User login
Eggs: A Weighty Matter for Postmenopausal Women?
TOPLINE:
such as processed and red meat, French fries, sweets, and deserts. Genetic predisposition for a high body mass index (BMI) also influences weight gain with higher egg intake.
METHODOLOGY:
- Egg consumption and elevated body weight are each linked to an increased risk for serious chronic diseases; however, whether elevated body weight mediates the association between egg intake and an elevated risk for serious chronic diseases needs further assessment.
- To investigate the association between eating eggs and weight gain, as well as the role of genetic susceptibility to an elevated BMI, researchers conducted a prospective study including 4439 postmenopausal women of European descent from the Women’s Health Initiative (WHI).
- They measured the participants’ consumption of egg and egg nutrients using a self-administered food frequency questionnaire.
- Changes in the consumption of eggs and egg nutrients such as cholesterol, choline, and betaine were assessed between baseline and follow-up visits at 1, 3, 6, and 9 years.
- The primary outcome was the change in body weight between baseline and each follow-up visit. Furthermore, an exploratory analysis evaluated how eating Western foods and genetic predisposition for a high BMI (assessed through a polygenic score) influenced weight change.
TAKEAWAY:
- An increased consumption of eggs was associated with weight gain, showing a positive linear trend at 1, 2, 3, and 6 years. By the third year, women whose egg consumption had increased by two eggs per week gained 0.70 kg more weight (P = .0002) than women whose egg consumption was reduced by 2.4 eggs per week (P-linear < .0001).
- An increase in the consumption of nutrients obtained from eggs, including cholesterol (P-linear < .0001) and choline (P-linear < .02), was positively associated with weight gain.
- Women with a higher consumption of Western foods showed significant associations between changes in egg, cholesterol, and choline intake and weight gain.
- A significant association was found between the BMI polygenic score and changes in body weight, with women most genetically predisposed to a higher BMI showing greater weight gain when their egg consumption increased by an average of 3.5 eggs per week.
IN PRACTICE:
“These results suggest that even relatively small increases or decreases in egg consumption could cause increases or decreases, respectively, in body weight among postmenopausal women, unless there are adequate compensating changes in factors such as dietary energy intake or physical activity,” the authors wrote. “Our results require confirmation,” they added.
SOURCE:
This study, led by James A. Greenberg, Department of Health and Nutrition Sciences, Brooklyn College, The City University of New York, was published online in Clinical Nutrition.
LIMITATIONS:
This observational study was susceptible to residual confounding, which suggests that the observed associations may not have established causality. Additionally, the results were according to data from a group of postmenopausal American women of European descent, which limited the generalizability to other populations.
DISCLOSURES:
The WHI program was funded by the National Heart, Lung, and Blood Institute, National Institutes of Health, Department of Health & Human Services. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
such as processed and red meat, French fries, sweets, and deserts. Genetic predisposition for a high body mass index (BMI) also influences weight gain with higher egg intake.
METHODOLOGY:
- Egg consumption and elevated body weight are each linked to an increased risk for serious chronic diseases; however, whether elevated body weight mediates the association between egg intake and an elevated risk for serious chronic diseases needs further assessment.
- To investigate the association between eating eggs and weight gain, as well as the role of genetic susceptibility to an elevated BMI, researchers conducted a prospective study including 4439 postmenopausal women of European descent from the Women’s Health Initiative (WHI).
- They measured the participants’ consumption of egg and egg nutrients using a self-administered food frequency questionnaire.
- Changes in the consumption of eggs and egg nutrients such as cholesterol, choline, and betaine were assessed between baseline and follow-up visits at 1, 3, 6, and 9 years.
- The primary outcome was the change in body weight between baseline and each follow-up visit. Furthermore, an exploratory analysis evaluated how eating Western foods and genetic predisposition for a high BMI (assessed through a polygenic score) influenced weight change.
TAKEAWAY:
- An increased consumption of eggs was associated with weight gain, showing a positive linear trend at 1, 2, 3, and 6 years. By the third year, women whose egg consumption had increased by two eggs per week gained 0.70 kg more weight (P = .0002) than women whose egg consumption was reduced by 2.4 eggs per week (P-linear < .0001).
- An increase in the consumption of nutrients obtained from eggs, including cholesterol (P-linear < .0001) and choline (P-linear < .02), was positively associated with weight gain.
- Women with a higher consumption of Western foods showed significant associations between changes in egg, cholesterol, and choline intake and weight gain.
- A significant association was found between the BMI polygenic score and changes in body weight, with women most genetically predisposed to a higher BMI showing greater weight gain when their egg consumption increased by an average of 3.5 eggs per week.
IN PRACTICE:
“These results suggest that even relatively small increases or decreases in egg consumption could cause increases or decreases, respectively, in body weight among postmenopausal women, unless there are adequate compensating changes in factors such as dietary energy intake or physical activity,” the authors wrote. “Our results require confirmation,” they added.
SOURCE:
This study, led by James A. Greenberg, Department of Health and Nutrition Sciences, Brooklyn College, The City University of New York, was published online in Clinical Nutrition.
LIMITATIONS:
This observational study was susceptible to residual confounding, which suggests that the observed associations may not have established causality. Additionally, the results were according to data from a group of postmenopausal American women of European descent, which limited the generalizability to other populations.
DISCLOSURES:
The WHI program was funded by the National Heart, Lung, and Blood Institute, National Institutes of Health, Department of Health & Human Services. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
such as processed and red meat, French fries, sweets, and deserts. Genetic predisposition for a high body mass index (BMI) also influences weight gain with higher egg intake.
METHODOLOGY:
- Egg consumption and elevated body weight are each linked to an increased risk for serious chronic diseases; however, whether elevated body weight mediates the association between egg intake and an elevated risk for serious chronic diseases needs further assessment.
- To investigate the association between eating eggs and weight gain, as well as the role of genetic susceptibility to an elevated BMI, researchers conducted a prospective study including 4439 postmenopausal women of European descent from the Women’s Health Initiative (WHI).
- They measured the participants’ consumption of egg and egg nutrients using a self-administered food frequency questionnaire.
- Changes in the consumption of eggs and egg nutrients such as cholesterol, choline, and betaine were assessed between baseline and follow-up visits at 1, 3, 6, and 9 years.
- The primary outcome was the change in body weight between baseline and each follow-up visit. Furthermore, an exploratory analysis evaluated how eating Western foods and genetic predisposition for a high BMI (assessed through a polygenic score) influenced weight change.
TAKEAWAY:
- An increased consumption of eggs was associated with weight gain, showing a positive linear trend at 1, 2, 3, and 6 years. By the third year, women whose egg consumption had increased by two eggs per week gained 0.70 kg more weight (P = .0002) than women whose egg consumption was reduced by 2.4 eggs per week (P-linear < .0001).
- An increase in the consumption of nutrients obtained from eggs, including cholesterol (P-linear < .0001) and choline (P-linear < .02), was positively associated with weight gain.
- Women with a higher consumption of Western foods showed significant associations between changes in egg, cholesterol, and choline intake and weight gain.
- A significant association was found between the BMI polygenic score and changes in body weight, with women most genetically predisposed to a higher BMI showing greater weight gain when their egg consumption increased by an average of 3.5 eggs per week.
IN PRACTICE:
“These results suggest that even relatively small increases or decreases in egg consumption could cause increases or decreases, respectively, in body weight among postmenopausal women, unless there are adequate compensating changes in factors such as dietary energy intake or physical activity,” the authors wrote. “Our results require confirmation,” they added.
SOURCE:
This study, led by James A. Greenberg, Department of Health and Nutrition Sciences, Brooklyn College, The City University of New York, was published online in Clinical Nutrition.
LIMITATIONS:
This observational study was susceptible to residual confounding, which suggests that the observed associations may not have established causality. Additionally, the results were according to data from a group of postmenopausal American women of European descent, which limited the generalizability to other populations.
DISCLOSURES:
The WHI program was funded by the National Heart, Lung, and Blood Institute, National Institutes of Health, Department of Health & Human Services. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Increasing Non–Candida albicans Yeasts in Vulvovaginal Candidiasis and Fluconazole Resistance in Leeds
TOPLINE:
Fluconazole resistance in yeast isolates from women with recurrent vulvovaginal candidiasis in Leeds, England, increased from 3.5% to 9.6% over 3 years. Non–Candida albicans yeasts also rose from 6.0% to 12.6% during the same period.
METHODOLOGY:
- Researchers conducted a retrospective data search of vaginal cultures from adult women in Leeds, England, between April 2018 and March 2021.
- A total of 5461 vaginal samples from women with clinical information indicating complicated/recurrent vulvovaginal candidiasis were included.
- Samples were processed on the WASPLAB automated platform, and species identification and antifungal susceptibility testing were performed in the Mycology Reference Centre by Matrix-assisted laser desorption ionization–time-of-flight mass spectrometry.
- Susceptibility to fluconazole was determined using disc diffusion and the Sensititre YeastOne microbroth dilution assay.
TAKEAWAY:
According to the authors, the prevalence of non–C albicans yeasts increased from 6.0% in 2018-2019 to 12.6% in 2020-2021 (P = .0003).
Fluconazole-sensitive (dose-dependent) and fluconazole-resistant isolates increased from 3.5% in 2018-2019 to 9.6% in 2020-2021 (P = .0001).
Most fluconazole resistance was observed in C albicans, with other species such as Nakaseomyces glabrata and Pichia kudriavzevii also showing resistance.
The authors state that the increase in fluconazole resistance and non–C albicans yeasts may be linked to a policy change encouraging empirical treatment of vulvovaginal candidiasis in primary care.
IN PRACTICE:
“This study shows that the rates of non–Candida albicans and fluconazole-resistant C albicans have increased year on year in the 3 years studied. The exact reasons for this increase remain unclear, but it follows the introduction of restricted access to fungal cultures for the diagnosis of vulvovaginal candidiasis by those working in primary care. A clinical diagnosis, followed by empirical treatment, has been recommended instead. Consequently, we believe this policy of encouraging empirical vaginitis treatment based on nonspecific symptoms and signs needs revisiting,” the authors wrote.
SOURCE:
The study was led by Jennifer C. Ratner, Leeds Teaching Hospitals NHS Trust, England. It was published online in Sexually Transmitted Infections.
LIMITATIONS:
The study’s limitations included a potential bias introduced by the reduced number of samples received from specialist sexual health clinics during the COVID-19 pandemic. Additionally, the study could not distinguish between cases of recurrent vulvovaginal candidiasis with complete resolution of symptoms and those with persistent symptoms despite treatment.
DISCLOSURES:
One coauthor disclosed receiving fees from Pfizer for contributing to webinar presentations in 2023. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Fluconazole resistance in yeast isolates from women with recurrent vulvovaginal candidiasis in Leeds, England, increased from 3.5% to 9.6% over 3 years. Non–Candida albicans yeasts also rose from 6.0% to 12.6% during the same period.
METHODOLOGY:
- Researchers conducted a retrospective data search of vaginal cultures from adult women in Leeds, England, between April 2018 and March 2021.
- A total of 5461 vaginal samples from women with clinical information indicating complicated/recurrent vulvovaginal candidiasis were included.
- Samples were processed on the WASPLAB automated platform, and species identification and antifungal susceptibility testing were performed in the Mycology Reference Centre by Matrix-assisted laser desorption ionization–time-of-flight mass spectrometry.
- Susceptibility to fluconazole was determined using disc diffusion and the Sensititre YeastOne microbroth dilution assay.
TAKEAWAY:
According to the authors, the prevalence of non–C albicans yeasts increased from 6.0% in 2018-2019 to 12.6% in 2020-2021 (P = .0003).
Fluconazole-sensitive (dose-dependent) and fluconazole-resistant isolates increased from 3.5% in 2018-2019 to 9.6% in 2020-2021 (P = .0001).
Most fluconazole resistance was observed in C albicans, with other species such as Nakaseomyces glabrata and Pichia kudriavzevii also showing resistance.
The authors state that the increase in fluconazole resistance and non–C albicans yeasts may be linked to a policy change encouraging empirical treatment of vulvovaginal candidiasis in primary care.
IN PRACTICE:
“This study shows that the rates of non–Candida albicans and fluconazole-resistant C albicans have increased year on year in the 3 years studied. The exact reasons for this increase remain unclear, but it follows the introduction of restricted access to fungal cultures for the diagnosis of vulvovaginal candidiasis by those working in primary care. A clinical diagnosis, followed by empirical treatment, has been recommended instead. Consequently, we believe this policy of encouraging empirical vaginitis treatment based on nonspecific symptoms and signs needs revisiting,” the authors wrote.
SOURCE:
The study was led by Jennifer C. Ratner, Leeds Teaching Hospitals NHS Trust, England. It was published online in Sexually Transmitted Infections.
LIMITATIONS:
The study’s limitations included a potential bias introduced by the reduced number of samples received from specialist sexual health clinics during the COVID-19 pandemic. Additionally, the study could not distinguish between cases of recurrent vulvovaginal candidiasis with complete resolution of symptoms and those with persistent symptoms despite treatment.
DISCLOSURES:
One coauthor disclosed receiving fees from Pfizer for contributing to webinar presentations in 2023. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Fluconazole resistance in yeast isolates from women with recurrent vulvovaginal candidiasis in Leeds, England, increased from 3.5% to 9.6% over 3 years. Non–Candida albicans yeasts also rose from 6.0% to 12.6% during the same period.
METHODOLOGY:
- Researchers conducted a retrospective data search of vaginal cultures from adult women in Leeds, England, between April 2018 and March 2021.
- A total of 5461 vaginal samples from women with clinical information indicating complicated/recurrent vulvovaginal candidiasis were included.
- Samples were processed on the WASPLAB automated platform, and species identification and antifungal susceptibility testing were performed in the Mycology Reference Centre by Matrix-assisted laser desorption ionization–time-of-flight mass spectrometry.
- Susceptibility to fluconazole was determined using disc diffusion and the Sensititre YeastOne microbroth dilution assay.
TAKEAWAY:
According to the authors, the prevalence of non–C albicans yeasts increased from 6.0% in 2018-2019 to 12.6% in 2020-2021 (P = .0003).
Fluconazole-sensitive (dose-dependent) and fluconazole-resistant isolates increased from 3.5% in 2018-2019 to 9.6% in 2020-2021 (P = .0001).
Most fluconazole resistance was observed in C albicans, with other species such as Nakaseomyces glabrata and Pichia kudriavzevii also showing resistance.
The authors state that the increase in fluconazole resistance and non–C albicans yeasts may be linked to a policy change encouraging empirical treatment of vulvovaginal candidiasis in primary care.
IN PRACTICE:
“This study shows that the rates of non–Candida albicans and fluconazole-resistant C albicans have increased year on year in the 3 years studied. The exact reasons for this increase remain unclear, but it follows the introduction of restricted access to fungal cultures for the diagnosis of vulvovaginal candidiasis by those working in primary care. A clinical diagnosis, followed by empirical treatment, has been recommended instead. Consequently, we believe this policy of encouraging empirical vaginitis treatment based on nonspecific symptoms and signs needs revisiting,” the authors wrote.
SOURCE:
The study was led by Jennifer C. Ratner, Leeds Teaching Hospitals NHS Trust, England. It was published online in Sexually Transmitted Infections.
LIMITATIONS:
The study’s limitations included a potential bias introduced by the reduced number of samples received from specialist sexual health clinics during the COVID-19 pandemic. Additionally, the study could not distinguish between cases of recurrent vulvovaginal candidiasis with complete resolution of symptoms and those with persistent symptoms despite treatment.
DISCLOSURES:
One coauthor disclosed receiving fees from Pfizer for contributing to webinar presentations in 2023. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Underutilized Mifepristone Shows Promise in Care of Early Pregnancy Loss
TOPLINE:
Mifepristone plus misoprostol reduces the need for subsequent uterine aspiration and emergency department visits in the management of early pregnancy loss. Despite its effectiveness, mifepristone remains underutilized, with 8.6% of patients receiving it in 2022.
METHODOLOGY:
- Researchers conducted a retrospective cohort study using national insurance claims data of US patients with commercial insurance.
- More than 31,000 pregnant women (mean age, 32.7 years) with a diagnosis of early pregnancy loss between 2015 and 2022 were included.
- The diagnosis of patients included having a missed abortion (72.3%), spontaneous abortion (26.9%), or both (0.8%).
- Researchers compared the outcomes of individuals who received a combination of mifepristone and misoprostol vs those who received misoprostol alone. The outcome measures included the need for subsequent procedural management (uterine aspiration), return visits to the emergency department or an outpatient clinic, hospitalizations, and complications within 6 weeks of initial diagnosis.
TAKEAWAY:
- The use of mifepristone was more common in outpatient clinics than in emergency departments (3.4% vs 0.9%; P < .001).
- The use of mifepristone plus misoprostol vs misoprostol alone was linked to a lower incidence of subsequent procedural management (10.5% vs 14.0%; P = .002) and fewer emergency department visits (3.5% vs 7.9%; P < .001).
- The multivariable analysis showed that the use of mifepristone was linked to decreased odds of subsequent procedural management (adjusted odds ratio, 0.71; 95% CI, 0.57-0.87).
- Despite its effectiveness, mifepristone was used in only 8.6% of those receiving medication management for early pregnancy loss in 2022.
IN PRACTICE:
“Continued efforts are needed to reduce barriers to mifepristone use for medication management of EPL,” the authors wrote.
“Any practitioner who cares for patients experiencing early pregnancy loss should consider mifepristone pretreatment to misoprostol to be the standard of care for medication management. Provision of the evidence-based standard of care with the use of mifepristone for early pregnancy loss is an opportunity to advocate for an essential strategy in improving sexual and reproductive health in the US,” wrote Sarita Sonalkar, MD, MPH, and Rachel McKean, MD, MPH, of the Perelman School of Medicine at the University of Pennsylvania, Philadelphia, in an invited commentary.
SOURCE:
The study was led by Lyndsey S. Benson, MD, MS, of the University of Washington School of Medicine, Seattle, and was published online in JAMA Network Open.
LIMITATIONS:
The study was limited by the accuracy of the diagnosis of early pregnancy loss and procedure codes because claims data are intended for billing purposes and may be incomplete or inaccurate. The use of de-identified data meant that specific gestational durations, exact dosing, or routes of misoprostol administration could not be determined. The findings may not be generalizable to those with public insurance or no insurance.
DISCLOSURES:
The study was supported in part by a grant from a Women’s Reproductive Health Research grant from the National Institutes of Health Eunice Kennedy Shriver National Institute for Child Health and Human Development. One author reported serving as an adviser and investigator, while another reported receiving personal fees and serving as an expert witness, contributing editor, and course instructor outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Mifepristone plus misoprostol reduces the need for subsequent uterine aspiration and emergency department visits in the management of early pregnancy loss. Despite its effectiveness, mifepristone remains underutilized, with 8.6% of patients receiving it in 2022.
METHODOLOGY:
- Researchers conducted a retrospective cohort study using national insurance claims data of US patients with commercial insurance.
- More than 31,000 pregnant women (mean age, 32.7 years) with a diagnosis of early pregnancy loss between 2015 and 2022 were included.
- The diagnosis of patients included having a missed abortion (72.3%), spontaneous abortion (26.9%), or both (0.8%).
- Researchers compared the outcomes of individuals who received a combination of mifepristone and misoprostol vs those who received misoprostol alone. The outcome measures included the need for subsequent procedural management (uterine aspiration), return visits to the emergency department or an outpatient clinic, hospitalizations, and complications within 6 weeks of initial diagnosis.
TAKEAWAY:
- The use of mifepristone was more common in outpatient clinics than in emergency departments (3.4% vs 0.9%; P < .001).
- The use of mifepristone plus misoprostol vs misoprostol alone was linked to a lower incidence of subsequent procedural management (10.5% vs 14.0%; P = .002) and fewer emergency department visits (3.5% vs 7.9%; P < .001).
- The multivariable analysis showed that the use of mifepristone was linked to decreased odds of subsequent procedural management (adjusted odds ratio, 0.71; 95% CI, 0.57-0.87).
- Despite its effectiveness, mifepristone was used in only 8.6% of those receiving medication management for early pregnancy loss in 2022.
IN PRACTICE:
“Continued efforts are needed to reduce barriers to mifepristone use for medication management of EPL,” the authors wrote.
“Any practitioner who cares for patients experiencing early pregnancy loss should consider mifepristone pretreatment to misoprostol to be the standard of care for medication management. Provision of the evidence-based standard of care with the use of mifepristone for early pregnancy loss is an opportunity to advocate for an essential strategy in improving sexual and reproductive health in the US,” wrote Sarita Sonalkar, MD, MPH, and Rachel McKean, MD, MPH, of the Perelman School of Medicine at the University of Pennsylvania, Philadelphia, in an invited commentary.
SOURCE:
The study was led by Lyndsey S. Benson, MD, MS, of the University of Washington School of Medicine, Seattle, and was published online in JAMA Network Open.
LIMITATIONS:
The study was limited by the accuracy of the diagnosis of early pregnancy loss and procedure codes because claims data are intended for billing purposes and may be incomplete or inaccurate. The use of de-identified data meant that specific gestational durations, exact dosing, or routes of misoprostol administration could not be determined. The findings may not be generalizable to those with public insurance or no insurance.
DISCLOSURES:
The study was supported in part by a grant from a Women’s Reproductive Health Research grant from the National Institutes of Health Eunice Kennedy Shriver National Institute for Child Health and Human Development. One author reported serving as an adviser and investigator, while another reported receiving personal fees and serving as an expert witness, contributing editor, and course instructor outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Mifepristone plus misoprostol reduces the need for subsequent uterine aspiration and emergency department visits in the management of early pregnancy loss. Despite its effectiveness, mifepristone remains underutilized, with 8.6% of patients receiving it in 2022.
METHODOLOGY:
- Researchers conducted a retrospective cohort study using national insurance claims data of US patients with commercial insurance.
- More than 31,000 pregnant women (mean age, 32.7 years) with a diagnosis of early pregnancy loss between 2015 and 2022 were included.
- The diagnosis of patients included having a missed abortion (72.3%), spontaneous abortion (26.9%), or both (0.8%).
- Researchers compared the outcomes of individuals who received a combination of mifepristone and misoprostol vs those who received misoprostol alone. The outcome measures included the need for subsequent procedural management (uterine aspiration), return visits to the emergency department or an outpatient clinic, hospitalizations, and complications within 6 weeks of initial diagnosis.
TAKEAWAY:
- The use of mifepristone was more common in outpatient clinics than in emergency departments (3.4% vs 0.9%; P < .001).
- The use of mifepristone plus misoprostol vs misoprostol alone was linked to a lower incidence of subsequent procedural management (10.5% vs 14.0%; P = .002) and fewer emergency department visits (3.5% vs 7.9%; P < .001).
- The multivariable analysis showed that the use of mifepristone was linked to decreased odds of subsequent procedural management (adjusted odds ratio, 0.71; 95% CI, 0.57-0.87).
- Despite its effectiveness, mifepristone was used in only 8.6% of those receiving medication management for early pregnancy loss in 2022.
IN PRACTICE:
“Continued efforts are needed to reduce barriers to mifepristone use for medication management of EPL,” the authors wrote.
“Any practitioner who cares for patients experiencing early pregnancy loss should consider mifepristone pretreatment to misoprostol to be the standard of care for medication management. Provision of the evidence-based standard of care with the use of mifepristone for early pregnancy loss is an opportunity to advocate for an essential strategy in improving sexual and reproductive health in the US,” wrote Sarita Sonalkar, MD, MPH, and Rachel McKean, MD, MPH, of the Perelman School of Medicine at the University of Pennsylvania, Philadelphia, in an invited commentary.
SOURCE:
The study was led by Lyndsey S. Benson, MD, MS, of the University of Washington School of Medicine, Seattle, and was published online in JAMA Network Open.
LIMITATIONS:
The study was limited by the accuracy of the diagnosis of early pregnancy loss and procedure codes because claims data are intended for billing purposes and may be incomplete or inaccurate. The use of de-identified data meant that specific gestational durations, exact dosing, or routes of misoprostol administration could not be determined. The findings may not be generalizable to those with public insurance or no insurance.
DISCLOSURES:
The study was supported in part by a grant from a Women’s Reproductive Health Research grant from the National Institutes of Health Eunice Kennedy Shriver National Institute for Child Health and Human Development. One author reported serving as an adviser and investigator, while another reported receiving personal fees and serving as an expert witness, contributing editor, and course instructor outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Maternal Immunization to Prevent Serious Respiratory Illness
Editor’s Note: Sadly, this is the last column in the Master Class Obstetrics series. This award-winning column has been part of Ob.Gyn. News for 20 years. The deep discussion of cutting-edge topics in obstetrics by specialists and researchers will be missed as will the leadership and curation of topics by Dr. E. Albert Reece.
Introduction: The Need for Increased Vigilance About Maternal Immunization
Viruses are becoming increasingly prevalent in our world and the consequences of viral infections are implicated in a growing number of disease states. It is well established that certain cancers are caused by viruses and it is increasingly evident that viral infections can trigger the development of chronic illness. In pregnant women, viruses such as cytomegalovirus can cause infection in utero and lead to long-term impairments for the baby.
Likewise, it appears that the virulence of viruses is increasing, whether it be the respiratory syncytial virus (RSV) in children or the severe acute respiratory syndrome (SARS) coronaviruses in adults. Clearly, our environment is changing, with increases in population growth and urbanization, for instance, and an intensification of climate change and its effects. Viruses are part of this changing background.

Vaccines are our most powerful tool to protect people of all ages against viral threats, and fortunately, we benefit from increasing expertise in vaccinology. Since 1974, the University of Maryland School of Medicine has a Center for Vaccine Development and Global Health that has conducted research on vaccines to defend against the Zika virus, H1N1, Ebola, and SARS-CoV-2.
We’re not alone. Other vaccinology centers across the country — as well as the National Institutes of Health at the national level, through its National Institute of Allergy and Infectious Diseases — are doing research and developing vaccines to combat viral diseases.
In this column, we are focused on viral diseases in pregnancy and the role that vaccines can play in preventing serious respiratory illness in mothers and their newborns. I have invited Laura E. Riley, MD, the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine, to address the importance of maternal immunization and how we can best counsel our patients and improve immunization rates.
As Dr. Riley explains, we are in a new era, and it behooves us all to be more vigilant about recommending vaccines, combating misperceptions, addressing patients’ knowledge gaps, and administering vaccines whenever possible.
Dr. Reece is the former Dean of Medicine & University Executive VP, and The Distinguished University and Endowed Professor & Director of the Center for Advanced Research Training and Innovation (CARTI) at the University of Maryland School of Medicine, as well as senior scientist at the Center for Birth Defects Research.
The alarming decline in maternal immunization rates that occurred in the wake of the COVID-19 pandemic means that, now more than ever, we must fully embrace our responsibility to recommend immunizations in pregnancy and to communicate what is known about their efficacy and safety. Data show that vaccination rates drop when we do not offer vaccines in our offices, so whenever possible, we should administer them as well.
The ob.gyn. is the patient’s most trusted person in pregnancy. When patients decline or express hesitancy about vaccines, it is incumbent upon us to ask why. Oftentimes, we can identify areas in which patients lack knowledge or have misperceptions and we can successfully educate the patient or change their perspective or misunderstanding concerning the importance of vaccination for themselves and their babies. (See Table 1.) We can also successfully address concerns about safety.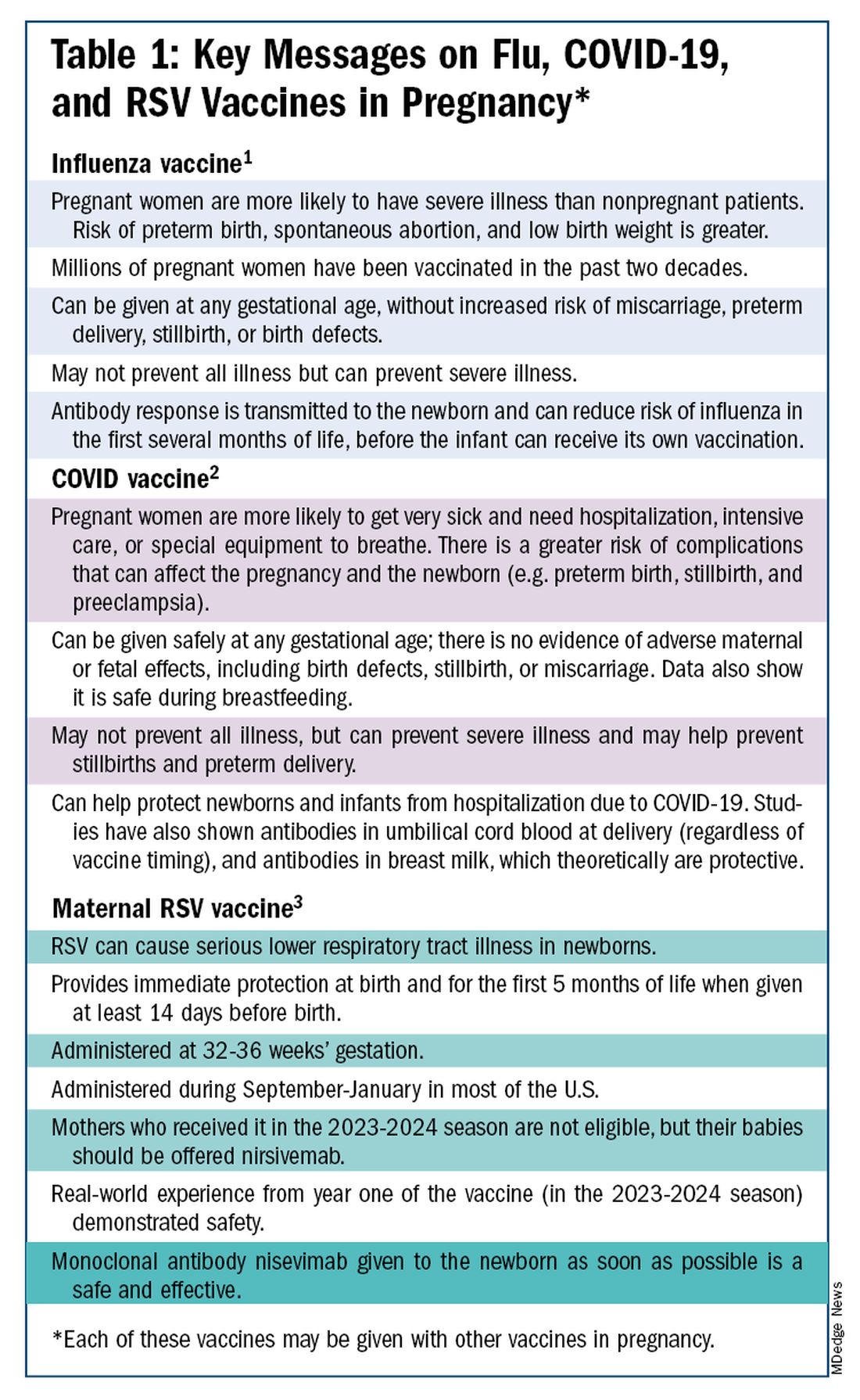
The safety of COVID-19 vaccinations in pregnancy is now backed by several years of data from multiple studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
Data also show that pregnant patients are more likely than patients who are not pregnant to need hospitalization and intensive care when infected with SARS-CoV-2 and are at risk of having complications that can affect pregnancy and the newborn, including preterm birth and stillbirth. Vaccination has been shown to reduce the risk of severe illness and the risk of such adverse obstetrical outcomes, in addition to providing protection for the infant early on.
Similarly, influenza has long been more likely to be severe in pregnant patients, with an increased risk of poor obstetrical outcomes. Vaccines similarly provide “two for one protection,” protecting both mother and baby, and are, of course, backed by many years of safety and efficacy data.

With the new maternal respiratory syncytial virus (RSV) vaccine, now in its second year of availability, the goal is to protect the baby from RSV-caused serious lower respiratory tract illness. The illness has contributed to tens of thousands of annual hospitalizations and up to several hundred deaths every year in children younger than 5 years — particularly in those under age 6 months.
The RSV monoclonal antibody nirsevimab is available for the newborn as an alternative to maternal immunization but the maternal vaccine is optimal in that it will provide immediate rather than delayed protection for the newborn. The maternal vaccine is recommended during weeks 32-36 of pregnancy in mothers who were not vaccinated during last year’s RSV season. With real-world experience from year one, the available safety data are reassuring.
Counseling About Influenza and COVID-19 Vaccination
The COVID-19 pandemic took a toll on vaccination interest/receptivity broadly in pregnant and nonpregnant people. Among pregnant individuals, influenza vaccination coverage declined from 71% in the 2019-2020 influenza season to 56% in the 2021-2022 season, according to data from the Centers for Disease Control and Prevention’s Vaccine Safety Datalink.4 Coverage for the 2022-2023 and 2023-2024 influenza seasons was even worse: well under 50%.5
Fewer pregnant women have received updated COVID-19 vaccines. Only 13% of pregnant persons overall received the updated 2023-2024 COVID-19 booster vaccine (through March 30, 2024), according to the CDC.6
Maternal immunization for influenza has been recommended in the United States since 2004 (part of the recommendation that everyone over the age of 6 months receive an annual flu vaccine), and flu vaccines have been given to millions of pregnant women, but the H1N1 pandemic of 2009 reinforced its value as a priority for prenatal care. Most of the women who became severely ill from the H1N1 virus were young and healthy, without co-existing conditions known to increase risk.7
It became clearer during the H1N1 pandemic that pregnancy itself — which is associated with physiologic changes such as decreased lung capacity, increased nasal congestion and changes in the immune system – is its own significant risk factor for severe illness from the influenza virus. This increased risk applies to COVID-19 as well.
As COVID-19 has become endemic, with hospitalizations and deaths not reaching the levels of previous surges — and with mask-wearing and other preventive measures having declined — patients understandably have become more complacent. Some patients are vaccine deniers, but in my practice, these patients are a much smaller group than those who believe COVID-19 “is no big deal,” especially if they have had infections recently.
This is why it’s important to actively listen to concerns and to ask patients who decline a vaccination why they are hesitant. Blanket messages about vaccine efficacy and safety are the first step, but individualized, more pointed conversations based on the patient’s personal experiences and beliefs have become increasingly important.
I routinely tell pregnant patients about the risks of COVID-19 and I explain that it has been difficult to predict who will develop severe illness. Sometimes more conversation is needed. For those who are still hesitant or who tell me they feel protected by a recent infection, for instance, I provide more detail on the unique risks of pregnancy — the fact that “pregnancy is different” — and that natural immunity wanes while the protection afforded by immunization is believed to last longer. Many women are also concerned about the safety of the COVID-19 vaccine, so having safety data at your fingertips is helpful. (See Table 2.)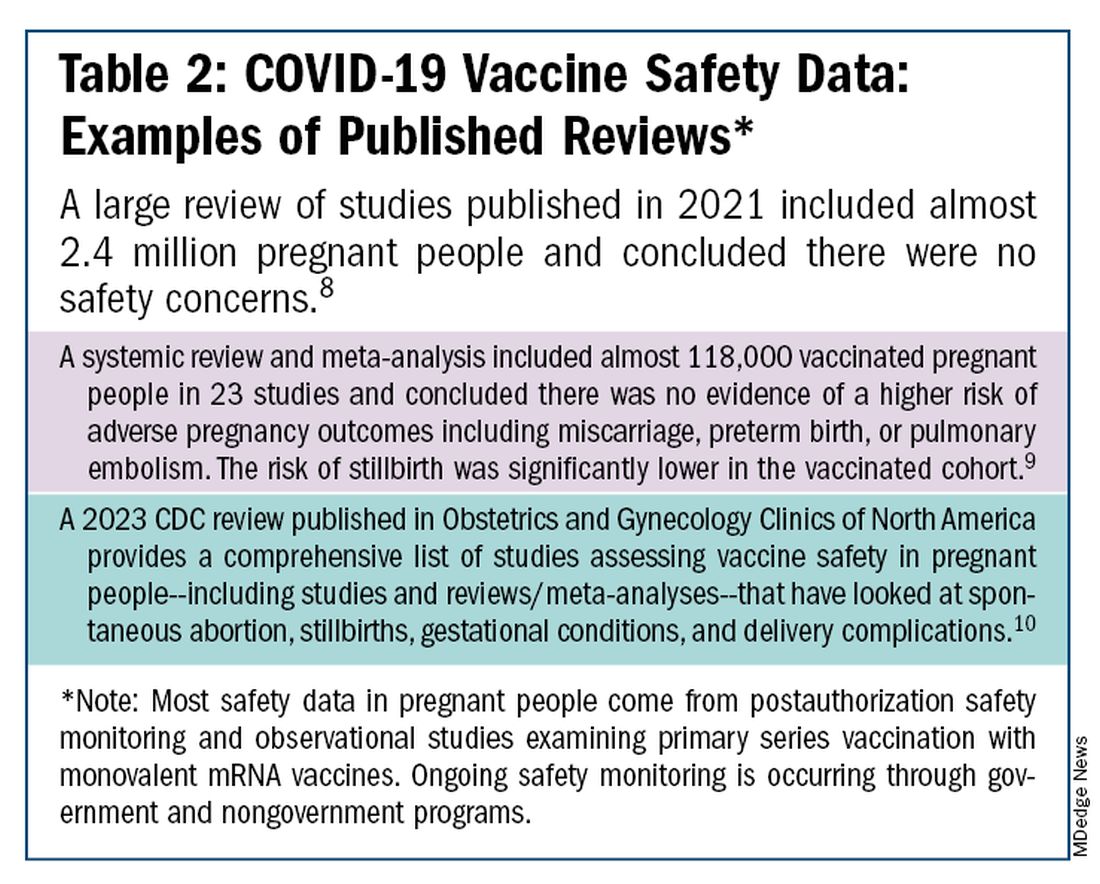
The fact that influenza and COVID-19 vaccination protect the newborn as well as the mother is something that I find is underappreciated by many patients. Explaining that infants likely benefit from the passage of antibodies across the placenta should be part of patient counseling.
Counseling About RSV Vaccination
Importantly, for the 2024-2025 RSV season, the maternal RSV vaccine (Abrysvo, Pfizer) is recommended only for pregnant women who did not receive the vaccine during the 2023-2024 season. When more research is done and more data are obtained showing how long the immune response persists post vaccination, it may be that the US Food and Drug Administration (FDA) will approve the maternal RSV vaccine for use in every pregnancy.
The later timing of the vaccination recommendation — 32-36 weeks’ gestation — reflects a conservative approach taken by the FDA in response to data from one of the pivotal trials showing a numerical trend toward more preterm deliveries among vaccinated compared with unvaccinated patients. This imbalance in the original trial, which administered the vaccine during 24-36 weeks of gestation, was seen only in low-income countries with no temporal association, however.
In our experience at two Weill Cornell Medical College–associated hospitals we did not see this trend. Our cohort study of almost 3000 pregnant patients who delivered at 32 weeks’ gestation or later found no increased risk of preterm birth among the 35% of patients who received the RSV vaccine during the 2023-2024 RSV season. We also did not see any difference in preeclampsia, in contrast with original trial data that showed a signal for increased risk.11
When fewer than 2 weeks have elapsed between maternal vaccination and delivery, the monoclonal antibody nirsevimab is recommended for the newborn — ideally before the newborn leaves the hospital. Nirsevimab is also recommended for newborns of mothers who decline vaccination or were not candidates (e.g. vaccinated in a previous pregnancy), or when there is concern about the adequacy of the maternal immune response to the vaccine (e.g. in cases of immunosuppression).
While there was a limited supply of the monoclonal antibody last year, limitations are not expected this year, especially after October.
The ultimate goal is that patients choose the vaccine or the immunoglobulin, given the severity of RSV disease. Patient preferences should be considered. However, given that it takes 2 weeks after vaccination for protection to build up, I stress to patients that if they’ve vaccinated themselves, their newborn will leave the hospital with protection. If nirsevimab is relied upon, I explain, their newborn may not be protected for some period of time.
Take-home Messages
- When patients decline or are hesitant about vaccines, ask why. Listen actively, and work to correct misperceptions and knowledge gaps.
- Whenever possible, offer vaccines in your practice. Vaccination rates drop when this does not occur.
- COVID-vaccine safety is backed by many studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
- Pregnant women are more likely to have severe illness from the influenza and SARS-CoV-2 viruses. Vaccines can prevent severe illness and can protect the newborn as well as the mother.
- Recommend/administer the maternal RSV vaccine at 32-36 weeks’ gestation in women who did not receive the vaccine in the 2023-2024 season. If mothers aren’t eligible their babies should be offered nirsevimab.
Dr. Riley is the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine and the obstetrician and gynecologist-in-chief at New York Presbyterian Hospital. She disclosed that she has provided one-time consultations to Pfizer (Abrysvo RSV vaccine) and GSK (cytomegalovirus vaccine), and is providing consultant education on CMV for Moderna. She is chair of ACOG’s task force on immunization and emerging infectious diseases, serves on the medical advisory board for MAVEN, and serves as an editor or editorial board member for several medical publications.
References
1. ACOG Committee Opinion No. 741: Maternal Immunization. Obstet Gynecol. 2018;131(6):e214-e217.
2. Centers for Disease Control and Prevention. COVID-19 Vaccination for People Who are Pregnant or Breastfeeding. https://www.cdc.gov/covid/vaccines/pregnant-or-breastfeeding.html.
3. ACOG Practice Advisory on Maternal Respiratory Syncytial Virus Vaccination, September 2023. (Updated August 2024).4. Irving S et al. Open Forum Infect Dis. 2023;10(Suppl 2):ofad500.1002.
5. Flu Vaccination Dashboard, CDC, National Center for Immunization and Respiratory Diseases.
6. Weekly COVID-19 Vaccination Dashboard, CDC. https://www.cdc.gov/covidvaxview/weekly-dashboard/index.html
7. Louie JK et al. N Engl J Med. 2010;362:27-35. 8. Ciapponi A et al. Vaccine. 2021;39(40):5891-908.
9. Prasad S et al. Nature Communications. 2022;13:2414. 10. Fleming-Dutra KE et al. Obstet Gynecol Clin North Am 2023;50(2):279-97. 11. Mouen S et al. JAMA Network Open 2024;7(7):e2419268.
Editor’s Note: Sadly, this is the last column in the Master Class Obstetrics series. This award-winning column has been part of Ob.Gyn. News for 20 years. The deep discussion of cutting-edge topics in obstetrics by specialists and researchers will be missed as will the leadership and curation of topics by Dr. E. Albert Reece.
Introduction: The Need for Increased Vigilance About Maternal Immunization
Viruses are becoming increasingly prevalent in our world and the consequences of viral infections are implicated in a growing number of disease states. It is well established that certain cancers are caused by viruses and it is increasingly evident that viral infections can trigger the development of chronic illness. In pregnant women, viruses such as cytomegalovirus can cause infection in utero and lead to long-term impairments for the baby.
Likewise, it appears that the virulence of viruses is increasing, whether it be the respiratory syncytial virus (RSV) in children or the severe acute respiratory syndrome (SARS) coronaviruses in adults. Clearly, our environment is changing, with increases in population growth and urbanization, for instance, and an intensification of climate change and its effects. Viruses are part of this changing background.
Vaccines are our most powerful tool to protect people of all ages against viral threats, and fortunately, we benefit from increasing expertise in vaccinology. Since 1974, the University of Maryland School of Medicine has a Center for Vaccine Development and Global Health that has conducted research on vaccines to defend against the Zika virus, H1N1, Ebola, and SARS-CoV-2.
We’re not alone. Other vaccinology centers across the country — as well as the National Institutes of Health at the national level, through its National Institute of Allergy and Infectious Diseases — are doing research and developing vaccines to combat viral diseases.
In this column, we are focused on viral diseases in pregnancy and the role that vaccines can play in preventing serious respiratory illness in mothers and their newborns. I have invited Laura E. Riley, MD, the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine, to address the importance of maternal immunization and how we can best counsel our patients and improve immunization rates.
As Dr. Riley explains, we are in a new era, and it behooves us all to be more vigilant about recommending vaccines, combating misperceptions, addressing patients’ knowledge gaps, and administering vaccines whenever possible.
Dr. Reece is the former Dean of Medicine & University Executive VP, and The Distinguished University and Endowed Professor & Director of the Center for Advanced Research Training and Innovation (CARTI) at the University of Maryland School of Medicine, as well as senior scientist at the Center for Birth Defects Research.
The alarming decline in maternal immunization rates that occurred in the wake of the COVID-19 pandemic means that, now more than ever, we must fully embrace our responsibility to recommend immunizations in pregnancy and to communicate what is known about their efficacy and safety. Data show that vaccination rates drop when we do not offer vaccines in our offices, so whenever possible, we should administer them as well.
The ob.gyn. is the patient’s most trusted person in pregnancy. When patients decline or express hesitancy about vaccines, it is incumbent upon us to ask why. Oftentimes, we can identify areas in which patients lack knowledge or have misperceptions and we can successfully educate the patient or change their perspective or misunderstanding concerning the importance of vaccination for themselves and their babies. (See Table 1.) We can also successfully address concerns about safety.
The safety of COVID-19 vaccinations in pregnancy is now backed by several years of data from multiple studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
Data also show that pregnant patients are more likely than patients who are not pregnant to need hospitalization and intensive care when infected with SARS-CoV-2 and are at risk of having complications that can affect pregnancy and the newborn, including preterm birth and stillbirth. Vaccination has been shown to reduce the risk of severe illness and the risk of such adverse obstetrical outcomes, in addition to providing protection for the infant early on.
Similarly, influenza has long been more likely to be severe in pregnant patients, with an increased risk of poor obstetrical outcomes. Vaccines similarly provide “two for one protection,” protecting both mother and baby, and are, of course, backed by many years of safety and efficacy data.
With the new maternal respiratory syncytial virus (RSV) vaccine, now in its second year of availability, the goal is to protect the baby from RSV-caused serious lower respiratory tract illness. The illness has contributed to tens of thousands of annual hospitalizations and up to several hundred deaths every year in children younger than 5 years — particularly in those under age 6 months.
The RSV monoclonal antibody nirsevimab is available for the newborn as an alternative to maternal immunization but the maternal vaccine is optimal in that it will provide immediate rather than delayed protection for the newborn. The maternal vaccine is recommended during weeks 32-36 of pregnancy in mothers who were not vaccinated during last year’s RSV season. With real-world experience from year one, the available safety data are reassuring.
Counseling About Influenza and COVID-19 Vaccination
The COVID-19 pandemic took a toll on vaccination interest/receptivity broadly in pregnant and nonpregnant people. Among pregnant individuals, influenza vaccination coverage declined from 71% in the 2019-2020 influenza season to 56% in the 2021-2022 season, according to data from the Centers for Disease Control and Prevention’s Vaccine Safety Datalink.4 Coverage for the 2022-2023 and 2023-2024 influenza seasons was even worse: well under 50%.5
Fewer pregnant women have received updated COVID-19 vaccines. Only 13% of pregnant persons overall received the updated 2023-2024 COVID-19 booster vaccine (through March 30, 2024), according to the CDC.6
Maternal immunization for influenza has been recommended in the United States since 2004 (part of the recommendation that everyone over the age of 6 months receive an annual flu vaccine), and flu vaccines have been given to millions of pregnant women, but the H1N1 pandemic of 2009 reinforced its value as a priority for prenatal care. Most of the women who became severely ill from the H1N1 virus were young and healthy, without co-existing conditions known to increase risk.7
It became clearer during the H1N1 pandemic that pregnancy itself — which is associated with physiologic changes such as decreased lung capacity, increased nasal congestion and changes in the immune system – is its own significant risk factor for severe illness from the influenza virus. This increased risk applies to COVID-19 as well.
As COVID-19 has become endemic, with hospitalizations and deaths not reaching the levels of previous surges — and with mask-wearing and other preventive measures having declined — patients understandably have become more complacent. Some patients are vaccine deniers, but in my practice, these patients are a much smaller group than those who believe COVID-19 “is no big deal,” especially if they have had infections recently.
This is why it’s important to actively listen to concerns and to ask patients who decline a vaccination why they are hesitant. Blanket messages about vaccine efficacy and safety are the first step, but individualized, more pointed conversations based on the patient’s personal experiences and beliefs have become increasingly important.
I routinely tell pregnant patients about the risks of COVID-19 and I explain that it has been difficult to predict who will develop severe illness. Sometimes more conversation is needed. For those who are still hesitant or who tell me they feel protected by a recent infection, for instance, I provide more detail on the unique risks of pregnancy — the fact that “pregnancy is different” — and that natural immunity wanes while the protection afforded by immunization is believed to last longer. Many women are also concerned about the safety of the COVID-19 vaccine, so having safety data at your fingertips is helpful. (See Table 2.)
The fact that influenza and COVID-19 vaccination protect the newborn as well as the mother is something that I find is underappreciated by many patients. Explaining that infants likely benefit from the passage of antibodies across the placenta should be part of patient counseling.
Counseling About RSV Vaccination
Importantly, for the 2024-2025 RSV season, the maternal RSV vaccine (Abrysvo, Pfizer) is recommended only for pregnant women who did not receive the vaccine during the 2023-2024 season. When more research is done and more data are obtained showing how long the immune response persists post vaccination, it may be that the US Food and Drug Administration (FDA) will approve the maternal RSV vaccine for use in every pregnancy.
The later timing of the vaccination recommendation — 32-36 weeks’ gestation — reflects a conservative approach taken by the FDA in response to data from one of the pivotal trials showing a numerical trend toward more preterm deliveries among vaccinated compared with unvaccinated patients. This imbalance in the original trial, which administered the vaccine during 24-36 weeks of gestation, was seen only in low-income countries with no temporal association, however.
In our experience at two Weill Cornell Medical College–associated hospitals we did not see this trend. Our cohort study of almost 3000 pregnant patients who delivered at 32 weeks’ gestation or later found no increased risk of preterm birth among the 35% of patients who received the RSV vaccine during the 2023-2024 RSV season. We also did not see any difference in preeclampsia, in contrast with original trial data that showed a signal for increased risk.11
When fewer than 2 weeks have elapsed between maternal vaccination and delivery, the monoclonal antibody nirsevimab is recommended for the newborn — ideally before the newborn leaves the hospital. Nirsevimab is also recommended for newborns of mothers who decline vaccination or were not candidates (e.g. vaccinated in a previous pregnancy), or when there is concern about the adequacy of the maternal immune response to the vaccine (e.g. in cases of immunosuppression).
While there was a limited supply of the monoclonal antibody last year, limitations are not expected this year, especially after October.
The ultimate goal is that patients choose the vaccine or the immunoglobulin, given the severity of RSV disease. Patient preferences should be considered. However, given that it takes 2 weeks after vaccination for protection to build up, I stress to patients that if they’ve vaccinated themselves, their newborn will leave the hospital with protection. If nirsevimab is relied upon, I explain, their newborn may not be protected for some period of time.
Take-home Messages
- When patients decline or are hesitant about vaccines, ask why. Listen actively, and work to correct misperceptions and knowledge gaps.
- Whenever possible, offer vaccines in your practice. Vaccination rates drop when this does not occur.
- COVID-vaccine safety is backed by many studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
- Pregnant women are more likely to have severe illness from the influenza and SARS-CoV-2 viruses. Vaccines can prevent severe illness and can protect the newborn as well as the mother.
- Recommend/administer the maternal RSV vaccine at 32-36 weeks’ gestation in women who did not receive the vaccine in the 2023-2024 season. If mothers aren’t eligible their babies should be offered nirsevimab.
Dr. Riley is the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine and the obstetrician and gynecologist-in-chief at New York Presbyterian Hospital. She disclosed that she has provided one-time consultations to Pfizer (Abrysvo RSV vaccine) and GSK (cytomegalovirus vaccine), and is providing consultant education on CMV for Moderna. She is chair of ACOG’s task force on immunization and emerging infectious diseases, serves on the medical advisory board for MAVEN, and serves as an editor or editorial board member for several medical publications.
References
1. ACOG Committee Opinion No. 741: Maternal Immunization. Obstet Gynecol. 2018;131(6):e214-e217.
2. Centers for Disease Control and Prevention. COVID-19 Vaccination for People Who are Pregnant or Breastfeeding. https://www.cdc.gov/covid/vaccines/pregnant-or-breastfeeding.html.
3. ACOG Practice Advisory on Maternal Respiratory Syncytial Virus Vaccination, September 2023. (Updated August 2024).4. Irving S et al. Open Forum Infect Dis. 2023;10(Suppl 2):ofad500.1002.
5. Flu Vaccination Dashboard, CDC, National Center for Immunization and Respiratory Diseases.
6. Weekly COVID-19 Vaccination Dashboard, CDC. https://www.cdc.gov/covidvaxview/weekly-dashboard/index.html
7. Louie JK et al. N Engl J Med. 2010;362:27-35. 8. Ciapponi A et al. Vaccine. 2021;39(40):5891-908.
9. Prasad S et al. Nature Communications. 2022;13:2414. 10. Fleming-Dutra KE et al. Obstet Gynecol Clin North Am 2023;50(2):279-97. 11. Mouen S et al. JAMA Network Open 2024;7(7):e2419268.
Editor’s Note: Sadly, this is the last column in the Master Class Obstetrics series. This award-winning column has been part of Ob.Gyn. News for 20 years. The deep discussion of cutting-edge topics in obstetrics by specialists and researchers will be missed as will the leadership and curation of topics by Dr. E. Albert Reece.
Introduction: The Need for Increased Vigilance About Maternal Immunization
Viruses are becoming increasingly prevalent in our world and the consequences of viral infections are implicated in a growing number of disease states. It is well established that certain cancers are caused by viruses and it is increasingly evident that viral infections can trigger the development of chronic illness. In pregnant women, viruses such as cytomegalovirus can cause infection in utero and lead to long-term impairments for the baby.
Likewise, it appears that the virulence of viruses is increasing, whether it be the respiratory syncytial virus (RSV) in children or the severe acute respiratory syndrome (SARS) coronaviruses in adults. Clearly, our environment is changing, with increases in population growth and urbanization, for instance, and an intensification of climate change and its effects. Viruses are part of this changing background.
Vaccines are our most powerful tool to protect people of all ages against viral threats, and fortunately, we benefit from increasing expertise in vaccinology. Since 1974, the University of Maryland School of Medicine has a Center for Vaccine Development and Global Health that has conducted research on vaccines to defend against the Zika virus, H1N1, Ebola, and SARS-CoV-2.
We’re not alone. Other vaccinology centers across the country — as well as the National Institutes of Health at the national level, through its National Institute of Allergy and Infectious Diseases — are doing research and developing vaccines to combat viral diseases.
In this column, we are focused on viral diseases in pregnancy and the role that vaccines can play in preventing serious respiratory illness in mothers and their newborns. I have invited Laura E. Riley, MD, the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine, to address the importance of maternal immunization and how we can best counsel our patients and improve immunization rates.
As Dr. Riley explains, we are in a new era, and it behooves us all to be more vigilant about recommending vaccines, combating misperceptions, addressing patients’ knowledge gaps, and administering vaccines whenever possible.
Dr. Reece is the former Dean of Medicine & University Executive VP, and The Distinguished University and Endowed Professor & Director of the Center for Advanced Research Training and Innovation (CARTI) at the University of Maryland School of Medicine, as well as senior scientist at the Center for Birth Defects Research.
The alarming decline in maternal immunization rates that occurred in the wake of the COVID-19 pandemic means that, now more than ever, we must fully embrace our responsibility to recommend immunizations in pregnancy and to communicate what is known about their efficacy and safety. Data show that vaccination rates drop when we do not offer vaccines in our offices, so whenever possible, we should administer them as well.
The ob.gyn. is the patient’s most trusted person in pregnancy. When patients decline or express hesitancy about vaccines, it is incumbent upon us to ask why. Oftentimes, we can identify areas in which patients lack knowledge or have misperceptions and we can successfully educate the patient or change their perspective or misunderstanding concerning the importance of vaccination for themselves and their babies. (See Table 1.) We can also successfully address concerns about safety.
The safety of COVID-19 vaccinations in pregnancy is now backed by several years of data from multiple studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
Data also show that pregnant patients are more likely than patients who are not pregnant to need hospitalization and intensive care when infected with SARS-CoV-2 and are at risk of having complications that can affect pregnancy and the newborn, including preterm birth and stillbirth. Vaccination has been shown to reduce the risk of severe illness and the risk of such adverse obstetrical outcomes, in addition to providing protection for the infant early on.
Similarly, influenza has long been more likely to be severe in pregnant patients, with an increased risk of poor obstetrical outcomes. Vaccines similarly provide “two for one protection,” protecting both mother and baby, and are, of course, backed by many years of safety and efficacy data.
With the new maternal respiratory syncytial virus (RSV) vaccine, now in its second year of availability, the goal is to protect the baby from RSV-caused serious lower respiratory tract illness. The illness has contributed to tens of thousands of annual hospitalizations and up to several hundred deaths every year in children younger than 5 years — particularly in those under age 6 months.
The RSV monoclonal antibody nirsevimab is available for the newborn as an alternative to maternal immunization but the maternal vaccine is optimal in that it will provide immediate rather than delayed protection for the newborn. The maternal vaccine is recommended during weeks 32-36 of pregnancy in mothers who were not vaccinated during last year’s RSV season. With real-world experience from year one, the available safety data are reassuring.
Counseling About Influenza and COVID-19 Vaccination
The COVID-19 pandemic took a toll on vaccination interest/receptivity broadly in pregnant and nonpregnant people. Among pregnant individuals, influenza vaccination coverage declined from 71% in the 2019-2020 influenza season to 56% in the 2021-2022 season, according to data from the Centers for Disease Control and Prevention’s Vaccine Safety Datalink.4 Coverage for the 2022-2023 and 2023-2024 influenza seasons was even worse: well under 50%.5
Fewer pregnant women have received updated COVID-19 vaccines. Only 13% of pregnant persons overall received the updated 2023-2024 COVID-19 booster vaccine (through March 30, 2024), according to the CDC.6
Maternal immunization for influenza has been recommended in the United States since 2004 (part of the recommendation that everyone over the age of 6 months receive an annual flu vaccine), and flu vaccines have been given to millions of pregnant women, but the H1N1 pandemic of 2009 reinforced its value as a priority for prenatal care. Most of the women who became severely ill from the H1N1 virus were young and healthy, without co-existing conditions known to increase risk.7
It became clearer during the H1N1 pandemic that pregnancy itself — which is associated with physiologic changes such as decreased lung capacity, increased nasal congestion and changes in the immune system – is its own significant risk factor for severe illness from the influenza virus. This increased risk applies to COVID-19 as well.
As COVID-19 has become endemic, with hospitalizations and deaths not reaching the levels of previous surges — and with mask-wearing and other preventive measures having declined — patients understandably have become more complacent. Some patients are vaccine deniers, but in my practice, these patients are a much smaller group than those who believe COVID-19 “is no big deal,” especially if they have had infections recently.
This is why it’s important to actively listen to concerns and to ask patients who decline a vaccination why they are hesitant. Blanket messages about vaccine efficacy and safety are the first step, but individualized, more pointed conversations based on the patient’s personal experiences and beliefs have become increasingly important.
I routinely tell pregnant patients about the risks of COVID-19 and I explain that it has been difficult to predict who will develop severe illness. Sometimes more conversation is needed. For those who are still hesitant or who tell me they feel protected by a recent infection, for instance, I provide more detail on the unique risks of pregnancy — the fact that “pregnancy is different” — and that natural immunity wanes while the protection afforded by immunization is believed to last longer. Many women are also concerned about the safety of the COVID-19 vaccine, so having safety data at your fingertips is helpful. (See Table 2.)
The fact that influenza and COVID-19 vaccination protect the newborn as well as the mother is something that I find is underappreciated by many patients. Explaining that infants likely benefit from the passage of antibodies across the placenta should be part of patient counseling.
Counseling About RSV Vaccination
Importantly, for the 2024-2025 RSV season, the maternal RSV vaccine (Abrysvo, Pfizer) is recommended only for pregnant women who did not receive the vaccine during the 2023-2024 season. When more research is done and more data are obtained showing how long the immune response persists post vaccination, it may be that the US Food and Drug Administration (FDA) will approve the maternal RSV vaccine for use in every pregnancy.
The later timing of the vaccination recommendation — 32-36 weeks’ gestation — reflects a conservative approach taken by the FDA in response to data from one of the pivotal trials showing a numerical trend toward more preterm deliveries among vaccinated compared with unvaccinated patients. This imbalance in the original trial, which administered the vaccine during 24-36 weeks of gestation, was seen only in low-income countries with no temporal association, however.
In our experience at two Weill Cornell Medical College–associated hospitals we did not see this trend. Our cohort study of almost 3000 pregnant patients who delivered at 32 weeks’ gestation or later found no increased risk of preterm birth among the 35% of patients who received the RSV vaccine during the 2023-2024 RSV season. We also did not see any difference in preeclampsia, in contrast with original trial data that showed a signal for increased risk.11
When fewer than 2 weeks have elapsed between maternal vaccination and delivery, the monoclonal antibody nirsevimab is recommended for the newborn — ideally before the newborn leaves the hospital. Nirsevimab is also recommended for newborns of mothers who decline vaccination or were not candidates (e.g. vaccinated in a previous pregnancy), or when there is concern about the adequacy of the maternal immune response to the vaccine (e.g. in cases of immunosuppression).
While there was a limited supply of the monoclonal antibody last year, limitations are not expected this year, especially after October.
The ultimate goal is that patients choose the vaccine or the immunoglobulin, given the severity of RSV disease. Patient preferences should be considered. However, given that it takes 2 weeks after vaccination for protection to build up, I stress to patients that if they’ve vaccinated themselves, their newborn will leave the hospital with protection. If nirsevimab is relied upon, I explain, their newborn may not be protected for some period of time.
Take-home Messages
- When patients decline or are hesitant about vaccines, ask why. Listen actively, and work to correct misperceptions and knowledge gaps.
- Whenever possible, offer vaccines in your practice. Vaccination rates drop when this does not occur.
- COVID-vaccine safety is backed by many studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
- Pregnant women are more likely to have severe illness from the influenza and SARS-CoV-2 viruses. Vaccines can prevent severe illness and can protect the newborn as well as the mother.
- Recommend/administer the maternal RSV vaccine at 32-36 weeks’ gestation in women who did not receive the vaccine in the 2023-2024 season. If mothers aren’t eligible their babies should be offered nirsevimab.
Dr. Riley is the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine and the obstetrician and gynecologist-in-chief at New York Presbyterian Hospital. She disclosed that she has provided one-time consultations to Pfizer (Abrysvo RSV vaccine) and GSK (cytomegalovirus vaccine), and is providing consultant education on CMV for Moderna. She is chair of ACOG’s task force on immunization and emerging infectious diseases, serves on the medical advisory board for MAVEN, and serves as an editor or editorial board member for several medical publications.
References
1. ACOG Committee Opinion No. 741: Maternal Immunization. Obstet Gynecol. 2018;131(6):e214-e217.
2. Centers for Disease Control and Prevention. COVID-19 Vaccination for People Who are Pregnant or Breastfeeding. https://www.cdc.gov/covid/vaccines/pregnant-or-breastfeeding.html.
3. ACOG Practice Advisory on Maternal Respiratory Syncytial Virus Vaccination, September 2023. (Updated August 2024).4. Irving S et al. Open Forum Infect Dis. 2023;10(Suppl 2):ofad500.1002.
5. Flu Vaccination Dashboard, CDC, National Center for Immunization and Respiratory Diseases.
6. Weekly COVID-19 Vaccination Dashboard, CDC. https://www.cdc.gov/covidvaxview/weekly-dashboard/index.html
7. Louie JK et al. N Engl J Med. 2010;362:27-35. 8. Ciapponi A et al. Vaccine. 2021;39(40):5891-908.
9. Prasad S et al. Nature Communications. 2022;13:2414. 10. Fleming-Dutra KE et al. Obstet Gynecol Clin North Am 2023;50(2):279-97. 11. Mouen S et al. JAMA Network Open 2024;7(7):e2419268.
How to Treat Cancer While Preserving Fertility
Thanks to the continuously improving treatment options for cancer, the number of cancer survivors is increasing, and a large proportion of survivors is confronted with the long-term effects of cancer treatment. Especially for young patients, the question of the impact of therapy on fertility arises.
Dose adjustment or modification of the treatment regimen can achieve a lot. But experts at the congress of the European Society for Medical Oncology (ESMO) 2024 noted that knowledge about newer treatment options like immunotherapies is still insufficient.
Therapy Selection
The question of preserving fertility must be considered when deciding on the appropriate treatment, said Matteo Lambertini, MD, PhD, medical oncology consultant at the University of Genoa in Genoa, Italy. “Preserving fertility is also an aim of cancer therapy,” he said.
Lambertini, who is also a member of the ESMO Guideline Group on fertility preservation in cancer patients, referred to the 2020 ESMO guidelines, which list the gonadotoxicity of a substance depending on the treatment regimen and the patient’s age.
Isabelle Demeestere, MD, PhD, director of the research lab for human reproduction at the Erasmus Hospital of the Free University of Brussels in Brussels, Belgium, pointed out the limitations of general guidelines. “Therapies change over time, and a classification must be updated regularly.”
Knowledge gaps related to well-known therapies and many novel options persist. “For many FDA-approved medications, there are either no fertility data or only preclinical data available,” she added.
Chemotherapies and Immunotherapies
Chemotherapies with alkylating or platinum-containing substances are known for their effects on oocytes, follicle maturation, and spermatogenesis, said Demeestere.
Chemotherapy is gonadotoxic and leads to a temporary decrease in sperm quality or temporary azoospermia in men.
These effects, however, can lead to permanent azoospermia and endocrine disorders, depending on the dose, duration, or combination with radiation, said Demeestere.
Cryopreservation of sperm should always be performed before starting treatment. For high-risk patients who are prepubertal, samples of testicular tissue are taken.
In women, chemotherapy affects primordial follicles and follicle maturation through DNA damage. This process results in severe or temporary amenorrhea, a temporary or permanent decrease in egg reserve, and ultimately premature egg insufficiency.
Novel immunotherapies also influence fertility, presumably through interactions of the immune system with the reproductive organs. But insufficient data are available, according to Lambertini, who emphasized that “these data are urgently needed, especially for young patients with cancer.”
In a mouse model, immune checkpoint inhibitors affected ovarian function, and the inflammatory reaction in humans can affect fertility. No long-term data are available for women yet, however, explained Demeestere. The effects of other therapeutics such as PARP, CDK4/6, or tyrosine kinase inhibitors, as well as monoclonal antibodies like trastuzumab, are only seen sporadically.
In the PENELOPE-B phase 3 study, the CDK4/6 inhibitor palbociclib did not affect ovarian function, even though the cyclin-dependent kinases play an important role in mitotic arrest, said Demeestere.
Adjusting the Regimen
In a PET-guided approach, Demeestere’s research team investigated the effects of dose reduction or adjustment of the treatment regimen of procarbazine and cyclophosphamide on the fertility of patients younger than 45 years with advanced Hodgkin lymphoma.
By regularly controlling tumor growth with PET, the treatment could be adjusted so that the effect on egg reserve or spermatogenesis was significantly reduced and loss of fertility could be prevented.
During the 5-year follow-up period, the ovarian function of participating women was assessed by the serum concentration of follicle-stimulating hormone (FSH), estradiol, and anti-Müllerian hormone (AMH) to evaluate egg reserve. In men, testicular function was assessed at the beginning of the study. At the end of treatment, sperm analysis and FSH and testosterone levels were checked.
Demeestere and colleagues demonstrated that dose reduction or altering the treatment regimen for patients who responded early to treatment (determined by PET-guided monitoring) reduced the risk for gonadotoxicity from 46% to 14.5%. That is, the risk was reduced by more than half.
FSH and AMH correlated with the patient’s age and the dose of the alkylating agent. In men, sperm parameters recovered after dose or agent adjustment compared with the unchanged treatment regimen.
Newer results from the PHERGain study in women with early human epidermal growth factor receptor 2–positive breast cancer also provided hope, according to Demeestere. Under PET-guided control, chemotherapy could be reduced.
More Data Needed
The new treatment options pose a challenge to preserving fertility during cancer treatment, said Demeestere.
For new targeted therapies, uniform recommendations cannot be issued because of the lack of data and varying treatment durations. Still, the new therapies are safer than chemotherapy.
The need to collect data on fertility and long-term effects in cancer survivors in clinical studies is also reflected in the literature, according to Demeestere. “There are more review articles on this topic than clinical studies.”
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Thanks to the continuously improving treatment options for cancer, the number of cancer survivors is increasing, and a large proportion of survivors is confronted with the long-term effects of cancer treatment. Especially for young patients, the question of the impact of therapy on fertility arises.
Dose adjustment or modification of the treatment regimen can achieve a lot. But experts at the congress of the European Society for Medical Oncology (ESMO) 2024 noted that knowledge about newer treatment options like immunotherapies is still insufficient.
Therapy Selection
The question of preserving fertility must be considered when deciding on the appropriate treatment, said Matteo Lambertini, MD, PhD, medical oncology consultant at the University of Genoa in Genoa, Italy. “Preserving fertility is also an aim of cancer therapy,” he said.
Lambertini, who is also a member of the ESMO Guideline Group on fertility preservation in cancer patients, referred to the 2020 ESMO guidelines, which list the gonadotoxicity of a substance depending on the treatment regimen and the patient’s age.
Isabelle Demeestere, MD, PhD, director of the research lab for human reproduction at the Erasmus Hospital of the Free University of Brussels in Brussels, Belgium, pointed out the limitations of general guidelines. “Therapies change over time, and a classification must be updated regularly.”
Knowledge gaps related to well-known therapies and many novel options persist. “For many FDA-approved medications, there are either no fertility data or only preclinical data available,” she added.
Chemotherapies and Immunotherapies
Chemotherapies with alkylating or platinum-containing substances are known for their effects on oocytes, follicle maturation, and spermatogenesis, said Demeestere.
Chemotherapy is gonadotoxic and leads to a temporary decrease in sperm quality or temporary azoospermia in men.
These effects, however, can lead to permanent azoospermia and endocrine disorders, depending on the dose, duration, or combination with radiation, said Demeestere.
Cryopreservation of sperm should always be performed before starting treatment. For high-risk patients who are prepubertal, samples of testicular tissue are taken.
In women, chemotherapy affects primordial follicles and follicle maturation through DNA damage. This process results in severe or temporary amenorrhea, a temporary or permanent decrease in egg reserve, and ultimately premature egg insufficiency.
Novel immunotherapies also influence fertility, presumably through interactions of the immune system with the reproductive organs. But insufficient data are available, according to Lambertini, who emphasized that “these data are urgently needed, especially for young patients with cancer.”
In a mouse model, immune checkpoint inhibitors affected ovarian function, and the inflammatory reaction in humans can affect fertility. No long-term data are available for women yet, however, explained Demeestere. The effects of other therapeutics such as PARP, CDK4/6, or tyrosine kinase inhibitors, as well as monoclonal antibodies like trastuzumab, are only seen sporadically.
In the PENELOPE-B phase 3 study, the CDK4/6 inhibitor palbociclib did not affect ovarian function, even though the cyclin-dependent kinases play an important role in mitotic arrest, said Demeestere.
Adjusting the Regimen
In a PET-guided approach, Demeestere’s research team investigated the effects of dose reduction or adjustment of the treatment regimen of procarbazine and cyclophosphamide on the fertility of patients younger than 45 years with advanced Hodgkin lymphoma.
By regularly controlling tumor growth with PET, the treatment could be adjusted so that the effect on egg reserve or spermatogenesis was significantly reduced and loss of fertility could be prevented.
During the 5-year follow-up period, the ovarian function of participating women was assessed by the serum concentration of follicle-stimulating hormone (FSH), estradiol, and anti-Müllerian hormone (AMH) to evaluate egg reserve. In men, testicular function was assessed at the beginning of the study. At the end of treatment, sperm analysis and FSH and testosterone levels were checked.
Demeestere and colleagues demonstrated that dose reduction or altering the treatment regimen for patients who responded early to treatment (determined by PET-guided monitoring) reduced the risk for gonadotoxicity from 46% to 14.5%. That is, the risk was reduced by more than half.
FSH and AMH correlated with the patient’s age and the dose of the alkylating agent. In men, sperm parameters recovered after dose or agent adjustment compared with the unchanged treatment regimen.
Newer results from the PHERGain study in women with early human epidermal growth factor receptor 2–positive breast cancer also provided hope, according to Demeestere. Under PET-guided control, chemotherapy could be reduced.
More Data Needed
The new treatment options pose a challenge to preserving fertility during cancer treatment, said Demeestere.
For new targeted therapies, uniform recommendations cannot be issued because of the lack of data and varying treatment durations. Still, the new therapies are safer than chemotherapy.
The need to collect data on fertility and long-term effects in cancer survivors in clinical studies is also reflected in the literature, according to Demeestere. “There are more review articles on this topic than clinical studies.”
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Thanks to the continuously improving treatment options for cancer, the number of cancer survivors is increasing, and a large proportion of survivors is confronted with the long-term effects of cancer treatment. Especially for young patients, the question of the impact of therapy on fertility arises.
Dose adjustment or modification of the treatment regimen can achieve a lot. But experts at the congress of the European Society for Medical Oncology (ESMO) 2024 noted that knowledge about newer treatment options like immunotherapies is still insufficient.
Therapy Selection
The question of preserving fertility must be considered when deciding on the appropriate treatment, said Matteo Lambertini, MD, PhD, medical oncology consultant at the University of Genoa in Genoa, Italy. “Preserving fertility is also an aim of cancer therapy,” he said.
Lambertini, who is also a member of the ESMO Guideline Group on fertility preservation in cancer patients, referred to the 2020 ESMO guidelines, which list the gonadotoxicity of a substance depending on the treatment regimen and the patient’s age.
Isabelle Demeestere, MD, PhD, director of the research lab for human reproduction at the Erasmus Hospital of the Free University of Brussels in Brussels, Belgium, pointed out the limitations of general guidelines. “Therapies change over time, and a classification must be updated regularly.”
Knowledge gaps related to well-known therapies and many novel options persist. “For many FDA-approved medications, there are either no fertility data or only preclinical data available,” she added.
Chemotherapies and Immunotherapies
Chemotherapies with alkylating or platinum-containing substances are known for their effects on oocytes, follicle maturation, and spermatogenesis, said Demeestere.
Chemotherapy is gonadotoxic and leads to a temporary decrease in sperm quality or temporary azoospermia in men.
These effects, however, can lead to permanent azoospermia and endocrine disorders, depending on the dose, duration, or combination with radiation, said Demeestere.
Cryopreservation of sperm should always be performed before starting treatment. For high-risk patients who are prepubertal, samples of testicular tissue are taken.
In women, chemotherapy affects primordial follicles and follicle maturation through DNA damage. This process results in severe or temporary amenorrhea, a temporary or permanent decrease in egg reserve, and ultimately premature egg insufficiency.
Novel immunotherapies also influence fertility, presumably through interactions of the immune system with the reproductive organs. But insufficient data are available, according to Lambertini, who emphasized that “these data are urgently needed, especially for young patients with cancer.”
In a mouse model, immune checkpoint inhibitors affected ovarian function, and the inflammatory reaction in humans can affect fertility. No long-term data are available for women yet, however, explained Demeestere. The effects of other therapeutics such as PARP, CDK4/6, or tyrosine kinase inhibitors, as well as monoclonal antibodies like trastuzumab, are only seen sporadically.
In the PENELOPE-B phase 3 study, the CDK4/6 inhibitor palbociclib did not affect ovarian function, even though the cyclin-dependent kinases play an important role in mitotic arrest, said Demeestere.
Adjusting the Regimen
In a PET-guided approach, Demeestere’s research team investigated the effects of dose reduction or adjustment of the treatment regimen of procarbazine and cyclophosphamide on the fertility of patients younger than 45 years with advanced Hodgkin lymphoma.
By regularly controlling tumor growth with PET, the treatment could be adjusted so that the effect on egg reserve or spermatogenesis was significantly reduced and loss of fertility could be prevented.
During the 5-year follow-up period, the ovarian function of participating women was assessed by the serum concentration of follicle-stimulating hormone (FSH), estradiol, and anti-Müllerian hormone (AMH) to evaluate egg reserve. In men, testicular function was assessed at the beginning of the study. At the end of treatment, sperm analysis and FSH and testosterone levels were checked.
Demeestere and colleagues demonstrated that dose reduction or altering the treatment regimen for patients who responded early to treatment (determined by PET-guided monitoring) reduced the risk for gonadotoxicity from 46% to 14.5%. That is, the risk was reduced by more than half.
FSH and AMH correlated with the patient’s age and the dose of the alkylating agent. In men, sperm parameters recovered after dose or agent adjustment compared with the unchanged treatment regimen.
Newer results from the PHERGain study in women with early human epidermal growth factor receptor 2–positive breast cancer also provided hope, according to Demeestere. Under PET-guided control, chemotherapy could be reduced.
More Data Needed
The new treatment options pose a challenge to preserving fertility during cancer treatment, said Demeestere.
For new targeted therapies, uniform recommendations cannot be issued because of the lack of data and varying treatment durations. Still, the new therapies are safer than chemotherapy.
The need to collect data on fertility and long-term effects in cancer survivors in clinical studies is also reflected in the literature, according to Demeestere. “There are more review articles on this topic than clinical studies.”
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Vitamin D in Pregnancy Results in Stronger Bones for Kids
TOPLINE:
Gestational supplementation of 1000 IU/d cholecalciferol (vitamin D3) from early pregnancy until delivery increases the bone mineral content, bone mineral density (BMD), and bone mineral apparent density in children at age 6-7 years.
METHODOLOGY:
- The double-blinded, placebo-controlled MAVIDOS trial of gestational vitamin D supplementation previously showed increased BMD at age 4 years (but no difference at birth), and it is unclear how the effect may persist or change over time.
- In the original trial, researchers randomized 1134 pregnant women with singleton pregnancy from three UK hospitals from 2008 to 2014, and the 723 children born to mothers recruited in Southampton were invited to continue in offspring follow-up.
- Mothers were randomly assigned to receive either 1000-IU/d vitamin D or placebo from 14-17 weeks’ gestation until delivery; women in the placebo arm could take up to 400-IU/d vitamin D.
- In this post hoc analysis, among 454 children who were followed up at age 6-7 years, 447 had a usable whole body and lumbar spine dual-energy x-ray absorptiometry scan (placebo group: n = 216; 48% boys; 98% White mothers and vitamin D group: n = 231; 56% boys; 96% White mothers).
- Offspring follow-up measures at birth and 4 and 6-7 years were bone area, bone mineral content, BMD, and bone mineral apparent density, derived from a dual-energy x-ray absorptiometry scan of whole body less head (WBLH), as well as fat and lean mass.
TAKEAWAY:
- The effect of gestational vitamin D supplementation on bone outcomes in children was similar at ages 4 and 6-7 years.
- At age 6-7 years, gestational vitamin D supplementation resulted in higher WBLH bone mineral content (0.15 SD; 95% CI, 0.04-0.26) and BMD (0.18 SD; 95% CI, 0.06-0.31) than placebo.
- The WBLH bone mineral apparent density (0.18 SD; 95% CI, 0.04-0.32) was also higher in the vitamin D group.
- The lean mass was greater in the vitamin D group (0.09 SD; 95% CI, 0.00-0.17) than in the placebo group.
IN PRACTICE:
“These findings suggest that pregnancy vitamin D supplementation may be an important population health strategy to improve bone health,” the authors wrote.
SOURCE:
This study was led by Rebecca J. Moon, PhD, MRC Lifecourse Epidemiology Centre, University of Southampton, Southampton General Hospital, England. It was published online in The American Journal of Clinical Nutrition.
LIMITATIONS:
Only individuals with baseline vitamin D levels of 25-100 nmol/L were eligible, excluding those with severe deficiency who might have benefited the most from supplementation. The participants were mostly White and well-educated, commonly overweight, which may have limited generalizability to other populations. Only 47% of the original cohort participated in the follow-up phase. Differences in maternal age, smoking status, and education between participants who remained in the study and those who did not may have introduced bias and affected generalizability.
DISCLOSURES:
The study was supported by Versus Arthritis UK, Medical Research Council, Bupa Foundation, and National Institute for Health and Care Research, Southampton Biomedical Research Centre, and other sources. Some authors disclosed receiving travel reimbursement, speaker or lecture fees, honoraria, research funding, or personal or consultancy fees from Alliance for Better Bone Health and various pharmaceutical, biotechnology, medical device, healthcare, and food and nutrition companies outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Gestational supplementation of 1000 IU/d cholecalciferol (vitamin D3) from early pregnancy until delivery increases the bone mineral content, bone mineral density (BMD), and bone mineral apparent density in children at age 6-7 years.
METHODOLOGY:
- The double-blinded, placebo-controlled MAVIDOS trial of gestational vitamin D supplementation previously showed increased BMD at age 4 years (but no difference at birth), and it is unclear how the effect may persist or change over time.
- In the original trial, researchers randomized 1134 pregnant women with singleton pregnancy from three UK hospitals from 2008 to 2014, and the 723 children born to mothers recruited in Southampton were invited to continue in offspring follow-up.
- Mothers were randomly assigned to receive either 1000-IU/d vitamin D or placebo from 14-17 weeks’ gestation until delivery; women in the placebo arm could take up to 400-IU/d vitamin D.
- In this post hoc analysis, among 454 children who were followed up at age 6-7 years, 447 had a usable whole body and lumbar spine dual-energy x-ray absorptiometry scan (placebo group: n = 216; 48% boys; 98% White mothers and vitamin D group: n = 231; 56% boys; 96% White mothers).
- Offspring follow-up measures at birth and 4 and 6-7 years were bone area, bone mineral content, BMD, and bone mineral apparent density, derived from a dual-energy x-ray absorptiometry scan of whole body less head (WBLH), as well as fat and lean mass.
TAKEAWAY:
- The effect of gestational vitamin D supplementation on bone outcomes in children was similar at ages 4 and 6-7 years.
- At age 6-7 years, gestational vitamin D supplementation resulted in higher WBLH bone mineral content (0.15 SD; 95% CI, 0.04-0.26) and BMD (0.18 SD; 95% CI, 0.06-0.31) than placebo.
- The WBLH bone mineral apparent density (0.18 SD; 95% CI, 0.04-0.32) was also higher in the vitamin D group.
- The lean mass was greater in the vitamin D group (0.09 SD; 95% CI, 0.00-0.17) than in the placebo group.
IN PRACTICE:
“These findings suggest that pregnancy vitamin D supplementation may be an important population health strategy to improve bone health,” the authors wrote.
SOURCE:
This study was led by Rebecca J. Moon, PhD, MRC Lifecourse Epidemiology Centre, University of Southampton, Southampton General Hospital, England. It was published online in The American Journal of Clinical Nutrition.
LIMITATIONS:
Only individuals with baseline vitamin D levels of 25-100 nmol/L were eligible, excluding those with severe deficiency who might have benefited the most from supplementation. The participants were mostly White and well-educated, commonly overweight, which may have limited generalizability to other populations. Only 47% of the original cohort participated in the follow-up phase. Differences in maternal age, smoking status, and education between participants who remained in the study and those who did not may have introduced bias and affected generalizability.
DISCLOSURES:
The study was supported by Versus Arthritis UK, Medical Research Council, Bupa Foundation, and National Institute for Health and Care Research, Southampton Biomedical Research Centre, and other sources. Some authors disclosed receiving travel reimbursement, speaker or lecture fees, honoraria, research funding, or personal or consultancy fees from Alliance for Better Bone Health and various pharmaceutical, biotechnology, medical device, healthcare, and food and nutrition companies outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Gestational supplementation of 1000 IU/d cholecalciferol (vitamin D3) from early pregnancy until delivery increases the bone mineral content, bone mineral density (BMD), and bone mineral apparent density in children at age 6-7 years.
METHODOLOGY:
- The double-blinded, placebo-controlled MAVIDOS trial of gestational vitamin D supplementation previously showed increased BMD at age 4 years (but no difference at birth), and it is unclear how the effect may persist or change over time.
- In the original trial, researchers randomized 1134 pregnant women with singleton pregnancy from three UK hospitals from 2008 to 2014, and the 723 children born to mothers recruited in Southampton were invited to continue in offspring follow-up.
- Mothers were randomly assigned to receive either 1000-IU/d vitamin D or placebo from 14-17 weeks’ gestation until delivery; women in the placebo arm could take up to 400-IU/d vitamin D.
- In this post hoc analysis, among 454 children who were followed up at age 6-7 years, 447 had a usable whole body and lumbar spine dual-energy x-ray absorptiometry scan (placebo group: n = 216; 48% boys; 98% White mothers and vitamin D group: n = 231; 56% boys; 96% White mothers).
- Offspring follow-up measures at birth and 4 and 6-7 years were bone area, bone mineral content, BMD, and bone mineral apparent density, derived from a dual-energy x-ray absorptiometry scan of whole body less head (WBLH), as well as fat and lean mass.
TAKEAWAY:
- The effect of gestational vitamin D supplementation on bone outcomes in children was similar at ages 4 and 6-7 years.
- At age 6-7 years, gestational vitamin D supplementation resulted in higher WBLH bone mineral content (0.15 SD; 95% CI, 0.04-0.26) and BMD (0.18 SD; 95% CI, 0.06-0.31) than placebo.
- The WBLH bone mineral apparent density (0.18 SD; 95% CI, 0.04-0.32) was also higher in the vitamin D group.
- The lean mass was greater in the vitamin D group (0.09 SD; 95% CI, 0.00-0.17) than in the placebo group.
IN PRACTICE:
“These findings suggest that pregnancy vitamin D supplementation may be an important population health strategy to improve bone health,” the authors wrote.
SOURCE:
This study was led by Rebecca J. Moon, PhD, MRC Lifecourse Epidemiology Centre, University of Southampton, Southampton General Hospital, England. It was published online in The American Journal of Clinical Nutrition.
LIMITATIONS:
Only individuals with baseline vitamin D levels of 25-100 nmol/L were eligible, excluding those with severe deficiency who might have benefited the most from supplementation. The participants were mostly White and well-educated, commonly overweight, which may have limited generalizability to other populations. Only 47% of the original cohort participated in the follow-up phase. Differences in maternal age, smoking status, and education between participants who remained in the study and those who did not may have introduced bias and affected generalizability.
DISCLOSURES:
The study was supported by Versus Arthritis UK, Medical Research Council, Bupa Foundation, and National Institute for Health and Care Research, Southampton Biomedical Research Centre, and other sources. Some authors disclosed receiving travel reimbursement, speaker or lecture fees, honoraria, research funding, or personal or consultancy fees from Alliance for Better Bone Health and various pharmaceutical, biotechnology, medical device, healthcare, and food and nutrition companies outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
ACS: Breast Cancer Incidence Rising, Mortality Disparities Persist
Breast cancer incidence has been on the rise, particularly among White women under age 50, but breast cancer deaths — for some, but not all, populations — have been steadily decreasing, according to a biennial update from the American Cancer Society (ACS).
The ACS update, which underscores the persistence of racial and ethnic disparities in breast cancer incidence and outcomes, noted an overall 1% annual increase in breast cancer incidence from 2012 to 2021. The additional cases were largely composed of localized-stage and hormone receptor (HR)–positive disease, which generally have better prognoses than more advanced and HR–negative disease.
Deaths from breast cancer, however, declined from 1989 to 2022, with an overall drop of 44%. That percentage drop “translates to almost 518,000 fewer women dying from breast cancer in the United States during this time,” Angela N. Giaquinto and ACS colleagues noted in the report, published in CA: A Cancer Journal for Clinicians.
“This progress is the result of advances in treatment and earlier detection through screening,” the authors wrote, while stressing that “these interventions have not been disseminated equally.”
The ACS also published an educational companion — Breast Cancer Facts & Figures 2024-2025 — that provides additional insights about trends in breast cancer and steps needed to bolster prevention, detection, and treatment advances.
Incidence and Mortality
Although the overall annual increase in breast cancer incidence from 2012 to 2021 was 1%, the increase was steeper among women under age 50, at 1.4% annually vs 0.7% among those aged 50 or older.
Asian American/Pacific Islander women had the greatest increases in breast cancer incidence among both age groups, with a 2.7% annual increase for those aged under 50 and a 2.5% increase for those aged 50 or older. This group, however, had the second lowest breast cancer rate in 2000 at 57.4 cases per 100,000 persons, but the highest rate in 2021 at 86.3 cases per 100,000, alongside White women (86.4 cases per 100,000). Black women were not far behind at 81.5 cases per 100,000.
Black women were least likely to be diagnosed with localized-stage breast cancer and most likely to be diagnosed with distant-stage or unstaged cancer, with American Indian/Alaska Native women not far behind.
Despite the rising incidence of breast cancer, death rates from the disease have gone down considerably overall from about 33 deaths per 100,000 women in 1989 to 19 deaths per 100,000 in 2022.
However, not all women have experienced these survival gains equally, Ms. Giaquinto and colleagues noted.
Since 1990, the mortality rate has remained unchanged among American Indian/Alaska Native women. Black women, however, have experienced a 38% higher mortality rate than White women, despite having a 5% lower incidence of breast cancer.
In fact, Black women have the lowest survival of any racial and ethnic group for every breast cancer subtype and stage of disease except localized disease.
Additional key findings from the report:
- In 2024, an estimated 310,720 new invasive breast cancers and 56,500 cases of ductal carcinoma in situ will be diagnosed among women in the United States, and an additional 2790 cases will be diagnosed in men.
- On the mortality front, in 2024, approximately 42,250 women are expected to die of breast cancer; 530 breast cancer deaths are anticipated in men.
- As for the lifetime risk for breast cancer, approximately one in eight women in the United States (13.1%) will be diagnosed with invasive breast cancer; 1 in 43 (2.3%) will die from the disease.
- The 5-year relative survival rate for breast cancer is 91%, but that drops to 86% at 10 years and 81% at 15 years.
- The 5-year relative survival rate is over 99% for breast cancer diagnosed at a localized stage but drops to 87% for regional-stage and 32% for distant-stage disease.
- American Indian/Alaska Native women have a 10% lower breast cancer incidence than White women but 6% higher mortality.
Similar to the ACS report, a recent study published in JAMA Network Open reported rising breast cancer incidence among US women aged 20-49 years of different races in different age groups over the past 2 decades.
The increased incidence of breast cancer in younger women “is an area of concern and an area where we really need to spend more effort trying to understand why,” said lead study author and breast surgeon Adetunji T. Toriola, MD, PhD, MPH, of Washington University in St Louis, Missouri.
Although reproductive and lifestyle factors, such as weight gain, diet, and physical activity, may contribute to the growing breast cancer incidence in younger women — and preliminary findings from Dr. Toriola’s own research suggest that reproductive factors may be a particularly strong driver — environmental factors, including exposure to forever chemicals, may also play a role.
Early-life factors, such as exposure to toxins, remain an underexplored area, Dr. Toriola noted, stressing the importance of teasing out the long-term effects of environmental exposures in puberty and during adolescence.
Overall, the trends observed both in this study and the ACS report highlight the need for enhanced prevention efforts that address racial disparities as well as the rising incidence in young women, said Dr. Toriola, also professor of surgery at the Washington University Institute of Public Health, St Louis.
For now, Dr. Toriola urges women to “engage with mammographic screening as soon as qualified” as per guidelines. Women at average risk should go for screening beginning at age 40, and those with a family history or other risk factors should talk to their physician about earlier screening, he said.
Ms. Giaquinto is employed by the ACS, which receives grants from private and corporate foundations, including foundations associated with companies in the health sector, for research outside of the submitted work. Dr. Toriola reported having no disclosures.
A version of this article first appeared on Medscape.com.
Breast cancer incidence has been on the rise, particularly among White women under age 50, but breast cancer deaths — for some, but not all, populations — have been steadily decreasing, according to a biennial update from the American Cancer Society (ACS).
The ACS update, which underscores the persistence of racial and ethnic disparities in breast cancer incidence and outcomes, noted an overall 1% annual increase in breast cancer incidence from 2012 to 2021. The additional cases were largely composed of localized-stage and hormone receptor (HR)–positive disease, which generally have better prognoses than more advanced and HR–negative disease.
Deaths from breast cancer, however, declined from 1989 to 2022, with an overall drop of 44%. That percentage drop “translates to almost 518,000 fewer women dying from breast cancer in the United States during this time,” Angela N. Giaquinto and ACS colleagues noted in the report, published in CA: A Cancer Journal for Clinicians.
“This progress is the result of advances in treatment and earlier detection through screening,” the authors wrote, while stressing that “these interventions have not been disseminated equally.”
The ACS also published an educational companion — Breast Cancer Facts & Figures 2024-2025 — that provides additional insights about trends in breast cancer and steps needed to bolster prevention, detection, and treatment advances.
Incidence and Mortality
Although the overall annual increase in breast cancer incidence from 2012 to 2021 was 1%, the increase was steeper among women under age 50, at 1.4% annually vs 0.7% among those aged 50 or older.
Asian American/Pacific Islander women had the greatest increases in breast cancer incidence among both age groups, with a 2.7% annual increase for those aged under 50 and a 2.5% increase for those aged 50 or older. This group, however, had the second lowest breast cancer rate in 2000 at 57.4 cases per 100,000 persons, but the highest rate in 2021 at 86.3 cases per 100,000, alongside White women (86.4 cases per 100,000). Black women were not far behind at 81.5 cases per 100,000.
Black women were least likely to be diagnosed with localized-stage breast cancer and most likely to be diagnosed with distant-stage or unstaged cancer, with American Indian/Alaska Native women not far behind.
Despite the rising incidence of breast cancer, death rates from the disease have gone down considerably overall from about 33 deaths per 100,000 women in 1989 to 19 deaths per 100,000 in 2022.
However, not all women have experienced these survival gains equally, Ms. Giaquinto and colleagues noted.
Since 1990, the mortality rate has remained unchanged among American Indian/Alaska Native women. Black women, however, have experienced a 38% higher mortality rate than White women, despite having a 5% lower incidence of breast cancer.
In fact, Black women have the lowest survival of any racial and ethnic group for every breast cancer subtype and stage of disease except localized disease.
Additional key findings from the report:
- In 2024, an estimated 310,720 new invasive breast cancers and 56,500 cases of ductal carcinoma in situ will be diagnosed among women in the United States, and an additional 2790 cases will be diagnosed in men.
- On the mortality front, in 2024, approximately 42,250 women are expected to die of breast cancer; 530 breast cancer deaths are anticipated in men.
- As for the lifetime risk for breast cancer, approximately one in eight women in the United States (13.1%) will be diagnosed with invasive breast cancer; 1 in 43 (2.3%) will die from the disease.
- The 5-year relative survival rate for breast cancer is 91%, but that drops to 86% at 10 years and 81% at 15 years.
- The 5-year relative survival rate is over 99% for breast cancer diagnosed at a localized stage but drops to 87% for regional-stage and 32% for distant-stage disease.
- American Indian/Alaska Native women have a 10% lower breast cancer incidence than White women but 6% higher mortality.
Similar to the ACS report, a recent study published in JAMA Network Open reported rising breast cancer incidence among US women aged 20-49 years of different races in different age groups over the past 2 decades.
The increased incidence of breast cancer in younger women “is an area of concern and an area where we really need to spend more effort trying to understand why,” said lead study author and breast surgeon Adetunji T. Toriola, MD, PhD, MPH, of Washington University in St Louis, Missouri.
Although reproductive and lifestyle factors, such as weight gain, diet, and physical activity, may contribute to the growing breast cancer incidence in younger women — and preliminary findings from Dr. Toriola’s own research suggest that reproductive factors may be a particularly strong driver — environmental factors, including exposure to forever chemicals, may also play a role.
Early-life factors, such as exposure to toxins, remain an underexplored area, Dr. Toriola noted, stressing the importance of teasing out the long-term effects of environmental exposures in puberty and during adolescence.
Overall, the trends observed both in this study and the ACS report highlight the need for enhanced prevention efforts that address racial disparities as well as the rising incidence in young women, said Dr. Toriola, also professor of surgery at the Washington University Institute of Public Health, St Louis.
For now, Dr. Toriola urges women to “engage with mammographic screening as soon as qualified” as per guidelines. Women at average risk should go for screening beginning at age 40, and those with a family history or other risk factors should talk to their physician about earlier screening, he said.
Ms. Giaquinto is employed by the ACS, which receives grants from private and corporate foundations, including foundations associated with companies in the health sector, for research outside of the submitted work. Dr. Toriola reported having no disclosures.
A version of this article first appeared on Medscape.com.
Breast cancer incidence has been on the rise, particularly among White women under age 50, but breast cancer deaths — for some, but not all, populations — have been steadily decreasing, according to a biennial update from the American Cancer Society (ACS).
The ACS update, which underscores the persistence of racial and ethnic disparities in breast cancer incidence and outcomes, noted an overall 1% annual increase in breast cancer incidence from 2012 to 2021. The additional cases were largely composed of localized-stage and hormone receptor (HR)–positive disease, which generally have better prognoses than more advanced and HR–negative disease.
Deaths from breast cancer, however, declined from 1989 to 2022, with an overall drop of 44%. That percentage drop “translates to almost 518,000 fewer women dying from breast cancer in the United States during this time,” Angela N. Giaquinto and ACS colleagues noted in the report, published in CA: A Cancer Journal for Clinicians.
“This progress is the result of advances in treatment and earlier detection through screening,” the authors wrote, while stressing that “these interventions have not been disseminated equally.”
The ACS also published an educational companion — Breast Cancer Facts & Figures 2024-2025 — that provides additional insights about trends in breast cancer and steps needed to bolster prevention, detection, and treatment advances.
Incidence and Mortality
Although the overall annual increase in breast cancer incidence from 2012 to 2021 was 1%, the increase was steeper among women under age 50, at 1.4% annually vs 0.7% among those aged 50 or older.
Asian American/Pacific Islander women had the greatest increases in breast cancer incidence among both age groups, with a 2.7% annual increase for those aged under 50 and a 2.5% increase for those aged 50 or older. This group, however, had the second lowest breast cancer rate in 2000 at 57.4 cases per 100,000 persons, but the highest rate in 2021 at 86.3 cases per 100,000, alongside White women (86.4 cases per 100,000). Black women were not far behind at 81.5 cases per 100,000.
Black women were least likely to be diagnosed with localized-stage breast cancer and most likely to be diagnosed with distant-stage or unstaged cancer, with American Indian/Alaska Native women not far behind.
Despite the rising incidence of breast cancer, death rates from the disease have gone down considerably overall from about 33 deaths per 100,000 women in 1989 to 19 deaths per 100,000 in 2022.
However, not all women have experienced these survival gains equally, Ms. Giaquinto and colleagues noted.
Since 1990, the mortality rate has remained unchanged among American Indian/Alaska Native women. Black women, however, have experienced a 38% higher mortality rate than White women, despite having a 5% lower incidence of breast cancer.
In fact, Black women have the lowest survival of any racial and ethnic group for every breast cancer subtype and stage of disease except localized disease.
Additional key findings from the report:
- In 2024, an estimated 310,720 new invasive breast cancers and 56,500 cases of ductal carcinoma in situ will be diagnosed among women in the United States, and an additional 2790 cases will be diagnosed in men.
- On the mortality front, in 2024, approximately 42,250 women are expected to die of breast cancer; 530 breast cancer deaths are anticipated in men.
- As for the lifetime risk for breast cancer, approximately one in eight women in the United States (13.1%) will be diagnosed with invasive breast cancer; 1 in 43 (2.3%) will die from the disease.
- The 5-year relative survival rate for breast cancer is 91%, but that drops to 86% at 10 years and 81% at 15 years.
- The 5-year relative survival rate is over 99% for breast cancer diagnosed at a localized stage but drops to 87% for regional-stage and 32% for distant-stage disease.
- American Indian/Alaska Native women have a 10% lower breast cancer incidence than White women but 6% higher mortality.
Similar to the ACS report, a recent study published in JAMA Network Open reported rising breast cancer incidence among US women aged 20-49 years of different races in different age groups over the past 2 decades.
The increased incidence of breast cancer in younger women “is an area of concern and an area where we really need to spend more effort trying to understand why,” said lead study author and breast surgeon Adetunji T. Toriola, MD, PhD, MPH, of Washington University in St Louis, Missouri.
Although reproductive and lifestyle factors, such as weight gain, diet, and physical activity, may contribute to the growing breast cancer incidence in younger women — and preliminary findings from Dr. Toriola’s own research suggest that reproductive factors may be a particularly strong driver — environmental factors, including exposure to forever chemicals, may also play a role.
Early-life factors, such as exposure to toxins, remain an underexplored area, Dr. Toriola noted, stressing the importance of teasing out the long-term effects of environmental exposures in puberty and during adolescence.
Overall, the trends observed both in this study and the ACS report highlight the need for enhanced prevention efforts that address racial disparities as well as the rising incidence in young women, said Dr. Toriola, also professor of surgery at the Washington University Institute of Public Health, St Louis.
For now, Dr. Toriola urges women to “engage with mammographic screening as soon as qualified” as per guidelines. Women at average risk should go for screening beginning at age 40, and those with a family history or other risk factors should talk to their physician about earlier screening, he said.
Ms. Giaquinto is employed by the ACS, which receives grants from private and corporate foundations, including foundations associated with companies in the health sector, for research outside of the submitted work. Dr. Toriola reported having no disclosures.
A version of this article first appeared on Medscape.com.
The Biology of ‘Precancer’: Stopping Cancer Before It Starts
Some breast cancer types are more likely than others to recur. Researchers have known this for more than a decade.
But they have long wondered why.
“How did those tumor types arise?” said Christina Curtis, PhD, a professor of medicine, genetics and biomedical data science at Stanford University in California. “They’re all breast cancers. They’re all estrogen receptor positive. But these groups are different. When did they become different, and how is that determined?”
Dr. Curtis and colleagues are finally starting to answer these questions. They recently broke new ground in a study linking differences in cancer-related genes to disease subtype and aggressiveness.
DNA inherited from our parents is known as the germline genome. It affects whether the immune system attacks or retreats when confronted with variations that may lead to breast cancer.
“It turns out, the germline genome sculpts tumor evolution,” said Dr. Curtis.
The study is part of a growing effort to understand “precancer” — the critical period after cells have started to grow abnormally but before they’ve developed into cancer — a research trend that could trigger a decisive shift in how cancer treatments are realized. Therapeutics could be designed on the basis of the biology of these precancerous cells.
While biotech start-ups push new tests to catch cancer early, researchers like Dr. Curtis hope to stop cancer before it even starts.
“This is a really exciting area of research,” said Susan Domchek, MD, executive director of the Basser Center for BRCA at the University of Pennsylvania, Philadelphia, who was not involved in the study. “What we hope for is that, over time, we’re going to have more and more biologically driven interception.”
‘We’re Basically Unearthing the Dark Matter of the Human Genome’
Of course, we already have mechanical ways of heading off cancer, like having a precancerous polyp removed. But for the Stanford researchers, biologic interception is the goal. They hope to figure out how to use the immune system to stop the cancer.
In their study, they looked at DNA variabilities known as somatic aberrations or single-nucleotide protein sequences (SNPs). The HER2 gene, for example, can contain SNPs — possibly affecting how the HER2 protein regulates breast cell growth and division.
“There’s been a huge effort through genomewide association studies to link SNPs to cancer outcomes and risk,” Dr. Curtis said.
Focusing on people with a genetic predisposition for breast cancer, Dr. Curtis used machine learning to show that these variabilities can occur in specific epitopes (protein features that can trigger an immune response).
They also found that heightened variability can show up in a region of the genome called the human leukocyte antigen (HLA). Each HLA molecule can contain many epitopes.
“We developed a whole new algorithm to compute this ‘germline epitope burden,’ ” Dr. Curtis said. “We’re basically unearthing the dark matter of the human genome to ask about the interplay between SNPs and HLA class one presentation.”
These aberration-rich regions can grab the immune system’s attention. Sometimes the immune system identifies and eradicates those epitopes.
In that case: “I have immunosurveillance. I’ve cured my cancer,” said Nora Disis, PhD, director of the Cancer Vaccine Institute and a professor of medicine at the University of Washington, Seattle. Dr. Disis was not involved in the study.
But other times, the immune system finds a way around the high “epitope burden,” and the tumors become more aggressive and immunosuppressive. That’s when cancer forms.
This suggests a “critical juncture between preinvasive and invasive disease,” Dr. Curtis said.
And that “critical juncture” may very well be the optimal time for intervention.
The Precancer Push
Stanford’s findings add information to prior biomarkers and may provide a way to identify “bad-acting tumors” from a simple blood draw measuring germline epitope burden, Dr. Curtis said. Looking further ahead, “this also reveals a new source of epitopes that might be immunogenic and might be informative for the development of vaccines.”
Many labs are trying to understand the biology of precancer and exploring possible vaccines.
The National Cancer Institute’s Human Tumor Atlas Network is building three-dimensional models of the evolution from precancerous to advanced disease. And researchers at the Cancer Vaccine Institute at the University of Washington are developing a vaccine for a precancerous lesion linked to many ovarian cancers.
Dr. Domchek’s research explores whether breast cancers caused by mutations in the BRCA 1 and 2 genes can be intercepted at very early stages. In a clinical trial of healthy people with those mutations, Dr. Domchek and colleagues are attempting to “rev up the immune system to tackle telomerase,” an enzyme that’s over-expressed in 95% of cancers. The hope is for this experimental vaccine to lower their risk of developing cancer.
At the Fred Hutch Cancer Center, Seattle, Ming Yu, PhD, is studying how senescent cells affect immune cells in precancer. As cells age and stop dividing, she said, they can accumulate and create a “tumor-promoting microenvironment” in older people.
Dr. Yu has found that the antiaging drug rapamycin can eliminate those “zombie cells” in mice. She’s studying whether the “cleanup” can help prevent cancer and expects results in a few months.
In the years and decades to come, all of this could lead to a new era in cancer treatment.
“Most drug development starts with people with advanced cancer and then goes into the earlier and earlier spaces,” said Dr. Domchek. “But it may be that we’re thinking about it all wrong and that you really have to understand the unique biology of early lesions to go after them.”
A version of this article first appeared on Medscape.com.
Some breast cancer types are more likely than others to recur. Researchers have known this for more than a decade.
But they have long wondered why.
“How did those tumor types arise?” said Christina Curtis, PhD, a professor of medicine, genetics and biomedical data science at Stanford University in California. “They’re all breast cancers. They’re all estrogen receptor positive. But these groups are different. When did they become different, and how is that determined?”
Dr. Curtis and colleagues are finally starting to answer these questions. They recently broke new ground in a study linking differences in cancer-related genes to disease subtype and aggressiveness.
DNA inherited from our parents is known as the germline genome. It affects whether the immune system attacks or retreats when confronted with variations that may lead to breast cancer.
“It turns out, the germline genome sculpts tumor evolution,” said Dr. Curtis.
The study is part of a growing effort to understand “precancer” — the critical period after cells have started to grow abnormally but before they’ve developed into cancer — a research trend that could trigger a decisive shift in how cancer treatments are realized. Therapeutics could be designed on the basis of the biology of these precancerous cells.
While biotech start-ups push new tests to catch cancer early, researchers like Dr. Curtis hope to stop cancer before it even starts.
“This is a really exciting area of research,” said Susan Domchek, MD, executive director of the Basser Center for BRCA at the University of Pennsylvania, Philadelphia, who was not involved in the study. “What we hope for is that, over time, we’re going to have more and more biologically driven interception.”
‘We’re Basically Unearthing the Dark Matter of the Human Genome’
Of course, we already have mechanical ways of heading off cancer, like having a precancerous polyp removed. But for the Stanford researchers, biologic interception is the goal. They hope to figure out how to use the immune system to stop the cancer.
In their study, they looked at DNA variabilities known as somatic aberrations or single-nucleotide protein sequences (SNPs). The HER2 gene, for example, can contain SNPs — possibly affecting how the HER2 protein regulates breast cell growth and division.
“There’s been a huge effort through genomewide association studies to link SNPs to cancer outcomes and risk,” Dr. Curtis said.
Focusing on people with a genetic predisposition for breast cancer, Dr. Curtis used machine learning to show that these variabilities can occur in specific epitopes (protein features that can trigger an immune response).
They also found that heightened variability can show up in a region of the genome called the human leukocyte antigen (HLA). Each HLA molecule can contain many epitopes.
“We developed a whole new algorithm to compute this ‘germline epitope burden,’ ” Dr. Curtis said. “We’re basically unearthing the dark matter of the human genome to ask about the interplay between SNPs and HLA class one presentation.”
These aberration-rich regions can grab the immune system’s attention. Sometimes the immune system identifies and eradicates those epitopes.
In that case: “I have immunosurveillance. I’ve cured my cancer,” said Nora Disis, PhD, director of the Cancer Vaccine Institute and a professor of medicine at the University of Washington, Seattle. Dr. Disis was not involved in the study.
But other times, the immune system finds a way around the high “epitope burden,” and the tumors become more aggressive and immunosuppressive. That’s when cancer forms.
This suggests a “critical juncture between preinvasive and invasive disease,” Dr. Curtis said.
And that “critical juncture” may very well be the optimal time for intervention.
The Precancer Push
Stanford’s findings add information to prior biomarkers and may provide a way to identify “bad-acting tumors” from a simple blood draw measuring germline epitope burden, Dr. Curtis said. Looking further ahead, “this also reveals a new source of epitopes that might be immunogenic and might be informative for the development of vaccines.”
Many labs are trying to understand the biology of precancer and exploring possible vaccines.
The National Cancer Institute’s Human Tumor Atlas Network is building three-dimensional models of the evolution from precancerous to advanced disease. And researchers at the Cancer Vaccine Institute at the University of Washington are developing a vaccine for a precancerous lesion linked to many ovarian cancers.
Dr. Domchek’s research explores whether breast cancers caused by mutations in the BRCA 1 and 2 genes can be intercepted at very early stages. In a clinical trial of healthy people with those mutations, Dr. Domchek and colleagues are attempting to “rev up the immune system to tackle telomerase,” an enzyme that’s over-expressed in 95% of cancers. The hope is for this experimental vaccine to lower their risk of developing cancer.
At the Fred Hutch Cancer Center, Seattle, Ming Yu, PhD, is studying how senescent cells affect immune cells in precancer. As cells age and stop dividing, she said, they can accumulate and create a “tumor-promoting microenvironment” in older people.
Dr. Yu has found that the antiaging drug rapamycin can eliminate those “zombie cells” in mice. She’s studying whether the “cleanup” can help prevent cancer and expects results in a few months.
In the years and decades to come, all of this could lead to a new era in cancer treatment.
“Most drug development starts with people with advanced cancer and then goes into the earlier and earlier spaces,” said Dr. Domchek. “But it may be that we’re thinking about it all wrong and that you really have to understand the unique biology of early lesions to go after them.”
A version of this article first appeared on Medscape.com.
Some breast cancer types are more likely than others to recur. Researchers have known this for more than a decade.
But they have long wondered why.
“How did those tumor types arise?” said Christina Curtis, PhD, a professor of medicine, genetics and biomedical data science at Stanford University in California. “They’re all breast cancers. They’re all estrogen receptor positive. But these groups are different. When did they become different, and how is that determined?”
Dr. Curtis and colleagues are finally starting to answer these questions. They recently broke new ground in a study linking differences in cancer-related genes to disease subtype and aggressiveness.
DNA inherited from our parents is known as the germline genome. It affects whether the immune system attacks or retreats when confronted with variations that may lead to breast cancer.
“It turns out, the germline genome sculpts tumor evolution,” said Dr. Curtis.
The study is part of a growing effort to understand “precancer” — the critical period after cells have started to grow abnormally but before they’ve developed into cancer — a research trend that could trigger a decisive shift in how cancer treatments are realized. Therapeutics could be designed on the basis of the biology of these precancerous cells.
While biotech start-ups push new tests to catch cancer early, researchers like Dr. Curtis hope to stop cancer before it even starts.
“This is a really exciting area of research,” said Susan Domchek, MD, executive director of the Basser Center for BRCA at the University of Pennsylvania, Philadelphia, who was not involved in the study. “What we hope for is that, over time, we’re going to have more and more biologically driven interception.”
‘We’re Basically Unearthing the Dark Matter of the Human Genome’
Of course, we already have mechanical ways of heading off cancer, like having a precancerous polyp removed. But for the Stanford researchers, biologic interception is the goal. They hope to figure out how to use the immune system to stop the cancer.
In their study, they looked at DNA variabilities known as somatic aberrations or single-nucleotide protein sequences (SNPs). The HER2 gene, for example, can contain SNPs — possibly affecting how the HER2 protein regulates breast cell growth and division.
“There’s been a huge effort through genomewide association studies to link SNPs to cancer outcomes and risk,” Dr. Curtis said.
Focusing on people with a genetic predisposition for breast cancer, Dr. Curtis used machine learning to show that these variabilities can occur in specific epitopes (protein features that can trigger an immune response).
They also found that heightened variability can show up in a region of the genome called the human leukocyte antigen (HLA). Each HLA molecule can contain many epitopes.
“We developed a whole new algorithm to compute this ‘germline epitope burden,’ ” Dr. Curtis said. “We’re basically unearthing the dark matter of the human genome to ask about the interplay between SNPs and HLA class one presentation.”
These aberration-rich regions can grab the immune system’s attention. Sometimes the immune system identifies and eradicates those epitopes.
In that case: “I have immunosurveillance. I’ve cured my cancer,” said Nora Disis, PhD, director of the Cancer Vaccine Institute and a professor of medicine at the University of Washington, Seattle. Dr. Disis was not involved in the study.
But other times, the immune system finds a way around the high “epitope burden,” and the tumors become more aggressive and immunosuppressive. That’s when cancer forms.
This suggests a “critical juncture between preinvasive and invasive disease,” Dr. Curtis said.
And that “critical juncture” may very well be the optimal time for intervention.
The Precancer Push
Stanford’s findings add information to prior biomarkers and may provide a way to identify “bad-acting tumors” from a simple blood draw measuring germline epitope burden, Dr. Curtis said. Looking further ahead, “this also reveals a new source of epitopes that might be immunogenic and might be informative for the development of vaccines.”
Many labs are trying to understand the biology of precancer and exploring possible vaccines.
The National Cancer Institute’s Human Tumor Atlas Network is building three-dimensional models of the evolution from precancerous to advanced disease. And researchers at the Cancer Vaccine Institute at the University of Washington are developing a vaccine for a precancerous lesion linked to many ovarian cancers.
Dr. Domchek’s research explores whether breast cancers caused by mutations in the BRCA 1 and 2 genes can be intercepted at very early stages. In a clinical trial of healthy people with those mutations, Dr. Domchek and colleagues are attempting to “rev up the immune system to tackle telomerase,” an enzyme that’s over-expressed in 95% of cancers. The hope is for this experimental vaccine to lower their risk of developing cancer.
At the Fred Hutch Cancer Center, Seattle, Ming Yu, PhD, is studying how senescent cells affect immune cells in precancer. As cells age and stop dividing, she said, they can accumulate and create a “tumor-promoting microenvironment” in older people.
Dr. Yu has found that the antiaging drug rapamycin can eliminate those “zombie cells” in mice. She’s studying whether the “cleanup” can help prevent cancer and expects results in a few months.
In the years and decades to come, all of this could lead to a new era in cancer treatment.
“Most drug development starts with people with advanced cancer and then goes into the earlier and earlier spaces,” said Dr. Domchek. “But it may be that we’re thinking about it all wrong and that you really have to understand the unique biology of early lesions to go after them.”
A version of this article first appeared on Medscape.com.
Hypothyroidism Treatment Does Not Affect Cognitive Decline in Menopausal Women
TOPLINE:
Women with hypothyroidism treated with levothyroxine show no significant cognitive decline across the menopausal transition compared with those without thyroid disease.
METHODOLOGY:
- Levothyroxine, the primary treatment for hypothyroidism, has been linked to perceived cognitive deficits, yet it is unclear whether this is due to the underlying condition being inadequately treated or other factors.
- Using data collected from the Study of Women’s Health Across the Nation, which encompasses five ethnic/racial groups from seven centers across the United States, researchers compared cognitive function over time between women with hypothyroidism treated with levothyroxine and those without thyroid disease.
- Participants underwent cognitive testing across three domains — processing speed, working memory, and episodic memory — which were assessed over a mean follow-up of 13 years.
- Further analyses assessed the impact of abnormal levels of thyroid-stimulating hormone on cognitive outcomes.
TAKEAWAY:
- Of 2033 women included, 227 (mean age, 49.8 years) had levothyroxine-treated hypothyroidism and 1806 (mean age, 50.0 years) did not have thyroid disease; the proportion of women with premenopausal or early perimenopausal status at baseline was higher in the hypothyroidism group (54.2% vs 49.8%; P = .010).
- At baseline, levothyroxine-treated women had higher scores for processing speed (mean score, 56.5 vs 54.4; P = .006) and working memory (mean score, 6.8 vs 6.4; P = .018) than those without thyroid disease; however, no difference in episodic memory was observed between the groups.
- Over the study period, there was no significant difference in cognitive decline between the groups.
- There was no significant effect of levothyroxine-treated hypothyroidism on working memory or episodic memory, although an annual decline in processing speed was observed (P < .001).
- Sensitivity analyses determined that abnormal levels of thyroid-stimulating hormone did not affect cognitive outcomes in women with hypothyroidism.
IN PRACTICE:
When cognitive decline is observed in these patients, the authors advised that “clinicians should resist anchoring on inadequate treatment of hypothyroidism as the cause of these symptoms and may investigate other disease processes (eg, iron deficiency, B12 deficiency, sleep apnea, celiac disease).”
SOURCE:
The study, led by Matthew D. Ettleson, Section of Endocrinology, Diabetes, and Metabolism, University of Chicago, was published online in Thyroid.
LIMITATIONS:
The cognitive assessments in the study were not designed to provide a thorough evaluation of all aspects of cognitive function. The study may not have been adequately powered to detect small effects of levothyroxine-treated hypothyroidism on cognitive outcomes. The higher levels of education attained by the study population may have acted as a protective factor against cognitive decline, potentially biasing the results.
DISCLOSURES:
The Study of Women’s Health Across the Nation was supported by grants from the National Institutes of Health (NIH), DHHS, through the National Institute on Aging, the National Institute of Nursing Research, and the NIH Office of Research on Women’s Health. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Women with hypothyroidism treated with levothyroxine show no significant cognitive decline across the menopausal transition compared with those without thyroid disease.
METHODOLOGY:
- Levothyroxine, the primary treatment for hypothyroidism, has been linked to perceived cognitive deficits, yet it is unclear whether this is due to the underlying condition being inadequately treated or other factors.
- Using data collected from the Study of Women’s Health Across the Nation, which encompasses five ethnic/racial groups from seven centers across the United States, researchers compared cognitive function over time between women with hypothyroidism treated with levothyroxine and those without thyroid disease.
- Participants underwent cognitive testing across three domains — processing speed, working memory, and episodic memory — which were assessed over a mean follow-up of 13 years.
- Further analyses assessed the impact of abnormal levels of thyroid-stimulating hormone on cognitive outcomes.
TAKEAWAY:
- Of 2033 women included, 227 (mean age, 49.8 years) had levothyroxine-treated hypothyroidism and 1806 (mean age, 50.0 years) did not have thyroid disease; the proportion of women with premenopausal or early perimenopausal status at baseline was higher in the hypothyroidism group (54.2% vs 49.8%; P = .010).
- At baseline, levothyroxine-treated women had higher scores for processing speed (mean score, 56.5 vs 54.4; P = .006) and working memory (mean score, 6.8 vs 6.4; P = .018) than those without thyroid disease; however, no difference in episodic memory was observed between the groups.
- Over the study period, there was no significant difference in cognitive decline between the groups.
- There was no significant effect of levothyroxine-treated hypothyroidism on working memory or episodic memory, although an annual decline in processing speed was observed (P < .001).
- Sensitivity analyses determined that abnormal levels of thyroid-stimulating hormone did not affect cognitive outcomes in women with hypothyroidism.
IN PRACTICE:
When cognitive decline is observed in these patients, the authors advised that “clinicians should resist anchoring on inadequate treatment of hypothyroidism as the cause of these symptoms and may investigate other disease processes (eg, iron deficiency, B12 deficiency, sleep apnea, celiac disease).”
SOURCE:
The study, led by Matthew D. Ettleson, Section of Endocrinology, Diabetes, and Metabolism, University of Chicago, was published online in Thyroid.
LIMITATIONS:
The cognitive assessments in the study were not designed to provide a thorough evaluation of all aspects of cognitive function. The study may not have been adequately powered to detect small effects of levothyroxine-treated hypothyroidism on cognitive outcomes. The higher levels of education attained by the study population may have acted as a protective factor against cognitive decline, potentially biasing the results.
DISCLOSURES:
The Study of Women’s Health Across the Nation was supported by grants from the National Institutes of Health (NIH), DHHS, through the National Institute on Aging, the National Institute of Nursing Research, and the NIH Office of Research on Women’s Health. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Women with hypothyroidism treated with levothyroxine show no significant cognitive decline across the menopausal transition compared with those without thyroid disease.
METHODOLOGY:
- Levothyroxine, the primary treatment for hypothyroidism, has been linked to perceived cognitive deficits, yet it is unclear whether this is due to the underlying condition being inadequately treated or other factors.
- Using data collected from the Study of Women’s Health Across the Nation, which encompasses five ethnic/racial groups from seven centers across the United States, researchers compared cognitive function over time between women with hypothyroidism treated with levothyroxine and those without thyroid disease.
- Participants underwent cognitive testing across three domains — processing speed, working memory, and episodic memory — which were assessed over a mean follow-up of 13 years.
- Further analyses assessed the impact of abnormal levels of thyroid-stimulating hormone on cognitive outcomes.
TAKEAWAY:
- Of 2033 women included, 227 (mean age, 49.8 years) had levothyroxine-treated hypothyroidism and 1806 (mean age, 50.0 years) did not have thyroid disease; the proportion of women with premenopausal or early perimenopausal status at baseline was higher in the hypothyroidism group (54.2% vs 49.8%; P = .010).
- At baseline, levothyroxine-treated women had higher scores for processing speed (mean score, 56.5 vs 54.4; P = .006) and working memory (mean score, 6.8 vs 6.4; P = .018) than those without thyroid disease; however, no difference in episodic memory was observed between the groups.
- Over the study period, there was no significant difference in cognitive decline between the groups.
- There was no significant effect of levothyroxine-treated hypothyroidism on working memory or episodic memory, although an annual decline in processing speed was observed (P < .001).
- Sensitivity analyses determined that abnormal levels of thyroid-stimulating hormone did not affect cognitive outcomes in women with hypothyroidism.
IN PRACTICE:
When cognitive decline is observed in these patients, the authors advised that “clinicians should resist anchoring on inadequate treatment of hypothyroidism as the cause of these symptoms and may investigate other disease processes (eg, iron deficiency, B12 deficiency, sleep apnea, celiac disease).”
SOURCE:
The study, led by Matthew D. Ettleson, Section of Endocrinology, Diabetes, and Metabolism, University of Chicago, was published online in Thyroid.
LIMITATIONS:
The cognitive assessments in the study were not designed to provide a thorough evaluation of all aspects of cognitive function. The study may not have been adequately powered to detect small effects of levothyroxine-treated hypothyroidism on cognitive outcomes. The higher levels of education attained by the study population may have acted as a protective factor against cognitive decline, potentially biasing the results.
DISCLOSURES:
The Study of Women’s Health Across the Nation was supported by grants from the National Institutes of Health (NIH), DHHS, through the National Institute on Aging, the National Institute of Nursing Research, and the NIH Office of Research on Women’s Health. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Severe Autoimmune Diseases Linked to Premature Ovarian Insufficiency
TOPLINE:
Women with premature ovarian insufficiency (POI) have a 2.6 times higher prevalence of severe autoimmune diseases before diagnosis and a 2- to 3-fold increased risk for these diseases after diagnosis.
METHODOLOGY:
- Researchers conducted a population-based registry study including 3972 women diagnosed with spontaneous POI between 1988 and 2017.
- A total of 15,708 female population controls matched by age and municipality of residence were included for comparison.
- Autoimmune disease diagnoses were evaluated from childhood until the end of 2017 using the Hospital Discharge Registry.
- Women with a history of cancer or bilateral oophorectomy were excluded from the study.
TAKEAWAY:
- Women with POI had a 2.6 times higher prevalence of severe autoimmune diseases before diagnosis compared to controls (odds ratio [OR], 2.6; 95% CI, 2.2-3.1).
- The prevalence of specific autoimmune diseases such as polyglandular autoimmune diseases (OR, 25.8; 95% CI, 9.0-74.1) and Addison disease (OR, 22.9; 95% CI, 7.9-66.1) was significantly higher in women with POI.
- The standardized incidence ratios for being diagnosed with a severe autoimmune disease after POI diagnosis was 2.8 (95% CI, 2.3-3.4) during the first 3 years, decreasing to 1.3 (95% CI, 1.1-1.6) after 12 years.
- No significant difference was found in the prevalence of diabetes type 1 and ankylosing spondylitis between women with POI and the reference cohort.
IN PRACTICE:
“The study results strengthen the hypothesis that autoimmune mechanisms play an important role in the pathogenesis of POI. Future studies should focus on the immunological mechanism of POI from preventative and curative perspectives,” wrote the authors of the study.
SOURCE:
The study was led by Susanna M. Savukoski, Oulu University Hospital in Finland. It was published online in Human Reproduction.
LIMITATIONS:
The study included only autoimmune disorders diagnosed in specialized health care, which may underestimate the overall prevalence of autoimmune disorders in women with POI. Additionally, the study did not account for confounders such as body mass index and smoking, which are associated with the risk for autoimmune disease and POI.
DISCLOSURES:
Ms. Savukoski received grants from the Finnish Menopause Society, the Finnish Medical Foundation, and the Juho Vainio Foundation. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Women with premature ovarian insufficiency (POI) have a 2.6 times higher prevalence of severe autoimmune diseases before diagnosis and a 2- to 3-fold increased risk for these diseases after diagnosis.
METHODOLOGY:
- Researchers conducted a population-based registry study including 3972 women diagnosed with spontaneous POI between 1988 and 2017.
- A total of 15,708 female population controls matched by age and municipality of residence were included for comparison.
- Autoimmune disease diagnoses were evaluated from childhood until the end of 2017 using the Hospital Discharge Registry.
- Women with a history of cancer or bilateral oophorectomy were excluded from the study.
TAKEAWAY:
- Women with POI had a 2.6 times higher prevalence of severe autoimmune diseases before diagnosis compared to controls (odds ratio [OR], 2.6; 95% CI, 2.2-3.1).
- The prevalence of specific autoimmune diseases such as polyglandular autoimmune diseases (OR, 25.8; 95% CI, 9.0-74.1) and Addison disease (OR, 22.9; 95% CI, 7.9-66.1) was significantly higher in women with POI.
- The standardized incidence ratios for being diagnosed with a severe autoimmune disease after POI diagnosis was 2.8 (95% CI, 2.3-3.4) during the first 3 years, decreasing to 1.3 (95% CI, 1.1-1.6) after 12 years.
- No significant difference was found in the prevalence of diabetes type 1 and ankylosing spondylitis between women with POI and the reference cohort.
IN PRACTICE:
“The study results strengthen the hypothesis that autoimmune mechanisms play an important role in the pathogenesis of POI. Future studies should focus on the immunological mechanism of POI from preventative and curative perspectives,” wrote the authors of the study.
SOURCE:
The study was led by Susanna M. Savukoski, Oulu University Hospital in Finland. It was published online in Human Reproduction.
LIMITATIONS:
The study included only autoimmune disorders diagnosed in specialized health care, which may underestimate the overall prevalence of autoimmune disorders in women with POI. Additionally, the study did not account for confounders such as body mass index and smoking, which are associated with the risk for autoimmune disease and POI.
DISCLOSURES:
Ms. Savukoski received grants from the Finnish Menopause Society, the Finnish Medical Foundation, and the Juho Vainio Foundation. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Women with premature ovarian insufficiency (POI) have a 2.6 times higher prevalence of severe autoimmune diseases before diagnosis and a 2- to 3-fold increased risk for these diseases after diagnosis.
METHODOLOGY:
- Researchers conducted a population-based registry study including 3972 women diagnosed with spontaneous POI between 1988 and 2017.
- A total of 15,708 female population controls matched by age and municipality of residence were included for comparison.
- Autoimmune disease diagnoses were evaluated from childhood until the end of 2017 using the Hospital Discharge Registry.
- Women with a history of cancer or bilateral oophorectomy were excluded from the study.
TAKEAWAY:
- Women with POI had a 2.6 times higher prevalence of severe autoimmune diseases before diagnosis compared to controls (odds ratio [OR], 2.6; 95% CI, 2.2-3.1).
- The prevalence of specific autoimmune diseases such as polyglandular autoimmune diseases (OR, 25.8; 95% CI, 9.0-74.1) and Addison disease (OR, 22.9; 95% CI, 7.9-66.1) was significantly higher in women with POI.
- The standardized incidence ratios for being diagnosed with a severe autoimmune disease after POI diagnosis was 2.8 (95% CI, 2.3-3.4) during the first 3 years, decreasing to 1.3 (95% CI, 1.1-1.6) after 12 years.
- No significant difference was found in the prevalence of diabetes type 1 and ankylosing spondylitis between women with POI and the reference cohort.
IN PRACTICE:
“The study results strengthen the hypothesis that autoimmune mechanisms play an important role in the pathogenesis of POI. Future studies should focus on the immunological mechanism of POI from preventative and curative perspectives,” wrote the authors of the study.
SOURCE:
The study was led by Susanna M. Savukoski, Oulu University Hospital in Finland. It was published online in Human Reproduction.
LIMITATIONS:
The study included only autoimmune disorders diagnosed in specialized health care, which may underestimate the overall prevalence of autoimmune disorders in women with POI. Additionally, the study did not account for confounders such as body mass index and smoking, which are associated with the risk for autoimmune disease and POI.
DISCLOSURES:
Ms. Savukoski received grants from the Finnish Menopause Society, the Finnish Medical Foundation, and the Juho Vainio Foundation. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.