User login
Daratumumab plus len-dex stalls myeloma progression in POLLUX trial
COPENHAGEN – In a classic case of clinical sibling rivalry, results of the POLLUX trial support the benefits of adding daratumumab to lenalidomide and dexamethasone in patients with relapsed/refractory multiple myeloma, echoing results reported a few days earlier by investigators in the twin (and archly named) CASTOR trial
Among 569 patients with relapsed/refractory multiple myeloma, the addition of the anti-CD38 monoclonal antibody daratumumab (Darzalex) to lenalidomide (Revlimid) and dexamethasone was associated with a 63% reduction in the risk of disease progress or death, compared with len-dex alone, reported Dr. Meletios A Dimopoulos of the National and Kapodistrian University of Athens.

With daratumumab and len-dex, “there is the highest-ever response rate seen in relapsed or refractory myeloma; 93% of the patients achieved at least a partial response, and more importantly, 43% of the patients achieved a complete response,” he said at a briefing prior to his presentation of the data at the annual congress of the European Hematology Association.
“The addition of daratumumab to lenalidomide and dexamethasone induces deep and durable responses. Data indicate that we can achieve minimal residual disease negativity status in a significant number of patients,” he added.
The trial was halted on May 20, 2016, after a preplanned interim analysis showed a significant improvement in the primary endpoint of a progression-free survival, compared with len-dex alone.
Dizygotic twins
Like their mythologic namesakes, who were twin sons from different fathers, the CASTOR and POLLUX trials differed somewhat in the patient populations treated and in trial design. The CASTOR trial is looking at the addition of daratumumab to bortezomib (Velcade) and dexamethasone, and excludes patients resistant to bortezomib. The POLLUX trial includes bortezomib-resistant patients, but excludes lenalidomide-resistant patients.
In addition, in CASTOR, patients were treated with the assigned regimen for a specified number of courses, followed by daratumumab maintenance, whereas patients in both arms in POLLUX continued on their assigned therapy until disease progression or unacceptable toxicity occurred.
POLLUX was a multicenter, randomized, open-label phase III trial in patients with relapsed/refractory multiple myeloma following one or more prior lines of therapy. They were randomized on a 1:1 basis to either len-dex (283 patients) or len-dex plus intravenous daratumumab at a dose of 16 mg/kg once a week during treatment cycles 1 and 2, every 2 weeks during cycles 3-6, and once only on day 1 of subsequent cycles.
After a median follow-up of 13.5 months, the median progression-free survival for patients treated with len-dex alone was 18.4 months, but the median was not yet reached among patients treated with daratumumab. The difference translated into a hazard ratio for progression-free survival with daratumumab of 0.37 (P less than .0001).
In addition, the antibody was associated with a significantly better overall response rate (93% for daratumumab vs. 76% for len-dex only; P less than .0001), as well as better rates of complete responses (43% vs. 19%, respectively; P less than .0001), and very good partial responses or better (76% vs. 44%, P less than .0001).
The combination was generally well tolerated, with adverse events consistent with the known safety profile of len-dex. Infusion reactions with daratumumab were generally mild, and tended to occur during the first infusion, Dr. Dimopoulos said.

Dr. Anton Hagenbeek, professor of hematology at the University of Amsterdam (the Netherlands), who moderated the briefing, commented that the progression-free survival curves with daratumumab appeared to plateau, and asked whether any patients in the trial could be considered to have been “cured.”
Dr. Dimopoulos replied that “although we believe that in the relapsed setting of myeloma, it is unlikely to achieve the cure rate, we are optimistic that there will be a sizable number of patients that will remain without progression for many months. Already from single-agent daratumumab where this patient population is far more heavily pretreated, there are patients who are without progression for several years.”
Dr. Dimopoulos has previously disclosed honoraria from Janssen, maker of daratumumab. Dr. Hagenbeek disclosed serving on an advisory board for Takeda, maker of bortezomib.
COPENHAGEN – In a classic case of clinical sibling rivalry, results of the POLLUX trial support the benefits of adding daratumumab to lenalidomide and dexamethasone in patients with relapsed/refractory multiple myeloma, echoing results reported a few days earlier by investigators in the twin (and archly named) CASTOR trial
Among 569 patients with relapsed/refractory multiple myeloma, the addition of the anti-CD38 monoclonal antibody daratumumab (Darzalex) to lenalidomide (Revlimid) and dexamethasone was associated with a 63% reduction in the risk of disease progress or death, compared with len-dex alone, reported Dr. Meletios A Dimopoulos of the National and Kapodistrian University of Athens.
With daratumumab and len-dex, “there is the highest-ever response rate seen in relapsed or refractory myeloma; 93% of the patients achieved at least a partial response, and more importantly, 43% of the patients achieved a complete response,” he said at a briefing prior to his presentation of the data at the annual congress of the European Hematology Association.
“The addition of daratumumab to lenalidomide and dexamethasone induces deep and durable responses. Data indicate that we can achieve minimal residual disease negativity status in a significant number of patients,” he added.
The trial was halted on May 20, 2016, after a preplanned interim analysis showed a significant improvement in the primary endpoint of a progression-free survival, compared with len-dex alone.
Dizygotic twins
Like their mythologic namesakes, who were twin sons from different fathers, the CASTOR and POLLUX trials differed somewhat in the patient populations treated and in trial design. The CASTOR trial is looking at the addition of daratumumab to bortezomib (Velcade) and dexamethasone, and excludes patients resistant to bortezomib. The POLLUX trial includes bortezomib-resistant patients, but excludes lenalidomide-resistant patients.
In addition, in CASTOR, patients were treated with the assigned regimen for a specified number of courses, followed by daratumumab maintenance, whereas patients in both arms in POLLUX continued on their assigned therapy until disease progression or unacceptable toxicity occurred.
POLLUX was a multicenter, randomized, open-label phase III trial in patients with relapsed/refractory multiple myeloma following one or more prior lines of therapy. They were randomized on a 1:1 basis to either len-dex (283 patients) or len-dex plus intravenous daratumumab at a dose of 16 mg/kg once a week during treatment cycles 1 and 2, every 2 weeks during cycles 3-6, and once only on day 1 of subsequent cycles.
After a median follow-up of 13.5 months, the median progression-free survival for patients treated with len-dex alone was 18.4 months, but the median was not yet reached among patients treated with daratumumab. The difference translated into a hazard ratio for progression-free survival with daratumumab of 0.37 (P less than .0001).
In addition, the antibody was associated with a significantly better overall response rate (93% for daratumumab vs. 76% for len-dex only; P less than .0001), as well as better rates of complete responses (43% vs. 19%, respectively; P less than .0001), and very good partial responses or better (76% vs. 44%, P less than .0001).
The combination was generally well tolerated, with adverse events consistent with the known safety profile of len-dex. Infusion reactions with daratumumab were generally mild, and tended to occur during the first infusion, Dr. Dimopoulos said.
Dr. Anton Hagenbeek, professor of hematology at the University of Amsterdam (the Netherlands), who moderated the briefing, commented that the progression-free survival curves with daratumumab appeared to plateau, and asked whether any patients in the trial could be considered to have been “cured.”
Dr. Dimopoulos replied that “although we believe that in the relapsed setting of myeloma, it is unlikely to achieve the cure rate, we are optimistic that there will be a sizable number of patients that will remain without progression for many months. Already from single-agent daratumumab where this patient population is far more heavily pretreated, there are patients who are without progression for several years.”
Dr. Dimopoulos has previously disclosed honoraria from Janssen, maker of daratumumab. Dr. Hagenbeek disclosed serving on an advisory board for Takeda, maker of bortezomib.
COPENHAGEN – In a classic case of clinical sibling rivalry, results of the POLLUX trial support the benefits of adding daratumumab to lenalidomide and dexamethasone in patients with relapsed/refractory multiple myeloma, echoing results reported a few days earlier by investigators in the twin (and archly named) CASTOR trial
Among 569 patients with relapsed/refractory multiple myeloma, the addition of the anti-CD38 monoclonal antibody daratumumab (Darzalex) to lenalidomide (Revlimid) and dexamethasone was associated with a 63% reduction in the risk of disease progress or death, compared with len-dex alone, reported Dr. Meletios A Dimopoulos of the National and Kapodistrian University of Athens.
With daratumumab and len-dex, “there is the highest-ever response rate seen in relapsed or refractory myeloma; 93% of the patients achieved at least a partial response, and more importantly, 43% of the patients achieved a complete response,” he said at a briefing prior to his presentation of the data at the annual congress of the European Hematology Association.
“The addition of daratumumab to lenalidomide and dexamethasone induces deep and durable responses. Data indicate that we can achieve minimal residual disease negativity status in a significant number of patients,” he added.
The trial was halted on May 20, 2016, after a preplanned interim analysis showed a significant improvement in the primary endpoint of a progression-free survival, compared with len-dex alone.
Dizygotic twins
Like their mythologic namesakes, who were twin sons from different fathers, the CASTOR and POLLUX trials differed somewhat in the patient populations treated and in trial design. The CASTOR trial is looking at the addition of daratumumab to bortezomib (Velcade) and dexamethasone, and excludes patients resistant to bortezomib. The POLLUX trial includes bortezomib-resistant patients, but excludes lenalidomide-resistant patients.
In addition, in CASTOR, patients were treated with the assigned regimen for a specified number of courses, followed by daratumumab maintenance, whereas patients in both arms in POLLUX continued on their assigned therapy until disease progression or unacceptable toxicity occurred.
POLLUX was a multicenter, randomized, open-label phase III trial in patients with relapsed/refractory multiple myeloma following one or more prior lines of therapy. They were randomized on a 1:1 basis to either len-dex (283 patients) or len-dex plus intravenous daratumumab at a dose of 16 mg/kg once a week during treatment cycles 1 and 2, every 2 weeks during cycles 3-6, and once only on day 1 of subsequent cycles.
After a median follow-up of 13.5 months, the median progression-free survival for patients treated with len-dex alone was 18.4 months, but the median was not yet reached among patients treated with daratumumab. The difference translated into a hazard ratio for progression-free survival with daratumumab of 0.37 (P less than .0001).
In addition, the antibody was associated with a significantly better overall response rate (93% for daratumumab vs. 76% for len-dex only; P less than .0001), as well as better rates of complete responses (43% vs. 19%, respectively; P less than .0001), and very good partial responses or better (76% vs. 44%, P less than .0001).
The combination was generally well tolerated, with adverse events consistent with the known safety profile of len-dex. Infusion reactions with daratumumab were generally mild, and tended to occur during the first infusion, Dr. Dimopoulos said.
Dr. Anton Hagenbeek, professor of hematology at the University of Amsterdam (the Netherlands), who moderated the briefing, commented that the progression-free survival curves with daratumumab appeared to plateau, and asked whether any patients in the trial could be considered to have been “cured.”
Dr. Dimopoulos replied that “although we believe that in the relapsed setting of myeloma, it is unlikely to achieve the cure rate, we are optimistic that there will be a sizable number of patients that will remain without progression for many months. Already from single-agent daratumumab where this patient population is far more heavily pretreated, there are patients who are without progression for several years.”
Dr. Dimopoulos has previously disclosed honoraria from Janssen, maker of daratumumab. Dr. Hagenbeek disclosed serving on an advisory board for Takeda, maker of bortezomib.
AT THE EHA CONGRESS
Key clinical point: The anti-CD38 monoclonal antibody daratumumab added to lenalidomide/dexamethasone improved progression-free survival in relapsed/refractory multiple myeloma.
Major finding: The hazard ratio for PFS with daratumumab plus len-dex was 0.37, compared with len-dex alone (P less than .0001).
Data source: An open-label phase III trial in 569 patients with relapsed or refractory multiple myeloma after one or more prior lines of therapy.
Disclosures: Dr. Dimopoulos has previously disclosed honoraria from Janssen, maker of daratumumab. Dr. Hagenbeek disclosed serving on an advisory board for Takeda, maker of bortezomib.

A new standard of care for relapsed/refractory MM?

COPENHAGEN—The combination of daratumumab, lenalidomide, and dexamethasone (DRd) could become a new standard of care for patients with relapsed or refractory multiple myeloma (MM), according to a speaker at the 21st Congress of the European Hematology Association.
In the phase 3 POLLUX study, DRd conferred the highest response rate reported to date in the treatment of relapsed/refractory MM.
DRd also significantly improved progression free survival (PFS) when compared to treatment with lenalidomide and dexamethasone (Rd).
In addition, the safety profile of DRd was manageable and consistent with results observed in previous studies, according to Meletios A. Dimopoulos, MD, of the National and Kapodistrian University of Athens in Greece.
Dr Dimopoulos presented these results at the congress as abstract LB2238. The POLLUX study was funded by Janssen Research & Development, LLC.
Treatment and patients
POLLUX was a randomized, double-blind study that enrolled 569 patients with relapsed or refractory MM. Patients had received 1 or more prior lines of therapy and had progressive disease.
The patients were randomized to receive DRd (n=286) or Rd (n=283). All patients received lenalidomide at 25 mg on days 1-21 of each cycle until disease progression. They also received dexamethasone at 40 mg weekly until disease progression.
Patients in the daratumumab arm also received daratumumab at 16 mg/kg once a week in cycles 1-2, every other week in cycles 3-6, and once every 4 weeks until disease progression.
Dr Dimopoulos noted that patient and disease features were equally distributed between the treatment arms. The median age was 65 in both arms (overall range, 34-89). About half of patients in each arm had ISS stage I disease, and patients were, roughly, a median of 4 years from diagnosis.
In both arms, patients had a median of 1 prior lines of therapy (overall range, 1-11). Roughly 60% of patients in both arms had received a prior transplant, 86% had received a proteasome inhibitor, 55% had received an immunomodulatory agent, 18% had prior lenalidomide, and 44% had received a proteasome inhibitor and an immunomodulatory agent.
Roughly 28% of patients in each arm were refractory to a proteasome inhibitor, and nearly 30% were refractory to their last line of therapy.
Results
At a median follow-up of 13.5 months, about 35% of patients had discontinued treatment—23% in the DRd arm and 47% in the Rd arm.
Reasons for discontinuation included disease progression (14% and 34%, respectively), adverse events (7% and 8%, respectively), non-compliance with study drug (0.4% and 2%, respectively), withdrawal by patient (0.4% and 2%, respectively), physician decision (1% and 0.7%, respectively), and death (0.7% and 0.4%, respectively).
The study’s primary endpoint was PFS. The median PFS has not been reached in the DRd arm and was 18.4 months in the Rd arm. The 12-month PFS was 83% and 60%, respectively, and the 18-month PFS was 78% and 52%, respectively.
“There is an unprecedented improvement of progression-free survival in favor of daratumumab with lenalidomide and dexamethasone, with a hazard ratio of 0.37 [95% CI, 0.27-0.52; P<0.0001], which corresponds to a 63% reduction in the risk of progressive disease or death in favor of DRd,” Dr Dimopoulos said.
He also pointed out that the improvement in PFS for the DRd arm was seen across all patient subgroups, regardless of age, ISS stage, prior treatment, and type of MM.
Furthermore, response rates were significantly higher in the DRd arm than in the Rd arm. The overall response rates were 93% and 76%, respectively (P<0.0001). And the complete response rates were 43% and 19%, respectively (P<0.0001).
“This trial was associated with the highest response ever reported—so far, at least—in the treatment of relapsed/refractory myeloma,” Dr Dimopoulos noted.
The median duration of response was not reached in the DRd arm and was 17.4 months in the Rd arm.
In addition, there was an overall survival advantage with DRd. The 18-month overall survival was 86% in the DRd arm and 76% in the Rd arm. The hazard ratio was 0.64 (95% CI, 0.40-1.01; P=0.0534).
As for safety, the most common hematologic adverse events (in the DRd and Rd arms, respectively) were neutropenia (59% and 43%), anemia (31% and 35%), thrombocytopenia (27% for both), lymphopenia (6% and 5%), and febrile neutropenia (6% and 3%).
The most common non-hematologic adverse events (in the DRd and Rd arms, respectively) were diarrhea (43% and 25%), fatigue (35% and 28%), upper respiratory tract infection (32% and 21%), constipation (29% and 25%), cough (29% and 13%), muscle spasms (26% and 19%), and pneumonia (14% and 13%).
“DRd has a manageable safety profile consistent with the known safety profile of daratumumab or Rd alone,” Dr Dimopoulos said. “And we believe the combination of daratumumab with lenalidomide and dexamethasone potentially represents a new standard of care for myeloma patients after 1 or more prior lines of therapy.” ![]()
COPENHAGEN—The combination of daratumumab, lenalidomide, and dexamethasone (DRd) could become a new standard of care for patients with relapsed or refractory multiple myeloma (MM), according to a speaker at the 21st Congress of the European Hematology Association.
In the phase 3 POLLUX study, DRd conferred the highest response rate reported to date in the treatment of relapsed/refractory MM.
DRd also significantly improved progression free survival (PFS) when compared to treatment with lenalidomide and dexamethasone (Rd).
In addition, the safety profile of DRd was manageable and consistent with results observed in previous studies, according to Meletios A. Dimopoulos, MD, of the National and Kapodistrian University of Athens in Greece.
Dr Dimopoulos presented these results at the congress as abstract LB2238. The POLLUX study was funded by Janssen Research & Development, LLC.
Treatment and patients
POLLUX was a randomized, double-blind study that enrolled 569 patients with relapsed or refractory MM. Patients had received 1 or more prior lines of therapy and had progressive disease.
The patients were randomized to receive DRd (n=286) or Rd (n=283). All patients received lenalidomide at 25 mg on days 1-21 of each cycle until disease progression. They also received dexamethasone at 40 mg weekly until disease progression.
Patients in the daratumumab arm also received daratumumab at 16 mg/kg once a week in cycles 1-2, every other week in cycles 3-6, and once every 4 weeks until disease progression.
Dr Dimopoulos noted that patient and disease features were equally distributed between the treatment arms. The median age was 65 in both arms (overall range, 34-89). About half of patients in each arm had ISS stage I disease, and patients were, roughly, a median of 4 years from diagnosis.
In both arms, patients had a median of 1 prior lines of therapy (overall range, 1-11). Roughly 60% of patients in both arms had received a prior transplant, 86% had received a proteasome inhibitor, 55% had received an immunomodulatory agent, 18% had prior lenalidomide, and 44% had received a proteasome inhibitor and an immunomodulatory agent.
Roughly 28% of patients in each arm were refractory to a proteasome inhibitor, and nearly 30% were refractory to their last line of therapy.
Results
At a median follow-up of 13.5 months, about 35% of patients had discontinued treatment—23% in the DRd arm and 47% in the Rd arm.
Reasons for discontinuation included disease progression (14% and 34%, respectively), adverse events (7% and 8%, respectively), non-compliance with study drug (0.4% and 2%, respectively), withdrawal by patient (0.4% and 2%, respectively), physician decision (1% and 0.7%, respectively), and death (0.7% and 0.4%, respectively).
The study’s primary endpoint was PFS. The median PFS has not been reached in the DRd arm and was 18.4 months in the Rd arm. The 12-month PFS was 83% and 60%, respectively, and the 18-month PFS was 78% and 52%, respectively.
“There is an unprecedented improvement of progression-free survival in favor of daratumumab with lenalidomide and dexamethasone, with a hazard ratio of 0.37 [95% CI, 0.27-0.52; P<0.0001], which corresponds to a 63% reduction in the risk of progressive disease or death in favor of DRd,” Dr Dimopoulos said.
He also pointed out that the improvement in PFS for the DRd arm was seen across all patient subgroups, regardless of age, ISS stage, prior treatment, and type of MM.
Furthermore, response rates were significantly higher in the DRd arm than in the Rd arm. The overall response rates were 93% and 76%, respectively (P<0.0001). And the complete response rates were 43% and 19%, respectively (P<0.0001).
“This trial was associated with the highest response ever reported—so far, at least—in the treatment of relapsed/refractory myeloma,” Dr Dimopoulos noted.
The median duration of response was not reached in the DRd arm and was 17.4 months in the Rd arm.
In addition, there was an overall survival advantage with DRd. The 18-month overall survival was 86% in the DRd arm and 76% in the Rd arm. The hazard ratio was 0.64 (95% CI, 0.40-1.01; P=0.0534).
As for safety, the most common hematologic adverse events (in the DRd and Rd arms, respectively) were neutropenia (59% and 43%), anemia (31% and 35%), thrombocytopenia (27% for both), lymphopenia (6% and 5%), and febrile neutropenia (6% and 3%).
The most common non-hematologic adverse events (in the DRd and Rd arms, respectively) were diarrhea (43% and 25%), fatigue (35% and 28%), upper respiratory tract infection (32% and 21%), constipation (29% and 25%), cough (29% and 13%), muscle spasms (26% and 19%), and pneumonia (14% and 13%).
“DRd has a manageable safety profile consistent with the known safety profile of daratumumab or Rd alone,” Dr Dimopoulos said. “And we believe the combination of daratumumab with lenalidomide and dexamethasone potentially represents a new standard of care for myeloma patients after 1 or more prior lines of therapy.” ![]()
COPENHAGEN—The combination of daratumumab, lenalidomide, and dexamethasone (DRd) could become a new standard of care for patients with relapsed or refractory multiple myeloma (MM), according to a speaker at the 21st Congress of the European Hematology Association.
In the phase 3 POLLUX study, DRd conferred the highest response rate reported to date in the treatment of relapsed/refractory MM.
DRd also significantly improved progression free survival (PFS) when compared to treatment with lenalidomide and dexamethasone (Rd).
In addition, the safety profile of DRd was manageable and consistent with results observed in previous studies, according to Meletios A. Dimopoulos, MD, of the National and Kapodistrian University of Athens in Greece.
Dr Dimopoulos presented these results at the congress as abstract LB2238. The POLLUX study was funded by Janssen Research & Development, LLC.
Treatment and patients
POLLUX was a randomized, double-blind study that enrolled 569 patients with relapsed or refractory MM. Patients had received 1 or more prior lines of therapy and had progressive disease.
The patients were randomized to receive DRd (n=286) or Rd (n=283). All patients received lenalidomide at 25 mg on days 1-21 of each cycle until disease progression. They also received dexamethasone at 40 mg weekly until disease progression.
Patients in the daratumumab arm also received daratumumab at 16 mg/kg once a week in cycles 1-2, every other week in cycles 3-6, and once every 4 weeks until disease progression.
Dr Dimopoulos noted that patient and disease features were equally distributed between the treatment arms. The median age was 65 in both arms (overall range, 34-89). About half of patients in each arm had ISS stage I disease, and patients were, roughly, a median of 4 years from diagnosis.
In both arms, patients had a median of 1 prior lines of therapy (overall range, 1-11). Roughly 60% of patients in both arms had received a prior transplant, 86% had received a proteasome inhibitor, 55% had received an immunomodulatory agent, 18% had prior lenalidomide, and 44% had received a proteasome inhibitor and an immunomodulatory agent.
Roughly 28% of patients in each arm were refractory to a proteasome inhibitor, and nearly 30% were refractory to their last line of therapy.
Results
At a median follow-up of 13.5 months, about 35% of patients had discontinued treatment—23% in the DRd arm and 47% in the Rd arm.
Reasons for discontinuation included disease progression (14% and 34%, respectively), adverse events (7% and 8%, respectively), non-compliance with study drug (0.4% and 2%, respectively), withdrawal by patient (0.4% and 2%, respectively), physician decision (1% and 0.7%, respectively), and death (0.7% and 0.4%, respectively).
The study’s primary endpoint was PFS. The median PFS has not been reached in the DRd arm and was 18.4 months in the Rd arm. The 12-month PFS was 83% and 60%, respectively, and the 18-month PFS was 78% and 52%, respectively.
“There is an unprecedented improvement of progression-free survival in favor of daratumumab with lenalidomide and dexamethasone, with a hazard ratio of 0.37 [95% CI, 0.27-0.52; P<0.0001], which corresponds to a 63% reduction in the risk of progressive disease or death in favor of DRd,” Dr Dimopoulos said.
He also pointed out that the improvement in PFS for the DRd arm was seen across all patient subgroups, regardless of age, ISS stage, prior treatment, and type of MM.
Furthermore, response rates were significantly higher in the DRd arm than in the Rd arm. The overall response rates were 93% and 76%, respectively (P<0.0001). And the complete response rates were 43% and 19%, respectively (P<0.0001).
“This trial was associated with the highest response ever reported—so far, at least—in the treatment of relapsed/refractory myeloma,” Dr Dimopoulos noted.
The median duration of response was not reached in the DRd arm and was 17.4 months in the Rd arm.
In addition, there was an overall survival advantage with DRd. The 18-month overall survival was 86% in the DRd arm and 76% in the Rd arm. The hazard ratio was 0.64 (95% CI, 0.40-1.01; P=0.0534).
As for safety, the most common hematologic adverse events (in the DRd and Rd arms, respectively) were neutropenia (59% and 43%), anemia (31% and 35%), thrombocytopenia (27% for both), lymphopenia (6% and 5%), and febrile neutropenia (6% and 3%).
The most common non-hematologic adverse events (in the DRd and Rd arms, respectively) were diarrhea (43% and 25%), fatigue (35% and 28%), upper respiratory tract infection (32% and 21%), constipation (29% and 25%), cough (29% and 13%), muscle spasms (26% and 19%), and pneumonia (14% and 13%).
“DRd has a manageable safety profile consistent with the known safety profile of daratumumab or Rd alone,” Dr Dimopoulos said. “And we believe the combination of daratumumab with lenalidomide and dexamethasone potentially represents a new standard of care for myeloma patients after 1 or more prior lines of therapy.” ![]()
Daratumumab yields “unprecedented” PFS benefit in refractory myeloma
CHICAGO – Adding daratumumab to the current two-drug standard of care for relapsed or refractory multiple myeloma dramatically improves outcomes, according to results of an interim analysis of the phase III CASTOR trial.
When added to bortezomib and dexamethasone, the anti-CD38 antibody, which has both direct and indirect antimyeloma activity, reduced the risk of progression or death by 61%, with little increase in toxicity, investigators reported in a plenary session and press briefing at the annual meeting of the American Society of Clinical Oncology.

This magnitude of benefit is “unprecedented in randomized studies that compare novel treatments for relapsed, refractory multiple myeloma,” contended lead investigator Dr. Antonio Palumbo, chief of the multiple myeloma unit at the University of Torino, Italy.
“We hope this [daratumumab combination for myeloma] will be the translation of R-CHOP for lymphoma,” he added, referring to the addition of rituximab to an established backbone regimen. “Daratumumab-DVd [bortezomib-dexamethasone] might be considered today a new standard of care for relapsed and refractory multiple myeloma.”
At present, daratumumab is approved by the Food and Drug Administration for use only after patients have received at least three other therapies, Dr. Palumbo said.
“This study will open the opportunity to have a combination approach after diagnosis, therefore, at first relapse,” he commented, while noting that sufficient evidence should be obtained before using a drug for a new indication. “It’s very important to move as fast as we can this combination into the early phases of disease, where there is the major impact, even from a cost-efficacy point of view.”
The CASTOR findings add to evidence suggesting that daratumumab is synergistic with other myeloma therapies, according to invited discussant Dr. Paul G. Richardson, the R.J. Corman Professor of Medicine, Harvard Medical School, Boston, and the clinical program leader and director of clinical research at the Jerome Lipper Multiple Myeloma Center, Dana-Farber Cancer Institute, Boston.
“What I think is particularly impressive is the effect on the one-prior-line-of-treatment stratum,” he said, where the reduction in risk of progression or death was 69% with the addition of daratumumab.
Findings from the POLLUX trial, soon to be presented at another meeting, show a similar benefit when daratumumab is added to lenalidomide and dexamethasone in this setting, yielding a 63% reduction in the risk of events, according to Dr. Richardson. Additionally, other anti-CD38 antibodies and immune checkpoint inhibitors are being studied in this disease.
“I would first and foremost emphasize that this is not a zero-sum game. We need all of these drugs and all of these combinations to fight this disease,” he maintained, reviewing the many options now available. “But truly, the advent of the monoclonal antibody platform in this setting has resulted in hazard ratios that are unprecedented,” he agreed.
In CASTOR, 498 patients were randomized evenly to eight cycles of bortezomib (Velcade) plus dexamethasone, either alone or with the addition of daratumumab (Darzalex) given concurrently and then as monotherapy after completion of those cycles.
In the interim analysis, conducted at a median follow-up of about 7 months, the trial met its primary endpoint of progression-free survival: the median time to an event had not been reached with the daratumumab three-drug therapy but was 7.2 months with the standard two-drug therapy (hazard ratio, 0.39; P less than .0001). The difference translated to a more than doubling of the 1-year rate of progression-free survival (60.7% vs. 26.9%).
Benefit was generally consistent across patient subgroups stratified by disease characteristics and previous treatments, although greater impact was seen among the subgroups having earlier-stage or less heavily pretreated disease.
On the basis of these interim findings, patients in the standard therapy arm were allowed to cross over to get daratumumab, according to Dr. Palumbo.
The triple regimen was also associated with a higher overall response rate (83% vs. 63%; P less than .0001) as well as deeper responses, with a doubling in rates of both very good partial response (VGPR) or better and complete response (CR) or better.
“More patients do achieve a profound cytoreduction,” Dr. Palumbo said. “The remission duration is almost [tripled] in patients with a CR or VGPR versus patients with a minimal response or partial response.”
Data for overall survival are not yet mature, but at the time of the analysis, there was also a trend toward fewer deaths with daratumumab than without it (hazard ratio, 0.77).
“Daratumumab did not significantly increase any toxicity that was already present with the combination of bortezomib and dexamethasone,” Dr. Palumbo reported.
The three-drug regimen yielded somewhat higher rates of treatment-emergent thrombocytopenia (59% vs. 44%) and sensory peripheral neuropathy (47% vs. 38%). However, “this was mainly due to the fact that the experimental arm was longer exposed to bortezomib in comparison to the control arm that had a higher proportion of early progressions,” he explained. Additionally, the increase in thrombocytopenia did not translate into increased bleeding.
Forty-five percent of patients in the daratumumab arm had an infusion-related reaction, but nearly all reactions were limited to the first infusion.
The rate of discontinuation because of treatment-emergent adverse events was 7% with daratumumab and 9% without it.
Dr. Palumbo disclosed that he has a consulting or advisory role with and receives honoraria and research funding (institutional) from Genmab, Janssen-Cilag, and Takeda. The trial was sponsored by Janssen Research & Development.
CHICAGO – Adding daratumumab to the current two-drug standard of care for relapsed or refractory multiple myeloma dramatically improves outcomes, according to results of an interim analysis of the phase III CASTOR trial.
When added to bortezomib and dexamethasone, the anti-CD38 antibody, which has both direct and indirect antimyeloma activity, reduced the risk of progression or death by 61%, with little increase in toxicity, investigators reported in a plenary session and press briefing at the annual meeting of the American Society of Clinical Oncology.
This magnitude of benefit is “unprecedented in randomized studies that compare novel treatments for relapsed, refractory multiple myeloma,” contended lead investigator Dr. Antonio Palumbo, chief of the multiple myeloma unit at the University of Torino, Italy.
“We hope this [daratumumab combination for myeloma] will be the translation of R-CHOP for lymphoma,” he added, referring to the addition of rituximab to an established backbone regimen. “Daratumumab-DVd [bortezomib-dexamethasone] might be considered today a new standard of care for relapsed and refractory multiple myeloma.”
At present, daratumumab is approved by the Food and Drug Administration for use only after patients have received at least three other therapies, Dr. Palumbo said.
“This study will open the opportunity to have a combination approach after diagnosis, therefore, at first relapse,” he commented, while noting that sufficient evidence should be obtained before using a drug for a new indication. “It’s very important to move as fast as we can this combination into the early phases of disease, where there is the major impact, even from a cost-efficacy point of view.”
The CASTOR findings add to evidence suggesting that daratumumab is synergistic with other myeloma therapies, according to invited discussant Dr. Paul G. Richardson, the R.J. Corman Professor of Medicine, Harvard Medical School, Boston, and the clinical program leader and director of clinical research at the Jerome Lipper Multiple Myeloma Center, Dana-Farber Cancer Institute, Boston.
“What I think is particularly impressive is the effect on the one-prior-line-of-treatment stratum,” he said, where the reduction in risk of progression or death was 69% with the addition of daratumumab.
Findings from the POLLUX trial, soon to be presented at another meeting, show a similar benefit when daratumumab is added to lenalidomide and dexamethasone in this setting, yielding a 63% reduction in the risk of events, according to Dr. Richardson. Additionally, other anti-CD38 antibodies and immune checkpoint inhibitors are being studied in this disease.
“I would first and foremost emphasize that this is not a zero-sum game. We need all of these drugs and all of these combinations to fight this disease,” he maintained, reviewing the many options now available. “But truly, the advent of the monoclonal antibody platform in this setting has resulted in hazard ratios that are unprecedented,” he agreed.
In CASTOR, 498 patients were randomized evenly to eight cycles of bortezomib (Velcade) plus dexamethasone, either alone or with the addition of daratumumab (Darzalex) given concurrently and then as monotherapy after completion of those cycles.
In the interim analysis, conducted at a median follow-up of about 7 months, the trial met its primary endpoint of progression-free survival: the median time to an event had not been reached with the daratumumab three-drug therapy but was 7.2 months with the standard two-drug therapy (hazard ratio, 0.39; P less than .0001). The difference translated to a more than doubling of the 1-year rate of progression-free survival (60.7% vs. 26.9%).
Benefit was generally consistent across patient subgroups stratified by disease characteristics and previous treatments, although greater impact was seen among the subgroups having earlier-stage or less heavily pretreated disease.
On the basis of these interim findings, patients in the standard therapy arm were allowed to cross over to get daratumumab, according to Dr. Palumbo.
The triple regimen was also associated with a higher overall response rate (83% vs. 63%; P less than .0001) as well as deeper responses, with a doubling in rates of both very good partial response (VGPR) or better and complete response (CR) or better.
“More patients do achieve a profound cytoreduction,” Dr. Palumbo said. “The remission duration is almost [tripled] in patients with a CR or VGPR versus patients with a minimal response or partial response.”
Data for overall survival are not yet mature, but at the time of the analysis, there was also a trend toward fewer deaths with daratumumab than without it (hazard ratio, 0.77).
“Daratumumab did not significantly increase any toxicity that was already present with the combination of bortezomib and dexamethasone,” Dr. Palumbo reported.
The three-drug regimen yielded somewhat higher rates of treatment-emergent thrombocytopenia (59% vs. 44%) and sensory peripheral neuropathy (47% vs. 38%). However, “this was mainly due to the fact that the experimental arm was longer exposed to bortezomib in comparison to the control arm that had a higher proportion of early progressions,” he explained. Additionally, the increase in thrombocytopenia did not translate into increased bleeding.
Forty-five percent of patients in the daratumumab arm had an infusion-related reaction, but nearly all reactions were limited to the first infusion.
The rate of discontinuation because of treatment-emergent adverse events was 7% with daratumumab and 9% without it.
Dr. Palumbo disclosed that he has a consulting or advisory role with and receives honoraria and research funding (institutional) from Genmab, Janssen-Cilag, and Takeda. The trial was sponsored by Janssen Research & Development.
CHICAGO – Adding daratumumab to the current two-drug standard of care for relapsed or refractory multiple myeloma dramatically improves outcomes, according to results of an interim analysis of the phase III CASTOR trial.
When added to bortezomib and dexamethasone, the anti-CD38 antibody, which has both direct and indirect antimyeloma activity, reduced the risk of progression or death by 61%, with little increase in toxicity, investigators reported in a plenary session and press briefing at the annual meeting of the American Society of Clinical Oncology.
This magnitude of benefit is “unprecedented in randomized studies that compare novel treatments for relapsed, refractory multiple myeloma,” contended lead investigator Dr. Antonio Palumbo, chief of the multiple myeloma unit at the University of Torino, Italy.
“We hope this [daratumumab combination for myeloma] will be the translation of R-CHOP for lymphoma,” he added, referring to the addition of rituximab to an established backbone regimen. “Daratumumab-DVd [bortezomib-dexamethasone] might be considered today a new standard of care for relapsed and refractory multiple myeloma.”
At present, daratumumab is approved by the Food and Drug Administration for use only after patients have received at least three other therapies, Dr. Palumbo said.
“This study will open the opportunity to have a combination approach after diagnosis, therefore, at first relapse,” he commented, while noting that sufficient evidence should be obtained before using a drug for a new indication. “It’s very important to move as fast as we can this combination into the early phases of disease, where there is the major impact, even from a cost-efficacy point of view.”
The CASTOR findings add to evidence suggesting that daratumumab is synergistic with other myeloma therapies, according to invited discussant Dr. Paul G. Richardson, the R.J. Corman Professor of Medicine, Harvard Medical School, Boston, and the clinical program leader and director of clinical research at the Jerome Lipper Multiple Myeloma Center, Dana-Farber Cancer Institute, Boston.
“What I think is particularly impressive is the effect on the one-prior-line-of-treatment stratum,” he said, where the reduction in risk of progression or death was 69% with the addition of daratumumab.
Findings from the POLLUX trial, soon to be presented at another meeting, show a similar benefit when daratumumab is added to lenalidomide and dexamethasone in this setting, yielding a 63% reduction in the risk of events, according to Dr. Richardson. Additionally, other anti-CD38 antibodies and immune checkpoint inhibitors are being studied in this disease.
“I would first and foremost emphasize that this is not a zero-sum game. We need all of these drugs and all of these combinations to fight this disease,” he maintained, reviewing the many options now available. “But truly, the advent of the monoclonal antibody platform in this setting has resulted in hazard ratios that are unprecedented,” he agreed.
In CASTOR, 498 patients were randomized evenly to eight cycles of bortezomib (Velcade) plus dexamethasone, either alone or with the addition of daratumumab (Darzalex) given concurrently and then as monotherapy after completion of those cycles.
In the interim analysis, conducted at a median follow-up of about 7 months, the trial met its primary endpoint of progression-free survival: the median time to an event had not been reached with the daratumumab three-drug therapy but was 7.2 months with the standard two-drug therapy (hazard ratio, 0.39; P less than .0001). The difference translated to a more than doubling of the 1-year rate of progression-free survival (60.7% vs. 26.9%).
Benefit was generally consistent across patient subgroups stratified by disease characteristics and previous treatments, although greater impact was seen among the subgroups having earlier-stage or less heavily pretreated disease.
On the basis of these interim findings, patients in the standard therapy arm were allowed to cross over to get daratumumab, according to Dr. Palumbo.
The triple regimen was also associated with a higher overall response rate (83% vs. 63%; P less than .0001) as well as deeper responses, with a doubling in rates of both very good partial response (VGPR) or better and complete response (CR) or better.
“More patients do achieve a profound cytoreduction,” Dr. Palumbo said. “The remission duration is almost [tripled] in patients with a CR or VGPR versus patients with a minimal response or partial response.”
Data for overall survival are not yet mature, but at the time of the analysis, there was also a trend toward fewer deaths with daratumumab than without it (hazard ratio, 0.77).
“Daratumumab did not significantly increase any toxicity that was already present with the combination of bortezomib and dexamethasone,” Dr. Palumbo reported.
The three-drug regimen yielded somewhat higher rates of treatment-emergent thrombocytopenia (59% vs. 44%) and sensory peripheral neuropathy (47% vs. 38%). However, “this was mainly due to the fact that the experimental arm was longer exposed to bortezomib in comparison to the control arm that had a higher proportion of early progressions,” he explained. Additionally, the increase in thrombocytopenia did not translate into increased bleeding.
Forty-five percent of patients in the daratumumab arm had an infusion-related reaction, but nearly all reactions were limited to the first infusion.
The rate of discontinuation because of treatment-emergent adverse events was 7% with daratumumab and 9% without it.
Dr. Palumbo disclosed that he has a consulting or advisory role with and receives honoraria and research funding (institutional) from Genmab, Janssen-Cilag, and Takeda. The trial was sponsored by Janssen Research & Development.
AT THE 2016 ASCO ANNUAL MEETING
Key clinical point: Daratumumab improves outcomes when added to the current standard of care in relapsed or refractory myeloma.
Major finding: Adding daratumumab to bortezomib and dexamethasone reduced the risk of progression or death by 61%.
Data source: An open-label randomized phase III trial among 498 patients with relapsed or refractory multiple myeloma.
Disclosures: Dr. Palumbo disclosed that he has a consulting or advisory role with and receives honoraria and research funding (institutional) from Genmab, Janssen-Cilag, and Takeda. The trial was sponsored by Janssen Research & Development.

‘Unprecedented’ efficacy for daratumumab in rel/ref MM

CHICAGO—The addition of the monoclonal antibody daratumumab to bortezomib and dexamethasone, the current standard of care for relapsed/refractory multiple myeloma (MM), has achieved progression-free survival that is “unprecedented in randomized studies that compared novel treatment” for this disease, according to Antonio Palumbo, MD, lead author of the phase 3 CASTOR study.
Dr Palumbo, of the University of Torino in Torino, Italy, presented the results on behalf of the CASTOR investigators during the plenary session of the 2016 ASCO Annual Meeting (abstract LBA4).
Daratumumab (Darzalex) is a human CD38 monoclonal antibody, which means it is targeted very specifically to the most relevant tumor antigen for plasma cells.
It also has direct major cytotoxic activity through the complement, which translates into major tumor reduction and a profound cytoreduction, Dr Palumbo said.
Even more important, he added, is that this is an immunomodulatory agent able to both increase the T-cell activity in the immune system, which controls the tumor, and also reduce the immunosuppressive regulatory cells that are suppressing the activity of the immune system.
Daratumumab is already approved by the US Food and Drug Administration and conditionally approved by the European Commission as a single agent for the treatment of relapsed/refractory multiple myeloma.
Study design
The CASTOR study was a multicenter, randomized, open-label, active-controlled phase 3 study.
Patients were eligible to enroll if they had relapsed or refractory MM with at least 1 prior line of therapy, which could include prior treatment with bortezomib, but they were not eligible if they were refractory to it.
Investigators randomized 251 patients to the experimental arm of daratumumab, bortezomib (Velcade), and dexamethasone (DVd) and 247 to the control arm of bortezomib and dexamethasone (Vd).
The dosing schedule was the same in both arms for bortezomib and dexamethasone. Patients in the experimental arm received daratumumab (16 mg/kg IV) every week for the first 3 cycles, on day 1 of cycles 4 – 8, and then every 4 weeks until progression.
The primary endpoint of the study was progression-free survival (PFS). Secondary endpoints included time to progression (TTP), overall survival (OS), overall response rate (ORR), very good partial response (VGPR), complete response (CR), minimal residual disease (MRD), time to response, and duration of response.
Patient demographics
Overall, patients had advanced stage disease with a long history of prior treatment.
They were a median age of 64 in both groups, and the time from diagnosis was a median 3.87 years in the experimental arm and 3.72 years in the control arm.
About 60% in both groups had had prior autologous stem cell transplant. Seventy-one percent in the experimental arm and 80% in the control arm had received a prior immunomodulatory drug, and 30% in the experimental arm and 34% in the control arm were refractory to their last line of therapy.
Dr Palumbo pointed out that accrual for the trial was rapid; 500 patients enrolled in 1 year, from September 2014 to September 2015.
“After 3 months, we already saw a difference in terms of efficacy,” he added, and the trial was stopped early. “So the median follow-up is short for this reason,” he explained, “and is around 7 months.”
The discontinuation rate was “as expected,” he said, “higher in the control arm,” with 44% discontinuing compared with 31% in the experimental arm.
Discontinuation for progressive disease was 25% in the control arm and 19% in the experimental arm, “showing already an advantage for the novel combination.”
Adverse events as reasons for discontinuation were 8% in the experimental arm and 10% in the control arm, “showing that the new agent is not adding any extra toxicity to the combination of bortezomib and dexamethasone.”
Efficacy
The “unprecedented” PFS, with a hazard ratio (HR) of 0.39 (95% CI, 0.28-0.53; P<0.0001), translated into a 61% reduction in the risk of disease progression or death for the experimental arm compared with the control arm.
The median PFS was not yet reached in the experimental arm, while the median PFS was 7.2 months in the control arm.
At 1 year, the PFS was 26.9% in the control arm and 60.7% in the experimental arm, “and this translates into a doubling in terms of remission duration for those patients,” Dr Palumbo stated.
“Even better was the outcome for the time to progression,” he said, with an HR of 0.30, “which means a 70% reduction in the risk of disease progression for DVd versus Vd, a more than doubling of time to disease progression.”
PFS by subgroup analysis showed that early intervention with daratumumab maximizes the efficacy of the combination.
For those patients who had received only 1 line of prior treatment, the HR was 0.31 (95% CI, 0.18 – 0.52; P<0.0001), which translated to a 69% reduction in the risk of progression or death for DVd compared with Vd.
The overall response rate revealed the profound cytoreduction achieved by the addition of daratumumab.
The CR rate increased from 9% in the control group to 19% in the experimental arm (P=0.0012), and the VGPR increased from 29% to 59%, in the control and experimental arms, respectively.
“So there is a doubling in the rate of CR and VGPR,” Dr Palumbo pointed out, “and this is quite relevant because more patients do achieve a profound cytoreduction.”
The rate of MRD negativity was 5 times higher for daratumumab-treated patients. Three percent of patients in the control arm were MRD negative (10-4) compared with 14% in the experimental arm.
Time to response, “in my opinion, is an important issue because . . . you can reach PR in around 1 month [with DVd] and this is clinically relevant because those patients are symptomatic,” he explained. “Reaching PR in 1 month means getting rid of pain in a quick way.”
“On the other hand, the achieving of CR requires a prolonged treatment,” he added. “CR is being achieved after 12 months of therapy, and MRD negativity might need even longer treatment.”
Safety
Daratumumab-treated patients experienced more thrombocytopenia and peripheral neuropathy (PN) of any grade than the control arm, 47% compared with 38%, respectively.
“But this is not due to the addition of the third agent,” Dr Palumbo clarified. “This is mainly the consequence, in the experimental arm, that treatment with bortezomib was longer in comparison to the control arm, and therefore, the typical toxicity of bortezomib—thrombocytopenia and PN—were slightly higher.”
There was also an increase in upper respiratory tract infections and cough in daratumumab-treated patients.
Grade 3-4 treatment-emergent adverse events occurring in more than 5% of patients included thrombocytopenia, anemia, neutropenia, lymphopenia, pneumonia, hypertension, and sensory PN.
However, grade 4 thrombocyotpenia, Dr Palumbo noted, did not translate into an increase in bleeding.
The major increase in toxicity due to daratumumab was in infusion-related reactions (IRRs), which occurred in 45% of patients. IRRs were consistent with the infusion of other monoclonal antibodies in cancer patients, he said, and 98% of patients with IRRs experienced them on the first infusion.
Conclusions
Dr Palumbo stressed that daratumumab did not increase the cumulative toxicity or the toxicity of the bortezomib-dexamethasone combination.
Daratumumab significantly improved PFS and the response rate; the experimental combination was associated with a 61% reduction in the risk of progression or death.
The benefit was maintained across different subgroups—whether younger, older, good prognosis, bad prognosis, previously exposed to bortezomib or not exposed to bortezomib.
And DVd doubled both VGPR rates and CR rates.
In a press briefing, Dr Palumbo said that in the myeloma field, “we hope to have our R-CHOP, that has been a major treatment for lymphoma now also available with a different antibody for multiple myeloma.”
So the final conclusion, he added, is that “daratumumab-Vd might be considered today a new standard of care for relapsed and refractory multiple myeloma.”
The study was funded by Janssen Research & Development. ![]()
CHICAGO—The addition of the monoclonal antibody daratumumab to bortezomib and dexamethasone, the current standard of care for relapsed/refractory multiple myeloma (MM), has achieved progression-free survival that is “unprecedented in randomized studies that compared novel treatment” for this disease, according to Antonio Palumbo, MD, lead author of the phase 3 CASTOR study.
Dr Palumbo, of the University of Torino in Torino, Italy, presented the results on behalf of the CASTOR investigators during the plenary session of the 2016 ASCO Annual Meeting (abstract LBA4).
Daratumumab (Darzalex) is a human CD38 monoclonal antibody, which means it is targeted very specifically to the most relevant tumor antigen for plasma cells.
It also has direct major cytotoxic activity through the complement, which translates into major tumor reduction and a profound cytoreduction, Dr Palumbo said.
Even more important, he added, is that this is an immunomodulatory agent able to both increase the T-cell activity in the immune system, which controls the tumor, and also reduce the immunosuppressive regulatory cells that are suppressing the activity of the immune system.
Daratumumab is already approved by the US Food and Drug Administration and conditionally approved by the European Commission as a single agent for the treatment of relapsed/refractory multiple myeloma.
Study design
The CASTOR study was a multicenter, randomized, open-label, active-controlled phase 3 study.
Patients were eligible to enroll if they had relapsed or refractory MM with at least 1 prior line of therapy, which could include prior treatment with bortezomib, but they were not eligible if they were refractory to it.
Investigators randomized 251 patients to the experimental arm of daratumumab, bortezomib (Velcade), and dexamethasone (DVd) and 247 to the control arm of bortezomib and dexamethasone (Vd).
The dosing schedule was the same in both arms for bortezomib and dexamethasone. Patients in the experimental arm received daratumumab (16 mg/kg IV) every week for the first 3 cycles, on day 1 of cycles 4 – 8, and then every 4 weeks until progression.
The primary endpoint of the study was progression-free survival (PFS). Secondary endpoints included time to progression (TTP), overall survival (OS), overall response rate (ORR), very good partial response (VGPR), complete response (CR), minimal residual disease (MRD), time to response, and duration of response.
Patient demographics
Overall, patients had advanced stage disease with a long history of prior treatment.
They were a median age of 64 in both groups, and the time from diagnosis was a median 3.87 years in the experimental arm and 3.72 years in the control arm.
About 60% in both groups had had prior autologous stem cell transplant. Seventy-one percent in the experimental arm and 80% in the control arm had received a prior immunomodulatory drug, and 30% in the experimental arm and 34% in the control arm were refractory to their last line of therapy.
Dr Palumbo pointed out that accrual for the trial was rapid; 500 patients enrolled in 1 year, from September 2014 to September 2015.
“After 3 months, we already saw a difference in terms of efficacy,” he added, and the trial was stopped early. “So the median follow-up is short for this reason,” he explained, “and is around 7 months.”
The discontinuation rate was “as expected,” he said, “higher in the control arm,” with 44% discontinuing compared with 31% in the experimental arm.
Discontinuation for progressive disease was 25% in the control arm and 19% in the experimental arm, “showing already an advantage for the novel combination.”
Adverse events as reasons for discontinuation were 8% in the experimental arm and 10% in the control arm, “showing that the new agent is not adding any extra toxicity to the combination of bortezomib and dexamethasone.”
Efficacy
The “unprecedented” PFS, with a hazard ratio (HR) of 0.39 (95% CI, 0.28-0.53; P<0.0001), translated into a 61% reduction in the risk of disease progression or death for the experimental arm compared with the control arm.
The median PFS was not yet reached in the experimental arm, while the median PFS was 7.2 months in the control arm.
At 1 year, the PFS was 26.9% in the control arm and 60.7% in the experimental arm, “and this translates into a doubling in terms of remission duration for those patients,” Dr Palumbo stated.
“Even better was the outcome for the time to progression,” he said, with an HR of 0.30, “which means a 70% reduction in the risk of disease progression for DVd versus Vd, a more than doubling of time to disease progression.”
PFS by subgroup analysis showed that early intervention with daratumumab maximizes the efficacy of the combination.
For those patients who had received only 1 line of prior treatment, the HR was 0.31 (95% CI, 0.18 – 0.52; P<0.0001), which translated to a 69% reduction in the risk of progression or death for DVd compared with Vd.
The overall response rate revealed the profound cytoreduction achieved by the addition of daratumumab.
The CR rate increased from 9% in the control group to 19% in the experimental arm (P=0.0012), and the VGPR increased from 29% to 59%, in the control and experimental arms, respectively.
“So there is a doubling in the rate of CR and VGPR,” Dr Palumbo pointed out, “and this is quite relevant because more patients do achieve a profound cytoreduction.”
The rate of MRD negativity was 5 times higher for daratumumab-treated patients. Three percent of patients in the control arm were MRD negative (10-4) compared with 14% in the experimental arm.
Time to response, “in my opinion, is an important issue because . . . you can reach PR in around 1 month [with DVd] and this is clinically relevant because those patients are symptomatic,” he explained. “Reaching PR in 1 month means getting rid of pain in a quick way.”
“On the other hand, the achieving of CR requires a prolonged treatment,” he added. “CR is being achieved after 12 months of therapy, and MRD negativity might need even longer treatment.”
Safety
Daratumumab-treated patients experienced more thrombocytopenia and peripheral neuropathy (PN) of any grade than the control arm, 47% compared with 38%, respectively.
“But this is not due to the addition of the third agent,” Dr Palumbo clarified. “This is mainly the consequence, in the experimental arm, that treatment with bortezomib was longer in comparison to the control arm, and therefore, the typical toxicity of bortezomib—thrombocytopenia and PN—were slightly higher.”
There was also an increase in upper respiratory tract infections and cough in daratumumab-treated patients.
Grade 3-4 treatment-emergent adverse events occurring in more than 5% of patients included thrombocytopenia, anemia, neutropenia, lymphopenia, pneumonia, hypertension, and sensory PN.
However, grade 4 thrombocyotpenia, Dr Palumbo noted, did not translate into an increase in bleeding.
The major increase in toxicity due to daratumumab was in infusion-related reactions (IRRs), which occurred in 45% of patients. IRRs were consistent with the infusion of other monoclonal antibodies in cancer patients, he said, and 98% of patients with IRRs experienced them on the first infusion.
Conclusions
Dr Palumbo stressed that daratumumab did not increase the cumulative toxicity or the toxicity of the bortezomib-dexamethasone combination.
Daratumumab significantly improved PFS and the response rate; the experimental combination was associated with a 61% reduction in the risk of progression or death.
The benefit was maintained across different subgroups—whether younger, older, good prognosis, bad prognosis, previously exposed to bortezomib or not exposed to bortezomib.
And DVd doubled both VGPR rates and CR rates.
In a press briefing, Dr Palumbo said that in the myeloma field, “we hope to have our R-CHOP, that has been a major treatment for lymphoma now also available with a different antibody for multiple myeloma.”
So the final conclusion, he added, is that “daratumumab-Vd might be considered today a new standard of care for relapsed and refractory multiple myeloma.”
The study was funded by Janssen Research & Development. ![]()
CHICAGO—The addition of the monoclonal antibody daratumumab to bortezomib and dexamethasone, the current standard of care for relapsed/refractory multiple myeloma (MM), has achieved progression-free survival that is “unprecedented in randomized studies that compared novel treatment” for this disease, according to Antonio Palumbo, MD, lead author of the phase 3 CASTOR study.
Dr Palumbo, of the University of Torino in Torino, Italy, presented the results on behalf of the CASTOR investigators during the plenary session of the 2016 ASCO Annual Meeting (abstract LBA4).
Daratumumab (Darzalex) is a human CD38 monoclonal antibody, which means it is targeted very specifically to the most relevant tumor antigen for plasma cells.
It also has direct major cytotoxic activity through the complement, which translates into major tumor reduction and a profound cytoreduction, Dr Palumbo said.
Even more important, he added, is that this is an immunomodulatory agent able to both increase the T-cell activity in the immune system, which controls the tumor, and also reduce the immunosuppressive regulatory cells that are suppressing the activity of the immune system.
Daratumumab is already approved by the US Food and Drug Administration and conditionally approved by the European Commission as a single agent for the treatment of relapsed/refractory multiple myeloma.
Study design
The CASTOR study was a multicenter, randomized, open-label, active-controlled phase 3 study.
Patients were eligible to enroll if they had relapsed or refractory MM with at least 1 prior line of therapy, which could include prior treatment with bortezomib, but they were not eligible if they were refractory to it.
Investigators randomized 251 patients to the experimental arm of daratumumab, bortezomib (Velcade), and dexamethasone (DVd) and 247 to the control arm of bortezomib and dexamethasone (Vd).
The dosing schedule was the same in both arms for bortezomib and dexamethasone. Patients in the experimental arm received daratumumab (16 mg/kg IV) every week for the first 3 cycles, on day 1 of cycles 4 – 8, and then every 4 weeks until progression.
The primary endpoint of the study was progression-free survival (PFS). Secondary endpoints included time to progression (TTP), overall survival (OS), overall response rate (ORR), very good partial response (VGPR), complete response (CR), minimal residual disease (MRD), time to response, and duration of response.
Patient demographics
Overall, patients had advanced stage disease with a long history of prior treatment.
They were a median age of 64 in both groups, and the time from diagnosis was a median 3.87 years in the experimental arm and 3.72 years in the control arm.
About 60% in both groups had had prior autologous stem cell transplant. Seventy-one percent in the experimental arm and 80% in the control arm had received a prior immunomodulatory drug, and 30% in the experimental arm and 34% in the control arm were refractory to their last line of therapy.
Dr Palumbo pointed out that accrual for the trial was rapid; 500 patients enrolled in 1 year, from September 2014 to September 2015.
“After 3 months, we already saw a difference in terms of efficacy,” he added, and the trial was stopped early. “So the median follow-up is short for this reason,” he explained, “and is around 7 months.”
The discontinuation rate was “as expected,” he said, “higher in the control arm,” with 44% discontinuing compared with 31% in the experimental arm.
Discontinuation for progressive disease was 25% in the control arm and 19% in the experimental arm, “showing already an advantage for the novel combination.”
Adverse events as reasons for discontinuation were 8% in the experimental arm and 10% in the control arm, “showing that the new agent is not adding any extra toxicity to the combination of bortezomib and dexamethasone.”
Efficacy
The “unprecedented” PFS, with a hazard ratio (HR) of 0.39 (95% CI, 0.28-0.53; P<0.0001), translated into a 61% reduction in the risk of disease progression or death for the experimental arm compared with the control arm.
The median PFS was not yet reached in the experimental arm, while the median PFS was 7.2 months in the control arm.
At 1 year, the PFS was 26.9% in the control arm and 60.7% in the experimental arm, “and this translates into a doubling in terms of remission duration for those patients,” Dr Palumbo stated.
“Even better was the outcome for the time to progression,” he said, with an HR of 0.30, “which means a 70% reduction in the risk of disease progression for DVd versus Vd, a more than doubling of time to disease progression.”
PFS by subgroup analysis showed that early intervention with daratumumab maximizes the efficacy of the combination.
For those patients who had received only 1 line of prior treatment, the HR was 0.31 (95% CI, 0.18 – 0.52; P<0.0001), which translated to a 69% reduction in the risk of progression or death for DVd compared with Vd.
The overall response rate revealed the profound cytoreduction achieved by the addition of daratumumab.
The CR rate increased from 9% in the control group to 19% in the experimental arm (P=0.0012), and the VGPR increased from 29% to 59%, in the control and experimental arms, respectively.
“So there is a doubling in the rate of CR and VGPR,” Dr Palumbo pointed out, “and this is quite relevant because more patients do achieve a profound cytoreduction.”
The rate of MRD negativity was 5 times higher for daratumumab-treated patients. Three percent of patients in the control arm were MRD negative (10-4) compared with 14% in the experimental arm.
Time to response, “in my opinion, is an important issue because . . . you can reach PR in around 1 month [with DVd] and this is clinically relevant because those patients are symptomatic,” he explained. “Reaching PR in 1 month means getting rid of pain in a quick way.”
“On the other hand, the achieving of CR requires a prolonged treatment,” he added. “CR is being achieved after 12 months of therapy, and MRD negativity might need even longer treatment.”
Safety
Daratumumab-treated patients experienced more thrombocytopenia and peripheral neuropathy (PN) of any grade than the control arm, 47% compared with 38%, respectively.
“But this is not due to the addition of the third agent,” Dr Palumbo clarified. “This is mainly the consequence, in the experimental arm, that treatment with bortezomib was longer in comparison to the control arm, and therefore, the typical toxicity of bortezomib—thrombocytopenia and PN—were slightly higher.”
There was also an increase in upper respiratory tract infections and cough in daratumumab-treated patients.
Grade 3-4 treatment-emergent adverse events occurring in more than 5% of patients included thrombocytopenia, anemia, neutropenia, lymphopenia, pneumonia, hypertension, and sensory PN.
However, grade 4 thrombocyotpenia, Dr Palumbo noted, did not translate into an increase in bleeding.
The major increase in toxicity due to daratumumab was in infusion-related reactions (IRRs), which occurred in 45% of patients. IRRs were consistent with the infusion of other monoclonal antibodies in cancer patients, he said, and 98% of patients with IRRs experienced them on the first infusion.
Conclusions
Dr Palumbo stressed that daratumumab did not increase the cumulative toxicity or the toxicity of the bortezomib-dexamethasone combination.
Daratumumab significantly improved PFS and the response rate; the experimental combination was associated with a 61% reduction in the risk of progression or death.
The benefit was maintained across different subgroups—whether younger, older, good prognosis, bad prognosis, previously exposed to bortezomib or not exposed to bortezomib.
And DVd doubled both VGPR rates and CR rates.
In a press briefing, Dr Palumbo said that in the myeloma field, “we hope to have our R-CHOP, that has been a major treatment for lymphoma now also available with a different antibody for multiple myeloma.”
So the final conclusion, he added, is that “daratumumab-Vd might be considered today a new standard of care for relapsed and refractory multiple myeloma.”
The study was funded by Janssen Research & Development. ![]()
VIDEO: Daratumumab dramatically improves outcomes of myeloma
CHICAGO – The phase III CASTOR trial tested addition of daratumumab—an anti-CD38 antibody—to bortezomib and dexamethasone in patients with relapsed or refractory multiple myeloma. Compared with the dual therapy, the triple therapy reduced the risk of progression or death by 61%, with little increase in toxicity, according to data reported at the annual meeting of the American Society of Clinical Oncology.
In an interview at the meeting, lead author Dr. Antonio Palumbo fielded key questions: Do some patients benefit more than others? Does the antibody prolong overall survival? And how much will it cost?
Dr. Palumbo is chief of the multiple myeloma Unit at the University of Torino, Italy.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – The phase III CASTOR trial tested addition of daratumumab—an anti-CD38 antibody—to bortezomib and dexamethasone in patients with relapsed or refractory multiple myeloma. Compared with the dual therapy, the triple therapy reduced the risk of progression or death by 61%, with little increase in toxicity, according to data reported at the annual meeting of the American Society of Clinical Oncology.
In an interview at the meeting, lead author Dr. Antonio Palumbo fielded key questions: Do some patients benefit more than others? Does the antibody prolong overall survival? And how much will it cost?
Dr. Palumbo is chief of the multiple myeloma Unit at the University of Torino, Italy.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – The phase III CASTOR trial tested addition of daratumumab—an anti-CD38 antibody—to bortezomib and dexamethasone in patients with relapsed or refractory multiple myeloma. Compared with the dual therapy, the triple therapy reduced the risk of progression or death by 61%, with little increase in toxicity, according to data reported at the annual meeting of the American Society of Clinical Oncology.
In an interview at the meeting, lead author Dr. Antonio Palumbo fielded key questions: Do some patients benefit more than others? Does the antibody prolong overall survival? And how much will it cost?
Dr. Palumbo is chief of the multiple myeloma Unit at the University of Torino, Italy.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE 2016 ASCO ANNUAL MEETING

Lenalidomide maintenance prolongs overall survival after ASCT
CHICAGO – Lenalidomide maintenance therapy significantly prolonged overall survival after autologous stem cell transplant in newly diagnosed multiple myeloma patients, including patients who had a complete response to ASCT, based on a meta-analysis presented at the annual meeting of the American Society of Clinical Oncology.
While several studies have indicated that lenalidomide maintenance reduces the risk of disease progression or death compared to a control group, none of the individual studies were powered to detect a significant improvement in overall survival, said Dr. Philip L. McCarthy, director of the Blood and Marrow Transplant Center at Roswell Park Cancer Institute, Buffalo, N.Y., who is a co-author of the meta-analysis and reported the results on behalf of Dr. Michel Attal of University Hospital, Toulouse, France.

The researchers found that three randomized controlled trials using lenalidomide post-ASCT (IFM 2005-02, CALGB 100104 [Alliance], GIMEMA RV-209) met the criteria of having patient-level data, a control arm, and primary efficacy data for newly-diagnosed patients with multiple myeloma.
After induction and single (82%) or tandem (18%) ASCT, 55% of patients in the meta-analysis had complete or very good partial responses.
From 2005 to 2009, 605 patients received lenalidomide either 10 mg/day on days 1-21 of a 28-day cycle (GIMEMA) or on days 1-28 of a 28-day cycle (IFM and CALGB); 604 patients were in a control group. With a median follow-up of 6.6 years, 491 patients (41%) had died.
Median overall survival was not reached in the lenolidamide group and was 86 months in the control group (HR = 0.74; 95% CI, 0.62-0.89; log-rank P = .001). Survival was longer in the lenolidamine group as compared to the control group at 5 years (71% vs 66%), 6 years (65% vs 58%), and 7 years (62% vs 50%), reported Dr. McCarthy.
Dr. McCarthy receives research funding from Celgene, the maker of Revlimid (lenalidomide); and is a consultant or advisor to and receives honoraria from Binding Site; Bristol-Myers Squibb; Celgene; Janssen; Karyopharm Therapeutics; and Sanofi. Dr. Attal had no disclosures.
On Twitter @maryjodales
CHICAGO – Lenalidomide maintenance therapy significantly prolonged overall survival after autologous stem cell transplant in newly diagnosed multiple myeloma patients, including patients who had a complete response to ASCT, based on a meta-analysis presented at the annual meeting of the American Society of Clinical Oncology.
While several studies have indicated that lenalidomide maintenance reduces the risk of disease progression or death compared to a control group, none of the individual studies were powered to detect a significant improvement in overall survival, said Dr. Philip L. McCarthy, director of the Blood and Marrow Transplant Center at Roswell Park Cancer Institute, Buffalo, N.Y., who is a co-author of the meta-analysis and reported the results on behalf of Dr. Michel Attal of University Hospital, Toulouse, France.
The researchers found that three randomized controlled trials using lenalidomide post-ASCT (IFM 2005-02, CALGB 100104 [Alliance], GIMEMA RV-209) met the criteria of having patient-level data, a control arm, and primary efficacy data for newly-diagnosed patients with multiple myeloma.
After induction and single (82%) or tandem (18%) ASCT, 55% of patients in the meta-analysis had complete or very good partial responses.
From 2005 to 2009, 605 patients received lenalidomide either 10 mg/day on days 1-21 of a 28-day cycle (GIMEMA) or on days 1-28 of a 28-day cycle (IFM and CALGB); 604 patients were in a control group. With a median follow-up of 6.6 years, 491 patients (41%) had died.
Median overall survival was not reached in the lenolidamide group and was 86 months in the control group (HR = 0.74; 95% CI, 0.62-0.89; log-rank P = .001). Survival was longer in the lenolidamine group as compared to the control group at 5 years (71% vs 66%), 6 years (65% vs 58%), and 7 years (62% vs 50%), reported Dr. McCarthy.
Dr. McCarthy receives research funding from Celgene, the maker of Revlimid (lenalidomide); and is a consultant or advisor to and receives honoraria from Binding Site; Bristol-Myers Squibb; Celgene; Janssen; Karyopharm Therapeutics; and Sanofi. Dr. Attal had no disclosures.
On Twitter @maryjodales
CHICAGO – Lenalidomide maintenance therapy significantly prolonged overall survival after autologous stem cell transplant in newly diagnosed multiple myeloma patients, including patients who had a complete response to ASCT, based on a meta-analysis presented at the annual meeting of the American Society of Clinical Oncology.
While several studies have indicated that lenalidomide maintenance reduces the risk of disease progression or death compared to a control group, none of the individual studies were powered to detect a significant improvement in overall survival, said Dr. Philip L. McCarthy, director of the Blood and Marrow Transplant Center at Roswell Park Cancer Institute, Buffalo, N.Y., who is a co-author of the meta-analysis and reported the results on behalf of Dr. Michel Attal of University Hospital, Toulouse, France.
The researchers found that three randomized controlled trials using lenalidomide post-ASCT (IFM 2005-02, CALGB 100104 [Alliance], GIMEMA RV-209) met the criteria of having patient-level data, a control arm, and primary efficacy data for newly-diagnosed patients with multiple myeloma.
After induction and single (82%) or tandem (18%) ASCT, 55% of patients in the meta-analysis had complete or very good partial responses.
From 2005 to 2009, 605 patients received lenalidomide either 10 mg/day on days 1-21 of a 28-day cycle (GIMEMA) or on days 1-28 of a 28-day cycle (IFM and CALGB); 604 patients were in a control group. With a median follow-up of 6.6 years, 491 patients (41%) had died.
Median overall survival was not reached in the lenolidamide group and was 86 months in the control group (HR = 0.74; 95% CI, 0.62-0.89; log-rank P = .001). Survival was longer in the lenolidamine group as compared to the control group at 5 years (71% vs 66%), 6 years (65% vs 58%), and 7 years (62% vs 50%), reported Dr. McCarthy.
Dr. McCarthy receives research funding from Celgene, the maker of Revlimid (lenalidomide); and is a consultant or advisor to and receives honoraria from Binding Site; Bristol-Myers Squibb; Celgene; Janssen; Karyopharm Therapeutics; and Sanofi. Dr. Attal had no disclosures.
On Twitter @maryjodales
AT ASCO 2016
Key clinical point: Lenalidomide maintenance therapy significantly prolonged overall survival after autologous stem cell transplant in newly diagnosed multiple myeloma patients.
Major finding: Median overall survival was not reached in the lenolidamide group and was 86 months in the control group (HR = 0.74; 95% CI, 0.62-0.89; log-rank P = .001).
Data source: Meta-analysis of 1,209 patients in three randomized controlled trials using lenalidomide post-ASCT (IFM 2005-02, CALGB 100104 [Alliance], GIMEMA RV-209).
Disclosures: Dr. McCarthy receives research funding from Celgene, the maker of Revlimid (lenalidomide); and is a consultant or advisor to and receives honoraria from Binding Site; Bristol-Myers Squibb; Celgene; Janssen; Karyopharm Therapeutics; and Sanofi. Dr. Attal had no disclosures.

Up-front ASCT superior for fit patients with newly diagnosed myeloma
CHICAGO – Up-front high-dose melphalan and autologous stem cell transplantation (ASCT) was superior to bortezomib-melphalan-prednisone (VMP) for fit patients younger than age 65 years with newly diagnosed multiple myeloma, based on the interim results from a randomized study of the European Myeloma Network.
With more than 1,200 patients, the study is the largest trial yet to show superior progression-free survival for ASCT. Follow-up has been too short to show significance for overall survival.
“Up-front ASCT was associated with a significant improvement in progression-free survival as compared to bortezomib-melphalan-prednisone in the overall patient population, (and the advantage) was retained across prespecified subgroups of patients at low and high risk … (as well as) in a multivariate analysis” of the overall population, Dr. Michele Cavo of the University of Bologna, Italy, reported at the annual meeting of the American Society of Clinical Oncology. “Up-front high-dose melphalan and ASCT continue to be the reference treatment choice for fit patients with newly diagnosed multiple myeloma, even in the novel agent era.”
ASCT was associated with higher rates of grade 3 or more adverse events in nearly every category, however, with the exception of peripheral nephropathy.
For the study, 1,266 patients, stratified by International Staging System stage and FISH (fluorescence in situ hybridization) analysis, were randomized to either VMP (512 pts) or to high-dose melphalan and ASCT (754 pts). At the meeting, Dr. Cavo reported on the study’s interim outcome results in 695 patients who had ASCT and 497 newly diagnosed patients who received VMP.
At 3 years, progression-free survival rates were 66.1% in the ASCT patients and 57.5% in the VMP patients. The median progression-free survival had not yet been reached in the ASCT patients and was 44 months in the bortezomib-melphalan-prednisone patients. (hazard ratio, 95% confidence interval, 0.73 [0.59-0.90]; P = .003).
Stringent complete responses were seen in 18.2% of patients in the VMP group and 17% of the ASCT group; Complete responses occurred in 25.3% of both groups. The main difference observed was in the number of very good partial responses, seen in 30.4% of the VMP group and in 43.2% of the ASCT group. Also, 11.2% of those in the VMP group had less than a partial response while that was the case for only 3.3% of the ASCT group.
Alternatively, the rate of grade 3 or more adverse events was higher in the ASCT group, with 17.5% experiencing febrile neutropenia, 15.6% mucositis, 3.2% sepsis, and 2.6% respiratory infections. The rates of these side effects in the VMP group were 0.2%, 0%, 0%, and 1.7%, respectively. The only grade 3 or more adverse event seen with greater frequency in the VMP group was peripheral neuropathy, seen in 13.8% as compared with 1.6% in the ASCT group.
Dr. Cavo receives honoraria from Amgen, Bristol-Myers Squibb, Celgene, Janssen, and Takeda. He serves as a consultant or advisor to and is on the speakers bureau for Amgen. Celgene, Janssen.
On Twitter @maryjodales
This story was updated on June 10, 2016.
Although novel drug combinations have become a standard of care for newly diagnosed multiple myeloma patients, high-dose melphalan and ASCT improve the depth of remission, regardless of the induction regimen. Four trials comparing differing induction and consolidation regimens to one or more ASCTs now have shown significantly improved progression-free survival. Two of the trials have more than 36 months of follow-up.
Dr. William Bensinger is with the Fred Hutchinson Cancer Research Center and the Swedish Cancer Institute in Seattle.
Although novel drug combinations have become a standard of care for newly diagnosed multiple myeloma patients, high-dose melphalan and ASCT improve the depth of remission, regardless of the induction regimen. Four trials comparing differing induction and consolidation regimens to one or more ASCTs now have shown significantly improved progression-free survival. Two of the trials have more than 36 months of follow-up.
Dr. William Bensinger is with the Fred Hutchinson Cancer Research Center and the Swedish Cancer Institute in Seattle.
Although novel drug combinations have become a standard of care for newly diagnosed multiple myeloma patients, high-dose melphalan and ASCT improve the depth of remission, regardless of the induction regimen. Four trials comparing differing induction and consolidation regimens to one or more ASCTs now have shown significantly improved progression-free survival. Two of the trials have more than 36 months of follow-up.
Dr. William Bensinger is with the Fred Hutchinson Cancer Research Center and the Swedish Cancer Institute in Seattle.
CHICAGO – Up-front high-dose melphalan and autologous stem cell transplantation (ASCT) was superior to bortezomib-melphalan-prednisone (VMP) for fit patients younger than age 65 years with newly diagnosed multiple myeloma, based on the interim results from a randomized study of the European Myeloma Network.
With more than 1,200 patients, the study is the largest trial yet to show superior progression-free survival for ASCT. Follow-up has been too short to show significance for overall survival.
“Up-front ASCT was associated with a significant improvement in progression-free survival as compared to bortezomib-melphalan-prednisone in the overall patient population, (and the advantage) was retained across prespecified subgroups of patients at low and high risk … (as well as) in a multivariate analysis” of the overall population, Dr. Michele Cavo of the University of Bologna, Italy, reported at the annual meeting of the American Society of Clinical Oncology. “Up-front high-dose melphalan and ASCT continue to be the reference treatment choice for fit patients with newly diagnosed multiple myeloma, even in the novel agent era.”
ASCT was associated with higher rates of grade 3 or more adverse events in nearly every category, however, with the exception of peripheral nephropathy.
For the study, 1,266 patients, stratified by International Staging System stage and FISH (fluorescence in situ hybridization) analysis, were randomized to either VMP (512 pts) or to high-dose melphalan and ASCT (754 pts). At the meeting, Dr. Cavo reported on the study’s interim outcome results in 695 patients who had ASCT and 497 newly diagnosed patients who received VMP.
At 3 years, progression-free survival rates were 66.1% in the ASCT patients and 57.5% in the VMP patients. The median progression-free survival had not yet been reached in the ASCT patients and was 44 months in the bortezomib-melphalan-prednisone patients. (hazard ratio, 95% confidence interval, 0.73 [0.59-0.90]; P = .003).
Stringent complete responses were seen in 18.2% of patients in the VMP group and 17% of the ASCT group; Complete responses occurred in 25.3% of both groups. The main difference observed was in the number of very good partial responses, seen in 30.4% of the VMP group and in 43.2% of the ASCT group. Also, 11.2% of those in the VMP group had less than a partial response while that was the case for only 3.3% of the ASCT group.
Alternatively, the rate of grade 3 or more adverse events was higher in the ASCT group, with 17.5% experiencing febrile neutropenia, 15.6% mucositis, 3.2% sepsis, and 2.6% respiratory infections. The rates of these side effects in the VMP group were 0.2%, 0%, 0%, and 1.7%, respectively. The only grade 3 or more adverse event seen with greater frequency in the VMP group was peripheral neuropathy, seen in 13.8% as compared with 1.6% in the ASCT group.
Dr. Cavo receives honoraria from Amgen, Bristol-Myers Squibb, Celgene, Janssen, and Takeda. He serves as a consultant or advisor to and is on the speakers bureau for Amgen. Celgene, Janssen.
On Twitter @maryjodales
This story was updated on June 10, 2016.
CHICAGO – Up-front high-dose melphalan and autologous stem cell transplantation (ASCT) was superior to bortezomib-melphalan-prednisone (VMP) for fit patients younger than age 65 years with newly diagnosed multiple myeloma, based on the interim results from a randomized study of the European Myeloma Network.
With more than 1,200 patients, the study is the largest trial yet to show superior progression-free survival for ASCT. Follow-up has been too short to show significance for overall survival.
“Up-front ASCT was associated with a significant improvement in progression-free survival as compared to bortezomib-melphalan-prednisone in the overall patient population, (and the advantage) was retained across prespecified subgroups of patients at low and high risk … (as well as) in a multivariate analysis” of the overall population, Dr. Michele Cavo of the University of Bologna, Italy, reported at the annual meeting of the American Society of Clinical Oncology. “Up-front high-dose melphalan and ASCT continue to be the reference treatment choice for fit patients with newly diagnosed multiple myeloma, even in the novel agent era.”
ASCT was associated with higher rates of grade 3 or more adverse events in nearly every category, however, with the exception of peripheral nephropathy.
For the study, 1,266 patients, stratified by International Staging System stage and FISH (fluorescence in situ hybridization) analysis, were randomized to either VMP (512 pts) or to high-dose melphalan and ASCT (754 pts). At the meeting, Dr. Cavo reported on the study’s interim outcome results in 695 patients who had ASCT and 497 newly diagnosed patients who received VMP.
At 3 years, progression-free survival rates were 66.1% in the ASCT patients and 57.5% in the VMP patients. The median progression-free survival had not yet been reached in the ASCT patients and was 44 months in the bortezomib-melphalan-prednisone patients. (hazard ratio, 95% confidence interval, 0.73 [0.59-0.90]; P = .003).
Stringent complete responses were seen in 18.2% of patients in the VMP group and 17% of the ASCT group; Complete responses occurred in 25.3% of both groups. The main difference observed was in the number of very good partial responses, seen in 30.4% of the VMP group and in 43.2% of the ASCT group. Also, 11.2% of those in the VMP group had less than a partial response while that was the case for only 3.3% of the ASCT group.
Alternatively, the rate of grade 3 or more adverse events was higher in the ASCT group, with 17.5% experiencing febrile neutropenia, 15.6% mucositis, 3.2% sepsis, and 2.6% respiratory infections. The rates of these side effects in the VMP group were 0.2%, 0%, 0%, and 1.7%, respectively. The only grade 3 or more adverse event seen with greater frequency in the VMP group was peripheral neuropathy, seen in 13.8% as compared with 1.6% in the ASCT group.
Dr. Cavo receives honoraria from Amgen, Bristol-Myers Squibb, Celgene, Janssen, and Takeda. He serves as a consultant or advisor to and is on the speakers bureau for Amgen. Celgene, Janssen.
On Twitter @maryjodales
This story was updated on June 10, 2016.
AT THE 2016 ASCO ANNUAL MEETING
Key clinical point: Up-front high-dose melphalan and autologous stem cell transplantation was superior to bortezomib-melphalan-prednisone for fit patients under age 65 years with newly diagnosed multiple myeloma.
Major finding: At 3 years of follow-up, progression-free survival rates were 66.1% in the ASCT patients and 57.5% in the bortezomib-melphalan-prednisone patients.
Data source: Interim results from a randomized study of over 1200 patients in the European Myeloma Network.
Disclosures: Dr. Cavo receives honoraria from Amgen, Bristol-Myers Squibb, Celgene, Janssen, and Takeda. He serves as a consultant or advisor to and is on the speakers bureau for Amgen. Celgene, Janssen.
CHMP advises against approving MM drug

multiple myeloma
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has advised the European Commission not to approve ixazomib (Ninlaro), an oral proteasome inhibitor, as a treatment for patients with relapsed and/or refractory multiple myeloma (MM).
Takeda Pharmaceutical Company Limited, the company developing ixazomib, said it intends to appeal this opinion and request a re-examination by the CHMP.
“We are disappointed by the CHMP’s opinion,” said Christophe Bianchi, MD, president of Takeda Oncology. “With the support of European key medical experts, we will continue our efforts working closely with the CHMP to make Ninlaro—the first oral proteasome inhibitor—available for patients in Europe.”
“We stand behind the TOURMALINE-MM1 trial data, which were recently published in the New England Journal of Medicine and demonstrated a significant extension in progression-free survival for Ninlaro plus lenalidomide and dexamethasone versus placebo plus lenalidomide and dexamethasone and a favorable benefit-risk profile.”
TOURMALINE-MM1
The trial enrolled 722 patients with relapsed (77%), refractory (11%), relapsed and refractory (12%), or primary refractory (6%) MM.
The patients were randomized to receive ixazomib, lenalidomide, and dexamethasone (IRd, n=360) or placebo, lenalidomide, and dexamethasone (Rd, n=362). Baseline patient characteristics were similar between the treatment arms.
The study’s primary endpoint was progression-free survival, which was significantly longer in the IRd arm than the Rd arm. The median progression-free survival was 20.6 months and 14.7 months, respectively. The hazard ratio was 0.74 (P=0.01).
At a median follow-up of about 23 months, the median overall survival had not been reached in either treatment arm.
Adverse events (AEs) occurred in 98% of patients in the IRd arm and 99% in the Rd arm. Grade 3 or higher AEs occurred in 74% and 69% of patients, respectively; serious AEs occurred in 47% and 49%, respectively; and on-study deaths occurred in 4% and 6%, respectively.
Grade 3 and 4 thrombocytopenia, rash, and gastrointestinal AEs were more frequent in the IRd arm than the Rd arm.
The incidence of peripheral neuropathy was similar in the 2 arms, as was the percentage patients who developed new primary malignant tumors. ![]()
multiple myeloma
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has advised the European Commission not to approve ixazomib (Ninlaro), an oral proteasome inhibitor, as a treatment for patients with relapsed and/or refractory multiple myeloma (MM).
Takeda Pharmaceutical Company Limited, the company developing ixazomib, said it intends to appeal this opinion and request a re-examination by the CHMP.
“We are disappointed by the CHMP’s opinion,” said Christophe Bianchi, MD, president of Takeda Oncology. “With the support of European key medical experts, we will continue our efforts working closely with the CHMP to make Ninlaro—the first oral proteasome inhibitor—available for patients in Europe.”
“We stand behind the TOURMALINE-MM1 trial data, which were recently published in the New England Journal of Medicine and demonstrated a significant extension in progression-free survival for Ninlaro plus lenalidomide and dexamethasone versus placebo plus lenalidomide and dexamethasone and a favorable benefit-risk profile.”
TOURMALINE-MM1
The trial enrolled 722 patients with relapsed (77%), refractory (11%), relapsed and refractory (12%), or primary refractory (6%) MM.
The patients were randomized to receive ixazomib, lenalidomide, and dexamethasone (IRd, n=360) or placebo, lenalidomide, and dexamethasone (Rd, n=362). Baseline patient characteristics were similar between the treatment arms.
The study’s primary endpoint was progression-free survival, which was significantly longer in the IRd arm than the Rd arm. The median progression-free survival was 20.6 months and 14.7 months, respectively. The hazard ratio was 0.74 (P=0.01).
At a median follow-up of about 23 months, the median overall survival had not been reached in either treatment arm.
Adverse events (AEs) occurred in 98% of patients in the IRd arm and 99% in the Rd arm. Grade 3 or higher AEs occurred in 74% and 69% of patients, respectively; serious AEs occurred in 47% and 49%, respectively; and on-study deaths occurred in 4% and 6%, respectively.
Grade 3 and 4 thrombocytopenia, rash, and gastrointestinal AEs were more frequent in the IRd arm than the Rd arm.
The incidence of peripheral neuropathy was similar in the 2 arms, as was the percentage patients who developed new primary malignant tumors. ![]()
multiple myeloma
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has advised the European Commission not to approve ixazomib (Ninlaro), an oral proteasome inhibitor, as a treatment for patients with relapsed and/or refractory multiple myeloma (MM).
Takeda Pharmaceutical Company Limited, the company developing ixazomib, said it intends to appeal this opinion and request a re-examination by the CHMP.
“We are disappointed by the CHMP’s opinion,” said Christophe Bianchi, MD, president of Takeda Oncology. “With the support of European key medical experts, we will continue our efforts working closely with the CHMP to make Ninlaro—the first oral proteasome inhibitor—available for patients in Europe.”
“We stand behind the TOURMALINE-MM1 trial data, which were recently published in the New England Journal of Medicine and demonstrated a significant extension in progression-free survival for Ninlaro plus lenalidomide and dexamethasone versus placebo plus lenalidomide and dexamethasone and a favorable benefit-risk profile.”
TOURMALINE-MM1
The trial enrolled 722 patients with relapsed (77%), refractory (11%), relapsed and refractory (12%), or primary refractory (6%) MM.
The patients were randomized to receive ixazomib, lenalidomide, and dexamethasone (IRd, n=360) or placebo, lenalidomide, and dexamethasone (Rd, n=362). Baseline patient characteristics were similar between the treatment arms.
The study’s primary endpoint was progression-free survival, which was significantly longer in the IRd arm than the Rd arm. The median progression-free survival was 20.6 months and 14.7 months, respectively. The hazard ratio was 0.74 (P=0.01).
At a median follow-up of about 23 months, the median overall survival had not been reached in either treatment arm.
Adverse events (AEs) occurred in 98% of patients in the IRd arm and 99% in the Rd arm. Grade 3 or higher AEs occurred in 74% and 69% of patients, respectively; serious AEs occurred in 47% and 49%, respectively; and on-study deaths occurred in 4% and 6%, respectively.
Grade 3 and 4 thrombocytopenia, rash, and gastrointestinal AEs were more frequent in the IRd arm than the Rd arm.
The incidence of peripheral neuropathy was similar in the 2 arms, as was the percentage patients who developed new primary malignant tumors. ![]()
Why patients don’t report possible cancer symptoms

Photo courtesy of NIH
Worrying about wasting their doctor’s time is stopping people from reporting symptoms that might be related to cancer, according to a small study published in the British Journal of General Practice.
The goal of the study was to determine why some people are more likely than others to worry about wasting a general practitioner’s (GP’s) time and delay reporting possible cancer symptoms.
“People worrying about wasting their doctor’s time is one of the challenges we need to tackle when thinking about trying to diagnose cancer earlier,” said study author Katriina Whitaker, PhD, of the University of Surrey in the UK.
“We need to get to the root of the problem and find out why people are feeling worried. Not a lot of work has been done on this so far. Our study draws attention to some reasons patients put off going to their GP to check out possible cancer symptoms.”
For this study, Dr Whitaker and her colleagues conducted interviews with subjects in London, South East England, and North West England.
The subjects were recruited from a sample of 2042 adults, age 50 and older, who completed a survey that included a list of “cancer alarm symptoms.”
Ultimately, the researchers interviewed 62 subjects who had reported symptoms at baseline, were still present at the 3-month follow-up, and had agreed to be contacted.
The interviews revealed a few reasons why subjects were hesitant to report symptoms to their GP.
Some subjects felt that long waiting times for appointments indicated GPs were very busy, so they shouldn’t bother making an appointment unless symptoms seemed very serious.
Other subjects felt that seeking help when their symptoms did not seem serious—ie, persistent, worsening, or life-threatening—was a waste of a doctor’s time.
Still other subjects were hesitant to seek help because their doctors had been dismissive about symptoms in the past.
On the other hand, subjects who reported positive interactions with GPs or good relationships with them were less worried about time-wasting.
And other subjects weren’t worried about wasting their doctor’s time because they think of GPs as fulfilling a service financed by taxpayers.
“We’ve all had times where we’ve wondered if we should go to see a GP, but getting unusual or persistent changes checked out is really important,” said Julie Sharp, head of health and patient information at Cancer Research UK, which funded this study.
“Worrying about wasting a GP’s time should not put people off. Doctors are there to help spot cancer symptoms early when treatment is more likely to be successful, and delaying a visit could save up bigger problems for later. So if you’ve noticed anything that isn’t normal for you, make an appointment to see your doctor.” ![]()
Photo courtesy of NIH
Worrying about wasting their doctor’s time is stopping people from reporting symptoms that might be related to cancer, according to a small study published in the British Journal of General Practice.
The goal of the study was to determine why some people are more likely than others to worry about wasting a general practitioner’s (GP’s) time and delay reporting possible cancer symptoms.
“People worrying about wasting their doctor’s time is one of the challenges we need to tackle when thinking about trying to diagnose cancer earlier,” said study author Katriina Whitaker, PhD, of the University of Surrey in the UK.
“We need to get to the root of the problem and find out why people are feeling worried. Not a lot of work has been done on this so far. Our study draws attention to some reasons patients put off going to their GP to check out possible cancer symptoms.”
For this study, Dr Whitaker and her colleagues conducted interviews with subjects in London, South East England, and North West England.
The subjects were recruited from a sample of 2042 adults, age 50 and older, who completed a survey that included a list of “cancer alarm symptoms.”
Ultimately, the researchers interviewed 62 subjects who had reported symptoms at baseline, were still present at the 3-month follow-up, and had agreed to be contacted.
The interviews revealed a few reasons why subjects were hesitant to report symptoms to their GP.
Some subjects felt that long waiting times for appointments indicated GPs were very busy, so they shouldn’t bother making an appointment unless symptoms seemed very serious.
Other subjects felt that seeking help when their symptoms did not seem serious—ie, persistent, worsening, or life-threatening—was a waste of a doctor’s time.
Still other subjects were hesitant to seek help because their doctors had been dismissive about symptoms in the past.
On the other hand, subjects who reported positive interactions with GPs or good relationships with them were less worried about time-wasting.
And other subjects weren’t worried about wasting their doctor’s time because they think of GPs as fulfilling a service financed by taxpayers.
“We’ve all had times where we’ve wondered if we should go to see a GP, but getting unusual or persistent changes checked out is really important,” said Julie Sharp, head of health and patient information at Cancer Research UK, which funded this study.
“Worrying about wasting a GP’s time should not put people off. Doctors are there to help spot cancer symptoms early when treatment is more likely to be successful, and delaying a visit could save up bigger problems for later. So if you’ve noticed anything that isn’t normal for you, make an appointment to see your doctor.” ![]()
Photo courtesy of NIH
Worrying about wasting their doctor’s time is stopping people from reporting symptoms that might be related to cancer, according to a small study published in the British Journal of General Practice.
The goal of the study was to determine why some people are more likely than others to worry about wasting a general practitioner’s (GP’s) time and delay reporting possible cancer symptoms.
“People worrying about wasting their doctor’s time is one of the challenges we need to tackle when thinking about trying to diagnose cancer earlier,” said study author Katriina Whitaker, PhD, of the University of Surrey in the UK.
“We need to get to the root of the problem and find out why people are feeling worried. Not a lot of work has been done on this so far. Our study draws attention to some reasons patients put off going to their GP to check out possible cancer symptoms.”
For this study, Dr Whitaker and her colleagues conducted interviews with subjects in London, South East England, and North West England.
The subjects were recruited from a sample of 2042 adults, age 50 and older, who completed a survey that included a list of “cancer alarm symptoms.”
Ultimately, the researchers interviewed 62 subjects who had reported symptoms at baseline, were still present at the 3-month follow-up, and had agreed to be contacted.
The interviews revealed a few reasons why subjects were hesitant to report symptoms to their GP.
Some subjects felt that long waiting times for appointments indicated GPs were very busy, so they shouldn’t bother making an appointment unless symptoms seemed very serious.
Other subjects felt that seeking help when their symptoms did not seem serious—ie, persistent, worsening, or life-threatening—was a waste of a doctor’s time.
Still other subjects were hesitant to seek help because their doctors had been dismissive about symptoms in the past.
On the other hand, subjects who reported positive interactions with GPs or good relationships with them were less worried about time-wasting.
And other subjects weren’t worried about wasting their doctor’s time because they think of GPs as fulfilling a service financed by taxpayers.
“We’ve all had times where we’ve wondered if we should go to see a GP, but getting unusual or persistent changes checked out is really important,” said Julie Sharp, head of health and patient information at Cancer Research UK, which funded this study.
“Worrying about wasting a GP’s time should not put people off. Doctors are there to help spot cancer symptoms early when treatment is more likely to be successful, and delaying a visit could save up bigger problems for later. So if you’ve noticed anything that isn’t normal for you, make an appointment to see your doctor.” ![]()
ASCT still a player for multiple myeloma
Even in this era of novel therapies for multiple myeloma, for patients with newly diagnosed disease, autologous stem cell transplant (ASCT) after chemotherapy provides benefits in terms of disease progression and extent of response, compared with chemotherapy alone. The benefit of ASCT was especially pronounced among certain groups of high-risk patients.
Novel proteasome inhibitors and immunomodulators “have dramatically increased the complete response rate and significantly extended progression-free survival and overall survival in previously untreated multiple myeloma patients,” Dr. Michele Cavo, head of the Seragnoli Institute of Hematology at the University of Bologna School of Medicine in Italy, said at a presscast in advance of the annual meeting of the American Society of Clinical Oncology.
But questions remain about how these newer agents perform, compared with high-dose melphalan (HDM) followed by ASCT, traditionally seen as the standard of care for younger and fit patients with newly diagnosed disease.
EMN02/HO95 is a large, prospective, multicenter, intergroup, randomized phase III study that addresses this question, as well as single vs. double ASCT and the use of consolidation therapy or not. The study includes patients 65 years old or younger, and the trial protocol involves induction therapy with bortezomib (Velcade)–cyclophosphamide-dexamethasone (VCD) and subsequent collection of peripheral blood stem cells.
Patients were then randomly assigned to receive bortezomib-melphalan-prednisone (VMP) or HDM as intensification therapy in centers that had a single ASCT policy. For those centers doing double (tandem) ASCT procedures, the randomization was to VMP vs. HDM + single ASCT vs. HDM + double ASCT.
Patients in each treatment arm then underwent another randomization to consolidation therapy with bortezomib-lenalidomide (Revlimid)–dexamethasone or no consolidation. All patients received lenalidomide maintenance until disease progression or toxicity. At the time of a preliminary analysis of trial data in January 2016, results from the second randomization to consolidation or no consolidation therapy were not yet complete. This first prespecified interim analysis was performed after at least 33% of the required events had occurred.
Early results show ASCT benefit
Early results on 1,266 patients (VMP, n = 512; HDM, n = 754) show that a median progression-free survival (PFS) was not yet reached after a median follow-up of 23.9 months from the first randomization (to VMP vs. HDM+ASCT), the primary endpoint of the trial.
In the overall patient population, patients achieved a significant 24% benefit in PFS when given HDM+ASCT up front (hazard ratio, 0.76 vs. VMP), and this benefit extended to certain patient subgroups, as well.
“PFS benefit with bortezomib-based ASCT was of relevance for patients at high risk of early relapse, in particular for those with revised ISS [International Staging System] stage III and high-risk cytogenetic profiles, who had a relative reduction in the risk of progression or death of 48% and 28%, respectively,” Dr. Cavo said.
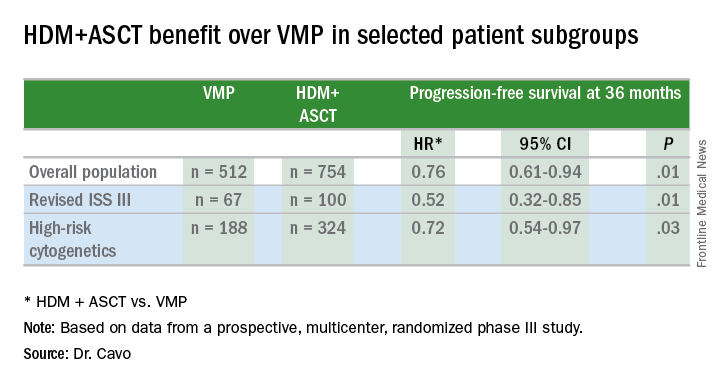
Other predictors of longer PFS were ISS stage I (HR, 0.44; 95% confidence interval, 0.28-067; P less than .0001), standard risk cytogenetics (HR, 0.57; 95% CI, 0.41-0.78; P less than .0001), randomization to the HDM+ASCT arm (HR, 0.61; 95% CI, 0.45-0.82; P = .001), and less than 60% bone marrow plasma cells (HR, 0.67; 95% CI, 0.48-0.99; P = .014).
More patients receiving ASCT up front had a significantly greater reduction in tumor volume of at least 90%, as indicated by the composite of very good partial remission, complete response, and stringent complete response, which was achieved in 74.0% in the VMP arm and in 84.4% of the HDM+ASCT arm (P less than .0001).
For patients at low risk of relapse, Dr. Cavo said longer follow up will be needed to compare the different arms of the study, and future analyses will delineate the effects of consolidation or no consolidation therapy and the use of the VMP regimen, compared with single or double ASCT.
ASCO president Dr. Julie Vose said that even with effective novel agents available, older, proven approaches still retain their value. “This study demonstrated that combining the best of both worlds – initial therapy with a novel agent followed by stem cell transplant – resulted in the best patient outcomes,” she said.
Even in this era of novel therapies for multiple myeloma, for patients with newly diagnosed disease, autologous stem cell transplant (ASCT) after chemotherapy provides benefits in terms of disease progression and extent of response, compared with chemotherapy alone. The benefit of ASCT was especially pronounced among certain groups of high-risk patients.
Novel proteasome inhibitors and immunomodulators “have dramatically increased the complete response rate and significantly extended progression-free survival and overall survival in previously untreated multiple myeloma patients,” Dr. Michele Cavo, head of the Seragnoli Institute of Hematology at the University of Bologna School of Medicine in Italy, said at a presscast in advance of the annual meeting of the American Society of Clinical Oncology.
But questions remain about how these newer agents perform, compared with high-dose melphalan (HDM) followed by ASCT, traditionally seen as the standard of care for younger and fit patients with newly diagnosed disease.
EMN02/HO95 is a large, prospective, multicenter, intergroup, randomized phase III study that addresses this question, as well as single vs. double ASCT and the use of consolidation therapy or not. The study includes patients 65 years old or younger, and the trial protocol involves induction therapy with bortezomib (Velcade)–cyclophosphamide-dexamethasone (VCD) and subsequent collection of peripheral blood stem cells.
Patients were then randomly assigned to receive bortezomib-melphalan-prednisone (VMP) or HDM as intensification therapy in centers that had a single ASCT policy. For those centers doing double (tandem) ASCT procedures, the randomization was to VMP vs. HDM + single ASCT vs. HDM + double ASCT.
Patients in each treatment arm then underwent another randomization to consolidation therapy with bortezomib-lenalidomide (Revlimid)–dexamethasone or no consolidation. All patients received lenalidomide maintenance until disease progression or toxicity. At the time of a preliminary analysis of trial data in January 2016, results from the second randomization to consolidation or no consolidation therapy were not yet complete. This first prespecified interim analysis was performed after at least 33% of the required events had occurred.
Early results show ASCT benefit
Early results on 1,266 patients (VMP, n = 512; HDM, n = 754) show that a median progression-free survival (PFS) was not yet reached after a median follow-up of 23.9 months from the first randomization (to VMP vs. HDM+ASCT), the primary endpoint of the trial.
In the overall patient population, patients achieved a significant 24% benefit in PFS when given HDM+ASCT up front (hazard ratio, 0.76 vs. VMP), and this benefit extended to certain patient subgroups, as well.
“PFS benefit with bortezomib-based ASCT was of relevance for patients at high risk of early relapse, in particular for those with revised ISS [International Staging System] stage III and high-risk cytogenetic profiles, who had a relative reduction in the risk of progression or death of 48% and 28%, respectively,” Dr. Cavo said.
Other predictors of longer PFS were ISS stage I (HR, 0.44; 95% confidence interval, 0.28-067; P less than .0001), standard risk cytogenetics (HR, 0.57; 95% CI, 0.41-0.78; P less than .0001), randomization to the HDM+ASCT arm (HR, 0.61; 95% CI, 0.45-0.82; P = .001), and less than 60% bone marrow plasma cells (HR, 0.67; 95% CI, 0.48-0.99; P = .014).
More patients receiving ASCT up front had a significantly greater reduction in tumor volume of at least 90%, as indicated by the composite of very good partial remission, complete response, and stringent complete response, which was achieved in 74.0% in the VMP arm and in 84.4% of the HDM+ASCT arm (P less than .0001).
For patients at low risk of relapse, Dr. Cavo said longer follow up will be needed to compare the different arms of the study, and future analyses will delineate the effects of consolidation or no consolidation therapy and the use of the VMP regimen, compared with single or double ASCT.
ASCO president Dr. Julie Vose said that even with effective novel agents available, older, proven approaches still retain their value. “This study demonstrated that combining the best of both worlds – initial therapy with a novel agent followed by stem cell transplant – resulted in the best patient outcomes,” she said.
Even in this era of novel therapies for multiple myeloma, for patients with newly diagnosed disease, autologous stem cell transplant (ASCT) after chemotherapy provides benefits in terms of disease progression and extent of response, compared with chemotherapy alone. The benefit of ASCT was especially pronounced among certain groups of high-risk patients.
Novel proteasome inhibitors and immunomodulators “have dramatically increased the complete response rate and significantly extended progression-free survival and overall survival in previously untreated multiple myeloma patients,” Dr. Michele Cavo, head of the Seragnoli Institute of Hematology at the University of Bologna School of Medicine in Italy, said at a presscast in advance of the annual meeting of the American Society of Clinical Oncology.
But questions remain about how these newer agents perform, compared with high-dose melphalan (HDM) followed by ASCT, traditionally seen as the standard of care for younger and fit patients with newly diagnosed disease.
EMN02/HO95 is a large, prospective, multicenter, intergroup, randomized phase III study that addresses this question, as well as single vs. double ASCT and the use of consolidation therapy or not. The study includes patients 65 years old or younger, and the trial protocol involves induction therapy with bortezomib (Velcade)–cyclophosphamide-dexamethasone (VCD) and subsequent collection of peripheral blood stem cells.
Patients were then randomly assigned to receive bortezomib-melphalan-prednisone (VMP) or HDM as intensification therapy in centers that had a single ASCT policy. For those centers doing double (tandem) ASCT procedures, the randomization was to VMP vs. HDM + single ASCT vs. HDM + double ASCT.
Patients in each treatment arm then underwent another randomization to consolidation therapy with bortezomib-lenalidomide (Revlimid)–dexamethasone or no consolidation. All patients received lenalidomide maintenance until disease progression or toxicity. At the time of a preliminary analysis of trial data in January 2016, results from the second randomization to consolidation or no consolidation therapy were not yet complete. This first prespecified interim analysis was performed after at least 33% of the required events had occurred.
Early results show ASCT benefit
Early results on 1,266 patients (VMP, n = 512; HDM, n = 754) show that a median progression-free survival (PFS) was not yet reached after a median follow-up of 23.9 months from the first randomization (to VMP vs. HDM+ASCT), the primary endpoint of the trial.
In the overall patient population, patients achieved a significant 24% benefit in PFS when given HDM+ASCT up front (hazard ratio, 0.76 vs. VMP), and this benefit extended to certain patient subgroups, as well.
“PFS benefit with bortezomib-based ASCT was of relevance for patients at high risk of early relapse, in particular for those with revised ISS [International Staging System] stage III and high-risk cytogenetic profiles, who had a relative reduction in the risk of progression or death of 48% and 28%, respectively,” Dr. Cavo said.
Other predictors of longer PFS were ISS stage I (HR, 0.44; 95% confidence interval, 0.28-067; P less than .0001), standard risk cytogenetics (HR, 0.57; 95% CI, 0.41-0.78; P less than .0001), randomization to the HDM+ASCT arm (HR, 0.61; 95% CI, 0.45-0.82; P = .001), and less than 60% bone marrow plasma cells (HR, 0.67; 95% CI, 0.48-0.99; P = .014).
More patients receiving ASCT up front had a significantly greater reduction in tumor volume of at least 90%, as indicated by the composite of very good partial remission, complete response, and stringent complete response, which was achieved in 74.0% in the VMP arm and in 84.4% of the HDM+ASCT arm (P less than .0001).
For patients at low risk of relapse, Dr. Cavo said longer follow up will be needed to compare the different arms of the study, and future analyses will delineate the effects of consolidation or no consolidation therapy and the use of the VMP regimen, compared with single or double ASCT.
ASCO president Dr. Julie Vose said that even with effective novel agents available, older, proven approaches still retain their value. “This study demonstrated that combining the best of both worlds – initial therapy with a novel agent followed by stem cell transplant – resulted in the best patient outcomes,” she said.
FROM THE 2016 ASCO ANNUAL MEETING
Key clinical point: ASCT bested bortezomib for newly diagnosed younger multiple myeloma patients.
Major finding: Multiple myeloma patients showed 24% PFS prolongation with up front HDM+ASCT.
Data source: EMN02/HO95, a prospective, multicenter, intergroup, randomized phase III study of 1,266 patients.
Disclosures: The study was funded by HOVON, the Hemato Oncology Foundation for Adults in the Netherlands. Dr. Cavo disclosed relationships with Janssen, Takeda, Amgen, Bristol-Myers Squibb, and Celgene. Dr. Vose disclosed relationships with Sanofi Aventis, Seattle Genetics, Acerta, Bristol-Myers Squibb, Celgene, Genentech, GlaxoSmithKline, Incyte, Janssen Biotech, Kite Pharma, Pharmacyclics, and Spectrum Pharmaceuticals.