User login
SHM Introduces Discounted PQRS Through New Learning Portal

First, SHM’s new Learning Portal was the one-stop shop for free and discounted continuing medical education (CME) credits online. Now, the Learning Portal can help hospitalists report into the physician quality reporting system (PQRS) at a discounted individual rate.
And the time to start reporting measures in PQRS is now.
The PQRS was developed by the Centers for Medicare & Medicaid Services (CMS) in 2007 as a voluntary reporting program that provides a financial incentive to physicians and other eligible professionals who report data on quality measures for covered services furnished to Medicare beneficiaries. Starting in 2013, reporting in PQRS becomes mandatory for all eligible professionals.
SHM has encouraged its members to participate in the PQRS since the system’s inception in 2007. With the exciting launch of the SHM Learning Portal, it is easier than ever to get started. If you or your group are not currently reporting, there are still incentive payments available in 2013 and 2014. Beginning in 2015, there will be a penalty for not reporting quality measures based on 2013 performance.
Access the PQRIwizard through the SHM Learning Portal
SHM has secured a significant discount for members to report PQRS through the PQRIwizard. Located within the SHM Learning Portal, this online tool is a fast, convenient, and cost-effective solution to help collect and report quality measures data for the PQRS program. Similar to online tax-preparation software, the PQRIwizard guides you through a few easy steps to help rapidly collect, validate, report, and submit your results to CMS. The tool is powered by the CECity Registry, a CMS-qualified registry for PQRS reporting.
What Measures Are Available?
The SHM PQRIwizard features six individual quality measures in the areas of stroke and stroke rehabilitation, including measures on screening for dysphagia and thrombolytic therapy. To report on any of these measures, simply select three measures and report on 80 percent of your Medicare Part B fee-for-services patients who apply to the measures you selected.
PQRIwizard has a built-in progress monitor that validates your report by checking for missing data. The monitor also tracks your data to provide you with continuous feedback regarding valid patients. The system even calculates your measures and provides a printable report of your measure results in real time.
First, SHM’s new Learning Portal was the one-stop shop for free and discounted continuing medical education (CME) credits online. Now, the Learning Portal can help hospitalists report into the physician quality reporting system (PQRS) at a discounted individual rate.
And the time to start reporting measures in PQRS is now.
The PQRS was developed by the Centers for Medicare & Medicaid Services (CMS) in 2007 as a voluntary reporting program that provides a financial incentive to physicians and other eligible professionals who report data on quality measures for covered services furnished to Medicare beneficiaries. Starting in 2013, reporting in PQRS becomes mandatory for all eligible professionals.
SHM has encouraged its members to participate in the PQRS since the system’s inception in 2007. With the exciting launch of the SHM Learning Portal, it is easier than ever to get started. If you or your group are not currently reporting, there are still incentive payments available in 2013 and 2014. Beginning in 2015, there will be a penalty for not reporting quality measures based on 2013 performance.
Access the PQRIwizard through the SHM Learning Portal
SHM has secured a significant discount for members to report PQRS through the PQRIwizard. Located within the SHM Learning Portal, this online tool is a fast, convenient, and cost-effective solution to help collect and report quality measures data for the PQRS program. Similar to online tax-preparation software, the PQRIwizard guides you through a few easy steps to help rapidly collect, validate, report, and submit your results to CMS. The tool is powered by the CECity Registry, a CMS-qualified registry for PQRS reporting.
What Measures Are Available?
The SHM PQRIwizard features six individual quality measures in the areas of stroke and stroke rehabilitation, including measures on screening for dysphagia and thrombolytic therapy. To report on any of these measures, simply select three measures and report on 80 percent of your Medicare Part B fee-for-services patients who apply to the measures you selected.
PQRIwizard has a built-in progress monitor that validates your report by checking for missing data. The monitor also tracks your data to provide you with continuous feedback regarding valid patients. The system even calculates your measures and provides a printable report of your measure results in real time.
First, SHM’s new Learning Portal was the one-stop shop for free and discounted continuing medical education (CME) credits online. Now, the Learning Portal can help hospitalists report into the physician quality reporting system (PQRS) at a discounted individual rate.
And the time to start reporting measures in PQRS is now.
The PQRS was developed by the Centers for Medicare & Medicaid Services (CMS) in 2007 as a voluntary reporting program that provides a financial incentive to physicians and other eligible professionals who report data on quality measures for covered services furnished to Medicare beneficiaries. Starting in 2013, reporting in PQRS becomes mandatory for all eligible professionals.
SHM has encouraged its members to participate in the PQRS since the system’s inception in 2007. With the exciting launch of the SHM Learning Portal, it is easier than ever to get started. If you or your group are not currently reporting, there are still incentive payments available in 2013 and 2014. Beginning in 2015, there will be a penalty for not reporting quality measures based on 2013 performance.
Access the PQRIwizard through the SHM Learning Portal
SHM has secured a significant discount for members to report PQRS through the PQRIwizard. Located within the SHM Learning Portal, this online tool is a fast, convenient, and cost-effective solution to help collect and report quality measures data for the PQRS program. Similar to online tax-preparation software, the PQRIwizard guides you through a few easy steps to help rapidly collect, validate, report, and submit your results to CMS. The tool is powered by the CECity Registry, a CMS-qualified registry for PQRS reporting.
What Measures Are Available?
The SHM PQRIwizard features six individual quality measures in the areas of stroke and stroke rehabilitation, including measures on screening for dysphagia and thrombolytic therapy. To report on any of these measures, simply select three measures and report on 80 percent of your Medicare Part B fee-for-services patients who apply to the measures you selected.
PQRIwizard has a built-in progress monitor that validates your report by checking for missing data. The monitor also tracks your data to provide you with continuous feedback regarding valid patients. The system even calculates your measures and provides a printable report of your measure results in real time.
Project BOOST Study Documents Modest Impact on 30-Day Hospital Readmissions

Initial research on outcomes following Project BOOST (Better Outcomes for Older Adults through Safe Transitions) implementation shows modest improvement in rehospitalization rates. Moreover, some experts suggest the real problem might lie in using 30-day hospital readmissions, now a target for Medicare reimbursement penalties, as the quality metric for care transitions out of the hospital.
Study data showed a 2% absolute reduction in all-patient, 30-day readmission rates at 11 of the original 30 BOOST sites (to 12.7% from 14.7%), according to an article in the August issue of the Journal of Hospital Medicine.1
“Everybody has talked about readmissions as the quality target, but really it should be about improving transitions of care for the patient going home,” says Ashish Jha, MD, MPH, of the Harvard School of Public Health, Health Policy and Management. “If we’re going to use readmissions as our quality measure, maybe we’re set up to fail. Can we do care transitions better? Yes, we can. Can we do better quality measures? Yes. My take-home message is that we should get clearer on what we are trying to achieve.”
Project BOOST (www.hospitalmedicine.org/boost) has been a major quality initiative for SHM since 2008 and one of several national programs aimed at helping hospitals improve care-transitions processes and patient outcomes. BOOST offers participating sites an online toolkit of strategies and interventions, along with the support of an expert mentor.
“Participation in Project BOOST appeared to be associated with a decrease in readmission rates,” the authors conclude. But two accompanying editorials in the journal expressed disappointment with a lack of “robustness” to these results and lack of participation by BOOST sites.2,3 The editorials also acknowledge the challenges of multisite, voluntary research on a topic that, so far, has largely resisted validated, generalizable research outcomes demonstrating what really works in preventing readmissions.
“I think people want a silver bullet on this issue,” says lead author Luke Hansen, MD, MHS, of the division of hospital medicine at Northwestern University Feinberg School of Medicine in Chicago. “They want to be able to define an intervention to take care of all of the avoidable fraction of rehospitalizations. But I don’t think that’s possible. The disappointment may come from the fact that this is a more complicated issue than we thought.”
Dr. Hansen says data reporting was voluntary and uncompensated, and the BOOST research team is trying to facilitate better reporting from subsequent cohorts. He says one of BOOST’s unique aspects—tailoring interventions to local circumstances—could be a drawback to outcomes research. “We have to incorporate the diversity of experience into our research methods and our expectations,” he says.
Hospitalist Bradley Flansbaum, DO, MPH, FACP, SFHM, of Lenox Hill Hospital in New York City says BOOST reinforces many of things hospitalists should be doing to provide optimal discharges and transitions
.
—Ashish Jha, MD, MPH, Harvard School of Public Health, Health Policy, and Management, Boston
“Like appropriate teaching and patient education, medication reconciliation, and setting up follow-up appointments,” says Dr. Flansbaum, a member of SHM’s Public Policy Committee and regular contributor to SHM’s Practice Management blog. “But if there was one thing I’d like hospitalists to take home from this research, it’s the cognitive dissonance—the challenge of matching the evidence with what the regulatory bodies expect from us and knowing that the evidence is falling short.
“As much as we might be held accountable for outcomes like readmissions, the reality is that we can’t control them. What we’re learning is that this is really hard to do.”
Amy Boutwell, MD, MPP, a hospitalist in Newton, Mass., and founder of Collaborative Healthcare Strategies, agrees transitions of care are difficult. However, she also thinks hospitals and hospitalists cannot wait for conclusive research that proves what works in preventing readmissions.
“The BOOST results reflect my own experience working with more than a hundred STAAR [State Action on Avoidable Readmissions] hospitals. We haven’t yet been able to sufficiently extract the data about readmissions from the field—and we need to figure out how to do that,” she says. “But when you look at the issue from a patient’s perspective and their desire for a safe transition, why would you not do the things recommended by Project BOOST and similar initiatives?”
Primary-care physicians (PCPs) need to know about major changes in a discharged patient’s plan of care in a timely manner, along with any results from pending lab tests, Dr. Boutwell explains. She emphasizes that patients and their caregivers need to be given clear discharge instructions when they leave the hospital.
“We have an obligation to do what we know to be best practices and standards of care. The BOOST toolkit of recommendations is very comprehensive and gives hospitals a lot of options to improve their internal processes,” Dr. Boutwell says. “It’s hard to argue against any of them, even if it’s hard to draw clear links between them and readmissions rates. These are the self-evident, basic tasks that I would want done for myself or my child or my parent, if we were in the hospital.”
Larry Beresford is a freelance writer in San Francisco.
References
- Hansen L, Greenwald J, Budnitz T, et al. Project BOOST: Effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8):421-427. doi: 10.1002/jhm.2054. Epub 2013 Jul 22.
- Auerbach A, Fang M, Glasheen J, Brotman D, O’Leary KJ, Horwitz LJ. BOOST: Evidence needing a lift. J Hosp Med. 2013;8(8):468-469. doi: 10.1002/jhm.2065. Epub 2013 Jul 22.
- Jha A. BOOST and readmissions: Thinking beyond the walls of the hospital. J Hosp Med. 2013;8(8):470-471. doi: 10.1002/jhm.2069. Epub 2013 Jul 22.
Initial research on outcomes following Project BOOST (Better Outcomes for Older Adults through Safe Transitions) implementation shows modest improvement in rehospitalization rates. Moreover, some experts suggest the real problem might lie in using 30-day hospital readmissions, now a target for Medicare reimbursement penalties, as the quality metric for care transitions out of the hospital.
Study data showed a 2% absolute reduction in all-patient, 30-day readmission rates at 11 of the original 30 BOOST sites (to 12.7% from 14.7%), according to an article in the August issue of the Journal of Hospital Medicine.1
“Everybody has talked about readmissions as the quality target, but really it should be about improving transitions of care for the patient going home,” says Ashish Jha, MD, MPH, of the Harvard School of Public Health, Health Policy and Management. “If we’re going to use readmissions as our quality measure, maybe we’re set up to fail. Can we do care transitions better? Yes, we can. Can we do better quality measures? Yes. My take-home message is that we should get clearer on what we are trying to achieve.”
Project BOOST (www.hospitalmedicine.org/boost) has been a major quality initiative for SHM since 2008 and one of several national programs aimed at helping hospitals improve care-transitions processes and patient outcomes. BOOST offers participating sites an online toolkit of strategies and interventions, along with the support of an expert mentor.
“Participation in Project BOOST appeared to be associated with a decrease in readmission rates,” the authors conclude. But two accompanying editorials in the journal expressed disappointment with a lack of “robustness” to these results and lack of participation by BOOST sites.2,3 The editorials also acknowledge the challenges of multisite, voluntary research on a topic that, so far, has largely resisted validated, generalizable research outcomes demonstrating what really works in preventing readmissions.
“I think people want a silver bullet on this issue,” says lead author Luke Hansen, MD, MHS, of the division of hospital medicine at Northwestern University Feinberg School of Medicine in Chicago. “They want to be able to define an intervention to take care of all of the avoidable fraction of rehospitalizations. But I don’t think that’s possible. The disappointment may come from the fact that this is a more complicated issue than we thought.”
Dr. Hansen says data reporting was voluntary and uncompensated, and the BOOST research team is trying to facilitate better reporting from subsequent cohorts. He says one of BOOST’s unique aspects—tailoring interventions to local circumstances—could be a drawback to outcomes research. “We have to incorporate the diversity of experience into our research methods and our expectations,” he says.
Hospitalist Bradley Flansbaum, DO, MPH, FACP, SFHM, of Lenox Hill Hospital in New York City says BOOST reinforces many of things hospitalists should be doing to provide optimal discharges and transitions
.
—Ashish Jha, MD, MPH, Harvard School of Public Health, Health Policy, and Management, Boston
“Like appropriate teaching and patient education, medication reconciliation, and setting up follow-up appointments,” says Dr. Flansbaum, a member of SHM’s Public Policy Committee and regular contributor to SHM’s Practice Management blog. “But if there was one thing I’d like hospitalists to take home from this research, it’s the cognitive dissonance—the challenge of matching the evidence with what the regulatory bodies expect from us and knowing that the evidence is falling short.
“As much as we might be held accountable for outcomes like readmissions, the reality is that we can’t control them. What we’re learning is that this is really hard to do.”
Amy Boutwell, MD, MPP, a hospitalist in Newton, Mass., and founder of Collaborative Healthcare Strategies, agrees transitions of care are difficult. However, she also thinks hospitals and hospitalists cannot wait for conclusive research that proves what works in preventing readmissions.
“The BOOST results reflect my own experience working with more than a hundred STAAR [State Action on Avoidable Readmissions] hospitals. We haven’t yet been able to sufficiently extract the data about readmissions from the field—and we need to figure out how to do that,” she says. “But when you look at the issue from a patient’s perspective and their desire for a safe transition, why would you not do the things recommended by Project BOOST and similar initiatives?”
Primary-care physicians (PCPs) need to know about major changes in a discharged patient’s plan of care in a timely manner, along with any results from pending lab tests, Dr. Boutwell explains. She emphasizes that patients and their caregivers need to be given clear discharge instructions when they leave the hospital.
“We have an obligation to do what we know to be best practices and standards of care. The BOOST toolkit of recommendations is very comprehensive and gives hospitals a lot of options to improve their internal processes,” Dr. Boutwell says. “It’s hard to argue against any of them, even if it’s hard to draw clear links between them and readmissions rates. These are the self-evident, basic tasks that I would want done for myself or my child or my parent, if we were in the hospital.”
Larry Beresford is a freelance writer in San Francisco.
References
- Hansen L, Greenwald J, Budnitz T, et al. Project BOOST: Effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8):421-427. doi: 10.1002/jhm.2054. Epub 2013 Jul 22.
- Auerbach A, Fang M, Glasheen J, Brotman D, O’Leary KJ, Horwitz LJ. BOOST: Evidence needing a lift. J Hosp Med. 2013;8(8):468-469. doi: 10.1002/jhm.2065. Epub 2013 Jul 22.
- Jha A. BOOST and readmissions: Thinking beyond the walls of the hospital. J Hosp Med. 2013;8(8):470-471. doi: 10.1002/jhm.2069. Epub 2013 Jul 22.
Initial research on outcomes following Project BOOST (Better Outcomes for Older Adults through Safe Transitions) implementation shows modest improvement in rehospitalization rates. Moreover, some experts suggest the real problem might lie in using 30-day hospital readmissions, now a target for Medicare reimbursement penalties, as the quality metric for care transitions out of the hospital.
Study data showed a 2% absolute reduction in all-patient, 30-day readmission rates at 11 of the original 30 BOOST sites (to 12.7% from 14.7%), according to an article in the August issue of the Journal of Hospital Medicine.1
“Everybody has talked about readmissions as the quality target, but really it should be about improving transitions of care for the patient going home,” says Ashish Jha, MD, MPH, of the Harvard School of Public Health, Health Policy and Management. “If we’re going to use readmissions as our quality measure, maybe we’re set up to fail. Can we do care transitions better? Yes, we can. Can we do better quality measures? Yes. My take-home message is that we should get clearer on what we are trying to achieve.”
Project BOOST (www.hospitalmedicine.org/boost) has been a major quality initiative for SHM since 2008 and one of several national programs aimed at helping hospitals improve care-transitions processes and patient outcomes. BOOST offers participating sites an online toolkit of strategies and interventions, along with the support of an expert mentor.
“Participation in Project BOOST appeared to be associated with a decrease in readmission rates,” the authors conclude. But two accompanying editorials in the journal expressed disappointment with a lack of “robustness” to these results and lack of participation by BOOST sites.2,3 The editorials also acknowledge the challenges of multisite, voluntary research on a topic that, so far, has largely resisted validated, generalizable research outcomes demonstrating what really works in preventing readmissions.
“I think people want a silver bullet on this issue,” says lead author Luke Hansen, MD, MHS, of the division of hospital medicine at Northwestern University Feinberg School of Medicine in Chicago. “They want to be able to define an intervention to take care of all of the avoidable fraction of rehospitalizations. But I don’t think that’s possible. The disappointment may come from the fact that this is a more complicated issue than we thought.”
Dr. Hansen says data reporting was voluntary and uncompensated, and the BOOST research team is trying to facilitate better reporting from subsequent cohorts. He says one of BOOST’s unique aspects—tailoring interventions to local circumstances—could be a drawback to outcomes research. “We have to incorporate the diversity of experience into our research methods and our expectations,” he says.
Hospitalist Bradley Flansbaum, DO, MPH, FACP, SFHM, of Lenox Hill Hospital in New York City says BOOST reinforces many of things hospitalists should be doing to provide optimal discharges and transitions
.
—Ashish Jha, MD, MPH, Harvard School of Public Health, Health Policy, and Management, Boston
“Like appropriate teaching and patient education, medication reconciliation, and setting up follow-up appointments,” says Dr. Flansbaum, a member of SHM’s Public Policy Committee and regular contributor to SHM’s Practice Management blog. “But if there was one thing I’d like hospitalists to take home from this research, it’s the cognitive dissonance—the challenge of matching the evidence with what the regulatory bodies expect from us and knowing that the evidence is falling short.
“As much as we might be held accountable for outcomes like readmissions, the reality is that we can’t control them. What we’re learning is that this is really hard to do.”
Amy Boutwell, MD, MPP, a hospitalist in Newton, Mass., and founder of Collaborative Healthcare Strategies, agrees transitions of care are difficult. However, she also thinks hospitals and hospitalists cannot wait for conclusive research that proves what works in preventing readmissions.
“The BOOST results reflect my own experience working with more than a hundred STAAR [State Action on Avoidable Readmissions] hospitals. We haven’t yet been able to sufficiently extract the data about readmissions from the field—and we need to figure out how to do that,” she says. “But when you look at the issue from a patient’s perspective and their desire for a safe transition, why would you not do the things recommended by Project BOOST and similar initiatives?”
Primary-care physicians (PCPs) need to know about major changes in a discharged patient’s plan of care in a timely manner, along with any results from pending lab tests, Dr. Boutwell explains. She emphasizes that patients and their caregivers need to be given clear discharge instructions when they leave the hospital.
“We have an obligation to do what we know to be best practices and standards of care. The BOOST toolkit of recommendations is very comprehensive and gives hospitals a lot of options to improve their internal processes,” Dr. Boutwell says. “It’s hard to argue against any of them, even if it’s hard to draw clear links between them and readmissions rates. These are the self-evident, basic tasks that I would want done for myself or my child or my parent, if we were in the hospital.”
Larry Beresford is a freelance writer in San Francisco.
References
- Hansen L, Greenwald J, Budnitz T, et al. Project BOOST: Effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8):421-427. doi: 10.1002/jhm.2054. Epub 2013 Jul 22.
- Auerbach A, Fang M, Glasheen J, Brotman D, O’Leary KJ, Horwitz LJ. BOOST: Evidence needing a lift. J Hosp Med. 2013;8(8):468-469. doi: 10.1002/jhm.2065. Epub 2013 Jul 22.
- Jha A. BOOST and readmissions: Thinking beyond the walls of the hospital. J Hosp Med. 2013;8(8):470-471. doi: 10.1002/jhm.2069. Epub 2013 Jul 22.
Patient Satisfaction Surveys Not Accurate Measure of Hospitalists’ Performance

Feeling frustrated with your group’s patient-satisfaction performance? Wondering why your chief (fill in the blank) officer glazes over when you try to explain why your hospitalist group’s Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) scores for doctor communication are in a percentile rivaling the numeric age of your children?
It is likely that the C-suite administrator overseeing your hospitalist group has a portion of their pay based on HCAHPS or other patient-satisfaction (also called patient experience) scores. And for good reason: The Centers for Medicare & Medicaid Services (CMS) Hospital Value-Based Purchasing (HVBP) program that started Oct. 1, 2012, has placed your hospital’s Medicare reimbursement at risk based on its HCAHPS scores.
HVBP and Patient Satisfaction
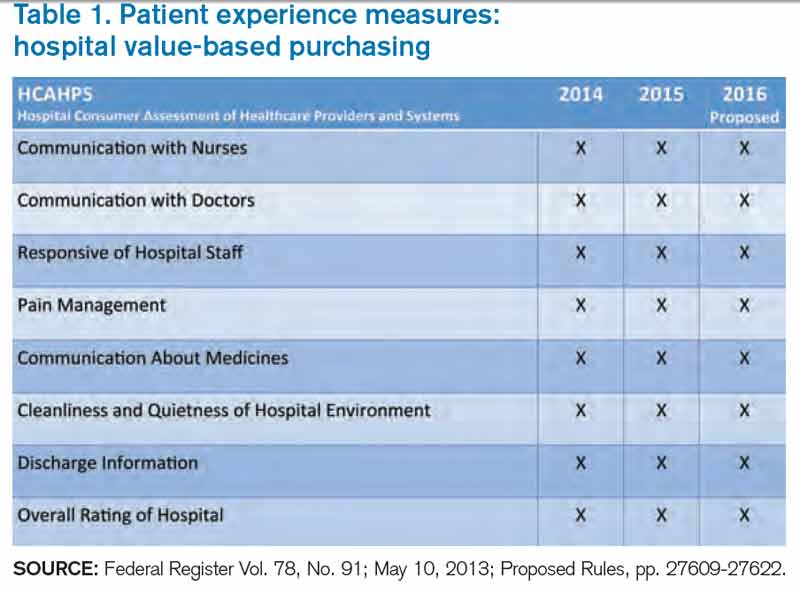
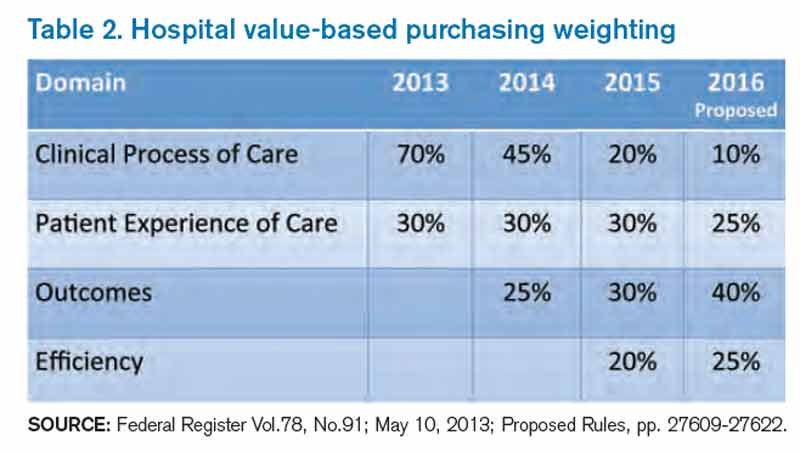
Patient satisfaction will remain an important part of HVBP in the coming years. Table 1 (below) shows the domains that will be included in fiscal years 2014 (which starts Oct. 1, 2013), 2015, and 2016. Table 2 (below) depicts the percent weighting the patient-satisfaction domain will receive through 2016. You may recall that HVBP is a program in which all hospitals place 1% to 2% (2013 through 2017, starting at 1% and increasing each year by 0.25% so that by 2017%, it is 2%) of their CMS inpatient payments in a withhold pool and, based on performance, can make back some, all, or an amount in excess of the amount placed in the withhold pool.
Source: Federal Register Vol. 78, No. 91; May 10, 2013; Proposed Rules, pp. 27609-27622.
Source: Federal Register Vol.78, No.91; May 10, 2013; Proposed Rules, pp. 27609-27622.
End In Itself
A colleague of mine recently asked, “Is an increase in patient satisfaction associated with higher quality of care and better patient safety?” The point here: It doesn’t matter. Patient satisfaction is an end in itself, and we should strive to maximize it, or at least put ourselves in the place of the patient and design care accordingly.
For Hospitalists: A Starting Point
There is a conundrum for hospitalists vis-à-vis patient satisfaction. Follow this chain of logic: The hospitals at which we work are incented to perform well on the HCAHPS domains. Hospitals pay a lot for hospitalists. Hospitalists can impact many of the HCAHPS domains. So shouldn’t hospitalists be judged according to HCAHPS scores?
Yes and no.
HCAHPS as a survey is intended to measure a patient’s overall experience of receiving care in the hospital. For example, from the “Doctor Communication” domain, we have questions like “how often did doctors treat you with courtesy and respect?” And “how often did doctors explain things in a way you could understand?”
These questions, like all in HCAHPS, are not designed to get at individual doctor performance, or even performance of a group of doctors, such as hospitalists. Instead, they are designed to measure a patient’s overall experience with the hospitalization, and “Doctor Communication” questions are designed to assess satisfaction with “doctors” collectively.
The Need for Hospitalist-Specific Satisfaction Surveys
So while HCAHPS is not designed to measure hospitalist performance with regard to patient satisfaction, it is a reasonable interim step for hospitals to judge hospitalists according to HCAHPS. However, this should be a bridge to a strategy that adopts hospitalist-specific patient-satisfaction questionnaires in the future and not an end in itself.
Why? Perhaps the biggest reason is that HCAHPS scores are neither specific nor timely enough to form the basis of improvement efforts for hospitalists. If a hospitalist receives a low score on the “Doctor Communication” domain, the scores are likely to be three to nine months old. How can we legitimately assign (and then modify) behaviors based on those scores?
Further, because the survey is not built to measure patient satisfaction specifically with hospitalists, the results are unlikely to engender meaningful and sustained behavior change. Hospitalists I talk to are generally bewildered and confused by HCAHPS scores attributed to them or their groups. Even if they understand the scores, I almost never see true quality improvement (plan-do-study-act) based on specific HCAHPS results. Instead, I see hospitalists trying to adhere to “best practices,” with no adjustments made along the way based on performance.
Nearly all the prominent patient satisfaction vendors have developed a survey instrument specifically designed for hospitalists. Each has an approach to appropriately attribute performance to the hospitalist in question, and each has a battery of questions that is designed to capture patient satisfaction with the hospitalist. Although use of these surveys involves an added financial commitment, I submit that because hospitalists have an unparalleled proximity to hospitalized patients, such an investment is worthy of consideration and has an accompanying business case, thanks to HVBP. The results of these surveys may form the basis of legitimate, targeted feedback to hospitalists, who may then adjust their approach to patient interactions. Such performance improvement should result in improved HCAHPS scores.
In sum, hospitalists should pay close attention to patient satisfaction and embrace HCAHPS. However, we should be looking beyond HCAHPS to survey instruments that fairly and accurately measure our performance. Such surveys will be more widely accepted by the hospitalists they are measuring, and will allow hospitalists to perform meaningful quality improvement based on the results. Although hospitalist-specific surveys will require an investment, the increased patient satisfaction that results should be the basis of a favorable return on that investment.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected].
Feeling frustrated with your group’s patient-satisfaction performance? Wondering why your chief (fill in the blank) officer glazes over when you try to explain why your hospitalist group’s Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) scores for doctor communication are in a percentile rivaling the numeric age of your children?
It is likely that the C-suite administrator overseeing your hospitalist group has a portion of their pay based on HCAHPS or other patient-satisfaction (also called patient experience) scores. And for good reason: The Centers for Medicare & Medicaid Services (CMS) Hospital Value-Based Purchasing (HVBP) program that started Oct. 1, 2012, has placed your hospital’s Medicare reimbursement at risk based on its HCAHPS scores.
HVBP and Patient Satisfaction
Patient satisfaction will remain an important part of HVBP in the coming years. Table 1 (below) shows the domains that will be included in fiscal years 2014 (which starts Oct. 1, 2013), 2015, and 2016. Table 2 (below) depicts the percent weighting the patient-satisfaction domain will receive through 2016. You may recall that HVBP is a program in which all hospitals place 1% to 2% (2013 through 2017, starting at 1% and increasing each year by 0.25% so that by 2017%, it is 2%) of their CMS inpatient payments in a withhold pool and, based on performance, can make back some, all, or an amount in excess of the amount placed in the withhold pool.
Source: Federal Register Vol. 78, No. 91; May 10, 2013; Proposed Rules, pp. 27609-27622.
Source: Federal Register Vol.78, No.91; May 10, 2013; Proposed Rules, pp. 27609-27622.
End In Itself
A colleague of mine recently asked, “Is an increase in patient satisfaction associated with higher quality of care and better patient safety?” The point here: It doesn’t matter. Patient satisfaction is an end in itself, and we should strive to maximize it, or at least put ourselves in the place of the patient and design care accordingly.
For Hospitalists: A Starting Point
There is a conundrum for hospitalists vis-à-vis patient satisfaction. Follow this chain of logic: The hospitals at which we work are incented to perform well on the HCAHPS domains. Hospitals pay a lot for hospitalists. Hospitalists can impact many of the HCAHPS domains. So shouldn’t hospitalists be judged according to HCAHPS scores?
Yes and no.
HCAHPS as a survey is intended to measure a patient’s overall experience of receiving care in the hospital. For example, from the “Doctor Communication” domain, we have questions like “how often did doctors treat you with courtesy and respect?” And “how often did doctors explain things in a way you could understand?”
These questions, like all in HCAHPS, are not designed to get at individual doctor performance, or even performance of a group of doctors, such as hospitalists. Instead, they are designed to measure a patient’s overall experience with the hospitalization, and “Doctor Communication” questions are designed to assess satisfaction with “doctors” collectively.
The Need for Hospitalist-Specific Satisfaction Surveys
So while HCAHPS is not designed to measure hospitalist performance with regard to patient satisfaction, it is a reasonable interim step for hospitals to judge hospitalists according to HCAHPS. However, this should be a bridge to a strategy that adopts hospitalist-specific patient-satisfaction questionnaires in the future and not an end in itself.
Why? Perhaps the biggest reason is that HCAHPS scores are neither specific nor timely enough to form the basis of improvement efforts for hospitalists. If a hospitalist receives a low score on the “Doctor Communication” domain, the scores are likely to be three to nine months old. How can we legitimately assign (and then modify) behaviors based on those scores?
Further, because the survey is not built to measure patient satisfaction specifically with hospitalists, the results are unlikely to engender meaningful and sustained behavior change. Hospitalists I talk to are generally bewildered and confused by HCAHPS scores attributed to them or their groups. Even if they understand the scores, I almost never see true quality improvement (plan-do-study-act) based on specific HCAHPS results. Instead, I see hospitalists trying to adhere to “best practices,” with no adjustments made along the way based on performance.
Nearly all the prominent patient satisfaction vendors have developed a survey instrument specifically designed for hospitalists. Each has an approach to appropriately attribute performance to the hospitalist in question, and each has a battery of questions that is designed to capture patient satisfaction with the hospitalist. Although use of these surveys involves an added financial commitment, I submit that because hospitalists have an unparalleled proximity to hospitalized patients, such an investment is worthy of consideration and has an accompanying business case, thanks to HVBP. The results of these surveys may form the basis of legitimate, targeted feedback to hospitalists, who may then adjust their approach to patient interactions. Such performance improvement should result in improved HCAHPS scores.
In sum, hospitalists should pay close attention to patient satisfaction and embrace HCAHPS. However, we should be looking beyond HCAHPS to survey instruments that fairly and accurately measure our performance. Such surveys will be more widely accepted by the hospitalists they are measuring, and will allow hospitalists to perform meaningful quality improvement based on the results. Although hospitalist-specific surveys will require an investment, the increased patient satisfaction that results should be the basis of a favorable return on that investment.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected].
Feeling frustrated with your group’s patient-satisfaction performance? Wondering why your chief (fill in the blank) officer glazes over when you try to explain why your hospitalist group’s Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) scores for doctor communication are in a percentile rivaling the numeric age of your children?
It is likely that the C-suite administrator overseeing your hospitalist group has a portion of their pay based on HCAHPS or other patient-satisfaction (also called patient experience) scores. And for good reason: The Centers for Medicare & Medicaid Services (CMS) Hospital Value-Based Purchasing (HVBP) program that started Oct. 1, 2012, has placed your hospital’s Medicare reimbursement at risk based on its HCAHPS scores.
HVBP and Patient Satisfaction
Patient satisfaction will remain an important part of HVBP in the coming years. Table 1 (below) shows the domains that will be included in fiscal years 2014 (which starts Oct. 1, 2013), 2015, and 2016. Table 2 (below) depicts the percent weighting the patient-satisfaction domain will receive through 2016. You may recall that HVBP is a program in which all hospitals place 1% to 2% (2013 through 2017, starting at 1% and increasing each year by 0.25% so that by 2017%, it is 2%) of their CMS inpatient payments in a withhold pool and, based on performance, can make back some, all, or an amount in excess of the amount placed in the withhold pool.
Source: Federal Register Vol. 78, No. 91; May 10, 2013; Proposed Rules, pp. 27609-27622.
Source: Federal Register Vol.78, No.91; May 10, 2013; Proposed Rules, pp. 27609-27622.
End In Itself
A colleague of mine recently asked, “Is an increase in patient satisfaction associated with higher quality of care and better patient safety?” The point here: It doesn’t matter. Patient satisfaction is an end in itself, and we should strive to maximize it, or at least put ourselves in the place of the patient and design care accordingly.
For Hospitalists: A Starting Point
There is a conundrum for hospitalists vis-à-vis patient satisfaction. Follow this chain of logic: The hospitals at which we work are incented to perform well on the HCAHPS domains. Hospitals pay a lot for hospitalists. Hospitalists can impact many of the HCAHPS domains. So shouldn’t hospitalists be judged according to HCAHPS scores?
Yes and no.
HCAHPS as a survey is intended to measure a patient’s overall experience of receiving care in the hospital. For example, from the “Doctor Communication” domain, we have questions like “how often did doctors treat you with courtesy and respect?” And “how often did doctors explain things in a way you could understand?”
These questions, like all in HCAHPS, are not designed to get at individual doctor performance, or even performance of a group of doctors, such as hospitalists. Instead, they are designed to measure a patient’s overall experience with the hospitalization, and “Doctor Communication” questions are designed to assess satisfaction with “doctors” collectively.
The Need for Hospitalist-Specific Satisfaction Surveys
So while HCAHPS is not designed to measure hospitalist performance with regard to patient satisfaction, it is a reasonable interim step for hospitals to judge hospitalists according to HCAHPS. However, this should be a bridge to a strategy that adopts hospitalist-specific patient-satisfaction questionnaires in the future and not an end in itself.
Why? Perhaps the biggest reason is that HCAHPS scores are neither specific nor timely enough to form the basis of improvement efforts for hospitalists. If a hospitalist receives a low score on the “Doctor Communication” domain, the scores are likely to be three to nine months old. How can we legitimately assign (and then modify) behaviors based on those scores?
Further, because the survey is not built to measure patient satisfaction specifically with hospitalists, the results are unlikely to engender meaningful and sustained behavior change. Hospitalists I talk to are generally bewildered and confused by HCAHPS scores attributed to them or their groups. Even if they understand the scores, I almost never see true quality improvement (plan-do-study-act) based on specific HCAHPS results. Instead, I see hospitalists trying to adhere to “best practices,” with no adjustments made along the way based on performance.
Nearly all the prominent patient satisfaction vendors have developed a survey instrument specifically designed for hospitalists. Each has an approach to appropriately attribute performance to the hospitalist in question, and each has a battery of questions that is designed to capture patient satisfaction with the hospitalist. Although use of these surveys involves an added financial commitment, I submit that because hospitalists have an unparalleled proximity to hospitalized patients, such an investment is worthy of consideration and has an accompanying business case, thanks to HVBP. The results of these surveys may form the basis of legitimate, targeted feedback to hospitalists, who may then adjust their approach to patient interactions. Such performance improvement should result in improved HCAHPS scores.
In sum, hospitalists should pay close attention to patient satisfaction and embrace HCAHPS. However, we should be looking beyond HCAHPS to survey instruments that fairly and accurately measure our performance. Such surveys will be more widely accepted by the hospitalists they are measuring, and will allow hospitalists to perform meaningful quality improvement based on the results. Although hospitalist-specific surveys will require an investment, the increased patient satisfaction that results should be the basis of a favorable return on that investment.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected].
Hospitalists’ Capitol Hill Advocacy Effort Produces Results
On May 12, 113 hospitalists descended on Capitol Hill for “Hospitalists on the Hill 2013,” the public-advocacy highlight of SHM’s annual meeting. Hospitalists from all parts of the country engaged with congressional representatives in a daylong series of meet-and-greets that may seem to some people useless in the face of political obstinacy in Washington. But the trip worked.
Josh Boswell, SHM’s senior manager of government relations, reports many Hill Day objectives were achieved:
- The number of legislators co-sponsoring a bill regarding the “three-day observation rule” more than tripled in the House of Representatives and doubled in the Senate. SHM officials note that the added support has come from both political parties.
- A Congressional Budget Office (CBO) review of the bill has been formally requested by those legislators.
- A congressman from Washington state asked for—and received—a letter of support for a proposed measure, the Improved Health Care at a Lower Cost Act of 2013 (H.R. 1487).
- Multiple reports of continued dialogue between congressional staffers and SHM members nationwide. When planning the advocacy day, SHM officials noted that one of the most valuable results is creating relationships at the local level.
Observation Legislation
One of the three talking points hospitalists took into their legislative meetings was solving the dilemmas surrounding observation status. Currently, time spent on observation status does not count toward the required three consecutive overnights an inpatient needs to qualify for Medicare benefits at a skilled nursing facility (SNF).
Hospitalists have been pushing to change that rule, in large part by supporting the Improving Access to Medicare Coverage Act of 2013 (H.R. 1179, S. 569), sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio).1 In addition to the status reclassification, the proposal would establish a 90-day appeal period for those who have been denied the benefit.
The issue is important to hospitalists because of the penalties hospitals face for readmissions—and also in part because hospitalists increasingly are providing care at SNFs and other post-acute-care facilities. SHM says that after the Hill visits—and the ensuing follow-up communications—the number of co-sponsors in the House jumped to 70 from 22. The Senate version doubled its list of co-sponsors.
And, perhaps more important, a CBO analysis has been requested for the observation bills. That review, known as a CBO score, weighs the financial impacts of proposed laws and is considered a necessary precursor to successfully passing any legislation.
All in all, SHM was pleased with the progress on the observation-status bill and will continue to push for its passage, whether it is in this congressional session or the next.
“Rep. Courtney’s bill is now getting significant traction,” Boswell says. “Hospitalists should be proud to know this is in no small part due to their advocacy efforts.”
Political Networking
Hospitalist David Ramenofsky, MD, who works at Northwest Hospital and Medical Center in Seattle, wasn’t sure how much traction he was going to be able to generate at his first Hill Day. SHM had arranged meetings with the offices of three local politicians: Rep. Jim McDermott (D-Wash.), Sen. Patty Murray (D-Wash.), and Sen. Maria Cantwell (D-Wash.).
Dr. Ramenofsky sat with two of McDermott’s staffers, one of whom sounded knowledgeable and enthused about health-care-policy issues. Although the congressman couldn’t sit in on the meeting, he knew Dr. Ramenofsky’s name and took the time to say hello.
“It was really interesting to me that these staffers wanted to hear what I had to say and learn about my experience,” Dr. Ramenofsky adds. “My views may affect how they work with their bosses to make policy changes. It was surprising to me how much my opinions mattered to them.”
After the meeting and another briefing SHM arranged with another local hospitalist, McDermott reached out to SHM. He asked for support for his proposed bill to expand protections from anti-kickback laws and regulations, to provide safe harbor protection for gainsharing, and other incentive-payment systems.
SHM responded in July with a letter of support that thanked the congressman for his efforts.2
“We look forward to working with you,” the letter ended.
Dr. Ramenofsky says he’s proud his efforts led to a working relationship between his professional society and his local legislator. He says he’s looking forward to participating in future Hill Day activities and acting as a local liaison for SHM.
He laments that he has not received much post-meeting feedback from his discussions with the senators’ offices, but says he understands how busy politicians are. And a 1-for-3 showing is pretty good, given his status as a political novice.
“Given overall public perception of Congress, I’m amazed that my visits caused one of three offices to engage in further policy discussions with SHM,” he says. “I’m encouraged to remain engaged in political activities through SHM.”
Richard Quinn is a freelance writer in New Jersey.
References
- Society of Hospital Medicine. Letter to Congress members. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_ Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=33169. Accessed July 15, 2013.
- Society of Hospital Medicine. Letter to Congressman Jim McDermott. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=34169. Accessed July 15, 2013.
On May 12, 113 hospitalists descended on Capitol Hill for “Hospitalists on the Hill 2013,” the public-advocacy highlight of SHM’s annual meeting. Hospitalists from all parts of the country engaged with congressional representatives in a daylong series of meet-and-greets that may seem to some people useless in the face of political obstinacy in Washington. But the trip worked.
Josh Boswell, SHM’s senior manager of government relations, reports many Hill Day objectives were achieved:
- The number of legislators co-sponsoring a bill regarding the “three-day observation rule” more than tripled in the House of Representatives and doubled in the Senate. SHM officials note that the added support has come from both political parties.
- A Congressional Budget Office (CBO) review of the bill has been formally requested by those legislators.
- A congressman from Washington state asked for—and received—a letter of support for a proposed measure, the Improved Health Care at a Lower Cost Act of 2013 (H.R. 1487).
- Multiple reports of continued dialogue between congressional staffers and SHM members nationwide. When planning the advocacy day, SHM officials noted that one of the most valuable results is creating relationships at the local level.
Observation Legislation
One of the three talking points hospitalists took into their legislative meetings was solving the dilemmas surrounding observation status. Currently, time spent on observation status does not count toward the required three consecutive overnights an inpatient needs to qualify for Medicare benefits at a skilled nursing facility (SNF).
Hospitalists have been pushing to change that rule, in large part by supporting the Improving Access to Medicare Coverage Act of 2013 (H.R. 1179, S. 569), sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio).1 In addition to the status reclassification, the proposal would establish a 90-day appeal period for those who have been denied the benefit.
The issue is important to hospitalists because of the penalties hospitals face for readmissions—and also in part because hospitalists increasingly are providing care at SNFs and other post-acute-care facilities. SHM says that after the Hill visits—and the ensuing follow-up communications—the number of co-sponsors in the House jumped to 70 from 22. The Senate version doubled its list of co-sponsors.
And, perhaps more important, a CBO analysis has been requested for the observation bills. That review, known as a CBO score, weighs the financial impacts of proposed laws and is considered a necessary precursor to successfully passing any legislation.
All in all, SHM was pleased with the progress on the observation-status bill and will continue to push for its passage, whether it is in this congressional session or the next.
“Rep. Courtney’s bill is now getting significant traction,” Boswell says. “Hospitalists should be proud to know this is in no small part due to their advocacy efforts.”
Political Networking
Hospitalist David Ramenofsky, MD, who works at Northwest Hospital and Medical Center in Seattle, wasn’t sure how much traction he was going to be able to generate at his first Hill Day. SHM had arranged meetings with the offices of three local politicians: Rep. Jim McDermott (D-Wash.), Sen. Patty Murray (D-Wash.), and Sen. Maria Cantwell (D-Wash.).
Dr. Ramenofsky sat with two of McDermott’s staffers, one of whom sounded knowledgeable and enthused about health-care-policy issues. Although the congressman couldn’t sit in on the meeting, he knew Dr. Ramenofsky’s name and took the time to say hello.
“It was really interesting to me that these staffers wanted to hear what I had to say and learn about my experience,” Dr. Ramenofsky adds. “My views may affect how they work with their bosses to make policy changes. It was surprising to me how much my opinions mattered to them.”
After the meeting and another briefing SHM arranged with another local hospitalist, McDermott reached out to SHM. He asked for support for his proposed bill to expand protections from anti-kickback laws and regulations, to provide safe harbor protection for gainsharing, and other incentive-payment systems.
SHM responded in July with a letter of support that thanked the congressman for his efforts.2
“We look forward to working with you,” the letter ended.
Dr. Ramenofsky says he’s proud his efforts led to a working relationship between his professional society and his local legislator. He says he’s looking forward to participating in future Hill Day activities and acting as a local liaison for SHM.
He laments that he has not received much post-meeting feedback from his discussions with the senators’ offices, but says he understands how busy politicians are. And a 1-for-3 showing is pretty good, given his status as a political novice.
“Given overall public perception of Congress, I’m amazed that my visits caused one of three offices to engage in further policy discussions with SHM,” he says. “I’m encouraged to remain engaged in political activities through SHM.”
Richard Quinn is a freelance writer in New Jersey.
References
- Society of Hospital Medicine. Letter to Congress members. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_ Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=33169. Accessed July 15, 2013.
- Society of Hospital Medicine. Letter to Congressman Jim McDermott. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=34169. Accessed July 15, 2013.
On May 12, 113 hospitalists descended on Capitol Hill for “Hospitalists on the Hill 2013,” the public-advocacy highlight of SHM’s annual meeting. Hospitalists from all parts of the country engaged with congressional representatives in a daylong series of meet-and-greets that may seem to some people useless in the face of political obstinacy in Washington. But the trip worked.
Josh Boswell, SHM’s senior manager of government relations, reports many Hill Day objectives were achieved:
- The number of legislators co-sponsoring a bill regarding the “three-day observation rule” more than tripled in the House of Representatives and doubled in the Senate. SHM officials note that the added support has come from both political parties.
- A Congressional Budget Office (CBO) review of the bill has been formally requested by those legislators.
- A congressman from Washington state asked for—and received—a letter of support for a proposed measure, the Improved Health Care at a Lower Cost Act of 2013 (H.R. 1487).
- Multiple reports of continued dialogue between congressional staffers and SHM members nationwide. When planning the advocacy day, SHM officials noted that one of the most valuable results is creating relationships at the local level.
Observation Legislation
One of the three talking points hospitalists took into their legislative meetings was solving the dilemmas surrounding observation status. Currently, time spent on observation status does not count toward the required three consecutive overnights an inpatient needs to qualify for Medicare benefits at a skilled nursing facility (SNF).
Hospitalists have been pushing to change that rule, in large part by supporting the Improving Access to Medicare Coverage Act of 2013 (H.R. 1179, S. 569), sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio).1 In addition to the status reclassification, the proposal would establish a 90-day appeal period for those who have been denied the benefit.
The issue is important to hospitalists because of the penalties hospitals face for readmissions—and also in part because hospitalists increasingly are providing care at SNFs and other post-acute-care facilities. SHM says that after the Hill visits—and the ensuing follow-up communications—the number of co-sponsors in the House jumped to 70 from 22. The Senate version doubled its list of co-sponsors.
And, perhaps more important, a CBO analysis has been requested for the observation bills. That review, known as a CBO score, weighs the financial impacts of proposed laws and is considered a necessary precursor to successfully passing any legislation.
All in all, SHM was pleased with the progress on the observation-status bill and will continue to push for its passage, whether it is in this congressional session or the next.
“Rep. Courtney’s bill is now getting significant traction,” Boswell says. “Hospitalists should be proud to know this is in no small part due to their advocacy efforts.”
Political Networking
Hospitalist David Ramenofsky, MD, who works at Northwest Hospital and Medical Center in Seattle, wasn’t sure how much traction he was going to be able to generate at his first Hill Day. SHM had arranged meetings with the offices of three local politicians: Rep. Jim McDermott (D-Wash.), Sen. Patty Murray (D-Wash.), and Sen. Maria Cantwell (D-Wash.).
Dr. Ramenofsky sat with two of McDermott’s staffers, one of whom sounded knowledgeable and enthused about health-care-policy issues. Although the congressman couldn’t sit in on the meeting, he knew Dr. Ramenofsky’s name and took the time to say hello.
“It was really interesting to me that these staffers wanted to hear what I had to say and learn about my experience,” Dr. Ramenofsky adds. “My views may affect how they work with their bosses to make policy changes. It was surprising to me how much my opinions mattered to them.”
After the meeting and another briefing SHM arranged with another local hospitalist, McDermott reached out to SHM. He asked for support for his proposed bill to expand protections from anti-kickback laws and regulations, to provide safe harbor protection for gainsharing, and other incentive-payment systems.
SHM responded in July with a letter of support that thanked the congressman for his efforts.2
“We look forward to working with you,” the letter ended.
Dr. Ramenofsky says he’s proud his efforts led to a working relationship between his professional society and his local legislator. He says he’s looking forward to participating in future Hill Day activities and acting as a local liaison for SHM.
He laments that he has not received much post-meeting feedback from his discussions with the senators’ offices, but says he understands how busy politicians are. And a 1-for-3 showing is pretty good, given his status as a political novice.
“Given overall public perception of Congress, I’m amazed that my visits caused one of three offices to engage in further policy discussions with SHM,” he says. “I’m encouraged to remain engaged in political activities through SHM.”
Richard Quinn is a freelance writer in New Jersey.
References
- Society of Hospital Medicine. Letter to Congress members. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_ Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=33169. Accessed July 15, 2013.
- Society of Hospital Medicine. Letter to Congressman Jim McDermott. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=34169. Accessed July 15, 2013.
Proposed Bill Would Open Door to Gainsharing Arrangements for Hospitals, Physicians
There is little dispute in the potential for cost savings when gainsharing arrangements incentivize things like product standardization, substitution of lower-cost products, and, most notably for hospitalists, medically appropriate decreases in length of stay. However, well-meaning but overly inclusive federal law makes the legal risk of establishing these arrangements so great that providers recoil at the prospect.
This doesn’t mean that gainsharing isn’t occurring. Currently, Medicare accountable-care organizations (ACOs) have been granted official waivers to establish such arrangements; smaller-scale pilot projects implemented by Medicare also have been granted similar waivers in the past. As availability is limited to participants within officially sanctioned programs, most providers are not able to tap into these cost-saving efforts, though this has not been for lack of trying.
Hospitals and physicians are engaging in a number of clinical joint ventures that have spurred them to seek their own gainsharing waivers by approaching the Office of the Inspector General (OIG). The OIG is the arm of the U.S. Department of Health and Human Services charged with enforcing the applicable laws affecting gainsharing. The OIG responded by cautioning that gainsharing arrangements violate the Social Security Act’s “Civil Monetary Penalty” prohibition against limitation of services to publicly insured patients, in addition to violating the federal Anti-Kickback Law and possibly the “Stark” law. Nonetheless, the OIG concluded it would not impose sanctions for the violations. In short, the OIG declared the proposals illegal but gave the go-ahead. The caveat, of course, is that these opinions are nonbinding, so providers remain understandably timid.
As a result, gainsharing currently remains more or less out of reach for those not participating in a Medicare ACO. This makes little sense at a time when Medicare and the entire health-care system are focusing on how to deliver high-quality, cost-conscious care. For example, if hospitalists are capable of reducing length of stay without detriment to the patient, they should not be legally prohibited from sharing any of the resulting cost savings. Fortunately, U.S. Rep. Jim McDermott (D-Wash.) agrees with this sentiment and has introduced legislation to address the problem.
McDermott introduced the Improved Health Care at Lower Cost Act of 2013 (H.R. 1487) in April. It seeks to exempt monetary incentive payments made by hospitals to physicians from federal anti-kickback and other sanctions. Such exemptions, or safe harbors, would be automatically granted to gainsharing arrangements that meet a pre-determined set of requirements. This means no formal application process or participation in a specific federal program would be required.
Passage of the bill would be a major step in the right direction for providers lacking the resources to navigate legal minefields or establish a full-scale ACO. If well-implemented, it could also generate significant cost savings for Medicare.
It is for these reasons that SHM supports H.R. 1487 and looks forward to working with McDermott in securing its passage.
In the coming months, members of SHM’s Grassroots Network will be encouraging Congress to make this important change to facilitate practice arrangements that provide high-value coordinated care for patients. Stay informed and take action when SHM issues Legislative Action Alerts by signing up for the Grassroots Network at www.hospitalmedicine.org/grassroots.
Josh Boswell is SHM’s senior manager of government relations.
There is little dispute in the potential for cost savings when gainsharing arrangements incentivize things like product standardization, substitution of lower-cost products, and, most notably for hospitalists, medically appropriate decreases in length of stay. However, well-meaning but overly inclusive federal law makes the legal risk of establishing these arrangements so great that providers recoil at the prospect.
This doesn’t mean that gainsharing isn’t occurring. Currently, Medicare accountable-care organizations (ACOs) have been granted official waivers to establish such arrangements; smaller-scale pilot projects implemented by Medicare also have been granted similar waivers in the past. As availability is limited to participants within officially sanctioned programs, most providers are not able to tap into these cost-saving efforts, though this has not been for lack of trying.
Hospitals and physicians are engaging in a number of clinical joint ventures that have spurred them to seek their own gainsharing waivers by approaching the Office of the Inspector General (OIG). The OIG is the arm of the U.S. Department of Health and Human Services charged with enforcing the applicable laws affecting gainsharing. The OIG responded by cautioning that gainsharing arrangements violate the Social Security Act’s “Civil Monetary Penalty” prohibition against limitation of services to publicly insured patients, in addition to violating the federal Anti-Kickback Law and possibly the “Stark” law. Nonetheless, the OIG concluded it would not impose sanctions for the violations. In short, the OIG declared the proposals illegal but gave the go-ahead. The caveat, of course, is that these opinions are nonbinding, so providers remain understandably timid.
As a result, gainsharing currently remains more or less out of reach for those not participating in a Medicare ACO. This makes little sense at a time when Medicare and the entire health-care system are focusing on how to deliver high-quality, cost-conscious care. For example, if hospitalists are capable of reducing length of stay without detriment to the patient, they should not be legally prohibited from sharing any of the resulting cost savings. Fortunately, U.S. Rep. Jim McDermott (D-Wash.) agrees with this sentiment and has introduced legislation to address the problem.
McDermott introduced the Improved Health Care at Lower Cost Act of 2013 (H.R. 1487) in April. It seeks to exempt monetary incentive payments made by hospitals to physicians from federal anti-kickback and other sanctions. Such exemptions, or safe harbors, would be automatically granted to gainsharing arrangements that meet a pre-determined set of requirements. This means no formal application process or participation in a specific federal program would be required.
Passage of the bill would be a major step in the right direction for providers lacking the resources to navigate legal minefields or establish a full-scale ACO. If well-implemented, it could also generate significant cost savings for Medicare.
It is for these reasons that SHM supports H.R. 1487 and looks forward to working with McDermott in securing its passage.
In the coming months, members of SHM’s Grassroots Network will be encouraging Congress to make this important change to facilitate practice arrangements that provide high-value coordinated care for patients. Stay informed and take action when SHM issues Legislative Action Alerts by signing up for the Grassroots Network at www.hospitalmedicine.org/grassroots.
Josh Boswell is SHM’s senior manager of government relations.
There is little dispute in the potential for cost savings when gainsharing arrangements incentivize things like product standardization, substitution of lower-cost products, and, most notably for hospitalists, medically appropriate decreases in length of stay. However, well-meaning but overly inclusive federal law makes the legal risk of establishing these arrangements so great that providers recoil at the prospect.
This doesn’t mean that gainsharing isn’t occurring. Currently, Medicare accountable-care organizations (ACOs) have been granted official waivers to establish such arrangements; smaller-scale pilot projects implemented by Medicare also have been granted similar waivers in the past. As availability is limited to participants within officially sanctioned programs, most providers are not able to tap into these cost-saving efforts, though this has not been for lack of trying.
Hospitals and physicians are engaging in a number of clinical joint ventures that have spurred them to seek their own gainsharing waivers by approaching the Office of the Inspector General (OIG). The OIG is the arm of the U.S. Department of Health and Human Services charged with enforcing the applicable laws affecting gainsharing. The OIG responded by cautioning that gainsharing arrangements violate the Social Security Act’s “Civil Monetary Penalty” prohibition against limitation of services to publicly insured patients, in addition to violating the federal Anti-Kickback Law and possibly the “Stark” law. Nonetheless, the OIG concluded it would not impose sanctions for the violations. In short, the OIG declared the proposals illegal but gave the go-ahead. The caveat, of course, is that these opinions are nonbinding, so providers remain understandably timid.
As a result, gainsharing currently remains more or less out of reach for those not participating in a Medicare ACO. This makes little sense at a time when Medicare and the entire health-care system are focusing on how to deliver high-quality, cost-conscious care. For example, if hospitalists are capable of reducing length of stay without detriment to the patient, they should not be legally prohibited from sharing any of the resulting cost savings. Fortunately, U.S. Rep. Jim McDermott (D-Wash.) agrees with this sentiment and has introduced legislation to address the problem.
McDermott introduced the Improved Health Care at Lower Cost Act of 2013 (H.R. 1487) in April. It seeks to exempt monetary incentive payments made by hospitals to physicians from federal anti-kickback and other sanctions. Such exemptions, or safe harbors, would be automatically granted to gainsharing arrangements that meet a pre-determined set of requirements. This means no formal application process or participation in a specific federal program would be required.
Passage of the bill would be a major step in the right direction for providers lacking the resources to navigate legal minefields or establish a full-scale ACO. If well-implemented, it could also generate significant cost savings for Medicare.
It is for these reasons that SHM supports H.R. 1487 and looks forward to working with McDermott in securing its passage.
In the coming months, members of SHM’s Grassroots Network will be encouraging Congress to make this important change to facilitate practice arrangements that provide high-value coordinated care for patients. Stay informed and take action when SHM issues Legislative Action Alerts by signing up for the Grassroots Network at www.hospitalmedicine.org/grassroots.
Josh Boswell is SHM’s senior manager of government relations.
Medicare Penalties Make Hospital-Acquired-Infection Solutions a Priority
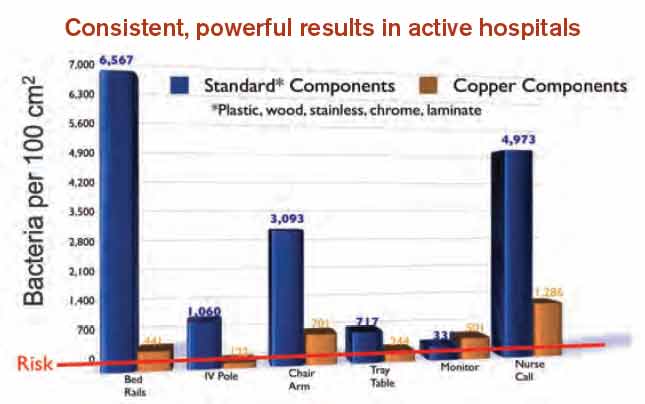
A shift in governmental regulations regarding reimbursement for hospital-acquired infections (HAIs) is forcing hospitals to take a closer look at how to reduce them. A recent study in Infection Control and Hospital Epidemiology shows that copper-alloy surfaces may be one such solution.3 According to the study, although only 9% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases.1
“Before these regulations, hospitals didn’t necessarily want technology to decrease HAI rates, because the more infections and complications, the longer the length of patient stay, the greater the reimbursement, and the better the bottom line,” says Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association.
Three regulations that have resulted in reimbursements to hospitals getting cut include:
- The Deficit Reduction Act of 2005, which was implemented on Oct. 1, 2008, which states that Medicare will not reimburse for certain types of HAIs;
- Section 3025 of the Affordable Care Act (signed into law in 2010), which incentivizes hospitals to decrease their readmission rates, which frequently are caused by HAIs. Beginning this fall, hospitals are getting reduced reimbursement when their readmission rates exceed a certain threshold. The maximum penalty in 2013 is 1% and will increase to 3% by 2015; and
- Section 1886 of the Affordable Care Act, which describes value-based purchasing and makes hospitals eligible to receive incentive payments for achieving better care on certain quality metrics. Funding for the program comes from withholding payment from poor-performing hospitals. The financial impact to hospitals started this year. In 2014, urinary tract infections and vascular-catheter-associated infections will be among the targeted conditions measured by CMS to calculate incentives and penalties.
“Hospitals are now feeling a direct impact from all of this,” Dr. Georgiou says. “Back in 2008, hospitals were noticing, but it was hard to get their attention since only one program was impacting their bottom line. But, pretty soon, hospitals risk losing upwards of 5% of their Medicare reimbursement for decreased quality.
“Reducing HAIs is clearly on the priority list of chief operating officers. They are very aware of the impact to their bottom line. They are looking to their vendors and suppliers to develop strategies to work with their hospitals to improve performance around these metrics.”
Karen Appold is a freelance writer in Pennsylvania.
A shift in governmental regulations regarding reimbursement for hospital-acquired infections (HAIs) is forcing hospitals to take a closer look at how to reduce them. A recent study in Infection Control and Hospital Epidemiology shows that copper-alloy surfaces may be one such solution.3 According to the study, although only 9% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases.1
“Before these regulations, hospitals didn’t necessarily want technology to decrease HAI rates, because the more infections and complications, the longer the length of patient stay, the greater the reimbursement, and the better the bottom line,” says Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association.
Three regulations that have resulted in reimbursements to hospitals getting cut include:
- The Deficit Reduction Act of 2005, which was implemented on Oct. 1, 2008, which states that Medicare will not reimburse for certain types of HAIs;
- Section 3025 of the Affordable Care Act (signed into law in 2010), which incentivizes hospitals to decrease their readmission rates, which frequently are caused by HAIs. Beginning this fall, hospitals are getting reduced reimbursement when their readmission rates exceed a certain threshold. The maximum penalty in 2013 is 1% and will increase to 3% by 2015; and
- Section 1886 of the Affordable Care Act, which describes value-based purchasing and makes hospitals eligible to receive incentive payments for achieving better care on certain quality metrics. Funding for the program comes from withholding payment from poor-performing hospitals. The financial impact to hospitals started this year. In 2014, urinary tract infections and vascular-catheter-associated infections will be among the targeted conditions measured by CMS to calculate incentives and penalties.
“Hospitals are now feeling a direct impact from all of this,” Dr. Georgiou says. “Back in 2008, hospitals were noticing, but it was hard to get their attention since only one program was impacting their bottom line. But, pretty soon, hospitals risk losing upwards of 5% of their Medicare reimbursement for decreased quality.
“Reducing HAIs is clearly on the priority list of chief operating officers. They are very aware of the impact to their bottom line. They are looking to their vendors and suppliers to develop strategies to work with their hospitals to improve performance around these metrics.”
Karen Appold is a freelance writer in Pennsylvania.
A shift in governmental regulations regarding reimbursement for hospital-acquired infections (HAIs) is forcing hospitals to take a closer look at how to reduce them. A recent study in Infection Control and Hospital Epidemiology shows that copper-alloy surfaces may be one such solution.3 According to the study, although only 9% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases.1
“Before these regulations, hospitals didn’t necessarily want technology to decrease HAI rates, because the more infections and complications, the longer the length of patient stay, the greater the reimbursement, and the better the bottom line,” says Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association.
Three regulations that have resulted in reimbursements to hospitals getting cut include:
- The Deficit Reduction Act of 2005, which was implemented on Oct. 1, 2008, which states that Medicare will not reimburse for certain types of HAIs;
- Section 3025 of the Affordable Care Act (signed into law in 2010), which incentivizes hospitals to decrease their readmission rates, which frequently are caused by HAIs. Beginning this fall, hospitals are getting reduced reimbursement when their readmission rates exceed a certain threshold. The maximum penalty in 2013 is 1% and will increase to 3% by 2015; and
- Section 1886 of the Affordable Care Act, which describes value-based purchasing and makes hospitals eligible to receive incentive payments for achieving better care on certain quality metrics. Funding for the program comes from withholding payment from poor-performing hospitals. The financial impact to hospitals started this year. In 2014, urinary tract infections and vascular-catheter-associated infections will be among the targeted conditions measured by CMS to calculate incentives and penalties.
“Hospitals are now feeling a direct impact from all of this,” Dr. Georgiou says. “Back in 2008, hospitals were noticing, but it was hard to get their attention since only one program was impacting their bottom line. But, pretty soon, hospitals risk losing upwards of 5% of their Medicare reimbursement for decreased quality.
“Reducing HAIs is clearly on the priority list of chief operating officers. They are very aware of the impact to their bottom line. They are looking to their vendors and suppliers to develop strategies to work with their hospitals to improve performance around these metrics.”
Karen Appold is a freelance writer in Pennsylvania.
Can Medicare Pay for Value?
Can quality measurement and comparisons serve as the backbone for a major shift in the Medicare payment system to reward value instead of volume? That is the question being explored over the next few years as the Physician Quality Reporting System (PQRS) and, by extension, the physician value-based payment modifier (VBPM) come fully into effect for all physicians.
There seems to be a consensus in the policy community that the fee-for-service model of payment is past its prime and needs to be replaced with a more dynamic and responsive payment system. Medicare hopes that PQRS and the VBPM will enable adjustments to physician payments to reward high-quality and low-cost care. Although these programs currently are add-ons to the fee-for-service system, they likely will serve as stepping stones to more radical departures from the existing payment system.
SHM advocates refinements to policies for PQRS and similar programs to make them more meaningful and productive for both hospitalists and the broader health-care system. Each year, SHM submits comments on the Physician Fee Schedule Rule, which creates and updates the regulatory framework for PQRS and the VBPM. SHM also provided feedback on Quality and Resource Use Reports (QRURs), the report cards for the modifier that were being tested over the past year.
From a practical standpoint, SHM engages with measure development and endorsement processes to ensure there are reportable quality measures in PQRS that fit hospitalist practice. In addition, SHM is helping to increase accessibility to PQRS reporting by offering members reduced fare access to registry reporting through the PQRI Wizard.
The comments range from the technical aspects of individual quality measures in PQRS to how hospitalists appear to be performing in these programs. SHM firmly believes that the unique positioning of hospitalists within the health-care system presents challenges for their identification and evaluation in Medicare programs. In some sense, hospitalists exist on the line between the inpatient and outpatient worlds, a location not adequately captured in pay-for-performance programs.
It’s imperative that pay-for-performance programs have reasonable and actionable outcomes for providers. If quality measures are not clinically meaningful and do not capture a plurality of the care provided by an individual hospitalist, it is difficult for the program to meet its stated aims. If payment is to be influenced by performance on quality measures, it follows that those measures should be relevant to the care provided.
There is a long way to go toward creating quality measurement and evaluation programs that are relevant and actionable for clinical quality improvement (QI). By becoming involved in SHM’s policy efforts, members are able to share their experiences and impressions of programs with SHM and lawmakers. This partnership helps create more responsive and intuitive programs, which in turn leads to greater participation and, hopefully, improved patient outcomes. As these programs continue to evolve and more health professionals are required to participate, SHM will be looking to its membership for their perspectives.
Join the grassroots network to stay involved and up to date by registering at www.hospitalmedicine.org/grassroots.
Joshua Lapps is SHM’s government relations specialist.
Can quality measurement and comparisons serve as the backbone for a major shift in the Medicare payment system to reward value instead of volume? That is the question being explored over the next few years as the Physician Quality Reporting System (PQRS) and, by extension, the physician value-based payment modifier (VBPM) come fully into effect for all physicians.
There seems to be a consensus in the policy community that the fee-for-service model of payment is past its prime and needs to be replaced with a more dynamic and responsive payment system. Medicare hopes that PQRS and the VBPM will enable adjustments to physician payments to reward high-quality and low-cost care. Although these programs currently are add-ons to the fee-for-service system, they likely will serve as stepping stones to more radical departures from the existing payment system.
SHM advocates refinements to policies for PQRS and similar programs to make them more meaningful and productive for both hospitalists and the broader health-care system. Each year, SHM submits comments on the Physician Fee Schedule Rule, which creates and updates the regulatory framework for PQRS and the VBPM. SHM also provided feedback on Quality and Resource Use Reports (QRURs), the report cards for the modifier that were being tested over the past year.
From a practical standpoint, SHM engages with measure development and endorsement processes to ensure there are reportable quality measures in PQRS that fit hospitalist practice. In addition, SHM is helping to increase accessibility to PQRS reporting by offering members reduced fare access to registry reporting through the PQRI Wizard.
The comments range from the technical aspects of individual quality measures in PQRS to how hospitalists appear to be performing in these programs. SHM firmly believes that the unique positioning of hospitalists within the health-care system presents challenges for their identification and evaluation in Medicare programs. In some sense, hospitalists exist on the line between the inpatient and outpatient worlds, a location not adequately captured in pay-for-performance programs.
It’s imperative that pay-for-performance programs have reasonable and actionable outcomes for providers. If quality measures are not clinically meaningful and do not capture a plurality of the care provided by an individual hospitalist, it is difficult for the program to meet its stated aims. If payment is to be influenced by performance on quality measures, it follows that those measures should be relevant to the care provided.
There is a long way to go toward creating quality measurement and evaluation programs that are relevant and actionable for clinical quality improvement (QI). By becoming involved in SHM’s policy efforts, members are able to share their experiences and impressions of programs with SHM and lawmakers. This partnership helps create more responsive and intuitive programs, which in turn leads to greater participation and, hopefully, improved patient outcomes. As these programs continue to evolve and more health professionals are required to participate, SHM will be looking to its membership for their perspectives.
Join the grassroots network to stay involved and up to date by registering at www.hospitalmedicine.org/grassroots.
Joshua Lapps is SHM’s government relations specialist.
Can quality measurement and comparisons serve as the backbone for a major shift in the Medicare payment system to reward value instead of volume? That is the question being explored over the next few years as the Physician Quality Reporting System (PQRS) and, by extension, the physician value-based payment modifier (VBPM) come fully into effect for all physicians.
There seems to be a consensus in the policy community that the fee-for-service model of payment is past its prime and needs to be replaced with a more dynamic and responsive payment system. Medicare hopes that PQRS and the VBPM will enable adjustments to physician payments to reward high-quality and low-cost care. Although these programs currently are add-ons to the fee-for-service system, they likely will serve as stepping stones to more radical departures from the existing payment system.
SHM advocates refinements to policies for PQRS and similar programs to make them more meaningful and productive for both hospitalists and the broader health-care system. Each year, SHM submits comments on the Physician Fee Schedule Rule, which creates and updates the regulatory framework for PQRS and the VBPM. SHM also provided feedback on Quality and Resource Use Reports (QRURs), the report cards for the modifier that were being tested over the past year.
From a practical standpoint, SHM engages with measure development and endorsement processes to ensure there are reportable quality measures in PQRS that fit hospitalist practice. In addition, SHM is helping to increase accessibility to PQRS reporting by offering members reduced fare access to registry reporting through the PQRI Wizard.
The comments range from the technical aspects of individual quality measures in PQRS to how hospitalists appear to be performing in these programs. SHM firmly believes that the unique positioning of hospitalists within the health-care system presents challenges for their identification and evaluation in Medicare programs. In some sense, hospitalists exist on the line between the inpatient and outpatient worlds, a location not adequately captured in pay-for-performance programs.
It’s imperative that pay-for-performance programs have reasonable and actionable outcomes for providers. If quality measures are not clinically meaningful and do not capture a plurality of the care provided by an individual hospitalist, it is difficult for the program to meet its stated aims. If payment is to be influenced by performance on quality measures, it follows that those measures should be relevant to the care provided.
There is a long way to go toward creating quality measurement and evaluation programs that are relevant and actionable for clinical quality improvement (QI). By becoming involved in SHM’s policy efforts, members are able to share their experiences and impressions of programs with SHM and lawmakers. This partnership helps create more responsive and intuitive programs, which in turn leads to greater participation and, hopefully, improved patient outcomes. As these programs continue to evolve and more health professionals are required to participate, SHM will be looking to its membership for their perspectives.
Join the grassroots network to stay involved and up to date by registering at www.hospitalmedicine.org/grassroots.
Joshua Lapps is SHM’s government relations specialist.
Bundled-Payment Program Basics

With general agreement that health-care costs in the U.S. are unsustainable, the Centers for Medicare & Medicaid Services (CMS), through the Center for Medicare and Medicaid Innovation (CMMI), and the private sector are embarking on new approaches to cost containment. On the one hand, we have value-based purchasing (VBP), which rests on the existing fee-for-service system and aims for incremental change. On the other hand, we have accountable-care organizations (ACOs), which provide a global payment for a population of patients, and bundled-payment programs, which provide a single payment for an episode of care. These reimbursement models represent a fundamental change in how we pay for health care.
On a broad scale, ACOs may be further along in development than bundled-payment programs, even though pockets of bundling prototypes have existed for years. Examples include the Prometheus payment system, Geisinger’s ProvenCare, and CMS’ Acute Care Episode demonstration project, which bundled Part A (hospital) and Part B (doctors, others) payments for cardiac and orthopedic surgery procedures. Over the past two years, we have seen a dramatic uptick in bundling activity, including programs in a number of states (including Arkansas, California, and Massachusetts). Here at Baystate Health in Massachusetts, we kicked off a total-hip-replacement bundle with our subsidiary health plan in January 2011.

Perhaps most notably, bundled payments are part of the Affordable Care Act. The Bundled Payments for Care Improvement initiative, launched earlier this year by CMMI, is enrolling traditional Medicare patients in bundled-payment programs across the country at more than 400 health systems.
How Bundled Payments Work
Bundled-payment programs provide a single payment to hospitals, doctors, post-acute providers, and other providers (for home care, lab, medical equipment, etc.) for a defined episode of care. Most bundles encompass at least an acute hospital episode and physician payments for the episode; many include some period after hospitalization, covering rehabilitation at a facility or at home and doctors’ visits during recovery. Bundling goes beyond Medicare’s diagnosis-related group (DRG) payments, which reimburse hospitals for all elements of an inpatient hospital stay for a given diagnosis but do not include services performed by nonhospital providers.
How do the finances work in a bundled-payment program? A single price for an episode of care is determined based on historical performance, factoring in all the services one wishes to include in a bundle (e.g. hospital, doctor visits in hospital, home physical therapy, follow-up doctor visits, follow up X-ray and labs for a defined time period). If the hospital, doctors, and others in the bundle generate new efficiencies in care (e.g. due to better care coordination, less wasteful test ordering, or lower implant/device costs), the savings are then distributed to these providers. What if spending exceeds the predetermined price? In some instances, the health plan bears the financial risk; in other instances, the hospital, physicians, and other bundle providers must pay back the shortfall. Important to note is that all sharing of savings is contingent on attainment of or improvement in demonstrated quality-of-care measures relevant to the bundle. In the future, bundling will evolve from shared savings to a single prospective payment for a care episode.
For now, most bundles encompass surgical procedures, although CMMI is working with health systems on several medical bundles, including acute MI, COPD, and stroke. All of these bundles are initiated by an acute hospitalization. Other types of bundles exist, such as with chronic conditions or with post-acute care only. In Massachusetts, a pediatric asthma bundle is being implemented through Medicaid, covering that population for a year or longer. The aim is to redirect dollars that normally would pay for ED visits and inpatient care to pay for interventions that promote better control of the disease and prevent acute flare-ups that lead to hospital visits.
How Hospitalists Fit In
To date, there has been little discussion of how physicians other than the surgeons doing the procedure (most bundles are for surgeries) fit into the clinical or financial model underpinning the program. However, with most patients in surgical or medical bundles being discharged to home, we now recognize that primary-care physicians (PCPs) will be essential to the success of a bundle.
Similarly, with medically complex patients enrolling in surgical bundles, hospitalists will be essential to the pre- and perioperative care of these patients. Also, transitioning bundle patients to home or to a rehabilitation will benefit from the involvement of a hospitalist.
What You Can Do Today
Although this might seem abstract for hospitalists practicing in the here and now, there are compelling opportunities for hospitalists who get involved in bundled-payment programs. Here’s what I suggest:
Find out if your hospital or post-acute facility is participating in bundling by looking at a map of CMMI bundle programs here: http://innovation.cms.gov/initiatives/bundled-payments;
- Get a seat at the table working on the bundle; and
- Negotiate a portion of the bundle’s shared savings on the basis of 1) increased efficiency and quality resulting from hospitalist involvement and 2) hospitalist direct oversight of bundled patients in post-acute facilities (if you choose).
Post-acute care may be new for your hospitalist program. Bundling programs are an important new business case for hospitalists in this setting.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected].
With general agreement that health-care costs in the U.S. are unsustainable, the Centers for Medicare & Medicaid Services (CMS), through the Center for Medicare and Medicaid Innovation (CMMI), and the private sector are embarking on new approaches to cost containment. On the one hand, we have value-based purchasing (VBP), which rests on the existing fee-for-service system and aims for incremental change. On the other hand, we have accountable-care organizations (ACOs), which provide a global payment for a population of patients, and bundled-payment programs, which provide a single payment for an episode of care. These reimbursement models represent a fundamental change in how we pay for health care.
On a broad scale, ACOs may be further along in development than bundled-payment programs, even though pockets of bundling prototypes have existed for years. Examples include the Prometheus payment system, Geisinger’s ProvenCare, and CMS’ Acute Care Episode demonstration project, which bundled Part A (hospital) and Part B (doctors, others) payments for cardiac and orthopedic surgery procedures. Over the past two years, we have seen a dramatic uptick in bundling activity, including programs in a number of states (including Arkansas, California, and Massachusetts). Here at Baystate Health in Massachusetts, we kicked off a total-hip-replacement bundle with our subsidiary health plan in January 2011.
Perhaps most notably, bundled payments are part of the Affordable Care Act. The Bundled Payments for Care Improvement initiative, launched earlier this year by CMMI, is enrolling traditional Medicare patients in bundled-payment programs across the country at more than 400 health systems.
How Bundled Payments Work
Bundled-payment programs provide a single payment to hospitals, doctors, post-acute providers, and other providers (for home care, lab, medical equipment, etc.) for a defined episode of care. Most bundles encompass at least an acute hospital episode and physician payments for the episode; many include some period after hospitalization, covering rehabilitation at a facility or at home and doctors’ visits during recovery. Bundling goes beyond Medicare’s diagnosis-related group (DRG) payments, which reimburse hospitals for all elements of an inpatient hospital stay for a given diagnosis but do not include services performed by nonhospital providers.
How do the finances work in a bundled-payment program? A single price for an episode of care is determined based on historical performance, factoring in all the services one wishes to include in a bundle (e.g. hospital, doctor visits in hospital, home physical therapy, follow-up doctor visits, follow up X-ray and labs for a defined time period). If the hospital, doctors, and others in the bundle generate new efficiencies in care (e.g. due to better care coordination, less wasteful test ordering, or lower implant/device costs), the savings are then distributed to these providers. What if spending exceeds the predetermined price? In some instances, the health plan bears the financial risk; in other instances, the hospital, physicians, and other bundle providers must pay back the shortfall. Important to note is that all sharing of savings is contingent on attainment of or improvement in demonstrated quality-of-care measures relevant to the bundle. In the future, bundling will evolve from shared savings to a single prospective payment for a care episode.
For now, most bundles encompass surgical procedures, although CMMI is working with health systems on several medical bundles, including acute MI, COPD, and stroke. All of these bundles are initiated by an acute hospitalization. Other types of bundles exist, such as with chronic conditions or with post-acute care only. In Massachusetts, a pediatric asthma bundle is being implemented through Medicaid, covering that population for a year or longer. The aim is to redirect dollars that normally would pay for ED visits and inpatient care to pay for interventions that promote better control of the disease and prevent acute flare-ups that lead to hospital visits.
How Hospitalists Fit In
To date, there has been little discussion of how physicians other than the surgeons doing the procedure (most bundles are for surgeries) fit into the clinical or financial model underpinning the program. However, with most patients in surgical or medical bundles being discharged to home, we now recognize that primary-care physicians (PCPs) will be essential to the success of a bundle.
Similarly, with medically complex patients enrolling in surgical bundles, hospitalists will be essential to the pre- and perioperative care of these patients. Also, transitioning bundle patients to home or to a rehabilitation will benefit from the involvement of a hospitalist.
What You Can Do Today
Although this might seem abstract for hospitalists practicing in the here and now, there are compelling opportunities for hospitalists who get involved in bundled-payment programs. Here’s what I suggest:
Find out if your hospital or post-acute facility is participating in bundling by looking at a map of CMMI bundle programs here: http://innovation.cms.gov/initiatives/bundled-payments;
- Get a seat at the table working on the bundle; and
- Negotiate a portion of the bundle’s shared savings on the basis of 1) increased efficiency and quality resulting from hospitalist involvement and 2) hospitalist direct oversight of bundled patients in post-acute facilities (if you choose).
Post-acute care may be new for your hospitalist program. Bundling programs are an important new business case for hospitalists in this setting.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected].
With general agreement that health-care costs in the U.S. are unsustainable, the Centers for Medicare & Medicaid Services (CMS), through the Center for Medicare and Medicaid Innovation (CMMI), and the private sector are embarking on new approaches to cost containment. On the one hand, we have value-based purchasing (VBP), which rests on the existing fee-for-service system and aims for incremental change. On the other hand, we have accountable-care organizations (ACOs), which provide a global payment for a population of patients, and bundled-payment programs, which provide a single payment for an episode of care. These reimbursement models represent a fundamental change in how we pay for health care.
On a broad scale, ACOs may be further along in development than bundled-payment programs, even though pockets of bundling prototypes have existed for years. Examples include the Prometheus payment system, Geisinger’s ProvenCare, and CMS’ Acute Care Episode demonstration project, which bundled Part A (hospital) and Part B (doctors, others) payments for cardiac and orthopedic surgery procedures. Over the past two years, we have seen a dramatic uptick in bundling activity, including programs in a number of states (including Arkansas, California, and Massachusetts). Here at Baystate Health in Massachusetts, we kicked off a total-hip-replacement bundle with our subsidiary health plan in January 2011.
Perhaps most notably, bundled payments are part of the Affordable Care Act. The Bundled Payments for Care Improvement initiative, launched earlier this year by CMMI, is enrolling traditional Medicare patients in bundled-payment programs across the country at more than 400 health systems.
How Bundled Payments Work
Bundled-payment programs provide a single payment to hospitals, doctors, post-acute providers, and other providers (for home care, lab, medical equipment, etc.) for a defined episode of care. Most bundles encompass at least an acute hospital episode and physician payments for the episode; many include some period after hospitalization, covering rehabilitation at a facility or at home and doctors’ visits during recovery. Bundling goes beyond Medicare’s diagnosis-related group (DRG) payments, which reimburse hospitals for all elements of an inpatient hospital stay for a given diagnosis but do not include services performed by nonhospital providers.
How do the finances work in a bundled-payment program? A single price for an episode of care is determined based on historical performance, factoring in all the services one wishes to include in a bundle (e.g. hospital, doctor visits in hospital, home physical therapy, follow-up doctor visits, follow up X-ray and labs for a defined time period). If the hospital, doctors, and others in the bundle generate new efficiencies in care (e.g. due to better care coordination, less wasteful test ordering, or lower implant/device costs), the savings are then distributed to these providers. What if spending exceeds the predetermined price? In some instances, the health plan bears the financial risk; in other instances, the hospital, physicians, and other bundle providers must pay back the shortfall. Important to note is that all sharing of savings is contingent on attainment of or improvement in demonstrated quality-of-care measures relevant to the bundle. In the future, bundling will evolve from shared savings to a single prospective payment for a care episode.
For now, most bundles encompass surgical procedures, although CMMI is working with health systems on several medical bundles, including acute MI, COPD, and stroke. All of these bundles are initiated by an acute hospitalization. Other types of bundles exist, such as with chronic conditions or with post-acute care only. In Massachusetts, a pediatric asthma bundle is being implemented through Medicaid, covering that population for a year or longer. The aim is to redirect dollars that normally would pay for ED visits and inpatient care to pay for interventions that promote better control of the disease and prevent acute flare-ups that lead to hospital visits.
How Hospitalists Fit In
To date, there has been little discussion of how physicians other than the surgeons doing the procedure (most bundles are for surgeries) fit into the clinical or financial model underpinning the program. However, with most patients in surgical or medical bundles being discharged to home, we now recognize that primary-care physicians (PCPs) will be essential to the success of a bundle.
Similarly, with medically complex patients enrolling in surgical bundles, hospitalists will be essential to the pre- and perioperative care of these patients. Also, transitioning bundle patients to home or to a rehabilitation will benefit from the involvement of a hospitalist.
What You Can Do Today
Although this might seem abstract for hospitalists practicing in the here and now, there are compelling opportunities for hospitalists who get involved in bundled-payment programs. Here’s what I suggest:
Find out if your hospital or post-acute facility is participating in bundling by looking at a map of CMMI bundle programs here: http://innovation.cms.gov/initiatives/bundled-payments;
- Get a seat at the table working on the bundle; and
- Negotiate a portion of the bundle’s shared savings on the basis of 1) increased efficiency and quality resulting from hospitalist involvement and 2) hospitalist direct oversight of bundled patients in post-acute facilities (if you choose).
Post-acute care may be new for your hospitalist program. Bundling programs are an important new business case for hospitalists in this setting.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at [email protected].
Congressional Budget Office Says Health-Care Inflation Is Slowing
The Congressional Budget Office in May sharply lowered its projections for the next decade’s outlays on Medicare, Medicaid, and the extension of coverage for 25 million uninsured Americans under the Affordable Care Act.1
“During the past several years, health-care spending has grown much more slowly, both nationally and for federal programs, than it did historically and more slowly than CBO had projected,” according to the CBO report.
Health-care spending in 2012 was 5% below the amount the nonpartisan budgetary analysts had estimated in a 2010 projection for 2012. If these trends continue, commentators note, that could lessen budgetary pressures and perhaps strengthen the economy, as well as reduce the urgency for Congress to achieve a “grand bargain” confronting national debt issues.
However, CBO notes, budgetary shortfalls are expected to increase later this decade under the pressures of an aging population, expanded federal subsidies for health insurance, and the resumption of health-care cost inflation.
Larry Beresford is a freelance writer in San Francisco.
Reference
The Congressional Budget Office in May sharply lowered its projections for the next decade’s outlays on Medicare, Medicaid, and the extension of coverage for 25 million uninsured Americans under the Affordable Care Act.1
“During the past several years, health-care spending has grown much more slowly, both nationally and for federal programs, than it did historically and more slowly than CBO had projected,” according to the CBO report.
Health-care spending in 2012 was 5% below the amount the nonpartisan budgetary analysts had estimated in a 2010 projection for 2012. If these trends continue, commentators note, that could lessen budgetary pressures and perhaps strengthen the economy, as well as reduce the urgency for Congress to achieve a “grand bargain” confronting national debt issues.
However, CBO notes, budgetary shortfalls are expected to increase later this decade under the pressures of an aging population, expanded federal subsidies for health insurance, and the resumption of health-care cost inflation.
Larry Beresford is a freelance writer in San Francisco.
Reference
The Congressional Budget Office in May sharply lowered its projections for the next decade’s outlays on Medicare, Medicaid, and the extension of coverage for 25 million uninsured Americans under the Affordable Care Act.1
“During the past several years, health-care spending has grown much more slowly, both nationally and for federal programs, than it did historically and more slowly than CBO had projected,” according to the CBO report.
Health-care spending in 2012 was 5% below the amount the nonpartisan budgetary analysts had estimated in a 2010 projection for 2012. If these trends continue, commentators note, that could lessen budgetary pressures and perhaps strengthen the economy, as well as reduce the urgency for Congress to achieve a “grand bargain” confronting national debt issues.
However, CBO notes, budgetary shortfalls are expected to increase later this decade under the pressures of an aging population, expanded federal subsidies for health insurance, and the resumption of health-care cost inflation.
Larry Beresford is a freelance writer in San Francisco.
Reference
Technology Developers Encouraged to Make Hospital Pricing More Transparent
In June, the Robert Wood Johnson Foundation announced a national competition for technology developers to help consumers understand and utilize data for comparing the prices of hospital procedures. Winners of the foundation’s Hospital Price Transparency Challenge, to be announced later this year, will share $120,000 in prizes for intuitive, actionable tools leading to more transparent hospital pricing in two categories.
One category involves the creation of visual aids that would help consumers and others better understand the Centers for Medicare & Medicaid Services’ (CMS) hospital-cost data, which was released in May and compares widely variable hospital prices for 100 common inpatient procedures. The other category involves developing applications and tools that could help consumers price-shop.
The foundation is offering support and opportunities for submitters to interact with experts and technical innovators. The deadline for applications is Aug. 25.
In June, the Robert Wood Johnson Foundation announced a national competition for technology developers to help consumers understand and utilize data for comparing the prices of hospital procedures. Winners of the foundation’s Hospital Price Transparency Challenge, to be announced later this year, will share $120,000 in prizes for intuitive, actionable tools leading to more transparent hospital pricing in two categories.
One category involves the creation of visual aids that would help consumers and others better understand the Centers for Medicare & Medicaid Services’ (CMS) hospital-cost data, which was released in May and compares widely variable hospital prices for 100 common inpatient procedures. The other category involves developing applications and tools that could help consumers price-shop.
The foundation is offering support and opportunities for submitters to interact with experts and technical innovators. The deadline for applications is Aug. 25.
In June, the Robert Wood Johnson Foundation announced a national competition for technology developers to help consumers understand and utilize data for comparing the prices of hospital procedures. Winners of the foundation’s Hospital Price Transparency Challenge, to be announced later this year, will share $120,000 in prizes for intuitive, actionable tools leading to more transparent hospital pricing in two categories.
One category involves the creation of visual aids that would help consumers and others better understand the Centers for Medicare & Medicaid Services’ (CMS) hospital-cost data, which was released in May and compares widely variable hospital prices for 100 common inpatient procedures. The other category involves developing applications and tools that could help consumers price-shop.
The foundation is offering support and opportunities for submitters to interact with experts and technical innovators. The deadline for applications is Aug. 25.