User login
Perinatal depression: what you can do to reduce its long-term effects
We’ve come a long way in our understanding of depression—and that’s a good thing. Consider the treatments popular in the late 18th and early 19th Centuries, for example, which included water immersion (short of drowning), spinning (to reorder the contents of the brain), and the induction of vomiting and administration of enemas, not to mention institutionalization.1 These modalities wouldn’t attract many patients (or clinicians) today.
And yet, even our distant forebears had some inkling of the potential for depression to continue from one generation to the next. As Trotula of Salerno noted around the 11th Century:
In other words, melancholy (aka depression) sometimes has its origins in the womb.
From our 21st Century vantage point, we understand this conclusion in more scientific terms. Data suggest than 14% to 23% of pregnant women will experience depressive symptoms during pregnancy,3 with the potential for long-term effects in the child. In the largest study to date on the effects of antenatal and postnatal parental depression on offspring, Pearson and colleagues found that children of mothers who are depressed during pregnancy are likely to experience depression themselves at age 18.4 Specifically, for each standard-deviation increase in the antenatal maternal depression score, offspring were 1.28 times more likely to have depression at age 18 (95% confidence interval [CI], 1.08–1.51; P = .003).4
Related Article: A talk about, then a plan for, antidepressants in pregnancy Danielle Carlin, MD, and Louann Brizendine, MD (May 2011)
Maternal depression in the postnatal period also was found to be a risk factor for depression in offspring, but only among mothers with “low education” (defined as either no education or compulsory education ending at or before age 16).4 For each standard-deviation increase in the postnatal maternal depression score in this population, offspring were 1.26 times more likely to have depression at age 18, compared with the children of nondepressed women (95% CI, 1.06–1.50; P = .01).4
Although antenatal depression in fathers was not associated with an increased incidence of depression in offspring, postnatal depression was—but only when the fathers had low education.4
As for the mechanism of transmission of depression from parent to child? Although Pearson and colleagues did not attempt to identify it, they did observe that the differential effects of maternal and paternal antenatal depression—with only maternal depression having an impact on offspring—suggest that, in pregnancy, maternal depression may be transmitted to her child “through the biological consequences of depression in utero.”4
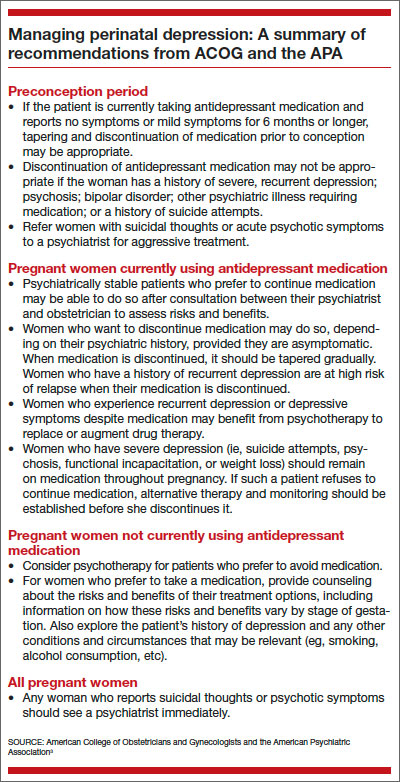
Clearly, if it goes unchecked during pregnancy, maternal depression has the potential to ravage the life of both mother and child. In this article, I review guidance on the management of depression in pregnancy from the American College of Obstetricians and Gynecologists (ACOG) and the American Psychiatric Association (APA), and I offer insights from a perinatal psychiatrist on how ObGyns might adjust their practices to reduce the impact of depression on both mother and infant.
COMPLICATIONS OF PERINATAL DEPRESSION
In a joint report on depression and pregnancy from ACOG and the APA, Yonkers and colleagues noted that low birth weight, neonatal irritability, and diminished neonatal activity and attentiveness are among the adverse reproductive outcomes that have been associated with untreated maternal depression.3 Reproductive outcomes are more dire if maternal depression is severe or if the mother has bipolar disorder or postpartum psychosis, potentially including infanticide or death from suicide.5
Pregnancy complications such as vomiting, nausea, hyperemesis gravidarum, and preeclampsia appear to occur more frequently in depressed women than in nondepressed women, according to the ACOG/APA report,3 although this finding is based on limited data, notes Leena P. Mittal, MD, director of the Reproductive Psychiatry Consultation Service at Brigham and Women’s Hospital in Boston and instructor in psychiatry at Harvard Medical School.
“The trouble with those studies in general is the difficulty of controlling for both the severity of depression and the effects of treatment of depression—or the effects of treatment versus effects of the illness itself,” she says.
That difficulty is compounded by the likely use of multiple medications—
including nonpsychiatric agents—during pregnancy, “which makes it difficult to assess the impact of a single compound, such as an antidepressant, on maternal and fetal outcomes,” according to ACOG and the APA.3 (More than 80% of pregnant women take at least one dose of a medication.3)
HOW THE OBGYN CAN MAKE A DIFFERENCE
Because of the potential for adverse short- and long-term effects of perinatal depression, “there is a need to identify it and attempt to address it prior to the postpartum period,” Dr. Mittal says. “If a woman has depressive symptoms during pregnancy, it is important to try to direct her toward treatment—either by initiating treatment yourself or referring her to a psychiatrist or psychiatric care provider before she enters the postpartum period.” Once she’s postpartum, she will be exposed to additional variables that will influence the severity and duration of her depression, Dr. Mittal says.
Screen all pregnant women for depression
Dr. Mittal recommends routine screening of all perinatal women.
“The data are not entirely clear about the intervals at which these women should be screened,” she says, “but the recommendation would be screening at least once during pregnancy and then again postpartum. Some clinicians screen for depression during each trimester of pregnancy.”
At Dr. Mittal’s institution, such screening usually takes place at the patient’s first prenatal visit.
The screening tools with the most high-quality data backing them include the:
- Edinburgh Postnatal Depression Scale (EPDS). “Despite its name, this tool has been validated for use during pregnancy and for use in the nonperinatal woman as well,” Dr. Mittal notes. It also is in the public domain (http://www.fresno.ucsf.edu/pediatrics/downloads/edinburghscale.pdf). “It’s particularly useful during pregnancy because it assesses the woman for symptoms of depression at the same time that it separates those symptoms from the physical symptoms of pregnancy—there can be some overlap.” The EPDS is self-administered, brief (10 questions), and easily assessed by the clinician, with a score of 10 or above indicating a likelihood of depression.6 It has been validated in more than a dozen languages, as well.
- Patient Health Questionnaire (PHQ-9).7 This is another public-domain tool validated for use during pregnancy (http://www.cqaimh.org/pdf/tool_phq9.pdf). It is utilized widely in primary care and closely associated with depression criteria listed in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders. Like the EPDS, it is self-administered, brief (9 questions), and easy to score. In general, PHQ-9 scores of 5, 10, 15, and 20 represent mild, moderate, moderately severe, and severe depression, respectively.8
Neither of these tools should override clinical judgment. Even with a positive score, clinical assessment is recommended. Nor are these tools designed to detect anxiety, personality disorders, and phobias.
Try to address the issue before conception
The best time to address perinatal depression, of course, with a conversation about prevention, is during the preconception period. Having time before pregnancy to determine the best perinatal management approach is especially valuable.
“What’s important for an ObGyn to consider when counseling someone who is contemplating pregnancy and who has a history of depression is the need to weigh the risks of treatment during pregnancy against the risks of nontreatment,” says Dr. Mittal. Two ways to do that are to assess the severity of her depressive symptoms—both currently and historically—and explore her response to treatment.
“Obviously, suicidality and psychosis suggest very severe illness, whether they are currently present or occurred in the past, and so does a history of psychiatric hospitalization,” says Dr. Mittal. “In such cases, the untreated illness itself carries significant risk, and when it is weighed against the perhaps smaller risk of antidepressant medication during pregnancy, the risk-benefit analysis likely is very different than it might be for someone with mild to moderate depression. I would definitely agree that addressing severity from the beginning is important.”
An understanding of the patient’s response to treatment also is beneficial. Has any treatment been helpful? If so, that information can guide the choice of treatment during pregnancy, says Dr. Mittal. Even knowing whether a woman has responded to nonpharmacologic therapy such as psychotherapy can help shape the treatment plan.
“It might mean that there’s a way to limit the risk of exposure to a variety of psychotropic medications,” Dr. Mittal says. “Or if the patient has had a good response to a particular medication, it might make sense to try that agent again—or, if she’s currently taking it, to stick with it.”
Even if preconception counseling is difficult to achieve, ObGyns see a large number of women of reproductive age during the course of routine gynecologic care.
“I do think it’s worth having a discussion about reproductive planning, especially in the context of their psychiatric illness or history, even if they aren’t currently planning a pregnancy,” says Dr. Mittal.
When to refer the patient to a psychiatrist
Again, the severity of symptoms comes into play.
“In severe mental illness—bipolar disorder, psychotic disorders, or a history of severe illness requiring psychiatric hospitalization—it is important to have a psychiatrist involved,” says Dr. Mittal.
“Even if the woman is stable during pregnancy, the postpartum risk—especially in bipolar disorder—is extremely high. The postpartum period is a vulnerable time, anyway, because obstetric care is coming to its end, and there’s a lot changing irrespective of mental illness. So a patient who’s at high risk for postpartum illness should have a psychiatrist on board as early as possible.”
Consultation with a psychiatrist is another option when managing women with severe depression, a significant psychiatric history, or refractory illness.
Should you prescribe antidepressant medication?
Dr. Mittal believes that ObGyns should feel fairly comfortable prescribing antidepressant medication to patients who have mild or moderate depression, provided that the initiation of such medication is the patient’s informed choice.
Once severe disease (including bipolar disorder and a history of suicidality or psychosis or psychiatric hospitalization) has been ruled out and a history indicates that the patient has mild to moderate symptoms and has responded to treatment, an ObGyn is well qualified to treat perinatal depression, says Dr. Mittal.
Typically, SSRIs are the first-line treatment for perinatal depression and generally have similar amounts of data about their risk in pregnancy. Paroxetine (Paxil) is the exception, as we have more data about the risk for cardiac defects in neonates exposed to it in utero, Dr. Mittal says.
SSRIs generally are found in low amounts in breast milk, although sertraline (Zoloft) generally is found in the smallest quantity, making it the most commonly used SSRI in pregnancy. Sertraline is followed by citalopram (Celexa), escitalopram (Lexapro), and fluoxetine (Prozac) in the respective amount of medication passed into breast milk.
The literature around the teratogenic risks of psychiatric medications is extremely diverse, she says. The “sum total” of the data suggests that SSRIs have relatively few teratogenic risks. “The overall story around SSRIs does not appear to suggest that they carry a risk of major malformations.”
Related Article: Antidepressants linked to pregnancy risks in infertility treatment (News for Your Practice, December 2012)
Dr. Mittal also recommends keeping in mind the possibility that psychotherapy alone is sometimes sufficient for a woman with mild to moderate depression.
“If she has a history of responding to psychotherapy alone and also has mild to moderate symptoms, I think a reasonable approach would be to try it again.”
“This is where preconception planning is especially useful,” she says. “If somebody with mild to moderate symptoms has never had a good trial of psychotherapy, the preconception period is a good time to determine whether it might be effective, to shape the optimal treatment plan.”
Two forms of psychotherapy have solid evidence of efficacy in perinatal depression:
- cognitive behavioral therapy (CBT) —an action-oriented approach that treats maladaptive thinking as the cause of pathologic behavior and “negative” emotions
- interpersonal psychotherapy (IPT)—a treatment in which the patient is educated about depression and its symptoms and her relation to the environment, especially social functioning. Unlike some other forms of therapy, IPT does not focus on underlying personality structures.
There are other forms of psychotherapy, but CBT and IPT have a large evidence base and are generally time-limited, rather than open-ended. They also are manualized and problem-focused, says Dr. Mittal.
How to prescribe an SSRI
SSRIs generally are initiated at a low dose and gradually titrated up (if necessary). A typical starting dose of sertraline, for example, would be 25 to 50 mg. The patient should be counseled about potential side effects, which include increased perspiration, somnolence or insomnia, nausea, diarrhea, headache, dizziness, and restlessness. These effects generally begin to subside the first week or two after initiation.
Sexual side effects such as reduced desire and difficulties with orgasm also may occur and generally do not diminish over time.
The patient also should be advised not to discontinue the SSRI abruptly, if at all possible, because of the risk that she might develop mild discontinuation syndrome. Although this syndrome is short-lived, self-limited, and non-life-threatening, it is uncomfortable. Symptoms include changes in mood or anxiety, shakiness, tremor, or gastrointestinal disturbance. If the patient elects to discontinue an SSRI, tapering over 4 to 7 days is preferable. However, in the event that the patient exhibits an adverse reaction or intolerance to antidepressant medication, immediate discontinuation may be appropriate, says Dr. Mittal.
After initiating SSRI therapy, follow-up in 2 weeks is appropriate, after which time oversight can be transferred to the patient’s primary care provider. In the United States, primary care physicians prescribe the bulk of SSRI medications.
It may take 6 to 8 weeks for the medication to begin to reduce depressive symptoms, although sleep and appetite sometimes improve within 1 or 2 weeks.
Avoid abrupt drug discontinuation in pregnancy
When asked to recommend one intervention that would have a big impact on reducing the burden of depression in pregnancy, Dr. Mittal zeroed in on the population of women who elect to discontinue antidepressant medication during pregnancy.
“I would suggest that ObGyns discourage these women against abrupt discontinuation,” she says. “There is a small body of literature that demonstrates that, in patients with significant illness—severe depression and bipolar disorder, certainly—abrupt discontinuation increases the likelihood of recurrence in the short period of time afterward. If medication is abruptly stopped when a woman discovers she’s pregnant, she’s likely to need to return to treatment during pregnancy because of recurrent symptoms. What happens in that case is that her pregnancy is exposed to both severe symptoms and the reinitiation of treatment, possibly including additional medications beyond the initial agent,” says Dr. Mittal.
Many women assume they should never get pregnant because of their mental health issues, their medications, or both, says Dr. Mittal. Or they believe they must stop their meds if they become pregnant. In fact, some patients report that they have been counseled to avoid medication in pregnancy by their psychiatrist or obstetrician!
“I have spoken to many psychiatrists who say they are not comfortable prescribing to pregnant women, so they either drop the patients or stop their meds!” she says.
When that happens, the patient should find another psychiatrist.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
- Nemade R, Reiss NS, Dombeck M. Historical understandings of depression. Mentalhelp.net. http://www.mentalhelp.net/poc/view_doc.php?type=doc&id=12995&cn=5. Published September 19, 2007. Accessed January 13, 2014.
- Brockington I. A historical perspective on the psychiatry of motherhood. In: Perinatal Stress, Mood, and Anxiety Disorders. Basel, Switzerland: S Karger AG; 2005.
- Yonkers KA, Wisner KL, Stewart DE, et al. The management of depression during pregnancy: A report from the American Psychiatric Association and the American College of Obstetricians and Gynecologists. Obstet Gynecol. 2009;114(3):703–713.
- Pearson RM, Evans J, Kounali D, et al. Maternal depression during pregnancy and the postnatal period. Risks and possible mechanisms for offspring depression at age 18 years [published online ahead of print October 9, 2013]. JAMA Psychiatry. doi:10.1001/jamapsychiatry.2013.2163.
- Hasser C, Brizendine L, Spielvogel A. SSRI use during pregnancy. Current Psychiatry. 2006;5(4):31–40.
- Edinburgh Postnatal Depression Scale. http://www.fresno.ucsf.edu/pediatrics/downloads/edinburghscale.pdf. Accessed January 14, 2014.
- Patient Health Questionnaire (PHQ-9). http://www.cqaimh.org/pdf/tool_phq9.pdf. Accessed January 14, 2014.
- Kroenke K, Spitzer R, Williams W. The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613.
We’ve come a long way in our understanding of depression—and that’s a good thing. Consider the treatments popular in the late 18th and early 19th Centuries, for example, which included water immersion (short of drowning), spinning (to reorder the contents of the brain), and the induction of vomiting and administration of enemas, not to mention institutionalization.1 These modalities wouldn’t attract many patients (or clinicians) today.
And yet, even our distant forebears had some inkling of the potential for depression to continue from one generation to the next. As Trotula of Salerno noted around the 11th Century:
In other words, melancholy (aka depression) sometimes has its origins in the womb.
From our 21st Century vantage point, we understand this conclusion in more scientific terms. Data suggest than 14% to 23% of pregnant women will experience depressive symptoms during pregnancy,3 with the potential for long-term effects in the child. In the largest study to date on the effects of antenatal and postnatal parental depression on offspring, Pearson and colleagues found that children of mothers who are depressed during pregnancy are likely to experience depression themselves at age 18.4 Specifically, for each standard-deviation increase in the antenatal maternal depression score, offspring were 1.28 times more likely to have depression at age 18 (95% confidence interval [CI], 1.08–1.51; P = .003).4
Related Article: A talk about, then a plan for, antidepressants in pregnancy Danielle Carlin, MD, and Louann Brizendine, MD (May 2011)
Maternal depression in the postnatal period also was found to be a risk factor for depression in offspring, but only among mothers with “low education” (defined as either no education or compulsory education ending at or before age 16).4 For each standard-deviation increase in the postnatal maternal depression score in this population, offspring were 1.26 times more likely to have depression at age 18, compared with the children of nondepressed women (95% CI, 1.06–1.50; P = .01).4
Although antenatal depression in fathers was not associated with an increased incidence of depression in offspring, postnatal depression was—but only when the fathers had low education.4
As for the mechanism of transmission of depression from parent to child? Although Pearson and colleagues did not attempt to identify it, they did observe that the differential effects of maternal and paternal antenatal depression—with only maternal depression having an impact on offspring—suggest that, in pregnancy, maternal depression may be transmitted to her child “through the biological consequences of depression in utero.”4
Clearly, if it goes unchecked during pregnancy, maternal depression has the potential to ravage the life of both mother and child. In this article, I review guidance on the management of depression in pregnancy from the American College of Obstetricians and Gynecologists (ACOG) and the American Psychiatric Association (APA), and I offer insights from a perinatal psychiatrist on how ObGyns might adjust their practices to reduce the impact of depression on both mother and infant.
COMPLICATIONS OF PERINATAL DEPRESSION
In a joint report on depression and pregnancy from ACOG and the APA, Yonkers and colleagues noted that low birth weight, neonatal irritability, and diminished neonatal activity and attentiveness are among the adverse reproductive outcomes that have been associated with untreated maternal depression.3 Reproductive outcomes are more dire if maternal depression is severe or if the mother has bipolar disorder or postpartum psychosis, potentially including infanticide or death from suicide.5
Pregnancy complications such as vomiting, nausea, hyperemesis gravidarum, and preeclampsia appear to occur more frequently in depressed women than in nondepressed women, according to the ACOG/APA report,3 although this finding is based on limited data, notes Leena P. Mittal, MD, director of the Reproductive Psychiatry Consultation Service at Brigham and Women’s Hospital in Boston and instructor in psychiatry at Harvard Medical School.
“The trouble with those studies in general is the difficulty of controlling for both the severity of depression and the effects of treatment of depression—or the effects of treatment versus effects of the illness itself,” she says.
That difficulty is compounded by the likely use of multiple medications—
including nonpsychiatric agents—during pregnancy, “which makes it difficult to assess the impact of a single compound, such as an antidepressant, on maternal and fetal outcomes,” according to ACOG and the APA.3 (More than 80% of pregnant women take at least one dose of a medication.3)
HOW THE OBGYN CAN MAKE A DIFFERENCE
Because of the potential for adverse short- and long-term effects of perinatal depression, “there is a need to identify it and attempt to address it prior to the postpartum period,” Dr. Mittal says. “If a woman has depressive symptoms during pregnancy, it is important to try to direct her toward treatment—either by initiating treatment yourself or referring her to a psychiatrist or psychiatric care provider before she enters the postpartum period.” Once she’s postpartum, she will be exposed to additional variables that will influence the severity and duration of her depression, Dr. Mittal says.
Screen all pregnant women for depression
Dr. Mittal recommends routine screening of all perinatal women.
“The data are not entirely clear about the intervals at which these women should be screened,” she says, “but the recommendation would be screening at least once during pregnancy and then again postpartum. Some clinicians screen for depression during each trimester of pregnancy.”
At Dr. Mittal’s institution, such screening usually takes place at the patient’s first prenatal visit.
The screening tools with the most high-quality data backing them include the:
- Edinburgh Postnatal Depression Scale (EPDS). “Despite its name, this tool has been validated for use during pregnancy and for use in the nonperinatal woman as well,” Dr. Mittal notes. It also is in the public domain (http://www.fresno.ucsf.edu/pediatrics/downloads/edinburghscale.pdf). “It’s particularly useful during pregnancy because it assesses the woman for symptoms of depression at the same time that it separates those symptoms from the physical symptoms of pregnancy—there can be some overlap.” The EPDS is self-administered, brief (10 questions), and easily assessed by the clinician, with a score of 10 or above indicating a likelihood of depression.6 It has been validated in more than a dozen languages, as well.
- Patient Health Questionnaire (PHQ-9).7 This is another public-domain tool validated for use during pregnancy (http://www.cqaimh.org/pdf/tool_phq9.pdf). It is utilized widely in primary care and closely associated with depression criteria listed in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders. Like the EPDS, it is self-administered, brief (9 questions), and easy to score. In general, PHQ-9 scores of 5, 10, 15, and 20 represent mild, moderate, moderately severe, and severe depression, respectively.8
Neither of these tools should override clinical judgment. Even with a positive score, clinical assessment is recommended. Nor are these tools designed to detect anxiety, personality disorders, and phobias.
Try to address the issue before conception
The best time to address perinatal depression, of course, with a conversation about prevention, is during the preconception period. Having time before pregnancy to determine the best perinatal management approach is especially valuable.
“What’s important for an ObGyn to consider when counseling someone who is contemplating pregnancy and who has a history of depression is the need to weigh the risks of treatment during pregnancy against the risks of nontreatment,” says Dr. Mittal. Two ways to do that are to assess the severity of her depressive symptoms—both currently and historically—and explore her response to treatment.
“Obviously, suicidality and psychosis suggest very severe illness, whether they are currently present or occurred in the past, and so does a history of psychiatric hospitalization,” says Dr. Mittal. “In such cases, the untreated illness itself carries significant risk, and when it is weighed against the perhaps smaller risk of antidepressant medication during pregnancy, the risk-benefit analysis likely is very different than it might be for someone with mild to moderate depression. I would definitely agree that addressing severity from the beginning is important.”
An understanding of the patient’s response to treatment also is beneficial. Has any treatment been helpful? If so, that information can guide the choice of treatment during pregnancy, says Dr. Mittal. Even knowing whether a woman has responded to nonpharmacologic therapy such as psychotherapy can help shape the treatment plan.
“It might mean that there’s a way to limit the risk of exposure to a variety of psychotropic medications,” Dr. Mittal says. “Or if the patient has had a good response to a particular medication, it might make sense to try that agent again—or, if she’s currently taking it, to stick with it.”
Even if preconception counseling is difficult to achieve, ObGyns see a large number of women of reproductive age during the course of routine gynecologic care.
“I do think it’s worth having a discussion about reproductive planning, especially in the context of their psychiatric illness or history, even if they aren’t currently planning a pregnancy,” says Dr. Mittal.
When to refer the patient to a psychiatrist
Again, the severity of symptoms comes into play.
“In severe mental illness—bipolar disorder, psychotic disorders, or a history of severe illness requiring psychiatric hospitalization—it is important to have a psychiatrist involved,” says Dr. Mittal.
“Even if the woman is stable during pregnancy, the postpartum risk—especially in bipolar disorder—is extremely high. The postpartum period is a vulnerable time, anyway, because obstetric care is coming to its end, and there’s a lot changing irrespective of mental illness. So a patient who’s at high risk for postpartum illness should have a psychiatrist on board as early as possible.”
Consultation with a psychiatrist is another option when managing women with severe depression, a significant psychiatric history, or refractory illness.
Should you prescribe antidepressant medication?
Dr. Mittal believes that ObGyns should feel fairly comfortable prescribing antidepressant medication to patients who have mild or moderate depression, provided that the initiation of such medication is the patient’s informed choice.
Once severe disease (including bipolar disorder and a history of suicidality or psychosis or psychiatric hospitalization) has been ruled out and a history indicates that the patient has mild to moderate symptoms and has responded to treatment, an ObGyn is well qualified to treat perinatal depression, says Dr. Mittal.
Typically, SSRIs are the first-line treatment for perinatal depression and generally have similar amounts of data about their risk in pregnancy. Paroxetine (Paxil) is the exception, as we have more data about the risk for cardiac defects in neonates exposed to it in utero, Dr. Mittal says.
SSRIs generally are found in low amounts in breast milk, although sertraline (Zoloft) generally is found in the smallest quantity, making it the most commonly used SSRI in pregnancy. Sertraline is followed by citalopram (Celexa), escitalopram (Lexapro), and fluoxetine (Prozac) in the respective amount of medication passed into breast milk.
The literature around the teratogenic risks of psychiatric medications is extremely diverse, she says. The “sum total” of the data suggests that SSRIs have relatively few teratogenic risks. “The overall story around SSRIs does not appear to suggest that they carry a risk of major malformations.”
Related Article: Antidepressants linked to pregnancy risks in infertility treatment (News for Your Practice, December 2012)
Dr. Mittal also recommends keeping in mind the possibility that psychotherapy alone is sometimes sufficient for a woman with mild to moderate depression.
“If she has a history of responding to psychotherapy alone and also has mild to moderate symptoms, I think a reasonable approach would be to try it again.”
“This is where preconception planning is especially useful,” she says. “If somebody with mild to moderate symptoms has never had a good trial of psychotherapy, the preconception period is a good time to determine whether it might be effective, to shape the optimal treatment plan.”
Two forms of psychotherapy have solid evidence of efficacy in perinatal depression:
- cognitive behavioral therapy (CBT) —an action-oriented approach that treats maladaptive thinking as the cause of pathologic behavior and “negative” emotions
- interpersonal psychotherapy (IPT)—a treatment in which the patient is educated about depression and its symptoms and her relation to the environment, especially social functioning. Unlike some other forms of therapy, IPT does not focus on underlying personality structures.
There are other forms of psychotherapy, but CBT and IPT have a large evidence base and are generally time-limited, rather than open-ended. They also are manualized and problem-focused, says Dr. Mittal.
How to prescribe an SSRI
SSRIs generally are initiated at a low dose and gradually titrated up (if necessary). A typical starting dose of sertraline, for example, would be 25 to 50 mg. The patient should be counseled about potential side effects, which include increased perspiration, somnolence or insomnia, nausea, diarrhea, headache, dizziness, and restlessness. These effects generally begin to subside the first week or two after initiation.
Sexual side effects such as reduced desire and difficulties with orgasm also may occur and generally do not diminish over time.
The patient also should be advised not to discontinue the SSRI abruptly, if at all possible, because of the risk that she might develop mild discontinuation syndrome. Although this syndrome is short-lived, self-limited, and non-life-threatening, it is uncomfortable. Symptoms include changes in mood or anxiety, shakiness, tremor, or gastrointestinal disturbance. If the patient elects to discontinue an SSRI, tapering over 4 to 7 days is preferable. However, in the event that the patient exhibits an adverse reaction or intolerance to antidepressant medication, immediate discontinuation may be appropriate, says Dr. Mittal.
After initiating SSRI therapy, follow-up in 2 weeks is appropriate, after which time oversight can be transferred to the patient’s primary care provider. In the United States, primary care physicians prescribe the bulk of SSRI medications.
It may take 6 to 8 weeks for the medication to begin to reduce depressive symptoms, although sleep and appetite sometimes improve within 1 or 2 weeks.
Avoid abrupt drug discontinuation in pregnancy
When asked to recommend one intervention that would have a big impact on reducing the burden of depression in pregnancy, Dr. Mittal zeroed in on the population of women who elect to discontinue antidepressant medication during pregnancy.
“I would suggest that ObGyns discourage these women against abrupt discontinuation,” she says. “There is a small body of literature that demonstrates that, in patients with significant illness—severe depression and bipolar disorder, certainly—abrupt discontinuation increases the likelihood of recurrence in the short period of time afterward. If medication is abruptly stopped when a woman discovers she’s pregnant, she’s likely to need to return to treatment during pregnancy because of recurrent symptoms. What happens in that case is that her pregnancy is exposed to both severe symptoms and the reinitiation of treatment, possibly including additional medications beyond the initial agent,” says Dr. Mittal.
Many women assume they should never get pregnant because of their mental health issues, their medications, or both, says Dr. Mittal. Or they believe they must stop their meds if they become pregnant. In fact, some patients report that they have been counseled to avoid medication in pregnancy by their psychiatrist or obstetrician!
“I have spoken to many psychiatrists who say they are not comfortable prescribing to pregnant women, so they either drop the patients or stop their meds!” she says.
When that happens, the patient should find another psychiatrist.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
We’ve come a long way in our understanding of depression—and that’s a good thing. Consider the treatments popular in the late 18th and early 19th Centuries, for example, which included water immersion (short of drowning), spinning (to reorder the contents of the brain), and the induction of vomiting and administration of enemas, not to mention institutionalization.1 These modalities wouldn’t attract many patients (or clinicians) today.
And yet, even our distant forebears had some inkling of the potential for depression to continue from one generation to the next. As Trotula of Salerno noted around the 11th Century:
In other words, melancholy (aka depression) sometimes has its origins in the womb.
From our 21st Century vantage point, we understand this conclusion in more scientific terms. Data suggest than 14% to 23% of pregnant women will experience depressive symptoms during pregnancy,3 with the potential for long-term effects in the child. In the largest study to date on the effects of antenatal and postnatal parental depression on offspring, Pearson and colleagues found that children of mothers who are depressed during pregnancy are likely to experience depression themselves at age 18.4 Specifically, for each standard-deviation increase in the antenatal maternal depression score, offspring were 1.28 times more likely to have depression at age 18 (95% confidence interval [CI], 1.08–1.51; P = .003).4
Related Article: A talk about, then a plan for, antidepressants in pregnancy Danielle Carlin, MD, and Louann Brizendine, MD (May 2011)
Maternal depression in the postnatal period also was found to be a risk factor for depression in offspring, but only among mothers with “low education” (defined as either no education or compulsory education ending at or before age 16).4 For each standard-deviation increase in the postnatal maternal depression score in this population, offspring were 1.26 times more likely to have depression at age 18, compared with the children of nondepressed women (95% CI, 1.06–1.50; P = .01).4
Although antenatal depression in fathers was not associated with an increased incidence of depression in offspring, postnatal depression was—but only when the fathers had low education.4
As for the mechanism of transmission of depression from parent to child? Although Pearson and colleagues did not attempt to identify it, they did observe that the differential effects of maternal and paternal antenatal depression—with only maternal depression having an impact on offspring—suggest that, in pregnancy, maternal depression may be transmitted to her child “through the biological consequences of depression in utero.”4
Clearly, if it goes unchecked during pregnancy, maternal depression has the potential to ravage the life of both mother and child. In this article, I review guidance on the management of depression in pregnancy from the American College of Obstetricians and Gynecologists (ACOG) and the American Psychiatric Association (APA), and I offer insights from a perinatal psychiatrist on how ObGyns might adjust their practices to reduce the impact of depression on both mother and infant.
COMPLICATIONS OF PERINATAL DEPRESSION
In a joint report on depression and pregnancy from ACOG and the APA, Yonkers and colleagues noted that low birth weight, neonatal irritability, and diminished neonatal activity and attentiveness are among the adverse reproductive outcomes that have been associated with untreated maternal depression.3 Reproductive outcomes are more dire if maternal depression is severe or if the mother has bipolar disorder or postpartum psychosis, potentially including infanticide or death from suicide.5
Pregnancy complications such as vomiting, nausea, hyperemesis gravidarum, and preeclampsia appear to occur more frequently in depressed women than in nondepressed women, according to the ACOG/APA report,3 although this finding is based on limited data, notes Leena P. Mittal, MD, director of the Reproductive Psychiatry Consultation Service at Brigham and Women’s Hospital in Boston and instructor in psychiatry at Harvard Medical School.
“The trouble with those studies in general is the difficulty of controlling for both the severity of depression and the effects of treatment of depression—or the effects of treatment versus effects of the illness itself,” she says.
That difficulty is compounded by the likely use of multiple medications—
including nonpsychiatric agents—during pregnancy, “which makes it difficult to assess the impact of a single compound, such as an antidepressant, on maternal and fetal outcomes,” according to ACOG and the APA.3 (More than 80% of pregnant women take at least one dose of a medication.3)
HOW THE OBGYN CAN MAKE A DIFFERENCE
Because of the potential for adverse short- and long-term effects of perinatal depression, “there is a need to identify it and attempt to address it prior to the postpartum period,” Dr. Mittal says. “If a woman has depressive symptoms during pregnancy, it is important to try to direct her toward treatment—either by initiating treatment yourself or referring her to a psychiatrist or psychiatric care provider before she enters the postpartum period.” Once she’s postpartum, she will be exposed to additional variables that will influence the severity and duration of her depression, Dr. Mittal says.
Screen all pregnant women for depression
Dr. Mittal recommends routine screening of all perinatal women.
“The data are not entirely clear about the intervals at which these women should be screened,” she says, “but the recommendation would be screening at least once during pregnancy and then again postpartum. Some clinicians screen for depression during each trimester of pregnancy.”
At Dr. Mittal’s institution, such screening usually takes place at the patient’s first prenatal visit.
The screening tools with the most high-quality data backing them include the:
- Edinburgh Postnatal Depression Scale (EPDS). “Despite its name, this tool has been validated for use during pregnancy and for use in the nonperinatal woman as well,” Dr. Mittal notes. It also is in the public domain (http://www.fresno.ucsf.edu/pediatrics/downloads/edinburghscale.pdf). “It’s particularly useful during pregnancy because it assesses the woman for symptoms of depression at the same time that it separates those symptoms from the physical symptoms of pregnancy—there can be some overlap.” The EPDS is self-administered, brief (10 questions), and easily assessed by the clinician, with a score of 10 or above indicating a likelihood of depression.6 It has been validated in more than a dozen languages, as well.
- Patient Health Questionnaire (PHQ-9).7 This is another public-domain tool validated for use during pregnancy (http://www.cqaimh.org/pdf/tool_phq9.pdf). It is utilized widely in primary care and closely associated with depression criteria listed in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders. Like the EPDS, it is self-administered, brief (9 questions), and easy to score. In general, PHQ-9 scores of 5, 10, 15, and 20 represent mild, moderate, moderately severe, and severe depression, respectively.8
Neither of these tools should override clinical judgment. Even with a positive score, clinical assessment is recommended. Nor are these tools designed to detect anxiety, personality disorders, and phobias.
Try to address the issue before conception
The best time to address perinatal depression, of course, with a conversation about prevention, is during the preconception period. Having time before pregnancy to determine the best perinatal management approach is especially valuable.
“What’s important for an ObGyn to consider when counseling someone who is contemplating pregnancy and who has a history of depression is the need to weigh the risks of treatment during pregnancy against the risks of nontreatment,” says Dr. Mittal. Two ways to do that are to assess the severity of her depressive symptoms—both currently and historically—and explore her response to treatment.
“Obviously, suicidality and psychosis suggest very severe illness, whether they are currently present or occurred in the past, and so does a history of psychiatric hospitalization,” says Dr. Mittal. “In such cases, the untreated illness itself carries significant risk, and when it is weighed against the perhaps smaller risk of antidepressant medication during pregnancy, the risk-benefit analysis likely is very different than it might be for someone with mild to moderate depression. I would definitely agree that addressing severity from the beginning is important.”
An understanding of the patient’s response to treatment also is beneficial. Has any treatment been helpful? If so, that information can guide the choice of treatment during pregnancy, says Dr. Mittal. Even knowing whether a woman has responded to nonpharmacologic therapy such as psychotherapy can help shape the treatment plan.
“It might mean that there’s a way to limit the risk of exposure to a variety of psychotropic medications,” Dr. Mittal says. “Or if the patient has had a good response to a particular medication, it might make sense to try that agent again—or, if she’s currently taking it, to stick with it.”
Even if preconception counseling is difficult to achieve, ObGyns see a large number of women of reproductive age during the course of routine gynecologic care.
“I do think it’s worth having a discussion about reproductive planning, especially in the context of their psychiatric illness or history, even if they aren’t currently planning a pregnancy,” says Dr. Mittal.
When to refer the patient to a psychiatrist
Again, the severity of symptoms comes into play.
“In severe mental illness—bipolar disorder, psychotic disorders, or a history of severe illness requiring psychiatric hospitalization—it is important to have a psychiatrist involved,” says Dr. Mittal.
“Even if the woman is stable during pregnancy, the postpartum risk—especially in bipolar disorder—is extremely high. The postpartum period is a vulnerable time, anyway, because obstetric care is coming to its end, and there’s a lot changing irrespective of mental illness. So a patient who’s at high risk for postpartum illness should have a psychiatrist on board as early as possible.”
Consultation with a psychiatrist is another option when managing women with severe depression, a significant psychiatric history, or refractory illness.
Should you prescribe antidepressant medication?
Dr. Mittal believes that ObGyns should feel fairly comfortable prescribing antidepressant medication to patients who have mild or moderate depression, provided that the initiation of such medication is the patient’s informed choice.
Once severe disease (including bipolar disorder and a history of suicidality or psychosis or psychiatric hospitalization) has been ruled out and a history indicates that the patient has mild to moderate symptoms and has responded to treatment, an ObGyn is well qualified to treat perinatal depression, says Dr. Mittal.
Typically, SSRIs are the first-line treatment for perinatal depression and generally have similar amounts of data about their risk in pregnancy. Paroxetine (Paxil) is the exception, as we have more data about the risk for cardiac defects in neonates exposed to it in utero, Dr. Mittal says.
SSRIs generally are found in low amounts in breast milk, although sertraline (Zoloft) generally is found in the smallest quantity, making it the most commonly used SSRI in pregnancy. Sertraline is followed by citalopram (Celexa), escitalopram (Lexapro), and fluoxetine (Prozac) in the respective amount of medication passed into breast milk.
The literature around the teratogenic risks of psychiatric medications is extremely diverse, she says. The “sum total” of the data suggests that SSRIs have relatively few teratogenic risks. “The overall story around SSRIs does not appear to suggest that they carry a risk of major malformations.”
Related Article: Antidepressants linked to pregnancy risks in infertility treatment (News for Your Practice, December 2012)
Dr. Mittal also recommends keeping in mind the possibility that psychotherapy alone is sometimes sufficient for a woman with mild to moderate depression.
“If she has a history of responding to psychotherapy alone and also has mild to moderate symptoms, I think a reasonable approach would be to try it again.”
“This is where preconception planning is especially useful,” she says. “If somebody with mild to moderate symptoms has never had a good trial of psychotherapy, the preconception period is a good time to determine whether it might be effective, to shape the optimal treatment plan.”
Two forms of psychotherapy have solid evidence of efficacy in perinatal depression:
- cognitive behavioral therapy (CBT) —an action-oriented approach that treats maladaptive thinking as the cause of pathologic behavior and “negative” emotions
- interpersonal psychotherapy (IPT)—a treatment in which the patient is educated about depression and its symptoms and her relation to the environment, especially social functioning. Unlike some other forms of therapy, IPT does not focus on underlying personality structures.
There are other forms of psychotherapy, but CBT and IPT have a large evidence base and are generally time-limited, rather than open-ended. They also are manualized and problem-focused, says Dr. Mittal.
How to prescribe an SSRI
SSRIs generally are initiated at a low dose and gradually titrated up (if necessary). A typical starting dose of sertraline, for example, would be 25 to 50 mg. The patient should be counseled about potential side effects, which include increased perspiration, somnolence or insomnia, nausea, diarrhea, headache, dizziness, and restlessness. These effects generally begin to subside the first week or two after initiation.
Sexual side effects such as reduced desire and difficulties with orgasm also may occur and generally do not diminish over time.
The patient also should be advised not to discontinue the SSRI abruptly, if at all possible, because of the risk that she might develop mild discontinuation syndrome. Although this syndrome is short-lived, self-limited, and non-life-threatening, it is uncomfortable. Symptoms include changes in mood or anxiety, shakiness, tremor, or gastrointestinal disturbance. If the patient elects to discontinue an SSRI, tapering over 4 to 7 days is preferable. However, in the event that the patient exhibits an adverse reaction or intolerance to antidepressant medication, immediate discontinuation may be appropriate, says Dr. Mittal.
After initiating SSRI therapy, follow-up in 2 weeks is appropriate, after which time oversight can be transferred to the patient’s primary care provider. In the United States, primary care physicians prescribe the bulk of SSRI medications.
It may take 6 to 8 weeks for the medication to begin to reduce depressive symptoms, although sleep and appetite sometimes improve within 1 or 2 weeks.
Avoid abrupt drug discontinuation in pregnancy
When asked to recommend one intervention that would have a big impact on reducing the burden of depression in pregnancy, Dr. Mittal zeroed in on the population of women who elect to discontinue antidepressant medication during pregnancy.
“I would suggest that ObGyns discourage these women against abrupt discontinuation,” she says. “There is a small body of literature that demonstrates that, in patients with significant illness—severe depression and bipolar disorder, certainly—abrupt discontinuation increases the likelihood of recurrence in the short period of time afterward. If medication is abruptly stopped when a woman discovers she’s pregnant, she’s likely to need to return to treatment during pregnancy because of recurrent symptoms. What happens in that case is that her pregnancy is exposed to both severe symptoms and the reinitiation of treatment, possibly including additional medications beyond the initial agent,” says Dr. Mittal.
Many women assume they should never get pregnant because of their mental health issues, their medications, or both, says Dr. Mittal. Or they believe they must stop their meds if they become pregnant. In fact, some patients report that they have been counseled to avoid medication in pregnancy by their psychiatrist or obstetrician!
“I have spoken to many psychiatrists who say they are not comfortable prescribing to pregnant women, so they either drop the patients or stop their meds!” she says.
When that happens, the patient should find another psychiatrist.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
- Nemade R, Reiss NS, Dombeck M. Historical understandings of depression. Mentalhelp.net. http://www.mentalhelp.net/poc/view_doc.php?type=doc&id=12995&cn=5. Published September 19, 2007. Accessed January 13, 2014.
- Brockington I. A historical perspective on the psychiatry of motherhood. In: Perinatal Stress, Mood, and Anxiety Disorders. Basel, Switzerland: S Karger AG; 2005.
- Yonkers KA, Wisner KL, Stewart DE, et al. The management of depression during pregnancy: A report from the American Psychiatric Association and the American College of Obstetricians and Gynecologists. Obstet Gynecol. 2009;114(3):703–713.
- Pearson RM, Evans J, Kounali D, et al. Maternal depression during pregnancy and the postnatal period. Risks and possible mechanisms for offspring depression at age 18 years [published online ahead of print October 9, 2013]. JAMA Psychiatry. doi:10.1001/jamapsychiatry.2013.2163.
- Hasser C, Brizendine L, Spielvogel A. SSRI use during pregnancy. Current Psychiatry. 2006;5(4):31–40.
- Edinburgh Postnatal Depression Scale. http://www.fresno.ucsf.edu/pediatrics/downloads/edinburghscale.pdf. Accessed January 14, 2014.
- Patient Health Questionnaire (PHQ-9). http://www.cqaimh.org/pdf/tool_phq9.pdf. Accessed January 14, 2014.
- Kroenke K, Spitzer R, Williams W. The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613.
- Nemade R, Reiss NS, Dombeck M. Historical understandings of depression. Mentalhelp.net. http://www.mentalhelp.net/poc/view_doc.php?type=doc&id=12995&cn=5. Published September 19, 2007. Accessed January 13, 2014.
- Brockington I. A historical perspective on the psychiatry of motherhood. In: Perinatal Stress, Mood, and Anxiety Disorders. Basel, Switzerland: S Karger AG; 2005.
- Yonkers KA, Wisner KL, Stewart DE, et al. The management of depression during pregnancy: A report from the American Psychiatric Association and the American College of Obstetricians and Gynecologists. Obstet Gynecol. 2009;114(3):703–713.
- Pearson RM, Evans J, Kounali D, et al. Maternal depression during pregnancy and the postnatal period. Risks and possible mechanisms for offspring depression at age 18 years [published online ahead of print October 9, 2013]. JAMA Psychiatry. doi:10.1001/jamapsychiatry.2013.2163.
- Hasser C, Brizendine L, Spielvogel A. SSRI use during pregnancy. Current Psychiatry. 2006;5(4):31–40.
- Edinburgh Postnatal Depression Scale. http://www.fresno.ucsf.edu/pediatrics/downloads/edinburghscale.pdf. Accessed January 14, 2014.
- Patient Health Questionnaire (PHQ-9). http://www.cqaimh.org/pdf/tool_phq9.pdf. Accessed January 14, 2014.
- Kroenke K, Spitzer R, Williams W. The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613.

Learning and feedback reduce cesarean section rate
NEW ORLEANS – A training program that continually reinforced best practices for labor and delivery reduced the risk of cesarean section by 10% overall, and by up to 32% in a subgroup of high-risk pregnancies.
The program also significantly improved newborn outcomes, with a 12% decrease in the rate of major neonatal morbidity, Dr. Nils Chaillet reported at the Pregnancy Meeting, sponsored by the Society of Maternal-Fetal Medicine. The neonatal benefit remained significant even after excluding all preterm births from the analysis, said Dr. Chaillet of the Sainte-Justine University Hospital Research Center, Montreal.
The QUARISMA (Quality of Care, Management of Obstetrical Risk, and Mode of Delivery in Quebec) study examined the effects of a clinician training program designed to promote optimal management of labor and delivery. QUARISMA was a multifaceted evidence-medicine program based on audit, feedback, and educational activities that followed the World Health Organization guidelines for quality obstetrical care.

A 2-day training session at each participating hospital introduced the program. Throughout the 3.5-year study, a local audit committee, headed by a peer-selected leader, regularly evaluated performance and provided feedback on results and suggestions on quality improvement. These audits were conducted every 3 months. They included an analysis of each cesarean case, centering on whether and how it could have been prevented.
The study randomized 32 public hospitals in Quebec to the intervention or to a control arm of usual practice. The hospitals all had a cesarean section rate of at least 17% and no prior program aimed at reducing that rate. They had to perform more than 300 deliveries annually. All women who gave birth to an infant of at least 500 grams and 24 weeks’ gestation were included in the study.
A total of 105,351 deliveries occurred. In the control group, the baseline rate of cesarean section was 23%; that remained unchanged. The rate did decrease in the intervention group, dropping from 22.5% at baseline to 21.8% at study’s end – a 10% risk reduction that was statistically significant.
Women with low-risk pregnancies experienced a considerable benefit, Dr. Chaillet noted, with an overall risk reduction of 20%. That varied among hospital type. It was smallest (2%) at community hospitals, followed by 21% at regional hospitals and 24% at tertiary care hospitals.
Among high-risk pregnancies, the risk of a cesarean decreased by 4% overall. It did not change in tertiary care centers, but decreased by 5% at regional hospitals and 32% at community hospitals.
Medical interventions were a secondary endpoint. There were no changes in the rates of episiotomy, epidurals, or artificial rupture of membranes. However, the risk of operative vaginal delivery dropped by 12%, and pharmacologic labor induction by 18%. The odds of using oxytocin during labor increased by16%.
There were no significant changes in the composite measures of minor or major maternal morbidities. But neonatal outcomes did improve. The risk of a minor neonatal morbidity decreased by a significant 12%; the risk of a major problem decreased by 19%.
Dr. Chaillet made no financial disclosures.
On Twitter @alz_gal
NEW ORLEANS – A training program that continually reinforced best practices for labor and delivery reduced the risk of cesarean section by 10% overall, and by up to 32% in a subgroup of high-risk pregnancies.
The program also significantly improved newborn outcomes, with a 12% decrease in the rate of major neonatal morbidity, Dr. Nils Chaillet reported at the Pregnancy Meeting, sponsored by the Society of Maternal-Fetal Medicine. The neonatal benefit remained significant even after excluding all preterm births from the analysis, said Dr. Chaillet of the Sainte-Justine University Hospital Research Center, Montreal.
The QUARISMA (Quality of Care, Management of Obstetrical Risk, and Mode of Delivery in Quebec) study examined the effects of a clinician training program designed to promote optimal management of labor and delivery. QUARISMA was a multifaceted evidence-medicine program based on audit, feedback, and educational activities that followed the World Health Organization guidelines for quality obstetrical care.
A 2-day training session at each participating hospital introduced the program. Throughout the 3.5-year study, a local audit committee, headed by a peer-selected leader, regularly evaluated performance and provided feedback on results and suggestions on quality improvement. These audits were conducted every 3 months. They included an analysis of each cesarean case, centering on whether and how it could have been prevented.
The study randomized 32 public hospitals in Quebec to the intervention or to a control arm of usual practice. The hospitals all had a cesarean section rate of at least 17% and no prior program aimed at reducing that rate. They had to perform more than 300 deliveries annually. All women who gave birth to an infant of at least 500 grams and 24 weeks’ gestation were included in the study.
A total of 105,351 deliveries occurred. In the control group, the baseline rate of cesarean section was 23%; that remained unchanged. The rate did decrease in the intervention group, dropping from 22.5% at baseline to 21.8% at study’s end – a 10% risk reduction that was statistically significant.
Women with low-risk pregnancies experienced a considerable benefit, Dr. Chaillet noted, with an overall risk reduction of 20%. That varied among hospital type. It was smallest (2%) at community hospitals, followed by 21% at regional hospitals and 24% at tertiary care hospitals.
Among high-risk pregnancies, the risk of a cesarean decreased by 4% overall. It did not change in tertiary care centers, but decreased by 5% at regional hospitals and 32% at community hospitals.
Medical interventions were a secondary endpoint. There were no changes in the rates of episiotomy, epidurals, or artificial rupture of membranes. However, the risk of operative vaginal delivery dropped by 12%, and pharmacologic labor induction by 18%. The odds of using oxytocin during labor increased by16%.
There were no significant changes in the composite measures of minor or major maternal morbidities. But neonatal outcomes did improve. The risk of a minor neonatal morbidity decreased by a significant 12%; the risk of a major problem decreased by 19%.
Dr. Chaillet made no financial disclosures.
On Twitter @alz_gal
NEW ORLEANS – A training program that continually reinforced best practices for labor and delivery reduced the risk of cesarean section by 10% overall, and by up to 32% in a subgroup of high-risk pregnancies.
The program also significantly improved newborn outcomes, with a 12% decrease in the rate of major neonatal morbidity, Dr. Nils Chaillet reported at the Pregnancy Meeting, sponsored by the Society of Maternal-Fetal Medicine. The neonatal benefit remained significant even after excluding all preterm births from the analysis, said Dr. Chaillet of the Sainte-Justine University Hospital Research Center, Montreal.
The QUARISMA (Quality of Care, Management of Obstetrical Risk, and Mode of Delivery in Quebec) study examined the effects of a clinician training program designed to promote optimal management of labor and delivery. QUARISMA was a multifaceted evidence-medicine program based on audit, feedback, and educational activities that followed the World Health Organization guidelines for quality obstetrical care.
A 2-day training session at each participating hospital introduced the program. Throughout the 3.5-year study, a local audit committee, headed by a peer-selected leader, regularly evaluated performance and provided feedback on results and suggestions on quality improvement. These audits were conducted every 3 months. They included an analysis of each cesarean case, centering on whether and how it could have been prevented.
The study randomized 32 public hospitals in Quebec to the intervention or to a control arm of usual practice. The hospitals all had a cesarean section rate of at least 17% and no prior program aimed at reducing that rate. They had to perform more than 300 deliveries annually. All women who gave birth to an infant of at least 500 grams and 24 weeks’ gestation were included in the study.
A total of 105,351 deliveries occurred. In the control group, the baseline rate of cesarean section was 23%; that remained unchanged. The rate did decrease in the intervention group, dropping from 22.5% at baseline to 21.8% at study’s end – a 10% risk reduction that was statistically significant.
Women with low-risk pregnancies experienced a considerable benefit, Dr. Chaillet noted, with an overall risk reduction of 20%. That varied among hospital type. It was smallest (2%) at community hospitals, followed by 21% at regional hospitals and 24% at tertiary care hospitals.
Among high-risk pregnancies, the risk of a cesarean decreased by 4% overall. It did not change in tertiary care centers, but decreased by 5% at regional hospitals and 32% at community hospitals.
Medical interventions were a secondary endpoint. There were no changes in the rates of episiotomy, epidurals, or artificial rupture of membranes. However, the risk of operative vaginal delivery dropped by 12%, and pharmacologic labor induction by 18%. The odds of using oxytocin during labor increased by16%.
There were no significant changes in the composite measures of minor or major maternal morbidities. But neonatal outcomes did improve. The risk of a minor neonatal morbidity decreased by a significant 12%; the risk of a major problem decreased by 19%.
Dr. Chaillet made no financial disclosures.
On Twitter @alz_gal
AT THE PREGNANCY MEETING
Major finding: Among high-risk pregnancies, the risk of a cesarean decreased by 4% overall. It did not change in tertiary care centers, but decreased by 5% at regional hospitals and 32% at community hospitals.
Data source: The study randomized 32 hospitals and tracked outcomes in more than 100,000 births.
Disclosures: Dr. Chaillet had no financial disclosures.

Video: Hospital births safer than home births
Babies delivered at home by midwives are almost four times more likely to die soon after birth than if they were delivered in a hospital, according to a database study. The difference appears to be more related to location than to attendant training, study investigator Dr. Amos Grunebaum explained in a video interview, because when home births go wrong, help is just too far away.
Babies delivered at home by midwives are almost four times more likely to die soon after birth than if they were delivered in a hospital, according to a database study. The difference appears to be more related to location than to attendant training, study investigator Dr. Amos Grunebaum explained in a video interview, because when home births go wrong, help is just too far away.
Babies delivered at home by midwives are almost four times more likely to die soon after birth than if they were delivered in a hospital, according to a database study. The difference appears to be more related to location than to attendant training, study investigator Dr. Amos Grunebaum explained in a video interview, because when home births go wrong, help is just too far away.

Intra-amniotic debris associated with preterm birth, not growth restriction
NEW ORLEANS – Intra-amniotic debris can portend a preterm birth, but doesn’t seem to be associated with any other adverse pregnancy outcomes, including small-for-gestational-age infants.
The debris – a mix of bacterial and inflammatory cells encased in an antibiotic-resistant biofilm – may actually trigger an early birth to help protect the fetus, Dr. George R. Saade said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.

The debris is associated with placental senescence, "which leads to preterm birth before there can be further fetal compromise and growth restriction," said Dr. Saade, director of maternal-fetal medicine at the University of Texas Medical Branch, Galveston.
He presented a secondary analysis of a study that examined the effect of progesterone injections to prevent preterm birth in nulliparous women with a short cervix.
The study was halted in October 2012, after preliminary results showed no treatment benefit.
The main outcome for the study was a composite of fetal death, small-for-gestational-age infants, placental abruption, and gestational hypertension/preeclampsia. Of the 657 randomized to progesterone or placebo, 78 were found to have intra-amniotic debris on ultrasound.
These women were significantly older than were those without debris (23 vs. 22 years), had a significantly higher prepregnancy body mass index (28 kg/m2 vs. 25 kg/m2), and a significantly shorter cervical length on ultrasound (19 vs. 24 cm).
There were significantly more infants born at less than 37 weeks’ gestation in women with debris (35% vs. 23%). But there was no significant between-group difference in the composite outcome. When Dr. Saade looked at the individual outcome measures, he found only one significant difference. Despite the larger number of preterm births, there were no small-for-gestational-age infants born to mothers with the debris. However, 5% of those without debris did have small-for-dates babies.
Dr. Saade had no financial declarations.
NEW ORLEANS – Intra-amniotic debris can portend a preterm birth, but doesn’t seem to be associated with any other adverse pregnancy outcomes, including small-for-gestational-age infants.
The debris – a mix of bacterial and inflammatory cells encased in an antibiotic-resistant biofilm – may actually trigger an early birth to help protect the fetus, Dr. George R. Saade said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
The debris is associated with placental senescence, "which leads to preterm birth before there can be further fetal compromise and growth restriction," said Dr. Saade, director of maternal-fetal medicine at the University of Texas Medical Branch, Galveston.
He presented a secondary analysis of a study that examined the effect of progesterone injections to prevent preterm birth in nulliparous women with a short cervix.
The study was halted in October 2012, after preliminary results showed no treatment benefit.
The main outcome for the study was a composite of fetal death, small-for-gestational-age infants, placental abruption, and gestational hypertension/preeclampsia. Of the 657 randomized to progesterone or placebo, 78 were found to have intra-amniotic debris on ultrasound.
These women were significantly older than were those without debris (23 vs. 22 years), had a significantly higher prepregnancy body mass index (28 kg/m2 vs. 25 kg/m2), and a significantly shorter cervical length on ultrasound (19 vs. 24 cm).
There were significantly more infants born at less than 37 weeks’ gestation in women with debris (35% vs. 23%). But there was no significant between-group difference in the composite outcome. When Dr. Saade looked at the individual outcome measures, he found only one significant difference. Despite the larger number of preterm births, there were no small-for-gestational-age infants born to mothers with the debris. However, 5% of those without debris did have small-for-dates babies.
Dr. Saade had no financial declarations.
NEW ORLEANS – Intra-amniotic debris can portend a preterm birth, but doesn’t seem to be associated with any other adverse pregnancy outcomes, including small-for-gestational-age infants.
The debris – a mix of bacterial and inflammatory cells encased in an antibiotic-resistant biofilm – may actually trigger an early birth to help protect the fetus, Dr. George R. Saade said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
The debris is associated with placental senescence, "which leads to preterm birth before there can be further fetal compromise and growth restriction," said Dr. Saade, director of maternal-fetal medicine at the University of Texas Medical Branch, Galveston.
He presented a secondary analysis of a study that examined the effect of progesterone injections to prevent preterm birth in nulliparous women with a short cervix.
The study was halted in October 2012, after preliminary results showed no treatment benefit.
The main outcome for the study was a composite of fetal death, small-for-gestational-age infants, placental abruption, and gestational hypertension/preeclampsia. Of the 657 randomized to progesterone or placebo, 78 were found to have intra-amniotic debris on ultrasound.
These women were significantly older than were those without debris (23 vs. 22 years), had a significantly higher prepregnancy body mass index (28 kg/m2 vs. 25 kg/m2), and a significantly shorter cervical length on ultrasound (19 vs. 24 cm).
There were significantly more infants born at less than 37 weeks’ gestation in women with debris (35% vs. 23%). But there was no significant between-group difference in the composite outcome. When Dr. Saade looked at the individual outcome measures, he found only one significant difference. Despite the larger number of preterm births, there were no small-for-gestational-age infants born to mothers with the debris. However, 5% of those without debris did have small-for-dates babies.
Dr. Saade had no financial declarations.
AT THE PREGNANCY MEETING
Major finding: Preterm birth occurred in 35% of women who had intra-amniotic debris, but none of those infants were small for gestational age.
Data source: The analysis comprised 657 women.
Disclosures: Dr. George Saade had no financial disclosures.

Fetal malformation after exposure to antiepileptics updated
Lamotrigine and carbamazepine yield lower rates of major fetal malformation than does valproate when pregnant women take one of them as monotherapy for epilepsy during the first trimester, according to an updated analysis of data from the U.K. Epilepsy and Pregnancy Register.
This supports previous findings. In recent years, lamotrigine and carbamazepine have come to be regarded as generally safer than valproate for pregnant women, and there has been a significant shift away from prescribing valproate. But some experts have raised concerns that taking high doses of the "safer" agents may be just as teratogenic as taking lower doses of valproate, according to the authors of the new analysis.
In the current study, first author Dr. Ellen Campbell of the department of neurology at Royal Victoria Hospital, Belfast, Ireland, and her colleagues analyzed data from the 5,206 pregnancies in the register exposed to valproate, carbamazepine, or lamotrigine as monotherapy during the first trimester among women residing in Ireland and the United Kingdom between 1996 and 2012. The outcome of interest was major congenital malformation, defined as any abnormality of an essential embryonic structure requiring significant treatment and present at birth or discovered during the first 6 weeks of life (J. Neurol. Neurosurg. Psychiatry 2014 Feb. 3 [doi:10.1136/jnnp-2013-306318]).
A total of 1,290 fetuses were exposed to valproate, 1,718 to carbamazepine, and 2,198 to lamotrigine. There were 248 pregnancy losses, including 17 in which the fetus had a major congenital malformation.
The odds ratios for having a child with a major congenital malformation after exposure to valproate or carbamazepine monotherapy were 3.0 and 2.7, respectively. There was no significant difference in risk between lamotrigine and carbamazepine, the investigators said.
In addition, the mean daily dose of valproate was significantly higher for mothers of infants with malformations (1,031.2 mg), compared with mothers of infants without malformations (897.9 mg). In contrast, there was no significant dose-related difference in risk of malformations among infants of mothers who took lamotrigine or carbamazepine.
"In contrast to previous data, the major congenital malformation rate with high-dose lamotrigine was reassuring and even appeared to be lower than that for low-dose valproate," the researchers noted.
The rates of all subtypes of malformation were higher after exposure to valproate than after exposure to the other agents. For example, the likelihood of neural tube defects and facial clefts was much greater after exposure to valproate than after exposure to carbamazepine (OR, 4.45), as well as after exposure to lamotrigine (OR, 11.29). There also were greater odds of hypospadias and genitourinary defects after exposure to valproate than after carbamazepine (OR, 4.11) or lamotrigine (OR, 2.60).
Similarly, skeletal defects were more common after exposure to valproate than after carbamazepine (OR, 3.41) or lamotrigine (OR, 5.77). Cardiac defects followed the same pattern.
"This large observational study confirms low overall rates of major congenital malformations among women taking an antiepileptic drug during pregnancy, with over 96% of pregnancies resulting in a child without a major congenital malformation. In keeping with previously published data, the overall major congenital malformation rates seen with exposure to lamotrigine and carbamazepine were not that different from background, particularly when taken in doses of less than 400 mg/day and 1,000 mg/day, respectively. This is likely to be of reassurance to women with epilepsy and those treating them," Dr. Campbell and her associates wrote.
They added that it remains important to control seizures as well as to minimize teratogenicity, so for some pregnant women, valproate may be the appropriate antiepileptic drug to use if other agents aren’t an option.
The U.K. Epilepsy and Pregnancy Register is supported by the Epilepsy Research Foundation and several pharmaceutical companies. Dr. Campbell reported no relevant financial conflicts of interest. Some of her coauthors reported ties to numerous industry sources.
Lamotrigine and carbamazepine yield lower rates of major fetal malformation than does valproate when pregnant women take one of them as monotherapy for epilepsy during the first trimester, according to an updated analysis of data from the U.K. Epilepsy and Pregnancy Register.
This supports previous findings. In recent years, lamotrigine and carbamazepine have come to be regarded as generally safer than valproate for pregnant women, and there has been a significant shift away from prescribing valproate. But some experts have raised concerns that taking high doses of the "safer" agents may be just as teratogenic as taking lower doses of valproate, according to the authors of the new analysis.
In the current study, first author Dr. Ellen Campbell of the department of neurology at Royal Victoria Hospital, Belfast, Ireland, and her colleagues analyzed data from the 5,206 pregnancies in the register exposed to valproate, carbamazepine, or lamotrigine as monotherapy during the first trimester among women residing in Ireland and the United Kingdom between 1996 and 2012. The outcome of interest was major congenital malformation, defined as any abnormality of an essential embryonic structure requiring significant treatment and present at birth or discovered during the first 6 weeks of life (J. Neurol. Neurosurg. Psychiatry 2014 Feb. 3 [doi:10.1136/jnnp-2013-306318]).
A total of 1,290 fetuses were exposed to valproate, 1,718 to carbamazepine, and 2,198 to lamotrigine. There were 248 pregnancy losses, including 17 in which the fetus had a major congenital malformation.
The odds ratios for having a child with a major congenital malformation after exposure to valproate or carbamazepine monotherapy were 3.0 and 2.7, respectively. There was no significant difference in risk between lamotrigine and carbamazepine, the investigators said.
In addition, the mean daily dose of valproate was significantly higher for mothers of infants with malformations (1,031.2 mg), compared with mothers of infants without malformations (897.9 mg). In contrast, there was no significant dose-related difference in risk of malformations among infants of mothers who took lamotrigine or carbamazepine.
"In contrast to previous data, the major congenital malformation rate with high-dose lamotrigine was reassuring and even appeared to be lower than that for low-dose valproate," the researchers noted.
The rates of all subtypes of malformation were higher after exposure to valproate than after exposure to the other agents. For example, the likelihood of neural tube defects and facial clefts was much greater after exposure to valproate than after exposure to carbamazepine (OR, 4.45), as well as after exposure to lamotrigine (OR, 11.29). There also were greater odds of hypospadias and genitourinary defects after exposure to valproate than after carbamazepine (OR, 4.11) or lamotrigine (OR, 2.60).
Similarly, skeletal defects were more common after exposure to valproate than after carbamazepine (OR, 3.41) or lamotrigine (OR, 5.77). Cardiac defects followed the same pattern.
"This large observational study confirms low overall rates of major congenital malformations among women taking an antiepileptic drug during pregnancy, with over 96% of pregnancies resulting in a child without a major congenital malformation. In keeping with previously published data, the overall major congenital malformation rates seen with exposure to lamotrigine and carbamazepine were not that different from background, particularly when taken in doses of less than 400 mg/day and 1,000 mg/day, respectively. This is likely to be of reassurance to women with epilepsy and those treating them," Dr. Campbell and her associates wrote.
They added that it remains important to control seizures as well as to minimize teratogenicity, so for some pregnant women, valproate may be the appropriate antiepileptic drug to use if other agents aren’t an option.
The U.K. Epilepsy and Pregnancy Register is supported by the Epilepsy Research Foundation and several pharmaceutical companies. Dr. Campbell reported no relevant financial conflicts of interest. Some of her coauthors reported ties to numerous industry sources.
Lamotrigine and carbamazepine yield lower rates of major fetal malformation than does valproate when pregnant women take one of them as monotherapy for epilepsy during the first trimester, according to an updated analysis of data from the U.K. Epilepsy and Pregnancy Register.
This supports previous findings. In recent years, lamotrigine and carbamazepine have come to be regarded as generally safer than valproate for pregnant women, and there has been a significant shift away from prescribing valproate. But some experts have raised concerns that taking high doses of the "safer" agents may be just as teratogenic as taking lower doses of valproate, according to the authors of the new analysis.
In the current study, first author Dr. Ellen Campbell of the department of neurology at Royal Victoria Hospital, Belfast, Ireland, and her colleagues analyzed data from the 5,206 pregnancies in the register exposed to valproate, carbamazepine, or lamotrigine as monotherapy during the first trimester among women residing in Ireland and the United Kingdom between 1996 and 2012. The outcome of interest was major congenital malformation, defined as any abnormality of an essential embryonic structure requiring significant treatment and present at birth or discovered during the first 6 weeks of life (J. Neurol. Neurosurg. Psychiatry 2014 Feb. 3 [doi:10.1136/jnnp-2013-306318]).
A total of 1,290 fetuses were exposed to valproate, 1,718 to carbamazepine, and 2,198 to lamotrigine. There were 248 pregnancy losses, including 17 in which the fetus had a major congenital malformation.
The odds ratios for having a child with a major congenital malformation after exposure to valproate or carbamazepine monotherapy were 3.0 and 2.7, respectively. There was no significant difference in risk between lamotrigine and carbamazepine, the investigators said.
In addition, the mean daily dose of valproate was significantly higher for mothers of infants with malformations (1,031.2 mg), compared with mothers of infants without malformations (897.9 mg). In contrast, there was no significant dose-related difference in risk of malformations among infants of mothers who took lamotrigine or carbamazepine.
"In contrast to previous data, the major congenital malformation rate with high-dose lamotrigine was reassuring and even appeared to be lower than that for low-dose valproate," the researchers noted.
The rates of all subtypes of malformation were higher after exposure to valproate than after exposure to the other agents. For example, the likelihood of neural tube defects and facial clefts was much greater after exposure to valproate than after exposure to carbamazepine (OR, 4.45), as well as after exposure to lamotrigine (OR, 11.29). There also were greater odds of hypospadias and genitourinary defects after exposure to valproate than after carbamazepine (OR, 4.11) or lamotrigine (OR, 2.60).
Similarly, skeletal defects were more common after exposure to valproate than after carbamazepine (OR, 3.41) or lamotrigine (OR, 5.77). Cardiac defects followed the same pattern.
"This large observational study confirms low overall rates of major congenital malformations among women taking an antiepileptic drug during pregnancy, with over 96% of pregnancies resulting in a child without a major congenital malformation. In keeping with previously published data, the overall major congenital malformation rates seen with exposure to lamotrigine and carbamazepine were not that different from background, particularly when taken in doses of less than 400 mg/day and 1,000 mg/day, respectively. This is likely to be of reassurance to women with epilepsy and those treating them," Dr. Campbell and her associates wrote.
They added that it remains important to control seizures as well as to minimize teratogenicity, so for some pregnant women, valproate may be the appropriate antiepileptic drug to use if other agents aren’t an option.
The U.K. Epilepsy and Pregnancy Register is supported by the Epilepsy Research Foundation and several pharmaceutical companies. Dr. Campbell reported no relevant financial conflicts of interest. Some of her coauthors reported ties to numerous industry sources.
FROM JOURNAL OF NEUROLOGY, NEUROSURGERY & PSYCHIATRY
Major Finding: The odds ratios for having a child with a major congenital malformation after exposure to valproate or carbamazepine monotherapy were 3.0 and 2.7, respectively.
Data Source: A 15-year, observational study of major congenital malformations occurring after exposure to antiepileptic drugs in 5,206 pregnancies in Ireland and the United Kingdom.
Disclosures: The U.K. Epilepsy and Pregnancy Register is supported by the Epilepsy Research Foundation and several pharmaceutical companies. Dr. Campbell reported no relevant financial conflicts of interest. Some of her coauthors reported ties to numerous industry sources.
For women with prior cesareans, 39-week delivery is not optimal
NEW ORLEANS – The safest time to deliver a woman with prior cesarean sections may be up to 2 weeks earlier than the current recommendation.
Guidelines from a number of national groups, including the Society for Maternal-Fetal Medicine, recommend planning a cesarean delivery at 39 weeks for these women. But a retrospective study has determined that maternal risk increases sharply after 37 weeks for women who have had three or more cesarean deliveries – a full 2 weeks before there is any increase in fetal risk.
"The data clearly show that the optimal time for delivery in women with three or more prior cesareans is 37 weeks," Dr. Laura Hart said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Dr. Hart of the University of Texas Health Science Center, Houston, extracted her data from the Maternal-Fetal Medicine Units (MFMU) Cesarean Section Registry. It contains prospective data on more than 24,000 deliveries performed after prior cesarean. She examined information on 6,435 deliveries that followed at least two prior cesareans (80% after two sections and 20% after three or more).

Dr. Hart analyzed both maternal and fetal outcomes. Each was a single composite comprising several endpoints. The maternal composite took into account transfusion, hysterectomy, operative injury, thromboembolic event, pulmonary edema, and death. The perinatal composite included respiratory distress syndrome, necrotizing enterocolitis (grade 2 or 3), intraventricular hemorrhage (grade 3 or 4), hypoxic ischemic injury, seizure, and stillbirth or neonatal death.
The results were expressed as a risk of the composite event relative to the number of ongoing pregnancies.
Less than half of the women who had two prior cesareans delivered at 39 weeks (46%); 11% delivered at 37 weeks, 31% at 38 weeks, and 13% at 40 weeks or more.
For these women, the risk of maternal complications was less than 5 per 1,000 ongoing pregnancies at 37 weeks. It remained low at 38 weeks (about 7/1,000). But between 38 and 39 weeks, it rose sharply, to 16/1,000. The risk remained similarly elevated at 40 weeks and beyond.
The perinatal outcomes risk was low at 37 weeks (7/1,000) and remained low at 38 and 39 weeks (7 and 9/1,000, respectively). The risk also increased sharply between 38 and 39 weeks, rising to about 20/1,000. The maternal and perinatal risk curves intersected between weeks 37 and 38, indicating that 38 weeks was probably the optimal time for delivery.
Less than half of women who had at least three prior cesareans also made it to 39 weeks (41%). About a third (35%) delivered at 38 weeks, 15% at 37 weeks, and 9% at 40 weeks or more.
Again, maternal risk was very low at 37 weeks (about 4/1,000 ongoing pregnancies). But in contrast to the risk for women with two prior deliveries, the risk for these women increased sharply and linearly over the final weeks of gestation. By 38 weeks, it had jumped to about 16/1,000. By 39 weeks, it was close to 50/1,000, and by 40 weeks and beyond, more than 50/1,000.
Conversely, perinatal risk remained fairly low in weeks 37, 38, and 39 (9, 7, and 10/1,000, respectively). Risk accelerated between weeks 39 and 40; by week 40 and beyond, it hovered just above 25/1,000. The risk curves intersected between weeks 37 and 38, indicating that 37 weeks is the optimal time for delivery.
Dr. Hart added that maternal transfusion was the main risk driver for women, followed closely by operative injury and hysterectomy.
These data were published in a supplement to the American Journal of Obstetrics and Gynecology (Amer. J. Obstet. Gynecol. 2014;210(suppl.):S27).
Dr. Hart had no financial disclosures.
NEW ORLEANS – The safest time to deliver a woman with prior cesarean sections may be up to 2 weeks earlier than the current recommendation.
Guidelines from a number of national groups, including the Society for Maternal-Fetal Medicine, recommend planning a cesarean delivery at 39 weeks for these women. But a retrospective study has determined that maternal risk increases sharply after 37 weeks for women who have had three or more cesarean deliveries – a full 2 weeks before there is any increase in fetal risk.
"The data clearly show that the optimal time for delivery in women with three or more prior cesareans is 37 weeks," Dr. Laura Hart said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Dr. Hart of the University of Texas Health Science Center, Houston, extracted her data from the Maternal-Fetal Medicine Units (MFMU) Cesarean Section Registry. It contains prospective data on more than 24,000 deliveries performed after prior cesarean. She examined information on 6,435 deliveries that followed at least two prior cesareans (80% after two sections and 20% after three or more).
Dr. Hart analyzed both maternal and fetal outcomes. Each was a single composite comprising several endpoints. The maternal composite took into account transfusion, hysterectomy, operative injury, thromboembolic event, pulmonary edema, and death. The perinatal composite included respiratory distress syndrome, necrotizing enterocolitis (grade 2 or 3), intraventricular hemorrhage (grade 3 or 4), hypoxic ischemic injury, seizure, and stillbirth or neonatal death.
The results were expressed as a risk of the composite event relative to the number of ongoing pregnancies.
Less than half of the women who had two prior cesareans delivered at 39 weeks (46%); 11% delivered at 37 weeks, 31% at 38 weeks, and 13% at 40 weeks or more.
For these women, the risk of maternal complications was less than 5 per 1,000 ongoing pregnancies at 37 weeks. It remained low at 38 weeks (about 7/1,000). But between 38 and 39 weeks, it rose sharply, to 16/1,000. The risk remained similarly elevated at 40 weeks and beyond.
The perinatal outcomes risk was low at 37 weeks (7/1,000) and remained low at 38 and 39 weeks (7 and 9/1,000, respectively). The risk also increased sharply between 38 and 39 weeks, rising to about 20/1,000. The maternal and perinatal risk curves intersected between weeks 37 and 38, indicating that 38 weeks was probably the optimal time for delivery.
Less than half of women who had at least three prior cesareans also made it to 39 weeks (41%). About a third (35%) delivered at 38 weeks, 15% at 37 weeks, and 9% at 40 weeks or more.
Again, maternal risk was very low at 37 weeks (about 4/1,000 ongoing pregnancies). But in contrast to the risk for women with two prior deliveries, the risk for these women increased sharply and linearly over the final weeks of gestation. By 38 weeks, it had jumped to about 16/1,000. By 39 weeks, it was close to 50/1,000, and by 40 weeks and beyond, more than 50/1,000.
Conversely, perinatal risk remained fairly low in weeks 37, 38, and 39 (9, 7, and 10/1,000, respectively). Risk accelerated between weeks 39 and 40; by week 40 and beyond, it hovered just above 25/1,000. The risk curves intersected between weeks 37 and 38, indicating that 37 weeks is the optimal time for delivery.
Dr. Hart added that maternal transfusion was the main risk driver for women, followed closely by operative injury and hysterectomy.
These data were published in a supplement to the American Journal of Obstetrics and Gynecology (Amer. J. Obstet. Gynecol. 2014;210(suppl.):S27).
Dr. Hart had no financial disclosures.
NEW ORLEANS – The safest time to deliver a woman with prior cesarean sections may be up to 2 weeks earlier than the current recommendation.
Guidelines from a number of national groups, including the Society for Maternal-Fetal Medicine, recommend planning a cesarean delivery at 39 weeks for these women. But a retrospective study has determined that maternal risk increases sharply after 37 weeks for women who have had three or more cesarean deliveries – a full 2 weeks before there is any increase in fetal risk.
"The data clearly show that the optimal time for delivery in women with three or more prior cesareans is 37 weeks," Dr. Laura Hart said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Dr. Hart of the University of Texas Health Science Center, Houston, extracted her data from the Maternal-Fetal Medicine Units (MFMU) Cesarean Section Registry. It contains prospective data on more than 24,000 deliveries performed after prior cesarean. She examined information on 6,435 deliveries that followed at least two prior cesareans (80% after two sections and 20% after three or more).
Dr. Hart analyzed both maternal and fetal outcomes. Each was a single composite comprising several endpoints. The maternal composite took into account transfusion, hysterectomy, operative injury, thromboembolic event, pulmonary edema, and death. The perinatal composite included respiratory distress syndrome, necrotizing enterocolitis (grade 2 or 3), intraventricular hemorrhage (grade 3 or 4), hypoxic ischemic injury, seizure, and stillbirth or neonatal death.
The results were expressed as a risk of the composite event relative to the number of ongoing pregnancies.
Less than half of the women who had two prior cesareans delivered at 39 weeks (46%); 11% delivered at 37 weeks, 31% at 38 weeks, and 13% at 40 weeks or more.
For these women, the risk of maternal complications was less than 5 per 1,000 ongoing pregnancies at 37 weeks. It remained low at 38 weeks (about 7/1,000). But between 38 and 39 weeks, it rose sharply, to 16/1,000. The risk remained similarly elevated at 40 weeks and beyond.
The perinatal outcomes risk was low at 37 weeks (7/1,000) and remained low at 38 and 39 weeks (7 and 9/1,000, respectively). The risk also increased sharply between 38 and 39 weeks, rising to about 20/1,000. The maternal and perinatal risk curves intersected between weeks 37 and 38, indicating that 38 weeks was probably the optimal time for delivery.
Less than half of women who had at least three prior cesareans also made it to 39 weeks (41%). About a third (35%) delivered at 38 weeks, 15% at 37 weeks, and 9% at 40 weeks or more.
Again, maternal risk was very low at 37 weeks (about 4/1,000 ongoing pregnancies). But in contrast to the risk for women with two prior deliveries, the risk for these women increased sharply and linearly over the final weeks of gestation. By 38 weeks, it had jumped to about 16/1,000. By 39 weeks, it was close to 50/1,000, and by 40 weeks and beyond, more than 50/1,000.
Conversely, perinatal risk remained fairly low in weeks 37, 38, and 39 (9, 7, and 10/1,000, respectively). Risk accelerated between weeks 39 and 40; by week 40 and beyond, it hovered just above 25/1,000. The risk curves intersected between weeks 37 and 38, indicating that 37 weeks is the optimal time for delivery.
Dr. Hart added that maternal transfusion was the main risk driver for women, followed closely by operative injury and hysterectomy.
These data were published in a supplement to the American Journal of Obstetrics and Gynecology (Amer. J. Obstet. Gynecol. 2014;210(suppl.):S27).
Dr. Hart had no financial disclosures.
AT THE PREGNANCY MEETING
Major finding: The optimal time for delivery of women with two prior cesarean sections is 38 weeks; for women with three or more prior sections, it is 37 weeks.
Data source: The retrospective analysis comprised 6,435 women.
Disclosures: Dr. Laura Hart had no financial disclosures.

Birth weight, not postterm delivery, puts a baby at risk for shoulder dystocia
Women who deliver a large infant before 40 weeks’ gestation have a higher risk of shoulder dystocia than those who deliver a large infant at 40 weeks’ gestation or later, according to a population-based study of all vaginal deliveries in Norway from 1969 to 2009 (n = 2,014,956).1 The increased risk of shoulder dystocia in deliveries before 40 weeks’ gestation was especially pronounced in pregnancies complicated by diabetes.
Large infants were defined as those weighing 3,500 g or more at delivery.
Related Article: You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial, May 2013)
DETAILS OF THE STUDY
Using the Medical Birth Registry of Norway, Overland and colleagues analyzed all vaginal deliveries of a singleton fetus in cephalic presentation over 30 years, calculating the incidence of shoulder dystocia by gestational age at delivery and estimating both crude and adjusted odds ratios.
Overall, the incidence of shoulder dystocia was 0.73%, and it increased along with gestational age at delivery. Using delivery at 40 to 41 weeks of gestation as the reference, Overland and colleagues found the following crude odds ratios (OR) for shoulder dystocia:
- delivery before 36 weeks: 0.27 (95% confidence interval [CI], 0.22–0.33)
- delivery at 42–43 weeks: 1.17 (95% CI, 1.11–1.22).
However, after adjustment for birth weight, the adjusted OR for shoulder dystocia was:
- delivery at 32–35 weeks: 2.92 (95% CI, 1.54–5.52)
- delivery at 42–43 weeks: 0.91 (95% CI, 0.50–1.66).
Among gestations affected by diabetes (n = 11,188), the incidence of shoulder dystocia was 3.95%.
Related Article: STOP all activities that may lead to further shoulder impaction when you suspect possible shoulder dystocia Ronald T. Burkman, MD (Stop/Start, March 2013)
LONGER PREGNANCIES MAY BE BETTER “PRIMED” FOR DELIVERY
The surprising finding that the risk of shoulder dystocia is lower in postterm infants than in infants delivered prior to 40 weeks at a given birth weight “is not easily explained,” write Overland and colleagues.1 “A successful delivery depends on a complex interplay between the uterus, the pelvis (the pelvic girdle and the pelvic floor muscles) and the offspring…. The physiological changes that occur during pregnancy to prime the pregnant woman and the offspring for delivery are likely to be complete by the estimated term. Hence, the risk for delivery complications, such as shoulder dystocia, may be increased in deliveries before term,” the investigators theorize.1
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
Reference
- Overland EA, Vatten, LJ, Eskild A. Pregnancy week at delivery and the risk of shoulder dystocia: a population study of 2,014,956 deliveries. BJOG. 2014;121:34–42.
Women who deliver a large infant before 40 weeks’ gestation have a higher risk of shoulder dystocia than those who deliver a large infant at 40 weeks’ gestation or later, according to a population-based study of all vaginal deliveries in Norway from 1969 to 2009 (n = 2,014,956).1 The increased risk of shoulder dystocia in deliveries before 40 weeks’ gestation was especially pronounced in pregnancies complicated by diabetes.
Large infants were defined as those weighing 3,500 g or more at delivery.
Related Article: You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial, May 2013)
DETAILS OF THE STUDY
Using the Medical Birth Registry of Norway, Overland and colleagues analyzed all vaginal deliveries of a singleton fetus in cephalic presentation over 30 years, calculating the incidence of shoulder dystocia by gestational age at delivery and estimating both crude and adjusted odds ratios.
Overall, the incidence of shoulder dystocia was 0.73%, and it increased along with gestational age at delivery. Using delivery at 40 to 41 weeks of gestation as the reference, Overland and colleagues found the following crude odds ratios (OR) for shoulder dystocia:
- delivery before 36 weeks: 0.27 (95% confidence interval [CI], 0.22–0.33)
- delivery at 42–43 weeks: 1.17 (95% CI, 1.11–1.22).
However, after adjustment for birth weight, the adjusted OR for shoulder dystocia was:
- delivery at 32–35 weeks: 2.92 (95% CI, 1.54–5.52)
- delivery at 42–43 weeks: 0.91 (95% CI, 0.50–1.66).
Among gestations affected by diabetes (n = 11,188), the incidence of shoulder dystocia was 3.95%.
Related Article: STOP all activities that may lead to further shoulder impaction when you suspect possible shoulder dystocia Ronald T. Burkman, MD (Stop/Start, March 2013)
LONGER PREGNANCIES MAY BE BETTER “PRIMED” FOR DELIVERY
The surprising finding that the risk of shoulder dystocia is lower in postterm infants than in infants delivered prior to 40 weeks at a given birth weight “is not easily explained,” write Overland and colleagues.1 “A successful delivery depends on a complex interplay between the uterus, the pelvis (the pelvic girdle and the pelvic floor muscles) and the offspring…. The physiological changes that occur during pregnancy to prime the pregnant woman and the offspring for delivery are likely to be complete by the estimated term. Hence, the risk for delivery complications, such as shoulder dystocia, may be increased in deliveries before term,” the investigators theorize.1
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
Women who deliver a large infant before 40 weeks’ gestation have a higher risk of shoulder dystocia than those who deliver a large infant at 40 weeks’ gestation or later, according to a population-based study of all vaginal deliveries in Norway from 1969 to 2009 (n = 2,014,956).1 The increased risk of shoulder dystocia in deliveries before 40 weeks’ gestation was especially pronounced in pregnancies complicated by diabetes.
Large infants were defined as those weighing 3,500 g or more at delivery.
Related Article: You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial, May 2013)
DETAILS OF THE STUDY
Using the Medical Birth Registry of Norway, Overland and colleagues analyzed all vaginal deliveries of a singleton fetus in cephalic presentation over 30 years, calculating the incidence of shoulder dystocia by gestational age at delivery and estimating both crude and adjusted odds ratios.
Overall, the incidence of shoulder dystocia was 0.73%, and it increased along with gestational age at delivery. Using delivery at 40 to 41 weeks of gestation as the reference, Overland and colleagues found the following crude odds ratios (OR) for shoulder dystocia:
- delivery before 36 weeks: 0.27 (95% confidence interval [CI], 0.22–0.33)
- delivery at 42–43 weeks: 1.17 (95% CI, 1.11–1.22).
However, after adjustment for birth weight, the adjusted OR for shoulder dystocia was:
- delivery at 32–35 weeks: 2.92 (95% CI, 1.54–5.52)
- delivery at 42–43 weeks: 0.91 (95% CI, 0.50–1.66).
Among gestations affected by diabetes (n = 11,188), the incidence of shoulder dystocia was 3.95%.
Related Article: STOP all activities that may lead to further shoulder impaction when you suspect possible shoulder dystocia Ronald T. Burkman, MD (Stop/Start, March 2013)
LONGER PREGNANCIES MAY BE BETTER “PRIMED” FOR DELIVERY
The surprising finding that the risk of shoulder dystocia is lower in postterm infants than in infants delivered prior to 40 weeks at a given birth weight “is not easily explained,” write Overland and colleagues.1 “A successful delivery depends on a complex interplay between the uterus, the pelvis (the pelvic girdle and the pelvic floor muscles) and the offspring…. The physiological changes that occur during pregnancy to prime the pregnant woman and the offspring for delivery are likely to be complete by the estimated term. Hence, the risk for delivery complications, such as shoulder dystocia, may be increased in deliveries before term,” the investigators theorize.1
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
Reference
- Overland EA, Vatten, LJ, Eskild A. Pregnancy week at delivery and the risk of shoulder dystocia: a population study of 2,014,956 deliveries. BJOG. 2014;121:34–42.
Reference
- Overland EA, Vatten, LJ, Eskild A. Pregnancy week at delivery and the risk of shoulder dystocia: a population study of 2,014,956 deliveries. BJOG. 2014;121:34–42.
Get same-day ultrasound if pregnant, bleeding
SAN FRANCISCO – Make sure a woman who has uterine bleeding or abdominal pain in the first trimester of pregnancy gets an ultrasound the same day you see her, whether you do the ultrasound yourself, refer her to another physician for a same-day ultrasound, or send her to the emergency department, Dr. Rebecca Jackson advised.
The same-day ultrasound is essential to diagnose ectopic pregnancy early, Dr. Jackson said at a conference on women’s health sponsored by the University of California, San Francisco. The ultrasound is unlikely to show an ectopic pregnancy, but if you see an intrauterine pregnancy, "you’re done," she said.
Ectopic pregnancy occurs in 2% of pregnancies and is the leading cause of U.S. maternal deaths in the first trimester. "The key thing about ectopic pregnancy is that two-thirds of the women dying from an ectopic pregnancy had recently seen a clinician, but had an incorrect or delayed diagnosis," said Dr. Jackson, professor of obstetrics and gynecology at the university and chief of obstetrics and gynecology at San Francisco General Hospital.

If an ultrasound doesn’t show the location of the pregnancy, obtain serial quantitative beta-HCG levels to determine whether the pregnancy is normal or abnormal, she advised. "If it rises appropriately, it’s likely normal, but ectopics can also rise in the same way" as beta-HCG levels with intrauterine pregnancies, she said. "But if it drops or rises very little you know it’s abnormal."
Get a uterine aspiration in women with an abnormal beta-HCG level to look for placental tissue in the uterus, which indicates an intrauterine pregnancy, she said. If there’s no placental tissue in the uterus, treat for ectopic pregnancy.
There’s a shortcut in all of this to keep in mind, she added. If a woman presents with abnormal uterine bleeding or abdominal pain and she tests positive for pregnancy, ask if she desires the pregnancy. If not, you can skip the ultrasound and beta-HCG levels and go straight to the uterine aspiration, Dr. Jackson said.
These steps to diagnosing ectopic pregnancy may sound simple but in reality take ob.gyn. residents years to master. "There are so many flavors of how women present, and you combine that with their desires and their fertility desires, and it’s a really hard thing to manage," she said.
Only approximately 2% of ultrasounds done for possible ectopic pregnancy will show a gestational sac with a yolk sac or fetal pole visible outside the uterus, and thus be diagnostic, Dr. Jackson said. A normal adnexal exam does not exclude an ectopic pregnancy. An empty uterus on ultrasound and a beta-HCG level above the discriminatory zone suggests an ectopic pregnancy, and will be in 86% of cases. An ultrasound showing a complex mass and fluid in a cul-de-sac will be an ectopic pregnancy in 94% of cases. The main role of the ultrasound is to rule in an intrauterine pregnancy.
Diagnosing ectopic pregnancy early decreases the risk of rupture, which has been associated with decreased fertility and increased morbidity and mortality. "Just as an aside, rupture can occur at any level of beta-HCG and whether beta-HCG is rising or falling or plateauing, so that doesn’t help you," she said.
More treatment options are available if ectopic pregnancy is diagnosed early, including methotrexate or conservative surgical treatment, and methotrexate is more efficacious in earlier than in later ectopic pregnancy, Dr. Jackson said.
Methotrexate treatment, which is relatively new for ectopic pregnancy, "is not for everyone," she added. "It involves a lot of follow-up. Patient compliance is incredibly important. There’s still 5% who will rupture despite methotrexate treatment. And all of these things need to be explained to the patient so she can make an informed choice." Methotrexate is less effective than salpingostomy, and the efficacy of the drug decreases with increasing beta-HCG levels. Fifteen percent of patients treated with methotrexate will require a second dose.
A decrease in future intrauterine pregnancy rates in women with ectopic pregnancy is no different in those treated with methotrexate than in those treated with surgery, and the risk of a future ectopic pregnancy is increased by 10%-15% in both groups, she said.
Dr. Jackson reported having no relevant financial disclosures.
On Twitter @sherryboschert
SAN FRANCISCO – Make sure a woman who has uterine bleeding or abdominal pain in the first trimester of pregnancy gets an ultrasound the same day you see her, whether you do the ultrasound yourself, refer her to another physician for a same-day ultrasound, or send her to the emergency department, Dr. Rebecca Jackson advised.
The same-day ultrasound is essential to diagnose ectopic pregnancy early, Dr. Jackson said at a conference on women’s health sponsored by the University of California, San Francisco. The ultrasound is unlikely to show an ectopic pregnancy, but if you see an intrauterine pregnancy, "you’re done," she said.
Ectopic pregnancy occurs in 2% of pregnancies and is the leading cause of U.S. maternal deaths in the first trimester. "The key thing about ectopic pregnancy is that two-thirds of the women dying from an ectopic pregnancy had recently seen a clinician, but had an incorrect or delayed diagnosis," said Dr. Jackson, professor of obstetrics and gynecology at the university and chief of obstetrics and gynecology at San Francisco General Hospital.
If an ultrasound doesn’t show the location of the pregnancy, obtain serial quantitative beta-HCG levels to determine whether the pregnancy is normal or abnormal, she advised. "If it rises appropriately, it’s likely normal, but ectopics can also rise in the same way" as beta-HCG levels with intrauterine pregnancies, she said. "But if it drops or rises very little you know it’s abnormal."
Get a uterine aspiration in women with an abnormal beta-HCG level to look for placental tissue in the uterus, which indicates an intrauterine pregnancy, she said. If there’s no placental tissue in the uterus, treat for ectopic pregnancy.
There’s a shortcut in all of this to keep in mind, she added. If a woman presents with abnormal uterine bleeding or abdominal pain and she tests positive for pregnancy, ask if she desires the pregnancy. If not, you can skip the ultrasound and beta-HCG levels and go straight to the uterine aspiration, Dr. Jackson said.
These steps to diagnosing ectopic pregnancy may sound simple but in reality take ob.gyn. residents years to master. "There are so many flavors of how women present, and you combine that with their desires and their fertility desires, and it’s a really hard thing to manage," she said.
Only approximately 2% of ultrasounds done for possible ectopic pregnancy will show a gestational sac with a yolk sac or fetal pole visible outside the uterus, and thus be diagnostic, Dr. Jackson said. A normal adnexal exam does not exclude an ectopic pregnancy. An empty uterus on ultrasound and a beta-HCG level above the discriminatory zone suggests an ectopic pregnancy, and will be in 86% of cases. An ultrasound showing a complex mass and fluid in a cul-de-sac will be an ectopic pregnancy in 94% of cases. The main role of the ultrasound is to rule in an intrauterine pregnancy.
Diagnosing ectopic pregnancy early decreases the risk of rupture, which has been associated with decreased fertility and increased morbidity and mortality. "Just as an aside, rupture can occur at any level of beta-HCG and whether beta-HCG is rising or falling or plateauing, so that doesn’t help you," she said.
More treatment options are available if ectopic pregnancy is diagnosed early, including methotrexate or conservative surgical treatment, and methotrexate is more efficacious in earlier than in later ectopic pregnancy, Dr. Jackson said.
Methotrexate treatment, which is relatively new for ectopic pregnancy, "is not for everyone," she added. "It involves a lot of follow-up. Patient compliance is incredibly important. There’s still 5% who will rupture despite methotrexate treatment. And all of these things need to be explained to the patient so she can make an informed choice." Methotrexate is less effective than salpingostomy, and the efficacy of the drug decreases with increasing beta-HCG levels. Fifteen percent of patients treated with methotrexate will require a second dose.
A decrease in future intrauterine pregnancy rates in women with ectopic pregnancy is no different in those treated with methotrexate than in those treated with surgery, and the risk of a future ectopic pregnancy is increased by 10%-15% in both groups, she said.
Dr. Jackson reported having no relevant financial disclosures.
On Twitter @sherryboschert
SAN FRANCISCO – Make sure a woman who has uterine bleeding or abdominal pain in the first trimester of pregnancy gets an ultrasound the same day you see her, whether you do the ultrasound yourself, refer her to another physician for a same-day ultrasound, or send her to the emergency department, Dr. Rebecca Jackson advised.
The same-day ultrasound is essential to diagnose ectopic pregnancy early, Dr. Jackson said at a conference on women’s health sponsored by the University of California, San Francisco. The ultrasound is unlikely to show an ectopic pregnancy, but if you see an intrauterine pregnancy, "you’re done," she said.
Ectopic pregnancy occurs in 2% of pregnancies and is the leading cause of U.S. maternal deaths in the first trimester. "The key thing about ectopic pregnancy is that two-thirds of the women dying from an ectopic pregnancy had recently seen a clinician, but had an incorrect or delayed diagnosis," said Dr. Jackson, professor of obstetrics and gynecology at the university and chief of obstetrics and gynecology at San Francisco General Hospital.
If an ultrasound doesn’t show the location of the pregnancy, obtain serial quantitative beta-HCG levels to determine whether the pregnancy is normal or abnormal, she advised. "If it rises appropriately, it’s likely normal, but ectopics can also rise in the same way" as beta-HCG levels with intrauterine pregnancies, she said. "But if it drops or rises very little you know it’s abnormal."
Get a uterine aspiration in women with an abnormal beta-HCG level to look for placental tissue in the uterus, which indicates an intrauterine pregnancy, she said. If there’s no placental tissue in the uterus, treat for ectopic pregnancy.
There’s a shortcut in all of this to keep in mind, she added. If a woman presents with abnormal uterine bleeding or abdominal pain and she tests positive for pregnancy, ask if she desires the pregnancy. If not, you can skip the ultrasound and beta-HCG levels and go straight to the uterine aspiration, Dr. Jackson said.
These steps to diagnosing ectopic pregnancy may sound simple but in reality take ob.gyn. residents years to master. "There are so many flavors of how women present, and you combine that with their desires and their fertility desires, and it’s a really hard thing to manage," she said.
Only approximately 2% of ultrasounds done for possible ectopic pregnancy will show a gestational sac with a yolk sac or fetal pole visible outside the uterus, and thus be diagnostic, Dr. Jackson said. A normal adnexal exam does not exclude an ectopic pregnancy. An empty uterus on ultrasound and a beta-HCG level above the discriminatory zone suggests an ectopic pregnancy, and will be in 86% of cases. An ultrasound showing a complex mass and fluid in a cul-de-sac will be an ectopic pregnancy in 94% of cases. The main role of the ultrasound is to rule in an intrauterine pregnancy.
Diagnosing ectopic pregnancy early decreases the risk of rupture, which has been associated with decreased fertility and increased morbidity and mortality. "Just as an aside, rupture can occur at any level of beta-HCG and whether beta-HCG is rising or falling or plateauing, so that doesn’t help you," she said.
More treatment options are available if ectopic pregnancy is diagnosed early, including methotrexate or conservative surgical treatment, and methotrexate is more efficacious in earlier than in later ectopic pregnancy, Dr. Jackson said.
Methotrexate treatment, which is relatively new for ectopic pregnancy, "is not for everyone," she added. "It involves a lot of follow-up. Patient compliance is incredibly important. There’s still 5% who will rupture despite methotrexate treatment. And all of these things need to be explained to the patient so she can make an informed choice." Methotrexate is less effective than salpingostomy, and the efficacy of the drug decreases with increasing beta-HCG levels. Fifteen percent of patients treated with methotrexate will require a second dose.
A decrease in future intrauterine pregnancy rates in women with ectopic pregnancy is no different in those treated with methotrexate than in those treated with surgery, and the risk of a future ectopic pregnancy is increased by 10%-15% in both groups, she said.
Dr. Jackson reported having no relevant financial disclosures.
On Twitter @sherryboschert
EXPERT ANALYSIS FROM A CONFERENCE ON WOMEN’S HEALTH

Shift in approach needed for managing inflammatory arthritis in pregnancy
SNOWMASS, COLO. – The common strategy of managing inflammatory arthritis during pregnancy by stopping all prepregnancy medications and prescribing prednisone is counterproductive, Dr. Megan E.B. Clowse said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
"This sort of safe approach is actually not the safest or best approach. We all need to shift our attitude and get comfortable with at least a couple of other medications in order to help our patients have better outcomes," asserted Dr. Clowse, director of the Duke Autoimmunity in Pregnancy (DAP) Registry at Duke University, Durham, N.C.

It’s often true that rheumatoid arthritis (RA) tends to get better in pregnancy. Nonetheless, pregnancy may not be enough to control disease activity in many women, as illustrated by a nationwide Dutch study in which half of RA patients had moderate to severe disease activity by their third trimester (Arthritis Rheum. 2008;59:1241-8).
"In my experience, the patients who were on tumor necrosis factor inhibitors prepregnancy do not do as well when they come off them. So pregnancy might be good for RA disease activity, but it’s definitely not as good as a tumor necrosis factor inhibitor," according to the rheumatologist.
Roughly one-quarter of the more than 230 prospectively studied pregnancies in the DAP Registry have been in women with RA or other inflammatory arthritides. The preterm birth rate in RA patients in DAP, as in other RA registries, is higher than in the general population. Notably, all of the DAP patients with RA who had preterm birth had moderate to severe disease activity in the first and second trimesters, compared with just a single RA patient with a term delivery.
"Allowing disease to flare may actually harm the pregnancy," Dr. Clowse commented.
Her two top recommendations for nonbiologic treatment of inflammatory arthritis during pregnancy are hydroxychloroquine and sulfasalazine. Hydroxychloroquine is effective for mild arthritis, and it’s rated by the Food and Drug Administration as Pregnancy Category C, with no reports of human toxicity. Sulfasalazine has a good safety profile in pregnancy – it is Pregnancy Category B – and has good efficacy for peripheral arthritis.
"These are two very important medications that are much better – and definitely much safer – options than prednisone. These are just great options, and I try to encourage patients to take them. It’s definitely better than letting patients flare while off methotrexate before they deliver," she continued.
"TNF [tumor necrosis factor] inhibitors are, I think, another reasonable option, particularly in the population with moderate to severe disease activity. If any of these medications help you avoid prednisone, then I think you come out ahead," Dr. Clowse said.
Reassuring data regarding the safety of anti-TNF biologics in pregnancy comes from several sources. A systematic literature review by Dr. Evelyne Vinet and her coworkers at McGill University, Montreal, found no evidence of excess risk of adverse pregnancy or fetal outcomes in women exposed to etanercept (Enbrel), infliximab (Remicade), or adalimumab (Humira) during pregnancy (Arthritis Rheum. 2009;61:587-92). A report from the Organization of Teratology Information Specialists (OTIS) Registry, presented at the 2012 annual meeting of the American College of Rheumatology, found no significant difference between RA patients exposed to adalimumab in pregnancy and RA controls in rates of live birth, miscarriage, stillbirth, congenital abnormalities, or serious infections in the first year of life.
Moreover, DAP Registry data support the notion that for some patients, anti-TNF biologics during pregnancy may be a good option. In Dr. Clowse’s series of 29 RA patients, disease activity during the first trimester neatly delineated three distinct groups. Eleven patients who had a 28-joint Disease Activity Score using C-reactive protein (DAS28-CRP) averaging 1.5 in the first trimester required neither TNF inhibitors nor prednisone during their pregnancy, and they had no abnormal outcomes. Seven patients with significant first-trimester disease activity as defined by an average DAS28-CRP score of 3.4 went back on their TNF inhibitor during pregnancy, and their disease essentially went into remission, with only one preterm birth. In contrast, 11 other patients with significant first-trimester disease activity went on prednisone because they rejected TNF inhibitor therapy; their disease activity remained substantial, and 6 of the 11 had a preterm birth and/or preeclampsia.
"All of the preeclampsia occurred in the prednisone group. They also had a lot of disease activity postpartum," Dr. Clowse observed.
Infliximab and adalimumab freely pass across the placenta; etanercept and certolizumab pegol (Cimzia) do not. Regardless, no infant exposed in utero to a TNF inhibitor should receive the rotavirus vaccine during the first 5 months of life. That’s the only live-virus vaccine given during infancy in the United States; all the other vaccines can safely be given according to schedule.
Dr. Clowse said there is essentially no published literature regarding psoriatic arthritis in pregnancy. The DAP registry experience includes seven pregnancies in women with psoriatic arthritis. There were no pregnancy losses, one preterm birth, and two cases of preeclampsia.
"What I see is dramatically increased disease activity when women with psoriatic arthritis stop their TNF inhibitor. The worst psoriasis I’ve ever seen is in pregnant patients; they are really miserable off their TNF inhibitors," she said.
There is also very little in the literature about axial spondyloarthritis in pregnancy. The DAP registry’s 10 cases constitute one of the largest series. There were no pregnancy losses, no preeclampsia, and one preterm birth. Eight of the women were delivered by C-section.
"That reflects my personal bias, which is that the position required for vaginal delivery is pretty horrible for sacroiliac joint pain and leads to significant flares postpartum. That’s particularly true if the patient has an epidural and doesn’t know how hard she’s pushing on those SI joints," according to the rheumatologist.
Dr. Clowse reported serving as a consultant to UCB, which markets certolizumab pegol.
SNOWMASS, COLO. – The common strategy of managing inflammatory arthritis during pregnancy by stopping all prepregnancy medications and prescribing prednisone is counterproductive, Dr. Megan E.B. Clowse said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
"This sort of safe approach is actually not the safest or best approach. We all need to shift our attitude and get comfortable with at least a couple of other medications in order to help our patients have better outcomes," asserted Dr. Clowse, director of the Duke Autoimmunity in Pregnancy (DAP) Registry at Duke University, Durham, N.C.
It’s often true that rheumatoid arthritis (RA) tends to get better in pregnancy. Nonetheless, pregnancy may not be enough to control disease activity in many women, as illustrated by a nationwide Dutch study in which half of RA patients had moderate to severe disease activity by their third trimester (Arthritis Rheum. 2008;59:1241-8).
"In my experience, the patients who were on tumor necrosis factor inhibitors prepregnancy do not do as well when they come off them. So pregnancy might be good for RA disease activity, but it’s definitely not as good as a tumor necrosis factor inhibitor," according to the rheumatologist.
Roughly one-quarter of the more than 230 prospectively studied pregnancies in the DAP Registry have been in women with RA or other inflammatory arthritides. The preterm birth rate in RA patients in DAP, as in other RA registries, is higher than in the general population. Notably, all of the DAP patients with RA who had preterm birth had moderate to severe disease activity in the first and second trimesters, compared with just a single RA patient with a term delivery.
"Allowing disease to flare may actually harm the pregnancy," Dr. Clowse commented.
Her two top recommendations for nonbiologic treatment of inflammatory arthritis during pregnancy are hydroxychloroquine and sulfasalazine. Hydroxychloroquine is effective for mild arthritis, and it’s rated by the Food and Drug Administration as Pregnancy Category C, with no reports of human toxicity. Sulfasalazine has a good safety profile in pregnancy – it is Pregnancy Category B – and has good efficacy for peripheral arthritis.
"These are two very important medications that are much better – and definitely much safer – options than prednisone. These are just great options, and I try to encourage patients to take them. It’s definitely better than letting patients flare while off methotrexate before they deliver," she continued.
"TNF [tumor necrosis factor] inhibitors are, I think, another reasonable option, particularly in the population with moderate to severe disease activity. If any of these medications help you avoid prednisone, then I think you come out ahead," Dr. Clowse said.
Reassuring data regarding the safety of anti-TNF biologics in pregnancy comes from several sources. A systematic literature review by Dr. Evelyne Vinet and her coworkers at McGill University, Montreal, found no evidence of excess risk of adverse pregnancy or fetal outcomes in women exposed to etanercept (Enbrel), infliximab (Remicade), or adalimumab (Humira) during pregnancy (Arthritis Rheum. 2009;61:587-92). A report from the Organization of Teratology Information Specialists (OTIS) Registry, presented at the 2012 annual meeting of the American College of Rheumatology, found no significant difference between RA patients exposed to adalimumab in pregnancy and RA controls in rates of live birth, miscarriage, stillbirth, congenital abnormalities, or serious infections in the first year of life.
Moreover, DAP Registry data support the notion that for some patients, anti-TNF biologics during pregnancy may be a good option. In Dr. Clowse’s series of 29 RA patients, disease activity during the first trimester neatly delineated three distinct groups. Eleven patients who had a 28-joint Disease Activity Score using C-reactive protein (DAS28-CRP) averaging 1.5 in the first trimester required neither TNF inhibitors nor prednisone during their pregnancy, and they had no abnormal outcomes. Seven patients with significant first-trimester disease activity as defined by an average DAS28-CRP score of 3.4 went back on their TNF inhibitor during pregnancy, and their disease essentially went into remission, with only one preterm birth. In contrast, 11 other patients with significant first-trimester disease activity went on prednisone because they rejected TNF inhibitor therapy; their disease activity remained substantial, and 6 of the 11 had a preterm birth and/or preeclampsia.
"All of the preeclampsia occurred in the prednisone group. They also had a lot of disease activity postpartum," Dr. Clowse observed.
Infliximab and adalimumab freely pass across the placenta; etanercept and certolizumab pegol (Cimzia) do not. Regardless, no infant exposed in utero to a TNF inhibitor should receive the rotavirus vaccine during the first 5 months of life. That’s the only live-virus vaccine given during infancy in the United States; all the other vaccines can safely be given according to schedule.
Dr. Clowse said there is essentially no published literature regarding psoriatic arthritis in pregnancy. The DAP registry experience includes seven pregnancies in women with psoriatic arthritis. There were no pregnancy losses, one preterm birth, and two cases of preeclampsia.
"What I see is dramatically increased disease activity when women with psoriatic arthritis stop their TNF inhibitor. The worst psoriasis I’ve ever seen is in pregnant patients; they are really miserable off their TNF inhibitors," she said.
There is also very little in the literature about axial spondyloarthritis in pregnancy. The DAP registry’s 10 cases constitute one of the largest series. There were no pregnancy losses, no preeclampsia, and one preterm birth. Eight of the women were delivered by C-section.
"That reflects my personal bias, which is that the position required for vaginal delivery is pretty horrible for sacroiliac joint pain and leads to significant flares postpartum. That’s particularly true if the patient has an epidural and doesn’t know how hard she’s pushing on those SI joints," according to the rheumatologist.
Dr. Clowse reported serving as a consultant to UCB, which markets certolizumab pegol.
SNOWMASS, COLO. – The common strategy of managing inflammatory arthritis during pregnancy by stopping all prepregnancy medications and prescribing prednisone is counterproductive, Dr. Megan E.B. Clowse said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
"This sort of safe approach is actually not the safest or best approach. We all need to shift our attitude and get comfortable with at least a couple of other medications in order to help our patients have better outcomes," asserted Dr. Clowse, director of the Duke Autoimmunity in Pregnancy (DAP) Registry at Duke University, Durham, N.C.
It’s often true that rheumatoid arthritis (RA) tends to get better in pregnancy. Nonetheless, pregnancy may not be enough to control disease activity in many women, as illustrated by a nationwide Dutch study in which half of RA patients had moderate to severe disease activity by their third trimester (Arthritis Rheum. 2008;59:1241-8).
"In my experience, the patients who were on tumor necrosis factor inhibitors prepregnancy do not do as well when they come off them. So pregnancy might be good for RA disease activity, but it’s definitely not as good as a tumor necrosis factor inhibitor," according to the rheumatologist.
Roughly one-quarter of the more than 230 prospectively studied pregnancies in the DAP Registry have been in women with RA or other inflammatory arthritides. The preterm birth rate in RA patients in DAP, as in other RA registries, is higher than in the general population. Notably, all of the DAP patients with RA who had preterm birth had moderate to severe disease activity in the first and second trimesters, compared with just a single RA patient with a term delivery.
"Allowing disease to flare may actually harm the pregnancy," Dr. Clowse commented.
Her two top recommendations for nonbiologic treatment of inflammatory arthritis during pregnancy are hydroxychloroquine and sulfasalazine. Hydroxychloroquine is effective for mild arthritis, and it’s rated by the Food and Drug Administration as Pregnancy Category C, with no reports of human toxicity. Sulfasalazine has a good safety profile in pregnancy – it is Pregnancy Category B – and has good efficacy for peripheral arthritis.
"These are two very important medications that are much better – and definitely much safer – options than prednisone. These are just great options, and I try to encourage patients to take them. It’s definitely better than letting patients flare while off methotrexate before they deliver," she continued.
"TNF [tumor necrosis factor] inhibitors are, I think, another reasonable option, particularly in the population with moderate to severe disease activity. If any of these medications help you avoid prednisone, then I think you come out ahead," Dr. Clowse said.
Reassuring data regarding the safety of anti-TNF biologics in pregnancy comes from several sources. A systematic literature review by Dr. Evelyne Vinet and her coworkers at McGill University, Montreal, found no evidence of excess risk of adverse pregnancy or fetal outcomes in women exposed to etanercept (Enbrel), infliximab (Remicade), or adalimumab (Humira) during pregnancy (Arthritis Rheum. 2009;61:587-92). A report from the Organization of Teratology Information Specialists (OTIS) Registry, presented at the 2012 annual meeting of the American College of Rheumatology, found no significant difference between RA patients exposed to adalimumab in pregnancy and RA controls in rates of live birth, miscarriage, stillbirth, congenital abnormalities, or serious infections in the first year of life.
Moreover, DAP Registry data support the notion that for some patients, anti-TNF biologics during pregnancy may be a good option. In Dr. Clowse’s series of 29 RA patients, disease activity during the first trimester neatly delineated three distinct groups. Eleven patients who had a 28-joint Disease Activity Score using C-reactive protein (DAS28-CRP) averaging 1.5 in the first trimester required neither TNF inhibitors nor prednisone during their pregnancy, and they had no abnormal outcomes. Seven patients with significant first-trimester disease activity as defined by an average DAS28-CRP score of 3.4 went back on their TNF inhibitor during pregnancy, and their disease essentially went into remission, with only one preterm birth. In contrast, 11 other patients with significant first-trimester disease activity went on prednisone because they rejected TNF inhibitor therapy; their disease activity remained substantial, and 6 of the 11 had a preterm birth and/or preeclampsia.
"All of the preeclampsia occurred in the prednisone group. They also had a lot of disease activity postpartum," Dr. Clowse observed.
Infliximab and adalimumab freely pass across the placenta; etanercept and certolizumab pegol (Cimzia) do not. Regardless, no infant exposed in utero to a TNF inhibitor should receive the rotavirus vaccine during the first 5 months of life. That’s the only live-virus vaccine given during infancy in the United States; all the other vaccines can safely be given according to schedule.
Dr. Clowse said there is essentially no published literature regarding psoriatic arthritis in pregnancy. The DAP registry experience includes seven pregnancies in women with psoriatic arthritis. There were no pregnancy losses, one preterm birth, and two cases of preeclampsia.
"What I see is dramatically increased disease activity when women with psoriatic arthritis stop their TNF inhibitor. The worst psoriasis I’ve ever seen is in pregnant patients; they are really miserable off their TNF inhibitors," she said.
There is also very little in the literature about axial spondyloarthritis in pregnancy. The DAP registry’s 10 cases constitute one of the largest series. There were no pregnancy losses, no preeclampsia, and one preterm birth. Eight of the women were delivered by C-section.
"That reflects my personal bias, which is that the position required for vaginal delivery is pretty horrible for sacroiliac joint pain and leads to significant flares postpartum. That’s particularly true if the patient has an epidural and doesn’t know how hard she’s pushing on those SI joints," according to the rheumatologist.
Dr. Clowse reported serving as a consultant to UCB, which markets certolizumab pegol.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM

2014 adult vaccine schedule includes recombinant flu vaccine
The recombinant influenza vaccine is now recommended as an option for adults with egg allergies, according to the 2014 recommended vaccine schedule for adults.
Approved last year, the recombinant influenza vaccine (RIV) is manufactured with the baculovirus. It contains no egg protein, and can be safely administered to those who have an egg allergy of any severity, according to the schedule published Feb. 3 (Ann. Int. Med. 2014;160:190-8).
RIV is a good addition to the schedule, Dr. Jonathan Temte, chair of the Centers for Disease Control and Prevention’s Advisory Committee of Immunization Practices (ACIP), said in an interview.
This provides an option for people who have a serious egg allergy. Many people with egg allergies have only mild allergies – hives – and can receive influenza vaccine," Dr. Temte said.
Other updates to the schedule include the following:
• Adults who have undergone successful hematopoietic stem cell transplant should get a three-dose series of Haemophilus influenzae type B vaccine (Hib) 6-12 months after the procedure, regardless of prior vaccination. Hib is no longer recommended for previously unvaccinated HIV-infected adults, because their risk of infection is low.
• Zoster and human papillomavirus vaccines (either HPV2 or HPV4) are no longer specifically indicated for health care workers; instead, each should be provided to health care professionals and other patients who meet age and other indications.
• Previously unvaccinated patients 11 years old or older should have a single dose of tetanus, diphtheria, and acellular pertussis (Tdap), with a tetanus, diphtheria (Td) booster every 10 years. Pregnant women should get a dose of Tdap during each pregnancy (preferably during 27-36 weeks’ gestation) regardless of when they last received Tdap or Td.
• Timing of the HPV vaccine series was clarified. Both HPV vaccines have a recommended three-dose series, with the second dose administered 4-8 weeks after the first and the third dose administered at least 12 weeks after the second.
• Recommendations on the meningococcal vaccine clarify which patients need either one or two doses as well as who should receive the meningococcal conjugate (MenACWY-D) and who should have the meningococcal polysaccharide (MenACWY-CRM) quadrivalent vaccines.
You can view the 2014 schedule at our Resources section here.
The recombinant influenza vaccine is now recommended as an option for adults with egg allergies, according to the 2014 recommended vaccine schedule for adults.
Approved last year, the recombinant influenza vaccine (RIV) is manufactured with the baculovirus. It contains no egg protein, and can be safely administered to those who have an egg allergy of any severity, according to the schedule published Feb. 3 (Ann. Int. Med. 2014;160:190-8).
RIV is a good addition to the schedule, Dr. Jonathan Temte, chair of the Centers for Disease Control and Prevention’s Advisory Committee of Immunization Practices (ACIP), said in an interview.
This provides an option for people who have a serious egg allergy. Many people with egg allergies have only mild allergies – hives – and can receive influenza vaccine," Dr. Temte said.
Other updates to the schedule include the following:
• Adults who have undergone successful hematopoietic stem cell transplant should get a three-dose series of Haemophilus influenzae type B vaccine (Hib) 6-12 months after the procedure, regardless of prior vaccination. Hib is no longer recommended for previously unvaccinated HIV-infected adults, because their risk of infection is low.
• Zoster and human papillomavirus vaccines (either HPV2 or HPV4) are no longer specifically indicated for health care workers; instead, each should be provided to health care professionals and other patients who meet age and other indications.
• Previously unvaccinated patients 11 years old or older should have a single dose of tetanus, diphtheria, and acellular pertussis (Tdap), with a tetanus, diphtheria (Td) booster every 10 years. Pregnant women should get a dose of Tdap during each pregnancy (preferably during 27-36 weeks’ gestation) regardless of when they last received Tdap or Td.
• Timing of the HPV vaccine series was clarified. Both HPV vaccines have a recommended three-dose series, with the second dose administered 4-8 weeks after the first and the third dose administered at least 12 weeks after the second.
• Recommendations on the meningococcal vaccine clarify which patients need either one or two doses as well as who should receive the meningococcal conjugate (MenACWY-D) and who should have the meningococcal polysaccharide (MenACWY-CRM) quadrivalent vaccines.
You can view the 2014 schedule at our Resources section here.
The recombinant influenza vaccine is now recommended as an option for adults with egg allergies, according to the 2014 recommended vaccine schedule for adults.
Approved last year, the recombinant influenza vaccine (RIV) is manufactured with the baculovirus. It contains no egg protein, and can be safely administered to those who have an egg allergy of any severity, according to the schedule published Feb. 3 (Ann. Int. Med. 2014;160:190-8).
RIV is a good addition to the schedule, Dr. Jonathan Temte, chair of the Centers for Disease Control and Prevention’s Advisory Committee of Immunization Practices (ACIP), said in an interview.
This provides an option for people who have a serious egg allergy. Many people with egg allergies have only mild allergies – hives – and can receive influenza vaccine," Dr. Temte said.
Other updates to the schedule include the following:
• Adults who have undergone successful hematopoietic stem cell transplant should get a three-dose series of Haemophilus influenzae type B vaccine (Hib) 6-12 months after the procedure, regardless of prior vaccination. Hib is no longer recommended for previously unvaccinated HIV-infected adults, because their risk of infection is low.
• Zoster and human papillomavirus vaccines (either HPV2 or HPV4) are no longer specifically indicated for health care workers; instead, each should be provided to health care professionals and other patients who meet age and other indications.
• Previously unvaccinated patients 11 years old or older should have a single dose of tetanus, diphtheria, and acellular pertussis (Tdap), with a tetanus, diphtheria (Td) booster every 10 years. Pregnant women should get a dose of Tdap during each pregnancy (preferably during 27-36 weeks’ gestation) regardless of when they last received Tdap or Td.
• Timing of the HPV vaccine series was clarified. Both HPV vaccines have a recommended three-dose series, with the second dose administered 4-8 weeks after the first and the third dose administered at least 12 weeks after the second.
• Recommendations on the meningococcal vaccine clarify which patients need either one or two doses as well as who should receive the meningococcal conjugate (MenACWY-D) and who should have the meningococcal polysaccharide (MenACWY-CRM) quadrivalent vaccines.
You can view the 2014 schedule at our Resources section here.
FROM ANNALS OF INTERNAL MEDICINE