiving grants from Roche Diagnostics, Abbott Laboratories, 4TEEN4, and Windtree Therapeutics; honoraria for lectures from Roche Diagnostics, Bayer, and Merck, Sharp & Dohme; and consulting for Corteria Pharmaceuticals, S-form Pharma, FIRE-1, Implicity, 4TEEN4, and Adrenomed; and to being a co-inventor on a patent involving combination therapy for patients having acute or persistent dyspnea.
Dr. Vest reports modest relationships with Boehringer Ingelheim, Corvia, and CareDx; and receiving research grants from the American Heart Association and the National Institutes of Health. Dr. Cleland discloses receiving honoraria from Idorsia; and research grants from Vifor Pharma, Medtronic, Bayer, and Bristol-Myers Squibb. Dr. Leon had no disclosures.
A version of this article first appeared on Medscape.com.
CHICAGO – Clinicians who prescribe heart failure meds are holding the best hand they’ve ever had, but with so much underuse and suboptimal dosing in actual practice, it seems many may not appreciate the value of their cards. But a major randomized trial that has captured the field’s attention may embolden them to go all in.
Results showed that a strategy of early, rapid up-titration of multiple guideline-directed meds in patients hospitalized with heart failure, compared with a usual-care approach, cut their 6-month risk for death or HF readmission by a steep 34% (P = .002).
The drugs had been started and partly up-titrated in the hospital with the goal of full up-titration within 2 weeks after discharge.
Patients well tolerated the high-intensity approach, researchers said. Their quality-of-life scores improved (P < .0001) compared with the usual-care group, and adverse events were considered few and manageable in the international trial with more than 1,000 patients.
Safety on the high-intensity strategy depended on close patient monitoring at frequently planned clinic visits along with guidance for the up-titrations from clinical signs and natriuretic peptide levels, observed Alexandre Mebazaa, MD, PhD, University of Paris and Public Hospitals of Paris.
Dr. Mebazaa is principal investigator on the trial, called STRONG-HF, which he presented at the American Heart Association scientific sessions, held in Chicago and virtually. He is also lead author on the study’s same-day publication in the Lancet.
The high-intensity strategy’s superiority emerged early in the trial, which was halted early on the data safety monitoring board’s recommendation, with about 90% of follow-ups completed. The board “felt it was unethical to keep patients in usual care,” Dr. Mebazaa said at a press conference.
A dramatic change
The next step, he said, will be to educate the heart failure community on the high-intensity care technique so it can swiftly enter clinical practice. Currently in acute heart failure, “very few patients are monitored after discharge and treated with full doses of heart failure therapies.”
Adoption of the strategy “would be a dramatic change from what’s currently being done,” said Martin B. Leon, MD, NewYork-Presbyterian/Columbia University Irving Medical Center, New York, who moderated the press conference.
Only an estimated 5% of patients with HF in the United States receive full guideline-directed medical therapy, Dr. Leon said, “so the generalizability of this strategy, with careful follow-up that has safety involved in it, is absolutely crucial.”
But the potential impact of this high-intensity approach on resource use is unknown, raising questions about how widely and consistently it could be implemented, said Dr. Leon, who is not connected with STRONG-HF.
The trial called for in-hospital initiation of the three distinct drug classes that, at the time, were the core of guideline-directed HF therapy, with up-titration to 50% of recommended dosage by hospital discharge, and then to 100% within 2 weeks later.
The meds included a beta-blocker, a mineralocorticoid receptor antagonist (MRA), and a renin-angiotensin system inhibitor (RASI). The latter could be an ACE inhibitor, angiotensin-receptor blocker (ARB), or angiotensin receptor-neprilysin inhibitor (ARNI).
How about a fourth drug?
Conspicuously absent from the list, for contemporary practice, was an SGLT2 inhibitor, a class that entered the HF guidelines well after STRONG-HF was designed. They would undoubtedly join the other three agents were the high-intensity strategy to enter practice, potentially changing its complexity and safety profile.
But Dr. Mebazaa and other experts don’t see that as a big challenge and would expect a smooth transition to a high-intensity approach that also includes the SGLT2 inhibitors.
STRONG-HF was necessary in part because many clinicians have been “reluctant” to take full advantage of three agents that had been the basis of guideline-directed therapy, he told this news organization.
That reluctance stemmed from concerns that beta-blockers might worsen the heart failure, ACE inhibitors could hurt the kidneys, or MRAs might cause hyperkalemia, Dr. Mebazaa said. The STRONG-HF high-intensity regimen, therefore, demanded multiple clinic visits for close follow-up.
But the SGLT2 inhibitors “are known to be rather safe drugs, at least much safer than the three others,” he said. So, it seems unlikely that their addition to a beta-blocker, RASI, and MRA in patients with HF would worsen the risk of adverse events.
John G.F. Cleland, MD, PhD, agrees. With addition of the fourth agent, “You may need to be a little bit more careful with renal function, just in that first couple of weeks,” he told this news organization. “But I think it would be easy to add an SGLT2 inhibitor into this regimen. And in general, there’s no titration with an SGLT2 inhibitor, so they’ll all be on full dose predischarge.”
Given the drugs’ diuretic-like action, moreover, some patients might be able to pull back on their loop diuretics, speculated Dr. Cleland, from the University of Glasgow’s School of Health and Wellbeing.
The prospect of a high-intensity strategy’s wide implementation in practice presents both “challenges and opportunities,” Amanda R. Vest, MBBS, MPH, Tufts University, Boston, told this news organization.
“There may be additional challenges in terms of ensuring we avoid hypotension or acute kidney injury in the up-titration phase,” said Dr. Vest, who is medical director of her center’s cardiac transplantation program but not connected with STRONG-HF.
“But it also gives us opportunities,” she added, “because there are some patients, especially in that vulnerable postdischarge phase, who are actually much more able to tolerate introduction of an SGLT2 inhibitor than, for example, an ACE inhibitor, ARB, or ARNI – or maybe a beta-blocker if they’ve been in a low cardiac-output state.” Effective dosing would depend on “the personalization and skill of the clinician in optimizing the medications in their correct sequence,” Dr. Vest said.
“It’s challenging to think that we would ever get to 100% up-titration,” she added, “and even in this excellent study, they didn’t get to 100%.” But as clinicians gain experience with the high-intensity strategy, especially as the SGLT2 inhibitors are included, “I think we can reasonably expect more progress to be made in these up-titration skills.”
No restrictions on LVEF
The researchers entered 1,078 patients hospitalized with acute HF in 14 countries across Africa, Europe, the Middle East, and South America, and randomly assigned them to the high-intensity management strategy or usual care.
About 60% of the patients were male and 77% were White. There were no entry restrictions based on left ventricular ejection fraction (LVEF), which exceeded 40% in almost a third of cases.
In the high-intensity care group’s 542 patients, the three agents were up-titrated to 50% of the maximum guideline-recommended dosage prior to hospital discharge, and to 100% within 2 weeks after discharge. Symptoms and laboratory biomarkers, including natriuretic peptides, were monitored closely at four planned clinical visits over the following 6 weeks.
The 536 patients assigned to usual care were discharged and managed according to local standards, with their meds handled by their own primary care doctors or cardiologists, the published report notes. They were reevaluated by STRONG-HF clinicians 90 days after discharge.
The number of clinic visits in the first 90 postdischarge days averaged 4.8 in the high-intensity care group and 1.0 for those receiving usual care. Full up-titration was far more likely in the high-intensity care group: 55% vs. 2% for RASI agents, 49% vs. 4% for beta-blockers, and 84% vs. 46% for MRAs.
They also fared significantly better on all measured parameters associated with decongestion, including weight, prevalence of peripheral edema, jugular venous pressure, NYHA functional class, and natriuretic peptide levels, the researchers said.
The primary endpoint of 180-day death from any cause or HF readmission was met by 15.2% of the high-intensity care group and 23.3% of usual-care patients, for an adjusted risk ratio (RR) of 0.66 (95% CI, 0.50-0.86; P = .0021).
Subgroup analyses saw no significant interactions by age, sex, race, geography, or baseline blood pressure, renal function, or LVEF. Patients with higher vs. lower baseline natriuretic peptide levels trend toward better responses to high-intensity care (P = .08)
The COVID effect
The group performed a sensitivity analysis that excluded deaths attributed to COVID-19 in STRONG-HF, which launched prior to the pandemic. The high-intensity strategy’s benefit for the primary endpoint grew, with an adjusted RR of 0.61 (95% CI, 0.46-0.82; P = .0005). There was no corresponding effect on death from any cause (P = .15).
Treatment-related adverse effects in the overall trial were seen in 41.1% of the high-intensity care group and in 29.5% of those assigned to usual care.
The higher rate in the high-intensity care arm “may be related to their higher number of [clinic] visits compared to usual care,” Dr. Mebazaa said. “However, serious adverse events and fatal adverse events were similar in both arms.”
Cardiac failure was the most common adverse event, developing in about 15% in both groups. It was followed by hypotension, hyperkalemia, and renal impairment, according to the published report.
Dr. Cleland cautioned that the risk of adverse events would potentially be higher should the high-intensity strategy become common clinical practice. The median age in STRONG-HF was 63, which is “10-15 years younger, on average, than the population with recently admitted heart failure that we see. There’s no doubt that older people have more multimorbidity.”
STRONG-HF was funded by Roche Diagnostics. Dr. Mebazaa discloses receiving grants from Roche Diagnostics, Abbott Laboratories, 4TEEN4, and Windtree Therapeutics; honoraria for lectures from Roche Diagnostics, Bayer, and Merck, Sharp & Dohme; and consulting for Corteria Pharmaceuticals, S-form Pharma, FIRE-1, Implicity, 4TEEN4, and Adrenomed; and to being a co-inventor on a patent involving combination therapy for patients having acute or persistent dyspnea.
Dr. Vest reports modest relationships with Boehringer Ingelheim, Corvia, and CareDx; and receiving research grants from the American Heart Association and the National Institutes of Health. Dr. Cleland discloses receiving honoraria from Idorsia; and research grants from Vifor Pharma, Medtronic, Bayer, and Bristol-Myers Squibb. Dr. Leon had no disclosures.
A version of this article first appeared on Medscape.com.
AT AHA 2022
Sham-controlled renal denervation trial for hypertension is a near miss
SPYRAL HTN–ON MED hits headwinds
CHICAGO – Renal denervation, relative to a sham procedure, was linked with statistically significant reductions in blood pressure in the newly completed SPYRAL HTN–ON MED trial, but several factors are likely to have worked in concert to prevent the study from meeting its primary endpoint.
Of these differences, probably none was more important than the substantially higher proportion of patients in the sham group that received additional BP-lowering medications over the course of the study, David E. Kandzari, MD, reported at the American Heart Association scientific sessions.

The SPYRAL HTN–ON MED pivotal trial followed the previously completed SPYRAL HTN–ON MED pilot study, which did show a significant BP-lowering effect on antihypertensive medications followed radiofrequency denervation. In a recent update of the pilot study, the effect was persistent out to 3 years.
In the SPYRAL HTN–ON MED program, patients on their second screening visit were required to have a systolic pressure of between 140 and 170 mm Hg on 24-hour ambulatory BP monitoring (ABPM) while taking up to three antihypertensive medications. Patients who entered the study were randomized to renal denervation or sham control while maintaining their baseline antihypertensive therapies.
The previously reported pilot study comprised 80 patients. The expansion pivotal trial added 257 more patients for a total cohort of 337 patients. The primary efficacy endpoint was based on a Bayesian analysis of change in 24-hour systolic ABPM at 6 months for those in the experimental arm versus those on medications alone. Participants from both the pilot and pivotal trials were included.
The prespecified definition of success for renal denervation was a 97.5% threshold for probability of superiority on the basis of this Bayesian analysis. However, the Bayesian analysis was distorted by differences in the pilot and expansion cohorts, which complicated the superiority calculation. As a result, the analysis only yielded a 51% probability of superiority, a level substantially below the predefined threshold.
Despite differences seen in BP control in favor of renal denervation, several factors were identified that likely contributed to the missed primary endpoint. One stood out.
“Significant differences in medication prescriptions were disproportionate in favor of the sham group,” reported Dr. Kandzari, chief of Piedmont Heart Institute, Atlanta. He said these differences, which were a violation of the protocol mandate, led to a “bias toward the null” for the primary outcome.
The failure to meet the primary outcome was particularly disappointing in the wake of the favorable pilot study and the SPYRAL HTN–OFF MED pivotal trial, which were both positive.
In the pilot study, which did not have a medication imbalance, a 7.3–mm Hg reduction (P = .004) in 24-hour ABPM was seen at 6 months. Relative reductions in office-based systolic pressure reductions for renal denervation versus sham were 6.6 mm Hg (P = .03) and 4.0 mm Hg (P = .03) for the pilot and expansions groups, respectively.
On the basis of a Win ratio derived from a hierarchical analysis of ABMP and medication burden reduction, the 1.50 advantage (P = .005) for the renal denervation arm in the newly completed SPYRAL HTN–ON MED trial was also compelling.
At study entry, the median number of medications was 1.9 in both the renal denervation and sham arms. At the end of 6 months, the median number of medications was unchanged in the experimental arm but rose to 2.1 (P = .01) in the sham group. Similarly, there was little change in the medication burden from the start to the end of the trial in the denervation group (2.8 vs. 3.0), but a statistically significant change in the sham group (2.9 vs. 3.5; P = .04).
Furthermore, the net percentage change of patients receiving medications favoring BP reduction over the course of the study did not differ between the experimental and control arms of the pilot cohort, but was more than 10 times higher among controls in the expansion group (1.9% vs. 21.8%; P < .0001).
Medication changes over the course of the SPYRAL HTN–ON MED trial were even greater in some specific subgroups. Among Black participants, for example, 14.2% of those randomized to renal denervation and 54.6% of those randomized to the sham group increased their antihypertensive therapies over the course of the study.
The COVID-19 epidemic is suspected of playing another role in the negative results, according to Dr. Kandzari. After a brief pause in enrollment, the SPYRAL HTN–ON MED trial was resumed, but approximately 80% of the expansion cohort data were collected during this period. When compared, variances in office and 24-hour ABPM were observed for participants who were or were not evaluated during COVID.
“Significant differences in 24-hour ABPM patterns pre- and during COVID may reflect changes in patient behavior and lifestyle,” Dr. Kandzari speculated.
The data from this study differ from essentially all of the other studies in the SPYRAL HTN program as well as several other sham-controlled studies with renal denervation, according to Dr. Kandzari.

The AHA-invited discussant, Ajay J. Kirtane, MD, director of the Cardiac Catheterization Laboratories at Columbia University, New York, largely agreed that several variables appeared to conspire against a positive result in this trial, but he zeroed in on the imbalance of antihypertensive medications.
“Any trial that attempts to show a difference between renal denervation and a sham procedure must insure that antihypertensive medications are the same in the two arms. They cannot be different,” he said.
As an active investigator in the field of renal denervation, Dr. Kirtane thinks the evidence does support a benefit from renal denervation, but he believes data are still needed to determine which patients are candidates.
“Renal denervation is not going to be a replacement for previous established therapies, but it will be an adjunct,” he predicted. The preponderance of evidence supports clinically meaningful reductions in BP with this approach, “but we need to determine who to consider [for this therapy] and to have realistic expectations about the degree of benefit.”
Dr. Kandzari reported financial relationships with Abbott Vascular, Ablative Solutions, Biotronik, Boston Scientific, CSI, Medtronic Cardiovascular, OrbusNeich, and Teleflex. Dr. Kirtane reported financial relationships with Abbott Vascular, Abiomed, Boston Scientific, Cardiovascular Systems, Cathworks, Chiesi, Medtronic, Opens, Philipps, Regeneron, ReCor Medical, Siemens, Spectranetics, and Zoll.
SPYRAL HTN–ON MED hits headwinds
SPYRAL HTN–ON MED hits headwinds
CHICAGO – Renal denervation, relative to a sham procedure, was linked with statistically significant reductions in blood pressure in the newly completed SPYRAL HTN–ON MED trial, but several factors are likely to have worked in concert to prevent the study from meeting its primary endpoint.
Of these differences, probably none was more important than the substantially higher proportion of patients in the sham group that received additional BP-lowering medications over the course of the study, David E. Kandzari, MD, reported at the American Heart Association scientific sessions.
The SPYRAL HTN–ON MED pivotal trial followed the previously completed SPYRAL HTN–ON MED pilot study, which did show a significant BP-lowering effect on antihypertensive medications followed radiofrequency denervation. In a recent update of the pilot study, the effect was persistent out to 3 years.
In the SPYRAL HTN–ON MED program, patients on their second screening visit were required to have a systolic pressure of between 140 and 170 mm Hg on 24-hour ambulatory BP monitoring (ABPM) while taking up to three antihypertensive medications. Patients who entered the study were randomized to renal denervation or sham control while maintaining their baseline antihypertensive therapies.
The previously reported pilot study comprised 80 patients. The expansion pivotal trial added 257 more patients for a total cohort of 337 patients. The primary efficacy endpoint was based on a Bayesian analysis of change in 24-hour systolic ABPM at 6 months for those in the experimental arm versus those on medications alone. Participants from both the pilot and pivotal trials were included.
The prespecified definition of success for renal denervation was a 97.5% threshold for probability of superiority on the basis of this Bayesian analysis. However, the Bayesian analysis was distorted by differences in the pilot and expansion cohorts, which complicated the superiority calculation. As a result, the analysis only yielded a 51% probability of superiority, a level substantially below the predefined threshold.
Despite differences seen in BP control in favor of renal denervation, several factors were identified that likely contributed to the missed primary endpoint. One stood out.
“Significant differences in medication prescriptions were disproportionate in favor of the sham group,” reported Dr. Kandzari, chief of Piedmont Heart Institute, Atlanta. He said these differences, which were a violation of the protocol mandate, led to a “bias toward the null” for the primary outcome.
The failure to meet the primary outcome was particularly disappointing in the wake of the favorable pilot study and the SPYRAL HTN–OFF MED pivotal trial, which were both positive.
In the pilot study, which did not have a medication imbalance, a 7.3–mm Hg reduction (P = .004) in 24-hour ABPM was seen at 6 months. Relative reductions in office-based systolic pressure reductions for renal denervation versus sham were 6.6 mm Hg (P = .03) and 4.0 mm Hg (P = .03) for the pilot and expansions groups, respectively.
On the basis of a Win ratio derived from a hierarchical analysis of ABMP and medication burden reduction, the 1.50 advantage (P = .005) for the renal denervation arm in the newly completed SPYRAL HTN–ON MED trial was also compelling.
At study entry, the median number of medications was 1.9 in both the renal denervation and sham arms. At the end of 6 months, the median number of medications was unchanged in the experimental arm but rose to 2.1 (P = .01) in the sham group. Similarly, there was little change in the medication burden from the start to the end of the trial in the denervation group (2.8 vs. 3.0), but a statistically significant change in the sham group (2.9 vs. 3.5; P = .04).
Furthermore, the net percentage change of patients receiving medications favoring BP reduction over the course of the study did not differ between the experimental and control arms of the pilot cohort, but was more than 10 times higher among controls in the expansion group (1.9% vs. 21.8%; P < .0001).
Medication changes over the course of the SPYRAL HTN–ON MED trial were even greater in some specific subgroups. Among Black participants, for example, 14.2% of those randomized to renal denervation and 54.6% of those randomized to the sham group increased their antihypertensive therapies over the course of the study.
The COVID-19 epidemic is suspected of playing another role in the negative results, according to Dr. Kandzari. After a brief pause in enrollment, the SPYRAL HTN–ON MED trial was resumed, but approximately 80% of the expansion cohort data were collected during this period. When compared, variances in office and 24-hour ABPM were observed for participants who were or were not evaluated during COVID.
“Significant differences in 24-hour ABPM patterns pre- and during COVID may reflect changes in patient behavior and lifestyle,” Dr. Kandzari speculated.
The data from this study differ from essentially all of the other studies in the SPYRAL HTN program as well as several other sham-controlled studies with renal denervation, according to Dr. Kandzari.
The AHA-invited discussant, Ajay J. Kirtane, MD, director of the Cardiac Catheterization Laboratories at Columbia University, New York, largely agreed that several variables appeared to conspire against a positive result in this trial, but he zeroed in on the imbalance of antihypertensive medications.
“Any trial that attempts to show a difference between renal denervation and a sham procedure must insure that antihypertensive medications are the same in the two arms. They cannot be different,” he said.
As an active investigator in the field of renal denervation, Dr. Kirtane thinks the evidence does support a benefit from renal denervation, but he believes data are still needed to determine which patients are candidates.
“Renal denervation is not going to be a replacement for previous established therapies, but it will be an adjunct,” he predicted. The preponderance of evidence supports clinically meaningful reductions in BP with this approach, “but we need to determine who to consider [for this therapy] and to have realistic expectations about the degree of benefit.”
Dr. Kandzari reported financial relationships with Abbott Vascular, Ablative Solutions, Biotronik, Boston Scientific, CSI, Medtronic Cardiovascular, OrbusNeich, and Teleflex. Dr. Kirtane reported financial relationships with Abbott Vascular, Abiomed, Boston Scientific, Cardiovascular Systems, Cathworks, Chiesi, Medtronic, Opens, Philipps, Regeneron, ReCor Medical, Siemens, Spectranetics, and Zoll.
CHICAGO – Renal denervation, relative to a sham procedure, was linked with statistically significant reductions in blood pressure in the newly completed SPYRAL HTN–ON MED trial, but several factors are likely to have worked in concert to prevent the study from meeting its primary endpoint.
Of these differences, probably none was more important than the substantially higher proportion of patients in the sham group that received additional BP-lowering medications over the course of the study, David E. Kandzari, MD, reported at the American Heart Association scientific sessions.
The SPYRAL HTN–ON MED pivotal trial followed the previously completed SPYRAL HTN–ON MED pilot study, which did show a significant BP-lowering effect on antihypertensive medications followed radiofrequency denervation. In a recent update of the pilot study, the effect was persistent out to 3 years.
In the SPYRAL HTN–ON MED program, patients on their second screening visit were required to have a systolic pressure of between 140 and 170 mm Hg on 24-hour ambulatory BP monitoring (ABPM) while taking up to three antihypertensive medications. Patients who entered the study were randomized to renal denervation or sham control while maintaining their baseline antihypertensive therapies.
The previously reported pilot study comprised 80 patients. The expansion pivotal trial added 257 more patients for a total cohort of 337 patients. The primary efficacy endpoint was based on a Bayesian analysis of change in 24-hour systolic ABPM at 6 months for those in the experimental arm versus those on medications alone. Participants from both the pilot and pivotal trials were included.
The prespecified definition of success for renal denervation was a 97.5% threshold for probability of superiority on the basis of this Bayesian analysis. However, the Bayesian analysis was distorted by differences in the pilot and expansion cohorts, which complicated the superiority calculation. As a result, the analysis only yielded a 51% probability of superiority, a level substantially below the predefined threshold.
Despite differences seen in BP control in favor of renal denervation, several factors were identified that likely contributed to the missed primary endpoint. One stood out.
“Significant differences in medication prescriptions were disproportionate in favor of the sham group,” reported Dr. Kandzari, chief of Piedmont Heart Institute, Atlanta. He said these differences, which were a violation of the protocol mandate, led to a “bias toward the null” for the primary outcome.
The failure to meet the primary outcome was particularly disappointing in the wake of the favorable pilot study and the SPYRAL HTN–OFF MED pivotal trial, which were both positive.
In the pilot study, which did not have a medication imbalance, a 7.3–mm Hg reduction (P = .004) in 24-hour ABPM was seen at 6 months. Relative reductions in office-based systolic pressure reductions for renal denervation versus sham were 6.6 mm Hg (P = .03) and 4.0 mm Hg (P = .03) for the pilot and expansions groups, respectively.
On the basis of a Win ratio derived from a hierarchical analysis of ABMP and medication burden reduction, the 1.50 advantage (P = .005) for the renal denervation arm in the newly completed SPYRAL HTN–ON MED trial was also compelling.
At study entry, the median number of medications was 1.9 in both the renal denervation and sham arms. At the end of 6 months, the median number of medications was unchanged in the experimental arm but rose to 2.1 (P = .01) in the sham group. Similarly, there was little change in the medication burden from the start to the end of the trial in the denervation group (2.8 vs. 3.0), but a statistically significant change in the sham group (2.9 vs. 3.5; P = .04).
Furthermore, the net percentage change of patients receiving medications favoring BP reduction over the course of the study did not differ between the experimental and control arms of the pilot cohort, but was more than 10 times higher among controls in the expansion group (1.9% vs. 21.8%; P < .0001).
Medication changes over the course of the SPYRAL HTN–ON MED trial were even greater in some specific subgroups. Among Black participants, for example, 14.2% of those randomized to renal denervation and 54.6% of those randomized to the sham group increased their antihypertensive therapies over the course of the study.
The COVID-19 epidemic is suspected of playing another role in the negative results, according to Dr. Kandzari. After a brief pause in enrollment, the SPYRAL HTN–ON MED trial was resumed, but approximately 80% of the expansion cohort data were collected during this period. When compared, variances in office and 24-hour ABPM were observed for participants who were or were not evaluated during COVID.
“Significant differences in 24-hour ABPM patterns pre- and during COVID may reflect changes in patient behavior and lifestyle,” Dr. Kandzari speculated.
The data from this study differ from essentially all of the other studies in the SPYRAL HTN program as well as several other sham-controlled studies with renal denervation, according to Dr. Kandzari.
The AHA-invited discussant, Ajay J. Kirtane, MD, director of the Cardiac Catheterization Laboratories at Columbia University, New York, largely agreed that several variables appeared to conspire against a positive result in this trial, but he zeroed in on the imbalance of antihypertensive medications.
“Any trial that attempts to show a difference between renal denervation and a sham procedure must insure that antihypertensive medications are the same in the two arms. They cannot be different,” he said.
As an active investigator in the field of renal denervation, Dr. Kirtane thinks the evidence does support a benefit from renal denervation, but he believes data are still needed to determine which patients are candidates.
“Renal denervation is not going to be a replacement for previous established therapies, but it will be an adjunct,” he predicted. The preponderance of evidence supports clinically meaningful reductions in BP with this approach, “but we need to determine who to consider [for this therapy] and to have realistic expectations about the degree of benefit.”
Dr. Kandzari reported financial relationships with Abbott Vascular, Ablative Solutions, Biotronik, Boston Scientific, CSI, Medtronic Cardiovascular, OrbusNeich, and Teleflex. Dr. Kirtane reported financial relationships with Abbott Vascular, Abiomed, Boston Scientific, Cardiovascular Systems, Cathworks, Chiesi, Medtronic, Opens, Philipps, Regeneron, ReCor Medical, Siemens, Spectranetics, and Zoll.
AT AHA 2022
Four-drug combo gets BP down in one step: QUARTET-USA
Use of a combination antihypertensive product containing quarter doses of four different drugs could be an effective strategy to get patients to target blood pressures in one step, a new study suggests.
The study, QUARTET-USA, showed a reduction in BP of almost 5 mm Hg more than the comparator of one antihypertensive agent at standard dose over the 12-week follow-up period in patients with mild to moderate hypertension.
The QUARTET-USA study was presented at the American Heart Association scientific sessions by Mark Huffman, MD, professor of medicine at Washington University in St. Louis.
It builds on a previous trial, QUARTET, conducted in Australia, which first showed benefits with this approach.
In the new U.S. study, which was considerably smaller than the Australian trial, the four-drug combination, including candesartan, amlodipine, indapamide, and bisoprolol, led to a –4.8/–4.9 mm Hg greater reduction in BP from baseline to 12 weeks, compared with standard-dose candesartan monotherapy.
Differences in systolic BP were not statistically significant, which is likely because of limited power related to the sample size, Dr. Huffman noted.
Adverse events were more common in the four-drug intervention group, but the rate of discontinuation was higher in the comparator group. No severe adverse events were deemed related to the study drug.
“The direction and magnitude of [the] blood pressure–lowering effect were similar between the previous Australian study and this American study, despite different populations with lower baseline blood pressure in the current study, thus strengthening the case for this new approach,” Dr. Huffman concluded.
“The two studies together show that the approach of using four drugs in quarter doses is more effective in lowering blood pressure than a single standard dose antihypertensive agent and has an acceptable safely profile,” he said in an interview.
He said the four-drug combination could be an effective way of getting patients to target without multiple appointments.
“If you think about how many visits to the doctor’s office it takes to get patients to goal blood pressures, this combination gets patients down to new guideline target levels in one step, whereas in the SPRINT trial it took three or more visits to get down to these levels. And in practice we lose people – they don’t come back,” he said.
Dr. Huffman explained that the rationale for the study was the persistently low hypertension control rate, which demonstrates the need for a new approach.
The previous Australian QUARTET study suggested that ultra–low-dose combination therapy has a favorable balance between blood pressure–lowering effect, tolerability, and adherence.
That study, conducted in 591 patients and reported in 2021, demonstrated a greater BP-lowering effect with a four-drug combination at quarter doses (irbesartan 37.5 mg, amlodipine 1.25 mg, indapamide 0.625 mg, bisoprolol 2.5 mg) at 12 weeks, compared with irbesartan 150 mg daily. Systolic BP was reduced by more than 6.9 mm Hg and diastolic BP by 5.8 mm Hg than full-dose irbesartan alone, both significant differences.
The current study, QUARTET-USA, aimed to see if a similar strategy could produce comparable results in a U.S. population.
The U.S. study included 62 patients from the Access Community Health Network, Chicago, who were either treatment naive with BPs above 140/90 mm Hg, or already taking antihypertensive monotherapy with BPs above 130/85 mm Hg.
The mean systolic BP at baseline was 138 mm Hg and the mean diastolic pressure was 84 mm Hg.
Study participants were mainly from ethnic minorities (90% Hispanic or Black) and over half were from low-income households (annual household income less than $25,000).
They were randomly assigned to daily administration of a four-drug combination at quarter doses (candesartan 2 mg, amlodipine 1.25 mg, indapamide 0.625 mg, bisoprolol 2.5 mg) or a full dose of candesartan 8 mg (the comparator arm).
Amlodipine 5 mg daily could be added on to treatment if BP remained above 130/80 mm Hg at 6 weeks. This occurred in 18% of the study group versus 53% of the comparator group.
Results showed that at 12 weeks the adjusted mean change in systolic BP weeks was –4.8 mm Hg (95% CI,–10.7 to 1.2), and the adjusted mean change in diastolic BP was –4.9 mm Hg (95% CI, –8.6 to –1.1) in the four-drug combination group, compared with the comparator arm.
Average BPs at the end of 12-week study period were 121 mm Hg systolic and 73 mm Hg diastolic in the four-drug intervention group, compared with 124 mm Hg systolic and 77 mm Hg diastolic in the comparator group.
Any adverse events that were possibly related to drug therapy occurred in 25% of the intervention group versus 10% of the comparator group. But adverse events leading to discontinuation occurred in 6.3% of the study group versus 26.7% of patients in the comparator arm.
“New approaches are needed to achieve lower blood pressure targets, especially for patients and communities with a high burden of hypertension and hypertension-related diseases. QUARTET-USA was the first trial of a four-drug, ultra–low-dose, blood pressure–lowering combination therapy in the U.S.,” Dr. Huffman said.
“We showed reductions in blood pressure similar in magnitude to those in the Australian study. It is useful to know that the direction of the effect is similar across varied populations. Now that we have that signal of efficacy and tolerability, we can move to actually getting it into the hands of patients and providers,” he added.
Noting that further studies will be required to attain marketing authorization, Dr. Huffman suggested that a pharmaceutical company would need to complete that process.
“These are promising results for companies who may be interested in partnering,” he said.
‘A more efficient approach’
LaPrincess C. Brewer, MD, assistant professor of medicine at the Mayo Clinic, Rochester, Minn., and discussant of the study, said the QUARTET-USA study suggests the four-drug, low-dose combination shows promise in lowering BP, compared with the standard dose, and while the reduction in systolic BP was not quite significant, it was clinically meaningful.
“Most U.S. adults with hypertension do not have it under control. This is due to unfavorable social and structural determinants of health which limit adherence to antihypertensive medication,” Dr. Brewer noted.
From a patient point of view, the multiple visits needed to attain goals are a burden and there is also the issue of clinical inertia and lack of medication intensification by clinicians, she commented.
“Of patients with uncontrolled hypertension, 40% are taking just one antihypertensive medication, so up-front, low-dose combination therapy is likely a more efficient approach,” she said.
“This study builds the evidence base for the need for tailored interventions that address the social determinants of health and the intentional prioritization of diverse population in clinical trials,” Dr. Brewer concluded.
QUARTET was an investigator-initiated study, Dr. Huffman reported a pending patent for a heart failure polypill. The George Institute for Global Health, Sydney, Australia, where Huffman has a secondary appointment, has a patent, license, and has received investment funding with intent to commercialize fixed-dose combination therapy. Dr. Brewer reported research support from the National Institutes of Health, Centers for Disease Control and Prevention, American Heart Association, and Bristol-Meyers Squibb Foundation.
A version of this article first appeared on Medscape.com.
Use of a combination antihypertensive product containing quarter doses of four different drugs could be an effective strategy to get patients to target blood pressures in one step, a new study suggests.
The study, QUARTET-USA, showed a reduction in BP of almost 5 mm Hg more than the comparator of one antihypertensive agent at standard dose over the 12-week follow-up period in patients with mild to moderate hypertension.
The QUARTET-USA study was presented at the American Heart Association scientific sessions by Mark Huffman, MD, professor of medicine at Washington University in St. Louis.
It builds on a previous trial, QUARTET, conducted in Australia, which first showed benefits with this approach.
In the new U.S. study, which was considerably smaller than the Australian trial, the four-drug combination, including candesartan, amlodipine, indapamide, and bisoprolol, led to a –4.8/–4.9 mm Hg greater reduction in BP from baseline to 12 weeks, compared with standard-dose candesartan monotherapy.
Differences in systolic BP were not statistically significant, which is likely because of limited power related to the sample size, Dr. Huffman noted.
Adverse events were more common in the four-drug intervention group, but the rate of discontinuation was higher in the comparator group. No severe adverse events were deemed related to the study drug.
“The direction and magnitude of [the] blood pressure–lowering effect were similar between the previous Australian study and this American study, despite different populations with lower baseline blood pressure in the current study, thus strengthening the case for this new approach,” Dr. Huffman concluded.
“The two studies together show that the approach of using four drugs in quarter doses is more effective in lowering blood pressure than a single standard dose antihypertensive agent and has an acceptable safely profile,” he said in an interview.
He said the four-drug combination could be an effective way of getting patients to target without multiple appointments.
“If you think about how many visits to the doctor’s office it takes to get patients to goal blood pressures, this combination gets patients down to new guideline target levels in one step, whereas in the SPRINT trial it took three or more visits to get down to these levels. And in practice we lose people – they don’t come back,” he said.
Dr. Huffman explained that the rationale for the study was the persistently low hypertension control rate, which demonstrates the need for a new approach.
The previous Australian QUARTET study suggested that ultra–low-dose combination therapy has a favorable balance between blood pressure–lowering effect, tolerability, and adherence.
That study, conducted in 591 patients and reported in 2021, demonstrated a greater BP-lowering effect with a four-drug combination at quarter doses (irbesartan 37.5 mg, amlodipine 1.25 mg, indapamide 0.625 mg, bisoprolol 2.5 mg) at 12 weeks, compared with irbesartan 150 mg daily. Systolic BP was reduced by more than 6.9 mm Hg and diastolic BP by 5.8 mm Hg than full-dose irbesartan alone, both significant differences.
The current study, QUARTET-USA, aimed to see if a similar strategy could produce comparable results in a U.S. population.
The U.S. study included 62 patients from the Access Community Health Network, Chicago, who were either treatment naive with BPs above 140/90 mm Hg, or already taking antihypertensive monotherapy with BPs above 130/85 mm Hg.
The mean systolic BP at baseline was 138 mm Hg and the mean diastolic pressure was 84 mm Hg.
Study participants were mainly from ethnic minorities (90% Hispanic or Black) and over half were from low-income households (annual household income less than $25,000).
They were randomly assigned to daily administration of a four-drug combination at quarter doses (candesartan 2 mg, amlodipine 1.25 mg, indapamide 0.625 mg, bisoprolol 2.5 mg) or a full dose of candesartan 8 mg (the comparator arm).
Amlodipine 5 mg daily could be added on to treatment if BP remained above 130/80 mm Hg at 6 weeks. This occurred in 18% of the study group versus 53% of the comparator group.
Results showed that at 12 weeks the adjusted mean change in systolic BP weeks was –4.8 mm Hg (95% CI,–10.7 to 1.2), and the adjusted mean change in diastolic BP was –4.9 mm Hg (95% CI, –8.6 to –1.1) in the four-drug combination group, compared with the comparator arm.
Average BPs at the end of 12-week study period were 121 mm Hg systolic and 73 mm Hg diastolic in the four-drug intervention group, compared with 124 mm Hg systolic and 77 mm Hg diastolic in the comparator group.
Any adverse events that were possibly related to drug therapy occurred in 25% of the intervention group versus 10% of the comparator group. But adverse events leading to discontinuation occurred in 6.3% of the study group versus 26.7% of patients in the comparator arm.
“New approaches are needed to achieve lower blood pressure targets, especially for patients and communities with a high burden of hypertension and hypertension-related diseases. QUARTET-USA was the first trial of a four-drug, ultra–low-dose, blood pressure–lowering combination therapy in the U.S.,” Dr. Huffman said.
“We showed reductions in blood pressure similar in magnitude to those in the Australian study. It is useful to know that the direction of the effect is similar across varied populations. Now that we have that signal of efficacy and tolerability, we can move to actually getting it into the hands of patients and providers,” he added.
Noting that further studies will be required to attain marketing authorization, Dr. Huffman suggested that a pharmaceutical company would need to complete that process.
“These are promising results for companies who may be interested in partnering,” he said.
‘A more efficient approach’
LaPrincess C. Brewer, MD, assistant professor of medicine at the Mayo Clinic, Rochester, Minn., and discussant of the study, said the QUARTET-USA study suggests the four-drug, low-dose combination shows promise in lowering BP, compared with the standard dose, and while the reduction in systolic BP was not quite significant, it was clinically meaningful.
“Most U.S. adults with hypertension do not have it under control. This is due to unfavorable social and structural determinants of health which limit adherence to antihypertensive medication,” Dr. Brewer noted.
From a patient point of view, the multiple visits needed to attain goals are a burden and there is also the issue of clinical inertia and lack of medication intensification by clinicians, she commented.
“Of patients with uncontrolled hypertension, 40% are taking just one antihypertensive medication, so up-front, low-dose combination therapy is likely a more efficient approach,” she said.
“This study builds the evidence base for the need for tailored interventions that address the social determinants of health and the intentional prioritization of diverse population in clinical trials,” Dr. Brewer concluded.
QUARTET was an investigator-initiated study, Dr. Huffman reported a pending patent for a heart failure polypill. The George Institute for Global Health, Sydney, Australia, where Huffman has a secondary appointment, has a patent, license, and has received investment funding with intent to commercialize fixed-dose combination therapy. Dr. Brewer reported research support from the National Institutes of Health, Centers for Disease Control and Prevention, American Heart Association, and Bristol-Meyers Squibb Foundation.
A version of this article first appeared on Medscape.com.
Use of a combination antihypertensive product containing quarter doses of four different drugs could be an effective strategy to get patients to target blood pressures in one step, a new study suggests.
The study, QUARTET-USA, showed a reduction in BP of almost 5 mm Hg more than the comparator of one antihypertensive agent at standard dose over the 12-week follow-up period in patients with mild to moderate hypertension.
The QUARTET-USA study was presented at the American Heart Association scientific sessions by Mark Huffman, MD, professor of medicine at Washington University in St. Louis.
It builds on a previous trial, QUARTET, conducted in Australia, which first showed benefits with this approach.
In the new U.S. study, which was considerably smaller than the Australian trial, the four-drug combination, including candesartan, amlodipine, indapamide, and bisoprolol, led to a –4.8/–4.9 mm Hg greater reduction in BP from baseline to 12 weeks, compared with standard-dose candesartan monotherapy.
Differences in systolic BP were not statistically significant, which is likely because of limited power related to the sample size, Dr. Huffman noted.
Adverse events were more common in the four-drug intervention group, but the rate of discontinuation was higher in the comparator group. No severe adverse events were deemed related to the study drug.
“The direction and magnitude of [the] blood pressure–lowering effect were similar between the previous Australian study and this American study, despite different populations with lower baseline blood pressure in the current study, thus strengthening the case for this new approach,” Dr. Huffman concluded.
“The two studies together show that the approach of using four drugs in quarter doses is more effective in lowering blood pressure than a single standard dose antihypertensive agent and has an acceptable safely profile,” he said in an interview.
He said the four-drug combination could be an effective way of getting patients to target without multiple appointments.
“If you think about how many visits to the doctor’s office it takes to get patients to goal blood pressures, this combination gets patients down to new guideline target levels in one step, whereas in the SPRINT trial it took three or more visits to get down to these levels. And in practice we lose people – they don’t come back,” he said.
Dr. Huffman explained that the rationale for the study was the persistently low hypertension control rate, which demonstrates the need for a new approach.
The previous Australian QUARTET study suggested that ultra–low-dose combination therapy has a favorable balance between blood pressure–lowering effect, tolerability, and adherence.
That study, conducted in 591 patients and reported in 2021, demonstrated a greater BP-lowering effect with a four-drug combination at quarter doses (irbesartan 37.5 mg, amlodipine 1.25 mg, indapamide 0.625 mg, bisoprolol 2.5 mg) at 12 weeks, compared with irbesartan 150 mg daily. Systolic BP was reduced by more than 6.9 mm Hg and diastolic BP by 5.8 mm Hg than full-dose irbesartan alone, both significant differences.
The current study, QUARTET-USA, aimed to see if a similar strategy could produce comparable results in a U.S. population.
The U.S. study included 62 patients from the Access Community Health Network, Chicago, who were either treatment naive with BPs above 140/90 mm Hg, or already taking antihypertensive monotherapy with BPs above 130/85 mm Hg.
The mean systolic BP at baseline was 138 mm Hg and the mean diastolic pressure was 84 mm Hg.
Study participants were mainly from ethnic minorities (90% Hispanic or Black) and over half were from low-income households (annual household income less than $25,000).
They were randomly assigned to daily administration of a four-drug combination at quarter doses (candesartan 2 mg, amlodipine 1.25 mg, indapamide 0.625 mg, bisoprolol 2.5 mg) or a full dose of candesartan 8 mg (the comparator arm).
Amlodipine 5 mg daily could be added on to treatment if BP remained above 130/80 mm Hg at 6 weeks. This occurred in 18% of the study group versus 53% of the comparator group.
Results showed that at 12 weeks the adjusted mean change in systolic BP weeks was –4.8 mm Hg (95% CI,–10.7 to 1.2), and the adjusted mean change in diastolic BP was –4.9 mm Hg (95% CI, –8.6 to –1.1) in the four-drug combination group, compared with the comparator arm.
Average BPs at the end of 12-week study period were 121 mm Hg systolic and 73 mm Hg diastolic in the four-drug intervention group, compared with 124 mm Hg systolic and 77 mm Hg diastolic in the comparator group.
Any adverse events that were possibly related to drug therapy occurred in 25% of the intervention group versus 10% of the comparator group. But adverse events leading to discontinuation occurred in 6.3% of the study group versus 26.7% of patients in the comparator arm.
“New approaches are needed to achieve lower blood pressure targets, especially for patients and communities with a high burden of hypertension and hypertension-related diseases. QUARTET-USA was the first trial of a four-drug, ultra–low-dose, blood pressure–lowering combination therapy in the U.S.,” Dr. Huffman said.
“We showed reductions in blood pressure similar in magnitude to those in the Australian study. It is useful to know that the direction of the effect is similar across varied populations. Now that we have that signal of efficacy and tolerability, we can move to actually getting it into the hands of patients and providers,” he added.
Noting that further studies will be required to attain marketing authorization, Dr. Huffman suggested that a pharmaceutical company would need to complete that process.
“These are promising results for companies who may be interested in partnering,” he said.
‘A more efficient approach’
LaPrincess C. Brewer, MD, assistant professor of medicine at the Mayo Clinic, Rochester, Minn., and discussant of the study, said the QUARTET-USA study suggests the four-drug, low-dose combination shows promise in lowering BP, compared with the standard dose, and while the reduction in systolic BP was not quite significant, it was clinically meaningful.
“Most U.S. adults with hypertension do not have it under control. This is due to unfavorable social and structural determinants of health which limit adherence to antihypertensive medication,” Dr. Brewer noted.
From a patient point of view, the multiple visits needed to attain goals are a burden and there is also the issue of clinical inertia and lack of medication intensification by clinicians, she commented.
“Of patients with uncontrolled hypertension, 40% are taking just one antihypertensive medication, so up-front, low-dose combination therapy is likely a more efficient approach,” she said.
“This study builds the evidence base for the need for tailored interventions that address the social determinants of health and the intentional prioritization of diverse population in clinical trials,” Dr. Brewer concluded.
QUARTET was an investigator-initiated study, Dr. Huffman reported a pending patent for a heart failure polypill. The George Institute for Global Health, Sydney, Australia, where Huffman has a secondary appointment, has a patent, license, and has received investment funding with intent to commercialize fixed-dose combination therapy. Dr. Brewer reported research support from the National Institutes of Health, Centers for Disease Control and Prevention, American Heart Association, and Bristol-Meyers Squibb Foundation.
A version of this article first appeared on Medscape.com.
FROM AHA 2022
Avoid routine early ECMO in severe cardiogenic shock: ECMO-CS
CHICAGO – Routine early, expeditious use of extracorporeal membrane oxygenation (ECMO) is a common strategy in patients with severe cardiogenic shock, but a less aggressive initial approach may be just as effective, a randomized trial suggests.
In the study that assigned patients with “rapidly deteriorating or severe” cardiogenic shock to one or the other approach, clinical outcomes were no better for those who received immediate ECMO than for those initially managed with inotropes and vasopressors, researchers said.
The conservative strategy, importantly, allowed for downstream ECMO in the event of hemodynamic deterioration, which occurred in a substantial 39% of cases, observed Petr Ostadal, MD, PhD, when presenting the results at the American Heart Association scientific sessions.
Dr. Ostadal of Na Homolce Hospital, Prague, is also first author on the published report of the study, called Extracorporeal Membrane Oxygenation in the Therapy of Cardiogenic Shock (ECMO-CS), which was published the same day in Circulation.
The trial makes a firm case for preferring the conservative initial approach over routine early ECMO in the kind of patients it entered, Larry A. Allen, MD, MHS, University of Coloradoat Denver, Aurora, told this news organization.
More than 60% of the trial’s 117 patients had shock secondary to an acute coronary syndrome; another 23% were in heart failure decompensation.
A preference for the conservative initial approach would be welcome, he said. The early aggressive ECMO approach is resource intensive and carries some important risks, such as stroke or coagulopathy, said Dr. Allen, who is not connected with ECMO-CS. Yet it is increasingly the go-to approach in such patients, based primarily on observational data.
Although early ECMO apparently didn’t benefit patients in this study in their specific stage of cardiogenic shock, Dr. Allen observed, it would presumably help some, but identifying them in practice presents challenges. “Defining where people are in the spectrum of early versus middle versus late cardiogenic shock is actually very tricky.”
It will therefore be important, he said, to identify ways to predict which conservatively managed patients do well with the strategy, and which are most at risk for hemodynamic deterioration and for whom ECMO should be readily available.
“I think part of what ECMO-CS tells us is that, if a patient is stable on intravenous inotropic and vasopressor support, you can defer ECMO while you’re thinking about the patient – about their larger context and the right medical decision-making for them.”
The trial randomly assigned 122 patients with rapidly deteriorating or severe cardiogenic shock to the immediate-ECMO or the conservative strategy at four centers in the Czech Republic. The 117 patients for whom informed consent could be obtained were included in the analysis, 58 and 59 patients, respectively. Their mean age was about 65 years and three-fourths were male.
The primary endpoint, the only endpoint for which the study was powered, consisted of death from any cause, resuscitated circulatory arrest, or use of a different form of mechanical circulatory support (MCS) by 30 days.
It occurred in 63.8% of patients assigned to immediate ECMO and 71.2% of those in the conservative strategy group, for a hazard ratio of 0.72 (95% confidence interval, 0.46-1.12; P = .21).
As individual endpoints, rates of death from any cause and resuscitated arrest did not significantly differ between the groups, but conservatively managed patients more often used another form of MCS. The HRs were 1.11 (95% CI, 0.66-1.87) for death from any cause, 0.79 (95% CI, 0.27-2.28) for resuscitated cardiac arrest, and 0.38 (95% CI, 0.18-0.79) for use of another MCS device.
The rates for serious adverse events – including bleeding, ischemia, stroke, pneumonia, or sepsis – were similar at 60.3% in the early-ECMO group and 61% in group with conservative initial management, Dr. Ostadal reported.
Other than the 23 patients in the conservative initial strategy group who went on to receive ECMO (1.9 days after randomization, on average), 1 went on to undergo implantation with a HeartMate (Abbott) ventricular assist device and 3 received an Impella pump (Abiomed).
Six patients in the early-ECMO group were already receiving intra-aortic balloon pump (IABP) support at randomization, two underwent temporary implantation with a Centrimag device (Abbott), and three went on to receive a HeartMate device, the published report notes.
ECMO is the optimal first choice for MCS in such patients with cardiogenic shock who need a circulatory support device, especially because it also oxygenates the blood, Dr. Ostadal told this news organization.
But ECMO doesn’t help with ventricular unloading. Indeed, it can sometimes reduce ventricular preload, especially if right-heart pressures are low. So MCS devices that unload the ventricle, typically an IABP, can complement ECMO.
Dr. Ostadal speculates, however, that there may be a better pairing option. “Impella plus ECMO, I think, is the combination which has a future,” he said, for patients in cardiogenic shock who need a short-term percutaneous hemodynamic support device. Impella “supports the whole circulation” and unloads the left ventricle.
“A balloon pump in combination with ECMO is still not a bad choice. It’s very cheap in comparison with Impella.” But in his opinion, Dr. Ostadal said, “The combination of Impella plus ECMO is more efficient from a hemodynamic point of view.”
As the published report notes, ongoing randomized trials looking at ECMO plus other MCS devices in cardiogenic shock include ECLS-SHOCK, with a projected enrollment of 420 patients, and EURO-SHOCK, aiming for a similar number of patients; both compare routine ECMO to conservative management.
In addition, ANCHOR, in which ECMO is combined with IABP, and DanShock, which looks at early use of Impella rather than ECMO, are enrolling patients with shock secondary to acute coronary syndromes.
Dr. Ostadal disclosed consulting for Getinge, Edwards, Medtronic, Biomedica, and Xenios/Fresenius, and receiving research support from Xenios/Fresenius. Dr. Allen disclosed modest or significant relationships with ACI Clinical, Novartis, UpToDate, Boston Scientific, and Cytokinetics.
A version of this article first appeared on Medscape.com.
CHICAGO – Routine early, expeditious use of extracorporeal membrane oxygenation (ECMO) is a common strategy in patients with severe cardiogenic shock, but a less aggressive initial approach may be just as effective, a randomized trial suggests.
In the study that assigned patients with “rapidly deteriorating or severe” cardiogenic shock to one or the other approach, clinical outcomes were no better for those who received immediate ECMO than for those initially managed with inotropes and vasopressors, researchers said.
The conservative strategy, importantly, allowed for downstream ECMO in the event of hemodynamic deterioration, which occurred in a substantial 39% of cases, observed Petr Ostadal, MD, PhD, when presenting the results at the American Heart Association scientific sessions.
Dr. Ostadal of Na Homolce Hospital, Prague, is also first author on the published report of the study, called Extracorporeal Membrane Oxygenation in the Therapy of Cardiogenic Shock (ECMO-CS), which was published the same day in Circulation.
The trial makes a firm case for preferring the conservative initial approach over routine early ECMO in the kind of patients it entered, Larry A. Allen, MD, MHS, University of Coloradoat Denver, Aurora, told this news organization.
More than 60% of the trial’s 117 patients had shock secondary to an acute coronary syndrome; another 23% were in heart failure decompensation.
A preference for the conservative initial approach would be welcome, he said. The early aggressive ECMO approach is resource intensive and carries some important risks, such as stroke or coagulopathy, said Dr. Allen, who is not connected with ECMO-CS. Yet it is increasingly the go-to approach in such patients, based primarily on observational data.
Although early ECMO apparently didn’t benefit patients in this study in their specific stage of cardiogenic shock, Dr. Allen observed, it would presumably help some, but identifying them in practice presents challenges. “Defining where people are in the spectrum of early versus middle versus late cardiogenic shock is actually very tricky.”
It will therefore be important, he said, to identify ways to predict which conservatively managed patients do well with the strategy, and which are most at risk for hemodynamic deterioration and for whom ECMO should be readily available.
“I think part of what ECMO-CS tells us is that, if a patient is stable on intravenous inotropic and vasopressor support, you can defer ECMO while you’re thinking about the patient – about their larger context and the right medical decision-making for them.”
The trial randomly assigned 122 patients with rapidly deteriorating or severe cardiogenic shock to the immediate-ECMO or the conservative strategy at four centers in the Czech Republic. The 117 patients for whom informed consent could be obtained were included in the analysis, 58 and 59 patients, respectively. Their mean age was about 65 years and three-fourths were male.
The primary endpoint, the only endpoint for which the study was powered, consisted of death from any cause, resuscitated circulatory arrest, or use of a different form of mechanical circulatory support (MCS) by 30 days.
It occurred in 63.8% of patients assigned to immediate ECMO and 71.2% of those in the conservative strategy group, for a hazard ratio of 0.72 (95% confidence interval, 0.46-1.12; P = .21).
As individual endpoints, rates of death from any cause and resuscitated arrest did not significantly differ between the groups, but conservatively managed patients more often used another form of MCS. The HRs were 1.11 (95% CI, 0.66-1.87) for death from any cause, 0.79 (95% CI, 0.27-2.28) for resuscitated cardiac arrest, and 0.38 (95% CI, 0.18-0.79) for use of another MCS device.
The rates for serious adverse events – including bleeding, ischemia, stroke, pneumonia, or sepsis – were similar at 60.3% in the early-ECMO group and 61% in group with conservative initial management, Dr. Ostadal reported.
Other than the 23 patients in the conservative initial strategy group who went on to receive ECMO (1.9 days after randomization, on average), 1 went on to undergo implantation with a HeartMate (Abbott) ventricular assist device and 3 received an Impella pump (Abiomed).
Six patients in the early-ECMO group were already receiving intra-aortic balloon pump (IABP) support at randomization, two underwent temporary implantation with a Centrimag device (Abbott), and three went on to receive a HeartMate device, the published report notes.
ECMO is the optimal first choice for MCS in such patients with cardiogenic shock who need a circulatory support device, especially because it also oxygenates the blood, Dr. Ostadal told this news organization.
But ECMO doesn’t help with ventricular unloading. Indeed, it can sometimes reduce ventricular preload, especially if right-heart pressures are low. So MCS devices that unload the ventricle, typically an IABP, can complement ECMO.
Dr. Ostadal speculates, however, that there may be a better pairing option. “Impella plus ECMO, I think, is the combination which has a future,” he said, for patients in cardiogenic shock who need a short-term percutaneous hemodynamic support device. Impella “supports the whole circulation” and unloads the left ventricle.
“A balloon pump in combination with ECMO is still not a bad choice. It’s very cheap in comparison with Impella.” But in his opinion, Dr. Ostadal said, “The combination of Impella plus ECMO is more efficient from a hemodynamic point of view.”
As the published report notes, ongoing randomized trials looking at ECMO plus other MCS devices in cardiogenic shock include ECLS-SHOCK, with a projected enrollment of 420 patients, and EURO-SHOCK, aiming for a similar number of patients; both compare routine ECMO to conservative management.
In addition, ANCHOR, in which ECMO is combined with IABP, and DanShock, which looks at early use of Impella rather than ECMO, are enrolling patients with shock secondary to acute coronary syndromes.
Dr. Ostadal disclosed consulting for Getinge, Edwards, Medtronic, Biomedica, and Xenios/Fresenius, and receiving research support from Xenios/Fresenius. Dr. Allen disclosed modest or significant relationships with ACI Clinical, Novartis, UpToDate, Boston Scientific, and Cytokinetics.
A version of this article first appeared on Medscape.com.
CHICAGO – Routine early, expeditious use of extracorporeal membrane oxygenation (ECMO) is a common strategy in patients with severe cardiogenic shock, but a less aggressive initial approach may be just as effective, a randomized trial suggests.
In the study that assigned patients with “rapidly deteriorating or severe” cardiogenic shock to one or the other approach, clinical outcomes were no better for those who received immediate ECMO than for those initially managed with inotropes and vasopressors, researchers said.
The conservative strategy, importantly, allowed for downstream ECMO in the event of hemodynamic deterioration, which occurred in a substantial 39% of cases, observed Petr Ostadal, MD, PhD, when presenting the results at the American Heart Association scientific sessions.
Dr. Ostadal of Na Homolce Hospital, Prague, is also first author on the published report of the study, called Extracorporeal Membrane Oxygenation in the Therapy of Cardiogenic Shock (ECMO-CS), which was published the same day in Circulation.
The trial makes a firm case for preferring the conservative initial approach over routine early ECMO in the kind of patients it entered, Larry A. Allen, MD, MHS, University of Coloradoat Denver, Aurora, told this news organization.
More than 60% of the trial’s 117 patients had shock secondary to an acute coronary syndrome; another 23% were in heart failure decompensation.
A preference for the conservative initial approach would be welcome, he said. The early aggressive ECMO approach is resource intensive and carries some important risks, such as stroke or coagulopathy, said Dr. Allen, who is not connected with ECMO-CS. Yet it is increasingly the go-to approach in such patients, based primarily on observational data.
Although early ECMO apparently didn’t benefit patients in this study in their specific stage of cardiogenic shock, Dr. Allen observed, it would presumably help some, but identifying them in practice presents challenges. “Defining where people are in the spectrum of early versus middle versus late cardiogenic shock is actually very tricky.”
It will therefore be important, he said, to identify ways to predict which conservatively managed patients do well with the strategy, and which are most at risk for hemodynamic deterioration and for whom ECMO should be readily available.
“I think part of what ECMO-CS tells us is that, if a patient is stable on intravenous inotropic and vasopressor support, you can defer ECMO while you’re thinking about the patient – about their larger context and the right medical decision-making for them.”
The trial randomly assigned 122 patients with rapidly deteriorating or severe cardiogenic shock to the immediate-ECMO or the conservative strategy at four centers in the Czech Republic. The 117 patients for whom informed consent could be obtained were included in the analysis, 58 and 59 patients, respectively. Their mean age was about 65 years and three-fourths were male.
The primary endpoint, the only endpoint for which the study was powered, consisted of death from any cause, resuscitated circulatory arrest, or use of a different form of mechanical circulatory support (MCS) by 30 days.
It occurred in 63.8% of patients assigned to immediate ECMO and 71.2% of those in the conservative strategy group, for a hazard ratio of 0.72 (95% confidence interval, 0.46-1.12; P = .21).
As individual endpoints, rates of death from any cause and resuscitated arrest did not significantly differ between the groups, but conservatively managed patients more often used another form of MCS. The HRs were 1.11 (95% CI, 0.66-1.87) for death from any cause, 0.79 (95% CI, 0.27-2.28) for resuscitated cardiac arrest, and 0.38 (95% CI, 0.18-0.79) for use of another MCS device.
The rates for serious adverse events – including bleeding, ischemia, stroke, pneumonia, or sepsis – were similar at 60.3% in the early-ECMO group and 61% in group with conservative initial management, Dr. Ostadal reported.
Other than the 23 patients in the conservative initial strategy group who went on to receive ECMO (1.9 days after randomization, on average), 1 went on to undergo implantation with a HeartMate (Abbott) ventricular assist device and 3 received an Impella pump (Abiomed).
Six patients in the early-ECMO group were already receiving intra-aortic balloon pump (IABP) support at randomization, two underwent temporary implantation with a Centrimag device (Abbott), and three went on to receive a HeartMate device, the published report notes.
ECMO is the optimal first choice for MCS in such patients with cardiogenic shock who need a circulatory support device, especially because it also oxygenates the blood, Dr. Ostadal told this news organization.
But ECMO doesn’t help with ventricular unloading. Indeed, it can sometimes reduce ventricular preload, especially if right-heart pressures are low. So MCS devices that unload the ventricle, typically an IABP, can complement ECMO.
Dr. Ostadal speculates, however, that there may be a better pairing option. “Impella plus ECMO, I think, is the combination which has a future,” he said, for patients in cardiogenic shock who need a short-term percutaneous hemodynamic support device. Impella “supports the whole circulation” and unloads the left ventricle.
“A balloon pump in combination with ECMO is still not a bad choice. It’s very cheap in comparison with Impella.” But in his opinion, Dr. Ostadal said, “The combination of Impella plus ECMO is more efficient from a hemodynamic point of view.”
As the published report notes, ongoing randomized trials looking at ECMO plus other MCS devices in cardiogenic shock include ECLS-SHOCK, with a projected enrollment of 420 patients, and EURO-SHOCK, aiming for a similar number of patients; both compare routine ECMO to conservative management.
In addition, ANCHOR, in which ECMO is combined with IABP, and DanShock, which looks at early use of Impella rather than ECMO, are enrolling patients with shock secondary to acute coronary syndromes.
Dr. Ostadal disclosed consulting for Getinge, Edwards, Medtronic, Biomedica, and Xenios/Fresenius, and receiving research support from Xenios/Fresenius. Dr. Allen disclosed modest or significant relationships with ACI Clinical, Novartis, UpToDate, Boston Scientific, and Cytokinetics.
A version of this article first appeared on Medscape.com.
AT AHA 2022
CRISPR gene editing takes next step in TTR amyloidosis
CHICAGO – Treatment with the investigational CRISPR-Cas9 gene-editing therapy, NTLA-2001, led to rapid responses in patients with transthyretin (TTR) amyloidosis with cardiomyopathy (ATTR-CM), interim phase 1 results show.
Serum levels of the disease-causing TTR protein were reduced by at least 90% at day 28 with a single infusion of NTLA-2001 at two different doses, with reductions sustained across 4-6 months’ follow-up.
NTLA-2001 was generally well-tolerated, and the results were similar in patients with New York Heart Association (NYHA) class I-III heart failure.
“These data further support and extend the early findings demonstrating the promise of CRISPR-based in vivo genome editing in humans,” said Julian Gillmore, MD, PhD, MBBS, who is leading the study at University College London.
“More specifically, the deep TTR reductions observed in patients with ATTR amyloidosis in this study provide a real possibility of genuine clinical improvement in a condition that has hitherto been ultimately progressive and invariably fatal,” he said.
The results were reported in a late-breaking session at the American Heart Association scientific sessions.
Mutations in the TTR gene and age-related changes in the stability of the TTR protein can cause misfolding of the TTR protein, resulting in amyloid deposits in skin and myocardial tissues.
An estimated 50,000 people worldwide are thought to have hereditary ATTR and up to 500,000 to have wild-type ATTR amyloidosis. Amyloid cardiomyopathy is underdiagnosed and fatal in 3-10 years without treatment. Current treatment options only slow progression and require lifelong administration, he said.
Results reported last year from the polyneuropathy arm of the study were hailed as a breakthrough and further proof-of-concept that CRISPR could be used to treat other diseases
CRISPR gene editing has shown success, for example, in beta-thalassemia and sickle cell disease but involved stem cells extracted from patients’ bone marrow, edited in the lab, and then replaced.
NTLA-2001 (Intellia Therapeutics/Regeneron) is an in vivo treatment that uses lipid nanoparticles containing messenger RNA for Cas9 and a single-guide RNA targeting TTR in the liver, where it’s almost exclusively produced.
The new analysis included 12 patients with heart failure: 3 in NYHA class I-II and 6 in NYHA class III who received a single dose of NTLA-2001 at 0.7 mg/kg, while the remaining 3 patients in NYHA class I-II received a single dose of 1.0 mg/kg.
During follow-up out to 6 months, TTR reductions averaged:
- 93% in the 0.7 mg/kg NYHA I-II group at 6 months.
- 94% in the 0.7 mg/kg NYHA III group at 4 months.
- 92% in the 1.0 mg/kg NYHA I-II group at 4 months.
Eight patients reported mild or moderate adverse events, and two patients experienced transient infusion reactions, including one grade 3 reaction in the 0.7 mg/kg NYHA class III group that resolved without clinical consequence. This group was expanded to six patients per study protocol. No additional treatment-related adverse events higher than grade 1 were reported, and no further dose escalation was undertaken, Dr. Gillmore reported.
There were no clinically relevant laboratory findings; one patient had a transient grade 1 liver enzyme elevation.
One disadvantage of CRISPR is the potential for off-target effects, but Dr. Gillmore said in an interview that the drug developers went through a “very rigorous process when selecting the guide RNA, which is what really targets the specificity of the TTR gene.”
“That’s a really, really important point,” he said. “When they did various studies using, for example, primary human hepatocytes, they found no evidence of off-target editing at concentrations of NTLA-2001 threefold greater than the EC90, the concentration at which one knocks down the protein by 90%. So, what we can say at the moment, is the specificity of NTLA-2001 for the TTR gene seems to be absolute.”
In terms of other challenges going forward, Dr. Gillmore added, “I think that it’s really to see whether the knockdown that is being achieved is going to translate into greater clinical benefit.”
Invited discussant Kevin M. Alexander, MD, of Stanford (Calif.) University, said therapies that stabilize or reduce TTR have recently emerged that have improved ATTR amyloidosis outcomes, including tafamidis and patisiran.
Nevertheless, there has been an unmet need to develop therapies that can halt or reverse disease, are effective in advanced ATTR, and have an improved route or frequency of administration, given that this is a chronic disease, he said.
Dr. Alexander noted that the reductions of greater than 90% were achieved with higher doses than used in the polyneuropathy arm reported last year but were well tolerated in patients that for the most part had wild-type ATTR (83%) and reflect the wild-type ATTR population in practice. “The data support consideration for subsequent efficacy trials for this compound.”
Unanswered questions in ongoing ATTR trials are whether TTR reductions translate into improved clinical outcomes, the long-term safety of TTR lowering, and the efficacy of NTLA-2001, particularly in higher-risk patients, such as those in NYHA class III and those with hereditary ATTR, Dr. Alexander said.
During a media briefing earlier in the day, invited discussant Kiran Musunuru, MD, University of Pennsylvania, Philadelphia, pointed out that, in the recent APOLLO-B trial of patisiran, patients with ATTR amyloidosis with cardiomyopathy had an average 87% TTR reduction but need intravenous infusions every 3 weeks for the rest of their lives.
“In contrast, gene editing is a one-and-done proposition,” he said. “You receive a single treatment that turns off the TTR gene permanently and the effects are durable and likely last a lifetime.”
Dr. Musunuru noted that patients who received patisiran also had significantly and substantially better functional capacity and quality of life, compared with those who received placebo. “Based on today’s results, we can expect future clinical trials for gene editing to have the same beneficial effects and possibly a mortality benefit as well.”
Today’s study is also important because it is part of the first wave of putting CRISPR into the body for an array of diseases, he commented.
“TTR gene editing stands out because it’s the very first CRISPR trial to show unequivocal success – you see that with a greater than 90% reduction in TTR,” Dr. Musunuru said. “So, in my view that makes it a milestone for modern medicine.”
Dosing at 55 mg, corresponding to a fixed 0.7 mg/kg dose, is ongoing in the dose-expansion portion of the trial, with enrollment across both arms expected to be completed by the end of 2022, Intellia Therapeutics reported.
The study was funded by Intellia Therapeutics and Regeneron Pharmaceuticals. Dr. Gillmore reports receiving consultancy fees from Alnylam, Ionis, AstraZeneca, Pfizer, Intellia, ATTRalus, and Novo Nordisk and has received grant support from Alnylam Pharmaceuticals. Dr. Alexander reports serving on advisory boards for Almylam and Arbor Biotechnologies; has consulted for Eidos, Ionis, Novo Nordisk, and Pfizer; and has received grants from AHA, Alnylam, Eidos, and the National Institutes of Health.
A version of this article first appeared on Medscape.com.
CHICAGO – Treatment with the investigational CRISPR-Cas9 gene-editing therapy, NTLA-2001, led to rapid responses in patients with transthyretin (TTR) amyloidosis with cardiomyopathy (ATTR-CM), interim phase 1 results show.
Serum levels of the disease-causing TTR protein were reduced by at least 90% at day 28 with a single infusion of NTLA-2001 at two different doses, with reductions sustained across 4-6 months’ follow-up.
NTLA-2001 was generally well-tolerated, and the results were similar in patients with New York Heart Association (NYHA) class I-III heart failure.
“These data further support and extend the early findings demonstrating the promise of CRISPR-based in vivo genome editing in humans,” said Julian Gillmore, MD, PhD, MBBS, who is leading the study at University College London.
“More specifically, the deep TTR reductions observed in patients with ATTR amyloidosis in this study provide a real possibility of genuine clinical improvement in a condition that has hitherto been ultimately progressive and invariably fatal,” he said.
The results were reported in a late-breaking session at the American Heart Association scientific sessions.
Mutations in the TTR gene and age-related changes in the stability of the TTR protein can cause misfolding of the TTR protein, resulting in amyloid deposits in skin and myocardial tissues.
An estimated 50,000 people worldwide are thought to have hereditary ATTR and up to 500,000 to have wild-type ATTR amyloidosis. Amyloid cardiomyopathy is underdiagnosed and fatal in 3-10 years without treatment. Current treatment options only slow progression and require lifelong administration, he said.
Results reported last year from the polyneuropathy arm of the study were hailed as a breakthrough and further proof-of-concept that CRISPR could be used to treat other diseases
CRISPR gene editing has shown success, for example, in beta-thalassemia and sickle cell disease but involved stem cells extracted from patients’ bone marrow, edited in the lab, and then replaced.
NTLA-2001 (Intellia Therapeutics/Regeneron) is an in vivo treatment that uses lipid nanoparticles containing messenger RNA for Cas9 and a single-guide RNA targeting TTR in the liver, where it’s almost exclusively produced.
The new analysis included 12 patients with heart failure: 3 in NYHA class I-II and 6 in NYHA class III who received a single dose of NTLA-2001 at 0.7 mg/kg, while the remaining 3 patients in NYHA class I-II received a single dose of 1.0 mg/kg.
During follow-up out to 6 months, TTR reductions averaged:
- 93% in the 0.7 mg/kg NYHA I-II group at 6 months.
- 94% in the 0.7 mg/kg NYHA III group at 4 months.
- 92% in the 1.0 mg/kg NYHA I-II group at 4 months.
Eight patients reported mild or moderate adverse events, and two patients experienced transient infusion reactions, including one grade 3 reaction in the 0.7 mg/kg NYHA class III group that resolved without clinical consequence. This group was expanded to six patients per study protocol. No additional treatment-related adverse events higher than grade 1 were reported, and no further dose escalation was undertaken, Dr. Gillmore reported.
There were no clinically relevant laboratory findings; one patient had a transient grade 1 liver enzyme elevation.
One disadvantage of CRISPR is the potential for off-target effects, but Dr. Gillmore said in an interview that the drug developers went through a “very rigorous process when selecting the guide RNA, which is what really targets the specificity of the TTR gene.”
“That’s a really, really important point,” he said. “When they did various studies using, for example, primary human hepatocytes, they found no evidence of off-target editing at concentrations of NTLA-2001 threefold greater than the EC90, the concentration at which one knocks down the protein by 90%. So, what we can say at the moment, is the specificity of NTLA-2001 for the TTR gene seems to be absolute.”
In terms of other challenges going forward, Dr. Gillmore added, “I think that it’s really to see whether the knockdown that is being achieved is going to translate into greater clinical benefit.”
Invited discussant Kevin M. Alexander, MD, of Stanford (Calif.) University, said therapies that stabilize or reduce TTR have recently emerged that have improved ATTR amyloidosis outcomes, including tafamidis and patisiran.
Nevertheless, there has been an unmet need to develop therapies that can halt or reverse disease, are effective in advanced ATTR, and have an improved route or frequency of administration, given that this is a chronic disease, he said.
Dr. Alexander noted that the reductions of greater than 90% were achieved with higher doses than used in the polyneuropathy arm reported last year but were well tolerated in patients that for the most part had wild-type ATTR (83%) and reflect the wild-type ATTR population in practice. “The data support consideration for subsequent efficacy trials for this compound.”
Unanswered questions in ongoing ATTR trials are whether TTR reductions translate into improved clinical outcomes, the long-term safety of TTR lowering, and the efficacy of NTLA-2001, particularly in higher-risk patients, such as those in NYHA class III and those with hereditary ATTR, Dr. Alexander said.
During a media briefing earlier in the day, invited discussant Kiran Musunuru, MD, University of Pennsylvania, Philadelphia, pointed out that, in the recent APOLLO-B trial of patisiran, patients with ATTR amyloidosis with cardiomyopathy had an average 87% TTR reduction but need intravenous infusions every 3 weeks for the rest of their lives.
“In contrast, gene editing is a one-and-done proposition,” he said. “You receive a single treatment that turns off the TTR gene permanently and the effects are durable and likely last a lifetime.”
Dr. Musunuru noted that patients who received patisiran also had significantly and substantially better functional capacity and quality of life, compared with those who received placebo. “Based on today’s results, we can expect future clinical trials for gene editing to have the same beneficial effects and possibly a mortality benefit as well.”
Today’s study is also important because it is part of the first wave of putting CRISPR into the body for an array of diseases, he commented.
“TTR gene editing stands out because it’s the very first CRISPR trial to show unequivocal success – you see that with a greater than 90% reduction in TTR,” Dr. Musunuru said. “So, in my view that makes it a milestone for modern medicine.”
Dosing at 55 mg, corresponding to a fixed 0.7 mg/kg dose, is ongoing in the dose-expansion portion of the trial, with enrollment across both arms expected to be completed by the end of 2022, Intellia Therapeutics reported.
The study was funded by Intellia Therapeutics and Regeneron Pharmaceuticals. Dr. Gillmore reports receiving consultancy fees from Alnylam, Ionis, AstraZeneca, Pfizer, Intellia, ATTRalus, and Novo Nordisk and has received grant support from Alnylam Pharmaceuticals. Dr. Alexander reports serving on advisory boards for Almylam and Arbor Biotechnologies; has consulted for Eidos, Ionis, Novo Nordisk, and Pfizer; and has received grants from AHA, Alnylam, Eidos, and the National Institutes of Health.
A version of this article first appeared on Medscape.com.
CHICAGO – Treatment with the investigational CRISPR-Cas9 gene-editing therapy, NTLA-2001, led to rapid responses in patients with transthyretin (TTR) amyloidosis with cardiomyopathy (ATTR-CM), interim phase 1 results show.
Serum levels of the disease-causing TTR protein were reduced by at least 90% at day 28 with a single infusion of NTLA-2001 at two different doses, with reductions sustained across 4-6 months’ follow-up.
NTLA-2001 was generally well-tolerated, and the results were similar in patients with New York Heart Association (NYHA) class I-III heart failure.
“These data further support and extend the early findings demonstrating the promise of CRISPR-based in vivo genome editing in humans,” said Julian Gillmore, MD, PhD, MBBS, who is leading the study at University College London.
“More specifically, the deep TTR reductions observed in patients with ATTR amyloidosis in this study provide a real possibility of genuine clinical improvement in a condition that has hitherto been ultimately progressive and invariably fatal,” he said.
The results were reported in a late-breaking session at the American Heart Association scientific sessions.
Mutations in the TTR gene and age-related changes in the stability of the TTR protein can cause misfolding of the TTR protein, resulting in amyloid deposits in skin and myocardial tissues.
An estimated 50,000 people worldwide are thought to have hereditary ATTR and up to 500,000 to have wild-type ATTR amyloidosis. Amyloid cardiomyopathy is underdiagnosed and fatal in 3-10 years without treatment. Current treatment options only slow progression and require lifelong administration, he said.
Results reported last year from the polyneuropathy arm of the study were hailed as a breakthrough and further proof-of-concept that CRISPR could be used to treat other diseases
CRISPR gene editing has shown success, for example, in beta-thalassemia and sickle cell disease but involved stem cells extracted from patients’ bone marrow, edited in the lab, and then replaced.
NTLA-2001 (Intellia Therapeutics/Regeneron) is an in vivo treatment that uses lipid nanoparticles containing messenger RNA for Cas9 and a single-guide RNA targeting TTR in the liver, where it’s almost exclusively produced.
The new analysis included 12 patients with heart failure: 3 in NYHA class I-II and 6 in NYHA class III who received a single dose of NTLA-2001 at 0.7 mg/kg, while the remaining 3 patients in NYHA class I-II received a single dose of 1.0 mg/kg.
During follow-up out to 6 months, TTR reductions averaged:
- 93% in the 0.7 mg/kg NYHA I-II group at 6 months.
- 94% in the 0.7 mg/kg NYHA III group at 4 months.
- 92% in the 1.0 mg/kg NYHA I-II group at 4 months.
Eight patients reported mild or moderate adverse events, and two patients experienced transient infusion reactions, including one grade 3 reaction in the 0.7 mg/kg NYHA class III group that resolved without clinical consequence. This group was expanded to six patients per study protocol. No additional treatment-related adverse events higher than grade 1 were reported, and no further dose escalation was undertaken, Dr. Gillmore reported.
There were no clinically relevant laboratory findings; one patient had a transient grade 1 liver enzyme elevation.
One disadvantage of CRISPR is the potential for off-target effects, but Dr. Gillmore said in an interview that the drug developers went through a “very rigorous process when selecting the guide RNA, which is what really targets the specificity of the TTR gene.”
“That’s a really, really important point,” he said. “When they did various studies using, for example, primary human hepatocytes, they found no evidence of off-target editing at concentrations of NTLA-2001 threefold greater than the EC90, the concentration at which one knocks down the protein by 90%. So, what we can say at the moment, is the specificity of NTLA-2001 for the TTR gene seems to be absolute.”
In terms of other challenges going forward, Dr. Gillmore added, “I think that it’s really to see whether the knockdown that is being achieved is going to translate into greater clinical benefit.”
Invited discussant Kevin M. Alexander, MD, of Stanford (Calif.) University, said therapies that stabilize or reduce TTR have recently emerged that have improved ATTR amyloidosis outcomes, including tafamidis and patisiran.
Nevertheless, there has been an unmet need to develop therapies that can halt or reverse disease, are effective in advanced ATTR, and have an improved route or frequency of administration, given that this is a chronic disease, he said.
Dr. Alexander noted that the reductions of greater than 90% were achieved with higher doses than used in the polyneuropathy arm reported last year but were well tolerated in patients that for the most part had wild-type ATTR (83%) and reflect the wild-type ATTR population in practice. “The data support consideration for subsequent efficacy trials for this compound.”
Unanswered questions in ongoing ATTR trials are whether TTR reductions translate into improved clinical outcomes, the long-term safety of TTR lowering, and the efficacy of NTLA-2001, particularly in higher-risk patients, such as those in NYHA class III and those with hereditary ATTR, Dr. Alexander said.
During a media briefing earlier in the day, invited discussant Kiran Musunuru, MD, University of Pennsylvania, Philadelphia, pointed out that, in the recent APOLLO-B trial of patisiran, patients with ATTR amyloidosis with cardiomyopathy had an average 87% TTR reduction but need intravenous infusions every 3 weeks for the rest of their lives.
“In contrast, gene editing is a one-and-done proposition,” he said. “You receive a single treatment that turns off the TTR gene permanently and the effects are durable and likely last a lifetime.”
Dr. Musunuru noted that patients who received patisiran also had significantly and substantially better functional capacity and quality of life, compared with those who received placebo. “Based on today’s results, we can expect future clinical trials for gene editing to have the same beneficial effects and possibly a mortality benefit as well.”
Today’s study is also important because it is part of the first wave of putting CRISPR into the body for an array of diseases, he commented.
“TTR gene editing stands out because it’s the very first CRISPR trial to show unequivocal success – you see that with a greater than 90% reduction in TTR,” Dr. Musunuru said. “So, in my view that makes it a milestone for modern medicine.”
Dosing at 55 mg, corresponding to a fixed 0.7 mg/kg dose, is ongoing in the dose-expansion portion of the trial, with enrollment across both arms expected to be completed by the end of 2022, Intellia Therapeutics reported.
The study was funded by Intellia Therapeutics and Regeneron Pharmaceuticals. Dr. Gillmore reports receiving consultancy fees from Alnylam, Ionis, AstraZeneca, Pfizer, Intellia, ATTRalus, and Novo Nordisk and has received grant support from Alnylam Pharmaceuticals. Dr. Alexander reports serving on advisory boards for Almylam and Arbor Biotechnologies; has consulted for Eidos, Ionis, Novo Nordisk, and Pfizer; and has received grants from AHA, Alnylam, Eidos, and the National Institutes of Health.
A version of this article first appeared on Medscape.com.
AT AHA 2022
No survival advantage for either torsemide or furosemide in HF: TRANSFORM-HF
CHICAGO – The choice of loop diuretic for decongestion in patients hospitalized with heart failure (HF) may make little difference to survival or readmission risk over the next year, at least when deciding between furosemide or torsemide, a randomized trial suggests.
Both drugs are old and widely used, but differences between the two loop diuretics in bioavailability, effects on potassium levels, and other features have led some clinicians to sometimes prefer torsemide. Until now, however, no randomized HF trials have compared the two drugs.
The new findings suggest clinicians can continue starting such patients with HF on either agent, at their discretion, without concern that the choice may compromise outcomes, say researchers from the TRANSFORM-HF trial, which compared furosemide-first and torsemide-first diuretic strategies in a diverse population of patients with HF.
Given that the two strategies were similarly effective for survival and rehospitalization, clinicians caring for patients with HF can focus more on “getting patients on the right dose for their loop diuretic, and prioritizing those therapies proven to improve clinical outcomes,” said Robert J. Mentz, MD, of Duke University Clinical Research Institute, Durham, N.C.
Dr. Mentz, a TRANSFORM-HF principal investigator, presented the primary results November 5 at the American Heart Association scientific sessions.
The trial had randomly assigned 2,859 patients hospitalized with HF and with a plan for oral loop diuretic therapy to initiate treatment with furosemide or torsemide. Clinicians were encouraged to maintain patients on the assigned diuretic, but crossovers to the other drug or other diuretic changes were allowed.
Rates of death from any cause, the primary endpoint, were about 26% in both groups over a median 17-month follow-up, regardless of ejection fraction (EF).
The composite rates of all-cause death or hospitalization at 12 months were also not significantly different, about 49% for those started on furosemide and about 47% for patients initially prescribed torsemide.
As a pragmatic comparative effectiveness trial, TRANSFORM-HF entered diverse patients with HF, broadly representative of actual clinical practice, who were managed according to routine practice and a streamlined study protocol at more than 60 U.S. centers, Dr. Mentz observed.
One of the pragmatic design’s advantages, he told this news organization, was “how efficient it was” as a randomized comparison of treatment strategies for clinical outcomes. It was “relatively low cost” and recruited patients quickly, compared with conventional randomized trials, “and we answered the question clearly.” The trial’s results, Dr. Mentz said, reflect “what happens in the real world.”
When might torsemide have the edge?
Although furosemide is the most commonly used loop diuretic in HF, and there are others besides it and torsemide, the latter has both known and theoretical advantages that set it apart. Torsemide is more than twice as potent as furosemide and more bioavailable, and its treatment effect lasts longer, the TRANSFORM-HF investigators have noted.
In addition, preclinical and small clinical studies suggest torsemide may have pleiotropic effects that might be theoretical advantages for patients with HF. For example, it appears to downregulate the renin-angiotensin-aldosterone system (RAAS) and reduce myocardial fibrosis and promote reverse ventricular remodeling, the group writes.
In practice, therefore, torsemide may be preferred in patients with furosemide resistance or “challenges with bioavailability, especially those with very advanced heart failure with congestion who may have gut edema, where oral furosemide and other loop diuretics are not effectively absorbed,” Biykem Bozkurt, MD, PhD, Baylor College of Medicine, Houston, told this news organization.
In such patients, she said, torsemide “is considered to be a better choice for individuals who have diuretic resistance with advanced congestion.”
The drug’s apparent pleiotropic effects, such as RAAS inhibition, may have less relevance to the TRANSFORM-HF primary endpoint of all-cause mortality than to clinical outcomes more likely associated with successful decongestion, such as HF hospitalization, Dr. Bozkurt proposed.
The trial’s pragmatic design, however, made it more feasible to focus on all-cause mortality and less practical to use measures of successful decongestion, such as volume loss or reduction in natriuretic peptide levels, she observed. Those are endpoints of special interest when diuretics are compared, “especially for the subgroup of patients who are diuretic resistant.”
Over the last 20 years or so, “we’ve learned that hospitalized heart failure is a very different disease process with a different natural history,” observed Clyde W. Yancy, MD, MSc, Northwestern University, Chicago, who was not part of the current study.
“So, the idea that something as nuanced as choice of one loop diuretic over the other, in that setting, would be sufficient to change the natural history, may be still a high bar for us,” he said in an interview.
“Based on these data, one would have to argue that whichever loop diuretic you select for the hospitalized patient – and a lot of that is driven by market exigencies right now – it turns out that the response is indistinguishable,” Dr. Yancy said. “That means if your hospital happens to have furosemide on the formulary, use it. If furosemide is not available but torsemide is available, use it.”
Dr. Yancy said he’d like to see a trial similar to TRANSFORM-HF but in outpatients receiving today’s guideline-directed medical therapy, which includes the sodium-glucose cotransporter 2 (SGLT2) inhibitors, drugs that increase the fractional excretion of sodium and have a “diureticlike” effect.
Such a trial, he said, would explore “the combination of not one, or two, but three agents with a diuretic effect – a loop diuretic, a mineralocorticoid antagonist, and an SGLT2 inhibitor – in ambulatory, optimized patients. It might make a difference.”
HF regardless of EF
The trial enrolled patients hospitalized with worsening or new-onset HF with a plan for long-term loop diuretic therapy who had either an EF of 40% or lower or, regardless of EF, elevated natriuretic peptide levels when hospitalized.
Of the 2,859 participants, whose mean age was about 65 years, about 36% were women and 34% African American. Overall, 1,428 were assigned to receive furosemide as their initial oral diuretic and 1,431 patients were assigned to the torsemide-first strategy.
The rate of death from any cause in both groups was 17 per 100 patient-years at a median of 17.4 months. The hazard ratio for torsemide vs. furosemide was 1.02 (95% confidence interval, 0.89-1.18; P = .77).
The corresponding HR at 12 months for all-cause death or hospitalization was 0.92 (95% CI, 0.83-1.02; P = .11). The relative risk for any hospitalization was 0.94 (95% CI, 0.84-1.07).
Pragmatic design: Other implications
Dosing was left to clinician discretion in the open-label study, as was whether patients maintained their assigned drug or switched over to the other agent. Indeed, 5.4% of patients crossed over to the other loop diuretic, and 2.8% went off loop diuretics entirely between in-hospital randomization and discharge, Dr. Mentz reported. By day 30, 6.7% had crossed over, and 7% had stopped taking loop diuretics.
The diuretic crossovers and discontinuations, Dr. Mentz said, likely biased the trial’s outcomes, such that the two strategies performed about equally well. Efforts were made, however, to at least partially overcome that limitation.
“We put measures in place to support adherence – sending letters to their primary doctors, giving them a wallet card so they would know which therapy they were on, having conversations about the importance of trying to stay on the randomized therapy,” Dr. Mentz said in an interview. Still, some clinicians saw differences between the two agents that prompted them, at some point, to switch patients from one loop diuretic to the other.
But interestingly, Dr. Mentz reported, the two strategies did not significantly differ in all-cause mortality or the composite of all-cause mortality or hospitalization in analysis by intention to treat.
Dr. Mentz discloses receiving honoraria from AstraZeneca, Bayer/Merck, Boehringer Ingelheim/Lilly, Cytokinetics, Pharmacosmos, Respicardia, Windtree Therapeutics, and Zoll; and research grants from American Regent and Novartis. Dr. Bozkurt discloses receiving honoraria from AstraZeneca, Baxter Health Care, and Sanofi Aventis and having other relationships with Renovacor, Respicardia, Abbott Vascular, Liva Nova, Vifor, and Cardurion. Dr. Yancy discloses a modest relationship with Abbott.
A version of this article first appeared on Medscape.com.
CHICAGO – The choice of loop diuretic for decongestion in patients hospitalized with heart failure (HF) may make little difference to survival or readmission risk over the next year, at least when deciding between furosemide or torsemide, a randomized trial suggests.
Both drugs are old and widely used, but differences between the two loop diuretics in bioavailability, effects on potassium levels, and other features have led some clinicians to sometimes prefer torsemide. Until now, however, no randomized HF trials have compared the two drugs.
The new findings suggest clinicians can continue starting such patients with HF on either agent, at their discretion, without concern that the choice may compromise outcomes, say researchers from the TRANSFORM-HF trial, which compared furosemide-first and torsemide-first diuretic strategies in a diverse population of patients with HF.
Given that the two strategies were similarly effective for survival and rehospitalization, clinicians caring for patients with HF can focus more on “getting patients on the right dose for their loop diuretic, and prioritizing those therapies proven to improve clinical outcomes,” said Robert J. Mentz, MD, of Duke University Clinical Research Institute, Durham, N.C.
Dr. Mentz, a TRANSFORM-HF principal investigator, presented the primary results November 5 at the American Heart Association scientific sessions.
The trial had randomly assigned 2,859 patients hospitalized with HF and with a plan for oral loop diuretic therapy to initiate treatment with furosemide or torsemide. Clinicians were encouraged to maintain patients on the assigned diuretic, but crossovers to the other drug or other diuretic changes were allowed.
Rates of death from any cause, the primary endpoint, were about 26% in both groups over a median 17-month follow-up, regardless of ejection fraction (EF).
The composite rates of all-cause death or hospitalization at 12 months were also not significantly different, about 49% for those started on furosemide and about 47% for patients initially prescribed torsemide.
As a pragmatic comparative effectiveness trial, TRANSFORM-HF entered diverse patients with HF, broadly representative of actual clinical practice, who were managed according to routine practice and a streamlined study protocol at more than 60 U.S. centers, Dr. Mentz observed.
One of the pragmatic design’s advantages, he told this news organization, was “how efficient it was” as a randomized comparison of treatment strategies for clinical outcomes. It was “relatively low cost” and recruited patients quickly, compared with conventional randomized trials, “and we answered the question clearly.” The trial’s results, Dr. Mentz said, reflect “what happens in the real world.”
When might torsemide have the edge?
Although furosemide is the most commonly used loop diuretic in HF, and there are others besides it and torsemide, the latter has both known and theoretical advantages that set it apart. Torsemide is more than twice as potent as furosemide and more bioavailable, and its treatment effect lasts longer, the TRANSFORM-HF investigators have noted.
In addition, preclinical and small clinical studies suggest torsemide may have pleiotropic effects that might be theoretical advantages for patients with HF. For example, it appears to downregulate the renin-angiotensin-aldosterone system (RAAS) and reduce myocardial fibrosis and promote reverse ventricular remodeling, the group writes.
In practice, therefore, torsemide may be preferred in patients with furosemide resistance or “challenges with bioavailability, especially those with very advanced heart failure with congestion who may have gut edema, where oral furosemide and other loop diuretics are not effectively absorbed,” Biykem Bozkurt, MD, PhD, Baylor College of Medicine, Houston, told this news organization.
In such patients, she said, torsemide “is considered to be a better choice for individuals who have diuretic resistance with advanced congestion.”
The drug’s apparent pleiotropic effects, such as RAAS inhibition, may have less relevance to the TRANSFORM-HF primary endpoint of all-cause mortality than to clinical outcomes more likely associated with successful decongestion, such as HF hospitalization, Dr. Bozkurt proposed.
The trial’s pragmatic design, however, made it more feasible to focus on all-cause mortality and less practical to use measures of successful decongestion, such as volume loss or reduction in natriuretic peptide levels, she observed. Those are endpoints of special interest when diuretics are compared, “especially for the subgroup of patients who are diuretic resistant.”
Over the last 20 years or so, “we’ve learned that hospitalized heart failure is a very different disease process with a different natural history,” observed Clyde W. Yancy, MD, MSc, Northwestern University, Chicago, who was not part of the current study.
“So, the idea that something as nuanced as choice of one loop diuretic over the other, in that setting, would be sufficient to change the natural history, may be still a high bar for us,” he said in an interview.
“Based on these data, one would have to argue that whichever loop diuretic you select for the hospitalized patient – and a lot of that is driven by market exigencies right now – it turns out that the response is indistinguishable,” Dr. Yancy said. “That means if your hospital happens to have furosemide on the formulary, use it. If furosemide is not available but torsemide is available, use it.”
Dr. Yancy said he’d like to see a trial similar to TRANSFORM-HF but in outpatients receiving today’s guideline-directed medical therapy, which includes the sodium-glucose cotransporter 2 (SGLT2) inhibitors, drugs that increase the fractional excretion of sodium and have a “diureticlike” effect.
Such a trial, he said, would explore “the combination of not one, or two, but three agents with a diuretic effect – a loop diuretic, a mineralocorticoid antagonist, and an SGLT2 inhibitor – in ambulatory, optimized patients. It might make a difference.”
HF regardless of EF
The trial enrolled patients hospitalized with worsening or new-onset HF with a plan for long-term loop diuretic therapy who had either an EF of 40% or lower or, regardless of EF, elevated natriuretic peptide levels when hospitalized.
Of the 2,859 participants, whose mean age was about 65 years, about 36% were women and 34% African American. Overall, 1,428 were assigned to receive furosemide as their initial oral diuretic and 1,431 patients were assigned to the torsemide-first strategy.
The rate of death from any cause in both groups was 17 per 100 patient-years at a median of 17.4 months. The hazard ratio for torsemide vs. furosemide was 1.02 (95% confidence interval, 0.89-1.18; P = .77).
The corresponding HR at 12 months for all-cause death or hospitalization was 0.92 (95% CI, 0.83-1.02; P = .11). The relative risk for any hospitalization was 0.94 (95% CI, 0.84-1.07).
Pragmatic design: Other implications
Dosing was left to clinician discretion in the open-label study, as was whether patients maintained their assigned drug or switched over to the other agent. Indeed, 5.4% of patients crossed over to the other loop diuretic, and 2.8% went off loop diuretics entirely between in-hospital randomization and discharge, Dr. Mentz reported. By day 30, 6.7% had crossed over, and 7% had stopped taking loop diuretics.
The diuretic crossovers and discontinuations, Dr. Mentz said, likely biased the trial’s outcomes, such that the two strategies performed about equally well. Efforts were made, however, to at least partially overcome that limitation.
“We put measures in place to support adherence – sending letters to their primary doctors, giving them a wallet card so they would know which therapy they were on, having conversations about the importance of trying to stay on the randomized therapy,” Dr. Mentz said in an interview. Still, some clinicians saw differences between the two agents that prompted them, at some point, to switch patients from one loop diuretic to the other.
But interestingly, Dr. Mentz reported, the two strategies did not significantly differ in all-cause mortality or the composite of all-cause mortality or hospitalization in analysis by intention to treat.
Dr. Mentz discloses receiving honoraria from AstraZeneca, Bayer/Merck, Boehringer Ingelheim/Lilly, Cytokinetics, Pharmacosmos, Respicardia, Windtree Therapeutics, and Zoll; and research grants from American Regent and Novartis. Dr. Bozkurt discloses receiving honoraria from AstraZeneca, Baxter Health Care, and Sanofi Aventis and having other relationships with Renovacor, Respicardia, Abbott Vascular, Liva Nova, Vifor, and Cardurion. Dr. Yancy discloses a modest relationship with Abbott.
A version of this article first appeared on Medscape.com.
CHICAGO – The choice of loop diuretic for decongestion in patients hospitalized with heart failure (HF) may make little difference to survival or readmission risk over the next year, at least when deciding between furosemide or torsemide, a randomized trial suggests.
Both drugs are old and widely used, but differences between the two loop diuretics in bioavailability, effects on potassium levels, and other features have led some clinicians to sometimes prefer torsemide. Until now, however, no randomized HF trials have compared the two drugs.
The new findings suggest clinicians can continue starting such patients with HF on either agent, at their discretion, without concern that the choice may compromise outcomes, say researchers from the TRANSFORM-HF trial, which compared furosemide-first and torsemide-first diuretic strategies in a diverse population of patients with HF.
Given that the two strategies were similarly effective for survival and rehospitalization, clinicians caring for patients with HF can focus more on “getting patients on the right dose for their loop diuretic, and prioritizing those therapies proven to improve clinical outcomes,” said Robert J. Mentz, MD, of Duke University Clinical Research Institute, Durham, N.C.
Dr. Mentz, a TRANSFORM-HF principal investigator, presented the primary results November 5 at the American Heart Association scientific sessions.
The trial had randomly assigned 2,859 patients hospitalized with HF and with a plan for oral loop diuretic therapy to initiate treatment with furosemide or torsemide. Clinicians were encouraged to maintain patients on the assigned diuretic, but crossovers to the other drug or other diuretic changes were allowed.
Rates of death from any cause, the primary endpoint, were about 26% in both groups over a median 17-month follow-up, regardless of ejection fraction (EF).
The composite rates of all-cause death or hospitalization at 12 months were also not significantly different, about 49% for those started on furosemide and about 47% for patients initially prescribed torsemide.
As a pragmatic comparative effectiveness trial, TRANSFORM-HF entered diverse patients with HF, broadly representative of actual clinical practice, who were managed according to routine practice and a streamlined study protocol at more than 60 U.S. centers, Dr. Mentz observed.
One of the pragmatic design’s advantages, he told this news organization, was “how efficient it was” as a randomized comparison of treatment strategies for clinical outcomes. It was “relatively low cost” and recruited patients quickly, compared with conventional randomized trials, “and we answered the question clearly.” The trial’s results, Dr. Mentz said, reflect “what happens in the real world.”
When might torsemide have the edge?
Although furosemide is the most commonly used loop diuretic in HF, and there are others besides it and torsemide, the latter has both known and theoretical advantages that set it apart. Torsemide is more than twice as potent as furosemide and more bioavailable, and its treatment effect lasts longer, the TRANSFORM-HF investigators have noted.
In addition, preclinical and small clinical studies suggest torsemide may have pleiotropic effects that might be theoretical advantages for patients with HF. For example, it appears to downregulate the renin-angiotensin-aldosterone system (RAAS) and reduce myocardial fibrosis and promote reverse ventricular remodeling, the group writes.
In practice, therefore, torsemide may be preferred in patients with furosemide resistance or “challenges with bioavailability, especially those with very advanced heart failure with congestion who may have gut edema, where oral furosemide and other loop diuretics are not effectively absorbed,” Biykem Bozkurt, MD, PhD, Baylor College of Medicine, Houston, told this news organization.
In such patients, she said, torsemide “is considered to be a better choice for individuals who have diuretic resistance with advanced congestion.”
The drug’s apparent pleiotropic effects, such as RAAS inhibition, may have less relevance to the TRANSFORM-HF primary endpoint of all-cause mortality than to clinical outcomes more likely associated with successful decongestion, such as HF hospitalization, Dr. Bozkurt proposed.
The trial’s pragmatic design, however, made it more feasible to focus on all-cause mortality and less practical to use measures of successful decongestion, such as volume loss or reduction in natriuretic peptide levels, she observed. Those are endpoints of special interest when diuretics are compared, “especially for the subgroup of patients who are diuretic resistant.”
Over the last 20 years or so, “we’ve learned that hospitalized heart failure is a very different disease process with a different natural history,” observed Clyde W. Yancy, MD, MSc, Northwestern University, Chicago, who was not part of the current study.
“So, the idea that something as nuanced as choice of one loop diuretic over the other, in that setting, would be sufficient to change the natural history, may be still a high bar for us,” he said in an interview.
“Based on these data, one would have to argue that whichever loop diuretic you select for the hospitalized patient – and a lot of that is driven by market exigencies right now – it turns out that the response is indistinguishable,” Dr. Yancy said. “That means if your hospital happens to have furosemide on the formulary, use it. If furosemide is not available but torsemide is available, use it.”
Dr. Yancy said he’d like to see a trial similar to TRANSFORM-HF but in outpatients receiving today’s guideline-directed medical therapy, which includes the sodium-glucose cotransporter 2 (SGLT2) inhibitors, drugs that increase the fractional excretion of sodium and have a “diureticlike” effect.
Such a trial, he said, would explore “the combination of not one, or two, but three agents with a diuretic effect – a loop diuretic, a mineralocorticoid antagonist, and an SGLT2 inhibitor – in ambulatory, optimized patients. It might make a difference.”
HF regardless of EF
The trial enrolled patients hospitalized with worsening or new-onset HF with a plan for long-term loop diuretic therapy who had either an EF of 40% or lower or, regardless of EF, elevated natriuretic peptide levels when hospitalized.
Of the 2,859 participants, whose mean age was about 65 years, about 36% were women and 34% African American. Overall, 1,428 were assigned to receive furosemide as their initial oral diuretic and 1,431 patients were assigned to the torsemide-first strategy.
The rate of death from any cause in both groups was 17 per 100 patient-years at a median of 17.4 months. The hazard ratio for torsemide vs. furosemide was 1.02 (95% confidence interval, 0.89-1.18; P = .77).
The corresponding HR at 12 months for all-cause death or hospitalization was 0.92 (95% CI, 0.83-1.02; P = .11). The relative risk for any hospitalization was 0.94 (95% CI, 0.84-1.07).
Pragmatic design: Other implications
Dosing was left to clinician discretion in the open-label study, as was whether patients maintained their assigned drug or switched over to the other agent. Indeed, 5.4% of patients crossed over to the other loop diuretic, and 2.8% went off loop diuretics entirely between in-hospital randomization and discharge, Dr. Mentz reported. By day 30, 6.7% had crossed over, and 7% had stopped taking loop diuretics.
The diuretic crossovers and discontinuations, Dr. Mentz said, likely biased the trial’s outcomes, such that the two strategies performed about equally well. Efforts were made, however, to at least partially overcome that limitation.
“We put measures in place to support adherence – sending letters to their primary doctors, giving them a wallet card so they would know which therapy they were on, having conversations about the importance of trying to stay on the randomized therapy,” Dr. Mentz said in an interview. Still, some clinicians saw differences between the two agents that prompted them, at some point, to switch patients from one loop diuretic to the other.
But interestingly, Dr. Mentz reported, the two strategies did not significantly differ in all-cause mortality or the composite of all-cause mortality or hospitalization in analysis by intention to treat.
Dr. Mentz discloses receiving honoraria from AstraZeneca, Bayer/Merck, Boehringer Ingelheim/Lilly, Cytokinetics, Pharmacosmos, Respicardia, Windtree Therapeutics, and Zoll; and research grants from American Regent and Novartis. Dr. Bozkurt discloses receiving honoraria from AstraZeneca, Baxter Health Care, and Sanofi Aventis and having other relationships with Renovacor, Respicardia, Abbott Vascular, Liva Nova, Vifor, and Cardurion. Dr. Yancy discloses a modest relationship with Abbott.
A version of this article first appeared on Medscape.com.
AT AHA 2022
Acute heart failure risk assessment in ED improves outcomes: COACH
CHICAGO – Systematic mortality-risk assessment of patients who presented to hospital emergency departments for acute heart failure led to better patient outcomes in a controlled Canadian trial with more than 5,000 patients.
Thirty days after patients presented, the incidence of death from any cause or hospitalization for cardiovascular causes – one of two primary endpoints in the COACH study – was 12.1% among patients who underwent acute risk assessment and 14.5% in control patients who did not undergo this assessment, which translated into an adjusted, significant 12% relative risk reduction for the patients who underwent systematic assessment, Douglas S. Lee, MD, PhD, said at the American Heart Association scientific sessions.

The study’s second primary endpoint, the incidence of the same combined outcome 20 months after initial presentation, was 54.4% among the 2,480 patients assessed with the risk-assessment tool and 56.2% in the 2,972 controls, a significant, adjusted relative risk reduction of 5%.
This benefit was primarily driven by reductions in cardiovascular hospitalizations, which fell by an adjusted 16% in the intervention group compared with controls, and more specifically by hospitalizations for heart failure, which tallied a relative 20% less with the intervention. Both were significant between-group differences.
The other portion of the combined endpoint, all-cause mortality, was not significantly different between the patients who underwent the systematic emergency department assessment and the controls who were managed using usual emergency-department protocols.
Simultaneous with the report, the results also appeared online in the New England Journal of Medicine.
A pathway for early discharge and improved outcomes
“Implementation of this approach may lead to a pathway for early discharge from the hospital or emergency department, and improved patient outcomes,” said Dr. Lee, a professor at the University of Toronto, and a senior core scientist at the ICES Cardiovascular Research Program in Toronto.

“The treatment effect on the primary process outcome – patients admitted or discharged – will add useful insights into how intervention may improve,” commented Harriette Van Spall, MD, who was designated discussant for the report. The findings “fill an important knowledge gap,” added Dr. Van Spall, a cardiologist at McMaster University in Hamilton, Ont. The results “have important implications for health resource utilization,” she said.
The risk assessment tool used in the study is called the Emergency Heart failure Mortality Risk Grade for 30-day mortality (EHMRG30-ST), which was devised and validated by Dr. Lee and his associates. The assessment tool uses 11 clinical variables that include age, systolic blood pressure, heart rate, oxygen saturation, potassium and creatinine levels, and presence of ST depression on a 12-lead ECG.
The study design recommended that patients be discharged early and receive standardized transitional care as outpatients if they had a low risk of death within 7 days and within 30 days as estimated by the EHMRG30-ST. The protocol recommended that patients scored as high risk should be admitted to the hospital, and that clinicians use their clinical judgment for intermediate-risk patients but favor admission for intermediate to high risk and discharge for low to intermediate risk. The study ran at 10 hospitals in Ontario. Initially, all 10 hospitals assessed patients by usual care, and then, over time, each hospital began using the tool so that by the end of the study all 10 hospitals employed it. Among the 2,480 patients seen during the active phase, 2,442 actually underwent assessment, with 24% rated as low risk, 32% rated as intermediate risk, and 44% judged to have high risk.
The researchers also ran risk assessments retrospectively on the controls, who showed a roughly similar risk distribution, with 18% low risk, 28% intermediate risk, and 54% high risk.
The patients averaged 78 years of age, 55% were men, about 40% had diabetes, and about 64% had a prior heart failure diagnosis.
Heart failure admissions have become ‘a big deal’
Emergency department clinicians and heart failure cardiologists “have worked together for a long time” when making decisions about which patients with acute heart failure need hospital admission, commented Mary N. Walsh, MD, medical director of the heart failure and cardiac transplantation programs at Ascension St. Vincent Heart Center in Indianapolis. These decisions “became a big deal” a decade ago when the U.S. Centers for Medicare & Medicaid Services launched the Hospital Readmissions Reduction Program that began to penalize hospitals for high rates of hospital readmissions for several conditions including heart failure, she said in an interview.

“If a heart failure patient is not admitted, they can’t be readmitted,” Dr. Walsh noted.
“Many risk-assessment tools exist for patients once they are hospitalized, but these tools have not been used in emergency departments. The take-home message is that we need to start risk assessment sooner, in the emergency department,” she said.
But the specific approach tested in the COACH trial needs more study and may need further tweaking to work in the United States, where it is not clear who would pay for a program like the one tested in the trial. Canada’s unified health care payment system makes the COACH approach more financially feasible, Dr. Walsh commented.
COACH received no commercial funding. Dr. Lee, Dr. Van Spall, and Dr. Walsh had no disclosures.
CHICAGO – Systematic mortality-risk assessment of patients who presented to hospital emergency departments for acute heart failure led to better patient outcomes in a controlled Canadian trial with more than 5,000 patients.
Thirty days after patients presented, the incidence of death from any cause or hospitalization for cardiovascular causes – one of two primary endpoints in the COACH study – was 12.1% among patients who underwent acute risk assessment and 14.5% in control patients who did not undergo this assessment, which translated into an adjusted, significant 12% relative risk reduction for the patients who underwent systematic assessment, Douglas S. Lee, MD, PhD, said at the American Heart Association scientific sessions.
The study’s second primary endpoint, the incidence of the same combined outcome 20 months after initial presentation, was 54.4% among the 2,480 patients assessed with the risk-assessment tool and 56.2% in the 2,972 controls, a significant, adjusted relative risk reduction of 5%.
This benefit was primarily driven by reductions in cardiovascular hospitalizations, which fell by an adjusted 16% in the intervention group compared with controls, and more specifically by hospitalizations for heart failure, which tallied a relative 20% less with the intervention. Both were significant between-group differences.
The other portion of the combined endpoint, all-cause mortality, was not significantly different between the patients who underwent the systematic emergency department assessment and the controls who were managed using usual emergency-department protocols.
Simultaneous with the report, the results also appeared online in the New England Journal of Medicine.
A pathway for early discharge and improved outcomes
“Implementation of this approach may lead to a pathway for early discharge from the hospital or emergency department, and improved patient outcomes,” said Dr. Lee, a professor at the University of Toronto, and a senior core scientist at the ICES Cardiovascular Research Program in Toronto.
“The treatment effect on the primary process outcome – patients admitted or discharged – will add useful insights into how intervention may improve,” commented Harriette Van Spall, MD, who was designated discussant for the report. The findings “fill an important knowledge gap,” added Dr. Van Spall, a cardiologist at McMaster University in Hamilton, Ont. The results “have important implications for health resource utilization,” she said.
The risk assessment tool used in the study is called the Emergency Heart failure Mortality Risk Grade for 30-day mortality (EHMRG30-ST), which was devised and validated by Dr. Lee and his associates. The assessment tool uses 11 clinical variables that include age, systolic blood pressure, heart rate, oxygen saturation, potassium and creatinine levels, and presence of ST depression on a 12-lead ECG.
The study design recommended that patients be discharged early and receive standardized transitional care as outpatients if they had a low risk of death within 7 days and within 30 days as estimated by the EHMRG30-ST. The protocol recommended that patients scored as high risk should be admitted to the hospital, and that clinicians use their clinical judgment for intermediate-risk patients but favor admission for intermediate to high risk and discharge for low to intermediate risk. The study ran at 10 hospitals in Ontario. Initially, all 10 hospitals assessed patients by usual care, and then, over time, each hospital began using the tool so that by the end of the study all 10 hospitals employed it. Among the 2,480 patients seen during the active phase, 2,442 actually underwent assessment, with 24% rated as low risk, 32% rated as intermediate risk, and 44% judged to have high risk.
The researchers also ran risk assessments retrospectively on the controls, who showed a roughly similar risk distribution, with 18% low risk, 28% intermediate risk, and 54% high risk.
The patients averaged 78 years of age, 55% were men, about 40% had diabetes, and about 64% had a prior heart failure diagnosis.
Heart failure admissions have become ‘a big deal’
Emergency department clinicians and heart failure cardiologists “have worked together for a long time” when making decisions about which patients with acute heart failure need hospital admission, commented Mary N. Walsh, MD, medical director of the heart failure and cardiac transplantation programs at Ascension St. Vincent Heart Center in Indianapolis. These decisions “became a big deal” a decade ago when the U.S. Centers for Medicare & Medicaid Services launched the Hospital Readmissions Reduction Program that began to penalize hospitals for high rates of hospital readmissions for several conditions including heart failure, she said in an interview.
“If a heart failure patient is not admitted, they can’t be readmitted,” Dr. Walsh noted.
“Many risk-assessment tools exist for patients once they are hospitalized, but these tools have not been used in emergency departments. The take-home message is that we need to start risk assessment sooner, in the emergency department,” she said.
But the specific approach tested in the COACH trial needs more study and may need further tweaking to work in the United States, where it is not clear who would pay for a program like the one tested in the trial. Canada’s unified health care payment system makes the COACH approach more financially feasible, Dr. Walsh commented.
COACH received no commercial funding. Dr. Lee, Dr. Van Spall, and Dr. Walsh had no disclosures.
CHICAGO – Systematic mortality-risk assessment of patients who presented to hospital emergency departments for acute heart failure led to better patient outcomes in a controlled Canadian trial with more than 5,000 patients.
Thirty days after patients presented, the incidence of death from any cause or hospitalization for cardiovascular causes – one of two primary endpoints in the COACH study – was 12.1% among patients who underwent acute risk assessment and 14.5% in control patients who did not undergo this assessment, which translated into an adjusted, significant 12% relative risk reduction for the patients who underwent systematic assessment, Douglas S. Lee, MD, PhD, said at the American Heart Association scientific sessions.
The study’s second primary endpoint, the incidence of the same combined outcome 20 months after initial presentation, was 54.4% among the 2,480 patients assessed with the risk-assessment tool and 56.2% in the 2,972 controls, a significant, adjusted relative risk reduction of 5%.
This benefit was primarily driven by reductions in cardiovascular hospitalizations, which fell by an adjusted 16% in the intervention group compared with controls, and more specifically by hospitalizations for heart failure, which tallied a relative 20% less with the intervention. Both were significant between-group differences.
The other portion of the combined endpoint, all-cause mortality, was not significantly different between the patients who underwent the systematic emergency department assessment and the controls who were managed using usual emergency-department protocols.
Simultaneous with the report, the results also appeared online in the New England Journal of Medicine.
A pathway for early discharge and improved outcomes
“Implementation of this approach may lead to a pathway for early discharge from the hospital or emergency department, and improved patient outcomes,” said Dr. Lee, a professor at the University of Toronto, and a senior core scientist at the ICES Cardiovascular Research Program in Toronto.
“The treatment effect on the primary process outcome – patients admitted or discharged – will add useful insights into how intervention may improve,” commented Harriette Van Spall, MD, who was designated discussant for the report. The findings “fill an important knowledge gap,” added Dr. Van Spall, a cardiologist at McMaster University in Hamilton, Ont. The results “have important implications for health resource utilization,” she said.
The risk assessment tool used in the study is called the Emergency Heart failure Mortality Risk Grade for 30-day mortality (EHMRG30-ST), which was devised and validated by Dr. Lee and his associates. The assessment tool uses 11 clinical variables that include age, systolic blood pressure, heart rate, oxygen saturation, potassium and creatinine levels, and presence of ST depression on a 12-lead ECG.
The study design recommended that patients be discharged early and receive standardized transitional care as outpatients if they had a low risk of death within 7 days and within 30 days as estimated by the EHMRG30-ST. The protocol recommended that patients scored as high risk should be admitted to the hospital, and that clinicians use their clinical judgment for intermediate-risk patients but favor admission for intermediate to high risk and discharge for low to intermediate risk. The study ran at 10 hospitals in Ontario. Initially, all 10 hospitals assessed patients by usual care, and then, over time, each hospital began using the tool so that by the end of the study all 10 hospitals employed it. Among the 2,480 patients seen during the active phase, 2,442 actually underwent assessment, with 24% rated as low risk, 32% rated as intermediate risk, and 44% judged to have high risk.
The researchers also ran risk assessments retrospectively on the controls, who showed a roughly similar risk distribution, with 18% low risk, 28% intermediate risk, and 54% high risk.
The patients averaged 78 years of age, 55% were men, about 40% had diabetes, and about 64% had a prior heart failure diagnosis.
Heart failure admissions have become ‘a big deal’
Emergency department clinicians and heart failure cardiologists “have worked together for a long time” when making decisions about which patients with acute heart failure need hospital admission, commented Mary N. Walsh, MD, medical director of the heart failure and cardiac transplantation programs at Ascension St. Vincent Heart Center in Indianapolis. These decisions “became a big deal” a decade ago when the U.S. Centers for Medicare & Medicaid Services launched the Hospital Readmissions Reduction Program that began to penalize hospitals for high rates of hospital readmissions for several conditions including heart failure, she said in an interview.
“If a heart failure patient is not admitted, they can’t be readmitted,” Dr. Walsh noted.
“Many risk-assessment tools exist for patients once they are hospitalized, but these tools have not been used in emergency departments. The take-home message is that we need to start risk assessment sooner, in the emergency department,” she said.
But the specific approach tested in the COACH trial needs more study and may need further tweaking to work in the United States, where it is not clear who would pay for a program like the one tested in the trial. Canada’s unified health care payment system makes the COACH approach more financially feasible, Dr. Walsh commented.
COACH received no commercial funding. Dr. Lee, Dr. Van Spall, and Dr. Walsh had no disclosures.
AT AHA 2022